Responsiveness of the Neck Disability Index in patients with mechanical neck disorders
Upload
independentCategory
view
1download
0
S
J
CcCTabTbat
Abhmwi
AD
M7
1
urgery of Melanoma of the Head and Neck
effery N. Myers, MD, PhD,1 and Hernan E. Gonzalez, MD, PhD2
fdels2wituaitwabtsdtgdTawsan
utaneous malignant melanoma (CMM) is an aggres-sive malignancy with an incidence rate that is in-
reasing by 5% each year. In about 30% of patients withMM, the primary site is located in the head and neck.he surgical management of CMM of the head and neck,s for other locations, is aimed to achieve disease control,oth at the primary site and of the regional lymphatics.herefore, detailed knowledge of factors that determineiologic behavior (ie, histologic type, depth of invasion,nd ulceration) and patterns of regional spread are essen-ial for proper surgical planning.
MANAGEMENT OF THEPRIMARY LESION
lthough the adequate width of resection for CMM haseen widely debated, surgical removal of CMM from theead and neck region is limited by the significant cos-etic and/or functional disabilities that result from veryide local excisions. In general, for thin (�1 mm) and
ntermediate thickness (1-4 mm) lesions located on the
From the 1Department of Head and Neck Surgery, The University of Texas MDnderson Cancer Center, Houston, TX; and 2Section of Head and Neck Surgery–ivision of Surgery, Pontificia Universidad Catolica de Chile, Santiago, Chile.Address reprint request to Jeffery N. Myers, MD, PhD, The University of TexasD Anderson Cancer Center, 1515 Holcombe Blvd, Unit 441, Houston, TX,
7030.© 2004 Elsevier Inc. All rights reserved.1524-153X/04/0602-0008$30.00/0doi:10.1053/j.optechgensurg.2004.05.003
24 Operative Te
ace, we recommend at least a 1-cm margin. For interme-iate thickness melanomas of the scalp and neck, thextent of the resection can be increased to 2 cm, particu-arly if there are adverse features such as ulceration oratellite lesions. For lesions greater than 4 mm, we favor-cm margins. For the depth of resection of thin lesions,e include a deep margin of subcutaneous tissue. For
ntermediate thickness lesions, depending on the loca-ion, we include all the subcutaneous tissue down to thenderlying fascia. In the scalp, we leave the galea intact tollow for skin grafting. For melanomas greater than 4-mmn thickness, depending on the location and greatesthickness, resection of the underlying facial muscles asell as the galea and pericranium may be necessary to
chieve a safe deep margin. After proper resection haseen achieved, the surgeon must determine the status ofhe surgical margins. In general, in pigmented lesionsuch as lentigo maligna, the true surgical margin can beifficult to determine on frozen sections; therefore, weend to perform reconstruction with a split thickness skinraft or leave the wound temporarily open and perform aefinitive reconstruction at a second stage, if necessary.he several alternatives for reconstruction of the defectsre beyond the scope of this article; however, in generale favor simple primary closure or rotation flaps, if pos-
ible. Split thickness skin grafting is also an excellentlternative for certain areas of the forehead, scalp, andose.
chniques in General Surgery, Vol 6, No 2 (June), 2004: pp 124-131

1aAlofirmajCP
125Surgery of Melanoma of the Head and Neck
MANAGEMENT OF THE REGIONAL LYMPHATICS
Although the lymphatic system of the head and neck is complex, regional spread to lymph nodes in general can be predictedccurately. Hence, the levels of lymph nodes to remove can be planned accordingly, depending on the location of the primary lesion.lthough elective neck dissection for the clinically negative neck is still an option for patients with intermediate thickness (1-4 mm)
esions, we favor radiotherapy or sentinel lymph node biopsy. In our opinion, the only formal indication for neck dissection in CMMf the head and neck is the presence of clinically or radiographically positive lymphadenopathy. Dissection comprises at least therst and second predicted echelons if it is an elective procedure, or one echelon beyond the location of nodal metastasis. If surgicalesection is the choice for a midline lesion, the neck dissection should be bilateral. Unless there is extensive disease involvingultiple levels or large lymph nodes, we perform selective neck dissections and preserve the sternocleidomastoid muscle, spinal
ccessory nerve, and internal jugular vein. Finally, because melanoma is a skin cancer, superficial nodes (buccal and externalugular vein nodes) should not be overlooked, and should be removed when indicated. (Used with permission from Byers RM:ervical and parotid node dissection, in Balch CM, Houghton AN, Milton GW, et al (eds): Cutaneous Melanoma (ed 2).hiladelphia, PA, JB Lippincott, 1992.)
