
Control of Allergic Rhinitis and Asthma Test (CARAT): dissemination and applications in primary care
Privileged Comm
unicationUteroglobin-related protein 1 and Clara cell protein in induced sputum of
patients with asthma and rhinitis
Journal: CHEST
Manuscript ID: CHEST-06-0835.R1
Manuscript Type: Manuscript
Date Submitted by the Author:
30-Jun-2006
Complete List of Authors: Claire, de Burbure; Catholic University of Louvain, School of Public Health Patrizia, Pignatti; Fondazione Salvatore Maugeri, Allergy Corradi, Massimo; University of Parma, Laboratory of Industrial Toxicology, Department of Clinical Medicine, Nephrology and Health Sciences Mario, Malerba; Universita of Brescia, department of Internal Medicine André, Clippe; Catholic University of Louvain, School of Public Health Xavier, Dumont; Catholic University of Louvain, School of Public Health Gianna, Moscato; Fondazione Salvatore Maugeri, Allergy Mutti, Antonio; University of Parma, Laboratorio di Tossicologie Industriale bernard, alfred; Catholic Universioty of Louvain, Public Health
Keywords: ALLERGY, ASTHMA, SPUTUM
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
Privileged Comm
unication
1
Uteroglobin-related protein 1 and Clara cell protein in induced sputum of patients with
asthma and rhinitis
de Burbure Claire1, Pignatti Patrizia2, Corradi Massimo3, Malerba Mario4, Clippe André1,
Dumont Xavier1, Moscato Gianna2, Mutti Antonio3, Bernard Alfred1
1Unit of Industrial Toxicology and Occupational Medicine, Faculty of Medicine, Université
Catholique de Louvain, Belgium
2Allergy and Immunology Unit, Fondazione Salvatore Maugeri, IRCCS, Pavia, Italy
3Laboratorio di Tossicologia Industriale, Universita degli Studi di Parma, Parma, Italy
4Department of Internal Medicine, University of Brescia, Spedali Civili, Brescia, Italy
Running title: Asthma/Rhinitis: New Sputum Proteins
Conflict of interest: none of the authors has a conflict of interest to disclose
Address correspondence to A. Bernard, Unit of Industrial Toxicology and Occupational
Medicine, Université Catholique de Louvain, Clos Chapelle-aux-Champs 30, bte 3054, B-
1200 Brussels Belgium Phone: 32-2-7643220, Fax: 32-2-7643228, e-mail:
Total word count = 3,216
Key words: induced sputum, uteroglobin-related protein 1, Clara cell protein, asthma, rhinitis.
Page 1 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Privileged Comm
unication
2
LIST OF ABBREVIATIONS
Alb: albumin
CC16 : Clara cell protein
DTT : dithiothreitol
FEV1: forced expiratory volume in one second
PD20FEV1: methacholine dose causing a 20% fall in FEV1
UGRP1: uteroglobin-related protein 1
VC: vital capacity
Page 2 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Privileged Comm
unication
3
ABSTRACT
(Word count: 217)
Rationale: uteroglobin-related protein 1 (UGRP1) and Clara cell protein (CC16), members of
the secretoglobin family, increasingly appear to play a role in airway inflammatory response.
Objectives: to explore levels of UGRP1 and CC16 in induced sputum of patients with asthma
and rhinitis.
Methods: induced sputum samples of patients suffering from asthma or rhinitis (n = 32 each,
atopics 24/32 and 20/32 respectively) and from 19 non-smoking non-atopic controls were
analyzed for cytology and levels of UGRP1, CC16 and albumin.
Measurements and main results: sputum UGRP1 increased in both asthma and rhinitis,
most strikingly so in asthma, where changes were most significant in atopic individuals. By
contrast, sputum CC16 did not change significantly in either condition although it was
positively correlated with UGRP1 in patients and controls. Changes in sputum UGRP1 in
atopic asthma were not linked to permeability changes reflected by increased albumin levels,
but correlated positively with sputum macrophages and negatively with eosinophils. The
observed differences in UGRP1 and CC16 may be linked to different cell populations being
responsible for their secretion, UGRP1 being mainly secreted in larger conducting airways
whereas CC16 is mainly secreted by the nasal and peripheral airways epithelium.
Conclusions: the increase in UGRP1 but not of CC16 in asthma and rhinitis suggests that
UGRP1 may play a role in these inflammatory diseases.
Page 3 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Privileged Comm
unication
4
INTRODUCTION
(Word count: 450)
Non-invasive methods for assessing the airway inflammatory response, which is central to the
pathogenesis of asthma and rhinitis, have been developed in the last decade with the hope to
reliably and accurately monitor patient progress and response to therapy. One such newly
developed and evolving tool consists in the study of lung-specific proteins secreted into the
airways lining fluid by both the conducting and the respiratory airway epithelial cells1.
The Clara cell protein, small 16kD protein secreted throughout the airways but mainly by the
bronchiolar Clara cell (hence called CC16), has been studied in relation to asthma and rhinitis
in particular as its gene is localized on the p12-q13 region of human chromosome 11 involved
in inflammation regulation. CC16 expression is indeed decreased in asthma2 and in case of
respiratory tract inflammation in both man3 and animals4,5. A38G gene polymorphism has
also been linked to lower serum CC16 levels and a higher risk of being asthmatic in some
populations6,7. A recent gene profiling study in allergic rhinitis furthermore reported CC16 to
have the most decreased anti-inflammatory gene expression among over 44,927 genes8.
CC16-deficient mice show increased sensitivity to hyperoxia or ozone damage, exaggerated
inflammatory responses1, with increased pulmonary eosinophilia when antigen-sensitized and
challenged9. CC16 has important immunosuppressive and antiinflammatory properties, which
include the inhibition of inflammatory mediators such as cytosolic phospholipase A2,
interferon-γ, tumor-necrosis factor α, as well as platelet-derived growth factor-induced
chemotaxis of fetal lung fibroblasts1. Measuring CC16 in bronchoalveolar lavage fluid, where
it reflects epithelial function, and in serum, bringing useful information on the permeability of
the alveolocapillary membrane, has therefore proven useful in assessing both acute and
chronic airway damage.
Page 4 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Privileged Comm
unication
5
Recently another small protein belonging to the same family as CC16, the secretoglobin
family10, has been discovered: uteroglobin-related protein 1 (UGRP1) is a 17 kDa
homodimeric lung-specific protein11,12,13 also called high in normal 2 protein (HIN2) or
secretoglobin SCGB3A212. As mouse UGRP1 has an overall aminoacid sequence identity of
25% to mouse Clara cell protein, including an area called antiflammin containing several
lysine residues, it is supposed to share some of its anti-inflammatory properties although its
precise functions are still unknown11. UGRP1 appears highly specific of the airways, and our
laboratory has been characterizing, sequencing and evaluating it along other pneumoproteins
as potential biomarker of lung damage since 1999 (GenBank deposit: UGRP2: AF436839-41;
UGRP1: AF439544-7)14. Expression of UGRP1 mRNA has been shown to decrease in mouse
lung after induction of inflammation by in situ hybridization11.
In this study, levels of CC16 and UGRP1 were analyzed for the first time in induced sputum
samples of patients with either asthma or rhinitis with a view to investigating the differential
diagnostic potential of the two pneumoproteins in these two conditions.
