Transient Cardiac BallooningâThe Syndrome
7
Transient Cardiac Ballooning — The Syndrome Raghav Gupta, MD; Candice Sech, MD; Ralph Lazzara, MD, FACC Section of Cardiovascular Diseases, Department of Internal Medicine, University of Oklahoma Health Sciences Center (Gupta, Sech, Lazzara), Oklahoma City, Oklahoma Address for correspondence: Raghav Gupta, MD 920 SL Young Blvd, WP 3010 Oklahoma City, OK 73104 [email protected] Transient cardiac ballooning is usually a reversible clinical entity. A patient typically presents with chest pain, electrocardiogram (ECG) abnormalities like ST-segment elevation (most commonly reported) or depression, and elevated cardiac enzymes, but has no or nonobstructive coronary artery disease. Left ventriculography reveals transient akinesis of the involved portion of the myocardial wall with compensatory hyperkinesis of the remaining myocardium, leading to ballooning of the noncontracting myocardial wall during systole. Acute regional myocardial dysfunction ensues, which normalizes on average within 1 to 6 weeks. The hypotheses for these pathophysiologic changes range from direct cardiac myocyte injury to postischemic myocardial stunning to neurotransmitter actions. The objective of this article is to present a succinct description of a small case series accompanied with various recently reported presentations and morphology by left ventriculogram and a detailed review of available data on underlying pathophysiology. In addition, a discussion on current diagnostic guidelines, treatment, prognosis, and potential future investigations is included. Introduction The differential diagnosis of reversible myocardial dys- function includes cardiotoxins, such as alcohol, cocaine, or antiretroviral agents; nutritional deficiencies (eg, thi- amine, selenium); endocrine disturbances (hyperthyroidism, hypothyroidism, pheochromocytoma); viral myocarditis; lyme carditis; hypersensitivity reactions; and infiltrative processes such as hemochromatosis, peripartum cardiomy- opathy, and tachycardia induced cardiomyopathy 1 and Takotsubo or stress-induced cardiomyopathy. It has been reported to account for as many as 1% of admissions for suspected acute myocardial infarction (MI). 2 Initially reported as transient apical dysfunction by Dote et al, 3 it can involve any part of the heart, but most commonly the left ventricle (LV). Takotsubo is a Japanese word used to describe a pot with a round bottom and narrow neck used for trapping octopi. In the last decade, the syndrome has been called by various names primarily based either on its most important inciting factor that is, stress, or its angio- graphic image—stress-induced cardiomyopathy, 4,5 broken heart syndrome, 6,7 ampulla cardiomyopathy, 8 or transient LV apical ballooning syndrome. 2,9 Clinical Discussion of Encountered Cases Three different encountered cases have been included in the review to enhance clinical understanding and are detailed (Table 1, Table 2, Figure 1, Figure 2). Our first patient presented with classic symptoms of chest pain with ST-segment elevation (Table 1, Figure 1) and cardiac enzyme elevation (Table 2) suggesting anterior infarction after a stressful trigger. Like all 3 encountered cases, she was found to have a normal coronary angiogram (Figure 1), but depicted an atypical left ventriculographic (LV gram) pattern with upper-anterior and mid-inferior wall hypokinesis and hence ballooning (Figure 2). The second patient was a young female contrary to the common norm of postmenopausal women. She was mentally handicapped and experienced acute shortness of breath, troponin, and ST-elevation (Table 2, Figure 1) during an arthroscopic procedure. Urgent cardiac catheterization revealed an unusual nonapical ballooning pattern during LV gram (Figure 2). Hers was a peculiar case altogether, as medical procedures inducing acute cardiac ballooning and dysfunction are an oddity, but her inability to properly understand an ongoing invasive procedure was thought to be the source of extreme stress eventually resulting in stress cardiomyopathy. The third case was the most typical for the syndrome, demonstrating ST-elevation in anterolateral leads (Figure 1) and chest pain after stress, but was one of the more severe cases as well. She had marked troponin elevation (Table 2) with a markedly low LV ejection fraction of < 20% (Table 1) and LV gram showing a larger ballooned area surrounding and involving the apex itself (Figure 2). This also correlates with her taking a longer duration of around 6 weeks to recover her cardiac function. All patients were cared for in the intensive care unit (ICU) during the acute phase while receiving high dose intravenous diuretics for the management of severe congestive heart failure. The second patient required vasopressor support with dobutamine for 1 day in ICU and therefore was not on β-blockers while the first patient received metoprolol tartrate (25 mg twice a day) and the third patient received carvedilol (6.25 mg twice a day). All were discharged on cardiac supportive medications including low dose angiotensin- converting enzyme (ACE) inhibitors and were followed up in the cardiology clinic every month for 3 months except for the second patient, who was lost to follow-up. The other 2 patients are healthy, maintaining normal cardiac function, and have not had any recurrence of symptoms. 614 Clin. Cardiol. 32, 11, 614 – 620 (2009) Received: March 19, 2009 Accepted with revision: June 15, 2009 Published online in Wiley InterScience. (www.interscience.wiley.com) DOI:10.1002/clc.20652 2009 Wiley Periodicals, Inc.
