World Journal of Gastroenterology - NET
259
World Journal of Gastroenterology World J Gastroenterol 2016 July 7; 22(25): 5623-5866 ISSN 1007-9327 (print) ISSN 2219-2840 (online) Published by Baishideng Publishing Group Inc
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of World Journal of Gastroenterology - NET

World Journal of GastroenterologyWorld J Gastroenterol 2016 July 7; 22(25): 5623-5866
ISSN 1007-9327 (print)ISSN 2219-2840 (online)
Published by Baishideng Publishing Group Inc

The World Journal of Gastroenterology Editorial Board consists of 1376 members, representing a team of worldwide experts in gastroenterology and hepatology. They are from 68 countries, including Algeria (2), Argentina (7), Australia (31), Austria (9), Belgium (11), Brazil (20), Brunei Darussalam (1), Bulgaria (2), Cambodia (1), Canada (26), Chile (4), China (164), Croatia (2), Cuba (1), Czech (6), Denmark (2), Egypt (9), Estonia (2), Finland (6), France (20), Germany (58), Greece (31), Guatemala (1), Hungary (15), Iceland (1), India (33), Indonesia (2), Iran (10), Ireland (9), Israel (18), Italy (194), Japan (149), Jordan (1), Kuwait (1), Lebanon (7), Lithuania (1), Malaysia (1), Mexico (11), Morocco (1), Netherlands (5), New Zealand (4), Nigeria (3), Norway (6), Pakistan (6), Poland (12), Portugal (8), Puerto Rico (1), Qatar (1), Romania (10), Russia (3), Saudi Arabia (2), Singapore (7), Slovenia (2), South Africa (1), South Korea (69), Spain (51), Sri Lanka (1), Sudan (1), Sweden (12), Switzerland (5), Thailand (7), Trinidad and Tobago (1), Tunisia (2), Turkey (55), United Kingdom (49), United States (180), Venezuela (1), and Vietnam (1).
Editorial Board2014-2017
EDITORS-IN-CHIEFStephen C Strom, StockholmAndrzej S Tarnawski, Long BeachDamian Garcia-Olmo, Madrid
ASSOCIATE EDITORSYung-Jue Bang, SeoulVincent Di Martino, BesanconDaniel T Farkas, BronxRoberto J Firpi, GainesvilleMaria Gazouli, AthensChung-Feng Huang, KaohsiungNamir Katkhouda, Los AngelesAnna Kramvis, JohannesburgWolfgang Kruis, ColognePeter L Lakatos, BudapestHan Chu Lee, SeoulChristine McDonald, ClevelandNahum Mendez-Sanchez, Mexico CityGeorge K Michalopoulos, PittsburghSuk Woo Nam, SeoulShu-You Peng, HangzhouDaniel von Renteln, MontrealAngelo Sangiovanni, MilanHildegard M Schuller, KnoxvilleDong-Wan Seo, SeoulAdrian John Stanley, GlasgowJurgen Stein, FrankfurtBei-Cheng Sun, NanjingYoshio Yamaoka, Yufu
GUEST EDITORIAL BOARD MEMBERSJia-Ming Chang, TaipeiJane CJ Chao, Taipei
Kuen-Feng Chen, TaipeiTai-An Chiang, TainanYi-You Chiou, TaipeiSeng-Kee Chuah, KaohsiungWan-Long Chuang, KaohsiungHow-Ran Guo, TainanMing-Chih Hou, TaipeiPo-Shiuan Hsieh, TaipeiChing-Chuan Hsieh, Chiayi countyJun-Te Hsu, TaoyuanChung-Ping Hsu, TaichungChien-Ching Hung, TaipeiChao-Hung Hung, KaohsiungChen-Guo Ker, KaohsiungYung-Chih Lai, TaipeiTeng-Yu Lee, Taichung CityWei-Jei Lee, TaoyuanJin-Ching Lee, KaohsiungJen-Kou Lin, TaipeiYa-Wen Lin, TaipeiHui-kang Liu, TaipeiMin-Hsiung Pan, TaipeiBor-Shyang Sheu, TainanHon-Yi Shi, KaohsiungFung-Chang Sung, TaichungDar-In Tai, TaipeiJung-Fa Tsai, KaohsiungYao-Chou Tsai, New Taipei CityChih-Chi Wang, KaohsiungLiang-Shun Wang, New Taipei CityHsiu-Po Wang, TaipeiJaw-Yuan Wang, KaohsiungYuan-Huang Wang, TaipeiYuan-Chuen Wang, Taichung
Deng-Chyang Wu, KaohsiungShun-Fa Yang, TaichungHsu-Heng Yen, Changhua
MEMBERS OF THE EDITORIAL BOARD
AlgeriaSaadi Berkane, AlgiersSamir Rouabhia, Batna
ArgentinaN Tolosa de Talamoni, CórdobaEduardo de Santibanes, Buenos AiresBernardo Frider, Capital FederalGuillermo Mazzolini, PilarCarlos Jose Pirola, Buenos AiresBernabé Matías Quesada, Buenos AiresMaría Fernanda Troncoso, Buenos Aires
AustraliaGolo Ahlenstiel, WestmeadMinoti V Apte, SydneyJacqueline S Barrett, MelbourneMichael Beard, AdelaideFilip Braet, SydneyGuy D Eslick, SydneyChristine Feinle-Bisset, AdelaideMark D Gorrell, SydneyMichael Horowitz, Adelaide
January 1, 2016IWJG|www.wjgnet.com

Gordon Stanley Howarth, RoseworthySeungha Kang, BrisbaneAlfred King Lam, Gold CoastIan C Lawrance, PerthFremantleBarbara Anne Leggett, BrisbaneDaniel A Lemberg, SydneyRupert W Leong, SydneyFinlay A Macrae, VictoriaVance Matthews, MelbourneDavid L Morris, SydneyReme Mountifield, Bedford ParkHans J Netter, MelbourneNam Q Nguyen, AdelaideLiang Qiao, WestmeadRajvinder Singh, AdelaideRoss Cyril Smith, StLeonardsKevin J Spring, SydneyDebbie Trinder, FremantleDaniel R van Langenberg, Box HillDavid Ian Watson, AdelaideDesmond Yip, GarranLi Zhang, Sydney
AustriaFelix Aigner, InnsbruckGabriela A Berlakovich, ViennaHerwig R Cerwenka, GrazPeter Ferenci, WienAlfred Gangl, ViennaKurt Lenz, LinzMarkus Peck-Radosavljevic, ViennaMarkus Raderer, ViennaStefan Riss, Vienna
BelgiumMichael George Adler, BrusselsBenedicte Y De Winter, AntwerpMark De Ridder, JetteOlivier Detry, LiegeDenis Dufrane Dufrane, BrusselsSven M Francque, EdegemNikos Kotzampassakis, LiègeGeert KMM Robaeys, GenkXavier Sagaert, LeuvenPeter Starkel, BrusselsEddie Wisse, Keerbergen
BrazilSMP Balzan, Santa Cruz do SulJLF Caboclo, Sao jose do rio pretoFábio Guilherme Campos, Sao PauloClaudia RL Cardoso, Rio de JaneiroRoberto J Carvalho-Filho, Sao PauloCarla Daltro, SalvadorJosé Sebastiao dos Santos, Ribeirao PretoEduardo LR Mello, Rio de JaneiroSthela Maria Murad-Regadas, FortalezaClaudia PMS Oliveira, Sao PauloJúlio C Pereira-Lima, Porto AlegreMarcos V Perini, Sao PauloVietla Satyanarayana Rao, Fortaleza
Raquel Rocha, SalvadorAC Simoes e Silva, Belo HorizonteMauricio F Silva, Porto AlefreAytan Miranda Sipahi, Sao PauloRosa Leonôra Salerno Soares, NiteróiCristiane Valle Tovo, Porto AlegreEduardo Garcia Vilela, Belo Horizonte
Brunei DarussalamVui Heng Chong, Bandar Seri Begawan
BulgariaTanya Kirilova Kadiyska, SofiaMihaela Petrova, Sofia
CambodiaFrancois Rouet, Phnom Penh
CanadaBrian Bressler, VancouverFrank J Burczynski, WinnipegWangxue Chen, OttawaFrancesco Crea, VancouverMirko Diksic, MontrealJane A Foster, HamiltonHugh J Freeman, VancouverShahrokh M Ghobadloo, OttawaYuewen Gong, WinnipegPhilip H Gordon, QuebecRakesh Kumar, EdmontonWolfgang A Kunze, HamiltonPatrick Labonte, LavalZhikang Peng, WinnipegJayadev Raju, OttawaMaitreyi Raman, CalgaryGiada Sebastiani, MontrealMaida J Sewitch, MontrealEldon A Shaffer, AlbertaChristopher W Teshima, EdmontonJean Sévigny, QuébecPingchang Yang, HamiltonPingchang Yang, HamiltonEric M Yoshida, VancouverBin Zheng, Edmonton
ChileMarcelo A Beltran, La SerenaFlavio Nervi, SantiagoAdolfo Parra-Blanco, SantiagoAlejandro Soza, Santiago
ChinaZhao-Xiang Bian, Hong Kong San-Jun Cai, ShanghaiGuang-Wen Cao, ShanghaiLong Chen, NanjingRu-Fu Chen, Guangzhou
George G Chen, Hong KongLi-Bo Chen, WuhanJia-Xu Chen, BeijingHong-Song Chen, BeijingLin Chen, BeijingYang-Chao Chen, Hong KongZhen Chen, ShanghaiYing-Sheng Cheng, ShanghaiKent-Man Chu, Hong KongZhi-Jun Dai, Xi’anJing-Yu Deng, TianjinYi-Qi Du, ShanghaiZhi Du, TianjinHani El-Nezami, Hong KongBao-Ying Fei, HangzhouChang-Ming Gao, NanjingJian-Ping Gong, ChongqingZuo-Jiong Gong, WuhanJing-Shan Gong, ShenzhenGuo-Li Gu, BeijingYong-Song Guan, ChengduMao-Lin Guo, LuoyangJun-Ming Guo, NingboYan-Mei Guo, ShanghaiXiao-Zhong Guo, ShenyangGuo-Hong Han, Xi’anMing-Liang He, Hong KongPeng Hou, Xi’anZhao-Hui Huang, WuxiFeng Ji, HangzhouSimon Law, Hong KongYu-Yuan Li, Guangzhou Meng-Sen Li, HaikouShu-De Li, Shanghai Zong-Fang Li, Xi’anQing-Quan Li, ShanghaiKang Li, LasaHan Liang, TianjinXing’e Liu, HangzhouZheng-Wen Liu, Xi’anXiao-Fang Liu, YantaiBin Liu, TianjinQuan-Da Liu, BeijingHai-Feng Liu, BeijingFei Liu, ShanghaiAi-Guo Lu, ShanghaiHe-Sheng Luo, WuhanXiao-Peng Ma, ShanghaiYong Meng, ShantouKe-Jun Nan, Xi’anSiew Chien Ng, Hong KongSimon SM Ng, Hong KongZhao-Shan Niu, QingdaoDi Qu, ShanghaiJu-Wei Mu, BeijingRui-Hua Shi, NanjingBao-Min Shi, ShanghaiXiao-Dong Sun, HangzhouSi-Yu Sun, ShenyangGuang-Hong Tan, HaikouWen-Fu Tang, ChengduAnthony YB Teoh, Hong KongWei-Dong Tong, ChongqingEric Tse, Hong KongHong Tu, Shanghai
January 1, 2016IIWJG|www.wjgnet.com

Rong Tu, HaikouJian-She Wang, ShanghaiKai Wang, JinanXiao-Ping Wang, XianyangXiu-Yan Wang, ShanghaiDao-Rong Wang, YangzhouDe-Sheng Wang, Xi’anChun-You Wang, WuhanGe Wang, ChongqingXi-Shan Wang, HarbinWei-hong Wang, BeijingZhen-Ning Wang, ShenyangWai Man Raymond Wong, Hong KongChun-Ming Wong, Hong KongJian Wu, ShanghaiSheng-Li Wu, Xi’anWu-Jun Wu, Xi’anQing Xia, ChengduYan Xin, ShenyangDong-Ping Xu, BeijingJian-Min Xu, ShanghaiWei Xu, ChangchunMing Yan, JinanXin-Min Yan, KunmingYi-Qun Yan, ShanghaiFeng Yang, ShanghaiYong-Ping Yang, BeijingHe-Rui Yao, GuangzhouThomas Yau, Hong KongWinnie Yeo, Hong KongJing You, KunmingJian-Qing Yu, WuhanYing-Yan Yu, ShanghaiWei-Zheng Zeng, ChengduZong-Ming Zhang, BeijingDian-Liang Zhang, QingdaoYa-Ping Zhang, ShijiazhuangYou-Cheng Zhang, LanzhouJian-Zhong Zhang, BeijingJi-Yuan Zhang, BeijingHai-Tao Zhao, BeijingJian Zhao, ShanghaiJian-Hong Zhong, NanningYing-Qiang Zhong, GuangzhouPing-Hong Zhou, ShanghaiYan-Ming Zhou, XiamenTong Zhou, NanchongLi-Ming Zhou, ChengduGuo-Xiong Zhou, NantongFeng-Shang Zhu, ShanghaiJiang-Fan Zhu, ShanghaiZhao-Hui Zhu, Beijing
CroatiaTajana Filipec Kanizaj, ZagrebMario Tadic, Zagreb
CubaDamian Casadesus, Havana
CzechJan Bures, Hradec KraloveMarcela Kopacova, Hradec Kralove
Otto Kucera, Hradec KraloveMarek Minarik, PraguePavel Soucek, PragueMiroslav Zavoral, Prague
DenmarkVibeke Andersen, OdenseE Michael Danielsen, Copenhagen
EgyptMohamed MM Abdel-Latif, AssiutHussein Atta, CairoAshraf Elbahrawy, CairoMortada Hassan El-Shabrawi, CairoMona El Said El-Raziky, CairoElrashdy M Redwan, New Borg AlrabZeinab Nabil Ahmed Said, CairoRagaa HM Salama, AssiutMaha Maher Shehata, Mansoura
EstoniaMargus Lember, TartuTamara Vorobjova, Tartu
FinlandMarko Kalliomäki, TurkuThomas Kietzmann, OuluKaija-Leena Kolho, HelsinkiEija Korkeila, TurkuHeikki Makisalo, HelsinkiTanja Pessi, Tampere
FranceArmando Abergel Clermont, FerrandElie K Chouillard, PolssyPierre Cordelier, ToulousePascal P Crenn, GarchesCatherine Daniel, LilleFanny Daniel, ParisCedric Dray, ToulouseBenoit Foligne, LilleJean-Noel Freund, StrasbourgHervé Guillou, ToulouseNathalie Janel, ParisMajid Khatib, BordeauxJacques Marescaux, StrasbourgJean-Claude Marie, ParisDriffa Moussata, Pierre BeniteHang Nguyen, Clermont-FerrandHugo Perazzo, ParisAlain L Servin, Chatenay-MalabryChang Xian Zhang, Lyon
GermanyStavros A Antoniou, MonchengladbachErwin Biecker, SiegburgHubert E Blum, Freiburg
Thomas Bock, BerlinKatja Breitkopf-Heinlein, MannheimElke Cario, EssenGüralp Onur Ceyhan, MunichAngel Cid-Arregui, HeidelbergMichael Clemens Roggendorf, MünchenChristoph F Dietrich, Bad MergentheimValentin Fuhrmann, HamburgNikolaus Gassler, AachenAndreas Geier, WuerzburgMarkus Gerhard, MunichAnton Gillessen, MuensterThorsten Oliver Goetze, OffenbachDaniel Nils Gotthardt, HeidelbergRobert Grützmann, DresdenThilo Hackert, HeidelbergClaus Hellerbrand, RegensburgHarald Peter Hoensch, DarmstadtJens Hoeppner, FreiburgRichard Hummel, MuensterJakob Robert Izbicki, HamburgGernot Maximilian Kaiser, EssenMatthias Kapischke, HamburgMichael Keese, FrankfurtAndrej Khandoga, MunichJorg Kleeff, MunichAlfred Koenigsrainer, TuebingenPeter Christopher Konturek, SaalfeldMichael Linnebacher, RostockStefan Maier, KaufbeurenOliver Mann, HamburgMarc E Martignoni, MunicThomas Minor, BonnOliver Moeschler, OsnabrueckJonas Mudter, EutinSebastian Mueller, HeidelbergMatthias Ocker, BerlinAndreas Ommer, EssenAlbrecht Piiper, FrankfurtEsther Raskopf, BonnChristoph Reichel, Bad BrückenauElke Roeb, GiessenUdo Rolle, FrankfurtKarl-Herbert Schafer, ZweibrückenPeter Schemmer, HeidelbergAndreas G Schreyer, RegensburgManuel A Silva, PenzbergGeorgios C Sotiropoulos, EssenUlrike S Stein, BerlinDirk Uhlmann, LeipzigMichael Weiss, Halle Hong-Lei Weng, MannheimKarsten Wursthorn, Hamburg
GreeceAlexandra Alexopoulou, AthensNikolaos Antonakopoulos, AthensStelios F Assimakopoulos, PatrasGrigoris Chatzimavroudis, ThessalonikiEvangelos Cholongitas, ThessalonikiGregory Christodoulidis, LarisaGeorge N Dalekos, LarissaUrania Georgopoulou, AthensEleni Gigi, Thessaloniki
January 1, 2016IIIWJG|www.wjgnet.com

Stavros Gourgiotis, AthensLeontios J Hadjileontiadis, ThessalonikiThomas Hyphantis, IoanninaIoannis Kanellos, ThessalonikiStylianos Karatapanis, RhodesMichael Koutsilieris, AthensSpiros D Ladas, AthensTheodoros K Liakakos, AthensEmanuel K Manesis, AthensSpilios Manolakopoulos, AthensGerassimos John Mantzaris, AthensAthanasios D Marinis, PiraeusNikolaos Ioannis Nikiteas, AthensKonstantinos X Papamichael, AthensGeorge Sgourakis, AthensKonstantinos C Thomopoulos, PatrasKonstantinos Triantafyllou, AthensChristos Triantos, PatrasGeorgios Zacharakis, AthensPetros Zezos, AlexandroupolisDemosthenes E Ziogas, Ioannina
GuatemalaCarlos Maria Parellada, Guatemala
HungaryMihaly Boros, SzegedTamás Decsi, PécsGyula Farkas, SzegedAndrea Furka, DebrecenY vette Mandi, SzegedPeter L Lakatos, BudapestPal Miheller, BudapestTamás Molnar, SzegedAttila Olah, GyorMaria Papp, DebrecenZoltan Rakonczay, SzegedFerenc Sipos, BudapestMiklós Tanyi, DebrecenTibor Wittmann, Szeged
IcelandTryggvi Bjorn Stefánsson, Reykjavík
IndiadBrij B Agarwal, New DelhiDeepak N Amarapurkar, Mumbai Shams ul Bari, SrinagarSriparna Basu, VaranasiRunu Chakravarty, KolkataDevendra C Desai, Mumbai Nutan D Desai, MumbaiSuneela Sunil Dhaneshwar, PuneRadha K Dhiman, ChandigarhPankaj Garg, MohaliUday C Ghoshal, LucknowKalpesh Jani, VadodaraPremashis Kar, New DelhiJyotdeep Kaur, ChandigarhRakesh Kochhar, Chandigarh
Pradyumna K Mishra, MumbaiAsish K Mukhopadhyay, KolkataImtiyaz Murtaza, SrinagarP Nagarajan, New DelhiSamiran Nundy, DelhiGopal Pande, HyderabadBenjamin Perakath, VelloreArun Prasad, New DelhiD Nageshwar Reddy, HyderabadLekha Saha, ChandigarhSundeep Singh Saluja, New DelhiMahesh Prakash Sharma, New DelhiSadiq Saleem Sikora, BangaloreSarman Singh, New DelhiRajeev Sinha, JhansiRupjyoti Talukdar, HyderabadRakesh Kumar Tandon, New DelhiNarayanan Thirumoorthy, Coimbatore
IndonesiaDavid Handojo Muljono, JakartaAndi Utama, Jakarta
IranArezoo Aghakhani, TehranSeyed Mohsen Dehghani, ShirazAhad Eshraghian, ShirazHossein Khedmat, TehranSadegh Massarrat, TehranMarjan Mohammadi, TehranRoja Rahimi, TehranFarzaneh Sabahi, TehranMajid Sadeghizadeh, TehranFarideh Siavoshi, Tehran
IrelandGary Alan Bass, DublinDavid J Brayden, DublinRonan A Cahill, DublinGlen A Doherty, DublinLiam J Fanning, CorkBarry Philip McMahon, DublinRossMcManus, DublinDervla O’Malley, CorkSinead M Smith, Dublin
IsraelDan Carter, Ramat GanJorge-Shmuel Delgado, MetarEli Magen, AshdodNitsan Maharshak, Tel AvivShaul Mordechai, Beer ShevaMenachem Moshkowitz, Tel AvivWilliam Bahij Nseir, NazarethShimon Reif, JerusalemRam Reifen, RehovotAriella Bar-Gil Shitrit, JerusalemNoam Shussman, JerusalemIgor Sukhotnik, HaifaNir Wasserberg, Petach Tiqwa
Jacob Yahav, RehovotDoron Levi Zamir, GederaShira Zelber-Sagi, HaifaRomy Zemel, Petach-Tikva
ItalyLudovico Abenavoli, CatanzaroLuigi Elio Adinolfi, NaplesCarlo Virginio Agostoni, MilanAnna Alisi, RomePiero Luigi Almasio, PalermoDonato Francesco Altomare, BariAmedeo Amedei, FlorencePietro Andreone, BolognaImerio Angriman, PadovaVito Annese, FlorencePaolo Aurello, RomeSalavtore Auricchio, NaplesGian Luca Baiocchi, BresciaGianpaolo Balzano, MilanAntonio Basoli, RomeGabrio Bassotti, San SistoMauro Bernardi, BolognaAlberto Biondi, RomeEnnio Biscaldi, GenovaMassimo Bolognesi, PaduaLuigi Bonavina, MilanoAldo Bove, ChietiRaffaele Bruno, PaviaLuigi Brusciano, NapoliGiuseppe Cabibbo, PalermoCarlo Calabrese, BolognaDaniele Calistri, MeldolaVincenza Calvaruso, PalermoLorenzo Camellini, Reggio EmiliaMarco Candela, Bologna Raffaele Capasso, NaplesLucia Carulli, ModenaRenato David Caviglia, RomeLuigina Cellini, ChietiGiuseppe Chiarioni, VeronaClaudio Chiesa, RomeMichele Cicala, RomaRachele Ciccocioppo, PaviaSandro Contini, ParmaGaetano Corso, FoggiaRenato Costi, ParmaAlessandro Cucchetti, BolognaRosario Cuomo, NapoliGiuseppe Currò, MessinaPaola De Nardi, MilanoGiovanni D De Palma, NaplesRaffaele De Palma, NapoliGiuseppina De Petro, BresciaValli De Re, AvianoPaolo De Simone, PisaGiuliana Decorti, TriesteEmanuele Miraglia del Giudice, NapoliIsidoro Di Carlo, CataniaMatteo Nicola Dario Di Minno, NaplesMassimo Donadelli, VeronaMirko D’Onofrio, VeronaMaria Pina Dore, SassariLuca Elli, MilanoMassimiliano Fabozzi, Aosta
January 1, 2016IVWJG|www.wjgnet.com

Massimo Falconi, AnconaEzio Falletto, TurinSilvia Fargion, MilanMatteo Fassan, VeronaGianfranco Delle Fave, RomaAlessandro Federico, NaplesFrancesco Feo, SassariDavide Festi, BolognaNatale Figura, SienaVincenzo Formica, RomeMirella Fraquelli, MilanMarzio Frazzoni, ModenaWalter Fries, MessinaGennaro Galizia, NaplesAndrea Galli, FlorenceMatteo Garcovich, RomeEugenio Gaudio, RomePaola Ghiorzo, GenoaEdoardo G Giannini, GenovaLuca Gianotti, MonzaMaria Cecilia Giron, PadovaAlberto Grassi, RiminiGabriele Grassi, TriesteFrancesco Greco, BergamoLuigi Greco, NaplesAntonio Grieco, RomeFabio Grizzi, RozzanoLaurino Grossi, PescaraSimone Guglielmetti, MilanTiberiu Hershcovici, JerusalemCalogero Iacono, VeronaEnzo Ierardi, BariAmedeo Indriolo, BergamoRaffaele Iorio, NaplesPaola Iovino, SalernoAngelo A Izzo, NaplesLoreta Kondili, RomeFilippo La Torre, RomeGiuseppe La Torre, RomeGiovanni Latella, L’AquilaSalvatore Leonardi, CataniaMassimo Libra, CataniaAnna Licata, PalermoC armela Loguercio, NaplesAmedeo Lonardo, ModenaCarmelo Luigiano, CataniaFrancesco Luzza, CatanzaroGiovanni Maconi, MilanoAntonio Macrì, MessinaMariano Malaguarnera, CataniaFrancesco Manguso, NapoliTommaso Maria Manzia, RomeDaniele Marrelli, SienaGabriele Masselli, RomeSara Massironi, MilanGiuseppe Mazzarella, AvellinoMichele Milella, RomeGiovanni Milito, RomeAntonella d’Arminio Monforte, MilanFabrizio Montecucco, GenoaGiovanni Monteleone, RomeMario Morino, TorinoVincenzo La Mura, MilanGerardo Nardone, NaplesRiccardo Nascimbeni, BresciaGabriella Nesi, FlorenceGiuseppe Nigri, Rome
Erica Novo, TurinVeronica Ojetti, RomeMichele Orditura, NaplesFabio Pace, SeriateLucia Pacifico, RomeOmero Alessandro Paoluzi, RomeValerio Pazienza, San Giovanni RotondoRinaldo Pellicano, TurinAdriano M Pellicelli, RomeNadia Peparini, CiampinoMario Pescatori, RomeAntonio Picardi, RomeAlberto Pilotto, PadovaAlberto Piperno, MonzaAnna Chiara Piscaglia, RomeMaurizio Pompili, RomeFrancesca Romana Ponziani, RomeCosimo Prantera, RomeGirolamo Ranieri, BariCarlo Ratto, TomeBarbara Renga, PerugiaAlessandro Repici, RozzanoMaria Elena Riccioni, RomeLucia Ricci-Vitiani, RomeLuciana Rigoli, MessinaMario Rizzetto, TorinoBallarin Roberto, ModenaRoberto G Romanelli, FlorenceClaudio Romano, MessinaLuca Roncucci, ModenaCesare Ruffolo, TrevisoL ucia Sacchetti, NapoliRodolfo Sacco, PisaLapo Sali, FlorenceRomina Salpini, RomeGiulio Aniello, Santoro TrevisoArmando Santoro, RozzanoEdoardo Savarino, PaduaMarco Senzolo, PaduaAnnalucia Serafino, RomeGiuseppe S Sica, RomePierpaolo Sileri, RomeCosimo Sperti, PaduaVincenzo Stanghellini, BolognaCristina Stasi, FlorenceGabriele Stocco, TriesteRoberto Tarquini, FlorenceMario Testini, BariGuido Torzilli, MilanGuido Alberto Massimo, Tiberio BresciaGiuseppe Toffoli, AvianoAlberto Tommasini, TriesteFrancesco Tonelli, FlorenceCesare Tosetti Porretta, TermeLucio Trevisani, ConaGuglielmo M Trovato, CataniaMariapia Vairetti, PaviaLuca Vittorio Valenti, MilanoMariateresa T Ventura, BariGiuseppe Verlato, VeronaMarco Vivarelli, AnconaGiovanni Li Volti, CataniaGiuseppe Zanotti, PaduaVincenzo Zara, LecceGianguglielmo Zehender, MilanAnna Linda Zignego, FlorenceRocco Antonio Zoccali, Messina
Angelo Zullo, Rome
JapanYasushi Adachi, SapporoTakafumi Ando, NagoyaMasahiro Arai, TokyoMakoto Arai, ChibaTakaaki Arigami, KagoshimaItaru Endo,YokohamaMunechika Enjoji, FukuokaShunji Fujimori, TokyoYasuhiro Fujino, AkashiToshiyoshi Fujiwara, OkayamaYosuke Fukunaga, TokyoToshio Fukusato, TokyoTakahisa Furuta, HamamatsuOsamu Handa, KyotoNaoki Hashimoto, OsakaYoichi Hiasa, ToonMasatsugu Hiraki, SagaSatoshi Hirano, SapporoKeiji Hirata, FukuokaToru Hiyama, HigashihiroshimaAkira Hokama, NishiharaShu Hoteya, TokyoMasao Ichinose, WakayamaTatsuya Ide, KurumeMasahiro Iizuka, AkitaToshiro Iizuka, TokyoKenichi Ikejima, TokyoTetsuya Ikemoto, TokushimaHiroyuki Imaeda, SaitamaAtsushi Imagawa, Kan-onjiHiroo Imazu, TokyoShuji Isaji, TsuToru Ishikawa, NiigataToshiyuki Ishiwata, TokyoSoichi Itaba, KitakyushuYoshiaki Iwasaki, OkayamaTatehiro Kagawa, IseharaSatoru Kakizaki, MaebashiNaomi Kakushima, ShizuokaTerumi Kamisawa, TokyoAkihide Kamiya, IseharaOsamu Kanauchi, TokyoTatsuo Kanda, ChibaShin Kariya, OkayamaShigeyuki Kawa, MatsumotoTakumi Kawaguchi, KurumeTakashi Kawai, TokyoSoo Ryang Kim, KobeShinsuke Kiriyama, GunmaTsuneo Kitamura, UrayasuMasayuki Kitano, OsakasayamaHirotoshi Kobayashi, TokyoHironori Koga, KurumeTakashi Kojima, SapporoSatoshi Kokura, KyotoShuhei Komatsu, KyotoTadashi Kondo, TokyoYasuteru Kondo, SendaiYasuhiro Kuramitsu, YamaguchiYukinori Kurokawa, OsakaShin Maeda, YokohamaKoutarou Maeda, Toyoake
January 1, 2016VWJG|www.wjgnet.com

Hitoshi Maruyama, ChibaAtsushi Masamune, SendaiHiroyuki Matsubayashi, SuntogunAkihisa Matsuda, InzaiHirofumi Matsui, TsukubaAkira Matsumori, KyotoYoichi Matsuo, NagoyaY Matsuzaki, AmiToshihiro Mitaka, SapporoKouichi Miura, AkitaShinichi Miyagawa, MatumotoEiji Miyoshi, SuitaToru Mizuguchi, SapporoNobumasa Mizuno, NagoyaZenichi Morise, NagoyaTomohiko Moriyama, FukuokaKunihiko Murase, Tusima Michihiro Mutoh, TsukijiAkihito Nagahara, TokyoHikaru Nagahara, TokyoHidenari Nagai, TokyoKoichi Nagata, Shimotsuke-shiMasaki Nagaya, KawasakiHisato Nakajima, Nishi-ShinbashiToshifusa Nakajima, TokyoHiroshi Nakano, KawasakiHiroshi Nakase, KyotoToshiyuki Nakayama, NagasakiTakahiro Nakazawa, NagoyaShoji Natsugoe, Kagoshima CityTsutomu Nishida, SuitaShuji Nomoto, NaogyaSachiyo Nomura, TokyoTakeshi Ogura, TakatsukishiNobuhiro Ohkohchi, TsukubaToshifumi Ohkusa, KashiwaHirohide Ohnishi, AkitaTeruo Okano, TokyoSatoshi Osawa, HamamatsuMotoyuki Otsuka, TokyoMichitaka Ozaki, SapporoSatoru Saito, YokohamaNaoaki Sakata, SendaiKen Sato, MaebashiToshiro Sato, TokyoTomoyuki Shibata, ToyoakeTomohiko Shimatani, KureYukihiro Shimizu, NantoTadashi Shimoyama, HirosakiMasayuki Sho, NaraIkuo Shoji, KobeAtsushi Sofuni, TokyoTakeshi Suda, NiigataM Sugimoto, HamamatsuKen Sugimoto, HamamatsuHaruhiko Sugimura, HamamatsuShoichiro Sumi, KyotoHidekazu Suzuki, TokyoMasahiro Tajika, NagoyaHitoshi Takagi, TakasakiToru Takahashi, NiigataYoshihisa Takahashi, TokyoShinsuke Takeno, FukuokaAkihiro Tamori, OsakaKyosuke Tanaka, TsuShinji Tanaka, Hiroshima
Atsushi Tanaka, TokyoYasuhito Tanaka, NagoyaShinji Tanaka, TokyoMinoru Tomizawa, Yotsukaido CityKyoko Tsukiyama-Kohara, KagoshimaTakuya Watanabe, NiigataKazuhiro Watanabe, SendaiSatoshi Yamagiwa, NiigataTakayuki Yamamoto, YokkaichiHiroshi Yamamoto, OtsuKosho Yamanouchi, NagasakiIchiro Yasuda, GifuYutaka Yata, Maebashi-cityShin-ichi Yokota, SapporoNorimasa Yoshida, KyotoHiroshi Yoshida, Tama-CityHitoshi Yoshiji, KashiharaKazuhiko Yoshimatsu, TokyoKentaro Yoshioka, ToyoakeNobuhiro Zaima, Nara
JordanKhaled Ali Jadallah, Irbid
KuwaitIslam Khan, Kuwait
LebanonBassam N Abboud, BeirutKassem A Barada, BeirutMarwan Ghosn, BeirutIyad A Issa, BeirutFadi H Mourad, BeirutAIa Sharara, BeirutRita Slim, Beirut
LithuaniaAntanas Mickevicius, Kaunas
MalaysiaHuck Joo Tan, Petaling Jaya
MexicoRichard A Awad, Mexico CityCarlos R Camara-Lemarroy, MonterreyNorberto C Chavez-Tapia, Mexico CityWolfgang Gaertner, Mexico CityDiego Garcia-Compean, MonterreyArturo Panduro, GuadalajaraOT Teramoto-Matsubara, Mexico CityFelix Tellez-Avila, Mexico CityOmar Vergara-Fernandez, Mexico CitySaúl Villa-Trevino, Cuidad de México
MoroccoSamir Ahboucha, Khouribga
NetherlandsRobert J de Knegt, RotterdamTom Johannes Gerardus Gevers, NijmegenMenno Hoekstra, LeidenBW Marcel Spanier, ArnhemKarel van Erpecum, Utrecht
New ZealandLeo K Cheng, AucklandAndrew Stewart Day, ChristchurchJonathan Barnes Koea, AucklandMax Petrov, Auckland
NigeriaOlufunmilayo Adenike Lesi, LagosJesse Abiodun Otegbayo, IbadanStella Ifeanyi Smith, Lagos
NorwayTrond Berg, OsloTrond Arnulf Buanes, KrokkleivaThomas de Lange, RudMagdy El-Salhy, StordRasmus Goll, TromsoDag Arne Lihaug Hoff, Aalesund
PakistanZaigham Abbas, KarachiUsman A Ashfaq, FaisalabadMuhammad Adnan Bawany, HyderabadMuhammad Idrees, LahoreSaeed Sadiq Hamid, KarachiYasir Waheed, Islamabad
PolandThomas Brzozowski, CracowMagdalena Chmiela, LodzKrzysztof Jonderko, SosnowiecAnna Kasicka-Jonderko, SosnowiecMichal Kukla, KatowiceTomasz Hubert Mach, KrakowAgata Mulak, WroclawDanuta Owczarek, KrakówPiotr Socha, WarsawPiotr Stalke, GdanskJulian Teodor Swierczynski, GdanskAnna M Zawilak-Pawlik, Wroclaw
PortugalMarie Isabelle Cremers, SetubalCeu Figueiredo, PortoAna Isabel Lopes, LIsbonM Paula Macedo, LisboaRicardo Marcos, PortoRui T Marinho, LisboaGuida Portela-Gomes, Estoril
January 1, 2016VIWJG|www.wjgnet.com

Filipa F Vale, Lisbon
Puerto RicoCaroline B Appleyard, Ponce
QatarAbdulbari Bener, Doha
RomaniaMihai Ciocirlan, BucharestDan LucianDumitrascu, Cluj-NapocaCarmen Fierbinteanu-Braticevici, BucharestRomeo G Mihaila, SibiuLucian Negreanu, BucharestAdrian Saftoiu, CraiovaAndrada Seicean, Cluj-NapocaIoan Sporea, TimisoaraLetiţia Adela Maria Streba, CraiovaAnca Trifan, Iasi
RussiaVictor Pasechnikov, StavropolVasiliy Ivanovich Reshetnyak, MoscowVitaly Skoropad, Obninsk
Saudi ArabiaAbdul-Wahed N Meshikhes, DammamM Ezzedien Rabie, Khamis Mushait
SingaporeBrian KP Goh, SingaporeRichie Soong, SingaporeKer-Kan Tan, SingaporeKok-Yang Tan, SingaporeYee-Joo Tan, SingaporeMark Wong, SingaporeHong Ping Xia, Singapore
SloveniaMatjaz Homan, LjubljanaMartina Perse, Ljubljana
South KoreaSang Hoon Ahn, SeoulSeung Hyuk Baik, SeoulSoon Koo Baik, WonjuSoo-Cheon Chae, IksanByung-Ho Choe, DaeguSuck Chei Choi, IksanHoon Jai Chun, SeoulYeun-Jun Chung, SeoulYoung-Hwa Chung, SeoulKi-Baik Hahm, SeongnamSang Young Han, Busan
Seok Joo Han, SeoulSeung-Heon Hong, IksanJin-Hyeok Hwang, SeoungnamJeong Won Jang, SeoulJin-Young Jang, SeoulDae-Won Jun, SeoulYoung Do Jung, KwangjuGyeong Hoon Kang, SeoulSung-Bum Kang, SeoulKoo Jeong Kang, DaeguKi Mun Kang, JinjuChang Moo Kang, Seodaemun-guGwang Ha Kim, BusanSang Soo Kim, Goyang-siJin Cheon Kim, SeoulTae Il Kim, SeoulJin Hong Kim, SuwonKyung Mo Kim, SeoulKyongmin Kim, SuwonHyung-Ho Kim, SeongnamSeoung Hoon Kim, GoyangSang Il Kim, SeoulHyun-Soo Kim, WonjuJung Mogg Kim, Seoul Dong Yi Kim, GwangjuKyun-Hwan Kim, SeoulJong-Han Kim, AnsanSang Wun Kim, SeoulJa-Lok Ku, SeoulKyu Taek Lee, SeoulHae-Wan Lee, ChuncheonInchul Lee, SeoulJung Eun Lee, SeoulSang Chul Lee, DaejeonSong Woo Lee, Ansan-siHyuk-Joon Lee, SeoulSeong-Wook Lee, YonginKil Yeon Lee, SeoulJong-Inn Lee, SeoulKyung A Lee, SeoulJong-Baeck Lim, SeoulEun-Yi Moon, SeoulSH Noh, SeoulSeung Woon Paik, SeoulWon Sang Park, SeoulSung-Joo Park, IksanKyung Sik Park, DaeguSe Hoon Park, SeoulYoonkyung Park, GwangjuSeung-Wan Ryu, DaeguIl Han Song, CheonanMyeong Jun Song, DaejeonYun Kyoung Yim, DaejeonDae-Yeul Yu Daejeon
SpainMariam Aguas, ValenciaRaul J Andrade, MálagaAntonio Arroyo, ElcheJosep M Bordas, BarcelonaLisardo Boscá, MadridRicardo Robles Campos, MurciaJordi Camps, ReusCarlos Cervera Barcelona
Alfonso Clemente, Granada Pilar Codoner-Franch, ValenciaFernando J Corrales, PamplonaFermin Sánchez de Medina, GranadaAlberto Herreros de Tejada, MajadahondaEnrique de-Madaria, AlicanteJE Dominguez-Munoz, Santiago de CompostelaVicente Felipo, ValenciaCM Fernandez-Rodriguez, MadridCarmen Frontela-Saseta, MurciaJulio Galvez, GranadaMaria Teresa García, VigoMI Garcia-Fernandez, MálagaEmilio Gonzalez-Reimers, La LagunaMarcel Jimenez, BellaterraAngel Lanas, ZaragozaJuan Ramón Larrubia, GuadalajaraAntonio Lopez-Sanroman, MadridVicente Lorenzo-Zuniga, BadalonaAlfredo J Lucendo, TomellosoVicenta Soledad Martinez-Zorzano, VigoJosé Manuel Martin-Villa, MadridJulio Mayol, MadridManuel Morales-Ruiz, BarcelonaAlfredo Moreno-Egea, MurciaAlbert Pares, BarcelonaMaria Pellise, BarcelonaJosé Perea, MadridMiguel Angel Plaza, ZaragozaMaría J Pozo, CáceresEnrique Quintero, La LagunaJose M Ramia, MadridFrancisco Rodriguez-Frias, BarcelonaSilvia Ruiz-Gaspa, BarcelonaXavier Serra-Aracil, BarcelonaVincent Soriano, MadridJavier Suarez, PamplonaCarlos Taxonera, MadridM Isabel Torres, JaénManuel Vazquez-Carrera, BarcelonaBenito Velayos, ValladolidSilvia Vidal, Barcelona
Sri LankaArjuna Priyadarsin De Silva, Colombo
SudanIshag Adam, Khartoum
SwedenRoland G Andersson, LundBergthor Björnsson, LinkopingJohan Christopher Bohr, ÖrebroMauro D’Amato, StockholmThomas Franzen, NorrkopingEvangelos Kalaitzakis, LundRiadh Sadik, GothenburgPer Anders Sandstrom, LinkopingErvin Toth, MalmöKonstantinos Tsimogiannis, VasterasApostolos V Tsolakis, Uppsala
January 1, 2016VIIWJG|www.wjgnet.com

SwitzerlandGieri Cathomas, LiestalJean Louis Frossard, GeneveChristian Toso, GenevaStephan Robert Vavricka, ZurichDominique Velin, Lausanne
ThailandThawatchai Akaraviputh, BangkokP Yoysungnoen Chintana, PathumthaniVeerapol Kukongviriyapan, MuangVijittra Leardkamolkarn, BangkokVarut Lohsiriwat, BangkokSomchai Pinlaor, Khaon KaenD Wattanasirichaigoon, Bangkok
Trinidad and TobagoB Shivananda Nayak, Mount Hope
TunisiaIbtissem Ghedira, SousseLilia Zouiten-Mekki, Tunis
TurkeyInci Alican, IstanbulMustafa Altindis, SakaryaMutay Aslan, AntalyaOktar Asoglu, IstanbulYasemin Hatice Balaban, IstanbulMetin Basaranoglu, AnkaraYusuf Bayraktar, Ankara Süleyman Bayram, AdiyamanAhmet Bilici, IstanbulAhmet Sedat Boyacioglu, AnkaraZüleyha Akkan Cetinkaya, Kocaeli Cavit Col, BoluYasar Colak, IstanbulCagatay Erden Daphan, KirikkaleMehmet Demir, HatayAhmet Merih Dobrucali, IstanbulGülsüm Ozlem Elpek, AntalyaAyse Basak Engin, AnkaraEren Ersoy, AnkaraOsman Ersoy, AnkaraYusuf Ziya Erzin, IstanbulMukaddes Esrefoglu, IstanbulLevent Filik, AnkaraOzgur Harmanci, AnkaraKoray Hekimoglu, AnkaraAbdurrahman Kadayifci, GaziantepCem Kalayci, IstanbulSelin Kapan, IstanbulHuseyin Kayadibi, AdanaSabahattin Kaymakoglu, IstanbulMetin Kement, IstanbulMevlut Kurt, BoluResat Ozaras, IstanbulElvan Ozbek, Adapazari
Cengiz Ozcan, MersinHasan Ozen, AnkaraHalil Ozguc, BursaMehmet Ozturk, IzmirOrhan V Ozkan, SakaryaSemra Paydas, AdanaOzlem Durmaz Suoglu, IstanbulIlker Tasci, AnkaraMüge Tecder-ünal, AnkaraMesut Tez, AnkaraSerdar Topaloglu, TrabzonMurat Toruner, AnkaraGokhan Tumgor, AdanaOguz Uskudar, AdanaMehmet Yalniz, ElazigMehmet Yaman, ElazigVeli Yazisiz, AntalyaYusuf Yilmaz, IstanbulOzlem Yilmaz, IzmirOya Yucel, IstanbulIlhami Yuksel, Ankara
United KingdomNadeem Ahmad Afzal, SouthamptonNavneet K Ahluwalia, StockportYeng S Ang, LancashireRamesh P Arasaradnam, CoventryIan Leonard Phillip Beales, NorwichJohn Beynon, SwanseaBarbara Braden, OxfordSimon Bramhall, BirminghamGeoffrey Burnstock, LondonIan Chau, SuttonThean Soon Chew, LondonHelen G Coleman, BelfastAnil Dhawan, LondonSunil Dolwani, CardiffPiers Gatenby, LondonAnil T George, LondonPasquale Giordano, LondonPaul Henderson, EdinburghGeorgina Louise Hold, AberdeenStefan Hubscher, BirminghamRobin D Hughes, LondonNusrat Husain, ManchesterMatt W Johnson, LutonKonrad Koss, MacclesfieldAnastasios Koulaouzidis, EdinburghSimon Lal, SalfordJohn S Leeds, AberdeenJK K Limdi, ManchesterHongxiang Liu, CambridgeMichael Joseph McGarvey, LondonMichael Anthony Mendall, LondonAlexander H Mirnezami, SouthamptonJ Bernadette Moore, GuildfordClaudio Nicoletti, NorwichSavvas Papagrigoriadis, LondonSylvia LF Pender, SouthamptonDavid Mark Pritchard, LiverpoolJames A Ross, EdinburghKamran Rostami, WorcesterXiong Z Ruan, LondonFrank I Tovey, LondonDhiraj Tripathi, Birmingham
Vamsi R Velchuru, Great YarmouthNicholas T Ventham, EdinburghDiego Vergani, LondonJack Westwood Winter, GlasgowTerence Wong, LondonLing Yang, Oxford
United StatesDaniel E Abbott, CincinnatiGhassan K Abou-Alfa, New YorkJulian Abrams, New YorkDavid William Adelson, Los AngelesJonathan Steven Alexander, ShreveportTauseef Ali, Oklahoma CityMohamed R Ali, SacramentoRajagopal N Aravalli, MinneapolisHassan Ashktorab, WashingtonShashi Bala, WorcesterCharles F Barish, RaleighP Patrick Basu, New YorkRobert L Bell, Berkeley HeightsDavid Bentrem, ChicagoHenry J Binder, New HavenJoshua Bleier, PhiladelphiaWojciech Blonski, Johnson CityKenneth Boorom, CorvallisBrian Boulay, ChicagoCarla W Brady, DurhamKyle E Brown, Iowa CityAdeel A Butt, PittsburghWeibiao Cao, ProvidenceAndrea Castillo, CheneyFernando J Castro, WestonAdam S Cheifetz, BostonXiaoxin Luke Chen, DurhamRamsey Cheung, Palo AltoParimal Chowdhury, Little RockEdward John Ciaccio, New YorkDahn L Clemens, OmahaYingzi Cong, GalvestonLaura Iris Cosen-Binker, BostonJoseph John Cullen, LowaMark J Czaja, BronxMariana D Dabeva, BronxChristopher James Damman, SeattleIsabelle G De Plaen, ChicagoPunita Dhawan, NashvilleHui Dong, La JollaWael El-Rifai, NashvilleSukru H Emre, New HavenPaul Feuerstadt, HamdenJosef E Fischer, BostonLaurie N Fishman, BostonJoseph Che Forbi, AtlantaTemitope Foster, AtlantaAmy E Foxx-Orenstein, ScottsdaleDaniel E Freedberg, New YorkShai Friedland, Palo AltoVirgilio George, IndianapolisAjay Goel, DallasOliver Grundmann, GainesvilleStefano Guandalini, ChicagoChakshu Gupta, St. JosephGrigoriy E Gurvits, New York
January 1, 2016VIIIWJG|www.wjgnet.com

Xiaonan Han, CincinnatiMohamed Hassan, JacksonMartin Hauer-Jensen, Little RockKoichi Hayano, BostonYingli Hee, AtlantaSamuel B Ho, San DiegoJason Ken Hou, HoustonLifang Hou, ChicagoK-Qin Hu, OrangeJamal A Ibdah, ColumbiaRobert Thomas Jensen, BethesdaHuanguang “Charlie” Jia, GainesvilleRome Jutabha, Los AngelesAndreas M Kaiser, Los AngelesAvinash Kambadakone, BostonDavid Edward Kaplan, PhiladelphiaRandeep Kashyap, RochesterRashmi Kaul, TulsaAli Keshavarzian, ChicagoAmir Maqbul Khan, MarshallNabeel Hasan Khan, New OrleansSahil Khanna, RochesterKusum K Kharbanda, OmahaHyun Sik Kim, PittsburghJoseph Kim, DuarteJae S Kim, GainesvilleMiran Kim, ProvidenceTimothy R Koch, WashingtonBurton I Korelitz, New YorkBetsy Kren, MinneapolisShiu-Ming Kuo, BuffaloMichelle Lai, BostonAndreas Larentzakis, BostonEdward Wolfgang Lee, Los AngelesDaniel A Leffler, BostonMichael Leitman, New YorkSuthat Liangpunsakul, IndianapolisJoseph K Lim, New HavenElaine Y Lin, BronxHenry C Lin, AlbuquerqueRohit Loomba, La JollaJames David Luketich, Pittsburgh
Li Ma, StanfordMohammad F Madhoun, Oklahoma CityThomas C Mahl, BuffaloAshish Malhotra, BettendorfPranoti Mandrekar, WorcesterJohn Marks, WynnewoodWendy M Mars, PittsburghJulien Vahe Matricon, San AntonioCraig J McClain, LouisvilleTamir Miloh, PhoenixAyse Leyla Mindikoglu, BaltimoreHuanbiao Mo, DentonKlaus Monkemuller, BirminghamJohn Morton, StanfordAdnan Muhammad, TampaMichael J Nowicki, JacksonPatrick I Okolo, BaltimoreGiusepp Orlando, Winston SalemNatalia A Osna, OmahaVirendra N Pandey, NewarkMansour A Parsi, Cleveland Michael F Picco, JacksonvilleDaniel S Pratt, BostonXiaofa Qin, NewarkJanardan K Reddy, ChicagoVictor E Reyes, GalvestonJon Marc Rhoads, HoustonGiulia Roda, New YorkJean-Francois Armand Rossignol, TampaPaul A Rufo, BostonMadhusudana Girija Sanal, New York Miguel Saps, ChicagoSushil Sarna, GalvestonAnn O Scheimann, BaltimoreBernd Schnabl, La JollaMatthew J Schuchert, PittsburghEkihiro Seki, La JollaChanjuan Shi, NashvilleDavid Quan Shih, Los AngelesShadab A Siddiqi, OrlandoWilliam B Silverman, Iowa CityShashideep Singhal, New York
Bronislaw L Slomiany, NewarkSteven F Solga, BethlehemByoung-Joon Song, BethesdaDario Sorrentino, RoanokeScott R Steele, Fort LewisBranko Stefanovic, TallahasseeArun Swaminath, New YorkKazuaki Takabe, RichmondNaoki Tanaka, BethesdaHans Ludger Tillmann, DurhamGeorge Triadafilopoulos, StanfordJohn Richardson Thompson, NashvilleAndrew Ukleja, WestonMiranda AL van Tilburg, Chapel HillGilberto Vaughan, AtlantaVijayakumar Velu, AtlantaGebhard Wagener, New YorkKasper Saonun Wang, Los AngelesXiangbing Wang, New BrunswickDaoyan Wei, HoustonTheodore H Welling, Ann ArborC Mel Wilcox, BirminghamJacqueline Lee Wolf, BostonLaura Ann Woollett, CincinnatiHarry Hua-Xiang Xia, East HanoverWen Xie, PittsburghGuang Yu Yang, ChicagoMichele T Yip-Schneider, IndianapolisSam Zakhari, BethesdaKezhong Zhang, DetroitHuiping Zhou, RichmondXiao-Jian Zhou, CambridgeRichard Zubarik, Burlington
VenezuelaMiguel Angel Chiurillo, Barquisimeto
VietnamVan Bang Nguyen, Hanoi
January 1, 2016IXWJG|www.wjgnet.com

S
EDITORIAL
5623 Symbioticchemo-andimmuno-therapyforhepatitisBandCviruses
Agrawal B, Kumar R
TOPIC HIGHLIGHT
5627 Liquidbiopsyinpatientswithpancreaticcancer:Circulatingtumorcellsandcell-freenucleicacids
Imamura T, Komatsu S, Ichikawa D, Kawaguchi T, Miyamae M, Okajima W, Ohashi T, Arita T, Konishi H, Shiozaki A,
Morimura R, Ikoma H, Okamoto K, Otsuji E
5642 Lightandsound-emergingimagingtechniquesforinflammatoryboweldisease
Knieling F, Waldner MJ
5655 Oralpathologyininflammatoryboweldisease
Muhvić-Urek M, Tomac-Stojmenović M, Mijandrušić-Sinčić B
5668 Genomicdiversityofcolorectalcancer:Changinglandscapeandemergingtargets
Ahn DH, Ciombor KK, Mikhail S, Bekaii-Saab T
5678 Newtrendsinmolecularandcellularbiomarkerdiscoveryforcolorectalcancer
Aghagolzadeh P, Radpour R
5694 Laparoscopicandrobot-assistedgastrectomyforgastriccancer:Currentconsiderations
Caruso S, Patriti A, Roviello F, De Franco L, Franceschini F, Coratti A, Ceccarelli G
5718 Preoperative,intraoperativeandpostoperativeriskfactorsforanastomoticleakageafterlaparoscopiclow
anteriorresectionwithdoublestaplingtechniqueanastomosis
Kawada K, Sakai Y
REVIEW
5728 Hepatopulmonarysyndrome:Whatweknowandwhatwewouldliketoknow
Grilo-Bensusan I, Pascasio-Acevedo JM
5742 GutdysfunctioninParkinson'sdisease
Mukherjee A, Biswas A, Das SK
Contents Weekly Volume 22 Number 25 July 7, 2016
� July 7, 2016|Volume 22|�ssue 25|WJG|www.wjgnet.com

ContentsWorld Journal of Gastroenterology
Volume 22 Number 25 July 7, 2016
MINIREVIEWS
5753 Aceticacidchromoendoscopy:ImprovingneoplasiadetectioninBarrett'sesophagus
Chedgy FJQ, Subramaniam S, Kandiah K, Thayalasekaran S, Bhandari P
ORIGINAL ARTICLE
Basic Study
5761 Roleofsexhormonesingastrointestinalmotilityinpregnantandnon-pregnantrats
Matos JF, Americo MF, Sinzato YK, Volpato GT, Corá LA, Calabresi MFF, Oliveira RB, Damasceno DC, Miranda JRA
5769 UrotensinⅡ-inducedinsulinresistanceismediatedbyNADPHoxidase-derivedreactiveoxygenspeciesin
HepG2cells
Li YY, Shi ZM, Yu XY, Feng P, Wang XJ
Retrospective Study
5780 Nationwidetrendsandpredictorsofinpatientmortalityin83884transjugularintrahepaticportosystemic
shunt
Lee EW, Kuei A, Saab S, Busuttil RW, Durazo F, Han SH, El-Kabany MM, McWilliams JP, Kee ST
5790 Clinicalanalysisofpatientswithhepatocellularcarcinomarecurrenceafterliving-donorliver
transplantation
Na GH, Hong TH, You YK, Kim DG
Observational Study
5800 Acceptanceoflivingliverdonationamongmedicalstudents:AmulticenterstratifiedstudyfromSpain
Ríos A, López-Navas AI, López-López AI, Gómez FJ, Iriarte J, Herruzo R, Blanco G, Llorca FJ, Asunsolo A, Sánchez-Gallegos P,
Gutiérrez PR, Fernández A, de Jesús MT, Martínez-Alarcón L, Lana A, Fuentes L, Hernández JR, Virseda J, Yelamos J, Bondía JA,
Hernández AM, Ayala MA, Ramírez P, Parrilla P
5814 LowexpressionofARID1Acorrelateswithpoorprognosisinintrahepaticcholangiocarcinoma
Yang SZ, Wang AQ, Du J, Wang JT, Yu WW, Liu Q, Wu YF, Chen SG
5822 Establishmentofanested-ASP-PCRmethodtodeterminetheclarithromycinresistanceofHelicobacter
pylori
Luo XF, Jiao JH, Zhang WY, Pu HM, Qu BJ, Yang BY, Hou M, Ji MJ
Randomized Controlled Trial
5831 Hemostaticeffectoftopicalhemocoagulasesprayindigestiveendoscopy
Wang T, Wang DN, Liu WT, Zheng ZQ, Chen X, Fang WL, Li S, Liang L, Wang BM
�� July 7, 2016|Volume 22|�ssue 25|WJG|www.wjgnet.com

ContentsWorld Journal of Gastroenterology
Volume 22 Number 25 July 7, 2016
SYSTEMATIC REVIEWS5837 TowardssafeinjectionpracticesforpreventionofhepatitisCtransmissioninSouthAsia:Challengesand
progress
Janjua NZ, Butt ZA, Mahmood B, Altaf A
5853 Gastrointestinalandliverinfectionsinchildrenundergoingantineoplasticchemotherapyintheyears2000
Castagnola E, Ruberto E, Guarino A
��� July 7, 2016|Volume 22|�ssue 25|WJG|www.wjgnet.com

NAMEOFJOURNALWorld Journal of Gastroenterology
ISSNISSN 1007-9327 (print)ISSN 2219-2840 (online)
LAUNCHDATEOctober 1, 1995
FREQUENCYWeekly
EDITORS-IN-CHIEFDamian Garcia-Olmo, MD, PhD, Doctor, Profes-sor, Surgeon, Department of Surgery, Universidad Autonoma de Madrid; Department of General Sur-gery, Fundacion Jimenez Diaz University Hospital, Madrid 28040, Spain
Stephen C Strom, PhD, Professor, Department of Laboratory Medicine, Division of Pathology, Karo-linska Institutet, Stockholm 141-86, Sweden
Andrzej S Tarnawski, MD, PhD, DSc (Med), Professor of Medicine, Chief Gastroenterology, VA
Long Beach Health Care System, University of Cali-fornia, Irvine, CA, 5901 E. Seventh Str., Long Beach, CA 90822, United States
EDITORIALOFFICEJin-Lei Wang, DirectorXiu-Xia Song, Vice DirectorWorld Journal of GastroenterologyRoom 903, Building D, Ocean International Center, No. 62 Dongsihuan Zhonglu, Chaoyang District, Beijing 100025, ChinaTelephone: +86-10-59080039Fax: +86-10-85381893E-mail: [email protected] Desk: http://www.wjgnet.com/esps/helpdesk.aspxhttp://www.wjgnet.com
PUBLISHERBaishideng Publishing Group Inc8226 Regency Drive, Pleasanton, CA 94588, USATelephone: +1-925-223-8242Fax: +1-925-223-8243E-mail: [email protected] Desk: http://www.wjgnet.com/esps/helpdesk.aspxhttp://www.wjgnet.com
Contents
EDITORS FOR THIS ISSUE
Responsible Assistant Editor: Xiang Li Responsible Science Editor: Jing YuResponsible Electronic Editor: Cai-Hong Wang Proofing Editorial Office Director: Jin-Lei WangProofing Editor-in-Chief: Lian-Sheng Ma
PUBLICATIONDATEJuly 7, 2016
COPYRIGHT© 2016 Baishideng Publishing Group Inc. Articles pub-lished by this Open-Access journal are distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license.
SPECIALSTATEMENTAll articles published in journals owned by the Baishideng Publishing Group (BPG) represent the views and opin-ions of their authors, and not the views, opinions or policies of the BPG, except where otherwise explicitly indicated.
INSTRUCTIONSTOAUTHORSFull instructions are available online at http://www.wjgnet.com/bpg/g_info_20160116143427.htm
ONLINESUBMISSIONhttp://www.wjgnet.com/esps/
World Journal of GastroenterologyVolume 22 Number 25 July 7, 2016
Editorial boardmember ofWorld Journal ofGastroenterology , Zhao-HuiZhu,MD,PhD,ChiefDoctor,Head,Professor,StaffPhysician,DepartmentofNuclearMedicine,PekingUnionMedicalCollegeHospital,ChineseAcademyofMedicalScienceandPekingUnionMedicalCollege,Beijing100730,China
World Journal of Gastroenterology (World J Gastroenterol, WJG, print ISSN 1007-9327, online ISSN 2219-2840, DOI: 10.3748) is a peer-reviewed open access journal. WJG was estab-lished on October 1, 1995. It is published weekly on the 7th, 14th, 21st, and 28th each month. The WJG Editorial Board consists of 1376 experts in gastroenterology and hepatology from 68 countries. The primary task of WJG is to rapidly publish high-quality original articles, reviews, and commentaries in the fields of gastroenterology, hepatology, gastrointestinal endos-copy, gastrointestinal surgery, hepatobiliary surgery, gastrointestinal oncology, gastroin-testinal radiation oncology, gastrointestinal imaging, gastrointestinal interventional ther-apy, gastrointestinal infectious diseases, gastrointestinal pharmacology, gastrointestinal pathophysiology, gastrointestinal pathology, evidence-based medicine in gastroenterol-ogy, pancreatology, gastrointestinal laboratory medicine, gastrointestinal molecular biol-ogy, gastrointestinal immunology, gastrointestinal microbiology, gastrointestinal genetics, gastrointestinal translational medicine, gastrointestinal diagnostics, and gastrointestinal therapeutics. WJG is dedicated to become an influential and prestigious journal in gas-troenterology and hepatology, to promote the development of above disciplines, and to improve the diagnostic and therapeutic skill and expertise of clinicians.
World Journal of Gastroenterology is now indexed in Current Contents®/Clinical Medicine, Science Citation Index Expanded (also known as SciSearch®), Journal Citation Reports®, Index Medi-cus, MEDLINE, PubMed, PubMed Central, Digital Object Identifier, and Directory of Open Access Journals. The 2015 edition of Journal Citation Reports® released by Thomson Reuters (ISI) cites the 2015 impact factor for WJG as 2.787 (5-year impact factor: 2.848), ranking WJG as 38 among 78 journals in gastroenterology and hepatology (quartile in category Q2).
I-IX EditorialBoard
ABOUT COVER
INDEXING/ABSTRACTING
AIMS AND SCOPE
FLYLEAF
�V July 7, 2016|Volume 22|�ssue 25|WJG|www.wjgnet.com

Symbiotic chemo- and immuno-therapy for hepatitis B and C viruses
Babita Agrawal, Rakesh Kumar
Babita Agrawal, Department of Surgery, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, AB T6G 2R3, Canada
Rakesh Kumar, Department of Laboratory Medicine and Pathology, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, AB T6G 2R3, Canada
Author contributions: Agrawal B and Kumar R wrote the manuscript.
Conflict-of-interest statement: Agrawal B and Kumar R have no conflict of interest to declare.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Manuscript source: Invited manuscript
Correspondence to: Dr. Rakesh Kumar, Professor, Depart-ment of Laboratory Medicine and Pathology, Faculty of Medicine and Dentistry, University of Alberta, 116 St and 85 Ave, Edmonton, AB T6G 2R3, Canada. [email protected]: +1-780-4927545
Received: May 4, 2016Peer-review started: May 4, 2016First decision: May 27, 2016Revised: May 31, 2016Accepted: June 13, 2016 Article in press: June 13, 2016Published online: July 7, 2016
AbstractHepatitis B and C viruses (HBV and HCV), both cause
serious chronic infections leading to fatal liver diseases. The prototype therapy for both HBV and HCV was based on IFN-α with or without ribavirin. The advent of direct-acting antivirals (DAA) for both HBV and HCV has remarkably improved the standard of treatment for both infections. While HCV can be eliminated following combination DAA therapy, HBV persists even after treatment, requiring life-long therapy with DAAs. Treatment with DAAs is also associated with high cost, the development of resistance and side effects. There is ample published evidence that both HBV and HCV can be eliminated from infected host cells through non-cytolytic immune mechanisms. We need to identify the mechanisms behind this successful elimination of replicating viruses and develop them into novel immunotherapeutic regimens. Moreover, a synergy of, chemo- and immuno-therapeutic strategies will be necessary to eradicate HBV or HCV from a host.
Key words: Hepatitis C virus; Hepatitis B virus; Direct-acting antiviral; Chemotherapy; Immunotherapy
© The Author(s) 2016. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Immune related mechanisms have been shown to eliminate both Hepatitis B and C viruses (HBV and HCV) from chronically infected host cells via non-cytolytic mechanisms. Current direct-acting antivirals against replication of both HBV and HCV are effective and provide significant viral suppression in a relatively short period of time. This time window should be harnessed to target host-mediated immune mechanisms to clear the host of the infection. This strategy would lead to a significant reduction in cost, duration, side effects and development of resistance associated with direct-acting antivirals therapy. In summary, regimens combining chemo- and immuno-therapy must be used in a mutually beneficial manner to eradicate HBV and/or HCV from a host.
EDITORIAL
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.3748/wjg.v22.i25.5623
5623 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
World J Gastroenterol 2016 July 7; 22(25): 5623-5626 ISSN 1007-9327 (print) ISSN 2219-2840 (online)
© 2016 Baishideng Publishing Group Inc. All rights reserved.

Agrawal B, Kumar R. Symbiotic chemo- and immuno-therapy for hepatitis B and C viruses. World J Gastroenterol 2016; 22(25): 5623-5626 Available from: URL: http://www.wjgnet.com/1007-9327/full/v22/i25/5623.htm DOI: http://dx.doi.org/10.3748/wjg.v22.i25.5623
INTRODUCTIONHepatitis B and C viruses (HBV and HCV) cause serious chronic infections globally in about 350 million and about 170 million people, respectively, leading to fatal liver diseases such as fibrosis, cirrhosis and hepatocellular carcinoma (HCC). In addition, 7-10 million people are co-infected with both HBV and HCV, resulting in more severe liver disease and increased risks of hepatocellular carcinoma and higher mortality rates compared to mono-infected people[1].
HBV and HCV belong to different families of viruses and have entirely different genomes and modes of replication: HBV belongs to the family Hepadnaviridae, has a partially double stranded circular DNA and replicates through an RNA intermediate via reverse transcription, whereas HCV belongs to the family Flaviviridae, has a single stranded + sense RNA genome and undergoes RNA replication[2,3]. Apart from these major genetic differences, they have many similarities including routes of transmission, hepato-tropism, ability to cause chronic infections, end-stage liver diseases and modulate host immunity. Importantly, both HBV and HCV can also trigger self-clearing acute infections by inducing protective and efficient immune responses in a fraction of infected individuals[2,3].
The very first successful therapy for HBV and HCV infections was immunotherapy with interferon-α (and peginterferon-α) and interferon-α plus ribavirin, respectively[4,5]. While these primitive immunotherapies have been used for decades, their exact mechanisms of action are still unclear and there are severe li-mitations associated with their use[4]. Nevertheless, they provide definitive proof of concept that both HBV and HCV are susceptible to immunotherapeutic regimens and their elimination can be associated with antiviral immune responses.
Great enthusiasm in HBV therapy was realized with the approval of direct acting antiviral (DAA) drug lamivudine, which was followed by the development of the next generation anti-HBV drugs entecavir, tenofovir, adefovir and telbivudine[6,7]. All of these are nucleoside analogs, which inhibit HBV DNA polymerase with varying potentials and have various resistance barriers[5-7]. These nucleosides efficiently suppress viral DNA replication in the majority of patients but seldom induce HBsAg seroconversion, a marker of a “functional cure” and eradication of intracellular virus[5,7]. Therefore, treatment of chronic HBV with these agents requires continued life-long therapy
to achieve sustained inhibition of viral replication. However, this is expensive, and can result in drug toxicities and development of resistant viral strains[5,7]. Long-term suppression of viral DNA replication does indeed lead to the beneficial effects of preventing or reversing liver diseases such as fibrosis, cirrhosis and HCC, and partial restoration of immune responses[5-7]. But while viral DNA synthesis is efficiently inhibited by antiviral nucleosides, they have limited effects on the levels and activity of cccDNA, which can persist for decades in hepatocytes[7,8]. Although it was hypothesized initially that with continued suppression of HBV DNA replication, the pool of cccDNA will eventually diminish to negligible levels that would provide a cure, this expectation has not withstood the test of time[7]. Efforts are continuing to seek new drugs targeted at other steps of the viral replication cycle such as inhibitors of entry, cccDNA formation, secretion, nucleocapsid formation etc[5-8]. Whether or not these approaches will lead to “cure” from chronic HBV infection remains to be seen.
For about 20 years, the combination of interferon and ribavirin (RBV) was the standard of care (SOC) therapy for chronic HCV. This treatment had limited success rates (< 50%) and had severe side effects, which at times discouraged patients to even get treated[9]. The first DAAs approved for HCV therapy were protease inhibitors boceprevir and telaprevir, which were given with the SOC (IFN-α + RBV). Within the last few years, the treatment for HCV has exploded tremendously with the approval of several DAAs, acting directly on various enzymes/steps of HCV replication such as NS3, NS5A, NS5B and NS4. As a result, several interferon-free treatment regimens have been approved for chronic HCV, which include various 2-3 drug combinations comprising of sofosbuvir, ledipasvir, ritonavir, dasabuvir, simeprevir, daclatasavir, ombitasvir, velpatasvir etc[10,11]. These combinations of DAAs lead to sustained viral response (SVR) in about 95% of the treated patients harboring all HCV genotypes except genotype 3. SVR is a clinical surrogate of treatment success defined as an undetectable HCV RNA (< 15 IU/mL) 12 wk (SVR12) and 24 wk (SVR24) after the end of treatment. The patients who achieved SVR did not relapse to HCVRNA+ status upon long-term follow-up (4-5 years), confirming SVR as an indication of cure[12,13]. Even with the 95% success rate, there are several limitations associated with the current all oral DAA regimens such as the very high cost of treatment, emergence of drug resistance, side effects, contraindications for patients with comorbidities, inefficacy in patients with genotype 3, the possibility of reinfection, etc[14]. Also, in real-life situations, patients may not comply with daily drug doses for 3 mo, especially if they are asymptomatic and are not feeling sick. Further, in a number of DAA combination regimens, ribavirin is still being recommended, suggesting that besides simultaneously targeting
5624 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Agrawal B et al . Symbiotic chemo- and immuno-therapy for HBV and HCV

several viral enzymes/processes by DAAs, an immu-nomodulatory component is required. At present, even in the United States, the DAA therapy is being used in < 20% of the diagnosed patients (in some cases, a triage system eliminates people with less-severe liver disease to reduce cost), and many more remain unaware of their infection status. Above all, the accessibility, affordability and questionable success of DAAs in resource-poor populations of the world, where the majority of the 170 million chronic HCV patients reside, remain major issues. Continued efforts are needed to search for more affordable, accessible, compliance-friendly approaches to cure HCV and eradicate it from the world.
Hepatocytes and hepatoma cell lines infected with HBV and/or HCV in cell culture and/or animal models have been investigated extensively to examine immune mediated viral clearance[15,16]. While there are ongoing debates and individual studies demonstrating the role of innate vs adaptive immunity and soluble vs. cellular immune components in viral clearance for both HBV and HCV, one aspect remains clear: non-cytolytic effector mechanisms induced by a number of cytokines and/or a combination of cytokines are most effective in clearing hepatocytes of HBV and/or HCV infections irrespective of whether they are produced by innate immune cells (e.g., NK, NKT) or adaptive immune (CD4+ and CD8+ T) cells. Notably, clearance of long-lived HBV cccDNA from infected hepatocytes has only been demonstrated through immune effector mechanisms mediated by a number of cytokines[16-20]. Obviously, treatment with combinations of effector cytokines is not foreseeable even in the future due to associated toxicities and systemic side effects. Consequently, the research focus must shift towards investigating more natural and balanced ways of inducing physiological levels of these effector molecules at the target organ - liver.
After the discovery of innate receptors such as TLRs, NLRs, RIG1 etc., and the observations that in cell cultures the agonists of the innate receptors such as TLR receptors demonstrate very promising antiviral effects against both HBV and HCV, several synthetic TLR agonists were tested in clinical trials. However, due to the ubiquitous presence of TLRs throughout the body and induction of systemic, non-physiological amounts of cytokines, so far TLR agonists have not succeeded in providing a safe and successful immunotherapeutic approach, which can be used universally[21,22]. Immunotherapeutic vaccine approaches for treatment of chronic HBV and HCV have also not been very attractive because of limitations associated with targeting specific viral epitopes by T cells due to mechanisms including T cell exhaustion, tolerance via anergy and deletion of antigen-specific T cells, viral immune escape mutants etc[5]. There is a need to investigate and discover more natural and regulated means of stimulating physiological levels of immune effector molecules,
which are induced and localized in the target organ, to obtain the viral eradication without associated immuno-toxicities and systemic inflammation.
Traditionally, research has been isolated in two camps with chemists and immunologists working in their own small silos. This approach has led to many groundbreaking discoveries, including the understanding of antiviral immune mechanisms and the direct acting antiviral treatments available to date. What has been remarkably demonstrated in animal models as well as in patients is that specific DAA regimens against both HBV and HCV are highly effective in suppressing viral replication in relatively short period of time. Importantly, this period of active suppression of extensive viral replication is associated with reduction in systemic viral antigens’ levels and associated immune suppression or immune blockade, and restoration of some of the immune components[23]. This time window should be exploited with an im-munotherapy administered on a weekly to monthly schedule that will help stimulate effector functions through innate and/or adaptive immune mechanisms and induce intrinsic non-cytolytic clearance of virus-infected hepatocytes. Such an approach should also allow substantial shortening of the DAA therapy in both HBV and HCV infections, leading to reduced costs, reduced emergence of drug-resistance, reduced side effects and improved compliance. This strategy, although attractive, is still far-sighted as there are not too many options available for immunotherapy. Consequently, there is an unprecedented need to identify a range of novel immunotherapies, which can be either combined or used sequentially with DAAs in a symbiotic relation to produce synergistic antiviral effects, if significant steps towards literal “cure” and “eradication” of HBV, HCV and HBV/HCV infections have to be realized.
REFERENCES1 Konstantinou D, Deutsch M. The spectrum of HBV/HCV co-
infection: epidemiology, clinical characteristics, viralinteractions and management. Ann Gastroenterol 2015; 28: 221-228 [PMID: 25830779]
2 Gish RG, Given BD, Lai CL, Locarnini SA, Lau JY, Lewis DL, Schluep T. Chronic hepatitis B: Virology, natural history, current management and a glimpse at future opportunities. Antiviral Res 2015; 121: 47-58 [PMID: 26092643 DOI: 10.1016/j.antiviral.2015.06.008]
3 Alter MJ. Epidemiology of hepatitis C virus infection. World J Gastroenterol 2007; 13: 2436-2441 [PMID: 17552026 DOI: 10.3748/wjg.v13.i17.2436 ]
4 Heim MH. 25 years of interferon-based treatment of chronic hepatitis C: an epoch coming to an end. Nat Rev Immunol 2013; 13: 535-542 [PMID: 23743475 DOI: 10.1038/nri3463]
5 Liang TJ, Block TM, McMahon BJ, Ghany MG, Urban S, Guo JT, Locarnini S, Zoulim F, Chang KM, Lok AS. Present and future therapies of hepatitis B: From discovery to cure. Hepatology 2015; 62: 1893-1908 [PMID: 26239691 DOI: 10.1002/hep.28025]
6 Jia H, Rai D, Zhan P, Chen X, Jiang X, Liu X. Recent advance of the hepatitis B virus inhibitors: a medicinal chemistry overview. Future Med Chem 2015; 7: 587-607 [PMID: 25921400 DOI:
5625 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Agrawal B et al . Symbiotic chemo- and immuno-therapy for HBV and HCV

5626 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
15 Guidotti LG, Chisari FV. Immunobiology and pathogenesis of viral hepatitis. Annu Rev Pathol 2006; 1: 23-61 [PMID: 18039107]
16 Pasquetto V, Wieland SF, Uprichard SL, Tripodi M, Chisari FV. Cytokine-sensitive replication of hepatitis B virus in immortalized mouse hepatocyte cultures. J Virol 2002; 76: 5646-5653 [PMID: 11991993]
17 Li HJ, Zhai NC, Song HX, Yang Y, Cui A, Li TY, Tu ZK. The Role of Immune Cells in Chronic HBV Infection. J Clin Transl Hepatol 2015; 3: 277-283 [PMID: 26807384 DOI: 10.14218/JCTH.2015.00026]
18 Rehermann B. Natural Killer Cells in Viral Hepatitis. Cell Mol Gastroenterol Hepatol 2015; 1: 578-588 [PMID: 26682281]
19 Li Y, Zhang T, Ho C, Orange JS, Douglas SD, Ho WZ. Natural killer cells inhibit hepatitis C virus expression. J Leukoc Biol 2004; 76: 1171-1179 [PMID: 15339939]
20 Rehermann B. Hepatitis C virus versus innate and adaptive immune responses: a tale of coevolution and coexistence. J Clin Invest 2009; 119: 1745-1754 [PMID: 19587449 DOI: 10.1172/JCI39133]
21 Baumert TF, Verrier ER, Nassal M, Chung RT, Zeisel MB. Host-targeting agents for treatment of hepatitis B virus infection. Curr Opin Virol 2015; 14: 41-46 [PMID: 26262886 DOI: 10.1016/j.coviro.2015.07.009]
22 Chang J, Guo JT. Treatment of chronic hepatitis B with pattern recognition receptor agonists: Current status and potential for a cure. Antiviral Res 2015; 121: 152-159 [PMID: 26205674 DOI: 10.1016/j.antiviral.2015.07.006]
23 Rehermann B, Bertoletti A. Immunological aspects of antiviral therapy of chronic hepatitis B virus and hepatitis C virus infections. Hepatology 2015; 61: 712-721 [PMID: 25048716 DOI: 10.1002/hep.27323]
P- Reviewer: Abdel-Fattah M, Farshadpour F, Purdy MA, Zeisel MB S- Editor: Qi Y L- Editor: A E- Editor: Wang CH
10.4155/fmc.15.19]7 Nassal M. HBV cccDNA: viral persistence reservoir and key
obstacle for a cure of chronic hepatitis B. Gut 2015; 64: 1972-1984 [PMID: 26048673 DOI: 10.1136/gutjnl-2015-309809]
8 Ohno M, Otsuka M, Kishikawa T, Yoshikawa T, Takata A, Koike K. Novel therapeutic approaches for hepatitis B virus covalently closed circular DNA. World J Gastroenterol 2015; 21: 7084-7088 [PMID: 26109795 DOI: 10.3748/wjg.v21.i23.7084]
9 Enomoto H, Nishiguchi S. Factors associated with the response to interferon-based antiviral therapies for chronic hepatitis C. World J Hepatol 2015; 7: 2681-2687 [PMID: 26609345 DOI: 10.4254/wjh.v7.i26.2681]
10 Zopf S, Kremer AE, Neurath MF, Siebler J. Advances in hepatitis C therapy: What is the current state - what come’s next? World J Hepatol 2016; 8: 139-147 [PMID: 26839638 DOI: 10.4254/wjh.v8.i3.139]
11 González-Grande R, Jiménez-Pérez M, González Arjona C, Mostazo Torres J. New approaches in the treatment of hepatitis C. World J Gastroenterol 2016; 22: 1421-1432 [PMID: 26819511 DOI: 10.3748/wjg.v22.i4.1421]
12 Burgess SV, Hussaini T, Yoshida EM. Concordance of sustained virologic response at weeks 4, 12 and 24 post-treatment of hepatitis c in the era of new oral direct-acting antivirals: A concise review. Ann Hepatol 2016; 15: 154-159 [PMID: 26845592 DOI: 10.5604/16652681.1193693]
13 Serfaty L. Follow-up of patients with chronic hepatitis C and a sustained viral response. Liver Int 2016; 36 Suppl 1: 67-71 [PMID: 26725900 DOI: 10.1111/liv.13016]
14 Banerjee D, Reddy KR. Review article: safety and tolerability of direct-acting anti-viral agents in the new era of hepatitis C therapy. Aliment Pharmacol Ther 2016; 43: 674-696 [PMID: 26787287 DOI: 10.1111/apt.13514]
Agrawal B et al . Symbiotic chemo- and immuno-therapy for HBV and HCV

Taisuke Imamura, Shuhei Komatsu, Daisuke Ichikawa, Tsutomu Kawaguchi, Mahito Miyamae, Wataru Okajima, Takuma Ohashi, Tomohiro Arita, Hirotaka Konishi, Atsushi Shiozaki, Ryo Morimura, Hisashi Ikoma, Kazuma Okamoto, Eigo Otsuji, Division of Digestive Surgery, Department of Surgery, Kyoto Prefectural University of Medicine, Kyoto 602-8566, Japan
Author contributions: Imamura T and Komatsu S equally contributed to this work; Imamura T and Komatsu S wrote the manuscript; Ichikawa D, Okamoto K and Otsuji E helped to draft the manuscript; Kawaguchi T, Miyamae M, Okajima W, Ohashi T, Arita T, Konishi H, Shiozaki A, Morimura R and Ikoma H collected the literatures.
Conflict-of-interest statement: The authors have no conflict of interest to report.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Manuscript source: Invited manuscript
Correspondence to: Shuhei Komatsu, MD, PhD, Division of Digestive Surgery, Department of Surgery, Kyoto Prefectural University of Medicine, 465 Kajii-cho, Kawaramachihirokoji, Kamigyo-ku, Kyoto 602-8566, Japan. [email protected]: +81-75-2515527 Fax: +81-75-2515522
Received: March 27, 2016 Peer-review started: March 28, 2016First decision: May 12, 2016
Revised: May 25, 2016 Accepted: June 15, 2016 Article in press: June 15, 2016Published online: July 7, 2016
AbstractDespite recent advances in surgical techniques and perioperative management, the prognosis of pancreatic cancer (PCa) remains extremely poor. To provide optimal treatment for each patient with Pca, superior biomarkers are urgently needed in all phases of management from early detection to staging, treatment monitoring, and prognosis. In the blood of patients with cancer, circulating tumor cells (CTCs) and cell-free nucleic acids (cfNAs), such as DNA, mRNA, and noncoding RNA have been recognized. In the recent years, their presence in the blood has encouraged researchers to investigate their potential use as novel blood biomarkers, and numerous studies have demonstrated their potential clinical utility as a biomarker for certain types of cancer. This concept, called “liquid biopsy” has been focused on as a less invasive, alternative approach to cancer tissue biopsy for obtaining genetic and epigenetic aberrations that contribute to oncogenesis and cancer progression. In this article, we review the available literature on CTCs and cfNAs in patients with cancer, particularly focusing on PCa, and discuss future perspectives in this field.
Key words: Pancreatic cancer; Biomarker; Liquid biopsy; Circulating tumor cells; Cell-free nucleic acids
© The Author(s) 2016. Published by Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.3748/wjg.v22.i25.5627
5627 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
World J Gastroenterol 2016 July 7; 22(25): 5627-5641 ISSN 1007-9327 (print) ISSN 2219-2840 (online)
© 2016 Baishideng Publishing Group Inc. All rights reserved.
Taisuke Imamura, Shuhei Komatsu, Daisuke Ichikawa, Tsutomu Kawaguchi, Mahito Miyamae, Wataru Okajima, Takuma Ohashi, Tomohiro Arita, Hirotaka Konishi, Atsushi Shiozaki, Ryo Morimura, Hisashi Ikoma, Kazuma Okamoto, Eigo Otsuji
TOPIC HIGHLIGHT
Liquid biopsy in patients with pancreatic cancer: Circulating tumor cells and cell-free nucleic acids
2016 Pancreatic Cancer: Global view

Core tip: In the blood of patients with cancer, cir-culating tumor cells (CTCs) and cell-free nucleic acids (cfNAs), such as DNA, mRNA, and noncoding RNA have been recognized. In the recent years, their presence in the blood has encouraged researchers to investigate their potential use as novel blood biomarkers. This concept, called “liquid biopsy” has been focused on as a less invasive, alternative approach to cancer tissue biopsy for obtaining genetic and epigenetic aberrations that contribute to oncogenesis and cancer progression. In this article, we review the available literature on CTCs and cfNAs in patients with cancer, particularly focusing on pancreatic cancer.
Imamura T, Komatsu S, Ichikawa D, Kawaguchi T, Miyamae M, Okajima W, Ohashi T, Arita T, Konishi H, Shiozaki A, Morimura R, Ikoma H, Okamoto K, Otsuji E. Liquid biopsy in patients with pancreatic cancer: Circulating tumor cells and cell-free nucleic acids. World J Gastroenterol 2016; 22(25): 5627-5641 Available from: URL: http://www.wjgnet.com/1007-9327/full/v22/i25/5627.htm DOI: http://dx.doi.org/10.3748/wjg.v22.i25.5627
INTRODUCTIONPancreatic cancer (PCa) is the fourth leading cause of cancer-related deaths in the United States, and the eighth worldwide[1]. In recent years, as a result of advances in surgical techniques and perioperative management, the perioperative mortality rate has decreased and perioperative chemotherapy and radiotherapy have greatly improved; however, prognostic outcomes for PCa remain poor[2,3]. Even now, the median survival time of patients with PCa is 5-8 mo and their 5-year survival rate is less than 10%[2,3].
Although surgical resection is the only option for macroscopic tumor clearance for PCa, most patients are diagnosed at an advanced and unresectable stage because PCa develops with no symptoms, local invasiveness, and metastases to distant organs in the early stage of its clinical course[1,4,5]. In addition, PCa shows resistance to conventional chemotherapies. Therefore, primary tumors must be detected at an early and resectable stage, whereas patients with far advanced disease must be preoperatively diagnosed to avoid surgical impairments and to select appropriate treatments to improve the quality of remaining life[6]. Consequently, to provide optimal management for each patient, biomarkers are urgently needed that are better than the conventional ones, such as carcinoembryonic antigen (CEA) and carbohydrate antigen 19-9 (CA19-9), in all phases of management from early detection to staging, treatment monitoring, and prognosis for PCa.
Numerous genetic and epigenetic aberrations contribute to oncogenesis and cancer progression, and the utility of these alterations for diagnostic,
prognostic, and therapeutic purposes in various cancers have been investigated. Conventionally, these cancer-related alterations are investigated using tissue samples from surgical or biopsy specimens. These methodologies for pancreatic tissue acquisition cannot always be performed and repeated because of their invasive nature and anatomical difficulties. Thus, conventional examinations may fail to reflect current tumor dynamics and drug sensitivities, which may change during the therapeutic process. Detection and examination of circulating tumor cells (CTCs) and/or cell-free nucleic acids (cfNAs) in the bloodstream by performing a so-called liquid biopsy, which allows repeated sampling, makes it possible to track the current status of a tumor and its heterogeneous characteristics, which single sampling may fail to capture.
In the past decades, numerous studies have shown the potential utility of novel blood-based biomarkers, such as CTCs and cfNAs, for various cancers including PCa[7-10]. These promising markers are considered to possess great potential and could facilitate the-rapeutic strategies for cancer. In this article, we review the histological backgrounds, characteristics, and developments among CTCs and cfNAs in cancer research and discuss future perspectives, particularly focusing on PCa.
BIOLOGY AND DETECTION OF CTCSIn 1869, Ashworth[11] identified the presence of CTCs for the first time in the blood of a metastatic breast cancer patient in whom cells similar to those in the primary tumors were found in the blood at autopsy. Since then, many groups have challenged and demonstrated the identification and characterization of CTCs in peripheral blood of patients with cancer in several cancers. It has been recognized that CTCs originate from the primary tumor and/or metastatic lesions and are therefore extremely rare in healthy subjects and patients with nonmalignant diseases but are present in various metastatic carcinomas with a wide range of frequencies[12].
CTCs are generally thought to be quite hetero-geneous in both phenotype and genotype, and only 2.5% of CTCs develop micrometastases and only 0.01% develop macrometastases[13-15]. During the journey toward the development of a metastatic lesion, some CTCs undergo epithelial-to-mesenchymal transition (EMT), which is characterized by decreased expression of epithelial markers and the acquisition of mesenchymal features[15] that could allow CTCs to escape from epithelial marker-based detection[16]. Furthermore, CTCs are present in peripheral blood at a low density among billions of blood cells in each milliliter of blood[17]. Consequently, accurate detection of CTCs with sufficient sensitivity and specificity has been a major technical challenge for researchers.
Currently, the CELLSEARCH system (Veridex) is
5628 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Imamura T et al . Liquid biopsy of pancreatic cancer

the most widely used CTC platform. In this platform, immunomagnetic beads coated with anti-epithelial cellular adhesion molecule (EpCAM) antibodies capture CTCs, followed by immunostaining with two positive markers: cytokeratins (CKs) 8/18/19 for cytoplasmic epithelium and 4′,6′-diamidino-2-phenylindole hydrochloride for nucleic acids, and a negative marker, leukocyte-specific CD45. The CELLSEARCH system is the only CTC platform to gain the approval of the United States Food and Drug Administration, and its clinical utility has been demonstrated as a diagnostic and prognostic indicator in patients with metastatic breast, prostate, and colon cancer[18-23]. In contrast, EpCAM-based enrichment of CTCs such as the CELLSEARCH system could fail to capture CTCs that have undergone EMT and increase the malignant potential. Several problems still remain regarding the detection and isolation capability and, thus, the clinical utility of CTCs. To improve sensitivity and specificity despite the heterogeneity of CTCs, new technology for the isolation and enrichment of CTCs has been developed. More recently, CTC-Chip[24] was demonstrated to increase the detection of CTCs by using tumor-specific markers, such as PSA in prostate cancer or HER2 in breast cancer, in addition to epithelial markers. Furthermore, Saucedo-Zeni et al[25] reported a new technology that enables the capture and enrichment of CTCs in vivo using a medical Seldinger guidewire inserted through a standard venous cannula into the cubital veins. Despite these advances, however, the isolation and enrichment of CTCs remains at the development stage.
After the isolation and enrichment of CTCs, identification procedures must be performed to ex-amine their genetic and biological features. Various methods, such as immunocytochemistry and mo-lecular techniques, have been commonly performed for identifying CTCs. Conventionally, immunostaining using 4′,6′-diamidino-2-phenylindole hydrochloride as a nuclear stain, CK as an epithelial marker, and CD45 as a hematopoietic marker have been widely used[26]. Among molecular approaches, quantitative reverse transcription-polymerase chain reaction (RT-PCR) has been generally employed to investigate the molecular characteristics of CKs, CEA, and other driver markers[27].
CTC DETECTION IN PATIENTS WITH PCA AND ITS CLINICAL RELEVANCETo date, many researchers have tried to detect CTCs in patients with PCa and have demonstrated its clinical utility using various approaches. Table 1 summarizes the previous reports about CTCs in patients with PCa. Early studies of CTCs in PCa employed tumor-specific and/or epithelial-related mRNAs as a molecular target for the detection of CTCs. Among these studies, RT-PCR techniques have been widely used for the
detection of mRNAs despite a low concentration. Funaki et al[28] first reported the clinical utility of CTCs in patients with PCa using RT-PCR. They demonstrated that the detection of CEA mRNA as a tumor-specific molecule in peripheral blood is useful in finding the hematogenous spreading of adenocarcinoma cells. Three of nine patients with PCa (33.3%) were positive for CEA mRNA, and none of the control patients was positive for CEA mRNA in peripheral blood. Following this study, some groups evaluated the clinical utility of CEA mRNA in the bloodstream for the detection of CTCs in PCa and reported its sensitivity (47.8%-75.0%) and specificity (94.6%-96%) for the detection of PCa[29-32]. Chausovsky et al[33] reported that the epithelial-associated molecule CK-20 mRNA is useful for the detection of CTCs in PCa. They successfully demonstrated RT-PCR of CK-20 as a potential biomarker for detecting metastases in blood samples from patients with PCa and in subsequent studies reported data supporting this result[34-36]. Other mRNAs, such as epithelial growth factor receptor mRNA[37], α1,4-N-acetylglucosaminyltransferase mRNA[38], and CK-19 mRNA[39] have also been reported as useful targets for the detection of CTCs using RT-PCR in patients with PCa. Regarding these mRNA-based studies, sensitivities varied widely and were relatively low despite high specificity. Furthermore, some of these studies used mononuclear cell fraction from density gradient enrichment or blood samples without enrichment techniques to extract total RNA for the investigation of mRNA expression; therefore, the approach cannot exclude the possible contamination of leukocyte-originated RNAs, an issue that should be considered in interpreting results. More recently, Zhou et al[40] suggested that the combined detection of c-Met, h-TERT, CK20, and CEA using RT-PCR following immunomagnetic bead enrichment could be used as an indicator for circulating cancer cells with 100% sensitivity and 100% specificity in patients with PCa.
Meanwhile, an immunocytochemical approach also has been used for identifying CTCs in patients with PCa. Although many studies have investigated the clinical utility of the CELLSEARCH platforms in PCa, a low detection rate ranging from 5% to 42% was reported[12,41,42]. In contrast, some of the studies demonstrated the clinical utility of CTCs as a predictor of disease recurrence and prognosis by reporting that a positive CTC finding was associated with disease recurrence and/or poor survival. To improve the detection rate of the CELLSEARCH system in PCa, several researchers have developed novel technolo-gies for the detection of CTCs, such as size-based isolation[43-46] and microfluidics[47,48], and reported favorable results.
Overall, a certain level of utility of CTCs as a biomarker in PCa may be practically guaranteed; however, there are several problems that remain to be solved before CTCs can be considered useful in a clinical setting. First, CTCs might not be suitable
5629 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Imamura T et al . Liquid biopsy of pancreatic cancer

5630 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Table 1 Circulating tumor cells in pancreatic cancer
Ref. Patient characteristics Number of patients with
PCa
Controls Enrichment/isolation method
Detection method Detection rate
Funaki et al[28], 1996 Pre- or post-treatment 9 NA None RT-PCR: CEA mRNA 33.3% of PCaFunaki et al[29], 1998 Preoperative 3 NA None RT-PCR: CEA-mRNAMiyazono et al[30], 1999 Intra-operative 21 15 HV Density gradient
enrichmentRT-PCR: CEA-mRNA 61.9% of PCa
Chausovsky et al[33], 1999 Metastatic PCa 28 22 BD Density gradient enrichment
RT-PCR: CK20 mRNA 78.6% of PCa
Z'graggen et al[124], 2001 All stages, preoperative
105 66 HV Density gradient enrichment
ICC: CK-AE1/AE3 Sensitivity: 26%, specificity: 96%
Lukyanchuk et al[34], 2003 NA 11 18 HV Density gradient enrichment
RT-PCR: CK-20 and PSCA
CK-20: 19 of 47 (40.4%), PSCA: 22 of 47 (46.8%)
Clarke et al[37], 2003 NA 11 23 HV Density gradient enrichment
RT-PCR: EGFR mRNA 18% of PCa, 0.0% of HV
Mataki et al[32], 2004 All stages 20 15 HV, 15 BD
Density gradient enrichment
RT-PCR: CEA mRNA Sensitivity: 75.0%, specificity: 94.6%
Zhang et al[35], 2005 Stages Ⅱ and Ⅲ 40 5 BD, 5 HV Not available RT-PCR: CK20 mRNA 57.5% of PCaSoeth et al[36], 2005 Preoperative 154 NA Density gradient
enrichmentRT-PCR: CK20 mRNA 33.8% of PCa
Ishizone et al[38], 2006 All stages 55 10 CP, 70 HV
Density gradient enrichment
RT-PCR: a4GnT 76.4% of PCa, 40.0% of CP, 17.1% of HV
Hoffmann et al[39], 2007 All stages 37 16 CP, 15 BD Density gradient enrichment
RT-PCR: CK-19 mRNA 64% of PCa
Kurihara et al[41], 2008 Stages Ⅱ, Ⅲ and Ⅳ 26 11 CP, 10 HV CELLSEARCH® 42% of PCaZhou et al[40], 2011 All stages 25 15 BD Immunomagnetic
separationRT-PCR: C-MET,
h-TERT, CK20, and CEA
Sensitivity: 100%, specificity: 93.3%
Khoja et al[125], 2012 Stages Ⅲ and Ⅳ 54 PCa NA Size-based selection RT-PCR: EpCAM, CK, vimentin, and CEA
ISET 49/54 (93%) vs CELLSEARCH® 21/54
(40%) de Albuquerque et al[126], 2012 Stages Ⅲ and Ⅳ 34 40 HV Immunomagnetic
separationRT-PCR: KRT19, MUC1, EpCAM,
CEACAM5, and BIRC5
Sensitivity: 47.1%, specificity: 100%
Kamande et al[127], 2013 All stages 12 5 HV Microfluidic; ICC DAPI+, CD45-, CK+ 100% of PCaBidard et al[42], 2013 Locally advanced PCa 79 NA CELLSEARCH® 11% of PCaIwanicki-Caron et al[43], 2013 All stages 40 NA Size-based selection Cell size and
cytopathologic criteriaSensitivity: 55.5%, specificity: 100%,
accuracy: 70%Bobek et al[45], 2014 All stages 24 NA Size-based selection DAPI, CK, CEA,
vimentin IHC66.7% of PCa
Sheng et al[48], 2014 Metastatic PCa 18 NA Multifluidic, "GEM"Chip
94.4% of PCa
Rhim et al[47], 2014 All stages 11 19 HV Geometrically enhanced
differential immunocapture
ICC for DAPI, CD45, CK, and PDX-1
73% of PCa
Catenacci et al[128], 2015 Stages Ⅱ, Ⅲ and Ⅳ 18 NA Immune-magnetic separation
CD45-negative and positive for CK8, -18, and/or -19 and DAPI
118.4 ± 36.8 CTCs/7.5 mL PVB, compared
with a mean of 0.8 ± 0.4 CTCs/7.5 mL PB
Earl et al[81], 2015 All stages 35 NA CELLSEARCH® 20% of PCaCauley et al[44], 2015 All stages 105 9 HV Size-based selection Cytomorphologic
criteria 48.6% of PCa
Kulemann et al[46], 2015 Preoperative 11 9 HV Size-based selection:
ScreenCell
Cytologic and detection of KRAS
mutation
75% of early PCa, 71.4% of advanced PCa
Zhang et al[129], 2015 All stages 32 30 HV ICC and FISH DAPI+, CD45-, and CK+, or CEP8 > 2+
Sensitivity: 63.6%, specificity: 94.4%
Bissolati et al[130], 2015 Intra-operative 20 NA CELLSEARCH® PVB: 40%, PB: 20%Zhang et al[131], 2015 15 15 HV Immunomagnetic
separationBC-15 aptamer or anti-
CK staining73.3% of PCa
BD: Benign disease; CEA: Carcinoembryonic antigen; CK: Cytokeratin; CP: Chronic pancreatitis; CTC: Circulating tumor cell; DAPI: 4′,6′-diamidino-2-phenylindole; EpCAM: Epithelial cellular adhesion molecule; FISH: Fluorescence in situ hybridization; HV: Healthy volunteer; ICC: Immunocytochemistry; IHC: Immunohistochemistry; NA: Not applicable; PB: Peripheral blood; PCa: Pancreatic cancer; PVB: Portal venous blood; RT-PCR: Reverse transcription polymerase chain reaction.
Imamura T et al . Liquid biopsy of pancreatic cancer

5631 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
in screening tests for early detection (which is de-sirable in PCa) owing to their low sensitivity. Novel technology with high sensitivity for the detection of CTCs is required to use CTCs in screening tests for early diagnosis. Second, the detection of CTCs has to overcome the challenge of the rarity and heterogeneity of CTCs, and because the methodology for the detection of CTCs remains in a developmental stage, the approach to CTCs and the results of studies have varied widely. Consequently, it is difficult to assess, compare, and interpret the results of multiple studies and establish the evidence and clinical relevance of CTCs. Establishment of a unified methodology and large-scale validation of their utility are required for wider clinical application.
BIOLOGY AND DETECTION OF CFNASFor many decades, cfNAs have been known to be pre-sent in peripheral blood. Mandel and Metais[49] first reported that nucleic acids were detectable in human plasma in 1948. In 1977, Leon et al[50] detected cell-free DNAs in the serum of patients with cancer. Since then, several studies have identified tumor-specific and/or tumor-associated alterations in the circulating cfNAs of patients with various cancers. In 1989, Vasioukhin et al[51] successfully detected cell-free DNA with neoplastic characteristics, providing the first evidence suggesting that tumors can shed DNA into the circulation. This hypothesis was further supported by a study in which a NRAS mutation in the plasma of patients with myelodysplastic syndrome or acute myelogenous leukemia[52] and KRAS mutation in the plasma or serum of patients with PCa were detected[53].
Cell-free RNA, which is thought to be more fragile than DNA because RNA is easily degraded by endogenous ribonuclease (RNase) in plasma/serum, has been successfully detected in blood. In 1999, tyrosinase mRNA in the serum of patients with malignant melanoma[54] and Epstein-Barr virus-associated RNA in nasopharyngeal carcinoma[55] was successfully detected. Subsequently, many studies have demonstrated the presence of specific mRNA in plasma/serum and its clinical utility in patients with various cancers[56-58].
Regarding noncoding RNA, Mitchell et al[59] firstly demonstrated that circulating microRNAs (miRNAs) had the potential to be novel biomarkers in patients with solid cancers in 2008. Since then, numerous studies examining circulating noncoding RNAs have been performed, with most studies focusing on miRNAs. Although other noncoding RNAs, such as small nucleolar RNA (snoRNA), small nuclear RNA (snRNA), piwi-interacting RNA (piRNA), and long noncoding RNA (lncRNA), have been recognized to have biological functions and may have great potential to be novel blood biomarkers, there are few reports of these noncoding RNAs. Further studies and
accumulation of evidence are required.
CIRCULATING CELL-FREE DNA IN PLASMA/SERUM AND PCAThe study of circulating cell-free DNA in the plasma/serum involves two major strategies: the mea-surement of the amount of cell-free DNA in the circulation and the detection of tumor-derived genetic aberrations such as point mutations, allelic imbalances, microsatellite instability, genetic polymorphisms, loss of heterozygosity, and methylation. Of these, many reports have demonstrated the detection of genetic and epigenetic alterations in circulating cell-free DNA in the bloodstream of patients with cancer[60-63].
Previous reports about circulating cell-free DNA in PCa are summarized in Table 2. In 1983, Shapiro et al[64] first reported the presence of circulating cell-free DNA in PCa. This study demonstrated that serum DNA concentration is markedly elevated in patients with PCa compared with normal controls using radioimmunoassay and that an abnormally high concentration of DNA in serum may have diagnostic and prognostic value. Since then, investigations of tumor-derived genetic alterations in plasma/serum have become mainstream. Only a few studies investigating the methylation[65,66], microsatellite instability, and allelic imbalance[67] can be found. In contrast, the detection of K-ras mutation in plasma/serum appears to be the most widely used approach in the diagnosis of PCa. It has been widely recognized that over 90% of pancreatic adenocarcinomas contain mutated K-ras genes[68-70], and the detection of mutant K-ras provides a definitive diagnosis of pancreatic adenocarcinoma in pancreatic tissue[70,71]. Based on the detection of K-ras mutation in tumor tissues, the detection of the tumor-derived genetic alterations in circulating cell-free DNA has been attempted for the diagnosis of PCa. In 1993, Yamada et al[72] demonstrated that detection of K-ras mutations in plasma may be clinically useful for evaluating tumor burden and efficacy of treatment for PCa. Subsequently, many groups have reported the possible clinical utility of K-ras mutations in circulating cell-free DNA in PCa[73-80].
PCR has been widely used to detect tumor-derived mutations in genes isolated from the serum and plasma of patients with cancer[51,53]. More recently, droplet digital PCR[81-84] and genome-wide high-throughput sequencing[84,85] has been demonstrated as a potential detection tool for rare mutations and multiple types of mutations in circulating DNA with great accuracy. Using these new technologies in several solid cancers such as colorectal, breast, and ovarian cancer, a correlation has been found between the acquisition of drug resistance and genetic aberrations in cell-free DNA in the blood of patients under treatment[86-88]. It is hoped that the potent utility
Imamura T et al . Liquid biopsy of pancreatic cancer

5632 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Table 2 Circulating cell-free DNA in pancreatic cancer
Ref. Patients Controls Sample Method Target candidate
Findings
Shapiro et al[64], 1983 201 MD 185 BD Serum Radioimmunoassay Circulating DNA levels
Serum DNA concentration is markedly elevated in 90% of patients with PCa as compared with HV
Yamada et al[72], 1998 21 PCa - Plasma Mutant allele-specific amplification method
K-ras mutation
In 9 of 15 (60%) patients with K-ras gene mutation-positive tumors, an identical mutation was detected in the plasma DNA. Detection of K-ras mutations in plasma may be clinically useful for evaluating tumor
burden and efficacy of treatmentGiacona et al[132], 1998 3 PCa 3 HV Plasma Gel electrophoresis and
measuring the variation in length by electron
microscopy
Length There are significant differences in non-cell-associated DNA in plasma between patients with PCa and HV
Theodor et al[73], 1999 20 PCa 6 CP, 5 HV
Serum PCR K-ras mutation
K-ras gene mutations at codon 12 were detected in the sera of 14 of 20 patients with PCa and in none of the 6
patients with CP, or in the 5 HVsCastells et al[74], 1999 44 PCa 37 CP Plasma Restriction fragment
length polymorphism-PCR and single-
strand conformation polymorphism techniques
K-ras mutation
Plasma K-ras analysis is a highly specific, low-sensitivity approach that has diagnostic and prognostic
clinical implications in patients with PCa
Zambon et al[75], 2000 29 PCa 12 HV Serum ME-PCR K-ras mutation
K-ras was amplifiable in 2 patients with PCa (6.9%), and K-ras was not amplifiable in any of the 12 serum
samples obtained from HVsMaire et al[76], 2002 47 PCa 31 CP Serum PCR and allele-specific
amplificationKRAS2
mutationsKRAS2 mutations were found in 22 patients (47%) with
PCa and in 4 controls with CP (13%) (P < 0.002)Melnikov et al[65], 2009 30 PCa 30 HV Plasma Multiplexed array-
mediated analysis of DNA methylation
Methylation Differential methylation profiling of plasma DNA can detect PCa with 76% sensitivity and 59% specificity
Liggett et al[66], 2010 30 PCa 30 CP, 30 HV
Plasma Microarray-mediated methylation analysis
Methylation Methylation analysis achieved 81.7% sensitivity and 78% specificity (P < 0.01) in the detection of CP (HV vs
CP) and 91.2% sensitivity and 90.8% specificity (P < 0.01) in the differential detection of PCa (PCa vs CP)
Chen et al[79], 2010 91 PCa - Plasma Direct sequencing K-ras K-ras codon 12 mutations were found in 30 of 91(33%) plasma DNA samples and significantly reflected the clinical parameters, including TNM tumor staging
and liver metastasis, and independent predict shorter survival time
Wu et al[80], 2014 24 PCa 25 HV Plasma COLD-PCR combined with an unlabeled-probe
HRM approach
K-ras KRAS mutations were identified in 26 of 36 PCa cases (72.2%), but none were detected in the disease control
and/or healthy groupEarl et al[81], 2015 31 PCa - Plasma Digital PCR KRAS KRAS mutant cfDNA was detected in 26% of patients
at all stages, which correlated strongly with OS, 60 d for KRAS mutation-positive vs 772 days for KRAS
mutation-negative patientsZill et al[85], 2015 26 PCa - Plasma Sequenced on an Illumina
Hi-Seq 2500KRAS, TP53,
APC, FBXW7, and SMAD4
The diagnostic accuracy of cfDNA sequencing was 97.7%, with 92.3% average sensitivity and 100%
specificity across 5 informative genesSingh et al[133], 2015 Plasma Levels of
ctDNA and K-ras mutation
Higher levels of plasma DNA were significantly associated with lower OS and advanced stage.
However, k-ras mutation did not correlate with any of the clinicopathological parameters or survival
Kinugasa et al[82], 2015 141 PCa 20 CP, 20 HV
Serum Digital PCR G12V, G12D, and G12R in codon 12 of K-ras gene
K-ras mutation rate in ctDNA was 62.6%. The survival of patients with K-ras mutations in ctDNA was
significantly shorter than that of patients without mutations
Sausen et al[83], 2015 77 PCa - Plasma Next-generation sequencing
The 43% of patients with localized disease had detectable ctDNA at diagnosis. Detection of ctDNA
after resection predicts clinical relapse and poor outcome, with recurrence by ctDNA detected 6.5
months earlier than with CT imagingTakai et al[84], 2015 259 PCa - Plasma Picoliter-droplet digital
PCR and targeted deep sequencing
KRAS mutation
KRAS mutations were identified in 14 of 48 patients (29.2%) examined by targeted deep sequencing of
cfDNA
BD: Benign disease; cfDNA: Cell-free DNA; COLD-PCR: Co-amplification at lower denaturation-temperature PCR; CP: Chronic pancreatitis; CT: Computed tomography; ctDNA: Circulating tumor DNA; HV: Healthy volunteer; ICC: Immunocytochemistry; PCa: Pancreatic cancer; MD: Malignant disease; OS: Overall survival; PCR: Polymerase chain reaction; ME-PCR: Mutant-enriched PCR.
Imamura T et al . Liquid biopsy of pancreatic cancer

5633 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
of cell-free DNA for the assessment of residual disease, recurrence, and acquisition of drug resistance as well as for the detection of disease can be proven in PCa.
CIRCULATING CELL-FREE MRNA IN PLASMA/SERUM AND PCAAlthough RNA is easily degraded by RNase and the concentration of RNase in blood is high in patients with cancer[89], many groups have demonstrated the stable presence of cell-free mRNAs in the blood of patients with cancer. Recently, it has been considered that these RNAs could be incorporated into exosomes, microvesicles, and multivesicles, which seem to be adequately protected against the degradation caused by the abundant RNases and released from the cellular surface to the bloodstream[90]. There are numerous studies investigating the correlation between cell-free mRNA in the bloodstream and several solid cancers, and these studies are mainly aimed at investigating the mRNAs in plasma/serum that are up-regulated in cancer tissues[56-58,91-93]. Regarding PCa, there are several studies investigating mRNA in peripheral blood mononuclear cells and CTCs[29,32,35,38] as a marker for the detection of CTCs; however, the number of cell-free mRNAs in plasma/serum is extremely small. Kang et al[94] recently demonstrated that type IV collagen (COL6A3) mRNA in serum might serve as a biomarker for the detection of PCa according to tumor-specific alternative splicing. Accumulation of evidence and understanding of cell-free mRNA in patients with cancer may have a potential to bring new insights into the field of liquid biopsy in PCa.
CIRCULATING NONCODING RNA IN PLASMA/SERUMIt has been revealed that as much as 80% of genomic DNA is transcribed into RNAs[95]. In contrast, the Human Genome Project discovered that the open reading frames of protein genes constitute less than 2% of the 3.2 billion bases[96,97]. Thus, a large portion of human genomic DNA does not code proteins. It is now becoming evident that a variety of noncoding RNAs (ncRNAs) play important roles in many cellular processes and are not just mere intermediates in the transfer of genetic information from DNA to proteins, which indicates that the ncRNAs expression patterns could be used as molecular markers in specific diagnostic methods[98].
For circulating ncRNAs, almost all of the studies have focused on miRNAs, which are short noncoding RNAs that play important roles in various physiologic and developmental processes. One strand (a guide strand) of mature miRNA is then incorporated into the RNA-induced silencing complex and subsequently hybridizes to the 3′-untranslated region of their target mRNAs to repress translation or degrade these mRNAs.
Thus, a single miRNA can influence the expression of hundreds of genes and allow them to function in a coordinated manner. Therefore, miRNAs have been implicated as key molecules in all cellular processes. Numerous studies have shown that alterations in miRNA expression correlate with various diseases, including the development and progression of cancer, and some miRNAs can function as oncogenes or tumor suppressors. Furthermore, several recent studies have demonstrated that some extracellular miRNAs occur not only through cell lysis but also through active secretion[8,99,100]. Cell-derived endogenous miRNAs are present in the blood in a remarkably stable form that is protected from endogenous RNase activity. Kosaka et al[100] demonstrated that a subset of miRNAs can be packaged into exosome vesicles and released through a ceramide-dependent secretory mechanism. Furthermore, most miRNAs are stable in plasma owing to their binding to proteins such as Argonaute2 and high-density lipoprotein[101]. All circulating miRNAs, regardless of whether they are incorporated into protein complexes and/or cell-derived microvesicles, seem to be adequately protected against the de-gradation caused by the abundant RNases in human plasma and serum. These findings have opened up a new and interesting field in the diagnosis of cancer and the treatments of patients with cancer.
Mitchell et al[59] first demonstrated that circulating miRNAs have the potential to be novel blood bio-markers in patients with solid cancers in 2008. Since then, numerous studies of circulating miRNAs in cancer have been performed to investigate their potential as candidate novel biomarkers. Regarding PCa, previous reports about circulating miRNAs are summarized in Table 3. Wang et al[102] first reported the plasma level of four candidate miRNAs (miR-21, -155, -196a, and -210) that were previously reported to be up-regulated in PCa tissue. Since then, several groups have reported the utility of circulating miRNAs as biomarkers for PCa, and the number of studies and the variety of miRNAs have been increasing. Many studies have demonstrated the clinical significance of deregulated expression of miRNA in plasma/serum, and more than 30 miRNAs have been reported as candidate novel blood biomarkers in PCa. As mentioned before, one miRNA can regulate multiple mRNAs and the numbers of discovered miRNAs and targeted mRNAs are still increasing owing to recent advances in analysis technology. Consequently, more recently, diagnosing PCa with higher sensitivity and specificity has been attempted by employing multiple miRNAs[103,104]. Schultz et al[103] reported that two diagnostic panels including four (miR-145, miR-150, miR-223, and miR-636) and 10 (miR-26b, miR-34a, miR-122, miR-126*, miR-145, miR-150, miR-223, miR-505, miR-636, and miR-885.5p) miRNAs based on the expression in whole blood could be used to detect PCa with high sensitivity and specificity. However, it should be considered that the study employed whole
Imamura T et al . Liquid biopsy of pancreatic cancer

5634 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
blood as a sample for extracting RNAs; therefore, the miRNAs found obviously included miRNAs derived from blood cells or CTCs other than cell-free miRNAs. Kojima et al[104] reported that a combination of eight miRNAs (miR-6075, miR-4294, miR-6880-5p, miR-6799-5p, miR-125a-3p, miR-4530, miR-6836-3p, and miR-4476) could achieve high sensitivity, specificity,
and accuracy for the detection of PCa.Furthermore, the studies of circulating cell-free
miRNAs in PCa have demonstrated the usefulness of circulating miRNAs as a staging marker, treatment marker, and prognostic marker as well as a biomarker for the detection of PCa. Kong et al[105] demonstrated that the serum miR-196a expression level had potential value for predicting median survival time of patients with PCa [high-level miR-196a, 6.1 mo (95%CI: 4.49-7.72), vs low-level miR-196a, 12.00 mo, (95%CI: 5.92-18.08), p = 0.007). Most recently, our group demonstrated that high expression of miR-744 in plasma might be a useful biomarker for screening PCa, monitoring, and predicting poor prognosis and chemoresistance in patients with PCa[106]. Although more evidence has been accumulating as we have been reviewing previous reports, several problems remain be solved for clinical application. There is no consensus regarding inter- and intra-individual variation, whether plasma or serum is more appropriate, and what molecule is optimal for the most sensitive detection and endogenous controls.
Some kinds of noncoding RNAs other than miRNA have been recognized to have biological functions. Especially in cancers, some noncoding RNAs have been demonstrated to have oncogenic or tumor-suppressive functions and to be deregulated in tumor tissue. Regarding PCa, HOTAIR[107], MALAT-1[108], MEG3[109], Gas5[110], HULC[111], PVT1[112], PPP3CB, MAP3K1, DAPK1[113], BC008363[114], ENST00000480739[115], and HSATII[116] have been reported to have tumor-associated functions and tumor-specific expression. However, there are no studies investigating these cell-free RNAs in the bloodstream of patients with PCa. The noncoding RNAs other than miRNAs, such as long noncoding RNA (lncRNA), small nucleolar RNA (snoRNA), small nuclear RNA (snRNA), and Piwi-interacting RNA (piRNA) in the bloodstream of patients with PCa remain largely unexplored. Most recently, Wang et al[117] demonstrated that the plasma fragments of lncRNA, HOTTIP-005, and RP11-567G11.1 have the potential to be used as diagnostic biomarkers of PCa. We believe that future studies of circulating noncoding RNAs in PCa will bring new insights to this field.
CURRENT ISSUES AND FUTURE PERSPECTIVEBlood-based biomarkers, evaluated using liquid biopsy, are attractive as diagnostic, staging, prognostic, and treatment markers for PCa owing to their less invasive nature, and the clinical relevance of using liquid biopsy to identify biomarkers in PCa has become practically guaranteed. However, several problems remain to be solved before application in a clinical setting. One of the important hurdles to overcome is the lack of consensus regarding a technical approach. The
Table 3 Circulating noncoding RNA in pancreatic cancer
Ref. Sample Candidate target Potential value
miRNAWang et al[102], 2009 Plasma miR-210 (↑), miR-21
(↑), miR-155 (↑), miR-196a (↑)
D
Ho et al[134], 2010 Plasma miR-210 (↑) DLi et al[135], 2010 Plasma miR-200a (↑), miR-
200b (↑)D
Ali et al[136], 2010 Plasma miR-21 (↑) D/PKong et al[105], 2011 Serum miR-196a (↑) D/S/PLaConti et al[137], 2011 Serum miR-155 (↑) DMorimura et al[138], 2011 Plasma miR-18a (↑) DLiu et al[139], 2012 Serum miR-16 (↑), miR-196a
(↑)D
Liu et al[140], 2012 Serum miR-20a (↑), miR-21 (↑), miR-24 (↑),
miR-25 (↑),
D/P
miR-99a (↑), miR-185 (↑), miR-191 (↑)
Li et al[141], 2012 Serum miR-1290 (↑) DWang et al[142], 2013 Whole blood miR-27a-3p (↑) DKawaguchi et al[143], 2013 Plasma miR-221 (↑), miR-375
(↓)D/S
Zhao et al[144], 2013 Serum miR-192 (↑) DLi et al[141], 2013 Serum miR-1290 (↑) DWang et al[145], 2013 Serum miR-21 (↑) T/PCarlsen et al[146], 2013 Plasma miR-375 (↑) DQue et al[147], 2013 Serum miR-17-5p (↑),
miR-21 (↑), miR-155 (↓), miR-196a (↓)
D/S
Schultz et al[103], 2014 Whole blood Multigene index DGao et al[148], 2014 Plasma miR-16 (↑) DChen et al[149], 2014 Plasma miR-182 (↑) D/S/PGanepola et al[150], 2015 Plasma miR-22 (↑), miR-642b
(↑), miR-885-5p (↑)D
Abue et al[151], 2015 Plasma miR-21 (↑), miR-483-3p (↑)
D/S/P
Slater et al[152], 2015 Serum miR-196a (↑), miR-196b (↑)
D
Kojima et al[104], 2015 Serum Multigene index DXu et al[153], 2015 Plasma miR-486-5p (↑),
miR-938 (↑)D
Madhavan et al[154], 2015 Serum miR-1246 (↑), miR-3976 (↑), miR-4306 (↑), miR-4644 (↑)
D
Komatsu et al[123], 2015 Plasma miR-223 (↑) D/PMiyamae et al[106], 2015 Plasma miR-744 (↑) D/S/P/T
Other noncoding RNAs
Wang et al[117], 2015 Plasma HOTTIP-005 (↑), RP11-567G11.1 (↑)
D/P
Baraniskin et al[155], 2013 Plasma/serum
U2 snRNA (↑) D
D: Diagnostic marker; miRNA: MicroRNA; P: Prognostic marker; S: Staging marker; T: Treatment marker.
Imamura T et al . Liquid biopsy of pancreatic cancer

5635 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
methodology for the detection and assessment of CTCs and circulating cfNAs remains in a developmental stage, and therefore, the techniques used, such as sample type, storage conditions, target molecules, and detection approach, have varied widely among research groups. The standardization and unification of techniques through all processes and the accumulation of many results under the same conditions or in large-scale studies should be emphasized. Meanwhile, recent technical advances allow us to detect a slight amount of circulating cell and nucleic acids even in the body fluid other than blood, and several recent studies have already reported the possible utility of CTC and cfNAs in body fluids other than blood[118-122]. These reports have suggested the possibility of even less invasive and even more effective biomarkers in near future.
For the development of the field, PCa seems to be the ideal cancer to investigate for several reasons. First, the investigation of tumor-associated genetic alterations using tissue samples obtained from surgical or biopsy specimens is costly and difficult owing to anatomical and clinical difficulties. Additionally, the utility of the current serum biomarkers is limited owing to insufficient sensitivity and specificity. Repeatable and less invasive testing with high sensitivity and specificity to obtain information about genetic alterations or tumor dynamics will considerably contribute to the improvement of management for PCa. Second, it has already been revealed that some genetic or epigenetic alterations, such as KRAS, p16, SMAD4, TP53, and CDKN2A are present in most pancreatic tumor cells, which might make it easy to confirm the targets as tumor-derived molecules. Third, a genetic evolutionary model[120] revealed that 10-30 years are required from initiating a mutation until a patient’s death. Furthermore, mucinous cystic neoplasms, intraductal papillary neoplasms, pancreatic intraepithelial neoplasia (IPMN), and intraductal tubular papillary neoplasms were identified as premalignant lesions of PCa[121] that develop to invasive PCa through stepwise progression with the accumulation of several genetic aberrations. If these important genetic aberrations could be captured by liquid biopsy, screening and monitoring tests for high-risk lesions or early detection could be realized. To date, there are few reports about the usefulness of liquid biopsy in these premalignant lesions of PCa[122]. Recently our study successfully demonstrated that plasma miR-223 could predict malignant potential of IPMN[123]. We believe that further studies of liquid biopsy in premalignant lesions of PCa could contribute to improve the prognostic outcomes of PCa patients and the biomarker for premalignant lesion is nearing the clinical application.
Overall, liquid biopsy has the potential to allow us to diagnose at an early stage, predict prognosis, track the current status such as therapeutic efficacy or resistance, and provide optimal, individual treatment strategies for patients with cancer, that is, tailor-made treatment. The development of liquid biopsy
could provide many benefits for patients with cancer, especially for patients with PCa.
REFERENCES1 Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics,
2009. CA Cancer J Clin 2009; 59: 225-249 [PMID: 19474385 DOI: 10.3322/caac.20006]
2 Stathis A, Moore MJ. Advanced pancreatic carcinoma: current treatment and future challenges. Nat Rev Clin Oncol 2010; 7: 163-172 [PMID: 20101258 DOI: 10.1038/nrclinonc.2009.236]
3 Wolfgang CL, Herman JM, Laheru DA, Klein AP, Erdek MA, Fishman EK, Hruban RH. Recent progress in pancreatic cancer. CA Cancer J Clin 2013; 63: 318-348 [PMID: 23856911 DOI: 10.3322/caac.21190]
4 Heinemann V, Boeck S, Hinke A, Labianca R, Louvet C. Meta-analysis of randomized trials: evaluation of benefit from gemcitabine-based combination chemotherapy applied in advanced pancreatic cancer. BMC Cancer 2008; 8: 82 [PMID: 18373843 DOI: 10.1186/1471-2407-8-82]
5 Sultana A, Tudur Smith C, Cunningham D, Starling N, Neoptolemos JP, Ghaneh P. Meta-analyses of chemotherapy for locally advanced and metastatic pancreatic cancer: results of secondary end points analyses. Br J Cancer 2008; 99: 6-13 [PMID: 18577990 DOI: 10.1038/sj.bjc.6604436]
6 Ozaka M, Matsumura Y, Ishii H, Omuro Y, Itoi T, Mouri H, Hanada K, Kimura Y, Maetani I, Okabe Y, Tani M, Ikeda T, Hijioka S, Watanabe R, Ohoka S, Hirose Y, Suyama M, Egawa N, Sofuni A, Ikari T, Nakajima T. Randomized phase II study of gemcitabine and S-1 combination versus gemcitabine alone in the treatment of unresectable advanced pancreatic cancer (Japan Clinical Cancer Research Organization PC-01 study). Cancer Chemother Pharmacol 2012; 69: 1197-1204 [PMID: 22249272 DOI: 10.1007/s00280-012-1822-1]
7 Alix-Panabières C, Pantel K. Circulating tumor cells: liquid biopsy of cancer. Clin Chem 2013; 59: 110-118 [PMID: 23014601 DOI: 10.1373/clinchem.2012.194258]
8 Schwarzenbach H, Hoon DS, Pantel K. Cell-free nucleic acids as biomarkers in cancer patients. Nat Rev Cancer 2011; 11: 426-437 [PMID: 21562580 DOI: 10.1038/nrc3066]
9 van de Stolpe A, Pantel K, Sleijfer S, Terstappen LW, den Toonder JM. Circulating tumor cell isolation and diagnostics: toward routine clinical use. Cancer Res 2011; 71: 5955-5960 [PMID: 21896640 DOI: 10.1158/0008-5472.can-11-1254]
10 Crowley E, Di Nicolantonio F, Loupakis F, Bardelli A. Liquid biopsy: monitoring cancer-genetics in the blood. Nat Rev Clin Oncol 2013; 10: 472-484 [PMID: 23836314 DOI: 10.1038/nrclinonc.2013.110]
11 Ashworth TR. A case of cancer in which cells similar to those in the tumours were seen in the blood after death. Aust Med J 1869; 14: 146-149
12 Allard WJ, Matera J, Miller MC, Repollet M, Connelly MC, Rao C, Tibbe AG, Uhr JW, Terstappen LW. Tumor cells circulate in the peripheral blood of all major carcinomas but not in healthy subjects or patients with nonmalignant diseases. Clin Cancer Res 2004; 10: 6897-6904 [PMID: 15501967 DOI: 10.1158/1078-0432.ccr-04-0378]
13 Fidler IJ. Metastasis: quantitative analysis of distribution and fate of tumor emboli labeled with 125 I-5-iodo-2’-deoxyuridine. J Natl Cancer Inst 1970; 45: 773-782 [PMID: 5513503]
14 O'Flaherty JD, Gray S, Richard D, Fennell D, O’Leary JJ, Blackhall FH, O’Byrne KJ. Circulating tumour cells, their role in metastasis and their clinical utility in lung cancer. Lung Cancer 2012; 76: 19-25 [PMID: 22209049 DOI: 10.1016/j.lungcan.2011.10.018]
15 Luzzi KJ, MacDonald IC, Schmidt EE, Kerkvliet N, Morris VL, Chambers AF, Groom AC. Multistep nature of metastatic inefficiency: dormancy of solitary cells after successful extravasation and limited survival of early micrometastases. Am J Pathol 1998; 153: 865-873 [PMID: 9736035 DOI: 10.1016/
Imamura T et al . Liquid biopsy of pancreatic cancer

5636 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
s0002-9440(10)65628-3]16 Gorges TM, Tinhofer I, Drosch M, Röse L, Zollner TM, Krahn T,
von Ahsen O. Circulating tumour cells escape from EpCAM-based detection due to epithelial-to-mesenchymal transition. BMC Cancer 2012; 12: 178 [PMID: 22591372 DOI: 10.1186/1471-2407-12-178]
17 Balic M, Lin H, Williams A, Datar RH, Cote RJ. Progress in circulating tumor cell capture and analysis: implications for cancer management. Expert Rev Mol Diagn 2012; 12: 303-312 [PMID: 22468820 DOI: 10.1586/erm.12.12]
18 Cristofanilli M, Budd GT, Ellis MJ, Stopeck A, Matera J, Miller MC, Reuben JM, Doyle GV, Allard WJ, Terstappen LW, Hayes DF. Circulating tumor cells, disease progression, and survival in metastatic breast cancer. N Engl J Med 2004; 351: 781-791 [PMID: 15317891 DOI: 10.1056/NEJMoa040766]
19 Danila DC, Heller G, Gignac GA, Gonzalez-Espinoza R, Anand A, Tanaka E, Lilja H, Schwartz L, Larson S, Fleisher M, Scher HI. Circulating tumor cell number and prognosis in progressive castration-resistant prostate cancer. Clin Cancer Res 2007; 13: 7053-7058 [PMID: 18056182 DOI: 10.1158/1078-0432.ccr-07-1506]
20 Hayes DF, Cristofanilli M, Budd GT, Ellis MJ, Stopeck A, Miller MC, Matera J, Allard WJ, Doyle GV, Terstappen LW. Circulating tumor cells at each follow-up time point during therapy of metastatic breast cancer patients predict progression-free and overall survival. Clin Cancer Res 2006; 12: 4218-4224 [PMID: 16857794 DOI: 10.1158/1078-0432.ccr-05-2821]
21 Riethdorf S, Fritsche H, Müller V, Rau T, Schindlbeck C, Rack B, Janni W, Coith C, Beck K, Jänicke F, Jackson S, Gornet T, Cristofanilli M, Pantel K. Detection of circulating tumor cells in peripheral blood of patients with metastatic breast cancer: a validation study of the CellSearch system. Clin Cancer Res 2007; 13: 920-928 [PMID: 17289886 DOI: 10.1158/1078-0432.ccr-06-1695]
22 Sastre J, Maestro ML, Puente J, Veganzones S, Alfonso R, Rafael S, García-Saenz JA, Vidaurreta M, Martín M, Arroyo M, Sanz-Casla MT, Díaz-Rubio E. Circulating tumor cells in colorectal cancer: correlation with clinical and pathological variables. Ann Oncol 2008; 19: 935-938 [PMID: 18212090 DOI: 10.1093/annonc/mdm583]
23 Shaffer DR, Leversha MA, Danila DC, Lin O, Gonzalez-Espinoza R, Gu B, Anand A, Smith K, Maslak P, Doyle GV, Terstappen LW, Lilja H, Heller G, Fleisher M, Scher HI. Circulating tumor cell analysis in patients with progressive castration-resistant prostate cancer. Clin Cancer Res 2007; 13: 2023-2029 [PMID: 17404082 DOI: 10.1158/1078-0432.ccr-06-2701]
24 Stott SL, Hsu CH, Tsukrov DI, Yu M, Miyamoto DT, Waltman BA, Rothenberg SM, Shah AM, Smas ME, Korir GK, Floyd FP, Gilman AJ, Lord JB, Winokur D, Springer S, Irimia D, Nagrath S, Sequist LV, Lee RJ, Isselbacher KJ, Maheswaran S, Haber DA, Toner M. Isolation of circulating tumor cells using a microvortex-generating herringbone-chip. Proc Natl Acad Sci USA 2010; 107: 18392-18397 [PMID: 20930119 DOI: 10.1073/pnas.1012539107]
25 Saucedo-Zeni N, Mewes S, Niestroj R, Gasiorowski L, Murawa D, Nowaczyk P, Tomasi T, Weber E, Dworacki G, Morgenthaler NG, Jansen H, Propping C, Sterzynska K, Dyszkiewicz W, Zabel M, Kiechle M, Reuning U, Schmitt M, Lücke K. A novel method for the in vivo isolation of circulating tumor cells from peripheral blood of cancer patients using a functionalized and structured medical wire. Int J Oncol 2012; 41: 1241-1250 [PMID: 22825490 DOI: 10.3892/ijo.2012.1557]
26 Lustberg MB, Balasubramanian P, Miller B, Garcia-Villa A, Deighan C, Wu Y, Carothers S, Berger M, Ramaswamy B, Macrae ER, Wesolowski R, Layman RM, Mrozek E, Pan X, Summers TA, Shapiro CL, Chalmers JJ. Heterogeneous atypical cell populations are present in blood of metastatic breast cancer patients. Breast Cancer Res 2014; 16: R23 [PMID: 24602188 DOI: 10.1186/bcr3622]
27 Pantel K, Alix-Panabières C, Riethdorf S. Cancer micrometastases. Nat Rev Clin Oncol 2009; 6: 339-351 [PMID: 19399023 DOI: 10.1038/nrclinonc.2009.44]
28 Funaki NO, Tanaka J, Kasamatsu T, Ohshio G, Hosotani R, Okino T, Imamura M. Identification of carcinoembryonic antigen mRNA
in circulating peripheral blood of pancreatic carcinoma and gastric carcinoma patients. Life Sci 1996; 59: 2187-2199 [PMID: 8950323]
29 Funaki NO, Tanaka J, Hosotani R, Kogire M, Suwa H, Imamura M. Quantitative analysis of carcinoembryonic antigen messenger RNA in peripheral venous blood and portal blood of patients with pancreatic ductal adenocarcinoma. Clin Cancer Res 1998; 4: 855-860 [PMID: 9563878]
30 Miyazono F, Takao S, Natsugoe S, Uchikura K, Kijima F, Aridome K, Shinchi H, Aikou T. Molecular detection of circulating cancer cells during surgery in patients with biliary-pancreatic cancer. Am J Surg 1999; 177: 475-479 [PMID: 10414697]
31 Uchikura K, Takao S, Nakajo A, Miyazono F, Nakashima S, Tokuda K, Matsumoto M, Shinchi H, Natsugoe S, Aikou T. Intraoperative molecular detection of circulating tumor cells by reverse transcription-polymerase chain reaction in patients with biliary-pancreatic cancer is associated with hematogenous metastasis. Ann Surg Oncol 2002; 9: 364-370 [PMID: 11986188]
32 Mataki Y, Takao S, Maemura K, Mori S, Shinchi H, Natsugoe S, Aikou T. Carcinoembryonic antigen messenger RNA expression using nested reverse transcription-PCR in the peripheral blood during follow-up period of patients who underwent curative surgery for biliary-pancreatic cancer: longitudinal analyses. Clin Cancer Res 2004; 10: 3807-3814 [PMID: 15173089 DOI: 10.1158/1078-0432.ccr-03-0130]
33 Chausovsky G, Luchansky M, Figer A, Shapira J, Gottfried M, Novis B, Bogelman G, Zemer R, Zimlichman S, Klein A. Expression of cytokeratin 20 in the blood of patients with disseminated carcinoma of the pancreas, colon, stomach, and lung. Cancer 1999; 86: 2398-2405 [PMID: 10590383]
34 Lukyanchuk VV, Friess H, Kleeff J, Osinsky SP, Ayuni E, Candinas D, Roggo A. Detection of circulating tumor cells by cytokeratin 20 and prostate stem cell antigen RT-PCR in blood of patients with gastrointestinal cancers. Anticancer Res 2003; 23: 2711-2716 [PMID: 12894563]
35 Zhang YL, Feng JG, Gou JM, Zhou LX, Wang P. Detection of CK20mRNA in peripheral blood of pancreatic cancer and its clinical significance. World J Gastroenterol 2005; 11: 1023-1027 [PMID: 15742407]
36 Soeth E, Grigoleit U, Moellmann B, Röder C, Schniewind B, Kremer B, Kalthoff H, Vogel I. Detection of tumor cell dissemination in pancreatic ductal carcinoma patients by CK 20 RT-PCR indicates poor survival. J Cancer Res Clin Oncol 2005; 131: 669-676 [PMID: 16136352 DOI: 10.1007/s00432-005-0008-1]
37 Clarke LE, Leitzel K, Smith J, Ali SM, Lipton A. Epidermal growth factor receptor mRNA in peripheral blood of patients with pancreatic, lung, and colon carcinomas detected by RT-PCR. Int J Oncol 2003; 22: 425-430 [PMID: 12527944]
38 Ishizone S, Yamauchi K, Kawa S, Suzuki T, Shimizu F, Harada O, Sugiyama A, Miyagawa S, Fukuda M, Nakayama J. Clinical utility of quantitative RT-PCR targeted to alpha1,4-N-acetylglucosaminyltransferase mRNA for detection of pancreatic cancer. Cancer Sci 2006; 97: 119-126 [PMID: 16441422 DOI: 10.1111/j.1349-7006.2006.00148.x]
39 Hoffmann K, Kerner C, Wilfert W, Mueller M, Thiery J, Hauss J, Witzigmann H. Detection of disseminated pancreatic cells by amplification of cytokeratin-19 with quantitative RT-PCR in blood, bone marrow and peritoneal lavage of pancreatic carcinoma patients. World J Gastroenterol 2007; 13: 257-263 [PMID: 17226905]
40 Zhou J, Hu L, Yu Z, Zheng J, Yang D, Bouvet M, Hoffman RM. Marker expression in circulating cancer cells of pancreatic cancer patients. J Surg Res 2011; 171: 631-636 [PMID: 20869080 DOI: 10.1016/j.jss.2010.05.007]
41 Kurihara T, Itoi T, Sofuni A, Itokawa F, Tsuchiya T, Tsuji S, Ishii K, Ikeuchi N, Tsuchida A, Kasuya K, Kawai T, Sakai Y, Moriyasu F. Detection of circulating tumor cells in patients with pancreatic cancer: a preliminary result. J Hepatobiliary Pancreat Surg 2008; 15: 189-195 [PMID: 18392713 DOI: 10.1007/s00534-007-1250-5]
42 Bidard FC, Huguet F, Louvet C, Mineur L, Bouché O, Chibaudel B, Artru P, Desseigne F, Bachet JB, Mathiot C, Pierga JY, Hammel P. Circulating tumor cells in locally advanced pancreatic
Imamura T et al . Liquid biopsy of pancreatic cancer
5637 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
adenocarcinoma: the ancillary CirCe 07 study to the LAP 07 trial. Ann Oncol 2013; 24: 2057-2061 [PMID: 23676420 DOI: 10.1093/annonc/mdt176]
43 Iwanicki-Caron I, Basile P, Toure E, Antonietti M, Lecleire S, Di Fiore A, Oden-Gangloff A, Blanchard F, Lemoine F, Di Fiore F, Sabourin JC, Michel P. Usefulness of circulating tumor cell detection in pancreatic adenocarcinoma diagnosis. Am J Gastroenterol 2013; 108: 152-155 [PMID: 23287955 DOI: 10.1038/ajg.2012.367]
44 Cauley CE, Pitman MB, Zhou J, Perkins J, Kuleman B, Liss AS, Fernandez-Del Castillo C, Warshaw AL, Lillemoe KD, Thayer SP. Circulating Epithelial Cells in Patients with Pancreatic Lesions: Clinical and Pathologic Findings. J Am Coll Surg 2015; 221: 699-707 [PMID: 26209458 DOI: 10.1016/j.jamcollsurg.2015.05.014]
45 Bobek V, Gurlich R, Eliasova P, Kolostova K. Circulating tumor cells in pancreatic cancer patients: enrichment and cultivation. World J Gastroenterol 2014; 20: 17163-17170 [PMID: 25493031 DOI: 10.3748/wjg.v20.i45.17163]
46 Kulemann B, Pitman MB, Liss AS, Valsangkar N, Fernández-Del Castillo C, Lillemoe KD, Hoeppner J, Mino-Kenudson M, Warshaw AL, Thayer SP. Circulating tumor cells found in patients with localized and advanced pancreatic cancer. Pancreas 2015; 44: 547-550 [PMID: 25822154 DOI: 10.1097/mpa.0000000000000324]
47 Rhim AD, Thege FI, Santana SM, Lannin TB, Saha TN, Tsai S, Maggs LR, Kochman ML, Ginsberg GG, Lieb JG, Chandrasekhara V, Drebin JA, Ahmad N, Yang YX, Kirby BJ, Stanger BZ. Detection of circulating pancreas epithelial cells in patients with pancreatic cystic lesions. Gastroenterology 2014; 146: 647-651 [PMID: 24333829 DOI: 10.1053/j.gastro.2013.12.007]
48 Sheng W, Ogunwobi OO, Chen T, Zhang J, George TJ, Liu C, Fan ZH. Capture, release and culture of circulating tumor cells from pancreatic cancer patients using an enhanced mixing chip. Lab Chip 2014; 14: 89-98 [PMID: 24220648 DOI: 10.1039/c3lc51017d]
49 Mandel P, Metais P. Les acides nucléiques du plasma sanguin chez l’homme. C R Seances Soc Biol Fil 1948; 142: 241-243 [PMID: 18875018]
50 Leon SA, Shapiro B, Sklaroff DM, Yaros MJ. Free DNA in the serum of cancer patients and the effect of therapy. Cancer Res 1977; 37: 646-650 [PMID: 837366]
51 Vasioukhin V, Anker P, Maurice P, Lyautey J, Lederrey C, Stroun M. Point mutations of the N-ras gene in the blood plasma DNA of patients with myelodysplastic syndrome or acute myelogenous leukaemia. Br J Haematol 1994; 86: 774-779 [PMID: 7918071]
52 Cachia PG, Taylor C, Thompson PW, Tennant GB, Masters G, Pettersson T, Whittaker JA, Burnett AK, Jacobs A, Padua RA. Non-dysplastic myelodysplasia? Leukemia 1994; 8: 677-681 [PMID: 8152265]
53 Sorenson GD, Pribish DM, Valone FH, Memoli VA, Bzik DJ, Yao SL. Soluble normal and mutated DNA sequences from single-copy genes in human blood. Cancer Epidemiol Biomarkers Prev 1994; 3: 67-71 [PMID: 8118388]
54 Kopreski MS, Benko FA, Kwak LW, Gocke CD. Detection of tumor messenger RNA in the serum of patients with malignant melanoma. Clin Cancer Res 1999; 5: 1961-1965 [PMID: 10473072]
55 Lo KW, Lo YM, Leung SF, Tsang YS, Chan LY, Johnson PJ, Hjelm NM, Lee JC, Huang DP. Analysis of cell-free Epstein-Barr virus associated RNA in the plasma of patients with nasopharyngeal carcinoma. Clin Chem 1999; 45: 1292-1294 [PMID: 10430801]
56 Dasí F, Martínez-Rodes P, March JA, Santamaría J, Martínez-Javaloyas JM, Gil M, Aliño SF. Real-time quantification of human telomerase reverse transcriptase mRNA in the plasma of patients with prostate cancer. Ann N Y Acad Sci 2006; 1075: 204-210 [PMID: 17108213 DOI: 10.1196/annals.1368.028]
57 Chen XQ, Bonnefoi H, Pelte MF, Lyautey J, Lederrey C, Movarekhi S, Schaeffer P, Mulcahy HE, Meyer P, Stroun M, Anker P. Telomerase RNA as a detection marker in the serum of breast cancer patients. Clin Cancer Res 2000; 6: 3823-3826 [PMID: 11051224]
58 Silva JM, Rodriguez R, Garcia JM, Muñoz C, Silva J, Dominguez G, Provencio M, España P, Bonilla F. Detection of epithelial tumour RNA in the plasma of colon cancer patients is associated with
advanced stages and circulating tumour cells. Gut 2002; 50: 530-534 [PMID: 11889075]
59 Mitchell PS, Parkin RK, Kroh EM, Fritz BR, Wyman SK, Pogosova-Agadjanyan EL, Peterson A, Noteboom J, O’Briant KC, Allen A, Lin DW, Urban N, Drescher CW, Knudsen BS, Stirewalt DL, Gentleman R, Vessella RL, Nelson PS, Martin DB, Tewari M. Circulating microRNAs as stable blood-based markers for cancer detection. Proc Natl Acad Sci USA 2008; 105: 10513-10518 [PMID: 18663219 DOI: 10.1073/pnas.0804549105]
60 Diehl F, Li M, Dressman D, He Y, Shen D, Szabo S, Diaz LA, Goodman SN, David KA, Juhl H, Kinzler KW, Vogelstein B. Detection and quantification of mutations in the plasma of patients with colorectal tumors. Proc Natl Acad Sci USA 2005; 102: 16368-16373 [PMID: 16258065 DOI: 10.1073/pnas.0507904102]
61 van 't Veer LJ, Dai H, van de Vijver MJ, He YD, Hart AA, Mao M, Peterse HL, van der Kooy K, Marton MJ, Witteveen AT, Schreiber GJ, Kerkhoven RM, Roberts C, Linsley PS, Bernards R, Friend SH. Gene expression profiling predicts clinical outcome of breast cancer. Nature 2002; 415: 530-536 [PMID: 11823860 DOI: 10.1038/415530a]
62 Dawson SJ, Tsui DW, Murtaza M, Biggs H, Rueda OM, Chin SF, Dunning MJ, Gale D, Forshew T, Mahler-Araujo B, Rajan S, Humphray S, Becq J, Halsall D, Wallis M, Bentley D, Caldas C, Rosenfeld N. Analysis of circulating tumor DNA to monitor metastatic breast cancer. N Engl J Med 2013; 368: 1199-1209 [PMID: 23484797 DOI: 10.1056/NEJMoa1213261]
63 Chan KC, Jiang P, Zheng YW, Liao GJ, Sun H, Wong J, Siu SS, Chan WC, Chan SL, Chan AT, Lai PB, Chiu RW, Lo YM. Cancer genome scanning in plasma: detection of tumor-associated copy number aberrations, single-nucleotide variants, and tumoral heterogeneity by massively parallel sequencing. Clin Chem 2013; 59: 211-224 [PMID: 23065472 DOI: 10.1373/clinchem.2012.196014]
64 Shapiro B, Chakrabarty M, Cohn EM, Leon SA. Determination of circulating DNA levels in patients with benign or malignant gastrointestinal disease. Cancer 1983; 51: 2116-2120 [PMID: 6188527]
65 Melnikov AA, Scholtens D, Talamonti MS, Bentrem DJ, Levenson VV. Methylation profile of circulating plasma DNA in patients with pancreatic cancer. J Surg Oncol 2009; 99: 119-122 [PMID: 19065635 DOI: 10.1002/jso.21208]
66 Liggett T, Melnikov A, Yi QL, Replogle C, Brand R, Kaul K, Talamonti M, Abrams RA, Levenson V. Differential methylation of cell-free circulating DNA among patients with pancreatic cancer versus chronic pancreatitis. Cancer 2010; 116: 1674-1680 [PMID: 20143430 DOI: 10.1002/cncr.24893]
67 Moriyama H, Matsubara N, Kanbara T, Mori M, Matsuoka J, Yoshino T, Takakura N, Shimizu K, Takaka N. Allelic imbalance and microsatellite instability in plasma DNA released from polyclonal pancreatic adenocarcinoma. Int J Oncol 2002; 21: 949-956 [PMID: 12370740]
68 Smit VT, Boot AJ, Smits AM, Fleuren GJ, Cornelisse CJ, Bos JL. KRAS codon 12 mutations occur very frequently in pancreatic adenocarcinomas. Nucleic Acids Res 1988; 16: 7773-7782 [PMID: 3047672]
69 Almoguera C, Shibata D, Forrester K, Martin J, Arnheim N, Perucho M. Most human carcinomas of the exocrine pancreas contain mutant c-K-ras genes. Cell 1988; 53: 549-554 [PMID: 2453289]
70 Tada M, Omata M, Ohto M. Clinical application of ras gene mutation for diagnosis of pancreatic adenocarcinoma. Gastroenterology 1991; 100: 233-238 [PMID: 1983826]
71 Lemoine NR, Jain S, Hughes CM, Staddon SL, Maillet B, Hall PA, Klöppel G. Ki-ras oncogene activation in preinvasive pancreatic cancer. Gastroenterology 1992; 102: 230-236 [PMID: 1309358]
72 Yamada T, Nakamori S, Ohzato H, Oshima S, Aoki T, Higaki N, Sugimoto K, Akagi K, Fujiwara Y, Nishisho I, Sakon M, Gotoh M, Monden M. Detection of K-ras gene mutations in plasma DNA of patients with pancreatic adenocarcinoma: correlation with clinicopathological features. Clin Cancer Res 1998; 4: 1527-1532 [PMID: 9626473]
Imamura T et al . Liquid biopsy of pancreatic cancer

5638 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
73 Theodor L, Melzer E, Sologov M, Idelman G, Friedman E, Bar-Meir S. Detection of pancreatic carcinoma: diagnostic value of K-ras mutations in circulating DNA from serum. Dig Dis Sci 1999; 44: 2014-2019 [PMID: 10548352]
74 Castells A, Puig P, Móra J, Boadas J, Boix L, Urgell E, Solé M, Capellà G, Lluís F, Fernández-Cruz L, Navarro S, Farré A. K-ras mutations in DNA extracted from the plasma of patients with pancreatic carcinoma: diagnostic utility and prognostic significance. J Clin Oncol 1999; 17: 578-584 [PMID: 10080602]
75 Zambon C, Navaglia F, Basso D, Gallo N, Greco E, Piva MG, Fogar P, Pasquali C, Pedrazzoli S, Plebani M. ME-PCR for the identification of mutated K-ras in serum and bile of pancreatic cancer patients: an unsatisfactory technique for clinical applications. Clin Chim Acta 2000; 302: 35-48 [PMID: 11074062]
76 Maire F, Micard S, Hammel P, Voitot H, Lévy P, Cugnenc PH, Ruszniewski P, Puig PL. Differential diagnosis between chronic pancreatitis and pancreatic cancer: value of the detection of KRAS2 mutations in circulating DNA. Br J Cancer 2002; 87: 551-554 [PMID: 12189555 DOI: 10.1038/sj.bjc.6600475]
77 Marchese R, Muleti A, Brozzetti S, Gandini O, Brunetti E, French D. Low value of detection of KRAS2 mutations in circulating DNA to differentiate chronic pancreatitis to pancreatic cancer. Br J Cancer 2004; 90: 2243 [PMID: 15150585 DOI: 10.1038/sj.bjc.6601854]
78 Magistrelli P, Neri M, Granone P, Cesario A, Paleari L, Russo P. K-ras mutations in circulating DNA from pancreatic and lung cancers: bridging methodology for a common validation of the molecular diagnosis value. Pancreas 2008; 37: 101-102 [PMID: 18580451 DOI: 10.1097/MPA.0b013e31815e72bc]
79 Chen H, Tu H, Meng ZQ, Chen Z, Wang P, Liu LM. K-ras mutational status predicts poor prognosis in unresectable pancreatic cancer. Eur J Surg Oncol 2010; 36: 657-662 [PMID: 20542658 DOI: 10.1016/j.ejso.2010.05.014]
80 Wu J, Zhou Y, Zhang CY, Song BB, Wang BL, Pan BS, Lou WH, Guo W. Co-amplification at lower denaturation-temperature PCR combined with unlabled-probe high-resolution melting to detect KRAS codon 12 and 13 mutations in plasma-circulating DNA of pancreatic adenocarcinoma cases. Asian Pac J Cancer Prev 2014; 15: 10647-10652 [PMID: 25605154]
81 Earl J , Garcia-Nieto S, Martinez-Avila JC, Montans J, Sanjuanbenito A, Rodríguez-Garrote M, Lisa E, Mendía E, Lobo E, Malats N, Carrato A, Guillen-Ponce C. Circulating tumor cells (Ctc) and kras mutant circulating free Dna (cfdna) detection in peripheral blood as biomarkers in patients diagnosed with exocrine pancreatic cancer. BMC Cancer 2015; 15: 797 [PMID: 26498594 DOI: 10.1186/s12885-015-1779-7]
82 Kinugasa H, Nouso K, Miyahara K, Morimoto Y, Dohi C, Tsutsumi K, Kato H, Matsubara T, Okada H, Yamamoto K. Detection of K-ras gene mutation by liquid biopsy in patients with pancreatic cancer. Cancer 2015; 121: 2271-2280 [PMID: 25823825 DOI: 10.1002/cncr.29364]
83 Sausen M, Phallen J, Adleff V, Jones S, Leary RJ, Barrett MT, Anagnostou V, Parpart-Li S, Murphy D, Kay Li Q, Hruban CA, Scharpf R, White JR, O’Dwyer PJ, Allen PJ, Eshleman JR, Thompson CB, Klimstra DS, Linehan DC, Maitra A, Hruban RH, Diaz LA, Von Hoff DD, Johansen JS, Drebin JA, Velculescu VE. Clinical implications of genomic alterations in the tumour and circulation of pancreatic cancer patients. Nat Commun 2015; 6: 7686 [PMID: 26154128 DOI: 10.1038/ncomms8686]
84 Takai E, Totoki Y, Nakamura H, Morizane C, Nara S, Hama N, Suzuki M, Furukawa E, Kato M, Hayashi H, Kohno T, Ueno H, Shimada K, Okusaka T, Nakagama H, Shibata T, Yachida S. Clinical utility of circulating tumor DNA for molecular assessment in pancreatic cancer. Sci Rep 2015; 5: 18425 [PMID: 26669280 DOI: 10.1038/srep18425]
85 Zill OA, Greene C, Sebisanovic D, Siew LM, Leng J, Vu M, Hendifar AE, Wang Z, Atreya CE, Kelley RK, Van Loon K, Ko AH, Tempero MA, Bivona TG, Munster PN, Talasaz A, Collisson EA. Cell-Free DNA Next-Generation Sequencing in Pancreatobiliary Carcinomas. Cancer Discov 2015; 5: 1040-1048 [PMID: 26109333 DOI: 10.1158/2159-8290.cd-15-0274]
86 Diaz LA, Williams RT, Wu J, Kinde I, Hecht JR, Berlin J, Allen B, Bozic I, Reiter JG, Nowak MA, Kinzler KW, Oliner KS, Vogelstein B. The molecular evolution of acquired resistance to targeted EGFR blockade in colorectal cancers. Nature 2012; 486: 537-540 [PMID: 22722843 DOI: 10.1038/nature11219]
87 Misale S, Yaeger R, Hobor S, Scala E, Janakiraman M, Liska D, Valtorta E, Schiavo R, Buscarino M, Siravegna G, Bencardino K, Cercek A, Chen CT, Veronese S, Zanon C, Sartore-Bianchi A, Gambacorta M, Gallicchio M, Vakiani E, Boscaro V, Medico E, Weiser M, Siena S, Di Nicolantonio F, Solit D, Bardelli A. Emergence of KRAS mutations and acquired resistance to anti-EGFR therapy in colorectal cancer. Nature 2012; 486: 532-536 [PMID: 22722830 DOI: 10.1038/nature11156]
88 Murtaza M, Dawson SJ, Tsui DW, Gale D, Forshew T, Piskorz AM, Parkinson C, Chin SF, Kingsbury Z, Wong AS, Marass F, Humphray S, Hadfield J, Bentley D, Chin TM, Brenton JD, Caldas C, Rosenfeld N. Non-invasive analysis of acquired resistance to cancer therapy by sequencing of plasma DNA. Nature 2013; 497: 108-112 [PMID: 23563269 DOI: 10.1038/nature12065]
89 Reddi KK, Holland JF. Elevated serum ribonuclease in patients with pancreatic cancer. Proc Natl Acad Sci USA 1976; 73: 2308-2310 [PMID: 1065880]
90 Houseley J, LaCava J, Tollervey D. RNA-quality control by the exosome. Nat Rev Mol Cell Biol 2006; 7: 529-539 [PMID: 16829983 DOI: 10.1038/nrm1964]
91 Silva JM, Dominguez G, Silva J, Garcia JM, Sanchez A, Rodriguez O, Provencio M, España P, Bonilla F. Detection of epithelial messenger RNA in the plasma of breast cancer patients is associated with poor prognosis tumor characteristics. Clin Cancer Res 2001; 7: 2821-2825 [PMID: 11555599]
92 Wong SC, Lo SF, Cheung MT, Ng KO, Tse CW, Lai BS, Lee KC, Lo YM. Quantification of plasma beta-catenin mRNA in colorectal cancer and adenoma patients. Clin Cancer Res 2004; 10: 1613-1617 [PMID: 15014011]
93 Garcia V, García JM, Peña C, Silva J, Domínguez G, Hurtado A, Alonso I, Rodriguez R, Provencio M, Bonilla F. Thymidylate synthase messenger RNA expression in plasma from patients with colon cancer: prognostic potential. Clin Cancer Res 2006; 12: 2095-2100 [PMID: 16609021 DOI: 10.1158/1078-0432.ccr-05-1644]
94 Kang CY, Wang J, Axell-House D, Soni P, Chu ML, Chipitsyna G, Sarosiek K, Sendecki J, Hyslop T, Al-Zoubi M, Yeo CJ, Arafat HA. Clinical significance of serum COL6A3 in pancreatic ductal adenocarcinoma. J Gastrointest Surg 2014; 18: 7-15 [PMID: 24002763 DOI: 10.1007/s11605-013-2326-y]
95 ENCODE Project Consortium. An integrated encyclopedia of DNA elements in the human genome. Nature 2012; 489: 57-74 [PMID: 22955616 DOI: 10.1038/nature11247]
96 Lander ES, Linton LM, Birren B, Nusbaum C, Zody MC, Baldwin J, Devon K, Dewar K, Doyle M, FitzHugh W, Funke R, Gage D, Harris K, Heaford A, Howland J, Kann L, Lehoczky J, LeVine R, McEwan P, McKernan K, Meldrim J, Mesirov JP, Miranda C, Morris W, Naylor J, Raymond C, Rosetti M, Santos R, Sheridan A, Sougnez C, Stange-Thomann Y, Stojanovic N, Subramanian A, Wyman D, Rogers J, Sulston J, Ainscough R, Beck S, Bentley D, Burton J, Clee C, Carter N, Coulson A, Deadman R, Deloukas P, Dunham A, Dunham I, Durbin R, French L, Grafham D, Gregory S, Hubbard T, Humphray S, Hunt A, Jones M, Lloyd C, McMurray A, Matthews L, Mercer S, Milne S, Mullikin JC, Mungall A, Plumb R, Ross M, Shownkeen R, Sims S, Waterston RH, Wilson RK, Hillier LW, McPherson JD, Marra MA, Mardis ER, Fulton LA, Chinwalla AT, Pepin KH, Gish WR, Chissoe SL, Wendl MC, Delehaunty KD, Miner TL, Delehaunty A, Kramer JB, Cook LL, Fulton RS, Johnson DL, Minx PJ, Clifton SW, Hawkins T, Branscomb E, Predki P, Richardson P, Wenning S, Slezak T, Doggett N, Cheng JF, Olsen A, Lucas S, Elkin C, Uberbacher E, Frazier M, Gibbs RA, Muzny DM, Scherer SE, Bouck JB, Sodergren EJ, Worley KC, Rives CM, Gorrell JH, Metzker ML, Naylor SL, Kucherlapati RS, Nelson DL, Weinstock GM, Sakaki Y, Fujiyama A, Hattori M, Yada T, Toyoda A, Itoh T, Kawagoe C, Watanabe H, Totoki
Imamura T et al . Liquid biopsy of pancreatic cancer

5639 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Y, Taylor T, Weissenbach J, Heilig R, Saurin W, Artiguenave F, Brottier P, Bruls T, Pelletier E, Robert C, Wincker P, Smith DR, Doucette-Stamm L, Rubenfield M, Weinstock K, Lee HM, Dubois J, Rosenthal A, Platzer M, Nyakatura G, Taudien S, Rump A, Yang H, Yu J, Wang J, Huang G, Gu J, Hood L, Rowen L, Madan A, Qin S, Davis RW, Federspiel NA, Abola AP, Proctor MJ, Myers RM, Schmutz J, Dickson M, Grimwood J, Cox DR, Olson MV, Kaul R, Raymond C, Shimizu N, Kawasaki K, Minoshima S, Evans GA, Athanasiou M, Schultz R, Roe BA, Chen F, Pan H, Ramser J, Lehrach H, Reinhardt R, McCombie WR, de la Bastide M, Dedhia N, Blöcker H, Hornischer K, Nordsiek G, Agarwala R, Aravind L, Bailey JA, Bateman A, Batzoglou S, Birney E, Bork P, Brown DG, Burge CB, Cerutti L, Chen HC, Church D, Clamp M, Copley RR, Doerks T, Eddy SR, Eichler EE, Furey TS, Galagan J, Gilbert JG, Harmon C, Hayashizaki Y, Haussler D, Hermjakob H, Hokamp K, Jang W, Johnson LS, Jones TA, Kasif S, Kaspryzk A, Kennedy S, Kent WJ, Kitts P, Koonin EV, Korf I, Kulp D, Lancet D, Lowe TM, McLysaght A, Mikkelsen T, Moran JV, Mulder N, Pollara VJ, Ponting CP, Schuler G, Schultz J, Slater G, Smit AF, Stupka E, Szustakowki J, Thierry-Mieg D, Thierry-Mieg J, Wagner L, Wallis J, Wheeler R, Williams A, Wolf YI, Wolfe KH, Yang SP, Yeh RF, Collins F, Guyer MS, Peterson J, Felsenfeld A, Wetterstrand KA, Patrinos A, Morgan MJ, de Jong P, Catanese JJ, Osoegawa K, Shizuya H, Choi S, Chen YJ, Szustakowki J. Initial sequencing and analysis of the human genome. Nature 2001; 409: 860-921 [PMID: 11237011 DOI: 10.1038/35057062]
97 Venter JC, Adams MD, Myers EW, Li PW, Mural RJ, Sutton GG, Smith HO, Yandell M, Evans CA, Holt RA, Gocayne JD, Amanatides P, Ballew RM, Huson DH, Wortman JR, Zhang Q, Kodira CD, Zheng XH, Chen L, Skupski M, Subramanian G, Thomas PD, Zhang J, Gabor Miklos GL, Nelson C, Broder S, Clark AG, Nadeau J, McKusick VA, Zinder N, Levine AJ, Roberts RJ, Simon M, Slayman C, Hunkapiller M, Bolanos R, Delcher A, Dew I, Fasulo D, Flanigan M, Florea L, Halpern A, Hannenhalli S, Kravitz S, Levy S, Mobarry C, Reinert K, Remington K, Abu-Threideh J, Beasley E, Biddick K, Bonazzi V, Brandon R, Cargill M, Chandramouliswaran I, Charlab R, Chaturvedi K, Deng Z, Di Francesco V, Dunn P, Eilbeck K, Evangelista C, Gabrielian AE, Gan W, Ge W, Gong F, Gu Z, Guan P, Heiman TJ, Higgins ME, Ji RR, Ke Z, Ketchum KA, Lai Z, Lei Y, Li Z, Li J, Liang Y, Lin X, Lu F, Merkulov GV, Milshina N, Moore HM, Naik AK, Narayan VA, Neelam B, Nusskern D, Rusch DB, Salzberg S, Shao W, Shue B, Sun J, Wang Z, Wang A, Wang X, Wang J, Wei M, Wides R, Xiao C, Yan C, Yao A, Ye J, Zhan M, Zhang W, Zhang H, Zhao Q, Zheng L, Zhong F, Zhong W, Zhu S, Zhao S, Gilbert D, Baumhueter S, Spier G, Carter C, Cravchik A, Woodage T, Ali F, An H, Awe A, Baldwin D, Baden H, Barnstead M, Barrow I, Beeson K, Busam D, Carver A, Center A, Cheng ML, Curry L, Danaher S, Davenport L, Desilets R, Dietz S, Dodson K, Doup L, Ferriera S, Garg N, Gluecksmann A, Hart B, Haynes J, Haynes C, Heiner C, Hladun S, Hostin D, Houck J, Howland T, Ibegwam C, Johnson J, Kalush F, Kline L, Koduru S, Love A, Mann F, May D, McCawley S, McIntosh T, McMullen I, Moy M, Moy L, Murphy B, Nelson K, Pfannkoch C, Pratts E, Puri V, Qureshi H, Reardon M, Rodriguez R, Rogers YH, Romblad D, Ruhfel B, Scott R, Sitter C, Smallwood M, Stewart E, Strong R, Suh E, Thomas R, Tint NN, Tse S, Vech C, Wang G, Wetter J, Williams S, Williams M, Windsor S, Winn-Deen E, Wolfe K, Zaveri J, Zaveri K, Abril JF, Guigó R, Campbell MJ, Sjolander KV, Karlak B, Kejariwal A, Mi H, Lazareva B, Hatton T, Narechania A, Diemer K, Muruganujan A, Guo N, Sato S, Bafna V, Istrail S, Lippert R, Schwartz R, Walenz B, Yooseph S, Allen D, Basu A, Baxendale J, Blick L, Caminha M, Carnes-Stine J, Caulk P, Chiang YH, Coyne M, Dahlke C, Mays A, Dombroski M, Donnelly M, Ely D, Esparham S, Fosler C, Gire H, Glanowski S, Glasser K, Glodek A, Gorokhov M, Graham K, Gropman B, Harris M, Heil J, Henderson S, Hoover J, Jennings D, Jordan C, Jordan J, Kasha J, Kagan L, Kraft C, Levitsky A, Lewis M, Liu X, Lopez J, Ma D, Majoros W, McDaniel J, Murphy S, Newman M, Nguyen T, Nguyen N, Nodell M, Pan S, Peck J, Peterson M, Rowe W, Sanders R, Scott J, Simpson M, Smith T,
Sprague A, Stockwell T, Turner R, Venter E, Wang M, Wen M, Wu D, Wu M, Xia A, Zandieh A, Zhu X. The sequence of the human genome. Science 2001; 291: 1304-1351 [PMID: 11181995 DOI: 10.1126/science.1058040]
98 Szymanski M, Barciszewska MZ, Erdmann VA, Barciszewski J. A new frontier for molecular medicine: noncoding RNAs. Biochim Biophys Acta 2005; 1756: 65-75 [PMID: 16125325 DOI: 10.1016/j.bbcan.2005.07.005]
99 Valadi H, Ekström K, Bossios A, Sjöstrand M, Lee JJ, Lötvall JO. Exosome-mediated transfer of mRNAs and microRNAs is a novel mechanism of genetic exchange between cells. Nat Cell Biol 2007; 9: 654-659 [PMID: 17486113 DOI: 10.1038/ncb1596]
100 Kosaka N, Iguchi H, Yoshioka Y, Takeshita F, Matsuki Y, Ochiya T. Secretory mechanisms and intercellular transfer of microRNAs in living cells. J Biol Chem 2010; 285: 17442-17452 [PMID: 20353945 DOI: 10.1074/jbc.M110.107821]
101 Arroyo JD, Chevillet JR, Kroh EM, Ruf IK, Pritchard CC, Gibson DF, Mitchell PS, Bennett CF, Pogosova-Agadjanyan EL, Stirewalt DL, Tait JF, Tewari M. Argonaute2 complexes carry a population of circulating microRNAs independent of vesicles in human plasma. Proc Natl Acad Sci USA 2011; 108: 5003-5008 [PMID: 21383194 DOI: 10.1073/pnas.1019055108]
102 Wang J, Chen J, Chang P, LeBlanc A, Li D, Abbruzzesse JL, Frazier ML, Killary AM, Sen S. MicroRNAs in plasma of pancreatic ductal adenocarcinoma patients as novel blood-based biomarkers of disease. Cancer Prev Res (Phila) 2009; 2: 807-813 [PMID: 19723895 DOI: 10.1158/1940-6207.capr-09-0094]
103 Schultz NA, Dehlendorff C, Jensen BV, Bjerregaard JK, Nielsen KR, Bojesen SE, Calatayud D, Nielsen SE, Yilmaz M, Holländer NH, Andersen KK, Johansen JS. MicroRNA biomarkers in whole blood for detection of pancreatic cancer. JAMA 2014; 311: 392-404 [PMID: 24449318 DOI: 10.1001/jama.2013.284664]
104 Kojima M, Sudo H, Kawauchi J, Takizawa S, Kondou S, Nobumasa H, Ochiai A. MicroRNA markers for the diagnosis of pancreatic and biliary-tract cancers. PLoS One 2015; 10: e0118220 [PMID: 25706130 DOI: 10.1371/journal.pone.0118220]
105 Kong X, Du Y, Wang G, Gao J, Gong Y, Li L, Zhang Z, Zhu J, Jing Q, Qin Y, Li Z. Detection of differentially expressed microRNAs in serum of pancreatic ductal adenocarcinoma patients: miR-196a could be a potential marker for poor prognosis. Dig Dis Sci 2011; 56: 602-609 [PMID: 20614181 DOI: 10.1007/s10620-010-1285-3]
106 Miyamae M, Komatsu S, Ichikawa D, Kawaguchi T, Hirajima S, Okajima W, Ohashi T, Imamura T, Konishi H, Shiozaki A, Morimura R, Ikoma H, Ochiai T, Okamoto K, Taniguchi H, Otsuji E. Plasma microRNA profiles: identification of miR-744 as a novel diagnostic and prognostic biomarker in pancreatic cancer. Br J Cancer 2015; 113: 1467-1476 [PMID: 26505678 DOI: 10.1038/bjc.2015.366]
107 Kim K, Jutooru I, Chadalapaka G, Johnson G, Frank J, Burghardt R, Kim S, Safe S. HOTAIR is a negative prognostic factor and exhibits pro-oncogenic activity in pancreatic cancer. Oncogene 2013; 32: 1616-1625 [PMID: 22614017 DOI: 10.1038/onc.2012.193]
108 Pang EJ, Yang R, Fu XB, Liu YF. Overexpression of long non-coding RNA MALAT1 is correlated with clinical progression and unfavorable prognosis in pancreatic cancer. Tumour Biol 2015; 36: 2403-2407 [PMID: 25481511 DOI: 10.1007/s13277-014-2850-8]
109 Modali SD, Parekh VI, Kebebew E, Agarwal SK. Epigenetic regulation of the lncRNA MEG3 and its target c-MET in pancreatic neuroendocrine tumors. Mol Endocrinol 2015; 29: 224-237 [PMID: 25565142 DOI: 10.1210/me.2014-1304]
110 Lu X, Fang Y, Wang Z, Xie J, Zhan Q, Deng X, Chen H, Jin J, Peng C, Li H, Shen B. Downregulation of gas5 increases pancreatic cancer cell proliferation by regulating CDK6. Cell Tissue Res 2013; 354: 891-896 [PMID: 24026436 DOI: 10.1007/s00441-013-1711-x]
111 Peng W, Gao W, Feng J. Long noncoding RNA HULC is a novel biomarker of poor prognosis in patients with pancreatic cancer. Med Oncol 2014; 31: 346 [PMID: 25412939 DOI: 10.1007/s12032-014-0346-4]
112 Huang C, Yu W, Wang Q, Cui H, Wang Y, Zhang L, Han F, Huang T. Increased expression of the lncRNA PVT1 is associated with poor prognosis in pancreatic cancer patients. Minerva Med 2015; 106:
Imamura T et al . Liquid biopsy of pancreatic cancer

