
Vascular Endothelial Growth Factor Gene Polymorphisms and Risk of Primary Lung Cancer
6
Vascular endothelial growth factor gene polymorphisms in North Indian patients with end stage renal disease Swayam Prakash a , Narayan Prasad b , Raj K. Sharma b , Rehan M. Faridi a , Suraksha Agrawal a,⇑ a Department of Medical Genetics, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, India b Department of Nephrology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, India article info Article history: Received 18 August 2011 Received in revised form 30 December 2011 Accepted 23 January 2012 Available online 26 February 2012 Keywords: End stage renal disease (ESRD) Single Nucleotide Polymorphism (SNP) Vascular endothelial growth factor (VEGF) abstract Context: Vascular endothelial growth factor (VEGF) is involved in the development and differentiation of the vascular system. VEGF is expressed constitutively by epithelial cells from embryonic to adult kidneys and may play a key role in progression of kidney diseases. It is required for the growth and proliferation of glomerular and peritubular endothelial cells. In the kidney VEGF expression is prominently found in glomerular podocytes and in tubular epithelial cells, while VEGF receptors are mainly seen on preglomerular, glomerular, and peritubular endothelial cells. Objectives: We have investigated the role of VEGF gene polymorphisms ( 2578C/A, 2549 18 bp I/D, 1154 G/A and +936 C/T) as a susceptibility marker for end stage renal disease (ESRD). Participants and methods: We genotyped VEGF gene polymorphism in three hundred patients and three hundred and fifty ethnically matched unrelated healthy controls free from any renal disease. These mark- ers were studied using ARMS-PCR and PCR-RFLP methods. Patients were categorized on the basis of the histo-pathological subtypes into chronic glomerulonephritis (CGN = 109), hypertensive nephrosclerosis (HTN = 106) and chronic interstitial nephritis (CIN = 60). Results: VEGF 2578C and 2549D alleles were found to be ESRD causative alleles. It was observed that there was significant differences in the frequencies of the T allele of +936C/T polymorphism among CGN, HTN and CIN respectively. VEGF 1154AA genotype and A allele were associated significantly with CGN. T–G–A–D, T–A–C–I,C–G–A–D,C–A–C–D,C–G–C–I,C–A–A–D and T–G–C–D were seven haplotypes concurred in all the ESRD patients irrespective of underlying disease. While C–G–C–D & C–G–A–I haplo- types showed risk association in CGN & CIN, C–A–C–I was observed to play predisposing role in HTN. Conclusion: The results highlight the role of studied VEGF polymorphisms in end stage renal disease at large and subsequently in the three primary kidney diseases among the North Indian population. Ó 2012 Elsevier Ltd. All rights reserved. 1. Introduction Kidney is a highly vascularized organ. Vascular endothelial growth factor (VEGF) which is constitutively expressed by epithe- lial cells from embryonic to adult kidneys might play a key role in progression of kidney diseases. VEGF expression has been demon- strated in the podocytes [1] and mesangial cells in kidneys of patients with glomerulonephritis [2]; VEGF receptors have been detected in the endothelium of glomeruli and peritubular capillar- ies [2] which prevent progression of kidney diseases. It acts as a survival factor that allows cells to survive and proliferate under conditions of extreme stress, both in vivo and in vitro [3]. Admin- istered in case of acute glomerular injury VEGF causes induction of glomerular repair & resolution of glomerulonephritis associated with stimulation of angiogenesis & vascular remodeling [4]. It is a potent regulator of vasculogenesis and angiogenesis which may amplify acute inflammatory reactions. Transcription factor is activated on exposure of endothelial cells and macrophages to VEGF. Additional abnormalities besides hyper proliferation of blood vessels are observed upon exposure of tissues to high VEGF concentration [5]. Upon reduction or total inhibition of VEGF sup- ply impaired angiogenesis may occur which leads to the inhibition of organ development [6]. The VEGF gene is located on chromosome 6p 21.3 [7] which is highly polymorphic, especially in the promoter region, 5’ untrans- lated region (UTR) and 3’UTR [8,9].The polymorphisms in these regions have been reported to be associated with VEGF levels [9,10]. The 2578 C/A, 1154 G/A, 2549 I/D polymorphisms are reported in the 5’UTR of promoter region while the +936 C/T 1043-4666/$ - see front matter Ó 2012 Elsevier Ltd. All rights reserved. doi:10.1016/j.cyto.2012.01.020 ⇑ Corresponding author. Address: Department of Medical Genetics, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Raebareli Road, Lucknow (UP) 226014, India. Tel.: +091 522 2668004 8x4338 (O), 4346, 4347, 4339 (R); fax: +091 522 26680973/6680017. E-mail addresses: [email protected], [email protected] (S. Agrawal). Cytokine 58 (2012) 261–266 Contents lists available at SciVerse ScienceDirect Cytokine journal homepage: www.elsevier.com/locate/issn/10434666
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Vascular Endothelial Growth Factor Gene Polymorphisms and Risk of Primary Lung Cancer

Cytokine 58 (2012) 261–266
Contents lists available at SciVerse ScienceDirect
Cytokine
journal homepage: www.elsevier .com/locate / issn/10434666
Vascular endothelial growth factor gene polymorphisms in North Indianpatients with end stage renal disease
Swayam Prakash a, Narayan Prasad b, Raj K. Sharma b, Rehan M. Faridi a, Suraksha Agrawal a,⇑a Department of Medical Genetics, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, Indiab Department of Nephrology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, India
a r t i c l e i n f o a b s t r a c t
Article history:Received 18 August 2011Received in revised form 30 December 2011Accepted 23 January 2012Available online 26 February 2012
Keywords:End stage renal disease (ESRD)Single Nucleotide Polymorphism (SNP)Vascular endothelial growth factor (VEGF)
1043-4666/$ - see front matter � 2012 Elsevier Ltd. Adoi:10.1016/j.cyto.2012.01.020
⇑ Corresponding author. Address: Department oGandhi Post Graduate Institute of Medical Sciences, R226014, India. Tel.: +091 522 2668004 8x4338 (O), 43522 26680973/6680017.
E-mail addresses: [email protected], su(S. Agrawal).
