Untitled - Philippine Journal of Otolaryngology Head and Neck ...
72
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Untitled - Philippine Journal of Otolaryngology Head and Neck ...


TABLE OF CONTENTS 3_..6,u-ri&3,_4a¢4, o92r-_,.66s_•,¥_" d_'n_, _,
VOL. 16, No. 2 (2001) "....................................................................
Editorial Stair
Guidelines for Authors
Original Studies
A Comparative Study on the Efficacy of Silica Gel versus Clotrimazole inOtomycosisMariel B. Conanan,M:D., VictorDino Alarva II1,M.D., OthelloRaymond S. Dave III, M.D .................................. 49-58
Alternative Method in Identification of Recurrent LaryngealNerveReinalyn Rosete-Pineda M_D.,Ronald delos Santos M.D_,Robie V.Zantua, .M.D................................................... 59-64
Ultrastructural Changes in Nasal Polyps with Exposure toMometasone Fnroate Monohydrate Aqueous Nasal SprayArlene Marie R. Cayelano M.D. , Jose B. Orosa M.D , Normando C. Gonzaga .M.D.,Ma. TeresaM. flondoc-Silvestre, M.D........................................................................................................................ 65-81
Surgical Innovation
The Composite Trapezius-Scapular Spine Flap: An Alternativein the Reconstruction of Oromandibular DefectsVictorDino A, Alarva III M.D. , Joseph Amado C. GalvezM.D., Armando 34. Chiong Ji:, M.D............................. 82-91
Su_ical Instrumentation
Feeding Obturators for Cleft Lip and Palate Patients: The
Experience of a Prosthesis Section of a Department ofOtorhinolaryngologySalvador V.Caslaneda M.D., Samantha R. Soriano M.D., Mariano B. Caparas M.D ............................................. 92-98
An Endoscopic Adaptor for Direct Laryngoscopy withMierolaryngeai SurgeryEfi'enA. GutierrezJr., M.D.., Ferdinand G. Pamintuan M.D..................................................................................... 99-106
Case Report
Alveolar Soft Part Sarcoma in the Malar Area: A Case ReportAna TeresaD. Licup M.D. , Christopher Malore S. CalaquianM,D ....................................................................... 107-112
A Floor of the Mouth Yolk Sac Tumor in Aicardi Syndrome: A Case ReportMaw. Jane C. T(paynoM.D ........................................................................................................................................113-117

Guidelines jbr Authors
THE PHILIPPINE JOURNAL OF OTOLARYNGOLOGYHEAD AND NECK SURGERY
Unit 1411 14thFloor
Espana Tower, Espana Blvd.Cor. Josefina St. Mataila
Tel/Fax: 3010551
Editor-in-chief Senior Associate Editors
Charlotte M. Chiong, MD Abner L. Chan, MDUniversity ofthePhilippines Jesus Randy O. Canal, MDDepartment of ORL
Philippine General HospitalTaft Avenue, Manila
Authors: Title page, Subtitle (if any).First name, middle initial, last name of each author (with highest academic degrees).Name of Departments and Institutions to which work should be attributed.Disclaimers (if any); and Acknowledgement of Financial Support.
Manuscript: Submit original copy and two duplicates (with diskette of manuscripts andfigures using Microsoft V_brd- Windows 98)Typed, double spaced (including references, legends, footnotes), unspecified
lengthInclude date of presentation at scientific meetingAuthor's telephone number and FAX nmnberReferences in the text should be superscripts in order of appearanceReferences with more than three authors should be presented as the first three
authors followed by et al.
Abstract: A 5-10 sentences abstract to precede article for case reports. Otherwise, there should be
a structured abstract including objective, design, setting subjects, result and conclusion.
All manuscripts and other editorial matter should be addressed to Charlotte M. Chiong,MD, Editor-in-chief. The Philippine Journal of Otolaryngology-Head and Neck Surgery,Department of Otolaryngology, UP-PGH, Taft Avenue, Manila.

Philippine JournaJ of Oto/ao,'ngolo,__l llead & .,Y,:'ck,_'u_,,3/iv
Vol. 16 No. 2 4!)-58.4_)2002 Philippine S(_cicty _)l'OtcHaryngology ['lead & Neck Surgery
A COMPARATIVE STUDY ON THE EFFICACYOF SILICA GEL VERSUS CLOTRIMAZOLE
IN OTOMYCOSIS*
MARIEL B. CONANAN, M.D. **VICTOR DINOALARVA Iii, M.D, **
OTHELLO RAYMOND S. DAVE III, M. D.**
ABSTRACT
Objectives:
1. To compare the efficacy of silica gel versus clotrimazole in the alleviation of the signs and symptomsof otomycosis or otitis externa of fungal etiology.
2. To determine the duration in the alleviation of signs and symptoms of otomycosis using clotrimazole.3. To determine the duration in the alleviation of signs and symptoms of otomycosis using silica gel_4. To determine if there is a significant statistical difference between the duration of signs and symptoms
of otomycosis using silica gel versus clotrimazole
Design: Random clinical trial
Setting: Tertiary hospital
Patients: 33 patients diagnosed to have otomycosis from October 1999 to April 2000
Conclusion:
The efficacy of silica gel versus clotrimazole in the alleviation of the signs and symptoms of otomycosiswas established by determining the duration after initiation of the respective treatment regimens. Statisticalanalysis was made using the two-tailed test of independence or T-test.
,w
Symptoms of otomycosis, namely: pruritus, otalgia, fullness, hearing loss and tinnitus, in patientstreated with silica gel exhibited a statistically significant shorter period of duration in comparison to those treatedwith clotrimazole.
Likewise, signs of otomycosis, namely: mycelial elements on otoscopy, erythema of external auditorycanal, edema, watery or serous discharge, and hyphae seen on KOH mount, in patients treated with silica gelexhibited a statistically significant shorter period of duration in comparison to those treated with clotrimazole.
The efficacy of silica gel in alleviating the signs and symptoms of otomycosis is greatly attributed to itsdessiccating property.
Despite the above-mentioned conclusions, the present study cannot conclude if silica gel is superior thanclotrimazole in treating otomycosis. The present study, however, strongly suggests that keeping the ear dryand free from cellular debris is still the best way to prevent otomycosis.
*Presented,PSOHNSAnalyticalResearchContest.November30,2000,PuntaBaluarte,Calatagan,Batangas**Resident,Departmentaf Qtorhinolaryngology,OspitalngMaynilaMedicalCenter

: : tili fi,::t:!igala d::oai::'A:(_!da! h"ffectiOnS Fu!_gai infeo.lion:iS i: :::::: .... ....i: : a :ii.:]::::_c "_ :i _"/_:!::g : _t _ _t ,s w ho: :i,trtdel:We h [ :
:
I: e' ':' te(,t o se (_1":_ lev be_, o _?P t_"toqe ](
ut,id@i;,})erlaii'.,icoliditO[lssi,l(:_tslasirlil_,lul,,_osupplessicii:il:: : : : .....
i
..... ai':'x:i afte_::':adormariI: :::: : : : :::: i: : : : ::: ;e (:5{"s ev ei"at:dai!s, t_,:::iwe eks L: : :::: : : : :: :: 0[,_ie !':p Iiysii::ai:at.,ld ct_eri'1leaI:p i'ope/'tle s is s :how_",i'_1[
: : : :
: fu:i:ii:iii::i!_ai,,mi:i::'i:{),ioi:i::_:mVCosis:,, .... : : ! :: : s\,,'mpti::_r_:is::of:ot,:on'wCosi,_or otit,is e:,,d:emsoi_ !,::::: : etiok::_gi,,.':: : :
: 8_{iadse I_m<ii:_i_"Ov_,:'Wi:ili fi_c:ii_i'i,:_iilVai/'!i,:and : :,:: ........ :
!!/::}):: iS::}{:_I!11::I:__'_:_/:wii:¸i)::,::,i::,_:_iC/e(_:'t!"a!_d:S,:_:_:_uiic::a_:;!_:,,'_,ie_i__!!:!_::__ILi/::_:{::::::: : :: ::::/_:,_!_:s_g_-,s_:_,_,__,:_,sy____t_::_m:s o_oto_,,,-_,v<:_:,s_:s:i :}:/ }::::gela!i i"l:(::i_,,,iSn,:iatel:'i:a wt:i e_i q (_l:::i,Sd_!ihi,,i::llated:,::!it: :i : : l:,.mi:i:"_q si!ica 9:te : .... :
i

:4 COMPd.Jbl HF£ STOIOY
3. To determine if there is a statisticallysignificant difference between the duration Group B patients had three silica gel pelletsin the alleviation of signs and symptoms inserted into their affected ears. These pellets wereof otomycosis using silica gel versus sandwiched between thin pieces of cotton and insertedclotrimazole, into the ear canal as far as the lateral two-thirds from
the opening. These were subsequently replaced or.,adaily basis by tile patients themselves and were asked
PATIENTSAND METHODS to return for follow-up every three days.
A. SUBJECT SELECTION Scrapings from the external auditory canalwere obtained with sterile cotton pledgets mounted on
This study includes patients seen in the Out- potassium hydroxide and examined under thePatient Department of Ospital ng Maynila Medical microscope to determine the presence of mycelialCenter diagnosed to have otomycosis from October elements prior to initiation of treatment, and during1999 to April 2000. The diagnosis of otomycosis was subsequent follow-up.based on the syrnptornatology and physicalexarn{r_ation consistent with otomycosis such as thepresence of the fungal elements in the external auditory RESULTScanal.
Thirty seven patients were initially included inPatients with perforated tympanic rnembrane, this study, however, 4 were subsequently dropped, all
purulent otorrhea, severe otalgia,, cellulitis of the of whom were diagnosed to have diabetes during theexternal auditory canal, patients who underwent duration of the treatment. There was a high index ofmastoid surgery, and irr_munocomprornised patients suspicion for diabetes when the condition of thewere excluded in the study, patient's ear worsened despite treatment. The
diagnosis was confirrned with fasting blood sugarB, EXPERIMENTAL INTERVENTION determination.
Prior to initiation of t;eatment, an informed All the patients diagnosed with otornycosis orconsent was secured from the subjects, who then fungal otitis externa were noted to be in its mildwere asked to fill up an information sheet regarding inflammatory stage. Bojrab et al classified thetheir demographic data (name, age, sex, and inflammatory stage of the otitis externa as mild,occupation). Medical history of diabetes, use of moderate, or severe. Increased itching and pain, intopical otic drops, and intake of irnmunosuppressive contrast to the pre-inflammatory state characterize thedrugs were elicited. Symptomatology such as otalgia, mild acute inflammatory stage. Mild erythema andpruritus, ear fullness, and hearing loss were obtained, edema are present on examination, and the externalInitial otoscopic _;ndings as well as presence ef other auditory canal is patent. Exfoli ,_ion of skin along withcutaneous and systemic infections were also noted, a minimal amount of clear or serous secretions mayTreatment proper began with thorough cleansing of the also be seen. 8ear canal of its accumulated infected debris either bymanual extraction, suctioning, or irrigation with normal Of the 33 patients, fifteen patients were treatedsaline solution After cleansing, patients cvererandomly with clotrimazole, and eighteen patients with silica gel.assigned into two groups: Group A (Control- For patients treated with clotrimazole,majority were .'.Clotrirnazc:::. Solution), and Group B (Experimental- female (66.67%), while for patients treated with silicaSilica Gel F, .iets}. gel, majority were male (72.22%), The average age
of patients treated with silica gel was found to beGroup A subjects were instilled with three slightly older than patients treated with clotrimazole
drops of 1% Clotrimazole solution to their affected ear. (35.61 years and 30.53 years, respectively).. PatientsThe solution was allowed to stay for three minutes, were rnostly vendor, drivers, and laborers, whoseThey were instructed to repeat the procedure ttqree nature of work exposes them to dust-containing fungaltimes daily and to follow-up every three day::_until they spores predisposing them for otomycosis..be.come asyrnptomatic. Subjective and objective'findings as well as microscopic e;<amination of mycehaleiernen:s were obtained and n.:,ted.

CONANAN EZ AL.
DISCUSSIONDuration of symptoms for both silica gel and
clotrimazolewere compared usinga two-tailed test of Fungi are ubiquitous, and consequently weindependence or T-test. This is synonymous with are constantly exposed to their infectious elements.clinical cure, which is the number of days when the In the present study, the majority of the patients werepatient became asymptomatic from the start of the vendors,drivers,and laborers,allof whomareexposedcorresponding treatment regimens. The period of to dust. This is similar to the study made by Tanet altreatment for silica gel was found to be significantly where majority of their patients was housewives whoshorter (10.05 +/- 4.22 days) as comparedto that for were continuously exposed to housedust. _0All fungiclotrimazole (16.60 +/- 3.11 days) with a p value of have three basic growth requirements: moisture,0_000. (Table1) warmth, and darkness. Altering any of these factors,
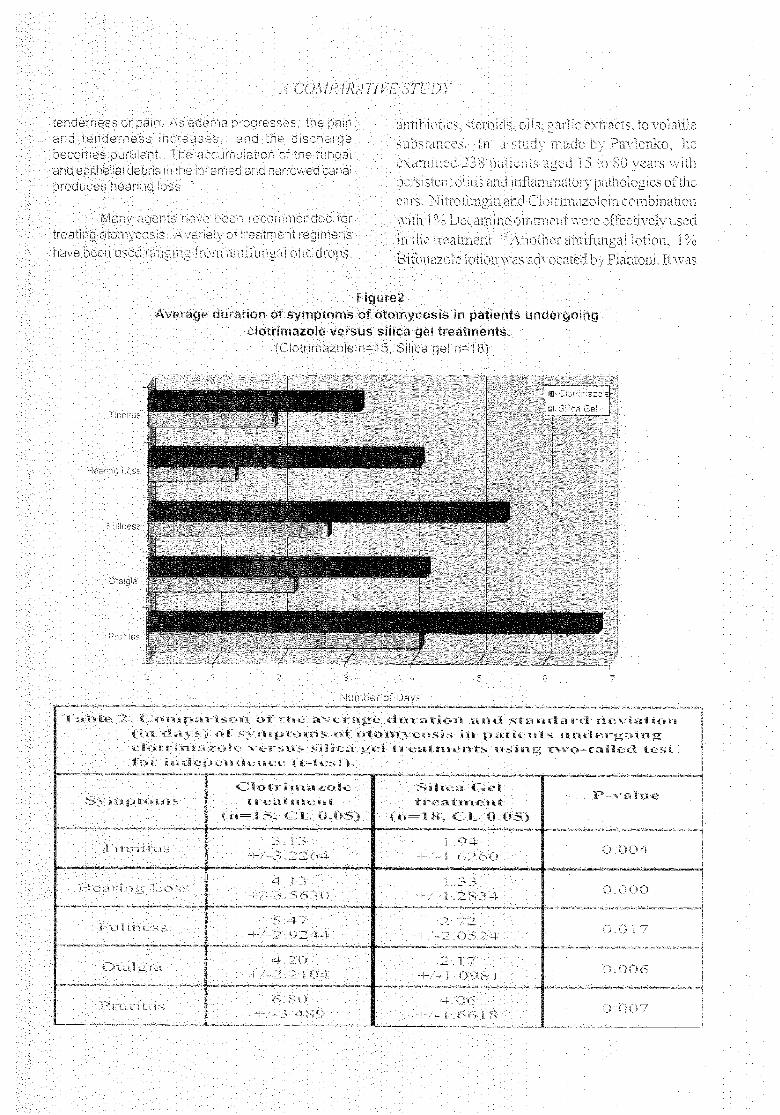
like moisture,willeventuallydiscouragefungal growth.Closer scrutiny of the specific symptoms The external canal being a moistwarm cavity coupled
(pruritus,otalgia,earfullness,hearinglossand tinnitus) with its epithelial debris serves as an ideal area forof otomycosis reveal that, on the average, patients fungal proliferation, especially Candida albicans andtreated with silica gel have shorter duration of Aspergillus sp. 11(Figure4)symptoms compared to patients treated withclotrimazole. (Figure2) Otomycosisor otitis externa offungal etiology
is a chronic or subacute infection of the pinna, theAlso, results of the individual t-test on the external auditory meatus, and the ear canal. It is a
average duration (in days) of specific symptoms rare clinical process but a relatively characteristicsexhibited by the patients reveal that, all patients concerningitsetiology andpresentationdependingontreated with silica gel exhibita statistically significant the geographic area, that, being a common conditionshorterperiodofdurationcomparedto patientstreated in the tropics due to high humidity. 8with clotrimazole. (Table2)
Senturia et al described several contributorySimilarly, data on the signs of otomycosis factors to this pathogenesis namely heat, humidity
(mycelial elements on otoscopy, erythema of canal, and trauma. Heatandhumidity increasesthe aqueousedema, serous ear discharge, and hyphal elements contentof the stratumcorneum producingintracellularon KOH) of the patients reveal that, on the average, edema of the external auditory canal. 12 The patientpatients treated with silica gel, were present for a perceives this condition as obstruction orshorter period of time compared to patients treated uncomfortablesense of fullness leading to the sensewith clotrimazole. (Figure3) of itching. Because the usual response to itching is
to scratch, and the act of scratching disrupts theResultsof the individual t-test on the number surfaceepithelium, thereby allowingcontaminationof
of days the specific signs of otomycosis persisted the epidermis and the dermis. This sets the stage forreveal that, patients treated with silica gel have a further edema allowing extravasation of fluidsstatisticallysignificantshorterperiodoftimecompared manifested as watery ear discharge, and slightto patients treated with clotrimazole. (Table 3)
I --
ITable l. Two-tailed test of Independence on OverallDuration of Treatment of Patients
i t i i
Clotrimazole Silica (;el P-Value
(n=15) (n--18)Overall ....
Standard StandardDuration Average Deviation Average Deviation
(Mean) (CL=0.05) (Mean) (CL=0.05)i • i i
Duration in16.6 3.1122 10.0556 4.2214 .000
Days
7:L:;:iji:/;::i!/::;i__ ! : : : : ::-:: . ;ii: ii/i::
::;ii/::_)):T/:ii!ii_:-k!:/{::::I//:U_:!!;I :i_I:I i :: :i ::i! :::i:v :f:u::::: : ..... : ....: ::: :.... _ _, .... __:_:" _ _ _ _/ i__ _ _ __'_:'_'-_tr'_ :_t_,c_:_,,_-_:C_?'_;i_:''_F_.... _ _: _: _ _ _:_ i _'::......... _:_ ::....... __:_ _i ...._....... _ _ __,-_c,O,L_:,_-:-L_u:d,.._,_.,_!.-L:_,b:_:<,'............_ _:....._.... _ _ __ _ ....
a',"c_the: ]: :i:i !_t:l;1.dT mSut,'.}:t_1,,,,_1_-_:_x,luu.]_.u,,"" .... !sc
::] : i"lde;:!;i:l.tieiiciebi;:i.s;ii:i::t.h_:i !:!:fir_-_rl_ted:a__ciri_rrox,,_,,e:d]ca_"_41 ]:: e£i:_:t:/:1:i:lit_1:.:,1!:]!_Jlt_._:i:](.T!11_;'_'_ii'lBI¢C]t.5i:O_(}]dcal"Sn.:'it]'_i,_rt_,dt_l@i,_ii],i,,_@4t,.ir.:_:_,i:k,,f,,_b:i: ] i:iiilii:<:_ru_:d)/_t:',/_i,.I'i-Ii'l'-I_i'l:('_t's,'j'_f:lthb'lO._icSofthe