Page 5 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Privileged Comm
unication
6
MATERIALS AND METHODS
(Word count = 667 + online supplement!)
Population studied
Patients gave their signed informed consent to participate into the study, which was approved
by the Ethical Committees of the Salvatore Maugeri Foundation IRCCS and the University
of Brescia and was conducted according to the Declaration of Helsinki. Induced sputum
specimens and lung function tests were obtained from 32 patients with intermittent to
moderate-persistent bronchial asthma, 32 rhinitis patients and 19 healthy volunteers
(men/women: 21/11, 10/22 and 10/9 respectively). Patients came from Pavia (Allergy and
Immunology Unit, Fondazione Salvatore Maugeri) and controls from Brescia or Parma
University (Internal Medicine and Industrial Toxicology respectively). Atopy was defined as
at least one positive skin prick test for common inhalant allergens (with positive histamine
prick). Bronchial asthma was diagnosed according to NHI Guidelines15. Allergic rhinitis was
diagnosed according to ARIA Guidelines16. Patients with rhinitis symptoms and negative skin
tests, after consultation with an ear, nose and throat specialist, received the diagnosis of non-
allergic rhinitis.
Sputum induction and processing
Sputum induction was obtained as previously described17. Sputum processing was performed
with 0.1% dithiothreitol (DTT), according to International guidelines17,18. After separation
from supernatant by centrifugation, cell count and viability by trypan blue exclusion were
determined by light microscopy. Cytospins were stained with Diff-Quick (Dade Diagnostika
GmbH, Unterscheiβheim), analyzed for differential cell count by counting 500 nonsquamous
cells minimum, and reported as percentages of total nonsquamous cells. Only sputum samples
with less than 30% squamous cells were considered acceptable.
Page 6 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Privileged Comm
unication
7
Sample analysis
Sputum supernatants were stored at –80 °C until evaluation. Sputum CC16 and albumin were
quantified by semi-automated non-isotopic latex immunoassay as previously described19,20.
The procedure for quantifying UGRP1 was similar to the above, using a combination of two
in-house polyclonal anti-UGRP1 antibodies. The between and within-run coefficients of
variation of both immunoassays in biological fluids, including sputum, were between 5 and
10%. The effect of DTT treatment on the concentrations of UGRP1 and CC16 was assessed
by adding DTT (0.1%) to six sputum samples with UGRP1 and CC16 concentrations ranging
from 20 to 3,980 µg/l and 27 to 2,170 µg/l, respectively. The concentrations of UGRP1 in
treated and untreated samples were highly correlated (Pearson’s r = 0.98, p<0.001) with post-
treatment values averaging 70 % of pretreatment values. Concentrations of CC16 in treated
and untreated samples were also highly correlated (Pearson’s r = 0.94, p<0.001) with no
systematic difference (post-treatment values averaged 102 % of the pre-treatment values).
Additional detail on the method for making UGRP1 measurements is provided in an online
data supplement. Due to the small volumes of some samples, all biological parameters could
not be determined in all subjects, exact numbers are indicated in the tables.
Lung function tests
Spirometry was performed according to European Respiratory Society guidelines21 with a
computerized water-sealed spirometer (BIOMEDIN, Padova). Measurements were expressed
as percentage of predicted normal values based on race, age, sex, and height. Methacholine
challenge testing was performed with a nebulizer (MEFAR, Brescia) connected to a dosimeter
as previously reported22. The methacholine dose causing a 20% fall in FEV1 (PD20FEV1)
was considered positive if PD20 was <1000 µg.
Page 7 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Privileged Comm
unication
8
Statistical analysis
Results are presented as means ± SEM. For statistical analysis, UGRP1, CC16, albumin and
absolute macrophage or eosinophil counts in sputum were normalized by log transformation,
and their results are presented as geometric means. Group means were compared by two-sided
unpaired Student’s t test or by ANOVA followed by Dunnett’s post hoc test. Associations
between sputum UGRP1, CC16, albumin and sputum cell counts were evaluated by simple
regression analysis and calculating Pearson’s correlation coefficient. Influence of age, gender
(male/female), diagnosis (asthma, 0/1; rhinitis, 0/1), smoking status (never-smoker/current
smoker) and atopy (0/1) was studied by stepwise multiple regression (entry: p = 0.25, staying
in model: p = 0.05). Three past-smokers were grouped with never-smokers. All statistical
analyses were performed using StatView® (StatView 5, SAS 2000-2001 © SAS Institute
Inc.). Figures were drawn with StatView or GraphPad Prism (GraphPad Prism 3.03, 2002, ©
GrapPad Prism Inc.). Statistical significance was set at 0.05.
Page 8 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Privileged Comm
unication
9
RESULTS
(Word count = 713)
The general characteristics, lung function and sputum cytology of controls, rhinitis and
asthmatic patients are given in Table 1, including disease duration, atopy and smoking status,
steroid treatment, methacholine sensitivity, sputum cytology and some lung function tests.
Whereas all 19 controls were non-smokers and non-atopic, about four in ten asthmatic and
rhinitis patients were smokers, and two thirds atopic. There were no significant differences in
lung function between patients and controls, indicating overall good control of the disease.
However, in comparison with rhinitis patients, asthmatics had significantly lower mean values
of FEV1, Tiffeneau index and vital capacity. Only one rhinitis patient (1/32, 3.1%) was
methacholine sensitive compared to 12/32 asthmatics (37.5%). The proportions of asthmatics
with a positive methacholine test were similar between those receiving inhaled corticosteroids
(7/19, 36.8%; low dose, 1/6; medium dose 4/9 and high dose, 1/6) and those who were not
under steroid medication (5/13, 38.5%). As expected, asthmatics had significantly raised
sputum eosinophil numbers but reduced macrophages compared to both controls and rhinitis
patients. Eosinophils were also raised in rhinitis compared to controls, though much less
dramatically so than in asthma. Epithelial cell numbers were increased in both groups of
patients compared to controls.
