
Circulating fatty acids in patients with head and neck cancer ...
8
Full Terms & Conditions of access and use can be found at https://www.tandfonline.com/action/journalInformation?journalCode=ioto20 Acta Oto-Laryngologica ISSN: (Print) (Online) Journal homepage: https://www.tandfonline.com/loi/ioto20 Circulating fatty acids in patients with head and neck cancer after treatment: an explorative study with a one-year perspective Constantina Nadia Christou, Ylva Tiblom Ehrsson, Erik Lampa, Ulf Risérus & Göran Laurell To cite this article: Constantina Nadia Christou, Ylva Tiblom Ehrsson, Erik Lampa, Ulf Risérus & Göran Laurell (2021) Circulating fatty acids in patients with head and neck cancer after treatment: an explorative study with a one-year perspective, Acta Oto-Laryngologica, 141:9, 878-884, DOI: 10.1080/00016489.2021.1959950 To link to this article: https://doi.org/10.1080/00016489.2021.1959950 © 2021 The Author(s). Published by Informa UK Limited, trading as Taylor & Francis Group. Published online: 15 Aug 2021. Submit your article to this journal Article views: 698 View related articles View Crossmark data
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Circulating fatty acids in patients with head and neck cancer ...

Full Terms & Conditions of access and use can be found athttps://www.tandfonline.com/action/journalInformation?journalCode=ioto20
Acta Oto-Laryngologica
ISSN: (Print) (Online) Journal homepage: https://www.tandfonline.com/loi/ioto20
Circulating fatty acids in patients with head andneck cancer after treatment: an explorative studywith a one-year perspective
Constantina Nadia Christou, Ylva Tiblom Ehrsson, Erik Lampa, Ulf Risérus &Göran Laurell
To cite this article: Constantina Nadia Christou, Ylva Tiblom Ehrsson, Erik Lampa, Ulf Risérus &Göran Laurell (2021) Circulating fatty acids in patients with head and neck cancer after treatment:an explorative study with a one-year perspective, Acta Oto-Laryngologica, 141:9, 878-884, DOI:10.1080/00016489.2021.1959950
To link to this article: https://doi.org/10.1080/00016489.2021.1959950
© 2021 The Author(s). Published by InformaUK Limited, trading as Taylor & FrancisGroup.
Published online: 15 Aug 2021.
Submit your article to this journal
Article views: 698
View related articles
View Crossmark data

RESEARCH ARTICLE
Circulating fatty acids in patients with head and neck cancer after treatment: anexplorative study with a one-year perspective
Constantina Nadia Christoua , Ylva Tiblom Ehrssona , Erik Lampab, Ulf Ris�erusc and G€oran Laurella
aDepartment of Surgical Sciences, Section of Otorhinolaryngology and Head & Neck Surgery, Uppsala University, Uppsala, Sweden; bUppsalaClinical Research Center, Uppsala University, Uppsala, Sweden; cDepartment of Public Health and Caring Sciences, Clinical Nutrition andMetabolism, Uppsala University, Uppsala, Sweden
ABSTRACTBackground: Unintended weight loss and nutritional problems are often seen in patients with headand neck cancer, but changes in lipid metabolism are poorly studied.Aim/Objectives: The present study aimed to explore the longitudinal changes in circulating fatty acid(FA) composition in patients with head and neck cancer.Materials and methods: This study included 27 patients with head and neck cancer. Treatment con-sisted of single modality or combined modality treatments. The patients were assessed by repeatedblood sampling and body weight assessments before treatment started and on three occasions afterthe start of treatment. FA profiling included gas chromatography analysis of unsaturated FAs and satu-rated FAs in serum.Results: The values of three fatty acids – FA 14:0, FA 18:3n3, and FA 20:3n6 – changed in a specificpattern over the course of the study and the change in FA 14:0 correlated with weight changes.Conclusions and significance: This study showed altered profiles of both saturated and unsaturatedFAs. An improved understanding of the metabolic pathways in patients with head and neck cancersupports the development of better nutritional surveillance and nutritional treatments.