Context: Vascular endothelial growth factor (VEGF) is involved in the development and differentiation ofthe vascular system. VEGF is expressed constitutively by epithelial cells from embryonic to adult kidneysand may play a key role in progression of kidney diseases. It is required for the growth and proliferation ofglomerular and peritubular endothelial cells. In the kidney VEGF expression is prominently found inglomerular podocytes and in tubular epithelial cells, while VEGF receptors are mainly seen onpreglomerular, glomerular, and peritubular endothelial cells.Objectives: We have investigated the role of VEGF gene polymorphisms (�2578C/A,�2549 18 bp I/D,�1154 G/A and +936 C/T) as a susceptibility marker for end stage renal disease (ESRD).Participants and methods: We genotyped VEGF gene polymorphism in three hundred patients and threehundred and fifty ethnically matched unrelated healthy controls free from any renal disease. These mark-ers were studied using ARMS-PCR and PCR-RFLP methods. Patients were categorized on the basis of thehisto-pathological subtypes into chronic glomerulonephritis (CGN = 109), hypertensive nephrosclerosis(HTN = 106) and chronic interstitial nephritis (CIN = 60).Results: VEGF �2578C and �2549D alleles were found to be ESRD causative alleles. It was observedthat there was significant differences in the frequencies of the T allele of +936C/T polymorphism amongCGN, HTN and CIN respectively. VEGF �1154AA genotype and A allele were associated significantly withCGN. T–G–A–D, T–A–C–I,C–G–A–D,C–A–C–D,C–G–C–I,C–A–A–D and T–G–C–D were seven haplotypesconcurred in all the ESRD patients irrespective of underlying disease. While C–G–C–D & C–G–A–I haplo-types showed risk association in CGN & CIN, C–A–C–I was observed to play predisposing role in HTN.Conclusion: The results highlight the role of studied VEGF polymorphisms in end stage renal disease atlarge and subsequently in the three primary kidney diseases among the North Indian population.
� 2012 Elsevier Ltd. All rights reserved.
1. Introduction
Kidney is a highly vascularized organ. Vascular endothelialgrowth factor (VEGF) which is constitutively expressed by epithe-lial cells from embryonic to adult kidneys might play a key role inprogression of kidney diseases. VEGF expression has been demon-strated in the podocytes [1] and mesangial cells in kidneys ofpatients with glomerulonephritis [2]; VEGF receptors have beendetected in the endothelium of glomeruli and peritubular capillar-ies [2] which prevent progression of kidney diseases. It acts as asurvival factor that allows cells to survive and proliferate under
ll rights reserved.
f Medical Genetics, Sanjayaebareli Road, Lucknow (UP)46, 4347, 4339 (R); fax: +091
conditions of extreme stress, both in vivo and in vitro [3]. Admin-istered in case of acute glomerular injury VEGF causes induction ofglomerular repair & resolution of glomerulonephritis associatedwith stimulation of angiogenesis & vascular remodeling [4]. It isa potent regulator of vasculogenesis and angiogenesis which mayamplify acute inflammatory reactions. Transcription factor isactivated on exposure of endothelial cells and macrophages toVEGF. Additional abnormalities besides hyper proliferation ofblood vessels are observed upon exposure of tissues to high VEGFconcentration [5]. Upon reduction or total inhibition of VEGF sup-ply impaired angiogenesis may occur which leads to the inhibitionof organ development [6].
The VEGF gene is located on chromosome 6p 21.3 [7] which ishighly polymorphic, especially in the promoter region, 5’ untrans-lated region (UTR) and 3’UTR [8,9].The polymorphisms in theseregions have been reported to be associated with VEGF levels[9,10]. The �2578 C/A, �1154 G/A, �2549 I/D polymorphisms arereported in the 5’UTR of promoter region while the +936 C/T

262 S. Prakash et al. / Cytokine 58 (2012) 261–266
polymorphism in the 3’UTR of promoter region. VEGF is expressedconstitutively in the adult kidney and over expressed in hypoxicand inflammatory renal disease. Genetically controlled variationin VEGF production may influence susceptibility to progression ofkidney diseases. Present study was aimed to investigate the rolesof �2578C/A, �1154 G/A, �2549 18 bp I/D and +936 C/T polymor-phisms and their haplotypes among ESRD patients, subsequentlystudying their incidence in primary kidney diseases namelychronic glomerulonephritis (CGN), chronic interstitial nephropathy(CIN) and hypertensive nephrosclerosis (HTN). This is the firststudy evaluating these polymorphisms among the North Indianpopulation.
2. Materials and methods
2.1. Subjects
Three hundred ESRD patients [Male = 244 (81%), Female = 56(19%)] and three hundred and fifty healthy age and sex matchedNorth Indians were included as controls [Male = 280 (80%), Fe-male = 70 (20%)] in this study. The inclusion criteria for patientselection was constantly elevated serum creatinine level above nor-mal range (ranging from 3.4 to 15.8 mg/dl) or creatinine clearance<15 ml/min/1.73 m2 and were recommended for renal transplanta-tion. We have used Cockcroft Gault for calculation of creatinineclearance. All the patients selected for the study were on regularhemodialysis. Patients were considered hypertensive if they wereon anti hypertensive medication or if systolic or diastolic bloodpressure was P140 or 90 mm Hg (blood pressure was measuredtwice with a mercury sphygmomanometer, in supine position, afterat least 10 min of rest, and results were averaged). For each patient,various information like age, gender, urinary protein level, bloodurea nitrogen, blood pressure and complete lipid profile were col-lected. The type of chronic kidney disease was established by doingultrasound and/or CT scan of the kidneys followed by histopathol-ogical evaluation of the renal biopsy specimen. Patients were cate-gorized on the basis of the histopathological subtypes intochronicglomerulonephritis (CGN = 109), chronic interstitial nephritis(CIN = 106), hypertensive nephrosclerosis (HTN = 60). All patientswith diabetic nephropathy were excluded from the study.
