
Pathophysiology of anemia and erythrocytosis
20
Critical Reviews in Oncology/Hematology 64 (2007) 139–158 Pathophysiology of anemia and erythrocytosis Vivien M. Hodges a,∗ , Susan Rainey a , Terence R. Lappin a , A. Peter Maxwell b a Haematology Research Group, Centre for Cancer Research and Cell Biology, Queen’s University, Belfast, United Kingdom b Regional Nephrology Unit, Belfast City Hospital and Queen’s University, Belfast, United Kingdom Accepted 12 June 2007 Contents 1. Introduction ......................................................................................................... 140 1.1. Erythropoiesis ................................................................................................. 140 1.2. Iron homeostasis ............................................................................................... 141 1.3. Cytokine regulation of erythropoiesis ............................................................................ 142 1.4. The erythropoietin receptor ..................................................................................... 143 1.5. Control of EPO gene expression ................................................................................. 144 2. Anemia ............................................................................................................. 146 2.1. Anemias with high Epo levels ................................................................................... 146 2.1.1. Anemias due to bone marrow failure ..................................................................... 146 2.1.2. Anemias due to substrate deficiencies or protein/enzyme defects of the red blood cell ......................... 147 2.2. Anemias with low Epo levels .................................................................................... 147 2.2.1. Anemia of chronic disease .............................................................................. 147 2.2.2. Anemia of chronic renal failure .......................................................................... 148 2.3. ESAs for anemia treatment ...................................................................................... 149 3. Erythrocytosis ....................................................................................................... 149 3.1. Erythrocytosis with low Epo levels ............................................................................... 150 3.2. Erythrocytosis with high Epo levels .............................................................................. 151 3.2.1. Appropriately elevated Epo ............................................................................. 151 3.2.2. Inappropriately elevated Epo ............................................................................ 152 4. Future directions ..................................................................................................... 152 Reviewers ........................................................................................................... 153 Acknowledgements ................................................................................................... 153 References .......................................................................................................... 153 Biographies .......................................................................................................... 158 Abstract An increasing understanding of the process of erythropoiesis raises some interesting questions about the pathophysiology, diagnosis and treatment of anemia and erythrocytosis. The mechanisms underlying the development of many of the erythrocytoses, previously characterised as idiopathic, have been elucidated leading to an increased understanding of oxygen homeostasis. Characterisation of anemia and erythrocytosis in relation to serum erythropoietin levels can be a useful addition to clinical diagnostic criteria and provide a rationale for treatment with erythropoiesis stimulating agents (ESAs). Recombinant human erythropoietin as well as other ESAs are now widely used to treat anemias associated with a range of conditions, including chronic kidney disease, chronic inflammatory disorders and cancer. There is also heightened awareness of the potential abuse of ESAs to boost athletic performance in competitive sport. The discovery of erythropoietin receptors outside of the erythropoietic compartment may herald future applications for ESAs in the management of neurological and cardiac diseases. The ∗ Corresponding author. E-mail address: [email protected] (V.M. Hodges). 1040-8428/$ – see front matter © 2007 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.critrevonc.2007.06.006
Transcript of Pathophysiology of anemia and erythrocytosis
C
1
2
3
4
A
taieaao
1d
Critical Reviews in Oncology/Hematology 64 (2007) 139–158
Pathophysiology of anemia and erythrocytosis
Vivien M. Hodges a,∗, Susan Rainey a, Terence R. Lappin a, A. Peter Maxwell b
a Haematology Research Group, Centre for Cancer Research and Cell Biology, Queen’s University, Belfast, United Kingdomb Regional Nephrology Unit, Belfast City Hospital and Queen’s University, Belfast, United Kingdom
Accepted 12 June 2007
ontents
. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1401.1. Erythropoiesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1401.2. Iron homeostasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1411.3. Cytokine regulation of erythropoiesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1421.4. The erythropoietin receptor . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1431.5. Control of EPO gene expression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 144
. Anemia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1462.1. Anemias with high Epo levels . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 146
2.1.1. Anemias due to bone marrow failure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1462.1.2. Anemias due to substrate deficiencies or protein/enzyme defects of the red blood cell . . . . . . . . . . . . . . . . . . . . . . . . . 147
2.2. Anemias with low Epo levels . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1472.2.1. Anemia of chronic disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1472.2.2. Anemia of chronic renal failure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 148
2.3. ESAs for anemia treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 149. Erythrocytosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 149
3.1. Erythrocytosis with low Epo levels . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1503.2. Erythrocytosis with high Epo levels . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 151
3.2.1. Appropriately elevated Epo . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1513.2.2. Inappropriately elevated Epo . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 152
. Future directions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 152Reviewers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 153Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 153References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 153Biographies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 158
bstract
An increasing understanding of the process of erythropoiesis raises some interesting questions about the pathophysiology, diagnosis andreatment of anemia and erythrocytosis. The mechanisms underlying the development of many of the erythrocytoses, previously characterised
s idiopathic, have been elucidated leading to an increased understanding of oxygen homeostasis. Characterisation of anemia and erythrocytosisn relation to serum erythropoietin levels can be a useful addition to clinical diagnostic criteria and provide a rationale for treatment withrythropoiesis stimulating agents (ESAs). Recombinant human erythropoietin as well as other ESAs are now widely used to treat anemiasssociated with a range of conditions, including chronic kidney disease, chronic inflammatory disorders and cancer. There is also heightenedwareness of the potential abuse of ESAs to boost athletic performance in competitive sport. The discovery of erythropoietin receptors outsidef the erythropoietic compartment may herald future applications for ESAs in the management of neurological and cardiac diseases. The∗ Corresponding author.E-mail address: [email protected] (V.M. Hodges).
040-8428/$ – see front matter © 2007 Elsevier Ireland Ltd. All rights reserved.oi:10.1016/j.critrevonc.2007.06.006

1
cct©
K
1
pcnSttptitbbalrrhsocd
F
40 V.M. Hodges et al. / Critical Reviews in Oncology/Hematology 64 (2007) 139–158
urrent controversy concerning optimal hemoglobin levels in chronic kidney disease patients treated with ESAs and the potential negativelinical outcomes of ESA treatment in cancer reinforces the need for cautious evaluation of the pleiotropic effects of ESAs in non-erythroidissues.
2007 Elsevier Ireland Ltd. All rights reserved.
; Iron h
1
ttmcmbertorekiitimatched to the demand for oxygen by the tissues. Complexregulatory mechanisms control the diverse events required to
eywords: Anemia; Erythrocytosis; Erythropoietin; Chuvash polycythemia
. Introduction
In human adults the process of erythropoiesis involves theroduction of 2 × 1011 red blood cells each day, or 2.3 × 106
ells every second, and is regulated by a feedback mecha-ism primarily involving the hormone erythropoietin (Epo).ince red blood cells are the essential transporters of oxygen
hroughout the body, it is vital that this continual produc-ion is tightly regulated. Normally, Epo is present in thelasma at a concentration of 10−11 M, maintaining a hema-ocrit (HCT) of approximately 0.45 at sea level. Changesn circulating levels of Epo, its function, or its action onarget cells can lead to major changes in red blood num-ers and subsequently the oxygen-carrying capacity of thelood. Disorders with excessively high levels of erythrocytesre termed erythrocytoses, while states with abnormally lowevels of red blood cells are known as anemias. Here weeview the process of erythropoiesis, with an emphasis onecent advances in the understanding of Epo signaling andypoxic control of EPO expression. Anemia and erythrocyto-is have been examined, and mechanistically classified basedn the levels of Epo present in the circulation. Finally, in the
ase of anemia, the use of recombinant ESAs as treatment isiscussed.ig. 1. The feedback loop mechanism of Epo production. The growth factor regulat
mT
omeostasis
.1. Erythropoiesis
Hematopoietic cell turnover in a human adult is estimatedo be close to 1 trillion cells per day including the forma-ion of 200 billion erythrocytes [1]. The circulating red cell
ass reflects a dynamic balance between Epo-regulated redell proliferation and the subsequent loss or destruction ofature erythrocytes. The production of Epo is controlled
y a classical feedback loop mechanism (see Fig. 1) and itsffects are mediated through the cell surface erythropoietineceptor (Epo-R). Factors which affect oxygen delivery tohe kidney, such as the inspired partial pressure of oxygenr defective cardio-pulmonary function perturbing normalenal perfusion, can increase Epo production and stimulaterythropoiesis. Conversely, increased oxygen supply to theidney reduces the stimulus to Epo synthesis. However, in ansolated perfused rat kidney model epo levels were found toncrease only moderately when renal blood flow was reducedo 10% of normal [2]. The optimal size of the red cell masss achieved when the rate of red cell production is closely
ed maturation of erythrocytes from HSC in the bone marrow is highlighted.
aintain a continuous population of maturing erythroid cells.his is achieved by the combined effects of growth factors

n Onco
ttoeheeEsEciuBtr[prmdEasap
ogDcacaipmlg
rTfarccc(1pvprcr
[T7p3epLettsaratdtoei
1
fmtsoimetrts
hciardpdie[occ
V.M. Hodges et al. / Critical Reviews i
hat permit cellular proliferation and transcription factorshat activate lineage-specific gene expression. The renewalf hematopoietic cells, including those of the erythroid lin-age, is supported by a small population of self-renewingematopoietic stem cells (HSCs) (see Fig. 1). The earli-st identifiable erythroid progenitors, burst-forming unitsrythroid (BFU-E) and colony forming units erythroid (CFU-) are characterised by their in vitro colony formation inemisolid culture [3]. Early BFU-Es are not responsive topo and do not express the Epo-R. In vitro culture of theseells for 48–72 h in the presence of stem cell factor (SCF),nterleukin-3 (IL-3) or granulocyte-macrophage colony stim-lating factor (GM-CSF) results in the formation of matureFU-Es which express Epo-R and are weakly responsive
o Epo [4]. After 4–5 days in culture BFU-Es give rise toapidly dividing CFU-Es which are highly responsive to Epo3]. CFU-Es in turn give rise to morphologically recognisedrogenitors (proerythroblasts and subsequent progeny). Epoesponsiveness declines slowly as the cells undergo terminalaturation and proceed beyond the Epo-dependent stage of
evelopment, with concomitant reduction in the number ofpo-Rs per cell [5]. Mature erythrocytes are enucleate, havelifespan of ∼120 days and ultimately undergo a process of
enescence associated with distinct morphological changesnd removal from the circulation by macrophage-mediatedhagocytosis.
During the past six decades the biochemistry and physiol-gy of Epo have been studied extensively. The human EPOene is a single-copy gene in a 5.4 kb region of genomicNA [6,7] localized on chromosome 7 (7pter-q22) [8]. It
ontains four introns and five exons encoding a 193 aminocid peptide. A hydrophobic 27 amino acid leader sequence isleaved during secretion which leaves a peptide of 166 aminocids, MW 18,398 [7]. The carboxy-terminal arginine is lostn urinary and recombinant Epo, due to post-translationalrocessing by an intracellular carboxypeptidase [9]. Theolecule has a carbohydrate content of ∼40% with one O-
inked (Ser 126) and three N-linked (Asn 24, 38 and 83)lycosylation sites [10].
In adults, Epo is primarily produced in the cells of theenal cortex, accounting for ∼90% of plasma Epo levels.he liver is the main secondary site of Epo production but
urther extra-renal sites include the spleen, lung, testis, brainnd erythroid progenitor cells [11–14]. In recent years a wideange of other tissues has been reported to express Epo and itsognate receptor (reviewed in [13]). In general, plasma Epooncentrations show an inverse relationship with the oxygen-arrying capacity of the blood [15]. Normal Epo levels<5–25 U/L) [16] can increase exponentially by as much as000-fold in severe anemia. Conversely, inappropriate over-roduction of Epo can lead to erythrocytosis, increased bloodiscosity and decreased blood flow [17]. The increase in Epo
roduction is dependent on the de novo synthesis of Epoather than release of pre-formed stores from Epo producingells. The hypoxia-induced increase in EPO mRNA levelsesults from a combination of increased gene transcriptioni[cd
logy/Hematology 64 (2007) 139–158 141
18] and stabilisation of EPO messenger RNA (EPO mRNA).he half-life of EPO mRNA during hypoxia is increased-fold due to decreased binding of the de-stabilising erythro-oietin mRNA-binding protein (ERBP) to the EPO mRNA′UTR [19]. The concentration of circulating Epo maintainsrythropoiesis by balancing the differentiation of erythroidrogenitor cells with the level of programmed cell death [20].argely quiescent early erythroid progenitors require Epo tonter the cell cycle while Epo acts as a survival factor forhe later progenitors, preventing their apoptosis and allowingerminal differentiation. In vivo physiological Epo levels areub-optimal, enabling only a fraction of progenitors to survivend proliferate; resulting in apoptosis of ∼20% of bone mar-ow erythroid cells [21]. The fine control of erythropoiesislso results from a graded response of erythroid progenitorso Epo, as cells with the same differentiation potential requireifferent concentrations of Epo to achieve terminal matura-ion [22]. Thus, the two key factors which determine the fatef individual cells are the concentration of Epo in the cellnvironment and the sensitivity of the cell to Epo (reviewedn [23]).
.2. Iron homeostasis
Iron is obligatory for erythropoiesis. In its ferrous (Fe2+)orm it is an essential component of heme in hemoglobin andany electron-transferring enzymes in the redox system of
he respiratory chain. The body balance of iron is regulatedolely by gastrointestinal absorption, which itself dependsn the bioavailability of iron in food. Dietary heme iron is anmportant nutritional source of iron and long recognised to be
ore readily absorbed than non-heme iron derived from veg-tables and grain. The protracted search for an intestinal hemeransporter recently identified a membrane protein, heme car-ier protein 1 (HCP 1), which is iron-regulated and localizedo the brush-border membrane of duodenal enterocytes intates of iron deficiency [24].
The principal regulator of systemic iron homeostasis isepcidin, a 25-amino acid peptide produced by hepato-ytes. Hepcidin controls the circulating iron concentration bynhibiting its efflux from duodenal enterocytes, macrophagesnd hepatocytes, by binding to the iron transporter, fer-eportin, on these cells. Whereas hepcidin production isecreased in anemia and hypoxia, it is increased in theresence of iron and inflammation. Consequently, in iron-eficiency anemia the hepcidin levels are low, but inron-loading anemias hepcidin levels reflect the divergentffects of the iron overload and ineffective erythropoiesis25,26]. Infection and inflammation induce the synthesisf hepcidin through a mechanism involving inflammatoryytokines. IL-6 alone causes rapid upregulation of hep-idin mRNA expression in primary hepatocytes in vitro and
ncreased urinary excretion of hepcidin in human volunteers27,28]. IL-1� and IL-1� are also capable of inducing hep-idin in vitro but in some cell models this effect is IL-6ependent [26]. Several proteins such as hemojuvelin, which
1 n Onco
ipr
rirtIpaeia(racttdtcmcb
cIvpsalctauivtspttmstcm
1
i(
tamlktdaooevToaeap[h
iTepmttdopwvItaFaetlmwc[t(oEsEs
42 V.M. Hodges et al. / Critical Reviews i
s highly expressed in skeletal muscle, and bone morphogenicroteins and their receptors appear to play major roles inegulating hepcidin expression [29].
At the cellular level the acquisition and storage of iron areeciprocally regulated by post-transcriptional mechanismsn which the expression of both ferritin and the transferrineceptor are co-ordinately regulated by a cytosolic protein,he iron-responsive element binding protein (IRE-BP) [30].RE-BP has a high affinity for specific stem-loop structuresresent in ferritin and transferrin receptor mRNAs. It hashigh degree of sequence similarity to the mitochrondrial
nzyme aconitase and a labile Fe-S cluster involved in sens-ng intracellular iron levels. When intracellular iron levelsre low the IRE-BP binds to stem-loop structures in the 5′upstream) region of ferritin and the 3′ region of the transfer-in receptor mRNA thereby preventing translation of ferritinnd prolonging the half-life of transferrin receptor mRNA. Inontrast, when intracellular iron levels are high the affinity ofhe IRE-BP for the stem-loop structures is reduced, leadingo production of ferritin and reduced transferrin receptor pro-uction. Thus, changes in intracellular iron availability alterhe affinity of the IRE-BP for its cognate RNAs, leading toontrol of iron uptake and storage by the cell. The divalentetal transporter 1 (DMT1) and ferroportin 1 (FPN1) which
ontribute to the regulation of intestinal iron absorption alsoear iron-responsive elements [31].