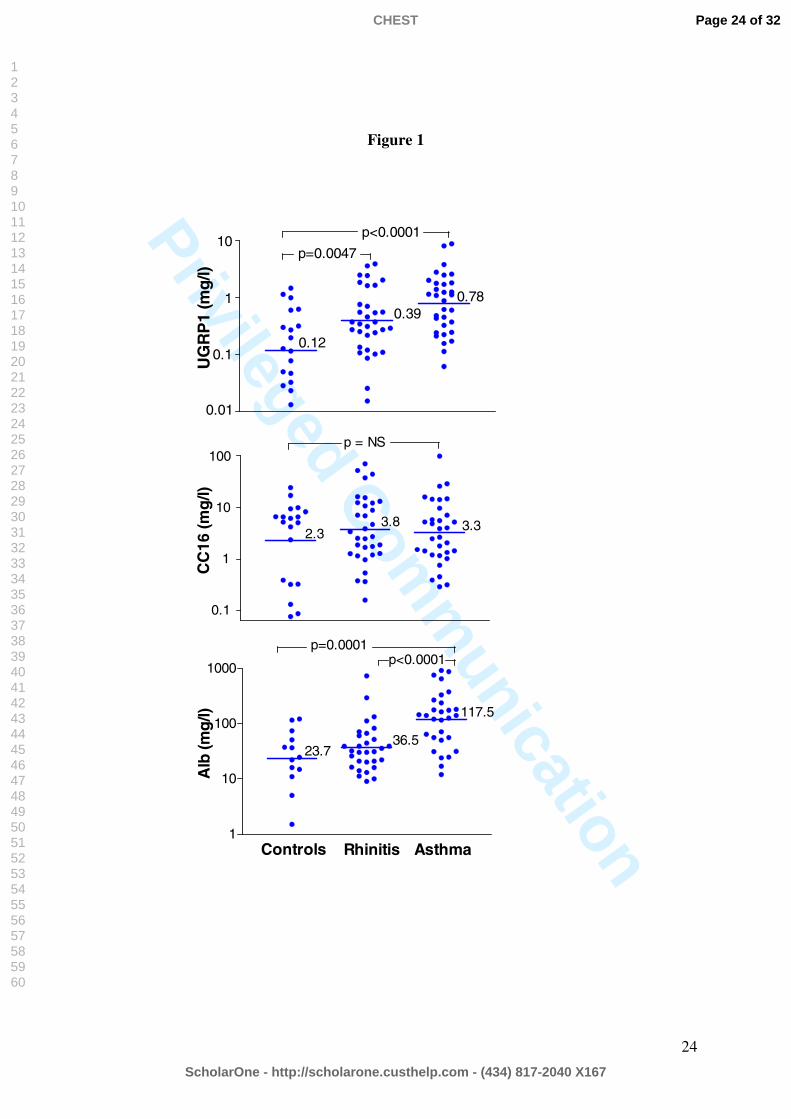
Concentrations of sputum UGRP1, CC16 and albumin in control, rhinitis and asthma subjects
are compared in Figure 1. Whereas variations in CC16 levels were not significantly different
between the three groups, UGRP1 was elevated in both rhinitis and asthma patients compared
to controls, particularly so in asthma. Sputum albumin levels only rose significantly in
asthma. Stepwise multiple regression analysis on the whole population taking age, gender,
smoking status, asthma and rhinitis into consideration confirmed the only significant
Page 9 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Privileged Comm
unication
10
determinants of sputum UGRP1 to be both asthma (partial r = 0.35, p = 0.013) and rhinitis
(partial r = 0.27, p = 0.011), while none of the tested predictors influenced sputum CC16.
Albumin levels were positively associated with asthma (partial r = 0.48, p < 0.0001), whereas
smoking status was a negative determinant (partial r = -0.26, p = 0.0112). Division by atopy
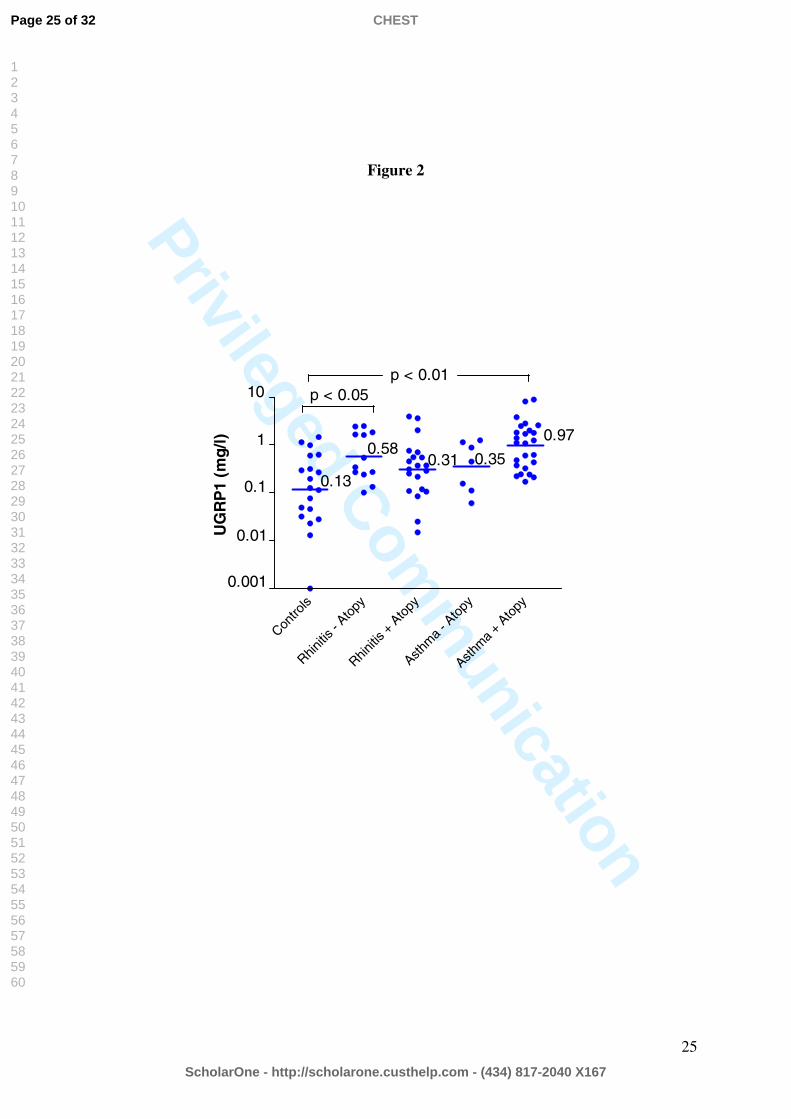
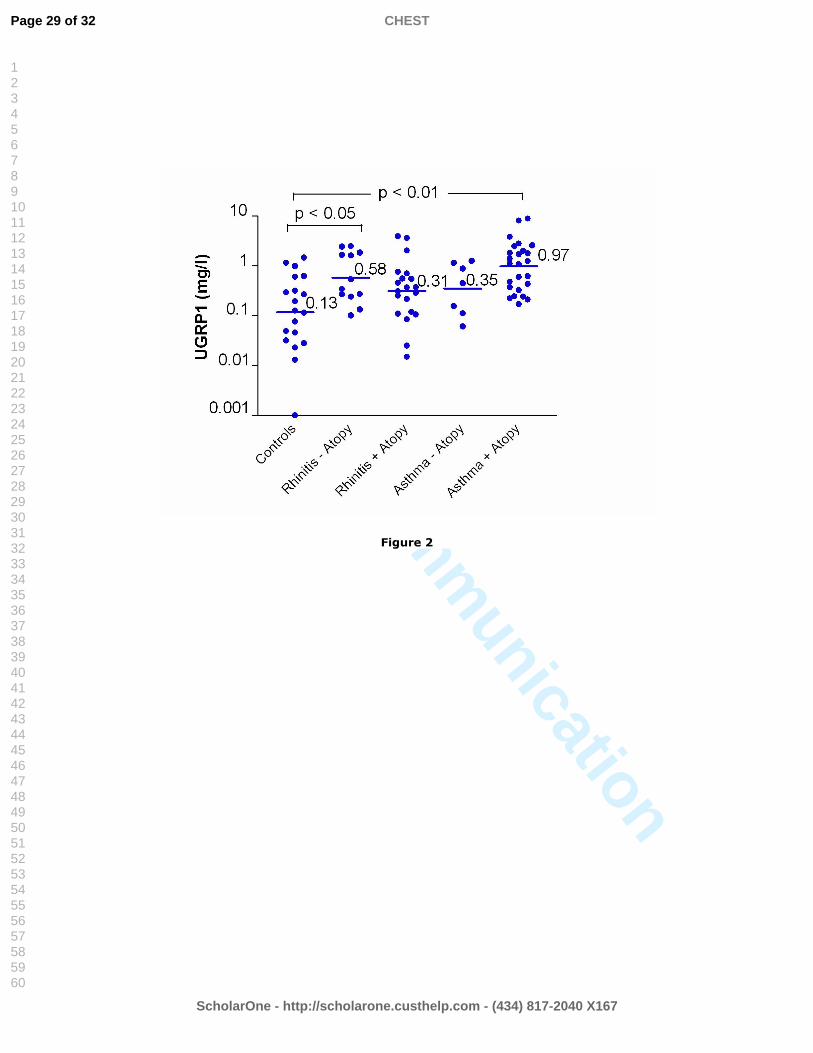
did not change results concerning CC16 and albumin. By contrast, this splitting revealed that
rhinitis determined UGRP1 levels in non-atopics only (partial r = 0.354, p = 0.029) while
asthma remained sole significant determinant in atopics (partial r = 0.415, p = 0.005). The
influence of atopy on sputum UGRP1 levels is illustrated in Figure 2.
