
World Journal of - Gastrointestinal Pathophysiology - NET
282
World Journal of Gastrointestinal Pathophysiology World J Gastrointest Pathophysiol 2015 February 15; 6(1): 1-28 ISSN 2150-5330 (online) Published by Baishideng Publishing Group Inc
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of World Journal of - Gastrointestinal Pathophysiology - NET

World Journal of Gastrointestinal PathophysiologyWorld J Gastrointest Pathophysiol 2015 February 15; 6(1): 1-28
ISSN 2150-5330 (online)
Published by Baishideng Publishing Group Inc

EDITOR-IN-CHIEFThomas Y Ma, Albuquerque
STRATEGY ASSOCIATE EDITOR-IN-CHIEFHirotada Akiho, FukuokaJean-Francois Beaulieu, SherbrookeMichael W Bradbury, ErieSharon DeMorrow, Temple
GUEST EDITORIAL BOARD MEMBERSJia-Ming Chang, TaipeiWai-Keung Chow, TaichungChien-Wei Hsu, KaohsiungMing-Tsan Lin, TaipeiBor-Shyang Sheu, TainanJin-Town Wang, Taipei
MEMBERS OF THE EDITORIAL BOARD
ArgentinaBernabé Matías Quesada, Buenos AiresMarcelo G Roma, Rosario
AustraliaChris Richard Abbiss, JoondalupGuy D Eslick, PenrithMontri Gururatsakul, AdelaideChandana Herath, Melbourne Michael Horowitz, AdelaidMustafa Khasraw, GeelongShu-Chuen Li, CallaghanAntonina Mikocka-Walus, AdelaideNam Quoc Nguyen, Adelaide
Kulmira Nurgali, St AlbansNicholas John Spencer, Flagstaff HillNick Spencer, AdelaideDeborah Verran, CamperdownShu-Feng Zhou, Melbourne
AustriaCord Langner, GrazDietmar Ofner-Velano, SalzburgMichael Trauner, Graz
Belgium
Kathleen Blondeau, LeuvenRobaeys Geert, GenkIlse Maria Hoffman, LeuvenMichael H J Maes, WilrijkTheodoor Abram Niewold, HeverleeXavier Sagaert, LeuvenJean-Marie Vanderwinden, BrusselsKristin Verbeke, LeuvenMathieu Vinken, Roeselare
BrazilUilian Andreis, BotucatuEverson L A Artifon, Vila MarianaJoão Batista Calixto, TrindadeNiels O Saraiva Câmara, Vila ClementinoJulio Chebli, Juiz de ForaFernando Fornari, Passo FundoClélia Akiko Hiruma-Lima, BotucatuMarcel C C Machado, Sao PauloJuarez Quaresma, BelemWagner Vilegas, Araraquara
Brunei Darussalam
Vui Heng Chong, Bandar Seri Begawan
Canada
Fernando Alvarez, MontréalFrancois Boudreau, SherbrookeGeorge A Bubenik, GuelphWang-Xue Chen, OttawaJan D Huizinga, PuslinchKusum K Kharbanda, OmahaWolfgang Kunze, HamiltoJian-Jun Li, OttawaRoderick John Macleod, KingstonMichele Molinari, HalifaxNathalie Rivard, SherbrookeKirill Rosen, HalifaxManuela Santos, MontrealCaroline Saucier, QuebecJean Sévigny, QuebecEldon A Shaffer, CalgaryManuel A Silva, HamiltonAlan B R Thomson, EdmontonPierre H Vachon, Sherbrooke
China
Kai-Xing Ai, ShanghaiZhao-Xiang Bian, Hong KongMin-Hu Chen, GuangzhouCH Cho, Hong KongZhong-Hong Gao, WuhanJun-Ming Guo, NingboJing-Yan Han, Beijing
I
Editorial Board2011-2015
The World Journal of Gastrointestinal Pathophysiology Editorial Board consists of 523 members, representing a team of worldwide experts in gastrointestinal pathophysiology. They are from 45 countries, including Argentina (2), Australia (14), Austria (3), Belgium (9), Brazil (10), Brunei Darussalam (1), Canada (20), China (30), Croatia (1), Czech Republic (2), Denmark (4), Egypt (1), Estonia (1), Finland (1), France (8), Germany (22), Greece (7), Hungary (5), India (10), Indonesia (1), Iran (2), Ireland (2), Israel (8), Italy (42), Japan (47), Lebanon (3), Malaysia (1), Mexico (2), Netherlands (8), Norway (1), Poland (4), Portugal (1), Romania (1), Russia (1), Singapore (4), South Korea (13), Spain (23), Sweden (11), Switzerland (4), Thailand (2), Turkey (6), Ukraine (1), United Kingdom (10), United States (173), and Venezuela (1).
February 15, 2013WJGP|www.wjgnet.com
World Journal ofGastrointestinal PathophysiologyW J G P

Jian-Dong Huang, Hong KongJia-Fu Ji, BeijingShi Liu, WuhanZhan-Ju Liu, ShanghaiXiao-Hong Wang, BeijingZhen-Ning Wang, ShenyangWei Wei, HefeiDong-Ping Xie, ShanghaiWen-Xie Xu, ShanghaiHua Yang, ChongqingXiao Yang, BeijingWei-Zhen Zhang, BeijingHua-Chuan Zheng, ShenyangDa-Ling Zhu, HarbinJin-Xia Zhu, BeijingMin-Sheng Zhu, NanjingYong-Liang Zhu, Hangzhou
Croatia
Alen Protic, Rijeka
Czech Republic
Pavel Hladik, SemilyMartin Vokurka, Prague
Denmark
Lars Arendt-Nielsen, AalborgFrank Vinholt Schiodt, CopenhagenJonas Worsoe, AarhusJing-Bo Zhao, Aalborg
Egypt
Mahmoud Aboelneen Khattab, Minia
Estonia
Enn Seppet, Tartu
Finland
Pauli Antero Puolakkainen, Turku
France
Bruno Bonaz, GrenoblePierre Marie Dechelotte, RouenJean-Paul Lallès, Saint-GillesCharles-Henri Malbert, Saint-GillesThierry Piche, NicePascale Plaisancié, LyonMichelina Plateroti, LyonVeronique Vitton, Marseille
Germany
Hans Gunter Beger, UlmCarsten Bergmann, IngelheimElke Cario, Essen
Arno J Dormann, KolnNikolaus Gassler, AachenWerner Hartwig, HeidelbergMarion Hewicker-Trautwein, HannoverJens Hoeppner, FreiburgTobias Keck, FreiburgJorg Kleeff, MunichPeter Malfertheiner, MagdeburgOliver Mann, HamburgChristoph Michalski, MunichAndreas Klaus Nussler, MunichChristian Pehl, VilsbiburgPeter Schemmer, HeidelbergMarc Stemmler, FreiburgFrank Tacke, AachenSya Nomna Ukena, HannoverBrigitte Vollmar, RostockThomas Michael Wex, MagdeburgMargot Zoller, Heidelberg
Greece
Stelios F Assimakopoulos, PatrasGeorge N Dalekos, LarissaAlkiviadis Efthymiou, thessalonikiMaria Gazouli, AthensIoannis E Koutroubakis, HeraklionGerassimos J Mantzaris, AthensGeorge Papatheodoridis, Athens
Hungary
Mária Bagyánszki, SzegedMihály Boros, SzegedLaszlo Czako, SzegedPal Miheller, BudapestZoltan Rakonczay, Szeged
India
Anil Kumar Agarwal, DelhiUday Bandyopadhyay, KolkataSriparna Basu, VaranasiChandra Kanti Chakraborti, RourkelaRajeev Garg, PunjabChandra P Sharma, ThiruvananthapuramShailesh V Shrikhande, MumbaiVirendra Singh, ChandigarhNicholas James Skill, IndianapolisPrabhakar R Veerareddy, Andhra Pradesh
Indonesia
Laurentius A Lesmana, Jakarta
Iran
Gholamreza Roshandel, GorganShahram Shahabi, Urmia
Ireland
Billy Bourke, DublinStephen Keely, Dublin
IsraelYosefa Avraham, JerusalemYaron Bar-Dayan, HolonShomron Ben-Horin, HashomerBoris Kirshtein, Beer ShevaStephen Malnick, RehovotYaakov Maor, Tel-HashomerRifaat Safadi, JerusalemNachum Vaisman, Tel Aviv
Italy
Rosaria Acquaviva, CataniaDario Acuna-Castroviejo, ArmillaAlessandro Antonelli, PisaGiacosa Attilio, GenovaSalvatore Auricchio, NaplesGuido Basilisco, MilanoAntonio Basoli, RomeClaudio Bassi, VeronaMassimo Bellini, PisaLuigi Bonavina, MilanoAlfio Brogna, CataniaGiuseppe Calamita, BariRaffaele Capasso, NaplesIgnazio Castagliuolo, PadovaEnrico Stefano Corazziari, RomeFrancesco Cresi, TorinoRosario Cuomo, NapoliSalvatore Cuzzocrea, GazziMario M D’Elios, FlorenceCinzia Domeneghini, MilanLuca Elli, MilanoCresi Francesco, TorinoWalter Fries, MessinaEugenio Gaudio, RomeMarco Gobbetti, BariFabio Grizzi, MilanEnzo Grossi, MilaneseEnzo Ierardi, FoggiaPietro Invernizzi, MilanAngelo A Izzo, NaplesAnna Kohn, RomeGiovanni Latella, L’AquilaMassimo Marignani, RomeSergio Morini, RomeRaffaele Pezzilli, BolognaCristiano Rumio, MilanGiovanni Sarnelli, NaplesEdoardo Vincenzo Savarino, GenoaPierpaolo Sileri, RomeAnnamaria Staiano, NaplesGiacomo Carlo Sturniolo, PadovaClaudio Tiribelli, Triest
Japan
Akihiro Asakawa, KagoshimaHisashi Aso, SendaiYasu-Taka Azuma, OsakaShotaro Enomoto, WakayamaMikihiro Fujiya, HokkaidoTakahisa Furuta, HamamatsuAkira Hokama, OkinawaRyota Hokari, SaitamaYuichi Hori, Kobe
II February 15, 2013WJGP|www.wjgnet.com

III February 15, 2013WJGP|www.wjgnet.com
Hideki Iijima, OsakaMasahiro Iizuka, AkitaMotohiro Imano, OsakaHajime Isomoto, NagasakiTatehiro Kagawa, IseharaTakumi Kawaguchi, KurumeHaruki Kitazawa, SendaiXiao-Kang Li, TokyoNoriaki Manabe, OkayamaAtsushi Masamune, SendaiHiroyuki Matsubayashi, ShizuokaKazuyuki Matsushita, Chuo-kuReiko Miyazawa, GunmaKazunari Murakami, OitaHikaru Nagahara, TokyoYuji Naito, KyotoAtsushi Nakajima, Atsushi NakajimaShoji Natsugoe, KagoshimaTsutomu Nishida, OsakaKoji Nomoto, TokyoNaoaki Sakata, MiyagiShouji Shimoyama, TokyoGoshi Shiota, YonagoIkuo Shoji, HyogoHidekazu Suzuki, TokyoHitoshi Takagi, GunmaToru Takahashi, OkayamaYoshihisa Takahashi, TokyoKan Uchiyama, ChibaTakato Ueno, KurumeYoshiyuki Ueno, SendaiHisayuki Uneyama, KwasakiMitsunori Yamakawa, YamagataTakayuki Yamamoto, MieYutaka Yata, GunmaNaohisa Yoshida, KyotoHitoshi Yoshiji, Nara
Lebanon
Costantine Fouad Daher, ByblosAssaad M Soweid, BeirutJulnar Usta, Beirut
Malaysia
Andrew Chua, Perak
Mexico
José María de la Roca-Chiapas, LeonMaria Raquel Huerta Franco, Guanajuato
Netherland
Wouter J de Jonge, AmsterdamAldo Grefhorst, GroningenRuben Hummelen, RotterdamDaniel Keszthelyi, MaastrichtCornelis F M Sier, LeidenPieter J Tanis, AmsterdamLuc JW van der Laan, RotterdamSander van der Marel, Leiden
NorwayAnne Marie Bakke, Oslo
Poland
Stanisław Hac, GdańskStanisław Jan Konturek, KrakówAgata Mulak, WroclawNapoleon Waszkiewicz, Choroszcz
Portugal
Ricardo Marcos, Porto
Romania
Mihai Ciocirlan, Bucharest
Russia
Ludmila Filaretova, Petersburg
Singapore
Madhav Bhatia, SingaporeBrian K P Goh, SingaporeKhek Yu Ho, SingaporeCliff K S Ong, Singapore
South Korea
Jae Hee Cheon, SeoulMyung Haing Cho, SeoulJae Bock Chung, SeoulKi-Baik Hahm, IncheonHo Jae Han, GwangjuChang Duk Jun, GwangjuHong Joo Kim, SeoulJin Kyung Kim, Gyeongsan-SiSang Geon Kim, SeoulWon Jae Lee, SeoulKwan Kyu Park, DaeguSeung Ha Park, BusanSung Joo Park, Jeonbuk
Spain
Raquel Abalo, AlcorcónJuan G Abraldes, BarcelonaAgustin Albillos, MadridMaria-Angeles Aller, MadridFernando Azpiroz, BarcelonaRamon Bataller, BarcelonaMarco Bustamante, ValenciaAndres Cardenas, BarcelonaDariao Acuna Castroviejo, ArmillaJoan Claria, BarcelonaPere Clave, BarcelonaManuel Giner, Madrid
Angel I Lanas, ZaragozaMaite Martin, BarcelonaMaria Teresa Martin, BarcelonaVicente Martinez, BarcelonaJose M Matés, MalagaJulio M Mayol, MadridMarçal Pastor-Anglada, BarcelonaMaría Eugenia Sáez, SevilleYolanda Sanz, BurjassotCarlos Taxonera, MadridMaria D Yago, Granada
Sweden
Marco Del Chiaro, StockholmFrida Fak, GothenburgGunnar FA Flemstrom, UppsalaEvangelos Kalaitzakis, GothenburgKristina Lamas, UmeaBob Roger Olsson, GöteborgSara Maria Regnér, MalmöPeter thelin Schmidt, StockholmXiao-Feng Sun, LinkopingHenrik Thorlacius, MalmöCurt Tysk, Orebro
Switzerland
Jyrki J Eloranta, ZurichAndreas Geier, ZurichRemy Meier, LiestalCatherine Pastor, Geneva
Thailand
Thawatchai Akaraviputh, BangkokWeekitt Kittisupamongkol, Bangkok
Turkey
Mehmet Bektas, AnkaraMukaddes Esrefoglu, MalatyaAhmet Guven, AnkaraMuammer Karadeniz, ManisaElvan Ozbek, ErzuruIlhami Yuksel, Ankara
Ukraine
Oksana S Zayavhkivska, Lviv
United Kingdom
Geoffrey Burnstock, LondonJanice E Drew, AberdeenGirish Gupte, BirminghamDavid C Hay, EdinburghNusrat Husain, CheshireMichael Leslie Lucas, GlasgowJamie Murphy, LondonVadim Sumbayev, KentWing-Kin Syn, Birmingham

IV February 15, 2013WJGP|www.wjgnet.com
Andrea Varro, Liverpool
United States
Sami Rene Achem, JacksonvilleTauseef Ali, OklahomaDavid H Alpers, St LouisGianfranco D Alpini, TempleShrikant Anant, OklahomaM Sawkat Anwer, North GraftonAndrew Aronsohn, ChicagoToms Augustin, SayreGyorgy Baffy, BostonMichael T Bailey, ColumbusKim Elaine Barrett, San DiegoMarc D Basson, LansingRobert L Bell, New HavenDavid H Berger, HoustonUrs A Boelsterli, StorrsRichard G Boles, Los AngelesEdward L Bradley III, SarasotaQiang Cai, AtlantaWei-Biao Cao, ProvidenceSubhash C Chauhan, Sioux FallsJian-De Chen, GalvestonTao-Sheng Chen, MemphisJohn Chiang, RootstownMashkoor A Choudhry, MaywoodParimal Chowdhury, Little RockEric Cohen, BostonRobert Cormier, DuluthSrinivasan Dasarathy, ClevelandEdwin A Deitch, NewarkDan A Dixon, ColumbiaJames P Dolan, PortlandH Henry Dong, PittsburghHui Dong, La JollaAshkan Farhadi, IrvineBin Feng, PittsburghJenifer Fenton, East LansingAlessandro Fichera, ChicagoMitchell P Fink, PittsburghP Marco Fisichella, MaywoodLeo R Fitzpatrick, HummelstownRobert Armour Forse, OmahaGlenn Tsuyoshi Furuta, AuroraJuan F Gallegos-Orozco, ScottsdalePandu R Gangula, NasvhilleTimothy Gardner, LebanonShannon Stroud Glaser, TempleFrancisco Gondim, St. LouisJohn R Grider, RichmondYan-Fang Guan, CincinnatiGregory M Holmes, Baton RougeAi-Xuan Le Holterman, ChicagoRichard Hu, Los AngelesHartmut Jaeschke, KansasRobert Thomas Jensen, Los AngelesSreenivasa S Jonnalagadda, LouisMichel Kahaleh, Charlottesville
Andreas Martin Kaiser, Los AngelesRandeep Singh Kashyap, RochesterLaurie Keefer, ChicagoRichard Kellermayer, HoustonChris Kevil, ShreveportSandeep Khurana, BaltimorePawel R Kiela, TucsonTammy Lyn Kindel, CincinnatGordana Kosutic, DurhamDavid Kravetz, San DiegoAshok Kumar, DetroitJohn H Kwon, ChicagoMuriel Larauche, Los AngelesI Michael Leitman, New YorkFelix W Leung, North HillsSuthat Liangpunsakul, IndianapolisFeng-Xin Lu, BostonPauline Kay Lund, Chapel HillGeorge Luo, LexingtonGuang-Xiang Luo, LexingtonJay Luther, Ann ArborRam I Mahato, MemphisAkhil Maheshwari, BirminghamKenneth Maiese, NewarkAdhip P N Majumdar, DetroitJose E Manautou, StorrsCraig J McClain, LouisvilleDermot McGovern, Los AngelesB Greenwood-van Meerveld, OklahomaDouglas Scott Merrel, BethesdaMurielle Mimeault, OmahaEmiko Mizoguchi, BostonHuan-Biao Mo, DentonAdam Moeser, RaleighRamzi M Mohammad, DetroitSatdarshan Singh Monga, PittsburghRoger Klein Moreira, New YorkSandeep Mukherjee, OmahaKarnam S Murthy, RichmondMichael J Nowicki, JacksonShuji Ogino, BostonMary Francis Otterson, WisconsinChung Owyang, Ann ArborHelieh S Oz, LexingtonMarco G Patti, ChicagoTimothy Michael Pawlik, BaltimoreSara Peleg, HoustonNicholas C Popescu, BethesdaLi-Ya Qiao, RichmondChao Qin, OklahomaParvaneh Rafiee, MilwaukeeSigrid A Rajasekaran, WilmingtonVazhaikkurichi M Rajendran, MorgantownJean Pierre Raufman, BaltimoreRamesh M Ray, MemphisArie Regev, IndianapolisDouglas K Rex, CarmelYehuda Ringel, Chapel HillRichard A Rippe, RockvilleChantal A Rivera, Bossier
Andrea Romani, ClevelandPraveen K Roy, AlbuquerquePaul A Rufo, BostonDavid B Sachar, New YorkBimaljit Singh Sandhu, RichmondSanjaya Kumar Satapathy, New Hyde ParkAnthony Senagore, Los AngelesMuhammad Y Sheikh, FresnoBo Shen, ClevelandLe Shen, ChicagoFrank A Simmen, Little RockSteven Mitchell Singer, WashingtonShailinder Jit Singh, WashingtonAdam Jan Smolka, CharlestonNed Snyder, HoustonZhen-Yuan Song, ChicagoGagan K Sood, HoustonRhonda F Souza, DallasStuart Jon Spechler, DallasSubbaramiah Sridha, AugustaCatia Sternini, Los AngelesVeedamali S Subramanian, Long BeachJun Sun, RochesterYvette Taché, Los AngelesXiao-Di Tan, ChicagoPaul Daniel Terry, AtlantaJennifer Tirnauer, FarmingtonAndrea Todisco, Ann ArborGeorge C Tsokos, BostonVic Velanovich, DetroitRaj Vuppalanchi, IndianapolisEstela Wajcberg, CranfordArnold Wald, MadisonLi-Xin Wang, Los AngelesHorst Christian Weber, BostonSteven D Wexner, WestonJackie D Wood, ColumbusGuo-Yao Wu, College StationChristian Wunder, BethesdaZuo-Liang Xiao, ClevelandGuang-Yin Xu, GalvestonGuo-Rong Xu, East OrangeGuang-Yu Yang, ChicagoJay A Yelon, ValhallaYamaoka Yoshio, HoustonShao-Yong Yu, HersheyYana Zavros, CincinnatiJoerg Zehetner, Los AngelesJian X Zhang, CharlotteZhi Zhong, CharlestonHui-Ping Zhou, RichmondZhan-Xiang Zhou, KannapolisQing Zhu, BethesdaYao-Hui Zhu, Stanford
Venezuela
Fabian Michelangeli, Caracas

Contents
February 15, 2015|Volume 6|Issue 1|WJGP|www.wjgnet.com I
Quarterly Volume 6 Number 1 February 15, 2015
REVIEW1 PathogenesisofCrohn’sdisease:Bugornobug
Bosca-Watts MM, Tosca J, Anton R, Mora M, Minguez M, Mora F
MINIREVIEWS13 Laboratorymarkersinulcerativecolitis:Currentinsightsandfutureadvances
Cioffi M, De Rosa A, Serao R, Picone I, Vietri MT
ORIGINAL ARTICLE
Basic Study23 Rabeprazoleiseffectiveforbilerefluxoesophagitisaftertotalgastrectomyinaratmodel
Hashimoto N

EditorialBoardMemberofWorld Journal of Gastrointestinal Pathophysiology ,Mitsunori Yamakawa,MD, PhD, Professor,Department of PathologicalDiag-nostics,YamagataUniversity, FacultyofMedicine, 2-2-2 Iida-Nishi, Yamagata990-9585,Japan
World Journal of Gastrointestinal Pathophysiology (World J Gastrointest Pathophysiol, WJGP, online ISSN 2150-5330, DOI: 10.4291), is a peer-reviewed open access academic journal that aims to guide clinical practice and improve diagnostic and therapeutic skills of clinicians.
WJGP is to report rapidly the most recent results in basic and clinical research on gastrointestinal pathophysiology, including all aspects of normal or abnormal function of the gastrointestinal tract, hepatobiliary system, and pancreas. WJGP specifically covers growth and development, digestion, secretion, absorption, metabolism and motility relative to the gastrointestinal organs, as well as immune and inflammatory processes, and neural, endocrine and circulatory control mechanisms that affect these organs. This journal will also report new methods and techniques in gastrointestinal pathophysiological research. We encourage authors to submit their manuscripts to WJGP. We will give priority to manuscripts that are supported by major national and international foundations and those that are of great basic and clinical significance.
World Journal of Gastrointestinal Pathophysiology is now indexed in PubMed Central, PubMed, Digital Object Identifier, and Directory of Open Access Journals.
I-IV EditorialBoard
ContentsWorld Journal of Gastrointestinal Pathophysiology
Volume 6 Number 1 February 15, 2015
FLYLEAF
EDITORS FOR THIS ISSUE
Responsible Assistant Editor: Xiang Li Responsible Science Editor: Yue-Li TianResponsible Electronic Editor: Huan-Liang Wu Proofing Editorial Office Director: Xiu-Xia Song Proofing Editor-in-Chief: Lian-Sheng Ma
NAMEOFJOURNALWorld Journal of Gastrointestinal Pathophysiology
ISSNISSN 2150-5330 (online)
LAUNCHDATEApril 15, 2010
FrequencyQuarterly
EDITOR-IN-CHIEFThomas Y Ma, MD, PhD, Professor, Chief, Division of Gastroenterology and Hepatology, University of New Mexico, MSC10 5550, 1 UNM, Albuquerque, NM 87131, United States
EDITORIALOFFICEJin-Lei Wang, DirectorXiu-Xia Song, Vice DirectorWorld Journal of Gastrointestinal Pathophysiology
Room 903, Building D, Ocean International Center, No. 62 Dongsihuan Zhonglu, Chaoyang District, Beijing 100025, ChinaTelephone: +86-10-85381891Fax: +86-10-85381893E-mail: [email protected] Desk: http://www.wjgnet.com/esps/helpdesk.aspxhttp://www.wjgnet.com
PUBLISHERBaishideng Publishing Group Inc8226 Regency Drive, Pleasanton, CA 94588, USATelephone: +1-925-223-8242Fax: +1-925-223-8243E-mail: [email protected] Desk: http://www.wjgnet.com/esps/helpdesk.aspxhttp://www.wjgnet.com
PUBLICATIONDATEFebruary 15, 2015
COPYRIGHT© 2015 Baishideng Publishing Group Inc. Articles pub-lished by this Open Access journal are distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license.
SPECIALSTATEMENTAll articles published in journals owned by the Baishideng Publishing Group (BPG) represent the views and opinionsof their authors, and not the views, opinions or policies of the BPG, except where other-wise explicitly indicated.
INSTRUCTIONSTOAUTHORSFull instructions are available online at http://www.wjgnet.com/2218-6182/g_info_20100722172951.htm
ONLINESUBMISSIONhttp://www.wjgnet.com/esps/
ABOUT COVER
February 15, 2015|Volume 6|Issue 1|WJGP|www.wjgnet.com II
AIM AND SCOPE
INDEXING/ABSTRACTING

bowel contents; severity of the disease is correlated with bacterial density in the mucosa; granulomas can contain bacteria; and susceptible mice raised in germ-free conditions develop inflammation when bacteria are introduced in the 1990’s, several studies sought to establish a relationship with viral infections and the onset of IBD, finally concluding that no direct link had been demonstrated. In the past fifteen years, evidence relating IBD pathogenesis to Mycobacterium avium paratuberculosis, salmonella, campylobacter, etc. , has been found. The tendency now under discussion to regard microbiota as the primary catalyst has led to the latest studies on microbiota as pathogens, focusing on Escherichia coli , mainly in ileal CD. The present review discusses the literature available on these “bugs”.
Key words: Inflammatory bowel disease; Crohn’s disease; Ulcerative colitis; Bacteria; Virus; Pathogenesis
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: The possibility of an infectious origin in inflammatory bowel disease (IBD) has been postulated since the first description of Crohn’s disease (CD). Many observations implicate bacteria as a trigger for the development of CD, and have tried to do so with virus. Inconclusive evidence relating IBD pathogenesis to Mycobacterium avium paratuberculosis, salmonella, campylobacter, etc. , has been found. The tendency now under discussion to regard microbiota as the primary catalyst, has led to the latest studies on microbiota as pathogens, focusing on Escherichia coli , mainly in ileal CD. The present review discusses the literature available on these “bugs”.
Bosca-Watts MM, Tosca J, Anton R, Mora M, Minguez M, Mora F. Pathogenesis of Crohn’s disease: Bug or no bug. World J Gastrointest Pathophysiol 2015; 6(1): 1-12 Available from: URL: http://www.wjgnet.com/2150-5330/full/v6/i1/1.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i1.1
Pathogenesis of Crohn’s disease: Bug or no bug
Marta Maia Bosca-Watts, Joan Tosca, Rosario Anton, Maria Mora, Miguel Minguez, Francisco Mora, IBD Unit, Digestive Disease Department, University of Valencia, University Clinic Hospital of Valencia and INCLIVA Health Research Institute, 46010 Valencia, SpainAuthor contributions: All authors contributed equally in the review of the medical literature and in writing the article; Bosca-Watts MM led the organization of the research and translated the final document from Spanish to English; Minguez M and Mora F supervised and corrected the review.Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/Correspondence to: Marta Maia Bosca-Watts, MD, IBD Unit, Digestive Disease Department, University of Valencia, University Clinic Hospital of Valencia and INCLIVA Health Research Institute, Avda. Blasco Ibañez 17, 46010 Valencia, Spain. [email protected]: +34-96-1973500 Fax: +34-96-1973500 Received: May 17, 2014 Peer-review started: May 18, 2014First decision: June 18, 2014Revised: November 1, 2014Accepted: November 7, 2014Article in press: November 10, 2014Published online: February 15, 2015
AbstractThe possibility of an infectious origin in inflammatory bowel disease (IBD) has been postulated since the first description of Crohn’s disease (CD). Many observations implicate bacteria as a trigger for the development of CD: lesions occur in regions with higher bacterial concentrations; aphthous ulcers occur in Peyer’s pat-ches; inflammation resolves when the fecal stream is diverted and is reactivated following reinfusion of
� February �5, 20�5|Volume 6|Issue �|WJGP|www.wjgnet.com
REVIEW
World J Gastrointest Pathophysiol 20�5 February �5; 6(�): �-�2ISSN 2�50-5330 (online)
© 20�5 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: �0.429�/wjgp.v6.i�.�
Marta Maia Bosca-Watts, Joan Tosca, Rosario Anton, Maria Mora, Miguel Minguez, Francisco Mora

INTRODUCTIONInflammatory bowel diseases (IBD), mainly Crohn’s disease (CD) and ulcerative colitis (UC), are chronic inflammatory disorders of the gastrointestinal tract[1]. Extensive studies in the past decades have suggested that the etiology of IBD involves environmental and genetic factors that lead to dysfunction of the epithelial barrier with consequent deregulation of the mucosal immune system and responses to gut microbiota[2].
Genome-wide association studies have shown that many genes correlate with the development of CD and UC, although not every individual presenting genetic abnormalities will develop the disease. Other factors, such as environmental triggers must play a role[3]. Dietary alterations in the Western populations have resulted in a shift in the composite gut microbiota. Colonic bacteria have a metabolic function, with a symbiotic relationship with human beings[4]. Gut microbiota, which outnumber human cells by nearly ten-fold and contain more than one million genes[4,5], have been shown to play an important role in complex disorders such as IBD. Historical animal models of CD initiated granulomatous change in both mice and rabbits by infiltrating healthy animal tissue with human Crohn’s tissue[6-8]. Work with animals has demonstrated the ability of an organism to induce colitis in immunodeficient but not immunocompetent mice[9]. This highlights the importance of genetics, and underlines the need to understand the hosts’ conditions, and might explain why studies have previously been unable to find a specific pathogen[4].
As mentioned, IBD is thought to be the result of a combination of genetic predisposition interacting with environmental factors that modify the gut micro-biota[3]. One of the explanations for the onset of IBD suggests a three-step scenario, in which bacteria penetrate the epithelial barrier, provoking a weak inflammatory response with impaired clearance, which in turn causes chronic inflammation, culminating in IBD[10].
It has become evident that IBD patients show an intestinal dysbiosis, with a decrease in the number of potentially beneficial bacteria such as Bifidobacteria, Lactobacilli and Firmicutes, and an increase in that of putative pathogenic bacteria such as Escherichia coli (E. coli) and other Enterobacteria[11,12]. Whether gut microbiota are responsible for the onset of IBD or a mere consequence of pathogenic microbial enteric-wall invasion, remains to be elucidated.
Over the years, many organisms have been pro-posed as etiological agents for IBD, to the extent of suggesting that CD, for example, is a manifestation of chronic mycobacterial infection[13-18] or E. coli adherence and invasion[19-23]. Many observations implicate bacteria as a trigger for the development of CD: lesions occur in regions with the highest bacterial concentrations; aphthous ulcers, the earli-
est lesion in CD, occur in Peyer’s patches, the site of bacterial sampling; inflammation resolves when the faecal stream is diverted and is reactivated following reinfusion of bowel contents[24]; severity of the disease is correlated with bacterial density in the mucosa; granulomas contain bacteria; and susceptible mice raised in germ-free conditions only develop inflammation when non-pathogenic bacteria are introduced[24-26].
The possibility of an infectious origin in IBD has been postulated since Dalziel’s first description of CD in 1913. He compared CD with Johne’s dise-ase in cattle, caused by Mycobacterium Avium Paratuberculosis[4]. Many studies have tried to find a germ that is responsible for IBD. The most recent papers focus on E. coli, especially in ileal CD, but there is literature for and against several bacteria (mycobacterias, helicobacters, campylobacter, etc.) and viruses (Ebstein-Barr virus, Cytomegalovirus, paramyxoviruses, etc.), as causative agents (Table 1). In this article, we will summarize the conclusions regarding these agents found in the medical literature.
ROLE OF BACTERIA IN THE ETIOLOGY OF IBDAdherent-invasive E. coliE. coli is the predominant aerobic Gram negative species of the normal intestinal flora, where it plays an important role in promoting the stability of the intestinal microbial flora and in maintaining the normal intestinal physiology. By acquisition of virulence factors, such as production of enterotoxins and cytotoxins, tissue invasion, and adherence to enterocytes, E. coli strains become pathogenic and become involved in intestinal diseases[27].
Interest in Escherichia coli as a pathogen in IBD began with the observation that organisms isolated from patients with CD had greater adherent properties to human cells than those from controls, and that previously unrecognized invasive E. coli were present in Crohn’s ileal tissue[4,19,25].
Higher E. coli antibody titres and E. coli antigens have been found in the blood and resection speci-mens, respectively, of CD patients[28,29]. In Darfeuille-Michaud’s study, E. coli was recovered from 65% of chronic lesions in resected ileum, and 100% of biopsies of early lesions, in postoperative endoscopic recurrence.
As mentioned, E. coli form a major component of the normal microflora of the gut. However, the E. coli prevalent in CD tissue was shown to have unique adherent and invasive properties, which enabled it to adhere to intestinal epithelial cells (IECs), invade the epithelial layer, and replicate within both IEC and macrophages[30]. These properties were used to designate it as a specific type of E. coli, adherent-
2 February �5, 20�5|Volume 6|Issue �|WJGP|www.wjgnet.com
Bosca-Watts MM et al . Bugs in the pathogenesis of CD

invasive E. coli [Adherent-invasive escherichia coli (AIEC)].
Studies on the adherence properties of E. coli have concluded that E. coli strains are able to adhere to various human cells or cell lines. 53%-62% of E. coli strains isolated from feces of CD were able to adhere to buccal cells, compared to only 5%-6% of those isolated from control subjects. A correlation between bacterial adhesion to intestinal cells and intestinal colonization has been observed. The presence of high levels of bacteria creates a biofilm on the surface of the gut mucosa in patients with CD and UC[31,32].
Analysis of E. coli strains isolated from early and chronic ileal lesions of patients with CD has revealed the presence of true invasive pathogens. Electron-microscopy of epithelial cells infected with CD-associated bacteria has revealed a macropinocytosis-like process of entry. Inside the host cells, CD-associated bacteria survive and replicate in the cytoplasm after lysis of the endocytic vacuole[26,31]. Glasser et al[21] demonstrated that AIEC was able to survive and replicate in macrophages, without inducing host cells and stimulating the infected cells to release high levels of tumor necrosis factor (TNF)-α.
Genetically related E. coli strains were shown to adhere and invade the intestinal wall in susceptible hosts[22]. These strains expressed type 1 pili, which presented point mutations, with amino acid substitutions in the type 1 pili FimH adhesion subunit, which contributed to the AIEC adhesion to the Carcinoembryonic antigen-related cell adhesion molecule 6 receptors (CEACAM6 receptor) in the
IEC. In contrast to non-AIEC isolates, AIEC isolates tended to carry FimH hotspot mutations that were of recent evolutionary origin and could be signatures of pathoadaptive mutations[30,33].
B2 and D E. coli strains are more frequently pathogenic, causing urinary tract and other extra-intestinal infections. AIEC isolated from CD patients were generally found to belong to the B2 and D phylotypes. This suggested that these isolates take advantage of a specific micro-environment found in the IBD gut[33-35].
AIEC genome sequencing revealed its similarity to uropathogenic E. coli (UPEC)[36]. Phylogenetic analysis of fimH sequences delineated a tight S70/N78 clade containing LF82, the reference strain for AIEC. Interestingly, UPEC and avian pathogenic E. coli were also found in the S70/N78 clade. As Dreux et al[33] remarked in their paper, this presence raises the possibility that IBD-isolated E. coli are members of a general pool of extraintestinal pathogenic E. coli that reside in the gut and have evolved specific potentialities dependent upon their microenvironment.
The Darfeuille-Michaud group highlighted potential pathological mechanisms for AIEC in CD: AIEC express type 1 pili which enables binding to CEACAM6 receptors that are increased in the ileal mucosa of CD patients; in ileal intestinal epithelial cells from CD patients, strong expression of the endoplasmic reticulum stress protein Gp96 facilitates invasion via recognition of the bacterial outer membrane protein OmpA of AIEC[37]; AIEC carriage of the long polar fimbriae (lpf) virulence
3 February �5, 20�5|Volume 6|Issue �|WJGP|www.wjgnet.com
Microorganism Main features
Bacteria Adherent-invasive Escherichia coli
The AIEC has adherente and invasive properties. They are found in macrophages of ileal CD tissue. It adheres with a type � pili to CEACAM6 receptors (increased in ileal tissue). Invasion is facilitated by endomasplic reticulum expresion of Gp96AIEC promotes translocation of bacteria and stimulates TNF production, promoting granuloma formation. CD mutations enhance intracellular replication. AIEC is very similar to the urologic UPEC
Mycobacterium avium paratuberculosis
MAP causes CD-like disease in animals. It has been found un blood and intestinal tissue of CD patients, mainly in spheroplast form (cell-wall deficient form which may take up to 18 mo to culture in special stains). Blood MAP DNA has been found in higher levels in controls, as a sign of exposure in the general population and maybe due to the treatment IBD patients receive, which has been shown to inhibit MAP. MAP antibodies have been found in IBD sera. MAP is a source for ASCA. In vitro, MAP impair macrophages to kill E. coli. Several CD genetic alterations can favor MAP infection
H. pylori Epidemiological studies have observed an inverse correlation between IBD and HP, that cannot only be explained by coincidence or by previous antibiotic treatment. It has been shown that HP’s DNA has the capacity to reduce type I IFN
C. difficile Up to �0% of the IBD patients will develop C. difficile infections, 40% of them without having had previous antibiotic treatment. It is considered a risk factor for exacerbations and should be screened in every IBD patient hospitalized for a flare
Campylobacter and salmonella
The risk of IBD after a Campylobacter or Salmonella positive test is high, but it is also high if a stool test has been done and it was negative, suggesting that IBD patients undergo stool tests in the years before diagnosis
Virus Measles and mumps Implication of these virus and their vaccines in the pathogenesis is uncertain, specially with respect to measles Rubella No relationship has been found Cytomegalovirus It reactivates underlying inflammatory disease. The intensity in which CMV is expressed in the intestinal mucosa relates to
the severity of the inflammation Epstein-Barr virus Like CMV, it has a modulating function, not an ethiological implication
Table 1 Microorganisms involved in inflammatory bowel disease
AIEC: Adherent-invasive Escherichia coli; MAP: Mycobacterium avium paratuberculosis; IBD: Inflammatory bowel disease; CD: Crohn’s disease; ASCA: Anti-bodies against saccharomyces cerevisiae; CMV: Cytomegalovirus.
Bosca-Watts MM et al . Bugs in the pathogenesis of CD

gene promotes translocation of the bacteria across Peyer’s patches[38]; and CD-associated mutations in autophagy genes enhance intracellular replication of AIEC[39]. AIEC have also been shown to induce the release of TNFα, a key cytokine in IBD inflammation. They survive and replicate inside macrophages inducing the release of large amounts of TNFα and motivating granuloma formation in vitro[21,40]. Recently, infection with AIEC was proven to up-regulate microRNAs (30C and MIR130A) to reduce expression of proteins required for autophagy (ATG5 and ATG16L1) and autophagy response in intestinal epithelial cells. In ileal samples from CD patients, these same microRNAs are augmented and the levels of ATG5 and ATG16L1 diminished[1].
Although AIEC has clearly been related to IBD, whether it is a single etiological invader or just the instigator is not clear. Chassaing et al[41] observed that T5KO mice, in early stages of microbiota development inoculated with AIEC, developed colitis that persisted beyond the period in which AIEC could be detected in feces. They observed that AIEC transient colonization altered the gut microbiota of the T5KO mice (not the wild type), by reducing its diversity, which resulted in greater levels of lipopolysaccharides and flagellin that gave the microbiota inherently greater proinflammatory potential, which was responsible for the development of chronic colitis in susceptible hosts. Therefore, the authors concluded from the findings that, in a genetically susceptible host, the presence of a pathobiont (as was AIEC in this case) in a developing microbiota, could result in lasting changes in microbiota composition that might eventuate in chronic inflammation[41]. The question that arises from this excellent study is if the AIEC was not detectable in faeces because it had been cleared or because it was caught in the macrophages and could not be detected.
Regarding urine infections from E. coli, fimH mutations were shown to confer significant advantages upon bacteria during bladder colonization in a murine model and to correlate with extraintestinal virulence of E. coli. In UPEC, blocking the binding of FimH to its natural receptor prevents bacterial colonization and subsequent inflammation of the urinary tract. Preventive treatments have been developed for UPEC infections: vaccines targeting FimH, mannoside compounds or biarylmannose-derivative FimH antagonists. Similar therapeutic strategies could be useful for preventing AIEC colonization in CD patients[33].
Organisms such as E. coli and Salmonellae that express the FimH protein of type 1 pilli have been shown to bind to M cells (microfold cells that overlie Peyer’s patches in the intestine and lymphoid follicles in the colon) by interaction between FimH and glycoprotein 2 (GP2), expressed on the apical plasma membrane of M cells; possession of FimH is
essential for invasion of M cells by these organisms to occur[42]. It has also been demonstrated that the same GP2 protein is the epitope for the “anti-pancreatic” antibody found in CD sera[43]. This raises the possibility that a combination of bacterial components, including FimH, linked to GP2, may be presented as a foreign antigen and thus lead to development of anti-GP2 antibodies, in a way analogous to the development of anti-tissue transglutaminase antibodies in celiac disease. As Friswell et al[44] highlight in their review of the role of bacteria in the pathogenesis of IBD, blockade of bacterial entry via M cells represents an important target for therapies. In a very recent paper[45], certain isolates of E. coli have been shown to be related both with colorectal cancer and IBD. The authors suggest that interventions that either reduce colonization by diffusely adherent E. coli or block their interaction with the mucosa may have preventive or therapeutic effects in colon cancer and CD.
Mycobacterium avium paratuberculosisMycobacterium avium subspecies paratuberculosis is an obligate pathogenic organism that causes Johne’s disease[44] in ruminants and other animals such as primates and rabbits. Johne’s disease is a chronic wasting diarrheal disease[18] with clinical and histological conditions that are highly evocative of CD[46]. Like in CD, Mycobacterium avium para-tuberculosis (MAP) infection causes segmental and fibrosing stenosis, as well as epithelial granulomata[47]. The link between CD and MAP was first postulated by Dalziel in 1913, before Crohn’s classic description of CD, when he noted the similarities with Johne’s disease.
MAP is historically considered not to be zoonotic, although case reports of infected human beings, with clinically relevant illness, have been published. Humans worldwide are highly exposed to MAP. MAP has been cultured from pasteurized milk, chlorinated potable water, meat products, breast milk from mothers with CD, and from the blood of IBD patients[46,48] and controls.
MAP is quite difficult to culture; it may be present in the cell-wall-deficient form (spheroplasts) and appear negative with Ziehl-Nielsen stain. Under appropriate culture conditions and over a prolonged period (weeks to years), these bacteria produce cell wall and become Ziehl-Nielsen positive. MAP lacks the iron-chelating agent mycobactin, so the infected host or the culture medium must provide the iron for it to grow. Detection of MAP DNA or RNA using PCR is generally preferred because of the shorter time scale and the increased sensitivity of the technique. Early PCR methods have been questioned because of the similarity of the primers for MAP to other non-MAP-mycobacterium which lead to false positives. An IS900-PCR method that gives more
4 February �5, 20�5|Volume 6|Issue �|WJGP|www.wjgnet.com
Bosca-Watts MM et al . Bugs in the pathogenesis of CD

reliable results is currently used. The flaws of the technique, as Greenstein points out, reside in the fact that, in the process of isolating the nucleus to obtain DNA, MAP DNA can be inadvertently removed if it is in the cytoplasm of the infected host (where MAP replicates) and that the presence of MAP DNA is not proof that MAP causes IBD, for it may have coincidentally been ingested without causing infection[18]. According to Greenstein, isolation of MAP RNA indicates that the organism was viable at the time of isolation; it is a technique that is easy to reproduce due to the smaller size of the RNA with respect to DNA, although the half-life of RNA is short (minutes) while DNA may survive for centuries.
In Naser’s series[49], MAP was cultured from blood in up to 50% of CD patients and 22% of UC patients, but no control patients. In Mendoza et al’s study using CD, UC and controls, MAP DNA was detected in all blood samples. No mycobacterial growth was observed using BACTEC MGTI cultures, but all of the 18-mo cultures from CD patients were positive by phenolic acridine orange staining, which suggested the presence of spheroplasts[15]. All the CD patients and one of the UC patients were observed to have cell-wall-deficient forms, but none of the non-IBD controls contained them.
Two studies carried out in the north of Spain have analyzed the MAP DNA, using IS900 nested PCR, in the blood of IBD and adult control patients. A higher prevalence of MAP infection was observed in healthy individuals than in IBD patients. Elguezabal et al[46] found a prevalence of 45.2% MAP DNA in the blood of healthy controls, compared to 21.38% and 19.04% in CD and UC patients respectively. The authors attributed the difference to therapy, as did Juste et al[48], who found an even bigger difference between healthy controls (47% MAP DNA in blood) and IBD (16%). Juste et al[48] found that 17% of the patients receiving mesalamine, 6% of those taking sulfasalazine, and none of the ones taking methotrexate, mercaptopurine, ciprofloxacin or tacrolimus had MAP DNA detectable in blood; no difference was observed with azathioprine or steroids.
Contrary to the previous finding of a higher MAP DNA prevalence in controls, Kirkwood et al[50] found more MAP IS900 DNA and live MAP (culture of gut biopsies) in naïve pediatric CD patients than in non-IBD. The non-IBD patients had lower levels of mucosal IS900 DNA, no MAP in tissue culture and no DNA in blood. The distinguishing characteristic of this study is that the CD patients were naïve, and, therefore, had not received IBD treatment and the disease had not yet evolved.
Another study by Greenstein’s group, performed in 1996 in resected intestinal tissue, found RNA of MAP in 100% of the cases. They concluded that, analogous to other mycobacterial infections, such as lepra and tuberculosis, which have different presen-
tations depending on the host’s genetic predisposition and immunological state, CD could be secondary to MAP and have two distinct presentations: fistulising and stenosing[51].
An alternative way to study the link between MAP and CD is to assess whether the CD patients have MAP antibodies that react to MAP antigens. Meta-analyses have shown reactivity in CD patients’ sera, to MAP p35 and p36 recombinant antigens. However, it should be noted that MAP p35 and p36 are similar to that of Mycobacterium avium, subspecies avium [MAA], so a specific reaction to MAP rather than MAA cannot be certain[44]. An increased presence of MAP-reactive T cells has also been found in CD patients but not in controls[52].
CD patients show increased levels of antibodies against saccharomyces cerevisiae (ASCA), the epitope of which is a mannose which is present in yeast walls. Studies have demonstrated that not only is MAP a possible source for the ASCA mannan epitope, but also that MAP release a mannose-containing glycoconjugate that impairs the in vitro ability of monocyte-derived macrophages to kill phagocytosed E. coli. Therefore, as Friswell suggests, MAP might be acting via an indirect pathogenic effect, which would explain its role in pathogenesis and yet not be greatly exacerbated by anti-TNF treatment[44,53]. ASCA may develop a long time before the diagnosis of CD is established. ASCA have a genetically modulated expression, found in 20%-25% of the relatives of CD patients, and not in their spouses[54].
Several studies highlight how genetic alterations found in CD can favor MAP infection. Ferwerda et al[55] demonstrated that NOD2 mutant patients show an ineffective recognition of MAP. Hansen et al[4]’s review explains that Gutierrez et al[56] showed that defective ATG16L1 function (which is found in CD patients) avoids Mycobacterium tuberculosis inhibition in mac-rophages, supporting the idea of a Mycobacterial pathogen in IBD[4,56]. Finally, Sechi et al[57] found a relationship between CD, MAP infection and SLC11A1 gene polymorphisms.
One of the puzzling aspects of MAP as a causa-tive agent was that IBD treatments were not worsening a possible MAP infection. To answer this question, Greenstein’s group published several studies in which they demonstrated that numerous IBD-drugs inhibited MAP growth in vitro: 5-ASA, mercaptopurine, methotrexate, cyclosporine, rapa-mycine and tacrolimus, most acting in a dose-dependent manner. The authors suggested that the medical profession had been treating MAP infections mistakenly since the introduction of sulfasalazine in 1942. This is supported by results like Juste’s et al’s, in which no DNA is found in peripheral blood of IBD patients treated with immunosuppressants.
An argument against MAP being clinically relevant in IBD is that antibiotic treatment does not cure
5 February �5, 20�5|Volume 6|Issue �|WJGP|www.wjgnet.com
Bosca-Watts MM et al . Bugs in the pathogenesis of CD

IBD. The authors who favor MAP as causative agent remark that most IBD antibiotic regimens are not fully effective for MAP and that good MAP treatments need to include macrolides, should include triple or quadruple therapies, or should be sustained for very long periods of time, as is done in tuberculosis treatment. Several long-term regimens have been performed, showing initial improvement, with steroid weaning, but concluding that the benefit is not sustained[58,59]. A two-year combination antibiotic therapy with clarithromycin, rifabutin, and clofazimine for CD was used in a study performed in Australia, in which significant improvement up to week 16 was observed, although subsequent follow-up results were not conclusive. However, correspondence in a Gastroenterology Journal in 2007 pointed out that less benefit was obtained with other IBD therapies and that none achieved uniform long-term sustained remission.
Greenstein and his group have frequently stated that MAP has met Koch’s four postulates, i.e., it is found in tissue of CD patients, can be cultured, can reproduce the disease when inoculated into other animals and can be re-isolated from the diseased subject. A paper by Momotani, among others, supported this idea by proving that MAP could cause CD-type necrotizing colitis in mice. However, as we have previously seen, MAP DNA can also be found in healthy controls, sometimes in higher proportions than in IBD patients. Whether this is a consequence of exposure and not infection, or if IBD treatment inhibits MAP but does not clear it up, or if MAP acts as a co-causative agent by impairing killing of bacteria, such as E. coli, all remain to be elucidated.
Helicobacter pyloriSeveral studies have postulated that Helicobacter pylori (HP) infection has a protective role against chronic inflammatory diseases, like IBD. These studies based their statements on the laboratory results that proved that HP could induce immune tolerance, limiting the inflammatory response[60]. Some preliminary studies suggested that patients infected with HP probably had less risk of developing IBD than the rest of the general population. The mechanisms for decreased prevalence of HP in IBD were not ascertained[61].
In 2001, Väre et al[62] published a study with 296 patients: 185 had UC, 94 CD and 17 had indeterminate colitis (IC). HP antibodies were determined. The results confirmed the low preva-lence of HP infection, especially in CD patients. Age of onset of IBD was higher in seropositive (mean 40 years) than in seronegative patients. The age of onset of IBD showed unimodal distribution in H. pylori seronegative patients, with a peak between 30 and 40 years. In contrast, H. pylori seropositive patients showed a clear bimodal pattern with peaks at 20-40 and 50-60 years of age. The results suggested that
HP could significantly modify the appearance of IBD, perhaps with a protective effect[62].
In 2010, Luther et al[60] carried out an extensive review of the papers published on HP, as well as a meta-analysis that evaluated the possible relationship between IBD and the presence or lack of HP infection. Five Thousand and ninety-three patients were evaluated. Twenty-seven percent of the IBD patients had HP infection, in comparison to 40% of the control group, with an estimated relative risk of infection of 0.64%. These results could suggest a protective role, but the authors emphasized that the heterogeneity in the studies included could not be accounted for by the method of IBD and H. pylori diagnosis, study location, or study population age, which limited the value of the results[60].
In 2011, the same authors published a study that tried to clarify the mechanism responsible for the inverse association of HP and IBD. The authors first assumed the postulate that bacterial DNA in distal intestine could influence mucosal immunity. Several papers have documented that HP DNA can be found both in the colon and feces of infected patients. The authors demonstrated that, contrary to what DNA from other bacteria such as E. coli do, which induce an inflammatory response from dendritic cells in vitro, HP DNA is unable to induce inflammatory reaction. On the other hand, it is capable of inhibiting the production of proinflammatory cytokines of the murine or human cells in vitro. They also demonstrated that HP infected patients have lower systemic levels of typeⅠIFN, in comparison to uninfected patients. The authors concluded that the inverse correlation between IBD and HP, observed in epidemiological studies, could be partially explained by HP DNA’s capacity to reduce typeⅠIFN[61].
More recently, in 2012 Sonnenberg et al[63,64], carried out a study in which they performed upper and lower endoscopy (on the same day) to a large sample of patients. Biopsies obtained in the upper endoscopy were examined for esophagitis, gastritis and HP infection. Biopsies obtained from colonoscopy were scrutinized for UC, CD and IC. IBD was identified in 1061 patients (1.6%), and the rest was used as control group. The analysis showed an inverse relationship between HP and IBD, both for UC and CD. On the other hand, a positive relationship was found between HP-negative chronic gastritis and IBD[63,64].
Data obtained in the different types of studies performed to date (epidemiological, clinical and experimental) suggest that HP infection reduces the risk of developing IBD, by producing a protective effect that hinders the appearance of IBD. Case reports and epidemiological studies have observed that IBD may appear quickly after HP eradication, possibly due to a shift in the Th pattern. However, other studies have exposed that this lower preva-
6 February �5, 20�5|Volume 6|Issue �|WJGP|www.wjgnet.com
Bosca-Watts MM et al . Bugs in the pathogenesis of CD

lence of HP in IBD might be secondary to HP “spontaneous eradication” with 5-ASA or antibiotic treatment[65].
Other Helicobacter species, like Helicobacter hepaticus, have shown their capability of inducing colitis in animals, mainly in immunocompromised ones. Studies need to be done to see if the same effect is seen in humans[9,66,67].
Clostridium difficileClostridium difficile (C. Difficile) is a gram positive anaerobic bacillus that forms spores and produces toxins, which can cause different degrees of intestinal disease. Classically, it has been considered a cause of colitis related to the use of antibiotics and of nosocomial diarrhea. In the last decades, its incidence has greatly increased. Nowadays, 20%-30% of antibiotic-related diarrheas and up to 50%-70% of the antibiotic-related colitis are con-sidered to be due to C. Difficile infection. A similar increase in the incidence of C. Difficile infection in IBD has been documented. Up to 10% of the IBD patients will develop C. Difficile infection at some point. IBD patients probably have a higher risk of infections due to increased antibiotic use and the consequent creation of a favorable environment for colonization, although in 40% of the cases in IBD patients, it can appear without previous use of antibiotic. Possible complications in these patients include colectomy and death. However, there are no conclusive data in the medical literature to support the idea of the bacteria as a cause of onset or reactivation of IBD, which could be merely a consequence of the existing inflammatory status[68,69].
As mentioned, many studies have observed an increased risk of C. Difficile infection in IBD, which may be due to a variety of factors that include the altered nutritional and immunological state, repeated hospitalizations, frequent and recurrent use of antibiotics and immunomodulators and even genetic predisposition. Although C. Difficile may not be a causative agent, it can produce superimposed colitis or induce reactivation, and, therefore, is nowadays considered a risk factor of exacerbations.
In 2013, Nitzan et al[70] published an extensive review regarding the role of C. Difficile in the patho-genesis of IBD, as well as its implications with respect to diagnosis and treatment. The review embraces the different risk factors, clinical chara-cteristics of the infection in IBD, special aspects of its presentation, diagnosis and treatment in IBD. The authors emphasize the necessary suspicion of diagnosis, recommending screening in every IBD patient hospitalized for a flare, as well as early treatment, especially in severe cases. They conclude that Clostridium Difficile most likely plays a role in the pathogenesis of exacerbations, although probably not in the development of IBD itself[70].
Campylobacter and salmonellaA recent study by Jess et al [71] analyzed the incidence of CD and UC in patients with positive and negative fecal Salmonella and Campylobacter tests, as well as the incidence of positive and negative cultures in those already diagnosed with IBD. To do so, the researchers analyzed the patients that had been included in the Danish national register in the previous 15 years, who had a positive or negative stool test for Salmonella and Campylobacter, and patients diagnosed with IBD[71]. Statistical analysis showed that the risk of developing IBD is relatively high (RR = of 5.4-9.8) the first year after a positive fecal test for Salmonella or Campylobacter. It rem-ains moderately high up to 10 years after the positive test (RR = 1.6-2.2) and becomes low after 10 years (0.8-1.8).
However, the first year after a negative stool test the relative risk of IBD was also high, and a decreasing incidence pattern over time was parallel to that following positive test results.
The risk of having IBD substantially increases, not only after an infection with Salmonella or Campylobacter, but also, and even more so, after a patient has a negative stool test. After 10 years of positive results, the relative risk of developing IBD is reduced to 1, but the risk remains quite high 10 years after having a stool test, in the case that the test had been negative. During the first year after a first hospitalization for IBD, the risk of a negative test is high and remains high.
In conclusion, the study confirmed the previous results of a higher risk of IBD after Salmonella or Campylobacter infection[72], but it revealed that the risk is perhaps surprisingly more pronounced after a negative stool test. These results might suggest that the risk which had previously been attributed to Salmonella and Campylobacter gastroenteritis could in fact be due to the fact that more tests are carried out, rather than to a casual effect.
ROLE OF VIRUSES IN THE ETIOLOGY OF IBDThe role of the different viruses in the pathogenesis of IBD is still not well understood. Two theories, based on many epidemiological studies with contr-adictory results, have been proposed to explain the relationship between viral infections and the development of IBD, which, in part, may be mutually exclusive. The first theory suggests that certain infections that occur during infancy may predispose to the appearance of IBD. The second theory points to the absence of infections in infancy and the lack of contact with certain antigens as the cause of subsequent intestinal inflammation (Hygiene Theory).
An example that supports infections as a risk
� February �5, 20�5|Volume 6|Issue �|WJGP|www.wjgnet.com
Bosca-Watts MM et al . Bugs in the pathogenesis of CD

factor is found in Ekbom’s case-control study, carried out in 1990 to determine the potential role of infections during infancy in the pathogenesis of IBD[73]. Analysis of perinatal events and risk of CD found postnatal infections to be the factor that was associated most strongly, both in the univariant analysis (OR = 9.5) and the multivariant (OR = 5.5). On the other hand, the fact that IBD appears more frequently in developed countries or in people who migrate from undeveloped to developed countries sustains the hygiene theory as the main etiological factor.
MeaslesThe possible role of the measles virus was stren-gthened in the 1990’s by the epidemiological studies that showed the incidence of CD, which was higher than expected, in children that had been born in the three months after measles outbreaks[74,75]. These studies observed that the virus was capable of producing an inflammatory reaction in the me-senteric endothelium that was quite similar to the one found in CD[75-77]. This finding stimulated the performance of numerous observational studies, which analyzed the relationship between measles infection or vaccination and the development of IBD. The studies, which in general were case-control or cohort, obtained heterogeneous results[78-85]. Some had limitations in data gathering and do not enable confirmation of an epidemiological relationship between measles virus and IBD.
A reasonable argument against the relationship between measles and IBD could be the increasing incidence of CD despite the progressive reduction of the measles virus infection. The increase could be due to a change in the virulence factors of the microorganism, as a consequence of widespread vaccination. The question arose if the effect of the attenuated vaccine was responsible for the increase in CD incidence, but again no relationship was found[79,81].
Several later attempts to isolate virus in tissue or blood with more specific techniques were unsu-ccessful[86]; the possibility of immunological cross reaction between intestinal or viral antigens was also discarded[87-89]. Consequently, since the minimum data necessary to establish a causal biological relationship has not been attained, the implication of the measles virus or its vaccine[90] in the path-ogenesis of IBD is uncertain.
Mumps (parotiditis)Similarly, during the same period of time, the hyp-othesis of the parotiditis virus as a pathogenic agent in IBD was proposed. Several studies were published evaluating the epidemiological association between mumps infection and IBD, both alone or with measles co-infection. Although some identified a higher IBD risk[91,92], viral parts were not isolated
from intestinal tissue[93] and the direct link with IBD could not be established. While it was suggested that the immunological response to the virus might be involved in the process of IBD presentation, as was observed with the measles virus, no concluding evidence was found[94].
CitomegalovirusThe role of Citomegalovirus (CMV) as an infectious agent that can reactivate underlying inflammatory disease has been accepted[95]. However, there is no proof of a CMV effect on the pathogenesis. Despite the association between the intensity of expression in the intestinal mucosa and the severity of the IBD inflammation, viral replication was also found in healthy mucosa[96]. A higher CMV infection rate was not observed in the IBD population with respect to the general population[97].
Virus de Epstein-BarrInterest in a potential etiopathogenic role of Virus de Epstein-Barr (VEB) in IBD arose when an increased number of B lymphocytes infected with VEB was found in mucosal samples from UC colons, and, to a lesser degree, in CD samples[98]. Epidemiological data indicate that frequency of infection is similar in IBD patients and healthy controls, both approximately 100%[99]. The intensity of replication has been related to increased bowel inflammation[100] and to serious complications such as lymphomas[95,101]. Therefore, as with CMV, a modulating function, rather than an etiological implication, was determined.
CONCLUSIONThe significant role of microorganisms in the pathogenesis of IBD seems apparent, although it is complex. Whether it is one pathogenic germ or more than one in unison with the gut microbiota as helper, main character or observer needs to be elucidated. Clinical suspicion, now widely supported by genetic and molecular studies, points to altered autophagy that may favor intracellular germs that trigger a cascade of events that produce the onset of IBD in predisposed individuals. Studies now implicating AIEC as pivotal in CD, mainly ileal CD, raise the question of if we have been discarding one of the main players, E. coli, as crucial because it was considered microbiota, without understanding its more adherent and invasive particularities in IBD patients and if the same is the case with other intestinal “bugs”. Or is CD caused, as happens with MAP, by chronic exposure to a slow-acting germ? Or are we simply in a “bacteria era” which will pass, as did the “virus era”, when more information is obtained and understood regarding the pathogenesis of CD? Many questions remain. Understanding the interaction of several germs together, as seen with E. coli and MAP, which may, in conjunction favor IBD, or
8 February �5, 20�5|Volume 6|Issue �|WJGP|www.wjgnet.com
Bosca-Watts MM et al . Bugs in the pathogenesis of CD

with HP, which may keep the balance away from IBD, might clarify the base of this complex disorder.
ACKNOWLEDGMENTSTo Frances Watts, Applied Linguistics, Polytechnic University of Valencia, for her language review.
REFERENCES1 Nguyen HT, Dalmasso G, Müller S, Carrière J, Seibold F,
Darfeuille-Michaud A. Crohn’s disease-associated adherent invasive Escherichia coli modulate levels of microRNAs in intestinal epithelial cells to reduce autophagy. Gastroenterology 2014; 146: 508-519 [PMID: 24148619]
2 Kaser A, Zeissig S, Blumberg RS. Inflammatory bowel disease. Annu Rev Immunol 2010; 28: 573-621 [PMID: 20192811 DOI: 10.1146/annurev-immunol-030409-101225]
3 Leone V, Chang EB, Devkota S. Diet, microbes, and host genetics: the perfect storm in inflammatory bowel diseases. J Gastroenterol 2013; 48: 315-321 [PMID: 23475322 DOI: 10.1007/s00535-013-0777-2]
4 Hansen R, Thomson JM, El-Omar EM, Hold GL. The role of infection in the aetiology of inflammatory bowel disease. J Gastroenterol 2010; 45: 266-276 [PMID: 20076977 DOI: 10.1007/s00535-009-0191-y]
5 Cani PD, Delzenne NM. The gut microbiome as therapeutic target. Pharmacol Ther 2011; 130: 202-212 [PMID: 21295072 DOI: 10.1016/j.pharmthera.2011.01.012]
6 Cave DR, Mitchell DN, Brooke BN. Experimental animal studies of the etiology and pathogenesis of Crohn’s disease. Gastroenterology 1975; 69: 618-624 [PMID: 1158079]
7 Cave DR, Mitchell DN, Kane SP, Brooke BN. Further animal evidence of a transmissible agent in Crohn’s disease. Lancet 1973; 2: 1120-1122 [PMID: 4128014]
8 Mitchell DN, Rees RJ, Goswami KK. Transmissible agents from human sarcoid and Crohn’s disease tissues. Lancet 1976; 2: 761-765 [PMID: 61441]
9 Kullberg MC, Ward JM, Gorelick PL, Caspar P, Hieny S, Cheever A, Jankovic D, Sher A. Helicobacter hepaticus triggers colitis in specific-pathogen-free interleukin-10 (IL-10)-deficient mice through an IL-12- and gamma interferon-dependent mechanism. Infect Immun 1998; 66: 5157-5166 [PMID: 9784517]
10 Sewell GW, Marks DJ, Segal AW. The immunopathogenesis of Crohn’s disease: a three-stage model. Curr Opin Immunol 2009; 21: 506-513 [PMID: 19665880 DOI: 10.1016/j.coi.2009.06.003]
11 Chassaing B, Darfeuille-Michaud A. The commensal microbiota and enteropathogens in the pathogenesis of inflammatory bowel diseases. Gastroenterology 2011; 140: 1720-1728 [PMID: 21530738 DOI: 10.1053/j.gastro.2011.01.054]
12 Manichanh C, Borruel N, Casellas F, Guarner F. The gut microbiota in IBD. Nat Rev Gastroenterol Hepatol 2012; 9: 599-608 [PMID: 22907164 DOI: 10.1038/nrgastro.2012.152]
13 Hudson MJ, Hill MJ, Elliott PR, Berghouse LM, Burnham WR, Lennard-Jones JE. The microbial flora of the rectal mucosa and faeces of patients with Crohn’s disease before and during antimicrobial chemotherapy. J Med Microbiol 1984; 18: 335-345 [PMID: 6334160]
14 Mendoza JL, Lana R, Díaz-Rubio M. Mycobacterium avium subspecies paratuberculosis and its relationship with Crohn’s disease. World J Gastroenterol 2009; 15: 417-422 [PMID: 19152445]
15 Mendoza JL, San-Pedro A, Culebras E, Cíes R, Taxonera C, Lana R, Urcelay E, de la Torre F, Picazo JJ, Díaz-Rubio M. High prevalence of viable Mycobacterium avium subspecies paratuberculosis in Crohn’s disease. World J Gastroenterol 2010; 16: 4558-4563 [PMID: 20857526]
16 Momotani E, Romona NM, Yoshihara K, Momotani Y, Hori M,
Ozaki H, Eda S, Ikegami M. Molecular pathogenesis of bovine paratuberculosis and human inflammatory bowel diseases. Vet Immunol Immunopathol 2012; 148: 55-68 [PMID: 22486997 DOI: 10.1016/j.vetimm.2012.03.005]
17 Greenstein RJ, Su L, Juste RA, Brown ST. On the action of cyclosporine A, rapamycin and tacrolimus on M. avium including subspecies paratuberculosis. PLoS One 2008; 3: e2496 [PMID: 18575598 DOI: 10.1371/journal.pone.0002496]
18 Greenstein RJ. Is Crohn’s disease caused by a mycobacterium? Comparisons with leprosy, tuberculosis, and Johne’s disease. Lancet Infect Dis 2003; 3: 507-514 [PMID: 12901893]
19 Darfeuille-Michaud A, Neut C, Barnich N, Lederman E, Di Martino P, Desreumaux P, Gambiez L, Joly B, Cortot A, Colombel JF. Presence of adherent Escherichia coli strains in ileal mucosa of patients with Crohn’s disease. Gastroenterology 1998; 115: 1405-1413 [PMID: 9834268]
20 Boudeau J, Glasser AL, Masseret E, Joly B, Darfeuille-Michaud A. Invasive ability of an Escherichia coli strain isolated from the ileal mucosa of a patient with Crohn’s disease. Infect Immun 1999; 67: 4499-4509 [PMID: 10456892]
21 Glasser AL, Boudeau J, Barnich N, Perruchot MH, Colombel JF, Darfeuille-Michaud A. Adherent invasive Escherichia coli strains from patients with Crohn’s disease survive and replicate within macrophages without inducing host cell death. Infect Immun 2001; 69: 5529-5537 [PMID: 11500426]
22 Masseret E, Boudeau J, Colombel JF, Neut C, Desreumaux P, Joly B, Cortot A, Darfeuille-Michaud A. Genetically related Escherichia coli strains associated with Crohn’s disease. Gut 2001; 48: 320-325 [PMID: 11171820]
23 Darfeuille-Michaud A, Boudeau J, Bulois P, Neut C, Glasser AL, Barnich N, Bringer MA, Swidsinski A, Beaugerie L, Colombel JF. High prevalence of adherent-invasive Escherichia coli associated with ileal mucosa in Crohn’s disease. Gastroenterology 2004; 127: 412-421 [PMID: 15300573]
24 Rutgeerts P, Goboes K, Peeters M, Hiele M, Penninckx F, Aerts R, Kerremans R, Vantrappen G. Effect of faecal stream diversion on recurrence of Crohn’s disease in the neoterminal ileum. Lancet 1991; 338: 771-774 [PMID: 1681159]
25 O’Brien CL, Pavli P, Gordon DM, Allison GE. Detection of bacterial DNA in lymph nodes of Crohn’s disease patients using high throughput sequencing. Gut 2014; 63: 1596-1606 [PMID: 24429583 DOI: 10.1136/gutjnl-2013-305320]
26 Baumgart M, Dogan B, Rishniw M, Weitzman G, Bosworth B, Yantiss R, Orsi RH, Wiedmann M, McDonough P, Kim SG, Berg D, Schukken Y, Scherl E, Simpson KW. Culture independent analysis of ileal mucosa reveals a selective increase in invasive Escherichia coli of novel phylogeny relative to depletion of Clostridiales in Crohn’s disease involving the ileum. ISME J 2007; 1: 403-418 [PMID: 18043660]
27 Nataro JP, Kaper JB. Diarrheagenic Escherichia coli. Clin Microbiol Rev 1998; 11: 142-201 [PMID: 9457432]
28 Cartun RW, Van Kruiningen HJ, Pedersen CA, Berman MM. An immunocytochemical search for infectious agents in Crohn’s disease. Mod Pathol 1993; 6: 212-219 [PMID: 8483893]
29 Tabaqchali S, O’Donoghue DP, Bettelheim KA. Escherichia coli antibodies in patients with inflammatory bowel disease. Gut 1978; 19: 108-113 [PMID: 344155]
30 Mann EA, Saeed SA. Gastrointestinal infection as a trigger for inflammatory bowel disease. Curr Opin Gastroenterol 2012; 28: 24-29 [PMID: 22080823 DOI: 10.1097/MOG.0b013e32834c453e]
31 Barnich N, Darfeuille-Michaud A. Role of bacteria in the etiopathogenesis of inflammatory bowel disease. World J Gastroenterol 2007; 13: 5571-5576 [PMID: 17948930]
32 Wine E, Ossa JC, Gray-Owen SD, Sherman PM. Adherent-invasive Escherichia coli target the epithelial barrier. Gut Microbes 2010; 1: 80-84 [PMID: 21326914]
33 Dreux N, Denizot J, Martinez-Medina M, Mellmann A, Billig M, Kisiela D, Chattopadhyay S, Sokurenko E, Neut C, Gower-Rousseau C, Colombel JF, Bonnet R, Darfeuille-Michaud A, Barnich N. Point mutations in FimH adhesin of Crohn’s disease-
9 February �5, 20�5|Volume 6|Issue �|WJGP|www.wjgnet.com
Bosca-Watts MM et al . Bugs in the pathogenesis of CD

associated adherent-invasive Escherichia coli enhance intestinal inflammatory response. PLoS Pathog 2013; 9: e1003141 [PMID: 23358328 DOI: 10.1371/journal.ppat.1003141]
34 Moulin-Schouleur M, Répérant M, Laurent S, Brée A, Mignon-Grasteau S, Germon P, Rasschaert D, Schouler C. Extraintestinal pathogenic Escherichia coli strains of avian and human origin: link between phylogenetic relationships and common virulence patterns. J Clin Microbiol 2007; 45: 3366-3376 [PMID: 17652485]
35 Wirth T, Falush D, Lan R, Colles F, Mensa P, Wieler LH, Karch H, Reeves PR, Maiden MC, Ochman H, Achtman M. Sex and virulence in Escherichia coli: an evolutionary perspective. Mol Microbiol 2006; 60: 1136-1151 [PMID: 16689791]
36 Miquel S, Peyretaillade E, Claret L, de Vallée A, Dossat C, Vacherie B, Zineb el H, Segurens B, Barbe V, Sauvanet P, Neut C, Colombel JF, Medigue C, Mojica FJ, Peyret P, Bonnet R, Darfeuille-Michaud A. Complete genome sequence of Crohn’s disease-associated adherent-invasive E. coli strain LF82. PLoS One 2010; 5: e12714 [PMID: 20862302 DOI: 10.1371/journal.pone.0012714]
37 Rolhion N, Barnich N, Bringer MA, Glasser AL, Ranc J, Hébuterne X, Hofman P, Darfeuille-Michaud A. Abnormally expressed ER stress response chaperone Gp96 in CD favours adherent-invasive Escherichia coli invasion. Gut 2010; 59: 1355-1362 [PMID: 20587550 DOI: 10.1136/gut.2010.207456]
38 Chassaing B, Rolhion N, de Vallée A, Salim SY, Prorok-Hamon M, Neut C, Campbell BJ, Söderholm JD, Hugot JP, Colombel JF, Darfeuille-Michaud A. Crohn disease--associated adherent-invasive E. coli bacteria target mouse and human Peyer’s patches via long polar fimbriae. J Clin Invest 2011; 121: 966-975 [PMID: 21339647]
39 Lapaquette P, Glasser AL, Huett A, Xavier RJ, Darfeuille-Michaud A. Crohn’s disease-associated adherent-invasive E. coli are selectively favoured by impaired autophagy to replicate intracellularly. Cell Microbiol 2010; 12: 99-113 [PMID: 19747213 DOI: 10.1111/j.1462-5822.2009.01381]
40 Matricon J, Barnich N, Ardid D. Immunopathogenesis of inflammatory bowel disease. Self Nonself 2010; 1: 299-309 [PMID: 21487504]
41 Chassaing B, Koren O, Carvalho FA, Ley RE, Gewirtz AT. AIEC pathobiont instigates chronic colitis in susceptible hosts by altering microbiota composition. Gut 2014; 63: 1069-1080 [PMID: 23896971 DOI: 10.1136/gutjnl-2013-304909]
42 Hase K, Kawano K, Nochi T, Pontes GS, Fukuda S, Ebisawa M, Kadokura K, Tobe T, Fujimura Y, Kawano S, Yabashi A, Waguri S, Nakato G, Kimura S, Murakami T, Iimura M, Hamura K, Fukuoka S, Lowe AW, Itoh K, Kiyono H, Ohno H. Uptake through glycoprotein 2 of FimH(+) bacteria by M cells initiates mucosal immune response. Nature 2009; 462: 226-230 [PMID: 19907495 DOI: 10.1038/nature08529]
43 Roggenbuck D, Hausdorf G, Martinez-Gamboa L, Reinhold D, Büttner T, Jungblut PR, Porstmann T, Laass MW, Henker J, Büning C, Feist E, Conrad K. Identification of GP2, the major zymogen granule membrane glycoprotein, as the autoantigen of pancreatic antibodies in Crohn’s disease. Gut 2009; 58: 1620-1628 [PMID: 19549613 DOI: 10.1136/gut.2008.162495]
44 Friswell M, Campbell B, Rhodes J. The role of bacteria in the pathogenesis of inflammatory bowel disease. Gut Liver 2010; 4: 295-306 [PMID: 20981205 DOI: 10.5009/gnl.2010.4.3.295]
45 Prorok-Hamon M, Friswell MK, Alswied A, Roberts CL, Song F, Flanagan PK, Knight P, Codling C, Marchesi JR, Winstanley C, Hall N, Rhodes JM, Campbell BJ. Colonic mucosa-associated diffusely adherent afaC+ Escherichia coli expressing lpfA and pks are increased in inflammatory bowel disease and colon cancer. Gut 2014; 63: 761-770 [PMID: 23846483 DOI: 10.1136/gutjnl-2013-304739]
46 Elguezabal N, Chamorro S, Molina E, Garrido JM, Izeta A, Rodrigo L, Juste RA. Lactase persistence, NOD2 status and Mycobacterium avium subsp. paratuberculosis infection associations to Inflammatory Bowel Disease. Gut Pathog 2012; 4: 6 [PMID: 22742424 DOI: 10.1186/1757-4749-4-6]
47 Lidar M, Langevitz P, Shoenfeld Y. The role of infection
in inflammatory bowel disease: initiation, exacerbation and protection. Isr Med Assoc J 2009; 11: 558-563 [PMID: 19960852]
48 Juste RA, Elguezabal N, Garrido JM, Pavon A, Geijo MV, Sevilla I, Cabriada JL, Tejada A, García-Campos F, Casado R, Ochotorena I, Izeta A, Greenstein RJ. On the prevalence of M. avium subspecies paratuberculosis DNA in the blood of healthy individuals and patients with inflammatory bowel disease. PLoS One 2008; 3: e2537 [PMID: 18596984 DOI: 10.1371/journal.pone.0002537]
49 Naser SA, Ghobrial G, Romero C, Valentine JF. Culture of Mycobacterium avium subspecies paratuberculosis from the blood of patients with Crohn’s disease. Lancet 2004; 364: 1039-1044 [PMID: 15380962]
50 Kirkwood CD, Wagner J, Boniface K, Vaughan J, Michalski WP, Catto-Smith AG, Cameron DJ, Bishop RF. Mycobacterium avium subspecies paratuberculosis in children with early-onset Crohn’s disease. Inflamm Bowel Dis 2009; 15: 1643-1655 [PMID: 19462429 DOI: 10.1002/ibd.20967]
51 Mishina D, Katsel P, Brown ST, Gilberts EC, Greenstein RJ. On the etiology of Crohn disease. Proc Natl Acad Sci USA 1996; 93: 9816-9820 [PMID: 8790414]
52 Olsen I, Tollefsen S, Aagaard C, Reitan LJ, Bannantine JP, Andersen P, Sollid LM, Lundin KE. Isolation of Mycobacterium avium subspecies paratuberculosis reactive CD4 T cells from intestinal biopsies of Crohn’s disease patients. PLoS One 2009; 4: e5641 [PMID: 19479064 DOI: 10.1371/journal.pone.0005641]
53 Mpofu CM, Campbell BJ, Subramanian S, Marshall-Clarke S, Hart CA, Cross A, Roberts CL, McGoldrick A, Edwards SW, Rhodes JM. Microbial mannan inhibits bacterial killing by macrophages: a possible pathogenic mechanism for Crohn’s disease. Gastroenterology 2007; 133: 1487-1498 [PMID: 17919633]
54 Tsianos EV, Katsanos K. Do we really understand what the immunological disturbances in inflammatory bowel disease mean? World J Gastroenterol 2009; 15: 521-525 [PMID: 19195052]
55 Ferwerda G, Kullberg BJ, de Jong DJ, Girardin SE, Langenberg DM, van Crevel R, Ottenhoff TH, Van der Meer JW, Netea MG. Mycobacterium paratuberculosis is recognized by Toll-like receptors and NOD2. J Leukoc Biol 2007; 82: 1011-1018 [PMID: 17652449]
56 Gutierrez MG, Master SS, Singh SB, Taylor GA, Colombo MI, Deretic V. Autophagy is a defense mechanism inhibiting BCG and Mycobacterium tuberculosis survival in infected macrophages. Cell 2004; 119: 753-766 [PMID: 15607973]
57 Sechi LA, Gazouli M, Sieswerda LE, Molicotti P, Ahmed N, Ikonomopoulos J, Scanu AM, Paccagnini D, Zanetti S. Relationship between Crohn’s disease, infection with Mycobacterium avium subspecies paratuberculosis and SLC11A1 gene polymorphisms in Sardinian patients. World J Gastroenterol 2006; 12: 7161-7164 [PMID: 17131479]
58 Gui GP, Thomas PR, Tizard ML, Lake J, Sanderson JD, Hermon-Taylor J. Two-year-outcomes analysis of Crohn’s disease treated with rifabutin and macrolide antibiotics. J Antimicrob Chemother 1997; 39: 393-400 [PMID: 9096189]
59 Selby W, Pavli P, Crotty B, Florin T, Radford-Smith G, Gibson P, Mitchell B, Connell W, Read R, Merrett M, Ee H, Hetzel D. Two-year combination antibiotic therapy with clarithromycin, rifabutin, and clofazimine for Crohn’s disease. Gastroenterology 2007; 132: 2313-2319 [PMID: 17570206]
60 Luther J, Dave M, Higgins PD, Kao JY. Association between Helicobacter pylori infection and inflammatory bowel disease: a meta-analysis and systematic review of the literature. Inflamm Bowel Dis 2010; 16: 1077-1084 [PMID: 19760778 DOI: 10.1002/ibd.21116]
61 Luther J, Owyang SY, Takeuchi T, Cole TS, Zhang M, Liu M, Erb-Downward J, Rubenstein JH, Chen CC, Pierzchala AV, Paul JA, Kao JY. Helicobacter pylori DNA decreases pro-inflammatory cytokine production by dendritic cells and attenuates dextran sodium sulphate-induced colitis. Gut 2011; 60: 1479-1486 [PMID: 21471567 DOI: 10.1136/gut.2010.220087]
62 Väre PO, Heikius B, Silvennoinen JA, Karttunen R, Niemelä SE, Lehtola JK, Karttunen TJ. Seroprevalence of Helicobacter pylori
�0 February �5, 20�5|Volume 6|Issue �|WJGP|www.wjgnet.com
Bosca-Watts MM et al . Bugs in the pathogenesis of CD

infection in inflammatory bowel disease: is Helicobacter pylori infection a protective factor? Scand J Gastroenterol 2001; 36: 1295-1300 [PMID: 11761020]
63 Sonnenberg A, Genta RM. Low prevalence of Helicobacter pylori infection among patients with inflammatory bowel disease. Aliment Pharmacol Ther 2012; 35: 469-476 [PMID: 22221289 DOI: 10.1111/j.1365-2036.2011.04969]
64 Sonnenberg A, Melton SD, Genta RM. Frequent occurrence of gastritis and duodenitis in patients with inflammatory bowel disease. Inflamm Bowel Dis 2011; 17: 39-44 [PMID: 20848539 DOI: 10.1002/ibd.21356]
65 Papamichael K, Konstantopoulos P, Mantzaris GJ. Helicobacter pylori infection and inflammatory bowel disease: is there a link? World J Gastroenterol 2014; 20: 6374-6385 [PMID: 24914359]
66 Kullberg MC, Jankovic D, Feng CG, Hue S, Gorelick PL, McKenzie BS, Cua DJ, Powrie F, Cheever AW, Maloy KJ, Sher A. IL-23 plays a key role in Helicobacter hepaticus-induced T cell-dependent colitis. J Exp Med 2006; 203: 2485-2494 [PMID: 17030948]
67 Morrison PJ, Bending D, Fouser LA, Wright JF, Stockinger B, Cooke A, Kullberg MC. Th17-cell plasticity in Helicobacter hepaticus-induced intestinal inflammation. Mucosal Immunol 2013; 6: 1143-1156 [PMID: 23462910]
68 Bien J, Palagani V, Bozko P. The intestinal microbiota dysbiosis and Clostridium difficile infection: is there a relationship with inflammatory bowel disease? Therap Adv Gastroenterol 2013; 6: 53-68 [PMID: 23320050 DOI: 10.1177/1756283X12454590]
69 Navaneethan U, Venkatesh PG, Shen B. Clostridium difficile infection and inflammatory bowel disease: understanding the evolving relationship. World J Gastroenterol 2010; 16: 4892-4904 [PMID: 20954275]
70 Nitzan O, Elias M, Chazan B, Raz R, Saliba W. Clostridium difficile and inflammatory bowel disease: role in pathogenesis and implications in treatment. World J Gastroenterol 2013; 19: 7577-7585 [PMID: 24282348]
71 Jess T, Simonsen J, Nielsen NM, Jørgensen KT, Bager P, Ethelberg S, Frisch M. Enteric Salmonella or Campylobacter infections and the risk of inflammatory bowel disease. Gut 2011; 60: 318-324 [PMID: 21193449 DOI: 10.1136/gut.2010.223396]
72 Gradel KO, Nielsen HL, Schønheyder HC, Ejlertsen T, Kristensen B, Nielsen H. Increased short- and long-term risk of inflammatory bowel disease after salmonella or campylobacter gastroenteritis. Gastroenterology 2009; 137: 495-501 [PMID: 19361507 DOI: 10.1053/j.gastro.2009.04.001]
73 Ekbom A, Adami HO, Helmick CG, Jonzon A, Zack MM. Perinatal risk factors for inflammatory bowel disease: a case-control study. Am J Epidemiol 1990; 132: 1111-1119 [PMID: 2260543]
74 Ekbom A, Wakefield AJ, Zack M, Adami HO. Perinatal measles infection and subsequent Crohn’s disease. Lancet 1994; 344: 508-510 [PMID: 7914614]
75 Wakefield AJ, Pittilo RM, Sim R, Cosby SL, Stephenson JR, Dhillon AP, Pounder RE. Evidence of persistent measles virus infection in Crohn’s disease. J Med Virol 1993; 39: 345-353 [PMID: 8492105]
76 Wakefield AJ, Ekbom A, Dhillon AP, Pittilo RM, Pounder RE. Crohn’s disease: pathogenesis and persistent measles virus infection. Gastroenterology 1995; 108: 911-916 [PMID: 7875495]
77 Wakefield AJ, Sim R, Akbar AN, Pounder RE, Dhillon AP. In situ immune responses in Crohn’s disease: a comparison with acute and persistent measles virus infection. J Med Virol 1997; 51: 90-100 [PMID: 9021538]
78 Van Damme W, Lynen L, Kegels G, Van Lerberghe W. Measles vaccination and inflammatory bowel disease. Lancet 1997; 350: 1774-1775 [PMID: 9413483]
79 Thompson NP, Montgomery SM, Pounder RE, Wakefield AJ. Is measles vaccination a risk factor for inflammatory bowel disease? Lancet 1995; 345: 1071-1074 [PMID: 7715338]
80 Morris DL, Montgomery SM, Thompson NP, Ebrahim S, Pounder RE, Wakefield AJ. Measles vaccination and inflammatory bowel
disease: a national British Cohort Study. Am J Gastroenterol 2000; 95: 3507-3512 [PMID: 11151885]
81 Feeney M, Ciegg A, Winwood P, Snook J. A case-control study of measles vaccination and inflammatory bowel disease. The East Dorset Gastroenterology Group. Lancet 1997; 350: 764-766 [PMID: 9297995]
82 Nielsen LL, Nielsen NM, Melbye M, Sodermann M, Jacobsen M, Aaby P. Exposure to measles in utero and Crohn’s disease: Danish register study. BMJ 1998; 316: 196-197 [PMID: 9468686]
83 Jones P, Fine P, Piracha S. Crohn’s disease and measles. Lancet 1997; 349: 473 [PMID: 9040582]
84 Hansen TS, Jess T, Vind I, Elkjaer M, Nielsen MF, Gamborg M, Munkholm P. Environmental factors in inflammatory bowel disease: a case-control study based on a Danish inception cohort. J Crohns Colitis 2011; 5: 577-584 [PMID: 22115378 DOI: 10.1016/j.crohns.2011.05.010]
85 Haslam N, Mayberry JF, Hawthorne AB, Newcombe RG, Holmes GK, Probert CS. Measles, month of birth, and Crohn’s disease. Gut 2000; 47: 801-803 [PMID: 11076878]
86 Ghosh S, Armitage E, Wilson D, Minor PD, Afzal MA. Detection of persistent measles virus infection in Crohn’s disease: current status of experimental work. Gut 2001; 48: 748-752 [PMID: 11358885]
87 Haga Y, Funakoshi O, Kuroe K, Kanazawa K, Nakajima H, Saito H, Murata Y, Munakata A, Yoshida Y. Absence of measles viral genomic sequence in intestinal tissues from Crohn’s disease by nested polymerase chain reaction. Gut 1996; 38: 211-215 [PMID: 8801199]
88 D’Souza Y, Dionne S, Seidman EG, Bitton A, Ward BJ. No evidence of persisting measles virus in the intestinal tissues of patients with inflammatory bowel disease. Gut 2007; 56: 886-888 [PMID: 17519494]
89 Koutsoumpas AL, Polymeros D, Tsiamoulos Z, Karamanolis G, Triantafyllou K, Bogdanos DP, Ladas SD. S1191 Molecular Mimicry and Immunological Crossreactivity Between Measles Virus and Human Intestinal Proteins is Not a Feature of Crohn’s Disease. Gastroenterol 2010; 138 (suppl 1): S-200
90 Davis RL, Bohlke K. Measles vaccination and inflammatory bowel disease: controversy laid to rest? Drug Saf 2001; 24: 939-946 [PMID: 11735650]
91 Montgomery SM, Morris DL, Pounder RE, Wakefield AJ. Paramyxovirus infections in childhood and subsequent inflammatory bowel disease. Gastroenterology 1999; 116: 796-803 [PMID: 10092301]
92 Ng SC, Woodrow S, Patel N, Subhani J, Harbord M. Role of genetic and environmental factors in British twins with inflammatory bowel disease. Inflamm Bowel Dis 2012; 18: 725-736 [PMID: 21557397 DOI: 10.1002/ibd.21747]
93 Folwaczny C, Jäger G, Schnettler D, Wiebecke B, Loeschke K. Search for mumps virus genome in intestinal biopsy specimens of patients with IBD. Gastroenterology 1999; 117: 1253-1255 [PMID: 10610334]
94 Iizuka M, Saito H, Yukawa M, Itou H, Shirasaka T, Chiba M, Fukushima T, Watanabe S. No evidence of persistent mumps virus infection in inflammatory bowel disease. Gut 2001; 48: 637-641 [PMID: 11302960]
95 Waters O, Ahmad T. Opportunistic infections and vaccinations in IBD patients. J Crohns Colitis 2011; 5: 263; author reply 264 [PMID: 21575894]
96 Sipponen T, Turunen U, Lautenschlager I, Nieminen U, Arola J, Halme L. Human herpesvirus 6 and cytomegalovirus in ileocolonic mucosa in inflammatory bowel disease. Scand J Gastroenterol 2011; 46: 1324-1333 [PMID: 21879802 DOI: 10.3109/00365521.2011.605466]
97 Lidar M, Langevitz P, Barzilai O, Ram M, Porat-Katz BS, Bizzaro N, Tonutti E, Maieron R, Chowers Y, Bar-Meir S, Shoenfeld Y. Infectious serologies and autoantibodies in inflammatory bowel disease: insinuations at a true pathogenic role. Ann N Y Acad Sci 2009; 1173: 640-648 [PMID: 19758210 DOI: 10.1111/j.1749-6632.2009.04673]
98 Yanai H, Shimizu N, Nagasaki S, Mitani N, Okita K. Epstein-Barr virus infection of the colon with inflammatory bowel disease. Am J
�� February �5, 20�5|Volume 6|Issue �|WJGP|www.wjgnet.com
Bosca-Watts MM et al . Bugs in the pathogenesis of CD

Gastroenterol 1999; 94: 1582-1586 [PMID: 10364028]99 Linton MS, Kroeker K, Fedorak D, Dieleman L, Fedorak RN.
Prevalence of Epstein-Barr Virus in a population of patients with inflammatory bowel disease: a prospective cohort study. Aliment Pharmacol Ther 2013; 38: 1248-1254 [PMID: 24053733 DOI: 10.1111/apt.12503]
100 Sankaran-Walters S, Ransibrahmanakul K, Grishina I, Hung J, Martinez E, Prindiville T, Dandekar S. Epstein-Barr virus
replication linked to B cell proliferation in inflamed areas of colonic mucosa of patients with inflammatory bowel disease. J Clin Virol 2011; 50: 31-36 [PMID: 21035384 DOI: 10.1016/j.jcv.2010.09.011]
101 Subramaniam K, D’Rozario J, Pavli P. Lymphoma and other lymphoproliferative disorders in inflammatory bowel disease: a review. J Gastroenterol Hepatol 2013; 28: 24-30 [PMID: 23094824 DOI: 10.1111/jgh.12015]
P- Reviewer: Fujimori S, Ierardi E, Schafer KH, Tsai HH S- Editor: Song XX L- Editor: A E- Editor: Wu HL
�2 February �5, 20�5|Volume 6|Issue �|WJGP|www.wjgnet.com
Bosca-Watts MM et al . Bugs in the pathogenesis of CD

response directed against normal constituents of the intestinal bacterial flora. Tests sometimes invasive are routine for the diagnosis and care of patients with IBD. Diagnosis of UC is based on clinical symptoms combined with radiological and endoscopic investigations. The employment of non-invasive biomarkers is needed. These biomarkers have the potential to avoid invasive diagnostic tests that may result in discomfort and potential complications. The ability to determine the type, severity, prognosis and response to therapy of UC, using biomarkers has long been a goal of clinical researchers. We describe the biomarkers assessed in UC, with special reference to acute-phase proteins and serologic markers and thereafter, we describe the new biological markers and the biological markers could be developed in the future: (1) serum markers of acute phase response: The laboratory tests most used to measure the acute-phase proteins in clinical practice are the serum concentration of C-reactive protein and the erythrocyte sedimentation rate. Other biomarkers of inflammation in UC include platelet count, leukocyte count, and serum albumin and serum orosomucoid concentrations; (2) serologic markers/antibodies: In the last decades serological and immunologic biomarkers have been studied extensively in immunology and have been used in clinical practice to detect specific pathologies. In UC, the presence of these antibodies can aid as surrogate markers for the aberrant host immune response; and (3) future biomarkers: The development of biomarkers in UC will be very important in the future. The progress of molecular biology tools (microarrays, proteomics and nanotechnology) have revolutionised the field of the biomarker discovery. The advances in bioinformatics coupled with cross-disciplinary collaborations have greatly enhanced our ability to retrieve, characterize and analyse large amounts of data generated by the technological advances. The techniques available for biomarkers development are genomics (single nucleotide polymorphism geno-typing, pharmacogenetics and gene expression analyses) and proteomics. In the future, the addition
Laboratory markers in ulcerative colitis: Current insights and future advances
Michele Cioffi, Antonella De Rosa, Rosalba Serao, Ilaria Picone, Maria Teresa Vietri, Department of Biochemistry, Biophysics and General Pathology, Second Medical School Naples, 80138 Naples, ItalyAuthor contributions: Cioffi M designed the research, analysed the data, and wrote the paper; De Rosa A contributed analytic tools, analysed the data; Serao R analysed the data; Picone I contributed analytic tools; Vietri MT designed the research, contributed analytic tools, and wrote the paper.Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/Correspondence to: Michele Cioffi, MD, Department of Biochemistry, Biophysics and General Pathology, Second Medical School Naples, Via L. De Crecchio 7, 80138 Naples, Italy. [email protected]: +39-08-15665680 Fax: +39-08-1450169Received: May 27, 2014 Peer-review started: May 27, 2014First decision: June 28, 2014Revised: October 3, 2014Accepted: December 29, 2014Article in press: December 31, 2014Published online: February 15, 2015
AbstractUlcerative colitis (UC) and Crohn’s disease (CD) are the major forms of inflammatory bowel diseases (IBD) in man. Despite some common features, these forms can be distinguished by different genetic predisposition, risk factors and clinical, endoscopic and histological characteristics. The aetiology of both CD and UC remains unknown, but several evidences suggest that CD and perhaps UC are due to an excessive immune
13 February 15, 2015|Volume 6|Issue 1|WJGP|www.wjgnet.com
MINIREVIEWS
World J Gastrointest Pathophysiol 2015 February 15; 6(1): 13-22ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i1.13
Michele Cioffi, Antonella De Rosa, Rosalba Serao, Ilaria Picone, Maria Teresa Vietri

of new serological markers will add significant benefit. Correlating serologic markers with genotypes and clinical phenotypes should enhance our understanding of pathophysiology of UC.
Key words: Inflammatory bowel diseases; Ulcerative colitis; Crohn’s disease; Serologic markers; Acute phase response
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Ulcerative colitis (UC) and Crohn’s disease are the major forms of inflammatory bowel diseases (IBD). Tests sometimes invasive are routine for the diagnosis and care of patients with IBD. The employment of non-invasive biomarkers is needed. We describe biomarkers assessed in UC, with special reference to acute-phase proteins and serologic markers and thereafter, we describe the new biological markers. The progress of molecular biology tools have revolutionised the field of the biomarker. The techniques available for biomarkers development are genomics and proteomics. Correlating serologic markers with genotypes and clinical phenotypes should enhance our understanding of pathophysiology of UC.
Cioffi M, De Rosa A, Serao R, Picone I, Vietri MT. Laboratory markers in ulcerative colitis: Current insights and future advances. World J Gastrointest Pathophysiol 2015; 6(1): 13-22 Available from: URL: http://www.wjgnet.com/2150-5330/full/v6/i1/13.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i1.13
INTRODUCTIONUlcerative colitis (UC) and Crohn’s disease (CD) are chronic, relapsing inflammatory diseases of the intestine. UC and CD can be differentiated by different genetic predisposition, risk factors, clinical, endoscopic and histological characteristics.
In UC pathogenesis are involved numerous mechanisms. The chronic inflammation of colonic mucosal in UC results from: (1) damage to the epithelial barrier; (2) equilibrium between tolerance to commensal microflora, dietary antigens and suitable sensitivity to enteric pathogens maintained by intestinal immune system; (3) dysregulation of immunological responses; and (4) genetic factors[1].
The inflammation in UC is limited to the mucosal surface. The illness starts in the rectum and generally extends proximally through the whole colon. However, some patients with proctitis or leftsided colitis might have a caecal patch of inflammation[2].
Although the precise cause of IBD is unknown, there seems to be a genetic predisposition. The risk is mainly high in firstdegree relatives: from 5.7% to
15.5% of patients with UC has a firstdegree relative with the same disease[3,4]. In addition, Ashkenazi Jews have a frequency of UC 35 times higher than other ethnic groups.
The frequency of UC is higher in developed countries and in urban vs rural areas. Numerous environmental factors act as predisposing or protective factors for UC, such as cigarette smoke. A metaanalysis showed that cigarettes smoking is protective against UC compared with nonsmoking[5]. The smoking UC patients have a milder course of the disease than nonsmokers, and disease activity is frequently improved in patients who have stopped smoking[6].
Previous gastrointestinal infections (e.g., Salmonella spp, Shigella spp and Campylobacter spp) double the risk of developing UC. This suggests that the acute intestinal infection could lead to changes in the intestinal flora triggering the onset of a chronic inflammatory process in genetically predisposed subjects[7,8].
Appendicectomy is protective against UC and a metaanalysis reported that reduces about 69% the risk of developing UC[9,10].
There are no data supporting psychological stress can promote the onset or relapse of UC[11]. The use of oral contraceptives is moderately associated with disease onset[12]. Breastfeeding is protective against later development of UC, but only when the duration of breastfeeding is more than 3 mo[13].
UC is more common than CD. In United States and in Northern Europe, the incidence of UC ranging from 920 cases per 100000 persons/years and prevalence rates from 156291 cases per 100000 people. The UC has the main peak of onset between 15 and 30 years old[14] and second peak in patients aged 5070 years. Previous studies have shown no preference for sex[14], if not a slight prevalence in men[15].
The goals of drug treatment for UC are treating the symptoms and inducing clinical remission. The ilealpouch anal anastomosis (IPAA) is the elective surgery treatment in about 20%30% of UC patients that eventually underwent surgery.
DIAGNOSISThe diagnosis of UC is based on clinical symptoms combined with radiological and endoscopic investigations. Employment of noninvasive biomarkers is needed. Noninvasive biomarkers have the potential to avoid invasive diagnostic tests and inhibit potential complications[16].
The ability to determine the type of UC, severity, prognosis and response to therapy, using biomarkers has long been the aim of clinical researchers[17,18]. A working group of the National Institute of Health, in 2001, defined biomarker as “a characteristic that is objectively measured and evaluated as an
14 February 15, 2015|Volume 6|Issue 1|WJGP|www.wjgnet.com
Cioffi M et al . Biomarkers in ulcerative colitis

indicator of normal biological processes, pathogenic processes, or pharmacologic responses to a therapeutic intervention”[19]. A good biomarker must be accurate, reproducible, standardized, easy to be interpreted by clinicians and with a high diagnostic sensitivity and specificity. Unfortunately, no single marker has all these features.
First we consider biomarkers assessed in UC, with special reference to acutephase proteins and serologic markers. Thereafter, we consider new biomarkers and which biological markers should be developed in the future. The main biomarkers in UC are the acutephase proteins and serologic markers (Table 1).
SERUM MARKERS OF ACUTE PHASE RESPONSEThe laboratory tests most used to measure the acutephase proteins in clinical practice are the serum concentration of Creactive protein (CRP) and the erythrocyte sedimentation rate. Other biomarkers of acute phase response in UC include platelet and leukocyte count, serum albumin, and orosomucoid concentrations.
CRPCRP is an acute phase protein produced by the liver in response to various acute and chronic inflammatory
15 February 15, 2015|Volume 6|Issue 1|WJGP|www.wjgnet.com
Serum markers of acute phase response Response
C-reactive protein Increased Erithrocyte sedimentation rate Increased Platelet count Increased White blood cell count Increased Alpha1-acid glycoprotein (Oromucoid) Increased Β2-microglobulin Increased Sialic acid Increased Serum amyloid A Increased Ferritin Increased Serum albumin Complement system Decreased Trasferrin Complement system Decreased C1s, C2, C3, C4, B Complement system Increased Haptoglogin Transport proteins Increased Haemopexin Transport proteins Increased Caeruloplasmin Transport proteins Increased Alpha1 Antitrypsin Proteinase inhibitors Increased Alpha 1 antichymotrypsin Proteinase inhibitors Increased Fibrinogen Coagulation and fibrinolytic proteins Increased Prothrombin Coagulation and fibrinolytic proteins Increased Plasminogen Coagulation and fibrinolytic proteins Increased Factor XII Coagulation and fibrinolytic proteins Decreased IL-6, IL-1 β- TNF-α, IL-8, IL-10, Interferon-β
Cytokines Increased
Serologic markers/antibodies Positive rate ANCAs Anti-neutrophil cytoplasmic antibodies
(cANCA, sANCA, pANCA)2%-28% CD
20%-85% UC ASCA Anti-saccharomyces cerevisiae antibodies 39%-69% CD
5%-15% UC Anti-OmpC Antibodies to outer membrane porin 24%-50% CD
5%-11% UC Anti-Cbir1 Flagellin related antigen 50% CD
5%-11% UC Anti-I2 Pseudomonas flourescens-associated
sequence I-230%-50% CD2%-10% UC
Flagellin A4-Fla2 and Fla-X antibodies Newly identified About 57% CD Antilaminaribioside carbohydrate IgG (ALCA)
Antiglycan antibody 17%-28% CD4%-7% UC
Antichitobioside carbohydrate IgA (ACCA)
Antiglycan antibody 20%-25% CD5%-15% UC
Anti-synthetic mannoside antibodies (ASMA or AMCA)
Antiglycan antibody 28% CD18% UC
Pancreatic antibodies Pancreatic secretion 30%-40% CD2%-6% UC
Serum p53 antibodies 9.3% UC
Table 1 Main biological markers in ulcerative colitis
CD: Crohn’s disease; UC: Ulcerative colitis; IL: Interleukin.
Cioffi M et al . Biomarkers in ulcerative colitis

conditions. CRP is produced mainly by hepatocytes in response to circulating interleukin6 (IL6), and to a lesser extent in response to IL1β and TNFα[20].
CRP levels range from 5 to 200 mg/L. During the onset of inflammatory response an increasingly number of hepatocytes are recruited to its synthesis. This recruitment is extremely rapid. The decrease of CRP concentration may be similarly rapid, with a decrease from peak with a half time of 48 h[21].
In literature are reported significant differences in the CRP response between CD and UC. In CD patients has been described a clear increase in CRP, whereas in UC the response is slight or absent[22,23]. There is no satisfactory explanation for these differences. Nevertheless, in literature is reported that serum IL6 concentrations were significantly increased in patients with CD compared with UC and healthy controls[24]. Another interpretation could be that the inflammation in UC is confined to the mucosa while in CD the inflammation is transmural, but not enough to explain all the differences.
Erythrocyte sedimentation rate The Erythrocyte sedimentation rate (ESR) determination reflects the changes in the various acute phase proteins. Although the usefulness of this test has decreased, it is still widely used. The test measures the distance that erythrocytes have fallen after one hour in a vertical column of noncoagulated blood under the influence of gravity[25].
ESR varies with plasma protein concentrations and haematocrit value, and in IBD provides a simple and rapid assessment of the plasma protein alterations of the acute phase response.
Thus, the ESR is greatly influenced by the size, shape, and number of erythrocytes as well as by other factors, including age, gender, anaemia, blood dyscrasias and pregnancy[26].
The ESR determination monitors satisfactorily the acutephase response of disease after the first 24 h. In contrast, during the first 24 h the CRP is a better indicator of the acute phase.
The ESR, compared with CRP, reaches the highest point less quickly, decreases more slowly and has a lesser degree of change.
PlateletsThe platelets also play an active role in several inflammatory processes[27]. The high platelet number correlates well with disease severity, and, interestingly, may persist even after bowel resection in IBD patients. Mean platelet volume has been proposed as a potential marker of clinical disease activity, being inversely proportional to the levels of CRP and ESR. The cause of the reduction in platelet volume in clinically active UC is unknown, but it may be a direct result of the thrombopoiesis disorder often observed in the early phases of systemic inflammatory
progression[28]. The platelets also relates to the increased incidence of thromboembolic phenomena in CD and UC. Some studies reported that spontaneous platelet aggregation is observed in more than 30% of IBD patients[29].
Other serum laboratory markersThe number of white blood cells increases during the acute phase response and is also influenced by the drugs utilized in IBD, such as glucocorticoids (increased) or azathioprine and 6mercaptopurine (decreased).
Albumin is a negative acute phase marker and decreased levels may be found during inflammation. Alpha 1acid glycoprotein or orosomucoid is another hepatocyte derived acute phase protein related with IBD activity[30], but the long halflife (5 d) reduced its usefulness.
Other acute phase markers include sialic acid, fibrinogen, lactoferrin, β2microglobulin, serum amyloid A, alpha 2globulin, and alpha 1antitrypsin. Most of these markers have not been extensively studied in IBD and the authors describe opposing results.
CytokinesThe cytokines are intercellular signalling polypeptides produced by activated cells. The cytokines produced during inflammatory processes are the chief stimulators of the production of acutephase proteins. The inflammationassociated cytokines include IL6, IL1β, TNFα, IFNβ, TGFβ, IL8 and possibly IL10[25].
For UC, the cellular events are less clear, but natural killer T cells may play an important role as initiating cells. The proinflammatory cytokines include TNFα, IL12, IL23, perhaps IL17 and IFNβ[31].
In the intestinal mucosa from UC patients the expression of proinflammatory cytokines was significantly increased. Future investigations will clarify the significance of impairments of cytokine network for the beginning and UC progression. Serum cytokines assessment has not correlated well with clinical activity.
SEROLOGIC MARKERS/ANTIBODIESIn previous years, serological and immunologic markers have been used in clinical practice. In UC, the presence of these antibodies can aid as alternate markers for the aberrant host immune response. New markers directed against microbial antigens have recently emerged (Table 1).
Anti-neutrophil cytoplasmic antibodiesSerologic antineutrophil cytoplasmic antibodies (ANCAs) are assessed by indirect immunofluorescence (IIF) and are detectable showed three main staining patterns: the cytoplasmic (cANCA), the speckled
16 February 15, 2015|Volume 6|Issue 1|WJGP|www.wjgnet.com
Cioffi M et al . Biomarkers in ulcerative colitis

(sANCA) and the perinuclear (pANCA). ANCAs are classically associated with vasculitis,
in which ANCA serum levels are used for diagnostic, monitoring, and prognostic aims. In addition, ANCAs are found in other chronic inflammatory disorders, such as rheumatoid arthritis and in UC[32]. While ANCA values ranges from 2%28% in CD patients, 20%85% of UC patients are positive for ANCA, resulting a sensitivity of 56% and a specificity of 89% in UC patients[33,34].
Anti-Saccharomyces cerevisiae antibodiesAntiSaccharomyces cerevisiae antibodies (ASCA) are found in 39%69% of CD patients and in 5%15% of UC patients[35]. It is interesting to note that ASCA IgA sensitivity is lower in Japanese and Chinese CD patients than Caucasian CD patients[33], suggesting that the ASCA response may be influenced by several distinct genetic determinants and/or environmental risk factors.
Antibodies to outer membrane porin, Flagellin, Pseudomonas flourescens-associated sequence I-2 and antibodies to Flagellin A4-Fla2 and Fla-XAntibodies to outer membrane porin (AntiOmpC) are a major outermembrane protein isolated first from Escherichia coli. The positivity of antiOmpC was very low in UC patients and in healthy subjects (5%11% and 5%, respectively). AntiOmpC may aid diagnosis of ASCA negative CD patients[36].
Antibodies to Cbir1 Flagellin (AntiCbir1) are positive in about 50% of CD patients, in contrast lower positivity was observed in UC patients (5%11%), other inflammatory gastrointestinal diseases (14%) and control subjects (8%). The positivity of antiCBir1 antibodies is greater in patients with increased antibody reactivity to ASCA, I2 and OmpC, without correlation between the level of response to CBir1 and the other antibodies[33]. Serum responses to CBir1 aid the differentiation between atypical pANCA positive CD and UC patients independently of ASCA[37].
Pseudomonas fluotescensassociated sequence I2 (AntiI2) has been studied and appears to be associated with CD[38]. IgA positivity against I2 has been reported in 30%50% in CD, 2%10% in UC[39], 36%42% in indeterminate colitis, 19% of patients with other inflammatory gastrointestinal diseases and 4%8% of healthy controls.
Flagellins A4Fla2 and FlaX have recently been found in CD patients. Flagellins A4Fla2 and FlaX positivity is more prevalent in subjects with postinfectious irritable bowel disease.
Anti-carbohydrate antibodies: Antilaminaribioside carbohydrate IgG, antichitobioside carbohydrate IgA, anti-synthetic mannoside antibodiesAntilaminaribioside carbohydrate IgG (ALCA), antichitobioside carbohydrate IgA (ACCA), and anti
synthetic mannoside antibodies (ASMA or AMCA) are new antiglycan antibodies. ALCA and ACCA are found respectively in 17%28% and 20%25% of CD patients. These antibodies may improve the sensitivity of diagnostic test since they are positive in 34%44% of ASCAnegative patients[40,41].
ASMA are antibodies against two major oligomannose epitopes that were positive in 28% of ASCAnegative CD patients. AntiC, antichitin carbohydrate, antiL, and antilaminarin carbohydrate antibodies have a low sensitivity but moderately high specificity in CD patients, related to UC patients[42,43].
Pancreatic antibodiesAntibodies directed against exocrine pancreas (PAbs) have been reported in patients affected with CD with a low prevalence (30%40%)[44,45]. Antipancreatic antibodies have been detected by IIF in UC patients (2%6%) and in healthy subjects (0%2%)[36,46].
Serum p53 antibodiesDuring the tumor progression, the genetic alterations are a key feature of malignant cells. The p53 gene is frequently mutated in human cancers. Cellular accumulation of mutated p53 protein can initiate an immune response with generation of circulating antip53 antibodies. Patients with UC have an increased risk of developing colorectal cancer, among the different genes involved in carcinogenesis, p53 may play a key role. Serum p53Ab were detectable in 9.3% of patients with UC. Serum p53Abs assessment could be used as a complementary test to improve surveillance program performance[47].
USEFULNESS OF SERUM MARKERS AND ANTIBODIES IN UCDiagnostic and differential diagnostic valuePrevious studies have valued the usefulness of routine laboratory testing in UC. CRP is a helpful index of UC activity, but its utility, as a screening test has not been totally evaluated.
CRP is the most sensitive compared to other serologic markers of inflammation in adult population for detecting IBD. The sensitivity of CRP ranges from 70%100% in the differential diagnosis between CD versus irritable bowel syndrome and from 50%60% in UC[32]. In high percentage of paediatric patients, the sensitivity of routine testing (anemia, ESR, CRP or platelet count), varies from 62%91% when evaluating the combination of ≥ 2 routine laboratory tests, whereas specificity ranged from 75%94%.
Levels of CRP are higher in active CD than in UC and this difference might be used to differentiate between CD and UC. The measurements of circulating levels of CRP, ESR, platelets count are not useful at all for differentiation between both types of IBD[48].
17 February 15, 2015|Volume 6|Issue 1|WJGP|www.wjgnet.com
Cioffi M et al . Biomarkers in ulcerative colitis

Orosomucoid is not useful test for screening healthy populations or differentiating patients with inflammatory vs functional disorders.
The clinical usefulness of pANCA or ASCA testing in patients with nonspecific gastrointestinal symptoms is limited, because of the low sensitivity. Assaying all the serum markers available for CD, the sensitivity for the diagnosis of CD is greater than 80% and the positive predictive value is over 90% but only when the prevalence of CD is > 38%[49].
Serum evaluation of ANCAs and ASCAs could help patients with indeterminate colitis. In these patients, early diagnosis could positively influence treatment decisions and prognosis[50]. Patients pANCApositive and ASCAnegative have a 19 times greater likelihood of developing UC, while patients ASCApositive and pANCAnegative are 16 times more likely to suffer CD[51].
Prediction of relapseIBD is characterized by acute episodes followed by remissions. The management of patients at high risk of relapse may be improved with early treatment. Previous studies about CD have investigated a panel of acute phase markers. Recently, a prospective study measured every six weeks, after recent weaning of steroids, some laboratory parameters (full blood count, CRP, ESR, a1 antitrypsin, orosomucoid) in CD patients[52]. The best predictor of shortterm relapse is the combination of CRP and ESR.
Patients with CRP > 20 mg/L and ESR > 15 mm had an eightfold increased risk of relapse with a negative predictive value of 97%, suggesting that normal CRP and ESR could almost exclude relapse in the next six weeks. In another study in which the patients were followed until relapse, the ESR, globulin and alpha1glycoprotein have been described like the best markers for discriminate relapse from nonrelapse.
It is clear that alone CRP cannot predict clinical relapse in IBD. ESR, CRP, IL1b, IL6 and IL15 are not predictive of clinical recurrence in UC[53]. In CD, serum IL6 and soluble IL2 receptor have been associated with a higher risk of relapse.
Association with clinical phenotypes and prognostic indicators In UC, very few studies have assessed acute phase markers in predicting outcome of disease or association with clinical phenotypes. In severe UC, after three days of intensive treatment (hydrocortisone and/or cyclosporine) patients with frequent stools (> 8/d), or 38 stools/d and CRP > 45 mg/L should be identified, as most of them will need to undergo colectomy. It is commonly accepted that the presence of ANCA in UC is not related to the duration and age of onset[54]. Previous studies agree that in patients affected with CD, the presence of atypical pANCAs in serum characterizes an UClike clinical phenotype[44].
Follow-up and response to treatmentCRP level is a good predictor of remission and response to treatment. Antiinflammatory or immunosuppressive drugs do not affect CRP production. Therefore, changes of CRP concentrations during treatment occur only as a result of the effect of the drug on the inflammation or disorder.
The serological markers are not useful for followup of disease activity. In UC the presence of atypical pANCAs have been associated with resistance to treatment of left sided UC and early surgery. These data suggest that pANCApositive UC patients may require earlier intervention with immunomodulators. In patients affected with UC pANCApositive and ASCAnegative at first infliximab infusion have been associated with a suboptimal early clinical response[55]. In patients ASCA, antiOmpC and antiI2 positive was observed a better response to antibiotic therapy, compared with negative patients[56].
FUTURE BIOMARKERSThe development of biomarkers in UC will be very important in the future. The progress of molecular biology tools (microarrays, proteomics and nanotechnology) has revolutionized the field of biomarker discovery[57]. The advances in bioinformatics associated with interdisciplinary collaborations have greatly improved the ability to collect, characterize and analyse large amounts of data.
The techniques available for biomarkers development are genomics [Single nucleotide polymorphism (SNP) genotyping, pharmacogenetics and gene expression analyses] and proteomics.
Metabolome biomarkersThe search for metabolic biomarkers in CD as evidence of microbial functions in the gut is a new and interesting diagnostic approach[58].
Recent studies described the role of Enzyme indoleamine 2,3 dioxygenase (IDO1) in gut inflammation and IBD. IDO1 is an enzyme that degrades the essential amino acid tryptophan. The concept that cells expressing IDO can suppress Tcell responses and promote tolerance is a relatively new paradigm in immunology[59]. IDO1 is significantly increased in the intestinal inflammation[60]. IDO induction might therefore contribute to a Tcellmediated negative feedbackloop by inhibition of their further activation. Thus, some papers hypothesized a potential antiinflammatory role of IDO in IBD, especially in CD, which is characterized by an exaggerated Th1cell response[61].
Larginine (LArg) serum levels are increased in patients with severe UC and LArg serum levels were highly correlated with disease activity index[62]. Metabolomics array studies have also identified high levels of LArg in colonic mucosal specimens of UC patients[63,64].
18 February 15, 2015|Volume 6|Issue 1|WJGP|www.wjgnet.com
Cioffi M et al . Biomarkers in ulcerative colitis

Gene expression profiling In the recent years there have been significant advances in understanding the genetics of UC. Gene expression profiling is considered a predictive marker in IBD.
Several studies explore the associations of UC with gene polymorphisms (i.e., vitamin D receptor, interleukin, interleukin receptor gene and OCT1). Genetic polymorphisms of VDR are significantly correlated with UC. Mutation of VDR is a protective factor for UC. Moreover, mutant genotype (TC/CC) of VDR and vitamin D deficiency may exert synergistic effects on the susceptibility to UC[65].
The cytokine network is highly complex with interactive cascades of gene activation and suppression. Not only the IL and ILR gene polymorphisms are in relation with UC pathogenesis but also the downstream signalling components of several ILs (i.e., JAKs, STATs), which could be potential targets of novel treatment strategies[66].
Several SNPs in the TNFα promoter region are known to affect the level of gene expression. The G → A polymorphism at position 238 in the TNF gene is associated with lower production of TNFα in UC patients. In contrast, the 308A polymorphism is associated with enhanced TNFα production in cells in vitro and in CD patients in vivo[67].
The 857 C → T SNP, located in promoter region of TNFα, is functional through binding to the transcription factor octamer transcription factor1 (OCT1). Carriers of the 857C allele show higher levels of circulating TNFα and was suggested that the TNF857C/T SNP increased the susceptibility to IBD in English population through it’s effects on the interaction between the OCT1 gene and the NFκB transcription factor[68].
In literature was reported in Australian subjects a possible association of TNFα857 variant with an increased CD risk. In another study was described an association of TNF857C with IBD overall and with subphenotypes in either UC or CD, only in patients not carrying other common mutations[69].
Genetic markers are associated with disease phenotype and longterm evolution, but their value in clinical practice is limited.
Proteomics The current advances in proteomic array profiling technology have sparked interest in using this technique for diagnosis of IBD.
Proteomic approaches for the identification of disease biomarkers are mainly based on the comparative analysis of protein expression in healthy and diseased tissues to identify aberrantly expressed proteins, analysis of secreted proteins (in cell lines and primary cultures) and direct serum protein profiling.
Recently has been published a study in patients with IBD, using the methodology of Surface Enhanced
Laser Desorption IonizationTime of FlightMass Spectrometer (SELDITOFMS). Four proteins of acute phase inflammation biomarkers were identified (PF4, MRP8, FIBA and Hpα2). PF4 and Hpα2 were also detected in serum by classical methods and their true diagnostic value should be confirmed. In the future, the application of protein interaction maps to intestinal cell models in IBD will produce a detailed photograph of protein dynamics regulating signalling homeostasis[17].
Furthermore, in inflammatory bowel diseases, proteomic arrays have shown promise for identify active disease, to differentiate between CD and UC and to study the pathogenesis of the diseases[17,70].
CONCLUSIONSeveral reliable serum biomarkers are currently used to aid in the diagnosis of IBD, to differentiate between CD and UC, to assess disease activity and to predict relapse. However, the available serological markers are limited in their capacity as predict longerrange disease course.
Advances in genomic, proteomic, and metabolomics array are easing biomarker finding in UC.
In the future, the addition of new serological markers will add significant benefit. In the last years have been identified 163 risk loci, which include a variety of immunologic functions. IBD is a highly heterogeneous disease for the onset, course and progression of the illness. Significant differences were also reported in the response to therapies and susceptibility to therapyrelated. Therefore, it is important identify predictors of the disease course, complications, probability of response to therapy and any adverse events, in order to enable a targeted therapeutic process. The genotype of an individual is constant and unchangeable, and thus could potentially play the role of important predictors of these outcomes.
Currently, the integration of serological markers with genetic markers may not be justified. However, with the increasing use of innovative methodological approaches such as genetics and proteomics, it is reasonable to expect that the aetiology of IBD could be clarified in the near future. In the future it is expected that all these biomarkers will be implemented in an integrated molecular diagnostic and prognostic approach of patients.
REFERENCES1 Ordás I, Eckmann L, Talamini M, Baumgart DC, Sandborn WJ.
Ulcerative colitis. Lancet 2012; 380: 1606-1619 [PMID: 22914296 DOI: 10.1016/S0140-6736(12)60150-0]
2 Silverberg MS, Satsangi J, Ahmad T, Arnott ID, Bernstein CN, Brant SR, Caprilli R, Colombel JF, Gasche C, Geboes K, Jewell DP, Karban A, Loftus EV, Peña AS, Riddell RH, Sachar DB, Schreiber S, Steinhart AH, Targan SR, Vermeire S, Warren BF. Toward an
19 February 15, 2015|Volume 6|Issue 1|WJGP|www.wjgnet.com
Cioffi M et al . Biomarkers in ulcerative colitis

integrated clinical, molecular and serological classification of inflammatory bowel disease: report of a Working Party of the 2005 Montreal World Congress of Gastroenterology. Can J Gastroenterol 2005; 19 Suppl A: 5A-36A [PMID: 16151544 DOI: 10.1067/mcp.2001.113989]
3 Monsén U, Broström O, Nordenvall B, Sörstad J, Hellers G. Prevalence of inflammatory bowel disease among relatives of patients with ulcerative colitis. Scand J Gastroenterol 1987; 22: 214-218 [PMID: 3576128]
4 Farmer RG, Michener WM, Mortimer EA. Studies of family history among patients with inflammatory bowel disease. Clin Gastroenterol 1980; 9: 271-277 [PMID: 7389171]
5 Mahid SS, Minor KS, Soto RE, Hornung CA, Galandiuk S. Smoking and inflammatory bowel disease: a meta-analysis. Mayo Clin Proc 2006; 81: 1462-1471 [PMID: 17120402 DOI: 10.4065/81.11.1462]
6 Beaugerie L, Massot N, Carbonnel F, Cattan S, Gendre JP, Cosnes J. Impact of cessation of smoking on the course of ulcerative colitis. Am J Gastroenterol 2001; 96: 2113-2116 [PMID: 11467641 DOI: 10.1111/j.1572-0241.2001.03944.x]
7 García Rodríguez LA, Ruigómez A, Panés J. Acute gastroenteritis is followed by an increased risk of inflammatory bowel disease. Gastroenterology 2006; 130: 1588-1594 [PMID: 16697722 DOI: 10.1053/j.gastro.2006.02.004]
8 Porter CK, Tribble DR, Aliaga PA, Halvorson HA, Riddle MS. Infectious gastroenteritis and risk of developing inflammatory bowel disease. Gastroenterology 2008; 135: 781-786 [PMID: 18640117 DOI: 10.1053/j.gastro.2008.05.081]
9 Andersson RE, Olaison G, Tysk C, Ekbom A. Appendectomy and protection against ulcerative colitis. N Engl J Med 2001; 344: 808-814 [PMID: 11248156 DOI: 10.1056/NEJM200103153441104]
10 Koutroubakis IE, Vlachonikolis IG. Appendectomy and the development of ulcerative colitis: results of a metaanalysis of published case-control studies. Am J Gastroenterol 2000; 95: 171-176 [PMID: 10638578 DOI: 10.1111/j.1572-0241.2000.01680.x]
11 Vidal A, Gómez-Gil E, Sans M, Portella MJ, Salamero M, Piqué JM, Panés J. Life events and inflammatory bowel disease relapse: a prospective study of patients enrolled in remission. Am J Gastroenterol 2006; 101: 775-781 [PMID: 16494590 DOI: 10.1111/j.1572-0241.2006.00476.x]
12 Cornish JA, Tan E, Simillis C, Clark SK, Teare J, Tekkis PP. The risk of oral contraceptives in the etiology of inflammatory bowel disease: a meta-analysis. Am J Gastroenterol 2008; 103: 2394-2400 [PMID: 18684177 DOI: 10.1111/j.1572-0241.2008.02064.x]
13 Klement E, Cohen RV, Boxman J, Joseph A, Reif S. Breastfeeding and risk of inflammatory bowel disease: a systematic review with meta-analysis. Am J Clin Nutr 2004; 80: 1342-1352 [PMID: 15531685]
14 Bernstein CN, Rawsthorne P, Cheang M, Blanchard JF. A population-based case control study of potential risk factors for IBD. Am J Gastroenterol 2006; 101: 993-1002 [PMID: 16696783 DOI: 10.1111/j.1572-0241.2006.00381.x]
15 Loftus EV, Sandborn WJ. Epidemiology of inflammatory bowel disease. Gastroenterol Clin North Am 2002; 31: 1-20 [PMID: 12122726]
16 Dubinsky MC, Ofman JJ, Urman M, Targan SR, Seidman EG. Clinical utility of serodiagnostic testing in suspected pediatric inflammatory bowel disease. Am J Gastroenterol 2001; 96: 758-765 [PMID: 11280547 DOI: 10.1111/j.1572-0241.2001.03618.x]
17 Meuwis MA, Fillet M, Geurts P, de Seny D, Lutteri L, Chapelle JP, Bours V, Wehenkel L, Belaiche J, Malaise M, Louis E, Merville MP. Biomarker discovery for inflammatory bowel disease, using proteomic serum profiling. Biochem Pharmacol 2007; 73: 1422-1433 [PMID: 17258689 DOI: 10.1016/j.bcp.2006.12.019]
18 Cellier C, Sahmoud T, Froguel E, Adenis A, Belaiche J, Bretagne JF, Florent C, Bouvry M, Mary JY, Modigliani R. Correlations between clinical activity, endoscopic severity, and biological parameters in colonic or ileocolonic Crohn’s disease. A prospective multicentre study of 121 cases. The Groupe d’Etudes
Thérapeutiques des Affections Inflammatoires Digestives. Gut 1994; 35: 231-235 [PMID: 7508411 DOI: 10.1136/gut.35.2.231]
19 Biomarkers Definitions Working Group. Biomarkers and surrogate endpoints: preferred definitions and conceptual framework. Clin Pharmacol Ther 2001; 69: 89-95 [PMID: 11240971 DOI: 10.1067/mcp.2001.113989]
20 Darlington GJ, Wilson DR, Lachman LB. Monocyte-conditioned medium, interleukin-1, and tumor necrosis factor stimulate the acute phase response in human hepatoma cells in vitro. J Cell Biol 1986; 103: 787-793 [PMID: 3017995]
21 Mazlam MZ, Hodgson HJ. Why measure C reactive protein? Gut 1994; 35: 5-7 [PMID: 8307448 DOI: 10.1136/gut.35.1.5]
22 Pepys MB, Druguet M, Klass HJ, Dash AC, Mirjah DD, Petrie A. Immunological studies in inflammatory bowel disease. Ciba Found Symp 1977; (46): 283-304 [PMID: 346325]
23 Saverymuttu SH, Hodgson HJ, Chadwick VS, Pepys MB. Differing acute phase responses in Crohn’s disease and ulcerative colitis. Gut 1986; 27: 809-813 [PMID: 3732890 DOI: 10.1136/gut.27.7.809]
24 Gross V, Andus T, Caesar I, Roth M, Schölmerich J. Evidence for continuous stimulation of interleukin-6 production in Crohn’s disease. Gastroenterology 1992; 102: 514-519 [PMID: 1370661]
25 Gabay C, Kushner I. Acute-phase proteins and other systemic responses to inflammation. N Engl J Med 1999; 340: 448-454 [PMID: 9971870 DOI: 10.1056/NEJM199902113400607]
26 Mendoza JL, Abreu MT. Biological markers in inflammatory bowel disease: practical consideration for clinicians. Gastroenterol Clin Biol 2009; 33 Suppl 3: S158-S173 [PMID: 20117339 DOI: 10.1016/S0399-8320(09)73151-3]
27 Danese S, Motte Cd Cde L, Fiocchi C. Platelets in inflammatory bowel disease: clinical, pathogenic, and therapeutic implications. Am J Gastroenterol 2004; 99: 938-945 [PMID: 15128364 DOI: 10.1111/j.1572-0241.2004.04129.x]
28 Kapsoritakis AN, Koukourakis MI, Sfiridaki A, Potamianos SP, Kosmadaki MG, Koutroubakis IE, Kouroumalis EA. Mean platelet volume: a useful marker of inflammatory bowel disease activity. Am J Gastroenterol 2001; 96: 776-781 [PMID: 11280550 DOI: 10.1111/j.1572-0241.2001.03621.x]
29 Webberley MJ, Hart MT, Melikian V. Thromboembolism in inflammatory bowel disease: role of platelets. Gut 1993; 34: 247-251 [PMID: 8432482 DOI: 10.1136/gut.34.2.247]
30 Andre C, Descos L, Landais P, Fermanian J. Assessment of appropriate laboratory measurements to supplement the Crohn’s disease activity index. Gut 1981; 22: 571-574 [PMID: 6973509 DOI: 10.1136/gut.22.7.571]
31 Roberts-Thomson IC, Fon J, Uylaki W, Cummins AG, Barry S. Cells, cytokines and inflammatory bowel disease: a clinical perspective. Expert Rev Gastroenterol Hepatol 2011; 5: 703-716 [PMID: 22017698 DOI: 10.1586/egh.11.74]
32 Vermeire S, Van Assche G, Rutgeerts P. Laboratory markers in IBD: useful, magic, or unnecessary toys? Gut 2006; 55: 426-431 [PMID: 16474109]
33 Peyrin-Biroulet L, Standaert-Vitse A, Branche J, Chamaillard M. IBD serological panels: facts and perspectives. Inflamm Bowel Dis 2007; 13: 1561-1566 [PMID: 17636565]
34 Reese GE, Constantinides VA, Simillis C, Darzi AW, Orchard TR, Fazio VW, Tekkis PP. Diagnostic precision of anti-Saccharomyces cerevisiae antibodies and perinuclear antineutrophil cytoplasmic antibodies in inflammatory bowel disease. Am J Gastroenterol 2006; 101: 2410-2422 [PMID: 16952282 DOI: 10.1111/j.1572-0241.2006.00840.x]
35 Vermeire S, Van Assche G, Rutgeerts P. C-reactive protein as a marker for inflammatory bowel disease. Inflamm Bowel Dis 2004; 10: 661-665 [PMID: 15472532]
36 Papp M, Norman GL, Altorjay I, Lakatos PL. Utility of serological markers in inflammatory bowel diseases: gadget or magic? World J Gastroenterol 2007; 13: 2028-2036 [PMID: 17465443 DOI: 10.3748/wjg.v13.i14.2028]
37 Targan SR, Landers CJ, Yang H, Lodes MJ, Cong Y, Papadakis KA, Vasiliauskas E, Elson CO, Hershberg RM. Antibodies to CBir1
20 February 15, 2015|Volume 6|Issue 1|WJGP|www.wjgnet.com
Cioffi M et al . Biomarkers in ulcerative colitis

flagellin define a unique response that is associated independently with complicated Crohn’s disease. Gastroenterology 2005; 128: 2020-2028 [PMID: 15940634 DOI: 10.1053/j.gastro.2005.03.046]
38 Wei B, Huang T, Dalwadi H, Sutton CL, Bruckner D, Braun J. Pseudomonas fluorescens encodes the Crohn’s disease-associated I2 sequence and T-cell superantigen. Infect Immun 2002; 70: 6567-6575 [PMID: 12438326 DOI: 10.1128/IAI.70.12.6567-6575.2002]
39 Landers CJ, Cohavy O, Misra R, Yang H, Lin YC, Braun J, Targan SR. Selected loss of tolerance evidenced by Crohn’s disease-associated immune responses to auto- and microbial antigens. Gastroenterology 2002; 123: 689-699 [PMID: 12198693 DOI: 10.1053/gast.2002.35379]
40 Dotan I, Fishman S, Dgani Y, Schwartz M, Karban A, Lerner A, Weishauss O, Spector L, Shtevi A, Altstock RT, Dotan N, Halpern Z. Antibodies against laminaribioside and chitobioside are novel serologic markers in Crohn’s disease. Gastroenterology 2006; 131: 366-378 [PMID: 16890590 DOI: 10.1053/j.gastro.2006.04.030]
41 Simondi D, Mengozzi G, Betteto S, Bonardi R, Ghignone RP, Fagoonee S, Pellicano R, Sguazzini C, Pagni R, Rizzetto M, Astegiano M. Antiglycan antibodies as serological markers in the differential diagnosis of inflammatory bowel disease. Inflamm Bowel Dis 2008; 14: 645-651 [PMID: 18240283 DOI: 10.1002/ibd.20368]
42 Rieder F, Schleder S, Wolf A, Dirmeier A, Strauch U, Obermeier F, Lopez R, Spector L, Fire E, Yarden J, Rogler G, Dotan N, Klebl F. Association of the novel serologic anti-glycan antibodies anti-laminarin and anti-chitin with complicated Crohn’s disease behavior. Inflamm Bowel Dis 2010; 16: 263-274 [PMID: 19653286 DOI: 10.1002/ibd.21046]
43 Lakatos PL, Papp M, Rieder F. Serologic antiglycan antibodies in inflammatory bowel disease. Am J Gastroenterol 2011; 106: 406-412 [PMID: 21245832 DOI: 10.1038/ajg.2010.505]
44 Bossuyt X. Serologic markers in inflammatory bowel disease. Clin Chem 2006; 52: 171-181 [PMID: 16339302 DOI: 10.1373/clinchem.2005.058560]
45 Klebl FH, Bataille F, Huy C, Hofstädter F, Schölmerich J, Rogler G. Association of antibodies to exocrine pancreas with subtypes of Crohn’s disease. Eur J Gastroenterol Hepatol 2005; 17: 73-77 [PMID: 15647645]
46 Joossens S, Vermeire S, Van Steen K, Godefridis G, Claessens G, Pierik M, Vlietinck R, Aerts R, Rutgeerts P, Bossuyt X. Pancreatic autoantibodies in inflammatory bowel disease. Inflamm Bowel Dis 2004; 10: 771-777 [PMID: 15626896]
47 Cioffi M, Riegler G, Vietri MT, Pilla P, Caserta L, Carratù R, Sica V, Molinari AM. Serum p53 antibodies in patients affected with ulcerative colitis. Inflamm Bowel Dis 2004; 10: 606-611 [PMID: 15472522]
48 Niederau C, Backmerhoff F, Schumacher B, Niederau C. Inflammatory mediators and acute phase proteins in patients with Crohn’s disease and ulcerative colitis. Hepatogastroenterology 1997; 44: 90-107 [PMID: 9058126]
49 Abreu MT. Serologies in Crohn’s disease: can we change the gray zone to black and white? Gastroenterology 2006; 131: 664-667 [PMID: 16890618 DOI: 10.1053/j.gastro.2006.06.040]
50 Joossens S, Reinisch W, Vermeire S, Sendid B, Poulain D, Peeters M, Geboes K, Bossuyt X, Vandewalle P, Oberhuber G, Vogelsang H, Rutgeerts P, Colombel JF. The value of serologic markers in indeterminate colitis: a prospective follow-up study. Gastroenterology 2002; 122: 1242-1247 [PMID: 11984510 DOI: 10.1053/gast.2002.32980]
51 Abreu MT. Controversies in IBD. Serologic tests are helpful in managing inflammatory bowel disease. Inflamm Bowel Dis 2002; 8: 224-226; discussion 223, 224-226 [PMID: 11979146]
52 Consigny Y, Modigliani R, Colombel JF, Dupas JL, Lémann M, Mary JY. A simple biological score for predicting low risk of short-term relapse in Crohn’s disease. Inflamm Bowel Dis 2006; 12: 551-557 [PMID: 16804391 DOI: 10.1097/01.ibd.0000225334.60990.5b]
53 Bitton A, Peppercorn MA, Antonioli DA, Niles JL, Shah S, Bousvaros A, Ransil B, Wild G, Cohen A, Edwardes MD, Stevens AC. Clinical, biological, and histologic parameters as predictors
of relapse in ulcerative colitis. Gastroenterology 2001; 120: 13-20 [PMID: 11208709 DOI: 10.1053/gast.2001.20912]
54 Reumaux D, Sendid B, Poulain D, Duthilleul P, Dewit O, Colombel JF. Serological markers in inflammatory bowel diseases. Best Pract Res Clin Gastroenterol 2003; 17: 19-35 [PMID: 12617880 DOI: 10.1053/bega.2002.0347]
55 Van Assche G, Vermeire S, Rutgeerts P. Inflimab therapy for patients with inflammatory bowel disease: 10 years on. Eur J Pharmacol 2009; 623 Suppl 1: S17-S25
56 Beaven SW, Abreu MT. Biomarkers in inflammatory bowel disease. Curr Opin Gastroenterol 2004; 20: 318-327 [PMID: 15703659]
57 Iskandar HN, Ciorba MA. Biomarkers in inflammatory bowel disease: current practices and recent advances. Transl Res 2012; 159: 313-325 [PMID: 22424434 DOI: 10.1016/j.trsl.2012.01.001]
58 Lin HM , Helsby NA, Rowan DD, Ferguson LR. Using metabolomic analysis to understand inflammatory bowel diseases. Inflamm Bowel Dis 2011; 17: 1021-1029 [PMID: 20629098 DOI: 10.1002/ibd.21426]
59 Mellor AL, Munn DH. IDO expression by dendritic cells: tolerance and tryptophan catabolism. Nat Rev Immunol 2004; 4: 762-774 [PMID: 15459668 DOI: 10.1038/nri1457]
60 Gupta NK, Thaker AI, Kanuri N, Riehl TE, Rowley CW, Stenson WF, Ciorba MA. Serum analysis of tryptophan catabolism pathway: correlation with Crohn’s disease activity. Inflamm Bowel Dis 2012; 18: 1214-1220 [PMID: 21823214 DOI: 10.1002/ibd.21849]
61 Wolf AM, Wolf D, Rumpold H, Moschen AR, Kaser A, Obrist P, Fuchs D, Brandacher G, Winkler C, Geboes K, Rutgeerts P, Tilg H. Overexpression of indoleamine 2,3-dioxygenase in human inflammatory bowel disease. Clin Immunol 2004; 113: 47-55 [PMID: 15380529]
62 Hong SK, Maltz BE, Coburn LA, Slaughter JC, Chaturvedi R, Schwartz DA, Wilson KT. Increased serum levels of L-arginine in ulcerative colitis and correlation with disease severity. Inflamm Bowel Dis 2010; 16: 105-111 [PMID: 19637336 DOI: 10.1002/ibd.21035]
63 Balasubramanian K, Kumar S, Singh RR, Sharma U, Ahuja V, Makharia GK, Jagannathan NR. Metabolism of the colonic mucosa in patients with inflammatory bowel diseases: an in vitro proton magnetic resonance spectroscopy study. Magn Reson Imaging 2009; 27: 79-86 [PMID: 18599242 DOI: 10.1016/j.mri.2008.05.014]
64 Martin FP, Rezzi S, Philippe D, Tornier L, Messlik A, Hölzlwimmer G, Baur P, Quintanilla-Fend L, Loh G, Blaut M, Blum S, Kochhar S, Haller D. Metabolic assessment of gradual development of moderate experimental colitis in IL-10 deficient mice. J Proteome Res 2009; 8: 2376-2387 [PMID: 19323467 DOI: 10.1021/pr801006e]
65 Wang L, Wang ZT, Hu JJ, Fan R, Zhou J, Zhong J. Polymorphisms of the vitamin D receptor gene and the risk of inflammatory bowel disease: a meta-analysis. Genet Mol Res 2014; 13: 2598-2610 [PMID: 24782048 DOI: 10.4238/2014.April.8.2]
66 Magyari L, Kovesdi E, Sarlos P, Javorhazy A, Sumegi K, Melegh B. Interleukin and interleukin receptor gene polymorphisms in inflammatory bowel diseases susceptibility. World J Gastroenterol 2014; 20: 3208-3222 [PMID: 24695754 DOI: 10.3748/wjg.v20.i12.3208]
67 Voleti B, Hammond DJ, Thirumalai A, Agrawal A. Oct-1 acts as a transcriptional repressor on the C-reactive protein promoter. Mol Immunol 2012; 52: 242-248 [PMID: 22750226 DOI: 10.1016/j.molimm.2012.06.005]
68 van Heel DA, Udalova IA, De Silva AP, McGovern DP, Kinouchi Y, Hull J, Lench NJ, Cardon LR, Carey AH, Jewell DP, Kwiatkowski D. Inflammatory bowel disease is associated with a TNF polymorphism that affects an interaction between the OCT1 and NF(-kappa)B transcription factors. Hum Mol Genet 2002; 11: 1281-1289 [PMID: 12019209 DOI: 10.1093/hmg/11.11.1281]
69 van Heel DA, Fisher SA, Kirby A, Daly MJ, Rioux JD, Lewis CM. Inflammatory bowel disease susceptibility loci defined by genome scan meta-analysis of 1952 affected relative pairs. Hum Mol Genet 2004; 13: 763-770 [PMID: 14976156 DOI: 10.1093/hmg/ddh090]
21 February 15, 2015|Volume 6|Issue 1|WJGP|www.wjgnet.com
Cioffi M et al . Biomarkers in ulcerative colitis

70 Nanni P, Parisi D, Roda G, Casale M, Belluzzi A, Roda E, Mayer L, Roda A. Serum protein profiling in patients with inflammatory bowel diseases using selective solid-phase bulk extraction, matrix-
assisted laser desorption/ionization time-of-flight mass spectrometry and chemometric data analysis. Rapid Commun Mass Spectrom 2007; 21: 4142-4148 [PMID: 18022963 DOI: 10.1002/rcm.3323]
P- Reviewer: Ahluwalia NK, de Silva AP, Yamakama M S- Editor: Yu J L- Editor: A E- Editor: Wu HL
22 February 15, 2015|Volume 6|Issue 1|WJGP|www.wjgnet.com
Cioffi M et al . Biomarkers in ulcerative colitis

Peer-review started: May 21, 2014First decision: June 27, 2014Revised: November 18, 2014Accepted: January 18, 2015 Article in press: January 18, 2015Published online: February 15, 2015
AbstractAIM: To elucidate the effect of a proton pump inhibitor (PPI, rabeparazole) on oesophageal bile reflux in oesophagitis after total gastrectomy.
METHODS: Twenty-one 8-week-old male Wistar rats were studied. They were performed oesophagoduodenostomy of total gastrectomy to induce oesophageal reflux of biliary and pancreatic juice. Five rats were performed the sham operation (Sham). On post-operative day 7, they were treated with saline (Control) (n = 8) or PPI (rabeprazole, 30 mg/kg per day, ip ) (n = 8) for 2 wk. On post-operative 21, all rats were sacrificed and each oesophagus was evaluated histologically. Oesophageal injury was evaluated by macroscopic and microscopic findings as well as the expression of cyclooxygenase-2 (COX2). We measured bile acid in the oesophageal lumen and the common bile duct.
RESULTS: At 3 wk after surgery, a histological study analysis revealed an increase in the thickness of the epithelium, elongation of the lamina propria and basal cell hyperplasia in the oesophageal mucosa. The macroscopic ulcer score and microscopic ulcer length of the control group were significantly higher compared to those of the rabeprazole- treated group. The expression of COX2 was significantly increased according to the immunostaining in the control group compared to rabeprazole- treated group. Although there was no difference between the control and PPI groups in the total bile acid in the common bile duct, the bile
Rabeprazole is effective for bile reflux oesophagitis after total gastrectomy in a rat model
Naoki Hashimoto, School of Medicine, Kinki University, Osaka 589-8511, JapanAuthor contributions: Hashimoto N solely contributed to this paper.Ethics approval: The study was reviewed and approved by Kinki University, School of Medicine.Institutional animal care and use committee: All procedures involving animals were reviewed and approved by the Institu-tional Animal Care and Use Committee of Kinki University (KAME21-005). The animal protocol was designed to minimize pain or discomfort to the animals. The animals were acclimatized to laboratory conditions (23℃,12 h/12 h light/dark, 50% humi-dity, ad libitum access to food and water) for two weeks prior to experimentation. Intragastric gavage administration was carried out with conscious animals, using straight gavage needles appropriate for the animal size (15-17 g body weight: 22 gauge, 1 inch length, 1.25 mm ball diameter). All animals were euthanized by barbiturate overdose (intravenous injection, 150 mg/kg pentobarbital sodium) for tissue collection.Conflict-of-interest: Naoki Hashimoto has not received fees for serving as a speaker. Naoki Hashimoto has not received research funding from any organizations. Naoki Hashimoto is not an employee of any organizations. Naoki Hashimoto does not own stocks and or shares. Naoki Hashimoto does not own patent.Data sharing: I declare data sharing statement in World Journal Gastrointestinal Pathophysiology. Technical appendix, statistical code, and dataset available from the corresponding author at email address or URL. Participants gave informed consent for data sharing.Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/Correspondence to: Naoki Hashimoto, MD, PhD, School of Medicine, Kinki University, 377-2 Ohnohigashi, Oosaka-sayama-shi, Osaka 589-8511, Japan. [email protected]: +81-723-660221Fax: +81-723-683382Received: May 21, 2014
23 February 15, 2015|Volume 6|Issue 1|WJGP|www.wjgnet.com
ORIGINAL ARTICLE
World J Gastrointest Pathophysiol 2015 February 15; 6(1): 23-28ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i1.23
Naoki Hashimoto
Basic Study

acid activity in the oesophageal lumen was significantly decreased in the rabeprazole- treated group due to augmentation of the duodenal motor complex.
CONCLUSION: With this model, rabeprazole is good effect for reflux esophagitis after total gastrectomy from bile reflux. Bile acid is an important factor in the mucosal lesion induced by duodenal reflux.
Key words: Oesophagoduodenostomy; Reflux oesoph-agitis; Proton pump inhibitor; Rabeprazole
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: To elucidate the effect of proton pump inhibitor (PPI, rabeparazole) on reflux oesophagitis. Sixteen 8-week-old male Wistar rats were studied. They were performed oesophagoduodenostomy of total gastrectomy to induce oesophageal reflux of biliary and pancreatic juice. Five rats were performed the sham operation (Sham). On post-operative day 7, they were treated with saline (Control) (n = 8) or PPI (rabeprazole, 30 mg/kg per day, ip) (n = 8) for 2 wk. On post-operative 21, all rats were sacrificed and each oesophagus was evaluated histologically. Oesophageal injury was evaluated by macroscopic and microscopic findings as well as the expression of cyclooxygenase-2 (COX2). We measured bile acid in the oesophageal lumen and the common bile duct. The macroscopic ulcer score and microscopic ulcer length of the control group were significantly higher compared to those of the rabeprazole- treated group. The expression of COX2 was significantly increased according to the immunostaining in the control group compared to rabeprazole- treated group. Although there was no difference between the control and PPI groups in the total bile acid in the common bile duct, the bile acid activity in the oesophageal lumen was significantly decreased in the rabeprazole- treated group due to augmentation of the duodenal motor complex. With this model, rabeprazole is good effect for reflux oesophagitis after total gastrectomy from bile reflux.
Hashimoto N. Rabeprazole is effective for bile reflux oesoph-agitis after total gastrectomy in a rat model. World J Gastrointest Pathophysiol 2015; 6(1): 23-28 Available from: URL: http://www.wjgnet.com/2150-5330/full/v6/i1/23.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i1.23
INTRODUCTIONReflux of duodenal contents contributes to the development of oesophageal mucosal lesion[1] Oesophagitis after total gastrectomy has been associated with the reflux of duodenal content (biliary and pancreatic juice) into the oesophagus.
Camostat mesilate[2] is commonly used in medical therapy for reflux oesophagitis after total gastrectomy. However, camostat mesilate therapy
alone may not result in complete recovery of reflux oesophagitis after total gastrectomy.
More than 10% of patients are reported to have relapses of oesophagitis, even if camostat mesilate is used for maintenance therapy. Proton pump inhibitors (PPIs) are considered the medical therapy for reflux oesophagitis. Although medications such as PPIs are thought to be efficacious in the treatment of reflux oesophagitis, the mechanism of the curative effect of such drugs remains unclear.
This study was to elucidate the effect of a PPI (rabeprazole, Eisai, Tokyo, Japan) on reflux oesophagitis.
MATERIALS AND METHODSEight week old male Wistar rats weighing 200250 g were used in this study. The animal care and use committee of Kinki University prospectively approved all procedures.
Surgical proceduresThe rats were permitted to acclimate for 2 wk before surgery. Prior to surgery, the animals were fasted for 24 h. An oesophagoduodenal anastomosis was performed under general anaesthesia (pentobarbital 50 mg/kg body wt intraperitoneal injection) through an upper midline incision. The gastroesophageal junction was ligated and the distal oesophagus was transected 2 mm above the ligature. Moreover, the gastroduodenal junction was also ligated, and the proximal duodenum was transected 3 mm distal to the pylorus. A total gastrectomy was performed with the removal of the entire stomach, and endtoend anastomosis of the oesophagus and duodenum. In the sham group, five rats underwent a sham operation, with a midline laparotomy alone without further surgical intervention.
Postoperatively, the rats were allowed to drink water after 6 h and were fed the following day. Feeding with a commercial chow (Oriental Co Ltd) was resumed on day 2.
Study Design and Drug AdministrationSeven days postoperatively, 16 operated rats with reflux oesophagitis were allocated into two groups, a control group (n = 8) that was treated with intraperitoneal injection of vehicle (physiological saline )/per day for 2 wk and a PPI group (n = 8) that was given rabeprazole sodium (Eisai, Tokyo,Japan) by intraperitoneal injection at a dose of 30 mg/kg per day for 2 wk. The Sham group (n = 5) was given regular rat chow to obtain normal control tissue. Fujisaki et al[3] reported that the subcutaneous injection of rabeprazole at doses of 130 mg/kg to rats was effective for reducing reflux esophagitis induced by ligation of both the boundary regions between the forestomach and the glandular portion as well as between the pylorus and the duodenum in
24 February 15, 2015|Volume 6|Issue 1|WJGP|www.wjgnet.com
Hashimoto N. Rabeprazole for reflux oesophagitis

SpragueDawley rats. Rabeprazole, at a dose of 30 mg/kg, inhibited reflux oesophagitis that had been induced by 10 h of ligation. In the present study, we selected a sufficient dose (30 mg/kg per day) of rabeprazole against rat oesophagitis (Figure 1).
Tissue preparationRats were evaluated at 21 d postoperatively under general anaesthesia. All the oesophagi were cut longitudinally; they were fixed in 10% buffered formalin. The formalinfixed oesophagus was Swissrolled, processed and embedded in paraffin. Five-micron sections were mounted onto glass slides and were used for the pathological and immunohistochemical analysis.
Macroscopic examinationA person who was blinded to the treatment scored the macroscopic ulcer lesions as follows: normal glistening mucosal appearance (score 0), oedematous mucosa with focal haemorrhagic spots (score 1); multiple erosions with haematins attached (score 2); linear ulcerations with yellowish exudates (score 3) or haemorrhagic coalesced ulcerations (score 4).
Microscopic examinationThe entire area of damage was collected and fixed in 10% formalin for the histological evaluation. The degree of epithelial loss was measured by micrometre as the ulcer length.
ImmunohistochemistryCOX2: Localisation of COX2 protein was determined by immunohistochemical staining using specific antibodies. The DAKO EnVision system (Dako Cytomation Japan Co. Ltd., Kyoto, Japan) was used with autoclave acceleration. After blocking with endogenous peroxidase, deparaffinized sections covered with a protein block and serumfree media (Dako) were incubated overnight at 4 ℃ with individual primary
antibodies, including antimouse COX2 (1:50, mouse monoclonal; BD Transduction Laboratories, San Jose, Calif). Sections were treated with a secondary biotinylated antibody (Dako). 3,3’diaminobenzidine tetrahydrochloride was used as the chromogen, and the sections were counterstained with haematoxylin.
Measurement of bile acid in the oesophageal lumen and the common bile duct The oesophagus was removed and lavaged with 0.5 mL of saline. The saline used for the lavage was centrifuged at 1500 g at 4 ℃ for 5 min. The supernatant was frozen and stored.
I cut down the common bile duct and insert PE 10 polyethylene tube to common bile duct to collect bile juice. The total bile acid concentration was measured with an ENZa BILE kit (Daiichi Chemical, Tokyo).
Statistical analysis Data are expressed as the mean ± SD of each group. The MannWhitney U test was used to compare each group. Differences were considered significant when the P value was < 0.05.
RESULTSMacroscopic findingsIn control rats, the oesophageal wall showed shortening and dilatation compared to PPI group and was covered with whitish nodular patches. However, the gross appearance of the oesophagus from the PPI group, showed only scattered erosions or mild haemorrhage spots along the oesophagus. The ulcer score was significantly (P < 0.05) decreased by treatment with a PPI (score 1: 2, score 2: 3, score 3: 3 and score 4: 0) compared with control (score 1: 0 score 2: 0 score 3: 1, and score 4: 7) (Figure 2).
Microscopic findingsThe control group had evident thickening of the epithelium, elongation of the lamina papillae, and basal cell hyperplasia in the oesophageal mucosa. Histological examination revealed much more severe oesophagitis in the control group compared to the PPI group. The microscopic ulcer length was significantly (P < 0.05) increased in the control group (8 ± 1 mm) compared to the PPI group (5 ± 1 mm) (Figure 2).
Total bile acid in the oesophageal lumen (μmol/L) The control group (175 ± 50) was significantly higher compared to the sham operated rats (35 ± 5) in the total bile acid in the oesophageal lumen. The treatment with a PPI (45 ± 5) significantly (P < 0.05) inhibited the increase in the total bile acid activity in the oesophageal lumen.
25 February 15, 2015|Volume 6|Issue 1|WJGP|www.wjgnet.com
Postoperative 7 d-21 d
Control group (n = 8): Physiological saline by intraperitoneal injectionRabeprazole group (n = 8): Rabeprazole sodium 30 mg/kg per day (Eisai) by intraperitoneal injection
Duodenum
Esophagus
OesophagoduodenostomyDuodenum
Esophagus
Stormach
Figure 1 Study design and Drug Administration.
Hashimoto N. Rabeprazole for reflux oesophagitis

Total bile acid (mmol/L) of bile juice in the common bile ductThere is no difference between the control group (26.5 ± 5.1) and the PPI group (22.9 ± 3.5). However, the control and PPI groups have significantly (P < 0.05) higher levels than the sham group (18.2 ± 2.4).
Expression of COX2COX2 was not detected in the normal oesophagus. However, COX2 was over expressed in the oesophageal mucosal lesion causing chronic duodenal esophageal reflux. The expression of COX2 was sig-nificantly (P < 0.05) increased according to immunostaining in the control group compared to the PPI group (Figure 3).
DISCUSSIONIt is well known that bile reflux plays an important role in the etiology of reflux esophagitis. In patients with gastroesophageal reflux disease, the concentration of bile acids in the oesophageal refluxate correlates with the degree of oesophageal mucosal injury[4]. In my experimental animals, the duodenoesophageal anastomosis led to reflux oesophagitis[5]. Bile acids is harmful and induce mucosal injury[6].
Helsingen[7] performed total gastrectomy and oesophagoduodenostomy on rats, examined the oesophageal mucosa from postoperative 4 d to 4 mo, and reported that the mucosal epithelium was destroyed and inflammation occurred inside the lamina muscularis mucosae relatively early. In our experiment on rats that underwent total
gastrectomy and oesophagoduodenostomy, erosion and ulceration of the oesophagus were noted 2 wk after the operation. Hyperplasia, ulceration and inflammation (polymorphonuclear and lymphocytic infiltration) of the mucosal epithelium were the histologic features of reflux oesophagitis in rats, which were same feature of Helsingen’s data.
This study provides concrete evidence that bile acid induces oesophageal mucosal lesions in rats by oesophagoduodenal reflux and that treatment with RPZ, a PPI, is decreasing histological findings of reflux oesophagitis as well as decreasing the expression of COX2 in affected oesophageal mucosa compared to saline treatment.
The most striking finding in the present study was that RPZ, PPI, attenuated oesophageal mucosal injury in duodenoesophageal reflux. Bile acid plays a significant role in the etiology of reflux esophagitis previously. Bile acid is one of the important factors of duodenal fluid. We observed overexpression of COX2 in inflamed oesophageal mucosa in an oesophagoduodenal anastomosis. However, we could not detect COX2 in normal oesophageal mucosa. Bile acid is harmful to the oesophagus, causing reflux esophagitis.
The precise mechanisms by which bile acid causes oesophageal injury remain unclear. Bile acids induce COX2 by both transcriptional and posttranscriptional mechanisms[8,9]. Protein kinase C was important factor for the bile acidmediating the induction of COX2. Bile acids can also stimulate PI3K activity[10]; this finding suggests that PI-3K could be involved in mediating the induction of COX2. We found that 2 inhibitors of PI3K activity blocked
26 February 15, 2015|Volume 6|Issue 1|WJGP|www.wjgnet.com
PPI Control
Figure 2 Macroscopic and microscopic finding. PPI: Proton pump inhibitor.
Hashimoto N. Rabeprazole for reflux oesophagitis

the induction of COX2 by bile acids. ERK1/2MAPK is downstream of PI3K and is important role of the regulation of COX2[11]. In fact, ERK1/2MAPK is involved in regulating both the transcription of COX2 and stability of COX2 mRNA. Treatment with bile acid induced ERK1/2 activity, and inhibiting the activation of ERK1/2 blocked the induction of COX2 by bile acid. These datas suggest that the bile acidmediated induction of COX2 involves a signaling cascade that consists of PKC, PI3K and ERK1/2MAPK.
Data on how RPZ reduces the degree of bile reflux are scarce. Champion et al[12] found a reduction in the percentage time of bilirubin absorbance > 0.14 from 32.8% to 4.7% with 40 mg of omeprazole daily in nine patients (3 GERD and 6 Barrett’s oesophagus). Administering the same dose of omeprazole to 11BO patients, Marshall et al observed a decrease in the oesophageal bilirubin exposure from a median of 28.9% to 2.4%[13].
There are two possible explanations for the reduction of DGER with acid suppressant therapy. First, PPIs generally reduce gastric secretion by approximately 40%, decreasing the volume of refluxate[14]. Second, PPIs have been shown to augment the antral and duodenal phase Ⅲ migrating motor complex in healthy individuals, accelerating antroduodenal passage of gastric contents, which should reduce duodenogastric reflux[15]. These findings show that PPIs can reduce the reflux of bile acids into the oesophagus. In our total gastrectomy model, gastric secretion was not affected by PPI. There was no difference between the control (26.5 ± 5.1 mmol/L) and PPI groups (22.9 ± 3.5 mmol/L) in bile acid concentration from the common bile duct. PPIs do not inhibit the secretion of bile acid from the common bile duct. Therefore, we speculate that PPIs accelerate the duodenal phase Ⅲ migrating motor complex, accelerating the duodenal passage of duodenal contents (bile acids), which should reduce duodenoesophageal reflux. Therefore, the bile acid activity in the oesophageal lumen was significantly
decreased in the rabeprazole treated group due to augmentation of the duodenal motor complex.
Recent studies suggest that PPIs have effects beyond acid suppression. Actually PPI reduced IL8 in the oesophageal mucosa of GERD patients[16]. Additionally, histological improvement may also implicate the cytoprotective properties of rabeprazole against bile induced oesophageal damage[17].
This evidence suggests that PPIs not only inhibit acid secretion but also reduce inflammation in the oesophageal mucosa. In our study described above, rabeprazole was good effect for reflux oesophagitis after total gastrectomy due to bile reflux.
In conclusion, we have demonstrated, with our model, that rabeprazole is good effect for reflux esophagitis after total gastrectomy from bile reflux. Bile acid is an important factor in the mucosal lesion induced by duodenal reflux.
COMMENTSBackgroundBile acid into the oesophagus has a role in the etiology of oesophageal lesions.Innovations and breakthroughsIn this study, Rabeprazole is good effect for reflux esophagitis after total gas-trectomy from bile reflux. Bile acid is an important factor in the mucosal lesion induced by duodenal reflux.Applications Rabeprazole is good effect for reflux oesophagitis.TerminologyHematoxylin eosin, cyclooxygenase-2 (COX2) and proton pump inhibitor (PPI).Peer-reviewIn the present study, the authors examined the effect of PPI on esophageal bile reflux in esophagitis after total gastrectomy in rat’s experimental model. They revealed that the macroscopic and microscopic reflux esophagitis were signifi-cantly reduced by rabeprazole treatment, and the COX2 expression was also markedly inhibited by rabeprazole treatment. Further, the bile acid activity in the esophageal lumen was significantly decreased by rabeprazole treatment. This study was well designed and the results were interesting.
REFERENCES1 Kauer WK, Peters JH, DeMeester TR, Ireland AP, Bremner CG,
Hagen JA. Mixed reflux of gastric and duodenal juices is more harmful to the esophagus than gastric juice alone. The need for
27 February 15, 2015|Volume 6|Issue 1|WJGP|www.wjgnet.com
Figure 3 Expression of cyclooxygenase-2. PPI: Proton pump inhibitor.
COMMENTS
Hashimoto N. Rabeprazole for reflux oesophagitis
PPI Control

surgical therapy re-emphasized. Ann Surg 1995; 222: 525-531; discussion 531-533 [PMID: 7574932 DOI: 10.1097/0000658-199522240-00010]
2 Tamura Y, Hirado M, Okamura K, Minato Y, Fujii S. Synthetic inhibitors of trypsin, plasmin, kallikrein, thrombin, C1r-, and C1 esterase. Biochim Biophys Acta 1977; 484: 417-422 [PMID: 143965]
3 Fujisaki H, Oketani K, Hirota K. Effects of Rabeprazole Sodium and Famotidine on Reflux Esophagitis in Rats. JNRC 2003; 52: 752-760
4 Nehra D, Howell P, Williams CP, Pye JK, Beynon J. Toxic bile acids in gastro-oesophageal reflux disease: influence of gastric acidity. Gut 1999; 44: 598-602 [PMID: 10205192 DOI: 10.1136/gut.44.5.598]
5 Goldstein SR, Yang GY, Curtis SK, Reuhl KR, Liu BC, Mirvish SS, Newmark HL, Yang CS. Development of esophageal metaplasia and adenocarcinoma in a rat surgical model without the use of a carcinogen. Carcinogenesis 1997; 18: 2265-2270 [PMID: 9395230]
6 Kivilaakso E, Fromm D, Silen W. Effect of bile salts and related compounds on isolated esophageal mucosa. Surgery 1980; 87: 280-285 [PMID: 6767288]
7 Helsingen N. Oesophageal lesions following total gastrectomy in rats. I. Development and nature. Acta Chir Scand 1960; 118: 202-216 [PMID: 14400939]
8 Galli J, Cammarota G, Calò L, Agostino S, D’Ugo D, Cianci R, Almadori G. The role of acid and alkaline reflux in laryngeal squamous cell carcinoma. Laryngoscope 2002; 112: 1861-1865 [PMID: 12368631 DOI: 10.1097/00005537-200210000-00030]
9 Galli J, Calò L, Agostino S, Cadoni G, Sergi B, Cianci R, Cammarota G. Bile reflux as possible risk factor in laryngopharyngeal inflammatory and neoplastic lesions. Acta Otorhinolaryngol Ital 2003; 23: 377-382 [PMID: 15108488]
10 Narisawa T, Magadia NE, Weisburger JH, Wynder EL. Promoting effect of bile acids on colon carcinogenesis after intrarectal instillation of N-methyl-N’-nitro-N-nitrosoguanidine in rats. J Natl Cancer Inst 1974; 53: 1093-1097 [PMID: 4427390]
11 Zhang F, Subbaramaiah K, Altorki N, Dannenberg AJ. Dihydroxy bile acids activate the transcription of cyclooxygenase-2. J Biol Chem 1998; 273: 2424-2428 [PMID: 9442092 DOI: 10.1074/jbc.273.4.2424]
12 Champion G, Richter JE, Vaezi MF, Singh S, Alexander R. Duodenogastroesophageal reflux: relationship to pH and importance in Barrett’s esophagus. Gastroenterology 1994; 107: 747-754 [PMID: 8076761 DOI: 10.1074/0016-5085(94)90123-6]
13 Marshall RE, Anggiansah A, Manifold DK, Owen WA, Owen WJ. Effect of omeprazole 20 mg twice daily on duodenogastric and gastro-oesophageal bile reflux in Barrett’s oesophagus. Gut 1998; 43: 603-606 [PMID: 9824338 DOI: 10.1136/gut.43.5.603]
14 Lind T, Cederberg C, Ekenved G, Haglund U, Olbe L. Effect of omeprazole--a gastric proton pump inhibitor--on pentagastrin stimulated acid secretion in man. Gut 1983; 24: 270-276 [PMID: 6832622 DOI: 10.1136/gut.24.4.270]
15 Vinter-Jensen L, Kraglund K, Pedersen SA. A double-blind placebo-controlled trial of omeprazole on characteristics of the migrating motor complex in healthy volunteers. Aliment Pharmacol Ther 1989; 3: 615-620 [PMID: 2518874 DOI: 10.1111/j.1365-2036.1989.tb00255.X]
16 Yoshida N, Yoshikawa T. Defense mechanism of the esophageal mucosa and esophageal inflammation. J Gastroenterol 2003; 38 Suppl 15: 31-34 [PMID: 12698868]
17 Miner PB. Review article: physiologic and clinical effects of proton pump inhibitors on non-acidic and acidic gastro-oesophageal reflux. Aliment Pharmacol Ther 2006; 23 Suppl 1: 25-32 [PMID: 16483267]
P- Reviewer: Osawa S S- Editor: Song XX L- Editor: A E- Editor: Wu HL
28 February 15, 2015|Volume 6|Issue 1|WJGP|www.wjgnet.com
Hashimoto N. Rabeprazole for reflux oesophagitis

© 2015 Baishideng Publishing Group Inc. All rights reserved.
Published by Baishideng Publishing Group Inc8226 Regency Drive, Pleasanton, CA 94588, USA
Telephone: +1-925-223-8242Fax: +1-925-223-8243
E-mail: [email protected] Desk: http://www.wjgnet.com/esps/helpdesk.aspx
http://www.wjgnet.com

World Journal of Gastrointestinal PathophysiologyWorld J Gastrointest Pathophysiol 2015 May 15; 6(2): 29-42
ISSN 2150-5330 (online)
Published by Baishideng Publishing Group Inc

EDITOR-IN-CHIEFThomas Y Ma, Albuquerque
STRATEGY ASSOCIATE EDITOR-IN-CHIEFHirotada Akiho, FukuokaJean-Francois Beaulieu, SherbrookeMichael W Bradbury, ErieSharon DeMorrow, Temple
GUEST EDITORIAL BOARD MEMBERSJia-Ming Chang, TaipeiWai-Keung Chow, TaichungChien-Wei Hsu, KaohsiungMing-Tsan Lin, TaipeiBor-Shyang Sheu, TainanJin-Town Wang, Taipei
MEMBERS OF THE EDITORIAL BOARD
ArgentinaBernabé Matías Quesada, Buenos AiresMarcelo G Roma, Rosario
AustraliaChris Richard Abbiss, JoondalupGuy D Eslick, PenrithMontri Gururatsakul, AdelaideChandana Herath, Melbourne Michael Horowitz, AdelaidMustafa Khasraw, GeelongShu-Chuen Li, CallaghanAntonina Mikocka-Walus, AdelaideNam Quoc Nguyen, Adelaide
Kulmira Nurgali, St AlbansNicholas John Spencer, Flagstaff HillNick Spencer, AdelaideDeborah Verran, CamperdownShu-Feng Zhou, Melbourne
AustriaCord Langner, GrazDietmar Ofner-Velano, SalzburgMichael Trauner, Graz
Belgium
Kathleen Blondeau, LeuvenRobaeys Geert, GenkIlse Maria Hoffman, LeuvenMichael H J Maes, WilrijkTheodoor Abram Niewold, HeverleeXavier Sagaert, LeuvenJean-Marie Vanderwinden, BrusselsKristin Verbeke, LeuvenMathieu Vinken, Roeselare
BrazilUilian Andreis, BotucatuEverson L A Artifon, Vila MarianaJoão Batista Calixto, TrindadeNiels O Saraiva Câmara, Vila ClementinoJulio Chebli, Juiz de ForaFernando Fornari, Passo FundoClélia Akiko Hiruma-Lima, BotucatuMarcel C C Machado, Sao PauloJuarez Quaresma, BelemWagner Vilegas, Araraquara
Brunei Darussalam
Vui Heng Chong, Bandar Seri Begawan
Canada
Fernando Alvarez, MontréalFrancois Boudreau, SherbrookeGeorge A Bubenik, GuelphWang-Xue Chen, OttawaJan D Huizinga, PuslinchKusum K Kharbanda, OmahaWolfgang Kunze, HamiltoJian-Jun Li, OttawaRoderick John Macleod, KingstonMichele Molinari, HalifaxNathalie Rivard, SherbrookeKirill Rosen, HalifaxManuela Santos, MontrealCaroline Saucier, QuebecJean Sévigny, QuebecEldon A Shaffer, CalgaryManuel A Silva, HamiltonAlan B R Thomson, EdmontonPierre H Vachon, Sherbrooke
China
Kai-Xing Ai, ShanghaiZhao-Xiang Bian, Hong KongMin-Hu Chen, GuangzhouCH Cho, Hong KongZhong-Hong Gao, WuhanJun-Ming Guo, NingboJing-Yan Han, Beijing
I
Editorial Board2011-2015
The World Journal of Gastrointestinal Pathophysiology Editorial Board consists of 523 members, representing a team of worldwide experts in gastrointestinal pathophysiology. They are from 45 countries, including Argentina (2), Australia (14), Austria (3), Belgium (9), Brazil (10), Brunei Darussalam (1), Canada (20), China (30), Croatia (1), Czech Republic (2), Denmark (4), Egypt (1), Estonia (1), Finland (1), France (8), Germany (22), Greece (7), Hungary (5), India (10), Indonesia (1), Iran (2), Ireland (2), Israel (8), Italy (42), Japan (47), Lebanon (3), Malaysia (1), Mexico (2), Netherlands (8), Norway (1), Poland (4), Portugal (1), Romania (1), Russia (1), Singapore (4), South Korea (13), Spain (23), Sweden (11), Switzerland (4), Thailand (2), Turkey (6), Ukraine (1), United Kingdom (10), United States (173), and Venezuela (1).
February 15, 2013WJGP|www.wjgnet.com
World Journal ofGastrointestinal PathophysiologyW J G P

Jian-Dong Huang, Hong KongJia-Fu Ji, BeijingShi Liu, WuhanZhan-Ju Liu, ShanghaiXiao-Hong Wang, BeijingZhen-Ning Wang, ShenyangWei Wei, HefeiDong-Ping Xie, ShanghaiWen-Xie Xu, ShanghaiHua Yang, ChongqingXiao Yang, BeijingWei-Zhen Zhang, BeijingHua-Chuan Zheng, ShenyangDa-Ling Zhu, HarbinJin-Xia Zhu, BeijingMin-Sheng Zhu, NanjingYong-Liang Zhu, Hangzhou
Croatia
Alen Protic, Rijeka
Czech Republic
Pavel Hladik, SemilyMartin Vokurka, Prague
Denmark
Lars Arendt-Nielsen, AalborgFrank Vinholt Schiodt, CopenhagenJonas Worsoe, AarhusJing-Bo Zhao, Aalborg
Egypt
Mahmoud Aboelneen Khattab, Minia
Estonia
Enn Seppet, Tartu
Finland
Pauli Antero Puolakkainen, Turku
France
Bruno Bonaz, GrenoblePierre Marie Dechelotte, RouenJean-Paul Lallès, Saint-GillesCharles-Henri Malbert, Saint-GillesThierry Piche, NicePascale Plaisancié, LyonMichelina Plateroti, LyonVeronique Vitton, Marseille
Germany
Hans Gunter Beger, UlmCarsten Bergmann, IngelheimElke Cario, Essen
Arno J Dormann, KolnNikolaus Gassler, AachenWerner Hartwig, HeidelbergMarion Hewicker-Trautwein, HannoverJens Hoeppner, FreiburgTobias Keck, FreiburgJorg Kleeff, MunichPeter Malfertheiner, MagdeburgOliver Mann, HamburgChristoph Michalski, MunichAndreas Klaus Nussler, MunichChristian Pehl, VilsbiburgPeter Schemmer, HeidelbergMarc Stemmler, FreiburgFrank Tacke, AachenSya Nomna Ukena, HannoverBrigitte Vollmar, RostockThomas Michael Wex, MagdeburgMargot Zoller, Heidelberg
Greece
Stelios F Assimakopoulos, PatrasGeorge N Dalekos, LarissaAlkiviadis Efthymiou, thessalonikiMaria Gazouli, AthensIoannis E Koutroubakis, HeraklionGerassimos J Mantzaris, AthensGeorge Papatheodoridis, Athens
Hungary
Mária Bagyánszki, SzegedMihály Boros, SzegedLaszlo Czako, SzegedPal Miheller, BudapestZoltan Rakonczay, Szeged
India
Anil Kumar Agarwal, DelhiUday Bandyopadhyay, KolkataSriparna Basu, VaranasiChandra Kanti Chakraborti, RourkelaRajeev Garg, PunjabChandra P Sharma, ThiruvananthapuramShailesh V Shrikhande, MumbaiVirendra Singh, ChandigarhNicholas James Skill, IndianapolisPrabhakar R Veerareddy, Andhra Pradesh
Indonesia
Laurentius A Lesmana, Jakarta
Iran
Gholamreza Roshandel, GorganShahram Shahabi, Urmia
Ireland
Billy Bourke, DublinStephen Keely, Dublin
IsraelYosefa Avraham, JerusalemYaron Bar-Dayan, HolonShomron Ben-Horin, HashomerBoris Kirshtein, Beer ShevaStephen Malnick, RehovotYaakov Maor, Tel-HashomerRifaat Safadi, JerusalemNachum Vaisman, Tel Aviv
Italy
Rosaria Acquaviva, CataniaDario Acuna-Castroviejo, ArmillaAlessandro Antonelli, PisaGiacosa Attilio, GenovaSalvatore Auricchio, NaplesGuido Basilisco, MilanoAntonio Basoli, RomeClaudio Bassi, VeronaMassimo Bellini, PisaLuigi Bonavina, MilanoAlfio Brogna, CataniaGiuseppe Calamita, BariRaffaele Capasso, NaplesIgnazio Castagliuolo, PadovaEnrico Stefano Corazziari, RomeFrancesco Cresi, TorinoRosario Cuomo, NapoliSalvatore Cuzzocrea, GazziMario M D’Elios, FlorenceCinzia Domeneghini, MilanLuca Elli, MilanoCresi Francesco, TorinoWalter Fries, MessinaEugenio Gaudio, RomeMarco Gobbetti, BariFabio Grizzi, MilanEnzo Grossi, MilaneseEnzo Ierardi, FoggiaPietro Invernizzi, MilanAngelo A Izzo, NaplesAnna Kohn, RomeGiovanni Latella, L’AquilaMassimo Marignani, RomeSergio Morini, RomeRaffaele Pezzilli, BolognaCristiano Rumio, MilanGiovanni Sarnelli, NaplesEdoardo Vincenzo Savarino, GenoaPierpaolo Sileri, RomeAnnamaria Staiano, NaplesGiacomo Carlo Sturniolo, PadovaClaudio Tiribelli, Triest
Japan
Akihiro Asakawa, KagoshimaHisashi Aso, SendaiYasu-Taka Azuma, OsakaShotaro Enomoto, WakayamaMikihiro Fujiya, HokkaidoTakahisa Furuta, HamamatsuAkira Hokama, OkinawaRyota Hokari, SaitamaYuichi Hori, Kobe
II February 15, 2013WJGP|www.wjgnet.com

III February 15, 2013WJGP|www.wjgnet.com
Hideki Iijima, OsakaMasahiro Iizuka, AkitaMotohiro Imano, OsakaHajime Isomoto, NagasakiTatehiro Kagawa, IseharaTakumi Kawaguchi, KurumeHaruki Kitazawa, SendaiXiao-Kang Li, TokyoNoriaki Manabe, OkayamaAtsushi Masamune, SendaiHiroyuki Matsubayashi, ShizuokaKazuyuki Matsushita, Chuo-kuReiko Miyazawa, GunmaKazunari Murakami, OitaHikaru Nagahara, TokyoYuji Naito, KyotoAtsushi Nakajima, Atsushi NakajimaShoji Natsugoe, KagoshimaTsutomu Nishida, OsakaKoji Nomoto, TokyoNaoaki Sakata, MiyagiShouji Shimoyama, TokyoGoshi Shiota, YonagoIkuo Shoji, HyogoHidekazu Suzuki, TokyoHitoshi Takagi, GunmaToru Takahashi, OkayamaYoshihisa Takahashi, TokyoKan Uchiyama, ChibaTakato Ueno, KurumeYoshiyuki Ueno, SendaiHisayuki Uneyama, KwasakiMitsunori Yamakawa, YamagataTakayuki Yamamoto, MieYutaka Yata, GunmaNaohisa Yoshida, KyotoHitoshi Yoshiji, Nara
Lebanon
Costantine Fouad Daher, ByblosAssaad M Soweid, BeirutJulnar Usta, Beirut
Malaysia
Andrew Chua, Perak
Mexico
José María de la Roca-Chiapas, LeonMaria Raquel Huerta Franco, Guanajuato
Netherland
Wouter J de Jonge, AmsterdamAldo Grefhorst, GroningenRuben Hummelen, RotterdamDaniel Keszthelyi, MaastrichtCornelis F M Sier, LeidenPieter J Tanis, AmsterdamLuc JW van der Laan, RotterdamSander van der Marel, Leiden
NorwayAnne Marie Bakke, Oslo
Poland
Stanisław Hac, GdańskStanisław Jan Konturek, KrakówAgata Mulak, WroclawNapoleon Waszkiewicz, Choroszcz
Portugal
Ricardo Marcos, Porto
Romania
Mihai Ciocirlan, Bucharest
Russia
Ludmila Filaretova, Petersburg
Singapore
Madhav Bhatia, SingaporeBrian K P Goh, SingaporeKhek Yu Ho, SingaporeCliff K S Ong, Singapore
South Korea
Jae Hee Cheon, SeoulMyung Haing Cho, SeoulJae Bock Chung, SeoulKi-Baik Hahm, IncheonHo Jae Han, GwangjuChang Duk Jun, GwangjuHong Joo Kim, SeoulJin Kyung Kim, Gyeongsan-SiSang Geon Kim, SeoulWon Jae Lee, SeoulKwan Kyu Park, DaeguSeung Ha Park, BusanSung Joo Park, Jeonbuk
Spain
Raquel Abalo, AlcorcónJuan G Abraldes, BarcelonaAgustin Albillos, MadridMaria-Angeles Aller, MadridFernando Azpiroz, BarcelonaRamon Bataller, BarcelonaMarco Bustamante, ValenciaAndres Cardenas, BarcelonaDariao Acuna Castroviejo, ArmillaJoan Claria, BarcelonaPere Clave, BarcelonaManuel Giner, Madrid
Angel I Lanas, ZaragozaMaite Martin, BarcelonaMaria Teresa Martin, BarcelonaVicente Martinez, BarcelonaJose M Matés, MalagaJulio M Mayol, MadridMarçal Pastor-Anglada, BarcelonaMaría Eugenia Sáez, SevilleYolanda Sanz, BurjassotCarlos Taxonera, MadridMaria D Yago, Granada
Sweden
Marco Del Chiaro, StockholmFrida Fak, GothenburgGunnar FA Flemstrom, UppsalaEvangelos Kalaitzakis, GothenburgKristina Lamas, UmeaBob Roger Olsson, GöteborgSara Maria Regnér, MalmöPeter thelin Schmidt, StockholmXiao-Feng Sun, LinkopingHenrik Thorlacius, MalmöCurt Tysk, Orebro
Switzerland
Jyrki J Eloranta, ZurichAndreas Geier, ZurichRemy Meier, LiestalCatherine Pastor, Geneva
Thailand
Thawatchai Akaraviputh, BangkokWeekitt Kittisupamongkol, Bangkok
Turkey
Mehmet Bektas, AnkaraMukaddes Esrefoglu, MalatyaAhmet Guven, AnkaraMuammer Karadeniz, ManisaElvan Ozbek, ErzuruIlhami Yuksel, Ankara
Ukraine
Oksana S Zayavhkivska, Lviv
United Kingdom
Geoffrey Burnstock, LondonJanice E Drew, AberdeenGirish Gupte, BirminghamDavid C Hay, EdinburghNusrat Husain, CheshireMichael Leslie Lucas, GlasgowJamie Murphy, LondonVadim Sumbayev, KentWing-Kin Syn, Birmingham

