
Trypanosoma cruzi activates mouse cardiac fibroblasts in vitro ...
Upload
independentCategory
view
1download
0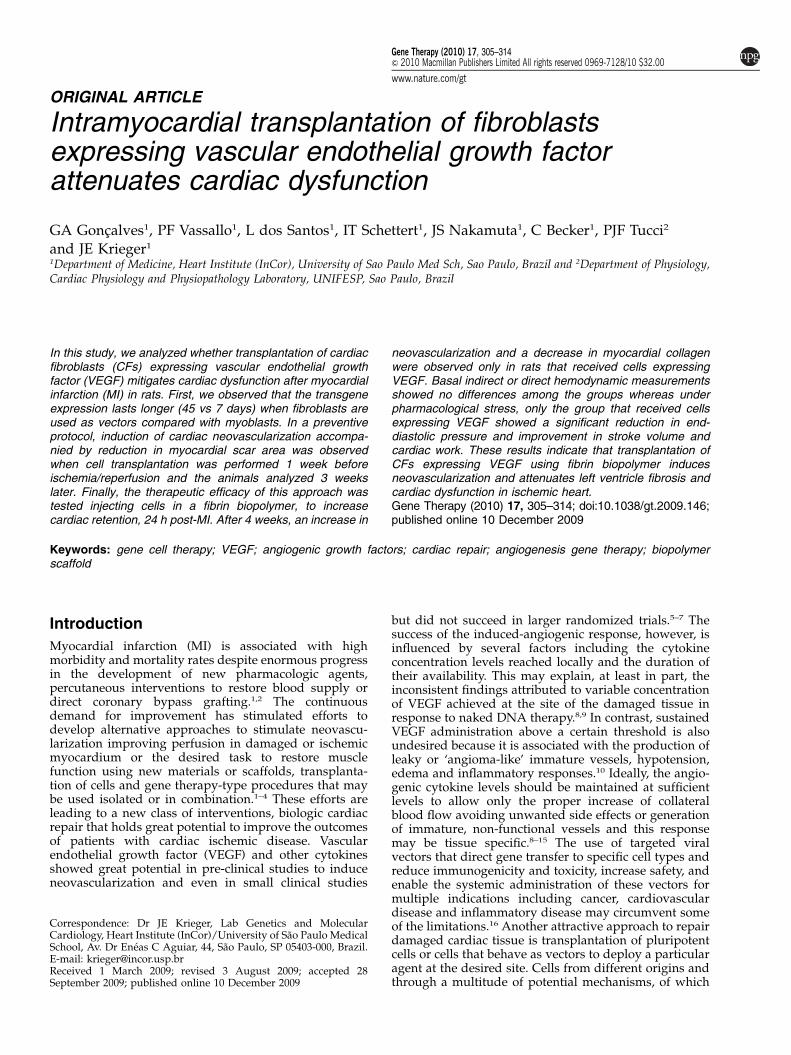
ORIGINAL ARTICLE
Intramyocardial transplantation of fibroblastsexpressing vascular endothelial growth factorattenuates cardiac dysfunction
GA Goncalves1, PF Vassallo1, L dos Santos1, IT Schettert1, JS Nakamuta1, C Becker1, PJF Tucci2
and JE Krieger1
1Department of Medicine, Heart Institute (InCor), University of Sao Paulo Med Sch, Sao Paulo, Brazil and 2Department of Physiology,Cardiac Physiology and Physiopathology Laboratory, UNIFESP, Sao Paulo, Brazil
In this study, we analyzed whether transplantation of cardiacfibroblasts (CFs) expressing vascular endothelial growthfactor (VEGF) mitigates cardiac dysfunction after myocardialinfarction (MI) in rats. First, we observed that the transgeneexpression lasts longer (45 vs 7 days) when fibroblasts areused as vectors compared with myoblasts. In a preventiveprotocol, induction of cardiac neovascularization accompa-nied by reduction in myocardial scar area was observedwhen cell transplantation was performed 1 week beforeischemia/reperfusion and the animals analyzed 3 weekslater. Finally, the therapeutic efficacy of this approach wastested injecting cells in a fibrin biopolymer, to increasecardiac retention, 24 h post-MI. After 4 weeks, an increase in
neovascularization and a decrease in myocardial collagenwere observed only in rats that received cells expressingVEGF. Basal indirect or direct hemodynamic measurementsshowed no differences among the groups whereas underpharmacological stress, only the group that received cellsexpressing VEGF showed a significant reduction in end-diastolic pressure and improvement in stroke volume andcardiac work. These results indicate that transplantation ofCFs expressing VEGF using fibrin biopolymer inducesneovascularization and attenuates left ventricle fibrosis andcardiac dysfunction in ischemic heart.Gene Therapy (2010) 17, 305–314; doi:10.1038/gt.2009.146;published online 10 December 2009
Keywords: gene cell therapy; VEGF; angiogenic growth factors; cardiac repair; angiogenesis gene therapy; biopolymerscaffold
Introduction
Myocardial infarction (MI) is associated with highmorbidity and mortality rates despite enormous progressin the development of new pharmacologic agents,percutaneous interventions to restore blood supply ordirect coronary bypass grafting.1,2 The continuousdemand for improvement has stimulated efforts todevelop alternative approaches to stimulate neovascu-larization improving perfusion in damaged or ischemicmyocardium or the desired task to restore musclefunction using new materials or scaffolds, transplanta-tion of cells and gene therapy-type procedures that maybe used isolated or in combination.1–4 These efforts areleading to a new class of interventions, biologic cardiacrepair that holds great potential to improve the outcomesof patients with cardiac ischemic disease. Vascularendothelial growth factor (VEGF) and other cytokinesshowed great potential in pre-clinical studies to induceneovascularization and even in small clinical studies
but did not succeed in larger randomized trials.5–7 Thesuccess of the induced-angiogenic response, however, isinfluenced by several factors including the cytokineconcentration levels reached locally and the duration oftheir availability. This may explain, at least in part, theinconsistent findings attributed to variable concentrationof VEGF achieved at the site of the damaged tissue inresponse to naked DNA therapy.8,9 In contrast, sustainedVEGF administration above a certain threshold is alsoundesired because it is associated with the production ofleaky or ‘angioma-like’ immature vessels, hypotension,edema and inflammatory responses.10 Ideally, the angio-genic cytokine levels should be maintained at sufficientlevels to allow only the proper increase of collateralblood flow avoiding unwanted side effects or generationof immature, non-functional vessels and this responsemay be tissue specific.8–15 The use of targeted viralvectors that direct gene transfer to specific cell types andreduce immunogenicity and toxicity, increase safety, andenable the systemic administration of these vectors formultiple indications including cancer, cardiovasculardisease and inflammatory disease may circumvent someof the limitations.16 Another attractive approach to repairdamaged cardiac tissue is transplantation of pluripotentcells or cells that behave as vectors to deploy a particularagent at the desired site. Cells from different origins andthrough a multitude of potential mechanisms, of which
Received 1 March 2009; revised 3 August 2009; accepted 28September 2009; published online 10 December 2009
Correspondence: Dr JE Krieger, Lab Genetics and MolecularCardiology, Heart Institute (InCor)/University of Sao Paulo MedicalSchool, Av. Dr Eneas C Aguiar, 44, Sao Paulo, SP 05403-000, Brazil.E-mail: [email protected]
Gene Therapy (2010) 17, 305–314& 2010 Macmillan Publishers Limited All rights reserved 0969-7128/10 $32.00
www.nature.com/gt
relative importance remains poorly understood, canimprove neovascularization and mitigate cardiac dys-function associated with cardiac ischemia.17–21 Alongwith others, we have shown earlier that geneticallymodified skeletal myoblasts (SKs) expressing VEGF usedas vectors and transplanted in a relative small numbercan increase capillary density and decreases myocardialscaring in rats when injected 1 week before ischemia/reperfusion injury.22 This early success occurs eventhough the expression of the transgene lasts only about7–14 days when myoblasts are used as vectors.22 In thisstudy, we hypothesized that transplantation of syngeneicfibroblasts as ‘vector’ to deliver angiogenic factors cansupport longer-lasting transgene expression and thatassociation of these cells with a fibrin biopolymer wouldincrease cell retention and the local levels of the growthfactors. First, we used a proof of principle-type approachand showed that the pre-emptive transplantation offibroblasts expressing VEGF produced similar improve-ments compared with the transplantation of genetic-modified myoblasts.22 Then, we provided evidencethat fibroblasts expressing VEGF can act therapeutically24 h post-MI to decrease cardiac scar area andmost importantly to reduce cardiac dysfunction 4 weekspost-treatment.
