Sudden cardiac death and polymorphous ventricular tachycardia in pationts with normal QT intervals...
6
Susan J. Eisenberg, MD, Melvin M. Scheinman, MD, Navneet K. Dullet, MBBS, Walter E. Finkbeiner, MD, Jerry C. Griffin, MD, Michael Eldar, MD, Michael R. Franz, MD, Roland0 Gonzalez, MD, Alan H. Kadish, MD, and Michael D. Lesh, MD This siudy d&e&es he clinical spectrum of 15 patients wifh &morphic venlriculw tuchycardii ad normal QT inbrvals in he absetws ob apparwi sfwc&ul hwi dimaJar, adverse + &cts, or &ch+te+ dishrr- bances. Pcdhls pmsad with eifhhsr palpitations (n = matic implctntable cardiovmlw d&brilkr intin. (Am J Cat&i lW5;75:687-692) T he clinical setting of polymorphic ventricular tachy- cardia (VT) is a subject of current interest. Published data have focused on the occurrence of polymorphic VT in the setting of either a long QT interval, organic heart disease, drug, or electrolyte abnormalities. There is a paucity of data describing the incidence and character- istics of polymorphic VT occurring in patients with nor- mal QT intervals and normal systolic function without drug exposure or metabolic abnormalities. Coumel et al described 4 patients who exhibited recurrent bouts of polymorphic VT with normal QT intervals.* He found that the arrhythmia occurred spontaneously, unrelated to psychological stress or exertion. Arrhythmia onset was initiated by closely coupled ventricular complexes, and verapamil was found to be consistently effective in con- trolling further episodes. To date, however, published reports have not defined a rational approach toward treat- from the Department of Medicine and the Cardiovascular Research Institute at the University of California, San Francisco, California. Manuscript received August 15, 1994; revised manuscript received and accepted December 22, 1994. Address for reprints: Susan J. Eisenberg, MD, De artment of Elec- trophysiolagy, Box 02 14, Raam M-323, Universiv o P California, San Francisco, San Francisco, California 94 143, ment, and have not been able to identify patients at high risk for sudden death. The current study attempts to fur- ther delineate the clinical spectrum of 15 patients who exhibit polymorphic VT in the setting of normal QT intervals, and in the absence of any clinical manifesta- tions of heart disease, drug, or electrolyte abnormalities. MEi’HODS Over the period 1984 to 1991, 11 patients with poly- morphic VT were identified from our arrhythmia center at the University of California, San Francisco. Four addi- tional patients were referred to our center from outside institutions (2 patients were studied and followed at Kaiser Permanente, Anaheim, California, 1 at the Uni- versity of Michigan, Ann Arbor, Michigan, and 1 at Duke University, Durham, North Carolina). All patients chosen for analysis originally presented for evaluation of asymptomatic polymorphic VT, palpitations, presyn- cope, syncope, or aborted sudden death. Patients were included in the series only if they had: (1) 22 episodes of polymorphic VT documented by ambulatory electro- cardiograms, or extensive in-hospital monitoring; (2) normal left ventricular systolic cardiac function deter- mined by either echocardiogram or left ventriculogra- PREVEN.llVE CARDIOLOGY/SUDDEN DEATH AND POLYMORPHIC VENTRICUWR TACHYCARDIA 687
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of Sudden cardiac death and polymorphous ventricular tachycardia in pationts with normal QT intervals...

Susan J. Eisenberg, MD, Melvin M. Scheinman, MD, Navneet K. Dullet, MBBS, Walter E. Finkbeiner, MD, Jerry C. Griffin, MD, Michael Eldar, MD,
Michael R. Franz, MD, Roland0 Gonzalez, MD, Alan H. Kadish, MD, and Michael D. Lesh, MD
This siudy d&e&es he clinical spectrum of 15 patients wifh &morphic venlriculw tuchycardii ad normal QT inbrvals in he absetws ob apparwi sfwc&ul hwi dimaJar, adverse + &cts, or &ch+te+ dishrr- bances. Pcdhls pmsad with eifhhsr palpitations (n =
matic implctntable cardiovmlw d&brilkr intin. (Am J Cat&i lW5;75:687-692)
T he clinical setting of polymorphic ventricular tachy- cardia (VT) is a subject of current interest. Published
data have focused on the occurrence of polymorphic VT in the setting of either a long QT interval, organic heart disease, drug, or electrolyte abnormalities. There is a paucity of data describing the incidence and character- istics of polymorphic VT occurring in patients with nor- mal QT intervals and normal systolic function without drug exposure or metabolic abnormalities. Coumel et al described 4 patients who exhibited recurrent bouts of polymorphic VT with normal QT intervals.* He found that the arrhythmia occurred spontaneously, unrelated to psychological stress or exertion. Arrhythmia onset was initiated by closely coupled ventricular complexes, and verapamil was found to be consistently effective in con- trolling further episodes. To date, however, published reports have not defined a rational approach toward treat-
from the Department of Medicine and the Cardiovascular Research
Institute at the University of California, San Francisco, California.
