
Rhinitis and sleep apnea
7
Rhinitis and Sleep Apnea Maria T. Staevska, MD, Mariana A. Mandajieva, MD, and Vasil D. Dimitrov, MD, PhD Address Clinic of Asthma, Allergology, and Clinical Immunology, Medical University–Sofia, University Hospital “Alexandrovska”, 1, St. George Sofiisky str., 1431, Sofia, Bulgaria. E-mail: [email protected] Current Allergy and Asthma Reports 2004, 4:193–199 Current Science Inc. ISSN 1529-7322 Copyright © 2004 by Current Science Inc. Introduction Allergic rhinitis (AR), the most prevalent allergic disorder, and nonallergic rhinitis affect more than 25% of the popu- lation [1]. AR is characterized by local symptoms, such as nasal obstruction, itching, sneezing, rhinorrhea, and post- nasal drip, as well as daytime sleepiness, fatigue, head- aches, and malaise [1]. The latter systemic symptoms are especially related to poor performance and concentration at school and work, and to overall impairment of quality of life. It is generally accepted that complaints of sleepi- ness, fatigue, and malaise are secondary to the action of high levels of inflammatory mediators, such as tumor necrosis factor (TNF)- α, interferon (IFN)- γ , and other cytokines on the hypothalamus [2]. There is an increasing body of evidence, however, that the disabilities might be partially due to nasal congestion and sleep-disordered breathing [3–5]. Obstructive sleep apnea syndrome (OSAS) is character- ized by: 1) complete or partial collapse of the upper air- ways during sleep, with consequent cessation of breathing, despite ongoing respiratory effort; and 2) coexistent day- time somnolence. OSAS is an important health problem, given its associated adverse consequences and its preva- lence of least 4%. Two kinds of clinical sequelae are associ- ated with the disorder. Neuropsychiatric complications include sleepiness; depression; cognitive dysfunction; dis- ruption of professional, family, and social life; and inatten- tion that can result in road and industrial accidents. Cardiovascular complications include pulmonary and sys- temic hypertension due to chronic sleep-related hypoventi- lation, congestive heart failure, coronary heart disease, myocardial infarction, and stroke [6]. Obesity, increased neck circumference, aging, male sex, acromegaly, hypothyroidism, and relatively rare craniofa- cial abnormalities are strong risk factors for sleep-disor- dered breathing (SDB). Currently, the most important clinical risk factors are those of high prevalence that poten- tially can be modified [7]. Rhinitis meets these criteria, because it is a syndrome of high and increasing prevalence with relatively easily modified nasal congestion as a major contributing factor. Although earlier studies failed to dem- onstrate a linear correlation between nasal resistance and the severity of OSA [7–9], in 2000, Lofaso et al. [10••] used stepwise multiple regression analysis to show that daytime nasal obstruction represented an independent risk factor for OSAS. Rhinitis had a weaker correlation than cephalo- metric landmarks, obesity, and male sex, but was stronger than age. Recently, several reviews discussing the role of nasal obstruction in the genesis of SDB have been pub- lished [11,12•,13]. Finally, OSA might be a chronic inflammatory condi- tion characterized by high levels of cytokines and inflam- matory mediators that are similar to those of allergic rhinitis and asthma. Asthma might be more severe and dif- ficult to control if OSA is present. Nasal continuous posi- tive airway pressure (nCPAP) therapy can improve both the OSA and asthma [14,15]. The inflammatory mediators generated by OSA could possibly account for the cardiovas- cular and asthmatic complications [16•]. The cause of the OSA-related inflammation and its role in rhinitis are still open to debate. Scope of Sleep-disordered Breathing Sleep-disordered breathing is a large entity encompassing a variety of conditions of sleep-related regular respiratory The nose and pharynx begin the upper airway system and represent a continuum. This is the biologic basis for the mutual influences of rhinitis and obstructive sleep apnea (OSA). Sleep-disordered breathing has a large differential diagnosis that includes snoring, upper airway resistance syndrome, and severe OSA. Nasal obstruction is an inde- pendent risk factor for OSA, but there is no correlation of daytime nasal resistance with the severity of OSA. How- ever, nasal resistance was an independent predictor of apnea–hypopnea index in a recent study of nonobese OSA patients. Rhinitis alone is associated with mild OSA, but commonly causes microarousals and sleep fragmentation. Reduction of nasal inflammation with topical treatment improves sleep quality and subsequent daytime sleepiness and fatigue. Patient compliance with the nasal continuous positive airway pressure (nCPAP) device is relatively low, in part due to adverse nasal effects.
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of Rhinitis and sleep apnea

Rhinitis and Sleep ApneaMaria T. Staevska, MD, Mariana A. Mandajieva, MD,
and Vasil D. Dimitrov, MD, PhD
AddressClinic of Asthma, Allergology, and Clinical Immunology, Medical University–Sofia, University Hospital “Alexandrovska”, 1, St. George Sofiisky str., 1431, Sofia, Bulgaria.E-mail: [email protected]
Current Allergy and Asthma Reports 2004, 4:193–199Current Science Inc. ISSN 1529-7322Copyright © 2004 by Current Science Inc.
IntroductionAllergic rhinitis (AR), the most prevalent allergic disorder,and nonallergic rhinitis affect more than 25% of the popu-lation [1]. AR is characterized by local symptoms, such asnasal obstruction, itching, sneezing, rhinorrhea, and post-nasal drip, as well as daytime sleepiness, fatigue, head-aches, and malaise [1]. The latter systemic symptoms areespecially related to poor performance and concentrationat school and work, and to overall impairment of qualityof life. It is generally accepted that complaints of sleepi-ness, fatigue, and malaise are secondary to the action ofhigh levels of inflammatory mediators, such as tumornecrosis factor (TNF)-α, interferon (IFN)-γ , and othercytokines on the hypothalamus [2]. There is an increasingbody of evidence, however, that the disabilities might bepartially due to nasal congestion and sleep-disorderedbreathing [3–5].