Results
‘Preventive’ studyThe transgene expression after intramyocardial trans-plantation of cardiac fibroblasts (CFs) lasted longer thanSKs despite the fact that both cells were transduced bythe same adenovirus vector (at least 45 days comparedwith 7 days) (Figure 1). Taking advantage of this finding,we then determined the efficacy of the transduced CFexpressing the angiogenic factor VEGF to increasecapillary density and to reduce MI scar area in a settingof cardiac ischemia without gross abnormality in cardiacfunction. Animals were first treated with vehicle, cells,cells transduced with an empty vector or cells trans-duced with a VEGF vector and, 7 days later, a smallischemia reperfusion injury was produced and theanimals followed for an additional 3-week period beforemorphometric analysis was performed. Cardiac VEGF
protein and capillary density increased only in groupstransplanted with VEGF expressing cells (VEGF protein:2090±11.4 vs Vehicle: 123.1±5.2, Cell: 104.2±7.4 andNull 73.2±2.4 positive cells/field, Po0.01 and capillarydensity: 543.8±52.1 vs 349.2±0.9, 288±19.0 and245±2.6 capillaries mm–2, Po0.01). Co-localization, re-vealed by immunostaining, of specific endothelial andsmooth muscle cell markers was significantly greater inthe VEGF group, suggesting maturation of newly formedvessels (45±3 vs 10±2, 8±1 and 16±3, vessels/fieldPo0.001). These responses were accompanied by asmall, but significant, reduction in myocardial scar areain VEGF vs Vehicle (3.0±1.3 vs 8.0±0.8%, Po0.05).
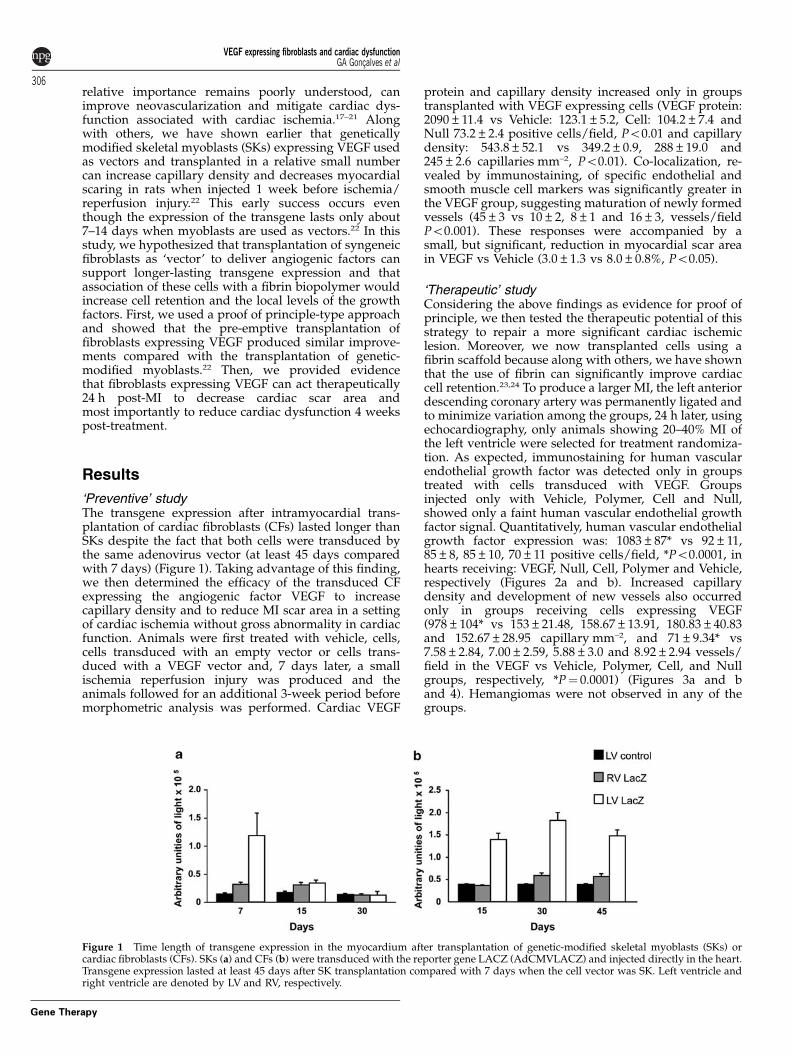
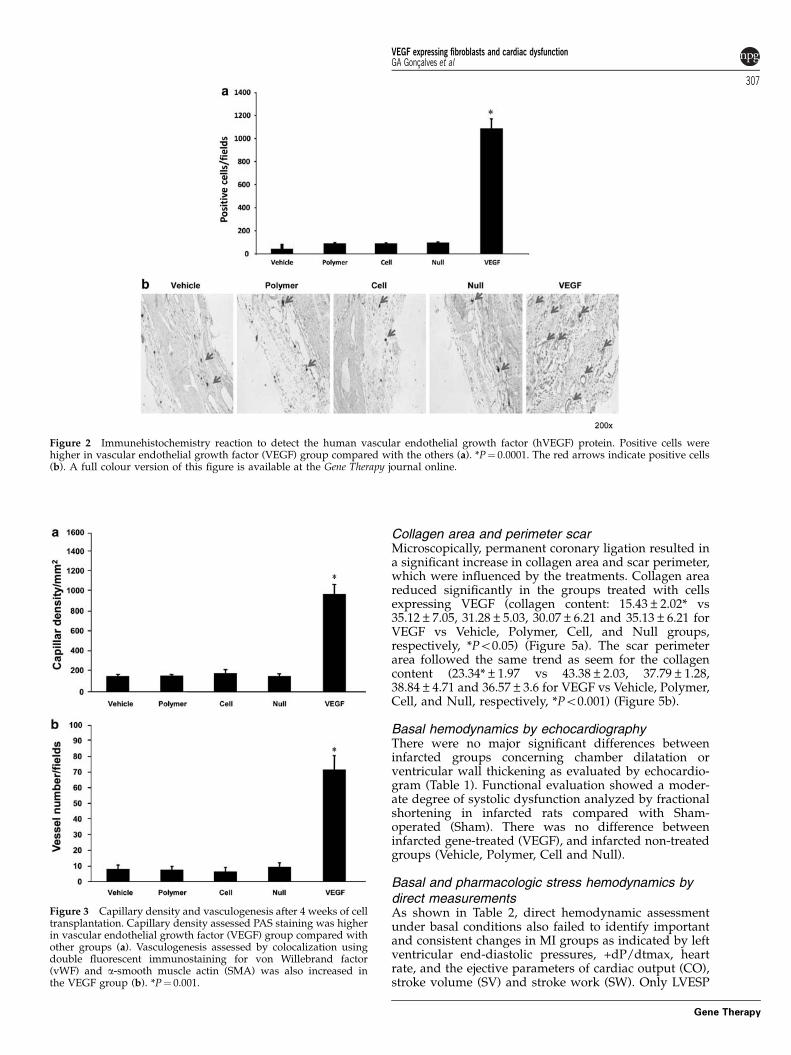
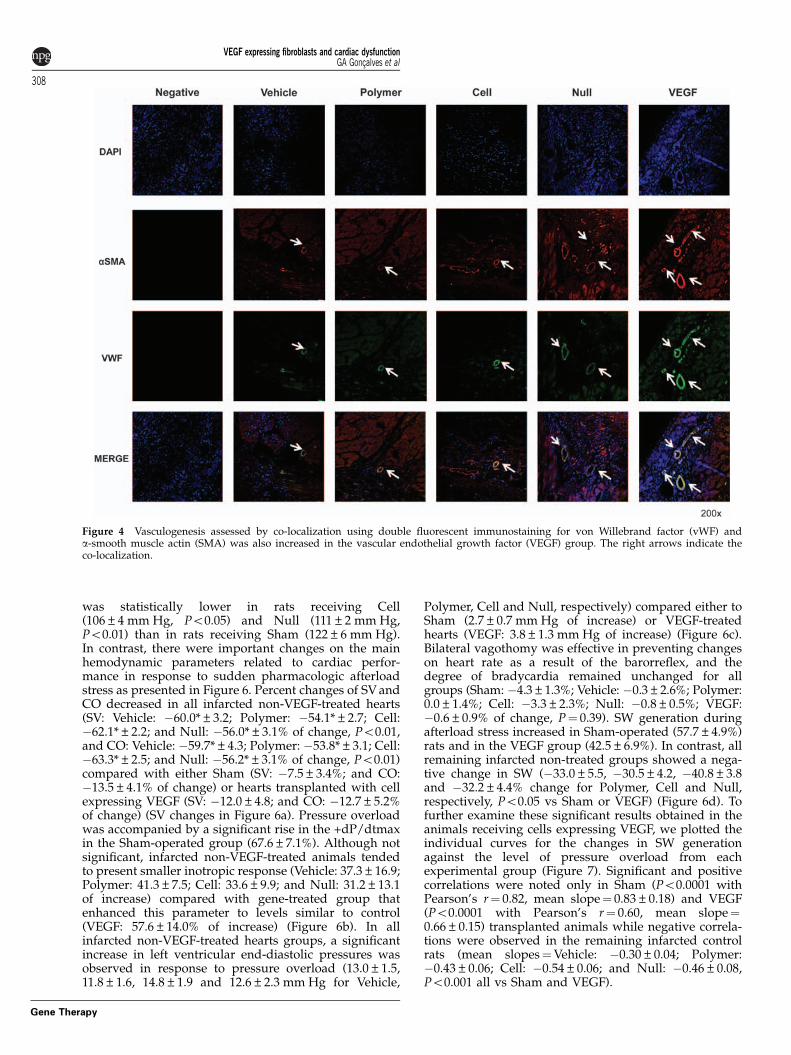
‘Therapeutic’ studyConsidering the above findings as evidence for proof ofprinciple, we then tested the therapeutic potential of thisstrategy to repair a more significant cardiac ischemiclesion. Moreover, we now transplanted cells using afibrin scaffold because along with others, we have shownthat the use of fibrin can significantly improve cardiaccell retention.23,24 To produce a larger MI, the left anteriordescending coronary artery was permanently ligated andto minimize variation among the groups, 24 h later, usingechocardiography, only animals showing 20–40% MI ofthe left ventricle