Methacholine sensitivity did not appear to affect either CC16 or UGRP1 sputum levels
globally. Among atopics, however, methacholine positive subjects had significantly increased
protein levels (CC16 and UGRP1: p = 0.045 and 0.009 respectively between 10 positive vs 28
negative subjects). Sputum albumin levels also increased with positive methacholine
challenge (12 positive vs 40 negative subjects: p = 0.024), but again this increase only
concerned atopics (9 positive vs 26 negative subjects: p = 0.008, p not significant for non-
atopic methacholine groups). Comparing the various inhaled steroid regimens in our small
number of treated subjects did not show any statistically significant differences in sputum
UGRP1 and CC16 (results not shown).
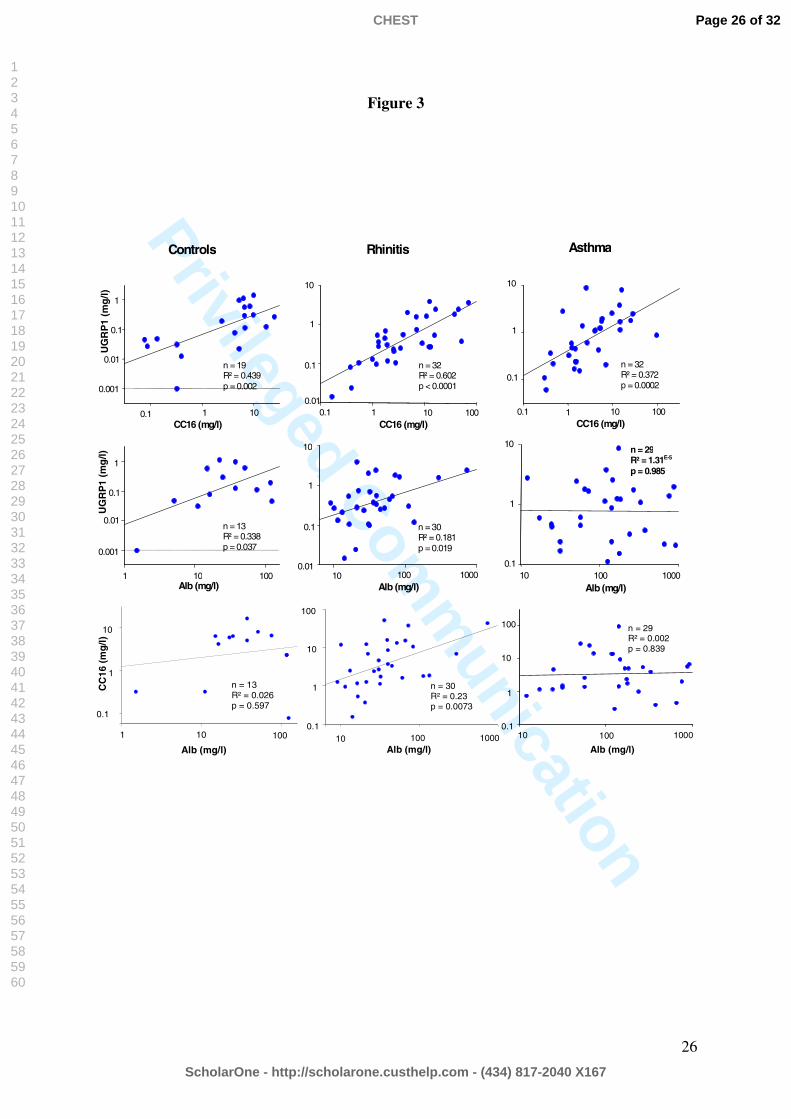
Sputum UGRP1 was significantly correlated to CC16 in all three subject groups whereas
correlations of these two proteins with albumin were weak and even non-existent in the case
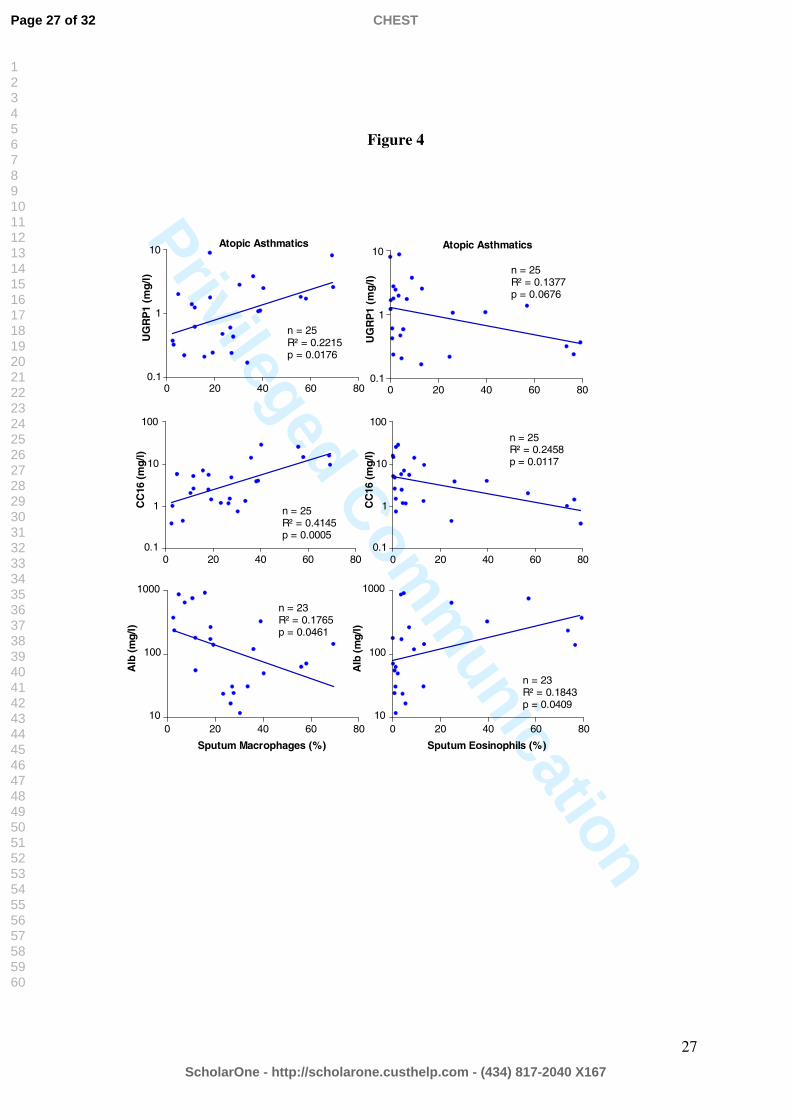
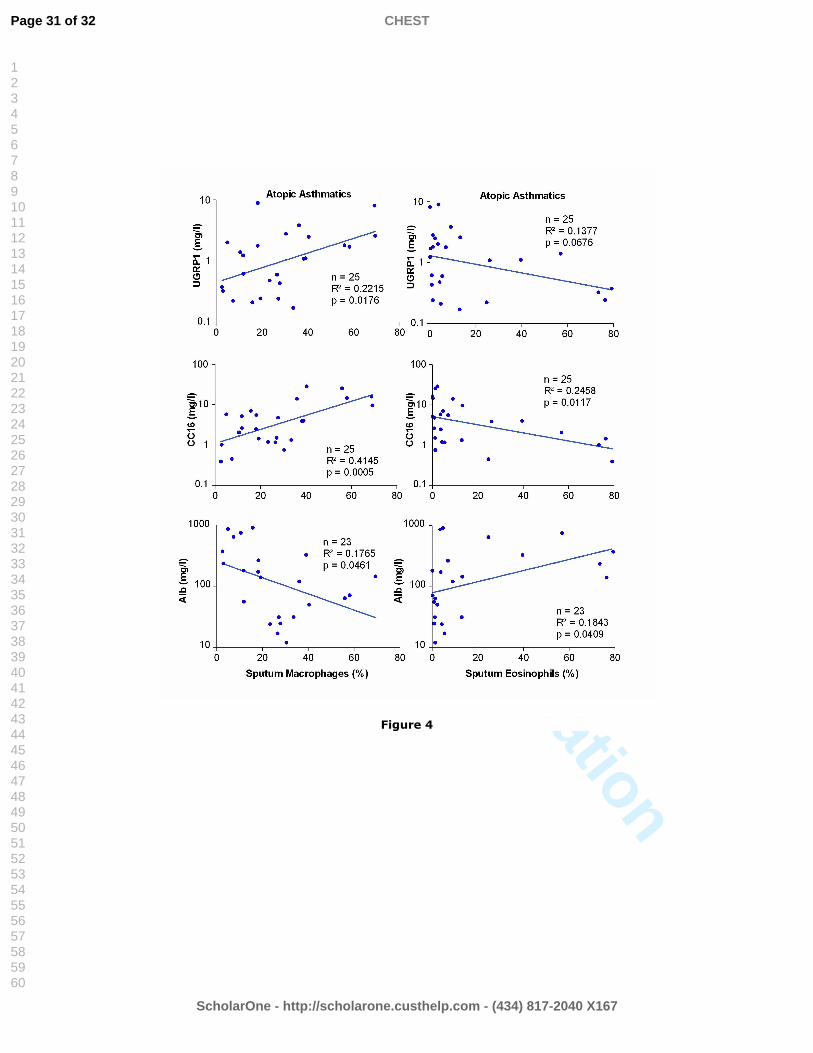
of asthma (Figure 3). In atopic asthmatics, sputum UGRP1 and CC16 correlated positively
with macrophages and negatively with eosinophils expressed as total cell percentage, whereas
albumin indicated opposite correlations (Figure 4). These correlations were confirmed when
using absolute cell numbers per milligram and more pertinently per milliliter of sputum, unit
Page 10 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Privileged Comm
unication
11
used for proteins. In particular, positive correlations with sputum macrophages were then also
observed for the whole population (UGRP1 (n=64): R2=0.165, p=0.0009 and R2=0.187,
p=0.0004; CC16 (n=64): R2=0.21, p=0.0001 and R2=0.234, p<0.0001 with macrophage
numbers per ml and mg of sputum, respectively). It is important to realize that correlations
emerging between URGP1 and CC16 as well as between these proteins and cells counts, were
calculated over very wide ranges of values, requiring logarithmic scales to be displayed.
Although statistically very significant, most of these correlations reflect associations that are
relatively weak. UGRP1 concentration in sputum, for instance, can show variations of more
than one order of magnitude for a given value of CC16 (Figure 3) while less than 25% of
UGRP1 or CC16 variations are related to changes in sputum eosinophils (Figure 4).
Page 11 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Privileged Comm
unication
12
DISCUSSION
(word count = 961)
To our knowledge this is the first report of UGRP1 protein being assayed in any human