-
Upload
independent -
Category
Documents
-
view
6 -
download
0
Transcript of Transient Cardiac BallooningâThe Syndrome

Transient Cardiac Ballooning—TheSyndrome
Raghav Gupta, MD; Candice Sech, MD; Ralph Lazzara, MD, FACCSection of Cardiovascular Diseases, Department of Internal Medicine, University of OklahomaHealth Sciences Center (Gupta, Sech, Lazzara), Oklahoma City, Oklahoma
Address for correspondence:Raghav Gupta, MD920 SL Young Blvd, WP 3010Oklahoma City, OK [email protected]
Transient cardiac ballooning is usually a reversible clinical entity. A patient typically presents with chest pain,electrocardiogram (ECG) abnormalities like ST-segment elevation (most commonly reported) or depression,and elevated cardiac enzymes, but has no or nonobstructive coronary artery disease. Left ventriculographyreveals transient akinesis of the involved portion of the myocardial wall with compensatory hyperkinesis ofthe remaining myocardium, leading to ballooning of the noncontracting myocardial wall during systole. Acuteregional myocardial dysfunction ensues, which normalizes on average within 1 to 6 weeks. The hypothesesfor these pathophysiologic changes range from direct cardiac myocyte injury to postischemic myocardialstunning to neurotransmitter actions. The objective of this article is to present a succinct description of a smallcase series accompanied with various recently reported presentations and morphology by left ventriculogramand a detailed review of available data on underlying pathophysiology. In addition, a discussion on currentdiagnostic guidelines, treatment, prognosis, and potential future investigations is included.
IntroductionThe differential diagnosis of reversible myocardial dys-function includes cardiotoxins, such as alcohol, cocaine,or antiretroviral agents; nutritional deficiencies (eg, thi-amine, selenium); endocrine disturbances (hyperthyroidism,hypothyroidism, pheochromocytoma); viral myocarditis;lyme carditis; hypersensitivity reactions; and infiltrativeprocesses such as hemochromatosis, peripartum cardiomy-opathy, and tachycardia induced cardiomyopathy1 andTakotsubo or stress-induced cardiomyopathy. It has beenreported to account for as many as 1% of admissionsfor suspected acute myocardial infarction (MI).2 Initiallyreported as transient apical dysfunction by Dote et al,3 itcan involve any part of the heart, but most commonly theleft ventricle (LV). Takotsubo is a Japanese word used todescribe a pot with a round bottom and narrow neck usedfor trapping octopi. In the last decade, the syndrome hasbeen called by various names primarily based either on itsmost important inciting factor that is, stress, or its angio-graphic image—stress-induced cardiomyopathy,4,5 brokenheart syndrome,6,7 ampulla cardiomyopathy,8 or transientLV apical ballooning syndrome.2,9
Clinical Discussion of Encountered Cases
Three different encountered cases have been includedin the review to enhance clinical understanding and aredetailed (Table 1, Table 2, Figure 1, Figure 2). Our firstpatient presented with classic symptoms of chest painwith ST-segment elevation (Table 1, Figure 1) and cardiacenzyme elevation (Table 2) suggesting anterior infarctionafter a stressful trigger. Like all 3 encountered cases,she was found to have a normal coronary angiogram(Figure 1), but depicted an atypical left ventriculographic(LV gram) pattern with upper-anterior and mid-inferiorwall hypokinesis and hence ballooning (Figure 2). The
second patient was a young female contrary to thecommon norm of postmenopausal women. She was mentallyhandicapped and experienced acute shortness of breath,troponin, and ST-elevation (Table 2, Figure 1) during anarthroscopic procedure. Urgent cardiac catheterizationrevealed an unusual nonapical ballooning pattern duringLV gram (Figure 2). Hers was a peculiar case altogether,as medical procedures inducing acute cardiac ballooningand dysfunction are an oddity, but her inability to properlyunderstand an ongoing invasive procedure was thought tobe the source of extreme stress eventually resulting in stresscardiomyopathy. The third case was the most typical forthe syndrome, demonstrating ST-elevation in anterolateralleads (Figure 1) and chest pain after stress, but was one ofthe more severe cases as well. She had marked troponinelevation (Table 2) with a markedly low LV ejection fractionof < 20% (Table 1) and LV gram showing a larger balloonedarea surrounding and involving the apex itself (Figure 2).This also correlates with her taking a longer duration ofaround 6 weeks to recover her cardiac function. All patientswere cared for in the intensive care unit (ICU) duringthe acute phase while receiving high dose intravenousdiuretics for the management of severe congestive heartfailure. The second patient required vasopressor supportwith dobutamine for 1 day in ICU and therefore was not onβ-blockers while the first patient received metoprolol tartrate(25 mg twice a day) and the third patient received carvedilol(6.25 mg twice a day). All were discharged on cardiacsupportive medications including low dose angiotensin-converting enzyme (ACE) inhibitors and were followedup in the cardiology clinic every month for 3 months exceptfor the second patient, who was lost to follow-up. The other2 patients are healthy, maintaining normal cardiac function,and have not had any recurrence of symptoms.
614 Clin. Cardiol. 32, 11, 614–620 (2009) Received: March 19, 2009Accepted with revision: June 15, 2009Published online in Wiley InterScience. (www.interscience.wiley.com)
DOI:10.1002/clc.20652 2009 Wiley Periodicals, Inc.