Obstructive sleep apnea syndrome (OSAS) is character-ized by: 1) complete or partial collapse of the upper air-
ways during sleep, with consequent cessation of breathing,despite ongoing respiratory effort; and 2) coexistent day-time somnolence. OSAS is an important health problem,given its associated adverse consequences and its preva-lence of least 4%. Two kinds of clinical sequelae are associ-ated with the disorder. Neuropsychiatric complicationsinclude sleepiness; depression; cognitive dysfunction; dis-ruption of professional, family, and social life; and inatten-tion that can result in road and industrial accidents.Cardiovascular complications include pulmonary and sys-temic hypertension due to chronic sleep-related hypoventi-lation, congestive heart failure, coronary heart disease,myocardial infarction, and stroke [6].
Obesity, increased neck circumference, aging, male sex,acromegaly, hypothyroidism, and relatively rare craniofa-cial abnormalities are strong risk factors for sleep-disor-dered breathing (SDB). Currently, the most importantclinical risk factors are those of high prevalence that poten-tially can be modified [7]. Rhinitis meets these criteria,because it is a syndrome of high and increasing prevalencewith relatively easily modified nasal congestion as a majorcontributing factor. Although earlier studies failed to dem-onstrate a linear correlation between nasal resistance andthe severity of OSA [7–9], in 2000, Lofaso et al. [10••] usedstepwise multiple regression analysis to show that daytimenasal obstruction represented an independent risk factorfor OSAS. Rhinitis had a weaker correlation than cephalo-metric landmarks, obesity, and male sex, but was strongerthan age. Recently, several reviews discussing the role ofnasal obstruction in the genesis of SDB have been pub-lished [11,12•,13].
Finally, OSA might be a chronic inflammatory condi-tion characterized by high levels of cytokines and inflam-matory mediators that are similar to those of allergicrhinitis and asthma. Asthma might be more severe and dif-ficult to control if OSA is present. Nasal continuous posi-tive airway pressure (nCPAP) therapy can improve both theOSA and asthma [14,15]. The inflammatory mediatorsgenerated by OSA could possibly account for the cardiovas-cular and asthmatic complications [16•]. The cause of theOSA-related inflammation and its role in rhinitis are stillopen to debate.
Scope of Sleep-disordered BreathingSleep-disordered breathing is a large entity encompassing avariety of conditions of sleep-related regular respiratory
The nose and pharynx begin the upper airway system and represent a continuum. This is the biologic basis for the mutual influences of rhinitis and obstructive sleep apnea (OSA). Sleep-disordered breathing has a large differential diagnosis that includes snoring, upper airway resistance syndrome, and severe OSA. Nasal obstruction is an inde-pendent risk factor for OSA, but there is no correlation of daytime nasal resistance with the severity of OSA. How-ever, nasal resistance was an independent predictor of apnea–hypopnea index in a recent study of nonobese OSA patients. Rhinitis alone is associated with mild OSA, but commonly causes microarousals and sleep fragmentation. Reduction of nasal inflammation with topical treatment improves sleep quality and subsequent daytime sleepiness and fatigue. Patient compliance with the nasal continuous positive airway pressure (nCPAP) device is relatively low, in part due to adverse nasal effects.

194 Rhinitis
disturbances. One could represent it as a continuum [17•]:Intermittent snoring → Persistent or habitual snoring →Upper airway resistance syndrome → Mild OSAS → SevereOSAS → Obesity–hypoventilation syndrome.
The mildest form is snoring, ranging from intermittentto persistent, with lack of any detrimental effect on indi-vidual health. Snoring affects 35% of the middle-aged pop-ulation, with a distribution of 44% men and 28% women.It becomes more common with age [18]. Snoring is pro-duced by vibration of the soft palate and partially col-lapsed pharyngeal walls due to turbulent airflow. Statescausing nasal obstruction, such as nasal polyps, hypertro-phied turbinates, and nasal septal deviation are ofteninvolved in this process. Recently, a population-basedcohort study showed that nasal congestion at night is astrong independent risk factor for habitual snoring with anodds ratio of 4.9 [18].
At the other end of the spectrum is Pickwick or obesity-hypoventilation syndrome. This is the most severe form ofSDB, and is characterized by persistent hypoxia and hyper-capnia, high morbidity, and mortality.
In the middle of the continuum is OSAS. Some addi-tional terms are needed to outline this disorder. Apnea isdefined as cessation of airflow for at least 10 seconds. Itcould be central, obstructive, or mixed. Central sleepapnea, which is rare and beyond the scope of this review, isdue to absence of brainstem-derived respiratory efforts.Obstructive sleep apnea is much more common andresults from complete obstruction of the upper airways,despite persistent ventilatory effort. Hypopnea results fromincomplete upper airway obstruction, and is defined by atleast a 30% reduction of airflow. The apnea–hypopneaindex (AHI) is the average number of apnea and hypopneaevents per hour of sleep. AHI less than 5 is considered nor-mal. OSA is characterized by an AHI of 5 or higher, and isassociated with a 4% decrease in oxygen saturation. OSA isdivided into three severity levels: mild with AHI of 5 to 15;moderate with AHI of 15 to 30; and severe with AHI higherthan 30. Apnea and hypopnea always cause arousal. Theserepetitive arousals underlie sleep fragmentation, resultingin daytime sleepiness. OSA, together with daytime sleepi-ness, constitutes OSAS [19].
Subgroups of patients have excessive daytime sleepi-ness because of repetitive nocturnal arousals, withoutapnea, hypopnea, or oxygen desaturation. In these cases,the airflow channel of the nocturnal polysomnogramshows less severe inspiratory flow limitation. Inspiratoryesophageal pressures show repetitive, increased upper air-way resistance. The respiratory efforts aimed at overcomingthis increased upper airway resistance result in transientarousals. The term respiratory effort-related arousal(RERA) is applied to this event.
