
High-Resolution Computed Tomography of Temporal Bone: Part IV: Coronal Postoperative Anatomy
Upload
khangminh22Category
view
2download
0
Journal ofNeurology, Neurosurgery, and Psychiatry, 1977, 40, 214-220
Value of computed tomography in the diagnosisof intracranial abscessM. D. M. SHAW AND J. A. RUSSELL
From the Institute ofNeurological Sciences, Southern General Hospital, Glasgow
SUMMARY The computed tomography (CT) scans of 60 patients with intracranial infection havebeen reviewed. Computed tomography, particularly if used with contrast enhancement, is a valuableadjunct to the investigation of patients with suspected intracranial abscess. The false negative rate is1 %, but despite this, mortality from intracranial abscess remains unchanged.
Mortality from intracranial abscess has remainedhigh, even since the introduction of antibiotics. Arecent retrospective study of 100 consecutive cases
reported a rate of 38% (van Alphen and Dreissen,1976). This is similar to Garfield's (1969) experiencefor supratentorial abscess (40 Y.), and to that of Shawand Russell (1975) for cerebellar abscess (41 %).Undoubtedly, there are several factors contributingto this mortality (Le Beau et al., 1973; Shaw andRussell, 1975; van Alphen and Dreissen, 1976;Bhatia et al., 1976), but one of the most important isthe delay in diagnosis, together with the difficulty oflocalisation, particularly in cases of metastaticinfection.
Clinically, intracranial infection may be suspectedbut its ultimate diagnosis depends upon investiga-tions. Keogh (1976) has shown that intracerebral andsubdural pus can be detected by computed tomo-graphy (CT scan; EMI scan), and that contrast en-
hancement is a useful adjunct. The question remainsas to whether the computed scan can exclude thepossibility of an abscess in a patient who is known tohave, or is suspected clinically of having, intracranialinfection. It is this question which we have tried toanswer by a retrospective survey of the patientsadmitted to the Institute of Neurological Sciencessince the installation of computed tomography inlate 1973.
Patients and Methods
Excluding obvious postoperative cases, 93 patientswith a diagnosis of intracranial infection were ad-mitted to the Institute between December 1973 andJuly 1976. Twenty-seven patients were not submittedto computed tomography, and 15 of these were in-Accepted 28 October 1976
vestigated radiologically to exclude a space occupyinglesion. It is not clear why they did not undergo com-puted tomography; the likely possibilities are 'down-time' on the scanner (both for maintenance andupgrading work), and, particularly in the early daysof computed tomography, clinical personal pref-erence. One of these patients had a cerebellar abscesswhich was diagnosed by positive contrast ventriculo-graphy. The remaining 12 cases were consideredclinically not to have space occupying lesions, but inone case with a persistent cerebrospinal fluid leakfrom the anterior fossa, a subdural empyema wasfound at surgery. Of the 25 patients who did not havean abscess, 18 were diagnosed as having meningitis,and seven encephalitis.Computed tomography was undertaken in 64
patients in the course of investigation to exclude anabscess, and in a further two patients after surgery forabscess. The study has been confined to thefindings in these patients who have been studiedretrospectively.The ages of the patients ranged from 10 months to
73 years. The male:female ratio was 32:34 over thewhole group, and was equal (10:10) for those withabscesses. The diagnoses are shown in Table 1, thesituation ofthe abscesses in Table 2, and their primarysources in Table 3. The mortality amongst the patientswith abscesses was 35 %, and for the remainingpatients 15%.The CT scans of six patients were not traceable.