IV February 15, 2013WJGP|www.wjgnet.com
Andrea Varro, Liverpool
United States
Sami Rene Achem, JacksonvilleTauseef Ali, OklahomaDavid H Alpers, St LouisGianfranco D Alpini, TempleShrikant Anant, OklahomaM Sawkat Anwer, North GraftonAndrew Aronsohn, ChicagoToms Augustin, SayreGyorgy Baffy, BostonMichael T Bailey, ColumbusKim Elaine Barrett, San DiegoMarc D Basson, LansingRobert L Bell, New HavenDavid H Berger, HoustonUrs A Boelsterli, StorrsRichard G Boles, Los AngelesEdward L Bradley III, SarasotaQiang Cai, AtlantaWei-Biao Cao, ProvidenceSubhash C Chauhan, Sioux FallsJian-De Chen, GalvestonTao-Sheng Chen, MemphisJohn Chiang, RootstownMashkoor A Choudhry, MaywoodParimal Chowdhury, Little RockEric Cohen, BostonRobert Cormier, DuluthSrinivasan Dasarathy, ClevelandEdwin A Deitch, NewarkDan A Dixon, ColumbiaJames P Dolan, PortlandH Henry Dong, PittsburghHui Dong, La JollaAshkan Farhadi, IrvineBin Feng, PittsburghJenifer Fenton, East LansingAlessandro Fichera, ChicagoMitchell P Fink, PittsburghP Marco Fisichella, MaywoodLeo R Fitzpatrick, HummelstownRobert Armour Forse, OmahaGlenn Tsuyoshi Furuta, AuroraJuan F Gallegos-Orozco, ScottsdalePandu R Gangula, NasvhilleTimothy Gardner, LebanonShannon Stroud Glaser, TempleFrancisco Gondim, St. LouisJohn R Grider, RichmondYan-Fang Guan, CincinnatiGregory M Holmes, Baton RougeAi-Xuan Le Holterman, ChicagoRichard Hu, Los AngelesHartmut Jaeschke, KansasRobert Thomas Jensen, Los AngelesSreenivasa S Jonnalagadda, LouisMichel Kahaleh, Charlottesville
Andreas Martin Kaiser, Los AngelesRandeep Singh Kashyap, RochesterLaurie Keefer, ChicagoRichard Kellermayer, HoustonChris Kevil, ShreveportSandeep Khurana, BaltimorePawel R Kiela, TucsonTammy Lyn Kindel, CincinnatGordana Kosutic, DurhamDavid Kravetz, San DiegoAshok Kumar, DetroitJohn H Kwon, ChicagoMuriel Larauche, Los AngelesI Michael Leitman, New YorkFelix W Leung, North HillsSuthat Liangpunsakul, IndianapolisFeng-Xin Lu, BostonPauline Kay Lund, Chapel HillGeorge Luo, LexingtonGuang-Xiang Luo, LexingtonJay Luther, Ann ArborRam I Mahato, MemphisAkhil Maheshwari, BirminghamKenneth Maiese, NewarkAdhip P N Majumdar, DetroitJose E Manautou, StorrsCraig J McClain, LouisvilleDermot McGovern, Los AngelesB Greenwood-van Meerveld, OklahomaDouglas Scott Merrel, BethesdaMurielle Mimeault, OmahaEmiko Mizoguchi, BostonHuan-Biao Mo, DentonAdam Moeser, RaleighRamzi M Mohammad, DetroitSatdarshan Singh Monga, PittsburghRoger Klein Moreira, New YorkSandeep Mukherjee, OmahaKarnam S Murthy, RichmondMichael J Nowicki, JacksonShuji Ogino, BostonMary Francis Otterson, WisconsinChung Owyang, Ann ArborHelieh S Oz, LexingtonMarco G Patti, ChicagoTimothy Michael Pawlik, BaltimoreSara Peleg, HoustonNicholas C Popescu, BethesdaLi-Ya Qiao, RichmondChao Qin, OklahomaParvaneh Rafiee, MilwaukeeSigrid A Rajasekaran, WilmingtonVazhaikkurichi M Rajendran, MorgantownJean Pierre Raufman, BaltimoreRamesh M Ray, MemphisArie Regev, IndianapolisDouglas K Rex, CarmelYehuda Ringel, Chapel HillRichard A Rippe, RockvilleChantal A Rivera, Bossier
Andrea Romani, ClevelandPraveen K Roy, AlbuquerquePaul A Rufo, BostonDavid B Sachar, New YorkBimaljit Singh Sandhu, RichmondSanjaya Kumar Satapathy, New Hyde ParkAnthony Senagore, Los AngelesMuhammad Y Sheikh, FresnoBo Shen, ClevelandLe Shen, ChicagoFrank A Simmen, Little RockSteven Mitchell Singer, WashingtonShailinder Jit Singh, WashingtonAdam Jan Smolka, CharlestonNed Snyder, HoustonZhen-Yuan Song, ChicagoGagan K Sood, HoustonRhonda F Souza, DallasStuart Jon Spechler, DallasSubbaramiah Sridha, AugustaCatia Sternini, Los AngelesVeedamali S Subramanian, Long BeachJun Sun, RochesterYvette Taché, Los AngelesXiao-Di Tan, ChicagoPaul Daniel Terry, AtlantaJennifer Tirnauer, FarmingtonAndrea Todisco, Ann ArborGeorge C Tsokos, BostonVic Velanovich, DetroitRaj Vuppalanchi, IndianapolisEstela Wajcberg, CranfordArnold Wald, MadisonLi-Xin Wang, Los AngelesHorst Christian Weber, BostonSteven D Wexner, WestonJackie D Wood, ColumbusGuo-Yao Wu, College StationChristian Wunder, BethesdaZuo-Liang Xiao, ClevelandGuang-Yin Xu, GalvestonGuo-Rong Xu, East OrangeGuang-Yu Yang, ChicagoJay A Yelon, ValhallaYamaoka Yoshio, HoustonShao-Yong Yu, HersheyYana Zavros, CincinnatiJoerg Zehetner, Los AngelesJian X Zhang, CharlotteZhi Zhong, CharlestonHui-Ping Zhou, RichmondZhan-Xiang Zhou, KannapolisQing Zhu, BethesdaYao-Hui Zhu, Stanford
Venezuela
Fabian Michelangeli, Caracas

Contents
May 15, 2015|Volume 6|Issue 2|WJGP|www.wjgnet.com I
Quarterly Volume 6 Number 2 May 15, 2015
EDITORIAL29 Cystictumorsofthepancreas:Opportunitiesandrisks
Del Chiaro M, Verbeke C
MINIREVIEWS33 CurrenttherapyofpediatricCrohn’sdisease
Lahad A, Weiss B

Editorial BoardMemberofWorld Journal of Gastrointestinal Pathophysiology ,YujiNaito,AssociateProfessor,DepartmentofGastroenterologyandHepatol-ogy,KyotoPrefecturalUniversityofMedicine,465-Kajiicho,Kamigyoku,Kyoto602-8566,Japan
World Journal of Gastrointestinal Pathophysiology (World J Gastrointest Pathophysiol, WJGP, online ISSN 2150-5330, DOI: 10.4291), is a peer-reviewed open access academic journal that aims to guide clinical practice and improve diagnostic and therapeutic skills of clinicians.
WJGP is to report rapidly the most recent results in basic and clinical research on gastrointestinal pathophysiology, including all aspects of normal or abnormal function of the gastrointestinal tract, hepatobiliary system, and pancreas. WJGP specifically covers growth and development, digestion, secretion, absorption, metabolism and motility relative to the gastrointestinal organs, as well as immune and inflammatory processes, and neural, endocrine and circulatory control mechanisms that affect these organs. This journal will also report new methods and techniques in gastrointestinal pathophysiological research. We encourage authors to submit their manuscripts to WJGP. We will give priority to manuscripts that are supported by major national and international foundations and those that are of great basic and clinical significance.
World Journal of Gastrointestinal Pathophysiology is now indexed in PubMed Central, PubMed, Digital Object Identifier, and Directory of Open Access Journals.
I-IV EditorialBoard
ContentsWorld Journal of Gastrointestinal Pathophysiology
Volume 6 Number 2 May 15, 2015
FLYLEAF
EDITORS FOR THIS ISSUE
NAMEOFJOURNALWorld Journal of Gastrointestinal Pathophysiology
ISSNISSN 2150-5330 (online)
LAUNCHDATEApril 15, 2010
FrequencyQuarterly
EDITOR-IN-CHIEFThomas Y Ma, MD, PhD, Professor, Chief, Division of Gastroenterology and Hepatology, University of New Mexico, MSC10 5550, 1 UNM, Albuquerque, NM 87131, United States
EDITORIALOFFICEJin-Lei Wang, DirectorXiu-Xia Song, Vice DirectorWorld Journal of Gastrointestinal Pathophysiology
Room 903, Building D, Ocean International Center, No. 62 Dongsihuan Zhonglu, Chaoyang District, Beijing 100025, ChinaTelephone: +86-10-85381891Fax: +86-10-85381893E-mail: [email protected] Desk: http://www.wjgnet.com/esps/helpdesk.aspxhttp://www.wjgnet.com
PUBLISHERBaishideng Publishing Group Inc8226 Regency Drive, Pleasanton, CA 94588, USATelephone: +1-925-223-8242Fax: +1-925-223-8243E-mail: [email protected] Desk: http://www.wjgnet.com/esps/helpdesk.aspxhttp://www.wjgnet.com
PUBLICATIONDATEMay 15, 2015
COPYRIGHT© 2015 Baishideng Publishing Group Inc. Articles pub-lished by this Open Access journal are distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license.
SPECIALSTATEMENTAll articles published in journals owned by the Baishideng Publishing Group (BPG) represent the views and opinionsof their authors, and not the views, opinions or policies of the BPG, except where other-wise explicitly indicated.
INSTRUCTIONSTOAUTHORSFull instructions are available online at http://www.wjgnet.com/2218-6182/g_info_20100722172951.htm
ONLINESUBMISSIONhttp://www.wjgnet.com/esps/
ABOUT COVER
May 15, 2015|Volume 6|Issue 2|WJGP|www.wjgnet.com II
AIM AND SCOPE
INDEXING/ABSTRACTING
Responsible Assistant Editor: Xiang Li Responsible Science Editor: Fang-Fang JiResponsible Electronic Editor: Ya-Jing Lu Proofing Editorial Office Director: Xiu-Xia Song Proofing Editor-in-Chief: Lian-Sheng Ma

neoplasms of the pancreas can be considered as the pancreatic analogon to colonic polyps. Treatment of these precursor lesions at an early stage can potentially reduce pancreas cancer mortality and introduce a new “era” of preemptive pancreatic surgery. However, only few of those lesions have an aggressive behavior. The accuracy of preoperative diagnosis, i.e. , the distinction between the various PCNs is around 60%, and the ability to predict the future outcome is also less accurate. For this reason, a significant number of patients are currently over-treated with an unnecessary, high-risk surgery. Furthermore, the majority of patients with PCN are on life-long follow-up with imaging modality, which has huge cost implications for the Health Care System for limited benefits considering that a significant proportion of PCNs are or behave like benign lesions. The current guidelines for the diagnosis and management of PCNs are more based on expert opinion than on evidence. For all those reasons, the management of cystic tumors of the pancreas remains a controversial area of pancreatology. On one hand, the detection of PCNs and the surgical treatment of pre-cancerous neoplasms can be considered a big opportunity to reduce pancreatic cancer related mortality. On the other hand, PCNs are associated with a considerable risk of under- or over- treatment of patients and incur high costs for the Health Care System.
Key words: Pancreatic cystic neoplasms; Mucinous cystic neoplasia; Preemptive pancreatic surgery; Pancreas; Intraductal papillary mucinous neoplasia
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: The present paper is an editorial focused on the critical problems regarding the management strategy of pancreatic cystic neoplasms (PCNs). Being a pre-cancerous condition in most of the cases, PCNs represent a unique opportunity to prevent pancreatic cancer and to develop preemptive pancreatic surgery programs. However, the lack of predictive factors of the behaviour of these lesions, the low accuracy of
Cystic tumors of the pancreas: Opportunities and risks
Marco Del Chiaro, Pancreatic Surgery Unit, Division of Surgery, Department of Clinical Science, Intervention and Technology (CLINTEC), Karolinska Institute at Center for Digestive Diseases, Karolinska University Hospital, 14186 Stockholm, SwedenCaroline Verbeke, Department of Pathology, Institute of Clinical Medicine, University of Oslo, 0316 Oslo, NorwayCaroline Verbeke, Department of Pathology, Karolinska Institute, 14186 Stockholm, SwedenAuthor contributions: Del Chiaro M and Verbeke C equally contributed to this paper. Conflict-of-interest: None.Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/Correspondence to: Marco Del Chiaro, MD, PhD, FACS, Associate Professor of Surgery, Head of Pancreatic Surgery Unit, Division of Surgery, Department of Clinical Science, Intervention and Technology (CLINTEC), Karolinska Institute at Center for Digestive Diseases, Karolinska University Hospital, K53, 14186 Stockholm, Sweden. [email protected]: +46-8-58580000Fax: +46-8-58586366Received: January 18, 2015 Peer-review started: January 20, 2015 First decision: February 7, 2015Revised: February 21, 2015Accepted: March 16, 2015Article in press: March 18, 2015Published online: May 15, 2015
AbstractPancreatic cystic neoplasms (PCNs) are a high prevalence disease. It is estimated that about 20% of the general population is affected by PCNs. Some of those lesions can progress till cancer, while others behave in a benign fashion. In particular intraductal papillary mucinous
29 May 15, 2015|Volume 6|Issue 2|WJGP|www.wjgnet.com
EDITORIAL
World J Gastrointest Pathophysiol 2015 May 15; 6(2): 29-32ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i2.29
Marco Del Chiaro, Caroline Verbeke

pre-operative diagnostics, and the limited knowledge regarding the natural history of those lesions, result in a substantial risk for under- and over-treatment of patients with PCN and represent a high cost factor for the Health Care organization. The paper underscores the critical importance of both the current management of PCNs and the need for future research.
Del Chiaro M, Verbeke C. Cystic tumors of the pancreas: Opportunities and risks. World J Gastrointest Pathophysiol 2015; 6(2): 29-32 Available from: URL: http://www.wjgnet.com/2150-5330/full/v6/i2/29.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i2.29
EDITORIALPancreatic cystic neoplasms (PCNs) represent disease with a high prevalence. Recent series report an overall prevalence of 20%[1,2], whereby the majority of these neoplasms are discovered incidentally. The most frequent PCNs are represented by three distinct tumor entities: Intraductal papillary mucinous neoplasia (IPMN), mucinous cystic neoplasia (MCN) and serous cystic neoplasia (SCN). The first two neoplastic entities can progress to cancer, whereas SCN is almost always benign.
The progression model of mucinous neoplasms, in particular of IPMN, is very similar to that of colonic polyps. The latter neoplasms can progress from a benign and non-invasive adenoma with mild dysplasia through stages with increasing grades of dysplasia and eventually transform into invasive cancer[3]. For this reason, PCNs, and in particular IPMNs, offer today an extraordinary opportunity to detect pancreatic cancer progression and perform preemptive pancreatic surgery[4].
PCNs are easy detectable with conventional and commonly used abdominal imaging modalities, i.e., computed tomography, magnetic resonance and ultra-sonography. They are frequently discovered at an early, often asymptomatic stage. Of particular interest is the fact that IPMNs are significantly more common in the subpopulation of patients that are at increased risk for pancreatic cancer, such as individuals with a positive family history[5]. Furthermore, data from the literature suggest that IPMN of the pancreas can be associated with an increased risk of extrapancreatic malignancies[6], hence their diagnosis can prompt the investigation and early detection of tumors in other organs. However, a recent multicentre study analyzing the incidence of extrapancreatic malignancies in IPMN patients seems to question this association[7].
In clinical practice, the concept that PCNs may be considered as the pancreatic analogon to colonic polyps, i.e., lesions suitable for preemptive surgery and cancer prevention, presents with many difficulties
and potential risks. First of all, considering the low incidence of pancreatic
cancer in the general population, it is obvious that only few of the PCNs really progress to invasive carcinoma. It is estimated that only about 24% of all resected BD-IPMNs are malignant[8]. In a recent series of 90 consecutive resected MCNs of the pancreas, only 4.4% were associated with invasive carcinoma[9]. The risk of progression to cancer is shown to be only 1.4% following 5 years’ surveillance of non-resected BD-IPMN[10]. The accuracy of pre-operative diagnosis remains poor, also in highly specialized tertiary referral centers. It is estimated that for PCNs the pre-operative diagnostic is around 63%, however, erroneous diagnosis has a clinical impact (for example unnecessary surgery) in only 8.5% of the cases[11]. Several recent studies demonstrate that even with the use of fine needle aspiration (FNA) during endoscopic ultrasound, the accuracy of the pre-operative diagnostic work-up does not significantly increase[11]. The sensitivity of FNA cytology is around 38%[12], while combined biochemistry and cytology provides a correct diagnosis in only 33%[13,14]. For this reason, there is a concrete danger of over- or under-estimation of the risk of malignant transformation in some lesions and, as a consequence, of over- or under-treatment of the patients. New diagnostic approaches based on molecular and genetic analysis of the cystic fluid seem to be promising for the future, but are not yet extensively used in clinical practice[15,16].
Unfortunately, this lack of accurate diagnostic modalities results for the majority of patients with PCNs in the need of frequent, expensive and life-long radiologic assessment.
In recent years, two new guidelines partially changed the management of patients with PCNs[8,17]. Even though both are similar in many aspects, there are also some significant differences. Limiting our attention to the treatment of IPMN and MCN, it can be said that the European Guidelines are less aggressive from a surgical point of view, and that they suggest a less aggressive surveillance program for patients who are not a candidate for resection. Of note, both guidelines are mostly based on expert opinion and - by default - founded on only a very low grade of evidence.
Today we know that IPMNs with involvement of main pancreatic duct (main-duct and mixed type) are associated with an increased cancer risk[8,17], and for this reason these tumors should be resected in every patient fit for surgery. However, the surgical approach and extent of resection is not well defined. In the near future, new endoscopic methods, such as pancreatoscopy, may possibly change our clinical practice[18]. The clinical decision process is also complex for patients with PCNs that do no involve the main pancreatic duct. IPMNs involving only the branch ducts are difficult to handle. The risk for cancer is lower than for main-duct or mixed type IPMN, and according to large studies the incidence of cancer during follow-
30 May 15, 2015|Volume 6|Issue 2|WJGP|www.wjgnet.com
Del Chiaro M et al . Cystic tumors of the pancreas: Opportunities and risks

up seems to be very low[10]. If there are multiple lesions, the diagnosis of IPMN is likely, and the current guidelines for the management of these patients seem to be safe. More challenging is the diagnosis of a single cystic lesion, as it may prove difficult to confidently exclude a series of differentials. For this reason, some authors suggested enucleation of these lesions as a combined diagnostic and therapeutic option in selected cases[19,20]. Currently, in absence of risk factors for malignancy and/or worrisome features on radiological assessment, cystic lesions of the pancreas (IPMN and MCN) can be conservatively treated as long as the diameter does not exceed 4 cm[17]. The timing of follow-up remains controversial, but considering that the cancer risk gradually increases over time, a more aggressive follow-up can be suggested after 5 years since initial diagnosis[17]. However, the majority of these patients remain nowadays under life-long follow-up with imaging modalities. Considering the prevalence of these neoplasms, it is obvious that patient surveillance represents a tremendous cost factor for the health care system. In view of the low rate of progression to cancer, the current follow-up approach is probably not cost effective.
In conclusion, PCNs offer today the only opportunity to reduce in the short to medium term the mortality related to pancreatic cancer. However, to realize this, we have to overcome obstacles and improve our current results. First and foremost, we need more accurate diagnostic tools in order to make a correct pre-operative diagnosis and overcome the problems of patient over-treatment and surgery-related mortality and morbidity. We need new markers that reliably predict the pro-gression of PCN to cancer, such that the indication for surgical treatment or follow-up can be tailored to the cancer risk in the individual patient. Less costly imaging modalities that are suitable for surveillance of large patient populations are urgently needed. Only when progress regarding these important issues has been achieved, may an effective preemptive surgical program for pancreatic cancer come into realization, which will require minimally invasive techniques performed at highly specialized centers[21].
REFERENCES1 Laffan TA, Horton KM, Klein AP, Berlanstein B, Siegelman SS,
Kawamoto S, Johnson PT, Fishman EK, Hruban RH. Prevalence of unsuspected pancreatic cysts on MDCT. AJR Am J Roentgenol 2008; 191: 802-807 [PMID: 18716113 DOI: 10.2214/AJR.07.3340]
2 Zhang XM, Mitchell DG, Dohke M, Holland GA, Parker L. Pancreatic cysts: depiction on single-shot fast spin-echo MR images. Radiology 2002; 223: 547-553 [PMID: 11997566 DOI: 10.1148/radiol.2232010815]
3 Shi C, Hruban RH. Intraductal papillary mucinous neoplasm. Hum Pathol 2012; 43: 1-16 [PMID: 21777948 DOI: 10.1016/j.humpath.2011.04.003]
4 Del Chiaro M, Segersvärd R, Lohr M, Verbeke C. Early detection and prevention of pancreatic cancer: is it really possible today? World J Gastroenterol 2014; 20: 12118-12131 [PMID: 25232247 DOI: 10.3748/wjg.v20.i34.12118]
5 Brune K, Abe T, Canto M, O’Malley L, Klein AP, Maitra A, Volkan Adsay N, Fishman EK, Cameron JL, Yeo CJ, Kern SE, Goggins M, Hruban RH. Multifocal neoplastic precursor lesions associated with lobular atrophy of the pancreas in patients having a strong family history of pancreatic cancer. Am J Surg Pathol 2006; 30: 1067-1076 [PMID: 16931950]
6 Larghi A, Panic N, Capurso G, Leoncini E, Arzani D, Salvia R, Del Chiaro M, Frulloni L, Arcidiacono PG, Zerbi A, Manta R, Fabbri C, Ventrucci M, Tarantino I, Piciucchi M, Carnuccio A, Boggi U, Costamagna G, Delle Fave G, Pezzilli R, Bassi C, Bulajic M, Ricciardi W, Boccia S. Prevalence and risk factors of extrapancreatic malignancies in a large cohort of patients with intraductal papillary mucinous neoplasm (IPMN) of the pancreas. Ann Oncol 2013; 24: 1907-1911 [PMID: 23676419 DOI: 10.1093/annonc/mdt184]
7 Marchegiani G, Malleo G, D’Haese JG, Wenzel P, Keskin M, Pugliese L, Borin A, Benning V, Nilsson L, Oruc N, Segersvärd R, Friess H, Schmid R, Löhr M, Maisonneuve P, Bassi C, Ceyhan GO, Salvia R, Del Chiaro M. Association Between Pancreatic Intraductal Papillary Mucinous Neoplasms and Extrapancreatic Malignancies. Clin Gastroenterol Hepatol 2014 Dec 2; Epub ahead of print [PMID: 25478920 DOI: 10.1016/j.cgh.2014.11.029]
8 Tanaka M, Fernández-del Castillo C, Adsay V, Chari S, Falconi M, Jang JY, Kimura W, Levy P, Pitman MB, Schmidt CM, Shimizu M, Wolfgang CL, Yamaguchi K, Yamao K. International consensus guidelines 2012 for the management of IPMN and MCN of the pancreas. Pancreatology 2012; 12: 183-197 [PMID: 22687371 DOI: 10.1016/j.pan.2012.04.004]
9 Park JW, Jang JY, Kang MJ, Kwon W, Chang YR, Kim SW. Mucinous cystic neoplasm of the pancreas: is surgical resection recommended for all surgically fit patients? Pancreatology 2014; 14: 131-136 [PMID: 24650968 DOI: 10.1016/j.pan.2013.12.006]
10 Malleo G, Marchegiani G, Borin A, Capelli P, Accordini F, Butturini G, Pederzoli P, Bassi C, Salvia R. Observational Study of the Incidence of Pancreatic and Extrapancreatic Malignancies During Surveillance of Patients With Branch-Duct Intraductal Papillary Mucinous Neoplasm. Ann Surg 2015; 261: 984-990 [PMID: 25493361]
11 Del Chiaro M, Segersvärd R, Pozzi Mucelli R, Rangelova E, Kartalis N, Ansorge C, Arnelo U, Blomberg J, Löhr M, Verbeke C. Comparison of preoperative conference-based diagnosis with histology of cystic tumors of the pancreas. Ann Surg Oncol 2014; 21: 1539-1544 [PMID: 24385209 DOI: 10.1245/s10434-013-3465-9]
12 Cizginer S, Turner BG, Bilge AR, Karaca C, Pitman MB, Brugge WR. Cyst fluid carcinoembryonic antigen is an accurate diagnostic marker of pancreatic mucinous cysts. Pancreas 2011; 40: 1024-1028 [PMID: 21775920 DOI: 10.1097/MPA.0b013e31821bd62f]
13 de Jong K, Poley JW, van Hooft JE, Visser M, Bruno MJ, Fockens P. Endoscopic ultrasound-guided fine-needle aspiration of pancreatic cystic lesions provides inadequate material for cytology and laboratory analysis: initial results from a prospective study. Endoscopy 2011; 43: 585-590 [PMID: 21611945 DOI: 10.1055/s-0030-1256440]
14 Jabbar KS, Verbeke C, Hyltander AG, Sjövall H, Hansson GC, Sadik R. Proteomic mucin profiling for the identification of cystic precursors of pancreatic cancer. J Natl Cancer Inst 2014; 106: djt439 [PMID: 24523528 DOI: 10.1093/jnci/djt439]
15 Al-Haddad MA, Kowalski T, Siddiqui A, Mertz HR, Mallat D, Haddad N, Malhotra N, Sadowski B, Lybik MJ, Patel SN, Okoh E, Rosenkranz L, Karasik M, Golioto M, Linder J, Catalano MF. Integrated molecular pathology accurately determines the malignant potential of pancreatic cysts. Endoscopy 2015; 47: 136-146 [PMID: 25314329 DOI: 10.1055/s-0034-1390742]
16 Kung JS, Lopez OA, McCoy EE, Reicher S, Eysselein VE. Fluid genetic analyses predict the biological behavior of pancreatic cysts: three-year experience. JOP 2014; 15: 427-432 [PMID: 25262708 DOI: 10.6092/1590-8577/2426]
17 Del Chiaro M, Verbeke C, Salvia R, Klöppel G, Werner J, McKay C, Friess H, Manfredi R, Van Cutsem E, Löhr M, Segersvärd R. European experts consensus statement on cystic tumours of the pancreas. Dig Liver Dis 2013; 45: 703-711 [PMID: 23415799 DOI: 10.1016/j.dld.2013.01.010]
18 Arnelo U, Siiki A, Swahn F, Segersvärd R, Enochsson L, del
31 May 15, 2015|Volume 6|Issue 2|WJGP|www.wjgnet.com
Del Chiaro M et al . Cystic tumors of the pancreas: Opportunities and risks

Chiaro M, Lundell L, Verbeke CS, Löhr JM. Single-operator pancreatoscopy is helpful in the evaluation of suspected intraductal papillary mucinous neoplasms (IPMN). Pancreatology 2014; 14: 510-514 [PMID: 25287157 DOI: 10.1016/j.pan.2014.08.007]
19 Del Chiaro M, Albiin N, Segersvärd R. Enucleation of branch duct-IPMN in a transplant patient. Pancreatology 2013; 13: 312-313 [PMID: 23858563]
20 Fritz S, Klauss M, Bergmann F, Hackert T, Hartwig W, Strobel O, Bundy BD, Büchler MW, Werner J. Small (Sendai negative) branch-duct IPMNs: not harmless. Ann Surg 2012; 256: 313-320 [PMID: 22791105 DOI: 10.1097/SLA.0b013e31825d355f]
21 Del Chiaro M, Segersvärd R. The state of the art of robotic pancreatectomy. Biomed Res Int 2014; 2014: 920492 [PMID: 24982913 DOI: 10.1155/2014/920492]
P- Reviewer: Eysselein VE, Guo XZ, Sumi S S- Editor: Ji FF L- Editor: A E- Editor: Lu YJ
32 May 15, 2015|Volume 6|Issue 2|WJGP|www.wjgnet.com
Del Chiaro M et al . Cystic tumors of the pancreas: Opportunities and risks

antibiotics, corticosteroids, immunomodulators and biological agents. Before the use of anti-tumor necrosis factor (TNF)-α became available to patients with IBD, the risk for surgery within five years of diagnosis was very high, however, with anti-TNF-α treatment the risk of surgery has decreased significantly. In the pediatric population a remission in disease can be achieved by exclusive enteral nutrition. Exclusive enteral nutrition also has an important role in the improvement of nutritional status and maintained growth. In this review we summarize the current therapeutic treatments in CD. The progress in the treatment options and the development of new drugs has led to optimized tactics for achieving the primary clinical goals of therapy - induction and maintenance of remission while improving the patient’s growth and overall well-being.
Key words: Pediatric Crohn’s disease; Immunomodulators; Antibiotics; Nutrition; Anti-tumor necrosis factor; Steroids; 5-aminosalicylic acid
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Inflammatory bowel diseases are chronic relapsing diseases of the bowel, with an unknown etiology, rising incidence in the pediatric population, and increasing therapeutic options. The therapeutic goal has changed over the last decade towards accelerated step up or top down therapy with a goal of achieving mucosal healing and perhaps changing the disease course. In this review we discuss these therapeutic approaches.
Lahad A, Weiss B. Current therapy of pediatric Crohn’s disease. World J Gastrointest Pathophysiol 2015; 6(2): 33-42 Available from: URL: http://www.wjgnet.com/2150-5330/full/v6/i2/33.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i2.33
INTRODUCTIONInflammatory bowel disease (IBD) is a phrase widely
Current therapy of pediatric Crohn’s disease
Avishay Lahad, Batia Weiss, Pediatric Gastroenterology, Hepatology and Nutrition Unit, Edmond and Lily Safra Children’s Hospital, Sheba Medical Center, Tel Hashomer 52661, IsraelAvishay Lahad, Batia Weiss, Tel-Aviv University, Tel-Aviv 69978, Israel Author contributions: Lahad A and Weiss B wrote the paper.Conflict-of-interest: The authors declare that they have no competing interests.Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/Correspondence to: Avishay Lahad, MD, Pediatric Gastro-enterology, Hepatology and Nutrition Unit, Edmond and Lily Safra Children’s Hospital, Sheba Medical Center, Ramat Gan, Tel Hashomer 52661, Israel. [email protected]: +972-3-5305006 Fax: +972-3-5302883Received: July 24, 2014Peer-review started: July 24, 2014First decision: August 15, 2014Revised: November 3, 2014Accepted: March 30, 2015 Article in press: April 2, 2015Published online: May 15, 2015
AbstractInflammatory bowel diseases (IBD), including Crohn’s disease (CD) and ulcerative colitis, are chronic relapsing and remitting diseases of the bowel, with an unknown etiology and appear to involve interaction between genetic susceptibility, environmental factors and the immune system. Although our knowledge and understanding of the pathogenesis and causes of IBD have improved significantly, the incidence in the pediatric population is still rising. In the last decade more drugs and treatment option have become available including 5-aminosalicylate,
33 May 15, 2015|Volume 6|Issue 2|WJGP|www.wjgnet.com
MINIREVIEWS
World J Gastrointest Pathophysiol 2015 May 15; 6(2): 33-42ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i2.33
Avishay Lahad, Batia Weiss

used to describe a diverse group of chronic inflammatory conditions of the gastrointestinal tract, including of the colon and small intestine. The major types of IBD can be characterized as Crohn’s disease (CD) and ulcerative colitis (UC), and about 10%-15% of the patients are diagnosed as having indeterminate colitis (IC). IC is typically exemplified by clinical, endoscopic and histological findings comprising elements which classically characterize those of both CD and UC. However, the differentiating characteristics between CD and those of UC are usually obvious, the main difference between these two conditions being the location and type of inflammatory changes. Thus, although CD and UC are both the result of an inflammatory condition of the gut they are clearly distinguished by the location of the disease and by disease conduct. CD normally affects any part of the gastrointestinal tract (GI), from mouth to anus, with any number of “skip areas” representing macroscopically and microscopically normal mucosa. Furthermore, the inflammation in CD is typically transmural, extending from the mucosa to the serosa, occasionally associated with granulomas, and may affect all of the layers of the bowel wall. The transmural inflammation may lead to perforating, fistulazing complications and to a stricturing disease. In sharp contrast, UC is restricted to the colon and rectum areas while the inflammation in UC is normally only restricted to the mucosal layer of the colon[1].
The etiologies of IBD remain unclear and appear to involve interplay between genetic susceptibility, environmental factors and the immune system. It should be noted that the intestinal epithelium and the enteric immune system act as the main “defense” barriers between the gastrointestinal tract, enteric bacteria, food antigens and noxious compounds that pass through it. Therefore, the gut mechanism of “defense” comprises the epithelial cell layer, mucus-secreting goblet cells, lymphoid tissue such as Peyer’s patches, nonimmune system mediators and cells of the immune system including the innate and the adaptive cells and their secreted mediators. The chronic stimulation by the intestinal microbiota and food antigens requires tight control mechanisms. An activation of the innate immune response and excessive inflammatory reaction or impaired innate immune response (i.e, NOD2, ATG16L1) can lead to the development of IBD. It is thought that alterations in the gut microbial environment also contribute to inflammatory bowel disease either by causing inflammation or by altered the immune system[1-5].
In 20%-25% of IBD patients, the disease has developed early in life, i.e., in childhood and adolescence, about 80% of the pediatric patients are diagnosed in adolescence (i.e., 10-18 years old children). The incidence of CD continues to increase worldwide. CD has a higher incidence in industrialized countries and higher rates have been noted in countries residing in the north and west as compared to countries residing in the south and east.
CD in children and adolescents can exemplify many similarities to the disease in adults, however, there may be clinical and pathological findings that are specific to children/adolescents as compared to adults. This can lead to different and specific treatment options. For instance, there is a difference between young children, aged less than 10 years, and adolescents in the location of the disease. In younger children the disease is more prevalent as isolated colonic inflammation while in adolescents the disease is more commonly detected in the terminal ileum and ileocecal regions. Young children and young adolescents have the potential for growth impairment due to the chronic inflammation and the low food intake. Furthermore, children and adolescents with CD experience greater levels of distress, emotional stress and the disease impacts their psychological well-being and reduces their quality of life. Quality of life is typically reduced due to pain, vomiting, diarrhea, and other socially unacceptable symptoms.
In pediatric CD patients, the main objective of therapy has been to induce and maintain clinical remission while optimizing the patient’s growth and well-being. Every effort needs to be made to choose a therapy that is effective with minimal adverse effect and easiest to use. The appropriate treatment plan should be based on disease activity and severity, disease location (i.e., in the gastrointestinal tract), phenotypic behavior, the patient’s linear growth and the patient’s psychosocial condition. After remission is achieved, the patient is usually switched to a lighter therapy with fewer potential side effects. However, disease flare-ups may occur any time between several weeks to several years resulting in an acute reappearance of disease symptoms. Depending on the situation, the flare-up may disappear on their own or may require a more intense therapy.
The treatment options summarized herein are used by pediatric gastroenterologists and are extrapolated from adult trials. As such, most doses and dosing interval are based on pharmacokinetic in adults and may be slightly different in children and adolescents. Furthermore, the therapeutic recommendations depend on the disease conduct, location, severity and related complications and further should take into consideration the type of treatment required, e.g., treatment of an acute disease, induction of a clinical remission or maintenance of remission.
5-AMINOSALICYLATE AGENTS5-aminosalicylic acid (5-ASA) agents are used often to manage mild to moderate cases of CD. They are currently considered by many physicians as first line therapy in cases of mild to moderate CD and in maintenance of disease remission. Conversely, 5-ASA agents are less effective in induction of remission as illustrated in randomized double blind, placebo controlled studies which did not illustrate any advantage of using 5-ASA over placebo[6]. Moreover a Cochrane review published in 2011 illustrated the modest efficacy of sulfasalazine as compared to placebo
34 May 15, 2015|Volume 6|Issue 2|WJGP|www.wjgnet.com
Lahad A et al . Current therapy of pediatric CD

in treatment of mild to moderate CD[7]. Furthermore, only two clinical trials have been carried out with 5-ASA in children[8,9] and the dosing in pediatric patients is thus extrapolated from adult treatment. The most convincing evidence for a beneficial treatment with 5-ASA has been the use of sulfazaline in the treatment of active CD involving the colon[10]. It should be noted, however, that 5-ASA are frequently being used as they are considered to have less adverse events and have some protective effect against cancer.
5-ASA exploits their therapeutic effect within the lumen of the gastrointestinal tract and is believed to have multiple anti-inflammatory effects. As unprotected 5-ASA is rapidly absorbed in the upper gastrointestinal tract, several slow release preparations have been developed to permit entrance of 5-ASA to the terminal ileum and to the colon. Currently there are several oral preparations of 5-ASA agents which differ from each other in the location of their therapeutic efficacy. These agents include pH-dependent delayed release formulations (e.g., Mesalamine), slow release formulations and azo-bound pro-drugs (e.g., Sulfasalazine), the later needing colonic bacteria to break the azo-bound drug and “activate” the drug. Azo-bound pro-drugs should mainly be used in patients with predominantly colonic disease. Furthermore, topical formulations (e.g., suppository and enema) can be used to treat or control mucosal inflammation in proctitis[11].
ANTIBIOTICSAlterations in the gut microbial environment are believed to be one of the contributing factors to CD and to flare-ups. This has lead to the use of antibiotic therapy in mild to moderate disease[12]. Antibiotic therapy is frequently used for the treatment of perianal disease, e.g., fistulae, and abscess. The two main antibiotics currently being used for treatment of acute CD and flare-ups of CD comprise Metronidazole (10-20 mg/kg per day) and Ciprofloxacin (20 mg/kg per day), either as monotherapy or as combination therapy. In 2011 Kahan et al[13] published a systemic review and meta-analysis wherein they determined that treatment with antibiotics is superior to placebo in patients with active CD. Metronidazole may be more effective in patients with active colonic involvement[14] while Ciprofloxacin may be effective in the treatment of ileitis. Furthermore, a combination of the two antibiotics may be preferentially used for a better efficacy.
In the long run, however, the clinical efficacy of an-tibiotics appears to be inadequate, and the majority of patients will experience flares in their disease after discontinuing antibiotic therapy[15]. Furthermore, it is not expected that antibiotic therapy will result in a successful remission in patients with moderate to severe CD.
SYSTEMIC CORTICOSTEROIDS AND BUDESONIDE Corticosteroids comprise a general potent anti-inflammatory effect for the treatment of CD. The mechanism of action of corticosteroids remains to be determined, however, it is generally accepted that corticosteroids attach to a cell’s cytoplasmic receptor, as a complex they enter the nuclease to interact with glucocorticoid response components on the chromosomal DNA. Corticosteroids comprise a wide variety of anti-inflammatory influences including inhibition of the proliferation and recruitment of monocytes, macrophages and lymphocytes; inhibition of migration of neutrophils to sites of inflammation; and decreased production of inflammatory mediators including prostaglandins, cytokines and leukotrienes[16].
In CD patients, systemic corticosteroids are considered to be very effective in the treatment of active disease and in achieving clinical remission. Corticosteroids continue to be the basic treatment to control acute disease that has not responded to first line therapy (e.g., antibiotics and 5-ASA)[17]. As previously reported by Bousvaros et al[18], only a minority of patients responding clinically to corticosteroid therapy exhibit endoscopic mucosal healing. A paper published by Canani in 2006 teaches endoscopic improvement in 4 of 10 children treated with steroids however, none of the treated children showed mucosal healing[19]. Oral therapy (with prednisone) is typically initiated at a dose of 1-2 mg/kg per day with a maximal daily dose of 40-60 mg/d for 2 to 4 wk. Conventional corticosteroid therapy is commonly used for short term treatment of moderate to severe symptoms and is typically used for achieving a quick relief of symptoms. It is important to minimize the use of corticosteroids as long term use results in adverse effects including hypertension, glucose intolerance, bone osteopenia, cataracts, decreased linear growth and increased risk of infections. Therefore, once the patient has improved clinically the daily corticosteroid dose should be reduced slowly over an 8 to 10 wk period until complete discontinuation. The induction and the tapering time of steroids relies on the physician’s experience and the patient’s respond (as illustrated clinically and in laboratory tests)[20,21].
About 10%-20% of moderate to severe CD patients will not respond to oral corticosteroids and will need parenteral administration. In severe cases of CD, parenteral administration should be immediately recommended. Furthermore, approximately 30% of CD patients become dependent on corticosteroid treatment and dose reduction results in clinical flares[21,22]. Thus, alternative therapies should be considered to replace corticosteroid use.
Budesonide is a glucocorticoid steroid that demonstrates a high affinity for the intestinal glucocorticoid receptor, enhances hepatic first-pass metabolism and lowers the systemic corticosteroid absorption[23]. Budesonide
35 May 15, 2015|Volume 6|Issue 2|WJGP|www.wjgnet.com
Lahad A et al . Current therapy of pediatric CD

is known for its lower risk of systemic corticosteroid related complications due to its high topical activity and low systemic bioavailability (10%)[24]. Furthermore, budesonide is efficient in the treatment of mild to moderate CD locating to the ileum and/or ascending colon[10]. The starting dose of oral budesonide is 9 mg/d and it is typically reduced by 3 mg increments (i.e., to 6 mg/d followed by 3 mg/d) over several weeks. A Cochrane systemic review evaluating the efficacy of budesonide illustrated budesonide to be superior to placebo and mesalamine in induction of remission in CD patients after 8 wk of treatment[25]. In two pediatric trials the efficacy of budesonide in induced remission was 42%-55%[26,27]. Previous work illustrated that administration of a daily dose of 6 mg budesonide was not efficient in preventing relapse and was only efficient in maintaining remission for a period of several months[28]. Moreover, data from several small studies comparing treatment with prednisone to budesonide illustrated no superiority of budesonide over traditional corticosteroids[26,29,30]. In fact, prednisone may be more effective for inducing remission in patients who failed budesonide therapy. Therefore, the use of budesonide should be recommended in specific CD cases.
NUTRITIONGut rest and total parenteral nutrition (TPN) were discovered to be efficient for improved nutritional status and induced remission in children with CD[31]. Children with CD are at high risk of nutrition malabsorbtion and weight loss, therefore, special nutrition has two goals: first, to improve malabsorption and gain weight, and second, exclusive enteral nutrition (EEN) can induce remission in active disease. EEN is a special liquid formula which is administered as a sole nutrition without the addition of a regular diet. The EEN formula may contain whole proteins (polymeric) or modified proteins (e.g., elemental). The advantage of the polymeric formula over the elemental formula is the better compliance and less need for using nasogastric tube.
EEN can be administered at first diagnosis of CD[32], but may also be considered as a mode of treating CD relapse patients, however, its efficiency tends to decrease. In many pediatric European centers, children with CD are treated with EEN as the first line treatment, however, the use of EEN in North America is less common[33]. There are a few trials comparing EEN to steroids in induction of remission in CD. Their results illustrate that the rate of remission and mucosal healing with EEN is about 75%[20,34]. Some of these trials also demonstrate significantly higher mucosal healing with EEN as compared to steroids[19,35]. Wilschanski et al published in 2006 that nutritional therapy has a role in maintaining disease remission in pediatric patients with CD. The duration of remission is controversial, some trials show relapse after three months and others demonstrate remission for 2 years. It is advisable to initiate an immunomodulatory treatment early or
shortly after EEN to maintain remission[36]. The duration of exclusive feeding as treatment for induction of remission is typically 6 to 8 wk[37]. Towards the end of the exclusive feeding period, reintroduction of regular diet should be started gradually over a period of several weeks. However, if exclusive nutrition does not induce clinical improvement after 2 wk or if disease activity is aggravated it is advisable to initiate other treatment options.
Monitoring nutrition is an important part of handling children with CD. As mentioned, children with CD, are at high risk of nutrient malabsorbtion and growth impairment. Deficiencies of iron, vitamin B12, folic acid, vitamin D, zinc, impaired calcium absorption all need to be monitored. Many children with CD need enhanced caloric intake due to disease activity, and therefore may need about 120% reference nutrient intake to overcome nutrient deficiencies and for normal growth[38]. Furthermore, administration of any deficient micronutrient and/or daily multivitamin supplements is advisable in all pediatric CD patients.
IMMUNOMUDOLATOR AGENTS Following an induction of remission with EEN or with corticosteroids, as mentioned above, maintaining remission may be carried out by administration of immunomodulatory drugs.
Azathioprine and 6-mercaptopurine The immunomodulatory drugs azathioprine (AZA) and 6-mercaptopurine (6-MP) are closely related chemical compounds classified as thiopurine anti-metabolites. AZA is a prodrug that is quickly converted to 6-MP via a nonenzymatic reaction following administration. 6-MP is subsequently metabolized to its active metabolite 6-thioguanine (6-TG) through a series of reactions.
The clinical effects of AZA and 6-MP are probably indistinguishable, although their exact form of action is still unclear. Both AZA and 6-MP inhibit inflammatory response in several ways including inhibition of pathways in the nucleic acid biosynthesis and by causing damage to DNA through the integration of thiopurine analogues. AZA and 6-MP are further known to alter lymphocyte function, interfere with clonal expansion, reduce the number of lamina propria plasma cells and affect natural killer cell function[39].
AZA and 6-MP are both slow acting drugs, which is why clinical efficacy cannot be expected until 8 to 12 wk or even months after initiation of treatment. After induction of remission with prednisone, the use of AZA and 6-MP demonstrated maintained remission in a higher rate compared to placebo in CD patients. In the known trial of Markowitz et al[40], adolescents who were randomized to 6-MP after induction of remission by steroids, were more likely to remain in steroid free remission with 6-MP maintenance treatment over an eighteen months follow-up than the placebo group. Also the relapse rate was significantly lower with
36 May 15, 2015|Volume 6|Issue 2|WJGP|www.wjgnet.com
Lahad A et al . Current therapy of pediatric CD

6-MP as compared to placebo treatment. A Cochrane review assessing seven trials of AZA illustrate that the use of AZA is associated with decreased rates of hospitalization and surgery and with decreased use of corticosteroids. Moreover, higher doses of AZA (2.5 mg/kg per day) were more effective than lower dose of AZA (1 mg/kg per day or 2 mg/kg per day) for decreased flare-ups of the disease[41]. Today, AZA and 6-MP are the most commonly used immunomodulatory drugs in the treatment of CD due to their steroid sparing effect and in maintained remission.
The general guidelines for weight-based dosing of thiopurines, based on clinical trials, demonstrated efficacy for AZA at 2-2.5 mg/kg per day and 6-MP at 1-1.5 mg/kg per day. It is recommended to initiate therapy at low doses and escalate dosing within several weeks.
Severe adverse effects of AZA and 6-MP include bone marrow suppression, leukopenia, acute pancreatitis and hepatitis. In addition, other adverse effects include dizziness, diarrhea, fatigue, skin rashes and increased risk of infections. Therefore, regular blood count checkups are advisable during treatment. If leukopenia occurs or if there is an increase in liver function test, discontinuation or tapering AZA/6-MP treatment is recommended until white blood cell count and liver enzymes normalize. Then, treatment should commence with lower dose. In cases of pancreatitis, it is recommended to discontinue treatment and alternate to other treatment options. Other serious but rare side effects of long term AZA and 6-MP treatment include the development of malignancies including the uncommon Hepatosplenic T cell lymphoma (HSTCL) and non Hodgkin lymphoma[42]. In a single center long-term follow-up, patients with CD who responded to AZA had an increased risk of malignancies twice that of patients who did not receive AZA[43].
AZA and 6-MP are prodrugs that metabolize to the active drug, while thiopurine S-methyltransferase (TPMT) is a rate limiting enzyme involved in AZA/6-MP metabolism. Genetic polymorphisms of TPMT lead to decreased methylation and decreased inactivation of 6-MP which can result in life threatening bone marrow suppression. An assay of TPMT in red blood cells or a TPMT gene test can avoid this complication. Therefore, it is most advisable to check the TPMT enzyme levels or activity prior to initiation of treatment with AZA or 6-MP. If assessing TPMT enzyme levels or activity is not possible, one should start with low dose AZA/6-MP and check complete blood count within seven days of treatment and increase the dose gradually every 1 to 2 wk[44,45].
Combination therapy comprising AZA/6-MP with 5-ASA can be used to increase treatment efficacy. Specifically, 5-ASA therapy can inhibit TPMT activity and thereby increase the potential for 6-TG[46].
AZA and 6-MP are among a small number of treatments of CD that have been demonstrated to clinical remission as well as induce mucosal healing[47].
MethotrexateThe immunomodulatory drug methotrexate (MTX) is an antimetabolite and antifolate drug. MTX is a folic acid antagonist that inhibits purine synthesis, DNA and RNA formation, and eventually inhibits the S phase of the cell cycle. MTX also has multiple anti-inflammatory effects including decreased pro-inflammatory cytokine production and lymphocyte apoptosis.
MTX has been used as an immunomodulatory drug in the treatment of several other autoimmune disorders including lupus and rheumatoid arthritis. It is still not widely used for the treatment of CD mostly due to the need for parenteral administration (intramuscular or subcutaneous) and due to concerns about it’s possible toxicity (e.g., liver fibrosis, hypersensitivity pneumonitis, and teratogenicity). However, while thiopurines remain the most widely used immunomodulatory drugs, there is a need for alternative drugs such as MTX, especially for the 10%-20% of patients who cannot tolerate these drugs.
In placebo-controlled studies in adult CD patients, remission and maintenance was achieved after MTX administration as a dose of 25 mg intramuscularly per week (for remission) and 15 mg intramuscularly per week for maintenance. Significantly more remained in remission on MTX (65%) as compared to placebo (39%)[48-50]. Deducing these adult studies to pediatric patients, MTX should be administered at a dose of 15 mg/m2 per week with a maximum of 25 mg per week. A few pediatric trials demonstrated induction and maintenance of remission of 40%-60% at six months and at a lower rate at twelve months[51-53]. In a retrospective analysis, Turner et al[54] demonstrated that 42% of 60 patients that did not respond to AZA/6-MP achieved and maintain remission when administered MTX therapy.
MTX can be administered by an intramuscular injection or subcutaneously, the effective dose of MTX is 15 mg/m2 weekly with a maximal dose of 25 mg. Supplement of 5 mg folate 2 d after administration of MTX is advisable to reduce the adverse events[50].
Typically patients respond to parenteral MTX treatment within 3 to 4 wk and treatment should continue for at least four to six months. Responders to treatment may then alternate to oral dosing[52], and the lowest effective dose should be maintained. However, if patients relapse on oral treatment, it is advisable to switch from oral treatment back to parenteral administration or alternatively to increase dosing[53].
In low doses, MTX is generally a safe and well tolerated drug. Some side effects such as fatigue, hair loss, diarrhea, nausea, anorexia, headaches, and skin pigmentation are common. However adverse effects, which should be monitored more closely, include bone marrow toxicity, hepatitis and pulmonary disease. Supplemental folate can diminish the severity and the incidence of these adverse effects[54].
37 May 15, 2015|Volume 6|Issue 2|WJGP|www.wjgnet.com
Lahad A et al . Current therapy of pediatric CD

BIOLOGIC AGENTS (ANTI-TUMOR NECROSIS FACTOR THERAPY)Tumor necrosis factor (TNF), also known as TNF-α, is a monocyte-derived pro-inflammatory cytokine that has diverse pro-inflammatory effects within the intestinal mucosa and is a pivotal cytokine in the inflammatory cascade. TNF-α been implicated in various autoimmune diseases including rheumatoid arthritis and psoriasis and has emerged as a key cytokine involved in pathogenesis of CD. Consequently, constant efforts have been made to control TNF-α’s harmful effects in CD. Anti-TNF antibodies neutralize this pro-inflammatory cytokine and thus interrupt the inflammatory cascade.
So far two anti-TNF agents have been approved by the FDA and EMA for the induction of remission and maintenance of remission in CD: infliximab (IFX) and adalimumab (ADA). These monoclonal antibodies differ in their structure and in their mode of administration.
IFX (trade name Remicade) is a chimeric IgG1 monoclonal antibody against TNF-α comprising 75% human and 25% murine sequences. IFX is typically used for the treatment of patients with moderately to severely acute CD and patients with fistulizing CD, who have had an inadequate response to conventional therapy. IFX is also recommended as primary induction therapy for patients with penetrating disease.
ADA (trade name Humira) is a complete human recombinant human IgG1 monoclonal antibody directed against TNF-α. ADA is typically used to decrease signs and symptoms of CD, and to achieve and maintain clinical remission in patients with moderate to severe acute luminal CD who have not responded well to conventional treatments. ADA is also used to treat patients who have lost response to IFX, are unable to tolerate or have an allergic to IFX.
ACCENT I, a large multicenter randomized, double blind trial, clearly demonstrated a statistically significant improvement in the response and remission rates of adult patients who were treated with a scheduled IFX maintenance therapy. These patients further showed a higher rate of free steroid remission at 54 wk and fewer hospitalizations and surgeries[55,56]. In adults with moderate to severe CD it was demonstrated that IFX is effective in induction and maintenance of remission[57]. In pediatric patients, a multi-center international study (REACH) demonstrated that 88% of children with acute CD who were treated with IFX achieved response and 60% were in clinical remission at 54 wk. REACH study also demonstrated the efficacy of IFX in maintaining remission in patients receiving IFX every 8 wk[58].
IFX is administered via an intravenous infusion at a dose of 5 mg/kg at zero, 2 and 6 wk followed by maintenance infusions every 8 wk. Dose of IFX may be increased to 10 mg/kg as needed. Dose escalation (to 10 mg/kg) and/or interval shortening (from 8 wk to 6 wk or 4 wk) may be implemented as needed[59].
In adults, the efficacy of ADA was first evaluated
in the CLASSIC Ⅰ study. This study demonstrated that ADA can be used for the induction of remission in moderate to severe CD[59]. The CLASSIC Ⅱ study demonstrated clinical remission at 56 wk in 88% of patients who maintained ADA treatment every other week[60], similar results have been demonstrated in the CHARM study[61,62]. In pediatrics patients, a few studies demonstrate the efficacy of ADA in inducing and maintaining remission in acute CD. The efficacy of ADA treatment was also illustrated after treatment failure with IFX[57,63-65].
ADA is administered via subcutaneous injection at an initial injection of 160 mg followed by a 80 mg dose given 2 wk later, initiation of maintenance is administered 2 wk later at a dose of 40 mg followed by maintenance treatment every 2 wk at a dose of 40 mg.
Typically patients respond to anti-TNF therapy within a few days to 3 wk. It should be noted that therapy with anti-TNF antibodies, IFX and ADA, has been proven effective in achieving mucosal healing with a more rapid effect compared to immumomodulants.
Adverse effects of anti-TNF therapy, including IFX and ADA, include increased risk for serious infections including hepatitis, tuberculosis (TB) and unusual infections caused by viruses, fungi, bacteria, and other opportunistic infections. Anti-TNF therapy is also associated with allergic reactions and new or worsening psoriasis. Anti-TNF therapy also increases the risk of lymphoma, such as the extremely rare HSTCL, in adolescents and young adults primarily in male patients. The risk of HSTCL increases in patients being treated with anti-TNF therapy in combination with thiopurines (e.g., azathioprine and/or mercaptopurine). Therefore, the benefits of such a combination therapy must be weight against the risk of HSTCL in young patients, especially in males[65-67].
Due to these adverse effects, every patient must be tested before initiation of anti-TNF therapy for hepatitis B, tuberculosis (TB) and varicella. It is advisable to begin anti-TNF therapy only after proper immunization of the patients.
It is advisable that patients with sustained remission will continue with their scheduled anti-TNF therapy. In case the patients were previously immunemodulator naïve they may be switched to an immunomodulatory drug. Moreover, discontinuing anti-TNF therapy may be considered in cases of longstanding sustained remission.
As mentioned, ADA and IFX are the only two biological drugs which were approved for the treatment of Crohn’s disease in pediatric patients. Currently there are two additional biological drugs that have been used off-label for the treatment of Crohn’s disease in patients who do not respond to ADA and IFX.
The first of these off-label drugs is Certolizumab pegol (CZP) (trade name Cimzia), a monoclonal antibody to TNF-α, which comprises the Fab portion of the antibody conjugated to a polyethylene glycol (PEG) moiety, which prolongs the drug’s half-life. The fact that Certolizumab pegol lacks an Fc region minimizes
38 May 15, 2015|Volume 6|Issue 2|WJGP|www.wjgnet.com
Lahad A et al . Current therapy of pediatric CD

potential Fc-mediated effects such as complement-dependent cytotoxicity (CDC) or antibody dependent cell-mediated cytotoxicity (ADCC). Four different studies (PRECiSE 1-4) were performed to evaluate the effectiveness of Certolizumab in CD patients. The PRECiSE studies illustrate that Certolizumab pegol administered subcutaneously at a dosage of 400 mg at weeks 0, 2 and 4 and every 4 wk afterwards (at the same dosage) significantly improved the patient’s response rates in comparison with placebo, and to a lesser extent improved remission rates. However, from these studies it is evident that administration of Certolizumab is much more efficient in achieving remission in patients receiving treatment within one year of diagnosis and the efficacy of Certolizumab is more pronounced in patients receiving it as a first anti-TNF-α treatment as compared to a prior infliximab therapy. Furthermore, remission rates decrease as administration of Certo-lizumab is postponed[68-71].
The second drug, Vedolizumab (VDZ) (trade name Entyvio), is a humanized monoclonal antibody to integrin α4β7. VDZ attaches to the integrin α4β7, a mucosal vascular addressin cell adhesion molecule 1 (MAdCAM-1). MAdCAM-1 is typically expressed on the endothelium of venules in the lamina propria of the small intestine and colon, as well as in Peyer’s patches[72]. The attachment of VDZ to integrin α4β7 inhibits adhesion and migration
of leukocytes into the gastrointestinal tract. The GEMINI 2 study illustrates that administration of vedolizumab (VDZ) at a dose of 300 mg at weeks 0 and 2 and afterwards every 8 wk demonstrates remission of Crohn’s disease. In the GEMINI 3 study, patients with previous failure to TNF-α antagonist treatment were recruited to assess the efficacy of VDZ treatment. The primary endpoint of clinical remission at week 6 in the population tested was not met. However, secondary endpoints, including clinical remission at week 10 and clinical response at week 6 and week 10, were partially met. This finding implies a modest effect and slow onset of action of VDZ in active CD. VDZ treatment has a better remission rate in Ulcerative colitis as compared to Crohn’s disease[73,74].
CONCLUSIONIn conclusion, we summarize herein the current treatments for pediatric Crohn’s disease and describe the risk and benefits of each (Figures 1 and 2). While 30 years ago only 2 medications were commonly utilized for the treatment of Crohn’s disease, currently there are more than 15 different therapeutic options of various efficacies and potencies. It should be appreciated that in children as well as in adults CD encompasses a varied range of disease phenotypes and severities and therefore optimal patient selection, timing and therapy requires clinical judgment.
Our knowledge and understanding of CD, its causes and pathogenesis is improving significantly alongside improvement in treatment options. In the near future, we may recognize more specific causes of the disease which will ultimately result in more specific therapeutics.
Although CD is incurable its adverse effects on health and quality of life can be considerably improved by appropriate treatment. Thus, pediatric patients who would otherwise experience chronic illness, symptoms, poor growth and reduced quality of life can benefit from early introduction of proper therapy and may become healthy and thriving. Clinical response is anticipated in pediatric patients but attention must be paid to
39 May 15, 2015|Volume 6|Issue 2|WJGP|www.wjgnet.com
Mild
Moderate
Severe
AminosalicylateAntibioticNutritional therapyBudesonide
Nutritional therapyBudesonideSystemic steroidsMethotrexateThiopurins
I.V steroidsAnti TNF αSurgery
Antibiotics
Anti TNF α
Surgery procedure
Perianal/fistulating disease
Figure 1 Medication used in the treatment of pediatric Crohn’s disease. I.V: Intravenous; TNF: Tumor necrosis factor.
Maintenance
AZA/6-MP
Aminosalicylates
Anti TNF α
Methotrexate
Figure 2 Medication for maintenance of remission. TNF: Tumor necrosis factor; AZA: Azathiopurine; 6-MP: 6-mercaptopurine.
Lahad A et al . Current therapy of pediatric CD

maintaining it to decreasing adverse events.
REFERENCES1 Abraham C, Cho JH. Inflammatory bowel disease. N Engl J
Med 2009; 361: 2066-2078 [PMID: 19923578 DOI: 10.1056/NEJMra0804647]
2 Gersemann M, Wehkamp J, Fellermann K, Stange EF. Crohn‘s disease--defect in innate defence. World J Gastroenterol 2008; 14: 5499-5503 [PMID: 18810765 DOI: 10.3748/wjg.14.5499]
3 Wallace KL, Zheng LB, Kanazawa Y, Shih DQ. Immunopathology of inflammatory bowel disease. World J Gastroenterol 2014; 20: 6-21 [PMID: 24415853 DOI: 10.3748/wjg.v20.i1.6]
4 Glocker E, Grimbacher B. Inflammatory bowel disease: is it a primary immunodeficiency? Cell Mol Life Sci 2012; 69: 41-48 [PMID: 21997382 DOI: 10.1007/s00018-011-0837-9]
5 Andreu-Ballester JC, Amigó-García V, Catalán-Serra I, Gil-Borrás R, Ballester F, Almela-Quilis A, Millan-Scheiding M, Peñarroja-Otero C. Deficit of gammadelta T lymphocytes in the peripheral blood of patients with Crohn’s disease. Dig Dis Sci 2011; 56: 2613-2622 [PMID: 21374064 DOI: 10.1007/s10620-011-1636-8]
6 Hanauer SB, Strömberg U. Oral Pentasa in the treatment of active Crohn’s disease: A meta-analysis of double-blind, placebo-controlled trials. Clin Gastroenterol Hepatol 2004; 2: 379-388 [PMID: 15118975 DOI: 10.1016/S1542-3565(04)00122-3]
7 Ford AC, Kane SV, Khan KJ, Achkar JP, Talley NJ, Marshall JK, Moayyedi P. Efficacy of 5-aminosalicylates in Crohn’s disease: systematic review and meta-analysis. Am J Gastroenterol 2011; 106: 617-629 [PMID: 21407190 DOI: 10.1038/ajg.2011.71]
8 Griffiths A, Koletzko S, Sylvester F, Marcon M, Sherman P. Slow-release 5-aminosalicylic acid therapy in children with small intestinal Crohn’s disease. J Pediatr Gastroenterol Nutr 1993; 17: 186-192 [PMID: 8229546 DOI: 10.1097/00005176-199308000-00010]
9 Cezard JP, Munck A, Mouterde O, Morali A, Lenaerts C, Lachaux A, Turck D, Schmitz J, Maurage C, Girardet JP, Belli D, Lamireau T, Sarles J, Chouraqui JP, Descos B, Dabadi A, Meyer M, Olives JP, Mary JY. Prevention of relapse by mesalazine (Pentasa) in pediatric Crohn’s disease: a multicenter, double-blind, randomized, placebo-controlled trial. Gastroenterol Clin Biol 2009; 33: 31-40 [PMID: 19118966 DOI: 10.1016/j.gcb.2008.07.007]
10 Lichtenstein GR, Hanauer SB, Sandborn WJ. Management of Crohn‘s disease in adults. Am J Gastroenterol 2009; 104: 465-483; quiz 464, 484 [PMID: 19174807 DOI: 10.1038/ajg.2008.168]
11 Desreumaux P, Ghosh S. Review article: mode of action and delivery of 5-aminosalicylic acid - new evidence. Aliment Pharmacol Ther 2006; 24 Suppl 1: 2-9 [PMID: 16939423 DOI: 10.1111/j.1365-2036.2006.03069.x]
12 Friswell M, Campbell B, Rhodes J. The role of bacteria in the pathogenesis of inflammatory bowel disease. Gut Liver 2010; 4: 295-306 [PMID: 20981205 DOI: 10.5009/gnl.2010.4.3.295]
13 Khan KJ, Ullman TA, Ford AC, Abreu MT, Abadir A, Marshall JK, Talley NJ, Moayyedi P. Antibiotic therapy in inflammatory bowel disease: a systematic review and meta-analysis. Am J Gastroenterol 2011; 106: 661-673 [PMID: 21407187 DOI: 10.1038/ajg.2011.72]
14 Ursing B, Alm T, Bárány F, Bergelin I, Ganrot-Norlin K, Hoevels J, Huitfeldt B, Järnerot G, Krause U, Krook A, Lindström B, Nordle O, Rosén A. A comparative study of metronidazole and sulfasalazine for active Crohn’s disease: the cooperative Crohn’s disease study in Sweden. II. Result. Gastroenterology 1982; 83: 550-562 [PMID: 6124474]
15 Hildebrand H, Berg NO, Hoevels J, Ursing B. Treatment of Crohn’s disease with metronidazole in childhood and adolescence. Evaluation of a six months trial. Gastroenterol Clin Biol 1980; 4: 19-25 [PMID: 6989700]
16 Katz JA. Treatment of inflammatory bowel disease with corticosteroids. Gastroenterol Clin North Am 2004; 33: 171-189, vii [PMID: 15177533 DOI: 10.1016/j.gtc.2004.02.002]
17 Faubion WA, Loftus EV, Harmsen WS, Zinsmeister AR, Sandborn
WJ. The natural history of corticosteroid therapy for inflammatory bowel disease: a population-based study. Gastroenterology 2001; 121: 255-260 [PMID: 11487534 DOI: 10.1053/gast.2001.26279]
18 Bousvaros A. Mucosal healing in children with Crohn’s disease: appropriate therapeutic goal or medical overkill? Inflamm Bowel Dis 2004; 10: 481-483 [PMID: 15475762 DOI: 10.1097/00054725-200407000-00025]
19 Berni Canani R, Terrin G, Borrelli O, Romano MT, Manguso F, Coruzzo A, D’Armiento F, Romeo EF, Cucchiara S. Short- and long-term therapeutic efficacy of nutritional therapy and corticosteroids in paediatric Crohn’s disease. Dig Liver Dis 2006; 38: 381-387 [PMID: 16301010 DOI: 10.1016/j.dld.2005.10.005]
20 Wilson DC, Thomas AG, Croft NM, Newby E, Akobeng AK, Sawczenko A, Fell JM, Murphy MS, Beattie RM, Sandhu BK, Mitton SG, Casson D, Elawad M, Heuschkel R, Jenkins H, Johnson T, Macdonald S, Murch SH. Systematic review of the evidence base for the medical treatment of paediatric inflammatory bowel disease. J Pediatr Gastroenterol Nutr 2010; 50 Suppl 1: S14-S34 [PMID: 20081542 DOI: 10.1097/MPG.0b013e3181c92caa]
21 Benchimol EI, Seow CH, Steinhart AH, Griffiths AM. Traditional corticosteroids for induction of remission in Crohn’s disease. Cochrane Database Syst Rev 2008; (2): CD006792 [PMID: 18425970 DOI: 10.1002/14651858.CD006792]
22 Lichtenstein GR. Approach to corticosteroid-dependent and corticosteroid-refractory Crohn‘s disease. Inflamm Bowel Dis 2001; 7 Suppl 1: S23-S29 [PMID: 11380040 DOI: 10.1002/ibd.3780070506]
23 McKeage K, Goa KL. Budesonide (Entocort EC Capsules): a review of its therapeutic use in the management of active Crohn’s disease in adults. Drugs 2002; 62: 2263-2282 [PMID: 12381231 DOI: 10.2165/00003495-200262150-00015]
24 Dignass A, Van Assche G, Lindsay JO, Lémann M, Söderholm J, Colombel JF, Danese S, D’Hoore A, Gassull M, Gomollón F, Hommes DW, Michetti P, O’Morain C, Oresland T, Windsor A, Stange EF, Travis SP. The second European evidence-based Consensus on the diagnosis and management of Crohn’s disease: Current management. J Crohns Colitis 2010; 4: 28-62 [PMID: 21122489 DOI: 10.1016/j.crohns.2009.12.002]
25 Kuenzig ME, Rezaie A, Seow CH, Otley AR, Steinhart AH, Griffiths AM, Kaplan GG, Benchimol EI. Budesonide for maintenance of remission in Crohn’s disease. Cochrane Database Syst Rev 2014; 8: CD002913 [PMID: 25141071 DOI: 10.1002/14651858.CD002913.pub3]
26 Levine A, Weizman Z, Broide E, Shamir R, Shaoul R, Pacht A, Dinari G, On A, Weiss B, Bujanover Y. A comparison of budesonide and prednisone for the treatment of active pediatric Crohn disease. J Pediatr Gastroenterol Nutr 2003; 36: 248-252 [PMID: 12548062 DOI: 10.1097/00005176-200302000-00017]
27 Escher JC. Budesonide versus prednisolone for the treatment of active Crohn’s disease in children: a randomized, double-blind, controlled, multicentre trial. Eur J Gastroenterol Hepatol 2004; 16: 47-54 [PMID: 15095852 DOI: 10.1097/00042737-200401000-00008]
28 Sandborn WJ, Löfberg R, Feagan BG, Hanauer SB, Campieri M, Greenberg GR. Budesonide for maintenance of remission in patients with Crohn’s disease in medically induced remission: a predetermined pooled analysis of four randomized, double-blind, placebo-controlled trials. Am J Gastroenterol 2005; 100: 1780-1787 [PMID: 16086715 DOI: 10.1111/j.1572-0241.2005.41992.x]
29 Levine A, Broide E, Stein M, Bujanover Y, Weizman Z, Dinari G, Pacht A, Branski D, Zahavi I. Evaluation of oral budesonide for treatment of mild and moderate exacerbations of Crohn’s disease in children. J Pediatr 2002; 140: 75-80 [PMID: 11815767 DOI: 10.1067/mpd.2002.119992]
30 Benchimol EI, Seow CH, Otley AR, Steinhart AH. Budesonide for maintenance of remission in Crohn’s disease. Cochrane Database Syst Rev 2009; (1): CD002913 [PMID: 19160212 DOI: 10.1002/14651858.CD002913.pub2]
31 Strobel CT, Byrne WJ, Ament ME. Home parenteral nutrition in children with Crohn’s disease: an effective management alternative. Gastroenterology 1979; 77: 272-279 [PMID: 109347]
40 May 15, 2015|Volume 6|Issue 2|WJGP|www.wjgnet.com
Lahad A et al . Current therapy of pediatric CD

32 Heuschkel RB, Menache CC, Megerian JT, Baird AE. Enteral nutrition and corticosteroids in the treatment of acute Crohn‘s disease in children. J Pediatr Gastroenterol Nutr 2000; 31: 8-15 [PMID: 10896064 DOI: 10.1097/00005176-200007000-00005]
33 Buchanan E, Gaunt WW, Cardigan T, Garrick V, McGrogan P, Russell RK. The use of exclusive enteral nutrition for induction of remission in children with Crohn’s disease demonstrates that disease phenotype does not influence clinical remission. Aliment Pharmacol Ther 2009; 30: 501-507 [PMID: 19549288 DOI: 10.1111/j.1365-2036.2009.04067.x]
34 Day AS, Whitten KE, Sidler M, Lemberg DA. Systematic review: nutritional therapy in paediatric Crohn’s disease. Aliment Pharmacol Ther 2008; 27: 293-307 [PMID: 18045244 DOI: 10.1111/j.1365-2036.2007.03578.x]
35 Borrelli O, Cordischi L, Cirulli M, Paganelli M, Labalestra V, Uccini S, Russo PM, Cucchiara S. Polymeric diet alone versus corticosteroids in the treatment of active pediatric Crohn’s disease: a randomized controlled open-label trial. Clin Gastroenterol Hepatol 2006; 4: 744-753 [PMID: 16682258 DOI: 10.1016/j.cgh.2006.03.010]
36 Vernier-Massouille G, Balde M, Salleron J, Turck D, Dupas JL, Mouterde O, Merle V, Salomez JL, Branche J, Marti R, Lerebours E, Cortot A, Gower-Rousseau C, Colombel JF. Natural history of pediatric Crohn’s disease: a population-based cohort study. Gastroenterology 2008; 135: 1106-1113 [PMID: 18692056 DOI: 10.1053/j.gastro.2008.06.079]
37 Whitten KE, Rogers P, Ooi CY, Day AS. International survey of enteral nutrition protocols used in children with Crohn’s disease. J Dig Dis 2012; 13: 107-112 [PMID: 22257479 DOI: 10.1111/j.1751-2980.2011.00558]
38 Sandhu BK, Fell JM, Beattie RM, Mitton SG, Wilson DC, Jenkins H. Guidelines for the management of inflammatory bowel disease in children in the United Kingdom. J Pediatr Gastroenterol Nutr 2010; 50 Suppl 1: S1-13 [PMID: 20081543 DOI: 10.1097/MPG.0b013e3181c92c53]
39 Nielsen OH, Vainer B, Rask-Madsen J. Review article: the treatment of inflammatory bowel disease with 6-mercaptopurine or azathioprine. Aliment Pharmacol Ther 2001; 15: 1699-1708 [PMID: 11683683 DOI: 10.1046/j.1365-2036.2001.01102.]
40 Markowitz J, Grancher K, Kohn N, Lesser M, Daum F. A multicenter trial of 6-mercaptopurine and prednisone in children with newly diagnosed Crohn’s disease. Gastroenterology 2000; 119: 895-902 [PMID: 11040176 DOI: 10.1053/gast.2000.18144]
41 Prefontaine E, Sutherland LR, Macdonald JK, Cepoiu M. Azathioprine or 6-mercaptopurine for maintenance of remission in Crohn’s disease. Cochrane Database Syst Rev 2009; (1): CD000067 [PMID: 19160175 DOI: 10.1002/14651858.CD000067.pub2]
42 Kotlyar DS, Osterman MT, Diamond RH, Porter D, Blonski WC, Wasik M, Sampat S, Mendizabal M, Lin MV, Lichtenstein GR. A systematic review of factors that contribute to hepatosplenic T-cell lymphoma in patients with inflammatory bowel disease. Clin Gastroenterol Hepatol 2011; 9: 36-41.e1 [PMID: 20888436 DOI: 10.1016/j.cgh.2010.09.016]
43 Camus M, Seksik P, Bourrier A, Nion-Larmurier I, Sokol H, Baumer P, Beaugerie L, Cosnes J. Long-term outcome of patients with Crohn’s disease who respond to azathioprine. Clin Gastroenterol Hepatol 2013; 11: 389-394 [PMID: 23142207 DOI: 10.1016/j.cgh.2012.10.038]
44 Weinshilboum RM, Sladek SL. Mercaptopurine pharmacogenetics: monogenic inheritance of erythrocyte thiopurine methyltransferase activity. Am J Hum Genet 1980; 32: 651-662 [PMID: 7191632]
45 Reuther LO, Sonne J, Larsen N, Dahlerup JF, Thomsen OO, Schmiegelow K. Thiopurine methyltransferase genotype distribution in patients with Crohn’s disease. Aliment Pharmacol Ther 2003; 17: 65-68 [PMID: 12492733 DOI: 10.1046/j.1365-2036.2003.01403]
46 Szumlanski CL, Weinshilboum RM. Sulphasalazine inhibition of thiopurine methyltransferase: possible mechanism for interaction with 6-mercaptopurine and azathioprine. Br J Clin Pharmacol 1995; 39: 456-459 [PMID: 7640156 DOI: 10.1111/j.1365-2125.1995.tb04478.x]
47 D'Haens G. Mucosal healing in pediatric Crohn’s disease: the goal
of medical treatment. Inflamm Bowel Dis 2004; 10: 479-480 [PMID: 15475761 DOI: 10.1097/00054725-200407000-00024]
48 Hawthorne AB. Methotrexate: a useful alternative in Crohn’s disease? Gut 2001; 49: 9-10 [PMID: 11413103 DOI: 10.1136/gut.49.1.9]
49 Alfadhli AA, McDonald JW, Feagan BG. Methotrexate for induction of remission in refractory Crohn’s disease. Cochrane Database Syst Rev 2005; (1): CD003459 [PMID: 15674908 DOI: 10.1002/14651858.CD003459.pub2]
50 Patel V, Macdonald JK, McDonald JW, Chande N. Methotrexate for maintenance of remission in Crohn’s disease. Cochrane Database Syst Rev 2009; (4): CD006884 [PMID: 19821390 DOI: 10.1002/14651858.CD006884.pub2]
51 Uhlen S, Belbouab R, Narebski K, Goulet O, Schmitz J, Cézard JP, Turck D, Ruemmele FM. Efficacy of methotrexate in pediatric Crohn’s disease: a French multicenter study. Inflamm Bowel Dis 2006; 12: 1053-1057 [PMID: 17075346 DOI: 10.1097/01.mib.0000235103.47280.bb]
52 Weiss B, Lerner A, Shapiro R, Broide E, Levine A, Fradkin A, Bujanover Y. Methotrexate treatment in pediatric Crohn disease patients intolerant or resistant to purine analogues. J Pediatr Gastroenterol Nutr 2009; 48: 526-530 [PMID: 19412004 DOI: 10.1097/MPG.0b013e318196df3e]
53 Willot S, Noble A, Deslandres C. Methotrexate in the treatment of inflammatory bowel disease: an 8-year retrospective study in a Canadian pediatric IBD center. Inflamm Bowel Dis 2011; 17: 2521-2526 [PMID: 21337668 DOI: 10.1002/ibd.21653]
54 Turner D, Grossman AB, Rosh J, Kugathasan S, Gilman AR, Baldassano R, Griffiths AM. Methotrexate following unsuccessful thiopurine therapy in pediatric Crohn’s disease. Am J Gastroenterol 2007; 102: 2804-2812; quiz 2803, 2813 [PMID: 18042110 DOI: 10.1111/j.1572-0241.2007.01474]
55 Hanauer SB, Feagan BG, Lichtenstein GR, Mayer LF, Schreiber S, Colombel JF, Rachmilewitz D, Wolf DC, Olson A, Bao W, Rutgeerts P. Maintenance infliximab for Crohn’s disease: the ACCENT I randomised trial. Lancet 2002; 359: 1541-1549 [PMID: 12047962 DOI: 10.1016/S0140-6736(02)08512-4]
56 Hanauer SB, Wagner CL, Bala M, Mayer L, Travers S, Diamond RH, Olson A, Bao W, Rutgeerts P. Incidence and importance of antibody responses to infliximab after maintenance or episodic treatment in Crohn’s disease. Clin Gastroenterol Hepatol 2004; 2: 542-553 [PMID: 15224278 DOI: 10.1016/S1542-3565(04)00238-1]
57 Hyams JS, Griffiths A, Markowitz J, Baldassano RN, Faubion WA, Colletti RB, Dubinsky M, Kierkus J, Rosh J, Wang Y, Huang B, Bittle B, Marshall M, Lazar A. Safety and efficacy of adalimumab for moderate to severe Crohn’s disease in children. Gastroenterology 2012; 143: 365-374.e2 [PMID: 22562021 DOI: 10.1053/j.gastro.2012.04.046]
58 Hyams J, Crandall W, Kugathasan S, Griffiths A, Olson A, Johanns J, Liu G, Travers S, Heuschkel R, Markowitz J, Cohen S, Winter H, Veereman-Wauters G, Ferry G, Baldassano R. Induction and maintenance infliximab therapy for the treatment of moderate-to-severe Crohn’s disease in children. Gastroenterology 2007; 132: 863-873; quiz 1165-1166 [PMID: 17324398 DOI: 10.1053/j.gastro.2006.12.003]
59 Hanauer SB, Sandborn WJ, Rutgeerts P, Fedorak RN, Lukas M, MacIntosh D, Panaccione R, Wolf D, Pollack P. Human anti-tumor necrosis factor monoclonal antibody (adalimumab) in Crohn’s disease: the CLASSIC-I trial. Gastroenterology 2006; 130: 323-333; quiz 591 [PMID: 16472588 DOI: 10.1053/j.gastro.2005.11.030]
60 Sandborn WJ, Hanauer SB, Rutgeerts P, Fedorak RN, Lukas M, MacIntosh DG, Panaccione R, Wolf D, Kent JD, Bittle B, Li J, Pollack PF. Adalimumab for maintenance treatment of Crohn’s disease: results of the CLASSIC II trial. Gut 2007; 56: 1232-1239 [PMID: 17299059 DOI: 10.1136/gut.2006.106781]
61 Colombel JF, Sandborn WJ, Rutgeerts P, Enns R, Hanauer SB, Panaccione R, Schreiber S, Byczkowski D, Li J, Kent JD, Pollack PF. Adalimumab for maintenance of clinical response and remission in patients with Crohn’s disease: the CHARM trial. Gastroenterology 2007; 132: 52-65 [PMID: 17241859 DOI: 10.1053/j.gastro.2006.11.041]
41 May 15, 2015|Volume 6|Issue 2|WJGP|www.wjgnet.com
Lahad A et al . Current therapy of pediatric CD

62 Feagan BG, Panaccione R, Sandborn WJ, D’Haens GR, Schreiber S, Rutgeerts PJ, Loftus EV, Lomax KG, Yu AP, Wu EQ, Chao J, Mulani P. Effects of adalimumab therapy on incidence of hospitalization and surgery in Crohn’s disease: results from the CHARM study. Gastroenterology 2008; 135: 1493-1499 [PMID: 18848553 DOI: 10.1053/j.gastro.2008.07.069]
63 Rosh JR, Lerer T, Markowitz J, Goli SR, Mamula P, Noe JD, Pfefferkorn MD, Kelleher KT, Griffiths AM, Kugathasan S, Keljo D, Oliva-Hemker M, Crandall W, Carvalho RS, Mack DR, Hyams JS. Retrospective Evaluation of the Safety and Effect of Adalimumab Therapy (RESEAT) in pediatric Crohn’s disease. Am J Gastroenterol 2009; 104: 3042-3049 [PMID: 19724267 DOI: 10.1038/ajg.2009.493]
64 Rosenbach Y, Hartman C, Shapiro R, Hirsch A, Avitzur Y, Shamir R. Adalimumab treatment in children with refractory Crohn’s disease. Dig Dis Sci 2010; 55: 747-753 [PMID: 19333754 DOI: 10.1007/s10620-009-0791-7]
65 Russell RK, Wilson ML, Loganathan S, Bourke B, Kiparissi F, Mahdi G, Torrente F, Rodrigues A, Davies I, Thomas A, Akobeng AK, Fagbemi A, Hyer W, Spray C, Vaish S, Rogers P, McGrogan P, Heuschkel RB, Ayub N, Fell JM, Afzal NA, Green M, Murphy MS, Rao P, Shah N, Ho GT, Naik S, Wilson DC. A British Society of Paediatric Gastroenterology, Hepatology and Nutrition survey of the effectiveness and safety of adalimumab in children with inflammatory bowel disease. Aliment Pharmacol Ther 2011; 33: 946-953 [PMID: 21342211 DOI: 10.1111/j.1365-2036.2011.04603]
66 Viget N, Vernier-Massouille G, Salmon-Ceron D, Yazdanpanah Y, Colombel JF. Opportunistic infections in patients with inflammatory bowel disease: prevention and diagnosis. Gut 2008; 57: 549-558 [PMID: 18178610 DOI: 10.1136/gut.2006.114660]
67 Colombel JF, Loftus EV, Tremaine WJ, Egan LJ, Harmsen WS, Schleck CD, Zinsmeister AR, Sandborn WJ. The safety profile of infliximab in patients with Crohn’s disease: the Mayo clinic experience in 500 patients. Gastroenterology 2004; 126: 19-31 [PMID: 14699483 DOI: 10.1053/j.gastro.2003.10.047]
68 Sandborn WJ, Feagan BG, Stoinov S, Honiball PJ, Rutgeerts P, Mason D, Bloomfield R, Schreiber S. Certolizumab pegol for the treatment of Crohn’s disease. N Engl J Med 2007; 357: 228-238 [PMID: 17634458 DOI: 10.1056/NEJMoa067594]
69 Schreiber S, Khaliq-Kareemi M, Lawrance IC, Thomsen OØ, Hanauer SB, McColm J, Bloomfield R, Sandborn WJ. Maintenance therapy with certolizumab pegol for Crohn’s disease. N Engl J Med 2007; 357: 239-250 [PMID: 17634459 DOI: 10.1056/NEJMoa062897]
70 Sandborn WJ, Schreiber S, Hanauer SB, Colombel JF, Bloomfield R, Lichtenstein GR. Reinduction with certolizumab pegol in patients with relapsed Crohn‘s disease: results from the PRECiSE 4 Study. Clin Gastroenterol Hepatol 2010; 8: 696-702.e1 [PMID: 20363366 DOI: 10.1016/j.cgh.2010.03.024]
71 Hanauer SB, Panes J, Colombel JF, Bloomfield R, Schreiber S, Sandborn WJ. Clinical trial: impact of prior infliximab therapy on the clinical response to certolizumab pegol maintenance therapy for Crohn’s disease. Aliment Pharmacol Ther 2010; 32: 384-393 [PMID: 20491747 DOI: 10.1111/j.1365-2036.2010.04360]
72 Souza HS, Elia CC, Spencer J, MacDonald TT. Expression of lymphocyte-endothelial receptor-ligand pairs, alpha4beta7/MAdCAM-1 and OX40/OX40 ligand in the colon and jejunum of patients with inflammatory bowel disease. Gut 1999; 45: 856-863 [PMID: 10562584 DOI: 10.1136/gut.45.6.856]
73 Sandborn WJ, Feagan BG, Rutgeerts P, Hanauer S, Colombel JF, Sands BE, Lukas M, Fedorak RN, Lee S, Bressler B, Fox I, Rosario M, Sankoh S, Xu J, Stephens K, Milch C, Parikh A. Vedolizumab as induction and maintenance therapy for Crohn’s disease. N Engl J Med 2013; 369: 711-721 [PMID: 23964933 DOI: 10.1056/NEJMoa1215739]
74 Sands BE, Feagan BG, Rutgeerts P, Colombel JF, Sandborn WJ, Sy R, D’Haens G, Ben-Horin S, Xu J, Rosario M, Fox I, Parikh A, Milch C, Hanauer S. Effects of vedolizumab induction therapy for patients with Crohn’s disease in whom tumor necrosis factor antagonist treatment failed. Gastroenterology 2014; 147: 618-627.e3 [PMID: 24859203 DOI: 10.1053/j.gastro.2014.05.008]
P- Reviewer: Ballester JCA, Ciccone MM, Ierardi E, Naito Y S- Editor: Tian YL L- Editor: A E- Editor: Lu YJ
42 May 15, 2015|Volume 6|Issue 2|WJGP|www.wjgnet.com
Lahad A et al . Current therapy of pediatric CD

© 2015 Baishideng Publishing Group Inc. All rights reserved.
Published by Baishideng Publishing Group Inc8226 Regency Drive, Pleasanton, CA 94588, USA
Telephone: +1-925-223-8242Fax: +1-925-223-8243
E-mail: [email protected] Desk: http://www.wjgnet.com/esps/helpdesk.aspx
http://www.wjgnet.com

World Journal of Gastrointestinal PathophysiologyWorld J Gastrointest Pathophysiol 2015 August 15; 6(3): 43-85
ISSN 2150-5330 (online)
Published by Baishideng Publishing Group Inc

EDITOR-IN-CHIEFThomas Y Ma, Albuquerque
STRATEGY ASSOCIATE EDITOR-IN-CHIEFHirotada Akiho, FukuokaJean-Francois Beaulieu, SherbrookeMichael W Bradbury, ErieSharon DeMorrow, Temple
GUEST EDITORIAL BOARD MEMBERSJia-Ming Chang, TaipeiWai-Keung Chow, TaichungChien-Wei Hsu, KaohsiungMing-Tsan Lin, TaipeiBor-Shyang Sheu, TainanJin-Town Wang, Taipei
MEMBERS OF THE EDITORIAL BOARD
ArgentinaBernabé Matías Quesada, Buenos AiresMarcelo G Roma, Rosario
AustraliaChris Richard Abbiss, JoondalupGuy D Eslick, PenrithMontri Gururatsakul, AdelaideChandana Herath, Melbourne Michael Horowitz, AdelaidMustafa Khasraw, GeelongShu-Chuen Li, CallaghanAntonina Mikocka-Walus, AdelaideNam Quoc Nguyen, Adelaide
Kulmira Nurgali, St AlbansNicholas John Spencer, Flagstaff HillNick Spencer, AdelaideDeborah Verran, CamperdownShu-Feng Zhou, Melbourne
AustriaCord Langner, GrazDietmar Ofner-Velano, SalzburgMichael Trauner, Graz
Belgium
Kathleen Blondeau, LeuvenRobaeys Geert, GenkIlse Maria Hoffman, LeuvenMichael H J Maes, WilrijkTheodoor Abram Niewold, HeverleeXavier Sagaert, LeuvenJean-Marie Vanderwinden, BrusselsKristin Verbeke, LeuvenMathieu Vinken, Roeselare
BrazilUilian Andreis, BotucatuEverson L A Artifon, Vila MarianaJoão Batista Calixto, TrindadeNiels O Saraiva Câmara, Vila ClementinoJulio Chebli, Juiz de ForaFernando Fornari, Passo FundoClélia Akiko Hiruma-Lima, BotucatuMarcel C C Machado, Sao PauloJuarez Quaresma, BelemWagner Vilegas, Araraquara
Brunei Darussalam
Vui Heng Chong, Bandar Seri Begawan
Canada
Fernando Alvarez, MontréalFrancois Boudreau, SherbrookeGeorge A Bubenik, GuelphWang-Xue Chen, OttawaJan D Huizinga, PuslinchKusum K Kharbanda, OmahaWolfgang Kunze, HamiltoJian-Jun Li, OttawaRoderick John Macleod, KingstonMichele Molinari, HalifaxNathalie Rivard, SherbrookeKirill Rosen, HalifaxManuela Santos, MontrealCaroline Saucier, QuebecJean Sévigny, QuebecEldon A Shaffer, CalgaryManuel A Silva, HamiltonAlan B R Thomson, EdmontonPierre H Vachon, Sherbrooke
China
Kai-Xing Ai, ShanghaiZhao-Xiang Bian, Hong KongMin-Hu Chen, GuangzhouCH Cho, Hong KongZhong-Hong Gao, WuhanJun-Ming Guo, NingboJing-Yan Han, Beijing
I
Editorial Board2011-2015
The World Journal of Gastrointestinal Pathophysiology Editorial Board consists of 523 members, representing a team of worldwide experts in gastrointestinal pathophysiology. They are from 45 countries, including Argentina (2), Australia (14), Austria (3), Belgium (9), Brazil (10), Brunei Darussalam (1), Canada (20), China (30), Croatia (1), Czech Republic (2), Denmark (4), Egypt (1), Estonia (1), Finland (1), France (8), Germany (22), Greece (7), Hungary (5), India (10), Indonesia (1), Iran (2), Ireland (2), Israel (8), Italy (42), Japan (47), Lebanon (3), Malaysia (1), Mexico (2), Netherlands (8), Norway (1), Poland (4), Portugal (1), Romania (1), Russia (1), Singapore (4), South Korea (13), Spain (23), Sweden (11), Switzerland (4), Thailand (2), Turkey (6), Ukraine (1), United Kingdom (10), United States (173), and Venezuela (1).
February 15, 2013WJGP|www.wjgnet.com
World Journal ofGastrointestinal PathophysiologyW J G P
Jian-Dong Huang, Hong KongJia-Fu Ji, BeijingShi Liu, WuhanZhan-Ju Liu, ShanghaiXiao-Hong Wang, BeijingZhen-Ning Wang, ShenyangWei Wei, HefeiDong-Ping Xie, ShanghaiWen-Xie Xu, ShanghaiHua Yang, ChongqingXiao Yang, BeijingWei-Zhen Zhang, BeijingHua-Chuan Zheng, ShenyangDa-Ling Zhu, HarbinJin-Xia Zhu, BeijingMin-Sheng Zhu, NanjingYong-Liang Zhu, Hangzhou
Croatia
Alen Protic, Rijeka
Czech Republic
Pavel Hladik, SemilyMartin Vokurka, Prague
Denmark
Lars Arendt-Nielsen, AalborgFrank Vinholt Schiodt, CopenhagenJonas Worsoe, AarhusJing-Bo Zhao, Aalborg
Egypt
Mahmoud Aboelneen Khattab, Minia
Estonia
Enn Seppet, Tartu
Finland
Pauli Antero Puolakkainen, Turku
France
Bruno Bonaz, GrenoblePierre Marie Dechelotte, RouenJean-Paul Lallès, Saint-GillesCharles-Henri Malbert, Saint-GillesThierry Piche, NicePascale Plaisancié, LyonMichelina Plateroti, LyonVeronique Vitton, Marseille
Germany
Hans Gunter Beger, UlmCarsten Bergmann, IngelheimElke Cario, Essen
Arno J Dormann, KolnNikolaus Gassler, AachenWerner Hartwig, HeidelbergMarion Hewicker-Trautwein, HannoverJens Hoeppner, FreiburgTobias Keck, FreiburgJorg Kleeff, MunichPeter Malfertheiner, MagdeburgOliver Mann, HamburgChristoph Michalski, MunichAndreas Klaus Nussler, MunichChristian Pehl, VilsbiburgPeter Schemmer, HeidelbergMarc Stemmler, FreiburgFrank Tacke, AachenSya Nomna Ukena, HannoverBrigitte Vollmar, RostockThomas Michael Wex, MagdeburgMargot Zoller, Heidelberg
Greece
Stelios F Assimakopoulos, PatrasGeorge N Dalekos, LarissaAlkiviadis Efthymiou, thessalonikiMaria Gazouli, AthensIoannis E Koutroubakis, HeraklionGerassimos J Mantzaris, AthensGeorge Papatheodoridis, Athens
Hungary
Mária Bagyánszki, SzegedMihály Boros, SzegedLaszlo Czako, SzegedPal Miheller, BudapestZoltan Rakonczay, Szeged
India
Anil Kumar Agarwal, DelhiUday Bandyopadhyay, KolkataSriparna Basu, VaranasiChandra Kanti Chakraborti, RourkelaRajeev Garg, PunjabChandra P Sharma, ThiruvananthapuramShailesh V Shrikhande, MumbaiVirendra Singh, ChandigarhNicholas James Skill, IndianapolisPrabhakar R Veerareddy, Andhra Pradesh
Indonesia
Laurentius A Lesmana, Jakarta
Iran
Gholamreza Roshandel, GorganShahram Shahabi, Urmia
Ireland
Billy Bourke, DublinStephen Keely, Dublin
IsraelYosefa Avraham, JerusalemYaron Bar-Dayan, HolonShomron Ben-Horin, HashomerBoris Kirshtein, Beer ShevaStephen Malnick, RehovotYaakov Maor, Tel-HashomerRifaat Safadi, JerusalemNachum Vaisman, Tel Aviv
Italy
Rosaria Acquaviva, CataniaDario Acuna-Castroviejo, ArmillaAlessandro Antonelli, PisaGiacosa Attilio, GenovaSalvatore Auricchio, NaplesGuido Basilisco, MilanoAntonio Basoli, RomeClaudio Bassi, VeronaMassimo Bellini, PisaLuigi Bonavina, MilanoAlfio Brogna, CataniaGiuseppe Calamita, BariRaffaele Capasso, NaplesIgnazio Castagliuolo, PadovaEnrico Stefano Corazziari, RomeFrancesco Cresi, TorinoRosario Cuomo, NapoliSalvatore Cuzzocrea, GazziMario M D’Elios, FlorenceCinzia Domeneghini, MilanLuca Elli, MilanoCresi Francesco, TorinoWalter Fries, MessinaEugenio Gaudio, RomeMarco Gobbetti, BariFabio Grizzi, MilanEnzo Grossi, MilaneseEnzo Ierardi, FoggiaPietro Invernizzi, MilanAngelo A Izzo, NaplesAnna Kohn, RomeGiovanni Latella, L’AquilaMassimo Marignani, RomeSergio Morini, RomeRaffaele Pezzilli, BolognaCristiano Rumio, MilanGiovanni Sarnelli, NaplesEdoardo Vincenzo Savarino, GenoaPierpaolo Sileri, RomeAnnamaria Staiano, NaplesGiacomo Carlo Sturniolo, PadovaClaudio Tiribelli, Triest
Japan
Akihiro Asakawa, KagoshimaHisashi Aso, SendaiYasu-Taka Azuma, OsakaShotaro Enomoto, WakayamaMikihiro Fujiya, HokkaidoTakahisa Furuta, HamamatsuAkira Hokama, OkinawaRyota Hokari, SaitamaYuichi Hori, Kobe
II February 15, 2013WJGP|www.wjgnet.com

III February 15, 2013WJGP|www.wjgnet.com
Hideki Iijima, OsakaMasahiro Iizuka, AkitaMotohiro Imano, OsakaHajime Isomoto, NagasakiTatehiro Kagawa, IseharaTakumi Kawaguchi, KurumeHaruki Kitazawa, SendaiXiao-Kang Li, TokyoNoriaki Manabe, OkayamaAtsushi Masamune, SendaiHiroyuki Matsubayashi, ShizuokaKazuyuki Matsushita, Chuo-kuReiko Miyazawa, GunmaKazunari Murakami, OitaHikaru Nagahara, TokyoYuji Naito, KyotoAtsushi Nakajima, Atsushi NakajimaShoji Natsugoe, KagoshimaTsutomu Nishida, OsakaKoji Nomoto, TokyoNaoaki Sakata, MiyagiShouji Shimoyama, TokyoGoshi Shiota, YonagoIkuo Shoji, HyogoHidekazu Suzuki, TokyoHitoshi Takagi, GunmaToru Takahashi, OkayamaYoshihisa Takahashi, TokyoKan Uchiyama, ChibaTakato Ueno, KurumeYoshiyuki Ueno, SendaiHisayuki Uneyama, KwasakiMitsunori Yamakawa, YamagataTakayuki Yamamoto, MieYutaka Yata, GunmaNaohisa Yoshida, KyotoHitoshi Yoshiji, Nara
Lebanon
Costantine Fouad Daher, ByblosAssaad M Soweid, BeirutJulnar Usta, Beirut
Malaysia
Andrew Chua, Perak
Mexico
José María de la Roca-Chiapas, LeonMaria Raquel Huerta Franco, Guanajuato
Netherland
Wouter J de Jonge, AmsterdamAldo Grefhorst, GroningenRuben Hummelen, RotterdamDaniel Keszthelyi, MaastrichtCornelis F M Sier, LeidenPieter J Tanis, AmsterdamLuc JW van der Laan, RotterdamSander van der Marel, Leiden
NorwayAnne Marie Bakke, Oslo
Poland
Stanisław Hac, GdańskStanisław Jan Konturek, KrakówAgata Mulak, WroclawNapoleon Waszkiewicz, Choroszcz
Portugal
Ricardo Marcos, Porto
Romania
Mihai Ciocirlan, Bucharest
Russia
Ludmila Filaretova, Petersburg
Singapore
Madhav Bhatia, SingaporeBrian K P Goh, SingaporeKhek Yu Ho, SingaporeCliff K S Ong, Singapore
South Korea
Jae Hee Cheon, SeoulMyung Haing Cho, SeoulJae Bock Chung, SeoulKi-Baik Hahm, IncheonHo Jae Han, GwangjuChang Duk Jun, GwangjuHong Joo Kim, SeoulJin Kyung Kim, Gyeongsan-SiSang Geon Kim, SeoulWon Jae Lee, SeoulKwan Kyu Park, DaeguSeung Ha Park, BusanSung Joo Park, Jeonbuk
Spain
Raquel Abalo, AlcorcónJuan G Abraldes, BarcelonaAgustin Albillos, MadridMaria-Angeles Aller, MadridFernando Azpiroz, BarcelonaRamon Bataller, BarcelonaMarco Bustamante, ValenciaAndres Cardenas, BarcelonaDariao Acuna Castroviejo, ArmillaJoan Claria, BarcelonaPere Clave, BarcelonaManuel Giner, Madrid
Angel I Lanas, ZaragozaMaite Martin, BarcelonaMaria Teresa Martin, BarcelonaVicente Martinez, BarcelonaJose M Matés, MalagaJulio M Mayol, MadridMarçal Pastor-Anglada, BarcelonaMaría Eugenia Sáez, SevilleYolanda Sanz, BurjassotCarlos Taxonera, MadridMaria D Yago, Granada
Sweden
Marco Del Chiaro, StockholmFrida Fak, GothenburgGunnar FA Flemstrom, UppsalaEvangelos Kalaitzakis, GothenburgKristina Lamas, UmeaBob Roger Olsson, GöteborgSara Maria Regnér, MalmöPeter thelin Schmidt, StockholmXiao-Feng Sun, LinkopingHenrik Thorlacius, MalmöCurt Tysk, Orebro
Switzerland
Jyrki J Eloranta, ZurichAndreas Geier, ZurichRemy Meier, LiestalCatherine Pastor, Geneva
Thailand
Thawatchai Akaraviputh, BangkokWeekitt Kittisupamongkol, Bangkok
Turkey
Mehmet Bektas, AnkaraMukaddes Esrefoglu, MalatyaAhmet Guven, AnkaraMuammer Karadeniz, ManisaElvan Ozbek, ErzuruIlhami Yuksel, Ankara
Ukraine
Oksana S Zayavhkivska, Lviv
United Kingdom
Geoffrey Burnstock, LondonJanice E Drew, AberdeenGirish Gupte, BirminghamDavid C Hay, EdinburghNusrat Husain, CheshireMichael Leslie Lucas, GlasgowJamie Murphy, LondonVadim Sumbayev, KentWing-Kin Syn, Birmingham

IV February 15, 2013WJGP|www.wjgnet.com
Andrea Varro, Liverpool
United States
Sami Rene Achem, JacksonvilleTauseef Ali, OklahomaDavid H Alpers, St LouisGianfranco D Alpini, TempleShrikant Anant, OklahomaM Sawkat Anwer, North GraftonAndrew Aronsohn, ChicagoToms Augustin, SayreGyorgy Baffy, BostonMichael T Bailey, ColumbusKim Elaine Barrett, San DiegoMarc D Basson, LansingRobert L Bell, New HavenDavid H Berger, HoustonUrs A Boelsterli, StorrsRichard G Boles, Los AngelesEdward L Bradley III, SarasotaQiang Cai, AtlantaWei-Biao Cao, ProvidenceSubhash C Chauhan, Sioux FallsJian-De Chen, GalvestonTao-Sheng Chen, MemphisJohn Chiang, RootstownMashkoor A Choudhry, MaywoodParimal Chowdhury, Little RockEric Cohen, BostonRobert Cormier, DuluthSrinivasan Dasarathy, ClevelandEdwin A Deitch, NewarkDan A Dixon, ColumbiaJames P Dolan, PortlandH Henry Dong, PittsburghHui Dong, La JollaAshkan Farhadi, IrvineBin Feng, PittsburghJenifer Fenton, East LansingAlessandro Fichera, ChicagoMitchell P Fink, PittsburghP Marco Fisichella, MaywoodLeo R Fitzpatrick, HummelstownRobert Armour Forse, OmahaGlenn Tsuyoshi Furuta, AuroraJuan F Gallegos-Orozco, ScottsdalePandu R Gangula, NasvhilleTimothy Gardner, LebanonShannon Stroud Glaser, TempleFrancisco Gondim, St. LouisJohn R Grider, RichmondYan-Fang Guan, CincinnatiGregory M Holmes, Baton RougeAi-Xuan Le Holterman, ChicagoRichard Hu, Los AngelesHartmut Jaeschke, KansasRobert Thomas Jensen, Los AngelesSreenivasa S Jonnalagadda, LouisMichel Kahaleh, Charlottesville
Andreas Martin Kaiser, Los AngelesRandeep Singh Kashyap, RochesterLaurie Keefer, ChicagoRichard Kellermayer, HoustonChris Kevil, ShreveportSandeep Khurana, BaltimorePawel R Kiela, TucsonTammy Lyn Kindel, CincinnatGordana Kosutic, DurhamDavid Kravetz, San DiegoAshok Kumar, DetroitJohn H Kwon, ChicagoMuriel Larauche, Los AngelesI Michael Leitman, New YorkFelix W Leung, North HillsSuthat Liangpunsakul, IndianapolisFeng-Xin Lu, BostonPauline Kay Lund, Chapel HillGeorge Luo, LexingtonGuang-Xiang Luo, LexingtonJay Luther, Ann ArborRam I Mahato, MemphisAkhil Maheshwari, BirminghamKenneth Maiese, NewarkAdhip P N Majumdar, DetroitJose E Manautou, StorrsCraig J McClain, LouisvilleDermot McGovern, Los AngelesB Greenwood-van Meerveld, OklahomaDouglas Scott Merrel, BethesdaMurielle Mimeault, OmahaEmiko Mizoguchi, BostonHuan-Biao Mo, DentonAdam Moeser, RaleighRamzi M Mohammad, DetroitSatdarshan Singh Monga, PittsburghRoger Klein Moreira, New YorkSandeep Mukherjee, OmahaKarnam S Murthy, RichmondMichael J Nowicki, JacksonShuji Ogino, BostonMary Francis Otterson, WisconsinChung Owyang, Ann ArborHelieh S Oz, LexingtonMarco G Patti, ChicagoTimothy Michael Pawlik, BaltimoreSara Peleg, HoustonNicholas C Popescu, BethesdaLi-Ya Qiao, RichmondChao Qin, OklahomaParvaneh Rafiee, MilwaukeeSigrid A Rajasekaran, WilmingtonVazhaikkurichi M Rajendran, MorgantownJean Pierre Raufman, BaltimoreRamesh M Ray, MemphisArie Regev, IndianapolisDouglas K Rex, CarmelYehuda Ringel, Chapel HillRichard A Rippe, RockvilleChantal A Rivera, Bossier
Andrea Romani, ClevelandPraveen K Roy, AlbuquerquePaul A Rufo, BostonDavid B Sachar, New YorkBimaljit Singh Sandhu, RichmondSanjaya Kumar Satapathy, New Hyde ParkAnthony Senagore, Los AngelesMuhammad Y Sheikh, FresnoBo Shen, ClevelandLe Shen, ChicagoFrank A Simmen, Little RockSteven Mitchell Singer, WashingtonShailinder Jit Singh, WashingtonAdam Jan Smolka, CharlestonNed Snyder, HoustonZhen-Yuan Song, ChicagoGagan K Sood, HoustonRhonda F Souza, DallasStuart Jon Spechler, DallasSubbaramiah Sridha, AugustaCatia Sternini, Los AngelesVeedamali S Subramanian, Long BeachJun Sun, RochesterYvette Taché, Los AngelesXiao-Di Tan, ChicagoPaul Daniel Terry, AtlantaJennifer Tirnauer, FarmingtonAndrea Todisco, Ann ArborGeorge C Tsokos, BostonVic Velanovich, DetroitRaj Vuppalanchi, IndianapolisEstela Wajcberg, CranfordArnold Wald, MadisonLi-Xin Wang, Los AngelesHorst Christian Weber, BostonSteven D Wexner, WestonJackie D Wood, ColumbusGuo-Yao Wu, College StationChristian Wunder, BethesdaZuo-Liang Xiao, ClevelandGuang-Yin Xu, GalvestonGuo-Rong Xu, East OrangeGuang-Yu Yang, ChicagoJay A Yelon, ValhallaYamaoka Yoshio, HoustonShao-Yong Yu, HersheyYana Zavros, CincinnatiJoerg Zehetner, Los AngelesJian X Zhang, CharlotteZhi Zhong, CharlestonHui-Ping Zhou, RichmondZhan-Xiang Zhou, KannapolisQing Zhu, BethesdaYao-Hui Zhu, Stanford
Venezuela
Fabian Michelangeli, Caracas

Contents
August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com I
Quarterly Volume 6 Number 3 August 15, 2015
EDITORIAL43 Emergingrolesofmyeloidderivedsuppressorcellsinhepaticinflammationandfibrosis
Hammerich L, Tacke F
51 Gutregion-dependentalterationsofnitrergicmyentericneuronsafterchronicalcoholconsumption
Bagyánszki M, Bódi N
58 Canhighresolutionmanometryparametersforachalasiabeobtainedbyconventionalmanometry?
Herbella FAM, Patti MG
MINIREVIEWS62 Irondeficiencyanemiaininflammatoryboweldisease
Kaitha S, Bashir M, Ali T
73 Designerprobiotics:Developmentandapplicationsingastrointestinalhealth
Sleator RD
79 Humanmicrobiome:Fromthebathroomtothebedside
Malnick S, Melzer E

Editorial BoardMemberofWorld Journal of Gastrointestinal Pathophysiology ,Arno JDormann,MD, Associate Professor, Kliniken der Stadt KölngGmbH,KrankenhausHolweide,MedizinischeKlinik,NeufelderStrasse32,51058Koln,Germany
World Journal of Gastrointestinal Pathophysiology (World J Gastrointest Pathophysiol, WJGP, online ISSN 2150-5330, DOI: 10.4291), is a peer-reviewed open access academic journal that aims to guide clinical practice and improve diagnostic and therapeutic skills of clinicians.
WJGP is to report rapidly the most recent results in basic and clinical research on gastrointestinal pathophysiology, including all aspects of normal or abnormal function of the gastrointestinal tract, hepatobiliary system, and pancreas. WJGP specifically covers growth and development, digestion, secretion, absorption, metabolism and motility relative to the gastrointestinal organs, as well as immune and inflammatory processes, and neural, endocrine and circulatory control mechanisms that affect these organs. This journal will also report new methods and techniques in gastrointestinal pathophysiological research. We encourage authors to submit their manuscripts to WJGP. We will give priority to manuscripts that are supported by major national and international foundations and those that are of great basic and clinical significance.
World Journal of Gastrointestinal Pathophysiology is now indexed in PubMed Central, PubMed, Digital Object Identifier, and Directory of Open Access Journals.
I-IV EditorialBoard
ContentsWorld Journal of Gastrointestinal Pathophysiology
Volume 6 Number 3 August 15, 2015
FLYLEAF
EDITORS FOR THIS ISSUE
NAMEOFJOURNALWorld Journal of Gastrointestinal Pathophysiology
ISSNISSN 2150-5330 (online)
LAUNCHDATEApril 15, 2010
FrequencyQuarterly
EDITOR-IN-CHIEFThomas Y Ma, MD, PhD, Professor, Chief, Division of Gastroenterology and Hepatology, University of New Mexico, MSC10 5550, 1 UNM, Albuquerque, NM 87131, United States
EDITORIALOFFICEJin-Lei Wang, DirectorXiu-Xia Song, Vice DirectorWorld Journal of Gastrointestinal Pathophysiology
Room 903, Building D, Ocean International Center, No. 62 Dongsihuan Zhonglu, Chaoyang District, Beijing 100025, ChinaTelephone: +86-10-85381891Fax: +86-10-85381893E-mail: [email protected] Desk: http://www.wjgnet.com/esps/helpdesk.aspxhttp://www.wjgnet.com
PUBLISHERBaishideng Publishing Group Inc8226 Regency Drive, Pleasanton, CA 94588, USATelephone: +1-925-223-8242Fax: +1-925-223-8243E-mail: [email protected] Desk: http://www.wjgnet.com/esps/helpdesk.aspxhttp://www.wjgnet.com
PUBLICATIONDATEAugust 15, 2015
COPYRIGHT© 2015 Baishideng Publishing Group Inc. Articles pub-lished by this Open Access journal are distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license.
SPECIALSTATEMENTAll articles published in journals owned by the Baishideng Publishing Group (BPG) represent the views and opinionsof their authors, and not the views, opinions or policies of the BPG, except where other-wise explicitly indicated.
INSTRUCTIONSTOAUTHORSFull instructions are available online at http://www.wjgnet.com/2218-6182/g_info_20100722172951.htm
ONLINESUBMISSIONhttp://www.wjgnet.com/esps/
ABOUT COVER
August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com II
AIM AND SCOPE
INDEXING/ABSTRACTING
Responsible Assistant Editor: Xiang Li Responsible Science Editor: Xue-Mei GongResponsible Electronic Editor: Huan-Liang Wu Proofing Editorial Office Director: Xiu-Xia Song Proofing Editor-in-Chief: Lian-Sheng Ma

marrow or spleen, especially in conditions of cancer, infections or inflammation. MDSC usually express CD11b, CD33, and low levels of human leukocyte antigen-DR in humans or CD11b and Gr1 (Ly6C/G) in mice, and they can be further divided into granulocytic or monocytic MDSC. The liver is an important organ for MDSC induction and accumulation in hepatic as well as extrahepatic diseases. Different hepatic cells, especially hepatic stellate cells, as well as liver-derived soluble factors, including hepatocyte growth factor and acute phase proteins (SAA, KC), can promote the differentiation of MDSC from myeloid cells. Importantly, hepatic myeloid cells like neutrophils, monocytes and macrophages fulfill essential roles in acute and chronic liver diseases. Recent data from patients with liver diseases and animal models linked MDSC to the pathogenesis of hepatic inflammation, fibrosis and hepatocellular carcinoma (HCC). In settings of acute hepatitis, MDSC can limit immunogenic T cell responses and subsequent tissue injury. In patients with chronic hepatitis C, MDSC increase and may favor viral persistence. Animal models of chronic liver injury, however, have not yet conclusively clarified the involvement of MDSC for hepatic fibrosis. In human HCC and mouse models of liver cancer, MDSC are induced in the tumor environment and suppress anti-tumoral immune responses. Thus, the liver is a primary site of MDSC in vivo , and modulating MDSC functionality might represent a promising novel therapeutic target for liver diseases.
Key words: Myeloid derived suppressor cells; Inter-leukin-10; Treg; Liver cirrhosis; Macrophage; Hepatitis C virus
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Myeloid derived suppressor cells (MDSC) are a heterogeneous population of immune-suppressive cells with important roles during inflammation, infection and cancer. The liver is a primary site for MDSC induction
Emerging roles of myeloid derived suppressor cells in hepatic inflammation and fibrosis
Linda Hammerich, Frank Tacke, Department of Medicine III, University Hospital Aachen, 52074 Aachen, Germany
Author contributions: Hammerich L and Tacke F wrote this editorial.
Supported by The German Research Foundation (DFG Ta434/3-1 and SFB/TRR57); and by the Interdisciplinary Center for Clinical Research (IZKF) Aachen.
Conflict-of-interest statement: The authors declare no conflict of interest.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Correspondence to: Frank Tacke, MD, PhD, Department of Medicine III, University Hospital Aachen, Pauwelsstrasse 30, 52074 Aachen, Germany. [email protected]: +49-241-8035848Fax: +49-241-8082455
Received: January 9, 2015Peer-review started: January 10, 2015 First decision: March 6, 2015Revised: March 16, 2015 Accepted: June 1, 2015Article in press: June 2, 2015Published online: August 15, 2015
AbstractMyeloid derived suppressor cells (MDSC) are a hetero-geneous population of immune cells that are potent suppressors of immune responses. MDSC emerge in various compartments in the body, such as blood, bone
43 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
EDITORIAL
World J Gastrointest Pathophysiol 2015 August 15; 6(3): 43-50ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i3.43
Linda Hammerich, Frank Tacke

and accumulation, and recent studies linked these cells to the pathogenesis of hepatic inflammation, fibrosis and hepatocellular carcinoma. MDSC can limit tissue injury during acute hepatitis, while they may favor viral persistence in chronic hepatitis. MDSC are also induced during development of liver cancer and suppress anti-tumoral immunity, but their involvement in hepatic fibrosis is less clear. Thus, modulating MDSC functionality might represent a promising novel therapeutic target for liver diseases.
Hammerich L, Tacke F. Emerging roles of myeloid derived suppressor cells in hepatic inflammation and fibrosis. World J Gastrointest Pathophysiol 2015; 6(3): 43-50 Available from: URL: http://www.wjgnet.com/2150-5330/full/v6/i3/43.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i3.43
INTRODUCTIONMyeloid-derived suppressor cells (MDSC) are a hetero-geneous cell population of myeloid origin originally described in tumor-bearing hosts[1] that are also induced under various inflammatory conditions - including sepsis[2], hepatitis[3,4] and viral infections[5-7]. MDSC regulate immune responses by potently suppressing T cell function[8]; although these T cell suppressive activities have been functionally linked to tumor pro-gression or evasion from immune responses, the exact roles of MDSC appear to be context-dependent and vary between infectious, autoimmune or malignant diseases. MDSC are usually identified as CD11b+ CD33+ HLA-DRlow cells in humans and CD11b+ Gr1+ cells in mice[9]. However, a specific marker for MDSC has not been described so far, which can make identification of these cells difficult as all those surface molecules are shared with other myeloid cell types such as neutrophils, monocytes or myeloid dendritic cells. Therefore, the most reliable feature to distinguish MDSC from other myeloid cells seems to be their suppressive function.
MDSC consist of at least two major subpopulations that are termed monocytic MDSC (mMDSC) and granu-locytic MDSC (gMDSC) according to their side scatter (SSC) profile and Gr1 (Ly6C/G) expression in mice[10]. Whereas murine mMDSC have a low SSC profile and are Ly6Chi Ly6G-, gMDSC are Ly6Clo Ly6Ghi and show a higher SSC profile. In humans, CD14 and CD15 have been suggested as markers for mMDSC and gMDSC, respectively, but further investigation is needed to verify this hypothesis[11]. The two subsets seem to differ in their suppressive capacity and functional mechanism(s) depending on the disease studied.
As MDSC are heterogeneous myeloid cells with immune suppressive functions, several mechanisms of T cell suppression have been described. These mechanisms include L-arginine depletion by the enzymes arginase 1 (Arg1) or inducible nitric oxide synthase (iNOS) and generation of reactive oxygen
species (ROS)[8,10,12]. Furthermore, MDSC have also been shown to secrete anti-inflammatory cytokines like IL-10[13]. Again, the suppressive mechanisms used by the different subsets as well as the requirement of cell-cell-contacts vs secretion of soluble factors seem to be highly dependent on the underlying pathology (Table 1). A recent study on the development of murine MDSC suggested that the two subsets depend on the expression of distinct anti-apoptotic proteins and that T cell suppressive functions are restricted to the mMDSC subset[14].
THE LIVER AS A SITE OF MDSC ACCUMULATION AND INDUCTIONThe liver has been shown to be a site of MDSC accu-mulation, and this seems to apply to hepatic and also to extrahepatic diseases. Different hepatic cell types as well as liver-derived soluble factors have been implicated in the recruitment and differentiation of MDSC under various conditions (Figure 1). In tumor-bearing mice with various types of cancer - including breast, lung and skin cancer - MDSC numbers increased in the liver irrespective of whether the mice had tumor manifestation in the liver, namely hepatic metastasis, or not[15]. Furthermore, adoptively transferred MDSC homed to livers and spleens of tumor-bearing mice in a comparable fashion. Ilkovitch et al[15] could show that this increase in hepatic MDSC is at least in part due to elevated levels of GM-CSF, a hematopoietic growth factor produced by many different types of tumors and associated with splenic accumulation of MDSC.
Additionally, hepatic stellate cells (HSC), a cell type associated with various immune-modulatory func-tions[16], have been shown to induce MDSC from myeloid cells in mice and men. Primary human HSC were able to induce differentiation of MDSC from PBMC in vitro[17]. This induction was dependent on direct cell-cell contacts as well as on the expression of CD44 by HSC and led to generation of CD14+ HLA-DRlo cells able to suppress T cell responses in an arginase 1-dependent manner. Similarly, murine hepatic stellate cells were proven to induce CD11b+Gr1+ MDSC from bone marrow-derived cells[18,19]. However, this induction seems to be mediated by soluble factors rather than cell-cell contact. Chou et al[18] implicated a critical role for IFNγ signaling in HSC, and an additional study from the same group showed that MDSC induction was mediated by complement component C3 released by HSC[19]. In addition, both studies demonstrated that HSC could also induce MDSC in vivo in the context of islet cell transplantation and therefore contribute to allograft survival.
Furthermore, liver-derived soluble factors can also promote the generation of MDSC (Figure 1). Human mesenchymal stromal cells and an osteosarcoma cell line are able to induce the expansion of CD11b+ CD33+ CD14- MDSC from peripheral blood leukocytes in vitro, an effect that is mediated by hepatocyte growth
44 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Hammerich L et al . MDSC in liver disease

factor (HGF) and its receptor c-Met[20]. Since the liver usually harbors high levels of HGF this might be an explanation for the high numbers of MDSC present in the liver even under steady state conditions. Indeed, inhibition of the HGF/c-Met pathway in mice led to a significant reduction in hepatic but not splenic MDSC[20]. In the context of polymicrobial sepsis in mice hepatic acute-phase proteins play a critical role for controlling the inflammatory reaction to infection. Both serum amyloid A (SAA) and the chemokine CXCL1/KC work synergistically to mobilize MDSC from the bone marrow and induce their accumulation in the spleen[2]. Mice lacking the production of acute phase proteins due to the deletion of the IL-6 cytokine family receptor gp130 in hepatocytes showed less accumulation of MDSC and increased mortality during sepsis, which could be reversed by adoptive transfer of MDSC or administration of recombinant SAA and KC[2]. Consistently, the ectopic expression of IL-6 in the liver induced accumulation of MDSC in liver and spleen, which protected mice from CD8+ T cell-mediated liver injury[21].
Another factor that may contribute to for the accumulation of MDSC in the liver is activation of inflammasomes, proteolytic complexes activated by pattern recognition receptors (PRR), and resulting in the production of IL-1β and IL-18. In murine cancer models activation of the Nlrp3 inflammasome has been associated with the accumulation of MDSC and sup-pression of anti-tumor immune responses[22,23]. This may also apply to liver diseases as inflammasome acti-vation is important in a wide range of conditions[24,25].
Chronic human liver diseases are often associated with changes in the intestinal microbiome with the resulting inflammation leading to disruption and enhanced permeability of the intestinal epithelial barrier[26,27]. This enables the translocation of microbial products, which can travel to the liver via the portal vein and activate the inflammasome complex through PRRs. So far, this process has mainly been described for liver macrophages[28], but considering what has been observed for tumor-associated MDSC, inflammasome activation might also induce accumulation of hepatic MDSC.
MDSC IN THE REGULATION OF HUMAN LIVER DISEASESWhile the above mentioned data demonstrated that the liver is an important site of MDSC induction for extrahepatic infections and cancer, more recent data implied hepatic MDSC as essential regulators of liver diseases as well. Several studies have concordantly reported that patients with hepatocellular carcinoma (HCC) or chronic hepatitis C virus (HCV) infection show increased frequencies of MDSC in the peripheral blood[6,7,29-32]. Human MDSC in HCC patients are mainly CD14+ HLA-DR-/low and able to inhibit T cell proliferation in an arginase dependent manner[29]. Furthermore, these cells induce a regulatory phenotype in CD4+ T cells and inhibit natural killer (NK) cell function in vitro[29,33]. Likewise, MDSC in the blood of patients
45 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
CD11c+Gr1+ cell
Bonemarrow
Blood
M-MDSC G-MDSC gd TC Hepatocyte Cancer cell Hepatic stellate cell
gd TC Live
r pa
renc
hym
aSi
nuso
ids
CD44
HSC
HCC
SAA
KC
KC
Spleen Liver
GM
-CSF
IL6
HG
F
IL6
HG
FKC
SAA
CXCL
5
IL17
IL17
IL23IL1β
C3
Figure 1 Myeloid derived suppressor cells in liver disease. Left: Myeloid derived suppressor cells (MDSC) accumulate during infectious, inflammatory or malignant diseases in several compartments of the body, including the liver. MDSC potently suppress immunogenic T cell responses, which is also relevant for liver diseases such as hepatic inflammation, fibrosis or HCC. Right: The induction of monocytic (mMDSC) or granulocytic (gMDSC) MDSC in the liver is promoted by different cell types in the liver via cell-cell-contact dependent mechanisms (e.g., CD44) as well as via various soluble mediators. Details are provided in the main text. GM-CSF: Granulocyte-macrophage colony-stimulating factor; HCC: Hepatocellular carcinoma; hepa: Hepatocyte; HGF: Hepatocyte growth factor; HSC: Hepatic stellate cell; IL: Interleukin; SAA: Serum amyloid A; TC: T cell.
Hammerich L et al . MDSC in liver disease
hepa

with chronic HCV were shown to be CD11b+ HLA-DRlow CD14+ CD33+ and suppress T cells using arginase[6]. In addition, ROS production may contribute to T cell inhibition by MDSC, and HCV-infected hepatocytes were found to promote MDSC differentiation from PBMC[7]. This might represent a mechanism of HCV-mediated immune suppression that leads to persistent infection.
ROLE OF MDSC FOR HEPATOCELLULAR CARCINOMASeveral studies have addressed the function of MDSC in liver cancer by investigating murine models of HCC. Mice bearing liver tumors show increased numbers of MDSC in liver, spleen, and bone marrow[34-37]. Remark-ably, the timing of MDSC accumulation seems to be highly dependent on the tumor model studied. Mice with diethylnitrosamine (DEN) or transgenic myc-overexpression induced liver tumors, in which primary liver cancer develops slowly in the “normal” hepatic microenvironment, showed increased MDSC numbers only during late stages of the disease, while mice with orthotopic or subcutaneous tumors displayed increased MDSC numbers early on[34]. In addition, MDSC from mice with transplantable tumors showed higher sup-pressive capacity than MDSC from mice with DEN-
induced HCC. Several studies showed that treatment with the multi-kinase inhibitor sorafenib[34,35] or an agonistic anti-CD137 antibody[37] decreased frequency of MDSC in mice bearing HCC, thereby contributing to anti-tumoral immunity.
Several soluble factors have been implicated in the recruitment of MDSC during HCC development. Tumor derived GM-CSF and KC mediated the accumulation of MDSC during hepatocarcinogenesis, and neutralization of these molecules reduced hepatic MDSC numbers[34]. Interleukin-17 (IL-17) produced by gamma/delta T cells (gd T cells) also indirectly mediated MDSC accu-mulation[38]. Ma et al[38] showed that gd T cell-derived IL-17 induced secretion of CXCL5 by tumor cells, which then recruited MDSC via engagement of CXCR2. Moreover, IL-17 also acted on the MDSC directly by enhancing their suppressive capacity and MDSC enhanced the production of IL-17 by gd T cells through release of IL-23 and IL-1β. Similarly, gd T cell-derived IL-17 has also been shown to recruit MDSC to the liver in HBV-transgenic mice, where they induce CD8 T cell exhaustion and HBV tolerance[5].
In DEN-induced liver carcinogenesis IL-18, is also involved in recruitment of MDSC to the liver. Li et al[39] demonstrated recently that TLR2-deficient mice develop more aggressive HCC than wildtype (wt) mice
46 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Species Type of disease Surface phenotype Function of MDSC Mechanism Ref.
Human Chronic HCV infection CD11b+ HLA-DRlo CD33+ CD14+ Inhibition of T cell proliferation and IFNg production Arginase1 [6] Human HCV-infected hepatocytes CD11b+/lo HLA-DRlo/- CD33+
CD14+Inhibition of T cell cytokine production ROS
Cell-cell-contact
[7]
Human HCC CD11b+ HLA-DR- CD33+ CD14- Long-lasting inhibition of effector T cells [22-30] Human HCC HLA-DRlo/- CD14+ Inhibition of natural killer cells Cell-cell-
contactNKp30
[33]
Human HCC HLA-DRlo/- CD14+ Induction of Treg and inhibition of effector T cells Arginase [29] Mouse CCl4-mediated fibrosis CD11b+Ly6G-Ly6ChiF4/80+ Amelioration of fibrosis through inhibition of HSC IL-10
production[13]
CD11b+Ly6G+Ly6CloF4/80-
Mouse Th1-mediated inflammation
CD11b+Ly6G-Ly6Chi Inhibition of T cell proliferation (CD4+ and CD8+) iNOScell-cell-contact
[48]CD11b+Ly6G+Ly6Clo
Mouse Sepsis CD11b+Gr1+ Inhibition of IL-12 and induction of IL-10 release by macrophages
Cell-cell-contact
[2]
Mouse Immune-mediated hepatitis
CD11b+Ly6GloLy6Chi Suppression of CD4+ T cell proliferation iNOS [46,47]CD11b+Ly6G+Ly6Clo
Mouse ConA-mediated hepatitis CD11b+Ly6G-Ly6C+ Protection against liver injury through inhibition of T cells
Arginase [4]CD11b+Ly6G+Ly6C+(int)
Mouse ConA/LPS-mediated hepatitis
CD11b+Ly6GloLy6Chi Suppression of CD4+ T cell proliferation and cytokine production
iNOScell-cell-contact
[3,45]CD11b+Ly6GhiLy6Cint
Mouse CTL-mediated liver injury CD11b+Gr1+ Suppression of CTL proliferation and IFNg production [21] Mouse HBV (transgenics) CD11b+Gr1+ Suppression of HBV-specific CTL Arginase
iNOS[5]
Mouse HCC/primary liver tumors
CD11b+Gr1+ Suppression of anti-tumor CTL [35,36,38]
Mouse Gastrointestinal cancer with liver metastasis
CD11b+Gr1+/int Inhibition of T cell proliferation and tumor cell lysis [40]
Table 1 Functional role of myeloid derived suppressor cells in the regulation of human and murine liver diseases
ConA: Concanavalin A; CTL: Cytotoxic T lymphocyte; HCC: Hepatocellular carcinoma; HCV: Hepatitis C virus; IFN: Interferon; IL: Interleukin; iNOS: Inducible nitric oxide synthase; ROS: Reactive oxygen species; Treg: Regulatory T cell; MDSC: Myeloid derived suppressor cells.
Hammerich L et al . MDSC in liver disease

associated with increased numbers of MDSC in the liver. This was mediated by IL-18 produced by hepatocytes and could be reversed through silencing of IL-18.
Interestingly, MDSC have also been associated with the development of liver metastasis. Mice with different types of intra-abdominal tumors showed a significant accumulation of MDSC in the liver that were able to potently suppress cytotoxic T cells and induce regulatory T cells[40]. Hepatic MDSC also differed from splenic MDSC in these models, expressing higher levels of immune-modulatory cytokines and being primarily of a monocytic phenotype. Similarly to HCC development, hepatic accumulation of MDSC was mediated by tumor-derived KC. This suggests that MDSC promote the development of liver metastases and may provide an explanation why human intra-abdominal cancers metastasize preferentially to the liver[41].
ROLE OF MDSC IN MOUSE MODELS OF LIVER INFLAMMATION AND FIBROSISThe accumulation of neutrophils, monocytes and macrophages is a hallmark of acute and chronic liver inflammation. For instance, hepatic neutrophils are associated with drug-induced liver injury, alcoholic hepatitis or ischemia-reperfusion injury[42]. Hepatic macrophages are a remarkably heterogeneous popu-lation comprising myeloid cells with different origins (e.g., resident Kupffer cells vs infiltrating monocyte-derived macrophages) and distinct properties[43]. Some of these neutrophils and macrophages have a clear immunosuppressive phenotype, prompting research on MDSC in acute and chronic liver injury.
Recently, MDSC have been studied in the context of acute liver inflammation and are usually associated with protective functions in this setting. We and others could show that MDSC accumulate in the liver during Concanavalin A (ConA)-, D-galactosamine (D-gal) and picryl chloride-induced hepatitis[3,4,44-47] and protect the liver from excessive damage. However, there seems to be controversy about which subsets are preferentially involved and which suppressive mechanisms they use. Two independent studies showed that administration of cannabidiol[4] or IL-25[3] increases the number of hepatic CD11b+ Gr1+ cells that ameliorated organ damage upon immune-mediated hepatitis. In this setting, the ratio of gMDSC to mMDSC was about 2:1, and T cell responses were inhibited in an arginase-dependent manner with mMDSC being more suppressive than gMDSC[4]. Consistently, we have shown that inhibiting the suppressive capacity specifically in the mMDSC subset led to severely aggravated hepatitis upon ConA-challenge[44]. Similar observations were also made by another group studying the role of FTY720, a sphingosine-1-phosphate receptor agonist, in recruitment of MDSC to the liver[46,47]. However, the suppressive function of these cells was dependent on iNOS and NO production rather than arginine depletion
by Arg1. Furthermore, these studies also provided some insight into how MDSC are recruited to the liver. Similarly to what has been observed in liver cancer, MDSC accumulation was mediated via CXCR2[46,47]. In contrast to the aforementioned studies, Zhu et al[45] showed that, although both MDSC subtypes were recruited, only mMDSC were able to suppress T cell responses and limit liver damage in ConA-mediated hepatitis. This was also observed in acutely inflamed livers of Tgfβ1-/- mice[48], where both subtypes of MDSC accumulated but only mMDSC were capable of suppressing T cells utilizing iNOS.
Overall, the liver provides a unique tolerogenic micro-environment, and several antigen-presenting cells contribute to the suppression of immunogenic T cell responses in the liver[49]. It has become increasingly clear that immune tolerance can also occur during chro-nic liver diseases. On the one hand, such tolerogenic mechanisms may limit intrahepatic immune responses and subsequent tissue injury, but on the other hand, immune tolerance may restrain eradication of pathogens and favor chronic infections[50]. Only limited data is available on the involvement of MDSC in chronic liver injury and the development of liver fibrosis. A recent study by Suh et al[13] indicates that bone marrow-derived MDSC can ameliorate hepatofibrogenesis through the production of IL-10, which downregulates pro-fibrotic functions of activated HSC. Interestingly, IL-10 production was induced upon contact with activated HSC in vitro, suggesting a mechanism for the beneficial effects observed in patients and mice with hepatic fibrosis treated with infusion of bone marrow cells[51]. On the contrary, liver fibrosis development upon chronic injury was not affected in a mouse model of transgenic overexpression of the transcription factor crem-alpha, which impairs the functionality of hepatic mMDSC[44]. Thus, more data are needed to define the possible role of MDSC in chronic inflammatory settings in the liver, and their involvement may likely vary depending on the etiology of the underlying disease, e.g., autoimmunity, chronic viral hepatitis or metabolic injury.
MDSC AS THERAPEUTIC TARGETS FOR THE TREATMENT OF LIVER DISEASESGiven that MDSC are mainly associated with pathoge-nic functions in human chronic liver diseases such as chronic viral infections or liver cancer development, depletion of these cells and/or inhibition of their deve-lopment may hold high potential in the treatment of such diseases. It has been shown that MDSC can be differentiated from murine bone-marrow cells and human PBMC in vitro in the presence of GM-CSF and IL-6[52-54]. Thus, these cytokines might be therapeutically targeted to avoid development of MDSC in vivo, but due to the various other functions of these cytokines, systemic inhibition might not be feasible and methods of local inhibition should be explored. In tumor bearing
47 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Hammerich L et al . MDSC in liver disease

mice depletion of MDSC using a Gr-1 specific antibody has proven to help with eradication of tumors and prevention of recurrence[55,56]. However, a more recent study reported that this antibody failed to completely eliminate hepatic MDSC[57], challenging the feasibility of this approach for liver disease therapy. Since MDSC are considered immature cells, influencing the differentiation of these cells into other myeloid cells that promote rather than inhibit immune responses could be a differ-ent therapeutic approach. Retinoic acid and vitamin D3 have both been implicated in the differentiation of MDSC to dendritic cells in vitro and administrations of these agents to tumor-bearing mice or cancer patients resulted in the significant improvement of anti-tumor immune responses[58-61].
In murine models of acute liver inflammation MDSC have been associated with protective rather than pathogenic functions. Therefore, it might be helpful to enhance hepatic MDSC numbers for the treatment of patients with acute inflammation or autoimmunity in the liver. The previously mentioned induction of MDSC from PBMC using GM-CSF and IL-6 would allow for the generation and expansion of autologous MDSC that can then be retransferred to the patient. The fact that adoptively transferred MDSC preferentially home to the liver[15] acts in favor of this approach allowing directed delivery of MDSC to the site of inflammation. However, migration of MDSC and “off-target” T cell suppression cannot be ruled out and should be considered in this setting.
Taken together, MDSC represent promising thera-peutic targets in the treatment of liver diseases, but more extensive research is needed before these appro-aches can be used in clinical settings.
REFERENCES1 Talmadge JE, Gabrilovich DI. History of myeloid-derived
suppressor cells. Nat Rev Cancer 2013; 13: 739-752 [PMID: 24060865 DOI: 10.1038/nrc3581]
2 Sander LE, Sackett SD, Dierssen U, Beraza N, Linke RP, Müller M, Blander JM, Tacke F, Trautwein C. Hepatic acute-phase proteins control innate immune responses during infection by promoting myeloid-derived suppressor cell function. J Exp Med 2010; 207: 1453-1464 [PMID: 20530204 DOI: 10.1084/jem.20091474]
3 Sarra M, Cupi ML, Bernardini R, Ronchetti G, Monteleone I, Ranalli M, Franzè E, Rizzo A, Colantoni A, Caprioli F, Maggioni M, Gambacurta A, Mattei M, Macdonald TT, Pallone F, Monteleone G. IL-25 prevents and cures fulminant hepatitis in mice through a myeloid-derived suppressor cell-dependent mechanism. Hepatology 2013; 58: 1436-1450 [PMID: 23564603 DOI: 10.1002/hep.26446]
4 Hegde VL, Nagarkatti PS, Nagarkatti M. Role of myeloid-derived suppressor cells in amelioration of experimental autoimmune hepatitis following activation of TRPV1 receptors by cannabidiol. PLoS One 2011; 6: e18281 [PMID: 21483776 DOI: 10.1371/journal.pone.0018281]
5 Kong X, Sun R, Chen Y, Wei H, Tian Z. γδT cells drive myeloid-derived suppressor cell-mediated CD8+ T cell exhaustion in hepatitis B virus-induced immunotolerance. J Immunol 2014; 193: 1645-1653 [PMID: 25015833 DOI: 10.4049/jimmunol.1303432]
6 Cai W, Qin A, Guo P, Yan D, Hu F, Yang Q, Xu M, Fu Y, Zhou J, Tang X. Clinical significance and functional studies of myeloid-derived suppressor cells in chronic hepatitis C patients. J Clin
Immunol 2013; 33: 798-808 [PMID: 23354838 DOI: 10.1007/s10875-012-9861-2]
7 Tacke RS, Lee HC, Goh C, Courtney J, Polyak SJ, Rosen HR, Hahn YS. Myeloid suppressor cells induced by hepatitis C virus suppress T-cell responses through the production of reactive oxygen species. Hepatology 2012; 55: 343-353 [PMID: 21953144 DOI: 10.1002/hep.24700]
8 Youn JI, Gabrilovich DI. The biology of myeloid-derived suppressor cells: the blessing and the curse of morphological and functional heterogeneity. Eur J Immunol 2010; 40: 2969-2975 [PMID: 21061430 DOI: 10.1002/eji.201040895]
9 Poschke I, Kiessling R. On the armament and appearances of human myeloid-derived suppressor cells. Clin Immunol 2012; 144: 250-268 [PMID: 22858650 DOI: 10.1016/j.clim.2012.06.003]
10 Movahedi K, Guilliams M, Van den Bossche J, Van den Bergh R, Gysemans C, Beschin A, De Baetselier P, Van Ginderachter JA. Identification of discrete tumor-induced myeloid-derived suppressor cell subpopulations with distinct T cell-suppressive activity. Blood 2008; 111: 4233-4244 [PMID: 18272812 DOI: 10.1182/blood-2007-07-099226]
11 Greten TF, Manns MP, Korangy F. Myeloid derived suppressor cells in human diseases. Int Immunopharmacol 2011; 11: 802-807 [PMID: 21237299 DOI: 10.1016/j.intimp.2011.01.003]
12 Youn JI, Nagaraj S, Collazo M, Gabrilovich DI. Subsets of myeloid-derived suppressor cells in tumor-bearing mice. J Immunol 2008; 181: 5791-5802 [PMID: 18832739]
13 Suh YG, Kim JK, Byun JS, Yi HS, Lee YS, Eun HS, Kim SY, Han KH, Lee KS, Duester G, Friedman SL, Jeong WI. CD11b(+) Gr1(+) bone marrow cells ameliorate liver fibrosis by producing interleukin-10 in mice. Hepatology 2012; 56: 1902-1912 [PMID: 22544759 DOI: 10.1002/hep.25817]
14 Haverkamp JM, Smith AM, Weinlich R, Dillon CP, Qualls JE, Neale G, Koss B, Kim Y, Bronte V, Herold MJ, Green DR, Opferman JT, Murray PJ. Myeloid-derived suppressor activity is mediated by monocytic lineages maintained by continuous inhibition of extrinsic and intrinsic death pathways. Immunity 2014; 41: 947-959 [PMID: 25500368 DOI: 10.1016/j.immuni.2014.10.020]
15 Ilkovitch D, Lopez DM. The liver is a site for tumor-induced myeloid-derived suppressor cell accumulation and immunosuppression. Cancer Res 2009; 69: 5514-5521 [PMID: 19549903 DOI: 10.1158/0008-5472.CAN-08-4625]
16 Weiskirchen R, Tacke F. Cellular and molecular functions of hepatic stellate cells in inflammatory responses and liver immunology. Hepatobiliary Surg Nutr 2014; 3: 344-363 [PMID: 25568859]
17 Höchst B, Schildberg FA, Sauerborn P, Gäbel YA, Gevensleben H, Goltz D, Heukamp LC, Türler A, Ballmaier M, Gieseke F, Müller I, Kalff J, Kurts C, Knolle PA, Diehl L. Activated human hepatic stellate cells induce myeloid derived suppressor cells from peripheral blood monocytes in a CD44-dependent fashion. J Hepatol 2013; 59: 528-535 [PMID: 23665041 DOI: 10.1016/j.jhep.2013.04.033]
18 Chou HS, Hsieh CC, Yang HR, Wang L, Arakawa Y, Brown K, Wu Q, Lin F, Peters M, Fung JJ, Lu L, Qian S. Hepatic stellate cells regulate immune response by way of induction of myeloid suppressor cells in mice. Hepatology 2011; 53: 1007-1019 [PMID: 21374665 DOI: 10.1002/hep.24162]
19 Hsieh CC, Chou HS, Yang HR, Lin F, Bhatt S, Qin J, Wang L, Fung JJ, Qian S, Lu L. The role of complement component 3 (C3) in differentiation of myeloid-derived suppressor cells. Blood 2013; 121: 1760-1768 [PMID: 23299310 DOI: 10.1182/blood-2012-06-440214]
20 Yen BL, Yen ML, Hsu PJ, Liu KJ, Wang CJ, Bai CH, Sytwu HK. Multipotent human mesenchymal stromal cells mediate expansion of myeloid-derived suppressor cells via hepatocyte growth factor/c-met and STAT3. Stem Cell Reports 2013; 1: 139-151 [PMID: 24052949 DOI: 10.1016/j.stemcr.2013.06.006]
21 Cheng L, Wang J, Li X, Xing Q, Du P, Su L, Wang S. Interleukin-6 induces Gr-1+CD11b+ myeloid cells to suppress CD8+ T cell-mediated liver injury in mice. PLoS One 2011; 6: e17631 [PMID:
48 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Hammerich L et al . MDSC in liver disease

21394214 DOI: 10.1371/journal.pone.0017631]22 van Deventer HW, Burgents JE, Wu QP, Woodford RM, Brickey
WJ, Allen IC, McElvania-Tekippe E, Serody JS, Ting JP. The inflammasome component NLRP3 impairs antitumor vaccine by enhancing the accumulation of tumor-associated myeloid-derived suppressor cells. Cancer Res 2010; 70: 10161-10169 [PMID: 21159638 DOI: 10.1158/0008-5472.CAN-10-1921]
23 Bruchard M, Mignot G, Derangère V, Chalmin F, Chevriaux A, Végran F, Boireau W, Simon B, Ryffel B, Connat JL, Kanellopoulos J, Martin F, Rébé C, Apetoh L, Ghiringhelli F. Chemotherapy-triggered cathepsin B release in myeloid-derived suppressor cells activates the Nlrp3 inflammasome and promotes tumor growth. Nat Med 2013; 19: 57-64 [PMID: 23202296 DOI: 10.1038/nm.2999]
24 Mehal WZ. The inflammasome in liver injury and non-alcoholic fatty liver disease. Dig Dis 2014; 32: 507-515 [PMID: 25034283 DOI: 10.1159/000360495]
25 Bieghs V, Trautwein C. Innate immune signaling and gut-liver interactions in non-alcoholic fatty liver disease. Hepatobiliary Surg Nutr 2014; 3: 377-385 [PMID: 25568861 DOI: 10.3978/j.issn.2304-3881.2014.12.04]
26 Schnabl B, Brenner DA. Interactions between the intestinal microbiome and liver diseases. Gastroenterology 2014; 146: 1513-1524 [PMID: 24440671 DOI: 10.1053/j.gastro.2014.01.020]
27 Qin N, Yang F, Li A, Prifti E, Chen Y, Shao L, Guo J, Le Chatelier E, Yao J, Wu L, Zhou J, Ni S, Liu L, Pons N, Batto JM, Kennedy SP, Leonard P, Yuan C, Ding W, Chen Y, Hu X, Zheng B, Qian G, Xu W, Ehrlich SD, Zheng S, Li L. Alterations of the human gut microbiome in liver cirrhosis. Nature 2014; 513: 59-64 [PMID: 25079328 DOI: 10.1038/nature13568]
28 Szabo G, Csak T. Inflammasomes in liver diseases. J Hepatol 2012; 57: 642-654 [PMID: 22634126 DOI: 10.1016/j.jhep.2012.03.035]
29 Hoechst B, Ormandy LA, Ballmaier M, Lehner F, Krüger C, Manns MP, Greten TF, Korangy F. A new population of myeloid-derived suppressor cells in hepatocellular carcinoma patients induces CD4(+)CD25(+)Foxp3(+) T cells. Gastroenterology 2008; 135: 234-243 [PMID: 18485901 DOI: 10.1053/j.gastro.2008.03.020]
30 Kalathil S, Lugade AA, Miller A, Iyer R, Thanavala Y. Higher frequencies of GARP(+)CTLA-4(+)Foxp3(+) T regulatory cells and myeloid-derived suppressor cells in hepatocellular carcinoma patients are associated with impaired T-cell functionality. Cancer Res 2013; 73: 2435-2444 [PMID: 23423978 DOI: 10.1158/0008-5472.CAN-12-3381]
31 Mundy-Bosse BL, Young GS, Bauer T, Binkley E, Bloomston M, Bill MA, Bekaii-Saab T, Carson WE, Lesinski GB. Distinct myeloid suppressor cell subsets correlate with plasma IL-6 and IL-10 and reduced interferon-alpha signaling in CD4⁺ T cells from patients with GI malignancy. Cancer Immunol Immunother 2011; 60: 1269-1279 [PMID: 21604071 DOI: 10.1007/s00262-011-1029-z]
32 Liu Y, She LH, Wang XY, Zhang GL, Yan Y, Lin CS, Zhao ZX, Gao ZL. Expansion of myeloid-derived suppressor cells from peripheral blood decreases after 4-week antiviral treatment in patients with chronic hepatitis C. Int J Clin Exp Med 2014; 7: 998-1004 [PMID: 24955173]
33 Hoechst B, Voigtlaender T, Ormandy L, Gamrekelashvili J, Zhao F, Wedemeyer H, Lehner F, Manns MP, Greten TF, Korangy F. Myeloid derived suppressor cells inhibit natural killer cells in patients with hepatocellular carcinoma via the NKp30 receptor. Hepatology 2009; 50: 799-807 [PMID: 19551844 DOI: 10.1002/hep.23054]
34 Kapanadze T, Gamrekelashvili J, Ma C, Chan C, Zhao F, Hewitt S, Zender L, Kapoor V, Felsher DW, Manns MP, Korangy F, Greten TF. Regulation of accumulation and function of myeloid derived suppressor cells in different murine models of hepatocellular carcinoma. J Hepatol 2013; 59: 1007-1013 [PMID: 23796475 DOI: 10.1016/j.jhep.2013.06.010]
35 Cao M, Xu Y, Youn JI, Cabrera R, Zhang X, Gabrilovich D, Nelson DR, Liu C. Kinase inhibitor Sorafenib modulates immunosuppressive cell populations in a murine liver cancer model. Lab Invest 2011; 91: 598-608 [PMID: 21321535 DOI: 10.1038/labinvest.2010.205]
36 Schneider C, Teufel A, Yevsa T, Staib F, Hohmeyer A, Walenda G, Zimmermann HW, Vucur M, Huss S, Gassler N, Wasmuth HE, Lira SA, Zender L, Luedde T, Trautwein C, Tacke F. Adaptive immunity suppresses formation and progression of diethylnitrosamine-induced liver cancer. Gut 2012; 61: 1733-1743 [PMID: 22267597 DOI: 10.1136/gutjnl-2011-301116]
37 Gauttier V, Judor JP, Le Guen V, Cany J, Ferry N, Conchon S. Agonistic anti-CD137 antibody treatment leads to antitumor response in mice with liver cancer. Int J Cancer 2014; 135: 2857-2867 [PMID: 24789574 DOI: 10.1002/ijc.28943]
38 Ma S, Cheng Q, Cai Y, Gong H, Wu Y, Yu X, Shi L, Wu D, Dong C, Liu H. IL-17A produced by γδ T cells promotes tumor growth in hepatocellular carcinoma. Cancer Res 2014; 74: 1969-1982 [PMID: 24525743 DOI: 10.1158/0008-5472.CAN-13-2534]
39 Li S, Sun R, Chen Y, Wei H, Tian Z. TLR2 limits development of hepatocellular carcinoma by reducing IL18-mediated immuno-suppression. Cancer Res 2015; 75: 986-995 [PMID: 25600646 DOI: 10.1158/0008-5472.CAN-14-2371]
40 Connolly MK, Mallen-St Clair J, Bedrosian AS, Malhotra A, Vera V, Ibrahim J, Henning J, Pachter HL, Bar-Sagi D, Frey AB, Miller G. Distinct populations of metastases-enabling myeloid cells expand in the liver of mice harboring invasive and preinvasive intra-abdominal tumor. J Leukoc Biol 2010; 87: 713-725 [PMID: 20042467 DOI: 10.1189/jlb.0909607]
41 McMillan DC, McArdle CS. Epidemiology of colorectal liver metastases. Surg Oncol 2007; 16: 3-5 [PMID: 17493802 DOI: 10.1016/j.suronc.2007.04.008]
42 Moles A, Murphy L, Wilson CL, Chakraborty JB, Fox C, Park EJ, Mann J, Oakley F, Howarth R, Brain J, Masson S, Karin M, Seki E, Mann DA. A TLR2/S100A9/CXCL-2 signaling network is necessary for neutrophil recruitment in acute and chronic liver injury in the mouse. J Hepatol 2014; 60: 782-791 [PMID: 24333183 DOI: 10.1016/j.jhep.2013.12.005]
43 Tacke F, Zimmermann HW. Macrophage heterogeneity in liver injury and fibrosis. J Hepatol 2014; 60: 1090-1096 [PMID: 24412603 DOI: 10.1016/j.jhep.2013.12.025]
44 Hammerich L, Warzecha KT, Stefkova M, Bartneck M, Ohl K, Gassler N, Luedde T, Trautwein C, Tenbrock K, Tacke F. Cyclic adenosine monophosphate-responsive element modulator alpha overexpression impairs function of hepatic myeloid-derived suppressor cells and aggravates immune-mediated hepatitis in mice. Hepatology 2015; 61: 990-1002 [PMID: 25330465 DOI: 10.1002/hep.27571]
45 Zhu K, Zhang N, Guo N, Yang J, Wang J, Yang C, Yang C, Zhu L, Xu C, Deng Q, Zhu R, Wang H, Chen X, Shi Y, Li Y, Leng Q. SSC(high)CD11b(high)Ly-6C(high)Ly-6G(low) myeloid cells curtail CD4 T cell response by inducible nitric oxide synthase in murine hepatitis. Int J Biochem Cell Biol 2014; 54: 89-97 [PMID: 25035167 DOI: 10.1016/j.biocel.2014.07.005]
46 Liu G, Bi Y, Wang R, Yang H, Zhang Y, Wang X, Liu H, Lu Y, Zhang Z, Chen W, Chu Y, Yang R. Targeting S1P1 receptor protects against murine immunological hepatic injury through myeloid-derived suppressor cells. J Immunol 2014; 192: 3068-3079 [PMID: 24567529 DOI: 10.4049/jimmunol.1301193]
47 Zhang Y, Bi Y, Yang H, Chen X, Liu H, Lu Y, Zhang Z, Liao J, Yang S, Chu Y, Yang R, Liu G. mTOR limits the recruitment of CD11b+Gr1+Ly6Chigh myeloid-derived suppressor cells in protecting against murine immunological hepatic injury. J Leukoc Biol 2014; 95: 961-970 [PMID: 24569105 DOI: 10.1189/jlb.0913473]
48 Cripps JG, Wang J, Maria A, Blumenthal I, Gorham JD. Type 1 T helper cells induce the accumulation of myeloid-derived suppressor cells in the inflamed Tgfb1 knockout mouse liver. Hepatology 2010; 52: 1350-1359 [PMID: 20803559 DOI: 10.1002/hep.23841]
49 Thomson AW, Knolle PA. Antigen-presenting cell function in the tolerogenic liver environment. Nat Rev Immunol 2010; 10: 753-766 [PMID: 20972472 DOI: 10.1038/nri2858]
50 Crispe IN. Immune tolerance in liver disease. Hepatology 2014; 60: 2109-2117 [PMID: 24913836 DOI: 10.1002/hep.27254]
51 Thomas JA, Pope C, Wojtacha D, Robson AJ, Gordon-Walker TT, Hartland S, Ramachandran P, Van Deemter M, Hume DA, Iredale
49 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Hammerich L et al . MDSC in liver disease

JP, Forbes SJ. Macrophage therapy for murine liver fibrosis recruits host effector cells improving fibrosis, regeneration, and function. Hepatology 2011; 53: 2003-2015 [PMID: 21433043 DOI: 10.1002/hep.24315]
52 Lechner MG, Liebertz DJ, Epstein AL. Characterization of cytokine-induced myeloid-derived suppressor cells from normal human peripheral blood mononuclear cells. J Immunol 2010; 185: 2273-2284 [PMID: 20644162 DOI: 10.4049/jimmunol.1000901]
53 Marigo I, Bosio E, Solito S, Mesa C, Fernandez A, Dolcetti L, Ugel S, Sonda N, Bicciato S, Falisi E, Calabrese F, Basso G, Zanovello P, Cozzi E, Mandruzzato S, Bronte V. Tumor-induced tolerance and immune suppression depend on the C/EBPbeta transcription factor. Immunity 2010; 32: 790-802 [PMID: 20605485 DOI: 10.1016/j.immuni.2010.05.010]
54 Highfill SL, Rodriguez PC, Zhou Q, Goetz CA, Koehn BH, Veenstra R, Taylor PA, Panoskaltsis-Mortari A, Serody JS, Munn DH, Tolar J, Ochoa AC, Blazar BR. Bone marrow myeloid-derived suppressor cells (MDSCs) inhibit graft-versus-host disease (GVHD) via an arginase-1-dependent mechanism that is up-regulated by interleukin-13. Blood 2010; 116: 5738-5747 [PMID: 20807889 DOI: 10.1182/blood-2010-06-287839]
55 Seung LP, Rowley DA, Dubey P, Schreiber H. Synergy between T-cell immunity and inhibition of paracrine stimulation causes tumor rejection. Proc Natl Acad Sci USA 1995; 92: 6254-6258 [PMID: 7603979]
56 Terabe M, Matsui S, Park JM, Mamura M, Noben-Trauth N, Donaldson DD, Chen W, Wahl SM, Ledbetter S, Pratt B, Letterio
JJ, Paul WE, Berzofsky JA. Transforming growth factor-beta production and myeloid cells are an effector mechanism through which CD1d-restricted T cells block cytotoxic T lymphocyte-mediated tumor immunosurveillance: abrogation prevents tumor recurrence. J Exp Med 2003; 198: 1741-1752 [PMID: 14657224 DOI: 10.1084/jem.20022227]
57 Ma C, Kapanadze T, Gamrekelashvili J, Manns MP, Korangy F, Greten TF. Anti-Gr-1 antibody depletion fails to eliminate hepatic myeloid-derived suppressor cells in tumor-bearing mice. J Leukoc Biol 2012; 92: 1199-1206 [PMID: 23077247 DOI: 10.1189/jlb.0212059]
58 Young MR, Ihm J, Lozano Y, Wright MA, Prechel MM. Treating tumor-bearing mice with vitamin D3 diminishes tumor-induced myelopoiesis and associated immunosuppression, and reduces tumor metastasis and recurrence. Cancer Immunol Immunother 1995; 41: 37-45 [PMID: 7641218]
59 Young MR, Lathers DM. Myeloid progenitor cells mediate immune suppression in patients with head and neck cancers. Int J Immunopharmacol 1999; 21: 241-252 [PMID: 10408632]
60 Hengesbach LM, Hoag KA. Physiological concentrations of retinoic acid favor myeloid dendritic cell development over granulocyte development in cultures of bone marrow cells from mice. J Nutr 2004; 134: 2653-2659 [PMID: 15465762]
61 Mirza N, Fishman M, Fricke I, Dunn M, Neuger AM, Frost TJ, Lush RM, Antonia S, Gabrilovich DI. All-trans-retinoic acid improves differentiation of myeloid cells and immune response in cancer patients. Cancer Res 2006; 66: 9299-9307 [PMID: 16982775 DOI: 10.1158/0008-5472.CAN-06-1690]
P- Reviewer: Gassler N, Morini S S- Editor: Ji FF L- Editor: A E- Editor: Wu HL
50 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Hammerich L et al . MDSC in liver disease

brain, the liver and the pancreas are well documented. Although chronic alcohol consumption causes serious impairments also in the gastrointestinal tract like altered motility, mucosal damage, impaired absorption of nutrients and inflammation, the effects of chronically consumed ethanol on the enteric nervous system are less detailed. While the nitrergic myenteric neurons play an essential role in the regulation of gastrointestinal peristalsis, it was hypothesised, that these neurons are the first targets of consumed ethanol or its metabolites generated in the different gastrointestinal segments. To reinforce this hypothesis the effects of ethanol on the gastrointestinal tract was investigated in different rodent models with quantitative immunohistochemistry, in vivo and in vitro motility measurements, western blot analysis, evaluation of nitric oxide synthase enzyme activity and bioimaging of nitric oxide synthesis. These results suggest that chronic alcohol consumption did not result significant neural loss, but primarily impaired the nitrergic pathways in gut regiondependent way leading to disturbed gastrointestinal motility. The gut segmentspecific differences in the effects of chronic alcohol consumption highlight the significance the ethanolinduced neuronal microenvironment involving oxidative stress and intestinal microbiota.
Key words: Chronic ethanol consumption; Nitrergic myenteric neurons; Enteric nervous system; Nitric oxide synthase; Gut motility disorders; Intestinal microbiota
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Chronic ethanol administration causes neurodegeneration in the central nervous system. In the enteric nervous system neurodegeneration was not demonstrated, however alcoholinduced quantitative, functional and neurochemical changes of nitrergic myenteric neurons were observed in gut regiondependent way. These suggest that disturbed gastrointestinal transit characteristic to alcoholic patients due to an impairment
Gut region-dependent alterations of nitrergic myenteric neurons after chronic alcohol consumption
Mária Bagyánszki, Nikolett Bódi, Department of Physiology, Anatomy and Neuroscience, University of Szeged, 6726 Szeged, Hungary
Author contributions: Both of the authors contributed to this paper.
Supported by The János Bolyai Research Scholarship of the Hungarian Academy of Sciences (Mária Bagyánszki); by the Hungarian Scientific Research Fund, OTKA grant PD 108309 (Nikolett Bódi).
Conflict-of-interest statement: The authors have no conflict of interest related to the manuscript.
OpenAccess: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Correspondence to: Mária Bagyánszki, PhD, Department of Physiology, Anatomy and Neuroscience, University of Szeged, Közép fasor 52, 6726 Szeged, Hungary. [email protected]: +36-62-343103Fax: +36-62-544149
Received: January 28, 2015Peerreview started: February 1, 2015First decision: March 6, 2015Revised: March 27, 2015Accepted: June 1, 2015 Article in press: June 2, 2015Published online: August 15, 2015
AbstractChronic alcohol abuse damages nearly every organ in the body. The harmful effects of ethanol on the
51 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
EDITORIAL
World J Gastrointest Pathophysiol 2015 August 15; 6(3): 51-57ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i3.51
Mária Bagyánszki, Nikolett Bódi

of a nitric oxidemediated descending inhibition during peristalsis. The better understanding of the effects of chronic ethanol administration on enteric neurons may reveal new targets for therapy.
Bagyánszki M, Bódi N. Gut region-dependent alterations of nitrergic myenteric neurons after chronic alcohol consumption. World J Gastrointest Pathophysiol 2015; 6(3): 51-57 Available from: URL: http://www.wjgnet.com/2150-5330/full/v6/i3/51.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i3.51
INTRODUCTIONAlcoholism is one of the world’s leading risk factor for morbidity, disability and mortality. In 2012, 5.9% of all global deaths in the world were attributable to alcohol abuse. Chronic alcohol consumption is a component cause of more than 200 disease and injury conditions[1].
The majority of absorbed ethanol is metabolized in the liver, but disassembly of ethanol also occurs in the whole length of the gastrointestinal (GI) tract, including the oral cavity, the esophagus, the stomach, and the small and large intestines. Ethanol is metabolized oxidatively into acetaldehyde by alcohol dehydrogenase, by the microsomal ethanol oxidizing system cytochrome P4502E1, and by catalase in the peroxisomes[2,3].
Ethanol and its oxidative and non-oxidative metabo-lites can be found throughout the GI tract, where they can interfere with several functions, including the intestinal barrier[2], GI motility and absorption of nutrients[4-6].
Animal models are available to investigate alcohol-related diseases[7-20], however there is still a need for animal models resembling more the human condition. It is well documented that alcohol ingestion results neuroinflammation and neurodegeneration in humans and animals[19]. In the induction of neuronal apoptosis, oxidative stress plays an important role[21]. Toxic and metabolic effects of ethanol vary in brain regions, the most affected regions are the frontal lobes, the cortical limbic-circuits and the cerebellum. Skeletal muscle, and peripheral nerves are also important targets of chronic alcohol-related metabolic injury and degeneration[22,23].
In this review the effects of chronic ethanol con-sumption on the enteric nervous system (ENS) are highlighted, particular the changes in the quantitative properties of nitrergic myenteric neurons and related motility disturbances in the different parts of the GI tract.
ALCOHOL AND NOS CONTAINING NEURONSIn the ENS, nitric oxide (NO) plays a critical role in mediating non-adrenergic, non-cholinergic relaxation of the intestinal smooth muscle in a gut regionally different way[24-26]. High concentrations of ethanol are reached
only in the duodenum and jejunum[5,27,28], however the concentration of ethanol reached in the ileum is not significantly different to the levels in the blood[27]. Therefore, the neuronal NO may be altered directly by the ethanol in the duodenum, while by the different oxidative and reductive metabolites in the different intestinal segments after chronic ethanol consumption. More findings provide evidence that effects of ethanol on NO system of intestinal relaxation[6,29] is responsible to the impaired motor function leading gut motility disorders[5,30,31]. NO is synthesized by the neuronal (n), endothelial (e) and inducible (i) nitric oxide synthases (NOSs)[32], and now, numerous investigations have already confirmed that all the NOSs are constitutively expressed in the myenteric neurons[33,34]. However, the effects of chronic alcohol intake on the density of nitrergic myenteric neurons, the amount of the three NOSs and/or their activity in different parts of the GI tract have been poorly investigated.
Therefore, in the last ten years we concentrated our research on the alcohol-induced alterations of nitrergic myenteric neurons in different gut regions[6,31,35,36]. We established a model suitable to study the NOS activities, protein content and the number of total and nNOS-immunoreactive myenteric neurons (Figure 1) in the duodenum, jejunum, ileum and colon of control and ethanol-exposed animals[35]. The activity of constitutive NOS (cNOS, both neuronal and endothelial) was 20 times higher in the proximal colon than in any part of the small intestine in control animals. Except of duodenum cNOS activity decreased significantly after chronic ethanol consumption. Under physiological conditions, the iNOS activity was also higher in the distal gut segments, but it did not change by the effects of ethanol. Similar results were observed in NOS protein content of tissue samples; the nNOS density of colonic fractions was more than twice as high as those of the samples prepared from the other gut segments and it also decreased after chronic ethanol consumption. The densities of eNOS-fractions were very weak and differences were not revealed in different intestinal samples and conditions. In intestinal whole-mount preparations from control rats, the number of nNOS-immunoreactive neurons was the highest in the colon. After ethanol exposure the decrease in the nitrergic cell number was significant in the whole length of the gut (Figure 2), however the greatest decrease in density of nitrergic neurons was observed in the colon[35]. The total number of myenteric neurons labelled with HuC/HuD pan-neuronal marker did not differ between controls and ethanol-drinking rats which suggest that chronic alcohol administration did not result in significant cell loss, but primarily impaired the nitrergic pathways in regionally different way.
Reduced number of nNOS-expressing neurons after chronic alcohol intake was also demonstrated in the murine jejunum[31] without changing in the total neuronal number. Both results indicate that chronic alcohol consumption leads to reduced nNOS expression
52 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Bagyánszki M et al . Chronic alcohol consumption impairs nitrergic neurons

resulting in motility disorders. In another study[6], the bio-imaging of basal NO synthesis of individual myenteric neurons was validated by loading the whole-mount preparations with the fluorescent indicator DAF-FM[37,38]. Based on DAF-FM recordings, chronic alcohol consumption induced a markedly increased basal NO synthesis in myenteric neurons as well as in glial cells or smooth muscle cells, indicates that chronic alcohol intake caused a general overproduction of NO in the jejunal gut wall. They confirmed reduced proportion of nNOS-expressing myenteric neurons and an increase of the proportion of iNOS-immunoreactive neurons was also revealed in murine small intestine[6]. Interestingly, the percentage of iNOS-containing neurons is in reasonable agreement with the measured percentages of neurons that produced NO but were not immunoreactive for nNOS. Others has also demonstrated that ethanol increased the amount of intestinal iNOS[36,39] and content of NO[39] in rats. Ethanol-induced NO overproduction appears to be relevant to the intestinal barrier dysfunc-tion and alcoholic gut leakiness[40].
Besides myenteric neurons, the presence of the three NOSs shows characteristic cell type-specific distribution in enteric smooth muscle cells and capillary endothelium[34]. In accord with recent studies[41,42], we hypothesized that the presence of the three NOSs with similar functions in the same type of cells, the gut wall is able to adapt to different pathological conditions. To evaluate the possible rearrangement of the cellular and subcellular NOS compartments in response to chronic ethanol treatment post-embedding immuno-electron microscopy was used in different gut segments and cell types. Counting gold particles labelling different NOSs, the nNOS labels were in general the most numerous under normal conditions[36] which is in agreement with the finding of an earlier study[43] and strengthen that in the GI tract, nNOS is the main source of NO. However in the different intestinal segments and cellular compartments, well-pronounced differences were observed in the number of nNOS labels under physiological and alcoholic conditions. After chronic ethanol consumption, the numbers of nNOS labels are decreased in one intestinal segment and increased
in another suggest significant differences in the microenvironment in different gut regions. Interestingly, the quantitative features of eNOS labels were changed in the opposite way to those in nNOS signing after ethanol intake. For example, while the number of nNOS gold particles decreased by more than 50% in the ganglia of duodenum, the eNOS labels approximately doubled here[36]. Depending on the investigated gut segment and type of NOS, a pronounced subcellular realignment of NOS labels was also found in ethanol-treated rats. The opposite alterations of eNOS and nNOS and subcellular rearrangement of NOS compartments may reflect a functional plasticity, in which different NOSs can replace each other to help maintenance the optimum NO level even under pathological condition.
CHRONIC ETHANOL ADMINISTRATION AFFECTS GASTROINTESTINAL MOTILITYAlthough the effects of ethanol consumption on gas-trointestinal motility is well documented[44-49], even the opposite effects of acute and chronic administration of alcohol on GI transit have demonstrated, the mech-anisms underlying impaired smooth muscle contractility are poorly understood and several conflicting data are present.
To reinforce the pathogenic role of NO in the ENS during chronic alcohol treatment, we investigated possible changes in the proportion of nitrergic myenteric neurons in relation to GI motility disturbances observed after chronic alcohol consumption in a murine model[31].
We demonstrated that chronic alcohol consumption affects gastric emptying and small intestinal transit in vivo (Figure 3). Migration of an Evans blue bolus throughout the stomach and small intestine was significantly delayed in chronic alcohol-treated mice when compared with controls receiving tap water. These findings point to an effect of chronic alcohol treatment on both stomach and small intestinal motility.
To elucidate whether this delay in intestinal transit could be associated with altered nitrergic relaxation of smooth muscle, we performed in vitro organ bath
53 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
A B
Figure 1 Representative light micrographs of whole mount preparation on the myenteric neurons of rat ileum after neuronal nitric oxide synthase immunohistochemistry. A: × 100; B: × 400.
Bagyánszki M et al . Chronic alcohol consumption impairs nitrergic neurons

experiments. Jejunal muscle strips relaxed to electrical field stimulation (EFS) and these relaxations were mimicked by exogenous NO. Relaxations to EFS were blocked by the NOS inhibitor L-NNA, confirming that they are mediated by NO[50]. In chronic alcohol-treated mice, the nitrergic relaxations to EFS were significantly decreased, whereas those to increasing concentrations of exogenous NO did not differ between chronic alcohol-treated and control mice. This finding indicates that the effect exerted by chronic alcohol consumption on smooth muscle relaxation is not because of a defective responsiveness of the smooth muscle to NO but appears to originate from impaired nitrergic neuronal activity[31].
Recently Yazir et al[51] found that chronic alcohol consumption impairs relaxant and contractile responses of both esophageal tunica muscularis mucosae and lower esophageal sphincter smooth muscle. Similarly to our results they found decreased nNOS immuno-reactivity in esophageal myenteric plexus in alcohol-exposed group compared to control groups[51].
ALCOHOL AND GUT MICROBIOTAIt is well documented that the anatomical, functional, and pathological regionality of the gastrointestinal tract develops under strict genetic control[52,53], which itself result in the unique susceptibility of the neurons to pathological conditions in different intestinal segments. The gut region-specific neuronal damage demonstrated in rats with chronic ethanol consumption[6,31,35,36] indi-cates the importance of the molecular differences in the microenvironment of nitrergic neurons located in different gut segments[36]. It has recently evidenced that after chronic ethanol consumption, the three NOS isoforms were affected differentially not only in the myenteric neurons but also in mesenteric capil-laries running in the vicinity of myenteric ganglia and smooth muscle cells[36]. Among the many factors that are implicated in this regionally distinct pathologic
microenvironment of neurons in different gut segments, the intestinal microbiota got recently in the focus of research gastrointestinal diseases[54,55].
The composition of gut microbiome and the amount of bacteria is also unique along the oro-anal gut axis. The upper gastrointestinal tract does not harbour a rich of microbial concentration due to gastric acid, biliary and pancreatic secretion, while in the colon the highest density of bacterial community is found[56,57] with potential role in prevention, several metabolic activities and gut permeability[58-60]. Alcohol has been shown to increase in total number of bacteria in jejunum[61] and also result in duodenal bacterial overgrowth[62,63]. Others[64] also demonstrated that chronic ethanol feeding caused an increase in the abundance of the gram negative Proteobacteria including several pathogenic species and gram positive Actinobacteria, as well as resulted in a decline of Bacteroidetes and Firmicutes phyla. The balance in the composition of microbiome is critical to maintain gut homeostasis, therefore the breakdown of it associated with endotoxemia, lipopolysaccharides translocation and several immunological reactions[65]. Elevation of the growth of gram negative bacteria results in augmentation of lipopolysaccharides like endotoxins, a component of gram negative bacterial wall. Endotoxins release several pro-inflammatory cytokines from acti-vated macrophages[66,67] which lead the alteration of intestinal barrier through disruption of tight junctions[68] and contribute to the progression of alcoholic liver disease, cirrhosis or alcoholic pancreatitis[55,69]. Increased gut permeability allows to endotoxins passing into the bloodstream creating harmful cycles[70]. However, Zhong et al[71] found that the gut leakiness after chronic alcohol exposure occurs in the ileum but not in the duodenum or jejunum. They also observed that alcohol exposure caused ROS accumulation in the small intestine with strongest labelling in the ileum. In parallel with oxidative stress, the zinc dyshomeostasis was also found gut region-specific as a consequence of ethanol exposure; the zinc status (an important trace element of all the major cell functions) was not affected in the duodenum
54 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
80
70
60
50
40
30
20
10
0Control Alcoholtreated Control Alcoholtreated
% gastric emptying % small intestinal transit
b
b
nNO
Sim
mun
orea
ctiv
e ne
uron
s/m
m2
120
100
80
60
40
20
0
b da
dControl
Ethanoltreated
Duodenum Jejunum Ileum Colon
Figure 2 In vivo measurement of % gastric emptying and % small intestinal transit in control and alcohol-treated mice (Bagyánszki et al[6] 2010). bP < 0.0001 vs control.
Figure 3 Gut-region-specific changes in the density of nNOS-immunor-eactive myenteric neurons after chronic ethanol consumption (Krecsmarik et al[35] 2006). aP < 0.05, bP < 0.01, dP < 0.001 vs control.
Bagyánszki M et al . Chronic alcohol consumption impairs nitrergic neurons

and jejunum but significantly decreased in the ileum[71]. Besides oxidative stress, alcohol reactive metabolites also have been suggested to critically mediate alcohol-induced intestinal barrier dysfunction[72,73]. Acetaldehyde is produced in a high concentration through ethanol metabolism by bacterial alcohol dehydrogenase[74,75] mediated mainly by aerobic or facultative anaerobic bacteria in the colon[76-78]. Based on these findings, further investigations on the region-specific composition of gut microbiome and alcohol-related alterations of intestinal microbiota in different gut segments should be performed to reveal the underlying events.
DISCUSSIONEndogenous NO is largely involved in the regulation of gut motility, secretion and blood flow[79-81]. More findings provide evidence that nitrergic subpopulation of the myenteric neurons is especially susceptible to different pathological conditions[35,36,81-85]. Furthermore, the NOS neurons are more sensitive to damage than other enteric neurons[86]. Among the possible reasons involving NOS neurons in enteric neuropathies, intracellular Ca+ concentration is thought to be critical[87]. In stress, neurons cannot maintain the optimal intracellular Ca+ level. Elevated Ca+ activates NOSs result in excessive production of free radicals as NO or peroxynitrite which lead cytotoxicity of neurons[86,87]. It has also been demonstrated that impairment of nitrergic myenteric neurons after chronic ethanol consumption is strictly gut region-dependent[35,36], which emphasize the importance of neuronal microenvironment. Therefore, to reveal the region-specific structural and molecular differences along the whole length of GI tract is essential to outline new directions in the diagnosis and the therapies GI diseases in chronic alcoholism.
ACKNOWLEDGMENTSWe thank our colleague and teacher, Professor Éva Fekete for her valuable comments on the manuscript.
REFERENCES1 WHO Global status report on alcohol and health, 2014. Available
from: URL: http://www.who.int/substance_abuse/publications/global_alcohol_report/en/
2 Elamin EE, Masclee AA, Dekker J, Jonkers DM. Ethanol metabolism and its effects on the intestinal epithelial barrier. Nutr Rev 2013; 71: 483-499 [PMID: 23815146 DOI: 10.1111/nure.12027]
3 Seth D, D’Souza El-Guindy NB, Apte M, Mari M, Dooley S, Neuman M, Haber PS, Kundu GC, Darwanto A, de Villiers WJ, Vonlaufen A, Xu Z, Phillips P, Yang S, Goldstein D, Pirola RM, Wilson JS, Moles A, Fernández A, Colell A, García-Ruiz C, Fernández-Checa JC, Meyer C, Meindl-Beinker NM. Alcohol, signaling, and ECM turnover. Alcohol Clin Exp Res 2010; 34: 4-18 [DOI: 10.1111/j.1530-0277.2009.01060.x]
4 Papa A, Tursi A, Cammarota G, Certo M, Cuoco L, Montalto M, Cianci R, Papa V, Fedeli P, Fedeli G, Gasbarrini G. Effect of moderate and heavy alcohol consumption on intestinal transit time.
Panminerva Med 1998; 40: 183-185 [PMID: 9785913]5 Bode C, Bode JC. Effect of alcohol consumption on the gut. Best
Pract Res Clin Gastroenterol 2003; 17: 575-592 [PMID: 12828956 DOI: 10.1016/S1521-6918(03)00034-9]
6 Bagyánszki M, Krecsmarik M, De Winter BY, De Man JG, Fekete E, Pelckmans PA, Adriaensen D, Kroese AB, Van Nassauw L, Timmermans JP. Chronic alcohol consumption affects gastrointestinal motility and reduces the proportion of neuronal NOS-immunoreactive myenteric neurons in the murine jejunum. Anat Rec (Hoboken) 2010; 293: 1536-1542 [PMID: 20648573 DOI: 10.1002/ar.21192]
7 Siegmund S, Haas S, Schneider A, Singer MV. Animal models in gastrointestinal alcohol research-a short appraisal of the different models and their results. Best Pract Res Clin Gastroenterol 2003; 17: 519-542 [PMID: 12828953 DOI: 10.1016/S1521-6918(03)00033-7]
8 Siegmund SV, Haas S, Singer MV. Animal models and their results in gastrointestinal alcohol research. Dig Dis 2005; 23: 181-194 [PMID: 16508282 DOI: 10.1159/000090165]
9 Patten AR, Fontaine CJ, Christie BR. A comparison of the different animal models of fetal alcohol spectrum disorders and their use in studying complex behaviors. Front Pediatr 2014; 2: 93 [DOI: 10.3389/fped.2014.00093]
10 Bates ME, Bowden SC, Barry D. Neurocognitive impairment associated with alcohol use disorders: implications for treatment. Exp Clin Psychopharmacol 2002; 10: 193-212 [PMID: 12233981 DOI: 10.1037/1064-1297.10.3.193]
11 Nixon K, Crews FT. Binge ethanol exposure decreases neurogenesis in adult rat hippocampus. J Neurochem 2002; 83: 1087-1093 [PMID: 12437579 DOI: 10.1046/j.1471-4159.2002.01214.x]
12 Monje ML, Toda H, Palmer TD. Inflammatory blockade restores adult hippocampal neurogenesis. Science 2003; 302: 1760-1765 [PMID: 14615545 DOI: 10.1126/science.1088417]
13 Ding J, Eigenbrodt ML, Mosley TH, Hutchinson RG, Folsom AR, Harris TB, Nieto FJ. Alcohol intake and cerebral abnormalities on magnetic resonance imaging in a community-based population of middle-aged adults: the Atherosclerosis Risk in Communities (ARIC) study. Stroke 2004; 35: 16-21 [PMID: 14657449 DOI: 10.1161/01.STR.0000105929.88691.8E]
14 Harper C. The neuropathology of alcohol-related brain damage. Alcohol Alcohol 2009; 44: 136-140 [PMID: 19147798 DOI: 10.1093/alcalc/agn102]
15 Crews FT, Nixon K. Mechanisms of neurodegeneration and regeneration in alcoholism. Alcohol Alcohol 2009; 44: 115-127 [PMID: 18940959 DOI: 10.1093/alcalc/agn079]
16 Zou J, Crews F. Induction of innate immune gene expression cascades in brain slice cultures by ethanol: key role of NF-κB and proinflammatory cytokines. Alcohol Clin Exp Res 2010; 34: 777-789 [PMID: 20201932 DOI: 10.1111/j.1530-0277.2010.01150.x]
17 Wang HJ, Zakhari S, Jung MK. Alcohol, inflammation, and gut-liver-brain interactions in tissue damage and disease development. World J Gastroenterol 2010; 16: 1304-1313 [PMID: 20238396 DOI: 10.3748/wjg.v16.i11.1304]
18 Ponomarev I. Epigenetic control of gene expression in the alcoholic brain. Alcohol Res 2013; 35: 69-76 [PMID: 24313166]
19 Szabo G, Lippai D. Converging actions of alcohol on liver and brain immune signaling. Int Rev Neurobiol 2014; 118: 359-80 [DOI: 10.1016/B978-0-12-801284-0.00011-7]
20 González-Reimers E, Santolaria-Fernández F, Martín-González MC, Fernández-Rodríguez CM, Quintero-Platt G. Alcoholism: a systemic proinflammatory condition. World J Gastroenterol 2014; 20: 14660-14671 [PMID: 25356029 DOI: 10.3748/wjg.v20.i40.14660]
21 Zou JY, Crews FT. Release of neuronal HMGB1 by ethanol through decreased HDAC activity activates brain neuroimmune signaling. PLoS One 2014; 9: e87915 [PMID: 24551070 DOI: 10.1371/journal.pone.0087915.]
22 de la Monte SM, Kril JJ. Human alcohol-related neuropathology. Acta Neuropathol 2014; 127: 71-90 [DOI: 10.1007/s00401-013-1233-3]
23 Bernardin F, Maheut-Bosser A, Paille F. Cognitive impairments in alcohol-dependent subjects. Front Psychiatry 2014; 5: 78 [PMID: 25076914 DOI: 10.3389/fpsyt.2014.00078]
55 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Bagyánszki M et al . Chronic alcohol consumption impairs nitrergic neurons

24 Takahashi T, Owyang C. Vagal control of nitric oxide and vasoactive intestinal polypeptide release in the regulation of gastric relaxation in rat. J Physiol 1995; 484 (Pt 2): 481-492 [PMID: 7602539 DOI: 10.1113/jphysiol.1995.sp020680]
25 Takahashi T, Owyang C. Regional differences in the nitrergic innervation between the proximal and the distal colon in rats. Gastroenterology 1998; 115: 1504-1512 [PMID: 9834278 DOI: 10.1016/S0016-5085(98)70029-0]
26 Nakao K, Takahashi T, Utsunomiya J, Owyang C. Extrinsic neural control of nitric oxide synthase expression in the myenteric plexus of rat jejunum. J Physiol 1998; 507 (Pt 2): 549-560 [PMID: 9518712 DOI: 10.1111/j.1469-7793.1998.549bt.x]
27 Bode JC. Alcohol and the gastrointestinal tract. Ergeb Inn Med Kinderheilkd 1980; 45: 1-75 [PMID: 7002540 DOI: 10.1007/978-3-642-67632-1_1]
28 Mezey E. Effect of ethanol on intestinal morphology, metabolism, and function. In: Alcohol Related Diseases in Gastroentreology. Seitz HK, Kommerell B, editors. Berlin: Springer, 1985: 342-360 [DOI: 10.1007/978-3-642-70048-4_19]
29 Wang SL, Xie DP, Liu KJ, Qin JF, Feng M, Kunze W, Liu CY. Nitric oxide mediates the inhibitory effect of ethanol on the motility of isolated longitudinal muscle of proximal colon in rats. Neurogastroenterol Motil 2007; 19: 515-521 [PMID: 17564633 DOI: 10.1111/j.1365-2982.2007.00918.x]
30 Addolorato G, Montalto M, Capristo E, Certo M, Fedeli G, Gentiloni N, Stefanini GF, Gasbarrini G. Influence of alcohol on gastrointestinal motility: lactulose breath hydrogen testing in orocecal transit time in chronic alcoholics, social drinkers and teetotaler subjects. Hepatogastroenterology 1997; 44: 1076-1081 [PMID: 9261602]
31 Bagyánszki M, Torfs P, Krecsmarik M, Fekete E, Adriaensen D, Van Nassauw L, Timmermans JP, Kroese AB. Chronic alcohol consumption induces an overproduction of NO by nNOS- and iNOS-expressing myenteric neurons in the murine small intestine. Neurogastroenterol Motil 2011; 23: e237-e248 [PMID: 21470341 DOI: 10.1111/j.1365-2982.2011.01707.x]
32 Bredt DS, Glatt CE, Hwang PM, Fotuhi M, Dawson TM, Snyder SH. Nitric oxide synthase protein and mRNA are discretely localized in neuronal populations of the mammalian CNS together with NADPH diaphorase. Neuron 1991; 7: 615-624 [PMID: 1718335 DOI: 10.1016/0896-6273(91)90374-9]
33 Vannucchi MG, Corsani L, Bani D, Faussone-Pellegrini MS. Myenteric neurons and interstitial cells of Cajal of mouse colon express several nitric oxide synthase isoforms. Neurosci Lett 2002; 326: 191-195 [PMID: 12095654 DOI: 10.1016/S0304-3940(02)00338-5]
34 Talapka P, Bódi N, Battonyai I, Fekete E, Bagyánszki M. Subcellular distribution of nitric oxide synthase isoforms in the rat duodenum. World J Gastroenterol 2011; 17: 1026-1029 [PMID: 21448354 DOI: 10.3748/wjg.v17.i8.1026]
35 Krecsmarik M, Izbéki F, Bagyánszki M, Linke N, Bódi N, Kaszaki J, Katarova Z, Szabó A, Fekete E, Wittmann T. Chronic ethanol exposure impairs neuronal nitric oxide synthase in the rat intestine. Alcohol Clin Exp Res 2006; 30: 967-973 [PMID: 16737454 DOI: 10.1111/j.1530-0277.2006.00110.x]
36 Bódi N, Jancsó Z, Talapka P, Pál A, Poles MZ, Bagyánszki M, Hermesz E, Fekete É. Gut region-specific rearrangement of the cellular and subcellular compartments of nitric oxide synthase isoforms after chronic ethanol consumption in rats. Histol Histopathol 2014; 29: 1547-1555 [PMID: 24848356]
37 Nagano T, Yoshimura T. Bioimaging of nitric oxide. Chem Rev 2002; 102: 1235-1270 [PMID: 11942795 DOI: 10.1021/cr010152s]
38 Itoh Y, Ma FH, Hoshi H, Oka M, Noda K, Ukai Y, Kojima H, Nagano T, Toda N. Determination and bioimaging method for nitric oxide in biological specimens by diaminofluorescein fluorometry. Anal Biochem 2000; 287: 203-209 [PMID: 11112265 DOI: 10.1006/abio.2000.4859]
39 Wang C, Wang S, Qin J, Lv Y, Ma X, Liu C. Ethanol upregulates iNOS expression in colon through activation of nuclear factor-kappa B in rats. Alcohol Clin Exp Res 2010; 34: 57-63 [PMID: 19860806 DOI: 10.1111/j.1530-0277.2009.01066.x]
40 Tang Y, Forsyth CB, Farhadi A, Rangan J, Jakate S, Shaikh M, Banan A, Fields JZ, Keshavarzian A. Nitric oxide-mediated intestinal injury is required for alcohol-induced gut leakiness and liver damage. Alcohol Clin Exp Res 2009; 33: 1220-1230 [PMID: 19389191 DOI: 10.1111/j.1530-0277.2009.00946.x]
41 Giaroni C, De Ponti F, Cosentino M, Lecchini S, Frigo G. Plasticity in the enteric nervous system. Gastroenterology 1999; 117: 1438-1458 [PMID: 10579986 DOI: 10.1016/S0016-5085(99)70295-7]
42 Giaroni C, Marchet S, Carpanese E, Prandoni V, Oldrini R, Bartolini B, Moro E, Vigetti D, Crema F, Lecchini S, Frigo G. Role of neuronal and inducible nitric oxide synthases in the guinea pig ileum myenteric plexus during in vitro ischemia and reperfusion. Neurogastroenterol Motil 2013; 25: e114-e126 [PMID: 23279126 DOI: 10.1111/nmo.12061]
43 Qu XW, Wang H, Rozenfeld RA, Huang W, Hsueh W. Type I nitric oxide synthase (NOS) is the predominant NOS in rat small intestine. Regulation by platelet-activating factor. Biochim Biophys Acta 1999; 1451: 211-217 [PMID: 10446403 DOI: 10.1016/S0167-4889(99)00076-2]
44 Charles F, Evans DF, Castillo FD, Wingate DL. Daytime ingestion of alcohol alters nighttime jejunal motility in man. Dig Dis Sci 1994; 39: 51-58 [PMID: 8281867 DOI: 10.1007/BF02090060]
45 Schmidt T, Eberle R, Pfeiffer A, Kaess H. Effect of ethanol on postprandial duodenojejunal motility in humans. Dig Dis Sci 1997; 42: 1628-1633 [PMID: 9286227]
46 Addolorato G, Capristo E, Gasbarrini G, Stefanini GF. Depression, alcohol abuse and orocaecal transit time. Gut 1997; 41: 417-418 [PMID: 9378406 DOI: 10.1136/gut.41.3.417a]
47 Lu G, Sarr MG, Szurszewski JH. Effects of ethyl alcohol on canine jejunal circular smooth muscle. Dig Dis Sci 1997; 42: 2403-2410 [PMID: 9440612]
48 Izbéki F, Wittmann T, Csáti S, Jeszenszky E, Lonovics J. Opposite effects of acute and chronic administration of alcohol on gastric emptying and small bowel transit in rat. Alcohol Alcohol 2001; 36: 304-308 [PMID: 11468129 DOI: 10.1093/alcalc/36.4.304]
49 Teyssen S, Singer MV. Alcohol-related diseases of the oesophagus and stomach. Best Pract Res Clin Gastroenterol 2003; 17: 557-573 [PMID: 12828955 DOI: 10.1016/S1521-6918(03)00049-0]
50 De Man JG, De Winter BY, Herman AG, Pelckmans PA. Study on the cyclic GMP-dependency of relaxations to endogenous and exogenous nitric oxide in the mouse gastrointestinal tract. Br J Pharmacol 2007; 150: 88-96 [PMID: 17115067 DOI: 10.1038/sj.bjp.0706964]
51 Yazir Y, Tugay M, Utkan Z, Utkan T. Effects of chronic ethanol consumption on rat upper gastrointestinal system: functional and histologic findings. Alcohol 2012; 46: 649-655 [PMID: 22818204 DOI: 10.1016/j.alcohol.2012.06.003]
52 Gao N, White P, Kaestner KH. Establishment of intestinal identity and epithelial-mesenchymal signaling by Cdx2. Dev Cell 2009; 16: 588-599 [PMID: 19386267 DOI: 10.1016/j.devcel.2009.02.010]
53 Doodnath R, Wride M, Puri P. The spatio-temporal patterning of Hoxa9 and Hoxa13 in the developing zebrafish enteric nervous system. Pediatr Surg Int 2012; 28: 115-121 [PMID: 21971947 DOI: 10.1007/s00383-011-2992-3]
54 Zhong W, Zhou Z. Alterations of the gut microbiome and metabolome in alcoholic liver disease. World J Gastrointest Pathophysiol 2014; 5: 514-522 [PMID: 25400995 DOI: 10.4291/wjgp.v5.i4.514]
55 Vonlaufen A, Spahr L, Apte MV, Frossard JL. Alcoholic pancreatitis: A tale of spirits and bacteria. World J Gastrointest Pathophysiol 2014; 5: 82-90 [PMID: 24891979 DOI: 10.4291/wjgp.v5.i2.82]
56 Wirth R, Bódi N, Maróti G, Bagyánszki M, Talapka P, Fekete É, Bagi Z, Kovács KL. Regionally distinct alterations in the composition of the gut microbiota in rats with streptozotocin-induced diabetes. PLoS One 2014; 9: e110440 [PMID: 25469509 DOI: 10.1371/journal.pone.0110440]
57 Schoster A, Arroyo LG, Staempfli HR, Weese JS. Comparison of microbial populations in the small intestine, large intestine and feces of healthy horses using terminal restriction fragment length polymorphism. BMC Res Notes 2013; 6: 91 [PMID: 23497580
56 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Bagyánszki M et al . Chronic alcohol consumption impairs nitrergic neurons

