
Occupational sleep medicine
15
CHAPTER 12 Occupational sleep medicine: Practice and promise Gregory Belenky*, Lora J. Wu and Melinda L. Jackson Sleep and Performance Research Center, Washington State University, Spokane, WA, USA Abstract: Occupational sleep medicine is a new field within sleep medicine. Occupational sleep medicine applies (1) the science of sleep, frequently as instantiated into mathematical modeling; (2) the tactics, techniques, and procedures of sleep and performance measurement in the operational environment; and (3) the clinical practice of sleep medicine to reduce the risks of poor performance, lost productivity, and error, incident, and accident in the workplace. As envisioned here, occupational sleep medicine will play a crucial role in fatigue risk management to, in the short term, improve performance, productivity, and safety and in the longer term improve worker health and well-being. Keywords: sleep; sleep loss; sleep deprivation; split sleep; fatigue; performance; fatigue risk management. Introduction to occupational sleep medicine Occupational sleep medicine applies sleep science and the clinical practice of sleep medicine to reduce fatigue and improve performance, produc- tivity, safety, health, and well-being in the work- place (Belenky and Akerstedt, 2011). Occupational sleep medicine, by mitigating the “fog of fatigue,” enables the management of fatigue risk (Moore-Ede, 1995). Error, incident, and accident causation in any particular case is multifactorial, complex, and tightly coupled (involving multiple, interdependent, linked processes; Perrow, 1999). Thus, with respect to any particular accident, ascribing a causal role to fatigue is difficult (Hersman, 2010). Nevertheless, an increase in fatigue appears to shift the perfor- mance distribution toward increased risk, making error, incident, and accident more probable and decreasing the likelihood of recovery even if the error is detected (Thomas et al., 2007; Van Dongen et al., 2010). Applying the science of sleep enables fatigue- friendly rostering and scheduling and other fatigue-related “antifogmatics,” otherwise known as fatigue countermeasures, that blunt the adverse effect of extended work hours, shift work, and cumulative fatigue on performance, productivity, health, and well-being. Applying the clinical prac- tice of sleep medicine in the occupational setting *Corresponding author. Tel.: þ 1-509-358-7738; Fax: þ 1-509-358-7810 E-mail: [email protected] 189 DOI: 10.1016/B978-0-444-53817-8.00012-8 H. P. A. Van Dongen and G. A. Kerkhof (Eds.) Progress in Brain Research, Vol. 190 ISSN: 0079-6123 Copyright Ó 2011 Elsevier B.V. All rights reserved.
Transcript of Occupational sleep medicine

H. P. A. Van Dongen and G. A. Kerkhof (Eds.)Progress in Brain Research, Vol. 190ISSN: 0079-6123Copyright � 2011 Elsevier B.V. All rights reserved.
CHAPTER 12
Occupational sleep medicine: Practice and promise
Gregory Belenky*, Lora J. Wu and Melinda L. Jackson
Sleep and Performance Research Center, Washington State University, Spokane, WA, USA
Abstract: Occupational sleep medicine is a new field within sleep medicine. Occupational sleepmedicine applies (1) the science of sleep, frequently as instantiated into mathematical modeling; (2)the tactics, techniques, and procedures of sleep and performance measurement in the operationalenvironment; and (3) the clinical practice of sleep medicine to reduce the risks of poor performance,lost productivity, and error, incident, and accident in the workplace. As envisioned here, occupationalsleep medicine will play a crucial role in fatigue risk management to, in the short term, improveperformance, productivity, and safety and in the longer term improve worker health and well-being.
Keywords: sleep; sleep loss; sleep deprivation; split sleep; fatigue; performance; fatigue riskmanagement.
Introduction to occupational sleep medicine
Occupational sleep medicine applies sleep scienceand the clinical practice of sleep medicine toreduce fatigue and improve performance, produc-tivity, safety, health, and well-being in the work-place (Belenky and Akerstedt, 2011).Occupational sleep medicine, by mitigating the“fog of fatigue,” enables the management offatigue risk (Moore-Ede, 1995). Error, incident,and accident causation in any particular case ismultifactorial, complex, and tightly coupled(involving multiple, interdependent, linked
*Corresponding author.Tel.: þ1-509-358-7738; Fax: þ1-509-358-7810E-mail: [email protected]
189DOI: 10.1016/B978-0-444-53817-8.00012-8
processes; Perrow, 1999). Thus, with respect toany particular accident, ascribing a causal role tofatigue is difficult (Hersman, 2010). Nevertheless,an increase in fatigue appears to shift the perfor-mance distribution toward increased risk, makingerror, incident, and accident more probable anddecreasing the likelihood of recovery even if theerror is detected (Thomas et al., 2007; VanDongen et al., 2010).
Applying the science of sleep enables fatigue-friendly rostering and scheduling and otherfatigue-related “antifogmatics,” otherwise knownas fatigue countermeasures, that blunt the adverseeffect of extended work hours, shift work, andcumulative fatigue on performance, productivity,health, and well-being. Applying the clinical prac-tice of sleep medicine in the occupational setting

190
enables the assessment of sleep disorders and theireffects on alertness, performance, productivity,and safety in the workplace and their detection,treatment, and evaluation of treatment outcome.
Occupational sleep medicine in application infatigue risk management has both short- andlong-term horizons. The short-term horizon isframed in terms of reducing the immediate riskof error, incident, and accident (Gander et al.,2011). The long-term horizon is framed in termsof improving health and well-being across a per-son's working life, particularly in reducing obe-sity, insulin resistance, metabolic syndrome, typeII diabetes, hypertension, cardiovascular disease,and cognitive decline (Mullington et al., 2009;Van Cauter et al., 2008).
One way of applying the science of sleep to cre-ate fatigue-friendly rosters and schedules involvesintegrating sleep and fatigue-related experimentalfindings, technologies, and metrics as componentsof personal biomedical status monitoring. In thenot too distant future, personal biomedical statusmonitoring will be available to measure and inte-grate a plethora of parameters, including meta-bolic indices (e.g., blood glucose, caloricexpenditure), cardiovascular parameters (e.g.,blood pressure, EKG, and arterial intima func-tion), inflammatory markers (e.g., leukocytes,IL-6, and high sensitivity C-reactive protein),behavioral metrics (e.g., sleep/wake history, circa-dian rhythm phase, and amplitude), metrics ofcognitive performance (e.g., reaction times, mem-ory), and workload (e.g., time on task and metricsof task intensity). Personal biomedical statusmonitoring will form the basis of open- andclosed-loop systems to monitor and intervenewhen necessary, in order to sustain human health,well-being, and operational performance. Withrespect to operational performance, biomedicalstatus monitoring will provide diagnostics andprognostics for the person in the operational loopby supplying inputs (e.g., sleep/wake history, cir-cadian phase, and workload) to mathematicalmodels to predict individual performance in realtime. These predictions will be benchmarked
against, and individually adjusted to predict,actual performance (Olofsen et al., 2004), andused as the evidence-base for real-time fatiguerisk management.
To make a military analogy, sleep can beviewed as an item of logistic resupply with respectto sustaining operational performance. In manag-ing fuel consumption, a battalion logistics officercan measure how much fuel the battalion has onhand, apply a simple mathematical model takingas input miles to be driven and estimated mileageby vehicle type to estimate how long this fuel willlast, and with this estimate in hand, plan fortimely resupply. Similarly in managing sleep-loss-related fatigue, one can measure sleep/wakehistory in operational personnel using actigraphy,and use this sleep/wake history as input to amathematical model predicting how long thissleep will sustain individual performance. In lightof these predictions, one can adjust operations toensure timely resupply of sleep, by arrangingsleep opportunities of adequate length andsleep-conducive circadian placement. Eventually,models will integrate individual performance pre-dictions to predict work group performance.