biological sample, and the first time CC16 is measured in induced sputum. Most interestingly,
UGRP1 levels were significantly increased in both asthma and rhinitis compared to controls,
the rise in atopic asthma being the most remarkable. CC16 levels, although correlated to
UGRP1, were by contrast not observed to change significantly in either asthma or rhinitis.
These increases in UGRP1 cannot be explained by epithelial permeability changes, known to
occur in both asthma and rhinitis23. UGRP1 levels were indeed only weakly or not at all
correlated with sputum albumin. Furthermore, as UGRP1was undetectable in serum samples
of this study (see materials and methods) transepithelial leakage from blood is unlikely to be
the cause of the high sputum UGRP1 levels. The only plausible mechanism for increased
UGRP1 in sputum appears therefore to be an increased synthesis and secretion of the protein
in those areas contributing to sputum collection.
Our findings concerning CC16 in sputum were rather unexpected from several points of view.
According to the literature, a decrease in CC16 could have been expected both in asthma and
in rhinitis. Indeed, patients who suffered from asthma for longer than 10 years have decreased
serum CC1624, in correlation with decreased populations of Clara cells in their airways2.
Furthermore, children suffering from allergic rhinitis were recently shown to have decreased
CC16 levels in nasal fluid25 and highly reduced CC16 gene expression8. The lack of changes
of sputum CC16 in asthma or rhinitis probably stems from the fact that induced sputum
mainly originates from central airways, with little or no recovery from the peripheral
respiratory system where CC16 is predominantly produced26. By contrast, serum levels of
CC16 mainly originate from distal and peripheral airways, which offer a vast surface area for
Page 12 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Privileged Comm
unication
13
transepithelial leakage into the bloodstream1. In comparison with sputum, serum might
therefore be a more reliable indicator of the amount of CC16 secreted in the lower respiratory
tract. Even though sputum CC16 levels in atopic asthmatics were overall unchanged, they
were found to correlate positively with macrophage and negatively with eosinophil
percentages. The correlation with macrophages might simply reflect their role in the
respiratory tract defense mechanisms, and maybe also tie up with the known role of
macrophages in phagocytosis and recycling of surfactant and other lung secretory proteins27.
