
University of Groningen Imaging in dermal fillers Grippaudo ...

Targeted delivery of adipose-derived stem cells viaacellular dermal matrix enhances wound repair indiabetic ratsChunlei Nie1,2†, Guoyou Zhang3,4†, Daping Yang2,5, Tong Liu1, Dan Liu5, Jin Xu6 and Jiewu Zhang1*1Department of Head and Neck Surgery, Third Affiliated Hospital of Harbin Medical University, People’s Republic of China2Tissue Repair and Engineering Laboratory, Harbin Medical University, People’s Republic of China3Department of Dermatology, University of Lübeck, Germany4Department of Hand and Plastic Surgery, Second Affiliated Hospital of Wenzhou Medical College, Zhejiang, People’s Republic of China5Department of Plastic Surgery, Second Affiliated Hospital of Harbin Medical University, People’s Republic of China6Department of Cell Biology, Harbin Medical University, People’s Republic of China
Abstract
Cell-based therapeutic intervention has emerged as a new approach to accelerate wound closure.Adipose-derived stem cells (ASCs), as a fascinating cell source, have received much attention in tissuerepair and regeneration. In this study we evaluated the potential of acellular dermal matrix (ADM)scaffold serving as a carrier for the delivery of ASCs and investigated its therapeutic effects on woundhealing. First, ASCswere isolated and characterized for multidifferentiation potential. ASCs–ADM graftswere then prepared, and ADM scaffold was shown to support the in vitro growth and proliferation ofASCs. Next, we analysed paracrine factors in conditioned medium and found that ASCs–ADM graftssecreted various cytokines, including VEGF, HGF, TGFb and bFGF. Moreover, ASCs–ADM conditionedmedium notably stimulated the migration and proliferation of fibroblasts. In vivo, we established anexcisional wound model in diabetic rats which received phosphate-buffered saline (PBS), ADM orASCs–ADM grafts, respectively. Our results demonstrated that implantation of ASCs–ADM significantlyenhanced tissue regeneration and increased epithelialization, resulting in accelerated wound closure.Immunofluorescence analysis further indicated that capillary density was evidently increased in theASCs–ADM group compared with the control or ADM group. In addition, western blot analysis showedthat ASCs–ADM significantly increased the expression of angiogenic factors, which was consistent within vitrodata. Taken together, our results suggest that targeted delivery of ASCs via ADMscaffold acceleratediabetic wound healing through a paracrinemechanism, with enhanced granulation tissue formation andincreased re-epithelialization and neovascularization. Copyright © 2012 John Wiley & Sons, Ltd.
Received 27 October 2011; Revised 4 July 2012; Accepted 25 August 2012
Keywords adipose-derived stem cells; acellular dermal matrix; scaffold; diabetic wounds; repair;paracrine effect
1. Introduction
Wound repair is a complex and highly ordered cellular andbiochemical response to tissue injury. Wound healing isessential to the prevention of the invasion of damaged tissue
by pathogens and the gradual restoration of the damagedtissues (Martin, 1997). Normal wound healing proceeds inthe majority of clinical patients. However, the progression ofhealing is significantly impaired and delayed inmany chronicdiseases, such as diabetes mellitus. Currently, 15% of diabeticpatients worldwide suffer from foot ulcerations, which oftenbecome non-healing chronic wounds (Boulton et al., 2005).Impairment of wound healing in diabetic environment ismultifactorial and mainly involves prolonged inflammation,decreased synthesis of collagen, reduced growth factors andimpaired neovascularization (Falanga, 2005).
*Correspondence to: J. Zhang, Department of Head and NeckSurgery, Third Affiliated Hospital of Harbin Medical University,150 Ha Ping Road, Harbin 150040, People’s Republic of China.E-mail: [email protected]†These authors contributed equally to this study.
Copyright © 2012 John Wiley & Sons, Ltd.
JOURNAL OF TISSUE ENGINEERING AND REGENERATIVE MEDICINE RESEARCH ARTICLEJ Tissue Eng Regen Med (2012)Published online in Wiley Online Library (wileyonlinelibrary.com) DOI: 10.1002/term.1622
Journal Code Article ID Dispatch: 22.09.12 CE:T E R M 1 6 2 2 No. of Pages: 12 ME:
12345678910111213141516171819202122232425262728293031323334353637383940414243444546474849505152535455565758596061626364
6566676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127128

Current therapies for diabetic wounds, including topicalapplication of growth factors, can not achieve satisfactoryoutcomes. Recently, stem cell therapy has emerged as anattractive approach for enhancingwound healing (Herdrichet al., 2008). It has been reported that bone marrow-derived stem cells (BMSCs) accelerate the rate of healing incutaneous wounds (McFarlin et al., 2006; Wu et al., 2007).However, due to difficulties in obtaining sufficientBMSCs, adipose-derived stem cells (ASCs) lately representan alternative source of pluripotent cells (Kern et al.,2006; Goh et al., 2007). ASCs not only possess the abilityto maintain self-renewal and differentiate into various celltypes but also secrete many growth factors, includingvascular endothelial growth factor (VEGF), hepatocytegrowth factor (HGF), transforming growth factor-b (TGFb),and fibroblast growth factor (FGF) (Rehman et al., 2004;Nakagami et al., 2005; Kim et al., 2007). In addition, ASCsare easier to obtain in abundance through minimallyinvasive procedures. Therefore, ASCs have emerged as afascinating cell source for impaired wound healing (Gimbleet al., 2007; Schäffler and Büchler, 2007).
Traditional approaches to cell transplantation includesystemic administration via a vein and direct injectionaround the injured tissue. We previously demonstrated thatlocal injection of ASCs promoted wound healing throughdifferentiation and vasculogenesis (Nie et al., 2011).However, it had been shown that the therapeutic capabili-ties of stem cells were not fully utilized upon in vivotransplantation because of their poor bio-distribution andlow cell survival (Aicher et al., 2003). Previous studiesrevealed that only a few stem cells, which had been injecteddirectly, migrated and participated in tissue regeneration(Suh et al., 2005; Bonaros et al., 2008). To overcome theselimitations of conventional transplantation methods, thepresent study aimed to apply acellular dermal matrix(ADM) as a scaffold, which might promote cell adhesionand introduce stem cells to the local environment. ADMhas many advantages over synthetic materials, includingfavourable handling properties and resistance to infection,which can usually be applied within local wounds (Bottinoet al., 2009; Formigli et al., 2011). This biological scaffoldalso facilitates host cell infiltration and revascularizationand results in integration of the implant into the autologoustissue at the injured site. Moreover, ADM provides a three-dimensional (3D) structure into which seeded stem cellscould incorporate and contribute to the formation of regen-erative tissues (Schönmeyr et al., 2009; Xu et al., 2009).
Previously we hypothesized that local administration ofASCs via an acellular matrix scaffold could acceleratewound healing (Nie et al., 2009). To test this, here weexplored the potential of the ADM scaffold serving as acarrier for the delivery of ASCs and evaluated its therapeu-tic effects on an excisional wound-healing model in diabeticrats. ASCs–ADM grafts were prepared and characterizedin vitro. In addition, we analysed paracrine factors secretedby ASCs–ADM grafts and determined their effects on themigration and proliferation of fibroblasts. Moreover, weinvestigated the underlying mechanisms by whichASCs–ADM grafts regulate diabetic wound repair in vivo.