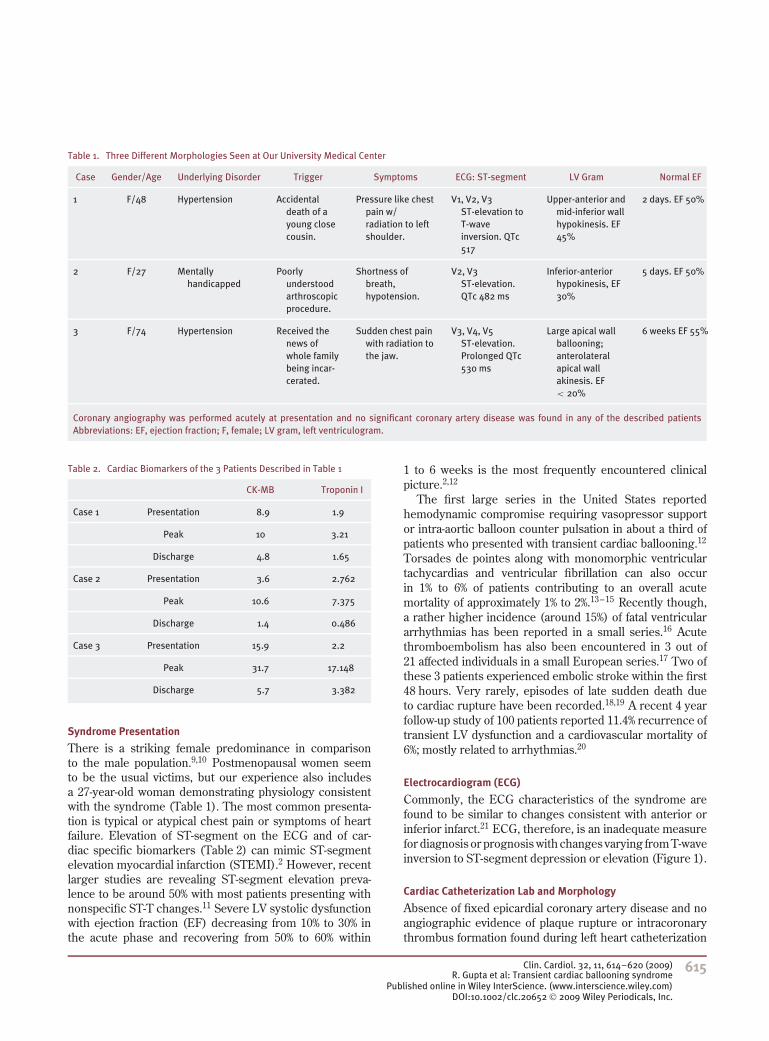
Table 1. Three Different Morphologies Seen at Our University Medical Center
Case Gender/Age Underlying Disorder Trigger Symptoms ECG: ST-segment LV Gram Normal EF
1 F/48 Hypertension Accidentaldeath of ayoung closecousin.
Pressure like chestpain w/radiation to leftshoulder.
V1, V2, V3ST-elevation toT-waveinversion. QTc517
Upper-anterior andmid-inferior wallhypokinesis. EF45%
2 days. EF 50%
2 F/27 Mentallyhandicapped
Poorlyunderstoodarthroscopicprocedure.
Shortness ofbreath,hypotension.
V2, V3ST-elevation.QTc 482 ms
Inferior-anteriorhypokinesis, EF30%
5 days. EF 50%
3 F/74 Hypertension Received thenews ofwhole familybeing incar-cerated.
Sudden chest painwith radiation tothe jaw.
V3, V4, V5ST-elevation.Prolonged QTc530 ms
Large apical wallballooning;anterolateralapical wallakinesis. EF< 20%
6 weeks EF 55%
Coronary angiography was performed acutely at presentation and no significant coronary artery disease was found in any of the described patientsAbbreviations: EF, ejection fraction; F, female; LV gram, left ventriculogram.
Table 2. Cardiac Biomarkers of the 3 Patients Described in Table 1
CK-MB Troponin I
Case 1 Presentation 8.9 1.9
Peak 10 3.21
Discharge 4.8 1.65
Case 2 Presentation 3.6 2.762
Peak 10.6 7.375
Discharge 1.4 0.486
Case 3 Presentation 15.9 2.2
Peak 31.7 17.148
Discharge 5.7 3.382
Syndrome Presentation
There is a striking female predominance in comparisonto the male population.9,10 Postmenopausal women seemto be the usual victims, but our experience also includesa 27-year-old woman demonstrating physiology consistentwith the syndrome (Table 1). The most common presenta-tion is typical or atypical chest pain or symptoms of heartfailure. Elevation of ST-segment on the ECG and of car-diac specific biomarkers (Table 2) can mimic ST-segmentelevation myocardial infarction (STEMI).2 However, recentlarger studies are revealing ST-segment elevation preva-lence to be around 50% with most patients presenting withnonspecific ST-T changes.11 Severe LV systolic dysfunctionwith ejection fraction (EF) decreasing from 10% to 30% inthe acute phase and recovering from 50% to 60% within
1 to 6 weeks is the most frequently encountered clinicalpicture.2,12
The first large series in the United States reportedhemodynamic compromise requiring vasopressor supportor intra-aortic balloon counter pulsation in about a third ofpatients who presented with transient cardiac ballooning.12
Torsades de pointes along with monomorphic ventriculartachycardias and ventricular fibrillation can also occurin 1% to 6% of patients contributing to an overall acutemortality of approximately 1% to 2%.13–15 Recently though,a rather higher incidence (around 15%) of fatal ventriculararrhythmias has been reported in a small series.16 Acutethromboembolism has also been encountered in 3 out of21 affected individuals in a small European series.17 Two ofthese 3 patients experienced embolic stroke within the first48 hours. Very rarely, episodes of late sudden death dueto cardiac rupture have been recorded.18,19 A recent 4 yearfollow-up study of 100 patients reported 11.4% recurrence oftransient LV dysfunction and a cardiovascular mortality of6%; mostly related to arrhythmias.20
Electrocardiogram (ECG)
Commonly, the ECG characteristics of the syndrome arefound to be similar to changes consistent with anterior orinferior infarct.21 ECG, therefore, is an inadequate measurefor diagnosis or prognosis with changes varying from T-waveinversion to ST-segment depression or elevation (Figure 1).
