
Study of matrix metalloproteinases and their tissue inhibitors in ductal in situ carcinomas of the...
13
Study of matrix metalloproteinases and their tissue inhibitors in ductal in situ carcinomas of the breast L O Gonzalez, 1,2,3 M D Corte, 1 J Vazquez, 1,2 S Junquera, 1 R Sanchez, 1 A Vin ˜ a, 1 J C Rodriguez, 1,2,4 M L Lamelas 1,2,5 & F Vizoso 1,2,4 1 Unidad de Investigacio ´n, Hospital de Jove, Gijo ´n, Spain, 2 Instituto Universitario de Oncologı ´a del Principado de Asturias, Oviedo, Spain, 3 Servicio de Anatomı ´a Patolo ´gica, 4 Servicio de Cirugı ´a General, and 5 Servicio de Ginecologı ´a, Hospital de Jove, Gijo ´n, Spain Date of submission 6 August 2007 Accepted for publication 24 April 2008 Gonzalez L O, Corte M D, Vazquez J, Junquera S, Sanchez R, Vin ˜ a A, Rodriguez J C, Lamelas M L & Vizoso F (2008) Histopathology 53, 403–415 Study of matrix metalloproteinases and their tissue inhibitors in ductal in situ carcinomas of the breast Aims: To analyse the expression of metalloproteinases (MMPs) and their inhibitors (TIMPs) in ductal carcin- oma in situ of the breast (DCIS). Methods and results: An immunohistochemical study was performed in 56 patients with pure DCIS, in 39 with DCIS adjacent to invasive carcinoma (IDC) and 63 patients with T1 IDC, using tissue microarrays and specific antibodies against MMPs and TIMPs. Immuno- histochemical results were categorized using a spe- cific software program. The data were analysed by unsupervised hierarchical cluster analysis by each cellular type. IDC showed a higher expression rate of MMP-7 and TIMP-1 than pure DCIS, as well as a higher expression rate of MMP-9 and TIMP-3 than the DCIS component of mixed cases, whereas pure DCIS showed a higher rate of expression of MMP-9 and -11 and TIMP-3 than in the DCIS component of mixed cases. Pure DCIS with a periductal inflamma- tory infiltrate showed significantly higher MMP-2, -14 and TIMP-1. Dendograms identified two cluster groups with distinct MMP ⁄ TIMP expression profiles in neo- plastic cells and fibroblastic or mononuclear inflamma- tory cells surrounding the neoplastic ducts of pure DCIS. Conclusions: The results indicate the distinct variability in MMP ⁄ TIMP expression by DCIS, which may be of potential biological and clinical interest in breast cancer. Keywords: breast cancer, ductal carcinoma in situ, matrix metalloproteinase, prognosis, tissue inhibitor of metalloproteinase, tissue arrays, tumour invasion Abbreviations: BCS, breast conservative surgery; BM, basement membrane; DCIS, ductal carcinoma in situ; ER, oestrogen receptor; H&E, haematoxylin and eosin; IDC, invasive ductal carcinoma; MIC, mononuclear inflammatory cell; MMP, matrix metalloproteinase; PR, progesterone receptor; TIMP, tissue inhibitor of metalloproteinase; TMA, tissue microarray Introduction With the adoption of screening mammography, the incidence of ductal carcinoma in situ (DCIS) has risen dramatically and DCIS now accounts for about 25% of new cases of breast carcinoma annually. 1 DCIS of the breast represents a neoplastic proliferation of epithelial cells that is confined to the ductal system and has not extended through the basement membrane (BM). Therefore, in principle, it has no metastatic potential. However, about 16–22% of DCIS cases develop recur- rence after breast-conserving surgery and about half of them recur in the form of invasive cancer that is more difficult to cure. 2 Even with radiotherapy, there is a 7–9% recurrence rate, 3–5 of which about half are invasive. 5,6 However, little is known about the biology of these preinvasive cancers. Combinations of nuclear Address for correspondence: Dr Francisco J Vizoso, Unidad de Investigacio ´ n, Hospital de Jove, Avda Eduardo Castro s ⁄ n, 33920 Gijo ´n, Asturias, Spain. e-mail: [email protected] ȑ 2008 The Authors. Journal compilation ȑ 2008 Blackwell Publishing Limited. Histopathology 2008, 53, 403–415. DOI: 10.1111/j.1365-2559.2008.03136.x
Transcript of Study of matrix metalloproteinases and their tissue inhibitors in ductal in situ carcinomas of the...