Components of fatigue and relation tofatigue risk management
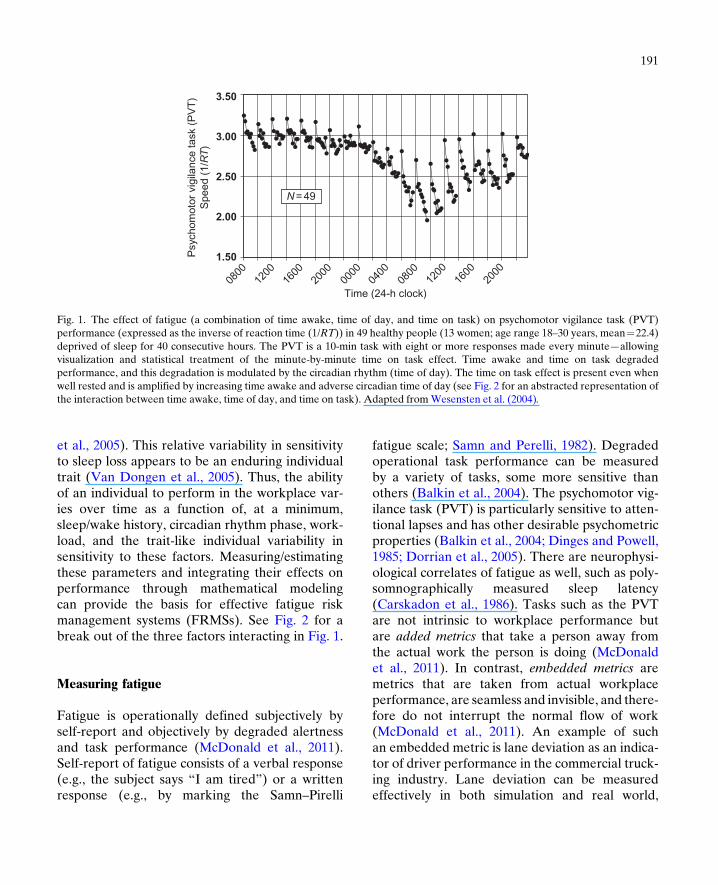
Fatigue is a function of the interaction of multiplefactors including sleep/wake history, circadianrhythm phase, and workload, and is modulatedby individual differences in response to thesefactors (Van Dongen et al., 2005; Wesenstenet al., 2004). A fatigue-inducing factor is one thatshifts the fatigue-risk distribution in the directionof increasing risk of error, incident, or accident.Figure 1 shows experimental data capturing theinteraction of sleep/wake history (in this instance,of total sleep deprivation), circadian rhythmphase, and time on task (a component of workload) on cognitive performance (Wesenstenet al., 2004). Individuals vary from one anotherin their sensitivity to these factors (Van Dongen
0800
1.50
2.00
Time (24-h clock)
Psy
chom
otor
vig
ilanc
e ta
sk (
PV
T)
Spe
ed (
1/R
T)
2.50
3.00
3.50
1200
1600
2000
0000
0400
0800
1200
1600
2000
N = 49
Fig. 1. The effect of fatigue (a combination of time awake, time of day, and time on task) on psychomotor vigilance task (PVT)performance (expressed as the inverse of reaction time (1/RT)) in 49 healthy people (13 women; age range 18–30 years, mean¼22.4)deprived of sleep for 40 consecutive hours. The PVT is a 10-min task with eight or more responses made every minute—allowingvisualization and statistical treatment of the minute-by-minute time on task effect. Time awake and time on task degradedperformance, and this degradation is modulated by the circadian rhythm (time of day). The time on task effect is present even whenwell rested and is amplified by increasing time awake and adverse circadian time of day (see Fig. 2 for an abstracted representation ofthe interaction between time awake, time of day, and time on task). Adapted fromWesensten et al. (2004).
191
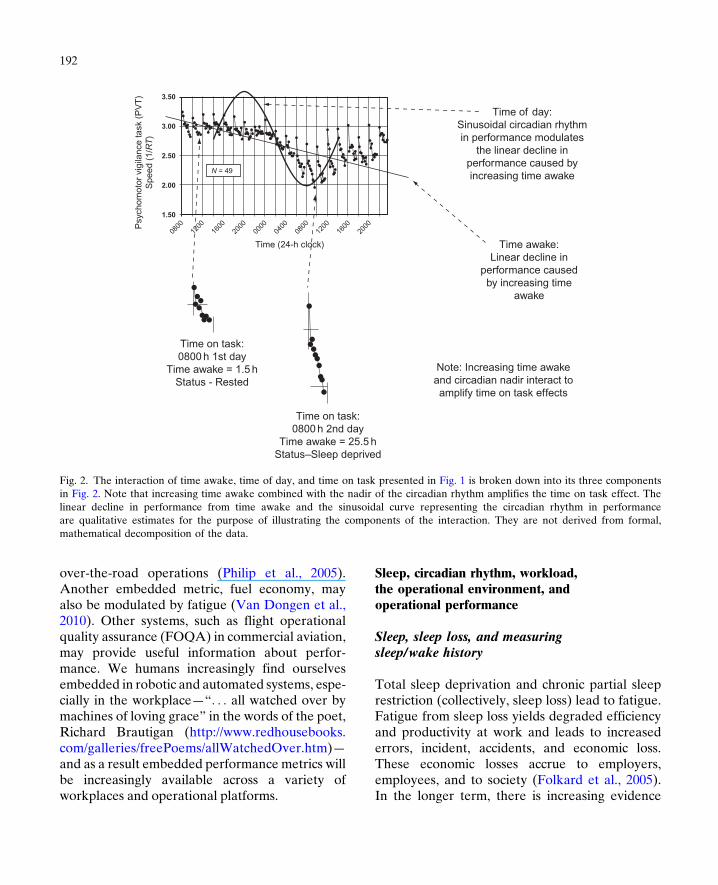
et al., 2005). This relative variability in sensitivityto sleep loss appears to be an enduring individualtrait (Van Dongen et al., 2005). Thus, the abilityof an individual to perform in the workplace var-ies over time as a function of, at a minimum,sleep/wake history, circadian rhythm phase, work-load, and the trait-like individual variability insensitivity to these factors. Measuring/estimatingthese parameters and integrating their effects onperformance through mathematical modelingcan provide the basis for effective fatigue riskmanagement systems (FRMSs). See Fig. 2 for abreak out of the three factors interacting in Fig. 1.