Approximately 85% of the patients were male hence care wastaken to include more number of male controls in order to ruleout gender bias. Controls with risk factors like family history ofhypertension, diabetes mellitus and hyperlipidemia were excludedfrom the study. The criterion of defining control sample as normalwas totally based on the absence of any kidney disease determinedfrom the serum creatinine level. The mean creatinine level of con-trols was found to be 0.74 ± 0.23 while that of patients was7.17 ± 3.1.Similar kind of proforma as for patients was also filledfor controls. The study was performed as per the ethical standardslaid down by the Declaration of Helsinki. Informed written consent
Fig. 1. Vegf +936C/T polymorphism Lane 1–50 bp ladder, Lane 2,3-TT genotype, Lane 4genotype, Lane 9,10-AA genotype, Lane 11,12-CC genotype; VEGF -1154G/A polymorph
was obtained from both the patients and controls prior to theirinclusion in the study. Further the study was approved by the insti-tute ethics committee.
2.2. Sample collection, DNA extraction and VEGF Genotyping
Blood samples for measuring the serum biochemical parame-ters were obtained in the morning after eight hours of fasting.For DNA extraction, 3.0 ml of venous blood from each study subjectwas collected in an EDTA vial. Genomic DNA was obtained usinggenomic DNA extraction kit from Quiagen (Brand GMbH and CoKG, Cat # 51104).
Amplification of the four regions of the VEGF gene containing thepolymorphisms �2578C/A, �1154G/A, �2549 I/D, and +936C/Twere carried out in a thermal cycler (Mastercycler gradient; Eppen-dorf, Hamburg, Germany).Genotype analyses of �2578 C/A and�1154G/A were based on ARMS PCR and RFLP was used for+936C/T polymorphisms as explained by Papazoglou et al. [11].Primers used for the genotyping purpose is shown in supplemen-tary table (Supplementary Table 1). In case of the VEGF + 936C/T,the PCR product was digested overnight with NlaIII restrictionenzyme (New England BioLabs, Beverly, MA,USA). The VEGF 936Tallele was cut into two fragments of 122 bp and 86 bp, whereasthe VEGF 936C allele remained uncut with a length of 208 bp(Fig. 1).
The �2549 I/D polymorphism was genotyped using a commonset of primers as mentioned by Buraczynska et al. [12]. PCR andRFLP products were run on 2% agarose and visualized using ethi-dium bromide (Fig. 2). The genotyping was done in a doubleblind manner by two investigators and after decoding nearly15% samples required re-genotyping.
2.3. Statistical analysis
The sample size for both the patients and controls was calcu-lated under the guidance of a statistician. Differences in the VEGFgenotypes, allele frequencies and haplotypes between the studyand control groups were analyzed with the Fisher exact test andp values <.05 were considered statistically significant. Bonferronicorrection to the p-value was applied. The Odds Ratio (OR) wasused as a measure of the strength of association between geno-types, allele frequencies and haplotypes. Haplotypes were gener-ated using Arlequin software and statistical analysis was doneusing SPSS software version 13.Allele frequencies were calculatedas the number of occurrences of the test allele in the populationdivided by the total number of alleles.
3. Results
Demographic characteristics and baseline laboratory data areprovided in Table 1. Two most important renal function
& 6-CT genotype, Lane 5-CC genotype; VEGF �2578C/A polymorphism Lane 7,8-CAism Lane 13,14-AA genotype, Lane 15,16-GA genotype.

Fig. 2. VEGF �2549 I/D polymorphism: lane A – 50 bp ladder, Lane B – DDgenotype, Lane C – ID genotype, Lane D – DD genotype D.
Table 1Biochemical parameters.
Parameters (SI) Patients = 300(Mean ± SD)
Controls = 350(Mean ± SD)
Age (years) 37.879 ± 11.09 33.95 ± 8.9Gender (male,female) 244 (81)/56 (19) 280(80)/70(20)Systolic Blood Pressure
(mmHg)149.7 ± 17.8 112.8 ± 8.4*
Diastolic Blood Pressure(mmHg)
88.66 ± 6.1 77.5 ± 5.4*
S.Creatinine (mg/dl) 7.17 ± 3.1 0.74 ± 0.23*
S.Albumin (mg/dl) 3.9 ± 1.4 3.97 ± 0.56*
Proteinurea (mg/mmol) 4.3 ± 1.2 0.54 ± 0.39*
S.Glucose (mg/dl) 104.4 ± 30.6 76.4 ± 6.8*
S.Uric (mg/dl) 8.52 ± 2.7 5.32 ± 1.04*
S.BUN (mg/dl) 47.30 ± 23.1 10.2 ± 3.1*
S.AKLP (U/l) 181.85 ± 15.4 86.7 ± 19.7*
S.Na (mmol/l) 153.73 ± 4.2 138.4 ± 2.5*
S.K (mmol/l) 5.9 ± 0.8 3.5 ± 0.3*
S.Phos (mg/dl) 4.9 ± 0.5 3.6 ± 0.3*
S.TG (mg/dl) 159.7 ± 61.4 144.3 ± 64.4*
S.TC (mg/dl) 158.2 ± 30.7 133.7 ± 34.2*
S.HDL (mg/dl) 37.8 ± 7.0 22.9 ± 7.1*
S.LDL (mg/dl) 104.6 ± 29.8 81.7 ± 27.2*
S.VLDL (mg/dl) 25.7 ± 9.3 34.7 ± 12.4*
Type of dialysis Hemodialysis NANumber of Dialysis(range) 1–230 NA
* Statistically significant (p 6 0.05); NA = not applicable; data are presented inmean ± SD.
S. Prakash et al. / Cytokine 58 (2012) 261–266 263
parameters namely serum creatinine level and protein ureashowed highly significant differences (p < 0.0001) between casesand controls, revealing that controls included in the present studywere true negative controls. Different genotypic, allele and allelecarriage frequency are shown in Table 2. Allele frequencies in pa-tients and controls were in Hardy Weinberg Equilibrium.
3.1. Genotypes and alleles frequency in cases and controls
The mutant homozygous genotype (AA) of the �1154G/A poly-morphism was significantly higher in cases (21%) as compared tocontrols (12%) showing almost two fold higher risk of ESRD. How-ever, we did not find any statistical significance against the GGgenotype of the �1154G/A polymorphism which was found sig-nificantly (55.3%) among ESRD patients. The frequency of CCand CA genotypes of �2578C/A polymorphism among caseswas 55% and 31%, while among control group it was 50.6%and 40%, respectively. In case of +936 C/T polymorphism thefrequency of homozygous TT and heterozygous CT genotype inpatient group was 18% and 9.3% respectively. In control groupit was 3.1% and 10% respectively and both the groups differedsignificantly. Similarly in�2549 I/D polymorphism the DD geno-type was found in 27.7% patients against 19.4% controls while
the D allele was figured in 80.6% of the patient and 75.4% ofthe control population. Significant difference at genotypic andallelic level was concurred between both the groups.