5640 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
143-149 [PMID: 25668599]113 Tahira AC, Kubrusly MS, Faria MF, Dazzani B, Fonseca RS,
Maracaja-Coutinho V, Verjovski-Almeida S, Machado MC, Reis EM. Long noncoding intronic RNAs are differentially expressed in primary and metastatic pancreatic cancer. Mol Cancer 2011; 10: 141 [PMID: 22078386 DOI: 10.1186/1476-4598-10-141]
114 Li J, Liu D, Hua R, Zhang J, Liu W, Huo Y, Cheng Y, Hong J, Sun Y. Long non-coding RNAs expressed in pancreatic ductal adenocarcinoma and lncRNA BC008363 an independent prognostic factor in PDAC. Pancreatology 2014; 14: 385-390 [PMID: 25200694 DOI: 10.1016/j.pan.2014.07.013]
115 Sun YW, Chen YF, Li J, Huo YM, Liu DJ, Hua R, Zhang JF, Liu W, Yang JY, Fu XL, Yan T, Hong J, Cao H. A novel long non-coding RNA ENST00000480739 suppresses tumour cell invasion by regulating OS-9 and HIF-1α in pancreatic ductal adenocarcinoma. Br J Cancer 2014; 111: 2131-2141 [PMID: 25314054 DOI: 10.1038/bjc.2014.520]
116 Ting DT, Lipson D, Paul S, Brannigan BW, Akhavanfard S, Coffman EJ, Contino G, Deshpande V, Iafrate AJ, Letovsky S, Rivera MN, Bardeesy N, Maheswaran S, Haber DA. Aberrant overexpression of satellite repeats in pancreatic and other epithelial cancers. Science 2011; 331: 593-596 [PMID: 21233348 DOI: 10.1126/science.1200801]
117 Wang Y, Li Z, Zheng S, Zhou Y, Zhao L, Ye H, Zhao X, Gao W, Fu Z, Zhou Q, Liu Y, Chen R. Expression profile of long non-coding RNAs in pancreatic cancer and their clinical significance as biomarkers. Oncotarget 2015; 6: 35684-35698 [PMID: 26447755 DOI: 10.18632/oncotarget.5533]
118 Záveský L, Jandáková E, Turyna R, Langmeierová L, Weinberger V, Záveská Drábková L, Hůlková M, Hořínek A, Dušková D, Feyereisl J, Minář L, Kohoutová M. Evaluation of Cell-Free Urine microRNAs Expression for the Use in Diagnosis of Ovarian and Endometrial Cancers. A Pilot Study. Pathol Oncol Res 2015; 21: 1027-1035 [PMID: 25827090 DOI: 10.1007/s12253-015-9914-y]
119 Erbes T, Hirschfeld M, Rücker G, Jaeger M, Boas J, Iborra S, Mayer S, Gitsch G, Stickeler E. Feasibility of urinary microRNA detection in breast cancer patients and its potential as an innovative non-invasive biomarker. BMC Cancer 2015; 15: 193 [PMID: 25886191 DOI: 10.1186/s12885-015-1190-4]
120 Yachida S, Jones S, Bozic I, Antal T, Leary R, Fu B, Kamiyama M, Hruban RH, Eshleman JR, Nowak MA, Velculescu VE, Kinzler KW, Vogelstein B, Iacobuzio-Donahue CA. Distant metastasis occurs late during the genetic evolution of pancreatic cancer. Nature 2010; 467: 1114-1117 [PMID: 20981102 DOI: 10.1038/nature09515]
121 Cooper CL, O’Toole SA, Kench JG. Classification, morphology and molecular pathology of premalignant lesions of the pancreas. Pathology 2013; 45: 286-304 [PMID: 23442735 DOI: 10.1097/PAT.0b013e32835f2205]
122 Permuth-Wey J, Chen DT, Fulp WJ, Yoder SJ, Zhang Y, Georgeades C, Husain K, Centeno BA, Magliocco AM, Coppola D, Malafa M. Plasma MicroRNAs as Novel Biomarkers for Patients with Intraductal Papillary Mucinous Neoplasms of the Pancreas. Cancer Prev Res (Phila) 2015; 8: 826-834 [PMID: 26314797 DOI: 10.1158/1940-6207.capr-15-0094]
123 Komatsu S, Ichikawa D, Miyamae M, Kawaguchi T, Morimura R, Hirajima S, Okajima W, Ohashi T, Imamura T, Konishi H, Shiozaki A, Ikoma H, Okamoto K, Taniguchi H, Otsuji E. Malignant potential in pancreatic neoplasm; new insights provided by circulating miR-223 in plasma. Expert Opin Biol Ther 2015; 15: 773-785 [PMID: 25819175 DOI: 10.1517/14712598.2015.1029914]
124 Z'graggen K, Centeno BA, Fernandez-del Castillo C, Jimenez RE, Werner J, Warshaw AL. Biological implications of tumor cells in blood and bone marrow of pancreatic cancer patients. Surgery 2001; 129: 537-546 [PMID: 11331445 DOI: 10.1067/msy.2001.113819]
125 Khoja L, Backen A, Sloane R, Menasce L, Ryder D, Krebs M, Board R, Clack G, Hughes A, Blackhall F, Valle JW, Dive C. A pilot study to explore circulating tumour cells in pancreatic cancer as a novel biomarker. Br J Cancer 2012; 106: 508-516 [PMID: 22187035 DOI: 10.1038/bjc.2011.545]
126 de Albuquerque A, Kubisch I, Breier G, Stamminger G, Fersis
N, Eichler A, Kaul S, Stölzel U. Multimarker gene analysis of circulating tumor cells in pancreatic cancer patients: a feasibility study. Oncology 2012; 82: 3-10 [PMID: 22270149 DOI: 10.1159/000335479]
127 Kamande JW, Hupert ML, Witek MA, Wang H, Torphy RJ, Dharmasiri U, Njoroge SK, Jackson JM, Aufforth RD, Snavely A, Yeh JJ, Soper SA. Modular microsystem for the isolation, enumeration, and phenotyping of circulating tumor cells in patients with pancreatic cancer. Anal Chem 2013; 85: 9092-9100 [PMID: 23947293 DOI: 10.1021/ac401720k]
128 Catenacci DV, Chapman CG, Xu P, Koons A, Konda VJ, Siddiqui UD, Waxman I. Acquisition of Portal Venous Circulating Tumor Cells From Patients With Pancreaticobiliary Cancers by Endoscopic Ultrasound. Gastroenterology 2015; 149: 1794-1803.e4 [PMID: 26341722 DOI: 10.1053/j.gastro.2015.08.050]
129 Zhang Y, Wang F, Ning N, Chen Q, Yang Z, Guo Y, Xu D, Zhang D, Zhan T, Cui W. Patterns of circulating tumor cells identified by CEP8, CK and CD45 in pancreatic cancer. Int J Cancer 2015; 136: 1228-1233 [PMID: 25042121 DOI: 10.1002/ijc.29070]
130 Bissolati M, Sandri MT, Burtulo G, Zorzino L, Balzano G, Braga M. Portal vein-circulating tumor cells predict liver metastases in patients with resectable pancreatic cancer. Tumour Biol 2015; 36: 991-996 [PMID: 25318603 DOI: 10.1007/s13277-014-2716-0]
131 Zhang J, Li S, Liu F, Zhou L, Shao N, Zhao X. SELEX aptamer used as a probe to detect circulating tumor cells in peripheral blood of pancreatic cancer patients. PLoS One 2015; 10: e0121920 [PMID: 25799539 DOI: 10.1371/journal.pone.0121920]
132 Giacona MB, Ruben GC, Iczkowski KA, Roos TB, Porter DM, Sorenson GD. Cell-free DNA in human blood plasma: length measurements in patients with pancreatic cancer and healthy controls. Pancreas 1998; 17: 89-97 [PMID: 9667526]
133 Singh N, Gupta S, Pandey RM, Chauhan SS, Saraya A. High levels of cell-free circulating nucleic acids in pancreatic cancer are associated with vascular encasement, metastasis and poor survival. Cancer Invest 2015; 33: 78-85 [PMID: 25647443 DOI: 10.3109/07357907.2014.1001894]
134 Ho AS, Huang X, Cao H, Christman-Skieller C, Bennewith K, Le QT, Koong AC. Circulating miR-210 as a Novel Hypoxia Marker in Pancreatic Cancer. Transl Oncol 2010; 3: 109-113 [PMID: 20360935]
135 Li A, Omura N, Hong SM, Vincent A, Walter K, Griffith M, Borges M, Goggins M. Pancreatic cancers epigenetically silence SIP1 and hypomethylate and overexpress miR-200a/200b in association with elevated circulating miR-200a and miR-200b levels. Cancer Res 2010; 70: 5226-5237 [PMID: 20551052 DOI: 10.1158/0008-5472.can-09-4227]
136 Ali S, Almhanna K, Chen W, Philip PA, Sarkar FH. Differentially expressed miRNAs in the plasma may provide a molecular signature for aggressive pancreatic cancer. Am J Transl Res 2010; 3: 28-47 [PMID: 21139804]
137 LaConti JJ, Shivapurkar N, Preet A, Deslattes Mays A, Peran I, Kim SE, Marshall JL, Riegel AT, Wellstein A. Tissue and serum microRNAs in the Kras(G12D) transgenic animal model and in patients with pancreatic cancer. PLoS One 2011; 6: e20687 [PMID: 21738581 DOI: 10.1371/journal.pone.0020687]
138 Morimura R, Komatsu S, Ichikawa D, Takeshita H, Tsujiura M, Nagata H, Konishi H, Shiozaki A, Ikoma H, Okamoto K, Ochiai T, Taniguchi H, Otsuji E. Novel diagnostic value of circulating miR-18a in plasma of patients with pancreatic cancer. Br J Cancer 2011; 105: 1733-1740 [PMID: 22045190 DOI: 10.1038/bjc.2011.453]
139 Liu J, Gao J, Du Y, Li Z, Ren Y, Gu J, Wang X, Gong Y, Wang W, Kong X. Combination of plasma microRNAs with serum CA19-9 for early detection of pancreatic cancer. Int J Cancer 2012; 131: 683-691 [PMID: 21913185 DOI: 10.1002/ijc.26422]
140 Liu R, Chen X, Du Y, Yao W, Shen L, Wang C, Hu Z, Zhuang R, Ning G, Zhang C, Yuan Y, Li Z, Zen K, Ba Y, Zhang CY. Serum microRNA expression profile as a biomarker in the diagnosis and prognosis of pancreatic cancer. Clin Chem 2012; 58: 610-618 [PMID: 22194634 DOI: 10.1373/clinchem.2011.172767]
141 Li A, Yu J, Kim H, Wolfgang CL, Canto MI, Hruban RH, Goggins M.
Imamura T et al . Liquid biopsy of pancreatic cancer

5641 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
MicroRNA array analysis finds elevated serum miR-1290 accurately distinguishes patients with low-stage pancreatic cancer from healthy and disease controls. Clin Cancer Res 2013; 19: 3600-3610 [PMID: 23697990 DOI: 10.1158/1078-0432.ccr-12-3092]
142 Wang WS, Liu LX, Li GP, Chen Y, Li CY, Jin DY, Wang XL. Combined serum CA19-9 and miR-27a-3p in peripheral blood mononuclear cells to diagnose pancreatic cancer. Cancer Prev Res (Phila) 2013; 6: 331-338 [PMID: 23430754 DOI: 10.1158/1940-6207.capr-12-0307]
143 Kawaguchi T, Komatsu S, Ichikawa D, Morimura R, Tsujiura M, Konishi H, Takeshita H, Nagata H, Arita T, Hirajima S, Shiozaki A, Ikoma H, Okamoto K, Ochiai T, Taniguchi H, Otsuji E. Clinical impact of circulating miR-221 in plasma of patients with pancreatic cancer. Br J Cancer 2013; 108: 361-369 [PMID: 23329235 DOI: 10.1038/bjc.2012.546]
144 Zhao C, Zhang J, Zhang S, Yu D, Chen Y, Liu Q, Shi M, Ni C, Zhu M. Diagnostic and biological significance of microRNA-192 in pancreatic ductal adenocarcinoma. Oncol Rep 2013; 30: 276-284 [PMID: 23612862 DOI: 10.3892/or.2013.2420]
145 Wang P, Zhuang L, Zhang J, Fan J, Luo J, Chen H, Wang K, Liu L, Chen Z, Meng Z. The serum miR-21 level serves as a predictor for the chemosensitivity of advanced pancreatic cancer, and miR-21 expression confers chemoresistance by targeting FasL. Mol Oncol 2013; 7: 334-345 [PMID: 23177026 DOI: 10.1016/j.molonc.2012.10.011]
146 Carlsen AL, Joergensen MT, Knudsen S, de Muckadell OB, Heegaard NH. Cell-free plasma microRNA in pancreatic ductal adenocarcinoma and disease controls. Pancreas 2013; 42: 1107-1113 [PMID: 24048453 DOI: 10.1097/MPA.0b013e318296bb34]
147 Que R, Ding G, Chen J, Cao L. Analysis of serum exosomal microRNAs and clinicopathologic features of patients with pancreatic adenocarcinoma. World J Surg Oncol 2013; 11: 219 [PMID: 24007214 DOI: 10.1186/1477-7819-11-219]
148 Gao L, He SB, Li DC. Effects of miR-16 plus CA19-9 detections on pancreatic cancer diagnostic performance. Clin Lab 2014; 60: 73-77 [PMID: 24600978]
149 Chen Q, Yang L, Xiao Y, Zhu J, Li Z. Circulating microRNA-182
in plasma and its potential diagnostic and prognostic value for pancreatic cancer. Med Oncol 2014; 31: 225 [PMID: 25326859 DOI: 10.1007/s12032-014-0225-z]
150 Ganepola GA, Rutledge JR, Suman P, Yiengpruksawan A, Chang DH. Novel blood-based microRNA biomarker panel for early diagnosis of pancreatic cancer. World J Gastrointest Oncol 2014; 6: 22-33 [PMID: 24578785 DOI: 10.4251/wjgo.v6.i1.22]
151 Abue M, Yokoyama M, Shibuya R, Tamai K, Yamaguchi K, Sato I, Tanaka N, Hamada S, Shimosegawa T, Sugamura K, Satoh K. Circulating miR-483-3p and miR-21 is highly expressed in plasma of pancreatic cancer. Int J Oncol 2015; 46: 539-547 [PMID: 25384963 DOI: 10.3892/ijo.2014.2743]
152 Slater EP, Strauch K, Rospleszcz S, Ramaswamy A, Esposito I, Klöppel G, Matthäi E, Heeger K, Fendrich V, Langer P, Bartsch DK. MicroRNA-196a and -196b as Potential Biomarkers for the Early Detection of Familial Pancreatic Cancer. Transl Oncol 2014; 7: 464-471 [PMID: 24956938 DOI: 10.1016/j.tranon.2014.05.007]
153 Xu J, Cao Z, Liu W, You L, Zhou L, Wang C, Lou W, Sun B, Miao Y, Liu X, Zhang T, Zhao Y. Plasma miRNAs Effectively Distinguish Patients With Pancreatic Cancer From Controls: A Multicenter Study. Ann Surg 2016; 263: 1173-1179 [PMID: 26114496 DOI: 10.1097/sla.0000000000001345]
154 Madhavan B, Yue S, Galli U, Rana S, Gross W, Müller M, Giese NA, Kalthoff H, Becker T, Büchler MW, Zöller M. Combined evaluation of a panel of protein and miRNA serum-exosome biomarkers for pancreatic cancer diagnosis increases sensitivity and specificity. Int J Cancer 2015; 136: 2616-2627 [PMID: 25388097 DOI: 10.1002/ijc.29324]
155 Baraniskin A, Nöpel-Dünnebacke S, Ahrens M, Jensen SG, Zöllner H, Maghnouj A, Wos A, Mayerle J, Munding J, Kost D, Reinacher-Schick A, Liffers S, Schroers R, Chromik AM, Meyer HE, Uhl W, Klein-Scory S, Weiss FU, Stephan C, Schwarte-Waldhoff I, Lerch MM, Tannapfel A, Schmiegel W, Andersen CL, Hahn SA. Circulating U2 small nuclear RNA fragments as a novel diagnostic biomarker for pancreatic and colorectal adenocarcinoma. Int J Cancer 2013; 132: E48-E57 [PMID: 22907602 DOI: 10.1002/ijc.27791]
P- Reviewer: Sawas T, Sica GS, Sperti C S- Editor: Ma YJ L- Editor: A E- Editor: Wang CH
Imamura T et al . Liquid biopsy of pancreatic cancer

Ferdinand Knieling, Clinic for Children and Adolescent Medicine, Friedrich-Alexander-Universität Erlangen-Nürnberg, 91054 Erlangen, Germany
Ferdinand Knieling, Maximilian J Waldner, Medical Department 1, Friedrich-Alexander-Universität Erlangen-Nürnberg, 91054 Erlangen, Germany
Maximilian J Waldner, Erlangen Graduate School of Advanced Optical Technologies, Friedrich-Alexander-Universität Erlangen-Nürnberg, 91054 Erlangen, Germany
Author contributions: Knieling F and Waldner MJ analyzed the literature and wrote the manuscript.
Supported by Interdisciplinary Center for Clinical Research of the University Medical Center of Erlangen (to Knieling F); Erlangen Graduate School in Advanced Optical Technologies by the German Research Foundation in the framework of the German excellence initiative (to Waldner MJ).
Conflict-of-interest statement: The authors have no conflict of interest to report.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Manuscript source: Invited manuscript
Correspondence to: Maximilian J Waldner, MD, Medical Department 1, Friedrich-Alexander-Universität Erlangen-Nürnberg, Ulmenweg 18, 91054 Erlangen, Germany. [email protected]: +49-9131-8545025Fax: +49-9131-8535959
Received: March 24, 2016 Peer-review started: March 25, 2016
First decision: April 14, 2016Revised: May 2, 2016 Accepted: May 23, 2016Article in press: May 23, 2016Published online: July 7, 2016
AbstractPatients with inflammatory bowel disease are known to have a high demand of recurrent evaluation for therapy and disease activity. Further, the risk of developing cancer during the disease progression is increasing from year to year. New, mostly non-radiant, quick to perform and quantitative methods are challenging, conventional endoscopy with biopsy as gold standard. Especially, new physical imaging approaches utilizing light and sound waves have facilitated the development of advanced functional and molecular modalities. Besides these advantages they hold the promise to predict personalized therapeutic responses and to spare frequent invasive procedures. Within this article we highlight their potential for initial diagnosis, assessment of disease activity and surveillance of cancer development in established techniques and recent advances such as wide-view full-spectrum endoscopy, chromoendoscopy, autofluorescence endoscopy, endo-cytoscopy, confocal laser endoscopy, multiphoton endoscopy, molecular imaging endoscopy, B-mode and Doppler ultrasound, contrast-enhanced ultrasound, ultrasound molecular imaging, and elastography.
Key words: Ulcerative colitis; Crohn’s disease; Endoscopy; Chromoendoscopy; Autofluorescence endoscopy; Full-view full-spectrum endoscopy; Confocal endomicroscopy; Multiphoton endoscopy; High-definition endoscopy; Ultrasound molecular imaging; B-mode ultrasound; Doppler ultrasound
© The Author(s) 2016. Published by Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.3748/wjg.v22.i25.5642
5642 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
World J Gastroenterol 2016 July 7; 22(25): 5642-5654 ISSN 1007-9327 (print) ISSN 2219-2840 (online)
© 2016 Baishideng Publishing Group Inc. All rights reserved.
Ferdinand Knieling, Maximilian J Waldner
TOPIC HIGHLIGHT
Light and sound - emerging imaging techniques for inflammatory bowel disease
2016 Inflammatory Bowel Disease: Global view

Core tip: Patients with inflammatory bowel disease are known to have a high demand of recurrent evaluation for therapy and disease activity. Further, the risk of developing cancer during disease progression is growing from year to year. Especially, new physical imaging approaches utilizing light and sound waves have facilitated the development of endoscopic tech-niques. Within this article we highlight their potential for initial diagnosis, assessment of disease activity and surveillance of cancer development in established techniques and recent advances such as wide-view full-spectrum endoscopy, chromoendoscopy, auto-fluorescence endoscopy, endocytoscopy, confocal laser endoscopy, multiphoton endoscopy, molecular imaging endoscopy, B-mode and Doppler ultrasound, contrast-enhanced ultrasound, ultrasound molecular imaging, and elastography.
Knieling F, Waldner MJ. Light and sound - emerging imaging techniques for inflammatory bowel disease. World J Gastroenterol 2016; 22(25): 5642-5654 Available from: URL: http://www.wjgnet.com/1007-9327/full/v22/i25/5642.htm DOI: http://dx.doi.org/10.3748/wjg.v22.i25.5642
INTRODUCTIONInflammatory bowel disease (IBD) is a group of chronic inflammatory diseases seen in 1 of 200 to 500 individuals[1]. The pathophysiology of the two major subtypes, Crohn’s Disease and ulcerative colitis, is still not completely understood[2]. The course of disease is marked by relapses of chronic inflammation and accompanied by severe symptoms, like bloody stool, abdominal pain and weight loss[3]. The assessment of disease extent is still a substantial challenge for clinicians, but it is crucial for successful treatment. The absence of endoscopic activity, e.g., mucosal healing or histologic remission, might even better guarantee long-term success compared to conventional clinical outcome measures[4-6]. Studies demonstrated that higher rates of mucosal healing might be achieved with higher frequency of assessment of endoscopic disease activity and adjustments to medical therapy[7,8]. It is still questionable, if patients adhere to intensive invasive endoscopic procedures[9]. Facing a high economic burden[10] together with globally increasing rates of pediatric IBD[11] raising concerns for potential risks and harmful procedures[12], we urgently need modalities to easily and quickly assess the extent of disease. Furthermore, these modalities need to account and detect precursor lesion in these patients knowing to bear an increasing risk of colitis associated cancer development[13,14]. As light and sound are very different waves in their physical behavior, both can be used to generate new insights into a bright variety of diseases. We provide a review focused on recent
imaging advances based on sound and light wave technologies, which are already or are about to be translated into routine clinical use for inflammatory bowel disease.
RECOMMENDATIONS AND STATE-OF-THE-ARTInternational consensus guidelines and recommen-dations for inflammatory bowel disease, including its surveillance and management of dysplasia, point out important aspects concerning imaging are summarized in Table 1[15-18].
Initial diagnosis, follow-up and surveillance are the major keys for clinical management of IBD. Up to now, endoscopy is representing the major backbone to compete in all disciplines. New imaging modalities are lining up to complement this technique with easy applicable, non-invasive and quantitative approaches, to individually improve patients’ care.
MACROSCOPIC ENDOSCOPIC TECHNOLOGIESSince the first endoscopy was performed by Kussmaul A in 1868, its technique and application has greatly expanded. Especially during recent years, new technological developments are further improving the diagnostic accuracy for wide-spread (pre-)clinical applications. Some of the most important techniques will be shortly described in this section:
High-definition endoscopyStandard definition (SD) endoscopy offers images in a 4:3 aspect ratio, reaching up to 270000 to 410000 pixels, while high definition (HD) or high resolution endoscopy presents images with 850000 to 1 million pixels. It is clear that high resolution endoscopy results in visualization of a more detailed mucosa[19].
Wide-view full-spectrum endoscopyUsually, standard forward-viewing colonoscopes visua-lize the intestinal surface using an optical system from tip with an angle of view up to 170°. The wide-view full-spectrum endoscopy provides an extended view with a 330° angle. This platform was first tested in an in vitro model, suggesting better detection rates for polyps[20]. Further, its applicability was also verified in small cohorts to show feasibility, performing at a 100% caecal intubation rate and providing high evaluation scores from patients and endoscopists[21].
ChromoendoscopyChromoendoscopy uses various dyes, endoscopic optical and computer-based software to enhance image quality and to visualize the mucosal architecture. One first approach was reported by Tada et al[22] and since
5643 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Knieling F et al . Emerging imaging techniques for IBD

then, different agents for topic application have been approved (methylene blue, toluidine blue, and cresyl violet, indigo carmine, acetic acid, Congo red, phenol red)[23]. By using this technique, an enhancement of the mucosal surface could be achieved to augment superficial patterns and the contrast of pathologic versus normal mucosa[24]. In order to further improve the visualization high-definition resolution was ad-ditionally introduced to this technique.
Narrow-band imaging (NBI) or virtual chromo-endoscopy, is a comparable software based approach utilizing light of specific wavelength in green and blue spectra to enhance the vascular pattern of the mucosa. As hemoglobin is known to have a peak light absorption at these wavelengths, an optical filtered image can then display the capillaries on the surface and in the submucosa in different colors[25,26].
Autofluorescence endoscopyDepended on the biochemical composition of the visualized tissue, this technique utilizes intensity laser light to induce and generate autofluorescent light spectra[27]. Strong endogenous fluorochromes such as collagen, elastin, nicotinamide adenine dinucleotide (NAD), flavin adenine dinucleotide (FAD), lipofuscin, tryptophan, and keratin can be detected[28]. Most studies used 370 nm excitation light and col-
lected fluorescence in the range 400-700 nm[29,30]. Fluorescence imaging is able to identify suspect lesion with high sensitivity, especially when it is used in the detection of suspect polyps[31,32].
MICROSCOPIC ENDOSCOPIC TECHNOLOGIESWhereas wide-field endoscopy enables the iden-tification of suspect lesions or inflamed areas of the mucosa during the endoscopic procedure, microscopic evaluation of tissue samples is still required for a definitive diagnosis. As this can delay a definitive treatment up to several days, the development of in vivo endomicroscopic imaging techniques has been one of the major aims of endoscopic research during recent years. Whereas some techniques are already used in clinical practice, others are still in development as subsequently described.
EndocytoscopyEndocytoscopy (EC) is based on contact light micro-scopy to the superficial layer of the mucosa. The technology uses fixed-focus and high-power objective lenses[33]. In order to prepare an ideal environment for imaging, washing the surface together with
5644 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Table 1 Recommendations and state-of-the-art in inflammatory bowel disease imaging according to international guidelines[15-18]
Initial diagnosis and follow-up
Colonoscopy with ileoscopy is recommended for the initial evaluation of inflammatory bowel disease (IBD) and for the differentiation IBD subtypesSampling of mucosal biopsy specimens from multiple sites during the initial endoscopic evaluation of IBD is recommendedFlexible sigmoidoscopy should be performed in patients with IBD when colonoscopy is contraindicatedRadiological imaging techniques are complementary to endoscopic assessment. Cross-sectional imaging offers the opportunity to detect and stage inflammatory, obstructive and fistulizing Crohn's disease (CD) and is fundamental at first diagnosis to stage disease and to monitor follow-upUltrasound (US) is a well-tolerated and radiation-free imaging technique, particularly for the terminal ileum and the colon. Examinations are impaired by gas-filled bowel and by large body habitusUS is able to detect signs of Crohn's disease and has high and comparable diagnostic accuracy at the initial presentation of terminal ileal CDUS can be used to assess disease activity in Crohn's disease of the terminal ileumUS imaging is an adjunct to endoscopy for diagnosis of colonic IBDTransabdominal US has a high accuracy for assessing the activity and severity of Crohn’s colitis; the performance in UC is less clear; the accuracy of monitoring therapy in colonic Crohn's disease is not well defined
Surveillance and management of dysplasia
It is recommended that all patients with UC or CD colitis undergo a screening colonoscopy 8 yr after disease onset to re-evaluate extent of disease and initiate surveillance for colorectal neoplasiaIt is recommended to perform surveillance colonoscopy every 1 to 3 yr beginning after 8 yr of disease in patients with UC with macroscopic or histologic evidence of inflammation proximal to and including the sigmoid colon and for patients with Crohn’s colitis with greater than one-third of colon involvementIf white-light colonoscopy is performed in case of surveillance, high definition (HD) is recommended rather than standard definition (SD)If surveillance is performed with SD colonoscopy, chromoendoscopy is recommended rather than white-lightIf performing surveillance with HD colonoscopy, chromoendoscopy is suggested rather than white-light colonoscopyIf performing surveillance with SD colonoscopy, narrow-band imaging (NBI) is not suggested in place of white-lightIf performing surveillance with high-definition colonoscopy, NBI is not suggested in place of white-lightIf performing surveillance with image-enhanced HD colonoscopy, NBI is not suggested in place of chromoendoscopy
Management of dysplasia discovered on surveillance colonoscopy
After complete removal of endoscopically resectable polypoid dysplastic lesions, surveillance colonoscopy is recommended rather than colectomyAfter complete removal of endoscopically resectable nonpolypoid dysplastic lesions, surveillance colonoscopy is suggested rather than colectomyFor patients with endoscopically invisible dysplasia (confirmed by a gastrointestinal pathologist), referral is suggested to an endoscopist with expertise in IBD surveillance using chromoendoscopy with high-definition colonoscopy
Knieling F et al . Emerging imaging techniques for IBD

5645 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
images. This general concept was also applied to adenomas/polyps, which are known to highly express the signaling molecule VEGF-A, which is supposed to be involved in vascular growth and maturation as well as tumor growth[45,46]. The feasibility to visualize small tumors in real time during colonoscopy could be demonstrated using NIR fluorescence endoscopy[47]. An overview of all described technologies for endoscopic imaging is given in Figure 1.
ULTRASOUND TECHNOLOGIESUltrasound (US) has an important role and great potential in imaging the intestine in children and adults[48]. In some countries, e.g., the United States, it is still far less important than CT imaging, which faces a relative increase of 47.3% from 2007-2010 for non-head application[49]. Compared to US, CT provides the rapid evaluation of bowel and mesentery as well cross-sectional assessment of abdominal and pelvic organs including major vessels[50]. In contrast, US is non-invasive, low cost, easily repeatable and does not rise concerns about radiation exposure in children and young adults[51].
B-mode and Doppler ultrasoundUS is a non-invasive, not radiant, and well tolerated modality. The window of imaging is limited by intestinal air or deep organs; therefore, fasting before imaging may be helpful[52].
US for IBD imaging requires the use of high-frequency (5-17 MHz) linear transducers in order to increase spatial resolution and to allow adequate assessment of bowel diameter and of different intestinal layers[53]. Authors recommend a systematic approach to visualize sites of inflammation including the upper and lower, right and left abdominal quadrants[51]. Usually the transabdominal imaging is less invasive, but endoscopic or endosonographic approaches have also been described in pre-clinical[54] and clinical settings[55].
Contrast-enhanced ultrasoundContrast-enhanced ultrasound utilized gas-filled coated microbubbles to image vascularity. Currently, its major domain is focal liver lesion diagnostics[56] and it is also frequently applied to vascular or cardiac diagnostics[57,58].
Due to its fast liver and renal independent pul-monary clearing, these microbubbles have superior pharmacologic profile in patients with a complicated medical history[59,60]. Diagnostic accuracy[56,61-64], pharmacological safety[65], and cost efficiency in comparison to other conventional imaging modalities[66] has been widely proven. Further, quantitative para-meters could be easily derived by secondary software quantification[67,68]. This technique was already applied in the follow-up of anti-vascular treatments in renal cell carcinoma[69], hepatocellular carcinoma[70,71] or
N-acetylcysteine for mucolysis is recommended[34]. EC requires prestaining with absorptive topic agents like the combination of crystal violet and methylene blue[35]. For example, EC was used to examine eso-phageal tissue to identify superficial esophageal carcinomas[36] or bladder cancer cells[37].
Confocal laser endoscopyConfocal laser colonoscopy (CLE) is either based on the integration of a confocal laser microscope into the distal tip (ISC-1000/EC3870CIK, Pentax Corporation, Tokyo, Japan) or the utilization of a small probe, which can be introduced through the working channel (Cellvizio, Mauna Kea Technologies, Paris, France). During the procedure, a laser is delivering the excitation light to the surface of the mucosa providing in-vivo histology at a magnification of 1000-fold[38]. As compared to chromoendoscopy, CLE also relies on the topic or systemic application of fluorescence agents[39]. Kiesslich et al[38] demonstrated that this technique may be helpful to avoid repeated colonoscopies, because target lesions could be analyzed more rapidly in vivo during colonoscopy. As a side note: Pentax has already discontinued its product.
Multiphoton endoscopyMultiphoton microscopy (MPM) has been widely used as an in vivo imaging technique for basic research. In comparison with single photon excitation during confocal microscopy, MPM provides a superior ef-fective resolution in thick tissue samples and an increased penetration depth[40]. Fluorescence imaging is therefore based on the molecular absorption of 2 infrared photons at the same time. First, by generating a second harmonic generation, a nonlinear scattering effect, fibers of collagen-I could be imaged. Second, autofluorescence can be detected from NADH-rich epithelial cells or FAD bearing immune cells. Because this effect is only occurring in a small volume of the focus images could be easily combined to a 3D-image stack[41]. Compared to confocal laser endomicroscopy, this technique is not restricted by the detection of exogenous fluorophores and can easily visualize the subcellular level of gastrointestinal diseases[41]. Until know, there is no MP-endoscope developed for clinical use, but pre-clinical systems have been already described[42].
Molecular imaging endoscopyTo further improve the quality of endoscopic imaging, subcellular/molecular information were acquired by adding molecular targeted compounds such as antibodies, peptides or nano particles for specific detection[43]. Liu et al[44] could show that a specific octapeptide conjugated with Cy5.5 excited at 671 nm allowed near infrared (NIR) fluorescence detection at 696 to 736 nm, which was supposed to be specific for colonic adenomas and achieved sub-cellular resolution
Knieling F et al . Emerging imaging techniques for IBD

5646 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
cholangiocellular carcinoma[72].
Ultrasound molecular imagingA further evolution of the aforementioned technique is ultrasound molecular imaging (UMI) or targeted molecular ultrasound. Both, CEUS and UMI, have in common that they use small gas-filled microbubbles to image vascularization. Further, UMI contrast agents have coupled a ligand to their outer shell to target specific endothelial molecules of interest[73]. Pre-clinical systems have been applied to detect cancer neovascularization in prostate using VEGFR-2[74] or P- and E-selectins in acute myocardial ischemia[75]. Until now, a clinical translation has not been achieved yet.
ElastographyAnother “contrast-agent-free” modality is ultrasound elastography. It is a non-invasive imaging approach to evaluate tissue hardness[76,77]. A transducer generates forced push pulses to displace targeted tissues at a
specified depth. This displacement causes orthogonal shear waves, which can be detected as they propagate through the tissue of interest[77]. The distance traveled by the generated shear and the time provides an estimate of shear wave velocity and tissue hardness (m/s)[78]. The shear wave velocity corresponds to the tissues’ ability to resist deformation and increases with increasing tissue hardness[77]. This has been exemplary studied in liver fibrosis[79], focal liver lesions[80], and thyroid nodules[81]. An overview all described technologies for ultrasound imaging is given in Figure 2.
CLINICAL EVIDENCE AND TRANSLATION OF ENDOSCOPIC TECHNIQUESFirst diagnosis of IBDThe identification of distinct patterns of mucosal inflammation has been one part of the initial diagnosis of IBD for decades. Whereas inflammation in Crohn’s disease (CD) presents with aphthous ulcers, cobble stoning,
Figure 1 Overview of existing and emerging endoscopic technologies to visualize macroscopic or microscopic features of the intestine. Macroscopic technologies include: high-definition endoscopy, wide-view full-spectrum endoscopy, chromoendoscopy, and autofluorescence endoscopy. Microscopic technologies include: endocytoscopy, confocal laser endoscopy, multiphoton endoscopy, and molecular imaging endoscopy. A detailed description for each modality is given in the text.
Topic applicationof dyes
Different wavelengthof light
Dye-basedchromoendoscopy
Virtualchromoendoscopy
Laser light
Fluorescenceemission
ChromoendoscopyWide-field full-spectrumendoscopy
170° 330°
High defintionendoscopy
Macroscopic techniques Autofluorescence endoscopy
Molecular imaging endoscopyMicroscopic techniquesEndocytoscopy
Magnificationlens
Topic applicationof dyes
Confocal laser endoscopy
Topic applicationof dyes
Systemic applicationof dyes
Fluorescenceemission
Infrared excitation
Topic applicationof fluorescent
probes
Excitationof fluorophor
Multiphoton endoscopy
Increased resolution
Knieling F et al . Emerging imaging techniques for IBD

5647 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
serpiginous ulcers, and the possibility of strictures in the terminal ileum; erythema, edema, bleeding and increased granularity of the colonic mucosa can be observed in UC. Despite these characteristic signs, endoscopy alone does not allow the definitive diagnosis of CD or UC and therefore relies on additional signs in microscopy such as granuloma formation in CD or crypt abscesses in UC. Despite the above-mentioned technological advantages of wide-field endoscopy during recent years, none of these technologies, including the techniques described above, have so far been shown to improve the initial diagnosis of IBD alone. However, first results show some advantage for the additional usage of confocal endomicroscopy. Although limited by its penetration depth, it is capable of visualizing disease-specific microscopic patterns, known from histopathology, to differentiate between UC and CD[82]. Findings in CD showed significantly more discontinuous inflammation, increased focal cryptitis, and discontinuous crypt architectural abnormality compared to UC, which was associated with severe, widespread crypt distortion, decreased crypt density, and frankly irregular surface[82]. In
addition to CLE, also EC has been used for the microscopic evaluation of IBD. However, although EC was able to reliably distinguish between single inflammatory cells, it is not clear, whether it can be used for the initial diagnosis and differentiation of IBD subtypes[83]. In conclusion, microscopic endoscopic techniques still lack in clear evidence to be able to visualize distinct disease patterns such as granulomas in CD.
Assessment of disease activityIn contrast to the initial diagnosis of IBD, more data are available regarding the use of new endoscopic imaging techniques for monitoring disease activity in IBD patients. Based on a prospective randomized trial, chromoendoscopy showed a higher diagnostic performance to assess the extent and severity of the inflammatory activity in UC when compared to conventional colonoscopy[84]. For NBI, Kudo et al[85] found that mucosal vascular patterns in UC presenting with obscure configuration showed significantly more inflammatory cell infiltrates, increased goblet cell depletion, and basal plasmacytosis. This group
Figure 2 Overview of existing and emerging ultrasound transabdominal and endoscopic technologies for visualizing the intestine. Besides B-mode and Doppler, technologies include: contrast-enhanced ultrasound, ultrasound molecular imaging, and elastography. A detailed description for each modality is given in the text.
Elastography
Push pulse
Shear waves
Contrast-enhanced ultrasound Ultrasound molecular imaging
Ligands
Gas core
Shell
Ultrasound waves
Microbubble harmonics
Contraction Expansion Contraction
Sign
al in
tens
ity
Time
Knieling F et al . Emerging imaging techniques for IBD

5648 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
also described the key features of different stages of activity in UC imaged with NBI[86]. In a small pilot study the concept of angiogenesis in IBD was also assessed to demonstrate that positive appearance on NBI showed increase in angiogenesis or vessel density[87]. By using the principle of digital post-processing in real-time (virtual chromoendoscopy, i-Scan), inflammatory extent and activity compared with histology showed an overall agreement of 48.71% and 53.85% (white-light) and 92.31% and 89.74% (i-Scan)[88]. Also endomicroscopic techniques have been tested to grade activity in IBD. For instance, CLE is able to provide information equivalent to conventional histology, showing distinct alterations in active and non-active UC patients compared to normal controls[89]. Li et al[90] demonstrated that a classification based on crypt architecture and fluorescein leakage with CLE showed good correlations with histological results in UC. The strong ability of visualizing abnormalities on a cellular level, underling the possibility to assess mucosal healing, was demonstrated by showing distinct vascular and tissue alterations in even endoscopically (magnified) normal appearing colonic mucosa in patients with UC in the state of remission[91].
For CD, a CD Endomicroscopic Activity Score (CDEAS) was proposed, which is consisting of six parameters: crypt number (increased or decreased), crypt distortion, micro erosions, cellular infiltrate, vascularity, and number of goblet cells (increased or decreased)[92]. Interestingly, the authors found a strong correlation of CDEAS and CRP to underline the potential as a disease activity predictor in CD[92]. EC is also capable to visualize different histopathological features. In a pilot trial Neumann et al[92] found a concordance with histopathology for grading intestinal disease activity reaching to 100%[83]. In order to visualize histology in real-time without the use of dies a comparable approach might be achieved with MPM[41]. The implementation into an endoscopic device shall be a helpful to create images of tissue in subcellular resolution[42,93,94]. An overview of selected studies is given in Table 2.
Prediction of therapeutic responseIn addition to monitoring disease activity, CLE tech-niques have also been used to predict the response to biological therapy in IBD. In a recent pilot study performed by Atreya et al[95], molecular-targeted confocal endomicroscopy prior to the initiation of anti-tumor necrosis factor (TNF) alpha therapy was used to evaluate the subsequent therapeutic response in 25 CD patients. The authors used a topical fluorescent anti-TNF-antibody to visualize membrane-bound TNF[95]. It was shown that patients with high numbers of membrane-bound TNF on inflammatory cells show higher short-term response rates, higher rates of mucosal healing and lower inflammatory scores during anti-TNF-therapy even after one year. This molecular targeted approach demonstrates an ideal example how personalized medicine, including innovative imaging strategies and targeted therapies, could be applied to IBD[6].
Surveillance, detection of precursor lesions and colon cancerOne main focus of the majority of new techniques is set to surveillance and detection of dysplasia in IBD. It is very well established that HD endoscopy is superior to SD endoscopy in detecting dysplastic lesions and cancer. In fact, a 3-fold higher detection rate with HD endoscopy was observed when compared to SD endoscopy in IBD[96].
Displaying an ever bigger field of view in high-resolution wide-view full-spectrum endoscopy could perform at an adenoma miss rate significantly lower compared to standard forward-viewing endoscopy: 5/67 (7%) vs 20/49 (41%) (p < 0.0001)[97]. By almost doubling the displayed window and reducing blind corners, this approach might also help to improve visualization of inflammation mucosa and suspects lesions in IBD. However, this approach is also not yet implemented for IBD and the greatest benefit is by now still attributed to chromoendoscopy in the setting of surveillance. In fact, chromoendoscopy allows the discrimination of hyperplastic/non-adenomatous
Table 2 Assessment of disease activity with advanced endoscopic imaging in the context of clinical trials
Ref. Technique No. of patients
Findings
Kiesslich et al[84], 2003 CE 165 Agreement with histology: 84.5% (72 of 84) vs 60% (49 of 81) Kudo et al[85], 2009 NBI 30 Obscure mucosal vascular pattern is associated with inflammatory cell infiltrates (26% vs 0%),
goblet cell depletion (32% vs 5%), and basal plasmacytosis (2% vs 21%)Danese et al[87], 2010 NBI 14 Positive appearance on NBI correlated with increase in angiogenesis or vessel density Neumann et al[88], 2013 Virtual CE
(i-Scan) 78 Inflammatory extent and activity accordance with the histological results: 48.71% and 53.85%
(white-light) and 92.31% and 89.74% (i-Scan)Watanabe et al[89], 2008 CLE 17 Distinct alterations in active and non-active UC patients compared to histologyLi et al[90], 2010 CLE 73 Crypt architecture and fluorescein leakage with CLE correlate with histological resultsNeumann et al[92], 2012 CLE 54 CDEAS consisting of six parameters: crypt number, crypt distortion, micro erosions, cellular
infiltrate, vascularity, and number of goblet cellsStrong correlation of CDEAS and CRP
CE: Chromoendoscopy; NBI: Narrow-band imaging; CLE: Confocal laser endomicroscopy.
Knieling F et al . Emerging imaging techniques for IBD

5649 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
polyps from adenomatous polyps at a sensitivity and specificity of 93% and 95% respectively[98]. A meta-analysis from six trials could show that dye-based chromoendoscopy has medium to high sensitivity and high diagnostic accuracy for detection of dysplastic lesions in UC[99]. This has led to the recommendation that this procedure together with targeted biopsies is preferred as a surveillance procedure in IBD patients in US and European guidelines[100-103].
In contrast, virtual chromoendoscopy (such as NBI) could not show any advantage to standard white-light endoscopy in terms of improved adenoma detection rate, e.g., authors concluded that this technique likely will not contribute to a reduction in adenoma miss rates[25]. On the other hand, NBI may improve pathology diagnosis for diminutive colorectal polyps were 92.8% (95%CI: 90.4%-94.8%) and patients could be already informed of the results at discharge[26]. Comparing this to dye-based tech-niques, NBI was found to have a lower dysplasia detection rate[15]. This is the reason why dye-based approaches still remain recommend by international guidelines[100-103]. Suspect polyps presented with different characteristics in autofluorescence endoscopy: they showed fluorescence intensity maxima at approximately 460 nm, while normal colon was found to have larger fluorescence intensity compared to adenoma by a factor varying between 2-9 x[29,30]. As demonstrated in patients with Barrett’s esophagus, CLE is highly capable in detecting intraepithelial neoplasia[104] 21741642. This approach combined with chromoendoscopy leads to an increase of 4.75-fold in detecting neoplasias while 50% fewer biopsy specimens (p = 0.008) were required in the colon[105]. As stated for wide-view full-spectrum endoscopy these techniques are not (yet) translated into clinical routine use; especially for patients with IBD.
CLINICAL EVIDENCE AND TRANSLATION OF ULTRASOUND TECHNIQUESAssessment of disease activityIn contrast to endoscopic imaging techniques, other imaging techniques including CT, MRI, scintigraphy and US are mainly used to evaluate the extend of disease and disease activity in IBD patients. All imaging strategies are based on the identification of distinct morphological characteristics. These include the assessment of mucosal alterations, transmural involvement and extra intestinal manifestations.
So far, no single imaging technique is considered as diagnostic gold standard[51]. Even if MRI seems to perform at a better sensitivity, US is a useful, non-invasive radiation free imaging technique for the initial diagnostic if IBD is suspected[106,107]. If ultrasound is compared to X-ray or endoscopic results by disease localization it shows higher diagnostic performance for inflammatory conditions of the ileum and sigmoid/
descending colon than in the rectum, duodenum and proximal jejunum[108]. There are no data published, but it has been estimated that approximately 6 mo and 100 examinations are needed to gain proficiency in performing bowel US[106,109]. A meta-analysis on different modalities for the diagnosis of IBD on a per-patient basis showed high sensitivity and specificity for US, MRI, scintigraphy, and CT as well[110]. In fact, the authors could not show significant differences in diagnostic accuracy among the imaging techniques and concluded that a diagnostic modality without ionizing radiation should be preferred if possible. By measuring the wall thickness and longitudinal extent of pathologically altered bowel segments it was found that US is not strictly associated with clinical activity[111]. In contrast, Limberg demonstrated that assessment with color Doppler/Duplex ultrasonography is helpful and offers a noninvasive and indirect mean of assessing disease activity in intestinal inflammation[112]. Active CD lesions were found to have increased blood flow on preoperative color Doppler US correlating with greater vascularity and numbers of inflammatory leukocytes upon histology[113]. The authors concluded that Doppler US is capable of characterizing the inflammatory activity of CD small-intestinal lesions. The same was shown in children, where mucosal or transmural hypervascularity was not specific and color Doppler sonography could be correlated with different etiological inflammatory bowel processes[114]. Taken away the advantage of being a transabdominal and non-invasive technique, but being closer to the mucosa, ultrasound can also be used to image from inside the body. In this way, endosonography was able to differentiate UC from CD by a sensitivity of 92.3% showing a good correlation with histological inflammation scores (UC: r = 0.43; CD: r = 0.69)[55].
Romanini et al[115] used a quantitative approach after ultrasound contrast application in order to visualize vascular changes and to correlate disease activity with histologic vascular density. The group described cut-off values to distinguish between active and inactive disease, such as peak enhancement (> 40.5%) or regional blood flow (> 54.8 mL/min)[115]. Further, perfusion analysis one month after starting treatment can provide prognostic information re-garding treatment efficiency in CD[116]. The major advantage of CEUS is that the use of this technique is already approved so it can already be used.
Furthermore, CEUS can be used for molecular targeted imaging, possibly allowing additional information regarding disease activity. Up to now, molecular approaches are limited to pre-clinical settings. Deshpande et al[117] could show that targeted contrast-enhanced US imaging enables noninvasive in vivo quantification and can be used for monitoring P-selectin expression in mice with induced chemical colitis. As selectins are glycoproteins expressed during the first phase of leukocyte adherence, it seems a favorable marker for detection of early inflammatory
Knieling F et al . Emerging imaging techniques for IBD

5650 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
processes[118]. Consequently, it has been shown that this approach might be a promising modality for assessing and monitoring active inflammation in IBD[119], both in early and chronic IBD models. The introduction of antibodies targeting α4β7-integrin leukocyte trafficking has now also become a new major target in IBD therapy[120]. That is why this approach seems to be an ideal tool to assess endothelial expression of emerging molecular targets aiming leukocyte trafficking in IBD therapy.
Assessment of tissue fibrosisAs ongoing inflammation drives intestinal fibrosis[121], ultrasonic electrography might have a valuable role in this scenario. As demonstrated in a rat model elastography, is feasible able to distinguish acutely inflamed from fibrotic intestine[78,122]. This has been translated to human ex vivo tissue[123] and clinical observations[124,125], which found that increased shear wave velocity corresponds to increase in tissue fibrosis and stricturing disease. In a pilot study in children, this modality combined with hydrosonography appears to be able to predict the presence of complications or increased disease activity[126].
CONCLUSIONIn the recent decade the utilization of light and sound waves has greatly expanded in imaging modalities for the evaluation of IBD. Many of them are still waiting to gain entrance into clinical studies and applications. If the focus has been initially set to detection of dysplastic lesions, now new modalities are coming up to also assess initial presentation of the disease or its activity in follow-up. Interestingly, more and more morphological approaches are silently replaced by functional or molecular imaging modalities, which resemble more closely the pathophysiology and therapeutic interventions in IBD.
REFERENCES1 Molodecky NA, Soon IS, Rabi DM, Ghali WA, Ferris M, Chernoff
G, Benchimol EI, Panaccione R, Ghosh S, Barkema HW, Kaplan GG. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology 2012; 142: 46-54.e42; quiz e30 [PMID: 22001864 DOI: 10.1053/j.gastro.2011.10.001]
2 Chidlow JH, Langston W, Greer JJ, Ostanin D, Abdelbaqi M, Houghton J, Senthilkumar A, Shukla D, Mazar AP, Grisham MB, Kevil CG. Differential angiogenic regulation of experimental colitis. Am J Pathol 2006; 169: 2014-2030 [PMID: 17148665 DOI: 10.2353/ajpath.2006.051021]
3 Abraham C, Cho JH. Inflammatory bowel disease. N Engl J Med 2009; 361: 2066-2078 [PMID: 19923578 DOI: 10.1056/NEJMra0804647]
4 Lichtenstein GR, Rutgeerts P. Importance of mucosal healing in ulcerative colitis. Inflamm Bowel Dis 2010; 16: 338-346 [PMID: 19637362 DOI: 10.1002/ibd.20997]
5 Rutgeerts P, Vermeire S, Van Assche G. Mucosal healing in inflammatory bowel disease: impossible ideal or therapeutic target? Gut 2007; 56: 453-455 [PMID: 17369375 DOI: 10.1136/
gut.2005.088732]6 Neurath MF, Travis SP. Mucosal healing in inflammatory bowel
diseases: a systematic review. Gut 2012; 61: 1619-1635 [PMID: 22842618 DOI: 10.1136/gutjnl-2012-302830]
7 Bouguen G, Levesque BG, Pola S, Evans E, Sandborn WJ. Endoscopic assessment and treating to target increase the likelihood of mucosal healing in patients with Crohn’s disease. Clin Gastroenterol Hepatol 2014; 12: 978-985 [PMID: 24246770 DOI: 10.1016/j.cgh.2013.11.005]
8 Bouguen G, Levesque BG, Pola S, Evans E, Sandborn WJ. Feasibility of endoscopic assessment and treating to target to achieve mucosal healing in ulcerative colitis. Inflamm Bowel Dis 2014; 20: 231-239 [PMID: 24351660 DOI: 10.1097/01.MIB.0000437985.00190.aa]
9 Rogler G, Vavricka SR, Biedermann L. Integrating Imaging into Clinical Practice in Inflammatory Bowel Disease. Dig Dis 2015; 33 Suppl 1: 37-43 [PMID: 26367115 DOI: 10.1159/000437063]
10 Benchimol EI, Fortinsky KJ, Gozdyra P, Van den Heuvel M, Van Limbergen J, Griffiths AM. Epidemiology of pediatric inflammatory bowel disease: a systematic review of international trends. Inflamm Bowel Dis 2011; 17: 423-439 [PMID: 20564651 DOI: 10.1002/ibd.21349]
11 Yu AP, Cabanilla LA, Wu EQ, Mulani PM, Chao J. The costs of Crohn’s disease in the United States and other Western countries: a systematic review. Curr Med Res Opin 2008; 24: 319-328 [PMID: 18067689 DOI: 10.1185/030079908X260790]
12 Haas K, Rubesova E, Bass D. Role of imaging in the evaluation of inflammatory bowel disease: How much is too much? World J Radiol 2016; 8: 124-131 [PMID: 26981221 DOI: 10.4329/wjr.v8.i2.124]
13 Bernstein CN, Blanchard JF, Kliewer E, Wajda A. Cancer risk in patients with inflammatory bowel disease: a population-based study. Cancer 2001; 91: 854-862 [PMID: 11241255]
14 Eaden JA, Abrams KR, Mayberry JF. The risk of colorectal cancer in ulcerative colitis: a meta-analysis. Gut 2001; 48: 526-535 [PMID: 11247898]
15 Laine L, Kaltenbach T, Barkun A, McQuaid KR, Subramanian V, Soetikno R. SCENIC international consensus statement on surveillance and management of dysplasia in inflammatory bowel disease. Gastrointest Endosc 2015; 81: 489-501.e26 [PMID: 25708752 DOI: 10.1016/j.gie.2014.12.009]
16 Laine L, Kaltenbach T, Barkun A, McQuaid KR, Subramanian V, Soetikno R. SCENIC international consensus statement on surveillance and management of dysplasia in inflammatory bowel disease. Gastroenterology 2015; 148: 639-651.e28 [PMID: 25702852 DOI: 10.1053/j.gastro.2015.01.031]
17 American Society for Gastrointestinal Endoscopy Standards of Practice Committee, Shergill AK, Lightdale JR, Bruining DH, Acosta RD, Chandrasekhara V, Chathadi KV, Decker GA, Early DS, Evans JA, Fanelli RD, Fisher DA, Fonkalsrud L, Foley K, Hwang JH, Jue TL, Khashab MA, Muthusamy VR, Pasha SF, Saltzman JR, Sharaf R, Cash BD, DeWitt JM. The role of endoscopy in inflammatory bowel disease. Gastrointest Endosc 2015; 81: 1101-1121.e1-13 [PMID: 25800660 DOI: 10.1016/j.gie.2014.10.030]
18 Panes J, Bouhnik Y, Reinisch W, Stoker J, Taylor SA, Baumgart DC, Danese S, Halligan S, Marincek B, Matos C, Peyrin-Biroulet L, Rimola J, Rogler G, van Assche G, Ardizzone S, Ba-Ssalamah A, Bali MA, Bellini D, Biancone L, Castiglione F, Ehehalt R, Grassi R, Kucharzik T, Maccioni F, Maconi G, Magro F, Martín-Comín J, Morana G, Pendsé D, Sebastian S, Signore A, Tolan D, Tielbeek JA, Weishaupt D, Wiarda B, Laghi A. Imaging techniques for assessment of inflammatory bowel disease: joint ECCO and ESGAR evidence-based consensus guidelines. J Crohns Colitis 2013; 7: 556-585 [PMID: 23583097 DOI: 10.1016/j.crohns.2013.02.020]
19 Udagawa T, Minami A, Okada F. Development of magnifying video endoscopes with high resolution. Dig Endosc 2001; 13: 163-169
20 Gralnek IM, Carr-Locke DL, Segol O, Halpern Z, Siersema PD, Sloyer A, Fenster J, Lewis BS, Santo E, Suissa A, Segev M. Comparison of standard forward-viewing mode versus ultrawide-viewing mode of a novel colonoscopy platform: a prospective,
Knieling F et al . Emerging imaging techniques for IBD

5651 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
multicenter study in the detection of simulated polyps in an in vitro colon model (with video). Gastrointest Endosc 2013; 77: 472-479 [PMID: 23410700 DOI: 10.1016/j.gie.2012.12.011]
21 Gralnek IM, Segol O, Suissa A, Siersema PD, Carr-Locke DL, Halpern Z, Santo E, Domanov S. A prospective cohort study evaluating a novel colonoscopy platform featuring full-spectrum endoscopy. Endoscopy 2013; 45: 697-702 [PMID: 23939509 DOI: 10.1055/s-0033-1344395]
22 Tada M, Misaki F, Kawai K. A new approach to the observation of minute changes of the colonic mucosa by means of magnifying colonoscope, type CF-MB-M (Olympus). Gastrointest Endosc 1978; 24: 146-147 [PMID: 648836]
23 Mönkemüller K, Fry LC, Zimmermann L, Mania A, Zabielski M, Jovanovic I. Advanced endoscopic imaging methods for colon neoplasia. Dig Dis 2010; 28: 629-640 [PMID: 21088415 DOI: 10.1159/000320065]
24 Wallace MB, Kiesslich R. Advances in endoscopic imaging of colorectal neoplasia. Gastroenterology 2010; 138: 2140-2150 [PMID: 20420951 DOI: 10.1053/j.gastro.2009.12.067]
25 Adler A, Aschenbeck J, Yenerim T, Mayr M, Aminalai A, Drossel R, Schröder A, Scheel M, Wiedenmann B, Rösch T. Narrow-band versus white-light high definition television endoscopic imaging for screening colonoscopy: a prospective randomized trial. Gastroenterology 2009; 136: 410-6.e1; quiz 715 [PMID: 19014944 DOI: 10.1053/j.gastro.2008.10.022]
26 Kaltenbach T, Rastogi A, Rouse RV, McQuaid KR, Sato T, Bansal A, Kosek JC, Soetikno R. Real-time optical diagnosis for diminutive colorectal polyps using narrow-band imaging: the VALID randomised clinical trial. Gut 2015; 64: 1569-1577 [PMID: 25387891 DOI: 10.1136/gutjnl-2014-307742]
27 Kapadia CR, Cutruzzola FW, O’Brien KM, Stetz ML, Enriquez R, Deckelbaum LI. Laser-induced fluorescence spectroscopy of human colonic mucosa. Detection of adenomatous transformation. Gastroenterology 1990; 99: 150-157 [PMID: 2160898]
28 Jocham D, Stepp H, Waidelich R. Photodynamic diagnosis in urology: state-of-the-art. Eur Urol 2008; 53: 1138-1148 [PMID: 18096307 DOI: 10.1016/j.eururo.2007.11.048]
29 Cothren RM, Richards-Kortum R, Sivak MV, Fitzmaurice M, Rava RP, Boyce GA, Doxtader M, Blackman R, Ivanc TB, Hayes GB. Gastrointestinal tissue diagnosis by laser-induced fluorescence spectroscopy at endoscopy. Gastrointest Endosc 1990; 36: 105-111 [PMID: 2335276]
30 Cothren RM, Sivak MV, Van Dam J, Petras RE, Fitzmaurice M, Crawford JM, Wu J, Brennan JF, Rava RP, Manoharan R, Feld MS. Detection of dysplasia at colonoscopy using laser-induced fluorescence: a blinded study. Gastrointest Endosc 1996; 44: 168-176 [PMID: 8858323]
31 Wang TD, Crawford JM, Feld MS, Wang Y, Itzkan I, Van Dam J. In vivo identification of colonic dysplasia using fluorescence endoscopic imaging. Gastrointest Endosc 1999; 49: 447-455 [PMID: 10202057]
32 McCallum AL, Jenkins JT, Gillen D, Molloy RG. Evaluation of autofluorescence colonoscopy for the detection and diagnosis of colonic polyps. Gastrointest Endosc 2008; 68: 283-290 [PMID: 18329642 DOI: 10.1016/j.gie.2007.10.039]
33 ASGE Technology Committee, Kwon RS, Wong Kee Song LM, Adler DG, Conway JD, Diehl DL, Farraye FA, Kantsevoy SV, Kaul V, Kethu SR, Mamula P, Pedrosa MC, Rodriguez SA, Tierney WM. Endocytoscopy. Gastrointest Endosc 2009; 70: 610-613 [PMID: 19788978 DOI: 10.1016/j.gie.2009.06.030]
34 Neumann H, Kudo SE, Kiesslich R, Neurath MF. Advanced colonoscopic imaging using endocytoscopy. Dig Endosc 2015; 27: 232-238 [PMID: 25311804 DOI: 10.1111/den.12395]
35 Ichimasa K, Kudo SE, Mori Y, Wakamura K, Ikehara N, Kutsukawa M, Takeda K, Misawa M, Kudo T, Miyachi H, Yamamura F, Ohkoshi S, Hamatani S, Inoue H. Double staining with crystal violet and methylene blue is appropriate for colonic endocytoscopy: an in vivo prospective pilot study. Dig Endosc 2014; 26: 403-408 [PMID: 24016362 DOI: 10.1111/den.12164]
36 Kumagai Y, Monma K, Kawada K. Magnifying chromoendoscopy
of the esophagus: in-vivo pathological diagnosis using an endocytoscopy system. Endoscopy 2004; 36: 590-594 [PMID: 15243880 DOI: 10.1055/s-2004-814533]
37 Ohigashi T, Kozakai N, Mizuno R, Miyajima A, Murai M. Endocytoscopy: novel endoscopic imaging technology for in-situ observation of bladder cancer cells. J Endourol 2006; 20: 698-701 [PMID: 16999630 DOI: 10.1089/end.2006.20.698]
38 Kiesslich R, Burg J, Vieth M, Gnaendiger J, Enders M, Delaney P, Polglase A, McLaren W, Janell D, Thomas S, Nafe B, Galle PR, Neurath MF. Confocal laser endoscopy for diagnosing intraepithelial neoplasias and colorectal cancer in vivo. Gastroenterology 2004; 127: 706-713 [PMID: 15362025]
39 Neumann H, Kiesslich R, Wallace MB, Neurath MF. Confocal laser endomicroscopy: technical advances and clinical applications. Gastroenterology 2010; 139: 388-92, 392.e1-2 [PMID: 20561523 DOI: 10.1053/j.gastro.2010.06.029]
40 Zipfel WR, Williams RM, Webb WW. Nonlinear magic: multiphoton microscopy in the biosciences. Nat Biotechnol 2003; 21: 1369-1377 [PMID: 14595365 DOI: 10.1038/nbt899]
41 Schürmann S, Foersch S, Atreya R, Neumann H, Friedrich O, Neurath MF, Waldner MJ. Label-free imaging of inflammatory bowel disease using multiphoton microscopy. Gastroenterology 2013; 145: 514-516 [PMID: 23850960 DOI: 10.1053/j.gastro.2013.06.054]
42 Rivera DR, Brown CM, Ouzounov DG, Pavlova I, Kobat D, Webb WW, Xu C. Compact and flexible raster scanning multiphoton endoscope capable of imaging unstained tissue. Proc Natl Acad Sci USA 2011; 108: 17598-17603 [PMID: 22006303 DOI: 10.1073/pnas.1114746108]
43 Goetz M, Wang TD. Molecular imaging in gastrointestinal endoscopy. Gastroenterology 2010; 138: 828-33.e1 [PMID: 20096697 DOI: 10.1053/j.gastro.2010.01.009]
44 Liu Z, Miller SJ, Joshi BP, Wang TD. In vivo targeting of colonic dysplasia on fluorescence endoscopy with near-infrared octapeptide. Gut 2013; 62: 395-403 [PMID: 22427239 DOI: 10.1136/gutjnl-2011-301913]
45 Waldner MJ, Wirtz S, Jefremow A, Warntjen M, Neufert C, Atreya R, Becker C, Weigmann B, Vieth M, Rose-John S, Neurath MF. VEGF receptor signaling links inflammation and tumorigenesis in colitis-associated cancer. J Exp Med 2010; 207: 2855-2868 [PMID: 21098094 DOI: 10.1084/jem.20100438]
46 Foersch S, Sperka T, Lindner C, Taut A, Rudolph KL, Breier G, Boxberger F, Rau TT, Hartmann A, Stürzl M, Wittkopf N, Haep L, Wirtz S, Neurath MF, Waldner MJ. VEGFR2 Signaling Prevents Colorectal Cancer Cell Senescence to Promote Tumorigenesis in Mice With Colitis. Gastroenterology 2015; 149: 177-189.e10 [PMID: 25797700 DOI: 10.1053/j.gastro.2015.03.016]
47 Tjalma JJ, Garcia-Allende PB, Hartmans E, Terwisscha van Scheltinga AG, Boersma-van Ek W, Glatz J, Koch M, van Herwaarden YJ, Bisseling TM, Nagtegaal ID, Timmer-Bosscha H, Koornstra JJ, Karrenbeld A, Kleibeuker JH, van Dam GM, Ntziachristos V, Nagengast WB. Molecular Fluorescence Endoscopy Targeting Vascular Endothelial Growth Factor A for Improved Colorectal Polyp Detection. J Nucl Med 2016; 57: 480-485 [PMID: 26678613 DOI: 10.2967/jnumed.115.166975]
48 Jasinski R, Rubin JM, Beezhold C, Aisen A. Ultrasound examination of the colon. J Clin Ultrasound 1981; 9: 206-208 [PMID: 6793643]
49 Hussein W, Mullins PM, Alghamdi K, Sarani B, Pines JM. Trends in advanced computed tomography use for injured patients in United States emergency departments: 2007-2010. Acad Emerg Med 2015; 22: 663-669 [PMID: 25996245 DOI: 10.1111/acem.12684]
50 Maturen KE, Wasnik AP, Kamaya A, Dillman JR, Kaza RK, Pandya A, Maheshwary RK. Ultrasound imaging of bowel pathology: technique and keys to diagnosis in the acute abdomen. AJR Am J Roentgenol 2011; 197: W1067-W1075 [PMID: 22109321 DOI: 10.2214/AJR.11.6594]
51 Strobel D, Goertz RS, Bernatik T. Diagnostics in inflammatory bowel disease: ultrasound. World J Gastroenterol 2011; 17: 3192-3197 [PMID: 21912467 DOI: 10.3748/wjg.v17.i27.3192]
52 Pinto PN, Chojniak R, Cohen MP, Yu LS, Queiroz-Andrade M,
Knieling F et al . Emerging imaging techniques for IBD

5652 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Bitencourt AG. Comparison of three types of preparations for abdominal sonography. J Clin Ultrasound 2011; 39: 203-208 [PMID: 21337584 DOI: 10.1002/jcu.20790]
53 Nylund K, Hausken T, Gilja OH. Ultrasound and inflammatory bowel disease. Ultrasound Q 2010; 26: 3-15 [PMID: 20216190 DOI: 10.1097/RUQ.0b013e3181ce0929]
54 de Britto MA, Soletti RC, Schanaider A, Madi K, de Souza HS, Machado JC. Endoluminal ultrasound biomicroscopy as a reliable tool for in vivo assessment of colonic inflammation in rats. Int J Colorectal Dis 2013; 28: 1613-1620 [PMID: 23925435 DOI: 10.1007/s00384-013-1755-0]
55 Ellrichmann M, Wietzke-Braun P, Dhar S, Nikolaus S, Arlt A, Bethge J, Kuehbacher T, Wintermeyer L, Balschun K, Klapper W, Schreiber S, Fritscher-Ravens A. Endoscopic ultrasound of the colon for the differentiation of Crohn’s disease and ulcerative colitis in comparison with healthy controls. Aliment Pharmacol Ther 2014; 39: 823-833 [PMID: 24612000 DOI: 10.1111/apt.12671]
56 Strobel D, Seitz K, Blank W, Schuler A, Dietrich C, von Herbay A, Friedrich-Rust M, Kunze G, Becker D, Will U, Kratzer W, Albert FW, Pachmann C, Dirks K, Strunk H, Greis C, Bernatik T. Contrast-enhanced ultrasound for the characterization of focal liver lesions--diagnostic accuracy in clinical practice (DEGUM multicenter trial). Ultraschall Med 2008; 29: 499-505 [PMID: 19241506 DOI: 10.1055/s-2008-1027806]
57 Piscaglia F, Nolsøe C, Dietrich CF, Cosgrove DO, Gilja OH, Bachmann Nielsen M, Albrecht T, Barozzi L, Bertolotto M, Catalano O, Claudon M, Clevert DA, Correas JM, D’Onofrio M, Drudi FM, Eyding J, Giovannini M, Hocke M, Ignee A, Jung EM, Klauser AS, Lassau N, Leen E, Mathis G, Saftoiu A, Seidel G, Sidhu PS, ter Haar G, Timmerman D, Weskott HP. The EFSUMB Guidelines and Recommendations on the Clinical Practice of Contrast Enhanced Ultrasound (CEUS): update 2011 on non-hepatic applications. Ultraschall Med 2012; 33: 33-59 [PMID: 21874631 DOI: 10.1055/s-0031-1281676]
58 Claudon M, Dietrich CF, Choi BI, Cosgrove DO, Kudo M, Nolsøe CP, Piscaglia F, Wilson SR, Barr RG, Chammas MC, Chaubal NG, Chen MH, Clevert DA, Correas JM, Ding H, Forsberg F, Fowlkes JB, Gibson RN, Goldberg BB, Lassau N, Leen EL, Mattrey RF, Moriyasu F, Solbiati L, Weskott HP, Xu HX. Guidelines and good clinical practice recommendations for contrast enhanced ultrasound (CEUS) in the liver--update 2012: a WFUMB-EFSUMB initiative in cooperation with representatives of AFSUMB, AIUM, ASUM, FLAUS and ICUS. Ultraschall Med 2013; 34: 11-29 [PMID: 23129518 DOI: 10.1055/s-0032-1325499]
59 Schneider M. SonoVue, a new ultrasound contrast agent. Eur Radiol 1999; 9 Suppl 3: S347-S348 [PMID: 10602926]
60 Morel DR, Schwieger I, Hohn L, Terrettaz J, Llull JB, Cornioley YA, Schneider M. Human pharmacokinetics and safety evaluation of SonoVue, a new contrast agent for ultrasound imaging. Invest Radiol 2000; 35: 80-85 [PMID: 10639039]
61 Friedrich-Rust M, Klopffleisch T, Nierhoff J, Herrmann E, Vermehren J, Schneider MD, Zeuzem S, Bojunga J. Contrast-Enhanced Ultrasound for the differentiation of benign and malignant focal liver lesions: a meta-analysis. Liver Int 2013; 33: 739-755 [PMID: 23432804 DOI: 10.1111/liv.12115]
62 Guang Y, Xie L, Ding H, Cai A, Huang Y. Diagnosis value of focal liver lesions with SonoVue®-enhanced ultrasound compared with contrast-enhanced computed tomography and contrast-enhanced MRI: a meta-analysis. J Cancer Res Clin Oncol 2011; 137: 1595-1605 [PMID: 21850382 DOI: 10.1007/s00432-011-1035-8]
63 Wang C, Yu C, Yang F, Yang G. Diagnostic accuracy of contrast-enhanced ultrasound for renal cell carcinoma: a meta-analysis. Tumour Biol 2014; 35: 6343-6350 [PMID: 24659450 DOI: 10.1007/s13277-014-1815-2]
64 D’Onofrio M, Biagioli E, Gerardi C, Canestrini S, Rulli E, Crosara S, De Robertis R, Floriani I. Diagnostic performance of contrast-enhanced ultrasound (CEUS) and contrast-enhanced endoscopic ultrasound (ECEUS) for the differentiation of pancreatic lesions: a systematic review and meta-analysis. Ultraschall Med 2014; 35: 515-521 [PMID: 25226455 DOI: 10.1055/s-0034-1385068]
65 Piscaglia F, Bolondi L; Italian Society for Ultrasound in Medicine and Biology (SIUMB) Study Group on Ultrasound Contrast Agents. The safety of Sonovue in abdominal applications: retrospective analysis of 23188 investigations. Ultrasound Med Biol 2006; 32: 1369-1375 [PMID: 16965977 DOI: 10.1016/j.ultrasmedbio.2006.05.031]
66 Westwood M, Joore M, Grutters J, Redekop K, Armstrong N, Lee K, Gloy V, Raatz H, Misso K, Severens J, Kleijnen J. Contrast-enhanced ultrasound using SonoVue® (sulphur hexafluoride microbubbles) compared with contrast-enhanced computed tomography and contrast-enhanced magnetic resonance imaging for the characterisation of focal liver lesions and detection of liver metastases: a systematic review and cost-effectiveness analysis. Health Technol Assess 2013; 17: 1-243 [PMID: 23611316 DOI: 10.3310/hta17160]
67 Girlich C, Jung EM, Iesalnieks I, Schreyer AG, Zorger N, Strauch U, Schacherer D. Quantitative assessment of bowel wall vascularisation in Crohn’s disease with contrast-enhanced ultrasound and perfusion analysis. Clin Hemorheol Microcirc 2009; 43: 141-148 [PMID: 19713608 DOI: 10.3233/CH-2009-1228]
68 Girlich C, Schacherer D, Jung EM, Schreyer A, Büttner R. Comparison between a clinical activity index (Harvey-Bradshaw-Index), laboratory inflammation markers and quantitative assessment of bowel wall vascularization by contrast-enhanced ultrasound in Crohn’s disease. Eur J Radiol 2012; 81: 1105-1109 [PMID: 21439749 DOI: 10.1016/j.ejrad.2011.02.054]
69 Lassau N, Koscielny S, Albiges L, Chami L, Benatsou B, Chebil M, Roche A, Escudier BJ. Metastatic renal cell carcinoma treated with sunitinib: early evaluation of treatment response using dynamic contrast-enhanced ultrasonography. Clin Cancer Res 2010; 16: 1216-1225 [PMID: 20145174 DOI: 10.1158/1078-0432.CCR-09-2175]
70 Lassau N, Koscielny S, Chami L, Chebil M, Benatsou B, Roche A, Ducreux M, Malka D, Boige V. Advanced hepatocellular carcinoma: early evaluation of response to bevacizumab therapy at dynamic contrast-enhanced US with quantification--preliminary results. Radiology 2011; 258: 291-300 [PMID: 20980447 DOI: 10.1148/radiol.10091870]
71 Knieling F, Waldner MJ, Goertz RS, Zopf S, Wildner D, Neurath MF, Bernatik T, Strobel D. Early response to anti-tumoral treatment in hepatocellular carcinoma--can quantitative contrast-enhanced ultrasound predict outcome? Ultraschall Med 2013; 34: 38-46 [PMID: 23258770 DOI: 10.1055/s-0032-1330387]
72 Wildner D, Pfeifer L, Goertz RS, Bernatik T, Sturm J, Neurath MF, Strobel D. Dynamic contrast-enhanced ultrasound (DCE-US) for the characterization of hepatocellular carcinoma and cholangiocellular carcinoma. Ultraschall Med 2014; 35: 522-527 [PMID: 25202903 DOI: 10.1055/s-0034-1385170]
73 Lindner JR. Contrast ultrasound molecular imaging of inflammation in cardiovascular disease. Cardiovasc Res 2009; 84: 182-189 [PMID: 19783842 DOI: 10.1093/cvr/cvp302]
74 Tardy I, Pochon S, Theraulaz M, Emmel P, Passantino L, Tranquart F, Schneider M. Ultrasound molecular imaging of VEGFR2 in a rat prostate tumor model using BR55. Invest Radiol 2010; 45: 573-578 [PMID: 20808233 DOI: 10.1097/RLI.0b013e3181ee8b83]
75 Hyvelin JM, Tardy I, Bettinger T, von Wronski M, Costa M, Emmel P, Colevret D, Bussat P, Lassus A, Botteron C, Nunn A, Frinking P, Tranquart F. Ultrasound molecular imaging of transient acute myocardial ischemia with a clinically translatable P- and E-selectin targeted contrast agent: correlation with the expression of selectins. Invest Radiol 2014; 49: 224-235 [PMID: 24442162 DOI: 10.1097/RLI.0000000000000018]
76 Ophir J, Céspedes I, Ponnekanti H, Yazdi Y, Li X. Elastography: a quantitative method for imaging the elasticity of biological tissues. Ultrason Imaging 1991; 13: 111-134 [PMID: 1858217]
77 Palmeri ML, Nightingale KR. Acoustic radiation force-based elasticity imaging methods. Interface Focus 2011; 1: 553-564 [PMID: 22419986 DOI: 10.1098/rsfs.2011.0023]
78 Dillman JR, Stidham RW, Higgins PD, Moons DS, Johnson LA, Rubin JM. US elastography-derived shear wave velocity helps
Knieling F et al . Emerging imaging techniques for IBD
5653 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
distinguish acutely inflamed from fibrotic bowel in a Crohn disease animal model. Radiology 2013; 267: 757-766 [PMID: 23401585 DOI: 10.1148/radiol.13121775]
79 Friedrich-Rust M, Nierhoff J, Lupsor M, Sporea I, Fierbinteanu-Braticevici C, Strobel D, Takahashi H, Yoneda M, Suda T, Zeuzem S, Herrmann E. Performance of Acoustic Radiation Force Impulse imaging for the staging of liver fibrosis: a pooled meta-analysis. J Viral Hepat 2012; 19: e212-e219 [PMID: 22239521 DOI: 10.1111/j.1365-2893.2011.01537.x]
80 Park H, Park JY, Kim do Y, Ahn SH, Chon CY, Han KH, Kim SU. Characterization of focal liver masses using acoustic radiation force impulse elastography. World J Gastroenterol 2013; 19: 219-226 [PMID: 23345944 DOI: 10.3748/wjg.v19.i2.219]
81 Liu BJ, Li DD, Xu HX, Guo LH, Zhang YF, Xu JM, Liu C, Liu LN, Li XL, Xu XH, Qu S, Xing M. Quantitative Shear Wave Velocity Measurement on Acoustic Radiation Force Impulse Elastography for Differential Diagnosis between Benign and Malignant Thyroid Nodules: A Meta-analysis. Ultrasound Med Biol 2015; 41: 3035-3043 [PMID: 26371402 DOI: 10.1016/j.ultrasmedbio.2015.08.003]
82 Tontini GE, Mudter J, Vieth M, Atreya R, Günther C, Zopf Y, Wildner D, Kiesslich R, Vecchi M, Neurath MF, Neumann H. Confocal laser endomicroscopy for the differential diagnosis of ulcerative colitis and Crohn’s disease: a pilot study. Endoscopy 2015; 47: 437-443 [PMID: 25521573 DOI: 10.1055/s-0034-1391226]
83 Neumann H, Vieth M, Neurath MF, Atreya R. Endocytoscopy allows accurate in vivo differentiation of mucosal inflammatory cells in IBD: a pilot study. Inflamm Bowel Dis 2013; 19: 356-362 [PMID: 22644957 DOI: 10.1002/ibd.23025]
84 Kiesslich R, Fritsch J, Holtmann M, Koehler HH, Stolte M, Kanzler S, Nafe B, Jung M, Galle PR, Neurath MF. Methylene blue-aided chromoendoscopy for the detection of intraepithelial neoplasia and colon cancer in ulcerative colitis. Gastroenterology 2003; 124: 880-888 [PMID: 12671882 DOI: 10.1053/gast.2003.50146]
85 Kudo T, Matsumoto T, Esaki M, Yao T, Iida M. Mucosal vascular pattern in ulcerative colitis: observations using narrow band imaging colonoscopy with special reference to histologic inflammation. Int J Colorectal Dis 2009; 24: 495-501 [PMID: 19145441 DOI: 10.1007/s00384-008-0631-9]
86 Esaki M, Kubokura N, Kudo T, Matsumoto T. Endoscopic findings under narrow band imaging colonoscopy in ulcerative colitis. Dig Endosc 2011; 23 Suppl 1: 140-142 [PMID: 21535220 DOI: 10.1111/j.1443-1661.2011.01110.x]
87 Danese S, Fiorino G, Angelucci E, Vetrano S, Pagano N, Rando G, Spinelli A, Malesci A, Repici A. Narrow-band imaging endoscopy to assess mucosal angiogenesis in inflammatory bowel disease: a pilot study. World J Gastroenterol 2010; 16: 2396-2400 [PMID: 20480525]
88 Neumann H, Vieth M, Günther C, Neufert C, Kiesslich R, Grauer M, Atreya R, Neurath MF. Virtual chromoendoscopy for prediction of severity and disease extent in patients with inflammatory bowel disease: a randomized controlled study. Inflamm Bowel Dis 2013; 19: 1935-1942 [PMID: 23839228 DOI: 10.1097/MIB.0b013e318290550e]
89 Watanabe O, Ando T, Maeda O, Hasegawa M, Ishikawa D, Ishiguro K, Ohmiya N, Niwa Y, Goto H. Confocal endomicroscopy in patients with ulcerative colitis. J Gastroenterol Hepatol 2008; 23 Suppl 2: S286-S290 [PMID: 19120913 DOI: 10.1111/j.1440-1746.2008.05559.x]
90 Li CQ, Xie XJ, Yu T, Gu XM, Zuo XL, Zhou CJ, Huang WQ, Chen H, Li YQ. Classification of inflammation activity in ulcerative colitis by confocal laser endomicroscopy. Am J Gastroenterol 2010; 105: 1391-1396 [PMID: 19935787 DOI: 10.1038/ajg.2009.664]
91 Macé V, Ahluwalia A, Coron E, Le Rhun M, Boureille A, Bossard C, Mosnier JF, Matysiak-Budnik T, Tarnawski AS. Confocal laser endomicroscopy: a new gold standard for the assessment of mucosal healing in ulcerative colitis. J Gastroenterol Hepatol 2015; 30 Suppl 1: 85-92 [PMID: 25827810 DOI: 10.1111/jgh.12748]
92 Neumann H, Vieth M, Atreya R, Grauer M, Siebler J, Bernatik T, Neurath MF, Mudter J. Assessment of Crohn’s disease activity
by confocal laser endomicroscopy. Inflamm Bowel Dis 2012; 18: 2261-2269 [PMID: 22344873 DOI: 10.1002/ibd.22907]
93 Myaing MT, MacDonald DJ, Li X. Fiber-optic scanning two-photon fluorescence endoscope. Opt Lett 2006; 31: 1076-1078 [PMID: 16625908]
94 Wu Y, Leng Y, Xi J, Li X. Scanning all-fiber-optic endomicroscopy system for 3D nonlinear optical imaging of biological tissues. Opt Express 2009; 17: 7907-7915 [PMID: 19434122]
95 Atreya R, Neumann H, Neufert C, Waldner MJ, Billmeier U, Zopf Y, Willma M, App C, Münster T, Kessler H, Maas S, Gebhardt B, Heimke-Brinck R, Reuter E, Dörje F, Rau TT, Uter W, Wang TD, Kiesslich R, Vieth M, Hannappel E, Neurath MF. In vivo imaging using fluorescent antibodies to tumor necrosis factor predicts therapeutic response in Crohn’s disease. Nat Med 2014; 20: 313-318 [PMID: 24562382 DOI: 10.1038/nm.3462]
96 Subramanian V, Ramappa V, Telakis E, Mannath J, Jawhari AU, Hawkey CJ, Ragunath K. Comparison of high definition with standard white light endoscopy for detection of dysplastic lesions during surveillance colonoscopy in patients with colonic inflammatory bowel disease. Inflamm Bowel Dis 2013; 19: 350-355 [PMID: 22552948 DOI: 10.1002/ibd.23002]
97 Gralnek IM, Siersema PD, Halpern Z, Segol O, Melhem A, Suissa A, Santo E, Sloyer A, Fenster J, Moons LM, Dik VK, D’Agostino RB, Rex DK. Standard forward-viewing colonoscopy versus full-spectrum endoscopy: an international, multicentre, randomised, tandem colonoscopy trial. Lancet Oncol 2014; 15: 353-360 [PMID: 24560453 DOI: 10.1016/S1470-2045(14)70020-8]
98 Axelrad AM, Fleischer DE, Geller AJ, Nguyen CC, Lewis JH, Al-Kawas FH, Avigan MI, Montgomery EA, Benjamin SB. High-resolution chromoendoscopy for the diagnosis of diminutive colon polyps: implications for colon cancer screening. Gastroenterology 1996; 110: 1253-1258 [PMID: 8613016]
99 Wu L, Li P, Wu J, Cao Y, Gao F. The diagnostic accuracy of chromoendoscopy for dysplasia in ulcerative colitis: meta-analysis of six randomized controlled trials. Colorectal Dis 2012; 14: 416-420 [PMID: 21073646 DOI: 10.1111/j.1463-1318.2010.02505.x]
100 Van Assche G, Dignass A, Bokemeyer B, Danese S, Gionchetti P, Moser G, Beaugerie L, Gomollón F, Häuser W, Herrlinger K, Oldenburg B, Panes J, Portela F, Rogler G, Stein J, Tilg H, Travis S, Lindsay JO. Second European evidence-based consensus on the diagnosis and management of ulcerative colitis part 3: special situations. J Crohns Colitis 2013; 7: 1-33 [PMID: 23040453 DOI: 10.1016/j.crohns.2012.09.005]
101 Farraye FA, Odze RD, Eaden J, Itzkowitz SH, McCabe RP, Dassopoulos T, Lewis JD, Ullman TA, James T, McLeod R, Burgart LJ, Allen J, Brill JV. AGA medical position statement on the diagnosis and management of colorectal neoplasia in inflammatory bowel disease. Gastroenterology 2010; 138: 738-745 [PMID: 20141808 DOI: 10.1053/j.gastro.2009.12.037]
102 Cairns SR, Scholefield JH, Steele RJ, Dunlop MG, Thomas HJ, Evans GD, Eaden JA, Rutter MD, Atkin WP, Saunders BP, Lucassen A, Jenkins P, Fairclough PD, Woodhouse CR. Guidelines for colorectal cancer screening and surveillance in moderate and high risk groups (update from 2002). Gut 2010; 59: 666-689 [PMID: 20427401 DOI: 10.1136/gut.2009.179804]
103 Annese V, Daperno M, Rutter MD, Amiot A, Bossuyt P, East J, Ferrante M, Götz M, Katsanos KH, Kießlich R, Ordás I, Repici A, Rosa B, Sebastian S, Kucharzik T, Eliakim R. European evidence based consensus for endoscopy in inflammatory bowel disease. J Crohns Colitis 2013; 7: 982-1018 [PMID: 24184171 DOI: 10.1016/j.crohns.2013.09.016]
104 Sharma P, Meining AR, Coron E, Lightdale CJ, Wolfsen HC, Bansal A, Bajbouj M, Galmiche JP, Abrams JA, Rastogi A, Gupta N, Michalek JE, Lauwers GY, Wallace MB. Real-time increased detection of neoplastic tissue in Barrett’s esophagus with probe-based confocal laser endomicroscopy: final results of an international multicenter, prospective, randomized, controlled trial. Gastrointest Endosc 2011; 74: 465-472 [PMID: 21741642 DOI: 10.1016/j.gie.2011.04.004]
105 Kiesslich R, Goetz M, Lammersdorf K, Schneider C, Burg J, Stolte
Knieling F et al . Emerging imaging techniques for IBD

5654 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
M, Vieth M, Nafe B, Galle PR, Neurath MF. Chromoscopy-guided endomicroscopy increases the diagnostic yield of intraepithelial neoplasia in ulcerative colitis. Gastroenterology 2007; 132: 874-882 [PMID: 17383417 DOI: 10.1053/j.gastro.2007.01.048]
106 Calabrese E, Maaser C, Zorzi F, Kannengiesser K, Hanauer SB, Bruining DH, Iacucci M, Maconi G, Novak KL, Panaccione R, Strobel D, Wilson SR, Watanabe M, Pallone F, Ghosh S. Bowel Ultrasonography in the Management of Crohn’s Disease. A Review with Recommendations of an International Panel of Experts. Inflamm Bowel Dis 2016; 22: 1168-1183 [PMID: 26958988 DOI: 10.1097/MIB.0000000000000706]
107 Castiglione F, Mainenti PP, De Palma GD, Testa A, Bucci L, Pesce G, Camera L, Diaferia M, Rea M, Caporaso N, Salvatore M, Rispo A. Noninvasive diagnosis of small bowel Crohn’s disease: direct comparison of bowel sonography and magnetic resonance enterography. Inflamm Bowel Dis 2013; 19: 991-998 [PMID: 23429465 DOI: 10.1097/MIB.0b013e3182802b87]
108 Parente F, Greco S, Molteni M, Cucino C, Maconi G, Sampietro GM, Danelli PG, Cristaldi M, Bianco R, Gallus S, Bianchi Porro G. Role of early ultrasound in detecting inflammatory intestinal disorders and identifying their anatomical location within the bowel. Aliment Pharmacol Ther 2003; 18: 1009-1016 [PMID: 14616167]
109 Condino G, Calabrese E, Zorzi F, Onali S, Lolli E, De Biasio F, Ascolani M, Pallone F, Biancone L. Anti-TNF-alpha treatments and obstructive symptoms in Crohn’s disease: a prospective study. Dig Liver Dis 2013; 45: 258-262 [PMID: 23195667 DOI: 10.1016/j.dld.2012.10.009]
110 Horsthuis K, Bipat S, Bennink RJ, Stoker J. Inflammatory bowel disease diagnosed with US, MR, scintigraphy, and CT: meta-analysis of prospective studies. Radiology 2008; 247: 64-79 [PMID: 18372465 DOI: 10.1148/radiol.2471070611]
111 Mayer D, Reinshagen M, Mason RA, Muche R, von Tirpitz C, Eckelt D, Adler G, Beckh K, Kratzer W. Sonographic measurement of thickened bowel wall segments as a quantitative parameter for activity in inflammatory bowel disease. Z Gastroenterol 2000; 38: 295-300 [PMID: 10820861 DOI: 10.1055/s-2000-14875]
112 Limberg B. [Diagnosis of chronic inflammatory bowel disease by ultrasonography]. Z Gastroenterol 1999; 37: 495-508 [PMID: 10427656]
113 Sasaki T, Kunisaki R, Kinoshita H, Kimura H, Kodera T, Nozawa A, Hanzawa A, Shibata N, Yonezawa H, Miyajima E, Morita S, Fujii S, Numata K, Tanaka K, Tanaka M, Maeda S. Doppler ultrasound findings correlate with tissue vascularity and inflammation in surgical pathology specimens from patients with small intestinal Crohn’s disease. BMC Res Notes 2014; 7: 363 [PMID: 24927748 DOI: 10.1186/1756-0500-7-363]
114 Quillin SP, Siegel MJ. Gastrointestinal inflammation in children: color Doppler ultrasonography. J Ultrasound Med 1994; 13: 751-756 [PMID: 7823336]
115 Romanini L, Passamonti M, Navarria M, Lanzarotto F, Villanacci V, Grazioli L, Calliada F, Maroldi R. Quantitative analysis of contrast-enhanced ultrasonography of the bowel wall can predict disease activity in inflammatory bowel disease. Eur J Radiol 2014; 83: 1317-1323 [PMID: 24908589 DOI: 10.1016/j.ejrad.2014.05.012]
116 Saevik F, Nylund K, Hausken T, Ødegaard S, Gilja OH. Bowel perfusion measured with dynamic contrast-enhanced ultrasound predicts treatment outcome in patients with Crohn’s disease. Inflamm Bowel Dis 2014; 20: 2029-2037 [PMID: 25185684 DOI: 10.1097/MIB.0000000000000159]
117 Deshpande N, Lutz AM, Ren Y, Foygel K, Tian L, Schneider M, Pai R, Pasricha PJ, Willmann JK. Quantification and monitoring of inflammation in murine inflammatory bowel disease with targeted contrast-enhanced US. Radiology 2012; 262: 172-180 [PMID: 22056689 DOI: 10.1148/radiol.11110323]
118 Vestweber D. How leukocytes cross the vascular endothelium. Nat Rev Immunol 2015; 15: 692-704 [PMID: 26471775 DOI: 10.1038/nri3908]
119 Machtaler S, Knieling F, Luong R, Tian L, Willmann JK. As-sessment of Inflammation in an Acute on Chronic Model of Inflammatory Bowel Disease with Ultrasound Molecular Imaging. Theranostics 2015; 5: 1175-1186 [PMID: 26379784 DOI: 10.7150/thno.13048]
120 Sandborn WJ, Feagan BG, Rutgeerts P, Hanauer S, Colombel JF, Sands BE, Lukas M, Fedorak RN, Lee S, Bressler B, Fox I, Rosario M, Sankoh S, Xu J, Stephens K, Milch C, Parikh A. Vedolizumab as induction and maintenance therapy for Crohn’s disease. N Engl J Med 2013; 369: 711-721 [PMID: 23964933 DOI: 10.1056/NEJMoa1215739]
121 Latella G, Di Gregorio J, Flati V, Rieder F, Lawrance IC. Mechanisms of initiation and progression of intestinal fibrosis in IBD. Scand J Gastroenterol 2015; 50: 53-65 [PMID: 25523556 DOI: 10.3109/00365521.2014.968863]
122 Kim K, Johnson LA, Jia C, Joyce JC, Rangwalla S, Higgins PD, Rubin JM. Noninvasive ultrasound elasticity imaging (UEI) of Crohn’s disease: animal model. Ultrasound Med Biol 2008; 34: 902-912 [PMID: 18294759 DOI: 10.1016/j.ultrasmedbio.2007.11.020]
123 Dillman JR, Stidham RW, Higgins PD, Moons DS, Johnson LA, Keshavarzi NR, Rubin JM. Ultrasound shear wave elastography helps discriminate low-grade from high-grade bowel wall fibrosis in ex vivo human intestinal specimens. J Ultrasound Med 2014; 33: 2115-2123 [PMID: 25425367 DOI: 10.7863/ultra.33.12.2115]
124 Baumgart DC, Müller HP, Grittner U, Metzke D, Fischer A, Guckelberger O, Pascher A, Sack I, Vieth M, Rudolph B. US-based Real-time Elastography for the Detection of Fibrotic Gut Tissue in Patients with Stricturing Crohn Disease. Radiology 2015; 275: 889-899 [PMID: 25668520 DOI: 10.1148/radiol.14141929]
125 Ishikawa D, Ando T, Watanabe O, Ishiguro K, Maeda O, Miyake N, Nakamura M, Miyahara R, Ohmiya N, Hirooka Y, El-Omar EM, Goto H. Images of colonic real-time tissue sonoelastography correlate with those of colonoscopy and may predict response to therapy in patients with ulcerative colitis. BMC Gastroenterol 2011; 11: 29 [PMID: 21453450 DOI: 10.1186/1471-230X-11-29]
126 Fufezan O, Asavoaie C, Tamas A, Farcau D, Serban D. Bowel elastography - a pilot study for developing an elastographic scoring system to evaluate disease activity in pediatric Crohn’s disease. Med Ultrason 2015; 17: 422-430 [PMID: 26649334 DOI: 10.11152/mu.2013.2066.174.bwe]
P- Reviewer: Manguso F, Jarry A S- Editor: Ma YJ L- Editor: A E- Editor: Wang CH
Knieling F et al . Emerging imaging techniques for IBD

Miranda Muhvić-Urek, Department of Oral Medicine and Periodontology, School of Dental Medicine, University of Rijeka, 51000 Rijeka, Croatia
Marija Tomac-Stojmenović, School of Medicine, University of Rijeka, 51000 Rijeka, Croatia
Brankica Mijandrušić-Sinčić, Division of Gastroenterology, Department of Internal Medicine, University Hospital Center Rijeka, 51000 Rijeka, Croatia
Author contributions: Muhvić-Urek M, Tomac-Stojmenović M and Mijandrušić-Sinčić B performed data acquisition and wrote the manuscript; Muhvić-Urek M and Mijandrušić-Sinčić B revised the manuscript; and Mijandrušić-Sinčić B approved the final manuscript.
Conflict-of-interest statement: No conflict of interest.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Manuscript source: Invited manuscript
Correspondence to: Mijandrušić-Sinčić Brankica, MD, PhD, Associate Professor, Division of Gastroenterology, Department of Internal Medicine, University Hospital Center Rijeka, Krešimirova 42, 51000 Rijeka, Croatia. [email protected]: +385-99-4366292Fax: +385-51-658826
Received: March 23, 2016 Peer-review started: March 24, 2016First decision: May 12, 2016Revised: May 27, 2016 Accepted: June 15, 2016 Article in press: June 15, 2016Published online: July 7, 2016
Abstract The incidence of inflammatory bowel diseases (IBD) - Crohn’s disease (CD) and ulcerative colitis (UC) - has been increasing on a global scale, and progressively, more gastroenterologists will be included in the diagnosis and treatment of IBD. Although IBD primarily affects the intestinal tract, extraintestinal manifestations of the disease are often apparent, including in the oral cavity, especially in CD. Specific oral manifestations in patients with CD are as follows: indurate mucosal tags, cobblestoning and mucogingivitis, deep linear ulcerations and lip swelling with vertical fissures. The most common non-specific manifestations, such as aphthous stomatitis and angular cheilitis, occur in both diseases, while pyostomatitis vegetans is more pronounced in patients with UC. Non-specific lesions in the oral cavity can also be the result of malnutrition and drugs. Malnutrition, followed by anemia and mineral and vitamin deficiency, affects the oral cavity and teeth. Furthermore, all of the drug classes that are applied to the treatment of inflammatory bowel diseases can lead to alterations in the oral cavity due to the direct toxic effects of the drugs on oral tissues, as well as indirect immunosuppressive effects with a risk of developing opportunistic infections or bone marrow suppression. There is a higher occurrence of malignant diseases in patients with IBD, which is related to the disease itself and to the IBD-related therapy with a possible oral pathology. Treatment of oral lesions includes treatment of the alterations in the oral cavity according to the etiology together with treatment of the primary intestinal disease, which requires adequate knowledge and a strong cooperation between gastroenterologists and specialists in oral medicine.
Key words: Crohn’s disease; Ulcerative colitis; Drug-related side effects and adverse reactions; Inflammatory bowel disease; Extraintestinal manifestations; Malnutrition
© The Author(s) 2016. Published by Baishideng Publishing Group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.3748/wjg.v22.i25.5655
5655 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
World J Gastroenterol 2016 July 7; 22(25): 5655-5667 ISSN 1007-9327 (print) ISSN 2219-2840 (online)
© 2016 Baishideng Publishing Group Inc. All rights reserved.
Miranda Muhvić-Urek, Marija Tomac-Stojmenović, Brankica Mijandrušić-Sinčić
TOPIC HIGHLIGHT
Oral pathology in inflammatory bowel disease2016 Inflammatory Bowel Disease: Global view

Core tip: Inflammatory bowel diseases (IBD), Crohn’s disease (CD) and ulcerative colitis affect the intestinal tract, but can also present with extraintestinal manifestations and complications. In CD, disease-specific lesions with granulomatous changes can occur in the oral cavity. However, non-specific lesions are more common in IBD and are mostly caused by malnutrition and medications. All of the drug classes that are applied in the treatment of IBD can lead to lesions in the oral cavity. This paper offers an overview of the oral pathology with a detailed description of the complications related to malnutrition and IBD therapy.
Muhvić-Urek M, Tomac-Stojmenović M, Mijandrušić-Sinčić B. Oral pathology in inflammatory bowel disease. World J Gastroenterol 2016; 22(25): 5655-5667 Available from: URL: http://www.wjgnet.com/1007-9327/full/v22/i25/5655.htm DOI: http://dx.doi.org/10.3748/wjg.v22.i25.5655
INTRODUCTION Crohn’s disease (CD) and ulcerative colitis (UC) belong to the group of chronic inflammatory bowel diseases (IBD). Although the etiology of these diseases has not been completely ascertained, it is well known that the factors contributing to disease pathogenesis include environmental aspects, intestinal microflora, genetic predisposition and pathological immune responses[1-3]. North America and North-Western Europe exhibit the highest incidence and prevalence of the disease, but an increase in the number of patients has been observed worldwide, indicating its emergence as a global disease[4,5]. It appears that the global increase in the disease is related to a “Western” lifestyle and diet, which shows the strong impact of the environment on the occurrence of the disease[1,3,6].
In addition to affecting the intestinal tract, the disease can manifest with extraintestinal symptoms in almost every organ system and significantly influence the quality of life and the functional state of the patient. There is a distinction between extraintestinal manifestations (EIM) and extraintestinal complications, although they are sometimes difficult to distinguish. EIMs occur in 6% to 47% of patients[7-10] with different rates of occurrence in relation to the primary disease. Peripheral arthropathy type I, aphthous stomatitis, erythema nodosum and episcleritis are usually related to an active disease. Ankylosing spondylitis and peripheral arthropathy type II have their own course of disease, independent of the activity of the bowel disease. Primary sclerosing cholangitis, uveitis and pyoderma gangrenosum have a variable course and can be associated with, but do not have to be related to, the activity of the bowel disease[10]. Patients with perianal CD, patients with colonic disease and smokers are at an increased risk of developing EIMs[9,10]. Furthermore, patients can develop several EIMs at the
same time, and the occurrence of one EIM increases the risk of developing another EIM[10].
The pathogenesis of EIMs is still not fully identified. It appears that the inflamed intestinal mucosa can trigger immunological responses by sharing common epitopes (e.g., intestinal bacteria and synovia). Bacteria that can translocate because of greater permeability of the intestinal mucosa trigger an acquired immune response that does not distinguish between a bacterial epitope and a joint or skin epitope[10]. In patients with extraintestinal disease manifestations, there is also a strong genetic predisposition; the connection between the EIMs and the major histocompatibility complex loci has been demonstrated, and there is a concordance for EIMs in 84% of siblings[8,9].
Extraintestinal complications of inflammatory bowel diseases frequently occur due to malnutrition, chronic inflammation and side effects of drugs[2,8-10].
Oral lesions are common in patients with IBD and epidemiology data vary over a wide range of 5%-50% due to contradictory studies[11,12]. The goal of our paper is to present the oral pathology of IBD, whether it includes extraintestinal manifestations of the disease or its complications.
ORAL MANIFESTATIONS OF INFLAMMATORY BOWEL DISEASEOral manifestations of CD include specific and non-specific lesions, while in patients with UC, only non-specific lesions in the oral cavity are observed. Characteristics of specific lesions include the presence of non-caseous granulomas, which occur only in CD patients. CD manifestations in the oral cavity can precede the intestinal manifestations, occur at the same time as the intestinal manifestations or occur after the occurrence of the intestinal manifestations. Oral lesions can be of significance when diagnosing CD because of a characteristic non-caseous granu-lomatous inflammation[12-17]. This condition can be easily confirmed by a histopathological examination of accessible lesions in the oral cavity. Turchi et al[18] described a rare case of tonsillar granuloma as a manifestation of CD. Oral manifestations of the disease are more common in males[15,19,20] and children[12,19,21,22]. They are also more common in patients with CD than in patients with UC[23,24], and their prevalence in CD patients ranges from 20%-50%[11], while in UC the prevalence is 8%[25]. However, some studies have not demonstrated a statistically significant difference[26]. Furthermore, data from the literature are contradictory; in some studies, it has been stated that the changes in the oral cavity are not related to the CD activity index[27] or to the localization of intestinal manifestations[23,24,28,29], although there are papers that do link and attribute the changes in the oral cavity to inflammatory responses following the exacerbation of CD[26,30].
5656 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Muhvić-Urek M et al . Oral pathology in IBD

Specific oral lesions in patients with CD include a cobblestone appearance of the oral mucosa; deep linear ulcerations; mucosal tags; swelling of the lips, cheeks and face; lip and tongue fissures; and mucogingivitis[15,19,21,22,25,31]. The mucosa of the oral cavity is hyperplastic and resembles a “cobblestone”, which marks the nodular, granulomatous swelling of the oral mucosa (Figure 1). In addition, there are also indurated polypoid fringe-like lesions of the vestibule and the retromolar region. Mucosal tags and deep ulcerations with hyperplastic edges, firm or boggy to palpation, are mostly present in the labial and buccal mucosa and in retromolar regions. Attached gingiva and alveolar mucosa become swollen, granulated and hyperplastic with or without ulcerations[19,32]. Edema of the face, of one or both lips and of the buccal mucosa may also occur. This condition is unpleasant for patients because it can lead to facial deformation[15,19,22,25]. Non-caseous granulomatous inflammation[33] can be histologically detected in such lesions. The lips are the most commonly affected, and they are usually painless, tender and firm to palpation[34]. Numerous patients with swollen lips also develop painful vertical fissures where many microorganisms can be isolated[35].
Furthermore, patients with CD often experience autoimmune changes of the minor salivary glands and dry mouth[23,36]. Mills et al[36] reported a case of patient with CD in which characteristic granulomatous lesions caused rupture of the excretory salivary duct leading to the formation of a cutaneous salivary duct fistula. Chronic inflammatory processes near the parotid duct resulted in partial to total duct obstruction and caused dilated ducts and cyst formation, which can lead to the formation of cutaneous fistula. All of these changes can cause reduction in saliva and dry mouth[23].
Non-specific oral lesions associated with CD and UC include aphthous stomatitis, angular che-ilitis, pyostomatitis vegetans, glossitis and lichen planus[13,17,19,23,31,37,38]. Non-specific lesions, present in both CD and UC patients, are more common than specific lesions, which makes the differential diagnosis very difficult[13]. Non-specific lesions occur due to
chronic inflammation, malnutrition and as a side effect of drugs. The occurrence of halitosis[23], dental erosion, dental caries[20,30,39,40], candidiasis, odynophagia and dysphagia[23,26] is more common in patients with IBD than in the general population. Furthermore, patients with UC exhibit diffuse pustules and non-specific gingivitis in the oral cavity[19].
Aphthous stomatitis, which occurs in both CD and UC patients, presents as shallow, round ulcers surrounded by an erythematous “halo” with a central fibrin membrane[19,31]. Aphthous stomatitis does not differ from the stomatitis that occurs in the general population. If aphthous ulcerations are present, the presence of inflammatory bowel disease must be suspected, although intestinal symptoms may not yet be present[28,29]. Because oral lesions are more common in children and can precede the development of inflammatory bowel disease, cooperation between a specialist in oral medicine and a gastroenterologist is crucial to detect the disease as early as possible[12,13].
Angular cheilitis is clinically manifested as erythema with or without painful fissures and sores at the corners of the mouth. It can occur due to anemia or as a manifestation of a fungal or bacterial infection[25,41-43].
Pyostomatitis vegetans is a rare benign chronic inflammatory mucocutaneous disorder characterized by pustules of an unknown etiology. It is related to inflammatory bowel disease, occurs more often in combination with UC (although it can occur in CD) and is more common in male patients. It represents a specific inflammatory marker of UC[19,33]. Only about fifty cases of this disorder have been described to-date[37,38,44-50]. Macroscopically, the disease manifests as small exophytic lesions with an erythematous perimeter and a creamy white or yellow surface. They are covered with vulnerable membranes and their cracking results in small superficial erosions or ulcers. The confluence of those lesions results in the characteristic morphology sign of a “snail track”[33]. The alterations occur in the upper and lower frontal vestibule, on the tongue (Figure 2) and gingiva, as well as on the soft and hard palate[33]. Microscopically, there are no granulomas in the lesions.
Although IBD complications lead to non-specific lesions in the oral cavity, the consequences of two of the most common complications, malnutrition and medications administered for the treatment of inflammatory bowel disease, must be emphasized. Table 1 summarizes the oral manifestations and complications of IBD.
ORAL PATHOLOGY CAUSED BY MALNUTRITION Malnutrition is present in 23% of outpatients and 85% of hospitalized patients suffering from IBD[51]. It is caused by a reduced food intake, reduced resorption of nutrients, gastrointestinal losses, increased metabolic
5657 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Figure 1 Cobblestoning and ulcerations in Crohn's disease.
Muhvić-Urek M et al . Oral pathology in IBD

Table 1 Oral manifestations and complications in inflammatory bowel disease
5658 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
jejunum) lead to a microcytic, hypochromic anemia, while the presence of proinflammatory cytokines causes chronic anemia with a high hyperferritinemia. The deficiency of B12 and folates leads to macrocytic anemia. The deficiency of B12 occurs most often in Crohn’s disease due to reabsorption deficiency in the terminal ileum, while the deficiency of folates can be caused by reduced reabsorption, inadequate dietary intake and as a side effect of methotrexate and sulfasalazine[7,54].
Anemia caused by an iron deficiency is manifested as paleness of the oral mucosa[55], generalized oral mucosal atrophy, pricking[56,57], atrophic glossitis with tongue pain[57] and angular cheilitis[43,55]. The deficiency of vitamin B12 is manifested in the oral cavity as a painful atrophy of the oral mucosa and the tongue, recurrent aphthous ulcerations[58,59], angular cheilitis, oral candidiasis, diffuse erythematous stomatitis and pale yellowish mucosa, especially on the palate[60]. Patients can also complain of altered taste, a burning sensation in the mouth and dysphagia[43]. If anemia is caused by a folate deficiency, the manifestations in the oral cavity are the same as in anemia caused by vitamin B12 deficiency but without neurological symptoms[43]. In more severe cases, ulcerative sto-matitis and pharyngitis[43] are also detected.
needs and as a side effect of drugs[51,52]. As a result of a nutrient deficiency, patients develop anemia due to lower iron, vitamin B12 and folate levels. In addition to anemia, a deficiency of electrolytes, trace elements and vitamins is also quite common[52,53]. Anemia is a common complication of inflammatory bowel disease, which can be manifested in oral pathology. Suffering from anemia can strongly influence the patient’s quality of life. Bleeding and reduced iron reabsorption (due to inflammatory changes in the duodenum and upper
Oral tissue Manifestations Etiology
Lips Lips swelling with or without fissures[12,15,16,21,22,34,36,156] Crohn's disease Angular cheilitis[15,22,31] Fungal and bacterial infections, nutritional deficiency
Erythema multiforme, Stevens-Johnson syndrome[143,144] Infliximab; adalimumabTongue Fissuring[23] Crohn's disease
Cobblestone plaques[17] Crohn's diseasePyostomatitis vegetans[17,37,38,45] Ulcerative colitis (more common) and Crohn's disease
Aphthous stomatitis[11,31] Nutritional deficiency; decreased heat shock protein 27 expressionTaste disturbance[17,23,147,155] Related to disease activity and nutritional habits; sulfasalazine;
metronidazole Candida infections[78,131,132,141] Corticosteroids; thiopurines; cyclosporin A; infliximab
Erythema multiforme, Stevens-Johnson syndrome[143,144] Infliximab; adalimumabOral mucosa Buccal edema[15,34,48] Crohn's disease(labial/buccal/ Cobblestoning[12,14,15,21,24,34] Crohn's diseasepalatal/vestibular) Deep linear ulceration[15,16,21-24,34,38] Crohn's disease
Mucosal tags[12,16,21,29,34] Crohn's diseaseBuccal sulcus ulcerations[20,34] Crohn's disease
Palatal ulcerations[20,44] Crohn's diseasePyostomatitis vegetans[33,37,45-47,49,50] Ulcerative colitis (more common) and Crohn's disease
Aphthous stomatitis[11,22,29,31,45] Nutritional deficiency; decreased heat shock protein 27 expressionLichen planus/lichenoid reaction[29,85,140,142] Sulfasalazine; mesalazine; infliximab;
certolizumab pegolErythema multiforme, Stevens-Johnson syndrome[143,144] Infliximab; adalimumab
Periodontal tissue Mucogingivitis[12,21,22,32,34] Crohn's diseaseCobblestoning[29,32] Crohn's disease
Pyostomatitis vegetans/pustular ulcerations[17,32,33,37,44,46,50] Ulcerative colitis (more common) and Crohn's disease Nonspecific gingivitis[13,19,147] Cause not clearly specified
Periodontal diseases/periodontitis[20,156] Cause not clearly specifiedAlveolar bone Periapical lesions[30] Related to disease activity
Alveolar bone loss[156] Cause not clearly specifiedTeeth Caries[20,30,39,40] Related to disease activity and malabsorption
Hypoplasia of enamel[40] Related to disease activity and malabsorptionSalivary glands Hyposalivation/dry mouth[23,36] Granulomatous inflammation
Autoimmune changes in minor salivary glandsSalivary duct fistula[36] Crohn's disease
Figure 2 Pyostomatitis vegetans in ulcerative colitis.
Muhvić-Urek M et al . Oral pathology in IBD

5659 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Today, it is well known that vitamin D not only plays an important role in the mineralization of bones and teeth but also contributes to numerous metabolic processes and has a protective role in immune-mediated diseases as well as allergies. A vitamin D deficiency, in addition to disorders in the metabolism of calcium and phosphate in the oral cavity, is accompanied by the development of bone hypomineralization and an increased risk of fractures[61]. Malabsorption of calcium, vitamin K and other nutrients, treatment with corticosteroids, inflammatory cytokines in IBD and hypogonadism caused by IBD are additional factors that contribute to the decreased bone mineral density[62]. A vitamin D deficiency is also associated with the increased prevalence of periodontal diseases (gingivitis and periodontitis), dental caries and tooth loss[63-65]. Vitamin D also exerts an immunomodulatory effect, and its deficiency increases the risk of infection, malignancy and autoimmune disease[66] with possible oral manifestations. Calcium is a mineral that plays an important role in tooth development and mineralization. Experimental studies have shown that a calcium deficiency causes a disorder affecting the mineralization of dentin and enamel[40,67]. A decreased mineralization of bones and teeth is expected in children, who have developed IBD with a deficiency of calcium and vitamin D. However, according to the literature, there are no studies addressing this issue.
Vitamin A and vitamin C deficiencies are also described in IBD patients. A vitamin A deficiency is manifested in the oral cavity as angular cheilitis, atrophy and dryness of oral mucosa. The lips are described as “retreating” because the mucosa contracts towards the oral cavity[68]. A vitamin C deficiency is manifested in the oral cavity as generalized gingival swelling and spontaneous bleeding, ulcerations, tooth mobility, increased severity of periodontal infections and bone loss[55,69]. Spontaneous bleeding of the mucosa can be observed as well[70]. The development of bones and teeth is disrupted in children because both dentin and osteoid depend on vitamin C.
A zinc deficiency is quite common in CD patients. It is manifested in the oral cavity with erosions, ulcers and fissures, a crusting and scaling rash on the lips[29,71],burning mouth syndrome[56] and altered taste[72].
ORAL PATHOLOGY CAUSED BY MEDICATIONTreatment of inflammatory bowel diseases includes 5-aminosalicylic acid (5-ASA) derivatives, corticos-teroids, immunomodulators, calcineurin inhibitors, biological therapy and antibiotics. The selection of treatment depends on the site of the disease, the disease activity and the course or behavior of the disease[73,74]. Currently, the personalized approach to
therapy is advocated, and “risk matrices” for assessing the risk of developing severe forms of the disease have been developed[75,76]. The therapy applied to treating inflammatory bowel diseases can lead to alterations in the oral cavity due to the direct toxic effect of the drug on the oral tissue, the indirect immunosuppressive effect which increases the risk for opportunistic infections or bone marrow suppression. The immunomodulators commonly used in IBD treatment include the following: corticosteroids (a total dose equivalent to ≥ 20 mg of prednisolone for ≥ 2 wk), thiopurines, methotrexate, anti-tumor necrosis factor alpha (anti-TNF) agents and other biologics, which increase the risk of op-portunistic infections[77]. The incidence of infection is higher if the patients simultaneously receive several immunosuppressive drugs, are malnourished, suffer from other associated diseases or have a prior history of serious infections[77-80]. The risk of infection also increases with age[77-79]. Potential myelotoxicity of the drugs, including the development of leucopenia and agranulocytosis, also increases the risk of developing opportunistic and serious infections[79-81]. In addition to the risk of developing gastrointestinal tumors, patients with inflammatory bowel diseases are at risk of developing hematological malignancies. Compared to the general population, patients suffering from CD are at risk of developing lymphoma, especially non-Hodgkin lymphoma, while patients with UC are more likely to develop leukemia[82]. Early disease onset, male gender and age > 65 are risk factors for developing hematological malignancies. With regard to malignancies related to IBD therapy, patients receiving thiopurines have an increased risk of developing cancer. The risk of developing lymphoma is also increased but can be reversed by thiopurine withdrawal. There is no evidence of an increased risk of developing cancer or lymphoma in patients who received monotherapy with anti TNF drugs[82].
Thus far, only one study addressing the risks of developing malignancies in the oral cavity of patients with IBD has been published[83]. Katsanos et al[83] have established that patients with IBD are at a higher risk of developing tumors in the oral cavity, especially on the tongue. The authors have also concluded that female IBD patients are at a higher risk than male patients. However, this study did not include a risk analysis based on the type of treatment.
Oral complications of aminosalicylates Sulfasalazine has been used to treat UC for 50 years[84]. It is a prodrug made of sulfapyridine and an active substance of 5-aminosalicylic acid (5-ASA). Sulfapyridine, or more precisely the sulfur component, is considered to be responsible for numerous side effects and allergic reactions caused by this drug. In the oral cavity, sulfasalazine causes an oral lichen planus/oral lichenoid reaction[85-87]. The occurrence of these lesions in the oral cavities of patients with IBD
Muhvić-Urek M et al . Oral pathology in IBD

5660 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
is rare, and only a few cases have been described[85]. Some patients receiving sulfasalazine may complain of a metallic taste in the mouth[72]. Patients suffering from inflammatory bowel diseases who are receiving sulfasalazine can also develop oral complications caused by myelotoxicity and hepatotoxicity due to the sulfasalazine treatment, presented through signs of aplastic anemia, bleeding (ecchymosis and petechiae) and oral infections. Side effects of 5-ASA derivatives (non-sulfa-containing drugs) are less numerous[88] but have been described in the literature[89]. Mesalazine can cause hematological side effects, such as leu-copenia, thrombocytopenia and aplastic anemia[89], resulting in alterations in the oral cavity. Alstead et al[85] presented a case of a patient who developed oral lichen as a reaction to sulfasalazine, which was replaced with mesalazine, but the lesions did not withdraw. After withdrawing the mesalazine, the oral lesions withdrew, and the authors concluded that the lesions were related to 5-ASA.
Oral complications of corticosteroidsDespite their efficiency, corticosteroids were declared unsuitable for long-term use due to a high percentage of side effects (reported in 50% of patients)[90]. Early adverse effects in the orofacial region, which occur as a result of a supra-physiological dose, include acne, moon face, petechiae and ecchymosis due to blood vessel vulnerability[90-92]. The long-term use
of corticosteroids increases the risk of opportunistic infection[78,79]. The risk of infection also depends on the dose[78]. The use of these drugs is related to the occurrence of candidiasis in the oral cavity, pharynx and esophagus[78]. Pseudomembranous candidiasis and chronic atrophic candidiasis are the most prevalent forms of oral candidiasis in such patients (Figure 3)[92,93]. Patients receiving corticosteroids and thiopurines simultaneously have an increased risk of developing opportunistic infections than patients who receive corticosteroids only[78]. Tourner et al[78] observed a 10% prevalence of Candida albicans infections in patients with IBD receiving corticosteroid therapy only. However, the clinical site of these infections was not specified. Numerous case reports and clinical studies on primary varicella zoster virus and herpes zoster virus infections[78,79,81,94] in patients with IBD were published, but checking the literature, no papers on these infections occurring in the oral cavity and orofacial region have been published. Herpes simplex virus (HSV) infections in such patients are also common, whether they are of primary or recurrent character[78,95-98]. Tourner et al[78] have described an 18% prevalence of HSV infections on the face, in the esophagus or on the extremities of patients with IBD.
In children with IBD, especially with CD, the disease itself[99] and the use of corticosteroids[100] can affect growth. There are no studies analyzing bone development in the orofacial region of children with IBD, especially in children who have received long-term corticosteroid therapy. Long-term corticosteroid use can also result in osteoporosis, affecting the patients’ jawbones and increasing the risk of peri-odontal diseases and fractures. Experimental and clinical studies have shown that the long-term use of corticosteroids leads to the occurrence of calcifications in the dental pulp and pulp obliteration[101-103].
Oral complications of thiopurines Azathioprine (AZA) and 6-mercaptopurine (6-MP) are thiopurine drugs that have been used in the treatment of IBD for the past 50 years, primarily for the maintenance of disease remission[90]. Unfortunately, in addition to the beneficial treatment effects in some patients with IBD, these drugs can also cause complications and lead to adverse effects. AZA has been shown to cause taste disturbances in the form of ageusia/hypogeusia and dysgeusia[72]. Other side effects of thiopurines include opportunistic infections, myelotoxicity and hepatotoxicity as well as a risk of developing malignant lymphomas, which can also lead to alterations in the oral cavity. The use of AZA/6-MP increases the risk of opportunistic infections for patients taking steroids from approximately 2-3-fold to approximately 15-fold[78]. Atypical clinical features and longer disease duration are characteristics of these infections. Cases of recurrent HSV infections with large and irregular ulcerations occurring in any region of the
Figure 3 Pseudomembranous candidiasis on the palatal mucosa and atrophic candidiasis on the tongue in a Crohn's disease patient treated with anti-TNF and prednisone.
Muhvić-Urek M et al . Oral pathology in IBD

5661 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
oral mucosa and lasting for weeks or months have been described. The lesions can also occur on non-keratinized mucosa (a region not usually affected) and are not easily distinguished from aphthous lesions[104]. Due to a potential myelotoxic effect of thiopurines, such as the development of leucopenia and neu-tropenia[105,106], the risk of developing opportunistic infections is increased.
It is well known that the use of thiopurines increases the risk of developing lymphoma and cancer[82,107,108]. However, clinical studies on the prevalence of malignant diseases in the oral cavity of patients with IBD receiving thiopurines are lacking. Only one clinical study was published on this subject. Pasternak et al[109] established that patients with IBD who are receiving thiopurines are at no greater risk of developing lip, oral cavity or pharynx cancer. Dojcinov et al[110] were the first to present the cases of two rheumatoid arthritis (RA) patients with an azathioprine-related lymphoproliferative disorder (LPD) in the oral cavity.
Oral complications of methotrexate Methotrexate is a stomatotoxic drug, which causes oral ulcers, ulcerative stomatitis and mucositis[87,111-113]. The occurrence of lesions in the oral cavity is associated with a folic acid deficiency and toxic effects of the drug[112]. The effects of the drug in the oral cavity depend on the administered dose. Lower doses cause ulcers and stomatitis, while higher doses, administered to treat malignant diseases, cause mucositis[114]. Several clinical studies and cases have described oral ulcers, stomatitis and mucositis in patients treated with methotrexate due to RA, psoriasis and malignancies[113,115,116]. Furthermore, methotrexate can cause agusea/hypogeusia in the oral cavity[72]. However, there are no published pa-pers on the occurrence of oral ulcers, stomatitis and taste disturbances in patients with IBD treated with methotrexate.
Bone marrow suppression (in the form of leu-copenia, thrombocytopenia or pancytopenia) is also described in patients receiving methotrexate (more often in patients treated with high doses and less often in patients treated with low doses)[117,118]. Oral alterations can develop as a consequence of bone marrow suppression. The only study on oral infections in patients receiving low doses of methotrexate that we found was published by Pedrazas et al[119]. The authors described a significantly higher prevalence of oral candidiasis (10.7%) and oral ulcers (60.7%) in patients with RA receiving methotrexate than in patients who were not treated with methotrexate.
Several clinical cases of methotrexate-related Epstein-Barr virus associated lymphoproliferative disorders in the oral cavity in patients with RA and Still’s disease[110,111,120-126] have been published. Clinical LPD is manifested in the oral cavity as swelling or painful ulcers of irregular edges on the gingiva, tongue, floor of the mouth and buccal mucosa[110,111,120-126]. In some cases,
the bone[111,122,125] was also affected. The common characteristic of these disorders is that the majority of lesions regress completely following the withdrawal of methotrexate[123]. According to the literature, there are no descriptions of these disorders in the oral cavity caused by methotrexate in patients with IBD.
Oral complications of calcineurin inhibitors (cyclosporine and tacrolimus) Gingival hyperplasia (or gingivae overgrowth) is common in patients receiving cyclosporine (CsA). The severity of gingival hyperplasia depends on the duration of CsA therapy, but its occurrence is also influenced by bacterial plaque, local irritants and possibly the simultaneous use of other drugs that cause gingival hyperplasia (e.g., nifedipine)[127,128]. Gingival hyperplasia can interfere with oral functions and speech and can cause delayed and/or ectopic dentition and difficulties in maintaining oral hygiene, increasing the risk of caries, infection and periodontal disease[129].
Furthermore, in patients receiving CsA, filiform papillae hypertrophy on the tongue[130], opportunistic infections (candidiasis)[131,132], squamous-cell carcinomas on the lip[133], non-Hodgkin lymphomas[134,135] and lymph-oproliferative disorders[110,136,137] have been described in the oral cavity. The side effects of tacrolimus are less common compared to cyclosporine[138], and currently there is no evidence of complications associated with tacrolimus treatment in the oral cavity.
Oral complications of biologic drugsIn addition to exerting a revolutionary effect in treating inflammatory bowel diseases, TNF alpha inhibitors have numerous side effects. These drugs can cause oral lichen/lichenoid reactions and opportunistic infections in the oral cavity[87,139-142]. Asarch et al[139] reported two cases of oral lichenoid reaction in patients with psoriasis receiving infliximab and adalimumab. Moss et al[140] described a case of a patient with CD receiving infliximab that resulted in an oral lichenoid reaction. Cases of erythema multiforme and Stevens-Johnson syndrome in the oral cavity and on the skin in patients with CD receiving infliximab and adalimumab[143,144] were also reported. Oral opportunistic infections (primarily candidiasis) can be expected in patients with IBD treated with anti-TNF drugs but so far only one case report has been published[141]. There are no clinical studies on the prevalence of opportunistic oral infections in these patients. One of the most often described side effects of vedolizumab (a gut selective anti-integrin) is pharyngitis[145,146].
Oral complications of antibiotics (metronidazole and ciprofloxacin) The most common side effect of metronidazole is a metallic taste in the mouth[147]. In addition to the metallic taste, there are no other described side effects
Muhvić-Urek M et al . Oral pathology in IBD

5662 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
of these antibiotics in the oral cavity.
TREATMENT OF THE ORAL LESIONS The goal of treating oral lesions in patients with IBD is to reduce pain, accelerate the healing of lesions and prevent secondary infections. The treatment depends on the etiology, severity of the clinical presentation and the symptoms of the oral lesions. Treatment options include topical or/and systemic medications. Although the first European evidence-based consensus on extraintestinal manifestations in inflammatory bowel disease has been recently published[148], there are still no statements on the treatment of oral manifestations and complications of IBD.
Treatment of specific oral lesions in Crohn’s disease and pyostomatitis vegetans (which occur in both diseases) is always aimed at treating and controlling the underlying disease, and lesions usually respond well to IBD treatment[37-39,41-43,46,50]. In addition to systemic therapy, topical agents can be used; therefore, a multidisciplinary approach is essential. Topical treatments include steroids (topical or intralesional injections), topical tacrolimus, 5-ASA mouthwashes, topical anesthetics for pain relief, non-steroidal anti-inflammatory pastes and antiseptic mouthwash for preventing secondary infections[11,14,19,33,34,149].
In IBD patients, the treatment of aphthous stomatitis includes nutrition supplements and topical or systemic medication therapy. The choice of therapy depends on the severity of symptoms and the type and numbers of aphthous lesions. Choices for therapy include steroids (topical, intralesional or systemic) as a first line of treatment, topical anesthetics, antiseptic mouthwash or non-steroidal anti-inflammatory pastes[150]. Furthermore, non-medical treatments, such as ozone therapy and low-level laser therapy, can be used for pain relief and to accelerate lesion healing[151,152]. When the aphthous lesions are numerous and very painful, systemic steroids, immunosuppressive agents and thalidomide are indicated[11,150].
Angular cheilitis and glossitis are frequently caused by anemia and malnutrition; in cases with specific deficiencies, the replacement of iron, B12, folate and zinc is necessary[52-54]. Angular cheilitis can also be caused by fungi (Candida spp.) and bacteria (Staphylococcus aureus or b-hemolytic streptococci). In the case of fungal etiology, treatment options include topical antifungals (e.g., nystatin, miconazole, ketoconazole or clotrimazole). When the infection is caused by Staphylococcus aureus, topical treatments include combinations of mupirocin or fusidic acid and 1% hydrocortisone cream[153].
Most often, oral infections occur as a consequence of immunosuppressive drug therapy, and candidiasis is the most commonly occurring infection. Oral candidiasis does not require the interruption of therapy[77]. Topical therapy options include nystatin, amphotericin B, miconazole, fluconazole, ketoconazole or clotrimazole.
In some cases, systemic therapy with fluconazole, itraconazole or ketoconazole is necessary[154].
HSV infection is not a contraindication for immuno-suppressive therapy. In recurrent oral HSV infections, oral antiviral therapy should be considered[77].
When oral lichen/oral lichenoid reactions or taste disturbances are present, the interruption and re-placement of medication can be considered.
The occurrence of erythema multiforme or Stevens-Johnson syndrome requires the prompt interruption of biologic drugs[143,144]. The patients with erythema multiforme can be treated as out-patients with systemic and topical steroids[143]. Stevens-Johnson syndrome requires treatment in a hospital setting[144].
CONCLUSIONOral lesions in patients with inflammatory bowel disease can be extraintestinal manifestations of the disease or can occur as complications of the disease and treatment. They occur more often in CD patients than in UC patients, although pyostomatitis vegetans is more common in UC patients. One or more oral lesions can simultaneously appear in the oral cavity. The severity of their clinical presentation can range from mild and painless to extensive and painful. The lesions can compromise oral functions. Cooperation between specialists in oral medicine and gastroenterologists is essential for the successful diagnosis of IBD (in cases when oral pathology precedes intestinal manifestations), as well as in the diagnosis and treatment of oral lesions in such patients.
REFERENCES1 Sartor RB. Mechanisms of disease: pathogenesis of Crohn’s disease
and ulcerative colitis. Nat Clin Pract Gastroenterol Hepatol 2006; 3: 390-407 [PMID: 16819502 DOI: 10.1038/ncpgasthep0528]
2 Danese S, Fiocchi C. Etiopathogenesis of inflammatory bowel diseases. World J Gastroenterol 2006; 12: 4807-4812 [PMID: 16937461]
3 Leone V, Chang EB, Devkota S. Diet, microbes, and host genetics: the perfect storm in inflammatory bowel diseases. J Gastroenterol 2013; 48: 315-321 [PMID: 23475322 DOI: 10.1007/s00535-013-0777-2]
4 Burisch J, Pedersen N, Čuković-Čavka S, Brinar M, Kaimakliotis I, Duricova D, Shonová O, Vind I, Avnstrøm S, Thorsgaard N, Andersen V, Krabbe S, Dahlerup JF, Salupere R, Nielsen KR, Olsen J, Manninen P, Collin P, Tsianos EV, Katsanos KH, Ladefoged K, Lakatos L, Björnsson E, Ragnarsson G, Bailey Y, Odes S, Schwartz D, Martinato M, Lupinacci G, Milla M, De Padova A, D'Incà R, Beltrami M, Kupcinskas L, Kiudelis G, Turcan S, Tighineanu O, Mihu I, Magro F, Barros LF, Goldis A, Lazar D, Belousova E, Nikulina I, Hernandez V, Martinez-Ares D, Almer S, Zhulina Y, Halfvarson J, Arebi N, Sebastian S, Lakatos PL, Langholz E, Munkholm P. East-West gradient in the incidence of inflammatory bowel disease in Europe: the ECCO-EpiCom inception cohort. Gut 2014; 63: 588-597 [PMID: 23604131 DOI: 10.1136/gutjnl-2013-304636]
5 Molodecky NA, Soon IS, Rabi DM, Ghali WA, Ferris M, Chernoff G, Benchimol EI, Panaccione R, Ghosh S, Barkema HW, Kaplan GG. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology
Muhvić-Urek M et al . Oral pathology in IBD

5663 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
2012; 142: 46-54.e42; quiz e30 [PMID: 22001864 DOI: 10.1053/j.gastro.2011.10.001]
6 Sincić BM, Vucelić B, Persić M, Brncić N, Erzen DJ, Radaković B, Mićović V, Stimac D. Incidence of inflammatory bowel disease in Primorsko-goranska County, Croatia, 2000-2004: A prospective population-based study. Scand J Gastroenterol 2006; 41: 437-444 [PMID: 16635912 DOI: 10.1080/00365520500320094]
7 Danese S, Semeraro S, Papa A, Roberto I, Scaldaferri F, Fedeli G, Gasbarrini G, Gasbarrini A. Extraintestinal manifestations in inflammatory bowel disease. World J Gastroenterol 2005; 11: 7227-7236 [PMID: 16437620 DOI: 10.3748/wjg.v11.i46.7227]
8 Rothfuss KS, Stange EF, Herrlinger KR. Extraintestinal manifestations and complications in inflammatory bowel diseases. World J Gastroenterol 2006; 12: 4819-4831 [PMID: 16937463]
9 Ardizzone S, Puttini PS, Cassinotti A, Porro GB. Extraintestinal manifestations of inflammatory bowel disease. Dig Liver Dis 2008; 40 Suppl 2: S253-S259 [PMID: 18598997 DOI: 10.1016/s1590-8658(08)60534-4]
10 Vavricka SR, Schoepfer A, Scharl M, Lakatos PL, Navarini A, Rogler G. Extraintestinal Manifestations of Inflammatory Bowel Disease. Inflamm Bowel Dis 2015; 21: 1982-1992 [PMID: 26154136 DOI: 10.1097/mib.0000000000000392]
11 Katsanos KH, Torres J, Roda G, Brygo A, Delaporte E, Colombel JF. Review article: non-malignant oral manifestations in inflammatory bowel diseases. Aliment Pharmacol Ther 2015; 42: 40-60 [PMID: 25917394 DOI: 10.1111/apt.13217]
12 Pittock S, Drumm B, Fleming P, McDermott M, Imrie C, Flint S, Bourke B. The oral cavity in Crohn’s disease. J Pediatr 2001; 138: 767-771 [PMID: 11343060 DOI: 10.1067/mpd.2001.113008]
13 Litsas G. Crohn’s disease of the mouth: report of a case. Eur J Paediatr Dent 2011; 12: 198-200 [PMID: 22077691]
14 Urek MM, Sinčić BM, Braut A. Oral manifestations of Crohn’s disease: a case report. Sanamed 2015; 10: 205-208
15 Dupuy A, Cosnes J, Revuz J, Delchier JC, Gendre JP, Cosnes A. Oral Crohn disease: clinical characteristics and long-term follow-up of 9 cases. Arch Dermatol 1999; 135: 439-442 [PMID: 10206051 DOI: 10.1001/archderm.135.4.439]
16 Ghandour K, Issa M. Oral Crohn’s disease with late intestinal manifestations. Oral Surg Oral Med Oral Pathol 1991; 72: 565-567 [PMID: 1745516 DOI: 10.1016/0030-4220(91)90495-X]
17 Ficarra G, Cicchi P, Amorosi A, Piluso S. Oral Crohn’s disease and pyostomatitis vegetans. An unusual association. Oral Surg Oral Med Oral Pathol 1993; 75: 220-224 [PMID: 8426722 DOI: 10.1016/0030-4220(93)90097-N]
18 Turchi RM, Soriano H, Rodgers GL. Tb or not TB: Crohn’s disease presenting with tonsillar granulomas. Otolaryngol Head Neck Surg 2006; 134: 528-530 [PMID: 16500459 DOI: 10.1016/j.otohns.2005.03.070]
19 Lankarani KB, Sivandzadeh GR, Hassanpour S. Oral manifestation in inflammatory bowel disease: a review. World J Gastroenterol 2013; 19: 8571-8579 [PMID: 24379574 DOI: 10.3748/wjg.v19.i46.8571]
20 Zbar AP, Ben-Horin S, Beer-Gabel M, Eliakim R. Oral Crohn’s disease: is it a separable disease from orofacial granulomatosis? A review. J Crohns Colitis 2012; 6: 135-142 [PMID: 22325167 DOI: 10.1016/j.crohns.2011.07.001]
21 Mays JW, Sarmadi M, Moutsopoulos NM. Oral manifestations of systemic autoimmune and inflammatory diseases: diagnosis and clinical management. J Evid Based Dent Pract 2012; 12: 265-282 [PMID: 23040353 DOI: 10.1016/s1532-3382(12)70051-9]
22 Galbraith SS, Drolet BA, Kugathasan S, Paller AS, Esterly NB. Asymptomatic inflammatory bowel disease presenting with mucocutaneous findings. Pediatrics 2005; 116: e439-e444 [PMID: 16099852 DOI: 10.1542/peds.2004-2281]
23 Katz J, Shenkman A, Stavropoulos F, Melzer E. Oral signs and symptoms in relation to disease activity and site of involvement in patients with inflammatory bowel disease. Oral Dis 2003; 9: 34-40 [PMID: 12617256]
24 Asquith P, Thompson RA, Cooke WT. Oral manifestations of Crohn’s disease. Gut 1975; 16: 249-254 [PMID: 1132799 DOI:
10.1136/gut.16.4.249]25 Siegel MA, Solomon LV, Majia LM. Diseases of Gastrointestinal
Tract. In: Glick M. Burket’s Oral Medicine. 12th ed. Shelton, Connecticut: People’s Medical Publishing House, 2015: 389-410
26 Laranjeira N, Fonseca J, Meira T, Freitas J, Valido S, Leitão J. Oral mucosa lesions and oral symptoms in inflammatory bowel disease patients. Arq Gastroenterol 2015; 52: 105-110 [PMID: 26039827 DOI: 10.1590/s0004-28032015000200006]
27 Best WR, Becktel JM, Singleton JW, Kern F. Development of a Crohn’s disease activity index. National Cooperative Crohn’s Disease Study. Gastroenterology 1976; 70: 439-444 [PMID: 1248701]
28 Veloso FT, Carvalho J, Magro F. Immune-related systemic manifestations of inflammatory bowel disease. A prospective study of 792 patients. J Clin Gastroenterol 1996; 23: 29-34 [PMID: 8835896 DOI: 10.1097/00004836-199607000-00009]
29 Plauth M, Jenss H, Meyle J. Oral manifestations of Crohn’s disease. An analysis of 79 cases. J Clin Gastroenterol 1991; 13: 29-37 [PMID: 2007740 DOI: 10.1097/00004836-199102000-00008]
30 Halme L, Meurman JH, Laine P, von Smitten K, Syrjänen S, Lindqvist C, Strand-Pettinen I. Oral findings in patients with active or inactive Crohn’s disease. Oral Surg Oral Med Oral Pathol 1993; 76: 175-181 [PMID: 8361727 DOI: 10.1016/0030-4220(93)90200-N]
31 Trost LB, McDonnell JK. Important cutaneous manifestations of inflammatory bowel disease. Postgrad Med J 2005; 81: 580-585 [PMID: 16143688 DOI: 10.1136/pgmj.2004.031633]
32 Ojha J, Cohen DM, Islam NM, Stewart CM, Katz J, Bhattacharyya I. Gingival involvement in Crohn disease. J Am Dent Assoc 2007; 138: 1574-181; quiz 1574-181; [PMID: 18056101]
33 Field EA, Allan RB. Review article: oral ulceration--aetiopatho-genesis, clinical diagnosis and management in the gastrointestinal clinic. Aliment Pharmacol Ther 2003; 18: 949-962 [PMID: 14616160]
34 Fatahzadeh M, Schwartz RA, Kapila R, Rochford C. Orofacial Crohn’s disease: an oral enigma. Acta Dermatovenerol Croat 2009; 17: 289-300 [PMID: 20021984]
35 Gibson J, Wray D, Bagg J. Oral staphylococcal mucositis: A new clinical entity in orofacial granulomatosis and Crohn’s disease. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000; 89: 171-176 [PMID: 10673652]
36 Mills CC, Amin M, Manisali M. Salivary duct fistula and recurrent buccal space infection: a complication of Crohn’s disease. J Oral Maxillofac Surg 2003; 61: 1485-1487 [PMID: 14663816 DOI: 10.1016/j.joms.2003.06.003]
37 Bens G, Laharie D, Beylot-Barry M, Vergier B, Noblesse I, Beylot C, Amouretti M. Successful treatment with infliximab and methotrexate of pyostomatitis vegetans associated with Crohn’s disease. Br J Dermatol 2003; 149: 181-184 [PMID: 12890215 DOI: 10.1046/j.1365-2133.2003.05385.x]
38 Mijandrusić-Sincić B, Licul V, Gorup L, Brncić N, Glazar I, Lucin K. Pyostomatitis vegetans associated with inflammatory bowel disease--report of two cases. Coll Antropol 2010; 34 Suppl 2: 279-282 [PMID: 21305742]
39 Grössner-Schreiber B, Fetter T, Hedderich J, Kocher T, Schreiber S, Jepsen S. Prevalence of dental caries and periodontal disease in patients with inflammatory bowel disease: a case-control study. J Clin Periodontol 2006; 33: 478-484 [PMID: 16820035 DOI: 10.1111/j.1600-051X.2006.00942.x]
40 Ansaldi N, Morabito A, Balocco P, Galleano E. [Dental changes in children with malabsorption]. Minerva Pediatr 1989; 41: 581-585 [PMID: 2699514]
41 Appleton SS. Candidiasis: pathogenesis, clinical characteristics, and treatment. J Calif Dent Assoc 2000; 28: 942-948 [PMID: 11323949]
42 Rogers RS, Bekic M. Diseases of the lips. Semin Cutan Med Surg 1997; 16: 328-336 [PMID: 9421227 DOI: 10.1016/S1085-5629(97)80025-9]
43 Huber MA, Sankar V. Hematologic diseases. In: Glick M. Burket’s Oral Medicine. 12th ed. Shelton, Connecticut: People’s Medical Publishing House, 2015: 463-488
44 Chaudhry SI, Philpot NS, Odell EW, Challacombe SJ, Shirlaw PJ. Pyostomatitis vegetans associated with asymptomatic ulcerative
Muhvić-Urek M et al . Oral pathology in IBD

5664 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
colitis: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999; 87: 327-330 [PMID: 10102594 DOI: 10.1016/S1079-2104(99)70217-9]
45 Ruiz-Roca JA, Berini-Aytés L, Gay-Escoda C. Pyostomatitis vegetans. Report of two cases and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005; 99: 447-454 [PMID: 15772593 DOI: 10.1016/j.tripleo.2003.08.022]
46 Ayangco L, Rogers RS, Sheridan PJ. Pyostomatitis vegetans as an early sign of reactivation of Crohn’s disease: a case report. J Periodontol 2002; 73: 1512-1516 [PMID: 12546102 DOI: 10.1902/jop.2002.73.12.1512]
47 Chan SW, Scully C, Prime SS, Eveson J. Pyostomatitis vegetans: oral manifestation of ulcerative colitis. Oral Surg Oral Med Oral Pathol 1991; 72: 689-692 [PMID: 1687483 DOI: 10.1016/0030-4220(91)90012-2]
48 Markiewicz M, Suresh L, Margarone J, Aguirre A, Brass C. Pyostomatitis vegetans: A clinical marker of silent ulcerative colitis. J Oral Maxillofac Surg 2007; 65: 346-348 [PMID: 17236948 DOI: 10.1016/j.joms.2005.07.020]
49 Wu YH, Chang JY, Chen HM, Wang YP. Pyostomatitis vegetans: An oral manifestation of inflammatory bowel disease. J Formos Med Assoc 2015; 114: 672-673 [PMID: 26049216 DOI: 10.1016/j.jfma.2015.05.001]
50 Femiano F, Lanza A, Buonaiuto C, Perillo L, Dell’Ermo A, Cirillo N. Pyostomatitis vegetans: a review of the literature. Med Oral Patol Oral Cir Bucal 2009; 14: E114-E117 [PMID: 19242389]
51 Triantafillidis JK, Vagianos C, Papalois AE. The role of enteral nutrition in patients with inflammatory bowel disease: current aspects. Biomed Res Int 2015; 2015: 197167 [PMID: 25793189 DOI: 10.1155/2015/197167]
52 Hartman C, Eliakim R, Shamir R. Nutritional status and nutritional therapy in inflammatory bowel diseases. World J Gastroenterol 2009; 15: 2570-2578 [PMID: 19496185]
53 Halmos EP, Gibson PR. Dietary management of IBD--insights and advice. Nat Rev Gastroenterol Hepatol 2015; 12: 133-146 [PMID: 25645969 DOI: 10.1038/nrgastro.2015.11]
54 Dignass AU, Gasche C, Bettenworth D, Birgegård G, Danese S, Gisbert JP, Gomollon F, Iqbal T, Katsanos K, Koutroubakis I, Magro F, Savoye G, Stein J, Vavricka S. European consensus on the diagnosis and management of iron deficiency and anaemia in inflammatory bowel diseases. J Crohns Colitis 2015; 9: 211-222 [PMID: 25518052 DOI: 10.1093/ecco-jcc/jju009]
55 Mulliken RA, Casner MJ. Oral manifestations of systemic disease. Emerg Med Clin North Am 2000; 18: 565-575 [PMID: 10967740 DOI: 10.1016/S0733-8627(05)70144-9]
56 Sun A, Wu KM, Wang YP, Lin HP, Chen HM, Chiang CP. Burning mouth syndrome: a review and update. J Oral Pathol Med 2013; 42: 649-655 [PMID: 23772971 DOI: 10.1111/jop.12101]
57 Wu YC, Wang YP, Chang JY, Cheng SJ, Chen HM, Sun A. Oral manifestations and blood profile in patients with iron deficiency anemia. J Formos Med Assoc 2014; 113: 83-87 [PMID: 24388269 DOI: 10.1016/j.jfma.2013.11.010]
58 Piskin S, Sayan C, Durukan N, Senol M. Serum iron, ferritin, folic acid, and vitamin B12 levels in recurrent aphthous stomatitis. J Eur Acad Dermatol Venereol 2002; 16: 66-67 [PMID: 11952294 DOI: 10.1046/j.1468-3083.2002.00369.x]
59 Adeyemo TA, Adeyemo WL, Adediran A, Akinbami AJ, Akanmu AS. Orofacial manifestations of hematological disorders: anemia and hemostatic disorders. Indian J Dent Res 2011; 22: 454-461 [PMID: 22048588 DOI: 10.4103/0970-9290.87070]
60 Derossi SS, Raghavendra S. Anemia. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003; 95: 131-141 [PMID: 12582350 DOI: 10.1067/moe.2003.13]
61 Turner AG, Anderson PH, Morris HA. Vitamin D and bone health. Scand J Clin Lab Invest Suppl 2012; 243: 65-72 [PMID: 22536765 DOI: 10.3109/00365513.2012.681963]
62 Vestergaard P. Prevalence and pathogenesis of osteoporosis in patients with inflammatory bowel disease. Minerva Med 2004; 95: 469-480 [PMID: 15785432]
63 Amano Y, Komiyama K, Makishima M. Vitamin D and periodontal
disease. J Oral Sci 2009; 51: 11-20 [PMID: 19325195 DOI: 10.2334/josnusd.51.11]
64 Zhan Y, Samietz S, Holtfreter B, Hannemann A, Meisel P, Nauck M, Völzke H, Wallaschofski H, Dietrich T, Kocher T. Prospective Study of Serum 25-hydroxy Vitamin D and Tooth Loss. J Dent Res 2014; 93: 639-644 [PMID: 24828383 DOI: 10.1177/0022034514534985]
65 Jimenez M, Giovannucci E, Krall Kaye E, Joshipura KJ, Dietrich T. Predicted vitamin D status and incidence of tooth loss and periodontitis. Public Health Nutr 2014; 17: 844-852 [PMID: 23469936 DOI: 10.1017/s1368980013000177]
66 Holick MF, Chen TC. Vitamin D deficiency: a worldwide problem with health consequences. Am J Clin Nutr 2008; 87: 1080S-1086S [PMID: 18400738]
67 Nanci A, Mocetti P, Sakamoto Y, Kunikata M, Lozupone E, Bonucci E. Morphological and immunocytochemical analyses on the effects of diet-induced hypocalcemia on enamel maturation in the rat incisor. J Histochem Cytochem 2000; 48: 1043-1058 [PMID: 10898799 DOI: 10.1177/002215540004800803]
68 Schlosser BJ, Pirigyi M, Mirowski GW. Oral manifestations of hematologic and nutritional diseases. Otolaryngol Clin North Am 2011; 44: 183-203, vii [PMID: 21093629 DOI: 10.1016/j.otc.2010.09.007]
69 Rubinoff AB, Latner PA, Pasut LA. Vitamin C and oral health. J Can Dent Assoc 1989; 55: 705-707 [PMID: 2676112]
70 Fontana M. Vitamin C (ascorbic acid): clinical implications for oral health--a literature review. Compendium 1994; 15: 916, 918, 920 passim; quiz 930 [PMID: 7728820]
71 Kambe T, Fukue K, Ishida R, Miyazaki S. Overview of Inherited Zinc Deficiency in Infants and Children. J Nutr Sci Vitaminol (Tokyo) 2015; 61 Suppl: S44-S46 [PMID: 26598882 DOI: 10.3177/jnsv.61.S44]
72 Spielman AI. Chemosensory function and dysfunction. Crit Rev Oral Biol Med 1998; 9: 267-291 [PMID: 9715366 DOI: 10.1177/10454411980090030201]
73 Van Assche G, Dignass A, Panes J, Beaugerie L, Karagiannis J, Allez M, Ochsenkühn T, Orchard T, Rogler G, Louis E, Kupcinskas L, Mantzaris G, Travis S, Stange E. The second European evidence-based Consensus on the diagnosis and management of Crohn’s disease: Definitions and diagnosis. J Crohns Colitis 2010; 4: 7-27 [PMID: 21122488 DOI: 10.1016/j.crohns.2009.12.003]
74 Dignass A, Lindsay JO, Sturm A, Windsor A, Colombel JF, Allez M, D’Haens G, D’Hoore A, Mantzaris G, Novacek G, Oresland T, Reinisch W, Sans M, Stange E, Vermeire S, Travis S, Van Assche G. Second European evidence-based consensus on the diagnosis and management of ulcerative colitis part 2: current management. J Crohns Colitis 2012; 6: 991-1030 [PMID: 23040451 DOI: 10.1016/j.crohns.2012.09.002]
75 Solberg IC, Cvancarova M, Vatn MH, Moum B. Risk matrix for prediction of advanced disease in a population-based study of patients with Crohn’s Disease (the IBSEN Study). Inflamm Bowel Dis 2014; 20: 60-68 [PMID: 24280875 DOI: 10.1097/01.mib.0000436956.78220.67]
76 Solberg IC, Høivik ML, Cvancarova M, Moum B. Risk matrix model for prediction of colectomy in a population-based study of ulcerative colitis patients (the IBSEN study). Scand J Gastroenterol 2015; 50: 1456-1462 [PMID: 26139389 DOI: 10.3109/00365521.2015.1064991]
77 Rahier JF, Magro F, Abreu C, Armuzzi A, Ben-Horin S, Chowers Y, Cottone M, de Ridder L, Doherty G, Ehehalt R, Esteve M, Katsanos K, Lees CW, Macmahon E, Moreels T, Reinisch W, Tilg H, Tremblay L, Veereman-Wauters G, Viget N, Yazdanpanah Y, Eliakim R, Colombel JF. Second European evidence-based consensus on the prevention, diagnosis and management of opportunistic infections in inflammatory bowel disease. J Crohns Colitis 2014; 8: 443-468 [PMID: 24613021 DOI: 10.1016/j.crohns.2013.12.013]
78 Toruner M, Loftus EV, Harmsen WS, Zinsmeister AR, Orenstein R, Sandborn WJ, Colombel JF, Egan LJ. Risk factors for opportunistic infections in patients with inflammatory bowel disease. Gastroenterology 2008; 134: 929-936 [PMID: 18294633 DOI:
Muhvić-Urek M et al . Oral pathology in IBD

5665 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
10.1053/j.gastro.2008.01.012]79 Naganuma M, Kunisaki R, Yoshimura N, Takeuchi Y, Watanabe
M. A prospective analysis of the incidence of and risk factors for opportunistic infections in patients with inflammatory bowel disease. J Gastroenterol 2013; 48: 595-600 [PMID: 23053426 DOI: 10.1007/s00535-012-0686-9]
80 Dave M, Purohit T, Razonable R, Loftus EV. Opportunistic infections due to inflammatory bowel disease therapy. Inflamm Bowel Dis 2014; 20: 196-212 [PMID: 24051931 DOI: 10.1097/MIB.0b013e3182a827d2]
81 Long MD, Martin C, Sandler RS, Kappelman MD. Increased risk of herpes zoster among 108 604 patients with inflammatory bowel disease. Aliment Pharmacol Ther 2013; 37: 420-429 [PMID: 23240738 DOI: 10.1111/apt.12182]
82 Annese V, Beaugerie L, Egan L, Biancone L, Bolling C, Brandts C, Dierickx D, Dummer R, Fiorino G, Gornet JM, Higgins P, Katsanos KH, Nissen L, Pellino G, Rogler G, Scaldaferri F, Szymanska E, Eliakim R. European Evidence-based Consensus: Inflammatory Bowel Disease and Malignancies. J Crohns Colitis 2015; 9: 945-965 [PMID: 26294789 DOI: 10.1093/ecco-jcc/jjv141]
83 Katsanos KH, Roda G, McBride RB, Cohen B, Colombel JF. Increased Risk of Oral Cancer in Patients With Inflammatory Bowel Diseases. Clin Gastroenterol Hepatol 2016; 14: 413-420 [PMID: 26499929 DOI: 10.1016/j.cgh.2015.09.041]
84 Hanauer SB. Review article: aminosalicylates in inflammatory bowel disease. Aliment Pharmacol Ther 2004; 20 Suppl 4: 60-65 [PMID: 15352896 DOI: 10.1111/j.1365-2036.2004.02048.x]
85 Alstead EM, Wilson AG, Farthing MJ. Lichen planus and mesalazine. J Clin Gastroenterol 1991; 13: 335-337 [PMID: 1676716 DOI: 10.1097/00004836-199106000-00018]
86 Ghosh S, Jain VK, Chaudhuri S, Mathur SK. Sulfasalazine induced lichen planus in a patient of rheumatoid arthritis. Indian J Dermatol Venereol Leprol 2013; 79: 541-544 [PMID: 23760333]
87 Yuan A, Woo SB. Adverse drug events in the oral cavity. Oral Surg Oral Med Oral Pathol Oral Radiol 2015; 119: 35-47 [PMID: 25442252 DOI: 10.1016/j.oooo.2014.09.009]
88 Jick H, Myers MW, Dean AD. The risk of sulfasalazine- and mesalazine-associated blood disorders. Pharmacotherapy 1995; 15: 176-181 [PMID: 7624265]
89 Farrell RJ, Peppercorn MA, Fine SN, Michetti P. Mesalamine-associated thrombocytopenia. Am J Gastroenterol 1999; 94: 2304-2306 [PMID: 10445572 DOI: 10.1111/j.1572-0241.1999.01324.x]
90 Carter MJ, Lobo AJ, Travis SP. Guidelines for the management of inflammatory bowel disease in adults. Gut 2004; 53 Suppl 5: V1-16 [PMID: 15306569 DOI: 10.1136/gut.2004.043372]
91 Sandborn WJ. Steroid-dependent Crohn’s disease. Can J Gastroenterol 2000; 14 Suppl C: 17C-22C [PMID: 11023556]
92 Akintoye SO, Collins MT, Ship JA. Diabetes mellitus and endocrine diseases. In: Greenberg MS, Glick M, Ship JA. Burket’s oral medicine: Diagnosis & treatment 11th ed. Hamilton: Bc Decker Inc, 2008: 509-536
93 Sharon V, Fazel N. Oral candidiasis and angular cheilitis. Dermatol Ther 2010; 23: 230-242 [PMID: 20597942 DOI: 10.1111/j.1529-8019.2010.01320.x]
94 Cullen G, Baden RP, Cheifetz AS. Varicella zoster virus infection in inflammatory bowel disease. Inflamm Bowel Dis 2012; 18: 2392-2403 [PMID: 22434654 DOI: 10.1002/ibd.22950]
95 Santos-Antunes J, Abreu C, Magro F, Coelho R, Vilas-Boas F, Andrade P, Lopes S, Macedo G. Disseminated cutaneous herpes simplex infection in a patient with Crohn’s disease under azathioprine and steroids: First case report and literature review. J Crohns Colitis 2014; 8: 326-330 [PMID: 24257435 DOI: 10.1016/j.crohns.2013.10.011]
96 Shlien RD, Meyers S, Lee JA, Dische R, Janowitz HD. Fulminant herpes simplex hepatitis in a patient with ulcerative colitis. Gut 1988; 29: 257-261 [PMID: 3345937]
97 Seksik P, Gozlan J, Guitton C, Galula G, Maury E, Offenstadt G. Fatal herpetic hepatitis in adult following short corticotherapy: a case report. Intensive Care Med 1999; 25: 415-417 [PMID: 10342519 DOI: 10.1007/s001340050869]
98 Alimohamadi SM, Malekzadeh R, Mirmadjless SH, Mohamadnejad M, Zamani F. Herpes simplex virus encephalistis during immunosuppressive treatment of ulcerative colitis. MedGenMed 2004; 6: 7 [PMID: 15775834]
99 Gasparetto M, Guariso G. Crohn’s disease and growth deficiency in children and adolescents. World J Gastroenterol 2014; 20: 13219-13233 [PMID: 25309059 DOI: 10.3748/wjg.v20.i37.13219]
100 Ezri J, Marques-Vidal P, Nydegger A. Impact of disease and treatments on growth and puberty of pediatric patients with inflammatory bowel disease. Digestion 2012; 85: 308-319 [PMID: 22688404 DOI: 10.1159/000336766]
101 Symons AL, Henry AC, Chang S, Daley TJ, Harbrow DJ, Joseph BK. The effect of glucocorticosteroid treatment on dentine formation in the Lewis rat, a histological study. Growth Factors 2000; 18: 157-167 [PMID: 11334052 DOI: 10.3109/08977190009003241]
102 Näsström K. Dentin formation after corticosteroid treatment. A clinical study and an experimental study on rats. Swed Dent J Suppl 1996; 115: 1-45 [PMID: 8804151]
103 van Hogezand RA, Hamdy NA. Skeletal morbidity in inflammatory bowel disease. Scand J Gastroenterol Suppl 2006; (243): 59-64 [PMID: 16782623 DOI: 10.1080/00365520600664276]
104 Atkinson JC, Moutsopoulos N, Pillemer SR, Imanguli MM. Transplantation Medicine. In: Glick M, Burket’s oral medicine. Shelton, Connecticut: People’s Medical publishing House, beaugertroelkuoogata 2015: 463-488
105 Sandborn WJ. Azathioprine: state of the art in inflammatory bowel disease. Scand J Gastroenterol Suppl 1998; 225: 92-99 [PMID: 9515759]
106 Cunliffe RN, Scott BB. Review article: monitoring for drug side-effects in inflammatory bowel disease. Aliment Pharmacol Ther 2002; 16: 647-662 [PMID: 11929382 DOI: 10.1046/j.1365-2036.2002.01216.x]
107 Subramaniam K, D’Rozario J, Pavli P. Lymphoma and other lymphoproliferative disorders in inflammatory bowel disease: a review. J Gastroenterol Hepatol 2013; 28: 24-30 [PMID: 23094824 DOI: 10.1111/jgh.12015]
108 Beaugerie L, Brousse N, Bouvier AM, Colombel JF, Lémann M, Cosnes J, Hébuterne X, Cortot A, Bouhnik Y, Gendre JP, Simon T, Maynadié M, Hermine O, Faivre J, Carrat F. Lymphoproliferative disorders in patients receiving thiopurines for inflammatory bowel disease: a prospective observational cohort study. Lancet 2009; 374: 1617-1625 [PMID: 19837455 DOI: 10.1016/s0140-6736(09)61302-7]
109 Pasternak B, Svanström H, Schmiegelow K, Jess T, Hviid A. Use of azathioprine and the risk of cancer in inflammatory bowel disease. Am J Epidemiol 2013; 177: 1296-1305 [PMID: 23514635 DOI: 10.1093/aje/kws375]
110 Dojcinov SD, Venkataraman G, Raffeld M, Pittaluga S, Jaffe ES. EBV positive mucocutaneous ulcer--a study of 26 cases associated with various sources of immunosuppression. Am J Surg Pathol 2010; 34: 405-417 [PMID: 20154586 DOI: 10.1097/PAS.0b013e3181cf8622]
111 Kalantzis A, Marshman Z, Falconer DT, Morgan PR, Odell EW. Oral effects of low-dose methotrexate treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005; 100: 52-62 [PMID: 15953917 DOI: 10.1016/j.tripleo.2004.08.020]
112 Deeming GM, Collingwood J, Pemberton MN. Methotrexate and oral ulceration. Br Dent J 2005; 198: 83-85 [PMID: 15702101 DOI: 10.1038/sj.bdj.4811972]
113 Troeltzsch M, von Blohn G, Kriegelstein S, Woodlock T, Gassling V, Berndt R, Troeltzsch M. Oral mucositis in patients receiving low-dose methotrexate therapy for rheumatoid arthritis: report of 2 cases and literature review. Oral Surg Oral Med Oral Pathol Oral Radiol 2013; 115: e28-e33 [PMID: 23601229 DOI: 10.1016/j.oooo.2012.12.008]
114 Stein RB, Hanauer SB. Comparative tolerability of treatments for inflammatory bowel disease. Drug Saf 2000; 23: 429-448 [PMID: 11085348 DOI: 10.2165/00002018-200023050-00006]
115 Kremer JM, Phelps CT. Long-term prospective study of the use of methotrexate in the treatment of rheumatoid arthritis. Update after
Muhvić-Urek M et al . Oral pathology in IBD

5666 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
a mean of 90 months. Arthritis Rheum 1992; 35: 138-145 [PMID: 1734902 DOI: 10.1002/art.1780350203]
116 Ince A, Yazici Y, Hamuryudan V, Yazici H. The frequency and clinical characteristics of methotrexate (MTX) oral toxicity in rheumatoid arthritis (RA): a masked and controlled study. Clin Rheumatol 1996; 15: 491-494 [PMID: 8894364 DOI: 10.1007/BF02229648]
117 Sosin M, Handa S. Low dose methotrexate and bone marrow suppression. BMJ 2003; 326: 266-267 [PMID: 12560282 DOI: 10.1136/bmj.326.7383.266]
118 Lang B, Riegel W, Peters T, Peter HH. Low dose methotrexate therapy for rheumatoid arthritis complicated by pancytopenia and Pneumocystis carinii pneumonia. J Rheumatol 1991; 18: 1257-1259 [PMID: 1941837]
119 Pedrazas CH, Azevedo MN, Torres SR. Oral events related to low-dose methotrexate in rheumatoid arthritis patients. Braz Oral Res 2010; 24: 368-373 [PMID: 20877977 DOI: 10.1590/S1806-83242010000300018]
120 Kikuchi K, Miyazaki Y, Tanaka A, Shigematu H, Kojima M, Sakashita H, Kusama K. Methotrexate-related Epstein-Barr Virus (EBV)-associated lymphoproliferative disorder--so-called “Hodgkin-like lesion”--of the oral cavity in a patient with rheumatoid arthritis. Head Neck Pathol 2010; 4: 305-311 [PMID: 20676828 DOI: 10.1007/s12105-010-0202-6]
121 Kojima M, Itoh H, Hirabayashi K, Igarashi S, Tamaki Y, Murayama K, Ogura H, Saitoh R, Kashiwabara K, Takimoto J, Masawa N, Nakamura S. Methtrexate-associated lymphoproliferative disorders. A clinicopathological study of 13 Japanese cases. Pathol Res Pract 2006; 202: 679-685 [PMID: 16859835 DOI: 10.1016/j.prp.2006.05.007]
122 Tanaka A, Shigematsu H, Kojima M, Sakashita H, Kusama K. Methotrexate-associated lymphoproliferative disorder arising in a patient with adult Still’s disease. J Oral Maxillofac Surg 2008; 66: 1492-1495 [PMID: 18571037 DOI: 10.1016/j.joms.2007.05.006]
123 Uneda S, Sonoki T, Nakamura Y, Matsuoka H, Nakakuma H. Rapid vanishing of tumors by withdrawal of methotrexate in Epstein-Barr virus-related B cell lymphoproliferative disorder. Intern Med 2008; 47: 1445-1446 [PMID: 18670155 DOI: 10.2169/internalmedicine.47.0989]
124 Ishida M, Hodohara K, Yoshii M, Okuno H, Horinouchi A, Nakanishi R, Harada A, Iwai M, Yoshida K, Kagotani A, Yoshida T, Okabe H. Methotrexate-related Epstein-Barr virus-associated lymphoproliferative disorder occurring in the gingiva of a patient with rheumatoid arthritis. Int J Clin Exp Pathol 2013; 6: 2237-2241 [PMID: 24133604]
125 Acero J, Navarro-Cuellar C, Menarguez J, Herencia H, Navarro-Vila C. Naso-maxillary non-Hodgkin lymphoma associated with methotrexate treatment in a patient with rheumatoid arthritis. J Oral Maxillofac Surg 2006; 64: 708-711 [PMID: 16546655 DOI: 10.1016/j.joms.2005.12.029]
126 Pastor-Nieto MA, Kilmurray LG, López-Chumillas A, O’Valle F, García-Del Moral R, Puig AM, Bautista P. [Methotrexate-associated lymphoproliferative disorder presenting as oral ulcers in a patient with rheumatoid arthritis]. Actas Dermosifiliogr 2009; 100: 142-146 [PMID: 19445880]
127 O’Valle F, Mesa F, Aneiros J, Gómez-Morales M, Lucena MA, Ramírez C, Revelles F, Moreno E, Navarro N, Caballero T. Gingival overgrowth induced by nifedipine and cyclosporin A. Clinical and morphometric study with image analysis. J Clin Periodontol 1995; 22: 591-597 [PMID: 8583014 DOI: 10.1111/j.1600-051X.1995.tb00810.x]
128 Ciavarella D, Guiglia R, Campisi G, Di Cosola M, Di Liberto C, Sabatucci A, Escudero N, Bascones A, Lo Muzio L. Update on gingival overgrowth by cyclosporine A in renal transplants. Med Oral Patol Oral Cir Bucal 2007; 12: E19-E25 [PMID: 17195822]
129 Hassell TM, Hefti AF. Drug-induced gingival overgrowth: old problem, new problem. Crit Rev Oral Biol Med 1991; 2: 103-137 [PMID: 1912141]
130 Rateitschak-Plüss EM, Hefti A, Lörtscher R, Thiel G. Initial observation that cyclosporin-A induces gingival enlargement in
man. J Clin Periodontol 1983; 10: 237-246 [PMID: 6575979 DOI: 10.1111/j.1600-051X.1983.tb01272.x]
131 King GN, Healy CM, Glover MT, Kwan JT, Williams DM, Leigh IM, Thornhill MH. Prevalence and risk factors associated with leukoplakia, hairy leukoplakia, erythematous candidiasis, and gingival hyperplasia in renal transplant recipients. Oral Surg Oral Med Oral Pathol 1994; 78: 718-726 [PMID: 7898908 DOI: 10.1016/0030-4220(94)90086-8]
132 Olczak-Kowalczyk D, Pawłowska J, Garczewska B, Smirska E, Grenda R, Syczewska M, Kowalczyk W. Oral candidiasis in immunosuppressed children and young adults after liver or kidney transplantation. Pediatr Dent 2010; 32: 189-194 [PMID: 20557701]
133 Seymour RA, Thomason JM, Nolan A. Oral lesions in organ transplant patients. J Oral Pathol Med 1997; 26: 297-304 [PMID: 9250928 DOI: 10.1111/j.1600-0714.1997.tb00219.x]
134 Kuo PC, Dafoe DC, Alfrey EJ, Sibley RK, Scandling JD. Posttransplant lymphoproliferative disorders and Epstein-Barr virus prophylaxis. Transplantation 1995; 59: 135-138 [PMID: 7839414 DOI: 10.1097/00007890-199501150-00024]
135 Maxymiw WG, Wood RE, Lee L. Primary, multi-focal, non-Hodgkin’s lymphoma of the jaws presenting as periodontal disease in a renal transplant patient. Int J Oral Maxillofac Surg 1991; 20: 69-70 [PMID: 2051050 DOI: 10.1016/S0901-5027(05)80708-8]
136 Cole-Hawkins H, Fyfe E, Price C, Pring M. Posttransplant lymphoproliferative disorder presenting as a nonhealing extraction socket: a case report and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol 2012; 113: e12-e18 [PMID: 22668635 DOI: 10.1016/j.oooo.2011.10.015]
137 León JE, Takahama Júnior A, Vassallo J, Soares FA, de Almeida OP, Lopes MA. EBV-associated polymorphic posttransplant lymphoproliferative disorder presenting as gingival ulcers. Int J Surg Pathol 2011; 19: 241-246 [PMID: 20034982 DOI: 10.1177/1066896909353599]
138 Ogata H, Matsui T, Nakamura M, Iida M, Takazoe M, Suzuki Y, Hibi T. A randomised dose finding study of oral tacrolimus (FK506) therapy in refractory ulcerative colitis. Gut 2006; 55: 1255-1262 [PMID: 16484504 DOI: 10.1136/gut.2005.081794]
139 Asarch A, Gottlieb AB, Lee J, Masterpol KS, Scheinman PL, Stadecker MJ, Massarotti EM, Bush ML. Lichen planus-like eruptions: an emerging side effect of tumor necrosis factor-alpha antagonists. J Am Acad Dermatol 2009; 61: 104-111 [PMID: 19539844 DOI: 10.1016/j.jaad.2008.09.032]
140 Moss AC, Treister NS, Marsee DK, Cheifetz AS. Clinical challenges and images in GI. Oral lichenoid reaction in a patient with Crohn’s disease receiving infliximab. Gastroenterology 2007; 132: 488, 829 [PMID: 17261307 DOI: 10.1053/j.gastro.2007.01.014]
141 Kaur N, Mahl TC. Pneumocystis carinii pneumonia with oral candidiasis after infliximab therapy for Crohn’s disease. Dig Dis Sci 2004; 49: 1458-1460 [PMID: 15481319 DOI: 10.1023/B:DDAS.0000042246.58984.98]
142 Mocciaro F, Orlando A, Renna S, Rizzuto MR, Cottone M. Oral lichen planus after certolizumab pegol treatment in a patient with Crohn’s disease. J Crohns Colitis 2011; 5: 173-174 [PMID: 21453892 DOI: 10.1016/j.crohns.2011.01.003]
143 Edwards D, Boritz E, Cowen EW, Brown RS. Erythema multiforme major following treatment with infliximab. Oral Surg Oral Med Oral Pathol Oral Radiol 2013; 115: e36-e40 [PMID: 23036796 DOI: 10.1016/j.oooo.2012.08.001]
144 Salama M, Lawrance IC. Stevens-Johnson syndrome complicating adalimumab therapy in Crohn’s disease. World J Gastroenterol 2009; 15: 4449-4452 [PMID: 19764100 DOI: 10.3748/wjg.15.4449]
145 Sandborn WJ, Feagan BG, Rutgeerts P, Hanauer S, Colombel JF, Sands BE, Lukas M, Fedorak RN, Lee S, Bressler B, Fox I, Rosario M, Sankoh S, Xu J, Stephens K, Milch C, Parikh A. Vedolizumab as induction and maintenance therapy for Crohn’s disease. N Engl J Med 2013; 369: 711-721 [PMID: 23964933 DOI: 10.1056/NEJMoa1215739]
146 Van Kemseke C, Louis E, Reenaers C. [Vedolizumab (Entyvio®) for the treatment of inflammatory bowel diseases]. Rev Med Liege
Muhvić-Urek M et al . Oral pathology in IBD

5667 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
2015; 70: 575-582 [PMID: 26738270]147 Frankel DH, Mostofi RS, Lorincz AL. Oral Crohn’s disease: report
of two cases in brothers with metallic dysgeusia and a review of the literature. J Am Acad Dermatol 1985; 12: 260-268 [PMID: 3973124 DOI: 10.1016/S0190-9622(85)80033-5]
148 Harbord M, Annese V, Vavricka SR, Allez M, Barreiro-de Acosta M, Boberg KM, Burisch J, De Vos M, De Vries AM, Dick AD, Juillerat P, Karlsen TH, Koutroubakis I, Lakatos PL, Orchard T, Papay P, Raine T, Reinshagen M, Thaci D, Tilg H, Carbonnel F. The First European Evidence-based Consensus on Extra-intestinal Manifestations in Inflammatory Bowel Disease. J Crohns Colitis 2016; 10: 239-254 [PMID: 26614685 DOI: 10.1093/ecco-jcc/jjv213]
149 Casson DH, Eltumi M, Tomlin S, Walker-Smith JA, Murch SH. Topical tacrolimus may be effective in the treatment of oral and perineal Crohn’s disease. Gut 2000; 47: 436-440 [PMID: 10940284 DOI: 10.1136/gut.47.3.436]
150 Jurge S, Kuffer R, Scully C, Porter SR. Mucosal disease series. Number VI. Recurrent aphthous stomatitis. Oral Dis 2006; 12: 1-21 [PMID: 16390463 DOI: 10.1111/j.1601-0825.2005.01143.x]
151 Dharmavaram AT, Reddy RS, Nallakunta R. “Ozone” - the new
NEMESIS of canker sore. J Clin Diagn Res 2015; 9: ZC01-ZC04 [PMID: 25954693 DOI: 10.7860/jcdr/2015/11911.5617]
152 Albrektson M, Hedström L, Bergh H. Recurrent aphthous stomatitis and pain management with low-level laser therapy: a randomized controlled trial. Oral Surg Oral Med Oral Pathol Oral Radiol 2014; 117: 590-594 [PMID: 24725989 DOI: 10.1016/j.oooo.2014.01.228]
153 Lamey PJ, Lewis MA. Oral medicine in practice: angular cheilitis. Br Dent J 1989; 167: 15-18 [PMID: 2775569 DOI: 10.1038/sj.bdj.4806892]
154 Garcia-Cuesta C, Sarrion-Pérez MG, Bagán JV. Current treatment of oral candidiasis: A literature review. J Clin Exp Dent 2014; 6: e576-e582 [PMID: 25674329 DOI: 10.4317/jced.51798]
155 Zopf Y, Rabe C, Kollmann S, Hahn EG, Thürauf N, Schwab D. Alterations of taste perception in Crohn’s disease and their dependency on disease activity and nutritional behavior. J Clin Gastroenterol 2009; 43: 617-621 [PMID: 19247206 DOI: 10.1097/MCG.0b013e31818acf91]
156 Sigusch BW. Periodontitis as manifestation of Crohn’s disease in primary dentition: a case report. J Dent Child (Chic) 2004; 71: 193-196 [PMID: 15871451]
P- Reviewer: Ahluwalia NK, Freeman HJ, Johnson MW S- Editor: Ma YJ L- Editor: A E- Editor: Wang CH
Muhvić-Urek M et al . Oral pathology in IBD

Daniel H Ahn, Tanios Bekaii-Saab, Division of Medical Oncology, Mayo Clinic, Phoenix, AZ 85054, United States
Kristen K Ciombor, Sameh Mikhail, Division of Medical Oncology, The Ohio State University Medical Center, Columbus, OH 43210, United States
Author contributions: All authors contributed to this paper with conception, drafting, revision and approval of the final version of the paper.
Conflict-of-interest statement: None of the authors have any potential conflicts of interest, and no financial support was used for the work of this paper.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Manuscript source: Invited manuscript
Correspondence to: Tanios Bekaii-Saab, MD, Division of Medical Oncology, Mayo Clinic, 5777 E Mayo Blvd, Phoenix, AZ 85054, United States. [email protected]: +1-480-3424800Fax: +1-480-3014675
Received: March 20, 2016Peer-review started: March 22, 2016First decision: May 12, 2016Revised: May 20, 2016Accepted: June 13, 2016Article in press: June 13, 2016Published online: July 7, 2016
AbstractImprovements in screening and preventive measures have led to an increased detection of early stage colorectal cancers (CRC) where patients undergo treatment with a curative intent. Despite these efforts, a high proportion of patients are diagnosed with advanced stage disease that is associated with poor outcomes, as CRC remains one of the leading causes of cancer-related deaths in the world. The development of next generation sequencing and collaborative multi-institutional efforts to characterize the cancer genome has afforded us with a comprehensive assessment of the genomic makeup present in CRC. This knowledge has translated into understanding the prognostic role of various tumor somatic variants in this disease. Additionally, the awareness of the genomic alterations present in CRC has resulted in an improvement in patient outcomes, largely due to better selection of personalized therapies based on an individual’s tumor genomic makeup. The benefit of various treatments is often limited, where recent studies assessing the genomic diversity in CRC have identified the development of secondary tumor somatic variants that likely contribute to acquired treatment resistance. These studies have begun to alter the landscape of treatment for CRC that include investigating novel targeted therapies, assessing the role of immunotherapy and prospective, dynamic assessment of changes in tumor genomic alterations that occur during the treatment of CRC.
Key words: Colorectal cancer; KRAS mutation; BRAF mutation; genomic diversity; Tumor DNA
© The Author(s) 2016. Published by Baishideng Publishing group Inc. All rights reserved.
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.3748/wjg.v22.i25.5668
5668 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
World J Gastroenterol 2016 July 7; 22(25): 5668-5677 ISSN 1007-9327 (print) ISSN 2219-2840 (online)
© 2016 Baishideng Publishing Group Inc. All rights reserved.
Daniel H Ahn, Kristen K Ciombor, Sameh Mikhail, Tanios Bekaii-Saab
TOPIC HIGHLIGHT
Genomic diversity of colorectal cancer: Changing landscape and emerging targets
2016 Colorectal Cancer: Global view