Measuring fatigue
Fatigue is operationally defined subjectively byself-report and objectively by degraded alertnessand task performance (McDonald et al., 2011).Self-report of fatigue consists of a verbal response(e.g., the subject says “I am tired”) or a writtenresponse (e.g., by marking the Samn–Pirelli
fatigue scale; Samn and Perelli, 1982). Degradedoperational task performance can be measuredby a variety of tasks, some more sensitive thanothers (Balkin et al., 2004). The psychomotor vig-ilance task (PVT) is particularly sensitive to atten-tional lapses and has other desirable psychometricproperties (Balkin et al., 2004; Dinges and Powell,1985; Dorrian et al., 2005). There are neurophysi-ological correlates of fatigue as well, such as poly-somnographically measured sleep latency(Carskadon et al., 1986). Tasks such as the PVTare not intrinsic to workplace performance butare added metrics that take a person away fromthe actual work the person is doing (McDonaldet al., 2011). In contrast, embedded metrics aremetrics that are taken from actual workplaceperformance, are seamless and invisible, and there-fore do not interrupt the normal flow of work(McDonald et al., 2011). An example of suchan embedded metric is lane deviation as an indica-tor of driver performance in the commercial truck-ing industry. Lane deviation can be measuredeffectively in both simulation and real world,
Time of day:Sinusoidal circadian rhythmin performance modulates
the linear decline inperformance caused byincreasing time awake
Time awake:Linear decline in
performance causedby increasing time
awake
Note: Increasing time awakeand circadian nadir interact toamplify time on task effects
Time on task:0800 h 2nd day
Time awake = 25.5 hStatus–Sleep deprived
Time on task:0800 h 1st day
Time awake = 1.5 hStatus - Rested
0800
1.50
2.00
N = 49
Time (24-h clock)
Psy
chom
otor
vig
ilanc
e ta
sk (
PV
T)
Spe
ed (
1/R
T)
2.50
3.00
3.50
1200
1600
2000
0000
0400
0800
1200
1600
2000
Fig. 2. The interaction of time awake, time of day, and time on task presented in Fig. 1 is broken down into its three componentsin Fig. 2. Note that increasing time awake combined with the nadir of the circadian rhythm amplifies the time on task effect. Thelinear decline in performance from time awake and the sinusoidal curve representing the circadian rhythm in performanceare qualitative estimates for the purpose of illustrating the components of the interaction. They are not derived from formal,mathematical decomposition of the data.
192
over-the-road operations (Philip et al., 2005).Another embedded metric, fuel economy, mayalso be modulated by fatigue (Van Dongen et al.,2010). Other systems, such as flight operationalquality assurance (FOQA) in commercial aviation,may provide useful information about perfor-mance. We humans increasingly find ourselvesembedded in robotic and automated systems, espe-cially in the workplace—“. . . all watched over bymachines of loving grace” in the words of the poet,Richard Brautigan (http://www.redhousebooks.com/galleries/freePoems/allWatchedOver.htm)—and as a result embedded performance metrics willbe increasingly available across a variety ofworkplaces and operational platforms.
Sleep, circadian rhythm, workload,the operational environment, andoperational performance
Sleep, sleep loss, and measuringsleep/wake history
Total sleep deprivation and chronic partial sleeprestriction (collectively, sleep loss) lead to fatigue.Fatigue from sleep loss yields degraded efficiencyand productivity at work and leads to increasederrors, incident, accidents, and economic loss.These economic losses accrue to employers,employees, and to society (Folkard et al., 2005).In the longer term, there is increasing evidence

193
that sleep loss is associated with adverse effectson mental and physical health, such as weightgain and obesity (Knutson et al., 2007), hyperten-sion and cardiovascular problems (Meier-Ewertet al., 2004), gastrointestinal disease, chronicfatigue, substance/alcohol abuse, family problems,and mood difficulties (Costa et al., 2004). Thus,the adverse effects of sleep loss include bothimmediate and longer-term effects.In laboratory studies, both acute, total sleep dep-
rivation and chronic, partial sleep restriction lead todecrements in task performance, well-being, andhealth. Acute, total sleep deprivation degradescognitive performance linearly over successivedays, modulated within days by the circadianrhythm, with an average of 17–25% loss of capacityto do useful work per day (Thomas et al., 2000;Thorne et al., 1983). Mild, moderate, and severesleep restriction (7, 5, or 3 h time in bed/night groupfor 7 days, respectively) leads to sleep-dose-dependent decreases in performance over time incomparison to baseline or to sleep augmentation(9 h time in bed/night) (Belenky et al., 2003). For7 and 5 h time in bed/night groups, performanceappears to stabilize at lower levels after 3–4 days,while for the 3 h time in bed/night group, perfor-mance continues to degrade across the 7 day exper-imental period. In a complementary study ofchronic sleep restriction, 6 and 4 h time in bed/nightfor 14 days led to sleep-dose-dependent degradedtask performance (Van Dongen et al., 2003). Ofclear operational importance is the finding thateven mild sleep restriction (7 h time in bed/night)degrades performance over time (Belenky et al.,2003). In the first mentioned study (Belenky et al.,2003), at the end of the 7-day sleep restrictionperiod participants were allowed 8 h time in bed/night recovery sleep for three nights. In contrastto acute total sleep deprivation, where recovery iscomplete in 1–2 days, performance in the 7, 5, and3 h time in bed groups did not recover to baselinetask performance over the 3-day recovery period.This is of operational importance as chronic sleeprestriction is common, not to say ubiquitous, andtotal sleep deprivation is rare. In a follow-on study
to the sleep restriction and recovery studydescribed above, it was found that preloading/augmenting sleep prior to the sleep restrictionyielded more rapid recovery (Rupp et al., 2008).
The laboratory standard for measuring sleep/wake history is polysomnography (PSG), whichuses the combination of electroencephalogram(EEG), electrooculogram (EOG), and electro-myogram (EMG) to score total sleep time, sleepefficiency (% of sleep opportunity spent asleep),and the stages of sleep (N1, N2, N3, and REM).While PSG has been applied to recording andscoring sleep/wake history in the field, its depen-dence on an electrode array makes it impracticalin most field settings. In field studies of sleepand performance, sleep diaries have been usedbut do not reliably measure total sleep time orsleep efficiency. In contrast to PSG and sleepdiaries, the actigraph (a wrist-worn device con-taining an accelerometer, signal processing hard-ware and software, and memory) is comparableto PSG in measuring total sleep time and sleepefficiency (Ancoli-Israel et al., 2003). Theactigraph is a device about the size of a sportswatch. Using its accelerometer, the actigraphmeasures arm movements and sums and recordsthem typically in 1-min bins. From this activityrecord, using a validated-against-PSG sleep-scoring algorithm, a sleep/wake history for 30consecutive days can usually be obtained beforethe device needs to be downloaded. Battery lifeand memory capacity are the limiting factors inthe length and temporal resolution of theactigraph in collecting sleep/wake history. Theactigraph is a useful tool for conducting fieldmeasurements over extended periods and mayhave utility applied to fatigue risk management.
The circadian rhythm and measuringcircadian rhythm phase
The circadian rhythm, an approximately sinusoi-dal, 24-h rhythm in core body temperature, sleep,and task performance, is set by the suprachiasmatic

194
nucleus (SCN) of the hypothalamus, the endoge-nous biological clock (Moore et al., 2002). TheSCN itself receives direct input from the retinaand responds most sensitively to blue light, asdescribed by a distinctive phase response curve(Wright et al., 2005; see further for explanation).Core body temperature peaks around 20:00 h andreaches its nadir between 04:00 and 06:00 h. Thecircadian rhythms in task performance and sleeppropensity parallel the circadian rhythm in corebody temperature. Task performance peaks inmid-evening just subsequent to the peak in thecircadian temperature rhythm and troughs inthe early morning just subsequent to the trough incircadian temperature rhythm. Sleep propensityfollows the circadian rhythm in core body tempera-ture, making it difficult to fall asleep and to stayasleep when core body temperature is rising orhigh and easy to fall asleep and to stay asleepwhen core body temperature is falling or low.The circadian rhythm modulates the risk of injury,a correlate of degraded performance. Risk ofinjury increases depending on the shift worked,with the lowest rates of injury risk on morningshifts and highest rates on night shifts (Folkardand Tucker, 2003). Thus, injury rates on the jobare highest during the late night/early morning cir-cadian low (Folkard and Tucker, 2003). Mild tomoderate sleep loss, common for night shiftworkers who typically experience restricted sleepduring the day (Akerstedt, 2003), leads todecrements in performance (Belenky et al., 2003).Sleep/wake history and the circadian rhythm inter-act to affect alertness, sleep propensity, andperformance.