.A COMt?ARATI I,"£ STUD I7
noted to be highly effective with complete resolution Some studies point to the possible irritatingof the clinical picture for all patients for a period of 4 to effect of otic solutions when applied to the ear canal15 days. 14 While some patients complain of burning sensation,
others complain of pain upon instillation, SuchJain et al evaluated the use of some oils complaints lead to doubts on the patient's compliance
against fungi-causing otornycosis. These oils from to treatment, whiclq may predispose to longermustard, groundnut, coconut, and amla showed treatment duration.sporos[atic effects. _ Two years later, he madefurther studies, this time using volatile substances Other drying agents such as merthiolate,such as ammonia, carbon disulfide, petroleum boric acid, and gentian violet have been discussed inbenzene, carbon dioxide, methanol, glacial acetic several literatures over and over again putting emphasisacid, and hydrogen peroxide. These substances were on its ability to keep the ear canal dry, aside from itsfound 1:oinhibit myceliaJ growth and sporulation or antimicrobial properties. The in vitro studies done bybudding. 15 Stern et al compared the effectiveness of 13 differentSenturia etal determined the usual pH ofthe external agents for treatment of otomycosis, one of whichauditory canal as mildly acidic at pH 4 to 5. In the merthiolate which showed effectivity against all thepresence of infection, the acidic pH gears toward organism tested. This again could point out its dryingalkalinity, allowing the growth of pathogenic capabilitythatpreventsthegrowthofthefungi. _8microorganisms. Using acetic acid solution, boricacid, or Burrow's solution specially in the early stage It cannot be overemphasized that the key toof infection, is sufficient enough to control the successful treatment of fungal otitis externa is gentledisease. 12 efficient cleaning of the ear canal carefully removing
its accumulated debris, followed by thorough drying,A local study done by Tan et al, compared because retained humidity promotes further fungal
two treatment regimens for otomycosis, that is, growth_ 8clotrimazole solution and guava leaf extract, of whichclotrimazole proved to be more effective. Whileclotrimazole continues to be the gold standard for CONCLUSIONotomycosis treatment, the guava leaf extract wasrecognized as an alternative mode of therapy. The The efficacy of silica gel versus clotrimazoleKirby-Bauer disc diffusion method was used to in the alleviation of the signs and symptoms ofdocument the antifungal properties of the treatment otomycosis was established by determining theregimens_ 10 duration after initiation of the respective treatment
regimens. Statistical analysis was made using theClotrimazole's mode of action is to alter the two-tailed test of independence or T-test.
cell membrane of the fungus so that the amino acidtransport is changed, thus impairing subsequent Symptoms of otomycosis, namely: pruritus,protein synthesis. It comes in different cornmerciallly- otalgia, fullness, hearing loss and tinnitus, in patientsavailable preparations such as cream, solutions, and treated with silica gel exhibited a statistically significantpowder. _ In the present study, we opted to use the shorter period of duration in comparison to thosesolution because of its availability. Kwok and Hawke treated with clotrimazole.reported a successful treatment of otomycosis using
the powder preparation and offered reasons for its Likewise, signs of otomycosis, namely:preference over the solution: (11)better coating of all mycelial elements on otoscopy, erythema of externalthe canal surfaces; (2) no increase in canal humidity; auditory canal, edema, watery or serous discharge,(3) avoidance of a carrier solution with possible and hyphae seen on K©H mount, in patients treatedcanal irritation; (4) ability to deliver higher drug with silica gel exhibited a statistically significant shorterconcentration, and (51)treatment is done by the period of duration in comparison to those treated withphysician himself avoiding the possible compliance clotrimazole.problems of patients. -,7The property of dryness or
being able to keep the ear canal dry makes it superior The efficacy of silica gel in alleviating the signsto the solution preparation, and symptoms of otomycosis is greatly attributed to
its desiccating property.

CONANAN ET AL.
5. Jain SK, Agrawal SC: Sporostatic EffectDespite the above-mentioned conclusions, the of Some Oils Against Fungi Causing
present study cannot conclude if silica gel is superior Otomycosis. Mycoses. 1994 July. Volumethan clotrimazole in treating otomycosis. 37 (7-8). 299-301
6. The New Encyclopaedia Britannica: SilicaThe present study, however, strongly suggests Gel. Volume IX. 15th Edition_ 1981. 202-
that keeping the ear dry and free from cellular debris is 203still the best way to prevent otomycosis. 7. Baker JT: Material Safety Data Sheet On
Silicic Acid, n-Hydrate, http://_w._w._.__y,jtl_ake__.qQmlm.s.d.s.Ls_l_.802.htm
RECOMMENDATION 8. Bojrab DI, Bruderly T,AbdulrazzakY: OtitisExterna. Otolaryngologic Clinics of North
In our search for cheaper alternatives for America. Volume 29. Number 5. October1996. 761-781currently used treatment regimens, we have started togive a second glance on materials not medically used 9. Garcia-Martos P, Delgado D, Marin P, Mirabut theoretically sound. This is true in the case of our J: Enferm Infecc Microbiol Clin. 1993 Nov.present study wherein we propose the possibility of 11 (9). 487-489using silica gel, a commercially available desiccant, 10. Tan GC, Del Rosario RA, Gonzales RE,as an alternative treatment for otomycosis. Reyes RT, Hardillo JU, Mijares JV, Abes
GT, Jamir JC: Otomycosis: Its Mycology
However, further studies are recommended to and a Comparison of Two-Treatment Regimen.ascertain if the compound will have any role in the Philippine Journal ofOtolaryngology-Headandmanagement of otomycosis: Neck Surgery. 1993. 63-66
11. Linstrom C J, Lucente FE: Infections of the
(1) Similar studies can be made on a larger External Ear, in Bailey, Johnson, Kohut,sample population to check the Pillsbury llI, Tardy Jr. (Eds); Head andNeckreproducibility of the results herein. Surgery-- Otolaryngology, Volume 2, 1993.
(2) Silica gel can be compared to other JB Lippincott Company. 1542-1556desiccants such as boric acid, 12. Senturia BH, Marcus MD, Lucente FE:merthiolate, and gentian violet. Diseases of the External Ear. New York,.
(3) Know the effectivity of silica gel in controlling Grun and Stratton, 1980other fungal pathogens. 13. Pavlenko SA: (Otmycoses in the Kuznetsk
(4) Determine the cost-effectivity of Region and Organization of Medical Servicessilica gel in comparison to other for this Group of Population. Vestntreatment regimens against Otorhinolaryngol. 1990 Jul. 4, 70.74
otomycosis. 14. Piantoni S, Narne S. Bottin R. et al. : 1%Bifonsaloe Lotion in the Therapy ofOtomycosis. Clin Te. 1989 Jul 15; 130(1),
REFERENCES 23-2715. Jain SK, Agrawal SC: Fungitoxic Effects of
1. Kelly EK, Mohs DC: The External Auditory Some Organic Volatile Substances AgainstCanal Anatomy and Physiology. Fur_giCausing Otomycosis. Mycoses. 1994Otolaryngologic Clinics of North America. July, Vo137 (7-8), 299-301Volume 29. Number 5. October 1996. 725- 16. Neibart E. Gumprecht: Antifungal Agents and739 Treatment of Fungal Infections of the Head
2. Conley JC: Evaluation of Fungous Disease of and Neck _ Otolaryngologic Clinics of Norththe External Auditory Canal. Archn America. Vol. 26., No. 6, December 1993,Otolaryngol. 47: 721-745. 1948 1123-1131.
3. Lucente FE: Fungal Infections of the External 17. Kwok P, Hawke M: Clotrimazole Powder inEar. Otolaryngologic Clinics of North America. the Treatment of Otomycosis. J Otolaryngol,Volume 26. Number6. December 1993. 995- 16:398, 19871005 18. Stern JC, Shah MK, Lucente FE: In Vitro
4. Manning SC: Mycoses. In Paparella, Effectiveness of13 Agents in Otomycosis andShumrick, Gluckman, Meyerhoff (Eds); Review ofthe Literature. Laryngoscope. 1988Otolaryngology. Volume 1. 3'_Edition 1991. November; 98 (11): 1173-1177.W.B. Saunders. 589.-.595
A COMPA.RA T1 VE STUD Y
APPENDICES
APPENDIXA
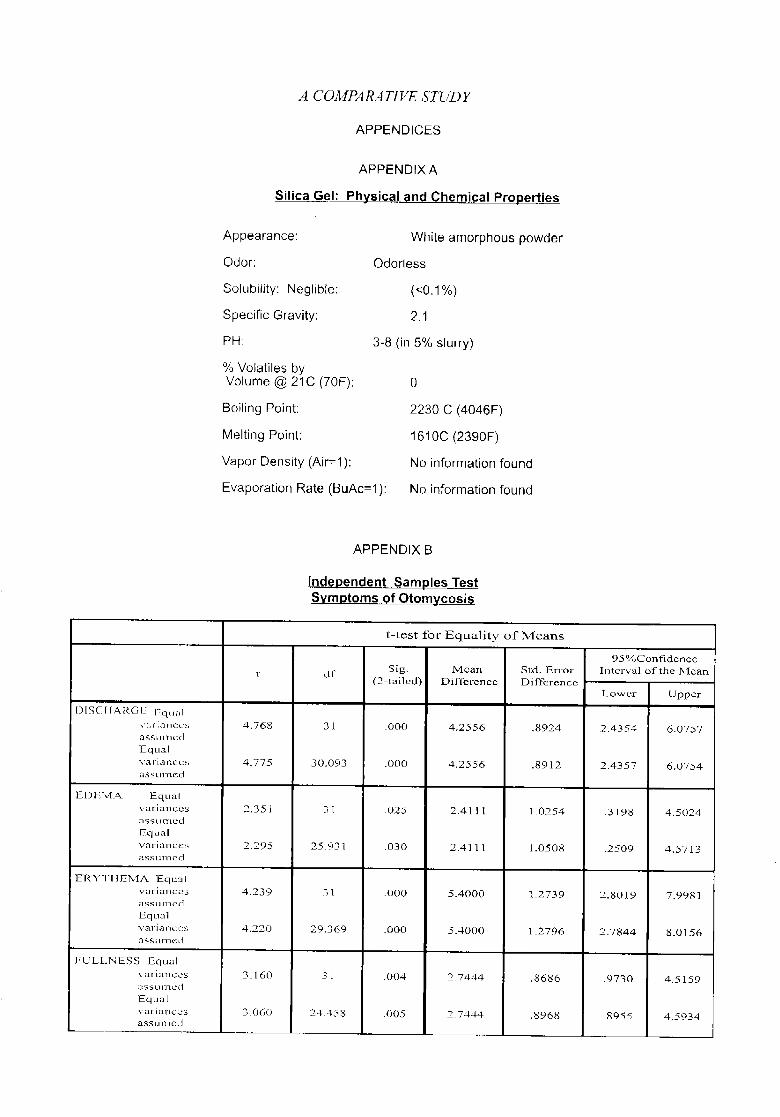
Silica Gel: Physical, and Chemical Properties
Appearance: White amorphous powder
Odor: Odorless
Solubility: Neglible: (<0,1%)
Specific Gravity: 2.1
PH: 3-8 (in 5% slurry)
% Volatiles byVolume @ 21C (70F): 0
Boiling Point: 2230 C (4046F)
Melting Point: 1610C (2390F)
Vapor Density (Air=l): No information found
Evaporation Rate (BuAc--1): No information found
APPENDIX B
Independent Samples TestSymptoms .of Otomyc .osis
t-test for Equality of Means
95%Confidence
t df Sig. Mean St:d• En-or Interval oftlne Nl:can(2-tailed) Difference Difference ....
l.,,owcr Upper
[) IS C I-[,;'l_,(-}I- l-qual .......
\':_r iariccs 4.768 3 t .000 4.2556 .8924 2.4354 6-0757,3SS kl lTlcd.
Equal
variances 4.775 30.093 .000 4.2556 .8912 2•4357 6.0754[|$s Llnled
.m,
IEl) I-';'MA. Equal
variances 2,351 31 .025 2.4[ 11 1.0254 -3198 4.5024asstJQlcd
F:.qual
variances 2.295 25.9-_ 1 ,030 2_4111 1.0508 .2509 4.5713_-'tSStlnlcd
ERYTIIENIA Equal
variances 4_239 3 I .000 5_4000 1._2739 2.8019 7.9981aSS kll'l'l_2d
Equal
varia ncos 4.220 29,369 .000 5,4000 1_2796 2_7844 8_0156a SS Ullled
,,, , • .....
FLJLLNESS Equal
variances 3.160 31 .004, 2_74,14 .8686 .9730 4.5159;;1S S L1131£_-d
]Equal
variarlccs 3.06() 24.458 .005 2.7444 .8968 ,8955 4•5934,ass L.ii1 Io_-J

A COMPARATIVE STUDY
APPENDIX C
Independent Samples TestSiclns of Otomycosis
t-test for Equality o:{-Means,., ., , ,
95%Confidence
t df Nig. Mean Sld. Error Interval of the Mean(2-tailed) Dift'erencc Difference
Lower Upperu
I I EARLOS S Equalvariar'_ccs 3.109 3 I .004 2.8000 .9006 .9632 4.6368
assLll I_d
Equalvariarlces 2.89 .I. 17.027 _010 2.8000 _9684 .7570 4.8430
abSt.lrl/ed
KO H E qua Ivariances 5.049 31 .000 5_8667 1. I 619 3.4970 8,2363
LISS tll'l/od
.F.qualvariances 5. I.96 30.531 .000 5.8667 1 _129 .t 3_5624 8.1710
asstlnaed
MYCEI_,I A L Equalvariances 4.827 31 .000 4.4889 .9300 2.592 [ 6.3857
assumed
Igqualvariances 5.0(19 29.555 .000 4.4889 .8961 2.6577 6.320.1.
aissumed . ,, , ....
()TALGIA Equalvariances 3_434 31 _002 2.0333 .5920 .8259 3.2408
assumed
Equalvariances 3.245 19.666 .004 2.0333 .6267 _7247 :3_3420
ass_llled
PRURITUS Equalvariances 2.965 3 I .006 2.7444 _9257 .8565 4,.6324
assurnod
Equalvariances 2.794 /9,228 .011 2,7444 .982,3 .6902 4_7987
assulrl_d
TIN2qlTU S Equalvmqanccs 1.371 31 .180 I .1889 _8671 -_5795 2.9572
aSS UI'l'led
Equalvariances 1.297 19.822 .210 1,1889 _9170 -.725(1 3_ 1028
as s Elrll k_,_"l

PI, "pph C,Jmtt n_d qJ'O/o] tt3vl_u/_J_ ' Hcn_/ _k-_\'_.[¢SJ','rgcr_;
V_4. I6 Nt_. 2 59- _-1.I,".,20(12l_l_ilil_pinc Sr_c c y o "Oto a -y 1_ ogy I-Ic_c _._.No:ok Surgcr'y
ALTERNATIVE METHOD IN IDENTIFICATION OFRECURRENTLARYNGEAL NERVE
REINALYN ROSETE-PINEDA, MD**RONAL.D DELOS SANTOS, MD**
ROBIE V. ZANTUA, MD***
ABSTRACT
Objective:To find an alternative and safe method in the identification of the recurrent laryngeal nerve.
Design:Experimental studies were done using periodic acid schiff as stain for the identification of the recurrent
laryngeal nerve in cadavers_
Setting:The study was done in the laboratory and morgue of a tertiary government hospital (Rizal Memorial
Medical Center).
Subjects:Frogs, cats and fresh cadavers were used in the study.
Results:The study revealed that the use of periodic acid schiff as a means of identifying the recurrent laryngeal
nerve showed no changed in the function; also, there was no alteration in the histology noted.
Conclusion:
The use of periodic acid schiff as a means of identification of the recurrent laryngeal nerve is safe andaccurate and could definitely be used as an alternative method in the identification of the recurrent laryngealnerve.
INTRODUCTION
Surgical therapy continues to be the primary The only way of identifying the recurrenttherapeutic modality for treating many thyroid laryngeal nerve is thru its anatomic location and itsdisorders, and is one of the more common surgical relation with the other structures in the cervical area.procedures done in our local setting. The technique This method however is not easy for many reasonsvaries and the procedure is tedious and difficult to do. such as: a) its size and color, b) the several anatomicIt has many inherent problems and what is more variations and c) even the distortion of the structurechallenglng is the identification of the recurrent as caused by the disease process or from previouslaryngeal nerve. In our institution, it has been the thyroid operation,practice of our residents in training to identify therecurrent laryngeal nerve in all thyroid surgeries and Failure in identifying the recurrent laryngealfailure of identification had resulted in injuries to the nerve can cause so much anxiety on the surgeon andabove mentioned nerve in 1% to 10% of the patients lead to permanent morbidity on the part of the patient.operated on. Injury to the recurrent laryngeal nerveresults in permanent change of voice or even worse, In this study, the authors chose to use the stainit mayleadtorespiratorydistress. Periodic Acid Schiff (PAS) as a means of
*Presented,AnalyticalResearchContest,November30,2000,PuntaBaluarte,Calatagan,Batangas**Resident,Departmentof Otorhinolaryr_gology,Sto.TomasUniversityHospital***Consultant,Departmentof Otorhinolaryngology,Sto.TomasUniversityHospital