2ipAitmpd
126 Myers and Gonzalez
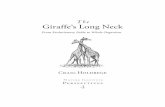
A patient with a 3-mm-thick melanoma located in the temple area, with adenopathy in the parotid gland. In this case, thencision is designed to allow continuity of resection with the primary lesion, given its close location to the first echelon (A). Therimary lesion is removed initially with a 2-cm margin, with a depth of resection carried down to the superficial temporal fascia. (B)superficial parotidectomy is performed that identifies and preserves the facial nerve and each of its branches. The white arrow
ndicates the main trunk of the facial nerve where it divides at the pes anserinus. A selective neck dissection is performed to removehe contents of levels II, III, and IV, and spare all the nonlymphatic structures. The star (�) indicates the sternocleidomastoiduscle, which is retracted posteriorly. The arrowhead indicates the spinal accessory nerve (cranial nerve XI) as it emerges below the
osterior belly of the digastric muscle. The arrow indicates where the internal jugular vein passes medial to the posterior belly ofigastric muscle.
3pi(
127Surgery of Melanoma of the Head and Neck
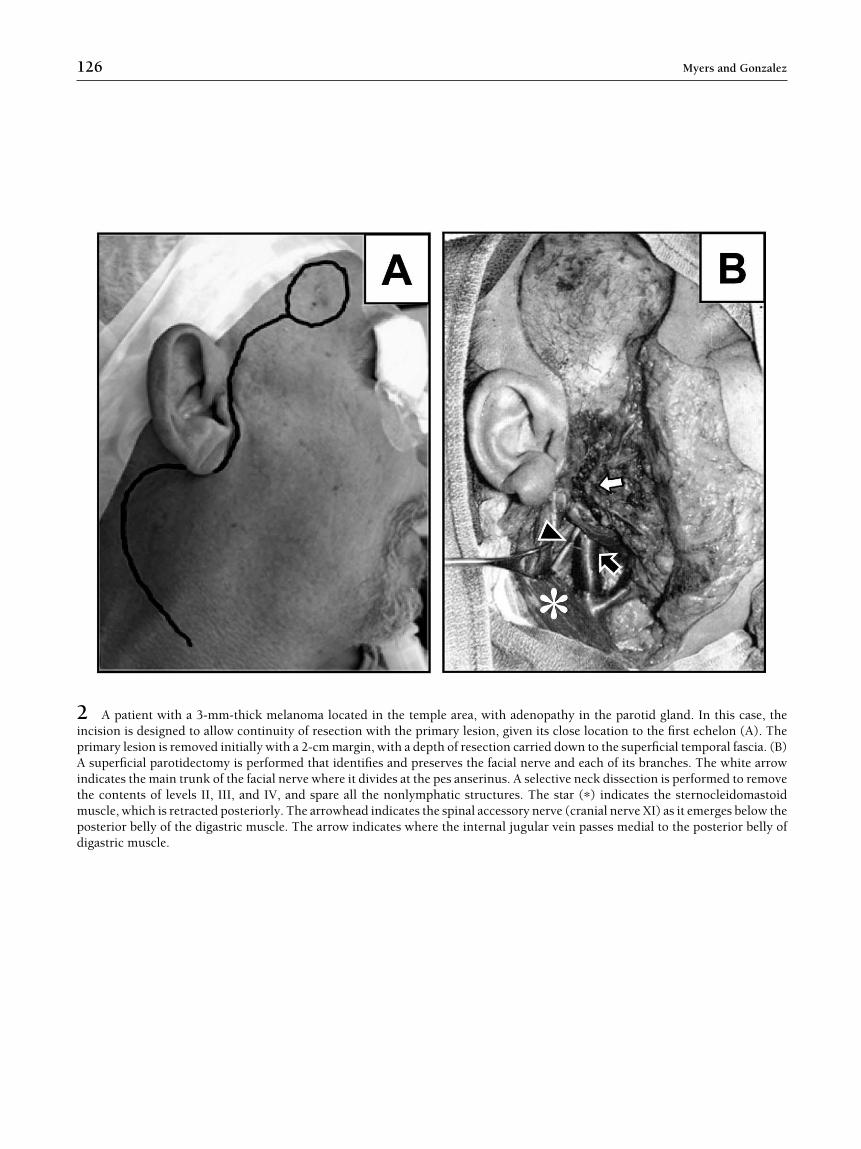