Cardiac Catheterization Lab and Morphology
Absence of fixed epicardial coronary artery disease and noangiographic evidence of plaque rupture or intracoronarythrombus formation found during left heart catheterization
Clin. Cardiol. 32, 11, 614–620 (2009) 615R. Gupta et al: Transient cardiac ballooning syndrome
Published online in Wiley InterScience. (www.interscience.wiley.com)DOI:10.1002/clc.20652 2009 Wiley Periodicals, Inc.

Reviews continued
Patient 1 Patient 2 Patient 3
I
II
III
VI
II
V5
aVR
aVL
aVF
V1
V2
V3
V4
V5
V6
I
II
III
VI
II
V5
aVR
aVL
aVF
V1
V2
V3
V4
V5
V6
I
II
III
VI
II
V5
aVR
aVL
aVF
V1
V2
V3
V4
V5
V6
Figure 1. Composite figure containing electrocardiograms (top row) and coronary angiogram (bottom row) images of 3 patients at our center. Patient 1:ST-segment elevation and T-wave inversion in anterior leads with QTc prolongation (V1, V2, V3). Patient 2: ST-elevation in V2 and V3. Patient 3: ST-elevationin V3, V4, and V5 (anterolateral) with QTc prolongation. Bottom row depicts non-destructive coronary angiograms of the three patients.
Patient 1 Patient 2 Patient 3
Left ventriculogram during diastole
Left ventriculogram during systole
Figure 2. Composite figure of 3 patients depicting right anterior oblique view (RAO) of left ventriculogram images during diastole (top row) and systole(bottom row): Patient 1: Inferobasal, upper-anterior ballooning during systole forming an inverted Takotsubo-like picture. Patient 2: Inferoanteriorhypokinesis during systole while the apex seems to contract well and hence is not visualized as are the basal segments. Patient 3: Classic and large apicalballooning during systole.
616 Clin. Cardiol. 32, 11, 614–620 (2009)R. Gupta et al: Transient cardiac ballooning syndromePublished online in Wiley InterScience. (www.interscience.wiley.com)DOI:10.1002/clc.20652 2009 Wiley Periodicals, Inc.

(LHC) is the characteristic feature. Acetylcholine provoca-tion during catheterization has also not revealed induciblecoronary spasms in this patient population.2,22 The LV gramduring the LHC demonstrates decreased or no motion ofa portion of the LV myocardial wall (most commonly theapex) with the remaining myocardium becoming hypercon-tractile and apparently compensating (Figure 2, Patient 3).This asynergy results in a decreased LVEF.
A variety of angiographic presentations have beenencountered with different areas of the heart beinginvolved. These LV grams have been called midventricu-lar ballooning23 (a variant in which the middle segments ofthe ventricle balloons during systole), inverted Takotsubopattern10 (Figure 2, Patient 1), or nonapical ballooning24
(Figure 2, Patient 2). Right ventricular involvement andbiventricular dysfunction have been recently reportedand were found to be associated with worse myocardialdysfunction.25,26 The presence of symptomatic cardiogenicshock was significantly more common in patients with api-cal ballooning rather than nonapical ballooning.24 It is alsonotable that apical vs midventricular LV dysfunction candiffer on recurrence in the same patient.27 The accumulateddata indicates that these are morphologic variants of a sin-gle syndrome and the term, transient cardiac ballooningsyndrome (TCBS), provides a consistent nomenclature28
unifying all variations of this reversible regional myocardialasynergy and dysfunction, both clinically and angiographi-cally (apical, midventricular, or right ventricular).
Guidelines for Diagnosis
Two sets of similar guidelines have been published: oneby the Mayo Clinic in the United States (Table 3)9 and theother by the Takotsubo Cardiomyopathy Study Group inJapan.29 The Japanese guidelines are more elaborate andcall the apical ballooning seen in cerebrovascular accidentsand pheochromocytoma, a Takotsubo-like myocardial dys-function. While the criteria can be extrapolated to includedifferent ballooning patterns, the most important aspect ofdocumented normalization of EF should not be overlooked.Therefore, the final diagnosis can only be concluded retro-spectively after the normalization of EF and should not bebased solely on the presence of a set of findings at a singlepoint in time.