Manuscript received August 15, 1994; revised manuscript received
and accepted December 22, 1994. Address for reprints: Susan J. Eisenberg, MD, De artment of Elec-
trophysiolagy, Box 02 14, Raam M-323, Universiv o P California, San Francisco, San Francisco, California 94 143,
ment, and have not been able to identify patients at high risk for sudden death. The current study attempts to fur- ther delineate the clinical spectrum of 15 patients who exhibit polymorphic VT in the setting of normal QT intervals, and in the absence of any clinical manifesta- tions of heart disease, drug, or electrolyte abnormalities.
MEi’HODS Over the period 1984 to 1991, 11 patients with poly-
morphic VT were identified from our arrhythmia center at the University of California, San Francisco. Four addi- tional patients were referred to our center from outside institutions (2 patients were studied and followed at Kaiser Permanente, Anaheim, California, 1 at the Uni- versity of Michigan, Ann Arbor, Michigan, and 1 at Duke University, Durham, North Carolina). All patients chosen for analysis originally presented for evaluation of asymptomatic polymorphic VT, palpitations, presyn- cope, syncope, or aborted sudden death. Patients were included in the series only if they had: (1) 22 episodes of polymorphic VT documented by ambulatory electro- cardiograms, or extensive in-hospital monitoring; (2) normal left ventricular systolic cardiac function deter- mined by either echocardiogram or left ventriculogra-
PREVEN.llVE CARDIOLOGY/SUDDEN DEATH AND POLYMORPHIC VENTRICUWR TACHYCARDIA 687
phy; (3) no clinical evidence of any other myocardial disease; and (4) a normal QT interval.
Polymorphic VT was defined as rapid (>150 beats/ min) irregular VT with continuous variation in QRS complexes of >4 beats’ duration. Torsades de pointes in- cludes as diagnostic criteria the presence of a prolonged QT interval; patients with this disease therefore were excluded from the study. QT intervals were defined as normal if they were co.42 second for men, ~0.43 sec- ond for women, and the QTc was ~0.46 second. The QT intervals were measured according to the methods sug-
gested by Lepeschkin.2 All patients were required to have normal physical
examinations and baseline 1Zlead electrocardiograms. QT intervals were measured on all available 12-lead electrocardiograms for each patient. All QT intervals measured were required to be normal, as previously de- fined, for inclusion in the study group, and an average
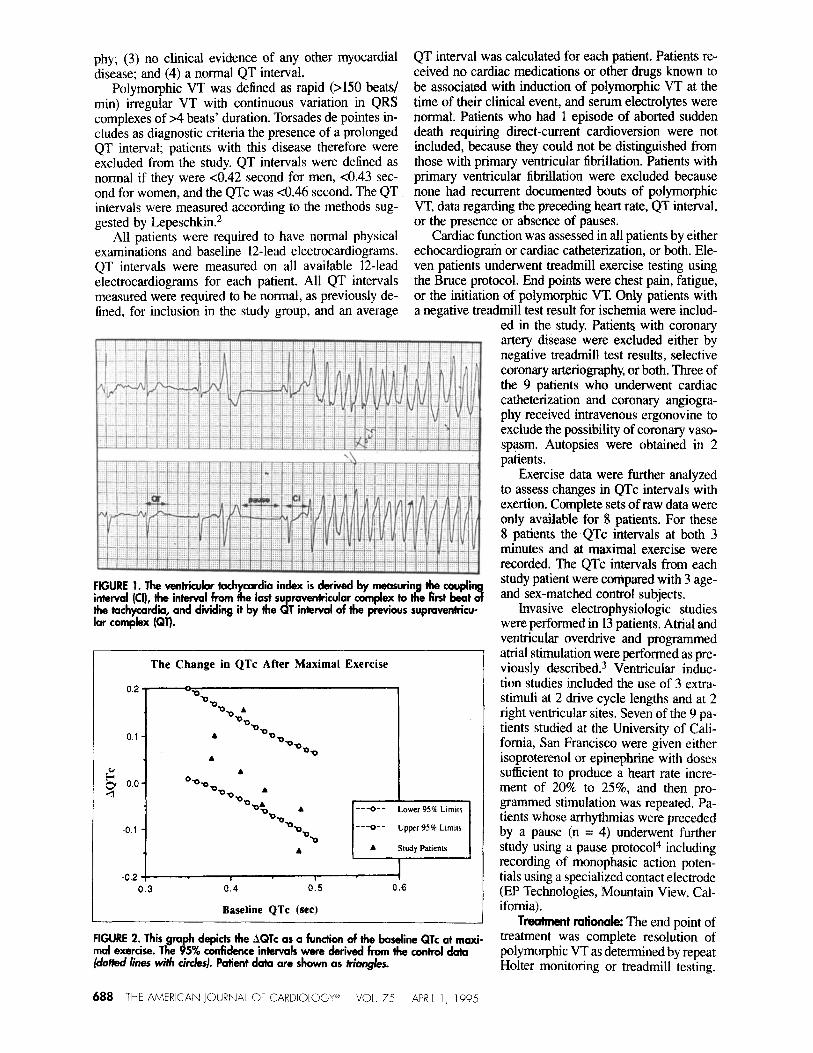
FIGURE 1. The ventricuiar tachycardia index is deriied by measuring the couph interval (Cl), the interval from the last supraventricular complex to the first beat 3 the tachycardia, and dividing it by the QT interval of the previous supmventricu- lar complex (QT).
The Change in QTc After Maximal Exercise