The approach for a 2.3-mm melanoma located on the posterior scalp for which the incision of the neck is tailored to include therimary lesion (A). In this case, a posterolateral neck dissection is performed to remove the suboccipital and retroauricular nodes
n addition to levels II-V. (B) Upon completion of the dissection, the trapezius muscle (�) is identified and the spinal accessory nerve
arrowhead) followed inferiorly to the trapezius muscle, which it innervates. The arrow indicates the internal jugular vein.
S
SpttiwAn
fpnwqopSb
4maio
128 Myers and Gonzalez
entinel Lymph Node Biopsy
entinel lymph node biopsy (SLNB) is based on therinciple that the sentinel lymph node is the first nodeo receive drainage from the primary tumor and isherefore at highest risk for metastasis. This procedures a staging procedure wherein patients are selectedho would potentially benefit from further treatment.lthough SLNB for melanoma arising in the head and
eck region has been shown to be feasible, long-term sbtained.
ollow-up showing that a negative SLNB accuratelyredicts the absence of microscopic metastasis in theeck is lacking. Therefore, our present use of SLNB isithin a prospective protocol designed to address thisuestion. Our protocol includes the following: (1) pre-perative lymphocintigraphy; (2) intraoperative lym-hatic mapping with a radiotracer; (3) separation of theLN from its basin ex vivo; and (4) histologic analysisy hematoxilin-eosin and immunohistochemistry of