Treatment and Follow-up
The armamentarium of LV systolic failure includingaspirin, β-blockers, diuretics, and ACE inhibitors have beenemployed in acute phase of TCBS. Although they have notshown any long-term benefit when compared to placebo,30
ethically and physiologically, it seems reasonable to aggres-sively manage an acute cardiac failure. The aim should be tomaintain supportive treatment in order to hopefully reducecardiovascular morbidity and short-term mortality. In theunusual case of severe hypotension requiring vasopressor
Table 3. Mayo Criteria for the Diagnosis of Apical Ballooning Syndrome9
1 Transient akinesis or dyskinesis of the left ventricular apical andmid-ventricular segments with regional wall motionabnormalities extending beyond a single epicardial vasculardistribution.
2 Absence of obstructive coronary disease or angiographic evidenceof acute plaque rupture.
3 Presence of new electrocardiographic abnormalities (eitherST-segment elevation or T-wave inversion).
4 Documented absence of:
1. recent significant head trauma
2. intracranial bleeding
3. pheochromocytoma
4. obstructive epicardial CAD (coronary artery disease)
5. myocarditis
6. hypertrophic cardiomyopathy
support, use of an intra-aortic balloon pump is preferableto inotropic agents as they have been reported to induceor worsen LV mid-ventricular and outflow obstruction inpatients with apical ballooning.12,31 Bedside echocardiog-raphy can rule out LV outflow tract obstruction beforeinotropes can be started.32
A recent systematic review reported the incidence of2.5% for LV thrombus formation in patients with TCBS, butthe thromboembolic complications were 0.8% and did notresult in any fatal outcomes or the need for surgery.17
Although life threatening, ventricular arrhythmias havebeen reported acutely,15,16 there is no data incorporating theuse of antiarrhythmic therapy or intracardiac defibrillator(ICD). The decision to implant an ICD could be consideredbased on other risk factors if the LVEF is still low after 6 to8 weeks on maximal medical therapy. Chronic managementshould be based on individual patient characteristics. Eventhough 4-year recurrence rate of 11.4% has been reported,the 4-year survival was not different from that in an age-matched and gender-matched population.15,20
Pathophysiology and Mechanisms
Multiple hypotheses have been proposed to explain thissyndrome, but the causal mechanisms remain uncertain.
The hypothesis of multivessel coronary spasm has beencountered by the inability of intracoronary acetylcholineto provoke it in a majority of patients.2,3,22,33 In addition,the duration of wall motion abnormality in TCBS is usuallylonger than expected in conventional cases of coronaryvasospasm. Endomyocardial biopsy has not revealed anyevidence of myocarditis.4 Those with MI due to occlusionof the left anterior descending coronary artery with a longapical-inferior segment (known as recurrent-LAD); depict an
Clin. Cardiol. 32, 11, 614–620 (2009) 617R. Gupta et al: Transient cardiac ballooning syndrome
Published online in Wiley InterScience. (www.interscience.wiley.com)DOI:10.1002/clc.20652 2009 Wiley Periodicals, Inc.

Reviews continued
extensive apical akinesia on the right anterior oblique (RAO)view on ventriculography.34 However, LAD ischemia wouldproduce dyskinesia along the anteroapical, anteroseptal, andinferior walls while sparing the lateral and posterior septalwalls (not seen in RAO view during ventriculography).Therefore, a uniform global apical akinesis, as seen inthe classic form of TCBS, is unlikely with recurrent-LADobstruction. In addition, a low EF concurrently documentedwith nonobstructive coronary arteries goes against thehypothesis.
A more plausible hypothesis is catecholamine inducedexcess sympathetic stimulation accounting for a reversiblystunned myocardium.4 Single photon emission computedtomography (SPECT) iodine-123 metaiodobenzylguanidine(MIBG) myocardial scintigraphy found an increase in heart-to-mediastinal ratio and global wash-out-rates of MIBGin patients with TCBS suggesting increased secretionand turnover of norepinephrine by sympathetic nerveterminals.22 There is higher norepinephrine content andgreater density of sympathetic nerves at the base of theheart35,36 and the distal LV apical wall has been shownto be particularly vulnerable to myocardial stunning incatecholamine-mediated toxicity. This neurohormonal stun-ning is comprised of supraphysiologic levels of plasmacatecholamines and other stress-related neuropeptides suchas serotonin and neuropeptide Y. According to a recenthypothesis, supraphysiologic circulating epinephrine levelstrigger a switch in the intracellular signal trafficking inventricular cardiomyocytes, from Gs protein to Gi proteinsignaling via the β2-adrenoceptor. These effects are nega-tively inotropic and are greatest at the apical myocardium,where the β2-adrenoceptor density is greatest.37 Corrobo-rative evidence of activation of the adrenomedullary systemalso comes from experiments on animal models of emotionalstress, such as immobilized (IMO) rats.38 ST-segment ele-vation and transient reduction in LV contraction, includingLV apical ballooning can be completely normalized by acombined blockade of α and β adrenoreceptors in IMOrats.38,39
Some indirect effects of catecholamine on the cardiomy-ocyte, though poorly explained, involve factors such as oxy-gen derived free radicals interfering with cation transportersin the myocardial sarcolemma.40,41 In addition, myocardialstunning has been explained by mechanisms involving tran-sient disturbances in calcium homeostasis culminating in adepressed contractile state. Transient intracellular calciumoverload has also been found in early reperfusion injury inin-vitro studies.42
Several observations, however, do not conform to thehypothesis of catecholamine excess. Severe or episodichypertension seen in 90% of pheochromocytoma patientshas not been observed as a feature of TCBS. Men seem toproduce higher levels of plasma catecholamines in responseto emotional stress and are more sensitive to catecholaminemediated vasoconstriction than women43,44; but women are
far more commonly affected. Recurrences are rare withrepetitive or worsening stress.