The negative correlation with eosinophils is likely linked to the anti-inflammatory role of
CC168,25.
With regard to UGRP1, similarly to CC16, genetic studies predicted lower uteroglobin-related
protein 1 levels in some asthmatics, following observations of reduced transcriptional activity
linked to a G-A point mutation at –112bp in the human UGRP1 gene promoter13. However,
studies in CC16-null mice demonstrated compensatory increases in UGRP1 and UGRP2
mRNA expression28. Assuming altered CC16 gene expression in asthma and rhinitis, as
suggested by the above-mentioned studies8,24, could therefore in part explain a compensatory
rise in UGRP1 as observed in our studies. Individual genetic differences linked to known
CC16 and UGRP1 gene polymorphism could further explain the differences observed,
notably the significant rise in UGRP1 in atopic asthmatics only29,13. Interestingly, although
weak and not specific of URGP1 (also found with CC16) the negative correlation in atopic
asthmatics between UGRP1 and eosinophil percentage is consistent with the downregulation
of UGRP1 expression observed in ovalbumin-challenged mice with high tissue eosinophilia
linked to high interleukin-5 levels30, as well as the very recent study by Chiba et al. (2006,
epub ahead of print)31 reporting that intranasal administration of adeno-UGRP1 markedly
reduced the number of infiltrating inflammatory cells, particularly eosinophils. As with CC16,
Page 13 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Privileged Comm
unication
14
correlations of UGRP1 with sputum macrophages may be linked to their role in defense
mechanisms, UGRP1 being a known ligand of the MARCO receptor (macrophage scavenger
receptor with collagenous structure) of alveolar macrophages32. Interestingly, although cell
numbers were overall in agreement with induced sputum reference values33,34, total cell
numbers were increased in our asthmatic patients, whereas macrophage percentages were
significantly reduced. Further studies would be required to fully comprehend the interactions
between UGRP1 and macrophages, particularly in asthma where macrophage function
alterations feature high in the recent literature35,36.
Morphological studies offer possible mechanistic clues for the observed differences between
UGRP1 and CC16: human UGRP1-secreting cells are located not only primarily in the larger
upper airways but in sub-mucosal glands in particular, whereas CC16 secretion is
predominant in the lower conducting airways although it also occurs in sub-mucosal acinar
and duct cells early in life11,28 and in some goblet cells37. Since asthma is known to lead to
airway remodeling, not only with goblet cell hyperplasia but with hypertrophy and
hyperplasia of the submucosal glands in particular38,39, the rise in UGRP1 observed in
asthmatic patients could reflect this hypersecretory state and therefore become an indirect
biomarker of airway remodeling. The significant rise in UGRP1 observed in rhinitis, albeit
smaller than in asthma, corroborates recent reports that remodeling occurs not only in asthma
but also in rhinitis and other conditions inducing chronic cough40,41. It would furthermore be
worth investigating how CC16 and UGRP1 levels would respond to corticosteroid treatment
recently shown to reverse airway remodeling in mice43, as the small number of patients in
each treatment category did not allow us to make conclusive observations.
Page 14 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Privileged Comm
unication
15
Finally, it appears from our study in asthma and rhinitis that induced sputum, clearly less
invasive than bronchial lavage, could prove a most helpful tool for monitoring inflammatory
cells and anti-inflammatory proteins such as UGRP1 and CC16. This could be practical for
clinicians keen to monitor treatment effect on remodeling in individual patients44. As this
study is the first report of UGRP1 and CC16 levels in induced sputum, further studies
conducted in larger numbers of atopic and non-atopic patients would be required to confirm
the differential levels of these two new biomarkers in asthma and rhinitis.
Page 15 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Privileged Comm
unication
16
ACKNOWLEDGMENTS
(word count = 35 words)
The authors wish to thank the staff members of the Internal Medicine and Industrial
Toxicology Departments of Brescia and Parma Universities respectively for volunteering to
provide the induced sputum control samples used in this study.
Page 16 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Privileged Comm
unication
17
REFERENCES
1. Hermans C, Bernard A. Lung epithelium-specific proteins: characteristics and potential
applications as markers. Am J Respir Crit Care Med. 1999 Feb;159(2):646-78.
2. Shijubo N, Itoh Y, Yamaguchi T et al. Clara cell protein-positive epithelial cells are
reduced in small airways of asthmatics. Am J Respir Crit Care Med. 1999
Sep;160(3):930-3.
3. Lensmar C, Nord M, Gudmundsson GH et al. Decreased pulmonary levels of the anti-
inflammatory Clara cell 16 kDa protein after induction of airway inflammation in
asthmatics. Cell Mol Life Sci. 2000 Jun;57(6):976-81.
4. Arsalane K, Broeckaert F, Knoops B, Wiedig M, Toubeau G, Bernard A. Clara cell
specific protein (CC16) expression after acute lung inflammation induced by intratracheal
lipopolysaccharide administration. Am J Respir Crit Care Med. 2000 May;161(5):1624-
30.
5. Hayashida S, Harrod KS, Whitsett JA. Regulation and function of CCSP during
pulmonary Pseudomonas aeruginosa infection in vivo. Am J Physiol Lung Cell Mol
Physiol. 2000 Sep;279(3):L452-9.
6. Laing IA, Hermans C, Bernard A, Burton PR, Goldblatt J, Le Souef PN. Association
between plasma CC16 levels, the A38G polymorphism, and asthma. Am J Respir Crit
Care Med. 2000 Jan;161(1):124-7.
7. Candelaria PV, Backer V, Laing IA et al. Association between asthma-related phenotypes
and the CC16 A38G polymorphism in an unselected population of young adult Danes.
Immunogenetics. 2005 Apr;57(1-2):25-32. Epub 2005 Mar 3.
8. Benson M, Jansson L, Adner M, Luts A, Uddman R, Cardell LO. Gene profiling reveals
decreased expression of uteroglobin and other anti-inflammatory genes in nasal fluid cells
from patients with intermittent allergic rhinitis. Clin Exp Allergy. 2005 Apr;35(4):473-8.
Page 17 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Privileged Comm
unication
18
9. Chen LC, Zhang Z, Myers AC, Huang SK. Cutting edge: altered pulmonary eosinophilic
inflammation in mice deficient for Clara cell secretory 10-kDa protein. J Immunol. 2001
Sep 15;167(6):3025-8.
10. Klug J, Beier HM, Bernard A et al. Uteroglobin/Clara cell 10-kDa family of proteins:
nomenclature committee report. Ann N Y Acad Sci. 2000;923:348-54.
11. Niimi T, Keck-Waggoner CL, Popescu NC, Zhou Y, Levitt RC, Kimura S. UGRP1, a
uteroglobin/Clara cell secretory protein-related protein, is a novel lung-enriched
downstream target gene for the T/EBP/NKX2.1 homeodomain transcription factor. Mol
Endocrinol. 2001 Nov;15(11):2021 -36.
12. Niimi T, Copeland NG, Gilbert DJ et al. Cloning, expression, and chromosomal
localization of the mouse gene (Scgb3a1, alias Ugrp2) that encodes a member of the novel
uteroglobin-related protein gene family. Cytogenet Genome Res. 2002a;97(1-2):120-7.