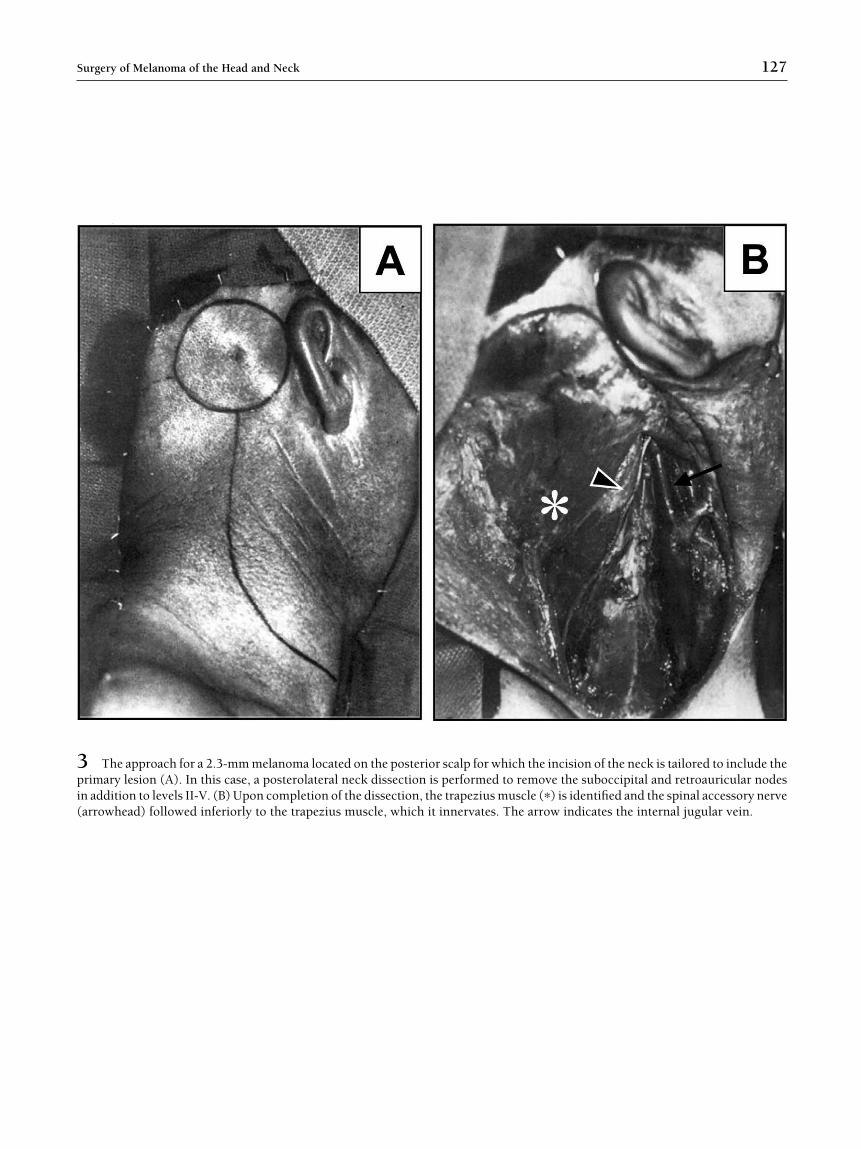
erial sections of the lymph nodes.(A,B) Preoperative lymphoscintigraphy scan of a patient with a 1.6-mm CMM of the skin overlying the left malar area. Oneilliliter of technetium-99 labeled sulfur colloid is injected around the periphery of the biopsy scar in a 4-quadrant fashion. Usinggamma camera with a low-energy, high-resolution collimator, dynamic images of the head and neck are taken 15 minutes after
njection and every 30 minutes thereafter until the SLN is visualized. At this point, transmission images of the head and neck are
5loiw(
129Surgery of Melanoma of the Head and Neck
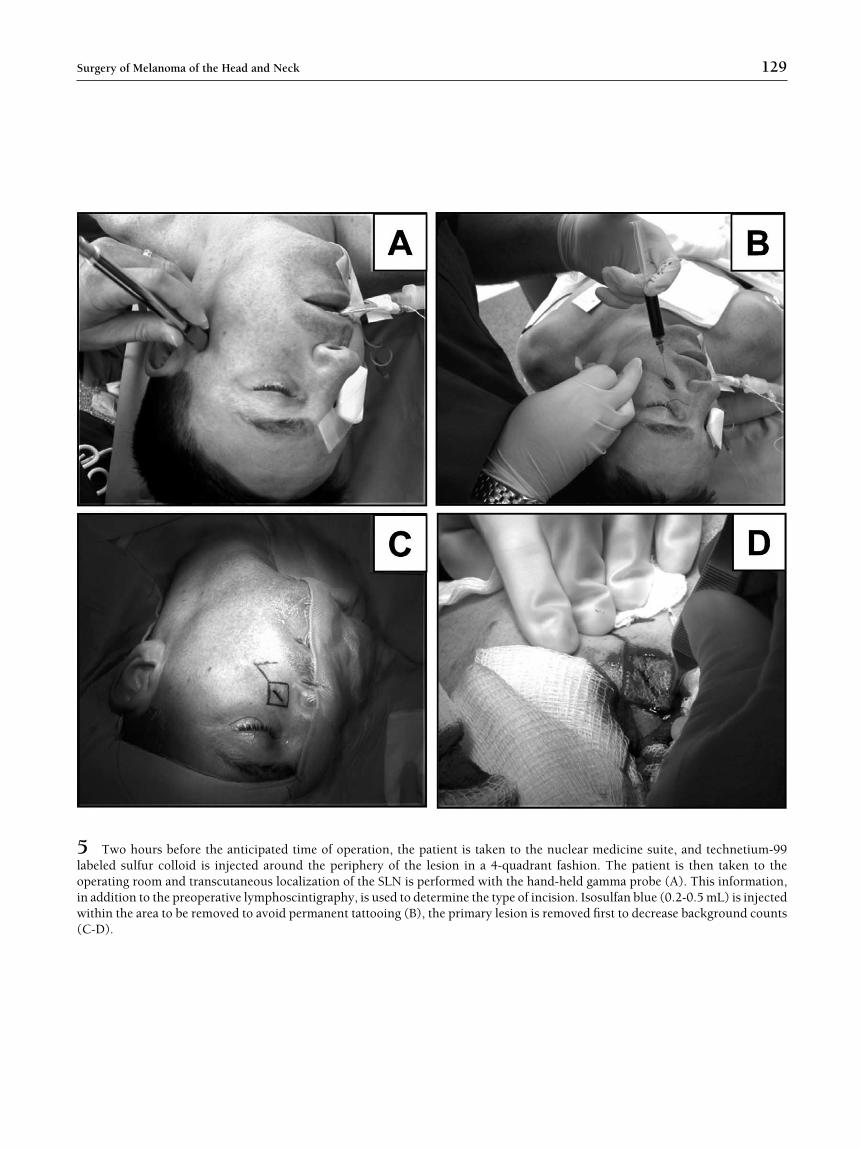
Two hours before the anticipated time of operation, the patient is taken to the nuclear medicine suite, and technetium-99abeled sulfur colloid is injected around the periphery of the lesion in a 4-quadrant fashion. The patient is then taken to theperating room and transcutaneous localization of the SLN is performed with the hand-held gamma probe (A). This information,n addition to the preoperative lymphoscintigraphy, is used to determine the type of incision. Isosulfan blue (0.2-0.5 mL) is injectedithin the area to be removed to avoid permanent tattooing (B), the primary lesion is removed first to decrease background counts