were selected for treatment randomiza-tion. As expected, immunostaining for human vascularendothelial growth factor was detected only in groupstreated with cells transduced with VEGF. Groupsinjected only with Vehicle, Polymer, Cell and Null,showed only a faint human vascular endothelial growthfactor signal. Quantitatively, human vascular endothelialgrowth factor expression was: 1083±87* vs 92±11,85±8, 85±10, 70±11 positive cells/field, *Po0.0001, inhearts receiving: VEGF, Null, Cell, Polymer and Vehicle,respectively (Figures 2a and b). Increased capillarydensity and development of new vessels also occurredonly in groups receiving cells expressing VEGF(978±104* vs 153±21.48, 158.67±13.91, 180.83±40.83and 152.67±28.95 capillary mm–2, and 71±9.34* vs7.58±2.84, 7.00±2.59, 5.88±3.0 and 8.92±2.94 vessels/field in the VEGF vs Vehicle, Polymer, Cell, and Nullgroups, respectively, *P¼ 0.0001) (Figures 3a and band 4). Hemangiomas were not observed in any of thegroups.
Figure 1 Time length of transgene expression in the myocardium after transplantation of genetic-modified skeletal myoblasts (SKs) orcardiac fibroblasts (CFs). SKs (a) and CFs (b) were transduced with the reporter gene LACZ (AdCMVLACZ) and injected directly in the heart.Transgene expression lasted at least 45 days after SK transplantation compared with 7 days when the cell vector was SK. Left ventricle andright ventricle are denoted by LV and RV, respectively.
VEGF expressing fibroblasts and cardiac dysfunctionGA Goncalves et al
306
Gene Therapy
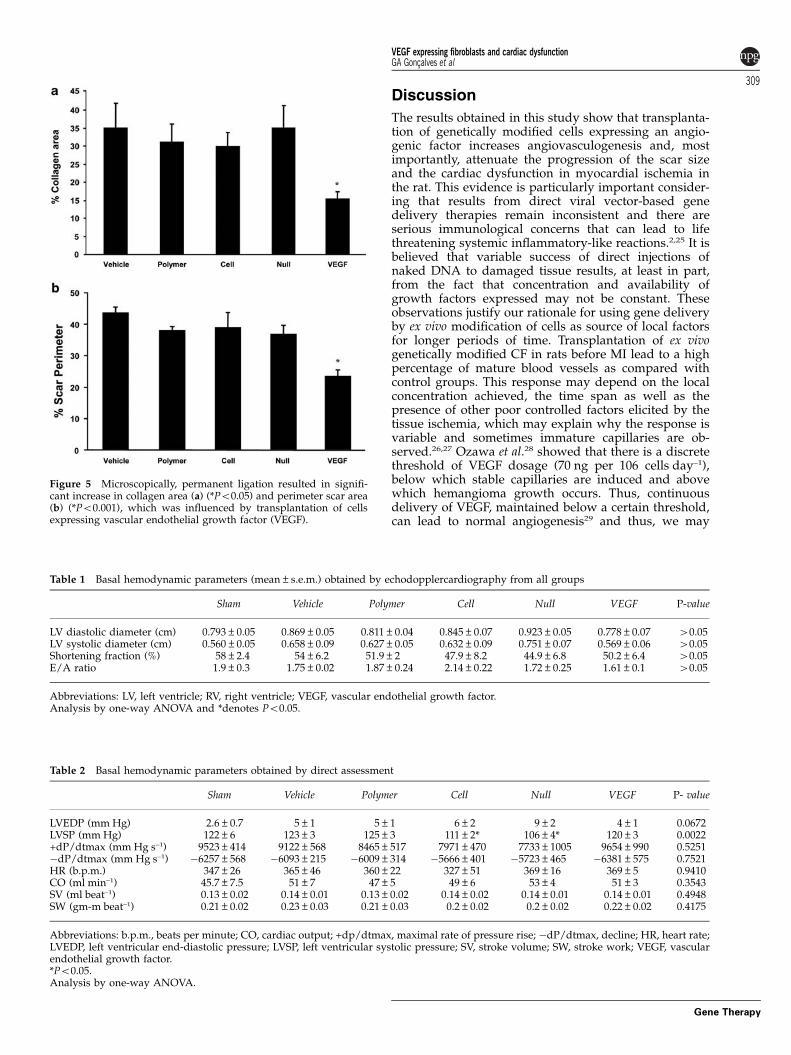
Collagen area and perimeter scarMicroscopically, permanent coronary ligation resulted ina significant increase in collagen area and scar perimeter,which were influenced by the treatments. Collagen areareduced significantly in the groups treated with cellsexpressing VEGF (collagen content: 15.43±2.02* vs35.12±7.05, 31.28±5.03, 30.07±6.21 and 35.13±6.21 forVEGF vs Vehicle, Polymer, Cell, and Null groups,respectively, *Po0.05) (Figure 5a). The scar perimeterarea followed the same trend as seem for the collagencontent (23.34*±1.97 vs 43.38±2.03, 37.79±1.28,38.84±4.71 and 36.57±3.6 for VEGF vs Vehicle, Polymer,Cell, and Null, respectively, *Po0.001) (Figure 5b).