Study of matrix metalloproteinases and their tissue inhibitorsin ductal in situ carcinomas of the breast
L O Gonzalez,1,2,3 M D Corte,1 J Vazquez,1,2 S Junquera,1 R Sanchez,1 A Vina,1
J C Rodriguez,1,2,4 M L Lamelas1,2,5 & F Vizoso1,2,4
1Unidad de Investigacion, Hospital de Jove, Gijon, Spain, 2Instituto Universitario de Oncologıa del Principado de Asturias,
Oviedo, Spain, 3Servicio de Anatomıa Patologica, 4Servicio de Cirugıa General, and 5Servicio de Ginecologıa, Hospital de
Jove, Gijon, Spain
Date of submission 6 August 2007Accepted for publication 24 April 2008
Gonzalez L O, Corte M D, Vazquez J, Junquera S, Sanchez R, Vina A, Rodriguez J C, Lamelas M L & Vizoso F
(2008) Histopathology 53, 403–415
Study of matrix metalloproteinases and their tissue inhibitors in ductal in situ carcinomasof the breast
Aims: To analyse the expression of metalloproteinases(MMPs) and their inhibitors (TIMPs) in ductal carcin-oma in situ of the breast (DCIS).Methods and results: An immunohistochemical studywas performed in 56 patients with pure DCIS, in 39with DCIS adjacent to invasive carcinoma (IDC) and 63patients with T1 IDC, using tissue microarrays andspecific antibodies against MMPs and TIMPs. Immuno-histochemical results were categorized using a spe-cific software program. The data were analysed byunsupervised hierarchical cluster analysis by eachcellular type. IDC showed a higher expression rate ofMMP-7 and TIMP-1 than pure DCIS, as well as ahigher expression rate of MMP-9 and TIMP-3 than the
DCIS component of mixed cases, whereas pureDCIS showed a higher rate of expression of MMP-9and -11 and TIMP-3 than in the DCIS componentof mixed cases. Pure DCIS with a periductal inflamma-tory infiltrate showed significantly higher MMP-2, -14and TIMP-1. Dendograms identified two cluster groupswith distinct MMP ⁄ TIMP expression profiles in neo-plastic cells and fibroblastic or mononuclear inflamma-tory cells surrounding the neoplastic ducts of pureDCIS.Conclusions: The results indicate the distinct variabilityin MMP ⁄ TIMP expression by DCIS, which may be ofpotential biological and clinical interest in breastcancer.
Keywords: breast cancer, ductal carcinoma in situ, matrix metalloproteinase, prognosis, tissue inhibitor ofmetalloproteinase, tissue arrays, tumour invasion
Abbreviations: BCS, breast conservative surgery; BM, basement membrane; DCIS, ductal carcinoma in situ;ER, oestrogen receptor; H&E, haematoxylin and eosin; IDC, invasive ductal carcinoma; MIC, mononuclearinflammatory cell; MMP, matrix metalloproteinase; PR, progesterone receptor; TIMP, tissue inhibitor ofmetalloproteinase; TMA, tissue microarray
Introduction
With the adoption of screening mammography, theincidence of ductal carcinoma in situ (DCIS) has risendramatically and DCIS now accounts for about 25% ofnew cases of breast carcinoma annually.1 DCIS of thebreast represents a neoplastic proliferation of epithelial
cells that is confined to the ductal system and has notextended through the basement membrane (BM).Therefore, in principle, it has no metastatic potential.However, about 16–22% of DCIS cases develop recur-rence after breast-conserving surgery and about half ofthem recur in the form of invasive cancer that is moredifficult to cure.2 Even with radiotherapy, there is a7–9% recurrence rate,3–5 of which about half areinvasive.5,6 However, little is known about the biologyof these preinvasive cancers. Combinations of nuclear
Address for correspondence: Dr Francisco J Vizoso, Unidad de
Investigacion, Hospital de Jove, Avda Eduardo Castro s ⁄ n, 33920
Gijon, Asturias, Spain. e-mail: [email protected]
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Limited.