2. Materials and methods
2.1. Animals
Adult male Sprague–Dawley (SD) rats, average weight200–250 g, were provided by the Vital River LaboratoryAnimal Co. (Beijing, China). All animals received humanecare in compliance with the National Institutes of Health’sGuide for the Care and Use of Laboratory Animals. Thefollowing experimental protocol was approved by the localethics committee. Thirty-six diabetic rats were inducedusing intraperitoneal (i.p.) injections of streptozotocin(STZ; Sigma, St. Louis, MO, USA). After overnight fasting,the animals were each injected with a single dose ofSTZ (75mg/kg) in 0.1M citrate buffer, pH 4.5, to inducediabetes. The blood glucose level was measured using aglucometer at days 0, 3 and 7. Animals showing a bloodglucose level> 15mM were considered diabetic. One weekafter the successful induction of diabetes, the animals wereused for the preparation of the wound-healing model.
2.2. Isolation and culture of ASCs
The normal SD rats were anaesthetized and shaved.Inguinal fat pads were excised and washed extensively withphosphate-buffered saline (PBS; Sigma-Aldrich). The fattissue was excised, finely minced and incubated with 5%antibiotic medium for 20min. The tissue was then rinsedthree times in PBS for 5min each, followed by digestionwith 0.075% type I collagenase (Sigma-Aldrich) andvigorous shaking for 1 h at 37�C in a 50ml centrifuge tube.Next, an equal volume of Dulbecco’s modified Eagle’smedium (DMEM) supplemented with 10% fetal bovineserum (FBS; Gibco) was added to neutralize the collage-nase. The cell suspension was centrifuged at 1200 rpm for10min and the cell pellet was resuspended in DMEM.Finally, the cells were plated onto 100mm2 tissue cultureplates and maintained at 37�C in 5% CO2. The growthmedium was changed 24h after the initial plating andevery 3days thereafter.When cells reached 90% confluence,they were passaged in a ratio of 1:2. Passage 3 ASCs used inthese experiments have previously been characterized byour group (Nie et al., 2011).
2.3. Multilineage differentiation of ASCs
To evaluate their differentiation potential, ASCs wereinduced to differentiate into adipocytes, osteoblasts andchondrocytes, as previously described. Briefly, for adipo-genic differentiation, the cultured cells were induced withdexamethasone, insulin, isobutyl-methylxanthine andindomethacine in DMEM containing 10% FBS. Then thecells were fixed in 10% formalin for 10min and stainedwithfresh oil red O solution (Sigma-Aldrich) to show lipiddroplets in induced cells. For osteogenic differentiation,the cultured cells were induced in osteogenic induction
2 C. Nie et al.
Copyright © 2012 John Wiley & Sons, Ltd. J Tissue Eng Regen Med (2012)DOI: 10.1002/term
12345678910111213141516171819202122232425262728293031323334353637383940414243444546474849505152535455565758596061626364
6566676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127128
medium (DMEM containing 10% FBS, dexamethasone,ascorbate-2-phosphate and b-glycerophosphate. Thecells were analysed by alkaline phosphatase (ALP) activ-ity detection and von Kossa staining (Sigma-Aldrich) toreveal osteogenic differentiation. For chondrogenicdifferentiation, the cultured cells were induced in chondro-genic induction medium (DMEM containing 10% FBS,insulin, ascorbate-2-phosphate and transforming growthfactor-b1 (TGFb1). After the culture period, chondrogenicdifferentiation was confirmed by Alcian blue staining(Sigma-Aldrich).
2.4. Preparation of ADM and ASCs–ADM grafts
Acellular dermal matrix graft sheets (10 � 40mm,0.3–0.5mm in thickness) derived from cadaveric skinsof human donors were utilized (Lot 992007, AlloDerm,LifeCell Corp., Branchburg, NJ, USA). ADM was washedin PBS and then cut into pieces using an 8mm punchbiopsy instrument (Premier Uni-Punch, Plymouth Meeting,PA, USA). The pieces were placed on the 24-well tissueculture plates with the papillary dermal surface facing up.In the ADM group, only 1ml DMEM was added into eachwell. Meanwhile, 1�106 ASCs suspended in 1ml DMEMwere added in the ASCs–ADM group. The unattached cellswere removed by aspiration of the medium after culturefor 48h, and the grafts in the culture plates were incubatedat 37�C in fresh complete medium that was replacedevery other day. Finally, the grafts were washed three timeswith PBS to remove remaining growth medium beforeoperative engraftment. All procedures were performedunder sterile conditions.
2.5. Assessment of the in vitro characteristicsof grafts
Following the preparation of ADM and ASCs–ADM grafts,their ultrastructures were examined under light microscopyand scanning electron microscopy (SEM). The graftsamples were fixed in 10% formalin, prepared as paraffinblocks, sectioned at 6mm and stained with haematoxylinand eosin (H&E). Histological evaluation was thenperformed under a light microscope (Olympus, Japan).For SEM examination (Hitachi S-3400N, Japan), thesamples were fixed with 0.25% glutaraldehyde solutionand sputter-coated with gold. Cell proliferation on ADMscaffolds was determined by methyltetrazolium (MTT)assay every day. Briefly, 100ml MTT solution (5mg/ml inPBS) was added into each well, and the cells were incu-bated for 4 h at 37�C. Next, the medium was removed and600ml dimethyl sulphoxide was added to dissolve the bluecrystals that formed in the cells by shaking for 15min.The optical density (OD) values were determined using amicroplate reader (Bio-Rad, USA) at 570nm wavelength.The experiments were repeated at least three times.
2.6. Enzyme-linked immunosorbent assay (ELIZA)
After ADM or ASCs–ADM grafts in the 24-well tissueculture plates had been incubated for 48h at 37�C in 5%CO2, the conditioned media were collected. VEGF andTGFb levels in the conditioned media were determinedusing ELISA kits (RRV00 and MB100B, R&D Systems).Rabbit polyclonal anti-HGF antibody (ab83760, Abcam)and rabbit anti-bFGF polyclonal antibody (250559,Abbiotec) were used as primary antibodies and incubatedwith conditioned media for 1 h at room temperature, thenincubated with goat anti-rabbit IgG-horseradish peroxidase(HRP; ab6721, Abcam). After the substrate solution ofhydrogen peroxide (R&D Systems) had been added, theoptical density of each well was determined by spectropho-tometry at 450nm wavelength and the concentrations ofgrowth factors were calculated.
2.7. Cell migration and proliferation assay
Fibroblasts were obtained from the rat dermis after diges-tion with 0.75% collagenase and cultured in DMEMsupplemented with 10% FBS. Passage 3 fibroblasts wereused for the experiments. Cell migration was assessed byscratch assay, as previously described (Liang et al., 2007).Briefly, fibroblasts were seeded on 24-well plates andmaintained at 37�C and 5% CO2 for 48 h to permit celladhesion and the formation of a confluent monolayer.The fibroblast sheets were scored with a sterile pipette tipto leave a scratch of approximately 0.2–0.4mm in width.The culture medium was then immediately removed, alongwith any dislodged cells, and the removed mediumwas replaced with control medium, ADM or ASCs–ADMconditioned medium. The cells were then incubated at37�C and 5% CO2 for 18 h. Wound closure images werecaptured on a microscope and analysed using ImagePro-Plus software. The proliferation rates of fibroblastscultured in different conditioned media were measuredby MTT assay as described above. All migration and prolif-eration assays were performed in triplicate.