All the polymorphisms were also analysed in ESRD patientswith different types of primary kidney diseases i.e. Chronic Glo-merulonephritis (CGN), Chronic Interstitial Nephritis (CIN), Hyper-tensive Nephrosclerosis (HTN) as shown in Table 3, but not inPolycystic Kidney Disease as the sample size was small. CGN wasfound to be the most common type (36.3%) followed by HTN(35.3%), CIN (20%) and PKD (8.3%). The homozygous genotype(AA) of �1154G/A polymorphism was found in 32 (29.3%) casessuffering from CGN and revealed three fold risk while �1154 A al-lele was associated with 39.9% CGN and 34% HTN cases respec-tively. In �2578C/A polymorphism, the risk associated AAhomozygous genotype was observed in 57 cases (53.7%) and A al-lele found in 68% HTN cases.
Considering the +936C/T polymorphism, the homozygous TTgenotype was observed to be statistically significant and risk asso-ciated among the CGN, HTN and CIN cases. Similarly three fold andtwofold risk were seen against the heterozygous CT genotype inCGN and HTN cases respectively. The distribution of T allele of+936C/T was 22.5% of CGN cases;22.7% of HTN cases and 19.1%of CIN cases. The DD genotype of �2549 I/D polymorphism wasfound to be twofold risk associated while the D allele was observedin 58% HTN cases and was susceptible to HTN.
3.2. Haplotype frequency in different kidney diseases
Fifteen haplotypes were found both in the ESRD group & con-trols. The more prevalent haplotypes and the one which occurredwith a frequency of more than 5% against CGN, HTN and CIN andrevealed protective or risk predisposing effect are shown in Table4.T–A–A–D was the unique haplotype found only in ESRD caseswhile T–A–A–I was observed only among controls. The T–G–A–D,T–A–C–I,C–G–A–D,C–A–C–D,C–G–C–I,C–A–A–D & T–G–C–Dwere risk associated haplotypes found in the North Indian ESRDpopulation. Some of the haplotypes as shown in Table 4 were ob-served to be risk associated in some of the diseases like C–G–C–D among CGN, HTN and CIN cases; C–A–C–I among HTN casesand C–G–A–I among CGN and CIN patients.
4. Discussion
The expression of different VEGF isoforms in normal humanglomeruli is variable. There exist inter and intra individual varia-tion [13].The function of constitutively expressed VEGF and VEGFreceptors in normal kidney is not known. It is suggested that VEGFis expressed by visceral epithelial cells and its binding sites arelocalized on glomerular endothelial cells. In the induction andmaintenance of the fenestrate in glomerular capillary endothelialcells, VEGF may be involved [14]. In the present study, we haveobserved significant association of VEGF gene polymorphisms withESRD among North Indians.
Various SNP’s located in the VEGF gene may alter gene tran-scription which affects the VEGF plasma level. Studies have shownthe association of VEGF polymorphisms with VEGF plasma levelsand demonstrated that mutant alleles of �1154 G/A, �2578 C/A,�2549 I/D and +936C/T lead to low VEGF expression [9,12,15].The exact mechanism for the development of ESRD with VEGFpolymorphism has not been established till date. However, thispolymorphism is associated with altered plasma VEGF levels whichmay cause ESRD. This is presumed to occur due to reduced tran-scription of the gene as a result of reduced binding of transcriptionfactor AP-4 to the polymorphic site [10].
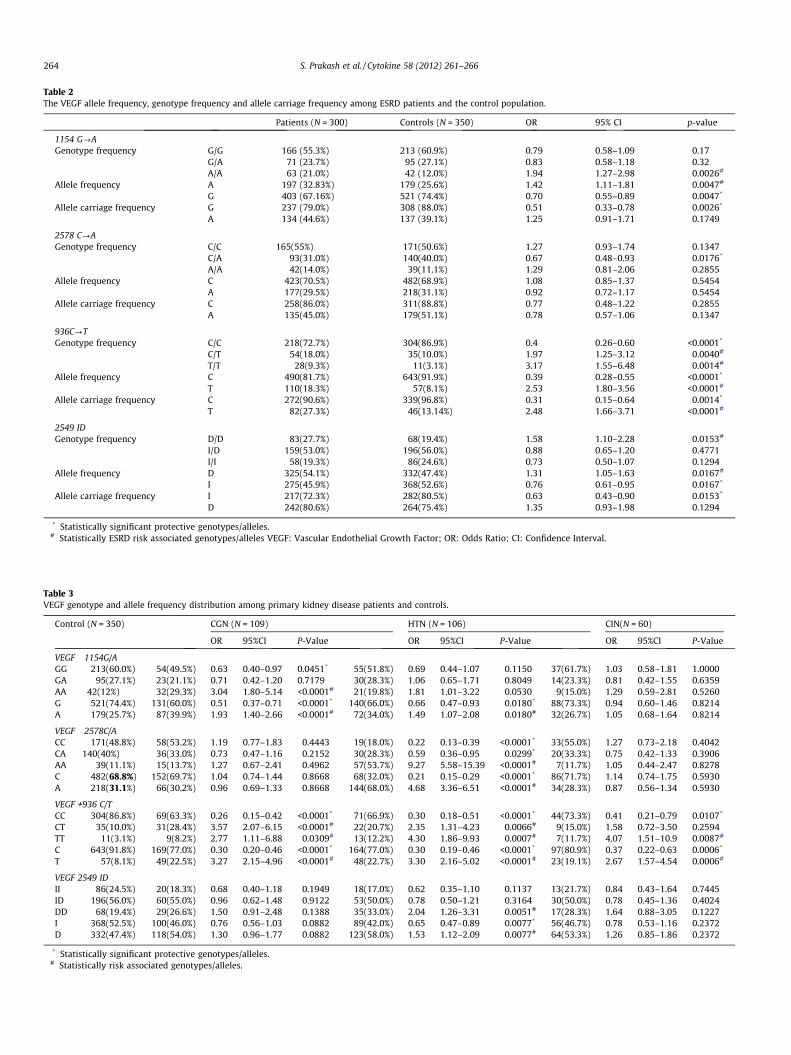
Table 2The VEGF allele frequency, genotype frequency and allele carriage frequency among ESRD patients and the control population.