Histopathology 2008, 53, 403–415. DOI: 10.1111/j.1365-2559.2008.03136.x

grade (low, intermediate or high), as well as thepresence of necrosis, margin width and tumour size,have all been used to predict the relative risk ofrecurrence and ⁄ or progression of disease.7 However,accuracy is not sufficient to identify patients at highrisk of recurrence as invasive cancer. During the pastdecade there has therefore been increased interest instudying various molecular markers as prognostic andpredictive factors in DCIS.8
Degradation of the connective tissue stroma andinvasion of the BM are key elements in tumour invasionand metastasis. The degradation of matrix componentsis executed by proteolytic enzymes of various classes.However, some components, particularly the interstitialcollagens, are very resistant to proteolytic attack andcan be degraded only by matrix metalloproteinases(MMPs).9 The activity of MMPs is specifically inhibitedby tissue inhibitors of metalloproteinase (TIMPs) or bynon-specific protease inhibitors (e.g., a2-macroglogu-lin). Currently, four different TIMPs are known to exist:TIMP-1, -2, -3 and -4. Nevertheless, it is now assumedthat TIMPs are multifactorial proteins also involved inthe induction of proliferation and inhibition of apopto-sis10,11 (TIMP-312 and TIMP-113). During the process oftumour invasion, the various groups of MMPs appearto have different functions. This may be due to theirsubstrate preference. It can be assumed that thegelatinases are primarily responsible for the destructionof BM collagen IV, whereas the stromelysins degradenon-collagenous proteins, such as laminins or entrac-tin ⁄ nidogen. When the tumour cells have destroyed theBM and have gained contact with the interstitial matrix,collagenases are required to disrupt the native intersti-tial collagen network, which is mainly made up ofcollagen types I, III and V and the microfibrillar colla-gen IV.14,15 In addition, there are data which clearlychallenge the classic dogma stating that MMPs promotemetastasis solely by modulating the remodelling ofextracellular matrix. MMPs have also been identifiedthat influence tumour cell behaviour in vivo as aconsequence of their ability to cleave growth factors,cell surface receptors, cell adhesion molecules orchemokines ⁄ cytokines.16–21 Furthermore, by cleavingof pro-apoptotic factors, MMPs may generate a moreaggressive phenotype by generation of apoptotic resis-tant cells.22 MMPs may also regulate angiogenesis incancer, both positively through their ability to mobilizeor activate pro-angiogenic factors,23,24 and negativelyvia generation of angiogenesis inhibitors, such asangiostatin and endostatin, cleaved from large proteinprecursors.25–27 Consequently, several MMPs, in par-ticular the gelatinases MMP-228–35 and MMP-9,34,36–38
have recently been studied as prognostic factors in
breast cancer and have been associated with a pooroutcome in various subsets of breast cancer. Likewise,it has been reported that several other MMPs andTIMPs may be overexpressed and ⁄ or related to clini-cal outcome in breast cancer, such as MMP-7,38
MMP-11,29,38 MT1-MMP (MMP-14),28,38,39 MMP-13,40 TIMP-138,41–45 and TIMP-2.38,41,46,47
Although the expression of MMPs and TIMPs hasbeen less investigated in DCIS, expression of MMP-1,MMP-2,48,49 MMP-3,49 MMP-949 and TIMP-148 hasbeen reported in the stroma around non-invasive breasttumours. In addition, it has recently been reported thatexpression of certain MMPs is not statistically differentbetween DCIS and invasive ductal carcinoma (IDC),50
suggesting that the invasive potential of breast carcin-oma has already been acquired before morphologicallyovert invasive growth. Thus, on the basis of all of thesedata it is a plausible hypothesis that the expression ofseveral MMPs and TIMPs in DCIS could combine todefine a more aggressive phenotype. In the presentstudy, tissue microarray (TMA) technology and immuno-histochemical techniques were used to determinewhether there is a differential pattern of expression ofMMPs and TIMPs in DCIS.