Guilleminault et al. [20] noted that the repetitiveRERAs were pathognomonic for the condition and intro-duced the term “upper airways resistance syndrome”(UARS). Because nasal resistance is responsible for at least
40% of total airway resistance, its increase could result inUARS. UARS is the mildest form of SDB and shows bettersleep fragmentation responses with treatment of nasal con-gestion than other OSA patients [12•,21]. Like OSA, UARSis characterized by excessive daytime sleepiness and fitfulsleep. However, snoring is not present in all patients.Although UARS was often placed between snoring andOSAS, it could be a distinct disorder [22]. Unlike OSA,UARS patients are predominantly nonobese, youngerwomen with histories of fainting, cold extremities, lowblood pressure, and postural hypotension [22]. Thesepatients frequently complain of sleep-onset insomnia,fatigue, headaches, depression, irritable bowel syndrome(IBS), bruxism (teeth grinding), gastroesophageal refluxdisease, and rhinitis [23]. The arousal threshold forincreased inspiratory effort is elevated in OSA, but is lowerthan normal in UARS. As a result, UARS patients wake upvery easily in response to even mild increases in respiratoryeffort. Guilleminault and Chowdhuri [22] hypothesizethat different functional arousal pathways are dysfunc-tional in the two syndromes. Blunted mechanoreceptorresponses predominate in OSA patients, whereas UARSpatients have intact or even increased sensitivity of mecha-noreceptor systems.
Electroencephalograms (EEGs) show that delta sleepand the percentage of sleep spent in alpha rhythms are rel-atively increased in UARS patients. Delta sleep is decreasedin OSA patients. UARS patients have evidence of “alpha–delta sleep.” This is the appearance of waking alpharhythms that intrude into the slow-wave delta rhythm thatcharacterizes deep sleep. This EEG finding is not a featureof OSA. Curiously, “alpha–delta sleep” is widespread indisorders characterized by chronic fatigue. These includechronic fatigue syndrome, fibromyalgia, migraine/tensionheadache syndrome, IBS, and temporomandibular jointsyndrome (TMJ). Gold et al. [23] demonstrated a correla-tion between UARS and increasing prevalence of alpha–delta rhythm, IBS, headache, and sleep-onset insomnia.Patients with OSA had low correlations with these condi-tions. Rhinitis was present in approximately 30% of UARSpatients in this study.
Levander [24], in a recent review on the pathophysiol-ogy of dysfunctional disorders, discussed the concept of“sensory sensitization dysfunctional disorder” that couldbe applied to the functional somatic syndromes men-tioned earlier and to dry eyes and mouth syndrome(SICCA syndrome), gastralgia, interstitial cystitis, chronicprostatitis, vestibulitis syndrome, and nonallergic rhinitis.Nonallergic rhinitis shows a significant overlap withchronic fatigue syndrome: 76% of chronic fatigue syn-drome patients have significant rhinosinusitis complaints[25]. It is tempting to speculate that UARS is part of thespectrum of sensory sensitization dysfunction disorders.Coexisting nonallergic rhinitis could be an additionalaggravating factor for UARS, resulting in increased inspira-tory effort due to nasal obstruction.

Rhinitis and Sleep Apnea • Staevska et al. 195
Pathophysiology of Sleep-disordered BreathingThe pharynx is a complex structure with opposing func-tions, such as breathing and swallowing, as well as phona-tion. It consists of three main compartments: thenasopharynx, oropharynx, and laryngopharynx. Thenasopharynx is the area between the nasal turbinates andhard palate. The oropharynx is the space between the hardpalate and epiglottis. The laryngopharynx is also called thehypopharynx. It is situated between the base of the tongueand the larynx. The narrowest portion of the pharynx isthe retropalatal region of the oropharynx, or velopharynx.The oropharynx has no bony structural support and is themost easily collapsible part of this airway. The normalpharynx has an elliptical cross-sectional area with a majorlateral diameter. The pharynx walls are made up of mus-cles (dilators and constrictors), lymphoid tissue, and pha-ryngeal mucosa. There are also parapharyngeal fat pads inthe velopharynx and in the retroglossal part of theoropharynx [17•,26,27]. Dilator muscles maintain upperairway patency. Normally, their activation precedes theactivation of the diaphragm and ensures upper airwaypatency, despite the negative intraluminal pressure duringinspiration [28,29]. The constrictor muscles participate inexpiration. During sleep, the dilator muscles are hypo-tonic. This results in a normal narrowing of the pharynx.This is normally compensated by the relative hypoventila-tion and higher PaCO2 setpoint for chemoreceptors duringsleep. These factors make upper airway stability vulnerableduring sleep.
Remmers et al. [30] first identified the oropharynx asthe exact location of collapse in OSA patients. He proposedthat this is caused by imbalance of the negative intralumi-nal pressure and opposing forces originated by the pharyn-geal dilator muscles. Unlike normal subjects, OSA patientshave narrower pharyngeal airways due to genetic or obe-sity-related structural abnormalities. Furthermore, thelongest diameter of the pharyngeal cross-sectional area isanterior–posterior, making it more round and susceptibleto lateral-wall collapse. Other factors that tend to narrowthe pharyngeal airway include neck flexion, jaw opening,gravidity, and surface adhesive forces. There are data thatOSA patients maintain their anatomically narrower airwaythrough higher activity of their dilator muscles [31]. How-ever, the physiologic dilator muscle hypotonia that occursduring sleep fails to prevent nocturnal pharyngeal obstruc-tion. Environmental factors that can further attenuate dila-tor muscle activation are alcohol, sleep deprivation,sedatives, and anesthesia.