Patients (N = 300) Controls (N = 350) OR 95% CI p-value
1154 G?AGenotype frequency G/G 166 (55.3%) 213 (60.9%) 0.79 0.58–1.09 0.17
G/A 71 (23.7%) 95 (27.1%) 0.83 0.58–1.18 0.32A/A 63 (21.0%) 42 (12.0%) 1.94 1.27–2.98 0.0026#
Allele frequency A 197 (32.83%) 179 (25.6%) 1.42 1.11–1.81 0.0047#
G 403 (67.16%) 521 (74.4%) 0.70 0.55–0.89 0.0047*
Allele carriage frequency G 237 (79.0%) 308 (88.0%) 0.51 0.33–0.78 0.0026*
A 134 (44.6%) 137 (39.1%) 1.25 0.91–1.71 0.1749
2578 C?AGenotype frequency C/C 165(55%) 171(50.6%) 1.27 0.93–1.74 0.1347
C/A 93(31.0%) 140(40.0%) 0.67 0.48–0.93 0.0176*
A/A 42(14.0%) 39(11.1%) 1.29 0.81–2.06 0.2855Allele frequency C 423(70.5%) 482(68.9%) 1.08 0.85–1.37 0.5454
A 177(29.5%) 218(31.1%) 0.92 0.72–1.17 0.5454Allele carriage frequency C 258(86.0%) 311(88.8%) 0.77 0.48–1.22 0.2855
A 135(45.0%) 179(51.1%) 0.78 0.57–1.06 0.1347
936C?TGenotype frequency C/C 218(72.7%) 304(86.9%) 0.4 0.26–0.60 <0.0001*
C/T 54(18.0%) 35(10.0%) 1.97 1.25–3.12 0.0040#
T/T 28(9.3%) 11(3.1%) 3.17 1.55–6.48 0.0014#
Allele frequency C 490(81.7%) 643(91.9%) 0.39 0.28–0.55 <0.0001*
T 110(18.3%) 57(8.1%) 2.53 1.80–3.56 <0.0001#
Allele carriage frequency C 272(90.6%) 339(96.8%) 0.31 0.15–0.64 0.0014*
T 82(27.3%) 46(13.14%) 2.48 1.66–3.71 <0.0001#
2549 IDGenotype frequency D/D 83(27.7%) 68(19.4%) 1.58 1.10–2.28 0.0153#
I/D 159(53.0%) 196(56.0%) 0.88 0.65–1.20 0.4771I/I 58(19.3%) 86(24.6%) 0.73 0.50–1.07 0.1294
Allele frequency D 325(54.1%) 332(47.4%) 1.31 1.05–1.63 0.0167#
I 275(45.9%) 368(52.6%) 0.76 0.61–0.95 0.0167*
Allele carriage frequency I 217(72.3%) 282(80.5%) 0.63 0.43–0.90 0.0153*
D 242(80.6%) 264(75.4%) 1.35 0.93–1.98 0.1294
* Statistically significant protective genotypes/alleles.# Statistically ESRD risk associated genotypes/alleles VEGF: Vascular Endothelial Growth Factor; OR: Odds Ratio; CI: Confidence Interval.
Table 3VEGF genotype and allele frequency distribution among primary kidney disease patients and controls.
Control (N = 350) CGN (N = 109) HTN (N = 106) CIN(N = 60)
OR 95%CI P-Value OR 95%CI P-Value OR 95%CI P-Value
VEGF �1154G/AGG 213(60.0%) 54(49.5%) 0.63 0.40–0.97 0.0451* 55(51.8%) 0.69 0.44–1.07 0.1150 37(61.7%) 1.03 0.58–1.81 1.0000GA 95(27.1%) 23(21.1%) 0.71 0.42–1.20 0.7179 30(28.3%) 1.06 0.65–1.71 0.8049 14(23.3%) 0.81 0.42–1.55 0.6359AA 42(12%) 32(29.3%) 3.04 1.80–5.14 <0.0001# 21(19.8%) 1.81 1.01–3.22 0.0530 9(15.0%) 1.29 0.59–2.81 0.5260G 521(74.4%) 131(60.0%) 0.51 0.37–0.71 <0.0001* 140(66.0%) 0.66 0.47–0.93 0.0180* 88(73.3%) 0.94 0.60–1.46 0.8214A 179(25.7%) 87(39.9%) 1.93 1.40–2.66 <0.0001# 72(34.0%) 1.49 1.07–2.08 0.0180# 32(26.7%) 1.05 0.68–1.64 0.8214
VEGF �2578C/ACC 171(48.8%) 58(53.2%) 1.19 0.77–1.83 0.4443 19(18.0%) 0.22 0.13–0.39 <0.0001* 33(55.0%) 1.27 0.73–2.18 0.4042CA 140(40%) 36(33.0%) 0.73 0.47–1.16 0.2152 30(28.3%) 0.59 0.36–0.95 0.0299* 20(33.3%) 0.75 0.42–1.33 0.3906AA 39(11.1%) 15(13.7%) 1.27 0.67–2.41 0.4962 57(53.7%) 9.27 5.58–15.39 <0.0001# 7(11.7%) 1.05 0.44–2.47 0.8278C 482(68.8%) 152(69.7%) 1.04 0.74–1.44 0.8668 68(32.0%) 0.21 0.15–0.29 <0.0001* 86(71.7%) 1.14 0.74–1.75 0.5930A 218(31.1%) 66(30.2%) 0.96 0.69–1.33 0.8668 144(68.0%) 4.68 3.36–6.51 <0.0001# 34(28.3%) 0.87 0.56–1.34 0.5930