QT interval was calculated for each patient. Patients re- ceived no cardiac medications or other drugs known to be associated with induction of polymorphic VT at the time of their clinical event, and serum electrolytes were normal. Patients who had 1 episode of aborted sudden death requiring direct-current cardioversion were not included, because they could not be distinguished from those with primary ventricular fibrillation. Patients with primary ventricular fibrillation were excluded because none had recurrent documented bouts of polymorphic VT, data regarding the preceding heart rate, QT interval, or the presence or absence of pauses.
Cardiac function was assessed in all patients by either echocardiogram or cardiac catheterization, or both. Ele- ven patients underwent treadmill exercise testing using the Bruce protocol. End points were chest pain, fatigue, or the initiation of polymorphic VT. Only patients with a negative treadmill test result for ischemia were includ-
ed in the study. Patients with coronary artery disease were excluded either by negative treadmill test results, selective coronary arteriography, or both. Three of the 9 patients who underwent cardiac catheterization and coronary angiogra- phy received intravenous ergonovine to exclude the possibility of coronary vaso- spasm. Autopsies were obtained in 2 patients.
Exercise data were further analyzed to assess changes in QTc intervals with exertion. Complete sets of raw data were only available for 8 patients. For these 8 patients the QTc intervals at both 3 minutes and at maximal exercise were recorded. The QTc intervals from each study patient were compared with 3 age- and sex-matched control subjects.
m--o-- Lower 956 Lmm
---o-- tipper 95% Lmwr
A Study Patients
-0.2 I
0.3 0.4 0.5 0.6
Baseline QTc (set)
Invasive electrophysiologic studies were performed in 13 patients. Atrial and ventricular overdrive and programmed atria1 stimulation were performed as pre- viously described.3 Ventricular induc- tion studies included the use of 3 extra- stimuli at 2 drive cycle lengths and at 2 right ventricular sites. Seven of the 9 pa- tients studied at the University of Cali- fornia, San Francisco were given either isoproterenol or epinephrine with doses sufficient to produce a heart rate incre- ment of 20% to 25%, and then pro- grammed stimulation was repeated. Pa- tients whose arrhythmias were preceded by a pause (n = 4) underwent further study using a pause protocol4 including recording of monophasic action poten- tials using a specialized contact electrode (EP Technologies, Mountain View, Cal- ifomia) .
FIGURE 2. This graph depicts the AQTc as a function of the bawline QTc at maxi- mal exercise. The 95% confidence intervals were der’ked from the control data (dotkd lines witi &/es). Patient data are shown as triangles.