Basal hemodynamics by echocardiographyThere were no major significant differences betweeninfarcted groups concerning chamber dilatation orventricular wall thickening as evaluated by echocardio-gram (Table 1). Functional evaluation showed a moder-ate degree of systolic dysfunction analyzed by fractionalshortening in infarcted rats compared with Sham-operated (Sham). There was no difference betweeninfarcted gene-treated (VEGF), and infarcted non-treatedgroups (Vehicle, Polymer, Cell and Null).
Basal and pharmacologic stress hemodynamics bydirect measurementsAs shown in Table 2, direct hemodynamic assessmentunder basal conditions also failed to identify importantand consistent changes in MI groups as indicated by leftventricular end-diastolic pressures, +dP/dtmax, heartrate, and the ejective parameters of cardiac output (CO),stroke volume (SV) and stroke work (SW). Only LVESP
Figure 2 Immunehistochemistry reaction to detect the human vascular endothelial growth factor (hVEGF) protein. Positive cells werehigher in vascular endothelial growth factor (VEGF) group compared with the others (a). *P¼ 0.0001. The red arrows indicate positive cells(b). A full colour version of this figure is available at the Gene Therapy journal online.
Figure 3 Capillary density and vasculogenesis after 4 weeks of celltransplantation. Capillary density assessed PAS staining was higherin vascular endothelial growth factor (VEGF) group compared withother groups (a). Vasculogenesis assessed by colocalization usingdouble fluorescent immunostaining for von Willebrand factor(vWF) and a-smooth muscle actin (SMA) was also increased inthe VEGF group (b). *P¼ 0.001.
VEGF expressing fibroblasts and cardiac dysfunctionGA Goncalves et al
307
Gene Therapy
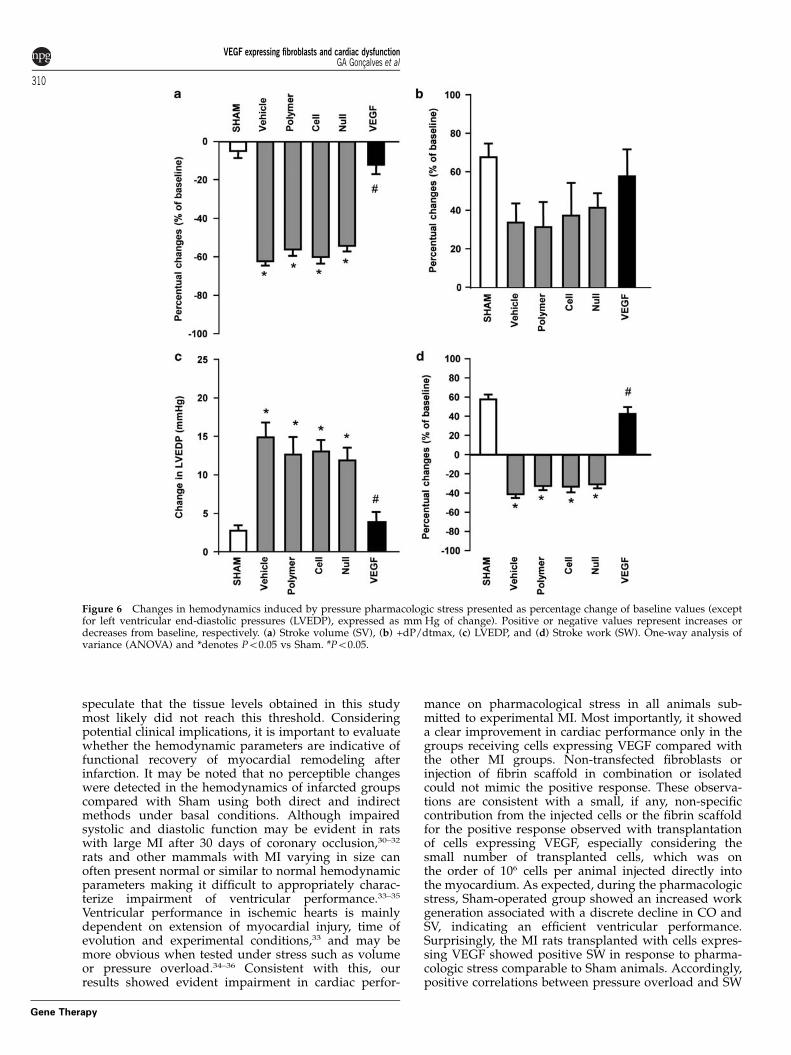
was statistically lower in rats receiving Cell(106±4 mm Hg, Po0.05) and Null (111±2 mm Hg,Po0.01) than in rats receiving Sham (122±6 mm Hg).In contrast, there were important changes on the mainhemodynamic parameters related to cardiac perfor-mance in response to sudden pharmacologic afterloadstress as presented in Figure 6. Percent changes of SV andCO decreased in all infarcted non-VEGF-treated hearts(SV: Vehicle: �60.0*±3.2; Polymer: �54.1*±2.7; Cell:�62.1*±2.2; and Null: �56.0*±3.1% of change, Po0.01,and CO: Vehicle: �59.7*±4.3; Polymer: �53.8*±3.1; Cell:�63.3*±2.5; and Null: �56.2*±3.1% of change, Po0.01)compared with either Sham (SV: �7.5±3.4%; and CO:�13.5±4.1% of change) or hearts transplanted with cellexpressing VEGF (SV: �12.0±4.8; and CO: �12.7±5.2%of change) (SV changes in Figure 6a). Pressure overloadwas accompanied by a significant rise in the +dP/dtmaxin the Sham-operated group (67.6±7.1%). Although notsignificant, infarcted non-VEGF-treated animals tendedto present smaller inotropic response (Vehicle: 37.3±16.9;Polymer: 41.3±7.5; Cell: 33.6±9.9; and Null: 31.2±13.1of increase) compared with gene-treated group thatenhanced this parameter to levels similar to control(VEGF: 57.6±14.0% of increase) (Figure 6b). In allinfarcted non-VEGF-treated hearts groups, a significantincrease in left ventricular end-diastolic pressures wasobserved in response to pressure overload (13.0±1.5,11.8±1.6, 14.8±1.9 and 12.6±2.3 mm Hg for Vehicle,
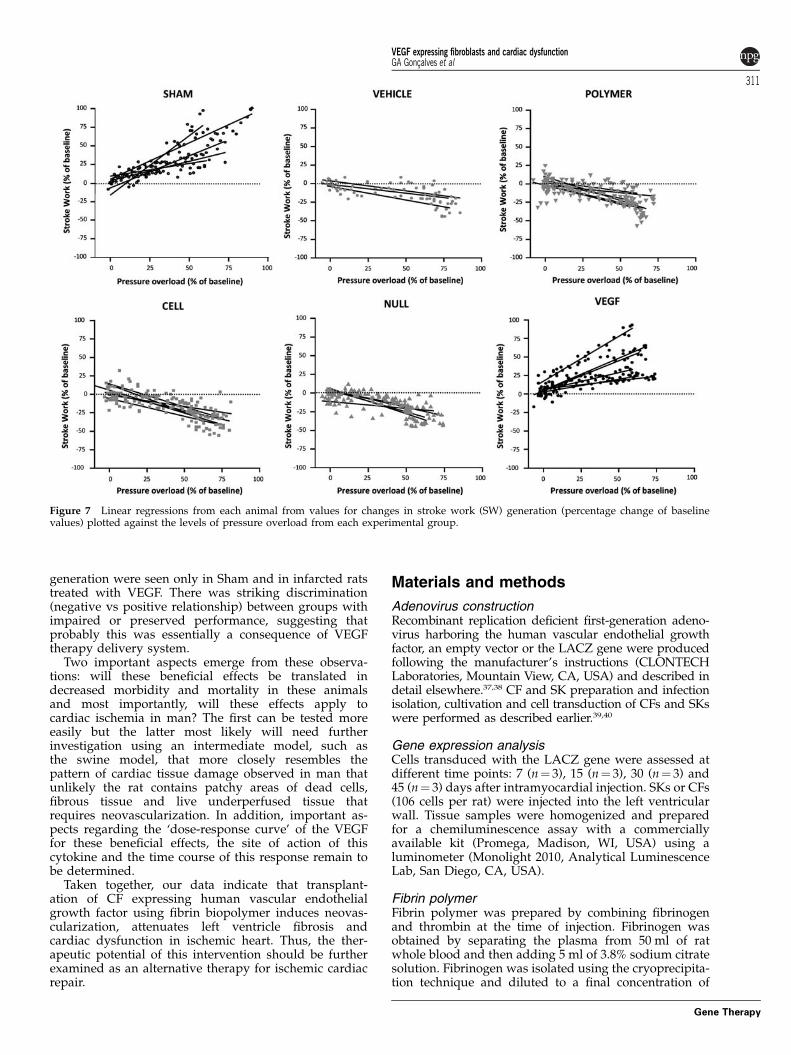
Polymer, Cell and Null, respectively) compared either toSham (2.7±0.7 mm Hg of increase) or VEGF-treatedhearts (VEGF: 3.8±1.3 mm Hg of increase) (Figure 6c).Bilateral vagothomy was effective in preventing changeson heart rate as a result of the barorreflex, and thedegree of bradycardia remained unchanged for allgroups (Sham: �4.3±1.3%; Vehicle: �0.3±2.6%; Polymer:0.0±1.4%; Cell: �3.3±2.3%; Null: �0.8±0.5%; VEGF:�0.6±0.9% of change, P¼ 0.39). SW generation duringafterload stress increased in Sham-operated (57.7±4.9%)rats and in the VEGF group (42.5±6.9%). In contrast, allremaining infarcted non-treated groups showed a nega-tive change in SW (�33.0±5.5, �30.5±4.2, �40.8±3.8and �32.2±4.4% change for Polymer, Cell and Null,respectively, Po0.05 vs Sham or VEGF) (Figure 6d). Tofurther examine these significant results obtained in theanimals receiving cells expressing VEGF, we plotted theindividual curves for the changes in SW generationagainst the level of pressure overload from eachexperimental group (Figure 7). Significant and positivecorrelations were noted only in Sham (Po0.0001 withPearson’s r¼ 0.82, mean slope¼ 0.83±0.18) and VEGF(Po0.0001 with Pearson’s r¼ 0.60, mean slope¼0.66±0.15) transplanted animals while negative correla-tions were observed in the remaining infarcted controlrats (mean slopes¼Vehicle: �0.30±0.04; Polymer:�0.43±0.06; Cell: �0.54±0.06; and Null: �0.46±0.08,Po0.001 all vs Sham and VEGF).