ARTICLE HISTORYReceived 18 April 2021Revised 14 July 2021Accepted 18 July 2021
KEYWORDSFatty acids; nutrition; headand neck cancer;radiotherapy;chemoradiotherapy
Introduction
For patients with head and neck cancer, the tumour andtreatment may affect the upper aerodigestive tract and causeswallowing problems, and even at the time of diagnosis crit-ical body weight loss (>5% in 1month or >10% in6months) is common [1]. Weight loss is associated with thenutritional status of the patients, which is often impairedbecause of loss of appetite, dysphagia, and odynophagia.Problems maintaining oral intake usually increase duringradiotherapy and combined modality treatment, and thisoften leads to weight loss [2].
Malnutrition is associated with alterations in a number ofmetabolic processes [3].
For example, inflammation is reported to be a commonaetiological factor for altered metabolism in cancer patients,which leads to a catabolic state and contributes to loss ofmuscle mass [4]. Cancer-associated malnutrition affects themetabolism of proteins, fats, and carbohydrates, and themost common metabolic abnormality observed in cancerpatients is increased mobilisation of peripheral fat andexcessive oxidation of fatty acids (FAs). Alterations in lipidmetabolism can lead to the depletion of adipose tissue andthus to weight loss [5].
Lipids are a group of water-insoluble molecules thatinclude triglycerides, phospholipids, sterols, and sphingoli-pids. FAs are the main component in the synthesis of trigly-cerides, which are mainly used for energy storage.Phospholipids also contain FAs, and together with sterolsand sphingolipids they represent the major structural com-ponents of biological membranes. Lipids also have essentialroles in signalling by functioning as second messengers andas hormones.
Lipids are found in the bloodstream as free FAs boundto albumin or complexed to proteins as low-density andhigh-density lipoproteins, e.g. cholesterol esters. An FA is acarboxylic acid and is either saturated or unsaturated. SomeFAs are obtained from dietary sources, while others are syn-thesised de novo mainly in the liver, adipose tissue, and lac-tating breast tissue. Depending on the type of FA,circulating FAs can reflect dietary intake and nutritional sta-tus and/or FA metabolism (e.g. de novo lipogenesis and FAdesaturation), both of which are pathways that may bealtered in cancer patients [6]. Tumour cells show high ratesof de novo lipid synthesis, and besides uptake of FAs fromblood circulation their ability to synthesize FAs plays a vitalrole in cancer pathogenesis [7].
CONTACT Constantina Nadia Christou [email protected] Department of Surgical Sciences, Section of Otorhinolaryngology and Head &Neck Surgery, Uppsala University, SE-751 85, Uppsala, Sweden� 2021 The Author(s). Published by Informa UK Limited, trading as Taylor & Francis Group.This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives License (http://creativecommons.org/licenses/by-nc-nd/4.0/),which permits non-commercial re-use, distribution, and reproduction in any medium, provided the original work is properly cited, and is not altered, transformed, or built upon inany way.
ACTA OTO-LARYNGOLOGICA2021, VOL. 141, NO. 9, 878–884https://doi.org/10.1080/00016489.2021.1959950

The plasma FA profile in patients with cancer has beenpoorly studied. The present study aimed to explore the lon-gitudinal changes in circulating fatty acids composition inpatients with head and neck cancer over the course of oneyear from the end of treatment. In addition, a secondaryaim was to investigate the relationship between circulatingfatty acids and the weight loss that is typically seen in thetreatment of head and neck cancer patients.
Materials and methods
This study included 27 patients with head and neck cancerwho underwent treatment at Uppsala, Umeå and OrebroUniversity Hospitals which are tertiary centres in Sweden.The inclusion criteria were patients with untreated head andneck cancer and a performance status of 0–2 according tothe WHO/ECOG Performance status. Patients with previouscancer history in the past 5 years (except skin cancer) andpatients with severe alcoholism, dementia, inability tounderstand Swedish, or any other inability to participate inthe study were excluded.