ROSETE- .PINEDA ET_.AL.
identifying the recurrent laryngeal nerve. The said with water. The results were thenstain is cheap, readily available and is safe as noted_
evidenced in the study. C. Postmortem ExperimentTo try to simulate the effects of PASon live patients, we did the same
OBJECTIVE staining procedure on fresh cadavers.The interval between the time of death
The experimental study was designed to find and the time of dissection was lessan easy, fast, safe and reliable method of identifying than 24 hours. After consent for
the recurrent laryngeal nerve intraoperatively. This could autopsy, we exposed the righthelp in making the operation easy, limit detailed cervical recurrent laryngeal nerve of theexploration, shorten the operating time and decrease cadaver using the same surgicalthe morbidity in thyroid surgery, procedure done on live patients.
Upon exposure of the thyroid gland,we lateralized it to expose the
MATERIALSANDMETHODOLOGY tracheoesophageal groove afterwhich we were able to expose the
This is a three-part study. The first part is the recurrent laryngeal structure. PASfrog experiment in which the sciatic nerve of the frog was applied to the structure and wewas exposed and stained with periodic acid schiff. The then noted for the results after rinsingsecond part of the experiment used a cat to note the it with distilled water. The dye wasfunction of the recurrent laryngeal nerve after staining also applied to the blood vessels andwith periodic acid schiff. The final part of the experiment fibrous tissues in the operative site.involved fresh cadavers. The recurrent laryngeal nerve
was exposed and stained with periodic acid schiff and Ii. Test for function of the stained nervethe stained nerve was sent to histopathology for
documentation. The second part of the experiment isto prove that the stain (PAS) when applied
I. Staining Procedure to the nerve is non-injurious and will notThe first part of the experiment was done affect its functions.to test whether PAS can really stain nerve
tissues grossly. .Frog Experiment- measurement ofnerve impulses before and after staining
A. Frog Experiment: of the sciatic nerve.The frog is one of the most commonexperimental animals used in medical One of the more important functionschools. We utilized the frog for its of nerve fibers is conduction of impulse.sciatic nerve. First we dissected the Electrical potentials exist across thesciatic nerve of both hindlegs, after membrane of nerve cells, and are "excitable"which we applied PAS over the
- nerve cells are capable of self-generation ofexposed area. After one minute, we electrochemical impulses are used at theirthen rinsed the area with sterile water
membranes and these impulses to transmitand noted the result, the signals along the nerve fiber.
B. Cat Experiment By measuring this membraneAfter the very encouraging results we potential generated in the nerve, we couldgot from the frog experiment, we
compare the function before and after stainingapplied the same method on the cat the nerve and test if PAS has affected the
but now we exposed the laryngeal conducting capacity of the nerve. To measurenerve. After anesthesia with ether gas, the conducting capacity of the nerve, we filledwe did a vertical incision on the neck a small pipette with a very strong electrolyteand with the help of a zoologist, we (KCL) that was imparted through tf,e cellwere able to identify and expose the membrane then to the interior of the fiber.laryngeal nerve. The chemical stain Another electrode called the "indifferentwas applied to the identified structure electrode" was placed in the interstitial fluidand after 1minute, the area was rinsed
ALTERNATIVE METftOD
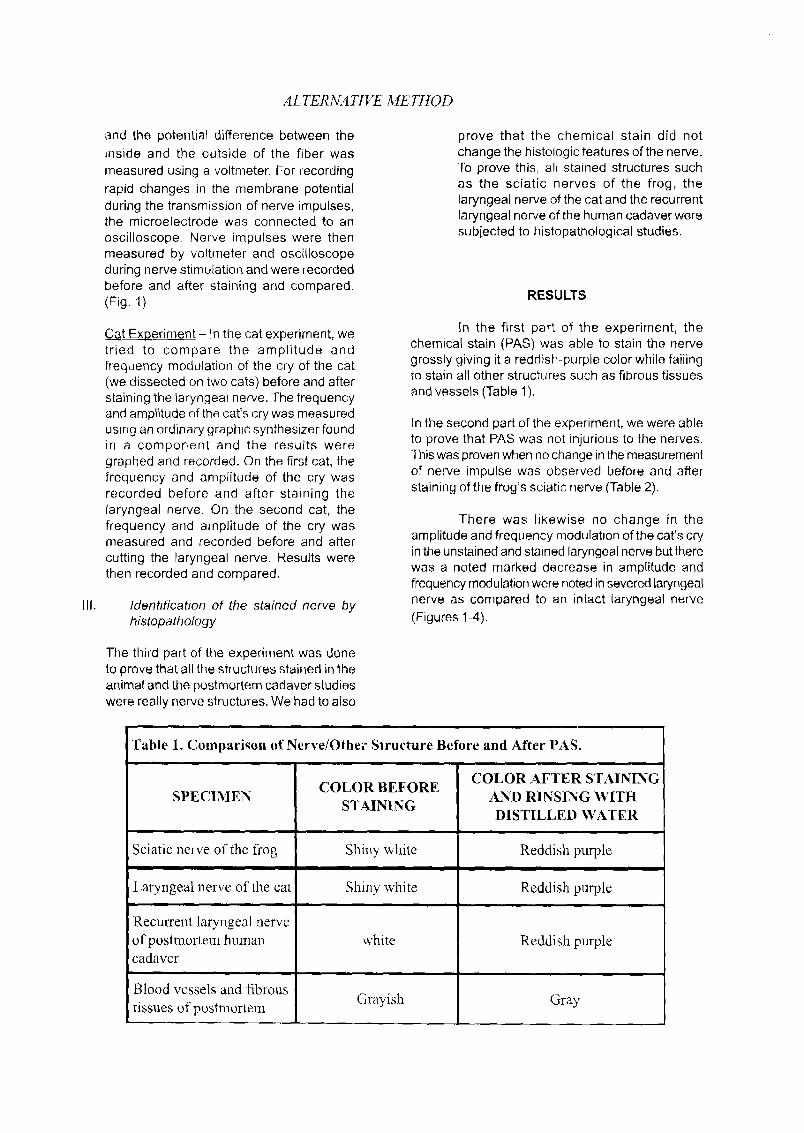
and the potential difference between the prove that the chemical stain did notreside and the outside of the fiber was change the histologicfeatures of the nerve.
measured using a voltmeter. For recording To prove this, all stained structures such
rapid changes in the membrane potential as the sciatic nerves of the frog, theduring the transmission of nerve impulses, laryngeal nerve of the cat and the recurrentthe microelectrode was connected to an laryngeal nerve of the human cadaver wereoscilloscope. Nerve impulses were then subjected to histopathological studies.measured by voltmeter and oscilloscopeduring nerve stimulation and were recordedbefore and after staining and compared.(Fig. 1) RESULTS
In the first part of the experiment, theCat Experiment- In the cat experiment, wetried to compare the amplitude and chemical stain (PAS) was able to stain the nervefrequency modulation of the cry of the cat grossly giving it a reddish-purple color while failing(we dissected on two cats) before and after to stain all other structures such as fibrous tissuesstaining the laryngeal nerve. The frequency and vessels (Table 1).and amplitude of the cat's cry was measuredusing an ordinary graphic synthesizer found in the second part of the experiment, we were able
to prove that PAS was not injurious to the nerves.in a component and the results wereThis was proven when no change inthe measurementgraphed and recorded. On the first cat, theof nerve impulse was observed before and afterfrequency and amplitude of the cry was
recorded before and after staining the staining of the frog's sciatic nerve (Table 2).laryngeal nerve, On the second cat, the
There was likewise no change in thefrequency and amplitude of the cry wasmeasured and recorded before and after amplitude and frequency modulation of the cat's cry
in the unstained and stained laryngeal nerve buttherecutting the laryngeal nerve. Results werethen recorded and compared, was a noted marked decrease in amplitude and
frequency modulation were noted insevered laryngeal
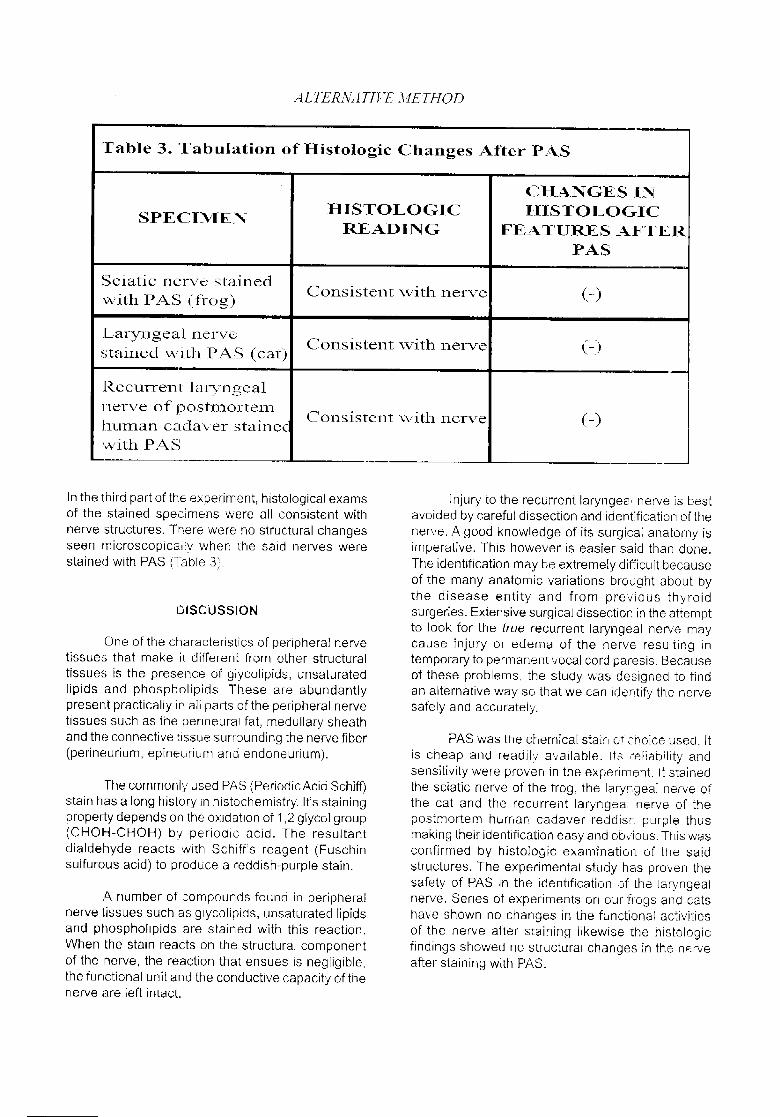
III. Identification of the stained nerve by nerve as compared to an intact laryngeal nervehistopathology (Figures 1-4).
The third part of the experiment was doneto prove that all the structures stained in theanimal and the postmortem cadaver studieswere really nerve structures. We had to also
Table 1. Comparison of Nerve/Other Structure Before and After PAS.
COLOR ,AFTER STAININGCOLOR BEFORE
SPECIMEN AND RINSING WITHSTAINING
DISTILLED WATER
Sciatic nerve of the frog Shiny white Reddish purple! I I
Laryngeal nerve of the cat Shiny white Reddish purplei i
Recto:rent laryngeal nerve
oFpostmorteln human white Reddish purplecadaver
Blood vessels and fibrous
tissues of postmortem Grayish Gray

_4LI-L_NATII,'E METHOD
Table 3. Tabulation of H istologic Changes A i_er PASi i
CHANGES IN
H I STOLOGIC I_.[ISTO LOGICSPECINIENREADING FEATURES AFTER
PASmll
Sciatic nerve stainedConsistent with nerve (-)with PAS (frog)
.Lary]:_gea.[ nerveConsistent with nerve (-)
stained wi.th PAS (cat)
'Recto:rent laryngeal
l:lerve of postm.ortena.human cada\,er staincc Consistent with nerve (-)
with PA 5;_
In the third part of the experiment, histological exams injury to the recurrent laryngeal nerve is bestof the stained specimens were aI[ consistent with avoided by careful dissection and identification of thenerve structures. There were no structural changes nerve. A good knowledge of its surgical anatomy isseen microscopical b, when the said nerves were imperative. This however is easier said than done.stained with PAS (q_bie 3). The identification may be extremely difficult because
of the many anatomic variations brought about bythe disease entity and from previous thyroid
DISCUSSION surgeries. Extensive surgical dissection in the attemptto look for the true recurrent laryngeal nerve may
One of the characteristics of peripheral nerve cause injury or edema of the nerve resulting intissues that make it different from other structural temporary to permanent vocal cord paresis. Becausetissues is the presence of glycolipids, unsaturated of these problems, the study was designed to findlipids and phospholipids. These are abundantly an alternative way so that we can identify the nervepresent practically in all parts of the peripheral nerve safely and accurately,tissues such as the penneural fat, medullary sheathand the connective tissue surrounding the nerve fiber PAS was the chemical stain of choice used. It
(perineurium, epineurium and endoneurium), is cheap and readilv a,_ailable. Its reliability andsensitivity were proven in the experiment. It stained
The commonly used PAS (PeriodicAcid Schiff) the sciatic nerve of the frog, the laryngeal nerve ofstain has a long history in histochemistry. It's staining the cat and the recurrent laryngeaJ nerve of theproperty depends on the oxidation of 1,2 glycol group postmortem hurt, at: cadaver reddistz purple thus(CHOH-CHOH) by periodic acid. The resultant making their identification easy and obv'ious. This wasdialdehyde reacts with Schiff's reagent (Fuschin confirmed by histoiogic examination of the saidsulfurous acid) to produce a reddish-purple stain, structures. The experimental study has proven the
safety of PAS in the identification of the laryngealA number of compounds found in peripheral nerve. Series of experinqents on our frogs and cats
nerve tissues such as giycolipids, unsaturated lipids have shown no changes in the functional activitiesand phospholipids are stained with this reaction, of the nerve after staining likewise the histologicWhen the stain reacts on the structural component findings showed no structural changes in the nerveof the nerve, the reaction that ensues is negligible, after staining with PAS_the functional unit and the conductive capacity of thenerve are left intact.
ROSETE- PINEDA ET.. AL_
CONCLUSION
We can therefore conclude that an easy and alternativeway of identifying the recurrent laryngeal nerve is bystaining it with PAS. W_th this method, we can avoid thenerve during dissection. This method would also preventextensive cervical dissection thus shortening theoperative time and ultimately avoiding possible morbidityin thyroid surgery.
RECOMMENDATIONS
We recommend to do further studies on PAS not only ondoing more cadaver and animal studies and eventuallywe can do this in live patients.
REFERENCES
1. Shah JP, Loree TR,Dhaknker D, et al. Surgicaltreatment in Thyroid CA. Am J Surgery 1992;164:658-661
2. Obar T, Itoy, et al. Complications of ThyroidSurgery. Ann Otol Rhinol Laryngol, 1977; 86:751-755
3. Okazaki H. Methodology in Neuropathology.Fundamentals of Neuropathology, 1't edition,1983:5-8
4. Hodgkin AL. The Conduction of the NerveImpulse. Springfield III, Charles C. Thomas,Publisher 1963
5. Livett BG. Anatomy of Cat. Zoology. New York,
Oxford University Press, 1975:125-127
vol. 16No 2 dS-,Sl.I'2002 PlHlippineSocletyolOloiaryllSoIo_yl l_.Ld_%NcckSui'_.ery
ULTRASTRUCTURAL CHANGES IN NASAL POLYPS
WITH EXPOSURE TO MOMETASONE FUROATE
MONOHYDRATE AQUEOUS NASAL SPRAY*
ARLENE MARIE R. CAYETANQ, MD**
JOSE B. ORQSA, MD***
MA. TERESA M. BONDOC-SlLVESTRE, MD*****
NORMANDQ C. GQNZAGA, MD, FPSP****
ABSTRACT
OBJECTIVES:
1. To describe the uitrastructurat changes in the nasal polyp of patients treated with Mometasone
Furoate Monohydrate aqueous nasal spray through the aid of electron microscopy
2. To describe through the use of transmission electron microscopy the ultrastructural appearance of the
nasal polyp
3_ To describe the uitrastructural changes in the nasal polyp of patients while undergoing
Treatment with Mometasone Furoate Monohydrate aqueous nasal spray after 4 and 8 weeks of exposure.
DESIGN: Descriptive Study
SETTING: Tertiary r_ospital
PATIENTS: 4 patients, ages 22 to 70,diagnosed to have nasal polyposis
CONCLUSION:
Tile ultrastructural changes seen in polyps are 1) the variability in the thickness of the surface epithelium
and cellular composition, 2) Extensive edema of the epithelial layer as evidenced by there widened and distended
intercellular spaces, and loosened junctional complexes. , 3) Presence of cells, which possessed large membrane
bound _acuoles containing flocculent material 4) Irregularities in the surface cilia such as the presence of thickened
ciliary membranes, disintegration and dissolution of ciliary components 5) The vacuolation of the mitochondria and
destruclion of intraorganelle crystals, 6) The basement membrane was thick and widened with the cell free zone
beneath it replaced by bands of edematous area containing loose collagen fibers and amorphous materials of low
electron density, 7) The mast cells showed exlensive degranulation, also occurring twice as much with a highly
variable morphology, 8) The granules were very small, very electron dense and amorphous with a crystalline matrix
and it lacked the outer lamellar content 9) The endoplasmic reticulum was distended and contained flocculent
materials of low eleclren density 10) The blood vessels seen had its endothelial ceils arranged in such a fashion
that the junctions in between provided spaces for the leakage of fluid, 11) The glands contained mucous elements
and the regular tall columnar lining was shifted to a flattened epithelium.
*Presented, PSOHNS Descriptive Research Contest, November 29, 2000, Punta Baluarte, Calatagan, Batangas**Third Year Resident, Department or O[orhinolaryngology-Head and Neck Surgery, Ospkal ng Maynila Medical Center"*'Diploma'.e, Department o1:Otorhinolaryngolo9y-Head and Neck Surgery, Qspital ng Maynila Medical Center
****Consukan[ and Chairmart, Dep_, of Pathology, Faculty or Medicine and Surgery, University of S[o, TomasHead of Electron Microsccpy bnit, Maka[i Medical Center,' UST
..... Fourth Year Resident, Dept, of Pathology, UST