The remaining 60 patients underwent 102 CT scans.These have been reviewed by two members of thesurgical staff who knew only that the CT scans werethose of patients with intracranial infection. Two CTscans on the same patient were reviewed by only onesurgeon as the second was directly involved at thetime of the study with the patient's management. The
14
Protected by copyright.
on July 19, 2022 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.40.3.214 on 1 M
arch 1977. Dow
nloaded from

Valiue ofcomputed tomography in the diagnosis of intracranial abscess
Table 1 Diagnoses in 66 patients undergoing computedtomography
Diagnoses Number ofpatients
Abscess 20Encephalitis 22Meningitis (pyogenic) 15Tuberculous meningitis 9
66
Table 2 Abscess sites
Sites Number ofpatients
Intracerebralfrontal 1temporal 5parietal occipital 4cerebellar 4multiple
pyogenic Ituberculous 2
Extracerebralsupratentorial 2infratentorial l
20
Table 3 Primary source ofabscesses
Source Number ofpatients
Ear 7Paranasal sinuses 2Chest
pyogenic 2tuberculous 2
Postoperativeearly 2late I
Injury 1Cyanotic heart disease 1Pelvic infection INo cause found 1
20
radiologist was asked to review any CT scan if therewas a marked disagreement between the surgeons'findings. Computed tomography was undertakenwith the EMI head scanner which is fitted with a 13mm collimator. The matrix was 80 x 80 in 30 in-stances, and from March 1975, the updated 160 x160, in 72. Before early 1976, the patient's head wasmoved by 2.5 cm between each paired CT scan. Sincethat time the technique has been modified such thatthe movement is now 2 cm. Intravenous sodiumiothalamate 70% w/v (Conray 420: May and Baker)is used for contrast enhancement in a dose of 50 mlfor adults and proportionally less for children.
Results
The radiological findings as reported at the time ofthe first CT scan for each patient are summarised inTable 4, and are related to the presence or absence ofan abscess.
Table 4 First CT scan report andpresence ofabscess
Report Number of Number ofpatients abscesses
Normal 30 0Abscess 8 8Hydrocephalus 9 0HydrocephalusNo post. fossa views 2 2
Reduced density 4 2Porencephalic cyst 1 0Recurrent post. fossa cholesteatoma I IUnsatisfactory 8 2Follow-up only 2 2Lost result 1 0
66 17
Table 5 First CTscan report in confirmed abscesses
CT Scan Number ofpatients
Positive diagnosis 8Unsatisfactory 2HydrocephalusNo post. fossa views 2
Recurrent cholesteatoma IReduced density 2
15
Of 15 patients who had an intracranial abscess(Table 5), nine (60%) were positively identifiedas having a localised space occupying mass, eventhough in one the previous history ofa posterior fossacholesteatoma was misleading preoperatively. Of theremaining 40%, two patients (13%Y.) had unsatisfac-tory scans due to patient movement; one patient(7%.) had hydrocephalus which was further investi-gated by ventriculography which confirmed thepresence of a posterior fossa lesion; and two patients(13%O) may not have had intracranial abscesses at thetime of their first CT scan. Of the latter group, onepatient, who had mild hydrocephalus which was notprogressive over three months (and in whom noposterior fossa views were taken), was found 10months after the first CT scan to have marked hydro-cephalus and a mass in the posterior fossa diagnosed,after removal, as a tuberculous abscess; the otherpatient's CT scan showed a questionable area ofreduced density (in relationship to an air-gun pellet)without displacement of the ventricles, but he diedsuddenly one month later when an abscess rupturedinto the ventricular system. In the final patient (7 %),
215
Protected by copyright.