Core tip: Tumor somatic variants have a prognostic role, in addition to treatment selection in patients with solid tumor malignancies, including colorectal cancer (CRC). The application of this knowledge in the development of novel, targeted therapies has resulted in improved patient outcomes in this disease. Our objective is to provide an overview of the genomic alterations present in CRC and its role in treatment implications, in addition to providing an overview of ongoing and future clinical trials.
Ahn DH, Ciombor KK, Mikhail S, Bekaii-Saab T. genomic diversity of colorectal cancer: Changing landscape and emerging targets. World J Gastroenterol 2016; 22(25): 5668-5677 Available from: URL: http://www.wjgnet.com/1007-9327/full/v22/i25/5668.htm DOI: http://dx.doi.org/10.3748/wjg.v22.i25.5668
INTRODUCTIONColorectal cancer (CRC) is the fourth most common cancer in the world, leading to more than 500000 deaths annually[1,2]. An increased awareness of the genomic makeup of CRC has allowed us to understand the prognostic role of certain tumor genomic alterations. This knowledge and its incorporation into the treatment of metastatic CRC has translated to significant improvements in patient outcomes, where patients’ median overall survival has approached 3 years[35]. The incorporation of our knowledge about the genomic landscape of CRC into treatment decisions with selected targeted agents has led to an improvement in patient outcomes. With this increased understanding, clinical trials are now being designed to assign treatment selection with novel therapies based upon identified specific tumor somatic variants in each individual. Herein we review the genomic landscape of CRC, its current role in treatment selection, and its integration in ongoing and future studies.
GENOMIC ALTERATIONS IN DOWNSTREAM SIGNALING PATHWAYS IN CRCRAS Mutations in CRCThe Kirsten Ras (KRAS) oncogene encodes for a guanosine triphosphate (GTP)/guanosine diphosphate binding protein downstream of the extracellular epidermal growth factor receptor in the RAS/RAF/MAPK signaling pathway. Activating KRAS exon 2 mutations occur in up to 45% of all CRC, and are involved in initiation, proliferation and progression of CRC[610]. While initial studies suggested a possible clinical benefit from antiepidermal growth factor receptor (EGFR) therapy for patients whose tumors
express KRAS codon 13 (G13D) mutations, a metaanalysis comprised of several large phase Ⅲ trials failed to demonstrate benefit from panitumumab, an antiEGFR monoclonal antibody, in CRC patients whose tumor harbored a KRAS codon 13 mutation[11]. In addition to KRAS exon 2, an approximate additional 10% of patients with other RAS mutations have been identified in CRC, including NRAS or nonexon 2 KRAS mutations[6]. In patients who exhibited activating nonexon 2 KRAS and NRAS mutations, an absence of clinical benefit, and perhaps a negative effect, was seen from the addition of antiEGFR therapy in combination with several chemotherapy regimens in various treatment settings[6,12,13]. On this basis, antiEGFR therapy should not be given to any patient with CRC exhibiting a RAS mutation.
While mutations in RAS as a predictive biomarker to antiEGFR therapy has been recognized, its relevance as a therapeutic target is unknown. Given the high incidence of RAS in CRC and its importance as an oncogene, targeting RAS represents an ideal and promising strategy. Developing strategies to directly block oncogenic RAS activity has remained a challenge due to several factors, including the high binding affinity of the oncoprotein to the GTPbound “on” state, as well as the lack of accessibility to active sites within KRAS to bind[14]. One alternative approach includes targeting pathways and its effectors downstream of RAS. The clinical benefit from targeting single pathways is often limited due to mechanisms of resistance including communication between signaling pathways and its resulting downstream effector activation and inhibition through a feedback loop mechanism[15,16]. Alternatively, secondary treatment resistance to antiEGFR treatment may result from the development of RAS mutations during a course of anti-EGFR therapy. Several studies have demonstrated up to 96% of patients who initially had RAS and BRAF wild-type CRC were later identified to have acquired activating RAS (KRAS or NRAS) or BRAF mutations on repeat tumor genomic assessment at the time of disease progression on antiEGFR therapy[1719].
Alternative treatment strategies in RAS mutant CRC include the combination of various therapeutic agents targeting several genes involved in the MAPK pathway that would cause sufficient suppression of activated RAS activity. Combining small molecule inhibitors of MEK to anti-EGFR therapies have demonstrated the reversal of acquired anti-EGFR therapy resistance, prompting ongoing clinical trials investigating the clinical utility of the combination of multiple signaling pathway inhibitors in the firstline setting, as well as in salvage therapy for refractory disease (Table 1). Targeting multiple signaling pathways may also be effective in overcoming resistance from se-condary activation of parallel signaling pathways[20]. Alternatively, administering anti-EGFR therapies in a pulsatile manner instead of to the point of clinical
5669 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Ahn DH et al . Colorectal cancer, genomics, targeted therapy

progression may prolong antiEGFR therapy efficacy. A recent study that performed dynamic monitoring of tumor somatic variants through circulating tumor DNA demonstrated a decrease in drug resistant KRAS clones upon withdraw of cetuximab, allowing for the reemergence of drug sensitivity to anti-EGFR therapy[21]. This suggests a rationale for intermittent EGFR blockade, and explains for the seldom efficacy seen with rechallenging antiEGFR therapies. Lastly, inhibitors of the MAPK and PI3K/Akt/mTOR pathway are considered to cause G1 cell cycle arrest through the suppression of Dtype cyclins and the upregulation of cell cycle inhibitors[22,23]. Pre-clinical studies have demonstrated potent inhibition of G1/S transition and phosphorylation of retinoblastoma (Rb) protein with the inhibition of the MAPK and PI3K/Akt pathway[24]. The combination of MEK and CDK inhibitors may be considered a potential strategy in treating RAS activated CRC or in tumors harboring mutations in CDK.
BRAF mutations in CRCBRAF V600E mutations occur in up to 5% of metastatic CRC[25,26] and are often associated with a more aggressive phenotype (with the exception in microsatellite instability high CRC, where the effect is attenuated). Patients with BRAF V600E mutations tend to respond poorly to conventional chemotherapy and have worse outcomes[6,2731]. The constitutive activation of BRAF evading any upstream inhibition of EGFR may explain the limited clinical benefit seen with anti-EGFR therapies in BRAF mutant metastatic CRC[6,32,33].
In metastatic melanoma, inhibition of BRAF with small molecule inhibitors has led to improvement in clinical outcomes in patients whose tumors exhibit mutations in BRAF[3437]. However, the clinical efficacy from single agent BRAF inhibition has not translated to patients with BRAF mutant metastatic CRC[36,38]. The lack of anti-tumor activity may be a result of insufficient inhibition of the MAPK pathway as a result of a feedback loop mechanism, resulting in the persistent activation of the MAPK signaling pathway[16,39] (Figure 1). To overcome this compensatory mechanism, the combination of tyrosine kinase inhibitors aimed at inhibiting the MAPK pathway has resulted in an improvement in treatment efficacy in comparison to singleagent BRAF small molecule inhibitor in metastatic melanoma[40]. Based on these results, a phase Ⅱ study investigating the clinical activity from the combination of BRAF and MEK inhibition with dabrafenib and trametinib was conducted in patients with BRAF mutant metastatic CRC[41]. While modest clinical activity was observed with the combination, with 12% of patients experiencing either a partial or complete response, correlative laboratory studies suggest an inhibition in MAPK signaling in patients receiving the combination[37]. The absence of significant anti-tumor activity may be attributed to insufficient suppression of MAPK signaling, which may be due to upstream activation of EGFR, leading to reactivation of MAPK and other integral signaling pathways[15]. Based on this rationale, ongoing studies are investigating the combination of antiEGFR therapies with BRAF tyrosine
5670 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Table 1 Ongoing combination targeted therapy trials for colorectal cancer
Agent(s) Class of agent Phase Trial number1 Misc
MEK162 + Panitumumab MEK tyrosine kinase inhibitor, anti-EGFR mAb
Ⅰb/Ⅱ NCT01927341 mCRC with mutant or wild-type RAS tumors
Dabrafenib + Trametinib + Panitumumab + 5-Fluorouracil
BRAF tyrosine kinase inhibitor, MEK tyrosine kinase inhibitor, anti-EGFR mAb
Ⅰ/Ⅱ NCT01750918 BRAF-V600E mutant + and in pts with secondary resistance to anti-EGFR mAb
LGX818 + Cetuximab ± BYL719 BRAF tyrosine kinase inhibitor, anti-EGFR mAb, PI3K tyrosine kinase inhibitor
Ⅰ/Ⅱ NCT01719380 BRAF mutant mCRC
Irinotecan + Cetuximab ± Vemurafenib
anti-EGFR mAb, BRAF tyrosine kinase inhibitor
Ⅱ NCT02164916 BRAF mutant mCRC
Neratinib + Cetuximab HER-2 tyrosine kinase inhibitor, anti-EGFR mAb
Ⅰ/Ⅱ NCT01960023 KRAS, NRAS, BRAF, PIK3CA wild type
1Utilizing the NCT number, clinical trial information can be obtained at https://clinicaltrials.gov. mAb: Monoclonal antibody; mCRC: Metastatic colorectal cancer; EGFR: Epidermal growth factor receptor; PIK3CA: Phosphatidylinositol-4,5-bisphosphate 3-kinase, catalytic subunit alpha; BRAF: v-Raf murine sarcoma viral oncogene homolog B.
Figure 1 RAS/RAF/MEK/ERK pathway and mechanisms of resistance to BRAF inhibition. The figure above shows the MAPK pathway and the compensatory feedback loop activation (arrow) despite BRAF inhibition, resulting in the upstream reactivation of the MAPK pathway.
Ahn DH et al . Colorectal cancer, genomics, targeted therapy
RAS
RAF
MEK 1/2
ERK 1/2
Feedback loop activation

5671 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
receptors consisting of four members (FGFR1, 2, 3 and 4). These receptors bind to one of 18 secreted glycoprotein ligands, or fibroblast growth factors (FGFs), to their extracellular domain[48]. Binding of the appropriate ligand results in FGFR dimerization, autophosphorylation and activation of downstream signaling pathways that include the MAPK, PI3K/Akt and signaling transducer and activator of transcription or STAT pathway, inducing cell differentiation, growth and survival[49]. FGFR overexpression has been identified in CRC samples, where the presence of FGFR signaling has been identified as playing an important role in the tumor microenvironment, with a correlation in FGFR overexpression with tumor invasion, advanced stage disease and chemotherapy resistance[5053]. Preclinical studies have demonstrated the reversal of chemotherapy resistance by combining small molecule FGFR inhibitors with chemotherapy in CRC cell lines, confirming the importance of targeting this receptor and representing a potential strategy in overcoming treatment resistance in CRC[54].
C-MET (MET)Hepatocyte growth factor receptor, also known as cMET, is a protooncogene that encodes the tyrosine kinase receptor for hepatocyte growth factor (HGF). Abnormal expression of cMET through somatic mutations or overexpression has been identified in up to 66.7% of CRC samples and its microenvironment and is a negative prognostic marker related to tumor
kinase inhibitors in patients with BRAF mutant mCRC (Table 1)[4245].
GENOMIC DIVERSITY AND ITS ROLE IN DEVELOPING PERSONALIZED THERAPIES WITH TARGETED AGENTS IN CRCWhile RAS mutations are the most common genomic alteration in CRC, recent efforts have allowed us to understand the genomic diversity and identify potential therapeutic targets of interest in this disease[46,47]. Through the efforts of The Cancer Genome Atlas (TCGA), 224 CRC cases underwent extensive molecular characterization to describe the genomic landscape present in CRC[46]. 24 genes were significantly mutated, where most were an actionable mutation, including ERBB2 (HER-2/neu) mutations, a therapeutic target in HER-2 positive gastric and breast cancer, were identified in 19% of tumors[46]. This comprehensive assessment allowed us to have a better understanding of the genomic landscape, in addition to identifying several potential targetable genes of interest that are essential for tumor growth and carcinogenesis that we will discuss in further detail below (Table 2).
Fibroblast growth factor receptor in CRCThe fibroblast growth factor receptors (FGFR) comprise a group of highly conserved tyrosine kinase
Table 2 Tumor genomic variants and potential targeted therapies of interest
Gene Agents of Interest
Mechanism of action Phase Trial number1 Comment
FGFR (FGFR1, FGFR2, FGFR3, FGFR4)
Ponatinib Multi-kinase small molecule inhibitor Ⅱ NCT02272998
BGJ398 Pan FGFR small molecule inhibitor Ⅰ NCT01928459RET Cabozantinib Multi-kinase small molecule inhibitor Ⅰ NCT02008383 Cabozantinib + panitumumab
Vandetanib Multi-kinase small molecule inhibitor Ⅰ NCT01582191Apatinib Multi-kinase small molecule inhibitorPonatinib Multi-kinase small molecule inhibitor Ⅱ NCT02272998RXDX-105 RET and BRAF small molecule inhibtor Ⅰ NCT01877811Sunitinib Multi-kinase small molecule inhibitorSorafenib Multi-kinase small molecule inhibitor Ⅰ NCT01531361
HER-2 AZD8931 Small molecule inhibitor of EGFR, HER-2, HER-3 Ⅰ/Ⅱ NCT01862003 AZD8931 + FOLFIRINeratinib Small molecule inhibitor of EGFR, HER-2, HER-3 Ⅱ NCT01953926
HER-2 vaccine B cell peptide vaccine Ⅰ NCT01376505T-DM1 Antibody-drug conjugate of traztuzumab and
DM1Ⅱ HERACLES-
RESCUEAt the time of traztumab
failurePertuzumab Anti HER-2 monoclonal antibody Ⅱ HERACLES Pertuzumab + trastuzumab
Lapatinib Anti HER-2 small molecule inhibitor Ⅱ HERACLES Lapatinib + trastuzumabc-MET (MET, HGFR) Crizotinib Multi-kinase small molecule inhibitor NCT02510001 Crizotinib + PD-0325901
Tivantinib c-MET inhibitor NCT01892527 Tivantinib + cetuximabCabozantinib c-MET and VEGFR2 inhibitor
INC280 Small molecule inhibitor of c-MET Ⅱ NCT2205398 INC280 + cetuximabAMG102 HGF inhibitorAV299 HGF inhibitor
1Utilizing the NCT number, clinical trial information can be obtained at https://clinicaltrials.gov. FGFR: Fibroblast growth factor receptor; EGFR: Epidermal growth factor receptor; BRAF: v-Raf murine sarcoma viral oncogene homolog B; HER-2: Human growth factor receptor 2; HGFR: Hepatocyte growth factor receptor; TDM-1: Ado-trastuzumab emtansine; VEGFR: Vascular endothelial growth factor receptor.
Ahn DH et al . Colorectal cancer, genomics, targeted therapy

5672 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
oncogenesis, invasiveness, local recurrence, and chemotherapy resistance[5558]. MET activation confers acquired anti-EGFR therapy resistance, through re-activation of anti-apoptotic signaling pathways, including the PI3K and MAPK pathways[5962]. Thus, inhibiting cMET represents an emerging target of interest in the development of novel agents in CRC. Pre-clinical studies have demonstrated that the blockade of cMET inhibits tumor growth in CRC cell lines[63,64], thus agents targeting MET, including small molecule multikinase inhibitors (e.g., crizotinib, tivantinib), HGF inhibitors (e.g., AMG102, AV299) and immunotherapeutic agents are of interest and under investigation in the treatment of CRC.
RETRET is located on chromosome 10q11.2 and encodes a transmembrane receptor tyrosine kinase that has three unique isoforms[65]. Four ligands can bind and activate RET, leading to the aberrant activity of several signaling pathways including PI3K/Akt and MAPK pathway[66]. While the aberrant expression of RET may function as an oncogene in certain solid tumor malignancies including papillary and medullary thyroid cancers[67], in colorectal cancer RET has been identified as a tumor suppressor and as an oncogene. Studies have shown that the hypermethylation and mutational inactivation of RET, as well as RET fusions, promote colorectal cancer formation[6870]. In several studies, RET mutations were identified in up to 7% of mCRC samples[46,71,72]. Regorafenib, an approved multi-target small molecule inhibitor in metastatic CRC[73], has demonstrated tumor growth inhibition in RET mutant cancer cells lines[70,74], and may explain part of its efficacy in this disease. Further studies investigating its activity in RET mutant CRC is warranted as it may provide further benefit in this specific cohort of CRC patients.
HER-2/NeuHuman growth factor receptor 2, also known as HER-2 or HER-2/neu, is part of the human epidermal growth factor receptor family and has been identified as an oncogene in several solid tumor malignancies, including CRC. Its overexpression has been a poor prognostic biomarker in breast cancer and is an effective therapeutic target in breast and gastric cancer[7577]. Studies evaluating HER-2 overexpression in CRC have identified HER-2 somatic mutations and amplification in 7% of patients with CRC[46], where preclinical studies have demonstrated its role in inducing resistance to antiEGFR therapy, and its inhibition showing durable tumor regression with antiHER-2 therapy[78]. Based on these findings, the HERACLES trial, a phase Ⅱ study investigated dual anti-HER-2 therapy blockade in patients with HER-2 amplified (immunohistochemistry staining 3+ or 2+ with FISH
positive (HER2:CEP17 ratio > 2) in > 50% of tumor cells) mCRC with previous anti-EGFR therapy. Patients received the combination of trastuzumab, an anti HER-2 monoclonal antibody with either lapatinib, a small molecule inhibitor of HER-2 or pertuzumab, an anti HER-2 monoclonal antibody. Early results from the lapatinib and trastuzumab arm demonstrated a 35% response rate and median progression free survival of 5.5 mo, despite being heavily pre-treated after failing multiple lines of therapy[79]. Based on these findings, anti HER-2 therapy may be an effective treatment option in a preselected patient population with mCRC.
DNA mismatch repair genes and their therapeutic relevance in advanced CRCMismatch repair (MMR) genes function to remove erroneous DNA nucleotides during mitosis. With deficient MMR activity, altered DNA nucleotides are incorporated into cells that increase their risk in forming into a neoplastic, hypermutated makeup[80], resulting in microsatellite instability. Deficient MMR activity is found in approximately 15% of CRC, in which 3% is attributed to Lynch Syndrome through germline mutations in MLH1, MSH2, MSH6, PMS2 or EPCAM3 genes[81,82]. The remaining 12% is due to sporadic inactivation of MLH1. While microsatellite instability (MSI) is a driver for tumor formation and proliferation in CRC, recent studies have demonstrated its relevance for potential novel therapeutic agents in this cohort of CRC. Tumors expressing MSI have been characterized by an intense immune infiltration, likely related to a high density of mutations, creating numerous neoantigens and targets for immune therapies. Based on this rationale, a singlearm phase Ⅱ study was conducted to assess the clinical efficacy of pembrolizumab, a programmed cell death protein (PD)1 inhibitor, in patients with treatment resistant, metastatic cancer that did or did not express mismatchrepair deficiency[83]. Individuals with deficient MMR colorectal cancer experienced a response rate of 40% and immunerelated PFS of 78% at 20 wk. Interestingly, a lack of activity was associated with mismatch repairproficient CRC patients, confirming that immunotherapeutic agents may be beneficial in only certain cohorts of CRC, unless alternative approaches can be developed to transform tumors into an immune-responsive phenotype[83]. Based on these findings, several ongoing clinical trials are investigating various novel, immunotherapeutic agents in the treatment of CRC that include studies in patients with MSI high tumors and those with positive PDL-1 expression (Table 3). While current trials will substantiate the role of immune therapy in CRC, a better understanding of mechanisms of acquired resistance, optimal duration of necessary treatment and predictive biomarkers associated with treatment efficacy are paramount.
Ahn DH et al . Colorectal cancer, genomics, targeted therapy

Table 3 Current ongoing immune therapy trials for colorectal cancer
5673 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Tumor genomic assessment at the time of acquired therapy resistance in mCRCWhile anti-tumor activity from targeted therapies can lead to dramatic responses, the clinical benefit is often limited due to inherent and acquired resistance through the acquisition of new tumor genomic alter-nations, including the oncogenic activation of MET or acquiring RAS mutations, as described above. While tumor genomic alterations are usually assessed through tumor samples, obtaining tissue can be challenging due to insufficient material from tumors only accessible through fine-needle aspirates, as well as the invasive nature of such procedures.
Tumor circulating free DNA can be non-invasively assessed in peripheral blood, a “liquid biopsy,” through the assessment of circulating tumor DNA (ctDNA) and tumor cells (CTCs) and are present in advanced malignancies[84,85]. CtDNA and CTCs can provide dynamic assessments of tumor specific mutations that may arise during the course of therapy. Although previous methodologies demonstrate low rates of sensitivity and concordance, the incorporation of new technology, including real time digital PCR has increased sensitivity (87.2%) and specificity (99.2%) in identifying tumor specific mutations responsible for treatment resistance in patients who initially responded to targeted therapies[18]. While there are limitations, including false negative results as well as the inability to identify genomic alterations from central nervous system (CNS) lesions, this non-invasive tool can monitor patients for resistanceconferring mutations as well as assessing all tumors concurrently, as heterogeneity can exist between different foci of disease.
CONCLUSIONAdvancements in genomic sequencing have resulted in our increased understanding of the genomic landscape of CRC, allowing us to develop and tailor personalized therapies for patients. Despite these improvements, future studies are needed to characterize and understand the functionality of the various different mutations of each gene, including mutational assessment at the time of treatment failure. This will allow us to improve therapies for patients with CRC
by assessing the prognostic and potential therapeutic implication of genes of interest, and to identify predictive biomarkers of response and resistance.
REFERENCES1 Siegel R, Desantis C, Jemal A. Colorectal cancer statistics, 2014. CA
Cancer J Clin 2014; 64: 104-117 [PMID: 24639052 DOI: 10.3322/caac.21220]
2 Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin 2014; 64: 9-29 [PMID: 24399786 DOI: 10.3322/caac.21208]
3 Tol J, Nagtegaal ID, Punt CJ. BRAF mutation in metastatic colorectal cancer. N Engl J Med 2009; 361: 98-99 [PMID: 19571295 DOI: 10.1056/NEJMc0904160]
4 Loupakis F, Cremolini C, Masi g, Lonardi S, Zagonel V, Salvatore L, Cortesi E, Tomasello g, Ronzoni M, Spadi R, Zaniboni A, Tonini g, Buonadonna A, Amoroso D, Chiara S, Carlomagno C, Boni C, Allegrini g, Boni L, Falcone A. Initial therapy with FOLFOXIRI and bevacizumab for metastatic colorectal cancer. N Engl J Med 2014; 371: 1609-1618 [PMID: 25337750 DOI: 10.1056/NEJMoa1403108]
5 Loupakis F, Cremolini C, Lonardi S, Tomasello g, Ronzoni M, Zaniboni A, Tonini g, Valsuani C, Chiara S, Boni C, Marcucci L, Negri F, Barone C, Vitello S, D’Amico M, granetto C, Fontanini g, Tomcikova D, Boni L, Falcone A. Subgroup analyses in RAS mutant, BRAF mutant and all-wt mCRC pts treated with FOLFOXIRI plus bevacizumab (bev) or FOLFIRI plus bev in the TRIBE study. J Clin Oncol 2014; 32: 3519
6 Douillard JY, Oliner KS, Siena S, Tabernero J, Burkes R, Barugel M, Humblet Y, Bodoky g, Cunningham D, Jassem J, Rivera F, Kocákova I, Ruff P, Błasińska-Morawiec M, Šmakal M, Canon JL, Rother M, Williams R, Rong A, Wiezorek J, Sidhu R, Patterson SD. Panitumumab-FOLFOX4 treatment and RAS mutations in colorectal cancer. N Engl J Med 2013; 369: 1023-1034 [PMID: 24024839 DOI: 10.1056/NEJMoa1305275]
7 Van Cutsem E, Köhne CH, Láng I, Folprecht g, Nowacki MP, Cascinu S, Shchepotin I, Maurel J, Cunningham D, Tejpar S, Schlichting M, Zubel A, Celik I, Rougier P, Ciardiello F. Cetuximab plus irinotecan, fluorouracil, and leucovorin as first-line treatment for metastatic colorectal cancer: updated analysis of overall survival according to tumor KRAS and BRAF mutation status. J Clin Oncol 2011; 29: 2011-2019 [PMID: 21502544 DOI: 10.1200/JCO.2010.33.5091]
8 Peeters M, Price TJ, Cervantes A, Sobrero AF, Ducreux M, Hotko Y, André T, Chan E, Lordick F, Punt CJ, Strickland AH, Wilson g, Ciuleanu TE, Roman L, Van Cutsem E, Tzekova V, Collins S, Oliner KS, Rong A, gansert J. Randomized phase III study of panitumumab with fluorouracil, leucovorin, and irinotecan (FOLFIRI) compared with FOLFIRI alone as second-line treatment in patients with metastatic colorectal cancer. J Clin Oncol 2010; 28: 4706-4713 [PMID: 20921462 DOI: 10.1200/JCO.2009.27.6055]
9 Maughan TS, Adams RA, Smith Cg, Meade AM, Seymour MT, Wilson RH, Idziaszczyk S, Harris R, Fisher D, Kenny SL, Kay E, Mitchell JK, Madi A, Jasani B, James MD, Bridgewater J, Kennedy MJ, Claes B, Lambrechts D, Kaplan R, Cheadle JP. Addition of
Agent Class of agent Phase Trial number1 Comment
MK-3475 Anti-PD-1 mAb Ⅱ NCT01876511 MSI-high tumorsMEDI4736 Anti-PD-L1 mAb Ⅰ/Ⅱ NCT01693562Nivolumab ± ipiliumumab Anti-PD-1 mAb/anti-CTLA-4 mAb Ⅰ/Ⅱ NCT02060188 Recurrent and metastatic CRCMK-3475 + mFOLFOX6 Anti-PD-1 mAb Ⅱ NCT02375672Tremelimumab + MEDI4736 Anti-CTLA-4 mAb + anti-PD-L1 mAb Ⅰ NCT01975831
1Utilizing the NCT number, clinical trial information can be obtained at https://clinicaltrials.gov. mAb: Monoclonal antibody; CRC: Colorectal cancer; MSI: Microsatellite instability; CTLA: Cytotoxic T associated lymphocyte protein; PD-1: Program cell death protein 1; PD-L1: Programmed cell death protein ligand 1; FOLFOX: Combination of 5-Flurouracil, folinic acid and oxaliplatin chemotherapy regimen.
Ahn DH et al . Colorectal cancer, genomics, targeted therapy

5674 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
cetuximab to oxaliplatin-based first-line combination chemotherapy for treatment of advanced colorectal cancer: results of the randomised phase 3 MRC COIN trial. Lancet 2011; 377: 2103-2114 [PMID: 21641636 DOI: 10.1016/S0140-6736(11)60613-2]
10 Tveit KM, guren T, glimelius B, Pfeiffer P, Sorbye H, Pyrhonen S, Sigurdsson F, Kure E, Ikdahl T, Skovlund E, Fokstuen T, Hansen F, Hofsli E, Birkemeyer E, Johnsson A, Starkhammar H, Yilmaz MK, Keldsen N, Erdal AB, Dajani O, Dahl O, Christoffersen T. Phase III trial of cetuximab with continuous or intermittent fluorouracil, leucovorin, and oxaliplatin (Nordic FLOX) versus FLOX alone in first-line treatment of metastatic colorectal cancer: the NORDIC-VII study. J Clin Oncol 2012; 30: 1755-1762 [PMID: 22473155 DOI: 10.1200/JCO.2011.38.0915]
11 Peeters M, Douillard JY, Van Cutsem E, Siena S, Zhang K, Williams R, Wiezorek J. Mutant KRAS codon 12 and 13 alleles in patients with metastatic colorectal cancer: assessment as prognostic and predictive biomarkers of response to panitumumab. J Clin Oncol 2013; 31: 759-765 [PMID: 23182985 DOI: 10.1200/JCO.2012.45.1492]
12 Heinemann V, von Weikersthal LF, Decker T, Kiani A, Vehling-Kaiser U, Al-Batran SE, Heintges T, Lerchenmüller C, Kahl C, Seipelt g, Kullmann F, Stauch M, Scheithauer W, Hielscher J, Scholz M, Müller S, Link H, Niederle N, Rost A, Höffkes Hg, Moehler M, Lindig RU, Modest DP, Rossius L, Kirchner T, Jung A, Stintzing S. FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab as first-line treatment for patients with metastatic colorectal cancer (FIRE-3): a randomised, open-label, phase 3 trial. Lancet Oncol 2014; 15: 1065-1075 [PMID: 25088940 DOI: 10.1016/S1470-2045(14)70330-4]
13 Schwartzberg LS, Rivera F, Karthaus M, Fasola g, Canon JL, Hecht JR, Yu H, Oliner KS, go WY. PEAK: a randomized, multicenter phase II study of panitumumab plus modified fluorouracil, leucovorin, and oxaliplatin (mFOLFOX6) or bevacizumab plus mFOLFOX6 in patients with previously untreated, unresectable, wild-type KRAS exon 2 metastatic colorectal cancer. J Clin Oncol 2014; 32: 2240-2247 [PMID: 24687833 DOI: 10.1200/JCO.2013.53.2473]
14 Gysin S, Salt M, Young A, McCormick F. Therapeutic strategies for targeting ras proteins. Genes Cancer 2011; 2: 359-372 [PMID: 21779505 DOI: 10.1177/1947601911412376]
15 Prahallad A, Sun C, Huang S, Di Nicolantonio F, Salazar R, Zecchin D, Beijersbergen RL, Bardelli A, Bernards R. Unresponsiveness of colon cancer to BRAF(V600E) inhibition through feedback activation of EgFR. Nature 2012; 483: 100-103 [PMID: 22281684 DOI: 10.1038/nature10868]
16 Corcoran RB, Ebi H, Turke AB, Coffee EM, Nishino M, Cogdill AP, Brown RD, Della Pelle P, Dias-Santagata D, Hung KE, Flaherty KT, Piris A, Wargo JA, Settleman J, Mino-Kenudson M, Engelman JA. EgFR-mediated re-activation of MAPK signaling contributes to insensitivity of BRAF mutant colorectal cancers to RAF inhibition with vemurafenib. Cancer Discov 2012; 2: 227-235 [PMID: 22448344 DOI: 10.1158/2159-8290.CD-11-0341]
17 Misale S, Yaeger R, Hobor S, Scala E, Janakiraman M, Liska D, Valtorta E, Schiavo R, Buscarino M, Siravegna g, Bencardino K, Cercek A, Chen CT, Veronese S, Zanon C, Sartore-Bianchi A, gambacorta M, gallicchio M, Vakiani E, Boscaro V, Medico E, Weiser M, Siena S, Di Nicolantonio F, Solit D, Bardelli A. Emergence of KRAS mutations and acquired resistance to anti-EgFR therapy in colorectal cancer. Nature 2012; 486: 532-536 [PMID: 22722830 DOI: 10.1038/nature11156]
18 Diaz LA, Williams RT, Wu J, Kinde I, Hecht JR, Berlin J, Allen B, Bozic I, Reiter Jg, Nowak MA, Kinzler KW, Oliner KS, Vogelstein B. The molecular evolution of acquired resistance to targeted EgFR blockade in colorectal cancers. Nature 2012; 486: 537-540 [PMID: 22722843 DOI: 10.1038/nature11219]
19 Bettegowda C, Sausen M, Leary RJ, Kinde I, Wang Y, Agrawal N, Bartlett BR, Wang H, Luber B, Alani RM, Antonarakis ES, Azad NS, Bardelli A, Brem H, Cameron JL, Lee CC, Fecher LA, gallia gL, gibbs P, Le D, giuntoli RL, goggins M, Hogarty MD, Holdhoff M, Hong SM, Jiao Y, Juhl HH, Kim JJ, Siravegna g, Laheru DA,
Lauricella C, Lim M, Lipson EJ, Marie SK, Netto gJ, Oliner KS, Olivi A, Olsson L, Riggins gJ, Sartore-Bianchi A, Schmidt K, Shih lM, Oba-Shinjo SM, Siena S, Theodorescu D, Tie J, Harkins TT, Veronese S, Wang TL, Weingart JD, Wolfgang CL, Wood LD, Xing D, Hruban RH, Wu J, Allen PJ, Schmidt CM, Choti MA, Velculescu VE, Kinzler KW, Vogelstein B, Papadopoulos N, Diaz LA. Detection of circulating tumor DNA in early- and late-stage human malignancies. Sci Transl Med 2014; 6: 224ra24 [PMID: 24553385 DOI: 10.1126/scitranslmed.3007094]
20 Schellens J, Van geel R, Bendell J, Spreafico A, Schuler M, Yoshino T, Delord J, Yamada Y, Lolkema MP, Faris JE, Eskens FALM, Sharma S, Yaeger R, Lenz H, Wainberg ZA, Avsar E, Chatterjee A, Jaeger S, Demuth T, Tabernero J. Final biomarker analysis of the pahse I study of the selective BRAF V600 inhibitor encorafenib (LGX818) combined with cetuximab with or without the α-specific PI3K inhibitor alpelisib (BYL719) in patients with advanced BRAF-mutant colorectal cancer. Presented at the 106th Annual Meeting of the American Association for Cancer Research, Philadelphia, PA, April 18-22, 2015
21 Siravegna G, Mussolin B, Buscarino M, Corti g, Cassingena A, Crisafulli g, Ponzetti A, Cremolini C, Amatu A, Lauricella C, Lamba S, Hobor S, Avallone A, Valtorta E, Rospo g, Medico E, Motta V, Antoniotti C, Tatangelo F, Bellosillo B, Veronese S, Budillon A, Montagut C, Racca P, Marsoni S, Falcone A, Corcoran RB, Di Nicolantonio F, Loupakis F, Siena S, Sartore-Bianchi A, Bardelli A. Clonal evolution and resistance to EgFR blockade in the blood of colorectal cancer patients. Nat Med 2015; 21: 827 [PMID: 26151329 DOI: 10.1038/nm0715-827b]
22 Leontieva OV, Demidenko ZN, Blagosklonny MV. MEK drives cyclin D1 hyperelevation during geroconversion. Cell Death Differ 2013; 20: 1241-1249 [PMID: 23852369 DOI: 10.1038/cdd.2013.86]
23 Liu B, Fang M, Lu Y, Mendelsohn J, Fan Z. Fibroblast growth factor and insulin-like growth factor differentially modulate the apoptosis and g1 arrest induced by anti-epidermal growth factor receptor monoclonal antibody. Oncogene 2001; 20: 1913-1922 [PMID: 11313939 DOI: 10.1038/sj.onc.1204277]
24 Paternot S, Roger PP. Combined inhibition of MEK and mammalian target of rapamycin abolishes phosphorylation of cyclin-dependent kinase 4 in glioblastoma cell lines and prevents their proliferation. Cancer Res 2009; 69: 4577-4581 [PMID: 19458076 DOI: 10.1158/0008-5472.CAN-08-3260]
25 Davies H, Bignell gR, Cox C, Stephens P, Edkins S, Clegg S, Teague J, Woffendin H, garnett MJ, Bottomley W, Davis N, Dicks E, Ewing R, Floyd Y, gray K, Hall S, Hawes R, Hughes J, Kosmidou V, Menzies A, Mould C, Parker A, Stevens C, Watt S, Hooper S, Wilson R, Jayatilake H, gusterson BA, Cooper C, Shipley J, Hargrave D, Pritchard-Jones K, Maitland N, Chenevix-Trench g, Riggins gJ, Bigner DD, Palmieri g, Cossu A, Flanagan A, Nicholson A, Ho JW, Leung SY, Yuen ST, Weber BL, Seigler HF, Darrow TL, Paterson H, Marais R, Marshall CJ, Wooster R, Stratton MR, Futreal PA. Mutations of the BRAF gene in human cancer. Nature 2002; 417: 949-954 [PMID: 12068308 DOI: 10.1038/nature00766]
26 Tie J, gibbs P, Lipton L, Christie M, Jorissen RN, Burgess AW, Croxford M, Jones I, Langland R, Kosmider S, McKay D, Bollag g, Nolop K, Sieber OM, Desai J. Optimizing targeted therapeutic development: analysis of a colorectal cancer patient population with the BRAF(V600E) mutation. Int J Cancer 2011; 128: 2075-2084 [PMID: 20635392 DOI: 10.1002/ijc.25555]
27 Samowitz WS, Sweeney C, Herrick J, Albertsen H, Levin TR, Murtaugh MA, Wolff RK, Slattery ML. Poor survival associated with the BRAF V600E mutation in microsatellite-stable colon cancers. Cancer Res 2005; 65: 6063-6069 [PMID: 16024606 DOI: 10.1158/0008-5472.CAN-05-0404]
28 Yokota T, Ura T, Shibata N, Takahari D, Shitara K, Nomura M, Kondo C, Mizota A, Utsunomiya S, Muro K, Yatabe Y. BRAF mutation is a powerful prognostic factor in advanced and recurrent colorectal cancer. Br J Cancer 2011; 104: 856-862 [PMID: 21285991 DOI: 10.1038/bjc.2011.19]
29 Price TJ, Hardingham JE, Lee CK, Weickhardt A, Townsend AR, Wrin JW, Chua A, Shivasami A, Cummins MM, Murone C,
Ahn DH et al . Colorectal cancer, genomics, targeted therapy

5675 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Tebbutt NC. Impact of KRAS and BRAF gene Mutation Status on Outcomes From the Phase III AgITg MAX Trial of Capecitabine Alone or in Combination With Bevacizumab and Mitomycin in Advanced Colorectal Cancer. J Clin Oncol 2011; 29: 2675-2682 [PMID: 21646616 DOI: 10.1200/JCO.2010.34.5520]
30 Morris V, Overman MJ, Jiang ZQ, garrett C, Agarwal S, Eng C, Kee B, Fogelman D, Dasari A, Wolff R, Maru D, Kopetz S. Progression-free survival remains poor over sequential lines of systemic therapy in patients with BRAF-mutated colorectal cancer. Clin Colorectal Cancer 2014; 13: 164-171 [PMID: 25069797 DOI: 10.1016/j.clcc.2014.06.001]
31 Tran B, Kopetz S, Tie J, gibbs P, Jiang ZQ, Lieu CH, Agarwal A, Maru DM, Sieber O, Desai J. Impact of BRAF mutation and microsatellite instability on the pattern of metastatic spread and prognosis in metastatic colorectal cancer. Cancer 2011; 117: 4623-4632 [PMID: 21456008 DOI: 10.1002/cncr.26086]
32 Douillard JY, Siena S, Cassidy J, Tabernero J, Burkes R, Barugel M, Humblet Y, Bodoky g, Cunningham D, Jassem J, Rivera F, Kocákova I, Ruff P, Błasińska-Morawiec M, Šmakal M, Canon JL, Rother M, Oliner KS, Wolf M, gansert J. Randomized, phase III trial of panitumumab with infusional fluorouracil, leucovorin, and oxaliplatin (FOLFOX4) versus FOLFOX4 alone as first-line treatment in patients with previously untreated metastatic colorectal cancer: the PRIME study. J Clin Oncol 2010; 28: 4697-4705 [PMID: 20921465 DOI: 10.1200/JCO.2009.27.4860]
33 Seymour MT, Brown SR, Middleton g, Maughan T, Richman S, gwyther S, Lowe C, Seligmann JF, Wadsley J, Maisey N, Chau I, Hill M, Dawson L, Falk S, O’Callaghan A, Benstead K, Chambers P, Oliver A, Marshall H, Napp V, Quirke P. Panitumumab and irinotecan versus irinotecan alone for patients with KRAS wild-type, fluorouracil-resistant advanced colorectal cancer (PICCOLO): a prospectively stratified randomised trial. Lancet Oncol 2013; 14: 749-759 [PMID: 23725851 DOI: 10.1016/S1470-2045(13)70163-3]
34 Sosman JA, Kim KB, Schuchter L, gonzalez R, Pavlick AC, Weber JS, McArthur gA, Hutson TE, Moschos SJ, Flaherty KT, Hersey P, Kefford R, Lawrence D, Puzanov I, Lewis KD, Amaravadi RK, Chmielowski B, Lawrence HJ, Shyr Y, Ye F, Li J, Nolop KB, Lee RJ, Joe AK, Ribas A. Survival in BRAF V600-mutant advanced melanoma treated with vemurafenib. N Engl J Med 2012; 366: 707-714 [PMID: 22356324 DOI: 10.1056/NEJMoa1112302]
35 Flaherty KT, Puzanov I, Kim KB, Ribas A, McArthur gA, Sosman JA, O’Dwyer PJ, Lee RJ, grippo JF, Nolop K, Chapman PB. Inhibition of mutated, activated BRAF in metastatic melanoma. N Engl J Med 2010; 363: 809-819 [PMID: 20818844 DOI: 10.1056/NEJMoa1002011]
36 Falchook GS, Long gV, Kurzrock R, Kim KB, Arkenau TH, Brown MP, Hamid O, Infante JR, Millward M, Pavlick AC, O’Day SJ, Blackman SC, Curtis CM, Lebowitz P, Ma B, Ouellet D, Kefford RF. Dabrafenib in patients with melanoma, untreated brain metastases, and other solid tumours: a phase 1 dose-escalation trial. Lancet 2012; 379: 1893-1901 [PMID: 22608338 DOI: 10.1016/S0140-6736(12)60398-5]
37 Hauschild A, grob JJ, Demidov LV, Jouary T, gutzmer R, Millward M, Rutkowski P, Blank CU, Miller WH, Kaempgen E, Martín-Algarra S, Karaszewska B, Mauch C, Chiarion-Sileni V, Martin AM, Swann S, Haney P, Mirakhur B, guckert ME, goodman V, Chapman PB. Dabrafenib in BRAF-mutated metastatic melanoma: a multicentre, open-label, phase 3 randomised controlled trial. Lancet 2012; 380: 358-365 [PMID: 22735384 DOI: 10.1016/S0140-6736(12)60868-X]
38 Kopetz S, Desai J, Chan E, Hecht JR, O’Dwyer PJ, Maru D, Morris V, Janku F, Dasari A, Chung W, Issa JP, gibbs P, James B, Powis g, Nolop KB, Bhattacharya S, Saltz L. Phase II Pilot Study of Vemurafenib in Patients With Metastatic BRAF-Mutated Colorectal Cancer. J Clin Oncol 2015; 33: 4032-4038 [PMID: 26460303 DOI: 10.1200/JCO.2015.63.2497]
39 Corcoran RB, Dias-Santagata D, Bergethon K, Iafrate AJ, Settleman J, Engelman JA. BRAF gene amplification can promote acquired resistance to MEK inhibitors in cancer cells harboring the BRAF V600E mutation. Sci Signal 2010; 3: ra84 [PMID: 21098728
DOI: 10.1126/scisignal.2001148]40 Flaherty KT, Infante JR, Daud A, gonzalez R, Kefford RF, Sosman
J, Hamid O, Schuchter L, Cebon J, Ibrahim N, Kudchadkar R, Burris HA, Falchook g, Algazi A, Lewis K, Long gV, Puzanov I, Lebowitz P, Singh A, Little S, Sun P, Allred A, Ouellet D, Kim KB, Patel K, Weber J. Combined BRAF and MEK inhibition in melanoma with BRAF V600 mutations. N Engl J Med 2012; 367: 1694-1703 [PMID: 23020132 DOI: 10.1056/NEJMoa1210093]
41 Corcoran RB, Atreya CE, Falchook gS, Kwak EL, Ryan DP, Bendell JC, Hamid O, Messersmith WA, Daud A, Kurzrock R, Pierobon M, Sun P, Cunningham E, Little S, Orford K, Motwani M, Bai Y, Patel K, Venook AP, Kopetz S. Combined BRAF and MEK Inhibition With Dabrafenib and Trametinib in BRAF V600-Mutant Colorectal Cancer. J Clin Oncol 2015; 33: 4023-4031 [PMID: 26392102 DOI: 10.1200/JCO.2015.63.2471]
42 Yaeger R, Cercek A, O’Reilly EM, Reidy DL, Kemeny N, Wolinsky T, Capanu M, gollub MJ, Rosen N, Berger MF, Lacouture ME, Vakiani E, Saltz LB. Pilot trial of combined BRAF and EgFR inhibition in BRAF-mutant metastatic colorectal cancer patients. Clin Cancer Res 2015; 21: 1313-1320 [PMID: 25589621 DOI: 10.1158/1078-0432.CCR-14-2779]
43 Hong DS, Morris VK, Fu S, Overman MJ, Piha-Paul SA, Kee BK, Zinner R, Fogelman DR, Mistry R, Shureiqi I, Meric-Bernstam F, Kopetz S. Phase 1B study of vemurafenib in combination with irinotecan and cetuximab in patients with BRAF-mutated advanced cancers and metastatic colorectal cancer. J Clin Oncol 2014; 32: 3516
44 Tabernero J, Chan E, Baselga J, Blay J-Y, Chau I, Hyman D, Raje N, Wolf J, Sirzen F, Veronese L, Mitchell L, Hidalgo M. VE-BASKET, a Simon 2-stage adaptive design, phase II, histology-independent study in nonmelanoma solid tumors harboring BRAF V600 mutations (V600m): Activity of vemurafenib (VEM) with or without cetuximab (CTX) in colorectal cancer (CRC). J Clin Oncol 2014; 32: 3518
45 Atreya CE, Van Cutsem E, Bendell JC, Schellens JHM, gordon MS, McRee A, O’Dwyer PJ, Muro K, Tabernero J, Van geel R, Sidhu R, greger Jg, Rangwala FA, Motwani M, Wu Y, Orford K, Corcoran RB. Updated efficacy of the MEK inhibitor trametinib (T), BRAF inhibitor dabrafenib (D), and anti-EgFR antibody panitumumab (P) in patients (pts) with BRAF V600E mutated (BRAFm) metastatic colorectal cancer (mCRC). J Clin Oncol 2015; 33: 103
46 Cancer Genome Atlas Network. Comprehensive molecular characterization of human colon and rectal cancer. Nature 2012; 487: 330-337 [PMID: 22810696 DOI: 10.1038/nature11252]
47 El-Deiry WS, Vijayvergia N, Xiu J, Scicchitano A, Lim B, Yee NS, Harvey HA, gatalica Z, Reddy S. Molecular profiling of 6,892 colorectal cancer samples suggests different possible treatment options specific to metastatic sites. Cancer Biol Ther 2015; 16: 1726-1737 [PMID: 26553611 DOI: 10.1080/15384047.2015.1113356]
48 Belov AA, Mohammadi M. Molecular mechanisms of fibroblast growth factor signaling in physiology and pathology. Cold Spring Harb Perspect Biol 2013; 5: [PMID: 23732477 DOI: 10.1101/cshperspect.a015958]
49 Kouhara H, Hadari YR, Spivak-Kroizman T, Schilling J, Bar-Sagi D, Lax I, Schlessinger J. A lipid-anchored grb2-binding protein that links FgF-receptor activation to the Ras/MAPK signaling pathway. Cell 1997; 89: 693-702 [PMID: 9182757]
50 Stevenson L, Allen WL, Turkington R, Jithesh PV, Proutski I, Stewart g, Lenz HJ, Van Schaeybroeck S, Longley DB, Johnston Pg. Identification of galanin and its receptor galR1 as novel determinants of resistance to chemotherapy and potential biomarkers in colorectal cancer. Clin Cancer Res 2012; 18: 5412-5426 [PMID: 22859720 DOI: 10.1158/1078-0432.CCR-12-1780]
51 Bange J, Prechtl D, Cheburkin Y, Specht K, Harbeck N, Schmitt M, Knyazeva T, Müller S, gärtner S, Sures I, Wang H, Imyanitov E, Häring HU, Knayzev P, Iacobelli S, Höfler H, Ullrich A. Cancer progression and tumor cell motility are associated with the FgFR4 Arg(388) allele. Cancer Res 2002; 62: 840-847 [PMID: 11830541]
52 Liu R, Li J, Xie K, Zhang T, Lei Y, Chen Y, Zhang L, Huang K,
Ahn DH et al . Colorectal cancer, genomics, targeted therapy

5676 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Wang K, Wu H, Wu M, Nice EC, Huang C, Wei Y. FgFR4 promotes stroma-induced epithelial-to-mesenchymal transition in colorectal cancer. Cancer Res 2013; 73: 5926-5935 [PMID: 23943801 DOI: 10.1158/0008-5472.CAN-12-4718]
53 Henriksson ML, Edin S, Dahlin AM, Oldenborg PA, Öberg Å, Van guelpen B, Rutegård J, Stenling R, Palmqvist R. Colorectal cancer cells activate adjacent fibroblasts resulting in FgF1/FgFR3 signaling and increased invasion. Am J Pathol 2011; 178: 1387-1394 [PMID: 21356388 DOI: 10.1016/j.ajpath.2010.12.008]
54 Turkington RC, Longley DB, Allen WL, Stevenson L, McLaughlin K, Dunne PD, Blayney JK, Salto-Tellez M, Van Schaeybroeck S, Johnston Pg. Fibroblast growth factor receptor 4 (FgFR4): a targetable regulator of drug resistance in colorectal cancer. Cell Death Dis 2014; 5: e1046 [PMID: 24503538 DOI: 10.1038/cddis.2014.10]
55 Al-Maghrabi J, Emam E, gomaa W, Saggaf M, Buhmeida A, Al-Qahtani M, Al-Ahwal M. c-MET immunostaining in colorectal carcinoma is associated with local disease recurrence. BMC Cancer 2015; 15: 676 [PMID: 26459369 DOI: 10.1186/s12885-015-1662-6]
56 Di Renzo MF, Olivero M, giacomini A, Porte H, Chastre E, Mirossay L, Nordlinger B, Bretti S, Bottardi S, giordano S. Overexpression and amplification of the met/HgF receptor gene during the progression of colorectal cancer. Clin Cancer Res 1995; 1: 147-154 [PMID: 9815967]
57 Osada S, Matsui S, Komori S, Yamada J, Sanada Y, Ihawa A, Tanaka Y, Tokuyama Y, Okumura N, Nonaka K, Hosono Y, Takahashi T, Yamaguchi K, Yoshida K. Effect of hepatocyte growth factor on progression of liver metastasis in colorectal cancer. Hepatogastroenterology 2010; 57: 76-80 [PMID: 20422876]
58 Gayyed MF, Abd El-Maqsoud NM, El-Hameed El-Heeny AA, Mohammed MF. c-MET expression in colorectal adenomas and primary carcinomas with its corresponding metastases. J Gastrointest Oncol 2015; 6: 618-627 [PMID: 26697193 DOI: 10.3978/j.issn.2078-6891.2015.072]
59 Bardelli A, Corso S, Bertotti A, Hobor S, Valtorta E, Siravegna g, Sartore-Bianchi A, Scala E, Cassingena A, Zecchin D, Apicella M, Migliardi g, galimi F, Lauricella C, Zanon C, Perera T, Veronese S, Corti g, Amatu A, gambacorta M, Diaz LA, Sausen M, Velculescu VE, Comoglio P, Trusolino L, Di Nicolantonio F, giordano S, Siena S. Amplification of the MET receptor drives resistance to anti-EgFR therapies in colorectal cancer. Cancer Discov 2013; 3: 658-673 [PMID: 23729478 DOI: 10.1158/2159-8290.CD-12-0558]
60 Liska D, Chen CT, Bachleitner-Hofmann T, Christensen Jg, Weiser MR. HgF rescues colorectal cancer cells from EgFR inhibition via MET activation. Clin Cancer Res 2011; 17: 472-482 [PMID: 21098338 DOI: 10.1158/1078-0432.CCR-10-0568]
61 Troiani T, Martinelli E, Napolitano S, Vitagliano D, Ciuffreda LP, Costantino S, Morgillo F, Capasso A, Sforza V, Nappi A, De Palma R, D’Aiuto E, Berrino L, Bianco R, Ciardiello F. Increased TGF-α as a mechanism of acquired resistance to the anti-EgFR inhibitor cetuximab through EgFR-MET interaction and activation of MET signaling in colon cancer cells. Clin Cancer Res 2013; 19: 6751-6765 [PMID: 24122793 DOI: 10.1158/1078-0432.CCR-13-0423]
62 Yonesaka K, Satoh T, Ueda S, Yoshida T, Takeda M, Shimizu T, Okamoto I, Nishio K, Tamura T, Nakagawa K. Circulating hepatocyte growth factor is correlated with resistance to cetuximab in metastatic colorectal cancer. Anticancer Res 2015; 35: 1683-1689 [PMID: 25750328]
63 Sun Y, Sun L, An Y, Shen X. Cabozantinib, a Novel c-Met Inhibitor, Inhibits Colorectal Cancer Development in a Xenograft Model. Med Sci Monit 2015; 21: 2316-2321 [PMID: 26255947 DOI: 10.12659/MSM.893590]
64 Song EK, Tai WM, Messersmith WA, Bagby S, Purkey A, Quackenbush KS, Pitts TM, Wang g, Blatchford P, Yahn R, Kaplan J, Tan AC, Atreya CE, Eckhardt g, Kelley RK, Venook A, Kwak EL, Ryan D, Arcaroli JJ. Potent antitumor activity of cabozantinib, a c-MET and VEgFR2 inhibitor, in a colorectal cancer patient-derived tumor explant model. Int J Cancer 2015; 136: 1967-1975 [PMID: 25242168 DOI: 10.1002/ijc.29225]
65 Runeberg-Roos P, Saarma M. Neurotrophic factor receptor RET:
structure, cell biology, and inherited diseases. Ann Med 2007; 39: 572-580 [PMID: 17934909 DOI: 10.1080/07853890701646256]
66 Arighi E, Borrello Mg, Sariola H. RET tyrosine kinase signaling in development and cancer. Cytokine Growth Factor Rev 2005; 16: 441-467 [PMID: 15982921 DOI: 10.1016/j.cytogfr.2005.05.010]
67 Phay JE, Shah MH. Targeting RET receptor tyrosine kinase activation in cancer. Clin Cancer Res 2010; 16: 5936-5941 [PMID: 20930041 DOI: 10.1158/1078-0432.CCR-09-0786]
68 Luo Y, Tsuchiya KD, Il Park D, Fausel R, Kanngurn S, Welcsh P, Dzieciatkowski S, Wang J, grady WM. RET is a potential tumor suppressor gene in colorectal cancer. Oncogene 2013; 32: 2037-2047 [PMID: 22751117 DOI: 10.1038/onc.2012.225]
69 Mokarram P, Kumar K, Brim H, Naghibalhossaini F, Saberi-firoozi M, Nouraie M, green R, Lee E, Smoot DT, Ashktorab H. Distinct high-profile methylated genes in colorectal cancer. PLoS One 2009; 4: e7012 [PMID: 19750230 DOI: 10.1371/journal.pone.0007012]
70 Le Rolle AF, Klempner SJ, garrett CR, Seery T, Sanford EM, Balasubramanian S, Ross JS, Stephens PJ, Miller VA, Ali SM, Chiu VK. Identification and characterization of RET fusions in advanced colorectal cancer. Oncotarget 2015; 6: 28929-28937 [PMID: 26078337 DOI: 10.18632/oncotarget.4325]
71 Seshagiri S, Stawiski EW, Durinck S, Modrusan Z, Storm EE, Conboy CB, Chaudhuri S, guan Y, Janakiraman V, Jaiswal BS, guillory J, Ha C, Dijkgraaf gJ, Stinson J, gnad F, Huntley MA, Degenhardt JD, Haverty PM, Bourgon R, Wang W, Koeppen H, gentleman R, Starr TK, Zhang Z, Largaespada DA, Wu TD, de Sauvage FJ. Recurrent R-spondin fusions in colon cancer. Nature 2012; 488: 660-664 [PMID: 22895193 DOI: 10.1038/nature11282]
72 Brannon AR, Vakiani E, Sylvester BE, Scott SN, McDermott g, Shah RH, Kania K, Viale A, Oschwald DM, Vacic V, Emde AK, Cercek A, Yaeger R, Kemeny NE, Saltz LB, Shia J, D’Angelica MI, Weiser MR, Solit DB, Berger MF. Comparative sequencing analysis reveals high genomic concordance between matched primary and metastatic colorectal cancer lesions. Genome Biol 2014; 15: 454 [PMID: 25164765 DOI: 10.1186/s13059-014-0454-7]
73 Grothey A, Van Cutsem E, Sobrero A, Siena S, Falcone A, Ychou M, Humblet Y, Bouché O, Mineur L, Barone C, Adenis A, Tabernero J, Yoshino T, Lenz HJ, goldberg RM, Sargent DJ, Cihon F, Cupit L, Wagner A, Laurent D. Regorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): an international, multicentre, randomised, placebo-controlled, phase 3 trial. Lancet 2013; 381: 303-312 [PMID: 23177514 DOI: 10.1016/S0140-6736(12)61900-X]
74 Wilhelm SM, Dumas J, Adnane L, Lynch M, Carter CA, Schütz g, Thierauch KH, Zopf D. Regorafenib (BAY 73-4506): a new oral multikinase inhibitor of angiogenic, stromal and oncogenic receptor tyrosine kinases with potent preclinical antitumor activity. Int J Cancer 2011; 129: 245-255 [PMID: 21170960 DOI: 10.1002/ijc.25864]
75 Verma S, Miles D, gianni L, Krop IE, Welslau M, Baselga J, Pegram M, Oh DY, Diéras V, guardino E, Fang L, Lu MW, Olsen S, Blackwell K. Trastuzumab emtansine for HER2-positive advanced breast cancer. N Engl J Med 2012; 367: 1783-1791 [PMID: 23020162 DOI: 10.1056/NEJMoa1209124]
76 Bang YJ, Van Cutsem E, Feyereislova A, Chung HC, Shen L, Sawaki A, Lordick F, Ohtsu A, Omuro Y, Satoh T, Aprile g, Kulikov E, Hill J, Lehle M, Rüschoff J, Kang YK. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (TogA): a phase 3, open-label, randomised controlled trial. Lancet 2010; 376: 687-697 [PMID: 20728210 DOI: 10.1016/S0140-6736(10)61121-X]
77 Janjigian YY, Werner D, Pauligk C, Steinmetz K, Kelsen DP, Jäger E, Altmannsberger HM, Robinson E, Tafe LJ, Tang LH, Shah MA, Al-Batran SE. Prognosis of metastatic gastric and gastroesophageal junction cancer by HER2 status: a European and USA International collaborative analysis. Ann Oncol 2012; 23: 2656-2662 [PMID: 22689179 DOI: 10.1093/annonc/mds104]
78 Kavuri SM, Jain N, galimi F, Cottino F, Leto SM, Migliardi g,
Ahn DH et al . Colorectal cancer, genomics, targeted therapy

5677 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Searleman AC, Shen W, Monsey J, Trusolino L, Jacobs SA, Bertotti A, Bose R. HER2 activating mutations are targets for colorectal cancer treatment. Cancer Discov 2015; 5: 832-841 [PMID: 26243863 DOI: 10.1158/2159-8290.CD-14-1211]
79 Siena S, Sartore-Bianchi A, Lonardi S, Trusolino L, Martino C, Bencardino K, Leone F, Zagonel V, Valtorta V, Torri V, Siravegna g, Amatu A, Bonazzina E, Rusconi F, ghezzi S, Ciardiello D, Veronese S, Comoglio P, Bardelli A, Marsoni S. Trastuzumab and lapatinib in HER2-amplified metastatic colorectal cancer patients (mCRC): The HERACLES trial. J Clin Oncol 2015; 33: 3508
80 Parsons R, Li gM, Longley MJ, Fang WH, Papadopoulos N, Jen J, de la Chapelle A, Kinzler KW, Vogelstein B, Modrich P. Hypermutability and mismatch repair deficiency in RER+ tumor cells. Cell 1993; 75: 1227-1236 [PMID: 8261516]
81 Hampel H, Frankel WL, Martin E, Arnold M, Khanduja K, Kuebler P, Nakagawa H, Sotamaa K, Prior TW, Westman J, Panescu J, Fix D, Lockman J, Comeras I, de la Chapelle A. Screening for the Lynch syndrome (hereditary nonpolyposis colorectal cancer). N Engl J Med 2005; 352: 1851-1860 [PMID: 15872200 DOI: 10.1056/NEJMoa043146]
82 Ligtenberg MJ, Kuiper RP, Chan TL, goossens M, Hebeda
KM, Voorendt M, Lee TY, Bodmer D, Hoenselaar E, Hendriks-Cornelissen SJ, Tsui WY, Kong CK, Brunner Hg, van Kessel Ag, Yuen ST, van Krieken JH, Leung SY, Hoogerbrugge N. Heritable somatic methylation and inactivation of MSH2 in families with Lynch syndrome due to deletion of the 3’ exons of TACSTD1. Nat Genet 2009; 41: 112-117 [PMID: 19098912 DOI: 10.1038/ng.283]
83 Le DT, Uram JN, Wang H, Bartlett BR, Kemberling H, Eyring AD, Skora AD, Luber BS, Azad NS, Laheru D, Biedrzycki B, Donehower RC, Zaheer A, Fisher gA, Crocenzi TS, Lee JJ, Duffy SM, goldberg RM, de la Chapelle A, Koshiji M, Bhaijee F, Huebner T, Hruban RH, Wood LD, Cuka N, Pardoll DM, Papadopoulos N, Kinzler KW, Zhou S, Cornish TC, Taube JM, Anders RA, Eshleman JR, Vogelstein B, Diaz LA. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N Engl J Med 2015; 372: 2509-2520 [PMID: 26028255 DOI: 10.1056/NEJMoa1500596]
84 Fleischhacker M, Schmidt B. Circulating nucleic acids (CNAs) and cancer--a survey. Biochim Biophys Acta 2007; 1775: 181-232 [PMID: 17137717 DOI: 10.1016/j.bbcan.2006.10.001]
85 Alix-Panabières C, Schwarzenbach H, Pantel K. Circulating tumor cells and circulating tumor DNA. Annu Rev Med 2012; 63: 199-215 [PMID: 22053740 DOI: 10.1146/annurev-med-062310-094219]
P- Reviewer: Cecchin E, Li YY, Meshikhes AW S- Editor: gong ZM L- Editor: A E- Editor: Wang CH
Ahn DH et al . Colorectal cancer, genomics, targeted therapy

detection using effective screening approaches, selection of appropriate therapeutic strategies and efficient follow-up programs are essential to reduce CRC mortalities. Biomarker discovery for CRC based on the personalized genotype and clinical information could facilitate the classification of patients with certain types and stages of cancer to tailor preventive and therapeutic approaches. These cancer-related biomarkers should be highly sensitive and specific in a wide range of specimen(s) (including tumor tissues, patients’ fluids or stool). Reliable biomarkers which enable the early detection of CRC, can improve early diagnosis, prognosis, treatment response prediction, and recurrence risk. Advances in our understanding of the natural history of CRC have led to the development of different CRC associated molecular and cellular biomarkers. This review highlights the new trends and approaches in CRC biomarker discovery, which could be potentially used for early diagnosis, development of new therapeutic approaches and follow-up of patients.
Key words: Colorectal cancer; Biomarkers; Cancer diagnosis; Cancer therapy; Predictive marker; Prognostic marker
© The Author(s) 2016. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Colorectal cancer (CRC) is one of the most common leading causes of cancer death in the world; therefore, any attempt in early diagnosis, selection of appropriate therapeutic strategies and efficient follow up can play an important role in reducing the disease related mortalities. Our review highlights the novel trends and approaches in CRC biomarker discovery, which are categorized as pathologic genetic or epigenetic changes within the tumor tissue as well as non-invasive biomarkers such as blood or stool based markers. These biomarkers could be used for the management of cancer patients.
Parisa Aghagolzadeh, Ramin Radpour, Department of Clinical Research, University Hospital of Bern, 3010 Bern, Switzerland
Author contributions: Aghagolzadeh R and Radpour R wrote the paper.
Conflict-of-interest statement: There is no conflict of interest.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Manuscript source: Invited manuscript
Correspondence to: Ramin Radpour, PhD, Department of Clinical Research, University Hospital of Bern, Murtenstrasse 35, 3010 Bern, Switzerland. [email protected]: +41-31-6320956Fax: +41-31-6323297
Received: March 21, 2016 Peer-review started: March 22, 2016First decision: May 12, 2016Revised: May 16, 2016Accepted: June 15, 2016 Article in press: June 15, 2016Published online: July 7, 2016
AbstractColorectal cancer (CRC) is the third leading cause of cancer death worldwide, which is consequence of multistep tumorigenesis of several genetic and epigenetic events. Since CRC is mostly asymptomatic until it progresses to advanced stages, the early
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.3748/wjg.v22.i25.5678
5678 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
World J Gastroenterol 2016 July 7; 22(25): 5678-5693 ISSN 1007-9327 (print) ISSN 2219-2840 (online)
© 2016 Baishideng Publishing Group Inc. All rights reserved.
Parisa Aghagolzadeh, Ramin Radpour
TOPIC HIGHLIGHT
New trends in molecular and cellular biomarker discovery for colorectal cancer
2016 Colorectal Cancer: Global view

Aghagolzadeh P, Radpour R. New trends in molecular and cellular biomarker discovery for colorectal cancer. World J Gastroenterol 2016; 22(25): 5678-5693 Available from: URL: http://www.wjgnet.com/1007-9327/full/v22/i25/5678.htm DOI: http://dx.doi.org/10.3748/wjg.v22.i25.5678
INTRODUCTIONColorectal cancer (CRC) is the third most common cancer worldwide and which is considered for 10% of new cancer diagnoses[1,2]. More than 10% of patients diagnosed with CRC, already have reached to the advanced stages of disease and could show metastasis to the other tissues and organs. Furthermore, about 30% of diagnosed patients with early-stage CRC, have the potential to develop metastatic disease[3].
CRC can be gradually developed through an accumulation of different somatic or inherited changes within genome and epigenome. These pathologic changes lead to the transformation of colonic mucosa into invasive cancer[4]. There are three most important molecular pathways leading to CRC development: (1) Somatic or germ line derived genomic instability due to inactivation of several tumor suppressor genes such as APC, SMAD4 and TP53; aberrant DNA methylation, DNA repair defects induced by mutations in mismatch repair genes (MMR); (2) Mutational inactivation of tumor suppressor genes (e.g., APC, TP53, TGFb, and MMR genes); and (3) Over activation of oncogenic pathways including BRAF, RAS (KRAS and NRAS), Phosphatidyl inositol 3-kinase (PIK-3)[5]. The growth and proliferation of metastatic CRC (mCRC) mainly depends on two signaling pathways: the vascular endothelial growth factor (VEGF) and the epidermal growth factor receptor (EGFR) pathways[6].
The risk of CRC increases with the higher age, as well as by carrying certain inherited genetic mutations (familial adenomatous polyposis and hereditary non-polyposis CRC)[7], a personal or family history of colorectal neoplasia, or having inflammatory bowel disease (IBD)[8].
Cancer related molecular and cellular markers can be classified in four groups: (1) Diagnostic markers, used for risk stratification and early detection; (2) Prognostic markers, give an indication of the likely progression of the disease; (3) Predictive markers, predict treatment response; and (4) Surveillance markers, used to monitor disease recurrence[9].
The increasing disease associated morbidity and mortality, is in part due to a lack of efficient early detection; therefore, earlier diagnosis and more efficient treatment could play a key role in reducing CRC mortality. The conventional examination techniques such as colonoscopy, are invasive; therefore, can affect the patients’ willingness for participation in screening programs. Our increasing knowledge about molecular and cellular mechanisms of CRC development, could
provide better objectives for management of the cancer patients using different potential biomarkers. Several marker classes have been evaluated for their use in CRC screening and have all shown potential in early phase biomarker studies (Figure 1). Importan-tly, non-invasive biomarkers derived from biological fluids (blood- or stool-based markers), due to their easy accessibility, could be considered as practical tools for CRC detection and monitoring (Figure 2A). Reliable biomarkers for early detection of CRC, could significantly improve patient prognosis, prediction of treatment response, and possible prediction of recurrence risk (Table 1). Figure 2B, illustrates the approved pipelines for CRC biomarker discovery and validation.
MICROSATELLITE INSTABILITYMicrosatellites are repeating units of DNA sequences (usually 1-6bp in length) that can be found in both non-coding or protein coding sequences of DNA. Microsatellite instability (MSI) is defined as somatic alterations in microsatellite sequences due to the insertion or deletion of those repeat units leading to genomic instability and subsequently increasing the susceptibility for the malformations. Tumors with 10%-29% of unstable microsatellite loci are considered MSI-low (MSI-L) while tumors showing ≥ 30% of unstable microsatellite loci are known as MSI-high (MSI-H).
MSI generally results from inactivation of the MMR genes through aberrant promoter hypermethylation (80% of MSI CRCs) or mutations in the genes MLH1, MSH2, MSH6, and PMS2 (20% of MSI CRCs)[10]. Inactivation of these genes results in the accumulation of DNA replication errors in microsatellite sequences, importantly those are located in the exons of potential tumor suppressor genes. In sporadic CRC, 10%-15% of tumors display MSI-high. The MLH1 gene silencing due to the aberrant DNA methylation is responsible for the majority of sporadic CRC with MSI-high[11,12]. A recent meta-analysis assessing the prognostic im-portance of the MSI in > 7500 patients, could show MSI-H tumors had a better prognosis than MSI-L tumors[13].
Currently, in order to detect MSI in CRC, a specific microsatellite screening panel (Bat-25, Bat-26, MONO-27, NR-21, and NR-24) is used by different clinical laboratories. Therefore, MSI status can serve as a useful predictive and prognostic biomarker for the CRC.
CHROMOSOMAL INSTABILITYChromosomal instability (CIN) is defined as the presence of multiple structural or numerical chromosome changes (losses or gains of large portions or whole of the chro-mosomes) within tumor cells resulting karyotypic
5679 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Aghagolzadeh P et al . Molecular and cellular biomarkers for CRC

variability[14]. CIN is the most common form of genetic instability in CRC that present in about 65%-70% of CRCs. The consequence of chromosomal instability is numerical imbalance for chromosomes (aneuploidy), sub-chromosomal amplifications, and also loss of heterozygosity (LOH).
DNA MUTATIONS AS BIOMARKERRecent data derived from many large-scale high-throughput DNA sequencing approaches, have identified different candidate genes which could have functional roles in the initiation and development of various human cancers[15,16]. Most of these mutations and genetic alterations occur at a relatively low frequency, while some are present in a high portion of tumors.
Analysis of somatic alterations in CRCs by the Cancer Genome Atlas included whole-genome sequencing that identified 24 significantly mutated genes. Commonly observed alterations enable a broad classification into (1) hypermutated tumors (about 15%), of which three-quarters show high-frequency
MSI (MSI-H) and one-quarter have somatic mutations in MMR genes and polymerase-ε (POLE) mutations; and (2) nonhypermutated tumors (about 85%) with multiple somatic copy number alterations and aneuploidy that contain activating mutations in KRAS and PIK3CA and loss of heterozygosity of APC and TP53 tumor-suppressor genes[17].
KRAS GENE MUTATIONSKRAS, a GTPase protein, is encoded by KRAS proto-oncogene, which is an early player in many biological pathways. Different point mutations in codons 12 and 13 of exon 2, or mutations in codon 61 of exon 3, lead to constitutive activation of RAS signaling pathway. Therefore, genetic disruption of the KRAS gene is one of the essential steps in development of many cancers including CRC.
KRAS is mutated in 30%-50% cases of CRC[18]. According to studies, the adverse impact of KRAS mutations on prognosis seems to be stronger in the distal compared with the proximal colon cancers[19]. More than 30% of CRCs carry mutations in exon 2 of
5680 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Figure 1 Different classes of colorectal cancer associated molecular and cellular biomarkers.
Aghagolzadeh P et al . Molecular and cellular biomarkers for CRC
Microsatelliteinstability (MSI)
Chromosomalinstability (CIN)
DNAmutation
Tumor specificmiR expression
patterns
Angiogenesisbiomarkers
Inflammatorybiomarkers
Non-invasivebiomarkers
(blood and stool)
Telomere lengthdynamics
Tumor specificgene expression
patterns
DNAmethylation
Lymph nodes Blood vessel
Metastasis
CRC development stages
Stage 0StageⅠ
Stage Ⅱ
Stage Ⅲ
Stage Ⅳ
Transverse colon Left
splenicflexure
Descendingcolon
Sigmoid colon
RectumAppendix
Cecum
Ascendingcolon
Righthepaticflexure

5681 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
protein kinases can activate MEK family proteins (including MEK1 and MEK2), which can further phosphorylate ERK1 and ERK2 proteins. ERK controls cell cycle process via regulating enzymes such as Cyclin D1[24]. BRAF is the direct downstream effector of KRAS within the Ras/Raf/MAPK signaling pathway. BRAF gene mutation is reported to be associated with CRC development and also with the poor prognosis of patients[25,26]. Based on the previous studies, BRAF gene mutations is associated with aging, female gender, proximal colon location, poor differentiation, mucinous histology, infiltrating lymphocytes and advanced stage of disease[27]. BRAF mutations occur more frequently in MSI-H cases of CRC[28].
A subset (about 8%) of CRCs carry a point mutation (V600E) in the BRAF oncogene that is mutually exclusive with mutation in KRAS[29]. Patients whose tumors carry BRAFV600E mutations have been consistently shown to have a poor prognosis in the metastatic setting[30]. In contrast to patients with BRAFV600 mutant melanoma[31],
KRAS, and an additional 15% of tumors were found to carry mutations at exons 3 and 4 of KRAS and also exons 2, 3, and exon 4 of NRAS gene[20-22].
Mutations detected in the KRAS gene is one of the most utilized predictive marker for response to the anti-EGFR antibody-based therapies using cetuximab and panitumumab[23]. In addition, approximately 60%-70% of metastatic CRC patients with no KRAS mutations, show poor response to EGFR antibody therapy, which highlights the contribution of additional mutations in different genes such as NRAS in resistance to anti-EGFR treatment[20]. Therefore, the expanded RAS (KRAS and NRAS) mutation screening is now recommended for all cancer patients before anti-EGFR antibody treatment.
BRAF GENE MUTATIONSThe Raf genes family includes three different serine/threonine kinases (ARAF, BRAF, and RAF1). These
Figure 2 Schematic view of biomarker secretion during different stages of colorectal cancer development (blood and stool biomarkers) (A) and pipelines of biomarker discovery for colorectal cancer (B).
Aghagolzadeh P et al . Molecular and cellular biomarkers for CRC
Plasma/Sera markers (vascular invasion)
Stages 0StagesⅠ
Stages Ⅱ
Stages Ⅲ
Stages Ⅳ
Metastasis
Stool markers (exfoliation)
Besic research Translational research Clinical aproval
Discovery Qualification Verification Validation
Number of analysis
Number of samples(large cohorts, quality assured samples)
Different OMICs approaches:Genomics EpigenomicsTranscriptomicsProteomicsMetabolomicsImaging technologies
Indegrated technologies
Multi-dimentional analysis
High-throughput assays
Development of clinical assays
Clinical assays andLarge cohort studies
A
B

5682 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
CRCs which harbor BRAFV600E mutations were found to be resistant to inhibition of the BRAF/MEK/ERK signaling pathway by vemurafenib[32]. Resistance to vemurafenib was later found to be caused by feedback activation of EGFR when BRAF is inhibited[33]. This finding has led to ongoing clinical trials that investigate combinations
of inhibitors of BRAF, EGFR, and MEK with or without chemotherapy[34].
TP53 GENE MUTATIONSTP53 gene is a very important tumor suppressor which
Table 1 Associated biomarkers for colorectal cancer and their predictive value
Biomarkers Molecular basis Predictive value Detection method
Category Type
Pathological characteristics
Tumor stage Diagnostic, prognostic and predictive markers
Diagnostic radiology and pathological/cytological
examinationLymph node statusGrade of differentiationAnatomy of invasion
Proliferation markers
Ki67 Nuclear antigen associated with proliferation
Diagnostic and prognostic markers
IHC
Cyclins Regulation of cell cycle phase transition Diagnostic and prognostic markers
IHC
Chromosome abnormalities
p53 Tumor suppressor gene which shows loss of function
Diagnostic, prognostic and predictive markers
IHC, RT-PCR, FISH
H-ras, K-ras, N-ras Membrane-associated GTPase integral to signal transduction cascade, if mutated, causes increased cellular proliferation
Diagnostic, prognostic and predictive markers
IHC, RT-PCR, FISH
Telomere length Pathologic telomere length dynamics Diagnostic and prognostic markers
RT-PCR, Flow cytometry
Telomerase activity Maintenance of telomeres and therefore chromosomal length
Diagnostic and prognostic markers
TRAP assay
enables progression through successive cell cycles
Hypoxia-regulated genes
HIF-1 HIF-1 transcription factor complex stabilized in hypoxic conditions,
leading to transcription of hypoxia-regulated genes
Diagnostic and prognostic markers
IHC
Glut-1 Increased Glut-1 expression caused by malignant transformation and
upregulated by hypoxia. Promotes switch to anaerobic glycolysis to
support hypoxic tumor
Diagnostic and prognostic markers
IHC
Angiogenesis VEGF Angiogenic growth factor Prognostic and predictive markers
IHC, FISH, immunoassay
PD-ECGF Angiogenic growth factor with thymidine phosphorylase activity
Prognostic and predictive markers
IHC
Vascularity New vasculature supports tumor growth
Prognostic and predictive markers
IHC staining for endothelial receptors e.g., CD31, CD34, von Willebrand (factor VIII)
combined with measurement of ICD or MVD using digital image
analysis techniquesEpigenetics Aberrant DNA
hypermethylationInactivation of key tumor suppressor genes including APC, ATM, BMP3, CDKN2A, SFRP2, GATA4, GSTP1,
HLTF, MLH1, MGMT, NDRG4, RASSF2A, SFRP2, TFPI2, VIM, and
WIF1
Diagnostic, prognostic and predictive markers
PCR-based methods and Pyrosequencing
Aberrant DNA hypomethylation
Lids to chromosomal instability and global loss of imprinting
Diagnostic and prognostic markers
PCR based methods and Pyrosequencing
Tumor specific expression patterns
Gene expression patterns
Unique signature of the dysregulated genes/pathways at different forms and
stages of CRC
Diagnostic, prognostic and predictive markers
Array-based methods, NGS, RT-PCR
MicroRNA expression patterns
Unique signature of the dysregulated microRNAs at different forms and
stages of CRC
Diagnostic, prognostic and predictive markers
Array-based methods, NGS, RT-PCR
FISH: Fluorescent in-situ hybridization; HIF-1: Hypoxia inducible factor-1; HPLC: High pressure liquid chromatography; ICD: Intercapillary distance; IGF-1: Insulin growth factor-1; IHC: Immunohistochemistry; MVD: Microvessel density; NGS: Next generation sequencing; PD-ECGF: Plateletderived endothelial cell growth factor; RT-PCR: Reverse transcription–polymerase chain reaction; RIA: Radioimmunoassay; VEGF: Vascular endothelial growth factor.
Aghagolzadeh P et al . Molecular and cellular biomarkers for CRC

5683 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
plays a role as a central regulator of different cellular processes including growth arrest and apoptosis, DNA damage, responses to stress, oxidative stress and aberrant proliferative signals[35]. TP53 stops cell cycle in damaged cells until alteration is properly repaired, otherwise it triggers the apoptosis cascade in those damaged cells.
TP53 protein dysfunction is one of the common hallmarks of human solid tumors which has been reported in more than 25% of adenomas, and in 50%-70% of patients with CRCs. TP53 dysfunction is also playing a critical role in the adenoma to carcinoma transition[36]. The majority (about 80%) of TP53 gene mutations are missense mutations leading to the synthesis of a dysfunctional protein with an abnormally long half-life. Those missense mutations mainly occur within five hotspot codons (175, 245, 248, 273, and 282)[37]. Different TP53 mutations are also reported in more than half of sporadic CRC patients[38].
APC/b-CATENIN MUTATIONSGenetic disruption of APC leading to the activation of Wnt pathway, is one of the important early genetic event in colorectal tumorigenesis[39]. The APC gene product is a large protein that regulates development, chromosomal segregation, cellular differentiation, polarity, adhesion, migration, and also apoptosis. The APC protein is interacting with glycogen synthase kinase-3b (GSK-3b ) and b-catenin (an important molecule of the Wnt pathway). Germline APC mu-tations are the cause for FAP (familial adenomatous polyposis)[40]. Somatic mutations in the APC gene are observed in 30%-70% of sporadic adenomas, and in around 70% of sporadic tumors[41]. These somatic mutations are mainly found between codons 1286 to 1513 (known as the mutation cluster region), while germline mutations are distributed throughout the entire gene[42]. As an alternative mechanism for APC gene dysfunction, APC promoter hypermethylation is also reported in more than 18% of primary colorectal carcinomas and adenomas[43].
DNA METHYLATION The most widely studied epigenetic alteration in cancer is aberrant DNA methylation. DNA methylation is one of the important epigenetic modifications that can regulate gene expression. In humans, DNA methylation occurs at cytosine residues that precede guanines, called CpG dinucleotides (C-phosphodiester-G)[44,45].
Recently, along with a growing understanding of cellular epigenetic mechanisms, the role of pathologic epigenetics changes in human cancer became more visible[46]. It is becoming more evident that epigenetic events might be central to the cancer initiation and progression[44,45,47-52].
ABERRANT DNA HYPERMETHYLATION IN CRCHypermethylation of promoter regions leading to gene silencing, is frequently found in different types of human cancers[45,50]. Recently a third class of CRCs characterized by a high frequency of DNA hyper-methylation has been reported. These cancers have been defined as having a “CpG island methylator phenotype (CIMP)”. Weisenberger et al[53] could show CIMP in CRC, is based on the methylation status of five genes (CACNA1G, IGF2, NEUROG1, RUNX3, and SOCS1). CIMP-positive tumors exhibit unique clinicopathological and molecular features, including a predilection for proximal location in the colon, poor and mucinous histology and the presence of frequent KRAS and BRAF mutations[54]. Approximately, 80% of sporadic CRCs with MSI-H harbor biallelic hypermethylated MLH1 alleles[53]. The transition from normal mucosa to adenomatous polyp is marked by both genetic and epigenetic alterations, which dysregulate important molecular pathways[55]. These epigenetic alterations include hypermethylation of a variety of genes, such as SLC5A8, ITGA4, SFRP2, PTCH1, CDKN2A, HLTF, and MGMT, and some of these play a role in the initiation and progression of adenomas to CRC[56,57].
To date, a large number of hypermethylated genes including APC, ATM, BMP3, CDKN2A, SFRP2, GATA4, GSTP1, HLTF, MLH1, MGMT, NDRG4, RASSF2A, SFRP2, TFPI2, VIM, and WIF1, have been found in stool DNA assays for the early detection of CRC[58].
The SEPT9 gene methylation assay has recently been developed as a novel blood-based test for CRC (Epi proColon 2.0, Epigenomics AG, Germany). Septins are a family of conserved GTP-binding proteins which are scaffolding proteins during compartmentalization and cell division[59]. In human, there are 13 known septin genes (SEPT1 to SEPT13). All septins can form heteromeric complexes; within terminal position of these octamer protein family, SEPT9 plays an important role in subunit stabilization and polymerization[60]. Therefore, abnormal SEPT9 or no SEPT9 may seriously affect cytokinesis. The crucial role of SEPT9 in the septin complex may be a key factor in CRC carcinogenesis when the promoter region of the SEPT9 gene is aberrantly hypermethylated and the transcription is compromised[61]. To date, several independent clinical trials have proved the aberrant SEPT9 gene methylation as a specific biomarker for CRC early detection and screening.
GENOME-WIDE DNA HYPOMETHYLATION IN CRCWhile DNA hypermethylation can silence tumor-suppressor genes, global DNA hypomethylation
Aghagolzadeh P et al . Molecular and cellular biomarkers for CRC

5684 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
can also influence CRC development by inducing chromosomal instability and global loss of im-printing[62]. Genome-wide hypomethylation occurs within repetitive transposable DNA elements, such as the long interspersed nuclear element-1 (LINE-1) or short interspersed nucleotide elements (SINE or Alu) sequences in many cancers, including CRC[63]. LINE-1 hypomethylation inversely associates with MSI-H phenotype and/or CIMP in colorectal cancer[63].
TUMOR SPECIFIC GENE EXPRESSION PATTERNSGene expression analyses of tumor derived cells/tissues in comparison to the normal tissue, reviled to a better understanding of interplay between dysregulated genes and the affected pathways in colorectal neoplasms. CRC is a very heterogenic disease and patients with even the same type of cancer, often have dissimilar genetic/epigenetic defects in their tumors which indicates why those patients respond heterogeneously to the anticancer agents. The use of DNA-microarray and next generation sequencing (NGS) technology have made it possible
to assess the expression of tens of thousands genes in a single experiment[64]. These gene-expression signatures can be used for the molecular classification of different tumors as well as cancer subtypes[65]. Those genes which their dysregulation is linked to CRC are summarized in the Figure 3.
Several groups have reported different molecular classifications of CRCs using gene expression data from NGS or expression arrays and in some cases, these subtypes could provide predictive values[66,67] or prognostic information[68,69]. Validation of a 23-gene microarray-based prognostic signature showed around 70% relapse predictive value for CRC patients[70]. High throughput gene expression profiling reveals tumor subtypes that show overlap with previous classification systems using MSI, CIN, CIMP or KRAS/BRAF mutation status[66], which cannot be identified only based on single mutations or epigenetic alterations.
TUMOR SPECIFIC MICRORNA EXPRESSION PATTERNSAbnormalities and dysregulations in non-coding regulatory RNAs can also contribute to tumorigenesis
Figure 3 Genes associated to colorectal cancer development. Dysregulation of these genes as a single or in cooperation (due to the DNA mutation, epigenetic changes or as a consequence of change in the regulatory upstream genes/pathways), has been shown in different forms and stages of colorectal cancer.
Aghagolzadeh P et al . Molecular and cellular biomarkers for CRC
Complex
Disease
Protein
Ligand
Protein kinase
Receptor
Transcription factor
MicroRNA
Protein phosphatase
Regulation
SMAD4 JUN
PPARD CDX2 FOXM1
TCF7L2 STAT3PMS2
TP53
VDR
MSH6
MUTYHMYC
PARP1
MSH2
ESR2HIF1A
PPARG
MLH1
MAPK1PRKC1
KRAS
TIAM1
CCND1
PTEN
MIF
AKT1
TYMS
MIR21
PTGER4 MET ERBB2
IGF1R TGFBR2 TLR4 CCR6
PTGS1
CTNNB1 LTF CDH1
TGFB1
VEGFC
ADIPOQ
CXCL8
PF4
MMP7
SPARC
MMP2
MMP9 GDF15
REG4 MMP1
MUC2
MMP3
HGF INS
IL17A
IGF1 TNFSF13 LEP IL6
GAST SPP1 NTN1 NTS IGFBP7
IL2 TNF VEGFA IGF2
TNFSF10
CD44 FAS DCC GHR
PTGS2 ABCB1
APC PLA2G2A CLDN1 CD82 EGFR CXCR4
PRKCBTelomerase
BCL2
BIRC5 SRC
PAK1CDKN1A FHIT
BAX NOS2
AXIN1
PIK3CABRAF
BCL2L1MTOR
PTP4A3
MTHFR
Colorectal neoplasms

5685 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
and cancer development[71,72]. A class of small cellular RNAs, termed microRNAs (miRNAs), can lead to silencing of their cognate target genes. MicroRNAs are key players in regulating diverse cellular pathways.
It is known that some miRNAs can function either as tumor suppressors or oncogene[72,73], and expression profiling of microRNAs have revealed the characteristic signatures of these small regulatory RNAs in different cancers including colorectal cancer[71,74].
Recently, the interest for miRNA biomarker re-search in human cancer has increased due to the unique characteristics of miRNAs. First, miRNAs are remarkably stable under a variety of experimental and laboratory conditions. Second, due to their small size and the hairpin-loop structure, miRNAs are protected from RNase-mediated degradation, and thus are easily extractable from a wide variety of clinical specimens, including formalin-fixed paraffin embedded (FFPE) tissues, and a variety of body fluids including blood, saliva, urine, feces etc. Third, cell-free miRNAs are often protected from degradation because of being in high density lipoprotein particles, apoptotic bodies, microvesicles, and exosomes[75].
MiRNAs can have a critical role in invasion, mi-gration and the progression of disease through epi-thelial mesenchymal transition (EMT) into metastases. Therefore, dysregulation of several miRNAs have been reported at different stages of CRC development and progress. More than 500 differentially expressed miRNAs have been associated with different stages of CRC. MiRNAs such as miR-20a, miR-21, miR-29a, miR-31, miR-34a, miR-92a, miR-200c, miR-215 and miR-375 were the most frequently dysregulated in CRC. Recent experimental analyses have validated a total of 530 miRNA-mRNA pairs in colorectal cancer, 200 unique miRNAs and 347 unique targets[76]. In BRAF mutated forms of CRC, a high expression of miR-31 was observed and suggested as a potential diagnostic/therapeutic biomarker[77]. A signature of miR-92a, miR-375 and miR-424 could discriminate invasive carcinoma from adenoma, representing a promising biomarker for the early diagnosis of CRC. The panel of six miRNA classifier (miR-21-5p, miR- 20a-5p, miR-103a-3p, miR-106b-5p, miR-143-5p, and miR-215) has potential to distinguish between high and low risk of disease progression[76].
The functional role of miR-34a and miR-200 family members have been shown in metastatic form of CRC. In addition, miR-34a can be used as an independent predictor of recurrence among patients[78]. Overexpression of miR-622 was induced by radiotherapy in rectal cancers, causing poor response to the therapy[79]. In metastatic CRC patients with wild-type KRAS that responded to anti-EGFR therapy, profiling the panel of miR-99a, let-7c and miR-125b could have a diagnostic potential[80]. In the other hand, reduced expression of miR-181a was associated with poor clinical outcome in CRC patients treated with anti-EGFR[81]. Whereas, down regulation of the miR-7, a
direct regulator of EGFR, was reported as a prognostic biomarker for tumors were resistant to targeted anti-EGFR therapy[82].
TELOMERE LENGTH DYNAMICSTelomeres, the ends of chromosomes in mammals, are composed of a 6-bp variable repeat sequence (TTAGGG), which is added on by the telomerase and has a crucial role in maintenance of chromosomal stability[83]. Telomeric DNA (tDNA) is progressively lost during each cell division due to the end replication mispairing, oxidative damage or other end processing events[84,85].
Telomerase activity and telomere length have a crucial role in malignant transformation. In the early stage of tumorigenesis, losing the telomere sequences (telomere shortening) limits cell proliferation, and telomerase activation protects the ends of chromosome and suppresses tumorigenesis. While, in the late stages of tumorigenesis, telomere shortening triggers instability in the genome, and telomerase activation induces immortalization of cancer cells[86,87]. Figure 4 summarizes the genes that regulate telomere length and also telomerase activity. Recent data proposed that the severe genomic instability exist in telomere crisis, accelerates secondary genetic alterations that lead to carcinogenesis and indeed highlights the implication of pathologic telomere length changes in cancer pathways. Therefore, telomere length dynamics can serve as a useful indicator and biomarker in risk assessment and prediction of different stages of cancer[88-92]. Telomere dysfunction has been indicated as a negative prognostic marker in solid tumors[90,93,94].
Several studies demonstrated telomeres are shorter in CRCs compared to the adjacent normal mucosa. In addition, malignant tumors have relatively shorter telomere length than benign tumors[95-98]. Since tumors in sporadic form of CRC appear relatively later compared with the hereditary nonpolyposis colorectal cancer (HNPCC), also the number of divisions between initiation and clinical presentation in sporadic may be more than HNPCC, therefore their base line telomere lengths at initiation are likely to be shorter in sporadic form of CRC[2,90,99].
The evidence that telomeres were shorter in CRCs, even in well-differentiated tumors, suggesting the telomere length shortening as an initial event in colorectal cancer which directly reflects pathologic cell proliferation[100,101].
ANGIOGENESIS BIOMARKERSAngiogenesis, critical step in cancer progression, is a new blood vessels generation from endothelial precursor, which is mediated through a group of ligands and receptors that work together[102]. A group of glycoproteins, including the placental growth factor (PIGF) and VEGF family (VEGF-A, VEGF-B, VEGF-C,
Aghagolzadeh P et al . Molecular and cellular biomarkers for CRC

5686 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
and VEGF-D), act as effectors of angiogenesis[102,103]. Several other factors including the PIGF, fibroblast growth factor (FGF), VEGF-C, VEGF-D, angiopoietin, hypoxia-inducible factor (HIF)-1α and HIF-2α, integrin, and platelet-derived growth factor, can overlap with the angiogenesis pathway, which makes the activation or inhibition outcomes very challenging[102].
The potential value for VEGF as a prediction or prognosis biomarker for metastatic CRC has been reported[104]. It is shown that the VEGF-1154G>A and VEGF405C>1 polymorphisms were associated with improved overall survival. This finding suggested that germline variants in VEGF-dependent and -independent angiogenesis can predict survival and treatment response to the first-line bevacizumab and oxaliplatin-based chemotherapy in patients with mCRC[105]. The importance of baseline levels of VEGF and soluble VEGFR-2 (sVEGFR-2) as predictive/prognostic biomarkers was shown in two independent phase-III studies evaluating the role of cediranib, an experimental angiogenesis inhibitor, in mCRC[106].
INFLAMMATORY BIOMARKERSIn patients with the inflammatory bowel diseases, chronic inflammation was suggested as a predisposing factor to CRC and the risk for developing CRC increa-ses with longer duration of colitis. Therefore, anti-inflammatory therapies, such as 5-aminosalicylates, can significantly reduce the development of colorectal neoplasia in those patients[107].
C-reactive protein (CRP) is a very sensitive but non-specific systemic marker of inflammation. CRP is mainly produced in the liver in response to cytokines released during infection, trauma, surgery, burns, tissue infarction, advanced cancer, and chronic inflammatory conditions[108]. According to a recent study, the concentrations of CRP, might have a positive correlation to the CRC risk[109].
Interleukin-6 (IL6) secreted by the hematopoietic or non-hematopoietic cells, is a multifunctional cytokine and has a pro-inflammatory function via
binding to a soluble IL6 receptor (sIL6R) or by acting on a transmembrane type 1 cytokine receptor[110]. IL6 upregulates several acute-phase proteins such as CRP, α1-antitrypsin, fibrinogen and serum amyloid A[111]. It is shown that IL6 is significantly augmented at the colonic tumor microenvironment[112].
TNFα is another pleiotropic cytokine which is secreted in response to any tissue damage or in-fection; some reports suggesting the role of TNFα in the pathogenesis of IBD[113]. The other inflammatory biomarker, macrophage inhibitory cytokine 1, is reported to be positively associated with CRC risk[114]. Certain inflammatory biomarkers from the CRC or tumor immune reaction, may lead to generation of individualized immune vaccines.
NON-INVASIVE BIOMARKERSBlood biomarkersAs non-invasive biomarkers for the screening of colorectal cancer, particularly at early stage of the disease initiation, blood biomarkers could show very promising value. Theses blood-based markers could be also used to monitor therapeutic response in CRC patients as well as the detection of disease recurrence or relapse.
Circulating tumor cells: Circulating tumor cells (CTCs) are tumor cells (mainly cancer stem cells) derived from either primary tumors or metastases which are circulating in the peripheral blood. The presence of CTCs in blood is associated with progressive or metastatic disease. Therefore, can be used to monitor advanced stage disease in patients without other measurable surveillance markers.
The CTCs in colorectal cancer have epithelial origin with defined immunephenotype signature (CD45-, EpCAM+)[115]. Using the immunephenotype markers and sensitive cell sorting technologies, it is now possible to isolate and assess the complete genetic/epigenetic profiles of tumor derived CTCs. This holds promise for the development of more efficient
Figure 4 Genes which are involved in the telomere maintenance and telomerase activity pathway. Any dysregulation in those genes will lead to the pathologic telomere length dynamics during colorectal cancer development stages.
Aghagolzadeh P et al . Molecular and cellular biomarkers for CRC
AKT1 ABL1 TP53 ATM
TINF2 NBN RAD50 XRCC5
TERF1 TERF2 TERF2IP
Telomere maintenance
MRE11APOT1TERTTERC
DKC1HNRNPA1TEP1
TEP1m_Tel1P
Telomerase(TTAGGG)n
End of telomereEnd of telomere
(TTAGGG)n
Cell process
Complex
Protein
Protein kinase
Transcription factor
Binding Direct regulation Promoter binding Prot modificationRegulation

5687 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
personalized treatment to eliminate cancer stem cells in CRC patients.
Circulating cell-free DNA: The discovery of circulating cell-free DNA (ccf-DNA) could open up a new possibility for non-invasive analysis of tumor derived genetic material, as it can be isolated from human body fluids[116]. The potential diagnostic/prognostic values of quantifying ccf-DNA in CRC patients compared to the healthy controls, have been assessed in different studies[117]. The ccf-DNA levels in those patients, could show significantly increase within the advanced disease stages and fluctuated during chemotherapy period[118].
Many studies have investigated MSI or LOH within ccf-DNA from the plasma/sera of CRC patients as very valuable non-invasive biomarkers[119]. Different studies have reported the diagnostic/prognostic value of mutated genes within ccf-DNA[120]. The detection of mutated TP53 or KRAS genes in the ccf-DNA of CRC patients could predictive disease recurrence as well as the clinical outcome[121]. Aberrant DNA methylation can also have a diagnostic or prognostic value in the plasma/sera of CRC patients. Relying on aberrant DNA methylation markers, promoter methylation of several genes have reported as biomarkers for CRC including ALX4, APC, CDKN2A/P16h, FRP2, MLH1, NGFR, NEUROG1, P16, RUNX3, SEPT9, TMEFF2, TP53 and TPEF/HPP1[122,123].
Circulating microRNAs: Due to the stability of circulating microRNAs as well as the potential role of the microRNA dysregulation at different stages of carcinogenesis, they have the potential to serve as very promising non-invasive biomarkers for different types of human cancers[124].
As a well-characterized oncogenic miRNA, miR-21 is considered one of the promising non-invasive biomarkers for the early detection of CRC. Dysregulation of miR-21 occurs frequently at early stages of the adenoma-carcinoma sequence; miR-21 is one of the most highly expressed miRNAs in CRC; and miR-21 is highly secreted by cancer cells, which can be measured in exosomes or as free miRNAs in plasma or serum[125].
As another potential circulating microRNA, the elevated serum level of miR-92a has been reported for the advanced adenoma and CRC[126]. There are also other studies showing the elevated circulating levels of miR-17-3p and miR-29a[127]. Significantly higher expression of miR-17-92 cluster and miR-135 were found in CRC patients in comparison to healthy controls which could discriminate CRC with an overall sensitivity and specificity of 74% and 79%[128].
Plasma levels of miR-92 could distinguish patients with CRC from gastric cancer, IBD and healthy control subjects[129]. A high diagnostic accuracy has been shown by a panel of miR-409-3p, miR-7, and miR-93 in discriminating CRC from controls with more than
90% sensitivity and specificity[130].
Circulating proteins: Shed or secreted proteins from different cancer cells into the bloodstream, can be detected by different methodological approaches like enzyme-linked immunosorbent assay (ELISA) or chromatographic and mass spectrometric (MS) technologies. Different protein-based biomarkers have been reported for CRC. These protein markers include circulating carcinoembryonales antigen (CEA), carbohydrate antigens (CA19-9, CA50, CA72-4), soluble Fas ligand (FasL), p53, and VEGF[131]. Of these markers, CEA could show a strong prognostic impact in CRC patients[132].
STOOL BIOMARKERSThe presence of tumor biomarkers in stool can be attributed to secretion, exfoliation or leakage[133]. Stool-based markers come from vital and apoptotic colonocytes, shed into the colorectal lumen. Since the stool markers are directly derived from the tumor cells, assumed to be highly specific biomarkers for CRC. These stool biomarkers include stool DNA (sDNA), which can be used for checking the MSI, aberrant DNA methylation or somatic mutation for specific cancer related genes, miRNAs, protein biomarkers as well as secretory molecules and biochemical materials resulted from metabolism of cancer cell. Considering the off-site testing and non-invasiveness together with the low potential costs, stool biomarkers gets more reappraisal. Recent advances in laboratory techniques, could introduce modern generation of stool tests with higher sensitivity and specificity rates for different subgroups of the colorectal cancer. These stool biomarkers should be very sensitive with higher specificity because positive test results lead to unnecessary, potentially morbid, and costly colonoscopies[134].
Human DNA is less than 0.01% of total DNA in stool and the vast majority (99.99%) of sDNA is derived from intestine bacterial or dietary; therefore, one of the important technical challenge of sDNA testing is specific detection of methylated or mutated human DNA within a pool of nontarget DNA[135,136]. Several panels of methylated genes within sDNA have been reported for different stages of CRC, involving BMP3, CDH1, CDH13, CRBP1, CXCL12, ESR1, HLTF, ID4, IRF8, ITGA4, MINT1, MINT31, NDRG4, P14, P16, RUNX3, SFRP1, SFRP2, SLC5A8, and TIMP3[137]. These panels were differing in the marker selection, assay methods, and patient populations studied which many of them could not be further validated in the bigger cohorts.
Although several stool-based tests (fecal im-munochemical test (FIT), guaiac fecal occult blood test (gFOBT), immunological fecal occult blood test (iFOBT), and sDNA test) are clinically available for the detection of CRC, the sensitivity and specificity for tests is not sufficient due to many factors such as inconvenience
Aghagolzadeh P et al . Molecular and cellular biomarkers for CRC

5688 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
in sampling or misinterpretation. Recently, the US food and drug administration (FDA) has approved the Cologuard® test (Exact Sciences Corporation, United States). Cologuard® is a panel of multi-target sDNA test, which combines molecular tests for KRAS and b-catenin mutation, aberrantly methylated BMP3 and NDRG4 gene promoters and human hemoglobin immunochemical assay[138].
CONCLUSION
The fast growing knowledge of cancer biology, par-ticularly in the field of genetic, epigenetic and molecular cell biology, could provide valuable objectives for the early detection of different malignancies including co-lorectal cancer. The poor outcome of advanced form of CRC, has prompted the need for reliable predictive and prognostic markers.
Circulating and stool-based tumor specific markers show promising potential as biomarkers. Additional biomarkers that have clinical applicability will continue to be proposed, tested, and developed from know-ledge of the genetic and epigenetic changes in CRCs. This would facilitate more individualized treatment approaches, relying the specific molecular signature of tumors. Sequencing of individual cancer genomes that provide a comprehensive picture of driver mutations within a CRC, may become commonplace when costs for this technology are lower and rapid analytic systems are employed. This will be most beneficial with simultaneous development and use of therapies that can address the personalized findings.
Unfortunately, most of the identified biomarkers in different tumor studies, failed in the validation studies. The lack of consistency between biomarker panels within independent studies, highlights a major obstacle for the development of robust CRC biomarkers. For being able to use CRC associated biomarkers in clinical care of patients, large-scale studies are needed to identify optimal marker panels and validate those biomarkers in more cross-sectional and prospective cohort studies.
ACKNOWLEDGMENTSWe thank Dr. Hiten D. Mistry for his valuable comments and kindly proofreading the text.
REFERENCES1 Koretz RL. Malignant polyps: are they sheep in wolves’ clothing?
Ann Intern Med 1993; 118: 63-68 [PMID: 8416159]2 González-González M, Garcia JG, Montero JA, Fernandez LM,
Bengoechea O, Muñez OB, Orfao A, Sayagues JM, Fuentes M. Genomics and proteomics approaches for biomarker discovery in sporadic colorectal cancer with metastasis. Cancer Genomics Proteomics 2013; 10: 19-25 [PMID: 23382583]
3 Böckelman C, Engelmann BE, Kaprio T, Hansen TF, Glimelius B. Risk of recurrence in patients with colon cancer stage II and III: a systematic review and meta-analysis of recent literature. Acta Oncol
2015; 54: 5-16 [PMID: 25430983 DOI: 10.3109/0284186x.2014.975839]
4 Burt RW, Bishop DT, Lynch HT, Rozen P, Winawer SJ. Risk and surveillance of individuals with heritable factors for colorectal cancer. WHO Collaborating Centre for the Prevention of Colorectal Cancer. Bull World Health Organ 1990; 68: 655-665 [PMID: 2289301]
5 Markowitz SD, Bertagnolli MM. Molecular origins of cancer: Molecular basis of colorectal cancer. N Engl J Med 2009; 361: 2449-2460 [PMID: 20018966 DOI: 10.1056/NEJMra0804588]
6 Schmoll HJ, Van Cutsem E, Stein A, Valentini V, Glimelius B, Haustermans K, Nordlinger B, van de Velde CJ, Balmana J, Regula J, Nagtegaal ID, Beets-Tan RG, Arnold D, Ciardiello F, Hoff P, Kerr D, Köhne CH, Labianca R, Price T, Scheithauer W, Sobrero A, Tabernero J, Aderka D, Barroso S, Bodoky G, Douillard JY, El Ghazaly H, Gallardo J, Garin A, Glynne-Jones R, Jordan K, Meshcheryakov A, Papamichail D, Pfeiffer P, Souglakos I, Turhal S, Cervantes A. ESMO Consensus Guidelines for management of patients with colon and rectal cancer. a personalized approach to clinical decision making. Ann Oncol 2012; 23: 2479-2516 [PMID: 23012255 DOI: 10.1093/annonc/mds236]
7 Whiffin N, Hosking FJ, Farrington SM, Palles C, Dobbins SE, Zgaga L, Lloyd A, Kinnersley B, Gorman M, Tenesa A, Broderick P, Wang Y, Barclay E, Hayward C, Martin L, Buchanan DD, Win AK, Hopper J, Jenkins M, Lindor NM, Newcomb PA, Gallinger S, Conti D, Schumacher F, Casey G, Liu T, Campbell H, Lindblom A, Houlston RS, Tomlinson IP, Dunlop MG. Identification of susceptibility loci for colorectal cancer in a genome-wide meta-analysis. Hum Mol Genet 2014; 23: 4729-4737 [PMID: 24737748 DOI: 10.1093/hmg/ddu177]
8 Hawk ET, Limburg PJ, Viner JL. Epidemiology and prevention of colorectal cancer. Surg Clin North Am 2002; 82: 905-941 [PMID: 12507200]
9 van de Vijver MJ, He YD, van’t Veer LJ, Dai H, Hart AA, Voskuil DW, Schreiber GJ, Peterse JL, Roberts C, Marton MJ, Parrish M, Atsma D, Witteveen A, Glas A, Delahaye L, van der Velde T, Bartelink H, Rodenhuis S, Rutgers ET, Friend SH, Bernards R. A gene-expression signature as a predictor of survival in breast cancer. N Engl J Med 2002; 347: 1999-2009 [PMID: 12490681]
10 Ward R, Meagher A, Tomlinson I, O’Connor T, Norrie M, Wu R, Hawkins N. Microsatellite instability and the clinicopathological features of sporadic colorectal cancer. Gut 2001; 48: 821-829 [PMID: 11358903]
11 Kane MF, Loda M, Gaida GM, Lipman J, Mishra R, Goldman H, Jessup JM, Kolodner R. Methylation of the hMLH1 promoter correlates with lack of expression of hMLH1 in sporadic colon tumors and mismatch repair-defective human tumor cell lines. Cancer Res 1997; 57: 808-811 [PMID: 9041175]
12 Montazer Haghighi M, Radpour R, Aghajani K, Zali N, Molaei M, Zali MR. Four novel germline mutations in the MLH1 and PMS2 mismatch repair genes in patients with hereditary nonpolyposis colorectal cancer. Int J Colorectal Dis 2009; 24: 885-893 [PMID: 19479271 DOI: 10.1007/s00384-009-0731-1]
13 Popat S, Hubner R, Houlston RS. Systematic review of microsatellite instability and colorectal cancer prognosis. J Clin Oncol 2005; 23: 609-618 [PMID: 15659508 DOI: 10.1200/jco.2005.01.086]
14 Lengauer C, Kinzler KW, Vogelstein B. Genetic instabilities in human cancers. Nature 1998; 396: 643-649 [PMID: 9872311 DOI: 10.1038/25292]
15 Greenman C, Stephens P, Smith R, Dalgliesh GL, Hunter C, Bignell G, Davies H, Teague J, Butler A, Stevens C, Edkins S, O’Meara S, Vastrik I, Schmidt EE, Avis T, Barthorpe S, Bhamra G, Buck G, Choudhury B, Clements J, Cole J, Dicks E, Forbes S, Gray K, Halliday K, Harrison R, Hills K, Hinton J, Jenkinson A, Jones D, Menzies A, Mironenko T, Perry J, Raine K, Richardson D, Shepherd R, Small A, Tofts C, Varian J, Webb T, West S, Widaa S, Yates A, Cahill DP, Louis DN, Goldstraw P, Nicholson AG, Brasseur F, Looijenga L, Weber BL, Chiew YE, DeFazio A, Greaves MF, Green AR, Campbell P, Birney E, Easton DF, Chenevix-Trench G,
Aghagolzadeh P et al . Molecular and cellular biomarkers for CRC

5689 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Tan MH, Khoo SK, Teh BT, Yuen ST, Leung SY, Wooster R, Futreal PA, Stratton MR. Patterns of somatic mutation in human cancer genomes. Nature 2007; 446: 153-158 [PMID: 17344846]
16 Wood LD, Parsons DW, Jones S, Lin J, Sjöblom T, Leary RJ, Shen D, Boca SM, Barber T, Ptak J, Silliman N, Szabo S, Dezso Z, Ustyanksky V, Nikolskaya T, Nikolsky Y, Karchin R, Wilson PA, Kaminker JS, Zhang Z, Croshaw R, Willis J, Dawson D, Shipitsin M, Willson JK, Sukumar S, Polyak K, Park BH, Pethiyagoda CL, Pant PV, Ballinger DG, Sparks AB, Hartigan J, Smith DR, Suh E, Papadopoulos N, Buckhaults P, Markowitz SD, Parmigiani G, Kinzler KW, Velculescu VE, Vogelstein B. The genomic landscapes of human breast and colorectal cancers. Science 2007; 318: 1108-1113 [PMID: 17932254]
17 Cancer Genome Atlas Network. Comprehensive molecular characterization of human colon and rectal cancer. Nature 2012; 487: 330-337 [PMID: 22810696 DOI: 10.1038/nature11252]
18 Santini D, Loupakis F, Vincenzi B, Floriani I, Stasi I, Canestrari E, Rulli E, Maltese PE, Andreoni F, Masi G, Graziano F, Baldi GG, Salvatore L, Russo A, Perrone G, Tommasino MR, Magnani M, Falcone A, Tonini G, Ruzzo A. High concordance of KRAS status between primary colorectal tumors and related metastatic sites: implications for clinical practice. Oncologist 2008; 13: 1270-1275 [PMID: 19056857 DOI: 10.1634/theoncologist.2008-0181]
19 Sinicrope FA, Mahoney MR, Yoon HH, Smyrk TC, Thibodeau SN, Goldberg RM, Nelson GD, Sargent DJ, Alberts SR. Analysis of Molecular Markers by Anatomic Tumor Site in Stage III Colon Carcinomas from Adjuvant Chemotherapy Trial NCCTG N0147 (Alliance). Clin Cancer Res 2015; 21: 5294-5304 [PMID: 26187617 DOI: 10.1158/1078-0432.ccr-15-0527]
20 Douillard JY, Oliner KS, Siena S, Tabernero J, Burkes R, Barugel M, Humblet Y, Bodoky G, Cunningham D, Jassem J, Rivera F, Kocákova I, Ruff P, Błasińska-Morawiec M, Šmakal M, Canon JL, Rother M, Williams R, Rong A, Wiezorek J, Sidhu R, Patterson SD. Panitumumab-FOLFOX4 treatment and RAS mutations in colorectal cancer. N Engl J Med 2013; 369: 1023-1034 [PMID: 24024839 DOI: 10.1056/NEJMoa1305275]
21 Bokemeyer C, Bondarenko I, Hartmann JT, de Braud F, Schuch G, Zubel A, Celik I, Schlichting M, Koralewski P. Efficacy according to biomarker status of cetuximab plus FOLFOX-4 as first-line treatment for metastatic colorectal cancer: the OPUS study. Ann Oncol 2011; 22: 1535-1546 [PMID: 21228335 DOI: 10.1093/annonc/mdq632]
22 De Roock W, Claes B, Bernasconi D, De Schutter J, Biesmans B, Fountzilas G, Kalogeras KT, Kotoula V, Papamichael D, Laurent-Puig P, Penault-Llorca F, Rougier P, Vincenzi B, Santini D, Tonini G, Cappuzzo F, Frattini M, Molinari F, Saletti P, De Dosso S, Martini M, Bardelli A, Siena S, Sartore-Bianchi A, Tabernero J, Macarulla T, Di Fiore F, Gangloff AO, Ciardiello F, Pfeiffer P, Qvortrup C, Hansen TP, Van Cutsem E, Piessevaux H, Lambrechts D, Delorenzi M, Tejpar S. Effects of KRAS, BRAF, NRAS, and PIK3CA mutations on the efficacy of cetuximab plus chemotherapy in chemotherapy-refractory metastatic colorectal cancer: a retrospective consortium analysis. Lancet Oncol 2010; 11: 753-762 [PMID: 20619739 DOI: 10.1016/s1470-2045(10)70130-3]
23 Cunningham D, Humblet Y, Siena S, Khayat D, Bleiberg H, Santoro A, Bets D, Mueser M, Harstrick A, Verslype C, Chau I, Van Cutsem E. Cetuximab monotherapy and cetuximab plus irinotecan in irinotecan-refractory metastatic colorectal cancer. N Engl J Med 2004; 351: 337-345 [PMID: 15269313 DOI: 10.1056/NEJMoa033025]
24 Pruitt K, Der CJ. Ras and Rho regulation of the cell cycle and oncogenesis. Cancer Lett 2001; 171: 1-10 [PMID: 11485822]
25 Fransén K, Klintenäs M, Osterström A, Dimberg J, Monstein HJ, Söderkvist P. Mutation analysis of the BRAF, ARAF and RAF-1 genes in human colorectal adenocarcinomas. Carcinogenesis 2004; 25: 527-533 [PMID: 14688025 DOI: 10.1093/carcin/bgh049]
26 Davies H, Bignell GR, Cox C, Stephens P, Edkins S, Clegg S, Teague J, Woffendin H, Garnett MJ, Bottomley W, Davis N, Dicks E, Ewing R, Floyd Y, Gray K, Hall S, Hawes R, Hughes J, Kosmidou V, Menzies A, Mould C, Parker A, Stevens C, Watt S, Hooper S, Wilson R, Jayatilake H, Gusterson BA, Cooper C, Shipley J, Hargrave D,
Pritchard-Jones K, Maitland N, Chenevix-Trench G, Riggins GJ, Bigner DD, Palmieri G, Cossu A, Flanagan A, Nicholson A, Ho JW, Leung SY, Yuen ST, Weber BL, Seigler HF, Darrow TL, Paterson H, Marais R, Marshall CJ, Wooster R, Stratton MR, Futreal PA. Mutations of the BRAF gene in human cancer. Nature 2002; 417: 949-954 [PMID: 12068308 DOI: 10.1038/nature00766]
27 Li WQ, Kawakami K, Ruszkiewicz A, Bennett G, Moore J, Iacopetta B. BRAF mutations are associated with distinctive clinical, pathological and molecular features of colorectal cancer independently of microsatellite instability status. Mol Cancer 2006; 5: 2 [PMID: 16403224 DOI: 10.1186/1476-4598-5-2]
28 de la Chapelle A, Palomaki G, Hampel H. Identifying Lynch syndrome. Int J Cancer 2009; 125: 1492-1493 [PMID: 19536819 DOI: 10.1002/ijc.24491]
29 Rajagopalan H, Bardelli A, Lengauer C, Kinzler KW, Vogelstein B, Velculescu VE. Tumorigenesis: RAF/RAS oncogenes and mismatch-repair status. Nature 2002; 418: 934 [PMID: 12198537 DOI: 10.1038/418934a]
30 Maughan TS, Adams RA, Smith CG, Meade AM, Seymour MT, Wilson RH, Idziaszczyk S, Harris R, Fisher D, Kenny SL, Kay E, Mitchell JK, Madi A, Jasani B, James MD, Bridgewater J, Kennedy MJ, Claes B, Lambrechts D, Kaplan R, Cheadle JP. Addition of cetuximab to oxaliplatin-based first-line combination chemotherapy for treatment of advanced colorectal cancer: results of the randomised phase 3 MRC COIN trial. Lancet 2011; 377: 2103-2114 [PMID: 21641636 DOI: 10.1016/s0140-6736(11)60613-2]
31 McArthur GA, Chapman PB, Robert C, Larkin J, Haanen JB, Dummer R, Ribas A, Hogg D, Hamid O, Ascierto PA, Garbe C, Testori A, Maio M, Lorigan P, Lebbé C, Jouary T, Schadendorf D, O’Day SJ, Kirkwood JM, Eggermont AM, Dréno B, Sosman JA, Flaherty KT, Yin M, Caro I, Cheng S, Trunzer K, Hauschild A. Safety and efficacy of vemurafenib in BRAF(V600E) and BRAF(V600K) mutation-positive melanoma (BRIM-3): extended follow-up of a phase 3, randomised, open-label study. Lancet Oncol 2014; 15: 323-332 [PMID: 24508103 DOI: 10.1016/s1470-2045(14)70012-9]
32 Kopetz S, Chang GJ, Overman MJ, Eng C, Sargent DJ, Larson DW, Grothey A, Vauthey JN, Nagorney DM, McWilliams RR. Improved survival in metastatic colorectal cancer is associated with adoption of hepatic resection and improved chemotherapy. J Clin Oncol 2009; 27: 3677-3683 [PMID: 19470929 DOI: 10.1200/jco.2008.20.5278]
33 Lito P, Pratilas CA, Joseph EW, Tadi M, Halilovic E, Zubrowski M, Huang A, Wong WL, Callahan MK, Merghoub T, Wolchok JD, de Stanchina E, Chandarlapaty S, Poulikakos PI, Fagin JA, Rosen N. Relief of profound feedback inhibition of mitogenic signaling by RAF inhibitors attenuates their activity in BRAFV600E melanomas. Cancer Cell 2012; 22: 668-682 [PMID: 23153539 DOI: 10.1016/j.ccr.2012.10.009]
34 Yaeger R, Cercek A, O’Reilly EM, Reidy DL, Kemeny N, Wolinsky T, Capanu M, Gollub MJ, Rosen N, Berger MF, Lacouture ME, Vakiani E, Saltz LB. Pilot trial of combined BRAF and EGFR inhibition in BRAF-mutant metastatic colorectal cancer patients. Clin Cancer Res 2015; 21: 1313-1320 [PMID: 25589621 DOI: 10.1158/1078-0432.ccr-14-2779]
35 Vogelstein B, Lane D, Levine AJ. Surfing the p53 network. Nature 2000; 408: 307-310 [PMID: 11099028]
36 Leslie A, Carey FA, Pratt NR, Steele RJ. The colorectal adenoma-carcinoma sequence. Br J Surg 2002; 89: 845-860 [PMID: 12081733 DOI: 10.1046/j.1365-2168.2002.02120.x]
37 Béroud C, Soussi T. The UMD-p53 database: new mutations and analysis tools. Hum Mutat 2003; 21: 176-181 [PMID: 12619103 DOI: 10.1002/humu.10187]
38 Wu W, Yang J, Feng X, Wang H, Ye S, Yang P, Tan W, Wei G, Zhou Y. MicroRNA-32 (miR-32) regulates phosphatase and tensin homologue (PTEN) expression and promotes growth, migration, and invasion in colorectal carcinoma cells. Mol Cancer 2013; 12: 30 [PMID: 23617834 DOI: 10.1186/1476-4598-12-30]
39 Powell SM, Zilz N, Beazer-Barclay Y, Bryan TM, Hamilton SR, Thibodeau SN, Vogelstein B, Kinzler KW. APC mutations occur early during colorectal tumorigenesis. Nature 1992; 359: 235-237
Aghagolzadeh P et al . Molecular and cellular biomarkers for CRC

5690 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
[PMID: 1528264 DOI: 10.1038/359235a0]40 Kinzler KW, Vogelstein B. Lessons from hereditary colorectal
cancer. Cell 1996; 87: 159-170 [PMID: 8861899]41 Otori K, Konishi M, Sugiyama K, Hasebe T, Shimoda T, Kikuchi-
Yanoshita R, Mukai K, Fukushima S, Miyaki M, Esumi H. Infrequent somatic mutation of the adenomatous polyposis coli gene in aberrant crypt foci of human colon tissue. Cancer 1998; 83: 896-900 [PMID: 9731892]
42 Miyoshi Y, Nagase H, Ando H, Horii A, Ichii S, Nakatsuru S, Aoki T, Miki Y, Mori T, Nakamura Y. Somatic mutations of the APC gene in colorectal tumors: mutation cluster region in the APC gene. Hum Mol Genet 1992; 1: 229-233 [PMID: 1338904]
43 Esteller M, Sparks A, Toyota M, Sanchez-Cespedes M, Capella G, Peinado MA, Gonzalez S, Tarafa G, Sidransky D, Meltzer SJ, Baylin SB, Herman JG. Analysis of adenomatous polyposis coli promoter hypermethylation in human cancer. Cancer Res 2000; 60: 4366-4371 [PMID: 10969779]
44 Barekati Z, Radpour R, Lu Q, Bitzer J, Zheng H, Toniolo P, Lenner P, Zhong XY. Methylation signature of lymph node metastases in breast cancer patients. BMC Cancer 2012; 12: 244 [PMID: 22695536 DOI: 10.1186/1471-2407-12-244]
45 Radpour R, Barekati Z, Kohler C, Holzgreve W, Zhong XY. New trends in molecular biomarker discovery for breast cancer. Genet Test Mol Biomarkers 2009; 13: 565-571 [PMID: 19814613 DOI: 10.1089/gtmb.2009.0060]
46 Feinberg AP, Tycko B. The history of cancer epigenetics. Nat Rev Cancer 2004; 4: 143-153 [PMID: 14732866]
47 Ramsahoye BH, Biniszkiewicz D, Lyko F, Clark V, Bird AP, Jaenisch R. Non-CpG methylation is prevalent in embryonic stem cells and may be mediated by DNA methyltransferase 3a. Proc Natl Acad Sci USA 2000; 97: 5237-5242 [PMID: 10805783]
48 Barekati Z, Radpour R, Kohler C, Zhang B, Toniolo P, Lenner P, Lv Q, Zheng H, Zhong XY. Methylation profile of TP53 regulatory pathway and mtDNA alterations in breast cancer patients lacking TP53 mutations. Hum Mol Genet 2010; 19: 2936-2946 [PMID: 20466735 DOI: 10.1093/hmg/ddq199]
49 Radpour R, Barekati Z, Kohler C, Lv Q, Bürki N, Diesch C, Bitzer J, Zheng H, Schmid S, Zhong XY. Hypermethylation of tumor suppressor genes involved in critical regulatory pathways for developing a blood-based test in breast cancer. PLoS One 2011; 6: e16080 [PMID: 21283676 DOI: 10.1371/journal.pone.0016080]
50 Radpour R, Barekati Z, Kohler C, Schumacher MM, Grussenmeyer T, Jenoe P, Hartmann N, Moes S, Letzkus M, Bitzer J, Lefkovits I, Staedtler F, Zhong XY. Integrated epigenetics of human breast cancer: synoptic investigation of targeted genes, microRNAs and proteins upon demethylation treatment. PLoS One 2011; 6: e27355 [PMID: 22076154 DOI: 10.1371/journal.pone.0027355]
51 Radpour R, Haghighi MM, Fan AX, Torbati PM, Hahn S, Holzgreve W, Zhong XY. High-throughput hacking of the methylation patterns in breast cancer by in vitro transcription and thymidine-specific cleavage mass array on MALDI-TOF silico-chip. Mol Cancer Res 2008; 6: 1702-1709 [PMID: 19010818 DOI: 10.1158/1541-7786.MCR-08-0262]
52 Radpour R, Kohler C, Haghighi MM, Fan AX, Holzgreve W, Zhong XY. Methylation profiles of 22 candidate genes in breast cancer using high-throughput MALDI-TOF mass array. Oncogene 2009; 28: 2969-2978 [PMID: 19503099 DOI: 10.1038/onc.2009.149]
53 Weisenberger DJ, Siegmund KD, Campan M, Young J, Long TI, Faasse MA, Kang GH, Widschwendter M, Weener D, Buchanan D, Koh H, Simms L, Barker M, Leggett B, Levine J, Kim M, French AJ, Thibodeau SN, Jass J, Haile R, Laird PW. CpG island methylator phenotype underlies sporadic microsatellite instability and is tightly associated with BRAF mutation in colorectal cancer. Nat Genet 2006; 38: 787-793 [PMID: 16804544 DOI: 10.1038/ng1834]
54 Toyota M, Ohe-Toyota M, Ahuja N, Issa JP. Distinct genetic profiles in colorectal tumors with or without the CpG island methylator phenotype. Proc Natl Acad Sci USA 2000; 97: 710-715 [PMID: 10639144]
55 Colussi D, Brandi G, Bazzoli F, Ricciardiello L. Molecular pathways involved in colorectal cancer: implications for disease behavior and
prevention. Int J Mol Sci 2013; 14: 16365-16385 [PMID: 23965959 DOI: 10.3390/ijms140816365]
56 Qi J, Zhu YQ, Luo J, Tao WH. Hypermethylation and expression regulation of secreted frizzled-related protein genes in colorectal tumor. World J Gastroenterol 2006; 12: 7113-7117 [PMID: 17131472 DOI: 10.3748/wjg.v12.i44.7113]
57 Li H, Myeroff L, Smiraglia D, Romero MF, Pretlow TP, Kasturi L, Lutterbaugh J, Rerko RM, Casey G, Issa JP, Willis J, Willson JK, Plass C, Markowitz SD. SLC5A8, a sodium transporter, is a tumor suppressor gene silenced by methylation in human colon aberrant crypt foci and cancers. Proc Natl Acad Sci USA 2003; 100: 8412-8417 [PMID: 12829793 DOI: 10.1073/pnas.1430846100]
58 Chen WD, Han ZJ, Skoletsky J, Olson J, Sah J, Myeroff L, Platzer P, Lu S, Dawson D, Willis J, Pretlow TP, Lutterbaugh J, Kasturi L, Willson JK, Rao JS, Shuber A, Markowitz SD. Detection in fecal DNA of colon cancer-specific methylation of the nonexpressed vimentin gene. J Natl Cancer Inst 2005; 97: 1124-1132 [PMID: 16077070 DOI: 10.1093/jnci/dji204]
59 Longtine MS, DeMarini DJ, Valencik ML, Al-Awar OS, Fares H, De Virgilio C, Pringle JR. The septins: roles in cytokinesis and other processes. Curr Opin Cell Biol 1996; 8: 106-119 [PMID: 8791410]
60 Kim MS, Froese CD, Estey MP, Trimble WS. SEPT9 occupies the terminal positions in septin octamers and mediates polymerization-dependent functions in abscission. J Cell Biol 2011; 195: 815-826 [PMID: 22123865 DOI: 10.1083/jcb.201106131]
61 Lee HS, Hwang SM, Kim TS, Kim DW, Park do J, Kang SB, Kim HH, Park KU. Circulating methylated septin 9 nucleic Acid in the plasma of patients with gastrointestinal cancer in the stomach and colon. Transl Oncol 2013; 6: 290-296 [PMID: 23730408]
62 Chen RZ, Pettersson U, Beard C, Jackson-Grusby L, Jaenisch R. DNA hypomethylation leads to elevated mutation rates. Nature 1998; 395: 89-93 [PMID: 9738504 DOI: 10.1038/25779]
63 Ogino S, Kawasaki T, Nosho K, Ohnishi M, Suemoto Y, Kirkner GJ, Fuchs CS. LINE-1 hypomethylation is inversely associated with microsatellite instability and CpG island methylator phenotype in colorectal cancer. Int J Cancer 2008; 122: 2767-2773 [PMID: 18366060 DOI: 10.1002/ijc.23470]
64 Schena M, Shalon D, Davis RW, Brown PO. Quantitative monitoring of gene expression patterns with a complementary DNA microarray. Science 1995; 270: 467-470 [PMID: 7569999]
65 van’t Veer LJ, Bernards R. Enabling personalized cancer medicine through analysis of gene-expression patterns. Nature 2008; 452: 564-570 [PMID: 18385730]
66 De Sousa E Melo F, Wang X, Jansen M, Fessler E, Trinh A, de Rooij LP, de Jong JH, de Boer OJ, van Leersum R, Bijlsma MF, Rodermond H, van der Heijden M, van Noesel CJ, Tuynman JB, Dekker E, Markowetz F, Medema JP, Vermeulen L. Poor-prognosis colon cancer is defined by a molecularly distinct subtype and develops from serrated precursor lesions. Nat Med 2013; 19: 614-618 [PMID: 23584090 DOI: 10.1038/nm.3174]
67 Sadanandam A, Lyssiotis CA, Homicsko K, Collisson EA, Gibb WJ, Wullschleger S, Ostos LC, Lannon WA, Grotzinger C, Del Rio M, Lhermitte B, Olshen AB, Wiedenmann B, Cantley LC, Gray JW, Hanahan D. A colorectal cancer classification system that associates cellular phenotype and responses to therapy. Nat Med 2013; 19: 619-625 [PMID: 23584089 DOI: 10.1038/nm.3175]
68 Budinska E, Popovici V, Tejpar S, D’Ario G, Lapique N, Sikora KO, Di Narzo AF, Yan P, Hodgson JG, Weinrich S, Bosman F, Roth A, Delorenzi M. Gene expression patterns unveil a new level of molecular heterogeneity in colorectal cancer. J Pathol 2013; 231: 63-76 [PMID: 23836465 DOI: 10.1002/path.4212]
69 Marisa L, de Reyniès A, Duval A, Selves J, Gaub MP, Vescovo L, Etienne-Grimaldi MC, Schiappa R, Guenot D, Ayadi M, Kirzin S, Chazal M, Fléjou JF, Benchimol D, Berger A, Lagarde A, Pencreach E, Piard F, Elias D, Parc Y, Olschwang S, Milano G, Laurent-Puig P, Boige V. Gene expression classification of colon cancer into molecular subtypes: characterization, validation, and prognostic value. PLoS Med 2013; 10: e1001453 [PMID: 23700391 DOI: 10.1371/journal.pmed.1001453]
70 Wang Y, Jatkoe T, Zhang Y, Mutch MG, Talantov D, Jiang J,
Aghagolzadeh P et al . Molecular and cellular biomarkers for CRC

5691 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
McLeod HL, Atkins D. Gene expression profiles and molecular markers to predict recurrence of Dukes’ B colon cancer. J Clin Oncol 2004; 22: 1564-1571 [PMID: 15051756 DOI: 10.1200/jco.2004.08.186]
71 Calin GA, Croce CM. MicroRNA signatures in human cancers. Nat Rev Cancer 2006; 6: 857-866 [PMID: 17060945]
72 Esquela-Kerscher A, Slack FJ. Oncomirs - microRNAs with a role in cancer. Nat Rev Cancer 2006; 6: 259-269 [PMID: 16557279]
73 Slack FJ, Weidhaas JB. MicroRNAs as a potential magic bullet in cancer. Future Oncol 2006; 2: 73-82 [PMID: 16556074 DOI: 10.2217/14796694.2.1.73]
74 Lu J, Getz G, Miska EA, Alvarez-Saavedra E, Lamb J, Peck D, Sweet-Cordero A, Ebert BL, Mak RH, Ferrando AA, Downing JR, Jacks T, Horvitz HR, Golub TR. MicroRNA expression profiles classify human cancers. Nature 2005; 435: 834-838 [PMID: 15944708]
75 Creemers EE, Tijsen AJ, Pinto YM. Circulating microRNAs: novel biomarkers and extracellular communicators in cardiovascular disease? Circ Res 2012; 110: 483-495 [PMID: 22302755 DOI: 10.1161/circresaha.111.247452]
76 Weissmann-Brenner A, Kushnir M, Lithwick Yanai G, Aharonov R, Gibori H, Purim O, Kundel Y, Morgenstern S, Halperin M, Niv Y, Brenner B. Tumor microRNA-29a expression and the risk of recurrence in stage II colon cancer. Int J Oncol 2012; 40: 2097-2103 [PMID: 22426940 DOI: 10.3892/ijo.2012.1403]
77 Li Y, Zhang Z. Potential microRNA-mediated oncogenic intercellular communication revealed by pan-cancer analysis. Sci Rep 2014; 4: 7097 [PMID: 25403569 DOI: 10.1038/srep07097]
78 Gao J, Li N, Dong Y, Li S, Xu L, Li X, Li Y, Li Z, Ng SS, Sung JJ, Shen L, Yu J. miR-34a-5p suppresses colorectal cancer metastasis and predicts recurrence in patients with stage II/III colorectal cancer. Oncogene 2015; 34: 4142-4152 [PMID: 25362853 DOI: 10.1038/onc.2014.348]
79 Liu H, Du L, Wen Z, Yang Y, Li J, Wang L, Zhang X, Liu Y, Dong Z, Li W, Zheng G, Wang C. Up-regulation of miR-182 expression in colorectal cancer tissues and its prognostic value. Int J Colorectal Dis 2013; 28: 697-703 [PMID: 23474644 DOI: 10.1007/s00384-013-1674-0]
80 Huynh C, Segura MF, Gaziel-Sovran A, Menendez S, Darvishian F, Chiriboga L, Levin B, Meruelo D, Osman I, Zavadil J, Marcusson EG, Hernando E. Efficient in vivo microRNA targeting of liver metastasis. Oncogene 2011; 30: 1481-1488 [PMID: 21102518 DOI: 10.1038/onc.2010.523]
81 Ma Y, Zhang P, Wang F, Zhang H, Yang J, Peng J, Liu W, Qin H. miR-150 as a potential biomarker associated with prognosis and therapeutic outcome in colorectal cancer. Gut 2012; 61: 1447-1453 [PMID: 22052060 DOI: 10.1136/gutjnl-2011-301122]
82 Ma W, Yu J, Qi X, Liang L, Zhang Y, Ding Y, Lin X, Li G, Ding Y. Radiation-induced microRNA-622 causes radioresistance in colorectal cancer cells by down-regulating Rb. Oncotarget 2015; 6: 15984-15994 [PMID: 25961730 DOI: 10.18632/oncotarget.3762]
83 Blackburn EH. Structure and function of telomeres. Nature 1991; 350: 569-573 [PMID: 1708110]
84 Harley CB. Telomere loss: mitotic clock or genetic time bomb? Mutat Res 1991; 256: 271-282 [PMID: 1722017]
85 Wright WE, Shay JW. Telomere dynamics in cancer progression and prevention: fundamental differences in human and mouse telomere biology. Nat Med 2000; 6: 849-851 [PMID: 10932210 DOI: 10.1038/78592]
86 Hahn WC. Role of telomeres and telomerase in the pathogenesis of human cancer. J Clin Oncol 2003; 21: 2034-2043 [PMID: 12743159]
87 Harley CB. Telomerase and cancer therapeutics. Nat Rev Cancer 2008; 8: 167-179 [PMID: 18256617 DOI: 10.1038/nrc2275]
88 Zhang A, Wang J, Zheng B, Fang X, Angström T, Liu C, Li X, Erlandsson F, Björkholm M, Nordenskjörd M, Gruber A, Wallin KL, Xu D. Telomere attrition predominantly occurs in precursor lesions during in vivo carcinogenic process of the uterine cervix. Oncogene 2004; 23: 7441-7447 [PMID: 15318175 DOI: 10.1038/sj.onc.1207527]
89 Gisselsson D, Jonson T, Petersén A, Strömbeck B, Dal Cin
P, Höglund M, Mitelman F, Mertens F, Mandahl N. Telomere dysfunction triggers extensive DNA fragmentation and evolution of complex chromosome abnormalities in human malignant tumors. Proc Natl Acad Sci USA 2001; 98: 12683-12688 [PMID: 11675499 DOI: 10.1073/pnas.211357798]
90 Muraki K, Nyhan K, Han L, Murnane JP. Mechanisms of telomere loss and their consequences for chromosome instability. Front Oncol 2012; 2: 135 [PMID: 23061048 DOI: 10.3389/fonc.2012.00135]
91 Haghighi MM, Aghagolzadeh P, Zadeh SM, Molaei M, Zali MR, Radpour R. Telomere shortening: a biological marker of sporadic colorectal cancer with normal expression of p53 and mismatch repair proteins. Genet Test Mol Biomarkers 2014; 18: 236-244 [PMID: 24495131 DOI: 10.1089/gtmb.2013.0436]
92 Radpour R, Barekati Z, Haghighi MM, Kohler C, Asadollahi R, Torbati PM, Holzgreve W, Zhong XY. Correlation of telomere length shortening with promoter methylation profile of p16/Rb and p53/p21 pathways in breast cancer. Mod Pathol 2010; 23: 763-772 [PMID: 20081803 DOI: 10.1038/modpathol.2009.195]
93 Bisoffi M, Heaphy CM, Griffith JK. Telomeres: prognostic markers for solid tumors. Int J Cancer 2006; 119: 2255-2260 [PMID: 16858685 DOI: 10.1002/ijc.22120]
94 Heaphy CM, Baumgartner KB, Bisoffi M, Baumgartner RN, Griffith JK. Telomere DNA content predicts breast cancer-free survival interval. Clin Cancer Res 2007; 13: 7037-7043 [PMID: 18056180]
95 Hastie ND, Dempster M, Dunlop MG, Thompson AM, Green DK, Allshire RC. Telomere reduction in human colorectal carcinoma and with ageing. Nature 1990; 346: 866-868 [PMID: 2392154 DOI: 10.1038/346866a0]
96 Takagi S, Kinouchi Y, Hiwatashi N, Chida M, Nagashima F, Takahashi S, Negoro K, Shimosegawa T, Toyota T. Telomere shortening and the clinicopathologic characteristics of human colorectal carcinomas. Cancer 1999; 86: 1431-1436 [PMID: 10526269]
97 Gertler R, Rosenberg R, Stricker D, Friederichs J, Hoos A, Werner M, Ulm K, Holzmann B, Nekarda H, Siewert JR. Telomere length and human telomerase reverse transcriptase expression as markers for progression and prognosis of colorectal carcinoma. J Clin Oncol 2004; 22: 1807-1814 [PMID: 15143073 DOI: 10.1200/JCO.2004.09.160]
98 Rial NS, Zell JA, Cohen AM, Gerner EW. Clinical end points for developing pharmaceuticals to manage patients with a sporadic or genetic risk of colorectal cancer. Expert Rev Gastroenterol Hepatol 2012; 6: 507-517 [PMID: 22928902 DOI: 10.1586/egh.12.23]
99 Meeker AK, Hicks JL, Gabrielson E, Strauss WM, De Marzo AM, Argani P. Telomere shortening occurs in subsets of normal breast epithelium as well as in situ and invasive carcinoma. Am J Pathol 2004; 164: 925-935 [PMID: 14982846]
100 O’Sullivan J, Risques RA, Mandelson MT, Chen L, Brentnall TA, Bronner MP, Macmillan MP, Feng Z, Siebert JR, Potter JD, Rabinovitch PS. Telomere length in the colon declines with age: a relation to colorectal cancer? Cancer Epidemiol Biomarkers Prev 2006; 15: 573-577 [PMID: 16537718 DOI: 10.1158/1055-9965.EPI-05-0542]
101 Raynaud CM, Jang SJ, Nuciforo P, Lantuejoul S, Brambilla E, Mounier N, Olaussen KA, André F, Morat L, Sabatier L, Soria JC. Telomere shortening is correlated with the DNA damage response and telomeric protein down-regulation in colorectal preneoplastic lesions. Ann Oncol 2008; 19: 1875-1881 [PMID: 18641004 DOI: 10.1093/annonc/mdn405]
102 Kerbel RS. Tumor angiogenesis. N Engl J Med 2008; 358: 2039-2049 [PMID: 18463380 DOI: 10.1056/NEJMra0706596]
103 Ebos JM, Lee CR, Bogdanovic E, Alami J, Van Slyke P, Francia G, Xu P, Mutsaers AJ, Dumont DJ, Kerbel RS. Vascular endothelial growth factor-mediated decrease in plasma soluble vascular endothelial growth factor receptor-2 levels as a surrogate biomarker for tumor growth. Cancer Res 2008; 68: 521-529 [PMID: 18199548 DOI: 10.1158/0008-5472.can-07-3217]
104 Tsai HL, Lin CH, Huang CW, Yang IP, Yeh YS, Hsu WH, Wu JY, Kuo CH, Tseng FY, Wang JY. Decreased peritherapeutic VEGF
Aghagolzadeh P et al . Molecular and cellular biomarkers for CRC

5692 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
expression could be a predictor of responsiveness to first-line FOLFIRI plus bevacizumab in mCRC patients. Int J Clin Exp Pathol 2015; 8: 1900-1910 [PMID: 25973082]
105 Gerger A, LaBonte M, Lenz HJ. Molecular predictors of response to antiangiogenesis therapies. Cancer J 2011; 17: 134-141 [PMID: 21427557 DOI: 10.1097/PPO.0b013e318212db3c]
106 Hoff PM, Hochhaus A, Pestalozzi BC, Tebbutt NC, Li J, Kim TW, Koynov KD, Kurteva G, Pintér T, Cheng Y, van Eyll B, Pike L, Fielding A, Robertson JD, Saunders MP. Cediranib plus FOLFOX/CAPOX versus placebo plus FOLFOX/CAPOX in patients with previously untreated metastatic colorectal cancer: a randomized, double-blind, phase III study (HORIZON II). J Clin Oncol 2012; 30: 3596-3603 [PMID: 22965965 DOI: 10.1200/jco.2012.42.6031]
107 Itzkowitz SH. Cancer prevention in patients with inflammatory bowel disease. Gastroenterol Clin North Am 2002; 31: 1133-1144 [PMID: 12489282]
108 Gabay C, Kushner I. Acute-phase proteins and other systemic responses to inflammation. N Engl J Med 1999; 340: 448-454 [PMID: 9971870 DOI: 10.1056/nejm199902113400607]
109 Zhou B, Shu B, Yang J, Liu J, Xi T, Xing Y. C-reactive protein, interleukin-6 and the risk of colorectal cancer: a meta-analysis. Cancer Causes Control 2014; 25: 1397-1405 [PMID: 25053407 DOI: 10.1007/s10552-014-0445-8]
110 Kishimoto T, Akira S, Narazaki M, Taga T. Interleukin-6 family of cytokines and gp130. Blood 1995; 86: 1243-1254 [PMID: 7632928]
111 Naka T, Nishimoto N, Kishimoto T. The paradigm of IL-6: from basic science to medicine. Arthritis Res 2002; 4 Suppl 3: S233-S242 [PMID: 12110143]
112 Becker C, Fantini MC, Wirtz S, Nikolaev A, Lehr HA, Galle PR, Rose-John S, Neurath MF. IL-6 signaling promotes tumor growth in colorectal cancer. Cell Cycle 2005; 4: 217-220 [PMID: 15655344]
113 Craven B, Zaric V, Martin A, Mureau C, Egan LJ. Effect of genetic deletion or pharmacological antagonism of tumor necrosis factor alpha on colitis-associated carcinogenesis in mice. Inflamm Bowel Dis 2015; 21: 485-495 [PMID: 25581824 DOI: 10.1097/mib.0000000000000303]
114 Mehta RS, Song M, Bezawada N, Wu K, Garcia-Albeniz X, Morikawa T, Fuchs CS, Ogino S, Giovannucci EL, Chan AT. A prospective study of macrophage inhibitory cytokine-1 (MIC-1/GDF15) and risk of colorectal cancer. J Natl Cancer Inst 2014; 106: dju016 [PMID: 24565956 DOI: 10.1093/jnci/dju016]
115 Akagi Y, Kinugasa T, Adachi Y, Shirouzu K. Prognostic significance of isolated tumor cells in patients with colorectal cancer in recent 10-year studies. Mol Clin Oncol 2013; 1: 582-592 [PMID: 24649214 DOI: 10.3892/mco.2013.116]
116 Utting M, Werner W, Dahse R, Schubert J, Junker K. Microsatellite analysis of free tumor DNA in urine, serum, and plasma of patients: a minimally invasive method for the detection of bladder cancer. Clin Cancer Res 2002; 8: 35-40 [PMID: 11801538]
117 Frattini M, Gallino G, Signoroni S, Balestra D, Battaglia L, Sozzi G, Leo E, Pilotti S, Pierotti MA. Quantitative analysis of plasma DNA in colorectal cancer patients: a novel prognostic tool. Ann N Y Acad Sci 2006; 1075: 185-190 [PMID: 17108210 DOI: 10.1196/annals.1368.025]
118 Schwarzenbach H, Stoehlmacher J, Pantel K, Goekkurt E. Detection and monitoring of cell-free DNA in blood of patients with colorectal cancer. Ann N Y Acad Sci 2008; 1137: 190-196 [PMID: 18837946 DOI: 10.1196/annals.1448.025]
119 Lazarev I, Leibovitch L, Czeiger D, Sion-Vardi N, Geffen DB, Douvdevani A, Ariad S. Cell-free DNA blood levels in colorectal cancer patients do not correlate with mismatch repair-proficiency. In Vivo 2014; 28: 349-354 [PMID: 24815837]
120 Diehl F, Schmidt K, Choti MA, Romans K, Goodman S, Li M, Thornton K, Agrawal N, Sokoll L, Szabo SA, Kinzler KW, Vogelstein B, Diaz LA. Circulating mutant DNA to assess tumor dynamics. Nat Med 2008; 14: 985-990 [PMID: 18670422 DOI: 10.1038/nm.1789]
121 Lefebure B, Charbonnier F, Di Fiore F, Tuech JJ, Le Pessot F, Michot F, Michel P, Frebourg T. Prognostic value of circulating mutant DNA in unresectable metastatic colorectal cancer. Ann
Surg 2010; 251: 275-280 [PMID: 20010083 DOI: 10.1097/SLA.0b013e3181c35c87]
122 Suzuki H, Yamamoto E, Maruyama R, Niinuma T, Kai M. Biological significance of the CpG island methylator phenotype. Biochem Biophys Res Commun 2014; 455: 35-42 [PMID: 25016183 DOI: 10.1016/j.bbrc.2014.07.007]
123 Tan SH, Ida H, Lau QC, Goh BC, Chieng WS, Loh M, Ito Y. Detection of promoter hypermethylation in serum samples of cancer patients by methylation-specific polymerase chain reaction for tumour suppressor genes including RUNX3. Oncol Rep 2007; 18: 1225-1230 [PMID: 17914577]
124 Berger F, Reiser MF. Micro-RNAs as potential new molecular biomarkers in oncology: have they reached relevance for the clinical imaging sciences? Theranostics 2013; 3: 943-952 [PMID: 24396505 DOI: 10.7150/thno.7445]
125 Schetter AJ, Leung SY, Sohn JJ, Zanetti KA, Bowman ED, Yanaihara N, Yuen ST, Chan TL, Kwong DL, Au GK, Liu CG, Calin GA, Croce CM, Harris CC. MicroRNA expression profiles associated with prognosis and therapeutic outcome in colon adenocarcinoma. JAMA 2008; 299: 425-436 [PMID: 18230780 DOI: 10.1001/jama.299.4.425]
126 Liu GH, Zhou ZG, Chen R, Wang MJ, Zhou B, Li Y, Sun XF. Serum miR-21 and miR-92a as biomarkers in the diagnosis and prognosis of colorectal cancer. Tumour Biol 2013; 34: 2175-2181 [PMID: 23625654 DOI: 10.1007/s13277-013-0753-8]
127 Huang Z, Huang D, Ni S, Peng Z, Sheng W, Du X. Plasma microRNAs are promising novel biomarkers for early detection of colorectal cancer. Int J Cancer 2010; 127: 118-126 [PMID: 19876917 DOI: 10.1002/ijc.25007]
128 Perilli L, Vicentini C, Agostini M, Pizzini S, Pizzi M, D’Angelo E, Bortoluzzi S, Mandruzzato S, Mammano E, Rugge M, Nitti D, Scarpa A, Fassan M, Zanovello P. Circulating miR-182 is a biomarker of colorectal adenocarcinoma progression. Oncotarget 2014; 5 : 6611-6619 [PMID: 25115394 DOI: 10.18632/oncotarget.2245]
129 Monzo M, Martínez-Rodenas F, Moreno I, Navarro A, Santasusagna S, Macias I, Muñoz C, Tejero R, Hernández R. Differential MIR-21 expression in plasma from mesenteric versus peripheral veins: an observational study of disease-free survival in surgically resected colon cancer patients. Medicine (Baltimore) 2015; 94: e145 [PMID: 25569638 DOI: 10.1097/md.0000000000000145]
130 Pu XX, Huang GL, Guo HQ, Guo CC, Li H, Ye S, Ling S, Jiang L, Tian Y, Lin TY. Circulating miR-221 directly amplified from plasma is a potential diagnostic and prognostic marker of colorectal cancer and is correlated with p53 expression. J Gastroenterol Hepatol 2010; 25: 1674-1680 [PMID: 20880178 DOI: 10.1111/j.1440-1746.2010.06417.x]
131 Hundt S, Haug U, Brenner H. Blood markers for early detection of colorectal cancer: a systematic review. Cancer Epidemiol Biomarkers Prev 2007; 16: 1935-1953 [PMID: 17932341 DOI: 10.1158/1055-9965.epi-06-0994]
132 Duffy MJ. Personalized treatment for patients with colorectal cancer: role of biomarkers. Biomark Med 2015; 9: 337-347 [PMID: 25808438 DOI: 10.2217/bmm.15.3]
133 Osborn NK, Ahlquist DA. Stool screening for colorectal cancer: molecular approaches. Gastroenterology 2005; 128: 192-206 [PMID: 15633136]
134 Dhaliwal A, Vlachostergios PJ, Oikonomou KG, Moshenyat Y. Fecal DNA testing for colorectal cancer screening: Molecular targets and perspectives. World J Gastrointest Oncol 2015; 7: 178-183 [PMID: 26483873 DOI: 10.4251/wjgo.v7.i10.178]
135 Diehl F, Schmidt K, Durkee KH, Moore KJ, Goodman SN, Shuber AP, Kinzler KW, Vogelstein B. Analysis of mutations in DNA isolated from plasma and stool of colorectal cancer patients. Gastroenterology 2008; 135: 489-498 [PMID: 18602395 DOI: 10.1053/j.gastro.2008.05.039]
136 Zou H, Taylor WR, Harrington JJ, Hussain FT, Cao X, Loprinzi CL, Levine TR, Rex DK, Ahnen D, Knigge KL, Lance P, Jiang X, Smith DI, Ahlquist DA. High detection rates of colorectal neoplasia by stool DNA testing with a novel digital melt curve assay.
Aghagolzadeh P et al . Molecular and cellular biomarkers for CRC

5693 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Gastroenterology 2009; 136: 459-470 [PMID: 19026650 DOI: 10.1053/j.gastro.2008.10.023]
137 Coppedè F, Lopomo A, Spisni R, Migliore L. Genetic and epigenetic biomarkers for diagnosis, prognosis and treatment of
colorectal cancer. World J Gastroenterol 2014; 20: 943-956 [PMID: 24574767 DOI: 10.3748/wjg.v20.i4.943]
138 A stool DNA test (Cologuard) for colorectal cancer screening. JAMA 2014; 312: 2566 [PMID: 25514307 DOI: 10.1001/jama.2014.15746]
P- Reviewer: Lakatos PL, Morris DL S- Editor: Ma YJ L- Editor: A E- Editor: Wang CH
Aghagolzadeh P et al . Molecular and cellular biomarkers for CRC

Stefano Caruso, Franco Franceschini, Department of General Surgery and Surgical Specialties, Unit of General Surgery, “Santa Maria Annunziata” Hospital, ASL Firenze, 50012 Florence, Italy
Alberto Patriti, Department of Surgery, General Minimally Invasive and Robotic Surgery, "San Matteo degli Infermi" Hospital, 06049 Spoleto (PG), Italy
Franco Roviello, Lorenzo De Franco, Department of Medical, Surgical and Neuroscience; Unit of General and Minimally Invasive Surgery, University of Siena, 53100 Siena, Italy
Andrea Coratti, Division of Oncological and Robotic General Surgery, “Careggi” University Hospital, 50134 Florence, Italy
Graziano Ceccarelli, Department of Medicine and General Surgery, Unit of Minimally Invasive and General Surgery, ASL8 Arezzo, “San Donato” Hospital, 52100 Arezzo, Italy
Author contributions: Caruso S wrote and conceived the design of the study; De Franco L and Franceschini F contributed to the search for the literature and acquisition of data; Patriti A, Roviello F, Coratti A and Ceccarelli G contributed to the critical appraisal of the work, revising the article critically for important intellectual content and supervising the interpretation of data.
Conflict-of-interest statement: The authors have no conflict of interest to report.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Manuscript source: Invited manuscript
Correspondence to: Stefano Caruso, MD, Department of General Surgery and Surgical Specialties, Unit of General Surgery, “Santa Maria Annunziata” Hospital, ASL Firenze, Via dell’Antella 58, Bagno a Ripoli, 50012 Florence, Italy. [email protected]: +39-55-9508373Fax: +39-349-8312397
Received: March 26, 2016 Peer-review started: March 26, 2016First decision: May 12, 2016Revised: May 20, 2016Accepted: June 15, 2016Article in press: June 15, 2016Published online: July 7, 2016
AbstractRadical gastrectomy with an adequate lymph-adenectomy is the main procedure which makes it possible to cure patients with resectable gastric cancer (GC). A number of randomized controlled trials and meta-analysis provide phase Ⅲ evidence that laparoscopic gastrectomy is technically safe and that it yields better short-term outcomes than conventional open gastrectomy for early-stage GC. While laparoscopic gastrectomy has become standard therapy for early-stage GC, especially in Asian countries such as Japan and South Korea, the use of minimally invasive techniques is still controversial for the treatment of more advanced tumours, principally due to existing concerns about its oncological adequacy and capacity to carry out an adequately extended lymphadenectomy. Some intrinsic drawbacks of the conventional laparoscopic technique have prevented the worldwide spread of laparoscopic gastrectomy
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.3748/wjg.v22.i25.5694
5694 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
World J Gastroenterol 2016 July 7; 22(25): 5694-5717 ISSN 1007-9327 (print) ISSN 2219-2840 (online)
© 2016 Baishideng Publishing Group Inc. All rights reserved.
Stefano Caruso, Alberto Patriti, Franco Roviello, Lorenzo De Franco, Franco Franceschini, Andrea Coratti, Graziano Ceccarelli
TOPIC HIGHLIGHT
Laparoscopic and robot-assisted gastrectomy for gastric cancer: Current considerations
2016 Laparoscopic Surgery: Global view

for cancer and, despite technological advances in recent year, it remains a technically challenging procedure. The introduction of robotic surgery over the last ten years has implied a notable mutation of certain minimally invasive procedures, making it possible to overcome some limitations of the traditional laparoscopic technique. Robot-assisted gastric resection with D2 lymph node dissection has been shown to be safe and feasible in prospective and retrospective studies. However, to date there are no high quality comparative studies investigating the advantages of a robotic approach to GC over traditional laparoscopic and open gastrectomy. On the basis of the literature review here presented, robot-assisted surgery seems to fulfill oncologic criteria for D2 dissection and has a comparable oncologic outcome to traditional laparoscopic and open procedure. Robot-assisted gastrectomy was associated with the trend toward a shorter hospital stay with a comparable morbidity of conventional laparoscopic and open gastrectomy, but randomized clinical trials and longer follow-ups are needed to evaluate the possible influence of robot gastrectomy on GC patient survival.
Key words: Gastric cancer; Gastric resection; Minimally invasive surgery; Laparoscopic gastrectomy; Robot-assisted gastrectomy
© The Author(s) 2016. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Laparoscopic gastrectomy has been de-monstrated to be feasible and oncologically adequate for early gastric cancer (GC). Major criticism arose instead towards the spread of the use of laparoscopy for advanced GC, principally due to its poor suitability to complex maneuvers, such as extended lymphadenectomy. In recent years, robotic surgery techniques have been shown to make certain laparoscopic procedures easier and safer, such as during D2 lymph node dissection. Authors increasingly cite robotic-assisted gastrectomy as one of the most promising tools to extend the minimally invasive surgical indications for advanced GC patients.
Caruso S, Patriti A, Roviello F, De Franco L, Franceschini F, Coratti A, Ceccarelli G. Laparoscopic and robot-assisted gastrectomy for gastric cancer: Current considerations. World J Gastroenterol 2016; 22(25): 5694-5717 Available from: URL: http://www.wjgnet.com/1007-9327/full/v22/i25/5694.htm DOI: http://dx.doi.org/10.3748/wjg.v22.i25.5694
INTRODUCTIONTotal and distal gastrectomy with D2 lymph node dissection is the recommended surgical procedure for resectable (curable) gastric cancer (gc) patients[1]. The current medical evidence shows that standardized
extended (D2) lymphadenectomy leads to better results than standardized limited (D1) lymphadenectomy in terms of lower loco-regional recurrence and gastric-cancer-related death rates, with equal postoperative mortality, morbidity and re-operation rates so far, thanks to the currently standard safer spleen-preserving D2 resection technique[1].
Laparoscopic surgery was introduced for the treat-ment of gc in 1991, when Kitano et al[2] performed the first laparoscopically assisted gastrectomy for gc. Since then laparoscopic assisted distal gastrectomy (LADg) for distal early-stage gc has progressively spread worldwide, especially in Eastern countries, such as Japan and South Korea[3,4]. During the years, reports have provided level Ⅲ evidence that LADg is technically safe and that it yields better short-term outcomes than conventional open gastrectomy for early-stage gc[5]. While laparoscopic gastrectomy (Lg) has become standard therapy for early-stage gc, especially in Asian countries, such as Japan and South Korea[5,6], a safer spleen-preserving Lg with D2 resection technique for the treatment of more advanced gc did not meet the same values and is currently available only in high-volume centers. The widespread diffusion of laparoscopic surgery to manage advanced gc[7,8] was limited, mainly by the technical difficulties posed by the total gastrectomy and the complexity of D2 lymphadenectomy, which entailed the removal of node stations along the celiac trunk, left gastric artery and hepatic pedicle. This gave rise to concern regarding the oncological feasibility and long-term outcomes of laparoscopic surgery for advanced gc.
The introduction of robot-assisted techniques improved some surgical procedures, especially when precise dissection is required, and gives them an advantage over conventional laparoscopy techniques. By making it possible to overcome some intrinsic limitations of the traditional laparoscopic approach, robot-assisted Lg is advocated by some authors as able to facilitate complex reconstruction after gastrectomy and the lymph node retrieval, so as to permit radical resection and adequate lymph node dissection also in advanced gc patients[9-11].
LAPAROSCOPIC GASTRECTOMY In the past decade, laparoscopic techniques have gained wide clinical acceptance in surgical practice. The principal advantages of laparoscopic over conventional open surgery are the reduction in stress, induced by minimal manipulation of the small bowel and the use of a small incision, accounting for earlier return to normal bowel function with earlier resumption of oral intake, less postoperative nausea, vomiting, and abdominal discomfort, reduction of postoperative pain and acceleration of discharge from hospital. Mitigating surgical stress reduces the generalized inflammatory reaction; consequently, it may lead to a reduction in
5695 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Caruso S et al . Robot-assisted laparoscopic gastrectomy for GC

the overall complication rate. Laparoscopic surgery was introduced for the
treatment of gc in 1994 by Kitano et al[2], who performed the first laparoscopically assisted distal gastrectomy (LADg) for early gc. Since then LADg for distal early-stage gc has progressively spread worldwide, especially in Eastern countries, such as Japan and South Korea[3,4].
During the years a large number of outcome variables were analyzed for individual series and comparative trials between laparoscopic assisted gastrectomy (LAg) and open gastrectomy (Og)[12]. Laparoscopic surgery was reported to give similar results to those with the open method regarding the oncological principles, with generally better postoperative patient comfort[12]. However, mainly due to the heterogeneity of available data and the extreme complexity of such a structured matter, comprising different topics on gc also worthy of being treated by different approaches, any meaningful conclusions regarding the advantages or disadvantages of LAg over conventional open procedures are difficult to draw. It was decided that this review strategy of discussion would divide the topic in main areas by the separation of two essentially different laparoscopic techniques, distal and total gastrectomy, and two fundamental oncological aspects, early and advanced gcs. Finally, we discussed the potential advantage of the newer introduction of the robotic assisted laparoscopic technique.
Laparoscopic assisted distal gastrectomy Several reports demonstrated that laparoscopic distal gastrectomy is a feasible and safe technical option in the treatment of gc, in particular for early gc[3].
However, the comparative data between this technique and the conventional open distal gastrectomy (ODg) originated mainly from retrospective and observational studies with a small number of patients, and limited essentially to early gc patients. Randomized controlled trials (RcTs) are few and have few patients. These studies largely represent the experience of Eastern countries.
In the last years, a number of meta-analysis on this topic have been published. There are 4 meta-analyses[3,13-15] based on few RcTs and a large number of retrospective and prospective studies that compare short-term outcomes of LADg and conventional ODg. The meta-analysis of Hosono et al[13] published in 2006 (12 retrospective studies, 4 RcTs) included patients with advanced gc, while Yakoub et al[3] (2009, 12 retrospective studies, 3 RcTs) and Zeng et al[15] (2012, 17 non-randomized studies, 5 RcTs) focused on early gc only. Finally, the more recent and large meta-analysis by Viñuela et al[14] (2012) included 6 RcTs and 19 high quality non-RcTs, with global 3055 patients (1658 LDg, 1397 ODg) studied, with a high proportion
of stage Ⅰ cancers. All these analyses reported that LADg for gastric
adenocarcinoma is associated with comparable or lower complications, reduction in the operative blood loss, less pain, faster bowel function recovery, and shorter hospital stay with respect to ODg. Moreover, all the meta-analysis demonstrated that LADg has a similar or lower overall morbidity rate, but that a higher number of lymph nodes were harvested by ODG, although this number did not become significant when less than D2 lymphadenectomy was performed.
Other 6 meta-analysis[4,16-20] focused on the comparative evaluation between LADg and ODg considering RcTs only. The meta-analysis of Memon et al[16] (2008) and Sun et al[17] (2012) focused on 4 and 8 RcTs respectively, including all gc patients independently from the tumour stage. The other 4 meta-analysis[4,18-20] focused their evaluation on respectively 4, 6, 6, and 7 RcTs comparing LADg and ODg restricted to early gc only. currently, other 2 meta-analysis[21,22], have been published in literature which included 6 and 8 randomized studies respectively, but they are both biased due to an inclusion criteria error. These authors, in fact, claimed to have conducted a meta-analysis of RcTs on LADg vs ODg for early gc, but effectively they included two studies (Huscher et al[7] and Varela et al[23]) the former is not limited to early cancer, and the latter is not a RcT .
However, all these studies showed essentially similar results, reporting a significant reduction of intraoperative blood loss in favor of LADg, at the expense of significantly longer duration of operating time and significant reduction in lymph nodes harvesting compared to the conventional open procedure. Length of hospital stay, complications, tumour recurrence and mortality rates were found to be similar in both groups or smaller in the laparoscopy group.
Thus, globally in all these meta-analysis, whether only data from RcTs is considered or data pooled by prospective studies, or whether gc unselectively from their stages is considered, or whether the analysis is limited to early gc only, the result of an inferior number of lymph nodes harvesting by LADg compared to ODg is always constant. Just only one recent meta-analysis[24] reported a dissimilar result in regards to number of lymph nodes dissected, but it focused only on non-randomized retrospective studies. In fact, the work of Ding et al[24] included studies comparing LADg and ODg for gc only associated to D2 lymphadenectomy, while all patients submitted to lymphadenectomy inferior (D1 or D1+α or D1+β) or superior (D2+ or D3) to D2, independently from the gc stage, were excluded from the final analysis. Eight retrospective nonrandomized studies, totaling 1065 distal gastrectomies (510 LADg and 555 ODg),
5696 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Caruso S et al . Robot-assisted laparoscopic gastrectomy for GC

5697 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
the patient’s attitude as well as the policy of practice of the surgical team. This may explain the significant heterogeneity between studies which could not be overcome by subgroup analyses.
Moreover, clinical evidence regarding long-term outcomes of LADg for gc is still lacking. Only 1 prospective randomized controlled trial (Huscher et al[7]) reported no significant difference in the 5-year overall survival and disease-free survival rate between LADg and ODg. Several retrospective studies reported comparable results[13], of which one of the largest is the study of gordon et al[30], that have the merit of focusing on patients with advanced gc, comparing LADg to ODg with quite a long follow-up period (mean of 49.2 mo). The study involved 201 patients, 66 of whom underwent LADg, and the authors did not find significant differences in terms of 5-year overall survival and disease specific compared to those submitted to ODg.
However, an overall shortage of statistical sig-nificance in the long-term outcomes of LADG still exists and may be attributable principally to the small sample size. Therefore, there was no sufficient data to allow a definitive conclusion on survival after LADG and long-term survival benefit remains to be proven by many high-quality RcTs with larger sample sizes.
Other limitations that warrant emphasis are the following. Most high quality data originates from Eastern experience. An intrinsic biological difference in gc tumour between Eastern and Western countries is well known. Molecular and biological evidence suggests that gastric adenocarcinoma can be divided into distinct sub-types based on the predominant histology and distinct patterns of gene expression[31,32]. Western patients typically present with more advanced lesions, have a higher proportion of proximal or gastro-oesophageal-junction tumours, and a greater proportion of diffuse-type histology[33]. Understanding geographic differences and the clinical and pathologic manifestations of various gc sub-types could in the future help to direct the surgical and medical management of this heterogeneous disease. Moreover, the advancements in diagnostic modalities and mass examination techniques employed in Eastern countries, together with nationwide screening and Helicobacter pylori eradication programs that have been in act for several years in Asia[34,35], have made the earlier detection of gc with respect to West possible. This meant more patients with early gc and an increase in the awareness of minimally invasive approaches for treatment. conversely, the disease incidence is much lower in the West and a greater proportion of patients present with locally advanced tumor that render laparoscopic resection less feasible. Notably, in many institutions in the United States and some in Western countries an extensive prophylactic lymphadenectomy D2 in advanced gc patients is not routinely performed,
were considered suitable for this meta-analysis. The final results were similar to the previous ones in terms of decreased blood loss, fewer complications, faster recovery, shorter hospitalization, as well as longer operating time in the LADg group, but no evident differences regarding the number of lymph nodes dissected were found between the two groups. Probably, the main reason for this discrepancy, other than the fact that all the included studies were retrospective and thus potentially leading to some selection bias, is that the meta-analysis of Ding et al included only gastrectomies with D2 lymphdenectomy, while previous meta-analysis on LADg[3,13-20] comprised different proportions of D1, D1+ ad D2 lymph nodes dissection. Extended D2 lymphadenectomy is a more complex procedure, principally indicated for advanced gc, and thus it is a procedure only more recently performed in highly experienced centers. In fact, the series included in the study of Ding et al are essentially newer compared to those in previous meta-analysis[3,13-20]. As the operative technique has developed, the number of lymph nodes dissected by LDg has gradually increased[25] and increasingly highly skilled surgeons will report adequate D2 lymphadenectomy[24,25]. The improvements in ins-truments and techniques could enable ever more surgeons to carry out an extended lymphadenectomy and decrease the operating time for LADg[13,26], which is essentially related to the knowledge of and familiarity with the laparoscopic system and the skill of the operating team[27].
Therefore, as lymph node metastasis has been considered one of the most significant predictive factors for recurrence and subsequently survival in patients with gc[3,28], concern has been raised regarding the oncological adequacy of LADg, which generally yields a lower number of lymph nodes with respect to ODg. The oncologic effect of procuring less nodes after LADg is understandable only if we separate early from advanced gc, treatment of which will occur in the following sections. Instead, with regards to the technical aspects, what must be outlined here is that laparoscopic systematic D2 lymphadenectomy is technically complicated. Large vessels have to be identified and extensive lymph node dissection has to be performed. In particular, this laparoscopic procedure is complex in the dissection of the perigastric lymph nodes along the major curvature and the second tier nodes along the celiac and splenic arteries[29]. Essentially, LADg with D2 lymphadenectomy remains a challenging and time-consuming procedure, and is significantly longer than ODg[3,13]. Another important point of potential heterogeneity and bias among results of different studies is that most postoperative recovery measures, such as time to oral intake and walking, as well as administration of analgesic drugs and length of hospital stay, are rather subjective and dependent on
Caruso S et al . Robot-assisted laparoscopic gastrectomy for GC

5698 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
firstly because complications of open gastrectomy with extended lymphadenectomy are still high enough to be considered disadvantageous in balance with oncologic benefit, and secondly because they are at low volume centers where experience with advanced laparoscopic gastric surgery is limited. A recent multi-center analysis[36] reported a median of 14 lymph nodes examined in a United States minimally invasive cohort, which is inadequate according to consensus guidelines. conversely, higher operative case volume was associated with the greatest odds of adequate lymph node staging, confirming the association between surgical volume and surgical quality[37,38]. As long as these differences between East and West exist, an appropriate comparison of the results among studies of different geographic origin is difficult, and in particular what is not strictly appropriate is to translate Asian results to western gc patients without proper confirmation.
In conclusion, LADg is associated with a similar or lower morbidity and better short-term outcomes compared to ODg. considering the literature evidence concerning its oncological adequacy, LADg is indicated for early gc and presently has become a routine option in South Korea and Japan for these early lesions. On the other hand, these results largely represent the Eastern experience and cannot be extrapolated to patients with advanced tumours. Significant limitations exist to draw definitive conclusions for all gc patients and for oncologic adequacy of laparoscopic D2 lymphadenectomy. The limited number of published RcTs, the small sample sizes to date and the limited duration of follow up does not make it possible to indicate the use of LADg as adequate for every advanced gc. Further large multi-center RcTs are required to increase statistical power and to delineate significantly quantifiable differences between LADg and ODg. In particular, well-designed RcTs which standardize postoperative measures and elucidate oncological clearance, including the quality of lymphadenectomy and long-term outcomes, are needed to establish whether LADg could be a standard treatment for advanced gc too.
Laparoscopic total gastrectomyIn contrast to LADg, there is not such a widespread acceptance of laparoscopic assisted total gastrectomy (LATg) as an alternative to the open approach, essentially due to its technical difficulty. In particular the procedure gives rise to concern about the com-plexity encountered in composite reconstruction of the alimentary tract, such as esophago-jejunal anastomosis, and potentially serious subsequent complications.
currently, there is no standard method for res-toration of continuity of the oesophagus and jejunum. In open surgery, an esophagojejunostomy is typically
performed end-to-side using a circular stapler. This procedure is very difficult to reproduce in conventional laparoscopy, because placing a purse-string suture on the esophageal stump requires particular skill.
Solutions to restore the digestive transit following LATg have been reported. The most common are to perform a laparoscopic intracorporeally esophago-jejunostomy using a linear stapler (side-to-side)[39] or with a circular stapler (end-to-end)[40]. Alternatively with a hybrid-open technique performing the eso-phagojejunostomy extra-corporeally through the same minilaparotomy used for specimen removal[41] or with a full robotic technique performing hand-sewn anastomosis[42]. The optimal method to perform anastomosis remains to be established and it is probable that there is not one single optimal method.
Opponents to LATg argue that there is a higher incidence of major intra- and post-operative com-plications due to the complexity of the procedure, made difficult also by the absence of tactile sensation, much longer anesthetic and operating times and insufficient surgical resection margins compared to conventional open gastrectomy[16]. The incidence of post-operative complications is reported to be higher when compared with distal gastrectomy too. The rates of infra-operative and post-operative complications in LATg were 2.6% and 21.8%, respectively[43], which is still high, despite the progressive development of laparoscopic techniques and while the complication rate in LADg is decreasing year by year.
Recently a systematic review[44] was conducted to research studies comparing LATg with open total gastrectomy (OTg) in gc. Only 8 non randomized comparative or case-control studies fulfilled quality criteria and were selected for this meta-analysis. LATg demonstrated compared with OTg a significant reduction of intra-operative blood loss, a reduced risk of post-operative complications, a shorter hospital stay, at the cost of longer operative time. Fewer lymph nodes were dissected in LATg than in OTg, even though the difference was not significant. Data on long-term survival were not sufficiently addressed in the included studies. In conclusion, thus far, no randomized clinical trials evaluating LATg have been conducted and studies available to date can be seen as pioneer work.
Recent meta-analyses[45,46] of LATg have shown that this procedure is feasible in terms of safety and survival, leading to a reduced risk of post-operative complications compared with OTg similar to the risk after LADg, despite the expense of longer operative time. But overall, data available in literature are poor. The sample sizes in these studies were small, there have been no high-quality RcTs, and the existing studies have limitations of potential bias and heterogeneity. The majority of the available studies focuses on early gc and originates from Asian countries[5,23,47-49]. Moreover, among the few reports which focused on the procedure
Caruso S et al . Robot-assisted laparoscopic gastrectomy for GC