Figure 4 Vasculogenesis assessed by co-localization using double fluorescent immunostaining for von Willebrand factor (vWF) anda-smooth muscle actin (SMA) was also increased in the vascular endothelial growth factor (VEGF) group. The right arrows indicate theco-localization.
VEGF expressing fibroblasts and cardiac dysfunctionGA Goncalves et al
308
Gene Therapy
Discussion
The results obtained in this study show that transplanta-tion of genetically modified cells expressing an angio-genic factor increases angiovasculogenesis and, mostimportantly, attenuate the progression of the scar sizeand the cardiac dysfunction in myocardial ischemia inthe rat. This evidence is particularly important consider-ing that results from direct viral vector-based genedelivery therapies remain inconsistent and there areserious immunological concerns that can lead to lifethreatening systemic inflammatory-like reactions.2,25 It isbelieved that variable success of direct injections ofnaked DNA to damaged tissue results, at least in part,from the fact that concentration and availability ofgrowth factors expressed may not be constant. Theseobservations justify our rationale for using gene deliveryby ex vivo modification of cells as source of local factorsfor longer periods of time. Transplantation of ex vivogenetically modified CF in rats before MI lead to a highpercentage of mature blood vessels as compared withcontrol groups. This response may depend on the localconcentration achieved, the time span as well as thepresence of other poor controlled factors elicited by thetissue ischemia, which may explain why the response isvariable and sometimes immature capillaries are ob-served.26,27 Ozawa et al.28 showed that there is a discretethreshold of VEGF dosage (70 ng per 106 cells day–1),below which stable capillaries are induced and abovewhich hemangioma growth occurs. Thus, continuousdelivery of VEGF, maintained below a certain threshold,can lead to normal angiogenesis29 and thus, we may
Table 1 Basal hemodynamic parameters (mean±s.e.m.) obtained by echodopplercardiography from all groups
Sham Vehicle Polymer Cell Null VEGF P-value
LV diastolic diameter (cm) 0.793±0.05 0.869±0.05 0.811±0.04 0.845±0.07 0.923±0.05 0.778±0.07 40.05LV systolic diameter (cm) 0.560±0.05 0.658±0.09 0.627±0.05 0.632±0.09 0.751±0.07 0.569±0.06 40.05Shortening fraction (%) 58±2.4 54±6.2 51.9±2 47.9±8.2 44.9±6.8 50.2±6.4 40.05E/A ratio 1.9±0.3 1.75±0.02 1.87±0.24 2.14±0.22 1.72±0.25 1.61±0.1 40.05
Abbreviations: LV, left ventricle; RV, right ventricle; VEGF, vascular endothelial growth factor.Analysis by one-way ANOVA and *denotes Po0.05.
Table 2 Basal hemodynamic parameters obtained by direct assessment
Sham Vehicle Polymer Cell Null VEGF P- value
LVEDP (mm Hg) 2.6±0.7 5±1 5±1 6±2 9±2 4±1 0.0672LVSP (mm Hg) 122±6 123±3 125±3 111±2* 106±4* 120±3 0.0022+dP/dtmax (mm Hg s–1) 9523±414 9122±568 8465±517 7971±470 7733±1005 9654±990 0.5251�dP/dtmax (mm Hg s–1) �6257±568 �6093±215 �6009±314 �5666±401 �5723±465 �6381±575 0.7521HR (b.p.m.) 347±26 365±46 360±22 327±51 369±16 369±5 0.9410CO (ml min–1) 45.7±7.5 51±7 47±5 49±6 53±4 51±3 0.3543SV (ml beat–1) 0.13±0.02 0.14±0.01 0.13±0.02 0.14±0.02 0.14±0.01 0.14±0.01 0.4948SW (gm-m beat–1) 0.21±0.02 0.23±0.03 0.21±0.03 0.2±0.02 0.2±0.02 0.22±0.02 0.4175
Abbreviations: b.p.m., beats per minute; CO, cardiac output; +dp/dtmax, maximal rate of pressure rise; �dP/dtmax, decline; HR, heart rate;LVEDP, left ventricular end-diastolic pressure; LVSP, left ventricular systolic pressure; SV, stroke volume; SW, stroke work; VEGF, vascularendothelial growth factor.*Po0.05.Analysis by one-way ANOVA.
Figure 5 Microscopically, permanent ligation resulted in signifi-cant increase in collagen area (a) (*Po0.05) and perimeter scar area(b) (*Po0.001), which was influenced by transplantation of cellsexpressing vascular endothelial growth factor (VEGF).