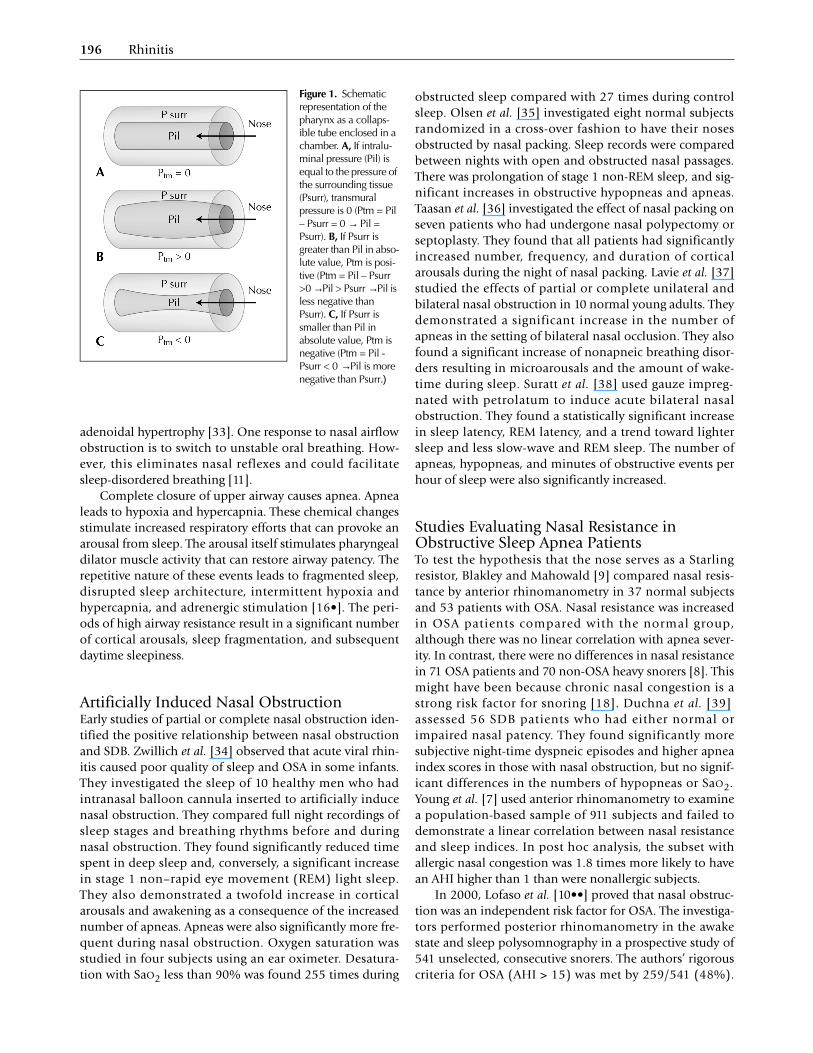
King et al. [32] showed that pharyngeal obstruction isthe primary defect in OSA, as opposed to reflex or arousalresponse abnormalities. These can be illustrated if thepharynx is represented as an elastic tube. The tube’spatency is determined by its transmural pressure (Ptm).Ptm is defined as the difference between the negativeintraluminal pressure (Pil) and the pressure created by the
surrounding dilator muscles (Psurr) (Fig. 1). Healthy sub-jects succeed in maintaining positive transmural pressuresof approximately 0 to +10 cm H2O during sleep, despitethe lower dilator muscle tone (Fig. 1B) [31]. Apneics, how-ever, fail to maintain positive pressure during sleep anddevelop airway collapse due to negative transmural pres-sure (Fig. 1C). This model can be further simplified. Ifthere is no flow through the airway, Pil = 0 = atmosphericpressure. In this situation, the absolute values of the trans-mural pressure and of the pressure of the surrounding tis-sue would be equal, but their mathematic signs would beopposite (Ptm = 0 – Psurr → Ptm = - Psurr). Hence, healthypeople can maintain positive transmural pressure by main-taining negative surrounding tissue pressures. The specificvalue of Psurr at the time of collapse is called the criticalclosure pressure (Pcrit). Pcrit exceeds -41 cm H20 inhealthy, awake subjects. In OSA patients, it ranges from -41to -17 cm H20 [6]. The dilator muscle hypotonia duringsleep causes Pcrit to rise to -13 cm H20 in normal subjects[6], to -6.5 cm H20 for asymptomatic snorers [6], -4.0 cmH20 in UARS patients [27], -1.6 cm H20 for patients withhypopneas but no apneas [6], and to +2.5 cm H20 forpatients with frank apneas [6]. As a result, OSA could beconsidered to be a condition resulting from pathologicallyelevated Pcrit during sleep. Pcrit is an important index,because it defines the lowest level of nCPAP that will keepthe upper airways patent [6].
The “Starling resistor” model can be applied to theupper airways. Under conditions of flow limitation, themaximal inspiratory flow is determined by the change inpressure between the upstream (ie, nasal passage) pressureand that at the most collapsible site of the upper airway.The downstream (tracheal) pressure generated by dia-phragmatic inspiration does not affect this relationship(Fig. 1). That means that in the beginning of an inspiratoryeffort, the pattern of airflow will increase in proportion tothe increase in the intraluminal pressure. However, whenthe critical intraluminal pressure is reached, airflow willremain constant, regardless of any continuing increase ofthe diaphragmatic driving pressure. This plateau leads tothe characteristic flattened shape of the pressure–flowcurve. Airway flow limitation is a very sensitive marker ofelevated intraluminal resistance. The maximal intralumi-nal pressure depends on two factors. The first is the trans-mural pressure discussed earlier. The second is theresistance of the upstream segment—that is, the nasal andnasopharyngeal part of the upper airways. An increase inairflow velocity in an attempt to maintain the intraluminalpressure actually results in paradoxical pharyngeal collapsedue to the Bernoulli effect [28].
Any pathologic event that increases nasal resistance canlimit maximal upper airway airflow and contribute to OSAor UARS. This includes all obstructive conditions of thenasal cavity, such as nasal septum deviation, hypertrophyof the inferior turbinates, stenosis of the nasal valve, nasalpolyps, the nasal congestion characteristic of rhinitis, and
196 Rhinitis
adenoidal hypertrophy [33]. One response to nasal airflowobstruction is to switch to unstable oral breathing. How-ever, this eliminates nasal reflexes and could facilitatesleep-disordered breathing [11].