on July 19, 2022 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.40.3.214 on 1 M
arch 1977. Dow
nloaded from
216
an area of oedema with ventricular shift, which didnot enhance on intravenous administration ofsodium iothalamate, was present on the CT scan, andpostmortem examination showed at least 12 wide-spread abscesses which varied in size from 1 mm indiameter to 1 x 1.5 x 3 cm. Two patients dido nothave CT scans as part of the initial investigation; itwas used as a method of follow-up after the installa-tion of a microsuspension of barium sulphate(Steripaque: Nicholas Laboratories).Three patients did not have abscesses at the time of
their CT scan: two were diagnosed by subsequentcomputed tomography, one 22 days after the originaldiagnosis of cortical thrombophlebitis complicatingmeningitis, and the other 20 days after the diagnosisof meningitis. The remaining patient had a technicallyunsatisfactory CT scan which was followed by carotidangiography, which suggested a temporal lobeswelling. This was biopsied and found to be due tocerebritis. One week later the patient deteriorated,and reneedling of the brain confirmed the presence ofan abscess at the same site.The results of the surgeons' review of the 102 CT
scans are presented in Tables 6 and 7, and the findingsin those patients who had an intracranial abscess atthe time of the investigation, in Table 8. There is goodcorrelation between the surgeons except in one case,in which Surgeon 1 diagnosed an abscess in the leftcerebellum and Surgeon 2 passed the CT scan asnormal. This CT scan was shown to the radiologistwho had not reported it previously, and he consideredit to be normal. In patients who had a technicallysatisfactory CT scan, there were none with abscesseswho did not have either the abscess shown clearlywith sodium iothalamate enhancement, or have anarea of reduced density together with ventricularshift. Only one patient, who proved to have menin-
Table 6 First CT scan 'blind' review
Finding Surgeon I Surgeon 2
Normal 21 22Abnormal
abscess 6 5reduced density with shift 4 4reduced density no shift 1 Iother
porencephalic cyst 1 Ihydrocephalus 4 4dense object 1 1
Unsatisfactorypatient movementnormal ventricles 7 6enlarged ventricles 3 3not completed 6 6
Hydrocephalusno post. fossa views 4 4
Follow-up 2 2
60 59
M. D. M. Shaw andJ. A. Russell
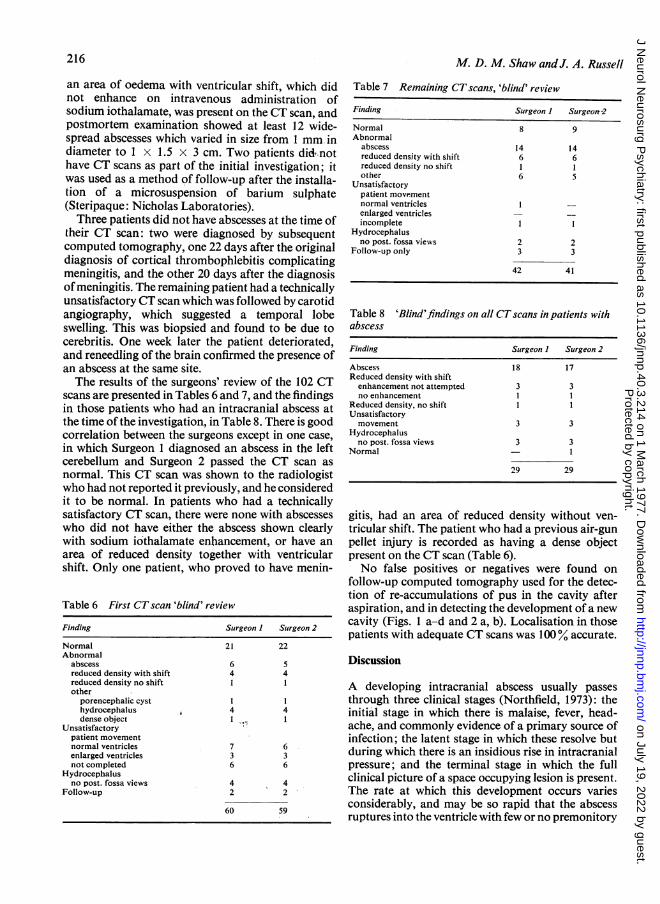
Table 7 Remaining CTscans, 'blind' review
Finding Surgeon 1 Surgeon-2
Normal 8 9Abnormal
abscess 14 14reduced density with shift 6 6reduced density no shift I Iother 6 5
Unsatisfactorypatient movementnormal ventricles I -
enlarged ventricles - -incomplete I I
Hydrocephalusno post. fossa views 2 2
Follow-up only 3 3
42 41
Table 8 'Blind'findings on all CTscans in patients withabscess
Finding Surgeon I Surgeon 2
Abscess 18 17Reduced density with shiftenhancement not attempted 3 3no enhancement I I
Reduced density, no shift I IUnsatisfactorymovement 3 3
Hydrocephalusno post. fossa views 3 3
Normal - I
29 29
gitis, had an area of reduced density without ven-tricular shift. The patient who had a previous air-gunpellet injury is recorded as having a dense objectpresent on the CT scan (Table 6).No false positives or negatives were found on
follow-up computed tomography used for the detec-tion of re-accumulations of pus in the cavity afteraspiration, and in detecting the development of a newcavity (Figs. 1 a-d and 2 a, b). Localisation in thosepatients with adequate CT scans was 100% accurate.