DOI: 10.1186/1756-0500-6-91]58 Guarner F. Enteric flora in health and disease. Digestion 2006; 73
Suppl 1: 5-12 [PMID: 16498248 DOI: 10.1159/000089775]59 Cummings JH, Beatty ER, Kingman SM, Bingham SA, Englyst
HN. Digestion and physiological properties of resistant starch in the human large bowel. Br J Nutr 1996; 75: 733-747 [PMID: 8695600 DOI: 10.1079/BJN19960177]
60 Gordon JI, Hooper LV, McNevin MS, Wong M, Bry L. Epithelial cell growth and differentiation. III. Promoting diversity in the intestine: conversations between the microflora, epithelium, and diffuse GALT. Am J Physiol 1997; 273: G565-G570 [PMID: 9316460]
61 Bode JC, Bode C, Heidelbach R, Dürr HK, Martini GA. Jejunal microflora in patients with chronic alcohol abuse. Hepatogastroenterology 1984; 31: 30-34 [PMID: 6698486]
62 Bode C, Kolepke R, Schäfer K, Bode JC. Breath hydrogen excretion in patients with alcoholic liver disease--evidence of small intestinal bacterial overgrowth. Z Gastroenterol 1993; 31: 3-7 [PMID: 8447153]
63 Gabbard SL, Lacy BE, Levine GM, Crowell MD. The impact of alcohol consumption and cholecystectomy on small intestinal bacterial overgrowth. Dig Dis Sci 2014; 59: 638-644 [PMID: 24323179 DOI: 10.1007/s10620-013-2960-y]
64 Bull-Otterson L, Feng W, Kirpich I, Wang Y, Qin X, Liu Y, Gobejishvili L, Joshi-Barve S, Ayvaz T, Petrosino J, Kong M, Barker D, McClain C, Barve S. Metagenomic analyses of alcohol induced pathogenic alterations in the intestinal microbiome and the effect of Lactobacillus rhamnosus GG treatment. PLoS One 2013; 8: e53028 [PMID: 23326376 DOI: 10.1371/journal.pone.0053028]
65 Malaguarnera G, Giordano M, Nunnari G, Bertino G, Malaguarnera M. Gut microbiota in alcoholic liver disease: pathogenetic role and therapeutic perspectives. World J Gastroenterol 2014; 20: 16639-16648 [PMID: 25469033 DOI: 10.3748/wjg.v20.i44.16639]
66 Fleming S, Toratani S, Shea-Donohue T, Kashiwabara Y, Vogel SN, Metcalf ES. Pro- and anti-inflammatory gene expression in the murine small intestine and liver after chronic exposure to alcohol. Alcohol Clin Exp Res 2001; 25: 579-589 [PMID: 11329499 DOI: 10.1111/j.1530-0277.2001.tb02253.x]
67 Thurman RG. II. Alcoholic liver injury involves activation of Kupffer cells by endotoxin. Am J Physiol 1998; 275: G605-G611 [PMID: 9756487]
68 Ma TY, Nguyen D, Bui V, Nguyen H, Hoa N. Ethanol modulation of intestinal epithelial tight junction barrier. Am J Physiol 1999; 276: G965-G974 [PMID: 10198341]
69 Gratz SW, Mykkanen H, El-Nezami HS. Probiotics and gut health: a special focus on liver diseases. World J Gastroenterol 2010; 16: 403-410 [PMID: 20101763 DOI: 10.3748/wjg.v16.i4.403]
70 Rao RK, Seth A, Sheth P. Recent Advances in Alcoholic Liver Disease I. Role of intestinal permeability and endotoxemia in alcoholic liver disease. Am J Physiol Gastrointest Liver Physiol 2004; 286: G881-G884 [PMID: 15132946 DOI: 10.1152/ajpgi.00006.2004]
71 Zhong W, McClain CJ, Cave M, Kang YJ, Zhou Z. The role of zinc deficiency in alcohol-induced intestinal barrier dysfunction. Am J Physiol Gastrointest Liver Physiol 2010; 298: G625-G633 [PMID: 20167873 DOI: 10.1152/ajpgi.00350.2009]
72 Forsyth CB , Farhadi A, Jakate SM, Tang Y, Shaikh M, Keshavarzian A. Lactobacillus GG treatment ameliorates alcohol-induced intestinal oxidative stress, gut leakiness, and liver injury in a rat model of alcoholic steatohepatitis. Alcohol 2009; 43: 163-172 [PMID: 19251117 DOI: 10.1016/j.alcohol.2008.12.009]
73 Keshavarzian A, Farhadi A, Forsyth CB, Rangan J, Jakate S, Shaikh
M, Banan A, Fields JZ. Evidence that chronic alcohol exposure promotes intestinal oxidative stress, intestinal hyperpermeability and endotoxemia prior to development of alcoholic steatohepatitis in rats. J Hepatol 2009; 50: 538-547 [PMID: 19155080 DOI: 10.1016/j.jhep.2008.10.028]
74 Seitz HK, Oneta CM. Gastrointestinal alcohol dehydrogenase. Nutr Rev 1998; 56: 52-60 [PMID: 9529900 DOI: 10.1111/j.1753-4887.1998.tb01692.x]
75 Visapää JP, Tillonen J, Salaspuro M. Microbes and mucosa in the regulation of intracolonic acetaldehyde concentration during ethanol challenge. Alcohol Alcohol 2002; 37: 322-326 [PMID: 12107032 DOI: 10.1093/alcalc/37.4.322]
76 Hill MJ, Drasar BS. The normal colonic bacterial flora. Gut 1975; 16: 318-323 [PMID: 1093952 DOI: 10.1136/gut.16.4.318]
77 Jokelainen K, Siitonen A, Jousimies-Somer H, Nosova T, Heine R, Salaspuro M. In vitro alcohol dehydrogenase-mediated acetaldehyde production by aerobic bacteria representing the normal colonic flora in man. Alcohol Clin Exp Res 1996; 20: 967-972 [PMID: 8892513 DOI: 10.1111/j.1530-0277.1996.tb01932.x]
78 Visapää JP, Jokelainen K, Nosova T, Salaspuro M. Inhibition of intracolonic acetaldehyde production and alcoholic fermentation in rats by ciprofloxacin. Alcohol Clin Exp Res 1998; 22: 1161-1164 [PMID: 9726290 DOI: 10.1111/j.1530-0277.1998.tb03716.x]
79 Bult H, Boeckxstaens GE, Pelckmans PA, Jordaens FH, Van Maercke YM, Herman AG. Nitric oxide as an inhibitory non-adrenergic non-cholinergic neurotransmitter. Nature 1990; 345: 346-347 [PMID: 1971425 DOI: 10.1038/345346a0]
80 Kubes P, McCafferty DM. Nitric oxide and intestinal inflammation. Am J Med 2000; 109: 150-158 [PMID: 10967157 DOI: 10.1016/S0002-9343(00)00480-0]
81 Barocelli E, Ballabeni V, Ghizzardi P, Cattaruzza F, Bertoni S, Lagrasta CA, Impicciatore M. The selective inhibition of inducible nitric oxide synthase prevents intestinal ischemia-reperfusion injury in mice. Nitric Oxide 2006; 14: 212-218 [PMID: 16504557 DOI: 10.1016/j.niox.2005.11.006]
82 Takahashi T. Pathophysiological significance of neuronal nitric oxide synthase in the gastrointestinal tract. J Gastroenterol 2003; 38: 421-430 [PMID: 12768383 DOI: 10.1007/s00535-003-1094-y]
83 Cellek S, Qu W, Schmidt AM, Moncada S. Synergistic action of advanced glycation end products and endogenous nitric oxide leads to neuronal apoptosis in vitro: a new insight into selective nitrergic neuropathy in diabetes. Diabetologia 2004; 47: 331-339 [PMID: 14676945]
84 Izbéki F, Wittman T, Rosztóczy A, Linke N, Bódi N, Fekete E, Bagyánszki M. Immediate insulin treatment prevents gut motility alterations and loss of nitrergic neurons in the ileum and colon of rats with streptozotocin-induced diabetes. Diabetes Res Clin Pract 2008; 80: 192-198 [PMID: 18242757 DOI: 10.1016/j.diabres.2007.12.013]
85 Talapka P, Nagy LI, Pál A, Poles MZ, Berkó A, Bagyánszki M, Puskás LG, Fekete É, Bódi N. Alleviated mucosal and neuronal damage in a rat model of Crohn’s disease. World J Gastroenterol 2014; 20: 16690-16697 [PMID: 25469038 DOI: 10.3748/wjg.v20.i44.16690]
86 Rivera LR, Poole DP, Thacker M, Furness JB. The involvement of nitric oxide synthase neurons in enteric neuropathies. Neurogastroenterol Motil 2011; 23: 980-988 [PMID: 21895878 DOI: 10.1111/j.1365-2982.2011.01780.x]
87 Dong Z, Saikumar P, Weinberg JM, Venkatachalam MA. Calcium in cell injury and death. Annu Rev Pathol 2006; 1: 405-434 [PMID: 18039121]
P- Reviewer: Boros M, Chiba T S- Editor: Song XX L- Editor: A E- Editor: Wu HL
57 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Bagyánszki M et al . Chronic alcohol consumption impairs nitrergic neurons

AbstractHigh resolution manometry (HRM) is a new technology that made important contributions to the field of gastrointestinal physiology. HRM showed clear advantages over conventional manometry and it allowed the creation of different manometric parameters. On the other side, conventional manometry is still wild available. It must be better studied if the new technology made possible the creation and study of these parameters or if they were always there but the colorful intuitive panoramic view of the peristalsis from the pharynx to the stomach HRM allowed the human eyes to distinguish subtle parameters unknown or uncomprehend so far and if HRM parameters can be reliably obtained by conventional manometry and data from conventional manometry still can be accepted in achalasia studies. Conventional manometry relied solely on the residual pressure to evaluate lower esophageal sphincter (LES) relaxation while HRM can obtain the Integrated Relaxation Pressure. Esophageal body HRM parameters defines achalasia subtypes, the Chicago classification, based on esophageal pressurization after swallows. The characterization of each subtype is very intuitive by HRM but also easy by conventional manometry since only wave amplitudes need to be measured. In conclusion, conventional manometry is still valuable to classify achalasia according to the Chicago classification. HRM permits a better study of the LES.
Key words: Achalasia; Esophagus; High resolution manometry; Conventional manometry; Lower esophageal sphincter; Esophageal body; Chicago classification
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: High resolution manometry is a new technology with clear advantages over conventional manometry. It is unclear; however, if new parameters created after this technology can be obtained by
Can high resolution manometry parameters for achalasia be obtained by conventional manometry?
Fernando AM Herbella, Hospital Sao Paulo, Surgical Gastroenterology, Division of Esophagus and Stomach, Federal University of Sao Paulo, Sao Paulo 04037-003, Brazil
Marco G Patti, Department of Surgery, Pritzker School of Medicine, University of Chicago, Chicago, IL 60637, United States
Author contributions: Herbella FAM contributed to conception and design, acquisition of data, analysis and interpretation of data, drafting the article, final approval of the version to be published; Patti MG contributed to analysis and interpretation of data, review for intellectual content, final approval of the version to be published.
Conflictofinterest statement: There are none. All authors contributed sufficiently to be named as authors and are responsible for the manuscript, no professional or ghost writer was hired.
OpenAccess: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Correspondence to: Dr. Fernando AM Herbella, MD, Hospital Sao Paulo, Surgical Gastroenterology, Division of Esophagus and Stomach, Federal University of Sao Paulo, Rua Diogo de Faria 1087 cj 301, Sao Paulo 04037-003, Brazil. [email protected]: +55-11-99922824Fax: +55-11-39267610
Received: March 20, 2015 Peerreview started: March 22, 2015 First decision: April 10, 2015Revised: April 22, 2015 Accepted: May 7, 2015Article in press: May 8, 2015Published online: August 15, 2015
58 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
EDITORIAL
World J Gastrointest Pathophysiol 2015 August 15; 6(3): 58-61ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i3.58
Fernando AM Herbella, Marco G Patti

conventional manometry especially in achalasia cases. We found that conventional manometry is still valuable to classify achalasia according to the Chicago classification but high resolution manometry permits a better study of the lower esophageal sphincter.
Herbella FAM, Patti MG. Can high resolution manometry parameters for achalasia be obtained by conventional manometry? World J Gastrointest Pathophysiol 2015; 6(3): 58-61 Available from: URL: http://www.wjgnet.com/2150-5330/full/v6/i3/58.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i3.58
High resolution manometry (HRM) made important contributions to the field of gastrointestinal physiology. HRM, in comparison to conventional manometry, not only brings more comfort and speediness to the test[1], a more intuitive comprehension of the plots compared to tracings[1] even for beginners[2], and a lesser degree of interobserver and intraobserver interpretation variability[3] but also HRM proved to be advantageous in the following parameters: (1) evaluation of gastric motility[4]; (2) the correct evaluation of the lower esophageal sphincter (LES) relaxation and esophagogastric junction flow avoiding movement artifacts and correlating it temporally with swallowing[5]; (3) the identification of segmental defects of peristalsis not covered by the spacing of sensors in conventional systems[6]; and (4) the motility and temporal correlation of the pharyngo-upper esophageal complex due to the rapid response and circunferentiality of the solid-state sensors, and compensation for movement artifacts[7].
The detailed view provided by HRM permitted the creation of new manometric parameters and a new classification of motility disorders, the Chicago classification[8], recently simplified and reviewed in his 3.0 version[9] with a 4.0 version under creation to incorporate intraluminal impedance as well. The Chicago classification made 3 major contributions: (1) defined an objective parameter to measure LES relaxation, the integrated relaxation pressure (IRP); (2) classified achalasia in 3 distinct subtypes; and (3) showed a prognostic value of manometry parameters[10].
It is still elusive; however, if the new technology made possible the creation and study of these para-meters or if they were always there but the colorful intuitive panoramic view of the peristalsis from the pharynx to the stomach HRM allowed the human eyes to distinguish subtle parameters unknown or uncomprehend so far (see examples on Figure 1). This lead to questioning if HRM parameters can be obtained by conventional manometry and data from conventional manometry still can be accepted in achalasia studies since HRM is not wildly available due to the high cost of the system and catheters.
Achalasia is a rare primary esophageal motor disorder characterized by aperistalsis and absent or incomplete relaxation of the LES[13]. Dysphagia and regurgitation are common symptoms of the disease that
59 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Herbella FAM et al . High resolution vs conventional manometry
Figure 1 Example of high resolution parameters identifiable at the conventional manometry. A: The peristaltic gap at transition zone (change from striated to smooth muscle in the proximal esophagus - arrow) has been fully explored with high resolution manometry[11] but it was well-known and identifiable as low amplitude waves at the proximal esophagus (arrow), although the clinical significance not comprehended, by conventional manometrists (B)[12]; C: The contractile deceleration point (CDP) represents the inflexion point in the contractile front propagation velocity in the distal esophagus representing the motility of the ampulla (arrow). Conventional manometry neglected time and privileged only amplitudes. A progressive latter onset of the distal wave (CDP) can be noticed from 3 to 1 cm above the lower esophageal sphincter upper border (D-F).
A
B
C
D
E
F

in association with a dilated esophagus on the barium esophagram makes the diagnoses of this disease not difficult[14]. Esophageal manometry; however, is useful not only for the diagnosis in difficult cases, especially without esophageal dilatation, but it seems to predict therapeutic outcomes[10], usually accomplished via endoscopic forced dilatation of the cardia or surgical Heller’s myotomy and fundoplication[15].
Conventional manometry relied solely on the residual pressure to evaluate LES relaxation[16]. IRP (Integrated Relaxation Pressure the average minimum esophagogastric junction pressure for 4 s of relaxation within 10 s of swallowing) is virtually impossible to be calculated in conventional tracings.
Esophageal body HRM parameters define achala-sia subtypes, the Chicago classification, based on
esophageal pressurization after swallows. The charac-terization of each subtype is very intuitive by HRM but also easy by conventional manometry since only wave amplitudes need to be measured (Figure 2). In fact, some well-known papers successfully applied the classification in patients submitted to conventional manometry[17,18]. Moreover, type III corresponds to the old terminology “vigorous achalasia”[8].
Different studies showed that achalasia type II shows the best response and type III the worst response to either Heller’s myotomy or endoscopic pneumatic dilatation[19]. The prognostic value of manometric parameters to define therapy outcomes is; however, not new to HRM. Long before Chicago classification, some Brazilians surgeons noticed poorer results for patients with lower amplitudes of the simultaneous waves observed at the conventional manometry (< 20 mmHg) precluding the choice of a Heller myotomy opting for an esophagectomy in these cases[20]. Very interestingly too, some authors found prognostic value for the basal pressure of the LES at conventional manometry[21], but this was never tested for HRM.
In conclusion, conventional manometry is still valuable to classify achalasia according to the Chicago classification. HRM permits a better study of the LES.
REFERENCES1 Salvador R, Dubecz A, Polomsky M, Gellerson O, Jones CE,
Raymond DP, Watson TJ, Peters JH. A new era in esophageal diagnostics: the image-based paradigm of high-resolution manometry. J Am Coll Surg 2009; 208: 1035-1044 [PMID: 19476889 DOI: 10.1016/j.jamcollsurg.2009.02.049]
2 Soudagar AS, Sayuk GS, Gyawali CP. Learners favour high resolution oesophageal manometry with better diagnostic accuracy over conventional line tracings. Gut 2012; 61: 798-803 [PMID: 21997554 DOI: 10.1136/gutjnl-2011-301145]
3 Bogte A, Bredenoord AJ, Oors J, Siersema PD, Smout AJ. Reproducibility of esophageal high-resolution manometry. Neurogastroenterol Motil 2011; 23: e271-e276 [PMID: 21496179 DOI: 10.1111/j.1365-2982.2011.01713.x]
4 Herbella FA, Aprile LR, Patti MG. High-resolution manometry for the evaluation of gastric motility. Updates Surg 2014; 66: 177-181 [PMID: 25106472 DOI: 10.1007/s13304-014-0261-4]
5 Kahrilas PJ, Peters JH. Evaluation of the esophagogastric junction using high resolution manometry and esophageal pressure topography. Neurogastroenterol Motil 2012; 24 Suppl 1: 11-19 [PMID: 22248103 DOI: 10.1111/j.1365-2982.2011.01829.x]
6 Vicentine FP, Herbella FA, Silva LC, Patti MG. High resolution manometry findings in patients with esophageal epiphrenic diverticula. Am Surg 2011; 77: 1661-1664 [PMID: 22273226]
7 Silva LC, Herbella FA, Neves LR, Vicentine FP, Neto SP, Patti MG. Anatomophysiology of the pharyngo-upper esophageal area in light of high-resolution manometry. J Gastrointest Surg 2013; 17: 2033-2038 [PMID: 24078388]
8 Kahrilas PJ, Ghosh SK, Pandolfino JE. Esophageal motility disorders in terms of pressure topography: the Chicago Classi-fication. J Clin Gastroenterol 2008; 42: 627-635 [PMID: 18364587 DOI: 10.1097/MCG.0b013e31815ea291]
9 Kahrilas PJ, Bredenoord AJ, Fox M, Gyawali CP, Roman S, Smout AJ, Pandolfino JE. The Chicago Classification of esophageal motility disorders, v3.0. Neurogastroenterol Motil 2015; 27: 160-174 [PMID: 25469569 DOI: 10.1111/nmo.12477]
10 Richter JE. High-resolution manometry in diagnosis and treatment of achalasia: help or hype. Curr Gastroenterol Rep 2014; 16: 420
60 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Type Ⅰ
Type Ⅱ
Type Ⅲ
Figure 2 Chicago classification subtypes at the light of high resolution manometry (left) and conventional manometry (right). Type Ⅰ (no distal pressurization), type Ⅱ (panesophageal pressurization), and type Ⅲ (premature spastic contractions).
Herbella FAM et al . High resolution vs conventional manometry

[PMID: 25543338]11 Ghosh SK, Pandolfino JE, Kwiatek MA, Kahrilas PJ. Oesophageal
peristaltic transition zone defects: real but few and far between. Neurogastroenterol Motil 2008; 20: 1283-1290 [PMID: 18662328 DOI: 10.1111/j.1365-2982.2008.01169.x]
12 Narawane NM, Bhatia SJ, Mistry FP, Abraham P, Dherai AJ. Manometric mapping of normal esophagus and definition of the transition zone. Indian J Gastroenterol 1998; 17: 55-57 [PMID: 9563221]
13 Herbella FA, Oliveira DR, Del Grande JC. Are idiopathic and Chagasic achalasia two different diseases? Dig Dis Sci 2004; 49: 353-360 [PMID: 15139481]
14 Patti MG, Herbella FA. Achalasia and other esophageal motility disorders. J Gastrointest Surg 2011; 15: 703-707 [PMID: 21394546 DOI: 10.1007/s11605-011-1478-x]
15 Allaix ME, Herbella FA, Patti MG. The evolution of the treatment of esophageal achalasia: a look at the last two decades. Updates Surg 2012; 64: 161-165 [PMID: 22847308 DOI: 10.1007/s13304-012-0169-9]
16 Patti MG, Diener U, Molena D. Esophageal achalasia: preoperative assessment and postoperative follow-up. J Gastrointest Surg 2001; 5: 11-12 [PMID: 11370614]
17 Salvador R, Costantini M, Zaninotto G, Morbin T, Rizzetto C,
Zanatta L, Ceolin M, Finotti E, Nicoletti L, Da Dalt G, Cavallin F, Ancona E. The preoperative manometric pattern predicts the outcome of surgical treatment for esophageal achalasia. J Gastrointest Surg 2010; 14: 1635-1645 [PMID: 20830530 DOI: 10.1007/s11605-010-1318-4]
18 Rohof WO, Salvador R, Annese V, Bruley des Varannes S, Chaussade S, Costantini M, Elizalde JI, Gaudric M, Smout AJ, Tack J, Busch OR, Zaninotto G, Boeckxstaens GE. Outcomes of treatment for achalasia depend on manometric subtype. Gastroenterology 2013; 144: 718-725; quiz e13-14 [PMID: 23277105 DOI: 10.1053/j.gastro.2012.12.027]
19 Müller M. Impact of high-resolution manometry on achalasia diagnosis and treatment. Ann Gastroenterol 2015; 28: 3-9 [PMID: 25608535]
20 Herbella FA, Aquino JL, Stefani-Nakano S, Artifon EL, Sakai P, Crema E, Andreollo NA, Lopes LR, de Castro Pochini C, Corsi PR, Gagliardi D, Del Grande JC. Treatment of achalasia: lessons learned with Chagas’ disease. Dis Esophagus 2008; 21: 461-467 [PMID: 18430188 DOI: 10.1111/j.1442-2050.2008.00811.x]
21 Arain MA, Peters JH, Tamhankar AP, Portale G, Almogy G, DeMeester SR, Crookes PF, Hagen JA, Bremner CG, DeMeester TR. Preoperative lower esophageal sphincter pressure affects outcome of laparoscopic esophageal myotomy for achalasia. J Gastrointest Surg 2004; 8: 328-334 [PMID: 15019930]
P- Reviewer: Jiang CM, Yamakawa M S- Editor: Ji FF L- Editor: A E- Editor: Wu HL
61 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Herbella FAM et al . High resolution vs conventional manometry

Article in press: June 16, 2015Published online: August 15, 2015
AbstractAnemia is a common extraintestinal manifestation of inflammatory bowel disease (IBD) and is frequently overlooked as a complication. Patients with IBD are commonly found to have iron deficiency anemia (IDA) secondary to chronic blood loss, and impaired iron absorption due to tissue inflammation. Patients with iron deficiency may not always manifest with signs and symptoms; so, hemoglobin levels in patients with IBD must be regularly monitored for earlier detection of anemia. IDA in IBD is associated with poor quality of life, necessitating prompt diagnosis and appropriate treatment. IDA is often associated with inflammation in patients with IBD. Thus, commonly used laboratory parameters are inadequate to diagnose IDA, and newer iron indices, such as reticulocyte hemoglobin content or percentage of hypochromic red cells or zinc protoporphyrin, are required to differentiate IDA from anemia of chronic disease. Oral iron preparations are available and are used in patients with mild disease activity. These preparations are inexpensive and convenient, but can produce gastrointestinal side effects, such as abdominal pain and diarrhea, that limit their use and patient compliance. These preparations are partly absorbed due to inflammation. Non-absorbed iron can be toxic and worsen IBD disease activity. Although costeffective intravenous iron formulations are widely available and have improved safety profiles, physicians are reluctant to use them. We present a review of the pathophysiologic mechanisms of IDA in IBD, improved diagnostic and therapeutic strategies, efficacy, and safety of iron replacement in IBD.
Key words: Iron deficiency anemia; Inflammatory bowel disease; Hepcidin; Ferritin; Oral iron; Intravenous iron
© The Author(s) 2015. Published by Baishideng Publishing
Iron deficiency anemia in inflammatory bowel disease
Sindhu Kaitha, Tauseef Ali, Department of Medicine, Section of Gastroenterology, Oklahoma University Health Sciences Center, Oklahoma City, OK 73104, United States
Muhammad Bashir, Department of Internal Medicine, Oklahoma University Health Sciences Center, Oklahoma City, OK 73104, United States
Author contributions: Kaitha S and Ali T conceived the idea; Kaitha S and Bashir M contributed to literature search and wrote the manuscript; Ali T supervised the project, performed critical review and proof reading of the manuscript.
Conflictofinterest statement: Sindhu Kaitha, MD and Muhammad Bashir, MD have neither received fees for serving as a speaker nor have received research funding from any organization for this review article. Sindhu Kaitha, MD and Muhammad Bashir, MD are employees of University of Oklahoma Health Sciences Center and the institute has no conflict of interest with the article. Sindhu Kaitha, MD and Muhammad Bashir, MD do not own stocks and/or shares and/or patents in any organization that would have conflict of interest with this review article. Tauseef Ali, MD has received honorarium for serving as an advisory board member for Luitpold pharmaceuticals.
OpenAccess: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Correspondence to: Tauseef Ali, MD, Assistant Professor, Department of Medicine, Section of Gastroenterology, Oklahoma University Health Sciences Center, Oklahoma, 601 NE 14th St, Oklahoma City, OK 73104, United States. [email protected]: +1-405-4712653Fax: +1-405-2715803
Received: January 29, 2015Peerreview started: January 29, 2015First decision: April 27, 2015Revised: May 9, 2015Accepted: June 15, 2015
62 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
MINIREVIEWS
World J Gastrointest Pathophysiol 2015 August 15; 6(3): 62-72ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i3.62
Sindhu Kaitha, Muhammad Bashir, Tauseef Ali

Group Inc. All rights reserved.
Core tip: Iron deficiency anemia (IDA) is increasingly recognized as a common complication in patients with inflammatory bowel disease (IBD). IDA has a significant impact on quality of life and health care costs. This comprehensive review article discusses the latest advances in understanding the pathophysiologic mechanisms involved in development of IDA in patients with IBD, and reviews new diagnostic tests and therapeutic options with high safety indexes for the management of IDA. This article aims at increasing physician awareness and understanding of the complex mechanisms involved in IDA, and the current cuttingedge approach for the management of IDA in patients with IBD.
Kaitha S, Bashir M, Ali T. Iron deficiency anemia in inflammatory bowel disease. World J Gastrointest Pathophysiol 2015; 6(3): 62-72 Available from: URL: http://www.wjgnet.com/2150-5330/full/v6/i3/62.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i3.62
INTRODUCTIONInflammatory bowel disease (IBD) describes a set of chronic gastrointestinal illnesses, including Crohn’s disease (CD) and ulcerative colitis (UC), of multifactorial etiology, which proceed with periods of relapse and remission. Extraintestinal complications are common in IBD, and are reported in more than 25% of patients[1]. Anemia is one of the most common manifestations of IBD[2]. One-third of patients with IBD have hemoglobin levels below 12 g/dL[3]. The anemic state is strongly correlated with quality of life, and is an important problem in the therapeutic management of patients with chronic disease[4].
ABSOLUTE AND FUNCTIONAL IRON DEFICIENCY Most cases of anemia in patients with IBD result from functional or absolute iron deficiency. Functional iron deficiency is a state in which there is insufficient availability of iron for incorporation into erythroid precursors despite normal or increased body iron stores[5,6]. In patients with absolute iron deficiency, iron is stored in the bone marrow. Other parts of the monocyte-macrophage system in the liver and spleen become depleted, making iron unavailable for normal or increased rates of erythropoiesis. This may occur as the result of poor dietary intake of iron, reduced iron absorption, and/or increased blood loss.
SIGNS AND SYMPTOMS OF IRON DEFICIENCY ANEMIASigns and symptoms of iron deficiency depend on the
severity and chronicity of the anemia, in addition to the usual signs of anemia, including fatigue, pallor, and reduced exercise capacity. Cheilosis and koilonychia are signs of advanced tissue iron deficiency which are not frequently seen in the modern world, due to early diagnosis and timely correction.
Key symptoms of anemia, such as dyspnea and tachycardia, are caused by decreased blood oxygen levels and peripheral hypoxia. Compensatory blood shifting from the mesenteric arteries may worsen perfusion of the intestinal mucosa[7]. Motility disorder, nausea, anorexia, and even malabsorption have been attributed to anemia. Reduced metabolic and energy efficiency during physical activity also contribute to weight loss in anemia[8].
Central hypoxia may lead to symptoms such as headache, dizziness, vertigo, or tinnitus. Several studies have confirmed that treatment of anemia improves cognitive function[9]. Iron is a component of hemoglobin myoglobin, cytochromes, and many other enzymes. Thus, anemia negatively impacts almost every aspect of daily life in patients with IBD. Men with iron deficiency anemia (IDA) may suffer from impotence. Loss of libido contributes to impaired quality of life in both sexes[10]. In addition, latent iron deficiency may be responsible for “non-hematological” symptoms such as hair loss, paresthesias of the hands and feet, and reduced cog-nitive function, and may also be significantly associated with restless leg syndrome.
CLINICAL RELEVANCEAnemia and iron deficiency have a dramatic impact on patients’ quality of life, yet anemia in patients with IBD is still underdiagnosed and undertreated. In the Uni-ted States, annual emergency room visits for anemia average around 209000[11], drastically maximizing health care costs. In a patient population with the predisposition for anemia, like patients with IBD, early diagnosis and management of iron deficiency can promptly reduce hospital visits, improve quality of life, reduce loss of work, and, ultimately, lower health care costs.
CAUSES OF IRON DEFICIENCY ANEMIA IN IBDAnemia in IBD patients involves multiple pathogenic mechanisms resulting in low hemoglobin levels and compromised quality of life. Although ongoing blood loss from chronically inflamed intestinal mucosa and micronutrient deficiency (iron and B12) are the main mechanisms underlying the development of anemia in patients with IBD, chronic inflammation, hemolysis, and medication-induced myelosuppression may also play important roles in both the development of anemia and the management of this condition[12,13]. Anemia of chronic disease (ACD) and IDA are the two most common causes of anemia in patients with IBD[14,15].
63 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Kaitha S et al . Iron and inflammatory bowel disease

Patients with IDA and concomitant ACD tend to have more severe anemia compared with patients with ACD alone[14]. Table 1 presents the causes of anemia in patients with IBD. Figure 1 outlines causes of IDA.
PATHOPHYSIOLOGY OF IRON DEFICIENCY ANEMIA IN IBDUp to 3-4 g of iron is stored in the human body. Around 1-2 mg of iron is lost every day through desquamation of epithelial cells of the skin, gastrointestinal tract, bile ducts, and urinary tract, and through blood loss in menstruating women[16].
Iron homeostasis is strictly maintained by iron absorption from the duodenal enterocytes, and is tightly regulated by hepcidin (Figure 2). Hepcidin is a 25-amino-acid peptide hormone, has intrinsic antimicrobial activity, and is an acute-phase protein that is primarily synthesized by hepatocytes[17]. Cellular targets for hepcidin and iron-exporting cells are villous enterocytes, reticuloendothelial macrophages, and hepatocytes. Hepcidin binds to the basolateral transporter and iron exporter ferroportin 1, leading to its phosphorylation, internalization by binding to JAK 2, and lysosomal degradation, thus preventing iron release into the plasma[16]. Increased hepcidin levels downregulate ferroportin, thereby reducing iron efflux from the enterocytes and macrophages, causing hypoferremia. The increase in enterocyte iron content reduces the expression of enterocyte brush border reductase (Dcytb) and divalent metal transporter 1 (DMT1) on villous enterocytes, inhibiting dietary iron absorption causing iron deficiency anemia[18]. Therefore, by regulating the expression of DMT1 and ferroportin, hepcidin acts as a negative regulator of iron absorption in the duodenum and of iron release from the enterocytes and macrophages.
Hepcidin expression is upregulated by iron overload, infection, and inflammation, through proinflammatory cytokines such as interleukin (IL)-6 via the JAK 2 mediated STAT 3 signaling, thus limiting iron absorp-tion[16,19]. Hepcidin expression is downregulated by hypoxia, oxidative stress, iron deficiency anemia,
and ineffective erythropoiesis, thus increasing iron availability (Figure 2)[20].
Hepcidin expression is mediated by two signaling pathways that involve bone morphogenetic protein (BMP) and transferrin receptor 2 (TfR2; Figure 3). The BMP signaling pathway includes BMP 6, hemojuvelin (HJV), and SMAD4, which constitute the major sig-naling pathway for hepcidin expression; TfR2 and the hereditary hemochromatosis protein (HFE)-dependent signaling pathway modulate this response[21,22]. In high iron conditions, transferrin-iron in the plasma forms a complex with HFE and TfR2 to promote hepcidin expression[21]. In iron-deficient conditions, there is downregulation of TfR2 and upregulation of TfR1. HFE is sequestered by TfR1, preventing its interaction with TfR2, thereby downregulating hepcidin expression (Figure 3)[21,23].
DIAGNOSTIC WORK-UP OF IRON DEFICIENCY ANEMIA IN IBD Healthcare providers screen for IDA by measuring hemoglobin, serum ferritin, and C-reactive protein (CRP). Based on expert opinion and common clinical practice, screening is recommended at least every 3 mo for outpatients with active disease, and once every 6 to 12 mo for patients in remission or with mild disease; screening is not applicable to hospitalized patients[24].
The World Health Organization (WHO) definitions of anemia also apply to patients with IBD. WHO defines anemia as hemoglobin levels < 13 g/dL (hematocrit < 39%) in males, < 12 g/dL (hematocrit < 36%) in nonpregnant females, and < 11 g/dL (hematocrit < 33%) in pregnant females[25]. Severe IDA is defined as hemoglobin levels < 10 g/dL.
If a patient meets WHO criteria for anemia, a basic anemia workup should be initiated to determine the cause of anemia. The basic workup includes serum ferritin, transferrin, transferrin saturation, and CRP levels. If the cause of anemia is unclear despite the results of the above workup, more extensive testing is recommended. Further tests include vitamin B12, folic acid, haptoglobin, lactate dehydrogenase, creatinine, and reticulocyte counts[24].
Both IDA and ACD often coexist with IBD, and the treatment for each differs. There is no single laboratory parameter that differentiates one from the other. Conse-quently, supplementary laboratory tests are required to differentiate IDA from ACD. These tests include soluble transferrin receptor, soluble transferrin receptor-ferritin index, reticulocyte hemoglobin concentration, zinc protoporphyrin, the percentage of hypochromic red cells, and hepcidin levels[16]. IDA in IBD is diagnosed based on a combination of factors, taking inflammation into account. The laboratory findings in IDA, ACD, mixed IDA, and ACD are shown in Table 2[16,22].
Serum ferritin is a measure of stored iron content in the reticuloendothelial system; in absolute iron
64 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Common causes Less common causes
Rare causes
Iron deficiency anemia
B12 deficiency Hemolysis
Anemia of chronic inflammation
Folic acid deficiency
Chronic renal insufficiency
Medications causing B12/Folate
deficiency
Myelodysplastic syndrome
Medication induced aplasia Congenital hemoglobinopathies
Protein starvation Anemia in liver disease
Table 1 Causes of anemia in inflammatory bowel disease
Kaitha S et al . Iron and inflammatory bowel disease

deficiency, the serum ferritin concentration is < 15 μg/L[16]. Serum ferritin is an acute-phase reactant; normal or high levels may be found in inflammatory conditions despite iron deficiency[26]. Therefore, the guidelines recommend that in patients with quiescent IBD without biochemical or clinical evidence of inflammation, iron deficiency is defined as serum ferritin < 30 g/L or transferrin saturation (TSAT) < 16%[24]. In the presence of active IBD with inflammation, as evidenced by elevated CRP, the guidelines give a cut-off level of serum ferritin < 100 g/L to increase sensitivity and specificity[24,27].
Microcytosis (low mean corpuscular volume, MCV) and hypochromia (low mean corpuscular hemoglobin, MCH), available from the complete blood count, are indicators of absolute iron deficiency. High MCV is found secondary to vitamin B12 and folate deficiency, the use of certain medications (thiopurines; azathioprine or 6-mercaptopurine), alcoholism, and hypothyroidism[24]. Therefore, normal or high MCV does not exclude IDA as a possibility. In patients with ACD, MCV may be low or
65 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Laboratory measures IDA ACD IDA and ACD
Serum iron ↓ ↓ ↓ Hemoglobin ↓ ↓ ↓ MCV ↓ ↓ or normal ↓ or normal CRP Normal ↑↑ ↑ Serum ferritin ↓ ↑ ↑ or normal Transferrin ↑ ↓ or normal ↓ Transferrin saturation ↓ ↓ ↓ sTfR ↑ ↓ ↑ or normal sTfR- Ferritin index High (> 2) Low (< 1) High (> 2) Reticulocyte Hb content (CHr, pg)
< 28 ≥ 28 < 28
Zinc protoporphyrin (μmol/mol heme)
> 40 < 40 > 40
Percentage of hypochromic RBC > 5 < 5 > 5 Hepcidin ↓ ↑ ↑
Table 2 Laboratory findings in iron deficiency anemia, anemia of chronic disease, mixed iron deficiency anem and anemia of chronic disease[16,31]
Causes of Iron Deficiency Anemia
Increased iron loss
Decreased iron absorption
Decreased iron intake
Increased demand for iron
Chronic blood loss
Acute blood loss
Phlebotomy
Malabsorptivediseases
Malabsorption from surgery
Drugs
Diet
Alcoholism
Low socioeconomic status
Inflammatory bowel diseaseGI tract ulcers
Gastritis
MedicationsColonic/gastric polypsDiverticular bleedingGI malignancy Intestinal parasitesMenses
Intraoperative blood loss
Trauma Internal bleeding
Polycythemia veraRegular blood donation
Inflammatory bowel disease
Chronic gastritisGastric lymphoma
AchlorhydriaGiardiasisHelicobacter pylori colonization
Bacterial overgrowth
Short bowel syndromeGastrectomy
Gastric bypass surgery
Iron bindersAntacids/decreased gastric acidity
Lack of balanced diet
VegansTea and toast diet
Ulcerative colitisCrohn's disease
Aspirin/NSAIDsPotassium supplements
Ulcerative colitis
Crohn's disease
Growing infants and childrenAdolescentsMenstruation
PregnancyLactationErythropoietin therapy
Figure 1 Causes of iron deficiency anemia. GI: Gastrointestinal; NSAIDs: Nonsteroidal anti-inflammatory drugs.
↓: Low/decreases; ↑: High/increases; ↑↑: Very high; IDA: Iron deficiency anemia; ACD: Anemia of chronic disease; MCV: Mean corpuscular volume; CRP: C-reactive protein; sTfR: Soluble transferrin receptor; Hb: Hemoglobin; RBC: Red blood cell.
Kaitha S et al . Iron and inflammatory bowel disease

66 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Duodenal villous enterocyte Reticuloendothelial macrophage
Dietary iron
Fe3+ Fe2+
Fe2+No Fe deficiencyFerritin
Hephaestin
Ferroportin
Lysosomal degradation
Fe2+ Fe3+ Transferrin
Hepcidin
Fe3+
Fe3+ Fe2+
Lysosomal degradation
Hepcidin
PlasmatransferrinFe3+
Hepcidin
Ferroportin
InfectionIron overloadInflammation
AnemiaOxidative stressHypoxiaIneffective erythropoiesis
Hepcidin synthesis
Hepatocyte
Senescent RBCs
+
HAMP
Figure 2 Role of hepcidin in the regulation of iron homeostasis. Fe3+ is reduced to Fe2+ by enterocyte brush border reductase Dcytb, transported across brush border membrane by DMT1. If iron demand is low, Fe2+ is stored as ferritin and sloughed with enterocytes. If iron demand is high, iron is oxidized by oxidase hephaestin and then exported into the plasma at the basolateral membrane by ferroportin[23]. Hepcidin binds to iron exporter, ferroportin 1, leading to its phosphorylation, internalization by binding to JAK 2 and lysosomal degradation, thus preventing iron release into the plasma[16]. DcytB: Duodenal ferric reductase; DMTI: Divalent metal transporter 1.
Blood Inflammation
IL6
IL6R
JAK 1/2
STAT 3
STAT 3
STAT 3
Nucleus
Matriptase2 HJV
BMP 6 sHJV
BMP 6
TFR2 HFE HFETF
TF
TF
TF
TFR1
SMAD1/5/8
SMAD1/5/8
SMAD 4
SMAD1/5/8SMAD 4
Cytoplasm
HAMP Hepcidin
Figure 3 Signaling pathways regulating hepcidin expression in the liver. Enterocyte iron induces BMP6 expression. BMP6 is released via the portal vein to act on cell-surface receptors in the liver, BMPR-I, BMPR-II, and HJV, a co-receptor of BMP, leading to phosphorylation of cytosolic transcription factors, SMAD 1/5/8, which complex with SMAD 4[16,21]. This heteromeric complex translocates to the nucleus and enhances transcription of hepcidin gene, HAMP. In iron deficiency, HJV is cleaved by matriptase-2 activation reducing BMP signaling, and BMP is sequestered by s-HJV, preventing its interaction with plasma membrane HJV, decreasing hepcidin expression[21]. IL-6: Interleukin 6; BMP: Bone morphogenetic protein; HJV: Hemojuvelin; s-HJV: Soluble HJV; TfR2: Transferrin receptor 2; HFE: Hereditary hemochromatosis protein.
P
P
P
P
Kaitha S et al . Iron and inflammatory bowel disease
FeTF
BMP I, II

normal. Serum transferrin carries Fe3+ in plasma and deli-
vers iron from the sites of iron absorption (duodenal enterocytes and macrophages) to all tissues. Therefore, its level is higher in IDA. However, as it is an acute-phase protein, its level can be decreased during inflammation, despite normal or low iron stores.
Transferrin saturation (TSAT), an indicator of the iron load of circulating transferrin, gives an indirect measure of extent of iron utilization[16]. TSAT is the ratio of serum iron and total iron-binding capacity, multiplied by 100. It is decreased in both IDA and ACD. Pregnancy and oral contraceptives increase plasma transferrin levels; therefore, TSAT may be low in such patients, despite normal iron stores[16]. Hepcidin is increased during inflammation and decreased in IDA. It prevents iron absorption, causes retention of iron in the macrophages, and inhibits erythropoiesis.
Soluble transferrin receptor (sTfR) is a measure of erythropoietic activity. It is directly proportional to erythropoietic activity and inversely proportional to tissue iron availability[28]. sTfR is used to differentiate iron deficiency (increased sTfR and low serum ferritin) from inflammation (normal sTfR and serum ferritin) and to diagnose a combination of iron deficiency and inflammation (increased sTfR and normal serum ferri-tin)[24,27]. However, its use is limited due to its cost and unavailability in many laboratories.
The sTfR/log ferritin ratio (sTfR-ferritin index) may be an early indicator of depletion of iron stores[29]. A ratio < 1 suggests ACD and excludes iron deficiency, while a ratio > 2 suggests either IDA or mixed IDA and ACD[27].
Functional iron deficiency is the imbalance between the iron requirements of the erythroid marrow and the iron supply, when the body cannot supply iron rapidly enough to maintain an increased erythropoietic rate. This leads to reduced reticulocyte and erythrocyte cellular hemoglobin (Hb) content[30]. Reticulocyte hemoglobin content (CHr) and the percentage of hypochromic RBC are indicators of red cell hemoglobinization and, thus, functional iron deficiency, regardless of inflammatory states[30]. In IDA, CHr > 40 and hypochromic RBCs > 5%[31].
Iron binds to protoporphyrin IX to form heme. In the absence of iron, zinc binds to protoporphyrin to form zinc protoporphyrin (ZPP). ZPP indicates iron levels in the bone marrow during erythropoiesis and is unaffected by ACD or inflammation[16].
MANAGEMENT OF IRON DEFICIENCY ANEMIA IN IBD Goals of therapyIt is important to realize that IDA commonly accom-panies IBD. The treatment of IDA should not be over-looked. Iron supplementation should be started as soon as a patient is found to have iron deficiency anemia. If a patient has iron deficiency without anemia, the decision
to initiate iron therapy depends on the clinical scenario and the patient’s preference[24]. The treatment options vs frequent laboratory monitoring should be discussed with the patient. The decision to initiate therapy and the type of therapy is determined by symptoms, severity of anemia, IBD disease activity, comorbidities, and risks associated with therapy[24]. Anemia impairs quality of life, even in the absence of specific symptoms, in patients with IBD. Iron therapy leads to significant improvement in the quality of life (QOL)[32]. Therefore, the therapeutic goals of IDA are to normalize hemoglobin, serum ferritin, and TSAT levels, replenish iron stores (serum ferritin > 100 g/L), avoid the need for blood transfusions, and improve the QOL. Three treatment options are available for iron deficiency anemia in IBD: oral iron, parenteral iron, and erythropoietin[33].
Response to therapyAfter starting iron therapy, an increase in reticulocyte count occurs within 2 wk, hemoglobin rises by 2 g/dL within 4 wk, and hemoglobin level returns to normal within 8 wk. Oral iron therapy should be continued for at least 6 mo after the hemoglobin has normalized, in order to replenish iron stores[34].
To assess the response to therapy, hemoglobin should be measured within 4 wk of the initiation of iron therapy. After 4 wk of iron therapy, response to treatment is considered appropriate or optimal, if hemoglobin rises by at least 2 g/dL; partial, if hemo-globin rises by 1-1.9 g/dL; absent, if hemoglobin rises less than 1 g/dL[24,35].
If the response to iron therapy is suboptimal, oral iron administration should be changed to intravenous iron therapy, erythropoietic agents should be added to intravenous iron therapy, or causes of anemia should be reassessed. A serum ferritin > 100 g/L indicates appropriate iron stores in a patient taking oral iron[24]. Serum ferritin is falsely high and is not useful for moni-toring intravenous iron supplementation, in such cases a TfS > 50% indicates iron overload[36].
Oral iron therapyIndications[16]: Anemia with hemoglobin > 10 g/dL, Quiescent or mildly active disease, in which oral iron absorption is not affected[37] in the absence of absolute indications for intravenous therapy (as mentioned below).
Advantages: There are some advantages, e.g., convenience and inexpensive, in oral iron therapy.
Limitations[33]: (1) intolerance and non-compliance due to side effects: abdominal pain, nausea, bloating, diarrhea; (2) impaired absorption due to duodenal inflammation, intestinal resection, severe disease activity; (3) partial or incomplete absorption; (4) non-absorbed iron can be toxic and worsen disease activity in IBD as a result of oxidative stress, neutrophilic infiltration, increased cytokines, and activation of NF-
67 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Kaitha S et al . Iron and inflammatory bowel disease

kappa B[38]; (5) experimental studies in animal models showed increased colon carcinogenesis with oral iron supplementation by inducing local oxidative stress at sites of active inflammation[39,40]; (6) slow response to therapy, cannot compensate for ongoing excessive blood loss; and (7) effective for short periods.
Available oral iron formulations: (1) ferrous fumarate has 106 mg elemental iron/tablet; (2) ferrous sulfate has 65 mg elemental iron/tablet; (3) ferrous gluconate has 28-36 mg iron/tablet; and (4) ferrous sulfate Elixir: 44 mg/5 mL (used if intolerant to oral iron tablets).
A maximum of 10-20 mg of oral iron can be absor-bed per day. The recommended maximum daily dose is up to 100 mg elemental iron per day, as higher doses do not increase its absorption and efficacy, and the side effects of oral iron are dose-related[24,26]. Oral iron should be started at a low dose after meals. If well tolerated, the dose can then be increased and should be taken on an empty stomach to increase absorption. Iron should be given two hours before, or four hours after, ingestion of antacids. Iron is best absorbed as the ferrous (Fe++) salt form in a mildly acidic medium, so a 250 mg ascorbic acid tablet or a half-glass of orange juice can be added at the time of iron administration to enhance the degree of iron absorption. Soy protein, dietary calcium, phytates (bran, oats, rye), cereals, tea, antacids such as H2 receptor blockers, and proton pump inhibitors prevent absorption of nonheme iron.
Intravenous iron therapyAccording to the international consensus statement, the preferred route of iron supplementation in IBD is intravenous[24].
Indications[24,41]: (1) severe anemia, hemoglobin < 10 g/dL; (2) intolerance to oral iron therapy; (3) failure of oral iron therapy; (4) need for quicker and prolonged response; and (5) active disease (CRP > 5 mg/L).
Advantages[34]: (1) repletion of iron stores in una-ffected by inflammation, intestinal resection; (2) rapid reversal of IDA; (3) relatively better tolerance and fewer side effects; (4) compliance can be monitored; (5) a single dose is sufficient for a few intravenous (IV) iron formulations (ferric carboxymaltose; low-molecular weight iron dextran); and (6) concurrent use of erythropoietin.
Limitations: (1) need for IV access and hospital staff for administration; (2) expensive; (3) inconvenience (travel, obtain IV access); and (4) iron dextran causes life-threatening anaphylactic reactions.
Available IV iron formulations: There are various IV iron preparations currently available for treatment of IDA. Their country-to-country availability, manufacturers,
dosing, maximum and minimum infusion times, adverse reactions, costs, and FDA pregnancy category are provided in Table 3. The use of high molecular weight iron dextran is obsolete, due to the associated high risk of life-threatening anaphylactic reactions.
Low molecular weight (LMW)-iron dextran (Cosmofer, INFeD) is more efficacious than oral iron in significantly raising hemoglobin levels within 8 wk[42]. LMW-iron dextran was associated with IgE-mediated anaphylactic reactions in up to 5.7% of patients during test dose infusion in a case-matched study[42,43]. Therefore, a black box warning that a test dose is required prior to its infusion is now included in the package insert. Its administration is time-consuming and infusions can take up to 4-6 h.
Iron gluconate (Ferrlecit) is indicated for patients with chronic kidney disease (CKD) receiving hemodia-lysis and supplemental epoetin therapy. A test dose is not required prior to its use. It has benzyl alcohol as a preservative.
Iron sucrose (Venofer) is indicated for IDA in CKD patients and requires a test dose only in Europe. It has been widely used for IDA due to its efficacy, safety, and better tolerability[44]. But, its use has been limited, due to an increased number of applications, and its infusion can take up to 3.5 h.
Ferric carboxymaltose (Ferinject, Injectafer) has been studied in patients with iron deficiency of diff-erent etiologies, such as non-dialysis and dialysis-dependent chronic kidney disease (CKD), IBD, heavy menstrual bleeding, post-partum IDA, or patients with chronic heart failure and IDA. It has been shown to be efficacious and welltolerated when compared with oral iron[45] and iron sucrose[46].
Ganzoni’s formula is useful to estimate individual iron requirements[47]: Iron deficit (mg) = body weight (kg) x [target Hb-actual Hb (g/dL) x 2.4] + stored iron (500 mg).
However, it is inconvenient, inconsistently applied in clinical practice, and underestimates iron require-ments[45]. A simplified method was used by the authors to calculate the cumulative iron dose (Table 4) for the ferric carboxymaltose group, instead of the traditional Ganzoni’s formula used in the iron sucrose group[46]. Ferric carboxymaltose is administered in 1-2 infusions, with each infusion given one week apart. It can be infused in 15 min, thus increasing the compliance rate. The use of ferric carboxymaltose for IDA was shown to be more cost effective and convenient than iron sucrose[48]. Transient hypophosphatemia, without clinical symptoms, was observed in a clinical study[46].
Ferumoxytol (Rienso, Feraheme) is indicated for IDA in patients with chronic kidney disease (CKD). It has a rapid administration time (minimum of 17 s for 510 mg dose), with a second dose given in 3-8 d. However, the safety and efficacy of infusion of 1020 mg of ferumoxytol over 15 min has been demonstrated in a single arm, open-label trial conducted at one center[49].
68 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Kaitha S et al . Iron and inflammatory bowel disease

Ferumoxytol is composed of superparamagnetic iron oxide nanoparticles coated with a low molecular weight semisynthetic carbohydrate. This agent may transiently interfere with the tissue diagnostic ability of MRI for up
to 3 mo, and with vascular MRI for up to 2 d, which is a limitation for patients with IBD who will need an MRI within 3 mo[50]. If MR imaging is required within 3 mo after ferumoxytol administration, T1- or proton density-weighted MR pulse sequences are used to minimize the effects of the agent, and the radiologist should also be notified.
Iron isomaltoside 1000 (Monofer) is the newest IV iron product, but it is not available in the United States. This agent has very low immunogenic potential and a very low content of labile and free iron, enabling
69 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Iron dextran (LMW)
Iron gluconate
Iron sucrose
Ferric carboxymaltose
Ferumoxytol Iron isomaltoside
Product/Europe Product/United States
CosmoFer®
INFeD® Ferrlecit®
Ferrlecit® Venofer®
Venofer® Ferinject®
Injectafer® Rienso®
Feraheme® Monofer®
Not available in United States
Manufacturer Pharmacosmos Sanofi-Aventis
Vifor Vifor AMAG Pharmacosmos
Test dose required Yes No Yes (in Europe)/No
No No No
Maximum approved dose 20 mg/kg 125 mg 200 mg(500 mg in few
countries)7 mg/kg
Ferinject- 1000 mg, or up to maximum of
20 mg/kgInjectafer-1500 mg if
patient’sweight > 50 kg
15 mg/kg if < 50 kg
1020 mg 20 mg/kg
Iron dextran (LMW)
Iron gluconate Iron sucrose Ferric carboxymaltose Ferumoxytol Iron isomaltoside
Maximum injectable single dose 100 mg(2 mL)
125 mg (10 mL)
200 mg (10 mL) Ferinject- 1000 mg or up to maximum of
20 mg/kgInjectafer- 750 mg
(15 mL)
510 mg (17 mL) 200 mg (2 mL)
Maximum infusion time 360 min (6 h) 30-60 min 210 min (3.5 h) 15 min 15 min 15 min Maximum injection time 2 min 10 min 5-10 min Bolus push over
7.5 min17 s
(1 mL/s)Bolus push
Dose-related reactions Dextran induced IgE -mediated anaphylaxis, hypotension,
edema
Hypotension, edema
Hypotension, edema
None reported None reported None reported
Relative risk of adverse side effects Moderate Low Very low None reported Very low None reported Costs per 500 mg in €1
Costs per maximum single injectable dose in United States dollars
84-86 €$37.70
52-56 €$76.32
105-100 €$120
170-175 €$993.75
82.12$658.54
170-175 €Not available
FDA Pregnancy category INFeD-category CCosmofer - no data available
B B C C Can be used in 2nd and 3rd trimester
Additional comments FDA approved for IDA in CKD
receiving hemodialysis
and supplemental
epoetin therapy
FDA approved for IDA in CKD
patients
Has been studied in patients with
IDA associated with CKD either dialysis
and nondialysis dependant, IBD, CHF,
post-partum and pregnancy patients.
Transient hypophosphatemia has been reported
FDA approved for IDA in CKD
patientsMay transiently interfere with
“tissue” diagnostic ability of MRI for up to 3 mo and “vascular” MRI
for up to 2 d
Very low immunogenic
potential
Table 3 Available preparations for intravenous iron supplementation[16,24,26]
1In Germany August 2012. Prescribing information of marketed products, package inserts. LMW: Low molecular weight; CKD: Chronic kidney disease; CHF: Congestive heart failure; IDA: Iron deficiency anemia; IBD: Inflammatory bowel disease.
Hemoglobin (g/dL) Body weight < 70 kg Body weight > 70 kg
> 10 1000 mg 1500 mg 7-10 1500 mg 2000 mg
Table 4 Determination of the Cumulative Iron Dose[46]
Kaitha S et al . Iron and inflammatory bowel disease
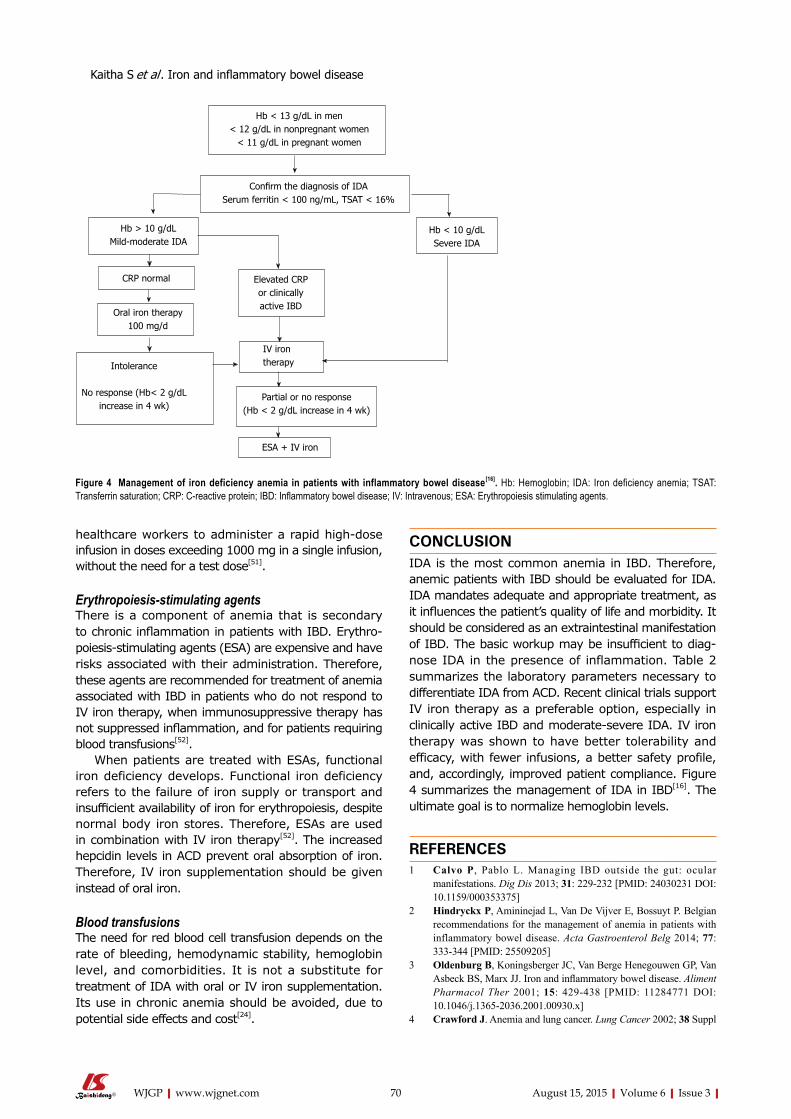
healthcare workers to administer a rapid high-dose infusion in doses exceeding 1000 mg in a single infusion, without the need for a test dose[51].
Erythropoiesis-stimulating agents There is a component of anemia that is secondary to chronic inflammation in patients with IBD. Erythropoiesis-stimulating agents (ESA) are expensive and have risks associated with their administration. Therefore, these agents are recommended for treatment of anemia associated with IBD in patients who do not respond to IV iron therapy, when immunosuppressive therapy has not suppressed inflammation, and for patients requiring blood transfusions[52].
When patients are treated with ESAs, functional iron deficiency develops. Functional iron deficiency refers to the failure of iron supply or transport and insufficient availability of iron for erythropoiesis, despite normal body iron stores. Therefore, ESAs are used in combination with IV iron therapy[52]. The increased hepcidin levels in ACD prevent oral absorption of iron. Therefore, IV iron supplementation should be given instead of oral iron.
Blood transfusions The need for red blood cell transfusion depends on the rate of bleeding, hemodynamic stability, hemoglobin level, and comorbidities. It is not a substitute for treatment of IDA with oral or IV iron supplementation. Its use in chronic anemia should be avoided, due to potential side effects and cost[24].
CONCLUSIONIDA is the most common anemia in IBD. Therefore, anemic patients with IBD should be evaluated for IDA. IDA mandates adequate and appropriate treatment, as it influences the patient’s quality of life and morbidity. It should be considered as an extraintestinal manifestation of IBD. The basic workup may be insufficient to diagnose IDA in the presence of inflammation. Table 2 summarizes the laboratory parameters necessary to differentiate IDA from ACD. Recent clinical trials support IV iron therapy as a preferable option, especially in clinically active IBD and moderate-severe IDA. IV iron therapy was shown to have better tolerability and efficacy, with fewer infusions, a better safety profile, and, accordingly, improved patient compliance. Figure 4 summarizes the management of IDA in IBD[16]. The ultimate goal is to normalize hemoglobin levels.
REFERENCES1 Calvo P, Pablo L. Managing IBD outside the gut: ocular
manifestations. Dig Dis 2013; 31: 229-232 [PMID: 24030231 DOI: 10.1159/000353375]
2 Hindryckx P, Amininejad L, Van De Vijver E, Bossuyt P. Belgian recommendations for the management of anemia in patients with inflammatory bowel disease. Acta Gastroenterol Belg 2014; 77: 333-344 [PMID: 25509205]
3 Oldenburg B, Koningsberger JC, Van Berge Henegouwen GP, Van Asbeck BS, Marx JJ. Iron and inflammatory bowel disease. Aliment Pharmacol Ther 2001; 15: 429-438 [PMID: 11284771 DOI: 10.1046/j.1365-2036.2001.00930.x]
4 Crawford J. Anemia and lung cancer. Lung Cancer 2002; 38 Suppl
70 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Hb < 13 g/dL in men< 12 g/dL in nonpregnant women
< 11 g/dL in pregnant women
Confirm the diagnosis of IDASerum ferritin < 100 ng/mL, TSAT < 16%
Hb < 10 g/dL Severe IDA
Hb > 10 g/dL Mildmoderate IDA
CRP normal
Oral iron therapy100 mg/d
Intolerance
No response (Hb< 2 g/dLincrease in 4 wk)
Elevated CRP or clinically active IBD
IV iron therapy
Partial or no response (Hb < 2 g/dL increase in 4 wk)
ESA + IV iron
Figure 4 Management of iron deficiency anemia in patients with inflammatory bowel disease[16]. Hb: Hemoglobin; IDA: Iron deficiency anemia; TSAT: Transferrin saturation; CRP: C-reactive protein; IBD: Inflammatory bowel disease; IV: Intravenous; ESA: Erythropoiesis stimulating agents.
Kaitha S et al . Iron and inflammatory bowel disease

3: S75-S78 [PMID: 12468152 DOI: 10.1016/S0169-5002(02)00275-1]5 Goodnough LT, Nemeth E, Ganz T. Detection, evaluation, and
management of iron-restricted erythropoiesis. Blood 2010; 116: 4754-4761 [PMID: 20826717 DOI: 10.1182/blood-2010-05-286260]
6 Thomas DW, Hinchliffe RF, Briggs C, Macdougall IC, Littlewood T, Cavill I. Guideline for the laboratory diagnosis of functional iron deficiency. Br J Haematol 2013; 161: 639-648 [PMID: 23573815 DOI: 10.1111/bjh.12311]
7 Vatner SF. Effects of hemorrhage on regional blood flow distribution in dogs and primates. J Clin Invest 1974; 54: 225-235 [PMID: 4211160 DOI: 10.1172/jci107757]
8 Daneryd P, Svanberg E, Körner U, Lindholm E, Sandström R, Brevinge H, Pettersson C, Bosaeus I, Lundholm K. Protection of metabolic and exercise capacity in unselected weight-losing cancer patients following treatment with recombinant erythropoietin: a randomized prospective study. Cancer Res 1998; 58: 5374-5379 [PMID: 9850068]
9 Pickett JL, Theberge DC, Brown WS, Schweitzer SU, Nissenson AR. Normalizing hematocrit in dialysis patients improves brain function. Am J Kidney Dis 1999; 33: 1122-1130 [PMID: 10352201 DOI: 10.1016/s0272-6386(99)70150-2]
10 Ludwig H, Strasser K. Symptomatology of anemia. Semin Oncol 2001; 28: 7-14 [PMID: 11395846 DOI: 10.1053/sonc.2001.25391]
11 National Hospital Ambulatory Medical Care Survey: 2010. Available from: URL: http://www.cdc.gov/nchs/data/ahcd/nhamcs_emergency/2010_ed_web_tables.pdf
12 Dallalio G, Law E, Means RT. Hepcidin inhibits in vitro erythroid colony formation at reduced erythropoietin concentrations. Blood 2006; 107: 2702-2704 [PMID: 16332970 DOI: 10.1182/blood-2005-07-2854]
13 Dieleman LA, Heizer WD. Nutritional issues in inflammatory bowel disease. Gastroenterol Clin North Am 1998; 27: 435-451 [PMID: 9650026 DOI: 10.1016/S0889-8553(05)70012-1]
14 Gomollón F, Gisbert JP. Anemia and inflammatory bowel diseases. World J Gastroenterol 2009; 15: 4659-4665 [PMID: 19787829 DOI: 10.3748/wjg.15.4659]
15 Semrin G, Fishman DS, Bousvaros A, Zholudev A, Saunders AC, Correia CE, Nemeth E, Grand RJ, Weinstein DA. Impaired intestinal iron absorption in Crohn’s disease correlates with disease activity and markers of inflammation. Inflamm Bowel Dis 2006; 12: 1101-1106 [PMID: 17119383 DOI: 10.1097/01.mib.0000235097.86360.04]
16 Stein J, Dignass AU. Management of iron deficiency anemia in inflammatory bowel disease - a practical approach. Ann Gastroenterol 2013; 26: 104-113 [PMID: 24714874]
17 Ganz T. Molecular control of iron transport. J Am Soc Nephrol 2007; 18: 394-400 [PMID: 17229910 DOI: 10.1681/asn.2006070802]
18 De Domenico I, Lo E, Ward DM, Kaplan J. Hepcidin-induced internalization of ferroportin requires binding and cooperative interaction with Jak2. Proc Natl Acad Sci USA 2009; 106: 3800-3805 [PMID: 19234114 DOI: 10.1073/pnas.0900453106]
19 Nemeth E, Rivera S, Gabayan V, Keller C, Taudorf S, Pedersen BK, Ganz T. IL-6 mediates hypoferremia of inflammation by inducing the synthesis of the iron regulatory hormone hepcidin. J Clin Invest 2004; 113: 1271-1276 [PMID: 15124018 DOI: 10.1172/jci20945]
20 Nicolas G, Chauvet C, Viatte L, Danan JL, Bigard X, Devaux I, Beaumont C, Kahn A, Vaulont S. The gene encoding the iron regulatory peptide hepcidin is regulated by anemia, hypoxia, and inflammation. J Clin Invest 2002; 110: 1037-1044 [PMID: 12370282 DOI: 10.1172/jci15686]
21 Knutson MD. Iron-sensing proteins that regulate hepcidin and enteric iron absorption. Annu Rev Nutr 2010; 30: 149-171 [PMID: 20415583 DOI: 10.1146/annurev.nutr.012809.104801]
22 Stein J, Hartmann F, Dignass AU. Diagnosis and management of iron deficiency anemia in patients with IBD. Nat Rev Gastroenterol Hepatol 2010; 7: 599-610 [PMID: 20924367 DOI: 10.1038/nrgastro.2010.151]
23 Anderson GJ, Frazer DM, McLaren GD. Iron absorption and metabolism. Curr Opin Gastroenterol 2009; 25: 129-135 [PMID: 19528880 DOI: 10.1097/MOG.0b013e32831ef1f7]
24 Gasche C, Berstad A, Befrits R, Beglinger C, Dignass A, Erichsen K, Gomollon F, Hjortswang H, Koutroubakis I, Kulnigg S, Oldenburg B, Rampton D, Schroeder O, Stein J, Travis S, Van Assche G. Guidelines on the diagnosis and management of iron deficiency and anemia in inflammatory bowel diseases. Inflamm Bowel Dis 2007; 13: 1545-1553 [PMID: 17985376 DOI: 10.1002/ibd.20285]
25 WHO/UNICEF/UNU. Iron Deficiency Anemia: Assessment, Prevention and Control. Accessed 1998. Available from: URL: http://www.who.int/nutrition/publications/en/ida_assessment_prevention_control.pdf
26 Gomollón F, Gisbert JP. Current management of iron deficiency anemia in inflammatory bowel diseases: a practical guide. Drugs 2013; 73: 1761-1770 [PMID: 24114623 DOI: 10.1007/s40265-013-0131-2]
27 Weiss G, Goodnough LT. Anemia of chronic disease. N Engl J Med 2005; 352: 1011-1023 [PMID: 15758012 DOI: 10.1056/NEJMra041809]
28 Lok CN, Loh TT. Regulation of transferrin function and expression: review and update. Biol Signals Recept 1998; 7: 157-178 [PMID: 9672759 DOI: 10.1159/000014542]
29 Punnonen K, Irjala K, Rajamäki A. Serum transferrin receptor, ferritin and TfR-F index in identification of latent iron deficiency. Eur J Haematol 1998; 60: 135-137 [PMID: 9508356 DOI: 10.1111/j.1600-0609.1998.tb01011.x]
30 Thomas C, Thomas L. Biochemical markers and hematologic indices in the diagnosis of functional iron deficiency. Clin Chem 2002; 48: 1066-1076 [PMID: 12089176]
31 Reinisch W, Staun M, Bhandari S, Muñoz M. State of the iron: how to diagnose and efficiently treat iron deficiency anemia in inflammatory bowel disease. J Crohns Colitis 2013; 7: 429-440 [PMID: 22917870 DOI: 10.1016/j.crohns.2012.07.031]
32 Wells CW, Lewis S, Barton JR, Corbett S. Effects of changes in hemoglobin level on quality of life and cognitive function in inflammatory bowel disease patients. Inflamm Bowel Dis 2006; 12: 123-130 [PMID: 16432377 DOI: 10.1097/01.MIB.0000196646.64615.db]
33 de la Morena F, Gisbert JP. Anemia and inflammatory bowel disease. Rev Esp Enferm Dig 2008; 100: 285-293 [PMID: 18662081]
34 Bayraktar UD, Bayraktar S. Treatment of iron deficiency anemia associated with gastrointestinal tract diseases. World J Gastroenterol 2010; 16: 2720-2725 [PMID: 20533591]
35 Gasche C. Anemia in IBD: the overlooked villain. Inflamm Bowel Dis 2000; 6: 142-150; discussion 151 [PMID: 10833075]
36 Ali M, Rigolosi R, Fayemi AO, Braun EV, Frascino J, Singer R. Failure of serum ferritin levels to predict bone-marrow iron content after intravenous iron-dextran therapy. Lancet 1982; 1: 652-655 [PMID: 6121967]
37 Lomer MC, Cook WB, Jan-Mohamed HJ, Hutchinson C, Liu DY, Hider RC, Powell JJ. Iron requirements based upon iron absorption tests are poorly predicted by haematological indices in patients with inactive inflammatory bowel disease. Br J Nutr 2012; 107: 1806-1811 [PMID: 22152498 DOI: 10.1017/s0007114511004971]
38 Carrier JC, Aghdassi E, Jeejeebhoy K, Allard JP. Exacerbation of dextran sulfate sodium-induced colitis by dietary iron supplementation: role of NF-kappaB. Int J Colorectal Dis 2006; 21: 381-387 [PMID: 16133010 DOI: 10.1007/s00384-005-0011-7]
39 Kulnigg S, Gasche C. Systematic review: managing anaemia in Crohn’s disease. Aliment Pharmacol Ther 2006; 24: 1507-1523 [PMID: 17206940 DOI: 10.1111/j.1365-2036.2006.03146.x]
40 Liao J, Seril DN, Lu GG, Zhang M, Toyokuni S, Yang AL, Yang GY. Increased susceptibility of chronic ulcerative colitis-induced carcinoma development in DNA repair enzyme Ogg1 deficient mice. Mol Carcinog 2008; 47: 638-646 [PMID: 18300266 DOI: 10.1002/mc.20427]
41 Gisbert JP, Gomollón F. Common misconceptions in the diagnosis and management of anemia in inflammatory bowel disease. Am J Gastroenterol 2008; 103: 1299-1307 [PMID: 18477354 DOI: 10.1111/j.1572-0241.2008.01846.x]
42 Khalil A, Goodhand JR, Wahed M, Yeung J, Ali FR, Rampton DS.
71 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Kaitha S et al . Iron and inflammatory bowel disease

Efficacy and tolerability of intravenous iron dextran and oral iron in inflammatory bowel disease: a case-matched study in clinical practice. Eur J Gastroenterol Hepatol 2011; 23: 1029-1035 [PMID: 21857526 DOI: 10.1097/MEG.0b013e32834a58d1]
43 Koutroubakis IE, Oustamanolakis P, Karakoidas C, Mantzaris GJ, Kouroumalis EA. Safety and efficacy of total-dose infusion of low molecular weight iron dextran for iron deficiency anemia in patients with inflammatory bowel disease. Dig Dis Sci 2010; 55: 2327-2331 [PMID: 19834803 DOI: 10.1007/s10620-009-1022-y]
44 Schröder O, Mickisch O, Seidler U, de Weerth A, Dignass AU, Herfarth H, Reinshagen M, Schreiber S, Junge U, Schrott M, Stein J. Intravenous iron sucrose versus oral iron supplementation for the treatment of iron deficiency anemia in patients with inflammatory bowel disease--a randomized, controlled, open-label, multicenter study. Am J Gastroenterol 2005; 100: 2503-2509 [PMID: 16279906 DOI: 10.1111/j.1572-0241.2005.00250.x]
45 Kulnigg S, Stoinov S, Simanenkov V, Dudar LV, Karnafel W, Garcia LC, Sambuelli AM, D’Haens G, Gasche C. A novel intravenous iron formulation for treatment of anemia in inflammatory bowel disease: the ferric carboxymaltose (FERINJECT) randomized controlled trial. Am J Gastroenterol 2008; 103: 1182-1192 [PMID: 18371137 DOI: 10.1111/j.1572-0241.2007.01744.x]
46 Evstatiev R, Marteau P, Iqbal T, Khalif IL, Stein J, Bokemeyer B, Chopey IV, Gutzwiller FS, Riopel L, Gasche C. FERGIcor, a randomized controlled trial on ferric carboxymaltose for iron deficiency anemia in inflammatory bowel disease. Gastroenterology
2011; 141: 846-853.e1-2 [PMID: 21699794 DOI: 10.1053/j.gastro.2011.06.005]
47 Ganzoni AM. Intravenous iron-dextran: therapeutic and experimental possibilities. Schweiz Med Wochenschr 1970; 100: 301-303 [PMID: 5413918]
48 Bager P, Dahlerup JF. The health care cost of intravenous iron treatment in IBD patients depends on the economic evaluation perspective. J Crohns Colitis 2010; 4: 427-430 [PMID: 21122539 DOI: 10.1016/j.crohns.2010.01.007]
49 Auerbach M, Strauss W, Auerbach S, Rineer S, Bahrain H. Safety and efficacy of total dose infusion of 1,020 mg of ferumoxytol administered over 15 min. Am J Hematol 2013; 88: 944-947 [PMID: 23828252 DOI: 10.1002/ajh.23534]
50 Bruining DH, Loftus EV. Technology Insight: new techniques for imaging the gut in patients with IBD. Nat Clin Pract Gastroenterol Hepatol 2008; 5: 154-161 [PMID: 18212778 DOI: 10.1038/ncpgasthep1028]
51 Jahn MR, Andreasen HB, Fütterer S, Nawroth T, Schünemann V, Kolb U, Hofmeister W, Muñoz M, Bock K, Meldal M, Langguth P. A comparative study of the physicochemical properties of iron isomaltoside 1000 (Monofer), a new intravenous iron preparation and its clinical implications. Eur J Pharm Biopharm 2011; 78: 480-491 [PMID: 21439379 DOI: 10.1016/j.ejpb.2011.03.016]
52 Moreno López R, Sicilia Aladrén B, Gomollón García F. Use of agents stimulating erythropoiesis in digestive diseases. World J Gastroenterol 2009; 15: 4675-4685 [PMID: 19787831]
P- Reviewer: Capasso R, Chow WK S- Editor: Tian YL L- Editor: A E- Editor: Wu HL
72 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Kaitha S et al . Iron and inflammatory bowel disease

their associated diarrhoeal complexes, to targeting HIV and application as novel mucosal vaccine delivery vehicles.
Key words: Gastrointestinal tract; Probiotics; BetL; Listeria monocytogenes ; Bifidobacterium; Lactobacillus
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Genetically engineered probiotic bacteria, with improved in vivo stress survival and persistence, have the potential to enhance, and in some instances replace, conventional prophylactic and therapeutic measures. This is particularly relevant in the developing world, where chronic and acute infections, and their associated sequelae impose a significant clinical and economic burden.
Sleator RD. Designer probiotics: Development and applications in gastrointestinal health. World J Gastrointest Pathophysiol 2015; 6(3): 73-78 Available from: URL: http://www.wjgnet.com/2150-5330/full/v6/i3/73.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i3.73
INTRODUCTIONProbiotics are commensal organisms that can be harnessed for therapeutic benefit[1]. In acute infections probiotics may enhance protection mediated by commensal flora through direct antagonism, i.e., completion for niches and nutrients, or via the production of antimicrobials, such as bacteriocins[2]. In chronic clinical conditions, such as immuno-suppression, microbe-host signalling is likely more relevant to effective probiotic function. This bacterialhost dialogue within the gut lumen, functions to maintain an effective mucosal barrier while also priming the host for further
Designer probiotics: Development and applications in gastrointestinal health
Roy D Sleator, Department of Biological Sciences, Cork Institute of Technology, Bishopstown, Cork, Ireland
Author contributions: Sleator RD conceived of the idea and wrote the paper.
Conflict-of-interest statement: There are no conflicts of interest.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Correspondence to: Roy D Sleator, Senior Lecturer and PI, Department of Biological Sciences, Cork Institute of Technology, Bishopstown, Cork, Ireland. [email protected]: +353-21-4335405
Received: March 11, 2015 Peer-review started: March 12, 2015First decision: April 13, 2015Revised: April 23, 2015 Accepted: July 11, 2015Article in press: July 14, 2015Published online: August 15, 2015
AbstractGiven the increasing commercial and clinical relevance of probiotics, improving their stress tolerance profile and ability to overcome the physiochemical defences of the host is an important biological goal. Herein, I review the current state of the art in the design of engineered probiotic cultures, with a specific focus on their utility as therapeutics for the developing world; from the treatment of chronic and acute enteric infections, and
73 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
MINIREVIEWS
World J Gastrointest Pathophysiol 2015 August 15; 6(3): 73-78ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i3.73
Roy D Sleator

responses to injury[3]. These health promoting benefits of probiotics, coupled with fact that they are cheap to produce, transport and store, makes them an attractive alternative to traditional therapies, especially in underdeveloped and wartorn territories.
Herein, I review key milestones in the development of probiotic based therapies, focusing particularly on problems encountered in developing countries such as acute and chronic enteric infections, as well HIV (AIDS) which continues to devastate subSaharan Africa[4]. Little or no access to appropriate medical care, often coupled with compromised immunity means that the malnourished are significantly more predisposed to infections by enteric pathogens, leading to inca-pacitating and dehydrating diarrhoea which in turn leads to a dramatic worsening of an already severely compromised nutritional status. Superimposing the HIV (AIDS) pandemic on an already distressed situation has created a state of affairs which needs to be urgently addressed[5].
Probiotic therapy, specifically the use of engineered probiotic strains, is a viable alternative to traditional approaches to alleviate suffering, to fight existing diseases and to protect against future infections[6]. Herein, I review the current state of the art in the design and application of probiotic cultures as therapeutics for the developing world.
Probiotics as therapeutics for the developing worldAlmost a third of the world’s population are malnurished[7], a quarter of which are children in the de-veloping world. Malnutrition significantly reduces cell-mediated immunity, immunoglobulin A (IgA) concentrations and cytokine production[7]. This in turn leads to an increased risk of infection, accompanied by bouts of acute and recurrent diarrhoea – which further exasperates an already depressed nutritional status. Indeed, almost half of all diarrhoea-related mortalities are linked to malnutrition[8], while morbidity is also disturbingly high (approximately 4 times more episodes per child per annum in developing countries than in the developed world). Diarrhoeal disorders exists as either acute diarrhoea; associated with sudden onset infections, characterized by recovery within two weeks, and chronic diarrhoea which lasts more than two weeks and usually arises as a symptom of malnutrition or immunodeficiency[9].
Probiotic bacteria have been shown to considerably limit the incidence and duration of diarrhoea associated with both acute infectious illness and chronic episodes linked to malnutrition[10]. Shornikova et al[11] showed that Lactobacillus reuteri can reduce the duration of acute diarrhoea in infants by one full day. Guandalini[12] observed similar effects with Lactobacillus rhamnosus, which also decreased the duration of hospital stays. Furthermore, in addition to alleviating the symptoms of malnutrition and diarrhoea, probiotics have also been used to specifically target bacterial and viral pathogens[1316]. Lb. casei Shirota, for example was
shown by Ogawa et al[17] to reduce Escherichia coli O157:H7 colonization, while Pascual et al[18] observed complete exclusion of Salmonella enteritidis by Lb. salivarius. Furthermore, even more impressive effects have been observed with mixed probiotic cocktails. Casey et al[19] reported significant amelioration of clinical symptoms of Salmonella Typhimurium infection in pigs using LIVE5; a cocktail of two Lactobacillus murinus strains with one strain each of Lb. salivarius subsp. salivarius, Lb. pentosus and Pediococcus pentosaceous. Pigs administered this mixture exhibited significantly lower levels of Salmonella infection, reduced frequency, severity and duration of diarrhoea, and enhanced weight gain relative to animals fed on a skim milk placebo. Nisbet et al[20] observed similar decreases in Salmonella gallinarum mediated mortality using a commercial probiotic mixture, while Johnson-Henry et al[21] showed that a Lactobacillus mixture reduced inflammation in Helicobacter pylori-infected animals. Furthermore, clinical trials in colonized humans revealed significantly lower levels of H. pylori, and decreased adverse side effects[22]. Probiotics are also effective against rotavirus, an enteric virus which accounts for approximately 60% of all diarrhoeal episodes in developing countries[23,24]. Specifically, Lactobacillus casei subsp. casei strain GG (LGG) has been shown to stimulate a rotavirus-specific IgA antibody response, which may confer immunity against future rotavirus infections[25].
However, one of the most significant limitations in the clinical application of probiotics is that the most clinically relevant probiotics are often the most physiologically fragile. Improving probiotic stress tolerance is thus a biological imperative. Below we describe the application of the “Pathobiotechnology” concept for the development of improved probiotic cultures[2629] (Figure 1).
DEVELOPMENT AND APPLICATION OF PROBIOTIC THERAPEUTICSFluctuations in temperature and water availability (aw) are the most common stresses associated with food production[30,31]. The ability to overcome these stresses is thus an important criterion in the selection of commercially viable and clinically effective probiotics[32]. A common strategy to overcome temperature and osmotic stress is the accumulation of compatible solutes, such as the plant derived trimethyl ammonium compound glycine betaine[33], which serves to stabilise cellular function under stressful conditions[34].
Improving compatible solutes accumulation is thus an important first step in the development of more physiologically robust probiotic strains[35]. Several sophisticated mechanisms for compatible solute accumulation have evolved over time[34]. Indeed, the intra-cellular pathogen L. monocytogenes, which serves as a useful model for Gram positive osmotolerance[36], has three compatible solute uptake systems (BetL, Gbu and OpuC[37]), the first to be identified being the secondary betaine transporter BetL[3840]. By cloning
74 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Sleator RD. Designer probiotics for improved gastrointestinal health

betL downstream of the nisin inducible promoter PnisA, we were able to assess the ability of BetL to contribute to probiotic survival under a variety of stresses[41,42]. As expected, the Lb. salivarius strain heterologously expressing BetL exhibited a significant increase in betaine uptake compared to the wild type, untrans-formed control. Indeed, the increased betaine uptake was sufficient to confer improved resistance to chill and cryotolerance, freeze-drying, spray-drying and barotolerance[41,43-46].
In addition to ex vivo stresses, probiotic bacteria must also overcome the in vivo defences of the host[30,31,47,48]. We demonstrated heterologous expres-sion of BetL in Bifidobacterium breve UCC2003, significantly improved survival of the probiotic in gastric juice[49]. In support of this, Termont et al[50] also reported similar effects in a L. lactis strain expressing the E. coli trehalose synthesis genes, suggesting a novel protective role for compatible solutes in the gastric environment. Furthermore, we have reported roles for carnitine and proline in contributing to bacterial gastrointestinal survival[5154]. Upon exiting the stomach, bacteria enter the upper small intestine where they are exposed to elevated osmolarity (equivalent to 0.3 mol/L NaCl). As was observed with L. salivarius[41], a significant osmoprotective effect was evident following BetL expression in B. breve, facilitating growth of the probiotic in conditions similar to those encountered in vivo. Furthermore, whilst stable colonisation of the murine intestine was achieved by oral administration of B. breve UCC2003, strains expressing BetL were recovered at significantly higher levels than the parent in the faeces, intestines and caecum of inoculated animals. Additionally, BetL significantly improved the clinical efficacy of the probiotic; resulting in significantly reduced levels of systemic infection following oral inoculation with L. monocytogenes, compared to the control.
In addition to improving physiological stress tolerance, “designer probiotics” have been designed to specifically inhibit enteric infections by blocking ligand-
receptor interactions between the pathogen and/or secreted toxins and the host[55]. Blocking receptor binding prevents infection, while toxin neutralization dampens clinical symptoms. Engineered to express receptormimic structures on their surface[56], orally administered probiotics neutralize toxins and inhibit pathogen adherence to the intestinal epithelium. Examples of such constructs include an E. coli strain expressing a chimeric lipopolysaccharide terminating in a shiga toxin (Stx) receptor, which binds to and neutralises Stx1 and Stx2[56], as well those with receptor blocking potential against cholera toxin (Ctx) and Enterotoxigenic E. coli (ETEC) toxin LT[57,58].
As well as treating enteric infections, “designer probiotics” have also been enlisted to target HIV. Every day approximately 14000 people become infected with HIV, a majority of which are in developing countries. Rao et al[59] recently described the construction of an E. coli strain engineered to secrete HIV-gp41-haemolysin A hybrid peptides, which block HIV fusion and entry into target cells. This “live microbicide”, administered either orally or via rectal suppository, colonizes the gut mucosa creating a protective barricade against HIV infection for four weeks[60]. Other anti-HIV probiotics include a human vaginal isolate of Lactobacillus jensenii engineered to secrete twodomain CD4 which inhibits HIV entry into target cells and Streptococcus gordonii modified to produce cyanovirin-N, a HIV-inactivating protein originally isolated from cyanobacterium[61].
PROBIOTICS BASED PROPHYLAXIS The most effective prophylaxis for infectious diseases is vaccination; resulting in the mobilisation of an immune response capable of specifically targeting invading pathogens[29]. In addition to the classical approach to vaccination, involving induction of acquired immunity to specific antigens, there is a growing awareness of the importance of innate immunity, associated primarily with our commensal microflora[2,62-64]. Indeed, optimal development and functioning of the mucosal immune
75 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
1 Delivery:Engineeringtechnologicalrobustness
2 Survival:Improved
competitivenessin the gastrointestinal tract
3 Efficacy: Improvedtherapeutic/prophylactic
properties
Figure 1 Overview the patho-biotechnology concept; enhancing probiotic delivery in the food matrix, gastrointestinal persistence and clinical efficacy.
Sleator RD. Designer probiotics for improved gastrointestinal health

response is dependent on microbial exposure early in postnatal life[65]. In the absence of such stimulation, development of the intestinalassociated lymphoid tissue is stunted and immune responses are suboptimal[66].
The development of efficient vaccine delivery vehi-cles remains challenging since traditional vaccines are typically based on either recombinant proteins or killed whole pathogens which, although safe, typically induce only weak immunity[6769]. The alternative is to use viable or attenuated pathogens[15]. However, while this approach improves targeted delivery, it carries with it the possibility of reversion to virulence[70]. Using a patho-biotechnology based approach, probiotics are being engineered to function as novel vaccine delivery vehicles which, lack the possibility of reversion to virulence, and effectively stimulate both the innate and acquired arms of the immune response[68,69]. In line with this approach, Guimarães et al[71] engineered a Lactococcus lactis strain capable of delivering either DNA or protein into the epithelial cells of the small intestine. Heterologous expression of inlA, encoding a listerial eukaryotic cell adhesion factor, converted the otherwise noninvasive L. lactis strain into a safe and effective vaccine delivery platform. Furthermore, the addition of hlyA (encoding listeriolysin) to L. lactis inlA+ enables phagosomal escape within the macrophage allowing MHC I and II stimulation[72].
Mucosal vaccine delivery, achieved using probiotic delivery platforms, has significant medical and metho-dical advantages, particularly for use in the developing world, including: reduced pain and the possibility of cross contamination associated with intramuscular injection, no requirement for expensive medically trained personnel and no cold chain requirement - a significant advantage in the tropical climes most often associated with the developing world.
CONCLUSIONWhile conventional medical research continues to provide effective prophylactics and therapeutics, these often remain beyond the reach of the developing world. In this context, probiotics provide a viable and cost effective alternative to fighting infection, modulating the immune response and alleviating the symptoms of malnutrition and its associated sequelae, all of which will ultimately contribute to health and social gain, particularly in the developing world.
REFERENCES1 Fuller R. Probiotics in man and animals. J Appl Bacteriol 1989; 66:
365-378 [PMID: 2666378]2 Sleator RD, Hill C. New frontiers in probiotic research. Lett Appl
Microbiol 2008; 46: 143-147 [PMID: 18028323 DOI: 10.1111/j.1472-765X.2007.02293.x]
3 Madara J. Building an intestine--architectural contributions of commensal bacteria. N Engl J Med 2004; 351: 1685-1686 [PMID: 15483290 DOI: 10.1056/NEJMcibr042621]
4 Sleator RD. Not so neglected diseases. J Infect Dev Ctries 2007; 1:
350-351 [PMID: 19734620]5 Sleator RD. Probiotics -- a viable therapeutic alternative for enteric
infections especially in the developing world. Discov Med 2010; 10: 119-124 [PMID: 20807472]
6 Sleator RD. Probiotic therapy - recruiting old friends to fight new foes. Gut Pathog 2010; 2: 5 [PMID: 20579345 DOI: 10.1186/1757-4749-2-5]
7 Solis B, Samartín S, Gómez S, Nova E, de la Rosa B, Marcos A. Probiotics as a help in children suffering from malnutrition and diarrhoea. Eur J Clin Nutr 2002; 56 Suppl 3: S57-S59 [PMID: 12142965 DOI: 10.1038/sj.ejcn.1601488]
8 Mittal SK. Chronic diarrhea in tropics. Indian J Pediatr 1999; 66: S4-15 [PMID: 11132468]
9 Thapar N, Sanderson IR. Diarrhoea in children: an interface between developing and developed countries. Lancet 2004; 363: 641-653 [PMID: 14987892 DOI: 10.1016/S0140-6736(04)15599-2]
10 Van Niel CW, Feudtner C, Garrison MM, Christakis DA. Lactobacillus therapy for acute infectious diarrhea in children: a meta-analysis. Pediatrics 2002; 109: 678-684 [PMID: 11927715]
11 Shornikova AV, Casas IA, Mykkänen H, Salo E, Vesikari T. Bacteriotherapy with Lactobacillus reuteri in rotavirus gastroenteritis. Pediatr Infect Dis J 1997; 16: 1103-1107 [PMID: 9427453]
12 Guandalini S. Treatment of acute diarrhea in the new millennium. J Pediatr Gastroenterol Nutr 2000; 30: 486-489 [PMID: 10817275]
13 Sleator RD, Hill C. Engineered pharmabiotics with improved therapeutic potential. Hum Vaccin 2008; 4: 271-274 [PMID: 18682694]
14 Sleator RD, Hill C. Designer probiotics: a potential therapeutic for Clostridium difficile? J Med Microbiol 2008; 57: 793-794 [PMID: 18480340 DOI: 10.1099/jmm.0.47697-0]
15 Sleator RD, Hill C. Rational design of improved pharmabiotics. J Biomed Biotechnol 2009; 2009: 275287 [PMID: 19753318 DOI: 10.1155/2009/275287]
16 Kechaou N, Chain F, Gratadoux JJ, Blugeon S, Bertho N, Chevalier C, Le Goffic R, Courau S, Molimard P, Chatel JM, Langella P, Bermúdez-Humarán LG. Identification of one novel candidate probiotic Lactobacillus plantarum strain active against influenza virus infection in mice by a large-scale screening. Appl Environ Microbiol 2013; 79: 1491-1499 [PMID: 23263960 DOI: 10.1128/AEM.03075-12]
17 Ogawa M, Shimizu K, Nomoto K, Takahashi M, Watanuki M, Tanaka R, Tanaka T, Hamabata T, Yamasaki S, Takeda Y. Protective effect of Lactobacillus casei strain Shirota on Shiga toxin-producing Escherichia coli O157: H7 infection in infant rabbits. Infect Immun 2001; 69: 1101-1108 [PMID: 11160007 DOI: 10.1128/IAI.69.2.1101-1108.2001]
18 Pascual M, Hugas M, Badiola JI, Monfort JM, Garriga M. Lactobacillus salivarius CTC2197 prevents Salmonella enteritidis colonization in chickens. Appl Environ Microbiol 1999; 65: 4981-4986 [PMID: 10543812]
19 Casey PG, Gardiner GE, Casey G, Bradshaw B, Lawlor PG, Lynch PB, Leonard FC, Stanton C, Ross RP, Fitzgerald GF, Hill C. A five-strain probiotic combination reduces pathogen shedding and alleviates disease signs in pigs challenged with Salmonella enterica Serovar Typhimurium. Appl Environ Microbiol 2007; 73: 1858-1863 [PMID: 17261517 DOI: 10.1128/AEM.01840-06]
20 Nisbet DJ, Tellez GI, Lowry VK, Anderson RC, Garcia G, Nava G, Kogut MH, Corrier DE, Stanker LH. Effect of a commercial competitive exclusion culture (Preempt) on mortality and horizontal transmission of Salmonella gallinarum in broiler chickens. Avian Dis 1998; 42: 651-656 [PMID: 9876831]
21 Johnson-Henry KC, Mitchell DJ, Avitzur Y, Galindo-Mata E, Jones NL, Sherman PM. Probiotics reduce bacterial colonization and gastric inflammation in H. pylori-infected mice. Dig Dis Sci 2004; 49: 1095-1102 [PMID: 15387328]
22 Gotteland M, Brunser O, Cruchet S. Systematic review: are probiotics useful in controlling gastric colonization by Helicobacter pylori? Aliment Pharmacol Ther 2006; 23: 1077-1086 [PMID: 16611267 DOI: 10.1111/j.1365-2036.2006.02868.x]
23 Cashman O, Lennon G, Sleator RD, Power E, Fanning S, O’Shea H. Changing profile of the bovine rotavirus G6 population in the south of Ireland from 2002 to 2009. Vet Microbiol 2010; 146: 238-244
76 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Sleator RD. Designer probiotics for improved gastrointestinal health

[PMID: 20541335 DOI: 10.1016/j.vetmic.2010.05.012]24 Collins PJ, Martella V, Sleator RD, Fanning S, O’Shea H.
Detection and characterisation of group A rotavirus in asymptomatic piglets in southern Ireland. Arch Virol 2010; 155: 1247-1259 [PMID: 20526785 DOI: 10.1007/s00705-010-0713-1]
25 Heyman M. Effect of lactic acid bacteria on diarrheal diseases. J Am Coll Nutr 2000; 19: 137S-146S [PMID: 10759139]
26 Sleator RD, Hill C. Battle of the bugs. Science 2008; 321: 1294-1295 [PMID: 18772416 DOI: 10.1126/science.321.5894.1294b]
27 Sleator RD, Hill C. Patho-biotechnology; using bad bugs to make good bugs better. Sci Prog 2007; 90: 1-14 [PMID: 17455762]
28 Sleator RD, Hill C. ‘Bioengineered Bugs’ - a patho-biotechnology approach to probiotic research and applications. Med Hypotheses 2008; 70: 167-169 [PMID: 17452084 DOI: 10.1016/j.mehy.2007.03.008]
29 Sleator RD, Hill C. Patho-biotechnology: using bad bugs to do good things. Curr Opin Biotechnol 2006; 17: 211-216 [PMID: 16459072 DOI: 10.1016/j.copbio.2006.01.006]
30 Sleator RD, Hill C. Food reformulations for improved health: A potential risk for microbial food safety? Med Hypotheses 2007; 69: 1323-1324 [PMID: 17452083 DOI: 10.1016/j.mehy.2007.03.007]
31 Sleator RD, Hill C. Molecular analysis of the microbial food safety implications of food reformulations for improved health. Foodborne Pathog Dis 2008; 5: 499-504 [PMID: 18666862 DOI: 10.1089/fpd.2008.0089]
32 Watson D, Sleator RD, Hill C, Gahan CG. Enhancing bile tolerance improves survival and persistence of Bifidobacterium and Lactococcus in the murine gastrointestinal tract. BMC Microbiol 2008; 8: 176 [PMID: 18844989 DOI: 10.1186/1471-2180-8-176]
33 Dreux N, Albagnac C, Sleator RD, Hill C, Carlin F, Morris CE, Nguyen-the C. Glycine betaine improves Listeria monocytogenes tolerance to desiccation on parsley leaves independent of the osmolyte transporters BetL, Gbu and OpuC. J Appl Microbiol 2008; 104: 1221-1227 [PMID: 17976173 DOI: 10.1111/j.1365-2672.2007.03623.x]
34 Sleator RD, Hill C. Bacterial osmoadaptation: the role of osmolytes in bacterial stress and virulence. FEMS Microbiol Rev 2002; 26: 49-71 [PMID: 12007642]
35 Sleator RD, Francis GA, O’Beirne D, Gahan CG, Hill C. Betaine and carnitine uptake systems in Listeria monocytogenes affect growth and survival in foods and during infection. J Appl Microbiol 2003; 95: 839-846 [PMID: 12969299]
36 Sleator RD, Gahan CG, Hill C. A postgenomic appraisal of osmotolerance in Listeria monocytogenes. Appl Environ Microbiol 2003; 69: 1-9 [PMID: 12513970]
37 Wemekamp-Kamphuis HH, Wouters JA, Sleator RD, Gahan CG, Hill C, Abee T. Multiple deletions of the osmolyte transporters BetL, Gbu, and OpuC of Listeria monocytogenes affect virulence and growth at high osmolarity. Appl Environ Microbiol 2002; 68: 4710-4716 [PMID: 12324311]
38 Sleator RD, Gahan CG, Abee T, Hill C. Identification and disruption of BetL, a secondary glycine betaine transport system linked to the salt tolerance of Listeria monocytogenes LO28. Appl Environ Microbiol 1999; 65: 2078-2083 [PMID: 10224004]
39 Sleator RD, Gahan CGM B, Hill C. Analysis of the role of betL in contributing to the growth and survival of Listeria monocytogenes LO28. Int J Food Microbiol 2000; 60: 261-268 [PMID: 11016615]
40 Hoffmann RF, McLernon S, Feeney A, Hill C, Sleator RD. A single point mutation in the listerial betL σ(A)-dependent promoter leads to improved osmo- and chill-tolerance and a morphological shift at elevated osmolarity. Bioengineered 2013; 4: 401-407 [PMID: 23478432 DOI: 10.4161/bioe.24094]
41 Sheehan VM, Sleator RD, Fitzgerald GF, Hill C. Heterologous expression of BetL, a betaine uptake system, enhances the stress tolerance of Lactobacillus salivarius UCC118. Appl Environ Microbiol 2006; 72: 2170-2177 [PMID: 16517668 DOI: 10.1128/AEM.72.3.2170-2177.2006]
42 Sleator RD, Wood JM, Hill C. Transcriptional regulation and posttranslational activity of the betaine transporter BetL in Listeria monocytogenes are controlled by environmental salinity. J Bacteriol 2003; 185: 7140-7144 [PMID: 14645273]
43 Considine KM, Kelly AL, Fitzgerald GF, Hill C, Sleator RD. High-pressure processing--effects on microbial food safety and food quality. FEMS Microbiol Lett 2008; 281: 1-9 [PMID: 18279335 DOI: 10.1111/j.1574-6968.2008.01084.x]
44 Considine KM, Sleator RD, Kelly AL, Fitzgerald GF, Hill C. Identification and characterization of an essential gene in Listeria monocytogenes using an inducible gene expression system. Bioeng Bugs 2013; 2: 150-159 [PMID: 21637009]
45 Considine KM, Sleator RD, Kelly AL, Fitzgerald GF, Hill C. A role for proline synthesis and transport in Listeria monocytogenes barotolerance. J Appl Microbiol 2011; 110: 1187-1194 [PMID: 21338448 DOI: 10.1111/j.1365-2672.2011.04982.x]
46 Considine KM, Sleator RD, Kelly AL, Fitzgerald GF, Hill C. Novel listerial genetic loci conferring enhanced barotolerance in Escherichia coli. J Appl Microbiol 2011; 110: 618-630 [PMID: 21223465 DOI: 10.1111/j.1365-2672.2010.04924.x]
47 Sleator RD, Clifford T, Hill C. Gut osmolarity: a key environmental cue initiating the gastrointestinal phase of Listeria monocytogenes infection? Med Hypotheses 2007; 69: 1090-1092 [PMID: 17433559 DOI: 10.1016/j.mehy.2007.02.028]
48 Culligan EP, Marchesi JR, Hill C, Sleator RD. Mining the human gut microbiome for novel stress resistance genes. Gut Microbes 1990; 3: 394-397 [PMID: 22688726 DOI: 10.4161/gmic.20984]
49 Sheehan VM, Sleator RD, Hill C, Fitzgerald GF. Improving gastric transit, gastrointestinal persistence and therapeutic efficacy of the probiotic strain Bifidobacterium breve UCC2003. Microbiology 2007; 153: 3563-3571 [PMID: 17906153 DOI: 10.1099/mic.0.2007/006510-0]
50 Termont S, Vandenbroucke K, Iserentant D, Neirynck S, Steidler L, Remaut E, Rottiers P. Intracellular accumulation of trehalose protects Lactococcus lactis from freeze-drying damage and bile toxicity and increases gastric acid resistance. Appl Environ Microbiol 2006; 72: 7694-7700 [PMID: 17028239 DOI: 10.1128/AEM.01388-06]
51 Sleator RD, Wouters J, Gahan CG, Abee T, Hill C. Analysis of the role of OpuC, an osmolyte transport system, in salt tolerance and virulence potential of Listeria monocytogenes. Appl Environ Microbiol 2001; 67: 2692-2698 [PMID: 11375182 DOI: 10.1128/AEM.67.6.2692-2698.2001]
52 Sleator RD, Gahan CG, Hill C. Identification and disruption of the proBA locus in Listeria monocytogenes: role of proline biosynthesis in salt tolerance and murine infection. Appl Environ Microbiol 2001; 67: 2571-2577 [PMID: 11375165 DOI: 10.1128/AEM.67.6.2571-2577.2001]
53 Sleator RD, Banville N, Hill C. Carnitine enhances the growth of Listeria monocytogenes in infant formula at 7 degrees C. J Food Prot 2009; 72: 1293-1295 [PMID: 19610343]
54 Feeney A, Sleator RD. Functional Screening of the Cronobacter sakazakii BAA-894 Genome reveals a role for ProP (ESA_02131) in carnitine uptake. Bioengineered 2015; 6: 161-165 [PMID: 25915804 DOI: 10.1080/21655979.2015.1043500]
55 Paton AW, Morona R, Paton JC. Designer probiotics for prevention of enteric infections. Nat Rev Microbiol 2006; 4: 193-200 [PMID: 16462752 DOI: 10.1038/nrmicro1349]
56 Paton AW, Morona R, Paton JC. A new biological agent for treatment of Shiga toxigenic Escherichia coli infections and dysentery in humans. Nat Med 2000; 6: 265-270 [PMID: 10700227 DOI: 10.1038/73111]
57 Paton AW, Jennings MP, Morona R, Wang H, Focareta A, Roddam LF, Paton JC. Recombinant probiotics for treatment and prevention of enterotoxigenic Escherichia coli diarrhea. Gastroenterology 2005; 128: 1219-1228 [PMID: 15887106]
58 Paton AW, Morona R, Paton JC. Neutralization of Shiga toxins Stx1, Stx2c, and Stx2e by recombinant bacteria expressing mimics of globotriose and globotetraose. Infect Immun 2001; 69: 1967-1970 [PMID: 11179385 DOI: 10.1128/IAI.69.3.1967-1970.2001]
59 Rao S, Hu S, McHugh L, Lueders K, Henry K, Zhao Q, Fekete RA, Kar S, Adhya S, Hamer DH. Toward a live microbial microbicide for HIV: commensal bacteria secreting an HIV fusion inhibitor peptide. Proc Natl Acad Sci USA 2005; 102: 11993-11998 [PMID:
77 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Sleator RD. Designer probiotics for improved gastrointestinal health

16040799 DOI: 10.1073/pnas.0504881102]60 Lagenaur LA, Berger EA. An anti-HIV microbicide comes alive.
Proc Natl Acad Sci USA 2005; 102: 12294-12295 [PMID: 16118279 DOI: 10.1073/pnas.0505960102]
61 Chang TL, Chang CH, Simpson DA, Xu Q, Martin PK, Lagenaur LA, Schoolnik GK, Ho DD, Hillier SL, Holodniy M, Lewicki JA, Lee PP. Inhibition of HIV infectivity by a natural human isolate of Lactobacillus jensenii engineered to express functional two-domain CD4. Proc Natl Acad Sci USA 2003; 100: 11672-11677 [PMID: 12972635 DOI: 10.1073/pnas.1934747100]
62 Sleator RD, Shortall C, Hill C. Metagenomics. Lett Appl Microbiol 2008; 47: 361-366 [PMID: 19146522 DOI: 10.1111/j.1472-765X.2008.02444.x]
63 Culligan EP, Hill C, Sleator RD. Probiotics and gastrointestinal disease: successes, problems and future prospects. Gut Pathog 2009; 1: 19 [PMID: 19930635 DOI: 10.1186/1757-4749-1-19]
64 Sleator RD. The human superorganism - of microbes and men. Med Hypotheses 2010; 74: 214-215 [PMID: 19836146 DOI: 10.1016/j.mehy.2009.08.047]
65 Newburg DS. Innate immunity and human milk. J Nutr 2005; 135: 1308-1312 [PMID: 15867330]
66 Forchielli ML, Walker WA. The role of gut-associated lymphoid tissues and mucosal defence. Br J Nutr 2005; 93 Suppl 1: S41-S48 [PMID: 15877894]
67 Johnston CD, Bannantine JP, Govender R, Endersen L, Pletzer D, Weingart H, Coffey A, O’Mahony J, Sleator RD. Enhanced expression
of codon optimized Mycobacterium avium subsp. paratuberculosis antigens in Lactobacillus salivarius. Front Cell Infect Microbiol 2014; 4: 120 [PMID: 25237653 DOI: 10.3389/fcimb.2014.00120]
68 Johnston C, Douarre PE, Soulimane T, Pletzer D, Weingart H, MacSharry J, Coffey A, Sleator RD, O’Mahony J. Codon optimisation to improve expression of a Mycobacterium avium ssp. paratuberculosis-specific membrane-associated antigen by Lactobacillus salivarius. Pathog Dis 2013; 68: 27-38 [PMID: 23620276 DOI: 10.1111/2049-632X.12040]
69 Johnston C, Coffey A, O’ Mahony J, Sleator RD. Development of a novel oral vaccine against Mycobacterium avium paratuberculosis and Johne disease: a patho-biotechnological approach. Bioeng Bugs 2010; 1: 155-163 [PMID: 21326921 DOI: 10.4161/bbug.1.3.10408]
70 Roland KL, Tinge SA, Killeen KP, Kochi SK. Recent advances in the development of live, attenuated bacterial vectors. Curr Opin Mol Ther 2005; 7: 62-72 [PMID: 15732531]
71 Guimarães VD, Gabriel JE, Lefèvre F, Cabanes D, Gruss A, Cossart P, Azevedo V, Langella P. Internalin-expressing Lactococcus lactis is able to invade small intestine of guinea pigs and deliver DNA into mammalian epithelial cells. Microbes Infect 2005; 7: 836-844 [PMID: 15878681 DOI: 10.1016/j.micinf.2005.02.012]
72 Bahey-El-Din M, Casey PG, Griffin BT, Gahan CG. Efficacy of a Lactococcus lactis ΔpyrG vaccine delivery platform expressing chromosomally integrated hly from Listeria monocytogenes. Bioeng Bugs 2010; 1: 66-74 [PMID: 21327128 DOI: 10.4161/bbug.1.1.10284]
P- Reviewer: Jia L, Julian S, Rahimi R S- Editor: Ma YJ L- Editor: A E- Editor: Wu HL
78 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Sleator RD. Designer probiotics for improved gastrointestinal health

years but only recently has been subjected to rigorous examination. We review the evidence regarding FMT for recurrent Clostridium difficile infection which has resulted in it being an approved treatment. In addition there is some evidence for its use in both irritable bowel syndrome and inflammatory bowel disease. Further research is needed in order to define the indications for FMT and the most appropriate method of administration.
Key words: Fecal microbial transplant; Clostridium difficile; Side-effects; Indications; Metabolic disorders
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Fecal microbial transplantation is approved for the treatment of recurrent Clostridium difficile infection by either nasojejunal administration or colonoscopy. In addition there is some evidence for its use in both irritable bowel syndrome and inflammatory bowel disease. There are, however, reports of side effects including weight gain, diverticulitis and development of autoimmune disease. Treatment for non-approved conditions should be performed in the framework of clinical research trials in order to better define the indications.
Malnick S, Melzer E. Human microbiome: From the bathroom to the bedside. World J Gastrointest Pathophysiol 2015; 6(3): 79-85 Available from: URL: http://www.wjgnet.com/2150-5330/full/v6/i3/79.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i3.79
INTRODUCTIONThe human microbiome is defined as the collection of organisms and their genomes inhabiting locations both in and on humans. Our understanding of the gastrointestinal microbiome (GIMb) has been assisted by the Human Microbiome Project[1] and the Metagenomics
Human microbiome: From the bathroom to the bedside
Stephen Malnick, Department of Internal Medicine C, Kaplan Medical Center, Affiliated to the Hebrew University, Rehovot 76100, Israel
Ehud Melzer, Institute of Gastroenterology and Liver Disease, Kaplan Medical Center, Affiliated to the Hebrew University, Rehovot 76100, Israel
Author contributions: Both authors contributed to this manu-script.
Conflict-of-interest statement: No potential conflicts of interest relevant to this article were reported.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Correspondence to: Stephen Malnick, MA (Oxon), MSc, MBBS (Lond), Director, Department of Internal Medicine C, Kaplan Medical Center, Affiliated to the Hebrew University, Jerusalem, Rehovot 76100, Israel. [email protected]: +972-8-9441371Fax: +972-8-9441852
Received: February 3, 2015 Peer-review started: February 4, 2015 First decision: March 20, 2015Revised: April 17, 2015 Accepted: April 28, 2015Article in press: April 30, 2015Published online: August 15, 2015
AbstractThe human gut contains trillions of bacteria, the major phylae of which include Bacteroidetes , Firmicutes, Actinobacteria and Proteobacteria . Fecal microbial transplantation (FMT) has been known of for many
79 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
MINIREVIEWS
World J Gastrointest Pathophysiol 2015 August 15; 6(3): 79-85ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i3.79
Stephen Malnick, Ehud Melzer

of the Human Intestinal Tract investigational groups.Trillions of bacteria are present in the human gas
trointestinal tract and encompass from 2000 to 4000 different species of bacteria, both aerobic and anaerobic. The major phyla include Bacteroidetes, Firmicutes, Actinobacteria and Proteobacteria.
The human GIMb is in many ways an additional organ of the body. It has ontogeny, anatomy and physiology and its function may be disturbed in certain pathological conditions. It is possible in some instances to restore normal GIMb function by fecal microbiota transplantation (FMT).
Although the concept of fecal transplantation has become more widely practiced in recent years, it has a long history. More than 2000 years ago Ge Hong used FMT to treat food poisoning and severe diarrhea[2]. Fabricius of Acquapendente in the 16th century described the transplantation of enteric bacteria. The first report of the use of FMT in recent times in more traditional medicine was that of Eiseman et al[3] in the form of a fecal enema obtained from a healthy donor in 4 cases of pseudomembranous colitis.
It is the purpose of this paper to review the current state of fecal transplantation.
FMT FOR CLOSTRIDIUM DIFFICILE INFECTIONClostridium difficile infection (CDI) is a gram positive anerobic bacillus that produces spores. It is present in the bowel of 4%13% of asymptomatic people[46]. CDI is an increasingly recognized cause of infectious hospitalacquired diarrhea in the developed world[7]. In healthy people it has been thought that it lacks the potential to produce toxins which can result in diarrhea. However, there is an increasing recognition of C. difficile in children, healthy adults and pregnant women[810]. Treatment consists of antibiotic therapy with metronidazole, vancomycin or fidaxomicin[11]. About 25% of those suffering from CDI have a recurrence after the first course of treatment[12]. For those patients with a recurrent episode of infection, there is a 40% chance of experiencing another recurrence and for those who have had more than 2 episodes there is a 60% chance of a further episode[12].
In view of the need for a more effective treatment for recurrent CDI, the use of FMT has been examined. In modern clinical research, there is usually an hypothesis that is examined in laboratory animals and then tried in placebocontrolled double blind clinical trials. However, for FMT as treatment for recurrent CDI this order has been reversed. The success of FMT for recurrent CDI has been demonstrated in case series[1315] and one randomized controlled trial[16].
Hamilton et al[13] have reported their experience with 43 consecutive patients treated with FMT for recurrent CDI at the University of Minnesota from 2009. The FMT was performed by colonoscopy. Fourteen of these
patients had inflammatory bowel disease (IBD). There was a mean of 5.9 relapses and the mean success rate was 86%.
Mattila et al[14] reported a retrospective review of 70 patients from 5 medical centers in Finland from 20072010. The FMT was performed by colonoscopy. Thirty six (51%) of the patients had the 027 ribotype strain that is more virulent and associated with a higher rate of relapse. All of the 34 patients with the non027 strain had a resolution within 12 wk compared to 32 of 36 patients (89%) with the 027 ribotype. The four nonresponders had serious comorbidity. Four of the patients who responded experienced a relapse after a year. Two were cured by repeat FMT and 2 by repeat antibiotic treatment.
Brandt et al[15] reported the multicenter United States experience of FMT for recurrent CDI. There were a total of 94 patients of whom there was followup data in 77. The primary cure rate was 91%. The secondary cure rate for the 7 patients that did not respond or relapsed was 98%. The mean followup period was 17 mo and was up to 68 mo.
There has recently been published a randomized controlled openlabel trial of patients with at least one episode of recurrent CDI from Holland and Finland. The numbers of patients involved was small13 in each of three groups. The groups were randomized to receive initial vancomycin for 4 d and then either bowel lavage, bowel lavage and donor feces through a nasoduodenal tube or just vancomycin alone. The study was stopped prematurely after an interim analysis revealed a resolution of CDI of 81% in the group receiving feces by nasoduodenal infusion as compared to 31% receiving vancomycin alone and 23% receiving vancomycin with bowel lavage[16] (Figure 1). These were much smaller numbers than initially planned for. Thus this study is consistent with previous case reports.
In view of the limited data from randomized controlled trials a systematic review of FMT involving 317 patients from 27 case series and reports has been published[17]. Two thirds of these were case series. There was resolution of the disease in 92% of cases, 89% after a single treatment. The lowest rate of resolution was by infusion via gastroscopy or nasojejunal tube. This is especially relevant regarding the above mentioned randomized trial[16], since the number of cases was very small due to the early termination of the trial mandated by the review committee. Although there is great heterogeneity between the various case reports and case series making up this systematic review, there was found to be a higher relapse rate in patients who received both bowel lavage and antibiotics before FMT (4/33, 12.1% vs 5/150, 3.3%).
In the light of this data FMT is now recognized as treatment for a third recurrence of CDI[18].
The rationale for use of FMT has been shown in a mouse model of mice treated with clindamycin and then infected with Clostridium difficile that had been
80 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Malnick S et al . Fecal microbial transplant

isolated from patients with CDI. The mice developed chronic disease and responded to the administration of homogenized feces from healthy mice[19]. Thus the data that is available support the use of FMT for the treatment of recurrent CDI.
FMT - HOW TO DO ITThe first issue to be addressed is the donor of the feces. Initially the donors of the feces were “healthy donors” with no other details provided[3]. In some case the stools of medical residents were used. Until 2011, a partner or family member was the most frequent source of donor. It was assumed that any infectious diseases would already have been transmitted between the donor and recipient. This has not been examined by evidencebased medicine. More recently the NIH in the United States has required that donor stool be examined for C difficile toxin, enteric bacterial pathogens (including Listeria monocytogenes, Vibrio cholera and Vibrio parahemolyticus), parasites including Giardia (via antigen test), Cryptosporidium (antigen test), Isospora (acidfast stain) and Rotavirus. In addition the donor blood needs to be screened for hepatitis A (IgM), B (HBsAg, anti-HBc-IgG and IgM, and anti-HBsAg) and C (HCV antibody) viruses, HIV type 1 and 2 and syphilis. In addition H. pylori should be tested for. The Israel Ministry of Health protocol is shown in Table 1. The tests for the donor may not be entirely covered by the medical insurance organizations since they may not be indicated for the routine medical care of the stool donor.
There is a growing trend for DIY stool transplants with instructions being available on the Internet for example www.thepoweerofpoop.com. There are cases when patients refer themselves to centers performing FMT after selfadministration of unscreened donor stool from a family member has failed[20]. The only systematic review of FMT suggested that stool from a related donor (spouse or intimate partner) resulted in a higher rate of cure (93.3%) as compared to an unrelated donor (84%).
The FMT program at the University of Minnesota
has reported their experience with frozen/thawed or fresh fecal preparations from universal donors[13] with cure rates of 90% for frozen material and 92% for fresh material. This is higher than those reported with patient selected donors (70%), although only small numbers of patients were included in each group 10 individual donors and 33 standard donors. A recent report of increase in weight after fecal transplantation from a related obese donor provides a note of caution[21]. For these reasons we believe that the use of individual donors should not be the first choice for obtaining feces for transplantation.
The donor needs to provide the stool sample into a clean plastic container. The amount is variable although 50 g in 250 mL of diluent is a common method. Different fluids have been used as the suspending fluid, including milk, water and saline. The resolution rates with saline and milk are 86.2% and 88.6%, with recurrence rates of 3.0% and 3.2%[17]. The use of water resulted in a resolution rate of 98.5% and recurrence of 7.8%. Three hundred milliliter is the usual dose for colonic FMT and 60 cc for upper GI tract FMT.
The patients who will receive the FMT need to have a large volume colonic lavage prior to the procedure. This is thought to cleanse the spores of C difficile that are responsible for the recurrence of the infection. There are different variations and some reports include loperamide if receiving a fecal enema[22], and proton pump inhibitor (to reduce the bactericidal effect of gastric acid) if the infusion of stools is via a nasogastric or nasojejunal route[23,24].
Some groups maintain the patient on vancomycin orally until the time of the FMT[16,25]. This practice is thought to reduce the vegetative forms of C. difficile since vancomycin has no action on the spores. However, the systematic analysis of Gough et al[17] found a higher relapse rate with the combination of bowel lavage and antibiotics. Our group policy is to discontinue antibiotics two days prior to FMT.
Recently, there has been a report of the use of capsules containing frozen stool. Twenty patients with recurrent CDI were treated with 15 FMT capsules daily for 2 d. The resolution rate was 70%. The 6 failures were retreated and 4 of these had resolution, resulting in an overall response rate of 90%. A total of 30% of the patients experienced mild abdominal complaints that resolved within 72 h. This is a preliminary study that needs to be repeated and expanded but is promising and if successful will probably replace the current methods of administration of the donor stools.
SAFETY AND COMPLICATIONSTwo studies have provided information regarding longterm follow up after FMT. A study from Finland of 70 patients had no data on complications[14], although the authors state “none of our patients had any serious adverse effects that could be related to fecal transplantation”. A multicenter North American study
81 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
1009080706050403020100
% c
ured
1st infusionOverallinfusion
V V + BL
% cured 81.3 93.8 30.8 23.1
Figure 1 Rates of cure after treatment of recurrent C. difficile infection by nasojejunal infusion of donor feces. The data show first infusion, overall infusion after retreatment for a treatment failure, vancomycin (V) treatment, and vancomycin treatment and bowel lavage (V + BL) (16).
Malnick S et al . Fecal microbial transplant

reported data from more than 3 mo follow up in 77 of the 94 eligible patients. Ninetyseven percent of the patients stated that they would choose FMT again as treatment for a recurrent CDI and 53% would prefer it as a first option. Twenty-seven percent of the patients developed abdominal pain following FMT but it was minor and resolved within 10 d. Four patients developed an autoimmune diseaseperipheral neuropathy, rheumatoid arthritis, Sjogrens and thrombocytopenia[15]. We have recently treated a patient with severe CDI who required 2 consecutive FMTs and developed thrombocytopenia after each transplantation. Recently, there has been a report of diverticulitis following FMT for CDI[26].
The field of FMT is rapidly developing and as experi-ence accumulates there are more reports of possible side effects or complications. Thus it is important to carry out these procedures in centers with approved protocols and to discourage patient or nonphysician supervised selfadministration.
CDI is common in patients who are immunosuppressed. Recently a retrospective study from 16 medical centers in the United States reported their experience in FMT in 80 immunosuppressed patients with severe or recurrent or refractory CDI[27]. The majority of the patients were immunosuppressed due to solid organ transplantation or treatment for IBD. The cure rate was 79% for the first time and 89% overall. There was a 15% incidence of serious adverse events within 12 wk. Five of the 36 IBD patients had post-FMT disease flare. Thus it appears that successful FMT is possible in immunosuppressed patients, although with a slightly reduced success rate and a higher rate of adverse
events.
OTHER USES FOR FMTIBDFMT appears to be an established treatment for CDI and attention has focused also on IBD. Gastrointestinal microbiome dysbiosis has an important role in the pathogenesis of IBD[28]. In addition a recent study employing the molecular biology technique of terminal restriction fragment length polymorphism (TRFLP) to profile the bacterial species in fecal samples has enabled the calculation of a discriminant score which was shown to be a biomarker for disease activity in UC[29]. The first FMT for ulcerative colitis (UC) was reported in 1989[30] and described the reversal of the UC that Bennet (one of the authors of the paper) had suffered from for 7 years by FMT administered as fecal enemas. Case series have suggested some role for FMT in UC[3133]. However, a recent report[34] of a prospective study of FMT in 5 adult patients with moderate to severe UC who had failed various immunosuppressive therapies adds a note of caution. None of the patients were receiving concomitant immunosuppressive therapy. None of the patients entered clinical remission after 12 wk of followup and only one had some clinical improvement. Additionally all of the 5 patients had fever and an elevation of CRP after the FMT and a worsening of the diarrhea the day after the procedure. In the patient who experienced some response there was an alteration of the fecal flora after FMT. Another recent trial of FMT for UC did not demonstrate a significant effect[35] in 6 patients but there was a change in the gut microbiota. The alteration of gut microbiota was temporary and it may be necessary to undergo repeated transplantation in order to maintain the altered gut microbiota. A phase 1 trial of FMT for 9 pediatric UC patients with mildtomoderate activity reported no serious adverse effects and found that 7 of these (79%) had responded within a week[36]. It may be that certain population subgroups suffering from UC will derive benefit from FMT. A recent systematic review and metaanalysis of FMT therapy for IBD showed a clinical remission of 22% for UC[37].
Crohn’s disease (CD) has also been treated by FMT. The data are limited to case reports and small case series[32,38]. The recent systematic review and meta-analysis of FMT as therapy for IBD found higher pooled estimate of clinical remission for CD, 60.5% as compared to UC 22%[37]. There have been 2 previous systematic reviews of FMT for IBD[39,40]. The success rate of FMT for adult IBD patients was 77.8%[39] but outcomes were measured by “success rates” only. There were also other methodological problems[37]. The other review[40] noted endoscopic and histologic remission of 63% in 24 patients but this too has been criticized for methodological flaws[37]. A note of caution is necessary following the report of bacteremia after FMT in a patient
82 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Patient eligibility for FMT 1 Questionnaire to exclude potentially transmissible diseases (1) Practices protected sexual intercourse (or in a monogamous relationship with a healthy partner) (2) Has not had tattooing in the previous six months (3) Does not have any known infectious diseases (4) No drug abuse (5) Has not travelled to the Far-East, India, Africa, Central or South America within the previous six months (6) Has no known autoimmune disease (7) There is no history of any gastrointestinal disease, including inflammatory bowel disease, celiac disease or irritable bowel disease (8) Has not had any previous bowel resection (9) There is no history of infectious diarrhea in the previous 12 mo (10) Has not received antibiotic therapy in the previous 2 mo 2 Laboratory tests (1) Negative stool culture (2) Negative stool microscopy, including Giardia, Cryptosporidium and Isospora beli (3) Negative Clostridium difficile toxin (4) Negative serological testing for HIV, HBV, HCV, HAV, VDRL, CMV (5) Negative test for Helicobacter pylori (either C13 urea breath testing, stool antigen or serum antibodies)
Table 1 The Israel Ministry of Health protocol for donor screening for fecal microbial transplantation
FMT: Fecal microbial transplantation. HCV: Hepatitis C virus; HBV: Hepatitis B virus; CMV: Cucumber mosaic virus; VDRL: Venereal disease research laboratory; HIV: Human immunodeficiency virus.
Malnick S et al . Fecal microbial transplant

with Crohns and CDI[41].Thus the jury is out regarding the utility of FMT for
IBD and further work is required in order to define the effect of different methods of delivery, changes on the microbiome and the interaction between phases of the illness (induction or maintenance) and the impact of additional therapies.
Irritable bowel disease There is evidence linking dysbiosis to irritable bowel disease (IBS)[42,43] and thus there is a question regarding the possibility of FMT for treatment. There have been reports of a favorable outcome after FMT in diarrhea - predominant IBS[32]. A recent report of singlecenter experience of 13 patients with IBS of whom 9 had diarrheapredominant, 3 constipationpredominant and one mixedtype[44], found resolution or improvement in symptoms in 70% of the patients overall. Presumably, the small sample size prevented the reporting of the response rate in each group separately. This subject has recently been reviewed[45]. There is a need for further research to define the role of FMT in the treatment of this common condition.
FMT and metabolic disordersIt is now apparent that there is an interaction between the microbiome of the intestinal tract and the metabolism of the human host and that there is a link to obesity[46]. Although there are reports of changes in the ratio of Firmicutes/Bacteroides with human obesity[47] other groups have not found such changes[48,49]. There are reports in mice of the induction of a phenotype of the metabolic syndrome via fecal transplants[50]. This complex subject has been reviewed[46,51,52]. Furthermore in mice the intestinal microbiota plays a role in the development of nonalcoholic fatty liver disease[53]. Recently stools from twins discordant for obesity has been shown to promote or impair the development of obesity in adult male germfree mice[54].
In humans there is a single study reporting that FMT using stool from lean donors improves insulin sensitivity in obese male individuals concomitant with an increase in butyrateproducing intestinal bacteria[55].
We are currently conducting a randomized controlled trial of FMT in obese individuals undergoing screening colonoscopy in order to determine if there is a clinical effect on obesity in humans (clinical trials.gov NCT02336789).
Other conditionsImmune thrombocytopenia (ITP) was reported to be reversed in a patient treated with FMT for UC but only published in an abstract form[55]. Other fields include autoimmune disease, allergic disorders, and neuropsychiatric disorders. This exciting field has recently been reviewed[56].
In summary, fecal microbial transplantation is now prime time treatment for refractory Cl. difficile infection. In addition, it may be of use for treating other disorders
of the gastrointestinal tract including irritable bowel syndrome and IBD. Further research is needed to define the optimal method of administration of the stools as well as the indications for treatment in other conditions. In addition there needs to be vigilance for the development of sideeffects related to this technique. For this reason it is important that treatments for other indications be conducted in the framework of research protocols.
REFERENCES1 Turnbaugh PJ, Ley RE, Hamady M, Fraser-Liggett CM, Knight
R, Gordon JI. The human microbiome project. Nature 2007; 449: 804-810 [PMID: 17943116 DOI: 10.1038/nature06244]
2 Zhang F, Luo W, Shi Y, Fan Z, Ji G. Should we standardize the 1,700-year-old fecal microbiota transplantation? Am J Gastroenterol 2012; 107: 1755; author reply p.1755-p.1756 [PMID: 23160295 DOI: 10.1038/ajg.2012.251]
3 Eiseman B, Silen W, Bascom GS, KauvaR AJ. Fecal enema as an adjunct in the treatment of pseudomembranous enterocolitis. Surgery 1958; 44: 854-859 [PMID: 13592638]
4 Stecher B, Hardt WD. Mechanisms controlling pathogen colonization of the gut. Curr Opin Microbiol 2011; 14: 82-91 [PMID: 21036098 DOI: 10.1016/j.mib.2010.10.003]
5 Vedantam G, Clark A, Chu M, McQuade R, Mallozzi M, Viswanathan VK. Clostridium difficile infection: toxins and non-toxin virulence factors, and their contributions to disease establishment and host response. Gut Microbes 2012; 3: 121-134 [PMID: 22555464 DOI: 10.4161/gmic.19399]
6 Sorg JA, Sonenshein AL. Inhibiting the initiation of Clostridium difficile spore germination using analogs of chenodeoxycholic acid, a bile acid. J Bacteriol 2010; 192: 4983-4990 [PMID: 20675492 DOI: 10.1128/JB.00610-10]
7 To KB, Napolitano LM. Clostridium difficile infection: update on diagnosis, epidemiology, and treatment strategies. Surg Infect (Larchmt) 2014; 15: 490-502 [PMID: 25314344 DOI: 10.1089/sur.2013.186]
8 Kim J, Smathers SA, Prasad P, Leckerman KH, Coffin S, Zaoutis T. Epidemiological features of Clostridium difficile-associated disease among inpatients at children’s hospitals in the United States, 2001-2006. Pediatrics 2008; 122: 1266-1270 [PMID: 19047244 DOI: 10.1542/peds.2008-0469]
9 Pituch H. Clostridium difficile is no longer just a nosocomial infection or an infection of adults. Int J Antimicrob Agents 2009; 33 Suppl 1: S42-S45 [PMID: 19303569]
10 Freeman J, Bauer MP, Baines SD, Corver J, Fawley WN, Goorhuis B, Kuijper EJ, Wilcox MH. The changing epidemiology of Clostridium difficile infections. Clin Microbiol Rev 2010; 23: 529-549 [PMID: 20610822 DOI: 10.1016/S0924-8579(09)70016-0]
11 Chahine EB, Sucher AJ, Mantei K. Fidaxomicin: a novel macrolide antibiotic for Clostridium difficile infection. Consult Pharm 2014; 29: 614-624 [PMID: 25203410 DOI: 10.4140/TCP.n.2014.614]
12 Kelly CP, LaMont JT. Clostridium difficile--more difficult than ever. N Engl J Med 2008; 359: 1932-1940 [PMID: 18971494 DOI: 10.1056/NEJMra0707500]
13 Hamilton MJ, Weingarden AR, Sadowsky MJ, Khoruts A. Standardized frozen preparation for transplantation of fecal microbiota for recurrent Clostridium difficile infection. Am J Gastroenterol 2012; 107: 761-767 [PMID: 22290405]
14 Mattila E, Uusitalo-Seppälä R, Wuorela M, Lehtola L, Nurmi H, Ristikankare M, Moilanen V, Salminen K, Seppälä M, Mattila PS, Anttila VJ, Arkkila P. Fecal transplantation, through colonoscopy, is effective therapy for recurrent Clostridium difficile infection. Gastroenterology 2012; 142: 490-496 [PMID: 22155369 DOI: 10.1053/j.gastro.2011.11.037]
15 Brandt LJ, Aroniadis OC, Mellow M, Kanatzar A, Kelly C, Park T, Stollman N, Rohlke F, Surawicz C. Long-term follow-up of
83 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Malnick S et al . Fecal microbial transplant

colonoscopic fecal microbiota transplant for recurrent Clostridium difficile infection. Am J Gastroenterol 2012; 107: 1079-1087 [PMID: 22450732 DOI: 10.1038/ajg.2012.60]
16 van Nood E, Vrieze A, Nieuwdorp M, Fuentes S, Zoetendal EG, de Vos WM, Visser CE, Kuijper EJ, Bartelsman JF, Tijssen JG, Speelman P, Dijkgraaf MG, Keller JJ. Duodenal infusion of donor feces for recurrent Clostridium difficile. N Engl J Med 2013; 368: 407-415 [PMID: 23323867 DOI: 10.1056/NEJMoa1205037]
17 Gough E, Shaikh H, Manges AR. Systematic review of intestinal microbiota transplantation (fecal bacteriotherapy) for recurrent Clostridium difficile infection. Clin Infect Dis 2011; 53: 994-1002 [PMID: 22002980 DOI: 10.1093/cid/cir632]
18 Surawicz CM, Brandt LJ, Binion DG, Ananthakrishnan AN, Curry SR, Gilligan PH, McFarland LV, Mellow M, Zuckerbraun BS. Guidelines for diagnosis, treatment, and prevention of Clostridium difficile infections. Am J Gastroenterol 2013; 108: 478-498; quiz 499 [PMID: 23439232 DOI: 10.1038/ajg.2013.4]
19 Lawley TD, Clare S, Walker AW, Stares MD, Connor TR, Raisen C, Goulding D, Rad R, Schreiber F, Brandt C, Deakin LJ, Pickard DJ, Duncan SH, Flint HJ, Clark TG, Parkhill J, Dougan G. Targeted restoration of the intestinal microbiota with a simple, defined bacteriotherapy resolves relapsing Clostridium difficile disease in mice. PLoS Pathog 2012; 8: e1002995 [PMID: 23133377 DOI: 10.1371/journal.ppat.1002995]
20 Brandt LJ. American Journal of Gastroenterology Lecture: Intestinal microbiota and the role of fecal microbiota transplant (FMT) in treatment of C. difficile infection. Am J Gastroenterol 2013; 108: 177-185 [PMID: 23318479 DOI: 10.1038/ajg.2012.450]
21 Alang N, Kelly CR. Weight Gain After Fecal Microbiota Transplantation. Open Forum Infect Dis 2015; 4: ofv004-ofv004 [DOI: 10.1093/ofid/ofv004]
22 Persky SE, Brandt LJ. Treatment of recurrent Clostridium difficile-associated diarrhea by administration of donated stool directly through a colonoscope. Am J Gastroenterol 2000; 95: 3283-3285 [PMID: 11095355 DOI: 10.1111/j.1572-0241.2000.03302.x]
23 Bakken JS, Borody T, Brandt LJ, Brill JV, Demarco DC, Franzos MA, Kelly C, Khoruts A, Louie T, Martinelli LP, Moore TA, Russell G, Surawicz C. Treating Clostridium difficile infection with fecal microbiota transplantation. Clin Gastroenterol Hepatol 2011; 9: 1044-1049 [PMID: 21871249 DOI: 10.1016/j.cgh.2011.08.014]
24 Aas J, Gessert CE, Bakken JS. Recurrent Clostridium difficile colitis: case series involving 18 patients treated with donor stool administered via a nasogastric tube. Clin Infect Dis 2003; 36: 580-585 [PMID: 12594638 DOI: 10.1086/367657]
25 Youngster I, Russell GH, Pindar C, Ziv-Baran T, Sauk J, Hohmann EL. Oral, capsulized, frozen fecal microbiota transplantation for relapsing Clostridium difficile infection. JAMA 2014; 312: 1772-1778 [PMID: 25322359 DOI: 10.1001/jama.2014.13875]
26 Mandalia A, Kraft CS, Dhere T. Diverticulitis after fecal microbiota transplant for C. difficile infection. Am J Gastroenterol 2014; 109: 1956-1957 [PMID: 25470590 DOI: 10.1038/ajg.2014.350]
27 Kelly CR, Ihunnah C, Fischer M, Khoruts A, Surawicz C, Afzali A, Aroniadis O, Barto A, Borody T, Giovanelli A, Gordon S, Gluck M, Hohmann EL, Kao D, Kao JY, McQuillen DP, Mellow M, Rank KM, Rao K, Ray A, Schwartz MA, Singh N, Stollman N, Suskind DL, Vindigni SM, Youngster I, Brandt L. Fecal microbiota transplant for treatment of Clostridium difficile infection in immunocompromised patients. Am J Gastroenterol 2014; 109: 1065-1071 [PMID: 24890442 DOI: 10.1038/ajg.2014.133]
28 Podolsky DK. Inflammatory bowel disease. N Engl J Med 2002; 347: 417-429 [PMID: 12167685 DOI: 10.1056/NEJMra020831]
29 Fukuda K, Fujita Y. Determination of the discriminant score of intestinal microbiota as a biomarker of disease activity in patients with ulcerative colitis. BMC Gastroenterol 2014; 14: 49 [PMID: 24641276 DOI: 10.1186/1471-230X-14-49]
30 Bennet JD, Brinkman M. Treatment of ulcerative colitis by implantation of normal colonic flora. Lancet 1989; 1: 164 [PMID: 2563083]
31 Borody TJ, Warren EF, Leis SM, Surace R, Ashman O, Siarakas S. Bacteriotherapy using fecal flora: toying with human motions. J
Clin Gastroenterol 2004; 38: 475-483 [PMID: 15220681]32 Borody TJ, George L, Andrews P, Brandl S, Noonan S, Cole P,
Hyland L, Morgan A, Maysey J, Moore-Jones D. Bowel-flora alteration: a potential cure for inflammatory bowel disease and irritable bowel syndrome? Med J Aust 1989; 150: 604 [PMID: 2783214]
33 Borody TJ, Warren EF, Leis S, Surace R, Ashman O. Treatment of ulcerative colitis using fecal bacteriotherapy. J Clin Gastroenterol 2003; 37: 42-47 [PMID: 12811208]
34 Angelberger S, Reinisch W, Makristathis A, Lichtenberger C, Dejaco C, Papay P, Novacek G, Trauner M, Loy A, Berry D. Temporal bacterial community dynamics vary among ulcerative colitis patients after fecal microbiota transplantation. Am J Gastroenterol 2013; 108: 1620-1630 [PMID: 24060759 DOI: 10.1038/ajg.2013.257]
35 Kump PK, Gröchenig HP, Lackner S, Trajanoski S, Reicht G, Hoffmann KM, Deutschmann A, Wenzl HH, Petritsch W, Krejs GJ, Gorkiewicz G, Högenauer C. Alteration of intestinal dysbiosis by fecal microbiota transplantation does not induce remission in patients with chronic active ulcerative colitis. Inflamm Bowel Dis 2013; 19: 2155-2165 [PMID: 23899544 DOI: 10.1097/MIB.0b013-e31829ea325]
36 Kunde S, Pham A, Bonczyk S, Crumb T, Duba M, Conrad H, Cloney D, Kugathasan S. Safety, tolerability, and clinical response after fecal transplantation in children and young adults with ulcerative colitis. J Pediatr Gastroenterol Nutr 2013; 56: 597-601 [PMID: 23542823 DOI: 10.1097/MPG.0b013e318292fa0d]
37 Colman RJ, Rubin DT. Fecal microbiota transplantation as therapy for inflammatory bowel disease: a systematic review and meta-analysis. J Crohns Colitis 2014; 8: 1569-1581 [PMID: 25223604 DOI: 10.1016/j.crohns.2014.08.006]
38 Gordon H, Harbord M. A patient with severe Crohn’s colitis responds to Faecal Microbiota Transplantation. J Crohns Colitis 2014; 8: 256-257 [PMID: 24239403 DOI: 10.1016/j.crohns.2013.10.007]
39 Sha S, Liang J, Chen M, Xu B, Liang C, Wei N, Wu K. Systematic review: faecal microbiota transplantation therapy for digestive and nondigestive disorders in adults and children. Aliment Pharmacol Ther 2014; 39: 1003-1032 [PMID: 24641570 DOI: 10.1111/apt.12699]
40 Anderson JL, Edney RJ, Whelan K. Systematic review: faecal microbiota transplantation in the management of inflammatory bowel disease. Aliment Pharmacol Ther 2012; 36: 503-516 [PMID: 22827693 DOI: 10.1111/j.1365-2036.2012.05220.x]
41 Quera R, Espinoza R, Estay C, Rivera D. Bacteremia as an adverse event of fecal microbiota transplantation in a patient with Crohn’s disease and recurrent Clostridium difficile infection. J Crohns Colitis 2014; 8: 252-253 [PMID: 24184170 DOI: 10.1016/j.crohns.2013.10.002]
42 Collins SM, Chang C, Mearin F. Postinfectious Chronic Gut Dysfunction: From Bench to Bedside. Am J Gastroenterol 2012; 1 Suppl: 2-8 [DOI: 10.1038/ajgsup.2012.2]
43 Mayer EA, Savidge T, Shulman RJ. Brain-gut microbiome interactions and functional bowel disorders. Gastroenterology 2014; 146: 1500-1512 [PMID: 24583088 DOI: 10.1053/j.gastro.2014.02.037]
44 Pinn DM, Aroniadis OC, Brandt LJ. Is fecal microbiota transplantation the answer for irritable bowel syndrome? A single-center experience. Am J Gastroenterol 2014; 109: 1831-1832 [PMID: 25373585 DOI: 10.1038/ajg.2014.295]
45 Pinn DM, Aroniadis OC, Brandt LJ. Is fecal microbiota transplantation (FMT) an effective treatment for patients with functional gastrointestinal disorders (FGID)? Neurogastroenterol Motil 2015; 27: 19-29 [PMID: 25424663]
46 Tilg H, Kaser A. Gut microbiome, obesity, and metabolic dysfunction. J Clin Invest 2011; 121: 2126-2132 [PMID: 21633181]
47 Ley RE, Turnbaugh PJ, Klein S, Gordon JI. Microbial ecology: human gut microbes associated with obesity. Nature 2006; 444: 1022-1023 [PMID: 17183309 DOI: 10.1038/4441022a]
48 Schwiertz A, Taras D, Schäfer K, Beijer S, Bos NA, Donus C, Hardt PD. Microbiota and SCFA in lean and overweight healthy subjects. Obesity (Silver Spring) 2010; 18: 190-195 [PMID: 19498350 DOI: 10.1038/oby.2009.167]
49 Duncan SH, Lobley GE, Holtrop G, Ince J, Johnstone AM, Louis P, Flint HJ. Human colonic microbiota associated with diet, obesity
84 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Malnick S et al . Fecal microbial transplant

and weight loss. Int J Obes (Lond) 2008; 32: 1720-1724 [PMID: 18779823 DOI: 10.1038/ijo.2008.155]
50 Turnbaugh PJ, Ley RE, Mahowald MA, Magrini V, Mardis ER, Gordon JI. An obesity-associated gut microbiome with increased capacity for energy harvest. Nature 2006; 444: 1027-1031 [PMID: 17183312 DOI: 10.1038/nature05414]
51 Shen J, Obin MS, Zhao L. The gut microbiota, obesity and insulin resistance. Mol Aspects Med 2013; 34: 39-58 [PMID: 23159341 DOI: 10.1016/j.mam.2012.11.001]
52 Gangarapu V, Yıldız K, Ince AT, Baysal B. Role of gut microbiota: obesity and NAFLD. Turk J Gastroenterol 2014; 25: 133-140 [PMID: 25003671 DOI: 10.5152/tjg.2014.7886]
53 Le Roy T, Llopis M, Lepage P, Bruneau A, Rabot S, Bevilacqua C, Martin P, Philippe C, Walker F, Bado A, Perlemuter G, Cassard-Doulcier AM, Gérard P. Intestinal microbiota determines development of non-alcoholic fatty liver disease in mice. Gut 2013; 62: 1787-1794 [PMID: 23197411 DOI: 10.1136/gutjnl-2012-303816]
54 Ridaura VK, Faith JJ, Rey FE, Cheng J, Duncan AE, Kau AL,
Griffin NW, Lombard V, Henrissat B, Bain JR, Muehlbauer MJ, Ilkayeva O, Semenkovich CF, Funai K, Hayashi DK, Lyle BJ, Martini MC, Ursell LK, Clemente JC, Van Treuren W, Walters WA, Knight R, Newgard CB, Heath AC, Gordon JI. Gut microbiota from twins discordant for obesity modulate metabolism in mice. Science 2013; 341: 1241214 [PMID: 24009397]
55 Vrieze A, Van Nood E, Holleman F, Salojärvi J, Kootte RS, Bartelsman JF, Dallinga-Thie GM, Ackermans MT, Serlie MJ, Oozeer R, Derrien M, Druesne A, Van Hylckama Vlieg JE, Bloks VW, Groen AK, Heilig HG, Zoetendal EG, Stroes ES, de Vos WM, Hoekstra JB, Nieuwdorp M. Transfer of intestinal microbiota from lean donors increases insulin sensitivity in individuals with metabolic syndrome. Gastroenterology 2012; 143: 913-6.e7 [PMID: 22728514 DOI: 10.1053/j.gastro.2012.06.031]
56 Xu MQ, Cao HL, Wang WQ, Wang S, Cao XC, Yan F, Wang BM. Fecal microbiota transplantation broadening its application beyond intestinal disorders. World J Gastroenterol 2015; 21: 102-111 [PMID: 25574083 DOI: 10.3748/wjg.v21.i1.102]
P- Reviewer: Oz HS, Saniabadi AR S- Editor: Ji FF L- Editor: A E- Editor: Wu HL
85 August 15, 2015|Volume 6|Issue 3|WJGP|www.wjgnet.com
Malnick S et al . Fecal microbial transplant

© 2015 Baishideng Publishing Group Inc. All rights reserved.
Published by Baishideng Publishing Group Inc8226 Regency Drive, Pleasanton, CA 94588, USA
Telephone: +1-925-223-8242Fax: +1-925-223-8243
E-mail: [email protected] Desk: http://www.wjgnet.com/esps/helpdesk.aspx
http://www.wjgnet.com

World Journal of Gastrointestinal PathophysiologyWorld J Gastrointest Pathophysiol 2015 November 15; 6(4): 86-248
ISSN 2150-5330 (online)
Published by Baishideng Publishing Group Inc

EDITOR-IN-CHIEFThomas Y Ma, Albuquerque
STRATEGY ASSOCIATE EDITOR-IN-CHIEFHirotada Akiho, FukuokaJean-Francois Beaulieu, SherbrookeMichael W Bradbury, ErieSharon DeMorrow, Temple
GUEST EDITORIAL BOARD MEMBERSJia-Ming Chang, TaipeiWai-Keung Chow, TaichungChien-Wei Hsu, KaohsiungMing-Tsan Lin, TaipeiBor-Shyang Sheu, TainanJin-Town Wang, Taipei
MEMBERS OF THE EDITORIAL BOARD
ArgentinaBernabé Matías Quesada, Buenos AiresMarcelo G Roma, Rosario
AustraliaChris Richard Abbiss, JoondalupGuy D Eslick, PenrithMontri Gururatsakul, AdelaideChandana Herath, Melbourne Michael Horowitz, AdelaidMustafa Khasraw, GeelongShu-Chuen Li, CallaghanAntonina Mikocka-Walus, AdelaideNam Quoc Nguyen, Adelaide
Kulmira Nurgali, St AlbansNicholas John Spencer, Flagstaff HillNick Spencer, AdelaideDeborah Verran, CamperdownShu-Feng Zhou, Melbourne
AustriaCord Langner, GrazDietmar Ofner-Velano, SalzburgMichael Trauner, Graz
Belgium
Kathleen Blondeau, LeuvenRobaeys Geert, GenkIlse Maria Hoffman, LeuvenMichael H J Maes, WilrijkTheodoor Abram Niewold, HeverleeXavier Sagaert, LeuvenJean-Marie Vanderwinden, BrusselsKristin Verbeke, LeuvenMathieu Vinken, Roeselare
BrazilUilian Andreis, BotucatuEverson L A Artifon, Vila MarianaJoão Batista Calixto, TrindadeNiels O Saraiva Câmara, Vila ClementinoJulio Chebli, Juiz de ForaFernando Fornari, Passo FundoClélia Akiko Hiruma-Lima, BotucatuMarcel C C Machado, Sao PauloJuarez Quaresma, BelemWagner Vilegas, Araraquara
Brunei Darussalam
Vui Heng Chong, Bandar Seri Begawan
Canada
Fernando Alvarez, MontréalFrancois Boudreau, SherbrookeGeorge A Bubenik, GuelphWang-Xue Chen, OttawaJan D Huizinga, PuslinchKusum K Kharbanda, OmahaWolfgang Kunze, HamiltoJian-Jun Li, OttawaRoderick John Macleod, KingstonMichele Molinari, HalifaxNathalie Rivard, SherbrookeKirill Rosen, HalifaxManuela Santos, MontrealCaroline Saucier, QuebecJean Sévigny, QuebecEldon A Shaffer, CalgaryManuel A Silva, HamiltonAlan B R Thomson, EdmontonPierre H Vachon, Sherbrooke
China
Kai-Xing Ai, ShanghaiZhao-Xiang Bian, Hong KongMin-Hu Chen, GuangzhouCH Cho, Hong KongZhong-Hong Gao, WuhanJun-Ming Guo, NingboJing-Yan Han, Beijing
I
Editorial Board2011-2015
The World Journal of Gastrointestinal Pathophysiology Editorial Board consists of 523 members, representing a team of worldwide experts in gastrointestinal pathophysiology. They are from 45 countries, including Argentina (2), Australia (14), Austria (3), Belgium (9), Brazil (10), Brunei Darussalam (1), Canada (20), China (30), Croatia (1), Czech Republic (2), Denmark (4), Egypt (1), Estonia (1), Finland (1), France (8), Germany (22), Greece (7), Hungary (5), India (10), Indonesia (1), Iran (2), Ireland (2), Israel (8), Italy (42), Japan (47), Lebanon (3), Malaysia (1), Mexico (2), Netherlands (8), Norway (1), Poland (4), Portugal (1), Romania (1), Russia (1), Singapore (4), South Korea (13), Spain (23), Sweden (11), Switzerland (4), Thailand (2), Turkey (6), Ukraine (1), United Kingdom (10), United States (173), and Venezuela (1).
February 15, 2013WJGP|www.wjgnet.com
World Journal ofGastrointestinal PathophysiologyW J G P

Jian-Dong Huang, Hong KongJia-Fu Ji, BeijingShi Liu, WuhanZhan-Ju Liu, ShanghaiXiao-Hong Wang, BeijingZhen-Ning Wang, ShenyangWei Wei, HefeiDong-Ping Xie, ShanghaiWen-Xie Xu, ShanghaiHua Yang, ChongqingXiao Yang, BeijingWei-Zhen Zhang, BeijingHua-Chuan Zheng, ShenyangDa-Ling Zhu, HarbinJin-Xia Zhu, BeijingMin-Sheng Zhu, NanjingYong-Liang Zhu, Hangzhou
Croatia
Alen Protic, Rijeka
Czech Republic
Pavel Hladik, SemilyMartin Vokurka, Prague
Denmark
Lars Arendt-Nielsen, AalborgFrank Vinholt Schiodt, CopenhagenJonas Worsoe, AarhusJing-Bo Zhao, Aalborg
Egypt
Mahmoud Aboelneen Khattab, Minia
Estonia
Enn Seppet, Tartu
Finland
Pauli Antero Puolakkainen, Turku
France
Bruno Bonaz, GrenoblePierre Marie Dechelotte, RouenJean-Paul Lallès, Saint-GillesCharles-Henri Malbert, Saint-GillesThierry Piche, NicePascale Plaisancié, LyonMichelina Plateroti, LyonVeronique Vitton, Marseille
Germany
Hans Gunter Beger, UlmCarsten Bergmann, IngelheimElke Cario, Essen
Arno J Dormann, KolnNikolaus Gassler, AachenWerner Hartwig, HeidelbergMarion Hewicker-Trautwein, HannoverJens Hoeppner, FreiburgTobias Keck, FreiburgJorg Kleeff, MunichPeter Malfertheiner, MagdeburgOliver Mann, HamburgChristoph Michalski, MunichAndreas Klaus Nussler, MunichChristian Pehl, VilsbiburgPeter Schemmer, HeidelbergMarc Stemmler, FreiburgFrank Tacke, AachenSya Nomna Ukena, HannoverBrigitte Vollmar, RostockThomas Michael Wex, MagdeburgMargot Zoller, Heidelberg
Greece
Stelios F Assimakopoulos, PatrasGeorge N Dalekos, LarissaAlkiviadis Efthymiou, thessalonikiMaria Gazouli, AthensIoannis E Koutroubakis, HeraklionGerassimos J Mantzaris, AthensGeorge Papatheodoridis, Athens
Hungary
Mária Bagyánszki, SzegedMihály Boros, SzegedLaszlo Czako, SzegedPal Miheller, BudapestZoltan Rakonczay, Szeged
India
Anil Kumar Agarwal, DelhiUday Bandyopadhyay, KolkataSriparna Basu, VaranasiChandra Kanti Chakraborti, RourkelaRajeev Garg, PunjabChandra P Sharma, ThiruvananthapuramShailesh V Shrikhande, MumbaiVirendra Singh, ChandigarhNicholas James Skill, IndianapolisPrabhakar R Veerareddy, Andhra Pradesh
Indonesia
Laurentius A Lesmana, Jakarta
Iran
Gholamreza Roshandel, GorganShahram Shahabi, Urmia
Ireland
Billy Bourke, DublinStephen Keely, Dublin
IsraelYosefa Avraham, JerusalemYaron Bar-Dayan, HolonShomron Ben-Horin, HashomerBoris Kirshtein, Beer ShevaStephen Malnick, RehovotYaakov Maor, Tel-HashomerRifaat Safadi, JerusalemNachum Vaisman, Tel Aviv
Italy
Rosaria Acquaviva, CataniaDario Acuna-Castroviejo, ArmillaAlessandro Antonelli, PisaGiacosa Attilio, GenovaSalvatore Auricchio, NaplesGuido Basilisco, MilanoAntonio Basoli, RomeClaudio Bassi, VeronaMassimo Bellini, PisaLuigi Bonavina, MilanoAlfio Brogna, CataniaGiuseppe Calamita, BariRaffaele Capasso, NaplesIgnazio Castagliuolo, PadovaEnrico Stefano Corazziari, RomeFrancesco Cresi, TorinoRosario Cuomo, NapoliSalvatore Cuzzocrea, GazziMario M D’Elios, FlorenceCinzia Domeneghini, MilanLuca Elli, MilanoCresi Francesco, TorinoWalter Fries, MessinaEugenio Gaudio, RomeMarco Gobbetti, BariFabio Grizzi, MilanEnzo Grossi, MilaneseEnzo Ierardi, FoggiaPietro Invernizzi, MilanAngelo A Izzo, NaplesAnna Kohn, RomeGiovanni Latella, L’AquilaMassimo Marignani, RomeSergio Morini, RomeRaffaele Pezzilli, BolognaCristiano Rumio, MilanGiovanni Sarnelli, NaplesEdoardo Vincenzo Savarino, GenoaPierpaolo Sileri, RomeAnnamaria Staiano, NaplesGiacomo Carlo Sturniolo, PadovaClaudio Tiribelli, Triest
Japan
Akihiro Asakawa, KagoshimaHisashi Aso, SendaiYasu-Taka Azuma, OsakaShotaro Enomoto, WakayamaMikihiro Fujiya, HokkaidoTakahisa Furuta, HamamatsuAkira Hokama, OkinawaRyota Hokari, SaitamaYuichi Hori, Kobe
II February 15, 2013WJGP|www.wjgnet.com

III February 15, 2013WJGP|www.wjgnet.com
Hideki Iijima, OsakaMasahiro Iizuka, AkitaMotohiro Imano, OsakaHajime Isomoto, NagasakiTatehiro Kagawa, IseharaTakumi Kawaguchi, KurumeHaruki Kitazawa, SendaiXiao-Kang Li, TokyoNoriaki Manabe, OkayamaAtsushi Masamune, SendaiHiroyuki Matsubayashi, ShizuokaKazuyuki Matsushita, Chuo-kuReiko Miyazawa, GunmaKazunari Murakami, OitaHikaru Nagahara, TokyoYuji Naito, KyotoAtsushi Nakajima, Atsushi NakajimaShoji Natsugoe, KagoshimaTsutomu Nishida, OsakaKoji Nomoto, TokyoNaoaki Sakata, MiyagiShouji Shimoyama, TokyoGoshi Shiota, YonagoIkuo Shoji, HyogoHidekazu Suzuki, TokyoHitoshi Takagi, GunmaToru Takahashi, OkayamaYoshihisa Takahashi, TokyoKan Uchiyama, ChibaTakato Ueno, KurumeYoshiyuki Ueno, SendaiHisayuki Uneyama, KwasakiMitsunori Yamakawa, YamagataTakayuki Yamamoto, MieYutaka Yata, GunmaNaohisa Yoshida, KyotoHitoshi Yoshiji, Nara
Lebanon
Costantine Fouad Daher, ByblosAssaad M Soweid, BeirutJulnar Usta, Beirut
Malaysia
Andrew Chua, Perak
Mexico
José María de la Roca-Chiapas, LeonMaria Raquel Huerta Franco, Guanajuato
Netherland
Wouter J de Jonge, AmsterdamAldo Grefhorst, GroningenRuben Hummelen, RotterdamDaniel Keszthelyi, MaastrichtCornelis F M Sier, LeidenPieter J Tanis, AmsterdamLuc JW van der Laan, RotterdamSander van der Marel, Leiden
NorwayAnne Marie Bakke, Oslo
Poland
Stanisław Hac, GdańskStanisław Jan Konturek, KrakówAgata Mulak, WroclawNapoleon Waszkiewicz, Choroszcz
Portugal
Ricardo Marcos, Porto
Romania
Mihai Ciocirlan, Bucharest
Russia
Ludmila Filaretova, Petersburg
Singapore
Madhav Bhatia, SingaporeBrian K P Goh, SingaporeKhek Yu Ho, SingaporeCliff K S Ong, Singapore
South Korea
Jae Hee Cheon, SeoulMyung Haing Cho, SeoulJae Bock Chung, SeoulKi-Baik Hahm, IncheonHo Jae Han, GwangjuChang Duk Jun, GwangjuHong Joo Kim, SeoulJin Kyung Kim, Gyeongsan-SiSang Geon Kim, SeoulWon Jae Lee, SeoulKwan Kyu Park, DaeguSeung Ha Park, BusanSung Joo Park, Jeonbuk
Spain
Raquel Abalo, AlcorcónJuan G Abraldes, BarcelonaAgustin Albillos, MadridMaria-Angeles Aller, MadridFernando Azpiroz, BarcelonaRamon Bataller, BarcelonaMarco Bustamante, ValenciaAndres Cardenas, BarcelonaDariao Acuna Castroviejo, ArmillaJoan Claria, BarcelonaPere Clave, BarcelonaManuel Giner, Madrid
Angel I Lanas, ZaragozaMaite Martin, BarcelonaMaria Teresa Martin, BarcelonaVicente Martinez, BarcelonaJose M Matés, MalagaJulio M Mayol, MadridMarçal Pastor-Anglada, BarcelonaMaría Eugenia Sáez, SevilleYolanda Sanz, BurjassotCarlos Taxonera, MadridMaria D Yago, Granada
Sweden
Marco Del Chiaro, StockholmFrida Fak, GothenburgGunnar FA Flemstrom, UppsalaEvangelos Kalaitzakis, GothenburgKristina Lamas, UmeaBob Roger Olsson, GöteborgSara Maria Regnér, MalmöPeter thelin Schmidt, StockholmXiao-Feng Sun, LinkopingHenrik Thorlacius, MalmöCurt Tysk, Orebro
Switzerland
Jyrki J Eloranta, ZurichAndreas Geier, ZurichRemy Meier, LiestalCatherine Pastor, Geneva
Thailand
Thawatchai Akaraviputh, BangkokWeekitt Kittisupamongkol, Bangkok
Turkey
Mehmet Bektas, AnkaraMukaddes Esrefoglu, MalatyaAhmet Guven, AnkaraMuammer Karadeniz, ManisaElvan Ozbek, ErzuruIlhami Yuksel, Ankara
Ukraine
Oksana S Zayavhkivska, Lviv
United Kingdom
Geoffrey Burnstock, LondonJanice E Drew, AberdeenGirish Gupte, BirminghamDavid C Hay, EdinburghNusrat Husain, CheshireMichael Leslie Lucas, GlasgowJamie Murphy, LondonVadim Sumbayev, KentWing-Kin Syn, Birmingham

IV February 15, 2013WJGP|www.wjgnet.com
Andrea Varro, Liverpool
United States
Sami Rene Achem, JacksonvilleTauseef Ali, OklahomaDavid H Alpers, St LouisGianfranco D Alpini, TempleShrikant Anant, OklahomaM Sawkat Anwer, North GraftonAndrew Aronsohn, ChicagoToms Augustin, SayreGyorgy Baffy, BostonMichael T Bailey, ColumbusKim Elaine Barrett, San DiegoMarc D Basson, LansingRobert L Bell, New HavenDavid H Berger, HoustonUrs A Boelsterli, StorrsRichard G Boles, Los AngelesEdward L Bradley III, SarasotaQiang Cai, AtlantaWei-Biao Cao, ProvidenceSubhash C Chauhan, Sioux FallsJian-De Chen, GalvestonTao-Sheng Chen, MemphisJohn Chiang, RootstownMashkoor A Choudhry, MaywoodParimal Chowdhury, Little RockEric Cohen, BostonRobert Cormier, DuluthSrinivasan Dasarathy, ClevelandEdwin A Deitch, NewarkDan A Dixon, ColumbiaJames P Dolan, PortlandH Henry Dong, PittsburghHui Dong, La JollaAshkan Farhadi, IrvineBin Feng, PittsburghJenifer Fenton, East LansingAlessandro Fichera, ChicagoMitchell P Fink, PittsburghP Marco Fisichella, MaywoodLeo R Fitzpatrick, HummelstownRobert Armour Forse, OmahaGlenn Tsuyoshi Furuta, AuroraJuan F Gallegos-Orozco, ScottsdalePandu R Gangula, NasvhilleTimothy Gardner, LebanonShannon Stroud Glaser, TempleFrancisco Gondim, St. LouisJohn R Grider, RichmondYan-Fang Guan, CincinnatiGregory M Holmes, Baton RougeAi-Xuan Le Holterman, ChicagoRichard Hu, Los AngelesHartmut Jaeschke, KansasRobert Thomas Jensen, Los AngelesSreenivasa S Jonnalagadda, LouisMichel Kahaleh, Charlottesville
Andreas Martin Kaiser, Los AngelesRandeep Singh Kashyap, RochesterLaurie Keefer, ChicagoRichard Kellermayer, HoustonChris Kevil, ShreveportSandeep Khurana, BaltimorePawel R Kiela, TucsonTammy Lyn Kindel, CincinnatGordana Kosutic, DurhamDavid Kravetz, San DiegoAshok Kumar, DetroitJohn H Kwon, ChicagoMuriel Larauche, Los AngelesI Michael Leitman, New YorkFelix W Leung, North HillsSuthat Liangpunsakul, IndianapolisFeng-Xin Lu, BostonPauline Kay Lund, Chapel HillGeorge Luo, LexingtonGuang-Xiang Luo, LexingtonJay Luther, Ann ArborRam I Mahato, MemphisAkhil Maheshwari, BirminghamKenneth Maiese, NewarkAdhip P N Majumdar, DetroitJose E Manautou, StorrsCraig J McClain, LouisvilleDermot McGovern, Los AngelesB Greenwood-van Meerveld, OklahomaDouglas Scott Merrel, BethesdaMurielle Mimeault, OmahaEmiko Mizoguchi, BostonHuan-Biao Mo, DentonAdam Moeser, RaleighRamzi M Mohammad, DetroitSatdarshan Singh Monga, PittsburghRoger Klein Moreira, New YorkSandeep Mukherjee, OmahaKarnam S Murthy, RichmondMichael J Nowicki, JacksonShuji Ogino, BostonMary Francis Otterson, WisconsinChung Owyang, Ann ArborHelieh S Oz, LexingtonMarco G Patti, ChicagoTimothy Michael Pawlik, BaltimoreSara Peleg, HoustonNicholas C Popescu, BethesdaLi-Ya Qiao, RichmondChao Qin, OklahomaParvaneh Rafiee, MilwaukeeSigrid A Rajasekaran, WilmingtonVazhaikkurichi M Rajendran, MorgantownJean Pierre Raufman, BaltimoreRamesh M Ray, MemphisArie Regev, IndianapolisDouglas K Rex, CarmelYehuda Ringel, Chapel HillRichard A Rippe, RockvilleChantal A Rivera, Bossier
Andrea Romani, ClevelandPraveen K Roy, AlbuquerquePaul A Rufo, BostonDavid B Sachar, New YorkBimaljit Singh Sandhu, RichmondSanjaya Kumar Satapathy, New Hyde ParkAnthony Senagore, Los AngelesMuhammad Y Sheikh, FresnoBo Shen, ClevelandLe Shen, ChicagoFrank A Simmen, Little RockSteven Mitchell Singer, WashingtonShailinder Jit Singh, WashingtonAdam Jan Smolka, CharlestonNed Snyder, HoustonZhen-Yuan Song, ChicagoGagan K Sood, HoustonRhonda F Souza, DallasStuart Jon Spechler, DallasSubbaramiah Sridha, AugustaCatia Sternini, Los AngelesVeedamali S Subramanian, Long BeachJun Sun, RochesterYvette Taché, Los AngelesXiao-Di Tan, ChicagoPaul Daniel Terry, AtlantaJennifer Tirnauer, FarmingtonAndrea Todisco, Ann ArborGeorge C Tsokos, BostonVic Velanovich, DetroitRaj Vuppalanchi, IndianapolisEstela Wajcberg, CranfordArnold Wald, MadisonLi-Xin Wang, Los AngelesHorst Christian Weber, BostonSteven D Wexner, WestonJackie D Wood, ColumbusGuo-Yao Wu, College StationChristian Wunder, BethesdaZuo-Liang Xiao, ClevelandGuang-Yin Xu, GalvestonGuo-Rong Xu, East OrangeGuang-Yu Yang, ChicagoJay A Yelon, ValhallaYamaoka Yoshio, HoustonShao-Yong Yu, HersheyYana Zavros, CincinnatiJoerg Zehetner, Los AngelesJian X Zhang, CharlotteZhi Zhong, CharlestonHui-Ping Zhou, RichmondZhan-Xiang Zhou, KannapolisQing Zhu, BethesdaYao-Hui Zhu, Stanford
Venezuela
Fabian Michelangeli, Caracas

Contents
November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com I
Quarterly Volume 6 Number 4 November 15, 2015
EDITORIAL86 Roleofcancerstemcellsinage-relatedriseincolorectalcancer
Nangia-Makker P, Yu Y, Majumdar APN
90 Alcoholichepatitis:ThepivotalroleofKupffercells
Suraweera DB, Weeratunga AN, Hu RW, Pandol SJ, Hu R
99 Starringroleoftoll-likereceptor-4activationinthegut-liveraxis
Carotti S, Guarino MPL, Vespasiani-Gentilucci U, Morini S
110 New-foundlinkbetweenmicrobiotaandobesity
Chakraborti CK
TOPIC HIGHLIGHTS120 Psychosocialimpactofirritablebowelsyndrome:Abriefreview
Ballou S, Bedell A, Keefer L
124 Structuralbrainlesionsininflammatoryboweldisease
Dolapcioglu C, Dolapcioglu H
REVIEW131 Elusiveliverfactorthatcausespancreaticαcellhyperplasia:Areviewofliterature
Yu R, Zheng Y, Lucas MB, Tong YG
140 Magneticresonanceimagingbiomarkersofgastrointestinalmotorfunctionandfluiddistribution
Khalaf A, Hoad CL, Spiller RC, Gowland PA, Moran GW, Marciani L
150 Eosinophilicesophagitis:Frompathophysiologytotreatment
D’Alessandro A, Esposito D, Pesce M, Cuomo R, De Palma GD, Sarnelli G
159 Host-microbiomeinteractioninCrohn’sdisease:Afamiliarorfamilialissue?
Michielan A, D’Incà R
169 GastrointestinaldysbiosisandtheuseoffecalmicrobialtransplantationinClostridiumdifficile infection
Schenck LP, Beck PL, MacDonald JA
181 Lymphoproliferativedisordersininflammatoryboweldiseasepatientsonimmunosuppression:Lessonsfrom
otherinflammatorydisorders
Lam GY, Halloran BP, Peters AC, Fedorak RN

ContentsWorld Journal of Gastrointestinal Pathophysiology
Volume 6 Number 4 November 15, 2015
November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com II
193 Currentunderstandingoftheneuropathophysiologyofpaininchronicpancreatitis
Atsawarungruangkit A, Pongprasobchai S
MINIREVIEWS203 Faecalcalprotectin:Managementininflammatoryboweldisease
Benítez JM, García-Sánchez V
210 Riskfactorsforosteoporosisininflammatoryboweldiseasepatients
Lima CA, Lyra AC, Rocha R, Santana GO
219 Promisingbiologicaltherapiesforulcerativecolitis:Areviewoftheliterature
Akiho H, Yokoyama A, Abe S, Nakazono Y, Murakami M, Otsuka Y, Fukawa K, Esaki M, Niina Y, Ogino H
ORIGINAL ARTICLEBasic Study
228 Predictivefactorsatbirthoftheseverityofgastroschisis
de Buys Roessingh AS, Damphousse A, Ballabeni P, Dubois J, Bouchard S
Retrospective Cohort Study
235 Roleofanti-stromalpolypharmacyinincreasingsurvivalafterpancreaticoduodenectomyforpancreatic
ductaladenocarcinoma
Tingle SJ, Moir JA, White SA
Case Report243 Energeticetiologiesofacutepancreatitis:Areportoffivecases
Shmelev A, Abdo A, Sachdev S, Shah U, Kowdley GC, Cunningham SC

EditorialBoardMemberofWorld Journalof GastrointestinalPathophysiology ,VazhaikkurichiMRajendran,PhD,Professor,DepartmentofBiochemistryandMolecular Biology,West VirginiaUniversity School ofMedicine,Morgantown,WV26506,UnitedStates
World Journal of Gastrointestinal Pathophysiology (World J Gastrointest Pathophysiol, WJGP, online ISSN 2150-5330, DOI: 10.4291), is a peer-reviewed open access academic journal that aims to guide clinical practice and improve diagnostic and therapeutic skills of clinicians.
WJGP is to report rapidly the most recent results in basic and clinical research on gastrointestinal pathophysiology, including all aspects of normal or abnormal function of the gastrointestinal tract, hepatobiliary system, and pancreas. WJGP specifically covers growth and development, digestion, secretion, absorption, metabolism and motility relative to the gastrointestinal organs, as well as immune and inflammatory processes, and neural, endocrine and circulatory control mechanisms that affect these organs. This journal will also report new methods and techniques in gastrointestinal pathophysiological research. We encourage authors to submit their manuscripts to WJGP. We will give priority to manuscripts that are supported by major national and international foundations and those that are of great basic and clinical significance.
World Journal of Gastrointestinal Pathophysiology is now indexed in PubMed Central, PubMed, Digital Object Identifier, and Directory of Open Access Journals.
I-IV EditorialBoard
ContentsWorld Journal of Gastrointestinal Pathophysiology
Volume 6 Number 4 November 15, 2015
FLYLEAF
EDITORS FOR THIS ISSUE
NAMEOFJOURNALWorld Journal of Gastrointestinal Pathophysiology
ISSNISSN 2150-5330 (online)
LAUNCHDATEApril 15, 2010
FrequencyQuarterly
EDITOR-IN-CHIEFThomas Y Ma, MD, PhD, Professor, Chief, Division of Gastroenterology and Hepatology, University of New Mexico, MSC10 5550, 1 UNM, Albuquerque, NM 87131, United States
EDITORIALOFFICEJin-Lei Wang, DirectorXiu-Xia Song, Vice DirectorWorld Journal of Gastrointestinal Pathophysiology
Room 903, Building D, Ocean International Center, No. 62 Dongsihuan Zhonglu, Chaoyang District, Beijing 100025, ChinaTelephone: +86-10-85381891Fax: +86-10-85381893E-mail: [email protected] Desk: http://www.wjgnet.com/esps/helpdesk.aspxhttp://www.wjgnet.com
PUBLISHERBaishideng Publishing Group Inc8226 Regency Drive, Pleasanton, CA 94588, USATelephone: +1-925-223-8242Fax: +1-925-223-8243E-mail: [email protected] Desk: http://www.wjgnet.com/esps/helpdesk.aspxhttp://www.wjgnet.com
PUBLICATIONDATENovember 15, 2015
COPYRIGHT© 2015 Baishideng Publishing Group Inc. Articles pub-lished by this Open Access journal are distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license.
SPECIALSTATEMENTAll articles published in journals owned by the Baishideng Publishing Group (BPG) represent the views and opinionsof their authors, and not the views, opinions or policies of the BPG, except where other-wise explicitly indicated.
INSTRUCTIONSTOAUTHORSFull instructions are available online at http://www.wjgnet.com/2218-6182/g_info_20100722172951.htm
ONLINESUBMISSIONhttp://www.wjgnet.com/esps/
ABOUT COVER
November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com III
AIM AND SCOPE
INDEXING/ABSTRACTING
Responsible Assistant Editor: Xiang Li Responsible Science Editor: Shui QiuResponsible Electronic Editor: Su-Qing Liu Proofing Editorial Office Director: Xiu-Xia Song Proofing Editor-in-Chief: Lian-Sheng Ma