2.8. Wound-healing model and treatment
The excisionalwound-healingmodel in diabetic ratswas gen-erated as described previously Q1(••••••••••••••••••••••••••••••).Briefly, the animals were anaesthetized with i.p. injection of10% chloral hydrate (350mg/kg). The dorsal surface wasshaved with an electric clipper and the skin was cleansedwith betadine solution. An 8mm punch biopsy tool was usedto create two circular, full-thickness cutaneous woundsbilaterally on the shaved dorsal skin of the rats. A donut-shaped silicone splint with an external diameter of 14mmand an internal diameter of 10mm was centred on thewound to prevent wound contraction. Then the 36 diabeticrats were randomly divided into three groups: the blankcontrol group, the ADMgraft group and the ASCs–ADMgraft
Effects of ASCs–ADM on diabetic wound healing 3
Copyright © 2012 John Wiley & Sons, Ltd. J Tissue Eng Regen Med (2012)DOI: 10.1002/term
12345678910111213141516171819202122232425262728293031323334353637383940414243444546474849505152535455565758596061626364
6566676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127128

group, which received PBS treatment, unseeded ADMscaffold or ADM graft seeded with ASCs, respectively.
2.9. Wound analysis
Digital photographs of wounds were taken at days 0, 3, 7, 10,14, 21 and 28. Time towound closurewas defined as the timeatwhich thewound bedwas completely re-epithelialized andfilled with new tissue. Wound area was measured by tracingthe wound margin and calculated using an image analysisprogram (Sigma Scan Pro Image). The percentage of woundclosure was calculated as follows:
area of original wound� area of actual woundð Þ=area of original wound � 100%
A wound was considered completely closed when thewound area was equal to 0.
2.10. Histological examination
At postoperative days 7, 14 and 21, rats were sacrificedand wound samples were excised and bisected. Thesamples were fixed in 10% formalin, paraffin-embeddedand sectioned at 6 mm on a microtome (Leica, Wetzlar,Germany). For histological evaluation, the sections werestained with H&E and photographed under phase-contrastmicroscopy, using a digital camera. The images wereanalysed for epithelial gap (EG) and total area of granula-tion tissue (GT), using digital analysis software. EG wasdefined as the distance between the advancing edges ofkeratinocyte migration. Area of GT was calculated bytracing regions of GT and calculating the pixel area. Threeanimals were analysed at each time point.
2.11. Capillary density determination
Wound samples, taken at days 7 and 14, were embeddedin OCT and immediately frozen in liquid nitrogen forfluorescent immunostaining. Frozen sections (6mm) wereincubated with primary monoclonal antibodies againstCD31 at 4�C overnight (mouse anti-CD31, 1:100, sc-53526;Santa Cruz, CA, USA). The sections were then rinsed withPBS and incubated with secondary antibody (goat anti-mouse IgG-TR, 1:200, sc-2781, Santa Cruz) for 1h at 37�C.Hoechst 33342 dye (C1026, Beyotime Institute of Biotech-nology, Shanghai, China) was used to stain the nuclei for2min. Capillary density was determined by counting forvascular structures positively stained with CD31 in threerandom fields/section.
2.12. Western blot analysis
The wound samples were homogenized using a Douncehomogenizer cooled to 4�C and incubated overnight ona rotary shaker. The homogenates were centrifuged at
13 000 rpm for 15min and the supernatant was collectedfor the determination of protein concentration, using aBSA kit (Bio-Rad). Equal amounts of protein were sepa-rated on 12% polyacrylamide gel electrophoresis andtransferred to nitrocellulose membranes. The membraneswere blocked with 10% non-fat dried milk in Tris-bufferedsaline (TBS) for 1 h and then incubated with primary anti-bodies against VEGF (1:1000, ab70612, Abcam), HGF(1:500, ab83760, Abcam), TGFb (1:500, ab66043, Abcam),bFGF (1:200, 250559, Abbiotec) and b-actin (1:1000,ab8227, Abcam) overnight at 4�C. Next the membraneswere incubated with HRP-conjugated goat anti-rabbit IgGsecondary antibody (1:2000, ab6721; Abcam) for 1 h atroom temperature. The immune complex was visualizedby photodetection. The reaction products were quantifiedusing digital scanning and scion image software.
2.13. Statistical analysis
Data were expressed as mean� SD (standard deviation).Statistical comparisons between the groupswere performedusing either student’s t-test or one-way analysis of variance(ANOVA) followed by SNK test for multiple comparisons.P<0.05 was considered statistically significant.
3. Results
3.1. Morphology and multilineage differentiationof ASCs
The adherent cultured ASCs exhibited a fibroblast-likemorphology when observed under a phase-contrastmicroscope (Figure F11A) and expanded efficiently in vitro.To investigate adipogenic differentiation potential ofASCs, cells were stained with oil red O to demonstratean intracellular accumulation of lipid droplets (Figure 1B).Osteogenic differentiation of ASCs was detected by posi-tive expression of ALP (Figure 1C). The von Kossa stainfurther indicated the deposition of calcified extracellularmatrix (ECM) (Figure 1D). Chondrogenic induction ofASCs was confirmed by Alcian blue staining to assessproteoglycan content (Figure 1E). These results confirmedthat ASCs we isolated possess proliferation capacity anddifferentiation potential.
3.2. Characteristics of ADMand ASCs–ADMgrafts
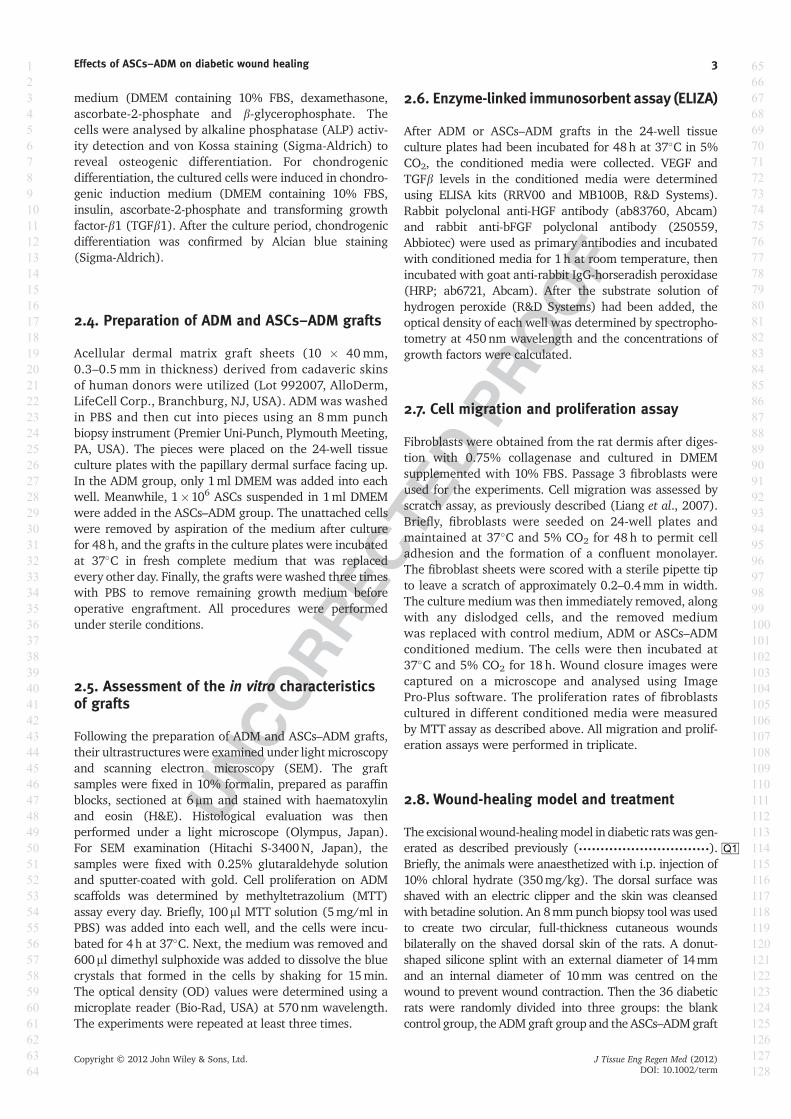
ADM scaffolds were characterized as having a microporousfibrous morphology. As shown in Figure F22A, schematicillustration depicted that ASCs were seeded into three-dimensional ADM scaffolds and cultured in fresh growthmedium. MTT assay showed that ASCs had an approxi-mate two-fold proliferation rate on day 7 compared today 1 (Figure 2B), suggesting that the scaffolds facilitateASCs proliferation. After one week of in vitro culture,SEM imaging showed that ASCs consistently attached to