The laboratory standard for measuring circa-dian rhythm phase is dim light melatonin onset(DLMO; Lewy and Sack, 1989). MeasuringDLMO requires laboratory control and dim lightand is not suitable for field measurement. Analternative metric to DLMO is core body temper-ature measured by swallowable temperature pillor rectal probe (Edwards et al., 2002). Becauseof masking effects of movement, core body tem-perature measurements require laboratory
control and constant routine and are also not suit-able for field measurement. In a personhabituated to a particular time zone, circadianphase can be estimated in the field by self-reporton the basis of the local time zone alone. How-ever, in crossing time zones any predictability byself-report is destroyed because of the sensitivityof the SCN to light exposure in the early morningand early evening hours. The cross over point ofthe phase response curve of the SCN in a personhabituated to a local time zone is in the temporalvicinity of 03:00 h, the midpoint of subjectivenight (Moore, 1997). In an individual habituated/synchronized to a time zone, exposure to lightbefore the crossover point of the phase responsecurve is seen by the SCN as a late sunset andstimulating a circadian phase delay, while expo-sure to light after the crossover point is seen bythe SCN as an early dawn stimulating a circadianphase advance. The maximum phase response tolight exposure is at dawn and dusk. Thisvariability in the phase response curve makesthe prediction of shifting phase angle when cross-ing multiple time zones difficult without exactknowledge of initial circadian phase and lightexposure at the level and position of the eye. Intheory, and perhaps in practice, accurate mea-surement of light exposure at the level and posi-tion of the eye combined with accuratemathematical models describing the SCN phaseresponse curve to light may enable the accurateprediction of circadian phase with shifting timezones (Bierman et al., 2005).
Workload
Workload is not satisfactorily operationallydefined and therefore not easily measured ineither laboratory or field. Some studies haveequated workload with time on task, a componentof workload. Fatigue as a result of time on taskhas been shown to be relieved by breaks withinshift (Knutson et al., 2007). Thus, fatigue fromtime on task recovers with simple rest, a break

195
from task performance, and does not require sleep(see Fig. 1). In contrast, fatigue and performancedecrements related to time awake are onlyreversed by sleep (Dawson and McCulloch, 2005).Fatigue resulting from working long hours or over-time shifts increases the risk of accident (Dembeet al., 2005). Workload, time of day, and sleep lossall interact to affect task performance.
The operational environment
The operational environment is defined as a worksetting in which human task performance is criti-cal, and if human performance degrades the sys-tem will fail. In the operational environment, thehuman-in-the-operational-loop has limited timeto decide and act (Wesensten et al., 2005). Thereis a large variety of operational settings. Theseinclude military operations, maritime operations,medicine, and the various modes of land transpor-tation, aviation, security work, energy generation,resource extraction (mining and drilling), finan-cial markets, and industrial production. In brief,any 24�7 operation and any operation involvingextended work hours or shift work is an opera-tional setting. In these settings, the operationalcharacteristics described previously (i.e., shifttiming and duration, work intensity, and difficultyand complexity of the work tasks) degrade per-formance directly through the effects of workloadand/or working through the circadian low andindirectly by reducing the amount of time avail-able for sleep or placing the sleep opportunity ata nonpropitious time for sleep, thus reducing totalsleep time, a primary determinant of alertnessand performance (Wesensten et al., 2005).The effects of fatigue on real world or realisticallysimulated operational performance can becomplex. In an aviation simulation study, aftercompleting a multiday international run (fatigued)versus coming into the simulation after a few daysat home (rested), Boeing 747 2-pilot crews werebetter able to detect errors but less able to managethem successfully (Petrilli et al., 2007).
Operational task performance
This finding of degradation in complex taskperformance seen in simulator studies iscomplemented by evidence from laboratory stud-ies in which some forms of complex task perfor-mance are degraded more than simple taskperformance (Harrison and Horne, 2000; Nilssonet al., 2005). There is however counter-evidencesuggesting further subtleties (Tucker et al.,2010). Evidence from imaging studies suggeststhat total sleep deprivation selectively deactivatesthe prefrontal cortex, as indicated by a largerdecrease in glucose uptake (regional cerebralmetabolic rate glucose (rCMRglu)) than the restof the brain as measured by positron emissiontomography using 18-fluoro-2-deoxyglucose astracer (Thomas et al., 2000). This decrease inrCMRglu reflects a general decrease in neuronalfiring as the brain depends on just-time deliveryof glucose and then oxygen (Magistretti et al.,1995). As the prefrontal cortex is responsible forcomplex task performance, including judgment,planning, situational awareness, and the integra-tion of reason with emotion, this physiologicalimaging evidence supports the behavioral findingsunder conditions of sleep loss (Harrison andHorne, 2000).
In complementary fashion, evidence from otherimaging studies suggests that the prefrontal cortexis selectively targeted for recuperation duringsleep, as the prefrontal cortex remains deactivatedduring both nonrapid eye movement (NREM)sleep and rapid eye movement (REM) sleep,while the rest of the brain returns to approxi-mately waking levels of activation during REMsleep.
A case example in which complex task perfor-mance degraded more than simple task perfor-mance comes from the debriefings conducted byone of the authors (G.B.) of friendly fire incidentsduring the 1990–1991 Gulf War (Operation Des-ert Storm). In one such incident, sleep restrictioncontributed to Bradley fighting vehicle crewslosing their orientation to the battlefield

196
(a complex task) and therefore causing them tomistake friend for foe while maintaining theirability to lay cross hairs on the target and shootaccurately (a simple task) resulting in the destruc-tion of a friendly Bradley (Belenky et al., 1996).
Consolidated sleep, split sleep,and sleep fragmentation
Split sleep, in the form of biphasic sleep, occursnaturally in cultures in which people regularlytake siestas (Webb and Dinges, 1989). Recentstudies have demonstrated that performance is afunction of total sleep time in 24 h, regardless ofwhether the sleep is consolidated or split(Belenky et al., 2008) and irrespective of sleepstages (e.g., NREM or REM sleep). Thus, it doesnot appear to matter whether sleep is obtained ina single, consolidated sleep bout or distributed intwo or three bouts over 24 h (split sleep). Givenequal total sleep time, split sleep appears to sus-tain performance as well as sleep consolidatedinto a single sleep bout (Belenky et al., 2008; seealso chapter 8 of volume 185). Thus, total sleeptime measured by actigraphy can be used to pre-dict performance in operational settings (Ancoli-Israel et al., 2003).
Similarly, in some work settings involving nightshift work and/or early starts, splitting sleep into amain sleep period and supplementary naps is com-mon. In a field study of physicians in training,assessing sleep (by actigraphy) and performanceand comparing when working night float versusday shift, physicians averaged about 7 h of totalsleep time per 24 h in both night float and day shifts(McDonald et al., 2009). However, they obtainedthis sleep quite differently depending onwhich typeof shift they were working. If working the day shift,the physicians obtained their 7 h of sleep at night ina consolidated main sleep. If working night float,the physicians split their sleep and obtained their7 h of sleep in a main morning sleep of �4 h,supplemented with nighttime naps totaling 3 h.Performance on the PVT, taken at approximately
the same clock times going on and going off shift,was the same on night float and day shift.
Split sleep (2–3 multihour sleep bouts across a24-h period) should be clearly distinguished fromfragmented sleep (sleep interrupted every fewminutes). Sleep fragmented with even subliminalarousals (change in sleep stage in response to astimulus) at a frequency of every 2–3 min can loseall recuperative value (Bonnet and Arand, 2003).In contrast, it appears that sleep bouts greaterthan 20 min in length have minute by minuterecuperative value equivalent to consolidatedsleep (Bonnet and Arand, 2003).