5699 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
of L
ATg
for
adva
nced
gc
the
maj
ority
includ
ed le
ss a
dvan
ced
dise
ase,
suc
h as
tho
se a
t st
age Ⅱ
or
stag
e Ⅲ
a[50,
51] , w
hile
the
effe
cts
of L
ATg
for
mor
e ad
vanc
ed g
c, s
uch
as s
tage
s Ⅲ
b an
d Ⅲ
c di
seas
e, h
ave
been
rar
ely
repo
rted
. Ju
st o
ne r
ecen
t re
tros
pect
ive
sing
le in
stitu
tion
stud
y[52] f
ocus
ed o
n la
paro
scop
ic t
otal
gas
trec
tom
y (L
Tg)
for
adva
nced
gc,
includ
ing
quite
a la
rge
prop
ortio
n of
sta
ge Ⅲ
b an
d Ⅲ
c tu
mou
rs a
lso.
The
aut
hors
dem
onst
rate
d th
at in
the
se p
atie
nts
LTg
(n
= 9
76)
yiel
d co
mpa
rabl
e on
colo
gica
l and
sur
gica
l out
com
es c
ompa
red
to L
ADg
(n
= 6
46).
Fin
ally,
mos
t of
the
se s
tudi
es d
ocum
ente
d th
e su
cces
s of
lapa
rosc
opic-a
ssiste
d ga
stric
res
ectio
n, w
hile
on
ly a
few
stu
dies
hav
e ex
amin
ed the
tot
ally
lapa
rosc
opic a
ppro
ach[5
3], a
nd p
rosp
ectiv
e st
udie
s co
mpa
ring
tota
lly la
paro
scop
ic tot
al g
astr
ecto
my
to the
ope
n m
etho
ds a
re
lack
ing.
Thu
s th
e re
sults
wer
e no
t con
clus
ive.
Early
GC
Sinc
e it
was
intr
oduc
ed, t
he la
paro
scop
ic te
chni
que
has
been
pro
gres
sive
ly u
sed
by s
ever
al s
pecial
ized
cen
ters
for th
e tr
eatm
ent o
f ear
ly g
c. P
hase
Ⅲ tr
ials (
Tabl
e 1)
[54-
60] ,
all o
rigin
ated
fro
m E
aste
rn s
erie
s, a
nd a
num
ber
of m
eta-
anal
ysis
[3,4
,14,
15,1
8-20
] dem
onst
rate
d be
nefit
s on
sho
rt-t
erm
pos
tope
rativ
e ou
tcom
es (
incl
udin
g le
ss b
lood
loss
, le
ss p
ain,
low
er in
cide
nce
of p
osto
pera
tive
com
plic
atio
ns, s
hort
er h
ospi
tal s
tay
and
rapi
d re
cove
ry)
of L
ADg
com
pare
d to
OD
g in
the
tre
atm
ent of
gc
at e
arly
sta
ge. A
s di
scus
sed
in the
“La
paro
copi
c di
stal
gas
trec
tom
y” s
ectio
n to
dat
e, s
ever
al in
vest
igat
ions
hav
e re
port
ed n
o di
ffere
nces
in r
ecur
renc
e or
sur
viva
l fol
low
ing
LAD
g a
nd O
Dg
fo
r ea
rly g
c lo
ng ter
m[5
,7,2
5,61
] , alth
ough
all
the
avai
labl
e m
eta-
anal
ysis
on
mor
e re
leva
nt p
oole
d da
ta s
how
ed tha
t th
e ov
eral
l num
ber
of ly
mph
nod
es r
etrie
ved
was
less
in
LAD
g c
ompa
red
to O
Dg
[4,1
6,18
] . An
Asi
an m
eta-
anal
ysis
invo
lved
stu
dies
com
parin
g LA
g v
s O
g,
inde
pend
ently
fro
m t
he t
ype
of g
astr
ecto
my
(tot
al o
r su
btot
al)
for
early
gc[6
2] in
clud
ed 5
RcT
s an
d 11
cas
e co
ntro
ls a
nd rep
orte
d es
sent
ially
com
para
ble
resu
lts to
thos
e of
pre
viou
s m
eta-
anal
ysis
. W
hy lo
wer
num
ber
of h
arve
sted
lym
ph n
odes
did
not
affe
ct lo
ng-t
erm
sur
viva
l in
early
gc
patie
nts
can
be e
xpla
ined
by
the
fact
tha
t su
rviv
al o
utco
me
is li
kely
to
be
mor
e to
lera
nt t
o a
less
ext
ensi
ve ly
mph
aden
ecto
my
com
pare
d to
adv
ance
d g
c st
ages
. In
fac
t, t
he p
atte
rn o
f ly
mph
nod
e m
etas
tasi
s to
the
2nd
tie
r (N
2) o
f no
des
is
only
3.5
% e
ven
in s
ubm
ucos
al c
ance
r[63] a
nd th
e pr
eval
ence
of d
ista
nt m
etas
tasi
s in
rec
urre
nce
patie
nts
indi
cate
s th
at tr
eatm
ent f
ailu
re m
ay b
e du
e to
sys
tem
ic tu
mou
r sp
read
rat
her
than
loca
l spr
ead[3
] . Ac
cord
ingl
y, t
he J
apan
ease
gc
Asso
ciat
ion
(JG
CA)
reco
mm
ende
d a
cons
erva
tive
sub-
D2
lym
phad
enec
tom
y, d
esig
nate
d m
odifi
ed
gast
rect
omy
A an
d B,
to S
tage
s IA
and
IB
gcs
[64].
Thus
, fo
r ea
rly g
cs,
part
icul
arly
for
tho
se w
ith in
freq
uent
lym
ph n
ode
met
asta
sis,
LAD
g h
as b
ecom
e a
wid
ely
acce
pted
alte
rnat
ive
trea
tmen
t op
tion
and
in A
sian
co
untr
ies,
suc
h as
Jap
an a
nd S
outh
Kor
ea, i
t has
bec
ome
a st
anda
rd th
erap
y[5,6
] .In
con
clus
ion,
des
pite
the
low
er n
umbe
r of
ret
rieve
d ly
mph
nod
es in
LAD
g c
ompa
red
to O
Dg
, a le
ss e
xten
sive
lym
phad
enec
tom
y in
LAD
g is
onc
olog
ical
ly a
dequ
ate
for
early
gc
and
thus
LAD
g w
ill n
ot c
ompr
omis
e su
rviv
al in
the
se p
atie
nts
even
whe
n pe
rfor
med
with
a s
ub-D
2 ly
mph
aden
ecto
my.
On
the
cont
rary
, th
is c
oncl
usio
n ca
nnot
be
extr
apol
ated
for
cas
es w
ith m
ore
adva
nced
sta
ge,
in w
hich
the
sur
viva
l ben
efit
for
radi
cal l
ymph
aden
ecto
my
is w
ell e
stab
lishe
d[1] .
How
ever
, on
e im
port
ant
aspe
ct s
houl
d be
out
lined
: it
is v
ery
diffi
cult
to d
iagn
ose
early
gc
accu
rate
ly b
efor
e op
erat
ion
and
the
unde
rest
imat
ion
of t
he p
reop
erat
ive
stag
e is
a w
ell k
now
n pr
oble
m[6
5]. A
risk
of u
nder
sta
ging
gc
has
been
rep
orte
d to
occ
ur in
up
to 2
5% o
f pat
ient
s di
agno
sed
preo
pera
tivel
y as
ear
ly g
c[66-
68] .
For
this
rea
son,
car
e sh
ould
be
Tabl
e 1 Ran
dom
ized
con
trol
led
tria
ls c
ompa
ring
lapa
rosc
opy-
assist
ed d
ista
l gas
trec
tom
y w
ith
open
dista
l gas
trec
tom
y in
the
tre
atm
ent
early
gast
ric
canc
er
Ref
.Yea
rC
ount
ryPa
tien
ts (n
)O
pera
tive
tim
e1 (
mea
n ±
SD
, m
in)
Blo
od lo
ss1 (
mea
n ±
SD
, m
L)H
arve
sted
nod
es1 (
mea
n ±
SD
, n)
Com
plic
atio
ns r
ate
(%)
Hos
pita
l sta
y1 (
mea
n ±
SD
, d)
LDG
OD
GLD
GO
DG
P v
alue
LDG
OD
GP
val
ueLD
GO
DG
P v
alue
LDG
OD
GP
val
ueLD
GO
DG
P v
alue
Kita
no et
al[5
4]
2002
Japa
n14
1422
7 ±
717
1 ±
13<
0.05
177
± 30
258
± 53
< 0.
0520
.2 ±
3.6
24.9
± 3
.5<
0.05
14.3
28.6
< 0.
0517
.6 ±
2.6
1
6 ±
0.4
< 0.
05Fu
jii et
al[5
5]20
03Ja
pan
1010
225
± 3
517
9 ±
37<
0.05
134
± 1
1020
5 ±
75<
0.05
NR
NR
- 2
.0 2
.0N
SN
RN
R-
Hay
ashi
et a
l[56]
2005
Japa
n14
14 3
78 ±
97
235
± 71
< 0.
05 3
27 ±
245
489
± 2
81<
0.05
28
± 14
27
± 10
NS
28.6
57.1
< 0.
0512
± 2
18
± 6
< 0.
05Le
e et
al[5
7]20
05So
uth
Kor
ea24
23 3
19 ±
16
235
± 71
< 0.
05 3
36 ±
180
294
± 1
56N
S 3
1.8
± 13
.5 3
8.1
± 15
.9<
0.05
12.5
43.5
< 0.
0511
± 4
17
± 1
5<
0.05
Kim
et a
l[58]
2008
Sout
h K
orea
8282
252
± 4
817
0 ±
27<
0.05
111
± 85
267
± 1
55<
0.05
3
9 ±
11.9
45.
1 ±
13.8
< 0.
05 0
.0 4
.9<
0.05
7.2
± 1
.48.
6 ±
2N
SSa
kura
mot
o et
al[5
9]20
13Ja
pan
3132
182
± 3
711
3 ±
21<
0.05
64
± 48
167
± 1
35<
0.05
31.
6 ±
12.2
33.
8 ±
13.4
NS
3.2
15.6
< 0.
05 9
.1 ±
1.1
1
0 ±
3.1
NS
Taki
guch
i et a
l[60]
2013
Japa
n20
20 1
85 ±
23
119
± 17
< 0.
05 6
5 ±
51 1
80 ±
111
< 0.
05 3
3.0
± 13
.7
32 ±
5.2
NS
0.0
10.0
< 0.
05
10 ±
0.2
1
1 ±
0.7
NS
1 Mea
n va
lue.
LD
G: L
apar
osco
pic
dist
al g
astr
ecto
my;
OD
G: O
pen
dist
al g
astr
ecto
my;
NS:
Not
sta
tistic
ally
sig
nific
ant;
NR:
Not
repo
rted
.
Caruso S et al . Robot-assisted laparoscopic gastrectomy for GC

5700 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
taken to increase the accuracy of the preoperative diagnosis before performing minimally invasive gastrectomy by selecting properly indicated patients; conversely, on the basis of this risk, other investigators emphasized the routine need for D2 dissection, even in cases preoperatively suspected as early gc[66,67].
Advanced GC The use of laparoscopic surgery in the management of advanced gc, contrary to early gc, has not yet met analogous widespread acceptance, mainly due to the controversial issue on the technical difficulty of carrying out D2 lymphadenectomy and insufficient data related to the procedure’s oncological adequacy[69-71]. As treatment options differ for these different stages of gc, the results of laparoscopic surgery for early stage cannot be directly applied to advanced gc.
Even experienced minimally-invasive surgeons reported the technical difficulty of laparoscopic extra-perigastric lymphadenectomy[72]. While a number RcTs and meta-analysis have been published for early gc patients (as discussed in “Laparoscopic distal gastrectomy” and “Early gc” sections), such studies have not been conducted for the majority of cases with advanced gastric tumour.
Since Uyama et al[8] first reported laparoscopy assisted total gastrectomy with D2 lymphadenectomy and distal pancreaticosplenectomy for advanced upper-third gcs in 1999, several studies have been reported to determine the technical feasibility of D2 lymphadenectomy in patients with advanced gc[66,73-78]. Although most of these series are retrospective and small, the first results have shown no differences in terms of oncological adequacy, recurrence, morbidity and survival rates of LAg compared with the open approach, confirming at the same time the well known advantages of minimally invasive surgery in improvement of postoperative outcomes[7,71,73,76,79-82].
In 2013, Qiu et al[83] conducted a systematic review and meta-analysis on LADg vs ODg for advanced gc. No RcTs were found by the authors’ search. con-clusively, 7 case-control studies involving 1271 patients (626 LADg and 645 ODg) were considered eligible for the final pooled analysis. The meta-analysis revealed that LADg patients had longer operative time, less estimated blood loss, fewer analgesic requirements, and a shorter hospital stay compared to ODg. There were no significant differences between the 2 groups in number of lymph node dissections, post-operative mortality and complication rates, and 3-year overall survival rate.
Recently, 2 meta-analysis have been conducted[84,85] comparing the clinical outcome of both partial and total LAg and Og for the treatment of advanced gc. In the first[84] overall 7 studies were selected for the analysis (1 prospective RcT, 1 comparative prospective study and 5 comparative retrospective studies), including a
total of 452 patients (174 in the LAg and 278 in the Og group). In the second one[85], overall 26 studies were included (1 prospective RcT, 1 comparative prospective study and 24 comparative retrospective studies), totaling 5061 patients, of which 2193 (43.3%) treated by LAg and 2868 (56.7%) underwent Og. The results of both these meta-analysis are overlapping. compared to Og, laparoscopic total and partial gas-trectomy demonstrated a longer operative time but lower blood loss and shorter postoperative hospital stay. Moreover, there were similar outcomes between both approaches in terms of number of dissected lymph nodes, and overall survival and disease-free survival.
The Korean Laparoscopic gastrointestinal Sur-gery Study group (KLASS) recently published their experience on long-term outcomes in patients undergoing laparoscopic resection for advanced lesions[86]. In this multi-center retrospective trial, the long-term outcomes of LAg for advanced gc was analyzed in a relatively large number of cases (n = 239). The median follow-up period was 55.4 mo with an overall 5-year survival rate of 78.8% and disease-specific 5-year survival rate of 85.6%, which were considered comparable to those previously reported for open gastrectomy.
These results make it possible to conclude that laparoscopic resection for advanced gc is feasible with oncologic equivalence to open resection. Although more time was needed to perform LAg, it had some advantages over Og in achieving faster postoperative recovery. However, most studies to date were retro-spective, their case volumes varied greatly, and a high heterogeneity between them can be recognized, which could significantly affect the final results of pooled data meta-analysis. Thus, these results are promising, but need to be confirmed in further prospective controlled randomized trials.
SPECIFIC CONSIDERATIONS ON LAPAROSCOPIC D2 LYMPHADENECTOMYAlthough only gradually accepted by Western in-vestigators, gastric resection with extended (D2) lymphadenectomy is the standard procedure for advanced gc. The long-term results of RcTs have reported superiority in the survival rate of patients who underwent D2 dissection relative to that of limited (D1) lymphadenectomy[1,87].
Thus, extended D2 lymph node dissection has its proper indication for advanced gc and the ability to perform an adequate D2 lymphadenectomy, with low morbidity and mortality, is crucial for the treatment of local advanced gc.
gradually, with the passing of time, together with
Caruso S et al . Robot-assisted laparoscopic gastrectomy for GC

5701 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
the improvement of laparoscopic technology, an increasing number of surgeons have demonstrated their ability to perform an adequate laparoscopic D2 lymphadenectomy. For example, Huang et al[88] respectively compared 66 vs 69 advanced gc patients who underwent LADg and ODg with D2 lymphadenectomy, and found that similar numbers of lymph nodes were collected in the two groups. Furthermore, the LADg group showed less infra-operative blood loss, earlier bowel recovery, and shorter hospital stays, without increasing the risk of postoperative morbidity and mortality. Zhao et al[89] objectively compare the surgical outcomes of 133 LADg and 133 ODg in a well-matched design trial, showing that LADg with D2 lymphadenectomy is comparable to open surgery in terms of its technical feasibility and safety, and with total numbers of collected lymph nodes similar in the two groups.
Recently two prospective RcTs[65,90] have been conducted to better elucidate the proficiency in performing D2 lymphadenectomy by laparoscopic tool. cai et al[90] focused their analysis on only advanced gc, comparing open vs laparoscopy-assisted D2 radical gastrectomy: 96 patients were randomly assigned to the LAg group (n = 49) and to the Og group (n = 47) cases. A similar number of harvested lymph nodes was obtained in both groups (22.98 ± 2.704 vs 22.87 ± 2.428, p = 0.839), at the price of significantly longer mean operating time for the LAg group. The postoperative morbidity rate was similar in the two groups, however pulmonary infection was observed more frequently in the Og group. Moreover, after a mean follow-up of 22 mo, the authors did not find a statistically significant difference in the overall estimated survival rate for patients in both groups. The second RcT[65] was conducted again with the specific aim of evaluating the radicalness and safety of laparoscopic D2 dissection, but in this case with unselective criteria for gc stage. The authors included 270 patients (128 in LAg and 142 in Og) with either early and advanced gc, submitted to either subtotal or total gastrectomy. Similir to cai et al[90], the authors did not find significant differences in the number of harvested lymph nodes and morbidity rates between the two groups.
In adjunct to these above mentioned studies, 2 meta-analysis[91,92] have been published which included pooled data on this issue and which reproduced essentially similar results. The more recent meta-analysis published in 2014 by Zou et al[91] focused on studies comparing open and laparoscopic D2 gastrectomy for the treatment of advanced gc. The analysis included only one RcT, that of cai et al, and 13 non-RcTs, with a total of 2596 eligible for the meta-analysis. Instead, the analysis of Wei et al[92] involved trials comparing laparoscopic and open gastrectomy with D2 lymphadenectomy for gc unselectively from
the tumor stage, thus including also early gc. The authors found 10 trials eligible for inclusion in the meta-analysis, of which one (i.e., a work of Lee et al[25] that is restricted to early gc) partially conducted in a randomized way and the rest case-control retrospective studies. In both this 2 meta-analysis, the authors concluded that LAg associated to laparoscopic D2 gastrectomy in comparison to the open procedure showed no significant differences regarding number of harvested lymph nodes, and tumour recurrence, disease-free and overall survival rates. However, laparoscopic gastrectomy had a longer operative time.
On the basis of these results, all the authors concluded that LAg with D2 lymph node dissection, despite being a technically demanding and time-consuming procedure, is a safe and feasible procedure with adequate lymphadenectomy, good curability and survival rate for the treatment of gc. With regard to lymph nodes harvested, this conclusion is slightly discordant with respect to the result of meta-analysis restricted to RcTs on LADg: as discussed in the “Laparoscopic distal gastrectomy” section, ODg demonstrated essentially to be associated with a major number of harvested lymph nodes than LADg. In order to explain this a main reason could be hypothesized. Laparoscopic procedures, in particular those as complex as extended lymphadenectomy and total gastrectomy, are characterized by a typical steep learning-curve. The discrepancy on results of previous meta-analysis regarding the number of harvested lymph nodes may be due to the combination of data from studies with different lymphadenectomy levels and from different periods of publication, other than the heterogeneity and low quality of studies involved which could lead to bias. In fact, a similar discrepancy in the number of lymph nodes retrieved was revealed also for the results of LADg when the procedure is meta-analyzed associated with D2 lymphadenectomy only, while excluding LADg with lymphadenectomies inferior to D2[24]. As confirmed by the meta-analysis of Ding et al[24], if this type of restriction is applied, the number of lymph node harvested by laparoscopy tended to become similar to those retrieved by open procedure. On the other hand, the RcTs of cai et al[90] and cui et al[65] introduced in their analysis a significant proportion of total gastrectomies. Both these procedures, i.e. laparoscopic extended D2 lymphadenectomy and laparoscopic total gastrectomy, are more complex, and only recently more frequently performed in highly experienced centres, than LADg with D1+ lymphadenectomy, which conversely are typically performed for early gc. Thus, these tech-niques are described in essentially newer series on advanced gc with respect to the meta-analysis limited to LADg and early gc[3,4,14,15,18-20]. So the heterogeneity is founded on the different skills among different surgical teams achieved during the years.
Caruso S et al . Robot-assisted laparoscopic gastrectomy for GC

5702 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
The increasingly reported adequacy of D2 dissection in literature is indeed probably due to the progressively higher number of surgeons reaching the plateau of the traditionally steep learning curve of LAg.
In other words, as the operative technique has developed, the number of lymph nodes dissected during either distal and total laparoscopic gas-trectomies has gradually increased and ever more highly skilled surgeons will report an adequate D2 lymphadenectomy[24,25,57]. Thus, while laparoscopic D2 dissection is probably not adequate at the beginning of the experience of every surgeon at the initial phase of the learning curve, it progressively increases and the number of retrieved lymph nodes in LADg tends to be close to or even greater than that in ODg[15].
The importance of the learning curve for LAg has been confirmed by other indications. Kim et al[27] found that LADg with systemic lymph node dissection for early gc requires a long learning curve, at least 50 cases, a surgeon’s familiarity with the endoscopic instruments, and the cooperation of the whole operation team. Ikeda et al[93], with the aim of assessing the oncological quality of laparoscopic D2 lympadenectomy, reported no significant differences in the viewpoint of lymph node dissection between 102 patients treated by LADg and 90 treated by ODg if the LADg was performed by an experienced laparoscopic surgeon. Kunisaki et al[94] demonstrated that the number of harvested lymph nodes during LADg did not differ significantly from that under open surgery, or better still was greater after experience of over 80 cases for an institution or over 40 cases for a surgeon. Moreover, it is reported that optimum proficiency can be achieved with experience in 40 to 60 cases and that a well executed educational system minimizes the steep learning curve[27,94,95].
Thus, in conclusion, the quality of laparoscopic lymph node dissection differs between institutes and depends essentially on the surgeon’s technical proficiency. In future years, increasing numbers of medical institutions will be capable of performing adequate laparoscopic D2 dissections, also for cases of advanced gc. Thanks to the development of laparoscopic technique, the use of LAg for treating gc has expanded also in the historically poor proficient West, such as in the United States, Europe, and other countries[7,43]. globally, these reasons could explain why the passing of time and more trials demonstrate the oncological adequacy of laparoscopic D2 lymphadenectomy compared with traditional open procedure and the reason for the slight variation from results of earlier meta-analysis with respect to the newer ones.
ROBOT-ASSISTED LAPAROSCOPIC GASTRECTOMYTo achieve wider application, new minimally invasive
techniques will necessarily demonstrate that they do not represent a disadvantage with respect to oncologic outcome. In order for gc treatment to be considered oncologically sound, the minimally invasive laparoscopic procedures need to include an appropriate lymphadenectomy. The concern is mainly due to the technical difficulties posed by laparoscopic D2 lymphadenectomy, which requires a highly skilled laparoscopic surgeon, effort and time.
The anatomic complexity of the vascular struc-tures and the technical limits of the conventional laparoscopic instrumentation can make this procedure quite complex even for minimally-invasive well-trained surgeons, and can be associated with significant bleeding during dissection around the hepatic, celiac, and splenic arteries. Relatively difficult areas to access during laparoscopic lymphadenectomy include lymph node stations 4, 6, 9, and 11p[29]. For advanced gc, the Japanese gc Association[64] indicated as the standard therapy complete D2 lymphadenectomy including lymph nodes along the hepatic artery (No. 12a), along the proximal splenic artery (No. 11p), and when carcinoma is located in the lower third of the stomach along the superior mesenteric vein (No. 14v). These are traditionally difficult points of the laparoscopic dissections. Miura et al[29] reported a lower compliance (i.e., no nodal tissue documented at a node station that should have been resected) rate for nodes along the hepatic, celiac, and splenic arteries and a significantly lower number of harvested lymph nodes for the perigastric lymph nodes along the major curvature (Nos. 4 and 6) and second tier nodes along the celiac and splenic arteries (Nos. 9 and 11) when laparoscopic D2 dissection was performed, as compared to open surgery. In a similar station-specific lymph node yield analysis, Bouras et al[96] revealed a statistically significant lower number of lymph nodes retrieved for LDg than for ODg in the common hepatic artery station, and Son et al[97] reported a statistically significant higher mean number of lymph nodes harvested around splenic vessels through a robotic spleen-preserving total gastrectomy with D2 dissection compared to those obtained by a laparoscopic approach. These areas contain the suprapancreatic or splenic hilar lymph nodes and are crucial for D2 lymph node dissection.
It is in this context that robotics is worth looking at, being a potentially valid tool which, within the laparoscopic procedure itself, could allow significant improvement. Robotic technology has been employed in areas of surgery in which precise movements are required and in 1994 it gained the approval of the United States Food and Drug Administration (FDA)[98]. The robotic surgical system can overcome some of the intrinsic drawbacks of conventional laparoscopy surgery, improving maneuverability and vision. The main specific technical disadvantages of conventional laparoscopy are, in fact, the unstable positioning of
Caruso S et al . Robot-assisted laparoscopic gastrectomy for GC

5703 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
the two-dimensional (2D) camera; instruments with restricted degrees of motion, increasing the physiologic tremor of surgeon’s hand, with limited manipulation and ergonomic discomfort; and the “fulcrum effect” (i.e., the need for the surgeon to move his/her hand in the opposite direction to that in which the tip of the instrument is intended to go in the abdominal cavity). In particular, the not ideal and often shallow angulation, together with the traditional non ergonomic nature of laparoscopic instrumentation, make the laparoscopic D2 dissection difficult, requiring particular ability. Moreover, the difficulty is associated with the need for all the members of the operating team to be skilled in laparoscopic procedures, including accurate maneuvering of the camera to view the site of dis-section, as well as very careful handling of forceps to prevent accidental bleeding from adipose tissue and lymph nodes.
While robotic surgery is poorly suited for dissections involving multiple quadrants and heavy structures, such as in gastric surgery for omentectomy, conversely, when precise dissection is needed, especially in a relatively small field of the abdomen, its superiority compared to a traditional laparoscopic technique is crucial. The hand movements of the surgeon, who sits at the master console, are transmitted to the robotic arms through a computerized interface software that removes the natural tremor of the hand. At the same time, the system provides improved dexterity with an internal articulated endoscopic wrist (EndoWristTM System) that allows 7 degrees of freedom, via 180º articulation and 540º rotation and enabling the hand movements of the surgeon into the abdomen to a scale motions filtered at a ratio of 3:1 or 5:1. Finally, the system provides magnified three-dimensional (3D) high-resolution images and stereoscopic vision supported by a dual light supply and dual three-
chipped camera[98]. The view system is characterized by a particular stability of the camera platform, which is held by a robotic arm controller by the first surgeon, that overcomes the physiologic human handling tremor of the traditional laparoscopic camera.
Another advantages of robotic surgery is to facilitate the technical limitation of traditional lapa-roscopy to perform the digestive restoration after total gastrectomy. To place a hand-sewn purse-string suture on the esophagus is simpler using robotic assistance and the esophageal anastomosis can then be performed using a circular stapler, just as with open surgery[9,41]. An alternative is to perform a full robotic hand-sewn esophagojejunal anastomosis, thanks to the ability of the robotic system to provide surgeons to perform precise sutures, even in deep and narrow spaces, which would otherwise be impossible with traditional laparoscopic tools. Finally, although the experience of laparoscopic surgery could affect the learning process of robotic gastrectomy, robotic surgery seems to require globally earlier adaptation with respect to a laparoscopic procedure that tra-ditionally has a steep learning curve. Operation time analysis showed that an experienced laparoscopic surgeon requires fewer cases of robotic gastrectomy to reach a steady state[99-102].
Robotic D2 lymphadenectomyIt is widely accepted that D2 lymph node (along the hepatic, celiac, and splenic vessels) dissection is the more critical part of the minimally invasive gastrectomy procedure for cancer patients. Thanks to significant technical advantages in performing the dissection of the lymphatic tissue around the portal vein, common hepatic artery, celiac trunk, and splenic artery, the D2 lymph node dissection can be a primary indication for the robot assisted procedure.
Figure 1 Adipose tissue including the station No. 8a lymph nodes (white arrow) is pulled up by the 2nd robotic (R2) arm dissected by the 1st robotic (R1) arm. Clipped on Hem-o-lock is Left gastric vein (LGV). Provided by Roviello F, University of Siena.
Caruso S et al . Robot-assisted laparoscopic gastrectomy for GC
R2
R1
LGV

5704 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
The robotic extended lymphadenectomy begins at the hepatic pedicle, along the common hepatic artery above the pancreas, and continues into the portal hepatis distally. The first assistant provides a gentle pressure on the pancreatic head to obtain an optimal tension of the hepato-duodenal ligament and to allow a complete dissection of the lymphatic tissue of the proper hepatic artery (station 12a). The dissection is prolonged above the pancreas along the common hepatic artery (station 8a) (Figure 1), which is exposed from the bifurcation of the gastroduodenal artery toward the root of the left gastric artery (Figure 2). The No. 8a lymph nodes and the right side of the No. 9 lymph nodes are dissected by exposing the right border of the celiac artery (Figure 2). Lymph nodes are removed ‘‘en bloc’’ until the left gastric artery is reached (station 7). Particularly in these sites the EndoWrist® function enables the surgeon to reach these deep areas that would otherwise be unreachable with the conventional straight forceps used in conventional laparoscopic surgery. Moreover, the convex body of the pancreas often interferes with the laparoscopic instruments and hinders surgeons from performing delicate dissection. conversely, the
robotic scope can provide a much more stable view of this narrow surgical field with better depth perception, and the articulating instruments of the robotic system could allow radical dissection over the pancreas with relative ease.
Proximally, the lymphatic dissection is continued along the celiac truck, the left gastric vessels are identified and, taking great care, the avascular space of the left gastric artery is dissected bilaterally. The left gastric artery is exposed (Figure 3) and ligated at the origin using endoclips (Hem-o-lock) or ties. Robotics make this maneuver easier to execute than with a typically straight laparoscopy tool, because during a laparoscopy the combination of surgeon tremors and flat two-dimensional imaging make it technically demanding to maintain appropriate tension between lymphatic tissue and the main artery. Over stretching of the suprapancreatic adipose tissue by the surgeon often leads to tissue laceration, hemorrhage, and inadequate nodal dissection.
Next, the left side of the celiac artery and the origin of the splenic artery are also exposed. The splenic artery is identified along its route and skeletonized by the surrounding lymphatic tissue (station 11p) (Figure
Figure 2 Dissection of No. 8 lymph nodes (white arrow) continues medially, through the traction of the 2nd robotic arm (R2), exposing (A) the proper hepatic artery and (B) the common hepatic artery. Provided by A: Coratti A, University of Florence; B: Patriti A. USL2 Spoleto. PHA: Proper hepatic artery; CHA: Common hepatic artery; GDA: Gastroduodenal artery.
Caruso S et al . Robot-assisted laparoscopic gastrectomy for GC
A
B
PHA
R2
PHA
GDA
CHA

5705 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
4) up to the splenic helium (station 10). During the dissection of the splenic vessels the small branches can be more easily visualized by the larger robotic 3D stereoscopic imaging compared to the traditional laparoscopic technique, allowing vascular dissection under the tunica adventitia, completely clearing the lymphatic tissue and identifying and preserving the vascular supply of the pancreas and spleen. That makes it safer and easier to complete the spleen-pancreatic-preserving D2 lymph node dissection (Figure 5). Moreover, similar to the proper hepatic (station 12a), the splenic arteries lymph nodes (station 11p) are located in the dorsal plane and the approach to these target nodes by laparoscopic forceps lacking articulation is troublesome. The robot assisted technique makes it easier to accomplish this phase laparoscopically, as robotic instruments can easily overcome this typical laparoscopic drawback when the dissection is driven circumferentially around the major vessels. The EndoWrist property of robotic arms is particularly useful to enable these movements and makes it easier to perform the dissection, during which conversely the conventional straight laparoscopic instrument does not provide the surgeon with enough freedom. In conventional laparoscopy it is very difficult to effectively reach the posterior side of the suprapancreatic node-bearing area, even with excessive downward compression of the pancreas. Further, this may cause pancreatic injuries and pancreatitis.
Moreover, the significant technical advantage of robotic capacity permits a safer control of eventual bleeding vessel injury. In fact, the infra pyloric area and the inferior mesenteric vein, including stations 6 and 14, and the supra pancreatic area including stations 7, 8, and 9 are reported in literature as the most frequent sources of intra operative bleeding[72]. Moreover, in cases of vascular injury, the recovery from
bleeding is easier than with conventional laparoscopy. The surgeon has direct control of vision and can use three surgical tools for clamping and suturing. In the meantime, the assistant surgeon can maintain a clean operating field using a sponge, suction, and irrigation. It is impossible to reproduce these same working conditions during a conventional laparoscopic procedure.
Literature evidenceAfter the earliest experiences of robot-assisted gastrectomy (RAg) published in 2003 by Hashizume et al[103] and giulianotti et al[104], in recent years several reports have demonstrated the safety and feasibility of robotic gastrectomy in the treatment of gc[105,106]. Most of the experience thus far comes from small, non randomized, retrospective studies. Table 2 summarizes some of the published data[9-11,42,66,105-122].
The studies prevalently originate from Asian countries. The Western experience with robotic gas-trectomy is limited to smaller series that assess feasibility and safety. In the United States, Anderson et al[10] were the first, in 2007, to report on outcomes after robot-assisted subtotal gastrectomy, in a pilot series of 7 patients. While no direct comparison was made with laparoscopy, the authors showed that robotic gastrectomy was feasible, with acceptable length of stay and low morbidity[10].
Among the largest single institution robotic series on short-term oncological and clinical outcomes to date are (Table 2): Woo et al[106] in 2011, Kim et al[116] in 2012, Kim et al[122] in 2016, Park et al[119] in 2013, and Junfeng et al[105] in 2014. They included respectively 236, 436, 223, 200 and 120 patients who underwent robot-assisted Lg for cancer. All these studies confirmed the safety and feasibility of RAG with lymphadenectomy for the treatment of gc, but they did not provide data on long-term survival.
Figure 3 Exposition of left gastric artery after No. 7 lymph nodes dissection. Clipped on Hem-o-lock is the left gastric vein (LGV). Provided by Coratti A, University of Florence. LGA: Left gastric artery.
Caruso S et al . Robot-assisted laparoscopic gastrectomy for GC
LGA
LGV

5706 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
While there are so many reports about the fea-sibility of RAg, only few robotic studies reported a high quality comparative analysis of RAg vs laparoscopic and/or open gastrectomy. Preliminary results showed better short-term surgical outcomes of RAg than those of open and laparoscopic methods. Kim et al[107] were the first to compare post-operative outcomes between robotic, laparoscopic and open gastrectomy in a small pilot series of (16 robotic, 11 laparoscopic, 12 open) patients with early stage disease. The robotic group demonstrated longer operative times, but lower blood loss and shorter hospital stay. There was no difference in terms of number of harvested lymph nodes or post-operative morbidity or mortality between groups.
The largest comparative study to date was conducted by Kim et al[116]. They retrospectively reviewed data on surgical complications of a pros-pectively collected gc patients data-base. In a total
of 5839 patients (4542 open, 861 laparoscopic and 436 robotic gastrectomies), overall complication, re-operation and mortality rates significant differences between the three groups were not found. The results of this study should be interpreted with some caution, as any retrospective comparison has its limitations and selection bias. In particular, the work included different surgical modalities of gastrectomy in a wide heterogeneous groups of patients. Patients in the Og group had more proximally located, more poorly differentiated and more locally advanced gcs, and so the proportion of total gastrectomies and adjacent organ resections was significantly higher in this group. Thus, consequently, it is obvious that a more positive lymph nodes harvested and intra operative blood loss were significantly greater in open operations, most likely attributable to higher rates of total gastrectomy and more extensive surgery for more advanced tumours. On the other hand, it is quite probable that
Caruso S et al . Robot-assisted laparoscopic gastrectomy for GC
Figure 4 Dissection of 11p lymph nodes. Provided by Coratti A, University of Florence. SpA: Splenic artery.
Figure 5 Exposure of the supra pancreatic area after supra pancreatic lymph nodes dissection. Provided by Coratti A, University of Florence.
11p
SpA

5707 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
patients who were expected to need a more radical operation based on preoperative evaluation did not undergo laparoscopic or robotic surgery, and even within the same pathological stage patients in the Og group may have had more advanced disease and more extensive surgery. The intrinsic bias which necessarily originates from such a heterogeneity study cohort, and specifically the different level of learning curve at which every group was treated, could determine why in this comparative analysis anastomotic leaks were significantly more common with the minimally invasive approach (twice as high after laparoscopic and robotic procedures than after an open approach), despite the more advanced stage of cancer in this last group. For these reasons, the work of Kim et al should be seen more as a study of feasibility rather than a comparative analysis of RAg vs LAg and Og.
Another among the largest single institute com-parative series, prospectively collecting patients who underwent curative resection of gc, compared robotic surgery with open and laparoscopic surgery respectively in 39, 586 and 64 patients[113] (Table 2).
Robotic gastrectomy was associated with less blood loss and shorter hospital stay, at the price of longer operative time than both open and laparoscopic gastrectomy. Postoperative morbidity rates were similar among the three groups. The number of retrieved lymph nodes was similar between the open and robotic groups, while the laparoscopic group had fewer retrieved lymph nodes than the open and robotic. In particular, the authors noted how much easier it was with the aid of robotic instruments to perform lymphadenectomy than the traditional laparoscopic gastrectomy, especially in the infra-pyloric and supra-pancreatic area. Similar results were reported by Junfeng et al[105] in an another of the largest comparative studies, which retrospectively compared 120 vs 394 gc patients who underwent to RAg and LAg respectively. In addition to showing once more less intraoperative blood loss and longer operative time of RAg with respect to LAg, interestingly the authors revealed that the numbers of collected lymph nodes were significantly higher in the RAg group at tier 2. Similarly, Kim et al[123] revealed in
Caruso S et al . Robot-assisted laparoscopic gastrectomy for GC
Table 2 Robot-assisted laparoscopic gastrectomy series for treatment of gastric cancer
Ref. Year Country Patients (n )
Resection type Operative time1 (mean ± SD, min)
Blood loss1 (mean ± SD,
mL)
Open conversion
(%)
Harvested nodes1
(mean ± SD, n )
Morbidity (%)
Mortality (%)
Hospital staya
(mean ± SD, d)
Total Subtotal
Anderson et al[10]
2007 United States
7 - 7 420 ± NR 300 ± NR 0 24 ± NR 11.1 0 4 ± NR
Patriti et al[9] 2008 Italy 13 4 9 286 ± 32.6 103 ± 87.5 0 28.1 ± 8.3 7.7 0 11.2 ± 4.3Song et al[11] 2009 South Korea 100 33 67 231.3 ± 43.2 128.2 ± 217.5 0 36.7 ± NR 13.0 1 7.8 ± 17.1Pugliese et al[66]
2010 Italy 16 - 16 344 ± 62 90 ± 48 12 25 ± 4.5 6.0 6 10 ± 3
Kim et al[107] 2010 South Korea 16 - 16 259.2 ± 38.9 30.3 ± 15.1 0 41.1 ± 10.9 0.0 0 5.1 ± 0.3Eom et al[108] 2011 South Korea 30 - 30 229.1 ± NR 152.8 ± NR 0 30.2 ± NR 13.3 0 7.9 ± NRLee et al[109] 2011 South Korea 12 - 12 253.7 ± 53.0 135.8 ± 133.9 0 46.0 ± 25.5 8.3 0 6.6 ± 1.6D’Annibale et al[110]
2011 Italy 24 11 13 267.5 ± NR 30 ± NR 0 28 ± NR 8.3 0 6 ± NR
Woo et al[106] 2011 South Korea 236 64 172 219.5 ± 46.8 91.6 ± 152.6 0 39.0 ± 15.2 11.0 0.4 7.7 ± 17.2Caruso et al[111]
2011 Italy 29 12 17 290 ± 67 197.6 ± 202.1 0 28.0 ± 11.2 41.4 (13.8)2 0 9.6 ± 2.8
Isogaki et al[112]
2011 Japan 61 14 47 520 ± 177 TG 150 ± 234 TG 0 43 ± 14 TG 4.9 1.6 13.3 ± NR 388 ± 85 SDG 61.8 ± 46.5
SDG42 ± 18 SDG
Huang et al[113]
2012 Taiwan 39 7 32 430 ± NR 50 ± NR 0 32.0 ± 13.7 15.4 2.6 7 ± NR
Uyama et al[114]
2012 Japan 25 - 25 361 ± 58.1 51.8 ± 38.2 0 44.3 ± 18.4 8.0 0 12.1 ± NR
Kang et al[115] 2012 South Korea 100 16 84 202.05 ± 52.31 93.25 ± 84.59 0 NR 14.0 0 9.81 ± 12.16Kim et al[116] 2012 South Korea 436 109 327 226 ± 54 85 ± 60 NR 40.2 ± 5.5 10.1 0.5 7.5 ± 13.7Yoon et al[117] 2012 South Korea 36 36 - 305.8 ± 115.8 NR 0 42.8 ± 12.7 16.7 0 8.8 ± 3.3Liu et al[42] 2013 China 104 54 50 272.52 ± 53.91 80.78 ± 32.37 2 23.1 ± 5.3 11.5 0 6.2 ± 2.5Hyun et al[118] 2013 South Korea 38 9 29 234.4 ± 48.0 131.3 ± 10.1 0 32.8 ± 13.8 47.3 (13.1)2 0 10.5 ± 5.9Park et al[119] 2013 South Korea 200 46 154 248.8 ± 55.6 146.1 ± 130.3 7 37.9 ± NR 10.0 0.5 8.0 ± 3.7Son et al[120] 2014 South Korea 51 51 - 264.1 ± 46.7 163.4 ± 255.1 0 47.2 ± NR 15.7 1.9 8.6 ± NRJunfeng et al[105]
2014 China 120 26 94 234.8 ± 42.4 118.3 ± 55.8 0 34.6 ± 10.9 5.8 0 7.8 ± 3.0
Shen et al[121] 2015 China 93 23 70 257.1 ± 74.5 176.6 ± 217.2 0 33 ± 8.5 9.8 NR 9.4 ± 7.5Kim et al[122] 2016 South Korea 223 43 180 226 ± NR 50 ± NR 2 33 ± NR 13.5 (1.3)2 0 4 ± NR
1Mean value; 2Total morbidity rate, including minor and major complications; between parenthesis major complications rate base on Clavien-Dindo classification ≥ 3, such as anastomotic and duodenal lekeage. NR: Not reported; TG: Total gastrectomy; SDG: Subtotal distal gastrectom.

5708 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
a series of 87 patients who underwent robot-assisted distal gastrectomy (RADg) compared to 288 patients who underwent to LADg that RADg could provide an advantage over LADg in the dissection of the D2 area lymph nodes, especially around the splenic artery area. Son’s study[120] found that robotic gastric surgery yielded significantly greater number of retrieved lymph nodes around splenic vessels and splenic hilum compared with those obtained by a laparoscopic approach.
These results would confirm the advantage of robotic surgery over LAg in the D2 dissection, in particular providing a better exposure and wider operating field visualization of the second tier lymph node stations (No. 7, No. 8a, No. 9, and No. 11) which are traditionally the more difficult sites to be laparoscopically harvested.
To date, 9 meta-analysis[124-132] have been published in literature to elucidate the issue of RAg in the treatment of gc patients. Of these meta-analysis, 1 included selected reports comparing RAg with Og[124]; 5 recruited high quality studies comparing RAg and Lg[125-129]; the other 3 consists of a systematic review and meta-analysis of trials evaluating the safety and short-term efficacy of RAG compared with laparoscopic and open gastrectomy[130-133]. Only non-randomized comparative controlled trials were found eligible for inclusion in these meta-analysis. These meta-analysis demonstrated that the short-term clinical outcomes of RAg were essentially comparable to those of Lg and OG. Specifically, RAG was superior to LG and OG in terms of blood loss, despite an increased operative time; there were no differences between RAg and Lg groups in the number of retrieved lymph nodes and conversion to open; hospital stay for RAg was slightly inferior or similar to that for LAg, but significantly shorter than Og; postoperative complications were similar for all three operative approaches.
The advantage of RAg with respective blood loss may be mainly attributable to the typical features of the robotic device which, compared to conventional laparoscopy, enable better detection of vessels, due to the greater field of vision and stereoscopic vision, and facilitate control of intra abdominal bleeding with tremor filtration and stable hemostatic pressure supplied by the robotic arms. On the other hand, the longer duration of robotic surgical procedure is mainly because of the additional setup- and docking-time required for the robotic system. However, the operating time significantly decreased with the accumulation of surgical experience in robotic gastrectomy[11,100,119].
However, significant limitations exist in the inter-pretation of the comparative data among RAg vs Lg and Og available so far, due to the lack of RcTs, the limited number of published high quality observational and retrospective studies, the small sample sizes to date, and the limited duration of follow up. Large
multi-centre prospective RcTs are required to delineate significantly quantifiable advantages of RAG over LAG and Og, thus to draw conclusive considerations. Due to this shortfall of studies, at the present time, the real, long-term benefits of RAg for the treatment of gc remain unreported. Pugliese et al[66] in Italy are one of the few groups to study long term outcomes in patients with early and locally advanced lesions undergoing minimally invasive subtotal gastrectomy. Of the 70 patients included (37 early and 33 advanced lesions), all patients had a D2 lymphadenectomy and 18 underwent robotic surgery. Short-term results were similar between laparoscopic and robotic surgery groups. The 5-year overall survival for the entire cohort was 81% (97% for early and 67% for advanced lesions). Recently, coratti et al[133] reported the long-term results of 98 consecutive patients submitted to RAg for early and advanced gc, with a mean follow-up of 46.9 mo and 5-year overall survival of 73.3%. Son et al[120] reported the longest follow-up study after RAg for gc, with a median follow-up of 70 mo, and found no difference in overall survival or disease-free survival. The 5-year overall survival rate was 89.5% in the RAg group and 91.1% in the LgS group while the 5-year disease-free survival rate was 90.2% in the RAg group and 91.2% in the LAg group. These results are promising, but these studies included limited numbers of cases and selection bias is a concern as the study design was non-randomized. To demonstrate oncologic outcomes follow-up periods longer than 5 years are needed, thus definitive conclusions need to be validated by further RcTs.
A recent prospective multi-centre comparative study[122] comparing short-term surgical outcomes of robotic (n = 223) and laparoscopic (n = 211) gastrectomy introduced also financial cost analysis. Both groups showed similar overall complication rates, estimated blood loss, and length of hospital-stay. The Robotic group showed significantly longer operative time and significantly higher total cost (robotic US$ 13.432 vs laparoscopic US$ 8090; p < 0.001). Other studies underlined the higher costs for RAg than those for LADg owing to the substantial expense of the robotic system itself[100].
globally, on the basis of the literature evidence available so far, the following preliminary conclusions could be drawn. Robotic gastrectomy shows short-term outcomes comparable to open and laparoscopic series, with essentially satisfactory results in terms of peri-operative outcomes and oncological adequacy. To date, RAg appears to be a valid alternative to conventional open or laparoscopic resection for the treatment of gastric carcinoma, thus essentially making some difficult traditional laparoscopy procedures easier and safer, also making it possible at the same time to maintain the typical advantages of minimally invasive surgery with respect to open. Although these initial
Caruso S et al . Robot-assisted laparoscopic gastrectomy for GC

5709 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
results are promising, solid evidence of superiority of robotic gastric surgery over the conventional laparoscopic approach is not determined. Moreover, the considerable expenses remain a major drawback of robotic surgery. The role of robotic gastrectomy for gc and its long-term oncologic benefits remain poorly investigated. Only in recent years have the first studies on long-term oncological outcomes of gc patients treated with RAg been reported. Larger and randomized prospective trials are needed before robotic resection can be considered to be an acceptable alternative for all patients with resectable gc. We believe that carefully selected patients may be considered for robotic resection by experienced gc surgeons.
DISCUSSION
The introduction of a new technological modality for the treatment of cancer is acceptable if it is as oncologically sound as the traditional procedure. Minimally invasive procedures would be a valid alternative to open surgery, with best short-term outcomes, if oncologic criteria could be respected as in the open approach, and long-term survival remain uncompromised. Although overall survival represents the prime oncologic parameter, wide margin resection and number of resected lymph nodes accurately reflect the adequacy of gastric resection for adenocarcinoma. Indeed, in order for laparoscopic gastric surgery to be accepted for the surgical treatment of gc and to not represent a disadvantage with regard to oncologic outcome, the quality of lymphadenectomy is the most important factor to be considered. When a laparoscopic or robotic-assisted laparoscopic approach is used for the surgical treatment of gc, the same extent of lymph node dissection as in traditional surgery should be performed, and postoperative outcomes should also be favorable.
Laparoscopic gastrectomy with lymph node dissection has developed as a minimally invasive surgery for gc over the past 20 years. This surgery has been used mainly for early-stage gc. Sufficient data is available on the feasibility of LADg and this approach has essentially been validated for early gc, as several level Ⅲ studies and meta-analysis demonstrated that laparoscopic gastrectomy with limited lymphadenectomy for patients with early gc had non-inferior oncologic outcome relative to open surgery, with instead better short-term results[3,14,18]. The potential benefits of laparoscopic gastrectomy compared to conventional open surgery include faster postoperative recovery, quicker return of gastrointestinal function, shorter hospital stay, less postoperative pain, and better cosmesis[54,79]. The incidence of operative complications is less than or the same as that with conventional open surgery.
conversely, few reports, all containing small
patient series, describe the safety of laparoscopic assisted distal and total gastrectomy with D2 lym-phadenectomy for advanced gc. During the last years, some meta-analysis on this topic have been published, but conflicting results were found in particular for postoperative complications and number of collected lymph nodes[14,18-20,24,84]. The majority of the comparative trials between Lg and traditional open technique are too heterogeneous to be globally evaluated. The main reasons for this heterogeneity were the different levels of laparoscopic expertise; the issue related to the learning curve; different levels of lymphadenectomy; nonblinded assessment of outcomes; lack of randomization; predominance of Asian studies. If individually taken, most of the studies on Lg including advanced gastric tumour are too small to reach the necessary statistical power to draw definitive conclusions and the majority of these contain a greater proportion of patients operated upon for early distal gc, thus making it implausible to obtain results generalized to all gc stages. Several meta-analysis on Lg vs Og, as discussed in the previous sections (laparoscopic assisted distal gastrectomy, laparo-scopic assisted total gastrectomy, early gc, advanced gc, laparoscopic D2 lymphadenectomy sections), have been conducted to address the controversy on potential advantage of the laparoscopic procedure, yet sample size of those analysis are not large enough and homogeneous. Some authors only included the few available RcTs[18-20]; others performed meta-analyses that combined RcTs also with retrospective comparative studies, which have the advantage of potentiating the statistical power of the study but at the price of the possibility to introduce bias for potential intrinsic flaws of non-randomization[14,24,84]. Some authors focused the meta-analysis on only one type of gastrectomies, usually LADg, others included all LAg procedure; some of them combined data from RcTs of different lymphadenectomy levels, others are restricted to one type of lymphadenectomy only; some included studies restricted to early gc only, while conversely some included studies that enrolled high ratio of advanced cases; and some even synthesized duplicated publication data. All of which would introduce bias.
Recently, a meta-analysis[134] has been conducted which enclosed all the available RcTs regarding the effectiveness of Lg vs Og for resectable gc, independently either of the type of gastrectomy (LADg and LATg) and gastric tumour stage; therefore, this study was not commented in the previous sections that are restricted to a specific topic. The strategy of this last meta-analysis has the advantage of increasing the study’s statistical power, expanding as much as possible the cohort patients for the analysis, but with the disadvantage of mixing different technical procedures towards different stages of cancer. Ultimately, 8 RcTs, totaling 784 patients (402 LAg
Caruso S et al . Robot-assisted laparoscopic gastrectomy for GC

5710 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
and 382 open gastrectomy), were considered eligible. The study included the largest sample sizes among the meta-analyses available to date, thanks to the above mentioned non selective inclusion criteria, but again the limits of previous meta-analysis were not overcome. In fact, the results again largely represent the experience of East Asian countries (included studies from South Korea = 3, Japan = 3, Italy = 1, china = 1), mostly cases were early gc (the advanced gc patients were from 2 trials only), the laparoscopic approach was mainly focused on LADg (87.5%), and the long-term survival rate was not available because of insufficient follow-up time. Overall, even if all of the RcTs comparing Lg vs Og available in literature are enclosed in this meta-analysis, they remain few and singularly small. Essentially this meta-analysis did not achieve significant superiority respect to the previous ones. Regarding the adequacy of lymph node dissection, no differences were found in the overall mean number of collected lymph nodes between the Lg and Og group, but as is known for the reasons above mentioned the meta-analysis is characterized by a significant heterogeneity of type of lymphadenectomy among RcTs. In fact, subgroup analysis depending on the level of lymph node dissection revealed a not so linear concordance. Subgroup analysis showed that the number of collected lymph nodes in Lg arm tended to be smaller than that in open gastrectomy arm in either the D1+ surgery or the D2 surgery subgroups, even though the differences were not statistically significant.
Thus, in conclusion, although LADg has been widely developed for early gc, many problems and controversies still exist. The therapeutic efficacy of LG in general and specifically LADG has not yet been widely investigated for the treatment of advanced gcs around the world. Although a totally Lg and an extended D2 lymphadenectomy might be possible to perform laparoscopically in some patients[7,8,48,50,71], owing to the intrinsic difficulty of execution, one of the major oncologic concerns is the ability to perform a radical and suitable D2 lymph node dissection. In fact, the meta-analysis of the randomized evidence shows that when data restricted to LADg are pooled from gcs not only in the early stage but also from advanced gc the same extent of lymph node dissection as in traditional surgery could not be guaranteed[13,16].
The technical challenge of performing this me-ticulous procedure (D2 lymphadenectomy) is well recognized, especially in patients with abundant intrabdominal fat[135]. Precisely in order to elucidate the efficacy of LADg with D2 lymphadenectomy for patients who are clinically diagnosed with locally advanced gc, with respect to conventional open subtotal gastrectomy and D2 lymphadenectomy, currently the Korean Laparoscopic Surgical Society (KLASS) group launched the multi-centre RcT[136] (KLASS-02 RcT; registered at www.clinicaltrials.gov as
NcT01456598), comparing the oncologic and surgical outcomes of these two procedures. Other ongoing studies, are being awaited, but until definitive evidence is obtained, doubts still persist on the routine use of laparoscopic procedure for advanced gc. Moreover, the operating time for LG in general remains significantly longer compared to its open counterpart and, as yet, there is little high-level evidence based on long-term outcome and oncologic outcome of Lg as a treatment of advanced gc[7,76,80].
Thus, conclusively, for all these reasons, although Lg for cancer is a safe and feasible technique, whereas laparoscopic sub-D2 lymphadenectomy can be con-sidered adequate for almost of all early gc and to date is the standard procedure in Asian countries, the same claim could not be made for advanced gc and Lg cannot be recommended as a routine approach for all gc patients.
Accordingly, Japanese gc Association (JgcA) treatment guidelines still indicate Lg as an ex-perimental procedure in the context of advanced gc[137], while on the other hand sub-D2 dissection is considered oncologically sufficient for most early gc, as lymph node metastases occur in 2%-20% of these[13]. In fact, the guidelines by the Japanese gc Association[64,137] recommend for early stage gc D1 or D1+α, β lymphadectomy in function of the tumour diameter, depth of wall infiltration and suspected nodal metastasis at preoperative investigation work-up (D1+α resection is defined as D1 plus No. 7 lymph node resection, D1+β is defined as D1 plus No. 7, 8, 9 lymph nodes resection).
However, some final considerations could be made. The correct assessment of tumour invasiveness through the gastric wall is sometimes difficult and underestimated at the preoperative investigation, thus, the role of D2 nodal clearance in early gc from some authors is emphasized[8,138]. Moreover, the applicability of Eastern evidence to Western countries remains uncertain and, to date, western literature has been limited to retrospective single-institution series and small nonrandomized trials. gc in the West is characterized by more advanced disease at initial diagnosis and a larger proportion of proximal tumors[33]. Intrinsic differences in gastric tumor biological aggressiveness, genetic arrangement and geographic spread between eastern and western countries are well known. These factors, in conjunction with the lower overall incidence of gc and increased prevalence of obesity in the West, and significant length of the learning curve associated with Lg, may account for the widespread low acceptance of minimally invasive approaches for gastrectomy.
In the future, a well-designed RcT with a large sample size would be required to aptly compare the controversial outcome measures of Lg over tradi-tional open procedure, particularly for the quality of
Caruso S et al . Robot-assisted laparoscopic gastrectomy for GC

5711 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
lymphadenectomy.Robotic surgery probably may overcome some
intrinsic limitations of traditional laparoscopy, expanding the application of minimally invasive procedures, in particular for the D2 lymphadenectomy. As long as drawbacks of laparoscopic gastrectomy technique exist, such as in extended lymphadenetomy, the introduction of new technologies and medical devices, such as robotic gastrectomy, that would be able to improve health care and patients' outcome, are desirable. When precise dissection is needed, such as during the lymphadenectomy along major abdominal vessels, robotic technology takes advantage of the excellent stereoscopic visualization, and the improved dexterity, stability (tremor filter) and superior movements of the robotic arm whose internal articulated endoscopic wrist makes it possible to perform the dissection with greater ease. For these reasons the use of the robotic techniques represents a technical advantage for a minimally invasive approach by making it possible to carry out a safe and effective lymphadenectomy. The median number of nodes retrieved reported by many investigators who used robotic techniques for D2 lymph node dissection is similar to that of open and in some cases superior to that laparoscopic[10,111,124-132].
Possible disadvantages of robot assisted lapa-roscopy could be decreased sense of touch, and a lack of sense of the tissue tension forces. Therefore, particular attention should be made during movements of the robotic instruments and traction with the robotic arms to avoid tissue damage.
The use of the robot is indeed a valuable adjunct facilitating some traditional difficult laparoscopic procedures. However, although it probably may overcame some intrinsic limitations of traditional laparoscopy, expanding the application of minimally invasive procedure, recent years have seen steady improvements in dissection techniques with the spread of those purely laparoscopic (without the aid of robot) and some medical institutions are now capable of performing laparoscopic D2 dissection with safe outcomes.
Moreover, the superiority of robot assisted la-paroscopic gastric surgery regarding laparoscopic oncological outcomes has not yet shown clear benefit for early gc patients, for whom an increasing number of harvested lymph nodes does not necessarily improve overall survival, but does at least influence accurate staging, for which highly experienced surgeons’ present levels of proficiency with con-ventional LG procedure seem to be sufficient.
Thus, there is expected to be a major impact of the robotic system on procedures that are technically demanding by laparoscopy rather than those that are relatively simple, such as overcoming the technical difficulties of laparoscopic total gastrectomy and
extended D2 lymphadenectomy, with particular re-ference to reconstruction of the alimentary tract and the supra-pancreatic area lymph nodes dissection respectively. Therefore, it is expected that the major area of research in robotic gastric surgery in the near future will be on advanced gc, and in Western countries where gc is mainly detected in advanced stages, for which the importance of D2 lymph node dissection has been advocated in order to improve long-term survival. This fact may justify the application of a robotic system.
It must be considered that robotic surgery re-quires an experienced operative team, additional surgical space and high costs of the procedure are still superior to conventional open or laparoscopic gastrectomy. From the point of view of technological development, and diffusion of laparoscopic and robotic instruments that could in the near future reduce costs, it is necessary to clarify the important controversy on the cost-effectiveness of robotic surgery. In fact, the main criticism to the robotic approach is the low ratio between the advantage over classic laparoscopic minimally invasive technique in spite of the clear cost-effectiveness gap. Other still persistent disadvantages of using the robot include the relatively restricted field of vision when compared with laparoscopy, increased operative times, and lack of data on long term on-cologic equivalency. Due to inadequate long-term follow-up results and a limited number of studies, it is still too early to draw definite conclusions. Randomized controlled studies are required for long-term survival outcomes.
Thus, although robot assisted laparoscopic surgery has evident benefits, it is difficult to assess and compare some advantages at the moment with respect to traditional surgery. Larger randomized prospective trials are needed before robotic resection can be considered an acceptable alternative for patients with local advanced resectable gc. Probably, the main indication for robotic gastrectomy is when it serves as an adjunct to laparoscopic resection in selected patients with locally advanced tumors requiring a D2 lymphadenectomy. However, what should be borne in mind is that robotic procedures are not independent from traditional laparoscopic ones, but are technically an adjunctive tool which can improve the effectiveness of laparoscopic technique and overcome some of its limits. Thus, well designed cost-effectiveness analysis, and high-quality comparative-effectiveness research are required to assess the strengths and disadvantages of robotic surgery compared with laparoscopic more than open surgery, in order to demonstrate if the addition of robotics to laparoscopy is truly beneficial.
CONCLUSIONThe available clinical evidence implies that Lg with
Caruso S et al . Robot-assisted laparoscopic gastrectomy for GC

5712 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
less than D2 or D2 lymphadenectomy may be a valid option to open surgery for the treatment of early gc. Level Ⅲ evidence of safety and oncological adequacy of this procedure has been reported. Principally the evidence originated from Eastern studies and at present LADg is routinely used for early gc in countries as Japan and South Korea. conversely, data available on the advantages of Lg for advanced gc are not so consistent. LAg with D2 lymphadenectomy is a time-consuming procedure even in the experienced surgeon’s hands. The reports are once more pre-valently from Eastern studies, where the patient population and disease biology may differ with respect to the West. Due to clinicopathological dissimilarities between Eastern and Western gc population, not all high quality and large amount of results from Asian studies can be applied to Europe and Unite States.
Oncological outcome such as lymph node yield and margin status appear similar between open and laparoscopic approaches, but a slight superiority of open surgery still exists regarding capacity to obtain a major, complete and extended (D2) lymphadenectomy. The first RcT recruiting a large number of patients to compare laparoscopic D2 lymphadenectomy with open conventional lymphadenectomy in patients preoperatively diagnosed with locally advanced gc is ongoing and its results are being awaited[136]. Emerging long-term data on survival after Lg suggest that out-comes are similar to open surgery, but high quality RCTs are needed to claim definitive conclusions.
At present, minimally invasive approaches to gc are currently indicated for patients with T1 and T2N0 adenocarcinomas, while careful selection of patients with locally advanced tumours (T3/4 or N+ disease) should be made only in high volume centers with advanced laparoscopic skills, and in a clinical research setting. Thanks to the improvements on minimally invasive techniques, the diffusion of neoadjuvant chemotherapy protocols and the introduction of robotic surgery, the indications for laparoscopic gastrec-tomy are expected to expand to all stages of gastric adenocarcinoma.
In general, RAg demonstrates it has overcome some intrinsic limitations of conventional laparoscopic techniques for gc, however the full potential of robotic surgery still remains to be balanced against the lack of a clear oncological superiority to its counterpart. The major technical advantages of the robot-assisted approach are appreciated in routine reproduction of D2-lymphadenectomy and complex reconstructions, such as intracorporeal reconstruction following total gastrectomy. These demanding procedures are not easily overcome by the surgeon’s experience or current laparoscopic instruments, thus representing the best indication for the use of the robot, particularly in radical gastrectomy for advanced gc for which the D2 dissection is crucial.
The learning curve and reproducibility of RAg seems to be shorter and more feasible than con-ventional laparoscopy, so that probably robotic surgery could permit major diffusion of minimally invasive surgery for gc in the near future. With acceptable complications and radical resection, RAg is a promising approach that improves LAg. Larger comparative series comparing robotic surgery with conventional laparoscopic procedure are needed to definitely elucidate eventual advantages in terms of long-term oncological results, in spite of more cost-effectiveness of the robotic procedure to date. An impartial assessment should be made in order to determine whether the progress so far identified in favor of robotic gastrectomy is really worth the higher expense.
REFERENCES1 Songun I, Putter H, Kranenbarg EM, Sasako M, van de Velde CJ.
Surgical treatment of gastric cancer: 15-year follow-up results of the randomised nationwide Dutch D1D2 trial. Lancet Oncol 2010; 11: 439-449 [PMID: 20409751 DOI: 10.1016/S1470-2045(10)70070-X]
2 Kitano S, Iso Y, Moriyama M, Sugimachi K. Laparoscopy-assisted Billroth I gastrectomy. Surg Laparosc Endosc 1994; 4: 146-148 [PMID: 8180768]
3 Yakoub D, Athanasiou T, Tekkis P, Hanna GB. Laparoscopic assisted distal gastrectomy for early gastric cancer: is it an alternative to the open approach? Surg Oncol 2009; 18: 322-333 [PMID: 18922689 DOI: 10.1016/j.suronc.2008.08.006]
4 Deng Y, Zhang Y, Guo TK. Laparoscopy-assisted versus open distal gastrectomy for early gastric cancer: A meta-analysis based on seven randomized controlled trials. Surg Oncol 2015; 24: 71-77 [PMID: 25791201 DOI: 10.1016/j.suronc.2015.02.003]
5 Kitano S, Shiraishi N, Uyama I, Sugihara K, Tanigawa N; Japanese Laparoscopic Surgery Study Group. A multicenter study on oncologic outcome of laparoscopic gastrectomy for early cancer in Japan. Ann Surg 2007; 245: 68-72 [PMID: 17197967]
6 Kim MC, Kim HH, Jung GJ. Surgical outcome of laparoscopy-assisted gastrectomy with extraperigastric lymph node dissection for gastric cancer. Eur J Surg Oncol 2005; 31: 401-405 [PMID: 15837047]
7 Huscher CG, Mingoli A, Sgarzini G, Sansonetti A, Di Paola M, Recher A, Ponzano C. Laparoscopic versus open subtotal gastrectomy for distal gastric cancer: five-year results of a randomized prospective trial. Ann Surg 2005; 241: 232-237 [PMID: 15650632]
8 Uyama I, Sugioka A, Fujita J, Komori Y, Matsui H, Hasumi A. Laparoscopic total gastrectomy with distal pancreatosplenectomy and D2 lymphadenectomy for advanced gastric cancer. Gastric Cancer 1999; 2: 230-234 [PMID: 11957104]
9 Patriti A, Ceccarelli G, Bellochi R, Bartoli A, Spaziani A, Di Zitti L, Casciola L. Robot-assisted laparoscopic total and partial gastric resection with D2 lymph node dissection for adenocarcinoma. Surg Endosc 2008; 22: 2753-2760 [PMID: 18813994 DOI: 10.1007/s00464-008-0129-0]
10 Anderson C, Ellenhorn J, Hellan M, Pigazzi A. Pilot series of robot-assisted laparoscopic subtotal gastrectomy with extended lymphadenectomy for gastric cancer. Surg Endosc 2007; 21: 1662-1666 [PMID: 17345142]
11 Song J, Oh SJ, Kang WH, Hyung WJ, Choi SH, Noh SH. Robot-assisted gastrectomy with lymph node dissection for gastric cancer: lessons learned from an initial 100 consecutive procedures. Ann Surg 2009; 249: 927-932 [PMID: 19474671 DOI:
Caruso S et al . Robot-assisted laparoscopic gastrectomy for GC

5713 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
10.1097/01.sla.0000351688.64999.73]12 Sato H, Shimada M, Kurita N, Iwata T, Nishioka M, Morimoto
S, Yoshikawa K, Miyatani T, Goto M, Kashihara H, Takasu C. Comparison of long-term prognosis of laparoscopy-assisted gastrectomy and conventional open gastrectomy with special reference to D2 lymph node dissection. Surg Endosc 2012; 26: 2240-2246 [PMID: 22311300 DOI: 10.1007/s00464-012-2167-x]
13 Hosono S, Arimoto Y, Ohtani H, Kanamiya Y. Meta-analysis of short-term outcomes after laparoscopy-assisted distal gastrectomy. World J Gastroenterol 2006; 12: 7676-7683 [PMID: 17171799]
14 Viñuela EF, Gonen M, Brennan MF, Coit DG, Strong VE. Laparoscopic versus open distal gastrectomy for gastric cancer: a meta-analysis of randomized controlled trials and high-quality nonrandomized studies. Ann Surg 2012; 255: 446-456 [PMID: 22330034 DOI: 10.1097/SLA.0b013e31824682f4]
15 Zeng YK, Yang ZL, Peng JS, Lin HS, Cai L. Laparoscopy-assisted versus open distal gastrectomy for early gastric cancer: evidence from randomized and nonrandomized clinical trials. Ann Surg 2012; 256: 39-52 [PMID: 22664559 DOI: 10.1097/SLA.0b013e3182583e2e]
16 Memon MA, Khan S, Yunus RM, Barr R, Memon B. Meta-analysis of laparoscopic and open distal gastrectomy for gastric carcinoma. Surg Endosc 2008; 22: 1781-1789 [PMID: 18437472 DOI: 10.1007/s00464-008-9925-9]
17 Sun J, Li J, Wang J, Pan T, Zhou J, Fu X, Zhang S. Meta-analysis of randomized controlled trials on laparoscopic gastrectomy vs. open gastrectomy for distal gastric cancer. Hepatogastroenterology 2012; 59: 1699-1705 [PMID: 22626787 DOI: 10.5754/hge12259]
18 Ohtani H, Tamamori Y, Noguchi K, Azuma T, Fujimoto S, Oba H, Aoki T, Minami M, Hirakawa K. A meta-analysis of randomized controlled trials that compared laparoscopy-assisted and open distal gastrectomy for early gastric cancer. J Gastrointest Surg 2010; 14: 958-964 [PMID: 20354807 DOI: 10.1007/s11605-010-1195-x]
19 Chen XZ, Hu JK, Yang K, Wang L, Lu QC. Short-term evaluation of laparoscopy-assisted distal gastrectomy for predictive early gastric cancer: a meta-analysis of randomized controlled trials. Surg Laparosc Endosc Percutan Tech 2009; 19: 277-284 [PMID: 19692873 DOI: 10.1097/SLE.0b013e3181b080d3]
20 Liang Y, Li G, Chen P, Yu J, Zhang C. Laparoscopic versus open gastrectomy for early distal gastric cancer: a meta-analysis. ANZ J Surg 2011; 81: 673-680 [PMID: 22295306]
21 Peng JS, Song H, Yang ZL, Xiang J, Diao DC, Liu ZH. Meta-analysis of laparoscopy-assisted distal gastrectomy and conventional open distal gastrectomy for early gastric cancer. Chin J Cancer 2010; 29: 349-354 [PMID: 20346206]
22 Wang Y, Wang S, Huang ZQ, Chou WP. Meta-analysis of laparoscopy assisted distal gastrectomy and conventional open distal gastrectomy for EGC. Surgeon 2014; 12: 53-58 [PMID: 23806307 DOI: 10.1016/j.surge.2013.03.006]
23 Varela JE, Hiyashi M, Nguyen T, Sabio A, Wilson SE, Nguyen NT. Comparison of laparoscopic and open gastrectomy for gastric cancer. Am J Surg 2006; 192: 837-842 [PMID: 17161104]
24 Ding J, Liao GQ, Liu HL, Liu S, Tang J. Meta-analysis of laparoscopy-assisted distal gastrectomy with D2 lymph node dissection for gastric cancer. J Surg Oncol 2012; 105: 297-303 [PMID: 21952834 DOI: 10.1002/jso.22098]
25 Lee JH, Yom CK, Han HS. Comparison of long-term outcomes of laparoscopy-assisted and open distal gastrectomy for early gastric cancer. Surg Endosc 2009; 23: 1759-1763 [PMID: 19057958 DOI: 10.1007/s00464-008-0198-0]
26 Lee SI, Choi YS, Park DJ, Kim HH, Yang HK, Kim MC. Comparative study of laparoscopy-assisted distal gastrectomy and open distal gastrectomy. J Am Coll Surg 2006; 202: 874-880 [PMID: 16735200]
27 Kim MC, Jung GJ, Kim HH. Learning curve of laparoscopy-assisted distal gastrectomy with systemic lymphadenectomy for early gastric cancer. World J Gastroenterol 2005; 11: 7508-7511 [PMID: 16437724]
28 Isozaki H, Tanaka N, Okajima K. General and specific prognostic factors of early gastric carcinoma treated with curative surgery. Hepatogastroenterology 1999; 46: 1800-1808 [PMID: 10430349]
29 Miura S, Kodera Y, Fujiwara M, Ito S, Mochizuki Y, Yamamura Y, Hibi K, Ito K, Akiyama S, Nakao A. Laparoscopy-assisted distal gastrectomy with systemic lymph node dissection: a critical reappraisal from the viewpoint of lymph node retrieval. J Am Coll Surg 2004; 198: 933-938 [PMID: 15194075]
30 Gordon AC, Kojima K, Inokuchi M, Kato K, Sugihara K. Long-term comparison of laparoscopy-assisted distal gastrectomy and open distal gastrectomy in advanced gastric cancer. Surg Endosc 2013; 27: 462-470 [PMID: 22890478 DOI: 10.1007/s00464-012-2459-1]
31 Shah MA, Khanin R, Tang L, Janjigian YY, Klimstra DS, Gerdes H, Kelsen DP. Molecular classification of gastric cancer: a new paradigm. Clin Cancer Res 2011; 17: 2693-2701 [PMID: 21430069 DOI: 10.1158/1078-0432.CCR-10-2203]
32 Deng N, Goh LK, Wang H, Das K, Tao J, Tan IB, Zhang S, Lee M, Wu J, Lim KH, Lei Z, Goh G, Lim QY, Tan AL, Sin Poh DY, Riahi S, Bell S, Shi MM, Linnartz R, Zhu F, Yeoh KG, Toh HC, Yong WP, Cheong HC, Rha SY, Boussioutas A, Grabsch H, Rozen S, Tan P. A comprehensive survey of genomic alterations in gastric cancer reveals systematic patterns of molecular exclusivity and co-occurrence among distinct therapeutic targets. Gut 2012; 61: 673-684 [PMID: 22315472 DOI: 10.1136/gutjnl-2011-301839]
33 Strong VE, Song KY, Park CH, Jacks LM, Gonen M, Shah M, Coit DG, Brennan MF. Comparison of gastric cancer survival following R0 resection in the United States and Korea using an internationally validated nomogram. Ann Surg 2010; 251: 640-646 [PMID: 20224369 DOI: 10.1097/SLA.0b013e3181d3d29b]
34 Inoue M, Tsugane S. Epidemiology of gastric cancer in Japan. Postgrad Med J 2005; 81: 419-424 [PMID: 15998815]
35 Wong J, Jackson P. Gastric cancer surgery: an American perspective on the current options and standards. Curr Treat Options Oncol 2011; 12: 72-84 [PMID: 21274666 DOI: 10.1007/s11864-010-0136-y]
36 Spolverato G, Kim Y, Ejaz A, Valero V, Squires MH, Poultsides G, Fields RC, Bloomston M, Weber SM, Acher AW, Votanopoulos K, Schmidt C, Cho CS, Maithel SK, Pawlik TM. A multi-institutional analysis of open versus minimally-invasive surgery for gastric adenocarcinoma: results of the US gastric cancer collaborative. J Gastrointest Surg 2014; 18: 1563-1574 [PMID: 24912915 DOI: 10.1007/s11605-014-2562-9]
37 Bilimoria KY, Talamonti MS, Wayne JD, Tomlinson JS, Stewart AK, Winchester DP, Ko CY, Bentrem DJ. Effect of hospital type and volume on lymph node evaluation for gastric and pancreatic cancer. Arch Surg 2008; 143: 671-68; discussion 678 [PMID: 18645110 DOI: 10.1001/archsurg.143.7.671]
38 Birkmeyer JD, Sun Y, Wong SL, Stukel TA. Hospital volume and late survival after cancer surgery. Ann Surg 2007; 245: 777-783 [PMID: 17457171]
39 Okabe H, Obama K, Tsunoda S, Tanaka E, Sakai Y. Advan-tage of completely laparoscopic gastrectomy with linear stapled reconstruction: a long-term follow-up study. Ann Surg 2014; 259: 109-116 [PMID: 23549426 DOI: 10.1097/SLA.0b013e31828dfa5d]
40 Bracale U, Marzano E, Nastro P, Barone M, Cuccurullo D, Cutini G, Corcione F, Pignata G. Side-to-side esophagojejunostomy during totally laparoscopic total gastrectomy for malignant disease: a multicenter study. Surg Endosc 2010; 24: 2475-2479 [PMID: 20396906 DOI: 10.1007/s00464-010-0988-z]
41 Coratti A, Annecchiarico M, Di Marino M, Gentile E, Coratti F, Giulianotti PC. Robot-assisted gastrectomy for gastric cancer: current status and technical considerations. World J Surg 2013; 37: 2771-2781 [PMID: 23674257 DOI: 10.1007/s00268-013-2100-z]
42 Liu XX, Jiang ZW, Chen P, Zhao Y, Pan HF, Li JS. Full robot-assisted gastrectomy with intracorporeal robot-sewn anastomosis produces satisfying outcomes. World J Gastroenterol 2013; 19: 6427-6437 [PMID: 24151361 DOI: 10.3748/wjg.v19.i38.6427]
Caruso S et al . Robot-assisted laparoscopic gastrectomy for GC

5714 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
43 Etoh T, Inomata M, Shiraishi N, Kitano S. Minimally invasive approaches for gastric cancer-Japanese experiences. J Surg Oncol 2013; 107: 282-288 [PMID: 22504947 DOI: 10.1002/jso.23128]
44 Haverkamp L, Weijs TJ, van der Sluis PC, van der Tweel I, Ruurda JP, van Hillegersberg R. Laparoscopic total gastrectomy versus open total gastrectomy for cancer: a systematic review and meta-analysis. Surg Endosc 2013; 27: 1509-1520 [PMID: 23263644 DOI: 10.1007/s00464-012-2661-1]
45 Chen K, Xu XW, Zhang RC, Pan Y, Wu D, Mou YP. Systematic review and meta-analysis of laparoscopy-assisted and open total gastrectomy for gastric cancer. World J Gastroenterol 2013; 19: 5365-5376 [PMID: 23983442 DOI: 10.3748/wjg.v19.i32.5365]
46 Shen H, Shan C, Liu S, Qiu M. Laparoscopy-assisted versus open total gastrectomy for gastric cancer: a meta-analysis. J Laparoendosc Adv Surg Tech A 2013; 23: 832-840 [PMID: 23980591 DOI: 10.1089/lap.2013.0152]
47 Dulucq JL, Wintringer P, Stabilini C, Solinas L, Perissat J, Mahajna A. Laparoscopic and open gastric resections for malignant lesions: a prospective comparative study. Surg Endosc 2005; 19: 933-938 [PMID: 15920691]
48 Pugliese R, Maggioni D, Sansonna F, Scandroglio I, Ferrari GC, Di Lernia S, Costanzi A, Pauna J, de Martini P. Total and subtotal laparoscopic gastrectomy for adenocarcinoma. Surg Endosc 2007; 21: 21-27 [PMID: 17031743]
49 Usui S, Yoshida T, Ito K, Hiranuma S, Kudo SE, Iwai T. Laparoscopy-assisted total gastrectomy for early gastric cancer: comparison with conventional open total gastrectomy. Surg Laparosc Endosc Percutan Tech 2005; 15: 309-314 [PMID: 16340559]
50 Tanimura S, Higashino M, Fukunaga Y, Takemura M, Tanaka Y, Fujiwara Y, Osugi H. Laparoscopic gastrectomy for gastric cancer: experience with more than 600 cases. Surg Endosc 2008; 22: 1161-1164 [PMID: 18322744 DOI: 10.1007/s00464-008-9786-2]
51 Kim KH, Kim MC, Jung GJ, Kim HH. Long-term outcomes and feasibility with laparoscopy-assisted gastrectomy for gastric cancer. J Gastric Cancer 2012; 12: 18-25 [PMID: 22500260 DOI: 10.5230/jgc.2012.12.1.18]
52 Lin JX, Huang CM, Zheng CH, Li P, Xie JW, Wang JB, Jun L, Chen QY, Lin M, Tu R. Evaluation of laparoscopic total gastrectomy for advanced gastric cancer: results of a comparison with laparoscopic distal gastrectomy. Surg Endosc 2016; 30: 1988-1998 [PMID: 26208499]
53 Moisan F, Norero E, Slako M, Varas J, Palominos G, Crovari F, Ibañez L, Pérez G, Pimentel F, Guzmán S, Jarufe N, Boza C, Escalona A, Funke R. Completely laparoscopic versus open gastrectomy for early and advanced gastric cancer: a matched cohort study. Surg Endosc 2012; 26: 661-672 [PMID: 22011940 DOI: 10.1007/s00464-011-1933-5]
54 Kitano S, Shiraishi N, Fujii K, Yasuda K, Inomata M, Adachi Y. A randomized controlled trial comparing open vs laparoscopy-assisted distal gastrectomy for the treatment of early gastric cancer: an interim report. Surgery 2002; 131: S306-S311 [PMID: 11821829]
55 Fujii K, Sonoda K, Izumi K, Shiraishi N, Adachi Y, Kitano S. T lymphocyte subsets and Th1/Th2 balance after laparoscopy-assisted distal gastrectomy. Surg Endosc 2003; 17: 1440-1444 [PMID: 12820059]
56 Hayashi H , Ochiai T, Shimada H, Gunji Y. Prospective randomized study of open versus laparoscopy-assisted distal gastrectomy with extraperigastric lymph node dissection for early gastric cancer. Surg Endosc 2005; 19: 1172-1176 [PMID: 16132323]
57 Lee JH, Han HS, Lee JH. A prospective randomized study comparing open vs laparoscopy-assisted distal gastrectomy in early gastric cancer: early results. Surg Endosc 2005; 19: 168-173 [PMID: 15580441]
58 Kim YW, Baik YH, Yun YH, Nam BH, Kim DH, Choi IJ, Bae JM. Improved quality of life outcomes after laparoscopy-assisted distal gastrectomy for early gastric cancer: results of a prospective
randomized clinical trial. Ann Surg 2008; 248: 721-727 [PMID: 18948798 DOI: 10.1097/SLA.0b013e318185e62e]
59 Sakuramoto S, Yamashita K, Kikuchi S, Futawatari N, Katada N, Watanabe M, Okutomi T, Wang G, Bax L. Laparoscopy versus open distal gastrectomy by expert surgeons for early gastric cancer in Japanese patients: short-term clinical outcomes of a randomized clinical trial. Surg Endosc 2013; 27: 1695-1705 [PMID: 23247737 DOI: 10.1007/s00464-012-2658-9]
60 Takiguchi S, Fujiwara Y, Yamasaki M, Miyata H, Nakajima K, Sekimoto M, Mori M, Doki Y. Laparoscopy-assisted distal gastrectomy versus open distal gastrectomy. A prospective randomized single-blind study. World J Surg 2013; 37: 2379-2386 [PMID: 23783252 DOI: 10.1007/s00268-013-2121-7]
61 Fujiwara M, Kodera Y, Misawa K, Kinoshita M, Kinoshita T, Miura S, Ohashi N, Nakayama G, Koike M, Nakao A. Longterm outcomes of early-stage gastric carcinoma patients treated with laparoscopy-assisted surgery. J Am Coll Surg 2008; 206: 138-143 [PMID: 18155579]
62 Zhang CD, Chen SC, Feng ZF, Zhao ZM, Wang JN, Dai DQ. Laparoscopic versus open gastrectomy for early gastric cancer in Asia: a meta-analysis. Surg Laparosc Endosc Percutan Tech 2013; 23: 365-377 [PMID: 23917592 DOI: 10.1097/SLE.0b013e31828e3e6e]
63 Folli S, Morgagni P, Roviello F, De Manzoni G, Marrelli D, Saragoni L, Di Leo A, Gaudio M, Nanni O, Carli A, Cordiano C, Dell’Amore D, Vio A; Italian Research Group for Gastric Cancer (IRGGC). Risk factors for lymph node metastases and their prognostic significance in early gastric cancer (EGC) for the Italian Research Group for Gastric Cancer (IRGGC). Jpn J Clin Oncol 2001; 31: 495-499 [PMID: 11696619]
64 Nakajima T. Gastric cancer treatment guidelines in Japan. Gastric Cancer 2002; 5: 1-5 [PMID: 12021853]
65 Cui M, Li Z, Xing J, Yao Z, Liu M, Chen L, Zhang C, Yang H, Zhang N, Tan F, Jiang B, Di J, Wang Z, Ji J, Su X. A prospective randomized clinical trial comparing D2 dissection in laparoscopic and open gastrectomy for gastric cancer. Med Oncol 2015; 32: 241 [PMID: 26350550 DOI: 10.1007/s12032-015-0680-1]
66 Pugliese R, Maggioni D, Sansonna F, Costanzi A, Ferrari GC, Di Lernia S, Magistro C, De Martini P, Pugliese F. Subtotal gastrectomy with D2 dissection by minimally invasive surgery for distal adenocarcinoma of the stomach: results and 5-year survival. Surg Endosc 2010; 24: 2594-2602 [PMID: 20414682 DOI: 10.1007/s00464-010-1014-1]
67 Shimizu S, Uchiyama A, Mizumoto K, Morisaki T, Nakamura K, Shimura H, Tanaka M. Laparoscopically assisted distal gastrectomy for early gastric cancer: is it superior to open surgery? Surg Endosc 2000; 14: 27-31 [PMID: 10653231]
68 Kitano S, Shiraishi N. Minimally invasive surgery for gastric tumors. Surg Clin North Am 2005; 85: 151-64, xi [PMID: 15619536]
69 Memon MA, Butler N, Memon B. The issue of lymphadenectomy during laparoscopic gastrectomy for gastric carcinoma. World J Gastrointest Oncol 2010; 2: 65-67 [PMID: 21160923 DOI: 10.4251/wjgo.v2.i2.65]
70 Huscher C, Mingoli A, Sgarzini G, Sansonetti A, Piro F, Ponzano C, Brachini G. Value of extended lymphadenectomy in laparoscopic subtotal gastrectomy for advanced gastric cancer. J Am Coll Surg 2005; 200: 314 [PMID: 15664111]
71 Uyama I, Sugioka A, Fujita J, Komori Y, Matsui H, Soga R, Wakayama A, Okamoto K, Ohyama A, Hasumi A. Completely laparoscopic extraperigastric lymph node dissection for gastric malignancies located in the middle or lower third of the stomach. Gastric Cancer 1999; 2: 186-190 [PMID: 11957094]
72 Kim MC , Choi HJ, Jung GJ, Kim HH. Techniques and complications of laparoscopy-assisted distal gastrectomy (LADG) for gastric cancer. Eur J Surg Oncol 2007; 33: 700-705 [PMID: 17399938]
73 Noshiro H, Nagai E, Shimizu S, Uchiyama A, Tanaka M. Laparoscopically assisted distal gastrectomy with standard radical
Caruso S et al . Robot-assisted laparoscopic gastrectomy for GC

5715 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
lymph node dissection for gastric cancer. Surg Endosc 2005; 19: 1592-1596 [PMID: 16247578]
74 Song KY, Kim SN, Park CH. Laparoscopy-assisted distal gastrectomy with D2 lymph node dissection for gastric cancer: technical and oncologic aspects. Surg Endosc 2008; 22: 655-659 [PMID: 17593447]
75 Ziqiang W, Feng Q, Zhimin C, Miao W, Lian Q, Huaxing L, Peiwu Y. Comparison of laparoscopically assisted and open radical distal gastrectomy with extended lymphadenectomy for gastric cancer management. Surg Endosc 2006; 20: 1738-1743 [PMID: 17024529]
76 Hur H, Jeon HM, Kim W. Laparoscopic pancreas- and spleen-preserving D2 lymph node dissection in advanced (cT2) upper-third gastric cancer. J Surg Oncol 2008; 97: 169-172 [PMID: 18095269]
77 Shinohara T, Kanaya S, Taniguchi K, Fujita T, Yanaga K, Uyama I. Laparoscopic total gastrectomy with D2 lymph node dissection for gastric cancer. Arch Surg 2009; 144: 1138-1142 [PMID: 20026832 DOI: 10.1001/archsurg.2009.223]
78 Haverkamp L, Ruurda JP, Offerhaus GJ, Weijs TJ, van der Sluis PC, van Hillegersberg R. Laparoscopic gastrectomy in Western European patients with advanced gastric cancer. Eur J Surg Oncol 2016; 42: 110-115 [PMID: 26603678 DOI: 10.1016/j.ejso.2015.09.018]
79 Lee SW, Nomura E, Bouras G, Tokuhara T, Tsunemi S, Tanigawa N. Long-term oncologic outcomes from laparoscopic gastrectomy for gastric cancer: a single-center experience of 601 consecutive resections. J Am Coll Surg 2010; 211: 33-40 [PMID: 20610246 DOI: 10.1016/j.jamcollsurg.2010.03.018]
80 Hwang SI, Kim HO, Yoo CH, Shin JH, Son BH. Laparoscopic-assisted distal gastrectomy versus open distal gastrectomy for advanced gastric cancer. Surg Endosc 2009; 23: 1252-1258 [PMID: 18855063 DOI: 10.1007/s00464-008-0140-5]
81 Li HT, Han XP, Su L, Zhu WK, Xu W, Li K, Zhao QC, Yang H, Liu HB. Short-term efficacy of laparoscopy-assisted vs open radical gastrectomy in gastric cancer. World J Gastrointest Surg 2014; 6: 59-64 [PMID: 24829623 DOI: 10.4240/wjgs.v6.i4.59]
82 Kim HH, Hyung WJ, Cho GS, Kim MC, Han SU, Kim W, Ryu SW, Lee HJ, Song KY. Morbidity and mortality of laparoscopic gastrectomy versus open gastrectomy for gastric cancer: an interim report--a phase III multicenter, prospective, randomized Trial (KLASS Trial). Ann Surg 2010; 251: 417-420 [PMID: 20160637 DOI: 10.1097/SLA.0b013e3181cc8f6b]
83 Qiu J , Pankaj P, Jiang H, Zeng Y, Wu H. Laparoscopy versus open distal gastrectomy for advanced gastric cancer: a systematic review and meta-analysis. Surg Laparosc Endosc Percutan Tech 2013; 23: 1-7 [PMID: 23386142 DOI: 10.1097/SLE.0b013e3182747af7]
84 Martínez-Ramos D, Miralles-Tena JM, Cuesta MA, Escrig-Sos J, Van der Peet D, Hoashi JS, Salvador-Sanchís JL. Laparoscopy versus open surgery for advanced and resectable gastric cancer: a meta-analysis. Rev Esp Enferm Dig 2011; 103: 133-141 [PMID: 21434716]
85 Quan Y, Huang A, Ye M, Xu M, Zhuang B, Zhang P, Yu B, Min Z. Comparison of laparoscopic versus open gastrectomy for advanced gastric cancer: an updated meta-analysis. Gastric Cancer 2016; 19: 939-950 [PMID: 26216579]
86 Park do J, Han SU, Hyung WJ, Kim MC, Kim W, Ryu SY, Ryu SW, Song KY, Lee HJ, Cho GS, Kim HH; Korean Laparoscopic Gastrointestinal Surgery Study (KLASS) Group. Long-term outcomes after laparoscopy-assisted gastrectomy for advanced gastric cancer: a large-scale multicenter retrospective study. Surg Endosc 2012; 26: 1548-1553 [PMID: 22170319 DOI: 10.1007/s00464-011-2065-7]
87 Degiuli M, Sasako M, Ponti A, Vendrame A, Tomatis M, Mazza C, Borasi A, Capussotti L, Fronda G, Morino M; Italian Gastric Cancer Study Group. Randomized clinical trial comparing survival after D1 or D2 gastrectomy for gastric cancer. Br J Surg 2014; 101: 23-31 [PMID: 24375296 DOI: 10.1002/bjs.9345]
88 Huang JL, Wei HB, Zheng ZH, Wei B, Chen TF, Huang Y, Guo WP, Hu B. Laparoscopy-assisted D2 radical distal gastrectomy for advanced gastric cancer. Dig Surg 2010; 27: 291-296 [PMID: 20689290 DOI: 10.1159/000281818]
89 Zhao XF, Jeong O, Jung MR, Ryu SY, Park YK. A propensity score-matched case-control comparative study of laparoscopic and open extended (D2) lymph node dissection for distal gastric carcinoma. Surg Endosc 2013; 27: 2792-2800 [PMID: 23389075 DOI: 10.1007/s00464-013-2809-7]
90 Cai J, Wei D, Gao CF, Zhang CS, Zhang H, Zhao T. A prospective randomized study comparing open versus laparoscopy-assisted D2 radical gastrectomy in advanced gastric cancer. Dig Surg 2011; 28: 331-337 [PMID: 21934308 DOI: 10.1159/000330782]
91 Zou ZH, Zhao LY, Mou TY, Hu YF, Yu J, Liu H, Chen H, Wu JM, An SL, Li GX. Laparoscopic vs open D2 gastrectomy for locally advanced gastric cancer: a meta-analysis. World J Gastroenterol 2014; 20: 16750-16764 [PMID: 25469048 DOI: 10.3748/wjg.v20.i44.16750]
92 Wei HB, Wei B, Qi CL, Chen TF, Huang Y, Zheng ZH, Huang JL, Fang JF. Laparoscopic versus open gastrectomy with D2 lymph node dissection for gastric cancer: a meta-analysis. Surg Laparosc Endosc Percutan Tech 2011; 21: 383-390 [PMID: 22146158 DOI: 10.1097/SLE.0b013e31822d02dc]
93 Ikeda O, Sakaguchi Y, Toh Y, Oogaki K, Oki E, Minami K, Okamura T, Baba H. Evaluation of oncological adequacy of laparoscopic distal gastrectomy with special attention to lymph node dissection: a comparison with conventional open gastrectomy. Hepatogastroenterology 2012; 59: 627-632 [PMID: 22353532 DOI: 10.5754/hge10089]
94 Kunisaki C, Makino H, Yamamoto N, Sato T, Oshima T, Nagano Y, Fujii S, Akiyama H, Otsuka Y, Ono HA, Kosaka T, Takagawa R, Shimada H. Learning curve for laparoscopy-assisted distal gastrectomy with regional lymph node dissection for early gastric cancer. Surg Laparosc Endosc Percutan Tech 2008; 18: 236-241 [PMID: 18574408 DOI: 10.1097/SLE.0b013e31816aa13f]
95 Jin SH, Kim DY, Kim H, Jeong IH, Kim MW, Cho YK, Han SU. Multidimensional learning curve in laparoscopy-assisted gastrectomy for early gastric cancer. Surg Endosc 2007; 21: 28-33 [PMID: 16960676]
96 Bouras G, Lee SW, Nomura E, Tokuhara T, Tsunemi S, Tanigawa N. Comparative analysis of station-specific lymph node yield in laparoscopic and open distal gastrectomy for early gastric cancer. Surg Laparosc Endosc Percutan Tech 2011; 21: 424-428 [PMID: 22146165 DOI: 10.1097/SLE.0b013e3182367dee]
97 Son T, Kwon IG, Hyung WJ. Minimally invasive surgery for gastric cancer treatment: current status and future perspectives. Gut Liver 2014; 8: 229-236 [PMID: 24827617 DOI: 10.5009/gnl.2014.8.3.229]
98 Alimoglu O, Atak I, Eren T. Robot-assisted laparoscopic (RAL) surgery for gastric cancer. Int J Med Robot 2014; 10: 257-262 [PMID: 24375986 DOI: 10.1002/rcs.1566]
99 Kim HI , Park MS, Song KJ, Woo Y, Hyung WJ. Rapid and safe learning of robotic gastrectomy for gastric cancer: multidimensional analysis in a comparison with laparoscopic gastrectomy. Eur J Surg Oncol 2014; 40: 1346-1354 [PMID: 24080199 DOI: 10.1016/j.ejso.2013.09.011]
100 Park JY, Jo MJ, Nam BH, Kim Y, Eom BW, Yoon HM, Ryu KW, Kim YW, Lee JH. Surgical stress after robot-assisted distal gastrectomy and its economic implications. Br J Surg 2012; 99: 1554-1561 [PMID: 23027072 DOI: 10.1002/bjs.8887]
101 Obama K, Sakai Y. Current status of robotic gastrectomy for gastric cancer. Surg Today 2016; 46: 528-534 [PMID: 26019020]
102 Terashima M, Tokunaga M, Tanizawa Y, Bando E, Kawamura T, Miki Y, Makuuchi R, Honda S, Tatsubayashi T, Takagi W, Omori H, Hirata F. Robotic surgery for gastric cancer. Gastric Cancer 2015; 18: 449-457 [PMID: 25899666 DOI: 10.1007/s10120-015-0501-4]
103 Hashizume M, Sugimachi K. Robot-assisted gastric surgery. Surg Clin North Am 2003; 83: 1429-1444 [PMID: 14712877]
Caruso S et al . Robot-assisted laparoscopic gastrectomy for GC

5716 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
104 Giulianotti PC, Coratti A, Angelini M, Sbrana F, Cecconi S, Balestracci T, Caravaglios G. Robotics in general surgery: personal experience in a large community hospital. Arch Surg 2003; 138: 777-784 [PMID: 12860761]
105 Junfeng Z, Yan S, Bo T, Yingxue H, Dongzhu Z, Yongliang Z, Feng Q, Peiwu Y. Robotic gastrectomy versus laparoscopic gastrectomy for gastric cancer: comparison of surgical performance and short-term outcomes. Surg Endosc 2014; 28: 1779-1787 [PMID: 24385251 DOI: 10.1007/s00464-013-3385-6]
106 Woo Y, Hyung WJ, Pak KH, Inaba K, Obama K, Choi SH, Noh SH. Robotic gastrectomy as an oncologically sound alternative to laparoscopic resections for the treatment of early-stage gastric cancers. Arch Surg 2011; 146: 1086-1092 [PMID: 21576595 DOI: 10.1001/archsurg.2011.114]
107 Kim MC, Heo GU, Jung GJ. Robotic gastrectomy for gastric cancer: surgical techniques and clinical merits. Surg Endosc 2010; 24: 610-615 [PMID: 19688399 DOI: 10.1007/s00464-009-0618-9]
108 Eom BW, Yoon HM, Ryu KW, Lee JH, Cho SJ, Lee JY, Kim CG, Choi IJ, Lee JS, Kook MC, Rhee JY, Park SR, Kim YW. Comparison of surgical performance and short-term clinical outcomes between laparoscopic and robotic surgery in distal gastric cancer. Eur J Surg Oncol 2012; 38: 57-63 [PMID: 21945625 DOI: 10.1016/j.ejso.2011.09.006]
109 Lee HH, Hur H, Jung H, Jeon HM, Park CH, Song KY. Robot-assisted distal gastrectomy for gastric cancer: initial experience. Am J Surg 2011; 201: 841-845 [PMID: 21741513 DOI: 10.1016/j.amjsurg.2010.05.013]
110 D’Annibale A, Pende V, Pernazza G, Monsellato I, Mazzocchi P, Lucandri G, Morpurgo E, Contardo T, Sovernigo G. Full robotic gastrectomy with extended (D2) lymphadenectomy for gastric cancer: surgical technique and preliminary results. J Surg Res 2011; 166: e113-e120 [PMID: 21227455 DOI: 10.1016/j.jss.2010.11.881]
111 Caruso S, Patriti A, Marrelli D, Ceccarelli G, Ceribelli C, Roviello F, Casciola L. Open vs robot-assisted laparoscopic gastric resection with D2 lymph node dissection for adenocarcinoma: a case-control study. Int J Med Robot 2011; 7: 452-458 [PMID: 21984205 DOI: 10.1002/rcs.416]
112 Isogaki J, Haruta S, Man-I M, Suda K, Kawamura Y, Yoshimura F, Kawabata T, Inaba K, Ishikawa K, Ishida Y, Taniguchi K, Sato S, Kanaya S, Uyama I. Robot-assisted surgery for gastric cancer: experience at our institute. Pathobiology 2011; 78: 328-333 [PMID: 22104204 DOI: 10.1159/000330172]
113 Huang KH, Lan YT, Fang WL, Chen JH, Lo SS, Hsieh MC, Li AF, Chiou SH, Wu CW. Initial experience of robotic gastrectomy and comparison with open and laparoscopic gastrectomy for gastric cancer. J Gastrointest Surg 2012; 16: 1303-1310 [PMID: 22450954 DOI: 10.1007/s11605-012-1874-x]
114 Uyama I, Kanaya S, Ishida Y, Inaba K, Suda K, Satoh S. Novel integrated robotic approach for suprapancreatic D2 nodal dissection for treating gastric cancer: technique and initial experience. World J Surg 2012; 36: 331-337 [PMID: 22131088 DOI: 10.1007/s00268-011-1352-8]
115 Kang BH , Xuan Y, Hur H, Ahn CW, Cho YK, Han SU. Comparison of Surgical Outcomes between Robotic and Laparoscopic Gastrectomy for Gastric Cancer: The Learning Curve of Robotic Surgery. J Gastric Cancer 2012; 12: 156-163 [PMID: 23094227 DOI: 10.5230/jgc.2012.12.3.156]
116 Kim KM, An JY, Kim HI, Cheong JH, Hyung WJ, Noh SH. Major early complications following open, laparoscopic and robotic gastrectomy. Br J Surg 2012; 99: 1681-1687 [PMID: 23034831 DOI: 10.1002/bjs.8924]
117 Yoon HM, Kim YW, Lee JH, Ryu KW, Eom BW, Park JY, Choi IJ, Kim CG, Lee JY, Cho SJ, Rho JY. Robot-assisted total gastrectomy is comparable with laparoscopically assisted total gastrectomy for early gastric cancer. Surg Endosc 2012; 26: 1377-1381 [PMID: 22083338 DOI: 10.1007/s00464-011-2043-0]
118 Hyun MH, Lee CH, Kwon YJ, Cho SI, Jang YJ, Kim DH, Kim JH, Park SH, Mok YJ, Park SS. Robot versus laparoscopic
gastrectomy for cancer by an experienced surgeon: comparisons of surgery, complications, and surgical stress. Ann Surg Oncol 2013; 20: 1258-1265 [PMID: 23080320 DOI: 10.1245/s10434-012-2679-6]
119 Park JY, Kim YW, Ryu KW, Eom BW, Yoon HM, Reim D. Emerging Role of Robot-assisted Gastrectomy: Analysis of Consecutive 200 Cases. J Gastric Cancer 2013; 13: 255-262 [PMID: 24511422 DOI: 10.5230/jgc.2013.13.4.255]
120 Son T, Lee JH, Kim YM, Kim HI, Noh SH, Hyung WJ. Robotic spleen-preserving total gastrectomy for gastric cancer: comparison with conventional laparoscopic procedure. Surg Endosc 2014; 28: 2606-2615 [PMID: 24695982 DOI: 10.1007/s00464-014-3511-0]
121 Shen W, Xi H, Wei B, Cui J, Bian S, Zhang K, Wang N, Huang X, Chen L. Robotic versus laparoscopic gastrectomy for gastric cancer: comparison of short-term surgical outcomes. Surg Endosc 2016; 30: 574-580 [PMID: 26208497 DOI: 10.1007/s00464-015-4241-7]
122 Kim HI, Han SU, Yang HK, Kim YW, Lee HJ, Ryu KW, Park JM, An JY, Kim MC, Park S, Song KY, Oh SJ, Kong SH, Suh BJ, Yang DH, Ha TK, Kim YN, Hyung WJ. Multicenter Prospective Comparative Study of Robotic Versus Laparoscopic Gastrectomy for Gastric Adenocarcinoma. Ann Surg 2016; 263: 103-109 [PMID: 26020107 DOI: 10.1097/SLA.0000000000001249]
123 Kim YW, Reim D, Park JY, Eom BW, Kook MC, Ryu KW, Yoon HM. Role of robot-assisted distal gastrectomy compared to laparoscopy-assisted distal gastrectomy in suprapancreatic nodal dissection for gastric cancer. Surg Endosc 2016; 30: 1547-1552 [PMID: 26169636]
124 Liao G, Chen J, Ren C, Li R, Du S, Xie G, Deng H, Yang K, Yuan Y. Robotic versus open gastrectomy for gastric cancer: a meta-analysis. PLoS One 2013; 8: e81946 [PMID: 24312610 DOI: 10.1371/journal.pone.0081946]
125 Xiong B , Ma L, Zhang C. Robotic versus laparoscopic gastrectomy for gastric cancer: a meta-analysis of short outcomes. Surg Oncol 2012; 21: 274-280 [PMID: 22789391 DOI: 10.1016/j.suronc.2012.05.004]
126 Xiong J, Nunes QM, Tan C, Ke N, Chen Y, Hu W, Liu X, Mai G. Comparison of short-term clinical outcomes between robotic and laparoscopic gastrectomy for gastric cancer: a meta-analysis of 2495 patients. J Laparoendosc Adv Surg Tech A 2013; 23: 965-976 [PMID: 24093968 DOI: 10.1089/lap.2013.0279]
127 Liao GX, Xie GZ, Li R, Zhao ZH, Sun QQ, Du SS, Ren C, Li GX, Deng HJ, Yuan YW. Meta-analysis of outcomes compared between robotic and laparoscopic gastrectomy for gastric cancer. Asian Pac J Cancer Prev 2013; 14: 4871-4875 [PMID: 24083761]
128 Shen WS, Xi HQ, Chen L, Wei B. A meta-analysis of robotic versus laparoscopic gastrectomy for gastric cancer. Surg Endosc 2014; 28: 2795-2802 [PMID: 24789136 DOI: 10.1007/s00464-014-3547-1]
129 Chuan L, Yan S, Pei-Wu Y. Meta-analysis of the short-term outcomes of robotic-assisted compared to laparoscopic gastrectomy. Minim Invasive Ther Allied Technol 2015; 24: 127-134 [PMID: 25467019 DOI: 10.3109/13645706.2014.985685]
130 Hyun MH, Lee CH, Kim HJ, Tong Y, Park SS. Systematic review and meta-analysis of robotic surgery compared with conventional laparoscopic and open resections for gastric carcinoma. Br J Surg 2013; 100: 1566-1578 [PMID: 24264778 DOI: 10.1002/bjs.9242]
131 Marano A, Choi YY, Hyung WJ, Kim YM, Kim J, Noh SH. Robotic versus Laparoscopic versus Open Gastrectomy: A Meta-Analysis. J Gastric Cancer 2013; 13: 136-148 [PMID: 24156033 DOI: 10.5230/jgc.2013.13.3.136]
132 Zong L, Seto Y, Aikou S, Takahashi T. Efficacy evaluation of subtotal and total gastrectomies in robotic surgery for gastric cancer compared with that in open and laparoscopic resections: a meta-analysis. PLoS One 2014; 9: e103312 [PMID: 25068955 DOI: 10.1371/journal.pone.0103312]
133 Coratti A, Fernandes E, Lombardi A, Di Marino M, Annecchiarico M, Felicioni L, Giulianotti PC. Robot-assisted surgery for gastric carcinoma: Five years follow-up and beyond: A single western
Caruso S et al . Robot-assisted laparoscopic gastrectomy for GC

5717 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
center experience and long-term oncological outcomes. Eur J Surg Oncol 2015; 41: 1106-1113 [PMID: 25796984 DOI: 10.1016/j.ejso.2015.01.014]
134 Jiang L, Yang KH, Guan QL, Cao N, Chen Y, Zhao P, Chen YL, Yao L. Laparoscopy-assisted gastrectomy versus open gastrectomy for resectable gastric cancer: an update meta-analysis based on randomized controlled trials. Surg Endosc 2013; 27: 2466-2480 [PMID: 23361259 DOI: 10.1007/s00464-012-2758-6]
135 Lee J, Kim YM, Woo Y, Obama K, Noh SH, Hyung WJ. Robotic distal subtotal gastrectomy with D2 lymphadenectomy for gastric cancer patients with high body mass index: comparison with conventional laparoscopic distal subtotal gastrectomy with D2 lymphadenectomy. Surg Endosc 2015; 29: 3251-3260 [PMID: 25631106 DOI: 10.1007/s00464-015-4069-1]
136 Hur H, Lee HY, Lee HJ, Kim MC, Hyung WJ, Park YK, Kim W, Han SU. Efficacy of laparoscopic subtotal gastrectomy with D2 lymphadenectomy for locally advanced gastric cancer: the protocol of the KLASS-02 multicenter randomized controlled clinical trial. BMC Cancer 2015; 15: 355 [PMID: 25939684 DOI: 10.1186/s12885-015-1365-z]
137 Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2010 (ver. 3). Gastric Cancer 2011; 14: 113-123 [PMID: 21573742 DOI: 10.1007/s10120-011-0042-4]
138 Mochiki E, Nakabayashi T, Kamimura H, Haga N, Asao T, Kuwano H. Gastrointestinal recovery and outcome after laparoscopy-assisted versus conventional open distal gastrectomy for early gastric cancer. World J Surg 2002; 26: 1145-1149 [PMID: 12209244]
P- Reviewer: El Nakeeb A, Hou X, Noshiro H S- Editor: Ma YJ L- Editor: A E- Editor: Wang CH
Caruso S et al . Robot-assisted laparoscopic gastrectomy for GC

complications after rectal cancer surgery. The double stapling technique has greatly facilitated intestinal reconstruction especially for anastomosis after low anterior resection (LAR). Risk factor analyses for AL after open LAR have been widely reported. However, a few studies have analyzed the risk factors for AL after laparoscopic LAR. Laparoscopic rectal surgery provides an excellent operative field in a narrow pelvic space, and enables total mesorectal excision surgery and preservation of the autonomic nervous system with greater precision. However, rectal transection using a laparoscopic linear stapler is relatively difficult compared with open surgery because of the width and limited performance of the linear stapler. Moreover, laparoscopic LAR exhibits a different postoperative course compared with open LAR, which suggests that the risk factors for AL after laparoscopic LAR may also differ from those after open LAR. In this review, we will discuss the risk factors for AL after laparoscopic LAR.
Key words: Risk factor; Laparoscopic low anterior resection; Anastomotic leakage
© The Author(s) 2016. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Recently, many studies have reported that laparoscopic rectal surgery is becoming popular and exhibits favorable outcomes compared with open surgery. However, the anastomotic leakage (AL) rate after laparoscopic low anterior resection (LAR) is yet about 10%, and AL remains a huge challenge despite many surgical and technological advances. Here we review the current literature published with respect to the risk factors for AL after laparoscopic LAR.
Kawada K, Sakai Y. Preoperative, intraoperative and postoperative risk factors for anastomotic leakage after laparoscopic low
Kenji Kawada, Yoshiharu Sakai, Department of Surgery, Graduate School of Medicine, Kyoto University, Kyoto 606-8507, Japan
Author contributions: Kawada K wrote the paper; Sakai Y contributed critical revision of the manuscript for important intellectual content.
Conflict-of-interest statement: No potential conflicts of interest exist.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Manuscript source: Invited manuscript
Correspondence to: Kenji Kawada, MD, PhD, Department of Surgery, Graduate School of Medicine, Kyoto University, 54 Shogoin- Kawara-cho, Sakyo-ku, Kyoto 606-8507, Japan. [email protected]: +81-75-3667595Fax: +81-75-3667642
Received: April 7, 2016Peer-review started: April 8, 2016First decision: May 27, 2016Revised: May 30, 2016Accepted: June 13, 2016 Article in press: June 13, 2016Published online: July 7, 2016
AbstractAnastomotic leakage (AL) is one of the most devastating
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.3748/wjg.v22.i25.5718
5718 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
World J Gastroenterol 2016 July 7; 22(25): 5718-5727 ISSN 1007-9327 (print) ISSN 2219-2840 (online)
© 2016 Baishideng Publishing Group Inc. All rights reserved.
Kenji Kawada, Yoshiharu Sakai
TOPIC HIGHLIGHT
Preoperative, intraoperative and postoperative risk factors for anastomotic leakage after laparoscopic low anterior resection with double stapling technique anastomosis
2016 Laparoscopic Surgery: Global view

anterior resection with double stapling technique anastomosis. World J Gastroenterol 2016; 22(25): 5718-5727 Available from: URL: http://www.wjgnet.com/1007-9327/full/v22/i25/5718.htm DOI: http://dx.doi.org/10.3748/wjg.v22.i25.5718
INTRODUCTIONLaparoscopic surgery for colon cancer was introduced in the 1990s, and has shown promising results. Laparoscopic low anterior resection (LAR) for rectal cancer is technically more difficult than laparoscopic colectomy because of the difficulties related to a narrow pelvic space. A higher incidence of positive circumferential margins after laparoscopic LAR was reported in an initial randomized controlled trial (RCT)[1], but an increasing number of studies have shown that laparoscopic surgery for rectal cancer provides surgical safety and oncological outcomes equivalent to open surgery[26]. Recent largescale RCTs such as COLOR II[7] and COREAN[8] have reported favorable outcomes for laparoscopic surgery compared with open surgery for rectal cancer.
The double stapling technique (DST) has greatly facilitated intestinal reconstruction, especially for anastomosis after LAR. Anastomotic leakage (AL) is one of the most devastating complications after rectal cancer surgery. AL impairs not only shortterm outcomes (morbidity, mortality, length of hospital stay, and financial cost) but also long-term oncological outcomes (survival and local recurrence)[911]. Therefore, it is important to identify the patients who are at high risk of AL for improving overall outcomes. Despite technical improvements and instrumental developments, recent studies have reported that the AL rate ranges from 3% to 19%[9,1215]; the most commonly reported rate is approximately 10%13% from recent large population databases in the United States[12] and Japan[15]. AL after rectal resection is influenced by many factors including not only surgical factors but also medical factors related to the systemic conditions in patients.
Several risk factors, including age, sex, intraoperative bleeding, obesity, preoperative chemoradiotherapy, protective diverting stoma, pelvic drainage, tumor size, tumor location and the level of anastomosis have been reported to be risk factors for AL after open LAR[1621]. In contrast, only a few studies have examined risk factors for AL after laparoscopic LAR[2231] (Table 1). In addition, the rates of protective diverting stoma, preoperative chemoradiotherapy (CRT), and total mesorectal excision (TME) in each study were not consistent, which might produce different results. Several studies reported that laparoscopic surgery and open surgery for rectal cancer did not differ in terms of the AL rate[1,2,4]. Laparoscopic rectal surgery provides an excellent operative field in a narrow pelvic space, and enables
the preservation of autonomic nerves more precisely. However, rectal transection using a laparoscopic linear stapler is relatively difficult when compared with open surgery because of the width and limited performance of the linear stapler. The devices and techniques used for laparoscopic LAR are different from those used for open LAR. Moreover, laparoscopic LAR exhibits a different postoperative course compared with open LAR, including less blood loss, faster recovery of peristalsis, faster initiation of oral intake, and shorter hospital stay. Notably, multicenter, prospective and cohort studies using propensity score matching analysis have reported that risk factors for AL after laparoscopic or robotic LAR are different from those after open LAR[30,31]. Factors related to technical difficulty such as male sex, previous abdominal sur-gery, lower location of tumor and the use of more than 2 cartridges for rectal transection were found to be significant only in laparoscopic or robotic LAR groups[31].
In this review, we will discuss the risk factors for AL after laparoscopic LAR. Risk factors are categorized into (1) preoperative; (2) intraoperative; and (3) postoperative factors. The identification of highrisk patients has great clinical relevance and ultimately improves patient outcomes. Although more prospective studies are needed, this review provides major insight into identifying important risk factors for AL after laparoscopic LAR.
PREOPERATIVE RISK FACTORS Male genderMales have a narrow pelvis, which makes rectal dissection and anastomosis more difficult and more prone to surgical complications. In fact, male gender has been reported as an increased risk factor for AL after open LAR[16,17,1921] as well as laparoscopic LAR[28,30,31]. The influence of androgenrelated differences in the intestinal microcirculation may be involved[32].
Body mass indexSome studies have shown that obesity measured by body mass index (BMI) can increase the risk of AL[3335]. Yamamoto et al[27] reported that BMI was independently predictive for AL after laparoscopic LAR. In place of BMI, waist circumference and waist/hip ratio may predict the risk of AL[36]. In addition, measuring visceral fat area may be more sensitive than BMI in predicting AL after laparoscopic surgery[37].
Preoperative radiotherapy/chemoradiotherapyPreoperative radiotherapy (RT) with or without concomitant chemotherapy is generally recommended for patients with locally advanced rectal cancer followed by TME surgery. It is accepted that these therapeutic modalities can reduce the local recurrence
5719 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Kawada K et al . Risk factors for AL after laparoscopic LAR

rate[3840]. Although effective in targeting cancer cells, RT has a wide array of detrimental effects on intestinal tissue and wound healing and has long been believed to be a risk factor for AL. There are many retrospective studies that have reported the relationship between preoperative RT and AL[20,21,28]. However, prospective trials and cohort studies have shown contradictory results. The MRC CR07 RCT[41] reported that there was no difference in AL between preoperative RT and selective postoperative CRT. A Dutch TME trial[42] reported that there was no significant difference in AL rates (TME plus preoperative RT vs TME alone). A recent report using propensity score matching analysis have also reported that preoperative CRT does not increase the risk of AL after LAR[43]. Most surgeons perform a temporary protective diverting stoma to minimize the consequences of AL in patients who have received preoperative CRT or RT.
Preoperative chemotherapyPreoperative chemotherapy is a wellknown risk factor for AL[13]; however, the mechanism underlying this association is poorly understood. Recent use of antiangiogenic agents also increases the risk of AL. The first studies examining bevacizumab (Avastin), a humanized antivascular endothelial growth factor antibody, reported several patients with bowel perforation[44,45]. The mechanism of this perforation is proposed to be arterial microthromboembolic disease leading to bowel ischemia. The same mechanism can cause AL. Bevacizumab has a halflife of 20 days, and the manufacturer recommends stopping its treatment at least 4 wk before surgery.
AntibioticsA metaanalysis of eight RCTs reported that combining preoperative intestinal decontamination with oral antibiotics and perioperative intravenous antibiotics reduced postoperative infection including AL, com
pared with use of intravenous antibiotics alone[46]. Notably, a recent RCT showed that intravenous plus oral antibiotics (cefmetazole, kanamycin and metronidazole) significantly reduced the risk of surgical site infection (SSI) compared with intravenous antibiotics alone (7.3% vs 12.8%, P = 0.028), while no significant difference was seen in the rate of AL[47]. Further studies are required to elucidate the effect of preoperative oral antibiotics on AL.
MedicationsAlthough it is assumed that impaired healing with corticosteroid use would affect the AL rate, it is difficult to find an absolute correlation. Prolonged use of corticosteroids can be a risk factor for AL, particularly when combined with other immunosuppressive drugs[4850]. A recent systematic review reported that the AL rate after lower gastrointestinal surgery was 6.8% in the corticosteroid group compared with 3.3% in the noncorticosteroid group, although the duration and dose of corticosteroid treatment were heterogeneous[51]. A metaanalysis with six RCTs reported that perioperative use of nonsteroidal antiinflammatory drugs (NSAIDs) had no statistically significant effect on the AL rate[52]. However, nonselective NSAIDs and nonselective cyclooxygenase (COX) 2 inhibitors were reported to be associated with a higher AL rate[53]. Therefore, NSAIDs should be used with caution in the postoperative period. In general, the postoperative pain after laparoscopic surgery is less than that after open surgery, which may result in the decreased usage of NSAIDs and decreased rate of AL in laparoscopic surgery.
Other factors, such as smoking and alcohol, have also been reported to be risk factors for AL after LAR[31,5457]. The effect of smoking might be secondary to ischemia caused by smokingrelated microvascular disease. Large quantities of alcohol consumption might be a surrogate for poor nutritional status.
5720 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Table 1 Selected studies to investigate the risk factors for Anastomotic leakage after laparoscopic low anterior resection
Ref. Year Sample AL Tumor Covering Risk factors
size rate Location1 stoma
Ito et al[22] 2008 180 5.0% R, RS + Anastomosis level, multiple stapler firingsKim et al[23] 2009 270 6.3% R, RS, S + Tumor locationHuh et al[24] 2010 223 8.5% R - Tumor location, operation timeChoi et al[25] 2010 156 10.3% R, RS - Anastomosis level, operation timeAkiyoshi et al[26] 2011 363 3.6% R, RS + Tumor location, abdominal drainYamamoto et al[27] 2012 111 5.4% R + BMIPark et al[28] 2013 1187 6.3% R, RS - Male, stage, transfusion, tumor location
preoperative CRT, multiple stapler firingsKawada et al[29] 2014 154 12.3% R - Tumor size, precompression before
stapler firingsKatsuno et al[30] 2015 209 15.3% R + MaleKim et al[31] 2016 1154 6.7% R + Male, smoking, alcohol intake, previous
abdominal surgery, operation time,tumor location, multiple stapler firings
1R: Rectum; RS: Rectosigmoid colon; S: Sigmoid colon.
Kawada K et al . Risk factors for AL after laparoscopic LAR

5721 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
operatorassistant movement, and that removal of the crossing point of staple lines was important to delete the potential source of AL. In a clinical setting, we previously analyzed whether the remnant crossing point could increase the AL rate, and found that it was not significantly associated with AL[29]. Therefore, we assume that surgeons do not need to persist in removal of the crossing point, especially when the crossing point is placed near the edge of the rectal stump and so removal of the crossing point is technically difficult.
It is notable that intracorporeal[68] or transanal[69] reinforcing sutures could effectively reduce AL after LAR, but the results of these studies are not conclusive. DST is inevitably associated with bilateral intersecting staple lines at the rectal stump, socalled dog ears. The dog ears are the weak spots associated with potential AL[70]. Recently, a combined laparoscopic LAR and eversion technique without dog ear formation was reported to be useful to reduce AL for mid and distal rectal cancer[71].
Precompression before stapler firingsWe previously reported that a sufficient amount of precompression time before stapler firings resulted in reduced intestinal wall thickness and proper staple formation in animal models[7274]. In addition, we recently reported that precompression before stapler firings and tumor size (≥ 5.0 cm) were associated with AL after laparoscopic LAR in a clinical setting, and that precompression before stapler firing tended to reduce the AL occurring in the early postoperative period[29]. Precompression time before stapler firings and proper cartridge selection according to the wall thickness are critical to achieve secure staple formation.
Diameter of circular stapler Kim et al[23] reported the association between a larger diameter circular stapler and increased rates of AL. They speculated that a larger diameter circular stapler made the distal rectum more distended. A distended rectum with thinned rectal wall may cause inadequate blood supply to the anastomosis site. We previously analyzed whether the diameter of a circular stapler could affect the AL rate, and found that it was not significantly associated with AL[29]. Further studies are required to elucidate the effect of diameter of a circular stapler.
Tumor characteristicsTumor size is a wellknown risk factor for AL after laparoscopic LAR[13,29,30]. A bulky tumor could adversely affect the ease of rectal transection and anastomosis in the limited pelvic space. Some studies demonstrated that tumor size greater than 5 cm was independently predictive of AL[13,29]. Advanced stage is also a risk factor for AL after laparoscopic LAR[28].
Mechanical bowel preparationMechanical bowel preparation (MBP) is performed before colorectal surgery to reduce massive bowel contents, which can be a source of colorectal AL and infectious bacterial pathogens. However, the routine use of MBP is being abandoned gradually, because some RCT studies and metaanalyses have concluded that omitting MBP before surgery has fewer postoperative morbidities including AL and SSI[5861]. The practice of omitting MBP is further promoted because MBP causes some discomforts to patients, such as nausea, vomiting, dehydration and electrolyte abnormalities. However, recent some studies from the United States databases have reported that combining MBP and oral antibiotics results in a significantly lower incidence of AL, incisional SSI and hospital readmission compared with no preoperative bowel preparation in colorectal surgery[6264]. Moreover, regarding the longterm effect of MBP, the 10year cancerspecific survival rate was recently reported to be significantly better in MBP group than in nonMBP group[65,66]. Further studies are required to elucidate the effect of MBP on AL.
INTRAOPERATIVE RISK FACTORSLevel of anastomosisIt is widely accepted that the risk of AL increases with more distal anastomosis. Although it is well accepted that a low anastomosis has a higher incidence of AL, the mechanism remains unknown. It is hypothesized that the height of the anastomosis or the tumor location can reflect technical difficulties of LAR, resulting in local tissue trauma, increased tension, or poor blood supply. A number of studies reported that lower anastomosis level is an important risk factor for AL after open LAR[1621] as well as laparoscopic LAR[2326,28,31].
Surgical technique and multiple stapler firings Surgical technique has a substantial impact on postoperative complications including AL. In laparoscopic LAR, optimal port placement is important to reduce the number of linear stapler firings for rectal transection in a narrow pelvis. The use of multiple staplers (e.g., ≥ 3 cartridges) for rectal transection is a major cause of AL after laparoscopic LAR[22,23,26,28,29,31]. When the number of stapler cartridges increases, there is a concern that an increased number of stapler firings can lead to small defects between the staple lines and, in turn, cause AL. Therefore, laparoscopic surgeons need to make efforts to reduce the number of linear stapler firings to two or less. Several different techniques have been proposed to reduce AL. Ito et al[22] reported that vertical rectal transection through an additional suprapubic site was useful for avoiding multiple stapler firings and decreasing the AL rate. Kuroyanagi et al[67] reported that rectal transection was performed using two cartridges in most cases, with coordinated
Kawada K et al . Risk factors for AL after laparoscopic LAR

5722 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Blood supplyDespite the multifactorial etiology of AL, insufficient perfusion and technical factors are considered to play a substantial role in the development of AL[9,7577]. For this reason, surgeons often assess intestinal perfusion by several clinical checks, such as the color of the bowel wall, palpable pulsation, and bleeding from marginal arteries. These checks are subjective and based on the surgeon’s experience, and may well lead to misinterpretations even by experienced surgeons[78]. In recent years, nearinfrared (NIR) fluorescence technology with indocyanine green (ICG) has been the most promising method that provides a realtime assessment of intestinal perfusion[7983]. The first study to use fluorescence imaging for colorectal surgery was published by Kudszus et al[79]. They reported that fluorescence imaging resulted in a proximal change of the initially planned transection line in 13.9% (28/201), and that intraoperative fluorescence imaging reduced AL by 4% compared with a control group (7.5% vs 3.5%). These data have been confirmed by Jafari et al[80] during roboticassisted laparoscopic rectal surgery. Moreover, a multiinstitutional prospective study, PILLARII, recently reported that fluorescence imaging changed surgical plans in 8% (11/139), and that the AL rate was 1.4% (2/139) in laparoscopic leftsided/anterior resection[82]. In addition, Sherwinter et al[84] evaluated the intraluminal aspect of the anastomosis transanally after DST construction using a transanal NIR imaging system. The assessment of rectal stump perfusion by transanal ICG imaging can be a promising method, although further studies are needed to correlate this technique to the clinical outcome. However, another recent another report stated that the intraoperative fluorescence imaging does not reduce the AL rate in colorectal surgery from a casematched retrospective study with the use of historical control subjects[85]. Because of the limited number of patients and the likely multifactorial nature of AL, it is hard to draw robust conclusions concerning the beneficial effect of fluorescence imaging on the AL rate.
The concept of high ligation of the inferior mesenteric artery to achieve optimal oncological results suppresses the vascular supply from the left colic artery, and vascularization of the proximal colon is dependent on marginal vessels from the middle colic artery. The preservation of the left colonic artery in laparoscopic LAR was reported to be associated with lower risk of AL[86]. With the progressive increase in the aging population, vascular disease can also be a factor contributing to insufficient blood supply, even in the case of low ligation.
Blood lossBlood loss greater than 100 mL and blood transfusion are independent risk factors for AL[2830,87,88], but it is unclear whether this is a specific manifestation due to
blood loss or whether blood loss is a surrogate for poor operative technique or challenging surgery.
Operation timeAlthough operation time is well known to be one of the risk factors for AL after laparoscopic LAR[2325,28,29,31], the experienced skill of the surgeon is also thought to act as a confounding variable. In patients with severe obesity, narrow pelvis, bulky tumor, and in cases with adverse intraoperative events, the operation time is prolonged. When the operation time is long, bacterial exposure and tissue damage can increase, which may cause inflammation and ultimately increase AL.
Anastomotic tensionMany surgeons assume that sufficient mobilization of the splenic flexure is necessary to lower anastomotic tension, especially when the anastomotic site is very low. Minimal anastomotic tension is thought to be one of the requirements of proper surgical technique; yet, this concept remains largely hypothetical. To our knowledge, there have been no experimental studies investigating the role of tension during an intestinal anastomosis. Lack of data likely stems from the difficulty in designing studies that investigate anastomotic tension in a clinical setting.
POSTOPERATIVE RISK FACTORSDiverting stomaFecal diversion is one of the most widely used methods to prevent AL. However, there is still debate as to whether the creation of a diverting stoma (DS) can reduce AL. Some randomized controlled trials reported that DS could reduce the rate of symptomatic AL[89,90], while a recent large multicenter cohort study using propensity score matching analysis indicated that DS was not associated with symptomatic AL[14]. A considerable number of retrospective studies also described the beneficial effect of DS on AL[16,20,91], while some studies stated that the creation of a DS did not reduce the rate of AL[21,92]. It is generally agreed that the creation of a DS can reduce the incidence of the severe complications of AL, including fecal peritonitis and septicemia. We need to bear in mind that even a temporarilyintended stoma can induce dehydration and renal impairment[93]. Moreover, reoperation for reversal of stoma may also be associated with morbidity and even death[94].
Transanal drainage tubeThe safety and efficacy of transanal drainage tube (TDT) placement to decrease the risk of AL after rectal cancer surgery has not been validated. In theory, TDT decreases the intraluminal pressure around the anastomotic site, and protects the anastomosis from watery stool and flatus when intestinal motility improves. There are only a few reports to investigate
Kawada K et al . Risk factors for AL after laparoscopic LAR

5723 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
whether TDT can prevent AL after open LAR, but the results are inconsistent, with some studies indicating favorable outcomes[9597], while other studies reported unfavorable outcomes[98]. Moreover, it has been reported that TDT can reduce the rate of AL after laparoscopic LAR[99]. There are slight differences in each study such as material and diameter of TDT, length of TDT insertion and duration of TDT placement. A standardized procedure for TDT should be validated and further investigation is required to elucidate its usefulness. With regard to reducing the intraluminal pressure around the anastomotic site, the concept of creating a DS is nearly the same as that for TDT. However, a DS increases patient discomfort and overall cost, and requires further surgery for closure of the DS. If the efficacy of prevention of AL is nearly equal for both procedures, it follows that TDT is superior to DS for this reason.
TDT can also be useful to cure localized peritonitis related to AL. Several reports have stated that the TDT is effective for localizing AL and controlling sepsis following LAR[100,101]. Shrinkage of an abscess by a TDT inserted into the cavity can localize inflammation, which results in a reduced incidence of reoperation.
Abdominal drainsThe use of an abdominal drain has been debated widely in terms of early detection of complications as well as preventing AL. After TME surgery, a large presacral space in which a hematoma or seroma may develop constitutes a nidus for bacterial growth, which may extend to the anastomosis and cause AL. Pelvic drainage can prevent this process and help to control AL. A systematic review including several RCTs reported no significant difference in the rate of AL, concluding there was insufficient evidence to support routine drainage[102]. However, a recent metaanalysis indicated a reduction of AL rate with pelvic drainage[103]. Akiyoshi et al[26] reported that the presence of an abdominal drain was an independent predictive factor for AL after laparoscopic LAR. The current evidence does not support drainage of a colonic anastomosis, but the LAR case for abdominal drains is less clear.
Intestinal microbes The human intestinal microbiome is thought to play a key ley role in the pathogenesis of obesity, gastrointestinal malignancies, and Crohn’s disease[104]. Recently, the role of microflora in anastomotic healing is attracting more attention[105]. One powerful modality contributing to major alterations in composition and virulence of the gastrointestinal microflora is radiation. The susceptibility to RTinduced diarrhea could be linked to differential initial microbial colonization[106]. In a rat model of LAR, Olivas et al[107] demonstrated that the combination of preoperative RT and intestinal inoculation with Pseudomonas aeruginosa
resulted in a higher rate of AL, whereas radiation alone or Pseudomonas aeruginosa alone did not cause AL. In an AL rat model, it has been recently reported that Enterococcus faecalis contributes to the pathogenesis of AL through collagen degradation and matrix metalloproteinase 9 (MMP9) activation in host intestinal tissues, and that either elimination of Enterococcus faecalis through direct topical antibiotics or pharmacological suppression of MMP9 could prevent AL[108]. Patients undergoing colectomy are at a unique risk of Clostridium difficile because of the additional physical disruption of the colonic microflora. The impact of postoperative Clostridium difficile infection is being increasingly reported with overall worse outcome after colon resection[109]. It was reported that postoperative diarrhea or high stoma output regardless of Clostridium difficile infection could increase significantly more superficial surgical site infections including AL[110], which may indicate the interaction between AL and the intraluminal pressure increased by postoperative diarrhea. Further investigation focusing on intestinal microbes could be important for uncovering the elusive causes of AL.
CONCLUSIONAL remains a huge challenge despite many surgical and technological advances. Our review identified several risk factors for AL after laparoscopic LAR, all of which are readily available in clinical settings. Continued highquality research is of paramount importance to reduce the risk and subsequent effects associated with AL.
REFERENCES1 Guillou PJ, Quirke P, Thorpe H, Walker J, Jayne DG, Smith AM,
Heath RM, Brown JM. Short-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial): multicentre, randomised controlled trial. Lancet 2005; 365: 1718-1726 [PMID: 15894098 DOI: 10.1016/S0140-6736(05)66545-2]
2 Zhou ZG, Hu M, Li Y, Lei WZ, Yu YY, Cheng Z, Li L, Shu Y, Wang TC. Laparoscopic versus open total mesorectal excision with anal sphincter preservation for low rectal cancer. Surg Endosc 2004; 18: 1211-1215 [PMID: 15457380 DOI: 10.1007/s00464-003-9170-1]
3 Lelong B, Bege T, Esterni B, Guiramand J, Turrini O, Moutardier V, Magnin V, Monges G, Pernoud N, Blache JL, Giovannini M, Delpero JR. Short-term outcome after laparoscopic or open restorative mesorectal excision for rectal cancer: a comparative cohort study. Dis Colon Rectum 2007; 50: 176-183 [PMID: 17180257 DOI: 10.1007/s10350-006-0751-7]
4 Lujan J, Valero G, Hernandez Q, Sanchez A, Frutos MD, Parrilla P. Randomized clinical trial comparing laparoscopic and open surgery in patients with rectal cancer. Br J Surg 2009; 96: 982-989 [PMID: 19644973 DOI: 10.1002/bjs.6662]
5 Milsom JW, de Oliveira O, Trencheva KI, Pandey S, Lee SW, Sonoda T. Long-term outcomes of patients undergoing curative laparoscopic surgery for mid and low rectal cancer. Dis Colon Rectum 2009; 52: 1215-1222 [PMID: 19571696 DOI: 10.1007/DCR0b013e3181a73e81]
6 Arezzo A, Passera R, Scozzari G, Verra M, Morino M. Laparoscopy for rectal cancer reduces short-term mortality and morbidity: results
Kawada K et al . Risk factors for AL after laparoscopic LAR

5724 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
of a systematic review and meta-analysis. Surg Endosc 2013; 27: 1485-1502 [PMID: 23183871 DOI: 10.1007/s00464-012-2649-x]
7 Bonjer HJ, Deijen CL, Abis GA, Cuesta MA, van der Pas MH, de Lange-de Klerk ES, Lacy AM, Bemelman WA, Andersson J, Angenete E, Rosenberg J, Fuerst A, Haglind E. A randomized trial of laparoscopic versus open surgery for rectal cancer. N Engl J Med 2015; 372: 1324-1332 [PMID: 25830422 DOI: 10.1056/NEJMoa1414882]
8 Jeong SY, Park JW, Nam BH, Kim S, Kang SB, Lim SB, Choi HS, Kim DW, Chang HJ, Kim DY, Jung KH, Kim TY, Kang GH, Chie EK, Kim SY, Sohn DK, Kim DH, Kim JS, Lee HS, Kim JH, Oh JH. Open versus laparoscopic surgery for mid-rectal or low-rectal cancer after neoadjuvant chemoradiotherapy (COREAN trial): survival outcomes of an open-label, non-inferiority, randomised controlled trial. Lancet Oncol 2014; 15: 767-774 [PMID: 24837215 DOI: 10.1016/S1470-2045(14)70205-0]
9 Kingham TP, Pachter HL. Colonic anastomotic leak: risk factors, diagnosis, and treatment. J Am Coll Surg 2009; 208: 269-278 [PMID: 19228539 DOI: 10.1016/j.jamcollsurg.2008.10.015]
10 Branagan G, Finnis D. Prognosis after anastomotic leakage in colorectal surgery. Dis Colon Rectum 2005; 48: 1021-1026 [PMID: 15789125 DOI: 10.1007/s10350-004-0869-4]
11 Mirnezami A, Mirnezami R, Chandrakumaran K, Sasapu K, Sagar P, Finan P. Increased local recurrence and reduced survival from colorectal cancer following anastomotic leak: systematic review and meta-analysis. Ann Surg 2011; 253: 890-899 [PMID: 21394013 DOI: 10.1097/SLA.0b013e3182128929]
12 Kang CY, Halabi WJ, Chaudhry OO, Nguyen V, Pigazzi A, Carmichael JC, Mills S, Stamos MJ. Risk factors for anastomotic leakage after anterior resection for rectal cancer. JAMA Surg 2013; 148: 65-71 [PMID: 22986932 DOI: 10.1001/2013.jamasurg.2]
13 Qu H, Liu Y, Bi DS. Clinical risk factors for anastomotic leakage after laparoscopic anterior resection for rectal cancer: a systematic review and meta-analysis. Surg Endosc 2015; 29: 3608-3617 [PMID: 25743996 DOI: 10.1007/s00464-015-4117-x]
14 Shiomi A, Ito M, Maeda K, Kinugasa Y, Ota M, Yamaue H, Shiozawa M, Horie H, Kuriu Y, Saito N. Effects of a diverting stoma on symptomatic anastomotic leakage after low anterior resection for rectal cancer: a propensity score matching analysis of 1,014 consecutive patients. J Am Coll Surg 2015; 220: 186-194 [PMID: 25529899 DOI: 10.1016/j.jamcollsurg.2014.10.017]
15 Matsubara N, Miyata H, Gotoh M, Tomita N, Baba H, Kimura W, Nakagoe T, Simada M, Kitagawa Y, Sugihara K, Mori M. Mortality after common rectal surgery in Japan: a study on low anterior resection from a newly established nationwide large-scale clinical database. Dis Colon Rectum 2014; 57: 1075-1081 [PMID: 25101603 DOI: 10.1097/DCR.0000000000000176]
16 Peeters KC, Tollenaar RA, Marijnen CA, Klein Kranenbarg E, Steup WH, Wiggers T, Rutten HJ, van de Velde CJ. Risk factors for anastomotic failure after total mesorectal excision of rectal cancer. Br J Surg 2005; 92: 211-216 [PMID: 15584062 DOI: 10.1002/bjs.4806]
17 Rullier E, Laurent C, Garrelon JL, Michel P, Saric J, Parneix M. Risk factors for anastomotic leakage after resection of rectal cancer. Br J Surg 1998; 85: 355-358 [PMID: 9529492 DOI: 10.1046/j.1365-2168.1998.00615.x]
18 Yeh CY, Changchien CR, Wang JY, Chen JS, Chen HH, Chiang JM, Tang R. Pelvic drainage and other risk factors for leakage after elective anterior resection in rectal cancer patients: a prospective study of 978 patients. Ann Surg 2005; 241: 9-13 [PMID: 15621985]
19 Jung SH, Yu CS, Choi PW, Kim DD, Park IJ, Kim HC, Kim JC. Risk factors and oncologic impact of anastomotic leakage after rectal cancer surgery. Dis Colon Rectum 2008; 51: 902-908 [PMID: 18408971 DOI: 10.1007/s10350-008-9272-x]
20 Eriksen MT, Wibe A, Norstein J, Haffner J, Wiig JN. Anastomotic leakage following routine mesorectal excision for rectal cancer in a national cohort of patients. Colorectal Dis 2005; 7: 51-57 [PMID: 15606585 DOI: 10.1111/j.1463-1318.2004.00700.x]
21 Matthiessen P, Hallböök O, Andersson M, Rutegård J, Sjödahl R. Risk factors for anastomotic leakage after anterior resection of the rectum. Colorectal Dis 2004; 6: 462-469 [PMID: 15521937 DOI:
10.1111/j.1463-1318.2004.00657.x]22 Ito M, Sugito M, Kobayashi A, Nishizawa Y, Tsunoda Y, Saito N.
Relationship between multiple numbers of stapler firings during rectal division and anastomotic leakage after laparoscopic rectal resection. Int J Colorectal Dis 2008; 23: 703-707 [PMID: 18379795 DOI: 10.1007/s00384-008-0470-8]
23 Kim JS, Cho SY, Min BS, Kim NK. Risk factors for anastomotic leakage after laparoscopic intracorporeal colorectal anastomosis with a double stapling technique. J Am Coll Surg 2009; 209: 694-701 [PMID: 19959036 DOI: 10.1016/j.jamcollsurg.2009.09.021]
24 Huh JW , Kim HR, Kim YJ. Anastomotic leakage after laparoscopic resection of rectal cancer: the impact of fibrin glue. Am J Surg 2010; 199: 435-441 [PMID: 19481197 DOI: 10.1016/j.amjsurg.2009.01.018]
25 Choi DH, Hwang JK, Ko YT, Jang HJ, Shin HK, Lee YC, Lim CH, Jeong SK, Yang HK. Risk factors for anastomotic leakage after laparoscopic rectal resection. J Korean Soc Coloproctol 2010; 26: 265-273 [PMID: 21152228 DOI: 10.3393/jksc.2010.26.4.265]
26 Akiyoshi T, Ueno M, Fukunaga Y, Nagayama S, Fujimoto Y, Konishi T, Kuroyanagi H, Yamaguchi T. Incidence of and risk factors for anastomotic leakage after laparoscopic anterior resection with intracorporeal rectal transection and double-stapling technique anastomosis for rectal cancer. Am J Surg 2011; 202: 259-264 [PMID: 21871980 DOI: 10.1016/j.amjsurg.2010.11.014]
27 Yamamoto S, Fujita S, Akasu T, Inada R, Moriya Y, Yamamoto S. Risk factors for anastomotic leakage after laparoscopic surgery for rectal cancer using a stapling technique. Surg Laparosc Endosc Percutan Tech 2012; 22: 239-243 [PMID: 22678320 DOI: 10.1097/SLE.0b013e31824fbb56]
28 Park JS, Choi GS, Kim SH, Kim HR, Kim NK, Lee KY, Kang SB, Kim JY, Lee KY, Kim BC, Bae BN, Son GM, Lee SI, Kang H. Multicenter analysis of risk factors for anastomotic leakage after laparoscopic rectal cancer excision: the Korean laparoscopic colorectal surgery study group. Ann Surg 2013; 257: 665-671 [PMID: 23333881 DOI: 10.1097/SLA.0b013e31827b8ed9]
29 Kawada K, Hasegawa S, Hida K, Hirai K, Okoshi K, Nomura A, Kawamura J, Nagayama S, Sakai Y. Risk factors for anastomotic leakage after laparoscopic low anterior resection with DST anastomosis. Surg Endosc 2014; 28: 2988-2995 [PMID: 24853855 DOI: 10.1007/s00464-014-3564-0]
30 Katsuno H, Shiomi A, Ito M, Koide Y, Maeda K, Yatsuoka T, Hase K, Komori K, Minami K, Sakamoto K, Saida Y, Saito N. Comparison of symptomatic anastomotic leakage following laparoscopic and open low anterior resection for rectal cancer: a propensity score matching analysis of 1014 consecutive patients. Surg Endosc 2016; 30: 2848-2856 [PMID: 26487228 DOI: 10.1007/s00464-015-4566-2]
31 Kim CW, Baek SJ, Hur H, Min BS, Baik SH, Kim NK. Anastomotic Leakage After Low Anterior Resection for Rectal Cancer Is Different Between Minimally Invasive Surgery and Open Surgery. Ann Surg 2016; 263: 130-137 [PMID: 25692355 DOI: 10.1097/SLA.0000000000001157]
32 Ba ZF, Yokoyama Y, Toth B, Rue LW, Bland KI, Chaudry IH. Gender differences in small intestinal endothelial function: inhibitory role of androgens. Am J Physiol Gastrointest Liver Physiol 2004; 286: G452-G457 [PMID: 14563675 DOI: 10.1152/ajpgi.00357.2003]
33 Volk A, Kersting S, Held HC, Saeger HD. Risk factors for morbidity and mortality after single-layer continuous suture for ileocolonic anastomosis. Int J Colorectal Dis 2011; 26: 321-327 [PMID: 20697722 DOI: 10.1007/s00384-010-1040-4]
34 Biondo S, Parés D, Kreisler E, Ragué JM, Fraccalvieri D, Ruiz AG, Jaurrieta E. Anastomotic dehiscence after resection and primary anastomosis in left-sided colonic emergencies. Dis Colon Rectum 2005; 48: 2272-2280 [PMID: 16228841 DOI: 10.1007/s10350-005-0159-9]
35 Senagore AJ, Delaney CP, Madboulay K, Brady KM, Fazio VW. Laparoscopic colectomy in obese and nonobese patients. J Gastrointest Surg 2003; 7: 558-561 [PMID: 12763416 DOI: 10.1016/S1091-255X(02)00124-5]
36 Kartheuser AH, Leonard DF, Penninckx F, Paterson HM, Brandt
Kawada K et al . Risk factors for AL after laparoscopic LAR

5725 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
D, Remue C, Bugli C, Dozois E, Mortensen N, Ris F, Tiret E. Waist circumference and waist/hip ratio are better predictive risk factors for mortality and morbidity after colorectal surgery than body mass index and body surface area. Ann Surg 2013; 258: 722-730 [PMID: 24096768 DOI: 10.1097/SLA.0b013e3182a6605a]
37 Watanabe J, Tatsumi K, Ota M, Suwa Y, Suzuki S, Watanabe A, Ishibe A, Watanabe K, Akiyama H, Ichikawa Y, Morita S, Endo I. The impact of visceral obesity on surgical outcomes of laparoscopic surgery for colon cancer. Int J Colorectal Dis 2014; 29: 343-351 [PMID: 24297037 DOI: 10.1007/s00384-013-1803-9]
38 Bosset JF, Collette L, Calais G, Mineur L, Maingon P, Radosevic-Jelic L, Daban A, Bardet E, Beny A, Ollier JC. Chemotherapy with preoperative radiotherapy in rectal cancer. N Engl J Med 2006; 355: 1114-1123 [PMID: 16971718 DOI: 10.1056/NEJMoa060829]
39 Roh MS, Colangelo LH, O’Connell MJ, Yothers G, Deutsch M, Allegra CJ, Kahlenberg MS, Baez-Diaz L, Ursiny CS, Petrelli NJ, Wolmark N. Preoperative multimodality therapy improves disease-free survival in patients with carcinoma of the rectum: NSABP R-03. J Clin Oncol 2009; 27: 5124-5130 [PMID: 19770376 DOI: 10.1200/JCO.2009.22.0467]
40 Heald RJ, Husband EM, Ryall RD. The mesorectum in rectal cancer surgery--the clue to pelvic recurrence? Br J Surg 1982; 69: 613-616 [PMID: 6751457 DOI: 10.1002/bjs.1800691019]
41 Sebag-Montefiore D, Stephens RJ, Steele R, Monson J, Grieve R, Khanna S, Quirke P, Couture J, de Metz C, Myint AS, Bessell E, Griffiths G, Thompson LC, Parmar M. Preoperative radiotherapy versus selective postoperative chemoradiotherapy in patients with rectal cancer (MRC CR07 and NCIC-CTG C016): a multicentre, randomised trial. Lancet 2009; 373: 811-820 [PMID: 19269519 DOI: 10.1016/S0140-6736(09)60484-0]
42 Marijnen CA, Kapiteijn E, van de Velde CJ, Martijn H, Steup WH, Wiggers T, Kranenbarg EK, Leer JW. Acute side effects and complications after short-term preoperative radiotherapy combined with total mesorectal excision in primary rectal cancer: report of a multicenter randomized trial. J Clin Oncol 2002; 20: 817-825 [PMID: 11821466 DOI: 10.1200/JCO.20.3.817]
43 Chang JS, Keum KC, Kim NK, Baik SH, Min BS, Huh H, Lee CG, Koom WS. Preoperative chemoradiotherapy effects on anastomotic leakage after rectal cancer resection: a propensity score matching analysis. Ann Surg 2014; 259: 516-521 [PMID: 23598382 DOI: 10.1097/SLA.0b013e31829068c5]
44 Heinzerling JH, Huerta S. Bowel perforation from bevacizumab for the treatment of metastatic colon cancer: incidence, etiology, and management. Curr Surg 2006; 63: 334-337 [PMID: 16971205 DOI: 10.1016/j.cursur.2006.06.002]
45 Saif MW, Elfiky A, Salem RR. Gastrointestinal perforation due to bevacizumab in colorectal cancer. Ann Surg Oncol 2007; 14: 1860-1869 [PMID: 17356952 DOI: 10.1245/s10434-006-9337-9]
46 Roos D, Dijksman LM, Tijssen JG, Gouma DJ, Gerhards MF, Oudemans-van Straaten HM. Systematic review of perioperative selective decontamination of the digestive tract in elective gastrointestinal surgery. Br J Surg 2013; 100: 1579-1588 [PMID: 24264779 DOI: 10.1002/bjs.9254]
47 Hata H, Yamaguchi T, Hasegawa S, Nomura A, Hida K, Nishitai R, Yamanokuchi S, Yamanaka T, Sakai Y. Oral and Parenteral Versus Parenteral Antibiotic Prophylaxis in Elective Laparoscopic Colorectal Surgery (JMTO PREV 07-01): A Phase 3, Multicenter, Open-label, Randomized Trial. Ann Surg 2016; 263: 1085-1091 [PMID: 26756752 DOI: 10.1097/SLA.0000000000001581]
48 Golub R, Golub RW, Cantu R, Stein HD. A multivariate analysis of factors contributing to leakage of intestinal anastomoses. J Am Coll Surg 1997; 184: 364-372 [PMID: 9100681]
49 Slieker JC, Komen N, Mannaerts GH, Karsten TM, Willemsen P, Murawska M, Jeekel J, Lange JF. Long-term and perioperative corticosteroids in anastomotic leakage: a prospective study of 259 left-sided colorectal anastomoses. Arch Surg 2012; 147: 447-452 [PMID: 22249852 DOI: 10.1001/archsurg.2011.1690]
50 Konishi T, Watanabe T, Kishimoto J, Nagawa H. Risk factors for anastomotic leakage after surgery for colorectal cancer: results of prospective surveillance. J Am Coll Surg 2006; 202: 439-444 [PMID:
16500248 DOI: 10.1016/j.jamcollsurg.2005.10.019]51 Eriksen TF, Lassen CB, Gögenur I. Treatment with corticosteroids
and the risk of anastomotic leakage following lower gastrointestinal surgery: a literature survey. Colorectal Dis 2014; 16: O154-O160 [PMID: 24215329 DOI: 10.1111/codi.12490]
52 Burton TP, Mittal A, Soop M. Nonsteroidal anti-inflammatory drugs and anastomotic dehiscence in bowel surgery: systematic review and meta-analysis of randomized, controlled trials. Dis Colon Rectum 2013; 56: 126-134 [PMID: 23222290 DOI: 10.1097/DCR.0b013e31825fe927]
53 Gorissen KJ, Benning D, Berghmans T, Snoeijs MG, Sosef MN, Hulsewe KW, Luyer MD. Risk of anastomotic leakage with non-steroidal anti-inflammatory drugs in colorectal surgery. Br J Surg 2012; 99: 721-727 [PMID: 22318712 DOI: 10.1002/bjs.8691]
54 Bertelsen CA, Andreasen AH, Jørgensen T, Harling H. Anastomotic leakage after anterior resection for rectal cancer: risk factors. Colorectal Dis 2010; 12: 37-43 [PMID: 19175624 DOI: 10.1111/j.1463-1318.2008.01711.x]
55 Richards CH, Campbell V, Ho C, Hayes J, Elliott T, Thompson-Fawcett M. Smoking is a major risk factor for anastomotic leak in patients undergoing low anterior resection. Colorectal Dis 2012; 14: 628-633 [PMID: 21749605 DOI: 10.1111/j.1463-1318.2011.02718.x]
56 Kruschewski M, Rieger H, Pohlen U, Hotz HG, Buhr HJ. Risk factors for clinical anastomotic leakage and postoperative mortality in elective surgery for rectal cancer. Int J Colorectal Dis 2007; 22: 919-927 [PMID: 17260142 DOI: 10.1007/s00384-006-0260-0]
57 Sørensen LT, Jørgensen T, Kirkeby LT, Skovdal J, Vennits B, Wille-Jørgensen P. Smoking and alcohol abuse are major risk factors for anastomotic leakage in colorectal surgery. Br J Surg 1999; 86: 927-931 [PMID: 10417567 DOI: 10.1046/j.1365-2168.1999.01165.x]
58 Contant CM, Hop WC, van’t Sant HP, Oostvogel HJ, Smeets HJ, Stassen LP, Neijenhuis PA, Idenburg FJ, Dijkhuis CM, Heres P, van Tets WF, Gerritsen JJ, Weidema WF. Mechanical bowel preparation for elective colorectal surgery: a multicentre randomised trial. Lancet 2007; 370: 2112-2117 [PMID: 18156032 DOI: 10.1016/S0140-6736(07)61905-9]
59 Slim K, Vicaut E, Launay-Savary MV, Contant C, Chipponi J. Updated systematic review and meta-analysis of randomized clinical trials on the role of mechanical bowel preparation before colorectal surgery. Ann Surg 2009; 249: 203-209 [PMID: 19212171 DOI: 10.1097/SLA.0b013e318193425a]
60 Van't Sant HP, Weidema WF, Hop WC, Oostvogel HJ, Contant CM. The influence of mechanical bowel preparation in elective lower colorectal surgery. Ann Surg 2010; 251: 59-63 [PMID: 20009750 DOI: 10.1097/SLA.0b013e3181c0e75c]
61 Dahabreh IJ, Steele DW, Shah N, Trikalinos TA. Oral Mechanical Bowel Preparation for Colorectal Surgery: Systematic Review and Meta-Analysis. Dis Colon Rectum 2015; 58: 698-707 [PMID: 26200685 DOI: 10.1097/DCR.0000000000000375]
62 Scarborough JE, Mantyh CR, Sun Z, Migaly J. Combined Mechanical and Oral Antibiotic Bowel Preparation Reduces Incisional Surgical Site Infection and Anastomotic Leak Rates After Elective Colorectal Resection: An Analysis of Colectomy-Targeted ACS NSQIP. Ann Surg 2015; 262: 331-337 [PMID: 26083870 DOI: 10.1097/SLA.0000000000001041]
63 Moghadamyeghaneh Z, Hanna MH, Carmichael JC, Mills SD, Pigazzi A, Nguyen NT, Stamos MJ. Nationwide analysis of outcomes of bowel preparation in colon surgery. J Am Coll Surg 2015; 220: 912-920 [PMID: 25907871 DOI: 10.1016/j.jamcollsurg.2015.02.008]
64 Kim EK, Sheetz KH, Bonn J, DeRoo S, Lee C, Stein I, Zarinsefat A, Cai S, Campbell DA, Englesbe MJ. A statewide colectomy experience: the role of full bowel preparation in preventing surgical site infection. Ann Surg 2014; 259: 310-314 [PMID: 23979289 DOI: 10.1097/SLA.0b013e3182a62643]
65 Jung B, Påhlman L, Nyström PO, Nilsson E. Multicentre randomized clinical trial of mechanical bowel preparation in elective colonic resection. Br J Surg 2007; 94: 689-695 [PMID: 17514668 DOI: 10.1002/bjs.5816]
Kawada K et al . Risk factors for AL after laparoscopic LAR

5726 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
66 Collin Å, Jung B, Nilsson E, Påhlman L, Folkesson J. Impact of mechanical bowel preparation on survival after colonic cancer resection. Br J Surg 2014; 101: 1594-1600 [PMID: 25204295 DOI: 10.1002/bjs.9629]
67 Kuroyanagi H, Oya M, Ueno M, Fujimoto Y, Yamaguchi T, Muto T. Standardized technique of laparoscopic intracorporeal rectal transection and anastomosis for low anterior resection. Surg Endosc 2008; 22: 557-561 [PMID: 18193475 DOI: 10.1007/s00464-007-9626-9]
68 Maeda K, Nagahara H, Shibutani M, Ohtani H, Sakurai K, Toyokawa T, Muguruma K, Tanaka H, Amano R, Kimura K, Sugano K, Ikeya T, Iseki Y, Hirakawa K. Efficacy of intracorporeal reinforcing sutures for anastomotic leakage after laparoscopic surgery for rectal cancer. Surg Endosc 2015; 29: 3535-3542 [PMID: 25673349 DOI: 10.1007/s00464-015-4104-2]
69 Baek SJ, Kim J, Kwak J, Kim SH. Can trans-anal reinforcing sutures after double stapling in lower anterior resection reduce the need for a temporary diverting ostomy? World J Gastroenterol 2013; 19: 5309-5313 [PMID: 23983434 DOI: 10.3748/wjg.v19.i32.5309]
70 Roumen RM, Rahusen FT, Wijnen MH, Croiset van Uchelen FA. “Dog ear” formation after double-stapled low anterior resection as a risk factor for anastomotic disruption. Dis Colon Rectum 2000; 43: 522-525 [PMID: 10789750 DOI: 10.1007/BF02237198]
71 Zhuo C, Liang L, Ying M, Li Q, Li D, Li Y, Peng J, Huang L, Cai S, Li X. Laparoscopic Low Anterior Resection and Eversion Technique Combined With a Nondog Ear Anastomosis for Mid- and Distal Rectal Neoplasms: A Preliminary and Feasibility Study. Medicine (Baltimore) 2015; 94: e2285 [PMID: 26683958 DOI: 10.1097/MD.0000000000002285]
72 Nakayama S, Hasegawa S, Nagayama S, Kato S, Hida K, Tanaka E, Itami A, Kubo H, Sakai Y. The importance of precompression time for secure stapling with a linear stapler. Surg Endosc 2011; 25: 2382-2386 [PMID: 21184102 DOI: 10.1007/s00464-010-1527-7]
73 Nakayama S, Hasegawa S, Hida K, Kawada K, Sakai Y. Obtaining secure stapling of a double stapling anastomosis. J Surg Res 2015; 193: 652-657 [PMID: 25277356 DOI: 10.1016/j.jss.2014.08.044]
74 Hasegawa S, Nakayama S, Hida K, Kawada K, Sakai Y. Effect of Tri-Staple Technology and Slow Firing on Secure Stapling Using an Endoscopic Linear Stapler. Dig Surg 2015; 32: 353-360 [PMID: 26228297 DOI: 10.1159/000437216]
75 Vignali A, Gianotti L, Braga M, Radaelli G, Malvezzi L, Di Carlo V. Altered microperfusion at the rectal stump is predictive for rectal anastomotic leak. Dis Colon Rectum 2000; 43: 76-82 [PMID: 10813128 DOI: 10.1007/BF02237248]
76 Sheridan WG, Lowndes RH, Young HL. Tissue oxygen tension as a predictor of colonic anastomotic healing. Dis Colon Rectum 1987; 30: 867-871 [PMID: 3677962 DOI: 10.1007/BF02555426]
77 Kologlu M, Yorganci K, Renda N, Sayek I. Effect of local and remote ischemia-reperfusion injury on healing of colonic anastomoses. Surgery 2000; 128: 99-104 [PMID: 10876192 DOI: 10.1067/msy.2000.107414]
78 Karliczek A, Harlaar NJ, Zeebregts CJ, Wiggers T, Baas PC, van Dam GM. Surgeons lack predictive accuracy for anastomotic leakage in gastrointestinal surgery. Int J Colorectal Dis 2009; 24: 569-576 [PMID: 19221768 DOI: 10.1007/s00384-009-0658-6]
79 Kudszus S, Roesel C, Schachtrupp A, Höer JJ. Intraoperative laser fluorescence angiography in colorectal surgery: a noninvasive analysis to reduce the rate of anastomotic leakage. Langenbecks Arch Surg 2010; 395: 1025-1030 [PMID: 20700603 DOI: 10.1007/s00423-010-0699-x]
80 Jafari MD, Lee KH, Halabi WJ, Mills SD, Carmichael JC, Stamos MJ, Pigazzi A. The use of indocyanine green fluorescence to assess anastomotic perfusion during robotic assisted laparoscopic rectal surgery. Surg Endosc 2013; 27: 3003-3008 [PMID: 23404152 DOI: 10.1007/s00464-013-2832-8]
81 Hellan M, Spinoglio G, Pigazzi A, Lagares-Garcia JA. The influence of fluorescence imaging on the location of bowel transection during robotic left-sided colorectal surgery. Surg Endosc 2014; 28: 1695-1702 [PMID: 24385249 DOI: 10.1007/s00464-013-3377-6]
82 Jafari MD, Wexner SD, Martz JE, McLemore EC, Margolin DA,
Sherwinter DA, Lee SW, Senagore AJ, Phelan MJ, Stamos MJ. Perfusion assessment in laparoscopic left-sided/anterior resection (PILLAR II): a multi-institutional study. J Am Coll Surg 2015; 220: 82-92.e1 [PMID: 25451666 DOI: 10.1016/j.jamcollsurg.2014.09.015]
83 Degett TH, Andersen HS, Gögenur I. Indocyanine green fluorescence angiography for intraoperative assessment of gastrointestinal anastomotic perfusion: a systematic review of clinical trials. Langenbecks Arch Surg 2016; Epub ahead of print [PMID: 26968863 DOI: 10.1007/s00423-016-1400-9]
84 Sherwinter DA, Gallagher J, Donkar T. Intra-operative transanal near infrared imaging of colorectal anastomotic perfusion: a feasibility study. Colorectal Dis 2013; 15: 91-96 [PMID: 22632448 DOI: 10.1111/j.1463-1318.2012.03101.x]
85 Kin C, Vo H, Welton L, Welton M. Equivocal effect of intraoperative fluorescence angiography on colorectal anastomotic leaks. Dis Colon Rectum 2015; 58: 582-587 [PMID: 25944430 DOI: 10.1097/DCR.0000000000000320]
86 Hinoi T, Okajima M, Shimomura M, Egi H, Ohdan H, Konishi F, Sugihara K, Watanabe M. Effect of left colonic artery preservation on anastomotic leakage in laparoscopic anterior resection for middle and low rectal cancer. World J Surg 2013; 37: 2935-2943 [PMID: 24005279 DOI: 10.1007/s00268-013-2194-3]
87 Leichtle SW, Mouawad NJ, Welch KB, Lampman RM, Cleary RK. Risk factors for anastomotic leakage after colectomy. Dis Colon Rectum 2012; 55: 569-575 [PMID: 22513436 DOI: 10.1097/DCR.0b013e3182423c0d]
88 Mäkelä JT, Kiviniemi H, Laitinen S. Risk factors for anastomotic leakage after left-sided colorectal resection with rectal anastomosis. Dis Colon Rectum 2003; 46: 653-660 [PMID: 12792443 DOI: 10.1007/s10350-004-6627-9]
89 Matthiessen P, Hallböök O, Rutegård J, Simert G, Sjödahl R. Defunctioning stoma reduces symptomatic anastomotic leakage after low anterior resection of the rectum for cancer: a randomized multicenter trial. Ann Surg 2007; 246: 207-214 [PMID: 17667498 DOI: 10.1097/SLA.0b013e3180603024]
90 Chude GG, Rayate NV, Patris V, Koshariya M, Jagad R, Kawamoto J, Lygidakis NJ. Defunctioning loop ileostomy with low anterior resection for distal rectal cancer: should we make an ileostomy as a routine procedure? A prospective randomized study. Hepatogastroenterology 2008; 55: 1562-1567 [PMID: 19102343]
91 Lefebure B, Tuech JJ, Bridoux V, Costaglioli B, Scotte M, Teniere P, Michot F. Evaluation of selective defunctioning stoma after low anterior resection for rectal cancer. Int J Colorectal Dis 2008; 23: 283-288 [PMID: 17768630 DOI: 10.1007/s00384-007-0380-1]
92 Enker WE, Merchant N, Cohen AM, Lanouette NM, Swallow C, Guillem J, Paty P, Minsky B, Weyrauch K, Quan SH. Safety and efficacy of low anterior resection for rectal cancer: 681 consecutive cases from a specialty service. Ann Surg 1999; 230: 544-552; discussion 552-554 [PMID: 10522724 DOI: 10.1097/00000658-199910000-00010]
93 Gessler B, Haglind E, Angenete E. A temporary loop ileostomy affects renal function. Int J Colorectal Dis 2014; 29: 1131-1135 [PMID: 25026894 DOI: 10.1007/s00384-014-1949-0]
94 Sharma A, Deeb AP, Rickles AS, Iannuzzi JC, Monson JR, Fleming FJ. Closure of defunctioning loop ileostomy is associated with considerable morbidity. Colorectal Dis 2013; 15: 458-462 [PMID: 22974343 DOI: 10.1111/codi.12029]
95 Xiao L, Zhang WB, Jiang PC, Bu XF, Yan Q, Li H, Zhang YJ, Yu F. Can transanal tube placement after anterior resection for rectal carcinoma reduce anastomotic leakage rate? A single-institution prospective randomized study. World J Surg 2011; 35: 1367-1377 [PMID: 21437746 DOI: 10.1007/s00268-011-1053-3]
96 Zhao WT, Hu FL, Li YY, Li HJ, Luo WM, Sun F. Use of a transanal drainage tube for prevention of anastomotic leakage and bleeding after anterior resection for rectal cancer. World J Surg 2013; 37: 227-232 [PMID: 23052807 DOI: 10.1007/s00268-012-1812-9]
97 Nishigori H, Ito M, Nishizawa Y, Nishizawa Y, Kobayashi A, Sugito M, Saito N. Effectiveness of a transanal tube for the prevention of anastomotic leakage after rectal cancer surgery.
Kawada K et al . Risk factors for AL after laparoscopic LAR

5727 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
World J Surg 2014; 38: 1843-1851 [PMID: 24378550 DOI: 10.1007/s00268-013-2428-4]
98 Cong ZJ, Fu CG, Wang HT, Liu LJ, Zhang W, Wang H. Influencing factors of symptomatic anastomotic leakage after anterior resection of the rectum for cancer. World J Surg 2009; 33: 1292-1297 [PMID: 19363687 DOI: 10.1007/s00268-009-0008-4]
99 Hidaka E, Ishida F, Mukai S, Nakahara K, Takayanagi D, Maeda C, Takehara Y, Tanaka J, Kudo SE. Efficacy of transanal tube for prevention of anastomotic leakage following laparoscopic low anterior resection for rectal cancers: a retrospective cohort study in a single institution. Surg Endosc 2015; 29: 863-867 [PMID: 25052128 DOI: 10.1007/s00464-014-3740-2]
100 Sirois-Giguère E, Boulanger-Gobeil C, Bouchard A, Gagné JP, Grégoire RC, Thibault C, Bouchard P. Transanal drainage to treat anastomotic leaks after low anterior resection for rectal cancer: a valuable option. Dis Colon Rectum 2013; 56: 586-592 [PMID: 23575397 DOI: 10.1097/DCR.0b013e31827687a4]
101 Okoshi K, Masano Y, Hasegawa S, Hida K, Kawada K, Nomura A, Kawamura J, Nagayama S, Yoshimura T, Sakai Y. Efficacy of transanal drainage for anastomotic leakage after laparoscopic low anterior resection of the rectum. Asian J Endosc Surg 2013; 6: 90-95 [PMID: 23228055 DOI: 10.1111/ases.12010]
102 Karliczek A, Jesus EC, Matos D, Castro AA, Atallah AN, Wiggers T. Drainage or nondrainage in elective colorectal anastomosis: a systematic review and meta-analysis. Colorectal Dis 2006; 8: 259-265 [PMID: 16630227 DOI: 10.1111/j.1463-1318.2006.00999.x]
103 Rondelli F, Bugiantella W, Vedovati MC, Balzarotti R, Avenia N, Mariani E, Agnelli G, Becattini C. To drain or not to drain extraperitoneal colorectal anastomosis? A systematic review and meta-analysis. Colorectal Dis 2014; 16: O35-O42 [PMID: 24245821 DOI: 10.1111/codi.12491]
104 Morowitz MJ, Babrowski T, Carlisle EM, Olivas A, Romanowski KS, Seal JB, Liu DC, Alverdy JC. The human microbiome and surgical disease. Ann Surg 2011; 253: 1094-1101 [PMID: 21422915 DOI: 10.1097/sla.0b013e31821175d7]
105 Manichanh C, Varela E, Martinez C, Antolin M, Llopis M, Doré J, Giralt J, Guarner F, Malagelada JR. The gut microbiota predispose to the pathophysiology of acute postradiotherapy diarrhea. Am J Gastroenterol 2008; 103: 1754-1761 [PMID: 18564125 DOI: 10.1111/j.1572-0241.2008.01868.x]
106 Shogan BD, An GC, Schardey HM, Matthews JB, Umanskiy K, Fleshman JW, Hoeppner J, Fry DE, Garcia-Granereo E, Jeekel H, van Goor H, Dellinger EP, Konda V, Gilbert JA, Auner GW, Alverdy JC. Proceedings of the first international summit on intestinal anastomotic leak, Chicago, Illinois, October 4-5, 2012. Surg Infect (Larchmt) 2014; 15: 479-489 [PMID: 25215465 DOI: 10.1089/sur.2013.114]
107 Olivas AD, Shogan BD, Valuckaite V, Zaborin A, Belogortseva N, Musch M, Meyer F, Trimble WL, An G, Gilbert J, Zaborina O, Alverdy JC. Intestinal tissues induce an SNP mutation in Pseudomonas aeruginosa that enhances its virulence: possible role in anastomotic leak. PLoS One 2012; 7: e44326 [PMID: 22952955 DOI: 10.1371/journal.pone.0044326]
108 Shogan BD, Belogortseva N, Luong PM, Zaborin A, Lax S, Bethel C, Ward M, Muldoon JP, Singer M, An G, Umanskiy K, Konda V, Shakhsheer B, Luo J, Klabbers R, Hancock LE, Gilbert J, Zaborina O, Alverdy JC. Collagen degradation and MMP9 activation by Enterococcus faecalis contribute to intestinal anastomotic leak. Sci Transl Med 2015; 7: 286ra68 [PMID: 25947163 DOI: 10.1126/scitranslmed.3010658]
109 Damle RN, Cherng NB, Flahive JM, Davids JS, Maykel JA, Sturrock PR, Sweeney WB, Alavi K. Clostridium difficile infection after colorectal surgery: a rare but costly complication. J Gastrointest Surg 2014; 18: 1804-1811 [PMID: 25091840 DOI: 10.1007/s11605-014-2600-7]
110 Gaertner WB, Madoff RD, Mellgren A, Kwaan MR, Melton GB. Postoperative diarrhea and high ostomy output impact postoperative outcomes after elective colon and rectal operations regardless of Clostridium difficile infection. Am J Surg 2015; 210: 759-765 [PMID: 26117432 DOI: 10.1016/j.amjsurg.2015.03.032]
P- Reviewer: Konishi T, Morris DLL S- Editor: Qi Y L- Editor: A E- Editor: Wang CH
Kawada K et al . Risk factors for AL after laparoscopic LAR