The mean age of the patients was 67 years (range50–81 years) with a male-to-female ratio of 2.4:1 (19 males,8 females). The most common tumour site was the orophar-ynx (n¼ 10) followed by the oral cavity (n¼ 9). Treatmentconsisted of single-modality surgery or radiotherapy orcombined modality treatment. The patients’ characteristicsare described in Table 1.
The patients were assessed by blood sampling and bodyweight measurements before treatment started (i.e. pre-treat-ment) and at 7weeks after the start of treatment and at3months and 1 year after the termination of treatment. Thenutritional status of all patients was followed according tolocal routines, and supplemental nutritional therapy wasoffered when indicated. Two patients did not provide bloodsamples at 7 weeks after the start of treatment. The bloodsamples at 1 year after the termination of treatment werenot collected in three patients. Two patients had died, andone patient was unable to give a blood sample due to
fatigue. Body weight was measured in kilograms, and thepatients did not wear outdoor clothing or shoes when beingweighed. Body mass index (BMI) was calculated using theformula kg/m2. The patients were divided into underweight,normal weight and overweight according to GlobalLeadership Initiative on Malnutrition (GLIM), as shown inTable 2. It was also recorded if the patients had oral intakeor nutritional support (total or partial use ofenteral nutrition).
FA analysis
Blood samples were stored at �70 �C at the UppsalaUniversity Hospital Biobank, Sweden, until analysis of FAcomposition. FA profiling included unsaturated FAs 16:1n-7, 18:1n-9, 18:2n-6, 18:3n-6, 18:3n-3, 20:3n-6, 20:4n-6,20:5n-3, and 22:6n-3 and saturated FAs 14:0, 15:0, 16:0, and18:0 in serum cholesterol esters using gas chromatographyas previously described [8]. For the analyses, 50 ll of centri-fuged clarified serum (2000� g for 10min) was used as thesample. The values of the FAs are presented as percentagesof the total amount of FAs.
Ethical considerations
The Regional Ethical Review Board in Uppsala reviewed andapproved the study (No. 2014/447), and written informedconsent was obtained from all patients. All blood sampleswere coded in the Uppsala Biobank (approved RCC 2015-0025). The study is registered at ClinicalTrials.gov(NCT03343236).
Statistical analyses
Generalised estimating equations were used to model thetime trends of each FA. Values of the FAs were first trans-formed from their percentage scale to the log scale, andtime was fitted with a second-degree polynomial allowing
Table 1. Characteristics of patients with head and neck cancer. Numbers of patients are given (n).
Total numberof patients
Radiationtherapy
Chemoradiationtherapy Surgery
Surgery &Radiation therapy
Surgery &Chemoradiation
therapy
SexMale 19 5 4 3 5 2Female 8 1 0 1 3 3
Age, years, mean 67 63 60 75 70 66(range) (50� 81) (52� 74) (50� 69) (74� 78) (62� 81) (60� 71)Tumour site
Oropharynx 10 4 4 0 0 2Oral cavity 9 0 0 2 5 2Salivary glands 1 0 0 0 1 0Larynx 4 2 0 1 1 0Hypopharynx 1 0 0 0 0 1Cancer of unknown primary 1 0 0 0 1 0External auditory canal cancer 1 0 0 1 0 0
Tumour stage�I 7 2 0 4 1 0II 4 0 0 0 4 0III 5 1 0 0 1 3IV 11 3 4 0 2 2
�According to Union for International Cancer Control (UICC) version 7.