CAYETANO ET. AL,.
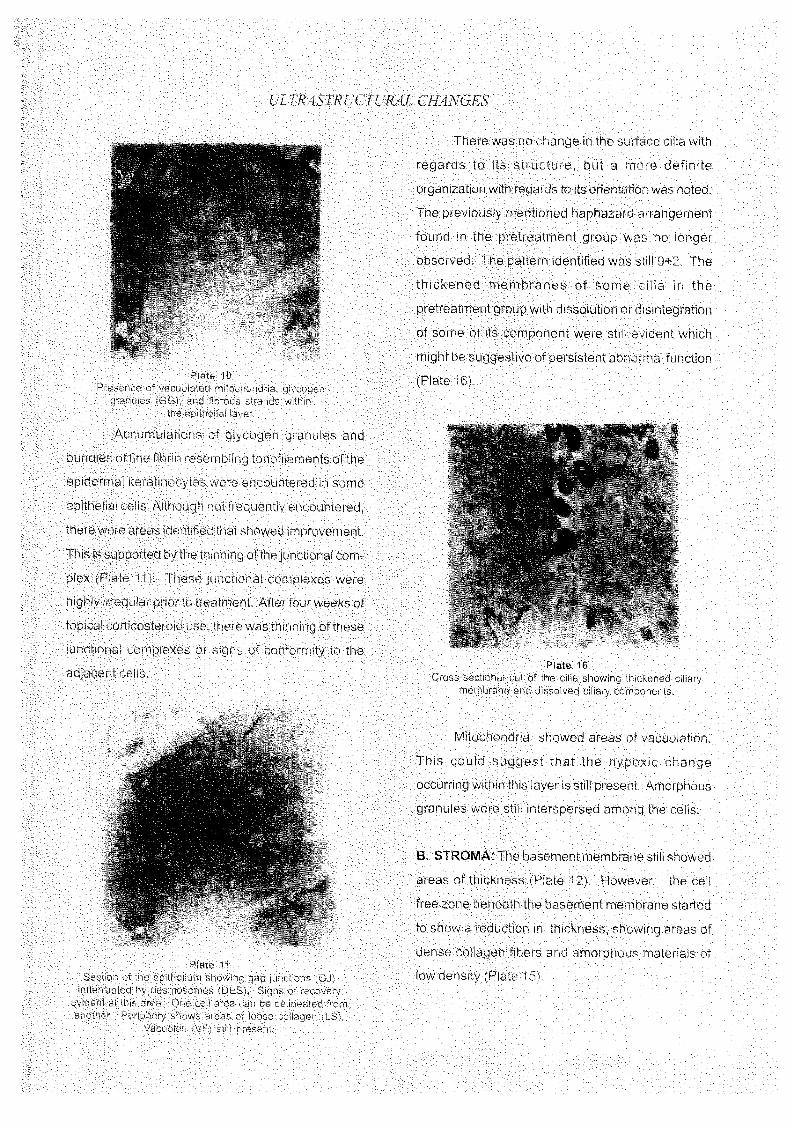
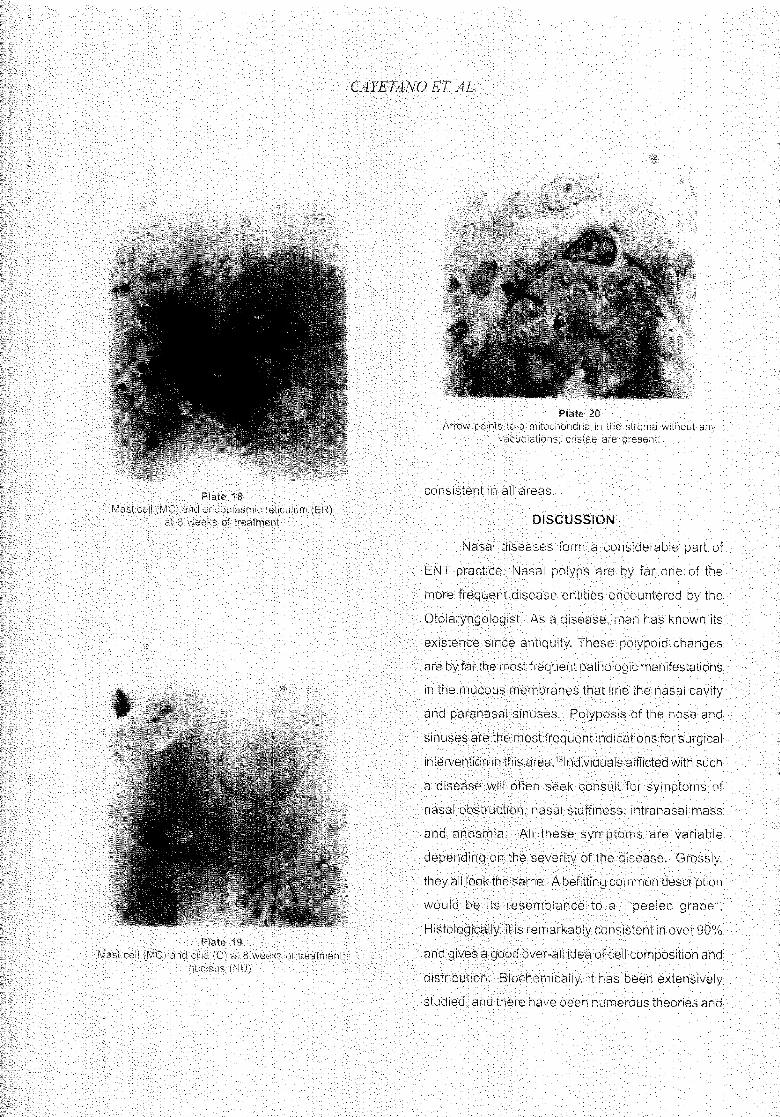
At four weeks of treatment the area beneath remain the essential morphologic features for
the basement membrane showed areas of less diagnosis.
edema. Mast cells were less degranulated and the Immunohistochemistry is a powerful tool for
granules showed the central core and the scroll pathologic diagnosis and is proved effective in the
pattern was already identified with tile presence of classification of the undifferentiated and/or small
crystalline inclusion bodies. The dilated cistern of lesions of the sinonasal tract. Briefly stated,
the endopiasmicreticulumwaslessprominentwith immunohistochemistry is the application of
a more uniform arrangement. Mitochondria had less immunologic principles and techniques to the study
vacuolation with reappearance of some intraorganelle of cells and tissues?
crystals. Other findings were 1) narrowing of the The main applications of electron microscopy
open endothelial junctions in the capillaries 2) portions to diagnostic pathology are in the fields of tumor
of the stroma demonstrated areas of necrosis 3) at pathology and renal pathology. In tumor pathology,
the epithelium, the junctional complexes showed ultrastructural examinations have proved to be very
thinning, useful in determining the histiogenesis of various
At eight weeks of treatment, there was tumors but unfortunately have not shown consistent
marked reduction in the edema atthe epithelial layer differences between reactive conditions, benign
wherein the junctional complexes were clearly tumors and malignant tumors of the same type? At
delineated from one cell to another. Ciliary present, the role of diagnostic electron microscopy
organization was more uniform. Mitochondria activity has diminished as a result of the advances in
was more prominent. There was narrowing of the immunohistochemistry. However, it remains a
basement membrane where collagen fibers were powerful diagnostic tool used selectively and
dense. Mast cells and thegranuleswere less dense intelligently, with full knowledge of its potential
and amorphous, contributions and limitations.
The polyps were devoid of sensory, vasomotor Nasal Polyposis is a disease known to man
and secretomotorinnervation, for over 5000 years. Nasal polyps are not true
neoplasms. They appear to be inflammatory swellings
INTRODUCTION of the nasal mucosa especially in the middle meatus
Lesions of the sinonasal region may have and anterior ethmoidal air cells rather than a true
similar or overlapping morphology, and pose a neoplastic growth. Many are still of obscure etiology.
challenge not just to the Otolaryngologist but also to Many hypotheses regarding its pathogenesis have
the Pathologist. With the advent of modern been proposed and debated upon, but there is still
technology in this present day and age, modern no clear-cut evidence for its cause. The pathologic
pathologic techniques including mechanism of polyp formation is still under
immunohistochemistry and electron microscopy, have investigation and current theories favor a connective
been employed and are commonly utilized in giving tissue dysfunction due to immunoglobulin E (IgE)-
us an accurate diagnosis and better understanding mediated response in the lamina propria, which results
of such lesions. Standard pathologic criteria for in fluid retention below the epithelial surface. Grossly,
architecture, nuclear configuration and mitotic rate nasal polyposis appears as soft polypoid translucent

UL TRASTR UCTUtL4L CHANGES
masses up to several centimeters in diameter, related to the functions of other hormones. Like any
Histologically, the surface mucosa is typically other steroid hormones, they act by controlling the
intact and covered by respiratory epithelium with rate of synthesis of proteins. It reacts with receptor
increased goblet cells and/or areas of squamous proteins in the cytoplasm of many sensitive cells to
metaplasia. The basement membrane is frequently form a steroid receptor complex. The complex
thickened and eosinophilic. The stroma is edematous undergoes sedimentation then moves into the nucleus
and myxomatous with scattered fibroblasts and and regulates transcription although most of the time
variable vascularity, it is enhanced as manifested by many mRNA. It then
There have been extensive histological and releases a protein, which plays a major part in the
biochemical studies of nasal polyps and a few studies receptor complex then proceeds to the nucleus where
were made with [he aid of electron it interacts with theDNA.
microscopy? ,4,s,6,7,°,9,r°Electron microscopy has Glucocorticoids act by preventing or
revealed that tissues of polyps are devoid of sensory, suppressing the development of the manifestations of
vasomotor and secretomotor innervation. Eosinophils inflammation. Although the effects may be palliative,
and neutrophils are increased in number in all layers_ the suppression of inflammation and its consequences
Plasma cells exhibit activity in the endoptasmic have madethemofgreatcIinicalvalue. Corticosteroids
reticulum and Golgi zone and that mast cells are do not onlyinhibitthe phenomena ofthe inflammatory
depleted oftheirgranules. The venules of polyps reveal process but also the later manifestations such as
open endothelial junctions, which signify vascular proliferation offibroblastsandcapillariesand deposition
leakage. 3 of collagen. It also inhibits the recruitment of
The increasing popularity of topical leukocytes, monocytes-macrophage into affected
corticosteroids has led to several studies on its clinical, areas. It also exerts actions on the various elements
biochemical and histological effects on nasal polyps, of the circulatory system, including the capillaries and
Studies showed thatthe numberofeosinophils in nasal arterioles. In the absence of corticosteroids, there
smears, concentrations of albumin, IgG and IgE, is increased capillary permeability, inadequate
number of goblet cells, degree of tissue edema and vasomotor response of the small vessels to
symptomatology in nasal polyps decrease significantly catecholamines.
with the use of topical corticosteroids. :',9,1_,17 No literature was encountered on the
Mometasone furoate aqueous nasal spray in the ultrastructural changes of nasal polyps that are being
treatment of perennial rhinitis led to an improved treated with topical corticosteroids. Thus, with the
appearance of the epithelium and reduced extent of aid of electron microscopy, this study aims to give a
inflammatory cell infiltrate, especially eosinophils and description of the nasal mucosa in the subcellular level
mast cells. _1 in patients with nasal polyps being treated with
The effects of corticosteroids are widespread mometasone furoate aqueous nasal spray.
and numerous. They not only influence carbohydrate, The management of nasal polyposis, both
lipid and protein metabolism but also water and medical and surgical presents as a challenge in the
electrolyte balance. Its actions are often complexly field of Otorhinolaryngology. Its therapy is one of the

CAYETANO ET AL,
major challenges for both medical and surgical bundles. All kinociliae had coordinated direction and
approaches including endoscopic sinus surgery, a morphologically evident function phase. There was
Polyps tend to recur as long as the underlying disease also a network of kinociliae without any function phase
is not eradicated, or coordinated direction. Thru their morphological
findings, it was concluded that there is an extensive
REVlEWOF LITERATURE: decrease in function of the mucociliary system in
It was in 1972 when Cauna et al. published cases of polyposis, and as a result of this, an infectious
their research, "Fine structure of nasal polyps". They origin is favored.With the increasing popularity of topicalpresented intimate details and descriptions of the
various structures seen in nasal polyps. The tissues corticosteroids, Sorensen et al. studied the effect of
Beclomethasone dipropionate on nasal polyps in 1976.of the polyps were noted to be devoid of sensory,The study showed a decreasing trend in the numbervasomotor and secretomotor innervation. Eosinophilsof eosinophils in nasal smears and falls in theand neutrophils were found to be increased in number
increased concentrations of albumin, IgG and IgE inin all layers. Plasma cells exhibit activity in thenasal secretions. No signs of adverse effects wereendoplasmic reticulum and Golgi zones, and mast
noted and with this, they regarded thatcells are depleted of their granules. The venules of
Beclomethasone dipropionate as a valuable drug inpolyps reveal open endothelial junctions, which signifythe treatment of nasal polyps. The same conclusionvascular leakage. It was suggested that the loss of
was reached in 1978 by Mygind et al. and added thatinnervation combined with allergic reactions, infection
the degree of tissue edema, number of infiltratingor inflammation is responsible for polyp formation.
Mygind et al. followed this in 1974 when they eosinophils, number of goblet cells decreased
published their findings regarding their studies in nasal significantly and that the use of the drug for a period
polyps thru scanning electron microscopy. The of few years will not cause atrophic rhinitis_
following year, Mygind described the human nasal However, in 1980, Baumgarte et al. in their
mucosa also thru scanning electron microscopy. He study of"Histopathological examination of nasal polyps
concluded that allergic reactions have only a slight of different etiology", claimed that it is impossible to
give a safe differentiation between an allergic and non-direct influence on the ultrastructure of the mucous
membranes and that the nasal mucosa is allergic polyp, whether it be studied under light or
electron microscopy. They noted, however, somecharacteristically altered in atrophic rhinitis.
Before 1975 ended, Lenz published his study, indications, which might lead to an allergic or non_
"The surface of nasal polyps in the scanning electron allergic origin. Eosinophils and round cell infiltrationsare present in all types of polyps. An index ofmicroscope", which revealed a domination of kinocilia-
free epithelium. There was evidence of transitional eosinophils to plasma cells below 5 is indicative of an
forms of epithelium, from a cylindrical to more cube- allergic origin while an index of above 5 correspondsto an infectious etiology. An increased number oflike and finally to squamous epithelium. The covered
surface showed bundle-like, long and mostly parallel glands and collagen fibers, especially under the
kinociliae together with short and thin kinociliae insmall epithelium indicate the age of the polyp.

UL 7"RASTR UCTURAL CHzlNGES
Drake_Lee made a series of descriptive and analytical shown that the administration of fluticasone propionate
studies about mast ceil ultrastructure. On his and Beclomethasone dipropionate are effective in the
preliminary report in 1987, he described mast cells treatment of nasal polyps, with some evidence that
from normal nasal mucosa, nasal polyps, inferior fluticasone propionate has a faster onset of action
turbinates and adenoid tissues. It was concluded and is tolerated as well as Beclomethasone at the
that almost all mast cells from nasal polyps showed same dose.
extensive degranulation, with occasional electron- Lund in 1998 discussed the effectivity of
dense granules and vacuoles and that the process of fluticasone spray in severe polyposis. The drug was
degranulation may extend throughout the rest of the found to be effective in treating the symptoms of severe
nose. Normal mast ceils have electron-dense polyposis. Evidence showed that the group treated
amorphous granules organized like a scroll or a less with FPANS responded more quickly and efficiently
dense crystalline matrix with a single nucleus and than in the group receiving Beclomethasone.
less degranulation. On his final paper in 1997 the Also in 1998, Minshall, et al. made a study
degree of degran ulation was evaluated. It confirmed on the "Assessment by nasal biopsy of long-term use
that mast cells are degranutated within the stroma of of mometasone furoate aqueous nasal spray (MFNS)
nasal polyps and that the changes there are more in the treatment of perennial rhinitis". In a study of 69
than those are found in the inferior turbinates. The patients with allergic rhinitis treated with mometasone
study also suggests that the degranulation in polyps furoate, they concluded that long-term use of MFNS
imply a co-existing inflammation occurring throughout appeared to improve the appearance of the epithe-
the nose. lium and reduced the extent of the inflammatory cell
Matthias and Merker (1997)investigated the infiltrate, particularly eosinophils and mast cells. It
morphology of the mucosa of Lhehuman paranasal had no untoward side effects on the nasal mucosa,
sinus by electron microscopy. The mucosa and there was complete absence ofatrophic changes.
represented a highly prismatic epithelium consisting By virtue of its effect on the nasal mucosa, they rec-
of kinociha-carrying and mucus producing (goblet) ammended MFNS as an effective treatment for pe-
cells. Other cell types, such as those occurring in rennial rhinitis.
the respiratory epithelium of other areas could not be
demonstrated. Electron microscopic and OBJECTIVES
immunomorphological investigations revealed collagen A. GENERAL OBJECTIVE:
type VII beneath the tamina densa of the basal To describethe ultrastructural changes in the
lamina, and only a small number of basophils and nasal polyp of patients treated with mometasone
eosinophils in the area. Pronounced acute reactions furoate monohydrate aqueous nasal spray through
of the mucosa in this area cannot be expected, which electron microscopy.
is in contrast to that of the nasal mucosa.
The response to steroid nasal sprays was B. SPECIFIC OBJECTIVES:
shown in the experiments of Holmberg et al. in 1997 To describe through the use of transmission
where they used fluticasone aqueous nasal spray electron microscopy the ultrastructural appearance
(FPANS) in the treatment of nasal polyposis. It was of the nasal polyp.