Hepatopulmonary syndrome: What we know and what we would like to know
Israel Grilo-Bensusan, Juan Manuel Pascasio-Acevedo
Israel Grilo-Bensusan, Digestive Diseases Department, HAR, Écija, APS Bajo Guadalquivir, Écija, 41400 Seville, Spain
Juan Manuel Pascasio-Acevedo, Unit for the Clinical Management of Digestive Diseases, IBIS, CIBERehd, Virgen del Rocío University Hospital, 41013 Seville, Spain
Author contributions: Grilo-Bensusan I and Pascasio-Acevedo JM wrote this paper.
Conflict-of-interest statement: The authors have no conflict of interest to report.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Manuscript source: Invited manuscript
Correspondence to: Israel Grilo-Bensusan, MD, PhD, Digestive Diseases Department, HAR, Écija, APS Bajo Guadalquivir, Avda, de los Emigrantes 24, Piso: 2º E, Écija, 41400 Seville, Spain. [email protected]: +34-676-278900Fax: +34-955-879090
Received: March 18, 2016Peer-review started: March 21, 2016First decision: May 12, 2016Revised: May 26, 2016Accepted: June 15, 2016Article in press: June 15, 2016Published online: July 7, 2016
AbstractHepatopulmonary syndrome (HPS) is characterized
by abnormalities in blood oxygenation caused by the presence of intrapulmonary vascular dilations (IPVD) in the context of liver disease, generally at a cirrhotic stage. Knowledge about the subject is still only partial. The majority of the information about the etiopathogenesis of HPS has been ob-tained through experiments on animals. Reported prevalence in patients who are candidates for a liver transplantation (LT) varies between 4% and 32%, with a predominance of mild or moderate cases. Although it is generally asymptomatic it does have an impact on their quality of life and survival. The diagnosis requires taking an arterial blood gas sample of a seated patient with alveolar-arterial oxygen gradient (AaO2) ≥ 15 mm Hg, or ≥ 20 mm Hg in those over 64 years of age. The IPVD are identified through a transthoracic contrast echocardiography or a macroaggregated albumin lung perfusion scan (99mTc-MAA). There is currently no effective medical treatment. LT has been shown to reverse the syndrome and improve survival rates, even in severe cases. Therefore the policy of prioritizing LT would appear to increase survival rates. This paper takes a critical and clinical look at the current understanding of HPS, as well as the controversies surrounding it and possible future research.
Key words: Hepatopulmonary syndrome; Liver cirrhosis; Liver transplantation; Contrast echocardiography; Macroaggregated albumin lung perfusion scan
© The Author(s) 2016. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Hepatopulmonary syndrome is a frequent complication which influences the quality of life and ultimately the survival of patients with cirrhosis. Knowledge about the condition is still limited and this complicates clinical decision making. The most widely used methods for establishing a diagnosis are an arterial blood gas analysis and a contrast echocardiography. There is currently no effective medical treatment and
REVIEW
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.3748/wjg.v22.i25.5728
5728 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
World J Gastroenterol 2016 July 7; 22(25): 5728-5741 ISSN 1007-9327 (print) ISSN 2219-2840 (online)
© 2016 Baishideng Publishing Group Inc. All rights reserved.

other means of supporting patients have barely been evaluated. Liver transplantation has been demonstrated to reverse it and improve survival levels, although there are controversies in the policies of prioritization in terms of the waiting lists for transplantation. This review examines current knowledge about the syndrome from a practical and analytical approach.
Grilo-Bensusan I, Pascasio-Acevedo JM. Hepatopulmonary syndrome: What we know and what we would like to know. World J Gastroenterol 2016; 22(25): 5728-5741 Available from: URL: http://www.wjgnet.com/1007-9327/full/v22/i25/5728.htm DOI: http://dx.doi.org/10.3748/wjg.v22.i25.5728
INTRODUCTIONHepatopulmonary syndrome (HPS) is defined as a defect in arterial oxygenation caused by the presence of intrapulmonary vascular dilatations (IPVD) in the context of liver disease[1,2].
It was in 1884 that Flückiger first described the case of a woman with liver cirrhosis, cyanosis and acropachy, which could correspond to a patient with HPS. The term HPS was coined by Kennedy and Knudson[3] in 1977. New definitions for the syndrome were suggested by Krowka, Cortese and Rodríguez Roisín at the beginning of the 90s. They described HPS as a syndrome characterized by a clinical triad comprising the presence of advanced chronic liver disease, gas exchange abnormalities, ultimately leading to hypoxemia, and the presence of IPVD, without the presence of intrinsic pulmonary diseases[4]. Krowka et al[5] added precision to the definition, observing that the syndrome can coexist with cardiopulmonary diseases and can also appear in cases of hepatitis, portal hypertension not associated with liver cirrhosis, alpha 1 antitrypsin deficiency and Wilson’s disease.
Until 1988 HPS was considered to be a contraindication for liver transplantation (LT). Later however, it was observed that transplantations led to a reversal in hypoxemia and that post LT survival stood at around 70%. This finding, combined with the lack of an effective medical treatment for the syndrome, the progressive nature of hypoxemia and the higher mortality levels in these patients, meant that HPS became an indication for LT[6].
ETIOPATHOGENESIS AND PHYSIOPATHOLOGYThe majority of the information about the etiopathogenesis of HPS has been obtained through experiments on animals. The most widely used is performing a common bile duct ligation in rats to provoke a secondary biliary cirrhosis. This results in
an alteration in the blood oxygenation and IPVD which can be measured in vivo and is similar to the changes in HPS in humans, although it is more common in animals[7]. Nevertheless, some of these findings have also been confirmed in humans.
The main mediators involved in the onset of IPVD, which are fundamental to the pathogenesis of HPS, are nitric oxide (NO) and carbon monoxide (CO). In the case of animals, the related molecules are: endothelin 1 (ET1) and its receptors A and B; the heme oxygenase1; TNFalpha and its effect on endothelial NO synthase (eNOS) and the inducible NO synthase (iNOS)[820]. In humans, it has been observed that the levels of exhaled NO are higher in patients with HPS and that the administration of LNAME and methylene blue as well as two nitric oxide synthase inhibitors (NOS) and their mediators, improve some HPS parameters[2126]. The exhaled nitric oxide reflects an excess in NO produced in the alveoli which does not come from the liver[21,27,28]. Angiogenesis is also considered to be an important phenomenon in the development of HPS. Endothelial growth factor and other related molecules may be associated with this phenomenon[17].
Studies in animals keep leading to the discovery of new molecules which offer innovative perspectives in terms of the understanding of the etiopathogenesis of HPS and which could provide future targets for medical treatment of the syndrome[2941]. There are a number of recent reviews which examine these developments in greater detail but this is not the aim of our review[4244].
The principal abnormality which defines HPS is the dilatation of pre and postcapillary pulmonary vessels in the alveolar regions. The diameter of these vessels in normal conditions ranges between 8 and 15 µm, whereas when HPS is present, this rises to between 15 and 500 µm[1,19,45].
With HPS there is an increase in the alveolararterial gradient of O2 (AaO2) and hypoxemia which is caused by three mechanisms. The main one is a mismatch between the ventilation and perfusion of alveolar units which is evident in even the mildest cases of HPS. The vasodilatation of alveolar capillaries results in an excessive amount of blood flowing into the normally ventilated alveoli, which causes a decline in the ventilation perfusion quotient, resulting in increased AaO2 and/or arterial hypoxemia[2]. The other two mechanisms are firstly the shunt effect, unventilated units which are still perfused and can be explained by the presence of arteriovenous communication, and secondly the alteration in oxygen diffusion, which is correlated with a reduction in the lung’s diffusing capacity for CO (DLCO), and could be explained by the distance between the alveoli and the central flow in blood capillaries. This distance is too great to permit correct gas exchange and could also be related to the depositing of collagen in the capillaries
5729 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Grilo-Bensusan I et al . Hepatopulmonary syndrome

and alveolar venules[1,4648]. These mechanisms can be seen in both moderate and severe cases of the disease.
PREVALENCE AND SEVERITYThe prevalence of the syndrome has not been fully established since figures depend on the method employed for the diagnosis and the profile of the patients studied.
In terms of diagnostic methodology, there are differences in the criteria of alteration of arterial oxygenation which define the syndrome[49]. There are also differences according to the method used for the diagnosis of IPVD.
Different results are obtained depending on whether a contrastenhanced echocardiography or macroaggregated albumin lung perfusion scan (99mTcMAA) is used and if the echocardiography is transthoracic or transoesophageal. They also depend on which agents are used to generate contrast bubbles in the echocardiography[50,51]. It is important to unify criteria for the diagnosis of HPS so as to obtain comparable results from the various different studies.
In terms of the profiles of the patients studied, in cirrhotic patients the average prevalence of HPS was 15%, in those with chronic viral hepatitis, with or without cirrhosis, it was approximately 10% and in BuddChiari syndrome, 28%[52,53]. In patients listed for LT the different studies have shown figures of between 4% and 32%[4951,5464].
Four degrees of severity can be distinguished according to levels of hypoxemia: mild [partial oxygen pressure (pO2) is ≥ 80 mmHg], moderate (pO2 < 80 mmHg and ≥ 60 mmHg), severe (pO2 < 60 mmHg and ≥ 50 mmHg) and very severe (pO2 < 50 mmHg,) which is often associated with pO2 < 300 mmHg when the patient is administered oxygen at 100%[1]. Systematic HPS screening in cirrhosis patients listed for LT shows that the majority of HPS patients are mild or moderate (77%88%). Severe cases (12%17%) and very severe cases (4%6.3%) are less common[56,65]. Previously it appeared that there were a higher number of more severe cases of HPS but this was due to the fact that in many earlier studies systematic screening was not used. Diagnosis was based on clinical criteria and this led to the more serious cases being selected rather than those which were less acute[57,59,6670].
CLINICAL FEATURESThe symptoms which have classically been associated with HPS are dyspnea and platypnea[71]. In the largest study covering patients listed for LT, dyspnea was present in 48% of HPS patients, and was more frequent than in patients without HPS, with significant differences[55]. In another study it was found that
dyspnea was more frequent in HPS patients with pO2 lower than 70 mmHg, (57%), compared with those who were diagnosed due to an increase in AaO2
[49]. Platypnea, which means a worsening in dyspnea when a patient is standing rather than lying down, is considered a pathognomonic characteristic of HPS. This phenomenon is associated with orthodeoxia or a decreased pO2 when the patient changes from the lying down to the standing position. It has been suggested that increased perfusion at the base of the lungs when the HPS patients are standing up increases the shunt effect, resulting in orthodeoxia and platypnea[19]. In a study with 20 HPS patients the orthodeoxia phenomenon showed a prevalence of 25% and a decrease ≥ 5% or ≥ 4 mmHg in arterial pO2 was established as the cut off value for its diagnosis[72]. However, a prospective study found a 30% prevalence of orthodeoxia in cirrhotic patients evaluated for LT, with no differences found between patients with or without HPS[56]. Furthermore, in another study it was found that the opposite phenomenon to platypnea, orthopnea, or the worsening in dyspnea when lying down, is more frequent in patients with HPS (25%) than in those without it, with significant differences[55].
Among the exploration findings, acropachy, cyanosis and asterixis were rare (lower than 20%) although there was a significant association in HPS patients[55]. The studies focusing on the presence of vascular spiders and their connection with HPS are contradictory[49,55,73,74].
Extrapulmonary complications as a result of the presence of lefttoright shunt, such as cerebral abscesses, intracranial hemorrhages and polycythemia have also been described[13,75,76].
HPS patients have a lower quality of life, rank higher in the New York Heart Association functional classification and suffer significant oxygen desaturation whilst sleeping[55,77].
The available data on the symptoms and exploration findings in HPS patients is mainly based on those with cirrhosis and therefore should not be extrapolated to all HPS patients. Nevertheless, the data reveals that most patients are asymptomatic, the most frequent symptom is dyspnea, and platypnea and orthodeoxia do not seem to be characteristic HPS phenomena. Therefore further studies are required to clarify these findings.
DIAGNOSISGasometric criteriaThe diagnostic criteria proposed for HPS are the presence of liver disease, an AaO2 ≥ 15 mmHg or ≥ 20 mmHg in patients over 64 years old detected by arterial blood gas analysis in a seating position, and the demonstration of IPVD by means of a positive contrastenhanced echocardiography[1].
Although these criteria were established in 2004,
5730 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Grilo-Bensusan I et al . Hepatopulmonary syndrome

5731 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
However, while in intracardiac shunts the transfer of bubbles occurs earlier, between the first and third heart beats, with HPS it takes place between the fourth and sixth beat[1].
The various agents used as a medium to produce bubbles offer different levels sensitivity for the diagnosis of IPVD. These include: saline solution, mannitol, polygeline, indocyanine green and other gelatinous solutions[50,8184]. Of these, a saline solution at 0.9% is currently recommended as the medium of choice[1].
The transthoracic contrast echocardiography is preferred to the transoesophageal option due to the potential risk of damage that the latter can cause to oesophageal varices, although the studies carried out to date have not found this complication[50,51,81]. There is greater technique sensitivity for the diagnosis of HPS against transthoracic ultrasound scan, although some interpretation discrepancies exist regarding very early stages of IPVD without HPS presence. The current recommendation is to use it in the event of poor echo window and high probability of HPS[50,51,81].
A recent study compared the performance of transcranial doppler ultrasonography for the diagnosis of IPVD with transthoracic echocardiography. It found that transcranial doppler ultrasonography was effective diagnostically with AUC = 0.813% (95%CI: 0.6660.959; p = 0.001), sensitivity: 76.2% (95%CI: 54.989.4) and specificity: 90% (95%CI: 63.996.5)[85]. Although the study was conducted with a small group of patients, it offers a new avenue of study for the diagnosis of HPS.
Macroaggregated albumin lung perfusion scanThe 99mTcMAA is another technique which is capable of detecting the presence of IPVD. The basis of this approach is similar to that of a contrast echocardiography. In this case, Tc99 tagged albumin particles are able to reach extrapulmonary sites due to the presence of IPVD. Cerebral uptake is considered to be pathological when greater than or equal to 6%[68]. However, some studies establish a cut off value at 5%, and others at 7% or even higher[8688]. Nevertheless, for better interpretation, the results of the lung perfusion scan should be reported in terms of uptake values rather than positive or negative.
Its main advantage is its capacity to quantify IPVD and determine its role in hypoxemia in patients with organic respiratory comorbidity. It has also been given a prognostic role, indicating that cerebral uptake ≥ 20% and/or hypoxemia ≤ 55 mmHg were associated with greater post LT mortality[67,68]. However, subsequent studies have not confirmed a correlation between 99mTcMAAbased cerebral uptake values and postransplantation survival[86]. Its main disadvantages on the other hand are its incapacity to differentiate IPVD from intracardiac shunting and its lower sensitivity in the diagnosis of IPVD. In this sense,
there were other previously existing parameters: the presence of an AaO2 > 20 mmHg, regardless of age, and/or a pO2 < 70 mmHg obtained in any position, lying down, sitting or standing, were the most widely accepted gasometric criteria[6668,70,78,79]. Other studies focused on the existence of an AaO2 greater than that theoretically established according to age. There are also differences in the formula used to calculate this value[58,59].
Arterial blood samples are obtained by radial artery puncture with the patient in a stable condition and breathing room air. There are also differences between studies in terms of the position of the patient when the sample was obtained: lying down, standing and/or sitting.
The establishing of standardized criteria allows us to unify the diagnostic methods and further our understanding of the disease. However these are based on a consensus of experts. There are hardly any studies on the application of different criteria for the diagnosis of HPS and how these might affect the prevalence or prognosis of the syndrome. A prospective study with 98 patients observed that prevalence of HPS is 32% when the cut off value for AaO2 is ≥ 15 mmHg, 31% when AaO2 > 20 mmHg and 28% when AaO2 was calculated according to age. This study also found that the prevalence is lower when pO2 rather than AaO2 was used in the diagnosis of HPS[49]. It is also worth noting an interesting study which proposed performing two arterial blood gas analyses to obtain a precise diagnosis of HPS and detect those cases in which the disease was more advanced. This study also analyzes different arterial gas criteria for the diagnosis of HPS[80]. In general, there are very few studies which have validated the arterial gas criteria which are currently used for the diagnosis of HPS as opposed to others. This is an issue which is extremely important to furthering our understanding of the disease, enabling us to compare studies.
Contrast echocardiography A contrast echocardiography is a sensitive, qualitative and noninvasive method which allows the screening of IPVD, which are the main characteristic of HPS. It is considered to be the gold standard technique for the diagnosis of HPS[1,2]. It consists of injecting a liquid medium with bubbles into a peripheral vein so as to observe the liquid entering the right auricle and ascertain whether or not it subsequently passes into the left cavities. Under physiological conditions, once the bubbles are visualized in the right auricle they become trapped in the pulmonary vascular bed and therefore cannot be visualized in the left heart. However, in HPS, bubbles bypass the pulmonary circulation and can be seen in the left cavities. The presence of an intracardiac shunt is another condition in which bubbles can be seen in the left cavities.
Grilo-Bensusan I et al . Hepatopulmonary syndrome

5732 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
the studies which have assessed this technique offer a variable sensitivity of between 20% and 96%, which seems to correlate with the severity of HPS, showing high sensitivity in severe and very severe cases and low in those which are mild and moderate[53,59,67,68,89,90]. These findings are consistent with the results of a subanalysis (unpublished) of our work[56]. Further studies are required to determine the influence of the severity of HPS and the sensitivity of this technique as well as its standardization and prognostic role.
Other diagnostic methods Pulse oximetry: Pulse oximetry is a cheap, rapid and painless method of estimating arterial pO2. This is the reason why it is considered a useful tool for the screening and monitoring of cirrhotic patients listed for LT, especially children[9193]. The selection of the cut off value for pulse oximetry is based on a study with a group of 120 patients listed for LT, which found that levels of saturation lower than 96% had 100% sensitivity and that specificity in detecting levels of hypoxemia lower than 60 mmHg was 88%[94]. This cut off value was considered to be optimum since it was especially relevant in terms of its influence on transplantation list priority and patient prognosis. However, in view of the latest survival studies, the clinical importance of using this or other cut off values as references need to be reevaluated[86,95]. Furthermore, the use of pulse oximetry, a cut off value lower than 97% to perform arterial blood gas analysis, and a contrast echocardiography for LT candidates seem to be costeffective measures for the screening of HPS, as opposed to the lack of screening, or the use of fatigue and dyspnea rates. There was no direct comparison with the use of arterial blood gas analysis[96].
However, some authors believe that this would not be sufficiently precise to replace arterial blood gas analysis, since pulse oximetry overestimates arterial oxygenation, which is not dependant on liver disease[1,94].
In any case, pulse oximetry alone is insufficient for the diagnosis of HPS. Therefore a contrast echocardiography followed by an arterial blood gas analysis is proposed[91].
Thoracic X-ray: Thoracic Xrays can be used to effectively rule out other concomitant pulmonary diseases. In the case of HPS, they are mostly normal although interstitial markings are more frequently found[1,55].
Thorax computed tomography scan: Thoracic computed tomography (CT) scans are proposed as a complementary technique to rule out another underlying pulmonary pathology[1,91] although there is little information regarding their specific role in the diagnosis of HPS. It is suggested that measurement of
the caliber of the peripheral arteries and the bronchial/arterial relationship can be useful in the diagnosis of the syndrome[97,98]. Furthermore, CT scans offer the advantage of defining the vascular pattern of HPS in a similar manner to arteriography. A technique which combines the study of the pulmonary perfusion by means of a SPECT scan and fusion with CT (SPECTCT) imaging has been used in two HPS patients, thereby offering a possible alternative to the use of pulmonary arteriography for the location of IPVD[99].
Pulmonary arteriography: Pulmonary arteriography permits us to distinguish two different types of vascular patterns in HPS patients. Firstly type Ⅰ or diffuse, which is in turn divided into two subtypes. Subtype Ⅰ minimal is characterized by the presence of normal or minimally dilated vessels in the shape of diffuse vascular spiders. Subtype Ⅰ advanced presents more evident dilatations with a spongy, diffused and speckled appearance. Type Ⅱ or focal, is characterized by the presence of arteriovenous shunts similar to those present in hereditary telangiectasia[100]. The application of this technique is suggested for cases in which type Ⅱ HPS is suspected due to the presence of severe hypoxemia and lack of response to 100% oxygen supplement, and due to the possibility of embolotherapy[101]. However, the number of published cases of examples which were responsive to embolotherapy for both type Ⅰ and type Ⅱ HPS are insufficient to establish a strong recommendation in this respect[100,102106].
Respiratory function tests: In HPS patients both spirometry and static volumes have characteristically been found to be normal in the absence of concomitant pulmonary diseases. However, although this has been mentioned in various different HPS reviews, it is essentially based on theoretical assumptions about the disease rather than observational studies[83]. In fact, more recent studies suggest that a reduction in forced vital capacity and maximum forced expiratory volume during the first second (FEV1) is more frequent in HPS patients. However, there is no hypothesis to explain this finding and therefore further studies for its corroboration and analysis are required[55,56]. Frequently, there is a moderate to severe reduction in pulmonary capacity for the diffusion of CO (DLCO) and in that corrected for hemoglobin (DLCOco)[55,56,64,107]. This has been related to the increase in the distance between the alveolus and the capillary, due to vascular dilatation, and possible accumulation of collagen between the capillaries and pulmonary venules and the alveoli[19,4648]. However, its role in the diagnosis of HPS is limited, since it is more frequent in severe and very severe cases than in mild and moderate ones[56,64].
Laboratory tests: A study has found that the levels of the von Willebrand factor antigen in the blood of HPS patients are increased and that this is correlated
Grilo-Bensusan I et al . Hepatopulmonary syndrome

5733 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
with gasometric abnormalities[108]. This test could be useful for screening HPS although further studies are needed to confirm these findings (Table 1).
Differential diagnosisThe differential diagnosis of HPS in cirrhotic patients is essentially mandatory in the following situations: the presence of dyspnea, hypoxemia or abnormal AaO2. In these cases it is necessary to rule out the coexistence of other cardiopulmonary diseases or complications due to the cirrhosis itself such as ascitis, hepatic hydrothorax or portopulmonary hypertension. The differential diagnosis is particularly complex in the context of a pulmonary disease coexisting with IPVD. In this case the patient could be wrongly diagnosed as suffering from HPS, since the presence of IPVD is frequent in cirrhotic patients without HPS and gasometric abnormalities could be due to a coexisting pulmonary disease (false positive). Early definitions of HPS included the need to rule out the existence of cardiopulmonary diseases as a requirement to reach a diagnosis of the syndrome[4]. Later this requirement was ruled out, since from a physiopathological viewpoint, HPS can coexist with other processes[5]. Currently, the main recommendation in these cases is to complement studies with a 99mTcMAA so as to quantify the extent of the shunt[91,101]. However, no studies have demonstrated the validity of this strategy. As we said earlier, 99mTcMAA is a less sensitive technique and a positive result seems to be related to the severity of HPS, which means that mild cases of HPS may not be diagnosed as such (false negative). In view of this, it would be necessary to conduct further studies to validate the efficacy of 99mTcMAA or other techniques for the differential diagnosis. In view of this, it seems reasonable to recommend that patients with concomitant cardiopulmonary disease are
excluded from HPS research studies so as to prevent false positives and negatives.
NATURAL HISTORYThe natural history of HPS is unknown. Existing studies have been conducted in cirrhotic patients for whom the presence of HPS worsens their survival rate, independently of their age, sex, race, ChildPugh score, blood urea levels and MELD score[55,57,68]. The results regarding the influence on survival in terms of the severity of the HPS and the levels of hypoxemia or AaO2 are contradictory[55,57].
Based on data from cirrhotic patients, especially those listed for LT, we could establish the following hypothesis for the natural history of the disease. Firstly, IPVD develop, but this wouldn’t initially cause gasometric abnormalities. They have been found to be frequent in cirrhotic patients without HPS criteria[81]. Their significance has not been fully evaluated, but they may be associated with HPS in its initial or early stages and their presence can be detected by contrastenhanced echocardiography. The progression of the IPVD and hemodynamic changes in cirrhotic patients result in gasometric changes, initially including AaO2 abnormalities and mild levels of hypoxemia[109]. This corresponds to the asymptomatic period of HPS, at mild and moderate levels, in which survival may not be especially compromised[55,56]. However, pulse oximetry and 99mTcMAA imaging may not be able to diagnose this patient group[53,67,68,89,90,94]. If the disease progresses, hypoxemia becomes more severe and other abnormalities are detected in respiratory function tests, such as a decreased DLCOco or a positive 99mTcMAA[53,56,64,67,68,8990]. This is the symptomatic period of HPS, with severe to very severe cases in which survival would probably be compromised, resulting in death if
Table 1 Diagnosis methods for hepatopulmonary syndrome
Diagnosis methods Findings in HPS patients Limitations Aims
Arterial blood gas analysis AaO2 ≥ 15 mmHg or ≥ 20 mmHg in patients over 64 years old
Consensus criteria Diagnosis of HPSInvasive
Pulse oximetry O2 Saturation < 96% or 97% Low sensitivity Screening HPS and follow upContrast echocardiography Bubbles in the left cavities between the
fourth and sixth beatVarious agents used Diagnosis of IPVD
Transthoracic vs transoesophageal99mTc-MAA Cerebral uptake ≥ 6% Low sensitivity Diagnosis and quantify of IPVDThoracic X-ray Interstitial markings Unspecific Rule out other concomitant pulmonary
diseasesThorax CT scan Measurement of the caliber of the
peripheral arteries and the bronchial/arterial relationship
More studies needed Rule out other concomitant pulmonary diseases
Vascular patterns Location of IPVDPulmonary arteriography Vascular patterns Low sensitivity Type Ⅱ HPS suspected
Invasive Embolotherapy?Respiratory function tests Normal or reduction FVC or FEV1 Unspecific Rule out other concomitant pulmonary
diseasesReduction in DLCOco Low sensitivityLaboratory tests von Willebrand factor antigen elevated More studies needed Screening HPS
AaO2: Alveolar-arterial oxygen gradient; DLCOco: Corrected diffusing capacity for carbon monoxide; FEV1: Maximum forced expiratory volume during the first second; FVC: Forced vital capacity; HPS: Hepatopulmonary syndrome; 99mTc-MAA: Macroaggregated albumin lung perfusion scan.
Grilo-Bensusan I et al . Hepatopulmonary syndrome

5734 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
the patient does not receive an LT[55,57,68] (Figure 1).
TREATMENTMedical treatmentDifferent substances have been used to treat HPS. Nevertheless the majority of studies have been carried out on animals and the studies carried out on humans lack the necessary design and sufficient sample numbers to allow them to be applied to clinical practice. Substances which have been tested without producing any clearly favourable results include somatostatin analogues[100,110], norfloxacin[12,13,111], inhaled nitric oxide[112], cyclooxygenase inhibitors such as aspirin[113] and indomethacin[114], immunosuppressants such as mycophenolate mofetil[115], cyclophosphamide[116] and sorafenib[117,118], quercetin[20,119], beta blockers[120], paroxetine[121], rosuvastatin[122], caspase3 inhibitors[37], methylene blue[26,123,124] and inhaled iloprost[125]. Amongst the substances used in human tests are pentoxifylline and garlic. Pentoxifylline, which has been seen to yield positive results in animal tests[11,17], has also been tried on adults and children. However, samples in each study have been fewer than 10 patients, with contradictory results in terms of improvements in oxygenation and frequent gastrointestinal side effects[126128]. The use of garlic as a treatment for HPS has not been tested on animals and its active mechanism is not understood. Nevertheless, in a comparative study using garlic oil capsules and a salt capsule placebo, with a total sample of 41 HPS patients, and in another study without a placebo involving 15 patients, favorable results were observed, with improvements in oxygenation and other symptoms[129,130]. For pharmaceutical studies it would be necessary to carry out multicentre controlled trials using these and other substances against placebos. A study is currently taking place to evaluate the safety of sorafenib vs placebo, and its effects in blood oxygenation (ClinicalTrials.gov Identifier: NCT02021929).
Oxygen therapyIt is recommended that HPS patients with severe hypoxemia at rest receive oxygen therapy[1,131]. Nevertheless, there is no available data concerning effectiveness, tolerance, costeffectiveness, compliance and effects on survival rates of this therapy[1]. Only 2 case studies have been published involving
the long term treatment of HPS with mild and severe hypoxemia using oxygen therapy in a home environment. In both cases an improvement in liver function and oxygenation was observed[132].
Transjugular intrahepatic portosystemic shuntThere are very few published cases of HPS patients being treated with a transjugular intrahepatic portosystemic shunt (TIPS), and those which do exist have shown varied shortterm results regarding pulmonary oxygen exchange. 12 cases have been studied, and the largest series is 3 patients[133139]. As such, there is not sufficient data to propose the compassionate use of TIPS in cases of HPS[1,138].
Surgery BuddChiari syndrome shows a high prevalence of HPS and there are descriptions of improvements in cases where the obstruction is resolved through cavoplasty or other methods[87,139].
As has been described in a few isolated cases, embolization has also been used for the treatment of type 1 and type 2 HPS with positive results[100,102106].
In both instances the information has been obtained from reports about isolated cases and therefore it is not possible to make recommendations about their use.
LTThe most widely studied treatment is LT. At the moment it is the only effective treatment for HPS and is proven to improve survival rates[68,86].
When evaluating a patient listed for LT, it is recommended that they are tested for the presence of HPS. This can be done through arterial blood gas analysis, contrastenhanced echocardiography or pulse oximetry, the latter being proposed more frequently as the option of choice[1,42,91,101]. In patients with oxygen saturation lower than 96%, the most effective way of confirming the existence of HPS is through an arterial blood gas analysis, followed by a contrast echocardiography, or vice versa[42,91]. These screening models are based on the detection through pulse oximetry of HPS patients with significant hypoxemia, due to existing implications in prioritization and posttransplantation survival of these patients. As we have already mentioned, the findings of new studies could question this form of screening[86,95].
Diagnosis No HPS Early HPS? HPS
Severity Mild Moderate Severe Very severeSymptoms Asymptomatic Symptomatic
Findings Liver cirrhosis Early stages of IVD Strong evidence ofIVD
Alteration in AaO2 Mild-moderate hypoxemia
Decreased DLCOco
Severe hypoxemia
Diagnostic Transoesophageal contrast
echocardiography
Transthoracic contrast
echocardiography
Arterial gas blood analysis
Pulse oximetryTests Respiratory function tests
99mTc-MAA
Figure 1 Hypothesis for the natural history of hepatopulmonary syndrome. HPS: Hepatopulmonary syndrome; AaO2: Alveolar-arterial oxygen gradient; DLCOco: Corrected diffusing capacity for carbon monoxide; 99mTc-MAA: Macroaggregated albumin lung perfusion scan.
Grilo-Bensusan I et al . Hepatopulmonary syndrome

5735 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
In terms of mortality rates for those on the active transplantation list, in a prospective study, no differences were observed between patients who had HPS and those who did not. In the study, the majority of cases were mild or moderate and MELD scores were not taken into account. This means that the survival of HPS patients was evaluated without the “distorting” effect associated with the inclusion of these scores[56]. Other retrospective studies, which include large samples, have found that mortality rates for HPS patients on the list are lower than those for patients without HPS, a situation which is explained by the addition of MELD points to severe or very severe cases of HPS, thereby favoring transplantations in these patients as opposed to those who do not have HPS[86,95].
Hypoxemia can worsen in HPS patients who are on the active transplantation list, with a median decrease in pO2 of 5.2 mmHg per year[68]. It has been suggested that an arterial blood gas analysis should be carried out every 6 mo, although there are no studies which have evaluated the method for carrying out this followup process (arterial blood gas analysis vs pulse oximetry) nor how frequently it should be
carried out[42,91] (Figure 2).
Anesthetics and post LT intensive care: There are very few studies concerning the influence of HPS in anesthetic procedures or in the intensive care unit immediately following a LT and those that do exist are based on very small samples. It would appear that inhaled general anesthetics have a worse immediate effect on hypoxemia than intravenous anesthetics, but after an hour there is no apparent difference[140]. Inhaled nitric oxide, methylene blue, extracorporeal membrane oxygenation and noninvasive ventilation have all been suggested as ways of improving oxygenation in immediate postsurgery[141143]. More studies are required in order to increase our understanding of HPS in terms of both anesthetics and immediate postsurgery so as to improve patient care.
Post LT survival: Ten years survival after LT in HPS patients stands at 64%[86]. The majority of published studies analyze gross mortality rate of transplanted HPS patients retrospectively. Post LT mortality rates obtained in these studies range between 7.7% and 33%. Retrospective and later prospective studies show
Figure 2 Hepatopulmonary syndrome screening model and diagnosis in liver transplantation candidates. AaO2: Alveolar-arterial oxygen gradient; HPS: Hepatopulmonary syndrome; LT: Liver transplantation; pO2: Partial oxygen pressure; Sat O2: Arterial oxygen saturation; 99mTc-MAA: Macroaggregated albumin lung perfusion scan.
LT candidate
Pulse oximetryO2 Sat < 96%
Arterial gasblood analysis
AaO2 < 15 mmHgpO2 > 80 mmHg
No HPS
AaO2 ≥ 15 mmHgpO2 ≤ 80 mmHg
Contrast echocardiography
Negative
Investigate another pulmonary disease
Positive
HPS
Only HPS
Respiratory function tests
Normal
Pathological
O2 Sat ≥ 96%
Pulse oximetry every 12 mo
HPS + pulmonary disease
99mTc-MAA
≥ 6%
HPS
< 6%
HPS?- mild moderate
HPS?
Transplantation(Individualized)
pO2 < 50 mmHgpO2 ≥ 50 - < 60 mmHg
Transplantation(Prioritization)
pO2 > 60 mmHg
Follow-uparterial gas blood analysis/6 mo
Grilo-Bensusan I et al . Hepatopulmonary syndrome

5736 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
that hypoxemia ≤ 50 mmHg and cerebral uptake on 99mTcMAA ≥ 20% are predictors of post operative mortality, but patient sample figures have been small[66,67,79,83]. Since 2007, in the United States, as a result of these findings, and due to the progression of hypoxemia on the transplantation list, it has been recommended to assign a 22 MELD score to HPS patients with pO2 < 60 mmHg, with increases every 3 mo[144]. Nevertheless, later studies have failed to confirm these findings[86,145].
Recently, a number of comparative studies have been carried out comparing survival rates for patients who have HPS and those who do not. In the majority of retrospective studies there were no statistically significant differences[65,69,146] and this was also true in a prospective study[56]. Finally, two prospective studies analyzing transplantation data of the UNOS, and therefore a larger sample of HPS patients, showed a better rate of survival in HPS patients, probably due to lower waiting list mortality and a similar level of posttransplantation mortality, influenced by the MELD score, as a previous study suggested[86,95,147]. Another finding from one of the studies was greater mortality when pO2 is ≤ 44 mmHg, but this was not the case in lower levels of hypoxemia to which MELD scores are currently being applied in an exceptional manner[95]. These recent findings have opened a debate concerning the suitability of the MELD scoring system as applied to HPS, which prioritizes patients for LT, and there could well be changes to this policy in the near future[134].
Reversibility after LT: The improvement in the parameters which define HPS after LT has mainly been evaluated in retrospective studies which have shown total reversibility figures ranging from 52% to 100% over a 6 to 12 mo period. The definition of reversibility has used a range of different criteria[58,6770,145,148,149].
There is a prospective study which analyzes HPS reversibility at 6, 9 and 12 mo after LT based on the different criteria used to define the syndrome. It shows that full reversibility of HPS can be seen after 12 mo and that the process is rapid, since even after 6 mo, in mainly mild and moderate cases there is a 95.8% reversal. In terms of the evolution of the characteristic parameters of HPS, pO2 and AaO2 levels improve more quickly than in intrapulmonary shunt demonstrated by means of a contrast echocardiography.
It has also been observed that there is a post transplantation improvement in DLCO, although not in all patients[56]. Previously, the reversibility of this parameter was not described[148]. It should be noted that the sample in both studies was small.
CONCLUSIONCurrent knowledge about HPS is limited and is essentially based on studies of cirrhotic patients listed for LT or animal experiments. These studies have
enabled us to establish the fact that HPS is a frequent complication for these patients, and although it is generally asymptomatic it does have an impact on their quality of life and survival. It has also been established that LT is an efficient method of treating the syndrome and has positive posttransplantation survival results, even in severe cases. Nevertheless, there is still much to do, particularly in terms of increasing the number of multicentre studies which confirm the etiopathogenic findings of animal models in humans and aid the development of pharmacological treatments. It is also important to focus on improving the clinical use of diagnostic or screening techniques as well as clarifying the prioritization and selection of patients for LT.
REFERENCES1 Rodríguez-Roisin R, Krowka MJ, Hervé P, Fallon MB. Pulmonary-
Hepatic vascular Disorders (PHD). Eur Respir J 2004; 24: 861-880 [PMID: 15516683 DOI: 10.1183/09031936.04.00010904]
2 Rodríguez-Roisin R, Krowka MJ. Hepatopulmonary syndrome--a liver-induced lung vascular disorder. N Engl J Med 2008; 358: 2378-2387 [PMID: 18509123 DOI: 10.1097/SA.0b013e3181a8a39c]
3 Kennedy TC, Knudson RJ. Exercise-aggravated hypoxemia and orthodeoxia in cirrhosis. Chest 1977; 72: 305-309 [PMID: 891282]
4 Rodriguez-Roisin R, Roca J. Hepatopulmonary syndrome: the paradigm of liver-induced hypoxaemia. Baillieres Clin Gastroenterol 1997; 11: 387-406 [PMID: 9395754]
5 Krowka MJ, Cortese DA. Hepatopulmonary syndrome. Chest 1990; 98: 1053-1054 [PMID: 2225941]
6 Krowka MJ. Hepatopulmonary syndrome: recent literature (1997 to 1999) and implications for liver transplantation. Liver Transpl 2000; 6: S31-S35 [PMID: 10915189]
7 Fallon MB, Abrams GA, McGrath JW, Hou Z, Luo B. Common bile duct ligation in the rat: a model of intrapulmonary vasodilatation and hepatopulmonary syndrome. Am J Physiol 1997; 272: G779-G784 [PMID: 9142908]
8 Zhang J, Ling Y, Tang L, Luo B, Pollock DM, Fallon MB. Attenuation of experimental hepatopulmonary syndrome in endothelin B receptor-deficient rats. Am J Physiol Gastrointest Liver Physiol 2009; 296: G704-G708 [PMID: 19196949 DOI: 10.1152/ajpgi.90627.2008]
9 Ling Y, Zhang J, Luo B, Song D, Liu L, Tang L, Stockard CR, Grizzle WE, Ku DD, Fallon MB. The role of endothelin-1 and the endothelin B receptor in the pathogenesis of hepatopulmonary syndrome in the rat. Hepatology 2004; 39: 1593-1602 [PMID: 15185300 DOI: 10.1002/hep.20244]
10 Zhang M, Luo B, Chen SJ, Abrams GA, Fallon MB. Endothelin-1 stimulation of endothelial nitric oxide synthase in the pathogenesis of hepatopulmonary syndrome. Am J Physiol 1999; 277: G944-G952 [PMID: 10564099]
11 Sztrymf B, Libert JM, Mougeot C, Lebrec D, Mazmanian M, Humbert M, Herve P. Cirrhotic rats with bacterial translocation have higher incidence and severity of hepatopulmonary syndrome. J Gastroenterol Hepatol 2005; 20: 1538-1544 [PMID: 16174071 DOI: 10.1111/j.1440-1746.2005.03914.x]
12 Rabiller A, Nunes H, Lebrec D, Tazi KA, Wartski M, Dulmet E, Libert JM, Mougeot C, Moreau R, Mazmanian M, Humbert M, Hervé P. Prevention of gram-negative translocation reduces the severity of hepatopulmonary syndrome. Am J Respir Crit Care Med 2002; 166: 514-517 [PMID: 12186830 DOI: 10.1164/rccm.200201-027OC]
13 Añel RM, Sheagren JN. Novel presentation and approach to management of hepatopulmonary syndrome with use of antimicrobial agents. Clin Infect Dis 2001; 32: E131-E136 [PMID: 11317264 DOI: 10.1086/320149]
14 Sztrymf B, Rabiller A, Nunes H, Savale L, Lebrec D, Le Pape
Grilo-Bensusan I et al . Hepatopulmonary syndrome

5737 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
A, de Montpreville V, Mazmanian M, Humbert M, Hervé P. Prevention of hepatopulmonary syndrome and hyperdynamic state by pentoxifylline in cirrhotic rats. Eur Respir J 2004; 23: 752-758 [PMID: 15176692 DOI: 10.1183/09031936.04.00080404]
15 Luo B, Liu L, Tang L, Zhang J, Ling Y, Fallon MB. ET-1 and TNF-alpha in HPS: analysis in prehepatic portal hypertension and biliary and nonbiliary cirrhosis in rats. Am J Physiol Gastrointest Liver Physiol 2004; 286: G294-G303 [PMID: 14715521 DOI: 10.1152/ajpgi.00298.2003]
16 Arguedas MR, Drake BB, Kapoor A, Fallon MB. Carboxy-hemoglobin levels in cirrhotic patients with and without hepatopulmonary syndrome. Gastroenterology 2005; 128: 328-333 [PMID: 15685544]
17 Zhang J, Luo B, Tang L, Wang Y, Stockard CR, Kadish I, Van Groen T, Grizzle WE, Ponnazhagan S, Fallon MB. Pulmonary angiogenesis in a rat model of hepatopulmonary syndrome. Gastroenterology 2009; 136: 1070-1080 [PMID: 19109954 DOI: 10.1053/j.gastro.2008.12.001]
18 Tumgor G, Berdeli A, Arikan C, Levent E, Aydogdu S. Mcp-1, eNOS, tPA and PAI-1 gene polymorphism and correlation of genotypes and phenotypes in hepatopulmonary syndrome. Dig Dis Sci 2008; 53: 1345-1351 [PMID: 17934860 DOI: 10.1007/s10620-007-0002-3]
19 Zhang XJ, Katsuta Y, Akimoto T, Ohsuga M, Aramaki T, Takano T. Intrapulmonary vascular dilatation and nitric oxide in hypoxemic rats with chronic bile duct ligation. J Hepatol 2003; 39: 724-730 [PMID: 14568253]
20 Tieppo J, Cuevas MJ, Vercelino R, Tuñón MJ, Marroni NP, González-Gallego J. Quercetin administration ameliorates pulmonary complications of cirrhosis in rats. J Nutr 2009; 139: 1339-1346 [PMID: 19494027 DOI: 10.3945/jn.109.105353]
21 Rolla G. Is nitric oxide the ultimate mediator in hepatopulmonary syndrome? J Hepatol 2003; 38: 668-670 [PMID: 12713879]
22 Matsumoto A, Ogura K, Hirata Y, Kakoki M, Watanabe F, Takenaka K, Shiratori Y, Momomura S, Omata M. Increased nitric oxide in the exhaled air of patients with decompensated liver cirrhosis. Ann Intern Med 1995; 123: 110-113 [PMID: 7778822]
23 Cremona G, Higenbottam TW, Mayoral V, Alexander G, Demoncheaux E, Borland C, Roe P, Jones GJ. Elevated exhaled nitric oxide in patients with hepatopulmonary syndrome. Eur Respir J 1995; 8: 1883-1885 [PMID: 8620957 DOI: 10.1183/09031936.95.08111883]
24 Dinh-Xuan AT, Texereau J. Measuring exhaled nitric oxide: Not only a matter of how - But also why - Should we do it? Eur Respir J 1998; 12: 1005-1007 [DOI: 10.1183/09031936.98.12051005]
25 Brussino L, Bucca C, Morello M, Scappaticci E, Mauro M, Rolla G. Effect on dyspnoea and hypoxaemia of inhaled N(G)-nitro-L-arginine methyl ester in hepatopulmonary syndrome. Lancet 2003; 362: 43-44 [PMID: 12853200 DOI: 10.1016/S0140-6736(03)13807-X]
26 Schenk P, Madl C, Rezaie-Majd S, Lehr S, Müller C. Methylene blue improves the hepatopulmonary syndrome. Ann Intern Med 2000; 133: 701-706 [PMID: 11074903]
27 Gómez FP, Barberà JA, Roca J, Burgos F, Gistau C, Rodríguez-Roisin R. Effects of nebulized N(G)-nitro-L-arginine methyl ester in patients with hepatopulmonary syndrome. Hepatology 2006; 43: 1084-1091 [PMID: 16628648 DOI: 10.1002/hep.21141]
28 Delclaux C, Mahut B, Zerah-Lancner F, Delacourt C, Laoud S, Cherqui D, Duvoux C, Mallat A, Harf A. Increased nitric oxide output from alveolar origin during liver cirrhosis versus bronchial source during asthma. Am J Respir Crit Care Med 2002; 165: 332-337 [PMID: 11818316 DOI: 10.1164/rccm2107017]
29 Zeng J, Chen L, Chen B, Lu K, Belguise K, Wang X, Yi B. MicroRNA-199a-5p Regulates the Proliferation of Pulmonary Microvascular Endothelial Cells in Hepatopulmonary Syndrome. Cell Physiol Biochem 2015; 37: 1289-1300 [PMID: 26430741 DOI: 10.1159/000430252]
30 Wang L, Zhuang L, Rong H, Guo Y, Ling X, Wang R, Yu X, Zhang W. MicroRNA-101 inhibits proliferation of pulmonary microvascular endothelial cells in a rat model of hepatopulmonary syndrome by
targeting the JAK2/STAT3 signaling pathway. Mol Med Rep 2015; 12: 8261-8267 [PMID: 26498873 DOI: 10.3892/mmr.2015.4471]
31 Gao J, Chen L, Zeng J, Cui J, Ning JL, Wang GS, Belguise K, Wang X, Qian GS, Lu KZ, Yi B. The involvement of aquaporin 1 in the hepatopulmonary syndrome rat serum-induced migration of pulmonary arterial smooth muscle cells via the p38-MAPK pathway. Mol Biosyst 2015; 11: 3040-3047 [PMID: 26315345 DOI: 10.1039/c5mb00347d]
32 Liu C, Chen L, Zeng J, Cui J, Ning JN, Wang GS, Belguise K, Wang X, Qian GS, Lu KZ, Yi B. Bone morphogenic protein-2 regulates the myogenic differentiation of PMVECs in CBDL rat serum-induced pulmonary microvascular remodeling. Exp Cell Res 2015; 336: 109-118 [PMID: 26071935 DOI: 10.1016/j.yexcr.2015.05.025]
33 Yeh DY, Yang YC, Wang JJ. Hepatic Warm Ischemia-Reperfusion-Induced Increase in Pulmonary Capillary Filtration Is Ameliorated by Administration of a Multidrug Resistance-Associated Protein 1 Inhibitor and Leukotriene D4 Antagonist (MK-571) Through Reducing Neutrophil Infiltration and Pulmonary Inflammation and Oxidative Stress in Rats. Transplant Proc 2015; 47: 1087-1091 [PMID: 26036526 DOI: 10.1016/j.transproceed.2014.10.061]
34 Oswald-Mammosser M, Rashid S, Boehm N, Agin A, Geny B, Schini-Kerth V, Charloux A. Effect of the oestrogen receptor antagonist fulvestrant on the cirrhotic rat lung. Fundam Clin Pharmacol 2015; 29: 269-277 [PMID: 25753092 DOI: 10.1111/fcp.12114]
35 Chen L, Li YS, Cui J, Ning JN, Wang GS, Qian GS, Lu KZ, Yi B. MiR-206 controls the phenotypic modulation of pulmonary arterial smooth muscle cells induced by serum from rats with hepatopulmonary syndrome by regulating the target gene, annexin A2. Cell Physiol Biochem 2014; 34: 1768-1779 [PMID: 25427750 DOI: 10.1159/000366377]
36 Yang W, Hu B, Wu W, Batra S, Blackburn MR, Alcorn JL, Fallon MB, Zhang J. Alveolar type II epithelial cell dysfunction in rat experimental hepatopulmonary syndrome (HPS). PLoS One 2014; 9: e113451 [PMID: 25419825 DOI: 10.1371/journal.pone.0113451]
37 Chen B, Ning JL, Gu JT, Cui J, Yang Y, Wang Z, Zeng J, Yi B, Lu KZ. Caspase-3 inhibition prevents the development of hepatopulmonary syndrome in common bile duct ligation rats by alleviating pulmonary injury. Liver Int 2015; 35: 1373-1382 [PMID: 25113058 DOI: 10.1111/liv.12655]
38 Zhang H, Lv M, Zhao Z, Jia J, Zhang L, Xiao P, Wang L, Li C, Ji J, Tian X, Li X, Fan Y, Lai L, Liu Y, Li B, Zhang C, Liu M, Guo J, Han D, Ji C. Glucose-regulated protein 78 may play a crucial role in promoting the pulmonary microvascular remodeling in a rat model of hepatopulmonary syndrome. Gene 2014; 545: 156-162 [PMID: 24768185 DOI: 10.1016/j.gene.2014.04.041]
39 Nacif LS, Andraus W, Kubrusly MS, Molan N, Chaib E, D’Albuquerque LA. Myeloperoxidase activity is increased in hepatopulmonary syndrome in rats. Arq Bras Cir Dig 2013; 26: 293-295 [PMID: 24510037]
40 Chen Y, Yi B, Wang Z, Gu J, Li Y, Cui J, Lu K. Paxillin suppresses the proliferation of HPS rat serum treated PASMCs by up-regulating the expression of cytoskeletal proteins. Mol Biosyst 2014; 10: 759-766 [PMID: 24457422 DOI: 10.1039/c3mb70391f]
41 Zhang H, Lv M, Jia J, Zhao Z, Zhang L, Lai L, Wu Y, Li B, Li C, Ji J, Tian X, Liu Y, Li X, Pang H, Guo J, Wang L, Fan Y, Zhang C, Han D, Ji C. Expression of the 78 kD glucose-regulated protein is induced by endoplasmic reticulum stress in the development of hepatopulmonary syndrome. Gene 2014; 537: 115-119 [PMID: 24334118 DOI: 10.1016/j.gene.2013.11.065]
42 Raevens S, Geerts A, Van Steenkiste C, Verhelst X, Van Vlierberghe H, Colle I. Hepatopulmonary syndrome and portopulmonary hypertension: recent knowledge in pathogenesis and overview of clinical assessment. Liver Int 2015; 35: 1646-1660 [PMID: 25627425 DOI: 10.1111/liv.12791]
43 Lv Y, Fan D. Hepatopulmonary Syndrome. Dig Dis Sci 2015; 60: 1914-1923 [PMID: 25732713 DOI: 10.1007/s10620-015-3593-0]
44 Tumgor G. Cirrhosis and hepatopulmonary syndrome. World J Gastroenterol 2014; 20: 2586-2594 [PMID: 24627594 DOI: 10.3748/wjg.v20.i10.2586]
Grilo-Bensusan I et al . Hepatopulmonary syndrome

5738 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
45 Schraufnagel DE, Kay JM. Structural and pathologic changes in the lung vasculature in chronic liver disease. Clin Chest Med 1996; 17: 1-15 [PMID: 8665783]
46 Berthelot P, Walker JG, Sherlock S, Reid L. Arterial changes in the lungs in cirrhosis of the liver--lung spider nevi. N Engl J Med 1966; 274: 291-298 [PMID: 5903210 DOI: 10.1056/NEJM196602102740601]
47 Krowka MJ, Cortese DA. Hepatopulmonary syndrome. Current concepts in diagnostic and therapeutic considerations. Chest 1994; 105: 1528-1537 [PMID: 8181347]
48 Stanley NN, Williams AJ, Dewar CA, Blendis LM, Reid L. Hypoxia and hydrothoraces in a case of liver cirrhosis: correlation of physiological, radiographic, scintigraphic, and pathological findings. Thorax 1977; 32: 457-471 [PMID: 929488]
49 Schenk P, Fuhrmann V, Madl C, Funk G, Lehr S, Kandel O, Müller C. Hepatopulmonary syndrome: prevalence and predictive value of various cut offs for arterial oxygenation and their clinical consequences. Gut 2002; 51: 853-859 [PMID: 12427789 DOI: 10.1136/gut.51.6.853]
50 Aller R, Moya JL, Moreira V, García-Lledo A, Sanromán AL, Paino C, Boixeda D. Diagnosis and grading of intrapulmonary vascular dilatation in cirrhotic patients with contrast transesophageal echocardiography. J Hepatol 1999; 31: 1044-1052 [PMID: 10604578]
51 Aller R, Moya JL, Moreira V, Boixeda D, Cano A, Picher J, García-Rull S, de Luis DA. Diagnosis of hepatopulmonary syndrome with contrast transesophageal echocardiography: advantages over contrast transthoracic echocardiography. Dig Dis Sci 1999; 44: 1243-1248 [PMID: 10389704]
52 Rodríguez-Roisin R, Agustí AG, Roca J. The hepatopulmonary syndrome: new name, old complexities. Thorax 1992; 47: 897-902 [PMID: 1465744]
53 Fallon MB, Abrams GA. Pulmonary dysfunction in chronic liver disease. Hepatology 2000; 32: 859-865 [PMID: 11003635 DOI: 10.1053/jhep.2000.7519]
54 Lima BL, França AV, Pazin-Filho A, Araújo WM, Martinez JA, Maciel BC, Simões MV, Terra-Filho J, Martinelli AL. Frequency, clinical characteristics, and respiratory parameters of hepatopulmonary syndrome. Mayo Clin Proc 2004; 79: 42-48 [PMID: 14708947]
55 Fallon MB, Krowka MJ, Brown RS, Trotter JF, Zacks S, Roberts KE, Shah VH, Kaplowitz N, Forman L, Wille K, Kawut SM. Impact of hepatopulmonary syndrome on quality of life and survival in liver transplant candidates. Gastroenterology 2008; 135: 1168-1175 [PMID: 18644373 DOI: 10.1053/j.gastro.2008.06.038]
56 Pascasio JM, Grilo I, López-Pardo FJ, Ortega-Ruiz F, Tirado JL, Sousa JM, Rodriguez-Puras MJ, Ferrer MT, Sayago M, Gómez-Bravo MA, Grilo A. Prevalence and severity of hepatopulmonary syndrome and its influence on survival in cirrhotic patients evaluated for liver transplantation. Am J Transplant 2014; 14: 1391-1399 [PMID: 24730359 DOI: 10.1111/ajt.12713]
57 Schenk P, Schöniger-Hekele M, Fuhrmann V, Madl C, Silberhumer G, Müller C. Prognostic Significance of the Hepatopulmonary Syndrome in. Gastroenterology 2003; 5085: 1042-1052 [DOI: 10.1053/S0016-5085(03)01207-1]
58 Stoller JK, Lange PA, Westveer MK, Carey WD, Vogt D, Henderson JM. Prevalence and reversibility of the hepatopulmonary syndrome after liver transplantation. The Cleveland Clinic experience. West J Med 1995; 163: 133-138 [PMID: 7571560]
59 Abrams GA, Nanda NC, Dubovsky EV, Krowka MJ, Fallon MB. Use of macroaggregated albumin lung perfusion scan to diagnose hepatopulmonary syndrome: a new approach. Gastroenterology 1998; 114: 305-310 [PMID: 9453490]
60 Abrams GA, Sanders MK, Fallon MB. Utility of pulse oximetry in the detection of arterial hypoxemia in liver transplant candidates. Liver Transpl 2002; 8: 391-396 [PMID: 11965585 DOI: 10.1053/jlts.2002.32252]
61 Yang YY, Lin HC, Lee WC, Hou MC, Lee FY, Chang FY, Lee SD. Portopulmonary hypertension: distinctive hemodynamic and clinical manifestations. J Gastroenterol 2001; 36: 181-186 [PMID:
11291881 DOI: 10.1007/s005350170126]62 De BK, Sen S, Biswas PK, Biswas J, Maity AK. Clinical and
haemodynamic aspects of hepatopulmonary syndrome in Indian patients with cirrhosis. J Gastroenterol Hepatol 2000; 15: 412-416 [PMID: 10824886]
63 Przybyłowski T, Krenke R, Fangrat A, Nasilowski J, Grabczak EM, Styczynski G, Pruszczyk P, Krawczyk M, Chazan R. Gas exchange abnormalities in patients listed for liver transplantation. J Physiol Pharmacol 2006; 57 Suppl 4: 313-323 [PMID: 17072060]
64 Martínez GP, Barberà JA, Visa J, Rimola A, Paré JC, Roca J, Navasa M, Rodés J, Rodriguez-Roisin R. Hepatopulmonary syndrome in candidates for liver transplantation. J Hepatol 2001; 34: 651-657 [PMID: 11434610]
65 Deberaldini M, Arcanjo AB, Melo E, da Silva RF, Felício HC, Arroyo PC, Duca WJ, Cordeiro JA, da Silva RC. Hepatopulmonary syndrome: morbidity and survival after liver transplantation. Transplant Proc 2008; 40: 3512-3516 [PMID: 19100426 DOI: 10.1016/j.transproceed.2008.08.134]
66 Krowka MJ, Wiseman GA, Burnett OL, Spivey JR, Therneau T, Porayko MK, Wiesner RH. Hepatopulmonary syndrome: a prospective study of relationships between severity of liver disease, PaO(2) response to 100% oxygen, and brain uptake after (99m)Tc MAA lung scanning. Chest 2000; 118: 615-624 [PMID: 10988181 DOI: 10.1378/chest.118.3.615]
67 Arguedas MR, Abrams GA, Krowka MJ, Fallon MB. Prospective evaluation of outcomes and predictors of mortality in patients with hepatopulmonary syndrome undergoing liver transplantation. Hepatology 2003; 37: 192-197 [PMID: 12500204 DOI: 10.1053/jhep.2003.50023]
68 Swanson KL, Wiesner RH, Krowka MJ. Natural history of hepatopulmonary syndrome: Impact of liver transplantation. Hepatology 2005; 41: 1122-1129 [PMID: 15828054 DOI: 10.1002/hep.20658]
69 Schiffer E, Majno P, Mentha G, Giostra E, Burri H, Klopfenstein CE, Beaussier M, Morel P, Hadengue A, Pastor CM. Hepa-topulmonary syndrome increases the postoperative mortality rate following liver transplantation: a prospective study in 90 patients. Am J Transplant 2006; 6: 1430-1437 [PMID: 16686767 DOI: 10.1111/j.1600-6143.2006.01334.x]
70 Taillé C, Cadranel J, Bellocq A, Thabut G, Soubrane O, Durand F, Ichaï P, Duvoux C, Belghiti J, Calmus Y, Mal H. Liver transplantation for hepatopulmonary syndrome: a ten-year experience in Paris, France. Transplantation 2003; 75: 1482-1489; discussion 1446-1447 [PMID: 12792501 DOI: 10.1097/01.TP.0000061612.78954.6C]
71 Lange PA, Stoller JK. The hepatopulmonary syndrome. Ann Intern Med 1995; 122: 521-529 [PMID: 7872588]
72 Gómez FP, Martínez-Pallí G, Barberà JA, Roca J, Navasa M, Rodríguez-Roisin R. Gas exchange mechanism of orthodeoxia in hepatopulmonary syndrome. Hepatology 2004; 40: 660-666 [PMID: 15349905 DOI: 10.1002/hep.20358]
73 Andrivet P, Cadranel J, Housset B, Herigault R, Harf A, Adnot S. Mechanisms of impaired arterial oxygenation in patients with liver cirrhosis and severe respiratory insufficiency. Effects of indomethacin. Chest 1993; 103: 500-507 [PMID: 8432144]
74 Rodriguez-Roisin R, Roca J, Agusti AG, Mastai R, Wagner PD, Bosch J. Gas exchange and pulmonary vascular reactivity in patients with liver cirrhosis. Am Rev Respir Dis 1987; 135: 1085-1092 [PMID: 3579008 DOI: 10.1164/arrd.1987.135.5.1085]
75 Molleston JP, Kaufman BA, Cohen A, Shackelford PG, Keating JP, Lowell JA, Howard TK. Brain abscess in hepatopulmonary syndrome. J Pediatr Gastroenterol Nutr 1999; 29: 225-226 [PMID: 10435665]
76 Shijo H, Sasaki H, Nishimaru K, Okumura M. Recurrent intracranial hemorrhagic episodes in hepatopulmonary syndrome. Intern Med 1992; 31: 786-790 [PMID: 1392183]
77 Palma DT, Philips GM, Arguedas MR, Harding SM, Fallon MB. Oxygen desaturation during sleep in hepatopulmonary syndrome. Hepatology 2008; 47: 1257-1263 [PMID: 18311748 DOI: 10.1002/hep.22143]
Grilo-Bensusan I et al . Hepatopulmonary syndrome

5739 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
78 Collisson EA, Nourmand H, Fraiman MH, Cooper CB, Bellamy PE, Farmer DG, Vierling JM, Ghobrial RM, Busuttil RW. Retrospective analysis of the results of liver transplantation for adults with severe hepatopulmonary syndrome. Liver Transpl 2002; 8: 925-931 [PMID: 12360435 DOI: 10.1053/jlts.2002.35544]
79 Krowka MJ, Mandell MS, Ramsay MA, Kawut SM, Fallon MB, Manzarbeitia C, Pardo M, Marotta P, Uemoto S, Stoffel MP, Benson JT. Hepatopulmonary syndrome and portopulmonary hypertension: a report of the multicenter liver transplant database. Liver Transpl 2004; 10: 174-182 [PMID: 14762853 DOI: 10.1002/lt.20016]
80 Gupta S, Nayyar D, Pomier-Layrargues G. Variability of oxy-genation in possible hepatopulmonary syndrome: effects of requiring two abnormal arterial blood gas results for diagnosis. Dig Dis Sci 2015; 60: 1848-1855 [PMID: 25586084 DOI: 10.1007/s10620-014-3506-7]
81 Vedrinne JM, Duperret S, Bizollon T, Magnin C, Motin J, Trepo C, Ducerf C. Comparison of transesophageal and transthoracic contrast echocardiography for detection of an intrapulmonary shunt in liver disease. Chest 1997; 111: 1236-1240 [PMID: 9149575]
82 Kim BJ, Lee SC, Park SW, Choi MS, Koh KC, Paik SW, Lee SH, Hong KP, Park JE, Seo JD. Characteristics and prevalence of intrapulmonary shunt detected by contrast echocardiography with harmonic imaging in liver transplant candidates. Am J Cardiol 2004; 94: 525-528 [PMID: 15325947 DOI: 10.1016/j.amjcard.2004.04.074]
83 Krowka MJ, Porayko MK, Plevak DJ, Pappas SC, Steers JL, Krom RA, Wiesner RH. Hepatopulmonary syndrome with progressive hypoxemia as an indication for liver transplantation: case reports and literature review. Mayo Clin Proc 1997; 72: 44-53 [PMID: 9005286]
84 Krowka MJ, Tajik AJ, Dickson ER, Wiesner RH, Cortese DA. Intrapulmonary vascular dilatations (IPVD) in liver transplant candidates. Screening by two-dimensional contrast-enhanced echocardiography. Chest 1990; 97: 1165-1170 [PMID: 2331913]
85 Ramírez Moreno JM, Millán Núñez MV, Rodríguez Carrasco M, Ceberino D, Romaskevych-Kryvulya O, Constantino Silva AB, Muñoz-Vega P, García-Corrales C, Guiberteau-Sánchez A, Roa Montero A, Márquez-Lozano P, Narváez Rodríguez I. [Detection of an intrapulmonary shunt in patients with liver cirrhosis through contrast-enhanced transcranial Doppler. A study of prevalence, pattern characterization, and diagnostic validity]. Gastroenterol Hepatol 2015; 38: 475-483 [PMID: 25841632 DOI: 10.1016/j.gastrohep.2015.02.006]
86 Iyer VN, Swanson KL, Cartin-Ceba R, Dierkhising RA, Rosen CB, Heimbach JK, Wiesner RH, Krowka MJ. Hepatopulmonary syndrome: favorable outcomes in the MELD exception era. Hepatology 2013; 57: 2427-2435 [PMID: 22996424 DOI: 10.1002/hep.26070]
87 Kaymakoglu S, Kahraman T, Kudat H, Demir K, Cakaloglu Y, Adalet I, Dincer D, Besisik F, Boztas G, Sözen AB, Mungan Z, Okten A. Hepatopulmonary syndrome in noncirrhotic portal hypertensive patients. Dig Dis Sci 2003; 48: 556-560 [PMID: 12757170 DOI: 10.1023/A:1022549018807]
88 de Queirós AS, Brandão SC, Macedo LG, Ourem MS, Mota VG, Leite LA, Lopes EP, Domingues AL. Evaluation of normality and reproducibility parameters of scintigraphy with (99m)Tc-MAA in the diagnosis of intrapulmonary vascular dilatations. Ann Nucl Med 2015; 29: 46-51 [PMID: 25326249 DOI: 10.1007/s12149-014-0915-9]
89 Zhao H, Tsauo J, Ma HY, Li X. The role of macroaggregated albumin lung perfusion scan in hepatopulmonary syndrome: are we ready to draw conclusions? Liver Int 2015; 35: 1918-1919 [PMID: 25688443 DOI: 10.1111/liv.12810]
90 Abrams GA, Jaffe CC, Hoffer PB, Binder HJ, Fallon MB. Diagnostic utility of contrast echocardiography and lung perfusion scan in patients with hepatopulmonary syndrome. Gastroenterology 1995; 109: 1283-1288 [PMID: 7557096]
91 Machicao VI , Balakrishnan M, Fallon MB. Pulmonary complications in chronic liver disease. Hepatology 2014; 59: 1627-1637 [PMID: 24089295 DOI: 10.1002/hep.26745]
92 Kochar R, Tanikella R, Fallon MB. Serial pulse oximetry in
hepatopulmonary syndrome. Dig Dis Sci 2011; 56: 1862-1868 [PMID: 21327708 DOI: 10.1007/s10620-011-1600-7]
93 Noli K, Solomon M, Golding F, Charron M, Ling SC. Prevalence of hepatopulmonary syndrome in children. Pediatrics 2008; 121: e522-e527 [PMID: 18310172 DOI: 10.1542/peds.2007-1075]
94 Arguedas MR, Singh H, Faulk DK, Fallon MB. Utility of pulse oximetry screening for hepatopulmonary syndrome. Clin Gastroenterol Hepatol 2007; 5: 749-754 [PMID: 17392034 DOI: 10.1016/j.cgh.2006.12.003]
95 Goldberg DS, Krok K, Batra S, Trotter JF, Kawut SM, Fallon MB. Impact of the hepatopulmonary syndrome MELD exception policy on outcomes of patients after liver transplantation: an analysis of the UNOS database. Gastroenterology 2014; 146: 1256-1265.e1 [PMID: 24412528 DOI: 10.1053/j.gastro.2014.01.005]
96 Roberts DN, Arguedas MR, Fallon MB. Cost-effectiveness of screening for hepatopulmonary syndrome in liver transplant candidates. Liver Transpl 2007; 13: 206-214 [PMID: 17205561 DOI: 10.1002/lt.20931]
97 Köksal D, Kaçar S, Köksal AS, Tüfekçioğlu O, Küçükay F, Okten S, Saşmaz N, Arda K, Sahin B. Evaluation of intrapulmonary vascular dilatations with high-resolution computed thorax tomography in patients with hepatopulmonary syndrome. J Clin Gastroenterol 2006; 40: 77-83 [PMID: 16340638 DOI: 10.1097/01.mcg.0000190775.57903.86]
98 Lee KN, Lee HJ, Shin WW, Webb WR. Hypoxemia and liver cirrhosis (hepatopulmonary syndrome) in eight patients: comparison of the central and peripheral pulmonary vasculature. Radiology 1999; 211: 549-553 [PMID: 10228541 DOI: 10.1148/radiology.211.2.r99ma46549]
99 Suga K, Kawakami Y, Iwanaga H, Tokuda O, Matsunaga N. Findings of hepatopulmonary syndrome on breath-hold perfusion SPECT-CT fusion images. Ann Nucl Med 2009; 23: 413-419 [PMID: 19396512 DOI: 10.1007/s12149-009-0250-8]
100 Krowka MJ, Dickson ER, Cortese DA. Hepatopulmonary syndrome. Clinical observations and lack of therapeutic response to somatostatin analogue. Chest 1993; 104: 515-521 [PMID: 8101797]
101 Porres-Aguilar M, Altamirano JT, Torre-Delgadillo A, Charlton MR, Duarte-Rojo A. Portopulmonary hypertension and hepatopulmonary syndrome: a clinician-oriented overview. Eur Respir Rev 2012; 21: 223-233 [PMID: 22941887 DOI: 10.1183/09059180.00007211]
102 Grady K, Gowda S, Kingah P, Soubani AO. Coil embolization of pulmonary arteries as a palliative treatment of diffuse type I hepatopulmonary syndrome. Respir Care 2015; 60: e20-e25 [PMID: 25185147 DOI: 10.4187/respcare.03198]
103 Ryu JK, Oh JH. Hepatopulmonary syndrome: angiography and therapeutic embolization. Clin Imaging 2003; 27: 97-100 [PMID: 12639774]
104 Saad NE, Lee DE, Waldman DL, Saad WE. Pulmonary arterial coil embolization for the management of persistent type I hepatopulmonary syndrome after liver transplantation. J Vasc Interv Radiol 2007; 18: 1576-1580 [PMID: 18057294 DOI: 10.1016/j.jvir.2007.08.008]
105 Lee HW, Suh KS, Kim J, Shin WY, Yi NJ, Jae HJ, Chung JW, Oh SW, Kang KW, Lee KU. Pulmonary artery embolotherapy in a patient with type I hepatopulmonary syndrome after liver transplantation. Korean J Radiol 2010; 11: 485-489 [PMID: 20592935 DOI: 10.3348/kjr.2010.11.4.485]
106 Poterucha JJ, Krowka MJ, Dickson ER, Cortese DA, Stanson AW, Krom RA. Failure of hepatopulmonary syndrome to resolve after liver transplantation and successful treatment with embolotherapy. Hepatology 1995; 21: 96-100 [PMID: 7806175]
107 Márquez Martín E, Jara Palomares L, Ortega Ruiz F, Grilo Bensusán I, López-Campos JL, Cejudo Ramos P, Pascasio JM, Rodríguez Becerra E. [Hepatopulmonary syndrome in patients with advanced hepatic disease: study of a series of 24 cases]. Med Clin (Barc) 2008; 130: 98-102 [PMID: 18261381]
108 Horvatits T, Drolz A, Roedl K, Herkner H, Ferlitsch A, Perkmann T, Müller C, Trauner M, Schenk P, Fuhrmann V. Von Willebrand factor antigen for detection of hepatopulmonary syndrome in patients with cirrhosis. J Hepatol 2014; 61: 544-549 [PMID: 24798623 DOI:
Grilo-Bensusan I et al . Hepatopulmonary syndrome

5740 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
10.1016/j.jhep.2014.04.025]109 Alonso Martínez JL, Zozaya Urmeneta JM, García Sanchotena
JL, Olaz-Preciado F, Estébanez-Estébanez C, Berjón-Reyero J. [Hepatopulmonary syndrome: relationship with liver dysfunction and systemic hemodynamic disorder]. Med Clin (Barc) 2004; 123: 721-725 [PMID: 15574284 DOI: 10.1016/S0025-7753(04)74648-5]
110 Söderman C, Juhlin-Dannfelt A, Lagerstrand L, Eriksson LS. Ventilation-perfusion relationships and central haemodynamics in patients with cirrhosis. Effects of a somatostatin analogue. J Hepatol 1994; 21: 52-57 [PMID: 7963422]
111 Gupta S, Faughnan ME, Lilly L, Hutchison S, Fowler R, Bayoumi AM. Norfloxacin therapy for hepatopulmonary syndrome: a pilot randomized controlled trial. Clin Gastroenterol Hepatol 2010; 8: 1095-1098 [PMID: 20816858 DOI: 10.1016/j.cgh.2010.08.011]
112 Jounieaux V, Leleu O, Mayeux I. Cardiopulmonary effects of nitric oxide inhalation and methylene blue injection in hepatopulmonary syndrome. Intensive Care Med 2001; 27: 1103-1104 [PMID: 11497151]
113 Song JY, Choi JY, Ko JT, Bae EJ, Kim HS, Noh CI, Yoon YS. Long-term aspirin therapy for hepatopulmonary syndrome. Pediatrics 1996; 97: 917-920 [PMID: 8657540]
114 Shijo H, Sasaki H, Yuh K, Sakaguchi S, Okumura M. Effects of indomethacin on hepatogenic pulmonary angiodysplasia. Chest 1991; 99: 1027-1029 [PMID: 2009756]
115 Moreira Silva H, Reis G, Guedes M, Cleto E, Vizcaíno JR, Kelly D, Gennery AR, Santos Silva E. A case of hepatopulmonary syndrome solved by mycophenolate mofetil (an inhibitor of angiogenesis and nitric oxide production). J Hepatol 2013; 58: 630-633 [PMID: 23104163 DOI: 10.1016/j.jhep.2012.10.021]
116 Cadranel JL, Milleron BJ, Cadranel JF, Fermand JP, Andrivet P, Brouet JC, Adnot S, Akoun GM. Severe hypoxemia-associated intrapulmonary shunt in a patient with chronic liver disease: improvement after medical treatment. Am Rev Respir Dis 1992; 146: 526-527 [PMID: 1489152 DOI: 10.1164/ajrccm/146.2.526]
117 Yang W, Zhang J, Hu B, Wu W, Venter J, Alpini G, Fallon MB. The role of receptor tyrosine kinase activation in cholangiocytes and pulmonary vascular endothelium in experimental hepatopulmonary syndrome. Am J Physiol Gastrointest Liver Physiol 2014; 306: G72-G80 [PMID: 24200956 DOI: 10.1152/ajpgi.00178.2013]
118 Chang CC, Chuang CL, Lee FY, Wang SS, Lin HC, Huang HC, Teng TH, Hsu SJ, Hsieh HG, Lee SD. Sorafenib treatment improves hepatopulmonary syndrome in rats with biliary cirrhosis. Clin Sci (Lond) 2013; 124: 457-466 [PMID: 23043394 DOI: 10.1042/CS20120052]
119 Vercelino R, Tieppo J, Forgiarini Junior LA, Dias AS, Marroni CA, Marroni NP. Experimental models for assessment of pulmonary alterations in hepatopulmonary syndrome. J Bras Pneumol 2008; 34: 453-460 [PMID: 18695789]
120 Lambrecht GL, Malbrain ML, Coremans P, Verbist L, Verhaegen H. Orthodeoxia and platypnea in liver cirrhosis: effects of propranolol. Acta Clin Belg 1994; 49: 26-30 [PMID: 7514828]
121 Yilmaz S, Dursum M, Canoruç F, Bayan K, Karabulut A, Akay H. A severe (type II) hepatopulmonary syndrome in a patient with idiopathic portal hypertension and treatment with paroxetine. Neth J Med 2005; 63: 448-452 [PMID: 16397315]
122 Chang CC, Wang SS, Hsieh HG, Lee WS, Chuang CL, Lin HC, Lee FY, Lee SD, Huang HC. Rosuvastatin improves hepatopulmonary syndrome through inhibition of inflammatory angiogenesis of lung. Clin Sci (Lond) 2015; 129: 449-460 [PMID: 25940601 DOI: 10.1042/CS20140622]
123 Rolla G , Bucca C, Brussino L. Methylene blue in the hepatopulmonary syndrome. N Engl J Med 1994; 331: 1098 [PMID: 8090178 DOI: 10.1056/NEJM199410203311617]
124 Miyamoto A, Katsuta Y, Zhang XJ, Li HL, Ohsuga M, Komeichi H, Shimizu S, Akimoto T, Mizuno K. Effect of chronic methylene blue administration on hypoxemia in rats with common bile duct ligation. Hepatol Res 2010; 40: 622-632 [PMID: 20412326 DOI: 10.1111/j.1872-034X.2010.00640.x]
125 Krug S, Seyfarth HJ, Hagendorff A, Wirtz H. Inhaled iloprost for hepatopulmonary syndrome: improvement of hypoxemia. Eur J
Gastroenterol Hepatol 2007; 19: 1140-1143 [PMID: 17998841 DOI: 10.1097/MEG.0b013e328220ed72]
126 Tanikella R, Philips GM, Faulk DK, Kawut SM, Fallon MB. Pilot study of pentoxifylline in hepatopulmonary syndrome. Liver Transpl 2008; 14: 1199-1203 [PMID: 18668653 DOI: 10.1002/lt.21482]
127 Gupta LB, Kumar A, Jaiswal AK, Yusuf J, Mehta V, Tyagi S, Tempe DK, Sharma BC, Sarin SK. Pentoxifylline therapy for hepatopulmonary syndrome: a pilot study. Arch Intern Med 2008; 168: 1820-1823 [PMID: 18779471 DOI: 10.1001/archinte.168.16.1820]
128 Kianifar HR, Khalesi M, Mahmoodi E, Afzal Aghaei M. Pentoxifylline in hepatopulmonary syndrome. World J Gastroenterol 2012; 18: 4912-4916 [PMID: 23002364 DOI: 10.3748/wjg.v18.i35.4912]
129 De BK, Dutta D, Pal SK, Gangopadhyay S, Das Baksi S, Pani A. The role of garlic in hepatopulmonary syndrome: a randomized controlled trial. Can J Gastroenterol 2010; 24: 183-188 [PMID: 20352147]
130 Abrams GA, Fallon MB. Treatment of hepatopulmonary syndrome with Allium sativum L. (garlic): a pilot trial. J Clin Gastroenterol 1998; 27: 232-235 [PMID: 9802451]
131 Porres-Aguilar M, Gallegos-Orozco JF. Hepatopulmonary syndrome: Is it time to redefine the MELD exception score for better organ allocation and outcomes? Ann Hepatol 2014; 13: 468-470 [PMID: 24927621]
132 Fukushima KY, Yatsuhashi H, Kinoshita A, Ueki T, Matsumoto T, Osumi M, Matsuoka Y. Two cases of hepatopulmonary syndrome with improved liver function following long-term oxygen therapy. J Gastroenterol 2007; 42: 176-180 [PMID: 17351808 DOI: 10.1007/s00535-006-1965-0]
133 Corley DA, Scharschmidt B, Bass N, Somberg K, Gold W. Lack of efficacy of TIPS for hepatopulmonary syndrome. Gastroenterology 1997; 113: 728-730 [PMID: 9247498]
134 Allgaier HP, Haag K, Ochs A, Hauenstein KH, Jeserich M, Krause T, Heilmann C, Gerok W, Rössle M. Hepato-pulmonary syndrome: successful treatment by transjugular intrahepatic portosystemic stent-shunt (TIPS) J Hepatol 1995; 23: 102 [PMID: 8530801]
135 Lasch HM, Fried MW, Zacks SL, Odell P, Johnson MW, Gerber DA, Sandhu FS, Fair JH, Shrestha R. Use of transjugular intrahepatic portosystemic shunt as a bridge to liver transplantation in a patient with severe hepatopulmonary syndrome. Liver Transpl 2001; 7: 147-149 [PMID: 11172400 DOI: 10.1053/jlts.2001.21287]
136 Riegler JL, Lang KA, Johnson SP, Westerman JH. Transjugular intrahepatic portosystemic shunt improves oxygenation in hepatopulmonary syndrome. Gastroenterology 1995; 109: 978-983 [PMID: 7657128]
137 Selim KM, Akriviadis EA, Zuckerman E, Chen D, Reynolds TB. Transjugular intrahepatic portosystemic shunt: a successful treatment for hepatopulmonary syndrome. Am J Gastroenterol 1998; 93: 455-458 [PMID: 9517657 DOI: 10.1111/j.1572-0241.1998.00455.x]
138 Siramolpiwat S. Transjugular intrahepatic portosystemic shunts and portal hypertension-related complications. World J Gastroenterol 2014; 20: 16996-17010 [PMID: 25493012 DOI: 10.3748/wjg.v20.i45.16996]
139 De BK, Sen S, Biswas PK, Sanyal R, Majumdar D, Biswas J. Hepatopulmonary syndrome in inferior vena cava obstruction responding to cavoplasty. Gastroenterology 2000; 118: 192-196 [PMID: 10611168]
140 Kim JA, Lee JJ, Kim CS, Chung IS, Gwak MS, Kim GS. Does general anesthesia with inhalation anesthetics worsen hypoxemia in patients with end-stage liver disease and an intrapulmonary shunt? Transplant Proc 2011; 43: 1665-1668 [PMID: 21693254 DOI: 10.1016/j.transproceed.2011.03.056]
141 Monsel A, Mal H, Brisson H, Luo R, Eyraud D, Vézinet C, Do CH, Lu Q, Vaillant JC, Hannoun L, Houssel P, Durand F, Rouby JJ. Extracorporeal membrane oxygenation as a bridge to liver transplantation for acute respiratory distress syndrome-induced life-threatening hypoxaemia aggravated by hepatopulmonary syndrome. Crit Care 2011; 15: R234 [PMID: 21958549 DOI: 10.1186/cc10476]
142 Chihara Y, Egawa H, Tsuboi T, Oga T, Handa T, Yamamoto K,
Grilo-Bensusan I et al . Hepatopulmonary syndrome

5741 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Mishima M, Tanaka K, Uemoto S, Chin K. Immediate noninvasive ventilation may improve mortality in patients with hepatopulmonary syndrome after liver transplantation. Liver Transpl 2011; 17: 144-148 [PMID: 21280187 DOI: 10.1002/lt.22207]
143 Fleming GM, Cornell TT, Welling TH, Magee JC, Annich GM. Hepatopulmonary syndrome: use of extracorporeal life support for life-threatening hypoxia following liver transplantation. Liver Transpl 2008; 14: 966-970 [PMID: 18581508 DOI: 10.1002/lt.21477]
144 Fallon MB, Mulligan DC, Gish RG, Krowka MJ. Model for end-stage liver disease (MELD) exception for hepatopulmonary syndrome. Liver Transpl 2006; 12: S105-S107 [PMID: 17123282 DOI: 10.1002/lt.20971]
145 Gupta S, Castel H, Rao RV, Picard M, Lilly L, Faughnan ME, Pomier-Layrargues G. Improved survival after liver transplantation in patients with hepatopulmonary syndrome. Am J Transplant 2010; 10: 354-363 [PMID: 19775311 DOI: 10.1111/j.1600-6143.2009.02822.x]
146 Kim HY, Choi MS, Lee SC, Park SW, Lee JH, Koh KC, Paik SW, Yoo BC, Rhee JC. Outcomes in patients with hepatopulmonary
syndrome undergoing liver transplantation. Transplant Proc 2004; 36: 2762-2763 [PMID: 15621142 DOI: 10.1016/j.transproceed.2004.10.002]
147 Sulieman BM, Hunsicker LG, Katz DA, Voigt MD. OPTN policy regarding prioritization of patients with hepatopulmonary syndrome: does it provide equitable organ allocation? Am J Transplant 2008; 8: 954-964 [PMID: 18416736 DOI: 10.1111/j.1600-6143.2007.02124.x]
148 Martínez-Palli G, Gómez FP, Barberà JA, Navasa M, Roca J, Rodríguez-Roisin R, Burgos F, Gistau C. Sustained low diffusing capacity in hepatopulmonary syndrome after liver transplantation. World J Gastroenterol 2006; 12: 5878-5883 [PMID: 17007057 DOI: 10.3748/wjg.v12.i36.5878]
149 Egawa H, Kasahara M, Inomata Y, Uemoto S, Asonuma K, Fujita S, Kiuchi T, Hayashi M, Yonemura T, Yoshibayashi M, Adachi Y, Shapiro JA, Tanaka K. Long-term outcome of living related liver transplantation for patients with intrapulmonary shunting and strategy for complications. Transplantation 1999; 67: 712-717 [PMID: 10096527]
P- Reviewer: Ramsay MA, Tumgor G S- Editor: Gong ZM L- Editor: A E- Editor: Wang CH
Grilo-Bensusan I et al . Hepatopulmonary syndrome

Adreesh Mukherjee, Atanu Biswas, Shyamal Kumar Das, Department of Neurology, Bangur Institute of Neurosciences and Institute of Post Graduate Medical Education and Research, Kolkata, West Bengal 700025, India
Author contributions: All authors equally contributed to this paper with conception and design of the study, literature review and analysis, drafting and critical revision and editing, and final approval of the final version.
Conflict-of-interest statement: Authors declare no conflict of interests for this article.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Manuscript source: Invited manuscript
Correspondence to: Shyamal Kumar Das, MD, DM, Professor, Head, Department of Neurology, Bangur Institute of Neurosciences and Institute of Post Graduate Medical Education and Research, 52/1A Sambhu Nath Pandit Street, Kolkata, West Bengal 700025, India. [email protected]: +91-33-22230003Fax: +91-33-22236677
Received: March 27, 2016 Peer-review started: March 28, 2016First decision: May 12, 2016Revised: May 30, 2016 Accepted: June 15, 2016 Article in press: June 15, 2016Published online: July 7, 2016
AbstractEarly involvement of gut is observed in Parkinson’s
disease (PD) and symptoms such as constipation may precede motor symptoms. α-Synuclein pathology is extensively evident in the gut and appears to follow a rostrocaudal gradient. The gut may act as the starting point of PD pathology with spread toward the central nervous system. This spread of the synuclein pathology raises the possibility of prion-like propagation in PD pathogenesis. Recently, the role of gut microbiota in PD pathogenesis has received attention and some phenotypic correlation has also been shown. The extensive involvement of the gut in PD even in its early stages has led to the evaluation of enteric α-synuclein as a possible biomarker of early PD. The clinical manifestations of gastrointestinal dysfunction in PD include malnutrition, oral and dental disorders, sialorrhea, dysphagia, gastroparesis, constipation, and defecatory dysfunction. These conditions are quite distressing for the patients and require relevant investigations and adequate management. Treatment usually involves both pharmacological and non-pharmacological measures. One important aspect of gut dysfunction is its contribution to the clinical fluctuations in PD. Dysphagia and gastroparesis lead to inadequate absorption of oral anti-PD medications. These lead to response fluctuations, particularly delayed-on and no-on, and there is significant relationship between levodopa pharmacokinetics and gastric emptying in patients with PD. Therefore, in such cases, alternative routes of administration or drug delivery systems may be required.
Key words: Parkinson’s disease; Gut dysfunction; Sialorrhea; Dysphagia; Gastroparesis; Constipation; Gut microbiota
© The Author(s) 2016. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Gut is involved in early Parkinson’s disease (PD) with extensive synuclein pathology, following a rostrocaudal gradient along the gastrointestinal system. It may act as the starting point of PD pathology with
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.3748/wjg.v22.i25.5742
5742 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
World J Gastroenterol 2016 July 7; 22(25): 5742-5752 ISSN 1007-9327 (print) ISSN 2219-2840 (online)
© 2016 Baishideng Publishing Group Inc. All rights reserved.
Gut dysfunction in Parkinson's disease
Adreesh Mukherjee, Atanu Biswas, Shyamal Kumar Das
REVIEW

prion-like spread toward the central nervous system. The clinical manifestations include malnutrition, oral and dental disorders, sialorrhea, dysphagia, gastroparesis, constipation, and defecatory dysfunction. These are distressing for the patients and need to be managed properly by pharmacological or non-pharmacological measures. Gut dysfunction also leads to response fluctuations in PD and this may require alternative routes of administration or drug delivery systems for anti-PD medications.
Mukherjee A, Biswas A, Das SK. Gut dysfunction in Parkinson’s disease. World J Gastroenterol 2016; 22(25): 5742-5752 Available from: URL: http://www.wjgnet.com/1007-9327/full/v22/i25/5742.htm DOI: http://dx.doi.org/10.3748/wjg.v22.i25.5742
INTRODUCTIONParkinson’s disease (PD) is a common neurodegenerative disorder affecting people across the globe. It is clinically defined by its motor features such as bradykinesia, rigidity, rest tremor, and postural impairment[1]. However, “nonmotor” features of PD play a vital role in the disease process, and recently this has gained increasing significance, clinically as well as from the etiopathogenesis point of view. Nonmotor manifestations such as loss of sense of smell and taste, rapid eye movement sleep behavior disorder, and clinical evidence of autonomic dysfunction can predate motor features by years and sometimes can dominate the clinical picture[2].
Gastrointestinal (GI) or gut dysfunction in PD can be because of both motor and nonmotor (dysautonomic) impairment. A better description of gut dysfunction in PD is available, and it is now established that GI disturbances are common and affect virtually all levels of the GI system[3]. Although initially considered to be late manifestations of PD, GI disturbances are present early in the course of the disease in relatively high frequency[4]. The gut dysfunction includes drooling, dental problems, diminished taste, swallowing disorders, impaired gastric emptying, weight loss, and constipation. Other than clinical gut manifestations, the GI system is a significant contributor to the pathogenesis of PD and gut may even act as route for the spread of pathology to the central nervous system (CNS). Moreover, early involvement of gut is considered a possible presymptomatic stage of PD.
In this review, we aim to discuss gut dysfunction in PD including the role of gut synuclein as biomarker for early PD. We also summarize various GI manifestations along with their management.
GUT PATHOLOGY IN PDPD is classified as synucleinopathy. It is pathologically
characterized by the presence of Lewy neurites and Lewy bodies in the brain, which are abnormal inclusions consisting of nearly insoluble aggregates within cellular processes and somata of involved neurons. These are chiefly made of αsynuclein along with ubiquitin and phosphorylated neurofilaments[5]. Until now, postmortem detection of αsynuclein aggregation in brain by immunohistochemistry along with neuronal loss in substantia nigra is considered gold standard for definite diagnosis of PD[6]. For pathological diagnosis of PD in early stages, alternative approaches are studied including identification of Lewy bodies and αsynuclein in extraCNS locations , and the gut appears to be a promising area because of its accessibility.
Distribution of gut pathologyDistribution of αsynuclein pathology in gut in relation to its nature, appearance, staining properties, and distribution along the GI system has been documented (Table 1). A rostrocaudal gradient of αsynuclein associated histopathology within GI system is likely. Earlier studies showed characteristic inclusions that were histologically and ultrastructurally identical to Lewy bodies in Auerbach’s and Meissner’s plexuses, which were abundant in the lower esophagus[7]. Another study confirmed the highest involvement in lower esophagus and submandibular gland followed by stomach and small intestine, whereas colon and rectum had the lowest involvement[8]. This rostrocaudal gradient along enteric nervous system (ENS) coincides with the distribution of vagal innervation from dorsal motor nucleus of vagus (DMV)[9]. However, this gradient is not unequivocally evident in all studies[10]. Interestingly, a recent study on patients with no history of neurological disease showed vermiform appendix enriched in αsynuclein in its mucosal plexus. The authors concluded that appendix may be used as candidate anatomical locus for the initiation of enteric αsynuclein aggregation[11].
Spreading from the gut?As the pathological involvement of gut is unfolding, a hypothesis that gut/ENS may act as initiation point of PD pathology or route to centripetal involvement of CNS has gained importance. Braak et al[12] suggested
5743 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Mukherjee A et al . Gut dysfunction in Parkinson’s disease
Table 1 Gut pathology in Parkinson’s disease
Distribution of gut pathology
Pathology spreading from the gut
Gut microbiota
Rostrocaudal gradient of α-synuclein pathology
Crossing the gut barrier
Modulation of gut-brain axis
Place of colon and vermiform appendix
Dual-hit hypothesis Helicobacter pylori and small intestinal bacterial
overgrowthPrion-like
propagationClinical phenotypic
correlation

that pathology may be caused by a pathogen that can penetrate the mucosal barrier of the GI tract and, via postganglionic enteric neurons, reaches the CNS along preganglionic fibers derived from the vagus by retrograde axonal and transneuronal transport, thus reaching selectively vulnerable subcortical nuclei.
In addition, a dualhit hypothesis is proposed, which suggests that a neurotropic pathogen, probably viral, enters the brain via two routesnasal and gastricfollowing swallowing of nasal secretions in saliva. These secretions might contain a neurotropic pathogen that penetrates the epithelial lining and reaches preganglionic parasympathetic motor neurons of the vagus nerve by transsynaptic transmission through axons of Meissner’s plexus. This would allow retrograde transport into the medulla, followed by caudorostral propagation to substantia nigra[13]. The early involvement of ENS has also been demonstrated in an animal study, which concluded that ENS abnormalities preceded CNS changes[14].
This hypothesis of spread of synuclein pathology across various sections of nervous system has suggested another aspect of PD pathogenesis, that is, the possibility of prionlike propagation. This is based on two recent reports showing Lewy bodies in grafted neurons in subjects with PD suggesting probable spread of αsynuclein aggregates from host to graft neurons[15,16]. Studies on animal models of PD have shown that intracerebral injection of exogenous αsynuclein induces a progressive αsynuclein immunoreactive staining pattern suggestive of αsynuclein pathology propagation via a prionlike process[6].
Role of gut microbiotaFurthermore, the emerging role of gut microbiota adds to the contribution of GI system in PD. Microbiota may interact with gutbrain axis through different mechanisms, most importantly via modulation of intestinal barrier[17]. In PD, gut microbiota changes associated with intestinal inflammation may contribute to αsynuclein misfolding. Moreover, priming of the innate immune system by gut microbiota may enhance the inflammatory response to αsynuclein. The role of peripherally-induced inflammation inflicting damage on dopaminergic neurons has also been studied in animals[18]. The role of Helicobacter pylori (H. pylori) in PD has been investigated. A Cochrane review concluded that there is limited evidence to suggest that H. pylori eradication improves absorption of levodopa and consequently motor symptoms[19]. However, a recent study showed that H. pylori infection is linked with worse motor severity of PD[20]. The study investigating the contribution of small intestinal bacterial overgrowth (SIBO) to pathophysiology of motor fluctuations in PD showed that SIBO eradication resulted in improved motor fluctuations without affecting pharmacokinetics of levodopa[21]. Recently, a study explored the relation
of gut microbiota with clinical phenotype of PD and compared fecal microbiomes of patients with PD with control subjects and showed a reduction of Prevotellaceae in PD. Moreover, the relative abundance of Enterobacteriaceae was positively related with the severity of postural instability and gait difficulty[22]. These findings offer some insight into the possible effect of gut microbiota on PD.
enteric α -synuclein as a biomarker of early pDBecause of extensive involvement of the GI tract and its easy accessibility, there is growing interest to utilize enteric αsynuclein as a possible biomarker of early PD. However, some reports were critical about gut biopsy utilization. A study showed that there was no neuronal loss in myenteric plexus in PD and that Lewy body pathology parallels parasympathetic autonomic input from DMV[23]. Pathologic species or strain of αsynuclein, considered to be responsible for PD pathology, have been detected using immunoreactive staining of αsynuclein, and future studies should concentrate on αsynuclein immunoreactivity for identifying these specific species. However, although studies have utilized antibodies reactive for phosphorylated αsynuclein as a marker of pathologic αsynuclein in the GI tract[24], αsynuclein phosphorylation may be a normal event in adult human brain[25]. Based on recent evidence that soluble, oligomeric aggregates of αsynuclein may ultimately be pathogenic, it was suggested that antibodies reactive to oligomeric forms of α-synuclein could improve specificity and sensitivity for pathological staining in the GI tract[6]. The other concern about gut sampling is the appropriate site for biopsy. Although colonic biopsy shows positive results, a recent evaluation of the procedure has questioned its applicability in the current form[26]. Another recent study on colonic mucosal biopsy showed elevated levels of aggregated hyperphosphorylated αsynuclein in both PD and control subjects and suggested that the colonic deposition of αsynuclein cannot be a useful diagnostic test for PD[27]. One option may be to use vagally innervated segments of the GI tract for biopsy. Conversely, biopsy of submandibular salivary glands appears to be useful. These glands have high intensity of PD pathology, and their feasibility and applicability have been demonstrated[28,29]. Thus, further studies for evaluating the role of enteric αsynuclein as a biomarker for PD should be conducted, including search for optimal biopsy site as well as methods of tissue sampling/preparation and possible pathological αsynuclein targets.
CLINICAL MANIFESTATIONS OF GI DYSFUNCTIONMalnutritionPD is associated with weight alteration, which maybe either loss or gain of weight. Unintended weight loss
5744 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Mukherjee A et al . Gut dysfunction in Parkinson’s disease

5745 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
dopamine dysregulation[45]. A patient was found to develop burning mouth syndrome with carbidopa/levodopa, which improved when this was replaced with pramipexole[46].
SialorrheaDrooling is an important component of PD, which leads to worse QOL and significant social and emotional consequences[47,48]. Its frequency varies from 10% to 84% probably because of lack of standard definition and criteria for diagnosing drooling[49]. Drooling in PD has been linked to dysphagia with less efficient swallowing[5052] rather than increased salivary production (Table 2). Studies have reported decrease in salivary production in PD[53]. Drooling was correlated with unintentional mouth opening because of hypomimia, abnormal head posture[52], and dysarthria[54]. Other features associated with drooling are longer disease duration[55], disease severity[56], dementia[57], hallucinations[47],orthostatic hypotension, and a history of using antidepressants[49].
Drooling increases the risk of silent aspiration and laryngeal penetration of saliva in patients with PD[58], therefore, this must be addressed in all affected patients. Its treatment consists of pharmacological and nonpharmacological measures. Glycopyrrolate is effective in reducing sialorrhea in patients with PD[59]. Studies have demonstrated benefit from anticholinergics used as topical preparations with less systemic adverse effects. These include sublingual ipratropium bromide spray[60] and intraoral tropicamide films[61]. Another effective and safe option is the use of ultrasoundguided intrasalivary gland injection of botulinum neurotoxin (both botulinum toxin A and B)[62,63]. The nonpharmacological approaches include chewing gum and behavioral modification[49]. Radiotherapy is effective in the treatment of sialorrhea and it can be used in cases refractory to medical therapy[64,65].
DysphagiaDysphagia is an important component of PD, which adversely affects QOL[66]. As shown by a metaanalysis, patients are less likely to voluntarily complain about dysphagia, which revealed a pooled frequency estimate of 35% for subjective dysphagia and of 82% for objectively measured dysphagia[67]. Dysphagia in PD may be due to dysfunction of oral, pharyngeal, and esophageal phases of swallowing[68]. Several abnormalities have been described and oropharyngeal bradykinesia and incoordination plays an important role in PD[69]. However, contributors to pathophysiology of dysphagia are much widespread. Recent studies have shown the involvement of cortical areas in dysphagia[70,71]. The role of central cholinergic dysfunction in dysphagia has also been suggested[72]. Pathology has also been demonstrated in pharyngeal motor and sensory nerves[73,74]. Dysphagia has been
is common[30] and correlates with worsened quality of life (QOL)[31]. Malnourishment in PD is linked to reduced food intake because of loss of appetite and GI dysfunction such as dysphagia, constipation, and early satiety[32]. It is associated with increased severity and duration of disease, psychiatric symptoms such as depression or anxiety, and fatigue[30,33,34]. The decreased body mass index during initial 6 mo of followup in PD was an indicator for future risk of dementia[35]. Increasing levodopa dosages were associated with the risk of malnutrition[36]. Micronutrient deficiencies, particularly vitamin D deficiency/insufficiency are common in PD[37] and these may be related to malnutrition, immobility, and sunlight deprivation. Patients with PD may have low bone mineral density and osteoporosis. Levodopa therapy causes vitamin B12 and folic acid deficiency with hyperhomocysteinemia and may contribute to osteoporosis[38]. Increasing evidence suggests that impaired insulin signaling and mitochondrial dysfunction lead to neurodegeneration, and these processes might also contribute to weight loss in PD.
Recent studies have shown that PD may be associated with weight gain[39,40]. Moreover, compulsive eating and weight gain have been related to dopamine agonist use[41]. Also deep brain stimulation (DBS) of subthalamic nucleus (STN) has been associated with postoperative weight gain[42].
Malnutrition in PD needs early intervention and patients should be advised regarding lifestyle changes, exercise, and dietary supplementation. Adverse effects of dopaminergic therapy must also be considered. Bisphosphonates, supplementation of vitamin D and calcium is useful in osteoporosis in PD[38].
Oral and dental disordersPatients with PD have poor oral hygiene. They have fewer remaining teeth, more caries, gingival recession, and increased tooth mobility. The poor oral health may be because of lower frequencies of tooth brushing, motor impairment, apathy, depression, and cognitive impairment[43,44]. There are reports of PD being associated with bruxism, temporomandibular disorders, and subjective taste impairment. Burning mouth syndrome is more common in PD and this could be because of decreased dopamine levels and
Table 2 Sialorrhea
Mechanism Treatment
Swallowing dysfunction Oral GlycopyrrolateAbnormal head posture Sublingual Ipratropium bromide spray Unintentional mouth opening due to hypomimia
Intra-oral Tropicamide films
Behavioral modificationIntra-salivary gland Botulinum
neurotoxin injectionRadiotherapy
Mukherjee A et al . Gut dysfunction in Parkinson’s disease

5746 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
associated with male gender, older age, longer disease duration, dementia, depression, and severity of motor symptoms[7577]. Although dysphagia is considered to arise in later parts of the disease, it is present in early stages of PD, particularly when a multimodal approach is used for its assessment[78,79]. This can be evaluated by bedside screening such as swallow trial, videofluoroscopy of swallowing act, fiberoptic endoscopic evaluation of swallowing, manometry, modified barium swallow studies, and cough reflex testing (Table 3)[8083].
Besides causing difficulty in ingesting food and medicine, dysphagia in PD with prolonged swallowing time is associated with the risk of aspiration pneumonia[84,85]. Therefore, dysphagia needs to be diagnosed and treated early. Treatment options include compensatory maneuvers such as thickening liquids to nectar or honey consistency, chintuck maneuver, frequency/multiple swallowing technique, and rehabilitation maneuvers such as exercises of tongue strengthening and control along with vocal exercises[86]. Logopedic dysphagia treatment by an experienced speech therapist consists of oral motor exercises, airwayprotecting maneuvers, and postural compensation[87]. Other options such as expiratory muscle strength training and videoassisted swallowing therapy may be effective[88]. Percutaneous endoscopic gastrostomy placement may be rarely needed in severe dysphagia[3]. Role of levodopa in improving dysphagia has been found conflicting[89,90]. A recent study showed that rotigotine transdermal patch improved swallowing in PD patients with dysphagia[91]. Effect of DBS on dysphagia in PD remains debatable[92]. However, unilateral STNDBS appears to have adverse effect on the swallowing function in contrast to unilateral globus pallidus internus DBS[93].
Gastric dysfunctionGastroparesis is quite common in PD, observed in about 70%100% of subjects and may be present in both early and advanced stages of the disease[9496]. The severity of motor impairment is correlated with gastroparesis in PD[97]. The symptoms of delayed gastric emptying include nausea, vomiting, early satiety, and postprandial fullness, and can lead to weight loss, malnutrition and dehydration. Delayed gastric emptying is defined as > 60% retention at 2 h
postprandially and/or > 10% retention at 4 h, using 4h imaging protocol after ingestion of a radioactive technetium Tc 99mlabeled solid food[98]. Alternatively, breath tests using nonradioactive 13Csodium octanoate bound into solid meal may be employed for evaluating gastric emptying[99]. Other methods used to assess gastric motility in PD are real time visualization by magnetic resonance imaging[100] and electrogastrography[101].
A major impact of gastroparesis on PD is the occurrence of response fluctuations, particularly delayedon (delay in onset of “onphase”) to noon (without “onphase”) with levodopa, and significant relationship were indicated between levodopa pharmacokinetics and gastric emptying[102,103]. In contrast, it has been suggested that levodopa itself can lead to the development of delayed gastric emptying[96]. Therefore, management of gastroparesis is essential. Other than dietary changes and exercise, one may use pharmacotherapy using domperidone. Although domperidone is useful in treating gastroparesis without interference with antiparkinsonism treatment[104], concerns have been raised about its arrhythmogenic potential with risk of long QT syndrome[105]. Recent studies have shown improvement of gastroparesis with Nizatidine[106], and the role of ghrelin agonist needs further evaluation[107]. Moreover, low levels of vitamin D has been suggested to contribute to gastric dysmotility in PD, but this finding needs further corroboration[108]. Benefits from botulinum neurotoxin injection in the pyloric sphincter[109] and STNDBS[110]
have been reported. In refractory cases, gastric electrical stimulation may be attempted (Table 4)[111].
To circumvent levodopa pharmacokinetic derangements associated with gastroparesis, several options have been studied. These include orally dissolving or soluble formulations[112,113]. Levodopacarbidopa intestinal gel, subcutaneous apomorphine, and rotigotine patch are beneficial in gastroparesis as well as severe dysphagia[114,115]. STNDBS is a useful surgical option[116].
H. pylori infection and small intestinal bacterial overgrowth The other aspect of gastric involvement in motor fluctuations is the putative role of H. pylori. Investigations for H. pylori infection include serology, urea breath test, and stool antigen test[117]. There are mixed views on effect of H. pylori infection; however, recent studies show that H. pylori infection is associated with worse motor severity of PD[20]. Therefore, H. pylori eradication preferably using a combination regimen is indicated. Similarly, the role of SIBO has been evaluated. SIBO is diagnosed by culture of intestinal aspirates, or more practically, by hydrogen lactulose, and glucose breath tests[118]. Treatment for SIBO in PD is indicated as recent studies show improvement in motor fluctuations following eradication of SIBO[21].
Table 3 Dysphagia
Evaluation Treatment
Bedside screening Compensatory maneuversCough reflex testing Rehabilitation maneuversModified barium swallow studies Expiratory muscle strength trainingVideofluoroscopy Video-assisted swallowing therapyManometry Rotigotine transdermal patchFiberoptic endoscopic evaluation of swallowing
Percutaneous endoscopic gastrostomy placement
Mukherjee A et al . Gut dysfunction in Parkinson’s disease

5747 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Constipation and defecatory dysfunctionConstipation is probably the commonest GI manifestation in PD and is present in more than 50% of the cases. It is approximately two to four times commoner in patients with PD than in controls[119]. Constipation and defecatory dysfunction is found in early stages of PD[120], and in fact, studies have shown that constipation can predate motor symptoms of PD by even 20 years[121]. Thus, constipation is one of the earliest manifestations of PD. Interestingly, studies have shown increased occurrence of future PD in persons with constipation, which may be in a dosedependent manner[122,123].
One mechanism is prolonged colon transit time[124]. Another dysfunction is defecatory pelvic floor dyssynergia or functional pelvic outlet obstruction by paradoxical contraction of striated anal sphincter muscles during straining for defecation, which is considered dystonia in some studies[120,125]. Constipation is a known adverse effect of drugs used in PD, such as anticholinergics and dopaminergic agents; however, intrinsic disease pathophysiology may be responsible for it. The use of betablockers in PD is associated with lower risk of constipation, whereas dopaminergic treatments tend to increase it[126]. Conversely, levodopa improves paradoxical sphincter contraction and anorectal constipation in patients with PD[127] supporting the presence of more than one mechanism for constipation in PD[128]. Likewise, symptoms include infrequent bowel movements, unsuccessful attempts at defecation, and a sense of incomplete rectal emptying at defecation[129].
In general, evaluation of chronic constipation usually comprises clinical assessment by digital anorectal examination followed by relevant investigations (Table 5). Colonic transit is evaluated by radiopaque markers, scintigraphy, or wireless motility capsule, and defecatory disorder is assessed by anorectal manometry, rectal balloon expulsion, or defecography[130]. In patients with PD, mostly colon transit time and manometry are utilized. Additionally, electromyography of external anal sphincter has
been used to demonstrate neurogenic changes[124]. The treatment starts with high fiber diet, proper fluid intake, psyllium, and physiotherapy. However, many patients require additional treatment. The effective options for slow transit constipation in PD are Macrogol and lubiprostone; Nizatidine was also effective (Table 5)[131133]. Other drugs such as prucalopride needs to be considered in PD. Treatment for dyssynergic defecation include biofeedback therapy and levodopa or apomorphine injections[134,135]. Botulinum neurotoxin type A injection into puborectalis muscle under ultrasonographic guidance is useful for dyssynergic outletobstruction constipation[134,136].
Apart from constipation and defecatory dysfunction, existence of fecal incontinence in PD has been described and its frequency may be significant[119].
CONCLUSIONIn PD, gut is affected early and extensively. It appears to participate in pathogenesis of the disease. Further studies are required to understand whether it indeed acts as an initiation point in PD pathology and if so, its mechanism of involvement including the role of gut microbiota. To establish the potential role of enteric αsynuclein as a biomarker of early PD, studies are needed with adequate reproducibility regarding optimal sampling site and technique and appropriate pathogenic targets. The GI manifestations in PD are distressing for patients with significant morbidity and complications. Therefore, these should be identified promptly and treated. This requires the clinician to pay due attention to these symptoms during the evaluation of PD patient. The management of these conditions may be tricky as it includes not only symptomatic treatment but also optimization of antiParkinsonian drugs, particularly anticholinergics and dopaminergic agents. Studies on novel therapeutic agents and nonpharmacotherapeutic interventions would be helpful. Moreover, newer dopaminergic drug delivery systems should be studied to circumvent dysfunctional gut.
Table 4 Gastroparesis
Evaluation Treatment Modifications of dopaminergic agents
Gastric emptying scintigraphy
Domperidone Orally dissolving or soluble formulations
13C-sodium octanoate breath test
Nizatidine Levodopa-carbidopa intestinal gel
Electrogastrography Ghrelin agonist Rotigotine patchBotulinum neurotoxin
injection into the pyloric sphincter
Subcutaneous Apomorphine
STN DBSGastric electrical
stimulation
STN: Subthalamic nucleus; DBS: Deep brain stimulation.
Table 5 Constipation and defecatory dysfunction
Mechanism Evaluation Treatment
Slow transit constipation
Radiopaque marker study for colonic transit
High fiber diet, psyllium, proper fluid intake
Wireless motility capsule
Adjustment of anticholinergics and dopaminergic agents
Macrogol1
Lubiprostone2
Dyssynergic defecation
Anorectal manometry Biofeedback therapy
Rectal balloon expulsion Botulinum neurotoxin injection into the puborectalis
Defecography
1Macrogol-polyethylene glycol (an osmotic laxative); 2Lubiprostone-chloride channel activator (increases fluid secretion in the intestine).
Mukherjee A et al . Gut dysfunction in Parkinson’s disease

5748 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
The role of DBS in these conditions needs further evaluation.
REFERENCES1 Kalia LV, Lang AE. Parkinson’s disease. Lancet 2015; 386: 896-912
[PMID: 25904081 DOI: 10.1016/S0140-6736(14)61393-3]2 Goldstein DS, Sewell L, Sharabi Y. Autonomic dysfunction in PD: a
window to early detection? J Neurol Sci 2011; 310: 118-122 [PMID: 21529844 DOI: 10.1016/j.jns.2011.04.011]
3 Pfeiffer RF. Gastrointestinal dysfunction in Parkinson’s disease. Parkinsonism Relat Disord 2011; 17: 10-15 [PMID: 20829091 DOI: 10.1016/j.parkreldis.2010.08.003]
4 Sung HY, Park JW, Kim JS. The frequency and severity of gastrointestinal symptoms in patients with early Parkinson’s disease. J Mov Disord 2014; 7: 7-12 [PMID: 24926404 DOI: 10.14802/jmd.14002]
5 Del Tredici K, Rüb U, De Vos RA, Bohl JR, Braak H. Where does parkinson disease pathology begin in the brain? J Neuropathol Exp Neurol 2002; 61: 413-426 [PMID: 12030260 DOI: 10.1093/jnen/61.5.413]
6 Ruffmann C, Parkkinen L. Gut Feelings About α-Synuclein in Gastrointestinal Biopsies: Biomarker in the Making? Mov Disord 2016; 31: 193-202 [PMID: 26799450 DOI: 10.1002/mds.26480]
7 Wakabayashi K, Takahashi H, Takeda S, Ohama E, Ikuta F. Parkinson’s disease: the presence of Lewy bodies in Auerbach’s and Meissner’s plexuses. Acta Neuropathol 1988; 76: 217-221 [PMID: 2850698 DOI: 10.1007/BF00687767]
8 Beach TG, Adler CH, Sue LI, Vedders L, Lue L, White Iii CL, Akiyama H, Caviness JN, Shill HA, Sabbagh MN, Walker DG. Multi-organ distribution of phosphorylated alpha-synuclein histopathology in subjects with Lewy body disorders. Acta Neuropathol 2010; 119: 689-702 [PMID: 20306269 DOI: 10.1007/s00401-010-0664-3]
9 Cersosimo MG, Benarroch EE. Pathological correlates of gastrointestinal dysfunction in Parkinson’s disease. Neurobiol Dis 2012; 46: 559-564 [PMID: 22048068 DOI: 10.1016/j.nbd.2011.10.014]
10 Hilton D, Stephens M, Kirk L, Edwards P, Potter R, Zajicek J, Broughton E, Hagan H, Carroll C. Accumulation of α-synuclein in the bowel of patients in the pre-clinical phase of Parkinson’s disease. Acta Neuropathol 2014; 127: 235-241 [PMID: 24240814 DOI: 10.1007/s00401-013-1214-6]
11 Gray MT, Munoz DG, Gray DA, Schlossmacher MG, Woulfe JM. Alpha-synuclein in the appendiceal mucosa of neurologically intact subjects. Mov Disord 2014; 29: 991-998 [PMID: 24352892 DOI: 10.1002/mds.25779]
12 Braak H, Rüb U, Gai WP, Del Tredici K. Idiopathic Parkinson’s disease: possible routes by which vulnerable neuronal types may be subject to neuroinvasion by an unknown pathogen. J Neural Transm (Vienna) 2003; 110: 517-536 [PMID: 12721813 DOI: 10.1007/s00702-002-0808-2]
13 Hawkes CH, Del Tredici K, Braak H. Parkinson’s disease: a dual-hit hypothesis. Neuropathol Appl Neurobiol 2007; 33: 599-614 [PMID: 17961138 DOI: 10.1111/j.1365-2990.2007.00874.x]
14 Kuo YM, Li Z, Jiao Y, Gaborit N, Pani AK, Orrison BM, Bruneau BG, Giasson BI, Smeyne RJ, Gershon MD, Nussbaum RL. Extensive enteric nervous system abnormalities in mice transgenic for artificial chromosomes containing Parkinson disease-associated alpha-synuclein gene mutations precede central nervous system changes. Hum Mol Genet 2010; 19: 1633-1650 [PMID: 20106867 DOI: 10.1093/hmg/ddq038]
15 Kordower JH, Chu Y, Hauser RA, Freeman TB, Olanow CW. Lewy body-like pathology in long-term embryonic nigral transplants in Parkinson’s disease. Nat Med 2008; 14: 504-506 [PMID: 18391962 DOI: 10.1038/nm1747]
16 Li JY, Englund E, Holton JL, Soulet D, Hagell P, Lees AJ, Lashley T, Quinn NP, Rehncrona S, Björklund A, Widner H, Revesz T, Lindvall O, Brundin P. Lewy bodies in grafted neurons in subjects with
Parkinson’s disease suggest host-to-graft disease propagation. Nat Med 2008; 14: 501-503 [PMID: 18391963 DOI: 10.1038/nm1746]
17 Carabotti M, Scirocco A, Maselli MA, Severi C. The gut-brain axis: interactions between enteric microbiota, central and enteric nervous systems. Ann Gastroenterol 2015; 28: 203-209 [PMID: 25830558]
18 Mulak A, Bonaz B. Brain-gut-microbiota axis in Parkinson’s disease. World J Gastroenterol 2015; 21: 10609-10620 [PMID: 26457021 DOI: 10.3748/wjg.v21.i37.10609]
19 Rees K, Stowe R, Patel S, Ives N, Breen K, Clarke CE, Ben-Shlomo Y. Helicobacter pylori eradication for Parkinson’s disease. Cochrane Database Syst Rev 2011; (11): CD008453 [PMID: 22071847 DOI: 10.1002/14651858.CD008453.pub2]
20 Tan AH, Mahadeva S, Marras C, Thalha AM, Kiew CK, Yeat CM, Ng SW, Ang SP, Chow SK, Loke MF, Vadivelu JS, Ibrahim N, Yong HS, Tan CT, Fox SH, Lang AE, Lim SY. Helicobacter pylori infection is associated with worse severity of Parkinson’s disease. Parkinsonism Relat Disord 2015; 21: 221-225 [PMID: 25560322 DOI: 10.1016/j.parkreldis.2014.12.009]
21 Fasano A, Bove F, Gabrielli M, Petracca M, Zocco MA, Ragazzoni E, Barbaro F, Piano C, Fortuna S, Tortora A, Di Giacopo R, Campanale M, Gigante G, Lauritano EC, Navarra P, Marconi S, Gasbarrini A, Bentivoglio AR. The role of small intestinal bacterial overgrowth in Parkinson’s disease. Mov Disord 2013; 28: 1241-1249 [PMID: 23712625 DOI: 10.1002/mds.25522]
22 Scheperjans F, Aho V, Pereira PA, Koskinen K, Paulin L, Pekkonen E, Haapaniemi E, Kaakkola S, Eerola-Rautio J, Pohja M, Kinnunen E, Murros K, Auvinen P. Gut microbiota are related to Parkinson’s disease and clinical phenotype. Mov Disord 2015; 30: 350-358 [PMID: 25476529 DOI: 10.1002/mds.26069]
23 Annerino DM, Arshad S, Taylor GM, Adler CH, Beach TG, Greene JG. Parkinson’s disease is not associated with gastrointestinal myenteric ganglion neuron loss. Acta Neuropathol 2012; 124: 665-680 [PMID: 22941241 DOI: 10.1007/s00401-012-1040-2]
24 Lebouvier T, Chaumette T, Damier P, Coron E, Touchefeu Y, Vrignaud S, Naveilhan P, Galmiche JP, Bruley des Varannes S, Derkinderen P, Neunlist M. Pathological lesions in colonic biopsies during Parkinson’s disease. Gut 2008; 57: 1741-1743 [PMID: 19022934 DOI: 10.1136/gut.2008.162503]
25 Muntané G , Ferrer I, Martinez-Vicente M. α-synuclein phosphorylation and truncation are normal events in the adult human brain. Neuroscience 2012; 200: 106-119 [PMID: 22079575 DOI: 10.1016/j.neuroscience.2011.10.042]
26 Visanji NP, Marras C, Hazrati LN, Liu LW, Lang AE. Alimentary, my dear Watson? The challenges of enteric α-synuclein as a Parkinson’s disease biomarker. Mov Disord 2014; 29: 444-450 [PMID: 24375496 DOI: 10.1002/mds.25789]
27 Visanji NP, Marras C, Kern DS, Al Dakheel A, Gao A, Liu LW, Lang AE, Hazrati LN. Colonic mucosal a-synuclein lacks specificity as a biomarker for Parkinson disease. Neurology 2015; 84: 609-616 [PMID: 25589666 DOI: 10.1212/WNL.0000000000001240]
28 Beach TG, Adler CH, Dugger BN, Serrano G, Hidalgo J, Henry-Watson J, Shill HA, Sue LI, Sabbagh MN, Akiyama H; Arizona Parkinson’s Disease Consortium. Submandibular gland biopsy for the diagnosis of Parkinson disease. J Neuropathol Exp Neurol 2013; 72: 130-136 [PMID: 23334596 DOI: 10.1097/NEN.0b013e3182805c72]
29 Adler CH, Dugger BN, Hinni ML, Lott DG, Driver-Dunckley E, Hidalgo J, Henry-Watson J, Serrano G, Sue LI, Nagel T, Duffy A, Shill HA, Akiyama H, Walker DG, Beach TG. Submandibular gland needle biopsy for the diagnosis of Parkinson disease. Neurology 2014; 82: 858-864 [PMID: 24500652 DOI: 10.1212/WNL.0000000000000204]
30 van der Marck MA, Dicke HC, Uc EY, Kentin ZH, Borm GF, Bloem BR, Overeem S, Munneke M. Body mass index in Parkinson’s disease: a meta-analysis. Parkinsonism Relat Disord 2012; 18: 263-267 [PMID: 22100523 DOI: 10.1016/j.parkreldis.2011.10.016]
31 Akbar U, He Y, Dai Y, Hack N, Malaty I, McFarland NR, Hess C, Schmidt P, Wu S, Okun MS. Weight loss and impact on quality of life in Parkinson’s disease. PLoS One 2015; 10: e0124541 [PMID: 25938478 DOI: 10.1371/journal.pone.0124541]
32 Sheard JM, Ash S, Mellick GD, Silburn PA, Kerr GK. Malnutrition
Mukherjee A et al . Gut dysfunction in Parkinson’s disease

5749 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
in a sample of community-dwelling people with Parkinson’s disease. PLoS One 2013; 8: e53290 [PMID: 23326408 DOI: 10.1371/journal.pone.0053290]
33 Fereshtehnejad SM, Ghazi L, Shafieesabet M, Shahidi GA, Delbari A, Lökk J. Motor, psychiatric and fatigue features associated with nutritional status and its effects on quality of life in Parkinson’s disease patients. PLoS One 2014; 9: e91153 [PMID: 24608130 DOI: 10.1371/journal.pone.0091153]
34 Pilhatsch M, Kroemer NB, Schneider C, Ebersbach G, Jost WH, Fuchs G, Odin P, Reifschneider G, Bauer M, Reichmann H, Storch A. Reduced body mass index in Parkinson’s disease: contribution of comorbid depression. J Nerv Ment Dis 2013; 201: 76-79 [PMID: 23274301 DOI: 10.1097/NMD.0b013e31827ab2cc]
35 Kim HJ, Oh ES, Lee JH, Moon JS, Oh JE, Shin JW, Lee KJ, Baek IC, Jeong SH, Song HJ, Sohn EH, Lee AY. Relationship between changes of body mass index (BMI) and cognitive decline in Parkinson’s disease (PD). Arch Gerontol Geriatr 2012; 55: 70-72 [PMID: 21763014 DOI: 10.1016/j.archger.2011.06.022]
36 Laudisio A, Vetrano DL, Meloni E, Ricciardi D, Franceschi F, Bentivoglio AR, Bernabei R, Zuccalà G. Dopaminergic agents and nutritional status in Parkinson’s disease. Mov Disord 2014; 29: 1543-1547 [PMID: 25214286 DOI: 10.1002/mds.25991]
37 Lv Z, Qi H, Wang L, Fan X, Han F, Wang H, Bi S. Vitamin D status and Parkinson’s disease: a systematic review and meta-analysis. Neurol Sci 2014; 35: 1723-1730 [PMID: 24847960 DOI: 10.1007/s10072-014-1821-6]
38 van den Bos F, Speelman AD, Samson M, Munneke M, Bloem BR, Verhaar HJ. Parkinson’s disease and osteoporosis. Age Ageing 2013; 42: 156-162 [PMID: 23132148 DOI: 10.1093/ageing/afs161]
39 Morales-Briceño H, Cervantes-Arriaga A, Rodríguez-Violante M, Calleja-Castillo J, Corona T. Overweight is more prevalent in patients with Parkinson’s disease. Arq Neuropsiquiatr 2012; 70: 843-846 [PMID: 23175195 DOI: 10.1590/S0004-282X2012001100004]
40 Vikdahl M, Carlsson M, Linder J, Forsgren L, Håglin L. Weight gain and increased central obesity in the early phase of Parkinson’s disease. Clin Nutr 2014; 33: 1132-1139 [PMID: 24423747 DOI: 10.1016/j.clnu.2013.12.012]
41 Nirenberg MJ, Waters C. Compulsive eating and weight gain related to dopamine agonist use. Mov Disord 2006; 21: 524-529 [PMID: 16261618 DOI: 10.1002/mds.20757]
42 Strowd RE, Herco M, Passmore-Griffin L, Avery B, Haq I, Tatter SB, Tate J, Siddiqui MS. Association between subthalamic nucleus deep brain stimulation and weight gain: Results of a case-control study. Clin Neurol Neurosurg 2016; 140: 38-42 [PMID: 26619034 DOI: 10.1016/j.clineuro.2015.11.002]
43 Hanaoka A, Kashihara K. Increased frequencies of caries, periodontal disease and tooth loss in patients with Parkinson’s disease. J Clin Neurosci 2009; 16: 1279-1282 [PMID: 19570683 DOI: 10.1016/j.jocn.2008.12.027]
44 Müller T, Palluch R, Jackowski J. Caries and periodontal disease in patients with Parkinson’s disease. Spec Care Dentist 2011; 31: 178-181 [PMID: 21950532 DOI: 10.1111/j.1754-4505.2011.00205.x]
45 Zlotnik Y, Balash Y, Korczyn AD, Giladi N, Gurevich T. Disorders of the oral cavity in Parkinson’s disease and parkinsonian syndromes. Parkinsons Dis 2015; 2015: 379482 [PMID: 25685594 DOI: 10.1155/2015/379482]
46 Coon EA, Laughlin RS. Burning mouth syndrome in Parkinson’s disease: dopamine as cure or cause? J Headache Pain 2012; 13: 255-257 [PMID: 22322657 DOI: 10.1007/s10194-012-0421-1]
47 Leibner J, Ramjit A, Sedig L, Dai Y, Wu SS, Jacobson C, Okun MS, Rodriguez RL, Malaty IA, Fernandez HH. The impact of and the factors associated with drooling in Parkinson’s disease. Parkinsonism Relat Disord 2010; 16: 475-477 [PMID: 20064737 DOI: 10.1016/j.parkreldis.2009.12.003]
48 Kalf JG, Smit AM, Bloem BR, Zwarts MJ, Munneke M. Impact of drooling in Parkinson’s disease. J Neurol 2007; 254: 1227-1232 [PMID: 17671806 DOI: 10.1007/s00415-007-0508-9]
49 Srivanitchapoom P, Pandey S, Hallett M. Drooling in Parkinson’s disease: a review. Parkinsonism Relat Disord 2014; 20: 1109-1118 [PMID: 25200111 DOI: 10.1016/j.parkreldis.2014.08.013]
50 Nóbrega AC, Rodrigues B, Torres AC, Scarpel RD, Neves CA, Melo A. Is drooling secondary to a swallowing disorder in patients with Parkinson’s disease? Parkinsonism Relat Disord 2008; 14: 243-245 [PMID: 17892967 DOI: 10.1016/j.parkreldis.2007.08.003]
51 Nicaretta DH, Rosso AL, Mattos JP, Maliska C, Costa MM. Dysphagia and sialorrhea: the relationship to Parkinson’s disease. Arq Gastroenterol 2013; 50: 42-49 [PMID: 23657306 DOI: 10.1590/S0004-28032013000100009]
52 Kalf JG, Munneke M, van den Engel-Hoek L, de Swart BJ, Borm GF, Bloem BR, Zwarts MJ. Pathophysiology of diurnal drooling in Parkinson’s disease. Mov Disord 2011; 26: 1670-1676 [PMID: 21484876 DOI: 10.1002/mds.23720]
53 Proulx M, de Courval FP, Wiseman MA, Panisset M. Salivary production in Parkinson’s disease. Mov Disord 2005; 20: 204-207 [PMID: 15389996 DOI: 10.1002/mds.20189]
54 Ou R, Guo X, Wei Q, Cao B, Yang J, Song W, Shao N, Zhao B, Chen X, Shang H. Prevalence and clinical correlates of drooling in Parkinson disease: a study on 518 Chinese patients. Parkinsonism Relat Disord 2015; 21: 211-215 [PMID: 25537930 DOI: 10.1016/j.parkreldis.2014.12.004]
55 Kalf JG, Bloem BR, Munneke M. Diurnal and nocturnal drooling in Parkinson’s disease. J Neurol 2012; 259: 119-123 [PMID: 21698387 DOI: 10.1007/s00415-011-6138-2]
56 Ou R, Guo X, Wei Q, Cao B, Yang J, Song W, Chen K, Zhao B, Chen X, Shang H. Diurnal drooling in Chinese patients with Parkinson’s disease. J Neurol Sci 2015; 353: 74-78 [PMID: 25896289 DOI: 10.1016/j.jns.2015.04.007]
57 Rana AQ, Khondker S, Kabir A, Owalia A, Khondker S, Emre M. Impact of cognitive dysfunction on drooling in Parkinson’s disease. Eur Neurol 2013; 70: 42-45 [PMID: 23711510 DOI: 10.1159/000348571]
58 Rodrigues B, Nóbrega AC, Sampaio M, Argolo N, Melo A. Silent saliva aspiration in Parkinson’s disease. Mov Disord 2011; 26: 138-141 [PMID: 21322025 DOI: 10.1002/mds.23301]
59 Arbouw ME, Movig KL, Koopmann M, Poels PJ, Guchelaar HJ, Egberts TC, Neef C, van Vugt JP. Glycopyrrolate for sialorrhea in Parkinson disease: a randomized, double-blind, crossover trial. Neurology 2010; 74: 1203-1207 [PMID: 20385892 DOI: 10.1212/WNL.0b013e3181d8c1b7]
60 Thomsen TR, Galpern WR, Asante A, Arenovich T, Fox SH. Ipratropium bromide spray as treatment for sialorrhea in Parkinson’s disease. Mov Disord 2007; 22: 2268-2273 [PMID: 17876852 DOI: 10.1002/mds.21730]
61 Lloret SP, Nano G, Carrosella A, Gamzu E, Merello M. A double-blind, placebo-controlled, randomized, crossover pilot study of the safety and efficacy of multiple doses of intra-oral tropicamide films for the short-term relief of sialorrhea symptoms in Parkinson’s disease patients. J Neurol Sci 2011; 310: 248-250 [PMID: 21636098 DOI: 10.1016/j.jns.2011.05.021]
62 Petracca M, Guidubaldi A, Ricciardi L, Ialongo T, Del Grande A, Mulas D, Di Stasio E, Bentivoglio AR. Botulinum Toxin A and B in sialorrhea: Long-term data and literature overview. Toxicon 2015; 107: 129-140 [PMID: 26327120 DOI: 10.1016/j.toxicon.2015.08.014]
63 Egevad G, Petkova VY, Vilholm OJ. Sialorrhea in patients with Parkinson’s disease: safety and administration of botulinum neurotoxin. J Parkinsons Dis 2014; 4: 321-326 [PMID: 24919823 DOI: 10.3233/JPD-140379]
64 Postma AG, Heesters M, van Laar T. Radiotherapy to the salivary glands as treatment of sialorrhea in patients with parkinsonism. Mov Disord 2007; 22: 2430-2435 [PMID: 17960826 DOI: 10.1002/mds.21752]
65 Hawkey NM, Zaorsky NG, Galloway TJ. The role of radiation therapy in the management of sialorrhea: A systematic review. Laryngoscope 2016; 126: 80-85 [PMID: 26152655 DOI: 10.1002/lary.25444]
66 Carneiro D, das Graças Wanderley de Sales Coriolano M, Belo LR, de Marcos Rabelo AR, Asano AG, Lins OG. Quality of life related to swallowing in Parkinson’s disease. Dysphagia 2014; 29: 578-582 [PMID: 24952632 DOI: 10.1007/s00455-014-9548-3]
Mukherjee A et al . Gut dysfunction in Parkinson’s disease

5750 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
67 Kalf JG, de Swart BJ, Bloem BR, Munneke M. Prevalence of oropharyngeal dysphagia in Parkinson’s disease: a meta-analysis. Parkinsonism Relat Disord 2012; 18: 311-315 [PMID: 22137459 DOI: 10.1016/j.parkreldis.2011.11.006]
68 Suttrup I, Warnecke T. Dysphagia in Parkinson’s Disease. Dysphagia 2016; 31: 24-32 [PMID: 26590572 DOI: 10.1007/s00455-015-9671-9]
69 Kim YH, Oh BM, Jung IY, Lee JC, Lee GJ, Han TR. Spatiotemporal characteristics of swallowing in Parkinson’s disease. Laryngoscope 2015; 125: 389-395 [PMID: 25093527 DOI: 10.1002/lary.24869]
70 Suntrup S, Teismann I, Bejer J, Suttrup I, Winkels M, Mehler D, Pantev C, Dziewas R, Warnecke T. Evidence for adaptive cortical changes in swallowing in Parkinson’s disease. Brain 2013; 136: 726-738 [PMID: 23412935 DOI: 10.1093/brain/awt004]
71 Kikuchi A, Baba T, Hasegawa T, Kobayashi M, Sugeno N, Konno M, Miura E, Hosokai Y, Ishioka T, Nishio Y, Hirayama K, Suzuki K, Aoki M, Takahashi S, Fukuda H, Itoyama Y, Mori E, Takeda A. Hypometabolism in the supplementary and anterior cingulate cortices is related to dysphagia in Parkinson’s disease: a cross-sectional and 3-year longitudinal cohort study. BMJ Open 2013; 3: [PMID: 23457325 DOI: 10.1136/bmjopen-2012-002249]
72 Lee KD, Koo JH, Song SH, Jo KD, Lee MK, Jang W. Central cholinergic dysfunction could be associated with oropharyngeal dysphagia in early Parkinson’s disease. J Neural Transm (Vienna) 2015; 122: 1553-1561 [PMID: 26199040 DOI: 10.1007/s00702-015-1427-z]
73 Mu L, Sobotka S, Chen J, Su H, Sanders I, Adler CH, Shill HA, Caviness JN, Samanta JE, Beach TG; Arizona Parkinson’s Disease Consortium. Alpha-synuclein pathology and axonal degeneration of the peripheral motor nerves innervating pharyngeal muscles in Parkinson disease. J Neuropathol Exp Neurol 2013; 72: 119-129 [PMID: 23334595 DOI: 10.1097/NEN.0b013e3182801cde]
74 Mu L, Sobotka S, Chen J, Su H, Sanders I, Nyirenda T, Adler CH, Shill HA, Caviness JN, Samanta JE, Sue LI, Beach TG; Arizona Parkinson’s Disease Consortium. Parkinson disease affects peripheral sensory nerves in the pharynx. J Neuropathol Exp Neurol 2013; 72: 614-623 [PMID: 23771215 DOI: 10.1097/NEN.0b013e3182965886]
75 Cereda E, Cilia R, Klersy C, Canesi M, Zecchinelli AL, Mariani CB, Tesei S, Sacilotto G, Meucci N, Zini M, Isaias IU, Cassani E, Goldwurm S, Barichella M, Pezzoli G. Swallowing disturbances in Parkinson’s disease: a multivariate analysis of contributing factors. Parkinsonism Relat Disord 2014; 20: 1382-1387 [PMID: 25456827 DOI: 10.1016/j.parkreldis.2014.09.031]
76 Han M, Ohnishi H, Nonaka M, Yamauchi R, Hozuki T, Hayashi T, Saitoh M, Hisahara S, Imai T, Shimohama S, Mori M. Relationship between dysphagia and depressive states in patients with Parkinson’s disease. Parkinsonism Relat Disord 2011; 17: 437-439 [PMID: 21458355 DOI: 10.1016/j.parkreldis.2011.03.006]
77 Kim JS, Youn J, Suh MK, Kim TE, Chin J, Park S, Cho JW. Cognitive and Motor Aspects of Parkinson’s Disease Associated with Dysphagia. Can J Neurol Sci 2015; 42: 395-400 [PMID: 26551089 DOI: 10.1017/cjn.2015.304]
78 Jones CA, Ciucci MR. Multimodal Swallowing Evaluation with High-Resolution Manometry Reveals Subtle Swallowing Changes in Early and Mid-Stage Parkinson Disease. J Parkinsons Dis 2016; 6: 197-208 [PMID: 26891176]
79 Sung HY, Kim JS, Lee KS, Kim YI, Song IU, Chung SW, Yang DW, Cho YK, Park JM, Lee IS, Kim SW, Chung IS, Choi MG. The prevalence and patterns of pharyngoesophageal dysmotility in patients with early stage Parkinson’s disease. Mov Disord 2010; 25: 2361-2368 [PMID: 20669313 DOI: 10.1002/mds.23290]
80 Speyer R. Oropharyngeal dysphagia: screening and assessment. Otolaryngol Clin North Am 2013; 46: 989-1008 [PMID: 24262955 DOI: 10.1016/j.otc.2013.08.004]
81 Correa-Flores M, Arch-Tirado E, Villeda-Miranda A, Rocha-Cacho KE, Verduzco-Mendoza A, Hernández-López X. Analysis of oropharyngeal dysphagia through fibroendoscopy evaluation of swallowing in patients with Parkinson’s disease. Cir Cir 2012; 80: 31-37 [PMID: 22472150]
82 Argolo N , Sampaio M, Pinho P, Melo A, Nóbrega AC.
Videofluoroscopic Predictors of Penetration-Aspiration in Parkinson’s Disease Patients. Dysphagia 2015; 30: 751-758 [PMID: 26492880 DOI: 10.1007/s00455-015-9653-y]
83 Ellerston JK, Heller AC, Houtz DR, Kendall KA. Quantitative Measures of Swallowing Deficits in Patients With Parkinson’s Disease. Ann Otol Rhinol Laryngol 2016; 125: 385-392 [PMID: 26602905]
84 Troche MS, Brandimore AE, Okun MS, Davenport PW, Hegland KW. Decreased cough sensitivity and aspiration in Parkinson disease. Chest 2014; 146: 1294-1299 [PMID: 24968148 DOI: 10.1378/chest.14-0066]
85 Lin CW, Chang YC, Chen WS, Chang K, Chang HY, Wang TG. Prolonged swallowing time in dysphagic Parkinsonism patients with aspiration pneumonia. Arch Phys Med Rehabil 2012; 93: 2080-2084 [PMID: 22846454 DOI: 10.1016/j.apmr.2012.07.010]
86 Luchesi KF, Kitamura S, Mourão LF. Dysphagia progression and swallowing management in Parkinson’s disease: an observational study. Braz J Otorhinolaryngol 2015; 81: 24-30 [PMID: 25450106 DOI: 10.1016/j.bjorl.2014.09.006]
87 Heijnen BJ, Speyer R, Baijens LW, Bogaardt HC. Neuromuscular electrical stimulation versus traditional therapy in patients with Parkinson’s disease and oropharyngeal dysphagia: effects on quality of life. Dysphagia 2012; 27: 336-345 [PMID: 22081122 DOI: 10.1007/s00455-011-9371-z]
88 van Hooren MR, Baijens LW, Voskuilen S, Oosterloo M, Kremer B. Treatment effects for dysphagia in Parkinson’s disease: a systematic review. Parkinsonism Relat Disord 2014; 20: 800-807 [PMID: 24794097 DOI: 10.1016/j.parkreldis.2014.03.026]
89 Melo A, Monteiro L. Swallowing improvement after levodopa treatment in idiopathic Parkinson’s disease: lack of evidence. Parkinsonism Relat Disord 2013; 19: 279-281 [PMID: 23231973 DOI: 10.1016/j.parkreldis.2012.11.017]
90 Sutton JP. Dysphagia in Parkinson’s disease is responsive to levodopa. Parkinsonism Relat Disord 2013; 19: 282-284 [PMID: 23333537 DOI: 10.1016/j.parkreldis.2012.11.007]
91 Hirano M, Isono C, Sakamoto H, Ueno S, Kusunoki S, Nakamura Y. Rotigotine Transdermal Patch Improves Swallowing in Dysphagic Patients with Parkinson’s Disease. Dysphagia 2015; 30: 452-456 [PMID: 25966655 DOI: 10.1007/s00455-015-9622-5]
92 Troche MS, Brandimore AE, Foote KD, Okun MS. Swallowing and deep brain stimulation in Parkinson’s disease: a systematic review. Parkinsonism Relat Disord 2013; 19: 783-788 [PMID: 23726461 DOI: 10.1016/j.parkreldis.2013.05.001]
93 Troche MS, Brandimore AE, Foote KD, Morishita T, Chen D, Hegland KW, Okun MS. Swallowing outcomes following unilateral STN vs. GPi surgery: a retrospective analysis. Dysphagia 2014; 29: 425-431 [PMID: 24652582 DOI: 10.1007/s00455-014-9522-0]
94 Tanaka Y, Kato T, Nishida H, Yamada M, Koumura A, Sakurai T, Hayashi Y, Kimura A, Hozumi I, Araki H, Murase M, Nagaki M, Moriwaki H, Inuzuka T. Is there a delayed gastric emptying of patients with early-stage, untreated Parkinson’s disease? An analysis using the 13C-acetate breath test. J Neurol 2011; 258: 421-426 [PMID: 20938781 DOI: 10.1007/s00415-010-5769-z]
95 Marrinan S, Emmanuel AV, Burn DJ. Delayed gastric emptying in Parkinson’s disease. Mov Disord 2014; 29: 23-32 [PMID: 24151126 DOI: 10.1002/mds.25708]
96 Heetun ZS, Quigley EM. Gastroparesis and Parkinson’s disease: a systematic review. Parkinsonism Relat Disord 2012; 18: 433-440 [PMID: 22209346 DOI: 10.1016/j.parkreldis.2011.12.004]
97 Goetze O, Nikodem AB, Wiezcorek J, Banasch M, Przuntek H, Mueller T, Schmidt WE, Woitalla D. Predictors of gastric emptying in Parkinson’s disease. Neurogastroenterol Motil 2006; 18: 369-375 [PMID: 16629864 DOI: 10.1111/j.1365-2982.2006.00780.x]
98 Pasricha PJ, Parkman HP. Gastroparesis: definitions and diagnosis. Gastroenterol Clin North Am 2015; 44: 1-7 [PMID: 25667018 DOI: 10.1016/j.gtc.2014.11.001]
99 Goetze O, Wieczorek J, Mueller T, Przuntek H, Schmidt WE, Woitalla D. Impaired gastric emptying of a solid test meal in patients with Parkinson’s disease using 13C-sodium octanoate breath test. Neurosci Lett 2005; 375: 170-173 [PMID: 15694254 DOI: 10.1016/
Mukherjee A et al . Gut dysfunction in Parkinson’s disease

5751 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
j.neulet.2004.11.007]100 Unger MM, Hattemer K, Möller JC, Schmittinger K, Mankel K,
Eggert K, Strauch K, Tebbe JJ, Keil B, Oertel WH, Heverhagen JT, Knake S. Real-time visualization of altered gastric motility by magnetic resonance imaging in patients with Parkinson’s disease. Mov Disord 2010; 25: 623-628 [PMID: 20213819 DOI: 10.1002/mds.22841]
101 Naftali T, Gadoth N, Huberman M, Novis B. Electrogastrography in patients with Parkinson’s disease. Can J Neurol Sci 2005; 32: 82-86 [PMID: 15825551 DOI: 10.1017/S0317167100016929]
102 Müller T, Erdmann C, Bremen D, Schmidt WE, Muhlack S, Woitalla D, Goetze O. Impact of gastric emptying on levodopa pharmacokinetics in Parkinson disease patients. Clin Neuropharmacol 2006; 29: 61-67 [PMID: 16614536 DOI: 10.1097/00002826-200603000-00001]
103 Doi H, Sakakibara R, Sato M, Masaka T, Kishi M, Tateno A, Tateno F, Tsuyusaki Y, Takahashi O. Plasma levodopa peak delay and impaired gastric emptying in Parkinson’s disease. J Neurol Sci 2012; 319: 86-88 [PMID: 22632782 DOI: 10.1016/j.jns.2012.05.010]
104 Soykan I, Sarosiek I, Shifflett J, Wooten GF, McCallum RW. Effect of chronic oral domperidone therapy on gastrointestinal symptoms and gastric emptying in patients with Parkinson’s disease. Mov Disord 1997; 12: 952-957 [PMID: 9399220 DOI: 10.1002/mds.870120618]
105 Rossi M, Giorgi G. Domperidone and long QT syndrome. Curr Drug Saf 2010; 5: 257-262 [PMID: 20394569 DOI: 10.2174/157488610791698334]
106 Doi H, Sakakibara R, Sato M, Hirai S, Masaka T, Kishi M, Tsuyusaki Y, Tateno A, Tateno F, Takahashi O, Ogata T. Nizatidine ameliorates gastroparesis in Parkinson’s disease: a pilot study. Mov Disord 2014; 29: 562-566 [PMID: 24375669 DOI: 10.1002/mds.25777]
107 Karasawa H, Pietra C, Giuliano C, Garcia-Rubio S, Xu X, Yakabi S, Taché Y, Wang L. New ghrelin agonist, HM01 alleviates constipation and L-dopa-delayed gastric emptying in 6-hydroxydopamine rat model of Parkinson’s disease. Neurogastroenterol Motil 2014; 26: 1771-1782 [PMID: 25327342 DOI: 10.1111/nmo.12459]
108 Kwon KY, Jo KD, Lee MK, Oh M, Kim EN, Park J, Kim JS, Youn J, Oh E, Kim HT, Oh MY, Jang W. Low Serum Vitamin D Levels May Contribute to Gastric Dysmotility in de novo Parkinson’s Disease. Neurodegener Dis 2016; 16: 199-205 [PMID: 26735311]
109 Gil RA, Hwynn N, Fabian T, Joseph S, Fernandez HH. Botulinum toxin type A for the treatment of gastroparesis in Parkinson’s disease patients. Parkinsonism Relat Disord 2011; 17: 285-287 [PMID: 21296606 DOI: 10.1016/j.parkreldis.2011.01.007]
110 Arai E, Arai M, Uchiyama T, Higuchi Y, Aoyagi K, Yamanaka Y, Yamamoto T, Nagano O, Shiina A, Maruoka D, Matsumura T, Nakagawa T, Katsuno T, Imazeki F, Saeki N, Kuwabara S, Yokosuka O. Subthalamic deep brain stimulation can improve gastric emptying in Parkinson’s disease. Brain 2012; 135: 1478-1485 [PMID: 22522940 DOI: 10.1093/brain/aws086]
111 Soffer EE. Gastric electrical stimulation for gastroparesis. J Neurogastroenterol Motil 2012; 18: 131-137 [PMID: 22523722 DOI: 10.5056/jnm.2012.18.2.131]
112 Ondo WG, Shinawi L, Moore S. Comparison of orally dissolving carbidopa/levodopa (Parcopa) to conventional oral carbidopa/levodopa: A single-dose, double-blind, double-dummy, placebo-controlled, crossover trial. Mov Disord 2010; 25: 2724-2727 [PMID: 20925074 DOI: 10.1002/mds.23158]
113 Stocchi F, Zappia M, Dall’Armi V, Kulisevsky J, Lamberti P, Obeso JA; Melevodopa Plus Carbidopa Study Group. Melevodopa/carbidopa effervescent formulation in the treatment of motor fluctuations in advanced Parkinson’s disease. Mov Disord 2010; 25: 1881-1887 [PMID: 20669296 DOI: 10.1002/mds.23206]
114 Olanow CW, Kieburtz K, Odin P, Espay AJ, Standaert DG, Fernandez HH, Vanagunas A, Othman AA, Widnell KL, Robieson WZ, Pritchett Y, Chatamra K, Benesh J, Lenz RA, Antonini A. Continuous intrajejunal infusion of levodopa-carbidopa intestinal gel for patients with advanced Parkinson’s disease: a randomised, controlled, double-blind, double-dummy study. Lancet Neurol
2014; 13: 141-149 [PMID: 24361112 DOI: 10.1016/S1474-4422(13)70293-X]
115 Trenkwalder C, Chaudhuri KR, García Ruiz PJ, LeWitt P, Katzenschlager R, Sixel-Döring F, Henriksen T, Sesar Á, Poewe W, Baker M, Ceballos-Baumann A, Deuschl G, Drapier S, Ebersbach G, Evans A, Fernandez H, Isaacson S, van Laar T, Lees A, Lewis S, Martínez Castrillo JC, Martinez-Martin P, Odin P, O’Sullivan J, Tagaris G, Wenzel K; Expert Consensus Group for Use of Apomorphine in Parkinson’s Disease. Expert Consensus Group report on the use of apomorphine in the treatment of Parkinson’s disease--Clinical practice recommendations. Parkinsonism Relat Disord 2015; 21: 1023-1030 [PMID: 26189414 DOI: 10.1016/j.parkreldis.2015.06.012]
116 Liu Y, Li W, Tan C, Liu X, Wang X, Gui Y, Qin L, Deng F, Hu C, Chen L. Meta-analysis comparing deep brain stimulation of the globus pallidus and subthalamic nucleus to treat advanced Parkinson disease. J Neurosurg 2014; 121: 709-718 [PMID: 24905564 DOI: 10.3171/2014.4.JNS131711]
117 Miftahussurur M, Yamaoka Y. Diagnostic Methods of Helicobacter pylori Infection for Epidemiological Studies: Critical Importance of Indirect Test Validation. Biomed Res Int 2016; 2016: 4819423 [PMID: 26904678 DOI: 10.1155/2016/4819423]
118 Gabrielli M, D’Angelo G, Di Rienzo T, Scarpellini E, Ojetti V. Diagnosis of small intestinal bacterial overgrowth in the clinical practice. Eur Rev Med Pharmacol Sci 2013; 17 Suppl 2: 30-35 [PMID: 24443065]
119 Jost WH. Gastrointestinal dysfunction in Parkinson’s Disease. J Neurol Sci 2010; 289: 69-73 [PMID: 19717168 DOI: 10.1016/j.jns.2009.08.020]
120 Bassotti G, Maggio D, Battaglia E, Giulietti O, Spinozzi F, Reboldi G, Serra AM, Emanuelli G, Chiarioni G. Manometric investigation of anorectal function in early and late stage Parkinson’s disease. J Neurol Neurosurg Psychiatry 2000; 68: 768-770 [PMID: 10811703 DOI: 10.1136/jnnp.68.6.768]
121 Savica R, Carlin JM, Grossardt BR, Bower JH, Ahlskog JE, Maraganore DM, Bharucha AE, Rocca WA. Medical records documentation of constipation preceding Parkinson disease: A case-control study. Neurology 2009; 73: 1752-1758 [PMID: 19933976 DOI: 10.1212/WNL.0b013e3181c34af5]
122 Abbott RD, Petrovitch H, White LR, Masaki KH, Tanner CM, Curb JD, Grandinetti A, Blanchette PL, Popper JS, Ross GW. Frequency of bowel movements and the future risk of Parkinson’s disease. Neurology 2001; 57: 456-462 [PMID: 11502913 DOI: 10.1212/WNL.57.3.456]
123 Lin CH, Lin JW, Liu YC, Chang CH, Wu RM. Risk of Parkinson’s disease following severe constipation: a nationwide population-based cohort study. Parkinsonism Relat Disord 2014; 20: 1371-1375 [PMID: 25293395 DOI: 10.1016/j.parkreldis.2014.09.026]
124 Jost WH , Schrank B. Defecatory disorders in de novo Parkinsonians--colonic transit and electromyogram of the external anal sphincter. Wien Klin Wochenschr 1998; 110: 535-537 [PMID: 9782572]
125 Mathers SE, Kempster PA, Swash M, Lees AJ. Constipation and paradoxical puborectalis contraction in anismus and Parkinson’s disease: a dystonic phenomenon? J Neurol Neurosurg Psychiatry 1988; 51: 1503-1507 [PMID: 3221217 DOI: 10.1136/jnnp.51.12.1503]
126 Pagano G, Tan EE, Haider JM, Bautista A, Tagliati M. Constipation is reduced by beta-blockers and increased by dopaminergic medications in Parkinson’s disease. Parkinsonism Relat Disord 2015; 21: 120-125 [PMID: 25483722 DOI: 10.1016/j.parkreldis.2014.11.015]
127 Tateno F, Sakakibara R, Yokoi Y, Kishi M, Ogawa E, Uchiyama T, Yamamoto T, Yamanishi T, Takahashi O. Levodopa ameliorated anorectal constipation in de novo Parkinson’s disease: The QL-GAT study. Parkinsonism Relat Disord 2011; 17: 662-666 [PMID: 21705259 DOI: 10.1016/j.parkreldis.2011.06.002]
128 Sakakibara R, Odaka T, Uchiyama T, Asahina M, Yamaguchi K, Yamaguchi T, Yamanishi T, Hattori T. Colonic transit time and rectoanal videomanometry in Parkinson’s disease. J Neurol
Mukherjee A et al . Gut dysfunction in Parkinson’s disease

5752 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Neurosurg Psychiatry 2003; 74: 268-272 [PMID: 12531969 DOI: 10.1136/jnnp.74.2.268]
129 Krogh K, Christensen P. Neurogenic colorectal and pelvic floor dysfunction. Best Pract Res Clin Gastroenterol 2009; 23: 531-543 [PMID: 19647688 DOI: 10.1016/j.bpg.2009.04.012]
130 Bharucha AE, Dorn SD, Lembo A, Pressman A. American Gastroenterological Association medical position statement on constipation. Gastroenterology 2013; 144: 211-217 [PMID: 23261064 DOI: 10.1053/j.gastro.2012.10.029]
131 Zangaglia R, Martignoni E, Glorioso M, Ossola M, Riboldazzi G, Calandrella D, Brunetti G, Pacchetti C. Macrogol for the treatment of constipation in Parkinson’s disease. A randomized placebo-controlled study. Mov Disord 2007; 22: 1239-1244 [PMID: 17566120 DOI: 10.1002/mds.21243]
132 Ondo WG, Kenney C, Sullivan K, Davidson A, Hunter C, Jahan I, McCombs A, Miller A, Zesiewicz TA. Placebo-controlled trial of lubiprostone for constipation associated with Parkinson disease.
Neurology 2012; 78: 1650-1654 [PMID: 22573627 DOI: 10.1212/WNL.0b013e3182574f28]
133 Sakakibara R, Doi H, Sato M, Hirai S, Masaka T, Kishi M, Tsuyusaki Y, Tateno A, Tateno F, Aiba Y, Ogata T, Suzuki Y. Nizatidine ameliorates slow transit constipation in Parkinson’s disease. J Am Geriatr Soc 2015; 63: 399-401 [PMID: 25688620 DOI: 10.1111/jgs.13279]
134 Rossi M, Merello M, Perez-Lloret S. Management of constipation in Parkinson’s disease. Expert Opin Pharmacother 2015; 16: 547-557 [PMID: 25539892 DOI: 10.1517/14656566.2015.997211]
135 Stern T, Davis AM. Evaluation and Treatment of Patients With Constipation. JAMA 2016; 315: 192-193 [PMID: 26757468 DOI: 10.1001/jama.2015.16995]
136 Cadeddu F, Bentivoglio AR, Brandara F, Marniga G, Brisinda G, Maria G. Outlet type constipation in Parkinson’s disease: results of botulinum toxin treatment. Aliment Pharmacol Ther 2005; 22: 997-1003 [PMID: 16268975 DOI: 10.1111/j.1365-2036.2005.02669.x]
P- Reviewer: Franceschi F, Garcia-Mena J S- Editor: Ma YJ L- Editor: A E- Editor: Wang CH
Mukherjee A et al . Gut dysfunction in Parkinson’s disease

Acetic acid chromoendoscopy: Improving neoplasia detection in Barrett's esophagus
Fergus JQ Chedgy, Sharmila Subramaniam, Kesavan Kandiah, Sreedhari Thayalasekaran, Pradeep Bhandari
Fergus JQ Chedgy, Sharmila Subramaniam, Kesavan Kandiah, Sreedhari Thayalasekaran, Pradeep Bhandari, Department of Gastroenterology, Queen Alexandra Hospital, PO6 3LY Portsmouth, United Kingdom
Author contributions: Chedgy FJQ was the lead author on the article and contributed to all sections of the manuscript and performed a literature review; Subramaniam S performed a literature review and wrote the section on acetic acid in the surveillance population; Kandiah K performed a literature review and wrote the section on acetic acid for the diagnosis of non-neoplastic Barrett’s esophagus; Thayalasekaran S performed a literature review and critically appraised the meta-analysis data of acetic acid for Barrett’s esophagus; Bhandari P provided critical revision of article and is senior author.
Conflict-of-interest statement: No potential conflicts of interest relevant to this article were reported.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Manuscript source: Invited manuscript
Correspondence to: Pradeep Bhandari, MBBS, MD, FRCP, Department of Gastroenterology, Queen Alexandra Hospital, Southwick Hill Rd, PO6 3LY Portsmouth, United Kingdom. [email protected] Telephone: +44-2392-286255Fax: +44-2392-286822
Received: March 11, 2016Peer-review started: March 12, 2016First decision: April 14, 2016Revised: April 26, 2016Accepted: May 23, 2016 Article in press: May 23, 2016Published online: July 7, 2016
AbstractBarrett’s esophagus (BE) is an important condition given its significant premalignant potential and dismal five-year survival outcomes of advanced esophageal adenocarcinoma. It is therefore suggested that patients with a diagnosis of BE undergo regular surveillance in order to pick up dysplasia at an earlier stage to improve survival. Current “gold-standard” surveillance protocols suggest targeted biopsy of visible lesions followed by four quadrant random biopsies every 2 cm. However, this method of Barrett’s surveillance is fraught with poor endoscopist compliance as the procedures are time consuming and poorly tolerated by patients. There are also significant miss-rates with this technique for the detection of neoplasia as only 13% of early neoplastic lesions appear as visible nodules. Despite improvements in endoscope resolution these problems persist. Chromoendoscopy is an extremely useful adjunct to enhance mucosal visualization and characterization of Barrett’s mucosa. Acetic acid chromoendoscopy (AAC) is a simple, non-proprietary technique that can significantly improve neoplasia detection rates. This topic highlight summarizes the current evidence base behind AAC for the detection of neoplasia in BE and provides an insight into the direction of travel for further research in this area.
Key words: Barrett’s esophagus; Acetic acid; Esophageal adenocarcinoma; Chromoendoscopy; Dysplasia
© The Author(s) 2016. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Neoplasia detection in surveillance of Barrett’s esophagus (BE) remains challenging as current gold-standard four quadrant biopsies have a high miss-rate and are poorly adhered to. Evidence to support the use of acetic acid chromoendoscopy (AAC) is growing. We discuss the current evidence of AAC in BE and the direction of travel for future research.
MINIREVIEWS
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.3748/wjg.v22.i25.5753
5753 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
World J Gastroenterol 2016 July 7; 22(25): 5753-5760 ISSN 1007-9327 (print) ISSN 2219-2840 (online)
© 2016 Baishideng Publishing Group Inc. All rights reserved.