Treatment rationale: The end point of treatment was complete resolution of polymorphic VT as determined by repeat Holter monitoring or treadmill testing.
688 l-HE AMERICAN JOURNAL OF CARDIOIOG’i- VOL. 75 APRIL I, 1995
Most patients continued to have frequent ventricular pre- mature complexes, and this was not considered to be a treatment failure. Patients who had polymorphic VT induced by exertion were treated initially with J.3 block- ers.5.6 If unable to tolerate the p blockers, therapy was changed to calcium channel blocking agents5a6 Those with polymorphic VT associated with coronary artery spasm were treated with calcium channel blocking agents. Patients with spontaneous polymorphic VT preceded by pauses were treated with chronic cardiac pacing using either atrial or dual chamber pacemakers. If pacing alone was insufficient to control the arrhythmia, S-blocking drugs were added first. Failure to suppress the arrhyth- mia with pacing and p blockers resulted in the addition of a second drug, which was usually a calcium channel blocker or, in 1 patient, a type Ib antiarrhythmic drug. Treatment for the patients with spontaneous poIymor- phic VT without pauses was not uniform, but always included initial trials of either p blockers or calcium channel blockers, and 1 patient was treated with a type Ia antiarrhythmic drug. Any patient who experienced aborted sudden death, either at presentation or during the follow-up period, received an automatic defibrillator in addition to the regimen previously detailed.
Fdbw-up: Patients were followed at regular intervals by either their referring physician or our arrhythmia clin- ic. Follow-up electrocardiograms and 24-hour Holter recordings were obtained twice yearly or as clinically indicated to assess drug efficacy and pacemaker func- tion. Patients were followed for a mean of 50.4 months (range 5 to 144).
DC&J andyEis: All available episodes of polymorphic VT were analyzed with reference to QT interval, base- line heart rate, length of the initiating pause (if present), and by the coupling interval introducing the episode of polymorphic VT. The QT interval was measured from 12-lead electrocardiograms obtained in closest temporal relation to the episodes of tachycardia. QTc intervals were calculated by dividing the QT interval by the square root of the RR interval. A pause was defined as the last RR interval immediately preceding tachycardia onset, which is longer than preceding RR intervals by Z%lO ms. To better characterize and quantify arrhythmia onset a VT index was derived for each episode of polymorphic VT The index was calculated by measuring the interval from the last supraventricular complex before polymor- phic VT onset to the first complex of the tachycardia. This interval was called the coupling interval To com- pare the coupling interval between patients with varying heart rates and QT intervals, the coupling interval was then expressed as a fraction of the patient’s own QT interval. The VT index would then equal the coupling interval divided by the QT interval of the last normally conducted complex immediately before arrhythmia onset (VT index = coupling interval/QT)7 (Figure 1). If the tachycardia was initiated during inscription of the T wave (R on T phenomenon), the value would be ~1.0. and is referred to as short-coupled polymorphic VT Con- versely, if the tachycardia began with a late-coupled ven- tricular complex, the VT index would be >l.O.