13. Niimi T, Munakata M, Keck-Waggoner CL et al. A polymorphism in the human UGRP1
gene promoter that regulates transcription is associated with an increased risk of asthma.
Am J Hum Genet. 2002b;70(3):718-25. Epub 2002 Jan 25.
14. HELIOS Project Final Report, Research and Technological Development Programme
“Quality of Life and Management of Living Resources” Key action 4 “Environment and
Health” QLK4-CT-1999-01308, 2003; pp 1-63; http://airnet.iras.uu.nl/products/
reports_and_annexes/HELIOS/HELIOS_final_report_Part_A.pdf
15. National Asthma Education and Prevention Program, Guidelines for the diagnosis and
management of Asthma, Expert Panel Report 2, National Institute of Health, National
Heart, Lung, and Blood Institute, 1997.
16. Bousquet J, Van Cauwenberge P, Khaltaev N; Aria Workshop Group; World Health
Organization. Allergic rhinitis and its impact on asthma J Allergy Clin Immunol. 2001 (5
Suppl):S147-334.
Page 18 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Privileged Comm
unication
19
17. Djukanovic R, Sterk P, Fahy JV, Hargreave FE. Standardized methodology of sputum
induction and processing. Eur Resp J 2002;20 supp.37:1s-55s.
18. Pignatti P, Delmastro M, Perfetti L et al. Is dithiothreitol affecting cells and soluble
mediators during sputum processing? A modified methodology to process sputum. J
Allergy Clin Immunol 2002;110:667-8.
19. Bernard AM, Lauwerys RR. Continuous-flow system for automation of latex
immunoassay by particle counting. Clin Chem. 1983;29:1007-11.
20. Bernard A, Marchandise FX, Depelchin S, Lauserys R, Sibille Y. Clara cell protein in
serum and bronchoalveolar lavage. Eur Respir J. 1992;5:1231-8.
21. Quanjer PH. Standardization of lung function testing. Bull Europ Physiopathol Resp
1983;19 (Suppl 5):45-51.
22. Crapo RO, Casaburi R, Enright PL et al. Guidelines for methacholine and exercise
challenge testing-1999. Am J Respir Crit Care Med 2000;161:309-29.
23. Svensson C, Andersson M, Greiff L, Alkner U, Persson CG. Exudative
hyperresponsiveness of the airway microcirculation in seasonal allergic rhinitis. Clin Exp
Allergy. 1995 Oct;25(10):942-50.
24. Shijubo N, Itoh Y, Yamaguchi T et al. Serum levels of Clara cell 10-kDa protein are
decreased in patients with asthma. Lung. 1999;177(1):45-52.
25. Johansson S, Keen C, Stahl A, Wennergren G, Benson M. Low levels of CC16 in nasal
fluid of children with birch pollen-induced rhinitis. Allergy. 2005 May;60(5):638-42.
26. Alexis NE, Hu SC, Zeman K, Alter T, Bennett WD. Induced sputum derives from the
central airways: confirmation using a radiolabeled aerosol bolus delivery technique. Am J
Respir Crit Care Med. 2001 Nov 15;164(10 Pt 1):1964-70.
27. Wright JR. Clearance and recycling of pulmonary surfactant. Am J Physiol. 1990
Aug;259(2 Pt 1):L1-12.
Page 19 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Privileged Comm
unication
20
28. Reynolds SD, Reynolds PR, Pryhuber GS, Finder JD, Stripp BR. Secretoglobins
SCGB3A1 and SCGB3A2 define secretory cell subsets in mouse and human airways. Am
J Respir Crit Care Med. 2002 Dec 1;166(11):1498-509. Epub 2002 Aug 01.
29. Sengler C, Heinzmann A, Jerkic SP et al. Clara cell protein 16 (CC16) gene
polymorphism influences the degree of airway responsiveness in asthmatic children. J
Allergy Clin Immunol. 2003 Mar;111(3):515-9.
30. Chiba Y, Srisodsai A, Supavilai P, Kimura S. Interleukin- 5 reduces the expression of
uteroglobin-related protein (UGRP) 1 gene in allergic airway inflammation. Immunol Lett.
2005 Feb 15;97(1):123-9.
31. Chiba Y, Kurotani R, Kusakabe T, Miura T, Link BW, Misawa M, Kimura S.
Uteroglobin-related Protein 1 Expression Suppresses Allergic Airway Inflammation in
Mice. Am J Respir Crit Care Med. 2006 Feb 2; [Epub ahead of print]
32. Bin LH, Nielson LD, Liu X, Mason RJ, Shu HB. Identification of uteroglobin-related
protein 1 and macrophage scavenger receptor with collagenous structure as a lung-specific
ligand-receptor pair. J Immunol. 2003 Jul 15;171(2):924-30.
33. Belda J, Leigh R, Parameswaran K, O'Byrne PM, Sears MR, Hargreave FE. Induced
sputum cell counts in healthy adults. Am J Respir Crit Care Med. 2000 Feb;161(2 Pt
1):475-8.
34. Spanevello A, Confalonieri M, Sulotto F et al. Induced sputum cellularity. Reference
values and distribution in normal volunteers. Am J Respir Crit Care Med. 2000 Sep;162(3
Pt 1):1172-4.
35. Alexis NE, Soukup J, Nierkens S, Becker S. Association between airway hyperreactivity
and bronchial macrophage dysfunction in individuals with mild asthma. Am J Physiol
Lung Cell Mol Physiol. 2001 Feb;280(2):L369-75.
Page 20 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Privileged Comm
unication
21
36. Peters-Golden M. The alveolar macrophage: the forgotten cell in asthma. Am J Respir
Cell Mol Biol. 2004 Jul;31(1):3-7.
37. Boers JE, Ambergen AW, Thunnissen FB. Number and proliferation of Clara cells in
normal human airway epithelium. Am J Respir Crit Care Med. 1999 May;159(5 Pt
1):1585-91.
38. Morcillo EJ, Cortijo J. Mucus and MUC in asthma. Curr Opin Pulm Med. 2006
Jan;12(1):1-6.
39. Boser SR, Park H, Perry SF, Menache MG, Green FH. Fractal geometry of airway
remodeling in human asthma. Am J Respir Crit Care Med. 2005 Oct 1;172(7):817-23.
Epub 2005 Jun 23.
40. Frieri M. Inflammatory issues in allergic rhinitis and asthma. Allergy Asthma Proc. 2005
May-Jun;26(3):163-9.
41. Niimi A, Torrego A, Nicholson AG, Cosio BG, Oates TB, Chung KF. Nature of airway
inflammation and remodeling in chronic cough. J Allergy Clin Immunol. 2005
Sep;116(3):565-70.
42. Bernard AM, Gonzalez-Lorenzo JM, Siles E, Trujillano G, Lauwerys R. Early decrease of
serum Clara cell protein in silica-exposed workers. Eur Respir J. 1994 Nov;7(11):1932-7.
43. Cho JY, Miller M, McElwain K, McElwain S, Broide DH. Combination of corticosteroid
therapy and allergen avoidance reverses allergen-induced airway remodeling in mice. J
Allergy Clin Immunol. 2005 Nov;116(5):1116-22. Epub 2005 Oct 10.