4 C. Nie et al.
Copyright © 2012 John Wiley & Sons, Ltd. J Tissue Eng Regen Med (2012)DOI: 10.1002/term
12345678910111213141516171819202122232425262728293031323334353637383940414243444546474849505152535455565758596061626364
6566676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127128

the ADM scaffolds in ASCs–ADM grafts (Figure 2C). Inaddition, histological staining demonstrated large numbersof attached cells in ASCs–ADM grafts, indicating that thescaffold has the potential to deliver considerable numbersof ASCs. Although most cells grew primarily on the surfaceof the scaffolds, numerous cells were also detected indeeper sections of the structures (Figure 2D).
3.3. Effects of ASCs–ADM conditioned mediumon cell migration and proliferation
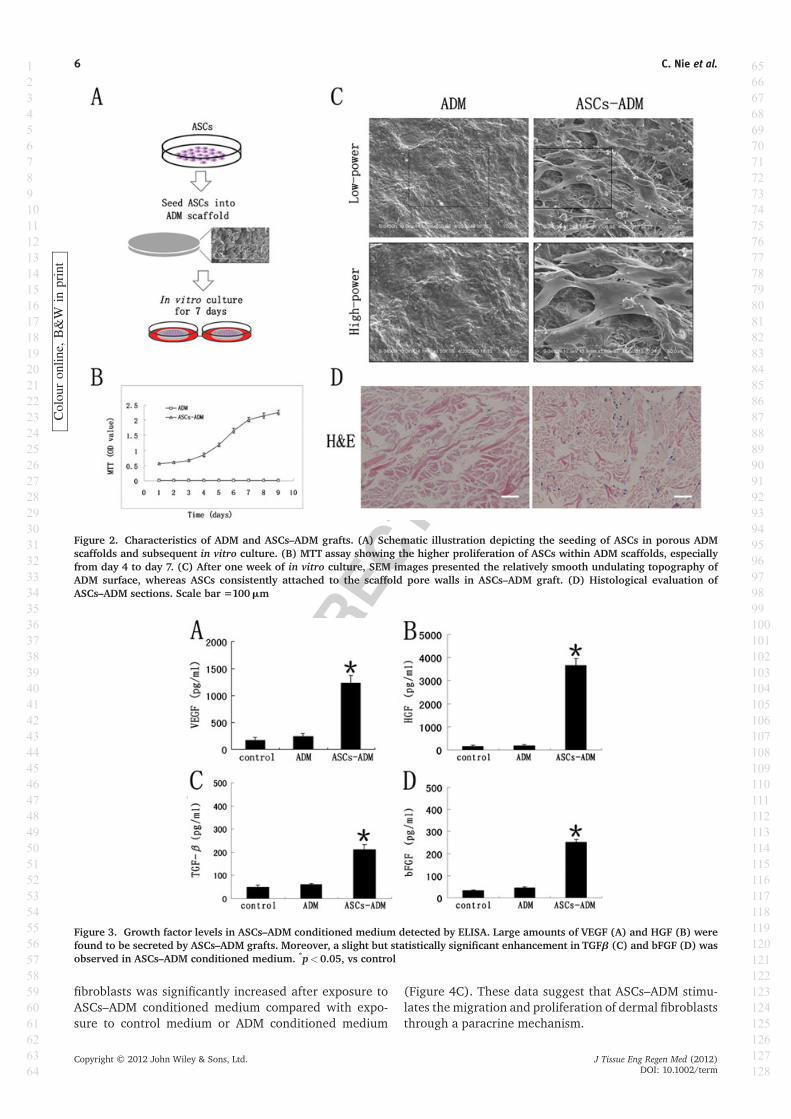
To determine whether ASCs–ADM could enhance woundhealing through a paracrine effect, we examined the levelsof various growth factors in ASCs–ADM conditionedmedium. ELISA assay showed that ASCs–ADM grafts in vitrosecreted significant amounts of VEGF (1230�126pg/ml)
and HGF (3666�189 pg/ml) (Figure F33A, B). Meanwhile,slight but statistically significant higher levels of TGFb(212� 20 pg/ml) and bFGF (252� 29 pg/ml) weredetected in ASCs–ADM conditioned medium comparedto control medium or ADM conditioned medium(Figure 3C, D).
Since fibroblasts play an important role inwound healing,we next measured the effects of ASCs–ADM conditionedmedium on the migration and proliferation of dermalfibroblasts. In vitro scratch assay showed that fibroblaststreated with control medium or ADM conditioned mediumfailed to migrate significantly toward the gap. Treatmentof ASCs–ADM conditioned medium considerably promotedwound closure, whereas ADM conditioned medium hadno influence on scratch wounds (Figure F44A, B). Further-more, fibroblasts were cultured with different mediaand cell proliferation was evaluated. The number of
Figure 1. Multilineage differentiation of ASCs. (A) The cultured ASCs exhibited a fibroblast-like morphology as observed under aphase-contrast microscope. (B) For adipogenic differentiation, an intracellular accumulation of lipid droplets was observed afteroil red O staining. (C) For osteogenic differentiation, positive expression of alkaline phosphatase was observed in ASCs and(D) von Kossa staining showed the deposition of calcified extracellular matrix. (E) For chondrogenic differentiation, chondrocytesin pellet culture were stained as blue in ASCs after Alcian blue staining. Scale bar =100mm
Colou
ron
line,
B&W
inprint
Effects of ASCs–ADM on diabetic wound healing 5
Copyright © 2012 John Wiley & Sons, Ltd. J Tissue Eng Regen Med (2012)DOI: 10.1002/term
12345678910111213141516171819202122232425262728293031323334353637383940414243444546474849505152535455565758596061626364
6566676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127128
fibroblasts was significantly increased after exposure toASCs–ADM conditioned medium compared with expo-sure to control medium or ADM conditioned medium
(Figure 4C). These data suggest that ASCs–ADM stimu-lates the migration and proliferation of dermal fibroblaststhrough a paracrine mechanism.