Nutritional deficiencies of iron, vitamin B12 and folatean be limiting factors in the production of red blood cells.ron is required as a substrate for hemoglobin production;itamin B12 and folate are needed for DNA synthesis androliferation of progenitor cells. To maintain iron homeosta-is an adult requires the absorption of 1 mg iron per day. Andditional 1000 mg of iron is required in pregnancy and fol-owing blood donation or trauma 1 mg of iron is required toompensate for each mL of erythrocytes. Vitamin B12 referso a group of cobalt-containing compounds known as cobal-mines. Cyanocobaltamin, formed as the result of the cyanidesed in its purification, is the principal form of B12 utilisedn nutrient supplements and foods. Although the incidence ofitamin B12 deficiency in the general population is unknown,he risk of deficiency appears to increase with age [32]. Onetudy provided laboratory evidence of B12 deficiency in 15ercent of adults older than 65 years. Medication, such as pro-on pump inhibitors, that reduce gastric acidity can also leado decreased vitamin B12 levels [33]. The body stores nor-ally contain 3–5 years supply of B12 and several months’
upply of folate. Consequently, symptoms of deficiency mayake months to years to develop in adults but in infants andhildren with lower established reserves signs of deficiencyay become manifest more rapidly.
.3. Cytokine regulation of erythropoiesis
Erythropoiesis is a finely tuned balance between the pos-tive signals generated mainly by Epo and stem cell factorSCF)/c-kit ligand and the negative signals from death recep-
eirt
logy/Hematology 64 (2007) 139–158
or ligands and inhibitory cytokines. SCF and its receptor c-kitre essential for normal erythropoiesis as SCF or c-kit nullice (the Sl and W, mutants, respectively) exhibit embryonic
ethality associated with severe macrocytic anemia [34]. C-it is expressed on high numbers of CD34+ cells and duringhe differentiation of BFU-Es through to CFU-Es but declinesuring terminal differentiation. Sl and W mutant mice showsevere reduction in CFU-E numbers, confirming the role
f c-kit in BFU-E to CFU-E transition. The combined actionf SCF and Epo results in the synergistic proliferation andxpansion of progenitors ([35]; reviewed in [36]) with acti-ation of the JAK-STAT, PI3K and MAPK pathways [37].hrombopoietin (Tpo) is the major regulator of megakary-poiesis but can synergise with early acting cytokines suchs SCF, IL-3, IL-6, IL-11 and G-CSF to support the prolif-ration of primitive hemopoietic progenitors [38]. Tpo alsocts in late stage erythropoiesis, acting in synergy with Epo toromote the proliferation and differentiation of progenitors39]. Insulin-like growth factor 1 (IGF-1) and insulin alsoave roles as positive erythropoietic regulators [40,41].
Chronic inflammation can inhibit erythropoiesis mediatedn part through the effects of IL-1, TNF�, TGF� and IFN�.hese pro-inflammatory cytokines are powerful inhibitors ofrythropoiesis in vivo and in vitro [42]. IL-1 and TNF� sup-ress Epo mRNA expression [43]. IL-1 inhibition may beediated in part by induction of NF-kB which can bind to
he Epo promoter [44] and negatively regulate Epo produc-ion [45]. TGF� reduces the proliferation and accelerates theifferentiation of late erythroid progenitors [42]. The actionf the pro-inflammatory cytokine IL-6 is less clear, with aroposed role in the onset of anemia of chronic disease butith positive effects also demonstrated in vitro [46] and in
ivo, as IL-6 deficient mice demonstrate severe anemia [47].L-6 may exert its effects on erythropoiesis though regula-ion of iron metabolism [48]. Erythroid differentiation canlso be negatively regulated by death receptor ligands, e.g.as, a classic pro-apoptotic activator of the caspase cascade,nd TRAIL (TNF-related apoptosis-inducing ligand). Withinrythroblastic islands of the bone marrow immature ery-hroid cells express death receptors which are activated byigands produced by mature erythroblasts leading to caspase
ediated apoptosis [49]. The action of death receptors, asith Epo-deprivation, is mediated in part by caspase-induced
leavage of the major erythroid transcription factor, GATA-150]. GATA-1 is a zinc finger protein which plays a cen-ral role in erythroid development. GATA-1 binding motifsWGATAR) have been identified in the promoters/enhancersf virtually all erythroid genes [51,52] including Epo andpo-R. Signaling through the Epo-R can increase the expres-ion and activation of GATA-1 which in turn upregulatespo-R resulting in increased receptor and GATA-1 expres-ion in late CFU-E/proerythroblast progenitors. GATA-1−/−
mbryonic stem (ES) cells undergo rapid apoptosis suggest-ng a key role for GATA-1 in erythroid survival [53]. Theate of proliferation and differentiation of progenitors is con-rolled by the balance between GATA-1 levels and caspase
n Onco
aGceheI[TiibFpRtaon
1
atTot
espewecidirvP
srtptbigaa
FYsS
V.M. Hodges et al. / Critical Reviews i
ctivity [50]. Another transcription factor Scl (TAL-1), likeATA-1, is rapidly cleaved after activation of the caspase
ascade but precedes GATA-1 downregulation [54]. Zeunert al. have demonstrated that caspase resistant cells maintainigh levels of bcl-XL which in turn exerts an anti-apoptoticffect by inhibiting amplification of the caspase cascade [54].FN� promotes apoptosis of erythroid progenitors via Fas55] with additional upregulation of multiple members of theNF family including TRAIL and TWEAK [56]. Maximal
nhibition by IFN� is seen at the BFU-E stage [57]. Interest-ngly, in this system SCF can overcome the effects mediatedy IFN� [57] and Nishio et al. [58] propose that SCF preventsas-mediated apoptosis by preventing activation of the cas-ase cascade. Rubiolo et al. [59] suggest that Fas, along withaf-1, acts as a key regulator of the balance between differen-
iation and proliferation of erythroid progenitors. TRAIL canlso negatively regulate erythropoiesis, reducing the numbersf erythroblasts [60] however, Epo can protect against theegative effects of TRAIL via induction of PKC epsilon [61].
.4. The erythropoietin receptor
Epo promotes the viability, proliferation and differenti-tion of mammalian erythroid progenitor cells via signals
ransduced by the specific cell surface Epo receptor (Epo-R).he Epo-R is a 508 amino acid protein and is a memberf the cytokine receptor superfamily. Bone marrow ery-hroid progenitors are the major Epo target cells. Duringsaei
ig. 2. Epo signaling pathways. The three main Epo signaling pathways are highlig401, STAT3 binding to Y431, activation of the MAPK pathway following assoc
ubunit to Y479. Negative regulation occurs via SHP-1 binding to Y429 and Y431OC3 can directly bind to JAK2 (signaling reviewed in [249]).
logy/Hematology 64 (2007) 139–158 143
rythroid differentiation cells become progressively moreensitive to Epo due to the appearance of Epo-Rs, with laterogenitors CFU-E and proerythroblasts having the high-st Epo-R expression (∼1000 receptors/cell) [4,62]. Miceith null mutations of the Epo-R die during embryogen-
sis at E12.5–13.5, a critical stage for increased erythroidell expansion [63]. Interestingly normal levels of progen-tors are still observed, indicating that Epo-R signaling isispensable at the earlier stages of erythropoiesis, includ-ng BFU-E formation [63]. Upon Epo binding, preformedeceptor dimers undergo a conformational change which acti-ates three major signal transduction pathways (JAK-STAT,I3K-Akt, Ras-MAPK) (see Fig. 2) [64].
Pre-associated JAK2 autophosphorylates and is respon-ible for phosphorylation of tyrosines in the cytoplasmicegion of the Epo-R [65]. Phosphorylated tyrosine residueshen act as docking sites for Src homology 2 (SH2) domainroteins including the signal transducers and activators ofranscription (STATs) 1, 3 and 5. STAT5a and STAT5become tyrosine phosphorylated, dimerize and the result-ng complex is translocated to the nucleus where it activatesene expression. The importance of STAT5 in both primitivend definitive erythropoiesis is highlighted as STAT5a−/−nd STAT5b−/− embryos are severely anemic with impaired
urvival of liver erythroid progenitors. Although only moder-tely anemic at birth the adult mice later exhibit a poor stressrythropoietic response. In stress erythropoiesis, for examplen acute anemia, splenic rather than bone marrow progenitorshted. Positive signaling is associated with STAT5 binding to Mu Y343 andiation of the adaptor protein Grb2 withY464 and binding of the p85 PI3Kand CIS and SOCS3 competition for STAT5 binding at Y401. SOCS1 and

1 n Onco
agaoacaehcaooesJmg
noaAsikgarbpM
ttESiitndwieagSvEanuolm
ppTmuqaItnrictmtEnstaIne
1
sECptbarbt(ctahdstHiaiI
44 V.M. Hodges et al. / Critical Reviews i
re responsible for the erythropoietic response. One of theenes activated by Epo-induced STAT5 is bcl-XL, an anti-poptotic gene. Bcl-XL is activated through direct bindingf STAT5 to a consensus sequence in the bcl-XL promoternd studies using mice deficient in bcl-XL also indicate aritical role for this protein in terminal erythroid differenti-tion [66]. Bcl-XL is also induced by GATA-1 and is a keyrythroid progenitor survival factor, as bcl-XL
−/− mice showigh levels of apoptosis in fetal liver cells and bcl-XL
−/− ESells fail to generate mature erythroblasts [67,68]. Menon etl. [69] postulate that STAT5 can distinguish between home-static and stress-induced Epo-R signaling with activationf the cytokine oncostatin M, rather than bcl-XL, promotingrythroid survival. Roles for STAT1 and STAT3 in Epo-Rignaling have also been proposed [70]. The importance ofAK2 in Epo signaling is also highlighted as JAK2 knockoutice have an almost identical phenotype to Epo and Epo-R
ene disruptions with embryonic lethality [71,72].In addition to the JAK/STAT pathway the phosphatidyli-
ositol 3 (PI3)-kinase-Akt pathway is activated by bindingf the SH2 domain of the p85 subunit to Epo-R Tyr479,nd is associated with erythroblast survival signaling [73,74].kt phosphorylates the pro-apoptotic factor BAD, which dis-
ociates from the cell survival factor bcl-XL, resulting innhibition of apoptosis [75]. The mitogen activated proteininase (MAPK) pathway is required for expansion of pro-enitors in response to Epo and SCF [37]. Following receptorctivation Src-homology and collagen (SHC) is phospho-ylated and forms a complex with growth factor receptorinding protein (Grb2), son of sevenless (SOS) and the G-rotein Ras with the resulting activation of the Raf, MEK,APK pathway.Epo-induced signaling via tyrosine phosphorylation is
ransient and returns to basal levels within 30 min of stimula-ion suggesting rapid dephosphorylation [76]. Termination ofpo signaling occurs when hematopoietic cell phosphatase,HP-1 catalyses the dephosphorylation of JAK2 [77] by bind-
ng to Epo-R Tyr 429 via its SH2 domain. Signaling is alsonhibited by cytokine (including Epo) regulated SOCS pro-eins (suppressor of cytokine signaling), which operate via aegative feedback loop to suppress Epo-induced signal trans-uction. Negative Epo signaling is associated with SOCS-3hich associates with the Epo-R and JAK2 [78]; mice lack-
ng SOCS3 show embryonic lethality associated with massiverythrocytosis [79]. SOCS-1 inhibits JAK2 by binding to thectivation loop, recruiting ubiquitination machinery and tar-eting JAK2 for degradation [80]. CIS (Cytokine InducibleH2 containing protein) is also induced by Epo signalingia STAT5 and represses proliferation when recruited to thepo-R, negatively regulating STAT5 activation [81]. Lnk, andaptor protein implicated in cytokine receptor signaling,egatively regulates Epo-mediated erythropoiesis by atten-
ating JAK2 activation [82]. Epo signaling increases the ratef Epo-R internalisation and the receptor is degraded byysosomal and proteasomal targeting using JAK2 dependentechanisms [83].
ncoa
logy/Hematology 64 (2007) 139–158
Epo-R is expressed primarily in bone marrow erythroidrogenitors but is also found on myocytes, cortical neurons,rostatic cells and vascular, breast and ovarian epithelia [84].he presence of the Epo-R outside of the erythroid compart-ent remains controversial as the validity of the antibody
sed in many of the localisation studies has been called intouestion [85,86]. Epo exhibits neuroprotective effects and ispotent promoter of neuronal survival (reviewed in [87,88]).
nterestingly, transgenic mice with exclusive expression ofhe Epo-R in hematopoietic cells develop normally with noeurological abnormalities [89]. However, conditional neu-onal Epo-R knock down has demonstrated a role for Epo-Rn adult neurogenesis [90]. It has been reported that systemi-ally delivered recombinant human Epo (rHuEpo) can crosshe blood brain barrier, reducing tissue damage in animal
odels of ischemic stroke [91,92] and may have potentialherapeutic use for neuroprotection. CEPO, a carbamylatedpo derivative which is not erythropoietic, may also haveeuroprotective therapeutic potential [93]. Brines et al. [93]uggest that tissue protective signals in non-hematopoieticissues may be mediated by heterodimerization of the Epo-Rnd the common �-receptor (�cR), a subunit of the GM-CSF,L-3 and IL-5 receptors. Interestingly, �cR null mice exhibitormal development with only relatively minor haematopoi-tic alterations [94].
.5. Control of EPO gene expression
The EPO promoter, 117 bp 5′ to the transcription startite, acts synergistically with a 3′ enhancer to regulate thepo gene [18]. There are several important elements in theIS acting EPO enhancer, which lies 120 bp 3′ to the EPOolyadenylation signal (reviewed in [15]). The most impor-ant of these elements is a hypoxia inducible factor (HIF)inding site (HBS) with the sequence CACGTGCT. HIFcts as a global regulator of oxygen homeostasis (reviewedecently in [95]). Transcriptional regulation occurs throughinding of HIF heterodimers, consisting of the oxygen sensi-ive HIF-� subunit and the constitutively expressed HIF-1�ARNT), to hypoxia-responsive elements (a core pentanu-leotide sequence RCGTG) in target genes [96,97]. There arehree main isoforms of HIF-� (HIF-1�, -2� and -3�) whichre members of the PAS (Per/ARNT/Sim) family of basic-elix-loop-helix transcription factors. The isoforms can allimerise with HIF-1� in hypoxia but differ in their tissue-pecific expression pattern [98]. It is not yet clear whetherhe EPO gene is regulated primarily by HIF-1� or HIF-2�.IF-1� was the first isoform demonstrated to be involved
n EPO gene regulation in vitro [99]. Recently, Warnecke etl. have shown that the Epo response is HIF-2� dependentn hepatoma (Hep3B) and neuroblastoma (Kelly) cells [100].nterestingly, in both the kidney and liver it is the HIF-2� and
ot the HIF-1� isoform that is expressed in Epo-producingells [101,98]. All three HIF-� proteins contain a centralxygen-dependent degradation domain (ODD) as well as N-nd C-terminal transactivation domains (TADs) [102].
V.M. Hodges et al. / Critical Reviews in Oncology/Hematology 64 (2007) 139–158 145
Fig. 3. Hypoxic regulation of EPO expression In normoxia HIF-� is hydroxylated by PHDs in the presence of the co-substrates Fe2+ and 2-oxoglutarate leadingt by the pl nucleuE
oh(�rldOhahHpbsfa1sci8mtdtsp
d
feaypvirs
waouPtaaprpPtaEhf
o association with a VHL-E3 ligase complex and ultimately degradationigases. In hypoxia, HIF-� remains unhydroxylated and is translocated to thePO.