Materials and methods
patients’ characteristics and tissue specimen
handling
Formalin-fixed paraffin-embedded breast tissue sectionswere obtained from 56 patients with pure DCIS, from39 cases of DCIS adjacent to invasive breast cancer and63 patients with IDC of the breast with T1 tumours,who underwent surgery at Fundacion Hospital de Joveof Gijon (Spain) between 1995 and 2006. The tissuesamples were obtained at the time of surgery. Patientswith DCIS were usually treated with lumpectomy,quadrantic or segmental resection and the correspond-ing archived histological slides were reviewed andreclassified according to the Consensus Conference of1997 51 for architectural subtypes and according to theclassification of Van Nuys for histological grade.52 Theexpression of oestrogen (ER) and progesterone recep-tors (PR) was evaluated by immunohistochemicaltechniques using mouse anti-ER clone 1D5 and anti-PR clone PgR 636 respectively (both Dako, Glostrup,Denmark). Allred scoring 53 was used for quantifica-tion (score 0–3, negative; score 4–8, positive). Tissuesamples from the tumours were obtained with theinformed consent of the patients. The study adhered toNational regulations and was approved by our Institu-tion’s Ethics and Investigation Committee.
404 L O Gonzalez et al.
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd, Histopathology, 53, 403–415.

tissue microarrays and
immunohistochemistry
Routinely fixed (overnight in 10% buffered formalin),paraffin-embedded tumour samples stored in the patho-logy laboratory files were used. Histopathologicallyrepresentative tumour areas were defined on haema-toxylin and eosin (H&E)-stained sections and marked onthe slide. Tumour TMA blocks were obtained bypunching a tissue cylinder (core) with a diameter of1.5 mm through a histologically representative area ofeach ‘donor’ tumour block, which was then insertedinto an empty ‘recipient’ tissue array paraffin blockusing a manual tissue arrayer (Beecher Instruments,Sun Prairie, WI, USA), as described elsewhere.54
Collection of tissue cores was carried out under highlycontrolled conditions. Areas of non-necrotic canceroustissue were selected for arraying by two experiencedpathologists (L.O.G. and A. M. Merino). Two cores wereemployed for each case. Two TMA cores of mixed caseswere taken from each case separately from both DCISand invasive components. From the 158 tumoursamples available, tissue array blocks were prepared,each containing 33 tumour samples, as well as internalcontrols including four normal breast tissue samplesfrom two healthy women who had undergone reductivemammary surgery. These latter samples containedepithelial components, in which immunoreactivitywas not seen with any of the antibodies used.
Six composite high-density TMA blocks were designedand serial 5-lm sections were consecutively cut with amicrotome (Leica Microsystems GmbH, Wetzlar, Ger-many) and transferred to adhesive-coated slides. Onesection from each tissue array block was stained withH&E and these slides were then reviewed to confirm thatthe sample was representative of the original tumour.Immunohistochemistry was done on these sections ofTMA fixed in 10% buffered formalin and embedded inparaffin using a TechMate TM50 autostainer (Dako).Antibodies for MMPs and TIMPs were obtained fromNeomarker (Lab Vision Corp., Fremont, CA, USA). Thedilution for each antibody was established based onnegative and positive controls (1:50 for MMP-2, -7, 14and TIMP-2; 1:100 for MMP-9, -13, TIMP-1 and -3;1:200 for MMP-1 and -11). The following positivecontrols were used: placenta for MMP-1, -2, -7, -11, -14and TIMP-3; breast carcinoma for MMP-9, -13 andTIMP-1; and colonic carcinoma for TIMP-2.
Tissue sections were deparaffinized in xylene and thenrehydrated in graded concentrations of ethyl alcohol(100%, 96%, 80%, 70%, then water). To enhanceantigen retrieval only for some antibodies, TMA sectionswere microwave treated in a H2800 Microwave
Processor (EBSciences, East Granby, CT, USA) in citratebuffer (Target Retrieval Solution; Dako) at 99�C for16 min. Endogenous peroxidase activity was blocked byincubating the slides in peroxidase-blocking solution(Dako) for 5 min. The EnVision Detection Kit (Dako)was used as the reactivity detection system. Sectionswere counterstained with haematoxylin, dehydratedwith ethanol and permanently coverslipped.