Complete closure of upper airway causes apnea. Apnealeads to hypoxia and hypercapnia. These chemical changesstimulate increased respiratory efforts that can provoke anarousal from sleep. The arousal itself stimulates pharyngealdilator muscle activity that can restore airway patency. Therepetitive nature of these events leads to fragmented sleep,disrupted sleep architecture, intermittent hypoxia andhypercapnia, and adrenergic stimulation [16•]. The peri-ods of high airway resistance result in a significant numberof cortical arousals, sleep fragmentation, and subsequentdaytime sleepiness.
Artificially Induced Nasal ObstructionEarly studies of partial or complete nasal obstruction iden-tified the positive relationship between nasal obstructionand SDB. Zwillich et al. [34] observed that acute viral rhin-itis caused poor quality of sleep and OSA in some infants.They investigated the sleep of 10 healthy men who hadintranasal balloon cannula inserted to artificially inducenasal obstruction. They compared full night recordings ofsleep stages and breathing rhythms before and duringnasal obstruction. They found significantly reduced timespent in deep sleep and, conversely, a significant increasein stage 1 non–rapid eye movement (REM) light sleep.They also demonstrated a twofold increase in corticalarousals and awakening as a consequence of the increasednumber of apneas. Apneas were also significantly more fre-quent during nasal obstruction. Oxygen saturation wasstudied in four subjects using an ear oximeter. Desatura-tion with SaO2 less than 90% was found 255 times during
obstructed sleep compared with 27 times during controlsleep. Olsen et al. [35] investigated eight normal subjectsrandomized in a cross-over fashion to have their nosesobstructed by nasal packing. Sleep records were comparedbetween nights with open and obstructed nasal passages.There was prolongation of stage 1 non-REM sleep, and sig-nificant increases in obstructive hypopneas and apneas.Taasan et al. [36] investigated the effect of nasal packing onseven patients who had undergone nasal polypectomy orseptoplasty. They found that all patients had significantlyincreased number, frequency, and duration of corticalarousals during the night of nasal packing. Lavie et al. [37]studied the effects of partial or complete unilateral andbilateral nasal obstruction in 10 normal young adults. Theydemonstrated a significant increase in the number ofapneas in the setting of bilateral nasal occlusion. They alsofound a significant increase of nonapneic breathing disor-ders resulting in microarousals and the amount of wake-time during sleep. Suratt et al. [38] used gauze impreg-nated with petrolatum to induce acute bilateral nasalobstruction. They found a statistically significant increasein sleep latency, REM latency, and a trend toward lightersleep and less slow-wave and REM sleep. The number ofapneas, hypopneas, and minutes of obstructive events perhour of sleep were also significantly increased.
Studies Evaluating Nasal Resistance in Obstructive Sleep Apnea PatientsTo test the hypothesis that the nose serves as a Starlingresistor, Blakley and Mahowald [9] compared nasal resis-tance by anterior rhinomanometry in 37 normal subjectsand 53 patients with OSA. Nasal resistance was increasedin OSA patients compared with the normal group,although there was no linear correlation with apnea sever-ity. In contrast, there were no differences in nasal resistancein 71 OSA patients and 70 non-OSA heavy snorers [8]. Thismight have been because chronic nasal congestion is astrong risk factor for snoring [18]. Duchna et al. [39]assessed 56 SDB patients who had either normal orimpaired nasal patency. They found significantly moresubjective night-time dyspneic episodes and higher apneaindex scores in those with nasal obstruction, but no signif-icant differences in the numbers of hypopneas or SaO2.Young et al. [7] used anterior rhinomanometry to examinea population-based sample of 911 subjects and failed todemonstrate a linear correlation between nasal resistanceand sleep indices. In post hoc analysis, the subset withallergic nasal congestion was 1.8 times more likely to havean AHI higher than 1 than were nonallergic subjects.
In 2000, Lofaso et al. [10••] proved that nasal obstruc-tion was an independent risk factor for OSA. The investiga-tors performed posterior rhinomanometry in the awakestate and sleep polysomnography in a prospective study of541 unselected, consecutive snorers. The authors’ rigorouscriteria for OSA (AHI > 15) was met by 259/541 (48%).
Figure 1. Schematic representation of the pharynx as a collaps-ible tube enclosed in a chamber. A, If intralu-minal pressure (Pil) is equal to the pressure of the surrounding tissue (Psurr), transmural pressure is 0 (Ptm = Pil – Psurr = 0 → Pil = Psurr). B, If Psurr is greater than Pil in abso-lute value, Ptm is posi-tive (Ptm = Pil – Psurr >0 → Pil > Psurr → Pil is less negative than Psurr). C, If Psurr is smaller than Pil in absolute value, Ptm is negative (Ptm = Pil - Psurr < 0 → Pil is more negative than Psurr.)

Rhinitis and Sleep Apnea • Staevska et al. 197
OSA patients had significantly higher nasal resistance thanthe non-OSA patients. Subjects with nasal resistances 3hPa/L/s or more were more prevalent in the OSA group,with a significant odds ratio of 2.2. Stepwise multiple lin-ear regression analysis ranked the explained variances (R2)of AHI as hyoid bone position 6.2%, obesity 4.6%, malesex 3.0%, nasal obstruction 2.3%, increasing age 1.3%,and mandibular characteristics 0.9%.
De Vito et al. [33] used anterior rhinomanometry in theseated and supine positions and demonstrated that 44% of36 consecutive OSA patients had nasal obstruction. Again,there was no significant correlation between nasal resis-tance and the degree of OSA. Virkkula et al. [40••] foundan association between nasal resistance and the cross-sec-tional area of the pharyngeal airway at the base of thetongue in the supine position. Nasal resistance and thechange into a relaxed mandibular position during recum-bency were independent predictors of AHI among patientswith normal body mass index (BMI). The authors consid-ered the possibility that there are several subtypes of OSAwith different pathogenic factors. In some, nasal mucosalreceptors might regulate pharyngeal dilator muscle activity.Impaired nasal breathing could lead to OSA.