Increases in Epo production are controlled by sensingf oxygen levels in the kidney by oxygen-dependent prolylydroxylases (PHDs) which regulate the stability of HIF-�see Fig. 3). There is continuous expression of HIF-� and
with mRNA levels remaining unchanged by hypoxia, andegulation of HIF activity occurring exclusively at the proteinevel. Under normoxic conditions, HIF-1� is not normallyetected since the protein has a half-life of <5 min at 21%2 [103]. In the presence of oxygen the HIF-1� protein isydroxylated at prolines 402 and 564 in the ODD [104,105],n oxygen-dependent process catalysed by PHDs. Prolyl-ydroxylated HIF-1� is then bound by a pVHL (the vonippel-Lindau tumor suppressor protein) multiprotein com-lex which functions as an E3 ubiquitin ligase [106]. HIF-�ecomes poly-ubiquitinated and is degraded by the protea-ome. In hypoxia, however, oxygen becomes rate-limitingor PHD mediated hydroxylation and HIF-� is stabilisednd translocated to the nucleus where it binds to HIF-� and activates transcription of hypoxia response genesuch as EPO. HIF-1� expression can be demonstrated inells exposed to hypoxia in as little as 30 min [103]. Dur-ng normoxia HIF-1� is also hydroxylated at asparagine03 by factor inhibiting HIF (FIH) in the c-TAD. Thisodification results in a decreased ability of the carboxy-
erminus of HIF-� to bind to its co-activator p300/CPBue to steric hindrance and prevents activation of the HIFranscriptional cascade [107,108]. Accumulating evidence
uggests that HIF-2� and HIF-3� are degraded by similarrocesses.PHDs belong to a superfamily of iron and 2-oxoglutarateependent dioxygenases and in mammalian cells three iso-
kwme
roteasome. The levels of the PHDs are modulated in part by the Siah E3s, where it binds HIF-1� and stimulates expression of target genes including
orms of PHDs have been identified (PHD1, 2, and 3). Thesenzymes demonstrate an absolute requirement for dioxygens a co-substrate as well as ascorbate and Fe2+. The hydrox-lation reaction involves one oxygen atom inserted at theroline residues of HIF while the other is utilised in the con-ersion of 2-oxoglutarate (2-OG) to succinate and CO2. Fe2+
s crucial for activating oxygen and ascorbate functions in thee-activation process by reducing Fe3+ (for a recent reviewee [109]).
Oxygen sensing involves complex regulatory mechanismsith potentially 2–5% of the genome responsive to hypoxia
nd under HIF-1 regulation [95]. Unsurprisingly, the actionsf the PHDs are therefore modulated in a number of wayssing both HIF-dependent and independent mechanisms. TheHD enzymes only catalyse the hydroxylation of HIF and not
he reverse reaction so the actual protein levels determine thectivity at distinct oxygen tensions. The expression of PHD2nd PHD3 is induced by hypoxia in a HIF-dependent mannerromoting a negative feedback loop [110] with hypoxia-esponsive elements identified in the PHD2 and PHD3 generomoters [111,112]. The levels of the other hydroxylases,HD1 and FIH, are unaffected by hypoxia [113,114]. In addi-
ion, PHD1 and PHD3 are degraded by the proteasome, inHIF-independent mechanism, using the Siah1 and Siah23 ligases with Siah protein expression also induced duringypoxia [115]. The role of individual PHDs remains to beully elucidated. Berra et al. [116] report that PHD2 is the
ey oxygen sensor as siRNA silencing of this single proteinas sufficient to stabilise HIF-1� in normoxia. In addition, autation in PHD2 resulting in increased HIF stability, causesrythrocytosis suggesting that PHDs 1 and 3 fail to compen-

1 n Onco
saPcH
albadtiaiPoiwradTivsiu
2
cicdqaadctccbitla
aEsai
uidDban
2
2
oalatrbwesatetrEbhfIkiwfm
uatiMtnanDiicS
46 V.M. Hodges et al. / Critical Reviews i
ate [117]. Appelhoff et al. [114] however suggested a role forll three PHDs to reflect the known variation in tissue-specificHD protein expression levels, with all three PHD proteinsontributing in a non-redundant manner to regulation of theIF system.An additional level of regulation of PHD activity has
lso been suggested at the levels of transcription and trans-ation. Two alternatively processed PHD3 transcripts haveeen identified [118] with the expression of one splice vari-nt restricted to primary cancer tissues. Tian et al. [119] haveemonstrated two PHD1 isoforms, resulting from differentranslation start sites, which exhibit similar hydoxylase activ-ty but different protein stabilities. Cellular localization maylso influence activity as PHD1 is almost exclusively foundn the nucleus; PHD2 is predominantly cytoplasmic whereasHD3 is found in both compartments [113]. The translocationf PHD2 to the nucleus was however demonstrated by Jok-lehto et al. [120] and along with increased PHD2 expressionas associated with tumor aggressiveness. The finely tuned
egulation of the hypoxic response allowing regulation overwide range of oxygen tensions may also be attributed to aifference in the oxygen dependence of PHD2 and FIH [121].he flexibility of regulation is demonstrated by differences
n preferences for the HIF isoforms by PHDs [114] and byariation in the specific activity for the HIF hydroxylationite [122]. The complex levels of regulation of hypoxia-nduced gene expression are only beginning to be fullynderstood.
. Anemia
Anemia is a deficiency of functional mature red bloodells, which leads to a decreased oxygen-carrying capac-ty of the blood, tissue hypoxia, and a variety of clinicalonsequences including weakness, fatigue, increased car-iac output, increased morbidity and mortality, and decreaseduality of life. Anemia is a very common disorder and prob-bly still quite under-recognised. Anemias may be classifiedccording to mechanisms such as levels of red blood cell pro-uction, destruction, or loss, and by parameters of red bloodell morphology, such as the size, color and shape, as well ashe RBC indicies, mean corpuscular volume (MCV), meanorpuscular hemoglobin concentration (MCHC) and meanorpuscular hemoglobin (MCH). Here, we consider anemiasased on levels of Epo present in the circulation, since Epos the primary hormone responsible for the maintenance ofhe erythroid lineage. Classifying anemias in relation to Epoevels is also useful in providing a rationale for treatment ofnemia by ESAs.
Epo concentrations will vary depending on both the degreend type of anemia. Availability of recombinant human
po (rHuEpo) has led to the replacement of in vitro bioas-ays, such as the ex-hypoxic mouse and mouse spleen cellssay, and the development of more sensitive and specificmmunoassays. Plasma/serum Epo levels are now measuredfilaw
logy/Hematology 64 (2007) 139–158
sing radioactive immunoassays (RIA) or more commonlymmunoassays using chemiluminescent (CLIA) or enzymaticetection methods (ELISA). Fully automated methods (e.g.PC Immunlite 2000) are also available. Samples are cali-rated against reference standards and concentrations of Epore expressed in International Units per liter (U/L) with aormal range of <5–25 U/L [16].
.1. Anemias with high Epo levels
.1.1. Anemias due to bone marrow failureFailure of the bone marrow to produce blood cells may
ccur at the level of the hemopoietic stem cell (HSC), ort later stages of hemopoietic cell development. The formereads to aplastic anemia, with a hypocellular bone marrow anddecrease in each of the blood cell subtypes. The main fea-
ures include anemia; leukopenia, which leads to an increasedisk of infection; and thrombocytopenia, which presents aleeding risk. Failure of blood cell production at later stagesill affect only distinct blood cell lineages. When only the
rythroid lineage is involved, it is termed pure red cell apla-ia (PRCA). These are usually acquired disorders, due to theutoimmune destruction of HSC or lineage-specific progeni-ors. This immune-mediated destruction may be due to priorxposure to toxins, viruses, or drugs, although in many caseshe cause is idiopathic. There has been an increase in theeported cases of red cell aplasia in patients treated withSAs, caused by the generation of autoantibodies againstoth the ESA and endogenous Epo [123–125]. Also, thereave been rare reports of aplastic anemia following therapyor chronic myelogenous leukemia (CML). In these cases,matinib, directed against bcr-abl positive CML cells, alsoills other blood cell types, presumably through less specificnteractions with other tyrosine kinase receptors [126]. Asith other forms of anemias, there is a varied clinical course,
rom patients with mild symptoms requiring little or no treat-ent to patients with severe life threatening pancytopenia.There are also rare congenital forms of bone marrow fail-
re. For example, Fanconi anemia (reviewed in [127]) isn autosomal recessive or X-linked form of aplastic anemiahat can also present with a variety of skeletal abnormalitiesncluding short stature and an increased risk of malignancies.
utations in at least eleven different genes are involved inhe pathogenesis of the disease. The treatment of choice isormally bone marrow transplantation. Diamond Blackfannemia (DBA) (reviewed in [128]) has an autosomal domi-ant inheritance pattern and is usually diagnosed in infancy.BA presents with a variety of congenital abnormalities,
ncluding facial, limb and urogenital malformations, and anncreased risk of developing leukemias. About 25% of theases are associated with a mutation in the ribosome protein19; others have been associated with an as yet unidenti-
ed gene on chromosome 8p, as well as at least one otherocus. Recently, mutations in telomerase enzymes, leading tobnormally shortened telomeres, have also been associatedith marrow failure [129].

n Onco
2p
rSawi[alaioBl
hdotpparaAiamgticop
s[batdamti
sattmlcm
adtIhi
dfcacoasqhcrdltsntbmt
2
2
pcderktrmcalAbuouda
V.M. Hodges et al. / Critical Reviews i
.1.2. Anemias due to substrate deficiencies orrotein/enzyme defects of the red blood cell
Many proteins and substrates are required for normaled blood cell maturation and hemoglobin production (seeection 1.2), and a deficit in any one of these can lead tonemia. Iron deficiency is the most common cause of anemiaorldwide (reviewed in [130]). Substrate deficiencies also
nclude lack of vitamin B12 or folate (megaloblastic anemia)131,132] in the diet, but can also be due to problems affectingbsorption of these compounds. Malabsorption may be due toiver, pancreatic, or intestinal disease. Pernicious anemia is anutoimmune disorder where antibodies are directed againstntrinsic factor (a glycoprotein produced by the parietal cellsf the stomach which is needed for absorption of vitamin12 in the intestine) or against the parietal cells themselves,
eading to impaired vitamin B12 absorption [133].Anemia can be caused by a failure or insufficiency of
emoglobin production. This can be due to a heme synthesisefect (usually because of lack of iron, as described above),r a globin synthesis defect. One of the most common ofhese is thalassemia, a condition in which there is defectiveroduction of one of the globin chains of the hemoglobinrotein. This leads to an overall deficiency of hemoglobinnd toxicity caused by the unassembled globin chains whicheduces the red cell life span. This is usually inherited in anutosomal recessive manner but may also be acquired [134].nother type of hemoglobinopathy, sickle cell anemia, is also
nherited in an autosomal recessive manner, and has persistedt abnormally high levels because heterozygotes carrying theutant gene have significant resistance to malaria [135]. The
enetic defect leads to a single amino acid substitution andhe production of a hemoglobin molecule that can polymerizen the cell under conditions of low oxygen. These red bloodells undergo a change in shape and consistency which cancclude vessels (vaso-occulsive crisis), leading to ischemia,ain, and organ damage.
Other problems with red blood cell proteins includepherocytosis, which may be hereditary or non-hereditary136,137]. Here, defects in various red blood cell mem-rane proteins lead to abnormally shaped (round) cells, whichre rapidly removed from the circulation and destroyed byhe spleen. Sideroblastic anemias (characterised by largeeposits of iron in erythroid mitochondria) can also becquired or inherited [138], and may be seen in someyelodysplastic syndromes. Here, defects within HSCs lead
o impaired cellular differentiation and the production ofmmature blasts which are filled with iron.
Hemolytic anemias are characterised by shortened red cellurvival. Whereas senescent red cells normally undergo lysisfter approximately 120 days, in severe hemolytic disordershe red cell lifespan can be as a short as a few days. There arehree principal causes: (i) intracellular defects arising from
etabolic enzyme dysfunction and hemoglobinopathies; (ii)oss of structural integrity of the red cell membrane andytoskeleton as occurs in hereditary spherocytosis, paroxys-al nocturnal hemoglobinuria (PNH), autoimmune disorders
1ctm
logy/Hematology 64 (2007) 139–158 147
nd drug-associated antibody damage; (iii) extracellularamage arising from chemical toxins, mechanical trauma,hrombocytopenic purpura and microangiopathic conditions.n general in hemolytic conditions the plasma Epo levels areigher than normal, and treatment of these patients with ESAss seldom justified [139].
In all of these anemias Epo levels are high, as the defects lieownstream of Epo production. In the cases of bone marrowailure, the defect is in the inability of the immature erythro-ytes to appropriately respond to the Epo signal, because theyre destroyed or damaged. In nutritional deficiencies or redell protein disorders, there is either an inadequate supplyf substrates required for erythrocyte maturation, or therere functionally important mutations in essential enzymes ortructural proteins. In all of these cases, the lack of an ade-uate supply of red blood cells leads to a continued state ofypoxia, loss of negative feedback to the kidney, and thus aontinued stimulus to Epo production in an attempt to cor-ect the hypoxia. Therefore, treatment with ESAs in theseisorders is neither logical nor effective. Even a very highevel of Epo is unable to overcome the underlying defects inhe erythropoietic pathway. These anemias are largely treatedymptomatically with transfusion as indicated by clinicaleed. Nutritional supplementation can be highly effective forhe substrate deficiency anemias, and steroid therapy can beeneficial in immune-related anemias. For some disordersore radical therapy such as splenectomy and bone marrow
ransplants must be undertaken.
.2. Anemias with low Epo levels
.2.1. Anemia of chronic diseaseThe anemia of chronic disease (ACD) is the second most
revalent cause of anemia, after iron deficiency. In someases it can still be difficult to distinguish ACD from iron-eficiency anemia [140], except that ACD patients normallyxhibit normal or increased serum ferritin levels, rather thaneduced serum ferritin levels. Recently, is has also becomenown as the anemia of inflammation (AI), which includeshe rapid onset anemia of acute critical illness [141]. Theesult of an acute or chronic immune system activation, ACDay be seen in over 75% of patients with hematological can-
ers or solid tumors, viral infections (including HIV), andutoimmune diseases such as rheumatoid arthritis, systemicupus erythematosus and irritable bowel syndrome [142].nemia is also a common finding in diabetes, which cane associated with renal tubular failure, but also arises fromnknown causes [143]. ACD often co-exists with other typesf anemia, and is believed to be widely under-diagnosed andnder-treated. Infections, malignant cells, and autoimmuneysregulation all lead to activation of the immune systemnd the production of cytokines, most notably TNF�, IL-
, IL-6, IL-10, and IL-� (reviewed in [142]). Inflammatoryytokines can depress Epo production (Section 1.3) leadingo the development of anemia. Suppression of erythropoiesisay also be mediated in part by the generation of oxygen and

1 n Onco
nc
iaotisdtroowEe
oiutlstiitcomcr
atse[taro
2
prlacwtctd
tlopt
([ftmttpacabismcaroao[tbsp(oldioalbaa
mrtcrlrt
48 V.M. Hodges et al. / Critical Reviews i
itrogen free radicals, which can directly damage progenitorells [144].
Present evidence indicates that hepcidin is the key factorn the development of the hypoferremia associated with thenemia of inflammation. IL-6 can upregulate the productionf hepcidin in the liver [26]. Higher levels of hepcidin leado decreased iron absorption, and the iron that is absorbeds sequestered for storage in the reticuloendothelial system,o that there is reduced iron availability for hemoglobin pro-uction in maturing erythrocytes. Hepcidin may contributeo the anemia of chronic inflammation by decreasing theesponsiveness of bone marrow erythroid cells to low levelsf erythropoietin [145]. However, the relative contributionf hepcidin to the pathogenesis of this anemia comparedith other factors such as decreased Epo production, bluntedpo response and shortened red cell survival remains to bestablished.
In ACD, Epo levels are inappropriately low for the degreef anemia and there is a blunted response to any Epo thats produced. The total iron binding capacity of the blood issually normal, but the reticulocyte count is low. Ultimatelyhe best way to treat ACD is to identify and cure the under-ying cause of the chronic inflammatory disease. However,ince this may not be immediately possible, it is importanto alleviate the ACD. Hepcidin antagonists are being exam-ned as a possible treatment for ACD, but currently rHuEpos the usual treatment. This exogenous Epo is administeredo counteract the antiproliferative effects of the endogenousytokines being produced and rHuEpo reduces dependencen blood transfusions. However, the effects of long-term ane-ia treatment with ESAs on the underlying disease are less
lear with some clinical concerns raised over the safety ofHuEpo therapy for cancer-related anemias.