SWisiics: A VT index was derived for each episode of polymorphic VT, and a mean index and SD were cal-
PREVENTIVE CARDIOLOGY/SUDDFN DEATH AND POLYMORPHIC VENTRICUIAR TACHYCARDIA 689

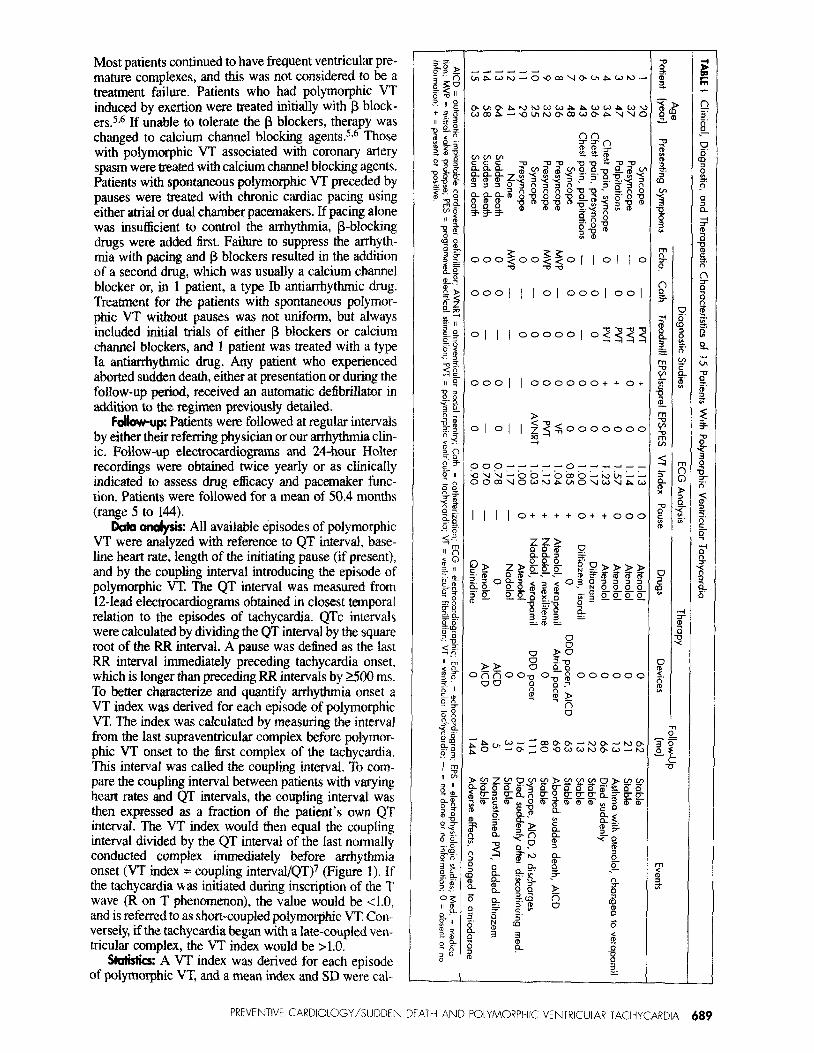
FIGURE 3. An exam* of initiation of tachycardia in patients with exercise- induced tochycardia. There is no preceding pause, and the ventricular tachycardia index is ~1.0. The lead depicted is lead II.
culated for each patient. QTc data recorded during tread- mill tests from both study patients and the age- and sex- matched control subjects were compared using paired t test and linear regression analysis. Probability was con- sidered significant at p ~0.05.
RESULTS Baseline characteristics: Results from the 15 patients
(8 women and 7 men, mean age 41 years [range 20 to 641) are recorded in Table I. All baseline electrocardio- grams were normal with an average QT interval of 0.41 second for men, and 0.41 + 0.02 second for women at heart rates of 53 to 100 beats/mm The QTc of all patients who underwent a treadmill test went from 0.443 f 0.043 at rest to 0.473 + 0.044 with exertion. There was no sta- tistically significant difference in the AQTc with exer- tion at either 3 minutes or at maximal exertion between study patients and age- and sex-matched control sub- jects. Linear regression analysis was used to see if the
QTc or the AQTc was predictable from any of the baseline characteristics. Re- gression lines were obtained from the control subjects with 95% confidence intervals to show the predictive value of the AQTc as a function of the base- line QTc (Figure 2). The 95% confi- dence intervals of the study patients were all found to lie within that of the control group. QT intervals were also analyzed before and after isoproterenol infusion in 6 patients. QT intervals all shortened from 0.433 second at base- line to 0.417 after an increase of at least 10% to 15% in heart rate.
All patients had normal systolic car- diac function, and 3 patients had evi- dence of mild mitral valve prolapse which was not hemodynamically sig- nificant.
Exercise-induced ~dymwphic ventricular tachycardii: Treadmill testing reproducibly induced polymorphic VT in 4 patients (Figure 3). Three of these 4 patients had no pause preceding the onset of polymorphic VT, and the fourth patient occasionally had episodes which were pause-dependent. The polymorphic VT indexes were all >1.13 in this group (range 1.13 to 1.57). None of these patients experienced spontaneous, nonexertional episodes of polymorphic VT, as documented by ambulatory elec- trocardiographic monitoring.
Baseline programmed electrical stimulation included atria1 and ventricular overdrive pacing at rates of >2OO beats/min and failed to provoke the arrhythmia. The infusion of isoproterenol alone, without pacing, induced short bursts of polymorphic VT in 3 of 4 patients.