VEGF expressing fibroblasts and cardiac dysfunctionGA Goncalves et al
309
Gene Therapy
speculate that the tissue levels obtained in this studymost likely did not reach this threshold. Consideringpotential clinical implications, it is important to evaluatewhether the hemodynamic parameters are indicative offunctional recovery of myocardial remodeling afterinfarction. It may be noted that no perceptible changeswere detected in the hemodynamics of infarcted groupscompared with Sham using both direct and indirectmethods under basal conditions. Although impairedsystolic and diastolic function may be evident in ratswith large MI after 30 days of coronary occlusion,30–32
rats and other mammals with MI varying in size canoften present normal or similar to normal hemodynamicparameters making it difficult to appropriately charac-terize impairment of ventricular performance.33–35
Ventricular performance in ischemic hearts is mainlydependent on extension of myocardial injury, time ofevolution and experimental conditions,33 and may bemore obvious when tested under stress such as volumeor pressure overload.34–36 Consistent with this, ourresults showed evident impairment in cardiac perfor-
mance on pharmacological stress in all animals sub-mitted to experimental MI. Most importantly, it showeda clear improvement in cardiac performance only in thegroups receiving cells expressing VEGF compared withthe other MI groups. Non-transfected fibroblasts orinjection of fibrin scaffold in combination or isolatedcould not mimic the positive response. These observa-tions are consistent with a small, if any, non-specificcontribution from the injected cells or the fibrin scaffoldfor the positive response observed with transplantationof cells expressing VEGF, especially considering thesmall number of transplanted cells, which was onthe order of 106 cells per animal injected directly intothe myocardium. As expected, during the pharmacologicstress, Sham-operated group showed an increased workgeneration associated with a discrete decline in CO andSV, indicating an efficient ventricular performance.Surprisingly, the MI rats transplanted with cells expres-sing VEGF showed positive SW in response to pharma-cologic stress comparable to Sham animals. Accordingly,positive correlations between pressure overload and SW
Figure 6 Changes in hemodynamics induced by pressure pharmacologic stress presented as percentage change of baseline values (exceptfor left ventricular end-diastolic pressures (LVEDP), expressed as mm Hg of change). Positive or negative values represent increases ordecreases from baseline, respectively. (a) Stroke volume (SV), (b) +dP/dtmax, (c) LVEDP, and (d) Stroke work (SW). One-way analysis ofvariance (ANOVA) and *denotes Po0.05 vs Sham. #Po0.05.
VEGF expressing fibroblasts and cardiac dysfunctionGA Goncalves et al
310
Gene Therapy
generation were seen only in Sham and in infarcted ratstreated with VEGF. There was striking discrimination(negative vs positive relationship) between groups withimpaired or preserved performance, suggesting thatprobably this was essentially a consequence of VEGFtherapy delivery system.
Two important aspects emerge from these observa-tions: will these beneficial effects be translated indecreased morbidity and mortality in these animalsand most importantly, will these effects apply tocardiac ischemia in man? The first can be tested moreeasily but the latter most likely will need furtherinvestigation using an intermediate model, such asthe swine model, that more closely resembles thepattern of cardiac tissue damage observed in man thatunlikely the rat contains patchy areas of dead cells,fibrous tissue and live underperfused tissue thatrequires neovascularization. In addition, important as-pects regarding the ‘dose-response curve’ of the VEGFfor these beneficial effects, the site of action of thiscytokine and the time course of this response remain tobe determined.
Taken together, our data indicate that transplant-ation of CF expressing human vascular endothelialgrowth factor using fibrin biopolymer induces neovas-cularization, attenuates left ventricle fibrosis andcardiac dysfunction in ischemic heart. Thus, the ther-apeutic potential of this intervention should be furtherexamined as an alternative therapy for ischemic cardiacrepair.
Materials and methods
Adenovirus constructionRecombinant replication deficient first-generation adeno-virus harboring the human vascular endothelial growthfactor, an empty vector or the LACZ gene were producedfollowing the manufacturer’s instructions (CLONTECHLaboratories, Mountain View, CA, USA) and described indetail elsewhere.37,38 CF and SK preparation and infectionisolation, cultivation and cell transduction of CFs and SKswere performed as described earlier.39,40
Gene expression analysisCells transduced with the LACZ gene were assessed atdifferent time points: 7 (n¼ 3), 15 (n¼ 3), 30 (n¼ 3) and45 (n¼ 3) days after intramyocardial injection. SKs or CFs(106 cells per rat) were injected into the left ventricularwall. Tissue samples were homogenized and preparedfor a chemiluminescence assay with a commerciallyavailable kit (Promega, Madison, WI, USA) using aluminometer (Monolight 2010, Analytical LuminescenceLab, San Diego, CA, USA).
Fibrin polymerFibrin polymer was prepared by combining fibrinogenand thrombin at the time of injection. Fibrinogen wasobtained by separating the plasma from 50 ml of ratwhole blood and then adding 5 ml of 3.8% sodium citratesolution. Fibrinogen was isolated using the cryoprecipita-tion technique and diluted to a final concentration of
Figure 7 Linear regressions from each animal from values for changes in stroke work (SW) generation (percentage change of baselinevalues) plotted against the levels of pressure overload from each experimental group.
VEGF expressing fibroblasts and cardiac dysfunctionGA Goncalves et al
311
Gene Therapy

90 UI ml–1. Human thrombin (Baxter Healthcare, Inc.,Deerfield, IL, USA) was used to catalyze fibrin polymer-ization. Cells were resuspended in 80 Pl of the fibrinogensolution and, a few seconds before the injection in thetissue; 20 Pl of thrombin (250 U ml–1) was added to thesyringe containing the cell suspension. This combinationallowed a suitable time window of 20 s to perform themyocardial injection before polymerization.
Cell transplantation and myocardial infarctionAll procedures involving animals were approved by theInstitutional Review Board of the University of Sao PauloMedical School, Brazil (SDC INCOR: 2256/03/050 – prot:397/03).
‘Preventive’ study. Male Lewis rats were submitted toMI as described earlier.22 This method produced adiscrete infarct area without compromising cardiacfunction. After 3 weeks, animals were anesthetized withsodium pentobarbital and hearts perfused with 10%formalin for morphometric and immunohistochemicalanalysis. Animals were divided into four experimentalgroups: Vehicle (DMEM/0.1 ml, n¼ 10); Cell (106cells/0.1 ml, n¼ 8); Null, (106cells transduced with an emptyvector/0.1 ml, n¼ 14) and VEGF, (106cells transducedwith adenovirus harboring the human vascular endothe-lial growth factor/0.1 ml, n¼ 18).
‘Therapeutic’ study. Myocardial infarction was in-duced by permanent ligation of the left anteriordescending coronary artery. Twenty-four hours afterthe procedure animals were subject to an echocardio-gram to estimate infarction size (animals with infarctionsize 20–40% of left ventricle were included in this study),106 cells or placebo are injected per animal into the freeventricular wall. Animals were divided into five groups:Sham, animals subjected to surgery without coronaryocclusion or therapy, n¼ 6, (used for functional evalua-tion); Vehicle, (DMEM/0.1 ml n¼ 6); Polymer, injectionof fibrin polymer (0.1 ml n¼ 6); Cell (106cells pluspolymer/0.1 ml, n¼ 6); Null (0.5� 106 cells transducedwith an empty vector plus polymer /0.1 ml, n¼ 6) andVEGF (0.5� 106cells transduced with AdVEGFEGFPplus polymer/0.1 ml, n¼ 5). After 4 weeks, animals weresubjected to direct and indirect hemodynamic analysis.At the end, the animals were anesthetized with sodiumpentobarbital and hearts perfused with 10% formalin formorphometric and immunohistochemical analysis.
HistologyHearts were fixed in 10% formalin for 24 h, embedded inparaffin and cut into 3 mm sections that were mountedonto slides and stained with Masson’s trichrome for scararea measurement (‘preventive’ study); Picrossirius Redfor collagen area and perimeter scar measurement(‘therapeutic’ study); and periodic Schiff acid forcapillary density quantification. A computerized imageacquisition system (Leica Imaging Systems, Bannock-burn, IL, USA) was used to measure scar areas. Infarctsize was quantified by the percentage of left ventriculararea or perimeter containing scar tissue.