Individual differences in response tofactors causing fatigue
There are substantial differences betweenindividuals in degree of performance degradationresulting from sleep loss (Van Dongen et al.,2005). These differences appear to be an enduringcharacteristic that is present on subsequent retest,and therefore trait-like. Recent work hasassociated this trait-like difference with geneticmarkers (Viola et al., 2007). There are also cohortdifferences associated with age. Older individualsperform less well than younger individuals whenboth are rested, but perform better than youngerindividuals when both are sleep restricted (Blieseet al., 2006). In addition, there are individualdifferences in phase angle and amplitude of circa-dian rhythm, such as age and morningness/eveningness, which are likely to affect fatigue asmeasured by self-report and objective perfor-mance measures (Brock, 1991; Kerkhof and VanDongen, 1996).
Predicting performance from thecomponents of fatigue
In the 1980s, one of the authors (G.B.) wasdirecting the U.S. Army's research program insleep and performance, measuring sleep in the

197
field environment by actigraphy. Actigraphy wasa young, developing technology. When presentedwith early field actigraph studies, US ArmyGeneral Maxwell Thurman (General “Max”)harrumphed and said, “I don't care how muchthey sleep, I want to know how well they per-form.” An actigraphically recorded sleep/wakehistory is a marvel of applied information technol-ogy, but in and of itself an actigraphically derivedsleep/wake history does not speak directly to thewearer's performance. Keeping General Max'sresponse in mind, we developed a mathematicalmodel taking sleep/wake history and estimatedcircadian phase as its inputs and yielding a min-ute-by-minute prediction of performance as itsoutput. Our model and other similar models havebecome commercial products with application inthe developing field of fatigue risk management(Mallis et al., 2004; Wesensten et al., 2005). Gen-eral Max would be pleased—with actigraphy wewill know how much people sleep, and applyingmathematical models to the actigraphic data, wewill be able to predict how well they will perform.
Systems of fatigue risk management
Outline of a fatigue risk management system
The traditional technique for managing fatiguerisk in the workplace has been, and still to a largeextent is, hours of service regulations. Hours ofservice rules were first promulgated in early nine-teenth century Britain in response to the indus-trial revolution (Cornish and Clark, 1989). Suchregulations typically specify the number of per-missible hours on duty in 24 h and sometimesweekly or other longer-term limits as well. Theytake into account homeostatic sleep drive butnot the effects of the circadian rhythm on perfor-mance and sleep propensity. Such rules are pre-scriptive and hence rigid and, as a defenseagainst fatigue risk, are brittle. As there is a neg-ative correlation between work hours and hoursof sleep, that is, longer-work hours predict less
sleep (Basner et al., 2007; McDonald et al.,2008), this approach, as a broad first cut, hasmerit for normal day shift work where the personworks during the day and sleeps at night. It isworth noting that employees who work afternoonshifts sleep more than employees working stan-dard day shifts (Lauderdale et al., 2006). Whenwork and sleep are in harmony with the circadianrhythm in sleep propensity and performance,hours of service regulations are a reasonableapproach. Where prescriptive rules break downare when the work schedule involves extendedwork hours, early morning starts, or night shifts,as simple prescriptive rules do not take intoaccount the circadian rhythms in performanceand sleep propensity.
The National Transportation Safety Board(NTSB) has taken an active role in working toreduce errors, incidents, and accidents in aviationby recommending a move away from simple pre-scriptive rules toward a system for managingfatigue risk that takes into account not just theeffects of timeawake, but seeks to“setworking hourlimits for flight crews, aviation mechanics, and airtraffic controllers based on fatigue research, circa-dian rhythms, and sleep and rest requirements”(http://www.ntsb.gov/recs/mostwanted/aviation_reduce_acc_inc_humanfatig.htm). More recently,The Honorable Deborah Hersman, the Chairmanof the NTSB, has expressed support for movingbeyond working hour limits to full-on fatiguerisk management (http://www.ntsb.gov/speeches/hersman/daph100305.html).
In contrast to prescriptive hours of service reg-ulation, evolving FRMSs are a flexible, multilayerdefense in depth against fatigue risk. In one con-ceptualization (Dawson and McCulloch, 2005),an organizational FRMS would include tactics,techniques, and procedures to ensure thatemployees have an adequate sleep opportunityboth in terms of total sleep opportunity durationover 24 h and in terms of placement relative tothe circadian rhythm in sleep propensity. Further,it would measure (e.g., by sleep diary or wrist-worn actigraph) the use made by employees of

198
the sleep opportunity that was available to them.Finally, given the sleep opportunity and the usemade of it, an FRMS would evaluate (e.g., by self-or coworker report, or with added or embeddedperformance metrics, or model-based perfor-mance predictions) how well employees areperforming in the workplace while on duty.
Creating and implementing fatigue-friendlyrosters and schedules
An FRMS can be implemented in a varietyof forms, from the technologically simple tothe technologically complex. FRMS in AirNew Zealand has been in use for around 15 years,overseen by a collaborative group with a combi-nation of management, crew member, and scien-tific/medical membership. The process originallyconsisted of soliciting and reviewing voluntaryfatigue reports from pilots and flight attendants,and undertaking specific studies on highlyreported trips or duties; these studies used acombination of subjective ratings such as theSamn–Perelli fatigue scale, along with reactiontime-based performance tests. More recently,studies have asked pilots to complete aSamn–Perelli assessment (Samn and Perelli, 1982)just prior to descent, on a routine basis (on somefleets this is being inputted directly into aircraftflight management computers). In FRMS, suchas the one used by Air New Zealand, the fatiguedata collected is typically used to refine specificflights and schedules within the framework ofexisting prescriptive hours of service regulations(Petrie et al., 2004; Powell et al., 2008). easyJethas evolved a more complex system involvinga detailed fatigue report form, as well asactigraphically measured sleep/wake history, andFOQA data that is used to obtain specificexceptions to prescriptive hours of serviceregulations (http://www.faa.gov/about/office_org/headquarters_offices/avs/offices/afs/afs200/media/aviation_fatigue_symposium/StewartComplete.pdf).
And, most recently Boeing has entered the FRMSfield by integrating mathematical modelingpredicting fatigue risk from sleep/wake historyand circadian rhythm phase into commercialrostering and scheduling software, to produce whatpotentially could be a turnkey FRMS (Romig andKlemets, 2009). In an FRMS of the sort beingdeveloped by Boeing, the model has the potentialto become the rule, completely replacing prescrip-tive hours of service regulations.
Whether modifying or replacing existingprescriptive rules, implementation of an FRMSoccurs within a complex context, for example,regulatory environment, labor/managementagreements, economic imperatives, and organiza-tional structure. There are synergies if FRMS isimplemented in the context of broader safetyand operational risk management. The aim ofFRMS is to maximize on shift performance andtotal sleep time in 24 h within existing operationalconstraints.