C-D).

6ohrcdsbn
130 Myers and Gonzalez
In this patient, a subplatysmal skin flap is elevated (A, arrows) and the greater auricular nerve (B, arrow) preserved as it passesver the sternocleidomastoid muscle. The sentinel lymph node is identified either by concentration of radiolabeled colloid with theand-held gamma probe (C) or by direct visualization of the blue dye-stained node. Each SLN is resected and ex vivo countsecorded. If the SLN cannot be directly identified because of its small size, encasement in fibro fatty tissue, or other factors, theomplete lymph node level is excised and the SLN identified ex vivo. As part of our protocol, we perform a comprehensive neckissection that includes all the predicted lymph nodes at risk. (D) A neck dissection is performed. The arrowhead indicates thepinal accessory nerve, the white arrow indicates the internal jugular vein, and the black arrow indicates the anterior and posteriorellies of the digastric muscle. Given the risk of damaging critical structures such as the spinal accessory, hypoglossal, or facial
erves, among others, we do not recommend “node plucking.”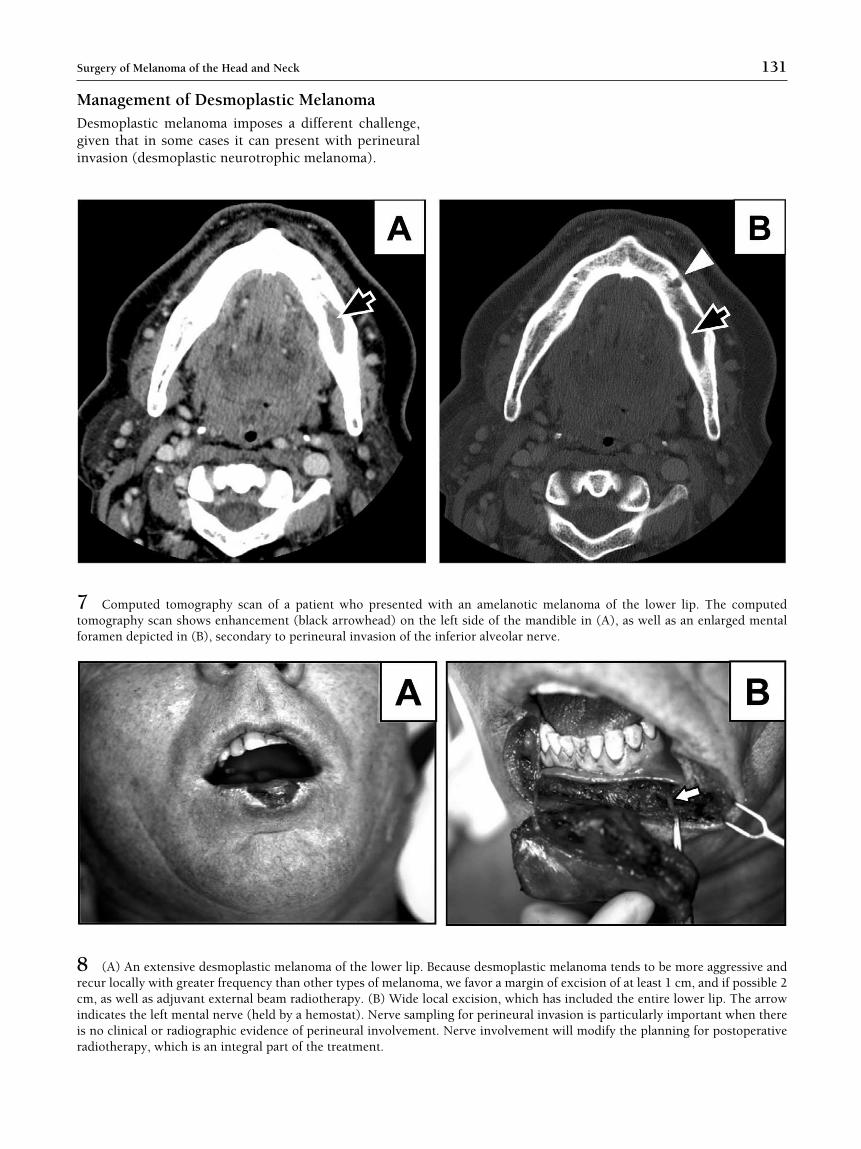
MDgi
7tf
8rciir
131Surgery of Melanoma of the Head and Neck
anagement of Desmoplastic Melanomaesmoplastic melanoma imposes a different challenge,iven that in some cases it can present with perineuralnvasion (desmoplastic neurotrophic melanoma).
adiotherapy, which is an integral part of the treatment.
h an amelanotic melanoma of the lower lip. The computedft side of the mandible in (A), as well as an enlarged mental
ferior alveolar nerve.
ause desmoplastic melanoma tends to be more aggressive andwe favor a margin of excision of at least 1 cm, and if possible 2l excision, which has included the entire lower lip. The arrowg for perineural invasion is particularly important when thereerve involvement will modify the planning for postoperative
Computed tomography scan of a patient who presented witomography scan shows enhancement (black arrowhead) on the leoramen depicted in (B), secondary to perineural invasion of the in
(A) An extensive desmoplastic melanoma of the lower lip. Bececur locally with greater frequency than other types of melanoma,m, as well as adjuvant external beam radiotherapy. (B) Wide locandicates the left mental nerve (held by a hemostat). Nerve samplins no clinical or radiographic evidence of perineural involvement. N
Copyright © 2022 FDOKUMEN