Figure 2. Characteristics of ADM and ASCs–ADM grafts. (A) Schematic illustration depicting the seeding of ASCs in porous ADMscaffolds and subsequent in vitro culture. (B) MTT assay showing the higher proliferation of ASCs within ADM scaffolds, especiallyfrom day 4 to day 7. (C) After one week of in vitro culture, SEM images presented the relatively smooth undulating topography ofADM surface, whereas ASCs consistently attached to the scaffold pore walls in ASCs–ADM graft. (D) Histological evaluation ofASCs–ADM sections. Scale bar =100mm
Colou
ron
line,
B&W
inprint
Figure 3. Growth factor levels in ASCs–ADM conditioned medium detected by ELISA. Large amounts of VEGF (A) and HGF (B) werefound to be secreted by ASCs–ADM grafts. Moreover, a slight but statistically significant enhancement in TGFb (C) and bFGF (D) wasobserved in ASCs–ADM conditioned medium. *p<0.05, vs control
6 C. Nie et al.
Copyright © 2012 John Wiley & Sons, Ltd. J Tissue Eng Regen Med (2012)DOI: 10.1002/term
12345678910111213141516171819202122232425262728293031323334353637383940414243444546474849505152535455565758596061626364
6566676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127128

3.4. Effects of ASCs–ADM on wound healing
In the diabetic rat model of wound healing, macroscopicevaluation showed that time to complete wound closurewas significantly shortened in the ASCs–ADM group.Wounds treated with ASCs–ADM exhibited improvedwound healing compared with control treatment at alltime points, with statistical significance at 3, 7, 10 and14days. Mean time to closure for ASCs–ADM-treatedwounds was 13� 0.37 days, compared with 20� 0.71days in the ADM group and 27� 0.44 days in the controlgroup (FigureF5 5A). Specifically, ASCs–ADM treatmentsignificantly accelerated wound closure at days 7, 10and 14, resulting in 55.5� 3.7%, 76.75�1.6% and99.5�1% closure, respectively. Compared with controls,ADM-treated wounds also exhibited an increased rate ofwound closure at days 10 and 14, with 50.5� 2.6% and71.7�2.4% closure. However, there was a statisticallysignificant difference in wound closure between ADM-and ASCs–ADM-treated wounds (Figure 5B).
The promotion of wound healing by ASCs–ADM wasalso evaluated by microscopic examination of the woundtissue. The histological observation showed that therewere significant differences between ASCs–ADM-treatedwounds and the control wounds at day 14 with respect toneo-tissue organization, cellular infiltration and collagenmatrix deposition. ASCs–ADM enormously enhancedtissue regeneration, with a well-differentiated epidermisand a noticeably thick dermis (FigureF6 6A). In addition,the epithelialization of wounds was significantly advancedin the ASCs–ADM-treated group. Although ADM treat-ment increased epithelialization at day 14 compared withcontrol, there was a significant difference in the epithelialregeneration between the ADM and ASCs–ADM groups
(Figure 6B). Moreover, ASCs–ADM therapy resulted in asignificant enhancement in granulation tissue formation,especially at days 10 and 14. Poorly formed tissue wasevidently delayed in control or ADM-treated wounds(Figure 6C). Taken together, these data demonstrate thatASCs–ADM significantly increase epithelialization andgranulation tissue deposition, and thus accelerate diabeticwound healing.
3.5. Effects of ASCs–ADM on angiogenesis
The paramount importance of blood supply in the healingof wounds has long been appreciated. Histologicalanalysis showed that ASCs–ADM treatment significantlyincreased neovascularization at postoperative day 7compared with the control or ADM treatment (Figure F77A).To investigate the correlation between angiogenesis andthe wound-healing process, immunostaining for endothe-lial protein CD31 was performed to show the vasculaturein wounds (Figure 7B). Capillary density assay revealedthat capillary density was evidently increased in theASCs–ADM group compared with the control group.Although a slight increase of vessel density was found inADM-treated wounds, there was no significant differencebetween control and ADM treatment (Figure 7C). Theseresults suggest that enhanced neovascularization playsan important role in ASCs–ADM-mediated acceleratedwound healing.
To further characterize the growth factors involved inangiogenesis, protein expression of VEGF, HGF, TGFb andbFGF in wound beds was analysed by western blotting.Consistent with the in vitro results, the expression of
Figure 4. Effects of ASCs–ADM conditioned medium on the migration and proliferation of fibroblasts. (A) Scratch migration assay offibroblasts exposed to ASCs–ADM conditioned medium showed increased migration of cells compared with the control. (B) Theclosure of scratch wound was significantly promoted by ASCs–ADM conditioned medium but not by control medium or ADMconditioned medium. (C) After 48h in vitro culture with ASCs–ADM conditioned medium, the number of fibroblasts was significantlyincreased. Scale bar =100mm. Abbreviations: CM, conditioned medium; p<0.05 vs control
Effects of ASCs–ADM on diabetic wound healing 7
Copyright © 2012 John Wiley & Sons, Ltd. J Tissue Eng Regen Med (2012)DOI: 10.1002/term
12345678910111213141516171819202122232425262728293031323334353637383940414243444546474849505152535455565758596061626364
6566676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127128

these growth factors was evidently enhanced by ASCs–ADMtreatment compared with control treatment. There wasno difference of VEGF protein expression between thecontrol and ADM groups, while expression of TGFbwas detected at a higher level in ADM group. A faint
baseline expression of HGF and bFGF could be detectedin both control and ADM groups (Figure F88). Collectively,these data indicate that ASCs–ADM could secrete signifi-cant amounts of angiogenic growth factors to acceleratewound angiogenesis.
Figure 5. Effects of ASCs–ADM on diabetic wound healing. (A) Images of wounds in diabetic rats which received implantation ofcontrol treatment, ADM graft or ASCs–ADM graft. Representative photographs of the wounds at days 0, 3, 10 and 14 exhibitedenhanced wound healing after treatment with ASCs–ADM grafts. (B) ASCs–ADM treatment significantly accelerated wound closureand the time to complete wound closure was shortened in the ADM group compared with the control group. *p<0.05 vs control;#p<0.05 vs ADM. Scale bar=5mm
Colou
ron
line,
B&W
inprint
Figure 6. Histological analysis of ASCs–ADM treated wounds. (A) Representative histological images of the wounds at day 14. Bluedotted line indicates the re-epithelialization of wounds, whereas red dotted line indicates epithelial gap of wounds. The histologicalanalysis showed that ASCs–ADM enormously enhanced tissue regeneration in diabetic wounds. (B) The epithelialization rate ofwounds was significantly elevated in the ASCs–ADM treated group compared with the control group. (C) ASCs–ADM promotedgranulation tissue formation in diabetic wounds, especially on days 10 and 14; *p<0.05 vs control. E, epidermis; EG, epithelialgap; GT, granulation tissue. Scale bar=400mm