tma analysis
For each antibody preparation studied, the location ofimmunoreactivity, percentage of reactive area andintensity were determined. Neoplastic ducts and sur-rounding stroma were evaluated independently. Atleast two neoplastic ducts were evaluated in the DCIScases. Each protein-reactive area was semiquantified inintraductal neoplastic areas of DCIS and IDC. An imageanalysis system with the Olympus BX51 microscopeand analysis software (analySIS�; Soft Imaging System,Munster, Germany) was employed as follows. Tumoursections were stained with antibodies according to themethod explained above and counterstained withhaematoxylin. Based on the phase analysis method, aquantitative evaluation was made of each core basedon separate colour phases. There are different opticalthresholds for both stains. Each core was scanned witha ·400 power objective in two fields per core. Fieldswere selected searching for the protein-reactive areas.The computer program selected and traced a linearound antibody-reactive areas (higher optical thresh-old: red spots), with the remaining, non-reactive areas(haematoxylin-stained tissue with lower optical thresh-old) standing out as a blue background. Any field had aratio of reactive (red) versus non-reactive (blue) areas.A final area ratio was obtained after averaging twofields. To evaluate the intensity of immunoreactivity, anumeric score ranging from 0 to 3 was used, reflectingthe intensity as follows: 0, no reactivity; 1, weakreactivity; 2, moderate reactivity; and 3, intensereactivity. Using an Excel spreadsheet, the mean scorewas obtained by multiplying the intensity score (I) bythe percentage of reactive area (PA) and the resultswere added together (total score: I · PA). This overallscore was then averaged with the number of cores thatwere done for each patient. If there was no tumour in aparticular core, then no score was given. In addition,for each tumour the mean score of two core biopsysamples was calculated.
Furthermore, whole-tissue sections from tumourblocks from a subset of 10 cases were compared withthe corresponding TMA discs, regarding MMP andTIMP expression in each. Those cases were selected
Study of MMPs and their tissue inhibitors in DCIS 405
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd, Histopathology, 53, 403–415.

randomly and the clinicopathological data obtainedwere similar to those of the whole series. Each whole-tissue section was scanned with a ·400 power lens in10 different fields. Fields were selected searching for theprotein-reactive areas, as described above.
data analysis and statistical methods
Differences in percentages were calculated with the v2
test. Immunoreactivity scores for each protein wereexpressed as a median (range). Comparison of immuno-reactivity values between groups was made with theMann–Whitney or Kruskall–Wallis tests. Statisticalresults were corrected applying Bonferroni’s correction.Expression profiles were analysed by an unsupervisedhierarchical clustering method that organizes proteinsin a tree structure, based on their similarity. Data were
reformatted as follows: three designated immunoneg-ativity, three immunopositivity and missing data wereleft blank. The score values were reformatted (positive–negative) choosing the median as cut-off value. TheCluster 3.0 (Human Genome Center, Institute of MedicalScience, University of Tokyo, Tokyo, Japan) programwas used (average linkage, uncentered correlation).Results were displayed with Treeview (Department ofGenetics, Stanford University School of Medicine,Stanford, CA, USA).55 The SPSS 11.5 program wasused for all calculations (SPSS Inc., Chicago, IL, USA).
Results
More than 3700 determinations in cancer specimensfrom 56 patients with pure DCIS, 39 with DCISadjacent to IDC and 63 patients with T1 IDC and
MMP-1 MMP-2 MMP-7 MMP-9 MMP-11
MMP-13 TIMP-1MMP-14 TIMP-2 TIMP-3
B C
A
Figure 1. A, Examples of tissue microarrays with immunostaining for all the proteins evaluated. B and C, Examples of tissue microarrays with
immunostaining for MMP-9 and 11 in fibroblastic cells (large arrows) and mononuclear inflammatory cells (small arrows).
406 L O Gonzalez et al.
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd, Histopathology, 53, 403–415.

controls, were performed on TMAs. Minimal internalvariance of score data between duplicate tissue coresfrom the same patients was detected in the tissuearrays, showing a high agreement for each protein(r > 0.95 and P < 0.0001 for each protein), in DCIS asin IDC. Likewise, in the validation study there was totalconcordance in global expression, as well as in theintensity of immunoreactivity, for each MMP and TIMPbetween TMA cases and the corresponding whole-tissue sections. In addition, there were highly signifi-cant correlations in the immunoreactivity scoresbetween these two paired sets (r > 0.90 andP < 0.0001 for each protein). We have previouslydescribed a validation study for MMPs and TIMPs inrespective IDCs.38 Is also of worthy of mention thatthere was uniformity of positivity of malignant epithe-lial cells in the whole sections of DCIS for each protein.