The microenvironments within tumors together with theirberrant blood supply create some areas within tumorshat are hypoxic. This phenomenon may be even moreevere in anemic patients. Tumor hypoxia can impair theffectiveness of radiation therapy and some chemotherapy146,147]. This has led to the hypothesis that strategieso diminish cancer-related anemia may not only allevi-te anemia-related symptoms but will also enhance tumoresponses to chemotherapy and radiotherapy and improveverall patient survival.
.2.2. Anemia of chronic renal failureAnemia associated with kidney failure may be present in
atients with acute or chronic renal failure. It is primarilyelated to an almost complete deficiency of Epo due to theoss of functional renal tissue. This may be compounded byn acute or chronic inflammatory state associated with theause of renal failure, e.g. glomerulonephritis. Many patientsith progressive kidney disease are treated with medication
hat inhibits the renin–angiotensin system such as angiotensinonverting enzyme inhibitors (ACEi) or angiotensin recep-or blockers (ARBs) that also blunts erythropoiesis. Theecrease in renal Epo production is inversely correlated with
bmep
logy/Hematology 64 (2007) 139–158
he glomerular filtration rate [148,149]. In addition to abso-ute Epo deficiency there is also a contribution to the anemiaf chronic renal failure from uremic inhibitors of erythro-oiesis. Adequate dialysis, that reduces the levels of uremicoxins, can improve the therapeutic response to ESAs.
If a patient has progressed to end-stage renal diseaseESRD), the treatment of choice is renal transplantation150]. However, the new kidney may not function optimally,ailing to produce an adequate supply of Epo, leading to post-ransplantation anemia (PTA). Over 30% of patients exhibit
oderate to severe anemia at some point within 5 years post-ransplantation [151–153], the prevalence increasing withime after the transplant. In most cases there is an initialeak of Epo levels on the first day post-transplantation [154];fter that, there is a strong correlation between hemoglobinoncentrations and graft function, as measured by serum cre-tinine levels [150]. Although a successful graft can restoreoth the excretory and endocrine functions of the kidney,ts function may still be sub-optimal [155]. Most evidenceuggests that impaired Epo production by the graft is theain cause of the anemia [149,150], but other factors may
ontribute. The drugs mycophenolate mofetil (MMF) andzathioprine (immunosuppressants used to prevent organejection) may exacerbate anemia. MMF is a selective blockerf the de novo or ribose derived purine synthesis pathway,nd is expected to have a major effect on the proliferationf lymphocytes, but not erythrocytes, from the bone marrow150]. Thus, its association with poor erythrocyte produc-ion is unclear. Azathioprine leads to a general depression ofone marrow cellular proliferation [156] and also shows someelective erythroid toxicity, although the mechanism of thehenomenon is not well understood [157]. ARBs and ACEiused as anti-hypertensives after transplant to reduce the riskf cardiovascular events) are also associated with a higherikelihood of anemia [150,158]. Other risk factors for theevelopment of PTA include recent infections and increas-ng age of the donor [150]. It has also been observed that solidrgan transplant patients receiving immunosuppressive ther-py are susceptible to parvovirus B19 infections which canead to red cell aplasia. This anemia can usually be alleviatedy a reduction in dosage of immunosuppressant drugs [159]nd administration of immunoglobulin therapy [160] but thenemia is often recurrent [161].
Patients with both chronic renal failure associated ane-ia and PTA can benefit from treatment with exogenous
HuEpo. Although there are few data available concerninghe outcomes of treatment of PTA with Epo, there is no indi-ation that patients treated with rHuEpo have any greaterisk of deterioration in their graft function [155]. Neverthe-ess it is reported that fewer than 10% of transplant recipientseceive this treatment [150,152,158]. Some reports suggesthat PTA patients treated with Epo may develop hypertension,
ut overall, treatment of PTA may be beneficial, since ane-ia can contribute significantly to the risk of cardiovascularvents, which are the main cause of death in renal trans-lant patients [162]. Treatment with Epo can improve left

n Onco
vlatatc
2
polmett(Bhuoi
tiltkepbsbrd
aiicb[iw[p[tata[lp
EHtmr
mcsErvkEtgh
tnpinmemdcsbttccs1taieVibetpn
3
V.M. Hodges et al. / Critical Reviews i
entricular structure and function as well as cardiac output,eading to a decrease in negative long-term outcomes as welln increased quality of life [163–165]. Recent studies suggesthat the presence of Epo receptors on normal kidney cellsllows Epo administration to have renal protective proper-ies, preventing ischemia-induced tissue damage in acute andhronic renal injuries [166,167].
.3. ESAs for anemia treatment
Treating anemia in patients can lead to decreased hos-italization times, quicker recoveries, improved clinicalutcomes, and better quality of life. Because Epo levels areow in patients with ACD and anemia of renal failure, ane-
ia can often be successfully treated by the administration ofxogenous Epo. One of the largest patient groups routinelyreated with ESAs are those with chronic kidney disease. Thearget hemoglobin values in these patients are 11–13 g/dLKDOQI guidelines [168]) or greater than 11 g/dL (Europeanest Practice Guidelines [169]), respectively. The optimumemoglobin in patients with renal anemia however remainsndetermined with recent reports demonstrating no benefitf rHuEpo therapy in maintaining higher target hemoglobinsn pre-dialysis or dialysis patients [168,170,171].
Originally, Epo was isolated and purified in small quanti-ies from the urine of patients with aplastic anemia [172], butn 1985, the human EPO gene was cloned [6,7] allowing thearge-scale production of the hormone by recombinant DNAechnology. Recombinant human Epo (rHuEpo), commonlynown as epoetin alpha, is highly effective at stimulatingrythropoiesis with a low immunogenicity. Only in a smallroportion of cases have patients developed neutralizing anti-odies that are also cross-reactive with native Epo, leading toevere pure red cell aplasia [173]. The increase in the num-er of PRCA cases has been attributed to leachates from theubber stoppers used in pre-filled syringe formulations of therug, which led to an increased immunogenicity [174,175].
For optimal efficacy and cost effectiveness epoetin isdministered 2–3 times per week by subcutaneous orntravenous injection. Novel Epo analogues with longer elim-nation half-lives, such as darbepoetin alfa (Aranesp) andontinuous erythropoietin receptor activator (CERA), haveeen developed which permit extended dosing schedules176–179]. A synthetic erythropoiesis protein (SEP), consist-ng of a 51 kDa protein–polymer, has also been developedhich stimulates activation of the erythropoietin receptor
180]. Biologically active erythropoietin dimers exhibitedrolonged half-life, but have not been clinically tested181]. Erythropoietin-mimetic peptides, which are struc-urally unrelated to Epo but are still able to activate the Epo-Rre also being investigated. These include Hematide, a pep-ide linked to polyethyleneglycol which increases solubility
nd circulation half-life, and is now entering phase II trials182,183]. Other strategies for alleviating anemia by stimu-ating erythropoiesis include inhibitors of hematopoietic cellhosphatases such as SHP-1, which negatively regulate theaBae
logy/Hematology 64 (2007) 139–158 149
po-induced JAK-STAT pathway [77,184] and stabilizers ofIF-1� [179]. However, the existence of more than 70 known
argets for HIF-1� may severely limit this approach. Further-ore, naturally occurring mutations in VHL and PHD2 which
esult in HIF stabilisation can cause erythrocytosis [185,117].There has been some experimental interest in treating ane-
ia via EPO gene therapy but this approach is tempered byoncerns about safety in clinical practice. It is potentially fea-ible to achieve hypoxia-regulated EPO gene expression if thePO transgene is driven by a promoter containing a hypoxia
esponse element (HRE). This has been demonstrated in an inivo model where erythropoiesis was reconstituted in an Eponockout mouse after adenoviral vector delivery of an HREPO transgene [186]. There are persisting concerns that gene
herapy may cause additional unpredictable insertional muta-enic events which limit the applicability of this technique touman disease.
Recently some concerns have been raised about the long-erm safety of Epo treatment both for renal anemia andon-renal anemias. Large pharmacological Epo doses giveneriodically to patients do not replicate normal physiolog-cal kinetics [187]. Epo may have a protective effect, ineural [188,189] and cardiac tissues [190]. Conversely, Epoay be harmful to some groups of cancer patients. Henke
t al. found that although Epo treatment corrected the ane-ia in head and neck cancer patients it was associated with
ecreased progression-free survival [191]. The Breast Can-er Erythropoietin Survival Trial (BEST), in which overallurvival was the primary end-point, was terminated earlyecause of poorer survival in the rHuEpo arm [192]. Fur-hermore, a Cochrane review of 9353 cancer patients in 57rials established that recombinant Epo or Aranesp signifi-antly reduced the requirement for blood transfusion but alsoarried an increased risk of thrombo-embolic events (such astroke and myocardial infarction) with a relative risk ratio of.67 [193]. Recently, rHuEpo administration during primaryreatment of locally advanced cervical carcinoma was associ-ted with a poorer response to radiation therapy, including anncreased recurrence rate, increased risk of death due to dis-ase, and decreased disease-free overall survival time [194].aupel et al. point out that raising the Hb level above 14 g/dL
n patients with cancer-related anemia causes an increase inlood viscosity which may lead to adverse cardiovascularvents [195]. These studies indicate a need for caution inreating cancer patients with rHuEpo and have led to the pro-osal that they may enhance thrombosis, tumor growth andeovascularization [196].
. Erythrocytosis
The term erythrocytosis defines a group of disorders char-
cterised by an increase in circulating red blood cells (RBCs).oth erythrocytosis and polycythemia are used interchange-bly to describe a condition in which the hematocrit (HCT)xceeds the upper limit of normal. The term erythrocytosis is
150 V.M. Hodges et al. / Critical Reviews in Oncology/Hematology 64 (2007) 139–158
Table 1Classification of erythrocytoses
Classification Epo levels Cause
PrimaryCongenital Low Epo-R mutationAcquired Low PV
SecondaryCongenital Inappropriately normal or elevated Chuvash/VHL-dependent polycythemia
PHD2 mutationHb variants2,3BPGM mutation
Acquired Appropriately elevated High altitudeChronic pulmonary diseaseSleep apnoeaRight to left cardiac shunts
Inappropriately elevated TumorsExogenous Epo
I
mtvpthspEralda
iilchituowtw[
idaEeta
rp
3
iab1stgIi[npabas[
blvaultp
diopathicCongenital or acquired Low or elevated
ore accurate when only the red cell lineage is involved whilehe term polycythemia can be confused with polycythemiaera (PV), a clonal stem cell disorder resulting in excessiveroduction of red cells, neutrophils and platelets. Erythrocy-osis is suspected in patients with an abnormally high HCT,emoglobin concentration or RBC count. All of these mea-urements are concentrations and are therefore dependent onlasma volume as well as circulating red cell mass (RCM).rythrocytosis can be further classified as relative, where the
ed cell mass is normal and the plasma volume is decreased orbsolute, where the red cell mass exceeds the normal upperimit. McMullin et al. [197] have provided guidelines foriagnosis, investigation and management of polycythemiand erythrocytosis.
Erythrocytosis may be classified as primary, secondary ordiopathic (see Table 1). In primary erythrocytosis there is anncrease in circulating RBC numbers caused by a molecu-ar defect in the erythroid lineage. Secondary erythrocytosisan arise due to appropriate changes such as adaptation toigh altitude, or inappropriate changes such as aberrantlyncreased circulating levels of Epo. The term idiopathic ery-hrocytosis denotes a heterogeneous group of rare disorders ofnknown etiology in which the cause may be either primaryr secondary. Similar to anemias, the treatment of patientsith erythrocytosis depends on the severity and cause of
he disorder. Some patients have a relatively benign diseasehilst others require venesection or cytoreductive therapy
197].Measurement of plasma Epo levels provides an important
nsight into the potential regulatory pathways which may beisrupted in the development of the erythrocytosis. Like thenemias, the erythrocytoses can also be classified using serum
po levels. Erythrocytosis with an inappropriately normal orlevated Epo level can be associated with abnormalities inhe oxygen sensing pathway or abnormal hemoglobin oxygenffinity while those with low Epo levels may be linked to dys-sTtp
Unknown
egulated Epo signaling and/or hypersensitivity of erythroidrecursors.
.1. Erythrocytosis with low Epo levels
Polycythemia vera (PV) is an acquired disorder lead-ng to clonal expansion of a single HSC containing ancquired mutation characterized by hyperplasia of threeone marrow lineages. It has an incidence of 2–3 per00,000 [198] and exhibits a risk of leukemic progres-ion. PV bone marrow progenitors can form colonies inhe absence of Epo in vitro, a criterion useful in distin-uishing PV from familial and congenital polycythemias.n 2005, an amino acid substitution V617F in JAK2 wasdentified in a high percentage of affected PV individuals199–202] and now forms a useful addition to PV diag-ostic criteria. This mutation is found in large numbers ofatients with myeloproliferative disorders, not only in PV butlso in essential thrombocytopenia and idiopathic myelofi-rosis. The mutation causes constitutive activation of JAK2nd downstream signaling pathways leading to erythrocyto-is. V617F is rare in patients with idiopathic erythrocytosis203].
Thirteen autosomal dominant mutations in the Epo-R haveeen described [204,205], which lead to erythrocytosis withow Epo levels and hypersensitivity of progenitors to Epo initro [206,207]. Mutation of the Epo-R was first described inlarge Finnish family (Trp439Ter) with thirty three individ-als over five generations demonstrating erythrocytosis withow Epo levels [208]. In total, ten Epo-R mutations cause aruncation of between 58 and 110 amino acids of the cyto-lasmic C-terminal of the receptor. This results in the loss of
ome of the Epo-R negative regulatory signaling pathways.he binding site for the phosphatase SHP-1 is lost in all of theruncated receptors, resulting in prolonged JAK2 autophos-horylation and STAT5 activation leading to enhanced Epo

n Onco
sdoaFaAaitce[e4e
3
fRpgata[hbtighhethbu(t
wAprhge1ratiV
emgmpcritolio�CTih
ihrgartrlttaeo[
3
aatap
fegatpha
V.M. Hodges et al. / Critical Reviews i
timulation and a proliferative advantage [209,210]. Partialownregulation of Epo signaling may still occur in somef the receptor truncations as the binding site for the neg-tive regulators CIS and SOCS3 (Y401) is still retained (seeig. 2). In addition, SOCS1 and SOCS3 can still bind to thectivation loop of JAK2 leading to suppression of signaling.rcasoy and Karayal [211] reported that the tyrosines which
re retained in one truncated Epo-R (HuY285 and Y344),ncluding a tyrosine which binds STAT5, both contribute tohe sensitivity of the progenitors to Epo. Congenital erythro-ytosis was replicated in a mouse model where the murinepo-R was replaced by a truncated mutant human Epo-R212]. The other three reported Epo-R mutations result inither an amino acid substitution or a base change in intronand are not associated with the development of familial
rythrocytosis [204].
.2. Erythrocytosis with high Epo levels
Recent studies of patients with inherited erythrocytosisrom the Chuvash population in the Upper Volga region ofussia have identified an abnormality in the oxygen sensingathway. A genome-wide screen of this ethnically homo-eneous population localized a region on chromosome 3ssociated with the disease. This led to identification of a Co T transition at nucleotide 598 of the VHL gene leading ton arginine to tryptophan change at amino acid 200 (R200W)185]. Affected individuals are homozygous and carriers areeterozygous. R200W leads to a reduction in the interactionetween VHL and HIF-1�, decreasing the levels of ubiqui-inated HIF-1�, leading to more active HIF dimer and anncrease in the expression of hypoxia inducible downstreamenes, including Epo. Indeed, Gordeuk et al. [213] reportemoglobin adjusted Epo levels were ∼10-fold higher inomozygotes compared to controls with Epo-hypersensitiverythroid progenitors. Unlike classical VHL syndrome noumorigenesis is found in Chuvash polycythemia, withomozygosity instead associated with varicose veins, lowlood pressure and elevated basal expression of the HIF reg-lated genes VEGF and plasminogen activator inhibitor 1PAI-1) associated with thrombosis and vascular abnormali-ies [214,215].