8 C. Nie et al.
Copyright © 2012 John Wiley & Sons, Ltd. J Tissue Eng Regen Med (2012)DOI: 10.1002/term
12345678910111213141516171819202122232425262728293031323334353637383940414243444546474849505152535455565758596061626364
6566676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127128

4. DiscussionChronic diabetic wounds are common diseases and difficultto heal (Boulton et al., 2005; Falanga, 2005). Previousstudies have shown that mesenchymal stromal cells (MSCs)such as BMSCs and ASCs possess the capacity to enhancewound healing (McFarlin et al., 2006; Wu et al., 2007; Nieet al., 2011). However, the amount of transplanted cells thatsurvived and participated in the tissue repair was relativelylow and the efficacy of MSC-based therapy appeared to bemarginal (Rosová et al., 2008). Thus, it is necessary tooptimize current cell transplantation methods to overcomethe poor bio-distribution and low in vivo survival of thetransplanted cells (Aicher et al., 2003). Recently, naturaland synthetic scaffolds have been employed as deliveryvehicles to attach or encapsulate the cells (Mooneyand Vandenburgh, 2008; Formigli et al., 2011). Becausethe ADM scaffold exhibited favourable biocompatibilityand promoted the adhesion and proliferation of seededcells (Bottino et al., 2009; Schönmeyr et al., 2009; Xuet al., 2009;), we hypothesized that application of ADMscaffold as a delivery carrier for stem cell therapy couldaccelerate cutaneous wound healing (Nie et al., 2009).
ASCs combined with atelocollagen matrix enhancedhealing-impaired wounds in a mouse model (Nambuet al., 2009). Other studies reported the use of ADM or
silk fibroin–chitosan scaffold for delivery of human ASCsto the site of soft tissue defects in an athymic murinecutaneous wound model (Altman et al., 2008, 2009).However, these studies have only examined the in vivoeffects of grafts on wound healing without detailedin vitro characteristics of ASCs grown on the scaffolds.In addition, the effect of ASCs–ADM transplantation onthe closure of diabetic wounds remains unclear.
In this study, ASCs were successfully isolated from rat fatpads and cultured in vitro. To test their multidifferentiationcapacity, ASCs were induced to differentiate into adipo-cytes, chondrocytes or osteoblasts under appropriate induc-ingmedia. Thereafter, we seeded ASCs on the ADM scaffoldfor the preparation of ASCs–ADM grafts. Consistent withprevious studies (Xu et al., 2009), the ADM scaffold wasfound to be an appropriate carrier that supported theadherence and proliferation of the transplanted ASCs.SEM and histological analysis of ASCs–ADM grafts alsorevealed that ASCs closely attached to the scaffold porewalls after 1week of in vitro culture. These results indicatethat ADM scaffolds are competent extracellular matrices forseeded ASCs because they provide a favourable structurefor ASCs growth and functional maintenance.
Differentiation and paracrine signalling have beenproposed as the mechanisms by which MSCs improvetissue repair (Kim et al., 2009). However, due to poor
Figure 7. Effects of ASCs–ADM on angiogenesis of wounds. (A) Cutaneous wounds harvested from each group on postoperative day 7were stained with H&E; yellow arrows, erythrocyte-filled vessels. (B) Immunostaining of endothelial protein CD31-positive bloodvessels (red) showed the vasculature in wounds, and the nuclei (blue) were counterstained with Hoechst 33342. (C) The numberof CD31-positive blood vessels in each section was counted and expressed as the number of vessels/high-power field. *p<0.05 vscontrol. Scale bar=100mm
Colou
ron
line,
B&W
inprint
Effects of ASCs–ADM on diabetic wound healing 9
Copyright © 2012 John Wiley & Sons, Ltd. J Tissue Eng Regen Med (2012)DOI: 10.1002/term
12345678910111213141516171819202122232425262728293031323334353637383940414243444546474849505152535455565758596061626364
6566676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127128

engraftment and low survival of MSCs at the site ofinjury, growing evidence indicates that MSC paracrinesignalling is the predominant mechanism responsiblefor enhanced wound repair (Kim et al., 2007; Gnecchiet al., 2008; Lee et al., 2009). To determine the paracrineeffects of ASCs–ADM grafts in vitro, ELISA assay wasused to detect the growth factor levels in ASCs–ADMconditioned medium. Similar to the secretome in ASCs-conditioned medium (Rehman et al., 2004; Kim et al.,2007; Lee et al., 2010), ASCs–ADM grafts secretedcertain cytokines, such as VEGF, HGF, TGFb and bFGF.It is well known that TGFb and bFGF are crucial for cellrecruitment, survival and proliferation during injuredtissue repair (Werner and Grose, 2003). Therefore, wefurther investigated the effects of ASCs–ADM condi-tioned medium on cell migration and proliferation. Ourdata revealed that ASCs–ADM conditioned mediumsignificantly increased the migration and proliferationof dermal fibroblasts in vitro. This would result inadvanced granulation tissue formation and acceleratedepithelialization. In the study, we showed that ASCs–ADMconditioned medium contained high levels of growthfactors, which might play a critical role in ASCs–ADMmediated wound healing.
Subsequently, ASCs–ADM grafts were implanted intoexcisional full-thickness wounds in diabetic rats and weobserved significantly acceleratedwound closure comparedwith the controls or ADM grafts. Histological analysis of thewounds further confirmed that ASCs–ADM grafts signifi-cantly enhanced granulation tissue formation and acceler-ated re-epithelialization. Importantly, the histologicalexamination of the implanted scaffolds revealed prominentinfiltration of fibroblasts and capillary ingrowth into ADMscaffolds, which indicates that the ADM scaffold can serveas the natural extracellular matrix for host cell infiltration,proliferation and revascularization (de Moya et al., 2008;Xu et al., 2009). Although using the ADM scaffold aloneincreased epithelialization compared to control, there wasa statistically significant difference in epithelial regenera-tion between ADM and ASCs–ADM treatment.
Neovascularization is an important process in woundhealing (Falanga, 2005; Suh et al., 2005; Blantonet al., 2009). The formation of new blood vessels isnecessary to sustain the newly formed granulation tissue.In our study, after implantation of ASCs–ADM grafts intothe diabetic wounds, increased capillary density wasobviously observed, which was confirmed by subsequenthistological and immunofluorescent analysis. ASCs–ADM
Figure 8. Protein levels of growth factors in wounds. Total protein extracted from wound samples on postoperative day 7 wasanalysed by western blot analysis. The results were presented as expression levels of VEGF, HGF, TGFb and bFGF in each group;*p<0.05 vs control
10 C. Nie et al.
Copyright © 2012 John Wiley & Sons, Ltd. J Tissue Eng Regen Med (2012)DOI: 10.1002/term
12345678910111213141516171819202122232425262728293031323334353637383940414243444546474849505152535455565758596061626364
6566676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127128

might enhance angiogenesis by secreting angiogenicgrowth factors and stimulating host endothelial cells.Western blot analysis showed that wounds treated withASCs–ADM had significantly higher levels of VEGF, HGF,TGFb and bFGF, consistent with our in vitro data thatASCs–ADM grafts secreted these growth factors in condi-tioned medium. It has been documented that VEGF andHGFare themost effective factors that regulate angiogenesis(Rehman et al., 2004; Cai et al., 2007; Blanton et al., 2009).Although our previous study showed that engrafted ASCsdifferentiated into endothelial lineage and contributed toneovascular structures in wound healing, only occasionalASC-incorporated vasculature was found despite substantialincreases in capillary density (Nie et al., 2011). Moreover,in situ differentiation of ASCs may be mediated byparacrine cytokines. Previous study reported that themajor contribution of transplanted ASCs in ischaemiclimbs might be due to increased paracrine secretion ofangiogenic growth factors (Bhang et al., 2009). Collectively,a paracrine effect may contribute to ASCs–ADM-mediatedenhanced neovascularization.