CAYETANO ET. AL.
To describe the ultrastructural changes in the mometasone furoate monohydrate aqueous nasal
nasal polyp of patients while undergoing treatment spray at two nasal puffs per nostril twice a day at
with mometasone furoate monohydrate aqueous nasal approximately 200 ug per day.
spray (Nasonex) after four weeks and eight weeks. Repeat biopsy was done every three to four
weeks, noting changes on the gross appearance of
SUBJECTS: the polyp. Patients were advised to note of any adverse
A. INCLUSION CRITERIA effects while continuously using mometasone furoate
monohydrate nasal spray (Nasonex).Patients 20 years up to 70 years of age
Patients belonging to both sexes
Patients with clinically-diagnosed Grade II and B. STUDY DESIGN:
Grade III nasal polyps A descriptive study.
Patients who have not undergone any treatment
prior to initial biopsy C. TISSUE PREPARATION:
Nasal polyps were obtained in the standard
B. EXCLUSION CRITERIA manner using Takahashi forceps from the right and
Patients who underwent functional endoscopic left nasal cavity of each subject, The nose had
sinus surgery previously been prepared with Oxymetazoline
Patients who received steroids in the last twelve hydrochloride (Drixine 0.05% nasal spray) and was
months subsequently anesthetized with lidocaine
Patients with known allergy to any of the hydrochloride (Xylocaine) 10% nasal spray, Nasal
components of the topical corticosteroid used biopsy specimens measuring 1-1.5 mm were
in this study immediately fixed in 2.5%-3.0% gluteraldehyde in
Pregnant women 0.2M Sorenson's sodium phosphate buffer. Biopsy
Lactating/breastfeeding women specimens were stored in the refrigerator at 4-5
Patients undergoing chemotherapy degrees Celsius, Specimens were later washed,
blocked and post-fixed in 1_% osmium tetroxide.
MATERIALS AND METHODOLOGY Processing of specimen was done automatically using
1-% uranyl acetate solution and ethyl alcohol before
A. PATIENT SELECTION: being placed in epoxy resin. Embedding of l-ram
Four adults diagnosed with nasal polyposis specimen was done in BEEM capsules. Biopsy
from our out patient department were selected for this specimens were sliced 0.5-1 um thick and stained
study. Ages range from twenty-two to seventy years, with 2% toluidine blue then examined under a light
A complete history and physical examination was microscope, to determine the areas of special interest.
done on all patients with emphasis on anterior Thin sectioningwasdoneandcollectedintrough, Thin
rhinoscopic findings, Voluntary consent to participate sections were examined using stereoscope binoculars
in the study was obtained_ Specimens were obtained to observe the "colors" of the section. The sections
thru punch biopsy. Patients were then subjected to were ascertained to be thin enough for adequate beam

UL TRASTR UCTUtL4L CHANGES
penetration to achievegood resolution. Ahigh quality The initial specimens served as the baseline with
thin section will have no chatter, knife lines, cracks, no exposure yet to mometasone furoate aqueous
folds or contamination. Manual grid staining was done nasal spray. These specimens were labeled as
with 35% methanol, 4% uranyl acetate in methanol EMRIA1, EMRIB1, EMRICl, and EMRID1. After
and leadcitrate.14Thespecimenswereobservedunder which, the prepared specimens were examined
the transmission electron microscope. The results under the light microscope,
were recorded and interpreted. Under light microscopy, polyps exhibited a
ciliated respiratory epithelium. The submucosa was
OBSERVATIONS composed of different degrees of loose myxomatous
or edematous stroma with varying numbers of mucous
A. CLINICAL FINDINGS glands. Interspersed within the stroma are numerous
infiltrates of inflammatory cells such as eosinophils,There were four adult patients involved in thislymphocytes, plasma cells, mast ceils andstudy. Two males and two females, with age range
from 22 to 70 years of age (mean of 41.5 years). All neutrophils. The basement membrane generally
of these patients had histories of mild to moderate appeared to be intact. Cellular cytoplasm varied inamount. The glands, which were mostly distended,rhinosinusitis. Their symptomatology included nasallost its usual lining from a columnar respiratoryobstruction, nasal stuffiness, difficulty in nasal
breathing, watery rhinorrhea, and headache. The epithelium to a flattened epithelium.
duration of symptoms ranged from 5 months to 4C. ELECTRON MICROSCOPIC FINDINGS
years. There was no history of epistaxis elicited_The succeeding specimens labeled asOn anterior rhinoscopy, all patients had
bilateral polyp formation, Conventional paranasal EMRIIA, EMRIIB, EMRIIC, EMRIID, EMRIIIA, EMRIIIB,EMRIIIC, and EMRIIID were the ones that were
sinus radiographs were done on these patients. The
overall clinical impression of these lesions was nasal exposed to Mometasone Furoate aqueous nasal
polyposis grades II to III, with no distinct features, spray. All three groups were examined under theelectron microscope.
which might be suggestive of unusual or malignant
changes.
GROUP I- PRETREATMENT GROUP
B. PATHOLOGIC FINDINGS A. EPITHELIUM: All reviewed specimens showed
On evaluation through anterior rhinoscopy, the varying thickness of its surface epithelium and cellular
polyps grossly appeared as smooth, soft, polypoid, composition. Numerous inflammatory infiltrates were
translucent, masses, sometimes pinkish in color, identified (eosinophils, neutrophils, lymphocytesand
rubbery and glistening masses. Focal hemorrhages mast cells). The epithelium showed extensive areas
and ulceration were observed in some areas, of edema characterized by the widened or distended
After obtaining the specimens through punch intercellular spaces. The cytoplasm contained
biopsy, the specimens were fixed in their proper media vacuoles with some lightly staining flocculent
and processed under the required manner for this study

_LL:L %.::L:L I:L ¸¸ :L:- -.:: : L L : .... L ............ ...... --- - ........... .....




: : : : ::p : : :: :............::::AffS_: _ :tt:i_.,.._iroma:wi:itso_.i.ar_v: :
:: [ : :::::::::[

CAYEI_NO ET. AL.
The fenestrated capillaries observed in this
study showed the presence of open endothelial cells, CONCLUSIONS
which could probably be responsible for the vascular The ultrastructural changes seen in polyps
leakage leading to edema aside from the reactions are variable in relation to the thickness of the surface
occurring in mast cells causing the release of epithelium and its cellular composition. There was
histamine. In nasal polyposis, the permeability of extensive edema of the epithelial layeras evidenced
capillaries is very high. The granules of these mast by the widened intercellular spaces and loosened junc-
cells are partly depleted, which may be an indication tional complexes. Presence of cells which possessed
that agents including histamine are being released large membrane bound vacuoles containing floccu-
from cells. This process is probably responsible for lent material was noted. Irregularities in the surface
the vascular leakage as manifested by the open cilia were observed, such as the presence of thick-
endothelial junctions found around the capillaries. The ened ciliary membranes, disintegration and dissolu-
reaction that happens thereby causes the surface tion of ciliary components, The vacuolation of the
membrane to alter causing the entry of calcium into mitochondria and destruction of intraorganelle crys-
the cells. This then initiates the formation of CAMP tals. The basement membrane was thick and wid-
from ATP. The initial response then is to release the ened with the cell free zone beneath it replaced by
preformed elements within the granules. Histamine bands of edematous area containing loose collagen
is then dissolved from the protein/heparin complex, fibers and amorphous materials of low electron den-
which can be seen as an electron dense matrix and sity. The mast cells showed a highly variable mor-
is either amorphous or organized as scrolls or crystals phology with extensive degranulation, occurring twice
within the granules. The granule swells and then as much of that in normal mucosa. The granules
becomes less electron dense, the end-results is were very small, very electron dense and amorphous
formation ofvacuoles.4Aside from the fenestrated type with a crystalline matrix and with its outer lamellar
of capillary, there is also the continuous type and the content lacking. The endoplasmic reticulum was dis-
discontinuous type. The layers of the basement tended and contained flocculent materials of low elec-
membrane may appear around this capillaries where tron density. The blood vessels had its endothelial
projections from these endothelial cells project into cells arranged in such a fashion that their junctions in
the interstitium. A well-developed basement, between provided spaces for the leakage of fluid. The
membrane prevents vascular leakage of large glands contained mucous elements and the regular
m°lecules-19 tall columnar lining was shifted to a flattened epithe-
Polyps seem to develop in areas where the lium.
lining of the nasal cavity joins the sinuses. These At four weeks of treatment the area beneath
areas may be mechanically more predisposed to the basement membrane showed areas of less
edema formation, edema. Mast cells were less degranulated and the
granules showed the central core and scroll pattern
together with the presence of crystalline inclusion
bodies. The dilated cistern of the endoplasmic reticu-

UL TRASTR UCTURAL CHANGES
lum was less prominent and had a more uniform ar- 3. To study the possible effects of other topical
rangement. Mitochondria had less vacuolation with corticosteroids versus anti-histamines and its effects
reappearance of some intraorganelle crystals. There at the subcellular level and to note of other possible
was narrowing of the open endothelial junctions in the changes that might occur.
capillaries. Portions of the stroma demonstrated ar-
eas of necrosis. At the epithelium, there was thinning References
of the junctional complexes.
At eightweeks of treatment, there was marked 1. Rosai J.: Akerman's Surgical Pathology
Eight-Edition volume 1 Copyright 1996 Mosby Yr. bookreduction in the edema at the epithelial layer with the
Inc. pp. 32-34
junctional complexes being clearly delineated from one 2. Cauna N., Hinderer KH. Manzetti GW.,
cell to another. Ciliary organization was more uniform Swanson EW.: Fine structure of Nasal polyps. Annals
of Otology, Rhinology, Laryngology. February 1972and mitochondrial activity was more prominent. There
volume 81 (1) pp. 41-58
was narrowing of the basement membrane where 3. Drake-Lee AB., Price JM. Milford CM.,
collagen fibers were dense. Mast cells and its granules Bickerton RC.: Nasal Mast Cells: a Preliminary report
on their Ultrastructure. Journal of Laryngology andwere less dense and amorphous.
Otology, Supplement 1987 volume 13 pp. 1-17
The polyps were devoid ofsensory, vasomotor 4. Drake-Lee AB., Price JM. Mast Cell
and secretomotor innervation. Ultrastructure in the Inferior Turbinate and Stroma of
Nasal Polyps. Journal of Laryngology and Otology, April
1997 volume 111pp. 340-345
RECOMMENDATIONS 5. Nakayama M., Wenig BM., Heffner DK.:This study was done to investigate the Atypical Stromal Cells in Inflammatory Nasal Polyps:
ultrastructural changes at the subcellular level of nasalImmunohistochemical and Ultrastructural Analysis in
polyps after there is exposure to a topical Defining Histogenesis. Laryngoscope February 1995
corticosteroid. Being a pilot study in this particular volume 105 pp. 127-134
area, the authors may have overlooked some details, 6. Lund VJ. Flood J., SykesAP., Richards DH:which to the reader of this paper might need further
Effect of fluticasone in Severe Polyposis. Archives ofimprovement. In this regard, the following are
Otolaryngology Head and Neck Surgery May 1998
recommended: volume 124 pp. 513-518
1. A longer period of time frame is suggested 7. Herzon FS. Upper Respiratory Tract Ciliaryto further evaluate and validate the ultrastructural
Ultrastructural Pathology. Annals of Otology, Rhinology
changes in nasal polyps once it is exposed to topical and Laryngology, Supplement 83 May-June 1981 vol-
corticosteroids, ume 90 no. 3 part 2 pp. 1-122. An increase in the number of patients to
8. Holmberg K., Juliusson S., Balder B_,Smith
point out a more definite association as to its probable DL. Richards DH, Karlsson G.: Fluticasone Propionateetiology.

CAYEI_,INO E.T.A.L_
aqueous nasal Spray in the treatment of nasal Histotechnology pp.257-263
polyps. Annals of Allergy, Asthma & Immunology. 15. Baumgarten C_, Kunkel G., Rudolph R.,
March 1997 volume 78 pp. 270_276 Staud RD., Sperner I., and Gelderblom H.:
9. Bernstein JM. Gorfien J., Noble B., Histopathological Examinations of Nasal Polyps of
Yankaskas JR.: Nasal Polyposis: different etiology. European Archives of
ImmunoMstochemistry and bioelectrical findings (a Otorhinolaryngology 1980 volume 226(3) pp 187-197
hypothesis for the development of nasal polyps). 16. Mygind N., Sorensen H., Pedersen CB,
Journal of Allergy and Clinical Immunology. February The nasal mucosa during long-term treatment with
1997 volume 99 no. 2 pp. 165-175 Beclomethasone dipropionate aerosol. A light-and
"10.Rosai J.: Akerman_s Surgical Pathology scanning electron microscopic study of nasal polyps.
Eight-Edition volume "1Copyright 1996 Mosby Yr. Acta Otolaryngologica May-June1978 volume 85(5-6)
book Inc. pp. 289-291 pp. 437-443
'11. Minshall E., Ghaffar O., Cameron L, 17. Sorensen H., Mygind N., Pedersen CB.
O'Brien F.,Quinn H, Rowe-Jones J., Davies RJ. Prior Prytz S.: Long-term treatment of nasal polyps with
A., Lunc VJ., Mackay IS., Nolop K., Lutsky B., beclomethasonedipropionateaerosolllI. Morphological
Durham SR.:Assessment by nasal biopsy of Iongterm studies and conclusions. Acta Otolaryngologica Sept.-
use of Mometasone Furoate aqueous nasal spray Oct 1976 volume 82(3-4) pp. 260-262
(Nasonex) in the treatment of perennial rhinitis. 18. Lenz H.: The Surface of nasal polyps in
Otolaryngology-Head and Neck Surgery May 1998 the scanning electron microscope. Laryngology,
volume 118 no.5 pp. 648-654 Rhinology, Otology. December1975 volume 54(12)pp.
12. Matthias C., De Souza P., Merker HJ. 950-964
Electron Microscopic and Irnmunomorphological 19. Watanabe K., Komatsuzaki A.:
investigations on the mucosa of human paranasal Ultrastructural findings of capillaries in nasal polyps.
sinuses. European Archives of Otorhinolaryngology Rhinology March 1992 volume 30(1) pp. 49-56
1997 volume 254:5 pp. 230_235
13. Stammberger H., Kopp W., Dekornfeld
TJ. Hawke M.: Functional Endoscopic Sinus Surgery:
The MesserklingerTechnique. Copyright 1991 Mosby
Yr. book tnc pp. 216-226
14. Hincherick FR.: Transmission Electron
Microscopy. AFIP Laboratory Methods in

PhEippilre Jou,-n_d qf Ot_l¢_3,11goloKv lft,a_! & _,cck Sur_'_y
VoL I6 No. 2 82-!_1. ¢.'.12002Philippine Society ol O_oia_ynL-'olo_y l l_;_d & Neck Sur6e_7
THE COMPOSITE TRAPEZIUS-SCAPULAR SPINE FLAP:AN ALTERNATIVE IN THE RECONSTRUCTION OF
OROMANDIBULAR DEFECTS*
VICTOR DINO A. ALARVA Iii, MD**JOSEPH AMADO C. GALVEZ, M D**
ARMANDO M. CHIONG JR., MD, DPBO ***
ABSTRACT
OBJECTIVES To present a new technique for mandibular reconstruction using pedicled spine of the scapula
DESIGN Case Report
SETTING Tertiary hospital
PATIENT 1 patient who underwent segmental mandibulectomy for ameloblastoma
CONCLUSION The trapezius_spine flap of the scapula offers a potential pedicled flap for immediate reconstructionof relatively large oro-mandibular defect resulting from tumor ablation. Because of its reliable blood supply, it offersthe following advantages: lesser chance of extrusion, non-union and bone resorption, rapid integration to recipienttissue, and high resistance to infection. Because of this advantages, early recovery, lesser morbidity, and goodcosmetic results are expected, and functional disability minimized.
INTRODUCTION or body can result to severe functional disability. Due
Mandibular defects resulting from post- to the loss of structural support for the tongue and
oncologic surgery, avulsive trauma, and inflammatory laryngeal apparatus, masticatory and deglutition
conditions pose a big problem for head and neck problems are also anticipated. In extreme cases, large
surgeons. Loss of a portion of the mandible will result anterior mandibular defects may cause airway
to a spectrum of aesthetic deformity and functional compromise secondary to posterior displacement of
disability depending on the size and location of the the tongue necessitating tracheostomy. Clearly, these
defect. Loss of a portion of the posterior body of the types of defects must be reconstructed to avoid
mandible or ramus causes slight malocclusion due functional disability.
to shifting of the remaining mandibleto the affected The primary goal of oromandibular
side, but rarely will result to cosmetic or functional reconstruction is to reliably, safely, and promptly restore
disturbance. On the other hand, extensive defects lower facial contour, occlusal relationship, functional
involving significant portions of the anterior mandible
*1st Place,PSOHNSPosterSessiononSurgicalInnovation,November30, 2000,PuntaBaluarte,Calatagan,Batangas**Resident,Departmentof Otolaryngology-Head& NeckSurgery,Ospitalng MaynilaMedicalCenter***Consultant,Departmentof Otolaryngology-Head& NeckSurgey,Ospitalng MaynilaMedicalCenter


ALAR VA III ET. AL.
lower dentition, deglutition and mastication. Immediate improved understanding of the vascular and skeletal
reconstruction as opposed to a staged-procedure will anatomy.
avoid major problems in secondary settings, which is Reconstruction of defects of the mandible and
related to the drifting of the remaining mandibular floor of the mouth remain to be one of the most
segments and soft tissue contracture. 1 Several challenging tasks in head and neck surgery. _ At
reconstructive techniques for mandibular defects have present, several options have been proposed for its
been described in literature. It commonly involves the reconstruction. Bone-containing free flaps are popular
use of different reconstruction materials such as not only for oromandibular reconstruction but also for
autogenous and allogenic bone grafts, prosthetic craniomaxillofacial surgery. Utilization of bone
devices, metallic plates and mesh. 2 containing free flaps for oromandibular reconstruction,
Ivy=reported the first attempt at mandibular however suffer the disadvantagesofrequiring prolonged
reconstruction with autogenous bone using femur and operating time, large number of operating room
tibia. World War I and WWII paved the way for major personnel and adequate microvascular skill for surgery.
advances in grafting techniques for mandibular Investigators found out that exposure to large salivary
reconstruction due to the significant increase in the fistula and oral flora contamination decreases the
number of patients with traumatic mandibular defects? anastomotic patency rate of free flaps.5
The recent introduction of myocutaneous flaps has Resistance to infection and extrusion make
kindled the enthusiasm in including bone in the flap the bone-containing pedicled flap suitable for
to reconstruct defects of the floor of the mouth and oromandibular reconstruction. The medial and lateral
mandible. During the 1970's and early 1980's, sides of the scapula were among the common donor
attention wasfocused on the transfer of vascularized sites. In 1976, Demergaso 6, B described the
bone to the oral cavity as a composite flap. McKee 5 incorporation of the scapular spine to a trapezius flap.
was the first to use vascularized bone containing free However, it was only in 1980 when the trapezius
flap to reconstruct the mandible followed by osteomyocutaneous flap appeared in American
Demergosso z6in 1976. In 1978, the first large series literature. The purpose of this paper is to present a
of mandibular reconstruction using vascularized bone- relatively new technique in reconstructing mandibular
containing free flap was published.5Since then, several defects with a pedicled trapezius osteomyofascial flap
refinements of surgical techniques have evolved with with the spine of the scapula.