Screening, diagnosing, and treatingsleep disorders
A common cause of degraded performance andexcessive day time sleepiness is inadequate sleep.Inadequate sleep can result from a number offactors including sleep disorders—in particular,obstructive sleep apnea (OSA). OSA, asdiscussed extensively elsewhere in this volume,is a respiratory impairment characterized byseverely disturbed breathing during sleep due tothe blockage of airflow in the upper airway(Carskadon and Dement, 1981). This results infrequent arousals triggered by the drive tobreathe, causing fragmentation of sleep whichdegrades its recuperative value, and leads to per-formance impairments and excessive day timesleepiness (Adams et al., 2001; Lavie, 1983). Forinstance, patients suffering from OSA oftenreport falling asleep briefly when stopped at traf-fic lights or while sitting quietly on the couch in

199
the afternoon (Johns, 1993; Johns and Hocking,1997). An increased risk of OSA is associatedwith male gender, increasing age, and being over-weight. A middle aged, overweight male whosnores loudly, has been witnessed choking,gasping, or having apneas (cessation of respira-tion movement) during sleep, and complainingof excessive daytime sleepiness or insomnia,likely has sleep apnea. It has been reported thatcommercial vehicle drivers have a higher inci-dence of OSA when compared to the generalpopulation (Horne and Reyner, 1995; Howardet al., 2001). Individuals who suffer from this dis-order are statistically more likely to be involvedin car crashes (George et al., 1997; Stoohs et al.,1994; Young et al., 1997) and are potentially at ahigher risk of other occupational accidents(Rodenstein, 2009). Notably, treatment of theOSA has been shown to reduce in motor vehicleaccidents (Mazza et al., 2006), highlighting theimportance of early diagnosis and effective treat-ment of the disorder.Age, gender, body mass index and neck cir-
cumference have been identified as independentpredictors of sleep-disordered breathing (Younget al., 2002). The multivariable apnea predictionscale (MAPS; Maislin et al., 1995) is one screen-ing tool that incorporates age, gender, body massindex, and responses to three questions into apredictive equation for sleep-disordered breath-ing. The questions relate to frequency of snortingor gasping; loud snoring; and episodes of choking,breathing stopping, or struggling for breath atnight. This questionnaire predicts sleep apnea riskusing a score between zero and one (low to highprobability of sleep-disordered breathing), withrelatively high sensitivity. In a clinical sample, theMAPS has been found to have a 95% sensitivityfor detecting sleep-disordered breathing (98% sen-sitivity for severe disease), with a specificity of68%, as compared to PSG (Gurubhagavatulaet al., 2001).Identification and treatment of OSA is an
important part of reducing excessive sleepiness
in workers, thereby reducing accident risk andincreasing productivity in the workplace.
Incorporated into an FRMS should be a mech-anism for screening for those at-risk for OSA andother sleep disorders, in order that the at-riskpopulation can be formally evaluated with anovernight sleep study and, if diagnosed, treated.A two-step screening process could involve an ini-tial screening questionnaire such as the MAPSand, depending on available funding, those whowere found to be at a higher risk for OSA couldundergo nocturnal oximetry or overnight PSGrecordings for formal diagnosis. Screening couldbe (1) routine as a part of a yearly physical exam,and/or (2) triggered by evidence of drowsiness orpoor performance (by observation or added orembedded performance metrics) given adequatesleep opportunity and good use made of it. Similarrecommendations have been made by the NTSB(http://www.ntsb.gov/recs/letters/2009/H09_15_16.pdf). Application of sleep apnea screening bySchneider Trucking according to DeborahHersman, Chairman of the NTSB, “reduced pre-ventable crashes by 30%, reduced the median costof crashes by 48%, improved fleet retention rateby 60% over fleet average, and achieved healthcaresavings of $539 per driver per month” (http://www.ntsb.gov/speeches/hersman/daph100526.html).
Evaluating effect of fatigue risk managementimplementations on error, incident, andaccident, performance, and productivity
An FRMS is data driven. It operates on the princi-ple of the process of iterative improvement,dubbed “test, operate, test, exit (TOTE)” (Milleret al., 1960), similar to the “observe, orient, decide,act (OODA) loop” posited by John Boyd (Coram,2002; Wesensten et al., 2005; http://en.wikipedia.org/wiki/John_Boyd_(military_strategist)). Forfatigue risk management, “test” involves monitor-ing of added or embedded measures of perfor-mance together with observation of error,

200
incident, or accident and/or loss of productivity,and making absolute or relative comparisons toprevious performance or some standard of perfor-mance, and thus detecting a drift away from nomi-nal. “Operate” involves changing something in thesystem, for example, the work schedule that opera-tional experience suggests will correct theobserved drift away from nominal performance.This is followed by another test to determinethe effectiveness of operate. This is an iterativeprocess, repeating asmany times as necessary, untiltest yields nominal values, at which point theprocess exits.
Error, incident, and accident reporting arefundamental to corporate safety managementsystems into which FRMS is logically folded.There is evidence that fatigue causes a decreasein productivity perhaps preceding an increase inerror, incident, and accident, making loss of pro-ductivity a leading indicator (in the economicsense of early indicator) of fatigue (Thomaset al., 1997; Van Dongen et al., 2010). Evaluatingproductivity and performance in the workplace isa critical component of fatigue risk management.
Summary of current practice and future promise
The current practice of fatigue risk managementincludes applying sleep science to reduce the riskof error, incident, or accident (1) within the con-text of the existing hours of service regulationsand (2) by gaining exceptions to the existingregulations. For its future promise, we predict thatfatigue risk management will replace the existinghours of service regulations (and associated labormanagement agreements) with sleep-science-derived mathematical models predicting individualand group performance from sleep/wake history,circadian rhythm phase, and workload, modelsderived from personal biomedical status monitor-ing, and integrated into rostering and schedulingsoftware. In the future, the model will becomethe rule.
References
Adams, N., Strauss, M., Schluchter, M., & Redline, S. (2001).Relation of measures of sleep-disordered breathing to neu-ropsychological functioning. American Journal of Respira-tory and Critical Care Medicine, 163, 1626–1631.
Akerstedt, T. (2003). Shift work and disturbed sleep/wakeful-ness. Occupational Medicine, 55, 89–94.
Ancoli-Israel, S., Cole, R., Alessi, C., Chambers, M.,Moorcroft, W., & Pollak, C. P. (2003). The role ofactigraphy in the study of sleep and circadian rhythms.American Academy of Sleep Medicine Review Paper. Sleep,26(3), 342–392.
Balkin, T. J., Bliese, P. D., Belenky, G., Sing, H.,Thorne, D. R., Thomas, M., et al. (2004). Comparative util-ity of instruments for monitoring sleepiness-related perfor-mance decrements in the operational environment. Journalof Sleep Research, 13, 219–227.
Basner, M., Fomberstein, K. M., Razavi, F. M., Banks, S.,William, J. H., Rosa, R. R., et al. (2007). American timeuse survey: Sleep time and its relationship to WakingActivities. Sleep, 30(9), 1085–1095.
Belenky, G., & Akerstedt, T. (2011). Introduction to occupa-tional sleep medicine. In M. Kryger, T. Roth & W. C.Dement (Eds.), Principles and practice of sleep medicine.(5th ed.). St Louis: Elsevier Saunders.
Belenky, G., Hursh, S. R., & Fitzpatrick, J. (2008). Split sleeperberth use and driver performance: A review of the literatureand application of a mathematical model predicting perfor-mance from sleep/wake history and circadian phase. Reportprepared for The American Trucking Associations, Sleepand Performance Research Center, Washington State Uni-versity, Spokane, WA.
Belenky, G., Marcy, S. C., & Martin, J. A. (1996). Debriefingsand battle reconstructions following combat. In J. A.Martin, L. Sparacino & G. Belenky (Eds.), The Gulf Warand mental health: A comprehensive guide. Westport, CT:Praeger.
Belenky, G., Wesensten, N. J., Thorne, D. R., Thomas, M. L.,Sing, M. L., Redmond, D. P., et al. (2003). Patterns of per-formance degradation and restoration during sleep restric-tion and subsequent recovery: A sleep dose-dependentstudy. Journal of Sleep Research, 12, 1–12.
Bierman, A., Klein, T. R., & Rea, M. S. (2005). Thedaysimeter: A device for measuring optical radiation asa stimulus for the human circadian system. MeasurementScience and Technology, 16, 2292–2299.
Bliese, P. D., Wesensten, N. J., & Balkin, T. J. (2006). Age andindividual variability in performance during sleep restric-tion. Journal of Sleep Research, 15(4), 376–385.
Bonnet, M. H., & Arand, D. L. (2003). Clinical effects of sleepfragmentation versus sleep deprivation. Sleep MedicineReviews, 7(4), 297–310.