Another hypothesis is microvascular postischemic stun-ning and it is supported by radionucleotide imaging studies.Myocardial perfusion scintigraphy has shown a more pro-nounced decrease in myocardial perfusion in patients withapical dysfunction. Fluorodeoxyglucose positron emissiontomography studies have revealed a significantly greaterdecrease in glucose metabolism than in perfusion in allcorresponding segments.45 The disease therefore seems topresent with an inverse mismatch typical for the appear-ance of postischemic stunned myocardium46 suggestive ofimpaired coronary microcirculation as a causative mecha-nism. This has been supported by abnormal ThrombolysisIn Myocardial Infarction (TIMI) frame counts (a methodof quantitating the time required for injected intracoro-nary contrast to reach predefined distal landmarks) in all 3major epicardial coronary arteries during the acute phaseof this syndrome.33,47 In contrast, Abe et al did not find anyabnormalities in coronary microcirculation using Dopplerguide wire technology and contrast echocardiography.48
The coronary flow reserve (CFR) was seemingly nor-mal, suggesting adequate coronary flow; however, nofollow-up studies were done. A recent study measuredpatients’ CFR in acute stage and compared that to CFRafter recovery phase and discovered that there was sig-nificant improvement in the recovery phase in the samepatients correlating well with improvement in LV wallmotion and LVEF.49 This gives credence to the micro-circulatory postischemic stunning hypothesis at least asa probable concurring phenomenon. A potential therapeu-tic study protocol based on the above platform could bethe use of dipyridamole during LHC to increase adeno-sine diphosphate and vasodilate the microcirculation,50
once the epicardial coronary angiogram is found to benonobstructive, while still in the acute phase of thesyndrome.
With multiple mechanisms demonstrated, it is difficultto determine which are causal and which epiphenomena.Not all stress gives stress cardiomyopathy, nor does repet-itive stress. Multiple mechanisms may actually representdifferent steps of a singular physiological cascade.
ConclusionThere have been a variety of clinical and angiographicpresentations of Takotsubo-like physiology with similar out-comes. This cardiomyopathy spectrum constitutes transientcardiac ballooning syndrome, essentially involving any partof the myocardium. Demonstration of normalization of EFis as important as LHC revealing nonobstructed coronaryflow. Short-term prognosis is favorable and long-term sur-vival was not different from that in an age-matched andgender-matched population. We therefore stress the impor-tance of follow-up in this patient population to reassess any
618 Clin. Cardiol. 32, 11, 614–620 (2009)R. Gupta et al: Transient cardiac ballooning syndromePublished online in Wiley InterScience. (www.interscience.wiley.com)DOI:10.1002/clc.20652 2009 Wiley Periodicals, Inc.

continued need or reconsideration of medical management;which, at this time, is tailored to individual patient charac-teristics. Acute care incorporates congestive heart failuremanagement. In severe cases, vasopressors can be usedonce LV outflow obstruction is not found on echocardiog-raphy. At this time, routine antiarrhythmic prophylaxis oracute or long-term anticoagulation is not justified. The roleof intense physiological/emotional stress as a precipitat-ing factor has been well documented and catecholaminesappear to play an important role but the mechanism cascadeis not fully elucidated.
AcknowledgementsOur sincere thanks to Dr. TA Hennebry and Dr. JF Saucedofor providing excellent angiographic images of left heartcatheterization of the described patients.
References1. Hollenberg SM, Paillo JE. Reversible causes of severe myocardial
dysfunction. J Heart Lung Transplant. 1997;16:S7–12.2. Tsuchihashi K, Ueshima K, Uchida T, et al. Transient left
ventricular apical ballooning without coronary artery stenosis:a novel heart syndrome mimicking acute myocardial infarction.Angina pectoris-myocardial infarction investigations in Japan. J AmColl Cardiol. 2001;38:11–18.
3. Dote K, Sato H, Tateishi H, Uchida T, Ishihara M. Myocardialstunning due to simultaneous multivessel coronary spasms: areview of 5 cases. J Cardiol. 1991;21:203–214.
4. Wittstein IS, Thiemann DR, Lima JA, et al. Neurohormonalfeatures of myocardial stunning due to sudden emotional stress. NEngl J Med. 2005;352:539–548.
5. Pavin D, Le Breton H, Daubert C. Human stress cardiomyopathymimicking acute myocardial syndrome. Heart. 1997;78:509–511.