All 4 of the patients were initially treated with a p blocker, and the treadmill test normalized. One patient (no. 4) died suddenly after running up a flight of stairs. She had been successfully treated with a p blocker for 66 months before her demise. Autopsy revealed a dilat-
ed right ventricle with full-thickness fatty re- placement of the right ventricular free wall. Microscopic analysis (Figure 4) revealed myo- cyte degeneration and widespread transmur- al replacement of myocardium with fat. These findings are consistent with arrhythmogenic right ventricular dysplasia. It is notable that this patient had serially normal echocardio- grams.
Polymaqhii wntiicular tochycardia in- duced by caronary artery spclsm: Two pa- tients had bouts of polymorphic VT clearly associated with chest pain. Both of these pa- tients denied any history of cocaine or ergo- tamine use. One patient (no. 5) had a pre- ceding pause and a VT index of 1.17, whereas the other (no. 6) had no pauses and a VT index of 1.00.
FIGURE 4. Patient 4. Whde mount showing marked fatty replacement of Marked focal coronary artery spasm was myocardium of the r’
pillary muscles an 3 ht ventricle. Only focal areas of the subendocardial produced in both patients after intravenous
p”
h&e&e contain significant numbers of myocyks. Hematoxykn-eosin stain, magnification x 5, reduced by 35%.)
ergonovine, and in patient 6 the left anteri- or descending artery spasm was followed by
690 THE AMERICAN JOURNAL OF CARDIOLOGY* ‘VOL 75 APRll 1, 1995

progressive ST-segment elevation and ultimately a sal- vo of polymorphic VT. Electrophysiologic studies were negative in both patients, including programmed stimu- lation after administration of epinephrine in patient 6. Both patients were treated with calcium channel block- ers and have had no further episodes.
sponkneor#rly octcming pdnorphic ventiubr twhy- cclrclia: Nine patients had spontaneously occurring epi- sodes of polymorphic VT associated with short VT in- dexes. The VT indexes were all 21.17 (range 0.70 to 1.17). This group could be further subdivided into pa- tients whose tachycardia was pause-related (Figure 5), and those in whom no pause preceded the onset of poly- m
tmmus tachycardi:
polpoqk vmiricubr Four patients had episodes of polymorphic
VT documented by ambulatory electrocardiographic re- cordings, and polymorphic VT was not inducible with exercise testing. Pauses were associated with ventricu- lar premature contractions in 3 patients and by extreme sinus bradycardia in 1. The duration of the pauses ranged from 0.5 to 2.9 seconds. Aborted sudden death occurred in 2 patients, and a third experienced a syncopal episode preceded by rapid palpitations.
Three of the 4 patients received pacemakers (dual chamber in 2, atria1 in 1) to prevent pauses from initiat- ing bouts of tachycardia. The fourth patient refused pace- maker therapy. Chronic pacing alone, however, was only effective for 1 patient (no. 7). The others (nos. 8,9, and 10) received a p blocker with or without chronic pacing. All 3 required the addition of a second agent to com- pletely control ongoing bursts of polymorphic VT. All patients who experienced either aborted sudden death or recurrent syncope either at presentation or during fol- low-up also received an implantable defibrillator.
Electrophysiologic studies were performed on all 4 of the patients in this group. With triple extrastimuli, 1 patient developed nonsustained polymorphic VT, where- as another had inducible ventricular fibrillation. The oth- er 2 patients had negative studies. Isoproterenol did not induce any additional arrhythmias. Monophasic action potential catheter recordings were obtained in 3 patients and did not reveal any early or late afterdepolarizations.
Non-pause-dependent spontaneous polymorphic ven- trkubr tachycardii: Five patients experienced sponta- neous polymorphic VT without preceding pauses, 3 of whom presented with aborted sudden death. All of these patients had repeated bouts of spontaneous polymorphic VT initiated by short-coupled ventricular complexes that were unrelated to exertion.
All of the 5 patients were treated with medications, and automatic defibrillators were implanted in 2 of the 3 patients who presented with aborted sudden death. The third patient refused device therapy. Four of the 5 pa- tients have done well, with no further symptoms or defib- rillator discharges. The fifth patient (no. 11) died sud- denly after discontinuing his medications. Autopsy revealed normal gross and histologic findings.