Discussion
A developing intracranial abscess usually passesthrough three clinical stages (Northfield, 1973): theinitial stage in which there is malaise, fever, head-ache, and commonly evidence of a primary source ofinfection; the latent stage in which these resolve butduring which there is an insidious rise in intracranialpressure; and the terminal stage in which the fullclinical picture of a space occupying lesion is present.The rate at which this development occurs variesconsiderably, and may be so rapid that the abscessruptures into the ventricle with few or no premonitory
Protected by copyright.
on July 19, 2022 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.40.3.214 on 1 M
arch 1977. Dow
nloaded from

Value ofcomputed tomography in the diagnosis of intracranial abscess
(a) (.U)
(C) (d)
Fig. la-d CTscans showing a left temporal abscess (a), before a negative re-aspiration two days later (b),re-accumulation some nine days later (c), and a return to normal 17 days later (d)
symptoms. While it is possible clinically to suspectthat a patient has intracranial infection, confirmationof the diagnosis depends upon investigations. Thatthe patient may have an intracranial abscess com-plicating the infection is suggested by the presence ofa local infected source, for example, a discharging ear.But in cases of metastatic abscess, which now appearto be relatively more common (Carey et al., 1972;Samson and Clark, 1973; Martin, 1973), the diagnosis
is more difficult. Investigation is required to confirmthe diagnosis, and to localise the abscess as accuratelyas possible before the terminal stage is reached.Lumbar puncture in the presence of an abscess is a
dangerous procedure (Garfield, 1969; Morgan et al.,1973; Samson and Clark, 1973), and analysis of thecerebrospinal fluid, either from the lumbar sac orfrom the lateral ventricles (Shaw and Russell, 1975),is not helpful in the diagnosis of intracranial abscess.
B
217
Protected by copyright.
on July 19, 2022 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.40.3.214 on 1 M
arch 1977. Dow
nloaded from

M. D. M. Shaw andJ. A. Russell
Fig. 2a and b CTscans showing a left temporal abscess(a), and 12 days later a new more anteriorly placedabscess (b)
Electroencephalography is of value both in diag-nosing and in localising supratentorial intracranialabscesses (Loeser and Scheinberg 1952; Morgan et al.,1973). Localisation is possible in approximately 50%of cases (Ziegler and Hoeffer, 1952; Garfield, 1969),but is misleading in 7% (Ziegler and Hoeffer, 1952).An accurate diagnosis is achieved in only 36%
(Garfield, 1969). Hass and Laubichler (1967) sug-gested that serial studies allowed appreciation of thedevelopment of an intracranial abscess.