Chedgy FJQ, Subramaniam S, Kandiah K, Thayalasekaran S, Bhandari P. Acetic acid chromoendoscopy: Improving neoplasia detection in Barrett’s esophagus. World J Gastroenterol 2016; 22(25): 5753-5760 Available from: URL: http://www.wjgnet.com/1007-9327/full/v22/i25/5753.htm DOI: http://dx.doi.org/10.3748/wjg.v22.i25.5753
INTRODUCTIONThe incidence of esophageal cancer is increasing[1], representing the ninth most common cancer in the United Kingdom. Seven thousand and eight hundred people are diagnosed with the condition every year, and it accounts for 5% of all cancer deaths in the United Kingdom[2]. It is well recognized that Barrett’s esophagus (BE) is a significant risk factor for the development of esophageal adenocarcinoma (EAC) and is present in 1.6% of the general population[3] and in up to 20% of patients with gastroesophageal reflux[4].
BE is defined as an esophagus in which any portion of the normal distal squamous epithelial lining has been replaced by metaplastic columnar epithelium, which is clearly visible endoscopically above the gastroesophageal junction[5]. It is universally recognized that the presence of intestinal metaplasia (IM) confers an increased risk of developing Barrett’srelated EAC and that IM is present in the vast majority of longsegment Barrett’s[6]. The development of Barrett’s EAC is postulated to occur in a progressive fashion from IM to low grade dysplasia (LGD) to high grade dysplasia (HGD) and then EAC. The annual rate of transformation into EAC in patients with nondysplastic BE is estimated to be between 0.07% and 0.82%[79]. However, the annual rate of progression from LGD to HGD or EAC is as high as 8.8% as demonstrated by the recent SURF trial[10] and from HGD to EAC is 12% to 40%[11,12]. The aim of endoscopic surveillance is to alter the natural history of the disease by identifying neoplasia at an earlier stage and thus instituting curative endoscopic therapy.
Established surveillance protocols suggest taking targeted biopsies of visible lesions and random four quadrant biopsies (4QBS) every 2 cm (Cleveland protocol) which reportedly proffers the maximum yield of dysplasia in comparison with other biopsy protocols[13]. However, there are several drawbacks to this technique. With only 13% of early neoplastic lesions appearing as visible nodules[14], a significant proportion of Barrett’s neoplasia is not visible on highdefinition whitelight endoscopy alone, with reported sensitivity in the range 40%64% and specificity 98%100%[15]. These nonvisible neoplastic foci can occupy areas as small as 0.5 cm2[16]. Unsurprisingly, there is a significant missrate with 4QBS. Studies comparing 4QBS with surgical resection specimen have shown that 41%66% of dysplastic lesions
are missed by 4QBS[17,18]. The total mucosal surface sampled with 4QBS is equivalent to 0.5 cm2 equating to sampling of only 3.5% of an averagelength BE. 4QBS are notoriously poorly adhered to[19], with worse adherence for longer segments, further compounding missrates. In addition, 4QBS are timeconsuming and poorly tolerated by patients. The cost of processing 4QBS is significant, with each cassette of tissue costing £58.90 ($90.61) to process[20].
These pitfalls in surveillance have prompted evaluation of more effective techniques to improve the diagnostic accuracy for the detection of IM and early Barrett’s neoplasia, the most promising of which is acetic acid chromoendoscopy (AAC). This review aims to summarize the current evidence for AAC in BE and provide insight into the direction of travel for further research in this area.
ACETIC ACID MECHANISM OF ACTIONThe use of acetic acid (AA) in the digestive tract was first reported by Guelrud and Herrera[21], to aid in the identification of small islands of BE following ablative therapy. The technique was derived from gynecology where AA instilled onto the cervix has been used to highlight dysplastic areas during screening for cervical intraepithelial neoplasia[22]. When AA is sprayed onto squamous epithelium, there is an acetowhitening reaction caused by masking of the submucosal capillaries and increasing opacity of the mucosal surface[23]. As AA (pH 2.53.0) infiltrates through the multilayered squamous epithelium it is neutralized, which protects the subepithelial stroma and vasculature[24]. In contrast, when sprayed on Barrett’s epithelium, at low concentrations (1%3%), AA initially eliminates the superficial mucus layer by breakage of glycoprotein disulphide bonds. The unbuffered acid then causes a reversible acetylation of cellular proteins and a change in the spatial properties of nuclear and cytoplasmic proteins, initially causing an acetowhitening reaction that highlights the surface pattern (Figure 1). With the disruption of the mucus layer, AA reaches stromal capillaries causing vascular congestion, leading to focal erythema but this is hidden under the acetowhite mucosa and only becomes visible after the loss of acetowhitening (LAW). This focal redness due to LAW was first described, by the Portsmouth group in 2010[2], as a strong predictor of neoplasia. The exact mechanism remains unclear but it is believed that the difference in acetowhitening reaction between nonneoplastic and neoplastic mucosa is due to the difference in the nucleocytoplasmic ratio between nonneoplastic and neoplastic cells. The low cytoplasmic content of neoplastic cells allows them to lose acetowhitening quicker than nonneoplastic cells. This reaction leads to focal erythema a pathognomic sign of neoplasia with AAC.
5754 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Chedgy FJQ et al . Acetic acid chromoendoscopy

ACETIC ACID FOR THE DIAGNOSIS OF NON-NEOPLASTIC BARRETT’S ESOPHAGUSThe diagnosis of Barrett’s esophagus, according to American society guidelines[25], is defined as the presence of esophageal IM. As IM is not readily identifiable by white light endoscopy, this diagnosis is made based on histology. Efforts have been made to visually identify IM by means of enhanced endoscopy. AA coupled with magnification endoscopy has been shown to accurately identify IM[21]. Guelrud et al[21] classified the surface pattern of Barrett’s mucosa into 4 categories: (1) round pits; (2) reticular (circular or oval pits); (3) villous (fine villiform appearance without visible pits); and (4) ridged (thick villi with convoluted, cerebriform appearance without visible pits).
They found that Pattern Ⅰ corresponded to fundic or cardiac type without IM and Patterns Ⅱ, Ⅲ, an Ⅳ each corresponded to IM with increasing sensitivities. The overall accuracy of AA with magnification endoscopy for the diagnosis of IM was 92.2%. These findings were reliably replicated by Toyoda et al[26] and Fortun et al[27].
A recent metaanalysis by Coletta et al[28] evaluated the use of AA for the detection of IM and HGD/EAC in patients with BE using histology as the reference standard. A total of 13 prospective studies (1690 patients) were included in the metaanalysis. Eight of the 13 studies, provided data on the diagnosis of IM. For the characterization of IM, the pooled sensitivity, specificity, positive likelihood ratio (LR+), and negative likelihood ratio (LR) for all the included studies (8 studies, 516 patients) were 0.96 (95%CI: 0.830.99), 0.69 (95%CI: 0.540.81), 3.0 (95%CI: 2.04.7) and 0.06 (95%CI: 0.010.26), respectively. No significant sources of heterogeneity were identified on subgroup analysis. AA may be helpful for the exclusion of specialized IM, however, histological confirmation remains critical due to low specificity (0.69). In our view, this is clinically not relevant when dealing with longsegment BE as presence of specialized IM would
not alter surveillance intervals.
ACETIC ACID IN THE DETECTION AND CHARACTERIZATION OF NEOPLASIA Use of AA to aid identification of IM in BE is important in the stratification of surveillance intervals[5]. However, the overriding utility of AA is the identification and characterization of Barrett’s neoplasia. There is a growing body of evidence to support the use of AA in this setting.
In 2006 Réaud et al[29], furthered Guelrud’s work aiming to define the neoplastic appearances of BE following 6% AA dye spray and magnification endoscopy. In their study of 28 patients, they noted that patients with HGD on biopsy displayed mucosal architectural disorganization and hypervascularity a phenomenon previously identified by Rey et al[30] in 2003. Using these parameters, they demonstrated a positive predictive value (PPV) of 75% for neoplasia. Camus et al[31] identified similar features when combining AA with FICE.
In their study of 62 patients in 2006, Fortun et al[27] examined whether the combination of magnification endoscopy and 3% AA could improve diagnostic accuracy in patients with BE. Patients underwent a repeat endoscopy having recently undergone surveillance endoscopy (mean 7 mo prior). Barrett’s neoplasia was identified in 9 patients: 5 LGD, 1 HGD and 3 EAC. The main drawback from this study is that the index endoscopy was used as a control, raising the question as to whether the neoplasia detected was de-novo or previously missed, with the total number of neoplasias being small. At the same time, Yagi et al[32] reported that Barrett’s EAC was associated with an irregular granular pattern or a minute grainlike pattern following 1.5% AA dye spray and magnification endoscopy.
A year later VázquezIglesias et al[33] reported on their prospective study of 100 patients undergoing Barrett’s surveillance, 13 of whom had neoplasia, using 3% AA and nonmagnification endoscopy. They proposed the following mucosal classification:
5755 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Figure 1 Acetic acid mechanism of action. A: Non-dysplastic Barrett’s with HDWL; B: Non dysplastic BE following AAC (Olympus Lucera ELITE processor, GIFHQ290 gastroscope).
A B
Chedgy FJQ et al . Acetic acid chromoendoscopy

5756 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
mL of simeticone, patients underwent conventional white light endoscopy followed by 2.5% AAC. The Barrett’s segment was assessed for the following features: (1) surface pattern: ridged, villous, round, irregular; (2) vascular pattern: regular or irregular; and (3) acetowhitening reaction: No loss of acetowhitening or focal early loss of acetowhitening.
Dysplastic Barrett’s was defined endoscopically as (Figure 2): (1) irregular surface patterns AND/OR; (2) increased vascularity or irregular vessels AND/OR; and (3) focal, early loss of acetowhitening was present.
Targeted biopsies were performed followed by 4QBS (unless area already sampled with targeted biopsy). Again, the combination of targeted and 4QBS was used as the reference for final histological diagnosis.
Seventyeight procedures were performed in patients with no prior neoplasia history (lowrisk group) and 112 procedures were performed in patients referred with a history of neoplasia (highrisk group). Neoplasia was histologically confirmed in 88/190 procedures: 21/88 EAC (T1a/b), 51/88 HGD, 16/88 LGD. AAC targeted biopsy demonstrated a sensitivity of 95.5% and specificity 80% for neoplasia detection. Significant correlation between the in vivo diagnosis of neoplasia and final histology was noted (r = 0.98). There was a 2.5fold increase in visible neoplasia detection with AAC as compared to white light alone (P = 0.001). The limitations of this study are similar to those of the Wiesbaden group: single center, expert endoscopist with a dysplasiaenriched population. What these studies cannot answer is how AAC would perform in the surveillance population where dysplasia prevalence is much lower and how AAC performs in nonexpert hands.
Another factor limiting the use of AAC is the additional skills required to interpret surface and vascular patterns and their subjective nature. To that end the Portsmouth group sought to develop an objective tool using the duration of acetowhitening for the diagnosis of neoplasia[2]. One hundred and thirtytwo patients underwent 2.5% AAC with targeted
(1) normal pattern: uniform reticulum along entire columnarlined esophagus; and (2) abnormal pattern: rough or irregular reticulum.
Applying these characteristics, they demonstrated 100% sensitivity and 97.7% specificity (PPV 86% NPV 100%) for the detection of early neoplasia. with the false positives arising in 2 patients; one with esophagitis, the other with an esophageal ulcer.
These results were a significant improvement on those reported by Mayinger et al[34] in 2006 who reported sensitivities for neoplasia recognition in the range 55.5% to 82.4% in endoscopists trained in interpretation of AA enhanced magnification endoscopy. The same study also demonstrated extremely low inter and intraobserver agreement for the technique.
The Wiesbaden group first reported their experiences of AAC for neoplasia detection in Barrett’s in 2007[35]. They performed a prospective randomized crossover tandem endoscopy study examining 57 patients with a history of Barrett’s neoplasia with AAC or virtual chromoendoscopy, using Fujinon Intelligent Chromoendoscopy (FICE), 46 wk apart. The patients had a known history of Barrett’s neoplasia (discrete mucosal alteration/ macroscopically occult lesions/ prior endoscopic treatment for neoplasia). Targeted biopsy of visible abnormalities was performed along with 4QBS. In 24 patients neoplasia was identified with the AAC achieving an 87% sensitivity. There are however, limitations with this study in that combined biopsies (targeted plus 4QBS) were used as the reference standard not surgical resection specimens. The study population was neoplasiaenriched in a tertiary center and thus results may not reflect the true performance of AAC in the community, surveillance population.
LongcroftWheaton et al[36] from Portsmouth reported on their cohort of patients undergoing Barrett’s examination with AAC with strikingly similar results. The study design was similar to the Wiesbaden group with 190 procedures performed in 119 patients. After esophageal cleansing, with a 50 mL solution containing 40 mL of water, 5 mL of 10% Nacetylcysteine and 5
Figure 2 Dysplastic Barrett’s was defined endoscopically. A: Barrett’s with HDWL; B: Same patient note dysplasia only visible post AAC with early loss of acetowhitening (Olympus Lucera ELITE processor, GIFHQ290 gastroscope).
A B
Chedgy FJQ et al . Acetic acid chromoendoscopy

5757 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
biopsies of neoplasia, followed by 4QBS. Time taken to lose acetowhitening effect was measured and analyzed for metaplasia, HGD and EAC. In cases of cancer, acetowhitening was lost in a median of 23 s (range 381 s), for HGD the median was 53 s (range 4288 s). In nondysplastic Barrett’s median time was 311 s (range 14992). They proved the concept of focal loss of acetowhitening (LAW) as a very effective tool in distinguishing metaplasia from HGD and HGD from EAC. The time differences to lose acetowhitening were statistically significant (P < 0.05). In order to further refine the tool, the authors plotted a receiver operating characteristic and determined that a time of 142 s yielded the optimum sensitivity of 98% and specificity of 84%. The benefit of this tool is that it provides endoscopists an objective measure of neoplasia, avoiding subjective interpretation of mucosal and vessel patterns. This is clinically very relevant as this phenomenon can be universally applied, regardless of endoscope manufacturer or definition, and requires minimal training. Their results reach the ASGE PIVI (preservation and incorporation of valuable endoscopic innovations) criteria[37] (sensitivity ≥ 90%, NPV ≥ 98% and specificity > 80%), reaching these thresholds eliminates the need for random 4QBs.
In the metaanalysis by Coletta et al[28], 9 studies (1379 patients) looked at AAC for the diagnosis of HGD/EAC. The pooled sensitivity, specificity, LR+, LR was 0.92 (95%CI: 0.830.97), 0.96 (95%CI: 0.850.99), 25.0(95%CI: 5.9105.3) and 0.08 (95%CI: 0.040.18), respectively. Subgroup analysis did not identify significant sources of heterogeneity. The results highlight, high sensitivity 92% and specificity 96% for AAC in the diagnosis of HGD/EAC.
ACETIC ACID IN THE SURVEILLANCE POPULATIONThe advent of advanced endoscopic imaging technologies such as NBI, FICE and iscan have improved the identification and characterization of neoplastic lesions, but these technologies require significant financial investment. Therefore, the role of AA in the surveillance population is of great interest as a potentially costeffective, accurate and nonproprietary tool for improving dysplasia detection.
Cost-effectiveness of acetic acid targeted biopsy protocolsIn 2010 the Wiesbaden group published a much larger AAC series[38]. In their study they enrolled 701 consecutive Barrett’s patients, 406 in a highrisk group (history of Barrett’s neoplasia) and 295 in a lowrisk group (no history of neoplasia). Each patient was examined with highresolution white light followed by 1.5% AAC. Targeted biopsy of visible lesions was performed followed by 4QBS every 12cm (unless area already sampled with targeted biopsy). To improve
visibility during 4QBS of long segment Barrett’s the drybiopsy technique[39] was employed spraying 1:20000 adrenaline onto the Barrett’s segment prior to biopsy. A total of 459 targeted biopsies were taken and 5485 4QBS. One hundred and thirtytwo early neoplastic lesions (HGD/EAC) were identified in 92 patients. AA was demonstrated to perform with a sensitivity of 96.7% and specificity of 66.5% overall with PPV 30.4% and NPV 99.3%. Only 3 additional patients (3.3%) with neoplasia were identified by 4QBS in the highrisk group. Their data suggested that there was minimal additional yield of 4QBS over AA targeted biopsy for the detection of dysplasia with the mean number of targeted biopsies required to yield one diagnosis of neoplasia being 5.2 vs 1828 for 4QBS. However, all HGD and EAC detected in this series were from the highrisk group, limiting applicability in the lowrisk surveillance population.
Bhandari et al[20] conducted a retrospective cohort study of all AAC procedures for BE performed from 20052010 to examine the efficacy and cost implications of this method in the identification of neoplasia. This study was done in a tertiarycenter with all procedures being performed by a single expert endoscopist. High definition white light endoscopy (HDWL) was used in all cases prior to 2.5% AAC. Targeted biopsies of all AAenhanced visible lesions were taken, followed by 4QBS. 197 highrisk patients underwent 263 procedures. Of these, 68 patients were referred with nonvisible HGD on random biopsy. Notably, there was a high proportion of highrisk neoplasia (HGD/EAC) in this cohort of patients (143/263 procedures; 54.4%). There was a twofold increase in neoplasia detection using AA (96%) as compared to HDWL (48%), P = 0.0001. HGD was missed with AA in 5/98 patients (5.1%) however, 4 of these were in the complex, postEMR follow up group.
They performed a cost modelling exercise of 3 alternative biopsy sampling protocols incorporating AA using their mean length BE of 4.5cm (Table 1). There was a 4% neoplasia missrate in the AAtargeted biopsies alone group. Nevertheless, the cost saving calculated is significant in the context of the highrisk population included in this study and if applied to the usual surveillance population with a lower neoplasia prevalence rate of < 5%, costeffectiveness increases 10 fold.
The Portsmouth group published another retrospective cohort study[40] comparing the neoplasia yield of AAC with 4QBS, in a routine BE surveillance population. Nine hundred and seventytwo patients were included in the study, with 655 (67%) undergoing 4QBS and 327 (33%) AAC. A gain in neoplasia detection was demonstrated in the AAC group on both per patient and per biopsy analysis. A significant (P = 0.0001) gain from 2% neoplasia rates in the 4QBS group to 12.5% in the AAC group was noted. When analyzed per biopsy, a 14.7fold increase in neoplasia detection was seen in the AAC group per biopsy
Chedgy FJQ et al . Acetic acid chromoendoscopy

5758 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
compared to 4QBS (0.025 vs 0.0017, P < 0.05). The number of biopsies required to detect one neoplasia was 15 times lower in the AAC cohort compared to the 4QBS cohort (40 biopsies vs 604 biopsies). This study was the first of its kind in a Barrett’s surveillance population and demonstrates a proof of concept that can be used to power a randomized controlled trial comparing 4QBS with AAC.
These data demonstrate that AAC targeted biopsy protocols are extremely costeffective in highrisk populations and suggest even greater gains are to be expected in the surveillance population.
The Portsmouth group is currently underway with the ABBA study[41]. This is a multicenter randomized, crossover, tandem endoscopy study comparing 4QBS versus AA targeted biopsies, in a Barrett’s surveillance population. The study will also focus on training the AAC technique by a webbased training program utilizing a comprehensive and wellvalidated image and video library. The results of this study (expected to complete in 2016) will add to the growing evidence base on the use of AAC in the surveillance population.
CONCLUSIONThe evidence for the use of AAC in the detection and characterization of Barrett’s neoplasia is compelling. The large studies from the Portsmouth and Wiesbaden groups demonstrate that experts are able to meet the ASGE PIVI criteria[40] (sensitivity ≥ 90%, NPV ≥ 98% and specificity > 80%) and are thus able to justifiably dispense with 4QBS. The technique is cheap and can be universally applied, regardless of endoscope manufacturer. However, further data from a wellpowered randomized controlled trial are required before completely abandoning 4QBS and it may be that the modified Portsmouth protocol provides optimum results for costeffective Barrett’s surveillance.
REFERENCES1 Wang KK, Sampliner RE. Updated guidelines 2008 for the
diagnosis, surveillance and therapy of Barrett’s esophagus. Am J
Gastroenterol 2008; 103: 788-797 [PMID: 18341497 DOI: 10.1111/j.1572-0241.2008.01835.x]
2 Longcroft-Wheaton G, Brown J, Basford P, Cowlishaw D, Higgins B, Bhandari P. Duration of acetowhitening as a novel objective tool for diagnosing high risk neoplasia in Barrett’s esophagus: a prospective cohort trial. Endoscopy 2013; 45: 426-432 [PMID: 23733726 DOI: 10.1055/s-0032-1326630]
3 Ronkainen J, Aro P, Storskrubb T, Johansson SE, Lind T, Bolling-Sternevald E, Vieth M, Stolte M, Talley NJ, Agréus L. Prevalence of Barrett’s esophagus in the general population: an endoscopic study. Gastroenterology 2005; 129: 1825-1831 [PMID: 16344051 DOI: 10.1053/j.gastro.2005.08.053]
4 Shaheen N, Ransohoff DF. Gastroesophageal reflux, barrett esophagus, and esophageal cancer: scientific review. JAMA 2002; 287: 1972-1981 [PMID: 11960540]
5 Fitzgerald RC, di Pietro M, Ragunath K, Ang Y, Kang JY, Watson P, Trudgill N, Patel P, Kaye PV, Sanders S, O’Donovan M, Bird-Lieberman E, Bhandari P, Jankowski JA, Attwood S, Parsons SL, Loft D, Lagergren J, Moayyedi P, Lyratzopoulos G, de Caestecker J. British Society of Gastroenterology guidelines on the diagnosis and management of Barrett’s oesophagus. Gut 2014; 63: 7-42 [PMID: 24165758 DOI: 10.1136/gutjnl-2013-305372]
6 Bhat S, Coleman HG, Yousef F, Johnston BT, McManus DT, Gavin AT, Murray LJ. Risk of malignant progression in Barrett’s esophagus patients: results from a large population-based study. J Natl Cancer Inst 2011; 103: 1049-1057 [PMID: 21680910 DOI: 10.1093/jnci/djr203]
7 de Jonge PJ, van Blankenstein M, Grady WM, Kuipers EJ. Barrett’s oesophagus: epidemiology, cancer risk and implications for management. Gut 2014; 63: 191-202 [PMID: 24092861 DOI: 10.1136/gutjnl-2013-305490]
8 Hvid-Jensen F, Pedersen L, Drewes AM, Sørensen HT, Funch-Jensen P. Incidence of adenocarcinoma among patients with Barrett’s esophagus. N Engl J Med 2011; 365: 1375-1383 [PMID: 21995385 DOI: 10.1056/NEJMoa1103042]
9 Yousef F, Cardwell C, Cantwell MM, Galway K, Johnston BT, Murray L. The incidence of esophageal cancer and high-grade dysplasia in Barrett’s esophagus: a systematic review and meta-analysis. Am J Epidemiol 2008; 168: 237-249 [PMID: 18550563 DOI: 10.1093/aje/kwn121]
10 Phoa KN, van Vilsteren FG, Weusten BL, Bisschops R, Schoon EJ, Ragunath K, Fullarton G, Di Pietro M, Ravi N, Visser M, Offerhaus GJ, Seldenrijk CA, Meijer SL, ten Kate FJ, Tijssen JG, Bergman JJ. Radiofrequency ablation vs endoscopic surveillance for patients with Barrett esophagus and low-grade dysplasia: a randomized clinical trial. JAMA 2014; 311: 1209-1217 [PMID: 24668102 DOI: 10.1001/jama.2014.2511]
11 Konda VJ, Ross AS, Ferguson MK, Hart JA, Lin S, Naylor K, Noffsinger A, Posner MC, Dye C, Cislo B, Stearns L, Waxman I. Is the risk of concomitant invasive esophageal cancer in high-grade dysplasia in Barrett’s esophagus overestimated? Clin Gastroenterol
Table 1 Projected histology costs by biopsy protocol
Biopsy protocols Cost of biopsies for cohort, n = 263 (£/$)
Cost per patient Cost reduction vs seattle protocol
Seattle protocol: £278832.60 £1060.204QBS every 1 cm individual cassettes $428929.60 $1630.91 Cleveland protocol: £139416.30 £530.10 50% reduction4QBS every 2 cm individual cassettes $214464.80 $815.46 Portsmouth protocol: £25032.50 £95.18 91% reductionAA-targeted and 4QBS (2 cassettes) $38507.62 $146.42 Modified portsmouth protocol: £15490.70 £58.90 95% reductionVisible neoplasia - AA-targeted or No neoplasia - 4QBS (1 cassette)
$23829.42 $90.61
Futuristic protocol: £9541.80 £30.91 97% reductionAA-targeted biopsies only $14678.20 $47.55
Chedgy FJQ et al . Acetic acid chromoendoscopy

5759 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Hepatol 2008; 6: 159-164 [PMID: 18096439 DOI: 10.1016/j.cgh.2007.09.013]
12 Heitmiller RF, Redmond M, Hamilton SR. Barrett’s esophagus with high-grade dysplasia. An indication for prophylactic esophagectomy. Ann Surg 1996; 224: 66-71 [PMID: 8678620 DOI: 10.1097/00000658-199607000-00010]
13 Fitzgerald RC, Saeed IT, Khoo D, Farthing MJ, Burnham WR. Rigorous surveillance protocol increases detection of curable cancers associated with Barrett’s esophagus. Dig Dis Sci 2001; 46: 1892-1898 [PMID: 11575441 DOI: 10.1023/A:1010678913481]
14 Pech O, Gossner L, Manner H, May A, Rabenstein T, Behrens A, Berres M, Huijsmans J, Vieth M, Stolte M, Ell C. Prospective evaluation of the macroscopic types and location of early Barrett’s neoplasia in 380 lesions. Endoscopy 2007; 39: 588-593 [PMID: 17611912 DOI: 10.1055/s-2007-966363]
15 Sturm MB, Wang TD. Emerging optical methods for surveillance of Barrett’s oesophagus. Gut 2015; 64: 1816-1823 [PMID: 25975605 DOI: 10.1136/gutjnl-2013-306706]
16 Rey JF, Inoue H, Guelrud M. Magnification endoscopy with acetic acid for Barrett’s esophagus. Endoscopy 2005; 37: 583-586 [PMID: 15933935 DOI: 10.1055/s-2005-861321]
17 Falk GW, Rice TW, Goldblum JR, Richter JE. Jumbo biopsy forceps protocol still misses unsuspected cancer in Barrett’s esophagus with high-grade dysplasia. Gastrointest Endosc 1999; 49: 170-176 [PMID: 9925694 DOI: 10.1016/S0016-5107(99)70482-7]
18 Edwards MJ, Gable DR, Lentsch AB, Richardson JD. The rationale for esophagectomy as the optimal therapy for Barrett’s esophagus with high-grade dysplasia. Ann Surg 1996; 223: 585-589; discussion 589-591 [PMID: 8651749 DOI: 10.1097/00000658-199605000-00014]
19 Peters FP, Curvers WL, Rosmolen WD, De Vries CE, Ten Kate FJW, Krishnadath KK, Fockens P, Bergman JJGHM. Surveillance history of endoscopically treated patients with early Barrett’s neoplasia: nonadherence to the Seattle biopsy protocol leads to sampling error. Dis Esophagus 2008; 21: 475-479 [DOI: 10.1111/j.1442-2050.2008.00813.x]
20 Bhandari P, Kandaswamy P, Cowlishaw D, Longcroft-Wheaton G. Acetic acid-enhanced chromoendoscopy is more cost-effective than protocol-guided biopsies in a high-risk Barrett’s population. Dis Esophagus 2012; 25: 386-392 [PMID: 21981061 DOI: 10.1111/j.1442-2050.2011.01267.x]
21 Guelrud M, Herrera I, Essenfeld H, Castro J. Enhanced mag-nification endoscopy: a new technique to identify specialized intestinal metaplasia in Barrett’s esophagus. Gastrointest Endosc 2001; 53: 559-565 [PMID: 11323579 DOI: 10.1067/mge.2001.114059]
22 Van Le L, Broekhuizen FF, Janzer-Steele R, Behar M, Samter T. Acetic acid visualization of the cervix to detect cervical dysplasia. Obstet Gynecol 1993; 81: 293-295 [PMID: 8423967]
23 Lambert R, Rey JF, Sankaranarayanan R. Magnification and chromoscopy with the acetic acid test. Endoscopy 2003; 35: 437-445 [PMID: 12701018 DOI: 10.1055/s-2003-38766]
24 Canto MI. Acetic-acid chromoendoscopy for Barrett’s esophagus: the “pros”. Gastrointest Endosc 2006; 64: 13-16 [PMID: 16813796 DOI: 10.1016/j.gie.2006.03.922]
25 Evans JA, Early DS, Fukami N, Ben-Menachem T, Chandrasekhara V, Chathadi KV, Decker GA, Fanelli RD, Fisher DA, Foley KQ, Hwang JH, Jain R, Jue TL, Khan KM, Lightdale J, Malpas PM, Maple JT, Pasha SF, Saltzman JR, Sharaf RN, Shergill A, Dominitz JA, Cash BD. The role of endoscopy in Barrett’s esophagus and other premalignant conditions of the esophagus. Gastrointest Endosc 2012; 76: 1087-1094 [PMID: 23164510 DOI: 10.1016/j.gie.2012.08.004]
26 Toyoda H, Rubio C, Befrits R, Hamamoto N, Adachi Y, Jaramillo E. Detection of intestinal metaplasia in distal esophagus and esophagogastric junction by enhanced-magnification endoscopy. Gastrointest Endosc 2004; 59: 15-21 [PMID: 14722541]
27 Fortun PJ, Anagnostopoulos GK, Kaye P, James M, Foley S, Samuel S, Shonde A, Badreldin R, Campbell E, Hawkey CJ,
Ragunath K. Acetic acid-enhanced magnification endoscopy in the diagnosis of specialized intestinal metaplasia, dysplasia and early cancer in Barrett’s oesophagus. Aliment Pharmacol Ther 2006; 23: 735-742 [PMID: 16556175 DOI: 10.1111/j.1365-2036.2006.02823.x]
28 Coletta M, Sami SS, Nachiappan A, Fraquelli M, Casazza G, Ragunath K. Acetic acid chromoendoscopy for the diagnosis of early neoplasia and specialized intestinal metaplasia in Barrett’s esophagus: a meta-analysis. Gastrointest Endosc 2016; 83: 57-67.e1 [PMID: 26371851 DOI: 10.1016/j.gie.2015.07.023]
29 Réaud S, Croue A, Boyer J. Diagnostic accuracy of magnifying chromoendoscopy with detection of intestinal metaplasia and dysplasia using acetic acid in Barrett’s esophagus. Gastroenterol Clin Biol 2006; 30: 217-223 [PMID: 16565653 DOI: 10.1016/S0399-8320(06)73156-6]
30 Rey JF, Kuznetsov K. Usefulness of chromoscopy with acetic acid and magnification for Barrett’s esophagus. Gastrointest Endosc 2003; AB91
31 Camus M, Coriat R, Leblanc S, Brezault C, Terris B, Pommaret E, Gaudric M, Chryssostalis A, Prat F, Chaussade S. Helpfulness of the combination of acetic acid and FICE in the detection of Barrett’s epithelium and Barrett’s associated neoplasias. World J Gastroenterol 2012; 18: 1921-1925 [PMID: 22563172 DOI: 10.3748/wjg.v18.i16.1921]
32 Yagi K , Nakamura A, Sekine A, Umezu H. Endoscopic diagnosis of mucosal adenocarcinomas and intestinal metap-lasia of columnar-lined esophagus using enhanced-magnifica-tion endoscopy. Dig Endosc 2006; 18: 21-26 [DOI: 10.1111/j.1443-1661.2006.00613.x]
33 Vázquez-Iglesias JL, Alonso-Aguirre P, Diz-Lois MT, Vázquez-Millán MA, Alvarez A, Lorenzo MJ. Acetic acid allows effective selection of areas for obtaining biopsy samples in Barrett’s esophagus. Eur J Gastroenterol Hepatol 2007; 19: 187-193 [PMID: 17301644 DOI: 10.1097/MEG.0b013e3280102f5e]
34 Mayinger B, Oezturk Y, Stolte M, Faller G, Benninger J, Schwab D, Maiss J, Hahn EG, Muehldorfer S. Evaluation of sensitivity and inter- and intra-observer variability in the detection of intestinal metaplasia and dysplasia in Barrett’s esophagus with enhanced magnification endoscopy. Scand J Gastroenterol 2006; 41: 349-356 [PMID: 16497625 DOI: 10.1080/00365520510024016]
35 Pohl J, May A, Rabenstein T, Pech O, Nguyen-Tat M, Fissler-Eckhoff A, Ell C. Comparison of computed virtual chromoendoscopy and conventional chromoendoscopy with acetic acid for detection of neoplasia in Barrett’s esophagus. Endoscopy 2007; 39: 594-598 [PMID: 17611913 DOI: 10.1055/s-2007-966649]
36 Longcroft-Wheaton G, Duku M, Mead R, Poller D, Bhandari P. Acetic acid spray is an effective tool for the endoscopic detection of neoplasia in patients with Barrett’s esophagus. Clin Gastroenterol Hepatol 2010; 8: 843-847 [PMID: 20601133 DOI: 10.1016/j.cgh.2010.06.016]
37 Sharma P, Savides TJ, Canto MI, Corley DA, Falk GW, Goldblum JR, Wang KK, Wallace MB, Wolfsen HC. The American Society for Gastrointestinal Endoscopy PIVI (Preservation and Incorporation of Valuable Endoscopic Innovations) on imaging in Barrett’s Esophagus. Gastrointest Endosc 2012; 76: 252-254 [PMID: 22817781 DOI: 10.1016/j.gie.2012.05.007]
38 Pohl J, Pech O, May A, Manner H, Fissler-Eckhoff A, Ell C. Incidence of macroscopically occult neoplasias in Barrett’s esophagus: are random biopsies dispensable in the era of advanced endoscopic imaging? Am J Gastroenterol 2010; 105: 2350-2356 [PMID: 20664531 DOI: 10.1038/ajg.2010.280]
39 Pohl J, Nguyen-Tat M, Manner H, Pech O, van Weyenberg SJ, Ell C. “Dry biopsies” with spraying of dilute epinephrine optimize biopsy mapping of long segment Barrett’s esophagus. Endoscopy 2008; 40: 883-887 [PMID: 18833509 DOI: 10.1055/s-2008-1077678]
40 Tholoor S, Bhattacharyya R, Tsagkournis O, Longcroft-Wheaton G, Bhandari P. Acetic acid chromoendoscopy in Barrett’s esophagus surveillance is superior to the standardized random biopsy protocol: results from a large cohort study (with video). Gastrointest
Chedgy FJQ et al . Acetic acid chromoendoscopy

5760 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Endosc 2014; 80: 417-424 [PMID: 24713305 DOI: 10.1016/j.gie.2014.01.041]
41 Portsmouth Hospitals NHS Trust. Using Dilute Vinegar to Find
Changes in Cells During Endoscopy for Patients With Barrett’s Oesophagus (The ABBA Study). Available from: URL: http://ClinicalTrials.gov
P- Reviewer: Cho YS, Lee SH, Rimbas M, Tantau M, Yu B S- Editor: Qi Y L- Editor: A E- Editor: Wang CH
Chedgy FJQ et al . Acetic acid chromoendoscopy

Juliana Fernandes Matos, Marcos Felipe de Freitas Calabresi, Yuri Karen Sinzato, Debora Cristina Damasceno, Jose Ricardo Arruda Miranda, Sao Paulo State University, Botucatu, SP 18618-970, Brazil
Madileine Francely Americo, Gustavo Tadeu Volpato, Instituto de Ciências Biológicas e da Saúde, Federal University of Mato Grosso, Barra do Garças, MT 78600-000, Brazil
Luciana Aparecida Corá, Universidade Estadual de Ciências da Saúde de Alagoas, Maceió, AL 57010-300, Brazil
Ricardo Brandt Oliveira, São Paulo University, Ribeirão Preto, SP 14049-900, Brazil
Author contributions: Americo MF, Sinzato YK, Damasceno DC and Miranda JRA designed the study; Matos JF and Calabresi MFF performed experiments; Americo MF, Matos JF, Calabresi MFF and Miranda JRA analyzed the data; Americo MF, Volpato GT and Oliveira RB wrote the paper; Americo MF, Sinzato YK, Volpato GT, Oliveira RB, Damasceno DC and Miranda JRA revised critically the paper; The final version of manuscript was read and approved by all authors.
Supported by Fundação de Amparo à Pesquisa do Estado de São Paulo (Fapesp), No. 2010/14845-4 and No. 2015/14923-9; Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), No. 150456/2009-3.
Institutional animal care and use committee statement: All procedures involving animals were reviewed and approved by the Institutional Animal Care and Use Committee of the Bioscience Institute/UNESP Ethics Committee on Use of Animals (CEUA Process 411).
Data sharing statement: No additional data are available.
Open-Access: This article is an open-access article which was
selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Manuscript source: Invited manuscript
Correspondence to: Madileine Francely Americo, PhD, Instituto de Ciências Biológicas e da Saúde, Federal University of Mato Grosso, Avenida Valdon Varjão 6390, Barra do Garças, MT 78600-000, Brazil. [email protected]: +55-66-34015317 Fax: +55-66-34015317
Received: March 7, 2016Peer-review started: March 8, 2016First decision: April 14, 2016Revised: May 7, 2016Accepted: June 2, 2016 Article in press: June 2, 2016Published online: July 7, 2016
Abstract AIM: To correlate gastric contractility, gastrointes-tinal transit, and hormone levels in non-pregnant (estrous cycle) and pregnant rats using noninvasive techniques.
METHODS: Female rats (n = 23) were randomly divided into (1) non-pregnant, (contractility, n =
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.3748/wjg.v22.i25.5761
5761 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
World J Gastroenterol 2016 July 7; 22(25): 5761-5768 ISSN 1007-9327 (print) ISSN 2219-2840 (online)
© 2016 Baishideng Publishing Group Inc. All rights reserved.
ORIGINAL ARTICLE
Role of sex hormones in gastrointestinal motility in pregnant and non-pregnant rats
Basic Study
Juliana Fernandes Matos, Madileine Francely Americo, Yuri Karen Sinzato, Gustavo Tadeu Volpato, Luciana Aparecida Corá, Marcos Felipe Freitas Calabresi, Ricardo Brandt Oliveira, Debora Cristina Damasceno, Jose Ricardo Arruda Miranda

6; transit, n = 6); and (2) pregnant (contractility, n = 5; transit, n = 6). In each estrous cycle phase or at 0, 7, 14, and 20 d after the confirmation of pregnancy, gastrointestinal transit was recorded by AC biosusceptometry (ACB), and gastric contractility was recorded by ACB and electromyography. After each recording, blood samples were obtained for progesterone and estradiol determination.
RESULTS: In the estrous cycle, despite fluctuations of sex hormone levels, no significant changes in gastrointestinal motility were observed. Days 7 and 14 of pregnancy were characterized by significant changes in the frequency of contractions (3.90 ± 0.42 cpm and 3.60 ± 0.36 cpm vs 4.33 ± 0.25 cpm) and gastric emptying (168 ± 17 min and 165 ± 15 min vs 113 ± 15 min) compared with day 0. On these same days, progesterone levels significantly increased compared with control (54.23 ± 15.14 ng/mL and 129.96 ± 30.52 ng/mL vs 13.25 ± 6.31 ng/mL). On day 14, we observed the highest level of progesterone and the lowest level of estradiol compared with day 0 (44.3 ± 15.18 pg/mL vs 24.96 ± 5.96 pg/mL).
CONCLUSION: Gastrointestinal motility was unaffected by the estrous cycle. In our data, high progesterone and low estradiol levels can be associated with decreased contraction frequency and slow gastric emptying.
Key words: Reproductive physiological process; Sex hormones; Gastrointestinal motility; Magnetic fields; Gastric emptying
© The Author(s) 2016. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: In female rats, the estrous cycle and pre-gnancy appear to disturb gastrointestinal motility because of variations in hormone levels, although data are conflicting. In vivo gastrointestinal studies during pregnancy are limited by the lack of safe and reliable methods. AC biosusceptometry and electromyography are appropriate for recording motility while adhering to ethical standards. Sex hormone variations were not sufficient to disturb gastrointestinal motility during the estrous cycle. In our data, high progesterone and low estradiol levels can be associated with decreased contraction frequency and slow gastric emptying. These data were obtained in vivo using harmless techniques during several reproductive stages.
Matos JF, Americo MF, Sinzato YK, Volpato GT, Corá LA, Calabresi MFF, Oliveira RB, Damasceno DC, Miranda JRA. Role of sex hormones in gastrointestinal motility in pregnant and non-pregnant rats. World J Gastroenterol 2016; 22(25): 5761-5768 Available from: URL: http://www.wjgnet.com/1007-9327/full/v22/i25/5761.htm DOI: http://dx.doi.org/10.3748/wjg.v22.i25.5761
INTRODUCTION Female rats typically exhibit distinct physiological changes, such as during the estrous cycle (proestrus, estrous, metestrus, and diestrus) and pregnancy. Gastrointestinal (GI) motility appears to be affected by both reproductive stages[1], but previous studies have reported conflicting results[2,3]. During the reproductive cycle, a delay in gastric emptying was observed during the luteal stage, which is characterized by high levels of estrogen and progesterone[4]. Irritable bowel syndrome, nausea, early satiety, and dysrhythmia were also observed during this phase[4-6]. In pregnancy, gastric emptying, GI transit, and contractility of the antral smooth muscle were reported to decrease[7]. Expansion of the uterus and the levels of such hormones as human chorionic gonadotropin, estradiol, progesterone, motilin, and relaxin have been implicated in the pathophysio-logy of GI disorders[8-10]. Furthermore, the effects of sex hormones depend on their levels and receptor sensitivity[5,11]. The inhibitory effect of progesterone on gastric smooth muscles may contribute to gastric dysmotility that is associated with such complaints as nausea during pregnancy[1,7,8]. Remarkable incon-sistency has been observed regarding the role of estrogen in modulating GI physiological function[3].
Studies on GI motility during pregnancy are scarce, especially in humans, because of the lack of safe and reliable methods[2,8]. Nevertheless, specific techniques can be used for each type of GI measurement, including gastric emptying, contractility, accommodation, and sensation[12,13]. AC biosusceptometry (ACB) has been shown to be valid for recording GI motor function in several species, including gastric contractility, gastric emptying, and GI transit[14,15]. ACB is appropriate for recording motility while adhering to ethical and physiological standards. Also, ACB has been combined with serosal electromyography (EMG) and cutaneous electrogastrography to simultaneously record me-chanical and electrical events in real time without invasiveness or radiation[16].
In rats, GI changes that are observed during pregnancy and the estrous cycle are comparable to those observed in humans[17,18]. Previous studies that had similar aims and used similar methodologies have reported discrepant results[2,3]. Few in vivo noninvasive studies have directly examined the relationship between sex hormones and GI motor parameters in female rats. Moreover, the effects of sex steroid hormones on transit in vivo cannot simply be determined according to their effects on contractility in vitro[19]. Our aim was to study the relationship between gastric electrical and mechanical contractility, GI transit, and hormone levels in non-pregnant rats (estrous cycle) and pregnant rats and to correlate these parameters in different reproductive stages.
5762 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Matos JF et al . Gastrointestinal motility in female rats

MATERIALS AND METHODSAnimals The protocol was planned to minimize pain and dis-comfort to the animals. Female Wistar rats, 90 d of age and 250-300 g, were obtained from the Animal Laboratory (ANILAB, Paulínia, SP, Brazil) and acclimatized to the laboratory conditions (24 ℃, 50% humidity, and 12 h/12 h light/dark cycle) with ad libitum access to food (Presence Nutrição Animal, Paulínia, SP, Brazil) and tap water. Rats were housed in individual cages for 2 wk prior to experimentation.
The procedures and animal handling were ex-ecuted in accordance with the guidelines provided by the NIH Guide for the Care and Use of Laboratory Animals and authorized by the Bioscience Institute/UNESP Ethics Committee on Use of Animals (CEUA Process 411). After the experimental procedures, all animals were euthanized by barbiturate overdose (via intravenous administration, 150 mg/kg pentobarbital sodium).
Experimental procedureThe animals were randomly distributed into the following groups: (I) estrous cycle or non-pregnant (n = 12); and (II) pregnant (n = 11). In both groups, two subgroups were formed: estrous cycle contractility (ECC; n = 6) and estrous cycle transit (ECT; n = 6) for group I and pregnancy contractility (PC; n = 5) and pregnancy transit (PT; n = 6) for group II. The reproductive cycle in female rats is characterized by proestrus, estrous, metestrus, and diestrus, based on the amount of three types of cells that are observed in vaginal smears: epithelial cells, cornified cells, and leukocytes[17]. For pregnancy, the female rats were mated with males overnight and vaginal smear was evaluated in the next morning. Presence of spermatozoa in the slides was indicative of gestational day 0.
Gastrointestinal recordingsOn the morning of each phase (estrous cycle) or established time points after pregnancy confirmation (0, 7, 14, and 20 d), GI transit was recorded by ACB, and gastric contractility was recorded by ACB and EGG according to the assigned groups.
An ACB sensor (Br4Science®, Brazil) with excitation coils (diameter = 3.5 cm) and detection coils (diameter = 2.9 cm) was used because of its high spatial resolution and sensitivity for rodents[14]. The ACB signal intensity depends on the amount of magnetic material and its distance to the sensor. Ferrite (MgZnFe2O3, Imag, Brazil) was used as the magnetic material, unabsorbed in GI tract which is unable to absorb it[20].
Gastric contractility A previous laparotomy was performed to implant the magnetic marker and electrode (Ethicon®, Johnson and Johnson, São Paulo, Brazil) in the gastric serosa, 3 cm from the pylorus[21]. Female rats were
anesthetized with ketamine/xylazine (30/15 mg/kg, intramuscularly) for the procedure. The lead wire from the electrode was exteriorized through the abdominal wall and tunneled subcutaneously to the neck. The animals were allowed at least 7 d to recover from surgery. Afterward, they were again anesthetized (30 mg/kg pentobarbital, Abbott Laboratories, Chicago, IL, United States) and placed in the supine position during 45-min recording period. The magnetic sensor was positioned on the anterior surface of the abdomen, and continuous ACB signal recording commenced. The electrode was connected to a BIOPAC system. Simultaneous signals were acquired at a sampling rate of 20 Hz/channel, digitized using a multi-channel recorder (MP100 System; BIOPAC, Santa Barbara, CA, United States), and stored for further analysis. The bipolar configuration implemented for EMG included electrodes implanted, reference, and ground (attached to the animal’s hind leg) that were connected to an amplifier system (Biopac EGG100C amplifier; set to 1000 gain, low pass filter at 1 Hz, high pass filter at 0.005 Hz)[21].
Gastrointestinal transitAfter fasting for 12 h, the rats ingested a solid magnetic pellet (0.5 g powder ferrite and 1.5 g laboratory chow) and were raised gently up by the neck to place the ACB sensor on the abdominal surface. The maximum magnetic intensity value obtained was registered and recognized as corresponding to the stomach. Sequentially, the ACB sensor was placed in the cecum projection (based on anatomical references), and the magnetic intensity value was also recorded[14]. Subsequent measurements were performed in awake rats at these two points at regular 15-min intervals for at least 6 h[22].
Hormone levelsAfter each GI recording, orbital sinus blood samples were obtained under ketamine/xylazine anesthesia (30/15 mg/kg, intramuscular). Blood samples from the four estrous cycle phases and 4 d of pregnancy were stored in a freezer at -80 ℃ for later analysis to determine progesterone and estradiol levels by chemiluminescence.
Data analysisTo quantify gastric contractility parameters, all ma-gnetic signals were analyzed in MatLab (Mathworks, Natick, MA, United States) by visual inspection and Fast Fourier Transform (FFT) with bi-directional Butter-worth band-pass filters with a cutoff frequency of 50-120 mHz. The highest frequency peak for each FFT was determined as the gastric dominant frequency, and the lowest frequency represented signal noise. The amplitude of contraction (A) was determined according to the relationship between power of gastric peak (P) and power of noise peak (P’) and expressed in decibels (dB) as the following: A = 10 log10 (P/P’)[19].
5763 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Matos JF et al . Gastrointestinal motility in female rats

0.01
-0.01
5764 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Statistical analysisThe statistical methods for the present study were reviewed by Jose Ricardo de Arruda Miranda. The normality of continuous variables was evaluated using the Kolmogorov-Smirnov test. The variables were normally distributed. Overall difference among groups was detected by ANOVA followed by Tukey’s multiple-comparison test. Pearson correlation coefficients were calculated to analyze the relationship between variables. A value of P < 0.05 was considered significant. The data are expressed as mean ± SD.
RESULTSFigure 1 and 2 show examples of gastric contractility and gastrointestinal transit during pregnancy and the estrous cycle in female rats, respectively. The control example in Figure 2 was obtained in estrous phase, although all stages of the estrous cycle and also day 0 of pregnancy have presented the same profile. Regarding to techniques, electrical (EMG) and mechanical (ACB) activities remained coordinated in all groups.
It is possible to observe associations among gastric emptying time, frequency of gastric contractions, and progesterone levels in female rats during pregnancy and the estrous cycle (Figure 3). Considering the estrous
Individual gastric emptying (GE) and orocecal transit (OCT) times were designed according to statistical moments using MatLab, defined as Mean Gastric Emptying Time (MGET) for GE and Mean Cecum Arrival Time (MCAT) for OCT[14,22].
Estrous cycleDiestrus
Inte
nsity
(m
V)
Proestrus
Estrous
Metestrus
0 1 2 3 4 t /min
1 2 3 4 5 6 7 8 Frequency (cpm)
1 2 3 4 5 6 7 8
1 2 3 4 5 6 7 8
1 2 3 4 5 6 7 8
0.01
0
PregnancyDay 0 (control)
Day 7
Day 14
Day 20
0 1 2 3 4 t /min
1 2 3 4 5 6 7 8 Frequency (cpm)
1 2 3 4 5 6 7 8
1 2 3 4 5 6 7 8
1 2 3 4 5 6 7 8
0.01
0
Figure 1 Profile of gastric contractility signals and their respective Fourier transform obtained in female rats during the estrous cycle (estrous phase) and pregnancy (day 14). The frequency values obtained were 4.3 and 3.6 cpm (71.7 and 60.0 mHz), respectively.
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0.0-30 0 30 60 90 120 150 180 210 240 270 300 330 360 390 t/min
Inte
nsity
(m
V)
GE in Estrous phaseCA in Estrous phaseGE in day 14 of pregnancyCA in day 14 of pregnancy
Figure 2 Profile of gastric emptying and cecum arrival obtained in estrous cycle (estrous phase) and pregnancy (day 14). Arrows indicate the statistical moment (minutes in X-axis), and consequently, mean gastric emptying time and mean cecum arrival time for each example.
Matos JF et al . Gastrointestinal motility in female rats

5765 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
cycle (group Ⅰ), despite an expected fluctuation in sex hormone levels, no significant changes in GI motility were observed. The estradiol peak that was observed in proestrus did not modify GI motility. During estrus and metestrus, increases in progesterone levels were observed compared with proestrus. The highest levels of estradiol were observed in proestrus, and the lowest levels were observed in diestrus/metestrus. In group Ⅱ, the most important days of pregnancy (days 7 and 14) were characterized by substantial changes in the frequency of contraction and gastric emptying. On these same days, progesterone levels increased compared with controls. On day 14, we observed both the highest level of progesterone and the lowest level of estradiol. This combination appeared to potentiate the effects on GI motility that were detected, including the reduction of contraction frequency that was observed by EMG. The amplitude of contractions and orocecal transit time were unaffected by pregnancy (Table 1).
An interest relationship was found among gastric emptying, the frequency of contractions, and proges-terone levels (Figure 3). Low frequencies of contraction were associated with slower gastric emptying during pregnancy (Figures 1 and 2). Negative correlations were
found between progesterone levels and the frequency of contractions by ACB and EMG (R = -0.93, P < 0.02, and R = -0.77, P < 0.05, respectively).
DISCUSSIONDespite several changes in body during pregnancy may contribute to impaired GI motility, our data show that high progesterone and low estradiol levels can also be associated with decreased contraction frequency and slow gastric emptying. During the estrous cycle, GI motility was unaltered, despite the occurrence of sex hormone variations. EMG and ACB were simultaneously employed, showing coordinated electric and mechanical gastric activities in female rats. Both methods can be employed in noninvasive approaches with magnetic tracer ingestion and surface electrodes[23]. Both of these techniques have enormous advantages when considering ethical issues, especially during gestation. The relatively short duration of the estrous cycle and pregnancy in rats makes these techniques ideal for investigating changes that occur during the reproductive cycle[17,24].
Previous studies have shown that progesterone
200
180
160
140
120
100
80
60
40
20
0Diestrus Proestrus Estrous Metestrus Phases
Freq
uenc
y of
con
trac
tion
(mH
z) p
roge
ster
one
(ng/
mL)
and
gas
tric
em
ptyi
ng (
min
)
Frequency of contractionGastric emptying ProgesteroneEstrogen
e f e f
e
ee
Estrous cycle200
180
160
140
120
100
80
60
40
20
00 7 14 20 Days
Freq
uenc
y of
con
trac
tion
(mH
z) p
roge
ster
one
(ng/
mL)
and
gas
tric
em
ptyi
ng (
min
)
aa
Pregnancy
aab c
b
d d
Figure 3 Associations among gastric emptying time (min), frequency of gastric contractions (mHz), and progesterone levels (ng/mL) in female rats during pregnancy and the estrous cycle. aP < 0.03, compared with control (day 0); bP < 0.002, compared with days 0 and 20; cP < 0.001, compared with day 14; dP < 0.001, compared with days 0 and 20; eP < 0.05, compared with proestrus; fP < 0.001 compared with estrous.
A B
Table 1 Gastrointestinal motility parameters recorded by AC biosusceptometry (cecum arrival and frequency of contractions) and by electromyography (frequency and amplitude of contractions) during pregnancy and the estrous cycle in female rats
Days/phases Frequency EMG (cpm) Amplitude ACB (dB) Amplitude EMG (dB) Cecum arrival (min)
Pregnancy 0 (control) 70.0 ± 7.0 66.79 ± 14.41 52.82 ± 7.02 254 ± 10.8 7 66.0 ± 6.0 72.12 ± 13.98 49.79 ± 9.64 244 ± 16.014 59.0 ± 7.0a 71.62 ± 18.97 48.41 ± 7.55 255 ± 14.820 65.0 ± 9.0 69.42 ± 12.75 52.97 ± 11.12 259 ± 19.9
Estrous cycle Diestrus 65.0 ± 11.0 62.10 ± 7.59 55.54 ± 11.69 260 ± 26.5Proestrus 64.0 ± 4.0 54.04 ± 10.16 54.99 ± 7.47 270 ± 16.7Estrous 65.0 ± 8.0 52.08 ± 13.09 57.20 ± 8.27 268 ± 17.1
Metestrus 68.0 ± 9.0 54.03 ± 10.79 54.66 ± 8.25 269 ± 21.2
Data are expressed as mean ± SD. aP < 0.03 vs control (day 0). EGM: Electromyography; ACB: AC biosusceptometry.
Matos JF et al . Gastrointestinal motility in female rats

5766 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
delays gastric emptying in female rats and women, particularly during the third trimester of pregnancy when progesterone levels substantially increase[25,26]. This finding is consistent with relatively higher tonus in the pylorus than in gastric muscles[25]. This presumed effect of progesterone on GI transit over long periods of time may at least partially account for the disturbances in GI function frequently related by pregnant women[26]. Other studies reported that estrogen administration inhibited gastric emptying in rats[3,11]. However, as-sessing the influence of estrogen or progesterone alone can be difficult when considering that both of these hormones act synergistically[27], especially in the uterus[25]. In the GI tract, progesterone provokes regional gastrointestinal sensitivity differences[28] and dose-dependency[11] which leads to a divergence in findings[5].
Delayed gastric emptying was observed in pregnant guinea pigs, with no changes in gastric smooth muscles contractile[25]. In the present study, gastric smooth muscles were affected, in which both techniques showed that the frequency of contractions decreased, whereas gastric emptying slowed (Table 1 and Figure 3). Gastric dysrhythmias include abnormalities in gastric tone, myoelectrical activity and contractility, representing a pathophysiologic mechanism by which nausea is experienced in pregnant women[29].
Phases of the estrous cycle can be differentiated due to changes in the serum levels of sex hormones at different stages of the estrous cycle[27]. Estradiol reaches peak levels during proestrus and returns to baseline in estrus. Progesterone secretion rises during metestrus and diestrus and subsequently decreases thereafter. Progesterone levels increase to a second peak toward the end of proestrus[17,24]. In the present study, we collected data at the beginning of this phase. However, sex hormone variations did not appear to be sufficient to disturb GI motility, which contrasts with other in vitro and ex vivo studies[4]. Gastrointestinal transit is reportedly prolonged during the luteal phase and pregnancy[5,26], but such a finding was not observed in the present study. Constipation is a common symptom in both stages[30] and can occur through a combination of mechanical and hormonal issues that affect GI function[5,30].
The uterus will gradually enlarge during pregnancy, and this gravid uterus may have a mechanical effect that can disturb GI motility[30]. However, on day 20 of pregnancy, despite the size of the uterus, no changes in GI motility were observed in pregnant rats, supporting the theory that hormonal factors are the major influence on GI motility[30]. It is difficult to draw definitive conclusions based on the few studies that have been conducted to analyze these issues, mainly because of the different experimental designs and methods that have been used to measure GI motility[5]. Much data have been obtained using isolated muscle strips[31], the stimulation of which does not always produce the propulsion of luminal contents[32]. In vivo
studies reflect a combination of factors that either stimulate or inhibit the rate of gastric emptying. Thus, contrasting effects of estrogen may be observed by increases in contractility in vitro but delayed gastric emptying[24]. Our model employed both ACB and EMG, clearly establishing the potential usefulness of such a combination as a minimally invasive monitoring system to improve clinical outcomes in obstetrics[33]. Employing such a combination of techniques allows researchers to follow the same animal over various reproductive stages.
Pregnancy in females per se is a major physiologic adjustment that affects many organ systems[9,33,34]. Understanding these physiologic adaptations is important for all clinicians because they have important implications for the diagnosis and management of various disorders[9]. When monitoring the oral intake of drugs or herbal substances, the day of pregnancy needs to be considered because changes in motility can alter the effects of such substances. In addition to the well-known elevation of sex hormones, pregnancy often alters the secretion of many hormones and peptides, including those that mediate GI motility[5,34-36]. Further investigations that utilize our model will allow us to characterize GI motility in females after different interventions, with important physiological and clinical implications.
COMMENTSBackgroundIn rats, gastrointestinal changes that are observed during pregnancy and the estrous cycle are comparable to those observed in humans. However, even studies that had similar aims and used similar methodologies have reported discrepant results. New studies, focusing on this traditional topic, are useful for definitely describe the physiology and for explaining certain symptoms. Few in vivo noninvasive studies have directly examined the relationship between sex hormones and gastrointestinal motor parameters in female rats. Moreover, the effects of sex steroid hormones on transit in vivo cannot simply be determined according to their effects on contractility in vitro.
Research frontiersStudies on gastrointestinal motility during pregnancy are scarce, especially in humans, because of the lack of safe and reliable methods. AC Bio-susceptometry is appropriate for recording motility while adhering to ethical and physiological standards. In the estrous cycle, despite fluctuations of sex hormone levels, no significant changes in gastrointestinal motility were observed. During pregnancy, there was a correlation between high progesterone level and slowed gastric emptying. In this context, it has been showed that gastrointestinal motor disturbance impairs drug oral treatment and intestinal nutrient absorption.
Innovations and breakthroughsThere are much controversies about which hormones provoke gastrointestinal symptoms during the estrous cycle and pregnancy. Presented data by authors data show that impaired gastrointestinal motor function is probably linked to both sex hormones: high progesterone levels accompanied by a reduction of estradiol. The major innovation is obtaining data in vivo using harmless techniques during several reproductive stages in the same animal. New studies can be exploited to refine and extend this idea toward clinical practice.
ApplicationsTraditional physiological aspects need to be revisited to draw general
COMMENTS
Matos JF et al . Gastrointestinal motility in female rats

5767 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
conclusions, due to methodological issues and different approaches. Thus, in vivo data are provided on the relationship between hormone level and motility, which is very important and has imminent clinical value. ACB is able to evaluate gastrointestinal contractility and transit in vivo. Besides, this approach allows analyzing the influence of hormone levels on motility parameters in an intact system.
TerminologyGastrointestinal motility includes transit (displacement of ingested material between gastrointestinal segments) and contractility (rhythmical variation of the smooth muscle and gastrointestinal wall). Both can be registered by AC Biosusceptometry through ingested or fixed (serous) magnetic material.
Peer-reviewThe authors have attempted to determine changes in GI motility in rats during various phases of the reproductive cycle and pregnancy using non-invasive novel methods. It is important to recognize that this study is not a validation of these novel methods. That was done in prior studies already and this study uses these previously validated tools to study differences in motility.
REFERENCES1 Bonapace ES, Fisher RS. Constipation and diarrhea in pregnancy.
Gastroenterol Clin North Am 1998; 27: 197-211 [PMID: 9546090 DOI: 10.1016/S0889-8553(05)70353-8]
2 Chiloiro M, Darconza G, Piccioli E, De Carne M, Clemente C, Riezzo G. Gastric emptying and orocecal transit time in pregnancy. J Gastroenterol 2001; 36: 538-543 [PMID: 11519832 DOI: 10.1007/s005350170056]
3 Hogan AM, Collins D, Baird AW, Winter DC. Estrogen and its role in gastrointestinal health and disease. Int J Colorectal Dis 2009; 24: 1367-1375 [PMID: 19655153 DOI: 10.1007/s00384-009-0785-0]
4 Verrengia M, Sachdeva P, Gaughan J, Fisher RS, Parkman HP. Variation of symptoms during the menstrual cycle in female patients with gastroparesis. Neurogastroenterol Motil 2011; 23: 625-e254 [PMID: 21332597 DOI: 10.1111/j.1365-2982.2011.01681.x]
5 Caballero-Plasencia AM, Valenzuela-Barranco M, Martín-Ruiz JL, Herrerías-Gutiérrez JM, Esteban-Carretero JM. Are there changes in gastric emptying during the menstrual cycle? Scand J Gastroenterol 1999; 34: 772-776 [PMID: 10499477 DOI: 10.1080/003655299750025697]
6 Güal O, Bozkurt A, Deniz M, Sungur M, Yeğen BC. Effect of sex steroids on colonic distension-induced delay of gastric emptying in rats. J Gastroenterol Hepatol 2004; 19: 975-981 [PMID: 15304112 DOI: 10.1111/j.1440-1746.2004.03409.x]
7 Wang F, Zheng TZ, Li W, Qu SY, He DY. Action of progesterone on contractile activity of isolated gastric strips in rats. World J Gastroenterol 2003; 9: 775-778 [PMID: 12679930 DOI: 10.3748/wjg.v9.i4.775]
8 Baron TH, Ramirez B, Richter JE. Gastrointestinal motility disorders during pregnancy. Ann Intern Med 1993; 118: 366-375 [PMID: 8257464 DOI: 10.7326/0003-4819-118-5-199303010-00008]
9 Chang J, Streitman D. Physiologic adaptations to pregnancy. Neurol Clin 2012; 30: 781-789 [PMID: 22840789 DOI: 10.1016/j.ncl.2012.05.001]
10 Speranzini LB, Lopasso PP, Laudanna AA. Progesterone, estrogen and pregnancy do not decrease colon myoelectric activity in rats: an in vivo study. Gynecol Obstet Invest 2008; 66: 53-58 [PMID: 18319603 DOI: 10.1159/000119643]
11 Liu CY, Chen LB, Liu PY, Xie DP, Wang PS. Effects of progesterone on gastric emptying and intestinal transit in male rats. World J Gastroenterol 2002; 8: 338-341 [PMID: 11925620 DOI: 10.3748/wjg.v8.i2.338]
12 Bratten J, Jones MP. New directions in the assessment of gastric function: clinical applications of physiologic measurements. Dig Dis 2006; 24: 252-259 [PMID: 16849852 DOI: 10.1159/000092878]
13 Szarka LA, Camilleri M. Stomach dysfunction in diabetes mellitus: emerging technology and pharmacology. J Diabetes Sci Technol
2010; 4: 180-189 [PMID: 20167183 DOI: 10.1177/193229681000400123]
14 Quini CC, Américo MF, Corá LA, Calabresi MF, Alvarez M, Oliveira RB, Miranda JR. Employment of a noninvasive magnetic method for evaluation of gastrointestinal transit in rats. J Biol Eng 2012; 6: 6 [PMID: 22587220 DOI: 10.1186/1754-1611-6-6]
15 Shahid M. [Alpha thalassemia]. J Med Liban 1971; 24: 571-583 [PMID: 5146844 DOI: 10.1007/s10620-014-3335-8]
16 Ramsey PL. The changing signs of congenital hip dislocation. J Pediatr Surg 1977; 12: 437-441 [PMID: 0874731 DOI: 10.1111/j.1365-2982.2010.01582.x]
17 Marcondes FK, Bianchi FJ, Tanno AP. Determination of the estrous cycle phases of rats: some helpful considerations. Braz J Biol 2002; 62: 609-614 [PMID: 12659010 DOI: 10.1590/S1519-69842002000400008]
18 Shah S, Hobbs A, Singh R, Cuevas J, Ignarro LJ, Chaudhuri G. Gastrointestinal motility during pregnancy: role of nitrergic component of NANC nerves. Am J Physiol Regul Integr Comp Physiol 2000; 279: R1478-R1485 [PMID: 11004018]
19 Chen TS, Doong ML, Chang FY, Lee SD, Wang PS. Effects of sex steroid hormones on gastric emptying and gastrointestinal transit in rats. Am J Physiol 1995; 268: G171-G176 [PMID: 7840200]
20 Corá LA, Américo MF, Romeiro FG, Oliveira RB, Miranda JR. Pharmaceutical applications of AC biosusceptometry. Eur J Pharm Biopharm 2010; 74: 67-77 [PMID: 19482083 DOI: 10.1016/j.ejpb.2009.05.011]
21 Marques RG, Americo MF, Spadella CT, Corá LA, Oliveira RB, Miranda JR. Different patterns between mechanical and electrical activities: an approach to investigate gastric motility in a model of long-term diabetic rats. Physiol Meas 2014; 35: 69-81 [PMID: 24345922 DOI: 10.1088/0967-3334/35/1/69]
22 Calabresi MF, Quini CC, Matos JF, Moretto GM, Americo MF, Graça JR, Santos AA, Oliveira RB, Pina DR, Miranda JR. Alternate current biosusceptometry for the assessment of gastric motility after proximal gastrectomy in rats: a feasibility study. Neurogastroenterol Motil 2015; 27: 1613-1620 [PMID: 26303680 DOI: 10.1111/nmo.12660]
23 Andreis U, Américo MF, Corá LA, Oliveira RB, Baffa O, Miranda JR. Gastric motility evaluated by electrogastrography and alternating current biosusceptometry in dogs. Physiol Meas 2008; 29: 1023-1031 [PMID: 18698113 DOI: 10.1088/0967-3334/29/9/002]
24 Spornitz UM, Socin CD, Dravid AA. Estrous stage determination in rats by means of scanning electron microscopic images of uterine surface epithelium. Anat Rec 1999; 254: 116-126 [PMID: 9892425 DOI: 10.1002/(SICI)1097-0185(19990101)254]
25 Coşkun T, Sevinç A, Tevetoğlu I, Alican I, Kurtel H, Yeğen BC. Delayed gastric emptying in conscious male rats following chronic estrogen and progesterone treatment. Res Exp Med (Berl) 1995; 195: 49-54 [PMID: 7784703 DOI: 10.1007/BF02576773]
26 Wald A, Van Thiel DH, Hoechstetter L, Gavaler JS, Egler KM, Verm R, Scott L, Lester R. Effect of pregnancy on gastrointestinal transit. Dig Dis Sci 1982; 27: 1015-1018 [PMID: 7140485 DOI: 10.1007/BF01391748]
27 Faccio L, Da Silva AS, Tonin AA, França RT, Gressler LT, Copetti MM, Oliveira CB, Sangoi MB, Moresco RN, Bottari NB, Duarte MM, Monteiro SG. Serum levels of LH, FSH, estradiol and progesterone in female rats experimentally infected by Trypanosoma evansi. Exp Parasitol 2013; 135: 110-115 [PMID: 23816642 DOI: 10.1016/j.exppara.2013.06.008]
28 Bruce LA, Behsudi FM. Differential inhibition of regional gastrointestinal tissue to progesterone in the rat. Life Sci 1980; 27: 427-434 [PMID: 7412484 DOI: 10.1016/0024-3205(80)90192-7]
29 Koch KL. Gastrointestinal factors in nausea and vomiting of pregnancy. Am J Obstet Gynecol 2002; 186: S198-S203 [PMID: 12011886 DOI: 10.1067/mob.2002.122598]
30 Cullen G, O’Donoghue D. Constipation and pregnancy. Best Pract Res Clin Gastroenterol 2007; 21: 807-818 [PMID: 17889809 DOI: 10.1016/j.bpg.2007.05.005]
31 Ryan JP, Bhojwani A. Colonic transit in rats: effect of ovariectomy, sex steroid hormones, and pregnancy. Am J Physiol 1986; 251: G46-G50 [PMID: 3728676]
Matos JF et al . Gastrointestinal motility in female rats

5768 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
32 Tsubouchi T, Saito T, Mizutani F, Yamauchi T, Iwanaga Y. Stimulatory action of itopride hydrochloride on colonic motor activity in vitro and in vivo. J Pharmacol Exp Ther 2003; 306: 787-793 [PMID: 12724347 DOI: 10.1124/jpet.102.048603]
33 Carlin A, Alfirevic Z. Physiological changes of pregnancy and monitoring. Best Pract Res Clin Obstet Gynaecol 2008; 22: 801-823 [PMID: 18760680 DOI: 10.1016/j.bpobgyn.2008.06.005]
34 Chang FY, Lee SD, Yeh GH, Lu CC, Wang PS, Wang SW. Disturbed small intestinal motility in the late rat pregnancy. Gynecol Obstet Invest 1998; 45: 221-224 [PMID: 9623784 DOI:
10.1159/000009971]35 Bani D, Baccari MC, Quattrone S, Nistri S, Calamai F, Bigazzi
M, Bani Sacchi T. Relaxin depresses small bowel motility through a nitric oxide-mediated mechanism. Studies in mice. Biol Reprod 2002; 66: 778-784 [PMID: 11870086 DOI: 10.1095/biolreprod66.3.778]
36 Shah S, Nathan L, Singh R, Fu YS, Chaudhuri G. E2 and not P4 increases NO release from NANC nerves of the gastrointestinal tract: implications in pregnancy. Am J Physiol Regul Integr Comp Physiol 2001; 280: R1546-R1554 [PMID: 11294780]
P- Reviewer: Arora Z S- Editor: Qi Y L- Editor: A E- Editor: Wang CH
Matos JF et al . Gastrointestinal motility in female rats

Ying-Ying Li, Zheng-Ming Shi, Xiao-Yong Yu, Ping Feng, Xue-Jiang Wang
Ying-Ying Li, Xiao-Yong Yu, Xue-Jiang Wang, Department of Physiology and Pathophysiology, School of Basic Medical Sciences, Capital Medical University, Beijing 100069, China
Ying-Ying Li, Xiao-Yong Yu, Xue-Jiang Wang, Beijing Key Laboratory for Cancer Invasion and Metastasis Research, Capital Medical University, Beijing 100069, China
Zheng-Ming Shi, Department of General Surgery, Beijing Jishuitan Hospital, Beijing 100069, China
Ping Feng, Department of Physiology and Pathophysiology, School of Basic Medical Sciences, Capital Medical University, Beijing 100069, China
Author contributions: Li YY and Shi ZM performed the experiments; Wang XJ contributed reagents/materials/analysis tools; Li YY, Yu XY and Feng P analyzed the data; Wang XJ conceived and designed the research; Li YY wrote the paper; all authors read and approved the final manuscript.
Supported by National Natural Science Foundation of China, No. 81272757; and the Project of Construction of Innovative Teams and Teacher Career Development for Universities and Colleges under Beijing Municipality, No. IDHT20150502.
Conflict-of-interest statement: The authors declare no conflicts of interest.
Data sharing statement: No additional unpublished data are available.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Correspondence to: Xue-Jiang Wang, Professor, Department
of Physiology and Pathophysiology, School of Basic Medical Sciences, Capital Medical University, No. 10 Xitoutiao, You An Men, Beijing 100069, China. [email protected]: +86-10-83911434Fax: +86-10-83911434
Received: March 2, 2016Peer-review started: March 4, 2016First decision: April 1, 2016Revised: April 12, 2016Accepted: May 4, 2016 Article in press: May 4, 2016Published online: July 7, 2016
AbstractAIM: To investigated the effects of urotensin Ⅱ (UII) on hepatic insulin resistance in HepG2 cells and the potential mechanisms involved.
METHODS: Human hepatoma HepG2 cells were cultured with or without exogenous UII for 24 h, in the presence or absence of 100 nmol/L insulin for the last 30 min. Glucose levels were detected by the glucose-oxidase method and glycogen synthesis was analyzed by glycogen colorimetric/fluorometric assay. Reactive oxygen species (ROS) levels were detected with a multimode reader using a 2′,7′-dichlorofluorescein diacetate probe. The protein expression and pho-sphorylation levels of c-Jun N-terminal kinase (JNK), insulin signal essential molecules such as insulin receptor substrate -1 (IRS-1), protein kinase B (Akt), glycogen synthase kinase-3β (GSK-3β), and glucose transporter-2 (Glut 2), and NADPH oxidase subunits such as gp91phox, p67phox, p47phox, p40phox, and p22phox were evaluated by Western blot.
RESULTS: Exposure to 100 nmol/L UII reduced the insulin-induced glucose consumption (P < 0.05)
ORIGINAL ARTICLE
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.3748/wjg.v22.i25.5769
World J Gastroenterol 2016 July 7; 22(25): 5769-5779 ISSN 1007-9327 (print) ISSN 2219-2840 (online)
© 2016 Baishideng Publishing Group Inc. All rights reserved.
5769 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Basic Study
Urotensin Ⅱ-induced insulin resistance is mediated by NADPH oxidase-derived reactive oxygen species in HepG2 cells

expression has been detected in various tissues and organs, including cardiac and vascular tissues, the central nervous system, spinal cord, kidney, liver, and pancreas[4]. In addition to its significant role in the cardiovascular system[5], UII is also involved in metabolic syndrome (MetS) and plays an important role in type Ⅱ diabetes mellitus (T2DM)[6]. Perfusion of rat pancreas with UII in vitro reduced glucose-induced insulin secretion[7]. The UII/UII receptor system was up-regulated, inhibiting insulin-stimulated 2-deoxyglucose uptake, in the skeletal muscle of diabetic mice[8], and impaired skeletal muscle glucose transport via the NADPH oxidase pathway[9]. In addition, UII expression was elevated in diethylnitrosamine-mediated pre-cancerous rat liver lesions[10], and UII knockout mice had significantly decreased low-density lipoprotein cholesterol profiles and hepatic steatosis, consistent with dyslipidemia[11], with lower plasma insulin and glucose levels and increased tolerance[12].
Insulin resistance is a common pathophysiological condition in which higher concentrations of insulin are required to maintain normal insulin actions in target tissues such as liver, muscle, and adipose tissues[13]. Recent studies have shown that insulin resistance is induced by multiple factors, such as high glucose, free fatty acids, tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6), and resistin[14-18]. Elevated plasma UII levels, which often accompany MetS and T2DM, may play a role in insulin resistance. However, the precise molecular mechanisms with regard to insulin resistance remain poorly understood.
Accumulating evidence suggests that oxidative stress associated with increased production of ROS, is an important trigger in the process of insulin resistance[19]. Much attention has been focused on NADPH oxidase as a primary source of ROS generation in insulin resistance[20]. Wei et al[21,22] found that NADPH oxidase activation played a crucial role in angiotensin Ⅱ-induced insulin resistance in skeletal muscle, and our preliminary studies[9] showed a similar effect. UII expression was increased in precancerous liver lesions in rats and in human liver tumor tissue[10,23] and associated with a high risk of insulin resistance. However, the role of UII in hepatic insulin resistance has not been explored. The present study investigated the role of UII in mediating insulin resistance in HepG2 cells, a frequently used in vitro system for studying insulin resistance in hepatic cells, and determined its involvement in the insulin signaling pathway.
MATERIALS AND METHODSCell culture and treatmentHuman hepatoma HepG2 cells (China Infrastructure of Cell Line Resources) were cultured in Dulbeccos’ modified Eagle’s medium (DMEM)/high glucose (Hyclone, Beijing, China) containing 200 mL/L fetal bovine serum (Gibco, New York, United States) and
Li YY et al . Urotensin Ⅱ induces insulin resistance in HepG2 cells
5770 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
and glycogen content (P < 0.01) in HepG2 cells compared with cells without UII. UII also abolished insulin-stimulated protein expression (P < 0.01) and phosphorylation of IRS-1 (P < 0.05), associated with down-regulation of Akt (P < 0.05) and GSK-3β (P < 0.05) phosphorylation levels, and the expression of Glut 2 (P < 0.001), indicating an insulin-resistance state in HepG2 cells. Furthermore, UII enhanced the phosphorylation of JNK (P < 0.05), while the activity of JNK, insulin signaling, such as total protein of IRS-1 (P < 0.001), phosphorylation of IRS-1 (P < 0.001) and GSK-3β (P < 0.05), and glycogen synthesis (P < 0.001) could be reversed by pretreatment with the JNK inhibitor SP600125. Besides, UII markedly improved ROS generation (P < 0.05) and NADPH oxidase subunit expression (P < 0.05). However, the antioxidant/NADPH oxidase inhibitor apocynin could decrease UII-induced ROS production (P < 0.05), JNK phosphorylation (P < 0.05), and insulin resistance (P < 0.05) in HepG2 cells.
CONCLUSION: UII induces insulin resistance, and this can be reversed by JNK inhibitor SP600125 and antioxidant/NADPH oxidase inhibitor apocynin targeting the insulin signaling pathway in HepG2 cells.
Key words: Urotensin Ⅱ; Insulin resistance; NADPH oxidase; Reactive oxygen species; HepG2 cells
© The Author(s) 2016. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: We report our results on urotensin Ⅱ (UII) in a newly developed insulin resistance model and the possible mechanisms involved. Exposure to UII may contribute to oxidative damage via the NADPH oxidase pathway and enhance the phosphorylation of c-Jun N-terminal kinase, which is associated with insulin signal transduction pathways. These may be the underlying mechanisms of UII-mediated insulin resistance in HepG2 cells. These findings confirm the important role of UII in hepatic insulin resistance, which shed light on new insight into hepatic insulin resistance.
Li YY, Shi ZM, Yu XY, Feng P, Wang XJ. Urotensin Ⅱ-induced insulin resistance is mediated by NADPH oxidase-derived reactive oxygen species in HepG2 cells. World J Gastroenterol 2016; 22(25): 5769-5779 Available from: URL: http://www.wjgnet.com/1007-9327/full/v22/i25/5769.htm DOI: http://dx.doi.org/10.3748/wjg.v22.i25.5769
INTRODUCTIONUrotensin Ⅱ (UII) is a vasoactive peptide first disco-vered in teleost fishes in 1985[1], and subsequently found in mammals and humans[2]. Ames identified a G protein-coupled UII receptor (GPR14) in 1999[3]. UII acts by binding to the UII receptor, and its

10 mL/L penicillin-streptomycin (Gibco). Cells were incubated at 37 ℃ in a humidified atmosphere of 50 mL/L CO2. Cells were incubated with recombinant human UII (Sigma-Aldrich, Missouri, United States), and in some experiments, cultured HepG2 cells were pretreated with apocynin (200 μmol/L, Sigma) or SP600125 (Selleck Chemicals, United States) to inhibit ROS and JNK, respectively.
Analysis of glucose consumptionHepG2 cells were cultured in serum- and phenol red-free DMEM (Gibco) with various concentrations (0, 1, 10, 100 nmol/L) of exogenous UII for 24 h, with the addition of 100 nmol/L insulin (Novolin30R, Novo Nordisk, North Carolina, United States) for the last 30 min. The supernatant was then removed and the glucose concentration was detected using the glucose-oxidase method (Applygen Technologies, Beijing, China). Glucose consumption was calculated as the glucose concentrations in the test wells subtracted from the concentration in the blank control wells, and normalized with cellular protein concentration[14,24].
Analysis of glycogen contentHepG2 cells were treated with or without 100 nmol/L UII for 24 h, followed by serum-free DMEM (Gibco) for 4 h in the presence or absence of 100 nmol/L insulin for the last 30 min[18]. Glycogen levels were measured using a glycogen colorimetric/fluorometric assay kit (Biovision, California, United States).
Determination of ROSThe dye 2′,7′-dichlorofluorescein diacetate (DCF-DA) (Nanjing Jiancheng Biotechnology, Jiangsu, China) was used to measure changes in ROS levels. Briefly, HepG2 cells were incubated with 5 μmol/L DCF-DA for 30 min at 37 ℃ in 96-well clear-bottom, black assay plates (Corning Incorporated, NY, United States), and washed three times with phosphate-buffered saline. ROS levels were determined by analyzing the fluorescence using a multimode reader (Molecular Devices SpectraMax M2/M2e, Highcreation, China), and expressed as the ratio of fluorescence intensity to cell proliferation.
Western blot analysisCell lysates (40-60 μg protein) were separated by 10% sodium dodecyl sulfate-polyacrylamide gel electrophoresis, transferred to polyvinylidene difluoride membranes (Millipore, Massachusetts, United States), and then incubated with primary antibodies at 4 ℃ overnight, after blocking with 50 g/L nonfat dry milk for 1 h. The blots were subsequently incubated with horseradish peroxidase-conjugated secondary antibodies, followed by detection with enhanced chemiluminescence (Applygen). Antibodies against SAPK/JNK, phospho (p)-SAPK/JNK (Thr183/Tyr185), insulin receptor substrate-1 (IRS-1), pIRS-1 (Tyr895), Akt, pAkt (Thr308), glycogen synthase kinase 3β (GSK-
3β), pGSK-3β (Ser9) and β-actin were all obtained from Cell Signaling. Antibodies against p22phox, p67phox, and p40phox were from Santa Cruz Biotechnology, and antibodies against glucose transporter-2 (Glut2), gp91phox, and p47phox were purchased from Bioworld Technology. Detailed information of all antibodies can be found in Supplementary Table 1.
Statistical analysisData from at least three independent experiments are presented as the mean ± SD. Statistical analyses were carried out by one-way analysis of variance followed by Bonferroni’s adjustment. The reference condition was set to 1. A P value < 0.05 was considered sig-nificant. Statistical analyses were performed using SPSS version 15.0 software (SPSS Inc., Chicago).
RESULTSUII decreases glucose consumption and glycogen synthesis in HepG2 hepatocytesWe examined the effect of UII on glucose consumption in human hepatoma HepG2 cells by incubating them with different concentrations of exogenous UII (0, 1, 10, or 100 nmol/L) for 24 h, with the addition of 100 nmol/L insulin for the last 30 min. UII decreased insulin-mediated glucose consumption in HepG2 cells in a dose-dependent manner (Figure 1A), in accord with the effect of UII on glucose transport in skeletal muscle[8]. Interestingly, glucose consumption was unaffected when HepG2 cells were treated with UII alone for 24 h (Supplementary Figure 1). To eliminate the possible influence of UII on apoptosis, we quantified cell viability by MTT assay and demonstrated no cytotoxic effect after exposure of HepG2 cells to UII for 24 h (Figure 1B). Previous studies demonstrated that 100 nmol/L UII inhibited glucose transport in C2C12 mouse myotube cells[9], and we therefore evaluated the effect of 100 nmol/L UII on glycogen synthesis, a metabolic endpoint of insulin action, in HepG2 cells. The insulin-induced glycogen content was significantly reduced in HepG2 cells after incubation with 100 nmol/L UII for 24 h, as analyzed using a glycogen-detection kit(Figure 1C).
UII inhibits insulin receptor-mediated signal transduction in HepG2 cellsTo determine if UII impairs the insulin signaling path-way in HepG2 cells, we subjected cell lysates to Western blot analysis. Expression levels of insulin-stimulated IRS-1 and tyrosine phosphorylation of IRS-1 were inhibited by UII treatment in HepG2 cells, while UII alone had no effect (Figure 2A). Downstream of IRS-1, insulin-mediated phosphorylation of Akt and GSK-3β was also impaired by 100 nmol/L UII, while total Akt and GSK-3β protein levels were unaffected (Figure 2B). Glut 2 is closely associated with glucose transport in liver cells. We observed that Glut 2 protein could be reduced by UII (Figure 2C), which potentially
5771 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Li YY et al . Urotensin Ⅱ induces insulin resistance in HepG2 cells

sidues of IRS-1/-2[25,26], thus impairing IRS tyrosine phosphorylation and reducing insulin receptor-induced signaling. Furthermore, UII has been shown to increase JNK activity in human pulmonary artery smooth muscle cells (PASMCs)[27]. We therefore determined the role of UII in JNK activation and its correlation with insulin resistance in HepG2 cells. UII increased JNK phosphorylation (Figure 3A), and this effect was abrogated by the JNK inhibitor SP600125 in a dose-dependent manner, indicating that UII activated JNK (Figure 3B). To determine if UII-mediated JNK activation induced insulin resistance, cells were pretreated with SP600125. In parallel with decreased JNK phosphorylation, SP600125 (20 μmol/L) increased insulin-induced phosphorylation of IRS-1 and IRS proteins, followed by rescue of GSK-3β phosphorylation in HepG2 cells exposed to UII (Figure 3C). Moreover, SP600125 reversed the UII-induced decrease in cellular glycogen levels (Figure 3D). These results suggest that JNK activation by UII contributes to UII-induced insulin resistance in HepG2 cells.
UII elevates ROS production and NADPH oxidase subunit expressionROS generation is an important component of insulin resistance[28]. We thus further elucidated the molecular mechanisms responsible for UII-induced insulin resistance in HepG2 cells by assessing the effects of UII on ROS levels. HepG2 cells were exposed to different concentrations UII for 12 or 24 h, stained with DCF, and detected using a multimode reader. ROS levels were both dose- and time-dependently increased by UII in HepG2 cells (Figure 4A and B).
We also evaluated the relationship between ROS generation and NADPH oxidase by investigating NADPH oxidase subunit expression in response to UII and apocynin. NADPH oxidase subunits gp91phox, p67phox, p47phox, and p40phox protein levels were up-regulated in HepG2 cells treated with 100 nmol/L UII for 24 h (Figure 4C). Pretreatment with the NADPH synthase inhibitor apocynin for 30 min significantly inhibited the UII-induced generation of ROS (Figure 4D). Taken together, these results suggest that UII enhanced ROS production, at least in part, by increasing NADPH oxidase in HepG2 cells, consistent with its effects in PASMCs[27].
UII interferes with the insulin signaling pathway, and this effect is reversed by apocyninWe investigated if JNK activation and ROS over-production plays causal roles in UII-induced insulin resistance in HepG2 cells. ROS are known to facilitate the activation of JNK, and deletion or inhibition of JNK improved insulin sensitivity in mice[29]. In addition, the JNK pathway has been reported to mediate ROS generation in PASMCs induced by UII[27]. It is therefore possible that JNK may mediate ROS-induced insulin resistance. Our results showed that UII elevated the
resulted in abnormal glucose metabolism. Overall, these results indicate that UII induces an insulin-resistant state in HepG2 cells.
JNK activation by UII contributes to UII-induced insulin resistanceJNK has been reported to phosphorylate serine re-
5772 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
1.5
1.0
0.5
0.0
Cont
rol
Ins
Ins +
1 nm
ol/L U
II
Ins +
10 nm
ol/L U
II
Ins +
100 n
mol/L U
II
Cell
prol
ifera
tion
(of
cont
rol)
Control Ins
a
Ins + UII
c
UII
2.5
2.0
1.5
1.0
0.5
0.0
Gly
coge
n le
vel
(of
cont
rol)
Figure 1 Urotensin Ⅱ decreases glucose consumption and glycogen synthesis in HepG2 hepatocytes. HepG2 cells were cultured in the presence of 0, 1, 10, or 100 nmol/L urotensin Ⅱ (UII) for 24 h prior to stimulation with insulin (100 nmol/L, 30 min). Glucose consumption decreased in a dose-dependent manner (A). There was no cytotoxic effect of UII after incubation for 24 h (B). Exposure of HepG2 cells to UII (100 nmol/L, 24 h) reduced the intracellular glycogen content (C). Data from at least three independent experiments are presented as mean ± SD. aP < 0.05, bP < 0.01 vs control group; cP < 0.05 vs insulin (Ins) treatment alone.
b
c
1.5
1.0
0.5
0.0
Cont
rol
Ins
Ins +
1 nm
ol/L U
II
Ins +
10 nm
ol/L U
II
Ins +
100 n
mol/L U
II
Glu
cose
leve
l/pro
tein
con
cent
ratio
n (o
f co
ntro
l)A
B
C
Li YY et al . Urotensin Ⅱ induces insulin resistance in HepG2 cells

phosphorylation of JNK, and that this effect could be attenuated by apocynin (Figure 5A).
To determine if ROS and JNK are signaling in-termediates in hepatic insulin resistance targeted by UII, HepG2 cells were pretreated with apocynin for 30 min. Inhibition of ROS by apocynin prevented UII-induced inhibition of insulin-stimulated total IRS-1 expression and IRS-1 tyrosine phosphorylation (Figure 5B). Similarly, pretreatment with apocynin abrogated UII-inhibited Akt and GSK-3β phosphorylation (Figure 5C) and Glut 2 expression (Figure 5D) in HepG2 cells. Overall, these results suggest that UII-induced insulin resistance is mediated by NADPH oxidase-derived ROS via JNK pathways in HepG2 cells, in accordance with previous studies of palmitate and TNF-α[24,30].
DISCUSSIONInsulin resistance is an essential factor in the patho-genesis of T2DM. Plasma UII levels were shown to be raised in diabetic mice and inhibit skeletal muscle glucose transport, suggesting a vital role for UII in the initiation and development of insulin resistance[8,9]. Insulin resistance involves decreased uptake and utilization of glucose promoted by insulin, and leads to impaired glucose consumption and glycogen synthesis in the liver, which is one of the main target organs of insulin resistance. Disruption of the liver microenvironment as a result of elevated UII levels may induce hepatic insulin resistance. However, animal models of insulin resistance are complex, and it is
5773 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
180
180
42
kD
P-IRS-1
IRS-1
β-actin
Ins
UII
-
-
+
-
+
+
-
+
A
60
60
46
kD
Ins
UII
-
-
+
-
+
+
-
+
46
42
p-Akt
Akt
p-GSK-3β
GSK-3β
β-actin
B
57
42
kDGlut 2
β-actin
Ins
UII
-
-
+
-
+
+
-
+
C
Prot
ein
leve
l (of
con
trol
)
2.5
2.0
1.5
1.0
0.5
0.0Control Ins Ins + UII UII
P-IRS-1/β-actin
IRS-1/β-actind
ba
f
Prot
ein
leve
l (of
con
trol
)
4
3
2
1
0Control Ins Ins + UII UII
p-Akt/Akt
p-GSK-3β/GSK-3βd
d
a
d
Control Ins
d
Ins + UII
h
UII
2.0
1.5
1.0
0.5
0.0
Glu
t 2/β-
actin
(of
con
trol
)
Figure 2 Urotensin Ⅱ inhibits insulin receptor-mediated signal transduction in HepG2 cells. HepG2 cells were exposed to 100 nmol/L urotensin Ⅱ (UII) for 24 h prior to stimulation with insulin (100 nmol/L, 30 min), and total cell lysates were then subjected to Western blot analysis. UII impaired IRS-1 and Glut 2 protein levels and reduced phosphorylation of IRS-1, Akt, and GSK-3β (A-C). Data from at least three independent experiments are presented as the mean ± SD. bP < 0.01, dP < 0.001 vs control group; aP < 0.05, fP < 0.01, hP < 0.001 vs insulin treatment alone.
Li YY et al . Urotensin Ⅱ induces insulin resistance in HepG2 cells
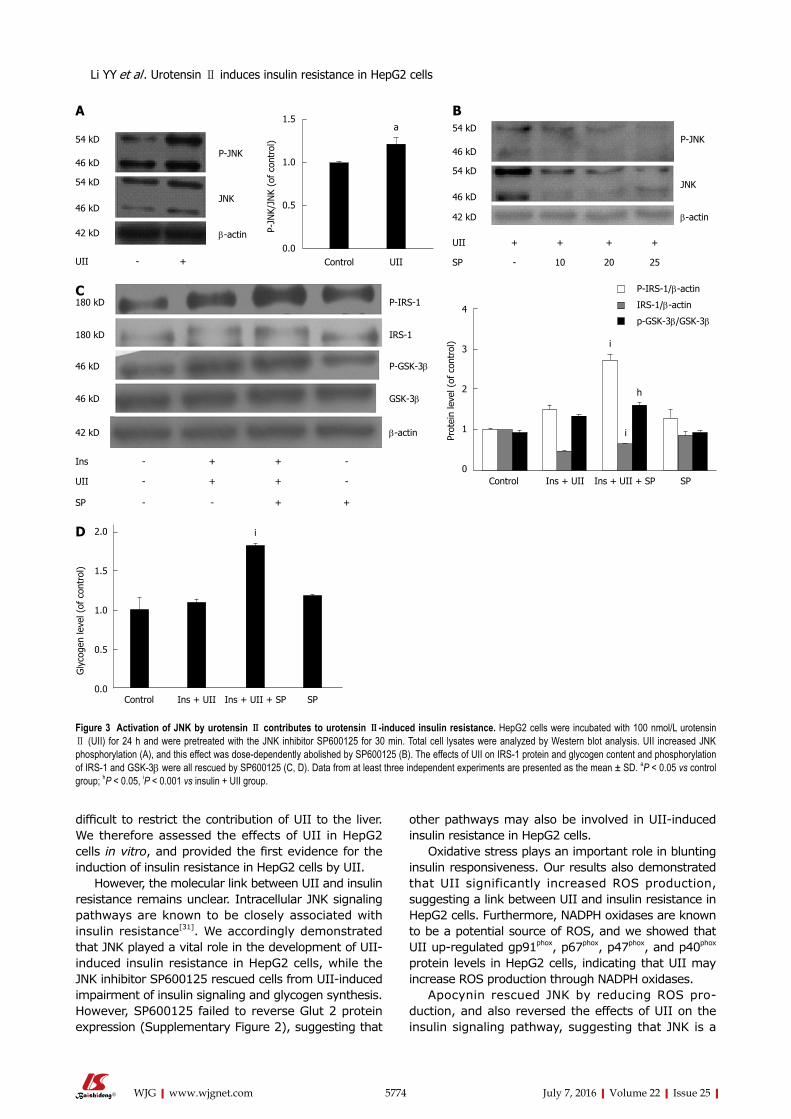
difficult to restrict the contribution of UII to the liver. We therefore assessed the effects of UII in HepG2 cells in vitro, and provided the first evidence for the induction of insulin resistance in HepG2 cells by UII.
However, the molecular link between UII and insulin resistance remains unclear. Intracellular JNK signaling pathways are known to be closely associated with insulin resistance[31]. We accordingly demonstrated that JNK played a vital role in the development of UII-induced insulin resistance in HepG2 cells, while the JNK inhibitor SP600125 rescued cells from UII-induced impairment of insulin signaling and glycogen synthesis. However, SP600125 failed to reverse Glut 2 protein expression (Supplementary Figure 2), suggesting that
other pathways may also be involved in UII-induced insulin resistance in HepG2 cells.
Oxidative stress plays an important role in blunting insulin responsiveness. Our results also demonstrated that UII significantly increased ROS production, suggesting a link between UII and insulin resistance in HepG2 cells. Furthermore, NADPH oxidases are known to be a potential source of ROS, and we showed that UII up-regulated gp91phox, p67phox, p47phox, and p40phox protein levels in HepG2 cells, indicating that UII may increase ROS production through NADPH oxidases.
Apocynin rescued JNK by reducing ROS pro-duction, and also reversed the effects of UII on the insulin signaling pathway, suggesting that JNK is a
5774 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Figure 3 Activation of JNK by urotensin Ⅱ contributes to urotensin Ⅱ-induced insulin resistance. HepG2 cells were incubated with 100 nmol/L urotensin Ⅱ (UII) for 24 h and were pretreated with the JNK inhibitor SP600125 for 30 min. Total cell lysates were analyzed by Western blot analysis. UII increased JNK phosphorylation (A), and this effect was dose-dependently abolished by SP600125 (B). The effects of UII on IRS-1 protein and glycogen content and phosphorylation of IRS-1 and GSK-3β were all rescued by SP600125 (C, D). Data from at least three independent experiments are presented as the mean ± SD. aP < 0.05 vs control group; hP < 0.05, iP < 0.001 vs insulin + UII group.
a
Control UII
1.5
1.0
0.5
0.0
P-JN
K/JN
K (o
f co
ntro
l)
54 kD
46 kD
54 kD
46 kD
42 kD
P-JNK
JNK
β-actin
UII + + + +
SP - 10 20 25
54 kD
46 kD
54 kD
46 kD
42 kD
P-JNK
JNK
β-actin
UII - +
A B
180 kD
180 kD
46 kD
46 kD
42 kD
P-IRS-1
IRS-1
β-actin
Ins - + + -
UII - + + -
SP - - + +
P-GSK-3β
GSK-3β
C
Control Ins + UII Ins + UII + SP
i
SP
2.0
1.5
1.0
0.5
0.0
Gly
coge
n le
vel (
of c
ontr
ol)
D
P-IRS-1/β-actin
IRS-1/β-actin
p-GSK-3β/GSK-3β
Prot
ein
leve
l (of
con
trol
)
4
3
2
1
0Control Ins + UII Ins + UII + SP SP
i
h
i
Li YY et al . Urotensin Ⅱ induces insulin resistance in HepG2 cells

5775 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
a1.5
1.0
0.5
0.0
ROS
leve
l/cel
l pro
lifer
atio
n (o
f co
ntro
l)
aa
Cont
rol
1 nmol/
L UII
10 nm
ol/L U
II
100 n
mol/L U
II
24 h
a
2.0
1.5
1.0
0.5
0.0
ROS
leve
l/cel
l pro
lifer
atio
n (o
f co
ntro
l)
a
Cont
rol
1 nmol/
L UII
10 nm
ol/L U
II
100 n
mol/L U
II
12 h
A B
65 kD
45 kD
67 kD
40 kD
22 kD
UII - +
42 kD
gp91phox
p47phox
p67phox
p40phox
p22phox
β-actin
Prot
ein
leve
l (of
con
trol
)
1.5
1.0
0.5
0.0gp91phox p47phox p67phox p22phox
Control
UIIb
aa
p40phox
b
C
g
1.5
1.0
0.5
0.0
ROS
leve
l/cel
l pro
lifer
atio
n (o
f co
ntro
l)
b
Control 100 nmol/L UII 100 nmol/L UII + Apo
D
Figure 4 Urotensin Ⅱ elevates reactive oxygen species production and NADPH oxidase subunit expression. HepG2 cells were cultured with 0, 1, 10, or 100 nmol/L urotensin Ⅱ (UII) for 24 h, with or without prior stimulation with apocynin (200 μmol/L, 30 min). Intracellular reactive oxygen species (ROS) production was elevated in a dose- and time-dependent manner (A, B). NADPH oxidase subunits gp91phox, p67phox, p47phox, and p40phox were significantly increased in response to UII (100 nmol/L, 24 h) (C). Apocynin pretreatment inhibited ROS generation (D). Data from at least three independent experiments are presented as the mean ± SD. aP < 0.05, bP < 0.01 vs control group; gP < 0.05 vs UII treatment alone.
Li YY et al . Urotensin Ⅱ induces insulin resistance in HepG2 cells

5776 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
54 kD46 kD
54 kD
46 kD
42 kD
P-JNK
JNK
β-actin
UII - + + -
Apo - - + +
180 kD
180 kD
42 kD
P-IRS-1
IRS-1
β-actin
Ins - + + +
UII - - + +
Apo - - - +
-
+
-
-
-
+
A B
Control UII UII + Apo
g
Apo
1.5
1.0
0.5
0.0
P-JN
K/JN
K (o
f co
ntro
l)
Prot
ein
leve
l (of
con
trol
)
3
2
1
0
Cont
rol
P-IRS-1/β-actin
IRS-1/β-actinh
Ins
Ins +
UII
Ins +
UII
+ Apo UI
IAp
o
h
60 kD
60 kD
46 kD
46 kD
42 kD
P-Akt
Akt
P-GSK-3β
Ins - + + +
UII - - + +
C
GSK-3β
β-actin
-
+
-
-
Apo - - - + - +
Prot
ein
leve
l (of
con
trol
)
4
3
2
1
0
Cont
rol
P-Akt/Akt
P-GSK-3β/GSK-3β
h
Ins
Ins +
UII
Ins +
UII
+ Apo UI
IAp
o
h
Li YY et al . Urotensin Ⅱ induces insulin resistance in HepG2 cells

downstream effector of ROS in UII-induced insulin resistance in HepG2 cells. In addition, the oxidative stress-induced decrease in insulin signaling contributes to inhibition of GSK-3β phosphorylation, the key enzyme in glycogen metabolism, and the facultative glucose transporter Glut2, which is located in/on the liver cell surface and transports molecules such as glucose and fructose in and out of the cells. These results are in accord with the findings in the liver of rats with high-fat diet-induced insulin resistance[32]. Our results demonstrated that UII alone did not alter GSK-3β phosphorylation and Glut 2 protein expression, but suppressed both of these in the presence of insulin, while pretreatment with either SP600125 or apocynin could reverse these effects. The changes in GSK-3β phosphorylation and/or Glut 2 expression suggest that the ability of insulin-stimulated HepG2 cells to take up glucose is partly blocked by exposure to UII, leading to decreased glucose consumption and hepatic glycogen synthesis. Collectively, these results demonstrate that UII impairs glucose consumption and glycogen synthesis in HepG2 cells, at least partly via a mechanism involving ROS production and the eventual occurrence of insulin resistance.
However, the effect of the ROS pathway may not be specific to UII, and chronic inflammation induced by adipokines and cytokines, associated with obesity or MetS, such as TNF-α and IL-6, is also known to
induce insulin resistance in the liver[33,34]. Indeed, UII has a strong proinflammatory effect[6], and the role of inflammatory cytokines accompanied by ROS in the development of insulin resistance should be further explored. Furthermore, ROS have been reported to affect various signaling pathways involving not only JNK, but also Foxo, JAK/signal transducer and activator of transcription, mitogen-activated protein kinase, p53, and phosphoinositide 3-kinase, depending on various factors including the types of ROS and cells, and the duration of exposure[35]. In addition to impairing glucose consumption and glycogen synthesis, hepatic insulin resistance could also suppress protein synthesis, lipogenesis, and increase hepatic gluconeo-genesis. However, further studies are needed to clarify the mechanisms responsible for UII-induced insulin resistance.
In summary, the results of the present study provide the first evidence demonstrating that UII enhances ROS levels by up-regulating NADPH oxidase subunits and promoting the phosphorylation of JNK, leading to reduced insulin sensitivity, glucose con-sumption, and glycogen synthesis in HepG2 cells. These results show that the effects of UII on insulin resistance are mediated by NADPH oxidase-derived ROS through the JNK pathway in HepG2 cells, and may be involved in the development of diabetes and MetS.
5777 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
57 kD
42 kD
Ins - + + +
Glut 2
β-actin
- -
UII - - + + + -
Apo - - - + - +
h
2.0
1.5
1.0
0.5
0.0
Glu
t 2/β-
actin
(of
con
trol
)
Cont
rol
Ins
Ins +
UII
Ins +
UII
+ Apo UI
IAp
o
D
Figure 5 Urotensin Ⅱ interferes with insulin signaling, and this effect is reversed by apocynin. HepG2 cells were exposed to 100 nmol/L urotensin Ⅱ (UII) for 24 h prior to stimulation with insulin (100 nmol/L, 30 min), and pretreatment with 200 μmol/L apocynin for 30 min. Total cell lysates were analyzed by Western blot. UII increased JNK phosphorylation, and this effect was abolished by apocynin (A); Protein levels of IRS-1 and Glut 2 and phosphorylation of IRS-1, Akt and GSK-3β were all reversed by apocynin (B-D). Data from at least three independent experiments are presented as the mean ± SD. gP < 0.05 vs UII treatment alone; hP < 0.05 vs insulin + UII group.
Li YY et al . Urotensin Ⅱ induces insulin resistance in HepG2 cells

COMMENTSBackgroundInsulin resistance is associated with many diseases, such as obesity, metabolic syndrome (MetS) and type Ⅱ diabetes mellitus (T2DM). Urotensin Ⅱ (UII) is also involved in MetS in addition to its significant role in the cardiovascular system, and plays an important role in the pathogenesis of insulin resistance and development of T2DM, but the exact mechanism remains unclear.
Research frontiersUII, a vasoactive peptide expressed in various tissues and organs, promotes endothelial cell proliferation, regulates blood pressure and is involved in glucose homeostasis. Recent studies show that UII gene polymorphism is positively correlated with insulin resistance. UII knockout mice had significantly decreased plasma insulin and glucose levels and increased tolerance. Moreover, elevated UII impairs insulin signaling in the muscle of diabetic model mice. The research hotspot is the mechanism of UII to induce insulin resistance.
Innovations and breakthroughsIn this article, the authors investigated the effects and mechanisms of UII in inducing insulin resistance in HepG2 cells. They provide the first evidence demonstrating that UII enhances ROS levels by up-regulating NADPH oxidase subunits and promotes the phosphorylation of JNK, which together lead to hepatic insulin resistance.
ApplicationsThe study results suggest that UII induces insulin resistance, and may be a new target for preventing the development of MetS and diabetes in future.
TerminologyUII, a vasoactive cyclic peptide, plays a variety of biological effects after binding to UII receptor. Studies have shown that UII participates in the pathological processes of many diseases, such as coronary heart disease, high blood pressure, diabetes and renal failure. In addition to its significant role in the cardiovascular system, the up-regulation of UII directly affects the pancreas, which results in impaired pancreatic beta cells, reduced glucose-induced insulin secretion, and damaged glucose tolerance.
Peer-reviewIn this study, Li and collaborators address, quite convincingly, that UII is an inducer of hepatic insulin resistance by studying the impact of a 24-h UII pre-treatment of hepatic cells HepG2 on subsequent insulin action. Authors show that pre-treatment of HepG2 cells with UII decreased hepatic glucose uptake, glycogen synthesis and diminished the activation of the key insulin-signaling molecules IRS1, PKB and GSK3 as assessed by the use of phospho-specific antibodies. Putative mechanisms are presented, including the upregulation of JNK activation and the NADPH oxidase compounds and consequent oxidative stress. This is a very well performed study, and the results are quite convincing.
REFERENCES1 Pearson D, Shively JE, Clark BR, Geschwind II, Barkley M,
Nishioka RS, Bern HA. Urotensin II: a somatostatin-like peptide in the caudal neurosecretory system of fishes. Proc Natl Acad Sci USA 1980; 77: 5021-5024 [PMID: 6107911 DOI: 10.1073/pnas.77.8.5021]
2 Coulouarn Y, Lihrmann I, Jegou S, Anouar Y, Tostivint H, Beauvillain JC, Conlon JM, Bern HA, Vaudry H. Cloning of the cDNA encoding the urotensin II precursor in frog and human reveals intense expression of the urotensin II gene in motoneurons of the spinal cord. Proc Natl Acad Sci USA 1998; 95: 15803-15808 [PMID: 9861051 DOI: 10.1073/pnas.95.26.15803]
3 Ames RS, Sarau HM, Chambers JK, Willette RN, Aiyar NV, Romanic AM, Louden CS, Foley JJ, Sauermelch CF, Coatney RW, Ao Z, Disa J, Holmes SD, Stadel JM, Martin JD, Liu WS, Glover GI, Wilson S, McNulty DE, Ellis CE, Elshourbagy NA, Shabon U, Trill JJ, Hay DW, Ohlstein EH, Bergsma DJ, Douglas SA. Human
urotensin-II is a potent vasoconstrictor and agonist for the orphan receptor GPR14. Nature 1999; 401: 282-286 [PMID: 10499587 DOI: 10.1038/45809]
4 Ross B, McKendy K, Giaid A. Role of urotensin II in health and disease. Am J Physiol Regul Integr Comp Physiol 2010; 298: R1156-R1172 [PMID: 20421634 DOI: 10.1152/ajpregu.00706.2009]
5 Watanabe T, Arita S, Shiraishi Y, Suguro T, Sakai T, Hongo S, Miyazaki A. Human urotensin II promotes hypertension and atherosclerotic cardiovascular diseases. Curr Med Chem 2009; 16: 550-563 [PMID: 19199921 DOI: 10.2174/092986709787458515]
6 Barrette PO, Schwertani AG. A closer look at the role of urotensin II in the metabolic syndrome. Front Endocrinol (Lausanne) 2012; 3: 165 [PMID: 23293629 DOI: 10.3389/fendo.2012.00165]
7 Silvestre RA, Egido EM, Hernández R, Marco J. Characterization of the insulinostatic effect of urotensin II: a study in the perfused rat pancreas. Regul Pept 2009; 153: 37-42 [PMID: 19101596 DOI: 10.1016/j.regpep.2008.11.008]
8 Wang HX, Zeng XJ, Liu Y, Wang J, Lu LQ, Hao G, Zhang LK, Tang CS. Elevated expression of urotensin II and its receptor in skeletal muscle of diabetic mouse. Regul Pept 2009; 154: 85-90 [PMID: 19323985 DOI: 10.1016/j.regpep.2009.01.004]
9 Wang HX, Wu XR, Yang H, Yin CL, Shi LJ, Wang XJ. Urotensin II inhibits skeletal muscle glucose transport signaling pathways via the NADPH oxidase pathway. PLoS One 2013; 8: e76796 [PMID: 24116164 DOI: 10.1371/journal.pone.0076796]
10 Wang H, Dong K, Xue X, Feng P, Wang X. Elevated expression of urotensin II and its receptor in diethylnitrosamine-mediated precancerous lesions in rat liver. Peptides 2011; 32: 382-387 [PMID: 21056072 DOI: 10.1016/j.peptides.2010.10.032]
11 Kiss RS, You Z, Genest J, Behm DJ, Giaid A. Urotensin II differentially regulates macrophage and hepatic cholesterol homeostasis. Peptides 2011; 32: 956-963 [PMID: 21376094 DOI: 10.1016/j.peptides.2011.02.016]
12 You Z, Genest J, Barrette PO, Hafiane A, Behm DJ, D’Orleans-Juste P, Schwertani AG. Genetic and pharmacological manipulation of urotensin II ameliorate the metabolic and atherosclerosis sequalae in mice. Arterioscler Thromb Vasc Biol 2012; 32: 1809-1816 [PMID: 22723440 DOI: 10.1161/ATVBAHA.112.252973]
13 Meshkani R, Adeli K. Hepatic insulin resistance, metabolic syndrome and cardiovascular disease. Clin Biochem 2009; 42: 1331-1346 [PMID: 19501581 DOI: 10.1016/j.clinbiochem.2009.05.018]
14 Yin J, Hu R, Chen M, Tang J, Li F, Yang Y, Chen J. Effects of berberine on glucose metabolism in vitro. Metabolism 2002; 51: 1439-1443 [PMID: 12404195 DOI: 10.1053/meta.2002.34715]
15 Pereira S, Park E, Mori Y, Haber CA, Han P, Uchida T, Stavar L, Oprescu AI, Koulajian K, Ivovic A, Yu Z, Li D, Bowman TA, Dewald J, El-Benna J, Brindley DN, Gutierrez-Juarez R, Lam TK, Najjar SM, McKay RA, Bhanot S, Fantus IG, Giacca A. FFA-induced hepatic insulin resistance in vivo is mediated by PKCδ, NADPH oxidase, and oxidative stress. Am J Physiol Endocrinol Metab 2014; 307: E34-E46 [PMID: 24824652 DOI: 10.1152/ajpendo.00436.2013]
16 Solomon SS, Buss N, Shull J, Monnier S, Majumdar G, Wu J, Gerling IC. Proteome of H-411E (liver) cells exposed to insulin and tumor necrosis factor-alpha: analysis of proteins involved in insulin resistance. J Lab Clin Med 2005; 145: 275-283 [PMID: 15902099 DOI: 10.1016/j.lab.2005.02.013]
17 Senn JJ, Klover PJ, Nowak IA, Mooney RA. Interleukin-6 induces cellular insulin resistance in hepatocytes. Diabetes 2002; 51: 3391-3399 [PMID: 12453891 DOI: 10.2337/diabetes.51.12.3391]
18 Luo Z, Zhang Y, Li F, He J, Ding H, Yan L, Cheng H. Resistin induces insulin resistance by both AMPK-dependent and AMPK-independent mechanisms in HepG2 cells. Endocrine 2009; 36: 60-69 [PMID: 19440859 DOI: 10.1007/s12020-009-9198-7]
19 Kaneto H, Katakami N, Matsuhisa M, Matsuoka TA. Role of reactive oxygen species in the progression of type 2 diabetes and atherosclerosis. Mediators Inflamm 2010; 2010: 453892 [PMID: 20182627 DOI: 10.1155/2010/453892]
20 Delbosc S, Paizanis E, Magous R, Araiz C, Dimo T, Cristol JP, Cros
5778 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
COMMENTS
Li YY et al . Urotensin Ⅱ induces insulin resistance in HepG2 cells

G, Azay J. Involvement of oxidative stress and NADPH oxidase activation in the development of cardiovascular complications in a model of insulin resistance, the fructose-fed rat. Atherosclerosis 2005; 179: 43-49 [PMID: 15721008 DOI: 10.1016/j.atherosclerosis.2004.10.018]
21 Wei Y, Sowers JR, Clark SE, Li W, Ferrario CM, Stump CS. Angiotensin II-induced skeletal muscle insulin resistance mediated by NF-kappaB activation via NADPH oxidase. Am J Physiol Endocrinol Metab 2008; 294: E345-E351 [PMID: 18073321 DOI: 10.1152/ajpendo.00456.2007]
22 Wei Y, Sowers JR, Nistala R, Gong H, Uptergrove GM, Clark SE, Morris EM, Szary N, Manrique C, Stump CS. Angiotensin II-induced NADPH oxidase activation impairs insulin signaling in skeletal muscle cells. J Biol Chem 2006; 281: 35137-35146 [PMID: 16982630 DOI: 10.1074/jbc.M601320200]
23 Yu XT, Wang PY, Shi ZM, Dong K, Feng P, Wang HX, Wang XJ. Up-regulation of urotensin II and its receptor contributes to human hepatocellular carcinoma growth via activation of the PKC, ERK1/2, and p38 MAPK signaling pathways. Molecules 2014; 19: 20768-20779 [PMID: 25514221 DOI: 10.3390/molecules191220768]
24 Gao D, Nong S, Huang X, Lu Y, Zhao H, Lin Y, Man Y, Wang S, Yang J, Li J. The effects of palmitate on hepatic insulin resistance are mediated by NADPH Oxidase 3-derived reactive oxygen species through JNK and p38MAPK pathways. J Biol Chem 2010; 285: 29965-29973 [PMID: 20647313 DOI: 10.1074/jbc.M110.128694]
25 Hirosumi J, Tuncman G, Chang L, Görgün CZ, Uysal KT, Maeda K, Karin M, Hotamisligil GS. A central role for JNK in obesity and insulin resistance. Nature 2002; 420: 333-336 [PMID: 12447443 DOI: 10.1038/nature01137]
26 Nakatani Y, Kaneto H, Kawamori D, Hatazaki M, Miyatsuka T, Matsuoka TA, Kajimoto Y, Matsuhisa M, Yamasaki Y, Hori M. Modulation of the JNK pathway in liver affects insulin resistance status. J Biol Chem 2004; 279: 45803-45809 [PMID: 15331609 DOI: 10.1074/jbc.M406963200]
27 Djordjevic T, BelAiba RS, Bonello S, Pfeilschifter J, Hess J,
Görlach A. Human urotensin II is a novel activator of NADPH oxidase in human pulmonary artery smooth muscle cells. Arterioscler Thromb Vasc Biol 2005; 25: 519-525 [PMID: 15618545 DOI: 10.1161/01.ATV.0000154279.98244.eb]
28 Henriksen EJ, Diamond-Stanic MK, Marchionne EM. Oxidative stress and the etiology of insulin resistance and type 2 diabetes. Free Radic Biol Med 2011; 51: 993-999 [PMID: 21163347 DOI: 10.1016/j.freeradbiomed.2010.12.005]
29 Kaneto H, Nakatani Y, Miyatsuka T, Kawamori D, Matsuoka TA, Matsuhisa M, Kajimoto Y, Ichijo H, Yamasaki Y, Hori M. Possible novel therapy for diabetes with cell-permeable JNK-inhibitory peptide. Nat Med 2004; 10: 1128-1132 [PMID: 15448687 DOI: 10.1038/nm1111]
30 Li L, He Q, Huang X, Man Y, Zhou Y, Wang S, Wang J, Li J. NOX3-derived reactive oxygen species promote TNF-alpha-induced reductions in hepatocyte glycogen levels via a JNK pathway. FEBS Lett 2010; 584: 995-1000 [PMID: 20102709 DOI: 10.1016/j.febslet.2010.01.044]
31 Pal M, Febbraio MA, Lancaster GI. The roles of c-Jun NH2-terminal kinases (JNKs) in obesity and insulin resistance. J Physiol 2016; 594: 267-279 [PMID: 26608096 DOI: 10.1113/JP271457]
32 Gan KX, Wang C, Chen JH, Zhu CJ, Song GY. Mitofusin-2 ameliorates high-fat diet-induced insulin resistance in liver of rats. World J Gastroenterol 2013; 19: 1572-1581 [PMID: 23538485 DOI: 10.3748/wjg.v19.i10.1572]
33 Khodabandehloo H, Gorgani-Firuzjaee S, Panahi G, Meshkani R. Molecular and cellular mechanisms linking inflammation to insulin resistance and β-cell dysfunction. Transl Res 2016; 167: 228-256 [PMID: 26408801 DOI: 10.1016/j.trsl.2015.08.011]
34 Xu L, Kitade H, Ni Y, Ota T. Roles of Chemokines and Chemokine Receptors in Obesity-Associated Insulin Resistance and Nonal-coholic Fatty Liver Disease. Biomolecules 2015; 5: 1563-1579 [PMID: 26197341 DOI: 10.3390/biom5031563]
35 Zephy D, Ahmad J. Type 2 diabetes mellitus: Role of melatonin and oxidative stress. Diabetes Metab Syndr 2015; 9: 127-131 [PMID: 25450812 DOI: 10.1016/j.dsx.2014.09.018]
P- Reviewer: Pirola L, Zhang J S- Editor: Yu J L- Editor: Wang TQ E- Editor: Ma S
5779 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Li YY et al . Urotensin Ⅱ induces insulin resistance in HepG2 cells

Edward Wolfgang Lee, Andrew Kuei, Sammy Saab, Ronald W Busuttil, Francisco Durazo, Steven-Huy Han, Mohamed M El-Kabany, Justin P McWilliams, Stephen T Kee
Edward Wolfgang Lee, Andrew Kuei, Justin P McWilliams, Stephen T Kee, Department of Radiology, Division of Interventional Radiology, Ronald Reagan Medical Center at UCLA, David Geffen School of Medicine at UCLA, Los Angeles, CA 90095, United States
Sammy Saab, Francisco Durazo, Steven-Huy Han, Mohamed M El-Kabany, Department of Medicine, Division of Hepatology, Pfleger Liver Institute, University of California at Los Angeles, Los Angeles, CA 90095, United States
Ronald W Busuttil, Dumont-UCLA Transplant Center, Pfleger Liver Institute, Division of Liver and Pancreas Transplantation, Department of Surgery, David Geffen School of Medicine at University of California, Los Angeles, Los Angeles, CA 90095, United States
Author contributions: Lee EW, Kuei A, Saab S, Busuttil RW, Durazo F, Han SH, El-Kabany MM, McWilliams JP and Kee ST equally contributed to this paper with conception and design of the study, literature review and analysis, drafting and critical revision and editing, and final approval of the final version.
Institutional review board statement: As this study used a national database with only deidentified patient and hospital data, this study meets the “Exempt” criteria by the Institutional Board Review.
Conflict-of-interest statement: No financial conflict-of-interest to disclose.
Data sharing statement: No additional data are available.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Correspondence to: Edward W Lee, MD, PhD, Department of Radiology, Division of Interventional Radiology, Ronald Reagan Medical Center at UCLA, David Geffen School of Medicine at UCLA, 757 Westwood Plaza, Suite 2125, Los Angeles, CA 90095, United States. [email protected]: +1-310-2678771Fax: +1-310-2061294
Received: March 14, 2016Peer-review started: March 15, 2016First decision: March 31, 2016Revised: April 21, 2016Accepted: May 4, 2016Article in press: May 4, 2016Published online: July 7, 2016
AbstractAIM: To evaluate and validate the national trends and predictors of in-patient mortality of transjugular intrahepatic portosystemic shunt (TIPS) in 15 years.
METHODS: Using the National Inpatient Sample which is a part of Health Cost and Utilization Project, we identified a discharge-weighted national estimate of 83884 TIPS procedures performed in the United States from 1998 to 2012 using international classification of diseases-9 procedural code 39.1. The demographic, hospital and co-morbility data were analyzed using a multivariant analysis. Using multi-nominal logistic regression analysis, we determined predictive factors related to increases in-hospital mortality. Comorbidity measures are in accordance to the Comorbidity Software designed by the Agency for Healthcare Research and Quality.
RESULTS: Overall, 12.3% of patients died during hospitalization with downward trend in-hospital
ORIGINAL ARTICLE
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.3748/wjg.v22.i25.5780
World J Gastroenterol 2016 July 7; 22(25): 5780-5789 ISSN 1007-9327 (print) ISSN 2219-2840 (online)
© 2016 Baishideng Publishing Group Inc. All rights reserved.
5780 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Retrospective Study
Nationwide trends and predictors of inpatient mortality in 83884 transjugular intrahepatic portosystemic shunt

INTRODUCTIONTransjugular intrahepatic portosystemic shunt, or TIPS, is currently the most commonly performed interventional procedure to treat complications of portal hypertension. TIPS achieves portal decompression through the placement of a stent bridging the hepatic and portal veins. The American Association for the Study of Liver Diseases indications for this procedure include refractory variceal bleeding and ascites[1]. Over 20 years of clinical experience have better defined TIPS candidacy and brought technical advancements such as polytetraflouroethylenne (PTFE) covered stents that have enhanced long term clinical outcomes[2]. However, TIPS remains a procedure full of clinical challenges. Patients are expected to be monitored overnight following the procedure for a number of complications including hemorrhage from extracapsular puncture, hepatic encephalopathy, injury to the bile duct, or hepatic artery and portal vein, shunt stenosis/thrombosis/occlusion, congestive heart failure, acute pulmonary edema and death[3].
Factors affecting patient survival following TIPS have been extensively studied in the past. Detailed patient markers proposed including Model for End-stage Liver Disease (MELD) scoring, Child-Pugh scoring, serum bilirubin, and serum creatinine have found use in daily clinical practice[48]. However, the majority of these studies are of (1) a limited sample size; (2) outside of directly measurable patient factors; and (3) lacking broadspectrum analysis. No contemporary nationwide analysis of patient demographic, hospital, and diagnostic data to inpatient mortality has been performed. Utilizing data from the National Inpatient Sample from 1998 to 2012, we aimed to investigate national trends in incidence and TIPS mortality and shed insight on new factors possibly associated with inpatient death.
MATERIALS AND METHODSThe National (Nationwide) Inpatient Sample (NIS) is a family of hospital discharge databases part of the Healthcare Cost and Utilization Project (HCUP). The NIS is the largest publically available allpayer inpatient health care database, containing unweighted data from over 7 million hospital stays each year. NIS data approximates a 20percent stratified sample of all discharges from United States community hospitals, excluding rehabilitation and longterm acute care hospitals. The samples are designed to facilitate dischargelevel weighting for producing national estimates. Used for this study are the 15years NIS data sets from year 1998 to 2012. This study uses only deidentified patient and hospital data and meets the
Lee EW et al . Nationwide trends of mortality in 83884 TIPS in United States
5781 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
mortality with the mean length of stay of 10.8 ± 13.1 d. Notable, African American patients (OR = 1.809 vs Caucasian patients, P < 0.001), transferred patients (OR = 1.347 vs non-transferred, P < 0.001), emergency admissions (OR = 3.032 vs elective cases, P < 0.001), patients in the Northeast region (OR = 1.449 vs West, P < 0.001) had significantly higher odds of in-hospital mortality. Number of diagnoses and number of procedures showed positive correlations with in-hospital death (OR = 1.249 per one increase in number of procedures). Patients diagnosed with acute respiratory failure (OR = 8.246), acute kidney failure (OR = 4.359), hepatic encephalopathy (OR = 2.217) and esophageal variceal bleeding (OR = 2.187) were at considerably higher odds of in-hospital death compared with ascites (OR = 0.136, P < 0.001). Comorbidity measures with the highest odds of in-hospital death were fluid and electrolyte disorders (OR = 2.823), coagulopathy (OR = 2.016), and lymphoma (OR = 1.842).
CONCLUSION: The overall mortality of the TIPS procedure is steadily decreasing, though the length of stay has remained relatively constant. Specific patient ethnicity, location, transfer status, primary diagnosis and comorbidities correlate with increased odds of TIPS in-hospital death.
Key words: Transjugular intrahepatic portosystemic shunt; Mortality; Inpatient; United States; National Inpatient Sample database; Health Cost and Utilization Project
© The Author(s) 2016. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: This is the first large-scale, national trends data investigating in-patient death following trans-jugular intrahepatic portosystemic shunt (TIPS) using the National Inpatient Sample database from 1998 to 2012. Over 80000 TIPS related data have been investigated. Overall in-patient mortality has been down-trending over the past 15 years. A significant decrease of mortality occurred after 2005 with an introduction of covered stent graft for TIPS which improved the patient survival and TIPS outcomes. Specific patient ethnicity, location, transfer status, primary diagnosis and comorbidities correlate with increased odds of in-hospital death after TIPS.
Lee EW, Kuei A, Saab S, Busuttil RW, Durazo F, Han SH, El-Kabany MM, McWilliams JP, Kee ST. Nationwide trends and predictors of inpatient mortality in 83884 transjugular intrahepatic portosystemic shunt. World J Gastroenterol 2016; 22(25): 5780-5789 Available from: URL: http://www.wjgnet.com/1007-9327/full/v22/i25/5780.htm DOI: http://dx.doi.org/10.3748/wjg.v22.i25.5780
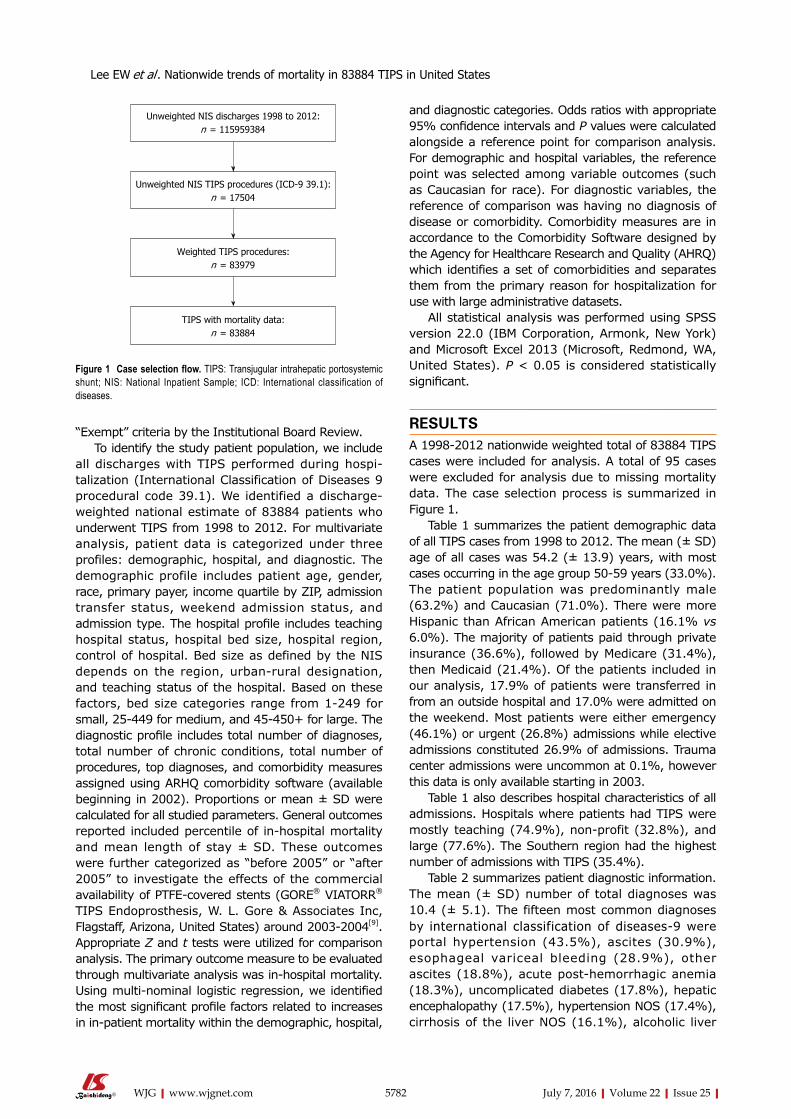
“Exempt” criteria by the Institutional Board Review. To identify the study patient population, we include
all discharges with TIPS performed during hospitalization (International Classification of Diseases 9 procedural code 39.1). We identified a discharge-weighted national estimate of 83884 patients who underwent TIPS from 1998 to 2012. For multivariate analysis, patient data is categorized under three profiles: demographic, hospital, and diagnostic. The demographic profile includes patient age, gender, race, primary payer, income quartile by ZIP, admission transfer status, weekend admission status, and admission type. The hospital profile includes teaching hospital status, hospital bed size, hospital region, control of hospital. Bed size as defined by the NIS depends on the region, urbanrural designation, and teaching status of the hospital. Based on these factors, bed size categories range from 1-249 for small, 25449 for medium, and 45450+ for large. The diagnostic profile includes total number of diagnoses, total number of chronic conditions, total number of procedures, top diagnoses, and comorbidity measures assigned using ARHQ comorbidity software (available beginning in 2002). Proportions or mean ± SD were calculated for all studied parameters. General outcomes reported included percentile of inhospital mortality and mean length of stay ± SD. These outcomes were further categorized as “before 2005” or “after 2005” to investigate the effects of the commercial availability of PTFE-covered stents (GORE® VIATORR® TIPS Endoprosthesis, W. L. Gore & Associates Inc, Flagstaff, Arizona, United States) around 2003-2004[9]. Appropriate Z and t tests were utilized for comparison analysis. The primary outcome measure to be evaluated through multivariate analysis was inhospital mortality. Using multinominal logistic regression, we identified the most significant profile factors related to increases in inpatient mortality within the demographic, hospital,
and diagnostic categories. Odds ratios with appropriate 95% confidence intervals and p values were calculated alongside a reference point for comparison analysis. For demographic and hospital variables, the reference point was selected among variable outcomes (such as Caucasian for race). For diagnostic variables, the reference of comparison was having no diagnosis of disease or comorbidity. Comorbidity measures are in accordance to the Comorbidity Software designed by the Agency for Healthcare Research and Quality (AHRQ) which identifies a set of comorbidities and separates them from the primary reason for hospitalization for use with large administrative datasets.
All statistical analysis was performed using SPSS version 22.0 (IBM Corporation, Armonk, New York) and Microsoft Excel 2013 (Microsoft, Redmond, WA, United States). p < 0.05 is considered statistically significant.
RESULTSA 19982012 nationwide weighted total of 83884 TIPS cases were included for analysis. A total of 95 cases were excluded for analysis due to missing mortality data. The case selection process is summarized in Figure 1.
Table 1 summarizes the patient demographic data of all TIPS cases from 1998 to 2012. The mean (± SD) age of all cases was 54.2 (± 13.9) years, with most cases occurring in the age group 50-59 years (33.0%). The patient population was predominantly male (63.2%) and Caucasian (71.0%). There were more Hispanic than African American patients (16.1% vs 6.0%). The majority of patients paid through private insurance (36.6%), followed by Medicare (31.4%), then Medicaid (21.4%). Of the patients included in our analysis, 17.9% of patients were transferred in from an outside hospital and 17.0% were admitted on the weekend. Most patients were either emergency (46.1%) or urgent (26.8%) admissions while elective admissions constituted 26.9% of admissions. Trauma center admissions were uncommon at 0.1%, however this data is only available starting in 2003.
Table 1 also describes hospital characteristics of all admissions. Hospitals where patients had TIPS were mostly teaching (74.9%), non-profit (32.8%), and large (77.6%). The Southern region had the highest number of admissions with TIPS (35.4%).
Table 2 summarizes patient diagnostic information. The mean (± SD) number of total diagnoses was 10.4 (± 5.1). The fifteen most common diagnoses by international classification of diseases9 were portal hypertension (43.5%), ascites (30.9%), esophageal variceal bleeding (28.9%), other ascites (18.8%), acute post-hemorrhagic anemia (18.3%), uncomplicated diabetes (17.8%), hepatic encephalopathy (17.5%), hypertension NOS (17.4%), cirrhosis of the liver NOS (16.1%), alcoholic liver
5782 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Unweighted NIS discharges 1998 to 2012:n = 115959384
Unweighted NIS TIPS procedures (ICD-9 39.1): n = 17504
Weighted TIPS procedures: n = 83979
TIPS with mortality data: n = 83884
Figure 1 Case selection flow. TIPS: Transjugular intrahepatic portosystemic shunt; NIS: National Inpatient Sample; ICD: International classification of diseases.
Lee EW et al . Nationwide trends of mortality in 83884 TIPS in United States

NOS (13.3%), esophageal varices with no bleeding (13.1%), and acute respiratory failure (12.8%). Liver disease (84.1%), fluid and electrolyte disorders (36.8%), and coagulopathy (35.7%), were the most common AHRQ comorbidity measures in the patient population.
Figure 2 demonstrates the overall mortality out-comes of TIPS cases from 19982012. In all cases, 12.3% of patients died during hospitalization. More patients died during hospitalization before 2005 (13.5%) than after 2005 (11.5%). The overall mean (± SD) length of stay of 10.83 (± 13.10) d has remained relatively unchanged before (10.78 ± 13.09 d) and after 2005 (10.89 ± 13.12 d). Figure 2A depicts number of TIPS admissions yearly. Figure 2B charts TIPS inhospital mortality by year and compares outcomes by common indications (ascites and esophageal variceal bleeding) and the complication of hepatic encephalopathy. As expected, overall mortality with TIPS is gradually declining (-0.22% yearly), more so in patients with ascites (-0.34% yearly) than esophageal variceal bleeding (-0.01% yearly). Patient mortality in those diagnosed with hepatic encephalopathy have shown a greater rate of decline
cirrhosis (15.3%), thrombocytopenia NOS (15.0%), varices of other sites (13.7%), acute kidney failure
5783 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Table 1 Demographic and hospital data1
Percent χ 2 P value
Age (yr) < 0.001 0-9 0.9% 10-19 1.3% 20-29 2.6% 30-39 6.3% 40-49 22.4% 50-59 33.0% 60-69 20.8% 70-79 10.4% 80-89 2.3% 90-99 0.1%Age > 70 11.4% < 0.001Sex < 0.001 Male 63.2% Female 36.8%Race < 0.001 White 71.0% Black 6.0% Hispanic 16.1% Asian/Pacific Islander 2.0% Native American 0.9% Other 3.5% Unknown 0.4%Primary payer < 0.001 Medicare 31.4% Medicaid 21.4% Private 36.6% Self-Pay 5.6%Income quartile by ZIP code < 0.001 (1) Quartile 1 28.3% (2) Quartile 2 26.9% (3) Quartile 3 24.5% (4) Quartile 4 19.4% Missing 0.8%Transfer status < 0.001 Transferred in from acute care hospital
17.9%
Not transfer 79.3%Weekend admission status < 0.001 Admitted on weekend (1) 17.0% Not admitted on weekend (0) 83.0%Admission type < 0.001 Emergency 46.1% Urgent 26.8% Elective 26.9% Trauma center 0.1%Hospital type < 0.001 Teaching hospital 74.9% Non-Teaching hospital 25.1%Hospital bed size < 0.001 Small 4.4% Medium 18.0% Large 77.6%Hospital region < 0.001 Northeast 17.8% Midwest 22.7% South 35.4% West 24.2%Control of hospital < 0.001 Private, non-profit 32.8% Private, investor owned 5.8%
1Number of cases (weighted): 83884; Age, mean ± SD: Mean 54.2 ± 13.9.
Table 2 Diagnostic data1
Percent χ 2 P value
Diagnosis (ICD-9 code) Portal hypertension (572.3) 43.5% < 0.001 Ascites (789.5) 30.9% Esophageal variceal bleeding (456.20) 28.9% Other ascites (789.59) 18.8% Acute post-hemorrhagic anemia (285.1) 18.3% Diabetes, uncomplicated (250.00) 17.8% Hepatic encephalopathy (572.2) 17.5% Hypertension NOS (401.9) 17.4% Cirrhosis of liver NOS (571.5) 16.1% Alcoholic Liver Cirrhosis (571.2) 15.3% Thrombocytopenia NOS (287.5) 15.0% Varices of other sites (456.8) 13.7% Acute kidney failure NOS (584.9) 13.3% Esophageal varices w/no bleeding (456.21) 13.1% Acute respiratory failure (518.81) 12.8%AHRQ comorbidity measure AIDS 0.7% < 0.001 CHF 5.2% < 0.001 Coagulopathy 35.7% < 0.001 Liver disease 84.1% < 0.001 Lymphoma 0.6% < 0.001 Fluid and electrolyte disorders 36.8% < 0.001 Metastatic cancer 1.3% < 0.001 Perivascular disease 3.7% < 0.001 Pulmonary circulation disorders 3.2% < 0.001 Renal failure 13.6% < 0.001 Solid tumor without mets 3.3% < 0.001 Valvular disease 2.4% < 0.001 Weight loss 14.0% < 0.001
1Number of diagnoses, mean ± SD: Mean 10.4 ± 5.1; Number of chronic conditions, mean ± SD: Mean 6.0 ± 2.6; Number of procedures, mean ± SD: Mean 4.8 ± 3.3. AIDS: Acquired immune deficiency syndrome; CHF: Congestive heart failure; ICD: International classification of diseases; AHRQ: Agency for Healthcare Research and Quality.
Lee EW et al . Nationwide trends of mortality in 83884 TIPS in United States

than average (-0.89% yearly). Through multivariate analysis using logistic re
gression and independent sample ttests, we were able to identify predictors correlated with increased inhospital death. Morbidity outcomes were directly compared to patient demographic factors (Table 3), hospital data (Table 3), and diagnostic factors (Table 4). Figure 3 compares odds of in-hospital mortality by age referenced to age group 50-59. Figure 4 depicts odds of in-hospital mortality in the presence of AHRQ comorbidity factors.
Compared to the most common cohort of patients age 5059, relative odds of inhospital mortality were significantly lower in patients below age 30 (OR = 0.439, p < 0.001). Beyond age 70, odds of death appeared to increase incrementally, though statistically significant odds data for patients 9099 years old is unavailable (p = 0.405). Males had at slightly higher odds of in-hospital mortality than females (OR = 1.072, p < 0.001). Black and Native American patients had markedly higher odds in-hospital death compared to Caucasians (OR = 1.809, p < 0.001 and OR = 1.696, p < 0.001). Self-paying patients had 1.610 times higher odds of in-hospital death than private payers (p < 0.001). Patient income did not appear to be a statistically significant
marker of inhospital mortality. Transfers from an acute care hospital were at 1.347
times higher odds of inhospital mortality than nontransfers (p < 0.001), while weekend admissions were at 1.423 times higher odds of inhospital death than weekday admissions (p < 0.001). Compared to elective admissions, those categorized by the hospital as emergency admissions were at 3.032 times higher risk of in-hospital death (p < 0.001).
Patients in teaching hospitals were at slightly higher odds of in-hospital death (OR = 1.149, p < 0.001). Patients admitted to hospitals in the Northeast had considerably higher odds of inhospital death to those in the West (OR = 1.449, p < 0.001), while patients in the South had slightly lower odds (OR = 0.917, p = 0.002). Patients in the Midwest had similar odds (OR = 0.982, p = 0.572).
The number of diagnoses and number of procedures show expectedly positive correlations with inhospital death, though the number of procedures exhibit a stronger relationship (OR = 1.249 per one increase in number of procedures, p < 0.001). Of the fifteen most common diagnoses, acute respiratory failure exhibited highest odds of in-hospital death (OR = 8.246, p < 0.001), followed by acute kidney failure NOS (OR =
5784 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Figure 2 Transjugular intrahepatic portosystemic shunt trends (A) and in-hospital mortality data (B).
8000
7000
6000
5000
4000
3000
2000
1000
01998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Number of TIPS YearlyA
30.00%
25.00%
20.00%
15.00%
10.00%
5.00%
0.00%1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Overall
Hepatic encephalopathy
Ascites
Bleeding esophageal varices
B
y = -0.0089x + 0.2785
y = -0.001x + 0.1967
y = -0.0021x + 0.1403
y = -0.0034x + 0.1444
TIPS in-hospital mortality by Year
Mean Before 2005 After 2005
Died during hospitalization (%) 12.32 13.15 11.5Length of stay (mean days ± SD) 10.83 ± 13.10 10.78 ± 13.09 10.89 ± 13.12
Lee EW et al . Nationwide trends of mortality in 83884 TIPS in United States

5785 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Table 3 Demographic and hospital predictors of in-hospital death
OR: Death in Hospital 95%CI: Lower 95%CI: Upper P value
DemographicAge (every 1 yr increase) 1.009 1.008 1.011 < 0.001Age group (Reference: Age 50-59) 0-9 0.354 0.252 0.498 < 0.001 10-19 0.529 0.417 0.672 < 0.001 20-29 0.427 0.354 0.515 < 0.001 30-39 1.076 0.986 1.175 0.100 40-49 1.085 1.027 1.147 0.004 50-59 REF REF REF REF 60-69 1.124 1.063 1.189 < 0.001 70-79 1.248 1.164 1.337 < 0.001 80-89 1.360 1.197 1.546 < 0.001 90-99 0.666 0.256 1.733 0.405Age > 70 (Ref: Age 0-70) 1.280 1.206 1.359 < 0.001Gender (Reference: Female) Male 1.072 1.028 1.118 0.001 Female REF REF REF REFRace (Reference: Caucasian) Caucasian REF REF REF REF Black 1.809 1.667 1.963 < 0.001 Hispanic 1.043 0.979 1.111 0.195 Asian/Pacific Islander 1.064 0.905 1.250 0.452 Native American 1.696 1.385 2.076 < 0.001 Other 1.470 1.314 1.644 < 0.001 Unknown 0.401 0.239 0.675 0.001Primary payer (Reference: Private) Medicare 1.140 1.085 1.199 < 0.001 Medicaid 1.113 1.052 1.177 < 0.001 Self-Pay 1.610 1.482 1.749 < 0.001 Private REF REF REF REFIncome quartile by ZIP (Reference: 1st quartile) 1st quartile REF REF REF REF 2nd quartile 0.948 1.210 2.430 0.297 3rd quartile 1.038 0.860 1.050 0.467 4th quartile 1.012 0.940 1.150 0.830 Missing income data 1.714 0.910 1.130 0.002Transfer status (Reference: Non-transfer) Transferred in from different acute care hospital 1.347 1.232 1.473 < 0.001 Non-transfer REF REF REF REFWeekend admission status (Reference: Weekday) Weekend admission 1.423 1.350 1.500 < 0.001 Weekday admission REF REF REF REFAdmission type (Reference: Elective) Emergency 3.032 2.835 3.244 < 0.001 Urgent 2.293 2.129 2.470 < 0.001 Elective REF REF REF REF Trauma center 4.541 2.772 7.440 < 0.001HospitalTeaching hospital status (Reference: Non-teaching hospital) Teaching Hospital 1.149 1.086 1.717 < 0.001 Non-Teaching Hospital REF REF REF REFHospital bed size (Reference: Large) Small 0.858 0.773 0.953 0.004 Medium 0.940 0.891 0.992 0.025 Large REF REF REF REFHospital region (Reference: West) Northeast 1.449 1.365 1.538 < 0.001 Midwest 0.982 0.925 1.043 0.572 South 0.917 0.868 0.969 0.002 West REF REF REF REFHospital control (Reference: Private, investor owned) Private, Non-profit 0.985 0.897 1.083 < 0.001 Private, Investor owned REF REF REF REF
Lee EW et al . Nationwide trends of mortality in 83884 TIPS in United States

4.359, p < 0.001) and hepatic encephalopathy (OR = 2.217, p < 0.001). Odds of death in patients diagnosed with ascites were not significantly different than those undiagnosed (OR = 1.020, p = 0.369). Patients diagnosed with bleeding esophageal varices had a mortality odds ratio of 2.217 (p < 0.001) compared to 0.445 (p < 0.001) in patients diagnosed with non-bleeding varices. Comorbidity measures at highest
odds of death were fluid and electrolyte disorders (OR = 2.823, p < 0.001), coagulopathy (OR = 2.016, p < 0.001), and lymphoma (OR = 1.842, p < 0.001) when compared to no comorbidity.
DISCUSSIONDetermining useful prognostic markers for mortality
5786 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Table 4 Diagnostic predictors of in-hospital death
OR: Death in Hospital 95%CI: Lower 95%CI: Upper P value
Number of diagnoses 1.095 1.091 1.099 < 0.000Number of procedures 1.249 1.242 1.256 < 0.000Diagnosis (Reference: No disease) Portal hypertension (5723) 0.689 0.660 0.719 0.000 Ascites (7895) 1.020 0.977 1.066 0.369 Esophageal variceal bleeding (45620) 2.187 2.098 2.279 0.000 Other ascites (78959) 0.783 0.741 0.827 0.000 Acute post-hemorrhagic anemia (2851) 2.011 1.920 2.105 0.000 Diabetes, uncomplicated (25000) 0.474 0.443 0.506 0.000 Hepatic encephalopathy (5722) 2.217 2.118 2.322 0.000 Hypertension NOS (4019) 0.597 0.561 0.635 0.000 Cirrhosis of liver NOS (5715) 0.836 0.789 0.886 0.000 Alcoholic liver cirrhosis (5712) 1.079 1.021 1.141 0.007 Thrombocytopenia NOS (2875) 1.081 1.022 1.142 0.006 Varices of other sites (4568) 0.784 0.736 0.835 0.000 Acute kidney failure NOS (5849) 4.359 4.162 4.566 0.000 Esophageal varices w/no bleeding (45621) 0.445 0.411 0.481 0.000 Acute respiratory failure (51881) 8.246 7.875 8.634 0.000AHRQ comorbidity measures (Reference: No disease) AIDS 1.579 1.216 2.050 0.001 CHF 1.437 1.300 1.587 < 0.001 Coagulopathy 2.016 1.918 2.119 < 0.001 Liver disease 1.051 0.981 1.125 0.156 Lymphoma 1.842 1.414 2.402 < 0.001 Fluid and electrolyte disorders 2.823 2.684 2.969 < 0.001 Metastatic cancer 1.412 1.167 1.708 < 0.001 Perivascular disease 1.527 1.292 1.806 <0.001 Pulmonary circulation disorders 1.496 1.249 1.792 < 0.001 Renal failure 1.036 0.933 1.151 0.506 Solid tumor without mets 1.491 1.322 1.681 < 0.001 Valvular disease 1.067 0.910 1.252 0.424 Weight loss 1.595 1.453 1.751 < 0.001
AIDS: Acquired immune deficiency syndrome; CHF: Congestive heart failure; ICD: International classification of diseases; AHRQ: Agency for healthcare research and quality.
1.600
1.400
1.200
1.000
0.800
0.600
0.400
0.200
0.0000-9
Odds of in-hospital death (Ref: Age 50-59)
10-19 20-29 30-39 40-49 50-59 60-69 70-79 80-89
Age
Figure 3 Odds of in-hospital death vs age 50-59.
Lee EW et al . Nationwide trends of mortality in 83884 TIPS in United States

is essential part of defining candidacy of any interven-tional procedure. A number of models for predicting TIPS outcomes have been implemented, with the most commonly applied in current practice being MELD[7,8]. Although these methods have been successful in stratifying patient risk based on biochemical markers such as bilirubin and creatinine, there remains interest on identifying new predictors that progress the way we monitor and follow up on patients[8,1017]. Our study is the first large-scale study to examine patient demographic, hospital, and diagnostic data as potential outcome markers for TIPS patients for all indications.
The sheer volume of patient data provided by the NIS brings unique statistical value to patient factors previously not associated with patient mortality. For example, although studies in the past have been unable to find clear associations between age and mortality, our data supports this relationship[16,17]. In our study, patients over 70 were at 1.28 times higher odds for inhospital mortality. Stepwise logistic regression analysis provided an odds ratio of 1.009 (1.008-1.011, p < 0.001) for every one year increase in age. At under 30, the odds of inpatient mortality dropped significantly (OR = 0.354-0.529, p < 0.001).
The role of ethnicity as predictor of clinical outcomes after TIPS has been controversial. One study on 643 patients finds patient ethnicity to be a poor indicator of early patient mortality[16], where another on 163 patients finds Hispanic patients to have a potential survival advantage[13]. In our study on 86,621 admissions, we found African-American (OR = 1.809, p < 0.001) and Native American (OR = 1.696, p < 0.001) patients to have statistically significant higher odds of in-hospital mortality than Caucasian patients. In contrast, Hispanic and Asian/Pacific Islander patients had similar in-house mortality as Caucasians.
Statistical relationships in any study should always
warrant careful consideration. For instance, although selfpayer patients were at considerably higher odds of in-patient mortality (OR = 1.610 vs private insurance), they were predominantly emergency admissions (61.1%) and therefore high risk (OR = 3.032 vs elective admissions, p < 0.001). One study on trauma victims finds a similar association between self-payers and a significantly higher mortality rate[18]. Similar to selfpayers, weekend admissions also had higher odds of inhospital mortality yet were comprised of mostly emergency admissions (65.8% vs 42.0% for weekday admissions).
Between hospital regions, the Northeast stood out with the highest mortality risk at odds 1.449 times higher than the Western region (p < 0.001). Further analysis of 2012 NIS data finds patients in the Northeast to have the highest mortality across all hospitalizations, just slightly but significantly at 1.095 times higher odds than in the West (p < 0.001).
Diagnosis as a predictive factor provides a different perspective than established clinical criteria. To illustrate, in a scenario where Child-Pugh and MELD scoring are unknown, we can anticipate a patient undergoing TIPS for esophageal variceal bleeding to be at roughly twice the odds of death in hospital following TIPS than for patients with other indications. Likewise, TIPS patients with hepatopulmonary syndrome, portopulmonary hypertension, or hepatic hydrothorax should be monitored closely for acute respiratory failure, which when diagnosed are expected to have around 8 times higher odds of inhospital death. The same ideology applies to patient comorbidity data, especially in the situation where a physician is evaluating a patient for an elective procedure. Based on our data, physicians should be especially wary of fluid and electrolyte disorders (OR = 2.823, p < 0.001), coagulopathy (OR = 2.016, p < 0.001), and
5787 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
3.000
2.500
2.000
1.500
1.000
0.500
0.000
Fluid
and e
lectro
lyte d
isord
ers
AHRQ comorbidity predictors of inhospital mortalityO
dds
ratio
for
in-h
ospi
tal m
orta
lity
Coag
ulopa
thy
Lymph
oma
Weig
ht lo
ssAI
DS
Periv
ascu
lar di
seas
e
Pulm
onary c
ircula
tion d
isord
ers
Solid
tumor
with
out m
ets CHF
Metasta
tic ca
ncer
Valvu
lar di
seas
e
Liver
dise
ase
Rena
l failu
re
Figure 4 Agency for Healthcare Research and Quality comorbidity predictors of in-hospital mortality.
Lee EW et al . Nationwide trends of mortality in 83884 TIPS in United States

lymphoma (OR = 1.842, p < 0.001). These data should alert physicians to implement closer monitoring before and during TIPS procedure and emphasize on closer following up on those patients with higher risk of postTIPS mortality.
From a trends perspective, NIS data supports improved clinical outcomes throughout the 15year study period (in-patient mortality declining on average -0.22% yearly), with the primary driving factor likely being the increasing use of PTFE covered stents[2,9]. This is particularly evident comparing inpatient mortality rates before widespread adoption of PTFE covered stents in 1998-2004 (13.15%) to after in 2005-2012 (11.50%).
Identifying subgroups with minimal reductions in mortality provides insight into potential areas of improvement. Although mortality in patients with ascites have declined overall (-0.34% yearly), mortality in patients with esophageal variceal bleeding have not changed substantially over the past 15 years (-0.01% yearly). In the same way, identifying subgroups that have shown sizable reductions in mortality highlight positives in the evolution of patient management. Hepatic encephalopathy is a frequent complication related to TIPS, with incidence rates ranging between 22%50%[1923]. For patients diagnosed with hepatic encephalopathy, the decline of inpatient mortality (-0.89% yearly) faster than the mean reinforces that management strategies have improved outcomes in this patient cohort.
Limitations of our study include those traditionally associated with retrospective research such as missing or incorrect data, selection bias, and the inability to control other sources of exposure. Also, NIS data is weighted and does not represent the entire cohort of patients undergoing TIPS in the United States. Changes in weighting with the NIS redesign in 2012 may impact the consistency of yeartoyear analysis. Associative factors are drawn from a nationwide perspective and both internal and external factors are not held constant. Details on outpatient mortality are not available using NIS data.
In the first 15year nationwide TIPS procedure mortality assessment, we outline inpatient mortality trends and provide comparison between demographic, regional, and diagnostic data as potential predictive markers. Results from this study are intended to aid practitioners in identifying populations that require closer monitoring to improve postTIPS mortality and clinical outcomes of TIPS.
COMMENTSBackgroundTransjugular intrahepatic portosystemic shunt (TIPS) became a main interventional procedure in treating patients with complications of portal hypertension. However, there is no large-scale, national trends data investigating in-patient death following TIPS. Using the National Inpatient Sample (NIS) database from 1998 to 2012, the authors demonstrated
downtrend in overall in-patient mortality associated with TIPS and they evaluated several factors including demographic, hospital and co-morbidities contributing to in-patient mortality in 83884 TIPS performed in the United States hospitals in 15 years.
Research frontiersUtilization of a nationwide, large database (NIS/HCUP) in assessing the mortality and predictors of TIPS procedure has not been fully studied. Especially, an evaluation of a large-scale database for 15 years has never been performed. In this study, the authors demonstrated the national trends of TIPS procedures and several predictors of in-patient mortality in TIPS procedures.
Innovations and breakthroughsUsing NIS/HCUP database in TIPS outcomes.
ApplicationsResults from this study are intended to aid hepatologists, gastroenterologists, internists, liver transplant surgeons and interventional radiologists in identifying populations that require closer monitoring and follow up to improve post-TIPS mortality and clinical outcomes of TIPS.
Peer-reviewIn this study, the authors evaluated several factors contributing to in-patient mortality in 83884 TIPS performed in the United States in 15 years using the NIS database from 1998 to 2012. In general, the main idea is interesting because this is a large-scale, national trends data investigating in-patient death following TIPS. Factors affecting patient survival following TIPS have been extensively studied.
REFERENCES1 Boyer TD, Haskal ZJ. The Role of Transjugular Intrahepatic
Portosystemic Shunt (TIPS) in the Management of Portal Hypertension: update 2009. Hepatology 2010; 51: 306 [PMID: 19902484 DOI: 10.1002/hep.23383]
2 Yang Z , Han G, Wu Q, Ye X, Jin Z, Yin Z, Qi X, Bai M, Wu K, Fan D. Patency and clinical outcomes of transjugular intrahepatic portosystemic shunt with polytetrafluoroethylene-covered stents versus bare stents: a meta-analysis. J Gastroenterol Hepatol 2010; 25: 1718-1725 [PMID: 21039832 DOI: 10.1111/j.1440-1746.2010.06400.x]
3 Quiroga J, Sangro B, Núñez M, Bilbao I, Longo J, García-Villarreal L, Zozaya JM, Betés M, Herrero JI, Prieto J. Transjugular intrahepatic portal-systemic shunt in the treatment of refractory ascites: effect on clinical, renal, humoral, and hemodynamic parameters. Hepatology 1995; 21: 986-994 [PMID: 7705810]
4 Ferral H. The evaluation of the patient undergoing an elective transjugular intrahepatic portosystemic shunt procedure. Semin Intervent Radiol 2005; 22: 266-270 [PMID: 21326704 DOI: 10.1055/s-2005-925552]
5 Ferral H, Gamboa P, Postoak DW, Albernaz VS, Young CR, Speeg KV, McMahan CA. Survival after elective transjugular intrahepatic portosystemic shunt creation: prediction with model for end-stage liver disease score. Radiology 2004; 231: 231-236 [PMID: 14990811 DOI: 10.1148/radiol.2311030967]
6 Richter GM, Noeldge G, Palmaz JC, Roessle M. The transjugular intrahepatic portosystemic stent-shunt (TIPSS): results of a pilot study. Cardiovasc Intervent Radiol 1990; 13: 200-207 [PMID: 2121348 DOI: 10.1007/BF02575474]
7 Angermayr B, Cejna M, Karnel F, Gschwantler M, Koenig F, Pidlich J, Mendel H, Pichler L, Wichlas M, Kreil A, Schmid M, Ferlitsch A, Lipinski E, Brunner H, Lammer J, Ferenci P, Gangl A, Peck-Radosavljevic M. Child-Pugh versus MELD score in predicting survival in patients undergoing transjugular intrahepatic portosystemic shunt. Gut 2003; 52: 879-885 [PMID: 12740346 DOI: 10.1136/gut.52.6.879]
8 Malinchoc M, Kamath PS, Gordon FD, Peine CJ, Rank J, ter
5788 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
COMMENTS
Lee EW et al . Nationwide trends of mortality in 83884 TIPS in United States

Borg PC. A model to predict poor survival in patients undergoing transjugular intrahepatic portosystemic shunts. Hepatology 2000; 31: 864-871 [PMID: 10733541 DOI: 10.1053/he.2000.5852]
9 Saad WE. The history and future of transjugular intrahepatic portosystemic shunt: food for thought. Semin Intervent Radiol 2014; 31: 258-261 [PMID: 25177087 DOI: 10.1055/s-0034-1382794]
10 Kim HK, Kim YJ, Chung WJ, Kim SS, Shim JJ, Choi MS, Kim do Y, Jun DW, Um SH, Park SJ, Woo HY, Jung YK, Baik SK, Kim MY, Park SY, Lee JM, Kim YS. Clinical outcomes of transjugular intrahepatic portosystemic shunt for portal hypertension: Korean multicenter real-practice data. Clin Mol Hepatol 2014; 20: 18-27 [PMID: 24757655 DOI: 10.3350/cmh.2014.20.1.18]
11 Harrod-Kim P, Waldman DL. Abnormal portal venous flow at sonography predicts reduced survival after transjugular intrahepatic portosystemic shunt creation. J Vasc Interv Radiol 2005; 16: 1459-1464 [PMID: 16319151 DOI: 10.1097/01.RVI.0000175328.72653.CA]
12 Harrod-Kim P, Saad WE, Waldman D. Predictors of early mortality after transjugular intrahepatic portosystemic shunt creation for the treatment of refractory ascites. J Vasc Interv Radiol 2006; 17: 1605-1610 [PMID: 17057001 DOI: 10.1097/01.RVI.0000240651.38289.4B]
13 Membreno F, Baez AL, Pandula R, Walser E, Lau DT. Differences in long-term survival after transjugular intrahepatic portosystemic shunt for refractory ascites and variceal bleed. J Gastroenterol Hepatol 2005; 20: 474-481 [PMID: 15740494 DOI: 10.1111/j.1440-1746.2005.03601.x]
14 Grunwald D, Tapper EB, Jiang ZG, Ahmed M, Malik R. A Standardized Assessment of Functional Disability Predicts 1-year Mortality in Patients Undergoing Transjugular Intrahepatic Portosystemic Shunt for Refractory Ascites. J Clin Gastroenterol 2016; 50: 75-79 [PMID: 25984975 DOI: 10.1097/MCG.0000000000000339]
15 Heinzow HS, Lenz P, Köhler M, Reinecke F, Ullerich H, Domschke W, Domagk D, Meister T. Clinical outcome and predictors of survival after TIPS insertion in patients with liver cirrhosis. World J Gastroenterol 2012; 18: 5211-5218 [PMID: 23066315 DOI: 10.3748/wjg.v18.i37.5211]
16 Dhanasekaran R, Gonzales P, West J, Subramanian R, Parekh S, Spivey JR, Reshamwala P, Martin LG, Kim HS. Predictors of
early mortality post transjugular intrahepatic portosystemic shunts and the role of hepatic venous pressure gradient. Gastrointest Inte 2012; 1: 63-68 [DOI: 10.1016/j.gii.2012.08.008]
17 Russo MW, Jacques PF, Mauro M, Odell P, Brown RS. Predictors of mortality and stenosis after transjugular intrahepatic portosystemic shunt. Liver Transpl 2002; 8: 271-277 [PMID: 11910573 DOI: 10.1053/jlts.2002.31653]
18 Chikani V, Salvino C, Hussaini K, Vossbrink A, Ng AR, Bobrow B, Skubic J, Martinez R. Self-pay trauma victims have a higher mortality rate than patients with different payment methods. Ann Adv Automot Med 2013; 57: 345-346 [PMID: 24406971]
19 Freedman AM, Sanyal AJ, Tisnado J, Cole PE, Shiffman ML, Luketic VA, Purdum PP, Darcy MD, Posner MP. Complications of transjugular intrahepatic portosystemic shunt: a comprehensive review. Radiographics 1993; 13: 1185-1210 [PMID: 8290720 DOI: 10.1148/radiographics.13.6.8290720]
20 Casadaban LC, Parvinian A, Minocha J, Lakhoo J, Grant CW, Ray CE, Knuttinen MG, Bui JT, Gaba RC. Clearing the Confusion over Hepatic Encephalopathy After TIPS Creation: Incidence, Prognostic Factors, and Clinical Outcomes. Dig Dis Sci 2015; 60: 1059-1066 [PMID: 25316553 DOI: 10.1007/s10620-014-3391-0]
21 Tripathi D, Ferguson J, Barkell H, Macbeth K, Ireland H, Redhead DN, Hayes PC. Improved clinical outcome with transjugular intrahepatic portosystemic stent-shunt utilizing polytetrafluo-roethylene-covered stents. Eur J Gastroenterol Hepatol 2006; 18: 225-232 [PMID: 16462534 DOI: 10.1097/00042737-200603000-00001]
22 Angeloni S, Merli M, Salvatori FM, De Santis A, Fanelli F, Pepino D, Attili AF, Rossi P, Riggio O. Polytetrafluoroethylene-covered stent grafts for TIPS procedure: 1-year patency and clinical results. Am J Gastroenterol 2004; 99: 280-285 [PMID: 15046218 DOI: 10.1111/j.1572-0241.2004.04056.x]
23 Bureau C, Pagan JC, Layrargues GP, Metivier S, Bellot P, Perreault P, Otal P, Abraldes JG, Peron JM, Rousseau H, Bosch J, Vinel JP. Patency of stents covered with polytetrafluoroethylene in patients treated by transjugular intrahepatic portosystemic shunts: long-term results of a randomized multicentre study. Liver Int 2007; 27: 742-747 [PMID: 17617116 DOI: 10.1111/j.1478-3231.2007.01522.x]
P- Reviewer: Alves A, Qiu B S- Editor: Gong ZM L- Editor: A E- Editor: Ma S
5789 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Lee EW et al . Nationwide trends of mortality in 83884 TIPS in United States

Gun Hyung Na, Tae Ho Hong, Young Kyoung You, Dong Goo Kim
Gun Hyung Na, Tae Ho Hong, Young Kyoung You, Dong Goo Kim, Department of Surgery, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul 137-701, South Korea
Author contributions: Na GH designed, performed the study, collected data, analyzed data, and wrote the paper; Hong TH and You YK designed the study; Kim DG designed, performed the study, analyzed data.
Institutional review board statement: This study was reviewed and approved by the Ethics Committee of the Catholic Medical Center.
Informed consent statement: Patients were not required to give informed consent to the study because the analysis used anonymous clinical data that were obtained after each patient agreed to treatment by written consent. For full disclosure, the details of the study are published on the home page of the Catholic Medical Center.
Conflict-of-interest statement: The authors have no conflicts of interest or financial associations to disclose.
Data sharing statement: No additional data are available.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Manuscript source: Unsolicited manuscript
Correspondence to: Dong Goo Kim, MD, PhD, Professor, Department of Surgery, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 505 Banpo-dong, Seocho-gu, Seoul 137-701, South Korea. [email protected]: +82-2-22586096Fax: +82-2-5952822
Received: March 2, 2016Peer-review started: March 4, 2016First decision: April 14, 2016Revised: April 26, 2016Accepted: May 23, 2016 Article in press: May 23, 2016Published online: July 7, 2016
AbstractAIM: To evaluated patterns and outcomes of hepa-tocellular carcinoma (HCC) recurrence after living donor liver transplantation (LDLT).
METHODS: From 2001 to 2014, 293 patients under-went LDLT for HCC at our transplant center. We retrospectively reviewed 54 (18.4%) patients with HCC recurrence after LDLT. We evaluated patterns and outcomes of HCC recurrence after LDLT, with particular attention to the Milan criteria at transplantation, treatments for HCC-recurrent patients, and factors related to survival after HCC recurrence. Furthermore, we evaluated the efficacy of combination treatment of sorafenib and an mTOR inhibitor.
RESULTS: The 1-, 2-, and 3-year overall survival rates after HCC recurrence were 41.1%, 20.5%, and 15.4%, respectively. The median time interval between LDLT and HCC recurrence was 6.5 mo. Although recurrence rates according to the Milan criteria at LDLT were significantly different, HCC recurrence patterns and survival rates after HCC recurrence were not significantly different between the two groups. Time to recurrence < 12 mo (P = 0.048), multiple recurrences at HCC recurrence (P = 0.038), and palliative treatment for recurrent tumors (P = 0.003) were significant independent prognostic factors for poor survival after HCC recurrence in a multivariate analysis. The combi-nation treatment of sorafenib and sirolimus showed
ORIGINAL ARTICLE
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.3748/wjg.v22.i25.5790
World J Gastroenterol 2016 July 7; 22(25): 5790-5799 ISSN 1007-9327 (print) ISSN 2219-2840 (online)
© 2016 Baishideng Publishing Group Inc. All rights reserved.
5790 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Retrospective Study
Clinical analysis of patients with hepatocellular carcinoma recurrence after living-donor liver transplantation

current treatment modalities other than LT[3], many centers are making efforts to expand the selection criteria[4,5]. For living-donor liver transplantation (LDLT), there has been a tendency to accept extended criteria in comparison with deceased-donor liver transplantation (DDLT)[6]. Thus, an evaluation of results after LDLT with such expanded criteria is important. In particular, it would be meaningful to compare HCC recurrence patterns and clinical outcome after LT according to the Milan criteria.
Treatment strategies for HCC-recurrence patients after LT are not well established, and treatment options are limited[7]. Due to the use of immunosuppressive agents, the prognosis of recurrent HCC after LT is poor, and its progression is typically very rapid. Additionally, recurrent HCC after LT tends to recur in multifocal and extra-hepatic sites. Nevertheless, some patients with HCC recurrence after LT have favorable prognoses and long-term survival after recurrence treatment[8]. However, few reports have examined patients with recurrent HCC after LT. Furthermore, LDLT differs from DDLT in terms of treatments after HCC recurrence, and there are a few reports about recurrent HCC after LDLT. Because currently used immunosuppressive agents, such as calcineurin inhibitors, make tumor cells proliferate, mammalian target of rapamycin (mTOR) inhibitors are recommended in patients at high risk of recurrent HCC after LT[9]. Due to compromised liver function in cirrhotic patients and the low efficacy of chemotherapy in HCC, chemotherapy treatments in HCC are not used commonly. Sorafenib is a small-molecule inhibitor of several tyrosine protein kinases (VEGFR and PDGFR) and Raf kinases. The SHARP trial showed the efficacy of sorafenib in HCC, with both median survival and time to progression showing 3-mo improvements[10]. Although combination treatments with mTOR inhibitors and sorafenib had some favorable results in HCC-recurrent patients after LT, there is currently no consensus on the most reliable treatment approach.
Thus, we examined patterns and outcomes of recurrent HCC after LDLT, particularly with regard to the Milan criteria at transplantation, treatments for HCC-recurrent patients after LDLT, and factors related to survival after HCC recurrence. Furthermore, we evaluated the effectiveness of combination treatment with sorafenib and mTOR inhibitors for recurrent HCC patients.
MATERIALS AND METHODSPatientsFrom January 2001 to June 2014, 293 patients underwent LDLT for HCC at our transplant center. Among them, 54 (18.4%) patients experienced HCC recurrence after LDLT. We retrospectively reviewed HCC recurrence patients after LDLT. This study was approved by the institutional review board of our center.
Na GH et al . HCC recurrence after LDLT
5791 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
survival benefits in the palliative treatment group (P = 0.005).
CONCLUSION: Curative treatment for recurrent HCC after LDLT is the most important factor in survival rates after HCC recurrence and combination treatments of sorafenib and an mTOR inhibitor could have survival benefits in patients with HCC recurrence after LT in the palliative treatment group.
Key words: Hepatocellular carcinoma; Living donor liver transplantation; mTOR inhibitor; Recurrence; Selection criteria
© The Author(s) 2016. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Although survival rates after liver transplan-tation (LT) have improved dramatically, hepatocellular carcinoma (HCC) recurrence remains a significant problem and studies regarding the clinical outcomes and treatments of patients with HCC recurrence after LT are rare. In this study, satisfying the Milan criteria at living donor liver transplantation (LDLT) was important for recurrence rates after LDLT, but was not important for survival rates after HCC recurrence. Curative treatment for recurrent HCC after LDLT is the most important factor in survival rates after HCC recurrence. Combination treatments of sorafenib and an mTOR inhibitor could have survival benefits in patients with HCC recurrence after LT in the palliative treatment group.
Na GH, Hong TH, You YK, Kim DG. Clinical analysis of patients with hepatocellular carcinoma recurrence after living-donor liver transplantation. World J Gastroenterol 2016; 22(25): 5790-5799 Available from: URL: http://www.wjgnet.com/1007-9327/full/v22/i25/5790.htm DOI: http://dx.doi.org/10.3748/wjg.v22.i25.5790
INTRODUCTIONAmong the several treatment modalities for hepato-cellular carcinoma (HCC), liver transplantation (LT) is a preferred treatment for selected patients with HCC because it targets not only the tumor but also the underlying liver disease. Since the introduction of the Milan criteria by Mazzaferro et al[1] in 1996, disease-free survival and overall survival after LT for patients HCC meeting the Milan criteria have been equivalent to those of non-HCC patients. HCC has become a major indication for LT, and due to the increasing number of HCC patients, the number of LTs will likely increase further[2]. However, although survival rates after LT have improved dramatically, HCC recurrence remains a significant problem. Furthermore, because the outcomes were disappointing when patients with HCC not meeting the Milan criteria were treated with

LT and post-transplant follow-upBecause of a shortage of deceased donor in my country, most patients with HCC could not undergo DDLT, and usually underwent LDLT. Therefore, For LDLT, relatively expanded selection criteria could be adopted, if liver transplantation was not contraindicated such as distant metastasis, regional lymph node metastasis, and macroscopic main portal vein invasion. The availability of liver donor is most important in LDLT. When a live donor is available, we performed LDLT. If not, we performed locoregional treatments regardless of the Milan criteria. In case of HCC patients within Milan criteria, we performed LT first, if the donor is available. In case of HCC patients beyond Milan criteria, when the tumor biology is expected to good and the donor is available, we performed LT first, but otherwise we performed locoregional treatments with the purpose of bridging or down-staging.
LDLT was performed according to a standard technique using a modified right lobe with middle hepatic vein reconstruction. For patients with ascites, aspiration and cytology were performed before the operation. When lymph node enlargement was present and in cases with suspected metastatic disease, an intraoperative biopsy was performed. The operation was performed only in cases with negative biopsy results. Immunosuppression regimens after LT consisted of a triple-drug regimen that included tacrolimus or cyclosporin, mycophenolate mofetil (MMF), and prednisolone. Steroids were withdrawn 3 mo after surgery, and MMF was withdrawn 6 mo after surgery. An interleukin-2 receptor blocker was administered on the day of surgery and on the fourth postoperative day. Patients were followed monthly for the first year, every 2 mo for 5 years, and then every 3 mo. Tumor markers such as AFP was measured monthly during the first year, and then every 2 mo. Abdomen CT, chest CT, and bone scintigraphy were performed routinely every 4 mo for the first year, every 6 mo for the second year, and then annually. When tumor recurrence was suspected, MRI and/or PET-CT were performed. The median follow up period was 18.5 mo (range: 3-170 mo).
Treatment of recurrent HCC after LDLTUpon HCC recurrence after LDLT, the immuno-suppressive agent was discontinued immediately or used at a reduced dose. Since the introduction of sorafenib in 2008 and sirolimus in 2012 in our hospital, the current standard treatment for recurrent HCC after LT has been a combination treatment of sorafenib and an mTOR inhibitor after locoregional treatment for suitable recurrent lesions. As an immunosuppressant, sirolimus was used instead of calcineurin inhibitors. The initial dose of sirolimus was 2 mg/d orally, and sirolimus whole blood concentrations were measured by immunoassay methodologies to adjust the dose to maintain whole blood trough concentrations at
5-10 ng/mL. The dose of sorafenib was 400 mg orally twice daily, and sorafenib was continued until the patient no longer benefitted or unacceptable toxicity emerged. Treatment modalities for recurrence were divided into curative intent and palliative intent treatments. Curative intent treatment was defined as surgical resection or ablation therapy, such as radiofrequency ablation (RFA) and percutaneous ethanol injection (PEI), intended to achieve no evi-dence of known recurrence. All patients considered unsuitable for curative treatment were enrolled in the palliative treatment group. Palliative treatments included transarterial chemoembolization (TACE), chemotherapy, and radiation.
Statistical analysisContinuous variables are reported as mean ± SD; they were compared using Student’s t-test. Categorical variables were analyzed using Pearson’s χ 2 test. Overall survival was calculated using the Kaplan-Meier method. To evaluate risk factors for survival in HCC recurrence patients, univariate analysis was performed using the Kaplan-Meier method and evaluated using the log-rank test. Candidate predictors associated with a P value < 0.2 in univariate analyses were entered into a multivariate analysis using Cox regression analysis. Furthermore, comparative study was done between recurrent HCC patients regarding Milan criteria at transplantation, also, in curative and palliative treatment groups, comparative studies were done between sorafenib and sirolimus treatment group and other treatment group. Statistical analyses were performed using the SPSS software (ver. 18.0 for Windows; SPSS, Inc., Chicago, IL, United States). A P value < 0.05 was considered to indicate statistical significance.
RESULTSClinicopathological characteristics and recurrence patterns of patients with HCC recurrence after LDLTThe mean age of patients with HCC recurrence after LDLT was 52.0 ± 8.1 years, and 46 (85.2%) patients were males. The most common reason for LT was hepatitis B (n = 46, 85.2%), followed by alcohol (n = 5, 9.3%), hepatitis C (n = 2, 3.7%), and other causes (n = 1, 1.9%). The mean Child-Pugh score was 7.5 ± 2.4, and the mean model for end-stage liver disease (MELD) score was 11.7 ± 8.5. Of the patients, 48 (88.9%) received pretransplant locoregional treatments. The mean tumor number and maximal tumor size at LT were 2.4 ± 1.9 and 4.85 ± 4.07 cm, respectively. Of the patients, 38 (70.4%) did not meet the Milan criteria. The median follow-up periods after LDLT and after HCC recurrence were 18.5 (range, 3-170) mo and 8.5 (range, 0-122) mo, respectively (Table 1).
The median time interval between LDLT and HCC recurrence was 6.5 mo (range, 1-150 mo, mean: 15.3
5792 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Na GH et al . HCC recurrence after LDLT

3.7%), and chest wall (n = 2, 3.7%).In this study, 15 (27.8%) patients were managed
with curative intent treatment, and the remaining 39 (72.2%) were managed with palliative intent treatments. Among the curative treatment group, 13 patients received only the operation for the first treatment of recurrent HCC, one patient underwent the operation and TACE, and one patient underwent TACE and RFA. Among the palliative group, TACE was the most common treatment modality for the first treatment of recurrent HCC: 10 patients received TACE as monotherapy or combined therapy (Table 2).
Patterns and treatment outcome of HCC recurrence after LDLT according to the Milan criteria at transplantationWe performed subgroup analysis to compare patterns of recurrent HCC according to the Milan criteria at LDLT. The Milam criteria were based on pathology results.
mo). Most HCC recurrence (n = 44, 81.5%) occurred within 2 years, with 37 (68.5%) patients experiencing HCC recurrence within 1 year (Figure 1A). At the time of HCC recurrence after LDLT, 14 (25.9%) patients had a solitary recurrent tumor, but 40 (74.1%) patients had multiple recurrent tumors. The most frequently involved organs were the lung (n = 24, 44.4%), followed by the liver (n = 17, 31.5%), bone (n = 10, 18.5%), lymph node (n = 6, 11.1%), brain (n = 2,
5793 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Table 1 Clinicopathological characteristics of patients with hepatocellular carcinoma recurrence after living donor liver transplantation
Factors Data, n (%)
Recipient age1 52.0 ± 8.1Recipient sex, male 46 (85.2)Etiology Hepatitis B 46 (85.2) Hepatitis C 2 (3.7) Alcohol 5 (9.3) Other 1 (1.9)MELD score1 11.7 ± 8.5GRWR1 1.28 ± 0.24Pre-transplant locoregional treatment 48 (88.9)Tumor marker at transplantation AFP1 717.3 ± 1748.1 (median: 43.3)HCC characteristics at pathology Number1 2.4 ± 1.9 (median: 2.0) Maximal tumor size (cm)1 4.85 ± 4.07 (median: 3.8) Microvascular invasion 30 (60.0) E-S grade Ⅲ-Ⅳ 25 (52.1) Beyond Milan criteria 38 (70.4)Patterns of HCC recurrence Time between LDLT and recurrence (mo)1
15.3 ± 23.9 (median: 6.5, range: 1-150)
Single vs multiple 14 (25.9) vs 40 (74.1) Intrahepatic vs extrahepatic vs both 12 (22.2) vs 37 (68.5) vs 5 (9.3)Recurrence organ Lung 24 (44.4) Liver 17 (31.3) Bone 10 (18.5)
1Values are shown as mean ± SD except where stated otherwise. MELD: Model for end-stage liver disease; GRWR: Graft-to-recipient body weight ratio; AFP: Alpha-fetoprotein; HCC: Hepatocellular carcinoma; E-S grade: Edmondson-Steiner grade; LDLT: Living donor liver transplantation.
Interval n % %
≤ 6 mo 27 50.0 50.0
≤ 12 mo 10 18.5 68.5
≤ 24 mo 7 13.0 81.5
> 24 mo 10 18.5 100.0
1.0
0.8
0.6
0.4
0.2
0.0
Prop
ortio
n of
rec
urre
nce
0 12 24 36 48 60 Time after LDLT (mo)
A
Median: 6.5 mo (1-150 mo)mean: 15.3 mo
1.0
0.8
0.6
0.4
0.2
0.0
Prop
ortio
n of
rec
urre
nce
0 12 24 36 48 60 Time after LDLT (mo)
Within milan group (n = 16)Median: 7.0 (1-150)mean: 24.1 ± 39.5
Beyond milan group (n = 38)Median: 6.0 (1-46)mean: 11.5 ± 11.9
B
Figure 1 Time interval between living donor liver transplantation and hepatocellular carcinoma recurrence. A: Whole study population; B: Comparison according to the Milan criteria at transplantation. HCC: Hepatocellular carcinoma; LDLT: Living donor liver transplantation.
Table 2 First treatment modalities for recurrent hepatocellular carcinoma after liver transplantation n (%)
Treatments Curative Palliative
(n = 15, 27.8%) (n = 39, 72.2%)
Operation 13 (86.7) 1 (2.6)Operation and radiation 1 (6.7) 4 (10.3)Operation and TACE 1 (2.6)TACE 8 (20.5)TACE and RFA 1 (6.7) 1 (2.6)Radiation 7 (17.9)Intravenous chemotherapy 5 (12.8)Sorafenib 8 (20.5)Conservative treatment 4 (10.3)
TACE: Transarterial chemoembolization; RFA: Radiofrequency ablation.
Na GH et al . HCC recurrence after LDLT

During the study period, 293 patients underwent LDLT for HCC at our transplant center. Among the 180 (61.4%) patients who met the Milan criteria at LDLT, 16 (8.9%) experienced HCC recurrence. Among the 113 (38.6%) patients who did not meet the Milan criteria, 38 (33.6%) experienced HCC recurrence. Recipient age in the group not meeting the Milan criteria was significantly higher than that in the group meeting them (P = 0.005). Tumor number (P < 0.001) and size (P < 0.001) and AFP (P = 0.043) in the outside-the-Milan group were significantly higher than those in the within Milan group. Other clinicopathological factors at transplantation, such as recipient gender, etiology for transplantation, MELD score, GRWR, and history of pre-transplant locoregional treatments, were not significantly different between the two groups. Recurrence rates according to the Milan criteria at LDLT were significantly different (P < 0.001). However, in terms of tumor recurrence patterns, the time interval between LDLT and HCC recurrence (P = 0.157, Figure 1B), tumor number at HCC recurrence (P = 0.735), and HCC recurrence site (P = 0.555), there was no significant difference between the groups (Table 3). Furthermore, survival rates after HCC recurrence were not significantly different between the groups (P = 0.245, Figure 2C).
Survival after HCC recurrence and factors related to itThe 6-, 12-, 24-, and 36-mo overall survivals after HCC recurrence were 63.0, 41.1, 20.5, and 15.4%,
respectively (Figure 2A). In univariate analysis, time to recurrence < 12 mo (P = 0.010), multiple HCC recurrences (P < 0.001), brain metastasis (P < 0.001), and palliative treatment for recurrent tumors (P < 0.001; Figure 2B) were statistically associated with poor overall survival after HCC recurrence. Among them, time to recurrence < 12 mo [hazard ratio = 2.408 (1.007-5.756), P = 0.048], multiple HCC recurrences [hazard ratio = 3.438 (1.072-11.025), P = 0.038], and palliative treatment for recurrent tumors [hazard ratio = 3.886 (1.591-9.490), P = 0.003] were independent predictors of poor survival in a multivariate analysis. However, tumor state at transplantation, such as meeting the Milan criteria (P = 0.245), microvascular invasion (P = 0.384), and tumor grade (P = 0.227), were not significantly associated with survival rate after HCC recurrence (Table 4).
Efficacy of combination treatments of sorafenib and sirolimus for HCC-recurrent patients after LDLTWe evaluated the efficacy of the combination treat-ment of sorafenib and sirolimus. We divided patients into a curative treatment group and a palliative group. In the palliative group, 12 patients received a combination treatment of sorafenib and sirolimus; the remaining 27 patients did not. Although tumor characteristics at transplantation and at HCC re-currence were not significantly different between the combination treatment group and the other treatment group (Table 5), survival rates after HCC recurrence
5794 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Table 3 Differences of hepatocellular carcinoma recurrence patterns according to the Milan criteria at transplantation n (%)
Factors Within Milan (n = 16) Beyond Milan (n = 38) P value
Recipient age1 47.4 ± 5.9 53.9 ± 8.1 0.005Recipient sex, male 13 (81.3) 33 (86.8) 0.682Etiology, hepatitis B 12 (75.0) 34 (89.5) 0.127MELD score1 10.9 ± 9.1 12.0 ± 8.2 0.692GRWR1 1.27 ± 0.20 1.28 ± 0.26 0.919Pre-transplant locoregional treatment 13 (81.3) 35 (92.1) 0.346Tumor marker at transplantation AFP1 213.0 ± 371.8 829.6 ± 2040.7 0.043HCC characteristics at pathology Number1 1.2 ± 0.6 2.9 ± 2.0 < 0.001 Maximal tumor size1 2.33 ± 1.10 5.93 ± 4.41 < 0.001 Microvascular invasion 7 (50.0) 23 (63.9) 0.368 E-S grade III-IV 6 (46.2) 19 (54.3) 0.616Recurrent HCC patterns Recurrence rates 8.90% 33.60% < 0.001 Time interval, median (mo) (LDLT-HCC recurrence) 7.0 (1-150) 6.0 (1-46) 0.157
mean: 24.1 ± 39.5 mean: 11.5 ± 11.9 Single or Multiple 0.735 Single 5 (31.3) 9 (23.7) Multiple 11 (68.7) 29 (76.3) Recurrence site 0.555 Intrahepatic 5 (31.3) 7 (18.4) Extrahepatic 10 (62.5) 27 (71.1) Both 1 (6.3) 4 (10.5)Survival after HCC recurrence, median (mo) 12.0 (3-122) 8.0 (1-62) 0.224
mean: 24.0 ± 33.5 mean: 10.4 ± 10.5
1Values are shown as mean ± SD except where stated otherwise. MELD: Model for end-stage liver disease; GRWR: Graft-to-recipient body weight ratio; AFP: Alpha-fetoprotein; HCC: Hepatocellular carcinoma; E-S grade: Edmondson-Steiner grade; LDLT: Living donor liver transplantation.
Na GH et al . HCC recurrence after LDLT

in the combination treatment group were significantly higher than in the other treatment group among the palliative group (P = 0.005; Figure 3A). However, combination treatment with sorafenib and sirolimus did not show survival benefits in the curative treatment group (P = 0.955; Figure 3B).
During the combination treatments of sorafenib and sirolimus, adverse effects included 8 cases of diarrhea and 3 cases of hand-foot syndrome. Although the combination treatment was generally well tolerated, there were adverse events exceeding grade 3 were 3 cases of diarrhea. Among them, one patient discontinued the combination treatment, the remaining
two patient reduced the dose of sorafenib.
DISCUSSIONLT is a preferred treatment for selected patients with HCC because it targets not only the tumor but also the underlying liver disease. The 5-year survival rate for HCC patients who meet the Milan criteria is 70%-85%, with a recurrence-free survival rate of 75%[1]. Many centers are making efforts to expand the selection criteria because of the strictness of the Milan criteria[4,5]. However, HCC recurrence after LT remains an important problem in clinical practice.
5795 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Time Survival rates
3 mo 83.3%
6 mo 63.0%
12 mo 41.1%
24 mo 20.5%
36 mo 15.4%
1.0
0.8
0.6
0.4
0.2
0.0
Surv
ival
rat
es a
fter
HCC
rec
urre
nce
0 12 24 36 48 60 Time after HCC recurrence (mo)
A1 yr 2 yr 3 yr
Curative 77.4% 50.2% 33.4%
Palliative 27.6% 7.7% 7.7%
1.0
0.8
0.6
0.4
0.2
0.0
Surv
ival
rat
es a
fter
HCC
rec
urre
nce
0 12 24 36 48 60 Time after HCC recurrence (mo)
Curative treatment group (n = 15)
Palliative treatment group (n = 39)
P < 0.001
B
1 yr 2 yr 3 yr
Within 56.3% 32.8% 21.9%
Beyond 34.0% 12.1% 14.1%
1.0
0.8
0.6
0.4
0.2
0.0
Surv
ival
rat
es a
fter
HCC
rec
urre
nce
0 12 24 36 48 60 Time after HCC recurrence (mo)
Within milan group (n = 16)
Beyond milan group (n = 38)
P = 0.245
C
Figure 2 Survival rates after hepatocellular carcinoma recurrence. A: Whole study population; B: Comparison between curative intent group and palliative intent group; C: Comparison according to the Milan criteria at living donor liver transplantation. HCC: Hepatocellular carcinoma.
Na GH et al . HCC recurrence after LDLT