Furthermore, we showed that paracrine cytokines in vitroreleased by ASCs–ADM significantly increased the migra-tion and proliferation of fibroblasts, and subsequentlyenhanced granulation tissue formation. MSC-conditionedmedium was reported to accelerate both dermal fibroblastand keratinocyte migration in vitro (Walter et al., 2010),although the paracrine effect of ASCs–ADM on the migra-tion of keratinocytes in vitro was not determined in ourstudy. In addition, paracrine factors such as VEGF andHGF play a crucial role in ASCs–ADM-mediated angiogene-sis during wound healing. Compared with unseeded ADMscaffold, ASCs–ADM grafts significantly accelerated exci-sional wound healing in diabetic rats. Moreover, becauseADM scaffold enhanced location and retention of ASCs at
injured tissue, the time to complete wound closure wasevidently shortened after ASCs–ADM treatment comparedwith direct injection of ASCs (data not shown). Theseresults confirm the therapeutic effects of ASCs–ADM graftsin cutaneous wound repair and regeneration.
5. Conclusions
ADM scaffolds successfully support the in vitro growth andproliferation of ASCs. These scaffolds also appear to beexcellent in vivo targeted delivery carriers of ASCs becausethey promote the location of seeded cells in a diabeticwound model. Furthermore, our in vivo data revealed thatthe targeted delivery of ASCs using the ADM scaffold wassuperior to the unseeded scaffold or local injection of ASCsin accelerating wound closure. Paracrine factors secretedfrom ASCs–ADM have potentially beneficial effects on cellmigration and proliferation, and on angiogenesis duringwound repair. These findings suggest that ASCs–ADMenhances diabetic wound healing via paracrine mechan-isms, with accelerated granulation tissue formation andincreased re-epithelialization and neovascularization.
Acknowledgements
This study was supported by the National Natural ScienceFoundation of China (Grant Nos 81101429 and 81101430), theScience and Technology Research Projects of Hei LongjiangProvince (Grant No. GC12C304-5), the Scientific Research Fundof Hei Longjiang Provincial Education Department (Grant No.12511173) and the Scientific Research Fund of the ThirdAffiliated Hospital of Harbin Medical University (Grant No.JJZ2010-02). The authors have no conflicts of interest.
References
Aicher A, Brenner W, Zuhayra M et al.2003; Assessment of the tissue distribu-tion of transplanted human endothelialprogenitor cells by radioactive labeling.Circulation 107: 2134–2139.
Altman AM, Matthias N, Yan Y et al. 2008;Dermal matrix as a carrier for in vivodelivery of human adipose-derived stemcells. Biomaterials 29: 1431–1442.
Altman AM, Yan Y, Matthias N et al. 2009;IFATS collection: Human adipose-derivedstem cells seeded on a silk fibroin–chitosanscaffold enhance wound repair in a murinesoft tissue injury model. Stem Cells 27:250–258.
Bhang SH, Cho SW, Lim JM et al. 2009;Locally delivered growth factor enhancesthe angiogenic efficacy of adipose-derivedstromal cells transplanted to ischemiclimbs. Stem Cells 27: 1976–1986.
Blanton MW, Hadad I, Johnstone BHet al. 2009; Adipose stromal cells andplatelet-rich plasma therapies synergis-tically increase revascularization duringwound healing. Plast Reconstr Surg123: 56–64S.
Bonaros N, Rauf R, Schachner T et al. 2008;Enhanced cell therapy for ischemic heartdisease. Transplantation 86: 1151–1160.
Bottino MC, Jose MV, Thomas V et al. 2009;Freeze-dried acellular dermal matrix graft:effects of rehydration on physical, chemi-cal, and mechanical properties. Dent Mater25: 1109–1115.
Boulton AJ, Vileikyte L, Ragnarson-Tennvall Get al. 2005; The global burden of diabeticfoot disease. Lancet 366: 1719–1724.
Cai L, Johnstone BH, Cook TG et al. 2007;Suppression of hepatocyte growthfactor production impairs the ability ofadipose-derived stem cells to promoteischemic tissue revascularization. StemCells 25: 3234–3243.
de Moya MA, Dunham M, Inaba K et al.2008; Long-term outcome of acellulardermalmatrix when used for large traumaticopen abdomen. J Trauma 65: 349–353.
Falanga V. 2005; Wound healing and itsimpairment in the diabetic foot. Lancet366: 1736–1743.
Formigli L, Benvenuti S, Mercatelli R et al.2011; Dermal matrix scaffold engineered
with adult mesenchymal stem cells andplatelet-rich plasma as a potential tool fortissue repair and regeneration. J TissueEng Regen Med Q2••: •••–•••; DOI: 10.1002/term.405.
Gimble JM, Katz AJ, Bunnell BA. 2007;Adipose-derived stem cells for regenera-tive medicine. Circ Res 100: 1249–1260.
GnecchiM, Zhang Z, Ni A et al. 2008; Paracrinemechanisms in adult stem cell signaling andtherapy. Circ Res 103: 1204–1219.
Goh BC, Thirumala S, Kilroy G et al. 2007;Cryopreservation characteristics of adipose-derived stem cells: maintenance of differen-tiation potential and viability. J Tissue EngRegen Med 1: 322–324.
Herdrich BJ, Lind RC, Liechty KW. 2008;Multipotent adult progenitor cells: theirrole in wound healing and the treat-ment of dermal wounds. Cytotherapy10: 543–550.
Kern S, Eichler H, Stoeve J et al. 2006;Comparative analysis of mesenchymalstem cells from bone marrow, umbilicalcord blood, or adipose tissue. Stem Cells24: 1294–1301.
Effects of ASCs–ADM on diabetic wound healing 11
Copyright © 2012 John Wiley & Sons, Ltd. J Tissue Eng Regen Med (2012)DOI: 10.1002/term
12345678910111213141516171819202122232425262728293031323334353637383940414243444546474849505152535455565758596061626364
6566676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127128

Kim WS, Park BS, Sung JH et al. 2007;Wound healing effect of adipose-derivedstem cells: a critical role of secretoryfactors on human dermal fibroblasts. JDermatol Sci 48: 15–24.
Kim WS, Park BS, Sung JH. 2009; Thewound-healing and antioxidant effects ofadipose-derived stem cells. Expert OpinBiol Ther 9: 879–887.
Lee EY, Xia Y, Kim WS et al. 2009; Hypoxia-enhanced wound-healing function ofadipose-derived stem cells: increase instem cell proliferation and up-regulationof VEGF and bFGF. Wound Repair Regen17: 540–547.
Lee MJ, Kim J, Kim MY et al. 2010; Proteomicanalysis of tumor necrosis factor-a-inducedsecretome of human adipose tissue-derivedmesenchymal stem cells. J Proteome Res9: 1754–1762.
Liang CC, Park AY, Guan JL. 2007; In vitroscratch assay: a convenient and inexpen-sive method for analysis of cell migrationin vitro. Nat Protoc 2: 329–333.
Martin P. 1997; Wound healing – aiming forperfect skin regeneration. Science 276: 75–81.