Isotope brain scanning has been found to be verysensitive in respect of the localisation of a lesionwhich takes up the isotope, but it lacks specificity(Jordan et al., 1972). In this series, for example, nineof the patients undergoing this investigation hadpositive scans; three of these had abscesses, twoherpes encephalitis, three meningitis, and onecerebritis. Of 16 patients with negative scans, one hada parietal abscess.Angiography and ventriculography have been
widely used. Krayenbuhl (1967) stated that the formerwas of great value in the diagnosis, and was indis-pensable for the localisation of a brain abscess.Garfield (1969) reported, however, that the accuracyof angiographic localisation supratentorially de-pended upon the site-temporal 100%, frontal 65 %,parietal 67 %, and subdural 68 %. He also found thatthe accuracy of ventriculography varied-temporal71 %, frontal 81 %, parietal 96%, and subdural 830%.Shaw and Russell (1975) showed it to be 97% accuratefor cerebellar abscess. Furthermore, Garfield (1969)found that the mortality among patients in whomlocalisation failed using arteriography or ventriculo-graphy was 81 %.
In a leading article in the British Medical Journal(1975), it was suggested that computed tomography,if it were more widely available, would greatly im-prove the results for abscess therapy. In this series,the overall mortality (35%) has not been reduced,presumably because it has not influenced either thetime at which the patient presents, or the other factorswhich are thought to affect the outcome (Le Beauet al., 1973; Shaw and Russell, 1975; van Alphen andDreissen, 1976). In the initial reporting by the radi-ologist, a definitive diagnosis was made in 60% ofcases who may have had an abscess at the time of theirfirst CT scan; although if the two who were unlikelyto have had abscesses at this time are excluded, thedetection rate was 69% (nine out of 13 patients). Ofthe remaining patients, one on computed tomographywas shown to have a marked hydrocephalus whichwas later shown to be due to a posterior fossa sub-dural abscess; one had an area of reduced densitywhich did not enhance with sodium iothalamate butwhich was associated with ventricular displacement;and there were two patients in whom the CT scan wastotally unsatisfactory because of patient movement.The latter underwent computed tomography in itsearly days, when it was not appreciated that generalanaesthesia was often required to obtain satisfactoryresults. Thus in no case was there a false negative CTscan. Similarly there were also no false negatives onthe follow-up CT scans.
218
Protected by copyright.
on July 19, 2022 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.40.3.214 on 1 M
arch 1977. Dow
nloaded from

Value ofcomputed tomography in the diagnosis of intracranial abscess
The degree of correlation between the findings onthe 'blind' random review on the CT scans by the twosurgeons was high. Surgeons were chosen to do thisbecause the question as to whether there is an abscessor not often arises out of normal hours when thesurgical staff are interpreting the CT scan. One CTscan was discussed with the radiologist because therewas disagreement as to whether it was normal orshowed evidence of a cerebellar abscess. The radiolo-gist felt that the CT scan was normal, and that theapparent rim which had appeared after the admin-istration of sodium iothalamate was not an abscesscapsule, but was more likely to be contrast mediumin normal blood vessels, as has been described byHuckman (1975). Ventriculography immediatelyafter the investigation demonstrated displacement ofthe fourth ventricle to the right, and surgical explora-tion revealed an area of cerebellitis with a smallamount of pus at its centre. It would, therefore,appear that observer error is of the order of 1% andmay result from the nature of the disease: for whendoes an area of inflammation become an abscess?