Pratima Nangia-Makker, Yingjie Yu, Adhip PN Majumdar
Pratima Nangia-Makker, Yingjie Yu, Adhip PN Majumdar, Veterans Affairs Medical Center, Department of Internal Medicine, Karmanos Cancer Institute, Wayne State University-School of Medicine, Research Service, Detroit, MI 48201, United States
Author contributions: Nangia-Makker P designed and wrote the editorial; Yu Y designed and performed the experiments; Majumdar APN was invited to contribute to the editorial, concep-tualized and wrote the editorial, and contributed to research design.
Supported by The National Institutes of Health AG014343, 1R21CA175916-01; the Department of Veterans Affairs (I101BX001927); and the Metropolitan Detroit Research and Education Foundation (to Adhip PN Majumdar).
Conflict-of-interest statement: The authors have no conflict of interest.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Correspondence to: Pratima Nangia-Makker, PhD, Veterans Affairs Medical Center, Department of Internal Medicine, Karmanos Cancer Institute, Wayne State University-School of Medicine, Research Service, 4646 John R, Room-B4238, Detroit, MI 48201, United States. [email protected]: +1-313-5754460 Fax: +1-313-5761112
Received: June 2, 2015Peer-review started: June 4, 2015First decision: July 6, 2015Revised: September 2, 2015Accepted: September 16, 2015Article in press: September 18, 2015Published online: November 15, 2015
AbstractColorectal cancer (CRC) that comprises about 50% of estimated gastrointestinal cancers remains a high mortality malignancy. It is estimated that CRC will result in 9% of all cancer related deaths. CRC is the third leading malignancy affecting both males and females equally; with 9% of the estimated new cancer cases and 9% cancer related deaths. Sporadic CRC, whose incidence increases markedly with advancing age, occurs in 80%-85% patients diagnosed with CRC. Little is known about the precise biochemical mechanisms responsible for the rise in CRC with aging. However, many probable reasons for this increase have been suggested; among others they include altered carcinogen metabolism and the cumulative effects of long-term exposure to cancer-causing agents. Herein, we propose a role for self-renewing, cancer stem cells (CSCs) in regulating these cellular events. In this editorial, we have briefly described the recent work on the evolution of CSCs in gastro-intestinal track especially in the colon, and how they are involved in the age-related rise in CRC. Focus of this editorial is to provide a description of (1) CSC; (2) epigenetic and genetic mechanisms giving rise to CSCs; (3) markers of CSC; (4) characteristics; and (5) age-related increase in CSC in the colonic crypt.
Key words: Cancer stem cells; Aging; Colorectal cancer; Colonospheres; Colonic crypt
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Sporadic colorectal cancer (CRC), an age-related disease, occurs in 80%-85% of patients with CRC. The changes that occur at the cellular and molecular levels during ageing leading to a rise in CRC are poorly understood. We have postulated a role for cancer stem/stem-like cells that are shown to possess self-renewing, pluripotent properties. These cells, which reside at the bottom of the colonic crypt, are thought to regulate the processes of carcinogenesis. In this
EDITORIAL
86 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Role of cancer stem cells in age-related rise in colorectal cancer
World J Gastrointest Pathophysiol 2015 November 15; 6(4): 86-89ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i4.86

editorial, we have briefly described the recent work on the evolution of cancer stem cells in gastro-intestinal tract with particular reference to the colon, and how they are involved in the development and progression of CRC, the incidence of which increases with advancing age.
Nangia-Makker P, Yu Y, Majumdar APN. Role of cancer stem cells in age-related rise in colorectal cancer. World J Gastrointest Pathophysiol 2015; 6(4): 86-89 Available from: URL: http://www.wjgnet.com/2150-5330/full/v6/i4/86.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i4.86
TEXTThe primary challenge in the study of aging is to gain an in-depth understanding of the intricate relationship between disease processes and aging. One of the most consistent pathological conditions with advancing age is a sharp rise in colorectal cancer (CRC), which typically occurs after the age of 50. It has been reported that a male in age group 70 years and above exhibits 54 times greater risk of developing CRC compared to younger male (birth to 39 years).
According to a well accepted model of CRC pro-gression by Vogelstein, this malignancy arises as a result of accumulation of mutations in tumor suppressor genes and oncogenes[1,2]. For a malignant tumor to be initiated mutations in at least 4-5 genes are required and it is the total number of mutations rather than their sequence that is important for malignant transformation to occur. Transformation from the initial events to an invasive carcinoma takes about 8-12 years. As colonic mucosa is a highly dynamic tissue and the mucosal surface epithelium cells are constantly replaced with cells derived from crypt stem cells; it is reasonable to assume that only the long-lived cells (stem cells) may serve as reservoirs for accumulation of such precancerous mutations. In a normal colon, these cells are typically present at the bottom of the colonic crypts[3]. Cancer stem cells (CSCs), that possess remarkable similarity with normal stem cells, are thought to be the result of accumulated mutations, specifically in tumor suppressor genes and/or oncogenes[4]. Like normal stem cells, CSCs are also able to proliferate indefinitely and also possess the property of pluripotency indicating their capability to differentiate into more than one cell lineages. Recent evidence show that CSCs are present in many malignancies, including CRC[4-6]. Self-renewing properties of CSCs allow these cells to form tumors representing the original tumor in immuno-compromised mice. Within the epithelial malignancies, CSCs were first identified in breast cancer and characterized by specific cell surface markers[4,6]. Since then, they have been reported in a multitude other human malignancies. It is suggested that these self-renewing, pluripotent cancer stem/stem-like cells may play a pivotal role in initiation, development
and progression of colorectal carcinoma.Data generated from several investigations from our
laboratory have revealed a progressive rise in CSCs in the colon with advancing age[7,8]. Stem cells, present in all vertebrates, are constantly replenishing dying cells or regenerating damaged or injured tissue. With aging, DNA repair system has been shown to be impaired that results in an increased DNA damage. DNA damage leading to reduction in some stem cells through apoptosis can result in genetic and epigenetic changes in stem cells that have survived the DNA repair mechanisms[9]. Both genetic and epigenetic alterations may affect stem cell function by altering transcriptome and lead to the processes of carcinogenesis (reviewed in[10]). Thus the age-related rise in CRC could partly be due a rise in CSCs.
CSCs can be identified by surface epitopes or their functional characteristics. Colon CSCs are characterized by the expression of several markers that represent the surface epitopes which among others include CD44, CD166, CD133 and EpCAM[11]. In addition, colonosphere formation is considered to be another functional assay for identification of CSCs.
Another characteristic of CSCs is the acquisition of epithelial to mesenchymal transition (EMT), which provides the cells ability to migrate, invade and metastasize. EMT can be determined by E-cadherin and vimentin expression, which are downstream targets of Wnt/β-catenin and notch signaling[12]. Our earlier data suggested a pivotal role fort Wnt/β-catenin signaling for proliferation and maintenance of CSCs in the colon[13]. Over-expression and/or induction of epidermal growth factor receptor (EGFR) signaling and/or other members of receptor tyrosine kinase family, especially ErbB-2 has also been shown to occur in many cancers including the colon and is considered to be an indicator of poor prognosis. We have postulated that activation of EGFR in the gastrointestinal tract may lead to stem cell proliferation and maintenance as inhibition of EGFR by cetuximab reduced CSCs in the colon[14].
In view of the recent evidence indicating the appearance of CSCs is one of the initial events in car-cinogenesis, we have investigated and confirmed that age-related increases in adenomatous polyps are associated with increases in mucosal CSCs[7]. We demon-strated that with advancing age there is a progressive rise in CSCs in the colon not only in adenomas, but also in normal appearing mucosa. This observation indicates that aging increases the risk of CRC[7]. The number of colonic mucosal cells showing CD44+, CD166+ or Ep-CAM was markedly higher in the isolated mucosal cells in subjects over 55 years of age with polyps than the younger ones.
We also reported an age-related rise in expression and activation of all members of EGFRs with the exception of EGFR-4, which was not studied[15-19]. In addition, our data also revealed that CD166 and EGFR were co-localized in normal appearing mucosa of patients with adenomas. Interestingly, the co-expression of CD166 and EGFR was found to be markedly higher in individuals over 60 years
87 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Nangia-Makker P et al . Colon cancer stem cells and aging
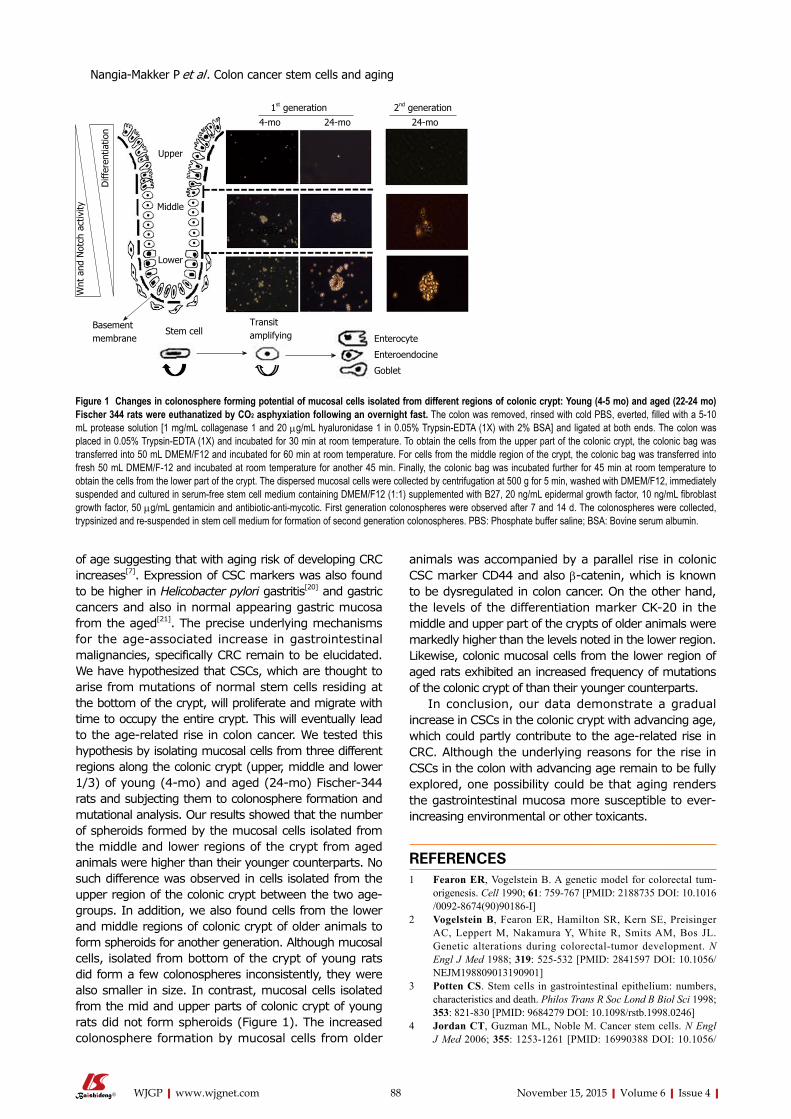
of age suggesting that with aging risk of developing CRC increases[7]. Expression of CSC markers was also found to be higher in Helicobacter pylori gastritis[20] and gastric cancers and also in normal appearing gastric mucosa from the aged[21]. The precise underlying mechanisms for the age-associated increase in gastrointestinal malignancies, specifically CRC remain to be elucidated. We have hypothesized that CSCs, which are thought to arise from mutations of normal stem cells residing at the bottom of the crypt, will proliferate and migrate with time to occupy the entire crypt. This will eventually lead to the age-related rise in colon cancer. We tested this hypothesis by isolating mucosal cells from three different regions along the colonic crypt (upper, middle and lower 1/3) of young (4-mo) and aged (24-mo) Fischer-344 rats and subjecting them to colonosphere formation and mutational analysis. Our results showed that the number of spheroids formed by the mucosal cells isolated from the middle and lower regions of the crypt from aged animals were higher than their younger counterparts. No such difference was observed in cells isolated from the upper region of the colonic crypt between the two age-groups. In addition, we also found cells from the lower and middle regions of colonic crypt of older animals to form spheroids for another generation. Although mucosal cells, isolated from bottom of the crypt of young rats did form a few colonospheres inconsistently, they were also smaller in size. In contrast, mucosal cells isolated from the mid and upper parts of colonic crypt of young rats did not form spheroids (Figure 1). The increased colonosphere formation by mucosal cells from older
animals was accompanied by a parallel rise in colonic CSC marker CD44 and also β-catenin, which is known to be dysregulated in colon cancer. On the other hand, the levels of the differentiation marker CK-20 in the middle and upper part of the crypts of older animals were markedly higher than the levels noted in the lower region. Likewise, colonic mucosal cells from the lower region of aged rats exhibited an increased frequency of mutations of the colonic crypt of than their younger counterparts.
In conclusion, our data demonstrate a gradual increase in CSCs in the colonic crypt with advancing age, which could partly contribute to the age-related rise in CRC. Although the underlying reasons for the rise in CSCs in the colon with advancing age remain to be fully explored, one possibility could be that aging renders the gastrointestinal mucosa more susceptible to ever-increasing environmental or other toxicants.
REFERENCES1 Fearon ER, Vogelstein B. A genetic model for colorectal tum-
origenesis. Cell 1990; 61: 759-767 [PMID: 2188735 DOI: 10.1016/0092-8674(90)90186-I]
2 Vogelstein B, Fearon ER, Hamilton SR, Kern SE, Preisinger AC, Leppert M, Nakamura Y, White R, Smits AM, Bos JL. Genetic alterations during colorectal-tumor development. N Engl J Med 1988; 319: 525-532 [PMID: 2841597 DOI: 10.1056/NEJM198809013190901]
3 Potten CS. Stem cells in gastrointestinal epithelium: numbers, characteristics and death. Philos Trans R Soc Lond B Biol Sci 1998; 353: 821-830 [PMID: 9684279 DOI: 10.1098/rstb.1998.0246]
4 Jordan CT, Guzman ML, Noble M. Cancer stem cells. N Engl J Med 2006; 355: 1253-1261 [PMID: 16990388 DOI: 10.1056/
88 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
1st generation 2nd generation
4-mo 24-mo 24-mo
Upper
Middle
Lower
Stem cellTransitamplifying Enterocyte
Enteroendocine
Goblet
Basementmembrane
Diff
eren
tiatio
n
Wnt
and
Not
ch a
ctiv
ity
Figure 1 Changes in colonosphere forming potential of mucosal cells isolated from different regions of colonic crypt: Young (4-5 mo) and aged (22-24 mo) Fischer 344 rats were euthanatized by CO2 asphyxiation following an overnight fast. The colon was removed, rinsed with cold PBS, everted, filled with a 5-10 mL protease solution [1 mg/mL collagenase 1 and 20 µg/mL hyaluronidase 1 in 0.05% Trypsin-EDTA (1X) with 2% BSA] and ligated at both ends. The colon was placed in 0.05% Trypsin-EDTA (1X) and incubated for 30 min at room temperature. To obtain the cells from the upper part of the colonic crypt, the colonic bag was transferred into 50 mL DMEM/F12 and incubated for 60 min at room temperature. For cells from the middle region of the crypt, the colonic bag was transferred into fresh 50 mL DMEM/F-12 and incubated at room temperature for another 45 min. Finally, the colonic bag was incubated further for 45 min at room temperature to obtain the cells from the lower part of the crypt. The dispersed mucosal cells were collected by centrifugation at 500 g for 5 min, washed with DMEM/F12, immediately suspended and cultured in serum-free stem cell medium containing DMEM/F12 (1:1) supplemented with B27, 20 ng/mL epidermal growth factor, 10 ng/mL fibroblast growth factor, 50 µg/mL gentamicin and antibiotic-anti-mycotic. First generation colonospheres were observed after 7 and 14 d. The colonospheres were collected, trypsinized and re-suspended in stem cell medium for formation of second generation colonospheres. PBS: Phosphate buffer saline; BSA: Bovine serum albumin.
Nangia-Makker P et al . Colon cancer stem cells and aging

89 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
10.1186/1476-4598-9-212]14 Nautiyal J, Du J, Yu Y, Kanwar SS, Levi E, Majumdar AP. EGFR
regulation of colon cancer stem-like cells during aging and in response to the colonic carcinogen dimethylhydrazine. Am J Physiol Gastrointest Liver Physiol 2012; 302: G655-G663 [PMID: 22281474 DOI: 10.1152/ajpgi.00323.2011]
15 Majumdar AP. Regulation of gastrointestinal mucosal growth during aging. J Physiol Pharmacol 2003; 54 Suppl 4: 143-154 [PMID: 15075456]
16 Majumdar AP, Du J. Phosphatidylinositol 3-kinase/Akt signaling stimulates colonic mucosal cell survival during aging. Am J Physiol Gastrointest Liver Physiol 2006; 290: G49-G55 [PMID: 16123202 DOI: 10.1152/ajpgi.00106.2005]
17 Majumdar AP, Du J, Yu Y, Xu H, Levi E, Patel BB, Rishi AK. Cell cycle and apoptosis regulatory protein-1: a novel regulator of apoptosis in the colonic mucosa during aging. Am J Physiol Gastrointest Liver Physiol 2007; 293: G1215-G1222 [PMID: 17932228]
18 Nautiyal J, Rishi AK, Majumdar AP. Emerging therapies in gastrointestinal cancers. World J Gastroenterol 2006; 12: 7440-7450 [PMID: 17167831]
19 Patel BB, Majumdar APN. HER family of receptors as treatment targets. In: Pancreatic cancer. Anderson Solid Tumor Oncology Series. 1st ed. Lowy AM, Leach SD, Phillip PA, editors. New York: Springer, 2008: 609-634
20 Bertaux-Skeirik N, Feng R, Schumacher MA, Li J, Mahe MM, Engevik AC, Javier JE, Peek RM, Ottemann K, Orian-Rousseau V, Boivin GP, Helmrath MA, Zavros Y. CD44 plays a functional role in Helicobacter pylori-induced epithelial cell proliferation. PLoS Pathog 2015; 11: e1004663 [PMID: 25658601 DOI: 10.1371/journal.ppat.1004663]
21 Levi E, Sochacki P, Khoury N, Patel BB, Majumdar AP. Cancer stem cells in Helicobacter pylori infection and aging: Implications for gastric carcinogenesis. World J Gastrointest Pathophysiol 2014; 5: 366-372 [PMID: 25133037]
P- Reviewer: Bonnet M, Rosales-Reynoso MA S- Editor: Gong XM L- Editor: A E- Editor: Liu SQ
NEJMra061808]5 Todaro M, Alea MP, Di Stefano AB, Cammareri P, Vermeulen L,
Iovino F, Tripodo C, Russo A, Gulotta G, Medema JP, Stassi G. Colon cancer stem cells dictate tumor growth and resist cell death by production of interleukin-4. Cell Stem Cell 2007; 1: 389-402 [PMID: 18371377 DOI: 10.1016/j.stem.2007.08.001]
6 Dick JE. Stem cell concepts renew cancer research. Blood 2008; 112: 4793-4807 [PMID: 19064739 DOI: 10.1182/blood-2008-08-077941]
7 Patel BB, Yu Y, Du J, Levi E, Phillip PA, Majumdar AP. Age-related increase in colorectal cancer stem cells in macroscopically normal mucosa of patients with adenomas: a risk factor for colon cancer. Biochem Biophys Res Commun 2009; 378: 344-347 [PMID: 19010307 DOI: 10.1016/j.bbrc.2008.10.179]
8 Patel BB, Yu Y, Du J, Rishi AK, Sarkar FH, Tarca AL, Wali A, Majumdar AP. Schlafen 3, a novel gene, regulates colonic mucosal growth during aging. Am J Physiol Gastrointest Liver Physiol 2009; 296: G955-G962 [PMID: 19228883 DOI: 10.1152/ajpgi.90726.2008]
9 Finkel T, Serrano M, Blasco MA. The common biology of cancer and ageing. Nature 2007; 448: 767-774 [PMID: 17700693 DOI: 10.1038/nature05985]
10 Roy S, Majumdar AP. Cancer Stem Cells in Colorectal Cancer: Genetic and Epigenetic Changes. J Stem Cell Res Ther 2012; Suppl 7: pii: 10342 [PMID: 23565347]
11 Sanders MA, Majumdar AP. Colon cancer stem cells: implications in carcinogenesis. Front Biosci (Landmark Ed) 2011; 16: 1651-1662 [PMID: 21196254 DOI: 10.2741/3811]
12 Morin PJ, Sparks AB, Korinek V, Barker N, Clevers H, Vogelstein B, Kinzler KW. Activation of beta-catenin-Tcf signaling in colon cancer by mutations in beta-catenin or APC. Science 1997; 275: 1787-1790 [PMID: 9065402 DOI: 10.1126/science.275.5307.1787]
13 Kanwar SS, Yu Y, Nautiyal J, Patel BB, Majumdar AP. The Wnt/beta-catenin pathway regulates growth and maintenance of colonospheres. Mol Cancer 2010; 9: 212 [PMID: 20691072 DOI:
Nangia-Makker P et al . Colon cancer stem cells and aging

Duminda B Suraweera, Ashley N Weeratunga, Robert W Hu, Stephen J Pandol, Richard Hu
Duminda B Suraweera, Department of Medicine, Olive View-UCLA Medical Center, Los Angeles, CA 91342, United States
Ashley N Weeratunga, Creighton University School of Medicine, Omaha, NE 68102, United States
Robert W Hu, College of Arts and Sciences, the University of Pennsylvania, Philadelphia, PA 19104, United States
Robert W Hu, Stephen J Pandol, Department of Gastroen-terology and Biomedical Sciences, Cedars-Sinai Medical Center, Los Angeles, CA 90048, United States
Richard Hu, Department of Gastroenterology, Olive View-UCLA Medical Center and David Geffen School of Medicine at UCLA, Los Angeles, CA 91342, United States
Author contributions: Suraweera DB designed the project, reviewed the articles and wrote the paper; Weeratunga AN and Hu RW reviewed the articles and analyzed data; Pandol SJ edited and reviewed the articles; Hu R contributed to developing the concept, editing and reviewing the article.
Conflict-of-interest statement: None of the authors of this paper have any conflict of interest to declare.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Correspondence to: Richard Hu, MD, Department of Gastro-enterology, Olive View-UCLA Medical Center and David Geffen School of Medicine at UCLA, 14445 Olive View Dr., 2B-182, Los Angeles, CA 91342, United States. [email protected]: +1-818-3643205Fax: +1-818-3644573
Received: May 26, 2015Peer-review started: May 27, 2015First decision: July 3, 2015
Revised: July 27, 2015 Accepted: September 7, 2015 Article in press: September 8, 2015Published online: November 15, 2015
AbstractKupffer cells play a central role in the pathogenesis of alcoholic hepatitis (AH). It is believed that alcohol increases the gut permeability that results in raised levels of serum endotoxins containing lipopolysaccharides (LPS). LPS binds to LPS-binding proteins and presents it to a membrane glycoprotein called CD14, which then activates Kupffer cells via a receptor called toll-like receptor 4. This endotoxin mediated activation of Kupffer cells plays an important role in the inflammatory process resulting in alcoholic hepatitis. There is no effective treatment for AH, although notable progress has been made over the last decade in understanding the underlying mechanism of alcoholic hepatitis. We specifically review the current research on the role of Kupffer cells in the pathogenesis of AH and the treatment strategies. We suggest that the imbalance between the pro-inflammatory and the anti-inflammatory process as well as the increased production of reactive oxygen species eventually lead to hepatocyte injury, the final event of alcoholic hepatitis.
Key words: Alcoholic liver disease; Alcoholic hepatitis; Macrophages; Kupffer cells
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: In this editorial we provide critical comments on the pivotal role of Kupffer cells on the development of alcoholic hepatitis with a focus on the pro-inflam-matory as well as the anti-inflammatory pathways. We propose that the anti-inflammatory pathway should be further explored as a potential alternative for novel treatment strategies. This editorial is significant as it provides a platform for the future basic and clinical
EDITORIAL
90 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Alcoholic hepatitis: The pivotal role of Kupffer cells
World J Gastrointest Pathophysiol 2015 November 15; 6(4): 90-98ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i4.90

research in elucidating the pathogenesis and developing the management strategies of this common clinical pathology - alcoholic hepatitis.
Suraweera DB, Weeratunga AN, Hu RW, Pandol SJ, Hu R. Alcoholic hepatitis: The pivotal role of Kupffer cells. World J Gastrointest Pathophysiol 2015; 6(4): 90-98 Available from: URL: http://www.wjgnet.com/2150-5330/full/v6/i4/90.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i4.90
INTRODUCTIONAlcoholic hepatitis (AH) is defined as an acute hepatic inflammatory response to excess alcohol ingestion. It is estimated that 56809 hospital admissions in 2007 in the United States had a primary diagnosis of AH, 0.71% of all admissions[1]. In addition, hospitalization for AH is a leading cause of healthcare utilization[1]. In spite of such high costs and mortality, there has been little progress in the treatment strategies over the past 20 years. Histologically, alcoholic hepatitis is characterized by hepatocellular necrosis and immune cell infiltration around damaged hepatocytes[2]. This inflammatory and immune response leads to further hepatic injury and acute liver failure. Thus understanding this inflammatory cascade is vital to understanding alcoholic hepatitis and developing a treatment strategy. Currently there are only two pharmacologic treatments of AH: Corticosteroids and pentoxifylline. However these treatments are limited in their effectiveness and severe cases of AH still carry a short term mortality of 30%-50%[3]. Hepatic macro-phages, called Kupffer cells, have been found to play a central role in hepatic inflammation[4]. Therefore, we will focus on providing a concise review of the role of Kupffer cells in AH, current treatments to disrupt this inflammatory pathway and potential basic and clinical research directions.
OVERVIEW OF THE PHYSIOLOGIC FUNCTION OF KUPFFER CELLSKupffer cells are macrophages found in the liver. They were first identified by Kupffer[5] in 1876. Monocytes in the blood stream migrate into the liver and differentiate into Kupffer cells[6]. Kupffer cells makeup about 15% of all cells in the liver and comprise 50% of the total population of macrophages in the body[7]. They function to clear foreign matter from the portal circulation and in animal models have been shown to clear about 80%-90% of all particulate injected[8]. The particulate include immune complexes, bacterial components, endotoxins and collagen fragments. Kupffer cells can kill ingested organisms using oxygen dependent and independent mechanisms[9]. Studies in Kupffer cell depleted mice have shown that Kupffer cells play a critical role in neutrophil recruitment and granulomatous
formation in the liver[10]. Kupffer cells are activated by endotoxins (Figure 1). Endotoxins are composed of the lipopolysaccharides (LPS) component of Gram-negative bacterial cell walls. LPS-binding proteins (LBPs), produced by hepatocytes, bind and present LPS to CD14, a membrane glycoprotein[9]. CD14 in turn activates Kupffer cells via a membrane complex that includes a pathogen recognition receptor called toll-like receptor 4 (TLR-4). Activated Kupffer cells release interleukin (IL)-1B, tumor necrosis factor (TNF)-α, IL-6, IL-8, macrophage chemotactic protein-1 and regulated normal T cell expressed and secreted. These cytokines, mainly TNF-α, then bind to hepatocyte receptors leading to tissue damage via oxidative stress and apoptosis[11].
ACTIVATION OF IMMUNE RESPONSE INALCOHOLIC HEPATITISGut bacterial translocation likely plays a key role in AH. In a healthy individual, only a small quotient of gut bacterial endotoxin gets translocated into the portal blood. Alcohol ingestion has been shown to increase this endotoxin translocation[12]. Alteration of gut microflora and increased gut permeability are the driving forces behind this process. Experimentally induced bacterial overgrowth in rats has been shown to lead to increased bacterial translocation and subsequent liver injury[13]. Furthermore, evidence suggests that alcohol can alter gut microflora[14]. Jejunal aspirates of chronic alcohol abuse patients have shown increased aerobic and anaerobic bacteria[15,16]. The pathophysiology of bacterial overgrowth in chronic alcoholic patients is not clearly identified. Possible etiologies include impaired bile flow, reduced gastrointestinal motility and increased gastric pH[14,17-19]. In addition to bacterial overgrowth, alcohol can lead to intestinal dysbiosis. Animal studies have shown an increased predominance of Gram-negative bacteria in alcohol fed subjects[20,21]. Mice with antibiotic induced eradication of gut flora had decreased alcohol induced liver injury as compared to mice with intact gut flora when exposed to ethanol[22]. Similar results were found in mice that were fed with lactobacillus[23]. Intestinal decontamination with rifaximin has also shown increased liver hemodynamics and decreased incidence of hepatic encephalopathy in patients with alcoholic liver disease (ALD)[24,25]. The second component of alcohol induced endotoxemia is increased gut permeability. Alcohol is metabolized into acetaldehyde, which has been shown to open tight junctions and increase gut epithelium permeability[26,27]. Several studies have suggested the association between endotoxins and alcoholic liver injury. It was found that endotoxin levels in mice directly correlated with the severity of alcoholic liver injury[28]. Rats that had LPS administered in addition to alcohol were also shown to have worse liver injury than those exposed to ethanol alone[29]. In humans, endotoxin levels have been shown to be measurably higher in acute and chronic alcohol use[30].
91 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Suraweera DB et al . Kupffer cells in alcoholic hepatitis

IMPORTANCE OF KUPFFER CELLS IN ALCOHOLIC HEPATITISSeveral lines of evidence suggest that Kupffer cells play an important role as inflammatory mediators in the setting of alcoholic hepatitis. TLR-4 defective rats exposed to ethanol were shown to have markedly less steatosis, inflammation, and necrosis as compared to wild-type rats[31]. Furthermore ethanol increased TNF-α in wild-type rats but failed to do so in the TLR-4 mutant rats[31]. In LBP and CD14 knockout mice, alcohol induced liver injury was also significantly reduced[31-33]. Mice in whom Kupffer cells were chemically destroyed had no alcohol induced liver injury[34]. Activated human Kupffer cells express CD163, a hemoglobin-haptoglobin scavenger surface receptor[35]. Although the function of CD163 is unknown, it has been used as a marker for macrophage activation. Studies have shown that CD163 is in fact not only elevated in ALD, but that the plasma concentration of CD163 also predicts mortality in acute liver failure[36]. In addition CD163 has been shown to be a predictor of clinical decompensation in the setting of liver cirrhosis, an independent prognostic indicator for variceal bleeds and a marker of portal hypertension[37-39]. It is important to note that a recent study comparing levels of CD163 in AH, chronic cirrhosis and healthy patients found that CD163 concentrations were 30% higher in AH patients than in chronic cirr-hotic patients and 10 times higher as compared to healthy individuals[40]. Therefore, CD163 could serve as a diagnostic marker of alcoholic hepatitis as well as a potential prognosticator for patients with alcoholic hepatitis.
Kupffer cell-mediated products have been extensively studied to further characterize their association in AH. TNF-α has been identified as a key mediator in AH. Serum TNF-α have been found to correlate with endo-
toxemia and development of inflammation and fibrosis in patients with AH. It can even be used as a biomarker for fibrosis[41,42]. Studies have confirmed that monocytes from patients with alcoholic hepatitis had greater levels of TNF-α than healthy subjects[43]. Furthermore, analysis of liver biopsies in patients with AH have shown increased staining for TNF-α, IL-1 and IL-6[44]. Kupffer cells can also contribute to liver injury via oxidant stress. Kupffer cells in animals fed with alcohol produce free radicals. This is further supported by studies showing nicotinamide adenine dinucleotide phosphate oxidase knocked out mice demonstrated to have decreased liver necrosis and inflammation in addition to decreased nuclear factor-kappa B and TNF-α[45].
In addition to the resident Kupffer cell-mediated hepatic injury, recruited macrophages have also been shown to play a part in liver injury[46]. Murine models have shown that there is an increased accumulation of infiltrating monocytes in the setting of liver injury[47]. Recruitment of these monocytes is highly dependent on the chemokines CCL1 and CCL2. Of note, one of the major sources of CCL2 is hepatic stellate cells, which in turn are activated by the TLR-4 ligands. Mice lacking CCL2 have been shown to incur less liver injury[48]. Furthermore mice lacking CCR8, a receptor for CCL1, were also shown to be more protected from liver injury[49]. Infiltrating monocytes have been divided into two groups depending on surface protein expression, Ly6Chi and Ly6Clow. Ly6Chi monocytes exhibit a pro-inflammatory phenotype while Ly6Clow monocytes exhibit an anti-inflammatory phenotype. Mice fed with ethanol had a shift towards more Ly6Chi monocytes, resulting in significantly increased liver injury[50]. There is still much to be learned about the role and function of infiltrating monocytes in liver injury.
Kupffer cells have been shown to play central roles in other causes of liver injury such as nonalcoholic
92 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
(1) Alcohol induced increase in gut permeability
(2) Gut bacterial translocation leading to endotoxemia
LPS
Kupffer cell
TLR-4
LPS
(3) LPS activates Kupffer cells via CD14 and TLR-4
(4) Activated Kupffer cells release cytokines and ROS leading to inflammatory dysregulation
(5) Hepatocyte injury
ROSIL-1TNF-α
IL-22IL-6
Figure 1 Central mediating role of Kupffer cells in alcoholic hepatitis. The dysregulation between the pro-inflammatory and the anti-inflammatory cytokines eventually leads to hepatocyte injury. Image components obtained from somersault 1824 online image library (http://www.somersault1824.com/). LPS: Lipopolysaccharides; TLR-4: Toll-like receptor 4; IL: Interleukin; TNF: Tumor necrosis factor; ROS: Reactive oxygen species.
Suraweera DB et al . Kupffer cells in alcoholic hepatitis

93 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
tality rates are predominantly due to a lack of effective treatment for severe AH. Multiple clinical trials for treatment of alcoholic hepatitis have been published (Table 1). The American Association for the Study of Liver Diseases (AASLD) guidelines for management of AH currently stratifies the management depending on severity. Low risk patients are managed conservatively with nutrition, supportive care and close monitoring. High-risk individuals, defined as those with a Maddrey’s discriminant function greater than or equal to 32 or a model for end-stage liver disease score greater than or equal to 18, may benefit from pharmacological intervention with either prednisolone or pentoxifylline. Corticosteroids have been extensively studied with mixed results[63-67]. This is likely due to the fact that study design, severity of AH and exclusions criteria vary greatly between studies. One meta-analysis showed survival rates of 80% at 28 d with corticosteroids vs 66% in the control group in patients with severe AH[63]. Corticosteroids presumably improved outcomes by decreasing pro-inflammatory cytokines. Pentoxifylline is a nonselective phosphodiesterase inhibitor that increases intracellular concentration of adenosine 3’, 5’-cyclic monophosphate, which in turn inhibits the expression of pro-inflammatory cytokines[68]. AASLD recommends pentoxifylline as an alternative to corticosteroids when the use of steroids is contraindicated or in the setting of early renal failure. According to one randomized, double-blinded, placebo controlled trial, patients treated with pentoxifylline had a survival benefit (24.5% mortality vs 46.1% in the placebo group)[69]. Although multiple clinical trials have shown some benefit of treatment with steroids or pentoxifylline, a recent well designed, multicenter, double-blinded, randomized trial found no statistically significant mortality benefit in treatment with either pentoxifylline or prednisolone[70]. The study involved 1053 patients who were randomized to four arms: A group that received a pentoxifylline-matched placebo and a prednisolone-matched placebo, a group that received prednisolone and a pentoxifylline-matched
steatohepatitis (NASH) and viral hepatitis that are often also present in AH patients. Using a murine model of NASH, several studies have shown that sequential depletion of Kupffer cells reduced the incidence of steatosis[51-53]. Furthermore, targeted knockdown of TNF-α also decreased the incidence of NASH develop-ment[51,54]. Current understanding of the role of Kupffer cells in viral hepatitis is limited. Identification of a specific pathogenesis has been difficult due to similar characteristics of recruited macrophages and resident Kupffer cells. A recent study suggests that Kupffer cell interaction with hepatitis B surface antigen leads to pro-inflammatory cytokine production, which may contribute to liver pathology[55]. Studies have shown increased numbers of Kupffer cells during hepatitis C viral (HCV) infection[56]. Incubation of HCV E2 envelop protein with human liver cells resulted in Kupffer cell binding in a CD81-dependent manner[57]. In addition HCV core and NS3 stimulate human CD14+ Kupffer cells and monocyte derived macrophages to produce IL-1β, IL-6 and TNF-α[58,59]. It is likely that Kupffer cell activation contributes to the progression of liver disease in viral hepatitis. Increased numbers of Kupffer cells have been found in regions of liver fibrosis in the setting of chronic viral hepatitis[60]. Viral hepatitis has also been shown to induce Kupffer cells to release cytotoxic molecules that kill not only infected hepatocytes but also non-infected cells[61,62]. It is likely that Kupffer cells are involved in the pathogenesis of many types of liver pathologies and it may be the case that their activation is multifactorial in patients with AH as well as other hepatic comorbidities.
CURRENT TREATMENT OF ALCOHOLIC HEPATITISAH is an acute process and most patients will recover with nutritional support and abstinence from alcohol. However severe AH carries a high mortality rate: 35% at 28 d without effective treatment[63]. These high mor-
Table 1 Randomized controlled trials evaluating the treatment of alcoholic hepatitis
Study Topic Methods Findings
Prednisolone or pentoxifylline Theodossi et al[99] PRED vs placebo Randomized control No difference in mortality Ramond et al[100] PRED vs placebo Double-blinded, randomized control Improved mortality with PRED Akriviadis et al[69] PTX vs placebo Double-blinded, randomized control Improved mortality with PTX Sidhu et al[101] PTX vs placebo Randomized control Improved mortality with PTX De et al[102] PTX vs PRED Double-blinded, randomized control Reduced mortality with PTX Park et al[103] PTX vs PRED Randomized control Reduced mortality with PRED Mathurin et al[104] PRED vs PRED + PTX Multicenter, double-blinded, randomized control No difference in mortality De et al[105] PTX vs PTX + PRED Double-blinded, randomized control No difference in mortality Thursz et al[70] PTX vs PRED vs placebo Multicenter, double-blinded, randomized control No difference in mortalityN-acetylcysteine Moreno et al[106] NAC vs placebo Multicenter, single-blinded, randomized control No difference in mortalityCytokine inhibitors Naveau et al[72] Infliximab vs placebo Double-blinded, randomized control Increased mortality with infliximab Boetticher et al[71] Etancercept vs placebo Multicenter, single-blinded, randomized control Increased mortality with etancercept
PTX: Pentoxifylline; PRED: Prednisiolone; NAC: N-acetylcysteine.
Suraweera DB et al . Kupffer cells in alcoholic hepatitis

94 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
placebo, a group that received pentoxifylline and a prednisolone-matched placebo, or a group that received both prednisolone and pentoxifylline. The prednisolone group was the only group associated with an initial reduction in 28-d mortality. However at 90 d and at 1 year there were no significant differences between the groups. There is no doubt that this well designed study certainly questions the currently established treatments of AH.
While cytokine inhibitors have great potential in theory, trials with both infliximab and etanercept have resulted in increased mortality, primarily due to infec-tion[71,72]. Liver transplantation is another treatment option in ALD. Most transplant centers require at least 6-months of abstinence[73,74]. This allows for disease regression in patients with recent alcohol use, time for proper counseling and demonstrates patients’ ability to abstain from alcohol. One meta-analysis comparing alcohol use in post-transplant patients showed no difference in the proportion of patients that used alcohol when comparing ALD to non-ALD patients, although ALD patients were more likely to drink excessively[75]. Risk of alcohol recurrence in ALD transplant patients continues to be an area of debate. In summary, treatment options for AH are limited with even the standard of care now being questioned, emphasizing the urgent need for effective and novel treatment strategies.
FUTURE AREAS OF RESEARCHIdentification of new therapeutic targets has been hampered by a lack of appropriate animal models. Current animal models do not develop severe liver injury as humans do. One possible area of future investigations would be the modulation of the LPS pathway. A recent study evaluating the effects of milk osteopontin on gut permeability found that milk osteopontin preserved gut architecture and prevented inflammation in ethanol fed mice[76]. Milk osteopontin has also been shown to directly bind to LPS and prevent Kupffer cell activation thereby disrupting the subsequent pro-inflammatory cascade[77]. Another study used probiotics to alter gut flora and TLR4 antagonists, which have been proposed for treatment of ALD[78].
Genetic factors leading to the predisposition for liver disease is another promising area of exploration in recent years. A number of studies have shown an association between variations in the PNPLA3 gene and liver fat content as well as plasma aspartate amino-transferase[79-82]. Furthermore two groups have inde-pendently found associations between the PNPLA3 single-nucleotide polymorphism rs738409 and ALD populations in Mexico and Germany[83,84]. During the last decade, a prominent area of research had been the inhibition of pro-inflammatory cytokines. However blocking TNF-α had led to unacceptable complications. More targeted inhibition using dexamethasone conjugates targeting the CD163 receptor on macrophages have shown some
success in rats[85,86]. Yet another unique way of managing inflammation in AH patients is apheresis. A recent case series and literature review of 35 cases concluded that leukocytapheresisand granulocytapheresiswere effective in controlling leukocytosis as wells as inflammatory cytokines[87].
In contrast to pro-inflammatory cytokines, Kupffer cells also produce anti-inflammatory or hepato-protective cytokines, such as IL-6 and IL-22[88] (Figure 1). Activated Kupffer cells release IL-6, which then stimulates signal transducer and activator of transcription 3 (STAT3) leading to increased expression of genes that are anti-apoptotic, anti-oxidative, and promote mitochondrial DNA repair[89,90]. Studies have shown that IL-6 deficient mice are in fact more susceptible to hepatic steatosis, cellular apoptosis and mitochondrial DNA damage when exposed to ethanol[89-91]. Furthermore STAT3 knockout mice have been shown to have greater degree of hepatic steatosis as compared to wild-type mice[92]. Ethanol induced liver injury was alleviated by treatment with IL-6[93]. IL-22 is another hepato-protective cytokine that has been found to ameliorate hepatocellular damage in fatty liver as well as acute and chronic alcoholic liver injury[94-97]. It is believed that both IL-6 and IL-22 share the same pathway, STAT3 mediated hepatoprotection[96].
Another potentially important observation relevant to alcoholic hepatitis is a recently reported finding that the administration of lactate reduced inflammation and organ injury in mice with an immune mediated hepa-titis[98]. Lactate interacted with the specific receptor G protein-coupled receptor 81 (GPR 81) to reduce inflam-mation and injury. Further, lactate and GPR 81 prevented LPS-induced macrophage activation (Kuppfer cells) suggesting that the beneficial effects were mediated by the effects of lactate on activated macrophages. These results suggest that hepatic injury due to macrophage activation may be treated by ligands including lactate that interact with GPR 81.
CONCLUSIONAH is a major cause of morbidity and mortality worldwide. The underlying mechanisms are poorly understood, which has resulted in a lack of specific treatments. The absence of animal models further hampered the progress in elucidating the molecular mechanisms which may provide scientific evidence for designing more targeted treatment strategies. Given the inconsistent results of currently available treatment strategies, which mainly target the pro-inflammatory process, we speculate that it is also important to recognize the potential effort of targeting the anti-inflammatory pathway or targeting both the anti and the pro-inflammatory pathways simul-taneously. With the recognition of the anti-inflamma-tory process mediated by Kupffer cells, it may be the prime time for a well-designed clinical trial to target the unique anti-inflammatory pathway. This may lead to the development of novel effective treatment strategies for
Suraweera DB et al . Kupffer cells in alcoholic hepatitis

95 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
this common clinical entity.
REFERENCES1 Liangpunsakul S. Clinical characteristics and mortality of
hospitalized alcoholic hepatitis patients in the United States. J Clin Gastroenterol 2011; 45: 714-719 [PMID: 21085006 DOI: 10.1097/MCG.0b013e3181fdef1d]
2 Lefkowitch JH. Morphology of alcoholic liver disease. Clin Liver Dis 2005; 9: 37-53 [PMID: 15763228 DOI: 10.1016/j.cld.2004.11.001]
3 O’Shea RS, Dasarathy S, McCullough AJ. Alcoholic liver disease. Hepatology 2010; 51: 307-328 [PMID: 20034030 DOI: 10.1002/hep.23258]
4 Chedid A, Arain S, Snyder A, Mathurin P, Capron F, Naveau S. The immunology of fibrogenesis in alcoholic liver disease. Arch Pathol Lab Med 2004; 128: 1230-1238 [PMID: 15504057 DOI: 10.1043/1543-2165(2004)128<1230:tiofia>2.0.co;2]
5 Kupffer C. Ueber Sternzellen der Leber. Archiv fmikrosk Anat 1876; 12: 353-358 [DOI: 10.1007/BF02933897]
6 van Furth R, Cohn ZA, Hirsch JG, Humphrey JH, Spector WG, Langevoort HL. The mononuclear phagocyte system: a new classification of macrophages, monocytes, and their precursor cells. Bull World Health Organ 1972; 46: 845-852 [PMID: 4538544]
7 Wisse E. Kupffer cell reactions in rat liver under various conditions as observed in the electron microscope. J Ultrastruct Res 1974; 46: 499-520 [PMID: 4363812]
8 Benacerraf B, Sebestyen MM, Schlossman S. A quantitative study of the kinetics of blood clearance of P32-labelled Escherichia coli and Staphylococci by the reticuloendothelial system. J Exp Med 1959; 110: 27-48 [PMID: 13664867]
9 Gao B, Seki E, Brenner DA, Friedman S, Cohen JI, Nagy L, Szabo G, Zakhari S. Innate immunity in alcoholic liver disease. Am J Physiol Gastrointest Liver Physiol 2011; 300: G516-G525 [PMID: 21252049 DOI: 10.1152/ajpgi.00537.2010]
10 Ebe Y, Hasegawa G, Takatsuka H, Umezu H, Mitsuyama M, Arakawa M, Mukaida N, Naito M. The role of Kupffer cells and regulation of neutrophil migration into the liver by macrophage inflammatory protein-2 in primary listeriosis in mice. Pathol Int 1999; 49: 519-532 [PMID: 10469395]
11 Bradham CA, Plümpe J, Manns MP, Brenner DA, Trautwein C. Mechanisms of hepatic toxicity. I. TNF-induced liver injury. Am J Physiol 1998; 275: G387-G392 [PMID: 9724248]
12 Fujimoto M, Uemura M, Nakatani Y, Tsujita S, Hoppo K, Tamagawa T, Kitano H, Kikukawa M, Ann T, Ishii Y, Kojima H, Sakurai S, Tanaka R, Namisaki T, Noguchi R, Higashino T, Kikuchi E, Nishimura K, Takaya A, Fukui H. Plasma endotoxin and serum cytokine levels in patients with alcoholic hepatitis: relation to severity of liver disturbance. Alcohol Clin Exp Res 2000; 24: 48S-54S [PMID: 10803780]
13 Lichtman SN, Sartor RB, Keku J, Schwab JH. Hepatic inflam-mation in rats with experimental small intestinal bacterial overgrowth. Gastroenterology 1990; 98: 414-423 [PMID: 2295397]
14 Bode C, Bode JC. Effect of alcohol consumption on the gut. Best Pract Res Clin Gastroenterol 2003; 17: 575-592 [PMID: 12828956]
15 Casafont Morencos F, de las Heras Castaño G, Martín Ramos L, López Arias MJ, Ledesma F, Pons Romero F. Small bowel bacterial overgrowth in patients with alcoholic cirrhosis. Dig Dis Sci 1996; 41: 552-556 [PMID: 8617135]
16 Bode JC, Bode C, Heidelbach R, Dürr HK, Martini GA. Jejunal microflora in patients with chronic alcohol abuse. Hepatogastroenterology 1984; 31: 30-34 [PMID: 6698486]
17 Inagaki T, Moschetta A, Lee YK, Peng L, Zhao G, Downes M, Yu RT, Shelton JM, Richardson JA, Repa JJ, Mangelsdorf DJ, Kliewer SA. Regulation of antibacterial defense in the small intestine by the nuclear bile acid receptor. Proc Natl Acad Sci USA 2006; 103: 3920-3925 [PMID: 16473946 DOI: 10.1073/pnas.0509592103]
18 Bauer TM, Steinbrückner B, Brinkmann FE, Ditzen AK, Schwacha
H, Aponte JJ, Pelz K, Kist M, Blum HE. Small intestinal bacterial overgrowth in patients with cirrhosis: prevalence and relation with spontaneous bacterial peritonitis. Am J Gastroenterol 2001; 96: 2962-2967 [PMID: 11693333 DOI: 10.1111/j.1572-0241.2001.04668.x]
19 Shindo K, Machida M, Miyakawa K, Fukumura M. A syndrome of cirrhosis, achlorhydria, small intestinal bacterial overgrowth, and fat malabsorption. Am J Gastroenterol 1993; 88: 2084-2091 [PMID: 8249977]
20 Mutlu E, Keshavarzian A, Engen P, Forsyth CB, Sikaroodi M, Gillevet P. Intestinal dysbiosis: a possible mechanism of alcohol-induced endotoxemia and alcoholic steatohepatitis in rats. Alcohol Clin Exp Res 2009; 33: 1836-1846 [PMID: 19645728 DOI: 10.1111/j.1530-0277.2009.01022.x]
21 Yan AW, Fouts DE, Brandl J, Stärkel P, Torralba M, Schott E, Tsukamoto H, Nelson KE, Brenner DA, Schnabl B. Enteric dysbiosis associated with a mouse model of alcoholic liver disease. Hepatology 2011; 53: 96-105 [PMID: 21254165 DOI: 10.1002/hep.24018]
22 Adachi Y, Moore LE, Bradford BU, Gao W, Thurman RG. Antibiotics prevent liver injury in rats following long-term exposure to ethanol. Gastroenterology 1995; 108: 218-224 [PMID: 7806045]
23 Nanji AA, Khettry U, Sadrzadeh SM. Lactobacillus feeding reduces endotoxemia and severity of experimental alcoholic liver (disease). Proc Soc Exp Biol Med 1994; 205: 243-247 [PMID: 8171045 DOI: 10.3181/00379727-205-43703]
24 Bass NM, Mullen KD, Sanyal A, Poordad F, Neff G, Leevy CB, Sigal S, Sheikh MY, Beavers K, Frederick T, Teperman L, Hillebrand D, Huang S, Merchant K, Shaw A, Bortey E, Forbes WP. Rifaximin treatment in hepatic encephalopathy. N Engl J Med 2010; 362: 1071-1081 [PMID: 20335583 DOI: 10.1056/NEJMoa0907893]
25 Vlachogiannakos J, Saveriadis AS, Viazis N, Theodoropoulos I, Foudoulis K, Manolakopoulos S, Raptis S, Karamanolis DG. Intestinal decontamination improves liver haemodynamics in patients with alcohol-related decompensated cirrhosis. Aliment Pharmacol Ther 2009; 29: 992-999 [PMID: 19210289 DOI: 10.1111/j.1365-2036.2009.03958.x]
26 Ma TY, Nguyen D, Bui V, Nguyen H, Hoa N. Ethanol modulation of intestinal epithelial tight junction barrier. Am J Physiol 1999; 276: G965-G974 [PMID: 10198341]
27 Rao R. Endotoxemia and gut barrier dysfunction in alcoholic liver disease. Hepatology 2009; 50: 638-644 [PMID: 19575462 DOI: 10.1002/hep.23009]
28 Nanji AA, Khettry U, Sadrzadeh SM, Yamanaka T. Severity of liver injury in experimental alcoholic liver disease. Correlation with plasma endotoxin, prostaglandin E2, leukotriene B4, and thromboxane B2. Am J Pathol 1993; 142: 367-373 [PMID: 8382006]
29 Mathurin P, Deng QG, Keshavarzian A, Choudhary S, Holmes EW, Tsukamoto H. Exacerbation of alcoholic liver injury by enteral endotoxin in rats. Hepatology 2000; 32: 1008-1017 [PMID: 11050051 DOI: 10.1053/jhep.2000.19621]
30 Parlesak A, Schäfer C, Schütz T, Bode JC, Bode C. Increased intestinal permeability to macromolecules and endotoxemia in patients with chronic alcohol abuse in different stages of alcohol-induced liver disease. J Hepatol 2000; 32: 742-747 [PMID: 10845660]
31 Uesugi T, Froh M, Arteel GE, Bradford BU, Thurman RG. Toll-like receptor 4 is involved in the mechanism of early alcohol-induced liver injury in mice. Hepatology 2001; 34: 101-108 [PMID: 11431739 DOI: 10.1053/jhep.2001.25350]
32 Yin M, Bradford BU, Wheeler MD, Uesugi T, Froh M, Goyert SM, Thurman RG. Reduced early alcohol-induced liver injury in CD14-deficient mice. J Immunol 2001; 166: 4737-4742 [PMID: 11254735]
33 Uesugi T, Froh M, Arteel GE, Bradford BU, Wheeler MD, Gäbele E, Isayama F, Thurman RG. Role of lipopolysaccharide-binding protein in early alcohol-induced liver injury in mice. J Immunol 2002; 168: 2963-2969 [PMID: 11884468]
Suraweera DB et al . Kupffer cells in alcoholic hepatitis

96 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
34 Adachi Y, Bradford BU, Gao W, Bojes HK, Thurman RG. Inactivation of Kupffer cells prevents early alcohol-induced liver injury. Hepatology 1994; 20: 453-460 [PMID: 8045507]
35 Møller HJ. Soluble CD163. Scand J Clin Lab Invest 2012; 72: 1-13 [PMID: 22060747 DOI: 10.3109/00365513.2011.626868]
36 Møller HJ, Grønbaek H, Schiødt FV, Holland-Fischer P, Schilsky M, Munoz S, Hassanein T, Lee WM. Soluble CD163 from activated macrophages predicts mortality in acute liver failure. J Hepatol 2007; 47: 671-676 [PMID: 17629586 DOI: 10.1016/j.jhep.2007.05.014]
37 Grønbaek H, Sandahl TD, Mortensen C, Vilstrup H, Møller HJ, Møller S. Soluble CD163, a marker of Kupffer cell activation, is related to portal hypertension in patients with liver cirrhosis. Aliment Pharmacol Ther 2012; 36: 173-180 [PMID: 22591184 DOI: 10.1111/j.1365-2036.2012.05134.x]
38 Rode A, Nicoll A, Møller HJ, Lim L, Angus PW, Kronborg I, Arachchi N, Gorelik A, Liew D, Kazankov K, Vilstrup H, Grønbæk H. Hepatic macrophage activation predicts clinical decompensation in chronic liver disease. Gut 2013; 62: 1231-1232 [PMID: 23442440 DOI: 10.1136/gutjnl-2012-304135]
39 Waidmann O, Brunner F, Herrmann E, Zeuzem S, Piiper A, Kronenberger B. Macrophage activation is a prognostic parameter for variceal bleeding and overall survival in patients with liver cirrhosis. J Hepatol 2013; 58: 956-961 [PMID: 23333526 DOI: 10.1016/j.jhep.2013.01.005]
40 Sandahl TD, Grønbaek H, Møller HJ, Støy S, Thomsen KL, Dige AK, Agnholt J, Hamilton-Dutoit S, Thiel S, Vilstrup H. Hepatic macrophage activation and the LPS pathway in patients with alcoholic hepatitis: a prospective cohort study. Am J Gastroenterol 2014; 109: 1749-1756 [PMID: 25155228 DOI: 10.1038/ajg.2014.262]
41 Kliaritskaia IL, Stilidi EI. [Pathogenetic importance of proinflammatory cytokines in the formation and progression of fibrosis in alcoholic hepatitis]. Eksp Klin Gastroenterol 2013; (4): 13-20 [PMID: 24294778]
42 Hanck C, Rossol S, Böcker U, Tokus M, Singer MV. Presence of plasma endotoxin is correlated with tumour necrosis factor receptor levels and disease activity in alcoholic cirrhosis. Alcohol Alcohol 1998; 33: 606-608 [PMID: 9872348]
43 McClain CJ, Barve S, Barve S, Deaciuc I, Hill DB. Tumor necrosis factor and alcoholic liver disease. Alcohol Clin Exp Res 1998; 22: 248S-252S [PMID: 9727645]
44 McClain CJ, Barve S, Deaciuc I, Kugelmas M, Hill D. Cytokines in alcoholic liver disease. Semin Liver Dis 1999; 19: 205-219 [PMID: 10422201 DOI: 10.1055/s-2007-1007110]
45 Nanji AA. Role of Kupffer cells in alcoholic hepatitis. Alcohol 2002; 27: 13-15 [PMID: 12062631]
46 Szabo G, Mandrekar P, Dolganiuc A. Innate immune response and hepatic inflammation. Semin Liver Dis 2007; 27: 339-350 [PMID: 17979071 DOI: 10.1055/s-2007-991511]
47 Karlmark KR, Weiskirchen R, Zimmermann HW, Gassler N, Ginhoux F, Weber C, Merad M, Luedde T, Trautwein C, Tacke F. Hepatic recruitment of the inflammatory Gr1+ monocyte subset upon liver injury promotes hepatic fibrosis. Hepatology 2009; 50: 261-274 [PMID: 19554540 DOI: 10.1002/hep.22950]
48 Galastri S, Zamara E, Milani S, Novo E, Provenzano A, Delogu W, Vizzutti F, Sutti S, Locatelli I, Navari N, Vivoli E, Caligiuri A, Pinzani M, Albano E, Parola M, Marra F. Lack of CC chemokine ligand 2 differentially affects inflammation and fibrosis according to the genetic background in a murine model of steatohepatitis. Clin Sci (Lond) 2012; 123: 459-471 [PMID: 22545719 DOI: 10.1042/cs20110515]
49 Heymann F, Hammerich L, Storch D, Bartneck M, Huss S, Rüsseler V, Gassler N, Lira SA, Luedde T, Trautwein C, Tacke F. Hepatic macrophage migration and differentiation critical for liver fibrosis is mediated by the chemokine receptor C-C motif chemokine receptor 8 in mice. Hepatology 2012; 55: 898-909 [PMID: 22031018 DOI: 10.1002/hep.24764]
50 Wang M, You Q, Lor K, Chen F, Gao B, Ju C. Chronic alcohol ingestion modulates hepatic macrophage populations and functions
in mice. J Leukoc Biol 2014; 96: 657-665 [PMID: 25030420 DOI: 10.1189/jlb.6A0114-004RR]
51 Tosello-Trampont AC, Landes SG, Nguyen V, Novobrantseva TI, Hahn YS. Kuppfer cells trigger nonalcoholic steatohepatitis development in diet-induced mouse model through tumor necrosis factor-α production. J Biol Chem 2012; 287: 40161-40172 [PMID: 23066023 DOI: 10.1074/jbc.M112.417014]
52 Huang W, Metlakunta A, Dedousis N, Zhang P, Sipula I, Dube JJ, Scott DK, O’Doherty RM. Depletion of liver Kupffer cells prevents the development of diet-induced hepatic steatosis and insulin resistance. Diabetes 2010; 59: 347-357 [PMID: 19934001 DOI: 10.2337/db09-0016]
53 Lanthier N, Molendi-Coste O, Cani PD, van Rooijen N, Horsmans Y, Leclercq IA. Kupffer cell depletion prevents but has no therapeutic effect on metabolic and inflammatory changes induced by a high-fat diet. FASEB J 2011; 25: 4301-4311 [PMID: 21873555 DOI: 10.1096/fj.11-189472]
54 Tomita K, Tamiya G, Ando S, Ohsumi K, Chiyo T, Mizutani A, Kitamura N, Toda K, Kaneko T, Horie Y, Han JY, Kato S, Shimoda M, Oike Y, Tomizawa M, Makino S, Ohkura T, Saito H, Kumagai N, Nagata H, Ishii H, Hibi T. Tumour necrosis factor alpha signalling through activation of Kupffer cells plays an essential role in liver fibrosis of non-alcoholic steatohepatitis in mice. Gut 2006; 55: 415-424 [PMID: 16174657 DOI: 10.1136/gut.2005.071118]
55 Boltjes A, van Montfoort N, Biesta PJ, Op den Brouw ML, Kwekkeboom J, van der Laan LJ, Janssen HL, Boonstra A, Woltman AM. Kupffer cells interact with hepatitis B surface antigen in vivo and in vitro, leading to proinflammatory cytokine production and natural killer cell function. J Infect Dis 2015; 211: 1268-1278 [PMID: 25362194 DOI: 10.1093/infdis/jiu599]
56 Khakoo SI, Soni PN, Savage K, Brown D, Dhillon AP, Poulter LW, Dusheiko GM. Lymphocyte and macrophage phenotypes in chronic hepatitis C infection. Correlation with disease activity. Am J Pathol 1997; 150: 963-970 [PMID: 9060834]
57 Petracca R, Falugi F, Galli G, Norais N, Rosa D, Campagnoli S, Burgio V, Di Stasio E, Giardina B, Houghton M, Abrignani S, Grandi G. Structure-function analysis of hepatitis C virus envelope-CD81 binding. J Virol 2000; 74: 4824-4830 [PMID: 10775621]
58 Tu Z, Pierce RH, Kurtis J, Kuroki Y, Crispe IN, Orloff MS. Hepatitis C virus core protein subverts the antiviral activities of human Kupffer cells. Gastroenterology 2010; 138: 305-314 [PMID: 19769973 DOI: 10.1053/j.gastro.2009.09.009]
59 Chang S, Dolganiuc A, Szabo G. Toll-like receptors 1 and 6 are involved in TLR2-mediated macrophage activation by hepatitis C virus core and NS3 proteins. J Leukoc Biol 2007; 82: 479-487 [PMID: 17595379 DOI: 10.1189/jlb.0207128]
60 Sandler NG, Koh C, Roque A, Eccleston JL, Siegel RB, Demino M, Kleiner DE, Deeks SG, Liang TJ, Heller T, Douek DC. Host response to translocated microbial products predicts outcomes of patients with HBV or HCV infection. Gastroenterology 2011; 141: 1220-1230, 1230.e1-3 [PMID: 21726511 DOI: 10.1053/j.gastro.2011.06.063]
61 Tordjmann T, Soulie A, Guettier C, Schmidt M, Berthou C, Beaugrand M, Sasportes M. Perforin and granzyme B lytic protein expression during chronic viral and autoimmune hepatitis. Liver 1998; 18: 391-397 [PMID: 9869393]
62 Kolios G, Valatas V, Kouroumalis E. Role of Kupffer cells in the pathogenesis of liver disease. World J Gastroenterol 2006; 12: 7413-7420 [PMID: 17167827]
63 Mathurin P, O’Grady J, Carithers RL, Phillips M, Louvet A, Mendenhall CL, Ramond MJ, Naveau S, Maddrey WC, Morgan TR. Corticosteroids improve short-term survival in patients with severe alcoholic hepatitis: meta-analysis of individual patient data. Gut 2011; 60: 255-260 [PMID: 20940288 DOI: 10.1136/gut.2010.224097]
64 Christensen E, Gluud C. Glucocorticoids are ineffective in alcoholic hepatitis: a meta-analysis adjusting for confounding variables. Gut 1995; 37: 113-118 [PMID: 7672658]
65 Daures JP, Peray P, Bories P, Blanc P, Yousfi A, Michel H, Gremy F. [Corticoid therapy in the treatment of acute alcoholic hepatitis.
Suraweera DB et al . Kupffer cells in alcoholic hepatitis

97 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Results of a meta-analysis]. Gastroenterol Clin Biol 1991; 15: 223-228 [PMID: 1828447]
66 Imperiale TF, McCullough AJ. Do corticosteroids reduce mortality from alcoholic hepatitis? A meta-analysis of the randomized trials. Ann Intern Med 1990; 113: 299-307 [PMID: 2142869]
67 Gao B, Bataller R. Alcoholic liver disease: pathogenesis and new therapeutic targets. Gastroenterology 2011; 141: 1572-1585 [PMID: 21920463 DOI: 10.1053/j.gastro.2011.09.002]
68 Strieter RM, Remick DG, Ward PA, Spengler RN, Lynch JP, Larrick J, Kunkel SL. Cellular and molecular regulation of tumor necrosis factor-alpha production by pentoxifylline. Biochem Biophys Res Commun 1988; 155: 1230-1236 [PMID: 2460096]
69 Akriviadis E, Botla R, Briggs W, Han S, Reynolds T, Shakil O. Pentoxifylline improves short-term survival in severe acute alcoholic hepatitis: a double-blind, placebo-controlled trial. Gastroenterology 2000; 119: 1637-1648 [PMID: 11113085]
70 Thursz MR, Richardson P, Allison M, Austin A, Bowers M, Day CP, Downs N, Gleeson D, MacGilchrist A, Grant A, Hood S, Masson S, McCune A, Mellor J, O’Grady J, Patch D, Ratcliffe I, Roderick P, Stanton L, Vergis N, Wright M, Ryder S, Forrest EH. Prednisolone or pentoxifylline for alcoholic hepatitis. N Engl J Med 2015; 372: 1619-1628 [PMID: 25901427 DOI: 10.1056/NEJMoa1412278]
71 Boetticher NC, Peine CJ, Kwo P, Abrams GA, Patel T, Aqel B, Boardman L, Gores GJ, Harmsen WS, McClain CJ, Kamath PS, Shah VH. A randomized, double-blinded, placebo-controlled multicenter trial of etanercept in the treatment of alcoholic hepatitis. Gastroenterology 2008; 135: 1953-1960 [PMID: 18848937 DOI: 10.1053/j.gastro.2008.08.057]
72 Naveau S, Chollet-Martin S, Dharancy S, Mathurin P, Jouet P, Piquet MA, Davion T, Oberti F, Broët P, Emilie D. A double-blind randomized controlled trial of infliximab associated with prednisolone in acute alcoholic hepatitis. Hepatology 2004; 39: 1390-1397 [PMID: 15122768 DOI: 10.1002/hep.20206]
73 Beresford TP, Everson GT. Liver transplantation for alcoholic liver disease: bias, beliefs, 6-month rule, and relapse--but where are the data? Liver Transpl 2000; 6: 777-778 [PMID: 11084067 DOI: 10.1053/jlts.2000.19027]
74 Consensus conference: Indications for Liver Transplantation, January 19 and 20, 2005, Lyon-Palais Des Congrès: text of recommendations (long version). Liver Transpl 2006; 12: 998-1011 [PMID: 16721776 DOI: 10.1002/lt.20765]
75 Bravata DM, Olkin I, Barnato AE, Keeffe EB, Owens DK. Employment and alcohol use after liver transplantation for alcoholic and nonalcoholic liver disease: a systematic review. Liver Transpl 2001; 7: 191-203 [PMID: 11244159 DOI: 10.1053/jlts.2001.22326]
76 Ge X, Lu Y, Leung TM, Sørensen ES, Nieto N. Milk osteopontin, a nutritional approach to prevent alcohol-induced liver injury. Am J Physiol Gastrointest Liver Physiol 2013; 304: G929-G939 [PMID: 23518682 DOI: 10.1152/ajpgi.00014.2013]
77 Ge X, Leung TM, Arriazu E, Lu Y, Urtasun R, Christensen B, Fiel MI, Mochida S, Sørensen ES, Nieto N. Osteopontin binding to lipopolysaccharide lowers tumor necrosis factor-α and prevents early alcohol-induced liver injury in mice. Hepatology 2014; 59: 1600-1616 [PMID: 24214181 DOI: 10.1002/hep.26931]
78 Mencin A, Kluwe J, Schwabe RF. Toll-like receptors as targets in chronic liver diseases. Gut 2009; 58: 704-720 [PMID: 19359436 DOI: 10.1136/gut.2008.156307]
79 Romeo S, Kozlitina J, Xing C, Pertsemlidis A, Cox D, Pennacchio LA, Boerwinkle E, Cohen JC, Hobbs HH. Genetic variation in PNPLA3 confers susceptibility to nonalcoholic fatty liver disease. Nat Genet 2008; 40: 1461-1465 [PMID: 18820647 DOI: 10.1038/ng.257]
80 Yuan X, Waterworth D, Perry JR, Lim N, Song K, Chambers JC, Zhang W, Vollenweider P, Stirnadel H, Johnson T, Bergmann S, Beckmann ND, Li Y, Ferrucci L, Melzer D, Hernandez D, Singleton A, Scott J, Elliott P, Waeber G, Cardon L, Frayling TM, Kooner JS, Mooser V. Population-based genome-wide association studies reveal six loci influencing plasma levels of liver enzymes. Am J Hum Genet 2008; 83: 520-528 [PMID: 18940312 DOI:
10.1016/j.ajhg.2008.09.012]81 Kotronen A, Johansson LE, Johansson LM, Roos C, Westerbacka
J, Hamsten A, Bergholm R, Arkkila P, Arola J, Kiviluoto T, Fisher RM, Ehrenborg E, Orho-Melander M, Ridderstråle M, Groop L, Yki-Järvinen H. A common variant in PNPLA3, which encodes adiponutrin, is associated with liver fat content in humans. Diabetologia 2009; 52: 1056-1060 [PMID: 19224197 DOI: 10.1007/s00125-009-1285-z]
82 Kollerits B, Coassin S, Beckmann ND, Teumer A, Kiechl S, Döring A, Kavousi M, Hunt SC, Lamina C, Paulweber B, Kutalik Z, Nauck M, van Duijn CM, Heid IM, Willeit J, Brandstätter A, Adams TD, Mooser V, Aulchenko YS, Völzke H, Kronenberg F. Genetic evidence for a role of adiponutrin in the metabolism of apolipoprotein B-containing lipoproteins. Hum Mol Genet 2009; 18: 4669-4676 [PMID: 19729411 DOI: 10.1093/hmg/ddp424]
83 Tian C, Stokowski RP, Kershenobich D, Ballinger DG, Hinds DA. Variant in PNPLA3 is associated with alcoholic liver disease. Nat Genet 2010; 42: 21-23 [PMID: 19946271 DOI: 10.1038/ng.488]
84 Stickel F, Buch S, Lau K, Meyer zu Schwabedissen H, Berg T, Ridinger M, Rietschel M, Schafmayer C, Braun F, Hinrichsen H, Günther R, Arlt A, Seeger M, Müller S, Seitz HK, Soyka M, Lerch M, Lammert F, Sarrazin C, Kubitz R, Häussinger D, Hellerbrand C, Bröring D, Schreiber S, Kiefer F, Spanagel R, Mann K, Datz C, Krawczak M, Wodarz N, Völzke H, Hampe J. Genetic variation in the PNPLA3 gene is associated with alcoholic liver injury in caucasians. Hepatology 2011; 53: 86-95 [PMID: 21254164 DOI: 10.1002/hep.24017]
85 Graversen JH, Svendsen P, Dagnæs-Hansen F, Dal J, Anton G, Etzerodt A, Petersen MD, Christensen PA, Møller HJ, Moestrup SK. Targeting the hemoglobin scavenger receptor CD163 in macrophages highly increases the anti-inflammatory potency of dexamethasone. Mol Ther 2012; 20: 1550-1558 [PMID: 22643864 DOI: 10.1038/mt.2012.103]
86 Granfeldt A, Hvas CL, Graversen JH, Christensen PA, Petersen MD, Anton G, Svendsen P, Sølling C, Etzerodt A, Tønnesen E, Moestrup SK, Møller HJ. Targeting dexamethasone to macrophages in a porcine endotoxemic model. Crit Care Med 2013; 41: e309-e318 [PMID: 23928834 DOI: 10.1097/CCM.0b013e31828a45ef]
87 Kamimura K, Imai M, Sakamaki A, Mori S, Kobayashi M, Mizuno K, Takeuchi M, Suda T, Nomoto M, Aoyagi Y. Granulocytapheresis for the treatment of severe alcoholic hepatitis: a case series and literature review. Dig Dis Sci 2014; 59: 482-488 [PMID: 24052196 DOI: 10.1007/s10620-013-2871-y]
88 Miller AM, Horiguchi N, Jeong WI, Radaeva S, Gao B. Molecular mechanisms of alcoholic liver disease: innate immunity and cytokines. Alcohol Clin Exp Res 2011; 35: 787-793 [PMID: 21284667 DOI: 10.1111/j.1530-0277.2010.01399.x]
89 Hong F, Kim WH, Tian Z, Jaruga B, Ishac E, Shen X, Gao B. Elevated interleukin-6 during ethanol consumption acts as a potential endogenous protective cytokine against ethanol-induced apoptosis in the liver: involvement of induction of Bcl-2 and Bcl-x(L) proteins. Oncogene 2002; 21: 32-43 [PMID: 11791174 DOI: 10.1038/sj.onc.1205016]
90 Zhang X, Tachibana S, Wang H, Hisada M, Williams GM, Gao B, Sun Z. Interleukin-6 is an important mediator for mitochondrial DNA repair after alcoholic liver injury in mice. Hepatology 2010; 52: 2137-2147 [PMID: 20931558 DOI: 10.1002/hep.23909]
91 El-Assal O, Hong F, Kim WH, Radaeva S, Gao B. IL-6-deficient mice are susceptible to ethanol-induced hepatic steatosis: IL-6 protects against ethanol-induced oxidative stress and mitochondrial permeability transition in the liver. Cell Mol Immunol 2004; 1: 205-211 [PMID: 16219169]
92 Horiguchi N, Wang L, Mukhopadhyay P, Park O, Jeong WI, Lafdil F, Osei-Hyiaman D, Moh A, Fu XY, Pacher P, Kunos G, Gao B. Cell type-dependent pro- and anti-inflammatory role of signal transducer and activator of transcription 3 in alcoholic liver injury. Gastroenterology 2008; 134: 1148-1158 [PMID: 18395093 DOI: 10.1053/j.gastro.2008.01.016]
93 Hong F, Radaeva S, Pan HN, Tian Z, Veech R, Gao B. Interleukin
Suraweera DB et al . Kupffer cells in alcoholic hepatitis

98 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
6 alleviates hepatic steatosis and ischemia/reperfusion injury in mice with fatty liver disease. Hepatology 2004; 40: 933-941 [PMID: 15382116 DOI: 10.1002/hep.20400]
94 Yang L, Zhang Y, Wang L, Fan F, Zhu L, Li Z, Ruan X, Huang H, Wang Z, Huang Z, Huang Y, Yan X, Chen Y. Amelioration of high fat diet induced liver lipogenesis and hepatic steatosis by interleukin-22. J Hepatol 2010; 53: 339-347 [PMID: 20452699 DOI: 10.1016/j.jhep.2010.03.004]
95 Xing WW, Zou MJ, Liu S, Xu T, Wang JX, Xu DG. Interleukin-22 protects against acute alcohol-induced hepatotoxicity in mice. Biosci Biotechnol Biochem 2011; 75: 1290-1294 [PMID: 21737938 DOI: 10.1271/bbb.110061]
96 Ki SH, Park O, Zheng M, Morales-Ibanez O, Kolls JK, Bataller R, Gao B. Interleukin-22 treatment ameliorates alcoholic liver injury in a murine model of chronic-binge ethanol feeding: role of signal transducer and activator of transcription 3. Hepatology 2010; 52: 1291-1300 [PMID: 20842630 DOI: 10.1002/hep.23837]
97 Aujla SJ, Kolls JK. IL-22: a critical mediator in mucosal host defense. J Mol Med (Berl) 2009; 87: 451-454 [PMID: 19219418 DOI: 10.1007/s00109-009-0448-1]
98 Hoque R, Farooq A, Ghani A, Gorelick F, Mehal WZ. Lactate reduces liver and pancreatic injury in Toll-like receptor- and inflammasome-mediated inflammation via GPR81-mediated suppression of innate immunity. Gastroenterology 2014; 146: 1763-1774 [PMID: 24657625 DOI: 10.1053/j.gastro.2014.03.014]
99 Theodossi A, Eddleston AL, Williams R. Controlled trial of methylprednisolone therapy in severe acute alcoholic hepatitis. Gut 1982; 23: 75-79 [PMID: 7035299]
100 Ramond MJ, Poynard T, Rueff B, Mathurin P, Théodore C, Chaput JC, Benhamou JP. A randomized trial of prednisolone in patients with severe alcoholic hepatitis. N Engl J Med 1992; 326: 507-512 [PMID: 1531090 DOI: 10.1056/nejm199202203260802]
101 Sidhu SS, Goyal O, Singla M, Bhatia KL, Chhina RS, Sood
A. Pentoxifylline in severe alcoholic hepatitis: a prospective, randomised trial. J Assoc Physicians India 2012; 60: 20-22 [PMID: 23029716]
102 De BK, Gangopadhyay S, Dutta D, Baksi SD, Pani A, Ghosh P. Pentoxifylline versus prednisolone for severe alcoholic hepatitis: a randomized controlled trial. World J Gastroenterol 2009; 15: 1613-1619 [PMID: 19340904]
103 Park SH, Kim DJ, Kim YS, Yim HJ, Tak WY, Lee HJ, Sohn JH, Yoon KT, Kim IH, Kim HS, Um SH, Baik SK, Lee JS, Suk KT, Kim SG, Suh SJ, Park SY, Kim TY, Jang JY. Pentoxifylline vs. corticosteroid to treat severe alcoholic hepatitis: a randomised, non-inferiority, open trial. J Hepatol 2014; 61: 792-798 [PMID: 24845609 DOI: 10.1016/j.jhep.2014.05.014]
104 Mathurin P, Louvet A, Duhamel A, Nahon P, Carbonell N, Boursier J, Anty R, Diaz E, Thabut D, Moirand R, Lebrec D, Moreno C, Talbodec N, Paupard T, Naveau S, Silvain C, Pageaux GP, Sobesky R, Canva-Delcambre V, Dharancy S, Salleron J, Dao T. Prednisolone with vs without pentoxifylline and survival of patients with severe alcoholic hepatitis: a randomized clinical trial. JAMA 2013; 310: 1033-1041 [PMID: 24026598 DOI: 10.1001/jama.2013.276300]
105 De B, Mandal S, Sau D, Mani S, Chatterjee S, Mondal S, Bhattacharya K, Sil K, Bhattacharya R. Pentoxifylline Plus Prednisolone versus Pentoxifylline Only for Severe Alcoholic Hepatitis: A Randomized Controlled Clinical Trial. Ann Med Health Sci Res 2014; 4: 810-816 [PMID: 25328799 DOI: 10.4103/2141-9248.141562]
106 Moreno C, Langlet P, Hittelet A, Lasser L, Degré D, Evrard S, Colle I, Lemmers A, Devière J, Le Moine O. Enteral nutrition with or without N-acetylcysteine in the treatment of severe acute alcoholic hepatitis: a randomized multicenter controlled trial. J Hepatol 2010; 53: 1117-1122 [PMID: 20801542 DOI: 10.1016/j.jhep.2010.05.030]
P- Reviewer: Baffy G, Morini S, Paydas S S- Editor: Tian YL L- Editor: A E- Editor: Liu SQ
Suraweera DB et al . Kupffer cells in alcoholic hepatitis

Simone Carotti, Michele Pier Luca Guarino, Umberto Vespasiani-Gentilucci, Sergio Morini
Simone Carotti, Sergio Morini, Laboratory of Microscopic and Ultrastructural Anatomy, School of Medicine, University Campus Bio-Medico of Rome, 00128 Rome, Italy
Michele Pier Luca Guarino, Gastroenterology Unit, School of Medicine, University Campus Bio-Medico of Rome, 00128 Rome, Italy
Umberto Vespasiani-Gentilucci, Clinical Medicine and Hepatology Unit, School of Medicine, University Campus Bio-Medico of Rome, 00128 Rome, Italy
Author contributions: Carotti S, Guarino MPL and Vespasiani-Gentilucci U contributed to the literature review and wrote the paper; Morini S contributed to the study conception, made revisions and helped with writing.
Conflict-of-interest statement: The author has no conflict of interests.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Correspondence to: Sergio Morini, MD, Laboratory of Microscopic and Ultrastructural Anatomy, School of Medicine, University Campus Bio-Medico of Rome, Via Alvaro Del Portillo, 21, 00128 Rome, Italy. [email protected]: +39-06-225419170Fax: +39-06-22541456
Received: May 28, 2015 Peer-review started: May 28, 2015 First decision: July 10, 2015Revised: July 21, 2015 Accepted: October 16, 2015Article in press: October 19, 2015Published online: November 15, 2015
AbstractSince the introduction of the term “gut-liver axis”, many studies have focused on the functional links of intestinal microbiota, barrier function and immune res-ponses to liver physiology. Intestinal and extra-intestinal diseases alter microbiota composition and lead to dysbiosis, which aggravates impaired intestinal barrier function via increased lipopolysaccharide translocation. The subsequent increased passage of gut-derived product from the intestinal lumen to the organ wall and bloodstream affects gut motility and liver biology. The activation of the toll-like receptor 4 (TLR-4) likely plays a key role in both cases. This review analyzed the most recent literature on the gut-liver axis, with a particular focus on the role of TLR-4 activation. Findings that linked liver disease with dysbiosis are evaluated, and links between dysbiosis and alterations of intestinal permeability and motility are discussed. We also examine the mechanisms of translocated gut bacteria and/or the bacterial product activation of liver inflammation and fibrogenesis via activity on different hepatic cell types.
Key words: Gut microbiota; Dysbiosis; Toll-like receptor 4; Gut motility; Lipopolysaccharide tolerance; Non-alcoholic fatty liver disease; Chronic hepatitis; Intestinal barrier function; Liver fibrosis
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Liver disease is associated with significant changes in intestinal microbiota, but whether liver disease modifies the complement of gut bacteria or dysbiosis causes liver disease is not clearly understood. This review outlines current knowledge on the gut-liver axis, with a particular focus on the role of toll-like receptor 4 activation in functional gastrointestinal disorders, liver inflammation and fibrosis.
EDITORIAL
99 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Starring role of toll-like receptor-4 activation in the gut-liver axis
World J Gastrointest Pathophysiol 2015 November 15; 6(4): 99-109ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i4.99

Carotti S, Guarino MPL, Vespasiani-Gentilucci U, Morini S. Starring role of toll-like receptor-4 activation in the gut-liver axis. World J Gastrointest Pathophysiol 2015; 6(4): 99-109 Available from: URL: http://www.wjgnet.com/2150-5330/full/v6/i4/99.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i4.99
INTRODUCTIONThe term gut-liver axis was introduced approximately 40 years ago, when Volta et al[1] described the pro-duction of IgA antibodies directed against intestinal microorganisms and food antigens in liver cirrhosis. The functional link between the gut and liver has been extensively investigated since this first report[1]. Intestinal microbiota, barrier function and immune responses that link the gut and liver are intriguing and promising research topics.
Growing evidence demonstrates that gut micro-biota play an important role in the gut-liver axis[2]. Disturbances in gut microbiota composition may con-tribute to many diseases and affect local and remote organ systems[3]. Several conditions are associated with specific microbial patterns and/or leaky gut. These disorders range from intestinal diseases, such as irritable bowel syndrome and inflammatory bowel diseases, to numerous extra-intestinal diseases[3], including diseases that affect the liver[4]. The intestinal mucosa exhibits impaired barrier function in the presence of abnormal microbiota, such as increased intestinal permeability and endotoxin translocation, with the subsequent increased passage of waste materials from the intestinal lumen to the organ wall and bloodstream[2,5]. The gut epithelium is a natural barrier that allows the selective entry of substances present in the lumen and avoids the entry of harmful elements, including bacteria and their bio-products[6].
Toll-like receptors (TLRs) are a family of highly conserved receptors that recognize pathogen-associated molecular patterns and allow the host to recognize bacteria, mycobacteria, yeast membrane/wall components and several gut-derived products. TLR-4 is one of the most intriguing of these receptors because it plays a key role in innate immunity by triggering inflammatory responses. TLR-4 initiates innate immune responses via nuclear factor kappa B (NF-κB) when it is activated by its primary ligand, Gram-negative bacterial lipopolysaccharides (LPS), which results in the transcription of several genes that encode inflammatory cytokines, chemokines and antimicrobial agents[7,8].
This review analyzed the most recent literature on the gut-liver axis, with a particular focus on the role of TLR-4 activation. First, we evaluated the evidence that links liver disease with the condition of dysbiosis. Second, we discuss the links between dysbiosis and alterations in intestinal permeability and motility. Finally, we examine the mechanisms of translocated gut bac-teria and/or the bacterial product activation of liver
inflammation and fibrogenesis via activity on different hepatic cell types.
DYSBIOSIS DURING CHRONIC LIVER DISEASE AND CIRRHOSISLiver disease is associated with significant qualitative and quantitative changes in intestinal microbiota, which is defined as “dysbiosis”. Dysbiosis is directly involved in the pathogenesis of several different forms of hepatic injury and many complications of advanced cirrhosis. Whether liver disease modifies the complement of gut bacteria or dysbiosis causes liver disease is not clearly understood. Existing evidence supports the need to contextualize the argument within the etiology of liver disease. Conversely, advanced liver disease is associated with dysbiosis that is independent from the original cause of hepatic damage. The hypothesis of a vicious circle in which microbiota alterations are supported by cirrhosis, which contributes to many cirrhosis com-plications seems appropriate and well structured.
Most of the research on dysbiosis during chronic liver disease investigated non-alcoholic fatty liver disease (NAFLD). Qualitative and quantitative dysbiotic changes are clearly documented during NAFLD in patients with simple fatty liver and non-alcoholic steatohepatitis (NASH). NAFLD patients exhibit a high prevalence of small intestinal bacterial overgrowth[9,10], and microbial samples from NAFLD and NASH patients exhibit a significantly lower proportion of members of the Ruminococcaceae family than healthy subjects[11]. Some conflicting results emerged in studies that compared the microbiota between NAFLD and NASH patients, and further studies are anticipated on this subject.
The feeding of a highfat/highpolysaccharide or a calorie-restricted diet to wild-type mice significantly alters microbial taxonomic composition in experimental models[12,13], and gut microbiota exacerbate NAFLD development via several different mechanisms. First, gut microbes participate in calorie extraction from food and regulate obesity and its complications, including NAFLD. Human enzymes cannot degrade most complex carbohydrates and plant polysaccharides, which are fermented in the colon by intestinal microbes. The resultant short-chain fatty acids account for approxi-mately 10% of daily energy intake[14] and stimulate de novo lipogenesis[15]. The intestinal microflora is also responsible for the increased endogenous ethanol production that is observed during NAFLD. An age-related increase in breath ethanol content was reported in ob/ob mice, and neomycin treatment abolished this effect[16]. Increased systemic ethanol levels were also confirmed in NASH patients[17], which may contribute to hepatocyte trygliceride accumulation and reactive oxygen species production. Bacterial conversion of dietary choline into methylamines experimentally produced similar effects of choline-deficient diets and caused NASH[18]. More recently, gut microbiota, which are responsible for
100 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Carotti S et al . TLR-4 and the gut-liver axis

the conversion of cholic and chenodeoxycholic acid into secondary bile acids, were suggested to control lipid and glucose metabolism through the regulation of bile acid pools. Bile acids also function as signaling molecules and bind to cellular receptors. For example, bile acid synthesis controls the activation of nuclear receptor farnesoid X receptor and the Takeda G-protein-coupled receptor 5[19,20], which are strongly implicated in the modulation of glucose metabolism[21,22]. Hepatotoxic bacterial products that pass across a dysregulated intestinal barrier trigger liver damage, as discussed below, and provoke systemic inflammation and insulin resistance[23], which is a primary event in NAFLD pathogenesis. Circulating levels of LPS, which is a component of the outer membrane of Gram-negative bacteria, are elevated in rodent NAFLD[24,25] and NAFLD patients[26,27].
Research on the role of the microbiome in alcoholic liver disease is not as advanced as NAFLD, but dysbiosis is clearly associated with alcohol-induced liver damage. Significant microbial alterations were observed in the Tsukamoto-French model of alcoholic liver disease in mice[28], and Lactobacilli administration reduced the features of alcoholic liver disease in several animal models[29,30]. Significant changes in the composition of the microbiome are also observed in alcoholic patients, which is consistent with these experimental results[31,32]. There are several mechanisms by which alcohol may contribute to dysbiosis. Commensal flora produce and metabolize ethanol, and alcohol intake may influence the complement of bacteria. Alcohol also produces intestinal dysmotility, alters gastric acid secretion and impairs the intestinal innate immune response[33].
Dysbiosis is closely associated with advanced liver disease, e.g., liver cirrhosis. An apparent increase in potentially pathogenic bacteria occurs during cirrhosis independently of the etiology of liver disease, with a greater abundance of Gram-negative taxa (Enterobacteriaceae, Bacteroidaceae)[34,35]. Similar to alcohol abuse, impaired intestinal motility and innate immunity may represent a basis for the dysbiosis that is observed during cirrhosis[36]. Cirrhotic patients are frequently exposed to hospitalization, antibiotics and dietary modi-fications, which are potential factors associated with alterations in the intestinal microbiome.
DYSBIOSIS: BARRIER DAMAGE, BACTERIAL TRANSLOCATION AND INTESTINAL DYSMOTILITYExperimental models suggest that dysbiosis itself contri-butes to intestinal inflammation and mucosal leakage, which favors the translocation of several inflammatory bacterial products[37,38]. Intestinal decontamination with non-absorbable antibiotics also significantly reduces intestinal inflammation and permeability[38].
Intestinal barrier damage allows bacterial trans-location, which is defined as the migration of viable microorganisms and microbial products (e.g., LPS, lipoteichoic
acid, bacterial DNA) across the intestinal barrier, from the intestinal lumen to mesenteric lymph nodes and other extra-intestinal organs and sites[39]. The translocation of viable bacteria may induce “spontaneous” bacterial infections in some cases, such as the spontaneous bacterial peritonitis that is observed during cirrhosis. The translocation of bacterial products that enter the systemic circulation via the portal vein and activate inflammatory pathways of hepatic cells contributes to the progression of liver damage in other cases, as discussed below. Viable microbes and bacterial fragments entering the systemic circulation via the portal vein or following the enteric lymphatic drainage trigger a proinflammatory state by provoking the release of cytokines, such as tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6) and IL-1β, which contributes to the hyperdynamic circulation and portal hypertension that are typical of advanced liver cirrhosis[40]. Recent evidence suggests that intestinal barrier damage is due to a microbial imbalance that influences gut motility[41]. The observations of intesti-nal dysmotility in germ-free animals further suggest that microbiota play a crucial role in the modulation of intestinal motility[42]. TLRs may explain how microbiota act on gut motility and the gut-liver axis because TLR activation during conditions of impaired intestinal barrier mediates intestinal and liver disorders. Intestinal dis-orders that are associated with impaired motility may be caused by intestinal dysbiosis[41], which further increases intestinal permeability and the translocation of bacterial substances, especially LPS, that may reach the liver[5] (Figure 1).
The importance of aberrant intestinal microbiota in the pathogenic mechanisms of several gastro-intestinal diseases was raised previously, in addition to its health-inducing effects[2]. Commensal microbiota provides beneficial effects, including neuroimmune and pain modulation, and a possible effect on intestinal motility modulation. Polymicrobial sepsis induces a complex inflammatory response within the intestinal muscularis with the recruitment of leukocytes and the production of mediators that inhibit intestinal muscle function[43]. Therefore, the intestine is a source of bacteremia and an important target of bacterial products that affect intestinal motility[43]. Barbara et al[42] suggested in a recent paper that one of the possible mechanisms of microbiota in-fluence on gut motor function occurs through the release of bacterial substances and the effects of mediators released by the gut immune response[42]. These inflammatory changes are partially determined by IL-1β mucosal expression, which is higher in patients suffering from post-infective irritable bowel syndrome (PI-IBS) than in patients without post-infectious symptoms[44]. Patients with IBS present increased IL-1β expression by peripheral blood mononuclear cells[45], and prolonged exposure to IL-1β alters neurotransmitter and electrically induced Ca2+ responses in the myenteric plexus[46]. The immune response also includes the release of histamine, tryptase and prostaglandins by mucosal-activated mast cells in PI-IBS[41] or activated macrophages during sepsis.
101 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Carotti S et al . TLR-4 and the gut-liver axis

102 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Notably, modulation of the intestinal microflora balance using probiotics likely plays an important role in the treatment and prevention of various gastrointestinal disorders[55]. The specific mechanisms underlying probiotic efficacy are not clearly elucidated, but most gastrointestinal diseases in which probiotics exhibit efficacy are associated with non-specific alterations of gastrointestinal motility, which suggests that the modulation of intestinal motility is another possible mechanism for the benefits of probiotic[55]. For example, Lactobacillus paracasei attenuated persistent muscle hypercontractility of jejunal strips in an animal model of PI-IBS[56], and Bifidobacterium and Lactobacillus, but not Streptococcus, alleviated visceral hypersensitivity and recovered intestinal barrier function and inflammation in a recent study in the PI-IBS mouse model, which correlated with an increase in tight junction proteins[57], such a claudin-1 and occludin. One of the mechanisms that underlies the altered permeability in IBS includes changes in the expression, localization and function of tight junctions[58]. Decreased levels of zonule occludin-1 (ZO-1) protein expression and disruption of claudin-1, occludin and ZO-1 expression were found in the apical region of the enterocytes during the course of IBS[59,60]. An increased risk of developing PI-IBS was also conferred by single nucleotide polymorphisms in the that gene encodes the tight junction protein E-cadherin[61].
Our group demonstrated that exposure of human colonic mucosa to Lactobacillus rhamnosus GG (LGG) may affect smooth muscle contraction, suggests that the modulation of muscle contractility represents a possible mechanism of action of these bacteria[62]. Notably, LGG acts through the direct activation of the Gram-positive sensing TLR-2, which is expressed on the surface of human colonic SMCs. We recently demonstrated that the surface expression of TLR-2 in resting cells was significantly decreased in cells exposed to LGG. This reduction in available receptors for monoclonal anti-TLR-2
Increased mucosal permeability was widely demon-strated during the course of sepsis and cases of severe mucosal inflammation[5], and impairment of contraction in these conditions seems to be related to the activation of normally quiescent intestinal muscularis macrophages by LPS or inflammatory mediators released by the mucosa[47-49]. Activated macrophages secrete several mediators, including prostaglandins, H2O2, cytokines and nitric oxide. Many of these mediators also alter the kinetic properties of smooth muscle cells (SMCs)[49-51]. Cyclooxygenase (COX)-1 and COX-2 are expressed in the neuromuscular compartment of the human colon, and these enzymes appear to modulate the cholinergic excitatory control of colonic motility at prejunctional and postjunctional sites, respectively[52]. IL-1β induces a decrease in tonic contraction in rat mesenteric lym-phatic muscle cells in a COX-2 dependent manner via prostaglandin E2
[53].Scirocco et al[54] demonstrated the constitutive ex-
pression of functionally active TLR-4 on primary human colonic SMCs in an in vitro model. Notably, exposure of SMCs to LPS caused contractile alterations[54]. This result suggests that the gastrointestinal dysmotility that occurs during acute infection is related to inflammation and a direct effect of circulating LPS on SMCs. TLR-4 activation following LPS binding leads to NF-κB activation, which participates in oxidative-dependent transcriptional changes in SMCs that modify the agonist-induced contraction[49,54]. LPS may also directly affect muscle cell contractility via alterations in electro-mechanical coupling[54], which could trigger a wide cascade of intracellular events that modify SMC integrity and function. Our group recently demonstrated that acute exposure of the human colonic mucosa to pathogenic LPS[49] impairs muscle cell contractility, and this effect was due to LPS translocation, which directly affects smooth muscle contractility, or the mucosal production of free radicals and inflammatory mediators that reach the muscle layer[49].
Normal microbiota
LPS
A
Microbiota imbalanceEarly inflammationMucosal leakage
LPS LPS
DysbiosisBarrier damageBacterial translocation
B C
Lamina propria
Submucosa
Muscle layer SMCs
TLR-4
BloodvesselContracted
SMCsReduced motility
LPS-TLR-4
MΦPGs H2O2NO
ContractedSMCs
LPS-TLR-4
LPSMΦ
Liver
Portal vein
Figure 1 The results of intestinal disorders that are associated with impaired motility. A: Normal conditions with intestinal mucosa tolerance; B: In the presence of microbiota imbalance, intestinal mucosa is characterized by a leak and mild inflammatory infiltrate. The subsequent passage of modest quantities of lipopolysaccharides (LPS) induces activation of resident macrophages (MΦ) with the release of inflammatory mediators, such as prostaglandins (PGs) and nitric oxide (NO). LPS can also reach the muscle layer and bind to smooth muscle cell (SMC) toll-like receptor 4 (TLR-4). Both conditions cause morpho-functional changes of SMCs. The reduced intestinal motility further induces intestinal microbiota imbalance, which leads to dysbiosis; C: Dysbiosis induces barrier damage and relevant bacterial and LPS translocation. The large amount of translocated LPS reaches the blood vessels through the portal vein and reaches the liver.
Carotti S et al . TLR-4 and the gut-liver axis

103 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
binding further suggests the occurrence of an interaction of LGG with TLR-2 receptors. TLR-2 activation likely induces transitory myogenic changes with alterations in morpho-functional parameters in muscle tissue and isolated SMCs[63]. TLR-2 activates an intrinsic myogenic response that likely counteracts the damage that is induced by the pro-inflammatory burst from pathogen LPS on human gastrointestinal smooth muscle[63]. LGG likely protects human SMCs from LPS-induced damage via LGG binding to TLR-2, and TLR-2 activation leads to IL10mediated antiinflammatory effects.
TLR-4-EXPRESSING CELLS AND SIGNALING IN THE LIVERInflammation during chronic liver damage correlates with fibrosis progression, but the molecular mechanism that links inflammation and fibrosis are not definitively understood. Several factors that participate in inflam-mation and liver fibrosis at the molecular and cellular levels were mentioned, regardless of the specific etiology involved. One of the pathways that has attracted the most attention in recent years as the putative link between liver inflammation and fibrosis is regulated by TLR-4 activation.
Several cell types express TLR-4 in the liver, including Kupffer cells, hepatic stellate cells (HSCs), biliary epithelial cells, hepatocytes and liver sinusoidal endothelial cell (LSECs)[64]. TLR-4 expression in healthy liver tissue is generally low because of the high degree of tolerance of this organ to the continuously incoming gut-derived TLR-4 ligands. The liver receives high concentrations of gut-derived endotoxin because of its location between the systemic and portal bloodstream and the connection with the intestine through the biliary tract. Kupffer cells and hepatocytes take up the incoming LPS, which removes it from the blood and places it into the bile[65-67]. Increased TLR-4 expression is induced in the injured liver, and inflammatory signaling cascades are triggered by this activation[68]. Two microRNAs are primarily involved in the regulation of “LPS tolerance”. TLR-4 activation increases miR-155 levels, which leads to the degradation of Src homology 2 domain-containing inositol-5-phosphatase 1, a down-regulator of TLR-4 signaling, and stimulation of the TLR-4 signaling pathway[69]. However, TLR-4 activation increases miR-21 expression, which upregulates IL-10 via programmed cell death protein 4 inhibition[70]. TLR-4-induces IL-10, which inhibits miR-155 and downgrades TRL-4 signaling. Therefore, the balance between miR-21 and miR-155 likely plays a pivotal role in the regulation of “LPS tolerance”. Other microRNAs are as fundamental in the control of the TLR-4-induced inflammatory response, particularly miR-146a and miR-9, which resolve the pro-inflammatory response by targeting key components in the TLR-4 signaling pathways, and miR-147, which promotes an antiinflammatory response via repression of cytokine production[71].
Once normal immune tolerance is exceeded, LPS directly activates the TLR-4 signaling pathway on Kupffer cells, HSCs, hepatocytes and cholangiocytes (Figure 2). LPS cooperates with circulating LPS-binding protein and binds to TLR-4 on the plasma membrane of cells with two co-receptors [CD14 and myeloid differentiation protein (MD)2] to activated TLR-4 signaling pathways in a myeloid differentiation factor (MyD)88-dependent or independent manner[72]. The MyD88 dependent signaling pathway primarily uses the iκB kinase and mitogen-activated protein kinase signaling pathways, which determines the activation of NF-κB and activator protein-1, respectively, and regulates the expression of proinflammatory cytokines and other genes related to immune functions[72]. The MyD88-independent signaling pathway is mediated by the Toll/interleukin1 receptor domain-containing adaptor inducing interferon-β, which activates interferon regulatory factor 3 and induces the expression of interferon (IFN)-β and genes that respond to IFN[72].
LPS, via activation of TLR-4 and the consequent inflammatory cascade in target cells, plays a key role in the pathogenesis and progression of fatty liver of alcoholic and non-alcoholic origin[24,73]. Szabo et al[73] recently suggested that alcohol and its metabolites regulate the intestinal barrier and allow increased LPS blood concentrations to reach the liver via the portal blood and promote TLR-4-induced inflammation and liver damage. The molecular mechanisms triggered by the LPS/TLR4 binding are likely crucial in NAFLD. Animal models of genetically induced obesity demonstrate an increased susceptibility to liver damage from endotoxin,and exposure to low doses of LPS also determines steato-hepatitis development[74]. Animal models of diet-induced steatohepatitis also exhibit increased levels of portal endotoxemia and TLR-4 hepatic hyperexpression[24]. Probiotic treatment prevents the histological features of NASH in genetically obese animal models[75], which supports the hypothesis of the pathogenetic role of intestinal-derived bacterial products.
TLR-4 likely plays a role in viral hepatitis C, but the relationship between hepatitis C virus (HCV) and TLR-4 is quite complex. HCV infection directly induces TLR-4 expression[76] and may determine the loss of tolerance to TLR-4 ligands by monocytes and macrophages[77]. The TLR-4 signal may also regulate HCV replication[78]. Variants of the TLR4 gene modulate the risk for liver fibrosis in Caucasian patients with chronic HCV infection[79,80]. TLR-4 was also involved in the cooperation between HCV and alcohol towards liver damage and hepatic oncogenesis in the liver progenitor cell trans-plantation model[81].
Inflammation (with secretion of TNF-α and IL-6) and anti-viral effects (with secretion of IFN-β) are determined by TLR-4 activation, depending on whether the MyD88-dependent or independent pathway is induced, respectively[82]. The function of TLR-4 in LPS-stimulated proinflammatory responses of Kupffer cells is well characterized[76,77], but new insights were proposed
Carotti S et al . TLR-4 and the gut-liver axis

104 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
recently. A TLR-4-driven metalloprotease expression has been postulated since matrix metalloproteinase (MMP)-10 was recently added to the list of genes that TLR-4 induces in liver macrophages[83]. MMP-10 was induced during hepatic injury and played a fundamental role in liver tissue repair[83]. Monocytes/macrophages represent the primary cellular targets of intestinal-derived endotoxin, and they are primary effectors of LPS-induced liver regeneration after partial hepatectomy and the experimental cholestatic liver disease, in which LPS promotes fibrogenesis[84,85].
TLR-4 expression by HSCs suggests a direct role of the receptor in hepatic fibrogenesis[72]. Transforming growth factor-β (TGF-β) signaling and liver fibrosis were enhanced by TLR-4 expression in HSCs[86], and the apoptotic threshold of HSCs is lowered by two TLR-4 polymorphisms that are protective against fibrosis[87].
The expression of chemokines and adhesion mole-cules in HSCs by TLR-4 signaling is likely also involved in macrophage recruitment to fibrogenesis sites[86].
LSECs and Kupffer cells play important roles in the clearance of gut-derived LPS without inducing local inflammatory reactions under physiological condi-tions. LPS tolerance in LSECs depends on reducing the nuclear translocation of NF-κB without a change in TRL4/CD14 surface expression or scavenger activity[88]. The C-X-C chemokine receptor type-(CXCR)4 was recently demonstrated to be a part of the LPS “sensing apparatus”, and inhibition of CXCR4 expression in endothelial cells (by RNA interference) decreased IL-6 production, LPS binding and chemotaxis[89]. CXCR4 over-
expression on the LSECs membrane is driven by chronic injury[90,91], and CXCR4 expression likely plays a central role in provoking fibrosis after chronic insult. CXCR4 downregulation (together with CXCR7 expression) stimulates regeneration immediately after injury. LSEC phenotype conversion from a CXCR7- to a CXCR4-expressing cell may enhance the response to gut-derived LPS, which provides a further mechanism for the induction of TLR-4 activation and profibrogenic cascade.
Hepatic progenitor cells, which were traditionally not described as TLR-4-expressing elements, were also recently demonstrated to be involved in TLR-4 signaling. TLR4 expression by hepatic progenitor cells and inflammatory cells at the porto-septal and interface level in patients with NAFLD, was supported by increased LPS activity and associated with the activation of fibrogenic cells and the degree of fibrosis[92]. Biliary cells of the interlobular bile ducts and liver progenitor cells exhibit the highest TLR-4 immunohistochemical expression in patients with chronic hepatitis C, which correlated with the degree of inflammation, portal/septal myofibroblasts activity and fibrosis stage[93].
Hepatic progenitor cells, which are bipotential stem cells that reside in human and animal livers, differen-tiate towards hepatocytic and cholangiocytic lineages, and proliferation leads to the so-called “ductular reac-tion”[93-96]. Studies in patients with biliary disorders and experimental models of biliary fibrosis demonstrated that the ductal epithelium expressed several profibrogenic and chemotactic proteins[97-100], and TLR-4 expression by biliary epithelial cells was associated with inflammation
Carotti S et al . TLR-4 and the gut-liver axis
Figure 2 Hepatic cell types express toll-like receptor-4. In the presence of the loss of lipopolysaccharides (LPS) tolerance, such as during non-alcoholic fatty liver disease, non-alcoholic steatohepatitis or HCV chronic hepatitis, TLR-4 is activated by gut-derived LPS and overexpressed. An altered balance of known miRNAs (miR155, miR21, let-7i) and chemokine receptors (CXCR4, CXCR7) could promote this condition. Then, activation and recruitment of inflammatory cells, ductular reaction and activation of endothelial and stellate cells drive liver inflammation and fibrosis. On the right, the mediators mainly involved in the fibrosis are presented (TGF-β, IGF-1, TNF-α, IL-6), on the left, mediators related to the inflammation are shown (TNF-α, IL-6, IL-1α, IL-8, GM-CSF, IFN-γ). TLR-4: Toll-like receptor-4; TNF-α: Tumor necrosis factor alpha; IL: Interleukin; GM-CSF: Granulocyte-macrophage colony-stimulating factor; IFN: Interferon; HCV: Hepatitis C virus; MMPs: Matrix metalloproteinases; NAFLD/NASH: Nonalcoholic fatty liver disease/nonalcoholic steatohepatitis.
Hepatic progenitor cells/cholangiocytes
↓ Let-7i↑ TLR-4
Ductular reaction
TNF-αIL-6IL-1βIL-8GM-CSFIFN-γ
TGF-βIGF-1TNF-αIL-6
Endothelial cells↑ TLR-4
↑ CXCR4/↓ CXCR7
↑ TLR-4
Hepatic stellate cells
Fibrosis
Collagen deposition
↑ TLR-4
T cells
B cells
Activation, recruitmentInflammation
Macrophages↑ TLR-4
Apoptotic hepatocyte
Hepatocytes
↑ TLR-4
Steatosis
Loss of LPS tolerance
↑ miR155/↓ miR21 MMPs dysregulation
NAFLD/NASHHCV chronic hepatitis

105 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
and fibrosis progression[93,101,102]. Proinflammatory cytokines produced in response to TLR-4 signaling may participate in the cross-talk between hepatic progenitor cells and proliferating cholangiocytes or inflammatory cells and portal/septal myofibroblasts[93].
Increased TLR-4 expression by cholangiocytes represents a marker of loss of tolerance to LPS, which contributes to chronic biliary inflammation[102]. TLR-4-expressing cholangiocytes produce high levels of IL-1β, IL-8, IFN-γ, TNF-α, granulocyte-macrophage colony-stimulating factor (GM-CSF) and TGF-β[101]. LPS treatment of cultured biliary epithelial cells induces nuclear translocation of NF-κB, NF-κB-DNA binding and the production of TNF-α[103]. Human cholangiocytes cultured under normal physiological conditions express let-7i (a family members of let-7 miRNA), which post-transcriptionally downregulates TLR-4 expression[104]. The formation of an NF-κB p50C/EBPβ silencer complex after LPS treatment or Cryptosporidium parvum infec-tion inhibits the transcription of Let-7i and leads to increased TLR-4 expression[104,105]. This mechanism was hypothesized to allow detection and response to microbes without enhancing the inflammatory response.
Activation of the hepatic progenitor cell compart-ment and the consequent ductular reaction are also associated with the severity of nonbiliary chronic liver disease[93,106-108], and endotoxin also exhibits a role in stem cell/progenitor activation in other organs. LPS directly induces the proliferation of embryonic stem cells and adult tissuespecific stem cells/progenitors[109], hematopoie-tic progenitors[110], bone marrow mesenchymal stem cells[111]. The transplantation of p53-deficient hepatic progenitor cells transduced with TLR-4 results in liver-tumor development in mice following repetitive LPS injection[80].
CONCLUSIONThe term “gut-liver axis” comes from the evidence of a strict interconnection between the gut and liver physiology and pathophysiology, and gut microbiota were recently claimed as a key mediator of this linkage. Chronic liver diseases are associated with qualitative and quantitative changes in the intestinal microbiota, which are partially dependent on the specific hepatic disease, and dysbiosis is almost always present during liver cirrhosis, regardless of the etiology of liver injury. Altered gut microflora contribute to intestinal dysmotility, inflammation and mucosal leakage. Finally, intestinal barrier damage allows the translocation of viable micro-organisms and bacterial products, which reach the liver through portal blood and activate inflammatory pathways on liver cells.
These bases suggest that the TLR-4 receptor for bacterial endotoxin plays a starring role in the gut-liver axis. TLR-4 is activated in intestinal muscolaris macrophages, which are stimulated to produce and release prostaglandins and cytokines, and intestinal SMCs, which exhibit altered contractility with resulting
dysmotility. TLR-4 activation in the gut exacerbates intestinal mucosal damage and bacterial translocation. Finally, most hepatic cell types express TLR-4, and LPS directly activates TLR-4 signaling in the liver once normal immune tolerance is exceeded. TLR-4 activation in Kupffer cells, HSCs, hepatocytes and cholangiocytes is implicated in most of inflammatory and fibrogenic pathways and activation contributes to the progression of liver disorders and complications of liver cirrhosis.
There are two promising strategies to hinder the deleterious effects of excessive TLR-4 activation: Modulation of gut microbiota to reduce the amount of TLR-4 ligand and direct interference with TLR-4 signaling. Drugs that are capable of attaining the first outcome, such as probiotics, prebiotics and antibiotics, already exist, and probiotic therapy produces beneficial effects on the liver, at least in the context of NAFLD[112]. Drugs of the second class are far from clinical application, but TLR-4 antagonism could weaken host immunity. However, some interesting evidence already comes from experimental studies, and the TLR-4 antagonist eritoran tetrasodium was recently demonstrated to attenuate liver damage in a liver ischemia/reperfusion injury model[113].
In conclusion, TLR-4 has emerged as a clear prota-gonist in the gut liver-axis over the past few years. Now that the pathophysiological basis is mostly known, it is time to see whether we can convert this knowledge into effective therapeutic interventions.
ACKNOWLEDGMENTSThanks are due to Mr. Mislav Dadic and Mr. Rocco Simone Flammia for their help in the artwork generation.
REFERENCES1 Volta U, Bonazzi C, Bianchi FB, Baldoni AM, Zoli M, Pisi E. IgA
antibodies to dietary antigens in liver cirrhosis. Ric Clin Lab 1987; 17: 235-242 [PMID: 3671996]
2 Minemura M, Shimizu Y. Gut microbiota and liver diseases. World J Gastroenterol 2015; 21: 1691-1702 [PMID: 25684933 DOI: 10.3748/wjg.v21.i6.1691]
3 Sekirov I, Russell SL, Antunes LC, Finlay BB. Gut microbiota in health and disease. Physiol Rev 2010; 90: 859-904 [PMID: 20664075 DOI: 10.1152/physrev.00045.2009]
4 Seki E, Schwabe RF. Hepatic inflammation and fibrosis: functional links and key pathways. Hepatology 2015; 61: 1066-1079 [PMID: 25066777 DOI: 10.1002/hep.27332]
5 Fukui H. Gut-liver axis in liver cirrhosis: How to manage leaky gut and endotoxemia. World J Hepatol 2015; 7: 425-442 [PMID: 25848468 DOI: 10.4254/wjh.v7.i3.425]
6 Barreau F, Hugot JP. Intestinal barrier dysfunction triggered by invasive bacteria. Curr Opin Microbiol 2014; 17: 91-98 [PMID: 24440560 DOI: 10.1016/j.mib.2013.12.003]
7 Beutler B. Inferences, questions and possibilities in Toll-like receptor signalling. Nature 2004; 430: 257-263 [PMID: 15241424]
8 Kawasaki T, Kawai T. Toll-like receptor signaling pathways. Front Immunol 2014; 5: 461 [PMID: 25309543 DOI: 10.3389/fimmu.2014.00461]
9 Miele L, Valenza V, La Torre G, Montalto M, Cammarota G, Ricci R, Mascianà R, Forgione A, Gabrieli ML, Perotti G, Vecchio FM, Rapaccini G, Gasbarrini G, Day CP, Grieco A. Increased intestinal permeability and tight junction alterations in nonalcoholic fatty
Carotti S et al . TLR-4 and the gut-liver axis

106 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
liver disease. Hepatology 2009; 49: 1877-1887 [PMID: 19291785 DOI: 10.1002/hep.22848]
10 Sabaté JM, Jouët P, Harnois F, Mechler C, Msika S, Grossin M, Coffin B. High prevalence of small intestinal bacterial overgrowth in patients with morbid obesity: a contributor to severe hepatic steatosis. Obes Surg 2008; 18: 371-377 [PMID: 18286348 DOI: 10.1007/s11695-007-9398-2]
11 Raman M, Ahmed I, Gillevet PM, Probert CS, Ratcliffe NM, Smith S, Greenwood R, Sikaroodi M, Lam V, Crotty P, Bailey J, Myers RP, Rioux KP. Fecal microbiome and volatile organic compound metabolome in obese humans with nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol 2013; 11: 868-75.e1-3 [PMID: 23454028 DOI: 10.1016/j.cgh.2013.02.015]
12 Turnbaugh PJ, Bäckhed F, Fulton L, Gordon JI. Diet-induced obesity is linked to marked but reversible alterations in the mouse distal gut microbiome. Cell Host Microbe 2008; 3: 213-223 [PMID: 18407065 DOI: 10.1016/j.chom.2008.02.015]
13 Ley RE, Turnbaugh PJ, Klein S, Gordon JI. Microbial ecology: human gut microbes associated with obesity. Nature 2006; 444: 1022-1023 [PMID: 17183309]
14 Conterno L, Fava F, Viola R, Tuohy KM. Obesity and the gut microbiota: does up-regulating colonic fermentation protect against obesity and metabolic disease? Genes Nutr 2011; 6: 241-260 [PMID: 21559992 DOI: 10.1007/s12263-011-0230-1]
15 Zambell KL, Fitch MD, Fleming SE. Acetate and butyrate are the major substrates for de novo lipogenesis in rat colonic epithelial cells. J Nutr 2003; 133: 3509-3515 [PMID: 14608066]
16 Cope K, Risby T, Diehl AM. Increased gastrointestinal ethanol production in obese mice: implications for fatty liver disease pathogenesis. Gastroenterology 2000; 119: 1340-1347 [PMID: 11054393]
17 Zhu L, Baker SS, Gill C, Liu W, Alkhouri R, Baker RD, Gill SR. Characterization of gut microbiomes in nonalcoholic steatohepatitis (NASH) patients: a connection between endogenous alcohol and NASH. Hepatology 2013; 57: 601-609 [PMID: 23055155 DOI: 10.1002/hep.26093]
18 Dumas ME, Barton RH, Toye A, Cloarec O, Blancher C, Rothwell A, Fearnside J, Tatoud R, Blanc V, Lindon JC, Mitchell SC, Holmes E, McCarthy MI, Scott J, Gauguier D, Nicholson JK. Metabolic profiling reveals a contribution of gut microbiota to fatty liver phenotype in insulin-resistant mice. Proc Natl Acad Sci USA 2006; 103: 12511-12516 [PMID: 16895997]
19 Hylemon PB, Zhou H, Pandak WM, Ren S, Gil G, Dent P. Bile acids as regulatory molecules. J Lipid Res 2009; 50: 1509-1520 [PMID: 19346331 DOI: 10.1194/jlr.R900007-JLR200]
20 Sinal CJ, Tohkin M, Miyata M, Ward JM, Lambert G, Gonzalez FJ. Targeted disruption of the nuclear receptor FXR/BAR impairs bile acid and lipid homeostasis. Cell 2000; 102: 731-744 [PMID: 11030617]
21 Prawitt J, Abdelkarim M, Stroeve JH, Popescu I, Duez H, Velagapudi VR, Dumont J, Bouchaert E, van Dijk TH, Lucas A, Dorchies E, Daoudi M, Lestavel S, Gonzalez FJ, Oresic M, Cariou B, Kuipers F, Caron S, Staels B. Farnesoid X receptor deficiency improves glucose homeostasis in mouse models of obesity. Diabetes 2011; 60: 1861-1871 [PMID: 21593203 DOI: 10.2337/db11-0030]
22 Thomas C, Gioiello A, Noriega L, Strehle A, Oury J, Rizzo G, Macchiarulo A, Yamamoto H, Mataki C, Pruzanski M, Pellicciari R, Auwerx J, Schoonjans K. TGR5-mediated bile acid sensing controls glucose homeostasis. Cell Metab 2009; 10: 167-177 [PMID: 19723493 DOI: 10.1016/j.cmet.2009.08.001]
23 Cani PD, Osto M, Geurts L, Everard A. Involvement of gut microbiota in the development of low-grade inflammation and type 2 diabetes associated with obesity. Gut Microbes 2012; 3: 279-288 [PMID: 22572877]
24 Rivera CA, Adegboyega P, van Rooijen N, Tagalicud A, Allman M, Wallace M. Toll-like receptor-4 signaling and Kupffer cells play pivotal roles in the pathogenesis of non-alcoholic steatohepatitis. J Hepatol 2007; 47: 571-579 [PMID: 17644211]
25 Kodama Y, Kisseleva T, Iwaisako K, Miura K, Taura K, De Minicis S, Osterreicher CH, Schnabl B, Seki E, Brenner DA. c-Jun
N-terminal kinase-1 from hematopoietic cells mediates progression from hepatic steatosis to steatohepatitis and fibrosis in mice. Gastroenterology 2009; 137: 1467-1477.e5 [PMID: 19549522 DOI: 10.1053/j.gastro.2009.06.045]
26 Alisi A, Manco M, Devito R, Piemonte F, Nobili V. Endotoxin and plasminogen activator inhibitor-1 serum levels associated with nonalcoholic steatohepatitis in children. J Pediatr Gastroenterol Nutr 2010; 50: 645-649 [PMID: 20400911 DOI: 10.1097/MPG.0b013e3181c7bdf1]
27 Harte AL, da Silva NF, Creely SJ, McGee KC, Billyard T, Youssef-Elabd EM, Tripathi G, Ashour E, Abdalla MS, Sharada HM, Amin AI, Burt AD, Kumar S, Day CP, McTernan PG. Elevated endotoxin levels in non-alcoholic fatty liver disease. J Inflamm (Lond) 2010; 7: 15 [PMID: 20353583 DOI: 10.1186/1476-9255-7-15]
28 Yan AW, Fouts DE, Brandl J, Stärkel P, Torralba M, Schott E, Tsukamoto H, Nelson KE, Brenner DA, Schnabl B. Enteric dysbiosis associated with a mouse model of alcoholic liver disease. Hepatology 2011; 53: 96-105 [PMID: 21254165 DOI: 10.1002/hep.24018]
29 Forsyth CB, Farhadi A, Jakate SM, Tang Y, Shaikh M, Keshav-arzian A. Lactobacillus GG treatment ameliorates alcohol-induced intestinal oxidative stress, gut leakiness, and liver injury in a rat model of alcoholic steatohepatitis. Alcohol 2009; 43: 163-172 [PMID: 19251117 DOI: 10.1016/j.alcohol.2008.12.009]
30 Wang Y, Liu Y, Sidhu A, Ma Z, McClain C, Feng W. Lactobacillus rhamnosus GG culture supernatant ameliorates acute alcohol-induced intestinal permeability and liver injury. Am J Physiol Gastrointest Liver Physiol 2012; 303: G32-G41 [PMID: 22538402 DOI: 10.1152/ajpgi.00024.2012]
31 Mutlu EA, Gillevet PM, Rangwala H, Sikaroodi M, Naqvi A, Engen PA, Kwasny M, Lau CK, Keshavarzian A. Colonic microbiome is altered in alcoholism. Am J Physiol Gastrointest Liver Physiol 2012; 302: G966-G978 [PMID: 22241860 DOI: 10.1152/ajpgi.00380.2011]
32 Bode JC, Bode C, Heidelbach R, Dürr HK, Martini GA. Jejunal microflora in patients with chronic alcohol abuse. Hepatogastroenterology 1984; 31: 30-34 [PMID: 6698486]
33 Bode C, Bode JC. Alcohol’s role in gastrointestinal tract disorders. Alcohol Health Res World 1997; 21: 76-83 [PMID: 15706765]
34 Chen Y, Yang F, Lu H, Wang B, Chen Y, Lei D, Wang Y, Zhu B, Li L. Characterization of fecal microbial communities in patients with liver cirrhosis. Hepatology 2011; 54: 562-572 [PMID: 21574172 DOI: 10.1002/hep.24423]
35 Wu ZW, Lu HF, Wu J, Zuo J, Chen P, Sheng JF, Zheng SS, Li LJ. Assessment of the fecal lactobacilli population in patients with hepatitis B virus-related decompensated cirrhosis and hepatitis B cirrhosis treated with liver transplant. Microb Ecol 2012; 63: 929-937 [PMID: 21965156 DOI: 10.1007/s00248-011-9945-1]
36 Chang CS, Chen GH, Lien HC, Yeh HZ. Small intestine dysmotility and bacterial overgrowth in cirrhotic patients with spontaneous bacterial peritonitis. Hepatology 1998; 28: 1187-1190 [PMID: 9794900]
37 Gómez-Hurtado I, Santacruz A, Peiró G, Zapater P, Gutiérrez A, Pérez-Mateo M, Sanz Y, Francés R. Gut microbiota dysbiosis is associated with inflammation and bacterial translocation in mice with CCl4-induced fibrosis. PLoS One 2011; 6: e23037 [PMID: 21829583 DOI: 10.1371/journal.pone.0023037]
38 Chen P, Stärkel P, Turner JR, Ho SB, Schnabl B. Dysbiosis-induced intestinal inflammation activates tumor necrosis factor receptor I and mediates alcoholic liver disease in mice. Hepatology 2015; 61: 883-894 [PMID: 25251280 DOI: 10.1002/hep.27489]
39 Benten D, Wiest R. Gut microbiome and intestinal barrier failure--the “Achilles heel” in hepatology? J Hepatol 2012; 56: 1221-1223 [PMID: 22406521 DOI: 10.1016/j.jhep.2012.03.003]
40 Quigley EM. Gastrointestinal dysfunction in liver disease and portal hypertension. Gut-liver interactions revisited. Dig Dis Sci 1996; 41: 557-561 [PMID: 8617136]
41 Quigley EM. Microflora modulation of motility. J Neurogastroenterol Motil 2011; 17: 140-147 [PMID: 21602990 DOI: 10.5056/jnm.2011.17.2.140]
42 Barbara G, Stanghellini V, Brandi G, Cremon C, Di Nardo G,
Carotti S et al . TLR-4 and the gut-liver axis

107 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
De Giorgio R, Corinaldesi R. Interactions between commensal bacteria and gut sensorimotor function in health and disease. Am J Gastroenterol 2005; 100: 2560-2568 [PMID: 16279914]
43 Overhaus M, Tögel S, Pezzone MA, Bauer AJ. Mechanisms of polymicrobial sepsis-induced ileus. Am J Physiol Gastrointest Liver Physiol 2004; 287: G685-G694 [PMID: 15331356]
44 Gwee KA, Collins SM, Read NW, Rajnakova A, Deng Y, Graham JC, McKendrick MW, Moochhala SM. Increased rectal mucosal expression of interleukin 1beta in recently acquired post-infectious irritable bowel syndrome. Gut 2003; 52: 523-526 [PMID: 12631663]
45 Liebregts T, Adam B, Bredack C, Röth A, Heinzel S, Lester S, Downie-Doyle S, Smith E, Drew P, Talley NJ, Holtmann G. Immune activation in patients with irritable bowel syndrome. Gastroenterology 2007; 132: 913-920 [PMID: 17383420]
46 Kindt S, Vanden Berghe P, Boesmans W, Roosen L, Tack J. Prolonged IL-1beta exposure alters neurotransmitter and electri-cally induced Ca(2+) responses in the myenteric plexus. Neurogastroenterol Motil 2010; 22: 321-e85 [PMID: 19796332 DOI: 10.1111/j.1365-2982.2009.01414.x]
47 Barona I, Fagundes DS, Gonzalo S, Grasa L, Arruebo MP, Plaza MÁ, Murillo MD. Role of TLR4 and MAPK in the local effect of LPS on intestinal contractility. J Pharm Pharmacol 2011; 63: 657-662 [PMID: 21492167 DOI: 10.1111/j.2042-7158.2011.01253.x]
48 Tomita M, Ohkubo R, Hayashi M. Lipopolysaccharide transport system across colonic epithelial cells in normal and infective rat. Drug Metab Pharmacokinet 2004; 19: 33-40 [PMID: 15499167]
49 Guarino MP, Sessa R, Altomare A, Cocca S, Di Pietro M, Carotti S, Schiavoni G, Alloni R, Emerenziani S, Morini S, Severi C, Cicala M. Human colonic myogenic dysfunction induced by mucosal lipopolysaccharide translocation and oxidative stress. Dig Liver Dis 2013; 45: 1011-1016 [PMID: 23891549 DOI: 10.1016/j.dld.2013.06.001]
50 Carotti S, Guarino MP, Cicala M, Perrone G, Alloni R, Segreto F, Rabitti C, Morini S. Effect of ursodeoxycholic acid on inflammatory infiltrate in gallbladder muscle of cholesterol gallstone patients. Neurogastroenterol Motil 2010; 22: 866-73, e232 [PMID: 20426797 DOI: 10.1111/j.1365-2982.2010.01510.x]
51 Guarino MP, Carotti S, Morini S, Perrone G, Behar J, Altomare A, Alloni R, Caviglia R, Emerenziani S, Rabitti C, Cicala M. Decreased number of activated macrophages in gallbladder muscle layer of cholesterol gallstone patients following ursodeoxycholic acid. Gut 2008; 57: 1740-1741 [PMID: 19022933 DOI: 10.1136/gut.2008.160333]
52 Fornai M, Blandizzi C, Colucci R, Antonioli L, Bernardini N, Segnani C, Baragatti B, Barogi S, Berti P, Spisni R, Del Tacca M. Role of cyclooxygenases 1 and 2 in the modulation of neuromuscular functions in the distal colon of humans and mice. Gut 2005; 54: 608-616 [PMID: 15831902 DOI: 10.1136/gut.2004.053322]
53 Al-Kofahi M, Becker F, Gavins FN, Woolard MD, Tsunoda I, Wang Y, Ostanin D, Zawieja DC, Muthuchamy M, von der Weid PY, Alexander JS. IL-1β reduces tonic contraction of mesenteric lymphatic muscle cells, with the involvement of cycloxygenase-2 and prostaglandin E2. Br J Pharmacol 2015; 172: 4038-4051 [PMID: 25989136 DOI: 10.1111/bph.13194]
54 Scirocco A, Matarrese P, Petitta C, Cicenia A, Ascione B, Mannironi C, Ammoscato F, Cardi M, Fanello G, Guarino MP, Malorni W, Severi C. Exposure of Toll-like receptors 4 to bacterial lipopolysaccharide (LPS) impairs human colonic smooth muscle cell function. J Cell Physiol 2010; 223: 442-450 [PMID: 20112289 DOI: 10.1002/jcp.22053]
55 Foxx-Orenstein AE, Chey WD. Manipulation of the Gut Microbiota as a Novel Treatment Strategy for Gastrointestinal Disorders. Am J Gastroenterol 2012; 1 Suppl: 41-46 [DOI: 10.1038/ajgsup.2012.8]
56 Verdú EF, Bercík P, Bergonzelli GE, Huang XX, Blennerhasset P, Rochat F, Fiaux M, Mansourian R, Corthésy-Theulaz I, Collins SM. Lactobacillus paracasei normalizes muscle hypercontractility in a murine model of postinfective gut dysfunction. Gastroenterology 2004; 127: 826-837 [PMID: 15362038]
57 Wang H, Gong J, Wang W, Long Y, Fu X, Fu Y, Qian W, Hou X.
Are there any different effects of Bifidobacterium, Lactobacillus and Streptococcus on intestinal sensation, barrier function and intestinal immunity in PI-IBS mouse model? PLoS One 2014; 9: e90153 [PMID: 24595218 DOI: 10.1371/journal.pone.0090153]
58 Hyland NP, Quigley EM, Brint E. Microbiota-host interactions in irritable bowel syndrome: epithelial barrier, immune regulation and brain-gut interactions. World J Gastroenterol 2014; 20: 8859-8866 [PMID: 25083059 DOI: 10.3748/wjg.v20.i27.8859]
59 Bertiaux-Vandaële N, Youmba SB, Belmonte L, Lecleire S, Antonietti M, Gourcerol G, Leroi AM, Déchelotte P, Ménard JF, Ducrotté P, Coëffier M. The expression and the cellular distribution of the tight junction proteins are altered in irritable bowel syndrome patients with differences according to the disease subtype. Am J Gastroenterol 2011; 106: 2165-2173 [PMID: 22008894 DOI: 10.1038/ajg.2011.257]
60 Martínez C, Lobo B, Pigrau M, Ramos L, González-Castro AM, Alonso C, Guilarte M, Guilá M, de Torres I, Azpiroz F, Santos J, Vicario M. Diarrhoea-predominant irritable bowel syndrome: an organic disorder with structural abnormalities in the jejunal epithelial barrier. Gut 2013; 62: 1160-1168 [PMID: 22637702 DOI: 10.1136/gutjnl-2012-302093]
61 Villani AC, Lemire M, Thabane M, Belisle A, Geneau G, Garg AX, Clark WF, Moayyedi P, Collins SM, Franchimont D, Marshall JK. Genetic risk factors for post-infectious irritable bowel syndrome following a waterborne outbreak of gastroenteritis. Gastroenterology 2010; 138: 1502-1513 [PMID: 20044998 DOI: 10.1053/j.ga-stro.2009.12.049]
62 Guarino MP, Altomare A, Stasi E, Marignani M, Severi C, Alloni R, Dicuonzo G, Morelli L, Coppola R, Cicala M. Effect of acute mucosal exposure to Lactobacillus rhamnosus GG on human colonic smooth muscle cells. J Clin Gastroenterol 2008; 42 Suppl 3 Pt 2: S185-S190 [PMID: 18685510 DOI: 10.1097/MCG.0b013e31817e1cac]
63 Ammoscato F, Scirocco A, Altomare A, Matarrese P, Petitta C, Ascione B, Caronna R, Guarino M, Marignani M, Cicala M, Chirletti P, Malorni W, Severi C. Lactobacillus rhamnosus protects human colonic muscle from pathogen lipopolysaccharide-induced damage. Neurogastroenterol Motil 2013; 25: 984-e777 [PMID: 24118564 DOI: 10.1111/nmo.12232]
64 Seki E, Brenner DA. Toll-like receptors and adaptor molecules in liver disease: update. Hepatology 2008; 48: 322-335 [PMID: 18506843 DOI: 10.1002/hep.22306]
65 Schwabe RF, Seki E, Brenner DA. Toll-like receptor signaling in the liver. Gastroenterology 2006; 130: 1886-1900 [PMID: 16697751]
66 Van Bossuyt H, De Zanger RB, Wisse E. Cellular and subcellular distribution of injected lipopolysaccharide in rat liver and its inactivation by bile salts. J Hepatol 1988; 7: 325-337 [PMID: 3235801]
67 Mimura Y, Sakisaka S, Harada M, Sata M, Tanikawa K. Role of hepatocytes in direct clearance of lipopolysaccharide in rats. Gastroenterology 1995; 109: 1969-1976 [PMID: 7498663]
68 Kitazawa T, Tsujimoto T, Kawaratani H, Fujimoto M, Fukui H. Expression of Toll-like receptor 4 in various organs in rats with D-galactosamine-induced acute hepatic failure. J Gastroenterol Hepatol 2008; 23: e494-e498 [PMID: 18070011]
69 O’Connell RM, Chaudhuri AA, Rao DS, Baltimore D. Inositol phosphatase SHIP1 is a primary target of miR-155. Proc Natl Acad Sci USA 2009; 106: 7113-7118 [PMID: 19359473 DOI: 10.1073/pnas.0902636106]
70 Sheedy FJ, Palsson-McDermott E, Hennessy EJ, Martin C, O’Leary JJ, Ruan Q, Johnson DS, Chen Y, O’Neill LA. Negative regulation of TLR4 via targeting of the proinflammatory tumor suppressor PDCD4 by the microRNA miR-21. Nat Immunol 2010; 11: 141-147 [PMID: 19946272 DOI: 10.1038/ni.1828]
71 O’Neill LA, Sheedy FJ, McCoy CE. MicroRNAs: the fine-tuners of Toll-like receptor signalling. Nat Rev Immunol 2011; 11: 163-175 [PMID: 21331081 DOI: 10.1038/nri2957]
72 Guo J, Friedman SL. Toll-like receptor 4 signaling in liver injury and hepatic fibrogenesis. Fibrogenesis Tissue Repair 2010; 3: 21
Carotti S et al . TLR-4 and the gut-liver axis

108 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
[PMID: 20964825 DOI: 10.1186/1755-1536-3-21]73 Szabo G, Bala S. Alcoholic liver disease and the gut-liver axis.
World J Gastroenterol 2010; 16: 1321-1329 [PMID: 20238398]74 Yang SQ, Lin HZ, Lane MD, Clemens M, Diehl AM. Obesity
increases sensitivity to endotoxin liver injury: implications for the pathogenesis of steatohepatitis. Proc Natl Acad Sci USA 1997; 94: 2557-2562 [PMID: 9122234]
75 Li Z, Yang S, Lin H, Huang J, Watkins PA, Moser AB, Desimone C, Song XY, Diehl AM. Probiotics and antibodies to TNF inhibit inflammatory activity and improve nonalcoholic fatty liver disease. Hepatology 2003; 37: 343-350 [PMID: 12540784]
76 Machida K, Cheng KT, Sung VM, Levine AM, Foung S, Lai MM. Hepatitis C virus induces toll-like receptor 4 expression, leading to enhanced production of beta interferon and interleukin-6. J Virol 2006; 80: 866-874 [PMID: 16378988]
77 Dolganiuc A, Norkina O, Kodys K, Catalano D, Bakis G, Marshall C, Mandrekar P, Szabo G. Viral and host factors induce macrophage activation and loss of toll-like receptor tolerance in chronic HCV infection. Gastroenterology 2007; 133: 1627-1636 [PMID: 17916356]
78 Broering R, Wu J, Meng Z, Hilgard P, Lu M, Trippler M, Szczeponek A, Gerken G, Schlaak JF. Toll-like receptor-stimulated non-parenchymal liver cells can regulate hepatitis C virus replication. J Hepatol 2008; 48: 914-922 [PMID: 18362039 DOI: 10.1016/j.jhep.2008.01.028]
79 Huang H, Shiffman ML, Friedman S, Venkatesh R, Bzowej N, Abar OT, Rowland CM, Catanese JJ, Leong DU, Sninsky JJ, Layden TJ, Wright TL, White T, Cheung RC. A 7 gene signature identifies the risk of developing cirrhosis in patients with chronic hepatitis C. Hepatology 2007; 46: 297-306 [PMID: 17461418]
80 Li Y, Chang M, Abar O, Garcia V, Rowland C, Catanese J, Ross D, Broder S, Shiffman M, Cheung R, Wright T, Friedman SL, Sninsky J. Multiple variants in toll-like receptor 4 gene modulate risk of liver fibrosis in Caucasians with chronic hepatitis C infection. J Hepatol 2009; 51: 750-757 [PMID: 19586676 DOI: 10.1016/j.jhep.2009.04.027]
81 Machida K, Tsukamoto H, Mkrtchyan H, Duan L, Dynnyk A, Liu HM, Asahina K, Govindarajan S, Ray R, Ou JH, Seki E, Deshaies R, Miyake K, Lai MM. Toll-like receptor 4 mediates synergism between alcohol and HCV in hepatic oncogenesis involving stem cell marker Nanog. Proc Natl Acad Sci USA 2009; 106: 1548-1553 [PMID: 19171902 DOI: 10.1073/pnas.0807390106]
82 Andreakos E, Foxwell B, Feldmann M. Is targeting Toll-like receptors and their signaling pathway a useful therapeutic approach to modulating cytokine-driven inflammation? Immunol Rev 2004; 202: 250-265 [PMID: 15546398]
83 Garcia-Irigoyen O, Carotti S, Latasa MU, Uriarte I, Fernández-Barrena MG, Elizalde M, Urtasun R, Vespasiani-Gentilucci U, Morini S, Banales JM, Parks WC, Rodriguez JA, Orbe J, Prieto J, Páramo JA, Berasain C, Ávila MA. Matrix metalloproteinase-10 expression is induced during hepatic injury and plays a fundamental role in liver tissue repair. Liver Int 2014; 34: e257-e270 [PMID: 24119197 DOI: 10.1111/liv.12337]
84 Isayama F, Hines IN, Kremer M, Milton RJ, Byrd CL, Perry AW, McKim SE, Parsons C, Rippe RA, Wheeler MD. LPS signaling enhances hepatic fibrogenesis caused by experimental cholestasis in mice. Am J Physiol Gastrointest Liver Physiol 2006; 290: G1318-G1328 [PMID: 16439470]
85 Strey CW, Markiewski M, Mastellos D, Tudoran R, Spruce LA, Greenbaum LE, Lambris JD. The proinflammatory mediators C3a and C5a are essential for liver regeneration. J Exp Med 2003; 198: 913-923 [PMID: 12975457]
86 Seki E, De Minicis S, Osterreicher CH, Kluwe J, Osawa Y, Brenner DA, Schwabe RF. TLR4 enhances TGF-beta signaling and hepatic fibrosis. Nat Med 2007; 13: 1324-1332 [PMID: 17952090]
87 Guo J, Loke J, Zheng F, Hong F, Yea S, Fukata M, Tarocchi M, Abar OT, Huang H, Sninsky JJ, Friedman SL. Functional linkage of cirrhosis-predictive single nucleotide polymorphisms of Toll-like receptor 4 to hepatic stellate cell responses. Hepatology 2009; 49: 960-968 [PMID: 19085953 DOI: 10.1002/hep.22697]
88 Uhrig A, Banafsche R, Kremer M, Hegenbarth S, Hamann A, Neurath M, Gerken G, Limmer A, Knolle PA. Development and functional consequences of LPS tolerance in sinusoidal endothelial cells of the liver. J Leukoc Biol 2005; 77: 626-633 [PMID: 15860798]
89 Triantafilou M, Lepper PM, Briault CD, Ahmed MA, Dmo-chowski JM, Schumann C, Triantafilou K. Chemokine receptor 4 (CXCR4) is part of the lipopolysaccharide “sensing apparatus”. Eur J Immunol 2008; 38: 192-203 [PMID: 18081034]
90 Ding BS, Nolan DJ, Butler JM, James D, Babazadeh AO, Rosenwaks Z, Mittal V, Kobayashi H, Shido K, Lyden D, Sato TN, Rabbany SY, Rafii S. Inductive angiocrine signals from sinusoidal endothelium are required for liver regeneration. Nature 2010; 468: 310-315 [PMID: 21068842 DOI: 10.1038/nature09493]
91 Ding BS, Cao Z, Lis R, Nolan DJ, Guo P, Simons M, Penfold ME, Shido K, Rabbany SY, Rafii S. Divergent angiocrine signals from vascular niche balance liver regeneration and fibrosis. Nature 2014; 505: 97-102 [PMID: 24256728 DOI: 10.1038/nature12681]
92 Vespasiani-Gentilucci U, Carotti S, Perrone G, Mazzarelli C, Galati G, Onetti-Muda A, Picardi A, Morini S. Hepatic toll-like receptor 4 expression is associated with portal inflammation and fibrosis in patients with NAFLD. Liver Int 2015; 35: 569-581 [PMID: 24649857 DOI: 10.1111/liv.12531]
93 Vespasiani-Gentilucci U, Carotti S, Onetti-Muda A, Perrone G, Ginanni-Corradini S, Latasa MU, Avila MA, Carpino G, Picardi A, Morini S. Toll-like receptor-4 expression by hepatic progenitor cells and biliary epithelial cells in HCV-related chronic liver disease. Mod Pathol 2012; 25: 576-589 [PMID: 22173288 DOI: 10.1038/modpathol.2011.197]
94 Roskams TA, Theise ND, Balabaud C, Bhagat G, Bhathal PS, Bioulac-Sage P, Brunt EM, Crawford JM, Crosby HA, Desmet V, Finegold MJ, Geller SA, Gouw AS, Hytiroglou P, Knisely AS, Kojiro M, Lefkowitch JH, Nakanuma Y, Olynyk JK, Park YN, Portmann B, Saxena R, Scheuer PJ, Strain AJ, Thung SN, Wanless IR, West AB. Nomenclature of the finer branches of the biliary tree: canals, ductules, and ductular reactions in human livers. Hepatology 2004; 39: 1739-1745 [PMID: 15185318]
95 Gaudio E, Carpino G, Cardinale V, Franchitto A, Onori P, Alvaro D. New insights into liver stem cells. Dig Liver Dis 2009; 41: 455-462 [PMID: 19403350 DOI: 10.1016/j.dld.2009.03.009]
96 Glaser SS, Gaudio E, Miller T, Alvaro D, Alpini G. Cholangiocyte proliferation and liver fibrosis. Expert Rev Mol Med 2009; 11: e7 [PMID: 19239726 DOI: 10.1017/S1462399409000994]
97 Yasoshima M, Kono N, Sugawara H, Katayanagi K, Harada K, Nakanuma Y. Increased expression of interleukin-6 and tumor necrosis factor-alpha in pathologic biliary epithelial cells: in situ and culture study. Lab Invest 1998; 78: 89-100 [PMID: 9461125]
98 Grappone C, Pinzani M, Parola M, Pellegrini G, Caligiuri A, DeFranco R, Marra F, Herbst H, Alpini G, Milani S. Expression of platelet-derived growth factor in newly formed cholangiocytes during experimental biliary fibrosis in rats. J Hepatol 1999; 31: 100-109 [PMID: 10424289]
99 Sedlaczek N, Jia JD, Bauer M, Herbst H, Ruehl M, Hahn EG, Schuppan D. Proliferating bile duct epithelial cells are a major source of connective tissue growth factor in rat biliary fibrosis. Am J Pathol 2001; 158: 1239-1244 [PMID: 11290541]
100 O’Hara SP, Tabibian JH, Splinter PL, LaRusso NF. The dynamic biliary epithelia: molecules, pathways, and disease. J Hepatol 2013; 58: 575-582 [PMID: 23085249 DOI: 10.1016/j.jhep.2012.10.011]
101 Karrar A, Broomé U, Södergren T, Jaksch M, Bergquist A, Björnstedt M, Sumitran-Holgersson S. Biliary epithelial cell antibodies link adaptive and innate immune responses in primary sclerosing cholangitis. Gastroenterology 2007; 132: 1504-1514 [PMID: 17408653]
102 Mueller T, Beutler C, Picó AH, Shibolet O, Pratt DS, Pascher A, Neuhaus P, Wiedenmann B, Berg T, Podolsky DK. Enhanced innate immune responsiveness and intolerance to intestinal endotoxins in human biliary epithelial cells contributes to chronic cholangitis. Liver Int 2011; 31: 1574-1588 [PMID: 22093333 DOI: 10.1111/j.1478-3231.2011.02635.x]
Carotti S et al . TLR-4 and the gut-liver axis

109 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
103 Harada K, Ohira S, Isse K, Ozaki S, Zen Y, Sato Y, Nakanuma Y. Lipopolysaccharide activates nuclear factor-kappaB through toll-like receptors and related molecules in cultured biliary epithelial cells. Lab Invest 2003; 83: 1657-1667 [PMID: 14615419]
104 Chen XM, Splinter PL, O’Hara SP, LaRusso NF. A cellular micro-RNA, let-7i, regulates Toll-like receptor 4 expression and contributes to cholangiocyte immune responses against Cryptosporidium parvum infection. J Biol Chem 2007; 282: 28929-28938 [PMID: 17660297]
105 O’Hara SP, Splinter PL, Gajdos GB, Trussoni CE, Fernandez-Zapico ME, Chen XM, LaRusso NF. NFkappaB p50-CCAAT/enhancer-binding protein beta (C/EBPbeta)-mediated transcriptional repression of microRNA let-7i following microbial infection. J Biol Chem 2010; 285: 216-225 [PMID: 19903813 DOI: 10.1074/jbc.M109.041640]
106 Lowes KN, Brennan BA, Yeoh GC, Olynyk JK. Oval cell numbers in human chronic liver diseases are directly related to disease severity. Am J Pathol 1999; 154: 537-541 [PMID: 10027411]
107 Carpino G, Renzi A, Onori P, Gaudio E. Role of hepatic progenitor cells in nonalcoholic fatty liver disease development: cellular cross-talks and molecular networks. Int J Mol Sci 2013; 14: 20112-20130 [PMID: 24113587 DOI: 10.3390/ijms141020112]
108 Carotti S, Vespasiani-Gentilucci U, Perrone G, Picardi A, Morini S. Portal inflammation during NAFLD is frequent and associated
with the early phases of putative hepatic progenitor cell activation. J Clin Pathol 2015; 68: 883-890 [PMID: 26124313]
109 Lee SH, Hong B, Sharabi A, Huang XF, Chen SY. Embryonic stem cells and mammary luminal progenitors directly sense and respond to microbial products. Stem Cells 2009; 27: 1604-1615 [PMID: 19544467 DOI: 10.1002/stem.75]
110 Nagai Y, Garrett KP, Ohta S, Bahrun U, Kouro T, Akira S, Takatsu K, Kincade PW. Toll-like receptors on hematopoietic progenitor cells stimulate innate immune system replenishment. Immunity 2006; 24: 801-812 [PMID: 16782035]
111 Pevsner-Fischer M, Morad V, Cohen-Sfady M, Rousso-Noori L, Zanin-Zhorov A, Cohen S, Cohen IR, Zipori D. Toll-like receptors and their ligands control mesenchymal stem cell functions. Blood 2007; 109: 1422-1432 [PMID: 17038530]
112 Ma YY, Li L, Yu CH, Shen Z, Chen LH, Li YM. Effects of probiotics on nonalcoholic fatty liver disease: a meta-analysis. World J Gastroenterol 2013; 19: 6911-6918 [PMID: 24187469 DOI: 10.3748/wjg.v19.i40.6911]
113 Mcdonald KA, Huang H, Tohme S, Loughran P, Ferrero K, Billiar T, Tsung A. Toll-like receptor 4 (TLR4) antagonist eritoran tetrasodium attenuates liver ischemia and reperfusion injury through inhibition of high-mobility group box protein B1 (HMGB1) signaling. Mol Med 2014; 20: 639-648 [PMID: 25375408 DOI: 10.2119/molmed.2014.00076]
P- Reviewer: Gafencu AV, Santos MM, Tanaka H S- Editor: Ji FF L- Editor: A E- Editor: Liu SQ
Carotti S et al . TLR-4 and the gut-liver axis

products) and lipopolysaccharides (LPS, an integral component of Gram negative microorganisms) play the key role in linking the two. Though several SCFAs are produced as microbiota-fermentation products, three of them, i.e. , butyrate, propionate and acetate have been found to be definitely involved in obesity; though individually they are neither purely obesogenic nor antiobesogenic. Out of these, butyrate and propionate are predominantly antiobesogenic. Butyrate, though a major energy source for colonocytes, has been found to increase mitochondrial activity, prevent metabolic endotoxemia, improve insulin sensitivity, possess anti-inflammatory potential, increase intestinal barrier function and protect against diet-induced obesity with-out causing hypophagia. Propionate has been found to inhibit cholesterol synthesis, thereby antagonizing the cholesterol increasing action of acetate, and to inhibit the expression of resistin in adipocytes. Moreover, both these SCFAs have been found to cause weight regulation through their stimulatory effect on anorexigenic gut hormones and to increase the synthesis of leptin. Unlike butyrate and propionate, acetate, which is substantially absorbed, shows more obesogenic potential, as it acts as a substrate for hepatic and adipocyte lipogenesis. High fat diet increases the absorption of LPS, which, in turn, has been found to be associated with metabolic endotoxemia and to induce inflammation resulting in obesity. Multiple independent and interrelated mechanisms have been found to be involved in such linking processes which are discussed in this review work along with some possible remedial measures for prevention of weight gain and obesity.
Key words: Microbiota; Obesity; Butyrate; Propionate; Acetate
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: The objective of this article is to relate gastro-intestinal microbiota with obesity positively. This idea itself is most innovative. In this article, probable mechanisms involved in relating microbiota with obesity
Chandra Kanti Chakraborti
Chandra Kanti Chakraborti, Department of Pharmacology,
Kanak Manjari Institute of Pharmaceutical Sciences, Rourkela 769015, Orissa, India
Author contributions: Chakraborti CK designed research, performed research, contributed new reagents or analytic tools, analyzed data and wrote the paper.
Conflict-of-interest statement: The author has no conflict of interests.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Correspondence to: Dr. Chandra Kanti Chakraborti, Professor, Department of Pharmacology, Kanak Manjari Institute of Pharmaceutical Sciences, Chhend, Rourkela 769015, Orissa, India. [email protected]: +91-661-2480752 Fax: +91-661-2480752
Received: May 26, 2015Peer-review started: May 29, 2015First decision: June 18, 2015Revised: September 26, 2015Accepted: October 20, 2015 Article in press: October 27, 2015Published online: November 15, 2015
AbstractDue to the grave pathological role of obesity, worldwide research is being continued to find out the causative factors involved in it. Recent advances in this field reveal a possible relationship between the compositional pattern of gut microbiota and genesis of obesity. Several study results have shown that short-chain fatty acids (SCFAs, microbiota-induced fermentation
EDITORIAL
110 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
New-found link between microbiota and obesity
World J Gastrointest Pathophysiol 2015 November 15; 6(4): 110-119ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i4.110

have been discussed. Its key findings are: (1) The gut microbiota play a definite role both in genesis and retardation of obesity; (2) Microbiota-derived lipopoly-saccharides and short-chain fatty acids mediate the obesogenic action; (3) Fatty diet not only adds calories but also shifts microbiota compositional pattern in favour of obesity; and (4) The obesogenic actions are mediated through receptor activation, modification of cytokine and endocrine function and gene expression.
Chakraborti CK. New-found link between microbiota and obesity. World J Gastrointest Pathophysiol 2015; 6(4): 110-119 Available from: URL: http://www.wjgnet.com/2150-5330/full/v6/i4/110.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i4.110
INTRODUCTIONObesity, in both males and females, was considered simply as a negative criterion while assessing beauty. But recently, in addition to its previous role, it is considered to be an important marker for several diseases; particularly, hypertension, type 2 diabetes mellitus (T2DM) and metabolic syndrome where it plays a definite and significant pathological role[1,2]. Multiple etiological factors have been attributed to the genesis of obesity, of which hereditary predisposition, wrong dietary habits (fatty food) and lifestyle (lack of exercise) are important[3]. Besides these, certain hormonal imbalances[4] and sideeffects of some drugs[5] also contribute towards its development. But unfortunately there are many obese individuals, in whom, these causative factors fail to explain the cause of their obesity. Therefore, because of its grave pathological role, research is still going on to find out the factors other than the abovementioned ones, so that a remedial measure can be taken to prevent the development as well as progression of this worldwide epidemic[6].
Recently, it has been observed that the composition of gut microbiota of healthy persons is different from that of obese T2DM patients. Such observations suggested a possible relationship between the compositional pattern of gut microbiota and pathology of metabolic disorders. Human colon harbours a vast number of microorganisms which are extremely diverse. Out of these, three phyla, Bacteroidetes (Gram negative), Firmicutes (Gram positive) and Actinobacteria (Gram positive), are most abundant and have been found to play a dominant role in the pathophysiology of metabolic disorders specifically, obesity. Other phyla also contribute, but to a lesser degree[6]. All these colonic microbiota cause fermentation of nondigestible carbohydrates resulting in the formation of shortchain fatty acids (SCFAs) along with gases like CO2 and H2
[7]. It has been shown that acetate and propionate are mainly produced by the phylum Bacteroidetes, whereas butyrate is the predominant product of the phylum Firmicutes[6]. Of these SCFAs, butyrate mainly serves as an energy
source for colonic epithelium[8,9], whereas propionate, getting absorbed through portal circulation, takes part in gluconeogenesis[8]. Acetate, on the other hand, reaches peripheral tissues after absorption through systemic circulation where it acts as a substrate for synthesis of cholesterol[8,10,11]. Butyrate, besides being an energy source for colonocytes, has been found to increase insulin sensitivity (in mice)[9], possesses obesityrelated antiinflammatory action (in humans)[12], can give protection against dietinduced obesity without causing hypophagia[13], may protect against colon carcinoma[8,10], and increase the leptin gene expression[11]. Propionate, in addition to contributing towards gluconeogenesis, also reduces the intake of food[13] and cholesterol synthesis[11] along with a favorable effect on leptin gene expression[11]. Acetate, in addition to serving as a substrate for synthesis of cholesterol, also takes part in the de novo synthesis of lipids in liver[14]. Because of the abovementioned functions of the microbiotaderived SCFAs, which appear to be closely related to obesity, both adversely as well as beneficially, an attempt has been made to review the workresults of several prominent investigators in this field, which may shed a light on the justification of “linking microbiota to obesity”.
MICROBIOTA IN NORMAL GUT AND OBESITYMicrobiota in normal gutThe gut harbours the greatest density of microorganisms in the body (e.g., about up to 1.5 kg of bacteria in the human gut) with Firmicutes, Bacteriodetes and Actinobacteria constituting the dominant phyla[7,15,16]. Generally, Firmicutes and Bacteroidetes are most abundant, followed by Proteobacteria and Actinobacteria with minor contributors like Verrucomicrobia and Fusobacteria[16].
Faecalibacterium prausnitzii (F. prausnitzii) is the most abundant bacterium in the human intestinal microbiota of healthy adults (Table 1). It represents more than 5% of the total bacterial population. F. prausnitzii species is a major representative of Firmicutes phylum, Clostridium class, Ruminococcaceae family[17]. While the Bacteroidetes phylum mainly produces acetate and propionate, the Firmicutes phylum has butyrate as its primary metabolic end product[7].
Microbiota in obesityGut microbiota have been found to be significantly changed in humans and animal models of obesity, comprising a decrease in bacterial diversity[15,18] as well as composition, such as a reduced abundance of Bacteroidetes with a proportional increase in Firmicutes phylum[6,9,1821].
In obese animals, Ley et al[22] found a difference in the ratio of Bacteroidetes and Firmicutes, where the obese mice displayed a decrease in Bacteroidetes with a corresponding increase in Firmicutes in comparison to their counterparts. In agreement with the results from
111 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Chakraborti CK. Microbiota and obesity

animal studies, it seems that human obesity is linked with a reduced abundance of intestinal Bacteroidetes associated with a high abundance of Firmicutes. However, these results have been contradicted by other studies[11]. Studies of Duncan et al[23] did not show any difference in the proportions of Bacteroidetes and Firmicutes in the feces of lean and obese subjects. In another investigation, overweight and obese subjects had a ratio of Bacteroidetes to Firmicutes in favour of Bacteroidetes. Moreover, many authors have shown no change or even an increase of Bacteroidetes in overweight[6]. Besides these two phyla, a higher level of Actinobacteria has been demonstrated in obese persons[24]. On the other hand, Clarke et al[25] reported that the gut microbiota of obese individuals contained a lower proportion Verrucomicrobia, i.e., abundance of this phylum in the gut is reduced in obese persons (Table 1). From these observations, it appears that the phylum level difference of the gut microbiota between obese and lean individuals may not be universally true[11]. But overall analysis of results point towards an increase in Firmicutes[6].
Methaneproducing Archaea, a domain of singlecelled microorganism, have been found to be present in greater abundance in obese mice and humans compared with lean subjects. Recently, in an investigation, germ-free mice were colonized with Bacteroides thetaiotaomicron (B. thetaiotaomicron) (an adaptive bacterial forager of dietary polysaccharides) alone or either with Methanobrevibacter smithii (M. smithii) or the sulfatereducing bacterium Desulfovibrio piger (D. piger). The results showed that cocolonization with M. smithii but not D. piger, induced B. thetaiotaomicron to ferment dietary fructans to acetate, resulting in a significant increase in host adiposity compared with monocolonized or B. thetaiotaomicron/D. piger cocolonized mice[20].
In an investigation, the numbers of hydrogenproducing Prevotellaceae, a family in the phylum Bacteroidetes, and Archaea, represented primarily by members of the order Methanobacteriales (hydrogenoxidizing methanogens), were at a higher level in obese individuals compared with lean subjects and with those after gastric bypass. The investigators hypothesized that hydrogen transfer between bacterial and archaeal species may raise energy uptake by the large intestine in obese individuals via methanogens removing fermentation intermediates, such as H2 or formate, thus relieving thermodynamic limitations and allowing greater production of SCFAs that are then available to be absorbed across the intestinal
epithelium[20]. On the contrary, Schwiertz et al[26] found no difference in the abundance of Archaea in overweight or obese humans, which brings into question the usefulness of Archaea as a potential biomarker of obesity.
The intestines of obese humans and mice have been found to be enriched with Erysipelotrichi, a class of bacteria within the phylum Firmicutes, and Clostridium ramosum (C. ramosum), a member of the Erysipelotrichi, is found to be linked with symptoms of the metabolic syndrome in humans. Thus, Woting et al[27] speculated that C. ramosum promotes obesity and related pathologies.
Obese children were found to display an elevated FirmicutestoBacteroidetes ratio compared with their lean counterparts. Furthermore, low relative proportions of Bacteroides vulgatus and high concentrations of Lactobacillus spp. were found in the obese children and were positively correlated with plasma highsensitivity Creactive protein[21]. Million et al[28] have shown that Lactobacillus reuteri was linked with obesity in adults. These results thus indicate a possible role of Lactobacillus species in body weight and obesity. Moreover, Staphylococcus spp. were found to be positively linked with energy intake in all children[21].
Obeseprone (OP) donor and germfree recipient animals have been found to harbour specific species from Oscillibacter and Clostridium clusters ⅩⅣa and Ⅳ, which were totally absent from their obeseresistant counterparts. Indeed, Duca et al[18] have reported high levels of bacteria from the Ruminococcus genus in OP rats, similar to that found in obese humans and high fatfed mice. It is known that Ruminococcus is phylogenetically heterogenous, and most of its species fall under several Clostridium clusters, including Clostridium clusters Ⅳ and ⅩⅣa. But peculiarly, Clostridium leptum (cluster Ⅳ) has been found to be associated with both obesity and weight loss (Table 2). From the above discussion, it may be mentioned that unfavourable microbiome seems to be a predisposing factor for development of obesity.
While some gut bacteria groups correlated with energy intake, obesity, and metabolic changes, others, such as F. prausnitzii, linked with alteration in the inflammatory state and diabetes[29]. The presence of F. prausnitzii species is directly associated with the reduction in low-grade inflammation state in obesity and diabetes (independently of calorie intake)[17,29] (Table 1).
SCFAsIt is well established that the human intestine harbours a vast number of microorganisms, known as gut microbiota, whose metabolic end products (mainly SCFAs) interfere with the absorption of digestion end products as well as energy homeostasis of the host[19].
In intestine, the sites of production of SCFAs are distal small intestine and colon where nondigestible carbohydrates like resistant starch, dietary fiber, and other lowdigestible polysaccharides are fermented
112 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Table 1 Prevalence of gut microbiota in health and disease
Microbiota in normal gut Microbiota in obesity
Firmicutes phylum Increase in Firmicutes phylumBacteriodetes phylum Reduced abundance of BacteroidetesActinobacteria phylum A higher level of Actinobacteria phylumVerrucomicrobia phylum Lower proportion of VerrucomicrobiaFaecalibacterium prausnitzii species
Reduced abundance of Faecalibacterium prausnitzii species
Chakraborti CK. Microbiota and obesity

113 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
distribution, metabolism and function. A substantial part of acetate is readily absorbed, reaches liver via portal circulation and subsequently, distributed throughout the whole body where it serves as a substrate for synthesis of cholesterol[11,13]. Because of the substantial absorption, plasma concentration of acetate is much more than the other two[30] and a small amount is available in the colon to be metabolized[10].
Propionate, like acetate, also reaches liver via portal circulation after absorption; but because of its primary utilization in gluconeogenesis (in the liver), its plasma concentration is less than that of acetate[10,11,30]. Butyrate, on the other hand, undergoes limited reabsorption, because it is primarily oxidized by the colonocytes and serves as a major source of energy for them[8,9,30].
It seems essential to mention here that absorption of these SCFAs through colonic epithelial cells alters the pH of colon, which in turn has an important influence on the composition and population of gut microbiota. It is so, because most of the SCFAs are absorbed in the colon being exchanged with bicarbonate and hence, the resultant luminal pH is determined by the rate of SCFA production by microbiota and the neutralizing capability of the bicarbonate. Due to its continuous absorption, decline in SCFA concentration from proximal to distal colon leads to a corresponding increase in pH from cecum to rectum. It has been demonstrated in animal and human fecal studies that gut pH has an important effect on the growth and composition of gut microbiota. Low luminal pH from ileum to cecum due to higher SCFA concentration, prevents the overgrowth of pHsensitive pathogenic bacteria (like Enterobacteriaceae and Clostridia) and at pH 5.5, butyrate producing bacteria (Firmicutes phylum) comprise 20% of the total population (mentioned earlier). But as the luminal pH increases to 6.5 in more distal colonic sites due to less production of SCFAs (as fermentable dietary fibers are less available here) and their absorption in exchange with bicarbonate, the butyrate producing bacteria practically disappear along with a concomitant rise in acetate and propionateproducing bacteria (Bacteroidetes phylum)[7].
A detailed discussion has been made above about the multiple bacterial phyla producing several metabolites, of which three SCFAs play a dominant role in the development, progression as well as retardation of obesity. These three SCFAs are butyrate, propionate and acetate, produced during the fermentation of complex dietary carbohydrates (polysaccharides and oligosaccharides), proteins, peptides, and glycoprotein precursors by the microbiota in the colon and distal small intestine[10,11,13]. Chemically, SCFAs are saturated aliphatic organic acids containing one to six carbons (Acetate C2, propionate C3 and butyrate C4)[7].
FACTORS CONTRIBUTING TOWARDS GENESIS OF OBESITYBesides the well known and established causes of
by the saccharolytic bacteria which include the phyla Bacteroidetes, Firmicutes and Actinobacteria. Acetate and propionate are the main products of Bacteroidetes phylum and butyrate is mainly produced by Firmicutes phylum. Most bacterial activity is found in the proximal colon where substrate availability is the highest. But towards the distal colon, the availability of substrate decreases, and the extraction of free water lowers the diffusion of substrates and microbial products. This makes the proximal colon to be the principal site of fermentation, where, mainly nondigestible carbohydrates are fermented by saccharolytic bacteria, primary fermenters being Bacteroidetes and the main fermentation products are SCFAs together with gases like CO2 and H2
[7]. Of the three SCFAs, butyrate is practically considered as a favourable marker (antiobesity) of obesity and its amount of production is determined by the composition of microbiota, population of the microorganisms producing it and the pH of the large intestine. Change in substrate bioavailability can alter the composition of butyrateproducing bacterial population and thus affect butyrate production[8]. It has been demonstrated that when the human fecal pH is 5.5; butyrate producing bacterial population (Firmicutes phylum) comprises 20% of the total bacterial population. But in the distal parts of large intestine, where fermentable dietary fiber availability is limited, the luminal pH is raised to 6.5. At this site, not only the bacteria producing butyrate, practically disappear completely, but also there occurs a significant increase in the population of acetate and propionateproducing bacteria, whose products are mainly obesogenic[7].
An analysis of the population data regarding the production of SCFAs in proximal and distal colon shows that the production is in the order of acetate > propionate > butyrate. When calculated in a molar ratio, it was found to be 60:20:20 or 3:1:1, respectively[10]. It has been observed that out of the total SCFAs present in the colon, 90%95% are constituted by acetate, propionate and butyrate together and their intraluminal individual concentrations have been found to be acetate 60%, propionate 25% and butyrate 15%[30].
After being produced in the colon, the abovementioned three SCFAs are absorbed through gut epithelial cells but follow different patterns of absorption,
Table 2 Microbiota having doubtful role in obesity
Microbiota
Archaea (a domain of microorganisms)Phylum Firmicutes: Erysipelotrichi (a class of bacteria)Methanobacteriales (an order of bacteria)Prevotellaceae (a family of bacteria)Ruminococcus (a genus of bacteria)Bacteroides thetaiotaomicron and Methanobrevibacter smithiiClostridium ramosum (a member of the Erysipelotrichi)Clustridium leptum (cluster Ⅳ) (associated with both obesity and weight loss)Specific species from Oscillibacter and Clostridium clusters ⅩⅣa and ⅣLactobacillus spp. - Lactobacillus reuteri
Chakraborti CK. Microbiota and obesity

114 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
obesity like genetic predisposition, excessive intake of high calorigenic diet (fatty food) and lack of exercise[3] which favours storage of calorie in the form of fat in adipocytes, recently researchers in the field have shown the contribution and involvement of several other factors, like hormonal imbalance[4]; inflammatory cytokines of adipocyte and nonadipocyte origin; adipocytokines like adiponectin[31], leptin[32], and resistin[33], etc., tolllike receptors (TLR)[34] and many others in the genesis of obesity[33].
In addition to these, multiple study results have shown a close link between the compositional patterns of “intestinal microbiota” and “obesity”- the microbiota affecting the above mentioned obesogenic factors through several mechanisms. A detailed account of the microbiota with their composition and population ratio and their metabolic end products (particularly SCFAs), have already been discussed. Here, an attempt has been made to discuss the various mechanisms involved in their obesogenic as well as antiobesity activity, although some of the observations appear to be controversial and inconclusive.
Though intestinal microflora comprises several phyla of microorganisms, focus has been made on three phyla, namely Bacteroidetes, Firmicutes and Actinobacteria. These three phyla generate multiple metabolites out of which three SCFAs butyrate, acetate and propionate have been shown to be definitely related with obesity. It may be mentioned in the beginning that none of these bacterial phyla is purely obesogenic or antiobesogenic. This is so, because individually they produce more than one SCFA, each of which possessing opposite actions as metabolites, which in turn possesses both the actions[7].
For this reason, while evaluating their obesogenic or the antiobesogenic potency, instead of taking the population of a single bacterial phylum, the population ratio of more than one phylum has been taken into consideration[6,7,19,21]. Several metabolic studies have suggested that imbalances in the intestinal bacterial population may result in obesity, systemic inflammation and metabolic dysfunction[14,35].
Gut microflora are involved in obesity through some of their constitutive structural materials and through some of their metabolic end products (SCFAs). Therefore, the mechanisms by which they contribute towards the development of obesity may be discussed under two headings: (1) The role of lipopolysaccharide (LPS) which is a structural component of bacteria; and (2) the role of SCFAs which are produced as bacterial metabolites of dietary compounds[11,14].
Role of LPSRecently, it has been shown that obesity is associated with a chronic and systemic lowgrade inflammation which is due to an innate immune response to LPS. It is an intrinsic constituent of Gram negative bacterial cell wall. It is considered as an endotoxin and found at low concentrations in the blood of healthy persons. But substantially high concentrations of LPS have been
demonstrated in obese individuals, where the obesity is dietinduced and has a genetic predisposition. High fat diet, both in animals and humans, has been found to alter the gut microbiota composition (more in favour of Gram negative phylum), which in turn increases the production and intestinal permeability of LPS, resulting in its high plasma concentration and development of “metabolic endotoxemia”[20]. Cani et al[36] have found that compositional pattern of microbiota, induced by a highfat diet, could increase gut permeability which is an important hallmark of endotoxemia. Such microbiota were found to reduce the expression of host genes which code for the intestinal tight junction proteins like ZO-1 and occludin necessary for normal gastrointestinal permeability character. Such microbiotainduced altered gastrointestinal epithelial integrity could result in intestinal absorption of the whole bacteria along with their products. It has been observed that in mice, taking a highfat, such bacterial absorption is higher than those taking a standard chow and was found to be reversed by administering an appropriate probiotic bacterium[37].
LPS has been found to induce inflammation resulting in development of obesity. In a comparative study, it has been shown that when low doses of LPS were administered to mice for 4 wk, they developed obesity similar to 4 wk of a highfat diet. LPSinduced inflammatory reactions are mediated through an immunoprotein called cluster of differentiation (CD) 14. When LPS was administered through CD14/ rats, there was no weight gain. It is interesting to note that high fat diet is not only directly responsible for obesity but also indirectly aggravates it by increasing the absorption of endotoxin LPS via lymph by integrating it to chylomicrons. As high fat diet in humans increases the formation of chylomicron, more chylomicron is available to be integrated with LPS and hence, more absorption of this endotoxin in comparison to low fat diet. Mice develop endotoxemia when they consume high fat diet. Studies have shown that when such mice were treated with ampicillin and neomycin, endotoxemia was found to be reduced because of the antimicrobialinduced altered gastrointestinal microbiota. High plasma concentration of LPS has been found to be associated with increased levels of CD14 and interleukin6 (IL6) the markers of inflammation. Because of these observations it may be inferred that regular intake of high fat diet, increases LPS absorption into systemic circulation, resulting in LPSinduced inflammation and obesity[37].
Chronic lowgrade inflammation found in endotoxemia has been demonstrated to be due to activation of TLR4 by LPS and dietary saturated fatty acids. TLR4 activation induces upregulation of common intracellular inflammatory pathways like c-Jun N-terminal kinase and nuclear factorkappa B in adipocytes and macrophages resulting in development of insulin resistance and increased adiposity[6]. Mice, lacking TLR4, have been found to be resistant to dietinduced obesity and insulin resistant[37].
de La Serre et al[38] have demonstrated that highfat
Chakraborti CK. Microbiota and obesity

115 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
diet not only alters the composition of gut microbiota, but also causes increased activation of intestinal TLR4. Such receptor activation results in gastrointestinal inflammation which in turn induces hyperphagia and thus, makes the animal an obese phenotype.
A neural mechanism has been suggested to explain LPSinduced obesity, in which the vagal afferents of dietinduced obese rats are found to be leptin resistant, and thus, develop hyperphagia and weight gain, which in turn, lead to increased food (fat) intake and LPS production, thereby increasing obesity and aggravating the inflammation further[37].
As mentioned earlier, LPS, which induces inflammation and increases adiposity resulting in obesity, is known to be a Gram negative bacterial product. But, there are confusing observations, where obese persons have more Firmicutes (Gram positive) and less Bacteroidetes (Gram negative) than lean individuals. Inspite of such confusions, recent observations show that obese person’s microbiota are rich in Prevotellaceae (a subgroup of Bacteroidetes), which is a good source of LPS[37].
Though microbiotaconstituent LPS is proinflammatory, some microbiota metabolite SCFAs possess immunoregulatory property and reduce inflammation. Studies have shown butyrate to have antiinflammatory action through inhibition of lymphocyte proliferation, and IL2 and interferonγ production. On the other hand, acetate and propionate increase interferonγ level. The resultant effect of these three SCFAs is immunoregulatory[37].
Role of SCFAsIt has already been mentioned about the production of three SCFAs by different phyla of gastrointestinal microflora[7] and the obesogenic as well as antiobesogenic property of individual SCFAs which make it difficult to categories each of them as purely obesogenic or antiobesogenic. Of course, a broad characterization can be made where acetate appears to be predominantly obesogenic, whereas butyrate and propionate are mainly antiobesogenic[813,39].
Interesting and novel mechanisms have been found to be involved in the causation and prevention of obesity by the abovementioned three SCFAs. It may be convenient to mention the contribution of individual SCFAs towards the genesis as well as prevention of obesity and subsequently, discuss the underlying mechanisms involved in such actions: (1) Butyrate has been found to be a major energy source for colo-nocytes[811,13,30]. In the colonocytemitochondria 70% to 90% of the SCFA (butyrate)[10] is oxidized into acetylCoA, which is subsequently processed through tricarboxylic acid cycle to generate large quantity of ATP[8]. It has been shown that in addition to producing butyrate, the butyrateproducing microbes also increase the expression of the enzymes taking part in the colonocytemitochondrial SCFAoxidative reactions[9]; (2)
Besides supplying energy, butyrate also has a controlling role over the mechanisms involved in cellular apoptosis, proliferation and differentiation[10]; (3) Butyrate has been shown to possess some mixed metabolic effects which include an increase in mitochondrial activity, prevention of metabolic endotoxemia and activation of intestinal gluconeogenesis. These actions are mediated through gene expression and regulation of hormonal activity[9]; (4) Butyrate, when given orally to mice, has been found to improve insulin sensitivity and increase energy expenditure by improving mitochondrial function which may result in reduction of obesity[9]; (5) Some studies have indicated the antiinflammatory potential of butyrate which may contribute towards a decrease in obesityassociated metabolic complication, because of its capability to increase intestinal barrier function[12]. These effects of butyrate support the observation that decreased population of intestinal butyrate producing bacteria is associated with metabolic risk in humans; (6) Butyrate has been found to be protective against dietinduced obesity without causing hypophagia. Acetate which is considered as obesogenic, also possesses this beneficial function like butyrate[13]; (7) Butyrate and propionate (beneficial SCFAs) cause weight regulation at least partially by controlling food intake; the action appears to be mediated through their stimulatory effect on the anorexigenic gut hormones. It may be mentioned here that acetate also inhibits weight gain, but through mechanisms which are independent of suppression of food intake and acute gut hormone effect[13]; (8) Xiong et al[40] had demonstrated the potential of butyrate and propionate to increase the expression of the gene coding for synthesis of leptin (Table 3); and (9) Besides these antiobesogenic properties, both butyrate and propionate have been shown to possess a definite protective role against colon carcinogenesis[8,10].
Like butyrate, propionate also possesses favourable some effects in obesity. They are as follows: (1) The SCFA has been found to reduce food intake and regulate body weight, similar to butyrate[13]; (2) It decreases cholesterol synthesis by inhibiting the activity of the enzyme acetylCoA synthetase (the enzyme converts acetate to acetylCoA), thereby antagonizing the cholesterol increasing action of acetate[10,11]; (3) Moreover, propionate has been found to be a precursor for gluconeogenesis in the liver[10,14]. This may decrease the hepatic synthesis of cholesterol because fatty acids necessary for cholesterol synthesis are diverted towards synthesis of glucose (gluconeogenesis)[14]; (4) It has been shown that like butyrate, propionate also stimulates the formation of the anorexigenic hormone leptin[40] (Table 3); and (5) However, propionate inhibits the expression of resistin in human adipose tissue[39].
Of all the three SCFAs, acetate seems to be more obesogenic than butyrate and propionate because: (1) It is a substrate for lipogenesis[8,14] and cholesterol synthesis in liver and other tissues[8,11]. This SCFA is readily and substantially absorbed by the colonocytes and though,
Chakraborti CK. Microbiota and obesity

116 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
some part of it is utilized in the liver for lipogenesis, a significant amount reaches systemic circulation and is delivered to the peripheral tissues[13] for synthesis of cholesterol (specifically in adipose tissues and mammary glands, whose cytosol contains acetylCoA synthetase, the enzyme essential for utilization of acetate for lipogenesis)[10]. Human studies have shown that when lactulose (synthetic nonabsorbable sugar, metabolized by microbiota to produce high amounts of acetate) was administered to the diets of six volunteers for two weeks, there was a significant increase in both total and lowdensity lipoprotein cholesterol, apolipoprotein B and plasma concentration of acetate in comparison to the control group[11]; and (2) Though predominantly obesogenic, some workers have demonstrated the obesityprotecting role of acetate, which is less than that of butyrate and propionate. Like butyrate, it gives protection against dietinduced obesity without causing hypophagia and thus, the action is independent of suppression of food intake and does not have any acute effect on gut hormones[13] (Table 3). It has been demonstrated that acetate increases cholesterol synthesis and propionate, though regulates it, does not affect serum cholesterol levels[8,11] and is primarily utilized for gluconeogenesis[8,10,14]. But when the two SCFAs are administered simultaneously, serum cholesterol level does not rise[11]. This may be due to increased gluconeogenesis by propionate consuming more fatty acids and thus diverting them from getting utilized by acetate for synthesis of cholesterol[14]. Therefore, though acetate increases fatty acid synthesis, they take part in gluconeogenesis rather than being used for synthesis of cholesterol and thus, plasma level of cholesterol does not rise[10,11].
It has been demonstrated that fecal concentration of SCFAs are 20% higher in obese individuals than their lean counterparts. But such higher SCFAs concentration in feces may reflect a compensatory protective mechanism against obesity, in which a greater amount is eliminated from the increased amount of SCFAs produced, thereby preventing increased accumulation
of SCFA in the intestinal lumen for obesogenic action[37].
MECHANISM OF ACTION OF SCFAS AT THE MOLECULAR LEVELSome important actions of these three SCFAs have been found to be mediated through activation of endogenous free fatty acid receptor (FFAR) like FFAR2 and FFAR3 which are otherwise designated as Gpr43 and Gpr41, respectively, because they belong to Gprotein coupled receptor family of receptors[13,37]. Presence of both these receptors has been demonstrated in adipocytes, epithelial cells and enteroendocrine cells. Activation of these two receptors leads to an increase in expression of satiety hormone polypeptide YY (PYY) and increase in intestinal motility. In addition to the above effect, Gpr41 activation also increases the expression of leptin in adipocytes. It has been observed that when SCFAproducing bacteria were administered to germfree mice, the mice gained weight along with an increase in body fat. But, mice (both germ-free and conventional), deficient in Gpr41 did not show such effects. Such observation indicates that weight gain occurs through activation of Gpr41[37]. Moreover, Samuel et al[41] have shown that the expression of PYY in the abovementioned mice was lower in the mice with intact Gpr41. Reduced production of PYY leads to decreased gut motility and hence, decreased dietary energy harvest[19]. Besides increasing leptin expression in adipocytes, Gpr41 activation also increases hepatic lipogenesis. Hence, this receptor is considered as a probable regulator of energy balance of the host[37].
SCFAs, like butyrate and propionate, increase the formation of the gut hormone glucagonlike peptide1 (GLP1). It reduces food intake by decreasing appetite. Maximal induction of GLP1 requires activation of Gpr41, but is not essential[13].
Nondigestible carbohydrates (NDC) are known to be antiobesogenic because they are not digested in the intestine but are fermented in the large bowel resulting in the formation of SCFAs. Ultimately, they (SCFAs) mediate some of the antiobesogenic actions of NDC.
Table 3 Gross mechanisms involved in short-chain fatty acids-induced obesity
Butyrate A major energy source for colonocytes Involved in cellular apoptosis, proliferation and differentiation Possesses metabolic effects like increase in mitochondrial activity, prevention of metabolic endotoxemia and activation of intestinal gluconeogenesis Improves insulin sensitivity and increases energy expenditure by improving mitochondrial function resulting in reduction of obesity Increases intestinal barrier function - an antiinflammatory potential Protects against diet-induced obesity without causing hypophagia - the action being mediated through stimulation of anorexigenic gut hormones Increases the expression of the gene coding for synthesis of leptinPropionate Increases the expression of the gene coding for synthesis of leptin Protects against diet-induced obesity without causing hypophagia - the mechanism being similar to butyrate Decreases cholesterol synthesis by inhibiting the activity of the enzyme acetyl-CoA synthetase Acts as a precursor for hepatic gluconeogenesis thereby decreasing the hepatic synthesis of cholesterol Inhibits the expression of resistin in human adipose tissueAcetate Acts as a substrate for lipogenesis and cholesterol synthesis in liver and other tissues Gives protection against diet-induced obesity without causing hypophagia
Chakraborti CK. Microbiota and obesity

117 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Propionate stimulates Gpr43 in caloric enteroendocrine cells leading to increased release of PYY and GLP1 (anorexigenic gut hormones). It also activates Gpr43 in adipocytes, which reduces output of FFAs into circulation and thus, it results in increased insulin sensitivity. Hence, the formation of more propionate in the colon, by consuming NDC, may be beneficial in obesity[42].
However, food rich in fermentable fibers are seemed to stimulate obesity through harvested energy by their SCFAs (metabolites). But epidemiological study results suggest that they prevent it rather than promoting. It may be explained by the fact that these SCFAs, by stimulating FFARs, cause satiety via increased production of GLP1 and PYY[18]. Thus, they are not obesogenic[14,18].
Certain study results have shown that mirobiotaderived SCFAs modulate (increase) the secretion and gene expression of GLP1 and PYY which are known to be satiety hormones[18,37]. Fastinginduced adipocyte factor (Fiaf) has been found to suppress the production of adipocyteLPL (hormone sensitive lipase) which leads to an increase in lipolysis of triglycerides in adipocytes and modulation of fatty acid oxidation in adipocytes and skeletal muscles. It has been shown that physiological appetite regulators regulate the expression of Fiaf in the hypothalamus and exert their anorexigenic effect through inhibition of hypothalamic AMPactivated protein kinase (AMPK) activity. This suggests a central regulatory role of Fiaf in energy metabolism[43].
Investigations on germfree and conventionalized mice have shown that one of the mechanisms of energy harvest and adipocyte hypertrophy by microbiota is through inhibition of enterocyte Fiaf, leading to suppression of the actions of intestinal LPL and increased activity of PYY[19,44].
Metabolic degradation of a given source of energy is more with Firmicutes than with Bacteroidetes, resulting in increased absorption of calories and hence more weight gain[45]. Increased population of Firmicutes has been found to raise the number of lipid droplets, thereby proportionately intensifying fatty acid absorption[46]. Such a finding seems to involve several mechanisms. Microbiota may increase the metabolism of the host along with modification and increase in bile salt production. It favours more fatty acid (FA) absorption and hence, increased bioavailability[47]. In addition, intestinal microbes may directly prevent the lipolytic activities of the host[48]. They may indirectly change the physiological responses in the gut of the host, resulting in increased absorption. Finally, microbes may lower the rate of FA oxidation, which increases FA absorption[46]. In addition to these, Firmicutesinduced increased FA absorption may involve other specific mechanisms[45].
Methanogen, like M. smithii is found in 70% of human beings. It generates methane through anaerobic fermentation. It has been found to enhance the fermentation of polysaccharides and other carbohydrates by removing hydrogen atoms, leading to greater production of SCFAs and hence, their increased absorption. These SCFAs function as an extra source of energy which contributes towards weight gain and subsequent
obesity[49].Some gastrointestinal microbiotacomponents have
been found to suppress the expression of the host genes which code for the synthesis of intestinal epithelial tight junction proteins and Fiaf, leading to increased adipocyte lipoprotein lipase (LPL) activity and hence, increased storage of liverderived triglyceride in host fat cells and weight gain[22,37,43]. Interesting experiments on mice has been conducted to demonstrate the combined effect of microbiota and diet resulting in development of obesity. When mice reared in germfree environment (hence absence of gastrointestinal microbiota) were fed with a westernstyle diet (high fat, high sugar), they did not gain weight as compared with colonized mice with similar diet. This may be due to suppression of microbiotainduced gene expression and hence, inhibition of Fiaf formation resulting in increased fat metabolism, lower fat storage and decreased sugar absorption. Such altered lipid metabolism and storage is supported by the fact that germfree mice were having higher levels of Fiaf and hence, lower LPL activity, higher muscle and hepatic levels of the key enzyme (phosphorylated AMPK) necessary for βoxidation and lesser monosaccharide absorption from the intestine in comparison with colonised mice[37]. Thus, gut microbiota may be considered as an important environmental factor increasing dietary energy harvest and energy storage in the host[19]. But such observations may not be taken conclusive, because another study has demonstrated that germfree mice significantly gained weight with westernstyle diet[37].
It has been shown that in the mucosa of small intestine of gnotobiotic mice, who harbour intestinal C. ramosum, there is upregulation of Glut2 and CD36 transcription. It suggests that this organism is responsible for more gain in body fat by an increase in intestinal absorption of glucose and lipid[27].
It may be mentioned here that though bacterial product LPS disrupts normal gastrointestinal integrity, bacterial SCFA metabolites acetate and butyrate strengthen it by increasing the secretion of mucin2 (MUC2) the mucus secreted by goblet cells, which plays an important role to maintain healthy intestinal epithelial barrier. It has been shown that butyrate, when added to goblet cell lines, increased the secretion of MUC2 23fold and, thus, considered as a protective SCFA against intestinal translocation of bacteria and their products[37].
As mentioned earlier, acetate is known to be obesogenic because of its peripheral action. However, it has been shown that it can also control weight gain through its central action, where it produces an anorexigenic signal in the hypothalamic arcuate nucleus, through increased generation of gammaaminobutyric acid (GABA), by augmenting the glutamateglutamine (transcellular) cycle involved in GABA production[50].
CONCLUSION The beneficial role of gastrointestinal microbiota for maintenance of proper health of the host is well
Chakraborti CK. Microbiota and obesity

118 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
established. From the above discussion, it seems that out of the millions of species harbouring the gastrointestinal tract, only a few are linked with the genesis of obesity. Moreover, individual species of these is not harmful entirely; each of them possessing obesogenic as well as antiobesogenic property, for which, ratio of two species (like Firmicutes and Bacteroidetes) are taken into consideration when grouping them into harmful or beneficial group. Several researchers have observed that it is the dietary habit (fatty food) of the host which alters the population and composition of the microbiome, thereby shifting the ratio of the concerned pair in favour of obesity. Hence, by altering the nature of the diet (less fat and more NDC), an individual, in addition to reducing the total calorie intake, may also be able to shift the ratio in the opposite direction (antiobesity).
As one of the causes of obesity has been attributed due to the structural components (LPS) and metabolic end products (SCFAs) of certain gastrointestinal microorganisms, it is not wrong to consider obesity (at least partially, if not fully) as an infectious disease. Further research in this respect is needed to confirm this possibility and to find out selective chemotherapeutic agents, which will reduce or abolish the more harmful bacterial population. Another possible mechanism, which can cause weight loss or decrease obesity, is to implant the useful bacterial species in appropriate ratio.
Probiotics and prebiotics are known to alter the compositional pattern and population of gastrointestinal microflora and are used to prevent or ameliorate some of the antimicrobial chemotherapyinduced gastrointestinal side effects and some other gastrointestinal diseases. Because of the new found link between these microflora and obesity (both obesogenic and antiobesogenic), pharmaceutical industries may focus more on manufacturing the required pre and probiotics which may be beneficial to counter this worldwide epidemic and its complications.
REFERENCES1 Steinberger J, Daniels SR. Obesity, insulin resistance, diabetes,
and cardiovascular risk in children: an American Heart Association scientific statement from the Atherosclerosis, Hypertension, and Obesity in the Young Committee (Council on Cardiovascular Disease in the Young) and the Diabetes Committee (Council on Nutrition, Physical Activity, and Metabolism). Circulation 2003; 107: 1448-1453 [PMID: 12642369 DOI: 10.1161/01.CIR.0000060923.07573.F2]
2 Kaur J. A comprehensive review on metabolic syndrome. Cardiol Res Pract 2014; 2014: 943162 [PMID: 24711954 DOI: 10.1155/2014/943162]
3 Rang HP, Dale MM, Ritter JM, Moore PK. Pharmacology. 5th ed. New Delhi: Churchill Livingstone, 2006: 394-403
4 Get Your Hormones Checked and Lose Weight. [Accessed 2013 Nov 20]. Available from: URL: http://www.dietdoctor.com/get-hormones-checked-lose-weight
5 Ness-Abramof R, Apovian CM. Drug-induced weight gain. Drugs Today (Barc) 2005; 41: 547-555 [PMID: 16234878 DOI: 10.1358/dot.2005.41.8.893630]
6 Abdallah Ismail N, Ragab SH, Abd Elbaky A, Shoeib AR, Alhosary Y, Fekry D. Frequency of Firmicutes and Bacteroidetes
in gut microbiota in obese and normal weight Egyptian children and adults. Arch Med Sci 2011; 7: 501-507 [PMID: 22295035 DOI: 10.5114/aoms.2011.23418]
7 den Besten G, van Eunen K, Groen AK, Venema K, Reijngoud DJ, Bakker BM. The role of short-chain fatty acids in the interplay between diet, gut microbiota, and host energy metabolism. J Lipid Res 2013; 54: 2325-2340 [PMID: 23821742 DOI: 10.1194/jlr.R036012]
8 Shoaie S, Karlsson F, Mardinoglu A, Nookaew I, Bordel S, Nielsen J. Understanding the interactions between bacteria in the human gut through metabolic modeling. Sci Rep 2013; 3: 2532 [PMID: 23982459 DOI: 10.1038/srep02532]
9 Hartstra AV, Bouter KE, Bäckhed F, Nieuwdorp M. Insights into the role of the microbiome in obesity and type 2 diabetes. Diabetes Care 2015; 38: 159-165 [PMID: 25538312 DOI: 10.2337/dc14-0769]
10 Hijova E, Chmelarova A. Short chain fatty acids and colonic health. Bratisl Lek Listy 2007; 108: 354-358 [PMID: 18203540]
11 Harris K, Kassis A, Major G, Chou CJ. Is the gut microbiota a new factor contributing to obesity and its metabolic disorders? J Obes 2012; 2012: 879151 [PMID: 22315672 DOI: 10.1155/2012/879151]
12 Brahe LK, Astrup A, Larsen LH. Is butyrate the link between diet, intestinal microbiota and obesity-related metabolic diseases? Obes Rev 2013; 14: 950-959 [PMID: 23947604 DOI: 10.1111/obr.12068]
13 Lin HV, Frassetto A, Kowalik EJ, Nawrocki AR, Lu MM, Kosinski JR, Hubert JA, Szeto D, Yao X, Forrest G, Marsh DJ. Butyrate and propionate protect against diet-induced obesity and regulate gut hormones via free fatty acid receptor 3-independent mechanisms. PLoS One 2012; 7: e35240 [PMID: 22506074 DOI: 10.1371/journal.pone.0035240]
14 Sanz Y, Santacruz A, Gauffin P. Gut microbiota in obesity and metabolic disorders. Proc Nutr Soc 2010; 69: 434-441 [PMID: 20540826 DOI: 10.1017/S0029665110001813]
15 Petriz BA, Castro AP, Almeida JA, Gomes CP, Fernandes GR, Kruger RH, Pereira RW, Franco OL. Exercise induction of gut microbiota modifications in obese, non-obese and hypertensive rats. BMC Genomics 2014; 15: 511 [PMID: 24952588 DOI: 10.1186/1471-2164-15-511]
16 Sun J, Chang EB. Exploring gut microbes in human health and disease: Pushing the envelope. Genes Dis 2014; 1: 132-139 [PMID: 25642449 DOI: 10.1016/j.gendis.2014.08.001]
17 Miquel S, Martín R, Rossi O, Bermúdez-Humarán LG, Chatel JM, Sokol H, Thomas M, Wells JM, Langella P. Faecalibacterium prausnitzii and human intestinal health. Curr Opin Microbiol 2013; 16: 255-261 [PMID: 23831042 DOI: 10.1016/j.mib.2013.06.003]
18 Duca FA, Sakar Y, Lepage P, Devime F, Langelier B, Doré J, Covasa M. Replication of obesity and associated signaling pathways through transfer of microbiota from obese-prone rats. Diabetes 2014; 63: 1624-1636 [PMID: 24430437 DOI: 10.2337/db13-1526]
19 Park JS, Seo JH, Youn HS. Gut microbiota and clinical disease: obesity and nonalcoholic Fatty liver disease. Pediatr Gastroenterol Hepatol Nutr 2013; 16: 22-27 [PMID: 24010102 DOI: 10.5223/pghn.2013.16.1.22]
20 DiBaise JK, Frank DN, Mathur R. Impact of the Gut Microbiota on the Development of Obesity: Current Concepts. Am J Gastroenterol Suppl 2012; 1: 22-27 [DOI: 10.1038/ajgsup.2012.5]
21 Bervoets L, Van Hoorenbeeck K, Kortleven I, Van Noten C, Hens N, Vael C, Goossens H, Desager KN, Vankerckhoven V. Differences in gut microbiota composition between obese and lean children: a cross-sectional study. Gut Pathog 2013; 5: 10 [PMID: 23631345 DOI: 10.1186/1757-4749-5-10]
22 Ley RE, Bäckhed F, Turnbaugh P, Lozupone CA, Knight RD, Gordon JI. Obesity alters gut microbial ecology. Proc Natl Acad Sci USA 2005; 102: 11070-11075 [PMID: 16033867 DOI: 10.1073/pnas.0504978102]
23 Duncan SH, Lobley GE, Holtrop G, Ince J, Johnstone AM, Louis P, Flint HJ. Human colonic microbiota associated with diet, obesity and weight loss. Int J Obes (Lond) 2008; 32: 1720-1724 [PMID: 18779823 DOI: 10.1038/ijo.2008.155]
24 Turnbaugh PJ, Hamady M, Yatsunenko T, Cantarel BL, Duncan A, Ley RE, Sogin ML, Jones WJ, Roe BA, Affourtit JP, Egholm
Chakraborti CK. Microbiota and obesity