McFarlin K, Gao X, Liu YB et al. 2006; Bonemarrow-derived mesenchymal stromalcells accelerate wound healing in the rat.Wound Repair Regen 14: 471–478.
Mooney DJ, Vandenburgh H. 2008; Celldelivery mechanisms for tissue repair. CellStem Cell 2: 205–213.
Nakagami H, Maeda K, Morishita R et al.2005; Novel autologous cell therapy inischemic limb disease through growthfactor secretion by cultured adiposetissue-derived stromal cells. ArteriosclerThromb Vasc Biol 25: 2542–2547.
Nambu M, Kishimoto S, Nakamura S et al.2009; Accelerated wound healing inhealing-impaired db/dbmice by autologousadipose tissue-derived stromal cells combinedwith atelocollagen matrix. Ann Plast Surg62: 317–321.
Nie C, Yang D, Morris SF. 2009; Local deliveryof adipose-derived stem cells via acellulardermal matrix as a scaffold: a new promis-ing strategy to accelerate wound healing.Med Hypoth 72: 679–682.
Nie C, Yang D, Xu J et al. 2011; Locallyadministered adipose-derived stem cellsaccelerate wound healing through differ-entiation and vasculogenesis. Cell Transpl20: 205–216.
Rehman J, Traktuev D, Li J et al. 2004; Secre-tion of angiogenic and antiapoptotic factorsby human adipose stromal cells. Circulation109: 1292–1298.
Rosová I, Dao M, Capoccia B et al. 2008; Hyp-oxic preconditioning results in increasedmotility and improved therapeutic potentialof human mesenchymal stem cells. StemCells 26: 2173–2182.
Schäffler A, Büchler C. 2007; Concisereview: adipose tissue-derived stromal
cells – basic and clinical implicationsfor novel cell-based therapies. Stem Cells25: 818–827.
Schönmeyr B, Clavin N, Avraham T et al.2009; Synthesis of a tissue-engineeredperiosteum with acellular dermal matrixand cultured mesenchymal stem cells.Tissue Eng Part A 15: 1833–1841.
Suh W, Kim KL, Kim JM et al. 2005;Transplantation of endothelial progenitorcells accelerates dermal wound healingwith increased recruitment of monocytes/macrophages and neovascularization. StemCells 23: 1571–1578.
Walter MN, Wright KT, Fuller HR et al.2010; Mesenchymal stem cell-condi-tioned medium accelerates skin woundhealing: an in vitro study of fibroblastand keratinocyte scratch assays. Exp CellRes 316: 1271–1281.
Werner S, Grose R. 2003; Regulation ofwound healing by growth factors andcytokines. Physiol Rev 83: 835–870.
Wu Y, Chen L, Scott PG et al. 2007;Mesenchymal stem cells enhance woundhealing through differentiation and angio-genesis. Stem Cells 25: 2648–2659.
Xu H, Wan H, Zuo W et al. 2009; A porcine-derived acellular dermal scaffold thatsupports soft tissue regeneration: removalof terminal galactose-a-(1,3)-galactose andretention of matrix structure. Tissue EngPart A 15: 1807–1819.
12 C. Nie et al.
Copyright © 2012 John Wiley & Sons, Ltd. J Tissue Eng Regen Med (2012)DOI: 10.1002/term
12345678910111213141516171819202122232425262728293031323334353637383940414243444546474849505152535455565758596061626364
6566676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127128

Author Query Form
Journal: Journal of Tissue Engineering and Regenerative Medicine
Article: term_1622
Dear Author,
During the copyediting of your paper, the following queries arose. Please respond to these by annotating your proofs withthe necessary changes/additions.• If you intend to annotate your proof electronically, please refer to the E-annotation guidelines.• If you intend to annotate your proof by means of hard-copy mark-up, please refer to the proof mark-up symbols guide-lines. If manually writing corrections on your proof and returning it by fax, do not write too close to the edge of the pa-per. Please remember that illegible mark-ups may delay publication.
Whether you opt for hard-copy or electronic annotation of your proofs, we recommend that you provide additional clar-ification of answers to queries by entering your answers on the query sheet, in addition to the text mark-up.
Query No. Query Remark
Q1 AUTHOR: Insert reference citation in name/date form (in MS given as 14).
Q2 AUTHOR: Published now? Insert volume and page numbers.

USING e-ANNOTATION TOOLS FOR ELECTRONIC PROOF CORRECTION
Required software to e-Annotate PDFs: Adobe Acrobat Professional or Adobe Reader (version 7.0 or above). (Note that this document uses screenshots from Adobe Reader X) The latest version of Acrobat Reader can be downloaded for free at: http://get.adobe.com/uk/reader/
Once you have Acrobat Reader open on your computer, click on the Comment tab at the right of the toolbar:
1. Replace (Ins) Tool – for replacing text.
Strikes a line through text and opens up a text box where replacement text can be entered.
How to use it
Highlight a word or sentence.
Click on the Replace (Ins) icon in the Annotations section.
Type the replacement text into the blue box that appears.
This will open up a panel down the right side of the document. The majority of tools you will use for annotating your proof will be in the Annotations section, pictured opposite. We’ve picked out some of these tools below:
2. Strikethrough (Del) Tool – for deleting text.
Strikes a red line through text that is to be deleted.
How to use it
Highlight a word or sentence.
Click on the Strikethrough (Del) icon in the Annotations section.
3. Add note to text Tool – for highlighting a section to be changed to bold or italic.
Highlights text in yellow and opens up a text box where comments can be entered.
How to use it
Highlight the relevant section of text.
Click on the Add note to text icon in the Annotations section.
Type instruction on what should be changed regarding the text into the yellow box that appears.
4. Add sticky note Tool – for making notes at specific points in the text.
Marks a point in the proof where a comment needs to be highlighted.
How to use it
Click on the Add sticky note icon in the Annotations section.
Click at the point in the proof where the comment should be inserted.
Type the comment into the yellow box that appears.

USING e-ANNOTATION TOOLS FOR ELECTRONIC PROOF CORRECTION
For further information on how to annotate proofs, click on the Help menu to reveal a list of further options:
5. Attach File Tool – for inserting large amounts of text or replacement figures.
Inserts an icon linking to the attached file in the appropriate pace in the text.
How to use it
Click on the Attach File icon in the Annotations section.
Click on the proof to where you’d like the attached file to be linked.
Select the file to be attached from your computer or network.
Select the colour and type of icon that will appear in the proof. Click OK.
6. Add stamp Tool – for approving a proof if no corrections are required.
Inserts a selected stamp onto an appropriate place in the proof.
How to use it
Click on the Add stamp icon in the Annotations section.
Select the stamp you want to use. (The Approved stamp is usually available directly in the menu that appears).
Click on the proof where you’d like the stamp to appear. (Where a proof is to be approved as it is, this would normally be on the first page).
7. Drawing Markups Tools – for drawing shapes, lines and freeform annotations on proofs and commenting on these marks.
Allows shapes, lines and freeform annotations to be drawn on proofs and for comment to be made on these marks..
How to use it
Click on one of the shapes in the Drawing Markups section.
Click on the proof at the relevant point and draw the selected shape with the cursor.
To add a comment to the drawn shape, move the cursor over the shape until an arrowhead appears.
Double click on the shape and type any text in the red box that appears.
Copyright © 2022 FDOKUMEN




