It has been suggested that, because there is an areaof hyperaemia around an intracerebral abscess, con-trast enhancement during computed tomographywill result in the development of a clearly defined haloof increased density (Huckman, 1975). In addition,Keogh (1976) found that in well developed abscessesthis halo was present before contrast enhancement.This phenomenon has recently been accepted as beingone of the features of an abscess on computed tomo-graphy although it is recognised that it is not specificfor the condition as it occurs in other lesions withnecrotic centres. This accounts for the lower positivediagnosis rate for abscesses in the 'blind' reviewing ofthe CT scans as opposed to the radiological reporting,because originally any evidence of a mass lesion onthe CT scan was accepted as being due to an abscess.However, it would appear that there are some intra-cerebral abscesses which do not enhance with contrastmedium but which are associated with ventriculardisplacement-for example, the patient who wasfound at postmortem examination to have more than12 abscesses. The largest of these was 1 x 1.5 x 3 cm.It is therefore just possible that, if the long axis of thisabscess was in the plane of the scan and the depth ofthe abscess at right angles to that plane was 1 cm, theenhancement could have been averaged out inadjacent scans. This explanation seems very unlikelybecause when the patient underwent computedtomography it had already been realised, (eventhough a 13 mm collimator had been used to controlthe depth of the X-ray beam), that the effective thick-ness of each slice was 10 mm, (Goodenough et al.,1975; New and Scott, 1975), and hence that therewere 5 mm gaps between each pair ofCT scans, if the
head was moved by 2.5 cm rather than 2 cm. Thus itwould seem that no part of this abscess could havebeen missed by the scan.During the period under review only three cases of
subdural empyema were admitted to the Institute,and in one of these the area of the empyema, theposterior fossa, was not seen on the CT scan. Fromthe remaining two cases, both supratentorial em-pyemas, we would agree with Keogh (1976) that thereis ventricular displacement with or without an area oflow density in the brain. We have not yet seen thesurface enhancement which he has described.
Localisation of the abscess as judged by computedtomography has been very good. The difficulties withlocalisation occur when follow-up is considered; forif the patient is not positioned identically, the relativeposition of the abscess may appear to have moved,even though in the case illustrated in Fig. 1 the re-current abscess was tapped in an identical fashionthrough the original burrhole. This may be over-come by inserting a small amount of suitablecontrast medium-for example, a microsuspensionof barium-which does not, at least on the 160 x 160matrix, cause a marked degree of interference.Furthermore, this allows routine skull radiographicfollow-up if the demand on computed tomography issuch that frequent follow-up CT scans are difficult toarrange. The advantage ofcomputed tomography forfollow-up is that it can detect multiple abscesses(Keogh, 1976), and in particular a new abscessdeveloping in relationship to the original one. Keoghhas also described a false positive result, on a follow-up CT scan. This was due to secondary infarctionfollowing the successful treatment of a subduralempyema. We have experienced a somewhat similarcase, though it was not misleading clinically. Thepatient, who was thought to be suffering from en-cephalitis, developed four small areas on the CT scan,which on contrast enhancement, showed the halophenomenon (Fig. 3). These appeared two weeks afterthe last normal CT scan at a time when the patientwas recovering from her illness, and gradually dis-appeared over the next month. It is not certain whatthese areas were as it was decided on clinical groundsnot to carry out a biopsy, but it was thought likelythat they represented areas of infarction.
Conclusion
Computed tomography is, therefore, a valuableaddition to the investigations available for the diag-nosis of intracranial abscess, particularly as the falsenegative rate is 1% or less. It is essential to achievegood CT scans, and it is often necessary to anaes-thetise the patient to prevent movement artefacts. Ifthe plain CT scan shows any abnormality, for example
219
Protected by copyright.
on July 19, 2022 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.40.3.214 on 1 M
arch 1977. Dow
nloaded from

M. D. M. Shaw andJ. A. Russell
Fig. 3 'False positive' CT scan.
ventricular distortion or an area of reduced density,contrast enhancement is necessary. If this reveals thehalo appearance then no further investigation isrequired. If enhancement does not occur, and par-ticularly if there is ventricular distortion, further in-vestigations are required: ventriculography for a
suspected infratentorial lesion, electroencephalo-graphy, and isotope brain scanning together withangiography, followed if necessary by burrholeexploration to exclude subdural pus or an intra-cerebral abscess supratentorially. It is disappointingthat the mortality has remained unchanged. Thepossibility that computed tomography facilitatesearly diagnosis is not yet proven, and cannot be so
until it is more generally available. Furthermore, theclinical diagnosis must be entertained early, and theneed for urgent treatment in neurosurgical unitsrecognised.