ACTA OTO-LARYNGOLOGICA 879
for non-linear temporal patterns. An AR (1) correlationstructure was assumed between the measurements, whichexpects a higher correlation between measurements fromthe same individual obtained closer in time than measure-ments obtained further apart. A comparison of the meanvalues on the log scale was conducted for each time pointversus the time point before, i.e. the mean value at 7weekswas compared to the mean value at baseline, the mean valueat 3months was compared to the mean value at 7weeks,and the mean value at 1 year was compared to the meanvalue at 3months. The confidence intervals and p-valueswere adjusted for these multiple comparisons. The freelyavailable statistical software R was used for the statisticalanalyses. Interaction terms were added to the models toassess the time trends in different pre-defined subgroups,and the p-values were adjusted for the additional tests inthose models. An additional analysis was performed toassess the association between FA14:0 and weight changefrom baseline. The association between FA changes andgender as well as treatment was analysed. A p-value �.05was considered statistically significant.
Results
Changes in FA levels over time
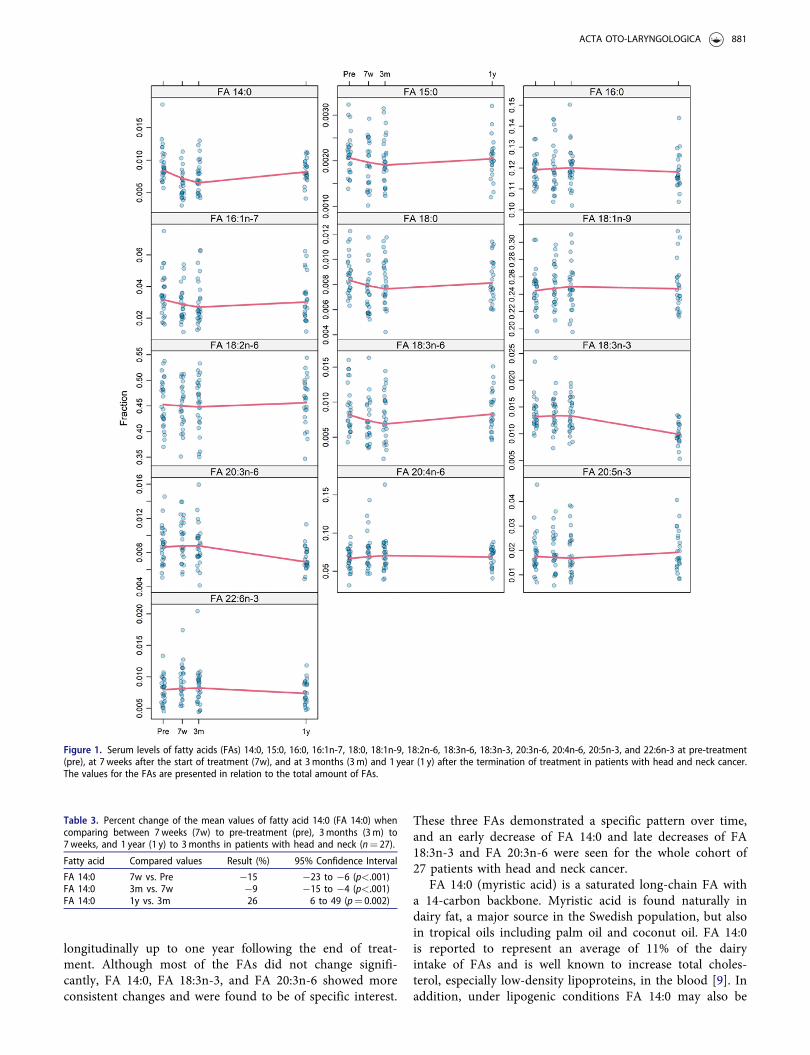
The levels of all studied FAs over the course of the studyare shown in Figure 1. For the whole cohort, FA 14:0 (myr-istic acid) showed a 15% decrease (p<.001) at 7 weeks, thussupporting a time-dependent association between pre-treatment and at 7weeks after the start of treatment. At3months after the end of treatment, FA 14:0 had decreasedeven further. The values then increased at 1 year after theend of treatment and were at nearly the same levels as thepre-treatment values, as shown in Table 3.