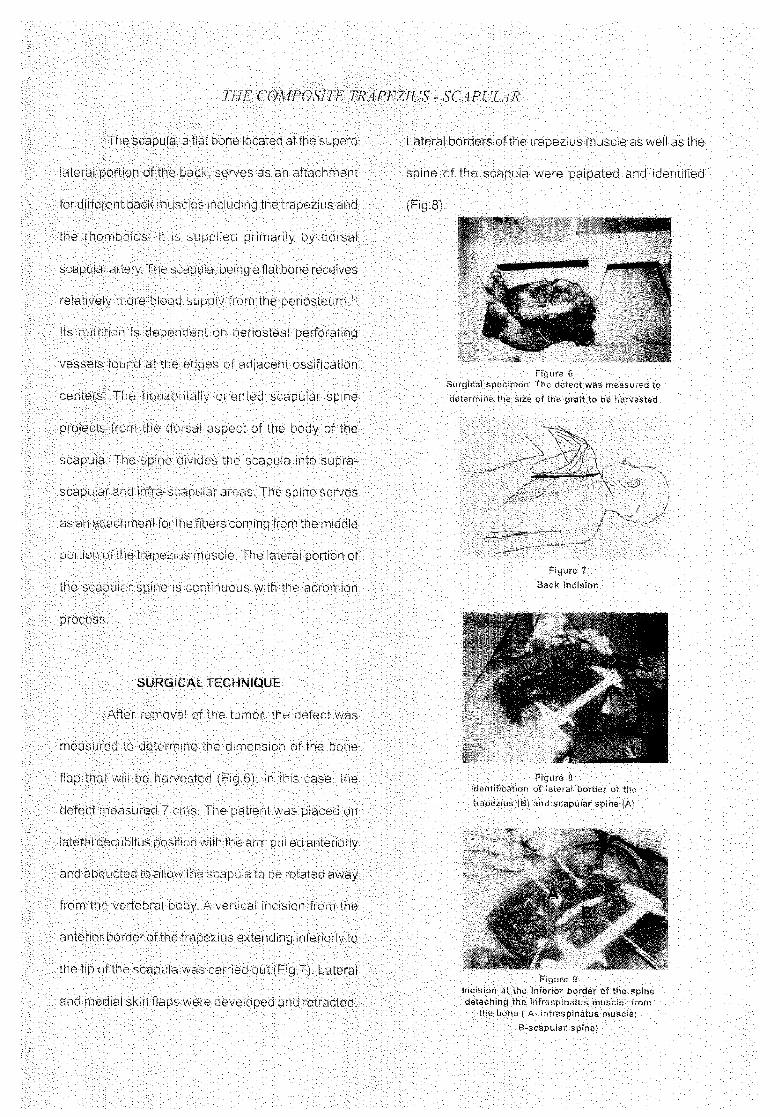


THE COMPOSITE TRAPEZIUS- SCAPULAR
attachment of the spine to the trapezius muscle. Usingvascularized corticocancellous bone for mandibular
blunt dissection, a skin tunnel was developed into thereconstruction. It does not only provide structural
neck and the flap was delivered through the tunnel tointegrity necessary to bridge the defect, but also
reach the mandibular defect(Fig 13). Multipleviable and immunocompatible osteoblastic cells, and
osteotomies were made on both cortices of the spine topleuripotential mesenchymal cells that can
facilitate contouring. The proximal portion of the spinedifferentiate into osteoblasts in the presence of
was attached to the condylar remnant using 2.4 mmmorphogenic proteins. 9 Owing to its vascular nature,
angled titanium mandibular plate and secured using 2this composite flap demonstrates increased rate of
titanium screws on each side. The distal segment ofhealing and graft incorporation. Among the
the spine was attached to the parasymphysis of the rightcomposite flaps, the trapezius spine flap has the
hemi-mandible using 2.4-ram straight titaniumhighest resistance to infection, making it a better
mandibular plate and secured using 2 titanium screwschoice for oromandibular reconstruction.
on each side(Fig.13). After determining the properAfter separation from the body of the scapula,
occlusion, mandibulo-maxillary fixation was achievedaccessory nutrient arteries coming from the trapezius
using Ivy loops. The trapezius muscle flap was securedmuscle will nourish the scapular spine? These
on soft tissues of the neck using chromic 3-0 suture toarteries penetrate the scapular spine at the fascial
prevent traction to the spine. The incision and the donorattachment of trapezius muscle to the spine. If the
sites were closed primarily, After adequate hemostasis,transverse cervical artery and vein is interrupted, such
separate suction drains were placed on the neck andas in irradiation and previous neck dissection, the
back. Mandibulo-maxillary fixation was maintained forflap can still survive based on paraspinous
six weeks, after the removal of which, regular diet wasperforators, with or without further blood supply
resumed.coming from the occipital artery(Fig.5). This event is
well documented by intravenous fluorescein perfusionDISCUSSION
studies. Vascularization of the pedicled trapezius
The pedicled trapezius osteomyofascialspine flap is also clearly demonstrated by extensive
composite flap using the scapular spine is a relativelyantibiotic incorporation by tetracycline labeling.
new technique for mandibular reconstruction. This isIn elevating the pedicled trapezius-spine flap,
the only pedicled flap [hat is able to transferPanje advocates the inclusion of at least three to four

theoveratlSi.iccess_ateWith:: :]

ALARVA III EZ AL.
Encyclopedia of Flaps, Vol. 1 1st Ed. LittleCONCLUSION Brown and Company, pg 508-11.
3. Ivy RH: Bone grafting for restoration of defectsThe pedicled scapular spine flap offers of mandible: a collective review. Plast Recons
Surg. 84:71,1989.an alternative viable source of autologous tissue for 4. Lindenmann A: Br Dent J, 38:201,1917.
5. McKee D: Microvascular bone transplantation.immediate reconstruction of mandibular defects Clin Plast Surg. 5:283,1978_
6. Dufresne C: reconstruction of mandible and floor
resulting from post ablative tumor surgery, particularly of the mouth defect with trapeziusosteomyocutaneous flap. Plast Reconstruct
those involving the anterior portion and the body of Surg, 1987 pg.687-95.7. Kenyeres Y: A new version of trapezius
the manaible. Because of the bulk oftrapezius muscle osteomyocutaneous flap for reconstruction ofthe lateral wall of the orbit and malar region.
that can be included in the flap, it can also be used to Plast Reconst Surg, 1984, Aug, 74:2,296-8.8. KrespiY: The rhombotrapezius myocutaneous
repair large soft tissue defects in the head and neck and osteomyocutaenous. Arch Otolar H and NSurg Vo1114, July 1988.
and cover the great vessels in region without 9. Arijan S: Neoplasms of head and neck. InJurkiewickz (ed.): Plastic Surgery Principles and
compromising the survival of the scapular spine flap. Practice Vol. 1,1990 CV Mosby Comp. pgs. 348-359.
As long as the periosteal attachment of the spine to 10. Gallrdo J., AM Chiong, VA Alarva II1: Theextended island trapezius myocutaneous flap:
the muscle is preserved, the survival of the composite Localization of the vascular pedicle based onFilipino cadaver dissection. Philippine Journal
flap is assured. Therefore, because of its independent of otolaryngology Head and Neck Surgery,1999.
and reliable vasculature, the trapezius spine flap is 11. Panje WR: Mandibular reconstruction withtrapezius osteomusculocutaneous flaps. Arch
an excellent choice for reconstructing mandibular and Otolaryn Vol 3, 1985 pgs. 223-29.12. Conley J : Use of composite flap containing bone
oral soft tissue defects, for major repairs in head and neck, Plast andReconst Surg, 1972; 49 : 522-26_
13. Shestak KC: JM Russavage. Scapular free flapREFERENCES and scapular osteocutaneous free flap. In Myers
(ed.) Operative Otolaryngology Head and Neck1. Llrken M: Oromandibular reconstruction. In Surgery, Vol 1,1999. WB Saunders pg.778-83.
Cumming's (ed.) Otolaryngology Head and 14. Eibling DE: Neck Dissection. In Myers (ed) :Neck Surgery Vol. 2 3rd ed. 1998. CV Operative Otolaryngology Head and NeckMosby pg. 1654-64. Surgery. Vol 1,1999. WB Saunders pg.778-83.
2. Panje WP: Trapezius 15. Tang YB : Pseudocystformation aftertrapeziusosteomusculocutaneous island flap for myocutaneous flap reconstruction :reconstruction of the floor of the mouth and management with chemical obliteration. Jmandible. In Strauch (ed.): Grabb's FormosaMedAssc_1995, Ju194:7, 435-7.
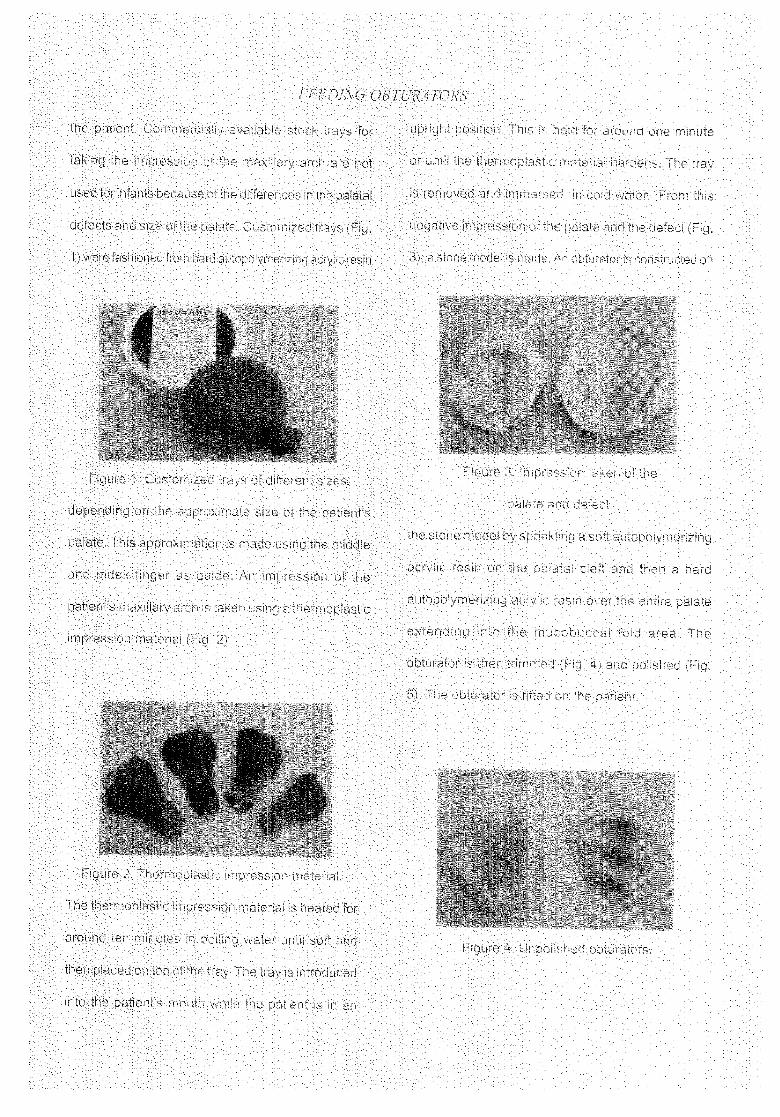
_ _:!_::iii::il_IIIi_i:i/ !_/!i_:!_I_/::_: : :: : i_: i_::.............. _,, , =.......(,,4_[ll_ t_,_:11__4_I(,-::............


FEEDING OBTURATORS
can be a hindrance for some parents. Also if thetime. This delay in the fitting of the feeding obturator
obturator do not seem to improve the appearance ofcan lead to poor nourishmer_t of the infant due to
their infant then some parents might not opt to comedifficult,./ in feeding and subsequent developmental
back. But first and foremost in the hindrance todelay (3). This can also lead to delay in surgical repair
of the palatal defect due to the nutritional deficiency, patient's follow-up is the economic factor. The cost of
the appliance if changed monthly would be a bigThere should be more information dissemination as
financial burden for most of the patients seen at ourto the timing of the application of the obturator
institution. Considering also that most of them comeespecially to the pediatricians who see the patients
from outlying provinces, then there would be the addedfirst even before the ENT specialist. They should be
cost of transportation to and from the hospital. If forinformed that prostheses can be safely used even by
the parents, the added benefits of the obturator donewborns and would be a benefit to their growth and
development, not outweigh the disadvantages then they will not
return for re4itting.There was also poor follow-up of the patients
noted (:32.5 % in 1999 and 31.5 % in 2000). In order
CONCLUSIONnot to interfere with the growth of the dental arch, the
border of the obturator must be trimmed regularly (9). AND
RECOMMENDATIONThe appliance is adjusted monthly to allow for maxillary
A process of fabricating the passive orthodonticgrowth (6). There could be a lot of factors for the poor
follow-up of the patients One factor could be feeding obturatorwas presented. There are numerous
satisfaction of the parents in the obturator in terms of ways of preparing feeding obturators. Some use
silicone as opposed to acrylic (9). Others use the Hotzdecrease in nasal regurgitation and increase in appetite
of the infant, retention of the prosthesis, care for the plate (10). Alpine et al advocated combined obturator
and palatal lift prosthesis (11). McKinstry suggestedprosthesis and added aesthetic appearance of the child.
The parents would be more disposed to bringing back pin and screw for added retention of the palatal
prosthesis especially for large defects (12). This methodtheir child for re-fitting if they see that there is an
of constructing the appliance was developed due toincrease in the amount of milk the child is taking in
the accessibility of the materials, ease in fabricatingand a gain in the patients weight. The added time
the appliance, good results noted as to retention,needed for the care and use of the feeding obturator

CASI21NEDA EZ A.L.
block in the milestones of normal development, can also be instrumental in the psychological and
Severe nutritional deficiencies further complicate social acceptance of the cleft palate patient (8)_
surgical closure at the right time ( 3).. A feeding
obturator is an intra-oral appliance which serves to OBJECTIVES
separate the oral cavity from the nasal cavity thus The objectives of this paper are as follows:
promoting betterdeglutition and mastication in a cleft 1. To describe the construction and
palate patient. Feeding obturators improve feeding maintenance of feeding obturators as
thereby contributing to weight gain and thriving state practiced in a Prosthesis Section of
of health, an important prerequisite for surgical repair a Department of Otorhinolaryngology
of the palatal defect (1), (ORL).
A second problem in cleft lip and palate 2. To determine the age offirst consult
patients is the protrusive and rotated premaxilla and follow-up behavior of the
especially in bilateral cleft lip patients which is caregivers of patients seen at a
challenging for the reconstructive team (4), Other Prosthesis Section.
deformities in cleft palate patients include 3. To identify the advantages and
malalignment of the alveolar arches which are often disadvantages of feeding obturators.
underdeveloped and are frequently collapsed in an
upward and inward direction (2). Feeding obturators METHODOLOGY
position the maxillary segments more ideally and then The list of patients was based on a Prosthesis
maintain their position while allowing growth to occur Section of a Department of ORL logbook entries from
(5). It encourages passive orthopedic guidance of Jan 1999 to October 15, 2000 and was compiled as
maxillary growth causing narrowing of the cleft and to number of patients seen per year, age of first consult
flattening of the steepness of the palatal slope (6). and number of patients with multiple follow-ups.
Furthermore, prosthetic intervention to rel3osition
segments before surgical correction may improve the The following steps were used in making the
bony base for tissue molding and avoid excessive feeding obturator per patient irrespective of the age of
tension at the surgical site (7). The aesthetic benefits

CASTANEDA E _I. AL.
decrease in nasal regurgitation and ease in care of Harker LA, Krause CJ, Schuller DE.
Otolaryngology-Head and Neck Surgery;the prosthesis. Further studies are in process to
3_'jEdition, 1998.
determine the above factors. 3. Nagda S, Deshpande OS, Mhatre SW.
A limitation of the study is [he deficiency of Infant Palatal Obturator. Journal of Indian
Social Pedontology and Preventivethe data from the records of the Prosthesis Section
Dentistry. 1996 March; 14 (1)24-5.
logbooks There could have been more patients seen 4. Figueroa AA, Reisbery DJ, Polley JW,
but not recorded. Some patients were logged in but Cohen M. Intraoral-appliance modification
to retract the premaxilla in patients withlacked in data such as age on consult. Dental stone
bilateral cleft lip. Cleft palate-Craniofacial
records were also noted to I)e incomplete since some Journal. 33 (6):497-500, 1996 Nov.
ofthem were damaged, des[royed or discarded during 5. Staggers J. Rigid-fixation palatal
appliances. Compendium of Continuingthe process of obturaLorfabrication.
Education in Dentistry (Jamesburg, NJ). 17
This is a preliminary study. As the census (9):902-7, 1996 Sept.
of the section increases, further studies can be made 6. Hochban W, Austermann Kt4. Presurgical
orthopedic treatment using hard plates.using the patients and data from this section.
Journal of Cranio-Maxillo-Facial Surgery.
Accurate and complete record keeping should be 17 Suppl, 1:2-4, 1989 Dec.
implemented in order- to rnaxirnlze the information 7. Wang RR. Thermoplastic resin used to
modify an alveolar orthopedic prosthesisgathered from the patients.
in a patient with cleft lip before
cheiloplasty:a clinical report. Journal of
Prosthetic Dentistry. 79(6):613-6, 1998REFERENCES
June., 1998
8. Abadi BJ, Johnson JD. The prosthodontic1.. Osunji OO. Preparaton of feeding
management of cleft palate patients..obturators for infants with cleft lip
Journal of Prosthetic Dentistry. 48(3):297-and palate. Journal of Clinical
302, 1982, Sept.
Pediatric Dentistry. 1995 Spring; 9. Chen HJ, Wang CH, Wang CC, Shieh TY.19(3): 211-4.
A modified technique of obturator fabrication2. Cummings CW, Fredrickson JM,