119 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
M, Henrissat B, Heath AC, Knight R, Gordon JI. A core gut microbiome in obese and lean twins. Nature 2009; 457: 480-484 [PMID: 19043404 DOI: 10.1038/nature07540]
25 Clarke SF, Murphy EF, Nilaweera K, Ross PR, Shanahan F, O’Toole PW, Cotter PD. The gut microbiota and its relationship to diet and obesity: new insights. Gut Microbes 2012; 3: 186-202 [PMID: 22572830 DOI: 10.4161/gmic.20168]
26 Schwiertz A, Taras D, Schäfer K, Beijer S, Bos NA, Donus C, Hardt PD. Microbiota and SCFA in lean and overweight healthy subjects. Obesity (Silver Spring) 2010; 18: 190-195 [PMID: 19498350 DOI: 10.1038/oby.2009.167]
27 Woting A, Pfeiffer N, Loh G, Klaus S, Blaut M. Clostridium ramosum promotes high-fat diet-induced obesity in gnotobiotic mouse models. MBio 2014; 5: e01530-e01514 [PMID: 25271283 DOI: 10.1128/mBio.01530-14]
28 Million M, Maraninchi M, Henry M, Armougom F, Richet H, Carrieri P, Valero R, Raccah D, Vialettes B, Raoult D. Obesity-associated gut microbiota is enriched in Lactobacillus reuteri and depleted in Bifidobacterium animalis and Methanobrevibacter smithii. Int J Obes (Lond) 2012; 36: 817-825 [PMID: 21829158 DOI: 10.1038/ijo.2011.153]
29 Furet JP, Kong LC, Tap J, Poitou C, Basdevant A, Bouillot JL, Mariat D, Corthier G, Doré J, Henegar C, Rizkalla S, Clément K. Differential adaptation of human gut microbiota to bariatric surgery-induced weight loss: links with metabolic and low-grade inflammation markers. Diabetes 2010; 59: 3049-3057 [PMID: 20876719 DOI: 10.2337/db10-0253]
30 Puddu A, Sanguineti R, Montecucco F, Viviani GL. Evidence for the gut microbiota short-chain fatty acids as key pathophysiological molecules improving diabetes. Mediators Inflamm 2014; 2014: 162021 [PMID: 25214711 DOI: 10.1155/2014/162021]
31 Lau CH, Muniandy S. Novel adiponectin-resistin (AR) and insulin resistance (IRAR) indexes are useful integrated diagnostic biomarkers for insulin resistance, type 2 diabetes and metabolic syndrome: a case control study. Cardiovasc Diabetol 2011; 10: 8 [PMID: 21251282 DOI: 10.1186/1475-2840-10-8]
32 Chakraborti CK. Possible links between obesity and type 2 diabetes mellitus. Int J Pharm Sci Res 2012; 3: 1935-1945
33 Bastard JP, Maachi M, Lagathu C, Kim MJ, Caron M, Vidal H, Capeau J, Feve B. Recent advances in the relationship between obesity, inflammation, and insulin resistance. Eur Cytokine Netw 2006; 17: 4-12 [PMID: 16613757]
34 vinh quốc Lu'o'ng K, Nguyễn LT. The beneficial role of vitamin D in obesity: possible genetic and cell signaling mechanisms. Nutr J 2013; 12: 89 [PMID: 23800102 DOI: 10.1186/1475-2891-12-89]
35 Escobedo G, López-Ortiz E, Torres-Castro I. Gut microbiota as a key player in triggering obesity, systemic inflammation and insulin resistance. Rev Invest Clin 2014; 66: 450-459 [PMID: 25695388]
36 Cani PD, Amar J, Iglesias MA, Poggi M, Knauf C, Bastelica D, Neyrinck AM, Fava F, Tuohy KM, Chabo C, Waget A, Delmée E, Cousin B, Sulpice T, Chamontin B, Ferrières J, Tanti JF, Gibson GR, Casteilla L, Delzenne NM, Alessi MC, Burcelin R. Metabolic endotoxemia initiates obesity and insulin resistance. Diabetes 2007; 56: 1761-1772 [PMID: 17456850 DOI: 10.2337/db06-1491]
37 Graham C, Mullen A, Whelan K. Obesity and the gastrointestinal microbiota: a review of associations and mechanisms. Nutr Rev 2015; 73: 376-385 [PMID: 26011912 DOI: 10.1093/nutrit/nuv004]
38 de La Serre CB, Ellis CL, Lee J, Hartman AL, Rutledge JC,
Raybould HE. Propensity to high-fat diet-induced obesity in rats is associated with changes in the gut microbiota and gut inflammation. Am J Physiol Gastrointest Liver Physiol 2010; 299: G440-G448 [PMID: 20508158 DOI: 10.1152/ajpgi.00098.2010]
39 Al-Lahham SH, Roelofsen H, Priebe M, Weening D, Dijkstra M, Hoek A, Rezaee F, Venema K, Vonk RJ. Regulation of adipokine production in human adipose tissue by propionic acid. Eur J Clin Invest 2010; 40: 401-407 [PMID: 20353437 DOI: 10.1111/j.1365-2362.2010.02278.x]
40 Xiong Y, Miyamoto N, Shibata K, Valasek MA, Motoike T, Kedzierski RM, Yanagisawa M. Short-chain fatty acids stimulate leptin production in adipocytes through the G protein-coupled receptor GPR41. Proc Natl Acad Sci USA 2004; 101: 1045-1050 [PMID: 14722361 DOI: 10.1073/pnas.2637002100]
41 Samuel BS, Shaito A, Motoike T, Rey FE, Backhed F, Manchester JK, Hammer RE, Williams SC, Crowley J, Yanagisawa M, Gordon JI. Effects of the gut microbiota on host adiposity are modulated by the short-chain fatty-acid binding G protein-coupled receptor, Gpr41. Proc Natl Acad Sci USA 2008; 105: 16767-16772 [PMID: 18931303 DOI: 10.1073/pnas.0808567105]
42 Frost GS, Dhillo WS, Ashby D, Bloom SR, Blundell JE, Murphy K. Increased propionate production in the colon is associated with reduced appetite body weight and improved insulin sensitivity. [Accessed 2015 Sep 23]. Available from: URL: http://gtr.rcuk.ac.uk/project/8FD29977-D6E2-4AFE-ADFA-D445CF5BB17C
43 Tilg H, Kaser A. Gut microbiome, obesity, and metabolic dysfunction. J Clin Invest 2011; 121: 2126-2132 [PMID: 21633181 DOI: 10.1172/JCI58109]
44 Zak-Gołąb A, Olszanecka-Glinianowicz M, Kocełak P, Chudek J. [The role of gut microbiota in the pathogenesis of obesity]. Postepy Hig Med Dosw (Online) 2014; 68: 84-90 [PMID: 24491899 DOI: 10.5604/17322693.1086419]
45 Kallus SJ, Brandt LJ. The intestinal microbiota and obesity. J Clin Gastroenterol 2012; 46: 16-24 [PMID: 22064556 DOI: 10.1097/MCG.0b013e31823711fd]
46 Semova I, Carten JD, Stombaugh J, Mackey LC, Knight R, Farber SA, Rawls JF. Microbiota regulate intestinal absorption and metabolism of fatty acids in the zebrafish. Cell Host Microbe 2012; 12: 277-288 [PMID: 22980325 DOI: 10.1016/j.chom.2012.08.003]
47 Swann JR, Want EJ, Geier FM, Spagou K, Wilson ID, Sidaway JE, Nicholson JK, Holmes E. Systemic gut microbial modulation of bile acid metabolism in host tissue compartments. Proc Natl Acad Sci USA 2011; 108 Suppl 1: 4523-4530 [PMID: 20837534 DOI: 10.1073/pnas.1006734107]
48 Ringø E, Strøm E, Tabachek JA. Intestinal microflora of salmonids: a review. Aquacult Res 1995; 26: 773-789 [DOI: 10.1111/j.1365-2109.1995.tb00870.x]
49 Basseri RJ, Basseri B, Pimentel M, Chong K, Youdim A, Low K, Hwang L, Soffer E, Chang C, Mathur R. Intestinal methane production in obese individuals is associated with a higher body mass index. Gastroenterol Hepatol (N Y) 2012; 8: 22-28 [PMID: 22347829]
50 Frost G, Sleeth ML, Sahuri-Arisoylu M, Lizarbe B, Cerdan S, Brody L, Anastasovska J, Ghourab S, Hankir M, Zhang S, Carling D, Swann JR, Gibson G, Viardot A, Morrison D, Louise Thomas E, Bell JD. The short-chain fatty acid acetate reduces appetite via a central homeostatic mechanism. Nat Commun 2014; 5: 3611 [PMID: 24781306 DOI: 10.1038/ncomms4611]
P- Reviewer: Bustamante-Balen M, Huerta-Franco MR S- Editor: Tian YL L- Editor: A E- Editor: Liu SQ
Chakraborti CK. Microbiota and obesity

Sarah Ballou, Alyse Bedell, Laurie Keefer
Sarah Ballou, Alyse Bedell, Laurie Keefer, Division of Gastroenterology, Department of Medicine, Northwestern University, Feinberg School of Medicine, Chicago, IL 60611, United States
Author contributions: Ballou S, Bedell A and Keefer L wrote the paper.
Conflict-of-interest statement: There are no conflicts of interest to be declared.
Open-Access: This article is an openaccess article which was selected by an inhouse editor and fully peerreviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work noncommercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: http://creativecommons.org/licenses/bync/4.0/
Correspondence to: Sarah Ballou, MD, Division of Gastroenterology, Department of Medicine, Northwestern University, Feinberg School of Medicine, 676 N Saint Clair, Suite 1400, Chicago, IL 60611, United States. [email protected]: +13126959317 Fax: +13126957095
Received: April 28, 2015 Peer-review started: May 5, 2015First decision: May 18, 2015Revised: June 11, 2015 Accepted: August 25, 2015 Article in press: August 28, 2015Published online: November 15, 2015
AbstractIrritable bowel syndrome (IBS) is a common disorder of the gastrointestinal tract with unclear etiology and no reliable biomarker. Like other chronic and functional disorders, medical treatments for IBS are suboptimal
and the overall illness burden is high. Patients with IBS report high rates of psychopathology, low quality of life, and increased suicidal ideation. These patients also miss more days of work, are less productive at work, and use many healthcare resources. However, little is known about the burden of IBS on daily functioning. The primary aim of this paper is to review the current literature on the burden of IBS and to highlight the need for further research to evaluate the impact of IBS on daily activities. This research would contribute to our existing understanding of the impact of IBS on overall quality of life and well-being.
Key words: Irritable bowel syndrome; Quality of life; Biopsychosocial; Burden of illness; Daily activities
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Little is known about the burden of irritable bowel syndrome (IBS) on daily functioning. The primary aim of this paper is to review the current literature on the overall burden of IBS.
Ballou S, Bedell A, Keefer L. Psychosocial impact of irritable bowel syndrome: A brief review. World J Gastrointest Pathophysiol 2015; 6(4): 120123 Available from: URL: http://www.wjgnet.com/21505330/full/v6/i4/120.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i4.120
IrrItable bowel SyndromeIrritable bowel syndrome (IBS) affects between 10%-15% of the population in North America with a 2:1 ratio of women to men[1,2]. It is classified as a functional gastrointestinal disorder, meaning that its symptoms are not associated with any structural or biochemical abnor-malities in the gut. Symptoms of IBS are characterized
120 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
World J Gastrointest Pathophysiol 2015 November 15; 6(4): 120-123ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i4.120
TOPIC HIGHLIGHT
psychosocial impact of irritable bowel syndrome: A brief review
2015 Advances in Irritable Bowel Syndrome

by abdominal pain and/or discomfort associated with diarrhea, constipation, or a mixture of both[3].
Although there are not currently any biological markers for IBS, recent research has identified physi-ological factors that contribute to the expression of IBS symptoms. One of the most commonly studied features of IBS is known as the braingut axis, which refers to neural and hormonal signaling between the central nervous system and the gastrointestinal tract. In the past decade, the pathophysiology of IBS has been attributed to dysregulation of the braingut axis primarily through a process known as visceral hypersensitivity (amplified pain signals originating in the neurons of the gut). In IBS patients, visceral hypersensitivity is believed to cause increased pain and stress symptoms in response to normal bowel activity, resulting in lower thresholds for colonic discomfort when compared to healthy controls[4,5].
Current medical treatments for IBS are relatively ineffective and do not address visceral hypersensitivity. Most available treatments are targeted at reducing specific IBS symptoms, especially symptoms associated with abnormal gut motility. These include laxatives, antidiarrheals, probiotics, antidepressants, and psychological interventions to enhance stressmanagement skills and to help patients cope with distress related to symptom experience[6,7]. The best and longest lasting treatment results for IBS have been found in a combination of medical and psychological interventions[8].
ComorbIdItyThe overall burden of IBS is affected in part by high comorbidity of other medical and psychological disorders. Approximately 65% of patients with IBS have comorbid extra-intestinal symptoms and disorders[9] such as fibromyalgia[10], back pain[11], urogenital pro-blems[12], sleep problems[13]. Additionally, 40%-60% of IBS patients (compared to 20% of the overall population) report comorbid psychiatric diagnoses such as anxiety disorders, depression, and Post Traumatic Stress Disorder[14,15]. Patients with IBS are also more likely to report low quality of life[16] and up to 38% of IBS patients in tertiary care settings have contemplated suicide as a result of their symptoms[17].
Given the high psychiatric comorbidity and increased stressreactivity associated with IBS, several psychological interventions have been tailored to specifically target psychosocial skills deficits in IBS patients. Cognitive behavioral therapy (CBT) is the most commonly used and most widely researched psychological treatment for IBS to date. In this treatment, patients are taught to evaluate the relationships between thoughts, behaviors, and emotions and to cope with stressors by learning to modify maladaptive behaviors and to reframe un-helpful cognitions with the goal of improving mood and decreasing stressreactivity. By doing so, patients can learn to decrease autonomic arousal, which may eventually decrease visceral hypersensitivity and reduce
IBS symptoms[18,19]. Newer adaptations of the CBT model have also begun to incorporate data that supports the role of braingut dysregulation and symptomspecific processes (i.e., symptom-specific anxiety) in the onset and maintenance of IBS[20,21]. These studies have supported the effectiveness of CBT in treating both physiological and psychological symptoms associated with IBS. For example, in a research study evaluating the effectiveness of 2 different types of CBT compared to Wait List Control, Lackner et al[21] demonstrated that 61%72% of patients who received CBT treatment reported adequate relief of symptoms compared to 7.4% of Wait List Control patients.
bUrden oF IbSDue to currently insufficient medical interventions for IBS, the burden of living with IBS is quite high. As mentioned above, research has established that patients with IBS have high rates of psychopathology, low quality of life, and increased suicidal ideation. In addition, these patients miss more days of work, are less productive at work, and use many healthcare resources.
PSyChologICal bUrdenThe primary goal of psychological interventions for IBS is to ease the overall burden of the illness. Decades of research using psychological parameters have provided a clear understanding of the psychological burden associated with IBS. As mentioned above, approximately 40%-60% of IBS patients have comorbid psychiatric diagnoses[14] and 38% contemplate suicide as a result of their symptoms[17]. Furthermore, these patients report lower quality of life than other patients with serious conditions such as endstage renal disease or diabetes mellitus[16]. Research studies evaluating the psychological burden of IBS typically rely on validated self-report quality of life measures to evaluate the impact of glycemicindex symptoms of overall wellbeing[16]. These measures evaluate emotional and physical functioning together, without providing a clear or specific picture of the impact of IBS on daily activities.
work ProdUCtIvIty and health-Care UtIlIzatIonA separate body of research has evaluated the burden of IBS on workproductivity and health care utilization[22,23]. This research reveals increased levels of both absenteeism and presenteeism in the workplace when com-pared to healthy controls. One study estimates that, assuming an IBS prevalence rate of 10%, an employer with 10000 employees could lose $7737600 per year in lost work-productivity due to IBS[22]. Furthermore, IBS accounts for 1.5-2.7 million physician visits a year, frequently resulting in unnecessary, expensive, and invasive diagnostics[24]. For example, 18%-33% of
121 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Ballou S et al . Psychosocial impact of irritable bowel syndrome

women with IBS have had a hysterectomy, compared to 12% to 17% of women without IBS who have had this same surgery[25,26].
daIly FUnCtIonIngWhile many studies have evaluated the costly effects of IBS on psychological functioning, healthcare utilization, and work productivity, relatively few studies have focused on overall daily functioning in patients with IBS. Survey studies have shown that IBS patients report higher levels of difficulty in a broad range of daily activities when compared to healthy controls[27]; that IBS negatively affects both mental and physical functioning[16]; and that the reported effect of IBS on daily living is almost as high as that of the flu[28]. Activities that appear to be particularly impaired by IBS include: Work, intimacy, leisure activities, personal relationships, and eating habits[1,28,29]. However, these findings typically come from large survey studies and only one study to our knowledge has sought to quantify functional impairment among IBS patients[29]. The findings from that study suggested high levels of avoidance in a range of daily activities, particularly when symptoms were present.
The existing body of research on the impact of IBS on daily activities has only just begun to address the issue of the burden of IBS on daily functioning. Although most clinicians who work with IBS would agree that many of their patients modify or limit certain activities due to IBS symptoms (or fear of symptoms), this has not been adequately measured or quantified in this population.
FUnCtIonal ImPaIrment In IbSExisting studies on functional impairment in IBS have offered, but not evaluated, two possible hypotheses for impaired daily functioning in IBS patients: (1) IBS symptoms may directly impact activities of daily living; and (2) emotional distress and/or maladaptive coping skills may primarily disrupt daily functioning.
These hypotheses are consistent with current research in chronic pain suggesting that daily functioning is influenced by both emotional distress and actual physical pain symptoms[30]. To our knowledge, no research study has systematically evaluated the impact of both symptom severity and emotional distress on daily functioning in IBS patients.
A preliminary evaluation of functional impairment in a small sample (n = 35) of women with IBS suggests that patients avoid or are unable to participate in a wide range of activities, which they attribute to IBS symptoms (Figure 1). Interestingly, this preliminary data revealed that although most participants attributed functional impairment to IBS, symptom severity was not a significant predictor of functional impairment. In fact, symptomspecific anxiety and depression were the only significant predictors of impairment in a regression model that included symptom-specific anxiety, psy-chological distress, and symptom severity[31]. These findings are inline with literature in pain and anxiety disorders suggesting that functional impairment may be independent of symptom severity. However, further research is required to evaluate the pathways that may lead to functional impairment.
ConClUSIonAlthough the psychosocial and economic burden of IBS has been well documented, further research is necessary to evaluate the impact of IBS on daily activities. As mentioned above, existing measures of quality of life evaluate emotional and physical functioning together and do not provide a clear or specific understanding of the behavioral consequences of IBS (e.g., avoiding social activities, avoiding work, avoiding travel, etc.). Existing research has alluded to behavioral avoidance or inability to participate in daily activities[27-30] but this concept has not yet been adequately or systematically characterized in IBS patients. Further research should evaluate and characterize functional impairment in IBS.
reFerenCeS1 Hungin AP, Chang L, Locke GR, Dennis EH, Barghout V. Irritable
bowel syndrome in the United States: prevalence, symptom patterns and impact. Aliment Pharmacol Ther 2005; 21: 13651375 [PMID: 15932367]
2 Thompson WG, Irvine EJ, Pare P, Ferrazzi S, Rance L. Functional gastrointestinal disorders in Canada: first populationbased survey using Rome II criteria with suggestions for improving the questionnaire. Dig Dis Sci 2002; 47: 225235 [PMID: 11837727 DOI: 10.1023/A:1013208713670]
3 Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional bowel disorders. Gastroenterology 2006; 130: 14801491 [PMID: 16678561 DOI: 10.1053/j.gastro.2005.11.061]
4 Fukudo S, Nomura T, Muranaka M, Taguchi F. Braingut response to stress and cholinergic stimulation in irritable bowel syndrome. A preliminary study. J Clin Gastroenterol 1993; 17: 133141 [PMID: 8031340 DOI: 10.1097/0000483619930900000009]
5 Schmulson M, Chang L, Naliboff B, Lee OY, Mayer EA. Correlation of symptom criteria with perception thresholds during rectosigmoid distension in irritable bowel syndrome patients. Am J
122 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Percent due to IBS100
90
80
70
60
50
40
3020
100
Wor
k
Socia
l
Activ
ity
Appe
aran
ce
House
hold
Intim
acy
Leisu
re
Trav
el
Eat a
lone
Eat in
grou
ps
7467
54
65
34
45
35
23
74
42
Figure 1 Percent of the sample (n = 35) that reported impairment in each area of daily living due to irritable bowel syndrome. IBS: Irritable bowel syndrome.
Ballou S et al . Psychosocial impact of irritable bowel syndrome

123 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
10.1159/000288012]20 Boyce PM, Talley NJ, Balaam B, Koloski NA, Truman G.
A randomized controlled trial of cognitive behavior therapy, relaxation training, and routine clinical care for the irritable bowel syndrome. Am J Gastroenterol 2003; 98: 22092218 [PMID: 14572570 DOI: 10.1111/j.15720241.2003.07716.x]
21 Lackner JM, Keefer L, Jaccard J, Firth R, Brenner D, Bratten J, Dunlap LJ, Ma C, Byroads M. The Irritable Bowel Syndrome Outcome Study (IBSOS): rationale and design of a randomized, placebocontrolled trial with 12 month follow up of self versus clinicianadministered CBT for moderate to severe irritable bowel syndrome. Contemp Clin Trials 2012; 33: 12931310 [PMID: 22846389 DOI: 10.1016/j.cct.2012.07.013]
22 Dean BB, Aguilar D, Barghout V, Kahler KH, Frech F, Groves D, Ofman JJ. Impairment in work productivity and healthrelated quality of life in patients with IBS. Am J Manag Care 2005; 11: S17S26 [PMID: 15926760]
23 Paré P, Gray J, Lam S, Balshaw R, Khorasheh S, Barbeau M, Kelly S, McBurney CR. Healthrelated quality of life, work productivity, and health care resource utilization of subjects with irritable bowel syndrome: baseline results from LOGIC (Longitudinal Outcomes Study of Gastrointestinal Symptoms in Canada), a naturalistic study. Clin Ther 2006; 28: 17261735; discussion 17101711 [PMID: 17157129 DOI: 10.1016/j.clinthera.2006.10.010]
24 Shih YC, Barghout VE, Sandler RS, Jhingran P, Sasane M, Cook S, Gibbons DC, Halpern M. Resource utilization associated with irritable bowel syndrome in the United States 19871997. Dig Dis Sci 2002; 47: 17051715 [PMID: 12184519 DOI: 10.1023/A:1016471923384]
25 Hasler WL, Schoenfeld P. Systematic review: Abdominal and pelvic surgery in patients with irritable bowel syndrome. Aliment Pharmacol Ther 2003; 17: 9971005 [PMID: 12694081 DOI: 10.1046/j.13652036.2003.01499.x]
26 Longstreth GF, Yao JF. Irritable bowel syndrome and surgery: a multivariable analysis. Gastroenterology 2004; 126: 16651673 [PMID: 15188159 DOI: 10.1053/j.gastro.2004.02.020]
27 Hungin AP, Whorwell PJ, Tack J, Mearin F. The prevalence, patterns and impact of irritable bowel syndrome: an international survey of 40,000 subjects. Aliment Pharmacol Ther 2003; 17: 643650 [PMID: 12641512 DOI: 10.1046/j.13652036.2003.01456.x]
28 Dapoigny M, Bellanger J, Bonaz B, Bruley des Varannes S, Bueno L, Coffin B, Ducrotté P, Flourié B, Lémann M, Lepicard A, Reigneau O. Irritable bowel syndrome in France: a common, debilitating and costly disorder. Eur J Gastroenterol Hepatol 2004; 16: 9951001 [PMID: 15371923 DOI: 10.1097/0004273720041000000008]
29 Corney RH, Stanton R. Physical symptom severity, psychological and social dysfunction in a series of outpatients with irritable bowel syndrome. J Psychosom Res 1990; 34: 483491 [PMID: 2231481 DOI: 10.1016/00223999(90)90022V]
30 Bass C. The role of emotion in determining pain. Dig Dis 2009; 27 Suppl 1: 1623 [PMID: 20203493 DOI: 10.1159/000268117]
31 Ballou S, Keefer L. Functional impairment in young adult women with irritable bowel syndrome (IBS): How and why does IBS affect daily functioning? Masters Thesis. Northwestern University. 2013
P- Reviewer: Chiarioni G, Ierardi E S- Editor: Ma YJ L- Editor: A E- Editor: Liu SQ
Gastroenterol 2000; 95: 152156 [PMID: 10638575 DOI: 10.1111/j.15720241.2000.01677.x]
6 Lesbros-Pantoflickova D, Michetti P, Fried M, Beglinger C, Blum AL. Metaanalysis: The treatment of irritable bowel syndrome. Aliment Pharmacol Ther 2004; 20: 12531269 [PMID: 15606387 DOI: 10.1111/j.13652036.2004.02267.x]
7 Tillisch K, Chang L. Diagnosis and treatment of irritable bowel syndrome: state of the art. Curr Gastroenterol Rep 2005; 7: 249256 [PMID: 16042907 DOI: 10.1007/s118940050016y]
8 Mahvi-Shirazi M, FathiAshtiani A, RasoolzadeTabatabaei SK, Amini M. Irritable bowel syndrome treatment: cognitive behavioral therapy versus medical treatment. Arch Med Sci 2012; 8: 123129 [PMID: 22457686 DOI: 10.5114/aoms.2012.27292]
9 Riedl A, Schmidtmann M, Stengel A, Goebel M, Wisser AS, Klapp BF, Mönnikes H. Somatic comorbidities of irritable bowel syndrome: a systematic analysis. J Psychosom Res 2008; 64: 573582 [PMID: 18501257 DOI: 10.1016/j.jpsychores.2008.02.021]
10 Sperber AD, Atzmon Y, Neumann L, Weisberg I, Shalit Y, AbuShakrah M, Fich A, Buskila D. Fibromyalgia in the irritable bowel syndrome: studies of prevalence and clinical implications. Am J Gastroenterol 1999; 94: 35413546 [PMID: 10606316 DOI: 10.1111/j.15720241.1999.01643.x]
11 Smith MD, Russell A, Hodges PW. How common is back pain in women with gastrointestinal problems? Clin J Pain 2008; 24: 199203 [PMID: 18287824 DOI: 10.1097/AJP.0b013e31815d3601]
12 Guo YJ, Ho CH, Chen SC, Yang SS, Chiu HM, Huang KH. Lower urinary tract symptoms in women with irritable bowel syndrome. Int J Urol 2010; 17: 175181 [PMID: 20088875 DOI: 10.1111/j.14422042.2009.02442.x]
13 Elsenbruch S, Harnish MJ, Orr WC. Subjective and objective sleep quality in irritable bowel syndrome. Am J Gastroenterol 1999; 94: 24472452 [PMID: 10484007 DOI: 10.1111/j.15720241.1999.01374.x]
14 Drossman DA, Camilleri M, Mayer EA, Whitehead WE. AGA technical review on irritable bowel syndrome. Gastroenterology 2002; 123: 21082131 [PMID: 12454866 DOI: 10.1053/gast.2002.37095S001650850200481X]
15 Cohen H, Jotkowitz A, Buskila D, PellesAvraham S, Kaplan Z, Neumann L, Sperber AD. Posttraumatic stress disorder and other comorbidities in a sample population of patients with irritable bowel syndrome. Eur J Intern Med 2006; 17: 567571 [PMID: 17142176 DOI: 10.1016/j.ejim.2006.07.011]
16 Koloski NA, Talley NJ, Boyce PM. The impact of functional gastrointestinal disorders on quality of life. Am J Gastroenterol 2000; 95: 6771 [PMID: 10638561 DOI: 10.1111/j.15720241.2000.01735.x]
17 Miller V, Hopkins L, Whorwell PJ. Suicidal ideation in patients with irritable bowel syndrome. Clin Gastroenterol Hepatol 2004; 2: 10641068 [PMID: 15625650 DOI: 10.1016/S15423565(04)005452]
18 van Dulmen AM, Fennis JF, Bleijenberg G. Cognitivebehavioral group therapy for irritable bowel syndrome: effects and longterm followup. Psychosom Med 1996; 58: 508514 [PMID: 8902902 DOI: 10.1097/0000684219960900000013]
19 Weiner H. Some unexplored regions of psychosomatic medicine. Psychother Psychosom 1987; 47: 153159 [PMID: 3333283 DOI:
Ballou S et al . Psychosocial impact of irritable bowel syndrome

early diagnosis and treatment, whereas unexplained manifestations might be linked with pathogenic mechanisms. This review focuses on both symptomatic and asymptomatic brain lesions detectable on imaging studies, as well as their frequency and potential mechanisms. A direct causal relationship between inflammatory bowel disease (IBD) and asymptomatic structural brain changes has not been demonstrated, but several possible explanations, including vasculitis, thromboembolism and malnutrition, have been proposed. IBD is associated with a tendency for thromboembolisms; therefore, cerebrovascular thromboembolism represents the most frequent and grave CNS complication. Vasculitis, demyelinating conditions and CNS infections are among the other CNS manifestations of the disease. Biological agents also represent a risk factor, particularly for demyelination. Identification of the nature and potential mechanisms of brain lesions detectable on imaging studies would shed further light on the disease process and could improve patient care through early diagnosis and treatment.
Key words: Inflammatory bowel disease; Ulcerative colitis; Crohn’s disease; Structural lesions; Magnetic resonance imaging; Brain lesions
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Central nervous system complications or manifestations of inflammatory bowel disease deserve particular attention because symptomatic conditions can require early diagnosis and treatment, whereas unexplained manifestations might be linked to pathogenic mechanisms. This review focuses on both symptomatic and asymptomatic brain lesions detectable on imaging studies, as well as their frequency and potential mechanisms. A direct causal relationship between inflammatory bowel disease and asymptomatic structural brain changes has not been demonstrated, but several possible explanations, including vasculitis, thromboembolism and malnutrition, have been proposed. Identification of the nature and potential mechanisms of
Can Dolapcioglu, Hatice Dolapcioglu
Can Dolapcioglu, Department of Gastroenterology, Dr. Lutfi Kirdar Kartal Research and Training Hospital, 34890 Istanbul, Turkey
Hatice Dolapcioglu, Department of Pathology, Fatih Sultan Mehmet Research and Training Hospital, 34752 Istanbul, Turkey
Author contributions: Both authors contributed to the conception and design of this work, to the acquisition and interpretation of the data, and to the drafting/writing of the manuscript.
Conflictofinterest statement: The authors do not report any conflict of interest regarding this manuscript.
OpenAccess: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Correspondence to: Dr. Can Dolapcioglu, Department of Gastroenterology, Dr. Lutfi Kirdar Kartal Research and Training Hospital, Şemsi Denizer Cad. E-5 Karayolu Cevizli Mevkii Kartal, 34890 Istanbul, Turkey. [email protected] Telephone: +90-532-2613919Fax: +90-216-4188752
Received: April 20, 2015 Peerreview started: April 21, 2015First decision: May 18, 2015Revised: July 7, 2015Accepted: August 30, 2015 Article in press: September 7, 2015Published online: November 15, 2015
AbstractCentral nervous system (CNS) complications or manifestations of inflammatory bowel disease deserve particular attention because symptomatic conditions can require
124 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
World J Gastrointest Pathophysiol 2015 November 15; 6(4): 124-130ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i4.124
TOPIC HIGHLIGHT
Structural brain lesions in inflammatory bowel disease2015 Advances in Inflammatory Bowel Disease

brain lesions on imaging studies would improve patient care through early diagnosis and treatment.
Dolapcioglu C, Dolapcioglu H. Structural brain lesions in inflammatory bowel disease. World J Gastrointest Pathophysiol 2015; 6(4): 124-130 Available from: URL: http://www.wjgnet.com/2150-5330/full/v6/i4/124.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i4.124
INTRODUCTIONInflammatory bowel diseases (IBDs), namely ulcerative colitis (UC) and Crohn’s disease (CD), are chronic, debilitating conditions with their onset at relatively young ages. CD is a transmural disease of gastrointestinal mucosa, and it has the potential to affect the entire gastrointestinal tract; in contrast, UC is not a transmural disease, and it affects the colon[1,2]. Both have relapsing and remitting courses. It is estimated that the total (UC plus CD) prevalence of IBD is approximately 0.4% in the Western populations[3].
Because IBD can involve body parts other than the gastrointestinal tract, it can be regarded as a systemic disease. Involvement of the skin, eyes, joints, liver, biliary tract, kidneys, and bone, as well as hematological, and neurological involvement, can occur, preceding, accompanying or following gastrointestinal symptoms. These extraintestinal manifestations are more common in CD patients, although a substantial number of IBD patients can develop these conditions[4-6].
Neurological manifestations are relatively rare but are of clinical importance, particularly in terms of the need for timely diagnosis and management. Several mechanisms, including thromboembolisms, immunologic abnormalities, drug side effects, malabsorption, and infections, have been suggested as pathogeneses[7]. Most central neurological manifestations of IBD can be detected by brain imaging studies because they cause structural alterations of neural structures to some extent. However, lesions of unknown clinical relevance have also been detected in these patients, with significantly higher prevalence than in the normal population.
This review focuses in particular on structural brain lesions with positive findings on imaging studies, includ-ing symptomatic conditions and asymptomatic situations with brain lesions as well (Table 1).
AsympTOmATIC sTRUCTURAl ChANges ON mAgNeTIC ResONANCe ImAgINgTo date, a small number of studies have examined the presence of white matter lesions and other structural alterations on imaging studies in patients with IBD. These lesions were asymptomatic with potential associations with IBD, and whether these structural changes re-
present a unique extraintestinal manifestation of the disease remains unclear. Figure 1 depicts white matter and gray matter (GM) on an magnetic resonance imaging (MRI) scan.
Initial reports examining the associations between IBD and asymptomatic brain lesions were conflicting[8,9]. In a study by Geissler et al[8], 72 patients with IBD (48 cases of CD and 24 of UC) and 50 healthy age-matched controls underwent magnetic resonance imaging with gadolinium-enhanced studies. In that series, hyper-intense focal white-matter lesions of 2-8 mm in diameter were found in 42% and 46% of patients with CD and UC, respectively, whereas such lesions were only present in 16% of healthy controls, resulting in relative risks of 2.6 for CD (95%CI: 1.3-5.3) and 2.9 for UC (95%CI: 1.3-6.2). A longer duration of disease and older age were associated with an increased tendency for the lesions, and none of the patients had neurological symptoms. In contrast to the study by Geissler et al[8], Hart et al[9] did not find a significantly increased frequency of asymptomatic brain white matter lesions on the MRIs of IBD patients (n = 40), compared to a control group consisting of 40 age- and sex-matched patients admitted for tension-type headache (12.5% vs 5%, p = 0.43). Although the relatively small sample size of the latter study might have prevented the differences from attaining statistical significance, the authors emphasized that such asymptomatic lesions had previously been reported consistently in healthy subjects[10], and they expressed concerns about the clinical relevance of these findings for patients with IBD. However, it should be emphasized that both reports dated from two decades ago. In contrast, a recent study with a relatively small sample size also could not find an increased rate of white matter lesions among patients with IBD, compared to healthy controls[11]. In that study, the frequencies of white matter lesions and other brainstem parenchymal lesions were similar, but among the subjects with white matter lesions, the number of lesions was significantly higher in IBD patients.
Two recent studies compared the frequency of white matter lesions between IBD patients and normal subjects using advanced magnetic resonance imaging techniques and equipment[12,13]. Chen et al[12] found a very high prevalence of hyperintense white matter lesions in patients with CD, compared to age-matched controls (75% vs 34%, p < 0.001). Their study had a relatively large sample size (54 Crohn’s patients and 100 age-matched controls). Similarly, Zikou et al[13] found a significantly increased frequency of white matter lesions among patients with IBD (Crohn’s and UC), compared to controls (66% vs 45%, p < 0.05). Both studies used fluid-attenuated inversion recovery images to evaluate white matter hyperintensities.
The development of advanced MRI techniques has allowed for better examination of brain structures, including estimation of volume differences and the evaluation of microstructural integrity. Voxel-based mor-phometry is a technique used to compare the regional
125 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Dolapcioglu C et al . Structural brain lesions in IBD

brain volumes of subjects, and it uses MRI data. Several studies using this technique have found a decreased GM volume among IBD patients, compared to controls. Agostini et al[14], in a study of CD patients, found decreased GM volume in parts of the frontal gyrus and in the anterior midcingulate cortex. In addition, negative correlations between disease duration and GM volume in several brain regions were found in the former study. In contrast, a recent study by the same lead author did not identify any decrease in GM volume in UC patients, compared to controls[15]. Zikou et al[13], however, found more diffuse GM volume decreases in a sample of IBD patients, consisting of subjects with CD and UC, involving the right and left fusiform gyri, the right and left temporal inferior gyri, the right precentral gyrus, the right superior motor area, the right middle frontal gyrus and the left superior parietal gyrus.
Diffusion tensor imaging (DTI) is an MRI technique that measures molecular diffusion. It is valuable for the identification of axonal injury and can be useful in differentiating between primary and Wallerian dege-neration[16]. To date, only a single study has examined the brains of IBD patients using DTI techniques and compared them with age-matched healthy controls[13]. That study found decreased white matter axial diffusivity in the right corticospinal tract and the right superior longitudinal fasciculus in IBD patients (Crohn’s and UC) compared to controls, indicating a possible degree of change in neural structures[17-21].
Several possible explanations have been proposed for the increased prevalence of white matter lesions, the decreased GM volume, and the decreased diffusivity in major tracks among patients with IBD. White matterlesions on brain MRI examinations have been associated with many conditions, including migraine headaches,hypertension, diabetes, celiac disease, and cerebro-vascular disease, as well as being found in healthy subjects[10,22-26]. The increased frequency of white matter hyperintensities in IBD patients might be due to central nervous system (CNS) vasculitis, likely secondary to coagulation and vessel obstruction[13]. IBD is known to be associated with thromboembolism and hyper-
coagulability[27-29]. Another possible explanation is malab-sorption because such lesions were previously described in celiac disease[26].
One explanation for decreased GM volume might be excito-toxicity due to chronic pain, which can result in neural atrophy or loss[14,30]. Structural changes of varying types have been observed in pain-related brain regions in other chronic pain syndromes[31-36], with GM decreases in the frontal and cingulate cortices being the most common anomalies[30]. Another possible mechanism might be increased inflammatory cytokines, resulting in astrocyte and oligodendrocyte apoptosis, decreased neurogenesis, and increased oxidative stress, thus leading to GM volume loss[37,38]. Similarly, cerebral small vessel vasculitis and the neurotoxic effects of cytokines could be responsible for the decreased axial diffusivity in major tracts[13].
Although a direct causal relationship between IBD and asymptomatic structural brain changes cannot be established, the available findings and their implications deserve further investigation, particularly in the context of the brain functional changes observed in patients with IBD[39].
CeRebROvAsCUlAR lesIONsPatients with IBD have an increased tendency for thrombotic events so that IBD could be considered a prothrombotic condition that increases the risk of cerebral arterial and venous thrombosis[40-44]. A recent meta-analysis found a modestly increased risk of cerebrovascular accidents among patients with IBD (OR = 1.18)[45]. The increased risk was more prominent among female patients and young patients. Venous thrombosis has also been seen in these patients with remarkable frequency[44,46-49]. Cerebrovascular events have been documented in up to 4% of IBD patients[50]. These cases are of particular clinical importance when the consequences of these conditions and the young age of the patient population are considered.
A number of pathological conditions have been linked to IBD in attempts to propose a mechanism for the increased tendency for thromboembolic events, including abnormalities of platelets and coagulation factors, genetic mutations, vitamin B6 deficiency due to hypercatabolism and malabsorption, antiphospholipid antibodies, hyperhomocystinemia, dehydration, and immobilization[4,7,40,49,51-58]. However, to date, the exact mechanism has not been fully understood.
126 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Table 1 Structural brain lesions
Asymptomatic structural changesSymptomatic structural changes Cerebrovascular lesions Demyelinating conditions Cerebral vasculitis CNS infections
Grey matterCorpus callosum
White matter
Ventricle
Figure 1 T1-weighted magnetic resonance image of a coronal section through the brain. Gray matter and white matter are indicated, as well as the ventricles.
Dolapcioglu C et al . Structural brain lesions in IBD
CNS: Central nervous system.

127 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
defects, mental impairment, confusion and personality changes, followed by motor weakness[57]. MRI is helpful in the diagnosis, showing white matter lesions with typical T1 and T2 signals[86]. Diagnosis can be confirmed by polymerase chain reaction for JCV DNA. Despite treatment, PML has a high mortality rate of 60%[87]. In addition, development/exacerbation of MS or demye-lination has been reported in association with anti-TNF-alpha therapy[88-90].
CeRebRAl vAsCUlITIsCerebral vasculitis has been reported in patients with UC in a number of studies[91-96]. In addition, a case of cerebral vasculitis was reported in association with CD[97]. Mostly immune-mediated mechanisms have been proposed for the development of vasculitis in UC. Magnetic re-sonance imaging is abnormal and shows hyperintense lesions[95,96], and magnetic resonance angiography can aid in diagnosis[97]. CNS vasculitis has also been reported in association with anti-TNF therapy[57]. The major symptoms of cerebral vasculitis are stroke, headache and encephalopathy. Other symptoms include seizures, cranial nerve palsies or myelopathies[98]. Cerebral vasculitis mimicking migraine with aura was reported in a case of CD, and the authors stated that migraine with aura can be the only finding in cerebral vasculitis[99]. Cerebral vasculitis resulting in stroke has been rarely reported in UC[61]. Cerebral vasculitis presented with right paresis and unbalanced gait in a 35-year-old woman with UC[93]. Another UC case was complicated by convulsions and was diagnosed as cerebral vasculitis on magnetic resonance imaging[96].
CNs INfeCTIONsAnti-TNF agents can suppress the immune system to such an extent that opportunistic infections develop, including of the CNS, in IBD patients. These patients present with meningeal signs, seizures, symptoms resembling stroke, and encephalopathy[100]; abnormal MRI findings and/or mass lesions are found on imaging studies. Among these opportunistic infections are fungal infections, cerebral tuberculosis, Epstein-Barr virus infection, nocardiosis, toxoplasmosis, herpes simplex virus infection, meningococcal infection, Campylobacter fetus infections, and listeria infections[57]. In a severe case of CD with ileocecal involvement, opportunistic meningitis with varicella zoster was reported after adalimumab and prednisone treatment[101]. In a patient with CD, meningococcal meningoencephalitis was reported after certolizumab pegol treatment[102].
RefeReNCes1 Baumgart DC, Sandborn WJ. Inflammatory bowel disease:
clinical aspects and established and evolving therapies. Lancet 2007; 369: 1641-1657 [PMID: 17499606 DOI: 10.1016/S0140-6736(07)60751-X]
2 Baumgart DC, Carding SR. Inflammatory bowel disease: cause
Cerebral arterial thromboembolism can present with headache, paresis, seizures or dysphagia, and it can result in high mortality and morbidity[51]. Large infarcts involving both the anterior and posterior circulation and lacunar infarcts have been reported in IBD[59-63]. In addition, UC has been associated with thrombotic thrombocytopenic purpura and small and large cerebral artery thrombosis risks[64-66]. Infarcts associated with IBD can be identified on computerized tomography and magnetic resonance imaging.
Cerebral venous thrombosis and sinus thrombosis seem to be more frequent in patients with UC than in CD patients[67]. Most often, the superior sagittal sinus and lateral sinuses are involved; however, thrombosis of the cortical venous sinuses has also been reported[68]. Young and male patients seem to be at greater risk[50,69,70]. The most common presenting symptom is headache, usually followed by neurological impairment, and cerebral infarction can develop due to extension of thrombus[71]. A combination of magnetic resonance imaging and magnetic resonance venography could identify venous occlusion[71]. The radiological characteristics, as well as the clinical course and prognosis of IBD-related cerebral venous thrombosis, seem to be similar to those in cases not related to IBD[44,72,73].
DemyelINATINg CONDITIONsDemyelinating conditions have been reported in the setting of IBD, in association or not with biological treatments.
Multiple sclerosis (MS) or MS-like conditions have long been reported in patients with IBD[74-77]. Such a relationship was first reported by Rang et al[74]. A retrospective study found an increased incidence of demyelinating disease among patients with IBD, parti-cularly in UC[77]. Nevertheless, MS has been reported in both UC and CD[78,79]. The findings of a recent meta-analysis supported a relationship between MS and IBD[80]. Both the development of an MS-like syndrome in the setting of IBD and the development of IBD in MS patients have been reported[81-83]. Because the diagnostic criteria for MS have evolved over time, some lesions found in previous studies might not actually be MS; rather, they could represent an MS-like syndrome, which might potentially be linked to IBD. The mechanism of these relationships has not been fully explained, but a role for impairments in functional T-cell subsets has been proposed[4,57].
Anti-tumor necrosis factor (TNF)-alpha drugs and anti-alpha4 integrin drugs (such as natalizumab), which are biological agents used in the treatment of IBD, can have adverse neurological effects[84,85]. Progressive multifocal leukoencephalopathy is the gravest compli-cation, particularly when associated with natalizumab therapy, although few cases have been reported in association with TNF-alpha drugs[85]. Reactivation of John Cunningham virus (JCV) is responsible for the development of PML, and it is associated with visual
Dolapcioglu C et al . Structural brain lesions in IBD

128 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
and immunobiology. Lancet 2007; 369: 1627-1640 [PMID: 17499605 DOI: 10.1016/S0140-6736(07)60750-8]
3 Watts DA, Satsangi J. The genetic jigsaw of inflammatory bowel disease. Gut 2002; 50 Suppl 3: III31-III36 [PMID: 11953330]
4 Morís G. Inflammatory bowel disease: an increased risk factor for neurologic complications. World J Gastroenterol 2014; 20: 1228-1237 [PMID: 24574797 DOI: 10.3748/wjg.v20.i5.1228]
5 Veloso FT. Extraintestinal manifestations of inflammatory bowel disease: do they influence treatment and outcome? World J Gastroenterol 2011; 17: 2702-2707 [PMID: 21734777 DOI: 10.3748/wjg.v17.i22.2702]
6 Bernstein CN, Blanchard JF, Rawsthorne P, Yu N. The prevalence of extraintestinal diseases in inflammatory bowel disease: a population-based study. Am J Gastroenterol 2001; 96: 1116-1122 [PMID: 11316157 DOI: 10.1111/j.1572-0241.2001.03756.x]
7 Zois CD, Katsanos KH, Kosmidou M, Tsianos EV. Neurologic manifestations in inflammatory bowel diseases: current knowledge and novel insights. J Crohns Colitis 2010; 4: 115-124 [PMID: 21122494]
8 Geissler A, Andus T, Roth M, Kullmann F, Caesar I, Held P, Gross V, Feuerbach S, Schölmerich J. Focal white-matter lesions in brain of patients with inflammatory bowel disease. Lancet 1995; 345: 897-898 [PMID: 7707814]
9 Hart PE, Gould SR, MacSweeney JE, Clifton A, Schon F. Brain white-matter lesions in inflammatory bowel disease. Lancet 1998; 351: 1558 [PMID: 10326545]
10 Horikoshi T, Yagi S, Fukamachi A. Incidental high-intensity foci in white matter on T2-weighted magnetic resonance imaging. Frequency and clinical significance in symptom-free adults. Neuroradiology 1993; 35: 151-155 [PMID: 8433794]
11 Dolapcioglu C, Guleryuzlu Y, Uygur-Bayramicli O, Ahishali E, Dabak R. Asymptomatic brain lesions on cranial magnetic resonance imaging in inflammatory bowel disease. Gut Liver 2013; 7: 169-174 [PMID: 23560152 DOI: 10.5009/gnl.2013.7.2.169]
12 Chen M, Lee G, Kwong LN, Lamont S, Chaves C. Cerebral white matter lesions in patients with Crohn’s disease. J Neuroimaging 2012; 22: 38-41 [PMID: 21091817 DOI: 10.1111/j.1552-6569.2010.00538.x]
13 Zikou AK, Kosmidou M, Astrakas LG, Tzarouchi LC, Tsianos E, Argyropoulou MI. Brain involvement in patients with inflammatory bowel disease: a voxel-based morphometry and diffusion tensor imaging study. Eur Radiol 2014; 24: 2499-2506 [PMID: 25001084 DOI: 10.1007/s00330-014-3242-6]
14 Agostini A, Benuzzi F, Filippini N, Bertani A, Scarcelli A, Farinelli V, Marchetta C, Calabrese C, Rizzello F, Gionchetti P, Ercolani M, Campieri M, Nichelli P. New insights into the brain involvement in patients with Crohn’s disease: a voxel-based morphometry study. Neurogastroenterol Motil 2013; 25: 147-e82 [PMID: 22998431 DOI: 10.1111/nmo.12017]
15 Agostini A, Campieri M, Bertani A, Scarcelli A, Ballotta D, Calabrese C, Rizzello F, Gionchetti P, Nichelli P, Benuzzi F. Absence of change in the gray matter volume of patients with ulcerative colitis in remission: a voxel based morphometry study. Biopsychosoc Med 2015; 9: 1 [PMID: 25614759 DOI: 10.1186/s13030-014-0028-7]
16 Pierpaoli C, Barnett A, Pajevic S, Chen R, Penix LR, Virta A, Basser P. Water diffusion changes in Wallerian degeneration and their dependence on white matter architecture. Neuroimage 2001; 13: 1174-1185 [PMID: 11352623 DOI: 10.1006/nimg.2001.0765]
17 Beaulieu C. The basis of anisotropic water diffusion in the nervous system - a technical review. NMR Biomed 2002; 15: 435-455 [PMID: 12489094 DOI: 10.1002/nbm.782]
18 Zivadinov R, Shucard JL, Hussein S, Durfee J, Cox JL, Bergsland N, Dwyer MG, Benedict RH, Ambrus J, Shucard DW. Multimodal imaging in systemic lupus erythematosus patients with diffuse neuropsychiatric involvement. Lupus 2013; 22: 675-683 [PMID: 23640981 DOI: 10.1177/0961203313486193]
19 Pievani M, Paternicò D, Benussi L, Binetti G, Orlandini A, Cobelli M, Magnaldi S, Ghidoni R, Frisoni GB. Pattern of structural and functional brain abnormalities in asymptomatic granulin mutation
carriers. Alzheimers Dement 2014; 10: S354-S363.e1 [PMID: 24418059 DOI: 10.1016/j.jalz.2013.09.009]
20 Padilla N, Junqué C, Figueras F, Sanz-Cortes M, Bargalló N, Arranz A, Donaire A, Figueras J, Gratacos E. Differential vulnerability of gray matter and white matter to intrauterine growth restriction in preterm infants at 12 months corrected age. Brain Res 2014; 1545: 1-11 [PMID: 24361462 DOI: 10.1016/j.brainres.2013.12.007]
21 Adamson C, Yuan W, Babcock L, Leach JL, Seal ML, Holland SK, Wade SL. Diffusion tensor imaging detects white matter abnormalities and associated cognitive deficits in chronic adolescent TBI. Brain Inj 2013; 27: 454-463 [PMID: 23472581 DOI: 10.3109/02699052.2012.750756]
22 Bryan RN, Manolio TA, Schertz LD, Jungreis C, Poirier VC, Elster AD, Kronmal RA. A method for using MR to evaluate the effects of cardiovascular disease on the brain: the cardiovascular health study. AJNR Am J Neuroradiol 1994; 15: 1625-1633 [PMID: 7847205]
23 Meguro K, Yamaguchi T, Hishinuma T, Miyazawa H, Ono S, Yamada K, Matsuzawa T. Periventricular hyperintensity on magnetic resonance imaging correlated with brain ageing and atrophy. Neuroradiology 1993; 35: 125-129 [PMID: 8433787]
24 Swartz RH, Kern RZ. Migraine is associated with magnetic resonance imaging white matter abnormalities: a meta-analysis. Arch Neurol 2004; 61: 1366-1368 [PMID: 15364681 DOI: 10.1001/archneur.61.9.1366]
25 Pavese N, Canapicchi R, Nuti A, Bibbiani F, Lucetti C, Collavoli P, Bonuccelli U. White matter MRI hyperintensities in a hundred and twenty-nine consecutive migraine patients. Cephalalgia 1994; 14: 342-345 [PMID: 7828192]
26 Kieslich M, Errázuriz G, Posselt HG, Moeller-Hartmann W, Zanella F, Boehles H. Brain white-matter lesions in celiac disease: a prospective study of 75 diet-treated patients. Pediatrics 2001; 108: E21 [PMID: 11483831]
27 Novacek G, Miehsler W, Kapiotis S, Katzenschlager R, Speiser W, Vogelsang H. Thromboembolism and resistance to activated protein C in patients with inflammatory bowel disease. Am J Gastroenterol 1999; 94: 685-690 [PMID: 10086652 DOI: 10.1111/j.1572-0241.1999.00937.x]
28 Lam A, Borda IT, Inwood MJ, Thomson S. Coagulation studies in ulcerative colitis and Crohn’s disease. Gastroenterology 1975; 68: 245-251 [PMID: 1116673]
29 Twig G, Zandman-Goddard G, Szyper-Kravitz M, Shoenfeld Y. Systemic thromboembolism in inflammatory bowel disease: mechanisms and clinical applications. Ann N Y Acad Sci 2005; 1051: 166-173 [PMID: 16126956 DOI: 10.1196/annals.1361.058]
30 May A. Chronic pain may change the structure of the brain. Pain 2008; 137: 7-15 [PMID: 18410991 DOI: 10.1016/j.pain.2008.02.034]
31 Kuchinad A, Schweinhardt P, Seminowicz DA, Wood PB, Chizh BA, Bushnell MC. Accelerated brain gray matter loss in fibromyalgia patients: premature aging of the brain? J Neurosci 2007; 27: 4004-4007 [PMID: 17428976 DOI: 10.1523/JNEUROSCI.0098-07.2007]
32 Apkarian AV, Sosa Y, Sonty S, Levy RM, Harden RN, Parrish TB, Gitelman DR. Chronic back pain is associated with decreased prefrontal and thalamic gray matter density. J Neurosci 2004; 24: 10410-10415 [PMID: 15548656 DOI: 10.1523/JNEUROSCI.2541-04.2004]
33 Schmidt-Wilcke T, Leinisch E, Straube A, Kämpfe N, Draganski B, Diener HC, Bogdahn U, May A. Gray matter decrease in patients with chronic tension type headache. Neurology 2005; 65: 1483-1486 [PMID: 16275843 DOI: 10.1212/01.wnl.0000183067.94400.80]
34 Blankstein U, Chen J, Diamant NE, Davis KD. Altered brain structure in irritable bowel syndrome: potential contributions of pre-existing and disease-driven factors. Gastroenterology 2010; 138: 1783-1789 [PMID: 20045701 DOI: 10.1053/j.gastro.2009.12.043]
35 Seminowicz DA, Labus JS, Bueller JA, Tillisch K, Naliboff BD, Bushnell MC, Mayer EA. Regional gray matter density changes in brains of patients with irritable bowel syndrome. Gastroenterology 2010; 139: 48-57.e2 [PMID: 20347816 DOI: 10.1053/j.gastro.2010.03.049]
Dolapcioglu C et al . Structural brain lesions in IBD

129 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
36 Schweinhardt P, Kuchinad A, Pukall CF, Bushnell MC. Increased gray matter density in young women with chronic vulvar pain. Pain 2008; 140: 411-419 [PMID: 18930351 DOI: 10.1016/j.pain.2008.09.014]
37 Miller AH, Maletic V, Raison CL. Inflammation and its dis-contents: the role of cytokines in the pathophysiology of major depression. Biol Psychiatry 2009; 65: 732-741 [PMID: 19150053 DOI: 10.1016/j.biopsych.2008.11.029]
38 Buntinx M, Moreels M, Vandenabeele F, Lambrichts I, Raus J, Steels P, Stinissen P, Ameloot M. Cytokine-induced cell death in human oligodendroglial cell lines: I. Synergistic effects of IFN-gamma and TNF-alpha on apoptosis. J Neurosci Res 2004; 76: 834-845 [PMID: 15160395 DOI: 10.1002/jnr.20118]
39 Agostini A, Filippini N, Cevolani D, Agati R, Leoni C, Tambasco R, Calabrese C, Rizzello F, Gionchetti P, Ercolani M, Leonardi M, Campieri M. Brain functional changes in patients with ulcerative colitis: a functional magnetic resonance imaging study on emotional processing. Inflamm Bowel Dis 2011; 17: 1769-1777 [PMID: 21744432 DOI: 10.1002/ibd.21549]
40 Canero A, Parmeggiani D, Avenia N, Atelli PF, Goffredi L, Peltrini R, Madonna I, Ambrosino P, Apperti S, Apperti M. Thromboembolic tendency (TE) in IBD (Inflammatory bowel disease) patients. Ann Ital Chir 2012; 83: 313-317 [PMID: 22759469]
41 Kappelman MD, Horvath-Puho E, Sandler RS, Rubin DT, Ullman TA, Pedersen L, Baron JA, Sørensen HT. Thromboembolic risk among Danish children and adults with inflammatory bowel diseases: a population-based nationwide study. Gut 2011; 60: 937-943 [PMID: 21339206 DOI: 10.1136/gut.2010.228585]
42 Barclay AR, Keightley JM, Horrocks I, Garrick V, McGrogan P, Russell RK. Cerebral thromboembolic events in pediatric patients with inflammatory bowel disease. Inflamm Bowel Dis 2010; 16: 677-683 [PMID: 19824070 DOI: 10.1002/ibd.21113]
43 Benavente L, Morís G. Neurologic disorders associated with inflammatory bowel disease. Eur J Neurol 2011; 18: 138-143 [PMID: 20500801 DOI: 10.1111/j.1468-1331.2010.03095.x]
44 Cognat E, Crassard I, Denier C, Vahedi K, Bousser MG. Cerebral venous thrombosis in inflammatory bowel diseases: eight cases and literature review. Int J Stroke 2011; 6: 487-492 [PMID: 22017824 DOI: 10.1111/j.1747-4949.2011.00620.x]
45 Singh S, Singh H, Loftus EV, Pardi DS. Risk of cerebrovascular accidents and ischemic heart disease in patients with inflammatory bowel disease: a systematic review and meta-analysis. Clin Gastroenterol Hepatol 2014; 12: 382-93.e1: quiz e22 [PMID: 23978350 DOI: 10.1016/j.cgh.2013.08.023]
46 Nudelman RJ, Rosen DG, Rouah E, Verstovsek G. Cerebral sinus thrombosis: a fatal neurological complication of ulcerative colitis. Patholog Res Int 2010; 2010: 132754 [PMID: 21152173 DOI: 10.4061/2010/132754]
47 Casella G, Spreafico C, Costantini M, Pagni F, Cortelezzi CC, Baldini V, DeLodovici ML, Bono G. Cerebral sinus thrombosis in ulcerative colitis. Inflamm Bowel Dis 2011; 17: 2214-2216 [PMID: 21351209 DOI: 10.1002/ibd.21659]
48 Katsanos AH, Katsanos KH, Kosmidou M, Giannopoulos S, Kyritsis AP, Tsianos EV. Cerebral sinus venous thrombosis in inflammatory bowel diseases. QJM 2013; 106: 401-413 [PMID: 23243293 DOI: 10.1093/qjmed/hcs229]
49 Ferro JM, Oliveira S. Neurologic manifestations of gastrointestinal and liver diseases. Curr Neurol Neurosci Rep 2014; 14: 487 [PMID: 25171900 DOI: 10.1007/s11910-014-0487-z]
50 Miehsler W, Reinisch W, Valic E, Osterode W, Tillinger W, Feichtenschlager T, Grisar J, Machold K, Scholz S, Vogelsang H, Novacek G. Is inflammatory bowel disease an independent and disease specific risk factor for thromboembolism? Gut 2004; 53: 542-548 [PMID: 15016749]
51 Saibeni S, Spina L, Vecchi M. Exploring the relationships between inflammatory response and coagulation cascade in inflammatory bowel disease. Eur Rev Med Pharmacol Sci 2004; 8: 205-208 [PMID: 15638231]
52 Dolapcioglu C, Soylu A, Kendir T, Ince AT, Dolapcioglu H, Purisa S, Bolukbas C, Sokmen HM, Dalay R, Ovunc O. Coagulation
parameters in inflammatory bowel disease. Int J Clin Exp Med 2014; 7: 1442-1448 [PMID: 24995109]
53 Tsiolakidou G, Koutroubakis IE. Thrombosis and inflammatory bowel disease-the role of genetic risk factors. World J Gastroenterol 2008; 14: 4440-4444 [PMID: 18680221]
54 Chamouard P, Grunebaum L, Wiesel ML, Freyssinet JM, Duclos B, Cazenave JP, Baumann R. Prevalence and significance of anticardiolipin antibodies in Crohn’s disease. Dig Dis Sci 1994; 39: 1501-1504 [PMID: 8026262]
55 Souto JC, Borrell M, Fontcuberta J, Roca M. Antiphospholipid antibodies in inflammatory bowel disease. Dig Dis Sci 1995; 40: 1524-1525 [PMID: 7628277]
56 Saibeni S, Cattaneo M, Vecchi M, Zighetti ML, Lecchi A, Lombardi R, Meucci G, Spina L, de Franchis R. Low vitamin B(6) plasma levels, a risk factor for thrombosis, in inflammatory bowel disease: role of inflammation and correlation with acute phase reactants. Am J Gastroenterol 2003; 98: 112-117 [PMID: 12526945 DOI: 10.1111/j.1572-0241.2003.07160.x]
57 Casella G, Tontini GE, Bassotti G, Pastorelli L, Villanacci V, Spina L, Baldini V, Vecchi M. Neurological disorders and inflammatory bowel diseases. World J Gastroenterol 2014; 20: 8764-8782 [PMID: 25083051 DOI: 10.3748/wjg.v20.i27.8764]
58 Danese S, Papa A, Saibeni S, Repici A, Malesci A, Vecchi M. Inflammation and coagulation in inflammatory bowel disease: The clot thickens. Am J Gastroenterol 2007; 102: 174-186 [PMID: 17100967 DOI: 10.1111/j.1572-0241.2006.00943.x]
59 Lossos A, Stener I. Cerebrovascular disease in inflammatory bowel disease. In: Bogousslavsky J, Kaplan L, editors. Uncommon causes of stroke. Cambridge: Cambridge University Press, 2001: 161-168
60 Keene DL, Matzinger MA, Jacob PJ, Humphreys P. Cerebral vascular events associated with ulcerative colitis in children. Pediatr Neurol 2001; 24: 238-243 [PMID: 11301230]
61 Mayeux R, Fahn S. Strokes and ulcerative colitis. Neurology 1978; 28: 571-574 [PMID: 565888]
62 Schneiderman JH, Sharpe JA, Sutton DM. Cerebral and retinal vascular complications of inflammatory bowel disease. Ann Neurol 1979; 5: 331-337 [PMID: 443768 DOI: 10.1002/ana.410050405]
63 Fukuhara T, Tsuchida S, Kinugasa K, Ohmoto T. A case of pontine lacunar infarction with ulcerative colitis. Clin Neurol Neurosurg 1993; 95: 159-162 [PMID: 8344017]
64 Scheid R, Hegenbart U, Ballaschke O, Von Cramon DY. Major stroke in thrombotic-thrombocytopenic purpura (Moschcowitz syndrome). Cerebrovasc Dis 2004; 18: 83-85 [PMID: 15178993 DOI: 10.1159/000078756]
65 Baron BW, Jeon HR, Glunz C, Peterson A, Cohen R, Hanauer S, Rubin D, Hart J, Baron JM. First two patients with ulcerative colitis who developed classical thrombotic thrombocytopenic purpura successfully treated with medical therapy and plasma exchange. J Clin Apher 2002; 17: 204-206 [PMID: 12494414 DOI: 10.1002/jca.10037]
66 Hisada T, Miyamae Y, Mizuide M, Shibusawa N, Iida T, Masuo T, Okada S, Sagawa T, Ishizuka T, Kusano M, Mori M. Acute thrombocytopenia associated with preexisting ulcerative colitis successfully treated with colectomy. Intern Med 2006; 45: 87-91 [PMID: 16484745]
67 Spina L, Saibeni S, Battaglioli T, Peyvandi F, de Franchis R, Vecchi M. Thrombosis in inflammatory bowel diseases: role of inherited thrombophilia. Am J Gastroenterol 2005; 100: 2036-2041 [PMID: 16128949 DOI: 10.1111/j.1572-0241.2005.42029.x]
68 Saadatnia M, Fatehi F, Basiri K, Mousavi SA, Mehr GK. Cerebral venous sinus thrombosis risk factors. Int J Stroke 2009; 4: 111-123 [PMID: 19383052 DOI: 10.1111/j.1747-4949.2009.00260.x]
69 Diakou M, Kostadima V, Giannopoulos S, Zikou AK, Argyropoulou MI, Kyritsis AP. Cerebral venous thrombosis in an adolescent with ulcerative colitis. Brain Dev 2011; 33: 49-51 [PMID: 20472378]
70 Benjilali L, Aidi S, El Mansouri H, Benabdejlil M, Jiddane M, El Alaoui Faris M. Cerebral thrombosis complicating Crohn’s disease: two cases. J Stroke Cerebrovasc Dis 2011; 20: 565-569 [PMID: 22078296]
71 Stam J. Thrombosis of the cerebral veins and sinuses. N Engl
Dolapcioglu C et al . Structural brain lesions in IBD

130 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
J Med 2005; 352: 1791-1798 [PMID: 15858188 DOI: 10.1056/NEJMra042354]
72 Ferro JM, Canhão P, Stam J, Bousser MG, Barinagarrementeria F. Prognosis of cerebral vein and dural sinus thrombosis: results of the International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT). Stroke 2004; 35: 664-670 [PMID: 14976332 DOI: 10.1161/01.STR.0000117571.76197.26]
73 Rodríguez S, Calleja S, Morís G. Cluster-like headache heralding cerebral venous thrombosis. Cephalalgia 2008; 28: 906-907 [PMID: 18540872 DOI: 10.1111/j.1468-2982.2007.01464.x]
74 Rang EH, Brooke BN, Hermon-Taylor J. Association of ulcerative colitis with multiple sclerosis. Lancet 1982; 2: 555 [PMID: 6125706]
75 Pandian JD, Pawar G, Singh GS, Abraham R. Multiple sclerosis in a patient with chronic ulcerative colitis. Neurol India 2004; 52: 282-283 [PMID: 15269508]
76 Bernstein CN, Wajda A, Blanchard JF. The clustering of other chronic inflammatory diseases in inflammatory bowel disease: a population-based study. Gastroenterology 2005; 129: 827-836 [PMID: 16143122 DOI: 10.1053/j.gastro.2005.06.021]
77 Gupta G, Gelfand JM, Lewis JD. Increased risk for demyelinating diseases in patients with inflammatory bowel disease. Gastroenterology 2005; 129: 819-826 [PMID: 16143121 DOI: 10.1053/j.gastro.2005.06.022]
78 Scheid R, Teich N. Neurologic manifestations of ulcerative colitis. Eur J Neurol 2007; 14: 483-493 [PMID: 17437605]
79 Purrmann J, Arendt G, Cleveland S, Borchard F, Fürst W, Gemsa R, Bertrams J, Hengels KJ. Association of Crohn’s disease and multiple sclerosis. Is there a common background? J Clin Gastroenterol 1992; 14: 43-46 [PMID: 1556407]
80 Dobson R, Giovannoni G. Autoimmune disease in people with multiple sclerosis and their relatives: a systematic review and meta-analysis. J Neurol 2013; 260: 1272-1285 [PMID: 23315260 DOI: 10.1007/s00415-012-6790-1]
81 Buccino GP, Corrente G, Visintini D. Crohn’s disease and multiple sclerosis: a single case report. Ital J Neurol Sci 1994; 15: 303-306 [PMID: 7843946]
82 Kitchin LI, Knobler RL, Friedman LS. Crohn’s disease in a patient with multiple sclerosis. J Clin Gastroenterol 1991; 13: 331-334 [PMID: 2066551]
83 Beaugerie L, Lamy P, Ganne N, Carbonnel F, Le Quintrec Y, Cosnes J, Gendre JP. [Morbid associations in Crohn’s disease. Study of a series of 832 patients]. Presse Med 1997; 26: 892-894 [PMID: 9232057]
84 Deepak P, Stobaugh DJ, Ehrenpreis ED. Infectious complications of TNF-α inhibitor monotherapy versus combination therapy with immunomodulators in inflammatory bowel disease: analysis of the Food and Drug Administration Adverse Event Reporting System. J Gastrointestin Liver Dis 2013; 22: 269-276 [PMID: 24078983]
85 Van Assche G, Van Ranst M, Sciot R, Dubois B, Vermeire S, Noman M, Verbeeck J, Geboes K, Robberecht W, Rutgeerts P. Progressive multifocal leukoencephalopathy after natalizumab therapy for Crohn’s disease. N Engl J Med 2005; 353: 362-368 [PMID: 15947080 DOI: 10.1056/NEJMoa051586]
86 Yousry TA, Major EO, Ryschkewitsch C, Fahle G, Fischer S, Hou J, Curfman B, Miszkiel K, Mueller-Lenke N, Sanchez E, Barkhof F, Radue EW, Jäger HR, Clifford DB. Evaluation of patients treated with natalizumab for progressive multifocal leukoencephalopathy. N Engl J Med 2006; 354: 924-933 [PMID: 16510746 DOI: 10.1056/NEJMoa054693]
87 Singh S, Kumar N, Loftus EV, Kane SV. Neurologic complications in patients with inflammatory bowel disease: increasing relevance in the era of biologics. Inflamm Bowel Dis 2013; 19: 864-872 [PMID: 22552994 DOI: 10.1002/ibd.23011]
88 Lozeron P, Denier C, Lacroix C, Adams D. Long-term course of demyelinating neuropathies occurring during tumor necrosis factor-alpha-blocker therapy. Arch Neurol 2009; 66: 490-497 [PMID: 19364934 DOI: 10.1001/archneurol.2009.11]
89 Pfueller CF, Seipelt E, Zipp F, Paul F. Multiple sclerosis following etanercept treatment for ankylosing spondylitis. Scand J Rheumatol 2008; 37: 397-399 [PMID: 18720264 DOI: 10.1080/03009740802136164]
90 Lees CW, Ali AI, Thompson AI, Ho GT, Forsythe RO, Marquez L, Cochrane CJ, Aitken S, Fennell J, Rogers P, Shand AG, Penman ID, Palmer KR, Wilson DC, Arnott ID, Satsangi J. The safety profile of anti-tumour necrosis factor therapy in inflammatory bowel disease in clinical practice: analysis of 620 patient-years follow-up. Aliment Pharmacol Ther 2009; 29: 286-297 [PMID: 19132970 DOI: 10.1111/j.1365-2036.2008.03882.x]
91 Nelson J, Barron MM, Riggs JE, Gutmann L, Schochet SS. Cerebral vasculitis and ulcerative colitis. Neurology 1986; 36: 719-721 [PMID: 3703273]
92 Carmona MA, Jaume Anselmi F, Ramírez Rivera J. Cerebral thrombosis and vasculitis: an uncommon complication of ulcerative colitis. Bol Asoc Med P R 2000; 92: 9-11 [PMID: 10846281]
93 Pandian JD, Henderson RD, O’Sullivan JD, Rajah T. Cerebral vasculitis in ulcerative colitis. Arch Neurol 2006; 63: 780 [PMID: 16682552 DOI: 10.1001/archneur.63.5.780]
94 Friol-Vercelletto M, Mussini JM, Bricout JH, Magne C. [Ulcero-hemorrhagic rectocolitis. Possible manifestation, angiitis of the central nervous system]. Presse Med 1984; 13: 1218 [PMID: 6232576]
95 Druschky A, Heckmann JG, Druschky K, Huk WJ, Erbguth F, Neundörfer B. Severe neurological complications of ulcerative colitis. J Clin Neurosci 2002; 9: 84-86 [PMID: 11749027 DOI: 10.1054/jocn.2001.0972]
96 Masaki T, Muto T, Shinozaki M, Kuroda T. Unusual cerebral complication associated with ulcerative colitis. J Gastroenterol 1997; 32: 251-254 [PMID: 9085177]
97 Schluter A, Krasnianski M, Krivokuca M, Spielmann RP, Neudecker S, Hirsch W. Magnetic resonance angiography in a patient with Crohn’s disease associated cerebral vasculitis. Clin Neurol Neurosurg 2004; 106: 110-113 [PMID: 15003300 DOI: 10.1016/j.clineuro.2003.09.004]
98 Berlit P. Diagnosis and treatment of cerebral vasculitis. Ther Adv Neurol Disord 2010; 3: 29-42 [PMID: 21180634 DOI: 10.1177/1756285609347123]
99 Holzer K, Esposito L, Stimmer H, Hemmer B, Poppert H. Cerebral vasculitis mimicking migraine with aura in a patient with Crohn’s disease. Acta Neurol Belg 2009; 109: 44-48 [PMID: 19402574]
100 Viget N, Vernier-Massouille G, Salmon-Ceron D, Yazdanpanah Y, Colombel JF. Opportunistic infections in patients with inflammatory bowel disease: prevention and diagnosis. Gut 2008; 57: 549-558 [PMID: 18178610 DOI: 10.1136/gut.2006.114660]
101 Ma C, Walters B, Fedorak RN. Varicella zoster meningitis complicating combined anti-tumor necrosis factor and corticosteroid therapy in Crohn’s disease. World J Gastroenterol 2013; 19: 3347-3351 [PMID: 23745038 DOI: 10.3748/wjg.v19.i21.3347]
102 Majumder S, Kumar A. Meningococcal meningoencephalitis after certolizumab pegol treatment in a patient with Crohn’s disease. J Crohns Colitis 2013; 7: e19 [PMID: 22742971]
P- Reviewer: Lakatos PL, Swaminath A S- Editor: Ma YJ L- Editor: A E- Editor: Liu SQ
Dolapcioglu C et al . Structural brain lesions in IBD

Run Yu, Yun Zheng, Matthew B Lucas, Yun-Guang Tong
Run Yu, Carcinoid and Neuroendocrine Tumor Center, Cedars-Sinai Medical Center, Los Angeles, CA 90048, United States
Yun Zheng, Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangzhou 510060, Guangdong Province, China
Matthew B Lucas, Princeton University, Princeton, NJ 08544, United States
Yun-Guang Tong, Department of Medicine, Cedars-Sinai Medical Center, UCLA School of Medicine, Los Angeles, CA 90048, United States
Yun-Guang Tong, Department of Pathology, Xinxiang Medical University, Xinxiang 453003, Henan Province, China
Author contributions: All authors contributed to this paper.
Supported by National Cancer Institute of the National Institutes of Health, No. R00CA138914 (YT); and by National Natural Science Foundation, No. 81372216 (YT).
Conflict-of-interest statement: The authors have no conflicts of interest to disclose. Dr. Yunguang Tong is supported by the National Cancer Institute of the National Institutes of Health under award number R00CA138914 (YT) and National Natural Science Foundation under grant number 81372216 (YT). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Correspondence to: Run Yu, MD, PhD, Carcinoid and Neuroendocrine Tumor Center, Cedars-Sinai Medical Center, 8700 Beverly Blvd, B-131, Los Angeles, CA 90048, United States. [email protected]
Telephone: +1-310-4234774Fax: +1-310-4230440
Received: April 1, 2015 Peer-review started: April 2, 2015 First decision: June 18, 2015Revised: July 3, 2015 Accepted: July 24, 2015Article in press: July 27, 2015Published online: November 15, 2015
AbstractTumors and cancers of the gastrointestinal tract and pancreas are commonly derived from precursor lesions so that understanding the physiological, cellular, and molecular mechanisms underlying the pathogenesis of precursor lesions is critical for the prevention and treatment of those neoplasms. Pancreatic neuro-endocrine tumors (PNETs) can also be derived from precursor lesions. Pancreatic α cell hyperplasia (ACH), a specific and overwhelming increase in the number of α cells, is a precursor lesion leading to PNET pathogenesis. One of the 3 subtypes of ACH, reactive ACH is caused by glucagon signaling disruption and invariably evolves into PNETs. In this article, the existing work on the mechanisms underlying reactive ACH pathogenesis is reviewed. It is clear that the liver secretes a humoral factor regulating α cell numbers but the identity of the liver factor remains elusive. Potential approaches to identify the liver factor are discussed.
Key words: Pancreatic α cell hyperplasia; Humoral factor; Pancreatic neuroendocrine tumors; Digestive system hormone; Liver
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Tumors and cancers of the gastrointestinal tract and pancreas are commonly derived from precursor
REVIEW
131 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Elusive liver factor that causes pancreatic α cell hyperplasia: A review of literature
World J Gastrointest Pathophysiol 2015 November 15; 6(4): 131-139ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i4.131

lesions. One of the precursor lesions, reactive pancreatic α cell hyperplasia is caused by glucagon signaling disruption and invariably evolves into pancreatic neuroendocrine tumors. In this article, the existing work on the mechanisms underlying the novel precursor lesion is reviewed. It is clear that the liver secretes a humoral factor regulating pancreatic α cell numbers but the identity of the liver factor remains elusive. Potential approaches to identify the liver factor are discussed.
Yu R, Zheng Y, Lucas MB, Tong YG. Elusive liver factor that causes pancreatic α cell hyperplasia: A review of literature. World J Gastrointest Pathophysiol 2015; 6(4): 131-139 Available from: URL: http://www.wjgnet.com/2150-5330/full/v6/i4/131.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i4.131
INTRODUCTION Tumors and cancers of the gastrointestinal tract and pancreas are commonly derived from precursor lesions[1-3]. For example, colon cancer is derived from polypoid or non-polypoid pre-neoplastic lesions in the colon, and pancreatic ductal carcinoma from pancreatic intraepithelial neoplasia. Neuroendocrine tumors in the gastrointestinal tract and pancreas (GEP-NETs) are relatively rare and indolent tumors with variable biological behaviors[4-6]. GEP-NETs can also be derived from precursor lesions[7-9]. In atrophic gastritis, hypergastrinemia drives entero-chromaffin-like cell hyperplasia, which in turn can give rise to gastric carcinoids[7,10]. In ulcerative colitis, microscopic neuroendocrine tumors can arise after long disease duration, probably in response to inflammation[7,11]. Recently, precursor lesions giving rise to pancreatic neuroendocrine tumors (PNETs) have drawn much attention and become more understood. It is well known now that diffuse precursor lesions including endocrine cell hyperplasia, dysplasia, and microadenomas are present in the pancreata of patients with familial tumor syndromes such as multiple endocrine neoplasia syndrome type 1 (MEN1) and von Hippel-Lindau disease, and of animal models of PNETs[12-16]. In the pancreata of patients with MEN1 and mice with heterozygous MEN1 inactivation, the hyperplastic endocrine cells are polyclonal and multi-hormonal and contain the normal menin allele, while microadenomas have to first lose the normal menin allele[17,18]. In contrast, uni-hormonal pancreatic endocrine cell hyperplasia such as pancreatic α cell hyperplasia (ACH) and pancreatic polypeptide cell hyperplasia has only been recognized in the last several years[8,9,19]. Although pancreatic polypeptide cell hyperplasia may be a physiological variation of normal pancreatic polypeptide cell distribution, ACH is clearly a pathologic precursor lesion leading to PNET pathogenesis[19].
In this article, we will summarize how the discovery of a novel hereditary tumor syndrome, Mahvash disease, has stimulated interest in the pathogenesis of ACH, and discuss the possible identify of an elusive liver factor that
may cause the ACH.The data we review are based on work in our
own laboratories and PubMed and major endocrine conferences search using key words pancreatic α cell hyperplasia, glucagon receptor mutation, glucagon receptor antagonism, and hyperglucagonemia.
PANCREATIC ACHACH is defined as an overwhelming and specific increase of pancreatic α cell numbers[8,19]. Based on etiology and glucagon levels, 3 types of ACH are observed. Reactive ACH is caused in humans by inactivating glucagon receptor mutations and is associated with marked hyper-glucagonemia. Because the glucagon receptor is inactive, the severe hyperglucagonemia in reactive ACH does not result in glucagonoma syndrome. Non-functional ACH has an unknown cause and is associated with normal glucagon levels. Functional ACH also has an unknown cause but is associated with hyperglucagonemia that results in glucagonoma syndrome.
Reactive ACH is most extensively studied due to the novel Mahvash disease and the existence of multiple animal models. We first described the Mahvash disease which is hyperglucagonemia, ACH, and PNETs but without glucagonoma syndrome, caused by an inactivating glucagon receptor mutation[20,21]. Later, we and others have confirmed the Mahvash disease (Tang L and Yu R, unpublished results)[19,22]. Currently, 8 inactivating glucagon receptor mutations are known.
We further established that the glucagon receptor knockout (Gcgr-/-) mice are a murine model of Mahvash disease[23-25]. The Gcgr-/- mice exhibit ACH throughout their lifespan. Dysplastic islets consisted of mostly α cells are evident from 5-7 mo on and glucagonomas are detected from 10-12 mo to death. Hyperplasia is also observed in the exocrine compartment but dysplasia, carcinoma in situ, or frank exocrine carcinoma is not found. Large PNETs contribute at least partially to the premature demise of the Gcgr-/- mice. Three other murine models also mimic the Mahvash disease in some aspects. The prohormone convertase 2 knockout (PC-/-) mice cannot make mature glucagon; they exhibit ACH and eventually develop PNETs[26,27]. The preproglucagon knockout (Gcg-/-) mice cannot make any proglucagon- derived peptide hormones, including mature glucagon; they also exhibit ACH and eventually develop PNETs[28,29]. The liver-specific Gsα knockout mice cannot transduce the glucagon signaling in hepatocytes; they exhibit hyperglucagonemia and ACH, and eventually develop PNETs as well[30,31].
Thus both in humans and in mice, reactive ACH ensues whenever glucagon signaling is disrupted and evolves into PNETs eventually. Reactive ACH thus is clearly a precursor lesion leading to PNET pathogenesis.
PATHOGENESIS OF REACTIVE ACHThe pathogenesis of reactive ACH in Gcgr-/- mice is
132 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Yu R et al . The elusive liver factor

studied in detail. As increased pancreatic endocrine cell numbers can be due to proliferation, neogenesis, or reduced apoptosis, they are each examined at 6-7 mo[23]. α cell proliferation measured by proliferating cell nuclear antigen or Ki-67 labeling is very low and not significantly different in WT and Gcgr-/- mice. α cell neogenesis measured by counting singlet and doublet α cells and exocrine ducts harboring glucagon-positive cells is much higher in Gcgr-/- than in WT mice. α cell apoptosis measured by TUNEL labeling is very low in both Gcgr-/- and WT mice and not significantly different. While upregulated α cell neogenesis is also seen in the PC-/- mice throughout their lifespan, higher α cell proliferation is found at 3 mo[27].
The hyperplastic α cells in the Gcgr-/- mice exhibit abnormal differentiation. A few of these cells are posi-tively labeled with both glucagon and insulin, and some express pancreatic and duodenal homeobox 1, a β cell marker[23]. Most α cells express embryonic α cell markers such as GLUT2[32]. Abnormal α cell differentiation is also seen in humans with mutated Gcgr and in the PC-/- mice as they both express glucagon-like peptide 1, which is normally not expressed in the α cells[21,27].
REACTIVE ACH AND THE LIVERAs reactive ACH universally occurs after glucagon signaling inhibition (see above), it is logical to hypothesize that glucagon signaling negatively feeds back on α cell number regulation and loss of the negative feedback causes the ACH[33]. A number of lines of evidence point to the liver as the organ which sends inhibitory signals to the α cells during normal glucagon signaling and a stimulatory signal to them when glucagon signaling is disrupted. First, liver is the natural target organ of glucagon signaling. Second, liver-specific Gsα deletion in mice recapitulates ACH pathogenesis[30]. Third, liver-specific glucagon receptor deletion in mice results in a phenotype very similar to that of mice with global glucagon receptor deletion[34]. Fourth, glucagon receptor re-expression in the liver of Gcgr-/- mice reduces glucagon levels by almost 99%[35]. Therefore, if the liver does not respond to glucagon but all other organs do, reactive ACH ensues; conversely, if the liver does respond to
glucagon but all other organs do not, reactive ACH likely reverses. In other words, the liver is likely necessary and sufficient to be the organ regulating the number of α cells in response to glucagon signaling.
THE ELUSIVE LIVER FACTORThe liver communicates with the pancreas via neuronal and humoral signals. It has been shown that the liver can regulate insulin secretion and pancreatic β cell proliferation through neuronal signals[36-38]. In a similarmanner, the liver may regulate glucagon secretion and pancreatic α cell proliferation through neuronal connection, but there has not been any direct experimen-tal evidence supporting or disputing that. In contrast, there is strong evidence that the liver regulates glucagon secretion and pancreatic α cell proliferation through a humoral factor as shown by islet transplantation experiments[34]. Transplanted wildtype islets in Gcgr-/- recipient mice exhibit higher α/β cell ratio and increased α cell proliferation, compared with those in wildtype recipient animals. Conversely, transplanted Gcgr-/- islets in wildtype recipient mice exhibited reduced α-cell proliferation compared with those in Gcgr-/- recipient animals.
The nature and identity of the liver factor that causes reactive ACH have been sought after. As the liver gene expression must be different between the wildtype and the Gcgr-/- mice, systems approaches such as DNA microarray studies are done to efficiently provide systemic and novel insights into the nature of the liver factor. We compared gene expression profile of 4 WT and 4 Gcgr-/- mouse livers at 2.5 mo (2 females and 2 males in each group) by Affymetrix GeneChip Mouse Gene 1.0 ST Array. The microarray data were analyzed using Genespring 11 (Tables 1 and 2). A total of 125 genes were significantly differentially expressed (> 2 fold change and P < 0.05). Since ACH occurs regardless of sex, we eliminated 47 genes with differential expression only limited in one sex, leaving 35 genes upregulated and 43 genes downregulated in both female and male Gcgr-/- mouse liver. The differential expression of some of the 78 genes was validated by realtime polymerase chain reaction (Figure 1). We reason that potential candidate genes should encode secretory proteins. Of the genes overexpressed in Gcgr-/- liver, Igfbp1, Defb1, Serpina7, Inhba, Cxcl13, Il1b, and Cxcl9 are secretory proteins and may stimulate α-cell differentiation and proliferation. Defb1 is particularly interesting as it is very significantly overexpressed in the Gcgr-/- liver (Table 1). Defensins are a group of cysteine-rich antimicrobial peptides that function to help defend against microbial infections[39]. They are mostly secreted by leukocytes and epithelial cells and their anti-microbial mechanisms are multiple. There are a few families of defensins according to their structures in mice and humans. Originally, defensin β1 (DB1, encoded by Defb1) is found to be expressed in the lung and urogenital epithelials cells[40-42]. Later, DB1 is also found
133 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Rela
tive
expr
essi
on le
vels
(fo
ld)
7
6
5
4
3
2
1
0Defb1 Il22ra1 Lpl Creld2 Oat Mmd2
Wildtype
Gcgr-/-
Figure 1 Realtime polymerase chain reaction of several genes differentially expressed in the Gcgr/ mice. See text for details.
Yu R et al . The elusive liver factor

134 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Table 1 Genes significantly overexpressed in the Gcgr-/- mouse liver
Gene symbol mRNA description GO biological process term Fold increase
Cdkn1a Cyclin-dependent kinase inhibitor 1A (P21), transcript variant 1
Response to DNA damage stimulus/cell cycle/cell cycle arrest/negative regulation of cell proliferation
5.6
Igfbp1 Insulin-like growth factor binding protein 1 Regulation of cell growth 5.5Defb1 Defensin beta 1 Defense response/response to bacterium/defense response to bacterium/
innate immune response 5.2
Gpr64 G protein-coupled receptor 64, transcript variant 1
Signal transduction/cell surface receptor linked signaling pathway/G-protein coupled receptor protein signaling pathway/neuropeptide signaling pathway
5.1
Serpina7 Serine (or cysteine) peptidase inhibitor, clade A (alpha-1 antiproteinase, antitrypsin),
member 7
Post-embryonic development/response to vitamin A/response to drug 4.9
Cpt1b Carnitine palmitoyltransferase 1b, muscle, nuclear gene encoding mitochondrial protein
Lipid metabolic process/fatty acid metabolic process/transport/long-chain fatty acid transport/long-chain fatty acid transport
4.6
Chac1 ChaC, cation transport regulator-like 1 (E. coli)
Apoptosis/response to unfolded protein/biological_process 4.3
Npas2 Neuronal PAS domain protein 2 Transcription/regulation of transcription, DNA-dependent/signal transduction/circadian sleep/wake cycle/regulation of transcription/
locomotor rhythm/positive regulation of transcription from RNA polymerase Ⅱ promoter/rhythmic process
3.9
Slc34a2 Solute carrier family 34 (sodium phosphate), member 2
In utero embryonic development/transport/ion transport/sodium ion transport/phosphate transport/phosphate transport/phosphate transport
3.6
Fabp5 Fatty acid binding protein 5, epidermal Glucose metabolic process/lipid metabolic process/phosphatidylcholine biosynthetic process/transport/glucose transport
3.5
BC023105 cDNA sequence BC023105 Unknown 3.1Cav1 Caveolin 1, caveolae protein MAPKKK cascade/inactivation of MAPK activity/vasculogenesis/response
to hypoxia/negative regulation of endothelial cell proliferation/negative regulation of cytokine-mediated signaling pathway/triglyceride metabolic process/calcium ion transport/cellular calcium ion homeostasis/cellular
calcium ion homeostasis/endocytosis/regulation of smooth muscle contraction
2.8
Lpl Lipoprotein lipase Lipid metabolic process/positive regulation of macrophage derived foam cell differentiation/lipid catabolic process/triglyceride biosynthetic process/
triglyceride catabolic process
2.7
Il22ra1 Interleukin 22 receptor, alpha 1 Blood coagulation 2.6Acaca Acetyl-Coenzyme A carboxylase alpha Tissue homeostasis/acetyl-CoA metabolic process/lipid metabolic process/
fatty acid biosynthetic process/metabolic process/lipid biosynthetic process/response to organic cyclic substance/multicellular organismal protein
metabolic process
2.6
Inhba Inhibin beta-A Mesoderm formation/hemopoietic progenitor cell differentiation/growth/positive regulation of transcription from RNA polymerase Ⅱ promoter/
mesodermal cell differentiation/negative regulation of hair follicle development
2.6
Gadd45b Growth arrest and DNA-damage-inducible 45 beta
Activation of MAPKK activity/negative regulation of protein kinase activity/apoptosis/multicellular organismal development/cell differentiation/
regulation of cell cycle
2.4
Tgtp1 T-cell specific GTPase 1 Immune response/response to virus 2.4Rassf4 Ras association (RalGDS/AF-6) domain
family member 4 Cell cycle/signal transduction 2.4
Cxcl13 Chemokine (C-X-C motif) ligand 13 Chemotaxis/inflammatory response/immune response/lymph node development
2.4
Il1b Interleukin 1 beta Angiogenesis/fever/inflammatory response/immune response/elevation of cytosolic calcium ion concentration/aging
2.4
Tgtp1 T-cell specific GTPase 1 Immune response/response to virus 2.3Asns Asparagine synthetase Asparagine biosynthetic process/glutamine metabolic process/metabolic
process/cellular amino acid biosynthetic process 2.3
Socs2 Suppressor of cytokine signaling 2, transcript variant 1
Lactation/regulation of growth/regulation of multicellular organism growth/negative regulation of multicellular organism growth/negative
regulation of multicellular organism growth/positive regulation of neuron differentiation/negative regulation of JAK-STAT cascade/mammary gland
alveolus development
2.3
Meig1 Meiosis expressed gene 1 Meiosis 2.3Cxcl9 Chemokine (C-X-C motif) ligand 9 Inflammatory response/immune response 2.2Vtcn1 V-set domain containing T cell activation
inhibitor 1 Negative regulation of T cell activation 2.2
H2-Ab1 Histocompatibility 2, class Ⅱ antigen A, beta 1
Antigen processing and presentation of peptide or polysaccharide antigen via MHC class Ⅱ/immune response/antigen processing and presentation/antigen processing and presentation of exogenous peptide antigen via MHC
class Ⅱ
2.2
Yu R et al . The elusive liver factor

135 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
in the liver, especially in the biliary epithelial cells under obstructive jaundice[40,43,44]. DB1 released in circulation may result in ACH. Serpina7 encodes thyroxine-binding globulin (TBG) which binds thyroxine and increases total thyroxine levels[45]. As the index patient with Mahvash disease has normal thyroid functions, suggesting normal TBG levels, it is unlikely that TBG is the liver factor that causes ACH. For Cxcl13, Il1b, and Cxcl9, please see below. Literature review does not give us any clues on which underexpressed genes in Gcgr-/- mouse liver might encode a secretory protein that acts as inhibitor of α-cell differentiation and proliferation.
Pathway analysis suggested that WT and Gcgr-/- liver exhibit different metabolic profiles. As expected, genes involved in gluconeogenesis, glycogen synthesis, and glycogenolysis were downregulated in the Gcgr-/- liver, compared with those in WT (Table 3). Interestingly, genes involved in inflammation and cell proliferation were upregulated in the Gcgr-/- liver. The protein products of genes regulating cell proliferation unlikely diffuse out of the liver thus are improbable signals for regulating α cell mass. In contrast, the protein products of genes regulating inflammation are mostly cytokines which are secreted into the circulation and can reach the α cells, such as Cxcl13, Il1b, and Cxcl9. Interestingly, interleukin-6 (IL6), a cytokine secreted by T cells and macrophages (but not by the liver), upregulates α-cell mass but circulating IL6 levels are normal in the Gcgr-/- mice[34,46]. Alternatively, multiple liver-elaborated cytokines may act synergistically to cause ACH.
The liver may indirectly regulate α cell differentiation and proliferation by metabolic signals. Not surprisingly, the metabolic profile of Gcgr-/- mice and wildtype counterparts are vastly different, as shown by polyomic metabolic profiling[47]. Similar to our results, genes involved in gluconeogenesis and amino acid catabolism are downregulated. Furthermore, genes involved in fatty acid oxidation processes are also downregulated and genes involved in glycolysis, fatty acid synthesis, and cholesterol synthesis are upregulated. More pertinent to the potential mechanisms for ACH pathogenesis are the dramatic changes in the levels of metabolites[47]. As reported before[21,23], glucose levels are decreased by 1.4-fold. Consistent with decreased gluconeogenesis in the Gcgr-/- mice, amino acids and amino acid derivatives
levels are significantly elevated. The most upregulated amino acids are threonine (9.6-fold), serine (8.7-fold), and asparagine (8.1-fold). Amino acid derivatives levels are also higher in the Gcgr-/- mice, the highest being 2-aminodipic acid and ornithine (both 5.4-fold). Levels of certain nucleotides and their derivatives are elevated, e.g., pyridoxine levels are 3.6-fold elevated. Levels of some vitamins are different; those of dihydrofolic acid are 5.3-fold elevated. Glycerol and glycerol derivatives levels are about 2-fold lower. Intriguingly, the levels of cholic acid and glycocholic acid, two bile acids, are markedly and unexpectedly elevated (244- and 154-fold, respectively). There have been only a few studies addressing glucagon signaling and bile acids. In the rats, glucagon increases cholic acid levels[48]; in cultured cells, one bile acid, chenodeoxycholic acid, desensitizes the glucagon receptor[49]. Bile acids, however, are recognized recently as metabolic regulators[50]. Wildtype mice fed with cholic acid exhibit markedly elevated bile acid levels but their pancreas weight and glucagon levels are not changed[34]. Interestingly, α cell mass is somewhat increased (approximately 80%) by cholic acid feeding. Thus a metabolic signal that causes ACH has not been identified yet.
FUTURE DIRECTIONSThe elusive, yet-to-be identified liver factor that causes ACH fulfills the definition of a novel digestive system hormone (Figure 2). The liver factor is produced by the liver and released into the circulation; it then acts remotely on the pancreas to result in ACH. The liver factor could be more than one molecule but we use singular form here for conciseness. To identify this liver factor, the process of discovering leptin may offer some insights. When the first obese mouse models were described, it was not clear why they are obese. A circulating factor was hypothesized[51]. In the obese mouse models, the factor may either stimulate appetite and be overproduced or inhibit appetite and be under-produced. The circulating factor hypothesis was tested by parabiosis which joins the circulation of two mice of various lean and obese phenotypes. Eventually it was found that the ob/ob obese mice lack an inhibitor of appetite (leptin) and the db/db obese mice lack the
Spon2 Spondin 2, extracellular matrix protein Cell adhesion/innate immune response 2.2Rgs16 Regulator of G-protein signaling 16 G-protein coupled receptor protein signaling pathway/negative regulation of
signal transduction 2.1
Il2rg Interleukin 2 receptor, gamma chain Regulation of gene expression/positive regulation of CD4-positive, CD25-positive, alpha-beta regulatory T cell differentiation/positive regulation of T cell differentiation in the thymus/positive regulation of B cell differentiation
2.1
Wdr67 WD repeat domain 67, transcript variant 1 Regulation of Rab GTPase activity 2.1Prss8 Protease, serine, 8 (prostasin) Hair follicle development/proteolysis 2.1Bach2 BTB and CNC homology 2 Transcription/regulation of transcription, DNA-dependent/regulation of
transcription 2.0
Serpina12 Serine (or cysteine) peptidase inhibitor, clade A (alpha-1 antiproteinase, antitrypsin),
member 12
Unknown 2.0
E. coli: Escherichia coli.
Yu R et al . The elusive liver factor

136 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Table 2 Genes significantly underexpressed in the Gcgr-/- mouse liver
Gene symbol mRNA description GO biological process term Fold decrease
Mmd2 Monocyte to macrophage differentiation-associated 2
Cytolysis 9.7
Nnmt Nicotinamide N-methyltransferase Unknown 6.2Gcgr Glucagon receptor Exocytosis/signal transduction/cell surface receptor linked signaling pathway/
G-protein coupled receptor protein signaling pathway/G-protein signaling, coupled to cAMP nucleotide second messenger/activation of adenylate cyclase
activity by G-protein signaling pathway
5.3
Mfsd2a Major facilitator superfamily domain containing 2A
Transport/transmembrane transport 4.2
Oat Ornithine aminotransferase, nuclear gene encoding mitochondrial protein
Unknown 4.1
Slc10a2 Solute carrier family 10, member 2 Transport/ion transport/sodium ion transport/organic anion transport/bile acid and bile salt transport
3.9
A1bg Alpha-1-B glycoprotein Unknown 3.5Gm129 Gene model 129 (NCBI) Unknown 3.3Sds Serine dehydratase Gluconeogenesis/cellular amino acid metabolic process/metabolic process 3.1Pck1 Phosphoenolpyruvate carboxykinase
1, cytosolic Gluconeogenesis/gluconeogenesis/oxaloacetate metabolic process/lipid
metabolic process/glycerol biosynthetic process from pyruvate 3.0
Lrtm1 Leucine-rich repeats and transmembrane domains 1
Unknown 3.0
Ntrk2 Neurotrophic tyrosine kinase, receptor, type 2, transcript variant 1
Vasculogenesis/protein amino acid phosphorylation/transmembrane receptor protein tyrosine kinase signaling pathway/multicellular organismal
development/nervous system development/feeding behavior/glutamate secretion/regulation of metabolic process/cell differentiation/brain-derived
neurotrophic factor receptor signaling pathway/mechanoreceptor differentiation
3.0
Gls2 Glutaminase 2 (liver, mitochondrial), nuclear gene encoding mitochondrial
protein
Gutamine metabolic process 3.0
Susd4 Sushi domain containing 4 Unknown 2.9Slc16a5 Solute carrier family 16
(monocarboxylic acid transporters), member 5
Unknown 2.9
Ccrn4l CCR4 carbon catabolite repression 4-like (S. cerevisiae)
Rhythmic process 2.9
Lhpp Phospholysine phosphohistidine inorganic pyrophosphate
phosphatase
Metabolic process 2.7
Neb Nebulin Regulation of actin filament length/sarcomere organization 2.6Got1 Glutamate oxaloacetate transaminase
1, soluble Oxaloacetate metabolic process/glycerol biosynthetic process/cellular amino
acid metabolic process/aspartate metabolic process/aspartate biosynthetic process/biosynthetic process/glutamate catabolic process to aspartate/glutamate catabolic process to 2-oxoglutarate/dicarboxylic acid metabolic process/fatty acid
homeostasis
2.6
Sult5a1 Sulfotransferase family 5A, member 1 Unknown 2.6Hapln1 Hyaluronan and proteoglycan link
protein 1 Cell adhesion 2.5
Mt2 Metallothionein 2 Cellular zinc ion homeostasis/nitric oxide mediated signal transduction/detoxification of copper ion
2.5
Mt1 Metallothionein 1 Cellular metal ion homeostasis/cellular zinc ion homeostasis/nitric oxide mediated signal transduction/detoxification of copper ion
2.4
Slc3a1 Solute carrier family 3, member 1 Amino acid transport 2.4Trdn Triadin Cellular calcium ion homeostasis/regulation of release of sequestered calcium
ion into cytosol by sarcoplasmic reticulum/negative regulation of calcium ion transport via store-operated calcium channel activity
2.4
Bhlhe41 Basic helix-loop-helix family, member e41
Negative regulation of transcription from RNA polymerase Ⅱ promoter/transcription/regulation of transcription, DNA-dependent/circadian rhythm/
entrainment of circadian clock/regulation of transcription
2.3
Usp2 Ubiquitin specific peptidase 2, transcript variant 3
Ubiquitin-dependent protein catabolic process 2.3
Derl3 Der1-like domain family, member 3 Unknown 2.3Mrap2 Melanocortin 2 receptor accessory
protein 2, transcript variant 1 Unknown 2.2
Ncam2 Neural cell adhesion molecule 2, transcript variant 1
Cell adhesion 2.2
S1pr5 Sphingosine-1-phosphate receptor 5 Signal transduction/G-protein coupled receptor protein signaling pathway 2.21810046K07Rik RIKEN cDNA 1810046K07 gene Unknown 2.2Nrg4 Neuregulin 4 Unknown 2.2
Yu R et al . The elusive liver factor

137 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
receptor for the inhibitor (leptin receptor). Analogously, the Gcgr-/- mice liver could produce a stimulator or lack an inhibitor of α cell mass. Whether the liver factor is a stimulator or an inhibitor in nature is critical in guiding the search for the identity of the liver factor that causes ACH. As parabiosis is technically challenging, it probably should be used as a last resort. Alternative approaches such as primary pancreatic islet culture[52,53] may be used first to resolve the stimulator/inhibitor question and
later used as a high-throughput model for identifying the factor. For example, if a 10:1 mixture of wildtype and Gcgr-/- serum stimulates α cell proliferation of the wildtype islets, then it is likely that the Gcgr-/- mice have a stimulator of α cell mass. Another potential systems approach is to compare the liver gene expression and metabolic profile of multiple animal models of reactive ACH. As all the models develop reactive ACH, any differentially expressed genes unlikely encode the liver
Gas2 Growth arrest specific 2 Apoptosis/cell cycle/cell cycle arrest/regulation of cell shape 2.2Ttc39b Tetratricopeptide repeat domain 39B Unknown 2.2Cyp17a1 Cytochrome P450, family 17,
subfamily a, polypeptide 1 Steroid biosynthetic process/glucocorticoid biosynthetic process/oxidation
reduction 2.1
Creld2 cysteine-rich with EGF-like domains 2
Unknown 2.1
Upp2 Uridine phosphorylase 2 Nucleoside metabolic process/nucleotide catabolic process 2.1Ar Androgen receptor In utero embryonic development/transcription/regulation of transcription, DNA-
dependent/regulation of transcription from RNA polymerase Ⅱ promoter/male gonad development/cellular process/regulation of gene expression/male
somatic sex determination/androgen receptor signaling pathway/androgen receptor signaling pathway/positive regulation of estrogen receptor signaling
pathway/positive regulation of MAPKKK cascade/positive regulation of insulin-like growth factor receptor signaling pathway
2.1
Gm10419 Lung RCB-0558 LLC cDNA, RIKEN full-length enriched library, clone:G730014J15 product: Hypothetical
protein
Unknown 2.1
Sdf2l1 Stromal cell-derived factor 2-like 1 Unknown 2.0Trdn Triadin Cellular calcium ion homeostasis/regulation of release of sequestered calcium
ion into cytosol by sarcoplasmic reticulum/negative regulation of calcium ion transport via store-operated calcium channel activity
2.0
Antxr2 Anthrax toxin receptor 2 Unknown 2.0
S. cerevisiae: Saccharomyces cerevisiae.
Table 3 Pathway analysis of differentially expressed genes in the Gcgr-/- mouse liver
Glucose homeostasis Inflammation Cell proliferation Metabolism
Underexpressed in Gcgr-/- mouse liver
Nnmt, Got1, Sds, Pck1 Gas2 Slc10a2, Ntrk2, Gls2, Lhpp, Sult5a1, Mt2, Mt1, Slc3a1,
Trdn, Usp2, Cyp17a1, Upp2Overexpressed in Gcgr-/- mouse liver
Il1b, Cxcl13, Tgtp1, Cxcl9, Defb1, Vtcn1, H2-Ab1, Spon2, Il2rg
Cdkn1a, Igfbp1, Chac1, Cav1, Inhba, Gadd45b, Rassf4, Socs2, Meig1
Serpina7, Cpt1b, Slc34a2, Fabp5, Lpl, Acaca, Asns
(2)(1)
(3)
(4) (5)
(6)
(7) (8)
(9)
?
Gs cAMP Glucose
Live
Pancreas
Glucagon
Gcgr
Figure 2 Schematic drawing of regulation of pancreatic α cell number by a humoral liver factor. The numbers indicate specific ways to disrupt glucagon signaling. (1) Glucagon deletion; (2) PC2 deletion; (3) Glucagon receptor (Gcgr) global deletion; (4) Gcgr liver-specific deletion; (5) Gcgr inactivating mutation; (6) Gcgr antisense RNA; (7) Gcgr antagonists; (8) Gcgr antibodies; and (9) Gsa liver-specific deletion. See text for details.
Yu R et al . The elusive liver factor

138 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
factor and metabolites of various levels unlikely cause ACH, thus greatly narrowing down the list of candidate genes or metabolites. It is also important to point out that other subtypes of ACH exist and not all ACH is associated with glucagon receptor mutation[22,54].
CONCLUSIONPancreatic ACH is a precursor lesion that gives rise to PNETs. Reactive ACH is associated with hyper-glucagonemia and invariably evolves into PNETs in both humans and animal models. The glucagon receptor knockout (Gcgr-/-) mice are one of the murine model of reactive ACH and current research has shown that the liver produces a factor that regulates pancreatic α cell mass. Liver gene expression arrays and metabolic profiling suggest a number of potential candidates for the novel liver hormone but none of them so far tested has been confirmed. As understanding the physiological, cellular, and molecular mechanisms underlying reactive ACH pathogenesis is important to the prevention and treatment of PNETs, the search for the elusive liver factor is worthwhile but may require a substantial effort to find it.
REFERENCES1 Geboes K, Ectors N, Geboes KP. Pathology of early lower GI
cancer. Best Pract Res Clin Gastroenterol 2005; 19: 963-978 [PMID: 16338652]
2 Vieth M, Stolte M. Pathology of early upper GI cancers. Best Pract Res Clin Gastroenterol 2005; 19: 857-869 [PMID: 16338646]
3 Scarlett CJ, Salisbury EL, Biankin AV, Kench J. Precursor lesions in pancreatic cancer: morphological and molecular pathology. Pathology 2011; 43: 183-200 [PMID: 21436628 DOI: 10.1097/PAT.0b013e3283445e3a]
4 Klöppel G. Classification and pathology of gastroenteropancreatic neuroendocrine neoplasms. Endocr Relat Cancer 2011; 18 Suppl 1: S1-16 [PMID: 22005112 DOI: 10.1530/ERC-11-0013]
5 Díez M, Teulé A, Salazar R. Gastroenteropancreatic neuroendocrine tumors: diagnosis and treatment. Ann Gastroenterol 2013; 26: 29-36 [PMID: 24714698]
6 Ro C, Chai W, Yu VE, Yu R. Pancreatic neuroendocrine tumors: biology, diagnosis,and treatment. Chin J Cancer 2013; 32: 312-324 [PMID: 23237225 DOI: 10.5732/cjc.012.10295]
7 Klöppel G, Anlauf M, Perren A. Endocrine precursor lesions of gastroenteropancreatic neuroendocrine tumors. Endocr Pathol 2007; 18: 150-155 [PMID: 18058264]
8 Ouyang D, Dhall D, Yu R. Pathologic pancreatic endocrine cell hyperplasia. World J Gastroenterol 2011; 17: 137-143 [PMID: 21245985 DOI: 10.3748/wjg.v17.i2.137]
9 Klöppel G, Anlauf M, Perren A, Sipos B. Hyperplasia to neoplasia sequence of duodenal and pancreatic neuroendocrine diseases and pseudohyperplasia of the PP-cells in the pancreas. Endocr Pathol 2014; 25: 181-185 [PMID: 24718881 DOI: 10.1007/s12022-014-9317-8]
10 Bordi C, Yu JY, Baggi MT, Davoli C, Pilato FP, Baruzzi G, Gardini G, Zamboni G, Franzin G, Papotti M. Gastric carcinoids and their precursor lesions. A histologic and immunohistochemical study of 23 cases. Cancer 1991; 67: 663-672 [PMID: 1702355]
11 Stewart CJ, Matsumoto T, Jo Y, Mibu R, Hirahashi M, Yao T, Iida M. Multifocal microcarcinoid tumours in ulcerative colitis. J Clin Pathol 2005; 58: 111-1112; author reply 1112 [PMID: 15623500]
12 Thompson NW, Lloyd RV, Nishiyama RH, Vinik AI, Strodel WE, Allo MD, Eckhauser FE, Talpos G, Mervak T. MEN I pancreas: a
histological and immunohistochemical study. World J Surg 1984; 8: 561-574 [PMID: 6207668]
13 Lubensky IA, Pack S, Ault D, Vortmeyer AO, Libutti SK, Choyke PL, Walther MM, Linehan WM, Zhuang Z. Multiple neuroendocrine tumors of the pancreas in von Hippel-Lindau disease patients: histopathological and molecular genetic analysis. Am J Pathol 1998; 153: 223-231 [PMID: 9665483]
14 Jensen RT, Berna MJ, Bingham DB, Norton JA. Inherited pancreatic endocrine tumor syndromes: advances in molecular pathogenesis, diagnosis, management, and controversies. Cancer 2008; 113: 1807-1843 [PMID: 18798544]
15 Vinik AI, Gonzales MR. New and emerging syndromes due to neuroendocrine tumors. Endocrinol Metab Clin North Am 2011; 40: 19-63, vii [PMID: 21349410 DOI: 10.1016/j.ecl.2010.12.010]
16 Babu V, Paul N, Yu R. Animal models and cell lines of pancreatic neuroendocrine tumors. Pancreas 2013; 42: 912-923 [PMID: 23851429 DOI: 10.1097/MPA.0b013e31827ae993]
17 Anlauf M, Perren A, Henopp T, Rudolf T, Garbrecht N, Schmitt A, Raffel A, Gimm O, Weihe E, Knoefel WT, Dralle H, Heitz PU, Komminoth P, Klöppel G. Allelic deletion of the MEN1 gene in duodenal gastrin and somatostatin cell neoplasms and their precursor lesions. Gut 2007; 56: 637-644 [PMID: 17135306]
18 Crabtree JS, Scacheri PC, Ward JM, Garrett-Beal L, Emmert-Buck MR, Edgemon KA, Lorang D, Libutti SK, Chandrasekharappa SC, Marx SJ, Spiegel AM, Collins FS. A mouse model of multiple endocrine neoplasia, type 1, develops multiple endocrine tumors. Proc Natl Acad Sci USA 2001; 98: 1118-1123 [PMID: 11158604]
19 Yu R. Pancreatic α-cell hyperplasia: facts and myths. J Clin Endocrinol Metab 2014; 99: 748-756 [PMID: 24285676 DOI: 10.1210/jc.2013-2952]
20 Yu R, Nissen NN, Dhall D, Heaney AP. Nesidioblastosis and hyperplasia of alpha cells, microglucagonoma, and nonfunctioning islet cell tumor of the pancreas: review of the literature. Pancreas 2008; 36: 428-431 [PMID: 18437091 DOI: 10.1097/MPA.0b013e31815ceb23]
21 Zhou C, Dhall D, Nissen NN, Chen CR, Yu R. Homozygous P86S mutation of the human glucagon receptor is associated with hyperglucagonemia, alpha cell hyperplasia, and islet cell tumor. Pancreas 2009; 38: 941-946 [PMID: 19657311 DOI: 10.1097/MPA.0b013e3181b2bb03]
22 Sipos B, Sperveslage J, Anlauf M, Hoffmeister M, Henopp T, Buch S, Hampe J, Weber A, Hammel P, Couvelard A, Höbling W, Lieb W, Boehm BO, Klöppel G. Glucagon cell hyperplasia and neoplasia with and without glucagon receptor mutations. J Clin Endocrinol Metab 2015; 100: E783-E788 [PMID: 25695890]
23 Yu R, Dhall D, Nissen NN, Zhou C, Ren SG. Pancreatic neuro-endocrine tumors in glucagon receptor-deficient mice. PLoS One 2011; 6: e23397 [PMID: 21853126 DOI: 10.1371/journal.pone.0023397]
24 Yu R, Ren SG, Mirocha J. Glucagon receptor is required for long-term survival: a natural history study of the Mahvash disease in a murine model. Endocrinol Nutr 2012; 59: 523-530 [PMID: 22951296 DOI: 10.1016/j.endonu.2012.06.006]
25 Yu R, Nissen NN, Dhall D. Exocrine pancreas hyperplasia without dysplasia in glucagon receptor knockout mice. Pancreas 2014; 43: 143-145 [PMID: 24326371 DOI: 10.1097/MPA.0b013e3182a5dc77]
26 Furuta M, Yano H, Zhou A, Rouillé Y, Holst JJ, Carroll R, Ravazzola M, Orci L, Furuta H, Steiner DF. Defective prohormone processing and altered pancreatic islet morphology in mice lacking active SPC2. Proc Natl Acad Sci USA 1997; 94: 6646-6651 [PMID: 9192619]
27 Jones HB, Reens J, Brocklehurst SR, Betts CJ, Bickerton S, Bigley AL, Jenkins RP, Whalley NM, Morgan D, Smith DM. Islets of Langerhans from prohormone convertase-2 knockout mice show α-cell hyperplasia and tumorigenesis with elevated α-cell neogenesis. Int J Exp Pathol 2014; 95: 29-48 [PMID: 24456331 DOI: 10.1111/iep.12066]
28 Hayashi Y, Yamamoto M, Mizoguchi H, Watanabe C, Ito R, Yamamoto S, Sun XY, Murata Y. Mice deficient for glucagon gene-derived peptides display normoglycemia and hyperplasia of islet
Yu R et al . The elusive liver factor

139 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
{alpha}-cells but not of intestinal L-cells. Mol Endocrinol 2009; 23: 1990-1999 [PMID: 19819987 DOI: 10.1210/me.2009-0296]
29 Hayashi Y, Takano Y, Kasai K, Imai T, Murata Y. Pancreatic Neuroendocrine Tumors in Mice Deficient in Glucagon Gene. Endocrine Society’s 96th Annual Meeting and Expo, Chicago, 2014
30 Chen M, Gavrilova O, Zhao WQ, Nguyen A, Lorenzo J, Shen L, Nackers L, Pack S, Jou W, Weinstein LS. Increased glucose tolerance and reduced adiposity in the absence of fasting hypo-glycemia in mice with liver-specific Gs alpha deficiency. J Clin Invest 2005; 115: 3217-3227 [PMID: 16239968]
31 Weinstein LS. Role of the Gnas Gene in Metabolic Regulation. 2012
32 Vuguin PM, Kedees MH, Cui L, Guz Y, Gelling RW, Nejathaim M, Charron MJ, Teitelman G. Ablation of the glucagon receptor gene increases fetal lethality and produces alterations in islet development and maturation. Endocrinology 2006; 147: 3995-4006 [PMID: 16627579]
33 Lucas MB, Yu VE, Yu R. Mahvash disease: pancreatic neuro-endocrine tumor syndrome caused by inactivating glucagon receptor mutation. J Mol Genet Med 2013; 7: 84
34 Longuet C, Robledo AM, Dean ED, Dai C, Ali S, McGuinness I, de Chavez V, Vuguin PM, Charron MJ, Powers AC, Drucker DJ. Liver-specific disruption of the murine glucagon receptor produces α-cell hyperplasia: evidence for a circulating α-cell growth factor. Diabetes 2013; 62: 1196-1205 [PMID: 23160527 DOI: 10.2337/db11-1605]
35 Lee Y, Berglund ED, Wang MY, Fu X, Yu X, Charron MJ, Burgess SC, Unger RH. Metabolic manifestations of insulin deficiency do not occur without glucagon action. Proc Natl Acad Sci USA 2012; 109: 14972-14976 [PMID: 22891336 DOI: 10.1073/pnas.1205983109]
36 Imai J, Katagiri H, Yamada T, Ishigaki Y, Suzuki T, Kudo H, Uno K, Hasegawa Y, Gao J, Kaneko K, Ishihara H, Niijima A, Nakazato M, Asano T, Minokoshi Y, Oka Y. Regulation of pancreatic beta cell mass by neuronal signals from the liver. Science 2008; 322: 1250-1254 [PMID: 19023081 DOI: 10.1126/science.1163971]
37 Imai J, Oka Y, Katagiri H. Identification of a novel mechanism regulating β-cell mass: neuronal relay from the liver to pancreatic β-cells. Islets 2009; 1: 75-77 [PMID: 21084852 DOI: 10.4161/isl.1.1.8615]
38 Demir IE, Schäfer KH, Tieftrunk E, Friess H, Ceyhan GO. Neural plasticity in the gastrointestinal tract: chronic inflammation, neurotrophic signals, and hypersensitivity. Acta Neuropathol 2013; 125: 491-509 [PMID: 23417735 DOI: 10.1007/s00401-013-1099-4]
39 Lehrer RI. Primate defensins. Nat Rev Microbiol 2004; 2: 727-738 [PMID: 15372083]
40 Bals R, Goldman MJ, Wilson JM. Mouse beta-defensin 1 is a salt-sensitive antimicrobial peptide present in epithelia of the lung and urogenital tract. Infect Immun 1998; 66: 1225-1232 [PMID:
9488417]41 McCray PB, Bentley L. Human airway epithelia express a beta-
defensin. Am J Respir Cell Mol Biol 1997; 16: 343-349 [PMID: 9070620]
42 Valore EV, Park CH, Quayle AJ, Wiles KR, McCray PB, Ganz T. Human beta-defensin-1: an antimicrobial peptide of urogenital tissues. J Clin Invest 1998; 101: 1633-1642 [PMID: 9541493]
43 Huang YH, Wang PW, Tiao MM, Chou MH, Du YY, Huang CC, Chuang JH. Glucocorticoid modulates high-mobility group box 1 expression and Toll-like receptor activation in obstructive jaundice. J Surg Res 2011; 170: e47-e55 [PMID: 21737101 DOI: 10.1016/j.jss.2011.05.033]
44 Harada K, Ohba K, Ozaki S, Isse K, Hirayama T, Wada A, Nakanuma Y. Peptide antibiotic human beta-defensin-1 and -2 contribute to antimicrobial defense of the intrahepatic biliary tree. Hepatology 2004; 40: 925-932 [PMID: 15382127]
45 Schussler GC. The thyroxine-binding proteins. Thyroid 2000; 10: 141-149 [PMID: 10718550]
46 Ellingsgaard H, Ehses JA, Hammar EB, Van Lommel L, Quintens R, Martens G, Kerr-Conte J, Pattou F, Berney T, Pipeleers D, Halban PA, Schuit FC, Donath MY. Interleukin-6 regulates pancreatic alpha-cell mass expansion. Proc Natl Acad Sci USA 2008; 105: 13163-13168 [PMID: 18719127 DOI: 10.1073/pnas.0801059105]
47 Yang J, MacDougall ML, McDowell MT, Xi L, Wei R, Zavadoski WJ, Molloy MP, Baker JD, Kuhn M, Cabrera O, Treadway JL. Polyomic profiling reveals significant hepatic metabolic alterations in glucagon-receptor (GCGR) knockout mice: implications on anti-glucagon therapies for diabetes. BMC Genomics 2011; 12: 281 [PMID: 21631939 DOI: 10.1186/1471-2164-12-281]
48 Guettet C, Mathe D, Riottot M, Lutton C. Effects of chronic glucagon administration on cholesterol and bile acid metabolism. Biochim Biophys Acta 1988; 963: 215-223 [PMID: 3058212]
49 Ikegami T, Krilov L, Meng J, Patel B, Chapin-Kennedy K, Bouscarel B. Decreased glucagon responsiveness by bile acids: a role for protein kinase Calpha and glucagon receptor phosphory-lation. Endocrinology 2006; 147: 5294-5302 [PMID: 16916948]
50 Hylemon PB, Zhou H, Pandak WM, Ren S, Gil G, Dent P. Bile acids as regulatory molecules. J Lipid Res 2009; 50: 1509-1520 [PMID: 19346331 DOI: 10.1194/jlr.R900007-JLR200]
51 Coleman DL. A historical perspective on leptin. Nat Med 2010; 16: 1097-1099 [PMID: 20930752 DOI: 10.1038/nm1010-1097]
52 Andersson A. Tissue culture of isolated pancreatic islets. Acta Endocrinol Suppl (Copenh) 1976; 205: 283-294 [PMID: 826064]
53 Andersson A, Eriksson U, Ostenson CG. Glucagon production by cultured pancreatic islets: effects of different culture conditions and media. In Vitro 1981; 17: 378-384 [PMID: 6166539]
54 Al-Sarireh B, Haidermota M, Verbeke C, Rees DA, Yu R, Griffiths AP. Glucagon cell adenomatosis without glucagon receptor mutation. Pancreas 2013; 42: 360-362 [PMID: 23407487]
P- Reviewer: Barreto S, Welsch T, Zielinski J S- Editor: Ji FF L- Editor: A E- Editor: Liu SQ
Yu R et al . The elusive liver factor

AbstractMagnetic resonance imaging (MRI) is a well established technique that has revolutionized diagnostic radiology. Until recently, the impact that MRI has had in the assessment of gastrointestinal motor function and bowel fluid distribution in health and in disease has been more limited, despite the novel insights that MRI can provide along the entire gastrointestinal tract. MRI biomarkers include intestinal motility indices, small bowel water content and whole gut transit time. The present review discusses new developments and applications of MRI in the upper gastrointestinal tract, the small bowel and the colon reported in the literature in the last 5 years.
Key words: Magnetic resonance imaging; Stomach; Small bowel; Colon; Motility
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Magnetic resonance imaging (MRI) of gastrointestinal motor function and fluids distribution is coming of age, with a range of MRI biomarkers that can be measured noninvasively. The novel MRI biomarkers include intestinal motility indexes, the small bowel water content and whole gut transit time. Future research directions will focus on small and large bowel motility and on gut transit. Further validation of the methods and automation of data analysis will finally translate the MRI biomarkers into clinical routine.
Khalaf A, Hoad CL, Spiller RC, Gowland PA, Moran GW, Marciani L. Magnetic resonance imaging biomarkers of gastrointestinal motor function and fluid distribution. World J Gastrointest Pathophysiol 2015; 6(4): 140149 Available from: URL: http://www.wjgnet.com/21505330/full/v6/i4/140.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i4.140
Asseel Khalaf, Caroline L Hoad, Robin C Spiller, Penny A Gowland, Gordon W Moran, Luca Marciani
Asseel Khalaf, Robin C Spiller, Gordon W Moran, Luca Marciani, Nottingham Digestive Diseases Centre and NIHR Nottingham Digestive Diseases Biomedical Research Unit, Nottingham University Hospitals NHS Trust and University of Nottingham, Nottingham NG7 2UH, United Kingdom
Caroline L Hoad, Penny A Gowland, Sir Peter Mansfield Imaging Centre, School of Physics and Astronomy, University of Nottingham, Nottingham NG7 2RD, United Kingdom
Author contributions: Khalaf A and Marciani L collected the data and all authors revised the final manuscript.
Conflictofinterest statement: The authors declare that they do not have any conflict of interest for this review article.
OpenAccess: This article is an openaccess article which was selected by an inhouse editor and fully peerreviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work noncommercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: http://creativecommons.org/licenses/bync/4.0/
Correspondence to: Dr. Luca Marciani, PhD, Associate Professor, Nottingham Digestive Diseases Centre and NIHR Nottingham Digestive Diseases Biomedical Research Unit, Nottingham University Hospitals NHS Trust and University of Nottingham, University Park street, Nottingham NG7 2UH, United Kingdom. [email protected]: +441158231248Fax: +441158231409
Received: June 26, 2015Peerreview started: June 27, 2015First decision: September 17, 2015Revised: September 28, 2015Accepted: October 20, 2015 Article in press: October 27, 2015Published online: November 15, 2015
REVIEW
140 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Magnetic resonance imaging biomarkers of gastrointestinal motor function and fluid distribution
World J Gastrointest Pathophysiol 2015 November 15; 6(4): 140-149ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i4.140

INTRODUCTIONThe first demonstrations of the use of dynamic, serial and cine magnetic resonance imaging (MRI) to investigate organ motor function and fluid distribution in the gastrointestinal (GI) tract were reported nearly three decades ago[1,2]. For a long period of time this niche field was explored in a handful of MRI research laboratories and dedicated researchers that put up with the very laborious and lengthy manual data processing, often carried out image by image. Recent advances in imaging methods and data analysis tools are now bringing MRIbased assessments of GI function and fluids into the clinical arena. The number of MRI biomarkers, as indicators of GI function that can be objectively measured, has broadened (Table 1). MRI is often perceived as an expensive technique; however the cost of a short MRI scan compares favorably with more invasive procedures such as, for example, manometric intubation. This review focuses only on the last 5 years of relevant literature using MRI to study gastrointestinal motor function and bowel fluid distribution in the upper GI tract, the small bowel and the colon in health and in disease. Previous years were covered by preceding reviews[35].
MRI OF GASTROINTESTINAL MOTOR FUNCTIONEsophagusThe dynamic of swallowing has been investigated with high temporal resolution MRI, providing functional information[68]. The images nicely delineate the motor action, and further work to validate these observations and establish clinical indications for “MR esophagography” would be welcome. One study showed a morphofunctional application to the study of achalasia[9] and another showed motility disturbances in some patients after Nissen fundoplication[10]. Gastroesophageal reflux was elegantly visualized using MRI and concomitant high resolution manometry[11] (Figure 1) with a view to improve understanding of reflux suppression by a raft-forming alginate, compared to a different antacid formulation. The same group provided a detailed biophysical analysis of the function and structure of the gastroesophageal junction[1214] hypothesizing that components of a “flap valve” contribute to reflux protection, and that this is impaired in patients with gastro esophageal reflux disease. These are unprecedented biomechanical insights into the function of the upper GI tract.
StomachThere has been continuing interest in the effect of manipulating the physical properties of food components on gastric motor function and appetite. Aerated foams were imaged for the first time in vivo demonstrating their effect on increasing gastric volumes and reducing appetite compared to isocaloric, nonaerated bever
ages[15]. It was also shown that fat emulsions of varying droplet size can modulate gastric emptying[16,17]. The data processing required to monitor gastric volumes and emptying can still be a burden. Developments were made in modeling the emptying curves including gastric secretion[18,19] and in automating the analysis[1921], with a view to creating a protocol that would be acceptable in clinical practice. Gastric motility was evaluated by simple review of cine MRI series across the stomach after laparoscopic sleeve gastrectomy[22]. The sleeve was found to have little peristaltic function whilst the antrum showed accelerated propulsion. Comparison between manual and automated analysis of gastric motility[23], concluded that the semiautomated procedure for segmentation had comparable accuracy and much better efficiency than the manual method.
Small bowelThe MRI assessment of small bowel motility is the field that has seen some of the most interesting developments over the last 5 years. A number of publications reported developments towards increased automation of analysis and quantitation of small bowel motility biomarkers. The task is still challenging. Good bowel distention is generally required; this is achieved by either infusing a large amount of liquid contrast directly in the small bowel using a catheter (MR enteroclysis) or by ingesting it [magnetic resonance enterography (MRE)]. MRE has been more popular because it is less demanding on both staff and patients. There is however little consensus. Based on local preferences, different contrast media, prone or supine position as well as different acquisition protocols and analysis strategies are used.
In terms of data acquisition, different MRI protocols have been proposed. Qualitatively, many MRI units nowadays add a short cine sequence to small bowel protocols, before injection of spasmolytics, for an overall visual assessment or operator’s grading of motility[24,25]. Robust biomarkers however require objective quantitation and their translation requires improvements in data processing. There are two distinct schools of thoughts: One prefers breathhold acquisitions whilst the other favors acquiring data for longer periods of time, freebreathing. The former minimizes diaphragmatic displacement thus making the data analysis easier. Multiple breathholds can be acquired to sample motility for longer periods. Displacement of the small bowel by abdominal or diaphragmatic movement can affect the analysis during prolonged observation; this was evaluated in the prone position finding that craniocaudal displacement is predominant but the amplitude of the displacement is modest[26]. The second school of thought seeks to acquire for longer periods of time with the patient breathing freely and gently. In this case respiratory motion affects the quantitation of motility substantially and techniques are needed to correct for this in the time series before analysis. Robust Data Decomposition Registration (RRDR)[27] was used as a preprocessing step to remove respiratory motion; after
141 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Khalaf A et al . MRI of GI function and fluids

this step global small bowel motility[28] was determined using an optic flow registration method[29]. The motility biomarker is based on the standard deviation of the Jacobian calculated from the displacement fields of the image pixels. This biomarker is based on the pixel intensity changes that the software uses to derive the registration parameters; hence it is not exactly anchored “biomechanically” to the bowel walls. On the other hand, the method provides an elegant and operatorindependent assessment of global motility from long, free breathing timeseries and yields motility maps that are easy to interpret (Figure 2). Another automated approach based on the optic flow registration technique was implemented, without the dual registration prestep, in studies in IBD patients[30,31]. An alternative MRI approach to monitor motility is the continuous tagging, as is common in cardiac MRI. A global tagging motility index biomarker was used[32] with the motility analysis subdivided in low, medium and high frequency bands[33]. The index was able to detect a decrease in motility due to intravenous antiperistaltic agent. The tagging method
is region of interest (ROI)independent. Tagging may also depend less on bowel distension, as suggested by the authors suggest[32].
In terms of data analysis, there was a limited use of visual, consensus analysis[34], mean change in signal amplitude[35] and manual luminal caliber measurements[36]. Software assisted methods were applied to both breathhold and freebreathing acquisitions[23,37,38] and performed better than manual measurements[39]. The choice of intrasegmental location for the softwareassisted analysis did not influence substantially the mea-surements substantially[40]. Region of interest analysis of small bowel motility showed however intersegmental variation and modest repeatability[41], which would favor global, operator independent methods[42]. The frequency band analysis of continuously tagged images was also assessed automatically[33].
The MRI assessment of motility has found interesting applications in Crohn’s disease (CD), a particularly vulnerable population. These patients are likely to undergo serial imaging examination over the course
142 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Table 1 Magnetic resonance imaging biomarkers of gastrointestinal motor function and fluid distribution
Biomarker Method Ref.
Gastric emptying Time courses of gastric volumes, ROI analysis [18-21]Gastric secretion volume T1 mapping, dilution of a meal labeled with gadolinium contrast agent [19,67]Gastric motility Cine-MRI [23]Small bowel motility Cine-MRI, image registration, standard deviation of the Jacobian [28,29]Small bowel water content Heavily T2 weighted imaging, ROI analysis using calibrated threshold [61]Oro-cecal transit time Arrival of the head of a meal in the cecum [65]Colonic volumes ROI analysis [58,59]Colon water content Heavily T2 weighted imaging, ROI analysis using calibrated threshold [74]Colon motility Cine-MRI, image registration, line ROI analysis [28]Whole gut transit T1-weighted imaging, capsules filled with water and gadolinium contrast agent [65]Colonic chyme relaxometry T1 and T2 measurements [61,74]
MRI: Magnetic resonance imaging; ROI: Region of interest.
t1 = 132 s t2 = 139 s t3 = 150 s t4 = 153 s
Proximal esophagusReflux event
Distal esophagus
LES
Stomach t1 t2 t3 t4
SwallowPr
essu
re (
mm
Hg)
Dis
tanc
e fr
om n
ares
(m
m)
195
220240260280300320340360380400420440
110
100
90
80
70
60
50454035302520151062261015
Figure 1 Concurrent high-resolution manometry and magnetic resonance imaging. Representative image demonstrates concurrent high-resolution manometry and magnetic resonance imaging detection of reflux. Note that shortening of the esophagus in the dynamic magnetic resonance images appears to draw the proximal stomach upwards relative to the catheter (above). Reproduced with permission from ref. [11].
Khalaf A et al . MRI of GI function and fluids

143 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
test was shown to accelerate intestinal motility after laparoscopic sleeve gastrectomy[25]. Another interesting application of cine MRI was in chronic intestinal pseudoobstruction (CIPO), showing contractility impairments in the CIPO patients compared to healthy volunteers and patients with irritable bowel syndrome[55]. It is worth noting that MRI of small bowel motility has also found some applications in animal models[56,57] although those are beyond the scope of this review. MRI was also used to study postprandial colon volumes as another biomarker of function[58]. Manual colon segmentation is lengthy and methods to semiautomate the processing have been proposed recently[59].
Despite the lack of standardization and the need for some further validation, the emerging biomarkers of small bowel motility are very promising and the body of recent work demonstrates that cine MRI of small bowel motility is coming of age. The data acquisition can translate to the clinics relatively easily. The highend image registration and data processing methods may however require implementation in the scanner viewing platforms or dedicated cloud computing services for the technique to move into routine use.
ColonDespite the flourishing of MRI publications on small bowel motility, so far little attention has been given
of their treatment and the cumulative radiation dose from repeated computed tomography is undesirable[43]. Reduced motility was associated with small bowel segments affected by CD[24], correlating well with histopathology[44] and inflammatory markers in the blood and stools[45]. Notably the MRI motility biomarker reflected disease activity. Motility scores were associated negatively with disease activity score[46,47], using a multivariate analysis based on mural thickness, mural T2 signal, perimural T2 signal and enhancement[48]. Another finding of great interest is the demonstration that small bowel motility is not only impaired at the site of the lesion but also proximally[4951]. The availability of cine MRE images was shown to aid the reader’s evaluation of questionable segments in a less ordinary CD exam protocol without the use of antiperistaltic agents[52].
Beyond specific CD applications, cine MRI of small bowel motility was used to compare intravenous and intramuscular delivery routes for antiperistaltic agents[53]. The data showed that intravenous administration had a faster and more reliable onset, whilst a combination of different agents and delivery routes provided early onset and high degree, sustained spasmolysis. The effectiveness of sublingual hyoscyamine sulphate as an alternative to antiperistaltic intravenous agents was also investigated using cine MRI[54]. The treatment effect of the sublingual agent was modest. The oral glucose tolerance
A B C
D E F
Figure 2 Small bowel motility maps. Example of small bowel regions (contoured) in the upper panel and motility biomarker maps in the lower panel. Respectively: breath-hold ground truth (A and D), dual-registration of abdominal motion (B and E) and free breathing optical flow registration alone (C and F), respectively. Respiratory motion compensation is visible as reduced motility in the transverse colon closest to the diaphragm and systemically over the small bowel. The effect of robust data decomposition registration is less apparent in the lower bowel further from the diaphragm where the effects of free breathing are less pronounced. The color coding I the motility maps shows black as lower motility and white as higher. Reprinted with permission from ref. [28].
Khalaf A et al . MRI of GI function and fluids

144 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
to colonic motility. One possible reason for this is that colonic motility is inherently erratic so that an observation based on a single breathhold cine slab may not be very informative. A longer acquisition time of a cine MRI sequence would characterize motility better. However, the same respiratory motion problems detailed above for the small bowel will affect the data.
The published studies used a variety of approaches. Visual inspection of cine MRI stacks showed reduced or absent peristalsis in involved colonic segments of 3 patients with ulcerative colitis, compared to other bowel segments[34]. In one elegant study bisacodyl instillation was used to induce high amplitude propagated pressure waves in the (cleansed) descending colon of 10 healthy volunteers and motility was monitored by concomitant MRI and manometry[60]. Three perpendicular imaging planes were acquired at 4 s intervals at baseline and for 24 min post bisacodyl instillation. The MRI images in each plane were played as a cine loop identifying changes of 50% in the largest diameter of the haustras. Eleven of these larger amplitude contractions were detected and these had an excellent 100% correlation with the manometry readings.
In a different study a subjective colonic motility index score was assessed by an operator in response to an oral polyethylene glycol (PEG) stimulus that distended the ascending colon and stimulated motility in healthy volunteers[61]. A single sagittal slice was acquired every second for 2 min of free breathing. No motion correction was applied and the operator inspected the data by dividing the ascending colon in three regions, estimating for how long each region showed contractility. This applied to any visible contractility not just high amplitude propagated waves. Using this relatively basic method the authors showed a marked increase in motility upon ingestion of PEG and that the increase was dosedependent.
More quantitative approaches can clearly benefit from the registration of abdominal motion as discussed for the small bowel. A recent study applied the optic flow and RRDR dualregistration method to MRI data from the ascending colon of 6 healthy volunteers who ingested an oral PEG stimulus[28]. A single sagittal slice was again acquired every second for 2 min of free breathing. The study then compared simple line ROIs analysis results with and without application of the motion correction and showed the importance of correcting for abdominal motion to remove ambiguity. Optic flow methods were also used to quantify effectively hypomotility of colonic segments affected by CD using the static images as guide to define regions of interest in global motility maps[30].
Work this area is likely to continue in the next few years and the focus for new developments will expand from the small bowel towards MRI of colonic motility.
Flow and transitBowel luminal flow has been overlooked whilst MRI of gastrointestinal transit has been the subject of a few new
technical development studies. Three studies by Hahn et al[62] sought to use 19F imaging and MRI “transit capsule markers”. This is an interesting approach as there is basically no endogenous fluorine MRI signal in the human body, so any signal detected can be attributed to the capsules. Moreover the 19F nucleus has particularly good MRI visibility with 100% natural abundance and a gyromagnetic ratio close to the one of the hydrogen proton. The authors were able to show simultaneous, realtime tracking of one and two capsules in the GI tract of two healthy volunteers using 19F projection imaging superimposed to a proton anatomical reference[62] (Figure 3). In subsequent studies the “3D golden angle radial projection” 19F imaging was deployed[63]. Using this acquisition they tracked capsules either embedded in a nasogastric catheter (to enable tracking of the catheter) or ingested (to track the transit of the capsules in the GI tract) by one healthy volunteer. The 19F MRI catheter tracking methodology was further improved which allowed real time visualization and manipulation of the catheter[64]. The idea of using 19F to monitor GI transit is elegant; however there are significant barriers to translation including the need to use high field (≥ 3T), multinuclear transmit and receive hardware and a dedicated abdominal 19F transmit/receive coil, of which at the moment there are only few worldwide. The capsules are also relatively large (12 mm × 7 mm) and so unlikely to empty from the fed stomach. They are more likely to remain within the stomach until expelled by the migrating motor complex which will not develop until the fasting state is reached. Thus propulsion of these capsules along the GI tract is unlikely to mirror physiological transit of food. A different approach has been to use the proton MRI and MRI “transit capsule markers” filled with water doped with trace amounts of gadolinium contrast agent. Measurement of whole gut transit based on ingestion of 5 such markers and T1weighted imaging was validated against standard radiopaque marker Xray methods with repeated studies in 21 healthy volunteers[65]. The MRI method performed well against Xray methodology and does not require high field or additional hardware. However the capsules are again relatively large (20 mm × 7 mm) and gastric sieving is likely to retain them during the fed state so they will only leave the stomach after the food has left. Furthermore their signal could be confused with high T1 food residue particularly at the terminal ileum/proximal colon. Within the same study, a simple method to measure orocecal transit time (OCTT) based on imaging the arrival of the “head of a meal” in the cecum was also evaluated against concomitant standard lactose ureide 13C breath test[65]. Correlation between the two methods was weak. Another major limitation of this MRI method is the need to continue imaging at intervals until the arrival of the “head of the meal” in the cecum is detected. This limits the time resolution of OCTT to the sampling frequency which is unsatisfactory. Furthermore the repeated scanning until detection is achieved would make its routine use expensive. Another study sought to evaluate OCTT by
Khalaf A et al . MRI of GI function and fluids

145 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
similar MRI methods comparing the results to concomitant standard lactulose hydrogen breath test[66]. The passing of the lactulose fluid bolus through the small bowel was followed visually on T2 weighted images until its arrival in the cecum was detected.
These studies show an increasing interest in developing non invasive MRI biomarkers for both orocecal and whole gut transit. Further work is needed to improve such methods and make them more physiological if they are to translate to the clinics effectively.
MRI OF GASTROINTESTINAL FLUID DISTRIBUTIONStomachThe investigation of fluids in the upper GI was predominantly focused on gastric secretion as measured by T1 mapping of a test meal doped with traces of a Gdbased contrast agent[19,67]. This showed a layer above the liquid meal in the stomach containing a lower concentration of contrast agent[68]. This is consistent with the concept of the “acid pocket” and could provide a target for gastroesophageal reflux treatments. Another study assessed the effect of pharmacologically enhanced gastric secretion on 13Cacetate breath test for gastric emptying[69]. There was new interest from the point of view of pharmaceutical sciences and drug dissolution. Two new studies investigated gastric fluid content under the standard fasting[70] and fed oral dosage form
conditions[71] with a view to improving in vitro/in vivo correlation of drug dissolution modeling.
Small bowelA number of studies evaluated the fluid content of the small bowel. Some monitored the effect of nutritional interventions[16,17,72,73]. These showed that the effect of physicochemical modifications in food microstructure (such as for example fat emulsion stability and droplet size) can markedly modulate small bowel postprandial fluid inflow. One study demonstrated the effect of a bowel preparation containing polyethylene glycol and electrolytes in generating inflow of fluid in the lumen[61]. By contrast another study showed the ability of a common antidiarrheal agent, loperamide, to reduce the small bowel water content after a mannitol challenge model of secretory diarrhea[74]. Bowel fluid was also shown to be increased by an essential amino acid[75]. Other MRI studies showed that experimental stress reduced small bowel water content[76]. The effect of poorly absorbed and non absorbable carbohydrates on bowel fluid inflow and accumulation was also studied; these included fructose[77] (Figure 4) and lactulose[78]. The presence of separate small water pockets in the fasting small bowel was confirmed and the distribution and volume of the bowel pockets measured before and after ingestion of the standard fasting drug testing dose of 240 mL of water[70] with the same pharmaceutical sciences rationale as described above. The main finding
Figure 3 19F magnetic resonance imaging tracking of transit marker capsule in two healthy subjects. The panel shows anatomical reference images, 19F capsules positions and the fitted intestinal course for subjects (A) and (B). The labels on the figure denote the stomach (S), gall bladder (G) and small intestine (I) and the time course of the two capsules is color coded. Reprinted with permission from ref. [62]. LR: Left-right; FH: Feet-head.
150
0
150
F H
(m
m)
1500
150L R (mm)
F H
(m
m)
L R (mm)
150
0
0 150
GSG
t /min
t /min
51
38
26
13
0
39
29
20
10
0
SS
150
0
150
F H
(m
m)
150
0
150
L R (m
m)
150
0
110
F H
(m
m)
L R (mm)150 0
A
B
I
I
I
I
Khalaf A et al . MRI of GI function and fluids

146 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
was that the small bowel water pockets are discontinuous and their number and volume is small.
ColonTwo studies addressed colon fluid distribution using MRI. One study used an oral mannitol challenge and showed inflow of water from the small bowel into the ascending colon[74], quantifying the amount of freely mobile water in the ascending colon using similar methods as those used for the small bowel. The study found that there was only a small amount of freely mobile water detectable in the ascending colon. T2 relaxometry was also used in that study to characterize physicochemical changes in the chyme upon arrival of the fluid bolus, which showed an increase in T2 reflecting increased fluid mobility in the chyme. The other study showed that ingestion of a bowel preparation containing polyethylene glycol and electrolytes reached the colon rapidly increasing its size twofold[61]. The study also used T1 relaxometry to characterize physicochemical changes in the chyme upon arrival of the fluid bolus. The relaxation time T1 of the ascending colon contents increased upon arrival of the fluid in the chyme as expected. Given the growing interest in bowel fluid dynamics and the work conducted so far more proximally, one can predict that MRI of colonic fluids will be an expanding field in the near future.
CONCLUSIONMRI of gastrointestinal function is coming of age. The development of more automated analysis methods will aid translation into clinical routine although further work on validating the MRI biomarkers is needed. The novel insights provided on bowel fluid volumes and distribution will improve understanding of disease and predictive models of drug dissolution. Further trials are needed to prove the value of the MRI biomarkers in clinical practice.
REFERENCES1 The British Society of Gastroenterology, 49th meeting. Sheffield,
1416 September 1988. Abstracts. Gut 1988; 29: A1429A1496 [PMID: 3197976]
2 Stehling MK, Evans DF, Lamont G, Ordidge RJ, Howseman AM, Chapman B, Coxon R, Mansfield P, Hardcastle JD, Coupland RE. Gastrointestinal tract: dynamic MR studies with echoplanar imaging. Radiology 1989; 171: 4146 [PMID: 2928545 DOI: 10.1148/radiology.171.1.2928545]
3 Schwizer W, Steingoetter A, Fox M. Magnetic resonance imaging for the assessment of gastrointestinal function. Scand J Gastroenterol 2006; 41: 12451260 [PMID: 17060117 DOI: 10.1080/00365520600827188]
4 Schwizer W, Fox M, Steingötter A. Noninvasive investigation of gastrointestinal functions with magnetic resonance imaging: towards an “ideal” investigation of gastrointestinal function. Gut 2003; 52 Suppl 4: iv34iv39 [PMID: 12746267 DOI: 10.1136/gut.52.suppl_4.iv34]
5 Marciani L. Assessment of gastrointestinal motor functions by MRI: a comprehensive review. Neurogastroenterol Motil 2011; 23: 399407 [PMID: 21276139 DOI: 10.1111/j.13652982.2011.01670.x]
6 Zhang S, Olthoff A, Frahm J. Realtime magnetic resonance imaging of normal swallowing. J Magn Reson Imaging 2012; 35: 13721379 [PMID: 22271426 DOI: 10.1002/jmri.23591]
7 Kulinna-Cosentini C, Schima W, Lenglinger J, Riegler M, Kölblinger C, BaSsalamah A, Bischof G, Weber M, Kleinhansl P, Cosentini EP. Is there a role for dynamic swallowing MRI in the assessment of gastroesophageal reflux disease and oesophageal motility disorders? Eur Radiol 2012; 22: 364370 [PMID: 21894565 DOI: 10.1007/s0033001122584]
8 Zhang J, Hu W, Zang L, Yao Y, Tang Y, Qian Z, Gao P, Wu X, Li S, Xie Z, Yuan X. Clinical investigation on application of water swallowing to MR esophagography. Eur J Radiol 2012; 81: 19801985 [PMID: 21645980 DOI: 10.1016/j.ejrad.2011.05.010]
9 Miyazaki Y, Nakajima K, Sumikawa M, Yamasaki M, Takahashi T, Miyata H, Takiguchi S, Kurokawa Y, Tomiyama N, Mori M, Doki Y. Magnetic resonance imaging for simultaneous morphological and functional evaluation of esophageal motility disorders. Surg Today 2014; 44: 668676 [PMID: 23689949 DOI: 10.1007/s0059501306172]
10 Kulinna-Cosentini C, Schima W, BaSsalamah A, Cosentini EP. MRI patterns of Nissen fundoplication: normal appearance and mechanisms of failure. Eur Radiol 2014; 24: 21372145 [PMID: 24965508 DOI: 10.1007/s003300143267x]
11 Sweis R, Kaufman E, Anggiansah A, Wong T, Dettmar P, Fried M, Schwizer W, Avvari RK, Pal A, Fox M. Postprandial reflux suppression by a raftforming alginate (Gaviscon Advance) compared to a simple antacid documented by magnetic resonance imaging and pHimpedance monitoring: mechanistic assessment in healthy volunteers and randomised, controlled, doubleblind study in reflux patients. Aliment Pharmacol Ther 2013; 37: 10931102 [PMID: 23600790 DOI: 10.1111/apt.12318]
12 Curcic J, Roy S, Schwizer A, Kaufman E, ForrasKaufman Z, Menne D, Hebbard GS, Treier R, Boesiger P, Steingoetter A, Fried M, Schwizer W, Pal A, Fox M. Abnormal structure and function of the esophagogastric junction and proximal stomach in gastroesophageal reflux disease. Am J Gastroenterol 2014; 109: 658667 [PMID: 24589669 DOI: 10.1038/ajg.2014.25]
13 Roy S, Fox MR, Curcic J, Schwizer W, Pal A. The gastroesophageal reflux barrier: biophysical analysis on 3D models of anatomy from magnetic resonance imaging. Neurogastroenterol Motil 2012; 24: 61625, e269 [PMID: 22417158 DOI: 10.1111/j.13652982.2012.01909.x]
14 Curcic J, Schwizer A, Kaufman E, ForrasKaufman Z, Banerjee S, Pal A, Hebbard GS, Boesiger P, Fried M, Steingoetter A, Schwizer W, Fox M. Effects of baclofen on the functional anatomy of the oesophagogastric junction and proximal stomach in
Stomach Small bowel
FructoseGlucose
Callbladder
A B
Figure 4 Small bowel water imaging. Representative example of coronal images of the small bowel water from a single volunteer acquired 75 min after drinking 40 g of glucose (A) or 40 g fructose (B) in 500 mL water. Glucose is rapidly absorbed so the small bowel has very little water in it despite the large drink. Conversely fructose is poorly absorbed and osmotically active as shown by the large amount of water in the small bowel. Adapted with authors’ own copyright from ref. [77].
Khalaf A et al . MRI of GI function and fluids

147 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
healthy volunteers and patients with GERD assessed by magnetic resonance imaging and highresolution manometry: a randomised controlled doubleblind study. Aliment Pharmacol Ther 2014; 40: 12301240 [PMID: 25230154 DOI: 10.1111/apt.12956]
15 Murray K, Placidi E, Schuring EA, Hoad CL, Koppenol W, Arnaudov LN, Blom WA, Pritchard SE, Stoyanov SD, Gowland PA, Spiller RC, Peters HP, Marciani L. Aerated drinks increase gastric volume and reduce appetite as assessed by MRI: a randomized, balanced, crossover trial. Am J Clin Nutr 2015; 101: 270278 [PMID: 25646323 DOI: 10.3945/ajcn.114.096974]
16 Hussein MO, Hoad CL, Wright J, Singh G, Stephenson MC, Cox EF, Placidi E, Pritchard SE, Costigan C, Ribeiro H, Ciampi E, Nandi A, Hedges N, Sanderson P, Peters HP, Rayment P, Spiller RC, Gowland PA, Marciani L. Fat emulsion intragastric stability and droplet size modulate gastrointestinal responses and subsequent food intake in young adults. J Nutr 2015; 145: 11701177 [PMID: 25926408 DOI: 10.3945/jn.114.204339]
17 Steingoetter A, Radovic T, Buetikofer S, Curcic J, Menne D, Fried M, Schwizer W, Wooster TJ. Imaging gastric structuring of lipid emulsions and its effect on gastrointestinal function: a randomized trial in healthy subjects. Am J Clin Nutr 2015; 101: 714724 [PMID: 25833970 DOI: 10.3945/ajcn.114.100263]
18 Fruehauf H, Menne D, Kwiatek MA, ForrasKaufman Z, Kaufman E, Goetze O, Fried M, Schwizer W, Fox M. Interobserver reproducibility and analysis of gastric volume measurements and gastric emptying assessed with magnetic resonance imaging. Neurogastroenterol Motil 2011; 23: 854861 [PMID: 21740482 DOI: 10.1111/j.13652982.2011.01743.x]
19 Hoad CL, Parker H, Hudders N, Costigan C, Cox EF, Perkins AC, Blackshaw PE, Marciani L, Spiller RC, Fox MR, Gowland PA. Measurement of gastric meal and secretion volumes using magnetic resonance imaging. Phys Med Biol 2015; 60: 13671383 [PMID: 25592405 DOI: 10.1088/00319155/60/3/1367]
20 Banerjee S, Dixit S, Fox M, Pal A. Validation of a rapid, semiautomatic image analysis tool for measurement of gastric accommodation and emptying by magnetic resonance imaging. Am J Physiol Gastrointest Liver Physiol 2015; 308: G652G663 [PMID: 25540229 DOI: 10.1152/ajpgi.00095.2014]
21 Bharucha AE, Karwoski RA, Fidler J, Holmes DR, Robb RA, Riederer SJ, Zinsmeister AR. Comparison of manual and semiautomated techniques for analyzing gastric volumes with MRI in humans. Am J Physiol Gastrointest Liver Physiol 2014; 307: G582G587 [PMID: 25012844 DOI: 10.1152/ajpgi.00048.2014]
22 Baumann T, Kuesters S, Grueneberger J, Marjanovic G, Zimmermann L, Schaefer AO, Hopt UT, Langer M, Karcz WK. Timeresolved MRI after ingestion of liquids reveals motility changes after laparoscopic sleeve gastrectomypreliminary results. Obes Surg 2011; 21: 95101 [PMID: 21088924 DOI: 10.1007/s1169501003176]
23 Bickelhaupt S, Froehlich JM, Cattin R, Raible S, Bouquet H, Bill U, Patak MA. Softwaresupported evaluation of gastric motility in MRI: a feasibility study. J Med Imaging Radiat Oncol 2014; 58: 1117 [PMID: 24131557 DOI: 10.1111/17549485.12097]
24 Guglielmo FF, Mitchell DG, O’Kane PL, Deshmukh SP, Roth CG, Burach I, Burns A, Dulka S, Parker L. Identifying decreased peristalsis of abnormal small bowel segments in Crohn’s disease using cine MR enterography: the frozen bowel sign. Abdom Imaging 2015; 40: 11501156 [PMID: 25326259 DOI: 10.1007/s002610140258y]
25 Trung VN, Yamamoto H, Furukawa A, Yamaguchi T, Murata S, Yoshimura M, Murakami Y, Sato S, Otani H, Ugi S, Morino K, Maegawa H, Tani T. Enhanced Intestinal Motility during Oral Glucose Tolerance Test after Laparoscopic Sleeve Gastrectomy: Preliminary Results Using Cine Magnetic Resonance Imaging. PLoS One 2013; 8: e65739 [PMID: 23823622 DOI: 10.1371/journal.pone.0065739]
26 Bickelhaupt S, Froehlich JM, Wentz KU, von Weymarn C, Patak MA. Smallbowel dislocation during longterm MRI observation insights in intestinal physiology. Clin Physiol Funct Imaging 2015; 35: 4148 [PMID: 24418110 DOI: 10.1111/cpf.12124]
27 Hamy V, Dikaios N, Punwani S, Melbourne A, Latifoltojar A, Makanyanga J, Chouhan M, Helbren E, Menys A, Taylor S, Atkinson D. Respiratory motion correction in dynamic MRI using robust data decomposition registration application to DCEMRI. Med Image Anal 2014; 18: 301313 [PMID: 24322575 DOI: 10.1016/j.media.2013.10.016]
28 Menys A, Hamy V, Makanyanga J, Hoad C, Gowland P, Odille F, Taylor SA, Atkinson D. Dual registration of abdominal motion for motility assessment in freebreathing data sets acquired using dynamic MRI. Phys Med Biol 2014; 59: 46034619 [PMID: 25079109 DOI: 10.1088/00319155/59/16/4603]
29 Odille F, Menys A, Ahmed A, Punwani S, Taylor SA, Atkinson D. Quantitative assessment of small bowel motility by nonrigid registration of dynamic MR images. Magn Reson Med 2012; 68: 783793 [PMID: 22234983 DOI: 10.1002/mrm.23298]
30 Hahnemann ML, Nensa F, Kinner S, Gerken G, Lauenstein TC. Motility mapping as evaluation tool for bowel motility: initial results on the development of an automated colorcoding algorithm in cine MRI. J Magn Reson Imaging 2015; 41: 354360 [PMID: 24399576 DOI: 10.1002/jmri.24557]
31 Hahnemann ML, Nensa F, Kinner S, Maderwald S, Umutlu L, Gerken G, Lauenstein TC. Improved detection of inflammatory bowel disease by additional automated motility analysis in magnetic resonance imaging. Invest Radiol 2015; 50: 6772 [PMID: 25260093 DOI: 10.1097/RLI.0000000000000097]
32 Sprengers AM, van der Paardt MP, Zijta FM, Caan MW, Lamerichs RM, Nederveen AJ, Stoker J. Use of continuously MR tagged imaging for automated motion assessment in the abdomen: a feasibility study. J Magn Reson Imaging 2012; 36: 492497 [PMID: 22411355 DOI: 10.1002/jmri.23637]
33 van der Paardt MP, Sprengers AM, Zijta FM, Lamerichs R, Nederveen AJ, Stoker J. Noninvasive automated motion assessment of intestinal motility by continuously tagged MR imaging. J Magn Reson Imaging 2014; 39: 916 [PMID: 23553805 DOI: 10.1002/Jmri.24094]
34 Heye T, Stein D, Antolovic D, Dueck M, Kauczor HU, Hosch W. Evaluation of bowel peristalsis by dynamic cine MRI: detection of relevant functional disturbancesinitial experience. J Magn Reson Imaging 2012; 35: 859867 [PMID: 22267053 DOI: 10.1002/jmri.22851]
35 Farghal A, Kasmai B, Malcolm PN, Graves MJ, Toms AP. Developing a new measure of small bowel peristalsis with dynamic MR: a proof of concept study. Acta Radiol 2012; 53: 593600 [PMID: 22761345 DOI: 10.1258/ar.2012.110634]
36 Wakamiya M, Furukawa A, Kanasaki S, Murata K. Assessment of small bowel motility function with cineMRI using balanced steadystate free precession sequence. J Magn Reson Imaging 2011; 33: 12351240 [PMID: 21509884 DOI: 10.1002/jmri.22529]
37 Bickelhaupt S, Froehlich JM, Cattin R, Raible S, Bouquet H, Bill U, Patak MA. Softwareassisted small bowel motility analysis using freebreathing MRI: feasibility study. J Magn Reson Imaging 2014; 39: 1723 [PMID: 23553910 DOI: 10.1002/jmri.24099]
38 Bickelhaupt S, Cattin R, Froehlich JM, Raible S, Bouquet H, Bill U, Patak MA. Automatic detection of small bowel contraction frequencies in motility plots using lombscargle periodogram and sinusfitting methodinitial experience. Magn Reson Med 2014; 71: 628634 [PMID: 23467927 DOI: 10.1002/mrm.24708]
39 Bickelhaupt S, Froehlich JM, Cattin R, Raible S, Bouquet H, Bill U, Patak MA. Softwareassisted quantitative analysis of small bowel motility compared to manual measurements. Clin Radiol 2014; 69: 363371 [PMID: 24424326 DOI: 10.1016/j.crad.2013.11.004]
40 Bickelhaupt S, Froehlich JM, Patak MA. Automated small bowel motility measurements in MRI using 2D coronal slices does the intrasegmental location matter? A pilot study. Clin Imaging 2015; 39: 8993 [PMID: 25457530 DOI: 10.1016/j.clinimag.2014.10.003]
41 Menys A, Plumb A, Atkinson D, Taylor SA. The challenge of segmental small bowel motility quantitation using MR enterography. Br J Radiol 2014; 87: 20140330 [PMID: 24919500]
42 Menys A, Taylor SA, Emmanuel A, Ahmed A, Plumb AA, Odille F, Alam A, Halligan S, Atkinson D. Global small bowel motility:
Khalaf A et al . MRI of GI function and fluids

148 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
assessment with dynamic MR imaging. Radiology 2013; 269: 443450 [PMID: 23801770 DOI: 10.1148/radiol.13130151]
43 Gee MS, Harisinghani MG. MRI in patients with inflammatory bowel disease. J Magn Reson Imaging 2011; 33: 527534 [PMID: 21512607 DOI: 10.1002/jmri.22504]
44 Cullmann JL, Bickelhaupt S, Froehlich JM, SzucsFarkas Z, Tutuian R, Patuto N, Dawson H, Patak MA. MR imaging in Crohn’s disease: correlation of MR motility measurement with histopathology in the terminal ileum. Neurogastroenterol Motil 2013; 25: 749e577 [PMID: 23741963 DOI: 10.1111/nmo.12162]
45 Bickelhaupt S, Pazahr S, Chuck N, Blume I, Froehlich JM, Cattin R, Raible S, Bouquet H, Bill U, Rogler G, Frei P, Boss A, Patak MA. Crohn’s disease: small bowel motility impairment correlates with inflammatoryrelated markers Creactive protein and calprotectin. Neurogastroenterol Motil 2013; 25: 467473 [PMID: 23495824 DOI: 10.1111/Nmo.12088]
46 Menys A, Atkinson D, Odille F, Ahmed A, Novelli M, RodriguezJusto M, Proctor I, Punwani S, Halligan S, Taylor SA. Quantified terminal ileal motility during MR enterography as a potential biomarker of Crohn’s disease activity: a preliminary study. Eur Radiol 2012; 22: 24942501 [PMID: 22661057 DOI: 10.1007/s0033001225142]
47 Hahnemann ML, Nensa F, Kinner S, Köhler J, Gerken G, Umutlu L, Lauenstein TC. Quantitative assessment of small bowel motility in patients with Crohn‘s disease using dynamic MRI. Neurogastroenterol Motil 2015; 27: 841848 [PMID: 25808321 DOI: 10.1111/nmo.12558]
48 Steward MJ, Punwani S, Proctor I, AdjeiGyamfi Y, Chatterjee F, Bloom S, Novelli M, Halligan S, RodriguezJusto M, Taylor SA. Nonperforating small bowel Crohn’s disease assessed by MRI enterography: derivation and histopathological validation of an MRbased activity index. Eur J Radiol 2012; 81: 20802088 [PMID: 21924572 DOI: 10.1016/j.ejrad.2011.07.013]
49 Menys A, Helbren E, Makanyanga J, Emmanuel A, Forbes A, Windsor A, Punwani S, Halligan S, Atkinson D, Taylor SA. Small bowel strictures in Crohn’s disease: a quantitative investigation of intestinal motility using MR enterography. Neurogastroenterol Motil 2013; 25: 967e775 [PMID: 24028647 DOI: 10.1111/nmo.12229]
50 Bickelhaupt S, Wurnig M, Boss A, Patak MA. Correlation between morphological expansion and impairment of intra and prelesionary motility in inflammatory small bowel lesions in patients with Crohn’s disease preliminary data. Eur J Radiol 2014; 83: 10441050 [PMID: 24794863 DOI: 10.1016/j.ejrad.2014.03.009]
51 Bickelhaupt S, Froehlich JM, Cattin R, Patuto N, Tutuian R, Wentz KU, Culmann JL, Raible S, Bouquet H, Bill U, Patak MA. Differentiation between active and chronic Crohn’s disease using MRI smallbowel motility examinations initial experience. Clin Radiol 2013; 68: 12471253 [PMID: 23973163 DOI: 10.1016/j.crad.2013.06.024]
52 Grand DJ, Beland MD, Machan JT, MayoSmith WW. Detection of Crohn’s disease: Comparison of CT and MR enterography without antiperistaltic agents performed on the same day. Eur J Radiol 2012; 81: 17351741 [PMID: 21645982 DOI: 10.1016/j.ejrad.2011.04.068]
53 Gutzeit A, Binkert CA, Koh DM, Hergan K, von Weymarn C, Graf N, Patak MA, Roos JE, Horstmann M, Kos S, Hungerbühler S, Froehlich JM. Evaluation of the antiperistaltic effect of glucagon and hyoscine on the small bowel: comparison of intravenous and intramuscular drug administration. Eur Radiol 2012; 22: 11861194 [PMID: 22270141 DOI: 10.1007/s0033001123661]
54 Ghobrial PM, Neuberger I, Guglielmo FF, Mitchell DG, Parker L, O’Kane PL, Roth CG, Deshmukh SP, Borowski A. Cine MR enterography grading of small bowel peristalsis: evaluation of the antiperistaltic effectiveness of sublingual hyoscyamine sulfate. Acad Radiol 2014; 21: 8691 [PMID: 24331269 DOI: 10.1016/j.acra.2013.09.024]
55 Ohkubo H, Kessoku T, Fuyuki A, Iida H, Inamori M, Fujii T, Kawamura H, Hata Y, Manabe N, Chiba T, Kwee TC, Haruma K, Matsuhashi N, Nakajima A, Takahara T. Assessment of small bowel motility in patients with chronic intestinal pseudoobstruction
using cineMRI. Am J Gastroenterol 2013; 108: 11301139 [PMID: 23511458 DOI: 10.1038/Ajg.2013.57]
56 Ailiani AC, Neuberger T, Brasseur JG, Banco G, Wang Y, Smith NB, Webb AG. Quantifying the effects of inactin vs Isoflurane anesthesia on gastrointestinal motility in rats using dynamic magnetic resonance imaging and spatiotemporal maps. Neurogastroenterol Motil 2014; 26: 14771486 [PMID: 25257924 DOI: 10.1111/nmo.12410]
57 Bickelhaupt S, Wurnig MC, Lesurtel M, Patak MA, Boss A. Quantitative in vivo analysis of small bowel motility using MRI examinations in miceproof of concept study. Lab Anim 2015; 49: 5764 [PMID: 25266965 DOI: 10.1177/0023677214553321]
58 Pritchard SE, Marciani L, Garsed KC, Hoad CL, Thongborisute W, Roberts E, Gowland PA, Spiller RC. Fasting and postprandial volumes of the undisturbed colon: normal values and changes in diarrheapredominant irritable bowel syndrome measured using serial MRI. Neurogastroenterol Motil 2014; 26: 124130 [PMID: 24131490 DOI: 10.1111/nmo.12243]
59 Sandberg TH, Nilsson M, Poulsen JL, Gram M, Frøkjær JB, Østergaard LR, Drewes AM. A novel semiautomatic segmentation method for volumetric assessment of the colon based on magnetic resonance imaging. Abdom Imaging 2015; 40: 22322241 [PMID: 26054979 DOI: 10.1007/s002610150475z]
60 Kirchhoff S, Nicolaus M, Schirra J, Reiser MF, Göke B, Lienemann A. Assessment of colon motility using simultaneous manometric and functional cineMRI analysis: preliminary results. Abdom Imaging 2011; 36: 2430 [PMID: 20151304 DOI: 10.1007/s0026101095993]
61 Marciani L, Garsed KC, Hoad CL, Fields A, Fordham I, Pritchard SE, Placidi E, Murray K, Chaddock G, Costigan C, Lam C, JalankaTuovinen J, De Vos WM, Gowland PA, Spiller RC. Stimulation of colonic motility by oral PEG electrolyte bowel preparation assessed by MRI: comparison of split vs single dose. Neurogastroenterol Motil 2014; 26: 14261436 [PMID: 25060551 DOI: 10.1111/nmo.12403]
62 Hahn T, Kozerke S, Schwizer W, Fried M, Boesiger P, Steingoetter A. Visualization and quantification of intestinal transit and motor function by realtime tracking of 19F labeled capsules in humans. Magn Reson Med 2011; 66: 812820 [PMID: 21381105 DOI: 10.1002/mrm.22822]
63 Hahn T, Kozerke S, Schwizer W, Fried M, Boesiger P, Steingoetter A. 19F MR imaging golden anglebased capsule tracking for intestinal transit and catheter tracking: initial in vivo experience. Radiology 2012; 265: 917925 [PMID: 22996747 DOI: 10.1148/radiol.12120297]
64 Hahn T, Kozerke S, Schwizer W, Fried M, Boesiger P, Steingoetter A. Realtime multipoint gastrointestinal 19fluorine catheter tracking. Magn Reson Med 2014; 71: 302307 [PMID: 23400935 DOI: 10.1002/mrm.24654]
65 Chaddock G, Lam C, Hoad CL, Costigan C, Cox EF, Placidi E, Thexton I, Wright J, Blackshaw PE, Perkins AC, Marciani L, Gowland PA, Spiller RC. Novel MRI tests of orocecal transit time and whole gut transit time: studies in normal subjects. Neurogastroenterol Motil 2014; 26: 205214 [PMID: 24165044 DOI: 10.1111/nmo.12249]
66 Savarino E, Savarino V, Fox M, Di Leo G, Furnari M, Marabotto E, Gemignani L, Bruzzone L, Moscatelli A, De Cassan C, Sardanelli F, Sconfienza LM. Measurement of orocaecal transit time by magnetic resonance imaging. Eur Radiol 2015; 25: 15791587 [PMID: 25576231 DOI: 10.1007/s0033001435751]
67 Curcic J, Sauter M, Schwizer W, Fried M, Boesiger P, Steingoetter A. Validation of a golden angle radial sequence (GOLD) for abdominal T1 mapping during free breathing: demonstrating clinical feasibility for quantifying gastric secretion and emptying. J Magn Reson Imaging 2015; 41: 157164 [PMID: 24391022 DOI: 10.1002/jmri.24530]
68 Sauter M, Curcic J, Menne D, Goetze O, Fried M, Schwizer W, Steingoetter A. Measuring the interaction of meal and gastric secretion: a combined quantitative magnetic resonance imaging and pharmacokinetic modeling approach. Neurogastroenterol Motil
Khalaf A et al . MRI of GI function and fluids

149 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
2012; 24: 632638, e272273 [PMID: 22452723 DOI: 10.1111/j.13652982.2012.01916.x]
69 Kuyumcu S, Goetze O, Menne D, Treier R, Boesiger P, Fox M, Fried M, Schwizer W, Steingoetter A. Gastric secretion does not affect the reliability of the 13Cacetate breath test: A validation of the 13Cacetate breath test by magnetic resonance imaging. Neurogastroenterol Motil 2013; 25: 176e87 [PMID: 23066987 DOI: 10.1111/nmo.12025]
70 Mudie DM, Murray K, Hoad CL, Pritchard SE, Garnett MC, Amidon GL, Gowland PA, Spiller RC, Amidon GE, Marciani L. Quantification of gastrointestinal liquid volumes and distribution following a 240 mL dose of water in the fasted state. Mol Pharm 2014; 11: 30393047 [PMID: 25115349 DOI: 10.1021/mp500210c]
71 Koziolek M, Grimm M, Garbacz G, Kühn JP, Weitschies W. Intragastric volume changes after intake of a highcaloric, highfat standard breakfast in healthy human subjects investigated by MRI. Mol Pharm 2014; 11: 16321639 [PMID: 24697247 DOI: 10.1021/mp500022u]
72 Marciani L, Hall N, Pritchard SE, Cox EF, Totman JJ, Lad M, Hoad CL, Foster TJ, Gowland PA, Spiller RC. Preventing gastric sieving by blending a solid/water meal enhances satiation in healthy humans. J Nutr 2012; 142: 12531258 [PMID: 22649258 DOI: 10.3945/jn.112.159830]
73 Marciani L, Pritchard SE, HellierWoods C, Costigan C, Hoad CL, Gowland PA, Spiller RC. Delayed gastric emptying and reduced postprandial small bowel water content of equicaloric whole meal bread versus rice meals in healthy subjects: novel MRI insights. Eur J Clin Nutr 2013; 67: 754758 [PMID: 23594839
DOI: 10.1038/ejcn.2013.78]74 Placidi E, Marciani L, Hoad CL, Napolitano A, Garsed KC,
Pritchard SE, Cox EF, Costigan C, Spiller RC, Gowland PA. The effects of loperamide, or loperamide plus simethicone, on the distribution of gut water as assessed by MRI in a mannitol model of secretory diarrhoea. Aliment Pharmacol Ther 2012; 36: 6473 [PMID: 22582872 DOI: 10.1111/j.13652036.2012.05127.x]
75 Baruffol C, Jordi J, Camargo S, Radovic T, Herzog B, Fried M, Schwizer W, Verrey F, Lutz TA, Steingoetter A. Llysine dose dependently delays gastric emptying and increases intestinal fluid volume in humans and rats. Neurogastroenterol Motil 2014; 26: 9991009 [PMID: 24890878 DOI: 10.1111/nmo.12354]
76 Pritchard SE, Garsed KC, Hoad CL, Lingaya M, Banwait R, Thongborisute W, Roberts E, Costigan C, Marciani L, Gowland PA, Spiller RC. Effect of experimental stress on the small bowel and colon in healthy humans. Neurogastroenterol Motil 2015; 27: 542549 [PMID: 25703609 DOI: 10.1111/nmo.12529]
77 Murray K, WilkinsonSmith V, Hoad C, Costigan C, Cox E, Lam C, Marciani L, Gowland P, Spiller RC. Differential effects of FODMAPs (fermentable oligo, di, monosaccharides and polyols) on small and large intestinal contents in healthy subjects shown by MRI. Am J Gastroenterol 2014; 109: 110119 [PMID: 24247211 DOI: 10.1038/ajg.2013.386]
78 Undseth R, Berstad A, Kløw NE, Arnljot K, Moi KS, Valeur J. Abnormal accumulation of intestinal fluid following ingestion of an unabsorbable carbohydrate in patients with irritable bowel syndrome: an MRI study. Neurogastroenterol Motil 2014; 26: 16861693 [PMID: 25271767 DOI: 10.1111/nmo.12449]
P- Reviewer: Landsman MJ, Lee SH, Sun XT S- Editor: Qi Y L- Editor: A E- Editor: Liu SQ
Khalaf A et al . MRI of GI function and fluids

AbstractEosinophilic esophagitis (EoE) is a chronic immune disease, characterized by a dense eosinophilic infiltrate in the esophagus, leading to bolus impaction and reflux-like symptoms. Traditionally considered a pediatric disease, the number of adult patients with EoE is continuously increasing, with a relatively higher incidence in western countries. Dysphagia and food impaction represent the main symptoms complained by patients, but gastroesophageal reflux-like symptoms may also be present. Esophageal biopsies are mandatory for the diagnosis of EoE, though clinical manifestations and proton pump inhibitors responsiveness must be taken into consideration. The higher prevalence of EoE in patients suffering from atopic diseases suggests a common background with allergy, however both the etiology and pathophysiology are not completely understood. Elimination diets are considered the first-line therapy in children, but this approach appears less effective in adults patients, who often require steroids; despite medical treatments, EoE is complicated in some cases by esophageal stricture and stenosis, that require additional endoscopic treatments. This review summarizes the evidence on EoE pathophysiology and illustrates the safety and efficacy of the most recent medical and endoscopic treatments.
Key words: Eosinophilic esophagitis; Eotaxin; Immune system; Proton pump inhibitors-responsive eosinophilia; Endoscopic dilation
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Eosinophilic esophagitis (EoE) is a chronic immune disease, characterized by a dense eosinophilic infiltrate in the esophagus, leading to bolus impaction and reflux-like symptoms. The pathophysiology of this
Alessandra D’Alessandro, Dario Esposito, Marcella Pesce, Rosario Cuomo, Giovanni Domenico De Palma, Giovanni Sarnelli
Alessandra D’Alessandro, Marcella Pesce, Rosario Cuomo, Giovanni Sarnelli, Department of Clinical Medicine and Surgery, Gastroenterology Unit, Federico II University, 80131 Naples, Italy
Dario Esposito, Giovanni Domenico De Palma, Department of Clinical Medicine and Surgery, Endoscopy Unit, Federico II University, 80131 Naples, Italy
Author contributions: D’Alessandro A, Esposito D and Pesce M reviewed literature data and wrote the manuscript; Cuomo R and De Palma GD participate to the critical revision of the manuscript; Sarnelli G designed, coordinated and revised the manuscript.
Conflict-of-interest statement: All the authors declare that they have no competing interests.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Correspondence to: Giovanni Sarnelli, MD, PhD, Department of Clinical Medicine and Surgery, Gastroenterology Unit, Federico II University of Naples, Via Sergio Pansini, 5, 80131 Naples, Italy. [email protected]: +39-081-7464290Fax: +39-081-7464290
Received: May 25, 2015Peer-review started: May 28, 2015First decision: July 27, 2015Revised: July 30, 2015Accepted: September 25, 2015Article in press: September 28, 2015Published online: November 15, 2015
REVIEW
150 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Eosinophilic esophagitis: From pathophysiology to treatment
World J Gastrointest Pathophysiol 2015 November 15; 6(4): 150-158ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i4.150

entity is still unclear, however the involvement of both genetic and immune factors have been suggested. In this review we summarize the evidence on EoE pathophysiology and illustrate the safety and efficacy of the most recent medical and endoscopic treatments.
D’Alessandro A, Esposito D, Pesce M, Cuomo R, De Palma GD, Sarnelli G. Eosinophilic esophagitis: From pathophysiology to treatment. World J Gastrointest Pathophysiol 2015; 6(4): 150-158 Available from: URL: http://www.wjgnet.com/2150-5330/full/v6/i4/150.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i4.150
INTRODUCTIONThe eosinophilic esophagitis (EoE) is a chronic immune disease, characterized by a dense eosinophilic infiltrate into the esophagus. Dysphagia and food impaction episodes are recognized as the main symptoms of EoE in adults, however regurgitation, chest pain and heartburn may also be referred[1].
Considered as a pediatric disease until few years ago, it is now clear that EoE may also occur in adults, especially young Caucasian man[2]. A rapid increase of incidence in the last decades has been registered, however a retrospective study[3] on biopsies collected between 1982 and 1999 revealed that the incidence of EoE appears stable, suggesting that the higher rate of new diagnosis depends, almost in part, on the improved disease recognition. African, West Asian and South American population share a low prevalence rate, but the real incidence of EoE in these countries remains unclear[4,5].
The EoE-symptoms pattern is heterogeneous and although dysphagia and food impaction are frequently reported, patients may also complain of typical and atypical gastroesophageal reflux disease (GERD) symptoms, leading to a delay in the diagnosis.
Endoscopic features, such as esophageal rings, white exudates or plaques, longitudinal furrows, diffuse esophageal narrowing, and mucosal fragility, may help the diagnosis, but histological identification of predo-minant eosinophilic-inflammation, with more than 15 eosinophils for high power field, represents the main diagnostic criterion for EoE (Figure 1 and Table 1). Nevertheless, the histological evidence of esophageal eosinophilia in a subset of proton pump inhibitors (PPI) responder patients further complicates the diagnosis. Previously considered a GERDsubtype, actually, PPIresponsive esophageal eosinophilia (PPIREE) is considered a different entity, not distinguishable from EoE[1,6]; in the Figure 2 it is summarized the diagnostic algorithm in case of suspected EoE.
The pathogenesis of EoE is unknown, but it is supposed to be multifactorial with genetic, immunologic and environmental factors being all involved. There is evidence that EoE is more prevalent in patients suffering from food-allergy, rhinitis, asthma or atopic
dermatitis[7,8]. Interestingly, all these pathologies share an altered immune response to common antigens, which determinates an aberrant Th2-response, and, hence, the uncontrolled activation of eosinophils, mast cells and basophils[9-13].
Specific allergy testing, or empiric elimination diets represent the first line therapy in children with EoE[1,14]. Topical corticosteroids are considered the mainstay of therapy for adult patients[1,15], while systemic steroids are reserved to patients with persistent eosinophilia[1]. Besides its central role in the diagnosis of EoE, endo-scopy has also of great impact on the treatment of EoE fibrotic complications[1,16].
This review summarizes the most recent evidence on the pathogenesis of EoE, focusing on the role of genetic and immunologic factors and illustrates the safety and efficacy of the most recent medical and endoscopic treatments.
PATHOPHYSIOLOGYGenetic factorsThe higher risk of EoE in familiars of affected patients supports the hypothesis of genetic predisposition. The latest familial study[17] estimated that 2.4% of proband siblings’ also had EoE, with a 40-folds higher risk, than general population.
The incidence of EoE is higher in monozygotic twins (41%), but the observation that the disease also occurs in 21% of dizygotic twins suggests a role for environ-mental factors, especially in the early-life[17]; by using a complex statistical model it has been estimated that the contribution to the familiar risk depends by hereditability and exposure to common environment for 14.5% and 80%, respectively[17].
Three different approaches have been used to identify the genes involved in EoE predisposition: The association with Mendelian syndromes, the search for a specific gene and the genome-wide association studies[18] (Table 2).
An increased prevalence of EoE has been reported in patients affected by hypermobile connective tissue diseases, like Marfan, Ehler-Danlos and Loeys-Dietz Syndromes; interestingly, these pathologies are cha-racterized by a defective transforming growth factor (TGF)β pathway, and the observation that this factor is increased in the esophagus of both syndromic and not EoE likely supports its causative role[19-21]. A major risk of EoE has been also described in some pro-allergenic Mendelian diseases, like the “Iper-IgE syndrome”[18] andan autosomal dominant disease belong to Mast-cell Activation syndromes, characterized by high levels of mast cell tryptase, this association strongly suggests the pathogenic association between EoE and atopic disea-ses[22]. This concept is further supported by the association between EoE and a rare syndrome characterized by severe atopic dermatitis, multiple allergies and metabolic syndrome (SAM); this syndrome is characterized by a mutation of desmoglein-1 gene’s[18,23], whose expression
151 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
D’Alessandro A et al . Pathological mechanisms underlying therapy of EoE

is significantly reduced in idiopathic EoE[24].Candidate-gene identification studies allowed iden-
tifying the putative factors associated with EoE in non-Mendelian syndromes. A single-nucleotide poly-morphism (SNP) in the gene CCL26, encoding for the eotaxin3, was associated with EoE[25]. This protein is overexpressed in esophageal epithelial cells of affected patients, and plays an important role in the chemotaxis of eosinophils[26,27]. Similarly, a SNP in the gene encoding for the filagrin, a structural membrane protein involved in epithelial cellsextracellular matrix interaction has also been identified[18]. Several genes were found to be associated with EoE by genoma wide association studies. In one of the most recent report[28] a significant association between a locus on 5q22, encoding for the cytokine thymic stromal limphopoietin (TSLP) and EoE was reported. Although the specific mechanism remains, yet, to be clarified, TSLP has been demonstrated to have
a pivotal role in the activation of basophils in human and animal models of EoE[29,30]. In the same study[28] also the CAPN14 gene, encoding for the calpain subfamily of proteolytic systems, was identified; more precisely this protein, that is specifically expressed by epithelial cells of the esophagus, is activated by interleukin (IL)-13 and participates to inflammatory process[28].
Immune system factorsThe EoE is characterized by a prevalent eosinophilic infiltrate in the lamina propria and submucosa of the esophagus. The precise mechanisms of such localized inflammatory reactions are not recognized yet, but it is suggested that different cytokines are involved in the maturation and migration of eosinophils. In particu-lar, IL-5, IL-13 and granulocyte-macrophage colony-stimulating factor are produced by different cell types, included esophageal epithelial cells, after an appropriate stimulation by the antigen-presenting cells (APCs)[31]. As shown in Figure 3, the evidence that in EoE patients there is desmoglein-1-dependent altered barrier function[23] have led some authors to hypothesize that the increased permeability of esophageal epithelium could facilitate the passage of different antigens, that causes the activation of APCs and invariant natural killer T-cells. These cells, if properly stimulated, are able to prime a Th2 immune response, by the production of IL-13 and IL-4[32]. However, whether the barrier impair-ment represents a primum movens, or an epipheno-menon in the context of the eosinophilicinflammation remains unclear. Sherrill et al[33] have demonstrated that esophageal epithelial cells express tolllike receptors, whose antigens-mediated activation, through the production of IL-5 and IL-13[34], is able to trigger a Th2-
152 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
A B
C D
Figure 1 Endoscopic and microscopic findings in eosinophilic esophagitis. A: Esophageal rings; B: White exudates, longitudinal furrows and mucosal fragility; C and D: Esophageal mucosa infiltrated by several eosinophils (red cells) (C: Original magnification HE 150 ×; D: HE 400 ×).
Table 1 Endoscopic and histological features of eosinophilic esophagitis
Endoscopic features Esophageal rings White exudates or plaques Longitudinal furrows Diffuse esophageal narrowing Mucosal fragilityHistological features Eosinophilic infiltration (≥ 15 eos/hpf) Eosinophilic degranulation Basal zone hyperplasia Eosinophilic micro-abscesses Spongiosis or dilated intercellular spaces Intramucosal lymphocytes
D’Alessandro A et al . Pathological mechanisms underlying therapy of EoE

153 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
basophils[31].The increased release of these cytokines in both
the esophagus and the blood of EoE patients has been demonstrated in different studies[35,36], and, although need to be further clarified, their role in the pathogenesis of EoE appears to be fundamental.
IL-4 and IL-13 are able to prolong the T-cell survival and to increase eosinophilic migration through the release of Eotaxin3 and TSLP by epithelial cells[37]; recently, Zhu et al[38] found that IL-15 is also enhanced in EoE and, most interestingly, they demonstrated that IL-15 receptor deficient mice are protected from EoE, but not from other allergic diseases, supporting a specific role of IL-15 in the “allergic-pathway” of esophagus. Although the eosinophilic infiltration represents the main characteristic, it is of relevance that other immune cells, like basophils and mast cells, are also involved in the
response with the production of other cytokines and the proliferation of eosinophils, T-cells, mast cells and
Absence of eosinophilic inflammation Eosinophilic inflammation
PPI bid for 4 wk
Persistent eosinophiliaHistological remission
PPI-responsive esophageal eosinophilia Eosinophilic esophagitis
Specific diet or steroidsPPI-therapy
Proximal and distal esophageal biopsies
EGD
Dysphagia - food impaction - atypical GERD symptoms
Endoscopic EoE-features or no lesionsMacroscopic evidence of specific disease
Specific treatment
Figure 2 Diagnostic flow-chart of eosinophilic esophagitis. GERD: Gastroesophageal reflux disease; EoE: Eosinophilic esophagitis; PPI: Proton pump inhibitors; EGD: Esophagogastroduodenoscopy.
Table 2 Genetic factors involved in eosinophilic esophagitis
Genes Encoded protein Mechanism of action Ref.
Mendelian syndromes FBN1 (Marfan syndrome) Fibrillin Alteration of TGF-β pathway [19] COL (Elher-Danlos syndrome) Collagen Alteration of TGF-β pathway [19] TGFBR (Loeys-Dietz syndrome) TGF-β-promoters Alteration of TGF-β pathway [21] STAT3 (Iper-IgE syndrome) Transcription activator 3 Aberrant cytokines production [18] DSG1 (SAM) Desmoglein1 Loss of cell-cell adhesion [23]EoE-associated genetic variants CCL26 Eotaxin-3 Eosinophilic chemo-attraction [25] FLG Filaggrin Epithelium-ECM interaction [18] TSLP (5q22) TSLP Basophils chemo-attraction [28,29] CAPN14 Calpain 14 Proteolytic effects [28]
TGF: Transforming growth factor; ECM: Extracellular matrix; SAM: Severe atopic dermatitis, multiple allergies and metabolic syndrome.
D’Alessandro A et al . Pathological mechanisms underlying therapy of EoE
IL-4IL-13IL-5
Eotaxin
IL-4
Altered barrierfunction
APC Th2-cellsMastcells
Basophils
Eosinophils
Foods
Antigens
IL-4 IL-13 IL-5
Figure 3 Pathophysiological mechanism involved in eosinophilic infiltration of esophageal mucosa. IL: Interleukin; APC: Antigen-presenting cell.