Capillary density evaluationWe estimated capillary density in slides treated withperiodic acid Schiff using a 10� 10 grid optically super-
imposed on each of 25 non-overlapping fields at 400�magnification distributed in a random manner at theantero–septal side of the left ventricle. The capillarydensity was evaluated adjacent to the cardiac scars as atotal of capillaries in the area of the fields, calculating thenumber of capillaries per field (units mm–2) in allexperimental groups in a blinded manner.22
ImmunohistochemistryCross-sections embedded in paraffin were first treatedwith antigenic exposure, and then blocked with 2% milksolution in phosphate-buffered saline. Tissue sectionswere then incubated with anti-human VEGF antibody(1:150; R&D) for 1 h at 37 1C. Sections were incubatedwith a biotinylated goat secondary antibody (1:400,Vector Laboratories; Burlingame, CA, USA) and thenwith streptavidin peroxides followed by the peroxidasesubstrate diaminobenzidine tetrahydrochoride accordingto manufacturer’s instructions. Negative control slideswere incubated with normal goat serum; and thesecondary antibody alone. Dual-fluorescence immunos-taining was performed for blood vessel quantification.For that, cross-sections were pre-incubated with 5%bovine serum albumin followed by human anti-rabbitvon Willebrand factor (1:20, Dako Laboratories, Glostr-up, Denmark) and goat anti-mouse smooth muscle actin(1:400, Sigma Laboratories, Saint Louis, MO, USA)overnight at 4 1C. Sections were subsequently incubatedwith the secondary antibody anti-mouse CY3 (1:700,Sigma Laboratories) and anti- rabbit Fitc (1:50 DakoLaboratories) for 45 min as well as with DAPI to identifythe cell nuclei. For each tissue section the number ofblood vessels (in which red fluorescence for smoothmuscle actin co-localized with green fluorescent for vonWillebrand factor and blue fluorescent for DAPI) werecounted from four randomly selected microscopic fieldsunder a 200� objective. A total of four different tissuesections from three animals in each group were used tomeasure the final blood vessel number.
Echodopplercardiography examinationDoppler echocardiogram was performed by one obser-ver; using a HP SONOS 5500 instrument (PhilipsMedical System, Amsterdam, Netherlands) under an-esthesia with a 12-MHz transducer at a depth of 2 cm asdescribed earlier.41 In brief, end-diastolic and systolic leftventricle diameters were measured from the transverseparasternal view using M-mode images. Systolic func-tion was estimated using the fractional area shortening.End-diastolic and systolic transverse ventricular areaswere obtained by tracing the endocardial border of basal,middle and apical images. Diastolic function wasanalyzed using parameters derived from mitral diastolicinflow and ventricular outflow tract velocity curves bypulsed-wave Doppler. Peak of E and A-wave velocitieswere measured, and E/A ratios calculated.
Hemodynamic study under pharmacologic stressThe direct hemodynamic analysis was performed asdescribed before.42 In brief, invasive hemodynamicevaluation was performed on a heated rodent operatingtable (37 1C), under adjusted anesthesia (urethane1.2 g kg–1), and oxygen-enriched mechanic ventilation.Left femoral vein was accessed to supplement anesthesiaand drugs or saline administration. Bilateral vagothomy
VEGF expressing fibroblasts and cardiac dysfunctionGA Goncalves et al
312
Gene Therapy
was produced to prevent changes on heart rate as aresult of the barorreflex in response to pharmacologicstress. A Millar micro manometer (MikroTip 2F, MillarInstruments Inc., Houston, TX, USA) was inserted fromthe right carotid artery to the left ventricle cavity toaccess intraventricular pressure. A blood flow ultra-sound probe (Transonic Systems Inc., Ithaca, NY, USA)was positioned on the ascending aorta to access CO(excluding coronary flow), through right thoracotomy.Data were acquired by the software acknowledge forwindows (Biopac Systems, Goleta, CA, USA) to getsystolic (LV systolic pressure) and left ventricular end-diastolic pressures, rate of LV pressure rise (dP/dt), heartrate, CO and SV. SW was estimated offline as a productof SV�developed pressure (LVSP�LVEDP)� constant0.0136. After baseline evaluation, a sudden afterloadstress was induced by sudden pressure overloadwith a vasoconstrictive phenylephrine bolus injection(25–75 mg kg–1 body weight) through the left femoralvein. Phenylephrine doses were adjusted for each animalto produce comparable blood pressure increases (60–80%of baseline).
Statistical analysisResults were expressed as mean±standard error of themean (s.e.m.). One-way analysis of variance with post hocTukey’s test was used to compare groups as appropriate.Linear regression analyses with comparison of slopeswere used to evaluate the effect of afterload stress oncardiac function and Po0.05 was considered significant.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgements
This study was funded by grants from public BrazilianAgencies Fundacao de Amparo a Pesquisa do Estado deSao Paulo (FAPESP #01/00090), Ministerio da Ciencia eTecnologia/Conselho Nacional de DesenvolvimentoCientifico e Tecnologico/Ministerio da Saude/Departa-mento Ciencia e Tecnologia (MCT/CNPq/MS/DECIT#552324/20005-1 and 10120104096700). JSN, CB, andGAG were recipients of fellowships from FAPESP(04/06784-4, 03/02671-8 and 03/02672-4, respectively).
References
1 Huang C, Ding W, Li L, Zhao D. Differences in the aging-associated trends of the monophasic action potential durationand effective refractory period of the right and left atria of therat. Circ J 2006; 70: 352–357.
2 Miyahara Y, Nagaya N, Kataoka M, Yanagawa B, Tanaka K, HaoH et al. Monolayered mesenchymal stem cells repair scarredmyocardium after MI. Nat Med 2006; 12: 459–465.
3 Pachori AS, Melo LG, Zhang L, Solomon SD, Dzau VJ. Chronicrecurrent myocardial ischemic injury is significantly attenuatedby pre-emptive adenoassociated virus heme oxygenase-1 genedelivery. J Am Coll Cardiol 2006; 47: 635–643.
4 Frangogiannis NG, Entman ML. Chemokines in myocardialischemia. Trends Cardiovasc Med 2005; 15: 163–169.
5 Udelson JE, Dilsizian V, Laham RJ, Chronos N, Vansant J,Blais M et al. Therapeutic angiogenesis with recombinant
fibroblast growth factor-2 improves stress and rest myocardialperfusion abnormalities in patients with severe symptomaticchronic coronary artery disease. Circulation 2000; 102: 1605–1610.
6 Laham RJ, Sellke FW, Edelman ER, Pearlman JD, Ware JA,Brown DL et al. Local perivascular delivery of basic fibroblastgrowth factor in patients undergoing coronary bypass surgery:results of a phase I randomized, double-blind, placebo-con-trolled trial. Circulation 1999; 100: 1865–1871.
7 Simons M. Integrative signaling in angiogenesis. Mol CellBiochem 2004; 264: 99–102.
8 Grines CL, Watkins MW, Helmer G, Penny W, Brinker J,Marmur JD et al. Angiogenic Gene Therapy (AGENT) trialin patients with stable angina pectoris. Circulation 2002; 105:1291–1297.
9 Vale PR, Losordo DW, Milliken CE, McDonald MC, GravelinLM, Curry CM et al. Randomized, single blind, placebocontrolled pilot study of catheter-based myocardial gene transferfor therapeutic angiogenesis using left ventricle electromecha-nical mapping in patients with chronic myocardial ischemia.Circulation 2001; 103: 2138–2143.
10 Yla-Herttuala S, Rissanen TT, Vajanto I, Hartikainen J. Vascularendothelial growth factors: biology and current status of clinicalapplications in cardiovascular medicine. J Am Coll Cardiol 2007;10: 1015–1026.
11 Pettersson A, Nagy JA, Brown LF, Sundberg C, Morgan E,Jungles S et al. Heterogeneity of the angiogenic response inducedin different normal adult tissues by vascular permeabilityfactor/vascular endothelial growth factor. Lab Invest 2000; 80:99–115.
12 Lee RJ, Springer ML, Blanco-Bose WE, Shaw R, Ursell PC, BlauHM. VEGF gene delivery to myocardium: deleterious effects ofunregulated expression. Circulation 2000; 102: 898–901.