6. Brandspiegel HZ, Marinchak RA, Rials SJ, Kowey PR. A brokenheart. Circulation. 1998;98(13):1349.
7. Flavahan NA. A farewell kiss triggers a broken heart? Circ Res.2006;98:1117–1119.
8. Kawai S, Suzuki H, Yamaguchi H, Tanaka K, Sawada H, Aizawa T.Ampulla cardiomyopathy (Takotsubo cardiomyopathy) reversibleLV dysfunction with ST segment elevation. Jpn Circ J.2000;64:156–159.
9. Bybee KA, Kara T, Prasad A, et al. Systematic review: transientleft ventricular apical ballooning: a syndrome that mimics ST-segment elevation myocardial infarction. Ann Intern Med. 2004;141:858–865.
10. Lee Y-P, Poh K-K, Razak A, et al. Diverse clinical spectrum of stressinduced cardiomyopathy. Int J Cardiol. 2009;133(2):272–275.
11. Sharkey SW, Lesser JR, Menon M, Parpart M, Maron MS,Maron BJ. Spectrum and significance of electrocardiographicpatterns, troponin levels, and thrombolysis in myocardial infarctionframe count in patients with stress (tako-tsubo) cardiomyopathyand comparison to those in patients with ST-elevation anterior wallmyocardial infarction. Am J Cardiol. 2008;101(12):1723–1728.
12. Sharkey SW, Lesser JR, Zenovich AG, et al. Acute and reversiblecardiomyopathy provoked by stress in women from United States.Circulation. 2005;111:472–479.
13. Denney SD, Lakkireddy DR, Khan IA. Long QT syndrome andtorsade de pointe in transient left ventricular apical ballooningsyndrome. Int J Cardiol. 2005;100:499–501.
14. Gianni M, Dentali F, Grandi AM, Sumner G, Hiralal R, Lonn E.Apical ballooning syndrome or Takotsubo cardiomyopathy: asystematic review. Eur Heart J. 2006;27:1523–1529.
15. Dib C, Prasad A, Friedman PA, et al. Malignant arrhythmia inapical ballooning syndrome: risk factors and outcomes. IndianPacing Electrophysiol J. 2008;8(3):182–192.
16. Bonello L, Com O, Ait-Moktar O, et al. Ventricular arrhythmiasduring tako-tsubo syndrome. Int J Cardiol. 2008;128(2):e50–53.
17. de Gregorio C, Grimaldi P, Lentini C. Left ventricular thrombusformation and cardioembolic complications in patients withTakotsubo-like syndrome: a systematic review. Int J Cardiol.2008;131(1):18–24.
18. Akshi Y, Tejima T, Sakurada H, et al. Left ventricular ruptureassociated with Takotsubo cardiomyopathy. Mayo Clin Proc.2004;79:821–824.
19. Ohara Y, Hiasa Y, Hosokawa S, et al. Left ventricular free wallrupture in transient left ventricular apical ballooning. Circ J.2005;69:621–623.
20. Elesber AA, Prasad A, Lennon RJ, Wright RS, Lerman A, Rihal CS.Four-year recurrence rate and prognosis of the apical ballooningsyndrome. J Am Coll Cardiol. 2007;50:448–452.
21. Bybee KA, Motiei A, Syed IS, et al. Electrocardiography cannotreliably differentiate transient left ventricular apical ballooningsyndrome from anterior ST-segment elevation myocardialinfarction. J Electrocardiol. 2007;40(1):38.e1–6.
22. Akashi YJ, Nakazawa K, Sakakibara M, Miyake F, Musha H,Sasaka K. 123I-MIBG myocardial scintigraphy in patients with‘‘Takotsubo’’ cardiomyopathy. J Nucl Med. 2004;45:1121–1127.
23. Hurst RT, Askew JW, Reuss CS, et al. Transient midventricularballooning syndrome: a new variant. J Am Coll Cardiol. 2006; 48:579–583.
24. Hahn J-Y, Gwon H-C, Park SW, et al. The clinical features of tran-sient left ventricular nonapical ballooning syndrome: comparisonwith apical ballooning syndrome. Am Heart J. 2007;154:1166–1173.
25. Haghi D, Athanasiadis A, Papavassiliu T, et al. Right ventricu-lar involvement in Takotsubo cardiomyopathy. Eur Heart J.2006;27(20):2433–2439.
26. Novak G, Kross K, Follmer K, Brofferio A, Shirani J. Transientbiventricular apical ballooning: a unique presentation of the ‘‘bro-ken heart.’’ Clin Cardiol. 2007;30(7):355–358.
27. Blessing E, Steen H, Rosenberg M, Katus H, Frey N. Recurrenceof Takotsubo cardiomyopathy with variant forms of left ventriculardysfunction. J Am Soc Echocardiogr. 2007;439:e11–12.
28. Sharkey SW, Lesser JR, Maron MS, Maron BJ. Stress cardiomy-opathy. J Am Coll Cardiol. 2007;49(8):921; author reply 921–292.
29. Kawai S, Kitabatake A, Tomoike H; Takotsubo CardiomyopathyStudy Group. Guidelines for diagnosis of Takotsubo (ampulla)cardiomyopathy. Circ J. 2007;71:990–992.