44. Woodruff PG, Fahy JV. Airway remodeling in asthma. Semin Respir Crit Care Med. 2002
Aug;23(4):361-7.
Page 21 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Privileged Comm
unication
22
FIGURE LEGENDS
Figure 1: Observed concentrations of uteroglobin-related protein 1 (UGRP1), Clara cell
protein (CC16) and albumin (Alb) in sputum samples of controls, rhinitis and asthma patients
(geometric means and relevant significant ANOVA results are indicated).
Figure 2: Levels of uteroglobin-related protein 1 (UGRP1) in sputum samples of controls,
rhinitis and asthma patients divided according to atopic status (geometric means and relevant
significant Dunnett test results are indicated).
Figure 3: Simple correlations of uteroglobin-related protein 1 (UGRP1) with Clara cell
protein (CC16) then those of UGRP1 and CC16 with albumin in induced sputum samples of
controls, rhinitis and asthma patients. Note the very strong correlations between UGRP1 and
CC16 and the weaker or absent correlations of both UGRP1 and CC16 with albumin, notably
in asthma.
Figure 4: Correlations between uteroglobin-related protein 1 (UGRP1), Clara cell protein
(CC16) and albumin (Alb) with macrophage and eosinophil percentages in induced sputum of
atopic asthmatics.
Page 22 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Privileged Comm
unication
23
Table 1: Population characteristics, sputum parameters and lung function tests according to
diagnosis (exact numbers are indicated between brackets if different from total).
Controls Rhinitis Asthma
Population studied
Total number 19 32 32
Men/Women 10/9 10/22 21/11
Age (years) 39.4 ± 3.4 35.2 ± 2.1 43.9 ± 2.5°
Disease length (months) - 51.7 ± 12.3 128.2 ± 30.0°
Inhaled steroids 0 0 6 high, 9 medium,
4 low doses
Atopics 0 20 24
Smokers 0 13 13
Pack-years 0 13.1 ± 4.3 15.8 ± 3.8
Lung function tests
Methacholine test not evaluated 1/32 12/32
PD20FEV1 (µg) - 584 538 ± 92.3
FEV1 % 100.4 ± 1.9 (13) 107.4 ± 1.8 (31) 95.3 ± 4.1 (31)°
VC % 105.4 ± 1.8 (13) 109.9 ± 2.4 (29) 102.6 ± 3.6 (30)°
Tiffeneau Index - 102.4 ± 1.2 (31) 93.1 ± 2.2 (31)°
Sputum parameters
Cells/mg 5,356 ± 581 (12) 5,301 ± 905 10,320 ± 2,320
Vitality % - 77.2 ± 2.2 74.7 ± 2.5
Macrophages % 45.3 ± 3.6 (12) 43.5 ± 4.4 26.6 ± 3.3*°
Neutrophils % 51.2 ± 3.6 (12) 44.1 ± 4.8 46.8 ± 5.1
Eosinophils % 0.08 ± 0.08 (12) 5.3 ± 2.5* 19.4 ± 4.7*°
Lymphocytes % 2.4 ± 0.4 (12) 2.9 ± 0.6 1.6 ± 0.3
Epithelial cells % 1.1 ± 0.4 (12) 4.3 ± 1.2* 5.4 ± 1.1*
*: p < 0.05 between patients and controls
°: p < 0.05 between asthma and rhinitis patients
Arithmetic means ± SEM. PD20FEV1: methacholine dose causing a 20% fall in FEV1;
FEV1: forced expiratory volume in 1 second; VC: vital capacity.
Page 23 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Privileged Comm
unication
24
Figure 1
p = NS
10
1
0.1
2.33.33.8
100
CC
16 (m
g/l)
p=0.0047
p<0.0001
1
0.1
0.01
10
0.12
0.780.39
UG
RP
1 (m
g/l)
1
10
100
1000p<0.0001
p=0.0001
23.7
117.5
36.5
Controls Rhinitis Asthma
Alb
(mg
/l)
Page 24 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Privileged Comm
unication
25
Figure 2
Contro
ls
Rhinitis
- Ato
py
Rhinitis
+ A
topy
Asthm
a - A
topy
Asthm
a + A
topy
p < 0.0110
1
0.1
0.01
0.001
p < 0.05
0.13
0.970.58
0.31 0.35
UG
RP
1 (m
g/l)
Page 25 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Privileged Comm
unication
26
Figure 3
Controls
0.001
0.01
0.1
1
0.1 1 10
UG
RP
1 (m
g/l)
CC16 (mg/l)
n = 19R² = 0.439p = 0.002
Rhinitis
0.01
0.1
1
10
0.1 1 10 100CC16 (mg/l)
n = 32R² = 0.602p < 0.0001
Asthma
0.1
1
10
0.1 10 100CC16 (mg/l)
n = 32R² = 0.372p = 0.0002
1
0.001
0.1
1
1 10 100Alb (mg/l)
n = 13R² = 0.338p = 0.037
UG
RP
1 (m
g/l)
0.01
0.01
0.1
1
10
10 100 1000Alb (mg/l)
n = 30R² = 0.181p = 0.019
0.1
1
10
10 100 1000Alb (mg/l)
n = 29R² = 1.31E-5
p = 0.985
0.1
1
10
1 10 100
Alb (mg/l)
n = 13R² = 0.026p = 0.597
CC
16 (
mg
/l)
0.1
1
10
100
10 100 1000
Alb (mg/l)
n = 29R² = 0.002p = 0.839
0.1
1
10
100
10 100 1000Alb (mg/l)
n = 30R² = 0.23p = 0.0073
Page 26 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Privileged Comm
unication
27
Figure 4
0 20 40 60 80
n = 25R² = 0.1377p = 0.0676
Atopic Asthmatics10
1
0.1U
GR
P1
(mg/
l)
0 20 40 60 80
n = 25R² = 0.2458p = 0.0117
100
1
0.1
10
CC
16 (
mg/
l)
0 20 40 60 80
n = 25R² = 0.4145p = 0.0005
100
1
0.1
10
CC
16 (
mg/
l)
0 20 40 60 80
n = 25R² = 0.2215p = 0.0176
Atopic Asthmatics10
1
0.1
UG
RP
1 (m
g/l)
0 20 40 60 80
n = 23R² = 0.1765p = 0.0461
1000
10
100
Sputum Macrophages (%)
Alb
(m
g/l)
0 20 40 60 80
n = 23R² = 0.1843p = 0.0409
1000
10
100
Sputum Eosinophils (%)
Alb
(m
g/l)
Page 27 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Privileged Comm
unicationFigure 1
Page 28 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Privileged Comm
unication
Figure 2
Page 29 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Privileged Comm
unication
Figure 3
Page 30 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Privileged Comm
unication
Figure 4
Page 31 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Privileged Comm
unicationLIST OF ABBREVIATIONS
Alb: albumin
CC16 : Clara cell protein
DDT : dithiothreitol
FEV1: forced expiratory volume in one second
PD20FEV1: methacholine dose causing a 20% fall in FEV1
UGRP1: uteroglobin-related protein 1
VC: vital capacity
Page 32 of 32
ScholarOne - http://scholarone.custhelp.com - (434) 817-2040 X167
CHEST
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Copyright © 2022 FDOKUMEN




