We would like to acknowledge the advice given byDr J. L. Steven, consultant neuroradiologist, and thekindness of the consultant staff at the Institute ofNeurological Sciences, Glasgow for allowing us
access to their case material, and to thank Miss H.Wilson, Mrs W. McDermid, and Mrs J. Rubythonfor typing the manuscript.
References
Bhatia, R., Tandon, P. N., Banerji, A. K., and Prakash, B.(1976). Brain abscess and congenital heart disease.Acta Neurochirurgica, 33, 233-239.
British Medical Journal (1975). Leading article. Brainabscess. British Medical Journal, 3, 504-505.
Carey, M. E., Chou, S. N., and French, L. A. (1972).Experience with brain abscesses. Journal of Neuro-surgery, 36, 1-9.
Garfield, J. (1969). Management of supratentorialabscess: A review of 200 cases. British Medical Journal,2, 7-11.
Goodenough, D. J., Weaver, K. E., and Davis, D. 0.(1975). Potential artifacts associated with the scanningpattern of the EMI scanner. Radiology, 117, 615-620.
Hass, R., and Laubichler, W. (1967). Die Bedeutung derElektroenzephalographie fur die Diagnose vonHirnabszessen. Acta Neurochirurgica, 16, 79-96.
Huckman, M. S. (1975). Clinical experience with theintravenous infusion of iodinated contrast material asan adjunct to computed tomography. Surgical Neurol-ogy, 3, 297-318.
Jordan, C. E., James, A. E., and Hodgess, F. J. (1972).Comparison of the cerebral angiogram and the brainradionuclide image in brain abscess. Radiology, 104,327-331.
Keogh, A. J. (1976). Computerised transverse axial tomo-graphy for the early diagnosis and follow-up ofintracranial abscess. Presented at the combined meetingof Nederlandse Vereniging Van Neurochirurgen andthe Society of British Neurological Surgeons: Amster-dam, Netherlands.
Krayenbiihl, H. A. (1967). Abscess of the brain. ClinicalNeurosurgery, 14, 25-44.
Le Beau, J., Creissard, P., Harispe, L., and Redondo, A.(1973). Surgical treatment of brain abscess andsubdural empyema. Journal of Neurosurgery, 38,198-203.
Loeser, E., and Scheinberg, L. (1957). Brain abscess: Areview of ninety-nine cases. Neurology (Minneap.), 7,601-609.
Martin, G. (1973). Non-otogenic cerebral abscess. Journalof Neurology, Neurosurgery, and Psychiatry, 36,607-610.
Morgan, H., Wood, M. W., and Murphey, F. (1973).Experience with 88 consecutive cases of brain abscess.Journal ofNeurosurgery, 38, 698-704.
New, P. F. J., and Scott, W. R. (1975). ComputedTomography of the Brain and Orbit (EMI Scanning).Williams and Wilkins: Baltimore.
Northfield, D. W. G. (1973). The Surgery of the CentralNervous System. Blackwell: Oxford.
Samson, D S., and Clark, K. (1973). A current review ofbrain abscess. American Journal of Medicine, 54,201-210.
Shaw, M. D. M., and Russell, J. A. (1975). Cerebellarabscess: A review of 47 cases. Journal of Neurology,Neurosurgery, and Psychiatry, 38,429-435.
Van Alphen, H. A. M., and Dreissen, J. J. R. (1976).Brain abscess and subdural empyema: factors influenc-ing mortality and the results of various surgicaltechniques. Journal of Neurology, Neurosurgery, andPsychiatry, 39, 481-490.
Ziegler, D. K., and Hoeffer, P. F. A. (1952). Electro-encephalographic and clinical findings in twenty-eightverified cases of brain abscess. Electroencephalographyand Clinical Neurophysiology, 4, 41-44.
220
Protected by copyright.
on July 19, 2022 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.40.3.214 on 1 M
arch 1977. Dow
nloaded from
Copyright © 2022 FDOKUMEN




