30. Fazio G, Pizzuto C, Barbaro G, et al. Chronic pharmacologicaltreatment in Takotsubo cardiomyopathy. Int J Cardiol. 2008;127(1):121–123.
31. Previtali M, Repetto A, Scuteri L. Dobutamine induced severe mid-ventricular obstruction and mitral regurgitation in left ventricularapical ballooning syndrome. Heart. 2005;91:353.
32. Mahmoud RE, Mansencal N, Pilliere R, et al. Prevalence and char-acteristics of left ventricular outflow tract obstruction in tako-tsubosyndrome. Am Heart J. 2008;156:543–548.
33. Kurisu S, Sato H, Kawagoe T, et al. Tako-tsubo-like left ventric-ular dysfunction with ST-segment elevation: a novel cardiacsyndrome mimicking acute myocardial infarction. Am Heart J.2002;143:448–455.
34. Ibanez B, Navarro F, Farre; J, et al. Tako-tsubo syndrome associ-ated with a long course of the left anterior descending coronaryartery along the apical diaphragmatic surface of the left ventricle.Rev Esp Cardiol. 2004;57(3):209–216.
35. Pierpont GL, DeMaster EG, Cohn JN. Regional differences inadrenergic function within the left ventricle. Am J Physiol. 1984;246:H824–H829.
Clin. Cardiol. 32, 11, 614–620 (2009) 619R. Gupta et al: Transient cardiac ballooning syndrome
Published online in Wiley InterScience. (www.interscience.wiley.com)DOI:10.1002/clc.20652 2009 Wiley Periodicals, Inc.

Reviews continued
36. Kawano H, Okada R, Yano K. Histological study on the distri-bution of autonomic nerves in the human heart. Heart Vessels.2003;18:32–39.
37. Lyon AR, Rees PS, Prasad S, Poole-Wilson PA, Harding SE. Stress(Takotsubo) cardiomyopathy—a novel pathophysiological hypoth-esis to explain catecholamine-induced acute myocardial stunning.Nat Clin Pract Cardiovasc Med. 2008;5(1):22–29.
38. Ueyama T, Yoshida K, Senba E. Stress induced elevation ofthe ST segment in the rat electrocardiogram in normalized byan adrenorector blocker. Clin Exp Pharmacol Physiol. 2000;27:384–386.
39. Ueyama T, Kasamatsu K, Hano T, Yamamoto K, Tsuruo Y, Nishio I.Emotional stress induces transient left ventricular hypocontrac-tion in the rat via activation of cardiac adrenoreceptors. Circ J.2002;66:712–713.
40. Bolli R, Marban E. Molecular and cellular mechanisms of myocar-dial stunning. Physiol Rev. 1999;79:609–634.
41. Singal PK, Kapur N, Dhillon KS, Beamish RE, Dhalla NS. Role offree radicals in catecholamine-induced cardiomyopathy. Can JPhysiol Pharmacol. 1982;60:1390–1397.
42. Bolli R. Mechanism of myocardial ‘‘stunning.’’ Circulation. 1990;82(3):723–738.
43. Frankenhaeuser M, Dunne E, Lundberg U. Sex differences insympathetic-adrenal medullary reactions induced by differentstressors. Psychopharmacology (Berl). 1976;47:1–5.
44. Kneale BJ, Chowienczyk PJ, Brett SE, Coltart DJ, Ritter JM. Gen-der differences in sensitivity to adrenergic agonists of forearmresistance vasculature. J Am Coll Cardiol. 2000;36:1233–1238.
45. Kurowski V, Kaiser A, Hof K, et al. Apical and midventricular tran-sient left ventricular dysfunction syndrome (tako-tsubo cardiomy-opathy)—frequency, mechanisms, and prognosis. Chest. 2007;132:809–816.
46. Trevi GP, Sheiban I. Chronic ischemic (‘‘hibernating’’) and postis-chemic (‘‘stunned’’) dysfunctional but viable myocardium. EurHeart J. 1991;12(suppl G):20–26.
47. Bybee KA, Prasad A, Barsness GW, et al. Clinical characteristicsand thrombolysis in myocardial infarction frame counts in womenwith transient left ventricular apical ballooning syndrome. Am JCardiol. 2004;94:343–346.
48. Abe Y, Kondo M, Matsuoka R, Araki M, Dohyama K, Tanio H.Assessment of clinical features in transient left ventricular apicalballooning. J Am Coll Cardiol. 2003;41:737–742.
49. Meimoun P, Malaquin D, Sayah S, et al. The coronary flow reserveis transiently impaired in tako-tsubo cardiomyopathy: a prospectivestudy using serial Doppler transthoracic echocardiography. J AmSoc Echocardiogr. 2008;21(1):72–77.
50. Saya S, Hennebry TA, Lozano P, Lazzara R, Schechter E. Coronaryslow flow phenomenon and risk for sudden cardiac death due toventricular arrhythmias: a case report and review of literature. ClinCardiol. 2008;31(8):352–355.
620 Clin. Cardiol. 32, 11, 614–620 (2009)R. Gupta et al: Transient cardiac ballooning syndromePublished online in Wiley InterScience. (www.interscience.wiley.com)DOI:10.1002/clc.20652 2009 Wiley Periodicals, Inc.