Outside of Chuvashia, other families have been describedith this mutation including those of Caucasian, Africanmerican and Asian ancestries [198,216]. VHL-dependentolycythemia, with the Chuvash haplotype, has also beeneported as endemic on the island of Ischia with non-affectedeterozygotes also showing an increase in HIF-1 activity sug-esting a mutation maintenance advantage [217]. A founderffect has been established which arose in a single ancestor4,000–62,000 years ago [218], although Cario et al. [219]ecently reported a single case where the Chuvash mutation
rose on a separate genetic background. VHL mutations in allhree exons have now been described [217,219,220] includ-ng compound heterozygotes displaying Chuvash and otherHL mutations [221].Enci
logy/Hematology 64 (2007) 139–158 151
However, a substantial number of patients with congenitalrythrocytosis with normal or elevated Epo do not have VHLutations but may have other defects in oxygen-dependent
ene regulation. Recently, Percy et al. [117] described autation in the hydroxylase PHD2 also leading to inap-
ropriate regulation of HIF and increased Epo expressionausing erythrocytosis. The C to G transition at base 950esults in a proline to arginine change in an evolutionar-ly conserved residue (P317R). This residue lies close tohe iron-chelating residue asparagine 315 in the active sitef the enzyme. The PHD2 mutation results in a markedoss of function by reducing binding to HIF and decreas-ng the prolyl-hydroxylase activity in vitro. Overexpressionf the mutant PHD was less effective at suppressing HIF-induced activation of a reporter gene. Unlike the recessivehuvash mutation this PHD mutation is autosomal dominant.hese studies of patients with erythrocytosis have provided
mportant insights into the regulatory mechanisms of oxygenomeostasis.
Hereditary erythrocytoses are extremely rare but alsonclude a wide range (>100) of hemoglobin variants ([222];ttp://globin.cse.psu.edu). The mutations are localized toegions of the hemoglobin molecule associated with oxy-en transport leading to an increased affinity for oxygen andcharacteristically abnormal “left-shifted” oxygen equilib-
ium curve. The red cell mass is increased to respond tohe resulting tissue hypoxia. In addition, deficiencies in theed cell enzyme bisphosphoglycerate mutase leading to lowevels of 2,3-bisphosphoglycerate (2,3 BPG) may cause ery-hrocytosis [223]. Reduced levels of 2,3 BPG, which bindso the central cavity of the hemoglobin molecule, lead to
failure to convert to a low oxygen affinity state. Thesenzyme deficiencies may be inherited in autosomal dominantr recessive traits depending on the severity of the deficiency224].
.2.1. Appropriately elevated EpoA number of relatively common clinical conditions are
ssociated with an elevated hematocrit secondary to anppropriately elevated serum Epo in the setting of chronicissue hypoxia. These include chronic respiratory diseasesssociated with hypoxia, right-to-left circulatory shunting,ost-renal transplant and residence at high altitude levels.
Chronic obstructive lung disease associated with loss ofunctional lung parenchyma and impaired pulmonary gasxchange results in chronic arterial hypoxia. This will trig-er increased renal Epo secretion to expand the red cell massnd enhance tissue oxygen delivery [225]. The rise in hema-ocrit may be compounded by smoking related reduction inlasma volume [226]. Alternatively, recurrent episodes ofypoventilation associated with sleep apnoea syndrome willlso result in decreased arterial oxygenation that will cause an
po-induced expansion in red cell mass, although the mag-itude of this response is disputed [227–229]. In congenitalyanotic heart disease a significant right-to-left cardiac shunts also associated with erythrocytosis [230] and in some cases
1 n Onco
mleic
ois[enpptAoaaah[
crpeifGiitcctE
3
oplecctemammd
ac
p[otoitna
thlvwaast
4
mhoDstTlctbp[kitoIbo
fiacotw
52 V.M. Hodges et al. / Critical Reviews i
ay be complicated by thrombotic events [231]. Serum Epoevels are high, driving an increase in red cell mass in affort to correct chronic tissue hypoxia caused by the shunt-ng of deoxygenated erythrocytes from the pulmonary arterialirculation directly into the systemic circulation.
Post-transplant erythrocytosis (PTE) occurs in up to 15%f renal transplant recipients [232]. Predisposing factorsnclude male gender, smoking, transplant renal artery steno-is, retention of native kidneys and a well-functioning graft233,234]. The source of Epo has been reported to be fromither the diseased native kidneys or the transplanted kid-ey itself [232,234,235]. Although Epo levels in most PTEatients are within the normal range the level is still inap-ropriate given the degree of erythrocytosis suggesting thathe normal physiological feedback regulation is disrupted.dditional stimuli to erythropoiesis may include the actionf factors such as androgens, insulin-like growth factor andngiotensin II [236,237]. This may explain the efficacy ofgents such as angiotensin converting enzyme inhibitors orngiotensin II type 1 receptor blockers that can reduce theaematocrit by inhibition of the renin–angiotensin system238,239].
A compensatory erythropoietin-induced increase in redell mass occurs secondary to hypoxia associated withesidence at high altitude. This contributes to the patho-hysiology of chronic mountain sickness. Some individualsxperience symptoms such as dizziness, headache, lethargy,nsomnia and paraesthesia described as burning hands andeet [240], and may develop cerebral or pulmonary edema.enetic and environmental adaptive factors are believed to
nfluence susceptibility to chronic mountain sickness since its more common in men than women, in post-menopausalhan premenopausal women and newcomers rather thanhronic mountain dwellers [241–243] although, Mejia et al.ould not show any genetic association between severe ery-hrocytosis and a number of candidate genes including EPO,PO-R, HIF-1α, VHL and PHDs [244].
.2.2. Inappropriately elevated EpoOne area of concern is the potential and actual misuse
f recombinant human erythropoietin to enhance athleticerformance. Epo doping is suspected in 3–7% of the top ath-etes involved in endurance sports [245] with an anticipatednhancement in performance by increasing the oxygen-arrying capacity of the blood. Numerous, often high-profile,ases have been detected in routine anti-doping controls buthe detection of recombinant proteins is challenging. Azzazyt al. [245] suggest that despite potential risks gene dopingay be in practice as soon as the Beijing 2008 Olympics. In
ddition, Lippi et al. [246] suggest that cobalt chloride abuseay become an alternative, currently undetectable, dopingethod as cobalt chloride administration can inhibit HIF-1�
egradation and thus lead to increased erythropoiesis.Erythrocytosis as a paraneoplastic syndrome has been
ssociated with a range of malignancies including renalell carcinoma, hepatoma, cerebellar hemangioblastoma,
ni
a
logy/Hematology 64 (2007) 139–158
heochromocytomas, ovarian tumors and Wilm’s tumor197] and can be attributed to Epo production by the tumorr by normal parenchyma in response to hypoxia-inducedumor growth [247]. Erythrocytosis is reported in up to 5%f patients with renal cell carcinomas. The mechanism forncreased Epo production may be linked in the majority ofhese tumours to mutations in the VHL gene that disrupt theormal regulation of hypoxia-induced proteins resulting inbnormal sensing of the renal tissue oxygen tension [248].
Since most dialysis units treating renal disease will attempto achieve an audited standard of >80% of patients withaemoglobin values within the target range or above the targetevel it is inevitable that some ESA-treated patients inad-ertently end up with haemoglobin values above 13 g/dL. Itould however be extremely rare that a patient would be
ccidentally treated to a hemoglobin level that would qualifys erythrocytosis. Usually cessation of the ESA treatment isufficient to allow the haemoglobin concentration to fall backo the target level.
. Future directions
Identification of the mechanisms underpinning the nor-al physiology, cell and molecular biology of erythropoiesis
as been crucial to our understanding of the pathophysiologyf anemias and erythrocytoses. Development of recombinantNA-derived erythropoiesis stimulating agents represents a
pectacular example of translational research providing novelherapies for the anemias associated with low Epo levels.hese treatments have literally transformed the quality of
ife for millions of anemia sufferers, especially those withhronic kidney disease. Nevertheless there are some concernshat ESA therapy may have limits reflecting the differencesetween normal physiological erythropoiesis compared withharmacological doses of ESAs in maintaining red cell mass187]. The ideal target hemoglobin in patients with chronicidney disease remains controversial despite 20 years of clin-cal trials with ESAs. The effects of ESAs on cells outside ofhe erythroid lineage are also being explored with the promisef beneficial effects on injured cardiac and neural tissues.nterest in such novel indications is tempered by the possi-le adverse effects of ESA treatment on tumor biology andverall cardiovascular risk.
It is also interesting to contrast the fate of persons with dif-erent mechanisms resulting in erythrocytosis. The probandn the original Finnish study of erythrocytosis caused by
truncated Epo-R was an Olympic gold medal-winningross-country skier with a naturally advantageous increasedxygen-carrying capacity [208]. In contrast, the VHL muta-ion causing Chuvash polycythemia, whilst not associatedith the risk of tumor formation seen in VHL syndrome, is
onetheless linked with premature mortality in part due to anncreased risk of arterial thrombosis [213].Future examination of the pathophysiology of anemiasnd erythrocytoses is likely to yield more surprising insights

n Onco
ie
R
t4S
iD
BDo1
A
csFt
R
V.M. Hodges et al. / Critical Reviews i
nto the complex inter-relationships of erythropoiesis andrythropoietin with overall human health.
eviewers
Josef Prchal, Professor of Medicine, Division of Hema-ology, University of Utah School of Medicine, RoomC416-SOM, 30N 1900E, Salt Lake City, UT 84132, Unitedtates.
Joachim Fandrey, Professor, Director, Institute for Phys-ology, University of Duisburg-Essen, Hufelandstrasse 55,-45122 Essen, Germany.Dr. Constance Tom Noguchi, PhD, Chief, Molecular Cell
iology Section, Molecular Medicine Branch, National Inst.iabetes & Digestive & Kidney Disease, National Institutesf Health, Building 10, Room 9N307, Bethesda, MD 20892-822, United States.
cknowledgements
The authors would like to thank Dr. Melanie Percy forritical reading of the manuscript and also to acknowledgeupport from RoFAR, the Northern Ireland Kidney Researchund, the Northern Ireland Leukaemia Research Fund and
he R&D Office, Northern Ireland.
eferences
[1] Ogawa M. Differentiation and proliferation of hematopoietic stemcells. Blood 1993;81:2844–53.
[2] Pagel H, Jelkmann W, Weiss C. O2-supply to the kidneys and theproduction of erythropoietin. Respir Physiol 1989;77:111–7.
[3] Gregory CJ, Eaves AC. Three stages of erythropoietic progenitor celldifferentiation distinguished by a number of physical and biologicproperties. Blood 1978;51:527–37.
[4] Sawada K, Krantz SB, Dai CH, et al. Purification of human bloodburst-forming units-erythroid and demonstration of the evolution oferythropoietin receptors. J Cell Physiol 1990;142:219–30.
[5] Koury MJ, Bondurant MC. Maintenance by erythropoietin of viabilityand maturation of murine erythroid precursor cells. J Cell Physiol1988;137:65–74.
[6] Jacobs K, Shoemaker C, Rudersdorf R, et al. Isolation and characteri-zation of genomic and cDNA clones of human erythropoietin. Nature1985;313:806–10.
[7] Lin FK, Suggs S, Lin CH, et al. Cloning and expression of the humanerythropoietin gene. Proc Natl Acad Sci USA 1985;82:7580–4.
[8] Watkins PC, Eddy R, Hoffman N, et al. Regional assignment of theerythropoietin gene to human chromosome region 7pter q22. Cyto-genet Cell Genet 1986;42:214–8.
[9] Recny MA, Scoble HA, Kim Y. Structural characterization ofnatural human urinary and recombinant DNA-derived erythropoi-etin. Identification of des-arginine 166 erythropoietin. J Biol Chem1987;262:17156–63.
[10] Egrie JC, Strickland TW, Lane J, et al. Characterization and biolog-
ical effects of recombinant human erythropoietin. Immunobiology1986;172:213–24.[11] Tan CC, Eckardt KU, Firth JD, Ratcliffe PJ. Feedback modulation ofrenal and hepatic erythropoietin mRNA in response to graded anemiaand hypoxia. Am J Physiol 1992;263:F474–81.
logy/Hematology 64 (2007) 139–158 153
[12] Fandrey J, Bunn HF. In vivo and in vitro regulation of erythropoi-etin mRNA: measurement by competitive polymerase chain reaction.Blood 1993;81:617–23.
[13] Lappin TR, Maxwell AP, Johnston PG. Epo’s alter ego: erythropoietinhas multiple actions. Stem Cells 2002;20:485–92.
[14] Stopka T, Zivny JH, Stopkova P, Prchal JF, Prchal JT.Human hematopoietic progenitors express erythropoietin. Blood1998;91:3766–72.
[15] Fandrey J. Oxygen-dependent and tissue-specific regulation of ery-thropoietin gene expression. Am J Physiol Regul Integr ComputPhysiol 2004;286:R977–88.
[16] Marsden JT. Erythropoietin—measurement and clinical applications.Ann Clin Biochem 2006;43:97–104.
[17] Erslev AJ, Caro J. Pure erythrocytosis classified according to erythro-poietin titers. Am J Med 1984;76:57–61.
[18] Blanchard KL, Acquaviva AM, Galson DL, Bunn HF. Hypoxicinduction of the human erythropoietin gene: cooperation betweenthe promoter and enhancer, each of which contains steroid receptorresponse elements. Mol Cell Biol 1992;12:5373–85.
[19] McGary EC, Rondon IJ, Beckman BS. Post-transcriptional regulationof erythropoietin mRNA stability by erythropoietin mRNA-bindingprotein. J Biol Chem 1997;272:8628–34.
[20] Koury MJ, Bondurant MC. The molecular mechanism of erythropoi-etin action. Eur J Biochem 1992;210:649–63.
[21] Shetty V, Hussaini S, Broady-Robinson L, et al. Intramedullary apop-tosis of hematopoietic cells in myelodysplastic syndrome patients canbe massive: apoptotic cells recovered from high-density fraction ofbone marrow aspirates. Blood 2000;96:1388–92.
[22] Kelley LL, Koury MJ, Bondurant MC, Koury ST, Sawyer ST, Wick-rema A. Survival or death of individual proerythroblasts results fromdiffering erythropoietin sensitivities: a mechanism for controlled ratesof erythrocyte production. Blood 1993;82:2340–52.
[23] Koury MJ, Kelley LL, Bondurant MC. The fate of erythroid progenitorcells. Ann N Y Acad Sci 1994;718:259–67 (discussion 267–70).
[24] Shayeghi M, Latunde-Dada GO, Oakhill JS, et al. Identification of anintestinal heme transporter. Cell 2005;122:789–801.
[25] Nemeth E, Ganz T. Regulation of iron metabolism by hepcidin. AnnuRev Nutr 2006;26:323–42.
[26] Nemeth E, Ganz T. Hepcidin and iron-loading anemias. Haematolog-ica 2006;91:727–32.
[27] Nemeth E, Valore EV, Territo M, Schiller G, Lichtenstein A, Ganz T.Hepcidin, a putative mediator of anemia of inflammation, is a type IIacute-phase protein. Blood 2003;101:2461–3.
[28] Nemeth E, Rivera S, Gabayan V, et al. IL-6 mediates hypoferremia ofinflammation by inducing the synthesis of the iron regulatory hormonehepcidin. J Clin Invest 2004;113:1271–6.
[29] Truksa J, Peng H, Lee P, Beutler E. Bone morphogenetic proteins2.4 and 9 stimulate murine hepcidin 1 expression independently ofhfe, transferrin receptor 2 (Tfr2), and IL-6. Proc Natl Acad Sci USA2006;103:10289–93.
[30] Haile DJ, Rouault TA, Tang CK, Chin J, Harford JB, Klausner RD.Reciprocal control of RNA-binding and aconitase activity in the reg-ulation of the iron-responsive element binding protein: role of theiron-sulfur cluster. Proc Natl Acad Sci USA 1992;89:7536–40.