Physical examination of 202 subjects showed a higherprevalence of nasal obstruction in OSAS compared withnon-OSAS subjects [41]. The relative risk of OSA with ahigh Mallampati class (3 and 4) was 1.95 for all OSApatients and 2.45 if nasal obstruction was present. Theyconcluded that Mallampati score was associated with OSAonly if there was concomitant nasal obstruction. Thesefindings endorsed the hypothesis that impaired nasal andoral patency were risk factors for OSA.
Studies on Patients with Allergic RhinitisThe influence of disordered nasal breathing on sleep wasfirst investigated in 14 allergic rhinitis patients [3]. Allshowed periodic breathing, hypo- and hyperpneic epi-sodes, and microarousals. The microarousals were 10 timesmore frequent than in normal subjects. Increased upperairway resistance and nasal discharge were thought tocause these problems. Several of these patients had difficul-ties falling asleep, nocturnal awakenings, and excessivedaytime sleepiness. Changes during and after the ragweedseason were evaluated in seven seasonal AR subjects [42].Nasal resistance and the number of obstructive apneaswere significantly higher during ragweed season comparedwith after the season. Males had a correlation between theseasonal change in nasal resistance and the correspondingfrequencies of obstructive sleep apnea episodes. Rhinitis-induced apneas were associated with only mild decreasesin SaO2. The number of obstructive apneas in AR patientswas still fewer than in the typical OSAS patient. They con-clude, however, that nasal resistance due to allergic rhinitiscould be an important factor in the pathogenesis of OSA.This led to a comparison of allergic rhinitis patients with or
without mild OSA [43]. Nasal obstruction was measuredby acoustic rhinometry before and after topical nasaldecongestion. The minimal cross-sectional area at the ante-rior nasal valve was significantly smaller in the OSA thanthe non-OSA group (P = 0.03). The non-OSA patients hada significant subjective improvement in nasal congestionafter vasoconstriction, whereas the OSA patients did not.This indicated that reversible, allergic nasal obstructionwas associated with mild OSA.
Effect of Local Treatment of Nasopharynx on Sleep-disordered BreathingSleep fragmentation and microarousals can unfavorablyinfluence daytime energy levels, mood, and daytime func-tion [44]. Nasal steroids were used to treat 20 perennialallergic rhinitis patients in a double-blind, placebo-con-trolled trial [4]. Subjective scores of nasal congestion andsleep were significantly improved in the topical corticoster-oid-treated patients compared with placebo group. Day-time sleepiness also improved, but did not achievesignificance (P = 0.08). Unfortunately, no objective mea-surements of sleep and nasal obstruction were included inthe study. Azelastine was also found to significantlyimprove subjective sleep scores in 24 allergic rhinitis sub-jects [45]. However, there were no differences in nasal con-gestion and daytime sleepiness. The effects of nasalfluticasone on OSA related to adenoidal and tonsillarhypertrophy were assessed in 13 children [46]. AHIdecreased significantly from 10.7 to 5.8. The frequencies ofhemoglobin desaturation and respiratory movement/sleeparousals were also improved compared with the placebotreatment. There were no changes in adenoid sizes. Theeffects of budesonide were assessed using the EpworthSleepiness Scale, Functional Outcomes of Sleep Quest-ionnaire, Rhinoconjunctivitis Quality of Life Question-naire, and a daily diary for nasal symptoms, sleepproblems, and daytime fatigue records [47]. Budesonidesignificantly improved daytime fatigue, somnolence, andquality of sleep
The Impact of Obstructive Sleep Apnea on the Nose: Does Obstructive Sleep Apnea Impact Nasal Mucosa?Rubinstein [48] demonstrated that patients with OSAwithout clinical symptoms of rhinitis have nasal inflam-mation. They had a significantly increased number of cells,percentages of neutrophils, and higher concentrations ofbradykinin and vasoactive intestinal peptide (VIP) in nasallavage fluid. Intracellular adhesion molecule-1 (ICAM-1),interleukin-6 (IL-6), IL-8, and monocyte chemoattractantprotein-1 (MCP-1) are also elevated. Exhaled air conden-sates also showed increased indicators of inflammationand oxidant stress including nitric oxide, pentane, and 8-isoprostane in OSA patients compared with normal con-

198 Rhinitis
trol subjects [16•,49]. All these changes can be reversed byapplication of nCPAP therapy. Similar mediators act inallergic rhinitis and asthma. There is some evidence thatOSA is associated with more severe asthma, and that bothimprove with nCPAP therapy [14,15]. A proinflammatoryeffect of OSA could also be related to the cardiovascularcomplications of sleep apnea [16•].
The Impact of Continuous Positive Airway Pressure on Nasal MucosaNight ventilation with nCPAP is the gold standard for treat-ment of moderate and severe OSA. The flow generator pro-vides air under positive pressure through a nasal or facialmask. This provides a “pneumatic splint” of the upper air-ways. Polysomnography is used to measure Pcrit, which setsthe necessary pressure within a range of 4 to 20 cm H2O[16•,50]. Compliance with nCPAP treatment is relatively lowbecause of undesirable side effects. These include nasal con-gestion, rhinorrhea, crusted nose, epistaxis, sneezing, anddryness. Although nasal disturbances are very common inOSA, nCPAP treatment can aggravate their rhinitis. Nasalcongestion depends on the temperature and humidity of theair being breathed. Cold, dry air can induce inflammatorymediator release. Heated, humidified air often reduces thenasal complaints and improves compliance. Nasal steroids,decongestants, anticholinergic agents, allergy shots, and sur-gical correction of nasal cavity anatomical obstructionsmight still be necessary to obtain satisfactory compliancewith nCPAP therapy [16•,50].