154 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
pathogenesis of EoE and they likely contribute to the amplification of the esophageal inflammatory response and mucosal damage[18,20,29].
Mechanisms of mucosal damage and fibrosisFood impaction and dysphagia are the main symptoms in patients with EoE and these are a direct consequence of the esophageal mucosa remodeling and fibrosis.
Eosinophils synthetize and release many proteins and mediators, in particular major basic protein (MBP), eosinophil cationic protein, eosinophil peroxidase, eosinophilderived neurotoxin, TGFβ, IL-13 and platelet-activating factor. Although all these mediators play a key role in the tissue damage and remodeling, the most robust data are about MBP and TGFβ[37].
MBP is able to directly damage epithelial cells, but also to induce mast cells degranulation, increasing the release of proteolytic enzymes, tryptase and chymase, that further participate to the deconstruction of the extracellular matrix[39]; MBP is also able to stimulate the production of fibroblast growth factor9, leading to fibroblasts proliferation and activation[40]. Similarly, TGFβ induces both fibroblasts activation and contraction, causing their transformation into myofibroblasts[41]; in addition at high concentration TGFβ stimulates epithelial cells to assume phenotypical characteristic of fibroblasts, a process named epithelial-mesenchymal transition[42]. These mechanisms act synergistically, determining the altered synthesis of extracellular matrix proteins, such as collagen, tenascin-C and metalloproteinases[43]. In recent studies the periostin, that is highly expressed in the esophagus of EoE patients, has been proposed as a major determinant of extracellular matrix alteration and epithelial barrier function impairment, because of its ability to determine collagen cross-linking and to bind several matrix proteins and integrins[44].
As mentioned above, other immune cells rather than eosinophils participate to the inflammatory response described in the EoE; recently, the ability of epithelial and mesenchymal cells to synthetize and release different molecules has been also suggested to contribute to tissue damage[12,20,45]. In addition, some authors found a correlation between the inflammatory cells infiltrate and enteric neurons alterations, but the role of enteric nervous system impairment in the process of mucosal damage has not been clarified, yet[46].
THERAPEUTIC OPTIONS The “3 D-approach” summarizes the three major treat-ments for EoE: Diet, drugs and dilation. Although clinical remission represents a good parameter to evaluate the effectiveness of therapy, the endoscopic and histological response is required. The main endpoint of diet and drug therapies is the resolution of both symptoms and inflammation, however the complete remission is rare, and the relief of esophageal symptoms in association with a significant reduction of mucosal eosinophilia should be considered a good response[1].
Dietary therapySpecific dietary approaches are considered the firstline therapy in the treatment of EoE in children, due to the lack of adverse effects and the high rate of response. Three different dietary patterns may be used: (1) ele-mental diet; (2) allergy test-based diet; and (3) empiric elimination diet[47].
The elemental diet demonstrates the high rate of response (almost 90% in children, 70% in adults), with a rapid relief of symptoms associated with histological remission. This diet contemplates the use of amino-acid based liquid formulas for 4-6 wk, followed by the histological evaluation of response. If the remission is achieved, foods are slowly reintroduced, following a strict scheme which contemplates four different food groups, based on their allergenic potential. A single food of each group should be reintroduced every 5-7 d; in absence of symptoms’ recurrence, the endoscopic and histological evaluation should be performed before starting the reintroduction of foods from another group. If a specific food determinates esophageal symptoms, it should be excluded and the next food of the same group tested. Despite the high rate of response, this diet is rarely accepted by patients[48,49].
The allergic-test driven diets showed a rate of response of 70% in children, using the combination of both skin prick and patch tests to identify trigger-foods; this dietary pattern allows the elimination of specific foods, enhancing the compliance, however atopy patch test are not universally accepted for food allergy[50,51]. Moreover, given that the rate of response to this diet in adults is lower, this approach is not recommended in this patients.
The empiric diets, instead, are based on the exclusion of the most allergenic foods, such as cow’s milk protein, soy, wheat, egg, peanut/tree nut, and fish/shellfish, independently on allergic tests. This dietary therapy has shown a rate of response of almost 70% in both children and adults. However, if the remission is achieved, an endoscopic and histological evaluation should be performed after the reintroduction of each food[52,53].
In conclusion, although the exclusion of triggerfoods allows a long-term remission without drugs, the high cost of such diets, especially aminoacid based-formulas, the poor compliance and the need for multiple endoscopies, represent important disadvantages for dietary therapy.
CorticosteroidsSeveral studies have demonstrated the efficacy of systemic corticosteroids, such as prednisolone or methyl-prednisolone, in the remission of both symptoms and eosinophilic infiltration, however the recurrence after the tapering is usually observed. Long-term therapy with corticosteroids is limited by the important adverse effects, hence systemic steroids may be used to rapidly induce remission, but a different maintenance therapy has to be set[54]. Topical steroids, in particular fluticasone
D’Alessandro A et al . Pathological mechanisms underlying therapy of EoE

155 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
and budesonide, have shown a good rate of response, reducing adverse effects also during long-term treat-ment[55,56]. Due to the lack of specific dispenser, multidose inhalers should be used, and patients have to be instructed to swallow, rather than inhale, the product[57]. A viscous compound of budesonide and sucralose, has also been tested, obtaining excellent results[58]. Topical steroids have shown a good safety profile, and are actually considered the first-line therapy, after the PPI trial, in EoE patients. However, some cases of eso-phageal candidiasis and herpes infections have been described[59,60].
PPI When the first consensus guidelines for EoE was published in 2007, a physiological 24h-pH-metry and the persistence of symptoms despite PPI therapy were considered major criteria for diagnosis of EoE. In the last years, several studies have shown that almost 40% of patients with clinical, endoscopic and histological features of EoE responds to PPI therapy, independently on the results of 24 h-pH-metry[61,62].
These data questioned the relationship between GERD and EoE, introducing a novel entity, named PPIREE, in the consensus of 2011[63]. Actually considered more a subtype of EoE, rather than atypical GERD, this pathology is defined by the presence of all hallmarks (clinical, endoscopic and histological) of EoE, associated with a complete (clinical, endoscopic and histological) remission during PPI therapy[1]. Considering that different studies have demonstrated that patients with PPIREE share the same genetic and phenotypic background of EoEsubjects, nowadays PPI bid is considered the firstline therapy in all patients with EoE features[1,64].
PPIREE opened a new field of research, focused on the role of reflux in the pathogenesis of esophageal eosinophilia[65]. The hypothesis that gastroesophageal reflux, even if not pathologic, could enhance epithelial barrier dysfunction, allowing the passage of multiple antigens through the mucosa, has been proposed and evaluated. Different studies have demonstrated that gastric reflux is able to enlarge intracellular space, and the increased transit of molecules through esophageal epithelium has also been observed in both GERD and EoE[66,67]. Accordingly, the exposition of several antigens to APC may induce, in predisposed subjects, a cascade of events, triggering a Th2-response, and, consequently, the eosinophilic infiltration. In this case the therapeutic effects of PPIs, will depend on their ability to favorite the regeneration of epithelial barrier, reducing the antigen exposition and, hence, the amplification of immune response.
According to others, also GERD, as EoE, represents an immunemediated pathology, in which acid reflux stimulates the release of cytokines, inducing a specific Th1-response. Therefore, the activation of immune system and the production of toxic mediators determinates mucosal erosions, rather than the direct caustic action of acid[68]. These authors suggest that in “atopic-subjects”,
the typical response to acid reflux switch to a Th2-response, causing an EoE-like damage of the esophagus. Therefore, the reduction of immunogenic trigger, by the inhibition of acid secretion, will determinate the resolution of damage. Furthermore, a direct anti-inflammatory effect of PPIs has been recently demonstrated. In particular, different studies have pointed out the reduction of eotaxin 3 and Th2-mediators, after treatment with PPI in the mucosa of patients with diagnosis of both EoE and PPIREE. These events have been observed both in vitro and in vivo experiments, suggesting that PPIs antiinflammatory action is acidindependent[69-71].
Summarizing, at the baseline, is not possible to discriminate between EoE and PPIREE, and, although the probability of PPI response in patients with pathologic 24 h-pH-metria is higher, PPIs trial still represents the only instrument to differentiate these entities (Figure 2)[72,73].
Other pharmacological treatmentsGiven the association with other atopic diseases, leukotriene antagonist and mast cells stabilizers, such as montelukast and cromolym, have been tested in the treatment of EoE, however all studies showed a poor efficacy of these drugs in both symptomatic and histological remission[74].
Specific antibodies against IL-5 and IgE were also tested, especially for treating steroid-refractory patients. However, despite the initial promising results, the controlled clinical trials have shown a similar response in treated and placebo subgroups[75-78]. Interestingly, a recent trial testing a human antibody against IL-13 showed a significant improvement of symptoms and eosinophilic infiltration, however the primary endpoint, the reduction of 75% of esophageal eosinophils, have been not achieved[79].
The failure of such specific therapy likely depends on the redundancy, in fact multiple cytokines share similar effects, allowing the persistence of inflammation after the blockage of single molecules.
Endoscopic treatmentDue to the fibro-stenotic evolution, strictures are frequently found in patients affected by EoE, hence endoscopic dilation have a key role in the treatment of this entity[1]. Several studies have shown the efficacy and safety of esophageal dilation, independently on the chosen technique. Wire-guided bougies, through-the-scope balloons, and non-wire-guided bougies have been indistinctly used[80,81]. Nowadays, there are not available data on the best endoscopic technique, because comparing studies are lacking.
Due to the long-term efficacy of this procedure in the treatment of EoE-related dysphagia, some authors have proposed dilation as initial therapy, however a recent study have demonstrated that fluticasone inhaler, followed by dilation if necessary, is the most economical initial strategy. Moreover, although dilation rapidly improve symptoms, this procedure did not influenced
D’Alessandro A et al . Pathological mechanisms underlying therapy of EoE

156 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
esophageal inflammation, hence further therapies should be set after the treatment[82].
CONCLUSIONEoE represents a multifactorial disease, in which both genetic predisposition and environmental factors con-tribute to disease manifestations. Although in the last years many studies have been performed, its pathophysiology remains unclear, likely reflecting the heterogeneity of disease phenotype.
The EoE-symptoms pattern is heterogeneous, dysphagia and food impaction are frequently referred, however also atypical GERD symptoms may be reported. The histological identification of a prevalent eosinophilic esophageal infiltrate represents the major diagnostic criterion for EoE, however only the PPI-trial allows to distingue EoE from PPIREE.
The good response to diet therapy in children, supports the role of food as a major trigger factor, leading to define EoE a subtype of foodallergy. For this reason, elimination diets and corticosteroids represent the mainstay of EoE-therapy, while endoscopic dilation have a key role in the treatment of fibrotic complication.
REFERENCES1 Dellon ES, Gonsalves N, Hirano I, Furuta GT, Liacouras CA,
Katzka DA; DAM American College of Gastroenterology. ACG clinical guideline: Evidenced based approach to the diagnosis and management of esophageal eosinophilia and eosinophilic esophagitis (EoE). Am J Gastroenterol 2013; 108: 679-92; quiz 693 [PMID: 23567357 DOI: 10.1038/ajg.2013.71]
2 Dellon ES. Epidemiology of eosinophilic esophagitis. Gastroenterol Clin North Am 2014; 43: 201-218 [PMID: 24813510 DOI: 10.1016/j.gtc.2014.02.002]
3 DeBrosse CW, Collins MH, Buckmeier Butz BK, Allen CL, King EC, Assa’ad AH, Abonia JP, Putnam PE, Rothenberg ME, Franciosi JP. Identification, epidemiology, and chronicity of pediatric esophageal eosinophilia, 1982-1999. J Allergy Clin Immunol 2010; 126: 112-119 [PMID: 20620567 DOI: 10.1016/j.jaci.2010.05.027]
4 Ishimura N, Shimura S, Jiao D, Mikami H, Okimoto E, Uno G, Aimi M, Oshima N, Ishihara S, Kinoshita Y. Clinical features of eosinophilic esophagitis: differences between Asian and Western populations. J Gastroenterol Hepatol 2015; 30 Suppl 1: 71-77 [PMID: 25827808 DOI: 10.1111/jgh.12746]
5 Weiler T, Mikhail I, Singal A, Sharma H. Racial differences in the clinical presentation of pediatric eosinophilic esophagitis. J Allergy Clin Immunol Pract 2014; 2: 320-325 [PMID: 24811024 DOI: 10.1016/j.jaip.2014.01.011]
6 Asher Wolf W, Dellon ES. Eosinophilic esophagitis and proton pump inhibitors: controversies and implications for clinical practice. Gastroenterol Hepatol (N Y) 2014; 10: 427-432 [PMID: 25904830]
7 Philpott H, Nandurkar S, Royce SG, Thien F, Gibson PR. Risk factors for eosinophilic esophagitis. Clin Exp Allergy 2014; 44: 1012-1019 [PMID: 24990069 DOI: 10.1111/cea.12363]
8 Virchow JC. Eosinophilic esophagitis: asthma of the esophagus? Dig Dis 2014; 32: 54-60 [PMID: 24603381 DOI: 10.1159/000357010]
9 Simon D, Straumann A, Simon HU. Eosinophilic esophagitis and allergy. Dig Dis 2014; 32: 30-33 [PMID: 24603377 DOI: 10.1159/000357006]
10 Straumann A, Bauer M, Fischer B, Blaser K, Simon HU. Idio-pathic eosinophilic esophagitis is associated with a T(H)2-type allergic inflammatory response. J Allergy Clin Immunol 2001; 108:
954-961 [PMID: 11742273]11 Lucendo AJ. Cellular and molecular immunological mechanisms
in eosinophilic esophagitis: an updated overview of their clinical implications. Expert Rev Gastroenterol Hepatol 2014; 8: 669-685 [PMID: 24742298 DOI: 10.1586/17474124.2014.909727]
12 Rieder F, Nonevski I, Ma J, Ouyang Z, West G, Protheroe C, DePetris G, Schirbel A, Lapinski J, Goldblum J, Bonfield T, Lopez R, Harnett K, Lee J, Hirano I, Falk G, Biancani P, Fiocchi C. T-helper 2 cytokines, transforming growth factor β1, and eosinophil products induce fibrogenesis and alter muscle motility in patients with eosinophilic esophagitis. Gastroenterology 2014; 146: 1266-77.e1-9 [PMID: 24486052 DOI: 10.1053/j.gastro.2014.01.051]
13 Abdulnour-Nakhoul SM, Al-Tawil Y, Gyftopoulos AA, Brown KL, Hansen M, Butcher KF, Eidelwein AP, Noel RA, Rabon E, Posta A, Nakhoul NL. Alterations in junctional proteins, inflammatory mediators and extracellular matrix molecules in eosinophilic esophagitis. Clin Immunol 2013; 148: 265-278 [PMID: 23792687 DOI: 10.1016/j.clim.2013.05.004]
14 Arias A, Lucendo AJ. Dietary therapies for eosinophilic esophagitis. Expert Rev Clin Immunol 2014; 10: 133-142 [PMID: 24236700 DOI: 10.1586/1744666X.2014.856263]
15 Alexander JA. Steroid treatment of eosinophilic esophagitis in adults. Gastroenterol Clin North Am 2014; 43: 357-373 [PMID: 24813521 DOI: 10.1016/j.gtc.2014.02.001]
16 Dellon ES, Liacouras CA. Advances in clinical management of eosinophilic esophagitis. Gastroenterology 2014; 147: 1238-1254 [PMID: 25109885 DOI: 10.1053/j.gastro.2014.07.055]
17 Alexander ES, Martin LJ, Collins MH, Kottyan LC, Sucharew H, He H, Mukkada VA, Succop PA, Abonia JP, Foote H, Eby MD, Grotjan TM, Greenler AJ, Dellon ES, Demain JG, Furuta GT, Gurian LE, Harley JB, Hopp RJ, Kagalwalla A, Kaul A, Nadeau KC, Noel RJ, Putnam PE, von Tiehl KF, Rothenberg ME. Twin and family studies reveal strong environmental and weaker genetic cues explaining heritability of eosinophilic esophagitis. J Allergy Clin Immunol 2014; 134: 1084-1092.e1 [PMID: 25258143 DOI: 10.1016/j.jaci.2014.07.021]
18 Rothenberg ME. Molecular, genetic, and cellular bases for treating eosinophilic esophagitis. Gastroenterology 2015; 148: 1143-1157 [PMID: 25666870 DOI: 10.1053/j.gastro.2015.02.002]
19 Abonia JP, Wen T, Stucke EM, Grotjan T, Griffith MS, Kemme KA, Collins MH, Putnam PE, Franciosi JP, von Tiehl KF, Tinkle BT, Marsolo KA, Martin LJ, Ware SM, Rothenberg ME. High prevalence of eosinophilic esophagitis in patients with inherited connective tissue disorders. J Allergy Clin Immunol 2013; 132: 378-386 [PMID: 23608731 DOI: 10.1016/j.jaci.2013.02.030]
20 Cheng E , Souza RF, Spechler SJ. Tissue remodeling in eosinophilic esophagitis. Am J Physiol Gastrointest Liver Physiol 2012; 303: G1175-G1187 [PMID: 23019192 DOI: 10.1152/ajpgi.00313.2012]
21 Frischmeyer-Guerrerio PA, Guerrerio AL, Oswald G, Chichester K, Myers L, Halushka MK, Oliva-Hemker M, Wood RA, Dietz HC. TGFβ receptor mutations impose a strong predisposition for human allergic disease. Sci Transl Med 2013; 5: 195ra94 [PMID: 23884466 DOI: 10.1126/scitranslmed.3006448]
22 Lyons JJ, Sun G, Stone KD, Nelson C, Wisch L, O’Brien M, Jones N, Lindsley A, Komarow HD, Bai Y, Scott LM, Cantave D, Maric I, Abonia JP, Rothenberg ME, Schwartz LB, Milner JD, Wilson TM. Mendelian inheritance of elevated serum tryptase associated with atopy and connective tissue abnormalities. J Allergy Clin Immunol 2014; 133: 1471-1474 [PMID: 24472624]
23 Samuelov L, Sarig O, Harmon RM, Rapaport D, Ishida-Yamamoto A, Isakov O, Koetsier JL, Gat A, Goldberg I, Bergman R, Spiegel R, Eytan O, Geller S, Peleg S, Shomron N, Goh CS, Wilson NJ, Smith FJ, Pohler E, Simpson MA, McLean WH, Irvine AD, Horowitz M, McGrath JA, Green KJ, Sprecher E. Desmoglein 1 deficiency results in severe dermatitis, multiple allergies and metabolic wasting. Nat Genet 2013; 45: 1244-1248 [PMID: 23974871 DOI: 10.1038/ng.2739]
24 Sherrill JD, Kc K, Wu D, Djukic Z, Caldwell JM, Stucke EM, Kemme KA, Costello MS, Mingler MK, Blanchard C, Collins MH, Abonia JP, Putnam PE, Dellon ES, Orlando RC, Hogan SP, Rothenberg ME. Desmoglein-1 regulates esophageal epithelial
D’Alessandro A et al . Pathological mechanisms underlying therapy of EoE

157 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
barrier function and immune responses in eosinophilic esophagitis. Mucosal Immunol 2014; 7: 718-729 [PMID: 24220297 DOI: 10.1038/mi.2013.90]
25 Blanchard C, Wang N, Stringer KF, Mishra A, Fulkerson PC, Abonia JP, Jameson SC, Kirby C, Konikoff MR, Collins MH, Cohen MB, Akers R, Hogan SP, Assa’ad AH, Putnam PE, Aronow BJ, Rothenberg ME. Eotaxin-3 and a uniquely conserved gene-expression profile in eosinophilic esophagitis. J Clin Invest 2006; 116: 536-547 [PMID: 16453027]
26 Fujiwara H, Morita A, Kobayashi H, Hamano K, Fujiwara Y, Hirai K, Yano M, Naka T, Saeki Y. Infiltrating eosinophils and eotaxin: their association with idiopathic eosinophilic esophagitis. Ann Allergy Asthma Immunol 2002; 89: 429-432 [PMID: 12392390]
27 Blanchard C, Stucke EM, Burwinkel K, Caldwell JM, Collins MH, Ahrens A, Buckmeier BK, Jameson SC, Greenberg A, Kaul A, Franciosi JP, Kushner JP, Martin LJ, Putnam PE, Abonia JP, Wells SI, Rothenberg ME. Coordinate interaction between IL-13 and epithelial differentiation cluster genes in eosinophilic esophagitis. J Immunol 2010; 184: 4033-4041 [PMID: 20208004 DOI: 10.4049/jimmunol.0903069]
28 Kottyan LC, Davis BP, Sherrill JD, Liu K, Rochman M, Kaufman K, Weirauch MT, Vaughn S, Lazaro S, Rupert AM, Kohram M, Stucke EM, Kemme KA, Magnusen A, He H, Dexheimer P, Chehade M, Wood RA, Pesek RD, Vickery BP, Fleischer DM, Lindbad R, Sampson HA, Mukkada VA, Putnam PE, Abonia JP, Martin LJ, Harley JB, Rothenberg ME. Genome-wide association analysis of eosinophilic esophagitis provides insight into the tissue specificity of this allergic disease. Nat Genet 2014; 46: 895-900 [PMID: 25017104 DOI: 10.1038/ng.3033]
29 Noti M, Wojno ED, Kim BS, Siracusa MC, Giacomin PR, Nair MG, Benitez AJ, Ruymann KR, Muir AB, Hill DA, Chikwava KR, Moghaddam AE, Sattentau QJ, Alex A, Zhou C, Yearley JH, Menard-Katcher P, Kubo M, Obata-Ninomiya K, Karasuyama H, Comeau MR, Brown-Whitehorn T, de Waal Malefyt R, Sleiman PM, Hakonarson H, Cianferoni A, Falk GW, Wang ML, Spergel JM, Artis D. Thymic stromal lymphopoietin-elicited basophil responses promote eosinophilic esophagitis. Nat Med 2013; 19: 1005-1013 [PMID: 23872715 DOI: 10.1038/nm.3281]
30 Cianferoni A, Spergel J. The importance of TSLP in allergic disease and its role as a potential therapeutic target. Expert Rev Clin Immunol 2014; 10: 1463-1474 [PMID: 25340427 DOI: 10.1586/1744666X.2014.967684]
31 Rosenberg HF, Dyer KD, Foster PS. Eosinophils: changing perspectives in health and disease. Nat Rev Immunol 2013; 13: 9-22 [PMID: 23154224 DOI: 10.1038/nri334]
32 Jyonouchi S, Smith CL, Saretta F, Abraham V, Ruymann KR, Modayur-Chandramouleeswaran P, Wang ML, Spergel JM, Cianferoni A. Invariant natural killer T cells in children with eosinophilic esophagitis. Clin Exp Allergy 2014; 44: 58-68 [PMID: 24118614 DOI: 10.1111/cea.12201]
33 Sherrill JD, Gao PS, Stucke EM, Blanchard C, Collins MH, Putnam PE, Franciosi JP, Kushner JP, Abonia JP, Assa’ad AH, Kovacic MB, Biagini Myers JM, Bochner BS, He H, Hershey GK, Martin LJ, Rothenberg ME. Variants of thymic stromal lymphopoietin and its receptor associate with eosinophilic esophagitis. J Allergy Clin Immunol 2010; 126: 160-5.e3 [PMID: 20620568]
34 Lim DM, Narasimhan S, Michaylira CZ, Wang ML. TLR3-mediated NF-{kappa}B signaling in human esophageal epithelial cells. Am J Physiol Gastrointest Liver Physiol 2009; 297: G1172-G1180 [PMID: 19779021 DOI: 10.1152/ajpgi.00065.2009]
35 Bhardwaj N, Ghaffari G. Biomarkers for eosinophilic esophagitis: a review. Ann Allergy Asthma Immunol 2012; 109: 155-159 [PMID: 22920068 DOI: 10.1016/j.anai.2012.06.014]
36 Konikoff MR, Blanchard C, Kirby C, Buckmeier BK, Cohen MB, Heubi JE, Putnam PE, Rothenberg ME. Potential of blood eosinophils, eosinophil-derived neurotoxin, and eotaxin-3 as biomarkers of eosinophilic esophagitis. Clin Gastroenterol Hepatol 2006; 4: 1328-1336 [PMID: 17059896]
37 Travers J, Rothenberg ME. Eosinophils in mucosal immune responses. Mucosal Immunol 2015; 8: 464-475 [PMID: 25807184 DOI: 10.1038/mi.2015.2]
38 Zhu X, Wang M, Mavi P, Rayapudi M, Pandey AK, Kaul A, Putnam PE, Rothenberg ME, Mishra A. Interleukin-15 expression is increased in human eosinophilic esophagitis and mediates pathogenesis in mice. Gastroenterology 2010; 139: 182-93.e7 [PMID: 20381491 DOI: 10.1053/j.gastro.2010.03.057]
39 Gleich GJ, Frigas E, Loegering DA, Wassom DL, Steinmuller D. Cytotoxic properties of the eosinophil major basic protein. J Immunol 1979; 123: 2925-2927 [PMID: 501097]
40 Mulder DJ, Pacheco I, Hurlbut DJ, Mak N, Furuta GT, MacLeod RJ, Justinich CJ. FGF9-induced proliferative response to eosino-philic inflammation in oesophagitis. Gut 2009; 58: 166-173 [PMID: 18978176 DOI: 10.1136/gut.2008.157628]
41 Vaughan MB, Howard EW, Tomasek JJ. Transforming growth factor-beta1 promotes the morphological and functional differen-tiation of the myofibroblast. Exp Cell Res 2000; 257: 180-189 [PMID: 10854066]
42 Piera-Velazquez S, Li Z, Jimenez SA. Role of endothelial-mesenchymal transition (EndoMT) in the pathogenesis of fibrotic disorders. Am J Pathol 2011; 179: 1074-1080 [PMID: 21763673 DOI: 10.1016/j.ajpath.2011.06.001]
43 Roberts AB, McCune BK, Sporn MB. TGF-β: Regulation of extracellular matrix. Kidney International 1999; 41: 557-559 [DOI: 10.1038/ki.1992.81]
44 Blanchard C, Mingler MK, McBride M, Putnam PE, Collins MH, Chang G, Stringer K, Abonia JP, Molkentin JD, Rothenberg ME. Periostin facilitates eosinophil tissue infiltration in allergic lung and esophageal responses. Mucosal Immunol 2008; 1: 289-296 [PMID: 19079190 DOI: 10.1038/mi.2008.15]
45 Flavahan NA, Slifman NR, Gleich GJ, Vanhoutte PM. Human eosinophil major basic protein causes hyperreactivity of respiratory smooth muscle. Role of the epithelium. Am Rev Respir Dis 1988; 138: 685-688 [PMID: 3202421]
46 Hogan SP, Mishra A, Brandt EB, Royalty MP, Pope SM, Zimmermann N, Foster PS, Rothenberg ME. A pathological function for eotaxin and eosinophils in eosinophilic gastrointestinal inflammation. Nat Immunol 2001; 2: 353-360 [PMID: 11276207]
47 Vashi R, Hirano I. Diet therapy for eosinophilic esophagitis: when, why and how. Curr Opin Gastroenterol 2013; 29: 407-415 [PMID: 23689524 DOI: 10.1097/MOG.0b013e328362285d]
48 Peterson KA, Byrne KR, Vinson LA, Ying J, Boynton KK, Fang JC, Gleich GJ, Adler DG, Clayton F. Elemental diet induces histologic response in adult eosinophilic esophagitis. Am J Gastroenterol 2013; 108: 759-766 [PMID: 23381017 DOI: 10.1038/ajg.2012.468]
49 Peterson KA, Boynton KK. Which patients with eosinophilic esophagitis (EoE) should receive elemental diets versus other therapies? Curr Gastroenterol Rep 2014; 16: 364 [PMID: 24338572 DOI: 10.1007/s11894-013-0364-y]
50 Spergel JM, Andrews T, Brown-Whitehorn TF, Beausoleil JL, Liacouras CA. Treatment of eosinophilic esophagitis with specific food elimination diet directed by a combination of skin prick and patch tests. Ann Allergy Asthma Immunol 2005; 95: 336-343 [PMID: 16279563]
51 Ballmer-Weber BK. Value of allergy tests for the diagnosis of food allergy. Dig Dis 2014; 32: 84-88 [PMID: 24603386 DOI: 10.1159/000357077]
52 Rodríguez-Sánchez J, Gómez Torrijos E, López Viedma B, de la Santa Belda E, Martín Dávila F, García Rodríguez C, Feo Brito F, Olmedo Camacho J, Reales Figueroa P, Molina-Infante J. Efficacy of IgE-targeted vs empiric six-food elimination diets for adult eosinophilic oesophagitis. Allergy 2014; 69: 936-942 [PMID: 24816218 DOI: 10.1111/all.12420]
53 Lucendo AJ, Arias Á, González-Cervera J, Yagüe-Compadre JL, Guagnozzi D, Angueira T, Jiménez-Contreras S, González-Castillo S, Rodríguez-Domíngez B, De Rezende LC, Tenias JM. Empiric 6-food elimination diet induced and maintained prolonged remission in patients with adult eosinophilic esophagitis: a prospective study on the food cause of the disease. J Allergy Clin Immunol 2013; 131: 797-804 [PMID: 23375693 DOI: 10.1016/j.jaci.2012.12.664]
54 Mukkada VA, Furuta GT. Management of refractory eosinophilic esophagitis. Dig Dis 2014; 32: 134-138 [PMID: 24603397 DOI:
D’Alessandro A et al . Pathological mechanisms underlying therapy of EoE

158 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
10.1159/000357296]55 Contreras EM, Gupta SK. Steroids in pediatric eosinophilic
esophagitis. Gastroenterol Clin North Am 2014; 43: 345-356 [PMID: 24813520 DOI: 10.1016/j.gtc.2014.02.008]
56 Schaefer ET, Fitzgerald JF, Molleston JP, Croffie JM, Pfefferkorn MD, Corkins MR, Lim JD, Steiner SJ, Gupta SK. Comparison of oral prednisone and topical fluticasone in the treatment of eosinophilic esophagitis: a randomized trial in children. Clin Gastroenterol Hepatol 2008; 6: 165-173 [PMID: 18237866 DOI: 10.1016/j.cgh.2007.11.008]
57 Konikoff MR, Noel RJ, Blanchard C, Kirby C, Jameson SC, Buckmeier BK, Akers R, Cohen MB, Collins MH, Assa’ad AH, Aceves SS, Putnam PE, Rothenberg ME. A randomized, double-blind, placebo-controlled trial of fluticasone propionate for pediatric eosinophilic esophagitis. Gastroenterology 2006; 131: 1381-1391 [PMID: 17101314]
58 Zur E. Eosinophilic esophagitis: treatment with oral viscous budesonide. Int J Pharm Compd 2012; 16: 288-293 [PMID: 23050387]
59 Gupta SK, Vitanza JM, Collins MH. Efficacy and safety of oral budesonide suspension in pediatric patients with eosinophilic esophagitis. Clin Gastroenterol Hepatol 2015; 13: 66-76.e3 [PMID: 24907502 DOI: 10.1016/j.cgh.2014.05.021]
60 Chuang MY, Chinnaratha MA, Hancock DG, Woodman R, Wong GR, Cock C, Fraser RJ. Topical Steroid Therapy for the Treatment of Eosinophilic Esophagitis (EoE): A Systematic Review and Meta-Analysis. Clin Transl Gastroenterol 2015; 6: e82 [PMID: 25809314 DOI: 10.1038/ctg.2015.9]
61 Molina-Infante J, Katzka DA, Dellon ES. Proton pump inhibitor-responsive esophageal eosinophilia: a historical perspective on a novel and evolving entity. Rev Esp Enferm Dig 2015; 107: 29-36 [PMID: 25603329]
62 Munday W, Zhang X. Proton pump inhibitor responsive esophageal eosinophilia, a distinct disease entity? World J Gastroenterol 2014; 20: 10419-10424 [PMID: 25132757 DOI: 10.3748/wjg.v20.i30.10419]
63 Liacouras CA, Furuta GT, Hirano I, Atkins D, Attwood SE, Bonis PA, Burks AW, Chehade M, Collins MH, Dellon ES, Dohil R, Falk GW, Gonsalves N, Gupta SK, Katzka DA, Lucendo AJ, Markowitz JE, Noel RJ, Odze RD, Putnam PE, Richter JE, Romero Y, Ruchelli E, Sampson HA, Schoepfer A, Shaheen NJ, Sicherer SH, Spechler S, Spergel JM, Straumann A, Wershil BK, Rothenberg ME, Aceves SS. Eosinophilic esophagitis: updated consensus recommendations for children and adults. J Allergy Clin Immunol 2011; 128: 3-20.e6; quiz 21-2 [PMID: 21477849 DOI: 10.1016/j.jaci.2011.02.040]
64 Wen T, Dellon ES, Moawad FJ, Furuta GT, Aceves SS, Rothen-berg ME. Transcriptome analysis of proton pump inhibitor-responsive esophageal eosinophilia reveals proton pump inhibitor-reversible allergic inflammation. J Allergy Clin Immunol 2015; 135: 187-197 [PMID: 25441638 DOI: 10.1016/j.jaci.2014.08.043]
65 Katzka DA. The complex relationship between eosinophilic esophagitis and gastroesophageal reflux disease. Dig Dis 2014; 32: 93-97 [PMID: 24603388 DOI: 10.1159/000357080]
66 Katzka DA, Ravi K, Geno DM, Smyrk TC, Iyer PG, Alexander JA, Mabary JE, Camilleri M, Vaezi MF. Endoscopic Mucosal Impedance Measurements Correlate With Eosinophilia and Dilation of Intercellular Spaces in Patients With Eosinophilic Esophagitis. Clin Gastroenterol Hepatol 2015; 13: 1242-1248.e1 [PMID: 25592662 DOI: 10.1016/j.cgh.2014.12.032]
67 Weijenborg PW, Smout AJ, Verseijden C, van Veen HA, Verheij J, de Jonge WJ, Bredenoord AJ. Hypersensitivity to acid is associated with impaired esophageal mucosal integrity in patients with gastroesophageal reflux disease with and without esophagitis. Am J Physiol Gastrointest Liver Physiol 2014; 307: G323-G329 [PMID: 24924748 DOI: 10.1152/ajpgi.00345.2013]
68 Souza RF, Huo X, Mittal V, Schuler CM, Carmack SW, Zhang
HY, Zhang X, Yu C, Hormi-Carver K, Genta RM, Spechler SJ. Gastroesophageal reflux might cause esophagitis through a cytokine-mediated mechanism rather than caustic acid injury. Gastroenterology 2009; 137: 1776-1784 [PMID: 19660463 DOI: 10.1053/j.gastro.2009.07.055]
69 Park JY, Zhang X, Nguyen N, Souza RF, Spechler SJ, Cheng E. Proton pump inhibitors decrease eotaxin-3 expression in the proximal esophagus of children with esophageal eosinophilia. PLoS One 2014; 9: e101391 [PMID: 24988451 DOI: 10.1371/journal.pone.0101391]
70 Molina-Infante J, Rivas MD, Hernandez-Alonso M, Vinagre-Rodríguez G, Mateos-Rodríguez JM, Dueñas-Sadornil C, Perez-Gallardo B, Ferrando-Lamana L, Fernandez-Gonzalez N, Bañares R, Zamorano J. Proton pump inhibitor-responsive oesophageal eosinophilia correlates with downregulation of eotaxin-3 and Th2 cytokines overexpression. Aliment Pharmacol Ther 2014; 40: 955-965 [PMID: 25112708 DOI: 10.1111/apt.12914]
71 Zhang X, Cheng E, Huo X, Yu C, Zhang Q, Pham TH, Wang DH, Spechler SJ, Souza RF. Omeprazole blocks STAT6 binding to the eotaxin-3 promoter in eosinophilic esophagitis cells. PLoS One 2012; 7: e50037 [PMID: 23185525 DOI: 10.1371/journal.pone.0050037]
72 Kia L, Hirano I. Distinguishing GERD from eosinophilic oesophagitis: concepts and controversies. Nat Rev Gastroenterol Hepatol 2015; 12: 379-386 [PMID: 25986303 DOI: 10.1038/nrgastro.2015.75]
73 Warners MJ, van Rhijn BD, Curvers WL, Smout AJ, Bredenoord AJ. PPI-responsive esophageal eosinophilia cannot be distin-guished from eosinophilic esophagitis by endoscopic signs. Eur J Gastroenterol Hepatol 2015; 27: 506-511 [PMID: 25822858 DOI: 10.1097/MEG.0000000000000331]
74 Kern E, Hirano I. Emerging drugs for eosinophilic esophagitis. Expert Opin Emerg Drugs 2013; 18: 353-364 [PMID: 23937314 DOI: 10.1517/14728214.2013.829039]
75 Cianferoni A, Spergel JM. Immunotherapeutic approaches for the treatment of eosinophilic esophagitis. Immunotherapy 2014; 6: 321-331 [PMID: 24762076 DOI: 10.2217/imt.14.3]
76 Otani IM, Anilkumar AA, Newbury RO, Bhagat M, Beppu LY, Dohil R, Broide DH, Aceves SS. Anti-IL-5 therapy reduces mast cell and IL-9 cell numbers in pediatric patients with eosinophilic esophagitis. J Allergy Clin Immunol 2013; 131: 1576-1582 [PMID: 23623266 DOI: 10.1016/j.jaci.2013.02.042]
77 Straumann A, Conus S, Grzonka P, Kita H, Kephart G, Bussmann C, Beglinger C, Smith DA, Patel J, Byrne M, Simon HU. Anti-interleukin-5 antibody treatment (mepolizumab) in active eosinophilic oesophagitis: a randomised, placebo-controlled, double-blind trial. Gut 2010; 59: 21-30 [PMID: 19828470]
78 Stein ML, Collins MH, Villanueva JM, Kushner JP, Putnam PE, Buckmeier BK, Filipovich AH, Assa’ad AH, Rothenberg ME. Anti-IL-5 (mepolizumab) therapy for eosinophilic esophagitis. J Allergy Clin Immunol 2006; 118: 1312-1319 [PMID: 17157662]
79 Rothenberg ME, Wen T, Greenberg A, Alpan O, Enav B, Hirano I, Nadeau K, Kaiser S, Peters T, Perez A, Jones I, Arm JP, Strieter RM, Sabo R, Gunawardena KA. Intravenous anti-IL-13 mAb QAX576 for the treatment of eosinophilic esophagitis. J Allergy Clin Immunol 2015; 135: 500-507 [PMID: 25226850]
80 Bohm ME, Richter JE. Review article: oesophageal dilation in adults with eosinophilic oesophagitis. Aliment Pharmacol Ther 2011; 33: 748-757 [PMID: 21320137 DOI: 10.1111/j.1365-2036.2011.04593.x]
81 Schoepfer A. Treatment of eosinophilic esophagitis by dilation. Dig Dis 2014; 32: 130-133 [PMID: 24603396 DOI: 10.1159/000357091]
82 Kavitt RT, Penson DF, Vaezi MF. Eosinophilic esophagitis: dilate or medicate? A cost analysis model of the choice of initial therapy. Dis Esophagus 2014; 27: 418-423 [PMID: 22947137 DOI: 10.1111/j.1442-2050.2012.01409.x]
P- Reviewer: Hokama A S- Editor: Song XX L- Editor: A E- Editor: Liu SQ
D’Alessandro A et al . Pathological mechanisms underlying therapy of EoE

Andrea Michielan, Renata D’Incà
Andrea Michielan, Renata D’Incà, Department of Surgical, Oncological and Gastroenterological Sciences, Azienda Ospedaliera Università degli Studi di Padova, 35128 Padova, Italy
Author contributions: Michielan A contributed to concept and drafting of the manuscript; D’Incà R contributed to critical revision for important intellectual content.
Conflict-of-interest statement: Authors declare no conflict of interests for this article.
Open-Access: This article is an openaccess article which was selected by an inhouse editor and fully peerreviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work noncommercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: http://creativecommons.org/licenses/bync/4.0/
Correspondence to: Andrea Michielan, MD, Department of Surgical, Oncological and Gastroenterological Sciences, Azienda Ospedaliera Università degli Studi di Padova, Via Giustiniani 2, 35128 Padova, Italy. [email protected]: +390498212893Fax: +390498760820
Received: June 24, 2015 Peer-review started: June 24, 2015First decision: August 25, 2015Revised: September 13, 2015 Accepted: October 23, 2015 Article in press: October 27, 2015Published online: November 15, 2015
AbstractAn impaired interaction between the gut and the intes-tinal microbiome is likely to be the key element in the pathogenesis of Crohn’s disease (CD). Family studies have provided invaluable information on CD pathogenesis and on its etiology. Relatives share the same genetic
risk of developing the disease as affected subjects. Relatives also exhibit similar features relating to their host-microbiome interaction, namely genetic variants in loci involved in detecting bacteria, a greater sero-reactivity to microbial components, and an impaired intestinal permeability. The burden of environmental factors such as cigarette smoking and dysbiosis also seems to be particularly relevant in these genetically predisposed subjects. Diet is emerging as an important factor and could account for the changing epidemiology of CD in recent years. Despite the pivotal role of genetics in the disease’s pathogenesis (especially in familial CD), screening tests in healthy relatives cannot be recom-mended.
Key words: Crohn’s disease; Genetics; Environment; Microbiome; Relatives
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Family studies support a host-microbiome interaction in the development of Crohn’s disease (CD). Unaffected relatives reveal genetic variants in loci involved in detecting bacteria, a greater sero-reactivity to microbial components, an impaired intestinal permeability, and a greater susceptibility to environ-mental factors. Whether genetic or environmental factors drive these conditions is still under investigation, but CD pathogenesis is very likely multifactorial. A genetic burden may be hypothesized in familial CD, while environmental factors may be predominant in sporadic CD.
Michielan A, D’Incà R. Hostmicrobiome interaction in Crohn’sdisease: A familiar or familial issue? World J Gastrointest Pathophysiol 2015; 6(4): 159168 Available from: URL: http://www.wjgnet.com/21505330/full/v6/i4/159.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i4.159
REVIEW
159 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Host-microbiome interaction in Crohn’s disease: A familiar or familial issue?
World J Gastrointest Pathophysiol 2015 November 15; 6(4): 159-168ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i4.159

INTRODUCTIONThe pathogenesis of inflammatory bowel disease (IBD) remains unclear, but is likely to be multifactorial and driven by an aberrant immune response to the gut microbiome in genetically susceptible hosts[1]. The genetic hypothesis to explain the pathogenesis of IBD, and Crohn’s disease (CD) in particular, has been intriguing researchers ever since familial clustering was first described by Crohn et al[2] himself in the 1930s, but the identification of the genes potentially involved has been hampered by the lack of a classical Mendelian inheritance. The rate of concordance in monozygotic twins is relatively low[3]. There is also a growing body of evidence to support an environmental burden in IBD epidemiology, now that the incidence of IBD is increasing in developing countries such as Asia and Africa[4], in migrants in Western countries[5], and in patients’ spouses[6].
Family studies have generated invaluable data regarding the pathogenesis of CD, as relatives may share both genetic and environmental factors with patients. These studies have shed light on the role of hostmicrobiome interaction in the disease’s development. The gut microbiome is involved in general homeostasis, with a crucial role in nutrition, energy metabolism and host defense[7]. The relationship between human organisms and their gut microbiome is regulated by the intestinal mucosal barrier, the permeability of which is a functional property that enables coexistence with bacterial symbionts, while preventing penetration by luminal macromolecules and pathogens[811]. Changes in the gut microbiome and intestinal permeability lead to an abnormal mucosal immune system response, which is the final step in the pathogenesis of IBD[1215]. Both innate and acquired gut immunity participate in maintening a state of chronic inflammation, with activated dendritic cells and mucosal T CD4+ cells apparently playing a key part in antigen presentation and response to the gut microbiome[16,17].
Changes in hostmicrobiome interactions have been welldocumented in both CD patients and their unaffected relatives.
FAMILIAL RISK IN CDEpidemiological studies have shown that almost 30% of IBD patients have a positive family history of the disease[1821], which is the most important risk factor for the onset of IBD; the lifetime risk for firstdegree relatives of CD patients is as high as 7.8% among Jewish people[20,2225]. It has been demonstrated that having a sibling with CD coincides with a 30fold increase in the odds of developing the same illness[16,22], or the other major form of IBD, ulcerative colitis (UC), and viceversa[20,26,27]. This crossdisease effect supports the evidence for a common genetic background in the onset of the two forms of IBD. There is also a cumulative effect since the risk increases when more than one relative or
both parents are affected[6,28,29]. Familial CD seems to be a distinct entity from sporadic cases of the disease because it becomes manifest at a younger age and has a different phenotypic expression, with a higher prevalence of ileal involvement[23,2932], a complicated course with penetrating or extraintestinal manifestations[33], and a strong concordance in terms of the site of disease and its behavior[21,33]. Although not all subsequent studies matched these results[34,35], a recent prospective study on more than six thousand CD patients confirmed them[36]. In families with CD, the children affected also have an earlier age of onset and a more aggressive course of the disease than their affected parents. Some authors suggested that genetic anticipation might explain this picture[37], but genetic anticipation is usually associated with monogenic diseases, and several further studies reveal potential biases due to a greater awareness of the condition[3841], or generated contradictory results[21,4244]. Irrespective of family history, pediatriconset CD has a more aggressive behavior, a higher rate of resistance to therapy, and a particular phenotype and genetic susceptibility[4547]; hence the Paris pediatric modification of the classical Montreal classification of IBD, which takes the influence of a very early onset on the disease’s history into account[48].
Twin studies on the concordance in the disease’sdevelopment and phenotype have identified a genetic predisposition that is stronger for CD than for UC[45,49,50].The concordance rate ranges from only 30% to 50% in monozygotic twins, however, meaning that environmental factors cannot be overlooked, as discussed below.
FAMILY STUDIES ON NOD2/CARD15 AND OTHER GENESThe nucleotide oligomerization domain 2 (NOD2) gene, later termed caspase recruitment domain 15 (CARD15), was the first to be identified as CDsusceptible in 2001[51,52]. Since then, more than a hundred polymorphisms and mutations have been reported in this gene, but only three of them are independently associated with CD, namely alleles R720W, G908R and L1007finsC[53,54]. Alone, these alleles each confer a risk of CD development that ranges from 1.5 to 3 fold, which rises to more than 40 when there are two of them in homozygosis or compound heterozygosis[55]. NOD2/CARD15 is a putative intracellular pattern recognition receptor expressed in several cells (monocytes, macrophages, intestinal epithelial and Paneth cells) and, when mutated, its ability to detect bacteria by recognizing peptidoglycan is impaired[53,56,57].
NOD2/CARD15 probably has a broader range of action in hostmicrobiome interactions, however, because its genotype affects gut microbiota composition[58], and its mutations have also been associated with defensin deficiency and an increased mucosal permeability in CD patients[5962].
NOD2/CARD15 mutations have been seen equally
160 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Michielan A et al . Familial Crohn’s disease

often in patients with sporadic and familial CD[6365], with the exception of one report of a higher frequency in the latter[66]. No differences have been found between relatives from multiplex and simplex families either[67], while they carry mutations significantly more frequently than in the general population[63,6870].
An Italian multicentric study found that, irrespective of family status, CD patients carrying at least one NOD2/CARD15 variant had a clinically aggressive disease that had been diagnosed at a younger age; they featured ileal involvement, a stenosing pattern and a history of surgical resections[54].
It is worth noting that the prevalence of NOD2/CARD15 mutations in CD patients is less than 50%, while it reaches 20% in healthy controls. This goes to show that, though important, it explains only a minor part of the variance in the development of CD[53]. A recent metaanalysis confirmed that NOD2/CARD15 mutations have little power in predicting the course of the disease[71].
The hypothesis of a genetic predisposition in the onset of CD is nonetheless consistent with the previousmentioned family studies, and with epidemiological evidence of ethnic differences[72,73]. In recent years, populationbased genomewide association studies (GWAS), and subsequent GWAS metaanalyses have also led to the detection of more than 160 IBDassociated loci, with more than 30 loci related to CD, and nearly 300 potential candidate genes[3,4,45,74].
These genetic studies have underscored the importance of hostmicrobiome interactions, highlighting the role of genes involved in barrier function, Tcell subsets, cytokine signaling, autophagy and mycobacteria recognition[7476]. These novel genetic markers have not been studied as extensively as NOD2/CARD15, but current data do not support any familial association[7780]. On the other hand, a large international multicentric study on IBD4 (a CDrelated locus containing several candidate genes) identified a greater genetic concordance in CD families where at least one member smoked than in nonsmoking CD families[81]. This important finding again suggests that the expression of CD in a given patient is the result of interaction not only between the gene products of several susceptibility loci, but also between these products and certain environmental factors.
Currently known variants can predict less than 14% of the IBD risk and they are quite common in the general population too, and associated with other inflammatory diseases[82]. In fact, the limited sensitivity and specificity of these mutations make a genetic screening for relatives unfeasible.
FAMILY STUDIES ON SEROLOGICAL MARKERSA hyperresponsive adaptive immunological response to microbial antigens is characteristic of CD and several
antibodies have already been correlated with this condition, including: Antiglycans (ASCA directed against mannan of Saccharomyces cervisiae, ACCA against chitobioside, ALCA against laminaribioside, AMCA against mannobioside, antiL against laminarin, and antiC against chitin), antibacterial sequence I2 of Pseudomonas fluorescens (antiI2), antibacterial flagellins (CBir, A4Fla2, FlaX) and antiouter membrane porin C of Escherichia coli (OMPc)[83,84]. Their clinical utility lies in their noninvasiveness, their ability to differentiate IBD phenotypes, and their prognostic value in CD. No current guidelines recommend their routine detection, however, given their low sensitivity, even though recent works have underscored their diagnostic and prognostic value when used in combination[84,85].
Family studies have demonstrated that some of these antibodies are more expressed in unaffected firstdegree relatives of CD patients than in the general population, with a prevalence that reaches 20%25% for ASCA, 15%19% for antiOmpC, 62% for ACCA, and 89% for ALCA[83,8688]. Using a quantitative detection assay, we also found that serum levels of ACCA, ALCA and AMCA were similar in firstdegree relatives and CD patients, and significantly higher than in healthy controls[83]. When we tested the magnitude of the total serological response to microbial antigens (the four antiglycans and antiOmpC), we found that firstdegree relatives had a weaker response than patients, but a stronger response than healthy controls. Being uninfluenced by household conditions, these results support the hypothesis that CD are genetically predisposed to the development of antibodies against microbiota[83]. These antibodies cannot be an epiphenomenon of immune activation because they are not associated with abnormal intestinal permeability or active disease[85,89]. On the other hand, a genetic background as a predisposing factor for seroreactivity has emerged from studies on ethnicity[90], and on the heritability of ASCA positivity in twins[91] and multiplex families[67], and from works correlating NOD2/CARD15 with serological markers. Several authors have reported that the aforementioned NOD2/CARD15 polymorphisms predispose individuals to the development of antimicrobial antibodies development[54,9294], and one study even demonstrated that both CD patients and their unaffected relatives carrying any of these genetic variants, had a higher number of positive antibodies and increased serological semiquantitative levels[95].
The association between serological response and genetics is likely to be more complex, however, and influenced by other factors, as shown by Vasseur et al[67], who reported that the ASCA trait in multiplex families is due partly to CD itself, not just to the NOD2/CARD15 genotype. Two complementary reports have also shown that, while CD patients with a positive family history have a higher prevalence of antibody and serologic responses[96,97], each additional positive antibody increases the risk of CD, whatever the NOD2/CARD15 genotype[98].
161 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Michielan A et al . Familial Crohn’s disease

162 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
reported case of CD occurring in a relative as predicted by an abnormal permeability test[111], so there is still too little evidence to warrant intestinal permeability assessments in relatives for screening purposes.
FAMILY STUDIES ON ENVIRONMENTAL FACTORSSome environmental factors shared by family members may contribute to modulating the microbiome and its interaction with the gut immune system. CD patients have a particular dysbiosis involving a reduction in Clostridium and Bacteroides species[12]. Given the symbiotic relationship between the gut microbiome and the mucosal barrier’s integrity, this dysbiosis may aggravate any intestinal permeability impairment. In fact, the bacterial strains that diminish in CD are also the main producers of butyrate, which is fundamental to intestinal cell homeostasis and mucosal barrier integrity[12]. Several efforts have been made to manipulate the gut microbiome in order to restore homeostasis: probiotics, prebiotics and fecal transplantation have generated promising results but their efficacy is shortlived in CD, probably because other host characteristics affect the balance of the intestinal flora[112,113].
Siblings have the same dysbiotic features as CD patients, particularly involving a reduction in Faecalibacterium prausnitzii[114]. This may be genetically determined[115], to some degree at least, but a study performed on twins showed that the gut microbiome was associated more with disease phenotype (ileal vs colonic CD) than with genotype[116].
Similarly, childhood exposure to environmental factors influencing the intestinal microbiome, such as gastrointestinal infections, antibiotic use and hospitalization, may override the role of genetics, even in twins[117,118]. A recent longitudinal study identified a declining role of childhood exposure to such factors, whereas smoking and family history of the disease remained the main risk factors[119]. Smoking has proved particularly harmful in familial CD, raising its incidence and reducing the age of onset[120]. Together with its previouslymentioned effect on intestinal permeability, smoking may also affect the intestinal microbiome, leading to dysbiosis[121].
Epidemiologic data underscore the importance of environmentdriven pathways: The incidence of CD is rising (and more rapidly than that of UC)[122], the colonic phenotype is becoming more common than ileal CD[123,124], monozygotic twin concordance is declining, and pediatric studies have shown a reduction in familial CD and an increasing multiethnicity of cases[50,122]. Western diet is increasingly seen as a major contributor to the changing epidemiology of CD because numerous dietary factors may affect the microbiome and intestinal permeability, leading to an acquired bacterial clearance defect that would foster subsequent mucosal inflammation[125]. Several studies have identified highly
Since a study suggested that ASCA could predict the onset of IBD[99], there has been increasing interest in the seroreactivity of IBD patients’ relatives. No longitudinal studies on serological markers conducted to date have demonstrated which relatives will develop IBD, however[33]. Although antibody response may vary over time, the risk is probably higher the greater the intensity of the response[98], so quantitative tests on a number of antibodies might be helpful for stratifying the risk of disease in relatives.
FAMILY STUDIES ON INTESTINAL PERMEABILITYAn altered mucosal barrier function and greater intestinal permeability contribute to chronic inflammation in IBD, facilitating the interaction between the enteric immune system and the gut microbiome[13,14].
Several changes have been reported in the components of CD patients’ mucosal barrier, mainly involving the intercellular adhesion molecules[100,101]. These changes increase paracellular permeability, nearly by as much as 50% when assessed with sugar excretion tests[102].
A greater paracellular permeability may not just a consequence of mucosal inflammation. It can be seen in IBD patients with quiescent disease too, and it correlates with intestinal symptoms even in the absence of any endoscopic disease activity[103].
The hypothesis of a genetic predisposition to barrier impairment in CD is suggested by the association between genes involved in intestinal barrier homeostasis and IBD susceptibility[104], and supported by the observation that up to 40% of relatives have an altered small intestinal permeability[33,102,105]. We found permeability abnormal in both patients and their relatives, with a more frequent occurrence in familial than sporadic cases of CD, and an association with NOD2/CARD15 variants in multiplex patients[61]. Other authors found not such correlation between permeability and genetic polymorphisms[106108], but such studies mainly involved sporadic cases of CD.
The role of genetics has also been questioned in the light of an increased permeability being observed in spouses of CD patients[33], and after a recent study underscored the importance of age and environmental factors such as age and smoking, rather than genotype, as contributors to permeability in relatives[109]. Oddly enough, relatives who smoked did not seem to have an altered permeability in this latter study. This is a matter that will need further investigation, however, because smoking is a known risk factor for CD and has recently been associated with a greater permeability of the small intestine in experimental models[110].
In conclusion, the abnormal intestinal permeability found in CD patients’ relatives further confirms a link between genetics and environmental factors in the development of CD. Thus far, there has been one only
Michielan A et al . Familial Crohn’s disease

163 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
refined sugars as a major culprit[120], but a recent study suggested that the current burden of immunerelated diseases (including CD) may also be explained by the increasing consumption of other industrial food additives via an impaired intestinal permeability[126]. There are currently no family studies on the consumption of such dietary components (earlier research mainly addressed cereal intake and produced contradictory results[127]). There is therefore not enough evidence as yet to support a causal effect of diet on CD, although a proinflammatory effect may be postulated for certain dietary components[118]. As one of the environmental factors, diet is likely to be a major contributor to the increasing incidence of colonic CD, as suggested by twin studies[117,128].
CONCLUSIONDespite the accumulating evidence emerging from genetic studies, the numerous susceptibility loci identified to date explain only a part of the variance in CD risk. Hostmicrobiome interaction has a pivotal role in CD pathogenesis, although the factor capable of turning a symbiotic into a pathogenic relationship remains unknown[75].
Family studies have generated the strongest evidence of genetic and environmental factors being complementary contributors to microbiallydriven inflammation in CD. Maybe, familial and sporadic CD should be considered as different entities (Table 1): The genetic burden prevails in familial CD, in which the genetic background influences the disease’s phenotype and course, whereas environmental factors could be more important in the pathogenesis of sporadic cases[50].
Some degree of subclinical inflammation has beendemonstrated in healthy relatives of CD patients[117,129,130],but it does not necessarily develop into clinical disease over time[131,132]. This limits the value of noninvasive screening tests, even though such tests proved effective
in detecting CD even before it becomes symptomatic[133,134].
In conclusion, CD patients’ relatives should not undergo screening so long as they are symptomfree, but they deserve special attention because of the invaluable information they can provide on the disease’s pathogenesis.
ACKNOWLEDGMENTSWe would like to thank Rachel Healy and Frances Anne Coburn for language editing.
REFERENCES1 Cho JH. The genetics and immunopathogenesis of inflammatory
bowel disease. Nat Rev Immunol 2008; 8: 458466 [PMID: 18500230 DOI: 10.1038/nri2340]
2 Crohn BB, Ginzburg L, Oppenheimer GD. Regional ileitis; a pathologic and clinical entity. Am J Med 1952; 13: 583590 [PMID: 12996536]
3 Cooney R, Jewell D. The genetic basis of inflammatory bowel disease. Dig Dis 2009; 27: 428442 [PMID: 19897957 DOI: 10.1159/000234909]
4 Ek WE, D’Amato M, Halfvarson J. The history of genetics in inflammatory bowel disease. Ann Gastroenterol 2014; 27: 294303 [PMID: 25331623]
5 Montgomery SM, Morris DL, Pounder RE, Wakefield AJ. Asian ethnic origin and the risk of inflammatory bowel disease. Eur J Gastroenterol Hepatol 1999; 11: 543546 [PMID: 10755259]
6 Laharie D, Debeugny S, Peeters M, Van Gossum A, GowerRousseau C, Bélaïche J, Fiasse R, Dupas JL, Lerebours E, Piotte S, Cortot A, Vermeire S, Grandbastien B, Colombel JF. Inflammatory bowel disease in spouses and their offspring. Gastroenterology 2001; 120: 816819 [PMID: 11231934]
7 Borody TJ, Paramsothy S, Agrawal G. Fecal microbiota transplantation: indications, methods, evidence, and future directions. Curr Gastroenterol Rep 2013; 15: 337 [PMID: 23852569 DOI: 10.1007/s1189401303371]
8 Cummings JH, Antoine JM, Azpiroz F, BourdetSicard R, Brandtzaeg P, Calder PC, Gibson GR, Guarner F, Isolauri E, Pannemans D, Shortt C, Tuijtelaars S, Watzl B. PASSCLAIMgut health and immunity. Eur J Nutr 2004; 43 Suppl 2: II118II173 [PMID: 15221356]
Table 1 Characteristics of familial and sporadic Crohn’s disease in patients and healthy relatives
Familial CD Sporadic CD
Patients Younger age at presentation Onset al the classical peak age for IBD Predominantly ileal involvement Predominantly colonic involvement Penetrating/stenosing phenotype Less frequently complicated More frequent extraintestinal manifestations Less frequent extraintestinal manifestations More frequent NOD2/CARD15 mutations NOD2/CARD15 mutations < 50% of patients Higher prevalence of anti-glycan antibodies NOD2/CARD15 mutations associated with an increased sero-reactivity to
microbial antigens Impaired intestinal permeability associated with NOD2/CARD15 variants Impaired intestinal permeability in < 50% of patients Environmental factors: Smoking Environmental factors: Smoking, diet?Healthy relatives Genetic concordance of IBD4 locus in families with smokers No reported genetic concordance ASCA trait Increased sero-reactivity to microbial antigens, also correlating with
NOD2/CARD15 genotype Abnormal intestinal permeability Abnormal intestinal permeability in < 40% of relatives
IBD: Inflammatory bowel disease; NOD2/CARD15: Nucleotide oligomerization domain 2/caspase recruitment domain 15; ASCA: Anti-Saccharomyces antibodies; CD: Crohn’s disease.
Michielan A et al . Familial Crohn’s disease

164 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
9 Bischoff SC, Barbara G, Buurman W, Ockhuizen T, Schulzke JD, Serino M, Tilg H, Watson A, Wells JM. Intestinal permeabilitya new target for disease prevention and therapy. BMC Gastroenterol 2014; 14: 189 [PMID: 25407511 DOI: 10.1186/s1287601401897]
10 Hooper LV, Littman DR, Macpherson AJ. Interactions between the microbiota and the immune system. Science 2012; 336: 12681273 [PMID: 22674334 DOI: 10.1126/science.1223490]
11 Maynard CL, Elson CO, Hatton RD, Weaver CT. Reciprocal interactions of the intestinal microbiota and immune system. Nature 2012; 489: 231241 [PMID: 22972296 DOI: 10.1038/nature11551]
12 Fava F, Danese S. Intestinal microbiota in inflammatory bowel disease: friend of foe? World J Gastroenterol 2011; 17: 557566 [PMID: 21350704 DOI: 10.3748/wjg.v17.i5.557]
13 Mankertz J, Schulzke JD. Altered permeability in inflammatory bowel disease: pathophysiology and clinical implications. Curr Opin Gastroenterol 2007; 23: 379383 [PMID: 17545772]
14 Antoni L, Nuding S, Wehkamp J, Stange EF. Intestinal barrier in inflammatory bowel disease. World J Gastroenterol 2014; 20: 11651179 [PMID: 24574793 DOI: 10.3748/wjg.v20.i5.1165]
15 Jäger S, Stange EF, Wehkamp J. Inflammatory bowel disease: an impaired barrier disease. Langenbecks Arch Surg 2013; 398: 112 [PMID: 23160753 DOI: 10.1007/s0042301210309]
16 Xu XR, Liu CQ, Feng BS, Liu ZJ. Dysregulation of mucosal immune response in pathogenesis of inflammatory bowel disease. World J Gastroenterol 2014; 20: 32553264 [PMID: 24695798 DOI: 10.3748/wjg.v20.i12.3255]
17 Bates J, Diehl L. Dendritic cells in IBD pathogenesis: an area of therapeutic opportunity? J Pathol 2014; 232: 112120 [PMID: 24122796 DOI: 10.1002/path.4277]
18 Mayberry JF, Rhodes J, Newcombe RG. Familial prevalence of inflammatory bowel disease in relatives of patients with Crohn’s disease. Br Med J 1980; 280: 84 [PMID: 7353132]
19 Monsén U, Broström O, Nordenvall B, Sörstad J, Hellers G. Prevalence of inflammatory bowel disease among relatives of patients with ulcerative colitis. Scand J Gastroenterol 1987; 22: 214218 [PMID: 3576128]
20 Orholm M, Munkholm P, Langholz E, Nielsen OH, Sørensen TI, Binder V. Familial occurrence of inflammatory bowel disease. N Engl J Med 1991; 324: 8488 [PMID: 1984188]
21 Annese V, Andreoli A, Astegiano M, Campieri M, Caprilli R, Cucchiara S, D’Incà R, Giaccari S, Iaquinto G, Lombardi G, Napolitano G, Pera A, Riegler G, Valpiani D, Andriulli A. Clinical features in familial cases of Crohn’s disease and ulcerative colitis in Italy: a GISC study. Italian Study Group for the Disease of Colon and Rectum. Am J Gastroenterol 2001; 96: 29392945 [PMID: 11693330]
22 Fielding JF. The relative risk of inflammatory bowel disease among parents and siblings of Crohn’s disease patients. J Clin Gastroenterol 1986; 8: 655657 [PMID: 3805664]
23 Yang H, McElree C, Roth MP, Shanahan F, Targan SR, Rotter JI. Familial empirical risks for inflammatory bowel disease: differences between Jews and nonJews. Gut 1993; 34: 517524 [PMID: 8491401]
24 Peeters M, Nevens H, Baert F, Hiele M, de Meyer AM, Vlietinck R, Rutgeerts P. Familial aggregation in Crohn’s disease: increased ageadjusted risk and concordance in clinical characteristics. Gastroenterology 1996; 111: 597603 [PMID: 8780562]
25 Ahmad T, Satsangi J, McGovern D, Bunce M, Jewell DP. Review article: the genetics of inflammatory bowel disease. Aliment Pharmacol Ther 2001; 15: 731748 [PMID: 11380312]
26 Meucci G, Vecchi M, Torgano G, Arrigoni M, Prada A, Rocca F, Curzio M, Pera A, de Franchis R. Familial aggregation of inflammatory bowel disease in northern Italy: a multicenter study. The Gruppo di Studio per le Malattie Infiammatorie Intestinali (IBD Study Group). Gastroenterology 1992; 103: 514519 [PMID: 1634069]
27 Binder V. Genetic epidemiology in inflammatory bowel disease. Dig Dis 1998; 16: 351355 [PMID: 10207221]
28 Bennett RA, Rubin PH, Present DH. Frequency of inflammatory
bowel disease in offspring of couples both presenting with inflammatory bowel disease. Gastroenterology 1991; 100: 16381643 [PMID: 2019369]
29 Cottone M, Brignola C, Rosselli M, Oliva L, Belloli C, Cipolla C, Orlando A, De Simone G, Aiala MR, Di Mitri R, Gatto G, Buccellato A. Relationship between site of disease and familial occurrence in Crohn’s disease. Dig Dis Sci 1997; 42: 129132 [PMID: 9009127]
30 Colombel JF, Grandbastien B, GowerRousseau C, Plegat S, Evrard JP, Dupas JL, Gendre JP, Modigliani R, Bélaïche J, Hostein J, Hugot JP, van Kruiningen H, Cortot A. Clinical characteristics of Crohn’s disease in 72 families. Gastroenterology 1996; 111: 604607 [PMID: 8780563]
31 Polito JM, Childs B, Mellits ED, Tokayer AZ, Harris ML, Bayless TM. Crohn’s disease: influence of age at diagnosis on site and clinical type of disease. Gastroenterology 1996; 111: 580586 [PMID: 8780560]
32 Halme L, Turunen U, Heliö T, Paavola P, Walle T, Miettinen A, Järvinen H, Kontula K, Färkkilä M. Familial and sporadic inflammatory bowel disease: comparison of clinical features and serological markers in a genetically homogeneous population. Scand J Gastroenterol 2002; 37: 692698 [PMID: 12126248]
33 Russell RK, Satsangi J. IBD: a family affair. Best Pract Res Clin Gastroenterol 2004; 18: 525539 [PMID: 15157825]
34 Dorn SD, Abad JF, Panagopoulos G, Korelitz BI. Clinical characteristics of familial versus sporadic Crohn’s disease using the Vienna Classification. Inflamm Bowel Dis 2004; 10: 201206 [PMID: 15290912]
35 Henriksen M, Jahnsen J, Lygren I, Vatn MH, Moum B. Are there any differences in phenotype or disease course between familial and sporadic cases of inflammatory bowel disease? Results of a populationbased followup study. Am J Gastroenterol 2007; 102: 19551963 [PMID: 17573793]
36 Andreu M, Márquez L, Domènech E, Gisbert JP, García V, MarínJiménez I, Peñalva M, Gomollón F, Calvet X, Merino O, GarciaPlanella E, VázquezRomero N, Esteve M, Nos P, Gutiérrez A, Vera I, Cabriada JL, Martín MD, CañasVentura A, Panés J. Disease severity in familial cases of IBD. J Crohns Colitis 2014; 8: 234239 [PMID: 24016462 DOI: 10.1016/j.crohns.2013.08.010]
37 Polito JM, Rees RC, Childs B, Mendeloff AI, Harris ML, Bayless TM. Preliminary evidence for genetic anticipation in Crohn’s disease. Lancet 1996; 347: 798800 [PMID: 8622336]
38 Sachar DB. Crohn’s disease: a family affair. Gastroenterology 1996; 111: 813815 [PMID: 8780588]
39 Hugot JP, Colombel JF, Bélaïche J, Cézard JP, Peeters M, Van Gossum A, Löfberg R, Pallone F, Zouali H, GowerRousseau C, Gendre JP, Thomas G. Date of birth in familial Crohn’s disease suggests environmental factors. Gastroenterology 1998; 114: A4092
40 Lee JC, Bridger S, McGregor C, Macpherson AJ, Jones JE. Why children with inflammatory bowel disease are diagnosed at a younger age than their affected parent. Gut 1999; 44: 808811 [PMID: 10323881]
41 Hampe J, Heymann K, Kruis W, Raedler A, Fölsch UR, Schreiber S. Anticipation in inflammatory bowel disease: a phenomenon caused by an accumulation of confounders. Am J Med Genet 2000; 92: 178183 [PMID: 10817651]
42 Roma ES, Panayiotou J, Pachoula J, Constantinidou C, Polyzos A, Zellos A, Lagona E, Mantzaris GJ, Syriopoulou VP. Inflammatory bowel disease in children: the role of a positive family history. Eur J Gastroenterol Hepatol 2010; 22: 710715 [PMID: 19543100 DOI: 10.1097/MEG.0b013e32832e2bd8]
43 Kuwahara E, Asakura K, Nishiwaki Y, Inoue N, Watanabe M, Hibi T, Takebayashi T. Effects of family history on inflammatory bowel disease characteristics in Japanese patients. J Gastroenterol 2012; 47: 961968 [PMID: 22382632 DOI: 10.1007/s0053501205583]
44 Cabré E, Mañosa M, GarcíaSánchez V, Gutiérrez A, Ricart E, Esteve M, Guardiola J, Aguas M, Merino O, Ponferrada A, Gisbert JP, GarciaPlanella E, Ceña G, Cabriada JL, Montoro M, Domènech E. Phenotypic concordance in familial inflammatory
Michielan A et al . Familial Crohn’s disease

165 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
bowel disease (IBD). Results of a nationwide IBD Spanish database. J Crohns Colitis 2014; 8: 654661 [PMID: 24388046 DOI: 10.1016/j.crohns.2013.12.005]
45 Uhlig HH, Schwerd T, Koletzko S, Shah N, Kammermeier J, Elkadri A, Ouahed J, Wilson DC, Travis SP, Turner D, Klein C, Snapper SB, Muise AM. The diagnostic approach to monogenic very early onset inflammatory bowel disease. Gastroenterology 2014; 147: 9901007.e3 [PMID: 25058236 DOI: 10.1053/j.gastro.2014.07.023]
46 Levine A, Kugathasan S, Annese V, Biank V, LeshinskySilver E, Davidovich O, Kimmel G, Shamir R, Palmieri O, Karban A, Broeckel U, Cucchiara S. Pediatric onset Crohn’s colitis is characterized by genotypedependent agerelated susceptibility. Inflamm Bowel Dis 2007; 13: 15091515 [PMID: 17763471]
47 Essers JB, Lee JJ, Kugathasan S, Stevens CR, Grand RJ, Daly MJ. Established genetic risk factors do not distinguish early and later onset Crohn’s disease. Inflamm Bowel Dis 2009; 15: 15081514 [PMID: 19322901 DOI: 10.1002/ibd.20922]
48 Levine A, Griffiths A, Markowitz J, Wilson DC, Turner D, Russell RK, Fell J, Ruemmele FM, Walters T, Sherlock M, Dubinsky M, Hyams JS. Pediatric modification of the Montreal classification for inflammatory bowel disease: the Paris classification. Inflamm Bowel Dis 2011; 17: 13141321 [PMID: 21560194 DOI: 10.1002/ibd.21493]
49 Halme L, PaavolaSakki P, Turunen U, Lappalainen M, Farkkila M, Kontula K. Family and twin studies in inflammatory bowel disease. World J Gastroenterol 2006; 12: 36683672 [PMID: 16773682]
50 Halfvarson J, Bodin L, Tysk C, Lindberg E, Järnerot G. Inflammatory bowel disease in a Swedish twin cohort: a longterm followup of concordance and clinical characteristics. Gastroenterology 2003; 124: 17671773 [PMID: 12806610]
51 Hugot JP, Chamaillard M, Zouali H, Lesage S, Cézard JP, Belaiche J, Almer S, Tysk C, O’Morain CA, Gassull M, Binder V, Finkel Y, Cortot A, Modigliani R, LaurentPuig P, GowerRousseau C, Macry J, Colombel JF, Sahbatou M, Thomas G. Association of NOD2 leucinerich repeat variants with susceptibility to Crohn’s disease. Nature 2001; 411: 599603 [PMID: 11385576]
52 Ogura Y, Bonen DK, Inohara N, Nicolae DL, Chen FF, Ramos R, Britton H, Moran T, Karaliuskas R, Duerr RH, Achkar JP, Brant SR, Bayless TM, Kirschner BS, Hanauer SB, Nuñez G, Cho JH. A frameshift mutation in NOD2 associated with susceptibility to Crohn’s disease. Nature 2001; 411: 603606 [PMID: 11385577]
53 van der Linde K, Boor PP, HouwingDuistermaat JJ, Crusius BJ, Wilson PJ, Kuipers EJ, de Rooij FW. CARD15 mutations in Dutch familial and sporadic inflammatory bowel disease and an overview of European studies. Eur J Gastroenterol Hepatol 2007; 19: 449459 [PMID: 17489054]
54 Annese V, Lombardi G, Perri F, D’Incà R, Ardizzone S, Riegler G, Giaccari S, Vecchi M, Castiglione F, Gionchetti P, Cocchiara E, Vigneri S, Latiano A, Palmieri O, Andriulli A. Variants of CARD15 are associated with an aggressive clinical course of Crohn’s diseasean IGIBD study. Am J Gastroenterol 2005; 100: 8492 [PMID: 15654786]
55 Bonen DK, Cho JH. The genetics of inflammatory bowel disease. Gastroenterology 2003; 124: 521536 [PMID: 12557156]
56 Girardin SE, Boneca IG, Viala J, Chamaillard M, Labigne A, Thomas G, Philpott DJ, Sansonetti PJ. Nod2 is a general sensor of peptidoglycan through muramyl dipeptide (MDP) detection. J Biol Chem 2003; 278: 88698872 [PMID: 12527755]
57 Hisamatsu T, Suzuki M, Reinecker HC, Nadeau WJ, McCormick BA, Podolsky DK. CARD15/NOD2 functions as an antibacterial factor in human intestinal epithelial cells. Gastroenterology 2003; 124: 9931000 [PMID: 12671896]
58 Rehman A, Sina C, Gavrilova O, Häsler R, Ott S, Baines JF, Schreiber S, Rosenstiel P. Nod2 is essential for temporal development of intestinal microbial communities. Gut 2011; 60: 13541362 [PMID: 21421666 DOI: 10.1136/gut.2010.216259]
59 Wehkamp J, Harder J, Weichenthal M, Schwab M, Schäffeler E, Schlee M, Herrlinger KR, Stallmach A, Noack F, Fritz P, Schröder JM, Bevins CL, Fellermann K, Stange EF. NOD2 (CARD15)
mutations in Crohn’s disease are associated with diminished mucosal alphadefensin expression. Gut 2004; 53: 16581664 [PMID: 15479689]
60 Wehkamp J, Salzman NH, Porter E, Nuding S, Weichenthal M, Petras RE, Shen B, Schaeffeler E, Schwab M, Linzmeier R, Feathers RW, Chu H, Lima H, Fellermann K, Ganz T, Stange EF, Bevins CL. Reduced Paneth cell alphadefensins in ileal Crohn’s disease. Proc Natl Acad Sci USA 2005; 102: 1812918134 [PMID: 16330776]
61 D’Incà R, Annese V, di Leo V, Latiano A, Quaino V, Abazia C, Vettorato MG, Sturniolo GC. Increased intestinal permeability and NOD2 variants in familial and sporadic Crohn’s disease. Aliment Pharmacol Ther 2006; 23: 14551461 [PMID: 16669960]
62 Buhner S, Buning C, Genschel J, Kling K, Herrmann D, Dignass A, Kuechler I, Krueger S, Schmidt HH, Lochs H. Genetic basis for increased intestinal permeability in families with Crohn’s disease: role of CARD15 3020insC mutation? Gut 2006; 55: 342347 [PMID: 16000642]
63 Annese V, Palmieri O, Latiano A, Ardizzone S, Castiglione F, Cottone M, D’Incà R, Gionchetti P, Papi C, Riegler G, Vecchi M, Andriulli A. Frequency of NOD2/CARD15 variants in both sporadic and familial cases of Crohn’s disease across Italy. An Italian Group for Inflammatory Bowel Disease Study. Dig Liver Dis 2004; 36: 121124 [PMID: 15002819]
64 Lesage S, Zouali H, Cézard JP, Colombel JF, Belaiche J, Almer S, Tysk C, O’Morain C, Gassull M, Binder V, Finkel Y, Modigliani R, GowerRousseau C, Macry J, Merlin F, Chamaillard M, Jannot AS, Thomas G, Hugot JP. CARD15/NOD2 mutational analysis and genotypephenotype correlation in 612 patients with inflammatory bowel disease. Am J Hum Genet 2002; 70: 845857 [PMID: 11875755]
65 Vermeire S, Wild G, Kocher K, Cousineau J, Dufresne L, Bitton A, Langelier D, Pare P, Lapointe G, Cohen A, Daly MJ, Rioux JD. CARD15 genetic variation in a Quebec population: prevalence, genotypephenotype relationship, and haplotype structure. Am J Hum Genet 2002; 71: 7483 [PMID: 12019468]
66 Heliö T, Halme L, Lappalainen M, Fodstad H, PaavolaSakki P, Turunen U, Färkkilä M, Krusius T, Kontula K. CARD15/NOD2 gene variants are associated with familially occurring and complicated forms of Crohn’s disease. Gut 2003; 52: 558562 [PMID: 12631669]
67 Vasseur F, Sendid B, Jouault T, StandaertVitse A, Dubuquoy L, Francois N, GowerRousseau C, Desreumaux P, Broly F, Vermeire S, Colombel JF, Poulain D. Variants of NOD1 and NOD2 genes display opposite associations with familial risk of Crohn’s disease and antisaccharomyces cerevisiae antibody levels. Inflamm Bowel Dis 2012; 18: 430438 [PMID: 21739538 DOI: 10.1002/ibd.21817]
68 Halfvarson J, Bresso F, Tysk C. Genetic Crohn’s disease. A different entity than sporadic. A study in monozygotic twins. Gastroenterology 2004; 126: A359360
69 Jess T, Riis L, Jespersgaard C, Hougs L, Andersen PS, Orholm MK, Binder V, Munkholm P. Disease concordance, zygosity, and NOD2/CARD15 status: followup of a populationbased cohort of Danish twins with inflammatory bowel disease. Am J Gastroenterol 2005; 100: 24862492 [PMID: 16279904]
70 Linde Kv, Boor PP, HouwingDuistermaat JJ, Kuipers EJ, Wilson JH, de Rooij FW. Card15 and Crohn’s disease: healthy homozygous carriers of the 3020insC frameshift mutation. Am J Gastroenterol 2003; 98: 613617 [PMID: 12650796]
71 Adler J, Rangwalla SC, Dwamena BA, Higgins PD. The prognostic power of the NOD2 genotype for complicated Crohn’s disease: a metaanalysis. Am J Gastroenterol 2011; 106: 699712 [PMID: 21343918 DOI: 10.1038/ajg.2011.19]
72 Basu D, Lopez I, Kulkarni A, Sellin JH. Impact of race and ethnicity on inflammatory bowel disease. Am J Gastroenterol 2005; 100: 22542261 [PMID: 16181378]
73 Economou M, Pappas G. New global map of Crohn’s disease: Genetic, environmental, and socioeconomic correlations. Inflamm Bowel Dis 2008; 14: 709720 [PMID: 18095316]
74 Knights D, Lassen KG, Xavier RJ. Advances in inflammatory
Michielan A et al . Familial Crohn’s disease
166 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
bowel disease pathogenesis: linking host genetics and the microbiome. Gut 2013; 62: 15051510 [PMID: 24037875 DOI: 10.1136/gutjnl2012303954]
75 Jostins L, Ripke S, Weersma RK, Duerr RH, McGovern DP, Hui KY, Lee JC, Schumm LP, Sharma Y, Anderson CA, Essers J, Mitrovic M, Ning K, Cleynen I, Theatre E, Spain SL, Raychaudhuri S, Goyette P, Wei Z, Abraham C, Achkar JP, Ahmad T, Amininejad L, Ananthakrishnan AN, Andersen V, Andrews JM, Baidoo L, Balschun T, Bampton PA, Bitton A, Boucher G, Brand S, Büning C, Cohain A, Cichon S, D’Amato M, De Jong D, Devaney KL, Dubinsky M, Edwards C, Ellinghaus D, Ferguson LR, Franchimont D, Fransen K, Gearry R, Georges M, Gieger C, Glas J, Haritunians T, Hart A, Hawkey C, Hedl M, Hu X, Karlsen TH, Kupcinskas L, Kugathasan S, Latiano A, Laukens D, Lawrance IC, Lees CW, Louis E, Mahy G, Mansfield J, Morgan AR, Mowat C, Newman W, Palmieri O, Ponsioen CY, Potocnik U, Prescott NJ, Regueiro M, Rotter JI, Russell RK, Sanderson JD, Sans M, Satsangi J, Schreiber S, Simms LA, Sventoraityte J, Targan SR, Taylor KD, Tremelling M, Verspaget HW, De Vos M, Wijmenga C, Wilson DC, Winkelmann J, Xavier RJ, Zeissig S, Zhang B, Zhang CK, Zhao H, Silverberg MS, Annese V, Hakonarson H, Brant SR, RadfordSmith G, Mathew CG, Rioux JD, Schadt EE, Daly MJ, Franke A, Parkes M, Vermeire S, Barrett JC, Cho JH. Hostmicrobe interactions have shaped the genetic architecture of inflammatory bowel disease. Nature 2012; 491: 119124 [PMID: 23128233 DOI: 10.1038/nature11582]
76 Fujiya M, Inaba Y, Musch MW, Hu S, Kohgo Y, Chang EB. Cytokine regulation of OCTN2 expression and activity in small and large intestine. Inflamm Bowel Dis 2011; 17: 907916 [PMID: 20722056 DOI: 10.1002/ibd.21444]
77 Latiano A, Palmieri O, Pastorelli L, Vecchi M, Pizarro TT, Bossa F, Merla G, Augello B, Latiano T, Corritore G, Settesoldi A, Valvano MR, D’Incà R, Stronati L, Annese V, Andriulli A. Associations between genetic polymorphisms in IL33, IL1R1 and risk for inflammatory bowel disease. PLoS One 2013; 8: e62144 [PMID: 23634226 DOI: 10.1371/journal.pone.0062144]
78 Lu XC, Tao Y, Wu C, Zhao PL, Li K, Zheng JY, Li LX. Association between variants of the autophagy related geneIRGM and susceptibility to Crohn’s disease and ulcerative colitis: a metaanalysis. PLoS One 2013; 8: e80602 [PMID: 24232856 DOI: 10.1371/journal.pone.0080602]
79 Glas J, Seiderer J, Nagy M, Fries C, Beigel F, Weidinger M, Pfennig S, Klein W, Epplen JT, Lohse P, Folwaczny M, Göke B, Ochsenkühn T, Diegelmann J, MüllerMyhsok B, Roeske D, Brand S. Evidence for STAT4 as a common autoimmune gene: rs7574865 is associated with colonic Crohn’s disease and early disease onset. PLoS One 2010; 5: e10373 [PMID: 20454450 DOI: 10.1371/journal.pone.0010373]
80 Latiano A, Palmieri O, Latiano T, Corritore G, Bossa F, Martino G, Biscaglia G, Scimeca D, Valvano MR, Pastore M, Marseglia A, D’Incà R, Andriulli A, Annese V. Investigation of multiple susceptibility loci for inflammatory bowel disease in an Italian cohort of patients. PLoS One 2011; 6: e22688 [PMID: 21818367 DOI: 10.1371/journal.pone.0022688]
81 Pierik M, Yang H, Barmada MM, Cavanaugh JA, Annese V, Brant SR, Cho JH, Duerr RH, Hugot JP, McGovern DP, PaavolaSakki P, RadfordSmith GL, Pavli P, Silverberg MS, Schreiber S, Taylor KD, Vlietinck R. The IBD international genetics consortium provides further evidence for linkage to IBD4 and shows geneenvironment interaction. Inflamm Bowel Dis 2005; 11: 17 [PMID: 15674107]
82 Festen EA, Weersma RK. How will insights from genetics translate to clinical practice in inflammatory bowel disease? Best Pract Res Clin Gastroenterol 2014; 28: 387397 [PMID: 24913379 DOI: 10.1016/j.bpg.2014.04.002]
83 Michielan A, Basso D, Martinato M, Pathak S, Banerjee A, Oliva L, Plebani M, Sturniolo GC, D’Incà R. Increased antibody response to microbial antigens in patients with Crohn’s disease and their unaffected firstdegree relatives. Dig Liver Dis 2013; 45: 894898 [PMID: 23477870 DOI: 10.1016/j.dld.2013.01.017]
84 Bonneau J, DumestrePerard C, RinaudoGaujous M, Genin C, Sparrow M, Roblin X, Paul S. Systematic review: new serological markers (antiglycan, antiGP2, antiGMCSF Ab) in the prediction of IBD patient outcomes. Autoimmun Rev 2015; 14: 231245 [PMID: 25462578 DOI: 10.1016/j.autrev.2014.11.004]
85 Xiong Y, Wang GZ, Zhou JQ, Xia BQ, Wang XY, Jiang B. Serum antibodies to microbial antigens for Crohn’s disease progression: a metaanalysis. Eur J Gastroenterol Hepatol 2014; 26: 733742 [PMID: 24901819 DOI: 10.1097/MEG.0000000000000102]
86 Sendid B, Quinton JF, Charrier G, Goulet O, Cortot A, Grandbastien B, Poulain D, Colombel JF. AntiSaccharomyces cerevisiae mannan antibodies in familial Crohn’s disease. Am J Gastroenterol 1998; 93: 13061310 [PMID: 9707056]
87 Seibold F, Stich O, Hufnagl R, Kamil S, Scheurlen M. AntiSaccharomyces cerevisiae antibodies in inflammatory bowel disease: a family study. Scand J Gastroenterol 2001; 36: 196201 [PMID: 11252413]
88 Mei L, Targan SR, Landers CJ, Dutridge D, Ippoliti A, Vasiliauskas EA, Papadakis KA, Fleshner PR, Rotter JI, Yang H. Familial expression of antiEscherichia coli outer membrane porin C in relatives of patients with Crohn’s disease. Gastroenterology 2006; 130: 10781085 [PMID: 16618402]
89 Vermeire S, Peeters M, Vlietinck R, Joossens S, Den Hond E, Bulteel V, Bossuyt X, Geypens B, Rutgeerts P. AntiSaccharomyces cerevisiae antibodies (ASCA), phenotypes of IBD, and intestinal permeability: a study in IBD families. Inflamm Bowel Dis 2001; 7: 815 [PMID: 11233666]
90 Prideaux L, Kamm MA, De Cruz P, van Langenberg DR, Ng SC, Dotan I. Inflammatory bowel disease serology in Asia and the West. World J Gastroenterol 2013; 19: 62076213 [PMID: 24115818 DOI: 10.3748/wjg.v19.i37.6207]
91 Halfvarson J, StandaertVitse A, Järnerot G, Sendid B, Jouault T, Bodin L, Duhamel A, Colombel JF, Tysk C, Poulain D. AntiSaccharomyces cerevisiae antibodies in twins with inflammatory bowel disease. Gut 2005; 54: 12371243 [PMID: 15863472]
92 Henckaerts L, Pierik M, Joossens M, Ferrante M, Rutgeerts P, Vermeire S. Mutations in pattern recognition receptor genes modulate seroreactivity to microbial antigens in patients with inflammatory bowel disease. Gut 2007; 56: 15361542 [PMID: 17595233]
93 Papp M, Altorjay I, Norman GL, Shums Z, Palatka K, Vitalis Z, Foldi I, Lakos G, Tumpek J, Udvardy ML, Harsfalvi J, Fischer S, Lakatos L, Kovacs A, Bene L, Molnar T, Tulassay Z, Miheller P, Veres G, Papp J, Lakatos PL. Seroreactivity to microbial components in Crohn’s disease is associated with ileal involvement, noninflammatory disease behavior and NOD2/CARD15 genotype, but not with risk for surgery in a Hungarian cohort of IBD patients. Inflamm Bowel Dis 2007; 13: 984992 [PMID: 17417801]
94 Papp M, Altorjay I, Dotan N, Palatka K, Foldi I, Tumpek J, Sipka S, Udvardy M, Dinya T, Lakatos L, Kovacs A, Molnar T, Tulassay Z, Miheller P, Norman GL, Szamosi T, Papp J, Lakatos PL. New serological markers for inflammatory bowel disease are associated with earlier age at onset, complicated disease behavior, risk for surgery, and NOD2/CARD15 genotype in a Hungarian IBD cohort. Am J Gastroenterol 2008; 103: 665681 [PMID: 18047543]
95 Devlin SM, Yang H, Ippoliti A, Taylor KD, Landers CJ, Su X, Abreu MT, Papadakis KA, Vasiliauskas EA, Melmed GY, Fleshner PR, Mei L, Rotter JI, Targan SR. NOD2 variants and antibody response to microbial antigens in Crohn’s disease patients and their unaffected relatives. Gastroenterology 2007; 132: 576586 [PMID: 17258734]
96 Simondi D, Mengozzi G, Betteto S, Bonardi R, Ghignone RP, Fagoonee S, Pellicano R, Sguazzini C, Pagni R, Rizzetto M, Astegiano M. Antiglycan antibodies as serological markers in the differential diagnosis of inflammatory bowel disease. Inflamm Bowel Dis 2008; 14: 645651 [PMID: 18240283 DOI: 10.1002/ibd.20368]
97 Annese V, Andreoli A, Andriulli A, Dinca R, Gionchetti P, Latiano A, Lombardi G, Piepoli A, Poulain D, Sendid B, Colombel JF. Familial expression of antiSaccharomyces cerevisiae Mannan
Michielan A et al . Familial Crohn’s disease

167 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
antibodies in Crohn’s disease and ulcerative colitis: a GISC study. Am J Gastroenterol 2001; 96: 24072412 [PMID: 11513182]
98 Joossens M, Van Steen K, Branche J, Sendid B, Rutgeerts P, Vasseur F, Poulain D, Broly F, Colombel JF, Vermeire S, Chamaillard M. Familial aggregation and antimicrobial response dosedependently affect the risk for Crohn’s disease. Inflamm Bowel Dis 2010; 16: 5867 [PMID: 19504613 DOI: 10.1002/ibd.20985]
99 Israeli E, Grotto I, Gilburd B, Balicer RD, Goldin E, Wiik A, Shoenfeld Y. AntiSaccharomyces cerevisiae and antineutrophil cytoplasmic antibodies as predictors of inflammatory bowel disease. Gut 2005; 54: 12321236 [PMID: 16099791]
100 Salim SY, Söderholm JD. Importance of disrupted intestinal barrier in inflammatory bowel diseases. Inflamm Bowel Dis 2011; 17: 362381 [PMID: 20725949 DOI: 10.1002/ibd.21403]
101 Lee SH. Intestinal permeability regulation by tight junction: implication on inflammatory bowel diseases. Intest Res 2015; 13: 1118 [PMID: 25691839 DOI: 10.5217/ir.2015.13.1.11]
102 Fries W, Renda MC, Lo Presti MA, Raso A, Orlando A, Oliva L, Giofré MR, Maggio A, Mattaliano A, Macaluso A, Cottone M. Intestinal permeability and genetic determinants in patients, firstdegree relatives, and controls in a highincidence area of Crohn’s disease in Southern Italy. Am J Gastroenterol 2005; 100: 27302736 [PMID: 16393227]
103 Vivinus-Nébot M, FrinMathy G, Bzioueche H, Dainese R, Bernard G, Anty R, Filippi J, SaintPaul MC, Tulic MK, Verhasselt V, Hébuterne X, Piche T. Functional bowel symptoms in quiescent inflammatory bowel diseases: role of epithelial barrier disruption and lowgrade inflammation. Gut 2014; 63: 744752 [PMID: 23878165 DOI: 10.1136/gutjnl2012304066]
104 Khor B, Gardet A, Xavier RJ. Genetics and pathogenesis of inflammatory bowel disease. Nature 2011; 474: 307317 [PMID: 21677747 DOI: 10.1038/nature10209]
105 Hollander D, Vadheim CM, Brettholz E, Petersen GM, Delahunty T, Rotter JI. Increased intestinal permeability in patients with Crohn‘s disease and their relatives. A possible etiologic factor. Ann Intern Med 1986; 105: 883885 [PMID: 3777713]
106 May GR, Sutherland LR, Meddings JB. Is small intestinal permeability really increased in relatives of patients with Crohn’s disease? Gastroenterology 1993; 104: 16271632 [PMID: 8500719]
107 Munkholm P, Langholz E, Hollander D, Thornberg K, Orholm M, Katz KD, Binder V. Intestinal permeability in patients with Crohn’s disease and ulcerative colitis and their first degree relatives. Gut 1994; 35: 6872 [PMID: 8307453]
108 Peeters M, Geypens B, Claus D, Nevens H, Ghoos Y, Verbeke G, Baert F, Vermeire S, Vlietinck R, Rutgeerts P. Clustering of increased small intestinal permeability in families with Crohn’s disease. Gastroenterology 1997; 113: 802807 [PMID: 9287971]
109 Kevans D, Turpin W, Madsen K, Meddings J, Shestopaloff K, Xu W, MorenoHagelsieb G, Griffiths A, Silverberg MS, Paterson A, Croitoru K. Determinants of intestinal permeability in healthy firstdegree relatives of individuals with Crohn’s disease. Inflamm Bowel Dis 2015; 21: 879887 [PMID: 25734694 DOI: 10.1097/MIB.0000000000000323]
110 Zuo L, Li Y, Wang H, Wu R, Zhu W, Zhang W, Cao L, Gu L, Gong J, Li N, Li J. Cigarette smoking is associated with intestinal barrier dysfunction in the small intestine but not in the large intestine of mice. J Crohns Colitis 2014; 8: 17101722 [PMID: 25205553 DOI: 10.1016/j.crohns.2014.08.008]
111 Irvine EJ, Marshall JK. Increased intestinal permeability precedes the onset of Crohn’s disease in a subject with familial risk. Gastroenterology 2000; 119: 17401744 [PMID: 11113095]
112 Anderson JL, Edney RJ, Whelan K. Systematic review: faecal microbiota transplantation in the management of inflammatory bowel disease. Aliment Pharmacol Ther 2012; 36: 503516 [PMID: 22827693 DOI: 10.1111/j.13652036.2012.05220.x]
113 Cui B, Feng Q, Wang H, Wang M, Peng Z, Li P, Huang G, Liu Z, Wu P, Fan Z, Ji G, Wang X, Wu K, Fan D, Zhang F. Fecal microbiota transplantation through midgut for refractory Crohn’s disease: safety, feasibility, and efficacy trial results. J Gastroenterol Hepatol 2015; 30: 5158 [PMID: 25168749 DOI: 10.1111/jgh.12727]
114 Hedin CR, McCarthy NE, Louis P, Farquharson FM, McCartney S, Taylor K, Prescott NJ, Murrells T, Stagg AJ, Whelan K, Lindsay JO. Altered intestinal microbiota and blood T cell phenotype are shared by patients with Crohn’s disease and their unaffected siblings. Gut 2014; 63: 15781586 [PMID: 24398881 DOI: 10.1136/gutjnl2013306226]
115 Hedin C, van der Gast CJ, Rogers GB, Cuthbertson L, McCartney S, Stagg AJ, Lindsay JO, Whelan K. Siblings of patients with Crohn’s disease exhibit a biologically relevant dysbiosis in mucosal microbial metacommunities. Gut 2015; Epub ahead of print [PMID: 25856344 DOI: 10.1136/gutjnl2014308896]
116 Willing B, Halfvarson J, Dicksved J, Rosenquist M, Järnerot G, Engstrand L, Tysk C, Jansson JK. Twin studies reveal specific imbalances in the mucosaassociated microbiota of patients with ileal Crohn’s disease. Inflamm Bowel Dis 2009; 15: 653660 [PMID: 19023901 DOI: 10.1002/ibd.20783]
117 Zhulina Y, HahnStrömberg V, Shamikh A, Peterson CG, Gustavsson A, Nyhlin N, Wickbom A, Bohr J, Bodin L, Tysk C, Carlson M, Halfvarson J. Subclinical inflammation with increased neutrophil activity in healthy twin siblings reflect environmental influence in the pathogenesis of inflammatory bowel disease. Inflamm Bowel Dis 2013; 19: 17251731 [PMID: 23669399 DOI: 10.1097/MIB.0b013e318281f2d3]
118 Halfvarson J, Jess T, Magnuson A, Montgomery SM, Orholm M, Tysk C, Binder V, Järnerot G. Environmental factors in inflammatory bowel disease: a cotwin control study of a SwedishDanish twin population. Inflamm Bowel Dis 2006; 12: 925933 [PMID: 17012962]
119 Castiglione F, Diaferia M, Morace F, Labianca O, Meucci C, Cuomo A, Panarese A, Romano M, Sorrentini I, D’Onofrio C, Caporaso N, Rispo A. Risk factors for inflammatory bowel diseases according to the “hygiene hypothesis”: a casecontrol, multicentre, prospective study in Southern Italy. J Crohns Colitis 2012; 6: 324329 [PMID: 22405169 DOI: 10.1016/j.crohns.2011.09.003]
120 Tuvlin JA, Raza SS, Bracamonte S, Julian C, Hanauer SB, Nicolae DL, King AC, Cho JH. Smoking and inflammatory bowel disease: trends in familial and sporadic cohorts. Inflamm Bowel Dis 2007; 13: 573579 [PMID: 17345609]
121 Parkes GC, Whelan K, Lindsay JO. Smoking in inflammatory bowel disease: impact on disease course and insights into the aetiology of its effect. J Crohns Colitis 2014; 8: 717725 [PMID: 24636140 DOI: 10.1016/j.crohns.2014.02.002]
122 Chapman-Kiddell CA, Davies PS, Gillen L, RadfordSmith GL. Role of diet in the development of inflammatory bowel disease. Inflamm Bowel Dis 2010; 16: 137151 [PMID: 19462428 DOI: 10.1002/ibd.20968]
123 Lapidus A. Crohn’s disease in Stockholm County during 19902001: an epidemiological update. World J Gastroenterol 2006; 12: 7581 [PMID: 16440421]
124 Lakatos L, Mester G, Erdelyi Z, Balogh M, Szipocs I, Kamaras G, Lakatos PL. Striking elevation in incidence and prevalence of inflammatory bowel disease in a province of western Hungary between 19772001. World J Gastroenterol 2004; 10: 404409 [PMID: 14760767]
125 Pfeffer-Gik T, Levine A. Dietary clues to the pathogenesis of Crohn’s disease. Dig Dis 2014; 32: 389394 [PMID: 24969285 DOI: 10.1159/000358143]
126 Lerner A, Matthias T. Changes in intestinal tight junction permeability associated with industrial food additives explain the rising incidence of autoimmune disease. Autoimmun Rev 2015; 14: 479489 [PMID: 25676324 DOI: 10.1016/j.autrev.2015.01.009]
127 Spooren CE, Pierik MJ, Zeegers MP, Feskens EJ, Masclee AA, Jonkers DM. Review article: the association of diet with onset and relapse in patients with inflammatory bowel disease. Aliment Pharmacol Ther 2013; 38: 11721187 [PMID: 24118051 DOI: 10.1111/apt.12501]
128 Halfvarson J. Genetics in twins with Crohn’s disease: less pronounced than previously believed? Inflamm Bowel Dis 2011; 17: 612 [PMID: 20848478 DOI: 10.1002/ibd.21295]
129 Pham M, Leach ST, Lemberg DA, Day AS. Subclinical intestinal
Michielan A et al . Familial Crohn’s disease

168 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
inflammation in siblings of children with Crohn’s disease. Dig Dis Sci 2010; 55: 35023507 [PMID: 20931283 DOI: 10.1007/s1062001014348]
130 Thjodleifsson B, Sigthorsson G, Cariglia N, Reynisdottir I, Gudbjartsson DF, Kristjansson K, Meddings JB, Gudnason V, Wandall JH, Andersen LP, Sherwood R, Kjeld M, Oddsson E, Gudjonsson H, Bjarnason I. Subclinical intestinal inflammation: an inherited abnormality in Crohn’s disease relatives? Gastroenterology 2003; 124: 17281737 [PMID: 12806605]
131 Sorrentino D, Avellini C, Geraci M, Dassopoulos T, Zarifi D, Vadalaʼ di Prampero SF, Benevento G. Tissue studies in screened firstdegree relatives reveal a distinct Crohn’s disease phenotype. Inflamm Bowel Dis 2014; 20: 10491056 [PMID: 24788221 DOI: 10.1097/MIB.0000000000000051]
132 Courville EL, Siegel CA, Vay T, Wilcox AR, Suriawinata AA, Srivastava A. Isolated asymptomatic ileitis does not progress to overt Crohn disease on longterm followup despite features of chronicity in ileal biopsies. Am J Surg Pathol 2009; 33: 13411347 [PMID: 19606015 DOI: 10.1097/PAS.0b013e3181ad25b6]
133 Parrilli G, Orsini L, Corsaro M, Bianco MA, Coccoli P, Garofano ML, Rotondano GG, Cipolletta L. Is intestinal permeability test useful for asymptomatic Crohn’s disease? Inflamm Bowel Dis 2006; 12: 11891190 [PMID: 17119396]
134 Biancone L, Calabrese E, Petruzziello C, Capanna A, Zorzi F, Onali S, Condino G, Lolli E, Ciccacci C, Borgiani P, Pallone F. A family study of asymptomatic small bowel Crohn’s disease. Dig Liver Dis 2014; 46: 276278 [PMID: 24360029 DOI: 10.1016/j.dld.2013.11.003]
P- Reviewer: Koulaouzidis A, Malnick S, Zhu YL S- Editor: Ji FF L- Editor: A E- Editor: Liu SQ
Michielan A et al . Familial Crohn’s disease

Revised: August 28, 2015Accepted: October 12, 2015Article in press: October 13, 2015Published online: November 15, 2015
AbstractThe impact of antibiotics on the human gut microbiota is a significant concern. Antibiotic-associated diarrhea has been on the rise for the past few decades with the increasing usage of antibiotics. Clostridium difficile infections (CDI) have become one of the most prominent types of infectious diarrheal disease, with dramatically increased incidence in both the hospital and community setting worldwide. Studies show that variability in the innate host response may in part impact upon CDI severity in patients. That being said, CDI is a disease that shows the most prominent links to alterations to the gut microbiota, in both cause and treatment. With recurrence rates still relatively high, it is important to explore alternative therapies to CDI. Fecal microbiota transplantation (FMT) and other types of bacteriotherapy have become exciting avenues of treatment for CDI. Recent clinical trials have generated excitement for the use of FMT as a therapeutic option for CDI; however, the exact components of the human gut microbiota needed for protection against CDI have remained elusive. Additional investigations on the effects of antibiotics on the human gut microbiota and subsequent CDI will help reduce the socioeconomic burden of CDI and potentially lead to new therapeutic modalities.
Key words: human gut microbiota; Antibiotic-associated diarrhea; Fecal microbial transplant; bacteriotherapy; Dysbiosis
© The Author(s) 2015. Published by baishideng Publishing Group Inc. All rights reserved.
Core tip: Emergent literature demonstrates the critical
L Patrick Schenck, Paul L beck, Justin A MacDonald
L Patrick Schenck, Gastrointestinal Research Group at the Snyder Institute for Chronic Diseases, Cumming School of Medicine, University of Calgary, Calgary AB T2N 4Z6, Canada
Paul L beck, Gastrointestinal Research Group at the Snyder Institute for Chronic Diseases and Department of Medicine, Cumming School of Medicine, University of Calgary, Calgary AB T2N 4Z6, Canada
Justin A MacDonald, Gastrointestinal Research Group at the Snyder Institute for Chronic Diseases and Department of Biochemistry and Molecular Biology, Cumming School of Medicine, University of Calgary, Calgary, AB, T2N 4Z6, Canada
Author contributions: Schenck LP, Beck PL and MacDonald JA performed the literature review and wrote the paper.
Supported by Canadian Institutes of Health Research, No. MOP#98004.
Conflict-of-interest statement: The authors declare that they have no affiliation with or involvement in any organization or entity with any financial interest in the subject matter or materials discussed in this manuscript.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Correspondence to: Justin A MacDonald, Professor, Gastrointestinal Research Group at the Snyder Institute for Chronic Diseases and Department of Biochemistry and Molecular Biology, Cumming School of Medicine, University of Calgary, 3280 Hospital Drive NW, Calgary AB T2N 4Z6, Canada. [email protected]: +1-403-2108433
Received: June 25, 2015Peer-review started: June 26, 2015First decision: August 16, 2015
REVIEW
169 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Gastrointestinal dysbiosis and the use of fecal microbial transplantation in Clostridium difficile infection
World J Gastrointest Pathophysiol 2015 November 15; 6(4): 169-180ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i4.169

role of the human microbiota in the susceptibility to Clostridium difficile (C. difficile ) infection (CDI). Microbial communities may exert effects on the metabolic composition within the GI tract that influence CDI pathogenesis (e.g. , bile salt metabolism). The identification of protective and susceptible human gut microbiomes would enable the development of screening tools to identify at-risk patients. Ultimately, the rational design of probiotic cocktails could assist in attenuating C. difficile transmission in hospital or community settings. Prevention of CDI would lead to decreased morbidity and mortality, as well as reduction of hospitalization time and health care costs associated with treatment.
Schenck LP, Beck PL, MacDonald JA. Gastrointestinal dysbiosis and the use of fecal microbial transplantation in Clostridium difficile infection. World J Gastrointest Pathophysiol 2015; 6(4): 169-180 Available from: URL: http://www.wjgnet.com/2150-5330/full/v6/i4/169.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i4.169
INTRODUCTIONThe discovery and application of antibiotics in the early 20th century was one of the most influential breakthroughs in medical history. It has led to the treatment of many diseases and improved survival rates of serious wounds and surgeries. However, the antibiotics used to treat these infections are not always specifically targeted towards the diseasecausing bacteria, as broadspectrum antibiotics can target other bacteria, including the commensal bacteria in the human intestinal tract, known as the human gut microbiota (HGM). Furthermore, calls from various health agencies and ministries have been made for improved antibiotic stewardship, as overprescription of antibiotics has led to escalations in antibioticresistant bacteria[14], including Clostridium difficile (C. difficile)[5]. While the increases in antibiotic resistance cannot be over looked, the indirect impact of antibiotics on the HGM is a growing problem. Antibioticassociated diarrhea (AAD) has been on the rise for the past few decades with the increasing usage of antibiotics. C. difficile infection (CDI) has become one of the most prominent types of AAD with increasing rates in both the hospital and community setting worldwide[68]. This increased burden on both the patient population and healthcare costs has become an alarming predicament. Investigations into the effects of antibiotics on the HGM and subsequent CDI will help reduce this burden and potentially lead to new therapeutics to treat this emergent epidemic.
The hUmaN GUT mICRObIOTa The human gastrointestinal tract houses one of the most dynamic bacterial communities on the planet,
with hundreds of species and thousands of strains competing for nutrients while producing byproducts that can be beneficial to the host. Additionally, the HGM plays a key role in host defense, providing a protective and competitive layer to resist growth of different pathogens. However, dysbiosis and overgrowth of microbiota has been seen in several different diseases, including inflammatory bowel disease (IBD)[9] and irritable bowel syndrome[10], allergy and asthma[11], tumorigenesis[12], nonalcoholic fatty liver disease[13], cardiovascular disease[14], autism[15,16], and obesity[17,18]. It is clear that proper maintenance and turnover of the microbiota is essential for proper health.
The HGM plays a large role in health and disease, yet until recently much of its composition and function remained unknown[19]. The HGM has been shown to play important roles in early life development, including vitamin and nutrient absorption, stimulation of intestinal angiogenesis, protection from pathogens and immune development[20]. This complex ecosystem is rapidly responding to the harsh environment within the gastrointestinal tract, including nutrient and pH fluctuations, niche competition with other bacteria, and antimicrobial peptides being excreted by the host[21]. While specific bacterial pathogens are well known to cause discrete disease, overall bacterial dysbiosis has been linked to many chronic diseases that are prevalent in society[16]. The mutualism exhibited by the HGM and its human host is paralleled by few other hostmicrobe interactions. Ultimately, knowledge of the HGM could be utilized to analyze disease status and therapeutic responses.
meThODOlOGy fOR sTUDyING The hUmaN GUT mICRObIOTa The study of the gut microbiota has been ongoing for almost a century. The earliest studies isolated animals into a germfree state, allowing development without any influence from bacteria or their products. In answer to a challenge originally issued by Louis Pasteur, scientists at the University of Notre Dame were able to deliver guinea pigs by caesarean section and house them in germfree containment. These guinea pigs were then bred under germfree conditions, to provide axenic animals[22]. The hope was for the animals to be used in identifying bacterial roles in normal physiology, as well as their role in proper immune defense against bacteria, as antibiotic resistance was already a rising threat.
Bacteria from the HGM are difficult to isolate in culture, making it challenging to determine the overall microbial community. The study of the HGM has expanded in the last decade due to advances in cultureindependent methods of monitoring microbial diversity. Most techniques target the 16S ribosomal RNA (16S rRNA) gene, as it contains conserved and variable regions that can be used to distinguish different bacterial species[23]. The 16S rRNA gene is approximately 1500
170 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Schenck LP et al . Clostridium difficile infection

nucleotide base pairs in length, and contains nine conserved regions and nine variable regions (V1V9)[23]. These variable regions have been targeted for bacterial group and species identification via different techniques. Basic techniques that began the culture-independent revolution include denaturing gradient gel electrophoresis (DGGE) and terminal restriction fragment length polymorphism (TRFLP).
Introduced in 1993, DGGE provided a snapshot of overall microbial diversity within a sample. The 16S rRNA gene is amplified in a polymerase chain reaction (PCR) and subjected to separation in polyacrylamide containing a denaturing gradient of urea and formamide[24]. This allowed DNA fragments to be separated based on melting temperature, fragment length and guaninecytosine content, resulting in a unique band pattern. These band patterns can be compared to prepared bacterial standards, or bands can be excised and analyzed by sequencing[24]. However, multiple bacterial taxa could occupy one band in a gel such that underestimation of bacterial diversity frequently occurred[25].
TRFLP, first described in 1997, involves PCR amplification of the 16S rRNA gene using a fluorescently-labelled forward primer[26]. This reaction is followed by restriction digestion targeted towards a conserved sequence, which produces terminalrestriction fragments (TRFs). Fluorescent primers allow for quantification of the TRFs, giving an overall and relative abundance. Identification to the phyla or deeper levels was possible by comparing the TRFs to an in silico library, which was generated from the Ribosomal Database project[27].
The strengths of DGGE and TRFLP in the early 2000’sincluded relatively high throughput combined with lower costs in an age of expensive genomic sequencing technology. Both methods were able to provide a finger-print of the microbial community within a fecal sample and enabled intersample comparisons. However, both were also associated with relatively poor resolution of the HGM community members, sometimes failing to identify bacteria beyond the phyla level. With the development of new and more costeffective genomic sequencing [i.e., nextgeneration sequencing (NGS) methods[28]], the method is now at the forefront of HGM research. While sequencing of the HGM has become for readily available, the bioinformatic analysis still provides challenges for the facile interpretation of datasets. Several computing programs and pipelines have been assembled, primarily through the Human Microbiome Project, which aid in the analysis[29]. “Quantitative insights into microbial ecology”, or QIIME, has been the most prominent pipeline developed thus far, as it allows the input of thousands of sequences and navigates through sequence alignment to known databases and downstream community analysis[30]. With the development of rapid and feasible sequencing, as well as improved bioinformatic output, the study of the HGM has shifted to cultureindependent dominated processes. However, the cultivation of bacteria is still considered the gold standard, and microbial DNA in samples does not indicate whether the sample came
from an active or dead bacteria[31]. Nonetheless, the NGS technologies have allowed for new studies to examine the HGM in health and disease.
C. difficile C. difficile is an anaerobic, sporeforming bacterium that was originally identified as a natural part of the infant microbiota[32]. However, research since the 1970’shas linked C. difficile colonization as the primary cause of antibioticassociated and nosocomial diarrhea in the adult and elderly populations[33,34]. CDI symptoms vary amongst patients, ranging from mild to severe diarrhea (> 15 bowel movements per day), with severe cases resulting in toxic megacolon or death[35]. The CDI mortality rate has been increasing over the last decade, due to the development of hypervirulent and antibioticresistant strains[36,37]. C. difficile transmission has become a major problem in hospitals across the developed world, as C. difficile spores are highly resistant to normal cleaning agents, including alcoholbased hand washes.
epIDemIOlOGy aND RIsk faCTORs fOR CDIC. difficile has risen to prominence internationally, with several large breakouts within hospitals causing the death of many patients. In 2003, an outbreak of the hypervirulent C. difficile, strain North American pulsedfield gel electrophoresis type1 (NAP1), in Quebec hospitals caused the death of nearly 2000 people[38]. Recently, it was also demonstrated that the spread of the NAP1 strain worldwide originated from this Quebec breakout[37]. In the United States and Europe, hospitalassociated CDI is estimated to incur annual healthcare costs over $4 billion[36]. Furthermore, there is increasing incidence in developing countries in Asia, although not from the NAP1 strain[7]. There are several risk factors with high association with CDI, including recent antibiotic exposure, age (> 65 years), recent hospitalization, and proton pump inhibitor use[35]. Antibiotic exposure shows the highest correlation, with odds ratios ranging from 1.311.87[39]. Certain antibiotics also demonstrate higher correlations, such as clindamycin[39]; indeed, this finding correlates with the history of the disease since CDI was originally referred to as clindamycinassociated pseudomembranous colitis[33]. There is also an increased threat from communityacquired CDI (CACDI), which is less studied compared to hospitalacquired CDI (HACDI), and the corresponding incidents of CACDI have increased approximately 5fold over the last decade as well[40]. CA-CDI is normally defined as an outpatient presenting with C. difficile toxinpositive stool, or an inpatient presenting less than 2 d after admission. A recent study suggested that the risk factors in these patients were different compared to HACDI, as 36% of patients did not have recent antibiotic exposure[41]. Another investigation determined that advanced age is also not a factor, as CA-CDI patients were significantly
171 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Schenck LP et al . Clostridium difficile infection

172 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
changed germination dynamics. Indeed, mutated CspC led to decreased mortality in the hamster model of CDI. Germination results in the upregulation of several genes, and the entry into the vegetative state of the C. difficile lifecycle. This involves the breakdown of the spore cortex, core expansion and water uptake into the core, allowing an increase in enzymatic activity[50]. This complex process has not been well studied in C. difficile but has in related species[51]. Germination normally occurs within the cecum and colon as other factors in the small intestine, such as high concentration of chenodeoxycholic acid, act to suppress widescale germination[48].
Subsequently, C. difficile initiates the activation of the pathogenicity locus (PaLoc) in the genome. The PaLoc, approximately 19.6 kb in size, is composed of 5 genes, tcdA, tcdB, tcdC, tcdR, and tcdE, which are responsible for the production of two large clostridial toxins, A (TcdA) and B (TcdB)[52,53]. The gene tcdR, which is found upstream of the toxin genes, is a positive regulator of gene expression whereas tcdC is a negative regulator. A poreforming holin is encoded by tcdE, which allows the release of TcdA and TcdB. Literature has suggested that hypervirulent NAP1 C. difficile released more toxin due to decreased expression of tcdC; however, this has come into question due to recent evidence that demonstrates no change in toxin production[54]. Another gene regulator is CodY, which binds and represses tcdR and thus inhibits toxin production, when essential nutrients are not available[55].
Importantly, CDIinduced colitis only occurs when either of TcdA or TcdB is present[56]. Indeed, patients with pseudomembranous colitis are C. difficile toxinpositive > 96% of the time[57]. TcdA was originally believed to be the only toxin necessary for virulence until the discovery of TcdA/TcdB+ C. difficile strain in major breakouts worldwide[58]; however, TcdA+/TcdB strains are equally likely to cause disease[59]. Recent studies in animals have attempted to delineate the importance of each toxin in vivo; new animal model to study host response to intrarectal instillation of C. difficile toxins revealed that TcdA was important for the majority of the damage, whereas TcdB alone caused no damage to the mouse colon but could potentiate the effects of TcdA[60]. Interestingly, individuals infected with the same C. difficile strain can respond very differently. While the mechanism has not been elucidated, it has been linked to development of antibodies against TcdA and/or TcdB[61,62]. However, this theory has come into question due to the increasing recurrence rates, with recent literature demonstrating that asymptomatic carriers and diseased patients having similar antibody loads towards the toxins[63]. Differences in microbiota between patients with a single case vs recurrent CDI have been suggested to play a role in patient susceptibility and variability[64]. Different animal models have been employed to determine important bacterial and host factors involved in CDI.
younger compared to HACDI[40]. An interesting area of study is the source of C. difficile within the community, as hospitals are the normal “reservoir” Recent studies have revealed relatively common contamination of retail prepared foods, including meat, seafood and vegetables, with C. difficile spores[4245]. While CACDI risk factors and sources differ from HACDI, the increasing rates in both are alarming.
C. diffiCile paThOGeNesIs aND lIfeCyCle C. difficile, as a pathogen, has an interesting lifecycle that ensures its success. Although anaerobic, C. difficile can survive for months on aerobic surfaces (e.g., hospital walls, doors, surgical tools, cell phones, etc.) in spore form. The spore structure contains several layers, including an exosporium, coat, cortex, membrane, and a DNAcontaining core[46]. This makes the spores resistant to alcoholbased cleaning agents used commonly in hospitals. C. difficile pathogenesis involves germination of spores into vegetative cells, colonization within the gut microbiota, productions of toxins which lead to toxininduced intestinal damage and inflammation (Figure 1). When ingested, the multiple layers of the spore help protect it from stomach acids and digestive enzymes. Spore germination occurs upon interaction with the appropriate germinants within the intestinal tract, which include taurocholic acid, a taurineconjugated bile acid, and glycine[47,48]. The receptor for taurocholic acid on a C. difficile spore, CspC, was only recently discovered[49], and researchers demonstrated that mutations to this protein
C. difficile spore
Vegetative C. difficile
Intestinalepithelia
Colonicmicrobiota
TcdA Tcdb
Neutrophil
Legend
Taurocholic acid
(1) (2)
(3)
(4)
hO
hO Oh
OhO
SNh
O O
Figure 1 Pathogenesis of Clostridium difficile infections. Clostridium difficile (C. difficile) spores are ingested and pass through the stomach, upon which they can interact with taurocholate within the small intestine and germinate into vegetative cells (1); Vegetative cells then colonize within the gut microbiota (2) and begin to produce toxins, TcdA and TcdB (3); Toxins cause epithelial damage and pro-inflammatory cytokine release, leading to infiltration of neutrophils that cause pseudomembranous colitis (4).
Schenck LP et al . Clostridium difficile infection

173 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
The hOsT ImmUNe RespONse TO C. diffiCile INfeCTIONC. difficile toxins induce epithelial injury, barrier dysfunction and activation of the mucosal immune system[52]. The classic endoscopic and histological feature of CDI is pseudomembranous colitis, characterized by severe inflammation (neutrophilic/monocytic), ulceration and pseudomembranes[33]. CDI has a rapid onset and previous exposure does not confer protection. There is marked variability in disease severity in patients with similar risk factors who are infected with the same C. difficile strain. Some of the variability in responses might, in part, be due to altered innate immune pathways. For example, the nucleotidebinding domain leucinerich repeat family of genes contains a number of intracellular innate immune receptors that respond to a variety of microbial and nonmicrobial danger signals. Indeed, TcdA and TcdB can trigger pro-inflammatory interleukin-1B release by activating an intracellular inflammasome[65]. A number of studies also support the activation of humoral immune responses to C. difficile toxin proteins during CDI (reviewed in[66]). Most healthy adults have detectable serum antibody titers to TcdA and TcdB (as well as nontoxin antigens) that may originate from transient environmental exposure to C. difficile from infancy[67]. The antitoxin antibody responses (e.g., IgG) in relation to the clinical course of CDI, as well as disease recurrence, have been reported in a number of studies[62,6871]. Immunity to TcdB may be important in the early stages of CDI; however, antigenic variation in TcdB suggests that acquired immunity may not provide crossprotection among different C. difficile strains[62]. Researchers are now examining the efficacy of protective immunity provided by vaccines against C. difficile.
TReaTmeNT Of C. diffiCile INfeCTIONThe current therapeutic paradigm for CDI is the removal of the causative antibiotics (i.e., clindamycin) and treatment with vancomycin (complicated disease) or metronidazole (mild disease)[72]. Fidaxomicin is a therapeutic option for patients with recurrent CDI or a high risk of recurrence. Occasionally, when CDI progresses to toxic megacolon, colectomy is required. A recent study demonstrated that survival rates postcolectomy are low, identifying this as a lastresort in CDI treatment[73]. Oral metronidazole was the normal first-line treatment, where vancomycin is used in more severe cases or with metronidazole failure[74]. These guidelines were confirmed by a doubleblind, randomized, placebocontrolled clinical trial, showing equal efficacy with vancomycin being more successful in severe patients[75]. However, recurrence of CDI, caused by relapse or reinfection, occurs in about 20%35% of these patients[76]. Fidaxomicin is a recently introduced antibiotic that targets C. difficile more selectively and shows equal efficacy compared to vancomycin[77,78]. This is likely due to the fact that
fidaxomicin has reduced effects on the commensal gut microbiota compared to vancomycin. Importantly, there was also decreased CDI recurrence rates in patients taking fidaxomicin compared to vancomycin, highlighting its role as a superior alternative antibiotic[77,78]. However, with recurrence rates still relatively high, it is important to explore alternative therapies to CDI. In this regard, fecal microbiota transplantation (FMT) and other types of bacteriotherapy have become exciting avenues for the treatment for CDI.
COlONIzaTION ResIsTaNCe aGaINsT C. diffiCileIdentifying mechanisms by which the microbiota controls colonization by C. difficile and susceptibility to CDI, known as colonization resistance, has been pushed to the forefront of research[7983]. C. difficile pathogenesis requires spore germination, colonization, and toxin production, which lead to the host immune response. Hypotheses for colonization resistance mechanisms include inhibiting germination, limiting important nutrients for colonization, or stimulation of the host immune response. Germination of C. difficile spores into vegetative, toxinproducing cells can be inhibited via several pathways. As previously mentioned, taurocholate is a primary bile salt that is formed in the liver and is involved in initiating the germination of C. difficile spores[84]. There are a few mechanisms by which bacteria actively modify the structure of bile salts, rendering them unable to stimulate germination. Some bacteria produce bile salt hydrolases (BSH) that catalyze the deconjugation of the amino acid (taurine or glycine) from carbon24 (C24) of bile salts[85]. BSHs tend to be intracellular enzymes, though one species, Clostridium perfringens, produces extracellular BSH[86]. Bile hydrolysis is quite common for different gut bacteria and has been demonstrated in Clostridia, Bacteroides, Parabacteroides, Lactobacillus, Bifidobacterium, and Enterococcus[85,8789]. BSHs are hypothesized to be beneficial to commensal bacteria by liberating nutrients (e.g., amino acids[90]), possibly giving a competitive advantage to BSH-producing bacteria. Additional studies have demonstrated that increasing BSH gene copies in Listeria result in increased survival in vivo, while decreasing BSH expression results in decreased bacterial growth[91].
Specific members of Eubacterium and Clostridia genera have the ability to epimerize bile acids at the C7 position (conversion of 7α to 7βhydroxy), converting primary bile salts (cholate and chenodeoxycholate) into secondary bile acids (deoxycholic acid and lithocholic acid, respectively) via 7αdehydroxysteroid dehydrogenases (7αHSDH) and 7βHSDH[92]. These enzymes exist solely in the large intestine of humans[85]. HSDHs also exist for the C-3 and C-12 positions on bile salts. Bacteria also produce dehydroxylation enzymes, which are important in the excretion of bile salts. Interestingly, these enzymes
Schenck LP et al . Clostridium difficile infection

174 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
can only function on deconjugated bile acids, requiring the activity of BSHs first[93]. This requires the bacteria to either produce BSH, or live in close proximity to a microbe that does. Taurocholate is rarely available to allow C. difficile to germinate in a healthy gut given the constant catabolism of bile salts. However, recent studies have identified that exposure to antibiotics decreases the metabolism rate of primary bile salts. Naïve mouse cecal contents incubated with C. difficile spores are unable to permit germination of C. difficile in vitro[47]. However, intraperitoneal injections of clindamycin and subsequent cecal content incubation led to C. difficile germination. This was corroborated with increased primary bile salts and decreased secondary bile salts in the cecum[47]. Additionally, incubating taurocholate with isolated cecal microbiota from naïve mice resulted in breakdown of the majority of the primary bile salt, whereas clindamycintreated mice completely lost their ability to metabolize taurocholate. This was recently corroborated with a metabolomic study that assessed bile in cecal contents of mice[94]. Most recently, analyses of the HGM of hospitalized CDI patients identified resistanceassociated bacteria[80]. Clostridium scindens (C. scindens), a bile acid 7αdehydroxylating intestinal bacterium, was associated with colonization resistance. Probiotic administration of C. scindens provided resistance to CDI in a secondary bile acid dependent fashion. Taken together, these studies demonstrate a potential link between microbiota function, bile metabolism and CDI susceptibility.
Pharmacologic agents that target the interaction between C. difficile spores and taurocholate have also been investigated as a potential therapeutic option[95]. A bile salt analog, cholate metabenzene sulfonic acid (CamSA), was a strong inhibitor of C. difficile germination in vitro and in vivo. In this case, CamSA (50 mg/kg) was able to completely inhibit C. difficile germination in a mouse, resulting in no CDI pathology[95]. Interestingly, a bile salt sequestrant, cholestyramine, was previously used as an adjunct therapy with antibiotics for CDI[96]. The mechanism of action was considered to be binding of C. difficile toxins but could have also been associated with C. difficile spore germination. One case study also detailed a patient with recurring CDI who was cured after prolonged cholestyramine therapy, potentially due to decreased germination[97]. Clearly, alteration of C. difficile germination is able to play a protective role in CDI.
aNTaGONIsTIC aCTIvITy Of COmmeNsal baCTeRIa aGaINsT C. diffiCileIn recent years, the aim for developing treatment for CDI has been a narrowspectrum antibiotic against C. difficile (e.g., fidaxomicin) and microbiota sparing[7578]. However, treatment strategies that rely on antibiotics impose strong selection for resistance as well as the disruption of the normal microbiota. Members of the gut microbiota
can also produce antimicrobial compounds, termed bacteriocins, which target a narrow range of bacterial species. Researchers in Ireland identified a C. difficiletargeting bacteriocin, Thuricin CD, produced by Bacillus thuringensis[98]. Thuricin CD was shown to be as effective as antibiotics in vitro for the elimination of C. difficile, while also having limited impact on the host microbiota. The group recently published that intrarectal instillation of Thuricin CD into mice was able to reduce shed C. difficile in the feces, though showed low bioavailability when orally gavaged[99]. Another contractile bacteriocin protein complex (Rtype; diffocin) was engineered to kill specific C. difficile pathogens[81]. The diffocins (i.e., AvidocinCDs) prevented colonization of NAP1type C. difficile strains and limited their transmission. AvidocinCDs administered in drinking water survived passage through the mouse gastrointestinal tract, did not detectably alter the mouse intestinal microbiota and did not disrupt natural colonization resistance to C. difficile.
A group at the University of Michigan identified that antibiotictreated mice had reduced levels of Lachnospiraceae in their feces, which correlated with increased CDI severity[100]. Reeves et al[101] later demonstrated that, while germfree mice were extremely susceptible to CDI, the addition of multiple Lachnospiraceae family members suppressed the growth of C. difficile by 20fold, and decreased the toxin production by 25%. Only complete cecal microbiota transfer entirely inhibited CDI. This parallels with studies completed in the 1980’s, where Itoh et al[102] transferred several different species, but only a full fecal transfer conferred protection.
Different groups have looked at the ability of certain bacterial species to inhibit toxin production in vitro. Kolling et al[103] determined that Streptococcus thermophilus produced lactic acid, which was able to suppress the transcription of tcdA and release of TcdA in vitro. Furthermore, mice treated with Streptococcus thermophilus have less severe CDI with decreases in weight loss, tissue injury on pathology, diarrhea, detectable C. difficile bacteria and toxin levels. This study demonstrated the ability of bacteria and bacterial products to suppress C. difficile growth and toxin production.
A recent study by Lawley et al[104] identified a consortium of six bacterial species in mice that could treat a recurrent carriermodel of CDI. These species, Bacteroidetes sp. nov., Enterorhabdus sp. nov., Enterococcus hirae, Lactobacillus reuteri, Staphylococcus warneri, and Anaerostipes sp. nov., were able to reduce inflammatory parameters of CDI as well as fecal counts of C. difficile. Individually, these six species were unable to confer protection, and no metabolic pathways could be identified to rationalize the effectiveness of the treatment[104]. The addition of these species did lead to increased bacterial diversity within the mouse intestinal microbiota, which was suggested as the potential mechanism for restoring colonization resistance. However, these species are limited to mice and not seen in HGM, so its application to human CDI is not clear.
Schenck LP et al . Clostridium difficile infection

175 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
FMTFMT has risen to prominence in the past few years as an exciting therapeutic approach for CDI, especially recurrent CDI. However, FMT actually has a very extensive history and has been successfully used to treat diarrhea for over 50 years. Four patients were treated with fecal enemas in 1958 to resolve pseudomembranous colitis, and they exhibited dramatic resolution over 2448 h posttreatment[105]. This study was conducted before C. difficile was recognized as the primary cause of pseudomembranous colitis, but it has since been validated by other studies using fecal enema[106]. The current protocol for involves fairly intense screening followed by simple techniques[107,108]. First, the FMT recipient ceases antibiotics and an FMT donor is selected. A donor completes a questionnaire and is screened for different pathogens, including bacteria (C. difficile, Listeria monocytogenes, Vibrio cholera, Helicobacter pylori, Treponema pallidum), parasites (Giardia, Cryptosporidium), and viruses (rotavirus, hepatitis A/B/C, Creutzfeldt-Jakob, and human immunodeficiency virus)[109]. Donors can also be excluded if they have had recent antibiotics or tattoos, or a history of gastrointestinal disease. Stool is then collected and prepared for transplant (e.g., diluted and homogenized before filtration through gauze pads to remove large particulate matter), although a recent study has demonstrated that frozen/thawed stool works as well as fresh stool[110,111]. The fecal filtrate can then delivered by oral capsule, nasogastric tube, colonoscopy or rectal enema.
Many trials interrogating the efficacy of FMT for CDI have taken place worldwide over the past few years[112116]. Two healthy donors were used for 27 patients in a recent trial at McMaster University (Hamilton, Canada), showing an overall cure rate of 93%[112]. In this study, failure of FMT was linked to lack of retention of enema. A smaller study from the University of Toronto (Toronto, Canada) examined the different microbiota profiles involved in successful vs failed FMT[113]. The study identified several groups of bacteria (reduction in Bacteroidetes, increase in Proteobacteria) that were important in CDI cases, but indicated that overall diversity was important for success of FMT. The first controlled trial of nasogastric/duodenal infusion of fecal filtrate was published with encouraging results[114]. The FMT arm demonstrated 81% success (13/16 patients) after a single infusion of donor feces, and two of the three failed patients were later successfully treated after infusion of feces from a different donor, for an overall success rate of 94%. This was significantly better than the 31% success (4/13 patients) for standard vancomycin treatment. In a multicenter retrospective series, the use of FMT was examined in immunocompromised patients with CDI that was recurrent, refractory, or severe[115]. The cure rate after a single FMT was 78%, and 89% after repeat FMT in 99 patients in various states of immunosuppression (e.g., human immunodeficiency virus/acquired immune deficiency syndrome, solid organ transplant, chemotherapy, immunosuppressive therapy for IBD). Some
patients (14% of IBD patients) experienced disease flare post FMT. Importantly, there were no related infectious complications reported in these highrisk patients.
A systematic review in 2013 found that different forms of FMT had been used to treat 273 patients with confirmed CDI from 19462012[117] with an overall success rate of 89% for FMT in treating CDI. In this analysis, a higher FMT success was correlated with lower gastrointestinal delivery routes (colonoscopy and enema vs nasoduodenal), but that donor relationship with recipient was uncorrelated. A more recent systematic review completed in 2015 suggests that FMT was associated with symptom resolution of recurrent CDI but its role in primary and severe CDI was not established[72]. The report concludes that treatment strategies should be aligned with disease severity, history of prior CDI, and the patient’s risk of recurrence. The exact mechanism by which FMT works on CDI has remained elusive, though it has been suggested to act through the restoration of colonization resistance. Unfortunately, there are also significant drawbacks of FMT. The screening process for known bacterial and viral pathogens can be costly and accessibility to an appropriate donor in a timely manner may be challenging. Additionally, a recent case report of FMT treatment detailed a patient with CDI that resulted in flare of dormant ulcerative colitis[118]. This adverse event suggests that microbial species that are protective in some disease states may be deleterious in others. Furthermore, links between the HGM and extraintestinal diseases, including type Ⅱ diabetes, obesity and behavioural disorders, have suggested FMT could have longterm safety issues[119121]. Therefore, a defined and refined bacterial cocktail would be beneficial for treating CDI and avoiding deleterious effects.
Other bacteriotherapy attempts have been made to replace donor stool as the means of conveyance for HGM. These methods generally involve the development of defined bacterial mixtures from laboratory bioreactors. Tvede and RaskMadsen demonstrated that a mixture of ten different bacteria could be curative to five (out of five) CDI patients in 1989[122]. The investigators found that recurrent CDI patients had decreased Bacteroides spp. that recovered after bacteriotherapy. A more recent study, termed rePOOPulation, used a combination of 33 bacteria to successfully treat two CDI patients[123]. These bacteria were cultured from a stoolsample and grown in the laboratory, but study design allowed for the transfer of a reproducible, known quantity of bacteria. However, these studies have still not identified a key mechanism provided by FMT to cure CDI. Identifying how the microbiota interacts and resists colonization by C. difficile will result in rational design of probiotic prevention or treatment of CDI.
CONClUsIONThe excitement of FMT as a treatment for recurrent CDI is increasing. A recent commentary has suggested that FMT could potentially be used to treat all cases
Schenck LP et al . Clostridium difficile infection

176 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
of CDI, including a patient’s first case[124]. While this suggestion is exciting, detailed safety profiling is still required before FMT is a widespread therapy[108,125,126]. That being said, CDI is a disease that shows the most prominent links to alterations to the HGM, in both cause and treatment. Studies investigating the effectiveness of FMT for CDI are leading to a better understanding of the roles of the microbial community in both host health and disease. Nonetheless, elucidating a specific combination of bacteria that can treat or prevent future CDI cases would be an impactful discovery for the advancement of bacteriotherapy as a viable treatment.
aCkNOWleDGmeNTsThe authors apologize to all those researchers whose work could not be cited owing to space limitations. Justin A MacDonald is an Alberta Innovates Health Solutions (AIHS) Senior Scholar, and Paul L Beck is an AIHS Clinical Senior Scholar. L Patrick Schenck was funded by an AIHS Graduate Scholarship.
RefeReNCes1 So AD, Gupta N, Cars O. Tackling antibiotic resistance. BMJ 2010;
340: c2071 [PMID: 20483948 DOI: 10.1136/bmj.c2071]2 Johnson AP. Surveillance of antibiotic resistance. Philos Trans R
Soc Lond B Biol Sci 2015; 370: 20140080 [PMID: 25918439 DOI: 10.1098/rstb.2014.0080]
3 Blair JM, Webber MA, Baylay AJ, Ogbolu DO, Piddock LJ. Molecular mechanisms of antibiotic resistance. Nat Rev Microbiol 2015; 13: 42-51 [PMID: 25435309 DOI: 10.1038/nrmicro3380]
4 Woolhouse M, Ward M, van Bunnik B, Farrar J. Antimicrobial resistance in humans, livestock and the wider environment. Philos Trans R Soc Lond B Biol Sci 2015; 370: 20140083 [PMID: 25918441 DOI: 10.1098/rstb.2014.0083]
5 Amy J, Johanesen P, Lyras D. Extrachromosomal and integrated genetic elements in Clostridium difficile. Plasmid 2015; 80: 97-110 [PMID: 25929174 DOI: 10.1016/j.plasmid.2015.04.006]
6 O’Connor JR, Johnson S, Gerding DN. Clostridium difficile infection caused by the epidemic BI/NAP1/027 strain. Gastroenterology 2009; 136: 1913-1924 [PMID: 19457419 DOI: 10.1053/j.gastro.2009.02.073]
7 Burke KE, Lamont JT. Clostridium difficile infection: a worldwide disease. Gut Liver 2014; 8: 1-6 [PMID: 24516694 DOI: 10.5009/gnl.2014.8.1.1]
8 Lessa FC, Winston LG, McDonald LC. Burden of Clostridium difficile infection in the United States. N Engl J Med 2015; 372: 2369-2370 [PMID: 26061850 DOI: 10.1056/NEJMc1505190]
9 Schippa S, Conte MP. Dysbiotic events in gut microbiota: impact on human health. Nutrients 2014; 6: 5786-5805 [PMID: 25514560 DOI: 10.3390/nu6125786]
10 Collins SM. A role for the gut microbiota in IBS. Nat Rev Gastroenterol Hepatol 2014; 11: 497-505 [PMID: 24751910 DOI: 10.1038/nrgastro.2014.40]
11 Fujimura KE, Lynch SV. Microbiota in allergy and asthma and the emerging relationship with the gut microbiome. Cell Host Microbe 2015; 17: 592-602 [PMID: 25974301 DOI: 10.1016/j.chom.2015.04.007]
12 Schulz MD, Atay C, Heringer J, Romrig FK, Schwitalla S, Aydin B, Ziegler PK, Varga J, Reindl W, Pommerenke C, Salinas-Riester G, Böck A, Alpert C, Blaut M, Polson SC, Brandl L, Kirchner T, Greten FR, Polson SW, Arkan MC. High-fat-diet-mediated dysbio-sis promotes intestinal carcinogenesis independently of obesity. Nature 2014; 514: 508-512 [PMID: 25174708 DOI: 10.1038/nature13398]
13 van Best N, Jansen PL, Rensen SS. The gut microbiota of nonalcoholic fatty liver disease: current methods and their inter-pretation. Hepatol Int 2015; 9: 406-415 [PMID: 26067771 DOI: 10.1007/s12072-015-9640-2]
14 Org E, Mehrabian M, Lusis AJ. Unraveling the environmental and genetic interactions in atherosclerosis: Central role of the gut microbiota. Atherosclerosis 2015; 241: 387-399 [PMID: 26071662 DOI: 10.1016/j.atherosclerosis.2015.05.035]
15 Toh MC, Allen-Vercoe E. The human gut microbiota with reference to autism spectrum disorder: considering the whole as more than a sum of its parts. Microb Ecol Health Dis 2015; 26: 26309 [PMID: 25634609 DOI: 10.3402/mehd.v26.26309]
16 Williams BL, Hornig M, Buie T, Bauman ML, Cho Paik M, Wick I, Bennett A, Jabado O, Hirschberg DL, Lipkin WI. Impaired carbohydrate digestion and transport and mucosal dysbiosis in the intestines of children with autism and gastrointestinal disturbances. PLoS One 2011; 6: e24585 [PMID: 21949732 DOI: 10.1371/journal.pone.0024585]
17 Janssen AW, Kersten S. The role of the gut microbiota in meta-bolic health. FASEB J 2015; 29: 3111-3123 [PMID: 25921831 DOI: 10.1096/fj.14-269514]
18 Ridaura VK, Faith JJ, Rey FE, Cheng J, Duncan AE, Kau AL, Griffin NW, Lombard V, Henrissat B, Bain JR, Muehlbauer MJ, Ilkayeva O, Semenkovich CF, Funai K, Hayashi DK, Lyle BJ, Martini MC, Ursell LK, Clemente JC, Van Treuren W, Walters WA, Knight R, Newgard CB, Heath AC, Gordon JI. Gut microbiota from twins discordant for obesity modulate metabolism in mice. Science 2013; 341: 1241214 [PMID: 24009397 DOI: 10.1126/science.1241214]
19 Ding T, Schloss PD. Dynamics and associations of microbial community types across the human body. Nature 2014; 509: 357-360 [PMID: 24739969 DOI: 10.1038/nature13178]
20 Eckburg PB, Bik EM, Bernstein CN, Purdom E, Dethlefsen L, Sargent M, Gill SR, Nelson KE, Relman DA. Diversity of the human intestinal microbial flora. Science 2005; 308: 1635-1638 [PMID: 15831718 DOI: 10.1126/science.1110591]
21 Flint HJ, Duncan SH, Scott KP, Louis P. Interactions and competition within the microbial community of the human colon: links between diet and health. Environ Microbiol 2007; 9: 1101-1111 [PMID: 17472627 DOI: 10.1111/j.1462-2920.2007.01281.x]
22 Glimstedt G. The germfree animal as a research tool. Ann N Y Acad Sci 1959; 78: 281-284 [PMID: 13828472 DOI: 10.1111/j.1749-6632.1959.tb53112.x]
23 Winker S, Woese CR. A definition of the domains Archaea, Bacteria and Eucarya in terms of small subunit ribosomal RNA characteristics. Syst Appl Microbiol 1991; 14: 305-310 [PMID: 11540071 DOI: 10.1016/S0723-2020(11)80303-6]
24 Muyzer G, de Waal EC, Uitterlinden AG. Profiling of complex microbial populations by denaturing gradient gel electrophoresis analysis of polymerase chain reaction-amplified genes coding for 16S rRNA. Appl Environ Microbiol 1993; 59: 695-700 [PMID: 7683183]
25 Muyzer G, Smalla K. Application of denaturing gradient gel electrophoresis (DGGE) and temperature gradient gel electrophoresis (TGGE) in microbial ecology. Antonie Van Leeuwenhoek 1998; 73: 127-141 [PMID: 9602286 DOI: 10.1023/A:1000669317571]
26 Liu WT, Marsh TL, Cheng H, Forney LJ. Characterization of microbial diversity by determining terminal restriction fragment length polymorphisms of genes encoding 16S rRNA. Appl Environ Microbiol 1997; 63: 4516-4522 [PMID: 9361437]
27 Shyu C, Soule T, Bent SJ, Foster JA, Forney LJ. MiCA: a web-based tool for the analysis of microbial communities based on terminal-restriction fragment length polymorphisms of 16S and 18S rRNA genes. Microb Ecol 2007; 53: 562-570 [PMID: 17406775 DOI: 10.1007/s00248-006-9106-0]
28 Mardis ER. A decade’s perspective on DNA sequencing techn-ology. Nature 2011; 470: 198-203 [PMID: 21307932 DOI: 10.1038/nature09796]
29 Peterson J, Garges S, Giovanni M, McInnes P, Wang L, Schloss JA, Bonazzi V, McEwen JE, Wetterstrand KA, Deal C, Baker
Schenck LP et al . Clostridium difficile infection

177 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
CC, Di Francesco V, Howcroft TK, Karp RW, Lunsford RD, Wellington CR, Belachew T, Wright M, Giblin C, David H, Mills M, Salomon R, Mullins C, Akolkar B, Begg L, Davis C, Grandison L, Humble M, Khalsa J, Little AR, Peavy H, Pontzer C, Portnoy M, Sayre MH, Starke-Reed P, Zakhari S, Read J, Watson B, Guyer M. The NIH Human Microbiome Project. Genome Res 2009; 19: 2317-2323 [PMID: 19819907 DOI: 10.1101/gr.096651.109]
30 Caporaso JG, Kuczynski J, Stombaugh J, Bittinger K, Bushman FD, Costello EK, Fierer N, Peña AG, Goodrich JK, Gordon JI, Huttley GA, Kelley ST, Knights D, Koenig JE, Ley RE, Lozupone CA, McDonald D, Muegge BD, Pirrung M, Reeder J, Sevinsky JR, Turnbaugh PJ, Walters WA, Widmann J, Yatsunenko T, Zaneveld J, Knight R. QIIME allows analysis of high-throughput community sequencing data. Nat Methods 2010; 7: 335-336 [PMID: 20383131 DOI: 10.1038/nmeth.f.303]
31 Walker AW, Duncan SH, Louis P, Flint HJ. Phylogeny, culturing, and metagenomics of the human gut microbiota. Trends Microbiol 2014; 22: 267-274 [PMID: 24698744 DOI: 10.1016/j.tim.2014.03.001]
32 Hall IC, O’Toole E. Intestinal flora in new-born infants with a description of a new pathogenic anaerobe Bacillus difficilis. Am J Dis Child 1935; 49: 390-402 [DOI: 10.1001/archpedi.1935.01970020105010]
33 Tedesco FJ, Stanley RJ, Alpers DH. Diagnostic features of clin-damycin-associated pseudomembranous colitis. N Engl J Med 1974; 290: 841-843 [PMID: 4855527 DOI: 10.1056/NEJM197404112901508]
34 George RH, Symonds JM, Dimock F, Brown JD, Arabi Y, Shinagawa N, Keighley MR, Alexander-Williams J, Burdon DW. Identification of Clostridium difficile as a cause of pseudo-membranous colitis. Br Med J 1978; 1: 695 [PMID: 630301 DOI: 10.1136/bmj.1.6114.695]
35 Potter VA, Aravinthan A. Identifying patients at risk of severe Clostridium difficile-associated disease. Br J Hosp Med (Lond) 2012; 73: 265-270 [PMID: 22585325 DOI: 10.12968/hmed.2012.73.5.265]
36 Kuijper EJ, Coignard B, Tüll P. Emergence of Clostridium difficile-associated disease in North America and Europe. Clin Microbiol Infect 2006; 12 Suppl 6: 2-18 [PMID: 16965399 DOI: 10.1111/j.1469-0691.2006.01580.x]
37 He M, Miyajima F, Roberts P, Ellison L, Pickard DJ, Martin MJ, Connor TR, Harris SR, Fairley D, Bamford KB, D’Arc S, Brazier J, Brown D, Coia JE, Douce G, Gerding D, Kim HJ, Koh TH, Kato H, Senoh M, Louie T, Michell S, Butt E, Peacock SJ, Brown NM, Riley T, Songer G, Wilcox M, Pirmohamed M, Kuijper E, Hawkey P, Wren BW, Dougan G, Parkhill J, Lawley TD. Emergence and global spread of epidemic healthcare-associated Clostridium difficile. Nat Genet 2013; 45: 109-113 [PMID: 23222960 DOI: 10.1038/ng.2478]
38 Loo VG, Poirier L, Miller MA, Oughton M, Libman MD, Michaud S, Bourgault AM, Nguyen T, Frenette C, Kelly M, Vibien A, Brassard P, Fenn S, Dewar K, Hudson TJ, Horn R, René P, Monczak Y, Dascal A. A predominantly clonal multi-institutional outbreak of Clostridium difficile-associated diarrhea with high morbidity and mortality. N Engl J Med 2005; 353: 2442-2449 [PMID: 16322602 DOI: 10.1056/NEJMoa051639]
39 Slimings C, Riley TV. Antibiotics and hospital-acquired Clostri-dium difficile infection: update of systematic review and meta-analysis. J Antimicrob Chemother 2014; 69: 881-891 [PMID: 24324224 DOI: 10.1093/jac/dkt477]
40 Khanna S, Pardi DS, Aronson SL, Kammer PP, Orenstein R, St Sauver JL, Harmsen WS, Zinsmeister AR. The epidemiology of community-acquired Clostridium difficile infection: a population-based study. Am J Gastroenterol 2012; 107: 89-95 [PMID: 22108454 DOI: 10.1038/ajg.2011.398]
41 Chitnis AS, Holzbauer SM, Belflower RM, Winston LG, Bamberg WM, Lyons C, Farley MM, Dumyati GK, Wilson LE, Beldavs ZG, Dunn JR, Gould LH, MacCannell DR, Gerding DN, McDonald LC, Lessa FC. Epidemiology of community-associated Clostridium difficile infection, 2009 through 2011. JAMA Intern Med 2013; 173: 1359-1367 [PMID: 23780507 DOI: 10.1001/jamainternmed.2
013.7056]42 Metcalf D, Avery BP, Janecko N, Matic N, Reid-Smith R, Weese
JS. Clostridium difficile in seafood and fish. Anaerobe 2011; 17: 85-86 [PMID: 21376822 DOI: 10.1016/j.anaerobe.2011.02.008]
43 Metcalf DS, Costa MC, Dew WM, Weese JS. Clostridium difficile in vegetables, Canada. Lett Appl Microbiol 2010; 51: 600-602 [PMID: 21069911 DOI: 10.1111/j.1472-765X.2010.02933.x]
44 Weese JS, Avery BP, Rousseau J, Reid-Smith RJ. Detection and enumeration of Clostridium difficile spores in retail beef and pork. Appl Environ Microbiol 2009; 75: 5009-5011 [PMID: 19525267 DOI: 10.1128/AEM.00480-09]
45 Mooyottu S, Flock G, Kollanoor-Johny A, Upadhyaya I, Jayarao B, Venkitanarayanan K. Characterization of a multidrug resistant C. difficile meat isolate. Int J Food Microbiol 2015; 192: 111-116 [PMID: 25440554 DOI: 10.1016/j.ijfoodmicro.2014.10.002]
46 Lawley TD, Croucher NJ, Yu L, Clare S, Sebaihia M, Goulding D, Pickard DJ, Parkhill J, Choudhary J, Dougan G. Proteomic and genomic characterization of highly infectious Clostridium difficile 630 spores. J Bacteriol 2009; 191: 5377-5386 [PMID: 19542279 DOI: 10.1128/JB.00597-09]
47 Giel JL, Sorg JA, Sonenshein AL, Zhu J. Metabolism of bile salts in mice influences spore germination in Clostridium difficile. PLoS One 2010; 5: e8740 [PMID: 20090901 DOI: 10.1371/journal.pone.0008740]
48 Howerton A, Ramirez N, Abel-Santos E. Mapping interactions between germinants and Clostridium difficile spores. J Bacteriol 2011; 193: 274-282 [PMID: 20971909 DOI: 10.1128/JB.00980-10]
49 Francis MB, Allen CA, Shrestha R, Sorg JA. Bile acid recognition by the Clostridium difficile germinant receptor, CspC, is important for establishing infection. PLoS Pathog 2013; 9: e1003356 [PMID: 23675301 DOI: 10.1371/journal.ppat.1003356]
50 Setlow P. Spore germination. Curr Opin Microbiol 2003; 6: 550-556 [PMID: 14662349 DOI: 10.1016/j.mib.2003.10.001]
51 Paredes-Sabja D, Torres JA, Setlow P, Sarker MR. Clostridium perfringens spore germination: characterization of germinants and their receptors. J Bacteriol 2008; 190: 1190-1201 [PMID: 18083820 DOI: 10.1128/JB.01748-07]
52 Voth DE, Ballard JD. Clostridium difficile toxins: mechanism of action and role in disease. Clin Microbiol Rev 2005; 18: 247-263 [PMID: 15831824 DOI: 10.1128/CMR.18.2.247-263.2005]
53 Metcalf DS, Weese JS. Binary toxin locus analysis in Clostridium difficile. J Med Microbiol 2011; 60: 1137-1145 [PMID: 21459907 DOI: 10.1099/jmm.0.028498-0]
54 Cartman ST, Kelly ML, Heeg D, Heap JT, Minton NP. Precise manipulation of the Clostridium difficile chromosome reveals a lack of association between the tcdC genotype and toxin production. Appl Environ Microbiol 2012; 78: 4683-4690 [PMID: 22522680 DOI: 10.1128/AEM.00249-12]
55 Dineen SS, Villapakkam AC, Nordman JT, Sonenshein AL. Repression of Clostridium difficile toxin gene expression by CodY. Mol Microbiol 2007; 66: 206-219 [PMID: 17725558 DOI: 10.1111/j.1365-2958.2007.05906.x]
56 Kelly CP, LaMont JT. Clostridium difficile--more difficult than ever. N Engl J Med 2008; 359: 1932-1940 [PMID: 18971494 DOI: 10.1056/NEJMra0707500]
57 Bartlett JG. Clostridium difficile: history of its role as an enteric pathogen and the current state of knowledge about the organism. Clin Infect Dis 1994; 18 Suppl 4: S265-S272 [PMID: 8086574 DOI: 10.1093/clinids/18.Supplement_4.S265]
58 Freeman J, Bauer MP, Baines SD, Corver J, Fawley WN, Goorhuis B, Kuijper EJ, Wilcox MH. The changing epidemiology of Clostridium difficile infections. Clin Microbiol Rev 2010; 23: 529-549 [PMID: 20610822 DOI: 10.1128/CMR.00082-09]
59 Kuehne SA, Cartman ST, Heap JT, Kelly ML, Cockayne A, Minton NP. The role of toxin A and toxin B in Clostridium difficile infection. Nature 2010; 467: 711-713 [PMID: 20844489 DOI: 10.1038/nature09397]
60 Hirota SA, Iablokov V, Tulk SE, Schenck LP, Becker H, Nguyen J, Al Bashir S, Dingle TC, Laing A, Liu J, Li Y, Bolstad J, Mulvey GL, Armstrong GD, MacNaughton WK, Muruve DA, MacDonald
Schenck LP et al . Clostridium difficile infection

178 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
JA, Beck PL. Intrarectal instillation of Clostridium difficile toxin A triggers colonic inflammation and tissue damage: development of a novel and efficient mouse model of Clostridium difficile toxin exposure. Infect Immun 2012; 80: 4474-4484 [PMID: 23045481 DOI: 10.1128/IAI.00933-12]
61 Kelly CP, Kyne L. The host immune response to Clostridium difficile. J Med Microbiol 2011; 60: 1070-1079 [PMID: 21415200 DOI: 10.1099/jmm.0.030015-0]
62 Islam J, Taylor AL, Rao K, Huffnagle G, Young VB, Rajkumar C, Cohen J, Papatheodorou P, Aronoff DM, Llewelyn MJ. The role of the humoral immune response to Clostridium difficile toxins A and B in susceptibility to C. difficile infection: a case-control study. Anaerobe 2014; 27: 82-86 [PMID: 24708941 DOI: 10.1016/j.anaerobe.2014.03.011]
63 Sánchez-Hurtado K, Corretge M, Mutlu E, McIlhagger R, Starr JM, Poxton IR. Systemic antibody response to Clostridium difficile in colonized patients with and without symptoms and matched controls. J Med Microbiol 2008; 57: 717-724 [PMID: 18480328 DOI: 10.1099/jmm.0.47713-0]
64 Johnson S. Recurrent Clostridium difficile infection: causality and therapeutic approaches. Int J Antimicrob Agents 2009; 33 Suppl 1: S33-S36 [PMID: 19303567 DOI: 10.1016/S0924-8579(09)70014-7]
65 Ng J, Hirota SA, Gross O, Li Y, Ulke-Lemee A, Potentier MS, Schenck LP, Vilaysane A, Seamone ME, Feng H, Armstrong GD, Tschopp J, Macdonald JA, Muruve DA, Beck PL. Clostridium difficile toxin-induced inflammation and intestinal injury are mediated by the inflammasome. Gastroenterology 2010; 139: 542-52, 552.e1-3 [PMID: 20398664 DOI: 10.1053/j.gastro.2010.04.005]
66 Zhao S, Ghose-Paul C, Zhang K, Tzipori S, Sun X. Immune-based treatment and prevention of Clostridium difficile infection. Hum Vaccin Immunother 2014; 10: 3522-3530 [PMID: 25668664 DOI: 10.4161/21645515.2014.980193]
67 Viscidi R, Laughon BE, Yolken R, Bo-Linn P, Moench T, Ryder RW, Bartlett JG. Serum antibody response to toxins A and B of Clostridium difficile. J Infect Dis 1983; 148: 93-100 [PMID: 6886489 DOI: 10.1093/infdis/148.1.93]
68 Winckler J. [Fixation of enzymes in freeze-dried tissue with gases]. Acta Histochem Suppl 1976; 16: 259-264 [PMID: 830019]
69 Kyne L, Warny M, Qamar A, Kelly CP. Asymptomatic carriage of Clostridium difficile and serum levels of IgG antibody against toxin A. N Engl J Med 2000; 342: 390-397 [PMID: 10666429 DOI: 10.1056/NEJM200002103420604]
70 Kyne L, Warny M, Qamar A, Kelly CP. Association between antibody response to toxin A and protection against recurrent Clostridium difficile diarrhoea. Lancet 2001; 357: 189-193 [PMID: 11213096 DOI: 10.1016/S0140-6736(00)03592-3]
71 Leav BA, Blair B, Leney M, Knauber M, Reilly C, Lowy I, Gerding DN, Kelly CP, Katchar K, Baxter R, Ambrosino D, Molrine D. Serum anti-toxin B antibody correlates with protection from recurrent Clostridium difficile infection (CDI). Vaccine 2010; 28: 965-969 [PMID: 19941990 DOI: 10.1016/j.vaccine.2009.10.144]
72 Bagdasarian N, Rao K, Malani PN. Diagnosis and treatment of Clostridium difficile in adults: a systematic review. JAMA 2015; 313: 398-408 [PMID: 25626036 DOI: 10.1001/jama.2014.17103]
73 Dallas KB, Condren A, Divino CM. Life after colectomy for fulminant Clostridium difficile colitis: a 7-year follow up study. Am J Surg 2014; 207: 533-539 [PMID: 24674828 DOI: 10.1016/j.amjsurg.2013.04.008]
74 ASHP therapeutic position statement on the preferential use of metronidazole for the treatment of Clostridium difficile-associated disease. Am J Health Syst Pharm 1998; 55: 1407-1411 [PMID: 9659970]
75 Zar FA, Bakkanagari SR, Moorthi KM, Davis MB. A comparison of vancomycin and metronidazole for the treatment of Clostridium difficile-associated diarrhea, stratified by disease severity. Clin Infect Dis 2007; 45: 302-307 [PMID: 17599306 DOI: 10.1086/519265]
76 Kuipers EJ, Surawicz CM. Clostridium difficile infection. Lancet 2008; 371: 1486-1488 [PMID: 18456087 DOI: 10.1016/S0140-67
36(08)60635-2]77 Mullane KM, Miller MA, Weiss K, Lentnek A, Golan Y, Sears
PS, Shue YK, Louie TJ, Gorbach SL. Efficacy of fidaxomicin versus vancomycin as therapy for Clostridium difficile infection in individuals taking concomitant antibiotics for other concurrent infections. Clin Infect Dis 2011; 53: 440-447 [PMID: 21844027 DOI: 10.1093/cid/cir404]
78 Louie TJ, Miller MA, Mullane KM, Weiss K, Lentnek A, Golan Y, Gorbach S, Sears P, Shue YK. Fidaxomicin versus vancomycin for Clostridium difficile infection. N Engl J Med 2011; 364: 422-431 [PMID: 21288078 DOI: 10.1056/NEJMoa0910812]
79 Lewis BB, Buffie CG, Carter RA, Leiner I, Toussaint NC, Miller LC, Gobourne A, Ling L, Pamer EG. Loss of Microbiota-Mediated Colonization Resistance to Clostridium difficile Infection With Oral Vancomycin Compared With Metronidazole. J Infect Dis 2015; Epub ahead of print [PMID: 25920320 DOI: 10.1093/infdis/jiv256]
80 Buffie CG, Bucci V, Stein RR, McKenney PT, Ling L, Gobourne A, No D, Liu H, Kinnebrew M, Viale A, Littmann E, van den Brink MR, Jenq RR, Taur Y, Sander C, Cross JR, Toussaint NC, Xavier JB, Pamer EG. Precision microbiome reconstitution restores bile acid mediated resistance to Clostridium difficile. Nature 2015; 517: 205-208 [PMID: 25337874 DOI: 10.1038/nature13828]
81 Gebhart D, Lok S, Clare S, Tomas M, Stares M, Scholl D, Donskey CJ, Lawley TD, Govoni GR. A modified R-type bacteriocin specifically targeting Clostridium difficile prevents colonization of mice without affecting gut microbiota diversity. MBio 2015; 6: pii: e02368-14 [PMID: 25805733 DOI: 10.1128/mBio.02368-14]
82 Britton RA, Young VB. Role of the intestinal microbiota in resistance to colonization by Clostridium difficile. Gastroenterology 2014; 146: 1547-1553 [PMID: 24503131]
83 Jump RL, Polinkovsky A, Hurless K, Sitzlar B, Eckart K, Tomas M, Deshpande A, Nerandzic MM, Donskey CJ. Metabolomics analysis identifies intestinal microbiota-derived biomarkers of colonization resistance in clindamycin-treated mice. PLoS One 2014; 9: e101267 [PMID: 24988418 DOI: 10.1371/journal.pone.0101267]
84 Burns DA, Heap JT, Minton NP. Clostridium difficile spore germination: an update. Res Microbiol 2010; 161: 730-734 [PMID: 20863888 DOI: 10.1016/j.resmic.2010.09.007]
85 Begley M, Gahan CG, Hill C. The interaction between bacteria and bile. FEMS Microbiol Rev 2005; 29: 625-651 [PMID: 16102595 DOI: 10.1016/j.femsre.2004.09.003]
86 Kishinaka M, Umeda A, Kuroki S. High concentrations of conjugated bile acids inhibit bacterial growth of Clostridium perfringens and induce its extracellular cholylglycine hydrolase. Steroids 1994; 59: 485-489 [PMID: 7985210 DOI: 10.1016/0039-128X(94)90062-0]
87 Takamine F, Imamura T. 7 beta-dehydroxylation of 3,7-dihydroxy bile acids by a Eubacterium species strain C-25 and stimulation of 7 beta-dehydroxylation by Bacteroides distasonis strain K-5. Microbiol Immunol 1985; 29: 1247-1252 [PMID: 3831723 DOI: 10.1111/j.1348-0421.1985.tb00915.x]
88 Bateup JM, McConnell MA, Jenkinson HF, Tannock GW. Comparison of Lactobacillus strains with respect to bile salt hydrolase activity, colonization of the gastrointestinal tract, and growth rate of the murine host. Appl Environ Microbiol 1995; 61: 1147-1149 [PMID: 7793916]
89 Breton YL, Mazé A, Hartke A, Lemarinier S, Auffray Y, Rincé A. Isolation and characterization of bile salts-sensitive mutants of Enterococcus faecalis. Curr Microbiol 2002; 45: 434-439 [PMID: 12402085 DOI: 10.1007/s00284-002-3714-9]
90 Van Eldere J, Celis P, De Pauw G, Lesaffre E, Eyssen H. Tauro-conjugation of cholic acid stimulates 7 alpha-dehydroxylation by fecal bacteria. Appl Environ Microbiol 1996; 62: 656-661 [PMID: 8593067]
91 Dussurget O, Cabanes D, Dehoux P, Lecuit M, Buchrieser C, Glaser P, Cossart P. Listeria monocytogenes bile salt hydrolase is a PrfA-regulated virulence factor involved in the intestinal and hepatic phases of listeriosis. Mol Microbiol 2002; 45: 1095-1106 [PMID: 12180927 DOI: 10.1046/j.1365-2958.2002.03080.x]
Schenck LP et al . Clostridium difficile infection

179 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
92 Sutherland JD, Williams CN. Bile acid induction of 7 alpha- and 7 beta-hydroxysteroid dehydrogenases in Clostridium limosum. J Lipid Res 1985; 26: 344-350 [PMID: 3857290]
93 Stellwag EJ, Hylemon PB. 7alpha-Dehydroxylation of cholic acid and chenodeoxycholic acid by Clostridium leptum. J Lipid Res 1979; 20: 325-333 [PMID: 36438]
94 Theriot CM, Koenigsknecht MJ, Carlson PE, Hatton GE, Nelson AM, Li B, Huffnagle GB, Z Li J, Young VB. Antibiotic-induced shifts in the mouse gut microbiome and metabolome increase susceptibility to Clostridium difficile infection. Nat Commun 2014; 5: 3114 [PMID: 24445449 DOI: 10.1038/ncomms4114]
95 Howerton A, Patra M, Abel-Santos E. A new strategy for the prevention of Clostridium difficile infection. J Infect Dis 2013; 207: 1498-1504 [PMID: 23420906 DOI: 10.1093/infdis/jit068]
96 Chang TW, Onderdonk AB, Bartlett JG. Anion-exchange resins in antibiotic-associated colitis. Lancet 1978; 2: 258-259 [PMID: 79047 DOI: 10.1016/S0140-6736(78)91765-8]
97 Moncino MD, Falletta JM. Multiple relapses of Clostridium difficile-associated diarrhea in a cancer patient. Successful control with long-term cholestyramine therapy. Am J Pediatr Hematol Oncol 1992; 14: 361-364 [PMID: 1456403 DOI: 10.1097/00043426-199211000-00015]
98 Rea MC, Sit CS, Clayton E, O’Connor PM, Whittal RM, Zheng J, Vederas JC, Ross RP, Hill C. Thuricin CD, a posttranslationally modified bacteriocin with a narrow spectrum of activity against Clostridium difficile. Proc Natl Acad Sci USA 2010; 107: 9352-9357 [PMID: 20435915 DOI: 10.1073/pnas.0913554107]
99 Rea MC, Alemayehu D, Casey PG, O’Connor PM, Lawlor PG, Walsh M, Shanahan F, Kiely B, Ross RP, Hill C. Bioavailability of the anti-clostridial bacteriocin thuricin CD in gastrointestinal tract. Microbiology 2014; 160: 439-445 [PMID: 24287693 DOI: 10.1099/mic.0.068767-0]
100 Reeves AE, Theriot CM, Bergin IL, Huffnagle GB, Schloss PD, Young VB. The interplay between microbiome dynamics and pathogen dynamics in a murine model of Clostridium difficile Infection. Gut Microbes 2011; 2: 145-158 [PMID: 21804357 DOI: 10.4161/gmic.2.3.16333]
101 Reeves AE, Koenigsknecht MJ, Bergin IL, Young VB. Suppre-ssion of Clostridium difficile in the gastrointestinal tracts of germfree mice inoculated with a murine isolate from the family Lachnospiraceae. Infect Immun 2012; 80: 3786-3794 [PMID: 22890996 DOI: 10.1128/IAI.00647-12]
102 Itoh K, Lee WK, Kawamura H, Mitsuoka T, Magaribuchi T. Intestinal bacteria antagonistic to Clostridium difficile in mice. Lab Anim 1987; 21: 20-25 [PMID: 3560860 DOI: 10.1258/002367787780740662]
103 Kolling GL, Wu M, Warren CA, Durmaz E, Klaenhammer TR, Timko MP, Guerrant RL. Lactic acid production by Streptococcus thermophilus alters Clostridium difficile infection and in vitro Toxin A production. Gut Microbes 2012; 3: 523-529 [PMID: 22895082 DOI: 10.4161/gmic.21757]
104 Lawley TD, Clare S, Walker AW, Stares MD, Connor TR, Raisen C, Goulding D, Rad R, Schreiber F, Brandt C, Deakin LJ, Pickard DJ, Duncan SH, Flint HJ, Clark TG, Parkhill J, Dougan G. Targeted restoration of the intestinal microbiota with a simple, defined bacteriotherapy resolves relapsing Clostridium difficile disease in mice. PLoS Pathog 2012; 8: e1002995 [PMID: 23133377 DOI: 10.1371/journal.ppat.1002995]
105 Eiseman B, Silen W, Bascom GS, Kauvar AJ. Fecal enema as an adjunct in the treatment of pseudomembranous enterocolitis. Surgery 1958; 44: 854-859 [PMID: 13592638]
106 Schwan A, Sjölin S, Trottestam U, Aronsson B. Relapsing clostri-dium difficile enterocolitis cured by rectal infusion of homologous faeces. Lancet 1983; 2: 845 [PMID: 6137662 DOI: 10.1016/S0140-6736(83)90753-5]
107 Bakken JS, Borody T, Brandt LJ, Brill JV, Demarco DC, Franzos MA, Kelly C, Khoruts A, Louie T, Martinelli LP, Moore TA, Russell G, Surawicz C. Treating Clostridium difficile infection with fecal microbiota transplantation. Clin Gastroenterol Hepatol 2011; 9: 1044-1049 [PMID: 21871249 DOI: 10.1016/j.cgh.2011.08.014]
108 Kelly CR, Kahn S, Kashyap P, Laine L, Rubin D, Atreja A, Moore T, Wu G. Update on Fecal Microbiota Transplantation 2015: Indications, Methodologies, Mechanisms, and Outlook. Gastroenterology 2015; 149: 223-237 [PMID: 25982290 DOI: 10.1053/j.gastro.2015.05.008]
109 Paramsothy S, Borody TJ, Lin E, Finlayson S, Walsh AJ, Samuel D, van den Bogaerde J, Leong RW, Connor S, Ng W, Mitchell HM, Kaakoush N, Kamm MA. Donor Recruitment for Fecal Microbiota Transplantation. Inflamm Bowel Dis 2015; 21: 1600-1606 [PMID: 26070003 DOI: 10.1097/MIB.0000000000000405]
110 Hamilton MJ, Weingarden AR, Sadowsky MJ, Khoruts A. Standardized frozen preparation for transplantation of fecal micro-biota for recurrent Clostridium difficile infection. Am J Gastroenterol 2012; 107: 761-767 [PMID: 22290405 DOI: 10.1038/ajg.2011.482]
111 Costello SP, Conlon MA, Vuaran MS, Roberts-Thomson IC, Andrews JM. Faecal microbiota transplant for recurrent Clostridium difficile infection using long-term frozen stool is effective: clinical efficacy and bacterial viability data. Aliment Pharmacol Ther 2015; 42: 1011-1018 [PMID: 26264455 DOI: 10.1111/apt.13366]
112 Kassam Z, Hundal R, Marshall JK, Lee CH. Fecal transplant via retention enema for refractory or recurrent Clostridium difficile infection. Arch Intern Med 2012; 172: 191-193 [PMID: 22271132 DOI: 10.1001/archinte.172.2.191]
113 Shahinas D, Silverman M, Sittler T, Chiu C, Kim P, Allen-Vercoe E, Weese S, Wong A, Low DE, Pillai DR. Toward an understanding of changes in diversity associated with fecal microbiome transplantation based on 16S rRNA gene deep sequencing. MBio 2012; 3: pii: e00338-12 [PMID: 23093385 DOI: 10.1128/mBio.00338-12]
114 van Nood E, Vrieze A, Nieuwdorp M, Fuentes S, Zoetendal EG, de Vos WM, Visser CE, Kuijper EJ, Bartelsman JF, Tijssen JG, Speelman P, Dijkgraaf MG, Keller JJ. Duodenal infusion of donor feces for recurrent Clostridium difficile. N Engl J Med 2013; 368: 407-415 [PMID: 23323867 DOI: 10.1056/NEJMoa1205037]
115 Kelly CR, Ihunnah C, Fischer M, Khoruts A, Surawicz C, Afzali A, Aroniadis O, Barto A, Borody T, Giovanelli A, Gordon S, Gluck M, Hohmann EL, Kao D, Kao JY, McQuillen DP, Mellow M, Rank KM, Rao K, Ray A, Schwartz MA, Singh N, Stollman N, Suskind DL, Vindigni SM, Youngster I, Brandt L. Fecal microbiota transplant for treatment of Clostridium difficile infection in immunocompromised patients. Am J Gastroenterol 2014; 109: 1065-1071 [PMID: 24890442 DOI: 10.1038/ajg.2014.133]
116 Aroniadis OC, Brandt LJ, Greenberg A, Borody T, Kelly CR, Mellow M, Surawicz C, Cagle L, Neshatian L, Stollman N, Giovanelli A, Ray A, Smith R. Long-term Follow-up Study of Fecal Microbiota Transplantation for Severe and/or Complicated Clostridium difficile Infection: A Multicenter Experience. J Clin Gastroenterol 2015; Epub ahead of print [PMID: 26125460 DOI: 10.1097/MCG.0000000000000374]
117 Kassam Z, Lee CH, Yuan Y, Hunt RH. Fecal microbiota transplantation for Clostridium difficile infection: systematic review and meta-analysis. Am J Gastroenterol 2013; 108: 500-508 [PMID: 23511459 DOI: 10.1038/ajg.2013.59]
118 De Leon LM, Watson JB, Kelly CR. Transient flare of ulcerative colitis after fecal microbiota transplantation for recurrent Clostridium difficile infection. Clin Gastroenterol Hepatol 2013; 11: 1036-1038 [PMID: 23669309 DOI: 10.1016/j.cgh.2013.04.045]
119 Kassam Z, Lee CH, Yuan Y, Hunt RH. Navigating long-term safety in fecal microbiota transplantation. Am J Gastroenterol 2013; 108: 1538 [PMID: 24005359 DOI: 10.1038/ajg.2013.214]
120 Collins SM, Kassam Z, Bercik P. The adoptive transfer of behavioral phenotype via the intestinal microbiota: experimental evidence and clinical implications. Curr Opin Microbiol 2013; 16: 240-245 [PMID: 23845749 DOI: 10.1016/j.mib.2013.06.004]
121 Alang N, Kelly CR. Weight gain after fecal microbiota trans-plantation. Open Forum Infect Dis 2015; 2: ofv004 [PMID: 26034755 DOI: 10.1093/ofid/ofv004]
122 Tvede M, Rask-Madsen J. Bacteriotherapy for chronic relapsing Clostridium difficile diarrhoea in six patients. Lancet 1989; 1: 1156-1160 [PMID: 2566734 DOI: 10.1016/S0140-6736(89)92749-
Schenck LP et al . Clostridium difficile infection

180 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
9]123 Petrof EO, Gloor GB, Vanner SJ, Weese SJ, Carter D, Daigneault
MC, Brown EM, Schroeter K, Allen-Vercoe E. Stool substitute transplant therapy for the eradication of Clostridium difficile infection: ‘RePOOPulating’ the gut. Microbiome 2013; 1: 3 [PMID: 24467987 DOI: 10.1186/2049-2618-1-3]
124 Borody TJ, Peattie D, Kapur A. Could fecal microbiota trans-plantation cure all Clostridium difficile infections? Future Microbiol
2014; 9: 1-3 [PMID: 24328373 DOI: 10.2217/fmb.13.146]125 Vandenplas Y, Pierard D, De Greef E. Fecal Microbiota Trans-
plantation: Just a Fancy Trend? J Pediatr Gastroenterol Nutr 2015; 61: 4-7 [PMID: 25905546 DOI: 10.1097/MPG.0000000000000816]
126 Smith MB, Kelly C, Alm EJ. Policy: How to regulate faecal transplants. Nature 2014; 506: 290-291 [PMID: 24558658 DOI: 10.1038/506290a]
P- Reviewer: Hu S, Shimizu Y S- Editor: Gong XM L- Editor: A E- Editor: Liu SQ
Schenck LP et al . Clostridium difficile infection