Three of these patients had electrophysiologic studies. One patient (no. 14) had ventricular fibrillation inducible with burst pacing from the right ventricular apex. Pro- grammed stimulation failed to provoke any arrhythmias in the other patients despite the addition of epinephrine in 2. Simultaneous monophasic action potential recordings failed to show evidence of any afterdepolarizations.
DISCUSSION Polymorphous VT has been well described in the set-
ting of adverse drug reactions, metabolic abnormalities, ischemia and reperfusion, organic heart disease, or in the congenital long QT syndrome. We describe a cohort of patients with polymorphic VT in the setting of normal QT intervals, and no apparent heart disease. Our main findings include a very high incidence of sudden death and a limited role for ventricular programmed stimula- tion. We found that patients could be divided into those with apparent initiating factors, and those whose poly- morphic VT occurred spontaneously.
It has been previously suggested that abnormally long QTc intervals in response to exertion may be a marker for arrhythmogenic substrate.” We found no statistical- ly significant difference in QTc response to exertion between our study patients and a group of age- and sex- matched control subjects. QTc response to exercise was not predictive of arrhythmia risk in any subset of this study population.
FIGURE 6. An example Ot ~hycardia in a
pause, akd the v&k&r tkhycardii index is extwnely short (0.70).
PREVENTIVE CARDIOLOGY/SUDDEN DEATH AND POLYMORPHIC VENTRICULAR TACHYCARDIA 691

Although this arrhythmia usually responds to g blockade, 1 young patient with exercise-induced poly- morphic VT died suddenly.9 We previously reported the association of exercise-induced polymorphic VT in a patient with right ventricular dysplasia.l” We suggest that exercise-induced polymorphic VT mandates excluding right ventricular dysplasia with cardiac magnetic reso- nance imaging. A high incidence of sudden death due to right ventricular dysplasia has been reported in Ital- ian athletes. I1
Two patients had bouts of polymorphic VT associat- ed with coronary artery spasm. They both responded to treatment with chronic calcium channel blockade. Poly- morphic VT and sudden death have been described in the setting of coronary spasm.12
Patients with spontaneous polymorphic VT had a strikingly high incidence of sudden death events (67%). The data would suggest that short VT indexes are a mark- er for patients with increased risk. In addition, patients with spontaneous polymorphic VT preceded by a pause (n = 4) did not universally respond to pacing. The lack of a clear-cut response to pacing alone, or pacing com- bined with drug therapy, mandates consideration for an automatic defibrillator.
The clinical association between bradyca.rdia’3~14 and polymorphic VT has been well described.15p1’j This is seen in older patients with severe organic heart disease. Thus, our patients with pause-dependent polymorphic VT differ from those described in previous reports.
Another subset of patients with spontaneous poly- morphic VT (n = 5) did not exhibit any pause depen- dency. Eighty percent of these patients experienced either sudden or aborted sudden death either at presen- tation or during follow-up. The polymorphic VT index- es in this subset of patients were the shortest in the entire senes.
The electrophysiologic behavior of the arrhythmia described in this report mimics many features of the long QT syndrome. l7 Both groups have bouts of polymorphic VT and a very high incidence of syncope and sudden death. None of our patients exhibited a familial pattern; all had normal QT intervals and tended to present later in life.
It is our belief that this syndrome is more frequent than commonly appreciated (0.02% of our referrals). Since we excluded all patients with primary ventricular fibrillation, we cannot exclude the possibility that these patients had nonsustained polymorphic VT before ven- tricular fibrillation, or that the initial episode of poly- morphic VT deteriorated into ventricular fibrillation. We concur with Akhtar’s assumption that polymorphic VT may be a common cause of sudden cardiac death.18
A striking 47% of patients (7 of 15) in the entire study group experienced either sudden death or aborted sud- den death. This underscores the particularly malignant nature of polymorphic VT, and emphasizes the need for aggressive evaluation and treatment. This is significant- ly different from the benign nature of nonsustained
monomorphic VT. The presence of a preceding pause or a short VT index appears to predict increased risk for sudden death events.
Study limikhons: This study was partially retrospec- tive; therefore, not all patients were studied in a uniform manner. Specifically, not all patients underwent treadmill testing, and cardiac catheterization with ergonovine challenge was performed only when coronary spasm was suspected. Also, right ventricular dysplasia or subclini- cal left ventricular hypertrophy could have been missed. Finally, it could be argued that patients with mitral valve prolapse should not be considered to have structurally normal hearts. Indeed, there is a known association between mitral valve prolapse and sudden death,19 and our study raises the possibility that sudden death in pa- tients with mitral valve prolapse may be related to poly- morphic VT.