VEGF +936 C/TCC 304(86.8%) 69(63.3%) 0.26 0.15–0.42 <0.0001* 71(66.9%) 0.30 0.18–0.51 <0.0001* 44(73.3%) 0.41 0.21–0.79 0.0107*
CT 35(10.0%) 31(28.4%) 3.57 2.07–6.15 <0.0001# 22(20.7%) 2.35 1.31–4.23 0.0066# 9(15.0%) 1.58 0.72–3.50 0.2594TT 11(3.1%) 9(8.2%) 2.77 1.11–6.88 0.0309# 13(12.2%) 4.30 1.86–9.93 0.0007# 7(11.7%) 4.07 1.51–10.9 0.0087#
C 643(91.8%) 169(77.0%) 0.30 0.20–0.46 <0.0001* 164(77.0%) 0.30 0.19–0.46 <0.0001* 97(80.9%) 0.37 0.22–0.63 0.0006*
T 57(8.1%) 49(22.5%) 3.27 2.15–4.96 <0.0001# 48(22.7%) 3.30 2.16–5.02 <0.0001# 23(19.1%) 2.67 1.57–4.54 0.0006#
VEGF 2549 IDII 86(24.5%) 20(18.3%) 0.68 0.40–1.18 0.1949 18(17.0%) 0.62 0.35–1.10 0.1137 13(21.7%) 0.84 0.43–1.64 0.7445ID 196(56.0%) 60(55.0%) 0.96 0.62–1.48 0.9122 53(50.0%) 0.78 0.50–1.21 0.3164 30(50.0%) 0.78 0.45–1.36 0.4024DD 68(19.4%) 29(26.6%) 1.50 0.91–2.48 0.1388 35(33.0%) 2.04 1.26–3.31 0.0051# 17(28.3%) 1.64 0.88–3.05 0.1227I 368(52.5%) 100(46.0%) 0.76 0.56–1.03 0.0882 89(42.0%) 0.65 0.47–0.89 0.0077* 56(46.7%) 0.78 0.53–1.16 0.2372D 332(47.4%) 118(54.0%) 1.30 0.96–1.77 0.0882 123(58.0%) 1.53 1.12–2.09 0.0077# 64(53.3%) 1.26 0.85–1.86 0.2372
* Statistically significant protective genotypes/alleles.# Statistically risk associated genotypes/alleles.
264 S. Prakash et al. / Cytokine 58 (2012) 261–266

Tabl
e4
Com
pari
son
ofha
plot
ype
dist
ribu
tion
amon
gV
EGF
(115
4G
/A�
2578
C/A�
936
C/T�
2549
I/D
)in
ESRD
case
san
dco
ntro
lsan
dpr
imar
yki
dney
dise
ase
case
san
dco
ntro
ls.
Hap
loty
peC
ontr
ol(N
=35
0)ES
RD
(N=
300)
CG
N(N
=10
9)H
TN(N
=10
6)C
IN(N
=60
)
Freq
uen
cyO
R95
%C
IP-
Val
ue
Freq
uen
cyO
R95
%C
IP-
Val
ue
Freq
uen
cyO
R95
%C
IP-
Val
ue
Freq
uen
cyO
R95
%C
IP-
Val
ue
C–A
–A–I
57(1
6.2%
)36
(12.
0%)
0.72
0.46
–1.1
10.
1603
16(1
4.6%
)0.
890.
50–1
.59
0.77
5617
(16.
0%)
1.04
0.59
–1.8
41.
0000
––
––
T–G
–A–D
7(2
.0%
)18
(6.0
%)
3.06
1.27
–7.3
80.
0135
#12
(11.
0%)
5.76
2.24
–14.
840.
0002
#9
(8.4
%)
0.22
0.08
–0.6
10.
0041
*–
––
–T–
A–C
–I1
(0.2
%)
20(6
.6%
)24
.10
3.22
–180
.20.
0001
#–
––
––
––
–6
(10.
0%)
36.7
84.
38–3
08.5
8<0
.000
1#⁄
C–G
–A–D
47(1
3.4%
)58
(19.
3%)
1.48
0.99
–2.2
20.
0531
#14
(12.
8%)
0.95
0.51
–1.7
61.
0000
19(1
7.9%
)0.
730.
41–1
.27
0.28
9522
(36.
6%)
3.11
1.80
–5.4
00.
0001
#
C–A
–C–D
36(1
0.2%
)65
(21.
6%)
2.24
1.46
–3.4
2<0
.000
2#32
(29.
3%)
3.17
1.91
–5.2
4<0
.000
1#21
(19.
8%)
0.49
0.28
–0.8
60.
0153
*9
(15.
0%)
1.49
0.70
–3.1
90.
2812
T–G
–C–I
12(3
.4%
)17
(5.6
%)
1.67
0.79
–3.5
30.
1907
10(9
.1%
)2.
751.
17–6
.47
0.02
20#
10(9
.4%
)0.
350.
15–0
.82
0.01
96*
8(1
3.3%
)4.
091.
63–1
0.24
0.00
45#
C–A
–C–I
71(2
0.2%
)29
(9.6
%)
0.44
0.28
–0.7
00.
0003
*14
(12.
8%)
0.60
0.33
–1.1
00.
1088
8(7
.5%
)2.
871.
36–6
.08
0.00
31#
12(2
0.0%
)0.
980.
51–1
.87
1.00
00C
–G–C
–D20
8(5
9.4%
)10
7(3
5.6%
)0.
510.
39–0
.66
<0.0
001*
28(2
5.6%
)0.
340.
22–0
.53
<0.0
001*
35(3
3.0%
)2.
131.
43–3
.18
<0.0
001#
25(4
1.6%
)0.
620.
38–0
.99
0.04
88*
C–G
–C–I
124
(35.
4%)
146
(48.
6%)
1.49
1.14
–1.9
50.
0039
#47
(43.
1%)
1.27
0.87
–1.8
60.
2317
46(4
3.3%
)0.
770.
53–1
.13
0.19
2120
(33.
3%)
0.92
0.55
–1.5
50.
8967
T–A
–C–D
9(2
.5%
)–
––
–8
(7.3
%)
2.92
1.11
–7.6
70.
0384
#9
(8.4
%)
0.29
0.11
–0.7
50.
0193
*–
––
–C
–A–A
–D4(
1.1%
)13
(11.
0%)
10.1
23.