Indeed, the number of patients with HCC recurrence after LT continues to increase. In addition, for LDLT, there has been a tendency to accept extended criteria in comparison with DDLT[6]. In one meta-analysis, disease-free survival was significantly shorter in patients receiving LDLT[11]. The inferior oncological outcomes in the LDLT group may have been caused by more aggressive tumor biology and small-for-size graft injuries and regeneration[12]. In this study, 54 (18.4%) patients experienced HCC recurrence after LDLT. HCC recurrence rates after LDLT in this study were higher than that in previous DDLT studies, especially in the group that did not meet the Milan criteria (33.6% for the group outside the Milan criteria vs 8.9% for the group within them). Although the risk factors for HCC recurrence after LT have been studied, there are few studies about the clinical outcomes and treatments of patients with HCC recurrence after LT. Furthermore, studies about the effects of meeting the Milan criteria at transplantation on clinical outcomes after HCC recurrence are even rarer. Thus, the primary aim of this study was to assess the clinical outcome in patients with HCC recurrence after LDLT and to identify factors affecting survival after HCC recurrence following LDLT. A secondary aim was to compare recurrence patterns and outcomes according to the Milan criteria at transplantation. The last aim was to examine the effectiveness of new modalities for patients with HCC recurrence after LDLT.
Although HCC patients are selected for LT accor-
ding to standard criteria, previous studies have reported that 10%-40% of them experience HCC recurrence[13]. Most HCC recurrence develops within 2 years after LT, and the lung is the most frequent site of recurrence after LT[14,15]. Similarly, in this study, most HCC recurrence (n = 44, 81.5%) occurred within 2 years after LDLT, with 37 (68.5%) patients experiencing HCC recurrence within 1 year; where the most frequently involved organ was the lung (n = 24, 44.4%). The 1-, 2-, and 3-year overall survival rates after HCC recurrence were 41.1%, 20.5%, and 15.4%, respectively. These findings were consistent with previous studies. This study also showed that time to recurrence < 12 mo, multiple recurrences at HCC recurrence, and palliative treatment for recurrent tumors were significant independent predictors of poor survival after HCC recurrence. These findings reinforce previous studies suggesting that the time between LT and HCC recurrence and curative treatment for recurrent HCC after LT are keys for predicting out-comes after HCC recurrence[16-18]. This study provides an important guide for the management for recurrent HCC in patients after LT and supports our treatment policy indicating that when a patient is diagnosed with HCC recurrence after LT, resection or ablative treatments should be considered first in the treatment algorithm if possible.
Because previous reports about patients with HCC
5796 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Table 4 Factors related with survival rates after hepatocellular caricnoma recurrence
Factors Univariate analysis
Multivariate analysis
P value Harzard ratio (95%CI)
P value
Age > 60 yr 0.124Male sex 0.739Etiology 0.291MELD score > 15 0.153GRWR < 1.0 0.658Pre-transplant treatments 0.170Tumor state at transplantation AFP > 100 0.575 Beyond Milan criteria 0.245 Microvascular invasion 0.384 E-S grade Ⅲ-Ⅳ 0.227Time to recurrence < 12 mo 0.010 2.408 (1.007-5.756) 0.048Multiple recurrence < 0.001 3.438 (1.072-11.025) 0.038Recurrence site Liver 0.824 Lung 0.937 Bone 0.695 Brain < 0.001 2.966 (0.565-15.583) 0.199Palliative treatment for recurrent tumors
< 0.001 3.886 (1.591-9.490) 0.003
MELD: Model for end-stage liver disease; GRWR: Graft-to-recipient body weight ratio; AFP: Alpha-fetoprotein; E-S grade: Edmondson-Steiner grade.
Table 5 Clinicopathological characteristics in palliative treatment group between sorafenib and sirolimus treatment group and other treatment group n (%)
Factors Sorafenib + Sirolimus
Other treatments P value
Recipient age1 55.3 ± 9.1 51.6 ± 6.9 0.179Recipient sex, male 9 (75.0) 24 (88.9) 0.348Etiology, Hepatitis B 10 (83.3) 22 (81.5) 0.369MELD score1 9.3 ± 3.3 14.0 ± 9.7 0.033GRWR1 1.40 ± 0.27 1.23 ± 0.25 0.065AFP at transplantation1 1038.3 ± 1849.2 256.5 ± 361.1 0.173HCC characteristics at pathology Number1 2.42 ± 2.02 2.38 ± 2.09 0.965 Maximal tumor size1 4.20 ± 2.06 5.44 ± 5.36 0.444 Beyond Milan criteria 9 (75.0) 17 (65.4) 0.714Time between LDLT and recurrence, median
6 (range: 3-150) 5 (range: 1-46) 0.270
Patterns of HCC recurrence Single or Multiple 0.219 Single 2 (16.7) 1 (3.7) Multiple 10 (83.3) 26 (96.3) Intrahepatic or Extrahepatic 0.074 Intrahepatic 0 9 (33.3) Extrahepatic 10 (83.3) 15 (55.6) Both 2 (16.7) 3 (11.1)AFP at HCC recurrence1 7913.2 ± 16023.5 6139.5 ± 17794.2 0.772
1Values are shown as mean ± SD except where stated otherwise. MELD: Model for end-stage liver disease; GRWR: Graft-to-recipient body weight ratio; AFP: Alpha-fetoprotein; HCC: Hepatocellular carcinoma; LDLT: Living donor liver transplantation.
Na GH et al . HCC recurrence after LDLT

recurrence after LT involved patients receiving DDLT, most patients met the Milan criteria at transplantation. There are some differences between LDLT and DDLT, and there has been a tendency to accept extended criteria for LDLT compared with DDLT. Our transplant center mainly performs LDLT. Thus, this study included many HCC patients who did not meet the Milan criteria at transplantation in contrast with most previous reports. Additionally, previous studies comparing recurrence patterns and survival rates after HCC recurrence according to the Milan criteria at LT are rare. Thus, we analyzed clinical outcomes and HCC-recurrent patterns according to the Milan criteria at transplantation. Our study showed that although recurrence rates after LDLT were significantly different, HCC recurrence patterns and survival rates after HCC recurrence were not significantly different between the two groups. Because of the small number of patients included in this study and the scarcity of comparable previous studies, further prospective studies are needed.
Treatment of recurrent HCC after LT is difficult, and the prognosis is poor, with a median survival of less than 1 year[18]. In principal, all treatment options currently available for advanced HCC are also potentially feasible in recurrent HCC after LT. However, HCC recurrence after LT is considered a “systemic disease”, and the efficacy of locoregional treatment for a systemic disease is doubtful. Thus, new treatment strategies in recurrent HCC after LT are needed. Sorafenib is the treatment of choice for advanced HCC because survival in sorafenib patients with underlying liver cirrhosis is longer than that in placebo controls[10,19]. Theoretically, such a systemic therapy could be the best approach for HCC recurrence after LT. Sposito et al[20] reported that sorafenib seemed to be associated with an acceptable safety profile and
provided benefit in survival in HCC patients suffering recurrence after LT. Survival of patients in the sorafenib group was improved significantly (median survival from recurrence 21.3 mo vs 11.8 mo, HR = 5.2, P = 0.0009). The only factor associated with survival after HCC recurrence in a multivariate analysis was treatment with sorafenib (HR = 4.0; P = 0.0325).
The growth rate of recurrent HCC after LT is significantly faster than that in non-transplanted patients with HCC who underwent surgical resection, presumably due to ongoing immunosuppression and reduced host immunity against micrometastasis[21,22]. Over recent decades, the mTOR inhibitors everolimus and sirolimus has been introduced, and attention has turned to the question of whether their use could ameliorate the risk of post-transplant HCC recurrence. Combination treatments of sorafenib and an mTOR inhibitor as a new treatment modality have been studied, but data about combination treatments of sorafenib and mTOR inhibitors in patients with HCC recurrence after LT are limited. It has been hypothesized that combination treatments could have synergistic effects. Recently, some studies reported that combination treatments of sorafenib and mTOR inhibitors showed survival benefits in patients with HCC recurrence after LT. Gomez-Martin et al[23] reported that the combination treatment of sorafenib and an mTOR inhibitor could be effective in recurrent HCC after LT in the palliative treatment group. In a total of 26 patients, there was one partial response and 13 cases with disease stabilization as the best response. Our study also showed that combination treatments of sorafenib and mTOR inhibitors had significant survival benefits in the palliative treatment group (P = 0.005).
In conclusion, meeting the Milan criteria at LDLT is associated with significant less recurrence rates after LDLT, but is not associated with survival rates
5797 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
1.0
0.8
0.6
0.4
0.2
0.0
Surv
ival
rat
es a
fter
HCC
rec
urre
nce
0 6 12 18 24 Time after HCC recurrence (mo)
Sorafenib + Sirolimus group (n = 12)
P = 0.005
Other treatment group (n = 27)
1.0
0.8
0.6
0.4
0.2
0.0
Surv
ival
rat
es a
fter
HCC
rec
urre
nce
0 12 24 36 Time after HCC recurrence (mo)
Sorafenib + Sirolimus group (n = 7)
P = 0.995
Other treatments group (n = 8)
A B
Figure 3 Survival rates after hepatocellular carcinoma recurrence in palliative treatment group (A) and curative treatment group (B). HCC: Hepatocellular carcinoma.
Na GH et al . HCC recurrence after LDLT

after HCC recurrence. However, curative treatment for recurrent HCC after LDLT is the most important factor in survival rates after HCC recurrence. Furthermore, combination treatments of sorafenib and an mTOR inhibitor could have survival benefits in patients with HCC recurrence after LT in the palliative treatment group. Lastly, prospective studies with larger cohorts are required to address these issues more fully.
COMMENTSBackgroundLiver transplantation (LT) is a preferred treatment for selected patients with hepatocellular carcinoma (HCC). Many centers are making efforts to expand the selection criteria. For living donor liver transplantation (LDLT), there has been a tendency to accept extended criteria in comparison with deceased-donor liver transplantation. However, HCC recurrence remains an important problem, and studies regarding the clinical outcomes and treatments of patients with HCC recurrence after LT are rare.
Research frontiersThe authors evaluated patterns and outcomes of HCC recurrence after LDLT, with particular attention to the Milan criteria at transplantation, treatments for HCC-recurrent patients, and factors related to survival after HCC recurrence. Furthermore, we evaluated the efficacy of combination treatment of sorafenib and an mTOR inhibitor.
Innovations and breakthroughsIn present study, curative treatment for recurrent HCC after LDLT is the most important factor in survival rates after HCC recurrence and combination treatments of sorafenib and an mTOR inhibitor could have survival benefits in patients with HCC recurrence after LT in the palliative treatment group.
ApplicationsAlthough the risk factors for HCC recurrence after LT have been studied, there are few studies about the clinical outcomes and treatments of patients with HCC recurrence after LT. Therefore, our study may assist the treatments for patients with HCC recurrence after LT.
TerminologyMammalian target of rapamycin (mTOR) is a serine/threonine kinase, which belongs to phosphatidylinositol-3 kinase (PI3K) related kinases (PIKKs) family. Sorafenib is a small-molecule inhibitor of several tyrosine protein kinases (VEGFR and PDGFR) and Raf kinases.
Peer-reviewThis is a retrospective study of the recurrent (HCC after LDLT among 54 patients with recurrent HCC out of 293 LDLT recipients with HCC. The study followed the principle of retrospective clinical research with some useful information, and seems suitable for the future publication.
REFERENCES1 Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A,
Bozzetti F, Montalto F, Ammatuna M, Morabito A, Gennari L. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med 1996; 334: 693-699 [PMID: 8594428 DOI: 10.1056/NEJM199603143341104]
2 Ioannou GN, Perkins JD, Carithers RL. Liver transplantation for hepatocellular carcinoma: impact of the MELD allocation system and predictors of survival. Gastroenterology 2008; 134: 1342-1351 [PMID: 18471511 DOI: 10.1053/j.gastro.2008.02.013]
3 Marrero JA. Multidisciplinary management of hepatocellular carcinoma: where are we today? Semin Liver Dis 2013; 33 Suppl 1:
S3-10 [PMID: 23457037 DOI: 10.1055/s-0033-1333631]4 Yao FY, Ferrell L, Bass NM, Watson JJ, Bacchetti P, Venook A,
Ascher NL, Roberts JP. Liver transplantation for hepatocellular carcinoma: expansion of the tumor size limits does not adversely impact survival. Hepatology 2001; 33: 1394-1403 [PMID: 11391528 DOI: 10.1053/jhep.2001.24563]
5 Kaido T, Ogawa K, Mori A, Fujimoto Y, Ito T, Tomiyama K, Takada Y, Uemoto S. Usefulness of the Kyoto criteria as expanded selection criteria for liver transplantation for hepatocellular carcinoma. Surgery 2013; 154: 1053-1060 [PMID: 24074704 DOI: 10.1016/j.surg.2013.04.056]
6 Lee SG. A complete treatment of adult living donor liver transplan-tation: a review of surgical technique and current challenges to expand indication of patients. Am J Transplant 2015; 15: 17-38 [PMID: 25358749 DOI: 10.1111/ajt.12907]
7 Welker MW, Bechstein WO, Zeuzem S, Trojan J. Recurrent hepatocellular carcinoma after liver transplantation - an emerging clinical challenge. Transpl Int 2013; 26: 109-118 [PMID: 22994652 DOI: 10.1111/j.1432-2277.2012.01562.x]
8 Xiang ZW, Sun L, Li GH, Maharjan R, Huang JH, Li CX. Progress in the treatment of pulmonary metastases after liver transplantation for hepatocellular carcinoma. World J Hepatol 2015; 7: 2309-2314 [PMID: 26380655 DOI: 10.4254/wjh.v7.i20.2309]
9 Toso C, Merani S, Bigam DL, Shapiro AM, Kneteman NM. Sirolimus-based immunosuppression is associated with increased survival after liver transplantation for hepatocellular carcinoma. Hepatology 2010; 51: 1237-1243 [PMID: 20187107 DOI: 10.1002/hep.23437]
10 Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc JF, de Oliveira AC, Santoro A, Raoul JL, Forner A, Schwartz M, Porta C, Zeuzem S, Bolondi L, Greten TF, Galle PR, Seitz JF, Borbath I, Häussinger D, Giannaris T, Shan M, Moscovici M, Voliotis D, Bruix J. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med 2008; 359: 378-390 [PMID: 18650514 DOI: 10.1056/NEJMoa0708857]
11 Grant RC, Sandhu L, Dixon PR, Greig PD, Grant DR, McGilvray ID. Living vs. deceased donor liver transplantation for hepatocellular carcinoma: a systematic review and meta-analysis. Clin Transplant 2013; 27: 140-147 [PMID: 23157398 DOI: 10.1111/ctr.12031]
12 Man K, Fan ST, Lo CM, Liu CL, Fung PC, Liang TB, Lee TK, Tsui SH, Ng IO, Zhang ZW, Wong J. Graft injury in relation to graft size in right lobe live donor liver transplantation: a study of hepatic sinusoidal injury in correlation with portal hemodynamics and intragraft gene expression. Ann Surg 2003; 237: 256-264 [PMID: 12560784 DOI: 10.1097/01.SLA.0000048976.11824.67]
13 Clavien PA, Lesurtel M, Bossuyt PM, Gores GJ, Langer B, Perrier A. Recommendations for liver transplantation for hepatocellular carcinoma: an international consensus conference report. Lancet Oncol 2012; 13: e11-e22 [PMID: 22047762 DOI: 10.1016/S1470-2045(11)70175-9]
14 Toso C, Cader S, Mentha-Dugerdil A, Meeberg G, Majno P, Morard I, Giostra E, Berney T, Morel P, Mentha G, Kneteman NM. Factors predicting survival after post-transplant hepatocellular carcinoma recurrence. J Hepatobiliary Pancreat Sci 2013; 20: 342-347 [PMID: 22710887 DOI: 10.1007/s00534-012-0528-4]
15 Roayaie S, Schwartz JD, Sung MW, Emre SH, Miller CM, Gondolesi GE, Krieger NR, Schwartz ME. Recurrence of hepato-cellular carcinoma after liver transplant: patterns and prognosis. Liver Transpl 2004; 10: 534-540 [PMID: 15048797 DOI: 10.1002/lt.20128]
16 Taketomi A, Fukuhara T, Morita K, Kayashima H, Ninomiya M, Yamashita Y, Ikegami T, Uchiyama H, Yoshizumi T, Soejima Y, Shirabe K, Maehara Y. Improved results of a surgical resection for the recurrence of hepatocellular carcinoma after living donor liver transplantation. Ann Surg Oncol 2010; 17: 2283-2289 [PMID: 20204531 DOI: 10.1245/s10434-010-0999-y]
17 Shin WY, Suh KS, Lee HW, Kim J, Kim T, Yi NJ, Lee KU. Prognostic factors affecting survival after recurrence in adult living donor liver transplantation for hepatocellular carcinoma. Liver Transpl 2010; 16: 678-684 [PMID: 20440777 DOI: 10.1002/
5798 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
COMMENTS
Na GH et al . HCC recurrence after LDLT

lt.22047]18 Kornberg A, Küpper B, Tannapfel A, Katenkamp K, Thrum
K, Habrecht O, Wilberg J. Long-term survival after recurrent hepatocellular carcinoma in liver transplant patients: clinical patterns and outcome variables. Eur J Surg Oncol 2010; 36: 275-280 [PMID: 19857941 DOI: 10.1016/j.ejso.2009.10.001]
19 Cheng AL, Kang YK, Chen Z, Tsao CJ, Qin S, Kim JS, Luo R, Feng J, Ye S, Yang TS, Xu J, Sun Y, Liang H, Liu J, Wang J, Tak WY, Pan H, Burock K, Zou J, Voliotis D, Guan Z. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol 2009; 10: 25-34 [PMID: 19095497 DOI: 10.1016/S1470-2045(08)70285-7]
20 Sposito C, Mariani L, Germini A, Flores Reyes M, Bongini M, Grossi G, Bhoori S, Mazzaferro V. Comparative efficacy of sorafenib versus best supportive care in recurrent hepatocellular carcinoma
after liver transplantation: a case-control study. J Hepatol 2013; 59: 59-66 [PMID: 23500153 DOI: 10.1016/j.jhep.2013.02.026]
21 Yokoyama I, Carr B, Saitsu H, Iwatsuki S, Starzl TE. Accelerated growth rates of recurrent hepatocellular carcinoma after liver transplantation. Cancer 1991; 68: 2095-2100 [PMID: 1655200]
22 Cheng JW, Shi YH, Fan J, Huang XW, Qiu SJ, Xiao YS, Wang Z, Dai Z, Tang ZY, Zhou J. An immune function assay predicts post-transplant recurrence in patients with hepatocellular carcinoma. J Cancer Res Clin Oncol 2011; 137: 1445-1453 [PMID: 21809031 DOI: 10.1007/s00432-011-1014-0]
23 Gomez-Martin C, Bustamante J, Castroagudin JF, Salcedo M, Garralda E, Testillano M, Herrero I, Matilla A, Sangro B. Efficacy and safety of sorafenib in combination with mammalian target of rapamycin inhibitors for recurrent hepatocellular carcinoma after liver transplantation. Liver Transpl 2012; 18: 45-52 [PMID: 21932373 DOI: 10.1002/lt.22434]
P- Reviewer: Gad EH, Sugawara Y S- Editor: Yu J L- Editor: A E- Editor: Ma S
5799 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Na GH et al . HCC recurrence after LDLT

Antonio Ríos, Ana Isabel López-Navas, Ana Isabel López-López, Francisco Javier Gómez, Jorge Iriarte, Rafael Herruzo, Gerardo Blanco, Francisco Javier Llorca, Angel Asunsolo, Pilar Sánchez-Gallegos, Pedro Ramón Gutiérrez, Ana Fernández, María Teresa de Jesús, Laura Martínez-Alarcón, Alberto Lana, Lorena Fuentes, Juan Ramón Hernández, Julio Virseda, José Yelamos, José Antonio Bondía, Antonio Miguel Hernández, Marco Antonio Ayala, Pablo Ramírez, Pascual Parrilla
Antonio Ríos, Ana Isabel López-Navas, Laura Martínez-Alarcón, Marco Antonio Ayala, Pablo Ramírez, International Collaborative Donor Project (“Proyecto Colaborativo Internacional Donante” , 30007 Casillas, Murcia, Spain
Antonio Ríos, Pablo Ramírez, Parrilla Pascual, Department of Surgery, Paediatrics, Obstetrics and Gynaecology, University of Murcia, Avenida de las Fuerzas Armadas, 30800 Espinardo, Murcia, Spain
Antonio Ríos, Laura Martínez-Alarcón, Pablo Ramírez, Pascual Parrilla, Transplant Unit, Surgery Service, IMIB - Virgen de la Arrixaca University Hospital, Carretera Madrid-Cartagena s/n, 30120 El Palmar, Murcia, Spain
Antonio Ríos, Pablo Ramírez, Regional Transplant Centre, Consejería de Sanidad y Consumo de la Región de Murcia, 30008 Ronda de Levante, Murcia, Spain
Antonio Ríos, Hospital Clínico Universitario Virgen de la Arrixaca, Departamento de Cirugía General y del Aparato Digestivo, Unidad de Trasplantes, 30007 Casillas, Murcia, Spain
Ana Isabel López-Navas, Department of Psychology, Universidad Católica San Antonio (UCAM), Avenida de los Jerónimos, 30107 Guadalupe, Murcia, Spain
Ana Isabel López-López, Department of Urology, San Juan University Hospital of Alicante, 03010 Calle Pintor Baeza, Alicante, Spain Francisco Javier Gómez, Universidad de Granada, Avenida del Hospicio s/n, 18010 Granada, Spain Jorge Iriarte, Universidad de Navarra, Campus Universitario, 31080 Pamplona, Navarra, Spain
Rafael Herruzo, Universidad Autónoma de Madrid, Ciudad Universitaria de cantoblanco, 28049 Madrid, Spain
Gerardo Blanco, Servicio de Cirugía HBP y Trasplante Hepático, Complejo Hospitalario Universitario de Badajoz, Hospital Infanta Cristina, Avenida Elvas s/n, 06006 Badajoz, Spain
Francisco Javier Llorca, Universidad de Cantabria, Avenida los Castros s/n, 39005 Santander, Cantabria, Spain
Angel Asunsolo, Departamento de Cirugía, Ciencias Médicas y Sociales, Facultad de Medicina y Ciencias de la Salud, Universidad de Alcalá Campus Científico-Tecnológico, Plaza de San Diego s/n, 28801 Alcala de Henares, Madrid, Spain
Pilar Sánchez-Gallegos, José Antonio Bondía, Facultad de Medicina, Universidad de Málaga, 29071 Avenida de Cervantes, Málaga, Spain
Pedro Ramón Gutiérrez, Servicio de Urología (Complejo Hospitalario Universitario de Canarias, CHUC) y Departamento de Cirugía (Universidad de La Laguna, ULL), Calle Molinos de Agua s/n, 38207 San Cristóbal de La Laguna, Santa Cruz de Tenerife, Spain
Ana Fernández, Departamento de Ciencias Biomédicas Básicas, Facultad de Ciencias Biomédicas, Universidad Europea de Madrid, Avenida de Fernando Alonso, 28108 Madrid, Spain María Teresa de Jesús, Universidad Rey Juan Carlos, Calle Tulipán s/n, 28933 Mostoles, Madrid, Spain Alberto Lana, Facultad de Medicina y Ciencias de la Salud. Área de Medicina Preventiva y Salud Pública, Universidad de Oviedo, Calle San Francisco, 33003 Oviedo, Asturias, Spain
Lorena Fuentes, Departamento de Farmacología y Fisiología Facultad de Ciencias de la Salud y del Deporte, Universidad de Zaragoza, 50018 Calle Pedro Cerbuna, Zaragoza, Spain
Juan Ramón Hernández, Universidad de las Palmas de Gran Canaria, Calle Juan de Quesada s/n, 35001 Las Palmas de Gran
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.3748/wjg.v22.i25.5800
5800 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
World J Gastroenterol 2016 July 7; 22(25): 5800-5813 ISSN 1007-9327 (print) ISSN 2219-2840 (online)
© 2016 Baishideng Publishing Group Inc. All rights reserved.
ORIGINAL ARTICLE
Observational Study
Acceptance of living liver donation among medical students: A multicenter stratified study from Spain

Revised: May 8, 2016Accepted: June 15, 2016Article in press: June 15, 2016Published online: July 7, 2016
AbstractAIM: To analyze the attitude of Spanish medical students toward living liver donation (LLD) and to establish which factors have an influence on this attitude.
METHODS: Study type: A sociological, interdisciplinary, multicenter and observational study. Study population: Medical students enrolled in Spain (n = 34000) in the university academic year 2010-2011. Sample size: A sample of 9598 students stratified by geographical area and academic year. Instrument used to measure attitude: A validated questionnaire (PCID-DVH RIOS) was self-administered and completed anonymously. Data collection procedure: Randomly selected medical schools. The questionnaire was applied to each academic year at compulsory sessions. Statistical analysis: Student´s t test, χ 2 test and logistic regression analysis.
RESULTS: The completion rate was 95.7% (n = 9275). 89% (n = 8258) were in favor of related LLD, and 32% (n = 2937) supported unrelated LLD. The following variables were associated with having a more favorable attitude: (1) age (P = 0.008); (2) sex (P < 0.001); (3) academic year (P < 0.001); (4) geographical area (P = 0.013); (5) believing in the possibility of needing a transplant oneself in the future (P < 0.001); (6) attitude toward deceased donation (P < 0.001); (7) attitude toward living kidney donation (P < 0.001); (8) acceptance of a donated liver segment from a family member if one were needed (P < 0.001); (9) having discussed the subject with one's family (P < 0.001) and friends (P < 0.001); (10) a partner's opinion about the subject (P < 0.001); (11) carrying out activities of an altruistic nature; and (12) fear of the possible mutilation of the body after donation (P < 0.001).
CONCLUSION: Spanish medical students have a favorable attitude toward LLD.
Key words: Attitude; Living liver donation; Medical students; Transplantation; Organ donation; Psychosocial variables; Spain
© The Author(s) 2016. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: Students of medicine represent a new generation of physicians, although their attitude towards living liver donation (LLD) has not been studied to any great extent, and most of the studies carried out use measurement tools that have not been validated. The objective of the authors was to analyze the
Canaria, Las Palmas, Spain
Julio Virseda, Universidad de Castilla La Mancha, Campus Universitario de Albacete s/n, 02071 Albacete, Spain
José Yelamos, Department of Immunology, Hospital del Mar, 08003 Passeig Marítim, Barcelona, Spain
Antonio Miguel Hernández, Endocrinology and Nutrition Service, Hospital Clínico Universitario Virgen de la Arrixaca, Servicio Murciano de Salud, Carretera Madrid - Cartagena s/n, 30120 El Palmar, Murcia, Spain
Marco Antonio Ayala, Hospital Regional de Alta Especialidad del Bajío, San Carlos la Rocha, Guanajuato 37660, León, Mexico
Marco Antonio Ayala, HGSZ No. 10 del Instituto Mexicano del Seguro Social Delegación Guanajuato, Calle San Clemente, Guanajuato 36010, León, Mexico
Author contributions: Ríos A designed the study; Ríos A, López-Navas AI, López-López AI, Ayala MA, Ramírez P and Parrilla P analyzed and interpreted the data; Ríos A and López-Navas AI contributed to statistical expertise, drafted the manuscript, and supervised this program; Ríos A, López-Navas AI, Ayala MA, Ramírez P and Parrilla P critically revised the manuscript for important intellectual content; all authors contributed to acquisition of a substantial portion of data, obtaining funding for this project or study, and final approval of the version to be published.
Institutional review board statement: The study was reviewed and approved by the “Proyecto Colaborativo Internacional Donante” Institutional Review Board.
Informed consent statement: All study participants provided informed verbal consent prior to study enrollment.
Conflict-of-interest statement: All authors declared that there is no conflict of interest to disclose.
Data sharing statement: No additional data are available.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Manuscript source: Invited manuscript
Correspondence to: Dr. Antonio Ríos, Hospital Clínico Universitario Virgen de la Arrixaca, Departamento de Cirugía General y del Aparato Digestivo, Unidad de Trasplantes, Avenida de la Libertad No. 208, 30007 Casillas, Murcia, Spain. [email protected]: +34-968-270757Fax: +34-968-369716
Received: February 16, 2016Peer-review started: February 17, 2016First decision: March 21, 2016
5801 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Ríos A et al . Medical students and living liver donation in Spain

attitude of Spanish medical students towards LLD. The project is a sociological, interdisciplinary, multicentre and observational study. A sample of 9598 students is stratified by geographical area and academic year. The instrument is a validated questionnaire (PCID-DVH RIOS) it was self-administered and completed anonymously.
Ríos A, López-Navas AI, López-López AI, Gómez FJ, Iriarte J, Herruzo R, Blanco G, Llorca FJ, Asunsolo A, Sánchez-Gallegos P, Gutiérrez PR, Fernández A, de Jesús MT, Martínez-Alarcón L, Lana A, Fuentes L, Hernández JR, Virseda J, Yelamos J, Bondía JA, Hernández AM, Ayala MA, Ramírez P, Parrilla P. Acceptance of living liver donation among medical students: A multicenter stratified study from Spain. World J Gastroenterol 2016; 22(25): 5800-5813 Available from: URL: http://www.wjgnet.com/1007-9327/full/v22/i25/5800.htm DOI: http://dx.doi.org/10.3748/wjg.v22.i25.5800
INTRODUCTIONLiver transplantation offers long survival periods and improved quality of life for patients with liver disease whose vital prognosis is short if they do not have a transplant. However, the current transplant organ donation rates are insufficient for covering minimum transplant needs[1], and the shortage of available livers means that mortality on the waiting list is increasing[1]. Even in Spain in the 21st century, the country with the highest donation rates, mortality on the liver transplant waiting list has been increasing[1]. All of this is making it necessary to encourage alternatives to deceased liver donation. The transplantation of the right liver lobe from a living donor to an adult recipient has been successfully carried out and in countries such as Japan, the United States and some European countries it is becoming more common[2,3]. Even so, in many countries living liver donation (LLD) is at a very low level[1]. One of the possible barriers to its development could be the risk involved for the donor and the fact that the results of the transplant are slightly worse than when the liver is transplanted from a deceased donor[4,5]. However, in experienced centers the results are acceptable[6,7]. Nevertheless, it should be taken into account that professionals in healthcare centers do not always have a favorable attitude toward LLD, and consequently they do not create the right kind of social climate for its implementation[8-10]. Therefore, healthcare professionals have a fundamentally important role to play in its development, given that they have the capacity to generate favorable or unfavorable attitudes in other groups of the population. In fact, in the public it has been seen that attitude toward organ donation which is based on the information provided by healthcare workers, whether positive or negative, is very solid[11].
Students of medicine represent a new generation of physicians, although their attitude toward LLD has not been studied to any great extent[12]. It should be remembered, however, that the adequate training of future physicians in the transplantation and donation process involves specifically finding out those varia-bles that have an effect on certain attitudes toward donation from the stage of being a student. In this sense, a knowledge of the factors that influence attitudes toward donation will allow us to optimize the resources invested in carrying out donation and transplantation promotion campaigns and to act in a more specific way.
The objective of this study was to analyze the attitude of medical students from Spanish universities toward related and unrelated LLD.
MATERIALS AND METHODSType of studyA sociological, interdisciplinary, multicenter and ob-servational study carried out in Spain in the university academic year of 2010-2011.
Study populationThe study population comprised of students studying a degree in medicine in Spain. The number of students enrolled in the academic year of 2010-2011 was estimated using data published by the Spanish National Institute of Statistics (INE)[13]. The number of students in other medical schools not included in the information of the INE was obtained over the telephone. As a result, the estimated number of medical students enrolled in the academic year of 2010-2011 was 34000. It should be noted that in Spain a degree in medicine lasts for 6 years. Once the degree has been completed and in order to start specialist training, the students have to take the public competitive (MIR) exam which involves a training period lasting between 3 and 5 years.
Sample sizeThe sample size calculated for a population of 34000 students was 9598 students, considering an estimated proportion (attitude in favor of donation) of 76%, a confidence of 99% and a precision of ± 1%.
Sample stratificationGeographical stratification: In the academic year of 2010-2011 there were 40 medical schools in Spain with active teaching activity. These medical schools were grouped into four geographical regions covering the country: (1) The North: including the Autonomous communities (Ac) of Galicia, the Principality of Asturias, the Basque country, the Foral community of Navarra, La Rioja, cantabria and castilla León; (2) The central area: including the Acs of castilla-La Mancha, Extremadura and the community of Madrid; (3) The
5802 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Ríos A et al . Medical students and living liver donation in Spain

5803 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
of administered questionnaires) was greater than 80% of the students present at the aforementioned compulsory student sessions. After a brief explanation of the study was provided by the study personnel about the structure and content of the questionnaire, and after specifying the confidentiality of the data gathered, a questionnaire was handed out to each student at one of the compulsory sessions. The questionnaire was self-administered, and completed voluntarily and anonymously by each student in a period of 5-10 min.
The final selection of the participating groups was carried out using non-probabilistic convenience sampling until the necessary number of questionnaires for each academic year was reached according to the proportionality factor. Given that the questionnaires were handed out in compulsory student sessions, an academic year was considered to be full when the number of questionnaires administered had a range of ± 5% of the number of questionnaires calculated to be necessary.
Instrument for measuring attitudeThe instrument of measurement used was a validated questionnaire of attitude toward Organ Donation and Transplantation[8,9] [“PcID - DVH Rios”: A questionnaire of the International collaborative Donor Project about Living Liver Donation (“Proyecto colaborativo Internacional Donante sobre Donación de Vivo Hepático” in Spanish) developed by Dr. Ríos]. This questionnaire included items distributed into three subscales or factors, and it was validated in the Spanish population, presenting a total explained variance of 63.995% and a cronbach’s Alpha confidence coefficient of 0.778. Each factor has an internal consistency, measured by Cronbach’s Alpha Confidence coefficient of α = 0.801, 0.696, and 0.559 respectively, and an explained variance of 38.461%, 14.228%, and 11.306% res-pectively. In Addition an ad hoc questionnaire was applied including other variables.
Study variablesAs a dependent variable we studied attitude toward related and unrelated LLD. The independent variables studied were classified into the following groups: (1) Socio-personal: age and sex; (2) University: Type of university, academic year of the degree in medicine and geographical location; (3) Knowledge of, and attitude toward, organ donation and transplantation: knowing a transplant patient, knowing a donor, believing that one might need a transplant in the future, attitude toward deceased organ donation, attitude toward living kidney donation and acceptance of a liver segment from a living donor if it was needed; (4) Social interaction: discussion with family and friends about donation and transplantation, the respondent’s partner’s opinion about the donation of a family member’s organs; (5) Pro-social behavior:
East: including the Acs of catalonia, Aragon, Valencia and Murcia; and (4) The South: including the Acs of Andalucía, ceuta and Melilla, the canary Islands, and the Balearic Islands.
In order to obtain the sample, an initial sampling stage was planned which was stratified proportionately to the number of students enrolled in each geographical region. In the North, 14% of the students were enrolled, corresponding to a sample of 1343; in the central area there were 25% corresponding to 2400; in the South there were 23.5% corresponding to 2256; and in the East there were 37.5% corresponding to 3,599 respondents.
Stratification by academic year: In each geo-graphical area stratified sampling was carried out according to each academic year. In order to do this, the proportion of students from each year in each geographical area was calculated and the corresponding sample was obtained. The percentage and number of students in each area in each academic year were as follows: In the North: 28% of the students (corresponding to 376 respondents) were enrolled in the first year; 15.5% (n = 208) were enrolled in the second year; 16% (n = 215) in the third year; 14% (n = 188) in the fourth; 12% (161) in the fifth and 14.5%( n = 195) in the sixth year; In the central Area: 23% of the student (n = 552) were enrolled in the first year; 25.5% (n = 540) in the second year; 12% (n = 288) in the third year; 13% (n = 312) in the fourth year; 11.5% (n = 276) in the fifth year; and 18% (n = 432) in the sixth year; In the South: 21% of the students (n=474) were enrolled in the first year; 20% (n = 451) in the second year; 13% (n = 293) in the third year; 15% (n = 338) in the fourth year; 15% (n = 338) in the fifth year; and 16% (n = 362) in the sixth year; In the East: 21% of the students (n = 756) were enrolled in the first year; 22% (n = 791) in the second; 18% (n = 648) in the third; 14% (n = 504) in the fourth; 11% (n = 396) in the fifth; and 14% (n = 504) in the sixth.
Data collection procedureIn each geographical area, a number of randomly selected medical schools were formally invited to participate in the study. contact was made with the Dean of the school at each university to obtain authorization to conduct the research. The ques-tionnaires were administered to medical students by members or collaborators from the “International Donor collaborative Project” group in the selected medical schools that agreed to participate in the study.
With the aim of preventing selection bias, the questionnaire was applied to each academic year and in each selected school, at one or several compulsory sessions (lectures, seminars, or practical classes). A group was only considered as valid when the response rate (number of completed questionnaires/number
Ríos A et al . Medical students and living liver donation in Spain

5804 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
carrying out pro-social type activities; (6) Religious: the respondent’s religion and knowing the attitude of his or her religion toward donation and transplantation; and (7) Attitude toward the body: concern about possible mutilation of the body after donation.
Statistical analysisThe data were stored on a database and analyzed using the SPSS 21.0 statistical package (IBM Software Group, chicago, IL, United States). A descriptive statistical analysis was carried out and in order to compare the different variables Student’s t-test and the χ 2 test were applied complemented by an analysis of the remainders. For determining and assessing multiple risks, logistic regression analysis was under-taken using the variables that were statistically significant in the bivariate analysis. In all cases, p values below 0.05 were considered to be statistically significant. The statistical review of the study was performed by a biomedical statistician.
RESULTSMedical faculties included and the response rate obtainedThe 22 randomly selected medical schools agreed to
take part in the study. Of the 9688 selected students (the 9598 selected plus the 0.9% per type of sample) 9275 correctly completed the questionnaire (a res-ponse rate of 95.73%). In Table 1, the sampling and completion data is given for each university and academic year.
In the North, the lowest completion rate was found (84.4%) because one of the universities (N1) did not provide any respondents in the end. In the central area the completion rate was 96.56%. In this area, the third year of medical school c5 and the second of medical school c6 were excluded from the analysis because the 80% response rate was not reached in the compulsory sessions when the questionnaire was handed out. In the South the completion rate was 96.41%, with the resulting exclusion of the fourth year of medical school S1, together with the first and fifth year of medical school S2 due to a response rate of less than 80%. In the East the completion rate was 98.97%.
Attitude toward living liver donation89% (n = 8258) were in favor of related LLD, 1% (n = 78) against and 10% (n = 939) undecided. If the donation was unrelated, 32% (n = 2937) were in favor, 11% (n = 1001) were against and 57% (n =
Table 1 Sample and completion data for university medical students according to geographical area, university and academic year
1st 2nd 3rd 4th 5th 6th TN0 TNR TR
N0 NR N0 NR N0 NR N0 NR N0 NR N0 NR
N1 45 0 30 0 30 0 30 0 30 0 35 0 200 0N2 96 91 96 91N3 133 133 87 87 97 95 100 99 65 65 92 92 574 571N4 100 100 89 88 84 84 58 58 73 73 72 71 476 474NT 374 324 206 175 211 179 188 157 168 138 199 163 1346 1136 84.39%C1 32 29 32 29C2 107 107 116 116 61 61 73 73 62 52 77 77 496 486C3 87 86 139 139 94 94 172 171 58 58 124 124 674 672C4 95 93 128 128 53 53 42 42 62 62 123 123 503 501C5 53 53 48 48 23 0 124 101C6 120 120 29 0 23 22 172 142C7 108 107 95 94 43 43 28 28 64 62 103 93 441 427NT 570 566 555 525 297 273 315 314 278 263 427 417 2442 2358 96.56%S1 12 0 25 25 38 38 75 63S2 24 0 27 27 24 23 75 75 22 0 28 28 200 153S3 193 193 241 238 155 153 99 98 144 143 145 143 977 968S4 59 59 68 67 25 25 50 50 26 26 38 38 266 265S5 181 179 116 125 86 85 115 114 152 141 119 112 769 756NT 457 431 452 457 290 286 351 337 369 335 368 359 2287 2205 96.41%L1 114 114 148 145 116 114 156 151 101 92 113 112 748 728L2 69 69 122 122 98 98 76 76 84 84 110 110 559 559L3 261 261 265 265 284 284 123 123 114 114 133 133 1180 1180L4 83 82 57 57 140 139L5 199 195 195 192 145 141 144 143 87 87 139 137 909 895L6 49 48 28 27 77 75NT 775 769 815 808 643 637 499 493 386 377 495 492 3613 3576 98.97%NT 2176 2090 2028 1965 1441 1375 1353 1301 1201 1113 1489 1431 9688 9275 95.73%
N1 to N4: Medical schools in the North; C1 to C7: Medical schools in the Central Area; S1 to S5: Medical schools in the South; L1 to L6: Medical schools in the East; 1st to 6th years: Academic years; N0: Questionnaires administered; NR: Questionnaires obtained; TN0: Total number of questionnaires administered; TNR: Total number of questionnaires obtained; NT: Total questionnaires in the corresponding column; TR (%): Completion rate.
Ríos A et al . Medical students and living liver donation in Spain

5805 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
5337) were undecided.Of the students who were in favor of this type of
donation, 42% (n = 3506) believed that LLD involved a considerable amount of risk, 30% (n = 2484) quite a lot of risk, 10% (n = 817) hardly any, 9% (n = 799) had not considered this matter and 8% (n = 652) believed it to be a highly risky kind of donation.
Factors affecting attitude toward LLDSocio-personal variables: Regarding age, significant differences have been found in favorable attitudes toward LLD. In the related type of donation, the younger respondents had a more favorable attitude (p = 0.008), while in unrelated donation it was the older students who were more in favor (p < 0.001) (Table 2). With regard to sex, this factor has only been found to be associated with attitude toward related LLD, with females having a more favorable attitude toward related LLD than males (91% vs 86%, p < 0.001) (Table 2).
University variables: The respondent’s academic year was an influential factor on attitude toward LLD, with the latter years being the ones when a more favorable attitude has been observed. When considering related donation, for instance, attitude was more favorable among students in the fifth and sixth year compared to those in the first year (92% vs 87%, p < 0.001). The same was also true for unrelated donation; the fifth and sixth years had the students with the most favorable attitude compared
to those in the first year (40% and 37% vs 25%, p < 0.001) (Table 2). Finally, with regard to geographical location, significant differences have only been found in attitudes toward related LLD with the students from the central area and the South having a better attitude compared to those from the North and East (90% vs 88%, p = 0.013) (Table 2).
Variables of knowledge about, and attitude toward, organ donation and transplantation: Among the factors associated with a favorable attitude toward related LLD, we have found that a respondent’s belief that he or she might need a transplant in the future tended to encourage a favorable attitude as opposed to when he or she had not considered this possibility (90% vs 81%, p < 0.001) (Table 3). In addition, the acceptance of other types of donation, such as deceased (92% vs 79%, p < 0.001) or living kidney donation (96% vs 75%) (p < 0.001), was also associated with a more favorable attitude compared to when these other types of donation were rejected. Finally, it should be noted that the willingness to accept a liver segment from a family member also tended to be associated with a favorable attitude toward LLD compared to when there were doubts about this option or there was an unwillingness to accept it (96% vs 80%, p < 0.001) (Table 3).
With regard to attitudes toward unrelated LLD, significant relationships have been found with all the variables analyzed in this section. We can see that those who had had previous links with donation and
Table 2 Socio-personal and university variables related to organ donation and transplantation affecting the attitude of university medical students toward unrelated and related living liver donation n (%)
Unrelated living liver donation Related living liver donation
Variable In favor (n = 2937; 32%)
Not in favor (n = 6338; 68%)
P value In favor (n = 8258; 89%)
Not in favor (n = 1017; 11%)
P value
Socio-personal variables Age (21 ± 3 yr) 22 ± 4 yr 21 ± 3 yr < 0.001 21 ± 3 yr 22 ± 4 yr 0.008 Sex 0.195 < 0.001 Male (n = 2702) 830 (31) 1872 (69) 2310 (86) 392 (14) Female (n = 6499) 2086 (32) 4413 (68) 5889 (91) 610 (9) DS/DK (n = 74) 21 53 59 15University variables Type of university 0.68 0.103 Public university (n = 8192) 2600 (32) 5592 (68) 7278 (89) 914 (11) Private university (n = 1083) 337 (31) 746 (69) 980 (91) 103 (9) Year of medicine < 0.001 < 0.001 First (n = 2090) 521 (25) 1569 (75) 1811 (87) 279 (13) Second (n = 1965) 544 (28) 1421 (72) 1736 (88) 229 (12) Third (n = 1375) 422 (31) 953 (69) 1212 (88) 163 (12) Fourth (n = 1301) 480 (37) 821 (63) 1166 (90) 135 (10) Fifth (n = 1113) 443 (40) 670 (60) 1020 (92) 93 (8) Sixth (n = 1431) 527 (37) 904 (63) 1313 (92) 118 (8) Geographical location 0.109 0.013 North (n = 1136) 365 (32) 771 (68) 1002 (88) 134 (12) Central area (n = 2358) 718 (30) 1640 (70) 2118 (90) 240 (10) South (n = 2205) 741 (34) 1464 (66) 1993 (90) 212 (10) East (n = 3576) 1113 (31) 2463 (69) 3145 (88) 431 (12)
DS/DK: Does not say/does not know.
Ríos A et al . Medical students and living liver donation in Spain

5806 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
transplantation, that is, people who knew a transplant patient (36% vs 30%, p < 0.001), or donor (37% vs 31%, p < 0.001) (Table 3), had a more favorable attitude compared to those respondents who did not have this personal experience.
Variables of social interaction: As shown in Table 4, all of these variables were associated with attitude toward LLD. Accordingly, the students who had discussed the subject of donation and transplantation, both with their families and friends, had a more favorable attitude toward related and unrelated LLD. It has also been found that the favorable attitude of a respondent’s partner toward donation and transplantation had a favorable influence (Table 4).
Variables of pro-social behavior: Among the students surveyed, a more favorable attitude has been observed toward both related and unrelated LLD among those who carry out altruistic type activities or who would be prepared to take part in them (Table 4).
Religious variables: In the present study no sig-nificant relationships were found between attitude toward LLD and the religious variables analyzed (Table 5). However, it is notable that believers who considered that their doctrine was in favor of donation
and transplantation were more in favor of unrelated donation than those who believed their religion was against (35% vs 27%) (p < 0.001).
Variable of attitude toward the body: Finally, it has been seen that not being concerned about the possible mutilation of the organism after donation tended to be associated with a favorable attitude toward LLD unlike in the case of those who were concerned about this aspect (p < 0.001) (Table 5).
A multivariate analysis of the factors affecting attitude toward related LLDThe multivariate analysis has shown that the following independent factors affected attitude toward related LLD (Table 6): (1) Being a female (OR = 1.356; p < 0.001); (2) Studying in the last academic years of the degree in medicine (fifth and sixth year) (OR = 1.485; p = 0.005); (3) Being in favor of deceased organ donation (OR = 2.169; p < 0.001); (4) Being in favor of living kidney donation (OR = 3.278; p < 0.001); (5) Being willing to be a recipient of a liver segment from a living donor (OR = 6.493; p < 0.001); (6) Not having a partner, and therefore, not being influenced by this person’s opinion (OR = 1.569; p = 0.040); and (7) Being involved in regular pro-social activities (OR = 1.620; p = 0.012).
Table 3 Variables of the university medical students' knowledge about, and attitude toward, related and unrelated living liver donation n (%)
Unrelated living liver donation Related living liver donation
Variable In favor (n = 2937, 32%)
Not in favor (n = 6338, 68%)
P value In favor (n = 8258, 89%)
Not in favor (n = 1017, 11%)
P value
Knowing a transplant patient Yes (n = 2261) 813 (36) 1448 (64) < 0.001 2026 (90) 235 (10) 0.296 No (n = 6992) 2121 (30) 4871 (70) 6210 (89) 782 (11) DS/DK (n =22) 3 19 22 --Knowing a donor Yes (n = 1305) 482 (37) 823 (63) < 0.001 1180 (90) 125 (10) 0.086 No (n = 7943) 2451 (31) 5492 (69) 7055 (89) 888 (11) DS/DK (n = 27) 4 23 23 4Possibility of needing a transplant Yes (n = 7712) 2544 (33) 5168 (67) < 0.001 6951 (90) 761 (10) < 0.001 No (n = 118) 35 (30) 83 (70) 96 (81) 22 (19) Doubts (n = 1372) 341 (25) 1031 (75) 1159 (85) 213 (16) DS/DK (n = 73) 17 56 52 21Attitude toward deceased donation In favor (n = 7376) 2603 (35) 4773 (65) < 0.001 6761 (92) 615 (8) < 0.001 Against - undecided (n = 1899) 334 (18) 1565 (82) 1497 (79) 402 (21)Donating a living kidney Yes, I would donate one (n = 2784) 1965 (71) 819 (29) < 0.001 2684 (96) 100 (4) < 0.001 No, I would not donate one (n = 872) 111 (13) 761 (87) 656 (75) 216 (25) I do not know (n = 5619) 861 (15) 4758 (85) 4918 (88) 701 (12)Willingness to accept a living liver segment from a family member Yes, I would accept it (n = 5342) 2187 (41) 3155 (59) < 0.001 5146 (96) 196 (4) < 0.001 No, I would wait on the waiting list (n = 907) 224 (25) 683 (75) 751 (83) 156 (17) I do not know (n = 2932) 519 (18) 2413 (82) 2341 (80) 591 (20) DS/DK (n = 94) 7 87 20 74
DS/DK: Does not say/does not know.
Ríos A et al . Medical students and living liver donation in Spain

5807 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Table 4 Variables of social interaction and pro-social behavior affecting the attitude of university medical students toward unrelated and related living liver donation n (%)
Unrelated living liver donation Related living liver donation
Variable In favor (n = 2937, 32%)
Not in favor (n = 6338, 68%)
P value In favor (n = 8258, 89%)
Not in favor (n = 1017, 11%)
P value
Variables of social interaction Family discussion Yes (n = 6565) 2255 (34) 4310 (66) < 0.001 5946 (91) 619 (9) < 0.001 No (n = 2689) 675 (25) 2014 (75) 2297 (85) 392 (15) DS/DK (n = 21) 7 14 15 6 Discussion with friends Yes (n = 6841) 2307 (34) 4534 (66) < 0.001 6172 (90) 669 (10) < 0.001 No (n = 2418) 627 (26) 1791 (74) 2074 (86) 344 (14) DS/DK (n = 16) 3 13 12 4 A partner's opinion about donation and transplantation Yes, it is favorable (n = 2740) 1045 (38) 1695 (62) < 0.001 2511 (92) 229 (8) < 0.001 I do not know (n = 2451) 603 (25) 1848 (75) 2101 (86) 350 (14) Yes, he or she is against (n = 247) 71 (29) 176 (71) 204 (83) 43 (17) I do not have a boyfriend/girlfriend (n = 3654) 1162 (32) 2492 (68) 3281 (90) 373 (10) DS/DK (n = 183) 56 127 161 22 Donation of a family member's organs Yes (n = 8424) 2776 (33) 5648 (67) < 0.001 7592 (90) 832 (10) < 0.001 No (n = 667) 128 (19) 539 (81) 536 (80) 131 (20) DS/DK (n = 184) 33 151 130 54Variable of pro-social behaviour Participation in pro-social activities Yes, regularly (n = 882) 348 (40) 534 (60) < 0.001 778 (88) 104 (12) < 0.001 Yes, occasionally (n = 1968) 710 (36) 1258 (64) 1756 (89) 212 (11) No, nor am I going to (n = 598) 92 (15) 506 (85) 499 (84) 99 (16) No, but I would be willing to (n = 5766) 1774 (31) 3992 (69) 5201 (90) 565 (10) DS/DK (n = 61) 13 48 24 37
DS/DK: Does not say/does not know.
Table 5 Religious variables and attitude toward the body which affect the attitude of university medical students toward unrelated and related living liver donation n (%)
Unrelated living liver donation Related living liver donation
Variable In favor (n = 2937, 32%)
Not in favor (n = 6338, 68%)
P value In favor (n = 8258, 89%)
Not in favor (n = 1017, 11%)
P value
Religious variables Respondent's religion Catholic (n = 5102) 1629 (32) 3473 (68) 0.607 4603 (90) 499 (10) 0.138 Other religions (n = 266) 92 (35) 174 (65) 233 (88) 33 (12) Atheist/agnostic (n = 3726) 1179 (32) 2547 (68) 3322 (89) 404 (11) DS/DK (n = 181) 37 144 100 81 Knowing the attitude of one's religion toward donation and transplantation Yes, in favor (n = 3049) 1074 (35) 1975 (65) < 0.001 2755 (90) 1975 (65) 0.624 Yes, against (n = 723) 193 (27) 530 (73) 645 (89) 530 (73) I do not know (n = 1152) 325 (28) 827 (72) 1035 (90) 827 (72) DS/DK (n = 444) 129 315 401 43Variable of attitude toward the body Fear of mutilation or scars Yes, I am concerned about it a lot (n = 1004)
262 (26) 742 (74) < 0.001 860 (86) 144 (14) < 0.001
I do not mind (n = 6318) 2230 (35) 4088 (65) 5746 (91) 572 (9) I do not know (n = 1860) 427 (23) 1433 (77) 1582 (85) 278 (15) DS/DK (n = 93) 18 75 70 23
DS/DK: Does not say/does not know.
Ríos A et al . Medical students and living liver donation in Spain

5808 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
A multivariate analysis of the factors affecting attitude toward unrelated LLDThe multivariate analysis has shown the following independent factors to affect attitude toward unrelated LLD (Table 7): (1) Age (OR = 1.026; p < 0.001); (2) Studying in the final years of medicine (fourth, fifth and sixth years) (OR = 1.436 and p = 0.006; OR = 1.594 and p = 0.001; OR = 1.745 and p < 0.001); (3) Being in favor of deceased organ donation (OR = 1.724; p < 0.001); (4) Being in favor of living kidney donation (OR = 12.820; p < 0.001); (5) Being willing to be a recipient of a liver segment from a living donor (OR = 3.115; p < 0.001); (6) Having a partner who is in favor of organ donation (OR = 1.443; p < 0.001) or not having a partner, and therefore, not being influenced by that person (OR = 1.410; p < 0.001); (7) Regular participation in altruistic activities (OR = 1.992; p = 0.002); and (8) A respondent’s belief that his or her religion is in favor of donation and transplantation (OR = 1.398; p = 0.002).
DISCUSSIONKnowing about people’s attitude toward organ dona-tion allows us to determine which factors affect this attitude and to be able to create adequately designed
and cost-effective campaigns. The application of questionnaires is one of the most widely-used data collection techniques in social research, given that (1) it has a low cost; (2) it makes it possible to reach a larger number of participants; and (3) it facilitates the analysis of the results obtained[14]. However, questionnaires also have their limitations, such as the loss of verbal communication. Furthermore, it is fundamentally important for the questionnaire to be designed so that it can quantify and universalize this information, and thus standardize the inter-view process. Therefore, a questionnaire should be subjected to a creation and validation process to confirm to what degree it reflects the situation that we are trying to measure. This basic premise has not been fulfilled in research into attitude toward donation, given that most of the studies carried out and published use measurement tools that have not been designed for such a purpose and have not been validated. Finally, we should remember that the interpretation of the results should involve the recognition of certain limitations that arise in opinion questionnaires. The first of these is the result of the tendency of all the participants to respond according to what is considered to be “socially desirable” in the surroundings where they live. The second is caused by the distance
Table 6 Variables affecting the attitude of university medical students toward related living liver donation, a multivariate study
Variable Regression coefficient (b)
Standard error OR (CI) P value
Sex Male (n = 2702) 1 Female (n = 6499) 0.304 1.356 (1.602-1.146) < 0.001Academic year of degree in medicine: First (n = 2090) 1 Second (n = 1965) 0.090 0.111 1.095 (1.360-0.880) 0.416 Third (n = 1375) 0.096 0.127 1.101 (1.412-0.858) 0.449 Fourth (n = 1301) 0.078 0.135 1.081 (1.408-0.830) 0.561 Fifth (n = 1113) 0.396 0.157 1.485 (2.024-1.091) 0.012 Sixth (n = 1431) 0.396 0.143 1.485 (1.964-1.123) 0.005Attitude toward deceased donation Against – Undecided (n = 1899) 1 In favor (n = 7376) 0.774 0.088 2.169 (2.577-1.824) < 0.001Donating a living kidney I do not know (n = 5619) 1 Yes, I would donate one (n = 2784) 1.189 0.127 3.278 (4.219-2.557) < 0.001 No, I would not donate one (n = 872) 0.914 0.109 2.494 (2.016-3.086) < 0.001Willingness to accept a liver segment from a family member I do not know (n = 2932) 1 Yes, I would accept it (n = 5342) 1.872 0.096 6.493 (7.874-5.376) < 0.001 No, I would wait on the list (n = 907) 0.347 0.115 1.414 (1.769-1.129) 0.003The respondent's partner's opinion about donation and transplantation Yes, he or she is against (n = 247) 1 Yes, it is favorable (n = 2740) 0.383 0.225 1.466 (2.277-0.943) 0.089 I do not know it (n = 2451) 0.157 0.220 1.169 (1.801-0.759) 0.477 I have not got a boyfriend or girlfriend (n = 3654) 0.450 0.219 1.569 (2.409-1.021) 0.040Participation in pro-social activities No, I have no intention to participate (n = 598) 1 Yes, regularly (n = 882) 0.482 0.193 1.620 (1.110-2.364) 0.012 Yes, occasionally (n = 1968) 0.332 0.171 1.394 (0.997-1.948) 0.052 No, but I would be prepared to (n = 5766) 0.168 0.154 1.183 (0.875-1.599) 0.276
Ríos A et al . Medical students and living liver donation in Spain

5809 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
between the responses and the responent’s actual behavior if the situation under consideration were to occur in real life[15].
One of the main efforts of this sociological study was to achieve a representative sample of medical students in the whole of Spain. In addition, the response rate in any attitude study is an indicator of the quality of the data and it is desirable for it to be above 75% in order to prevent a positive bias given that those who tend to respond are those who are more interested in the topic[16].
LLD has been very controversial, although after a steep learning curve, there have been improved outcomes for both donors and recipients in specialist centers making this an acceptable therapeutic option[6,17,18]. This type of living donation has therefore become especially necessary because of the shortage of livers available for transplantation and the mortality on the transplant waiting list[1]. Until now LLD has not been developed to a great extent in Spain, where LLD rates are lower than 0.1 per million population[1].
With the objective of boosting LLD, it has become necessary to improve the social image of this do-nation[19]. In order to achieve this, it has become essential to find out the attitude of the population about the issue, because it is not free of fear and mistrust[19,20]. Furthermore, healthcare professionals should get involved in the matter, given that although they might not be directly involved in the donation and transplantation process, they are groups that generate opinions and therefore they influence the decisions of potential donors[8,9]. This study has shown that medical students, who will be physicians in a few years, have a clearly favorable attitude toward related LLD. This fact is very important, because it should be taken into account that for its development it is essential for healthcare professionals to encourage living donation. However, other factors should be analyzed given that donation rates are not increasing in spite of this positive attitude[1].
Attitude was favorable in 89% of the respondents, a percentage that is higher than the rate reported in
Table 7 Variables affecting the attitude of university medical students toward unrelated living liver donation, a multivariate study
Variable Regression coefficient (b)
Standard error OR (CI) P value
1Age (21 ± 3 yr) 0.026 0.012 1.026 (1.051-1.002) 0.037Year of medicine First (n = 2090) 1 Second (n = 1965) 0.082 0.120 1.085 (1.373-0.857) 0.496 Third (n = 1375) 0.205 0.131 1.226 (1.587-0.949) 0.118 Fourth (n = 1301) 0.362 0.131 1.436 (1.855-1.111) 0.006 Fifth (n = 1113) 0.467 0.141 1.594 (2.100-1.210) 0.001 Sixth (n = 1431) 0.556 0.138 1.745 (2.288-1.331) < 0.001Attitude toward deceased donation Against - Undecided (n = 1899) 1 In favor (n = 7376) 0.546 0.106 1.724 (2.123-1.402) < 0.001Donating a living kidney I do not know (n = 5619) Yes, I would donate one (n = 2784) 2.552 0.078 12.820 (14.925-10.989) < 0.001 No, I would not donate one (n = 872) 0.099 0.146 1.104 (0.830-1.469) 0.495Willingness to accept a liver segment from a family member I do not know (n = 2932) 1 Yes, I would accept it (n = 5342) 1.137 0.089 3.115 (3.717-2.617) < 0.001 No, I would wait on the waiting list (n = 907) 0.257 0.144 1.293 (1.715-0.974) 0.074A partner's opinion about donation and transplantation I do not know it (n = 2451) 1 Yes, it is favorable (n = 2740) 0.367 0.099 1.443 (1.751-1.187) < 0.001 Yes, he or she is against (n = 247) 0.336 0.227 1.398 (2.183-0.896) 0.139 I do not have a boyfriend/girlfriend (n = 3654) 0.344 0.094 1.410 (1.694-1.173) < 0.001Donating a family member's organs No (n = 667) 1 Yes (n = 8424) 0.395 0.162 1.483 (2.040-1.078) 0.015Participation in pro-social activities No, I do not intend to particpate in them (n = 598) 1 Yes, regularly (n = 882) 0.690 0.219 1.992 (3.067-1.297) 0.002 Yes, occasionally (n = 1968) 0.611 0.200 1.841 (2.724-1.243) 0.002 No, but I would be willing to (n = 5766) 0.518 0.190 1.677 (2.439-1.157) 0.006Knowing the attitude of one's religion toward donation and transplantation Yes, against (n = 723) 1 Yes, in favor (n = 3049) 0.336 0.110 1.398 (1.736-1.127) 0.002 I do not know it (n = 1152) 0.249 0.123 1.282 (1.633-1.008) 0.043
Ríos A et al . Medical students and living liver donation in Spain

5810 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
the Spanish general public[19] and in other European countries[21], where about 75% are in favor. In all of these cases it is related donation that is under consideration, that is, when there is some kind of connection between the donor and recipient. This is the reason why it has such a high acceptance level in every stratum, both in the population[12] and healthcare workers[8]. A lot of sensitivity toward unrelated living donation has also been found, with rates of more than 30% in favor. This differs from the data found in English speaking societies where there is a lower acceptance rate[21].
Attitudes toward LLD have not been studied very extensively and there have only been a few isolated studies on medical students. Among these the most notable is the one by Dahlke et al[12] which analyzed the attitude of students in the United States, Germany and Japan, and although the sample was small, it suggests that acceptance is mainly influenced by cultural factors. For example, they state that acceptance is greater in the United States compared to Germany and Japan, with a greater willingness for infant donation than adult donation, and therefore they suggest that socio-demographic differences should be taken into account to establish protocols of clinical practice in living donation. Although this is very important, this aspect is well-known in attitude studies, given that there are many cultural differences between the different continents. We should point out that there have not been any studies about this issue covering a whole country, or a specific geographical area, or even the whole degree in medicine. Instead of this, researchers have focused on a specific group of a specific university. Therefore, until today the only generalizable conclusions about the attitude of medical students toward LLD, in this case in Spain, are the ones presented in this study.
The student’s academic year has an effect on attitude toward LLD. As the student advances through the years there is a gradual progress in technical knowledge of the issue which allows students, mainly in the second half of their degree, to establish contact with the healthcare system and certain clinical services related to transplantation making it possible for students to develop a personal view of the subject[22,23]. In this way, it has been seen that students in the fifth and sixth years have a more favorable attitude than those in the earlier years.
Regardless of academic training and university progression, a close relationship has been observed between attitude toward LLD, and attitude toward the other kinds of human organ donation, both deceased and living kidney donation. This coincides with findings in the Spanish speaking population, where there is a clear association between attitude toward deceased and living donation[24]. Organ donation is an altruistic aspect of life, and if one is able to accept one type of donation then other kinds are also generally
acceptable. Furthermore, as reported in deceased organ donation, feelings of reciprocity also have an influence[14], that is, doing to others what we would like to be done to ourselves. Thus, the principal related factors that have been found have this component of reciprocity, such as the belief that one might need a transplant in the future and if this were the case, a respondent’s willingness to receive an organ from a living donor.
The variables of social interaction have a very clear association with attitude toward the donation of one’s own organs[25-28]. The way each respondent perceives opinions in his or her surroundings has a great influence on his or her ultimate decision on whether to donate or not. For instance, being in a family and social context in which there is a favorable attitude multiplies the chances of the student having a favorable attitude. In current times, when it is uncommon to live independently of the family during the university period, and when students tend to continue to depend on the family for financial support, this fact is becoming more evident.
Family factors should also be noted[29], in the sense that the respondent’s partner’s attitude toward donation has an important influence on the respondent’s attitude. This is a factor that has been typically reported in attitude toward deceased donation[14,30], and it has been seen that when one’s partner is against donation there is a significant increase in the percentage of respondents with doubts or who are against this kind of donation and vice versa. This aspect continues to reinforce the theory that we should keep talking about donation and transplantation, and underlines the importance of expressing favorable attitudes toward donation, because this simple act will have a promotional effect on donation which is generally greater than any organized campaign.
Finally, there is the fear of possible mutilation as a consequence of living donation. Healthcare professionals are just as sensitive as the general public with regard to feelings that arise due to the manipulation of the body, and it has been seen that they have greater difficulty in allowing action to be carried out on it even when there are well-accepted objectives such as in transplantation[19].
We have the basic pillars in place such as future professionals with a relatively high favorable attitude (when deceased donation was first encouraged in Spain, attitude toward this kind of donation was less favorable than current attitude toward LLD), and we also have a receptive population. If institutional and political support can be achieved, as occurred in deceased donation, it is hoped that in the coming years we could relaunch this kind of donation, so we could reach a point where we are able to prevent mortality on the waiting list.
However, we should be cautious about its deve-lopment and restrict it to experienced centers to
Ríos A et al . Medical students and living liver donation in Spain

5811 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
prevent unnecessary morbidity among donors[1]. Therefore, given that current mortality on the liver transplant waiting list in Spain ranges between 8%-10%, our objective should be to arrive at this percentage, and no more. If this is not achieved, we are going to create a healthy young population subjected to liver surgery with frequent morbidity and occasional mortality[31]. Moreover, we should remember that among all the potential liver donors for each recipient a series of invasive procedures need to be performed such as biopsy, arteriography, etc. that produce morbidity in people who do not even become donors[6]. On the other hand, it is well-known that there is an improvement in the bond between the donor and recipient and their self-esteem as a result of this kind of transplant, especially when it is donation from a parent to a child[32], while parents who have refused to donate to their children report consequent stress, anxiety, psychosomatic syndromes and feelings of guilt[32].
To conclude, the attitude of medical student toward related and unrelated LLD is very favorable, and is associated with factors directly and indirectly related to donation and transplantation, family and religious factors, and factors related to attitude toward the body.
COMMENTSBackgroundLiver transplantation offers long survival periods and improved quality of life. However, the current transplant organ donation rates are insufficient for covering minimum transplant needs. Even though living liver donation (LLD) has been successfully carried out in many countries it is at a very low level. One of the possible barriers to its development could be the risk involved for the donor. However, in experienced centers the results are acceptable. Nevertheless, it should be taken into account that professionals in healthcare centers do not always have a favorable attitude toward LLD. Students of medicine represent a new generation of physicians, although their attitude toward LLD has not been studied to any great extent. It should be remembered, however, that the adequate training of future physicians in the transplantation and donation process involves specifically finding out those variables that have an effect on certain attitudes toward donation from the stage of being a student. In this sense, a knowledge of the factors that influence attitudes toward donation will allow us to optimize the resources invested in carrying out donation and transplantation promotion campaigns and to act in a more specific way.
Research frontiersAttitudes toward LLD have not been studied very extensively and there have only been a few isolated studies on medical students. Among these the most notable is the one by Dahlke et al analyzing the attitude of students in the United States, Germany and Japan, and although the sample is small, it suggests that acceptance is mainly influenced by cultural factors. For example, they state that acceptance is greater in the United States compared to Germany and Japan, with a greater willingness for infant donation than adult donation, and therefore they suggest that socio-demographic differences should be taken into account to establish protocols of clinical practice in living donation. Although this is very important, this aspect is well-known in attitude studies, given that there are many cultural differences between the different continents. We should point out that there have not been any studies about this issue covering a whole country, or a specific geographical area, or even the whole degree in medicine. Instead of this, researchers have focused on a specific
group of a specific university. Therefore, until today the only generalizable conclusions about the attitude of medical students toward LLD, in this case in Spain, are the ones presented in this study.
Innovations and breakthroughsIn studies of attitude toward organ donation, there are few stratified studies that have stratified the study population so that generalizations can be made from the results obtained. The study presented in this article represents the first stratified and validated study carried out on medical students covering a whole country, in this case Spain. Attitude was favorable in 89% of the respondents, a percentage that is higher than the rate reported in the Spanish general public and in other European countries, where about 75% are in favor. In all of these cases it is related donation that is under consideration, that is, when there is some kind of connection between the donor and recipient. Attitudes toward LLD have not been studied very extensively in medical students. Dahlke et al analyzed the attitude of students in the United States, Germany and Japan, and although the sample was small, it suggests that acceptance is mainly influenced by cultural factors.
ApplicationsThe authors have the basic pillars in place such as future professionals with a relatively high favorable attitude (when deceased donation was first encouraged in Spain, attitude toward this kind of donation was less favorable than current attitude toward LLD), and the authors also have a receptive population. If institutional and political support can be achieved, as occurred in deceased donation, it is hoped that in the coming years this kind of donation could be relaunched, so that they could reach a point where they are able to prevent mortality on the waiting list. However, they should be cautious about its development and restrict it to experienced centers to prevent unnecessary morbidity among donors. Therefore, given that current mortality on the liver transplant waiting list in Spain ranges between 8%-10%, our objective should be to arrive at this percentage, and no more. If this is not achieved, the authors are going to create a healthy young population subjected to liver surgery with frequent morbidity and occasional mortality. Moreover, the authors should remember that among all the potential liver donors for each recipient a series of invasive procedures need to be performed such as biopsy, arteriography, etc. that produce morbidity in people who do not even become donors. On the other hand, it is well-known that there is an improvement in the bond between the donor and recipient and their self-esteem as a result of this kind of transplant, especially when it is donation from a parent to a child, while parents who have refused to donate to their children report consequent stress, anxiety, psychosomatic syndromes and feelings of guilt.
TerminologyLiver transplantation offers long survival periods and improved quality of life for patients with liver disease whose vital prognosis is short if they do not have a transplant. However, the current transplant organ donation rates are insufficient for covering minimum transplant needs, and the shortage in available livers means that mortality on the waiting list is increasing. Even in Spain in the 21st century, the country with the highest donation rates, mortality on the liver transplant waiting list has been increasing. All of this is making it necessary to encourage alternatives to deceased liver donation. The living liver transplantation has been successfully carried out and in some countries it is becoming more common.
Peer-reviewThis is a very interesting manuscript that explores the views of the next generation of Spanish doctors about living related liver donation. The study includes a large number of medical students with an excellent response rate.
REFERENCES1 Council of Europe. International Figures on Donation and
Transplantation 2013. Newsletter Transplant, 20142 Dutkowski P, Linecker M, DeOliveira ML, Müllhaupt B, Clavien
PA. Challenges to liver transplantation and strategies to improve outcomes. Gastroenterology 2015; 148: 307-323 [PMID: 25224524
COMMENTS
Ríos A et al . Medical students and living liver donation in Spain

5812 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
DOI: 10.1053/j.gastro.2014.08.045]3 Xu DW, Long XD, Xia Q. A review of life quality in living donors
after liver transplantation. Int J Clin Exp Med 2015; 8: 20-26 [PMID: 25784970]
4 Olthoff KM, Abecassis MM, Emond JC, Kam I, Merion RM, Gillespie BW, Tong L; Adult-to-Adult Living Donor Liver Transplantation Cohort Study Group. Outcomes of adult living donor liver transplantation: comparison of the Adult-to-adult Living Donor Liver Transplantation Cohort Study and the national experience. Liver Transpl 2011; 17: 789-797 [PMID: 21360649 DOI: 10.1002/lt.22288]
5 Wan P, Yu X, Xia Q. Operative outcomes of adult living donor liver transplantation and deceased donor liver transplantation: a systematic review and meta-analysis. Liver Transpl 2014; 20: 425-436 [PMID: 24478109 DOI: 10.1002/lt.23836]
6 Li KW, Wen TF, Yan LN, Li B, Zeng Y, Zhao JC, Wang WT, Xu MQ, Yang JY, Ma YK, Chen ZY, Huang B. Donor right hepatectomy in living donor liver transplantation: report of 143 cases. Hepatogastroenterology 2010; 57: 1232-1236 [PMID: 21410064]
7 Azoulay D, Bhangui P, Andreani P, Salloum C, Karam V, Hoti E, Pascal G, Adam R, Samuel D, Ichai P, Saliba F, Castaing D. Short- and long-term donor morbidity in right lobe living donor liver transplantation: 91 consecutive cases in a European Center. Am J Transplant 2011; 11: 101-110 [PMID: 21199351 DOI: 10.1111/j.1600-6143.2010.03284.x]
8 Ríos A, Ramírez P, Rodríguez MM, Martínez L, Rodríguez JM, Galindo PJ, Parrilla P. Attitude of hospital personnel faced with living liver donation in a Spanish center with a living donor liver transplant program. Liver Transpl 2007; 13: 1049-1056 [PMID: 17600353 DOI: 10.1002/lt.21226]
9 Ríos A, Ramírez P, Rodríguez MM, Martínez L, Montoya MJ, Lucas D, Parrilla P. Personnel in cadaveric organ transplant-related hospital units faced with living liver donation: an attitudinal study in a Spanish hospital with a cadaveric and living liver transplant programme. Liver Int 2007; 27: 687-693 [PMID: 17498255 DOI: 10.1111/j.1478-3231.2007.01464.x]
10 Castaing D, Azoulay D, Danet C, Thoraval L, Tanguy Des Deserts C, Saliba F, Samuel D, Adam R. Medical community preferences concerning adult living related donor liver transplantation. Gastroenterol Clin Biol 2006; 30: 183-187 [PMID: 16565648 DOI: 10.1016/S0399-8320(06)73151-7]
11 Conesa Bernal C, Ríos Zambudio A, Ramírez Romero P, Rodríguez Martínez MM, Canteras Jordana M, Parrilla Paricio P. [Importance of primary health-care professionals in the sanitary education about organ donation]. Aten Primaria 2004; 34: 528-533 [PMID: 15607055 DOI: 10.1157/1306958]
12 Dahlke MH, Popp FC, Eggert N, Hoy L, Tanaka H, Sasaki K, Piso P, Schlitt HJ. Differences in attitude toward living and postmortal liver donation in the United States, Germany, and Japan. Psychosomatics 2005; 46: 58-64 [PMID: 15765822 DOI: 10.1176/appi.psy.46.1.58]
13 Instituto Nacional de Estadistica. (Spanish Statistical Office). Available from: URL: http//www.ine.es/
14 Ríos A, Cascales P, Martínez L, Sánchez J, Jarvis N, Parrilla P, Ramírez P. Emigration from the British Isles to southeastern Spain: a study of attitudes toward organ donation. Am J Transplant 2007; 7: 2020-2030 [PMID: 17617867 DOI: 10.1111/j.1600-6143.2007.01879.x]
15 Tourangeau R, Rips LJ, Rasinski K. The Psychology of Survey Response. Cambridge University Press, 2000 [DOI: 10.1017/CBO9780511819322]
16 Ríos A, López-Navas A, Ayala-García MA, Sebastián MJ, Abdo-Cuza A, Alán J, Martínez-Alarcón L, Ramírez EJ, Muñoz G, Suárez-López J, Castellanos R, Ramírez R, González B, Martínez MA, Díaz E, Ramírez P, Parrilla P. Spanish-Latin American multicenter study of attitudes toward organ donation among personnel from hospital healthcare centers. Cir Esp 2014; 92: 393-403 [PMID: 24565516 DOI: 10.1016/j.ciresp.2013.12.017]
17 Morioka D, Egawa H, Kasahara M, Ito T, Haga H, Takada Y,
Shimada H, Tanaka K. Outcomes of adult-to-adult living donor liver transplantation: a single institution’s experience with 335 consecutive cases. Ann Surg 2007; 245: 315-325 [PMID: 17245187 DOI: 10.1097/01.sla.0000236600.24667.a4]
18 Lai JC, Pichardo EM, Emond JC, Brown RS. Resource utilization of living donor versus deceased donor liver transplantation is similar at an experienced transplant center. Am J Transplant 2009; 9: 586-591 [PMID: 19191773 DOI: 10.1111/j.1600-6143.2008.02511.x]
19 Conesa C, Ríos A, Ramírez P, del Mar Rodríguez M, Rivas P, Parrilla P. Socio-personal factors influencing public attitude towards living donation in south-eastern Spain. Nephrol Dial Transplant 2004; 19: 2874-2882 [PMID: 15316100 DOI: 10.1093/ndt/gfh466]
20 Popp FC, Eggert N, Hoy L, Lang SA, Obed A, Piso P, Schlitt HJ, Dahlke MH. Who is willing to take the risk? Assessing the readiness for living liver donation in the general German population. J Med Ethics 2006; 32: 389-894 [PMID: 16816037 DOI: 10.1136/jme.2005.013474]
21 Neuberger J, Farber L, Corrado M, O’Dell C. Living liver donation: a survey of the attitudes of the public in Great Britain. Transplantation 2003; 76: 1260-1264 [PMID: 14578769 DOI: 10.1097/01.TP.0000087835.09752.70]
22 Radunz S, Juntermanns B, Heuer M, Frühauf NR, Paul A, Kaiser GM. The effect of education on the attitude of medical students towards organ donation. Ann Transplant 2012; 17: 140-144 [PMID: 22466921 DOI: 10.12659/AOT.882648]
23 Schaeffner ES , Windisch W, Freidel K, Breitenfeldt K, Winkelmayer WC. Knowledge and attitude regarding organ donation among medical students and physicians. Transplantation 2004; 77: 1714-1718 [PMID: 15201671 DOI: 10.1097/00007890-200406150-00015]
24 Brown RS, Russo MW, Lai M, Shiffman ML, Richardson MC, Everhart JE, Hoofnagle JH. A survey of liver transplantation from living adult donors in the United States. N Engl J Med 2003; 348: 818-825 [PMID: 12606737 DOI: 10.1056/NEJMsa021345]
25 Ríos A, López-Navas AI, Navalón JC, Martínez-Alarcón L, Ayala-García MA, Sebastián-Ruiz MJ, Moya-Faz F, Garrido G, Ramirez P, Parrilla P. The Latin American population in Spain and organ donation. Attitude toward deceased organ donation and organ donation rates. Transpl Int 2015; 28: 437-447 [PMID: 25557362 DOI: 10.1111/tri.12511]
26 Wakefield CE, Watts KJ, Homewood J, Meiser B, Siminoff LA. Attitudes toward organ donation and donor behavior: a review of the international literature. Prog Transplant 2010; 20: 380-391 [PMID: 21265292 DOI: 10.7182/prtr.20.4.p54651601pg80183]
27 Ríos A, Ramírez P, del Mar Rodríguez M, Martínez L, Montoya MJ, Lucas D, Alcaraz J, Parrilla P. Attitude of ancillary personnel faced with living kidney donation in a hospital with a living donor kidney transplant program. Transplantation 2007; 83: 336-340 [PMID: 17297409 DOI: 10.1097/01.tp.0000247799.35846.b1]
28 Ríos Zambudio A, López-Navas A, Ayala-García M, Sebastián MJ, Abdo-Cuza A, Alán J, Martínez-Alarcón L, Ramírez EJ, Muñoz G, Palacios G, Suárez-López J, Castellanos R, González B, Martínez MA, Díaz E, Ramírez P, Parrilla P. Level of awareness of personnel in hospital services related to the donation process: A Spanish and Latin American multicenter study. J Heart Lung Transplant 2012; 31: 850-857 [PMID: 22551932 DOI: 10.1016/j.healun.2012.03.011]
29 Ríos A, Conesa C, Ramírez P, Galindo PJ, Martínez L, Pons JA, Rodríguez MM, Parrilla P. Attitudes toward living liver donation among hospital personnel in services not related to transplantation. Transplant Proc 2005; 37: 3636-3640 [PMID: 16386489 DOI: 10.1016/j.transproceed.2005.10.037]
30 Ríos A, Ramírez P, Martínez L, Montoya MJ, Lucas D, Alcaraz J, Rodríguez MM, Rodríguez JM, Parrilla P. Are personnel in transplant hospitals in favor of cadaveric organ donation? Multivariate attitudinal study in a hospital with a solid organ transplant program. Clin Transplant 2006; 20: 743-754 [PMID: 17100725 DOI: 10.1111/
Ríos A et al . Medical students and living liver donation in Spain

5813 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
j.1399-0012.2006.00562.x]31 Kaido T, Uemoto S. Does living donation have advantages
over deceased donation in liver transplantation? J Gastroenterol Hepatol 2010; 25: 1598-1603 [PMID: 20880167 DOI: 10.1111/j.1440-1746.2010.06418.x]
32 Kärrfelt HM, Berg UB, Lindblad FI, Tydén GE. To be or not to be a living donor: questionnaire to parents of children who have undergone renal transplantation. Transplantation 1998; 65: 915-918 [PMID: 9565094 DOI: 10.1097/00007890-199804150-00009]
P- Reviewer: Bramhall S, Gruttadauria S, Qin JM S- Editor: Gong ZM L- Editor: A E- Editor: Wang CH
Ríos A et al . Medical students and living liver donation in Spain

Song-Zhu Yang, An-Qiang Wang, Juan Du, Jian-Tao Wang, Wei-Wei Yu, Qing Liu, Yan-Fang Wu, Shu-Guang Chen
Song-Zhu Yang, Jian-Tao Wang, Wei-Wei Yu, Qing Liu, Yan-Fang Wu, Department of Hepatobiliary Surgery, Yantaishan Hospital, Yantai 264001, Shandong Province, China
An-Qiang Wang, Shu-Guang Chen, Department of Surgery, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing 100730, China
Juan Du, Department of Health Management, The General Hospital Rocket Forces of the Chinese People’s Liberation Army, Beijing 100088, China
Author contributions: Yang SZ and Wang AQ contributed equally to this work; Yang SZ, Wang AQ, Du J and Chen SG designed the research; Yang SZ, Wang AQ, Du J, Wang JT, Yu WW, Liu Q and Wu YF performed the research; Yu WW and Liu Q contributed new reagents and analytic tools; Yang SZ, Wang JT, Wu YF and Chen SG analyzed the data; and Yang SZ, Wang AQ and Chen SG wrote the paper.
Institutional review board statement: The study was reviewed and approved by the Yantaishan Hospital Institutional Review Board.
Informed consent statement: All study participants, or their legal guardian, provided informed written consent prior to study enrollment.
Conflict-of-interest statement: All authors have no conflict of interest to disclosure.
Data sharing statement: No additional data are available.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Manuscript source: Unsolicited manuscript
Correspondence to: Shu-Guang Chen, MD, Professor, Department of Surgery, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, 1 Shuaifuyuan, Wangfujing, Dongcheng District, Beijing 100730, China. [email protected] Telephone: +86-10-69155200 Fax: +86-10-69155201
Received: April 5, 2016Peer-review started: April 6, 2016First decision: May 12, 2016Revised: May 13, 2016Accepted: June 2, 2016 Article in press: June 2, 2016Published online: July 7, 2016
AbstractAIM: To investigate the relationship between ARID1A expression and clinicopathologic parameters, as well as its prognostic value, for patients with intrahepatic cholangiocarcinoma (IHCC).
METHODS: We assessed ARID1A protein and mRNA expression in IHCC tissues and paracarcinomatous (PC) tissues from 57 patients with IHCC using western blot and quantitative real-time reverse transcription polymerase chain reaction, respectively. We used Fisher’s exact and χ 2 tests to analyze relationships between clinicopathological parameters and ARID1A expression. The Kaplan-Meier method and Cox regression were used to analyze survival.
RESULTS: The mean ARID1A protein level in IHCC tissues was 1.16 ± 0.36 relative units (RU), which was significantly lower than that in PC tissues (1.26 ± 0.21 RU, P < 0.01) and NL tissues (1.11 ± 0.31, P < 0.001).
ORIGINAL ARTICLE
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.3748/wjg.v22.i25.5814
World J Gastroenterol 2016 July 7; 22(25): 5814-5821 ISSN 1007-9327 (print) ISSN 2219-2840 (online)
© 2016 Baishideng Publishing Group Inc. All rights reserved.
5814 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Observational Study
Low expression of ARID1A correlates with poor prognosis in intrahepatic cholangiocarcinoma

of IHCC is much higher in Asian countries than it is worldwide[7]. Although the incidence of IHCC is relatively low, it has been progressively and significantly increasing over the last 30 years[8]. Presently, surgical resection is the only option for treating IHCC. Despite surgery improving median survival when compared with conservative therapy alone (1.8 mo), the outcome is still poor, with a postoperative median survival of 12.2 mo[9,10]. Thus, in order to help develop diagnostic methods for enhanced therapeutic outcomes, information on somatic mutations that contribute to the oncogenesis of IHCC is an important first step.
The ATrich interactive domain 1A (ARID1A) protein (BAF250) is a member of the switching defective/sucrose nonfermenting (SWI/SNF) complexes, which function as ATPdependent chromatin remodelers[11,12]. The ARID1A gene is located at chromosome 1p36, which is related to the regulation of many cellular processes, including proliferation, DNA repair, development, differentiation, and tumor suppression[13]. Absence of ARID1A protein or gene expression has been found in the precursor stage of clear cell carcinoma of the ovary, ovarian endometrioid adenocarcinoma, breast cancer, and colorectal cancer, and correlates with tumor progression in these cancers[1417]. These findings indicate that ARID1A may be a tumorsuppressor gene.
Although correlations between ARID1A gene mutation and ARID1A protein expression with clinicopathologic parameters and prognosis in HCC have been recently reported[18], no study has examined its correlation with IHCC. In the current study, we investigated ARID1A gene and protein expression in surgically resected IHCC tumors in order to observe whether its expression status could be a prognostic biomarker for IHCC.
MATERIALS AND METHODSPatients and tissue specimensIHCC and adjacent paracarcinomatous (PC) liver specimens from 57 IHCC patients and normal liver tissues from 19 hepatic hemangioma patients (controls) were collected in the operation room. Samples were instantly frozen in liquid nitrogen and stored at 80 ℃ until testing. PC tissues were hepatic tissue collected 25 cm away from the tumor edge. All patients underwent surgery in the Department of Hepatobiliary Surgery, Yantaishan Hospital, from January 2012 to June 2013. Diagnoses were defined by pathological examination. The study protocol was approved by the Ethics Committee of Yantaishan Hospital. Informed written consent was obtained from each patient.
We collected clinicopathologic parameters, including age, gender, liver function, tumor size, tumor number, histopathological classification, vessel invasion, recurrence, and patient survival time. Vessel invasion was observed during pathological examination, which
Yang SZ et al . Low-expressed ARID1A and intrahepatic cholangiocarcinoma
5815 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
The mean ARID1A mRNA level in IHCC tissues (1.20 ± 0.18) was also lower than that in PC tissues (1.27 ± 0.15, P < 0.001) and normal liver tissues (1.15 ± 0.34, P < 0.001). Low ARID1A expression was significantly associated with tumor nodules, vein invasion, and recurrence. Median overall survival (OS) and disease-free survival (DFS) for the low ARID1A expression group was 15.0 and 7.0 mo, respectively, which were significantly shorter than those for the high ARID1A expression group at 25.0 and 22.0 mo (OS: P < 0.01; DFS: P < 0.001), respectively. Low ARID1A expression was significantly associated with worse OS (HR = 3.967, 95%CI: 1.299-12.118, P = 0.016) in multivariate analyses.
CONCLUSION: Low expression of ARID1A is associated with poor prognosis in patients with IHCC, and thus may be a potential prognostic biomarker candidate in IHCC.
Key words: ARID1A; Intrahepatic cholangiocarcinoma; Progression; Prognosis; Biomarker
© The Author(s) 2016. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: We investigated the relationship between ARID1A expression and clinicopathologic parameters, as well as its prognostic value, for patients with intrahepatic cholangiocarcinoma (IHCC). We examined ARID1A protein and mRNA expression in IHCC and paracarcinomatous (PC) tissue from 57 patients with IHCC. The mean ARID1A protein and mRNA expression levels in IHCC tissues were significantly lower than those in PC tissues and normal liver tissues. Low ARID1A expression was significantly associated with tumor nodules, vein invasion, and recurrence. Low ARID1A expression was significantly associated with worse overall survival in multivariate analyses. ARID1A may be a potential prognostic biomarker candidate in IHCC.
Yang SZ, Wang AQ, Du J, Wang JT, Yu WW, Liu Q, Wu YF, Chen SG. Low expression of ARID1A correlates with poor prognosis in intrahepatic cholangiocarcinoma. World J Gastroenterol 2016; 22(25): 5814-5821 Available from: URL: http://www.wjgnet.com/1007-9327/full/v22/i25/5814.htm DOI: http://dx.doi.org/10.3748/wjg.v22.i25.5814
INTRODUCTIONPrimary liver cancer (PLC) is the fifth most common cancer worldwide, causing around 600000 deaths annually[1,2]. Intrahepatic cholangiocarcinoma (IHCC) accounts for 5%10% of all PLCs in Western countries[3,4], with hepatocellular carcinoma (HCC) accounting for about 90%[5]. IHCC, a rare malignant tumor arising from the biliary tract, is aggressive and related to a very poor prognosis[6]. The incidence

indicated tumor infiltration in the portal and/or hepatic veins. We monitored recurrence via ultrasound, computed tomography scan, and magnetic resonance imaging.
Western blot analysisIHCC and PC tissues were homogenized and treated with RIPA lysis buffer (Dingguo, Beijing, China). Protein samples were resolved on a 4%12% acrylamide gradient gel. Samples were transferred to a polyvinylidene fluoride membrane using iBlot fast electric transfer (Invitrogen, IL, United States). Membranes were blocked at room temperature for 1 h in 5% milk and incubated with primary antibodies against ARID1A or GAPDH (1:1000, Abcam, MA, United States) at 4 ℃ overnight. Membranes were then washed with TBST three times, followed by incubation with appropriate secondary antibodies (1:8000, Abcam, MA, United States) at room temperature for 2 h. After a further three washes in TBST, the membranes were exposed to film using the ECL kit (Pierce, CA, United States). ARID1Aspecific signals were quantified from X-ray films using a scanner with BandScan 4.30 densitometry software and expressed as integrated intensity units relative to GAPDH signals[19]. The results were analyzed by physicians in a blinded manner.
Quantitative real-time reverse transcription-polymerase chain reactionTotal RNA was extracted from IHCC and PC tissues with TRIzol. The retroviral reverse transcriptase kit (Takara, Tokyo, Japan) was used to synthesize cDNA with the reaction conditions of 37 ℃ for 60 min and 95 ℃ for 3 min. Primers were sense: 5′- TTAACTCCAGCCACCAAAATGAAC-3′ and antisense: 5′- ATAGAGGCGATAGAGGTCCAGAGG-3′ for the ARID1A gene, and sense: 5′-GAAGGTGAAGGTCGGAGTC-3′ and antisense: 5′-GAAGATGGTGATGGGATTTC-3′ for GAPDH. Realtime polymerase chain reaction (PCR) was performed with the 7500 realtime quantitative PCR instrument (Applied Biosystems, CA, United States) using the following conditions: 95 ℃ for 15 s, 60 ℃ for 30 s, and 72 ℃ for 30 s for 40 cycles. Data were normalized using the GAPDH housekeeping gene and expressed as 2-ΔCt.
Patient follow-upWe obtained followup data after discharge for all 57 IHCC patients by direct communication with the patients or their relatives, or by reviewing hospital records. Diseasefree survival (DFS) was measured from the date of hepatectomy until tumor recurrence. Overall survival (OS) was measured from the date of hepatectomy until death or the last followup point. The last followup evaluation was set as August 31, 2015, or up to the time of death.
Statistical analysisQuantitative values are presented as mean ± SD or median (range). Student’s ttest was used to evaluate differences in ARID1A protein and mRNA expression between IHCC and PC tissues. Fisher’s exact and χ 2 tests were used to analyze the correlation between ARID1A expression level and clinicopathologic parameters in patients with IHCC. Survival curves were plotted by the KaplanMeier method and compared using the logrank test. Survival data were evaluated using the Cox proportional hazards model. All tests were twotailed; P < 0.05 was considered significant. SPSS package 17.0 (SPSS Inc., Chicago, IL, United States) was used for all analyses. The statistical methods of this study were reviewed by Prof. Xiaoqing Liu from Peking Union Medical College Hospital.
RESULTSPatient characteristicsThe mean age of the IHCC patients was 55.1 ± 9.3 years and 68.4% (39/57) were male. The mean age of the controls was 51.2 ± 6.6 years and 57.9% (11/19) were male. Forty patients with IHCC had at least one tumor nodule larger than 3 cm. Tumors were welldifferentiated in 22 patients, moderatelydifferentiated in 17 patients, and poorlydifferentiated in 18 patients. The median followup time was 20 mo (range: 228 mo). IHCC recurred in 33 patients over a median recurrence time of 15.0 mo. During the followup, 30 patients died, with a mean survival time of 19.0 ± 6.4 mo.
ARID1A protein and mRNA expression in IHCC and PC tissuesThe mean ARID1A protein level in IHCC tissues was 1.16 ± 0.36 relative units (RU). This was significantly lower than that in PC (1.26 ± 0.21 RU, P < 0.01) and normal liver (NL) tissues (1.11 ± 0.31, P < 0.001) (Figure 1). The mean ARID1A mRNA level in IHCC tissues (1.20 ± 0.18) was also lower than that in PC (1.27 ± 0.15, P < 0.001) and NL tissues (1.15 ± 0.34, P < 0.001) (Figure 2).
Correlations between ARID1A expression and clinicopathological featuresIHCC tissues were then divided according to ARID1A expression. IHCC tissues with ARID1A protein expression lower than that in NL tissues were defined as low expression tumors. Of the 57 total IHCC cases, 19 cases showed low ARID1A expression and 38 cases showed high ARID1A expression. The correlations of ARID1A mRNA and protein expression with clinicopathological parameters are shown in Table 1. Low ARID1A expression was significantly associated with tumor nodules, vein invasion, and recurrence.
ARID1A protein expression in IHCC tissues with
5816 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Yang SZ et al . Low-expressed ARID1A and intrahepatic cholangiocarcinoma

without recurrence (n = 24, 1.39 ± 0.27, P < 0.001). ARID1A mRNA levels in IHCC tissues with recurrence (1.20 ± 0.17) were also lower than in those without recurrence (1.25 ± 0.21), although without statistical significance.
Association of ARID1A expression with prognosisKaplanMeier survival curves and logrank tests showed that low ARID1A protein expression in IHCC tissues was associated with poor prognosis. The median OS for the low ARID1A expression group was 15.0 mo, which was significantly shorter than that of the high ARID1A expression group at 25.0 mo (P < 0.01; Figure 3A). The median DFS rates for the low and high ARID1A expression groups were 7.0 mo and 22.0 mo, respectively (P < 0.001; Figure 3B). Furthermore, multivariate analysis using the Cox proportional hazards model indicated that ARID1A expression levels, tumor nodules, and vein invasion were independent predictors of DFS in patients with IHCC (Table 2). However, ARID1A expression level was the only independent predictor of OS in a multivariate analysis. Low ARID1A expression was significantly associated with worse OS in patients with IHCC when compared with the results from high ARID1A expression (HR = 3.967, 95%CI: 1.29912.118, P =
multiple tumor nodules was significantly lower (n = 18, 0.93 ± 0.34 RU) than in those with solitary tumor nodules (n = 39, 1.27 ± 0.32, P < 0.001). ARID1A mRNA expression in IHCC tissues with multiple tumor nodules (n = 18, 1.13 ± 0.17) was also lower than in those with solitary tumor nodules (1.23 ± 0.16, P < 0.05).
ARID1A protein expression in IHCC tissues with vein invasion was significantly lower (n = 24, 0.93 ± 0.33 RU) than in those without vein invasion (n = 33, 1.33 ± 0.28, P < 0.001). ARID1A mRNA expression in IHCC tissues with vein invasion (1.18 ± 0.18) was also lower than in those without vein invasion (1.21 ± 0.17), although without statistical significance.
ARID1A protein levels in IHCC tissues from patients who experienced recurrence during followup (n = 33, 1.00 ± 0.33) were significantly lower than in those
5817 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
ARID1A
GAPDH
ARID1A
GAPDH
ARID1A
GAPDH
NL tissue
PC tissue
IHCC tissue
Figure 1 ARID1A protein expression in intrahepatic cholangiocarcinoma patients. Western blotting for ARID1A expression in intrahepatic cholangiocarcinoma tissues, paracarcinomatous tissues, and normal liver tissues. GAPDH was used as the internal loading control. IHCC: Intrahepatic cholangiocarcinoma; PC: Paracarcinomatous; NL: Normal liver.
IHCC PC NL
c1.6
1.4
1.2
1.0
0.8
0.6
0.4
0.2
0.0
ARID
1A m
RNA
leve
l
Figure 2 ARID1A mRNA level in intrahepatic cholangiocarcinoma patients. IHCC: Intrahepatic cholangiocarcinoma; PC: Paracarcinomatous; NL: Normal liver. cP < 0.001 vs PC and NL.
Table 1 Clinicopathological features of IHCC patients and the correlation between ARID1A protein expression and clinicopathological parameters
Characteristics ARID1A P value
Low expression High expression
n = 19 n = 38
Age (yr) 0.703 < 50 7 16 ≥ 50 12 22Sex 0.546 Female 7 11 Male 12 27Child-classification 0.500 A 15 34 B 4 4Differentiation 0.546 Well 10 12 Moderately 4 13 Poorly 5 13Tumor size (cm) 0.306 > 3 15 25 ≤ 3 4 13Tumor nodule < 0.001 Solitary 7 32 Multiple 12 6Vein invasion 0.004 Positive 13 11 Negative 6 27Recurrence status 0.004 Yes 16 17 No 3 21
Yang SZ et al . Low-expressed ARID1A and intrahepatic cholangiocarcinoma
IHCC: Intrahepatic cholangiocarcinoma.

0.016, Table 2).
DISCUSSIONARID1A/BAF250 is a component of the SWI/SNF family complexes and is extensively expressed in different human tissues[14,20,21]. The SWI/SNF chromatin remodeling complexes are recurrently mutated in various carcinomas[22]. Mutations in several subunits of these complexes have been identified, including BAF180, SNF5, BRM/SWI2related genes, and ARID1A[22,23]. ARID1A/BAF250 provides SNF/SWI complex specificity and facilitates proteinprotein or proteinDNA molecule interactions. Knockdown of ARID1A gene causes cell cycle arrest in osteoblasts cells, and previous studies have demonstrated a correlation of ARID1A loss and tumorigenesis[11]. Taken together, this supports the potential tumor suppressor function of ARID1A and suggests that ARID1A plays an important role in tumorigenesis and tumor progression.
Guichard et al[24] performed highresolution copynumber analysis on 125 tumor tissues of patients
with HCC, with wholeexome sequencing then being performed on 24 of these tumors. The author found new recurrent modifications in four genes (ARID1A, RPS6KA3, NFE2L2, and IRF2) that had not been formerly described in HCC. In a study by Fujimoto et al[25], the entire genomes of 27 HCCs were sequenced and analyzed. Twentyfive were associated with hepatitis B or C virus infections, including two groups of multicentric tumors. Statistical and functional analyses showed that ARID1A, ARID1B, ARID2, MLL, and MLL3 genes were mutated in about 50% of tumors. Huang et al[18] showed that ARID1A was mutated in 13% of HBVassociated HCC specimens. These studies suggested that ARID1A may be involved in advanced HCC.
IHCC is the second most common primary liver cancer after HCC, accounting for 5%10% of all cholangiocarcinomas[26]. The origin of IHCC is normally demarcated as grade Ⅱ intrahepatic bile duct epithelium[27,28]. The prognosis and mortality rate of IHCC is poor, as IHCC is usually diagnosed at terminal stages due to an absence of appropriate methods for early diagnosis, and surgical treatment only extends postoperative median survival to 12.2 mo[9,10]. A better understanding of the somatic mutations that contribute to the oncogenesis of IHCC is therefore critical for the development of diagnostic strategies. Through exome sequencing of 32 patients with IHCC, Jiao et al[29] found many inactivating mutations in various chromatinremodeling genes (PBRM1, ARID1A, and BAP1), with activating mutations in one of these genes being observed in nearly half of all cancers sequenced. Zou et al[30] sequenced carcinoma and paracancerous tissues in a large cohort of 103 patients with IHCC in China and found that IHCC-specific somatic mutation was correlated with liver inflammation, fibrosis, and cirrhosis. The authors identified 25 mutated genes with eight possible driver genes, including KRAS, TP53, IDH1, ARID1A, PTEN, ECE2, EPPK1, and FYN.
5818 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Low expression of ARID1A protein
High expression of ARID1A protein
1.0
0.8
0.6
0.4
0.2
0.0
Ove
rall
surv
ival
rat
e
5.00 10.00 15.00 20.00 25.00 30.00 35.00 Time after surgery (mo)
Low expression of ARID1A protein
High expression of ARID1A protein
1.0
0.8
0.6
0.4
0.2
0.0
Dis
ease
-fre
e su
rviv
al r
ate
0.00 5.00 10.00 15.00 20.00 25.00 30.00 Time after surgery (mo)
Figure 3 Overall survival (A) and disease-free survival (B) of patients with intrahepatic cholangiocarcinoma after surgical resection according to ARID1A protein expression in intrahepatic cholangiocarcinoma tissues (P < 0.01; log-rank test).
A B
Table 2 Multivariate analysis of overall survival and disease-free survival on ARID1A protein expression in patients with intrahepatic cholangiocarcinoma (Cox proportional hazards model)
Prognostic factors Overall survival Disease-free survival
Hazard ration (95%CI)
P value Hazard ration (95%CI)
P value
Tumor noduleSolitary vs multiple 0.292
(0.093-0.914) 0.034 1.092
(0.328-3.639)0.886
Vein invasionPositive vs negative 0.181
(0.079-0.413)< 0.001 1.207
(0.509-2.859)0.669
ARID1A expressionLow vs high 7.240
(2.281-22.980)< 0.001 3.967
(1.299-12.118)0.016
Yang SZ et al . Low-expressed ARID1A and intrahepatic cholangiocarcinoma

We observed that ARID1A may be a key point for the oncogenesis of IHCC; however, whether ARID1A status impacts clinical behavior has not been made clear. We performed this retrospective study in order to investigate the relationship between ARID1A expression and clinicopathologic parameters, as well as its predictive value for IHCC prognosis.
We found lower ARID1A protein in IHCC tumor tissues when compared with the PC tissues of patients with IHCC and the NL tissues of hepatic hemangioma patients. We also observed a significant difference between the expression level of ARID1A mRNA in IHCC samples and PC tissues.
An important result of the current study was that ARID1A protein expression was associated with tumor nodules, vein invasion, and tumor recurrence status. These factors are highly correlated with the invasion and metastasis of IHCC. Our results indicate that more invasive tumors have lower ARID1A protein expression, suggesting that ARID1A has a suppressive function in IHCC. ARID1A protein expression did not correlate with sex, age, liver function, tumor size, or tumor differentiation.
Many studies have examined the relevance of ARID1A mutation or protein loss to survival in several carcinomas, although the findings were varied. ARID1A mutation or protein loss was a predictor of poor prognosis in cervical carcinoma[31] and gastric cancer[21]. Other studies found no association between ARID1A mutation/protein loss and survival in endometrial clearcell carcinoma[32] and ovarian clear cell adenocarcinoma[33]. Other reports suggested that ARID1A mutation or protein loss may be related to survival in endometrial carcinoma[20] and gastric cancer[21]. Our study is the first to explore the relationship between ARID1A expression and IHCC survival. OS and DFS were significantly shorted in the low ARID1A expression group when compared to that of the high ARID1A expression group. These associations need to be verified and the mechanisms clarified in future investigations. In univariate analyses, ARID1A expression, tumor nodules, vein invasion, and recurrence status were found to be significant prognostic factors. In multivariate analysis, all of the above factors were independent prognostic factors of DFS, while only ARID1A expression was an independent prognostic factor of OS. Taken together, our findings suggest that ARID1A may be a potential prognostic biomarker candidate in IHCC.
This is the first investigation into the correlation between ARID1A gene and protein expression with clinicopathologic features of IHCC. Expressions of ARID1A protein and mRNA of IHCC tissues were lower than in that of PC tissues. ARID1A protein levels in IHCC tissues from patients with recurrence during follow-up were significantly lower than in those without recurrence. IHCC tissues with vein invasions had significantly lower ARID1A protein levels than in those without vein invasions. ARID1A protein expression
in IHCC tissues correlated with OS and DFS. Based on our results showing low ARID1A expression in IHCC, we speculate that the manipulation of ARID1A expression in IHCC patients might have therapeutic implications. However, the functions and mechanisms of ARID1A regulation in normal and IHCC tissues remain unclear and require further study.
COMMENTSBackgroundPrimary liver cancer (PLC) is the fifth most common cancer, with annually about 600000 deaths worldwide. Intrahepatic cholangiocarcinoma (IHCC) accounts for 5%10% of all PLCs in western countries, while hepatocellular carcinoma (HCC) accounts for about 90%.
Research frontiersThe authors investigated ARID1A gene and protein expression in surgically resected IHCC tumors to observe whether its expression status could be a prognostic biomarker for IHCC.
Innovations and breakthroughsThis is the first investigation into correlations between ARID1A gene and protein expression with clinicopathologic features of IHCC. Expressions of ARID1A protein and mRNA of IHCC tissues were lower than in that of paracarcinomatous (PC) tissues.
Peer-reviewIn this very interesting study, the authors investigated the relationship between ARID1A expression and clinicopathologic parameters, as well as its prognostic value, for patients with IHCC. ARID1A protein and mRNA expression in IHCC and PC tissues from 57 patients with IHCC were assessed. The authors found that the low ARID1A expression was associated with a poor prognosis in patients with IHCC, and that ARID1A may be a potential prognostic biomarker candidate in IHCC.
REFERENCES1 Miao R, Luo H, Zhou H, Li G, Bu D, Yang X, Zhao X, Zhang H,
Liu S, Zhong Y, Zou Z, Zhao Y, Yu K, He L, Sang X, Zhong S, Huang J, Wu Y, Miksad RA, Robson SC, Jiang C, Zhao Y, Zhao H. Identification of prognostic biomarkers in hepatitis B virus-related hepatocellular carcinoma and stratification by integrative multi-omics analysis. J Hepatol 2014; 61: 840-849 [PMID: 24859455 DOI: 10.1016/j.jhep.2014.05.025]
2 Zhang H, Zhu C, Zhao Y, Li M, Wu L, Yang X, Wan X, Wang A, Zhang MQ, Sang X, Zhao H. Long non-coding RNA expression profiles of hepatitis C virus-related dysplasia and hepatocellular carcinoma. Oncotarget 2015; 6: 43770-43778 [PMID: 26540467 DOI: 10.18632/oncotarget.6087]
3 Aljiffry M, Abdulelah A, Walsh M, Peltekian K, Alwayn I, Molinari M. Evidence-based approach to cholangiocarcinoma: a systematic review of the current literature. J Am Coll Surg 2009; 208: 134-147 [PMID: 19228515]
4 Wan X, Zhao H. New avenues to treatment of liver cirrhosis. Sci China Life Sci 2014; 57: 1049-1050 [PMID: 25231841 DOI: 10.1007/s11427-014-4751-x]
5 Chan SL, Johnson PJ, Mo F, Berhane S, Teng M, Chan AW, Poon MC, Lai PB, Yu S, Chan AT, Yeo W. International validation of the Chinese university prognostic index for staging of hepatocellular carcinoma: a joint United Kingdom and Hong Kong study. Chin J Cancer 2014; 33: 481-491 [PMID: 25223914 DOI: 10.5732/cjc.014.10133]
6 Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 2010; 127: 2893-2917 [PMID: 21351269 DOI:
5819 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
COMMENTS
Yang SZ et al . Low-expressed ARID1A and intrahepatic cholangiocarcinoma

10.1002/ijc.25516]7 Lo RC, Ng IO. Hepatocellular tumors: immunohistochemical
analyses for classification and prognostication. Chin J Cancer Res 2011; 23: 245-253 [PMID: 23359751 DOI: 10.1007/s11670-011-0245-6]
8 Shaib YH, Davila JA, McGlynn K, El-Serag HB. Rising incidence of intrahepatic cholangiocarcinoma in the United States: a true increase? J Hepatol 2004; 40: 472-477 [PMID: 15123362 DOI: 10.1016/j.jhep.2003.11.030]
9 Shaib Y, El-Serag HB. The epidemiology of cholangiocarcinoma. Semin Liver Dis 2004; 24: 115-125 [PMID: 15192785 DOI: 10.1055/s-2004-828889]
10 Soares KC, Kamel I, Cosgrove DP, Herman JM, Pawlik TM. Hilar cholangiocarcinoma: diagnosis, treatment options, and management. Hepatobiliary Surg Nutr 2014; 3: 18-34 [PMID: 24696835 DOI: 10.3978/j.issn.2304-3881.2014.02.05]
11 Nagl NG, Patsialou A, Haines DS, Dallas PB, Beck GR, Moran E. The p270 (ARID1A/SMARCF1) subunit of mammalian SWI/SNF-related complexes is essential for normal cell cycle arrest. Cancer Res 2005; 65: 9236-9244 [PMID: 16230384 DOI: 10.1158/0008-5472.CAN-05-1225]
12 Wang X, Nagl NG, Wilsker D, Van Scoy M, Pacchione S, Yaciuk P, Dallas PB, Moran E. Two related ARID family proteins are alternative subunits of human SWI/SNF complexes. Biochem J 2004; 383: 319-325 [PMID: 15170388 DOI: 10.1042/BJ20040524]
13 Ho L, Crabtree GR. Chromatin remodelling during development. Nature 2010; 463: 474-484 [PMID: 20110991 DOI: 10.1038/nature08911]
14 Wiegand KC, Shah SP, Al-Agha OM, Zhao Y, Tse K, Zeng T, Senz J, McConechy MK, Anglesio MS, Kalloger SE, Yang W, Heravi-Moussavi A, Giuliany R, Chow C, Fee J, Zayed A, Prentice L, Melnyk N, Turashvili G, Delaney AD, Madore J, Yip S, McPherson AW, Ha G, Bell L, Fereday S, Tam A, Galletta L, Tonin PN, Provencher D, Miller D, Jones SJ, Moore RA, Morin GB, Oloumi A, Boyd N, Aparicio SA, Shih IeM, Mes-Masson AM, Bowtell DD, Hirst M, Gilks B, Marra MA, Huntsman DG. ARID1A mutations in endometriosis-associated ovarian carcinomas. N Engl J Med 2010; 363: 1532-1543 [PMID: 20942669 DOI: 10.1056/NEJMoa1008433]
15 Ayhan A, Mao TL, Seckin T, Wu CH, Guan B, Ogawa H, Futagami M, Mizukami H, Yokoyama Y, Kurman RJ, Shih IeM. Loss of ARID1A expression is an early molecular event in tumor progression from ovarian endometriotic cyst to clear cell and endometrioid carcinoma. Int J Gynecol Cancer 2012; 22: 1310-1315 [PMID: 22976498 DOI: 10.1097/IGC.0b013e31826b5dcc]
16 Samartzis EP, Samartzis N, Noske A, Fedier A, Caduff R, Dedes KJ, Fink D, Imesch P. Loss of ARID1A/BAF250a-expression in endometriosis: a biomarker for risk of carcinogenic transformation? Mod Pathol 2012; 25: 885-892 [PMID: 22301703 DOI: 10.1038/modpathol.2011.217]
17 Mao TL, Ardighieri L, Ayhan A, Kuo KT, Wu CH, Wang TL, Shih IeM. Loss of ARID1A expression correlates with stages of tumor progression in uterine endometrioid carcinoma. Am J Surg Pathol 2013; 37: 1342-1348 [PMID: 24076775 DOI: 10.1097/PAS.0b013e3182889dc3]
18 Huang J, Deng Q, Wang Q, Li KY, Dai JH, Li N, Zhu ZD, Zhou B, Liu XY, Liu RF, Fei QL, Chen H, Cai B, Zhou B, Xiao HS, Qin LX, Han ZG. Exome sequencing of hepatitis B virus-associated hepatocellular carcinoma. Nat Genet 2012; 44: 1117-1121 [PMID: 22922871 DOI: 10.1038/ng.2391]
19 Sun Y, Yang H, Mao Y, Xu H, Zhang J, Li G, Lu X, Sang X, Zhao H, Zhong S, Huang J, Zhang H. Increased Golgi protein 73 expression in hepatocellular carcinoma tissue correlates with tumor aggression but not survival. J Gastroenterol Hepatol 2011; 26: 1207-1212 [PMID: 21443671 DOI: 10.1111/j.1440-1746.2011.06733.x]
20 Allo G, Bernardini MQ, Wu RC, Shih IeM, Kalloger S, Pollett A, Gilks CB, Clarke BA. ARID1A loss correlates with mismatch repair deficiency and intact p53 expression in high-grade endometrial carcinomas. Mod Pathol 2014; 27: 255-261 [PMID: 23887303 DOI: 10.1038/modpathol.2013.144]
21 Wang DD, Chen YB, Pan K, Wang W, Chen SP, Chen JG, Zhao JJ,
Lv L, Pan QZ, Li YQ, Wang QJ, Huang LX, Ke ML, He J, Xia JC. Decreased expression of the ARID1A gene is associated with poor prognosis in primary gastric cancer. PLoS One 2012; 7: e40364 [PMID: 22808142 DOI: 10.1371/journal.pone.0040364]
22 Wilson BG, Roberts CW. SWI/SNF nucleosome remodellers and cancer. Nat Rev Cancer 2011; 11: 481-492 [PMID: 21654818 DOI: 10.1038/nrc3068]
23 Yang X, Li M, Liu Q, Zhang Y, Qian J, Wan X, Wang A, Zhang H, Zhu C, Lu X, Mao Y, Sang X, Zhao H, Zhao Y, Zhang X. Dr.VIS v2.0: an updated database of human disease-related viral integration sites in the era of high-throughput deep sequencing. Nucleic Acids Res 2015; 43: D887-D892 [PMID: 25355513 DOI: 10.1093/nar/gku1074]
24 Guichard C, Amaddeo G, Imbeaud S, Ladeiro Y, Pelletier L, Maad IB, Calderaro J, Bioulac-Sage P, Letexier M, Degos F, Clément B, Balabaud C, Chevet E, Laurent A, Couchy G, Letouzé E, Calvo F, Zucman-Rossi J. Integrated analysis of somatic mutations and focal copy-number changes identifies key genes and pathways in hepatocellular carcinoma. Nat Genet 2012; 44: 694-698 [PMID: 22561517 DOI: 10.1038/ng.2256]
25 Fujimoto A, Totoki Y, Abe T, Boroevich KA, Hosoda F, Nguyen HH, Aoki M, Hosono N, Kubo M, Miya F, Arai Y, Takahashi H, Shirakihara T, Nagasaki M, Shibuya T, Nakano K, Watanabe-Makino K, Tanaka H, Nakamura H, Kusuda J, Ojima H, Shimada K, Okusaka T, Ueno M, Shigekawa Y, Kawakami Y, Arihiro K, Ohdan H, Gotoh K, Ishikawa O, Ariizumi S, Yamamoto M, Yamada T, Chayama K, Kosuge T, Yamaue H, Kamatani N, Miyano S, Nakagama H, Nakamura Y, Tsunoda T, Shibata T, Nakagawa H. Whole-genome sequencing of liver cancers identifies etiological influences on mutation patterns and recurrent mutations in chromatin regulators. Nat Genet 2012; 44: 760-764 [PMID: 22634756 DOI: 10.1038/ng.2291]
26 Cardinale V, Bragazzi MC, Carpino G, Torrice A, Fraveto A, Gentile R, Pasqualino V, Melandro F, Aliberti C, Bastianelli C, Brunelli R, Berloco PB, Gaudio E, Alvaro D. Cholangiocarcinoma: increasing burden of classifications. Hepatobiliary Surg Nutr 2013; 2: 272-280 [PMID: 24570958 DOI: 10.3978/j.issn.2304-3881.2013.10.02]
27 Choi SB , Kim KS, Choi JY, Park SW, Choi JS, Lee WJ, Chung JB. The prognosis and survival outcome of intrahepatic cholangiocarcinoma following surgical resection: association of lymph node metastasis and lymph node dissection with survival. Ann Surg Oncol 2009; 16: 3048-3056 [PMID: 19626372 DOI: 10.1245/s10434-009-0631-1]
28 Miwa S, Miyagawa S, Kobayashi A, Akahane Y, Nakata T, Mihara M, Kusama K, Soeda J, Ogawa S. Predictive factors for intrahepatic cholangiocarcinoma recurrence in the liver following surgery. J Gastroenterol 2006; 41: 893-900 [PMID: 17048054 DOI: 10.1007/s00535-006-1877-z]
29 Jiao Y, Pawlik TM, Anders RA, Selaru FM, Streppel MM, Lucas DJ, Niknafs N, Guthrie VB, Maitra A, Argani P, Offerhaus GJ, Roa JC, Roberts LR, Gores GJ, Popescu I, Alexandrescu ST, Dima S, Fassan M, Simbolo M, Mafficini A, Capelli P, Lawlor RT, Ruzzenente A, Guglielmi A, Tortora G, de Braud F, Scarpa A, Jarnagin W, Klimstra D, Karchin R, Velculescu VE, Hruban RH, Vogelstein B, Kinzler KW, Papadopoulos N, Wood LD. Exome sequencing identifies frequent inactivating mutations in BAP1, ARID1A and PBRM1 in intrahepatic cholangiocarcinomas. Nat Genet 2013; 45: 1470-1473 [PMID: 24185509 DOI: 10.1038/ng.2813]
30 Zou S, Li J, Zhou H, Frech C, Jiang X, Chu JS, Zhao X, Li Y, Li Q, Wang H, Hu J, Kong G, Wu M, Ding C, Chen N, Hu H. Mutational landscape of intrahepatic cholangiocarcinoma. Nat Commun 2014; 5: 5696 [PMID: 25526346 DOI: 10.1038/ncomms6696]
31 Cho H, Kim JS, Chung H, Perry C, Lee H, Kim JH. Loss of ARID1A/BAF250a expression is linked to tumor progression and adverse prognosis in cervical cancer. Hum Pathol 2013; 44: 1365-1374 [PMID: 23427874]
32 Fadare O, Gwin K, Desouki MM, Crispens MA, Jones HW, Khabele D, Liang SX, Zheng W, Mohammed K, Hecht JL, Parkash V. The clinicopathologic significance of p53 and BAF-250a
5820 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Yang SZ et al . Low-expressed ARID1A and intrahepatic cholangiocarcinoma

(ARID1A) expression in clear cell carcinoma of the endometrium. Mod Pathol 2013; 26: 1101-1110 [PMID: 23524907 DOI: 10.1038/modpathol.2013.35]
33 Yamamoto S, Tsuda H, Takano M, Tamai S, Matsubara O.
PIK3CA mutations and loss of ARID1A protein expression are early events in the development of cystic ovarian clear cell adeno-carcinoma. Virchows Arch 2012; 460: 77-87 [PMID: 22120431 DOI: 10.1007/s00428-011-1169-8]
P- Reviewer: Higuchi K, Ryan EM, Okada S S- Editor: Qi Y L- Editor: Rutherford A E- Editor: Ma S
5821 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Yang SZ et al . Low-expressed ARID1A and intrahepatic cholangiocarcinoma

Xiao-Feng Luo, Jian-Hua Jiao, Wen-Yue Zhang, Han-Ming Pu, Bao-Jin Qu, Bing-Ya Yang, Min Hou, Min-Jun Ji
Xiao-Feng Luo, Wen-Yue Zhang, Bing-Ya Yang, Min Hou, Min-Jun Ji, Department of Pathogen Biology, Nanjing Medical University, Nanjing 211166, Jiangsu Province, China
Jian-Hua Jiao, Bao-Jin Qu, Department of Gastroenterology, First Affiliated Hospital of Nanjing Medical University, Nanjing 210029, Jiangsu Province, China
Han-Ming Pu, Department of Gastroenterology, Nanjing Qixia District Hospital, Nanjing 210046, Jiangsu Province, China
Author contributions: Luo XF and Jiao JH contributed equally to this work; Luo XF and Zhang WY performed the nested-ASP-PCR experiments and analyzed the data; Pu HM and Qu BJ collected the samples; Hou M contributed new reagents and materials; Yang BY performed the bacterial culturing and DNA extraction; Jiao JH and Ji MJ conceived and designed the research; Luo XF, Jiao JH and Ji MJ drafted the manuscript; all authors read and approved the final version of the paper.
Institutional review board statement: The study was reviewed and approved by the Nanjing Medical University Institutional Review Board (No. (2015)-246).
Informed consent statement: All patients in this study provided a signed informed consent statement.
Conflict-of-interest statement: Each author certifies that he or she has no commercial associations that might pose a conflict of interest in connection with the submitted article.
Data sharing statement: No additional data are available.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Correspondence to: Dr. Min-Jun Ji, Department of Pathogen
Biology, Nanjing Medical University, No. 101 Longmian Dadao, Nanjing 211166, Jiangsu Province, China. [email protected] Telephone: +86-25-86869400
Received: December 21, 2015Peer-review started: December 31, 2015First decision: March 22, 2016Revised: April 8, 2016Accepted: April 20, 2016 Article in press: April 20, 2016Published online: July 7, 2016
AbstractAIM: To investigate clarithromycin resistance posi-tions 2142, 2143 and 2144 of the 23SrRNA gene in Helicobacter pylori (H. pylori ) by nested-allele specific primer-polymerase chain reaction (nested-ASP-PCR).
METHODS: The gastric tissue and saliva samples from 99 patients with positive results of the rapid urease test (RUT) were collected. The nested-ASP-PCR method was carried out with the external primers and inner allele-specific primers corresponding to the reference strain and clinical strains. Thirty gastric tissue and saliva samples were tested to determine the sensitivity of nested-ASP-PCR and ASP-PCR methods. Then, clarithromycin resistance was detected for 99 clinical samples by using different methods, including nested-ASP-PCR, bacterial culture and disk diffusion.
RESULTS: The nested-ASP-PCR method was success-fully established to test the resistance mutation points 2142, 2143 and 2144 of the 23SrRNA gene of H. pylori . Among 30 samples of gastric tissue and saliva, the H. pylori detection rate of nested-ASP-PCR was 90% and 83.33%, while the detection rate of ASP-PCR was just 63% and 56.67%. Especially in the saliva samples, nested-ASP-PCR showed much higher sensitivity in H. pylori detection and resistance mutation rates than
ORIGINAL ARTICLE
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.3748/wjg.v22.i25.5822
World J Gastroenterol 2016 July 7; 22(25): 5822-5830 ISSN 1007-9327 (print) ISSN 2219-2840 (online)
© 2016 Baishideng Publishing Group Inc. All rights reserved.
5822 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Observational Study
Establishment of a nested-ASP-PCR method to determine the clarithromycin resistance of Helicobacter pylori

gastrointestinal disorders, peptic ulcer diseases, gastric mucosa-associated lymphoid tissue lymphoma and gastric cancer[2]. In most regimens, clarithromycin (CLA) is the key ingredient of strategies to eradicate H. pylori. Bacterial susceptibility to CLA is significantly related to eradication rates of H. pylori by CLA-based therapy. However, this therapy has gradually come under questioning because of increased eradication failure rates. Many factors contribute to the increased risk of failure, such as ineffective penetration of antibiotics into the gastric mucosa, antibiotic inactivation by low stomach pH, and lack of patient compliance[3-5]. Another important cause of failure of H. pylori eradication therapy is resistance to antibiotics. According to many reports[6-8], the incidence of resistance to CLA has increased rapidly in different geographical regions, such as from 29% in 2004 to 77% in 2007 in France[9], from 6% to 55% in Belgium during two decades of observation (1990-2009)[10,11] and from 15% to 65% in 10 years (2000-2009) in China[12,13].
Many studies have confirmed that bacterial resistance of H. pylori to CLA is associated with structural change of the 23SrRNA. This structural change is caused by the single nucleotide polymorphism (SNP) of 23SrRNA[14]. A-to-G point mutations at three positions of 2142, 2143 and 2144 within domain V (A2142G, A2143G and A2144G) have been found to be associated with CLA resistance[2,15-21]. Generally, the assessment of CLA resistance is mainly based on phenotypic methods that are performed by sensitivity testing after bacterial culturing, including the agar diffusion for the E-test or the agar dilution method. However, these methods are time-consuming and lack sensitivity. Moreover, the E-test is unable to provide any information regarding the genetic mutations involved in the resistance mechanism. In the last decade, novel culture-free polymerase chain reaction (PCR)-based techniques have been established to detect these mutations, and they include the techniques of PCR-restriction fragment length polymorphism (RFLP), PCR-DNA-enzyme immunoassay[22], nested PCR[23-26] and so on. In this study, the nested-allele specific primer-polymerase chain reaction (nested-ASP-PCR) and ASP-PCR methods were implemented to determine SNPs of 23SrRNA in H. pylori. Furthermore, the feasibility of saliva as a noninvasive material for testing CLA resistance of H. pylori was evaluated, as compared to gastric tissue.
MATERIALS AND METHODSH. pylori reference strain and clinical isolate strainsThe standard strain NCTC11637 of H. pylori was kept in our laboratory. H. pylori isolates were collected from 99 patients at the Nanjing Qixia District Hospital (Nanjing, Jiangsu Province, China) from March 1, 2014 to December 30, 2014. The age range of these patients was from 18-years old to 65-years-old. All
Luo XF et al . Nested-ASP-PCR to determine CLR of H. pylori
5823 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
ASP-PCR. In the 99 RUT-positive gastric tissue and saliva samples, the H. pylori -positive detection rate by nested-ASP-PCR was 87 (87.88%) and 67 (67.68%), in which there were 30 wild-type and 57 mutated strains in gastric tissue and 22 wild-type and 45 mutated strains in saliva. Genotype analysis showed that three-points mixed mutations were quite common, but different resistant strains were present in gastric mucosa and saliva. Compared to the high sensitivity shown by nested-ASP-PCR, the positive detection of bacterial culture with gastric tissue samples was 50 cases, in which only 26 drug-resistant strains were found through analyzing minimum inhibitory zone of clarithromycin.
CONCLUSION: The nested-ASP-PCR assay showed higher detection sensitivity than ASP-PCR and drug sensitivity testing, which could be performed to evaluate clarithromycin resistance of H. pylori .
Key words: Helicobacter pylori ; Nested-allele specific primer-polymerase chain reaction; Rapid urease test; Clarithromycin resistance; Drug sensitivity testing
© The Author(s) 2016. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: In recent years, antibiotic resistance in Helico-bacter pylori (H. pylori ) has become a global problem, especially the resistances towards metronidazole, clarithromycin and amoxicillin. To combat this growing problem, it is important to determine antimicrobial resistance of a patient’s infection before treatment. Normally, the detection of clarithromycin resistance is based mainly on phenotypic methods performed after culturing. However, bacterial culture has many inherent disadvantages. In the present study, the nested-allele specific primer-polymerase chain reaction was established to detect the different mutations at positions 2142, 2143 and 2144 in the 23SrRNA gene of H. pylori , which can be completed within several hours. This method is expected to contribute towards improving the efficacy of H. pylori eradication therapy.
Luo XF, Jiao JH, Zhang WY, Pu HM, Qu BJ, Yang BY, Hou M, Ji MJ. Establishment of a nested-ASP-PCR method to determine the clarithromycin resistance of Helicobacter pylori. World J Gastroenterol 2016; 22(25): 5822-5830 Available from: URL: http://www.wjgnet.com/1007-9327/full/v22/i25/5822.htm DOI: http://dx.doi.org/10.3748/wjg.v22.i25.5822
INTRODUCTIONHelicobacter pylori (H. pylori) is a microaerobic, Gram-negative, spiral bacterium that colonizes the human stomach in a sustainable manner and is found in more than half of the world’s population[1]. Eradication of H. pylori infection is required for the treatment of upper

patients underwent gastroscopy examination and tested positive for H. pylori by the rapid urease test (RUT), in which the biopsy specimen was inoculated into the rapid urease reagent and a positive result was indicated when the color changed from yellow to pink within 15 min. Then, we collected the gastric tissue and saliva samples to detect 23SrRNA mutation points of CLA. All patients provided a signed informed consent form for study participation.
Design of the PCR primersPCR primers were designed by the Primer 5.0 software, according to 23S ribosomal gene sequence of H. pylori (GenBank Accession No. U27270). Primers External-F and External-R were used as the nested-PCR outer primers to amplify the 23SrRNA gene fragment (1962-2466 bp, 505 bp) of H. pylori. Allele-specific primers (WT2142-F, MUT2142-F, WT2143-F, MUT2143-F, WT2144-F, MUT2144-F and Inner-R) were used as the nested-PCR inner primers to amplify the resistance mutation gene (2122-2415 bp, 294 bp). The primers are listed in Table 1.
Establishment of a nested-ASP-PCR method to determine A2142G, A2143G and A2144G mutations of 23SrRNA of H. pyloriThe extracted DNA from the standard strain NCTC11637 was used as the positive control, while DNA extracted from H. pylori-negative samples determined by RUT and PCR as the negative control. Genomic DNAs extracted from gastric mucosa samples and saliva of 30 H. pylori-positive patients by RUT were used to evaluate the detection sensitivity between ASP-PCR and nested-ASP-PCR methods.
The ASP-PCR amplification reaction mixture (50 µL) contained 5 µL 10 × buffer, 1 µL dNTPs, 1 µL allele-specific primers (WT2142-F, MUT2142-F, WT2143-F, MUT2143-F, WT2144-F, MUT2144-F respectively and Inner-R), 1 µL rTaq DNA polymerase, 1 µL genomic DNA template and 40 µL double-distilled H2O. The PCR cycling conditions were 95 ℃ for 5 min, hot start,
followed by 35 cycles of denaturation at 95 ℃ for 30 s, annealing at 55 ℃ for 30 s and extension at 72 ℃ for 30 s, with a final extension step at 72 ℃ for 5 min. Amplified fragments were visualized by 1.5% agarose gel electrophoresis and staining with ethidium bromide.
The nested-ASP-PCR technique is carried out as a combination of nested-PCR and ASP-PCR, which improves detection sensitivity and specificity by using two rounds of the PCR procedure. The outer primers (External-F and External-R) were utilized to amplify the genomic DNA in the first round of PCR. Then, 1 µL outer PCR product was applied as a template to amplify the resistance mutations fragment with allele-specific primers in the second round of PCR. The reaction conditions for the two rounds of PCR were the same as outlined for the ASP-PCR. Finally, the amplified 23SrRNA gene fragments obtained by nested-ASP-PCR were sequenced in order to confirm the corresponding position’s mutation.
Detection of CLA resistance of clinical samples by nested-ASP-PCR, bacterial culturing and antimicrobial sensitivity testingThe CLA resistance of 99 RUT-positive H. pylori gastric mucosa and saliva samples was evaluated by various methods. The resistance mutation points were detected by nested-ASP-PCR. Gastric specimens were subjected to bacterial culturing and antimicrobial sensitivity testing. The biopsy samples were incubated at 37 ℃ under microaerobic conditions (5% O2, 10% CO2 and 85% N2) for 3 d to 5 d. Then, colonies were sub-cultured to determine the minimum inhibitory zone of CLA by the disk diffusion method (TianHe Microbial Ltd, Hangzhou, China). The minimum inhibitory zone used to define resistance to CLA was ≤ 13 mm.
RESULTSA nested-ASP-PCR method was successfully established to determine the gene mutation of CLA resistanceThe H. pylori reference strain was used to establish the nested-ASP-PCR method. Then, PCR products were amplified from patient samples of gastric mucosa (Figure 1) and saliva (Supplementary Figure 1). The wild-type bacteria strain was amplified into PCR products with 2142A, 2143A and 2144A primers, while the mutated primers were unable to produce any amplification. As Figure 1A and B shows, the 505 bp outer gene fragment of 23SrRNA and the 294 bp inner PCR product were amplifiable by the outer primers and inner primers of the wild-type strain respectively. Furthermore, we found that the result of nested-PCR after the two-round PCR exhibited a stronger band at 294 bp (Figure 1C) than the one-round PCR procedure (Figure 1B). A similar finding was obtained in the detection of saliva samples. Because the DNA content
5824 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Table 1 Primer sequences for the Helicobacter pylori 23SrRNA gene
Gene name Primer sequence, 5’-3’ Product length (bp)
External-F GCGTTGAATTGAAGCCCGAGTAAAC 505External-R CCGACTTTCGTCTCTGCTTGAWT2142-F TCCTACCCGCGGCAAGACGGA 294MUT2142-F TCCTACCCGCGGCAAGACGGGWT2143-F CCTACCCGCGGCAAGACGGAAMUT2143-F CCTACCCGCGGCAAGACGGAGWT2144-F CCTACCCGCGGCAAGACGGAAAMUT2144-F CCTACCCGCGGCAAGACGGAAGInner-R GCCATTACACTCAACTTGCGATTTC
The underlined primer is designed to match the single nucleotide polymorphism site. WT: Wild-type; MUT: Mutation; F: Forward primer; R: Reverse primer.
Luo XF et al . Nested-ASP-PCR to determine CLR of H. pylori

PCR methods. The H. pylori-positive detection includes the amplification detection of wild-type and mutated fragments of H. pylori strains. As shown in Table 2, among the 30 gastric tissue samples, the H. pylori-positive rate detected by nested-ASP-PCR was 90%, but only 63% by ASP-PCR. In the 30 saliva samples, the H. pylori-positive detection rates of nested-ASP-PCR and ASP-PCR were 83.33% and 56.67% respectively. Thus, the detection rate of nested-ASP-PCR was obviously higher than that of ASP-PCR. Furthermore, H. pylori-resistance mutation detection of 23SrRNA in the 30 gastric tissue and saliva samples by nested-ASP-PCR was 11 and 16 respectively, while the number of total mutation was 11 and 10 detected by ASP-PCR. These results suggested that nested-ASP-PCR was more suitable for the detection of low levels of H. pylori in saliva samples.
Nested-ASP-PCR results of 23SrRNA point mutationsFurthermore, 99 RUT-positive patients were analyzed by nested ASP-PCR. Among these patients, 87 (87/99, 87.88%) cases were detected as H. pylori-positive by testing gastric mucosa by nested-ASP-PCR, and included 30 patients (30/87, 34.48%) with wild-type strains and 57 patients (57/87, 65.52%) with 23SrRNA point mutations associated with CLA resistance. Fifty patients (50/87, 57.47%) were infected with strains with A2142G mutations, 52 patients (52/87, 59.77%) with A2143G mutations and 44 patients (44/87, 50.57%) with A2144G mutations. Among the 99 RUT-positive saliva samples, 67 (67/99, 67.68%) were detected as H. pylori-positive by nested-ASP-PCR, and included 22 patients (22/67, 32.84%) with wild-type strains and 45 patients (45/67, 67.16%) with
was very low in saliva, the one-round PCR produced no bands (Supplementary Figure 1B), whereas the nested-PCR amplified the relative bands at 294 bp (Supplementary Figure 1C). Thus, the nested-PCR presented more detection sensitivity than the one-round PCR, especially for the saliva samples.
Next, we used the allele-specific primers to perform the second PCR in order to identify each gene mutation’s position. As Figure 2 shows, in gastric mucosa, H. pylori-negative samples yielded no PCR product (Figure 2A). The A2142G, A2143G and A2144G mutated H. pylori strains were identified according to the corresponding PCR products using different mutated primers, while other positions showed no mutation (Figure 2B and C). Figure 2C shows the mixed bacteria strains of wild-type and A2143G mutation. The saliva samples (Supplementary Figure 2) showed similar results as the gastric mucosa samples, but the bands amplified from saliva were weaker than those from gastric mucosa. The amplified PCR products were sent for sequencing, and the results were consistent with those previously reported in the NCBI GenBank database (Accession No. U27270). The sequences of fragments with 2142, 2143, 2144 position A-to-G mutation are shown in the Supplementary Text 1.
The nested-ASP-PCR method showed higher detection sensitivity than ASP-PCRTo ascertain that the nested-ASP-PCR method has higher sensitivity compared to ASP-PCR, we imple-mented a small-sample experiment. The gastric mucosa and saliva samples from 30 RUT-positive patients were detected to determine the resistance mutation position by the nested-ASP-PCR and ASP-
5825 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
M N 1 M W2 W3 W4M2 M3 M4
500 bp300 bp
M
300 bp
A B
C W2 W3 W4M2 M3 M4
Figure 1 PCR products of wild-type Helicobacter pylori strain in gastric mucosa. A: PCR product amplified with the external primers (M: 1000 bp DNA marker, N: Helicobacter pylori negative sample, 1: Wild-type strains); B: PCR products amplified with the different inner primers; C: The products amplified by nested-ASP-PCR [M: 1000 bp DNA marker (1000, 750, 500, 400, 300, 200, 100), W2: 2142 wild-type primers (2142A), M2: 2142 mutation primers (2142G), W3: 2143 wild-type primers (2143A), M3: 2143 mutation primers (2143G), W4: 2144 wild-type primers (2144A), M4: 2144 mutation primers (2144G)]. ASP-PCR: Allele-specific primer-polymerase chain reaction.
Luo XF et al . Nested-ASP-PCR to determine CLR of H. pylori

23SrRNA point mutations. The numbers of patients with A2142G, A2143G and A2144G mutations were 35 (35/67, 52.24%), 39 (39/67, 58.21%) and 23 (23/67, 34.34%) respectively (Table 3). We observed all the
mutation sub-types in these patients (Figure 3). The results showed that the mixed mutations rate with 2142, 2143 and 2144 positions was relatively high, while patients with a single mutation were rare, which
5826 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
M
500 bp
W2 W3 W4M2 M3 M4E
300 bp
M W2 W3 W4M2 M3 M4
300 bp
A2142G mutation strain
W2 W3 W4M2 M3 M4
A2143G mutation strain
M W2 W3 W4M2 M3 M4
300 bp
A2144G mutation strain
W2 W3 W4M2 M3 M4
wt and A2143G mutation strain
A
B
C
Figure 2 PCR products of Helicobacter pylori clinical strains in gastric mucosa with 2142, 2143 and 2144 positions mutation assayed by nested-ASP-PCR. A: Helicobacter pylori-negative control; B: A2142G mutation and A2143G mutation strains; C: A2144G mutation; C: wild-type and A2143G mutation mixture strains [M: 1000 bp DNA marker (1000, 750, 500, 400, 300, 200, 100), E: Outer PCR primers, W2: 2142 wild-type primers (2142A), M2: 2142 mutation primers (2142G), W3: 2143 wild-type primers (2143A), M3: 2143 mutation primers (2143G), W4: 2144 wild-type primers (2144A), M4: 2144 mutation primers (2144G)]. ASP-PCR: Allele-specific primer-polymerase chain reaction.
Table 2 Results for the 23SrRNA point mutation in 30 gastric mucosa and saliva samples, as detected by ASP-PCR and nested-ASP-PCR
H. pylori -positive detection rate WT Total mutation, A-to-G 2142 G 2143 G 2144 G
Gastric mucosaASP-PCR 19 8 11 10 10 10Ratio 63% 42.11% 57.89 52.63% 52.63% 52.63%
(19/30) (8/30) (11/19) (10/19) (10/19) (10/19)Nested-ASP-PCR 27 16 11 11 10 11Ratio 90% 59.26% 40.74% 40.74% 37.04% 40.74%
(27/30) (16/30) (11/19) (11/19) (10/19) (10/19)SalivaASP-PCR 17 7 10 10 4 0Ratio 56.67% 41.18% 58.82% 58.82% 23.53% 0
(17/30) (7/30) (10/17) (10/17) (4/17)Nested-ASP-PCR 25 9 16 16 13 9Ratio 83.33% 36% 64% 64% 52% 36%
(25/30) (9/30) (16/25) (16/25) (13/25) (9/25)
ASP-PCR: Allele-specific primer-polymerase chain reaction.
Luo XF et al . Nested-ASP-PCR to determine CLR of H. pylori

suggested that the mixture strains existed commonly in gastric mucosa and saliva. We further analyzed the mutation genotypes in the gastric mucosa and saliva samples from each individual (Supplementary Table 1) and found that the rate of simultaneous mutation in gastric mucosa and saliva was 33. The mutation consistency rate was just 33.33% (11/33). In short, gastric mucosa and saliva samples exhibited different mutation genotypes.
Comparative analysis of H. pylori detection and CLA resistance by various methodsIn the 99 RUT-positive patients, the H. pylori detection
rate in gastric mucosa by the nested-ASP-PCR was 87.88% (87/99), for which the resistance site mutation rate was 65.52% (57/87). This finding suggested that RUT can give some false-positive results.
Next, H. pylori isolates were cultured from the gastric biopsy samples of 87 patients who had been identified as having H. pylori infection by nested-ASP-PCR, and only 50 H. pylori-positive strains were obtained by primary culture. The bacterial culture positive rate was 57.47% (50/87). Furthermore, we implemented the drug sensitivity test (DST) by disk diffusion method. Among these 50 cases, 26 (26/50, 52%) showing resistant strains of H. pylori, with the
5827 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
2142G, 2143G and 2144G
2143G and 2144G
2142G and 2144G
2142G and 2143G
Single 2144G
Single 2143G
Single 2142G
Total 2144G
Total 2143G
Total 2142G
0 20 40 60 Casas
Gastric mucosa
Saliva
Mutation subtypes
Figure 3 Mutation subtypes of each site in gastric mucosa and saliva. (1) “2142G, 2143G and 2144G” indicates the three-sites mutation sub-type; (2) “2142G and 2143G, 2142G and 2144G, 2143G and 2144G” indicate the two-sites mutation subtypes; (3) “Single 2142G, single 2143G and single 2144G” indicate the single-site mutation subtypes; (4) “Total 2142G, total 2143G and total 2144G” indicate the sum of corresponding site mutations in the single-site, two-sites and three-sites mutations.
Luo XF et al . Nested-ASP-PCR to determine CLR of H. pylori
Table 3 Results for the 23SrRNA point mutation in gastric mucosa and saliva samples of 99 RUT-positive clinical cases detected by nested-ASP-PCR
H. pylori: Helicobacter pylori; ASP-PCR: Allele-specific primer-polymerase chain reaction.
RUT-positive H. pylori -positive detection rate
WT Total mutation, A-to-G 2142 G 2143 G 2144 G
Gastric mucosa 99 87 30 57 50 52 44ratio 87.88% 34.48% 65.52% 57.47% 59.77% 50.57%
(87/99) (30/87) (57/87) (50/87) (52/87) (44/87)Saliva 99 67 22 45 35 39 23ratio 67.68% 32.84% 67.16% 52.24% 58.21% 34.34%
(67/99) (22/67) (45/67) (35/67) (39/67) (22/67)

remaining 24 (24/50, 48%) showing wild-type strains (Table 4).
DISCUSSIONIn recent years, antibiotic resistance in H. pylori infection has become a global problem, especially for resistance to amoxicillin, CLA and metronidazole. Some elements, including age, sex, in-house infection, colonization density, gastric pH and pre-exposure to antibiotics, are thought to be responsible for resistance development, which subsequently leads to failure of H. pylori eradication. It has been reported that CLA resistance doubled within a 5-year period, probably because of the wide usage of this antibiotic as treatment for community-based pneumonia[27]. To combat the growing problem of antibiotic resistance, it is important to choose the most appropriate first-line treatment regimen. This choice should be made on the basis of knowledge of the status of antimicrobial resistance before treatment[28].
A variety of diagnostic methods have been deve-loped for antibiotic resistance to H. pylori, including invasive tests (gastric biopsy for histology and culture) and noninvasive tests (urea breath and stool antigen tests). Normally, the detection of CLA resistance is based mainly on phenotypic methods that are performed after culturing, such as agar diffusion for the E-test or the agar dilution method. Bacterial culturing is a widely available method that allows for antimicrobial susceptibility testing, and it can require tissues obtained through endoscopy. However, bacterial culture has many inherent disadvantages, such as special transportation and culture conditions, special media and environments, restrictive timelines and lengthy incubation time. These factors directly influence the detection of H. pylori. Detection of point mutations conferring resistance to CLA by molecular methods may constitute a more reliable approach. Some PCR-based techniques have been developed to detect these mutations, such as PCR-RFLP, PCR-DNA-enzyme immunoassay, real-time PCR and reverse hybridization line probe assay[29]. In the present study, the nested-ASP-PCR was established to detect the different mutations at positions 2142, 2143 and 2144 in the 23SrRNA gene of H. pylori. This method can determine whether H. pylori strains are sensitive or resistant to CLA within several hours, while traditional culture testing for bacterial susceptibility to antibiotics is expensive and requires 7-10 d[30]. Thus, nested-ASP-
PCR molecular testing is a relatively rapid, sensitive and reliable technique to detect CLA resistance[31], which might help make an individualized treatment strategy feasible in daily clinical practice and contribute to H. pylori eradication therapy[27]. In our study, among 30 gastric tissue samples, the H. pylori-positive rates detected by nested-ASP-PCR and ASP-PCR were 90% and 63% respectively. Simultaneously, the H. pylori-positive detection rates for saliva samples by the two methods were 83.33% and 56.67%. Not only in H. pylori detection but also in resistance site mutation detection, the nested-ASP-PCR method exhibited much higher sensitivity than ASP-PCR, especially in saliva samples with low levels of H. pylori.
PCR detection of H. pylori has been reported using a variety of clinical samples, including gastric biopsy, gastric juice, saliva, dental plaque and stools. It has been reported that the oral cavity may be a reservoir for H. pylori, responsible for oral-to-oral transmission of this bacterium. Other studies have also shown that H. pylori infection in the oral cavity is closely related to that in the stomach and that the mouth is the first extra-gastric reservoir[32,33]. More recently, DNA present in saliva has been employed in PCR-based assays designed to detect mutations associated with fragile X syndrome[34,35]. DNA fingerprinting studies have suggested that the same H. pylori strain can colonize both the oral cavity and the stomach[36].
We sought to determine if genomic DNA recovered from whole saliva constitutes a reliable alternative for DNA isolated from gastric mucosa and can reflect the resistance site polymorphisms[37] of H. pylori. In our study, the CLA resistance rate in gastric mucosa and saliva was 65.52% and 67.16% respectively. On the one hand, the resistance to CLA in gastric mucosa and saliva is quite common now. Some studies in the literature have reported 72.44% CLA resistance in Italy[7], 65%-75% in Taiwan[8], and even as high as 84.9% in the children in Beijing, China[13]. On the other hand, we found that gastric mucosa and saliva samples can exhibit different mutation genotypes. Our results are similar to Wang and Song’s studies[38], which showed that DNA sequences of PCR products from saliva differed from those obtained from the gastric biopsy of the same individual, suggesting that different strains are present in the mouth and the stomach. However, more investigations with a larger number of patients are required to confirm this.
In conclusion, in the present study we established the nested-ASP-PCR method to increase the detection
5828 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Luo XF et al . Nested-ASP-PCR to determine CLR of H. pylori
Table 4 Results for Helicobacter pylori detection and clarithromycin resistance in gastric mucosa by different testing methods
RUT-positive Nested-ASP-PCR detection Nested-ASP-PCR mutation Bacterial culture H. pylori -positive Drug-resistant strains
Cases 99 87 57 50 26Ratio 87.88% (87/99) 65.52% (57/87) 57.47% (50/87) 52% (26/50)
H. pylori: Helicobacter pylori; ASP-PCR: Allele-specific primer-polymerase chain reaction.

sensitivity of resistance site mutations of the H. pylori 23SrRNA gene[39,40]. This study provides an inexpensive, reliable method for the evaluation of CLA resistance, which will likely contribute to improving the efficacy of H. pylori eradication therapy.
ACKNOWLEDGMENTSWe thank the Hospital of Qixia in Nanjing for providing sufficient financial support for this study.
COMMENTSBackgroundIn recent years, antibiotic resistance in Helicobacter pylori infection has become a global problem, especially of resistance to amoxicillin, clarithromycin (CLA) and metronidazole. According to many reports, CLA resistance increased from 29% in 2004 to 77% in 2007 in France and from 15% to 65% over a 10-year period (2000-2009) in China. Generally, the assessment of CLA resistance is based mainly on phenotypic methods performed by sensitivity testing after bacterial culturing, such as agar diffusion for the E-test or the agar dilution method. Furthermore, CLA resistance of H. pylori has been directly linked to the single nucleotide polymorphisms at positions 2142, 2143 and 2144 of 23SrRNA gene. Thus, in the last decade, novel culture-free polymerase chain reaction (PCR)-based techniques have been established to detect these mutations, and these include the PCR-restriction fragment length polymorphism, PCR-DNA-enzyme immunoassay and so on.
Research frontiersA variety of diagnostic methods have been developed for antibiotic resistance to H. pylori, including invasive tests (gastric biopsy for histology and culture) and noninvasive tests (urea breath and stool antigen tests). Bacterial culture is a widely available method that allows for antimicrobial susceptibility testing, but it is expensive and requires 7-10 d for results. In the present study, the nested-ASP-PCR technique was established to detect the CLA resistance mutations at positions 2142, 2143 and 2144 in the 23SrRNA gene of H. pylori. This method can determine whether H. pylori strains are sensitive or resistant to CLA within several hours.
Innovations and breakthroughsTraditional culture testing for bacterial susceptibility to antibiotics has many inherent disadvantages, such as special transportation and culture conditions, special media and environments, restrictive timelines and lengthy incubation time. These factors directly influence the detection of H. pylori. Detection of point mutations conferring resistance to CLA by molecular methods may constitute a more reliable approach. It has been reported that the oral cavity may be a reservoir for H. pylori, responsible for oral-to-oral transmission of this bacterium. Other studies have also showed that H. pylori infection in the oral cavity is closely related to that in the stomach and that the mouth is the first extra-gastric reservoir. In the present study, the feasibility of saliva as a noninvasive material for use in detecting CLA resistance of H. pylori was evaluated compared to gastric tissue. The nested-ASP-PCR molecular test is a relatively rapid, sensitive and reliable method to detect CLA resistance.
ApplicationsThe data in this study suggested that the nested-ASP-PCR method can increase the detection sensitivity of resistance site mutations of the 23SrRNA gene in H. pylori. The outcomes from this study are expected to contribute to improving the efficacy of H. pylori eradication therapy and to guide clinical treatment. Furthermore, this study also provided readers with some important information regarding CLA resistance of H. pylori in the populations of China.
TerminologyNested-ASP-PCR is nested-PCR combined with allele-specific primer-PCR.
Peer-reviewAvailable papers concerning CLA resistance of H. pylori in mainland China are common. However, articles describing the detection of CLA resistant strains using gastric and saliva samples simultaneously are rare. The authors in this study analyzed the CLA resistance rates for each site and the mutations consistency between the saliva and gastric samples. This study showed that gastric mucosa and saliva samples can exhibit different mutation genotypes. The results are interesting and provide important information concerning the background and trends of H. pylori treatments for people in China.
REFERENCES1 Agudo S, Pérez-Pérez G, Alarcón T, López-Brea M. High
prevalence of clarithromycin-resistant Helicobacter pylori strains and risk factors associated with resistance in Madrid, Spain. J Clin Microbiol 2010; 48: 3703-3707 [PMID: 20668128 DOI: 10.1128/JCM.00144-10]
2 Nakamura A, Furuta T, Shirai N, Sugimoto M, Kajimura M, Soya Y, Hishida A. Determination of mutations of the 23S rRNA gene of Helicobacter pylori by allele specific primer-polymerase chain reaction method. J Gastroenterol Hepatol 2007; 22: 1057-1063 [PMID: 17608851 DOI: 10.1111/j.1440-1746.2006.04546.x]
3 Schmitt BH, Regner M, Mangold KA, Thomson RB, Kaul KL. PCR detection of clarithromycin-susceptible and -resistant Helicobacter pylori from formalin-fixed, paraffin-embedded gastric biopsies. Mod Pathol 2013; 26: 1222-1227 [PMID: 23579617 DOI: 10.1038/modpathol.2013.48]
4 Furuta T, Shirai N, Takashima M, Xiao F, Hanai H, Sugimura H, Ohashi K, Ishizaki T, Kaneko E. Effect of genotypic differences in CYP2C19 on cure rates for Helicobacter pylori infection by triple therapy with a proton pump inhibitor, amoxicillin, and clarithromycin. Clin Pharmacol Ther 2001; 69: 158-168 [PMID: 11240980 DOI: 10.1067/mcp.2001.113959]
5 Maeda S, Yoshida H, Matsunaga H, Ogura K, Kawamata O, Shiratori Y, Omata M. Detection of clarithromycin-resistant helicobacter pylori strains by a preferential homoduplex formation assay. J Clin Microbiol 2000; 38: 210-214 [PMID: 10618089]
6 Mégraud F. H pylori antibiotic resistance: prevalence, importance, and advances in testing. Gut 2004; 53: 1374-1384 [PMID: 15306603 DOI: 10.1136/gut.2003.022111]
7 Di Giulio M , Di Campli E, Di Bartolomeo S, Cataldi V, Marzio L, Grossi L, Ciccaglione AF, Nostro A, Cellini L. In vitro antimicrobial susceptibility of Helicobacter pylori to nine antibiotics currently used in Central Italy. Scand J Gastroenterol 2016; 51: 263-269 [PMID: 26554617 DOI: 10.3109/00365521.2015.1092577]
8 Wu IT, Chuah SK, Lee CH, Liang CM, Lu LS, Kuo YH, Yen YH, Hu ML, Chou YP, Yang SC, Kuo CM, Kuo CH, Chien CC, Chiang YS, Chiou SS, Hu TH, Tai WC. Five-year sequential changes in secondary antibiotic resistance of Helicobacter pylori in Taiwan. World J Gastroenterol 2015; 21: 10669-10674 [PMID: 26457027 DOI: 10.3748/wjg.v21.i37.10669]
9 Raymond J, Lamarque D, Kalach N, Chaussade S, Burucoa C. High level of antimicrobial resistance in French Helicobacter pylori isolates. Helicobacter 2010; 15: 21-27 [PMID: 20302586 DOI: 10.1111/j.1523-5378.2009.00737.x]
10 Boltin D, Ben-Zvi H, Perets TT, Kamenetsky Z, Samra Z, Dickman R, Niv Y. Trends in secondary antibiotic resistance of Helicobacter pylori from 2007 to 2014: has the tide turned? J Clin Microbiol 2015; 53: 522-527 [PMID: 25428158 DOI: 10.1128/JCM.03001-14]
11 Miendje Deyi VY, Bontems P, Vanderpas J, De Koster E, Ntounda R, Van den Borre C, Cadranel S, Burette A. Multicenter survey of routine determinations of resistance of Helicobacter pylori to antimicrobials over the last 20 years (1990 to 2009) in Belgium. J Clin Microbiol 2011; 49: 2200-2209 [PMID: 21450969 DOI: 10.1128/JCM.02642-10]
12 Gao W, Cheng H, Hu F, Li J, Wang L, Yang G, Xu L, Zheng X. The evolution of Helicobacter pylori antibiotics resistance over 10
5829 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Luo XF et al . Nested-ASP-PCR to determine CLR of H. pylori
COMMENTS

years in Beijing, China. Helicobacter 2010; 15: 460-466 [PMID: 21083752 DOI: 10.1111/j.1523-5378.2010.00788.x]
13 Zhang YX, Zhou LY, Song ZQ, Zhang JZ, He LH, Ding Y. Primary antibiotic resistance of Helicobacter pylori strains isolated from patients with dyspeptic symptoms in Beijing: a prospective serial study. World J Gastroenterol 2015; 21: 2786-2792 [PMID: 25759550 DOI: 10.3748/wjg.v21.i9.2786]
14 Ioannidou S, Tassios PT, Kotsovili-Tseleni A, Foustoukou M, Legakis NJ, Vatopoulos A. Antibiotic resistance rates and macrolide resistance phenotypes of viridans group streptococci from the oropharynx of healthy Greek children. Int J Antimicrob Agents 2001; 17: 195-201 [PMID: 11282264]
15 Shen J, Zhang JZ, Ke Y, Deng D. Formation of A2143G mutation of 23S rRNA in progression of clarithromycin resistance in Helicobacter pylori 26695. Microb Drug Resist 2005; 11: 100-106 [PMID: 15910222 DOI: 10.1089/mdr.2005.11.100]
16 Pan ZJ , Su WW, Tytgat GN, Dankert J, van der Ende A. Assessment of clarithromycin-resistant Helicobacter pylori among patients in Shanghai and Guangzhou, China, by primer-mismatch PCR. J Clin Microbiol 2002; 40: 259-261 [PMID: 11773126]
17 Slinger R, Yan L, Chan F, Forward K, Cooper-Lesins G, Best L, Haldane D, Veldhuyzen van Zanten S. Pyrosequencing assay to rapidly detect clarithromycin resistance mutations in Canadian Helicobacter pylori isolates. Can J Gastroenterol 2009; 23: 609-612 [PMID: 19816623]
18 Liu G, Xu X, He L, Ding Z, Gu Y, Zhang J, Zhou L. Primary antibiotic resistance of Helicobacter pylori isolated from Beijing children. Helicobacter 2011; 16: 356-362 [PMID: 21923681 DOI: 10.1111/j.1523-5378.2011.00856.x]
19 Versalovic J, Osato MS, Spakovsky K, Dore MP, Reddy R, Stone GG, Shortridge D, Flamm RK, Tanaka SK, Graham DY. Point mutations in the 23S rRNA gene of Helicobacter pylori associated with different levels of clarithromycin resistance. J Antimicrob Chemother 1997; 40: 283-286 [PMID: 9301997]
20 de Francesco V, Margiotta M, Zullo A, Hassan C, Valle ND, Burattini O, Cea U, Stoppino G, Amoruso A, Stella F, Morini S, Panella C, Ierardi E. Primary clarithromycin resistance in Italy assessed on Helicobacter pylori DNA sequences by TaqMan real-time polymerase chain reaction. Aliment Pharmacol Ther 2006; 23: 429-435 [PMID: 16423002 DOI: 10.1111/j.1365-2036.2006.02769.x]
21 Kim JM, Kim JS, Kim N, Kim YJ, Kim IY, Chee YJ, Lee CH, Jung HC. Gene mutations of 23S rRNA associated with clarithromycin resistance in Helicobacter pylori strains isolated from Korean patients. J Microbiol Biotechnol 2008; 18: 1584-1589 [PMID: 18852516]
22 Elviss NC, Lawson AJ, Owen RJ. Application of 3’-mismatched reverse primer PCR compared with real-time PCR and PCR-RFLP for the rapid detection of 23S rDNA mutations associated with clarithromycin resistance in Helicobacter pylori. Int J Antimicrob Agents 2004; 23: 349-355 [PMID: 15081083 DOI: 10.1016/j.ijantimicag.2003.09.015]
23 Noguchi N, Rimbara E, Kato A, Tanaka A, Tokunaga K, Kawai T, Takahashi S, Sasatsu M. Detection of mixed clarithromycin-resistant and -susceptible Helicobacter pylori using nested PCR and direct sequencing of DNA extracted from faeces. J Med Microbiol 2007; 56: 1174-1180 [PMID: 17761479 DOI: 10.1099/jmm.0.47302-0]
24 Maeda S, Yoshida H, Ogura K, Kanai F, Shiratori Y, Omata M. Helicobacter pylori specific nested PCR assay for the detection of 23S rRNA mutation associated with clarithromycin resistance. Gut 1998; 43: 317-321 [PMID: 9863474]
25 Patel SK, Mishra GN, Pratap CB, Jain AK, Nath G. Helicobacter pylori is not eradicated after triple therapy: a nested PCR based study. Biomed Res Int 2014; 2014: 483136 [PMID: 25054141 DOI:
10.1155/2014/483136]26 Mishra S, Singh V, Rao GR, Dixit VK, Gulati AK, Nath G.
Prevalence of Helicobacter pylori in asymptomatic subjects--a nested PCR based study. Infect Genet Evol 2008; 8: 815-819 [PMID: 18771754 DOI: 10.1016/j.meegid.2008.08.001]
27 Karabiber H, Selimoglu MA, Otlu B, Yildirim O, Ozer A. Virulence factors and antibiotic resistance in children with Helicobacter pylori gastritis. J Pediatr Gastroenterol Nutr 2014; 58: 608-612 [PMID: 24792628 DOI: 10.1097/MPG.0000000000000273]
28 Oleastro M, Ménard A, Santos A, Lamouliatte H, Monteiro L, Barthélémy P, Mégraud F. Real-time PCR assay for rapid and accurate detection of point mutations conferring resistance to clarithromycin in Helicobacter pylori. J Clin Microbiol 2003; 41: 397-402 [PMID: 12517879]
29 Pina M, Occhialini A, Monteiro L, Doermann HP, Mégraud F. Detection of point mutations associated with resistance of Helicobacter pylori to clarithromycin by hybridization in liquid phase. J Clin Microbiol 1998; 36: 3285-3290 [PMID: 9774580]
30 Calvet X, Ducons J, Guardiola J, Tito L, Andreu V, Bory F, Guirao R. One-week triple vs. quadruple therapy for Helicobacter pylori infection - a randomized trial. Aliment Pharmacol Ther 2002; 16: 1261-1267 [PMID: 12144575]
31 Mahachai V, Sirimontaporn N, Tumwasorn S, Thong-Ngam D, Vilaichone RK. Sequential therapy in clarithromycin-sensitive and -resistant Helicobacter pylori based on polymerase chain reaction molecular test. J Gastroenterol Hepatol 2011; 26: 825-828 [PMID: 21251064 DOI: 10.1111/j.1440-1746.2011.06660.x]
32 Rimbara E, Sasatsu M, Graham DY. PCR detection of Heli-cobacter pylori in clinical samples. Methods Mol Biol 2013; 943: 279-287 [PMID: 23104297 DOI: 10.1007/978-1-60327-353-4_19]
33 Sugimoto M, Wu JY, Abudayyeh S, Hoffman J, Brahem H, Al-Khatib K, Yamaoka Y, Graham DY. Unreliability of results of PCR detection of Helicobacter pylori in clinical or environmental samples. J Clin Microbiol 2009; 47: 738-742 [PMID: 19129407 DOI: 10.1128/JCM.01563-08]
34 van Schie RC, Wilson ME. Saliva: a convenient source of DNA for analysis of bi-allelic polymorphisms of Fc gamma receptor IIA (CD32) and Fc gamma receptor IIIB (CD16). J Immunol Methods 1997; 208: 91-101 [PMID: 9433465]
35 Hagerman RJ, Wilson P, Staley LW, Lang KA, Fan T, Uhlhorn C, Jewell-Smart S, Hull C, Drisko J, Flom K. Evaluation of school children at high risk for fragile X syndrome utilizing buccal cell FMR-1 testing. Am J Med Genet 1994; 51: 474-481 [PMID: 7943023 DOI: 10.1002/ajmg.1320510436]
36 Parsonnet J, Shmuely H, Haggerty T. Fecal and oral shedding of Helicobacter pylori from healthy infected adults. JAMA 1999; 282: 2240-2245 [PMID: 10605976]
37 Adler I, Muiño A, Aguas S, Harada L, Diaz M, Lence A, Labbrozzi M, Muiño JM, Elsner B, Avagnina A, Denninghoff V. Helicobacter pylori and oral pathology: relationship with the gastric infection. World J Gastroenterol 2014; 20: 9922-9935 [PMID: 25110422 DOI: 10.3748/wjg.v20.i29.9922]
38 Song Q, Spahr A, Schmid RM, Adler G, Bode G. Helicobacter pylori in the oral cavity: high prevalence and great DNA diversity. Dig Dis Sci 2000; 45: 2162-2167 [PMID: 11215732]
39 Zhen-Hua Z, De-Qiang H, Yong X, Lin-Lin L, Nong-Hua L. Characterization of 23S rRNA gene mutation in primary and secondary clarithromycin-resistant Helicobacter pylori strains from East China. Turk J Gastroenterol 2013; 24: 5-9 [PMID: 23794337]
40 Juvonen R, Koivula T, Haikara A. Group-specific PCR-RFLP and real-time PCR methods for detection and tentative discrimination of strictly anaerobic beer-spoilage bacteria of the class Clostridia. Int J Food Microbiol 2008; 125: 162-169 [PMID: 18502530 DOI: 10.1016/j.ijfoodmicro.2008.03.042]
P- Reviewer: El-Zahaby SA, Pierzchalski P, Zalazar F S- Editor: Yu J L- Editor: Filipodia E- Editor: Ma S
5830 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Luo XF et al . Nested-ASP-PCR to determine CLR of H. pylori

Tao Wang, Dan-Na Wang, Wen-Tian Liu, Zhong-Qing Zheng, Xin Chen, Wei-Li Fang, Shu Li, Li Liang, Bang-Mao Wang, Department of Gastroenterology, Tianjin Medical University General Hospital, Tianjin 300052, China
Author contributions: Wang T, Wang DN, Liu WT and Wang BM designed the research; Wang T, Liu WT, Zheng ZQ, Chen X, Fang WL, Li S, Liang L and Wang BM took part in this study as endoscopic operators or assistants; Wang T, Wang DN, Liu WT and Wang BM analyzed the data; Wang T, Wang DN and Wang BM wrote the paper and gave final approval of the version to be published.
Institutional review board statement: The study was reviewed and approved by the Medical Ethics Committee of Tianjin Medical University General Hospital.
Clinical trial registration statement: This study has not been registered temporarily.
Informed consent statement: All study participants, or their legal guardian, provided informed written consent prior to study enrollment.
Conflict-of-interest statement: There are no conflicts of interest in relation to this manuscript.
Data sharing statement: No additional data are available.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Correspondence to: Bang-Mao Wang, Professor, Department of Gastroenterology, Tianjin Medical University General Hospital, Anshan Road 154, Heping District, Tianjin 300052, China. [email protected]: +86-22-60363800
Received: March 13, 2016 Peer-review started: March 13, 2016First decision: March 31, 2016Revised: April 21, 2016 Accepted: May 4, 2016Article in press: May 4, 2016Published online: July 7, 2016
AbstractAIM: To evaluate the hemostatic effect of topical hemocoagulase spray in digestive endoscopy.
METHODS: Eighty-nine patients who developed oozing bleeding during endoscopic treatment from September 2014 to October 2014 at Center for Digestive Endoscopy, Tianjin Medical University General Hospital were randomly divided into either a study group (n = 39) or a control group (n = 50). The study group was given topical hemocoagulase spray intraoperatively, while the control group was given traditional 8% norepinephrine spray. Hemostatic efficacy was compared between the two groups. Bleeding site, wound cleanliness and perforation were recorded, and the rates of perforation and late bleeding were compared.
RESULTS: Successful hemostasis was achieved in 39 (100%) patients of the study group and in 47 (94.0%) patients of the control group, and there was no significant difference in the rate of successful hemostasis between the two groups. Compared with the control group, after topical hemocoagulase spray in the study group, the surgical field was clearer, the bleeding site was more easily identified, and the wound was cleaner. There was no significant difference in the rate of perforation between the study and control groups (16.7% vs 35.0%, P = 0.477), but the rates of
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.3748/wjg.v22.i25.5831
5831 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
World J Gastroenterol 2016 July 7; 22(25): 5831-5836 ISSN 1007-9327 (print) ISSN 2219-2840 (online)
© 2016 Baishideng Publishing Group Inc. All rights reserved.
ORIGINAL ARTICLE
Hemostatic effect of topical hemocoagulase spray in digestive endoscopy
Randomized Controlled Trial
Tao Wang, Dan-Na Wang, Wen-Tian Liu, Zhong-Qing Zheng, Xin Chen, Wei-Li Fang, Shu Li, Li Liang, Bang-Mao Wang

late bleeding (0% vs 15.8%, P = 0.048) and overall complications (P = 0.032) were significantly lower in the study group.
CONCLUSION: Topical hemocoagulase spray has a definite hemostatic effect for oozing bleeding in digestive endoscopy, and this method is convenient, safe, and reliable. It is expected to become a new method for endoscopic hemostasis.
Key words: Hemocoagulase; Digestive endoscopy; Oozing bleeding; Spray; Hemostatic effect
© The Author(s) 2016. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: In this study, we evaluated the hemostatic effect of topical hemocoagulase spray in digestive endoscopy. There was no significant difference in the rate of perforation between the study and control groups. There was no significant difference in the rate of successful hemostasis between the two groups, but the rates of late bleeding and overall complications of the hemocoagulase group were significantly lower than the 8% norepinephrine group. The surgical field was clearer, the bleeding site was more easily identified, and the wound was cleaner in the study group.
Wang T, Wang DN, Liu WT, Zheng ZQ, Chen X, Fang WL, Li S, Liang L, Wang BM. Hemostatic effect of topical hemocoagulase spray in digestive endoscopy. World J Gastroenterol 2016; 22(25): 5831-5836 Available from: URL: http://www.wjgnet.com/1007-9327/full/v22/i25/5831.htm DOI: http://dx.doi.org/10.3748/wjg.v22.i25.5831
INTRODUCTIONWith the development of endoscopic techniques, more and more gastrointestinal diseases can be treated endoscopically, such as endoscopic resection of gastrointestinal polyps and endoscopic submucosal dissection (ESD) of tumors. Compared with traditional open surgery, endoscopic surgery can greatly reduce the trauma to patients. However, bleeding and perforation are the main complications of endoscopic treatment[1-3]. Effectively reducing the development of intraoperative bleeding and maintaining adequate visualization of the surgical field are the keys to reducing the incidence of complications with endoscopic treatment and ensuring successful endoscopic treatment.
Hemocoagulase for injection (Baquting), a he-mostatic agent extracted and purified from the venom of Bothrops jararacussu, has thrombin- and thrombokinase-like effects[4,5]. It can cause platelet aggregation at the bleeding site, accelerate the hydrolysis of fibrin to form fibrin I monomer and polymer, and promote the formation of white thrombi,
thereby achieving hemostatic effects[6]. Currently, hemocoagulase has been widely used to manage bleeding in various clinical settings, such as obstetrics, orthopaedics[7,8], and general surgery[9]. Hemocoagulase combined with proton pump inhibitors has been used to manage peptic ulcer bleeding. These studies indicated that hemocoagulase has a definite hemostatic effect. However, hemocoagulase was delivered via an intravenous route in most of previous studies. A study[10] showed that topical application of hemocoagulase at the bleeding site had dose-related effects in promoting fibrinogen polymerization, which was not inhibited by any plasma thrombin inhibitor or anticoagulant. Thus, hemocoagulase can be used as a topical hemostatic. A recent study[11] showed that local injection of hemo-coagulase can achieve rates of successful hemostasis of 100% and 88.9%, respectively, for portal veins with inner diameters of < 1 mm and 1-2 mm, and the maximum time to achieve hemostasis was 24.0 ± 7.2 s, suggesting that hemocoagulase has a more obvious hemostatic effect in tiny blood vessels (diameter < 1 mm).
The purpose of the present study was to evaluate the hemostatic effect of hemocoagulase spraying on oozing bleeding in digestive endoscopy.
MATERIALS AND METHODSPatientsEighty-nine patients who developed oozing bleeding (non-small artery or vein bleeding) during endoscopic treatment from September 2014 to October 2014 at Center for Digestive Endoscopy, Tianjin Medical University General Hospital were included in this study, including 32 patients who underwent ESD for gastric muscularis propria tumors, 22 patients who underwent esophageal tunneling techniques (including STER and POEM), and 35 patients who underwent ESD for gastric mucosal or submucosal tumors. Patients with coagulation disorders or drug allergies were excluded. The patients were randomly divided into a study group (n = 39) and a control group (n = 50). The study group was given topical hemocoagulase spray intraoperatively, while the control group was given traditional 8% norepinephrine (in normal saline) spray. There were no significant differences in demographic data between the two groups (Table 1).
MethodsAll patients were preoperatively given an intravenous drip of esomeprazole (40 mg + 0.9% normal saline 100 mL) once every 24 h. Patients who developed oozing bleeding (non-small artery or vein bleeding) during endoscopic treatment were randomly divided into a study group and a control group. The study group was treated with hemocoagulase for injection (Baquting).The hemocoagulase solution was prepared by dissolving 4U hemocoagulase in 60 mL normal
5832 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Wang T et al . Hemocoagulase spray in digestive endoscopy

saline. The solution (20 mL) was sprayed to the wound site at 30 s intervals until the bleeding stopped. The control group was treated with 8% norepinephrine spray at 30 s intervals. If active bleeding persisted 5 min after spraying, failed hemostasis was considered. For patients who had failed hemostasis and were found to have small artery or vein bleeding, electrocoagulation or clipping was performed to achieve hemostasis. Hemostatic efficacy was compared between the two groups. Bleeding site, wound cleanliness and perforation were observed. After wound processing was performed, the endoscope was withdrawn. Postoperatively, gastrointestinal decompression was carried out, and the patients were fasted and given parenteral nutrition support and an intravenous drip of esomeprazole (40 mg + 0.9% normal saline 100 mL) once every 12 h. Patients with perforation were treated with antibiotics to prevent wound infection. Late bleeding was observed and recorded. Statistical methods were then used to compare the rates of successful hemostasis, perforation and late bleeding between the two groups.
RESULTSThere were no significant differences in demographic data such as gender or age between the two groups.
Successful hemostasis was achieved in 39 (100%) patients of the study group and in 47 (94.0%) patients of the control group, and there was no significant difference in the rate of successful hemostasis between the two groups (χ2 = 3.541, P = 0.060) (Table 2). Three patients in the control group had failed hemostasis, and all of them underwent ESD for gastric mucosal or submucosa tumors. After endoscopic electrocoagulation or clipping was performed, successful hemostasis was achieved in all the three cases.
There were a total of nine cases of perforation, all of which occurred in the gastric muscularis propria, including 2 (16.7%) cases in the study group and 7 (35.0%) cases in the control group. Patients with perforation after clipping hemostasis did not show any sign of peritonitis such as obvious abdominal pain. There was no significant difference in the rate of perforation between the two groups (χ 2 = 0.505, P = 0.477) (Table 3). No late bleeding occurred in the study group, but there were 3 (15.8%) cases in the control group, all of which occurred in patients who underwent ESD for gastric mucosal or submucosal tumors. The rate of late bleeding was significantly lower in the study group than in the control group (χ 2 = 3.901, P = 0.048) (Table 3). The rate of overall complications was also significantly lower in the study group than in the control group (χ 2 = 4.576, P = 0.032) (Table 3).
Compared with the control group, after hemo-coagulase spray in the study group, bleeding stopped more rapidly, the surgical field was clearer, the bleeding site was more easily identified, and the world was cleaner (Figures 1 and 2).
DISCUSSIONWith the wide application of digestive endoscopy in clinical practice, minimally invasive endoscopic techniques have gradually been advocated by more and more patients. Bleeding and perforation are common complications of endoscopic treatment[1-3]. Therefore, effective, fast endoscopic hemostasisis is very important for endoscopic treatment. Currently commonly used endoscopic hemostatic methods include mechanical hemostasis methods (such as electrocoagulation and clipping), topical spray of drugs, and local injection of drugs[12-14].
Clipping hemostasis is achieved by using titanium clips to mechanically clamp the bleeding vessels and
5833 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Table 1 General data of patients in both groups
Study group Control group
Drug spray Hemocoagulase 8% norepinephrine
Patients 39 50 Gender Male 18 20 Female 21 30 Age 52.90 ± 1.73 53.10 ± 1.76Category of endoscopic treatments ESD 28 39 Submucosal tunneling 11 11 (POEM and STER)Hemostatic effect Successful 39 47 Failed 0 3Complication 2 10 Perforation 2 7 Late bleeding 0 3
ESD: Endoscopic submucosal dissection; POEM: Peroral endoscopic myo-tomy; STER: Submucosal tunneling endoscopic resection.
Table 2 Hemostatic efficacy between the two groups
Group Study Control Total
Successful hemostasis 39 (100) 47 (94) 86 (97)Failed hemostasis 0 (0) 3 (6) 3 (3)Total 39 50 89
χ 2 = 3.541, P = 0.060.
Table 3 Complications between the two groups
Group Study Control Total
Perforation 2 (5) 7 (14) 9 (10)Late bleeding 0a 3 (6) 3 (3)Total 2 (5)b 10 (20) 12 (13)
χ 2 = 3.901, aP = 0.048 vs control; χ 2 = 4.576, bP = 0.032 vs control.
Wang T et al . Hemocoagulase spray in digestive endoscopy