Another time-dependent association was observed for FA18:3n-3 (linolenic acid). The values of FA 18:3n-3 decreasedby 26% (p<.001) at 1 year after the end of treatment com-pared to 3months after the end of treatment. The values ofFA 18:3n-3 did not vary between pre-treatment, 7 weeksafter treatment start, and 3months after treatment termin-ation, as shown in Figure 1. FA 20:3n-6 showed the sametrend over time as FA 18:3n-3 with a 21% decrease at 1 year
after the end of treatment compared to the value at3months (p<.001) (Figure 1).
The compositions of the other studied FAs in serumwere different between patients, and the data do not suggestany clear time-dependent changes.
Weight change over time and nutritional status
At the time of their diagnosis, three patients were under-weight (BMI <20 (<22 if �70 years)), seven patients werenormal weight (BMI ¼ 20–25 (22–27 if �70 years)), and 17patients were overweight (BMI >25 (>27 if �70 years)).The mean pre-treatment weight of the patients was 78.1 kg(range 52.6–99.5 kg). There was a significant decrease inmean weight of 3.9 kg between pre-treatment and at7weeks, which corresponds to a weight loss of 5%. The per-centage weight change from start of treatment to 3monthsafter the end of treatment was 6.4%. At 1 year after the endof treatment, the mean weight of the patients was 74.3 kg(range 47–94 kg), which was at the same level as the meanweight at 7 weeks after the start of treatment (Table 2).
None of the patients needed partial or total parenteralnutrition during treatment or after treatment. A total ofseven patients needed enteral nutritional support during thestudy period as shown in Table 2.
Correlation of FA with weight, treatment, and gender
An association was found between FA 14:0 and weightchange from baseline. This association was seen at 7weeksafter the start of treatment and at 3months but not at 1 yearafter the end of treatment, as shown in Figure 2.
No association was seen in the FA profile between thepatients who received radiotherapy and the patients whoreceived chemo radiotherapy.
No association was observed in the FA profile betweenmen and women.
Discussion
The association between FAs and head and neck cancertreatment has not been reported earlier. In the presentexplorative study, serum levels of FAs were assessed
Table 2. Weight and nutritional data of patients with head and neck cancer.
Pre-treatmentn¼ 27
7 weeks after start of treatmentn¼ 27
3 months after end of treatmentn¼ 27
12 months after end of treatmentn¼ 25��
Body mass index� (BMI)Underweight 3 5 4 5Normal weight 7 10 14 11Overweight 17 12 9 8
Weight mean (kg) 78.1 74.2 73.1 74.3Range (52.6� 99.5) (49.9� 92.1) (47.3� 89) (47� 94)SD 12.2 12.3 12.9 13.6
NutritionTotal peroral 27 20 25 24Enteral nutrition��� 0 7 2 1
Numbers of patients are given (n).�Underweight: BMI <20 (BMI < 22 if �70 years); normal weight: BMI 20–24.99 (BMI 22–27 if �70years); overweight/obese: BMI >25 (BMI >27 if � 70 years).��Weight and BMI were not available for 1 patient at 12months.���Nutrition through nasogastric tube at 7 weeks and 3months and percutaneous endoscopic gastrostomy at 12months.
880 C. N. CHRISTOU ET AL.
longitudinally up to one year following the end of treat-ment. Although most of the FAs did not change signifi-cantly, FA 14:0, FA 18:3n-3, and FA 20:3n-6 showed moreconsistent changes and were found to be of specific interest.
These three FAs demonstrated a specific pattern over time,and an early decrease of FA 14:0 and late decreases of FA18:3n-3 and FA 20:3n-6 were seen for the whole cohort of27 patients with head and neck cancer.