ConclusionsObstructive sleep apnea is largely the result of nasal and pha-ryngeal abnormalities. The full differential diagnosis andpathogenic factors have not yet been fully discerned. Theinfluence of the nose on pharyngeal collapse is apparentfrom the “Starling resistor” model of the pharynx as a col-lapsible tube. Nasal reflexes could play a role in maintainingpharyngeal patency, but this is controversial. Studies showedthat artificial nasal obstruction clearly induced SDB. How-ever, there was no linear correlation of nasal resistance withapnea severity in either OSA or non-OSA patients. Overall,nasal obstruction is an independent but relatively weak riskfactor for OSA. However, increased nasal resistance was astronger, independent predictor of the AHI in a nonobesesubgroup of OSA patients with less severe sleep disorders[40••]. Also, within the continuum of SDB is UARS [20].UARS can be subdivided into two main subtypes: obese,heavy snorers at risk for OSA, and nonobese, nonsnoringpatients who might have functional somatic syndromes. Thelatter group appears to have a strong link with nonallergicrhinitis. Nasal steroid therapy and CPAP appear to be capa-ble of reducing nasal inflammation and improving sleepquality, nocturnal arousals, daytime sleepiness, and fatigue.
Allergic rhinitis subjects with coexisting OSA also improveafter successful immunotherapy.
AcknowledgmentsThe amount of literature in the area is extremely large. Weapologize for omitting some important studies for lack ofspace. We would like to thank Dr. Dora Popova for herindispensable help in reviewing the manuscript and Dr.Alexander Simidchiev, for his valuable help with the litera-ture search.
References and Recommended ReadingPapers of particular interest, published recently, have been highlighted as:• Of importance•• Of major importance
1. Bousquet J, Van Cauwenberge P, Khaltaev N: Allergic rhinitis and its impact on asthma. J Allergy Clin Immunol 2001, 108:147–334.
2. Baraniuk JN: Pathogenesis of allergic rhinitis. J Allergy Clin Immunol 1997, 99:S763–S772.
3. Lavie P, Gertner R, Zomer J, et al.: Breathing disorders in sleep associated with “microarousals” in patients with allergic rhinitis. Acta Otolaryngol 1981, 92:529–533.
4. Craig TJ, Teets S, Lehman EB, et al.: Nasal congestion second-ary to allergic rhinitis as a cause of sleep disturbance and daytime fatigue and the response to topical nasal corticoster-oids. J Allergy Clin Immunol 1998, 101:633–637.
5. Hughes K, Glass C, Ripchinski M, et al.: Efficacy of the topical nasal steroid budesonide on improving sleep and daytime somnolence in patients with perennial allergic rhinitis. Allergy 2003, 58:380–385.
6. Sher AE: An overview of sleep disordered breathing for the otolaryngologist. Ear Nose Throat J 1999, 78:694–708.
7. Young T, Finn L, Kim H: Nasal obstruction as a risk factor for sleep-disordered breathing. J Allergy Clin Immunol 1997, 99:S757–S762.
8. Atkins M, Taskar V, Clayton N, et al.: Nasal resistance in obstructive sleep apnea. Chest 1994, 105:1133–1135.
9. Blakley BW, Mahowald MW: Nasal resistance and sleep apnea. Laryngoscope 1987, 97:752–754.
10.•• Lofaso F, Coste A, d’Ortho MP, et al.: Nasal obstruction as a risk factor for sleep apnoea syndrome. Eur Respir J 2000, 16:639–643.
First study that, by means of stepwise multiple regression analysis, showed that daytime nasal obstruction represents an independent risk factor for OSAS, even though it is weaker than cephalometric landmarks, obesity, and male sex.11. Verse T, Pirsig W: Impact of impaired nasal breathing on
sleep-disordered breathing. Sleep Breath 2003, 7:63–76.12.• Chen W, Kushida CA: Nasal obstruction in sleep-disordered
breathing. Otolaryngol Clin North Am 2003, 36:437–460.A comprehensive review of the relation between nasal obstruction and sleep disordered breathing—pathophysiology of SDB, link with nasal obstruction, causes of nasal obstruction, and therapeutic modalities. It includes 102 references.13. Meltzer E: Does rhinitis compromise night-time sleep and
daytime productivity? Clin Exp All Rev 2002, 2:67–72.14. Chan CS, Woolcock AJ, Sullivan CE: Nocturnal asthma: role of
snoring and obstructive sleep apnea. Am Rev Respir Dis 1988, 137:1502–1504.
15. Bohadana AB, Hannhart B, Teculescu DB: Nocturnal worsen-ing of asthma and sleep-disordered breathing. J Asthma 2002, 39:85–100.
Rhinitis and Sleep Apnea • Staevska et al. 199
16.• Qureshi A, Ballard RD, Nelson HS: Obstructive sleep apnea. J Allergy Clin Immunol 2003, 112:643–651.
A comprehensive review of OSA that covers its pathophysiology, clini-cal features, clinical consequences, and therapeutic modalities. The authors suggested that the proinflammatory effect of OSA could be related to asthma severity.17.• Bonekat HW, Hardin KA: Severe upper airway obstruction
during sleep. Clin Rev Allergy Immunol 2003, 25:191–210.A very comprehensive review of OSA covering all its aspects and dis-cussing, in depth, the link between nocturnal asthma, sleep, and OSA.18. Young T, Finn L, Palta M: Chronic nasal congestion at night is
a risk factor for snoring in a population-based cohort study. Arch Intern Med 2001, 161:1514–1519.
19. American Academy of Sleep Medicine: Sleep related breathing disorders in adults: recommendations for syndrome defini-tion and measurement techniques in clinical research. Sleep 1999, 22:667–689.
20. Guilleminault C, Stoohs R, Clerk A, et al.: A cause of daytime sleepiness: the upper airway resistance syndrome. Chest 1993, 104:781–787.
21. Houser SM, Mamikoglu B, Aquino BF, et al.: Acoustic rhinome-try findings in patients with mild sleep apnea. Otolaryngol Head Neck Surg 2002, 126:475–480.