5834 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
the tissue, and after injection it can induce local vasoconstriction, swelling of the surrounding tissue to compress blood vessels, and platelet aggregation, thus achieving temporary hemostasis, with a rate of successful hemostasis of about 80%[20]. However, studies have shown that with the increase of the dose of adrenaline, it can lead to high blood pressure and increased heart rate. Therefore, its use in patients with cardiovascular diseases is restricted[22]. In addition, the hemostatic effect of adrenaline is short-acting, and it is associated with high rates of pseudo hemostasis and late bleeding.
Hemocoagulase is a hemostatic agent extracted and purified from the venom of Bothrops jararacussu, and it has advantages of high efficiency, rapid action, definite topical hemostatic effect, reduced local tissue inflammation and accelerated wound healing. It can not only promote the fibrin formation and result in rapid blood solidification to form blood clots, but also promote irreversible platelet aggregation and platelet release reaction, accelerate blood clotting, promote vascular epithelial cell growth, and accelerate wound healing, thus achieving a good hemostatic effect[11,23]. In this study, we used local hemocoagulase spray to manage oozing bleeding in digestive endoscopic treatment. The results showed that hemocoagulase had a comparable hemostatic effect to norepinephrine and
surrounding tissues[15], with a definite and reliable hemostatic effect. However, clipping hemostasis is mainly suitable for exposed large or deep blood vessels[16], and its application in endoscopic tunneling techniques (such as STER and POEM) is limited. Electrocoagulation hemostasis is achieved by using local high-frequency heat energy to make local tissue necrotic or coagulated[17], and this method is particularly effective for small blood vessel hemorrhage[18]. However, the above hemostatic methods have a high requirement for operation skill, are expensive and more suitable for local hemostasis, and are often associated with unclean wound, which makes it difficult to identify the bleeding site. Thus, their application value in diffuse oozing bleeding is limited.
Many studies[11,14,19-21] showed that endoscopic injection or spray of hemostatic drugs can be used for topical hemostasis, with a definite hemostatic effect. Common topical hemostatic drugs include hypertonic saline, Yunnan Baiyao, thrombin, adrenaline and so on. Hypertonic saline can induce tissue edema at the injection site, local compression, fibrosis of the vessel wall, and vascular lumen thrombosis, thus achieving hemostasis. However, the application of hypertonic saline affects the observation of the wound and bleeding site, and for this reason, hypertonic saline was less applied clinically. Adrenaline does not damage
A B
Figure 1 Gastric muscularis propria manifestations in endoscopic treatment. A: Before hemocoagulase spray; B: After hemocoagulase spray.
A B
Figure 2 Esophageal muscularis propria manifestations in endoscopic treatment. A: Before hemocoagulase spray; B: After hemocoagulase spray.
Wang T et al . Hemocoagulase spray in digestive endoscopy

5835 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
was associated with a lower incidence of complications. In addition, no systemic adverse reactions such as elevated blood pressure and heart rate were obser-ved. Compared with norepinephrine, hemocoagulase had a longer hemostatic effect. After endoscopic he-mocoagulase spray, the wound was cleaner and the broken ends of small blood vessels were clearly shown, which makes the identification of bleeding sites easier. Therefore, topical hemocoagulase spray can not only achieve hemostasis, but also help provide good wound conditions for other hemostatic methods such as electrocoagulation and clipping to improve the efficiency of hemostasis, increase the success rate of hemostasis, reduce the damage of electrocoagulation to the wound, and decrease the rates of perforation and late bleeding associated with electrocoagulation.
In conclusion, topical hemocoagulase spray has a definite hemostatic effect for oozing bleeding in digestive endoscopy, and this method is simple and has low cost. Since the wound after topical hemocoagulase spray is clean, the bleeding site is easily identified, which is conductive to postoperative recovery. Topical hemocoagulase spray is associated with a low rate of late bleeding, and it is expected to be widely used in endoscopic therapy. A study has shown that topical hemocoagulase spray can be used for the treatment of upper gastrointestinal mucosal bleeding in hepatitis B patients[24], but its curative effect needs further validation. However, topical hemocoagulase spray is more suitable for oozing non-small artery or vein bleeding, and its hemostatic effect in large vessel bleeding is poorer than clipping, which is the main limitation of topical hemocoagulase spray. In addition, the sample size of this study is small, and multicenter studies with larger sample sizes are warranted to confirm the hemostatic efficacy of topical hemocoagulase spray.
COMMENTSBackgroundBleeding and perforation are the main complications of endoscopic treatment, how to reduce the incidence of complications remains to be studied. Many studies indicated that hemocoagulase has a definite hemostatic effect and can be used as a topical hemostatic. The purpose of the present study was to evaluate the hemostatic effect of hemocoagulase spraying on oozing bleeding in digestive endoscopy.
Research frontiersHemocoagulase has thrombin- and thrombokinase-like effects, and it has been widely used to manage bleeding in various clinical settings. A study showed that topical application of hemocoagulase at the bleeding site had dose-related effects in promoting fibrinogen polymerization. However, no one has used it for endoscopic hemostasis, or explored its effectiveness.
Innovations and breakthroughsThe authors compared the rate of successful hemostasis between hemocoagulase spray and 8% norepinephrine spray, and showed that there was no significant difference in the rate of successful hemostasis, but the rates of late bleeding and overall complications of the hemocoagulase group were significantly lower than the 8% norepinephrine group. The surgical field was
clearer, the bleeding site was more easily identified, and the wound was cleaner in the study group.
Applications Topical hemocoagulase spray has a definite hemostatic effect for oozing bleeding in digestive endoscopy, and this method is convenient, safe, and reliable. It is expected to become a new method for endoscopic hemostasis.
TerminologyEndoscopic hemocoagulase spray is a method of spraying the hemocoagulase solution to the wound site at 30 s intervals until the bleeding stops.
Peer-reviewThis study is an interesting study about the hemostatic effect of topical hemocoagulase spray in digestive endoscopy. Compared with the control group, after topical hemocoagulase spray in the study group, the surgical field was clearer, the bleeding site was more easily identified, and the wound was cleaner. There was no significant difference in the rate of perforation between the study and control groups, but the rates of late bleeding and overall complications were significantly lower in the study group. Over all, the study is well designed and the manuscript can be accepted. Large-sample studies should be performed in the future.
REFERENCES1 Takeda S, Mitoro A, Namisaki T, Yoshida M, Sawai M, Yamao
J, Yoshiji H, Uejima M, Moriya K, Douhara A, Seki K, Ishida K, Morita K, Noguchi R, Kitade M, Kawaratani H, Okura Y, Takaya H, Fukui H. Gastric adenocarcinoma of fundic gland type (chief cell predominant type) with unique endoscopic appearance curatively treated by endoscopic submucosal resection. Acta Gastroenterol Belg 2015; 78: 340-343 [PMID: 26448418]
2 Zhang Y, Chen Y, Qu CY, Zhou M, Ni QW, Xu LM. Effects of medical adhesives in prevention of complications after endoscopic submucosal dissection. World J Gastroenterol 2013; 19: 2704-2708 [PMID: 23674879 DOI: 10.3748/wjg.v19.i17.2704]
3 Salah W, Faigel DO. When to puncture, when not to puncture: Submucosal tumors. Endosc Ultrasound 2014; 3: 98-108 [PMID: 24955339 DOI: 10.4103/2303-9027.131038]
4 Marsh N, Williams V. Practical applications of snake venom toxins in haemostasis. Toxicon 2005; 45: 1171-1181 [PMID: 15922782]
5 Braud S, Bon C, Wisner A. Snake venom proteins acting on hemostasis. Biochimie 2000; 82: 851-859 [PMID: 11086215]
6 Stocker KF. Snake venom proteins affecting hemostasis and fibrinolysis. In: Stocker KF. Medical Use of Snake Venom Proteins. Boca Raton: CRC Press Inc, 1990: 97-160
7 Hu HM, Chen L, Frary CE, Chang CC, Hui H, Zhang HP, Huang DG, Liu ZK, Zhao YT, He SM, Zhang XF, He BR, Hao DJ. The beneficial effect of Batroxobin on blood loss reduction in spinal fusion surgery: a prospective, randomized, double-blind, placebo-controlled study. Arch Orthop Trauma Surg 2015; 135: 491-497 [PMID: 25720848 DOI: 10.1007/s00402-015-2183-0]
8 Xu C, Wu A, Yue Y. Which is more effective in adolescent idiopathic scoliosis surgery: batroxobin, tranexamic acid or a combination? Arch Orthop Trauma Surg 2012; 132: 25-31 [PMID: 21909815 DOI: 10.1007/s00402-011-1390-6]
9 Zeng Z, Xiao P, Chen J, Wei Y. Are batroxobin agents effective for perioperative hemorrhage in thoracic surgery? A systematic review of randomized controlled trials. Blood Coagul Fibrinolysis 2009; 20: 101-107 [PMID: 19786937 DOI: 10.1097/MBC.0b013e3283254532]
10 Meier J, Stocker K. Effects of snake venoms on hemostasis. Crit Rev Toxicol 1991; 21: 171-182 [PMID: 2039593]
11 Luo Y, Liu Q, Jiao Z, Wu R, Tang J, Lv F. A comparison study of local injection and radiofrequency ablation therapy for traumatic portal vein injure guided by contrast-enhanced ultrasonography. Ann Hepatol 2012; 11: 249-256 [PMID: 22345343]
12 Barkun AN, Bardou M, Kuipers EJ, Sung J, Hunt RH, Martel M, Sinclair P. International consensus recommendations on the
COMMENTS
Wang T et al . Hemocoagulase spray in digestive endoscopy

5836 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
management of patients with nonvariceal upper gastrointestinal bleeding. Ann Intern Med 2010; 152: 101-113 [PMID: 20083829 DOI: 10.7326/0003-4819-152-2-201001190-00009]
13 Sung JJ, Chan FK, Chen M, Ching JY, Ho KY, Kachintorn U, Kim N, Lau JY, Menon J, Rani AA, Reddy N, Sollano J, Sugano K, Tsoi KK, Wu CY, Yeomans N, Vakil N, Goh KL. Asia-Pacific Working Group consensus on non-variceal upper gastrointestinal bleeding. Gut 2011; 60: 1170-1177 [PMID: 21471571 DOI: 10.1136/gut.2010.230292]
14 Holster IL, Kuipers EJ. Update on the endoscopic management of peptic ulcer bleeding. Curr Gastroenterol Rep 2011; 13: 525-531 [PMID: 21918857 DOI: 10.1007/s11894-011-0223-7]
15 Raju GS, Gajula L. Endoclips for GI endoscopy. Gastrointest Endosc 2004; 59: 267-279 [PMID: 14745407]
16 Ljubicic N. Efficacy of endoscopic clipping and long-term follow-up of bleeding Dieulafoy’s lesions in the upper gastrointestinal tract. Hepatogastroenterology 2006; 53: 224-227 [PMID: 16608029]
17 Lei KF, Chen KH, Tsui PH, Tsang NM. Real-time electrical impedimetric monitoring of blood coagulation process under temperature and hematocrit variations conducted in a microfluidic chip. PLoS One 2013; 8: e76243 [PMID: 24116099 DOI: 10.1371/journal.pone.0076243]
18 Hui AJ, Sung JJ. Endoscopic Treatment of Upper Gastrointestinal Bleeding. Curr Treat Options Gastroenterol 2005; 8: 153-162
[PMID: 15769437]19 Changela K, Papafragkakis H, Ofori E, Ona MA, Krishnaiah
M, Duddempudi S, Anand S. Hemostatic powder spray: a new method for managing gastrointestinal bleeding. Therap Adv Gastroenterol 2015; 8: 125-135 [PMID: 26082803 DOI: 10.1177/1756283X1557258]
20 Calvet X, Vergara M, Brullet E, Gisbert JP, Campo R. Addition of a second endoscopic treatment following epinephrine injection improves outcome in high-risk bleeding ulcers. Gastroenterology 2004; 126: 441-450 [PMID: 14762781]
21 Chung SC, Leong HT, Chan AC, Lau JY, Yung MY, Leung JW, Li AK. Epinephrine or epinephrine plus alcohol for injection of bleeding ulcers: a prospective randomized trial. Gastrointest Endosc 1996; 43: 591-595 [PMID: 8781939]
22 Liou TC, Lin SC, Wang HY, Chang WH. Optimal injection volume of epinephrine for endoscopic treatment of peptic ulcer bleeding. World J Gastroenterol 2006; 12: 3108-3113 [PMID: 16718798]
23 Jin Y. Hemostasis mechanism of Hemocoagulase atrox for injection. Zhongguo Yiyuan Yongyao Pingjia Yu Fenxi 2012; 12: 488-490
24 Wang X, Wang Z, Jin B, Xiang L, Li H, Han J. Efficacy of endoscopic spray blood coagulation in the treatment of patients with hepatitis B. Zhongguo Yiyao 2010; 11: 1092 [DOI: 10.3760/cma.j.issn.1673-4777.2010.11.058]
P- Reviewer: Sogabe I, Toth E S- Editor: Ma YJ L- Editor: Wang TQ E- Editor: Wang CH
Wang T et al . Hemocoagulase spray in digestive endoscopy

Towards safe injection practices for prevention of hepatitis C transmission in South Asia: Challenges and progress
Naveed Zafar Janjua, Zahid Ahmad Butt, Bushra Mahmood, Arshad Altaf
Naveed Zafar Janjua, Clinical Prevention Services, British Columbia Centre for Disease Control, Vancouver, BC V5Z 4R4, Canada
Naveed Zafar Janjua, Zahid Ahmad Butt, Bushra Mahmood, School of Population and Public Health, University of British Columbia, Vancouver, BC V6T 1Z3, Canada
Arshad Altaf, Service Delivery and Safety, World Health Organization, Geneva 27, Switzerland
Author contributions: Janjua NZ conceived the idea, designed the study and wrote first draft; all authors contributed to the literature review, critical revision and editing, and approval of the final version.
Conflict-of-interest statement: None to declare.
Data sharing statement: All data presented in this paper are available in the cited references.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Manuscript source: Invited manuscript
Correspondence to: Naveed Zafar Janjua, MBBS, MSc, DrPH, Senior Scientist, Clinical Associate Professor, Clinical Prevention Services, British Columbia Centre for Disease Control, 655 West 12th Avenue, Vancouver, BC V5Z 4R4, Canada. [email protected]: +1-604-7072514 Fax: +1-604-7072690
Received: March 27, 2016 Peer-review started: March 28, 2016First decision: May 12, 2016Revised: June 5, 2016
Accepted: June 15, 2016Article in press: June 15, 2016Published online: July 7, 2016
AbstractAIM: To summarize the available information about injection use and its determinants in the South Asian region.
METHODS: We searched published and unpublished literature on injection safety in South Asia published during 1995-2016 using the keywords “injection” “unsafe injection” and “immunization injection” and combined these with each of the countries and/or their respective states or provinces in South Asia. We used a standardized questionnaire to abstract the following data from the articles: the annual number of injections per capita, the proportion of injections administered with a reused syringe or needle, the distribution of injections with respect to prescribers and providers and determinants of injection use.
RESULTS: Although information is very limited for certain countries (i.e. , Bhutan, Maldives and Sri Lanka), healthcare injection use is very common across South Asia, with cross-country rates ranging from 2.4 to 13.6 injections/person/year. Furthermore, recent studies show that 5% to 50% of these injections are provided with reused syringes, thus creating potential to transmission of blood-borne pathogens. Qualified and unqualified practitioners, especially in the private sector, are the major drivers behind injection use, but patients also prefer injections, especially among the rural, poor or uneducated in certain countries. According to available data, Pakistan and India have recently taken steps towards achieving safe injection. Potential interventions include the introduction of reuse prevention devices, and patient-, community- and patient/community and provider-centered interventions
SYSTEMATIC REVIEWS
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.3748/wjg.v22.i25.5837
5837 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
World J Gastroenterol 2016 July 7; 22(25): 5837-5852 ISSN 1007-9327 (print) ISSN 2219-2840 (online)
© 2016 Baishideng Publishing Group Inc. All rights reserved.

to change population and practitioner behavior.
CONCLUSION: Injection use is common in South Asian countries. Multilevel interventions aiming at patients, providers and the healthcare system are needed to reduce injection use and reuse.
Key words: Unsafe injections; Hepatitis C; Hepatitis B; South Asia; Prescription practices
© The Author(s) 2016. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: The reuse of syringes in healthcare has been consistently identified as major route of hepatitis B and C transmission in Pakistan and India. Injection use and reuse is common in Pakistan, India and other South Asian countries. This paper synthesizes literature on injection use, re-use and potential interventions to reduce injection use and reuse to prevent hepatitis C transmission and hence overall disease burden. We also propose a multi-level model to guide further research, interventions and programs to prevent unnecessary injection use and reuse.
Janjua NZ, Butt ZA, Mahmood B, Altaf A. Towards safe injection practices for prevention of hepatitis C transmission in South Asia: Challenges and progress. World J Gastroenterol 2016; 22(25): 5837-5852 Available from: URL: http://www.wjgnet.com/1007-9327/full/v22/i25/5837.htm DOI: http://dx.doi.org/10.3748/wjg.v22.i25.5837
INTRODUCTIONHepatitis B virus (HBV) and hepatitis C virus (HCV) infections are global health concerns, particularly in South Asian countries where prevalence ranges from 2%-5% and 1.3%-4.8% for HBV and HCV, respectively[1-4]. Pakistan has second highest number of HCV infections in the world. HCV and HBV are associated with increasing morbidity and mortality in these countries. In Pakistan and India in 2015, there were 383301 and 455848 HCV infected people living with cirrhosis and about 16000 and 18000 died of HCV, respectively (Figure 1)[5].
During the early nineties, investigations of clusters of HBV and HCV infections in India and Pakistan revealed the reuse of glass and plastic syringes by unqualified and qualified practitioners as a major factor in occurrence of these outbreaks[6-8]. Later on, detailed investigations of HBV and HCV risk factors in well-planned studies from both countries revealed a consistent association of injections with these infections[9-13]. Based on these studies, reuse of syringes is major contributor to HBV and HCV transmission in India and Pakistan. More than 50% of HCV infections in Pakistan and about 38%
of HCV infections in India are attributed to unsafe injections[14,15].
Although use of unsafe and unnecessary in-jections has long been reported from India[16,17]; unsafe injections as a public health problem became a major concern only after the explosive outbreaks of HBV and HCV in India and Pakistan. Despite the enormity of the problem, the level of concern is not the same in all countries of South Asia, as shown by variations in data availability on injection use and its determinants, and the extent of preventative actions at government levels. However, since countries in South Asia have similar healthcare systems, culture, and people beliefs and behaviors, best practices in countries that have achieved significant progress towards safe injections, may provide valuable lessons to other countries in the region who are just beginning to address this issue.
In this paper we have summarized the situation of injection use in the South Asian region. Specifically we have reviewed the frequency of injection use in populations, reuse of syringes and distribution of injections with respect to prescribers and providers.
Health and development in South Asia South Asia, which includes Pakistan, India, Ban-gladesh, Nepal, Sri Lanka, Maldives and Bhutan (Figure 2), is home to about 1.7 billion people. After independence from the British Empire in 1947-1948, these countries had similar health and development indicators, but some did better than others in later decades. From 2005 to 2013, the adult literacy rate ranged from 52.8% in Bhutan to 98.4% in Maldives. Infant mortality ranged from 8.2/1000 live births in Sri Lanka to 69/1000 live births in Pakistan. In terms of overall human development, Sri Lanka is ranked top in the region with a worldwide human development index of 73, while Pakistan is ranked lowest in the region with an index of 147 (Table 1)[18]. The health and development indicators indicate that the overall health status of the population in South Asia is not very impressive, but there are examples of success from Sri Lanka and Kerala in India[19].
MATERIALS AND METHODSSearch methodsWe searched published literature in PubMed from Jan 1, 1995 - Feb 23, 2016 using keywords “injection”, “unsafe injection” “immunization injection” and combined these with each of the countries and/or their respective states or provinces in South Asia. In addition, we also searched the websites of WHO, UNICEF for each country for unpublished reports, including evaluations of the expanded program on immunization (EPI). We contacted researchers in each country for unpublished literature. We also reviewed relevant references cited in identified articles (Table 2).
5838 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Janjua NZ et al . Injection practices in South Asia

Data abstractionWe developed a questionnaire to standardize data abstraction from the articles. Indicators of injection use that were identified and assessed are: the annual number of injections per capita, the proportion of injections administered with a reused syringe or needle, and the distribution of injections with respect
to prescribers and providers. We also assessed determinants of injection use.
Annual number of injections per person: To estimate the annual number of injections per person, we selected population based surveys designed for estimating the frequency of injections. These studies
5839 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Figure 1 Number of hepatitis C virus cases in India and Pakistan over time with viremia and cirrhosis[5].
Figure 2 Map of South Asian countries.
Janjua NZ et al . Injection practices in South Asia
8
7
6
5
4
3
2
1
0
500000
450000
400000
350000
300000
250000
200000
150000
100000
50000
01999 2001 2003 2005 2007 2009 2011 2013 2015 Year
Num
ber
of v
irem
ic c
ases
(m
illio
ns)
Num
ber of cirrhotic cases
Cirrhosis Pakistan Cirrhosis India Viremic Pakistan Viremic India
India
Pakis
tan
NepalBhutan
Bangladesh
MaldivesSri Lanka

5840 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
we will refer to reuse of injection equipment in the absence of sterilization simply as “reuse of injection
equipment.” Some studies have assessed the unsafe use of injections using other parameters. We have elaborated these parameters while describing these studies.
Injection prescribers and injection providers: A public provider is defined as a health care provider, whether a physician or a dispenser, working in a public sector. A private provider was defined as a health care provider, whether a physician, dispenser or any other primary health care worker, running a clinic/hospital in the private sector[21]. We defined physician as a person with basic medical qualification (MBBS or MD) and a private provider with MBBS was called general practitioner. “Unqualified practitioners” were defined as those with no basic medical qualification (MBBS or MD) and who prescribe medications A prescriber is a person who provides consultation and prescribes injections and drugs while injection provider, also called dispenser in the region, is a persons who dispenses medicine and provides injection.
RESULTSFrom PubMed, we were able to retrieve 25 papers on injection safety for India, 25 for Pakistan, 8 for Nepal and 5 for Bangladesh. For the rest of the countries we searched through Google scholar and we found 7 additional articles that provided some evidence about injection use in India, Nepal, Bangladesh and Sri Lanka (Table 2). Table 3 lists the studies and their characteristics that are used in this review.
Injection use in PakistanInjection use and prescribers: Many studies re-ported an association between injections and HBV and HCV outbreaks during the 1990s[7,9,10]. This association led to a study of injection use among patients presenting to the Aga Khan University Hospital Community Health Center in 1999, which reported 8 injections per person per year[22]. This study was then followed by a population based survey in two districts of Sindh province in 2001 which reported an annual ratio of 13.6 injections per capita. After excluding the top 2% , the annual ratio was 8.2 per capita[23].
yield high quality estimates, although such studies are rare. If estimates from a national or well-designed population based survey using WHO standard methodology over large area of injection use were available, we presumed these to be the best estimates.
Proportion of injection reuse: To estimate the proportion of reuse of syringe or needle for each country, we restricted our selection to standardized observational studies, preferably based on WHO’s tool of injection practices. For each country, we presented the range of the estimates from the studies.
Distribution of injections with respect to prescribers: We reviewed the distribution of injections with respect to prescribers, injection providers and settings.
If no information was available about the annual ratio of injections per capita, proportion reuse or the prescribers for a country, we used circumstantial evidence to infer if there is an injection overuse or safety problem in the country. We used these evidences in the following order, if available: qualitative studies to assess injection practices; studies to describe prevalence and risk factor for HBV, HCV and HIV; and studies of prescription practices and health care seeking.
DefinitionsHealthcare injection: We defined a healthcare in-jection as a procedure that introduces a substance into the body through a piercing of the skin or mucosal membrane for the purposes of curative or preventive health care, whether administered in a formal healthcare setting (for example, a clinic or hospital) or other settings (such as homes or pharmacies)[20].
Injections of illicit drugs were not considered in this study.
Reuse of injection equipment in the absence of sterilization: We defined reuse of injection equipment in the absence of sterilization as the administration of an injection to a recipient with a syringe or a needle that had been used previously on another person and that was reused in the absence of sterilization.
Sterilization means a procedure that kills HBV, HCV and HIV in and on the syringe or needle. In this paper
Table 1 Human development statistics for South Asia: Human development report 2015[18]
Indicators Year Sri Lanka Maldives India Bhutan Pakistan Nepal Bangladesh
Total population (millions) 2014 21.4 0.4 1267.4 0.8 185.1 28.1 158.5GDP per capita (US$) 2011 9426 11283 5238 7167 4454 2173 2853Population living below $1.25 a day (%) 2002-2012 - 1.5 23.6 2.4 12.7 23.7 43.3Adult literacy rate (% ages ≥ 15) 2005-2013 91.2 98.4 62.8 52.8 54.7 57.4 58.8Public health expenditure (% of GDP) 2013 3.2 10.8 4.0 3.6 2.8 6.0 3.7Stunting (moderate or severe) (% under age 5) 2008-2013 14.7 20.3 47.9 33.6 45.0 40.5 41.4Infant Mortality rate per 1000 live births 2008-2013 8.2 8.4 41.4 29.7 69.0 32.2 33.2Overall human development index 2015 73.0 104 130 132 147 145 142
Janjua NZ et al . Injection practices in South Asia

5841 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
A more recent 2012-13 Pakistan Demographic and Health survey (PDHS), which included a nationally representative sample of men and women ages 15-49 years, reported 5 injections per person per year (women: 5.4 and men: 4.9). However, this survey only included those between 15 and 49 years of age, a group which generally has lower health care needs compared to younger and older population[24] (Table 4).
A national survey conducted in 2007-08 to assess HBV and HCV prevalence found that 48% respondents received < 5, 22% received 5-10 and 6% received > 10 intramuscular injections. However, this study may have underestimated injections as it only inquired about intramuscular injections[4].
In a Sindh survey, 96% injections were provided for therapeutic purposes, the majority (63.1%) of which were given at the private general practitioners (GP) clinics by dispensers (75%) who were often not qualified, a finding corroborated by another recent study[23,25]. A study of injection use at clinics of GPs, public health care facilities and unqualified practitioners in 2004-2005, selected randomly from three districts in Sindh province, indicated that 95.6% (95%CI: 93.9%-97.2%) of the administered injections were unnecessary[26]. In summary, a large number of injections are administered in Pakistan, with the majority being unnecessary and occurring in the private sector.
Safety of injection equipment: A study in a peri-urban community in Karachi conducted in 1995 reported that 94% of the 54 observed injections were provided with reused injection equipment[6]. In a population based survey in Sindh province, only 54% (454/1150) of the respondents had been injected with newly opened injection equipment[23]. A study at the
public and private sector in three districts of Sindh province revealed that 59.3% (677/1153) of injections are provided with a new syringe opened in front of a patient[23] (Table 4). The PDHS 2006-07 (women only) and 2012-2013 (both men and women) inquired about injection with newly opened syringes. In the 2012-2013 PDHS, 85% of women and 90% of men reported receiving an injection with a newly opened syringe. There were marked geographic differences in injections with new syringes ranging from 68% and 58% in Baluchistan province to 90% and 96% in Punjab among women and men, respectively[24]. Similar results were reported in the 2006-2007 PDHS[27]. In a national HBV and HCV survey, 49% of injections were provided with re-used syringes[4]. These data suggest some improvements in injection reuse in Pakistan, but still there is substantial reuse happening in Pakistan, calling for multilevel interventions.
Determinants of injection use: Injection use occurs because of preference of injections by both prescribers and patients (Table 5). A qualitative study for determinants of injection use in Sindh province reported that the practitioners take the initiative for injection prescription. However, some patients believe that disease can only be cured by injections. Quick relief, referred to as early relief from the disease was reported as the main reason for patients to prefer injections. Daily wage earners were concerned about loss of their working day and practitioners gave them assurance that injection could quickly relieve their symptoms allowing them to go back to work the next morning[28]. These results have been substantiated by an epidemiological study that quantified the beliefs of the general population in two districts of Sindh province regarding injection use. The study revealed
Table 2 Search and retrieval of information for injection use in South Asia 1995-2016
Key words India Pakistan Bangladesh Nepal Sri Lanka Maldives
PubMed - Retrieved Injection and country/state 189 51 12 14 13 5PubMed - selected/relevant 25 25 5 8 0 0Google Scholar1 Unsafe injections, injections, country 3 1 (419) 2 (329) 1 (242) 0 (40)Google Unsafe injections, injections, country 2 1 0 0WHO website 0 0 0 0 0 0PATH 2In country assessments by MoH 1Unpublished reports 1 2Other circumstantial evidence2
Risk factors studies suggesting injection use
Risk factors, HBV (HCV), country 1
Hepatitis B/C Hepatitis B, Hepatitis C, Country 19 (38) 13 (36)Health care utilization Health care seeking, Health care
utilization, Private practice, Country 15 (32) 6 (16)
(retrieved)Private practitioners health seeking (retrieved)
Health care seeking, Private practice, Country
5 (8) 3
Prescribing practices (retrieved) Prescription practices, Country 5 (5) 1
1Google scholar retrieved too many articles and most of them were not relevant: these were used mainly for countries for which information was not available through PubMed; 2Not used for countries for which data on injection use were available. Parenthesis represent retrieved and number represent the number that were relevant and reviewed. HBV: Hepatitis B virus; HCV: Hepatitis C virus.
Janjua NZ et al . Injection practices in South Asia

5842 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
that the majority of subjects (80.6%) were not aware of the risk associated with injection use. Multivariable logistic regression analysis for factors associated with receiving an injection revealed that those living
in rural areas who believe “injections act faster than oral drugs and symptoms are quickly relieved” were 15 times more likely to receive injection than those living in urban areas without this belief. Those who
Table 3 Characteristic of injection use studies in South Asia 1995-2016
Ref. Study type Setting Study base City/province n Sampling Year Year conducted published
India Rajasekaran et al[37] Population survey Both 3 areas Tamil Nadu 175 Convenience 2001 2003 IPEN study group[40] Population survey Both Whole
countrywhole country 23997 Cluster sampling 2002-2003 2004
IPEN study group[40] Patients exit interview and observations
Both Whole country
whole country 6015 Cluster sampling 2002-2004 2004
Murhekar et al[36] Population survey Island Nicobar Island
210 Cluster sampling - 2004
Kotwal et al[34] Population survey Both City Delhi 150 Cluster sampling random
2003 2004
Anand et al[38] Population survey Rural 1 village Haryana State 1280 Systematic sampling - 2001 Lakshman et al[35] Patients exit interview
and observationsBoth 15 miles
around a townTamil Nadu 400 Consecutive patients - 2000
Becker et al[66] Population survey Both 1 district Karnataka 4949 Cluster sampling 2003 2005 Kermode et al[67] Population survey Urban 2 cities New Delhi
and Imphal200 Convenience 2004 2006
Kermode et al[41] Patients and relatives survey
Rural 2 hospitals Bihar and Jharkhand
280 patients, Systematic sampling, convenience
2004-2005 2006120 relatives
Pandit et al[42] Population survey Both 1 District Anand 182 HF1 Stratified and simple random
2004 20082080
Shah et al[68] Providers interview Both 1 district Gujarat 251 Random sampling 2012-2013 2014 Bhargo et al[43] Providers interview Urban 1 district Gwalior 30 Convenience 2012-2013 2014 Garapati et al[44] Providers interview and
observationBoth 1 district Andhra
Pradeh300 Convenience 2010-2011 2014
Bendale et al[69] Hospital survey Urban 1 district Maharashtra 20 sites Random sampling 2015Pakistan Raglow et al[22] Survey of OPD patients Urban Patients Karachi 198 Consecutive patients 1995 2001 Janjua et al[23] Population survey Both 2 districts Sindh 1150 Cluster sampling
random2001 2005
Janjua et al[29] Population survey Both 2 districts Sindh 1150 Cluster sampling random
2001 2006
Janjua et al[26] Patients exit interview and observations
Both 3 districts Sindh 2124 Random sample of clinics
2004-2005 UP
Janjua et al[27] Population survey Both Whole country
Whole country
10023 Cluster sampling 2006-2007 2014
Yousafzai et al[25] Provider survey Urban City Karachi 317 Convenience 2006 2013 Khan et al[6] Patients exit interview
and observationsPeri-
urban1 village Sindh 203 consecutive patients 1995 2000
Mantel et al[70]2 Patients exit interview Both 8 districts 3 provinces Random sample of clinics
2002 UP
PDHS 2012-13[24] Population survey 15-49 years of age
Both National F: 13558 Cluster sampling random
2012-2013 2014M: 3134
Bangladesh Gibney et al[71] Risk factor study Urban Truck stand Dhaka 387 Cluster sampling
random1999 2001
Shill et al[51] Provider interviews and facility records
Rural Primary Health Care
Centres
Dhaka 6 Convenience sample 2009 2011
Chowdhury et al[50] Provider interviews, FGD, observations and
prescription review
Primary Health Care
Centres
National Prescription: 4320
Cluster sampling 2008-09 2013
Injection events: 480
Sri Lanka Rannan-Eliya et al[59] Patients exit interview Both National Sri Lanka 2100 Random sample of
clinics2000 2003
Nepal Gyawali et al[54] Survey of pharmacies Urban City Pokhara 54 Convenience sample 2012 2014 Gyawali et al[52] Population survey Both 1 district Kaski 2470 Stratified sampling 2012 2014
1Health Facilities; 2Included only public sector facilities. UP: Unpublished; F: Females; M: Males.
Janjua NZ et al . Injection practices in South Asia

5843 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
live in urban areas and believe in the quick action of injections were 2.5 times more likely to receive injections than those who did not believe in quick action of injections. Similarly those who believed that a disease can only be cured by injections were 2.2 times more likely to receive injections[29]. In a recent analysis, poor knowledge about blood borne pathogens was associated with receiving injections with used syringes[27].
The relative contribution of prescribers in injection overuse is greater than that of the population in-clination for injections. Patient exit interviews in a cross-sectional study at public and private clinics in three districts of Sindh province revealed that 60% of the 2124 patients surveyed left the choice for type of medication to the practitioner while 22.5% demanded injections in the current visit[26]. Another study in the community showed that of the 815 who remembered their last injection, 32% demanded injections at their contact with a health care provider while 62.2% left
the choice of prescription to the prescribers[29]. An exit interview study of patients in a peri-urban community of Karachi reported that 40% prefer injections if told oral and injectable drugs are equally effective[6]. A high proportion (28%) of injections are prescribed by unqualified practitioners as documented by two studies in Pakistan[23,29]. Hence, although some patients demand injections, these studies consistently report that providers’ decision to administer injection is major driving force for injection overuse in Pakistan. Economic incentives of the practitioners have been reported to play a role in injection overuse since practitioners earn more if they provide injections. In such circumstances, the use of reuse prevention devices (RUP) such as autodisable (AD) syringes could prevent the injection equipment reuse[23].
Progress towards addressing the injection problemAn assessment of a simple health education program through community outreach about the risks as-
Table 4 Injection use and safety of injections in South Asia 1995-2016
Ref. Annual ratio of injections per
capita
Received an injection
Therapeutic Injection reuse by Injection reuse by Overall unsafe interview7 observing
India Rajasekaran et al[37] 2.4 60.6%1 87% 64.6% IPEN study group[40] 2.91-5.8 27.1%1/44.1%3 82.5% 31.6% 62.9% Murhekar et al[36] 3 21.9%1 91% 6.5% Kotwal et al[34] 5.1 45.6%1 71.2% 56.5% 77.5% Anand et al[38] 2.45 35%4 40%-100% 45% Lakshman et al[35] 89%3 100% 73%-99% 99% Becker et al[66] 3.5 67.7%6
Kermode et al[67] 8.6 15%2 68% 31% Kermode et al[41] 43%2 (Patients) 100% 7.6%
13.3%1 (Relatives)Pandit NB 0.2 21.6%6 77% Shah et al[68] 64.1% Bhargo et al[43] 76.7% Garapati et al[44] 0.72 14.3%Pakistan Raglow et al[22] 8.4 51%5 100% 48% 16% Janjua et al[23] 13.6 68%1 94% 46% Janjua et al[26] 74%1
Janjua et al[23] 55%3 47% Janjua et al[27] 51%6 4% Yousafzai et al[25] 87% Khan et al[6] 81%3 90% 94% Mantel et al[70] 12% 65% PDHS 2012-13[24] F:5.4/M:4.9 F:61%/M: 53%6 F:15%/M:10%Bangladesh Gibney et al[71] 39.7%6 100% Shill et al[51] 4.88 Chowdhury et al[50] 77.7% 15.5%Sri Lanka Rannan-Eliya et al[59] 3%3
Nepal Gyawali et al[54]
Gyawali et al[52] 2.37 10.4%1 97.1%
1During last 3 mo; 2During last 4 wk; 3Current visit from prescription review; 4Six months; 5Past one week; 6Past one year; 7Syringe that has been used on multiple patients, not opened in front of patient is considered unsafe; some studies performed direct observations while other relied on the patient recall; F: Females; M: Males.
Janjua NZ et al . Injection practices in South Asia

5844 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
sociated with unnecessary and unsafe injections in Hafizabad (a town where an earlier study of injections and HCV infections were conducted) found that the use of new syringes increased from 24% in 1994 to 59% in 1998; however, the number of injections stayed the same[30]. Since injection prescribers are major drivers behind injection overuse, addressing their behaviors including behaviors of unqualified practitioners is also needed[31].
Another study at GP clinics in Karachi that used interactional group discussion (IGD) methodology, involving patients and prescribers discussing their choice for medication, resulted in: reduction in injection use by 33% from a baseline of 84%; an increase in the use of new syringes from 77 % to 92% in the intervention group; and dropped from 74% to 67% in control group[32]. The implementation of such intervention on a larger scale in national programs needs to be assessed.
A study conducted in 2011 in Sindh province assessed the community based interventions focusing on messages in large gatherings and discussions with key community influencers including teachers and religious leaders (Imams) along with messages on safe injection use in media. The study showed an increase in HBV and HCV knowledge and report of injection with new syringe from 15% to 29%[33].
In August 2004, the Ministry of Health Pakistan, Aga
Khan University, the World Health Organization’s local office and UNICEF organized a first national workshop/meeting to devise a national policy on injection safety in Pakistan. The workshop produced the National Policy on Injection Safety draft that highlighted the need for: population and provider behavior change, adequate supplies of injection devices, switching to reuse prevention injection devices and safe disposal of sharp waste. The syringe manufacturing industry has shown an interest in manufacturing Re-Use Prevention (RUP) injection devices for therapeutic injection to prevent reuse. Immunization injections in the EPI are already provided with AD syringes. Two manufacturers had shown an interest in supplying AD and RUP syringes for immunization and medical injections, but due to lack of progress on policy and legislation, this did not materialize.
In 2005, the government in Pakistan launched the National Program for Hepatitis B and C Prevention, with injection safety being one of its major components. The program included communication and behavior change and construction of incinerators throughout the country for disposal of syringes. However, there is still a need to develop and test methodologically sound interventions based on theories of behavior change to achieve reduction in injection use and reuse of injection equipment. Overall, two types of interventions, one focusing on providers and patients in small groups
Janjua NZ et al . Injection practices in South Asia
Table 5 Prescribers, providers, and preference of patients and practitioners for injections in South Asia 1995-2016
Ref. Prescribed by GP
Prescribed by unqualified practitioner
Provided at private clinic
Provider dispenser
Patient prefers Injection
Practitioner prefers injection
Practitioner says patient demand it
India Rajasekaran et al[37] 59% 37.6% 40% 87.2% IPEN study group[40] 42.6% 57.5% 77%1/34%2 93.5% 10.2% 70.6%3 88.6% Murhekar et al[36] 50.8% 54.8% Kotwal et al[34] 13.8% 58.8% 30% Anand et al[38] 18% Lakshman et al[35] 65% Kermode et al[67] 8% 35% Kermode et al[41] 55% (patients) 24.8% (patients) 7.7% (patients) 9.3% (relatives) Pandit et al[42] 57% 55% 17% Garapati et al[44] 48.7% Bendale et al[69] 8.16% 35% 65%Pakistan Raglow et al[22] 94% 94% Janjua et al[23] 63% 28% 69% 76% 16% Janjua et al[26] 63% 28% 63% 32% Janjua et al[23]
Janjua et al[27] 52% 16% Yousafzai et al[25] 7.9% 8.8% 71% Khan et al[6] 44%Bangladesh Gibney et al[71]
Shill et al[51] 50%Sri Lanka Rannan-Eliya et al[59]
Nepal Gyawali et al[54] 92.6% Gyawali et al[52] 12.6% 21.4% 5%
1Therapeutic; 2Preventive injections; 3Physician took prescription decision/in 15% cases practitioner promoted injection prescription.

5845 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
and the other focusing on the community as a whole, showed improvement in injection safety.
Injection use in India Injection use, prescribers and providers: Since the 1980’s, there has been an awareness of injection overuse in India[16,17]. During the 1990s, the medical/public health community became more concerned with the emergence of HIV/AIDS and the occurrence of injection associated outbreaks of HBV and HCV in many parts of India[8,11,12]. Since then, many injection use studies have been reported from various parts of India (Table 3)[34-39]. In India, the receipt of injections per person per year ranged from 0.2 to 8.6 injections (Table 4). In 2002-2003, a national assessment of injection practices was conducted using a population survey utilizing cluster sampling. The study involved interviews at home, observation at clinics and exit interviews of patients. The results revealed that each person received between 2.8 (based on 3 mo recall) to 5.8 (based on past 2 wk recall) injections per year with a higher number (9.5) for those ≤ 1 year of age. Overall, 17% injections were provided for vaccination purposes. At public facilities 68.0% of injections were for vaccination purposes compared to 31.9% in the private sector. The proportion of injections for vaccination is higher in India than other countries including Pakistan. Injections are provided by unqualified health workers (helper/trainee/assistant, yet-to- qualify) to qualified practitioners. Infacility survey, 44% of patients at private clinics and 38% of public clinics received an injection. A higher proportion of patients received injections at non-formal prescriber clinics (58%) and Indigenous Medicine clinics (53%). In the private sector, unqualified helpers/assistants provided most of the injections compared to health workers or nurses in the public sector. Public facilities prescribed 34% of all injections for fever, diarrhea or cough while 49.5% of private facilities provided injections for these complaints. However, most of these injections are not required as these conditions can be treated with oral drugs[40].
Private practitioners are more likely to provide injections as compared to public practitioners. Data from other studies suggest that injections are prescribed by a variety of practitioners ranging from unqualified dispensers who learned injection administration while working at a clinic to a qualified medical practitioner (MBBS)[34-38,41-43].
Safety of injection equipment: The national as-sessment of injection safety in 2002-2003, described above, found that glass syringes are still being used although less common (27.2%)[40]. Overall, 32% of the injections provided could potentially transmit blood borne pathogens and 62.9% were considered unsafe. The highest proportion of unsafe injections were reported from immunization clinics (74.0%)
followed by government (68.7%) and private health care facilities (59.9%)[40]. Other studies have reported varying proportion of unsafe injections (Table 4).
Determinants of injections: The majority of the injections were administered by private practitioners driven by economic benefits. Qualitative data from the National assessment suggest that injections are prescribed for money, for quick relief, and to maintain credibility among patients. Studies have consistently reported that prescribers, rather than patients, make the decision for injection most of the time (> 50%)[40], though more patients in rural areas (43.1%-47.8%) have shown preference for injections as compared to those in cities (19.4%) (Table 5)[37]. In a study from Car Nicobar Island, 54.8% of participants preferred injection for treatment of a fever while only 36.2% preferred oral medication[36]. In summary, practitioners reported that injections are provided because patients demand/prefer them while in reality only small numbers of patients prefer injections[40,44]. This common phenomenon of cognitive dissonance has also been reported from other parts of the world[45].
Progress towards promoting safe injection practices: India took a giant leap towards promoting safe injection practices once the injection problem was recognized at a high political level[46]. The Indian Medical Association (IMA) and the Indian Academy of Pediatrics (IAP) issued injection safety policies and endorsed the use of safe injections by its members in 2004[47]. IMA started a national project in which about 400 leaders of the IMA from five regions of the India were trained in injection safety issues in workshops with the expectation that they would address the issues at the local level among practitioners. IMA organized a special session in its national conference and distributed a CD of safe injection practices among 1500 participants. Andhra Pradesh state IMA took the lead and started a pilot project with Program for Appropriate Technologies in Health (PATH) to educate members at its local branches about injection safety. A “Model Injection Center” was developed by PATH in collaboration with Niloufer Hospital attached to Osmania Medical College, Hyderabad, to educate the medical community about the safe administration of injections[48]. In 2014, the National Centre for Disease Control issued guidelines on safe and appropriate use injections in medical practice[49].
A national assessment of injection practices 2003-2004 in India showed that 48% of the injections were provided with glass syringes in immunization programs, where the sterility of syringes is always uncertain. The government decided to switch to AD syringes that prevent reuse. This is a big step towards ensuring safety of immunization injection, however immunization injections are a fraction of all provided injections and most of the injections are provided in
Janjua NZ et al . Injection practices in South Asia

5846 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
the private sector. Local and international manufacturers of syringes
have started producing immunization and therapeutic RUP at an affordable price. With the implementation of the South Asia Free Trade Agreement, these syringes will be available to people in other countries in South Asia at the same low price (5 US Cents).
However, this is just the beginning of a journey towards safe injections for India. Strategies need to be developed for making injections safer in the private sector, and to encourage behavior change of prescribers, providers and the population.
Injection safety in BangladeshInjection use, prescribers and providers: We found two published articles on injection practices from Bangladesh. Chowdhury et al[50], conducted a study in 2008-09 at 24 primary health care centers (PHC) across Bangladesh and included three components: (1) a retrospective review of prescriptions; (2) systematic observation of PHCs facilities, injection providers, waste handlers, and injection administering events; and (3) six focus group discussions (FGDs) with prescribers and 38 in-depth interviews with doctors, nurses, and waste handlers on injection safety practices. In this study, 78% of 3354 prescriptions included at least one injection. The most commonly provided injections included antibiotics (78.3%), IV fluids (38.6%), analgesics/pain killers (29.4%), vitamins (26.7%), and anti-histamines (18.5%). About 85% of 480 observed injections were provided with new syringes and new needles. Reuse of syringes was higher in Sylhet (25%). Qualitative data revealed that decisions for injection prescriptions were influenced by: prescribers’ belief in efficacy of injections compared to oral medication; perception of the seriousness of the disease; quest to prove superiority over other doctors by using high-cost “powerful medications”; and the perception that patients want injection because patients do not consider prescriptions without injection as good as injections, and patients desire quick relief[50].
Shill et al[51] conducted a retrospective review of prescriptions at six primary health care units in Dhaka in 2009. This study found that about 60% of prescriptions included an injection. Major reasons for injection prescriptions by prescribers included seriousness of illness, patient’s demand, belief in injection efficacy, and injection prescription by an assistant in absence of physician.
The above mentioned studies reported high injection use in facilities, but did not report on population level injection frequency and distribution by public and private sector which is important for planning interventions to reduce injection use and re-use. Studies are needed to estimate the annual ratio of injections which could be accomplished by including questions on injection use in demographic and health survey similar to Pakistan.
Injection use in NepalData on injection use in Nepal has been reported recently. A population based study including a cross-sectional survey (2470 people from 600 households) and FGDs with those who reported receiving injections was conducted in 2012 in Western Nepal[52]. In this study, 10% of individuals received an injection during the last three months, and annual ratio of injection per capita was 2.37. About 3% of injections were provided for vaccination. Of the respondents who recalled their last injection, 77%, received their injection from a formal health provider (physicians, nurses or other trained healthcare worker) while 21% received injections from a medical dispenser. Of all injections, 95% were provided with a new single use syringe taken from a sealed packet. In this study, 79% of 714 respondent preferred oral drugs for fever, 5% preferred injection and 16% had no preference (Table 5). Data from this study suggest that injection use in this part of Nepal is low and most injections are provided with new syringes and population does not prefer injection. However, these data are in contrast to an earlier qualitative study conducted in 2000 in seven districts of Nepal’s central region. This earlier study included FGDs, secret shoppers interaction and in-depth interviews with consumers and providers[53]. The study indicates that injection use is common, as reported by both consumers and providers; however the exact magnitude is not known. Most of the injections are unnecessary, provided for weakness, pain, fever and flu and include multivitamin (7 of 50 observations), painkillers and antibiotics. Various types of practitioners prescribe injections ranging from those unqualified with no formal schooling at all to qualified physicians; most are administered by the unqualified practitioners. The majority of injections are provided at pharmacies and “medical shops” but also at homes, and grocery stores. The use of glass syringe has declined and disposable syringes are used most of the time, but reuse of these syringes is common. Reusing a syringe is more often done by unqualified practitioners and for poor and less educated people. Reuse of syringes has been reported consistently from observations, in-depth interviews and focus group discussions.
In most of the interactions with practitioners, patients did not request injection; practitioners made the decision for the medication especially for poor and less educated patients. However, at the same time many practitioners refused injections to secret shoppers. However, during in-depth interviews pro-viders reported that patients, especially the less educated, demand injections and that is why they provide injections. Most of the patients think that it is better to use oral drugs and use injections for serious conditions but some also believe that injections are fast acting and more efficacious then oral drugs. However, most consumers believe that children should be treated with injections. Most consumers are aware
Janjua NZ et al . Injection practices in South Asia

Last
inje
ctio
n w
ith n
ew s
yrin
ge
100
80
60
40
20
0No education Primary Middle Secondary Higher Wealth quintiles
Women Men
5847 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
of the risks associated with injections, like injection abscesses and even death either because of their own experience or that of family or friends.
An assessment of pharmacy and injection practices at pharmacies in Western Nepal revealed that 91% pharmacies dispensed and administered injections. About half of these pharmacies reported dumping sharp waste into municipal waste[54].
In summary, there is wide variation in injection use in Nepal. There is need to collect data on injection use from all regions of Nepal using standardized methodology to inform programs.
Sri Lanka- an exception to injection use in South AsiaNo published or unpublished report was available to describe the magnitude of injection use in Sri Lanka. The prevalence of HBV and HCV is low in Sri Lanka, although recent estimates from large, well designed studies are not available[55,56].The private sector played a negligible role in provision of health care until 1977 when the government allowed private practice physicians. Recently there has been growth of the private sector that is now providing about 45% of the outpatient care[57]. This is much less than the 80% provided by the private sector in
India and Pakistan. There have been some reports of malpractice of physicians in the private sector in terms of over prescription of drugs[58]. A national survey was conducted in 2000 to assess the size of the primary care private sector and the quality of their practice by the Institute of Policy Studies[59]. The study included clinics run by full time private practitioners and excluded private practice of government physicians (a substantial proportion) and traditional and unqualified practitioners. The study reported that the private practitioners provide about 15% of outpatient care in Sri Lanka. Assessment of prescriptions revealed that: no medication was prescribed in 14% of cases, the mean number of items prescribed per consultation was 2.7, and only 3% of the prescriptions contained an injection. The authors concluded that the quality of care is comparable to that provided by GPs in Australia[59].
The available evidence suggests that injection use is not very common in Sri Lanka. There are many plausible explanations for this. A large proportion of those in private practice have post graduate qualifications in family medicine. All of the practitioners receive their initial training and many years of post-internship practical experience in the public sector where rational prescription is a norm. Moreover, the literacy level of the population is also very high.
Injection use in Maldives and BhutanWe were not able to find any published or unpublished reports that relate to injection safety in these countries.
Disparities in injection use Limited data on socioeconomic disparities in injection use was available. In the 2012-13 PDHS, men and women in rural areas reported receiving more injections compared to those in urban areas of Pakistan (women: 5.8 vs 4.7; men: 5.2 vs 4.2)[24]. A similar finding of higher injection use in rural areas has been reported from Indian[40]. PDHS also reported a decreasing trend in number of injections received with increasing education level, with the number of injections being about twice as high among those with no formal schooling compared to those with higher education for both men and women (Figure 3). There was no clear relationship between wealth and injection use, however, injection with a new syringe increased with an increase in wealth of the patient for both men and women (Figure 4)[24,27]. Other data from both India and Pakistan support that people in rural areas, with low education level and those in lower quintiles of wealth are more likely to receive low quality health care including injections with use syringes[34,60].
DISCUSSION
This is the first paper to summarize evidence on injection use in South Asia. Overall, injection use is very common in South Asia with variation across
Figure 3 Annual ratio of injections per capita by education level in Pakistan, Pakistan Demographic and Health Survey 2012-2013.
Janjua NZ et al . Injection practices in South AsiaAn
nual
rat
io o
f in
ject
ions
per
cap
ita
8.0
7.0
6.0
5.0
4.0
3.0
2.0
1.0
0.0No education Primary Middle Secondary Higher Education level
Women Men
Figure 4 Receipt of injection with newly opened syringes in Pakistan by wealth quintiles, Pakistan Demographic and Health Survey 2012-2013.

5848 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
countries (2.4-13.6 injections/person per year) with a varying proportion of injections being unsafe in recent studies (5%-50%). In this regard, Sri Lanka is an exception where limited available reports suggest that very few injections are used. Studies to assess injection use are not available from Maldives and Bhutan. Injections are provided in formal and informal sectors, more so in the private than the public sector. Practitioners are the major driving force behind injection overuse, although patients from different parts of South Asia also prefer injections as a form of therapy. Countries for which ample injection use data is available (India and Pakistan), have taken major steps towards promotion of safe injection practices. Hence the availability of data about unsafe injections plays an important role in mobilizing political will to reduce unsafe injection practices. The paucity of information in the region from rest of the countries demands an immediate assessment of injection safety to inform optimal response.
Available evidence suggests some major similarities in injection use patterns across countries. Injection use is high and most of the curative injections are provided in the private sector and prescribed by a variety of prescribers that include unqualified as well as qualified practitioners. Similarly, injection providers range from qualified health workers to unqualified providers, with the latter being more common in the private sector. Reuse of injection equipment or unsafe injections are also more common in the private sector. Mostly prescribers make the decision for injections although there is demand for injections from consumers as well. Consumer demand varies from one place to another within a country as well as between countries.
In Pakistan, Nepal, and India, the poor and un-educated are more likely to be prescribed injections which are prone to be unsafe if they are being provided at an unqualified practitioner’s clinic, especially in rural areas[22,23,34]. Practitioners state that poor and uneducated people demand more injections, but in most cases the decision about injections is made by a practitioner not the consumer. Very few patients demand injections and the poor are less likely to do so because of the power differential. Choice of the practitioner made by the economically disadvantaged and uneducated patients may put them at a higher risk of unsafe and unnecessary injections. For example, in Pakistan those in the lowest income bracket were more likely to seek care from unqualified practitioners[60] and in India those with income < 5000 rupees were more likely to receive injections from informal health care workers[34]. Other reasons could be that poor and uneducated are not aware of the risks associated with injections or the reuse of syringes and are more concerned about getting better quickly and returning to work soon so as not to lose their wages[6,23,27,28,34,37,51]. In Pakistan, knowledge of bloodborne pathogens increased incrementally with education level and injection administration
with new syringes increased with this increase in knowledge. Furthermore, 70% of those who had no formal education and lacked knowledge on transmission of HCV with reused syringes received injections with a new syringe, while 94% of those who had some education and knowledge on HCV transmission with reused syringes received injections with a new syringe[27]. Thus, higher education level, wealth and knowledge are all associated with higher percentage of injections with a new syringe. Higher education level and socioeconomic status also provide empowerment and increases self-efficacy, enabling the patient to negotiate quality of care. Thus, large scale interventions on knowledge and awareness related to oral and injectable medication efficacy and harms associated with injections may reduce injection use and reuse among the general population with higher education and socioeconomic status. Mass awareness campaigns using low cost health education material on injection safety and information dissemination through community meetings and mosques etc., has been shown to reduce the reuse and overuse of injections[30,33].
People with low education levels and wealth are less empowered and there is a greater power differential with their healthcare provider. Thus, this segment of population has lower self-efficacy to negotiate care quality and injection prescription. Interventions to improve self-efficacy to negotiate injection prescription could be successful in reducing injection use and reuse. Tools to help in initiating discussions on different types of medications could be useful in this regards. Support structures to change overall prescription environment by empowerment of community and community expectation of safe injection practices from prescribers and providers could aid in the overall injection prescription negotiation and reducing injection use. Community education and involvement has been successful in increasing knowledge levels and injections with new syringes in rural area of Pakistan[33].
The discrepancy between patients’ preference for injections and prescribers’ beliefs that patients demand it is present in all the countries for which data is available. This gap is greater in urban than rural areas where a larger proportion of patients have shown preference for injections. A behavior change intervention - Interactional Group Discussion (IGD) - to convince prescribers that patients do not systematically prefer injectable medications has been successful in reducing injection use and reuse in Indonesia, Pakistan and India[32,45,61]. Hence, behavior change among practitioners and the population can reduce unsafe injection; however, these strategies need to be tested on a large scale in public health programs.
Since there is a concern among practitioners that if they do not provide injections their clients will shift to other practitioners, professional medical associations could play an important role in alleviating this concern. Dialogue and consensus at the local
Janjua NZ et al . Injection practices in South Asia

5849 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
level and endorsement at the national and local levels about appropriate use of injections and counseling of patients about the appropriateness of injection could allay the fear of losing clients and reduce injection use. These activities can have enormous impact over large areas without too much cost. Pilot projects should test the involvement of professional associations and practitioners in improving safety and reducing overall injection use.
A large proportion of injection use occurs in the private sector and many studies have indicated that the role of economic incentives in the reuse and overuse of needles/syringes by practitioners[6,22,23,32]. Structural interventions in the form of re-use pre-vention (RUP) injection devices can play a major role in reducing reuse of injection devices. However, their use in the private sector can only occur if the price is affordable (similar to or lower than conventional devices) and conventional devices are replaced with RUP injection devices. Partnerships between industry and governments can play a major role in providing these devices at an affordable price and assist with the phase-out of conventional devices from the market. The likely role of government is to establish a policy of RUP injection device use at all health care facilities and to provide incentives to manufacturers in the form of tax subsidies to lower initial cost. In India, industry has already started producing these devices at an affordable price. These ventures have implications for
the entire South Asian region especially for smaller countries where establishing a new plant may not be cost effective.
As highlighted above, injection use and safety is a complex issue and requires interventions at multiple levels and settings including individual patients, prescribers/providers, community, health system and broader policy level to have a major impact. We propose a framework based on social ecological model (SEM) and health belief model (HBM) to inform design of interventions targeting various components to promote rational injection use and eliminate reuse[62-64] (Figure 5). In this framework, the HBM is based on the understanding that at the individual level, a patient’s ability to avoid unnecessary and unsafe injections is based on the individual’s perceived susceptibility of getting an HCV/HIV infection, perceived severity, or his/her belief of how serious the consequences of getting this infection can be, the benefits of being able to avoid getting infected, the perceived barriers to being able to avoid unsafe and unnecessary injection, and self-efficacy in his/her abilities to negotiate with the provider to not administer unnecessary or unsafe injection with a used syringe. Self-efficacy is defined as people’s judgments of their capabilities to organize and execute a course of action required to attain designated types of performances[65]. Beliefs and behaviors, BBP knowledge, education, socioeconomic status and ethnicity influence beliefs on efficacy of
Figure 5 Social ecological model for reducing unsafe injection prescriptions.
Janjua NZ et al . Injection practices in South Asia
Community cohesion and social network:Learning about HCV/BBI in community and harms of injections from each otherCommunity social capital/empowerment: Leverage point for reducing injection use by collective action at provider and government levelNegotiation with providers for safe injection practices at community levelCommunity action for availability of syringes and proper disposal Socioeconomic position: Income, poverty, education, occupation→ influence service organization and quality (reuse/prescription)Organizational/system level factors: Workforce: Lack of trained providersProfessional associations and unions: Influence practice and best practices
Macro-level factors
Neighborhood and organizational or system
factors
Provider factors
Interpersonal (social environment)
Intrapersonal factors
Public health and healthcare: Provincial/national laws, policies, implementation strategies, practice guidelines rational injection/RUP use and regulations; funding allocation; Healthcare worker trainingGovernment and political structures and policies: Avaibility of SIP/RUP;Facilitation of SIP/RUP device introductionTrade policies and industry: Economic environment Societal and cultural norms and values: Media
Provider factors: Knowledge: of harms with syringe reuse and injection overuseBeliefs in injection efficacyPerceptions: patient wants injectionPatient-provider relationship:Trust, communication; Skills/motivation to counsel client;Provide type; economic factors
Social and cultural norms: Family, friends and peers attitude, preferences, knowledge, values, skills and behaviors related to injection useSocial support:Community support for influencing prescription practices
BBI knowledge: transmission, disease severity, treatment (availability,
curability, side effects)
Self efficacy innegotiating Injection
use
Injection prescription/Injection with used
syringe
Perceived susceptibility/perceived disease severity
Perceived disease threat
Intentions to get injection
Demographics and other factors: Age, sex, education, SEP, ethnicity, language, friend/family member disease status
Perceived benefits of injections/injection
efficacy

5850 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
injections and self-efficacy to negotiate injection pre-scription with a healthcare provider. Self-efficacy is an important factor for client/patient empowerment for demanding quality of care. To enhance self-efficacy to negotiate injection prescription, beliefs about injection efficacy have to be addressed. The SEM takes into account factors not just at the individual level, but also at interpersonal, community, organizational and policy levels that may impact prevalence of unnecessary or unsafe injection administration. For instance, at the interpersonal level, health care providers’ knowledge on harms related to reuse and rational prescription, beliefs on injection efficacy and patient expectation of an injection, communication skills, economic incentive and power imbalance play a major role in unnecessary injection prescription. Family and friends, and broader community also play a role in creating an environment for promoting injection safety. At the organization and community level, professional associations can influence safety of injections through creating code of conduct and standard of practice by their members at local level as was done in India. Community members together can negotiate and create a demand for safe injection practices. Finally, macro level factors including policies related to promotion and introduction of RUP injection devices, rational prescription guidelines, training of healthcare work force, and economic incentive for reuse prevention and sharp injury prevention devices could provide enabling environment.
In this paper, we included all available literature to synthesize evidence on injection practices in South Asia to provide a comprehensive picture. We did not rate quality of studies for methodological rigour. However, during evidence synthesis we commented on methodological quality and generalizability of studies.
In summary, although information is not available for all countries, injection use is common in South Asia with high levels of reuse of injection equipment and the potential to spread BBPs. Injections are prescribed and provided by qualified and unqualified practitioners mainly in the private sector. Practitioners mostly make decision for injection use although a small percentage of patients also prefer injections. Patient preference varies from one place to another and is higher in rural than urban areas. SEM model proposed above could guide design of multi- pronged interventions including: (1) introduction of RUP devices; (2) behavior change of the population th-rough education, enhancement of self-efficacy of patients and community empowerment to negotiate injection prescription; and (3) behavior change of practitioners through focused IGDs, involvement of community and medical associations in promoting and endorsing safe injection practices.
Knowledge gaps still exist in assessing the mag-nitude of the problem of injection use in some countries in South Asia which could be bridged by including questions on injection use in demographic and health
surveys (DHS). DHS will provide comparable data on injections at the national level to provide a baseline and to assess impact of interventions. Also, there is a need to develop and test new interventions for behavior change, to improve the currently known interventions and to test them in large scale public health programs. The impact of policy and regulation on the supply/availability of injection equipment, and other devices should also be documented. Greater collaboration among stakeholders could enhance achievement of safe injection practices in the region.
COMMENTSBackgroundAlthough, hepatitis B and C are global concern, prevalence in South Asian countries is particularly high. Reuse of syringes for healthcare injections have been consistently shown to transmit hepatitis B and C.
Research frontiersThis is the first paper to summarize evidence on injection use in South Asia. Overall, injection use is very common in South Asia with variation across countries (2.4-13.6 injections/person per year) with a varying proportion of injections being unsafe in recent studies (5%-50%). Studies to assess injection use are not available from Maldives and Bhutan. Injections are provided in formal and informal sectors, more so in the private than the public sector. Practitioners are the major driving force behind injection overuse, although patients from different parts of South Asia also prefer injections as a form of therapy.
Innovations and breakthroughsInterventions aimed at patients, providers and health system such as availability of re-use prevention injection devices have shown to reduce the injection re-use and overuse.
Applications Countries for which ample injection use data is available (India and Pakistan), have taken major steps towards promotion of safe injection practices. Hence the availability of data about unsafe injections plays an important role in mobilizing political will to reduce unsafe injection practices. The paucity of information in the region from rest of the countries demands an immediate assessment of injection safety to inform optimal response.
TerminologyRe-use prevention injection devices are syringes that have mechanical mechanism to prevent reuse after a single use. Social ecological model is a theory-based framework that proposes that individual behaviour is shaped within the context of broader interpersonal, community, organization and policy environment.
Peer-reviewTo provide a context to readers, reviewers highlighted need for inclusion of data on hepatitis B and C prevalence and association between injection and transmission of hepatitis B virus and hepatitis C virus.
REFERENCES 1 Gower E, Estes C, Blach S, Razavi-Shearer K, Razavi H. Global
epidemiology and genotype distribution of the hepatitis C virus infection. J Hepatol 2014; 61: S45-S57 [PMID: 25086286 DOI: 10.1016/j.jhep.2014.07.027]
2 Mohd Hanafiah K, Groeger J, Flaxman AD, Wiersma ST. Global epidemiology of hepatitis C virus infection: new estimates of age-specific antibody to HCV seroprevalence. Hepatology 2013; 57:
Janjua NZ et al . Injection practices in South Asia
COMMENTS

5851 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
1333-1342 [PMID: 23172780 DOI: 10.1002/hep.26141]3 Schweitzer A, Horn J, Mikolajczyk RT, Krause G, Ott JJ.
Estimations of worldwide prevalence of chronic hepatitis B virus infection: a systematic review of data published between 1965 and 2013. Lancet 2015; 386: 1546-1555 [PMID: 26231459 DOI: 10.1016/S0140-6736(15)61412-X]
4 Qureshi H, Bile KM, Jooma R, Alam SE, Afridi HU. Prevalence of hepatitis B and C viral infections in Pakistan: findings of a national survey appealing for effective prevention and control measures. East Mediterr Health J 2010; 16 Suppl: S15-S23 [PMID: 21495584]
5 Razavi H. Polaris Observatory: Hepatitis C disease burden in India and Pakistan. Centre for Data Analysis, 2016
6 Khan AJ, Luby SP, Fikree F, Karim A, Obaid S, Dellawala S, Mirza S, Malik T, Fisher-Hoch S, McCormick JB. Unsafe injections and the transmission of hepatitis B and C in a periurban community in Pakistan. Bull World Health Organ 2000; 78: 956-963 [PMID: 10994278]
7 Luby SP, Qamruddin K, Shah AA, Omair A, Pahsa O, Khan AJ, McCormick JB, Hoodbhouy F, Fisher-Hoch S. The relationship between therapeutic injections and high prevalence of hepatitis C infection in Hafizabad, Pakistan. Epidemiol Infect 1997; 119: 349-356 [PMID: 9440439]
8 Singh J, Gupta S, Khare S, Bhatia R, Jain DC, Sokhey J. A severe and explosive outbreak of hepatitis B in a rural population in Sirsa district, Haryana, India: unnecessary therapeutic injections were a major risk factor. Epidemiol Infect 2000; 125: 693-699 [PMID: 11218219]
9 Bari A, Akhtar S, Rahbar MH, Luby SP. Risk factors for hepatitis C virus infection in male adults in Rawalpindi-Islamabad, Pakistan. Trop Med Int Health 2001; 6: 732-738 [PMID: 11555441]
10 Pasha O, Luby SP, Khan AJ, Shah SA, McCormick JB, Fisher-Hoch SP. Household members of hepatitis C virus-infected people in Hafizabad, Pakistan: infection by injections from health care providers. Epidemiol Infect 1999; 123: 515-518 [PMID: 10694166]
11 Singh J, Bhatia R, Khare S, Patnaik SK, Biswas S, Lal S, Jain DC, Sokhey J. Community studies on prevalence of HBsAg in two urban populations of southern India. Indian Pediatr 2000; 37: 149-152 [PMID: 10745409]
12 Singh J, Bhatia R, Patnaik SK, Khare S, Bora D, Jain DC, Sokhey J. Community studies on hepatitis B in Rajahmundry town of Andhra Pradesh, India, 1997-8: unnecessary therapeutic injections are a major risk factor. Epidemiol Infect 2000; 125: 367-375 [PMID: 11117960]
13 Usman HR, Akhtar S, Rahbar MH, Hamid S, Moattar T, Luby SP. Injections in health care settings: a risk factor for acute hepatitis B virus infection in Karachi, Pakistan. Epidemiol Infect 2003; 130: 293-300 [PMID: 12729198]
14 Reid S. Estimating the Burden of Disease from Unsafe Injections in India: A Cost-benefit Assessment of the Auto-disable Syringe in a Country with Low Blood-borne Virus Prevalence. Indian J Community Med 2012; 37: 89-94 [PMID: 22654281 DOI: 10.4103/0970-0218.96093]
15 Hauri AM, Armstrong GL, Hutin YJ. The global burden of disease attributable to contaminated injections given in health care settings. Int J STD AIDS 2004; 15: 7-16 [PMID: 14769164]
16 Wyatt HV. The popularity of injections in the Third World: origins and consequences for poliomyelitis. Soc Sci Med 1984; 19: 911-915 [PMID: 6515426]
17 Greenhalgh T. Drug prescription and self-medication in India: an exploratory survey. Soc Sci Med 1987; 25: 307-318 [PMID: 3629304]
18 World Bank. World Development Indicators 2015. Washington, DC: World Bank, 2015
19 Bhutta ZA, Gupta I, de'Silva H, Manandhar D, Awasthi S, Hossain SM, Salam MA. Maternal and child health: is South Asia ready for change? BMJ 2004; 328: 816-819 [PMID: 15070640 DOI: 10.1136/bmj.328.7443.816]
20 Hutin Y, Hauri A, Chiarello L, Catlin M, Stilwell B, Ghebrehiwet T, Garner J. Best infection control practices for intradermal,
subcutaneous, and intramuscular needle injections. Bull World Health Organ 2003; 81: 491-500 [PMID: 12973641]
21 Hanson K, Berman P. Private health care provision in developing countries: a preliminary analysis of levels and composition. Health Policy Plan 1998; 13: 195-211 [PMID: 10187592]
22 Raglow GJ, Luby SP, Nabi N. Therapeutic injections in Pakistan: from the patients' perspective. Trop Med Int Health 2001; 6: 69-75 [PMID: 11263465]
23 Janjua NZ, Akhtar S, Hutin YJ. Injection use in two districts of Pakistan: implications for disease prevention. Int J Qual Health Care 2005; 17: 401-408 [PMID: 15883127]
24 Pakistan Demographic and Health Survey 2012-13. Islamabad: National Institute of Population Studies (NIPS) and Macro International Inc., 2013: 1-366
25 Yousafzai MT, Nisar N, Kakakhel MF, Qadri MH, Khalil R, Hazara SM. Injection practices among practitioners in private medical clinics of Karachi, Pakistan. East Mediterr Health J 2013; 19: 570-575 [PMID: 24975187]
26 Janjua NZ, Akhtar S, Hutin YJ. Economic burden of unnecessary Injections in Pakistan. Proceedings of the AIDS 2006 - XVI International AIDS Conference; 2006 August 13, 2006; Toronto, Canada. Geneva: International AIDS Society, TUPE0504
27 Janjua NZ, Mahmood B, Imran Khan M. Does knowledge about bloodborne pathogens influence the reuse of medical injection syringes among women in Pakistan? J Infect Public Health 2014; 7: 345-355 [PMID: 24861642 DOI: 10.1016/j.jiph.2014.04.001]
28 Altaf A, Fatmi Z, Ajmal A, Hussain T, Qahir H, Agboatwalla M. Determinants of therapeutic injection overuse among communities in Sindh, Pakistan. J Ayub Med Coll Abbottabad 2004; 16: 35-38 [PMID: 15631369]
29 Janjua NZ, Hutin YJ, Akhtar S, Ahmad K. Population beliefs about the efficacy of injections in Pakistan's Sindh province. Public Health 2006; 120: 824-833
30 Luby S, Hoodbhoy F, Jan A, Shah A, Hutin Y. Long-term improvement in unsafe injection practices following community intervention. Int J Infect Dis 2005; 9: 52-59 [PMID: 15603995]
31 Ahmad K, Raza SA, Janjua NZ, Bin Hamza H, Khan MI. Interventions for improvement in unsafe injection practices in Pakistan. Int J Infect Dis 2005; 9: 232-233 [PMID: 15936969 DOI: 10.1016/j.ijid.2005.02.001]
32 Agboatwalla M, Hutin Y, Luby S, Mussarat A. A pilot intervention to improve injection practices in the informal private sector in Karachi, Pakistan. Abstract #AC 112. Proceedings of the second International Conference on Improving Use of Medicines (ICIUM); 2004, 30 March-2 April; Chiang Mai, Thailand: ICIUM, 2004
33 Altaf A, Shah SA, Shaikh K, Constable FM, Khamassi S. Lessons learned from a community based intervention to improve injection safety in Pakistan. BMC Res Notes 2013; 6: 159 [PMID: 23607289 DOI: 10.1186/1756-0500-6-159]
34 Kotwal A, Priya R, Thakur R, Gupta V, Kotwal J, Seth T. Injection practices in a metropolis of North India: perceptions, determinants and issues of safety. Indian J Med Sci 2004; 58: 334-344 [PMID: 15345887]
35 Lakshman M, Nichter M. Contamination of medicine injection paraphernalia used by registered medical practitioners in south India: an ethnographic study. Soc Sci Med 2000; 51: 11-28 [PMID: 10817465]
36 Murhekar MV, Murhekar KM, Arankalle VA, Sehgal SC. Epidemiology of hepatitis B infection among the Nicobarese--a mongoloid tribe of the Andaman and Nicobar Islands, India. Epidemiol Infect 2002; 128: 465-471 [PMID: 12113491]
37 Rajasekaran M, Sivagnanam G, Thirumalaikolundusubramainan P, Namasivayam K, Ravindranath C. Injection practices in southern part of India. Public Health 2003; 117: 208-213 [PMID: 12825472]
38 Anand K, Pandav CS, Kapoor SK. Injection use in a village in north India. Natl Med J India 2001; 14: 143-144 [PMID: 11467141]
39 Kaipilyawar SB, Rao RG. Injection safety for immunisation--Andhra Pradesh experience. J Indian Med Assoc 2005; 103: 222-225 [PMID: 16173430]
40 IPEN Study Group. Injection practices in India. WHO South-East
Janjua NZ et al . Injection practices in South Asia

5852 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Asia Journal of Public Health 2012; 1: 189-20041 Kermode M, Muani V. Injection practices in the formal & amp;
informal healthcare sectors in rural north India. Indian J Med Res 2006; 124: 513-520 [PMID: 17213519]
42 Pandit NB, Choudhary SK. Unsafe injection practices in Gujarat, India. Singapore Med J 2008; 49: 936-939 [PMID: 19037563]
43 Bhargo L, Tiwari R, Jain S, Yuwane P, Rajpoot MB, Tiwari S. A study to assess injection practices at different levels of health care facilities in district Gwalior, MP, India. Int Res Med Sci 2014; 2: 1020-1025
44 Garapati S, Peethala S. Assessment of knowledge and practices on injection safety among service providers in east Godavari district of Andhra Pradesh. Indian J Community Health 2014; 26: 259-263
45 Hadiyono JE, Suryawati S, Danu SS, Sunartono B. Interactional group discussion: results of a controlled trial using a behavioral intervention to reduce the use of injections in public health facilities. Soc Sci Med 1996; 42: 1177-1183 [PMID: 8737436]
46 Hutin YJ. Acting upon evidence: progress towards the elimination of unsafe injection practices in India. Indian Pediatr 2005; 42: 111-115 [PMID: 15767704]
47 Kamath SS. IAP Workshop on Safe Injection Practices: recom-mendations and IAP plan of action. Indian Pediatr 2005; 42: 155-161 [PMID: 15767712]
48 Shankar U, Kanchan R. Model injection centre (MIC). J Indian Med Assoc 2005; 103: 226-227 [PMID: 16173431]
49 National Centre for Disease Control. Handbook on safe injection practices New Delhi. India: National Centre for Disease Control (NCDC), Ministry of Health & Family Welfare, 2014
50 Chowdhury AK, Roy T, Faroque AB, Bachar SC, Asaduzzaman M, Nasrin N, Akter N, Gazi HR, Lutful Kabir AK, Parvin M, Anderson C. A comprehensive situation assessment of injection practices in primary health care hospitals in Bangladesh. BMC Public Health 2011; 11: 779 [PMID: 21985397 DOI: 10.1186/1471-2458-11-779]
51 Shill MC, Fahad MB, Sarker S, Dev S, Rufaka H K, D AK. Injection practices at primary healthcare units in bangladesh: experience at six upazilla health complexes. Australas Med J 2011; 4: 26-42 [PMID: 23393500 DOI: 10.4066/AMJ.2011.471]
52 Gyawali S, Rathore DS, Shankar PR, Kumar VK, Maskey M, Jha N. Injection practice in Kaski district, Western Nepal: a community perspective. BMC Public Health 2015; 15: 435 [PMID: 25928311 DOI: 10.1186/s12889-015-1775-5]
53 Bhattarai M, Wittet S. Perceptions about Injections and Private Sector Injection Practices in Central Nepal. General Welfare Pratisthan and Gates Children’s Vaccine Program at PATH, 2000
54 Gyawali S, Rathore DS, Adhikari K, Shankar PR, K C VK, Basnet S. Pharmacy practice and injection use in community pharmacies in Pokhara city, Western Nepal. BMC Health Serv Res 2014; 14: 190 [PMID: 24774195 DOI: 10.1186/1472-6963-14-190]
55 Gunasekera HA, Sunil-Chandra NP, de Silva HJ. Low community seroprevalence of hepatitis C virus infection in the Gampaha district. Ceylon Med J 2002; 47: 122 [PMID: 12661342]
56 Premawardhena AP, Premaratne R, Jayaweera G, Costa S, Chandrasena LG, de Silva HJ. Hepatitis B and C virus markers
among new entrant medical students. Ceylon Med J 1999; 44: 120-122 [PMID: 10675996]
57 Hsiao WC, Li K. A preliminary assessment of Sri Lanka's health sector and steps forward: William Hsiao, 2000
58 Attanayake N, Siyambalagoda L. An inquiry into the regulation of pharmaceuticals and medical practice in Sri Lanka. HEFP working paper 05/03. London, UK: London School of Hygiene and Tropical Medicine, 2003: viii 70
59 Rannan-Eliya RP, Jayawardhane P. Private primary care practi-tioners in Sri Lanka. Health Policy Research in South Asia, 2003: 279
60 Janjua NZ, Khan MI, Usman HR, Azam I, Khalil M, Ahmad K. Pattern of health care utilization and determinants of care-seeking from GPs in two districts of Pakistan. Southeast Asian J Trop Med Public Health 2006; 37: 1242-1253 [PMID: 17333784]
61 Bhunia R, Hutin Y, Ramkrishnan R, Ghosh PK, Dey S, Murhekar M. Reducing use of injections through interactional group discussions: a randomized controlled trial. Indian Pediatr 2010; 47: 409-414 [PMID: 19736370]
62 Bronfenbrenner U. The ecology of human development: Ex-periments by design and nature. Cambridge, MA: Harvard University Press, 1979
63 Janjua NZ, Razaq M, Chandir S, Rozi S, Mahmood B. Poor knowledge--predictor of nonadherence to universal precautions for blood borne pathogens at first level care facilities in Pakistan. BMC Infect Dis 2007; 7: 81 [PMID: 17650331]
64 Sallis JF, Owen N, Fisher EB. Ecological models of health behavior. In: Glanz K, Rimer BK, Viswanath K, editors. Health behavior and health education: Theory, research, and practice. San Francisco: Jossey-Bass, 2008: 465-486
65 Bandura A. Self-efficacy. Wiley Online Library, 199466 Becker ML, Reza-Paul S, Ramesh B, Washington R, Moses S,
Blanchard JF. Association between medical injections and HIV infection in a community-based study in India. AIDS 2005; 19: 1334-1336 [PMID: 16052095]
67 Kermode M, Holmes W, Langkham B, Thomas MS, Gifford S. Safer injections, fewer infections: injection safety in rural north India. Trop Med Int Health 2005; 10: 423-432 [PMID: 15860088 DOI: 10.1111/j.1365-3156.2005.01421.x]
68 Shah HD, Mangal AD, Solanki HR, Parmar DV. Unsafe injection practices: An occupational hazard for health care providers and a potential threat for community: A detailed study on injection practices of health care providers. IJHAS 2014; 3: 28
69 Bendale N, Bhatkule P. Assessment of injection safety practices in tertiary institute in Maharashtra, India. Int J Recent Trends Sci Technol 2015; 15: 622-625
70 Mantel C. Survey on the safety of injections in Pakistan. Assignment report, 17 May 2002. Islamabad: Ministry of Health, Govrnment of Pakistan, 2002
71 Gibney L, Saquib N, Metzger J, Choudhury P, Siddiqui M, Hassan M. Human immunodeficiency virus, hepatitis B, C and D in Bangladesh’s trucking industry: prevalence and risk factors. Int J Epidemiol 2001; 30: 878-884 [PMID: 11511620]
P- Reviewer: Abenavoli L, Lee HC, Said Z, Waheed Y S- Editor: Ma YJ L- Editor: A E- Editor: Wang CH
Janjua NZ et al . Injection practices in South Asia

Gastrointestinal and liver infections in children undergoing antineoplastic chemotherapy in the years 2000
Elio Castagnola, Eliana Ruberto, Alfredo Guarino
Elio Castagnola, Infectious Diseases Unit, Istituto Giannina Gaslini, 16147 Genoa, Italy
Eliana Ruberto, Alfredo Guarino, Department of Translational Medical Science, Section of Pediatrics, University of Naples Federico II, 80131 Naples, Italy
Author contributions: All authors contributed to this paper with conception and design of the study, literature review and analysis, drafting and critical revision and editing, and approval of the final version.
Conflict-of-interest statement: All the authors declare that they have no competing interests.
Data sharing statement: No additional data are available.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Manuscript source: Invited manuscript
Correspondence to: Elio Castagnola, MD, PhD, Infectious Diseases Unit, Istituto Giannina Gaslini, Largo G. Gaslini 5, 16147 Genoa, Italy. [email protected]: +39-10-56362428 Fax: +39-10-384323
Received: March 24, 2016 Peer-review started: March 25, 2016First decision: May 12, 2016Revised: May 27, 2016 Accepted: June 15, 2016 Article in press: June 15, 2016Published online: July 7, 2016
Abstract AIM: To review gastrointestinal and liver infections in children undergoing antineoplastic chemotherapy. To look at gut microflora features in oncology children.
METHODS: We selected studies published after year 2000, excluding trials on transplanted pediatric patients. We searched English language publications in MEDLINE using the keywords: “gastrointestinal infection AND antineoplastic chemotherapy AND children”, “gastrointestinal infection AND oncology AND children”, “liver infection AND antineoplastic chemotherapy AND children”, “liver abscess AND chemotherapy AND child”, “neutropenic enterocolitis AND chemotherapy AND children”, “thyphlitis AND chemotherapy AND children”, “infectious diarrhea AND children AND oncology”, “abdominal pain AND infection AND children AND oncology”, “perianal sepsis AND children AND oncology”, “colonic pseudo-obstruction AND oncology AND child AND chemotherapy”, “microflora AND children AND malignancy”, “microbiota AND children AND malignancy”, “fungal flora AND children AND malignancy”. We also analysed evidence from several articles and book references.
RESULTS: Gastrointestinal and liver infections represent a major cause of morbidity and mortality in children undergoing antineoplastic chemotherapy. Antineoplastic drugs cause immunosuppression in addition to direct toxicity, predisposing to infections, although the specific risk is variable according to disease and host features. Common pathogens potentially induce severe diseases whereas opportunistic microorganisms may attack vulnerable hosts. Clinical manifestations can be subtle and not specific. In addition, several conditions are rare and diagnostic process and treatments are not standardized. Diagnosis may be challenging, however early diagnosis is needed for quick and appropriate interventions. Interestingly, the source of infection
SYSTEMATIC REVIEWS
Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.3748/wjg.v22.i25.5853
5853 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
World J Gastroenterol 2016 July 7; 22(25): 5853-5866 ISSN 1007-9327 (print) ISSN 2219-2840 (online)
© 2016 Baishideng Publishing Group Inc. All rights reserved.

in those children can be exogenous or endogenous. Indeed, mucosal damage may allow the penetrance of endogenous microbes towards the bowel wall and their translocation into the bloodstream. However, only limited knowledge of intestinal dysbiosis in oncology children is available.
CONCLUSION: The diagnostic work-up requires a multimodal approach and should be implemented (also by further studies on new biomarkers) for a prompt and individualized therapy.
Key words: Gastrointestinal tract; Liver; Microflora; Infection; Oncology; Chemotherapy; Children
© The Author(s) 2016. Published by Baishideng Publishing Group Inc. All rights reserved.
Core tip: The presence of an infectious complication should be always suspected in children with cancer who experience abdominal symptoms. Gastrointestinal and liver infections may be severe complications of chemotherapy that require early diagnosis and appropriate treatment. In these patients there are no absolute predictive markers of gastrointestinal infections, with the possible exception of viral hepatitis. Therefore diagnosis requires a comprehensive approach based on medical history, clinical examination, microbiological tests, imaging and sometimes also invasive procedures.
Castagnola E, Ruberto E, Guarino A. Gastrointestinal and liver infections in children undergoing antineoplastic chemotherapy in the years 2000. World J Gastroenterol 2016; 22(25): 5853-5866 Available from: URL: http://www.wjgnet.com/1007-9327/full/v22/i25/5853.htm DOI: http://dx.doi.org/10.3748/wjg.v22.i25.5853
INTRODUCTIONChildren with cancer often have gastrointestinal and liver symptoms and/or dysfunction. Risk factors include neoplastic infiltration, mechanical obstruction by tumor mass, abdominal tumor rupture, abdominal surgery, radiation therapy and, primarily, antineoplastic chemotherapy, with different effects according to drugs, dosing, schedule and associated treatments[1-6]. Antineoplastic chemotherapy may cause direct damage such as bowel motility disturbance and cytotoxic injury to gastrointestinal and liver tissue, in addition to immunosuppression and nutritional impairment[7-9]. Cancer children are prone to develop gastrointestinal and liver infections that may have a significant impact on morbidity and mortality[10-20].
Aim of the present paper was to describe the digestive and liver infections in children undergoing antineoplastic chemotherapy.
MATERIALS AND METHODSSearch of English language publications in MEDLINE from January 1st 2000 to December 31st 2015 was performed using the following keywords: “gastrointestinal infection AND antineoplastic chemotherapy AND children”, “gastrointestinal infection AND oncology AND children”, “liver infection AND antineoplastic chemotherapy AND children”, “liver abscess AND chemotherapy AND child”, “neutropenic enterocolitis AND chemotherapy AND children”, “thyphlitis AND chemotherapy AND children”,“infectious diarrhea AND children AND oncology”, “abdominal pain AND infection AND children AND oncology”, “perianal sepsis AND children AND oncology”, “colonic pseudo-obstruction AND oncology AND child AND chemotherapy”,“microflora AND children AND malignancy”, “microbiota AND children AND malignancy”, “fungal flora AND children AND malignancy”. Data from patients undergoing allogenic hemopoietic stem cell transplant were excluded due to the peculiarities of this patients’ population. Studies providing information unrelated to our search objective were excluded. In adjunct, we also considered re-ferences from several articles and several books. Major papers were critically reviewed to produce a summary of best available evidence.
RESULTSGastrointestinal infectionsGastrointestinal infections may present with hete-rogenous and non-specific signs and symptoms in children undergoing antineoplastic chemotherapy. These include hemorrhage, abdominal pain, with or without fever. On the other hand, gastrointestinal symptoms are described both in infectious and non-infectious diseases of abdominal and extra-abdominal sites.
Gastrointestinal hemorrhage: Gastrointestinal hemorrhage is not a frequent clinical condition in pediatric oncology, but it may be life threatening in cancer children because of thrombocytopenia, sometime associated with coagulopathy. Fever is generally absent and neutropenia (absolute granulocyte count < 500/cmm, or < 1000/cmm but rapidly declining) can be frequently but not consistently detected. Infections are a rare cause of isolated hemorrhage. Neutropenic enterocolitis has been associated with gastrointestinal bleeding[21-26]
induced by a number of pathogens. Helicobacter pylori (H. pylori) has been detected in gastrointestinal bleeding, mainly in leukemic adolescents receiving steroids[27,28]. Cytomegalovirus is an established enteric pathogen in transplanted patients, whereas it is rarely reported in non-transplanted patients with malignancy, mostly in adults[29,30]. Fungal infections can also cause
5854 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Castagnola E et al . Gut and liver infections in oncology

gastrointestinal hemorrhage. Candida-associated vasculitis (CAV) is a rare but challenging complication of Candida infection. This probably represents a broad spectrum of disease, whose severity ranges from a self-limiting condition to a diffuse life-threatening evolutive process requiring prolonged antifungal treatment, surgery, and quite paradoxically, high dose steroids for its treatment[31-33].Its pathogenesis is unclear, but immunomediated injury seems more plausible than direct fungal toxicity, since no agent is found near vessel walls and vasculitic damage is similar to that found in polyarteritis nodosa[31,32]. Hematemesis and melena are described when Aspergillus localizes in the gastrointestinal tract[33]. Mucorales infect the gut more frequently in children than in adults[34] and children with leukemia seem to be at higher risk of Zygomycetes infection than other oncology patients[35]. Mucorales species localize preferentially in the gastric rather than the intestinal tract. The fungus is angiotropic and invasive, and may cause massive and life-threatening hemorrhage[36].
Endoscopy is useful in case of gastrointestinal bleeding in cancer children both for its potential diagnostic value and for possible therapeutic inter-ventions. This procedure was safe and of great diagnostic usefulness in a large series of cancer children with gastrointestinal bleeding despite the presence of neutropenia and thrombocytopenia[37]. Finally, search for H. pylori antigen in the stools should be done in symptomatic subjects in order to early identify this pathogen[27,28] before the occurrence of severe bleeding.
Abdominal pain: Abdominal pain is a frequent condition in cancer children and may have different infectious and non-infectious causes. The presence or absence of neutropenia deeply affects the etiology and clinical management.
Neutropenic enterocolitis (NE) is a peculiar condition associated with abdominal pain and may be life-threatening. It encompasses a broad pathological and clinical spectrum of diseases with a multifactorial etiopathogenesis, but all characterised by mucosal injury and transmural microbial invasion in the absence of granulocyte infiltration (due to the presence of neutropenia). Typical features are abdominal pain usually generalized or localized to the right lower quadrant, fever (so mimicking an acute appendicitis), and bowel wall thickening documented by ultrasound or CT scan, in a neutropenic patient. Major symptoms may be nausea, vomiting, abdominal distension, constipation and diarrhea (also hemorrhagic),with abdominal pain and fever[22-26,38-44]. Although NE is sometimes termed “typhlitis” or “ileocecal syndrome”, any intestinal segments can be affected, despite its predilection for ileocecal wall[21,38,41-43,45-48]. The true incidence of NE is unknown, with reports ranging from 0.2% to 46%[7,21-23,26,38-42,47,49-51]. Such a wide range likely depends on intrinsic variability of the disease
and on heterogeneous study design. Definitions also play a role since nosographic definitions are based on autopsy findings rather than clinical features and diagnostic criteria are not uniform (Table 1). In addition, populations are different among studies, mainly for patients’ age (sometimes both adults and children) and underlying malignancy. However, the recently observed incidence increase could be at least partially explained by improved diagnostics[38,42] and intensification of antineoplastic regimens[25,52,53]. Anyway, NE is more frequently described in hematologic malignancies[7,22,23,38,40,42,50], in children on specific drugs or drug combinations (e.g., granulocyte-colony-stimulating factor and topotecan, topotecan and idarubicin, cyclophosphamide and hydrocortisone, cyclophosphamide and methotrexate, cyclophosphamide and carboplatin, carboplatin and methotrexate; anthracyclines, cytosine arabinoside, steroids)[42,51,53] administered in the 2-3 wk preceeding the onset of symptoms[38,54], and in the presence of mucositis[54]. Different factors are associated with severe clinical presentation[22,26,38,42,55-57], as summarized in Table 2. Before year 2000 50%-100% mortality was reported, but in the last years this proportion has been reduced from 50% to 30%,or even lesser[7,22,25,26,38,41,47], probably as a consequence of earlier diagnosis and improved treatment strategies. In most patients, a conservative multifaceted approach with the administration of broad-spectrum anti-infectious drugs (including agents against anaerobes and Candida), bowel rest, intravenous fluids, and drugs to limit cytopenia may be successful. Surgery may be considered in refractory or complicated cases. Differential diagnosis should include appendicitis[7,23,24,38,40-41,51,56,58-61], infectious colitis[7,23], Clostridium difficile (C. difficile) - induced diarrhea[38,41] and veno-occlusive disease[7,23].
Appendicitis has been described as a rare com-plication in neutropenic children with a frequency of about 1.5% in patients with severe abdominal pain[24,51,62].
Patients with hematologic malignancy may experience abdominal pain due to intestinal zygomycosis[63,64]. Intestinal aspergillosis is rare and available data mainly come from adult patients on intensive chemotherapy for hematologic malignancies and solid tumors[65-72]. This condition may be severe and even fatal, sometimes within a disseminated disease. Life-threatening complications include bowel infarction, toxic megacolon and bowel perforation.
Pancreatitis is another possible origin of abdominal pain in oncologic children, but is generally due to non-infectious etiologies, although it can be the cause of bloodstream infections especially in the presence of neutropenia[7,24,73]. Similarly, gallbladder disease is mainly related to therapy and not to infections[73].
Intestinal mechanical obstruction may occur due to tumor itself. Intussusception should be taken into account in patients with abdominal tumors[24,74,75]. Bowel adenocarcinoma is rare in pediatric oncology,
5855 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Castagnola E et al . Gut and liver infections in oncology

5856 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
abdominal distension and peritonism (sometimes also called “abdominal crisis”) may also indicate tumor rupture[80]. Gerota capsule distension, hemorrhage within the capsule, spontaneous rupture may cause abdominal pain in Wilms tumor[81]. Acute abdomen may be due to vascular complications such as aneurysm rupture[82]. Ovarian torsion is reported in children and adolescents with neoplasms, although it is not usually associated with malignancy[83,84].
Perianal infections: Perianal infections may be catastrophic in immunocompromised children. High-risk hematologic malignancies treated with aggressive protocols, use of diapers and neutropenia are associated with severe local infections[85]. Anal
however it should be suspected in children with familiar cancer predisposition[76]. A marked colon dilation without mechanical obstruction characterizes acute colonic pseudo-obstruction, otherwise named Ogilvie’s syndrome[77-79]. This gastrointestinal motility disorder is probably due to an imbalanced autonomic innervation of the bowel. Predisposing conditions include sepsis, dyselectrolytemia, drugs influencing gastrointestinal motility such as vincristine or major antidolorific drugs like morphine. Ogilvie’s syndrome is rare and awareness of this condition is minimal. The clinical presentation is characterized by abdominal pain, abdominal distention, nausea, vomiting and constipation, and it may progress to ischaemia and bowel perforation[77,78]. Sudden onset abdominal pain,
Table 1 Different definitions of neutropenic enterocolitisamong studies
Neutropenic enterocolitis definition Neutropenia (Neutrophil count/mm3)
Abnormal bowel wall thickness thresholds (imaging technique)
Ref.
Neutropenia in addition to fever and abdominal pain (generalized or localized to right lower quadrant) without any other obvious cause of abdominal discomfort
< 500 Not specified Jain et al[26], 2000
Al least 1 suggestive clinical sign (fever, abdominal tenderness, diarrhea, nausea, emesis, abdominal pain, and/or constipation) associated with bowel wall thickness ≥ 0.3 cm
< 500 ≥ 0.3 cm (either CT or US; CT and US findings were
significantly different)
McCarville et al[42], 2005
Abdominal pain, fever, and neutropenia associated with radiological abnormalities in the terminal ileum and/or ascending colon (comprising increased wall thickness, pericecal edema, pneumatosis intestinalis)
< 1000 Not specified (CT) Hobson et al[51], 2005
Recent abdominal pain (global or right lower quadrant), fever and severe neutropenia in absence of prior abdominal discomfort
< 500 > 5 mm (US and CT) Alioglu et al[24], 2007
One or more of clinical signs (fever, abdominal pain, diarrhea, abdominal tenderness, nausea, emesis, and/or evidence of peritonitis) and one or more imaging findings on US, CT, x-ray (bowel wall thickening, bowel edema, relative paucity of bowel gas, bowel mass, thumb printing of the mucosa or air in the bowel wall)
< 500 Not specified (x-ray or US or CT)
Moran et al[54], 2009
Clinical triad (abdominal pain, fever and neutropenia) or 2 clinical features with thickened bowel wall in imaging
< 1.65 Not specified (US or CT) Mullassery et al[23], 2009
1 or more signs and/or symptoms related to the effects of treatment (abdominal pain, abdominal distention, vomiting, diarrhea, fever defined as TC ≥ 38 ℃, gastrointestinal bleeding, or obstipation) associated with increased intestinal wall thickness in US
≤ 500 ≥ 3 mm (US) Rizzatti et al[22], 2010
Clinical triad (abdominal pain, high fever and neutropenia) associated with the evidence of image signs (thickened bowel wall) by abdominal US or CT scan
< 500 > 4 mm (US or CT) Li et al[40], 2011
Fever (TC > 38.5 ℃), abdominal pain, neutropenia associated with radiologically confirmed thickening of the bowel wall
< 500 > 3 mm (CT and US concordant)
Sundell et al[38], 2012
Clinical triad (abdominal pain, fever and neutropenia) or 2 clinical features with thickened bowel wall in imaging
< 500 > 5 mm (US/CT) Altinel et al[39], 2012
Proposed diagnostic criteria: Sachak et al[175], 2015Major criteria Compatible histology At least borderline neutropenia Gastrointestinal symptoms Immunosuppression Recent chemotherapy Exclusion of other treatable etiologies Minor criteria Fever of > 38 ℃ Bowel wall thickening of > 4 mm over > 30 mm Positive microbiologic studies“Definitive” NE satisfies the major criteria
US: Ultrasonography; CT: Computed tomography.
Castagnola E et al . Gut and liver infections in oncology

5857 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
fissuration is often the presenting manifestation, then local infection may progress towards deeper strata and cause bacteremia, severe disease and even death. Prevention is probably the most effective measure[7]. In case of perianal sepsis, conservative management is usually applied, although not always effective. Recently, early diverting colostomy has proved successful in a small group of children with acute leukemia[85].
Diarrhea: Diarrhea can be due to infections, although non-infectious causes, such as tumor itself[86-88] or drug toxicity, should be considered. Clinicians should consider three infectious disease scenarios, not mutually excluding: (1) common pathogens, which may be more aggressive in cancer patients; (2) nosocomial infections; and (3) opportunistic pathogens.
Rotavirus is a cause of diarrhea in cancer children. Prolonged shedding is observed among immu-nocompromised subjects and hygiene measures are essential for infection control[89]. Other viral agents responsible for diarrhea include adenovirus and calicivirus. Norovirus is the most common calicivirus detected in gastroenteritis and its shedding in immunocompromised patients is prolonged[90,91]. Sapovirus is an unfrequent cause of gastroenteritis, whose symptoms are usually milder than in Norovirus infection[90]. Bacteria and protozoa can be significant causes of diarrhea in oncology children, at least in specific regions. In a single-center Egyptian survey an infectious cause was found in 74/104 episodes (71.1%), with a not negligible mortality in presence of mixed etiology[13]. Lothstein et al[92] performed a 11-year retrospective study and found zoonotic diseases in 88/10197 acute leukemia children (0.86%). Intestinal pathogens (Campylobacter, Cryptosporidium, Giardia and Salmonella) were responsible for the vast majority (86.4%) of cases, and, despite rare, their individual incidence rates appeared to be higher than
in the general population. Cryptosporidiosis may be a cause of severe and/or prolonged diarrhea in children with acute leukemia and may be complicated by cholangitis[93]. Ehrlichiosis should be suspected in presence of fever and gastrointestinal symptoms associated with epidemiological criteria (living in an endemic area)[94].
Children with malignancy are at higher risk of developing C. difficile infection (CDI), the rate being 15 fold than in all other pediatric patients’ popu-lations[10,95]. Recent exposure to antibiotics, especially anti-pseudomonal B-lactams was associated with increased risk, also with a significant effect of total exposure time within the 30 d preceeding the symptoms[10,95]. Indeed, CDI in hospitalised children is associated with prolonged hospital stay, increased risk of death and costs[96,97]. Prolonged colonization (intermittent or persistent) has been found in more than 50% of oncology children after treatment[98]. In a recent study, malignancy was significantly associated with CDI recurrence (OR = 3.39, 95%CI: 1.52-7.85), but recent surgery and the number of antibiotic courses by class also were significant predictors of recurrence[99]. Crews and coworkers studied the epidemiology of CDI in children in Texas (both in the community and in hospital setting), excluding those under 1 year of age, due to the high rate of colonisation at this young age. Children with hematologic malignancies or undergoing solid organ transplantation had more frequently hospital-acquired CDI than community acquired-CDI. Authors also evaluated the risk factors for severe CDI, according to the following criteria: (1) presence of at least 2 clinical manifestations (fever, bloody stools, leukocytosis, hypoalbuminemia, elevated creatinine); and (2) CDI-related complications (pneumatosis intestinalis, pseudomembranous colitis, toxic megacolon, gastrointestinal perforation, surgical intervention, admission to intensive care unit, death). Fever was observed in 38% of cases, abdominal manifestations
Table 2 Clinical, laboratory and imaging factors associated with severe neutropenic enterocolitis
Factor Outcome Ref.
Previous therapy with cytarabine Higher death rate Rizzatti et al[22], 2010Age > 16 yr Worse response to medical therapy McCarville et al[42], 2005Presence of abdominal distention Higher risk of death Rizzatti et al[22], 2010Presence of abdominal tenderness Prolonged duration McCarville et al[42], 2005Presence of fever Prolonged duration McCarville et al[42], 20054 or more symptoms of enterocolitis Higher risk of death Rizzatti et al[22], 2010Severe (absolute neutrophil count < 108/L) or prolonged (> 7 d) neutropenia
Disease progression Jain et al[26], 2000
Duration of neutropenia Prolonged duration McCarville et al[42], 2005Increased serum Interleukin-8 levels on the first day of clinical illness
Higher risk of admission in Intensive Care Unit van de Wetering et al[55], 2008
Bowel wall tickness Prolonged duration Sundell et al[38], 2012Higher mortality rate Cartoni et al[57], 2001
Higher death rate Rizzatti et al[22], 2010Prolonged duration McCarville et al[42], 2005
Appendiceal thickening Higher risk of serious complications McCarville et al[56], 2004
Castagnola E et al . Gut and liver infections in oncology

5858 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
included diarrhea, bloody stools in 25%, abdominal pain in 46% and vomiting in 28%. Severe disease was observed in 21% of cases and gastrostomy tube and recent hospitalisation were identified as significant risk factors[96]. CDI is associated to higher mortality rate than other etiologies in cancer children with symptomatic gastroenteritis[13]. Neutrophils may have a role in the development of C. difficile-associated pseudomembranous colitis[100]. Fulminant colitis has been reported in 3% of cases of CDI, typically in patients suffering from high fever, abdominal pain, diarrhea orileus[16]. Furthermore, CDI is of concern also due to possible clusters of cases[100,101].
Strongyloides, despite rare, may be a cause of diarrhea (and disseminated infection) especially in high endemic areas and high-risk populations. In an American (Texas) 30-years survey, the frequency of Strongyloides stercoralis infection was 0.8 per 10000 new cancer cases (adults and children) but its frequency was 2.0 per 10000 new cases of leukemia. Interestingly, Authors observed that subjects with hematologic malignancy were at risk for persistent intestinal infestation, and infestation cannot be excluded in the absence of increased eosinophil counts[102].
Therefore, in specific settings, differential diagnosis of diarrhea in oncology children should include a broad pattern of classical and opportunistic agents. This may also be important for hospital infection control purposes due to the high diffusion of selected (especially viral and C. difficile) agents in pediatric hemato-oncology wards.
Liver infections: Liver disease in cancer children may be due to viral, bacterial or fungal pathogens, with clinical features varying from mild to fulminant disease.
A viral infection can be present before diagnosis and treatment of a neoplastic disease, with reactivation during immunosuppression[19,103] especially with drugs like rituximab[104], or may be acquired during treatment, generally through contaminated and poorly controlled blood transfusions[105,106]. Hepatitis B virus (HBV) and hepatitis C virus (HCV) are the most typical agents associated with hepatitis in cancer patients, but their infection pattern has changed over time. Before year 2000 HCV infection ranged from 3% to 9% of survivors of childhood malignancies[107,108], with higher frequencies in acute leukemias[105], with patients experiencing coinfections with HBV or HIV[107,109]. Immunisation programs have significantly influenced HBV epidemiology, while HCV (and HIV) infection incidence almost disappeared after the introduction of blood testing[110]. At present, even if there is no doubt that the risk is minimal, it is not null and it is important to consider viral hepatitis in the differential diagnosis of liver dysfunction in cancer children. In several settings, nosocomial outbreaks have been recently reported[111]. Serology can provide false negative
results in immunocompromised patients and molecular techniques should be used for the diagnosis[112,113].
Other viral agents may be responsible for severe hepatic complications in oncology children. Adenovirus-induced fulminant hepatitis and life-threatening illness have been rarely described in standard chemotherapy regimens[20,114], while Varicella Zoster Virus may be the cause of severe liver dysfunction in immunocompromised hosts[115-117].
Other etiologies, like Mycobacterium fortuitum[118], Aspergillus[34,119] and Mucorales[35] have been found from children with disseminated diseases. A few cases of isolated liver mucormycosis have also been reported[120]. Among disseminated infections hepatic candidiasis (frequently associated with spleen and/or kidney localization, producing the clinical picture of hepatosplenic, also defined as chronic disseminated candidiasis) plays a major role[121-126], particularly in children with acute leukemias. The clinical picture is characterized by long lasting fever and abdominal pain, mainly at the upper-right quadrant, in presence of prolonged neutropenia. Typical (owl’s eye) liver and spleen lesions become evident at imaging only after granulocyte recovery[122,124]. Steroids, quite paradoxically, may be effective in adjunct to antifungal as treatment of chronic disseminated candidiasis in the presence of persistent fever and abdominal pain since these symptoms are at least partially related to an immuno reconstitution syndrome[127,128]. Liver abscesses in children can be due to bacteria, fungi and parasites and sometimes present with abdominal and extra-abdominal complications[129-133]. Amebic and pyogenic abscesses are solitary and right-sided in the vast majority of cases[130,133]. Epidemiology, microbiological tests, imaging and response to treatment may support the diagnosis[129,130].
Differential diagnosis of liver infections may include underlying disease localizations, drug toxicity (methotrexate, thioguanine, dactinomycin, mercaptopurine and busulphan)[1,110], or other life-threatening conditions, like veno-occlusive disease. Imaging (ultrasound, computed tomography), anti-body and viral genome detection are pivotal tools for the diagnosis of these complications.
Microbes in the gastrointestinal tract: Friends or foe?Dysbiosis in oncology children: Intestinal microbiota is a dynamic organ composed by micro-organisms that live in the host with a symbiotic relationship, composing the microbiome. Microflora exerts local and systemic effects and significantly contribute to homeostasis. Dysbiosis, that defines any perturbation in healthy commensal communities, has been described in intestinal and extraintestinal diseases and represents an area of growing interest[134-137]. Quantitative and qualitative alterations of the normal microflorain cancer subjects depends on many factors, such as underlying disease, mucosal disruption, bowel motility disturbance,
Castagnola E et al . Gut and liver infections in oncology

5859 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
enteral/parenteral nutrition, broad-spectrum antibiotic administration. Antineoplastic drugs may also play an important role, that is different for different moieties as demonstrated by in vitro studies showing specific effects on bacterial growth depending on drug type and concentrations[138].
Microbiological analysis of fecal samples of children treated for acute myeloid leukemia demonstrated that the total number of bacteria was 100 fold lower in patients during chemotherapy compared to healthy controls. The microbiota composition was different and, in particular, a 10000-fold decrease in anaerobic bacteria was observed, in concomitance with a 100-fold increase of potentially pathogenic enterococci[138]. Huang et al[139] also found a decreased amount of microbial flora (and in particular of Bifidobacteria, Lactobacillus and E. coli) in acute lymphoblastic leukemia children treated with high dose methotrexate compared to healthy controls. Moreover, a study of fungal flora in stool samples from children receiving chemotherapy or stem cell transplant showed that the incidence of Candida non-albicans species was significantly higher in patients than in controls, with C.glabrata and C.kruzei being the most common non-albicans species. An increase in Candida non-albicans species was observed in prolonged hospital stay, suggesting a nosocomial origin. Interestingly, fungal colonisation was not associated with the type of underlying disease[140]. In another study, Candida colonisation rate resulted not significantly different between children with cancer and healthy subjects, and no difference was found between children with haematological cancer and solid tumours[141]. Also oral microbiota shows distinctive features in oncology patients compared to healthy subjects. Reduced richness, reduced diversity and higher abundance of Firmicutes/Bacilli/Lactobacillales/Carnobacteriaceae/Granullicatella and Firmicutes/Bacilli/Lactobacillales/Aerococcaceae/Abiotrophia were found in children with acute lymphoblastic leukemia compared with healthy controls[142]. Oral ecology changes have been reported both during radiation therapy[143] and chemotherapy[144-146], underlying again the dynamic nature of endogenous microflora. Unfortunately, at present, knowledge about dysbiosis in malignancy is limited, studied populations are heterogeneous and, in addition, study methodology is not uniform. Moreover, only few studies focused on microbiological and clinical outcomes and effects of microflora modifications in cancer children[147-149].
Gastrointestinal tract as a source of pathogens: Pathogens may originate from the gastrointestinal tract and invade the bloodstream through disrupted intestinal barriers. Therefore, intestinal microbial translocation may lead to systemic disease[34,35,140,150-164] with or without localization in other organs. For these reasons gut colonization with resistant phenotypes pose great concern. Carbapenem-resistant Enter-
obacteriaceae (CPE) colonization and infection re-present an emerging treat in oncology children[165-167]. Also Vancomycin-Resistant Enterococcus (VRE) co-lonization have been reported as a possible cause of severe disease in pediatric cancer patients[164,168]. The presence of gastrostomy or nasogastric tube and inadequate hygiene measures were associated with VRE acquisition. Reduced VRE positive screens were found after the implementation of infection control measures[168]. Similar considerations can be made for Candida species that may cause invasive disease in immunocompromised subjects and spread to one or more organs, frequently affecting the gastrointestinal tract, liver, lung and spleen[121,140,169-171].
DISCUSSIONIn summary, Children undergoing antineoplastic treatment are at risk of gastrointestinal or liver complications, including infections that may have a negative impact on quality of life and may preclude, delay or modify antineoplastic treatment. Moreover, they may be clinically severe in susceptible hosts and even be life threatening and sometimes, it may be difficult to distinguish between infectious and not infectious etiology. Furthermore, as the catalogue of antineoplastic agents increases, the infection profile in cancer children might change[103,172-174].
Prompt diagnostic workup must be implemented, even including invasive procedures, to set up ap-propriate interventions. Unfortunately, infectious etiologies of gastrointestinal diseases in cancer children are not frequently documented and therefore literature data are lacking and optimal management is unclear. In addition, studies are not uniform because of different definitions or non-comparable settings (different age of enrolled patients, cancer type, antineoplastic treatment, comorbidities), and therefore no generalisation is allowed for most infectious complications. The availability of new diagnostic criteria will improve knowledge and management strategies, at least for specific conditions[175]. Biomarkers may be used to support differential diagnosis. Miedema et al[176] analyzed several inflammatory markers (CRP, PCT, sTREM-1, IL8) in febrile neutropenic children with malignancy, founding that IL-8 (especially associated with clinical features or PCT) is the best marker for the early detection of bacterial infections, whereas, during mucositis, PCT might be more useful. However, based on available evidence, no ideal biomarker has been found, and undoubtedly diagnosis is multimodal. Medical history and physical examinations remain the best tools for the clinicians. Laboratory tests (inclu-ding local and blood cultures), imaging and invasive procedures may be helpful and sometimes also conclusive in the diagnostic process. New prediction models with items on medical history, clinical features and laboratory tests should be defined and applied to predict infectious risk in oncology children. Moreover,
Castagnola E et al . Gut and liver infections in oncology

5860 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
empirical therapy response could significantly help diagnosis and decision making in clinical practice.
However, children with malignancy are not all the same and the infectious risk might be influenced by exogenous and endogenous factors. Interestingly, in recent years, there is growing interest on genetic susceptibility to specific infections, and future studies may reveal the impact of genetic background on the infectious risk and severity, possibly leading a personalised approach. Similarly, more data on the gastrointestinal microecology modifications in children with malignancy might provide useful insights into gastrointestinal and liver complications. Further studies should characterize intestinal microflora in this setting with the aim of clarifying the cause-effect relationship between specific agents and mucositis, intestinal inflammation, colonisation and infection. Moreover, it could be interesting to look for micro-bial “signatures” (distinctive microbial patterns for specific conditions) as diagnostic tool and potential therapeutic target[136]. New approach such as the opportunity to restructure intestinal microbiota with the use of specific probiotics in combination with other approaches could open new opportunities for prevention of microbial infections.
COMMENTSBackgroundGastrointestinal and liver infections have a significant impact on morbidity and mortality in children undergoing antineoplastic chemotherapy. Infections may delay antineoplastic treatment, impair the quality of life and also jeopardise patients’ life. Unfortunately, diagnosis is often difficult, although a quick and appropriate intervention is needed. The first aim of this review was to critically analyze evidence on gastrointestinal and liver infections in children undergoing antineoplastic chemotherapy published in the years 2000. The authors also added some recent evidences on the role of dysbiosis as a possible risk factor for in cancer children.
Research frontiersThe management of infections needs implementation based on a multifaceted approach. Several nosological entities should be clearly and uniformly defined. Further studies should focus on the definition of the infectious risk and should assess the use of combined diagnostic markers towards precision medicine. Response to empirical treatment should be further investigated as indirect and practical diagnostic tool for differential diagnosis.
Innovations and breakthroughsInfections are a major threat to children with cancer, despite scientific advance. Furthermore, as a natural consequence of scientific progress, cancer survival will increase and new short- and long-term complications from antineoplastic therapies will emerge, including infections. Unfortunately, clinical presentation may be subtle and nonspecific, available evidence is heterogeneous, and data are lacking especially for rare diseases. Moreover, definite diagnosis of several diseases requires invasive procedures that are not easily appliable in vulnerable subjects. Advances from basic and applied science may provide key insight in the management of gastrointestinal and liver infections in children undergoing antineoplastic chemotherapy.
ApplicationsThis review should be considered for practical and research purposes. It analyses the wide differential diagnosis for gastrointestinal and liver infections in children undergoing antineoplastic chemotherapy based on available evidence
obtained in the last 15 years and suggests potential preventive and diagnostic tools to improve patients’ management.
TerminologyNeutropenia (or granulocytopenia) is a condition of bone marrow suppression induced by antineoplastic chemotherapy. It is defined by an absolute granulocyte count < 500/cmm, or < 1000/cmm but in rapid decrease. Neutropenic enterocolitis is a spectrum of diseases characterised by mucosal injury and transmural microbial invasion in the absence of granulocyte infiltration. Hepatosplenic (chronic) candidiasis is a deep organ localization of a disseminated Candida infection, that is acquired during neutropenia but that can be diagnosed by imaging only after granulocyte recovery. Dysbiosis can be defined as any imbalance in healthy commensal microbial communities.
Peer-reviewThis review paper has summarized data from abdominal symptoms, diagnostic methods and data from gut microbiota in oncology children with digestive infections. This is a very well done paper. And in this study, authors have edited the review on the evidences, diagnostic criteria and results of gastrointestinal and liver infections in children suffering from oncologic diseases. This study has achieved to present the factors contributing to infections and the procedures improving quality of life with exact diagnosis and prevention.
REFERENCES1 Altaf S, Enders F, Lyden E, Donaldson SS, Rodeberg D, Arndt
C. Age-related toxicity in patients with rhabdomyosarcoma: a report from the children’s oncology group. J Pediatr Hematol Oncol 2014; 36: 599-604 [PMID: 24936741 DOI: 10.1097/MPH.0000000000000192]
2 Dubowy R, Graham M, Hakami N, Kletzel M, Mahoney D, Newman E, Ravindranath Y, Camitta B. Sequential oral hydroxyurea and intravenous cytosine arabinoside in refractory childhood acute leukemia: a pediatric oncology group phase 1 study. J Pediatr Hematol Oncol 2008; 30: 353-357 [PMID: 18458568 DOI: 10.1097/MPH.0b013e318166247e]
3 Hijiya N, Stewart CF, Zhou Y, Campana D, Coustan-Smith E, Rivera GK, Relling MV, Pui CH, Gajjar A. Phase II study of topotecan in combination with dexamethasone, asparaginase, and vincristine in pediatric patients with acute lymphoblastic leukemia in first relapse. Cancer 2008; 112: 1983-1991 [PMID: 18318429 DOI: 10.1002/cncr.23395]
4 Horton TM, Ames MM, Reid JM, Krailo MD, Pendergrass T, Mosher R, Reaman GH, Seibel NL; Children’s Oncology Group. A Phase 1 and pharmacokinetic clinical trial of paclitaxel for the treatment of refractory leukemia in children: a Children’s Oncology Group study. Pediatr Blood Cancer 2008; 50: 788-792 [PMID: 17668866]
5 Rodriguez-Galindo C, Crews KR, Stewart CF, Furman W, Panetta JC, Daw NC, Cain A, Tan M, Houghton PH, Santana VM. Phase I study of the combination of topotecan and irinotecan in children with refractory solid tumors. Cancer Chemother Pharmacol 2006; 57: 15-24 [PMID: 16001174]
6 Daw NC, Santana VM, Iacono LC, Furman WL, Hawkins DR, Houghton PJ, Panetta JC, Gajjar AJ, Stewart CF. Phase I and pharmacokinetic study of topotecan administered orally once daily for 5 days for 2 consecutive weeks to pediatric patients with refractory solid tumors. J Clin Oncol 2004; 22: 829-837 [PMID: 14990638]
7 Chui CH. Surgical management of complications of multimodal therapy. Pediatr Blood Cancer 2012; 59: 405-409 [PMID: 22434785 DOI: 10.1002/pbc.24147]
8 Parbhoo DM, Tiedemann K, Catto-Smith AG. Clinical outcome after percutaneous endoscopic gastrostomy in children with malignancies. Pediatr Blood Cancer 2011; 56: 1146-1148 [PMID: 21488164 DOI: 10.1002/pbc.22873]
9 Sacks N, Hwang WT, Lange BJ, Tan KS, Sandler ES, Rogers PC, Womer RB, Pietsch JB, Rheingold SR. Proactive enteral tube feeding in pediatric patients undergoing chemotherapy. Pediatr
Castagnola E et al . Gut and liver infections in oncology
COMMENTS

5861 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Blood Cancer 2014; 61: 281-285 [PMID: 24019241 DOI: 10.1002/pbc.24759]
10 Fisher BT, Sammons JS, Li Y, de Blank P, Seif AE, Huang YS, Kavcic M, Klieger S, Harris T, Torp K, Rheam D, Shah A, Aplenc R. Variation in Risk of Hospital-Onset Clostridium difficile Infection Across β-Lactam Antibiotics in Children With New-Onset Acute Lymphoblastic Leukemia. J Pediatric Infect Dis Soc 2014; 3: 329-335 [PMID: 26625453 DOI: 10.1093/jpids/piu008]
11 Cortés JA, Cuervo S, Gómez CA, Bermúdez D, Martínez T, Arroyo P. Febrile neutropenia in the tropics: a description of clinical and microbiological findings and their impact on inappropriate therapy currently used at an oncological reference center in Colombia. Biomedica 2013; 33: 70-77 [PMID: 23715309 DOI: 10.1590/S0120-41572013000100009]
12 Wang A, Fan S, Yang Y, Shen X. Nosocomial infections among pediatric hematology patients: results of a retrospective incidence study at a pediatric hospital in China. J Pediatr Hematol Oncol 2008; 30: 674-678 [PMID: 18776759 DOI: 10.1097/MPH.0b013e3181758110]
13 El-Mahallawy HA, El-Din NH, Salah F, El-Arousy M, El-Naga SA. Epidemiologic profile of symptomatic gastroenteritis in pediatric oncology patients receiving chemotherapy. Pediatr Blood Cancer 2004; 42: 338-342 [PMID: 14966830]
14 Aksoylar S, Cetingül N, Kantar M, Karapinar D, Kavakli K, Kansoy S. Meropenem plus amikacin versus piperacillin-tazobactam plus netilmicin as empiric therapy for high-risk febrile neutropenia in children. Pediatr Hematol Oncol 2004; 21: 115-123 [PMID: 15160510]
15 Petrilli AS, Dantas LS, Campos MC, Tanaka C, Ginani VC, Seber A. Oral ciprofloxacin vs. intravenous ceftriaxone administered in an outpatient setting for fever and neutropenia in low-risk pediatric oncology patients: randomized prospective trial. Med Pediatr Oncol 2000; 34: 87-91 [PMID: 10657866]
16 Vaiphei K, Trehan A, Sachdeva MU, Malhotra P. A young leukemic patient with unusual catastrophic intestinal complication. Indian J Pathol Microbiol 2015; 58: 48-54 [PMID: 25673592 DOI: 10.4103/0377-4929.151187]
17 Asim M, Zaidi A, Ghafoor T, Qureshi Y. Death analysis of childhood acute lymphoblastic leukaemia; experience at Shaukat Khanum Memorial Cancer Hospital and Research Centre, Pakistan. J Pak Med Assoc 2011; 61: 666-670 [PMID: 22204242]
18 Gray TL, Ooi CY, Tran D, Traubici J, Gerstle JT, Sung L. Gastrointestinal complications in children with acute myeloid leukemia. Leuk Lymphoma 2010; 51: 768-777 [PMID: 20350277 DOI: 10.3109/10428191003695652]
19 Elkady A, Aboulfotuh S, Ali EM, Sayed D, Abdel-Aziz NM, Ali AM, Murakami S, Iijima S, Tanaka Y. Incidence and characteristics of HBV reactivation in hematological malignant patients in south Egypt. World J Gastroenterol 2013; 19: 6214-6220 [PMID: 24115819 DOI: 10.3748/wjg.v19.i37.6214]
20 Steiner I, Aebi C, Ridolfi Lüthy A, Wagner B, Leibundgut K. Fatal adenovirus hepatitis during maintenance therapy for childhood acute lymphoblastic leukemia. Pediatr Blood Cancer 2008; 50: 647-649 [PMID: 17278117]
21 de Lijster MS, Smets AM, van den Berg H, Reekers JA. Embolisation for caecal bleeding in a child with typhlitis. Pediatr Radiol 2015; 45: 283-285 [PMID: 24917127 DOI: 10.1007/s00247-014-3059-0]
22 Rizzatti M, Brandalise SR, de Azevedo AC, Pinheiro VR, Aguiar Sdos S. Neutropenic enterocolitis in children and young adults with cancer: prognostic value of clinical and image findings. Pediatr Hematol Oncol 2010; 27: 462-470 [PMID: 20578807 DOI: 10.3109/08880018.2010.489934]
23 Mullassery D, Bader A, Battersby AJ, Mohammad Z, Jones EL, Parmar C, Scott R, Pizer BL, Baillie CT. Diagnosis, incidence, and outcomes of suspected typhlitis in oncology patients--experience in a tertiary pediatric surgical center in the United Kingdom. J Pediatr Surg 2009; 44: 381-385 [PMID: 19231539 DOI: 10.1016/j.jpedsurg.2008.10.094]
24 Alioglu B, Avci Z, Ozcay F, Arda S, Ozbek N. Neutropenic enterocolitis in children with acute leukemia or aplastic anemia. Int J Hematol 2007; 86: 364-368 [PMID: 18055346]
25 Larsen TK, Qvist N, Bak M. Delayed neutropenic enterocolitis in a 12-year-old girl treated with total colectomy and J-pouch reservoir. J Pediatr Surg 2001; 36: 1066-1067 [PMID: 11431780]
26 Jain Y, Arya LS, Kataria R. Neutropenic enterocolitis in children with acute lymphoblastic leukemia. Pediatr Hematol Oncol 2000; 17: 99-103 [PMID: 10689720]
27 Castagnola E, Calvillo M, Gigliotti AR, Fioredda F, Hanau G, Caviglia I, Lanino E, Dufour C. Helicobacter pylori as cause of gastrointestinal disease in children with hemato-oncologic diseases. Pediatr Blood Cancer 2006; 47: 89-91 [PMID: 16007605]
28 Fioredda F, Haupt R, Castagnola E, Barabino A, Micalizzi C, Dini G, Dufour C. Helicobacter pylori-associated large gastric ulcer during treatment for childhood leukemia. J Pediatr Hematol Oncol 2002; 24: 759-762 [PMID: 12468920]
29 Papadopoulos IN, Konstantiadou I, Papantoni E. Enterocolitis with multiple ulcers of ileum and right colon in a patient with leukaemia attributed to cytomegalovirus. BMJ Case Rep 2012; 2012: [PMID: 22669855 DOI: 10.1136/bcr.01.2012.5651]
30 Torres HA, Kontoyiannis DP, Bodey GP, Adachi JA, Luna MA, Tarrand JJ, Nogueras GM, Raad II, Chemaly RF. Gastrointestinal cytomegalovirus disease in patients with cancer: a two decade experience in a tertiary care cancer center. Eur J Cancer 2005; 41: 2268-2279 [PMID: 16143517]
31 Kwon S, Ho JW, Drugas G, Avansino JR. Presentation and management of Candida-associated vasculitis with gastrointestinal involvement in a pediatric patient. J Pediatr Gastroenterol Nutr 2013; 56: e46-e48 [PMID: 22659888 DOI: 10.1097/MPG.0b013e318261030e]
32 Sargent J, O’Marcaigh A, Smith O, Butler K, Gavin P, O’Sullivan M. Candida albicans-associated necrotizing vasculitis producing life-threatening gastrointestinal hemorrhage. Hum Pathol 2010; 41: 602-604 [PMID: 20153510 DOI: 10.1016/j.humpath.2009.09.015]
33 Mantadakis E, Danilatou V, Stiakaki E, Kalmanti M. Infectious toxicity of dexamethasone during all remission-induction chemotherapy: report of two cases and literature review. Pediatr Hematol Oncol 2004; 21: 27-35 [PMID: 14660304]
34 Castagnola E, Viscoli C. Invasive aspergillosis in malignancy and stem cell transplant recipients. In: Latgé JP, Steinbach WJ, editors. Aspergillus fumigatus and Aspergillosis. Washington: ASM press, 2009: 519-530
35 Petrikkos G, Skiada A, Lortholary O, Roilides E, Walsh TJ, Kontoyiannis DP. Epidemiology and clinical manifestations of mucormycosis. Clin Infect Dis 2012; 54 Suppl 1: S23-S34 [PMID: 22247442 DOI: 10.1093/cid/cir866]
36 Dehority W, Willert J, Pong A. Zygomycetes infections in pediatric hematology oncology patients: a case series and review of the literature. J Pediatr Hematol Oncol 2009; 31: 911-919 [PMID: 19855304 DOI: 10.1097/MPH.0b013e3181bbc516]
37 Buderus S, Sonderkötter H, Fleischhack G, Lentze MJ. Diagnostic and therapeutic endoscopy in children and adolescents with cancer. Pediatr Hematol Oncol 2012; 29: 450-460 [PMID: 22612259 DOI: 10.3109/08880018.2012.678568]
38 Sundell N, Boström H, Edenholm M, Abrahamsson J. Management of neutropenic enterocolitis in children with cancer. Acta Paediatr 2012; 101: 308-312 [PMID: 21910749 DOI: 10.1111/j.1651-2227.2011.02465.x]
39 Altınel E, Yarali N, Isık P, Bay A, Kara A, Tunc B. Typhlitis in acute childhood leukemia. Med Princ Pract 2012; 21: 36-39 [PMID: 22024548 DOI: 10.1159/000331587]
40 Li K, Zheng S, Dong K, Gao Y, Wang H, Liu G, Gao J, Xiao X. Diagnosis and outcome of neutropenic enterocolitis: experience in a single tertiary pediatric surgical center in China. Pediatr Surg Int 2011; 27: 1191-1195 [PMID: 21667116 DOI: 10.1007/s00383-011-2938-9]
41 Ullery BW, Pieracci FM, Rodney JR, Barie PS. Neutropenic enterocolitis. Surg Infect (Larchmt) 2009; 10: 307-314 [PMID:
Castagnola E et al . Gut and liver infections in oncology

5862 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
19566419 DOI: 10.1089/sur.2008.061]42 McCarville MB, Adelman CS, Li C, Xiong X, Furman WL,
Razzouk BI, Pui CH, Sandlund JT. Typhlitis in childhood cancer. Cancer 2005; 104: 380-387 [PMID: 15952190]
43 Wilson DB, Rao A, Hulbert M, Mychaliska KP, Luchtman-Jones L, Hill DA, Foglia RP. Neutropenic enterocolitis as a presenting complication of acute lymphoblastic leukemia: an unusual case marked by delayed perforation of the descending colon. J Pediatr Surg 2004; 39: e18-e20 [PMID: 15213940]
44 Schlatter M, Snyder K, Freyer D. Successful nonoperative management of typhlitis in pediatric oncology patients. J Pediatr Surg 2002; 37: 1151-1155 [PMID: 12149691]
45 Ozgen U, Uzüm I, Mizrak B, Saraç K. “Typhlitis” in rectum. Pediatr Int 2010; 52: e32-e33 [PMID: 20158643 DOI: 10.1111/j.1442-200X.2009.02989.x]
46 Gupta S, Kapoor S, Ravi RN, Prakash A, Aggarwal SK. Rectal involvement in neutropenic enterocolitis. Indian J Pediatr 2012; 79: 535-537 [PMID: 21706240 DOI: 10.1007/s12098-011-0506-x]
47 Ozçay F, Kayiran SM, Ozbek N. Successful medical management of neutropenic enterocolitis (typhlitis) in a child with acute lymphoblastic leukemia. Turk J Pediatr 2003; 45: 248-250 [PMID: 14696805]
48 Gayer G, Apter S, Zissin R. Typhlitis as a rare cause of a psoas abscess. Abdom Imaging 2002; 27: 600-602 [PMID: 12173006]
49 El-Matary W, Soleimani M, Spady D, Belletrutti M. Typhlitis in children with malignancy: a single center experience. J Pediatr Hematol Oncol 2011; 33: e98-100 [PMID: 21127432 DOI: 10.1097/MPH.0b013e3181eda606]
50 Fike FB, Mortellaro V, Juang D, St Peter SD, Andrews WS, Snyder CL. Neutropenic colitis in children. J Surg Res 2011; 170: 73-76 [PMID: 21435655 DOI: 10.1016/j.jss.2011.01.041]
51 Hobson MJ, Carney DE, Molik KA, Vik T, Scherer LR, Rouse TM, West KW, Grosfeld JL, Billmire DF. Appendicitis in childhood hematologic malignancies: analysis and comparison with typhilitis. J Pediatr Surg 2005; 40: 214-29; discussion 214-29; [PMID: 15871157]
52 Yaniv I, Fischer S, Mor C, Stark B, Goshen Y, Stein J, Cohen IJ, Zaizov R. Improved outcome in childhood B-cell lymphoma with the intensified French LMB protocol. Med Pediatr Oncol 2000; 35: 8-12 [PMID: 10881001]
53 Kelly KM, Hutchinson RJ, Sposto R, Weiner MA, Lones MA, Perkins SL, Massey V; Children’s Oncology Group. Feasibility of upfront dose-intensive chemotherapy in children with advanced-stage Hodgkin’s lymphoma: preliminary results from the Children’s Cancer Group Study CCG-59704. Ann Oncol 2002; 13 Suppl 1: 107-111 [PMID: 12078889]
54 Moran H, Yaniv I, Ashkenazi S, Schwartz M, Fisher S, Levy I. Risk factors for typhlitis in pediatric patients with cancer. J Pediatr Hematol Oncol 2009; 31: 630-634 [PMID: 19644402 DOI: 10.1097/MPH.0b013e3181b1ee28]
55 van de Wetering MD, Caron HN, Biezeveld M, Taminiau JA, ten Kate FJ, Spanjaard L, Kuijpers TW. Severity of enterocolitis is predicted by IL-8 in paediatric oncology patients. Eur J Cancer 2004; 40: 571-578 [PMID: 14962725]
56 McCarville MB, Thompson J, Li C, Adelman CS, Lee MO, Alsammarae D, May MV, Jones SC, Rao BN, Sandlund JT. Significance of appendiceal thickening in association with typhlitis in pediatric oncology patients. Pediatr Radiol 2004; 34: 245-249 [PMID: 14722695]
57 Cartoni C, Dragoni F, Micozzi A, Pescarmona E, Mecarocci S, Chirletti P, Petti MC, Meloni G, Mandelli F. Neutropenic enterocolitis in patients with acute leukemia: prognostic significance of bowel wall thickening detected by ultrasonography. J Clin Oncol 2001; 19: 756-761 [PMID: 11157028]
58 McAteer JP, Sanchez SE, Rutledge JC, Waldhausen JH. Isolated appendiceal typhlitis masquerading as perforated appendicitis in the setting of acute lymphoblastic leukemia. Pediatr Surg Int 2014; 30: 561-564 [PMID: 24448913 DOI: 10.1007/s00383-014-3473-2]
59 Wiegering VA, Kellenberger CJ, Bodmer N, Bergstraesser E, Niggli
F, Grotzer M, Nadal D, Bourquin JP. Conservative management of acute appendicitis in children with hematologic malignancies during chemotherapy-induced neutropenia. J Pediatr Hematol Oncol 2008; 30: 464-467 [PMID: 18525466 DOI: 10.1097/MPH.0b013e318168e7cb]
60 Chui CH, Chan MY, Tan AM, Low Y, Yap TL, Jacobsen AS. Appendicitis in immunosuppressed children: Still a diagnostic and therapeutic dilemma? Pediatr Blood Cancer 2008; 50: 1282-1283 [PMID: 18306278 DOI: 10.1002/pbc.21554]
61 Ozyurek E, Arda S, Ozkiraz S, Alioglu B, Arikan U, Ozbek N. Febrile neutropenia as the presenting sign of appendicitis in an adolescent with acute myelogenous leukemia. Pediatr Hematol Oncol 2006; 23: 269-273 [PMID: 16517543]
62 Velez MC, Athale UH, Loe W, Warrier RP. Acute perforative appendicitis during preoperative chemotherapy for Wilms tumor. Pediatr Hematol Oncol 2003; 20: 147-150 [PMID: 12554525]
63 Radhakrishnan N, Yadav SP, Oberoi J, Kulshreshta R, Bhalla S, Sachdeva A. Intestinal mucormycosis: a rare entity in pediatric oncology. Pediatr Hematol Oncol 2013; 30: 178-183 [PMID: 23410194 DOI: 10.3109/08880018.2013.769286]
64 Cheng VC, Chan JF, Ngan AH, To KK, Leung SY, Tsoi HW, Yam WC, Tai JW, Wong SS, Tse H, Li IW, Lau SK, Woo PC, Leung AY, Lie AK, Liang RH, Que TL, Ho PL, Yuen KY. Outbreak of intestinal infection due to Rhizopus microsporus. J Clin Microbiol 2009; 47: 2834-2843 [PMID: 19641069 DOI: 10.1128/JCM.00908-09]
65 Enjoji M, Ohtsukasa S, Nagano H, Matsuki M, Kawachi Y, Kurisu A, Maruyama H, Kusakabe M, Nagata K, Hamaguchi H, Taki K. Localized small-bowel infarction caused by Aspergillus during chemotherapy for acute myeloid leukemia: report of a case. Surg Today 2008; 38: 449-452 [PMID: 18560970 DOI: 10.1007/s00595-007-3639-9]
66 Mohite U, Kell J, Haj MA, O’Brien C, Kundu S, Rees J, Burnett AK. Invasive aspergillosis localised to the colon presenting as toxic megacolon. Eur J Haematol 2007; 78: 270-273 [PMID: 17328784]
67 Saitoh T, Matsushima T, Matsuo A, Yokohama A, Irisawa H, Handa H, Tsukamoto N, Karasawa M, Nojima Y, Murakami H. Small-bowel perforation accompanied by Aspergillus endocarditis in a patient with angioimmunoblastic T-cell lymphoma. Ann Hematol 2007; 86: 71-73 [PMID: 17043778]
68 Eggimann P, Chevrolet JC, Starobinski M, Majno P, Totsch M, Chapuis B, Pittet D. Primary invasive aspergillosis of the digestive tract: report of two cases and review of the literature. Infection 2006; 34: 333-338 [PMID: 17180588]
69 Chaudhary A, Jain V, Dwivedi RS, Misra S. Invasive aspergillosis causing small bowel infarction in a patient of carcinoma breast undergoing chemotherapy. J Carcinog 2006; 5: 18 [PMID: 16753069]
70 Ouaïssi M, Moutardier V, Emungania O, Lelong B, Forel JM, Guiramand J, Turrini O, Delpero JR. Fatal bowel infarction due to aspergillosis after chemotherapy. Eur J Surg Oncol 2003; 29: 628 [PMID: 12943632]
71 Sousa AB, Ferreira G, Veiga J, Carvalho A. Clinical picture: Bowel infarction due to aspergillosis. Lancet 2002; 359: 210 [PMID: 11812556]
72 Chambon-Pautas C, Costa JM, Chaumette MT, Cordonnier C, Bretagne S. Galactomannan and polymerase chain reaction for the diagnosis of primary digestive aspergillosis in a patient with acute myeloid leukaemia. J Infect 2001; 43: 213-214 [PMID: 11798263]
73 Khoury NJ, Kanj V, Abboud M, Muwakkit S, Birjawi GA, Haddad MC. Abdominal complications of chemotherapy in pediatric malignancies: imaging findings. Clin Imaging 2009; 33: 253-260 [PMID: 19559346 DOI: 10.1016/j.clinimag.2008.10.029]
74 Ramdial PK, Sing Y, Hadley GP, Chotey NA, Mahlakwane MS, Singh B. Paediatric intussusception caused by acquired immunodeficiency syndrome-associated Kaposi sarcoma. Pediatr Surg Int 2010; 26: 783-787 [PMID: 20535484 DOI: 10.1007/s00383-010-2625-2]
75 Wang SM, Huang FC, Wu CH, Ko SF, Lee SY, Hsiao CC. Ileocecal Burkitt’s lymphoma presenting as ileocolic intussusception with
Castagnola E et al . Gut and liver infections in oncology

5863 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
appendiceal invagination and acute appendicitis. J Formos Med Assoc 2010; 109: 476-479 [PMID: 20610150 DOI: 10.1016/S0929-6646(10)60080-0]
76 Hryhorczuk AL, Lee EY. Imaging evaluation of bowel obstruction in children: updates in imaging techniques and review of imaging findings. Semin Roentgenol 2012; 47: 159-170 [PMID: 22370194 DOI: 10.1053/j.ro.2011.11.007]
77 Lee GE, Lim GY, Lee JW, Cho B. Acute colonic pseudo-obstruction complicating chemotherapy in paediatric oncohaematological patients: clinical and imaging features. Br J Radiol 2012; 85: 377-381 [PMID: 21828148 DOI: 10.1259/bjr/13281402]
78 Jessop M, Choo K, Little M. Acute colonic pseudo-obs-truction in paediatric oncology patients. J Paediatr Child Health 2010; 46: 698-699 [PMID: 21077980 DOI: 10.1111/j.1440-1754.2010.01906.x]
79 Kim TS, Lee JW, Kim MJ, Park YS, Lee DH, Chung NG, Cho B, Lee S, Kim HK. Acute colonic pseudo-obstruction in postchemotherapy complication of brain tumor treated with neostigmine. J Pediatr Hematol Oncol 2007; 29: 420-422 [PMID: 17551407]
80 Davies JQ, de la Hall PM, Kaschula RO, Sinclair-Smith CC, Hartley P, Rode H, Millar AJ. Hepatoblastoma--evolution of management and outcome and significance of histology of the resected tumor. A 31-year experience with 40 cases. J Pediatr Surg 2004; 39: 1321-1327 [PMID: 15359384]
81 Li A, Asch M, Lasky J, Sieger L, Lee SL. The surgical management of a stage III Wilms tumor presenting with perforated appendicitis. J Pediatr Hematol Oncol 2012; 34: e193-e194 [PMID: 22395216 DOI: 10.1097/MPH.0b013e3182425b72]
82 Guler N, Ozkara C, Kaya Y, Saglam E. Ruptured abdominal aortic aneurysm after resection of an infected cardiac myxoma. Tex Heart Inst J 2007; 34: 233-235 [PMID: 17622377]
83 Tsai TC, Wong LY, Wu HP. Ovarian torsion caused by teratoma masquerading as perforated appendicitis in a 5-year-old girl. Pediatr Neonatol 2011; 52: 51-54 [PMID: 21385659 DOI: 10.1016/j.pedneo.2010.12.002]
84 Correa-Rivas MS, Colón-González G, Lugo-Vicente H. Cavernous hemangioma presenting as a right adnexal mass in a child. P R Health Sci J 2003; 22: 311-313 [PMID: 14619460]
85 Pini Prato A, Castagnola E, Micalizzi C, Dufour C, Avanzini S, Pio L, Guida E, Mattioli G, Jasonni V, Disma N, Mameli L, Montobbio G, Buffa P. Early diverting colostomy for perianal sepsis in children with acute leukemia. J Pediatr Surg 2012; 47: e23-e27 [PMID: 23084226 DOI: 10.1016/j.jpedsurg.2012.05.034]
86 Nazir Z. Long-term follow-up of a child with primary lymph node gastrinoma and Zollinger-Ellison syndrome. J Pediatr Surg 2011; 46: 969-972 [PMID: 21616263 DOI: 10.1016/j.jpedsurg.2011.02.002]
87 Al-Saleem T, Al-Mondhiry H. Immunoproliferative small intestinal disease (IPSID): a model for mature B-cell neoplasms. Blood 2005; 105: 2274-2280 [PMID: 15542584]
88 Young G, Toretsky JA, Campbell AB, Eskenazi AE. Recognition of common childhood malignancies. Am Fam Physician 2000; 61: 2144-2154 [PMID: 10779255]
89 Rogers M, Weinstock DM, Eagan J, Kiehn T, Armstrong D, Sepkowitz KA. Rotavirus outbreak on a pediatric oncology floor: possible association with toys. Am J Infect Control 2000; 28: 378-380 [PMID: 11029139]
90 Moser O, Lück S, Dilloo D, Eis-Hübinger AM, Simon A. Sapovirus as a gastrointestinal pathogen in febrile pediatric patients with cancer. J Med Virol 2011; 83: 2233-2236 [PMID: 22012734 DOI: 10.1002/jmv.22219]
91 Ludwig A, Adams O, Laws HJ, Schroten H, Tenenbaum T. Quantitative detection of norovirus excretion in pediatric patients with cancer and prolonged gastroenteritis and shedding of norovirus. J Med Virol 2008; 80: 1461-1467 [PMID: 18551595 DOI: 10.1002/jmv.21217]
92 Lothstein K, Fisher B, Li Y, Seif A, Harris T, Torp K, Kavcic M, Huang YS, Rheingold SR, Aplenc R. Zoonotic infections in pediatric patients with acute leukemia. Pediatr Blood Cancer 2013; 60:
E160-E162 [PMID: 23956002 DOI: 10.1002/pbc.24596]93 Domenech C, Rabodonirina M, Bleyzac N, Pagès MP, Bertrand Y.
Cryptosporidiosis in children with acute lymphoblastic leukemia on maintenance chemotherapy. J Pediatr Hematol Oncol 2011; 33: 570-572 [PMID: 21941152 DOI: 10.1097/MPH.0b013e31820e2d3a]
94 Esbenshade A, Esbenshade J, Domm J, Williams J, Frangoul H. Severe ehrlichia infection in pediatric oncology and stem cell transplant patients. Pediatr Blood Cancer 2010; 54: 776-778 [PMID: 20052776 DOI: 10.1002/pbc.22392]
95 Chaudhry R, Joshy L, Kumar L, Dhawan B. Changing pattern of Clostridium difficile associated diarrhoea in a tertiary care hospital: a 5 year retrospective study. Indian J Med Res 2008; 127: 377-382 [PMID: 18577793]
96 Crews JD, Koo HL, Jiang ZD, Starke JR, DuPont HL. A hospital-based study of the clinical characteristics of Clostridium difficile infection in children. Pediatr Infect Dis J 2014; 33: 924-928 [PMID: 25361022 DOI: 10.1097/INF.0000000000000338]
97 Asensio A, Di Bella S, Lo Vecchio A, Grau S, Hart WM, Isidoro B, Scotto R, Petrosillo N, Watt M, Nazir J. The impact of Clostridium difficile infection on resource use and costs in hospitals in Spain and Italy: a matched cohort study. Int J Infect Dis 2015; 36: 31-38 [PMID: 26003403 DOI: 10.1016/j.ijid.2015.05.013]
98 Dominguez SR, Dolan SA, West K, Dantes RB, Epson E, Friedman D, Littlehorn CA, Arms LE, Walton K, Servetar E, Frank DN, Kotter CV, Dowell E, Gould CV, Hilden JM, Todd JK. High colonization rate and prolonged shedding of Clostridium difficile in pediatric oncology patients. Clin Infect Dis 2014; 59: 401-403 [PMID: 24785235 DOI: 10.1093/cid/ciu302]
99 Nicholson MR, Thomsen IP, Slaughter JC, Creech CB, Edwards KM. Novel risk factors for recurrent Clostridium difficile infection in children. J Pediatr Gastroenterol Nutr 2015; 60: 18-22 [PMID: 25199038 DOI: 10.1097/MPG.0000000000000553]
100 Castagnola E, Battaglia T, Bandettini R, Caviglia I, Baldelli I, Nantron M, Moroni C, Garaventa A. Clostridium difficile-associated disease in children with solid tumors. Support Care Cancer 2009; 17: 321-324 [PMID: 18802726 DOI: 10.1007/s00520-008-0507-0]
101 Warrack S, Duster M, Van Hoof S, Schmitz M, Safdar N. Clostridium difficile in a children’s hospital: assessment of environmental contamination. Am J Infect Control 2014; 42: 802-804 [PMID: 24751141 DOI: 10.1016/j.ajic.2014.03.008]
102 Safdar A, Malathum K, Rodriguez SJ, Husni R, Rolston KV. Strongyloidiasis in patients at a comprehensive cancer center in the United States. Cancer 2004; 100: 1531-1536 [PMID: 15042689]
103 Rapti IN, Hadziyannis SJ. Treatment of special populations with chronic hepatitis B infection. Expert Rev Gastroenterol Hepatol 2011; 5: 323-339 [PMID: 21651351 DOI: 10.1586/egh.11.7]
104 Oh MJ, Lee HJ. A study of hepatitis B virus reactivation associated with rituximab therapy in real-world clinical practice: a single-center experience. Clin Mol Hepatol 2013; 19: 51-59 [PMID: 23593610 DOI: 10.3350/cmh.2013.19.1.51]
105 Sevinir B, Meral A, Günay U, Ozkan T, Ozuysal S, Sinirtas M. Increased risk of chronic hepatitis in children with cancer. Med Pediatr Oncol 2003; 40: 104-110 [PMID: 12461794]
106 Fioredda F, Gigliotti AR, Haupt R, Calevo MG, Giudice CL, Bocciardo L, Giacchino R. HCV infection in very-long-term survivors after cancer chemotherapy and bone marrow transplantation: a single-center experience. J Pediatr Hematol Oncol 2005; 27: 481-485 [PMID: 16189441]
107 Karim B, Alex G, Smith AL, Hardikar W. Hepatitis C infection in children: a Melbourne perspective. J Paediatr Child Health 2000; 36: 385-388 [PMID: 10940177]
108 Matsuzaki A, Ishii E, Nagatoshi Y, Eguchi H, Koga H, Yanai F, Inada H, Nibu K, Tamai Y, Akiyoshi K, Nakayama H, Hara T, Take H, Miyazaki S, Okamura J. Long-term outcome of treatment with protocols AL841, AL851, and ALHR88 in children with acute lymphoblastic leukemia: results obtained by the Kyushu-Yamaguchi Children’s Cancer Study Group. Int J Hematol 2001; 73: 369-377 [PMID: 11345205]
109 Kołtan S, Wysocki M, Kołtan A, Swiatkiewicz V, Styczyński J,
Castagnola E et al . Gut and liver infections in oncology

5864 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Debski R, Balcar-Boroń A. Course of viral hepatitis B and combined B and C hepatitis in children treated for neoplastic diseases. Med Sci Monit 2002; 8: CR274-CR279 [PMID: 11951070]
110 Mulder RL, Kremer LC, Koot BG, Benninga MA, Knijnenburg SL, van der Pal HJ, Koning CC, Oldenburger F, Wilde JC, Taminiau JA, Caron HN, van Dalen EC. Surveillance of hepatic late adverse effects in a large cohort of long-term survivors of childhood cancer: prevalence and risk factors. Eur J Cancer 2013; 49: 185-193 [PMID: 22901831 DOI: 10.1016/j.ejca.2012.07.009]
111 Büchner A, Du Plessis NM, Reynders DT, Omar FE, Mayaphi SH, Haeri Mazanderani AF, Avenant T. Nosocomial outbreak of hepatitis B virus infection in a pediatric hematology and oncology unit in South Africa: Epidemiological investigation and measures to prevent further transmission. Pediatr Blood Cancer 2015; 62: 1914-1919 [PMID: 26047015 DOI: 10.1002/pbc.25605]
112 Durmaz O. Hepatitis C infection in childhood. Clin Res Hepatol Gastroenterol 2012; 36: 294-296 [PMID: 22521559 DOI: 10.1016/j.clinre.2012.03.024]
113 Swilley S, Strickland DK, Davila R, Levstik M, Ribeiro R, Hudson MM. Hepatitis C infection during treatment for childhood cancer: pitfalls in diagnosis and management. Med Pediatr Oncol 2002; 39: 58-59 [PMID: 12116084]
114 Hough R, Chetwood A, Sinfield R, Welch J, Vora A. Fatal adenovirus hepatitis during standard chemotherapy for childhood acute lymphoblastic leukemia. J Pediatr Hematol Oncol 2005; 27: 67-72 [PMID: 15701979]
115 Matsuzaki A, Suminoe A, Koga Y, Kusuhara K, Hara T, Ogata R, Sata T, Hara T. Fatal visceral varicella-zoster virus infection without skin involvement in a child with acute lymphoblastic leukemia. Pediatr Hematol Oncol 2008; 25: 237-242 [PMID: 18432508 DOI: 10.1080/08880010801938215]
116 Mantadakis E, Anagnostatou N, Danilatou V, Markaki EA, Spanaki AM, Briassoulis G, Kalmanti M. Fulminant hepatitis due to varicella zoster virus in a girl with acute lymphoblastic leukemia in remission: report of a case and review. J Pediatr Hematol Oncol 2005; 27: 551-553 [PMID: 16217259]
117 Müller I, Aepinus C, Beck R, Bültmann B, Niethammer D, Klingebiel T. Noncutaneous varicella-zoster virus (VZV) infection with fatal liver failure in a child with acute lymphoblastic leukemia (ALL). Med Pediatr Oncol 2001; 37: 145-147 [PMID: 11496356]
118 Zainal Muttakin AR, Tan AM. Mycobacterium fortuitum catheter-related sepsis in acute leukaemia. Singapore Med J 2006; 47: 543-545 [PMID: 16752025]
119 Hwang YK, Joo NH, Tee GY, Tan P, Tan L, Girija R. Clinical activity of the new triazole drug voriconazole (UK 109, 496) against disseminated hepatosplenic aspergillosis in a patient with relapsed leukemia. Haematologia (Budap) 2001; 31: 73-80 [PMID: 11345409]
120 Tuysuz G, Ozdemir N, Senyuz OF, Emre S, Kantarcioglu S, Adaletli I, Kepil N, Tutuncu C, Celkan T. Successful management of hepatic mucormycosis in an acute lymphoblastic leukaemia patient: a case report and review of the literature. Mycoses 2014; 57: 513-518 [PMID: 24635874 DOI: 10.1111/myc.12184]
121 Lewis RE, Cahyame-Zuniga L, Leventakos K, Chamilos G, Ben-Ami R, Tamboli P, Tarrand J, Bodey GP, Luna M, Kontoyiannis DP. Epidemiology and sites of involvement of invasive fungal infections in patients with haematological malignancies: a 20-year autopsy study. Mycoses 2013; 56: 638-645 [PMID: 23551865 DOI: 10.1111/myc.12081]
122 Yen TY, Huang LM, Lee PI, Lu CY, Shao PL, Chang LY. Clinical characteristics of hepatosplenic fungal infection in pediatric patients. J Microbiol Immunol Infect 2011; 44: 296-302 [PMID: 21524963 DOI: 10.1016/j.jmii.2010.08.005]
123 Ridola V, Chachaty E, Raimondo G, Corradini N, Brugieres L, Valteau-Couanet D, Hartmann O. Candida infections in children treated with conventional chemotherapy for solid tumors (transplant recipients excluded): The Institut Gustave Roussy Pediatrics Department experience. Pediatr Blood Cancer 2004; 42: 332-337 [PMID: 14966829]
124 Edwards JE. Candida Species. In: Mandell GL, Bennett JE, Dolin R, editors. Mandell, Douglas, and Bennett’s Principle and practice of infectious diseases, 7th ed. Philadelphia: Churchill Livingstone Elsevier, 2009: 3225-3240
125 Avci Z, Alioglu B, Anuk D, Ozbek OY, Azap OK, Ozbek N. Double invasive fungal infection and typhlitis in children with acute lymphoblastic leukemia. Pediatr Hematol Oncol 2008; 25: 99-106 [PMID: 18363175 DOI: 10.1080/08880010701885235]
126 Lin PC , Chang TT, Jang RC, Chiou SS. Hepatosplenic microabscesses in pediatric leukemia: a report of five cases. Kaohsiung J Med Sci 2003; 19: 368-374 [PMID: 12926524]
127 Legrand F, Lecuit M, Dupont B, Bellaton E, Huerre M, Rohrlich PS, Lortholary O. Adjuvant corticosteroid therapy for chronic disseminated candidiasis. Clin Infect Dis 2008; 46: 696-702 [PMID: 18230039 DOI: 10.1086/527390]
128 Saint-Faust M, Boyer C, Gari-Toussaint M, Deville A, Poiree M, Weintraub M, Sirvent N. Adjuvant corticosteroid therapy in 2 children with hepatosplenic candidiasis-related IRIS. J Pediatr Hematol Oncol 2009; 31: 794-796 [PMID: 19770685 DOI: 10.1097/MPH.0b013e3181b795ec]
129 Srivastava A, Yachha SK, Arora V, Poddar U, Lal R, Baijal SS. Identification of high-risk group and therapeutic options in children with liver abscess. Eur J Pediatr 2012; 171: 33-41 [PMID: 21537924 DOI: 10.1007/s00431-011-1481-y]
130 Mishra K, Basu S, Roychoudhury S, Kumar P. Liver abscess in children: an overview. World J Pediatr 2010; 6: 210-216 [PMID: 20706820 DOI: 10.1007/s12519-010-0220-1]
131 Rao S, Solaymani-Mohammadi S, Petri WA, Parker SK. Hepatic amebiasis: a reminder of the complications. Curr Opin Pediatr 2009; 21: 145-149 [PMID: 19242252 DOI: 10.1097/MOP.0b013e32831ef249]
132 Muorah M, Hinds R, Verma A, Yu D, Samyn M, Mieli-Vergani G, Hadzić N. Liver abscesses in children: a single center experience in the developed world. J Pediatr Gastroenterol Nutr 2006; 42: 201-206 [PMID: 16456416]
133 Sifri CD, Madoff LC. Infections of the liver and biliary system. In: Mandell GL, Bennett JE, Dolin R, editors. Mandell, Douglas, and Bennett’s Principle and practice of infectious diseases, 7th ed. Philadelphia: Churchill Livingstone Elsevier, 2009: 1035-1039
134 Wong M. What has happened in the last 50 years in immunology. J Paediatr Child Health 2015; 51: 135-139 [PMID: 25677480 DOI: 10.1111/jpc.12834]
135 Chan YK, Estaki M, Gibson DL. Clinical consequences of diet-induced dysbiosis. Ann Nutr Metab 2013; 63 Suppl 2: 28-40 [PMID: 24217034 DOI: 10.1159/000354902]
136 Buccigrossi V, Nicastro E, Guarino A. Functions of intestinal microflora in children. Curr Opin Gastroenterol 2013; 29: 31-38 [PMID: 23196853 DOI: 10.1097/MOG.0b013e32835a3500]
137 Döerffel Y, Pavel M, Loening-Baucke V, Swidsinski A. Common biostructure of the fecal flora in celiac disease, Crohn’s disease, and carcinoid tumors. Inflamm Bowel Dis 2008; 14: 1613-1614 [PMID: 18521905 DOI: 10.1002/ibd.20507]
138 van Vliet MJ, Tissing WJ, Dun CA, Meessen NE, Kamps WA, de Bont ES, Harmsen HJ. Chemotherapy treatment in pediatric patients with acute myeloid leukemia receiving antimicrobial prophylaxis leads to a relative increase of colonization with potentially pathogenic bacteria in the gut. Clin Infect Dis 2009; 49: 262-270 [PMID: 19514856 DOI: 10.1086/599346]
139 Huang Y, Yang W, Liu H, Duan J, Zhang Y, Liu M, Li H, Hou Z, Wu KK. Effect of high-dose methotrexate chemotherapy on intestinal Bifidobacteria, Lactobacillus and Escherichia coli in children with acute lymphoblastic leukemia. Exp Biol Med (Maywood) 2012; 237: 305-311 [PMID: 22362190 DOI: 10.1258/ebm.2011.011297]
140 Agirbasli H, Ozcan SA, Gedikoğlu G. Fecal fungal flora of pediatric healthy volunteers and immunosuppressed patients. Mycopathologia 2005; 159: 515-520 [PMID: 15983737]
141 Gammelsrud KW, Sandven P, Høiby EA, Sandvik L, Brandtzaeg P, Gaustad P. Colonization by Candida in children with cancer, children with cystic fibrosis, and healthy controls. Clin Microbiol
Castagnola E et al . Gut and liver infections in oncology

5865 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
Infect 2011; 17: 1875-1881 [PMID: 21745258 DOI: 10.1111/j.1469-0691.2011.03528.x]
142 Wang Y, Xue J, Zhou X, You M, Du Q, Yang X, He J, Zou J, Cheng L, Li M, Li Y, Zhu Y, Li J, Shi W, Xu X. Oral microbiota distinguishes acute lymphoblastic leukemia pediatric hosts from healthy populations. PLoS One 2014; 9: e102116 [PMID: 25025462 DOI: 10.1371/journal.pone.0102116]
143 Srithavaj T, Thaweboon S. Determination of oral microflora in irradiated ocular deformed children. Southeast Asian J Trop Med Public Health 2006; 37: 991-995 [PMID: 17333745]
144 Ye Y, Carlsson G, Agholme MB, Wilson JA, Roos A, Henriques-Normark B, Engstrand L, Modéer T, Pütsep K. Oral bacterial community dynamics in paediatric patients with malignancies in relation to chemotherapy-related oral mucositis: a prospective study. Clin Microbiol Infect 2013; 19: E559-E567 [PMID: 23829394 DOI: 10.1111/1469-0691.12287]
145 de Mendonça RM, de Araújo M, Levy CE, Morari J, Silva RA, Yunes JA, Brandalise SR. Prospective evaluation of HSV, Candida spp., and oral bacteria on the severity of oral mucositis in pediatric acute lymphoblastic leukemia. Support Care Cancer 2012; 20: 1101-1107 [PMID: 21597938 DOI: 10.1007/s00520-011-1190-0]
146 Sixou JL, Aubry-Leuliette A, De Medeiros-Battista O, Lejeune S, Jolivet-Gougeon A, Solhi-Pinsard H, Gandemer V, Barbosa-Rogier M, Bonnaure-Mallet M. Capnocytophaga in the dental plaque of immunocompromised children with cancer. Int J Paediatr Dent 2006; 16: 75-80 [PMID: 16430520]
147 Wada M, Nagata S, Saito M, Shimizu T, Yamashiro Y, Matsuki T, Asahara T, Nomoto K. Effects of the enteral administration of Bifidobacterium breve on patients undergoing chemotherapy for pediatric malignancies. Support Care Cancer 2010; 18: 751-759 [PMID: 19685085 DOI: 10.1007/s00520-009-0711-6]
148 Avcin SL, Pokorn M, Kitanovski L, Premru MM, Jazbec J. Bifidobacterium breve Sepsis in Child with High-Risk Acute Lymphoblastic Leukemia. Emerg Infect Dis 2015; 21: 1674-1675 [PMID: 26291071 DOI: 10.3201/eid2109.150097]
149 Cesaro S, Chinello P, Rossi L, Zanesco L. Saccharomyces cerevisiae fungemia in a neutropenic patient treated with Saccharomyces boulardii. Support Care Cancer 2000; 8: 504-505 [PMID: 11094997]
150 Kara A, Devrim İ, Bayram N, Katipoğlu N, Kıran E, Oruç Y, Demiray N, Apa H, Gülfidan G. Risk of vancomycin-resistant enterococci bloodstream infection among patients colonized with vancomycin-resistant enterococci. Braz J Infect Dis 2015; 19: 58-61 [PMID: 25529366 DOI: 10.1016/j.bjid.2014.09.010]
151 van der Velden WJ, Herbers AH, Netea MG, Blijlevens NM. Mucosal barrier injury, fever and infection in neutropenic patients with cancer: introducing the paradigm febrile mucositis. Br J Haematol 2014; 167: 441-452 [PMID: 25196917 DOI: 10.1111/bjh.13113]
152 Olczak-Kowalczyk D, Daszkiewicz M, Krasuska-Sławińska B, Gozdowski D, Daszkiewicz P, Fronc B, Semczuk K. Bacteria and Candida yeasts in inflammations of the oral mucosa in children with secondary immunodeficiency. J Oral Pathol Med 2012; 41: 568-576 [PMID: 23019688]
153 Brook I. The role of anaerobic bacteria in bacteremia. Anaerobe 2010; 16: 183-189 [PMID: 20025984 DOI: 10.1016/j.anaerobe.2009.12.001]
154 Sakaguchi S, Saito M, Tsuji H, Asahara T, Takata O, Fujimura J, Nagata S, Nomoto K, Shimizu T. Bacterial rRNA-targeted reverse transcription-PCR used to identify pathogens responsible for fever with neutropenia. J Clin Microbiol 2010; 48: 1624-1628 [PMID: 20351213 DOI: 10.1128/JCM.01724-09]
155 Huang WT, Chang LY, Hsueh PR, Lu CY, Shao PL, Huang FY, Lee PI, Chen CM, Lee CY, Huang LM. Clinical features and complications of viridans streptococci bloodstream infection in pediatric hemato-oncology patients. J Microbiol Immunol Infect 2007; 40: 349-354 [PMID: 17712470]
156 Alazmi W, Bustamante M, O’Loughlin C, Gonzalez J, Raskin JB. The association of Streptococcus bovis bacteremia and gastrointestinal diseases: a retrospective analysis. Dig Dis Sci 2006;
51: 732-736 [PMID: 16614996]157 Pasqualotto AC, Rosa DD, Medeiros LR, Severo LC. Candidaemia
and cancer: patients are not all the same. BMC Infect Dis 2006; 6: 50 [PMID: 16542444]
158 Butler KM. Enterococcal infection in children. Semin Pediatr Infect Dis 2006; 17: 128-139 [PMID: 16934707]
159 André N, Coze C, Gentet JC, Perez R, Bernard JL. Geotrichum candidum septicemia in a child with hepatoblastoma. Pediatr Infect Dis J 2004; 23: 86 [PMID: 14743060]
160 Posteraro B, Bruno S, Boccia S, Ruggiero A, Sanguinetti M, Romano Spica V, Ricciardi G, Fadda G. Candida parapsilosis bloodstream infection in pediatric oncology patients: results of an epidemiologic investigation. Infect Control Hosp Epidemiol 2004; 25: 641-645 [PMID: 15357154]
161 Safdar A, Armstrong D. Listeriosis in patients at a comprehensive cancer center, 1955-1997. Clin Infect Dis 2003; 37: 359-364 [PMID: 12884160]
162 Tunkel AR, Sepkowitz KA. Infections caused by viridans streptococci in patients with neutropenia. Clin Infect Dis 2002; 34: 1524-1529 [PMID: 12015700]
163 Moore DL. Essentials of paediatric infection control. Paediatr Child Health 2001; 6: 571-579 [PMID: 20084127]
164 Gray JW, George RH. Experience of vancomycin-resistant enterococci in a children’s hospital. J Hosp Infect 2000; 45: 11-18 [PMID: 10833339]
165 Caselli D, Cesaro S, Fagioli F, Carraro F, Ziino O, Zanazzo G, Meazza C, Colombini A, Castagnola E; Infectious Diseases Study Group of the Italian Association of Pediatric Hematology and Oncology (AIEOP). Incidence of colonization and bloodstream infection with carbapenem-resistant Enterobacteriaceae in children receiving antineoplastic chemotherapy in Italy. Infect Dis (Lond) 2016; 48: 152-155 [PMID: 26393496 DOI: 10.3109/23744235.2015.1087647]
166 Haeusler GM, Mechinaud F, Daley AJ, Starr M, Shann F, Connell TG, Bryant PA, Donath S, Curtis N. Antibiotic-resistant Gram-negative bacteremia in pediatric oncology patients--risk factors and outcomes. Pediatr Infect Dis J 2013; 32: 723-726 [PMID: 23838774 DOI: 10.1097/INF.0b013e31828aebc8]
167 Logan LK. Carbapenem-resistant enterobacteriaceae: an emerging problem in children. Clin Infect Dis 2012; 55: 852-859 [PMID: 22700827 DOI: 10.1093/cid/cis543]
168 Nolan SM, Gerber JS, Zaoutis T, Prasad P, Rettig S, Gross K, McGowan KL, Reilly AF, Coffin SE. Outbreak of vancomycin-resistant enterococcus colonization among pediatric oncology patients. Infect Control Hosp Epidemiol 2009; 30: 338-345 [PMID: 19239375 DOI: 10.1086/596202]
169 Kurucu N, Kul S, Tosun I, Erduran E, Köksal I. Fungemia and renal fungus ball formation with Candida norvegensis in a child with acute lymphoblastic leukemia. Turk J Pediatr 2011; 53: 448-451 [PMID: 21980850]
170 Lehrnbecher T, Frank C, Engels K, Kriener S, Groll AH, Schwabe D. Trends in the postmortem epidemiology of invasive fungal infections at a university hospital. J Infect 2010; 61: 259-265 [PMID: 20624423 DOI: 10.1016/j.jinf.2010.06.018]
171 Schwesinger G, Junghans D, Schröder G, Bernhardt H, Knoke M. Candidosis and aspergillosis as autopsy findings from 1994 to 2003. Mycoses 2005; 48: 176-180 [PMID: 15842333]
172 Roberts ME, Bishop JL, Fan X, Beer JL, Kum WW, Krebs DL, Huang M, Gill N, Priatel JJ, Finlay BB, Harder KW. Lyn deficiency leads to increased microbiota-dependent intestinal inflammation and susceptibility to enteric pathogens. J Immunol 2014; 193: 5249-5263 [PMID: 25339668 DOI: 10.4049/jimmunol.1302832]
173 Kobos R, Shukla N, Renaud T, Prockop SE, Boulad F, Steinherz PG. High-dose cyclophosphamide for the treatment of refractory T-cell acute lymphoblastic leukemia in children. J Pediatr Hematol Oncol 2014; 36: e265-e270 [PMID: 24327129 DOI: 10.1097/MPH.0000000000000080]
174 Trelinska J, Dachowska I, Kotulska K, Fendler W, Jozwiak S, Mlynarski W. Complications of mammalian target of rapamycin inhibitor anticancer treatment among patients with tuberous sclerosis
Castagnola E et al . Gut and liver infections in oncology

5866 July 7, 2016|Volume 22|Issue 25|WJG|www.wjgnet.com
complex are common and occasionally life-threatening. Anticancer Drugs 2015; 26: 437-442 [PMID: 25719621 DOI: 10.1097/CAD.0000000000000207]
175 Sachak T, Arnold MA, Naini BV, Graham RP, Shah SS, Cruise M, Park JY, Clark L, Lamps L, Frankel WL, Theodoropoulos N, Arnold CA. Neutropenic Enterocolitis: New Insights Into a Deadly Entity. Am J Surg Pathol 2015; 39: 1635-1642 [PMID: 26414225 DOI:
10.1097/PAS.0000000000000517]176 Miedema KG, de Bont ES, Elferink RF, van Vliet MJ, Nijhuis
CS, Kamps WA, Tissing WJ. The diagnostic value of CRP, IL-8, PCT, and sTREM-1 in the detection of bacterial infections in pediatric oncology patients with febrile neutropenia. Support Care Cancer 2011; 19: 1593-1600 [PMID: 20803037 DOI: 10.1007/s00520-010-0987-6]
P- Reviewer: Plaza MA, Yucel O S- Editor: Ma YJ L- Editor: A E- Editor: Wang CH
Castagnola E et al . Gut and liver infections in oncology

© 2016 Baishideng Publishing Group Inc. All rights reserved.
Published by Baishideng Publishing Group Inc8226 Regency Drive, Pleasanton, CA 94588, USA
Telephone: +1-925-223-8242Fax: +1-925-223-8243
E-mail: [email protected] Desk: http://www.wjgnet.com/esps/helpdesk.aspx
http://www.wjgnet.com
I S S N 1 0 0 7 - 9 3 2 7
9 7 7 1 0 07 9 3 2 0 45
2 5