FEEDING OBTURATORS
for cleft palate infants. Kao Hsiung
I Hsueh Ko Hsueh Tsa Chih. 1990,
Oct.; 6(10); 546-50 (Abstract only)
10. Mishima K, Sugahara T, Mori Y,
Minami K, Sakuda M. Efeects of
presurgical orthopedic treatment in
infants with complete bilateral cleft
lip and palate. Cleft palate-
Craniofacial Journal. 35(3): 227-32,
1998, May.
11. Alpine KD, Stone CR, Badr SE.
Combined obturator and palatal-lift
prosthesis: a case report.
Quintessence International. 21 (11): t
893-6, 1990, Nov.
12. McKinstry RE. Pin and screw
retained palatal prosthesis in cleft
palate patients. Journal of Pedontics.
13(4):355-65, 1989, Summer. t

Phihppint_ ,hmrnal q/'¢ 2mlm_l-n_JOi()_¢vHe¢ld ¢_ Neck ,S'uq:CuO'
Vul, 16 NC, 2 99-11)6. ,:)2h(12 Philil_pine Society of (7)_olal_ngology I-Ietld & Neck Surgery
AN ENDOSCOPIC ADAPTOR FORDIRECT LARYNGOSCOPY WITH MICROLARYNGEAL SURGERY*
EFREN A. GUTIERREZ JR., MD**FERDINAND G. PAMINTUAN, MD***
ABSTRACT
Direct laryngoscopy remains the mainstay in the visualization of the larynx as well as performing other
surgical procedures on tile larynx. Often when microlaryngeal surgery or biopsy needs to be done, a rigid laryngoscope
together with an operating microscope is necessary. An alternative to this set-up is endoscopic microlaryngeal
surgery. However, the cost to put up this current set-up is overwhelmingly high. The nasal endoscope adaptor
provides a stable and yet economical alternative in doing endoscopic microlaryngeal surgery without hindering the
surgeon's maneuverability. Through the use of this adaptor, the need for an operating microscope is obviated.
..................................................................................................................................................................
INTRODUCTION sacrificing the full use of the surgeon's hands and at
With the ever-growing advances intechnology the same time providing a means of teaching students.
in the field of Medicine and Surgery, it is not surprising
that the costs of surgical instruments and equipment MATERIALS AND METHODS
continue to soar. These instruments and equipment The basic instruments used for Microlaryngeal
are used in the different operative procedures, surgery are the following (Fig. 1):
Microlaryngeal surgery is one of the most common
procedures done by an otolaryngologist _.The surgeon Rigid Karl Storz Adult Laryngoscope
however occasionally encounters difficulties especially Rigid laryngoscopes come in different
when an operating microscope is unavailable whether sizes for both adults and children. These scopes
the reason is technical or financial, provide an excellent view of the larynx even in difficult
The objective of this instrument conditions such as small oral opening and short, thick
design is to provide a cheaper yet stable alternative and stiff necks _,
to the use of the operating microscope without
*3rdPlace,PSOHNSPos[erSessiononSurgicalInstrumentation,November30,2000PuntaBaluarte,Calatagan,Batangas
**Resident,Departmentof Otorhinolaryngology,Sto.TomasUniversityHospital***Consultant,Departmentof Otorhinolaryngology.Sto.TomasUniversityHospital

G UTIERREZ .EJI AL.
Suspension bar and laryngoscope holder clip for the handle of the rigid laryngoscope was
These support devices provide stability to the fashioned from a hard stainless steel 0.05 mm plate.
laryngoscope,, The chest support can be placed The carrier was made from a flat stainless steel 0.039
directly over the thorax without affecting respiration, mm plate. These were then riveted together using
two flat spring stainless steel pegs.
0 degree Nasal endoscope with protective sheath
The nasal endoscope provides a magnified Endocscopic Camera System (optional)
view ofthe structures to be visualized. These come This system is hooked-up to the nasal
in different degrees or angulations as to provide varied endoscope so that the surgeon can view the image
views. Common ones are the 0, 30, 70, 90 and 120 through a television or monitor.
degrees. The protective metal sheath comes with
the nasal endoscope. The device was tested on two patients, one
with a vocal cord nodule (Fig. 3) and another one
Light source and cable with laryngeal squamous papillomatosis (Fig. 4). The
The light cable and light source provide first patient was given general anesthesia via
illumination, orotracheal intubation and the second one via
tracheostomy. The rigid laryngoscope was then
Microlaryngeal instruments inserted until the laryngeal inlet was visualized. The
These different instruments are necessary for laryngoscope was then suspended. Ordinarily, an
precision surgery of the larynx particularly when operating microscope with a 400 mm lens would be
operating on the vocal folds of the larynx,, used at this point for a more detailed anatomy of
the larynx. In this operation however, the procedure
Nasal Endoscope Clip (Fig. 2) was done endoscopically The adaptor was clipped
This simple adaptor was made from a metal to the handle of the laryngoscope together with the
sheet, It is designed to be clipped-on to the handle of protective sheath (Fig. 1 and B). A 0 degree nasal
the laryngoscope with the long end inserted through endoscope was then inserted in the sheath. 1
the scope. The long end has three holders for carrying Microlaryngeal surgery then proceeded as usual with
the protective sheath of the nasal endoscope. The no complications post-operatively. The views and

: : :
: :



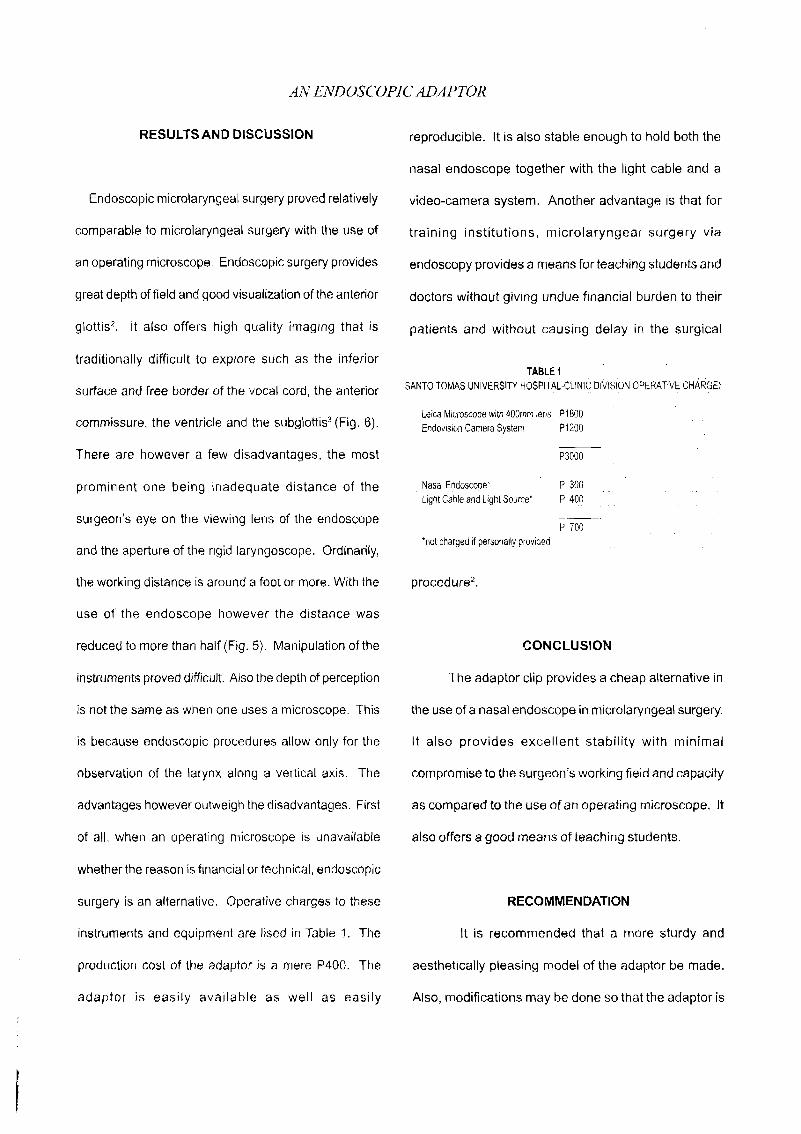
AN ENDOSCOPIC AI_APTOR
RESULTSAND DISCUSSION reproducible. It is also stable enough to hold both the
nasal endoscope together with the light cable and a
Endoscopic microlaryngeal surgery proved relatively video-camera system. Another advantage is that for
comparable to microlaryngeal surgery with the use of training institutions, microlaryngeal surgery via
an operating microscope. Endoscopic surgery provides endoscopy provides a means for teaching students and
great depth of field and good visualization of the anterior doctors without giving undue financial burden to their
glottis 2. It also offers high quality imaging that is patients and without causing delay in the surgical
traditionally difficult to explore such as the inferiorTABLE1
surface and free border of the vocal cord, the anterior SANTOTOMASUNIVERSITYHOSPI]:AL-CLINICDIVISIONOPERATIVEcHARGE_
LeicaMicroscopewith4OOmmler_s P1800
commissure, the ventricle and the subglottis _(Fig. 6). EndovisionCameraSystem P1200 : "
There are however a few disadvantages, the most P3000
prominent one being inadequate distance of the NasalE[_doscope_ P300 ....LightCablearidLightSource* P 400
surgeon's eye on the viewing lens of the endoscope P 700*notchargedif pe[sonallyprovided
and the aperture of the rigid laryngoscope. Ordinarily,
the working distance is around a foot or more. With the procedure 2.
use of the endoscope however the distance was
reduced to more than half (Fig. 5). Manipulation of the CONCLUSION
instruments proved difficult. Also the depth of perception The adaptor clip provides a cheap alternative in
is not the same as when one uses a microscope. This the use of a nasal endoscope in microlaryngeal surgery.
is because endoscopic procedures allow only for the It also provides excellent stability with minimal
observation of the larynx along a vertical axis. The compromise to the surgeon's working field and capacity
advantages however outweigh the disadvantages. First as compared to the use of an operating microscope. It
of all, when an operating microscope is unavailable also offers a good means ofteaching students.
whether the reason is financial or technical, endoscopic
surgery is an alternative. Operative charges to these RECOMMENDATION
instruments and equipment are lised in Table 1. The It is recommended that a more sturdy and
production cost of the adaptor is a mere P400. The aesthetically pleasing model of the adaptor be made.
adaptor is easily available as well as easily Also, modifications may be done so that the adaptor is

GUTIERREZ ET. AL.
made adjustable to the different sizes of rigid ACKNOWLEGEMENT
laryngoscopes. A longer scope such as a The author wishes to thank the advising consultant
cystoscope may also be used instead of a for his generous time and his support in the making of this
nasal endoscope so that the working space of paper. Likewise, to the residency staff most especially to
the surgeon is not minimized, the author's junior colleagues.
REFERENCES
1. Karl Storz - Endoskope, Endoscopes andInstruments for ENT, p. LA8
2. Bruce Benjamin, FRACS, Thirty-Five-MillimeterPhotography Using the Kantor-Berci VideoLaryngoscope, Annals of Otorhinolaryngology 107:1998, pp.775-778
3. Prof. Martin Andrea and Oscar Dias, RigidEndoscopy associated with Microlaryngeal Surgery(REMS)
4. Bruce Benjamin, O.B.E., Diagnostic Laryngology,1990
5. Jackson and Jackson, Bronchoesophagology,1950

o R,sor:T sARco.A NT.E.ALARAREA::: : ::::::: :: :A (,:A:SE:R" E.:PORT*:: : : .... ....
::: ..... : .... .... : :
::
:: :
:::ABSTRA:_::
: ,: ...::,.:"_:::"t_i_ii:i"w t: 7.i_:_,:;:i2q"esSv:6fea-tures Repeatec :_ _psesa '{ b & Estaii7g were incon-: : ckiS;_;i:e::1]::.)_if iiiii::ti_:hi:st<::ii:.._;i_:th:oio{::iV0f:i,{\lvco1;i:_1::S6iff;::o.Pat!t::Sarc0ma was:made:aft er:'PASand i1_7murlo-staininq, Wide:: ex:cisti(!;lfi0t!.i:.t.ie_:i;,t.laJi!t[::.1_::>_7evvas:perfb rmed wit:h:rei:onst:ructi0n tisin sy'nthe:tiCborle impJants (M:edpot"),Foilow-up
:: n::E:_:':_i'Vf:}."e:, 'viid 7 : is9?lsof ':,c :): :: :
: : Emb_'yo"_alRhabdomyOsarcoma(RB)versusIvlalignant
....... S,i_rC::0ma(::,i_SiiS):i:S:8ve_._#: F@:ousHist::iocytoma(MFH)oPASandblasso7-T"c7o77e: : :u..... : i,t:_re!_:,,t:,ltTlot"Wt:St(:h_S<}'J;t:'l,,,}{,__:rlEthql1_-1_1_,::'_,,DLt[ n lay ln_balJv stain were posit v:e
.... : L._.":I'"l:t_b,,ai',_.,nfol:a........:, ' ......: oF_lprotr:a:cted :: .... ........: : ht(::lOii:_,.ri!t:::pifi H&E: : CompUted:tomoqrapl:'iyreve,:._:ieda nodule on :
_._i.:::;:i_i:::iiiafstainh_q:ibrde:f:initedia@iosis{ : :: tt7eleft.malar:areawith bony erosionOfthe z.ygomatic ::A_:::! "i_dsutt:inuriderl:reatmenti_and :1 0os 7erlce, (:l'les:_.X-rayac otle_b ood w(!k.-ups
: ri:C_K_;:Wiliteqt:lir:_r_._oreextei,_sive:repe:_t:::were 7{ na :: .........< ' _*e_Ses 'lie a c t of.... .............[_ .,., _: , .....,, . [....... : ..... ,,,,, ...... ....... ....ca{_,::ii: andriTe _,arie:? _n-ttie:: : Figure l ; A×lal C I scar'l showu:_g malar mass : ::
t-n:,_]rff::ier:0iI: _.:i:./:_:=i:_dl:i:ii'_orld,::Sc.rv_.t:o Urid_4iinet!7_.): : : : ..... ........dii ii:l !_ii':iliiar::t:iases:itin:Ciin:i{:alqroi.:inds:::: : :
.......... ...... :i ....h/i::_l_e:i_:Se:i:lh ,f tJiesetumo's:
i
ii:_:di::i:erlceof i:i'iis:diaqnos;sartd provide a bas s fo" t 7e : : :..... _;:::ct 7:c_* {"ff::i:{-Y_:_"*,_eat 1 e 7tp :otOcoJs:..... : :: : ::: t _..t,.:,J:..... ......,:_ ,..:.-._.............. : :
: ......
..... i/{,,ii.t:h:a:rnasS_:iit:::l.hei_i2i:!i:n"l;:_l:i:,u"ai:eaoffive,yearsduratiOr/,:: :: : : : : :
....: "_ .............:....................." ...... "..... .....::FISI[OPATHOLOG_'] ::: t:w_"ii .....t-i_: :'__ei" -n_ teet tOtiqe S(7 ...... : .... :,.......... : 7ct::'i, de:::,v.!,:.:ti:! _t es "., e .T_asswas exc sed by ::" ' '


ALVEOLAR SOFT PART SARCOMA
Though these masses are more commonly inChildrenandAdolescents: ClinicalFeaturesandbenign, a suspicion of a malignancy is based on Outcome of 11 Patients.MEDICALPEDIATRICclinical behaviour which is usually confirmed by ONCOLOGY.26(2):81-4, 1996 FebnJary.microscopic examination of a biopsy specimen. 4. Jong Ret al. Alveolar Soft Part Sarcoma:Most common of the malignant tumors comprise Reviewof NineCasesIncludingTwoCaseswiththe rhabdomyosarcoma group followed byfibrosarcoma, liposarcoma, malignant fibrous Unusual Histology. HISTOPATHOLOGY.histiocytoma, hemangiopericytoma and 32(1):63-8,1998,January.malignant neurofibrosarcoma. 5. Flieder DBet al. Primary Alveolar Soft-PartSarcoma of the Mediastinum: A
Alveolar Soft-Part Sarcoma has been ClinicopathologicalandlmmunohistochemicalStudy of Two Cases. HISTOPATHOLOGY.
diagnosed in a very small percentage of cases of 31(5):469-73,1997, November.soft tissue tumors, and is rarely considered in the 6_ Ordonez NGandMackayB.AlveolarSoft-Partdifferential diagnosis. It is a true malignancy with Sarcoma: A Review ofthe Pathologyandthe capacity to invade surrounding tissues and tometastasize. However, it usually presents as an _. ULTRASTRUCTURALPATHOLOGY.indolent lesion with little or no involvement of its 22(4):275-92, 1998July-Augustsurroundings and is prone to be mistaken as benign 7. Nakano H. Alveolar Soft-Partlesion. Improper surgical manipulation may result Sarcoma:Histogenesis. ANTICANCERRES.not only in change of aggressiveness of the lesion 18(6A):4207-1 1, 1998 Novemeber toDecember.but alsodisruption of the tissue planesand possible & DeSautel Met al.AlveolarSoft-Part Sarcoma:seeding. Delay in adequate treatment may alsoensue. Most important is the failure to advise the Reportofa Case Occuring in the
Larynx.OTOLARYNGOLOGY-HEADANDNECKpatient on the severity of the disease,asthe survival SURGERY.117(6):$95-7, 1997 December.rates have been dismal in the few cases reported, 9. Lorigan, J.G., O'Keeffe F.N., Evans, H.L.,regardlessof clinicalbehavior. Wallace,S.The RadiologicManifestations of
Specialstains are required to demonstrate Alveolar Soft Part Sarcoma. AMERICANthe characteristic intracellular glycogen. Variable .EIJRNALOFRADIOLOGY.153:335-339,August1989.
immunoreactivityto S-100, musclespecificActin and 10. Rubenfield S. RadiationTherapy in AlveolarVimentin has been described in the literature.Soft Part Sarcoma. CANCER.28:577-580,
Histopathologic findings save for PAS-staining September,1971intracellular glycogen are not uniqueto ASPSalone
11. Evans, H.L. Alveolar Soft Part Sarcoma: Aandmust be correlated with clinical evidence.Study of 13 TypicalExamplesandOnewith aHistologicallyAtypical Component. CANCER.
With the few casesof ASPSreported so far, 55:912-917,1985.it is difficult to pinpoint identifying characteristics inthe clinicalhistory and physicalfindings.Surgery still ] 2. I ieberrnan,P.H.,Brennan,M.F.et al. Alveolarappears to be the treatment modality of choice in Soft PartSarcoma:A Clinico-PathologicStudy
of Halfa Century. CANCER.63:1-13, 1989.the literature and the case presented hasremained 13. Auerbach H.E.andBrooks, J.J.Alveolar Softtumor free after two years with minimalcosmetic or Part Sarcoma: A Clinicopathologic andfunctional derangements.Resectabilitywas the best immunohistocheicalStudy. CANCER.60:66-prognosticating factor in the literature. Increased 73, ] 987.awareness of ASPSwill hopefully allow more casesto be properly identified, and as experience with 14. CastilloM, Lee Y, YamasakiS. Infratemporalthese malignanciesexpands, aproper diagnosticand Alveolar Soft Part Sarcoma: CT, MRI and
Angiographic Findings. NEURORADIOLOGY.treatment protocol may be arrived at. 34(5):367-369.1992.
15. CetikF, Ozsahinoglu C, Kivanc F, Secinti E.
REFERENCES Alveolar Soft Part Sarcoma of the Tongue.Joumalof LaryngologyabdOtology.103 (10):
1. SOFTTISSUETUMORS.929-936, 1992. 952-954,Oct1989.1G SimmonsWB,Haggerty HS,NganB,Anonsen2. Hunter BCet al. Alveolar Soft Sarcoma of
CK. Alveolar Soft Part Sarcomaof the headthe Head and Neack Region. ANNUAL OF
and Neck. A Disease of Children and YoungOTOLOGY, RHINOLOGY ANDAdults. INTERNATIONAL JOURNAL OF
LARYNGOLOGY.107 (9Ptl):810-4, 1998September. PEDIATRICOTORHINOLARYNGOLOGY.