[31] Zoller H, Theurl I, Koch R, Kaser A, Weiss G. Mechanisms of ironmediated regulation of the duodenal iron transporters divalent metaltransporter 1 and ferroportin 1. Blood Cells Mol Dis 2002;29:488–97.
[32] Pennypacker LC, Allen RH, Kelly JP, et al. High prevalence ofcobalamin deficiency in elderly outpatients. J Am Geriatr Soc1992;40:1197–204.
[33] Bradford GS, Taylor CT. Omeprazole and vitamin B12 deficiency.Ann Pharmacother 1999;33:641–3.
[34] Nocka K, Tan JC, Chiu E, et al. Molecular bases of dominant negativeand loss of function mutations at the murine c-kit/white spotting locus:W37, wv, W41 and W. EMBO J 1990;9:1805–13.
[35] Wu H, Klingmuller U, Besmer P, Lodish HF. Interaction of the ery-thropoietin and stem-cell-factor receptors. Nature 1995;377:242–6.

1 n Onco
54 V.M. Hodges et al. / Critical Reviews i[36] Munugalavadla V, Kapur R. Role of c-kit and erythropoietin receptorin erythropoiesis. Crit Rev Oncol Hematol 2005;54:63–75.
[37] Arcasoy MO, Jiang X. Co-operative signalling mechanisms requiredfor erythroid precursor expansion in response to erythropoietin andstem cell factor. Br J Haematol 2005;130:121–9.
[38] Itoh R, Katayama N, Kato T, et al. Activity of the ligand forc-mpl, thrombopoietin, in early haemopoiesis. Br J Haematol1996;94:228–35.
[39] Liu W, Wang M, Tang DC, Ding I, Rodgers GP. Thrombopoietinhas a differentiative effect on late-stage human erythropoiesis. Br JHaematol 1999;105:459–69.
[40] Sawada K, Krantz SB, Dessypris EN, Koury ST, Sawyer ST. Humancolony-forming units-erythroid do not require accessory cells, butdo require direct interaction with insulin-like growth factor I and/orinsulin for erythroid development. J Clin Invest 1989;83:1701–9.
[41] Muta K, Krantz SB, Bondurant MC, Wickrema A. Distinct rolesof erythropoietin, insulin-like growth factor I, and stem cell fac-tor in the development of erythroid progenitor cells. J Clin Invest1994;94:34–43.
[42] Zermati Y, Fichelson S, Valensi F, et al. Transforming growth fac-tor inhibits erythropoiesis by blocking proliferation and acceleratingdifferentiation of erythroid progenitors. Exp Hematol 2000;28:885–94.
[43] Faquin WC, Schneider TJ, Goldberg MA. Effect of inflamma-tory cytokines on hypoxia-induced erythropoietin production. Blood1992;79:1987–94.
[44] Lee-Huang S, Lin JJ, Kung HF, Huang PL, Lee L, Huang PL. Thehuman erythropoietin-encoding gene contains a CAAT box. TATAboxes and other transcriptional regulatory elements in its 5’ flankingregion. Gene 1993;128:227–36.
[45] Batmunkh C, Krajewski J, Jelkmann W, Hellwig-Burgel T. Erythro-poietin production: molecular mechanisms of the antagonistic actionsof cyclic adenosine monophosphate and interleukin-1. FEBS Lett2006;580:3153–60.
[46] Vreugdenhil G, Lowenberg B, van Eijk HG, Swaak AJ. Anaemia ofchronic disease in rheumatoid arthritis. Raised serum interleukin-6(IL-6) levels and effects of IL-6 and anti-IL-6 on in vitro erythro-poiesis. Rheumatol Int 1990;10:127–30.
[47] Bernad A, Kopf M, Kulbacki R, Weich N, Koehler G, Gutierrez-Ramos JC. Interleukin-6 is required in vivo for the regulation ofstem cells and committed progenitors of the hematopoietic system.Immunity 1994;1:725–31.
[48] Raja KBO, Latunde-Dada G, Peters TJ, McKie AT, Simpson RJ. Roleof interleukin-6 in hypoxic regulation of intestinal iron absorption. BrJ Haematol 2005;131:656–62.
[49] De Maria R, Testa U, Luchetti L, et al. Apoptotic role of Fas/Fas ligandsystem in the regulation of erythropoiesis. Blood 1999;93:796–803.
[50] De Maria R, Zeuner A, Eramo A, et al. Negative regulation oferythropoiesis by caspase-mediated cleavage of GATA-1. Nature1999;401:489–93.
[51] Orkin SH. GATA-binding transcription factors in hematopoietic cells.Blood 1992;80:575–81.
[52] Weiss MJ, Orkin SH. GATA transcription factors: key regulators ofhematopoiesis. Exp Hematol 1995;23:99–107.
[53] Weiss MJ, Orkin SH. Transcription factor GATA-1 permits survivaland maturation of erythroid precursors by preventing apoptosis. ProcNatl Acad Sci USA 1995;92:9623–7.
[54] Zeuner A, Eramo A, Testa U, et al. Control of erythroid cell productionvia caspase-mediated cleavage of transcription factor SCL/Tal-1. CellDeath Differ 2003;10:905–13.
[55] Dai CH, Price JO, Brunner T, Krantz SB. Fas ligand is present inhuman erythroid colony-forming cells and interacts with fas induced
by interferon gamma to produce erythroid cell apoptosis. Blood1998;91:1235–42.[56] Felli N, Pedini F, Zeuner A, et al. Multiple members of the TNFsuperfamily contribute to IFN-gamma-mediated inhibition of erythro-poiesis. J Immunol 2005;175:1464–72.
logy/Hematology 64 (2007) 139–158
[57] Dai CH, Krantz SB, Kollar K, Price JO. Stem cell factor can overcomeinhibition of highly purified human burst-forming units-erythroid byinterferon gamma. J Cell Physiol 1995;165:323–32.
[58] Nishio M, Oda A, Koizumi K, et al. Stem cell factor prevents fas-mediated apoptosis of human erythroid precursor cells with src-familykinase dependency. Exp Hematol 2001;29:19–29.
[59] Rubiolo C, Piazzolla D, Meissl K, et al. A balance between raf-1and fas expression sets the pace of erythroid differentiation. Blood2006;108:152–9.
[60] Zamai L, Secchiero P, Pierpaoli S, et al. TNF-related apoptosis-inducing ligand (TRAIL) as a negative regulator of normal humanerythropoiesis. Blood 2000;95:3716–24.
[61] Mirandola P, Gobbi G, Ponti C, Sponzilli I, Cocco L, Vitale M. PKCepsilon controls protection against TRAIL in erythroid progenitors.Blood 2006;107:508–13.
[62] D’Andrea AD, Zon LI. Erythropoietin receptor. Subunit structure andactivation. J Clin Invest 1990;86:681–7.
[63] Wu H, Liu X, Jaenisch R, Lodish HF. Generation of committed ery-throid BFU-E and CFU-E progenitors does not require erythropoietinor the erythropoietin receptor. Cell 1995;83:59–67.
[64] Constantinescu SN, Keren T, Socolovsky M, Nam H, Henis YI, LodishHF. Ligand-independent oligomerization of cell-surface erythropoi-etin receptor is mediated by the transmembrane domain. Proc NatlAcad Sci USA 2001;98:4379–84.
[65] Miura O, D’Andrea A, Kabat D, Ihle JN. Induction of tyrosinephosphorylation by the erythropoietin receptor correlates with mito-genesis. Mol Cell Biol 1991;11:4895–902.
[66] Motoyama N, Kimura T, Takahashi T, Watanabe T, Nakano T. Bcl-xprevents apoptotic cell death of both primitive and definitive erythro-cytes at the end of maturation. J Exp Med 1999;189:1691–8.
[67] Motoyama N, Wang F, Roth KA, et al. Massive cell death of imma-ture hematopoietic cells and neurons in bcl-x-deficient mice. Science1995;267:1506–10.
[68] Gregory T, Yu C, Ma A, Orkin SH, Blobel GA, Weiss MJ. GATA-1and erythropoietin cooperate to promote erythroid cell survival byregulating bcl-xL expression. Blood 1999;94:87–96.
[69] Menon MP, Karur V, Bogacheva O, Bogachev O, Cuetara B, Woj-chowski DM. Signals for stress erythropoiesis are integrated via anerythropoietin receptor-phosphotyrosine-343-Stat5 axis. J Clin Invest2006;116:683–94.
[70] Kirito K, Nakajima K, Watanabe T, et al. Identification of the humanerythropoietin receptor region required for Stat1 and Stat3 activation.Blood 2002;99:102–10.
[71] Parganas E, Wang D, Stravopodis D, et al. Jak2 is essential for sig-naling through a variety of cytokine receptors. Cell 1998;93:385–95.
[72] Neubauer H, Cumano A, Muller M, Wu H, Huffstadt U, PfefferK. Jak2 deficiency defines an essential developmental checkpoint indefinitive hematopoiesis. Cell 1998;93:397–409.
[73] Uddin S, Kottegoda S, Stigger D, Platanias LC, Wickrema A. Activa-tion of the Akt/FKHRL1 pathway mediates the antiapoptotic effectsof erythropoietin in primary human erythroid progenitors. BiochemBiophys Res Commun 2000;275:16–9.
[74] Myklebust JH, Blomhoff HK, Rusten LS, Stokke T, SmelandEB. Activation of phosphatidylinositol 3-kinase is important forerythropoietin-induced erythropoiesis from CD34(+) hematopoieticprogenitor cells. Exp Hematol 2002;30:990–1000.
[75] Datta SR, Dudek H, Tao X, et al. Akt phosphorylation of BADcouples survival signals to the cell-intrinsic death machinery. Cell1997;91:231–41.
[76] Constantinescu SN, Ghaffari S, Lodish HF. The erythropoietin recep-tor: structure, activation and intracellular signal transduction. Trends
Endocrinol Metab 1999;10:18–23.[77] Klingmuller U, Lorenz U, Cantley LC, Neel BG, Lodish HF. Spe-cific recruitment of SH-PTP1 to the erythropoietin receptor causesinactivation of JAK2 and termination of proliferative signals. Cell1995;80:729–38.
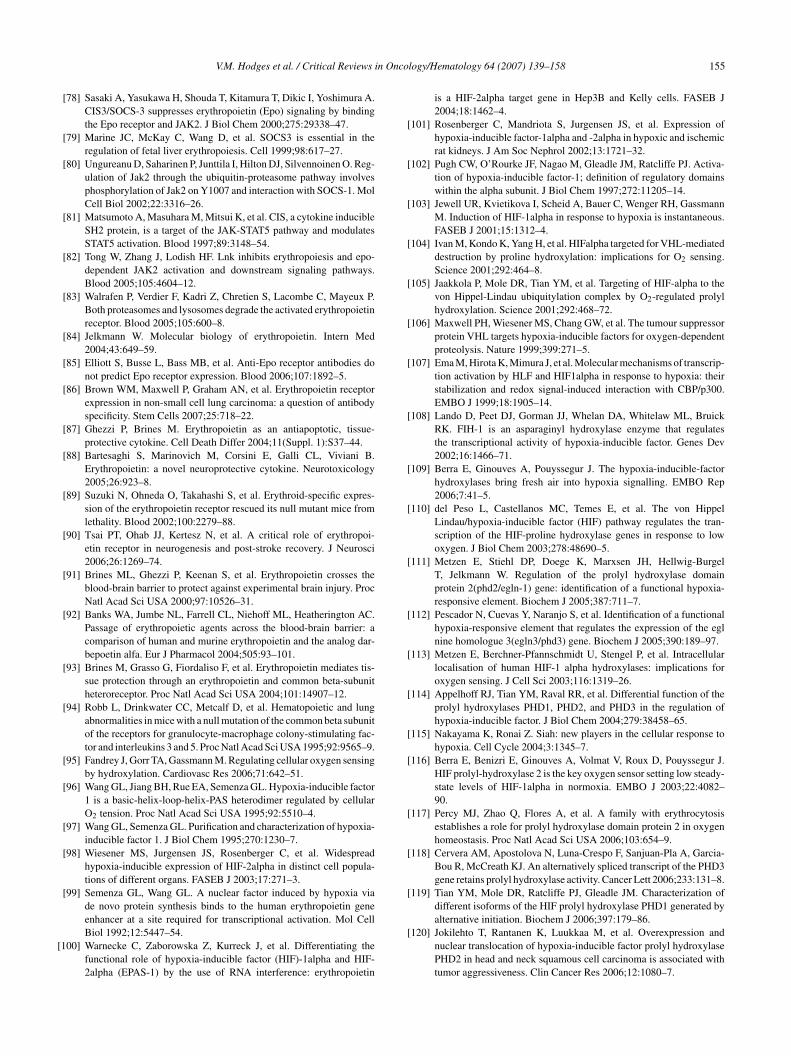
n Onco
V.M. Hodges et al. / Critical Reviews i[78] Sasaki A, Yasukawa H, Shouda T, Kitamura T, Dikic I, Yoshimura A.CIS3/SOCS-3 suppresses erythropoietin (Epo) signaling by bindingthe Epo receptor and JAK2. J Biol Chem 2000;275:29338–47.
[79] Marine JC, McKay C, Wang D, et al. SOCS3 is essential in theregulation of fetal liver erythropoiesis. Cell 1999;98:617–27.
[80] Ungureanu D, Saharinen P, Junttila I, Hilton DJ, Silvennoinen O. Reg-ulation of Jak2 through the ubiquitin-proteasome pathway involvesphosphorylation of Jak2 on Y1007 and interaction with SOCS-1. MolCell Biol 2002;22:3316–26.
[81] Matsumoto A, Masuhara M, Mitsui K, et al. CIS, a cytokine inducibleSH2 protein, is a target of the JAK-STAT5 pathway and modulatesSTAT5 activation. Blood 1997;89:3148–54.
[82] Tong W, Zhang J, Lodish HF. Lnk inhibits erythropoiesis and epo-dependent JAK2 activation and downstream signaling pathways.Blood 2005;105:4604–12.
[83] Walrafen P, Verdier F, Kadri Z, Chretien S, Lacombe C, Mayeux P.Both proteasomes and lysosomes degrade the activated erythropoietinreceptor. Blood 2005;105:600–8.
[84] Jelkmann W. Molecular biology of erythropoietin. Intern Med2004;43:649–59.
[85] Elliott S, Busse L, Bass MB, et al. Anti-Epo receptor antibodies donot predict Epo receptor expression. Blood 2006;107:1892–5.
[86] Brown WM, Maxwell P, Graham AN, et al. Erythropoietin receptorexpression in non-small cell lung carcinoma: a question of antibodyspecificity. Stem Cells 2007;25:718–22.
[87] Ghezzi P, Brines M. Erythropoietin as an antiapoptotic, tissue-protective cytokine. Cell Death Differ 2004;11(Suppl. 1):S37–44.
[88] Bartesaghi S, Marinovich M, Corsini E, Galli CL, Viviani B.Erythropoietin: a novel neuroprotective cytokine. Neurotoxicology2005;26:923–8.
[89] Suzuki N, Ohneda O, Takahashi S, et al. Erythroid-specific expres-sion of the erythropoietin receptor rescued its null mutant mice fromlethality. Blood 2002;100:2279–88.
[90] Tsai PT, Ohab JJ, Kertesz N, et al. A critical role of erythropoi-etin receptor in neurogenesis and post-stroke recovery. J Neurosci2006;26:1269–74.
[91] Brines ML, Ghezzi P, Keenan S, et al. Erythropoietin crosses theblood-brain barrier to protect against experimental brain injury. ProcNatl Acad Sci USA 2000;97:10526–31.
[92] Banks WA, Jumbe NL, Farrell CL, Niehoff ML, Heatherington AC.Passage of erythropoietic agents across the blood-brain barrier: acomparison of human and murine erythropoietin and the analog dar-bepoetin alfa. Eur J Pharmacol 2004;505:93–101.
[93] Brines M, Grasso G, Fiordaliso F, et al. Erythropoietin mediates tis-sue protection through an erythropoietin and common beta-subunitheteroreceptor. Proc Natl Acad Sci USA 2004;101:14907–12.