56–2
8.76
<0.0
001#
12(1
1.0%
)10
.13
3.23
–31.
77<0
.000
1#15
(14.
1%)
0.07
0.02
–0.2
3<0
.000
1*–
––
–C
–G–A
–I96
(27.
4%)
16(5
3.3%
)0.
170.
10–0
.29
<0.0
001*
6(5
.5%
)0.
170.
07–0
.41
<0.0
001*
––
––
6(1
0.0%
)0.
330.
14–0
.77
0.00
65*
T–G
–C–D
21(6
.0%
)30
(10.
0%)
1.70
0.96
–3.0
00.
8646
#10
(9.1
%)
1.55
0.72
–3.3
50.
2826
14(1
3.2%
)0.
430.
21–0
.87
0.02
36*
4(6
.6%
)1.
110.
37–3
.30
0.77
57
*St
atis
tica
lly
sign
ifica
nt
prot
ecti
veh
aplo
type
.#
Stat
isti
call
yri
skas
soci
ated
hap
loty
pe.
S. Prakash et al. / Cytokine 58 (2012) 261–266 265
In the present study, we have observed significant association ofthe VEGF gene polymorphisms with ESRD among North Indians.There was 1.94-fold risk against mutant homozygous genotype(AA) of the �1154G/A polymorphism among ESRD cases; homozy-gous TT genotype and heterozygous CT genotypes of +936 C/Tpolymorphism showed 3.17-fold and 1.97-fold risk associationsrespectively. The homozygous DD genotype of �2549 I/D polymor-phism revealed 1.58-fold risk as compared to healthy controlpopulation.
The association of these polymorphisms with graft survival wasalso observed in renal transplant recipients. When the recipientneutrophils and macrophages are exposed to reperfusion theninfiltration of the allograft occurs which leads to VEGF production.Increased expression of VEGF is observed in renal interstitiumduring renal allograft rejection. VEGF genotype is an independentpredicting factor for patient mortality [16].The �1154 G/A poly-morphism in the promoter region is believed to regulate geneexpression, with A allele leading to reduced plasma VEGF levels[8,15]. �1154 G allele is functionally associated with in vitro VEGFproduction & cells from �1154G/G homozygous individuals andproduce significantly more VEGF than �1154A/A homozygotes[15]. Among North Indian population we observed 1.42-fold riskassociation against the A allele of �1154 G/A polymorphism. The�2578C/A and �2549 I/D [8] polymorphisms are associated withdifferential gene expression which results into altered angiogene-sis. In a study of VEGF polymorphism on peritoneal dialysispatients, the AA genotype of VEGF promoter at �2578 positionwas associated with progressive increase in peritoneal transport.The CA/AA genotype at �2578 position revealed lower serum VEGFlevel but higher VEGF mRNA gene expression from peritoneal dial-ysis effluent in comparison to the wild-type CC genotype. Further-more, the CA/AA genotype at this position was also associated witha worse actuarial survival in peritoneal dialysis patients[16].�2578 C/C and C/A genotypes were associated with increasedrejection risk [15].
Our study has demonstrated the potential association of thestudied VEGF gene polymorphisms with basic kidney diseasesCGN, HTN and CIN, which are one of the underlying causes of ESRD.CGN is characterized by slowly progressive and irreversible glo-merular and tubuleinterstitial fibrosis, leading to a reduction inthe glomerular filtration rate (GFR) and retention of uremic toxins.Safrankova et al. [17] showed risk association against CC genotypeof �2578 C/A polymorphism. In our study the frequency distribu-tion of homozygous mutant homozygous AA and wild homozygousCC genotypes of VEGF �2578C/A polymorphism were significantlyhigher among CGN cases than in controls & the frequency of C al-lele was 69.72%, which was strikingly higher. The AA genotype of�1154G/A polymorphism was seen in most of the CGN cases(29.3%) and showed 3.04-fold risk association with CGN whilethe A allele figured a 1.93-fold risk association. The CC genotypeand C allele of the +936C/T polymorphism and D allele of�2549I/D polymorphism were susceptible to CGN.
Inflammatory pathways may be initiated due to hypertensionand this possibly act synergistically with alloantigen-dependentfactors on graft injury [18].Initiation of the immune response alongwith induction of growth factors traditionally caused may be thealloantigen dependent factors such as acute rejection. In an earlierstudy it has been demonstrated that homozygous mutant AA geno-type of VEGF �1154G/A occurred with a higher frequency as com-pared to homozygous wild GG genotype among HTN patientsthan in control population [19] which is in concordance with thecurrent study. Against A allele of the�1154G/A and�2578C/A poly-morphism 1.49-fold and 4.68-fold risk association respectivelywhile 3.3-fold risk against the T allele of +936C/T polymorphismand 1.5-fold risk against D allele of the �2549I/D polymorphismwere established among HTN cases as compared to the control

266 S. Prakash et al. / Cytokine 58 (2012) 261–266
population. We have seen that there is significant risk association ofCA & CC genotypes of�2578 C/A polymorphism and CC genotype of+936C/T polymorphism with HTN.
New local antigen expression, inflammatory cell infiltration, andactivation of pro-inflammatory and chemo-attractant cytokinesmay be due to lethal or sub lethal injury to renal cells which maylead to acute or chronic nephritis. It is observed that the nuclearfactor kappa B (NFjB) like nuclear transcription factors are acti-vated in injured kidney cells [20], and release pro-inflammatorycytokines in the interstitium which may cause chronic tubuleinter-stitial inflammation. None of the polymorphisms of VEGF haveshown any association with CIN except TT genotype and T alleleof +936 C/T.
VEGF haplotypes have been correlated with VEGF plasma levelsin one of the earlier study[21].Particular haplotypes especiallythose involving low expression alleles may predispose to ESRDdue to decrease in VEGF production [22]. While studying the vari-ous primary kidney diseases we obtained 15 haplotypes each forCGN and HTN while 14 haplotypes against CIN.C–G–C–D andC–G–A–I haplotypes showed causative effect in CGN & CIN.C–A–CI played predisposing role in HTN.
5. Conclusions
To conclude, our study has found the association of �2578C/Cand �2549D/D genotype in end stage renal disease patients. Fur-ther we have shown the association of T allele of +936C/T polymor-phism which was found to predispose CGN, CIN and HTN in theNorth Indian population. The limitation of our study remains aswe have not estimated the VEGF level and functional componentof this polymorphism.