FA 14:0 (myristic acid) is a saturated long-chain FA witha 14-carbon backbone. Myristic acid is found naturally indairy fat, a major source in the Swedish population, but alsoin tropical oils including palm oil and coconut oil. FA 14:0is reported to represent an average of 11% of the dairyintake of FAs and is well known to increase total choles-terol, especially low-density lipoproteins, in the blood [9]. Inaddition, under lipogenic conditions FA 14:0 may also be
Figure 1. Serum levels of fatty acids (FAs) 14:0, 15:0, 16:0, 16:1n-7, 18:0, 18:1n-9, 18:2n-6, 18:3n-6, 18:3n-3, 20:3n-6, 20:4n-6, 20:5n-3, and 22:6n-3 at pre-treatment(pre), at 7 weeks after the start of treatment (7w), and at 3months (3m) and 1 year (1 y) after the termination of treatment in patients with head and neck cancer.The values for the FAs are presented in relation to the total amount of FAs.
Table 3. Percent change of the mean values of fatty acid 14:0 (FA 14:0) whencomparing between 7weeks (7w) to pre-treatment (pre), 3months (3m) to7weeks, and 1 year (1 y) to 3months in patients with head and neck (n¼ 27).
Fatty acid Compared values Result (%) 95% Confidence Interval
FA 14:0 7w vs. Pre �15 �23 to �6 (p<.001)FA 14:0 3m vs. 7w �9 �15 to �4 (p<.001)FA 14:0 1y vs. 3m 26 6 to 49 (p¼ 0.002)
ACTA OTO-LARYNGOLOGICA 881

produced de novo in parallel with FA 16:0 [10]. FA 18:3n-3(linolenic acid) is an essential omega-3 FA found exclusivelyin plant oils, such as rapeseed oil, but it can be converted tovery long-chain n-3 polyunsaturated FAs (PUFAs) that arefound in seafood. Notably, despite being an essential FA,18:3n-3 as assessed in serum cholesterol esters does notappear to be a reliable biomarker of self-reported dietaryintake [11]. FA 20:3n-6 (dimoho-c-linolenic acid) is a poly-unsaturated omega-6 FA that is produced in the body byelongation and desaturation of FA 18:2n-6 (linoleic acid).Linolenic acid and linoleic acid are the two essential FAs forhumans that must be obtained through the diet.
The changes in the FA profile in serum over time inpatients with head and neck cancer are most probablymultifactorial. The pre-treatment body composition is onefactor to take into account, and dysphagia is a frequent con-tributor to reduced intake of nutrients, including essentialFAs, and thus contributes to weight loss. Seventeen patientsin the present cohort (63%) were overweight at baseline.Although 7 patients (26%) received enteral nutrition at7weeks after start of treatment, only 8 patients (32%) wereoverweight at 12months after termination of treatment.
In the present study, FA 14:0 in serum was consistentlycorrelated to weight change both at 7weeks after the start oftreatment and at 3months after the end of treatment, corre-sponding to the convalescent phase, but the correlation didnot remain at 1 year after the end of treatment, most
probably due to the limited sample size. In a study ofpatients with head and neck cancer, the patients’ meanweight changed over time with a nadir observed at5–6months after the start of radiotherapy and thereafterslowly recovered [12]. In the present study, weight loss wasmost severe at 3months after the termination of treatment.It can be speculated that the decrease in the serum concen-tration of FA 14:0 after treatment was associated with areduced dietary intake of saturated fat (e.g. high-fat dairyfoods) as indicated in elderly Swedish populations [13]. Inaddition to FA 14:0 being a potential marker of saturatedfat intake, it is also possible that the reduced FA 14:0 levelsto some extent reflect a decrease in de novo lipogenesis dueto lowered intake of energy from carbohydrates [14]. Thus,the associations between changes of serum FA 14:0 andbody weight observed here may suggest that this FA mayreflect the nutritional and consequently the anabolic/cata-bolic status in these patients post-treatment. Its use as anutritional marker is of high interest but needs furtherinvestigation.
Fourteen patients in the present study received radiother-apy and 9 patients underwent chemoradiotherapy. Anincrease of pro-inflammatory cytokines is reported in con-nection to chemoradiotherapy in patients with head andneck cancer, which was correlated to the T-stage of thetumour [15]. It is clear that inflammation and immune reac-tions play a role in cancer development, progression, and
Figure 2. Correlation between fatty acid 14:0 (FA 14:0) and body weight changes from baseline to 7weeks after start of treatment and to 3months and 1 yearpost-treatment in patients with head and neck cancer (n¼ 27).