22. Guilleminault C, Chowdhuri S: Upper airway resistance syn-drome is a distinct syndrome. Am J Respir Crit Care Med 2000, 161:1413–1416.
23. Gold AR, Dipalo F, Gold MS, et al.: The symptoms and signs of upper airway resistance syndrome: a link to the functional somatic syndromes. Chest 2003, 123:12–14.
24. Levander H: Sensory sensitization. Part II: Pathophysiology in dysfunctional disorders. Understanding the inner life of the nerve pathways may explain hitherto unexplainable symptoms [Swedish]. Lakartidningen 2003, 100:1618–1619, 1622–1624.
25. Baraniuk JN, Clauw DJ, Gaumond E: Rhinitis symptoms in chronic fatigue syndrome. Ann Allergy Asthma Immunol 1998 81:359–365.
26. Rama AN, Tekwani SH, Kushida CA: Sites of obstruction in obstructive sleep apnea. Chest 2002, 122: 1139–1147
27. Gold AR, Marcus CL, Dipalo F, Gold MS: Upper airway collaps-ibility during sleep in upper airway resistance syndrome. Chest 2002, 121:1531–1540.
28. Ayappa I, Rapoport DM: The upper airway in sleep: physiol-ogy of the pharynx. Sleep Med Rev 2003, 7:9–33.
29. Strohl KP, Hensley MJ, Hallett M, et al.: Activation of upper air-way muscle before onset of inspiration in normal humans. J Appl Physiol 1980, 49:638–642.
30. Remmers JE, de Groot WJ, Sauerland EK, et al.: Pathogenesis of upper airway occlusion during sleep. J Appl Physiol 1979, 46:931–938.
31. Mezzanote WS, Tangel DJ, White DP: Waking genioglossal electromyogram in sleep apnea patients versus normal con-trols (a neuromuscular compensatory mechanism). J Clin Invest 1992, 89:1571–1579.
32. King ED, O’Donnell CP, Smith PL, et al.: A model of obstruc-tive sleep apnea in normal humans. Am J Respir Crit Care Med 2000, 161:1979–1984.
33. De Vito A, Berrettini S, Carabelli A, et al.: The importance of nasal resistance in obstructive sleep apnea syndrome: a study with positional rhinomanometry. Sleep Breath 2001, 5:3–11.
34. Zwillich CW, Pickett C, Hanson FN, et al.: Disturbed sleep and prolonged apnea during nasal obstruction in normal men. Am Rev Respir Dis 1981, 124:158–160.
35. Olsen KD, Kern EB, Westbrook PR: Sleep and breathing distur-bance secondary to nasal obstruction. Otolaryngol Head Neck Surg 1981, 89:804–910.
36. Taasan V, Wynne JW, Cassisi N, et al.: The effect of nasal pack-ing on sleep-disordered breathing and nocturnal oxygen desaturation. Laryngoscope 1981, 91:1163–1172.
37. Lavie P, Fischel N, Zomer J, et al.: The effects of partial and complete mechanical occlusion of the nasal passages on sleep structure and breathing in sleep. Acta Otolaryngol 1983, 95:161–166.
38. Suratt PM, Turner BL, Wilhoit SC: Effect of intranasal obstruc-tion on breathing during sleep. Chest 1986, 90:324–329.
39. Duchna HW, Rasche K, Orth M, et al.: Anamnestic and poly-graphic parameters in obstructive sleep apnea syndrome patients with reduced nasal respiration during the day in comparison with obstructive sleep apnea patients with nor-mal nasal respiration [German]. Wien Med Wochenschr 1996, 146:348–349.
40.•• Virkkula P, Hurmerinta K, Loytonen M, et al.: Postural cephalo-metric analysis and nasal resistance in sleep-disordered breathing. Laryngoscope 2003, 113:1166–1174.
Must read. For the first time, the authors suggest that OSAS could be a complex disorder that could be subdivided into several subtypes with different contributing factors. By means of stepwise multiple regres-sion analysis, they estimated that combined nasal resistance is an independent predictor of OSA severity.41. Liistro G, Rombaux P, Belge C, et al.: High Mallampati score
and nasal obstruction are associated risk factors for obstruc-tive sleep apnoea. Eur Respir J 2003, 21:248–252.
42. McNicholas WT, Tarlo S, Cole P, et al.: Obstructive apneas dur-ing sleep in patients with seasonal allergic rhinitis. Am Rev Respir Dis 1982, 126:625–628.
43. Houser SM, Mamikoglu B, Aquino BF, et al.: Acoustic rhinome-try findings in patients with mild sleep apnea. Otolaryngol Head Neck Surg 2002, 126:475–480.
44. Martin SE, Wraith PK, Deary IJ, et al.: The effect of nonvisible sleep fragmentation on daytime function. Am J Resir Crit Care Med 1997, 155:1596–1601.
45. Golden S, Teets SJ, Lehman EB, et al.: Effect of topical nasal azelastine on the symptoms of rhinitis, sleep, and daytime somnolence in perennial allergic rhinitis. Ann Allergy Asthma Immunol 2000, 85:53–57.
46. Brouillette RT, Manoukian JJ, Ducharme FM, et al.: Efficacy of fluticasone nasal spray for pediatric obstructive sleep apnea. J Pediatr 2001, 138:838–844.
47. Hughes K, Glass C, Ripchinski M, et al.: Efficacy of the topical nasal steroid budesonide on improving sleep and daytime somnolence in patients with perennial allergic rhinitis. Allergy 2003, 58:380–385.
48. Rubinstein I: Nasal inflammation in patients with obstructive sleep apnea. Laryngoscope 1995, 105:175–177.
49. Lavie L: Obstructive sleep apnoea syndrome: an oxidative stress disorder. Sleep Med Rev 2003, 7:35–51.
50. Hollandt JH, Mahlerwein M: Nasal breathing and continuous positive airway pressure (CPAP) in patient with obstructive sleep apnea (OSA). Sleep Breath 2003, 7:87–94.




