Acknowledgements
We acknowledge the financial support to Department of Bio-technology, Government of India, New Delhi, India to carry out thiswork.
Appendix A. Supplementary data
Supplementary data associated with this article can be found, inthe online version, at doi:10.1016/j.cyto.2012.01.020.
References
[1] Shulman K, Rosen S, Tognazzi K, Manseau E, Brown L. Expression of vascularpermeability factor (VPF/VEGF) is altered in many glomerular diseases. J AmSoc Nephrol 1996;7:661–6.
[2] Noguchi K, Yoshikawa N, Ito-Kariya S, Inoue Y, Hayashi Y, Ito H, et al. Activatedmesangial cells produce vascular permeability factor in early-stage mesangialproliferative glomerulonephritis. J Am Soc Nephrol 1998;9:1815–25.
[3] Benjamin LE, Golijanin D, Itin A, Pode D, Keshet E. Selective ablation ofimmature blood vessels in established human tumors follows vascularendothelial growth factor withdrawal. J Clin Invest 1999;103:159–65.
[4] Kim ByungSoo, Goligorsky MichealS. Role of VEGF in kidney developmentmicrovascular maintenance and pathophysiology of renal disease. Korean JIntern Med 2003;18:65–75.
[5] Drake CJ, Little CD. Exogenous vascular endothelial growth factor inducesmalformed and hyperfused vessels during embryonic neovascularization. ProcNatl Acad Sci U S A 1995;92:7657–61.
[6] Ferrara N, Chen H, Davis-Smyth T, Gerber HP, Nguyen TN, Peers D, et al.Vascular endothelial growth factor is essential for corpus luteum angiogenesis.Nat Med 1998;4:336–40.
[7] Tischer E, Mitchell R, Hartman T, Silva M, Gospodarowicz D, Fiddes JC, et al. Thehuman gene for vascular endothelial growth factor. J Biol Chem1991;266:11947–54.
[8] Brogan IJ, Khan N, Isaac K, Hutchinson JA, Pravica V, Hutchinson IV. Novelpolymorphisms in the promoter and 5’UTR regions of the human vascularendothelial growth factor gene. Hum Immunol 1999;60:1245–9.
[9] Watson CJ, Webb NJ, Bottomley MJ, Brenchley PE. Identification ofpolymorphisms within the vascular endothelial growth factor (VEGF) gene:correlation with variation in VEGF protein production. Cytokine2000;12:1232–5.
[10] Renner W, Kotschan S, Hoffmann C, Obermayer-Pietsch B, Pilger E. A common936 C/T mutation in the gene for vascular endothelial growth factor isassociated with vascular endothelial growth factor plasma levels. J Vasc Res2000;37:443–8.
[11] Papazoglou D, Galazios G, Papatheodorou K, Liberis V, Papanas N, Maltezos E,et al. Vascular endothelial growth factor gene polymorphisms and idiopathicrecurrent pregnancy loss. Fertil Steril 2005;83(4):959–63.
[12] Buraczynska M, Ksiazek P, Baranowicz-Gaszczyk I, Jozwiak L. Association ofthe VEGF gene polymorphism with diabetic retinopathy in type 2 diabetespatients. Nephrol Dial Transplant 2007;22:827–32.
[13] Whittle C, Gillespie K, Harrison R, Mathieson PW, Harper SJ. Heterogeneousvascular endothelial growth factor (VEGF) isoform mRNA and receptor mRNAexpression in human glomeruli, and the identification of VEGF148 mRNA, anovel truncated splice variant. Clin Sci 1999;97:303–12.
[14] Eremina V, Sood M, Haigh J, Nagy A, Lajoie G, Ferrara N, et al. Glomerularspecific alterations of VEGF-A expression lead to distinct congenital andacquired renal diseases. J Clin Invest 2003;111:707–16.
[15] Shahbazi M, Fryer AA, Pravica V, Brogan IJ, Ramsay HM, Hutchinson IV, et al.Vascular endothelial growth factor gene polymorphisms are associated withacute renal allograft rejection. J Am Soc Nephrol 2002;13:260–4.
[16] Szeto Cheuk-Chun, Chow Kai-Ming, Poon Peter. Carol Yi-Ki Szeto, Teresa Yuk-Hwa Wong, Philip Kam-Taoli. Genetic polymorphism of VEGF: Impact onlongitudinal change of peritoneal transport and survival of peritoneal dialysispatients. Kidney Int 2004;65:1947–55.
[17] Safránková H, Merta M, Reiterová J, Stekrová J, Maixnerová D, Ryšavá R, et al.The influence of vascular endothelial growth factor (VEGF) polymorphism onthe progression of chronic glomerulonephritides. Folia Biol (Praha)2011;57(4):145–50.
[18] Luft FC, Haller H. Hypertension induced renal injury: is mechanically mediatedinterstitial inflammation involved? Nephrol Dial Transplant 1995;10(1):9–11.
[19] Yang JW, Hutchinson IV, Shah T, Fang J, Min DI. Gene polymorphism ofvascular endothelial growth factor �1154 G>A is associated with hypertensivenephropathy in a Hispanic population. Mol Biol Rep 2011;38(4):2417–25.
[20] Rangan GK, Wang Y, Tay YC, Harris DC. Inhibition of nuclear factor-kappaBactivation reduces cortical tubulointerstitial injury in proteinuric rats. KidneyInt 1999;56(1):118–34.
[21] Prior SJ, Hagberg JM, Paton CM, Douglass LW, Brown MD, McLenithan JC, et al.DNA sequence variation in the promoter region of the VEGF gene impactsVEGF gene expression and maximal oxygen consumption. Am J Physiol HeartCirc Physiol 2006;290:1848–55.
[22] Aggarwal Shagun, Parveen Farah, Faridi Rehan Mujeeb, Phadke Shubha, BorkarMinal, Agrawal Suraksha. Vascular endothelial growth factor genepolymorphisms in North Indian patients with recurrent miscarriages. ReprodBiomed Online 2011;22(1):59–64.




