201
Brock, M. A. (1991). Chronobiology and aging. Journal of theAmerican Geriatrics Society, 39, 74–91.
Carskadon, M. A., & Dement, W. C. (1981). Respiration dur-ing sleep in the aged human. Journal of Gerontology, 36,420–423.
Carskadon, M. A., Dement, W. C., Mitler, M. M., Roth, T.,Westbrook, P. R., & Keenan, S. (1986). Guidelines for themultiple sleep latency test (MSLT): A standard measure ofsleepiness. Sleep, 9(4), 519–524.
Coram, R. (2002). Boyd: The fighter pilot who changed the artof war. New York: Little, Brown and Co.
Cornish, W. R., & Clark, G. (1989). Law and society inEngland 1750–1950. London: Sweet Maxwell.
Costa, G., Akerstedt, T., Nachreiner, F., Baltieri, F.,Folkard, S., Dresen, M. F., et al. (2004). Flexible workinghours, health, and well-being in Europe: Some con-siderations from a SALTSA project. Chronobiology Interna-tional, 21, 831–844.
Dawson, D., & McCulloch, K. (2005). Managing fatigue: It'sabout sleep. Sleep Medicine Reviews, 9, 365–380.
Dembe, A., Erickson, J., Delbos, R., & Banks, S. (2005).The impact of overtime and long work hours on occupa-tional injuries and illnesses: New evidence from the UnitedStates. Occupational and Environmental Medicine, 62(9),588–597.
Dinges, D. F., & Powell, J. W. (1985). Microcomputer analysesof performance on a portable, simple visual RT task duringsustained operation. Behavior Research, Methods,Instruments and Computers, 17, 652–655.
Dorrian, J., Rogers, N. L., & Dinges, D. F. (2005). Psychomo-tor vigilance performance: Neurocognitive assay sensitive tosleep loss. In C. A. Kushida (Ed.), Sleep deprivation: Clinicalissues, pharmacology, and sleep loss effects (pp. 39–70).New York: Marcel Dekker.
Edwards, B., Waterhouse, J., Reilly, T., & Atkinson, G.(2002). A comparisons of the suitabilities of rectal, gut,and insulated axilla temperatures for measurement of thecircadian rhythm of core temperature in field studies. Chro-nobiology International, 19(3), 579–598.
Folkard, S., & Tucker, P. (2003). Shift work, safety, and pro-ductivity. Occupational Medicine, 53, 89–94.
Folkard, S., Lombardi, D. A., & Tucker, P. T. (2005).Shiftwork: Safety, sleepiness and sleep. Industrial Health,1, 20–23.
Gander, P. H., Graeber, R. C., & Belenky, G. (2011). Fatiguerisk management. In M. Kryger, T. Roth & W. C. Dement(Eds.), Principles and practice of sleep medicine. (5th ed.).St. Louis: Elsevier Saunders.
George, C. F., Boudreau, A. C., & Smiley, A. (1997). Effectsof nasal CPAP on simulated driving performance in patientswith obstructive sleep apnoea. Thorax, 52(7), 648–653.
Gurubhagavatula, I., Maislin, G., & Pack, A. I. (2001). Analgorithm to stratify sleep apnea risk in a sleep disorders
clinic population. American Journal of Respiratory and Crit-ical Care Medicine, 164, 1904–1909.
Harrison, Y., & Horne, J. A. (2000). The impact of sleep dep-rivation on decision making: A review. Journal of Experi-mental Psychology Applied, 6(3), 236–249.
Hersman, D. (2010). Remarks of Honorable Deborah A.P.Hersman, Chairman, National Transportation Safety BoardBefore the National Sleep Foundation,Washington,DC,March5, 2010. http://www.ntsb.gov/speeches/hersman/daph100305.html.
Horne, J. A., & Reyner, L. A. (1995). Sleep related vehicleaccidents. British Medical Journal, 310(6979), 565–567.
Howard, M., Worsnop, C., Campbell, D., Swann, P., &Pierce, R. (2001). Sleep disordered breathing in Victoriantransport drivers. American Journal of Respiratory and Crit-ical Care Medicine, 163(5), A933.
Johns, M. W. (1993). Daytime sleepiness, snoring, and obstruc-tive sleep apnea. The Epworth Sleepiness Scale. Chest, 103(1), 30–36.
Johns, M., & Hocking, B. (1997). Daytime sleepiness and sleephabits of Australian workers. Sleep, 20(10), 844–849.
Kerkhof, G. A., & Van Dongen, H. P. A. (1996). Morning-type and evening-type individuals differ in the phase posi-tion of their endogenous circadian oscillator. NeuroscienceLetters, 218, 153–156.
Knutson, K. L., Spiegel, K., Penev, P., & Van Cauter, E.(2007). The metabolic consequences of sleep deprivation.Sleep Medicine Reviews, 11, 163–178.
Lauderdale, D. S., Knutson, K. L., Yan, L. L., Rathouz, P. J.,Hulley, S. B., Sidney, S., et al. (2006). Objectively measuredsleep characteristics aomon early-middle-aged adults: TheCARDIA study. American Journal of Epidemiology, 164(1), 5–16.
Lavie, P. (1983). Incidence of sleep apnea in a presumablyhealthy working population: A significant relationship withexcessive daytime sleepiness. Sleep, 6, 312–318.
Lewy, A. J., & Sack, R. L. (1989). The dim light melatoninonset as a marker for circadian phase position. Chronobiol-ogy International, 6(1), 93–102.
Magistretti, P. J., Pellerin, L., & Martin, J. L. (1995).Brain energy metabolism, an integrated cellular perspective.In F. E. Bloom & D. J. Kupfer (Eds.), Psychopharmcology:The fourth generation of progress (pp. 657–670). New York:Raven Press Ltd.
Maislin, G., Pack, A. I., Kribbs, N. B., Smith, P. L.,Kline, L. R., Schwab, R. J., et al. (1995). A survey screenfor prediction of apnea. Sleep, 18(3), 158–166.
Mallis, M. M., Mejdal, S., Ngyuen, T. T., & Dinges, D. F.(2004). Summary of the key features of seven biomathemat-ical models of human fatigue and performance. AviationSpace and Environmental Medicine, 75, A4–A14.
Mazza, S., Pepin, J. L., Naegele, B., Rauch, E., Deschaux, C.,Ficheux, P., et al. (2006). Driving ability in sleep apnoea

202
patients before and after CPAP treatment: Evaluation on aroad safety platform. The European Respiratory Journal, 28,1020–1028.
McDonald, J. L., Lillis, T. A., Tompkins, L. A., VanDongen, H., & Belenky, G. (2008). Effects of extendedwork hours on objectively measured sleep and performancein industrial employees. Sleep, 31, A374.
McDonald, J., Patel, D., & Belenky, G. (2011). Sleep and per-formance monitoring in the workplace: The basis for fatiguerisk management. In M. Kryger, T. Roth & W. C. Dement(Eds.), Principles and practice of sleep medicine. (5th ed.).St. Louis: Elsevier Saunders.
McDonald, J. L., Tompkins, L. A., Lillis, T. A., Bowen, A. K.,Grant, D. A., Van Dongen, H. P. A., et al. (2009). Workhours, sleep, and performance in medical residents workingnight float vs. day shift. Sleep, 32, A394.
Meier-Ewert, H. K., Ridker, P. M., Rifai, N., Price, N.,Dinges, D., & Mullington, J. (2004). Effect of sleep loss onC-reactive protein, an inflammatory marker of cardiovascu-lar risk. Journal of the American College of Cardiology, 43,678–683.
Miller, G., Galanter, E., & Pribram, K. (1960). Plans and thestructure of behavior. New York: Holt, Rinehart andWinston.