Grace Y Lam, Brendan P Halloran, Anthea C Peters, Richard N Fedorak
Grace Y Lam, Department of Medicine, Division of Internal Medicine, University of Alberta, 8440 112 St NW Edmonton, Alberta, Canada
Brendan P Halloran, Richard N Fedorak, Department of Medicine, Division of Gastroenterology, University of Alberta, Zeidler Ledcor Centre, 8440 112 St NW Edmonton, Alberta, Canada
Anthea C Peters, Department of Medicine, Division of Hematology, University of Alberta, 8440 112 St NW Edmonton, Alberta, Canada
Author contributions: Lam GY, Halloran BP, Peters AC and Fedorak RN contributed equally to this work.
Conflict-of-interest statement: Lam GY has no conflicts of interest to declare. Peters AC has been an advisory board member for Janssen, Roche, Lundbeck and Seattle Genetics. Halloran BP is a consultant and/or advisory board member for Abbvie and Janssen. Fedorak RN is a consultant or advisory board member of Abbvie, Ferring, Janssen, Shire, VSL#3, Celltrion. He is also the recipient of the following clinical/basic science research grants: Abbvie, Alba, Bristol Myers Squibb, Centocor, GSK, Genentec, Janssen, Merck, Millennium, Novartis, Pfizer, Proctor and Gamble, Roche, VSL#3, Celltrion. Finally, he is also the owner/Shareholder of Metablolomic Technologies Inc (www.metabolomictechnologies.ca).
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Correspondence to: Dr. Brendan P Halloran, Department of Medicine, Division of Gastroenterology, University of Alberta, Zeidler Ledcor Centre, 130 University Campus NW, 8440 112 St NW Edmonton, Alberta, Canada. [email protected]
Telephone: +1-780-4928691Fax: +1-780-4928121
Received: March 31, 2015 Peer-review started: March 31, 2015First decision: April 23, 2015Revised: June 14, 2015Accepted: August 30, 2015 Article in press: September 28, 2015Published online: November 15, 2015
AbstractImmunosuppressive agents, such as thiopurines, methotrexate, and biologics, have revolutionized the treatment of inflammatory bowel disease (IBD). However, a number of case reports, case control studies and retrospective studies over the last decade have identified a concerning link between immunosuppression and lymphoproliferative disorders (LPDs), the onco-logical phenomenon whereby lymphocytes divide uncontrollably. These LPDs have been associated with Epstein-Barr virus (EBV) infection in which the virus provides the impetus for malignant transformation while immunosuppression hampers the immune system’s abilityto detect and clear these malignant cells. As such, the use of immunosuppressive agents may come at the cost of increased risk of developing LPD. While little is known about the LPD risk in IBD, more is known about immunosuppression in the post-transplantation setting and the development of EBV associated post-transplantation lymphoproliferative disorders (PTLD). In review of the PTLD literature, evidence is available to demonstrate that certain immune suppressants such as cyclosporine and T-lymphocyte modulators in particular are associated with an increased risk of PTLD development. As well, high doses of immunosuppressive agents and multiple immunosuppressive agent use are also linked to increased PTLD development. Here,
REVIEW
181 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Lymphoproliferative disorders in inflammatory bowel disease patients on immunosuppression: Lessons from other inflammatory disorders
World J Gastrointest Pathophysiol 2015 November 15; 6(4): 181-192ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i4.181

we discuss these findings in context of IBD and what future studies can be taken to understand and reduce the risk of EBV-associated LPD development from immunosuppression use in IBD.
Key words: Epstein-Barr virus; Immunosuppression; Post-transplantation lymphoproliferative disorders; Lymphoproliferative disorders; Inflammatory bowel disease
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Immunosuppressive agents, such as thiopu-rines, methotrexate, and biologics, have revolutionized the treatment and maintenance therapy of inflammatory bowel disease (IBD). However, their use may come at the cost of increased risk of developing lym-phoproliferative disorders (LPD). While little is known about this risk in IBD, more is known about immuno-suppression risk in the fields of rheumatoid arthritis and post-transplantation with regards to the development of Epstein-Barr virus (EBV) associated LPD. Here, we attempt to review lymphoma risk in the setting of immunosuppression use in various medical conditions, discuss what lessons may be translatable to the IBD field and what future directions can be taken to reduce the risk of EBV-associated LPD from immunosuppression use in IBD.
Lam GY, Halloran BP, Peters AC, Fedorak RN. Lympho-proliferative disorders in inflammatory bowel disease patients on immunosuppression: Lessons from other inflammatory disorders. World J Gastrointest Pathophysiol 2015; 6(4): 181-192 Available from: URL: http://www.wjgnet.com/2150-5330/full/v6/i4/181.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i4.181
INTRODUCTIONInflammatory bowel disease (IBD) is a term that describes a collection of autoimmune gastrointestinal conditions, most notably Crohn’s disease (CD) and ulcerative colitis (UC). While UC is confined to the colon, CD can involve the entire digestive tract from mouth to anus. The pathogenesis of IBD is currently thought to be the result of a combination of host/genetic, environmental and microbial factors that perpetuate chronic and inappropriate inflammation of the gastrointestinal tract[1]. IBD has a bimodal age distribution with first diagnoses occurring between 15 to 40 years of age or 50 to 80 years of age[2]. In addition to age, a range of other risk factors have been linked to the development of IBD including gender, ethnicity, smoking, gut microbiome and medications[3]. One concerning consequence of IBD, and its treatment, is the increased incidence of lymphoproliferative diseases (LPD). LPDs include B and Tcell lymphoma, the development of which can be the result of EpsteinBarr virus (EBV) mediated malignant
transformation of normal B and T lymphocytes to divide uncontrollably. Other pathogens, such as other human Tcell lymphotropic virus1, human herpesvirus8, hepatitis B and C, human papilloma virus, Kaposi’s sarcomaassociated herpesvirus, Merkel cell polyomavirus and Helicobacter pylori have also been implicated in malignant transformation of the infected host[4,5]. LPD encompasses a diverse group of hematological malignancies that can either be acute or chronic in nature; either leukemic or lymphoid in morphology. One unique group of LPD includes the posttransplantation lymphoproliferative disorders (PTLD), which can develop due to both primary and secondary immunosuppression[6]. IBD itself, even independent of immunosuppressive treatment, is thought to be associated with either no or a slight increase in the risk of LPD development[710]. However, an increase in rates of LPD development in those with IBD who are on immunosuppressive therapy has been noted by different groups worldwide, documented in a variety of populationbased, retrospective and case control studies[8,11,12]. Collectively, these studies point to the possibility that increased malignancy rates may be due the use of particular immunosuppressive therapies that inhibit normal host immunity and exposure to EBV, which in an immunosuppressed host, can infect host cells and result in malignant transformation. While limited data is available in the IBD population, there is a wealth of studies conducted on PTLD and rheumatoid arthritis patients. The development of PTLD primarily involves either reactivation of latent EBV infection or new EBV infection and as such, the development of PTLD is screened for in the most highrisk population (EBV negative recipient matched with EBV positive donor) by monitoring EBV viral load. In the rheumatoid arthritis population, the use of methotrexate is well described to confer a significant risk of lymphoma development. In this review, we first describe the well-established causal relationship between EBV infection and LPD development. Second, we explore the effect of immunosuppression, including biologics, in the posttransplantation and rheumatoid arthritis populations on EBVassociated LPD development. Third, we examine what is known currently about the risk of EBVassociated LPD development in patients treated with immune suppressants in IBD. Lastly, we discuss what can be translated from the posttransplantation literature to IBD to manage risks of EBVassociated LPD while on immune suppressants.
EBV CAUSES LPDEBV is a doublestranded DNA virus belonging to the herpesvirus family that is ubiquitously found worldwide in roughly 90%95% of adults[13]. The peak incidence by age is bimodal as roughly half of children under five years of age in developed countries acquire this relatively benign infection, often passing as a constellation of unremarkable upper respiratory tract infection symptom
182 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Lam GY et al . LPD risk with immunosuppression use in IBD

while the second peak of infections occurs in the 15 to 24 years old group[13]. EBV spreads via oral secretions and blood, capable of triggering Blymphocyte and epithelial cell uptake[13]. Once intracellular, EBV initiates the lytic phase of infection, resulting in the lysis of the cellular host and subsequent release of viral progenies. In an immunocompetent host, cellmediated immunity is activated as cytotoxic T lymphocytes (CTLs) target viral infected cells for apoptosis[13]. A proportion of EBV infected Blymphocytes escape CTLs detection and continues on to become longlived infected memory Blymphocytes where the virus persists in the latent phase of its life cycle[13].
In latent phase, viral proteins are capable of initiating host malignant transformation in a subset of individuals, resulting in uncontrolled memory Blymphocytes proliferation, or a LPD. A number of prospective and casecontrol studies worldwide have identified EBV infection as a risk factor to the development of LPDs such as Hodgkin lymphoma, Burkitt’s lymphoma, and a subset of aggressive nonHodgkin lymphomas[14,15]. Hodgkin lymphoma has been the best studied and remains the lymphoma with the strongest association between EBV[16]. A causal relationship has been established in in vitro studies where EBV infection of human Blymphocytes results in the uncontrolled proliferation of infected cells[17]. One study suggests that the rate of malignant transformation in EBV infected individuals occurs at a rate of 1:1000 over the span of four years from infection to Hodgkin lymphoma detection[14].
Certain risk factors have been associated with higher rates of LPDs. A casecontrol study from England revealed that the age of first infection is associated with a higher oddsratio of developing Hodgkin’s lymphoma with the highest oddsratio in the 1624 years of age group[18]. Immune deficient patients have increased susceptibility to LPD development in part due to an inability to mount an EBVspecific immune response. Those with compromised immunity[19] or those receiving immunosuppressive therapies[20,21] have been found to have an altered humoral immunity against EBV. As such, increased rates of EBVassociated LPD have been documented in patients with human immune-deficiency virus[22] those with inherited immunedeficiencies[23] and in posttransplanted patients receiving immunosuppressive therapy[24].
EFFECT OF POST-TRANSPLANTATION IMMUNOSUPPRESSION ON EBV-ASSOCIATED LPD DEVELOPMENT EBV is thought to be responsible for the majority of cases of PTLD, defined as uncontrolled lymphoid or plasma cell proliferation post solid organ or hematologic transplantation in the setting of immunosuppressive agents[25]. PTLDs include a range of subtypes. Early lesions, which include plasmacytic hyperplasia and infectious mononucleosis, and polymorphic PTLD typically
involve EBV and occur within the first year post transplant. On the other hand, monomorphic PTLDs, which are histologically identical to B or Tcell derived nontransplant malignant lymphomas, tend to occur late post transplant, involve EBV less often, and are clinically more aggressive. Hodgkin lymphoma type PTLD is the least common subtype[2630]. Similar to the risk factors for development of LPDs in immunocompetent patients infected with EBV, studies of posttransplant patients revealed the key risk factors for developing PTLD include the degree of Tlymphocyte immunosuppression and the EBV serostatus[31,32]. The risk of PTLD in renal transplant patients is thought to be 620 times higher than the general population while those receiving heart transplants have an estimated 200 times higher risk due to the relatively intensive immunosuppression that thoracic transplant recipients receive[29]. A number of multinational retrospective database review studies revealed the greatest yearly incidence rate was seen in the first year post transplantation with the number of new cases steadily declining over the five years of study[32,33], suggesting that the degree of immunosuppression, which typically is highest during the first year posttransplantation, may increase the risk for PTLD development[29]. Studies with longer followup, however, show a second peak in incidence at around 8 years posttransplant, suggesting that prolonged high doses of immunosuppression are also associated with increased rates of PTLD development[30,34].
Different immunesuppressive induction agents have been hypothesized to confer different risk for developing PTLD[29,35,36]. In addition, combination therapy, while most successful at preventing rejection, is associated with greater risk of PTLD development in one pediatric population[37]. Agents that suppress CTLs, such as belatacept and efalizumab[3840], and Tlymphocytes in general, such as OKT3 and thymoglobulin[36,38], were suggested to have a greater role in inducing PTLD than those that mediate general immunosuppression. Given that viral infected cells are cleared by activated CTLs, agents that hamper CTLs is thought to be permissive for viral infection and later malignant transformation of the infected host. The rates of PTLD were found to increase dramatically as well with the initial use of cyclosporine[41,42]. Fortunately, by implementing druglevel monitoring and dose reduction, rates of PTLD have dropped since the early days of cyclosporine use. Certain agents, such as mycophenolate mofetil, have not been associated with any increased risk of PTLD[38,43].
In addition to the degree and type of immunosuppression, EBV seronegativity is an independent risk factor for the development of PTLD. The risk of PTLD is greater in EBV seronegative patients who become infected while immune suppressed than in seropositive recipients reactivating latent EBV infection posttransplantation[24]. Numerous studies have identified EBVseroconversion after either solid organ or hematological transplantation as a risk factor for PTLD development[37,4448]. EBV naïve patients receiving immune
183 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Lam GY et al . LPD risk with immunosuppression use in IBD

184 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
increasing the relative risk for LPD development from 2.5 (RA without immunosuppression) to 10 (RA with immunosuppression)[76]. The highest incidence of LPD development typically occurs within the first year post treatment[77,78]. Various immune suppressive agents have been linked to an increased risk of malignancies. The beststudied immune suppressant in context of RA and LPD development is methotrexate (MTX). This immunosuppressive agent has such a strong association with LPD development that the 2008 World Health Organization Classification of Tumours of Haematopoietic and Lymphoid Tissues recognized MTXassociated LPD as in independent entity[79]. MTXassociated LPD is commonly characterized by the presence of EBV virus in the lymphoma tissue and that discontinuation of MTX in results in regression of LPD in many but not all patients[80,81]. Furthermore, this risk of MTXassociated LPD increases with higher treatment doses[82]. Thus, it has been proposed that should MTX treated RA patients develop LPD, they should then receive EBV serologic screening to determine if MTX should be discontinued[83] as the likelihood of regression post MTX discontinuation appear to be linked to EBV status[80].
Antitumor necrosis factor (TNF)a antibody therapy has also been shown to increase rates of LPD in RA patients compared to healthy controls in a systematic metaanalysis[84]. In one head to head comparison of antiTNFa (infliximab) against MTX treatment, antiTNFa agents were associated with higher rates of LPD than MTX[85]. The risk of LPD development is likewise correlated with higher doses of antiTNFa (either inflixi-mab or adalimumab)[84]. One recent report has even linked adalimumab to EBVassociated lymphoproliferative disorder development after two years of treatment[86].
EBV-ASSOCIATED LPD DEVELOPMENT IN IBD PATIENTS TREATED WITH IMMUNE SUPPRESSANTS EBV and IBDGiven the extensive data from the posttransplantation and RA literature that shows the risk of EBVassociated LPD increases with immunosuppression, one logical question to ask is whether similar immunosuppression in other disease states, such as IBD, is also associated with increased rates of LPD. Furthermore, given that IBD patients are often diagnosed and initiate treatment younger than 30 years of age (an age demographic with many unexposed to EBV), concern for LPD risk in EBV seronegative patients may be raised.
Even without treatment, IBD patients have higher rates of infections such as nonantibiotic associated Clostridium difficile colitis[87], cytomegalovirus[87,88], and infectious colitis[88]. It is unclear why IBD is associated with higher rates of these specific infections. Regardless, it is clear is that with the addition of immunosuppressive agents, this infectious risk increases substantially[8891]. However, with respect to EBV, Reijasse et al[92] did not
suppressants were found to be at a higher risk of developing PTLD compared to EBV positive patients in one landmark University of Alberta retrospective study[49]. Since then, others in different centers have likewise identified EBV seronegativity in the pretransplantation individual as a significant risk factor for developing PTLD post transplantation[44,45,50]. EBV seronegativity has a stronger impact on the risk of PTLD that occurs early (i.e., within 1 year) as opposed to late post transplant[30,34]. As such, EBV seronegative patients are subjected to monitoring during the first year post-transplantation to detect PTLD development (discussed in the “PTLD Prevention” section).
PTLD preventionTo address the increased risk of malignant transformation of PTLD in context of immunosuppression and EBV infection, some have recommended that routine monitoring of EBV viral load be undertaken in the posttransplant settings. Rising viral load raises the suspicion of PTLD development since a high EBV viral load has been documented in some studies to precede the development of EBVmediated PTLD[5155]. As such, the absolute viral load has been proposed as prognostic of PTLD development[47,53]. However, in part due to a number of technical challenges of the EBV viral load assay, including a lack of standardized reference ranges for instrument calibration across multiple assay platforms, the positive predictive value of this assay remains low as an elevated viral load has high sensitivity but lacks specificity for PTLD development[5661]. Thus, the utility of EBV viral load monitoring in a seropositive patient remains highly controversial[6264]. On the other hand, serial EBV viral load monitoring in the seronegative recipient is an effective tool to identify those at clear risk of developing PTLD[65,66]. By routine monitoring of EBV viral load in the seronegative recipient, preemptive interventions, such as antiviral treatment and rituximab therapy, may be undertaken to prevent PTLD development when rising EBV viral load is detected[55,65,6771].
EBV-ASSOCIATED LPD DEVELOPMENT IN RHEUMATOID ARTHRITIS PATIENTS TREATED WITH IMMUNE SUPPRESSANTS Several largescale population studies have demonstrated a mildly elevated risk of LPD and EBVassociated LPD in those with rheumatoid arthritis (RA) and an even higher risk in patients being actively immunosuppressed compared to the healthy population[7274]. Mechanistically, patients with RA have been shown to have defective EBVspecific T cell function, resulting in a greater number of infected lymphocytes and as such are at a higher risk than the general population for development of LPD[75]. The addition of an immunosuppressive agent further elevates the risk of EBVassociated LPD,
Lam GY et al . LPD risk with immunosuppression use in IBD

185 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
find a relationship between EBV viral load and severity of CD activity or the type of immunosuppression (infliximab infusion, corticosteroids, azathioprine and cyclosporine) used. Similarly, Fernandez Salazar et al[93] found that EBV seropositive CD patients in remission maintained on either no immunosuppression, azathioprine and/or infliximab did not have any significant changes to the viral load. However, interestingly patients with the most severe uncontrolled CD activity were found to have transient dramatic spikes in EBV viral load[92,94] with EBV DNA detected in colonic mucosal Blymphocytes[94].
EBV-associated LPD and IBDThe link between EBVassociated LPD and IBD remains somewhat controversial as there have been a number of conflicting major studies done to date. The majority of large populationbased studies have failed to find a significant association between IBD and LPD[95100]. On the other hand, studies based in tertiary referral centers, which may have an inherent a referral bias towards those with more severe disease, showed that after factoring in the type and dose of immune suppressants used, IBD by itself does confer a slightly elevated risk for LPD[7,101]. In addition, when subgroup analysis was undertaken in one populationbased study from the University of Manitoba, an increased risk of LPD in male patients with CD was found[102]. The difficulty in large population studies is that a number of factors, such as IBD disease severity and immune suppressant usage, are often not accounted for. Thus, it remains unclear how much IBD by itself, without the influence of immune suppressants, contributes to LPD development.
While the influence of IBD on EBVassociated LPD development has not been independently determined, analysis of IBD patients on immunosuppressive therapy demonstrates a clear risk for the development of EBVassociated LPD. An estimated 50% of IBD patients on immunosuppressive therapy with LPD were EBV seropositive[8,103] with a number of case reports identifying EBV DNA present in LPDs that developed post immunosuppression in IBD patients[104107]. In reviewing the posttransplantation literature, a major risk for the development of PTLD is EBV seroconversion or EBV naivety while on immune suppressants and those who were EBV seropositive prior to transplantation habouring a latent infection represents a minor risk factor[44,45,49,50].Currently, only a handful of case reports have documented the link between EBV seroconversion and LPD development in context of IBD and immunosuppression. Van Biervliet et al[108] reported the case of a young EBV seronegative CD patient who developed LPD shortly after treatment with azathioprine. Similarly, a 16yearold CD patient who became seropositive while on therapy of mesalamine, azathioprine and infliximab infusion consequently developed EBVassociated LPD[109]. Lastly, a 25yearold CD patient develops LPD after undergoing EBV seroconversion while on azathioprine[110]. Taken together, these reports may indicate a risk of LPD development from EBV seroconversion while on immune
suppressants in IBD patients on immune suppressants. Perhaps an argument can thus be made for EBV serological monitoring in the EBV naïve IBD population. However, more research is needed to determine the effectiveness and utility of such an approach.
Role of immune suppressants on EBV-associated LPD development in IBDMedical therapy for IBD is often individualized and there are nuanced differences between the management of CD and UC[111]. Regardless, typical immunosuppressive regimens may include prednisone, mesalazine, cyclosporine, thiopurines, such as azathioprine (AZA) and 6mercaptopurine (6MP), and infliximab[111]. (MTX is also used in IBD treatment, though much less frequently than in RA management and thus scant safety data is available in the IBD population). These therapies have been examined for a correlation with EBVassociated LPD development. Mechanistically, it is theorized that increased cancer risk may be conferred with a disturbed mucosal barrier and increased inflammation resulting in an accumulation of genetic mutations provides the opportunity for EBVmediated malignant transformation. Immunosuppressive agents hamper the innate and adaptive responses for tumor surveillance and clearance[95].
The best studied of all IBD treatment agents, AZA and 6MP, were associated with an increased risk of LPD when standard dosing (AZA 2.5 mg/kg per day; 6MP 1.5 mg/kg per day) were used[8,1012]. Dayharsh et al[112] found in a retrospective study that thiopurine use dramatically increased the rates of EBVassociated LPD in their IBD population (17% increase to 50%). Similarly, thiopurine treatment in a French nationwide prospective observational cohort study (CESAME) was associated with increased EBVassociated lymphomas[113]. A recent review of the Kaiser Permanente Cancer Registry of 16023 IBD patients revealed an increased incidence of lymphomas in thiopurine treated patients[9]. Finally, in a recent metaanalysis[114] and a retrospective cohort study of the United States Veteran Affairs database[11], both publications demonstrated a 4fold increased risk of lymphoma in AZA or 6MP treated IBD patients compared with the general population[11,114]. The metaanalysis found the lymphoma development risk increased with duration of immunosuppression and decrease with discontinuation of therapy[114]. In fact, one case report described lymphoma regression upon withdrawal of thiopurine[115]. Thus, given the higher risk of EBVassociated LPD development in young male IBD patients, some groups have proposed the avoidance of thiopurine use in this particular population altogether[116,117].
In addition to thiopurine, other IBD treatment agents have been studied, albeit to a lesser extent. MTX is one such agent. There has been scant data on MTX and EBVassociated LPD development in the IBD population. Kandiel et al[11] found that 2 of the 4 cases of lymphoma development in IBD patients involved treatment with MTX (31 patients of the 782 person study
Lam GY et al . LPD risk with immunosuppression use in IBD

186 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
received MTX in total). While studies in IBD are lacking, studies involving patients with rheumatoid arthritis found MTX treatment to be associated with increased risk of lymphoma development[118,119]. One case report documented the development of EBVassociated LPD in a patient with rheumatoid arthritis receiving MTX with lymphoma regression upon discontinuation of MTX use[120].
Another commonly used class of IBD agents is the antiTNFa antibody, including both adalimumab and infliximab[12]. Adalimumab has been linked to Hodgkin Lymphoma development[121] or recurrence[122]. However, the largest trial to date involving adalimumab use found no increased incidences of Tcell non Hodgkin Lymphoma development over control[123]. This study, however, did find increased risk of Tcell non Hodgkin Lymphoma development in those treated with antiTNFa agents (either adalimumab or infliximab) in combination with a thiopurine[123]. The link between infliximab and LPD is likewise controversial. There are a number of trials that have identified a small but significant risk of lymphoma development in IBD patients on infliximab. In the ACCENT Ⅰ maintenance infliximab infusion randomized placebocontrolled trial, two cases of EBVassociated nonHodgkin lymphoma were found out of 573 patients (all participants had a score of at least 220 on the CD activity index)[124]. A second study based at the Mayo Clinic found one case of EBVassociated lymphoma out of 500 patients[11]. A third smaller randomized, doubleblinded placebo controlled trial of 73 IBD patients who were either refractory to conventional treatments or responded suboptimally to treatment were initiated on a course of four infliximab infusions every 8 wk[125]. One patient developed Bcell lymphoma 9.5 mo post initial infusion[125]. A large retrospective chart review of the Kaiser Permanente Cancer Registry revealed an increased standardized incidence rate ratio (5.5 for past use; 4.4 for current use) of lymphoma development over nearly 6-year span in the IBD population treated with infliximab over those without[9]. Finally, a recent metaanalysis of 26 publications found, in subgroup analysis, an increased risk of nonHodgkin’s lymphoma development in antiTNFa agent treated IBD male patients aged 2054 years of age[12]. On the other hand, a number of studies have failed to find evidence of increased LPD risk from infliximab use. The large Crohn’s Therapy Resource, Evaluation, and Assessment Tool registry found no increased risk of lymphoma in IBD patients treated with infliximab over control population[126]. A selective small metaanalysis of randomized controlled trials failed to find an increased risk of lymphoma associated with infliximab over those that did not receive any anti-TNFa agents. Finally, a recent study of longterm safety of infliximab use found no increase LPD risk conferred by infliximab over control over the span of 14 years[127].
There are several inherent difficulties in establishing a role for infliximab in EBV-associated LPD development in IBD. First, most studies do not stratify the data based on disease severity. It may be reasonable to
suspect that those requiring treatment with an antiTNFa agent is associated with more refractory or severe disease as biologics are typically prescribed after other immune suppressants have failed. As such, more severe inflammatory disease may independently confer a higher LPD risk. Second, it maybe challenging to show the effect of anti-TNFα therapy alone in the development of LPD as the control group typically has received some form of immunosuppressive therapy. Third, very few patients will have received only antiTNFa therapy without prior exposure to any other immunosuppressive agents. As such, there may be an accumulated risk from multiple agent use. This raises the hypothesis that it may not be any specific immunosuppressive agent that may be the culprit for LPD development, but rather the combination or addition of the third or the fourth agent that statistically increases LPD risk[128]. One observation that supports this theory is the increasing rates of hepatosplenic Tcell lymphoma (HSTCL) where the majority of reported cases involve young male patients (average age midtwenties) receiving either prolonged thiopurine therapy (more than two years) or combination immunosuppression therapy of thiopurine and antiTNF therapy[129,130]. As such, some have proposed that male patients under 35 years of age on prolonged thiopurine treatment or combination therapy should be monitored carefully for signs of HSTCL[129,130].
In summary, EBVassociated LPD may not be elevated in IBD from a population perspective but appears to occur more frequently in the younger male population, possibly due to the fact that significant EBV exposure occurs during this time. What might be behind the gender differences is currently unclear. In addition, regardless of patient demographics, thiopurines appear to confer the greatest risk of EBVassociated LPD development when compared to the methotrexate or biologics.
LESSONS FROM IMMUNE SUPPRESSION USE: FUTURE DIRECTIONS FOR IBD RESEARCH Attempting to interpret findings from one field and apply them to another must be done with caution, as the dosing and treatment regimens of immune suppressants used in IBD are different than those used posttransplantation or in RA. Furthermore, the pathophysiology of these diseases, although incompletely elucidated, are likely quite different. However, given the sparse data available in the IBD field surrounding the risks of immune suppre-ssants, complications from their use in the context of other inflammatory diseases should also not be overlooked. Currently, there is a trend amongst IBD physicians to move towards increased use of MTX for the purposes of both primary immunosuppression and also for suppression of antibiologics antibody production. As the data linking lymphoma risk in MTX use in RA is mounting, the role of MTX in lymphoma development
Lam GY et al . LPD risk with immunosuppression use in IBD

187 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
in IBD should be examined more closely. Furthermore, it remains largely unclear what effect the dose, the combination and the duration of IBD immunosuppressive therapy has on EBVassociated LPD development. In review of the available data, more questions remain than answers. Is there a role for EBV serological screening as in the posttransplantation field and if so, who should be screened and for how long? The younger male population appears to have a higher risk of LPD development while on immune suppressants and given the second peak of EBV seroconversion is within the same age range, should males between the ages of 18 to 30 be selected for routine EBV viral load screening while on therapy? Are there certain combinations of drugs
or specific therapies that should be avoided or dose adjusted to minimize the risk of EBVassociated LPD? Should withdrawal of immunosuppressive therapy be initiated as soon as metrics of early remission is achieved to minimize LPD risk? How should this be balanced with the risk of disease flare or risk of subsequent surgery? The benefit of immunosuppressive therapies in IBD, much like in RA, is unequivocal but the risk of LPD development is a cost that while relatively small is one which not all patients are comfortable with. Many questions surrounding how best to utilize and discontinue these powerful immunosuppressive agents remain. As such, the development of an early screening tool to further minimize the risk of LPD may invaluable to all IBD patients on immunosuppressive treatment (Figure 1).
REFERENCES1 Loftus EV. Clinical epidemiology of inflammatory bowel
disease: Incidence, prevalence, and environmental influences. Gastroenterology 2004; 126: 1504-1517 [PMID: 15168363]
2 Ekbom A. Epidemiology of inflammatory bowel disease. Nestle Nutr Workshop Ser Clin Perform Programme 1999; 2: 7-18; discussion 18-21 [PMID: 11490629]
3 Baumgart DC, Carding SR. Inflammatory bowel disease: cause and immunobiology. Lancet 2007; 369: 1627-1640 [PMID: 17499605 DOI: 10.1016/S0140-6736(07)60750-8]
4 Jaffe ES, Harris NL, Stein H, Isaacson PG. Classification of lymphoid neoplasms: the microscope as a tool for disease discovery. Blood 2008; 112: 4384-4399 [PMID: 19029456 DOI: 10.1182/blood-2008-07-077982]
5 Morales-Sánchez A, Fuentes-Pananá EM. Human viruses and cancer. Viruses 2014; 6: 4047-4079 [PMID: 25341666 DOI: 10.3390/v6104047]
6 Campo E, Swerdlow SH, Harris NL, Pileri S, Stein H, Jaffe ES. The 2008 WHO classification of lymphoid neoplasms and beyond: evolving concepts and practical applications. Blood 2011; 117: 5019-5032 [PMID: 21300984 DOI: 10.1182/blood-2011-01-293050]
7 Lewis JD, Bilker WB, Brensinger C, Deren JJ, Vaughn DJ, Strom BL. Inflammatory bowel disease is not associated with an increased risk of lymphoma. Gastroenterology 2001; 121: 1080-1087 [PMID: 11677199]
8 Beaugerie L, Brousse N, Bouvier AM, Colombel JF, Lémann M, Cosnes J, Hébuterne X, Cortot A, Bouhnik Y, Gendre JP, Simon T, Maynadié M, Hermine O, Faivre J, Carrat F. Lymphoproliferative disorders in patients receiving thiopurines for inflammatory bowel disease: a prospective observational cohort study. Lancet 2009; 374: 1617-1625 [PMID: 19837455 DOI: 10.1016/S0140-6736(09)61302-7]
9 Herrinton LJ, Liu L, Weng X, Lewis JD, Hutfless S, Allison JE. Role of thiopurine and anti-TNF therapy in lymphoma in inflam-matory bowel disease. Am J Gastroenterol 2011; 106: 2146-2153 [PMID: 22031357 DOI: 10.1038/ajg.2011.283]
10 Vos AC, Bakkal N, Minnee RC, Casparie MK, de Jong DJ, Dijkstra G, Stokkers P, van Bodegraven AA, Pierik M, van der Woude CJ, Oldenburg B, Hommes DW; WInitiative on Crohn's and Colitis (ICC). Risk of malignant lymphoma in patients with inflammatory bowel diseases: a Dutch nationwide study. Inflamm Bowel Dis 2011; 17: 1837-1845 [PMID: 21830262 DOI: 10.1002/ibd.21582]
11 Kandiel A, Fraser AG, Korelitz BI, Brensinger C, Lewis JD. Increased risk of lymphoma among inflammatory bowel disease patients treated with azathioprine and 6-mercaptopurine. Gut 2005; 54: 1121-1125 [PMID: 16009685 DOI: 10.1136/gut.2004.049460]
12 Siegel CA, Marden SM, Persing SM, Larson RJ, Sands BE. Risk of lymphoma associated with combination anti-tumor necrosis
New diagnosis of IBD
No further EBV testing indicated. Monitor for signs
and symptoms of LPD
EBV serological testing (EBV IgG VCA and IgG EBNA)1 at time of IBD diagnosis
Avoid starting thiopurines if possible
Repeat EBV serological testing (EBV IgG VCA, IgG EBNA and IgM VCA every 3-6 mo while
on immunosuppression)
EBV seropositive EBV seronegative
Monitor EBV viral load2. If on a thiopurine, switch to a biologic agent. If on a biologic, consider dose
reduction. Monitor for signs and symptoms of LPD
Continue current immunosuppression Monitor for signs and symptoms of EBV infection. Immediate
EBV testing if symptomatic
EBV seropositive EBV seronegative
Figure 1 Proposed algorithm for treatment management of inflammatory bowel disease patients who are either Epstein-Barr virus seropositive or negative. 1EBV monospot or EBV IgM have not been shown to be helpful in in determining serostatus; 2EBV viral load should be done by polymerase chain reaction in whole blood in EDTA collection tube. EBV: Epstein-Barr virus; IBD: Inflammatory bowel disease; EBNA: Epstein-Barr virus-determined nuclear antigen; LPD: Lymphoproliferative disorders; VCA: Viral-capsid antigen; EDTA: Ethylenediaminetetraacetic acid.
Lam GY et al . LPD risk with immunosuppression use in IBD

188 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
factor and immunomodulator therapy for the treatment of Crohn’s disease: a meta-analysis. Clin Gastroenterol Hepatol 2009; 7: 874-881 [PMID: 19558997 DOI: 10.1016/j.cgh.2009.01.004]
13 Cohen JI. Epstein-Barr virus infection. N Engl J Med 2000; 343: 481-492 [PMID: 10944566 DOI: 10.1056/NEJM200008173430707]
14 Hjalgrim H, Askling J, Rostgaard K, Hamilton-Dutoit S, Frisch M, Zhang JS, Madsen M, Rosdahl N, Konradsen HB, Storm HH, Melbye M. Characteristics of Hodgkin’s lymphoma after infectious mononucleosis. N Engl J Med 2003; 349: 1324-1332 [PMID: 14523140 DOI: 10.1056/NEJMoa023141]
15 Glaser SL, Lin RJ, Stewart SL, Ambinder RF, Jarrett RF, Brousset P, Pallesen G, Gulley ML, Khan G, O’Grady J, Hummel M, Preciado MV, Knecht H, Chan JK, Claviez A. Epstein-Barr virus-associated Hodgkin’s disease: epidemiologic characteristics in international data. Int J Cancer 1997; 70: 375-382 [PMID: 9033642]
16 Coghill AE, Hildesheim A. Epstein-Barr virus antibodies and the risk of associated malignancies: review of the literature. Am J Epidemiol 2014; 180: 687-695 [PMID: 25167864 DOI: 10.1093/aje/kwu176]
17 Yates JL, Warren N, Sugden B. Stable replication of plasmids derived from Epstein-Barr virus in various mammalian cells. Nature 1985; 313: 812-815 [PMID: 2983224]
18 Alexander FE, Jarrett RF, Lawrence D, Armstrong AA, Freeland J, Gokhale DA, Kane E, Taylor GM, Wright DH, Cartwright RA. Risk factors for Hodgkin’s disease by Epstein-Barr virus (EBV) status: prior infection by EBV and other agents. Br J Cancer 2000; 82: 1117-1121 [PMID: 10737396 DOI: 10.1054/bjoc.1999.1049]
19 Henle W, Henle G, Andersson J, Ernberg I, Klein G, Horwitz CA, Marklund G, Rymo L, Wellinder C, Straus SE. Antibody responses to Epstein-Barr virus-determined nuclear antigen (EBNA)-1 and EBNA-2 in acute and chronic Epstein-Barr virus infection. Proc Natl Acad Sci USA 1987; 84: 570-574 [PMID: 3025881]
20 Grose C, Henle W, Horwitz MS. Primary Epstein-Barr virus infection in a renal transplant recipient. South Med J 1977; 70: 1276-1278 [PMID: 199946]
21 Lange B, Arbeter A, Hewetson J, Henle W. Longitudinal study of Epstein-Barr virus antibody titers and excretion in pediatric patients with Hodgkin’s disease. Int J Cancer 1978; 22: 521-527 [PMID: 82539]
22 Goedert JJ, Coté TR, Virgo P, Scoppa SM, Kingma DW, Gail MH, Jaffe ES, Biggar RJ. Spectrum of AIDS-associated malignant disorders. Lancet 1998; 351: 1833-1839 [PMID: 9652666]
23 Filipovich AH, Mathur A, Kamat D, Shapiro RS. Primary immunodeficiencies: genetic risk factors for lymphoma. Cancer Res 1992; 52: 5465s-5467s [PMID: 1327508]
24 Green M, Michaels MG. Epstein-Barr virus infection and post-transplant lymphoproliferative disorder. Am J Transplant 2013; 13 Suppl 3: 41-54; quiz 54 [PMID: 23347213 DOI: 10.1111/ajt.12004]
25 Hanto DW. Classification of Epstein-Barr virus-associated post-transplant lymphoproliferative diseases: implications for under-standing their pathogenesis and developing rational treatment strategies. Annu Rev Med 1995; 46: 381-394 [PMID: 7598473 DOI: 10.1146/annurev.med.46.1.381]
26 Zimmermann H, Trappe RU. EBV and posttransplantation lymphoproliferative disease: what to do? Hematology Am Soc Hematol Educ Program 2013; 2013: 95-102 [PMID: 24319169 DOI: 10.1182/asheducation-2013.1.95]
27 Na R, Grulich AE, Meagher NS, McCaughan GW, Keogh AM, Vajdic CM. De novo cancer-related death in Australian liver and cardiothoracic transplant recipients. Am J Transplant 2013; 13: 1296-1304 [PMID: 23464511 DOI: 10.1111/ajt.12192]
28 Kasiske BL, Kukla A, Thomas D, Wood Ives J, Snyder JJ, Qiu Y, Peng Y, Dharnidharka VR, Israni AK. Lymphoproliferative disorders after adult kidney transplant: epidemiology and comparison of registry report with claims-based diagnoses. Am J Kidney Dis 2011; 58: 971-980 [PMID: 21930332 DOI: 10.1053/j.ajkd.2011.07.015]
29 Opelz G, Döhler B. Lymphomas after solid organ transplantation:
a collaborative transplant study report. Am J Transplant 2004; 4: 222-230 [PMID: 14974943]
30 Caillard S, Lamy FX, Quelen C, Dantal J, Lebranchu Y, Lang P, Velten M, Moulin B; French Transplant Centers. Epidemiology of posttransplant lymphoproliferative disorders in adult kidney and kidney pancreas recipients: report of the French registry and analysis of subgroups of lymphomas. Am J Transplant 2012; 12: 682-693 [PMID: 22226336 DOI: 10.1111/j.1600-6143.2011.03896.x]
31 Smith JM, Rudser K, Gillen D, Kestenbaum B, Seliger S, Weiss N, McDonald RA, Davis CL, Stehmen-Breen C. Risk of lymphoma after renal transplantation varies with time: an analysis of the United States Renal Data System. Transplantation 2006; 81: 175-180 [PMID: 16436959 DOI: 10.1097/01.tp.0000188687.18972.a8]
32 Caillard S, Lelong C, Pessione F, Moulin B; French PTLD Working Group. Post-transplant lymphoproliferative disorders occurring after renal transplantation in adults: report of 230 cases from the French Registry. Am J Transplant 2006; 6: 2735-2742 [PMID: 17049061 DOI: 10.1111/j.1600-6143.2006.01540.x]
33 Opelz G, Henderson R. Incidence of non-Hodgkin lymphoma in kidney and heart transplant recipients. Lancet 1993; 342: 1514-1516 [PMID: 7902900]
34 van Leeuwen MT, Grulich AE, Webster AC, McCredie MR, Stewart JH, McDonald SP, Amin J, Kaldor JM, Chapman JR, Vajdic CM. Immunosuppression and other risk factors for early and late non-Hodgkin lymphoma after kidney transplantation. Blood 2009; 114: 630-637 [PMID: 19443660 DOI: 10.1182/blood-2009-02-202507]
35 Bustami RT, Ojo AO, Wolfe RA, Merion RM, Bennett WM, McDiarmid SV, Leichtman AB, Held PJ, Port FK. Immuno-suppression and the risk of post-transplant malignancy among cadaveric first kidney transplant recipients. Am J Transplant 2004; 4: 87-93 [PMID: 14678038]
36 Swinnen LJ, Costanzo-Nordin MR, Fisher SG, O’Sullivan EJ, Johnson MR, Heroux AL, Dizikes GJ, Pifarre R, Fisher RI. Increased incidence of lymphoproliferative disorder after immunosuppression with the monoclonal antibody OKT3 in cardiac-transplant recipients. N Engl J Med 1990; 323: 1723-1728 [PMID: 2100991 DOI: 10.1056/NEJM199012203232502]
37 McDonald RA, Smith JM, Ho M, Lindblad R, Ikle D, Grimm P, Wyatt R, Arar M, Liereman D, Bridges N, Harmon W; CCTPT Study Group. Incidence of PTLD in pediatric renal transplant recipients receiving basiliximab, calcineurin inhibitor, sirolimus and steroids. Am J Transplant 2008; 8: 984-989 [PMID: 18416737 DOI: 10.1111/j.1600-6143.2008.02167.x]
38 Kirk AD , Cherikh WS, Ring M, Burke G, Kaufman D, Knechtle SJ, Potdar S, Shapiro R, Dharnidharka VR, Kauffman HM. Dissociation of depletional induction and posttransplant lymphoproliferative disease in kidney recipients treated with alemtuzumab. Am J Transplant 2007; 7: 2619-2625 [PMID: 17868060 DOI: 10.1111/j.1600-6143.2007.01972.x]
39 Vincenti F, Larsen C, Durrbach A, Wekerle T, Nashan B, Blancho G, Lang P, Grinyo J, Halloran PF, Solez K, Hagerty D, Levy E, Zhou W, Natarajan K, Charpentier B; Belatacept Study Group. Costimulation blockade with belatacept in renal transplantation. N Engl J Med 2005; 353: 770-781 [PMID: 16120857 DOI: 10.1056/NEJMoa050085]
40 Vincenti F, Mendez R, Pescovitz M, Rajagopalan PR, Wilkinson AH, Butt K, Laskow D, Slakey DP, Lorber MI, Garg JP, Garovoy M. A phase I/II randomized open-label multicenter trial of efalizumab, a humanized anti-CD11a, anti-LFA-1 in renal transplantation. Am J Transplant 2007; 7: 1770-1777 [PMID: 17564637 DOI: 10.1111/j.1600-6143.2007.01845.x]
41 Beveridge T, Krupp P, McKibbin C. Lymphomas and lympho-proliferative lesions developing under cyclosporin therapy. Lancet 1984; 1: 788 [PMID: 6143097]
42 Starzl TE, Nalesnik MA, Porter KA, Ho M, Iwatsuki S, Griffith BP, Rosenthal JT, Hakala TR, Shaw BW, Hardesty RL. Reversibility of lymphomas and lymphoproliferative lesions developing under cyclosporin-steroid therapy. Lancet 1984; 1:
Lam GY et al . LPD risk with immunosuppression use in IBD

189 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
583-587 [PMID: 6142304]43 Funch DP, Ko HH, Travasso J, Brady J, Kew CE, Nalesnik MA,
Walker AM. Posttransplant lymphoproliferative disorder among renal transplant patients in relation to the use of mycophenolate mofetil. Transplantation 2005; 80: 1174-1180 [PMID: 16314782]
44 Walker RC, Paya CV, Marshall WF, Strickler JG, Wiesner RH, Velosa JA, Habermann TM, Daly RC, McGregor CG. Pretrans-plantation seronegative Epstein-Barr virus status is the primary risk factor for posttransplantation lymphoproliferative disorder in adult heart, lung, and other solid organ transplantations. J Heart Lung Transplant 1995; 14: 214-221 [PMID: 7779838]
45 Aris RM, Maia DM, Neuringer IP, Gott K, Kiley S, Gertis K, Handy J. Post-transplantation lymphoproliferative disorder in the Epstein-Barr virus-naïve lung transplant recipient. Am J Respir Crit Care Med 1996; 154: 1712-1717 [PMID: 8970360 DOI: 10.1164/ajrccm.154.6.8970360]
46 Shahinian VB, Muirhead N, Jevnikar AM, Leckie SH, Khakhar AK, Luke PP, Rizkalla KS, Hollomby DJ, House AA. Epstein-Barr virus seronegativity is a risk factor for late-onset posttransplant lymphoroliferative disorder in adult renal allograft recipients. Transplantation 2003; 75: 851-856 [PMID: 12660514 DOI: 10.1097/01.TP.0000055098.96022.F7]
47 Wheless SA, Gulley ML, Raab-Traub N, McNeillie P, Neuringer IP, Ford HJ, Aris RM. Post-transplantation lymphoproliferative disease: Epstein-Barr virus DNA levels, HLA-A3, and survival. Am J Respir Crit Care Med 2008; 178: 1060-1065 [PMID: 18755927 DOI: 10.1164/rccm.200804-531OC]
48 Bakker NA, Verschuuren EA, Erasmus ME, Hepkema BG, Veeger NJ, Kallenberg CG, van der Bij W. Epstein-Barr virus-DNA load monitoring late after lung transplantation: a surrogate marker of the degree of immunosuppression and a safe guide to reduce immunosuppression. Transplantation 2007; 83: 433-438 [PMID: 17318076 DOI: 10.1097/01.tp.0000252784.60159.96]
49 Cockfield SM, Preiksaitis JK, Jewell LD, Parfrey NA. Post-transplant lymphoproliferative disorder in renal allograft recipients. Clinical experience and risk factor analysis in a single center. Transplantation 1993; 56: 88-96 [PMID: 8333073]
50 Walker RC, Marshall WF, Strickler JG, Wiesner RH, Velosa JA, Habermann TM, McGregor CG, Paya CV. Pretransplantation assessment of the risk of lymphoproliferative disorder. Clin Infect Dis 1995; 20: 1346-1353 [PMID: 7620022]
51 Luskin MR, Heil DS, Tan KS, Choi S, Stadtmauer EA, Schuster SJ, Porter DL, Vonderheide RH, Bagg A, Heitjan DF, Tsai DE, Reshef R. The Impact of EBV Status on Characteristics and Outcomes of Posttransplantation Lymphoproliferative Disorder. Am J Transplant 2015; 15: 2665-2673 [PMID: 25988622 DOI: 10.1111/ajt.13324]
52 Wagner HJ, Wessel M, Jabs W, Smets F, Fischer L, Offner G, Bucsky P. Patients at risk for development of posttransplant lymphoproliferative disorder: plasma versus peripheral blood mononuclear cells as material for quantification of Epstein-Barr viral load by using real-time quantitative polymerase chain reaction. Transplantation 2001; 72: 1012-1019 [PMID: 11579293]
53 Stevens SJ, Verschuuren EA, Pronk I, van Der Bij W, Harmsen MC, The TH, Meijer CJ, van Den Brule AJ, Middeldorp JM. Frequent monitoring of Epstein-Barr virus DNA load in unfractionated whole blood is essential for early detection of posttransplant lym-phoproliferative disease in high-risk patients. Blood 2001; 97: 1165-1171 [PMID: 11222357]
54 Tsai DE, Douglas L, Andreadis C, Vogl DT, Arnoldi S, Kotloff R, Svoboda J, Bloom RD, Olthoff KM, Brozena SC, Schuster SJ, Stadtmauer EA, Robertson ES, Wasik MA, Ahya VN. EBV PCR in the diagnosis and monitoring of posttransplant lymphoproliferative disorder: results of a two-arm prospective trial. Am J Transplant 2008; 8: 1016-1024 [PMID: 18312608 DOI: 10.1111/j.1600-6143.2008.02183.x]
55 Green M, Bueno J, Rowe D, Mazariegos G, Qu L, Abu-Almagd K, Reyes J. Predictive negative value of persistent low Epstein-Barr virus viral load after intestinal transplantation in children. Transplantation 2000; 70: 593-596 [PMID: 10972215]
56 Wagner HJ, Cheng YC, Huls MH, Gee AP, Kuehnle I, Krance RA, Brenner MK, Rooney CM, Heslop HE. Prompt versus preemptive intervention for EBV lymphoproliferative disease. Blood 2004; 103: 3979-3981 [PMID: 14751931 DOI: 10.1182/blood-2003-12-4287]
57 Gärtner BC, Schäfer H, Marggraff K, Eisele G, Schäfer M, Dilloo D, Roemer K, Laws HJ, Sester M, Sester U, Einsele H, Mueller-Lantzsch N. Evaluation of use of Epstein-Barr viral load in patients after allogeneic stem cell transplantation to diagnose and monitor posttransplant lymphoproliferative disease. J Clin Microbiol 2002; 40: 351-358 [PMID: 11825941]
58 Loginov R, Aalto S, Piiparinen H, Halme L, Arola J, Hedman K, Höckerstedt K, Lautenschlager I. Monitoring of EBV-DNAemia by quantitative real-time PCR after adult liver transplantation. J Clin Virol 2006; 37: 104-108 [PMID: 16931140 DOI: 10.1016/j.jcv.2006.06.012]
59 Doesch AO, Konstandin M, Celik S, Kristen A, Frankenstein L, Sack FU, Schnabel P, Schnitzler P, Katus HA, Dengler TJ. Epstein-Barr virus load in whole blood is associated with immunosuppression, but not with post-transplant lymphoproliferative disease in stable adult heart transplant patients. Transpl Int 2008; 21: 963-971 [PMID: 18564989 DOI: 10.1111/j.1432-2277.2008.00709.x]
60 Hoshino Y, Kimura H, Tanaka N, Tsuge I, Kudo K, Horibe K, Kato K, Matsuyama T, Kikuta A, Kojima S, Morishima T. Prospective monitoring of the Epstein-Barr virus DNA by a real-time quantitative polymerase chain reaction after allogenic stem cell transplantation. Br J Haematol 2001; 115: 105-111 [PMID: 11722419]
61 van Esser JW, van der Holt B, Meijer E, Niesters HG, Trenschel R, Thijsen SF, van Loon AM, Frassoni F, Bacigalupo A, Schaefer UW, Osterhaus AD, Gratama JW, Löwenberg B, Verdonck LF, Cornelissen JJ. Epstein-Barr virus (EBV) reactivation is a frequent event after allogeneic stem cell transplantation (SCT) and quantitatively predicts EBV-lymphoproliferative disease following T-cell--depleted SCT. Blood 2001; 98: 972-978 [PMID: 11493441]
62 Kasiske BL, Zeier MG, Chapman JR, Craig JC, Ekberg H, Garvey CA, Green MD, Jha V, Josephson MA, Kiberd BA, Kreis HA, McDonald RA, Newmann JM, Obrador GT, Vincenti FG, Cheung M, Earley A, Raman G, Abariga S, Wagner M, Balk EM; Kidney Disease: Improving Global Outcomes. KDIGO clinical practice guideline for the care of kidney transplant recipients: a summary. Kidney Int 2010; 77: 299-311 [PMID: 19847156 DOI: 10.1038/ki.2009.377]
63 Costanzo MR, Dipchand A, Starling R, Anderson A, Chan M, Desai S, Fedson S, Fisher P, Gonzales-Stawinski G, Martinelli L, McGiffin D, Smith J, Taylor D, Meiser B, Webber S, Baran D, Carboni M, Dengler T, Feldman D, Frigerio M, Kfoury A, Kim D, Kobashigawa J, Shullo M, Stehlik J, Teuteberg J, Uber P, Zuckermann A, Hunt S, Burch M, Bhat G, Canter C, Chinnock R, Crespo-Leiro M, Delgado R, Dobbels F, Grady K, Kao W, Lamour J, Parry G, Patel J, Pini D, Towbin J, Wolfel G, Delgado D, Eisen H, Goldberg L, Hosenpud J, Johnson M, Keogh A, Lewis C, O’Connell J, Rogers J, Ross H, Russell S, Vanhaecke J. The International Society of Heart and Lung Transplantation Guidelines for the care of heart transplant recipients. J Heart Lung Transplant 2010; 29: 914-956 [PMID: 20643330 DOI: 10.1016/j.healun.2010.05.034]
64 EBPG Expert Group on Renal Transplantation. European best practice guidelines for renal transplantation. Section IV: Long-term management of the transplant recipient. Nephrol Dial Transplant 2002; 17 Suppl 4: 1-67 [PMID: 12484407]
65 Lee TC, Savoldo B, Rooney CM, Heslop HE, Gee AP, Caldwell Y, Barshes NR, Scott JD, Bristow LJ, O’Mahony CA, Goss JA. Quantitative EBV viral loads and immunosuppression alterations can decrease PTLD incidence in pediatric liver transplant recipients. Am J Transplant 2005; 5: 2222-2228 [PMID: 16095501 DOI: 10.1111/j.1600-6143.2005.01002.x]
66 Green M, Cacciarelli TV, Mazariegos GV, Sigurdsson L, Qu L, Rowe DT, Reyes J. Serial measurement of Epstein-Barr viral load in peripheral blood in pediatric liver transplant recipients
Lam GY et al . LPD risk with immunosuppression use in IBD

190 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
during treatment for posttransplant lymphoproliferative disease. Transplantation 1998; 66: 1641-1644 [PMID: 9884252]
67 Allen U, Hebert D, Petric M, Tellier R, Tran D, Superina R, Stephens D, West L, Wasfy S, Nelson S. Utility of semiquantitative polymerase chain reaction for Epstein-Barr virus to measure virus load in pediatric organ transplant recipients with and without posttransplant lymphoproliferative disease. Clin Infect Dis 2001; 33: 145-150 [PMID: 11418872 DOI: 10.1086/321806]
68 McDiarmid SV, Jordan S, Kim GS, Toyoda M, Goss JA, Vargas JH, Martín MG, Bahar R, Maxfield AL, Ament ME, Busuttil RW. Prevention and preemptive therapy of postransplant lymphoproliferative disease in pediatric liver recipients. Transplantation 1998; 66: 1604-1611 [PMID: 9884246]
69 Gridelli B, Spada M, Riva S, Colledan M, Segalin A, Lucianetti A, Sonzogni A, Furione M, Baldanti F, Torre G. Circulating Epstein-Barr virus DNA to monitor lymphoproliferative disease following pediatric liver transplantation. Transpl Int 2000; 13 Suppl 1: S399-S401 [PMID: 11112041]
70 Liu Q, Xuan L, Liu H, Huang F, Zhou H, Fan Z, Zhao K, Wu M, Xu L, Zhai X, Zhang F, Liu C, Sun J, Huang X. Molecular monitoring and stepwise preemptive therapy for Epstein-Barr virus viremia after allogeneic stem cell transplantation. Am J Hematol 2013; 88: 550-555 [PMID: 23564232 DOI: 10.1002/ajh.23452]
71 van der Velden WJ, Mori T, Stevens WB, de Haan AF, Stelma FF, Blijlevens NM, Donnelly JP. Reduced PTLD-related mortality in patients experiencing EBV infection following allo-SCT after the introduction of a protocol incorporating pre-emptive rituximab. Bone Marrow Transplant 2013; 48: 1465-1471 [PMID: 23749107 DOI: 10.1038/bmt.2013.84]
72 Askling J. Malignancy and rheumatoid arthritis. Curr Rheumatol Rep 2007; 9: 421-426 [PMID: 17915099]
73 Hemminki K, Liu X, Försti A, Ji J, Sundquist J, Sundquist K. Subsequent leukaemia in autoimmune disease patients. Br J Haematol 2013; 161: 677-687 [PMID: 23565673 DOI: 10.1111/bjh.12330]
74 Baecklund E, Smedby KE, Sutton LA, Askling J, Rosenquist R. Lymphoma development in patients with autoimmune and inflammatory disorders--what are the driving forces? Semin Cancer Biol 2014; 24: 61-70 [PMID: 24333759 DOI: 10.1016/j.semcancer.2013.12.001]
75 Tosato G, Steinberg AD, Blaese RM. Defective EBV-specific suppressor T-cell function in rheumatoid arthritis. N Engl J Med 1981; 305: 1238-1243 [PMID: 6270556 DOI: 10.1056/NEJM198111193052102]
76 Kinlen LJ. Incidence of cancer in rheumatoid arthritis and other disorders after immunosuppressive treatment. Am J Med 1985; 78: 44-49 [PMID: 3970040]
77 Chen YJ, Chang YT, Wang CB, Wu CY. The risk of cancer in patients with rheumatoid arthritis: a nationwide cohort study in Taiwan. Arthritis Rheum 2011; 63: 352-358 [PMID: 21279991 DOI: 10.1002/art.30134]
78 Ekström K, Hjalgrim H, Brandt L, Baecklund E, Klareskog L, Ekbom A, Askling J. Risk of malignant lymphomas in patients with rheumatoid arthritis and in their first-degree relatives. Arthritis Rheum 2003; 48: 963-970 [PMID: 12687538 DOI: 10.1002/art.10939]
79 Vardiman JW. The World Health Organization (WHO) classi-fication of tumors of the hematopoietic and lymphoid tissues: an overview with emphasis on the myeloid neoplasms. Chem Biol Interact 2010; 184: 16-20 [PMID: 19857474 DOI: 10.1016/j.cbi.2009.10.009]
80 Salloum E, Cooper DL, Howe G, Lacy J, Tallini G, Crouch J, Schultz M, Murren J. Spontaneous regression of lympho-proliferative disorders in patients treated with methotrexate for rheumatoid arthritis and other rheumatic diseases. J Clin Oncol 1996; 14: 1943-1949 [PMID: 8656264]
81 Feng WH, Cohen JI, Fischer S, Li L, Sneller M, Goldbach-Mansky R, Raab-Traub N, Delecluse HJ, Kenney SC. Reactivation of latent Epstein-Barr virus by methotrexate: a potential contributor to methotrexate-associated lymphomas. J Natl Cancer Inst 2004;
96: 1691-1702 [PMID: 15547182 DOI: 10.1093/jnci/djh313]82 Kameda T, Dobashi H, Miyatake N, Inoo M, Onishi I, Kurata N,
Mitsunaka H, Kawakami K, Fukumoto T, Susaki K, Izumikawa M, Nakashima S, Shimada H, Takeuchi Y, Haba R, Mano S, Onishi H, Imataki O, Matsunaga T. Association of higher methotrexate dose with lymphoproliferative disease onset in rheumatoid arthritis patients. Arthritis Care Res (Hoboken) 2014; 66: 1302-1309 [PMID: 24515570 DOI: 10.1002/acr.22306]
83 Starkebaum G. Rheumatoid arthritis, methotrexate, and lymp-homa: risk substitution, or cat and mouse with Epstein-Barr virus? J Rheumatol 2001; 28: 2573-2575 [PMID: 11764198]
84 Bongartz T, Sutton AJ, Sweeting MJ, Buchan I, Matteson EL, Montori V. Anti-TNF antibody therapy in rheumatoid arthritis and the risk of serious infections and malignancies: systematic review and meta-analysis of rare harmful effects in randomized controlled trials. JAMA 2006; 295: 2275-2285 [PMID: 16705109 DOI: 10.1001/jama.295.19.2275]
85 Wolfe F, Michaud K. Lymphoma in rheumatoid arthritis: the effect of methotrexate and anti-tumor necrosis factor therapy in 18,572 patients. Arthritis Rheum 2004; 50: 1740-1751 [PMID: 15188349 DOI: 10.1002/art.20311]
86 Ikeda T, Toyama S, Ogasawara M, Amano H, Takasaki Y, Morita H, Ishizuka T. Rheumatoid arthritis complicated with immunodeficiency-associated lymphoproliferative disorders during treatment with adalimumab. Mod Rheumatol 2012; 22: 458-462 [PMID: 21830047 DOI: 10.1007/s10165-011-0501-0]
87 Irving PM, Gibson PR. Infections and IBD. Nat Clin Pract Gastroenterol Hepatol 2008; 5: 18-27 [PMID: 18174904 DOI: 10.1038/ncpgasthep1004]
88 Epple HJ. Therapy- and non-therapy-dependent infectious complications in inflammatory bowel disease. Dig Dis 2009; 27: 555-559 [PMID: 19897974 DOI: 10.1159/000233297]
89 Lichtenstein GR, Feagan BG, Cohen RD, Salzberg BA, Diamond RH, Price S, Langholff W, Londhe A, Sandborn WJ. Serious infection and mortality in patients with Crohn’s disease: more than 5 years of follow-up in the TREAT™ registry. Am J Gastroenterol 2012; 107: 1409-1422 [PMID: 22890223 DOI: 10.1038/ajg.2012.218]
90 Marehbian J, Arrighi HM, Hass S, Tian H, Sandborn WJ. Adverse events associated with common therapy regimens for moderate-to-severe Crohn’s disease. Am J Gastroenterol 2009; 104: 2524-2533 [PMID: 19532125 DOI: 10.1038/ajg.2009.322]
91 Toruner M, Loftus EV, Harmsen WS, Zinsmeister AR, Orenstein R, Sandborn WJ, Colombel JF, Egan LJ. Risk factors for opportunistic infections in patients with inflammatory bowel disease. Gastroenterology 2008; 134: 929-936 [PMID: 18294633 DOI: 10.1053/j.gastro.2008.01.012]
92 Reijasse D, Le Pendeven C, Cosnes J, Dehee A, Gendre JP, Nicolas JC, Beaugerie L. Epstein-Barr virus viral load in Crohn’s disease: effect of immunosuppressive therapy. Inflamm Bowel Dis 2004; 10: 85-90 [PMID: 15168806]
93 Fernandez Salazar L, Rojo S, De Lejarazu RO, Castro E, Higuera E, González JM. No increase in Epstein-Barr virus viral load in a group of 30 asymptomatic patients with Crohn’s disease. Am J Gastroenterol 2013; 108: 1933-1935 [PMID: 24300873 DOI: 10.1038/ajg.2013.250]
94 Sankaran-Walters S, Ransibrahmanakul K, Grishina I, Hung J, Martinez E, Prindiville T, Dandekar S. Epstein-Barr virus replication linked to B cell proliferation in inflamed areas of colonic mucosa of patients with inflammatory bowel disease. J Clin Virol 2011; 50: 31-36 [PMID: 21035384 DOI: 10.1016/j.jcv.2010.09.011]
95 Aithal GP, Mansfield JC. Review article: the risk of lymphoma associated with inflammatory bowel disease and immunosuppressive treatment. Aliment Pharmacol Ther 2001; 15: 1101-1108 [PMID: 11472312]
96 Bebb JR, Logan RP. Review article: does the use of immuno-suppressive therapy in inflammatory bowel disease increase the risk of developing lymphoma? Aliment Pharmacol Ther 2001; 15: 1843-1849 [PMID: 11736713]
97 Ekbom A, Helmick C, Zack M, Adami HO. Extracolonic malignancies in inflammatory bowel disease. Cancer 1991; 67:
Lam GY et al . LPD risk with immunosuppression use in IBD

191 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
2015-2019 [PMID: 2004319]98 Karlén P, Löfberg R, Broström O, Leijonmarck CE, Hellers G,
Persson PG. Increased risk of cancer in ulcerative colitis: a population-based cohort study. Am J Gastroenterol 1999; 94: 1047-1052 [PMID: 10201481 DOI: 10.1111/j.1572-0241.1999.01012.x]
99 Palli D, Trallori G, Bagnoli S, Saieva C, Tarantino O, Ceroti M, d’Albasio G, Pacini F, Amorosi A, Masala G. Hodgkin’s disease risk is increased in patients with ulcerative colitis. Gastroenterology 2000; 119: 647-653 [PMID: 10982757]
100 Persson PG, Karlén P, Bernell O, Leijonmarck CE, Broström O, Ahlbom A, Hellers G. Crohn’s disease and cancer: a population-based cohort study. Gastroenterology 1994; 107: 1675-1679 [PMID: 7958678]
101 Greenstein AJ, Gennuso R, Sachar DB, Heimann T, Smith H, Janowitz HD, Aufses AH. Extraintestinal cancers in inflammatory bowel disease. Cancer 1985; 56: 2914-2921 [PMID: 4052961]
102 Bernstein CN, Blanchard JF, Kliewer E, Wajda A. Cancer risk in patients with inflammatory bowel disease: a population-based study. Cancer 2001; 91: 854-862 [PMID: 11241255]
103 Sokol H, Beaugerie L. Inflammatory bowel disease and lympho-proliferative disorders: the dust is starting to settle. Gut 2009; 58: 1427-1436 [PMID: 19749141 DOI: 10.1136/gut.2009.181982]
104 Allen PB, Laing G, Connolly A, O’Neill C. EBV-associated colonic B-cell lymphoma following treatment with infliximab for IBD: a new problem? BMJ Case Rep 2013; 2013: pii: bcr2013200423 [PMID: 24081592 DOI: 10.1136/bcr-2013-200423]
105 Bai M, Katsanos KH, Economou M, Kamina S, Balli C, Briasoulis E, Kappas AM, Agnantis N, Tsianos EV. Rectal Epstein-Barr virus-positive Hodgkin’s lymphoma in a patient with Crohn’s disease: case report and review of the literature. Scand J Gastroenterol 2006; 41: 866-869 [PMID: 16785203 DOI: 10.1080/00365520500529629]
106 Loiudice TA, Nemer W, Rosenblum S, Murray B, Batizy S, Fleming L, Mubashir B, Demeter S. Crohn’s disease (regional enteritis) in association with Hodgkin’s disease. J Am Osteopath Assoc 1989; 89: 519-523 [PMID: 2661509]
107 Castrellon A, Feldman PA, Suarez M, Spector S, Chua L, Byrnes J. Crohn’s disease complicated by primary gastrointestinal Hodgkin’s lymphoma presenting with small bowel perforation. J Gastrointestin Liver Dis 2009; 18: 359-361 [PMID: 19795032]
108 Van Biervliet S, Velde SV, De Bruyne R, De Looze D, De Vos M, Van Winckel M. Epstein-Barr virus related lymphoma in inflammatory bowel disease. Acta Gastroenterol Belg 2008; 71: 33-35 [PMID: 18396748]
109 Gidrewicz D, Lehman D, Rabizadeh S, Majlessipour F, Dubinsky M. Primary EBV infection resulting in lymphoproliferative disease in a teenager with Crohn disease. J Pediatr Gastroenterol Nutr 2011; 52: 103-105 [PMID: 20890216 DOI: 10.1097/MPG.0b013e3181e80410]
110 N’guyen Y, Andreoletti L, Patey M, Lecoq-Lafon C, Cornillet P, Léon A, Jaussaud R, Fieschi C, Strady C. Fatal Epstein-Barr virus primo infection in a 25-year-old man treated with azathioprine for Crohn’s disease. J Clin Microbiol 2009; 47: 1252-1254 [PMID: 19193838 DOI: 10.1128/JCM.02052-08]
111 Baumgart DC, Sandborn WJ. Inflammatory bowel disease: clinical aspects and established and evolving therapies. Lancet 2007; 369: 1641-1657 [PMID: 17499606 DOI: 10.1016/S0140-6736(07)60751-X]
112 Dayharsh GA, Loftus EV, Sandborn WJ, Tremaine WJ, Zinsmeister AR, Witzig TE, Macon WR, Burgart LJ. Epstein-Barr virus-positive lymphoma in patients with inflammatory bowel disease treated with azathioprine or 6-mercaptopurine. Gastroenterology 2002; 122: 72-77 [PMID: 11781282]
113 Sokol H, Beaugerie L, Maynadié M, Laharie D, Dupas JL, Flourié B, Lerebours E, Peyrin-Biroulet L, Allez M, Simon T, Carrat F, Brousse N; CESAME Study Group. Excess primary intestinal lymphoproliferative disorders in patients with inflammatory bowel disease. Inflamm Bowel Dis 2012; 18: 2063-2071 [PMID: 22271569 DOI: 10.1002/ibd.22889]
114 Khan N, Abbas AM, Lichtenstein GR, Loftus EV, Bazzano LA.
Risk of lymphoma in patients with ulcerative colitis treated with thio-purines: a nationwide retrospective cohort study. Gastroenterology 2013; 145: 1007-1015.e3 [PMID: 23891975 DOI: 10.1053/j.gastro.2013.07.035]
115 Larvol L, Soule JC, Le Tourneau A. Reversible lymphoma in the setting of azathioprine therapy for Crohn’s disease. N Engl J Med 1994; 331: 883-884 [PMID: 8078549 DOI: 10.1056/NEJM199409293311321]
116 Subramaniam K, D’Rozario J, Pavli P. Lymphoma and other lymphoproliferative disorders in inflammatory bowel disease: a review. J Gastroenterol Hepatol 2013; 28: 24-30 [PMID: 23094824 DOI: 10.1111/jgh.12015]
117 Schwartz LK, Kim MK, Coleman M, Lichtiger S, Chadburn A, Scherl E. Case report: lymphoma arising in an ileal pouch anal anastomosis after immunomodulatory therapy for inflammatory bowel disease. Clin Gastroenterol Hepatol 2006; 4: 1030-1034 [PMID: 16854631 DOI: 10.1016/j.cgh.2006.05.024]
118 Baecklund E, Askling J, Rosenquist R, Ekbom A, Klareskog L. Rheumatoid arthritis and malignant lymphomas. Curr Opin Rheumatol 2004; 16: 254-261 [PMID: 15103253]
119 Buchbinder R, Barber M, Heuzenroeder L, Wluka AE, Giles G, Hall S, Harkness A, Lewis D, Littlejohn G, Miller MH, Ryan PF, Jolley D. Incidence of melanoma and other malignancies among rheumatoid arthritis patients treated with methotrexate. Arthritis Rheum 2008; 59: 794-799 [PMID: 18512713 DOI: 10.1002/art.23716]
120 Kamel OW, van de Rijn M, Weiss LM, Del Zoppo GJ, Hench PK, Robbins BA, Montgomery PG, Warnke RA, Dorfman RF. Brief report: reversible lymphomas associated with Epstein-Barr virus occurring during methotrexate therapy for rheumatoid arthritis and dermatomyositis. N Engl J Med 1993; 328: 1317-1321 [PMID: 8385742 DOI: 10.1056/NEJM199305063281806]
121 Rodriguez AA, Kerner J, Luna-Fineman S, Berry GJ. Hodgkin lymphoma following adalimumab for the treatment of Crohn’s disease in an adolescent. Dig Dis Sci 2014; 59: 2403-2405 [PMID: 24817339 DOI: 10.1007/s10620-014-3191-6]
122 Cassaday RD, Malik JT, Chang JE. Regression of Hodgkin lymphoma after discontinuation of a tumor necrosis factor inhibitor for Crohn’s disease: a case report and review of the literature. Clin Lymphoma Myeloma Leuk 2011; 11: 289-292 [PMID: 21658658 DOI: 10.1016/j.clml.2011.03.018]
123 Deepak P, Sifuentes H, Sherid M, Stobaugh D, Sadozai Y, Ehrenpreis ED. T-cell non-Hodgkin’s lymphomas reported to the FDA AERS with tumor necrosis factor-alpha (TNF-α) inhibitors: results of the REFURBISH study. Am J Gastroenterol 2013; 108: 99-105 [PMID: 23032984 DOI: 10.1038/ajg.2012.334]
124 Hanauer SB, Feagan BG, Lichtenstein GR, Mayer LF, Schreiber S, Colombel JF, Rachmilewitz D, Wolf DC, Olson A, Bao W, Rutgeerts P; ACCENT I Study Group. Maintenance infliximab for Crohn's disease: the ACCENT I randomised trial. Lancet 2002; 359: 1541-1549 [PMID: 12047962 DOI: 10.1016/S0140-6736(02)08512-4]
125 Rutgeerts P, D’Haens G, Targan S, Vasiliauskas E, Hanauer SB, Present DH, Mayer L, Van Hogezand RA, Braakman T, DeWoody KL, Schaible TF, Van Deventer SJ. Efficacy and safety of retreatment with anti-tumor necrosis factor antibody (infliximab) to maintain remission in Crohn’s disease. Gastroenterology 1999; 117: 761-769 [PMID: 10500056]
126 Lichtenstein GR, Feagan BG, Cohen RD, Salzberg BA, Diamond RH, Langholff W, Londhe A, Sandborn WJ. Drug therapies and the risk of malignancy in Crohn’s disease: results from the TREAT™ Registry. Am J Gastroenterol 2014; 109: 212-223 [PMID: 24394749 DOI: 10.1038/ajg.2013.441]
127 Fidder H, Schnitzler F, Ferrante M, Noman M, Katsanos K, Segaert S, Henckaerts L, Van Assche G, Vermeire S, Rutgeerts P. Long-term safety of infliximab for the treatment of inflammatory bowel disease: a single-centre cohort study. Gut 2009; 58: 501-508 [PMID: 18832524 DOI: 10.1136/gut.2008.163642]
128 Subramaniam K, Cherian M, Jain S, Latimer M, Corbett M, D’Rozario J, Pavli P. Two rare cases of Epstein-Barr virus-associated
Lam GY et al . LPD risk with immunosuppression use in IBD

192 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
lymphoproliferative disorders in inflammatory bowel disease patients on thiopurines and other immunosuppressive medications. Intern Med J 2013; 43: 1339-1342 [PMID: 24330365]
129 Parakkal D, Sifuentes H, Semer R, Ehrenpreis ED. Hepatosplenic T-cell lymphoma in patients receiving TNF-α inhibitor therapy: expanding the groups at risk. Eur J Gastroenterol Hepatol 2011; 23: 1150-1156 [PMID: 21941193 DOI: 10.1097/MEG.0b013e3283
4bb90a]130 Kotlyar DS, Osterman MT, Diamond RH, Porter D, Blonski WC,
Wasik M, Sampat S, Mendizabal M, Lin MV, Lichtenstein GR. A systematic review of factors that contribute to hepatosplenic T-cell lymphoma in patients with inflammatory bowel disease. Clin Gastroenterol Hepatol 2011; 9: 36-41.e1 [PMID: 20888436 DOI: 10.1016/j.cgh.2010.09.016]
P- Reviewer: Grossi L, Maharshak N, Miheller P S- Editor: Ma YJ L- Editor: A E- Editor: Liu SQ
Lam GY et al . LPD risk with immunosuppression use in IBD

Amporn Atsawarungruangkit, Supot Pongprasobchai
Amporn Atsawarungruangkit, Department of Family Medicine, Rajavithi Hospital, Bangkok 10400, Thailand
Supot Pongprasobchai, Division of Gastroenterology, Department of Medicine, Siriraj Hospital, Bangkok 10700, Thailand
Author contributions: Atsawarungruangkit A and Pongprasopchai S contributed equally to this work including article reviewing and paper writing.
Conflict-of-interest statement: Authors declare no conflict of interests for this article.
Open-Access: This article is an openaccess article which was selected by an inhouse editor and fully peerreviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work noncommercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: http://creativecommons.org/licenses/bync/4.0/
Correspondence to: Supot Pongprasobchai, MD, Division of Gastroenterology, Department of Medicine, Siriraj Hospital, 2 PranNok Road, Bangkok 10700, Thailand. [email protected] Telephone: +6612070903 Fax: +6624115013
Received: April 10, 2015 Peer-review started: April 12, 2015 First decision: July 10, 2015Revised: July 22, 2015 Accepted: September 10, 2015 Article in press: September 16, 2015Published online: November 15, 2015
AbstractChronic pancreatitis (CP) is a chronic inflammatory disease of the pancreas. The main symptom of patients with CP is chronic and severe abdominal pain. However, the pathophysiology of pain in CP remains obscure.
Traditionally, researchers believed that the pain was caused by anatomical changes in pancreatic structure. However, treatment outcomes based on such beliefs are considered unsatisfactory. The emerging explanations of pain in CP are trending toward neurobiological theories. This article aims to review current evidence regarding the neuropathophysiology of pain in CP and its potential implications for the development of new treatments for pain in CP.
Key words: Neurobiology; Neuropathophysiology; Pain; Pancreatic pain; Chronic pancreatitis
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Abdominal pain is the main symptom of patients with chronic pancreatitis (CP), yet the under-lying mechanisms are not well understood. The emerging explanations of pain in CP are trending toward neurobiological theories. This article reviews these emerging concepts and their potential implications for the development of new treatments for pain in CP. Three major concepts attempting to explain the pathogenesis of CP pain: Pancreatic nociception and sensitization-induced pain, neuropathic remodeling, and central mechanism of pancreatitis pain are summarized, along with the specific molecules involved in each and potential therapeutic targets.
Atsawarungruangkit A, Pongprasobchai S. Current understanding of the neuropathophysiology of pain in chronic pancreatitis. World J Gastrointest Pathophysiol 2015; 6(4): 193202 Available from: URL: http://www.wjgnet.com/21505330/full/v6/i4/193.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i4.193
INTRODUCTIONChronic pancreatitis (CP) is a persistent and chronic inflammatory disease of the pancreas. Approximately,
REVIEW
193 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Current understanding of the neuropathophysiology of pain in chronic pancreatitis
World J Gastrointest Pathophysiol 2015 November 15; 6(4): 193-202ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i4.193

80%-90% of patients with CP typically suffer from pancreatic pain[1], which is commonly described as a constant, severe, and dull pain in the mid-epigastrium that radiates to the back and worsens by with high-fat meals. Unsurprisingly, the pancreatic pain can have substantial psychological and economic impact on patients. In addition, a recent study confirmed that the life quality of patients with CP is significantly worsened by pain severity and disease-related complications[2].
The pathogenesis of pancreatic pain is still not fully understood. Thus, management of this pain cannot be specific, leading to unnecessarily high treatment costs and ineffective outcomes. Many theories have been proposed to explain the pain mechanism based on anatomical changes including high pressure within the pancreatic duct, high pressure in the pancreatic parenchyma, and complications of pancreatic and extra-pancreatic structures (i.e., pseudocysts, duodenal and bile duct obstruction, and peptic ulcer). These anatomical changes are believed to be noxious stimuli that activate pancreatic pain via nociceptive pathways. However, a number of human studies of CP have demonstrated evidence against the above theories, finding, for example, no relationship between pain and pancreatic duct pressure reduction[3,4], no relationship between pain and increase of parenchymal pressure[5], no pancreatic duct dilation in some patients with severe pancreatic pain[6], and no relationship between pain and severity of CP-related structural changes on imaging[7]. Therefore, the pain of CP patients cannot be explained by mechanical stimulation of nociceptive pathways alone.
Since the late 1990s, investigators have been trend-ing toward neurobiological theories to explain pain in CP[8]. Therefore, the main objective of this paper was to review the current neurobiological theories and emerging concepts that might lead to the development of new treatment regimens for alleviating pain in CP patients.
NEUROPHYSIOLOGY OF THE PANCREATIC PAINThe pancreas is innervated by a complex structure of two groups of afferent fibers. The first group consists of branches of the abdominal vagus nerve, and the second fibers that run through the celiac plexus and reach the lower thoracic segments of the spinal cord via the splanchnic nerves[9]. The latter group is best known for stimulating visceral pain.
The nociceptive pathway in the pancreas begins with nociceptors located at the ends of the primary afferent neurons and function as afferent nerve endings[10]. Unlike those in other visceral organs, these primary afferent neurons convey only pain stimuli. One special subset of theses nociceptors contains a group called “silent nociceptors”, which are only activated during inflammatory processes[11]. Furthermore, the pancreatic nociceptors can be activated by various noxious stimuli through
mechanosensitive and chemosensitive mechanisms[12]. The former mechanism is located on blood vessels that supply the pancreas and pancreatic parenchyma and can be stimulated by stretching, ischemia, and necrosis. The latter mechanism can be stimulated by inflammatory mediators, but the exact location of this mechanism is not completely known.
The pathogenesis of CP is strongly related to prolonged exposure to noxious stimuli, which causes chronic inflammation. Noxious stimuli not only stimulate nociceptors, but can also damage pancreatic tissues and nerves surrounding the pancreas[13]. The injured tissues can release pro-inflammatory mediators such as prostanoid, bradykinin, tachykinin, serotonin, and growth factors[14]. Induced by the above mediators, primary sensory neurons then become more sensitive to further stimulation by either noxious (hyperalgesia) or non-noxious (allodynia) stimuli. This process is called peripheral sensitization[15], which indicates that the noxious stimuli can evoke nociceptor plasticity. Moreover, there is another mechanism by which pain can be exacerbated via peripheral sensitization, which begins with the activation of silent nociceptors by peripheral inflammation, and the silent nociceptors consequently facilitate and increase afferent activities in the spinal cord.
Once stimulated by pro-inflammatory mediators, the nociceptors will transform the stimuli into action potentials by unbalancing the Na and K currents on the neuronal membrane. The action potentials travel along both unmyelinated C-fibers and small myelinated Aδ fibers of primary sensory neurons[11,12]. These neurons traverse paravertebral and prevertebral ganglia to synapse with secondary sensory neurons at laminae Ⅰ, Ⅱ, Ⅴ, and Ⅹ of the dorsal horn of the spinal cord at the T5-L2 level. Based on an animal study, the secondary sensory neurons related to the pancreas are primarily located at the T10-T11 level[12]. Consequently, the primary sensory axons release glutamate, substance P, and calcitonin gene-related peptide (CGRP). Glutamate activates both α-amino-3-hydroxy-5-methyl-4-isoxazole propionate and N-methyl-D-aspartate (NMDA) receptors, while substance P activates NK1 receptors[16,17]. Thesethree receptors are located on secondary sensory neurons within the dorsal horn. At this level of stimu-lation, prolonged stimulation from peripheral sensitization can facilitate excitation of dorsal horn neurons, which can increase spontaneous activities, decrease the firing threshold, and expand the receptive field of the dorsal horn neurons. This process is called central sensitization and can result in hyperalgesia and allodynia[11].
After the activation of secondary sensory neurons, action potentials are generated and transmitted to the thalamus via the spinothalamic tract to activate tertiary sensory neurons. These tertiary sensory neurons then transmit the signal to the somatosensory cortex for cognitive integration of pain and the limbic system and hypothalamus for autonomic/affective integration of the pain[18].
194 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Atsawarungruangkit A et al . Neuropathophysiology of pain in chronic pancreatitis

Furthermore, the central nervous system (CNS) can modulate pain signaling at the spinal cord level via either facilitation, increasing the spinal transmission of pain impulses, or inhibition, decreasing the spinal trans-mission of pain impulses. The combination of facilitation and inhibition generates the signal that will determine the pain perception in the brain.
After the primary sensory neurons are activated, neurotransmitters (glutamate, substance P, and CGRP) are not only released to the dorsal horn of the spinal cord, but also to primary nerve endings located on the pancreas, where they act as inflammatory mediators that create pancreatic inflammation characterized by vasodilation, edema, and neutrophil infiltration. This process is also known as neurogenic inflammation[19-21]. Additionally, this neurogenic inflammation can facilitate the activation of peripheral sensitization[10].
NEUROPATHOPHYSIOLOGY OF PANCREATIC PAINChronic inflammation in the pancreas has been shown to spread to the pancreatic nerve[22,23]. Additionally, perineural inflammatory cells including eosinophils, CD4+ and CD8+ lymphocytes, macrophages, and mast cells are evidenced in patients with painful CP[24-27]. This finding is consistent with the increased percentage of eosinophils observed in perineural inflammatory cell infiltrates, which may be related to the release of a nociceptive substance[13]. In addition, numerous studies[28-34] have reported the increase of various perineural inflammatory mediators including histamine, serotonin, interleukin, bradykinin, substance P, CGRP, tumor necrosis factor-alpha, and several neurotrophins [i.e., growth-associated protein 43, brain-derived neurotrophic factor (BDNF), and nerve growth factor (NGF)]. Specifically, BDNF and NGF up-regulation has been shown in CP patients[24,26].
Such evidence has recently become the main focus of many studies attempting to explain the pathogenesis of pain based on three concepts: pancreatic nociception and sensitization-induced pain, neuropathic remodeling (neuropathic pain), and central mechanism of pan-creatitis pain. Each of these aspects is complex and involves specific molecules that are described in the following sections.
PANCREATIC NOCICEPTION AND SENSITIZATION-INDUCED PAINThere is much evidence to support that peripheral and central sensitization is largely associated with the pancreatic pain in CP. The evidence related to the mole-cules and receptors that have been found to be involved in the sensitization mechanisms will be discussed one-by-one in the following paragraphs.
The transient receptor potential (TRP) family is a group of ion channels localized mainly to the plasma membrane of neurons. Three molecules strongly related to pain and
inflammation in the TRP family are TRP vanilloid 1 (TRPV1), TRPV4, and TRP ankyrin 1 (TRPA1)[35]. These three TRP channels are also associated with pain in CP patients through the sensitization of pancreatic afferent neurons and development of neurogenic inflammation. The primary sensory nerve endings that supply the pancreas contain these three types of TRP, which can be stimulated by specific stimuli including inflammatory mediators. After the receptors are stimulated, primary sensory neurons then release substance P and CGRP at both the spinal cord and peripheral sites, thus causing pancreatic inflammation via neurogenic inflammation[36-40]. The mechanism of peripheral sensitization (Figure 1) is discussed below.
TRPV1TRPV1 can be directly activated by many factors, including heat, extra-cellular proton and tissue acidosis, capsaicin, biologically active compounds (anandamide and hydrogen sulfide), and endogenous lipid metabolites from the arachidonic acid pathway[41,42]. Furthermore, TRPV1 can be indirectly activated by pro-inflammatory bradykinin and pro-inflammatory leukotriene[43]. By modulating TRPV1 activity, pro-inflammatory bradykinin can indirectly activate TRPV1 via B2 receptors residing on primary sensory neurons. By binding to their leukotriene B4 receptors, pro-inflammatory leukotriene B4 can activate TRPV1 via an intra-neural signaling pathway. Furthermore, pro-inflammatory agents can sensitize TRPV1 by reducing the threshold of thermal stimuli (hyperalgesia)[44].
In animal and human studies, TRPV1 plays an important role in explaining pain in CP. After TRPV1 receptor activation by capsaicin in rats with induced CP, peripheral sensitization is evidenced by the significant upregulation of TRPV1 at both mRNA and protein levels in the dorsal root ganglion (DRG) and pancreas-specific sensory neurons[45]. Moreover, the same study found significant reduction of pain behavior and hyperalgesia after administration of a systemic TRPV1 antagonist. Significant upregulation of TRPV1 is also seen in the pancreatic tissue of patients with painful CP; however, no relationship was found between the pain score level and the level of TRPV1 expression[46].
TRPA1TRPA1 is responsive to various stimuli that can be categorized into five groups: The pungent ingredients of spices, environmental irritants, endogenous agonists of TRPA1[39], cyclopentenone prostaglandins, and general anesthetics[47]. The pungent ingredients of spices include mustard oil[48], garlic[48], and cinnamon[48,49], and enviro-nmental irritants include acrolein[48,50], formaldehyde[48,51], and cigarette smoke[36,48]. Cyclopentenone prostaglandins include PGA2, PGA1, and PGJ2[52,53]. Pro-inflammatory agents also sensitize TRPA1 leading to hyperalgesia[54-56].
TRPV4TRPV4 responds to changes in tonicity[57,58], moderate
195 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Atsawarungruangkit A et al . Neuropathophysiology of pain in chronic pancreatitis

196 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
detected in sensory neurons supplying the pancreas; in fact, primary sensory neurons could be activated and sensitized by administering PAR2-specific proteinase activating peptide and trypsin in an in vivo study[66,67]. Moreover, both PAR2-specific proteinase activating peptide and trypsin-induced behavioral pain response have been observed in awake rats[67]. Another study discovered that tryptase, a substance released from activated mast cells, can stimulate PAR2[27], which might explain the relationship between mast cells and pain in CP patients. In an experimental animal model of pancreatitis pain, the administration of two proteinase inhibitors (camostat mesylate and nafamostat mesylate) reduced sensitivity to abdominal pain[68]. Likewise, nafamostat was associated with a significant reduction of pain duration induced by acute pancreatitis[69].
Based on in vitro findings, PAR2 activation causes TRPV1 sensitization by enhancing capsaicin; con-sequently, this process leads to the significant release of CGRP[70]. Similarly, in in vivo studies, PAR2 activation resulted in pain-related behavior[55,70,71]. As additional supporting evidence that PAR2 is involved in the development of hyperalgesia, PAR2 was significantly upregulated in DRG neurons along with decreased thermal withdrawal latencies in a rat model of CP[72]. In short, PAR2 agonist peptides, trypsin and tryptase, are related to the pathogenesis of pain in CP via nociception and sensitization caused by the interaction between TRPV1 and PAR2.
heat (> 27 ℃)[37], and mechanical pain[37]. Changes in tonicity can cause cell swelling and activate phospholipase A2; this process leads to the generation of arachidonic acid[59], which is an endogenous agonist of TRPV4. In addition, 4α-phorbol 12,13-didecanoate (4αPDD) is a synthetic TRPV4 agonist[60,61]. Similar to TRPV1 and TRPA1, pro-inflammatory agents can sensitize TRPV4 causing hyperalgesia to mechanical stimuli[62-64].
To the best of our knowledge, the first evidence that TRPA1 and TRPV4 contribute to pancreatitis pain was reported in rats with induced acute pancreatitis[48]. Another study also demonstrated that TRPA1 mediates CP pain in mice[54]. In a recent study using mice in which CP was induced through repetitive cerulein injections, TRPV1 and TRPA1 antagonists were important in allevia-ting neurogenic inflammation in pancreatitis, reducing pain-related behavior, and preventing the transition from acute to chronic inflammation[65]. Therefore, TRPV1, TRPA1, and TRPV4 are likely to be targets for therapeutic pain management in CP patients by reducing peripheral sensitization and neuropathic inflammation.
Proteinase-activated receptor 2Proteinase-activated receptor 2 (PAR2) is one of the chief regulators of pancreatic exocrine secretion in pancreatic acinar cells and ductal epithelium. Notably, trypsin is recognized as the strongest activator of PAR2. There is also evidence supporting a relationship between PAR2 and pancreatic pain. PAR2 expression was
Atsawarungruangkit A et al . Neuropathophysiology of pain in chronic pancreatitis
Figure 1 The mechanism of peripheral sensitization. PAR2: Proteinase-activated receptor 2; NGF: Nerve growth factor; TRPA1: Transient receptor potential ankyrin 1; TRPV1: Transient receptor potential vanilloid 1; BDNF: Brain-derived neurotrophic factor; GAP43: Growth-associated protein 43; LTB4: Leukotriene B4.
Pancreatic acinar cells Mast cells
Trypsin
PAR2 TryptaseSpice, pungent ingredient,
anesthetics, irritants, prostaglandins NGF
Heat, H+, capsacin, anandamide
LTB4Bradykinin
TRPA1NGF/TrkA pathway
Kv Nav PAR2 TRPV1 LTB4 B2TRPV4
Arteminreceptor BDNF
receptor
Pressure osmolality
Artemin
BDNF
Pro-inflammatory agents
Neuropathy process GAP43
Fractalkine

197 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
NGFNGF, a type of neurotrophin, is a protein important for the growth, maintenance, regulation of survival, and specialization of sensory neurons. Moreover, NGF is an essential mediator of peripheral sensitization[73]. Although the islets of pancreatocytes typically generate NGF, NGF was found to be upregulated and surprisingly expressed in pancreatic acinar cells and ductal epithe-lium in a rat model of pancreatitis[74]. However, the upregulation of NGF returned to normal after the pan-creatic inflammation resolved[16]. Many studies have attempted to explain the mechanism of NGF-induced pancreatitis pain on sensitization via modulation of TRPV1 and excitability of K and Na currents[73,75-77]. Another hypothesized mechanism underlying pain in CP is activation of the NGF/trkA pathway[78,79]. In a study of rats with CP induced by trinitrobenzene sulfonic acid, both anti-NGF antibodies and trkA-immunoglobulin G substantially reduced hyperalgesia[80,81].
Artemin Artemin is a neurotrophin classified as a glial cell line-derived neurotrophic factor. Overexpression of artemin and its co-receptor GFR alpha 3 has been reported to strongly relate to the increased frequency and intensity of pain in rats with CP[82].
BDNFBDNF is also a member of the neurotrophin family found in the brain and periphery. An in vivo study reported that BDNF is upregulated in primary sensory neurons in rats with CP, and that BDNF antagonist treatment was associated with a reduction of pain-related behavior in these animals[83]. Another study of pancreatic tissue in patients with CP found that pain was positively related with BDNF levels and increased in CP patients compared to healthy control. These findings suggest that BDNF is essential to the nociceptive pathway of CP.
Other substances Studies have also reported associations between pain in CP and other substances that could be related to peripheral sensitization, for example, the over-expression of interleukin 1[84], interleukin 6[85], interleukin 8[86], and fractalkine[87].
Neurotransmitter expressionPrevious findings in patients with painful CP indicate overexpression of neurokinin 1[88], neurokinin 2[88], CGRP[16], and substance P[16,88]. Therefore, overexpression of these neurotransmitters may result from activation of nociceptive pathways and peripheral sensitization.
PANCREATIC NEUROPATHIC REMODELING-INDUCED PAIN In clinico-pathological studies, the intra-pancreatic nerves in patients with painful CP demonstrate immune
cell infiltration, indicating pancreatic neuritis[13,89], and characteristics of pancreatic neuropathy, which can be described as the increase of neural density, hypertrophy, and spouting[13,90-92]. Both pancreatic neuritis and pancreatic neuropathy are believed to relate with the inflammatory process, which is a key pathogenic factor in CP as indicated by the following evidence. The increase of fractalkine and its receptor is correlated with fibrosis, neuropathic changes, pain duration of CP and the degree of inflammatory cell infiltrate[87,91,92]. Moreover, the expression of growth-associated protein 43 (GAP43), which is a member of the neurotrophin family, is reported to have a relationship with pancreatic neuropathy, pancreatic neuritis, and pancreatic pain. Consequently, GAP43 may be considered a potential marker of neuronal plasticity during development and injury[87,89,91,92].
Patients with painful CP have been reported to demon-strate significant alterations in pancreatic innervation, with a marked decrease in sympathetic innervation but no statistically significant difference in cholinergic innervation[92]. In the same study, stronger expression of pain-related behavior was also noted in patients with painful CP, indicating neuronal regeneration after neuron injury.
In conclusion, the inflammatory process leaves pancreatic neurons damaged and characterized as showing either neuropathy or neuritis. Correspondingly, these neurons express GAP43, leading to the remodeling of pancreatic innervation. This process might explain pancreatic pain in CP patients. Such a process is similar to pancreatic nociception and sensitization-induced pain in the sense that both processes involve inflammatory mediators. However, the mechanism by which inflammatory mediators induce neuropathic pain is by destroying the neurons, leading to permanent neuronal lesions without involving noxious stimuli and the sensitization process.
CENTRAL MECHANISM OF PANCREATITIS-INDUCED PAINCentral sensitizationAs previously described, several factors can induce pain in CP by triggering the CNS, for instance, chronic stimulation of pain through nociceptive pathways, peri-pheral sensitization caused by inflammatory processes in the pancreas, and nerve damage. Consequently, prolonged peripheral sensitization can lead to central sensitization, which will be discussed next.
Using quantitative sensory testing in human experi-ments, researchers found that the brain activity of patients with CP demonstrated increased areas of referred pain and increased heterogeneity of referred pain location compared to the control group after electrical stimulation of the esophagus, stomach, and duodenum[93]. The sensitization caused by CP could decrease the pain threshold and increase the referred pain area[94,95].
Atsawarungruangkit A et al . Neuropathophysiology of pain in chronic pancreatitis

198 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
By using electroencephalography (EEG) to measure brain activities, studies of pain in CP can be categorized as either resting-state EEG or evoked potential (EP) tests[84,96]. In resting-state EEG, alpha activities were found to demonstrate increased amplitude strength in CP patients compared to healthy volunteers[97], and pain duration was negatively correlated with the average peak alpha frequency[98]. Notably, the relationship between chronic pain and the change in alpha activity could be the result of thalamocortical dysrhythmia, which is activated by T-type calcium channels[99]. In EP tests, constant electrical stimulation of the upper gastrointestinal tract significantly decreased latencies of the early EP components in CP patients compared to healthy volunteers[93]. Moreover, hyperalgesia and prolonged latencies of early visceral EPs components in the frontal region of the cortex were seen following electrical stimulation in CP patients compared to healthy subjects[100].
As observed with functional magnetic resonance imaging, pain sensation is processed and localized in somatosensory cortex, insula, anterior cingulate cortex, prefrontal cortex, and thalamus. Recently reported evidence indicates that plasticity, i.e., functional or structural changes, in the CNS may be associated with pain in chronic syndromes. The structural reduction of cortical thickness[101] and microstructural changes in the insula and frontal cortex[102] also have been observed in magnetic resonance imaging studies.
The above findings support the hypothesis that the pain experienced by CP patients can be triggered by central sensitization, which is derived from sustained and increased peripheral nociceptive drivers. Moreover, recent studies have demonstrated that descending inhibitory modulators are significantly impaired in patients with CP compared to healthy controls[95,103]. Descending facilitation from the brainstem was also reported to be a critical factor in pancreatic pain in rats with CP[20].
POTENTIAL APPLICATIONSGenerally, drug discovery involves finding a new drug with the ability to increase or decrease the activities of selected targets or unrelated targets. The greater our
understanding of the neuropathophysiology of pain in CP, the better our opportunity to identify potential treatment alternatives. Currently, there are two groups of potential treatment alternatives and their drug targets, which are summarized in Table 1. The first group of potential treatment alternatives is directed at attenuating the peripheral sensitization process by targeting related molecules and receptors, such as NGF, TRPV1, PAR2, trypsin, tryptase, interleukin 1, and interleukin 6. The second group of potential treatment alternatives focuses on attenuating the central sensitization process.
Anti-NGF antibody demonstrated a significant effect on attenuating the changes in the excitation of pancreatic nociceptors in rats with CP[81]. Tanezumab, a humanized monoclonal antibody with specific binding to NGF, is able to relieve chronic pain in many conditions, for instance, chronic low back pain[8,104], interstitial cystitis[8,105,106], and osteoarthritis knee pain[8,107,108]. However, to the best of our knowledge, there has not been any human study to date using anti-NGF in CP.
A TRPV1 antagonist remarkably reduced both visceral pain behavior and referred somatic hyperalgesia in rats with CP[45]. Since not only TRPA1 but also TRPV4 are related to the peripheral sensitization of pain in CP, theoretically both TRPV1 and TRPV4 antagonists should be able to attenuate pain in CP. Nevertheless, we have not seen any study using a TRPV4 antagonist in CP.
Although PAR2 is the receptor that induces peripheral sensitization of pain in CP, direct PAR2 antagonists are very difficult to create[8]. As already mentioned, both trypsin and tryptase are agonists of the PAR2 receptor. Therefore, one researcher proposed that PAR2-sensitized pain can be inhibited indirectly by using trypsin inhibitors and a mast cell stabilizer (ketotifen)[8].
In the inflammatory process, interleukin 1 and interleukin 6 are associated with pain in CP. As a result, antagonists of both these interleukins may be able to attenuate pain. Researchers found that a recombinant interleukin-1 receptor antagonist[109] and interleukin-6 antagonist[85] can have an effect on attenuating pan-creatitis-induced pain in rats with CP.
Central sensitization of pain in CP can be influenced by NMDA receptors, thalamocortical dysrhythmia, and impaired modulation pathways. Consequently, we can attenuate pain in CP by modifying the activities of these influencing factors. Several known drugs can reduce the effect of central sensitization, such as ketamine[8,110,111], dextromethrophan[8,112], pregabalin[113-115], tricyclic anti-depressants[84], and noradrenaline reuptake inhibitors[84].
CONCLUSION Chronic pain is an important issue that significantly lowers quality of life in patients with CP. The theories for underlying causes of pancreatic pain in CP have been shifting away from anatomical changes of pancreatic structure to changes in neurobiological structure, which include peripheral sensitization-induced pain, neuropathic remodeling, and central sensitization of
Table 1 Potential treatment alternatives and their drug targets
Drug target Potential treatment alternatives
NGF Tanezumab TRPV1 TRPV1 antagonistPAR2 Trypsin inhibitors Mast cell KetotifenInterleukin 1 Recombinant interleukin-1 receptor antagonistInterleukin 6 Interleukin-6 antagonistCentral sensitization Ketamine, dextromethrophan, pregabalin,
tricyclic antidepressants, and noradrenaline reuptake inhibitors
NGF: Nerve growth factor; TRPV1: Transient receptor potential vanilloid 1; PAR2: Proteinase-activated receptor 2.
Atsawarungruangkit A et al . Neuropathophysiology of pain in chronic pancreatitis

199 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
pancreatic pain. Furthermore, researchers have identi-fied numerous molecules related to pancreatic pain in CP, for example, TRPV1, TRPA1, TRPV4, PAR2, NGF, artemin, BDBF, GAP43, and fractalkine. As a result, the neuropathophysiological mechanisms of pain in CP show strong potential as targets for drug discovery to relieve the pain and improve quality of life in this patient population.
REFERENCES1 Andrén-Sandberg A, Hoem D, Gislason H. Pain management
in chronic pancreatitis. Eur J Gastroenterol Hepatol 2002; 14: 957970 [PMID: 12352215]
2 Olesen SS, Juel J, Nielsen AK, Frøkjær JB, WilderSmith OH, Drewes AM. Pain severity reduces life quality in chronic pancreatitis: Implications for design of future outcome trials. Pancreatology 2014; 14: 497502 [PMID: 25455540 DOI: 10.1016/j.pan.2014.09.009]
3 Okazaki K, Yamamoto Y, Ito K. Endoscopic measurement of papillary sphincter zone and pancreatic main ductal pressure in patients with chronic pancreatitis. Gastroenterology 1986; 91: 409418 [PMID: 3721126]
4 Renou C, Grandval P, Ville E, Laugier R. Endoscopic treatment of the main pancreatic duct: correlations among morphology, manometry, and clinical followup. Int J Pancreatol 2000; 27: 143149 [PMID: 10862513 DOI: 10.1385/IJGC:27:2:143]
5 Manes G, Büchler M, Pieramico O, Di Sebastiano P, Malfertheiner P. Is increased pancreatic pressure related to pain in chronic pancreatitis? Int J Pancreatol 1994; 15: 113117 [PMID: 8071569]
6 Walsh TN, Rode J, Theis BA, Russell RC. Minimal change chronic pancreatitis. Gut 1992; 33: 15661571 [PMID: 1452086]
7 Bahuva R, Walsh RM, Kapural L, Stevens T. Morphologic abnormalities are poorly predictive of visceral pain in chronic pancreatitis. Pancreas 2013; 42: 610 [PMID: 22750976 DOI: 10.1097/MPA.0b013e318258cd9c]
8 Pasricha PJ. Unraveling the mystery of pain in chronic pancreatitis. Nat Rev Gastroenterol Hepatol 2012; 9: 140151 [PMID: 22269952 DOI: 10.1038/nrgastro.2011.274]
9 Cervero F. Sensory innervation of the viscera: peripheral basis of visceral pain. Physiol Rev 1994; 74: 95138 [PMID: 8295936]
10 Barreto SG, Saccone GT. Pancreatic nociceptionrevisiting the physiology and pathophysiology. Pancreatology 2012; 12: 104112 [PMID: 22487519 DOI: 10.1016/j.pan.2012.02.010]
11 Olesen SS, Krarup AL, Brock C, Drewes AM. Gastrointestinal sensations and pain: a review on basic, experimental and clinical findings. Minerva Gastroenterol Dietol 2009; 55: 301313 [PMID: 19829286]
12 Knowles CH, Aziz Q. Basic and clinical aspects of gastrointestinal pain. Pain 2009; 141: 191209 [PMID: 19155134 DOI: 10.1016/j.pain.2008.12.011]
13 Keith RG, Keshavjee SH, Kerenyi NR. Neuropathology of chronic pancreatitis in humans. Can J Surg 1985; 28: 207211 [PMID: 3995416]
14 Vardanyan M, Rilo HL. Pathogenesis of chronic pancreatitisinduced pain. Discov Med 2010; 9: 304310 [PMID: 20423674]
15 Sandkühler J. Models and mechanisms of hyperalgesia and allodynia. Physiol Rev 2009; 89: 707758 [PMID: 19342617]
16 Winston JH, He ZJ, Shenoy M, Xiao SY, Pasricha PJ. Molecular and behavioral changes in nociception in a novel rat model of chronic pancreatitis for the study of pain. Pain 2005; 117: 214222 [PMID: 16098667 DOI: 10.1016/j.pain.2005.06.013]
17 Büchler M, Weihe E, Friess H, Malfertheiner P, Bockman E, Müller S, Nohr D, Beger HG. Changes in peptidergic innervation in chronic pancreatitis. Pancreas 1992; 7: 183192 [PMID: 1372738]
18 Lieb JG, Forsmark CE. Review article: pain and chronic pancreatitis. Aliment Pharmacol Ther 2009; 29: 706719 [PMID: 19284407 DOI: 10.1111/j.13652036.2009.03931.x]
19 Liddle RA, Nathan JD. Neurogenic inflammation and pancreatitis.
Pancreatology 2004; 4: 551559; discussion 559560 [PMID: 15550764 DOI: 10.1159/000082180]
20 Vera-Portocarrero L, Westlund KN. Role of neurogenic inflammation in pancreatitis and pancreatic pain. Neurosignals 2005; 14: 158165 [PMID: 16215298 DOI: 10.1159/000087654]
21 Anaparthy R, Pasricha PJ. Pain and chronic pancreatitis: is it the plumbing or the wiring? Curr Gastroenterol Rep 2008; 10: 101106 [PMID: 18462594]
22 Di Sebastiano P, di Mola FF, Buchler MW, Friess H. Pathogenesis of pain in chronic pancreatitis. Dig Dis 2004; 22: 267272 [PMID: 15753609]
23 Bornman PC, Marks IN, Girdwood AW, Berberat PO, Gulbinas A, Büchler MW. Pathogenesis of pain in chronic pancreatitis: ongoing enigma. World J Surg 2003; 27: 11751182 [PMID: 14574490 DOI: 10.1007/s002680037235x]
24 Shrikhande SV, Martignoni ME, Shrikhande M, Kappeler A, Ramesh H, Zimmermann A, Büchler MW, Friess H. Comparison of histological features and inflammatory cell reaction in alcoholic, idiopathic and tropical chronic pancreatitis. Br J Surg 2003; 90: 15651572 [PMID: 14648737 DOI: 10.1002/bjs.4353]
25 Goecke H, Forssmann U, Uguccioni M, Friess H, ConejoGarcia JR, Zimmermann A, Baggiolini M, Büchler MW. Macrophages infiltrating the tissue in chronic pancreatitis express the chemokine receptor CCR5. Surgery 2000; 128: 806814 [PMID: 11056444 DOI: 10.1067/msy.2000.108613]
26 Hunger RE, Mueller C, Z‘graggen K, Friess H, Büchler MW. Cytotoxic cells are activated in cellular infiltrates of alcoholic chronic pancreatitis. Gastroenterology 1997; 112: 16561663 [PMID: 9136845]
27 Hoogerwerf WA, Gondesen K, Xiao SY, Winston JH, Willis WD, Pasricha PJ. The role of mast cells in the pathogenesis of pain in chronic pancreatitis. BMC Gastroenterol 2005; 5: 8 [PMID: 15745445 DOI: 10.1186/1471230X58]
28 Detlefsen S, Sipos B, Feyerabend B, Klöppel G. Fibrogenesis in alcoholic chronic pancreatitis: the role of tissue necrosis, macrophages, myofibroblasts and cytokines. Mod Pathol 2006; 19: 10191026 [PMID: 16680157 DOI: 10.1038/modpathol.3800613]
29 Di Sebastiano P. The quality of life in chronic pancreatitis: the role of surgery. JOP 2006; 7: 120121 [PMID: 16407633]
30 Talukdar R, Saikia N, Singal DK, Tandon R. Chronic pancreatitis: evolving paradigms. Pancreatology 2006; 6: 440449 [PMID: 16847381 DOI: 10.1159/000094561]
31 Madro A, Celiński K, Słomka M. The role of pancreatic stellate cells and cytokines in the development of chronic pancreatitis. Med Sci Monit 2004; 10: RA166RA170 [PMID: 15232519]
32 Zhu ZW, Friess H, Wang L, Zimmermann A, Büchler MW. Brainderived neurotrophic factor (BDNF) is upregulated and associated with pain in chronic pancreatitis. Dig Dis Sci 2001; 46: 16331639 [PMID: 11508661]
33 DiMagno EP. Toward understanding (and management) of painful chronic pancreatitis. Gastroenterology 1999; 116: 12521257 [PMID: 10220520]
34 Friess H, Zhu ZW, di Mola FF, Kulli C, Graber HU, AndrenSandberg A, Zimmermann A, Korc M, Reinshagen M, Büchler MW. Nerve growth factor and its highaffinity receptor in chronic pancreatitis. Ann Surg 1999; 230: 615624 [PMID: 10561084]
35 Nilius B, Owsianik G, Voets T, Peters JA. Transient receptor potential cation channels in disease. Physiol Rev 2007; 87: 165217 [PMID: 17237345 DOI: 10.1152/physrev.00021.2006]
36 Andrè E, Campi B, Materazzi S, Trevisani M, Amadesi S, Massi D, Creminon C, Vaksman N, Nassini R, Civelli M, Baraldi PG, Poole DP, Bunnett NW, Geppetti P, Patacchini R. Cigarette smokeinduced neurogenic inflammation is mediated by alpha,betaunsaturated aldehydes and the TRPA1 receptor in rodents. J Clin Invest 2008; 118: 25742582 [PMID: 18568077]
37 Güler AD, Lee H, Iida T, Shimizu I, Tominaga M, Caterina M. Heatevoked activation of the ion channel, TRPV4. J Neurosci 2002; 22: 64086414 [PMID: 12151520]
38 Su HC, Bishop AE, Power RF, Hamada Y, Polak JM. Dual intrinsic and extrinsic origins of CGRP and NPYimmunoreactive nerves of rat gut and pancreas. J Neurosci 1987; 7: 26742687 [PMID:
Atsawarungruangkit A et al . Neuropathophysiology of pain in chronic pancreatitis

200 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
2442325]39 Trevisani M, Siemens J, Materazzi S, Bautista DM, Nassini R,
Campi B, Imamachi N, Andrè E, Patacchini R, Cottrell GS, Gatti R, Basbaum AI, Bunnett NW, Julius D, Geppetti P. 4Hydroxynonenal, an endogenous aldehyde, causes pain and neurogenic inflammation through activation of the irritant receptor TRPA1. Proc Natl Acad Sci USA 2007; 104: 1351913524 [PMID: 17684094]
40 Vergnolle N, Cenac N, Altier C, Cellars L, Chapman K, Zamponi GW, Materazzi S, Nassini R, Liedtke W, Cattaruzza F, Grady EF, Geppetti P, Bunnett NW. A role for transient receptor potential vanilloid 4 in tonicityinduced neurogenic inflammation. Br J Pharmacol 2010; 159: 11611173 [PMID: 20136846 DOI: 10.1111/j.14765381.2009.00590.x]
41 Hwang SW, Cho H, Kwak J, Lee SY, Kang CJ, Jung J, Cho S, Min KH, Suh YG, Kim D, Oh U. Direct activation of capsaicin receptors by products of lipoxygenases: endogenous capsaicinlike substances. Proc Natl Acad Sci USA 2000; 97: 61556160 [PMID: 10823958]
42 McVey DC, Vigna SR. The role of leukotriene B4 in Clostridium difficile toxin Ainduced ileitis in rats. Gastroenterology 2005; 128: 13061316 [PMID: 15887113]
43 Geppetti P, Bertrand C, Ricciardolo FL, Nadel JA. New aspects on the role of kinins in neurogenic inflammation. Can J Physiol Pharmacol 1995; 73: 843847 [PMID: 8846419]
44 Cesare P, McNaughton P. A novel heatactivated current in nociceptive neurons and its sensitization by bradykinin. Proc Natl Acad Sci USA 1996; 93: 1543515439 [PMID: 8986829]
45 Xu GY, Winston JH, Shenoy M, Yin H, Pendyala S, Pasricha PJ. Transient receptor potential vanilloid 1 mediates hyperalgesia and is upregulated in rats with chronic pancreatitis. Gastroenterology 2007; 133: 12821292 [PMID: 17698068]
46 Hartel M, di Mola FF, Selvaggi F, Mascetta G, Wente MN, Felix K, Giese NA, Hinz U, Di Sebastiano P, Büchler MW, Friess H. Vanilloids in pancreatic cancer: potential for chemotherapy and pain management. Gut 2006; 55: 519528 [PMID: 16174661 DOI: 10.1136/gut.2005.073205]
47 Matta JA, Cornett PM, Miyares RL, Abe K, Sahibzada N, Ahern GP. General anesthetics activate a nociceptive ion channel to enhance pain and inflammation. Proc Natl Acad Sci USA 2008; 105: 87848789 [PMID: 18574153 DOI: 10.1073/pnas.0711038105]
48 Ceppa E, Cattaruzza F, Lyo V, Amadesi S, Pelayo JC, Poole DP, Vaksman N, Liedtke W, Cohen DM, Grady EF, Bunnett NW, Kirkwood KS. Transient receptor potential ion channels V4 and A1 contribute to pancreatitis pain in mice. Am J Physiol Gastrointest Liver Physiol 2010; 299: G556G571 [PMID: 20539005 DOI: 10.1152/ajpgi.00433.2009]
49 Jordt SE, Bautista DM, Chuang HH, McKemy DD, Zygmunt PM, Högestätt ED, Meng ID, Julius D. Mustard oils and cannabinoids excite sensory nerve fibres through the TRP channel ANKTM1. Nature 2004; 427: 260265 [PMID: 14712238]
50 Bautista DM, Jordt SE, Nikai T, Tsuruda PR, Read AJ, Poblete J, Yamoah EN, Basbaum AI, Julius D. TRPA1 mediates the inflammatory actions of environmental irritants and proalgesic agents. Cell 2006; 124: 12691282 [PMID: 16564016 DOI: 10.1016/j.cell.2006.02.023]
51 McNamara CR, MandelBrehm J, Bautista DM, Siemens J, Deranian KL, Zhao M, Hayward NJ, Chong JA, Julius D, Moran MM, Fanger CM. TRPA1 mediates formalininduced pain. Proc Natl Acad Sci USA 2007; 104: 1352513530 [PMID: 17686976 DOI: 10.1073/pnas.0705924104]
52 Materazzi S, Nassini R, Andrè E, Campi B, Amadesi S, Trevisani M, Bunnett NW, Patacchini R, Geppetti P. Coxdependent fatty acid metabolites cause pain through activation of the irritant receptor TRPA1. Proc Natl Acad Sci USA 2008; 105: 1204512050 [PMID: 18687886]
53 Taylor-Clark TE, Undem BJ, Macglashan DW, Ghatta S, Carr MJ, McAlexander MA. Prostaglandininduced activation of nociceptive neurons via direct interaction with transient receptor potential A1 (TRPA1). Mol Pharmacol 2008; 73: 274281 [PMID: 18000030 DOI: 10.1124/mol.107.040832]
54 Cattaruzza F, Johnson C, Leggit A, Grady E, Schenk AK, Cevikbas F, Cedron W, Bondada S, Kirkwood R, Malone B, Steinhoff M, Bunnett N, Kirkwood KS. Transient receptor potential ankyrin 1 mediates chronic pancreatitis pain in mice. Am J Physiol Gastrointest Liver Physiol 2013; 304: G1002G1012 [PMID: 23558009 DOI: 10.1152/ajpgi.00005.2013]
55 Dai Y, Wang S, Tominaga M, Yamamoto S, Fukuoka T, Higashi T, Kobayashi K, Obata K, Yamanaka H, Noguchi K. Sensitization of TRPA1 by PAR2 contributes to the sensation of inflammatory pain. J Clin Invest 2007; 117: 19791987 [PMID: 17571167 DOI: 10.1172/JCI30951]
56 Wang S, Dai Y, Fukuoka T, Yamanaka H, Kobayashi K, Obata K, Cui X, Tominaga M, Noguchi K. Phospholipase C and protein kinase A mediate bradykinin sensitization of TRPA1: a molecular mechanism of inflammatory pain. Brain 2008; 131: 12411251 [PMID: 18356188 DOI: 10.1093/brain/awn060]
57 Liedtke W, Choe Y, MartíRenom MA, Bell AM, Denis CS, Sali A, Hudspeth AJ, Friedman JM, Heller S. Vanilloid receptorrelated osmotically activated channel (VROAC), a candidate vertebrate osmoreceptor. Cell 2000; 103: 525535 [PMID: 11081638]
58 Liedtke W, Friedman JM. Abnormal osmotic regulation in trpv4/ mice. Proc Natl Acad Sci USA 2003; 100: 1369813703 [PMID: 14581612]
59 Pedersen S, Lambert IH, Thoroed SM, Hoffmann EK. Hypotonic cell swelling induces translocation of the alpha isoform of cytosolic phospholipase A2 but not the gamma isoform in Ehrlich ascites tumor cells. Eur J Biochem 2000; 267: 55315539 [PMID: 10951212]
60 Watanabe H, Davis JB, Smart D, Jerman JC, Smith GD, Hayes P, Vriens J, Cairns W, Wissenbach U, Prenen J, Flockerzi V, Droogmans G, Benham CD, Nilius B. Activation of TRPV4 channels (hVRL2/mTRP12) by phorbol derivatives. J Biol Chem 2002; 277: 1356913577 [PMID: 11827975 DOI: 10.1074/jbc.M200062200]
61 Watanabe H, Vriens J, Prenen J, Droogmans G, Voets T, Nilius B. Anandamide and arachidonic acid use epoxyeicosatrienoic acids to activate TRPV4 channels. Nature 2003; 424: 434438 [PMID: 12879072]
62 Alessandri-Haber N, Yeh JJ, Boyd AE, Parada CA, Chen X, Reichling DB, Levine JD. Hypotonicity induces TRPV4mediated nociception in rat. Neuron 2003; 39: 497511 [PMID: 12895423]
63 Grant AD, Cottrell GS, Amadesi S, Trevisani M, Nicoletti P, Materazzi S, Altier C, Cenac N, Zamponi GW, BautistaCruz F, Lopez CB, Joseph EK, Levine JD, Liedtke W, Vanner S, Vergnolle N, Geppetti P, Bunnett NW. Proteaseactivated receptor 2 sensitizes the transient receptor potential vanilloid 4 ion channel to cause mechanical hyperalgesia in mice. J Physiol 2007; 578: 715733 [PMID: 17124270 DOI: 10.1113/jphysiol.2006.121111]
64 Sipe WE, Brierley SM, Martin CM, Phillis BD, Cruz FB, Grady EF, Liedtke W, Cohen DM, Vanner S, Blackshaw LA, Bunnett NW. Transient receptor potential vanilloid 4 mediates protease activated receptor 2induced sensitization of colonic afferent nerves and visceral hyperalgesia. Am J Physiol Gastrointest Liver Physiol 2008; 294: G1288G1298 [PMID: 18325985 DOI: 10.1152/ajpgi.00002.2008]
65 Schwartz ES, La JH, Scheff NN, Davis BM, Albers KM, Gebhart GF. TRPV1 and TRPA1 antagonists prevent the transition of acute to chronic inflammation and pain in chronic pancreatitis. J Neurosci 2013; 33: 56035611 [PMID: 23536075 DOI: 10.1523/JNEUROSCI.180612.2013]
66 Hoogerwerf WA, Zou L, Shenoy M, Sun D, Micci MA, LeeHellmich H, Xiao SY, Winston JH, Pasricha PJ. The proteinaseactivated receptor 2 is involved in nociception. J Neurosci 2001; 21: 90369042 [PMID: 11698614]
67 Hoogerwerf WA, Shenoy M, Winston JH, Xiao SY, He Z, Pasricha PJ. Trypsin mediates nociception via the proteinaseactivated receptor 2: a potentially novel role in pancreatic pain. Gastroenterology 2004; 127: 883891 [PMID: 15362043]
68 Kawabata A, Matsunami M, Tsutsumi M, Ishiki T, Fukushima O, Sekiguchi F, Kawao N, Minami T, Kanke T, Saito N. Suppression
Atsawarungruangkit A et al . Neuropathophysiology of pain in chronic pancreatitis

201 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
of pancreatitisrelated allodynia/hyperalgesia by proteinaseactivated receptor2 in mice. Br J Pharmacol 2006; 148: 5460 [PMID: 16520745 DOI: 10.1038/sj.bjp.0706708]
69 Takeda K, Matsuno S, Sunamura M, Kakugawa Y. Continuous regional arterial infusion of protease inhibitor and antibiotics in acute necrotizing pancreatitis. Am J Surg 1996; 171: 394398 [PMID: 8604829 DOI: 10.1016/S00029610(97)896171]
70 Amadesi S, Nie J, Vergnolle N, Cottrell GS, Grady EF, Trevisani M, Manni C, Geppetti P, McRoberts JA, Ennes H, Davis JB, Mayer EA, Bunnett NW. Proteaseactivated receptor 2 sensitizes the capsaicin receptor transient receptor potential vanilloid receptor 1 to induce hyperalgesia. J Neurosci 2004; 24: 43004312 [PMID: 15128844 DOI: 10.1523/JNEUROSCI.567903.2004]
71 Nishimura S, Ishikura H, Matsunami M, Shinozaki Y, Sekiguchi F, Naruse M, Kitamura T, Akashi R, Matsumura K, Kawabata A. The proteinase/proteinaseactivated receptor2/transient receptor potential vanilloid1 cascade impacts pancreatic pain in mice. Life Sci 2010; 87: 643650 [PMID: 20932849 DOI: 10.1016/j.lfs.2010.09.030]
72 Zhang W, Gao J, Zhao T, Wei L, Wu W, Bai Y, Zou D, Li Z. Proteinaseactivated receptor 2 mediates thermal hyperalgesia and is upregulated in a rat model of chronic pancreatitis. Pancreas 2011; 40: 300307 [PMID: 21311307]
73 Woolf CJ, SafiehGarabedian B, Ma QP, Crilly P, Winter J. Nerve growth factor contributes to the generation of inflammatory sensory hypersensitivity. Neuroscience 1994; 62: 327331 [PMID: 7530342]
74 Toma H, Winston J, Micci MA, Shenoy M, Pasricha PJ. Nerve growth factor expression is upregulated in the rat model of Larginineinduced acute pancreatitis. Gastroenterology 2000; 119: 13731381 [PMID: 11054396]
75 Djouhri L, Dawbarn D, Robertson A, Newton R, Lawson SN. Time course and nerve growth factor dependence of inflammationinduced alterations in electrophysiological membrane properties in nociceptive primary afferent neurons. J Neurosci 2001; 21: 87228733 [PMID: 11698584]
76 Lewin GR, Mendell LM. Maintenance of modalityspecific connections in the spinal cord after neonatal nerve growth factor deprivation. Eur J Neurosci 1996; 8: 16771684 [PMID: 8921258]
77 McMahon SB, Bennett DL, Priestley JV, Shelton DL. The biological effects of endogenous nerve growth factor on adult sensory neurons revealed by a trkAIgG fusion molecule. Nat Med 1995; 1: 774780 [PMID: 7585179]
78 Della Seta D, de Acetis L, Aloe L, Alleva E. NGF effects on hot plate behaviors in mice. Pharmacol Biochem Behav 1994; 49: 701705 [PMID: 7862726]
79 Lewin GR, Rueff A, Mendell LM. Peripheral and central mechanisms of NGFinduced hyperalgesia. Eur J Neurosci 1994; 6: 19031912 [PMID: 7704300]
80 Zhu Y, Colak T, Shenoy M, Liu L, Pai R, Li C, Mehta K, Pasricha PJ. Nerve growth factor modulates TRPV1 expression and function and mediates pain in chronic pancreatitis. Gastroenterology 2011; 141: 370377 [PMID: 21473865 DOI: 10.1053/j.gastro.2011.03.046]
81 Zhu Y, Mehta K, Li C, Xu GY, Liu L, Colak T, Shenoy M, Pasricha PJ. Systemic administration of antiNGF increases Atype potassium currents and decreases pancreatic nociceptor excitability in a rat model of chronic pancreatitis. Am J Physiol Gastrointest Liver Physiol 2012; 302: G176G181 [PMID: 22038828 DOI: 10.1152/ajpgi.00053.2011]
82 Ceyhan GO, Bergmann F, Kadihasanoglu M, Erkan M, Park W, Hinz U, Giese T, Müller MW, Büchler MW, Giese NA, Friess H. The neurotrophic factor artemin influences the extent of neural damage and growth in chronic pancreatitis. Gut 2007; 56: 534544 [PMID: 17047099 DOI: 10.1136/gut.2006.105528]
83 Hughes MS, Shenoy M, Liu L, Colak T, Mehta K, Pasricha PJ. Brainderived neurotrophic factor is upregulated in rats with chronic pancreatitis and mediates pain behavior. Pancreas 2011; 40: 551556 [PMID: 21499209]
84 Bouwense SA, de Vries M, Schreuder LT, Olesen SS, Frøkjær JB, Drewes AM, van Goor H, WilderSmith OH. Systematic
mechanismorientated approach to chronic pancreatitis pain. World J Gastroenterol 2015; 21: 4759 [PMID: 25574079 DOI: 10.3748/wjg.v21.i1.47]
85 Vardanyan M, Melemedjian OK, Price TJ, Ossipov MH, Lai J, Roberts E, Boos TL, Deschamps JR, Jacobson AE, Rice KC, Porreca F. Reversal of pancreatitisinduced pain by an orally available, small molecule interleukin6 receptor antagonist. Pain 2010; 151: 257265 [PMID: 20599324 DOI: 10.1016/j.pain.2010.05.022]
86 Di Sebastiano P, di Mola FF, Di Febbo C, Baccante G, Porreca E, Innocenti P, Friess H, Büchler MW. Expression of interleukin 8 (IL8) and substance P in human chronic pancreatitis. Gut 2000; 47: 423428 [PMID: 10940282]
87 Ceyhan GO, Deucker S, Demir IE, Erkan M, Schmelz M, Bergmann F, Müller MW, Giese T, Büchler MW, Giese NA, Friess H. Neural fractalkine expression is closely linked to pain and pancreatic neuritis in human chronic pancreatitis. Lab Invest 2009; 89: 347361 [PMID: 19153557]
88 Michalski CW, Shi X, Reiser C, Fachinger P, Zimmermann A, Büchler MW, Di Sebastiano P, Friess H. Neurokinin2 receptor levels correlate with intensity, frequency, and duration of pain in chronic pancreatitis. Ann Surg 2007; 246: 786793 [PMID: 17968170 DOI: 10.1097/SLA.0b013e318070d56e]
89 Di Sebastiano P, Fink T, Weihe E, Friess H, Innocenti P, Beger HG, Büchler MW. Immune cell infiltration and growthassociated protein 43 expression correlate with pain in chronic pancreatitis. Gastroenterology 1997; 112: 16481655 [PMID: 9136844]
90 Friess H, Shrikhande S, Shrikhande M, Martignoni M, Kulli C, Zimmermann A, Kappeler A, Ramesh H, Büchler M. Neural alterations in surgical stage chronic pancreatitis are independent of the underlying aetiology. Gut 2002; 50: 682686 [PMID: 11950816]
91 Ceyhan GO, Bergmann F, Kadihasanoglu M, Altintas B, Demir IE, Hinz U, Müller MW, Giese T, Büchler MW, Giese NA, Friess H. Pancreatic neuropathy and neuropathic paina comprehensive pathomorphological study of 546 cases. Gastroenterology 2009; 136: 177186.e1 [PMID: 18992743 DOI: 10.1053/j.gastro.2008.09.029]
92 Ceyhan GO, Demir IE, Rauch U, Bergmann F, Müller MW, Büchler MW, Friess H, Schäfer KH. Pancreatic neuropathy results in “neural remodeling” and altered pancreatic innervation in chronic pancreatitis and pancreatic cancer. Am J Gastroenterol 2009; 104: 25552565 [PMID: 19568227]
93 Dimcevski G, Sami SA, FunchJensen P, Le Pera D, Valeriani M, ArendtNielsen L, Drewes AM. Pain in chronic pancreatitis: the role of reorganization in the central nervous system. Gastroenterology 2007; 132: 15461556 [PMID: 17408654 DOI: 10.1053/j.gastro.2007.01.037]
94 Buscher HC, WilderSmith OH, van Goor H. Chronic pancreatitis patients show hyperalgesia of central origin: a pilot study. Eur J Pain 2006; 10: 363370 [PMID: 16087373]
95 Olesen SS, Brock C, Krarup AL, FunchJensen P, ArendtNielsen L, WilderSmith OH, Drewes AM. Descending inhibitory pain modulation is impaired in patients with chronic pancreatitis. Clin Gastroenterol Hepatol 2010; 8: 724730 [PMID: 20304100]
96 Olesen SS, Hansen TM, Graversen C, Steimle K, WilderSmith OH, Drewes AM. Slowed EEG rhythmicity in patients with chronic pancreatitis: evidence of abnormal cerebral pain processing? Eur J Gastroenterol Hepatol 2011; 23: 418424 [PMID: 21399506 DOI: 10.1097/MEG.0b013e3283457b09]
97 Olesen SS, Frøkjær JB, Lelic D, Valeriani M, Drewes AM. Painassociated adaptive cortical reorganisation in chronic pancreatitis. Pancreatology 2010; 10: 742751 [PMID: 21273802]
98 de Vries M, WilderSmith OH, Jongsma ML, van den Broeke EN, Arns M, van Goor H, van Rijn CM. Altered resting state EEG in chronic pancreatitis patients: toward a marker for chronic pain. J Pain Res 2013; 6: 815824 [PMID: 24379694 DOI: 10.2147/JPR.S50919]
99 Frøkjær JB, Olesen SS, Graversen C, Andresen T, Lelic D, Drewes AM. Neuroimaging of the human visceral pain systema methodoi: ogical review. Scand J Pain 2011; 2: 95104
100 Drewes AM, Gratkowski M, Sami SA, Dimcevski G, Funch
Atsawarungruangkit A et al . Neuropathophysiology of pain in chronic pancreatitis

202 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Jensen P, ArendtNielsen L. Is the pain in chronic pancreatitis of neuropathic origin? Support from EEG studies during experimental pain. World J Gastroenterol 2008; 14: 40204027 [PMID: 18609686]
101 Frøkjær JB, Bouwense SA, Olesen SS, Lundager FH, Eskildsen SF, van Goor H, WilderSmith OH, Drewes AM. Reduced cortical thickness of brain areas involved in pain processing in patients with chronic pancreatitis. Clin Gastroenterol Hepatol 2012; 10: 4348.e1 [PMID: 22155560 DOI: 10.1016/j.cgh.2011.11.024]
102 Frøkjær JB, Andersen LW, Brock C, Simrén M, Ljungberg M, Søfteland E, Dimcevski G, Yavarian Y, Gregersen H, Drewes AM. Altered brain microstructure assessed by diffusion tensor imaging in patients with diabetes and gastrointestinal symptoms. Diabetes Care 2013; 36: 662668 [PMID: 23139372 DOI: 10.2337/dc121131]
103 Bouwense SA, Olesen SS, Drewes AM, Frøkjær JB, van Goor H, WilderSmith OH. Is altered central pain processing related to disease stage in chronic pancreatitis patients with pain? An exploratory study. PLoS One 2013; 8: e55460 [PMID: 23405154]
104 Katz N, Borenstein DG, Birbara C, Bramson C, Nemeth MA, Smith MD, Brown MT. Efficacy and safety of tanezumab in the treatment of chronic low back pain. Pain 2011; 152: 22482258 [PMID: 21696889 DOI: 10.1016/j.pain.2011.05.003]
105 Te AE. A study to investigate tanezumab in patients with interstitial cystitis/painful bladder syndrome. Curr Urol Rep 2011; 12: 245246 [PMID: 21559849 DOI: 10.1007/s1193401101940]
106 Evans RJ, Moldwin RM, Cossons N, Darekar A, Mills IW, Scholfield D. Proof of concept trial of tanezumab for the treatment of symptoms associated with interstitial cystitis. J Urol 2011; 185: 17161721 [PMID: 21420111 DOI: 10.1016/j.juro.2010.12.088]
107 Lane NE, Schnitzer TJ, Birbara CA, Mokhtarani M, Shelton DL, Smith MD, Brown MT. Tanezumab for the treatment of pain from osteoarthritis of the knee. N Engl J Med 2010; 363: 15211531 [PMID: 20942668 DOI: 10.1056/NEJMoa0901510]
108 Schnitzer TJ, Lane NE, Birbara C, Smith MD, Simpson SL,
Brown MT. Longterm openlabel study of tanezumab for moderate to severe osteoarthritic knee pain. Osteoarthritis Cartilage 2011; 19: 639646 [PMID: 21251985 DOI: 10.1016/j.joca.2011.01.009]
109 Xu C, Shen J, Zhang J, Jia Z, He Z, Zhuang X, Xu T, Shi Y, Zhu S, Wu M, Han W. Recombinant interleukin1 receptor antagonist attenuates the severity of chronic pancreatitis induced by TNBS in rats. Biochem Pharmacol 2015; 93: 449460 [PMID: 25559498 DOI: 10.1016/j.bcp.2014.12.016]
110 Bouwense SA, Buscher HC, van Goor H, WilderSmith OH. Sketamine modulates hyperalgesia in patients with chronic pancreatitis pain. Reg Anesth Pain Med 2011; 36: 303307 [PMID: 21490522 DOI: 10.1097/AAP.0b013e3182177022]
111 Sprenger T, Valet M, Woltmann R, Zimmer C, Freynhagen R, Kochs EF, Tölle TR, Wagner KJ. Imaging pain modulation by subanesthetic S(+)ketamine. Anesth Analg 2006; 103: 729737 [PMID: 16931688 DOI: 10.1213/01.ane.0000231635.14872.40]
112 Ilkjaer S, Dirks J, Brennum J, Wernberg M, Dahl JB. Effect of systemic NmethylDaspartate receptor antagonist (dextromethorphan) on primary and secondary hyperalgesia in humans. Br J Anaesth 1997; 79: 600605 [PMID: 9422898]
113 Bouwense SA, Olesen SS, Drewes AM, Poley JW, van Goor H, WilderSmith OH. Effects of pregabalin on central sensitization in patients with chronic pancreatitis in a randomized, controlled trial. PLoS One 2012; 7: e42096 [PMID: 22879908 DOI: 10.1371/journal.pone.0042096]
114 Olesen SS, Graversen C, Olesen AE, Frøkjaer JB, WilderSmith O, van Goor H, Valeriani M, Drewes AM. Randomised clinical trial: pregabalin attenuates experimental visceral pain through subcortical mechanisms in patients with painful chronic pancreatitis. Aliment Pharmacol Ther 2011; 34: 878887 [PMID: 21848870]
115 Olesen SS, Bouwense SA, WilderSmith OH, van Goor H, Drewes AM. Pregabalin reduces pain in patients with chronic pancreatitis in a randomized, controlled trial. Gastroenterology 2011; 141: 536543 [PMID: 21683078 DOI: 10.1053/j.gastro.2011.04.003]
P- Reviewer: Drewes AM S- Editor: Ji FF L- Editor: A E- Editor: Liu SQ
Atsawarungruangkit A et al . Neuropathophysiology of pain in chronic pancreatitis

José Manuel Benítez, Valle García-Sánchez
José Manuel Benítez, Valle García-Sánchez, Department of Gastroenterology, University Hospital Reina Sofia (Córdoba), 14004 Córdoba, Spain
Author contributions: Benítez JM and García-Sánchez V contributed equally to this work.
Conflict-of-interest statement: The authors declare no have conflict of interest.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Correspondence to: José Manuel Benítez, MD, Department of Gastroenterology, University Hospital Reina Sofia (Córdoba), Avda.Menéndez Pidal s/n, 14004 Córdoba, Spain. [email protected]: +34-95-7010450Fax: +34-95-7012818
Received: June 30, 2015Peer-review started: July 5, 2015First decision: July 31, 2015Revised: September 11, 2015Accepted: October 23, 2015Article in press: October 27, 2015Published online: November 15, 2015
AbstractInflammatory bowel disease (IBD) is a chronic and relapsing disorder which leads to an inflammation of the gastrointestinal tract. A tailored therapy to achieve mucosal healing with the less adverse events has become a key issue in the management of IBD. In the past, the clinical remission was the most important
factor to consider for adapting diagnostic procedures and therapeutic strategies. However, there is no a good correlation between symptoms and intestinal lesions, so currently the goals of treatment are to achieve not only the control of symptoms, but deep remission, which is related with a favourable prognosis. Thus, the determination of biological markers or biomarkers of intestinal inflammation play a crucial role. Many biomarkers have been extensively evaluated in IBD showing significant correlation with endoscopic lesions, risk of recurrence and response to treatment. One of the most important markers is faecal calprotectin (FC). Despite calprotectin limitations, this biomarker represents a reliable and noninvasive alternative to reduce the need for endoscopic procedures. FC has demonstrated its performance for regular monitoring of IBD patients, not only to the diagnosis for discriminating IBD from non-IBD diagnosis, but for assessing disease activity, relapse prediction and response to therapy. Although, FC provides better results than other biomarkers such as C-reactive protein and erythrocyte sedimentation rate, these surrogate markers of intestinal inflammation should not be used isolation but in combination with other clinical, endoscopic, radiological or/and histological parameters enabling a comprehensive assessment of IBD patients.
Key words: Faecal calprotectin; Inflammatory bowel disease; Biomarkers; Ulcerative colitis; Crohn’s disease; Relapse
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: The surveillance of inflammatory bowel disease (IBD) course is needed to select the patients with worse prognosis and to adapt an early therapeutic strategy. Faecal calprotectin constitutes a surrogate marker of intestinal inflammation and a robust alternative to invasive procedures as endoscopy. This biomarker has been demonstrated reliable and accuracy in different aspects of IBD such as diagnosis of IBD, activity
MINIREVIEWS
203 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Faecal calprotectin: Management in inflammatory bowel disease
World J Gastrointest Pathophysiol 2015 November 15; 6(4): 203-209ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i4.203

assessment, response to treatment and relapse pre-diction. Although a cut-off level of calprotectin has not been fully established, the combination with other biomarkers allows an appropriate management of the patient.
Benítez JM, García-Sánchez V. Faecal calprotectin: Management in inflammatory bowel disease. World J Gastrointest Pathophysiol 2015; 6(4): 203-209 Available from: URL: http://www.wjgnet.com/2150-5330/full/v6/i4/203.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i4.203
INTRODUCTIONThe main forms of inflammatory bowel disease (IBD) are the ulcerative colitis (UC) and Crohn’s disease (CD). Both are chronic inflammatory disorders characterized by a relapsing-remitting clinical behavior. The course of IBD is unpredictable and can lead to cumulative intestinal tissue damage and complications which affect quality of life of patients[1]. The chronic nature of the disease requires a continuous assessment of activity to adapt the therapeutic strategy. Thus, physicians need reliable tools which allow to evaluate the disease activity and relapses risk.
Initially, the aim of therapy was to reach clinical remission, but this way is not enough to change the natural history of the disease. In recent years, the goal of treatment in IBD has changed and it is guided towards the mucosal healing, considered as a good predictor of the disease course, and associated with better patient outcomes[2,3].
Diagnosis and monitoring of IBD activity is based on a combination of clinical assessment, serologic and fecal markers of inflammation, cross-sectional imaging and endoscopy. Although endoscopy remains the gold standard for assessing IBD activity and mucosal healing, it has some risks and limitations: It is an invasive procedure, usually with low acceptance by the patient and potentially harmful, relatively high cost, it does not give information of the transmural inflammation, and finally is not well-known the timing of endoscopic evaluation. For this reason, numerous biomarkers have been proposed as surrogate markers of intestinal inflammation, and therefore also as potential markers of IBD activity. The biomarkers most extensively studied and commonly employed in clinical practice are C-reactive protein (CRP) and faecal calprotectin (FC).
This review offers a practical overview of the role of FC in several scenarios of clinical practice such as diagnosis of IBD, disease activity measurement, therapy response assessment and disease relapse prediction, describing its advantages and limitations (Table 1).
FAECAL CALPROTECTINCalprotectin is a calcium and zinc-binding protein which
constitutes 60% of neutrophil cytosolic proteins[4,5], and that has functions such as antibacterial activity and induction of apoptosis[6]. Granulocytes produce FC at the site of mucosal inflammation increasing levels of this protein in faeces[7].
The FC level is a marker more specific of mucosal inflammation than CRP or erythrocyte sedimentation rate (ESR), which is less influenced by other non-intestinal conditions[8]. FC determination can be performed by enzyme-linked immunosorbent assay[5], and shows great stability at room temperature for a week[7]. This easy and inexpensive determination becomes calprotectin in a useful tool for monitoring of IBD patients.
Calprotectin presents some limitations in clinical practice. FC concentrations can be increase in non-IBD disorders; a cut-off level has not been well-established, and some authors described significant variability in a same patient[9]. Although a concentration < 50 μg/g may be considered upper limit of normal[10], an optimal cut-off for distinguishing IBD from other entities has not been fully described. The cut-off level of FC most commonly used varies from 50 to 200 μg/g[11]. von Roon et al[12] evaluated the diagnostic accuracy of FC for IBD and demonstrated that a cut-off level of 100 μg/g had better accuracy than 50 μg/g. Even, others authors increased the cut-off up to 150 μg/g[13].
The role of faecal calprotectin in the diagnosis of IBDThe diagnosis of IBD is based not only on clinical data, because symptoms are unspecific and present in other organic or functional disorders, but also, endoscopic, radiological and histological criteria are needed to confirm or exclude the diagnosis. The use of biological markers capable to differentiate between organic and functional diseases, would select those patients with suspected IBD which needs further invasive procedures such as colonoscopy. The role of biomarkers in this setting is variable.
FC has a great diagnostic accuracy for discriminating IBD from non-organic entities like has been reported in the literature[14] and evaluated in multiple studies[15-19].
Gisbert et al[14] reported an overall sensitivity of 80% and specificity of 76% for the diagnosis of IBD, reaching a higher accuracy for CD (sensitivity 83%, specificity 85%) than for UC (sensitivity 72%; specificity 74%). In a meta-analysis, von Roon et al[12] assessed the diagnostic precision of FC for IBD, and showed higher FC levels than non-IBD patients with a sensitivity of 95% and a specificity of 91%. Similar results have been published by other meta-analysis which included adult and pediatric studies with patients suspected to have IBD, with sensitivity and specificity of FC for distinction between IBD and irritable bowel syndrome of 93% and 96%, respectively. In pediatric population, this accuracy is lower reaching a sensitivity of FC of 0.92 (95%CI: 0.84-0.96) and specificity slightly lower 0.76 (95%CI: 0.62-0.86), probably due to the higher FC levels in healthy children up to 9 years of age[20].
This diagnostic accuracy of FC would decrease the
204 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Benítez JM et al . Calprotectin in inflammatory bowel disease

numbers of endoscopies needed up to 3-fold in adults and 35% in children[21] and, therefore, significantly reduces costs[22].
Therefore, FC is a reliable marker for organic gastro-intestinal disorders, however, it is not specific for IBD, and other process can increase it such as neoplasms (colorectal cancer, polyps), gastrointestinal infections, other inflammatory entities (microscopic colitis, diver-ticulitis) and NSAID-induced enterocolitis[21]. A high value of FC constitutes a solid reason for performing a colonoscopy and confirming the diagnosis.
Although there is no established cut-off level to predict IBD, it is widely accepted that 50 μg/g is an accurate FC level to exclude organic intestinal disease with a high negative predictive value (NPV)[23]. Higher levels are not recommended because they would result in more false negative results and in this setting, the predictive negative value needs to be high in order to prevent delays in diagnosis. A normal value of FC makes unlikely the diagnosis of intestinal organic disease. The performance of FC with a cutoff of 50 μg/g as the first step to exclude organic disease seems reasonable, if the suspicion of IBD is not too high.
The diagnostic accuracy of FC for the diagnosis of IBD has been shown higher than other biomarkers such as CRP, ESR, anti-neutrophil cytoplasmic antibodies and anti-saccharomyces cerevisiae antibodies.
The role of faecal calprotectin in the monitoring of IBDThe role of faecal calprotectin to evaluate disease activity: The identification of inflammatory activity in a symptomatic IBD patient is crucial before changing the therapeutic strategy. Most of clinical indices employed to assess disease activity in IBD are based on patient symptoms and, therefore, subjective and poorly correlated with mucosal inflammation. The availability of biomarkers with a good correlation with clinical, endoscopic and histological activity is of capital relevance in daily clinical practice avoiding repeating invasive procedures. Moreover, fecal biomarkers are cheaper and easier, providing an important alternative to endoscopic procedures.
FC levels have shown a good correlation with the degree of inflammatory activity in IBD[24-26]. In CD, the median Pearson r correlation between the CD
Endoscopic Index of Severity (CDEIS) and FC was 0.49, and for lactoferrin was 0.77[27-29]; the correlation with the simple endoscopic score for CD was similar for both FC (0.53) and lactoferrin (0.62)[27,30]. A meta-analysis with 550 patients evaluated the accuracy of CRP, FC and endoscopic scores, and it showed that in symptomatic patients (CDAI > 220), the sensitivity and specificity of CRP ≤ 5 mg/L or FC ≤ 200 μg/g to anticipate a CDEIS ≤ 6 was 83% and 71%, respectively[31].
In UC, FC levels show a better association with disease activity than in CD, and its correlation with endoscopic May score[28,32], Rachmilevitz index, and modified Baron score[33] was 0.72 (0.49-0.83).
Although no cut-off level has been validated, a FC > 200-250 μg/g has shown to have good accuracy in predicting endoscopic activity[28]. However, in CD with exclusively small bowel location, the sensitivity of FC to detect endoscopic lesions might be lower[34].
CRP has shown a sensitivity and specificity lower than FC for endoscopic disease activity both in UC and CD, so FC constitutes a more valuable marker than CRP in this context. In an appropriate scenario, the performance of FC could prevent the need for colonoscopy to confirm or exclude endoscopy activity in a symptomatic patient.
The role of faecal calprotectin to confirm mucosal healing and predict disease relapse: The course of IBD varies over time and while some patients have a favourable course with long periods of remission, others have a more aggressive disease, with unpredictable activity flare-up. Predicting the course along with the risk of relapse is useful because would allow to clinicians to individualize the management of each patient, conducting a more personalized approach and optimizing therapeutic strategies, minimizing adverse effects. The prediction of relapses would allow an early and intensive treatment in patients with worse prognosis. Studies examining this issue prospectively are limited and with inconclusive results regarding the frequency of determination of these biomarkers.
The capability to predict IBD relapse is one of the potential of the FC[25,35]. High levels of calprotectin in remission are associated with an increased risk of clinical relapse, with a sensitivity of 90% and specificity of 83%[18]. So, patients in clinical remission with high
205 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Advantages Disadvantages
Relatively good acceptance Not always well accepted by patients (faecal samples)Non-invasive Subject to non-specific variationsRelatively low cost Predictive threshold values not fully establishedMay be combined to improve prediction Imperfect correlation with mucosal healing and transmural healingCan be repeated as a longitudinal monitoring toolPredictive value for Disease relapse Response to anti-TNF therapy Mucosal healing
Table 1 Monitoring of inflammatory bowel disease with biomarkers
TNF: Tumor necrosis factor.
Benítez JM et al . Calprotectin in inflammatory bowel disease

206 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
before clinical relapse, so determinations every 3-4 mo should be sufficient to detect high levels and allow to clinicians to tailor therapeutic strategies[38].
The FC determination could also be useful to assess diseases activity evolution. Thus, Casellas et al[39] studied patients with clinically quiescent UC for 1 year or until clinical relapse; and they observed that FC values remains stable in patients with inactive UC, and increased in relapsing patients.
Ho et al[40] reported as FC levels could predict the colectomy risk in patients with acute severe UC. They evaluated 90 patients hospitalized for acute severe colitis and showed as very high levels of FC on admission were associated with an increased risk of colectomy. An initial calprotectin over 1900 μg/g predicted colectomy of 87% patients in the first year.
The role of faecal calprotectin to evaluate response to treatment: Another feature of faecal biomarkers is the rapid confirmation of drug efficacy after initiation of therapy. Usually, the evaluation of the response to treatment is based on clinical assessment, while endoscopy is rarely performed. It would be of great interest to have markers that reliably estimate the probability of response to different therapies. Thus, it is possible to identify subgroups of patients who would benefit from a particular therapeutic strategy as well as patients will have a poor response to the treatment being able to avoid exposure to them and the risk of adverse events. The lack of response to treatment may affect the quality of life of patients and increase their mortality.
Nowadays, the goal of treatment in IBD is to achieve mucosal healing, which has been associated with better outcomes and fewer relapses. However, to confirm absence of endoscopic lesions would be needed repeated endoscopic procedures. Therefore, biomarkers able to indirectly estimate this healing are imperative.
FC has been suggested as surrogate faecal marker of response to therapy. Several studies have demon-strated that normalization of calprotectin levels in
concentrations of FC had a risk of relapse of 2 and 14 times higher in CD and UC, respectively, compared to patients without elevated calprotectin[36]. However, CRP and ESR are not as helpful to predict disease’s relapse, probably because theses biomarkers estimate intestinal inflammation indirectly.
It is necessary to clarify the predictive value of FC in UC and CD, its chronological relationship with the occurrence of relapse and the best cut-off point to determine relapse risk. D’Haens et al[28] showed that CD patients with a level of FC > 250 μg/g predicted the presence of large ulcers with a sensitivity of 60% and specificity of 80%, while a concentration of < 250 μg/gpredicted mucosal healing (CDEIS < 3) with a sensitivity and specificity of 94% and 62%, respectively. A recent subanalysis of STORI study[37] suggested that the combination of FC (with threshold < 250 μg/g) and PCR (with threshold < 5 mg/L) can improve the capacity to predict mucosal healing with reasonably good sensitivity and specificity, around 70%. When considering inactiveCD patients (CDAI ≤ 150), the association of a PCR ≤ 10 mg/L and a calprotectin ≤ 200 μg/g has a sensitivity of 78% and a specificity of 58% for pre-dicting no significant endoscopic activity (CDEIS ≤ 3), with a positive predictive value between 65%-88% and 40%-70% NPV. So, if a colonoscopy is performed to 100 patients with CD in clinical remission with both biomarkers below this threshold, 30-40 colonoscopies could have been avoided. Patients with higher calpro-tectin or CRP levels should be considered holders of active intestinal lesions (Figure 1).
García-Sánchez et al[35] showed that the predictive value of FC was similar in UC and CD with colon involve-ment, and considering FC > 120 μg/g as a predictor of relapse risk with a sensitivity of 80% and a specificity of 60%. This predictive value is lower in patients with ileal CD. Although the appropriate frequency of determination of these markers is not well-established to date, data from the GETAID-STORI cohort indicates that both CRP and FC begin to increase their concentrations 4-6 mo
Clinically active disease
No signs of complication or disease progression
Doubt about lesions location, severity or extent, complications
Endoscopy and/or cross-sectional imaging
FC ≥ 250 μg/g and/or CRP ≥ 5 mg/L
FC < 250 μg/g and CRP < 5 mg/L
Controlled disease close monitoring with repeated
FC and CRP
Uncontrolled disease
Clinically inactive disease
FC ≥ 250 μg/g and/or CRP ≥ 5 mg/L
FC < 250 μg/g and CRP < 5 mg/L
Clinical and biological remission
Endoscopy and/or cross-sectional imaging
Close monitoring with repeated FC and CRP
Figure 1 Algorithm for inflammatory bowel disease monitoring. A combination of clinical symptoms and biomarkers such as FC and CRP allow an individualized approach and a selection of patients for performing other invasive procedures and targeting treatment. FC: Faecalcalprotectin; CRP: C-reactive protein.
Benítez JM et al . Calprotectin in inflammatory bowel disease

207 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
IBD patients after medical treatment is a marker that predicts the endoscopic healing. Decreased levels of FC after therapy are associated with clinical, endoscopic and histological improvement[41]. The normalization of calprotectin (< 50 mg/g) is more difficult to reach than the CRP normalization, so a significant decrease of FC could represent a deeper remission and a higher tissue healing[42,43].
When a steroid-free remission is achieved, de-escalation therapy may be tried to optimize benefit/risk. The combination of CRP and FC represents a good option to predict the risk of relapse after infliximab with-drawal[43].
For de-escalation of any drug or cessation of corticos-teroids or mesalamine, a confirmation of biological remission with biomarkers such as CRP or FC can be sufficient. However, if we are willing to stop immuno-suppressants or anti-TNF drugs, a confirmation of mucosal healing by endoscopy seems desirable[44].
The role of faecal calprotectin in postoperative recurrence assessment: There are scarce and conflicting data regarding the value of biomarkers in the postoperative setting to predict disease recurrence. FC usually returns to normal level by 2 mo postoperatively and any increase of its concentrations are associated with inflammatory recurrence[45].
Lobatón et al[34] suggested that FC is a more accurate and better surrogate marker of endoscopy activity in recurrent CD than clinical or serological markers, allowing to distinguish between postoperative recurrence patients (Rutgeert’s score 2-4) and patients without recurrence (Rutgeert’s score 0-1). In this study, using a cut-off value of FC of 203 μg/g reached a sensitivity of 75% and a specificity of 72%.
Beltrán et al[46] reported that FC is a useful early noninvasive marker for assessing recurrence of CD. A cut-off of 175 μg/g for FC is proposed.
CONCLUSIONThe availability of biomarkers as FC represents a com-plementary tool to the clinical, endoscopic, radiological and histological procedures in the management of IBD patients. This surrogate marker is non-invasive, objective and non-expensive, and has a high accuracy for assessing different scenarios in IBD (to distinguish organic and functional disease, to evaluate disease activity, to predict risk of relapse, response to treatment and postoperative recurrence risk). FC can help to clinicians to avoid repeating invasive techniques selecting patients and to guide therapeutic decision. FC could be determined during follow-up allowing an early detection rather than just prediction of relapses. A combination of serological and faecal markers and endoscopy allow to the overall understanding of intestinal inflammation.
REFERENCES1 Peyrin-Biroulet L, Loftus EV, Colombel JF, Sandborn WJ.
The natural history of adult Crohn’s disease in population-based cohorts. Am J Gastroenterol 2010; 105: 289-297 [PMID: 19861953 DOI: 10.1038/ajg.2009.579]
2 Schnitzler F, Fidder H, Ferrante M, Noman M, Arijs I, Van Assche G, Hoffman I, Van Steen K, Vermeire S, Rutgeerts P. Mucosal healing predicts long-term outcome of maintenance therapy with infliximab in Crohn’s disease. Inflamm Bowel Dis 2009; 15: 1295-1301 [PMID: 19340881 DOI: 10.1002/ibd.20927]
3 Baert F, Moortgat L, Van Assche G, Caenepeel P, Vergauwe P, De Vos M, Stokkers P, Hommes D, Rutgeerts P, Vermeire S, D’Haens G. Mucosal healing predicts sustained clinical remission in patients with early-stage Crohn’s disease. Gastroenterology 2010; 138: 463-468; quiz e10-11 [PMID: 19818785 DOI: 10.1053/j.gastro.2009.09.056]
4 Nacken W, Roth J, Sorg C, Kerkhoff C. S100A9/S100A8: Myeloid representatives of the S100 protein family as prominent players in innate immunity. Microsc Res Tech 2003; 60: 569-580 [PMID: 12645005 DOI: 10.1002/jemt.10299]
5 Røseth AG, Fagerhol MK, Aadland E, Schjønsby H. Assessment of the neutrophil dominating protein calprotectin in feces. A methodologic study. Scand J Gastroenterol 1992; 27: 793-798 [PMID: 1411288 DOI: 10.3109/00365529209011186]
6 Sutherland AD, Gearry RB, Frizelle FA. Review of fecal biomarkers in inflammatory bowel disease. Dis Colon Rectum 2008; 51: 1283-1291 [PMID: 18543035 DOI: 10.1007/s10350-008-9310-8]
7 Angriman I, Scarpa M, D’Incà R, Basso D, Ruffolo C, Polese L, Sturniolo GC, D’Amico DF, Plebani M. Enzymes in feces: useful markers of chronic inflammatory bowel disease. Clin Chim Acta 2007; 381: 63-68 [PMID: 17368600 DOI: 10.1016/j.cca.2007.02.025]
8 Tibble JA, Sigthorsson G, Foster R, Forgacs I, Bjarnason I. Use of surrogate markers of inflammation and Rome criteria to distinguish organic from nonorganic intestinal disease. Gastroenterology 2002; 123: 450-460 [PMID: 12145798 DOI: 10.1053/gast.2002.34755]
9 Husebye E, Tøn H, Johne B. Biological variability of fecal calprotectin in patients referred for colonoscopy without colonic inflammation or neoplasm. Am J Gastroenterol 2001; 96: 2683-2687 [PMID: 11569695 DOI: 10.1016/s0002-9270(01)02688-0]
10 Tøn H, Brandsnes S, Holtlund J, Skuibina E, Schjønsby H, Johne B. Improved assay for fecal calprotectin. Clin Chim Acta 2000; 292: 41-54 [PMID: 10686275 DOI: 10.1016/S0009-8981(99)00206-5]
11 Abraham BP, Kane S. Fecal markers: calprotectin and lactoferrin. Gastroenterol Clin North Am 2012; 41: 483-495 [PMID: 22500530 DOI: 10.1016/j.gtc.2012.01.007]
12 von Roon AC, Karamountzos L, Purkayastha S, Reese GE, Darzi AW, Teare JP, Paraskeva P, Tekkis PP. Diagnostic precision of fecal calprotectin for inflammatory bowel disease and colorectal malignancy. Am J Gastroenterol 2007; 102: 803-813 [PMID: 17324124 DOI: 10.1111/j.1572-0241.2007.01126.x]
13 Tibble J, Teahon K, Thjodleifsson B, Roseth A, Sigthorsson G, Bridger S, Foster R, Sherwood R, Fagerhol M, Bjarnason I. A simple method for assessing intestinal inflammation in Crohn’s disease. Gut 2000; 47: 506-513 [PMID: 10986210 DOI: 10.1136/gut.47.4.506]
14 Gisbert JP, McNicholl AG. Questions and answers on the role of faecal calprotectin as a biological marker in inflammatory bowel disease. Dig Liver Dis 2009; 41: 56-66 [PMID: 18602356 DOI: 10.1016/j.dld.2008.05.008]
15 Otten CM, Kok L, Witteman BJ, Baumgarten R, Kampman E, Moons KG, de Wit NJ. Diagnostic performance of rapid tests for detection of fecal calprotectin and lactoferrin and their ability to discriminate inflammatory from irritable bowel syndrome. Clin Chem Lab Med 2008; 46: 1275-1280 [PMID: 18597588 DOI: 10.1515/CCLM.2008.246]
16 Dai J, Liu WZ, Zhao YP, Hu YB, Ge ZZ. Relationship between fecal lactoferrin and inflammatory bowel disease. Scand J Gastroenterol 2007; 42: 1440-1444 [PMID: 17852860 DOI: 10.1080/00365520701427094]
17 Schoepfer AM, Trummler M, Seeholzer P, Criblez DH, Seibold F.
Benítez JM et al . Calprotectin in inflammatory bowel disease

208 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Accuracy of four fecal assays in the diagnosis of colitis. Dis Colon Rectum 2007; 50: 1697-1706 [PMID: 17762964 DOI: 10.1007/s10350-007-0303-9]
18 Tibble JA, Sigthorsson G, Bridger S, Fagerhol MK, Bjarnason I. Surrogate markers of intestinal inflammation are predictive of relapse in patients with inflammatory bowel disease. Gastroenterology 2000; 119: 15-22 [PMID: 10889150 DOI: 10.1053/gast.2000.8523]
19 Wang S, Wang Z, Shi H, Heng L, Juan W, Yuan B, Wu X, Wang F. Faecal calprotectin concentrations in gastrointestinal diseases. J Int Med Res 2013; 41: 1357-1361 [PMID: 23723365 DOI: 10.1177/0300060513488499]
20 van Rheenen PF, Van de Vijver E, Fidler V. Faecal calprotectin for screening of patients with suspected inflammatory bowel disease: diagnostic meta-analysis. BMJ 2010; 341: c3369 [PMID: 20634346 DOI: 10.1136/bmj.c3369]
21 Kopylov U, Rosenfeld G, Bressler B, Seidman E. Clinical utility of fecal biomarkers for the diagnosis and management of inflammatory bowel disease. Inflamm Bowel Dis 2014; 20: 742-756 [PMID: 24562174 DOI: 10.1097/01.MIB.0000442681.85545.31]
22 Kim MK, Chae YN, Kim HD, Yang EK, Cho EJ, Choi SH, Cheong YH, Kim HS, Kim HJ, Jo YW, Son MH, Kim SH, Shin CY. DA-1229, a novel and potent DPP4 inhibitor, improves insulin resistance and delays the onset of diabetes. Life Sci 2012; 90: 21-29 [PMID: 22056373 DOI: 10.1016/j.clinbiochem.2011.10.015]
23 Yang Z, Clark N, Park KT. Effectiveness and cost-effectiveness of measuring fecal calprotectin in diagnosis of inflammatory bowel disease in adults and children. Clin Gastroenterol Hepatol 2014; 12: 253-262.e2 [PMID: 23883663 DOI: 10.1016/j.cgh.2013.06.028]
24 Tibble JA, Bjarnason I. Fecal calprotectin as an index of intestinal inflammation. Drugs Today (Barc) 2001; 37: 85-96 [PMID: 12783101 DOI: 10.1358/dot.2001.37.2.614846]
25 García Sánchez Mdel V, González R, Iglesias Flores E, Gómez Camacho F, Casais Juanena L, Cerezo Ruiz A, Montero Pérez-Barquero M, Muntané J, de Dios Vega JF. [Diagnostic value of fecal calprotectin in predicting an abnormal colonoscopy]. Med Clin (Barc) 2006; 127: 41-46 [PMID: 16801001 DOI: 10.1157/13090002]
26 Langhorst J, Elsenbruch S, Mueller T, Rueffer A, Spahn G, Michalsen A, Dobos GJ. Comparison of 4 neutrophil-derived proteins in feces as indicators of disease activity in ulcerative colitis. Inflamm Bowel Dis 2005; 11: 1085-1091 [PMID: 16306771 DOI: 10.1097/01.MIB.0000187980.08686.18]
27 Sipponen T, Kärkkäinen P, Savilahti E, Kolho KL, Nuutinen H, Turunen U, Färkkilä M. Correlation of faecal calprotectin and lactoferrin with an endoscopic score for Crohn’s disease and histological findings. Aliment Pharmacol Ther 2008; 28: 1221-1229 [PMID: 18752630 DOI: 10.1111/j.1365-2036.2008.03835.x]
28 D’Haens G, Ferrante M, Vermeire S, Baert F, Noman M, Moortgat L, Geens P, Iwens D, Aerden I, Van Assche G, Van Olmen G, Rutgeerts P. Fecal calprotectin is a surrogate marker for endoscopic lesions in inflammatory bowel disease. Inflamm Bowel Dis 2012; 18: 2218-2224 [PMID: 22344983 DOI: 10.1002/ibd.22917]
29 Meuwis MA, Vernier-Massouille G, Grimaud JC, Bouhnik Y, Laharie D, Piver E, Seidel L, Colombel JF, Louis E. Serum calprotectin as a biomarker for Crohn’s disease. J Crohns Colitis 2013; 7: e678-e683 [PMID: 23845231 DOI: 10.1016/j.crohns.2013.06.008]
30 Sipponen T, Savilahti E, Kolho KL, Nuutinen H, Turunen U, Färkkilä M. Crohn’s disease activity assessed by fecal calprotectin and lactoferrin: correlation with Crohn’s disease activity index and endoscopic findings. Inflamm Bowel Dis 2008; 14: 40-46 [PMID: 18022866 DOI: 10.1002/ibd.20312]
31 Bondjemah V, Mary JY, Jose J, Sandborn W, Schoepfer A, Louis E, Sipponen T, Vieira A, Colombel JF, Allez M. Fecal calprotectin and CRP as biomarkers of endoscopic activity in Crohn’s disease: a meta-study. J Crohn Colitis 2012; 6: P133 [DOI: 10.1016/S1873-9946(12)60153-6]
32 Langhorst J, Elsenbruch S, Koelzer J, Rueffer A, Michalsen A, Dobos GJ. Noninvasive markers in the assessment of intestinal inflammation in inflammatory bowel diseases: performance
of fecal lactoferrin, calprotectin, and PMN-elastase, CRP, and clinical indices. Am J Gastroenterol 2008; 103: 162-169 [PMID: 17916108]
33 Schoepfer AM, Beglinger C, Straumann A, Safroneeva E, Romero Y, Armstrong D, Schmidt C, Trummler M, Pittet V, Vavricka SR. Fecal calprotectin more accurately reflects endoscopic activity of ulcerative colitis than the Lichtiger Index, C-reactive protein, platelets, hemoglobin, and blood leukocytes. Inflamm Bowel Dis 2013; 19: 332-341 [PMID: 23328771 DOI: 10.1097/MIB.0b013e3182810066]
34 Lobatón T, López-García A, Rodríguez-Moranta F, Ruiz A, Rodríguez L, Guardiola J. A new rapid test for fecal calprotectin predicts endoscopic remission and postoperative recurrence in Crohn’s disease. J Crohns Colitis 2013; 7: e641-e651 [PMID: 23810085 DOI: 10.1016/j.crohns.2013.05.005]
35 García-Sánchez V, Iglesias-Flores E, González R, Gisbert JP, Gallardo-Valverde JM, González-Galilea A, Naranjo-Rodríguez A, de Dios-Vega JF, Muntané J, Gómez-Camacho F. Does fecal calprotectin predict relapse in patients with Crohn’s disease and ulcerative colitis? J Crohns Colitis 2010; 4: 144-152 [PMID: 21122498 DOI: 10.1016/j.crohns.2009.09.008]
36 Costa F, Mumolo MG, Ceccarelli L, Bellini M, Romano MR, Sterpi C, Ricchiuti A, Marchi S, Bottai M. Calprotectin is a stronger predictive marker of relapse in ulcerative colitis than in Crohn’s disease. Gut 2005; 54: 364-368 [PMID: 15710984 DOI: 10.1136/gut.2004.043406]
37 Lemann M, Colombel J-F, Grimaud J-C. Fecal calprotectin and high sensitivity c-reactive protein levels to predict mucosal healing in patients with Crohn’s disease. A subanalysis of the STORI study. Gut 2010; 59 Suppl III: A80
38 De Suray N, Salleron J, Vernier-Massouille G, Grimaud JC, Bouhnik Y, Laharie D, Dupas JL, Pillant H, Picon L, Veyrac M, Flamant M, Savoye G, Jian R, De Vos M, Piver E, Mary JY, Colombel JF, Louis E. Close monitoring of CRP and fecal calprotectin levels to predict relapse in Crohn’s disease patients. A sub-analysis of the STORI study. J Crohn Colitis 2012; 6: P274 [DOI: 10.1016/S1873-9946(12)60294-3]
39 Casellas F, Borruel N, Antolín M, Varela E, Torrejón A, Armadans L, Guarner F, Malagelada JR. Fecal excretion of deoxyribonucleic acid in long-term follow-up of patients with inactive ulcerative colitis. Inflamm Bowel Dis 2007; 13: 386-390 [PMID: 17206700 DOI: 10.1002/ibd.20042]
40 Ho GT, Lee HM, Brydon G, Ting T, Hare N, Drummond H, Shand AG, Bartolo DC, Wilson RG, Dunlop MG, Arnott ID, Satsangi J. Fecal calprotectin predicts the clinical course of acute severe ulcerative colitis. Am J Gastroenterol 2009; 104: 673-678 [PMID: 19262524 DOI: 10.1038/ajg.2008.119]
41 Røseth AG, Aadland E, Grzyb K. Normalization of faecal calprotectin: a predictor of mucosal healing in patients with inflam-matory bowel disease. Scand J Gastroenterol 2004; 39: 1017-1020 [PMID: 15513345]
42 Benitez JM, Meuwis MA, Reenaers C, Van Kemseke C, Meunier P, Louis E. Role of endoscopy, cross-sectional imaging and bio-markers in Crohn’s disease monitoring. Gut 2013; 62: 1806-1816 [PMID: 24203056 DOI: 10.1136/gutjnl-2012-303957]
43 Louis E, Mary JY, Vernier-Massouille G, Grimaud JC, Bouhnik Y, Laharie D, Dupas JL, Pillant H, Picon L, Veyrac M, Flamant M, Savoye G, Jian R, Devos M, Porcher R, Paintaud G, Piver E, Colombel JF, Lemann M. Maintenance of remission among patients with Crohn’s disease on antimetabolite therapy after infliximab therapy is stopped. Gastroenterology 2012; 142: 63-70.e5; quiz e31 [PMID: 21945953 DOI: 10.1053/j.gastro.2011.09.034]
44 Pittet V, Froehlich F, Maillard MH, Mottet C, Gonvers JJ, Felley C, Vader JP, Burnand B, Michetti P, Schoepfer A. When do we dare to stop biological or immunomodulatory therapy for Crohn’s disease? Results of a multidisciplinary European expert panel. J Crohns Colitis 2013; 7: 820-826 [PMID: 23664620 DOI: 10.1016/j.crohns.2013.04.013]
45 Lamb CA, Mohiuddin MK, Gicquel J, Neely D, Bergin FG,
Benítez JM et al . Calprotectin in inflammatory bowel disease
LPD

209 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Hanson JM, Mansfield JC. Faecal calprotectin or lactoferrin can identify postoperative recurrence in Crohn’s disease. Br J Surg 2009; 96: 663-674 [PMID: 19384912 DOI: 10.1002/bjs.6593]
46 Beltrán B, Cerrillo E, Iborra M. Fecal calprotectin is a useful early predictive marker for postoperative recurrence in Crohn’s disease. Gastroenterol 2012; 142: S659
P- Reviewer: Francesco C, Tsai HH S- Editor: Qiu S L- Editor: A E- Editor: Liu SQ
Benítez JM et al . Calprotectin in inflammatory bowel disease

Carla Andrade Lima, Andre Castro Lyra, Raquel Rocha, Genoile Oliveira Santana
Carla Andrade Lima, Pos-graduation program in medicine and health, Federal University of Bahia, Salvador, Bahia 40110-060, Brazil
Andre Castro Lyra, Genoile Oliveira Santana, Department of Gastroenterology, Federal University of Bahia, Salvador, Bahia 40110-060, Brazil
Raquel Rocha, Department of Sciences of Nutrition, School of Nutrition, Federal University of Bahia, Salvador, Bahia 40110-060, Brazil
Author contributions: Lima CA performed most of the writing and prepared the table; Lyra AC coordinated the writing of the paper; Rocha R coordinated the writing of the paper; Santana GO designed the outline and coordinated the writing of the paper.
Conflict-of-interest statement: There is no conflict of interest associated with any of the senior authors or coauthors who contributed their efforts to this manuscript.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Correspondence to: Raquel Rocha, DMSc, Department of Science of Nutrition, School of Nutrition, Federal University of Bahia, Salvador, Araujo Pinho Avenue, number 32, Bahia 40110-060, Brazil. [email protected]: +55-71-99749964
Received: April 18, 2015Peer-review started: April 18, 2015First decision: June 18, 2015Revised: August 22, 2015Accepted: September 16, 2015Article in press: September 18, 2015Published online: November 15, 2015
AbstractInflammatory bowel disease (IBD) patients exhibit higher risk for bone loss than the general population. The chronic inflammation causes a reduction in bone mineral density (BMD), which leads to osteopenia and osteoporosis. This article reviewed each risk factor for osteoporosis in IBD patients. Inflammation is one of the factors that contribute to osteoporosis in IBD patients, and the main system that is involved in bone loss is likely RANK/RANKL/osteoprotegerin. Smoking is a risk factor for bone loss and fractures, and many mechanisms have been proposed to explain this loss. Body composition also interferes in bone metabolism and increasing muscle mass may positively affect BMD. IBD patients frequently use corticosteroids, which stimulates osteoclastogenesis. IBD patients are also associated with vitamin D deficiency, which contributes to bone loss. However, infliximab therapy is associated with improvements in bone metabolism, but it is not clear whether the effects are because of inflammation improvement or infliximab use. Ulcerative colitis patients with proctocolectomy and ileal pouches and Crohn’s disease patients with ostomy are also at risk for bone loss, and these patients should be closely monitored.
Key words: Bone mineral density; Crohn’s disease; Osteoporosis; Ulcerative colitis; Inflammatory bowel disease; Risk factors
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Inflammatory bowel disease (IBD) is associated with bone loss. Some factors reduce bone mineral density and lead to osteopenia and osteoporosis. The major complication in osteoporosis is the increased risk of fracture, which may impact quality of life. This article reviews each risk factor for osteoporosis in IBD patients, like chronic inflammation, smoking, body composition, corticosteroid use, vitamin D deficiency, surgery, and
MINIREVIEWS
210 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Risk factors for osteoporosis in inflammatory bowel disease patients
World J Gastrointest Pathophysiol 2015 November 15; 6(4): 210-218ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i4.210

the effect of infliximab therapy.
Lima CA, Lyra AC, Rocha R, Santana GO. Risk factors for osteoporosis in inflammatory bowel disease patients. World J Gastrointest Pathophysiol 2015; 6(4): 210-218 Available from: URL: http://www.wjgnet.com/2150-5330/full/v6/i4/210.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i4.210
INTRODUCTIONInflammatory bowel disease (IBD), which is primarily comprised of ulcerative colitis (UC) and Crohn’s disease (CD), is associated with various systemic complications, such as extra-intestinal manifestations (EIMs)[1]. These complications are found in approximately 40% of IBD patients. The most widely known EIMs are skin lesions (erythema nodosum and pyoderma gangrenosum), articular manifestations and liver diseases (primary sclerosing cholangitis and primary biliary cirrhosis)[2,3].
IBD patients exhibit a higher risk for bone loss than the general population. Chronic inflammation causes a reduction in bone mineral density (BMD), which leads to osteopenia and osteoporosis. Cross-sectional studies reported a highly variable prevalence of low BMD in IBD patients. The prevalence of osteopenia and osteoporosis varies significantly depending on the study population, location, and design, but it ranges from 22%-77% and 17%-41%, respectively[4].
The incidence of inflammatory bowel disease seems stable in Western countries, but this disease has become more prevalent in Eastern countries, including Asia and Eastern Europe[5]. Extra-intestinal manifestations are also present in IBD patients in Eastern countries. Some studies demonstrated that these patients are at risk for bone loss and osteoporosis[6].
Dual-energy X-ray absorptiometry (DXA) is the current gold standard technique for the measurement of bone mass. Measurements are generally obtained at the femoral neck and lumbar spine. DXA results are typically expressed as the number of standard deviations (SD) above or below the expected mean for individuals of the same age, ethnicity and gender (Z score) or the mean of peak bone mass in young adults (T score)[7-9]. The World Health Organization reported formulated diagnostic ranges for osteoporosis based on T scores. Osteoporosis and osteopenia are defined by a T score below -2.5, and between -1 and -2.5, respectively. These re-commendations were derived from postmenopausal Caucasian females. Therefore, caution must be exercised when extrapolating these data to other groups[9,10]. The current guidelines recommend DXA screening in IBD patients with one or more of the following risk factors: History of vertebral fractures, postmenopausal, male > 50 years of age, chronic corticosteroid therapy, or hypogonadism[9-11].
The major complication of bone loss and osteoporosis
is the increased risk of fracture, especially non-traumatic fractures[12,13]. Bernstein et al[14] demonstrated that the incidence of fracture in persons with IBD is 40% greater than the general population. Other authors also reported similar findings[15-17]. Whether differences between IBD type (CD or UC) and BMD exist are not known. A cross-sectional population based study by Jahnsen et al[18] found that CD patients exhibited significantly reduced BMD compared to UC patients and healthy controls. A cohort of 3141 IBD patients in Taiwan also demonstrated a higher risk of osteoporosis in CD patients than UC patients[6]. However, these results are not consistent with other reports.
Whether gender interferes with BMD in IBD patients is not known. Ardizzone et al[19] demonstrated that spine and femur BMD Z and T scores were significantly lower in men than women UC patients, but this difference was not demonstrated in CD patients. A case control cross-sectional study of 113 CD patients found that female patients exhibited significantly decreased BMD of the femoral neck and the trochanteric region, but BMD was not significantly different from healthy controls in men[20].
Other risk factors associated to IBD or the general population are also related to the loss of bone mass with older age, postmenopausal status, smoking, malnu-trition, physical inactivity, corticosteroid use for more than three months and vitamin D deficiency[21].
This review describes the specific risk factors for osteoporosis in IBD patients.
INFLAMMATIONMany factors exert important effects on bone metabo-lism, but there is increasing evidence that inflammation per se contributes to osteoporosis in IBD. Some studies in patients with newly diagnosed IBD demonstrated a reduction of BMD, even without the use of medications, such as corticosteroids[22,23].
Several chronic inflammatory disorders are asso-ciated with osteoporosis and an increased number of fractures. Inflammation is characterized by the pro-duction of cytokines, which is associated with increased bone resorption and reduced bone formation. The main system involved in the development of osteoporosis in IBD and other inflammatory diseases is likely the RANK/RANKL/osteoprotegerin[24].
The receptor activator of nuclear factor-B (RANK) is a transmembrane protein that is expressed on the surface of cells of hematopoietic origin that belongs to the TNF receptor family. RANK is the primary cytokine receptor in the development of osteoclastogenesis[25-28]. The ligand for RANK receptor (RANKL) is expressed on the surface of osteoblasts, mesenchymal cells and other cells, such as T and B lymphocytes. The binding of RANKL to RANK induces the differentiation of osteoclast precursors. RANKL also increases the resorptive activity of osteoclasts and prolongs their survival by suppressing
211 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Lima CA et al . Risk factors/osteoporosis/in IBD

apoptosis[25-28].Osteoblasts produce osteoprotegerin (OPG) as a
control to maintain balance. OPG is a decoy receptor molecule that naturally binds RANKL to inhibit osteoclast activation and protect against bone loss[25-28]. Chronic inflammatory states mediated by T cell-produced cytokines affect osteoblasts and osteoclasts. Activated T cells produce RANKL and its soluble form, which directly triggers bone loss via the induction and activation of osteoclasts by RANK[29].
Several pro-inflammatory cytokines are involved in the activation of osteoclasts, such as interleukin-1 (IL-1), tumor necrosis factor alpha (TNF-α), IL-6, IL-11, IL-15 and IL-17[30]. IL-6 plays an important role in the mediation of inflammatory osteoporosis, and it may also be involved in the pathways that lead to osteoporosis but are not elicited by inflammation[31].
Turk et al[32] demonstrated that patients with newly diagnosed and untreated CD exhibited elevated proin-flammatory cytokines levels (IL-6, TNF-α, and IL-1) and increased free RANKL and OPG activity. These authors also observed a positive correlation between TNF-α and sRANK.
Disease activity interferes with bone metabolism. Some studies demonstrated that patients with disease in remission exhibit an increase in BMD. Reffitt et al[33] analyzed 137 IBD patients and demonstrated that patients with longer disease remission exhibited higher BMD.
SMOKINGSmoking has been recognized as a risk factor for bone loss and fractures for many years. Several mechanisms were proposed to explain the differences in BMD between smokers and non-smokers. However, the pathophysiological mechanisms underlying osteoporosis in cigarette smokers have not been fully explored[34,35].
Some studies demonstrated that the dose and duration of smoking may influence the effect of smoking on bone[35,36]. Smoking seems related to a vitamin D deficiency, and one possible explanation is that smoking alters the hepatic metabolism of vitamin D by influen-cing 25 hydroxylase in the liver, which lowers serum 25-hydroxyvitamin D[34,35]. There is also evidence that smoking alters gastrointestinal calcium absorption. Smokers lead an unhealthy lifestyle that includes low calcium/vitamin D intake, lack of exercise and alcohol ingestion, which affects bone health[34,35].
Whether smoking is associated with estradiol levels is controversial, but some studies demonstrated that smoking alters estrogen production and metabolism. There are some possible mechanisms. Nicotine may reduce estrogen production, and smoking enhances the hepatic metabolism of estradiol. Smokers exhibit higher serum sex-hormone binding globulin levels, which reduces free estradiol concentrations[34,35].
Few studies investigated the relationship between smoking and the RANK-RANKL-OPG system. Some
reports demonstrated that smokers exhibit lower OPG levels without a difference in RANKL levels[36]. A cross-sectional study of 126 UC and 39 CD Iranian IBD patients demonstrated that femoral neck T scores were predicted by age, body mass index (BMI), smoking, and corticosteroid use. However, the association between smoking and BMD was not observed in the lumbar spine in this study[37]. Silvennoinen et al[38] evaluated the effect of smoking on BMD in 152 IBD patients (67 UC, 78 CD, 7 indeterminate colitis) and 73 controls and found that female IBD patients who currently smoked or with a previous history of smoking exhibited lower Z scores for the lumbar spine and femoral neck than female patients who had never smoked.
Smoking is also associated with relapses and disease activity (especially CD) and the need for steroids, which also negatively interferes with bone metabolism. The suspension of smoking is associated with more flare-ups in UC patients. However, smoking cessation should be encouraged in all IBD patients because it reduces other complications, such as cardiovascular disease, lung cancer and changes in bone health[39].
BODY COMPOSITIONLow BMI is a well-documented risk factor for low BMD and fracture[40]. Azzopardi et al[41] analyzed the risk factors for osteoporosis in 83 CD patients and found a significant association between BMI and BMD.
Many others studies also identified a positive asso-ciation between BMD and BMI[42-44]. Atreja et al[45] also considered BMI a strong risk factor for altered bone metabolism and a way to identify osteoporotic patients who are missed by current guidelines. Leslie et al[46] studied 388 IBD patients and found that greater weight, height, and body mass measurements positively corre-lated with bone density at all sites. Fat and lean tissues exhibited positive relationships with BMD in this study, but lean tissue exhibited a much stronger correlation than fat tissue, especially for the total hip.
Low BMI is a risk factor for fractures, but whether obesity is a protective factor is not clear because obesity increases the risk of some osteoporotic fractures[47,48]. Johansson et al[49] published a recent meta-analysis of the association of fracture risk and BMI in women and concluded that there is a slight increase in osteoporotic fracture risk with increasing BMI after adjustment for BMD. Therefore, body composition appears more important than BMI in bone metabolism.
Mechanical loading of the muscles that act on the bone produce an anabolic effect, which results in osteo-genesis[50,51]. Many IBD patients have reduced muscle (lean mass) because of nutritional factors, a sedentary lifestyle or medications, and these factors may lead to a reduced bone mass that is secondary to the decrease in mechanical stimulation of the skeleton[52].
A Canadian study analyzed the bone mass (bone mineral content) and muscle mass (lean mass) of 65 CD patients. Multiple regression analysis demonstrated
212 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Lima CA et al . Risk factors/osteoporosis/in IBD

213 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
status because GCs reduce estrogen and testosterone production. This negative effect of oral GCs on gonadal function may increase bone resorption[52,54].
GCs reduce intestinal calcium absorption and inhibit calcium reabsorption in the kidney, which indirectly leads to a negative net calcium balance and stimulates an increase in parathyroid hormone. These changes further increase the number of osteoclasts and stimulate bone resorption[57,58].
ROLE OF VITAMIN DThe role of vitamin D in IBD was not investigated in recent years. This vitamin primarily increases serum calcium and phosphate levels and promotes bone mine-ralization.
Vitamin D is available in two forms: Vitamin D3 (cho-lecalciferol), which is produced in the skin by exposure to sun light and obtained from animal sources, and vitamin D2 (ergocalciferol), which is obtained from plant sources. Vitamin D is metabolized in the liver to 25-hydroxyvitamin D [25-(OH) D], which circulates in the blood plasma and is stored in fat tissue and muscles. Metabolites of vitamin D are transported bound to albumin binding protein or vitamin D. This protein regulates the effects of the metabolites in target organs[61].
A study of 49 healthy young men demonstrated that free and bioavailable 25-(OH) D positively correlated with BMD, which suggests a possible benefit of vitamin D supplementation during deficiencies[62].
Vitamin D exerts its biological effects through the vitamin D receptor[61]. Multiple tissues and immune cells express this receptor, and these cells contain the enzyme that converts vitamin D into its active metabolite. Therefore, vitamin D appears to influence the innate immune response by inhibiting the maturation of dendritic cells and IL-12 and the adaptive immune response by inhibiting the production of IFN-γ, IL-17 and IL-21[63,64].
Several studies demonstrated a high prevalence of vitamin D deficiency in IBD patients. Many factors are attributed to this deficiency, and some of these factors are common to the general population, such as low sun exposure, inadequate intake, inactivity and other factors related to inflammatory disease, such as terminal ileum resection and low absorption due to the inflammatory process[64]. Disease activity is also associated with low levels of vitamin D in CD and UC patients[65,66].
Vitamin D deficiency leads to reduced calcium and secondary hyperparathyroidism, which stimulates osteoclastogenesis, increases bone resorption, and results in osteopenia and osteoporosis[64].
IS ANTI-TNF A PROTECTIVE FACTOR?Elevated TNF-α concentration may play a role in dysfunctional bone metabolism in IBD. TNF-α is a major factor in the inactivation of osteoclasts. This cytokine induces osteoclast differentiation, increases osteoclast
that only total lean mass was independently associated with lumbar bone mineral content (BMC), BMC in both hips and total BMC[52]. Lee et al[53] demonstrated a similar effect in a cohort of 61 CD patients. This study found that lean mass and muscle strength, but not fat mass, significantly correlated with regional and whole body BMD, but lean mass was the only independent predictor of hip BMD after multiple regression analysis. These authors concluded that maintaining or increasing muscle mass may positively affect BMD and prevent the development of osteopenia and osteoporosis.
GLUCOCORTICOID USEGlucocorticoids (GCs) are frequently used in the treat-ment of inflammatory conditions, such as rheumatoid arthritis, systemic lupus erythematous, asthma and IBD. GC exposure is common in IBD patients, and over 50% of patients are exposed to systemic GCs within 5 years of diagnosis, and 20% have used at least 3 g of prednisone in any 1-year period[54].
Many studies consistently identified systemic GC use as a risk factor for osteoporosis and bone mineral loss in IBD patients[54,55]. Abraham et al[56] studied 166 IBD patients and demonstrated that the risk of osteoporosis was twice as high in patients who used corticosteroids [OR = 2.4 (1.5-3.4), P = 0.001].
Osteoporosis attributed to GC exposure is the most common etiology of drug-induced osteoporosis. Approximately 50% of patients receiving chronic GC therapy will develop osteopenia and fractures, and 17% of these patients will develop fractures within the first year of GC therapy[57].
Some risk factors for the development of fractures after steroid exposure were identified: Age older than 65 years, cumulative steroid dose (high GC dose and duration of treatment > 3 mo), positive family history of osteoporosis, low calcium intake, female sex, low bodyweight (BMI < 24 kg/m2) and low BMD[57,58].
The mechanism of this loss is not fully understood. GC exposure alters the balance between osteoclast and osteoblast activity in bone metabolism. One important mechanism for the effects of GC on bone is osteoblastic dysfunction. GC inhibits stem cell differentiation into osteoblasts and induces osteoblast apoptosis, which decreases the secretion of osteoid matrix and new bone formation[57,59].
GCs increase the expression of RANKL and decrease the expression of its soluble decoy receptor OPG in stromal and osteoblastic cells. These alterations caused a greater differentiation of precursors into osteoclasts, which increases their resorptive activity and enhances bone reabsorption. There is also evidence that GCs directly prolong the lifespan of mature osteoclasts[57,59,60]. The increase in RANKL is only transient. Therefore, the failure of bone formation, rather than increased bone resorption, is likely the main mechanism underlying glucocorticoid-associated bone loss[58].
GCs also exhibit a negative effect on sex hormones
Lima CA et al . Risk factors/osteoporosis/in IBD