13 Koh GY, Kim SJ, Klug MG, Park K, Soonpaa MH, Field LJ.Targeted expression of transforming growth factor-beta 1 inintracardiac grafts promotes vascular endothelial cell DNAsynthesis. J Clin Invest 1995; 95: 114–121.
14 Suzuki K, Murtuza B, Smolenski RT, Sammut IA, Suzuki N,Kaneda Y et al. Cell transplantation for the treatment of acute MIusing vascular endothelial growth factor-expressing skeletalmyoblasts. Circulation 2001; 104: 1207–1212.
15 Santini MP, Tsao L, Monassier L, Theodoropoulos C, Carter J,Lara-Pezzi E et al. Enhancing repair of the mammalian heart.Circ Res 2007; 12: 1732–1740.
16 Wickham TJ. Targeting adenovirus. Gene Therapy 2000; 7:110–114.
17 Freedman SB, Isner JM. Therapeutic angiogenesis for coronaryartery disease. Ann Intern Med 2002; 136: 54–71.
18 Udelson JE, Dilsizian V, Laham RJ, Chronos N, Vansant J,Blais M et al. Therapeutic angiogenesis with recombinantfibroblast growth factor-2 improves stress and rest myocardialperfusion abnormalities in patients with severe symptomaticchronic coronary artery disease. Circulation 2000; 102: 1605–1610.
19 Koh GY, Kim SJ, Klug MG, Park K, Soonpaa MH, Field LJ.Targeted expression of transforming growth factor-beta 1 inintracardiac grafts promotes vascular endothelial cell DNAsynthesis. J Clin Invest 1995; 95: 114–121.
20 Penn MS, Francis GS, Ellis SG, Young JB, McCarthy PM, TopolEJ. Autologous cell therapy for the treatment of damagedmyocardium. Prog Cardiovasc Dis 2002; 45: 21–32.
21 Anversa P, Leri A, Rota M, Hosoda T, Bearzi C, Urbanek K et al.Concise review: stem cells, myocardial regeneration, andmethodological artifacts. Stem Cells 2007; 25: 589–601.
22 Becker C, Lacchini S, Muotri AR, da Silva GJ, Castelli JB, VassalloPF et al. Skeletal muscle cells expressing VEGF induce capillaryformation and reduce cardiac injury in rats. Int J Cardiol 2006;113: 348–354.
23 Christman KL, Vardanian AJ, Fang Q, Sievers RE, Fok HH, LeeRJ. Injectable fibrin scaffold improves cell transplant survival,
VEGF expressing fibroblasts and cardiac dysfunctionGA Goncalves et al
313
Gene Therapy
reduces infarct expansion, and induces neovasculatureformation in ischemic myocardium. J Am Coll Cardiol 2004; 44:654–660.
24 Nakamuta JS, Danoviz ME, Marques FL, dos Santos L, Becker C,Goncalves GA et al. Cell therapy attenuates cardiac dysfunctionpost myocardial infarction: effect of timing, routes of injectionand a fibrin scaffold. PLoS One 2009; 4: e6005.
25 Halene S, Wang L, Cooper RM, Bockstoce DC, Robbins PB,Kohn DB. Improved expression in hematopoietic and lymphoidcells in mice after transplantation of bone marrow transducedwith a modified retroviral vector. Blood 1999; 94: 3349–3357.
26 Lee RJ, Springer ML, Blanco-Bose WE, Shaw R, Ursell PC,Blau HM. VEGF gene delivery to myocardium: deleteriouseffects of unregulated expression. Circulation 2000; 102: 898–901.
27 Askari A, Unzek S, Goldman CK, Ellis SG, Thomas JD, DiCorletoPE et al. Cellular, but not direct, adenoviral delivery of vascularendothelial growth factor results in improved left ventriclefunction and neovascularization in dilated ischemic cardiomyo-pathy. J Am Coll Cardiol 2004; 43: 1908–1914.
28 Ozawa CR, Banfi A, Glazer NL, Thurston G, Springer ML,Kraft PE et al. Microenvironmental VEGF concentration, not totaldose, determines a threshold between normal and aberrantangiogenesis. J Clin Invest 2004; 113: 516–527.
29 Ngan ES, Lee KY, Yeung WS, Ngan HY, Ng EH, Ho PC.Endocrine gland derived vascular endothelial growth factor isexpressed in human periimplantation endometrium, but not inendometrial carcinoma. Endocrinology 2006; 147: 88–95.
30 Suzuki K, Murtuza B, Smolenski RT, Sammut IA, Suzuki N,Kaneda Y et al. Cell transplantation for the treatment ofacute myocardial infarction using vascular endothelialgrowth factor expressing skeletal myoblasts. Circulation 2001;104: 1207–1212.
31 Anand IS, Liu D, Chugh SS, Prahash AJ, Gupta S, John R et al.Isolated myocyte contractile function is normal in postinfarctremodeled rat heart with systolic dysfunction. Circulation 1997;96: 3974–3984.
32 Fletcher PJ, Pfeffer JM, Pfeffer MA, Braunwald E. Leftventricular diastolic pressure-volume relations in rats withhealed myocardial infarction—Effects on systolic function.Circ Res 1981; 49: 618–626.
33 Pfeffer MA, Pfeffer JM, Fishbein MC, Fletcher PJ, Spadaro J,Kloner RA et al. Myocardial infarct size and ventricular functionin rats. Circ Res 1979; 44: 503–512.
34 Kumar R, Hood Jr WB, Joison J, Norman JC, Abelmann WH.Experimental myocardial infarction II. Acute depression andsubsequent recovery of left ventricular function: serial measure-ments in intact conscious dogs. J Clin Invest 1970; 49: 55–62.
35 Hood Jr WB. Experimental myocardial infarction. Recovery ofleft ventricular function in the healing phase. Contribution ofincreased fiber shortening in noninfarcted myocardium. AmHeart J 1970; 79: 531–538.
36 Bugge-Asperheim B, Kiil F. Cardiac response to increased aorticpressure. Changes in output and left ventricular pressurepattern at various levels of inotropy. Scand J Clin Lab Invest1969; 24: 345–360.
37 Riazi AM, Lee H, Hsu C, Van Arsdell G. CSX/Nkx2.5 modulatesdifferentiation of skeletal myoblasts and promotes differentia-tion into neuronal cells in vitro. J Biol Chem 2005; 280:10716–10720.
38 Retuerto MA, Beckmann JT, Carbray J, Patejunas G, Sarateanu S,Kane BJ et al. Angiogenic pretreatment to enhance myocardialfunction after cellular cardiomyoplasty with skeletal myoblasts.J Thorac Cardiovasc Surg 2007; 133: 478–484.
39 Ye L, Haider HK, Jiang S, Tan RS, Ge R, Law PK et al. Improvedangiogenic response in pig heart following ischaemic injuryusing human skeletal myoblast simultaneously expressingVEGF165 and angiopoietin-1. Eur J Heart Fail 2007; 9: 15–22.
40 Crabos M, Roth M, Hahn AW, Erne P. Characterization ofangiotensin II receptors in cultured adult rat cardiac fibroblasts-Coupling to signaling systems and gene expression. J. Clin Invest1994; 93: 2372–2378.
41 Nozawa E, Kanashiro RM, Murad N, Carvalho AC, Cravo SL,Campos O et al. Performance of two-dimensional Dopplerechocardiography for the assessment of infarct size and leftventricular function in rats. Braz J Med Biol Res 2006; 39: 687–695.
42 Dos Santos L, Santos AA, Goncalves GA, Krieger JE, Tucci PJ.Bone marrow cell therapy prevents infarct expansion andimproves border zone remodeling after coronary occlusion inrats. Int J Cardiol 2009 [e-pub ahead of print 2 July 2009; PMID:19577315].
VEGF expressing fibroblasts and cardiac dysfunctionGA Goncalves et al
314
Gene Therapy
Copyright © 2022 FDOKUMEN




