Moore, R. Y. (1997). Circadian rhythms: Basic neurobiologyand clinical applications. Annual Review of Medicine, 48,252–266.
Moore, R. Y., Speh, J. C., & Leak, R. K. (2002).Suprachiasmatic nucleus organization. Cell and TissueResearch, 309, 89–98.
Moore-Ede, M. (1995). Things that go bump in the night.American Bar Association, 81, 56–60.
Mullington, J. M., Haack, M., Toth, M., Serrador, J. M., &Meier-Ewert, H. K. (2009). Cardiovascular, inflammatory,and metabolic consequences of sleep deprivation. Progressin Cardiovascular Disease, 51(4), 294–302.
Nilsson, J. P., Soderstrom, M., Karlsson, A. U., Lenader, M.,Akerstedt, T., Lindroth, N. E., et al. (2005). Less effectiveexecutive functioning after one night's sleep deprivation.Journal of Sleep Research, 14(1), 1–6.
Olofsen, E., Dinges, D. F., & Van Dongen, H. P. A. (2004).Nonlinear mixed effects modeling: Individualization andprediction. Aviation, Space and Environmental Medicine,75(Suppl. 3), A134–A140.
Perrow, C. (1999). Normal accidents. Princeton: PrincetonUniversity Press.
Petrie, K. J., Powell, D. M. C., & Broadbent, E. A. (2004).Fatigue self-management strategies and reported fatigue ininternational pilots. Ergonomics, 47(5), 461–468.
Petrilli, R. M., Thomas, M. J. W., Lamond, N., Dawson, D., &Roach, G. (2007). Effect of flight duty and sleep on the deci-sion-making of commercial airline pilots. In J. M. Anca(Ed.), Multimodal safety management and human factors:
Crossing the borders of medical, aviation, road and railindustries (pp. 259–270). Burlington, Vermont: AshgatePublishing Company Ltd.
Philip, P., Sagaspe, P., Taillard, J., Valtat, C., Moore, N.,Akerstedt, T., et al. (2005). Fatigue, sleepiness, and perfor-mance in simulated versus real driving conditions. Sleep, 28(12), 1511–1516.
Powell, D., Spencer, M., Holland, D., & Petrie, K. (2008).Fatigue in two-pilot operations: Implications for flight andduty time limitations. Aviation Space and EnvironmentalMedicine, 79(11), 1047–1050.
Rodenstein, D. (2009). Sleep apnea: Traffic and occupationalaccidents—Individual risks, socioeconomic and legalimplications. Respiration, 78(3), 241–248.
Romig, E., & Klemets, T. (2009). Fatigue risk management inflight crew scheduling. Aviation Space and EnvironmentalMedicine, 80(12), 1073–1074.
Rupp, T. L., Wesensten, N. J., Bliese, P. D., & Balkin, T. J.(2008). Banking sleep: Realization of benefits duringsubsequent sleep restriction. Sleep, 32(3), 311–321.
Samn, S. W., & Perelli, L. P. (1982). Estimating aircrew fatigue:A technique with implications for airlift operations. TechRep SAM-TR-82-21, USAF School of Aerospace Medicine,Brooks AFB, TX.
Stoohs, R. A., Guilleminault, C., Itoi, A., & Dement, W. C.(1994). Traffic accidents in commercial long-haul truckdrivers: The influence of sleep-disordered breathing andobesity. Sleep, 17(7), 619–623.
Thomas, G. R., Raslear, T. G., & Kuehn, G. I. (1997). Theeffects of work schedule on train handling performance andsleep of locomotive engineers: A simulator study. FinalReport, DOT/FRA/ORD-97-09, Federal Railroad Adminis-tration, U.S. Department of Transportation, Washington,DC.
Thomas, M. J. W., Petrilli, R. M., & Roach, G. D. (2007). TheImpacts of Australian Transcontinental 'Back of Clock'Operations on Sleep and Performance in CommercialAviation Flight Crew. Transport Safety Report B2005/0121, Australian Transport Safety Bureau, ACT, Australia.
Thomas, M. L., Sing, H. C., Belenky, G., Holcomb, H.,Mayberg, H., Dannals, R., et al. (2000). Neural basis ofalertness and cognitive performance impairments duringsleepiness. I. Effects of 24 h of sleep deprivation on wakinghuman regional brain activity. Journal of Sleep Research,9(4), 335–352.
Thorne, D. R., Genser, S., Sing, H., & Hegge, F. (1983).Plumbing human performance limits during 72 hours of hightask load. In Proceedings of the 24th DRG seminar on thehuman as a limiting element in military systems (pp. 17–40).Toronto, Canada: Defense and Civil Institute of Environ-mental Medicine (DCIEM).
Tucker, A. M., Whitney, P., Belenky, G., Hinson, J. M., & VanDongen, H. P. A. (2010). Effects of sleep deprivation on

203
dissociated components of executive functioning. Sleep,33(1), 47–57.
Van Cauter, E., Spiegel, K., Tasali, E., & Leproult, R. (2008).Metabolic consequences of sleep and sleep loss. Sleep Medi-cine, 9(Suppl.), S23–S28.
Van Dongen, H., Belenky, G., Moore, J. M., Bender, A. M.,Huang, L., Mott, C. G., et al. (2010). Nighttime drivingand fuel use: A high-fidelity simulator study in a sleep labo-ratory. Sleep, 33, A308.
Van Dongen, H. P. A., Maislin, G., Mullington, J. M., &Dinges, D. F. (2003). The cumulative cost of additionalwakefulness: Dose-response effects on neurobehavioralfunctions and sleep physiology from chronic sleep restrictionand total sleep deprivation. Sleep, 26(2), 117–126.
Van Dongen, H. P. A., Vitellaro, K. M., & Dinges, D. F.(2005). Individual differences in adult human sleep andwakefulness: Leitmotif for a Research Agenda. Sleep,28(4), 1–18.
Viola, A. U., Archer, S. N., James, L. M., Groeger, J. A.,Lo, J. C. Y., Skene, D. J., et al. (2007). PER3 Polymorphismpredicts sleep structure and waking performance. CurrentBiology, 17, 613–618.
Webb,W.B.,&Dinges,D.F. (1989).Culturalperspectivesonnap-ping and the siesta. In D. F. Dinges & R. J. Broughton (Eds.),Sleep and alertness: Chronobiological, behavioral, and medicalaspects of napping (pp. 247–265). NewYork: Raven Press.
Wesensten, N. J., Belenky, G., & Balkin, T. J. (2005). Cogni-tive readiness in network centric operations. Parameters:US Army War College Quarterly, 35(1), 94–105.
Wesensten, N. J., Belenky, G., Thorne, D. R., Kautz, M. A., &Balkin, T. J. (2004). Modafinil versus caffeine: Effects onfatigue during sleep deprivation. Aviation Space and Envi-ronmental Medicine, 75, 520–525.
Wright, K. P., Gronfier, C., Duffy, J. F., & Czeisler, C. A.(2005). Intrinsic period and light intensity determine thephase relationship between melatonin and sleep in humans.Journal of Biological Rhythms, 20(2), 168–177.
Young, T., Blustein, J., Finn, L., & Palta, M. (1997). Sleep-disordered breathing and motor vehicle accidents in a popula-tion-based sample of employed adults. Sleep, 20(8), 608–613.
Young, T., Shahar, E., Nieto, F. J., Redline, S., Newman, A. B.,Gottlieb, D. J., et al. (2002). Predictors of sleep-disorderedbreathing in community-dwelling adults: The Sleep HeartHealth Study. Archives of Internal Medicine, 162, 893–900.




