[94] Robb L, Drinkwater CC, Metcalf D, et al. Hematopoietic and lungabnormalities in mice with a null mutation of the common beta subunitof the receptors for granulocyte-macrophage colony-stimulating fac-tor and interleukins 3 and 5. Proc Natl Acad Sci USA 1995;92:9565–9.
[95] Fandrey J, Gorr TA, Gassmann M. Regulating cellular oxygen sensingby hydroxylation. Cardiovasc Res 2006;71:642–51.
[96] Wang GL, Jiang BH, Rue EA, Semenza GL. Hypoxia-inducible factor1 is a basic-helix-loop-helix-PAS heterodimer regulated by cellularO2 tension. Proc Natl Acad Sci USA 1995;92:5510–4.
[97] Wang GL, Semenza GL. Purification and characterization of hypoxia-inducible factor 1. J Biol Chem 1995;270:1230–7.
[98] Wiesener MS, Jurgensen JS, Rosenberger C, et al. Widespreadhypoxia-inducible expression of HIF-2alpha in distinct cell popula-tions of different organs. FASEB J 2003;17:271–3.
[99] Semenza GL, Wang GL. A nuclear factor induced by hypoxia viade novo protein synthesis binds to the human erythropoietin gene
enhancer at a site required for transcriptional activation. Mol CellBiol 1992;12:5447–54.[100] Warnecke C, Zaborowska Z, Kurreck J, et al. Differentiating thefunctional role of hypoxia-inducible factor (HIF)-1alpha and HIF-2alpha (EPAS-1) by the use of RNA interference: erythropoietin
logy/Hematology 64 (2007) 139–158 155
is a HIF-2alpha target gene in Hep3B and Kelly cells. FASEB J2004;18:1462–4.
[101] Rosenberger C, Mandriota S, Jurgensen JS, et al. Expression ofhypoxia-inducible factor-1alpha and -2alpha in hypoxic and ischemicrat kidneys. J Am Soc Nephrol 2002;13:1721–32.
[102] Pugh CW, O’Rourke JF, Nagao M, Gleadle JM, Ratcliffe PJ. Activa-tion of hypoxia-inducible factor-1; definition of regulatory domainswithin the alpha subunit. J Biol Chem 1997;272:11205–14.
[103] Jewell UR, Kvietikova I, Scheid A, Bauer C, Wenger RH, GassmannM. Induction of HIF-1alpha in response to hypoxia is instantaneous.FASEB J 2001;15:1312–4.
[104] Ivan M, Kondo K, Yang H, et al. HIFalpha targeted for VHL-mediateddestruction by proline hydroxylation: implications for O2 sensing.Science 2001;292:464–8.
[105] Jaakkola P, Mole DR, Tian YM, et al. Targeting of HIF-alpha to thevon Hippel-Lindau ubiquitylation complex by O2-regulated prolylhydroxylation. Science 2001;292:468–72.
[106] Maxwell PH, Wiesener MS, Chang GW, et al. The tumour suppressorprotein VHL targets hypoxia-inducible factors for oxygen-dependentproteolysis. Nature 1999;399:271–5.
[107] Ema M, Hirota K, Mimura J, et al. Molecular mechanisms of transcrip-tion activation by HLF and HIF1alpha in response to hypoxia: theirstabilization and redox signal-induced interaction with CBP/p300.EMBO J 1999;18:1905–14.
[108] Lando D, Peet DJ, Gorman JJ, Whelan DA, Whitelaw ML, BruickRK. FIH-1 is an asparaginyl hydroxylase enzyme that regulatesthe transcriptional activity of hypoxia-inducible factor. Genes Dev2002;16:1466–71.
[109] Berra E, Ginouves A, Pouyssegur J. The hypoxia-inducible-factorhydroxylases bring fresh air into hypoxia signalling. EMBO Rep2006;7:41–5.
[110] del Peso L, Castellanos MC, Temes E, et al. The von HippelLindau/hypoxia-inducible factor (HIF) pathway regulates the tran-scription of the HIF-proline hydroxylase genes in response to lowoxygen. J Biol Chem 2003;278:48690–5.
[111] Metzen E, Stiehl DP, Doege K, Marxsen JH, Hellwig-BurgelT, Jelkmann W. Regulation of the prolyl hydroxylase domainprotein 2(phd2/egln-1) gene: identification of a functional hypoxia-responsive element. Biochem J 2005;387:711–7.
[112] Pescador N, Cuevas Y, Naranjo S, et al. Identification of a functionalhypoxia-responsive element that regulates the expression of the eglnine homologue 3(egln3/phd3) gene. Biochem J 2005;390:189–97.
[113] Metzen E, Berchner-Pfannschmidt U, Stengel P, et al. Intracellularlocalisation of human HIF-1 alpha hydroxylases: implications foroxygen sensing. J Cell Sci 2003;116:1319–26.
[114] Appelhoff RJ, Tian YM, Raval RR, et al. Differential function of theprolyl hydroxylases PHD1, PHD2, and PHD3 in the regulation ofhypoxia-inducible factor. J Biol Chem 2004;279:38458–65.
[115] Nakayama K, Ronai Z. Siah: new players in the cellular response tohypoxia. Cell Cycle 2004;3:1345–7.
[116] Berra E, Benizri E, Ginouves A, Volmat V, Roux D, Pouyssegur J.HIF prolyl-hydroxylase 2 is the key oxygen sensor setting low steady-state levels of HIF-1alpha in normoxia. EMBO J 2003;22:4082–90.
[117] Percy MJ, Zhao Q, Flores A, et al. A family with erythrocytosisestablishes a role for prolyl hydroxylase domain protein 2 in oxygenhomeostasis. Proc Natl Acad Sci USA 2006;103:654–9.
[118] Cervera AM, Apostolova N, Luna-Crespo F, Sanjuan-Pla A, Garcia-Bou R, McCreath KJ. An alternatively spliced transcript of the PHD3gene retains prolyl hydroxylase activity. Cancer Lett 2006;233:131–8.
[119] Tian YM, Mole DR, Ratcliffe PJ, Gleadle JM. Characterization ofdifferent isoforms of the HIF prolyl hydroxylase PHD1 generated by
alternative initiation. Biochem J 2006;397:179–86.[120] Jokilehto T, Rantanen K, Luukkaa M, et al. Overexpression andnuclear translocation of hypoxia-inducible factor prolyl hydroxylasePHD2 in head and neck squamous cell carcinoma is associated withtumor aggressiveness. Clin Cancer Res 2006;12:1080–7.

1 n Onco
56 V.M. Hodges et al. / Critical Reviews i[121] Stolze IP, Tian YM, Appelhoff RJ, et al. Genetic analysis of the roleof the asparaginyl hydroxylase factor inhibiting hypoxia-induciblefactor (HIF) in regulating HIF transcriptional target genes. J BiolChem 2004;279:42719–25.
[122] Huang J, Zhao Q, Mooney SM, Lee FS. Sequence determi-nants in hypoxia-inducible factor-1alpha for hydroxylation by theprolyl hydroxylases PHD1, PHD2, and PHD3. J Biol Chem2002;277:39792–800.
[123] Cournoyer D, Toffelmire EB, Wells GA, et al. Anti-erythropoietinantibody-mediated pure red cell aplasia after treatment with recombi-nant erythropoietin products: recommendations for minimization ofrisk. J Am Soc Nephrol 2004;15:2728–34.
[124] Boven K, Knight J, Bader F, Rossert J, Eckardt KU, Casade-vall N. Epoetin-associated pure red cell aplasia in patients withchronic kidney disease: solving the mystery. Nephrol Dial Transplant2005;20(Suppl. 3):iii33–40.
[125] Jacob A, Sandhu K, Nicholas J, et al. Antibody-mediated pure redcell aplasia in a dialysis patient receiving darbepoetin alfa as the soleerythropoietic agent. Nephrol Dial Transplant 2006;21:2963–5.
[126] Srinivas U, Pillai LS, Kumar R, Pati HP, Saxena R. Bone marrowaplasia-a rare complication of imatinib therapy in CML patients. AmJ Hematol 2006.
[127] Taniguchi T, D’Andrea AD. Molecular pathogenesis of Fanconi ane-mia: recent progress. Blood 2006;107:4223–33.
[128] Lipton JM. Diamond Blackfan anemia: new paradigms for a “notso pure” inherited red cell aplasia. Semin Hematol 2006;43:167–77.
[129] Xin ZT, Beauchamp AD, Calado RT, et al. Functional characterizationof natural telomerase mutations found in patients with hematologicaldisorders. Blood 2007;109:524–32.
[130] Umbreit J. Iron deficiency: a concise review. Am J Hematol2005;78:225–31.
[131] Whitehead VM. Acquired and inherited disorders of cobalamin andfolate in children. Br J Haematol 2006;134:125–36.
[132] Grasbeck R. Megaloblastic anaemia (MA). Hematology2005;10(Suppl. 1):227–8.
[133] Toh BH, Alderuccio F. Pernicious anaemia. Autoimmunity2004;37:357–61.
[134] Forget BG. De novo and acquired forms of alpha thalassemia. CurrHematol Rep 2006;5:11–4.
[135] Min-Oo G, Gros P. Erythrocyte variants and the nature of their malariaprotective effect. Cell Microbiol 2005;7:753–63.
[136] Shah S, Vega R. Hereditary spherocytosis. Pediatr Rev2004;25:168–72.
[137] Eber S, Lux SE. Hereditary spherocytosis-defects in proteins thatconnect the membrane skeleton to the lipid bilayer. Semin Hematol2004;41:118–41.
[138] Fleming MD. The genetics of inherited sideroblastic anemias. SeminHematol 2002;39:270–81.
[139] McMullin MF, Hillmen P, Elder GE, Lappin TR, Luzzatto L.Serum erythropoietin levels in paroxysmal nocturnal haemoglobin-uria: implications for therapy. Br J Haematol 1996;92:815–7.
[140] Fitzsimons EJ, Brock JH. The anaemia of chronic disease. BMJ2001;322:811–2.
[141] Ganz T. Molecular pathogenesis of anemia of chronic disease. PediatrBlood Cancer 2006;46:554–7.
[142] Weiss G, Goodnough LT. Anemia of chronic disease. N Engl J Med2005;352:1011–23.
[143] Thomas MC. The high prevalence of anemia in diabetes is linked tofunctional erythropoietin deficiency. Semin Nephrol 2006;26:275–82.
[144] Maciejewski JP, Selleri C, Sato T, et al. Nitric oxide suppressionof human hematopoiesis in vitro. Contribution to inhibitory action
of interferon-gamma and tumor necrosis factor-alpha. J Clin Invest1995;96:1085–92.[145] Dallalio G, Law E, Means Jr RT. Hepcidin inhibits in vitro erythroidcolony formation at reduced erythropoietin concentrations. Blood2006;107:2702–4.
logy/Hematology 64 (2007) 139–158
[146] Bohlius J, Weingart O, Trelle S, Engert A. Cancer-related anemiaand recombinant human erythropoietin-an updated overview. Nat ClinPract Oncol 2006;3:152–64.
[147] Vaupel P, Mayer A. Hypoxia and anemia: effects on tumor biologyand treatment resistance. Transfus Clin Biol 2005;12:5–10.
[148] Ritz E, Haxsen V. Diabetic nephropathy and anaemia. Eur J Clin Invest2005;35(Suppl. 3):66–74.
[149] Nangaku M, Eckardt KU. Pathogenesis of renal anemia. SeminNephrol 2006;26:261–8.
[150] Vanrenterghem Y, Ponticelli C, Morales JM, et al. Prevalence andmanagement of anemia in renal transplant recipients: a Europeansurvey. Am J Transplant 2003;3:835–45.
[151] Yorgin PD, Belson A, Sanchez J, et al. Unexpectedly high prevalenceof posttransplant anemia in pediatric and young adult renal transplantrecipients. Am J Kidney Dis 2002;40:1306–18.
[152] Yorgin PD, Scandling JD, Belson A, Sanchez J, Alexander SR,Andreoni KA. Late post-transplant anemia in adult renal trans-plant recipients. an under-recognized problem? Am J Transplant2002;2:429–35.
[153] Vanrenterghem Y. Anaemia after renal transplantation. Nephrol DialTransplant 2004;19(Suppl. 5):V54–8.
[154] Sun CH, Ward HJ, Paul WL, Koyle MA, Yanagawa N, Lee DB.Serum erythropoietin levels after renal transplantation. N Engl J Med1989;321:151–7.
[155] Muirhead N. Erythropoietin and renal transplantation. Kidney IntSuppl 1999;69:S86–92.
[156] Goldsmith D, Al-Khoury S, Shah N, Covic A. Anaemia after renaltransplantation—role of immunosuppressive drugs and a pathophys-iological appraisal. Nephron Clin Pract 2006;104:c69–74.
[157] Old CW, Flannery EP, Grogan TM, Stone WH. San AntonioRP. Azathioprine-induced pure red blood cell aplasia. JAMA1978;240:552–4.
[158] Winkelmayer WC, Kewalramani R, Rutstein M, Gabardi S, Vonvis-ger T, Chandraker A. Pharmacoepidemiology of anemia in kidneytransplant recipients. J Am Soc Nephrol 2004;15:1347–52.
[159] Bertoni E, Rosati A, Zanazzi M, et al. Unusual incidence of aplasticanaemia due to B-19 parvovirus infection in renal transplant recipi-ents. Transplant Proc 1997;29:818–9.
[160] Mareschal-Desandes R, Andre JL, Lesesve JF, Krier MJ, Bordigoni P,Humbert JC. Successful treatment of chronic parvovirus B19 infectionby high-dose immunoglobulin. Clin Nephrol 2003;59:311–2.
[161] Renoult E, Bachelet C, Krier-Coudert MJ, Diarrassouba A, AndreJL, Kessler M. Recurrent anemia in kidney transplant recipientswith parvovirus B19 infection. Transplant Proc 2006;38:2321–3.
[162] Kasiske BL, Guijarro C, Massy ZA, Wiederkehr MR, Ma JZ. Car-diovascular disease after renal transplantation. J Am Soc Nephrol1996;7:158–65.
[163] Gentil MA, Cabello V, Perez-Valdivia M, et al. Influence of the currentmanagement of renal transplant recipients on the prevalence of anemiaand related costs. Transplant Proc 2005;37:3823–4.
[164] Zalunardo N, Levin A. Anemia and the heart in chronic kidney dis-ease. Semin Nephrol 2006;26:290–5.
[165] Afzali B, Al-Khoury S, Shah N, Mikhail A, Covic A, Goldsmith D.Anemia after renal transplantation. Am J Kidney Dis 2006;48:519–36.
[166] Fliser D, Bahlmann FH, Haller H. Epo: renoprotection beyond anemiacorrection. Pediatr Nephrol 2006;21:1785–9.
[167] Sharples EJ, Yaqoob MM. Erythropoietin and acute renal failure.Semin Nephrol 2006;26:325–31.
[168] Steinbrook R. Haemoglobin concentrations in chronic kidney disease.Lancet 2006;368:2191–3.
[169] Locatelli F, Aljama P, Barany P, Canaud B, Carrera F, Eckardt KU,
Horl WH, Macdougal IC, Macleod A, Wiecek A, Cameron S, Euro-pean Best Practice Guidelines Working Group. Revised Europeanbest practice guidelines for the management of anaemia in patientswith chronic renal failure. Section II. Targets fro anaemia treatment.Nephrol Dial Transplant 2004;19(Suppl 2):ii6–15.
n Onco
V.M. Hodges et al. / Critical Reviews i[170] Drueke TB, Locatelli F, Clyne N, et al. Normalization of hemoglobinlevel in patients with chronic kidney disease and anemia. N Engl JMed 2006;355:2071–84.
[171] Singh AK, Szczech L, Tang KL, et al. Correction of anemia with Epo-etin alfa in chronic kidney disease. N Engl J Med 2006;355:2085–98.
[172] Miyake T, Kung CK, Goldwasser E. Purification of human erythro-poietin. J Biol Chem 1977;252:5558–64.