Acknowkdgment: We thank Gunnard Modin for his assistance with the statistical analysis of our data.
1. Coumel P, Leclercq JF, Lucet V. Possible mechanisms of the arrhythmias in the long QT syndrome. Ew Hearr J 19X5;6(suppI D):l15-129.
2. Lepeschkin E. The U wave of the electrocardiogram. Mod Concepts Cardiovasc Dis 1969;38:394. 3. Morady F, Wang YS, Scheinman MM, Sung RJ, Shen E, Shapiro WA. Extent of &al participation in atrioventricular-reciprocating tachycaniia. Circularion
1983;61:646-650.
4. Denker S, Lehman” M, Mabmud R, Gilbert C, Akbtar M. Effects of alternating cycle lengths on refractoriness of the His-Purkinje system. J Clin Invesr 1984,74: S5%-570. 5. Nguyen m, Scheinman MM, Seger J. Polymorphous ventricular tachywdia:
clinical characterization, therapy and the QT interval. Circularion 1986;74:34O-349.
6. Woelfel A, Foster JR, McAllister RGJ, Simpson RJJ, Gettes LS. Efficacy of ver-
apamil in exercise-induced ventriculw tachycardia. Am J Cwdiol 1985:X%292-297. 7. Low B, Fakbro AM, Hood WBJ. Thorn GW. The coronary care unit. New per-
spectives and directions. JAMA 1967;199:18%198. 8. Kadish AH, Weisman HF, V&I EP, Epstdn AE, Slepian MJ. Levme JH. Para-
doxical effects of exercise on the QT interval in patients with polymorphic ven-
tncular tachycardia receiving type la antianhythmic agents. Crr&arion 1990;8 I: 14-19.
9. Morgera T , Pivotti F. Gori P, Maras P. Mechanism of action and efficacy of ver-
apamil and beta-blockers in exercise-induced ventricular tachycardia. Eur Hem J 1987;8(suppl D):99--105.
10. Morady F, Shen EN, Scheinman MM. Unusual features of arrhythmogenic right ventricular dysplasia. Am .I Cmdiol I984:53:639-640.
11. Cormdo D. Thiene G, Nava A, Rossi L, Pen&Ii N. Sudden death in young
competitive athletes: clinicopatholog~c correlations in 22 cases. Am J Med 1990:89: 588-596.
12. Priori SG, Mantica M, Napolitano C, Schwaa PJ. Early afterdepolarizations
mduced in wvo by reperfusion of ischsmic myocardium. A possible mechanism for reperfusion arrhythmias. Cirrukuia~ l990;8 I : 191 l-1920.
13. Brugada P. Wellens HJ. The role of triggered activity in clinical ventricular
arrhythmias. PACE 1984:7:26&27 I.
14. Bmgada P, Wellens HJ. Early afterdepolarizations: role in conduction block,
“prolonged repolarizationdependent reexcitation.” and tachyarrhytbmias in the
human heart. PACE 1985$:889-X96. 15. Puddu PE, Bourdssa MG, Waters DD, ixspemnce J. Sudden death in two
patients with variant angina and apparently minimal fixed coronary stenoses. J Ek- rmwrdiol 1983; l6:2 13-220. 16. Strasberg B, Kusniec J, Erdman S, Lewn RF, Arditti A, Sclarovsky S, Agmon
J. Polymorphous ventricular tachycwlia and atriaventricular block. PACE I98h:9:
522-526. 17. Schwatr PJ. idiopathic long QT syndrome: progress and question\. Am Hecrrr
J 19X5;109:39WI I.
18. Akbta M. Clinical spectrum of ventrular tachycwdia. Ckularion 1990;82: 1561.-157.1.
19. Pratt CM, Young JB, Wierman AM, Borland RM, Seals AA, Leon CA, R&n-
er A, Quinones MA, Roberts R. Complex ventricular arrhythmias associated with the mitral valve prolapse syndrome. Effectiveness of moricizine (ethmozine) in
patients resistant to conventional antiarrhythmics. .4m J Med 3986;80:62&632.
692 THE AMERICAN JOURNAL OF CARDIOLOGY” VOL. 75 APRlt 1, 1995