882 C. N. CHRISTOU ET AL.

response to treatment [16]. Moreover, the tumour itself mayproduce pro-inflammatory cytokines that trigger an inflam-matory response that may contribute to a decrease in foodintake and thus to weight loss.
Lipid metabolism has been more extensively studied incancer cell progression in pre-clinical studies. Cancer devel-opment is dependent on the ability of the cancer cells toproduce lipids that are necessary for cell membrane forma-tion, protein modification, and transmission of oncogenicsignals [17]. Cancer cells also take advantage of exogenousFAs in order to carry out de novo lipogenesis [18].
In many cases, patients with head and neck cancer needessential nutrients and intake of surplus energy, especiallyduring periods of high energy expenditure, i.e. the treatmentphase . Among the various aspects to consider in nutritionalsurveillance are the nutritional and energy demands of can-cer cells in relation to energy intake and storage, which isan area of research that needs to be better explored in clin-ical studies. The present study indicates that supplementa-tion of the essential FA 18:3n-3 may be especially indicatedat 1 year after the termination of treatment.
Although no difference was found in the present studybetween patients receiving radiotherapy and chemoradio-therapy, the effect of treatment modality on FA profiles can-not be overlooked. It could be speculated that radiotherapyand chemotherapy affect FAs in different ways. An earlierstudy on three patients with advanced breast cancer sug-gested that chemotherapy is a possible cause of low levels ofplasma phospholipids [19]. A larger study on 42 men withsquamous cell carcinoma of the oesophagus demonstratedincreased levels of polyunsaturated FAs after platinum-basedchemoradiotherapy [20].
The limitations of the study are the size of the cohortand the heterogeneity of tumour site, stage, and treatment.The results of the current study should be regarded ashypothesis-generating, and a larger study cohort should pro-vide confirmatory and more detailed knowledge on thepotential importance of FA 14:0, FA 18:3n-3, and FA 20:3n-6 in patients with head and neck cancer.
Conclusion
An altered serum profile of FA 14:0, FA 18:3n-3, and FA20:3n-6 was observed within a year post-treatment inpatients with head and neck cancer. At the group level, FA14:0 was associated with weight change within the first3months after the end of treatment. Whether these FAsreflect nutritional and/or metabolic status is unclear, but ofpotentially high interest because FAs may be useful prog-nostic or indicative biomarkers in patients undergoing can-cer treatment. Our observations encourage furtherinvestigation of the association between FAs and nutritionalstatus in patients with head and neck cancer.
Acknowledgements
Thanks to research nurse Nilla West€o€o and specialist nurses BrithGranstr€om and Charlotte Ryman and all participating ENT clinics in
the Uppsala-€Orebro region and the Northern region. A special thanksalso to all participating patients.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Author contributions
All authors contributed to the work and the final version of the manu-script was approved by all authors. YTE and GL designed the study,YTE collected the data, CC drafted the manuscript, EL analysed thedata, and CC, YTE, GL, and UR critically revised the manuscript.
Funding
The study was supported by the Swedish Cancer Society, grant num-ber 2015/363 and 2018/502; The Kamprad Family Foundation forEntrepreneurship, Research & Charity, grant number 20150003. Thiswork was also supported by Scientific research for junior researchers,Uppsala University.
ORCID
Constantina Nadia Christou http://orcid.org/0000-0002-8347-7239Ylva Tiblom Ehrsson http://orcid.org/0000-0001-7435-167XUlf Ris�erus http://orcid.org/0000-0002-8620-4586G€oran Laurell http://orcid.org/0000-0002-7760-246X
References
[1] Jager-Wittenaar H, Dijkstra PU, Vissink A, et al. Critical weightloss in head and neck cancer–prevalence and risk factors atdiagnosis: an explorative study. Support Care Cancer. 2007;15(9) :1045–1050.