LICUP ET. AL.
3. Pappo AS et al. Alveolar Soft Part Sarcoma17(2);139-153, May 1989.
17. Rubenstein MI, Drake AF, McClatchey KD.AlveolarSoft PartSarcomaof the NasalCavity:Report of a Case and a Review of theLiterature. LARYNGOSCOPE.98 (11 ); 1246-IZ50Nov.1998.
18.DonaldPJ.AlveolarSoftPartSarcomaoftheTongue.HEAD AND NECKSURGERY9(3):172-178Jan1987.
19.KingW, FeeWE Jr.AlveolarSoftPartSarcomaof the Tongue. AMERICAN JOURNAL OFOTOLARYNGOLOGY.4(5):363-366,Sep.1983.
20.SpectorRA,TravisLW,SmithJ.AlveolarSoftPart Sarcoma of the Head and Neck.
LARYNGOSCOPE. 89 (8):1301-I306,Aug1979.

Philil_pine dourtlal o/'O._lat.wngoloKv Head & Neck Sul_eEv
VOl, 16 No. 2 113-117. _)2002 Philippine Society ofOtolaryngology IIead & Neck Surgery
A FLOOR OF THE MOUTH YOLK SAC TUMOR INAICARDI SYNDROME: A CASE REPORT*
MARY JANE C. TIPAYNO, M.D.**
ABSTRACT
Objectives:To present a rare case of yolk sac tumor inthe oral cavity of an infant diagnosed of the extremely rare congenitaldisorder of Aicardi Syndrome.To review the differential diagnoses of sublingual masses in the infant.To present options in the management of extragonadal yolk sac tumors.
Design: Case Report
Setting: Tertiary Hospital
Patients: One year old patient with sublingual mass
Results:
Afloor-of-the-mouth endodermal sinus (yolk sac) tumor (EST-YST) in a previously diagnosed case of Aicardi syndromeis reported. The patient is a one-year-old girl exhibiting a rapidly growing tumor in the sublingual and floor of themouth regions.
The lesion showed the typical microscopic features of YST including Schiller-Duval bodies. Alpha fet0proteinimmunoreactivity was expressed by the representative specimen slides. There was no clinical or ultrasonographicevidence of the presence of this tumor elsewhere in the body.
Conclusion:
The association of YST and genetic or environmental factors is little known except for its increased risk in Klinefelterand Swyer Syndrome. To date, no local or international literature has been published on the association or coexistenceof a yolk sac tumor in Aicardi sydrome. This may be the first reported case of a yolk sac Tumor in Aicardi syndromeworldwide.
Hemangiomas, ranula and dermoid cysts are the more common childhod tumors in the oral cavity, however aphysician should not discount a potential malignancy especially in cases where a coexisting congenital disorder ispresent.
Experts of pediatric oncology recommend total excision of primary tumor whenever possible and chemotherapy ishighly recommended. This case is however compounded by an existing congenital disorder that magnifies the risksinvolved with the standard management. Supportive therapy maybe the most humane management option.
* Presented,PSO-HNSClinicalCaseReportContest,October24,2000,EDSAShangri-LaHotel,MandaluyongCity
**Resident,BaguioGeneralHospital

TIPAYNO ET. AL.
INTRODUCTION diagnostic procedures, it was revealed that she wassuffering from microphthalmia, anisocoria and
Yolk sac tumors are malignant tumors that chorioretinal coloboma all on the left eye; agenesis ofoccur in the gonads of children and young adults and the Corpus Callosum, hemi vertebrae andat extragonadal sites in young children. Extragonadal dextroscoliosis; and a general seizure disorder notedlesions in the head and neck apart from the CNS are by EEG. After thorough evaluation, she was diagnosedhowever rare. with Aicardi Syndrome by certified pediatricians.
This is the first reported case of a Yolk Sac Family HistoryTumor in Aicardi Syndrome patient based on Medline Both parents were 46 years old during patient'ssearch, conception; healthy, unrelated by consanguinity. The
patient is the youngest among eight siblings of fourboys and four girls. Two of the male siblings had cleftpalate. The first male sibling died of severe pneumonia.
CASE REPORT No historyof malignancy was extracted from the lineageand there was no known blood relatives with similar
General Data signs and symptoms presented by the patient.This isthe case ofV. P., a one-year-old female
from Balsigan, Baguio City admitted for the second Physical Examinationtime inour medical center on February 8, 2000 due to On admission, the patient was awake, active,a left sublingual mass. in moderate respiratory distress with the fotlo_ng vital
signs: cardiac rate of 106/min, respiratory rate of 32/History of Present Illness min, body temperature of 37 deg. C., weight of 8.2kg
Five days prior to admission, the patient had (p25-50), length of 61 cms (-3sd), head circurrfferencemanifestations of fair oral intake, fever by palpation and 43 cms (p25), and chest circumference of 44 cms. (P10).a watery nasal discharge. Three days prior to She was normocephalic with closed fontanels, stillwithadmission, there was onset of stridor along with a sparse hair, grossly normal right eye, left microphthalmianotable pinkish, glistening mass on the left sublingual with anisocoria. There was an intact extraocular musclearea. A consult was made with the ENT-OPD, which movement on the right while the left was inferomediallyprompted subsequent admission, deviated. External ears were grossly normal with patent
auditory canals; tympanic membranes were intact withPerinatal History no discharge. The oral cavity showed elevation of the
She was born to a 46-year-old mother with an leftantero-lateral area of the tongue due to an underlyingOB score of G12P9 (9-0-3-8) and who had no previous bright pink glistening mass that extended to the floor ofhistory of viral infection, drug intake or exposure to the mouth. The mass approximated a size of 1.7 cmsradiations_ The patient was hospital- borne, by normal x 2cms x 3cms. There were no other palpable massesspontaneous delivery, term, with a good Apgar score, noted at the oral cavity and neck regions.
DevelopmentaIHistory Chest examination showed suprasternalThe smile was spontaneous at age one-month, retraction, symmetrical chest expansion with harsh
She was fully capable of moving her head from side to breath sounds. Heart findings revealed the point ofside and follows moving objects at 2 months. At 3 maximal impulse at the left 4th intercostal space withmonths she had a good head control, however, no further distinct heart sounds of regular rhythm and normal rate.sociopsychomotordevelopmentwasobservedfromthis The abdomen was soft, with no palpable mass ortime onwards, organomegaly. There was a grossly female genitalia.
No deformities of the extremities were seen and sheFeeding History had good muscle bulk, full pulses and acyanotic nail
She was breastfed from birth on a per demand beds.basis up to three months when formula feeding wasintroduced with good acceptance. Pertinent neurological examination revealed the
right pupil to be 2-3mm reactive to light; the left pupilPast Medical History was 3-4 mm and non-reactive to light. Extraocular
Nine months prior to admission, she movement was full on the right with inferomedial deviationmanifested upward rolling of eyeballs and ontheleft. There was shallowing of the left nasolabialhyperextension of both upper and lower extremities, fold on crying. All extremities had a motor grading of 5/This lead to her first admission to the medical center. 5. No nystagmus was appreciated; swallowing and gagAfter thorough physical examinations and a battery of


TIPAYNO ET. AL.
Aicardi syndrome is a rare genetic disorder REFERENCESdiscovered by a French neurologist Dr. Jean Aicardi in1965. This syndrome presents with the clinical tetrad of 1. Kusumakumari P, Geetha N, Chellam VG, Nairagenesis of corpus callosum, infantile spasms, MK:MedicalPediatricOncology19.Oct;29(40);chorioretinal lacunae and mental retardation. All of which 303-7.
were present in our patient. The number of identified 2. Lack, EE: Human Pathology 1985 Jan; 16(1):cases of girls is approximately 300-500 worldwide, 56-64.females mostly affected with lethality in hemizygous 3. Dexeus FH, Logothetis C J, Chong C, et al.:males. The treatment is primarily supportive and Genetic abnormalities in men with germprognosis varies. It affects ages from birth to mid-20s, celltumor. Joumal of urology 140(10:80-84) 1998.
4. Nichols CR, Heerema NA, Palmer C, et al.:A variety of uncommon benign and malignant Klinefelter's syndrome associated with
tumors have been associated with Aicardi syndrome, mediastinal germ cellThese are Choroid plexus papilloma with gastric 5. Lachman MF, Kim K, Koo BC: Mediastinalhyperplasic polyps described by Trifeletti et al. (1995), teratoma associated with Klinefelter's syndrome.scalp lipoma with cavernous hemangioma of the leg Archives of Pathology and Laboratory Medicinereported by Tsao et al. (1993) and the only oral cavity 110(11): 1067-1071,1986.tumor was that of Kiristioglu et al. (1999) who reported 6. CoutinAS, HamyA, Fondevilla M, etal.: Pureof a palatal hemangioma in a one day old female. No 46XY gonadal dysgenesis. Journal dereport of an YST in Aicardi Syndrome has yet been made Gynecologie, Obstetrique et Biologie de lafrom the available English medical literature reviewed to Reproduction (Paris) 25(8): 792-796, 1996.date. 7. Amice V, Amice J, Bercovici JP, et al.: Gonadal
tumor and H-Y antigen in 46,XY pure gonadalA treatment protocol released by both the dysgenesis. Cancer 57(7): 1313-1317, 1986
Pediatric Oncology Group and the Children's cancer 8. Hawkins EP, Finegold MJ, Hawkins HK, et al.:group on Yolk Sac Tumors recommends a complete Nongerminomatous malignant germ cell tumorsexcision of the primary tumor whenever possible, in children: a review of 89 cases from theDebulking procedures only may be appropriate with Pediatric Oncology Group, 1971-1984. Cancer
Planned secondary procedure for delayed excision 58(12): 2579-2584, 1986.following chemotherapy. 9. Marina N, Fontanesi J, Kun L, et al.: Treatment
of childhood germ cell tumors: review of the St.The outcome of children with malignant Jude experience from 1979 to 1988. Cancer
extracranial germ cell tumors was poor before the advent 70(10): 2568-2575, 1992.of effective chemotherapy. Although children with 10. Kurman RJ, Norris HJ: Endodermal sinustesticular tumors did well with surgical resection.8.9 for tumor of the ovary: a clinical and pathologicmost patients 3-year survival rates were 15% to 20% analysis of 71 cases. Cancer 38(8): 2404-with surgery and/or radiation therapy-10-12Chemotherapy 2419, 1976.has dramatically improved the outcome for these 11. Chretien PB, Milam JD, Foote FW, et al.:patients, with 5-year survival rates increasing to 60% to Embryonal adenocarcinomas (a type of90%. 9._.14The standard chemotherapy regimen for both malignant teratoma) of the sacrococcygealadults and children with malignant nonseminomatous region: clinical and pathologic aspects of 21germ cell tumors includes cisplatin, etoposide, and cases. Cancer_26(3): 522-535, 1970.bleomycin (PEB) at one cycle per month for four cycles 12. Billmire DF, Grosfeld JL: Teratomas inchildhood:1s.19.The combination of carboplatin, etoposide, and analysis of 142 cases. Journal of Pediatricbleomycin is also used for pediatric patients 20-21. Surgery_21(6): 548-551,1986.
The decision of patients or parents to refuse 13. Ablin AIR, Krailo MD, Ramsay NK, et al.:tumor extirpation in the oral cavity is largely on account Results of treatment of malignant germ cellof the inevitable sacrifice of essential functions of normal tumors in 93 children: a report from the
swallowing and speech not to mention the deformities it Children's Cancer Study Group. Journal ofleaves behind. On the other hand, the adverse effects of Clinical Oncology_9(10): 1782-1792, 1991chemotherapy remain a prime stumbling block in its 14.. Mann JR, Pearson D, Barrett A, et al.: Resultsuse among infant patients. Non-conformation to the of the United Kingdom Children's Cancer Studystandard treatment protocol may prove a wiser decision, Group's malignant germ cell tumor studies.keeping guard and addressing symptoms as they come Cancer 63(9): 1657-1667, 1989.has been the best choice in this case. 15. Gershenson DM, Morris M, Cangir A, et al.:

A FLOOR OF 17t£ MONTH YOLK SAC
Treatment of malignant germ cell tumors ofthe ovary with bleomycin, etoposide, andcisplatin. Journal of Clinical Oncology 8(4):715-720, 1990.
16. Williams SD, Birch R, Einhorn LH, et al.:Treatment of disseminated germ-cell tumorswith cisplatin, bleomycin, and eithervinblastine or etoposide. New England Journalof Medicine 316(23): 1435-1440, 1987.17.Nichols CR, Williams SD, Loehrer PJ, et al.:Randomized study of cisplatin dose intensityin poor-risk germ cell tumors: a SoutheasternCancer Study Group and a SouthwestOncology Group protocol. Journal of ClinicalOncology 9(7): 1163-1172, 1991.
18. Cushing B, Giller R, Marina N, et al.: Resultsof surgery alone or surgery plus cisplatin,etoposide and bleomycin (PEB) in childrenwith localized gonadal malignant germ celltumor (MGCT): a pediatric intergroup report(POG9048/CCG8891). Proceedings of theAmerican Society of Clinical Oncology16:A1840, 511a, 1997.
19. Cushing B, Giller R, Lauer S, et al.:Comparison of high dose or standard dosecisplatin with etoposide and bleomycin(HDPEB vs PEB) in children with stage I-IVextragonadal malignant germ cell tumors(MGCT): a Pediatric Intergroup report(POG9049/CCG8882). Proceedings of theAmerican Society of Clinical Oncology 17:A2017, 525a, 1998.
20. Pinkerton CR, Broadbent V, HorwichA, et al.:'JEB'--a carboplatin based regimen formalignant germ cell tumors in children. BritishJournal of Cancer 62(2): 257-262, 1990.
21. Mann JR, Raafat F,etal. on behalf of the UnitedKingdom Children's Cancer Study Group:UKCCSG's germ cell tumor (GCT) studies:improving outcome for children with malignantextra cranial non-gonadal tumors--carboplatin, etoposide, and bleomycin areeffective and less toxic than previous regimens.Medical and Pediatric Oncology 30(4): 217-227, 1998.
22. Kiristiologo I; Kilic N; GurpinarAN; DugroyulH.European Journal of Pediatric surgery 1999Oct; 9(5): 325-6.
23. Trifiletti RR; Incorpora G; Cocuzza MD; BolanEA; Paramano E. Brain development 1995July-August; 17(4): 283-5.
24, Tsao C.Y.; Sommer, A.; Hamoudi, A.B.-AicardiSyndrome, metastatic angiosarcoma of theleg, and scalp lipoma. Am. J.Med.Genet.45;594-596,1993.

The Philippine Journal of Otolaryngology Head and Neck Surgery
Founded in 1981
Editor-in-chief Previous Editors
Charlotte M. Chiong, MD Angel E. Enriquez, MD - 1981 to 1988Eusebio E. Llamas, MD - 1989
Alfredo Q.Y. Pontejos, Jr., MD - 1990Joselito C. Jamir, MD - 1991-1998Jose M. Acuin, MD - 1999 - 2000
Senior Associate Editors
Abner L. Chan, MDJesus Randy O. Canal, MD
Managing Editor
Rhodora A. del Rosario-Ocampo, MD
Associate Editors
Roberto M. Pangan, MD, DMD, PhD, Oral and Maxillofacial SurgeryRuzanne M. Caro, MD, Clinical EpidemiologyGil M. Vicente, MD, Rhinology
Eduardo C. Yap, MD, General OtolaryngologyNatividad A. Almazan-Aguilar, MD, Otology
Cecilia Gretchen S. Navarro-Locsin, MD, Pediatric OtolaryngologyMa. Clarissa S. Fortuna, MD, Laryngology
Cesar V. Villafuerte Jr., MD, Facial Plastic Surgery
EDITORIAL ADVISORY BOARD
Joselito C. Jamir, MD, Laryngology and BronchoesophagologyGeneroso %Abes, MD, Otology
Mariano B. Caparas, MD, Maxillofacial SurgeryEutrapio S. Guevara, Jr., MD, Facial Plastic Surgery
Adonis B. Jurado, MD. Pediatric OtolaryngologyDominador M. Almeda, Jr., MD, NeurotologyAlfredo Q.Y. Pontejos, Jr., MD, Head and Neck Surgery
Editorial Assistant: Melody T. Francisco