214 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
bone resorption, and protects these cells against apoptosis, which sensitizes osteoblasts to apoptosis and diminishes bone formation[67].
Infliximab (IFX) is a monoclonal antibody that exhibits high affinity and specificity for TNF-α. Anti-TNF therapy is an important IBD treatment because it allows for remission induction, relapse prevention and a decrease in corticosteroid use[68]. Some studies demonstrated the benefits of IFX use on BMD (Table 1). However, the exact mechanism of action of this anti-TNF in bone metabolism is not clear.
Miheller et al[69] investigated the effects of IFX on bone metabolism by measuring biochemical parameters in 29 CD patients and found that IFX increased osteocalcin levels (marker of bone formation) and reduced beta-Cross Laps levels (marker of bone resorption).
Abreu et al[70] observed increased bone alkaline phosphatase (bone formation marker) in 38 CD patients treated with IFX and no significant change in the dose of N-telopeptide of type Ⅰ collagen (NTX-marker of bone resorption). Franchimont et al[71] also examined the evolution of biochemical markers of bone metabolism after the first treatment with IFX in 71 CD patients. The authors of this study detected a normalization of bone markers after 8 wk of IFX treatment, with a median increase in formation markers of 14%-51%, according to the marker, and an approximately 10% reduction in bone resorption[71].
A retrospective study by Mauro et al[72] in 15 CD patients treated with IFX demonstrated significant increases in BMC and BMD in the lumbar spine compared to the control group.
The benefit of using IFX in BMD was also demon-strated with its associated use with bisphosphonates, as noted by Pazianas et al[73] in a retrospective cohort. They studied 61 CD patients, and patients who used bisphosphonates plus IFX experienced a greater increase in BMD than patients who used only bisphosphonate (6.7%/year vs 4.46%/year, P < 0.05).
The mechanism of action of IFX on bone metabolism is not well established, but its benefits in BMD may
occur via the alteration of bone markers, the reduction of GC utilization and the induction of clinical and endoscopic remission.
Adalimumab is a human monoclonal IgG1 antibody that is specific for human TNF. It is also used in the treatment of IBD and other inflammatory diseases, such as rheumatoid arthritis and spondyloarthritis[74]. Studies demonstrated benefits in BMD in some patients using this therapy. Durnez et al[75] studied 59 patients with spondylo arthropathy treated with anti-TNF (infliximab, adalimumab or etarnecept) during a follow up of 6.5 years and found an increase in BMD of 11.8% in the lumbar spine and 3.6% in the trochanter.
Wijbrandts et al[76] conducted a prospective, open-label study of 50 rheumatoid arthritis patients. They analyzed the mineral density of the lumbar spine and femoral neck before and 1 year after adalimumab treatment. The authors observed no significant changes in BMD in lumbar spine (0.3%) or femoral neck (0.3%) and concluded that therapy with this anti-TNF does not increase BMD, but it can stop bone loss.
Another study by Krieckaert et al[77] evaluated the effect of long-term adalimumab use on BMD of the lumbar spine, hip and hands of rheumatoid arthritis patients. A total of 184 patients were studied, and hip and lumbar spine BMD remained stable after 1 year of treatment, but BMD in the hands decreased significantly by 1.41%. The mean BMD change per year was -0.58% and 0.07% for hip and lumbar spine, respectively, after a mean follow-up of 4.0 years (overall P value of hip was < 0.0001 and spine was 0.67). The authors considered that the BMD changes were associated to disease activity.
However, there are currently no published data inves-tigating the effect of adalimumab on bone metabolism in IBD patients. There are also no data with certolizumab pegol.
EFFECT OF SURGERYProctocolectomy with ileal pouch-anal anastomosis
Table 1 Infliximab effects on bone mineral density in Crohn’s disease
Ref. Study design1 Participants number Endpoints Results
Miheller et al[69] Prospective 29 CD patients Determine the effects of IFX on bone metabolism in CD patients
IFX improves bone metabolism in CD independently from the behavior of the disease
Abreu et al[70] Prospective 38 CD patients Assess the ability of IFX to increase bone formation measured by markers of bone
turnover in active CD patients
Treatment with IFX was associated with increased markers of bone formation
Franchimont et al[71] Prospective 71 CD patients, 68 controls
Assess the evolution of markers of bone turnover after IFX treatment for active
CD
IFX induces improvement in biochemical markers of bone turnover
Mauro et al[72] Retrospective 15 CD patients, 30 controls
Assess whether treatment with IFX had a beneficial effect on lumbar bone mass
Treatment with IFX was associated with significant increases in lumbar bone area, BMC and BMD in
CD patientsPazianas et al[73] Retrospective 61 CD patients Evaluate the effects of IFX administration
on BMD in CD patients IFX may work in synergy with bisphosphonates to provide additional increases in BMD in CD patients
1All were cohort study. CD: Crohn disease; IFX: Infliximab; BMC: Bone mineral content; BMD: Bone mineral density.
Lima CA et al . Risk factors/osteoporosis/in IBD

215 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
(IPAA) is the procedure of choice for the treatment of most patients with refractory UC, UC with dysplasia and familial adenomatous polyposis[78-80]. Some studies demonstrated an increase in long-term BMD after total colectomy with IPAA[79]. This surgery may improve BMD in UC patients, possibly due to the discontinuation of corticosteroids, improvement in nutritional status and a decreased production of cytokines by the diseased colon[78,79].
However, it is unclear whether total colectomy with ileal pouch provides benefits or detriments to BMD. In a study of 327 UC patients who underwent this surgery, 32% had low BMD 4 years after surgery, which suggests that bone loss continues after colectomy[78].
Possible risk factors and mechanisms of bone loss are considered. An ileal pouch changes the anatomy and function of the small intestine by reducing the absorption of bile salts, which contributes to the reduced absorption of vitamin D. The stasis of stool in the ileum in UC patients with IPAA promotes bacterial overgrowth, which causes deconjugation of bile salts and leads to the malabsorption of vitamin D[79]. Another mechanism is inflammation of the ileal pouch, which increases inflammatory cytokines levels, such as IL-1, IL-6 and TNF-α, and stimulates osteoclast activity and promotes bone loss[79].
Navaneethan et al[81] also found a lower BMD in UC patients undergoing total proctocolectomy and ileal pouch compared to the control group (31.1% vs 15.1%, P < 0.001). They also found that BMD was already low before surgery in 13 patients, and 7 (53.8%) of these patients exhibited an increase in BMD after surgery. Some studies demonstrated a higher incidence of fractures in UC patients with IPAA, ranging from 7%-15%[78,81].
IBD patients, particularly CD, are at increased risk of surgery based on disease severity and duration. The most common surgery for CD patients involves removal of the terminal ileum, which is associated to a vitamin D deficiency and the consequent secondary hyperparathyroidism, which promotes bone mass reduction. However, the relationship of these factors with osteoporosis in CD is not well defined[54].
Gupta et al[82] analyzed 126 patients with ostomy, and 95% of these patients had CD and ileostomy. This study also demonstrated a high frequency of fractures (9.5%) in CD patients after ostomy, with significantly higher rates in patients with low BMD. IBD patients with ostomy and low BMD also exhibited low BMI. Fractures were also five times more frequent in IBD patients with ostomy and low BMD.
IBD patients with ostomy are at higher risk for bone loss, and these patients should be monitored closely, especially patients with risk factors, such as low BMI and a previous history of fractures.
CONCLUSIONIBD is associated with bone loss, and patients are at
increased risk of developing fractures. Many risk factors are associated with reductions in BMD in this population, including inflammation, smoking, body composition, glucocorticoid use, vitamin D deficiency and surgery. Infliximab seems to increase BMD, but the exact mechanism is not well established. More studies are needed to analyze the effect of other anti-TNF therapies in BMD.
REFERENCES1 Ott C, Schölmerich J. Extraintestinal manifestations and
complications in IBD. Nat Rev Gastroenterol Hepatol 2013; 10: 585-595 [PMID: 23835489 DOI: 10.1038/nrgastro.2013.117]
2 Miheller P, Gesztes W, Lakatos PL. Manipulating bone disease in inflammatory bowel disease patients. Ann Gastroenterol 2013; 26: 296-303 [PMID: 24714303]
3 Rothfuss KS, Stange EF, Herrlinger KR. Extraintestinal mani-festations and complications in inflammatory bowel diseases. World J Gastroenterol 2006; 12: 4819-4831 [PMID: 16937463]
4 Ali T, Lam D, Bronze MS, Humphrey MB. Osteoporosis in inflammatory bowel disease. Am J Med 2009; 122: 599-604 [PMID: 19559158 DOI: 10.1016/j.amjmed.2009.01.022]
5 Ng SC. Epidemiology of inflammatory bowel disease: focus on Asia. Best Pract Res Clin Gastroenterol 2014; 28: 363-372 [PMID: 24913377 DOI: 10.1016/j.bpg.2014.04.003]
6 Tsai MS, Lin CL, Tu YK, Lee PH, Kao CH. Risks and predictors of osteoporosis in patients with inflammatory bowel diseases in an Asian population: a nationwide population-based cohort study. Int J Clin Pract 2015; 69: 235-241 [PMID: 25472555 DOI: 10.1111/ijcp.12526]
7 Pinto Neto AM, Soares A, Urbanetz AA, Souza ACA, Ferrari AEM, Amaral B, Moreira C, Fernandes CE, Zerbini CAF, Baracat E, Freitas EC, Meirelles ES, Bandeira F, Gonçalves HT, Lemgruber I, Marques Neto JF, Borges JLC, Sisson de Castro JA, Fiat JC, Mendonça LMC, Oliveira L, Russo LAT, Gregório LH, Marone M, Castro ML, Abi Haidar M, Santos PRD, Plapler P, Carneiro R, Guarniero R, Machado RB, Pereira RMR, Lederman R, Radominski S, Eis SR, Pereira SRM, Szjenfeld V, Chahade W. Brasilian Consensus on osteoporosis 2002. Rev Bras Reumatol 2002; 42: 343-354
8 American Gastroenterological Association medical position statement: guidelines on osteoporosis in gastrointestinal diseases. Gastroenterology 2003; 124: 791-794 [PMID: 12612916]
9 Bernstein CN, Leslie WD, Leboff MS. AGA technical review on osteoporosis in gastrointestinal diseases. Gastroenterology 2003; 124: 795-841 [PMID: 12612917]
10 Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. Report of a WHO Study Group. World Health Organ Tech Rep Ser 1994; 843: 1-129 [PMID: 7941614]
11 Scott EM, Gaywood I, Scott BB. Guidelines for osteoporosis in coeliac disease and inflammatory bowel disease. British Society of Gastroenterology. Gut 2000; 46 Suppl 1: i1-i8 [PMID: 10647595 DOI: 10.1136/gut.46.suppl_1.I1]
12 Targownik LE, Bernstein CN, Leslie WD. Inflammatory bowel disease and the risk of osteoporosis and fracture. Maturitas 2013; 76: 315-319 [PMID: 24139749 DOI: 10.1016/j.maturitas.2013.09.009]
13 Miheller P, Lorinczy K, Lakatos PL. Clinical relevance of changes in bone metabolism in inflammatory bowel disease. World J Gastroenterol 2010; 16: 5536-5542 [PMID: 21105186 DOI: 10.3748/wjg.v16.i44.5536]
14 Bernstein CN, Blanchard JF, Leslie W, Wajda A, Yu BN. The incidence of fracture among patients with inflammatory bowel disease. A population-based cohort study. Ann Intern Med 2000; 133: 795-799 [PMID: 11085842 DOI: 10.7326/0003-4819-133-10-200011210-00012]
Lima CA et al . Risk factors/osteoporosis/in IBD

216 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
15 Card T, West J, Hubbard R, Logan RF. Hip fractures in patients with inflammatory bowel disease and their relationship to corticosteroid use: a population based cohort study. Gut 2004; 53: 251-255 [PMID: 14724159 DOI: 10.1136/gut.2003.026799]
16 van Staa TP, Cooper C, Brusse LS, Leufkens H, Javaid MK, Arden NK. Inflammatory bowel disease and the risk of fracture. Gastroenterology 2003; 125: 1591-1597 [PMID: 14724810 DOI: 10.1053/j.gastro.2003.09.027]
17 Hilmi I, Sunderesvaran K, Ananda V, Sarji SA, Arumugam K, Goh KL. Increased fracture risk and osteoporosis not associated with vitamin D levels in Malaysian patients with inflammatory bowel disease. J Clin Endocrinol Metab 2013; 98: 2415-2421 [PMID: 23553858 DOI: 10.1210/jc.2013-1147]
18 Jahnsen J, Falch JA, Aadland E, Mowinckel P. Bone mineral density is reduced in patients with Crohn’s disease but not in patients with ulcerative colitis: a population based study. Gut 1997; 40: 313-319 [PMID: 9135518 DOI: 10.1136/gut.40.3.313]
19 Ardizzone S, Bollani S, Bettica P, Bevilacqua M, Molteni P, Bianchi Porro G. Altered bone metabolism in inflammatory bowel disease: there is a difference between Crohn’s disease and ulcerative colitis. J Intern Med 2000; 247: 63-70 [PMID: 10672132 DOI: 10.1046/j.1365-2796.2000.00582.x]
20 Andreassen H, Hylander E, Rix M. Gender, age, and body weight are the major predictive factors for bone mineral density in Crohn’s disease: a case-control cross-sectional study of 113 patients. Am J Gastroenterol 1999; 94: 824-828 [PMID: 10086673 DOI: 10.1111/j.1572-0241.1999.00866.x]
21 Bernstein CN, Leslie WD. The pathophysiology of bone disease in gastrointestinal disease. Eur J Gastroenterol Hepatol 2003; 15: 857-864 [PMID: 12867794 DOI: 10.1097/00042737-200308000-00004]
22 Schoon EJ, Blok BM, Geerling BJ, Russel MG, Stockbrügger RW, Brummer RJ. Bone mineral density in patients with recently diagnosed inflammatory bowel disease. Gastroenterology 2000; 119: 1203-1208 [PMID: 11054377 DOI: 10.1053/gast.2000.19280]
23 Sakellariou GT, Moschos J, Berberidis C, Mpoumponaris A, Kadis S, Molyvas E, Kouklakis G. Bone density in young males with recently diagnosed inflammatory bowel disease. Joint Bone Spine 2006; 73: 725-728 [PMID: 17126059 DOI: 10.1016/j.jbspin.2006.01.017]
24 Reinshagen M. Osteoporosis in inflammatory bowel disease. J Crohns Colitis 2008; 2: 202-207 [PMID: 21172211 DOI: 10.1016/j.crohns.2008.01.005]
25 Boyce BF, Xing L. Functions of RANKL/RANK/OPG in bone modeling and remodeling. Arch Biochem Biophys 2008; 473: 139-146 [PMID: 18395508 DOI: 10.1016/j.abb.2008.03.018]
26 Hofbauer LC, Schoppet M. Clinical implications of the osteoprotegerin/RANKL/RANK system for bone and vascular diseases. JAMA 2004; 292: 490-495 [PMID: 15280347]
27 Tilg H, Moschen AR, Kaser A, Pines A, Dotan I. Gut, inflammation and osteoporosis: basic and clinical concepts. Gut 2008; 57: 684-694 [PMID: 18408105 DOI: 10.1136/gut.2006.117382]
28 Eriksen EF. Cellular mechanisms of bone remodeling. Rev Endocr Metab Disord 2010; 11: 219-227 [PMID: 21188536 DOI: 10.1007/s11154-010-9153-1]
29 Clowes JA, Riggs BL, Khosla S. The role of the immune system in the pathophysiology of osteoporosis. Immunol Rev 2005; 208: 207-227 [PMID: 16313351 DOI: 10.1111/j.0105-2896.2005.00334.x]
30 Mundy GR. Osteoporosis and inflammation. Nutr Rev 2007; 65: S147-S151 [PMID: 18240539 DOI: 10.1111/j.1753-4887.2007.tb00353.x]
31 Redlich K, Smolen JS. Inflammatory bone loss: pathogenesis and therapeutic intervention. Nat Rev Drug Discov 2012; 11: 234-250 [PMID: 22378270 DOI: 10.1038/nrd3669]
32 Turk N, Cukovic-Cavka S, Korsic M, Turk Z, Vucelic B. Proinflammatory cytokines and receptor activator of nuclear factor kappaB-ligand/osteoprotegerin associated with bone deterioration in patients with Crohn’s disease. Eur J Gastroenterol Hepatol
2009; 21: 159-166 [PMID: 19098682 DOI: 10.1097/MEG.0b013e3283200032]
33 Reffitt DM, Meenan J, Sanderson JD, Jugdaohsingh R, Powell JJ, Thompson RP. Bone density improves with disease remission in patients with inflammatory bowel disease. Eur J Gastroenterol Hepatol 2003; 15: 1267-1273 [PMID: 14624148 DOI: 10.1097/00042737-200312000-00003]
34 Wong PK, Christie JJ, Wark JD. The effects of smoking on bone health. Clin Sci (Lond) 2007; 113: 233-241 [PMID: 17663660 DOI: 10.1042/CS20060173]
35 Yoon V, Maalouf NM, Sakhaee K. The effects of smoking on bone metabolism. Osteoporos Int 2012; 23: 2081-2092 [PMID: 22349964 DOI: 10.1007/s00198-012-1940-y]
36 Ward KD, Klesges RC. A meta-analysis of the effects of cigarette smoking on bone mineral density. Calcif Tissue Int 2001; 68: 259-270 [PMID: 11683532 DOI: 10.1007/BF02390832]
37 Zali M, Bahari A, Firouzi F, Daryani NE, Aghazadeh R, Emam MM, Rezaie A, Shalmani HM, Naderi N, Maleki B, Sayyah A, Bashashati M, Jazayeri H, Zand S. Bone mineral density in Iranian patients with inflammatory bowel disease. Int J Colorectal Dis 2006; 21: 758-766 [PMID: 16463035 DOI: 10.1007/s00384-005-0084-3]
38 Silvennoinen JA, Lehtola JK, Niemelä SE. Smoking is a risk factor for osteoporosis in women with inflammatory bowel disease. Scand J Gastroenterol 1996; 31: 367-371 [PMID: 8726305 DOI: 10.3109/00365529609006412]
39 Cosnes J. Smoking, physical activity, nutrition and lifestyle: environmental factors and their impact on IBD. Dig Dis 2010; 28: 411-417 [PMID: 20926865 DOI: 10.1159/000320395]
40 De Laet C, Kanis JA, Odén A, Johanson H, Johnell O, Delmas P, Eisman JA, Kroger H, Fujiwara S, Garnero P, McCloskey EV, Mellstrom D, Melton LJ, Meunier PJ, Pols HA, Reeve J, Silman A, Tenenhouse A. Body mass index as a predictor of fracture risk: a meta-analysis. Osteoporos Int 2005; 16: 1330-1338 [PMID: 15928804]
41 Azzopardi N, Ellul P. Risk factors for osteoporosis in Crohn’s disease: infliximab, corticosteroids, body mass index, and age of onset. Inflamm Bowel Dis 2013; 19: 1173-1178 [PMID: 23511037 DOI: 10.1097/MIB.0b013e31828075a7]
42 Noble CL, McCullough J, Ho W, Lees CW, Nimmo E, Drummond H, Bear S, Hannan J, Millar C, Ralston SH, Satsangi J. Low body mass not vitamin D receptor polymorphisms predict osteoporosis in patients with inflammatory bowel disease. Aliment Pharmacol Ther 2008; 27: 588-596 [PMID: 18194505 DOI: 10.1111/j.1365-2036.2008.03599.x]
43 Habtezion A, Silverberg MS, Parkes R, Mikolainis S, Steinhart AH. Risk factors for low bone density in Crohn‘s disease. Inflamm Bowel Dis 2002; 8: 87-92 [PMID: 11854605]
44 Ezzat Y, Hamdy K. The frequency of low bone mineral density and its associated risk factors in patients with inflammatory bowel diseases. Int J Rheum Dis 2010; 13: 259-265 [PMID: 20704624 DOI: 10.1111/j.1756-185X.2010.01542.x]
45 Atreja A, Aggarwal A, Licata AA, Lashner BA. Low body mass index can identify majority of osteoporotic inflammatory bowel disease patients missed by current guidelines. ScientificWorldJournal 2012; 2012: 807438 [PMID: 22645457 DOI: 10.1100/2012/807438]
46 Leslie WD, Miller N, Rogala L, Bernstein CN. Body mass and composition affect bone density in recently diagnosed inflammatory bowel disease: the Manitoba IBD Cohort Study. Inflamm Bowel Dis 2009; 15: 39-46 [PMID: 18623166 DOI: 10.1002/ibd.20541]
47 Cawsey S, Padwal R, Sharma AM, Wang X, Li S, Siminoski K. Women with severe obesity and relatively low bone mineral density have increased fracture risk. Osteoporos Int 2015; 26: 103-111 [PMID: 25182230 DOI: 10.1007/s00198-014-2833-z]
48 Zhao LJ, Liu YJ, Liu PY, Hamilton J, Recker RR, Deng HW. Relationship of obesity with osteoporosis. J Clin Endocrinol Metab 2007; 92: 1640-1646 [PMID: 17299077 DOI: 10.1210/jc.2006-0572]
49 Johansson H, Kanis JA, Odén A, McCloskey E, Chapurlat RD,
Lima CA et al . Risk factors/osteoporosis/in IBD

217 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Christiansen C, Cummings SR, Diez-Perez A, Eisman JA, Fujiwara S, Glüer CC, Goltzman D, Hans D, Khaw KT, Krieg MA, Kröger H, LaCroix AZ, Lau E, Leslie WD, Mellström D, Melton LJ, O’Neill TW, Pasco JA, Prior JC, Reid DM, Rivadeneira F, van Staa T, Yoshimura N, Zillikens MC. A meta-analysis of the association of fracture risk and body mass index in women. J Bone Miner Res 2014; 29: 223-233 [PMID: 23775829 DOI: 10.1002/jbmr.2017]
50 Lee N, Radford-Smith G, Taaffe DR. Bone loss in Crohn’s disease: exercise as a potential countermeasure. Inflamm Bowel Dis 2005; 11: 1108-1118 [PMID: 16306774 DOI: 10.1097/01.MIB.0000192325.28168.08]
51 Turner CH, Robling AG. Exercise as an anabolic stimulus for bone. Curr Pharm Des 2004; 10: 2629-2641 [PMID: 15320750 DOI: 10.2174/1381612043383755]
52 Mauro M, Armstrong D. Evaluation of densitometric bone-muscle relationships in Crohn’s disease. Bone 2007; 40: 1610-1614 [PMID: 17433801 DOI: 10.1016/j.bone.2007.02.026]
53 Lee N, Radford-Smith GL, Forwood M, Wong J, Taaffe DR. Body composition and muscle strength as predictors of bone mineral density in Crohn’s disease. J Bone Miner Metab 2009; 27: 456-463 [PMID: 19333683 DOI: 10.1007/s00774-009-0059-5]
54 Targownik LE, Bernstein CN, Leslie WD. Risk factors and management of osteoporosis in inflammatory bowel disease. Curr Opin Gastroenterol 2014; 30: 168-174 [PMID: 24419292 DOI: 10.1097/MOG.0000000000000037]
55 Bernstein CN, Blanchard JF, Metge C, Yogendran M. The asso-ciation between corticosteroid use and development of fractures among IBD patients in a population-based database. Am J Gastroenterol 2003; 98: 1797-1801 [PMID: 12907335 DOI: 10.1111/j.1572-0241.2003.07590.x]
56 Abraham BP, Prasad P, Malaty HM. Vitamin D deficiency and corticosteroid use are risk factors for low bone mineral density in inflammatory bowel disease patients. Dig Dis Sci 2014; 59: 1878-1884 [PMID: 24619280 DOI: 10.1007/s10620-014-3102-x]
57 Mitra R. Adverse effects of corticosteroids on bone metabolism: a review. PM R 2011; 3: 466-471; quiz 471 [PMID: 21570035 DOI: 10.1016/j.pmrj.2011.02.017]
58 Canalis E, Mazziotti G, Giustina A, Bilezikian JP. Glucocorticoid-induced osteoporosis: pathophysiology and therapy. Osteoporos Int 2007; 18: 1319-1328 [PMID: 17566815 DOI: 10.1007/s00198-007-0394-0]
59 van Staa TP. The pathogenesis, epidemiology and management of glucocorticoid-induced osteoporosis. Calcif Tissue Int 2006; 79: 129-137 [PMID: 16969593 DOI: 10.1007/s00223-006-0019-1]
60 Rodríguez-Bores L, Barahona-Garrido J, Yamamoto-Furusho JK. Basic and clinical aspects of osteoporosis in inflammatory bowel disease. World J Gastroenterol 2007; 13: 6156-6165 [PMID: 18069754]
61 Garg M, Lubel JS, Sparrow MP, Holt SG, Gibson PR. Review article: vitamin D and inflammatory bowel disease--established concepts and future directions. Aliment Pharmacol Ther 2012; 36: 324-344 [PMID: 22686333 DOI: 10.1111/j.1365-2036.2012.05181.x]
62 Powe CE, Ricciardi C, Berg AH, Erdenesanaa D, Collerone G, Ankers E, Wenger J, Karumanchi SA, Thadhani R, Bhan I. Vitamin D-binding protein modifies the vitamin D-bone mineral density relationship. J Bone Miner Res 2011; 26: 1609-1616 [PMID: 21416506 DOI: 10.1002/jbmr.387]
63 Reich KM, Fedorak RN, Madsen K, Kroeker KI. Vitamin D improves inflammatory bowel disease outcomes: basic science and clinical review. World J Gastroenterol 2014; 20: 4934-4947 [PMID: 24803805 DOI: 10.3748/wjg.v20.i17.4934]
64 Mouli VP, Ananthakrishnan AN. Review article: vitamin D and inflammatory bowel diseases. Aliment Pharmacol Ther 2014; 39: 125-136 [PMID: 24236989 DOI: 10.1111/apt.12553]
65 Blanck S, Aberra F. Vitamin d deficiency is associated with ulcerative colitis disease activity. Dig Dis Sci 2013; 58: 1698-1702 [PMID: 23334382 DOI: 10.1007/s10620-012-2531-7]
66 Jørgensen SP, Hvas CL, Agnholt J, Christensen LA, Heickendorff L,
Dahlerup JF. Active Crohn’s disease is associated with low vitamin D levels. J Crohns Colitis 2013; 7: e407-e413 [PMID: 23403039 DOI: 10.1016/j.crohns.2013.01.012]
67 Kawai VK, Stein CM, Perrien DS, Griffin MR. Effects of anti-tumor necrosis factor α agents on bone. Curr Opin Rheumatol 2012; 24: 576-585 [PMID: 22810364 DOI: 10.1097/BOR.0b013e328356d212]
68 Lee KS, Kim IY, Kim PN. Dissecting intramural hematoma of the esophagus in Boerhaave syndrome: CT findings. AJR Am J Roentgenol 1991; 157: 197-198 [PMID: 2048525 DOI: 10.2214/ajr.157.1.2048525]
69 Miheller P, Muzes G, Rácz K, Blázovits A, Lakatos P, Herszényi L, Tulassay Z. Changes of OPG and RANKL concentrations in Crohn’s disease after infliximab therapy. Inflamm Bowel Dis 2007; 13: 1379-1384 [PMID: 17663430 DOI: 10.1002/ibd.20234]
70 Abreu MT, Geller JL, Vasiliauskas EA, Kam LY, Vora P, Martyak LA, Yang H, Hu B, Lin YC, Keenan G, Price J, Landers CJ, Adams JS, Targan SR. Treatment with infliximab is associated with increased markers of bone formation in patients with Crohn’s disease. J Clin Gastroenterol 2006; 40: 55-63 [PMID: 16340635 DOI: 10.1097/01.mcg.0000190762.80615.d4]
71 Franchimont N, Putzeys V, Collette J, Vermeire S, Rutgeerts P, De Vos M, Van Gossum A, Franchimont D, Fiasse R, Pelckmans P, Malaise M, Belaiche J, Louis E. Rapid improvement of bone metabolism after infliximab treatment in Crohn’s disease. Aliment Pharmacol Ther 2004; 20: 607-614 [PMID: 15352908 DOI: 10.1111/j.1365-2036.2004.02152.x]
72 Mauro M, Radovic V, Armstrong D. Improvement of lumbar bone mass after infliximab therapy in Crohn’s disease patients. Can J Gastroenterol 2007; 21: 637-642 [PMID: 17948133]
73 Pazianas M, Rhim AD, Weinberg AM, Su C, Lichtenstein GR. The effect of anti-TNF-alpha therapy on spinal bone mineral density in patients with Crohn‘s disease. Ann N Y Acad Sci 2006; 1068: 543-556 [PMID: 16831950 DOI: 10.1196/annals.1346.055]
74 Lapadula G, Marchesoni A, Armuzzi A, Blandizzi C, Caporali R, Chimenti S, Cimaz R, Cimino L, Gionchetti P, Girolomoni G, Lionetti P, Marcellusi A, Mennini FS, Salvarani C. Adalimumab in the treatment of immune-mediated diseases. Int J Immunopathol Pharmacol 2014; 27: 33-48 [PMID: 24774505]
75 Durnez A, Paternotte S, Fechtenbaum J, Landewé RB, Dougados M, Roux C, Briot K. Increase in bone density in patients with spondyloarthritis during anti-tumor necrosis factor therapy: 6-year followup study. J Rheumatol 2013; 40: 1712-1718 [PMID: 23950191 DOI: 10.3899/jrheum.121417]
76 Wijbrandts CA, Klaasen R, Dijkgraaf MG, Gerlag DM, van Eck-Smit BL, Tak PP. Bone mineral density in rheumatoid arthritis patients 1 year after adalimumab therapy: arrest of bone loss. Ann Rheum Dis 2009; 68: 373-376 [PMID: 18408246 DOI: 10.1136/ard.2008.091611]
77 Krieckaert CL, Nurmohamed MT, Wolbink G, Lems WF. Changes in bone mineral density during long-term treatment with adalimumab in patients with rheumatoid arthritis: a cohort study. Rheumatology (Oxford) 2013; 52: 547-553 [PMID: 23221326 DOI: 10.1093/rheumatology/kes320]
78 Shen B, Remzi FH, Oikonomou IK, Lu H, Lashner BA, Hammel JP, Skugor M, Bennett AE, Brzezinski A, Queener E, Fazio VW. Risk factors for low bone mass in patients with ulcerative colitis following ileal pouch-anal anastomosis. Am J Gastroenterol 2009; 104: 639-646 [PMID: 19262520 DOI: 10.1038/ajg.2008.78]
79 Gupta S, Shen B. Bone loss in patients with the ileostomy and ileal pouch for inflammatory bowel disease. Gastroenterol Rep (Oxf) 2013; 1: 159-165 [PMID: 24759961 DOI: 10.1093/gastro/got030]
80 Fazio VW, Ziv Y, Church JM, Oakley JR, Lavery IC, Milsom JW, Schroeder TK. Ileal pouch-anal anastomoses complications and function in 1005 patients. Ann Surg 1995; 222: 120-127 [PMID: 7639579]
81 Navaneethan U, Shen L, Venkatesh PG, Hammel J, Patel V, Remzi FH, Kiran RP. Influence of ileal pouch anal anastomosis on
Lima CA et al . Risk factors/osteoporosis/in IBD

218 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
bone loss in ulcerative colitis patients. J Crohns Colitis 2011; 5: 415-422 [PMID: 21939915 DOI: 10.1016/j.crohns.2011.04.008]
82 Gupta S, Wu X, Moore T, Shen B. Frequency, risk factors, and
adverse sequelae of bone loss in patients with ostomy for inflam-matory bowel diseases. Inflamm Bowel Dis 2014; 20: 259-264 [PMID: 24378598 DOI: 10.1097/01.MIB.0000439065.92211.d3]
P- Reviewer: Chow WK, Rajendran VM S- Editor: Tian YL L- Editor: A E- Editor: Liu SQ
Lima CA et al . Risk factors/osteoporosis/in IBD

Hirotada Akiho, Azusa Yokoyama, Shuichi Abe, Yuichi Nakazono, Masatoshi Murakami, Yoshihiro Otsuka, Kyoko Fukawa, Mitsuru Esaki, Yusuke Niina, Haruei Ogino
Hirotada Akiho, Azusa Yokoyama, Shuichi Abe, Yuichi Nakazono, Masatoshi Murakami, Yoshihiro Otsuka, Kyoko Fukawa, Mitsuru Esaki, Yusuke Niina, Haruei Ogino, Department of Gastroenterology, Kitakyushu Municipal Medical Center, Fukuoka 8020077, Japan
Author contributions: All authors contributed extensively to this manuscript; Akiho H provided a significant editorial and literature contribution; Yokoyama A, Abe S, Nakazono Y, Murakami M, Otsuka Y, Fukawa K, Esaki M, Niina Y and Ogino H provided literaturerelated comments and review.
Conflict-of-interest statement: All authors declare no conflict of interests for this article.
Open-Access: This article is an openaccess article which was selected by an inhouse editor and fully peerreviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work noncommercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: http://creativecommons.org/licenses/bync/4.0/
Correspondence to: Hirotada Akiho, MD, PhD, Department of Gastroenterology, Kitakyushu Municipal Medical Center, 211, Bashaku kokurakitaku, Kitakyushushi, Fukuoka 8020077, Japan. [email protected]u.ac.jpTelephone: +81935411831Fax: +81935338693
Received: June 22, 2015Peer-review started: June 22, 2015First decision: August 16, 2015Revised: September 2, 2015Accepted: October 23, 2015 Article in press: October 28, 2015Published online: November 15, 2015
AbstractUlcerative colitis (UC) is a chronic lifelong condition
characterized by alternating flare-ups and remission. There is no single known unifying cause, and the pathogenesis is multifactorial, with genetics, environmental factors, microbiota, and the immune system all playing roles. Current treatment modalities for UC include 5-aminosalicy-lates, corticosteroids, immunosuppressants (including purine antimetabolites, cyclosporine, and tacrolimus), and surgery. Therapeutic goals for UC are evolving. Medical treatment aims to induce remission and prevent relapse of disease activity. Infliximab, an anti-tumor necrosis factor (TNF)-α monoclonal antibody, is the first biological agent for the treatment of UC. Over the last decade, infliximab and adalimumab (anti-TNF-α agents) have been used for moderate to severe UC, and have been shown to be effective in inducing and maintaining remission. Recent studies have indicated that golimumab (another anti-TNF-α agent), tofacitinib (a Janus kinase inhibitor), and vedolizumab and etrolizumab (integrin antagonists), achieved good clinical remission and response rates in UC. Recently, golimumab and vedolizumab have been approved for UC by the United States Food and Drug Administration. Vedolizumab may be used as a first-line alternative to anti-TNF-α therapy in patients with an inadequate response to corticosteroids and/or immunosuppressants. Here, we provide updated information on various biological agents in the treatment of UC.
Key words: Ulcerative colitis; Biological therapy; Anti-tumor necrosis factor α agents; Janus kinase inhibitor; Anti-integrin agents
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Ulcerative colitis (UC) is a chronic lifelong condition characterized by alternating flare-ups and remission. Current treatment modalities for UC include 5-aminosalicylates, corticosteroids, immunosuppressants (e.g. , cyclosporine, tacrolimus), and surgery. Medical
MINIREVIEWS
219 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Promising biological therapies for ulcerative colitis: A review of the literature
World J Gastrointest Pathophysiol 2015 November 15; 6(4): 219-227ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i4.219

treatment aims to induce remission and prevent relapse of disease activity. Infliximab and adalimumab have been used for moderate to severe UC, and are effective in inducing and maintaining remission in UC. Recent studies have indicated that golimumab, tofacitinib, vedolizumab and etrolizumab achieved good clinical remission and response rates in UC. In this review, we provide updated information on various biological agents in the treatment of UC.
Akiho H, Yokoyama A, Abe S, Nakazono Y, Murakami M, Otsuka Y, Fukawa K, Esaki M, Niina Y, Ogino H. Promising biological therapies for ulcerative colitis: A review of the literature. World J Gastrointest Pathophysiol 2015; 6(4): 219227 Available from: URL: http://www.wjgnet.com/21505330/full/v6/i4/219.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i4.219
INTRODUCTIONUlcerative colitis (UC) is an inflammatory disorder of the gastrointestinal tract that affects the colon and rectum. The symptoms of UC are rectal bleeding, diarrhea, and abdominal pain. It is a chronic lifelong condition characterized by alternating flare-ups and remission. There is no single known unifying cause, and the pathogenesis is multifactorial, with genetics, environmental factors, microbiota, and immune system all playing roles[1,2].
Medical treatment aims to induce remission and prevent relapse of disease activity, thereby minimizing the impact on quality of life. Current treatment modalities for UC include 5-aminosalicylates, corticosteroids, immunosuppressants (including purine antimetabolites, cyclosporine, and tacrolimus), and surgery. Therapeutic goals for the treatment of UC are evolving. Over the past decade there has been increasing evidence in favor of more objective measures of biological disease activity, including biomarkers such as C-reactive protein, faecal calprotectin, and the histological resolution of active inflammation in UC[3,4].
Infliximab, an anti-tumor necrosis factor (TNF)-α monoclonal antibody, is the first biological agent to have received United States Food and Drug Administration (FDA) approval. Over the last decade, infliximab has been used for moderate to severe UC, and has been shown to be effective in inducing and maintaining remission in UC[5]. Recently the TNF-α antagonists adalimumab and golimumab have shown a significant effect on UC[6,7].
In 2014, integrin receptor antagonist vedolizumab was approved for UC by the United States FDA and European Commission. In this review, we provide updated information on various biological agents in the treatment of UC.
ANTI-TNF-α AGENTSTNF has been known to play a pivotal role in the
pathogenesis of inflammatory bowel disease (IBD)[8]. When released by active macrophages and T lym-phocytes, TNF initiates multiple biological reactions like modulates immune cell function, drives adaptive immune responses, triggers epithelium apoptosis and breaks epithelial barrier[9,10]. Anti-TNF-α agents have changed the treatment paradigm in the management of patients with UC.
InfliximabAs the first monoclonal TNF antibody approved for human treatment, infliximab is a purified, recombinant DNA-derived chimeric human-mouse IgG monoclonal antibody and contains murine heavy and light chain variable regions, ligated to genomic human heavy and light chain constant regions[11,12]. Infliximab can quickly form stable complexes with the human soluble or the membrane form of TNF and terminate the biological activity and signals of TNF[13]. With a serum half-life of 9.5 d and still detectable in serum of IBD patients 8 wk after infusion treatment, infliximab provides a useful strategy to neutralize TNF and to inhibit immune responses of IBD[14]. Infliximab is administered intravenously, and has been found to be effective for the treatment of moderate to severe UC in clinical trials[5,15]. Two randomized, double-blind, placebo-controlled studies-the Active UC Trials 1 and 2 (ACT 1 and ACT 2, respectively)-evaluated the efficacy of infliximab for induction and maintenance therapy in adults with UC[5]. Clinical response was defined as a decrease from baseline in the total Mayo score of ≥ 3 points and ≥ 30%, with an accompanying decrease in the subscore for rectal bleeding of ≥ 1 point or an absolute subscore for rectal bleeding of 0 or 1. Clinical remission was defined as a total Mayo score of ≤ 2 points, with no individual subscore exceeding 1 point. In ACT 1, 69.4% of patients who received 5 mg infliximab and 61.5% of those who received 10 mg had a clinical response at week 8, as compared with 37.2% of those who received placebo (P < 0.001 for both comparisons with placebo). In ACT 2, 64.5% of patients who received 5 mg infliximab and 69.2% of those who received 10 mg had a clinical response at week 8, as compared with 29.3% of those who received placebo (P < 0.001 for both comparisons with placebo). In both studies, patients who received infliximab were more likely to have a clinical response at week 30 (P ≤ 0.002 for all comparisons). In ACT 1, more patients who received 5 or 10 mg infliximab had a clinical response at week 54 (45.5% and 44.3%, respectively) than did those who received placebo[5]. The results of ACT 1 and ACT 2 showed that infliximab had superior clinical efficacy compared with placebo, both in induction and maintenance phases.
AdalimumabAdalimumab is a complete human IgG1 anti-TNF-α mono-clonal Ab that has been generated through repertoire cloning. It binds to the soluble and transmembrane forms of TNF-α with high affinity, thereby preventing
220 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Akiho H et al . Biological therapies for UC

TNF-α from binding to its receptors. In vitro studies have also demonstrated its effect on the induction of cell lysis and apoptosis[16]. It is generally administered at a dose of 40 mg subcutaneously every 2 wk, or at higher doses administered once a week. It is indicated for use in rheumatoid arthritis, psoriasis, ankylosing spondylitis, and moderate to severe Crohn’s disease. Adalimumab can be self-administered by patients at home. Two randomized, double-blind, placebo-controlled studies-UC long-term remission and maintenance with adali-mumab 1 and 2 (ULTRA 1 and ULTRA 2, respectively)-evaluated the efficacy of adalimumab for induction and maintenance therapy in UC patients[6,17]. ULTRA 1 was an 8-wk clinical trial investigating the use of adalimumab as induction therapy in patients with moderate to severe UC despite conventional therapy[17]. In this trial, 576 patients were divided into 160/80 mg and 80/40 mg groups, based on the loading dose, and then compared with the placebo group. At the end of 8 wk, the clinical remission rate of patients receiving adalimumab was twice that of the placebo group (P = 0.031). There was no significant difference in remission rates between patients receiving adalimumab 80/40 mg and placebo (P = 0.833). In ULTRA 2, a 52-wk randomized controlled study investigating the use of adalimumab as mainte-nance therapy, 494 patients were divided into 160/80 mg adalimumab and placebo groups. Overall rates of clinical remission at week 8 were 16.5% on adalimumab and 9.3% on placebo (P = 0.019); corresponding values for week 52 were 17.3% and 8.5% (P = 0.004). Among anti-TNF-α-naïve patients, rates of remission at week 8 were 21.3% on adalimumab and 11% on placebo (P = 0.017); corresponding values for week 52 were 22% and 12.4% (P = 0.029). Among patients who had previously received anti-TNF-α agents, rates of remission at week 8 were 9.2% on adalimumab and 6.9% on placebo (P = 0.559); corresponding values for week 52 were 10.2% and 3% (P = 0.039). Importantly, on sub-analysis, it was observed that the anti-TNF-α-naïve group exhibited approximately two times higher clinical remission rates at week 8 and week 52, compared with the placebo group. Though it is not direct comparison, infliximab is more likely to induce a favorable clinical outcome than adalimumab. The dose of adalimumab trough level might not enough to induce remission and maintenance for UC. More date are needed for dose escalation of adalimumab.
Up to 4 years of data for adalimumab-treated patients from ULTRA 1 and 2, and the open-label extension ULTRA 3 have been presented[18]. A total of 600/1094 patients enrolled in ULTRA 1 or 2 were ran-domized to receive adalimumab and induced in the intent to treat analyses. Of these, 199 patients remained on adalimumab after 4 years follow-up. Rates of remission according to partial Mayo score, remission according to inflammatory bowel disease questionnaire score, mucosal healing, and corticosteroid discontinuation at week 208 were 24.7%, 26.3%, 27.7% (nonresponder imputation), and 59.2% (observed), respectively. Of the
patients who were followed up in ULTRA 3 (588/1094), a total of 360 patients remained on adalimumab 3 years later. Remission according to partial Mayo score and mucosal healing after ULTRA 1 or 2 to year 3 of ULTRA 3 were maintained by 63.6% and 59.9% of patients, respectively (nonresponder imputation). Nonresponder imputation method is used for dichotomous (“yes or no”) or categorical variables, if a subject drops out of a study, that subject is assumed to be a non-responder, regardless of whether or not the subject was responding to treatment at the time of dropout.
GolimumabGolimumab is a fully human IgG1 monoclonal antibody that targets TNF-α. It is subcutaneously administered and approved for use in rheumatoid arthritis, psoriatic arthritis, and ankylosing spondylitis. The affinity of golimumab for soluble TNF-α was similar to that of etanercept and greater than those of infliximab and adalimumab (2.4-fold and 7.1-fold, respectively). A similar pattern was observed regarding golimumab neutralization of soluble TNF-α in the cytotoxicity and endothelial cell activation assays. The IC50 values for golimumab were comparable to those for etanercept and ranged from 2.5- to 5.7-fold lower than those for infliximab and adalimumab. These in vitro bioassays suggest that a lower serum concentration of golimumab, compared with infliximab or adalimumab, would provide similar pharmacological effects in patients[19]. Two large, double-blinded, randomized, controlled trials have been conducted-the Program of UC Research Studies Utilizing an Investigation Treatment, which was divided into Subcutaneous and Maintenance phases (PURSUIT-SC, PURSUIT-M, respectively)[7,20]. In PURSUIT-SC, 774 patients were randomized to receive golimumab at week 6. The clinical response and remission rates showed a significant change in both the golimumab 200/100 mg and 400/200 mg groups (P < 0.0001)[10]. In PURSUIT-M, 464 patients who had responded to golimumab induction therapy in PURSUIT-SC were randomized to receive placebo or golimumab 50/100 mg every 4 wk for 52 wk. Clinical response was maintained through week 54 in 47.0% of patients receiving 50 mg golimumab, 49.7% of patients receiving 100 mg golimumab, and 31.2% of patients receiving placebo (P = 0.010 and P < 0.001, respectively). At weeks 30 and 54, a higher percentage of patients who received 100 mg golimumab were in clinical remission and had mucosal healing (27.8% and 42.4%) than patients given placebo (15.6% and 26.6%; P= 0.004 and P = 0.002, respectively) or 50 mg golimumab (23.2% and 41.7%, respectively)[7]. Though PURSUIT-M had included only persons who responded to induction in its maintenance phase, golimumab is more likely to induce a favorable clinical outcome than adalimumab (Table 1).
Janus kinase inhibitor: Various cytokines and intracellular messengers play a key role in pathogenesis of UC. Tyrosine kinases, such as Janus kinase 1 (JAK1)
221 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Akiho H et al . Biological therapies for UC

222 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
and 15 mg (P < 0.001), respectively, as compared with 42% of patients receiving placebo. Clinical remission at 8 wk occurred in 13%, 33%, 48% and 41% of patients receiving tofacitinib at a dose of 0.5 mg (P = 0.76), 3 mg (P = 0.01), 10 mg (P < 0.001), and 15 mg (P < 0.001), respectively, as compared with 10% of patients receiving placebo[21]. Though the study population is small, 15 mg of tofacitinib showed most superior clinical response rate in induction phase than the other biological agents for UC.
INTEGRIN ANTAGONISTSThe integrin inhibitors are currently under development and have shown promising results to date. This group of drugs targets the leukocyte adhesion and trafficking systems, thereby reducing inflammation.
and JAK3, are intracellular molecules for the signal transmission of interleukins.
TofacitinibTofacitinib (CP-690,550) is an oral inhibitor of JAK 1, 2 and 3 (with in vitro functional specificity for JAK1 and JAK3 over JAK2), which is expected to block signaling involving gamma-chain-containing cytokines including interleukins 2, 4, 7, 9, 15 and 21. In a double-blind, placebo-controlled, phase 2 trial, it was evaluated the efficacy of tofacitinib in 194 adults with moderate to severe active UC. Patients were randomly assigned to receive tofacitinib at a dose of 0.5, 3, 10 or 15 mg or placebo twice daily for 8 wk[21]. The primary outcome, clinical response at 8 wk, occurred in 32%, 48%, 61% and 78% of patients receiving tofacitinib at a dose of 0.5 mg (P = 0.39), 3 mg (P = 0.55), 10 mg (P = 0.10),
Table 1 Clinical trials evaluating the efficacy of anti-tumor necrosis factor α agents in ulcerative colitis patients
Drug Trial Study population Protocol Follow-up (wk) Outcome
Infliximab ACT 1 Rutgeerts et al[5] 121 5 mg/kg iv at 0, 2, 6, 54 69.4% (P < 0.001) clinical response at week 8and every 8 wk 45.5% (P < 0.001) clinical response at week 54
38.8% (P < 0.001) clinical remission at week 834.7% (P = 0.001) clinical remission at week 54
122 10 mg/kg iv at 0, 2, 6, 54 61.5% (P < 0.001) clinical response at week 8and every 8 wk 44.3% (P < 0.001) clinical response at week 54
32.0% (P = 0.002) clinical remission at week 834.4% (P = 0.001) clinical remission at week 54
ACT 2 Rutgeerts et al[5] 121 5 mg/kg iv at 0, 2, 6, 30 64.5% (P < 0.001) clinical response at week 8and every 8 wk 47.1% (P < 0.001) clinical response at week 30
33.9% (P < 0.001) clinical remission at week 825.6% (P = 0.003) clinical remission at week 30
120 10 mg/kg iv at 0, 2, 6, 30 69.2% (P < 0.001) clinical response at week 8and every 8 wk 60.0% (P < 0.001) clinical response at week 30
27.5% (P < 0.001) clinical remission at week 835.8% (P < 0.001) clinical remission at week 30
Adalimumab ULTRA1 Reinisch et al[17] 130 80/40 mg sc 8 51.5% clinical response at week 880 mg at week 0, 40 mg at
week 2, 4 and 610.0% (P = 0.833) clinical remission at week 8
130 160/80 mg sc 54.6% clinical response at week 8160 mg at week 0, 80 mg at
week 2, 40 mg at week 4 and 618.5% (P = 0.031) clinical remission at week 8
ULTRA2 Sandborn et al[6]
248 160/80 mg sc 52 16.5% (P = 0.019) clinical remission at week 8
160 mg at week 0, 80 mg at week 2, and then 40 mg every
other week
17.3% (P = 0.004) clinical remission at week 52
ULTRA3 Colombel et al[18]
360 40 mg sc every other week 208 63.6% remission per partial Mayo score at week 208
Golimumab PURSUIT-SC[20] 253 200/100 mg sc 2 wk apart 6 51.6% (P < 0.0001) clinical response at week 617.8% (P < 0.0001) clinical remission at week 6
257 400/200 mg sc 2 wk apart 6 54.9% (P < 0.0001) clinical response at week 617.9% (P < 0.0001) clinical remission at week 6
PURSUIT-M[7] 151 50 mg sc every 4 wk 54 47% (P = 0.010) clinical response at week 5423.2% clinical remission at week 54
151 100 mg sc every 4 wk 54 49.7% (P < 0.001) clinical response at week 5427.8% (P = 0.004) clinical remission at week 54
Clinical response was defined as a decrease from baseline in the total Mayo score of ≥ 3 points and ≥ 30%, with an accompanying decrease in the subscore for rectal bleeding of ≥ 1 point or an absolute subscore for rectal bleeding of 0 or 1. Clinical remission was defined as a total Mayo score of ≤ 2 points, with no individual subscore exceeding 1 point. iv: Intravenously; sc: Subcutaneously; ACT: Active Ulcerative Colitis Trials; ULTRA: Ulcerative Colitis Long-term Remission and Maintenance with Adalimumab; PURSUIT-SC: The Program of Ulcerative Colitis Research Studies Utilizing an Investigation Treatment, which was divided into Subcutaneous phases; PURSUIT-M: The Program of Ulcerative Colitis Research Studies Utilizing an Investigation Treatment, which was divided into Maintenance phases.
Akiho H et al . Biological therapies for UC

223 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
VedolizumabThe α4β7 integrin[22], a cell surface glycoprotein variably expressed on circulating B and T lymphocytes, inter-acts with mucosal addressin-cell adhesion molecule 1 (MAdCAM-1)[23] on the intestinal vasculature[24,25]. Vedolizumab, a humanized monoclonal antibody that specifically recognizes the α4β7 heterodimer, selectively blocks gut lymphocyte trafficking without interfering with trafficking to the central nervous system[26-28] (Figure 1).
A predecessor molecule (MLN02) showed proof-of-concept in a phase 2 trial[29]. Natalizumab, a monoclonal antibody with efficacy in multiple sclerosis and Crohn’sdisease, inhibits both α4β1 and α4β7 integrins and is associated with progressive multifocal leukoencepha-lopathy; a serious brain infection. Natalizumab and vedolizumab differ in that natalizumab blocks lymphocyte trafficking to multiple organs, including the brain and gut[30,31].
Randomized, double-blinded, placebo-controlled trials of vedolizumab in patients with active UC have been conducted[32]. In a trial of induction therapy, 374 patients (Cohort 1) received vedolizumab (300 mg) or placebo intravenously at weeks 0 and 2, and 521 patients (Cohort 2) received open-label vedolizumab at weeks 0 and 2, with disease evaluation at week 6. In a trial of maintenance therapy, patients in either cohort who had a response to vedolizumab at week 6 were randomly assigned to continue receiving vedolizumab every 8 or 4 wk or to switch to placebo for up to 52 wk.Response rates at week 6 were 47.1% and 25.5% among patients in the vedolizumab and placebo groups, respectively (difference with adjustment for stratification factors, 21.7% points; 95%CI: 11.6-31.7; P < 0.001). At week 52, 41.8% of patients who continued to receive vedolizumab every 8 wk and 44.8% of patients who
continued to receive vedolizumab every 4 wk were in clinical remission (Mayo Clinic score ≤ 2 and no subscore > 1), as compared with 15.9% of patients who switched to placebo [adjusted difference, 26.1% points for vedo-lizumab every 8 wk vs placebo (95%CI: 14.9-37.2; P < 0.001) and 29.1% points for vedolizumab every 4 wk vs placebo (95%CI: 17.9-40.4; P < 0.001)]. The frequency of adverse events was similar between the vedolizumab and placebo groups.
A network meta-analysis showed that in patients with moderate to severe active UC naïve to biological therapy, vedolizumab has similar efficacy to the anti-TNF-α antibodies, infliximab, adalimumab, and golimumab for induction of response and remission, and for main-tenance of response and remission, but only vedolizumab had an incidence of serious adverse events lower than that of placebo[33]. Thus, in UC, vedolizumab may be used as a first-line alternative to anti-TNF-α therapy in patients with an inadequate response to corticosteroids and/or immunosuppressants. Vedolizumab may also be used in patients with UC not responding to anti-TNF therapy (primary nonresponders and secondary loss of response), because the drug has shown efficacy for this particular subpopulation[32].
The United States FDA and European Commission approved vedolizumab (Entyvio) for treatment of adults with moderate to severe active UC or CD in 2014. Up to 2015, vedolizumab for UC is approved in the United States, European Union, Canada, Israel, Switzerland, Puerto Rico, and Bosnia and Herzegovina. A phase 3, multicenter, randomized, double-blinded, placebo-controlled, parallel-group study to examine the efficacy, safety, and pharmacokinetics of MLN0002 (vedolizumab) in induction and maintenance therapy in Japanese patients with moderate or severe active UC is ongoing.
Naïve T cellEffector/memoryT cell
T cell activated by antigen presenting cellIL-6
IL-12/23
Vedolizumabmechanism of action
Endothelium
α4β7 integrin binds to MAdCAM-1
VedolizumabCCR9:
Chemokine receptor
α4β7 integrin
T cell adhesion
MAdCAM-1
ChemokineGI tissue
IBDonset
Inflammatory cytokines (IL-17, IFN-γ) produced by T cell
T cell migration
Figure 1 A mechanism of action that works to reduce inflammation in the gastrointestinal tract (Reprinted with permission from Takeda Pharmaceutical Co.). Vedolizumab selectively inhibits the movement of a discrete subset of T lymphocytes that preferentially migrate into inflamed GI tissue. Vedolizumab specifically binds to the α4β7 integrin, blocking its interaction with MAdCAM-1, which is mainly expressed on gut endothelial cells. This interaction facilitates lymphocyte homing to the gut and is an important contributor to inflammation that is a hallmark of ulcerative colitis. GI: Gastrointestinal; MAdCAM-1: Mucosal addressin cell adhesion molecule-1; IBD: Inflammatory bowel disease; CCR: Chemokine receptor; IL: Interleukine; IFN-γ: Interferon-γ.
Akiho H et al . Biological therapies for UC

224 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
EtrolizumabEtrolizumab is an IgG1 humanized monoclonal anti-body that selectively binds the subunit of the α4β7 and the αEβ7 integrin heterodimers in the intestine. Etrolizumab antagonizes α4β7/MAdCAM-1-mediated leukocyte recruitment in the intestinal vasculature and αEβ7/E-cadherin interactions, which are believed to be involved in retention of α4β7 cells in the intraepithelial compartment and in the migration and function of retinoic acid-producing CD103+ dendritic cells expressing β7. The safety and pharmacology of etrolizumab were evaluated in a randomized phase 1 study in patients with moderate to severe UC. In the single ascending-dose stage, etrolizumab up to 10 mg/kg intravenously or 3.0 mg/kg subcutaneously showed no dose-limiting toxicity[34]. In a subsequent phase 2 study, patients with moderate to severe active UC were treated with three monthly doses of etrolizumab at 100 mg, a loading dose of etrolizumab at 420 mg and then 300 mg, or placebo[35]. Clinical remission occurred at week 10 in 20.5% of patients in the etrolizumab 100 mg group (P = 0.004), 10.3% of patients in the etrolizumab 420 mg loading dose group (P = 0.048), and no patients in the placebo group. The study population is so small, more studies are needed to confirm these data (Table 2).
Safety: Recent studies have shown that a few patients experience adverse events with biological agents. For adverse events, such as infections, neoplasms are related to the immunosuppressive effects of biological agents. Patients who are administered biological agents frequently develop antibodies against these drugs. This problem is more frequent with chimeric agents like infliximab than fully humanized agents like adalimumab.
Infliximab: Infliximab is a chimeric monoclonal antibody with a protein sequence that is 75% human and 25% mouse; therefore, human antichimeric antibody
formation can occur in the blood. The presence of human antichimeric antibody is associated with an increased risk of infusion reactions during administration and reduced clinical efficacy. The common adverse events of infliximab are acute infusion reaction, and infection such as reactivation of tuberculosis.
As with other immunomodulatory drugs, infliximab therapy increases the risk of developing non-serious infections (RR approximately equal to 2); however, the data on serious infections are inconsistent[36]. Examples of reported serious infections include sepsis, pneumonia, cellulitis and intra-abdominal abscess[37]. Thus, infliximab should not be administered to a patient who has a clinically active infection. Patients who are at a high risk of chronic hepatitis B infection should be screened before the initiation of infliximab therapy.
Approximately 10% of infliximab infusions are associated with mild reactions such as headache, dizziness, fever, chills, chest pain, cough dyspnea or pruritus. These reactions occur within 1-2 h after infusion and can be alleviated by reducing the rate of infusion or by pretreatment with an H1-receptor antagonist[36,37]. In the ACT 1 and ACT 2 trials, 11.4% of the patients receiving infliximab experienced infusion reactions (44 of 484), compared with 9.4% of those receiving a placebo (23 of 244)[5].
For reasons that are unclear, 1 in 1000 infliximab infusions results in a serious reaction[37]. Delayed hyper-sensitivity-like reactions (serum sickness-like disorders) can occur 3-14 d after episodic infliximab infusions and include, but are not limited to, myalgia, fever, rash, pruritus, dysphagia, urticaria and headache[37]. In the ACT 1 and ACT 2 trials, three patients who received either 5 or 10 mg/kg infliximab had delayed hypersensitivity reactions (n = 484), as compared with two patients in the placebo study group (n = 244)[5].
Cases of aplastic anemia, pancytopenia, vasculitis, hepatitis, reversible mono/polyneuropathy and demye-
Table 2 Clinical trials evaluating the efficacy of Janus kinase inhibitor and integrin antagonists in ulcerative colitis patients
Drug Trial Study population Protocol Follow-up (wk) Outcome
Tofacitinib Sandborn et al[21] 31 0.5 mg po twice daily 8 32% (P = 0.39) clinical response at week 813% (P = 0.76) clinical remission at week 8
33 3 mg po twice daily 8 48% (P = 0.55) clinical response at week 833% (P = 0.01) clinical remission at week 8
33 10 mg po twice daily 8 61% (P = 0.10) clinical response at week 848% (P < 0.001) clinical remission at week 8
49 15 mg po twice daily 8 78% (P < 0.001) clinical response at week 841% (P < 0.001) clinical remission at week 8
Vedolizumab GEMINI 1[32] 225 300 mg iv at weeks 0, 2 and 6 6 47.1% (P < 0.001) clinical response at week 616.9% (P = 0.00) clinical remission at week 6
122 300 mg iv at week 0, 2, 6 and every 4 wk
52 44.8% (P < 0.001) clinical remission at week 52
125 300 mg iv at week 0, 2, 6 and every 8 wk
52 41.8% (P < 0.001) clinical remission at week 52
Etrolizumab Vermeire et al[35] 39 100 mg sc at week 0, 4 and 8 10 21% (P = 0.0040) clinical remission at week 10 39 420 mg sc loading dose then 300 mg
at week 2, 4, and 810 10% (P = 0.048) clinical remission at week 10
po: Perorally; iv: Intravenously; sc: Subcutaneously.
Akiho H et al . Biological therapies for UC

225 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
lination have been attributed to infliximab therapy[38].At present, there is no consensus regarding the
estimated lymphoma risk for patients treated with infliximab[36]. However, most experts believe that immunosuppression does impart some small cumulative risk of malignancy. The development of hepatosplenic T-cell lymphoma, a rare malignancy, has been reported in pediatric patients receiving infliximab treatment for Crohn’s disease in the United States[38,39].
Adalimumab: A total of 1010 patients received at least one dose of adalimumab in the ULTRA 1, 2 and 3 trials. The most frequently reported serious adverse event was worsening or flare of UC. Two serious events of cytomegalovirus colitis were reported. After the double-blind study period, one serious infection of tuberculosis and two treatment-emergent fatal adverse events were reported. Three events of B-cell lymphoma occurred during ULTRA 3. All three patients had a history of smoking and either previous or concomitant azathioprine use[18].
Golimumab: The most commonly observed adverse events in golimumab- and placebo-treated patients were headache and nasopharyngitis. Overall, the incidences of serious adverse events (3.0% vs 6.1%), including serious infections (0.5% vs 1.8%), were also similar, respectively, for golimumab- and placebo-treated patients. The most common serious adverse event was the exacerbation of UC, reported by eight (1.1%) golimumab-treated and eight (2.4%) placebo-treated patients. The only serious infection reported by more than one patient was pneumonia (one receiving 200/100 mg golimumab and one placebo patient). One patient (400/200 mg) died from peritonitis and sepsis after surgical complications related to an ischiorectal abscess and subsequent bowel perforation after surgery;this patient was receiving concomitant 20 mg pred-nisolone. One patient (400/200 mg) had a demyelinating disorder reported after the patient completed PURSUIT-SC induction and subsequently was randomized toplacebo in the maintenance study. Two opportunistic infections were reported up to week 6: Esophageal candidiasis (400/200 mg golimumab) and cytome-galovirus infection (placebo). Neither event was reported as serious. No patient developed active tuberculosis[20].
Tofacitinib: The most commonly reported adverse events related to infection were influenza and naso-pharyngitis (in six patients each). During the study period, the absolute neutrophil count was < 1500 cells/mm3
in three patients receiving tofacitinib (one at a dose of 10 mg twice daily and two at a dose of 15 mg twice daily); it was < 1000 cells/mm3 in none of the patients[21].
Vedolizumab: In the large GEMINI Ⅰ study, no signi-ficant difference was observed among the study groups for the most commonly reported adverse events: Namely, flare of UC, headache, nasopharyngitis and
arthralgia. Serious infections were no more common with vedolizumab than with placebo. No cases of progressive multifocal leukoencephalopathy occurred[32].
Etrolizumab: Patients in the 100 mg etrolizumab group had higher rates of rash, influenza-like illness, and arthralgia than did those in the placebo or 300 mg etrolizumab plus loading dose (LD) groups; all of these events were regarded as mild to moderate in severity. Serious adverse events were reported in 12 patients; five of these were related to UC (two in the 100 mg etrolizumab group; one in the 300 mg etrolizumab plus LD group; and two in the placebo group; Appendix)[35].
CONCLUSIONA number of biological agents are currently available for treatment of UC. These agents serve as another appropriate treatment option for gastrointestinal clinicians in patients with moderate to severe UC who may not be effectively treated with conventional agents. Various cytokines and intracellular messengers are involved in the pathogenesis of UC; thus, further discovery and development of new agents are required.
REFERENCES1 Baumgart DC, Carding SR. Inflammatory bowel disease: cause
and immunobiology. Lancet 2007; 369: 16271640 [PMID: 17499605 DOI: 10.1016/S01406736(07)607508]
2 Engel MA, Neurath MF. New pathophysiological insights and modern treatment of IBD. J Gastroenterol 2010; 45: 571583 [PMID: 20213337 DOI: 10.1007/s0053501002193]
3 Hanauer SB, Kirsner JB. Treat the patient or treat the disease? Dig Dis 2012; 30: 400403 [PMID: 22796805 DOI: 10.1159/000338139]
4 Costa F, Mumolo MG, Ceccarelli L, Bellini M, Romano MR, Sterpi C, Ricchiuti A, Marchi S, Bottai M. Calprotectin is a stronger predictive marker of relapse in ulcerative colitis than in Crohn’s disease. Gut 2005; 54: 364368 [PMID: 15710984 DOI: 10.1136/gut.2004.043406]
5 Rutgeerts P, Sandborn WJ, Feagan BG, Reinisch W, Olson A, Johanns J, Travers S, Rachmilewitz D, Hanauer SB, Lichtenstein GR, de Villiers WJ, Present D, Sands BE, Colombel JF. Infliximab for induction and maintenance therapy for ulcerative colitis. N Engl J Med 2005; 353: 24622476 [PMID: 16339095 DOI: 10.1056/NEJMoa050516]
6 Sandborn WJ, van Assche G, Reinisch W, Colombel JF, D’Haens G, Wolf DC, Kron M, Tighe MB, Lazar A, Thakkar RB. Adalimumab induces and maintains clinical remission in patients with moderatetosevere ulcerative colitis. Gastroenterology 2012; 142: 25765.e13 [PMID: 22062358 DOI: 10.1053/j.gastro.2011.10.032]
7 Sandborn WJ, Feagan BG, Marano C, Zhang H, Strauss R, Johanns J, Adedokun OJ, Guzzo C, Colombel JF, Reinisch W, Gibson PR, Collins J, Järnerot G, Rutgeerts P. Subcutaneous golimumab maintains clinical response in patients with moderatetosevere ulcerative colitis. Gastroenterology 2014; 146: 96109.e1 [PMID: 23770005 DOI: 10.1053/j.gastro.2013.06.010]
8 Papadakis KA, Targan SR. Role of cytokines in the pathogenesis of inflammatory bowel disease. Annu Rev Med 2000; 51: 289298 [PMID: 10774465 DOI: 10.1146/annurev.med.51.1.289]
9 Apostolaki M, Armaka M, Victoratos P, Kollias G. Cellular mechanisms of TNF function in models of inflammation and autoimmunity. Curr Dir Autoimmun 2010; 11: 126 [PMID: 20173385 DOI: 10.1159/000289195]
10 Khor B, Gardet A, Xavier RJ. Genetics and pathogenesis of
Akiho H et al . Biological therapies for UC

226 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
inflammatory bowel disease. Nature 2011; 474: 307317 [PMID: 21677747 DOI: 10.1038/nature10209]
11 Rutgeerts P, Vermeire S, Van Assche G. Biological therapies for inflammatory bowel diseases. Gastroenterology 2009; 136: 11821197 [PMID: 19249397 DOI: 10.1053/j.gastro.2009.02.001]
12 Danese S. Mechanisms of action of infliximab in inflammatory bowel disease: an antiinflammatory multitasker. Dig Liver Dis 2008; 40 Suppl 2: S225S228 [PMID: 18598993 DOI: 10.1016/S15908658(08)605307]
13 Rutgeerts P, Van Assche G, Vermeire S. Optimizing antiTNF treatment in inflammatory bowel disease. Gastroenterology 2004; 126: 15931610 [PMID: 15168370 DOI: 10.1053/j.gastro.2004.02.070]
14 Cornillie F, Shealy D, D’Haens G, Geboes K, Van Assche G, Ceuppens J, Wagner C, Schaible T, Plevy SE, Targan SR, Rutgeerts P. Infliximab induces potent antiinflammatory and local immunomodulatory activity but no systemic immune suppression in patients with Crohn’s disease. Aliment Pharmacol Ther 2001; 15: 463473 [PMID: 11284774 DOI: 10.1046/j.13652036.2001.00956.x]
15 Panaccione R, Ghosh S, Middleton S, Márquez JR, Scott BB, Flint L, van Hoogstraten HJ, Chen AC, Zheng H, Danese S, Rutgeerts P. Combination therapy with infliximab and azathioprine is superior to monotherapy with either agent in ulcerative colitis. Gastroenterology 2014; 146: 392400.e3 [PMID: 24512909 DOI: 10.1053/j.gastro.2013.10.052]
16 Shen C, Assche GV, Colpaert S, Maerten P, Geboes K, Rutgeerts P, Ceuppens JL. Adalimumab induces apoptosis of human monocytes: a comparative study with infliximab and etanercept. Aliment Pharmacol Ther 2005; 21: 251258 [PMID: 15691299 DOI: 10.1111/j.13652036.2005.02309.x]
17 Reinisch W, Sandborn WJ, Hommes DW, D’Haens G, Hanauer S, Schreiber S, Panaccione R, Fedorak RN, Tighe MB, Huang B, Kampman W, Lazar A, Thakkar R. Adalimumab for induction of clinical remission in moderately to severely active ulcerative colitis: results of a randomised controlled trial. Gut 2011; 60: 780787 [PMID: 21209123 DOI: 10.1136/gut.2010.221127]
18 Colombel JF, Sandborn WJ, Ghosh S, Wolf DC, Panaccione R, Feagan B, Reinisch W, Robinson AM, Lazar A, Kron M, Huang B, Skup M, Thakkar RB. Fouryear maintenance treatment with adalimumab in patients with moderately to severely active ulcerative colitis: Data from ULTRA 1, 2, and 3. Am J Gastroenterol 2014; 109: 17711780 [PMID: 25155227 DOI: 10.1038/ajg.2014.242]
19 Shealy DJ, Cai A, Staquet K, Baker A, Lacy ER, Johns L, Vafa O, Gunn G, Tam S, Sague S, Wang D, BrighamBurke M, Dalmonte P, Emmell E, Pikounis B, Bugelski PJ, Zhou H, Scallon BJ, GilesKomar J. Characterization of golimumab, a human monoclonal antibody specific for human tumor necrosis factor α. MAbs 2010; 2: 428439 [PMID: 20519961 DOI: 10.4161/mabs.12304]
20 Sandborn WJ, Feagan BG, Marano C, Zhang H, Strauss R, Johanns J, Adedokun OJ, Guzzo C, Colombel JF, Reinisch W, Gibson PR, Collins J, Järnerot G, Hibi T, Rutgeerts P. Subcutaneous golimumab induces clinical response and remission in patients with moderatetosevere ulcerative colitis. Gastroenterology 2014; 146: 8595; quiz e1415 [PMID: 23735746 DOI: 10.1053/j.gastro.2013.05.048]
21 Sandborn WJ, Ghosh S, Panes J, Vranic I, Su C, Rousell S, Niezychowski W. Tofacitinib, an oral Janus kinase inhibitor, in active ulcerative colitis. N Engl J Med 2012; 367: 616624 [PMID: 22894574 DOI: 10.1056/NEJMoa1112168]
22 von Andrian UH, Engelhardt B. Alpha4 integrins as therapeutic targets in autoimmune disease. N Engl J Med 2003; 348: 6872 [PMID: 12510047 DOI: 10.1056/NEJMe020157]
23 Erle DJ, Briskin MJ, Butcher EC, GarciaPardo A, Lazarovits AI, Tidswell M. Expression and function of the MAdCAM1 receptor, integrin alpha 4 beta 7, on human leukocytes. J Immunol 1994; 153: 517528 [PMID: 7517418]
24 Arihiro S, Ohtani H, Suzuki M, Murata M, Ejima C, Oki M, Kinouchi Y, Fukushima K, Sasaki I, Nakamura S, Matsumoto T, Torii A, Toda G, Nagura H. Differential expression of mucosal addressin cell adhesion molecule1 (MAdCAM1) in ulcerative colitis and Crohn’s disease. Pathol Int 2002; 52: 367374 [PMID:
12100519 DOI: 10.1046/j.14401827.2002.01365.x]25 Briskin M, WinsorHines D, Shyjan A, Cochran N, Bloom S,
Wilson J, McEvoy LM, Butcher EC, Kassam N, Mackay CR, Newman W, Ringler DJ. Human mucosal addressin cell adhesion molecule1 is preferentially expressed in intestinal tract and associated lymphoid tissue. Am J Pathol 1997; 151: 97110 [PMID: 9212736]
26 Fedyk ER, Wyant T, Yang LL, Csizmadia V, Burke K, Yang H, Kadambi VJ. Exclusive antagonism of the α4 β7 integrin by vedolizumab confirms the gutselectivity of this pathway in primates. Inflamm Bowel Dis 2012; 18: 21072119 [PMID: 22419649 DOI: 10.1002/ibd.22940]
27 Haanstra KG, Hofman SO, Lopes Estêvão DM, Blezer EL, Bauer J, Yang LL, Wyant T, Csizmadia V, ‘t Hart BA, Fedyk ER. Antagonizing the α4β1 integrin, but not α4β7, inhibits leukocytic infiltration of the central nervous system in rhesus monkey experimental autoimmune encephalomyelitis. J Immunol 2013; 190: 19611973 [PMID: 23365083 DOI: 10.4049/jimmunol.1202490]
28 Soler D, Chapman T, Yang LL, Wyant T, Egan R, Fedyk ER. The binding specificity and selective antagonism of vedolizumab, an antialpha4beta7 integrin therapeutic antibody in development for inflammatory bowel diseases. J Pharmacol Exp Ther 2009; 330: 864875 [PMID: 19509315 DOI: 10.1124/jpet.109.153973]
29 Feagan BG, Greenberg GR, Wild G, Fedorak RN, Paré P, McDonald JW, Dubé R, Cohen A, Steinhart AH, Landau S, Aguzzi RA, Fox IH, Vandervoort MK. Treatment of ulcerative colitis with a humanized antibody to the alpha4beta7 integrin. N Engl J Med 2005; 352: 24992507 [PMID: 15958805 DOI: 10.1056/NEJMoa042982]
30 Tysabri. Cambridge, MA: Biogen Idec, 2012 (package insert)31 Ransohoff RM. Natalizumab and PML. Nat Neurosci 2005; 8:
1275 [PMID: 16189528 DOI: 10.1038/nn10051275]32 Feagan BG, Rutgeerts P, Sands BE, Hanauer S, Colombel JF,
Sandborn WJ, Van Assche G, Axler J, Kim HJ, Danese S, Fox I, Milch C, Sankoh S, Wyant T, Xu J, Parikh A. Vedolizumab as induction and maintenance therapy for ulcerative colitis. N Engl J Med 2013; 369: 699710 [PMID: 23964932 DOI: 10.1056/NEJMoa1215734]
33 Danese S, Fiorino G, PeyrinBiroulet L, Lucenteforte E, Virgili G, Moja L, Bonovas S. Biological agents for moderately to severely active ulcerative colitis: a systematic review and network metaanalysis. Ann Intern Med 2014; 160: 704711 [PMID: 24842416 DOI: 10.7326/M132403]
34 Rutgeerts PJ, Fedorak RN, Hommes DW, Sturm A, Baumgart DC, Bressler B, Schreiber S, Mansfield JC, Williams M, Tang M, Visich J, Wei X, Keir M, Luca D, Danilenko D, Egen J, O’Byrne S. A randomised phase I study of etrolizumab (rhuMAb β7) in moderate to severe ulcerative colitis. Gut 2013; 62: 11221130 [PMID: 22717454 DOI: 10.1136/gutjnl2011301769]
35 Vermeire S, O’Byrne S, Keir M, Williams M, Lu TT, Mansfield JC, Lamb CA, Feagan BG, Panes J, Salas A, Baumgart DC, Schreiber S, Dotan I, Sandborn WJ, Tew GW, Luca D, Tang MT, Diehl L, EasthamAnderson J, De Hertogh G, Perrier C, Egen JG, Kirby JA, van Assche G, Rutgeerts P. Etrolizumab as induction therapy for ulcerative colitis: a randomised, controlled, phase 2 trial. Lancet 2014; 384: 309318 [PMID: 24814090 DOI: 10.1016/S01406736(14)606619]
36 Desai SB, Furst DE. Problems encountered during antitumour necrosis factor therapy. Best Pract Res Clin Rheumatol 2006; 20: 757790 [PMID: 16979537 DOI: 10.1016/j.berh.2006.06.002]
37 Lichtenstein GR, Abreu MT, Cohen R, Tremaine W. American Gastroenterological Association Institute technical review on corticosteroids, immunomodulators, and infliximab in inflammatory bowel disease. Gastroenterology 2006; 130: 940987 [PMID: 16530532 DOI: 10.1053/j.gastro.2006.01.048]
38 Panaccione R, Fedorak RN, Aumais G, Bernard EJ, Bernstein CN, Bitton A, Croitoru K, Dieleman LA, Enns R, Feagan BG, Franchimont D, Greenberg GR, Griffiths AM, Marshall JK, Pare P, Patel S, Penner R, Render C, Seidman E, Steinhart AH. Review and clinical perspectives for the use of infliximab in ulcerative
Akiho H et al . Biological therapies for UC

227 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
colitis. Can J Gastroenterol 2008; 22: 261272 [PMID: 18354755]39 Mackey AC, Green L, Liang LC, Dinndorf P, Avigan M.
Hepatosplenic T cell lymphoma associated with infliximab use in
young patients treated for inflammatory bowel disease. J Pediatr Gastroenterol Nutr 2007; 44: 265267 [PMID: 17255842 DOI: 10.1097/MPG.0b013e31802f6424]
P- Reviewer: Hillman LC, Hokama A, HuertaFranco MR S- Editor: Gong ZM L- Editor: A E- Editor: Liu SQ
Akiho H et al . Biological therapies for UC

Anthony S de Buys Roessingh, Amélie Damphousse, Pierluigi Ballabeni, Josée Dubois, Sarah Bouchard
Anthony S de Buys Roessingh, Sarah Bouchard, Department of Pediatric Surgery, University Hospital, Hôpital Sainte-Justine, H3T1C5 Montréal, Canada
Amélie Damphousse, Josée Dubois, Department of Radiology, University Hospital, Hôpital Sainte-Justine, H3T1C5 Montréal, Canada
Anthony S de Buys Roessingh, Pierluigi Ballabeni, Department of Biostatistic, Centre Hospitalier Universitaire Vaudois, CH -1011 Lausanne, Switzerland
Author contributions: de Buys Roessingh AS and Bouchard S wrote the paper; Damphousse A and Dubois J did all the radiological lecture and Ballabeni P made the statistics.
Institutional review board statement: None.
Informed consent statement: All human studies have been reviewed by the appropriate ethics committee and all persons gave their informed consent prior to their inclusion in the study. Details that might disclose the identity of the subjects under study were omitted. Authors drew attention to the Code of Ethics of the World Medical Association (Declaration of Helsinki, 1964, as revised in 2004).
Conflict-of-interest statement: None of the authors have any financial or other relationships with other people or organizations that could inappropriately influence their work. There is no grant support for this research.
Data sharing statement: I declare data sharing statement in World Journal Gastrointestinal Pathophysiology; dataset available from the corresponding author at Email address or URL. Participants gave informed consent for data sharing.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Correspondence to: Anthony S de Buys Roessingh, MD, PhD, Department of Biostatistic, Centre Hospitalier Universitaire Vaudois, Rue du Bugnon 21, CH -1011 Lausanne, Switzerland. [email protected]: +41-21-3143126Fax: +41-21-3143076
Received: June 5, 2015Peer-review started: June 6, 2015First decision: August 10, 2015Revised: October 12, 2015Accepted: October 23, 2015Article in press: October 27, 2015Published online: November 15, 2015
AbstractAIM: To establish children born with gastroschisis (GS).
METHODS: We performed a retrospective study covering the period from January 2000 to December 2007. The following variables were analyzed for each child: Weight, sex, apgar, perforations, atresia, volvulus, bowel lenght, subjective description of perivisceritis, duration of parenteral nutrition, first nasogastric milk feeding, total milk feeding, necrotizing enterocolitis, average period of hospitalization and mortality. For statistical analysis, descriptive data are reported as mean ± standard deviation and median (range). The non parametric test of Mann-Whitney was used. The threshold for statistical significance was P < 0.05 (Two-Tailed).
RESULTS: Sixty-eight cases of GS were studied. We found nine cases of perforations, eight of volvulus, 12 of atresia and 49 children with subjective description of perivisceritis (72%). The mortality rate was 12% (eight deaths). Average duration of total parenteral nutrition was 56.7 d (8-950; median: 22), with five cases of necrotizing enterocolitis. Average length of hospitalization for 60 of our patients was 54.7 d (2-370;
228 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
World J Gastrointest Pathophysiol 2015 November 15; 6(4): 228-234ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i4.228
Predictive factors at birth of the severity of gastroschisisBasic Study
ORIGINAL ARTICLE

median: 25.5). The presence of intestinal atresia was the only factor correlated with prolonged parenteral nutrition, delayed total oral milk feeding and longer hospitalization.
CONCLUSION: In our study, intestinal atresia was our predictive factor of the severity of GS.
Key words: Gastroschisis; Perivisceritis; Bowel atresia; Volvulus
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Gastroschisis (GS) is defined as a full-thickness congenital abdominal wall defect usually situated on the right side of the umbilicus, with intestines protruding into the amniotic fluid without any protective membrane. The amniotic fluid creates an inflammation of the bowel wall, called perivisceritis. Associated with intestinal abnormalities are malrotation and a degree of short bowel: Volvulus, perforation and atresia may also be found. Our study shows that for babies born with GS, intestinal atresia is the only factor of prediction of the need for early and full enteral feeding, for its duration, and for the length of hospitalization.
de Buys Roessingh AS, Damphousse A, Ballabeni P, Dubois J, Bouchard S. Predictive factors at birth of the severity of gas-troschisis. World J Gastrointest Pathophysiol 2015; 6(4): 228-234 Available from: URL: http://www.wjgnet.com/2150-5330/full/v6/i4/228.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i4.228
INTRODUCTIONGastroschisis (GS) is defined as a full-thickness con-genital abdominal wall defect usually situated on the right side of the umbilicus, with intestines protruding into the amniotic fluid without any protective membrane[1]. The amniotic fluid creates an inflammation of the bowel wall, called perivisceritis[2]. Associated with intestinal abnormalities are malrotation and a degree of short bowel: Volvulus, perforation and atresia may also be found[3]. The degree of inflammation of the bowel and the presence of intestinal abnormalities are supposed to reflect the severity of the malformation, determining the surgical procedure and affecting the clinical outcome[4]. The duration of total parenteral nutrition (TPN), the timing of the introduction of normal feeding, the average length of hospitalization and in some cases death is all dependent on the severity of the malformation.
A prenatal ultrasound (US) diagnosis makes it possible to inform and prepare the parents, even though it remains difficult to predict whether the affected children will have a high or a low risk of abdominal complications, and how long they will need to be hospitalized[5,6]. If the defect closes by itself before birth, ischemia of the bowel may provoke total bowel necrosis. The prenatal closure
of the abdominal wall is therefore not always a good sign and may be associated with midgut infarction, short bowel or even vanishing midgut[7,8].
Surgical management starts with the clinical obser-vation of the anatomical anomalies accompanying GS and the search for associated malformations. Primary or delayed repair of the abdominal wall is then discussed[9]. Primary repair entails returning the bowel into its cavity soon after birth with a surgical procedure. But this primary abdominal closure is not always possible and depends on the age, weight and clinical condition of the baby, as well as on the amount of viscera protruding from the abdominal cavity: If it is too important, the immediate closure of the abdominal wall may cause excessive pressure. Delayed repair entails the use of a suspended pouch, called a “silo”, containing the externalized bowel loops, with a gradual return of the bowel into the abdominal cavity and the closure of the abdominal wall a few days later[10]. The “silo” reduces the risk of excessive pressure, hypothermia and dehydration.
Volvulus, perforation and atresia may require resection, anastomosis or the creation of a stoma. The presence of these associated intestinal anomalies influences surgical and post surgical clinical management, for instance regarding the decision to perform a stoma or delay oral feeding because of the risk of necrotizing enterocolitis (NEC).
We performed a retrospective review of all children born with GS in our hospital over an eightyear period. The aim of this study is to establish which parameters such as bowel volvulus and/or atresia may help to predict the duration of TPN before the initiation of milk intake and eventual total oral milk feeding, and also the length of hospitalization.
MATERIALS AND METHODSWe reviewed the files of all children admitted to our hospital with a diagnosis of GS from January 2000 to December 2007. Our records on the mothers indicate the duration of the pregnancy and the method of delivery. In our records on the children, we registered: weight, sex, apgar scores, acidosis at birth, length of intubation, bowel aspect, presence of necrosis, of perforation, of volvulus without necrosis, length of TPN, first milk feeding, total milk feeding, NEC, average length of hospitalization and, in some cases, time of death. Signed informed consent for this study was obtained from the appropriate local institutional Human Research Board.
Mothers were followed during the prenatal period by means of regular ultrasound exams. Bowel dilation, thickness of the abdominal wall, motility of the bowel, quantity of amniotic fluid, and fetal development were controlled during gestation. Vaginal delivery of the babies was proposed in our maternity department to avoid postnatal transfer. Scheduled vaginal provocation was planned, unless obstetric considerations led us to opt for caesarian delivery. When faced with fetal indications such
229 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
de Buys Roessingh AS et al . Severity of gastroschisis at birth

as worsening fetal status, progressive bowel dilation or loss of bowel movement, or with maternal problems, we performed an early delivery. Prenatal discussion sessions were organized between physicians of different specializations, and parents had the opportunity to meet with pediatric surgeons, neonatologists and geneticists.
The diagnosis of GS was confirmed immediately after delivery by neonatologists and pediatric surgeons. Primary surgery, if possible within the few hours following delivery, was our preferred mode of wall repair. After a rapid physical assessment, a nasogastric tube was placed in the stomach and intravenous fluid and antibiotics were given. The child was rapidly brought to the operating theater after routine resuscitation. The colon was irrigated with 5% n-acetyl cysteine diluted in warm normal saline solution to evacuate meconium. A Foley catheter was placed in the bladder for urinary drainage and for measurement of intra-abdominal pressure after closure of the abdominal wall.
Under total anaesthesia, the bowel loops were reduced gently into the abdominal cavity, fascia were separated from the skin and repaired with absorbable sutures. The abdominal wall was closed layer by layer. Urine production, absence of a compartment syndrome and good perfusion of both legs were controlled throu-ghout. A broviac catheter was placed for TPN. The babies were then taken to the intensive care ward with intubation/ventilation, and given pain killers and drugs for wall relaxation for as long as necessary. Bladder pressure was measured continuously and maintained below 15 mmHg. Pulse oxymetry was measured on the feet. Nasogastric suction was maintained until bowel function returned. TPN was provided until adequate oral nutrition became possible.
Primary closure was not always indicated, and the decision not to close the abdominal wall was taken either during surgery, when the introduction of the bowel into the abdominal cavity induced a compartment syndrome, or if the baby could not be brought to the operating room because of his weight or the presence of associated malformations. In these cases, we used a protective “silo” to allow staged reduction of the bowel over a period of several days. After this period of progressive bowel reintegration into the abdominal cavity, the abdominal wall was closed layer by layer as described above.
Short bowel syndrome normally defines a func-tional state dependent on the degree to which the normal absorbtive capacity of the small intestine is compromised[11]. In our paper, short bowel is defined according to either the length of small intestine present after abdominal closure, or the length left after intestinal resections in cases of intestinal atresia. We defined two categories: more than 100 cm or less than 50 cm.
Inflammation of the bowel was defined subjectively at birth and during surgery on the basis of the aspect of the bowel wall, the presence of large amount of fibrin, the abnormal thickness of the bowel wall and the absence of bowel movement or contraction after
stimulation. A less inflamed bowel was defined subjectively, on the basis of the presence of a small amount of fibrin, a practically normal appearance and thickness of the bowel wall, and bowel movement under stimulation.
Oral feeding was started as soon as possible through a gastric catheter. One milliliter per hour was given at the beginning, and this amount was gradually increased depending on the color and quantity of fluid aspiration, the abdominal distention and stools production. The amount needed for full feeding was determined by the weight of the baby.
For statistical analysis, descriptive data are reported as mean ± standard deviation and median (range). The non parametric test of Mann-Whitney was used as the distribution of different variables was not always regular. The threshold for statistical significance was P < 0.05 (Two-Tailed). All statistical analyses were performed by a biostatistician using the statistical software SAS for Windows (SAS release 8.2, 2002, Cupertino, California, United States).
RESULTSFrom January 2000 to December 2007, 72 babies were deemed eligible for the study. But four were immediately excluded because their records were incomplete. We therefore retained 68 cases of GS (n = 68) for our study.
The mean age of the mothers was 23.1 years, with a range from 15 to 34 years. The mean delivery time was 35.6 wk (median: 36 wk), with vaginal delivery in 67% of cases. A diagnosis of intrauterine growth restriction was made in 22.4% (n = 15) of cases, and confirmed at birth in all cases. No intrauterine deaths were reported for fetuses with intrauterine growth restriction. Oligohydramnios was observed in 24% (n = 16) of mothers. No complications were reported during delivery. Average weight at birth was 2501 g and 53% were girls.
We found eight volvulus, 12 atresia, nine perforations and six stenosis, 39 bowels less than 100 cm and 22 less than 50 cm (Table 1). Subjective description has done by the surgeon of the presence of a perivisceritis were found in 49 children (72%). We used silos in 17 cases (25%), for an average period of 5.94 d. Average age at surgery was 2.45 d.
A postnatal mortality rate of 12% (8/68) was observed. Three of these babies (3/68) showed concomitant fetal abnormalities incompatible with life; three (3/68) died, respectively from short bowel syndrome requiring a bowel transplant, NEC with fistula, and after surgery for a chylothorax; and two more (2/68), who presented small bowel necroses requiring multiple surgery, also died shortly after birth.
Mean duration of TPN was 56.7 d (range: 8-950 d; median: 22 d) with five NEC; four newborns (6%) received TPN for less than ten days; 20 patients (29.9%) required TPN for 30 d or more, including nine patients (n = 9) who presented no other complications besides GS. Of those 20 patients, eight (n = 8) required multiple
230 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
de Buys Roessingh AS et al . Severity of gastroschisis at birth

231 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
The etiology of GS has not yet been ascertained, but low socioeconomic status, poor maternal education, drug abuse, in particular with cocaine, abuse of tobacco and alcohol, and young maternal age (less than 20 years old) are associated with GS[11-14]. Although the survival rate for babies born with GS has improved and is now practically 85%, short and long-term morbidity is still a serious problem. The mortality rate reported in recent literature varies greatly (2.4% to 11%)[15,16]. but the mortality rate reported in our study (11.7%) tallies with the values reported in most studies. Prematurity, intrauterine growth retardation and the presence of a congenital circulatory or pulmonary anomaly are external factors associated with a poorer outcome for children born with GS[3]. In our study, three babies (3/68) showed concomitant fetal abnormalities incompatible with life; finally, five babies died from GS and associated bowel complications (5/68, 7.3%).
Many authors have attempted to establish a prognosis of post-natal morbidity in cases of GS by studying various prenatal US findings, such as amniotic fluid volume, small bowel diameter, maximum bowel diameter, maximum thickness of the bowel wall, intrauterine growth restriction, Doppler velocimetry of the superior mesenteric artery, and the presence of other anomalies. Other studies have tried, based either on prenatal US or on bowel examination at birth, to establish a prognosis for the length of hospitalization, the duration of TPN or the timing of introduction of normal feeding. It appears, however, that antenatal screening cannot reliably predict morbidity, and the fact that no consensus emerges from the different studies is due mainly to the small sample size, but also to the difficulty in correlating imaging findings with clinical outcome. Some studies found a significant association between intra-abdominal bowel dilation and bowel atresia[5,17,18]. Japaraj et al[6] found that the occurrence of polyhydramnios was significantly associated with a higher rate of severe bowel complications such as atresia, perforation and necrosis. Intestinal atresia has been described as a significant risk factor of morbidity and mortality, due to the fact that the dilated bowel causes increased abdominal pressure during and after abdominal closure[15]. While, in both our groups (with atresia and without atresia), nasogastric milk feeding was initiated after an equal number of days following surgery (11 d and 10 d respectively), the median duration of TPN was clearly and significantly greater in the “atresia group”, and the period of time before total milk feeding could be introduced was longer. The mortality rate in the “atresia group” was not higher, even though, in 12 cases, atresia was associated with three perforations and intestinal necrosis which required several surgical procedures. In one case, atresia was also associated with a chronic intestinal pseudo obstruction. The higher morbidity in this group also influenced the duration of hospitalization, which was definitely longer, due to surgical complications, prolonged TPN and delayed total milk feeding.
Short-term and long-term outcomes of GS are
surgery, six had atresia (n = 6), three NEC (n = 3), and three eventually died (n = 3).
Mean duration of intubation was 8.47 d (median: 5 d). Mean duration of hospitalization was 54.7 d (2-370; median: 25.5) for our 60 cases of GS (Table 1). Twenty-six patients (23.9%) were hospitalized for 50 d or more, among whom nine required (n = 9) multiple surgery, eight were cases of atresia (n = 8), three of volvulus (n = 3), three of NEC (n = 3), and the three who eventually died (n = 3).
The median period of time before initiation of naso-gastric milk, the median duration of TPN, the median period of time until the start of total oral milk intake and the median duration of hospitalization are summarized in Table 2.
There were a total of 12 cases with intestinal atresia and 48 without atresia. The median period of time before initiation of nasogastric milk, the median duration of TPN, the median period of time until the start of total oral milk intake and the median duration of hospitalization are summarized in Table 2.
There were eight cases of volvulus and 52 children without volvulus. The median period of time before initiation of nasogastric milk, the median duration of TPN, the median period of time until the start of total oral milk intake and the median duration of hospitalization are summarized in Table 2.
DISCUSSIONOur study shows that for babies born with GS, intestinal atresia is the only factor of prediction of the need for early and full enteral feeding, for its duration, and for the length of hospitalization.
Table 1 Summary of clinical conditions for the 68 cases of gastroschisis
Mean Median
Birth weight 2501 gGestational age 35.6 wk 36 wkFemale sex 53%Mother's age 23 yrTiming of closure 2.5 dSilo 25% (17)Severely inflamed 72% (49)Perforations 13.2% (9)Volvulus 11.7% (8)Atresia 17.6% (12)Bowel less than 100 cm 66% (39)Short bowel less than 50 cm 30% (21)Stenosis 8.8% (6)NEC 7.35% (5)Mortality 11.7% (8)For 60 children (68 minus eight deaths)Intubation in days 8.5 d 5 d1st feeding 17.3 d 11 dTiming of total milk feedingDays of TPN 56.7 d 22 dHospitalization 54.7 d 25.5 d
NEC: Necrotizing enterocolitis; TPN: Total parenteral nutrition.
de Buys Roessingh AS et al . Severity of gastroschisis at birth

232 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
wellknown but difficult to predict. Many studies have demonstrated that the presence of a compromised bowel is associated with a significant increase in the number of surgical procedures, a longer period of full enteral feeding and a prolonged hospitalization[15,19]. Prolonged TPN, with its risk of sepsis, is directly related to intestinal recuperation, and the morbidity of GS is closely related to intestinal damage[20]. While gastrointestinal complica-tions such as matting between the loops, malrotation, volvulus, perforations and atresia increase the complexity of early management[19,21], later management may be complicated by the presence of problems of absorption, intestinal dysmotility, obstruction, NEC, infarction and stenosis[1,3,9].
The pathogenesis of secondary bowel lesions is not fully understood, but both chemical and mechanical origins are concerned[2]. We know that prolonged contact with the amniotic fluid is deleterious for the bowel and may lead to inflammation of the bowel wall resulting in the production of a yellow fibrous tissue named perivisceritis[21,22]. This perivisceritis is accompanied by edema, cellular infiltration of epithelial cells and the presence of macrophages in the bowel wall. Specific therapeutic strategies, including amnio-exchange as a prenatal treatment, may be developed to prevent the resulting more serious bowel damage. Amnio-exchange has been tried for many years in some centers[22]. Amnio-infusion during pregnancy consists in replacing the amniotic fluid with a saline solution in order to reduce the inflammation of the bowel due to its contact with the amniotic fluid. In animal studies, amnio-exchange reduces the inflammation of the bowel wall by eliminating inflammatory compounds. However, since no prospective and randomized studies with human fetuses have yet been realized, we do not use this technique and none of our babies benefited from amnioinfusion. Inflammation of the bowel at birth, on the basis of the aspect of the bowel wall, the presence of large amount of fibrin, the abnormal thickness of the bowel wall and the absence of bowel movement or contraction after stimulation, does not help to predict the outcome of GS, and does not seem to correlate with the degree of bowel recuperation or bowel damage. The condition of the externalized bowel loops can be difficult to evaluate, and its appreciation is largely subjective and without
predictive value. The recommended mode and timing of delivery
remains a subject of debate[23-26]. Labor may be dele-terious to the externalized bowel loops, and may entail the risk of membrane rupture and of infection. However, most authors found that caesarean delivery presented no significant benefit and did not improve the outcome of infants with GS. It is therefore reserved for obstetric indications or acute fetal emergencies often related to other organ failure. Preterm delivery, in order to limit the period of intrauterine damage of the bowel due to contact with the amniotic fluid, was of no benefit and did not lessen the morbidity of GS[25].
Surgery is performed in our hospital under emer-gency conditions, in order to close the abdominal wall as quickly as possible[9,27]. We think that early repair leads to a lower incidence of perivisceritis[28]. Coughlin JP et al[29] also observed an absence of inflammatory desquamation on the bowels of babies operated immediately after birth. Nevertheless, the surgical procedure may have to be delayed if further investigation for associated anomalies is required or if the child is too small for the operation. The surgical procedure may also have to be postponed if the intra-abdominal pressure during reintegration of the loops is too high (more than 20 mmHg) and would require high ventilation pressure, myorelaxant drugs and diuretics[30]. In these cases, abdominal closure is deferred, and the intestinal loops are protected with a silo during their progressive reintegration into the abdominal cavity[7]. The use of a suspended “silo” for a few days, allowing the gradual return of the viscera into the naturally growing abdominal cavity, makes it possible to close the abdominal wall without undue pressure and with a relatively low risk of intestinal damage.
All our patients required TPN for at least 10 d. In the course of prenatal counseling, parents should be made aware that their newborn will need TPN, and therefore the placement of a central venous line to provide adequate intake until oral nutrition is possible.
Our study also shows that a long period of hospitalization should be expected (mean hospitalization time of 54.7 d) and that, not surprisingly, a prolonged hospitalization is associated with a less favorable outcome. Parents should also be made aware that the length of the hospital stay will depend on how long the
Table 2 Comparison in days between two groups of 60 children depending on the presence of atresia, volvulus and perivisceritis (68 minus eight deaths)
Atresia (n = 12)
Non atresia (n = 48)
Mann-Whitney test
Volvulus (n = 8)
No volvulus (n = 52)
Mann-Whitney test
Subjective perivisceritis (n = 49)
Subjective low perivisceritis (n = 19)
Mann-Whitney test
TPN duration 60 20 0.005 36 20 0.140 34.5 22 0.564Start of total oral milk intake
10 11 0.809 11 7.5 0.212 11 10.5 0.569
Total oral milk intake
56 20 0.05 22 17 0.468 36 21 0.196
Mean hospitalization
64 24.5 0.021 48 25.5 0.309 39 25.5 0.505
TPN: Total parenteral nutrition.
de Buys Roessingh AS et al . Severity of gastroschisis at birth

233 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
bowel needs to rest and on the duration of total enteral feeding, two elements which depend primarily on clinical conditions.
ACKNOWLEDGMENTSThe authors are grateful to Annette Wagnière for reviewing the English text.
COMMENTSBackgroundThe authors performed a retrospective study covering the period from January 2000 to December 2007.
Research frontiersThe median duration of total parenteral nutrition (TPN) was clearly and significantly greater in the “atresia group”, and the period of time before total milk feeding could be introduced was longer.
Innovations and breakthroughsAssociated with intestinal abnormalities are malrotation and a degree of short bowel: Volvulus, perforation and atresia may also be found.
ApplicationsThis study also shows that a long period of hospitalization should be expected (mean hospitalization time of 54.7 d) and a prolonged hospitalization is associated with a less favorable outcome.
TerminologyThe duration of TPN or the timing of introduction of normal feeding.
Peer-reviewThe authors showed that the predictive factor of babies with gastroschisis (GS) is intestinal atresia by analysing 60 babies with GS.
REFERENCES1 Axt R, Quijano F, Boos R, Hendrik HJ, Jessberger HJ, Schwaiger
C, Schmidt W. Omphalocele and gastroschisis: prenatal diagnosis and peripartal management. A case analysis of the years 1989-1997 at the Department of Obstetrics and Gynecology, University of Homburg/Saar. Eur J Obstet Gynecol Reprod Biol 1999; 87: 47-54 [PMID: 10579616 DOI: 10.1016/S0301-2115(99)00078-0]
2 Langer JC, Longaker MT, Crombleholme TM, Bond SJ, Finkbeiner WE, Rudolph CA, Verrier ED, Harrison MR. Etiology of intestinal damage in gastroschisis. I: Effects of amniotic fluid exposure and bowel constriction in a fetal lamb model. J Pediatr Surg 1989; 24: 992-997 [PMID: 2530329 DOI: 10.1016/S0022-3468(89)80200-3]
3 Lao OB, Larison C, Garrison MM, Waldhausen JH, Goldin AB. Outcomes in neonates with gastroschisis in U.S. children‘s hospitals. Am J Perinatol 2010; 27: 97-101 [PMID: 19866404 DOI: 10.1055/s-0029-1241729]
4 Snyder CL. Outcome analysis for gastroschisis. J Pediatr Surg 1999; 34: 1253-1256 [PMID: 10466606 DOI: 10.1016/S0022-3468(99)90162-8]
5 Bond SJ, Harrison MR, Filly RA, Callen PW, Anderson RA, Golbus MS. Severity of intestinal damage in gastroschisis: correlation with prenatal sonographic findings. J Pediatr Surg 1988; 23: 520-525 [PMID: 2971103 DOI: 10.1016/S0022-3468(88)80360-9]
6 Japaraj RP, Hockey R, Chan FY. Gastroschisis: can prenatal sonography predict neonatal outcome? Ultrasound Obstet Gynecol 2003; 21: 329-333 [PMID: 12704738 DOI: 10.1002/uog.85]
7 Houben C, Davenport M, Ade-Ajayi N, Flack N, Patel S. Closing gastroschisis: diagnosis, management, and outcomes. J Pediatr
Surg 2009; 44: 343-347 [PMID: 19231531 DOI: 10.1016/j.jped-surg.2008.10.084]
8 Vegunta RK, Wallace LJ, Leonardi MR, Gross TL, Renfroe Y, Marshall JS, Cohen HS, Hocker JR, Macwan KS, Clark SE, Ramiro S, Pearl RH. Perinatal management of gastroschisis: analysis of a newly established clinical pathway. J Pediatr Surg 2005; 40: 528-534 [PMID: 15793730 DOI: 10.1016/j.jpedsurg.2004.11.037]
9 Page R, Ferraro ZM, Moretti F, Fung KF. Gastroschisis: antenatal sonographic predictors of adverse neonatal outcome. J Pregnancy 2014; 2014: 239406 [PMID: 25587450 DOI: 10.1155/2014/239406]
10 Schwartz MZ, Tyson KR, Milliorn K, Lobe TE. Staged reduction using a Silastic sac is the treatment of choice for large congenital abdominal wall defects. J Pediatr Surg 1983; 18: 713-719 [PMID: 6229620 DOI: 10.1016/S0022-3468(83)80010-4]
11 Goldbaum G, Daling J, Milham S. Risk factors for gastroschisis. Teratology 1990; 42: 397-403 [PMID: 2147789 DOI: 10.1002/tera.1420420408]
12 Curry JI, McKinney P, Thornton JG, Stringer MD. The aetiology of gastroschisis. BJOG 2000; 107: 1339-1346 [PMID: 11117759 DOI: 10.1111/j.1471-0528.2000.tb11645.x]
13 Loane M, Dolk H, Bradbury I. Increasing prevalence of gastro-schisis in Europe 1980-2002: a phenomenon restricted to younger mothers? Paediatr Perinat Epidemiol 2007; 21: 363-369 [PMID: 17564594 DOI: 10.1111/j.1365-3016.2007.00820.x]
14 Zamakhshary M, Yanchar NL. Complicated gastroschisis and maternal smoking: a causal association? Pediatr Surg Int 2007; 23: 841-844 [PMID: 17618440 DOI: 10.1007/s00383-007-1926-6]
15 Driver CP, Bruce J, Bianchi A, Doig CM, Dickson AP, Bowen J. The contemporary outcome of gastroschisis. J Pediatr Surg 2000; 35: 1719-1723 [PMID: 11101722 DOI: 10.1053/jpsu.2000.19221]
16 Fratelli N, Papageorghiou AT, Bhide A, Sharma A, Okoye B, Thilaganathan B. Outcome of antenatally diagnosed abdominal wall defects. Ultrasound Obstet Gynecol 2007; 30: 266-270 [PMID: 17674424 DOI: 10.1002/uog.4086]
17 Heinig J, Müller V, Schmitz R, Lohse K, Klockenbusch W, Steinhard J. Sonographic assessment of the extra-abdominal fetal small bowel in gastroschisis: a retrospective longitudinal study in relation to prenatal complications. Prenat Diagn 2008; 28: 109-114 [PMID: 18186152 DOI: 10.1002/pd.1907]
18 Piper HG, Jaksic T. The impact of prenatal bowel dilation on clinical outcomes in neonates with gastroschisis. J Pediatr Surg 2006; 41: 897-900 [PMID: 16677878 DOI: 10.1016/j.jpedsurg.2006.01.005]
19 Henrich K, Huemmer HP, Reingruber B, Weber PG. Gastroschisis and omphalocele: treatments and long-term outcomes. Pediatr Surg Int 2008; 24: 167-173 [PMID: 17985136 DOI: 10.1007/s00383-007-2055-y]
20 Carvalho NS, Helfer TM, Serni PO, Terasaka OA, Boute T, Araujo Júnior E, Nardozza LM, Moron AF, Rolo LC. Postnatal outcomes of infants with gastroschisis: a 5-year follow-up in a tertiary referral center in Brazil. J Matern Fetal Neonatal Med 2015: 1-5 [PMID: 25747953 DOI: 10.3109/14767058.2014.1002764]
21 Goulet O, Ruemmele F, Lacaille F, Colomb V. Irreversible intestinal failure. J Pediatr Gastroenterol Nutr 2004; 38: 250-269 [PMID: 15076623 DOI: 10.1097/00005176-200403000-00006]
22 Luton D, de Lagausie P, Guibourdenche J, Oury J, Sibony O, Vuillard E, Boissinot C, Aigrain Y, Beaufils F, Navarro J, Blot P. Effect of amnioinfusion on the outcome of prenatally diagnosed gastroschisis. Fetal Diagn Ther 1999; 14: 152-155 [PMID: 10364666 DOI: 10.1159/000020910]
23 Ergün O, Barksdale E, Ergün FS, Prosen T, Qureshi FG, Reblock KR, Ford H, Hackam DJ. The timing of delivery of infants with gastroschisis influences outcome. J Pediatr Surg 2005; 40: 424-428 [PMID: 15750942 DOI: 10.1016/j.jpedsurg.2004.10.013]
24 Baud D, Lausman A, Alfaraj MA, Seaward G, Kingdom J, Windrim R, Langer JC, Kelly EN, Ryan G. Expectant management compared with elective delivery at 37 weeks for gastroschisis. Obstet Gynecol 2013; 121: 990-998 [PMID: 23635735 DOI: 10.1097/AOG.0b013e31828ec299]
25 Lausman AY, Langer JC, Tai M, Seaward PG, Windrim RC, Kelly EN, Ryan G. Gastroschisis: what is the average gestational age of spontaneous delivery? J Pediatr Surg 2007; 42: 1816-1821 [PMID:
de Buys Roessingh AS et al . Severity of gastroschisis at birth
COMMENTS

234 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
18022429 DOI: 10.1016/j.jpedsurg.2007.07.005]26 Logghe HL, Mason GC, Thornton JG, Stringer MD. A randomized
controlled trial of elective preterm delivery of fetuses with gastro-schisis. J Pediatr Surg 2005; 40: 1726-1731 [PMID: 16291160 DOI: 10.1016/j.jpedsurg.2005.07.047]
27 Savoie KB, Huang EY, Aziz SK, Blakely ML, Dassinger S, Dorale AR, Duggan EM, Harting MT, Markel TA, Moore-Olufemi SD, Shah SR, St Peter SD, Tsao K, Wyrick DL, Williams RF. Improving gastroschisis outcomes: does birth place matter? J Pediatr Surg 2014; 49: 1771-1775 [PMID: 25487481 DOI: 10.1016/j.jpedsurg.2014.09.019]
28 Blessed WB, Coughlin JP, Johnson MP, Evans MI, Jewell MR, Goyert GL, Schwartz DB, Klein MD. Immediate delivery room repair of fetal abdominal wall defects. Fetal Diagn Ther 1993; 8: 203-208 [PMID: 8240695 DOI: 10.1159/000263826]
29 Coughlin JP, Drucker DE, Jewell MR, Evans MJ, Klein MD. Delivery room repair of gastroschisis. Surgery 1993; 114: 822-826; discussion 826-827 [PMID: 8211700]
30 Kandasamy Y, Whitehall J, Gill A, Stalewski H. Surgical management of gastroschisis in North Queensland from 1988 to 2007. J Paediatr Child Health 2010; 46: 40-44 [PMID: 19943863 DOI: 10.1111/j.1440-1754.2009.01615.x]
P- Reviewer: Cordon JP, Germer CT, Woo SY S- Editor: Qiu S L- Editor: A E- Editor: Liu SQ
de Buys Roessingh AS et al . Severity of gastroschisis at birth

Samuel J Tingle, John A Moir, Steven A White
Samuel J Tingle, Faculty of Medical Sciences, Newcastle Medical School, Newcastle, Tyne and Wear NE2 4HH, United Kingdom
John A Moir, Newcastle Medical School Fibrosis Lab, Tyne and Wear NE2 4HH, United Kingdom
Steven A White, HPB and Transplant Consultant, HPB Unit, Freeman Hospital, Newcastle upon Tyne, Tyne and Wear NE7 7DN, United Kingdom
Author contributions: Tingle SJ performed the research and wrote the paper; Moir JA and White SA supervised and designed the project.
Institutional review board statement: The study was reviewed and approved for publication by our institutional reviewer, NUTH trust.
Informed consent statement: All cases were anonymised during data collection therefore informed consent was not required.
Conflict-of-interest statement: No authors have any conflict of interest.
Data sharing statement: The original anonymised database is available for collaborative studies via the corresponding author, [email protected].
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Correspondence to: Steven A White, Professor, HPB and Transplant Consultant, HPB Unit, Freeman Hospital, Freeman Road, Newcastle upon Tyne, Tyne and Wear NE7 7DN,
United Kingdom. [email protected]: +44-191-2137074
Received: June 2, 2015 Peer-review started: June 5, 2015 First decision: July 6, 2015Revised: September 9, 2015Accepted: October 16, 2015Article in press: October 19, 2015Published online: November 15, 2015
AbstractAIM: To investigate the survival impact of common pharmaceuticals, which target stromal interactions, following a pancreaticoduodenectomy for pancreatic ductal adenocarcinoma.
METHODS: Data was collected retrospectively for 164 patients who underwent a pancreaticoduodenectomy for pancreatic ductal adenocarcinoma (PDAC). Survival analysis was performed on patients receiving the follow-ing medications: angiotensin-converting enzyme inhibitors (ACEI)/angiotensin Ⅱ receptor blockers (ARB), calcium channel blockers (CCB), aspirin, and statins. Statistical analysis included Kaplan-meier survival estimates and cox multivariate regression; the latter of which allowed for any differences in a range of prognostic indicators between groups. Medications showing a significant survival benefit were investigated in combination with other medications to evaluate synergistic effects.
RESULTS: No survival benefit was observed with respect to ACEI/ARB (n = 41), aspirin or statins on individual drug analysis (n = 39). However, the entire CCB group (n = 26) showed a significant survival benefit on multivariate cox regression; hazard ratio (HR) of 0.475 (CI = 0.250-0.902, P = 0.023). Further analysis
235 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
World J Gastrointest Pathophysiol 2015 November 15; 6(4): 235-242ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i4.235
Role of anti-stromal polypharmacy in increasing survival after pancreaticoduodenectomy for pancreatic ductal adenocarcinoma
Retrospective Cohort Study
ORIGINAL ARTICLE

revealed that this was influenced by a group of patients who were taking aspirin in combination with CCB; median survival was significantly higher in the CCB + aspirin group (n = 15) compared with the group taking neither drug (n = 98); 1414 d vs 601 d (P = 0.029, log-rank test). Multivariate cox regression revealed neither aspirin nor CCB had a statistically significant impact on survival when given alone, however in combination the survival benefit was significant; HR = 0.332 (CI = 0.126-0.870, P = 0.025). None of the other medications showed a survival benefit in any combination.
CONCLUSION: Aspirin + CCB in combination appears to increase survival in patients with PDAC, highlighting the potential clinical use of combination therapy to target stromal interactions in pancreatic cancer.
Key words: Pancreatic ductal adenocarcinoma; Stroma; Polypharmacy; Calcium channel blockers; Angiotensin Ⅱ receptor blockers; Angiotensin-converting enzyme inhibitors; Aspirin; Pancreaticoduodenectomy; Statins
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Stromal interactions play a large part in the dismal prognosis of pancreatic cancer. Recent laboratory studies have examined the potential use of common pharmaceuticals, such as calcium channel blocker (CCB), aspirin, angiotensin-converting enzyme inhibi-tors/angiotensin Ⅱ receptor blockers and statins, in inhibiting these protumorigenic stromal interactions. We retrospectively collected data from 164 patients whom underwent a pancreaticoduodenectomy to remove a pancreatic ductal adenocarcinoma, to see if the potential benefits of these drugs translated into increased survival. Our finding that those taking a combination of aspirin and CCB survived over twice as long as those on neither drug, highlights the potential of novel drug combinations to increase survival in pancreatic cancer.
Tingle SJ, Moir JA, White SA. Role of anti-stromal polypharmacy in increasing survival after pancreaticoduodenectomy for pancreatic ductal adenocarcinoma. World J Gastrointest Pathophysiol 2015; 6(4): 235-242 Available from: URL: http://www.wjgnet.com/2150-5330/full/v6/i4/235.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i4.235
INTRODUCTIONPancreatic cancer is one of the most aggressive malignancies with a dismal prognosis. In the United Kingdom it is the 5th most common cause of cancer death, with 1 and 5year survival rates of 20.8% and 3.3% respectively[1]. The most common type of pancreatic cancer is pancreatic ductal adenocarcinoma (PDAC), making up 95% of cases. Given this poor prognosis, with
little improvement over the last 40 years, novel options for therapeutic targets are being investigated, in both the palliative setting to improve survival and the postresection setting to reduce recurrence rates. One such target is the complex interaction between pancreatic cancer and the surrounding tissue, which is termed stroma.
The stroma is the local microenvironment which surrounds the tumour and is made up of a variety of cellular (vascular, inflammatory and neural cells) and noncellular components. Most of these are present in the normal pancreas and aid in regulating normal pancreatic function. In the presence of a pancreatic tumour stromal cells become activated, resulting in a desmoplastic reaction that increases tumour proliferation, chemotherapy resistance and metastasis[25]. PDAC has the most significant interactions with surrounding stroma out of all solid organ epithelial cancers, which may partly explain the aggressive nature of the disease, and as such is currently a hot topic in pancreatic cancer research.
Patients who receive surgery benefit from improved outcomes, but surgical resection is only an option in around 20% of patients[6]. Previous studies have shown that despite the curative intent of surgery, the majority of patients experience recurrence[7]. This is largely due to incomplete R1 resection. However, the activated stroma which is left behind in the remnant pancreas, even in theoretically complete R0 resections, may have a role in creating a protumorigenic environment and encouraging recurrence of disease.
Various scientific studies have demonstrated that commonly used pharmaceutical agents may influence the protumorigenic cancerstroma relationship. Calcium channel blockers (CCB)[8], aspirin[9], statins[10,11], angiotensin converting enzyme inhibitors (ACEI) and angiotensin receptor blockers (ARB)[12,13] demonstrate inhibitory effects on stromal interactions, manifesting as reduced growth and/or metastasis of PDAC cells in a mixture of in-vitro and animal studies. This effect is enhanced in combination with gemcitabine (the current first line chemotherapeutic agent in pancreatic cancer), suggesting that these medications may work by improving chemo penetrance[9,14].
ACEI and ARBs, which affect stromal interactions via the local reninangiotensin system (RAS), have been shown to improve survival[15]. Furthermore aspirin[16] and statins[17] have been shown to reduce the risk of pancreatic cancer development, suggesting an inhibitory effect on carcinogenesis. The anticancer potential of these drugs has been examined in a whole range of other cancer types[1821].
This study aims to investigate whether the aforementioned laboratory findings translate into a significant clinical survival benefit in the postresection setting, and to observe if any of these medications could act in combination to give a synergistically beneficial effect on survival.
236 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Tingle SJ et al . Anti-stromal polypharmacy in pancreatic ductal adenocarcinoma

MATERIALS AND METHODSPatientsAll patients included in the study had a histologically confirmed PDAC removed from the head of the pancreas by Whipple’s pancreaticoduodenectomy between December 2004 and March 2013. Data was retrospectively collected from hand held and electronic patient notes. This included whether they were taking ACEI/ARB (which were grouped as they both affect the local RAS), CCB, aspirin or statins as regular medications upon discharge after their operation.
Any drug which offered a significant benefit in survival was then investigated in combination with the other drugs to determine if any synergistic benefits were present.
Statistical analysisKaplanMeier was used to calculate estimated median overall survival, which was measured in days after surgery, and the logrank test was applied to compare groups. As some of the patients were still alive at the end of the study, censoring was applied, allowing these patients to be included in the analysis. χ 2 test was used to compare categorical variables. A P < 0.05 was considered significant.
Cox regression was used to exclude possible cofounding factors, and estimate the hazard ratios for various drug groups, adjusting for prognostic indicators. Prognostic indicators included sex, age (< 60 or ≥ 60 years), blood pressure status (hypertensive or normotensive), preoperative body mass index (< 18.5, 18.525, > 25), postoperative adjuvant chemotherapy, CA199 level at diagnosis (< 47, 471000, > 1000), American Society of Anesthesiologists (ASA) grade (12 or 34), resection margin status and TNM staging.
SPSS was used for all of the statistical analysis.
RESULTSIn total, 195 patients had a Whipple’s pancreaticoduodenectomy to remove a PDAC at the Newcastle Freeman Hospital between December 2004 and March 2013. Of these data could be collected for 164 patients with a median follow up time of 23.9 mo.
Individual drug analysisDrugs were initially looked at on an individual basis,
creating four groups; ACEI/ARB (n = 30/11 = 41), CCB (n = 26), aspirin (n = 55), and statins (n = 39). Median daily dose of the various drugs were as follows; aspirin 75 mg, CCB 10 mg (range: 5180 mg), statin 40 mg (540 mg), ACEI 10 mg (1.2540 mg) and ARBs 60 mg (4300 mg). Information on adjuvant chemotherapy could be collected for 153 patients. In total 110 (71.9%) received postoperative adjuvant chemotherapy. Of these 53 (48.2%) received 5FU treatment in the MAYO regime, 53 received Gemcitabine (48.2%), and the remaining 4 (3.6%) received other chemotherapeutic agents. Of the 53 patients taking Gemcitibine, 4 were also receiving Capecitabine and 2 were also receiving Carboplatin. None of the patients received radiotherapy.
Initial analysis compared median survival of every patient taking a particular drug, with those not taking that drug (Table 1). This initial analysis did not investigate whether the drug was being taken in combination with any of the other medications. None of the medications showed a statistically significant impact on survival when a Log rank test was applied. The only drug which showed an increase in median survival was CCB, (Figure 1) with those taking the drug having a median survival of 815 d compared with 528 d in those not taking the drug (P = 0.061). At this stage, the CCB group included every person taking CCB, some of which were also taking other medications such as aspirin, statins or ACEI/ARBs in various combinations.
When multivariate analysis was applied, being in the CCB group was an independent predictor of improved survival with a hazard ratio of 0.475 (P = 0.023) as can be seen in Table 2. All of the other drugs resulted in worsened survival, but this was not statistically significant.
Combination therapyAfter observing a statistically significant benefit in the entire CCB group, this drug was analysed in combination with the other drugs in the study, as seen at the top of Table 3. Both KaplainMeier median survival estimates and multivariate cox regression showed that there was no significant survival benefit in people taking either statins or ACEI/ARBs along with CCB (Table 3). However, the CCB + aspirin group (n = 15) had a significantly improved median survival; 1414 d compared to 528 d in those not on this drug combination (P = 0.012 Log rank test). This benefit was confirmed in the multivariate cox regression analysis; being in the CCB + aspirin group
237 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Table 1 Differences in Kaplan-Meier estimated median survival between individual drugs groups
Drug name Number taking the drug out of 164 patients
Median survival estimate for those taking the drug (d)
Median survival for those not taking the drug (d)
P value (log rank test)
ACEI/ARB 41 539 611 0.652CCB 26 815 528 0.061Aspirin 55 504 546 0.846Statins 39 504 577 0.368
Significance calculated using log-rank tests. ACEI/ARB: Angiotensin-converting enzyme inhibitors/angiotensin Ⅱ receptor blockers; CCB: Calcium channel blockers.
Tingle SJ et al . Anti-stromal polypharmacy in pancreatic ductal adenocarcinoma

238 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
patients into four groups; those taking CCB + aspirin in combination (n = 15), those taking aspirin without CCB (n = 40), those taking CCB without aspirin (n = 11), and those taking neither drug which acted as the control group (n = 98). χ 2 tests were then used to compare differences in the various prognostic indicators between these drug groups (Table 4). None of these prognostic indicators showed statistically significant differences between groups, except blood pressure status, ASA grade, and resection value; those taking CCB and/or aspirin were more likely to suffer from hypertension (P
gave a HR of 0.300 (CI = 0.1220.735, P = 0.008). Further analysis later revealed that this CCB + aspirin group was solely responsible for the increase in median survival seen in the initial entire CCB group (Figure 2). No other combination of ACEI/ARB, statins or aspirin showed a significant improvement in survival as seen in Table 3.
CCB and aspirinFurther statistical analysis of patients taking CCB and/or aspirin was then performed. This divided the 164
Table 2 Univariate and multivariate cox regression comparing individual drug groups with those not taking the drug
Drug name Number taking the drug out of 164 patients Univariate analysis Multivariate analysis
HR (95%CI) P -value HR (95%CI) P -valueACEI/ARB 41 1.094 (0.741-1.614) 0.653 1.129 (0.617-2.065) 0.693CCB 26 0.635 (0.393-1.025) 0.063 0.475 (0.250-0.902) 0.023Aspirin 55 1.036 (0.726-1.479) 0.846 1.041 (0.651-1.667) 0.865Statins 39 1.200 (0.806-1.787) 0.369 1.055 (0.614-1.814) 0.845
ACEI/ARB: Angiotensin-converting enzyme inhibitors/angiotensin Ⅱ receptor blockers; CCB: Calcium channel blockers.
Table 3 Kaplan-Meier survival estimates and multivariate cox regression comparing patients taking a combination of medications with patients on one or neither drug
Drug combination Number of people on Kaplan-Meier estimated median survival Multivariate cox regressioncombination out of 164 For those on the drug
combinationFor those not on drug combination
P -value (log rank)
HR (95%CI) P -value
CCB + aspirin 15 1414 528 0.012 0.300 (0.122-0.735) 0.008CCB + statin 12 544 539 0.284 0.413 (0.155-1.101) 0.077CCB + ACEI/ARB 12 485 541 0.450 0.512 (0.194-1.348) 0.175Aspirin + statin 27 504 546 0.697 0.969 (0.509-1.844) 0.924Aspirin + ACEI/ARB 22 485 569 0.923 0.948 (0.438-2.054) 0.893Statin + ACEI/ARB 21 368 577 0.426 1.126 (0.533-2.379) 0.756
ACEI/ARB: Angiotensin-converting enzyme inhibitors/angiotensin Ⅱ receptor blockers; CCB: Calcium channel blockers.
Cum
sur
viva
l
1.0
0.8
0.6
0.4
0.2
0.0
0 1000 2000 3000 4000Days survival
Patients taking CCB
Patients not taking CCB
Figure 1 Kaplan-Meier curves showing overall survival in those taking calcium channel blockers and those not taking the drug. (P = 0.061 using log rank test). CCB: Calcium channel blockers.
Cum
sur
viva
l
1.0
0.8
0.6
0.4
0.2
0.0
0 1000 2000 3000 4000Days survival
CCB and aspirin
Aspirin without CCB
CCB without aspirin
Neither
Figure 2 Kaplan-Meier curves showing overall survival in those taking calcium channel blockers and aspirin in combination and taking one or neither drug. (P = 0.01 using log rank test). CCB: Calcium channel blockers.
Tingle SJ et al . Anti-stromal polypharmacy in pancreatic ductal adenocarcinoma

239 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
= 0.000), more likely to have a higher ASA grade (P = 0.008), and more likely to have a successful surgical resection (P = 0.020).
KaplanMeier estimated median survival was 601 d in those taking neither drug (Table 5). At 1414 d, combination of CCB + aspirin made a statistically significant improvement in median survival (P = 0.029 log rank test). Taking either drug alone led to a decrease in median survival time; median survival in the aspirin without CCB group was 392 d (P = 0.032), and was 343 d in the CCB without aspirin group (P = 0.563). Differences in survival between groups can be seen in Figure 2.
The previously observed benefit of taking CCB + aspirin remained statistically significant when multi
variate cox regression was used; this allowed for any differences in prognostic indicators, including resection status, and compared the CCB + aspirin group with those taking neither drug, to find a hazard ratio of 0.332 (CI = 0.1260.870, P = 0.025). Taking either of the drugs in isolation made no statistically significant impact on survival when multivariate cox regression was applied.
DISCUSSIONThis study interestingly demonstrates a greater than twofold increase in postoperative median survival in patients who take a combination of CCB and aspirin, as compared to those taking neither drug. The estimated
Table 4 Comparison of differences in prognostic indicators between drug groups
Characteristics No CCB/aspirin, n (%) CCB and aspirin, n (%) Aspirin without CCB, n (%) CCB without Aspirin, n (%) P value
n = 98 n = 15 n = 40 n = 11Sex Male 56 (57.1) 5 (33.3) 25 (62.5) 8 (72.7) 0.169Age (yr) < 60 39 (39.8) 5 (33.3) 8 (20.0) 3 (27.3) 0.157 ≥ 60 59 (60.2) 10 (66.7) 32 (80.0) 8 (72.7)Blood pressure status Hypertensive 27 (27.6) 13 (86.7) 22 (55.0) 11 (100.0) 0.000 Non-hypertensive 71 (72.4) 2 (13.3) 18 (45.0) 0 (0.0)BMI < 18.5 2 (2.0) 0 (0) 1 (2.5) 0 (0.0) 0.307 18.5-25 52 (53.1) 5 (33.3) 24 (60.0) 3 (27.3) > 25 41 (41.8) 9 (60.0) 14 (35.0) 8 (72.7)Adjuvant chemotherapy Received post-op 69 (70.4) 9 (60.0) 23 (57.5) 9 (81.8) 0.333 Not received 24 (24.5) 5 (33.3) 13 (32.5) 1 (9.1)CA19-9 < 47 27 (27.6) 3 (20.0) 9 (22.5) 1 (9.1) 0.437 47-1000 51 (52.0) 7 (46.7) 20 (50.0) 7 (63.6) > 1000 8 (8.2) 3 (20.0) 6 (15.0) 3 (27.3)ASA grade 1-2 81 (82.7) 12 (80.0) 22 (55.0) 8 (72.7) 0.008 3-4 17 (17.3) 3 (20.0) 18 (45.0) 3 (27.3)Resection value R0 14 (14.3) 6 (40.0) 9 (22.5) 5 (45.5) 0.020 R1 83 (84.7) 9 (60.0) 31 (77.5) 6 (54.5)T status T1-2 3 (3.1) 2 (13.3) 1 (2.5) 0 (0.0) 0.199 T3-4 95 (96.9) 13 (86.7) 39 (97.5) 11 (100.0)N status N0 7 (7.1) 3 (20.0) 5 (12.5) 0 (0.0) 0.242 N1 90 (91.8) 12 (80) 35 (87.5) 11 (100.0)
P-values were calculated using tests χ 2 tests. CCB: Calcium channel blockers; ASA: American society of anaesthesiologists; BMI: Body mass index.
Table 5 Kaplan-Meier survival estimates and multivariate cox regression comparing patients taking a combination of calcium channel blockers + aspirin with patients on one or neither drug
Drug group Number of people Estimated median P -value (log rank) Multivariate cox regression
in group survival (d) compared to control HR (95%CI) P -valueControl (no CCB/aspirin) 98 601 - 1 -CCB + aspirin 15 1414 0.029 0.332 (0.126-0.870) 0.025Aspirin without CCB 40 392 0.032 1.658 (0.968-2.840) 0.066CCB without Aspirin 11 343 0.563 1.039 (0.416-2.595) 0.935
CCB: Calcium channel blockers.
Tingle SJ et al . Anti-stromal polypharmacy in pancreatic ductal adenocarcinoma

240 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
median survival in patients taking neither drug was comparable to that in similar studies[2224]. These observations remained significant when allowing for a range of prognostic indicators using multivariate cox regression. In contrast taking any of these medications in isolation or other combinations did not impact on survival. One may therefore postulate that aspirin and CCB’s may act in synergy to inhibit cancerstromal interactions and thus improve survival.
It has been suggested that the dense desmoplastic reaction that surrounds tumours may account for up to 90% of tumour volume[25]. This represents an intriguing concept in tumour staging, as whilst one may theoretically achieve a tumourfree R0 resection margin, large amounts of activated tumour stroma may be left behind and act as a catalyst for recurrent disease. Therefore, in the context of this study’s findings, it may be that aspirin and CCB act in combination to inhibit any subsequent protumorigenic activity, thus reducing/slowing recurrence and improving survival.
A vast array of different signalling pathways exist which are involved in the development and progression of cancer. The benefits of inhibiting multiple pathways, or multiple points on a single pathway, via combination drug therapy is supported by clinical data showing the synergistic effects of combining anticancer therapies leading to improved outcomes compared to the sum of each individual drug’s benefits[26]. To the author’s knowledge, this is the first study looking at a combination of CCB and aspirin as a therapeutic option in pancreatic cancer. As a result, the mechanisms of action are poorly understood. However, we can consider some of the laboratory work which prompted this study, to appreciate some of the potential underlying mechanisms.
Aspirin’s role as an antiinflammatory, antiplatelet drug is well established through its inhibitory action on the inflammatory enzyme cyclooxygenase1 (COX1), and is known to have a key role in reducing the risk of cancer development in a variety of malignancies, including pancreatic cancer[16,27,28]. The mechanism of effect is likely due to the inhibition of stromalinteractions which interfere with local inflammation. This is particularly pertinent in PDAC given the significant inflammatory environment observed, with a weak and fragile extracellular matrix promoting cancer development[29]. The fact chronic pancreatitis is a key risk factor in PDAC supports this.
There are various pathways aspirin exerts an influence upon in this setting. Incorrect regulation of the transcription factor nuclear factor kappa B (NFκB) can lead to excess local inflammation and a positive feedback loop amplifying the activity of the local RAS to oncogenic levels[30]. NFκB is frequently activated in pancreatic cancer which suggests a link between local inflammation and progression of pancreatic cancer[31]. Aspirin’s inhibitory effect on inflammation and NFκB have been demonstrated in laboratory studies[31,32], and a resulting decrease in the progression and development of PDAC has been observed in mouse models[33].
Another molecule involved in inflammation is COX-2, an inflammatory enzyme which is also often raised in pancreatic cancer; the inhibition of which leads to decreased carcinogenesis[34]. Although aspirin has a greater effect on COX1, it may have a role in inhibiting COX2 in pancreatic cancer. The immune system also plays a role in inflammation, and immune inflammatory cells are one of the cellular components of pancreatic stroma. One such immune cell is the FOXP3 regulatory T cell, which aspirin has been shown to inhibit in the context of pancreatic stroma[9].
CCBs have also shown promise in the laboratory, with an earlier study showing that CCBs can inhibit growth and decrease the doubling time of pancreatic cancer cells[35]. Furthermore the stroma is known to represent a barrier to chemotherapy, and CCBs may have a role in improving chemo penetrance in a range of cancer types, including pancreatic[36]. CCBs have been shown to increase the effectiveness of chemotherapy on a resistant pancreatic adenocarcinoma via its effect on Pglycoprotein, which is also known as multidrug resistance protein[37].
Another possible mechanism of action involves cholecystokinin (CCK), an intracellular peptide hormone which has various roles in control of the pancreas[38]. It is known that high levels of CCK can cause both formation and progression of pancreatic cancer[39]. CCBs have the ability to limit the effects of CCK on pancreatic cells and lead to decreased carcinogenesis[40] and metastasis[41]. Alternatively CCBs have been shown to inhibit the proliferation of pancreatic cancer through the blockade of IK calciumactivated potassium channels[8].
This study is limited by the small sample size of patients taking aspirin and CCB in combination. It is also limited by the fact we looked at regular medications being taken on discharge from hospital, which did not allow any analysis into the effect of altering the duration of administration of these medications.
The retrospective nature of this work brings an inherent selection bias however this was countered through multivariate analysis including a range of prognostic indicators. The one key difference between groups related to the resection margin status, where those taking aspirin and CCB in combination were more likely to have an R0 resection. However, when allowed for using multivariate analysis, the benefits of combining aspirin and CCB still remained statistically significant. One may potentially hypothesise that the antistromal effects of taking this combination of medications preoperatively led to a less locally advanced tumour and therefore a higher chance of full resection.
It could be argued that it is simply the CCB which are having an effect on survival, as seen in our initial individual drug analysis, and that aspirin was only found as a coincidence as we were looking at combinations in the already beneficial CCB group. However, our statistics would suggest that the only reason that CCB showed a benefit on individual drug analysis was the presence of 15 people within the group who were also
Tingle SJ et al . Anti-stromal polypharmacy in pancreatic ductal adenocarcinoma

241 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
taking aspirin. Indeed, without those 15 patients, CCB in isolation showed no benefit.
In conclusion, this novel retrospective study has shown that the potential antistromal benefits of CCB and aspirin demonstrated by previous laboratory studies do translate into survival benefits in patients with pancreatic ductal adenocarcinoma. Laboratory studies would be useful to determine the mechanism of action of the synergistic effect observed. Further clinical studies with larger patient groups, as well as randomised prospective studies, will help to determine the true anticancer potential of these drugs. This study builds on previous laboratory research and represents an exciting new range of potential therapeutics for pancreatic cancer, especially given the cheap, accessible and safe nature of these drugs.
COMMENTSBackgroundThe complex interaction between pancreatic ductal adenocarcinoma and its surrounding tissue microenvironment (termed stroma) plays a large part in the dismal prognosis of pancreatic cancer. Recent laboratory studies have examined the potential use of common pharmaceuticals, such as calcium channel blockers (CCB), aspirin, angiotensin-converting enzyme inhibitors/angiotensin Ⅱ receptor blockers and statins, in inhibiting these protumorigenic stromal interactions. Further clinical research is required to look at the effects of these drugs on mortality.
Research frontiersStudies looking at whether the potential benefits suggested by laboratory research translates into increased survival in clinical research is a current hotspot in this field. There has also been growing interest into the effect of combining therapies to get a synergistic effect; an area which this study explores.
Innovations and breakthroughsThis study built on previous laboratory research to show survival benefits in the clinical setting. The authors demonstrated a statistically significant improvement in Kaplan-Meier estimated median survival in patients taking a combination of aspirin and CCB, a combination which has not been studied in this setting before. The twofold increase in estimated median survival seen in the aspirin + CCB group was confirmed by multivariate cox regression which found the increase in survival to remain significant when a range of prognostic indicators was allowed for.
ApplicationsIf the findings of this study are confirmed by further research, patients with pancreatic cancer could expect improvements in life expectancy, with the simple addition of extremely cheap, well tolerated, and readily available medications.
Terminology The stroma is the local microenvironment which surrounds the tumour and is made up of a variety of cellular (vascular, inflammatory and neural cells) and non-cellular components. Most of these are present in the normal pancreas and aid in regulating normal pancreatic function. In the presence of a pancreatic tumour stromal cells become activated, resulting in increased tumour proliferation, chemotherapy resistance and metastasis.
Peer-reviewThis is a novel look at a very interesting topic. In the clinical finding presented in this manuscript, the authors showed that combination CCB and aspirin can increase survival in patients with pancreatic cancer pancreatic ductal adenocarcinoma following pancreaticoduodenectomy although in a small number of patients. A potential mechanism related to targeting stromal
interactions in pancreatic cancer was proposed.
REFERENCES1 Cancer Research UK. Pancreatic cancer key stats. Cancer
Research UK, 20142 Maitra A, Hruban RH. Pancreatic cancer. Annu Rev Pathol
2008; 3: 157-188 [PMID: 18039136 DOI: 10.1146/annurev.path-mechdis.3.121806.154305]
3 Bissell MJ, Radisky D. Putting tumours in context. Nat Rev Cancer 2001; 1: 46-54 [PMID: 11900251 DOI: 10.1038/35094059]
4 Heldin CH, Rubin K, Pietras K, Ostman A. High interstitial fluid pressure - an obstacle in cancer therapy. Nat Rev Cancer 2004; 4: 806-813 [PMID: 15510161 DOI: 10.1038/nrc1456]
5 Vonlaufen A, Phillips PA, Xu Z, Goldstein D, Pirola RC, Wilson JS, Apte MV. Pancreatic stellate cells and pancreatic cancer cells: an unholy alliance. Cancer Res 2008; 68: 7707-7710 [PMID: 18829522 DOI: 10.1158/0008-5472.CAN-08-1132]
6 Hidalgo M. Pancreatic cancer. N Engl J Med 2010; 362: 1605-1617 [PMID: 20427809 DOI: 10.1056/NEJMra0901557]
7 Barugola G, Falconi M, Bettini R, Boninsegna L, Casarotto A, Salvia R, Bassi C, Pederzoli P. The determinant factors of recurrence following resection for ductal pancreatic cancer. JOP 2007; 8: 132-140 [PMID: 17228145]
8 Jäger H, Dreker T, Buck A, Giehl K, Gress T, Grissmer S. Blockage of intermediate-conductance Ca2+-activated K+ channels inhibit human pancreatic cancer cell growth in vitro. Mol Pharmacol 2004; 65: 630-638 [PMID: 14978241 DOI: 10.1124/mol.65.3.630]
9 Plassmeier L, Knoop R, Waldmann J, Kesselring R, Buchholz M, Fichtner-Feigl S, Bartsch DK, Fendrich V. Aspirin prolongs survival and reduces the number of Foxp3+ regulatory T cells in a genetically engineered mouse model of pancreatic cancer. Langenbecks Arch Surg 2013; 398: 989-996 [PMID: 23989613 DOI: 10.1007/s00423-013-1105-2]
10 Ishikawa S, Nagai Y, Masuda T, Koga Y, Nakamura T, Imamura Y, Takamori H, Hirota M, Funakosi A, Fukushima M, Baba H. The role of oxysterol binding protein-related protein 5 in pancreatic cancer. Cancer Sci 2010; 101: 898-905 [PMID: 20128820 DOI: 10.1111/j.1349-7006.2009.01475.x]
11 Kusama T, Mukai M, Iwasaki T, Tatsuta M, Matsumoto Y, Akedo H, Inoue M, Nakamura H. 3-hydroxy-3-methylglutaryl-coenzyme a reductase inhibitors reduce human pancreatic cancer cell invasion and metastasis. Gastroenterology 2002; 122: 308-317 [PMID: 11832446 DOI: 10.1053/gast.2002.31093]
12 Arafat HA, Gong Q, Chipitsyna G, Rizvi A, Saa CT, Yeo CJ. Antihypertensives as novel antineoplastics: angiotensin-I-converting enzyme inhibitors and angiotensin II type 1 receptor blockers in pancreatic ductal adenocarcinoma. J Am Coll Surg 2007; 204: 996-1005; discussion 1005-1006 [PMID: 17481528 DOI: 10.1016/j.jamcollsurg.2007.01.067]
13 Masamune A, Hamada S, Kikuta K, Takikawa T, Miura S, Nakano E, Shimosegawa T. The angiotensin II type I receptor blocker olmesartan inhibits the growth of pancreatic cancer by targeting stellate cell activities in mice. Scand J Gastroenterol 2013; 48: 602-609 [PMID: 23477656 DOI: 10.3109/00365521.2013.777776]
14 Bocci G, Fioravanti A, Orlandi P, Bernardini N, Collecchi P, Del Tacca M, Danesi R. Fluvastatin synergistically enhances the antiproliferative effect of gemcitabine in human pancreatic cancer MIAPaCa-2 cells. Br J Cancer 2005; 93: 319-330 [PMID: 16052215 DOI: 10.1038/sj.bjc.6602720]
15 Nakai Y, Isayama H, Ijichi H, Sasaki T, Sasahira N, Hirano K, Kogure H, Kawakubo K, Yagioka H, Yashima Y, Mizuno S, Yamamoto K, Arizumi T, Togawa O, Matsubara S, Tsujino T, Tateishi K, Tada M, Omata M, Koike K. Inhibition of renin-angiotensin system affects prognosis of advanced pancreatic cancer receiving gemcitabine. Br J Cancer 2010; 103: 1644-1648 [PMID: 20978506 DOI: 10.1038/sj.bjc.6605955]
16 Tan XL, Reid Lombardo KM, Bamlet WR, Oberg AL, Robinson DP, Anderson KE, Petersen GM. Aspirin, nonsteroidal anti-inflammatory drugs, acetaminophen, and pancreatic cancer risk: a clinic-based case-
COMMENTS
Tingle SJ et al . Anti-stromal polypharmacy in pancreatic ductal adenocarcinoma

242 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
control study. Cancer Prev Res (Phila) 2011; 4: 1835-1841 [PMID: 21803981 DOI: 10.1158/1940-6207.CAPR-11-0146]
17 Khurana V, Sheth A, Caldito G, Barkin JS. Statins reduce the risk of pancreatic cancer in humans: a case-control study of half a million veterans. Pancreas 2007; 34: 260-265 [PMID: 17312467 DOI: 10.1097/MPA.0b013e318030e963]
18 Corcos L, Le Jossic-Corcos C. Statins: perspectives in cancer therapeutics. Dig Liver Dis 2013; 45: 795-802 [PMID: 23490341 DOI: 10.1016/j.dld.2013.02.002]
19 Cuzick J, Thorat MA, Bosetti C, Brown PH, Burn J, Cook NR, Ford LG, Jacobs EJ, Jankowski JA, La Vecchia C, Law M, Meyskens F, Rothwell PM, Senn HJ, Umar A. Estimates of benefits and harms of prophylactic use of aspirin in the general population. Ann Oncol 2015; 26: 47-57 [PMID: 25096604 DOI: 10.1093/annonc/mdu225]
20 Chiang YY, Chen KB, Tsai TH, Tsai WC. Lowered cancer risk with ACE inhibitors/ARBs: a population-based cohort study. J Clin Hypertens (Greenwich) 2014; 16: 27-33 [PMID: 24304931 DOI: 10.1111/jch.12228]
21 Holmes MD, Chen WY. Hiding in plain view: the potential for commonly used drugs to reduce breast cancer mortality. Breast Cancer Res 2012; 14: 216 [PMID: 23227958 DOI: 10.1186/bcr3336]
22 Winter JM, Cameron JL, Campbell KA, Arnold MA, Chang DC, Coleman J, Hodgin MB, Sauter PK, Hruban RH, Riall TS, Schulick RD, Choti MA, Lillemoe KD, Yeo CJ. 1423 pancrea-ticoduodenectomies for pancreatic cancer: A single-institution experience. J Gastrointest Surg 2006; 10: 1199-1210; discussion 1210-1211 [PMID: 17114007 DOI: 10.1016/j.gassur.2006.08.018]
23 Eeson G, Chang N, McGahan CE, Khurshed F, Buczkowski AK, Scudamore CH, Warnock GL, Chung SW. Determination of factors predictive of outcome for patients undergoing a pancrea-ticoduodenectomy of pancreatic head ductal adenocarcinomas. HPB (Oxford) 2012; 14: 310-316 [PMID: 22487068 DOI: 10.1111/j.1477-2574.2012.00448.x]
24 Lewis R, Drebin JA, Callery MP, Fraker D, Kent TS, Gates J, Vollmer CM. A contemporary analysis of survival for resected pancreatic ductal adenocarcinoma. HPB (Oxford) 2013; 15: 49-60 [PMID: 23216779 DOI: 10.1111/j.1477-2574.2012.00571.x]
25 Neesse A, Michl P, Frese KK, Feig C, Cook N, Jacobetz MA, Lolkema MP, Buchholz M, Olive KP, Gress TM, Tuveson DA. Stromal biology and therapy in pancreatic cancer. Gut 2011; 60: 861-868 [PMID: 20966025 DOI: 10.1136/gut.2010.226092]
26 Alexis F. Nano-polypharmacy to treat tumors: coencapsulation of drug combinations using nanoparticle technology. Mol Ther 2014; 22: 1239-1240 [PMID: 24981439 DOI: 10.1038/mt.2014.96]
27 Ulrich CM, Bigler J, Potter JD. Non-steroidal anti-inflammatory drugs for cancer prevention: promise, perils and pharmacogenetics. Nat Rev Cancer 2006; 6: 130-140 [PMID: 16491072 DOI: 10.1038/nrc1801]
28 Ye X, Fu J, Yang Y, Gao Y, Liu L, Chen S. Frequency-risk and duration-risk relationships between aspirin use and gastric cancer: a systematic review and meta-analysis. PLoS One 2013; 8: e71522 [PMID: 23936269 DOI: 10.1371/journal.pone.0071522]
29 Frantz C, Stewart KM, Weaver VM. The extracellular matrix at a glance. J Cell Sci 2010; 123: 4195-4200 [PMID: 21123617 DOI: 10.1242/jcs.023820]
30 Daniluk J, Liu Y, Deng D, Chu J, Huang H, Gaiser S, Cruz-Monserrate Z, Wang H, Ji B, Logsdon CD. An NF-κB pathway-mediated positive feedback loop amplifies Ras activity to pathological levels in mice. J Clin Invest 2012; 122: 1519-1528 [PMID: 22406536 DOI: 10.1172/JCI59743]
31 Sclabas GM, Uwagawa T, Schmidt C, Hess KR, Evans DB, Abbruzzese JL, Chiao PJ. Nuclear factor kappa B activation is a potential target for preventing pancreatic carcinoma by aspirin. Cancer 2005; 103: 2485-2490 [PMID: 15861417 DOI: 10.1002/cncr.21075]
32 Yue W, Yang CS, DiPaola RS, Tan XL. Repurposing of metformin and aspirin by targeting AMPK-mTOR and inflammation for pancreatic cancer prevention and treatment. Cancer Prev Res (Phila) 2014; 7: 388-397 [PMID: 24520038 DOI: 10.1158/1940-6207.CAPR-13-0337]
33 Fendrich V, Chen NM, Neef M, Waldmann J, Buchholz M, Feldmann G, Slater EP, Maitra A, Bartsch DK. The angiotensin-I-converting enzyme inhibitor enalapril and aspirin delay progression of pancreatic intraepithelial neoplasia and cancer formation in a genetically engineered mouse model of pancreatic cancer. Gut 2010; 59: 630-637 [PMID: 19880966 DOI: 10.1136/gut.2009.188961]
34 Schuller HM, Zhang L, Weddle DL, Castonguay A, Walker K, Miller MS. The cyclooxygenase inhibitor ibuprofen and the FLAP inhibitor MK886 inhibit pancreatic carcinogenesis induced in hamsters by transplacental exposure to ethanol and the tobacco carcinogen NNK. J Cancer Res Clin Oncol 2002; 128: 525-532 [PMID: 12384795 DOI: 10.1007/s00432-002-0365-y]
35 Sato K, Ishizuka J, Cooper CW, Chung DH, Tsuchiya T, Uchida T, Rajaraman S, Townsend CM, Thompson JC. Inhibitory effect of calcium channel blockers on growth of pancreatic cancer cells. Pancreas 1994; 9: 193-202 [PMID: 8190721 DOI: 10.1097/00006676-199403000-00009]
36 Ford JM, Hait WN. Pharmacology of drugs that alter multidrug resistance in cancer. Pharmacol Rev 1990; 42: 155-199 [PMID: 2217530]
37 Liu B , Staren ED, Iwamura T, Appert HE, Howard JM. Mechanisms of taxotere-related drug resistance in pancreatic carcinoma. J Surg Res 2001; 99: 179-186 [PMID: 11469885 DOI: 10.1006/jsre.2001.6126]
38 Guo YS, Townsend CM. Roles of gastrointestinal hormones in pancreatic cancer. J Hepatobiliary Pancreat Surg 2000; 7: 276-285 [PMID: 10982627 DOI: 10.1007/s005340070049]
39 Smith JP, Solomon TE. Cholecystokinin and pancreatic cancer: the chicken or the egg? Am J Physiol Gastrointest Liver Physiol 2014; 306: G91-G101 [PMID: 24177032 DOI: 10.1152/ajpgi.00301.2013]
40 Nakaizumi A, Uehara H, Baba M, Iishi H, Tatsuta M. Inhibition by verapamil of cholecystokinin-enhancement of pancreatic carcinogenesis induced by azaserine in Wistar rats. Cancer Lett 1996; 105: 23-27 [PMID: 8689627 DOI: 10.1016/0304-3835(96)04256-5]
41 Matters GL, Cooper TK, McGovern CO, Gilius EL, Liao J, Barth BM, Kester M, Smith JP. Cholecystokinin mediates progression and metastasis of pancreatic cancer associated with dietary fat. Dig Dis Sci 2014; 59: 1180-1191 [PMID: 24817409 DOI: 10.1007/s10620-014-3201-8]
P- Reviewer: Lu Z, Reddy SS S- Editor: Gong XM L- Editor: A E- Editor: Liu SQ
Tingle SJ et al . Anti-stromal polypharmacy in pancreatic ductal adenocarcinoma

Revised: September 15, 2015Accepted: October 23, 2015Article in press: October 27, 2015Published online: November 15, 2015
AbstractThere are several common causes of acute pancreatitis, principally excessive alcohol intake and gallstones, and there are many rare causes. However, cases of pancreatitis still occur in the absence of any recognizable factors, and these cases of idiopathic pancreatitis suggest the presence of unrecognized etiologies. Five cases of acute pancreatitis in four patients came to attention due to a strong temporal association with exposure to nerve stimulators and energy drinks. Given that these cases of pancreatitis were otherwise unexplained, and given that these exposures were not clearly known to be associated with pancreatitis, we performed a search for precedent cases and for mechanistic bases. No clear precedent cases were found in PubMed and only scant, weak precedent cases were found in public-health databases. However, there was a coherent body of intriguing literature in support of a mechanistic basis for these exposures playing a role in the etiology of pancreatitis.
Key words: Pancreatitis; Energy drinks; Transcutaneous electric nerve stimulation; Etiology; Chronic pain
© The Author(s) 2015. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: This may be the first report of nerve stimu-lators or energy drinks playing an etiologic role in the development of pancreatitis. Five recent cases of otherwise unexplained pancreatitis recently came to attention due to a strong temporal association between pancreatitis and exposure to nerve stimulators (3 cases in 3 patients) and energy drinks (2 cases in 1 patient).
Artem Shmelev, Alain Abdo, Sarina Sachdev, Urvi Shah, Gopal C Kowdley, Steven C Cunningham
Artem Shmelev, Alain Abdo, Sarina Sachdev, Urvi Shah, Gopal C Kowdley, Steven C Cunningham, The Department of Surgery, Saint Agnes Hospital, Baltimore, MD 21229, United States
Author contributions: Shmelev A and Abdo A contributed equally to this work; Shmelev A, Abdo A, Sachdev S, Shah U, Kowdley GC and Cunningham SC participated in the acquisition, analysis, and interpretation of the data, and drafted the initial manuscript; Kowdley GC and Cunningham SC were the guarantors and designed the study; Shmelev A, Abdo A, Sachdeva S, Shah U, Kowdley GC and Cunningham SC revised the article critically for important intellectual content.
Institutional review board statement: Study of the acute pancreatitis patients was approved by SAH-IRB 2011-030.
Informed consent statement: Need for consent was waived by SAH-IRB 2011-030. There are no details that might identify the patients in this manuscript.
Conflict-of-interest statement: None of the authors have any conflict of interest regarding this manuscript.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Correspondence to: Steven C Cunningham, MD, FACS, Director of Pancreatic and Hepatobiliary Surgery and Research, The Department of Surgery, Saint Agnes Hospital, 900 Caton Avenue, MB 207, Baltimore, MD 21229, United States. [email protected]: +1-443-8146773Fax: +1-410-7190094
Received: March 26, 2015Peer-review started: March 28, 2015First decision: August 20, 2015
CASE REPORT
243 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Energetic etiologies of acute pancreatitis: A report of five cases
World J Gastrointest Pathophysiol 2015 November 15; 6(4): 243-248ISSN 2150-5330 (online)
© 2015 Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.4291/wjgp.v6.i4.243

Although causality is not shown, the temporal association is striking.
Shmelev A, Abdo A, Sachdev S, Shah U, Kowdley GC, Cunnin-gham SC. Energetic etiologies of acute pancreatitis: A report of five cases. World J Gastrointest Pathophysiol 2015; 6(4): 243-248 Available from: URL: http://www.wjgnet.com/2150-5330/full/v6/i4/243.htm DOI: http://dx.doi.org/10.4291/wjgp.v6.i4.243
INTRODUCTIONAcute pancreatitis is a common and potentially life-threatening disease, whose incidence is increasing[1]. While the etiology of the vast majority of cases is identified as either alcohol or biliary stones, many cases (10%-34%)[1,2] are labeled idiopathic or cryptogenic, due to unknown etiology, and this proportion too is increasing[2,3]. Other, less common causes of pancreatitis that are identifiable include hypertriglyceridemia, tumors and stones, autoimmune diseases, and medications.
Use of energy drinks and nerve stimulators is also on the rise. Use of energy drinks such as RedBull and RockStar is increasing due in part to aggressive marketing campaigns and other psychosocial factors. The range and relative concentrations of their various ingredients vary widely, and per capita consumption has recently doubled in the United States[4-6]. Electrical nerve stimulation, such as transcutaneous electrical nerve stimulation (TENS) are employed at various intensities and frequencies for pain suppression, a controversial use[7].
HypothesisVery few data on idiopathic or cryptogenic causes of pancreatitis are available. Some cases of so-called idiopathic pancreatitis are likely due to unrecognized, or poorly understood, genetic defects[3,8-13] and pancrea-ticobiliary malformations[14,15]. Yet, there still remains a group of patients with so-called true idiopathic pan-creatitis (TIP), whose etiology cannot be identified[16]. Three such patients with seemingly TIP, with no identified cause, were found to have a clear temporal association with the use of nerve-stimulation devices, and a fourth such patient was found to have a clear temporal asso-ciation between 2 separate episodes of pancreatitis and consumption of the popular energy drink, Rockstar™(Table 1). Other causes of pancreatitis, including gallstones, alcohol, autoimmune pancreatitis (elevated IgG4 levels), and hypertriglyceridemia, were ruled out, leading to the hypothesis that exposures to nerve stimulation or to energy drinks could play a role in the etiology of acute pancreatitis.
CASE REPORTThree nerve-stimulation cases A healthy female in her 40s underwent cholecystectomy
for suspected biliary pancreatitis based on a suspicion of gallbladder sludge, but then re-presented several months later with recurrent pancreatitis. Upon further questioning it became clear that she occasionally used TENS to treat pain, including prior to her current episode of interstitial edematous pancreatitis. She did not recall if she used it prior to her pre-cholecystectomy pancreatitis. She responded to standard nonoperative therapy and recovered well.
A healthy female in her 30s, with an implanted electrical nerve stimulator device for chronic back pain, developed interstitial edematous pancreatitis. She responded to standard nonoperative therapy and recovered well.
A healthy female in her 50s wore a TENS device for back pain during a 10-h car trip. Shortly after arrival she developed severe, extensive, necrotizing pan-creatitis and disconnected-duct syndrome, requiring necrosectomy, after which she recovered well. Although following her stay in the intensive-care unit, and her extensive operation and requisite recovery, she could not recall the exact settings she used for TENS, but thought that it was a moderate setting and that the pads were applied to her back for the vast majority of her 10-h car trip. Pathology following operation revealed extensive necrotic pancreatic and peripancreatic tissue.
Two energy-drink casesA healthy male in his 40s with a remote history of severe acute alcoholic pancreatitis with pseudocyst formation, all now resolved. He was thought certainly to be free of recent alcohol use, but developed 2 episodes of interstitial edematous pancreatitis, both following Rockstar™ consumption. He responded well to nonoperative therapy.
Literature searchTo inquire whether these could be two heretofore unappre-ciated etiologies of acute pancreatitis, a literature search was performed in PubMed looking for a mechanistic basis, using the title and abstract terms “pancreatitis” with either “idiopathic” or “etiology” and combined this with either “energy drink” or “nerve stimulation”. In addition, a search was performed of www.fda.gov for pancreatitis, nerve stimulation, energy drink, and several ingredients in common energy beverages (e.g., milk thistle, guarana, ginkgo, ginseng)[17].
The PubMed search revealed no case reports asso-ciating pancreatitis with either energy drinks or with nerve stimulation. Although energy drinks are associated with a variety of adverse signs and symptoms, such as nausea, vomiting, diarrhea, abdominal pain, hyperhi-drosis, tachycardia, irritability, insomnia, stroke, and psychotic and bipolar disorders, the Food and Drug Administration (FDA) search on www.fda.gov revealed only one report of pancreatitis (which required hospi-talization) associated with the energy drink Redbull™[18] and two reports of pancreatic disorders associated with 5-Hour Energy Booster™ and Monster Energy™[19]. Four
244 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Shmelev A et al . New etiologies of pancreatitis

reports of pancreatitis associated with ginkgo were found in www.fda-reports.com.
DISCUSSIONThe observation of five cases of pancreatitis in 4 patients without the usual risk factors for pancreatitis, but with other exposures, which themselves were notable, either because the exposure was unusually prolonged (patient #3, with exposure to nerve stimulation during the entirety of a 10 h car ride), or unusually recurrent (patient #4, with pancreatitis episodes occurring following each consumption of the energy drink Rockstar™) led us tohypothesize that these could conceivably be unreco-gnized etiologies of pancreatitis. Although some of the patients in Table 1 has confounding factors, such as medications loosely associated with AP, and pancreas divisum and genetic causes were not possible to rule out in each and every case, nevertheless it is striking that the patient with the most severe pancreatitis had the purest form of seemingly TIP (lacking any identifiable confounders) had the greatest exposure to TENS, and
had the most severe pancreatitis, necrotizing pancreatitis requiring multidisciplinary management[20]. Our search of the literature and FDA records revealed no published case reports and only scant FDA evidence, but did reveal supporting evidence of this hypothesis worthy of discussion.
Nerve stimulation and neurogenic inflammationIronically, nerve stimulation, such as TENS, has been used to treat pain of pancreatitis, as well as pain of many other sources[21-23] but the number of patients is too small, and the follow-up too inconsistent, for there to be any observed causal relationship between pancreatitis and nerve stimulation. Certainly it is well known that the pancreas is richly innervated, and mounting evidence suggests that pathologic activation of pancreatic neurons and the inflammatory sequelae of that activation (known as neurogenic inflammation) play a role in the development of pancreatitis (Table 2). The concept of neurogenic inflammation is additionally supported by the observation that most of the neurotransmitters of C and Aδ fibers of the pancreas have proinflammatory
245 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
Table 1 Patient characteristics
Pt Age Gender Type of exposure
Time gap between exposure and pancreatitis
Duration of exposure Severity of pancreatits
TG IgG4 Confounding factors
1 40s F TENS Narrow Short Mild Nl Nl3 CCB and PPI2 30s F IENS Narrow Unk Mild Unk Unk Unk2
3 50s F TENS Narrow Long Severe Nl Nl3 None1
4 40s M Energy drink Narrow Consumed Rockstar™ prior to 2 unexplained episodes
Both mild Nl Nl Initial episode due to alcohol, but abstinent for
1 yr prior to these 2 episodes
1No medications, no alcohol, no gallstones (by transabdominal and intraoperative, but not endoscopic, ultrasound), there was no evidence for or against genetic causes and pancreas divisum; 2No alcohol, and no gallstones (by transabdominal but not endoscopic ultrasound), but the patient could not recall her medication history; 3Total IgG, not IgG4, was sent. Pt: Patient; Nl: Normal; Unk: Unknown; TG: Triglyceride level; TENS: Transcutaneous electrical nerve stimulation; F: Female; M: Male; CCB: Calcium-channel blocker; PPI: Proton-pump inhibitor; IENS: Implanted electrical nerve stimulator.
Table 2 List of observations associating electrical nerve stimulations and the development of acute pancreatitis
Ref.
Observation All cases reported here were considered idiopathic N/A There was a strong temporal association of exposure and AP N/A There was a directly proportional relationship between duration of exposure and severity of subsequent AP N/A Neurogenic inflammation is increasingly recognized to play a role in development of AP, with sensory nerves in particular being considered a final common pathway in AP
[24,30,39,40]
TRPV1 and TRPA1 expression and function in pancreatic afferent neurons increases and blocking this pathway attenuates pancreatitis in a mouse model of AP
[25,26]
Over-stimulation of nerves associated with pancreatic disease (decrease in pancreatic blood flow and DNA synthesis) in rats [34] Neural cross talk between the duodenum and pancreas (duodeno-pancreatic reflex at T6-T13) can promote AP in a rat model [41]Possibly contradictory observations Stimulation by electroacupuncture of dorsal segmental points corresponding to levels that innervate pancreas (by splanchnic nerves; T9-T11) causes decrease in fasting blood glucose
[33]
Electroacupuncture protects against CCK-induced AP in rats [31] Electroacupuncture to paraumbilical point ST25 (dermatome T10) down-regulates pro-inflammatory cytokines (TNFa, IL-6) and attenuates the morphological damage to pancreas in a rat model of AP
[32]
AP: Acute pancreatitis; N/A: Not available; TNF: Tumor necrosis factor; IL- 6: Interleukin- 6; TRPV1: Transient receptor potential vanilloid 1; TRPA1: Transient receptor potential cation channel, subfamily A, member 1; CCK: Cholecystokinin.
Shmelev A et al . New etiologies of pancreatitis

246 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
of pancreatic tissue due to massive vasodilation and white blood cells infiltration. Remarkably, those changes in pancreas may be caused by irritation of SN in duodenal mucosa, because of axonal dichotomy and central convergence at spinal or higher levels (Table 2). Damage to pancreatic acinar cells may also be mediated by non-specific excitation of ryanodine or inositol-3-phosphate receptors with subsequent calcium release from endoplasmic reticulum and activation of enzymes in zymogen granules inside the cell.
Interestingly, there is also evidence that some forms of nerve stimulation, such as electroacupunture, seem to be protective against pancreatitis (Table 2)[31-33]. However, the concept of dose may well explain why a small amount of stimulation can have the opposite effect as a large amount, as is commonly observed in medicine, when a small amount of an exposure is safe and effective, such as acetaminophen (paracetamol) in therapeutic doses working as a safe antipyretic and analgesic, but a higher dose is toxic and can cause liver failure and death. Perhaps a very high dose of TENS, as in patient #3, can cause severe acute necrotizing pancreatitis, known to require prolonged multidisciplinary management[20], where as a small dose may be protec-tive, and a moderate dose may cause only a minor episode of pancreatitis.
Indeed, experimental neurochemical precedent exists for the notion that over-stimulation of nerves may cause pancreatic disease. In conscious rats, for example, stimulation of sensory nerves with low-dose capsaicin reduces basal pancreatic secretory function, while moderate doses increase this function, and large (neurotoxic) doses cause a 27% decrease in pancreatic blood flow accompanied by a decrease in DNA synthesis
actions[24].Further intriguing experimental evidence exists
linking neurogenic inflammation and pancreatitis. For example, sensory neurons of the pancreas express channels whose activation induces pancreatic inflam-mation, and whose blockade attenuates experimental pancreatitis[25-27]. Similarly, in a study of the modulatory role of bradykinin in neurogenic inflammation, a potent inhibitor of bradykinin was administered in an animal model of pancreatitis and this administration attenuated the hypotension, edema, and hypovolemia associated with the pancreatitis, suggesting modulation of nerve stimulation modulates severity of pancreatitis[28].
Studying the neuropeptide substance P (SP), a common neurotransmitter mediating pain and other nerve signals, Figini et al[29] found that administration of SP to mice stimulated plasma extravasation from postcapillary venules in the pancreas, and that this effect was blocked by the administration of antagonists to the SP receptor. More recently, in a neonatal model of pancreatitis, administration of the neuron-denervating agent capsaicin significantly reduced histological severity scores and abolished plasma extravasation associated with pancreatitis[30], findings which support the notion that primary sensory neurons constitute a common final pathway for pancreatitis.
Figure 1 illustrates in a schematic model some of these possible processes contributing to a neurogenic etiology of pancreatitis. Various stimuli may excite vanilloid receptor TRPV1 on primary sensory neurons (SN), which play the pivotal role in initiation of neuro-genic inflammation. Subsequent depolarization release various neuropeptides, such as SP, neurokinin A, and calcitonin gene related peptide. The result is edema
STTDRGTE
NSre
ferr
ed p
ain
T8-T9
Dorsalvagalcomplex
Vagus
NGWBC infiltration
Edema
IL-1IL-6TNFaNk-1R
SP
SP CGRP NkA
TRPV-1
1oSNZG
IP3R
CaCa
Acinar cell
RyRStrongstimuli
CaspazepineCapsaicinbradykinintrypsinPg, LTB4
Heat, H+
EtOH andmetabolites
Figure 1 Schematic model illustrating possible mechanisms of neurogenic pancreatitis. AP: Acute pancreatitis; STT: Spinothalamic tract; TENS: Transcutaneous electrical nerve stimulation; DRG: Dorsal root ganglion; IL: Interleukin; TNF: Tumor necrosis factor; NK-1R: Neurokinin receptor 1; 1oSN: Primary sensory neuron; NG: Nodose ganglion; Pg: Prostaglandins; SP: Substance P; TRPV-1: Transient receptor potential vanilloid 1; CGRP: Calcitonin gene related protein; NkA: Neurokinin A; IP3R: Inositol-3-phosphate receptor; RyR: Ryanodine receptor.
Shmelev A et al . New etiologies of pancreatitis

247 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
in pancreatic tissue[34].
Energy drinksSeveral aspects of the increasingly popular energy drinks are concerning. For example, because many energy drinks contain “natural” ingredients, such as ginseng, ginkgo, milk thistle, guarna-seed extract[17], these drinks are regulated as dietary supplements and not as medications, freeing manufacturers from the usual transparency associated with FDA-regulated pro-ducts[6]. Similarly, several of the ingredients have been linked to health problems, but these links are either weak or inconsistent, and indeed, several of these same ingredients are commonly taken as remedies or preventive supplements to combat various common ailments.
For example, while there is some weak evidence that ginkgo is protective against pancreatitis[35,36], there are four low-quality “FDA reports” of pancreatitis in patients taking ginkgo[37]. Search of the presumably more reliable www.fda.gov site reveals no reports of this association.
While the health benefits and risks of caffeine are well known, none of these risks appear to be related to pancreatitis, and at least weak data suggest that caffeinated coffee may protect against alcoholic pan-creatitis[38]. Similarly, no convincing association could be found between pancreatitis and other energy-drink ingredients, such as milk thistle and guarana. However, the FDA’s Center for Food Safety and Applied Nutrition Adverse Event Reporting System has reported several associations between pancreatitis and the cocktails of various energy drinks, such as RedBull™, 5-h Energy Booster™, and Monster Energy™[18,19]. Nevertheless, the possibility remains that what we have observed in patient #4 is merely a coincidence between exacerbations of autonomous alcoholic pancreatitis and the consumption of energy drinks. Still the fact that the otherwise unexplained pancreatitis occurred in this single patient twice, both times immediately following consumption of the energy drinks, is striking.
In conclusion, there is insufficient direct evidence to support causality between pancreatitis and exposures to nerve stimulators and to energy drinks. However, the observations presented here, coupled with the rising use of the offending products, are cause for concern and warrant further study. Possibilities for such study include either cellular or animal models of pancreatitis using these potentially offending agents, analyses of large databases, and the establishment of an international registry.
COMMENTSCase characteristicsFive cases of pancreatitis in four patients occurring after exposure to nerve stimulators or energy drinks.
Clinical diagnosisElevated lipase and/or imaging evidence of pancreatic inflammation.
Differential diagnosisPancreatitis could have been due to another cause not tested for, or missed, such as genetic polymorphisms or mutations.
Laboratory diagnosisElevated lipase, but normal IgG4 and triglycerides.
Imaging diagnosisComputed tomography or magnetic resonance imaging showed evidence of pancreatic inflammation. It was not possible to rule out pancreas divisum in each and every case.
Pathological diagnosisPancreatic debridement in patient #3 yielded only necrotic and saponified tissue, as expected.
TreatmentThe patients were treated with standard supportive care during their episodes of pancreatitis. Patient #3 required open pancreatic debridement and recovered well.
Related reportsThe causes of idiopathic pancreatitis remain, of course, unknown, by definition. The authors know no other cases associating nerve stimulators and pancreatitis, and only very weak evidence exists associating some ingredients in energy drinks with pancreatitis.
Experiences and lessonsThis case report presents several cases that suggest the possibility of new etiologies of pancreatitis. However, this observation should be interpreted with caution, as it is impossible to rule out every possible systemic, structural, and genetic cause of pancreatitis. In no way does this report prove any cause.
Peer-reviewThis is a very interesting manuscript from the clinical point of view. Both hypotheses are interesting.
REFERENCES1 Yadav D, Lowenfels AB. Trends in the epidemiology of the first attack
of acute pancreatitis: a systematic review. Pancreas 2006; 33: 323-330 [PMID: 17079934 DOI: 10.1097/01.mpa.0000236733.31617.52]
2 Lankisch PG, Schirren CA, Schmidt H, Schönfelder G, Creutz-feldt W. Etiology and incidence of acute pancreatitis: a 20-year study in a single institution. Digestion 1989; 44: 20-25 [PMID: 2599279 DOI: 10.1159/000199888]
3 Joergensen M, Brusgaard K, Crüger DG, Gerdes AM, de Muckadell OB. Incidence, prevalence, etiology, and prognosis of first-time chronic pancreatitis in young patients: a nationwide cohort study. Dig Dis Sci 2010; 55: 2988-2998 [PMID: 20108119 DOI: 10.1007/s10620-009-1118-4]
4 Wolk BJ, Ganetsky M, Babu KM. Toxicity of energy drinks. Curr Opin Pediatr 2012; 24: 243-251 [PMID: 22426157 DOI: 10.1097/MOP.0b013e3283506827]
5 Sepkowitz KA. Energy drinks and caffeine-related adverse effects. JAMA 2013; 309: 243-244 [PMID: 23330171 DOI: 10.1001/jama.2012.173526]
6 Reissig CJ, Strain EC, Griffiths RR. Caffeinated energy drinks--a growing problem. Drug Alcohol Depend 2009; 99: 1-10 [PMID: 18809264 DOI: 10.1016/j.drugalcdep.2008.08.001]
7 Khadilkar A, Odebiyi DO, Brosseau L, Wells GA. Transcutaneous electrical nerve stimulation (TENS) versus placebo for chronic low-back pain. Cochrane Database Syst Rev 2008; (4): CD003008 [PMID: 18843638 DOI: 10.1002/14651858.cd003008.pub3]
8 Wang W, Sun XT, Weng XL, Zhou DZ, Sun C, Xia T, Hu LH, Lai XW, Ye B, Liu MY, Jiang F, Gao J, Bo LM, Liu Y, Liao Z, Li ZS. Comprehensive screening for PRSS1, SPINK1, CFTR, CTRC
Shmelev A et al . New etiologies of pancreatitis
COMMENTS

248 November 15, 2015|Volume 6|Issue 4|WJGP|www.wjgnet.com
and CLDN2 gene mutations in Chinese paediatric patients with idiopathic chronic pancreatitis: a cohort study. BMJ Open 2013; 3: e003150 [PMID: 24002981 DOI: 10.1136/bmjopen-2013-003150]
9 Sun XT, Xia T, Hu LH, Zhou DZ, Li ZS, Liao Z. Identification of a novel deletion of CFTR in a 13-year-old: patient with idiopathic chronic pancreatitis. Pancreas 2014; 43: 659-660 [PMID: 24713676 DOI: 10.1097/MPA.0000000000000071]
10 Rai P , Sharma A, Gupta A, Aggarwal R. Frequency of SPINK1 N34S mutation in acute and recurrent acute pancreatitis. J Hepatobiliary Pancreat Sci 2014; 21: 663-668 [PMID: 24844923]
11 Masson E, Chen JM, Audrézet MP, Cooper DN, Férec C. A conservative assessment of the major genetic causes of idiopathic chronic pancreatitis: data from a comprehensive analysis of PRSS1, SPINK1, CTRC and CFTR genes in 253 young French patients. PLoS One 2013; 8: e73522 [PMID: 23951356 DOI: 10.1371/journal.pone.0073522]
12 LaRusch J, Barmada MM, Solomon S, Whitcomb DC. Whole exome sequencing identifies multiple, complex etiologies in an idiopathic hereditary pancreatitis kindred. JOP 2012; 13: 258-262 [PMID: 22572128]
13 Audrézet MP, Chen JM, Le Maréchal C, Ruszniewski P, Robaszkiewicz M, Raguénès O, Quéré I, Scotet V, Férec C. Determination of the relative contribution of three genes-the cystic fibrosis transmembrane conductance regulator gene, the cationic trypsinogen gene, and the pancreatic secretory trypsin inhibitor gene-to the etiology of idiopathic chronic pancreatitis. Eur J Hum Genet 2002; 10: 100-106 [PMID: 11938439 DOI: 10.1038/sj.ejhg.5200786]
14 Takuma K, Kamisawa T, Hara S, Tabata T, Kuruma S, Chiba K, Kuwata G, Fujiwara T, Egashira H, Koizumi K, Fujiwara J, Arakawa T, Momma K, Igarashi Y. Etiology of recurrent acute pancreatitis, with special emphasis on pancreaticobiliary malformation. Adv Med Sci 2012; 57: 244-250 [PMID: 23183766]
15 Gonoi W, Akai H, Hagiwara K, Akahane M, Hayashi N, Maeda E, Yoshikawa T, Tada M, Uno K, Ohtsu H, Koike K, Ohtomo K. Pancreas divisum as a predisposing factor for chronic and recurrent idiopathic pancreatitis: initial in vivo survey. Gut 2011; 60: 1103-1108 [PMID: 21325173 DOI: 10.1136/gut.2010.230011]
16 Lee JK, Enns R. Review of idiopathic pancreatitis. World J Gastroenterol 2007; 13: 6296-6313 [PMID: 18081217 DOI: 10.3748/wjg.v13.i47.6296]
17 Higgins JP, Tuttle TD, Higgins CL. Energy beverages: content and safety. Mayo Clin Proc 2010; 85: 1033-1041 [PMID: 21037046 DOI: 10.4065/mcp.2010.0381]
18 USDHHS/FDA/CFSAN. Voluntary Reports on Red Bull Energy Drink. 2012
19 USDHHS/FDA/CFSAN. Voluntary and Mandatory Reports on 5-Hour Energy, Monster Energy and Rockstar Energy Drink. 2012
20 Sabo A, Goussous N, Sardana N, Patel S, Cunningham SC. Necrotizing pancreatitis: a review of multidisciplinary management. JOP 2015; 16: 125-135 [PMID: 25791545]
21 Nielson KD, Adams JE, Hosobuchi Y. Experience with dorsal column stimulation for relief of chronic intractable pain: 1968-1973. Surg Neurol 1975; 4: 148-152 [PMID: 1080899]
22 Roberts HJ. Transcutaneous electrical nerve stimulation in the management of pancreatitis pain. South Med J 1978; 71: 396-398 [PMID: 76340 DOI: 10.1097/00007611-197804000-00016]
23 Ballegaard S, Christophersen SJ, Dawids SG, Hesse J, Olsen NV. Acupuncture and transcutaneous electric nerve stimulation in the treatment of pain associated with chronic pancreatitis. A randomized study. Scand J Gastroenterol 1985; 20: 1249-1254 [PMID: 3912961 DOI: 10.3109/00365528509089285]
24 Liddle RA, Nathan JD. Neurogenic inflammation and pancreatitis. Pancreatology 2004; 4: 551-559; discussion 559-560 [PMID: 15550764 DOI: 10.1159/000082180]
25 Schwartz ES, Christianson JA, Chen X, La JH, Davis BM,
Albers KM, Gebhart GF. Synergistic role of TRPV1 and TRPA1 in pancreatic pain and inflammation. Gastroenterology 2011; 140: 1283-1291.e1-2 [PMID: 21185837]
26 Schwartz ES, La JH, Scheff NN, Davis BM, Albers KM, Gebhart GF. TRPV1 and TRPA1 antagonists prevent the transition of acute to chronic inflammation and pain in chronic pancreatitis. J Neurosci 2013; 33: 5603-5611 [PMID: 23536075 DOI: 10.1523/JNEUROSCI.1806-12.2013]
27 Liddle RA. The role of Transient Receptor Potential Vanilloid 1 (TRPV1) channels in pancreatitis. Biochim Biophys Acta 2007; 1772: 869-878 [PMID: 17428642]
28 Félétou M, Lonchampt M, Robineau P, Jamonneau I, Thurieau C, Fauchère JL, Villa P, Ghezzi P, Prost JF, Canet E. Effects of the bradykinin B2 receptor antagonist S 16118 (p-guanidobenzoyl-[Hyp3,Thi5,D-Tic7,Oic8]bradykinin) in different in vivo animal models of inflammation. J Pharmacol Exp Ther 1995; 273: 1078-1084 [PMID: 7791078]
29 Figini M, Emanueli C, Grady EF, Kirkwood K, Payan DG, Ansel J, Gerard C, Geppetti P, Bunnett N. Substance P and bradykinin stimulate plasma extravasation in the mouse gastrointestinal tract and pancreas. Am J Physiol 1997; 272: G785-G793 [PMID: 9142909]
30 Nathan JD, Peng RY, Wang Y, McVey DC, Vigna SR, Liddle RA. Primary sensory neurons: a common final pathway for inflammation in experimental pancreatitis in rats. Am J Physiol Gastrointest Liver Physiol 2002; 283: G938-G946 [PMID: 12223354 DOI: 10.1152/ajpgi.00105.2002]
31 An HJ, Lee JH, Lee HJ, Yang WM, Park SK, Hong SH, Kim HM, Um JY. Electroacupuncture protects against CCK-induced acute pancreatitis in rats. Neuroimmunomodulation 2007; 14: 112-118 [PMID: 17804915 DOI: 10.1159/000107793]
32 Xue QM, Huang L, Li N. [Effects of electroacupuncture at Tianshu (ST25) on pro- and anti-inflammatory cytokines in rats with severe acute pancreatitis]. Zhongxiyi Jiehe Xuebao 2011; 9: 658-664 [PMID: 21669171 DOI: 10.3736/jcim20110613]
33 Belivani M, Lundeberg T, Cummings M, Dimitroula C, Belivani N, Vasilakos D, Hatzitolios A. Immediate effect of three different electroacupuncture protocols on fasting blood glucose in obese patients: a pilot study. Acupunct Med 2015; 33: 110-114 [PMID: 25522743]
34 Warzecha Z, Dembiński A, Jaworek J, Ceranowicz P, Szlachcic A, Walocha J, Konturek SJ. Role of sensory nerves in pancreatic secretion and caerulein-induced pancreatitis. J Physiol Pharmacol 1997; 48: 43-58 [PMID: 9098825]
35 Zeybek N, Gorgulu S, Yagci G, Serdar M, Simsek A, Kaymak-cioglu N, Deveci S, Ozcelik H, Tufan T. The effects of gingko biloba extract (EGb 761) on experimental acute pancreatitis. J Surg Res 2003; 115: 286-293 [PMID: 14697296 DOI: 10.1016/S0022-4804(03)00190-2]
36 Xu XW, Yang XM, Bai YH, Zhao YR, Shi GS, Zhang JG, Zheng YH. Treatment with ginkgo biloba extract protects rats against acute pancreatitis-associated lung injury by modulating alveolar macrophage. Prz Gastroenterol 2014; 9: 43-48 [PMID: 24868298 DOI: 10.5114/pg.2014.40850]
37 Schwartz PI, La A. FDA Reports. 201238 Morton C, Klatsky AL, Udaltsova N. Smoking, coffee, and
pancreatitis. Am J Gastroenterol 2004; 99: 731-738 [PMID: 15089909 DOI: 10.1111/j.1572-0241.2004.04143.x]
39 Hegde A, Bhatia M. Neurogenic inflammation in acute pancreatitis. JOP 2005; 6: 417-421 [PMID: 16186661]
40 Li Q, Peng J. Sensory nerves and pancreatitis. Gland Surg 2014; 3: 284-292 [PMID: 25493260]
41 Li C, Zhu Y, Shenoy M, Pai R, Liu L, Pasricha PJ. Anatomical and functional characterization of a duodeno-pancreatic neural reflex that can induce acute pancreatitis. Am J Physiol Gastrointest Liver Physiol 2013; 304: G490-G500 [PMID: 23306082]
P- Reviewer: BoettoR, Shen HN, Vujasinovic M S- Editor: Qiu S L- Editor: A E- Editor: Liu SQ
Shmelev A et al . New etiologies of pancreatitis

© 2015 Baishideng Publishing Group Inc. All rights reserved.
Published by Baishideng Publishing Group Inc8226 Regency Drive, Pleasanton, CA 94588, USA
Telephone: +1-925-223-8242Fax: +1-925-223-8243
E-mail: [email protected] Desk: http://www.wjgnet.com/esps/helpdesk.aspx
http://www.wjgnet.com

© 2015 Baishideng Publishing Group Inc. All rights reserved.
Published by Baishideng Publishing Group Inc8226 Regency Drive, Pleasanton, CA 94588, USA
Telephone: +1-925-223-8242Fax: +1-925-223-8243
E-mail: [email protected] Desk: http://www.wjgnet.com/esps/helpdesk.aspx
http://www.wjgnet.com




