[2] Arribas L, Hurt�os L, Taberna M, et al. Nutritional changes inpatients with locally advanced head and neck cancer duringtreatment. Oral Oncol. 2017; 71:67–74.
[3] Van Cutsem E, Arends J. The causes and consequences ofcancer-associated malnutrition. Eur J Oncol Nurs. 2005; 9Suppl 2(Suppl 2):S51–S63.
[4] Ryan AM, Power DG, Daly L, et al. Cancer-associated malnu-trition, cachexia and sarcopenia: the skeleton in the hospitalcloset 40 years later. Proc Nutr Soc. 2016;75(2):199–211.
[5] McAndrew PF. Fat metabolism and cancer. Surg Clin NorthAm. 1986;66(5):1003–1012.
[6] Vriens K, Christen S, Parik S, et al. Evidence for an alternativefatty acid desaturation pathway increasing cancer plasticity.Nature. 2019;566(7744):403–406.
[7] Santos CR, Schulze A. Lipid metabolism in cancer. Febs J.2012;279(15):2610–2623.
[8] Fisk HL, West AL, Childs CE, et al. The use of gas chromatog-raphy to analyze compositional changes of fatty acids in ratliver tissue during pregnancy. JoVE. 2014;(85)51445
[9] Ohlsson L. Dairy products and plasma cholesterol levels. FoodNutr Res. 2010;54:1–9.
[10] Roberts R, Hodson L, Dennis AL, et al. Markers of de novolipogenesis in adipose tissue: associations with small adipocytesand insulin sensitivity in humans. Diabetologia. 2009;52(5):882–890.
[11] Iggman D, €Arnl€ov J, Cederholm T, et al. Association of adiposetissue fatty acids with cardiovascular and all-cause mortality inelderly men. JAMA Cardiol. 2016;1(7):745–753.
ACTA OTO-LARYNGOLOGICA 883

[12] Einarsson S, Laurell G, Tiblom Ehrsson Y.An explorative studyon energy balance in patients with head and neck cancer. NutrCancer. 2020;72(7):1191–1199.
[13] Rosell M, Johansson G, Berglund L, et al. The relation betweenalcohol intake and physical activity and the fatty acids 14: 0,15: 0 and 17: 0 in serum phospholipids and adipose tissue usedas markers for dairy fat intake. Br J Nutr. 2005; 93(1) :115–121.
[14] Song X, et al. Dietary long-chain fatty acids and carbohydratebiomarker evaluation in a controlled feeding study in partici-pants from the women’s health initiative cohort. Am J ClinNutr. 2017; 105(6) :1272–1282.
[15] Astradsson T, Sellberg F, Berglund D, et al. Systemic inflamma-tory reaction in patients with head and neck cancer-an explora-tive study. Front Oncol. 2019; 9:1177.
[16] Bonomi M, et al. The role of inflammation in head and neckcancer. Adv Exp Med Biol. 2014;816:107–127.
[17] Hanahan D, Weinberg RA. Hallmarks of cancer: the next gen-eration. Cell. 2011;144(5):646–674.
[18] Louie SM, Roberts LS, Mulvihill MM, et al. Cancer cells incorp-orate and remodel exogenous palmitate into structural andoncogenic signaling lipids. Biochim Biophys Acta. 2013;1831(10):1566–1572.
[19] Pratt VC, Watanabe S, Bruera E, et al. Plasma and neutrophilfatty acid composition in advanced cancer patients and responseto fish oil supplementation. Br J Cancer. 2002;87(12):1370–1378.
[20] Zemanova M, Vecka M, Petru�zelka L, et al. Plasma phosphati-dylcholines fatty acids in men with squamous cell esophagealcancer: chemoradiotherapy improves abnormal profile. Med SciMonit. 2016;22:4092–4099.
884 C. N. CHRISTOU ET AL.




