[173] Casadevall N, Nataf J, Viron B, et al. Pure red-cell aplasia andantierythropoietin antibodies in patients treated with recombinanterythropoietin. N Engl J Med 2002;346:469–75.
[174] Sharma B, Bader F, Templeman T, Lisi P, Ryan M, Heavner GA.Technical investigations into the cause of the increased indiidence ofantibody-mediated pure red cell aplasia assoicated with EPREX. EurJ Hosp Pharm 2004;5:86–91.
[175] Boven K, Stryker S, Knight J, et al. The increased incidence of purered cell aplasia with an eprex formulation in uncoated rubber stoppersyringes. Kidney Int 2005;67:2346–53.
[176] Egrie JC, Browne JK. Development and characterization of novel ery-thropoiesis stimulating protein (NESP). Br J Cancer 2001;84(Suppl.1):3–10.
[177] Maxwell AP. Novel erythropoiesis-stimulating protein in the man-agement of the anemia of chronic renal failure. Kidney Int2002;62:720–9.
[178] Macdougall IC. CERA (continuous erythropoietin receptor activator):a new erythropoiesis-stimulating agent for the treatment of anemia.Curr Hematol Rep 2005;4:436–40.
[179] Macdougall IC, Eckardt KU. Novel strategies for stimulatingerythropoiesis and potential new treatments for anaemia. Lancet2006;368:947–53.
[180] Kochendoerfer GG, Chen SY, Mao F, et al. Design and chemicalsynthesis of a homogeneous polymer-modified erythropoiesis protein.Science 2003;299:884–7.
[181] Sytkowski AJ, Lunn ED, Davis KL, Feldman L, Siekman S. Humanerythropoietin dimers with markedly enhanced in vivo activity. ProcNatl Acad Sci USA 1998;95:1184–8.
[182] Fan Q, Leuther KK, Holmes CP, et al. Preclinical evaluation ofhematide, a novel erythropoiesis stimulating agent, for the treatmentof anemia. Exp Hematol 2006;34:1303–11.
[183] Stead RB, Lambert J, Wessels D, et al. Evaluation of the safety andpharmacodynamics of hematide, a novel erythropoietic agent, in aphase 1, double-blind, placebo-controlled, dose-escalation study inhealthy volunteers. Blood 2006;108:1830–4.
[184] Akagi S, Ichikawa H, Okada T, et al. The critical role of SRC homol-ogy domain 2-containing tyrosine phosphatase-1 in recombinanthuman erythropoietin hyporesponsive anemia in chronic hemodial-ysis patients. J Am Soc Nephrol 2004;15:3215–24.
[185] Ang SO, Chen H, Gordeuk VR, et al. Endemic polycythemia in Rus-sia: mutation in the VHL gene. Blood Cells Mol Dis 2002;28:57–62.
[186] Binley K, Askham Z, Iqball S, et al. Long-term reversal of chronicanemia using a hypoxia-regulated erythropoietin gene therapy. Blood2002;100:2406–13.
[187] Fishbane S. Recombinant human erythropoietin: has treatmentreached its full potential? Semin Dial 2006;19:1–4.
[188] Brines M, Cerami A. Emerging biological roles for erythropoietin inthe nervous system. Nat Rev Neurosci 2005;6:484–94.
[189] Pacary E, Petit E, Bernaudin M, Erythropoietin. a cytoprotectiveand regenerative cytokine, and the hypoxic brain. Neurodegener Dis2006;3:87–93.
[190] Schwartzenberg S, Ben-Shoshan J, Keren G, George J. The role oferythropoietin in myocardial protection: potential mechanisms andapplications. Expert Rev Cardiovasc Ther 2006;4:41–50.
[191] Henke M, Laszig R, Rube C, et al. Erythropoietin to treat
head and neck cancer patients with anaemia undergoing radio-therapy: randomised, double-blind, placebo-controlled trial. Lancet2003;362:1255–60.[192] Leyland-Jones B, et al. Breast cancer trial with erythropoietin termi-nated unexpectedly. Lancet Oncol 2003;4:459–60.
logy/Hematology 64 (2007) 139–158 157
[193] Bohlius J, Wilson J, Seidenfeld J, et al. Recombinant human ery-thropoietins and cancer patients: updated meta-analysis of 57 studiesincluding 9353 patients. J Natl Cancer Inst 2006;98:708–14.
[194] Temkin SM, Hellmann M, Serur E, Lee YC, Abulafia O. Erythro-poietin administration during primary treatment for locally advancedcervical carcinoma is associated with poor response to radiation. IntJ Gynecol Cancer 2006;16:1855–61.
[195] Vaupel P, Dunst J, Engert A, et al. Effects of recombinant humanerythropoietin (rHuEPO) on tumor control in patients with cancer-induced anemia. Onkologie 2005;28:216–21.
[196] Bunn HF. New agents that stimulate erythropoiesis. Blood2007;109:868–73.
[197] McMullin MF, Bareford D, Campbell P, et al. Guidelinesfor the diagnosis, investigation and management of poly-cythaemia/erythrocytosis. Br J Haematol 2005;130:174–95.
[198] Maran J, Prchal J. Polycythemia and oxygen sensing. Pathol Biol(Paris) 2004;52:280–4.
[199] Baxter EJ, Scott LM, Campbell PJ, et al. Acquired mutation of thetyrosine kinase JAK2 in human myeloproliferative disorders. Lancet2005;365:1054–61.
[200] James C, Ugo V, Le Couedic JP, et al. A unique clonal JAK2 mutationleading to constitutive signalling causes polycythaemia vera. Nature2005;434:1144–8.
[201] Jones AV, Kreil S, Zoi K, et al. Widespread occurrence of theJAK2 V617F mutation in chronic myeloproliferative disorders. Blood2005;106:2162–8.
[202] Kralovics R, Teo SS, Buser AS, et al. Altered gene expression inmyeloproliferative disorders correlates with activation of signalingby the V617F mutation of Jak2. Blood 2005;106:3374–6.
[203] Percy MJ, Jones FG, Green AR, Reilly JT, McMullin MF. Theincidence of the JAK2 V617F mutation in patients with idiopathicerythrocytosis. Haematologica 2006;91:413–4.
[204] Kralovics R, Prchal JT. Genetic heterogeneity of primary familial andcongenital polycythemia. Am J Hematol 2001;68:115–21.
[205] Petersen KB, Hokland P, Petersen GB, Nyvold CG. Erythropoietinreceptor defect: a cause of primary polycythaemia. Br J Haematol2004;125:537–8.
[206] Prchal JT, Crist WM, Goldwasser E, Perrine G, Prchal JF. Autosomaldominant polycythemia. Blood 1985;66:1208–14.
[207] Juvonen E, Ikkala E, Fyhrquist F, Ruutu T. Autosomal dominant ery-throcytosis caused by increased sensitivity to erythropoietin. Blood1991;78:3066–9.
[208] de la Chapelle A, Traskelin AL, Juvonen E. Truncated erythropoietinreceptor causes dominantly inherited benign human erythrocytosis.Proc Natl Acad Sci USA 1993;90:4495–9.
[209] Arcasoy MO, Harris KW, Forget BG. A human erythropoietin recep-tor gene mutant causing familial erythrocytosis is associated withderegulation of the rates of Jak2 and Stat5 inactivation. Exp Hematol1999;27:63–74.
[210] Watowich SS, Xie X, Klingmuller U, et al. Erythropoietin receptormutations associated with familial erythrocytosis cause hypersensitiv-ity to erythropoietin in the heterozygous state. Blood 1999;94:2530–2.
[211] Arcasoy MO, Karayal AF. Erythropoietin hypersensitivity in pri-mary familial and congenital polycythemia: role of tyrosines Y285and Y344 in erythropoietin receptor cytoplasmic domain. BiochimBiophys Acta 2005;1740:17–28.
[212] Divoky V, Liu Z, Ryan TM, Prchal JF, Townes TM, Prchal JT.Mouse model of congenital polycythemia: homologous replacementof murine gene by mutant human erythropoietin receptor gene. ProcNatl Acad Sci USA 2001;98:986–91.
[213] Gordeuk VR, Stockton DW, Prchal JT. Congenital poly-
cythemias/erythrocytoses. Haematologica 2005;90:109–16.[214] Gordeuk VR, Sergueeva AI, Miasnikova GY, et al. Congenital dis-order of oxygen sensing: association of the homozygous Chuvashpolycythemia VHL mutation with thrombosis and vascular abnor-malities but not tumors. Blood 2004;103:3924–32.

1 n Onco
B
LCU
pfB
58 V.M. Hodges et al. / Critical Reviews i
[215] Gordeuk VR, Prchal JT. Vascular complications in Chuvash poly-cythemia. Semin Thromb Hemost 2006;32:289–94.
[216] Percy MJ, McMullin MF, Jowitt SN, et al. Chuvash-type congenitalpolycythemia in 4 families of Asian and Western European ancestry.Blood 2003;102:1097–9.
[217] Perrotta S, Nobili B, Ferraro M, et al. Von Hippel-Lindau-dependentpolycythemia is endemic on the island of ischia: identification of anovel cluster. Blood 2006;107:514–9.
[218] Liu E, Percy MJ, Amos CI, et al. The worldwide distribution ofthe VHL 598C>T mutation indicates a single founding event. Blood2004;103:1937–40.
[219] Cario H, Schwarz K, Jorch N, et al. Mutations in the von Hippel-Lindau (VHL) tumor suppressor gene and VHL-haplotype analysisin patients with presumable congenital erythrocytosis. Haematologica2005;90:19–24.
[220] Bento MC, Chang KT, Guan Y, et al. Congenital polycythemia withhomozygous and heterozygous mutations of von Hippel-Lindau gene:five new caucasian patients. Haematologica 2005;90:128–9.
[221] Pastore Y, Jedlickova K, Guan Y, et al. Mutations of von Hippel-Lindau tumor-suppressor gene and congenital polycythemia. Am JHum Genet 2003;73:412–9.
[222] Hardison RC, Chui DH, Giardine B, et al. HbVar: a relational databaseof human hemoglobin variants and thalassemia mutations at the globingene server. Hum Mutat 2002;19:225–33.
[223] Rosa R, Prehu MO, Beuzard Y, Rosa J. The first case of a completedeficiency of diphosphoglycerate mutase in human erythrocytes. JClin Invest 1978;62:907–15.
[224] Hoyer JD, Allen SL, Beutler E, Kubik K, West C, Fairbanks VF.Erythrocytosis due to bisphosphoglycerate mutase deficiency withconcurrent glucose-6-phosphate dehydrogenase (G-6-PD) deficiency.Am J Hematol 2004;75:205–8.
[225] Fitzpatrick MF, Mackay T, Whyte KF, et al. Nocturnal desaturationand serum erythropoietin: a study in patients with chronic obstruc-tive pulmonary disease and in normal subjects. Clin Sci (Lond)1993;84:319–24.
[226] Isbister JP. The contracted plasma volume syndromes (relative poly-cythaemias) and their haemorheological significance. Baillieres ClinHaematol 1987;1:665–93.
[227] Hoffstein V, Herridge M, Mateika S, Redline S, Strohl KP. Hematocritlevels in sleep apnea. Chest 1994;106:787–91.
[228] Eisensehr I, Noachtar S. Haematological aspects of obstructive sleepapnoea. Sleep Med Rev 2001;5:207–21.
[229] Choi JB, Loredo JS, Norman D, et al. Does obstructive sleep apneaincrease hematocrit? Sleep Breath 2006;10:155–60.
[230] Goncalves RC, Buschpigell CA, Lopes AA. Circulating blood vol-umes in pulmonary hypertension associated with erythrocytosis—theeffects of therapeutic hemodilution. Cardiol Young 2003;13:544–50.
[231] Oechslin E. Hematological management of the cyanotic adult withcongenital heart disease. Int J Cardiol 2004;97(Suppl. 1):109–15.
[232] Vlahakos DV, Marathias KP, Agroyannis B, Madias NE. Posttrans-plant erythrocytosis. Kidney Int 2003;63:1187–94.
[233] Bacon BR, Rothman SA, Ricanati ES, Rashad FA. Renal artery steno-sis with erythrocytosis after renal transplantation. Arch Intern Med1980;140:1206–11.
[234] Aeberhard JM, Schneider PA, Vallotton MB, Kurtz A, Leski M. Mul-tiple site estimates of erythropoietin and renin in polycythemic kidneytransplant patients. Transplantation 1990;50:613–6.
[235] Ilan Y, Dranitzki-Elhallel M, Rubinger D, Silver J, Popovtzer MM.Erythrocytosis after renal transplantation. The response to theo-phylline treatment. Transplantation 1994;57:661–4.
[236] Brox AG, Mangel J, Hanley JA, St Louis G, Mongrain S, Gagnon RF.Erythrocytosis after renal transplantation represents an abnormality of
U
Q
logy/Hematology 64 (2007) 139–158
insulin-like growth factor-I and its binding proteins. Transplantation1998;66:1053–8.
[237] Gossmann J, Burkhardt R, Harder S, et al. Angiotensin II infusionincreases plasma erythropoietin levels via an angiotensin II type 1receptor-dependent pathway. Kidney Int 2001;60:83–6.
[238] Julian BA, Brantley Jr RR, Barker CV, et al. Losartan, an angiotensinII type 1 receptor antagonist, lowers hematocrit in posttransplanterythrocytosis. J Am Soc Nephrol 1998;9:1104–8.
[239] Montanaro D, Groupuzzo M, Boscutti G, Risaliti A, Bresadola F,Mioni G. Long-term therapy for postrenal transplant erythrocytosiswith ACE inhibitors: efficacy, safety and action mechanisms. ClinNephrol 2000;53(Suppl.):47–51.
[240] Thomas PK, King RH, Feng SF, et al. Neurological manifestations inchronic mountain sickness: the burning feet-burning hands syndrome.J Neurol Neurosurg Psychiatry 2000;69:447–52.
[241] Leon-Velarde F, Ramos MA, Hernandez JA, et al. The role ofmenopause in the development of chronic mountain sickness. AmJ Physiol 1997;272:R90–4.
[242] Leon-Velarde F, Rivera-Chira M, Tapia R, Huicho L, Monge CC.Relationship of ovarian hormones to hypoxemia in women res-idents of 4.300 m. Am J Physiol Regul Integr Comput Physiol2001;280:R488–93.
[243] Moore LG. Human genetic adaptation to high altitude. High Alt MedBiol 2001;2:257–79.
[244] Mejia OM, Prchal JT, Leon-Velarde F, Hurtado A, Stockton DW.Genetic association analysis of chronic mountain sickness in anandean high-altitude population. Haematologica 2005;90:13–9.
[245] Azzazy HM, Mansour MM, Christenson RH. Doping in therecombinant era: strategies and counterstrategies. Clin Biochem2005;38:959–65.
[246] Lippi G, Franchini M, Guidi GC. Blood doping by cobalt. Should wemeasure cobalt in athletes? J Occup Med Toxicol 2006;1:18.
[247] Gross AJ, Wolff M, Fandrey J, Miersch WD, Dieckmann KP, Jelk-mann W. Prevalence of paraneoplastic erythropoietin production byrenal cell carcinomas. Clin Investig 1994;72:337–40.
[248] Wiesener MS, Seyfarth M, Warnecke C, et al. Paraneoplastic ery-throcytosis associated with an inactivating point mutation of the vonhippel-lindau gene in a renal cell carcinoma. Blood 2002;99:3562–5.
[249] Richmond TD, Chohan M, Barber DL. Turning cells red: sig-nal transduction mediated by erythropoietin. Trends Cell Biol2005;15:146–55.
iographies
Vivien M. Hodges is Post-doctoral Fellow in Professorappin’s Laboratory in the Haematology Research Group,entre for Cancer Research and Cell Biology at Queen’sniversity, Belfast.
Susan Rainey is Post-doctoral Fellow in Professor Lap-in’s Laboratory in the Haematology Research Group, Centreor Cancer Research and Cell Biology at Queen’s University,elfast.
Terence R. Lappin is Professor of Haematology at Queen’sniversity, Belfast.
A. Peter Maxwell is Professor of Renal Medicine atueen’s University, Belfast.




