Figure 1A shows examples of TMAs with immuno-reactivity for each protein evaluated. Immunoreactivityfor all the proteins studied was localized into neoplasticducts in neoplastic cells. Table 1 shows the percentageof DCIS showing the crude expression (positive versusnegative) for each protein in neoplastic cells, as wellas in consecutive cases of DCIS seen admixed withinvasive disease and in their corresponding IDCs, and
in consecutive T1 pure IDC, for which respectivepatients were treated in the same period. As can beseen in Table 1, there were significant differences inMMP-7, -9 and -11 and TIMP-3 expression betweenthese groups of tumours. IDC showed a higher
Table 1. MMP and TIMP expression by neoplastic cells inDCIS and DCIS component of mixed cases and in invasiveductal carcinoma of the breast
Pure DCIS(n = 56)
Mixed cases (n = 39)
T1 IDC(n = 63)DCIS
AdjacentIDC
MMP-1()) 8 (15.7) 1 (2.7) 12 (30.8) 9 (14)
(+) 43 (84.3) 36 (97.3) 27 (69.2) 54 (86)
MMP-2()) 41 (73.2) 27 (69.2) 26 (66.7) 42 (66)
(+) 15 (26.8) 12 (30.8) 13 (33.3) 21 (34)
MMP-7()) 18 (34.6) 7 (18.9) 4 (10.3) 8 (13)
(+) 34 (65.4) 30 (81.1) 35 (89.7) 55 (87)
MMP-9()) 10 (18.9) 23 (63.9) 11 (28.2) 20 (32)
(+) 43 (81.1) 13 (36.1) 28 (71.8) 43 (68)
MMP-11()) 3 (5.6) 9 (23.7) 9 (23.1) 9 (15)
(+) 51 (94.4) 29 (76.3) 30 (76.9) 54 (85)
Table 1. (Continued)
Pure DCIS(n = 56)
Mixed cases (n = 39)
T1 IDC(n = 63)DCIS
AdjacentIDC
MMP-13()) 17 (32.1) 20 (51.3) 6 (15.4) 17 (27)
(+) 36 (67.9) 19 (48.7) 33 (84.6) 46 (73)
MMP-14()) 14 (25) 11 (29.7) 8 (20.5) 7 (11)
(+) 42 (75) 26 (70.3) 31 (79.5) 56 (89)
TIMP-1()) 12 (22.2) 5 (12.8) 5 (12.8) 4 (6)
(+) 42 (77.8) 34 (87.2) 34 (87.2) 59 (94)
TIMP-2()) 6 (10.9) 7 (17.9) 4 (10.3) 9 (14)
(+) 49 (89.1) 32 (82.1) 35 (89.7) 54 (86)
TIMP-3()) 15 (28.3) 24 (61.5) 15 (38.5) 12 (19)
(+) 38 (71.7) 15 (38.5) 24 (61.5) 51 (81)
Data are expressed as number of cases (percentage).
MMP-1: mixed DCIS versus adjacent IDC, P = 0.002; MMP-7: pure DCIS versus T1 invasive carcinoma, P = 0.008;MMP-9: pure versus mixed DCIS, P < 0.001; Mixed DCISversus T1 invasive carcinoma, P = 0.004; Mixed DCIS versusadjacent IDC, P = 0.004. MMP-11: pure DCIS versus mixedDCIS, P = 0.026; MMP-13: mixed DCIS versus adjacentIDC, P = 0.002; TIMP-1: pure DCIS versus T1 invasivecarcinoma, P = 0.029; TIMP-3: pure DCIS versus mixedDCIS, P = 0.003; Mixed DCIS versus T1 invasive carcinoma,P < 0.001.
Samples of tissue sections were either insufficient or lost inpure DCIS cases for analysis in five cases for MMP-1, fourcases for MMP-7, three for MMP-9, MMP-13 and TIMP-3,two for MMP-11 and TIMP-1, one for TIMP-2. For DCIScomponent of mixed cases, samples of tissue sections wereeither insufficient or lost for analysis in two cases for MMP-1,MMP-7 and MMP-14, three for MMP-9, one for MMP-11.The values shown correspond to the total of cases analysedfor each protein.
DCIS, Ductal carcinoma in situ; IDC, invasive ductal carcin-oma; MMP, matrix metalloproteinase; TIMP, tissue inhibitorof metalloproteinase.
Study of MMPs and their tissue inhibitors in DCIS 407
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd, Histopathology, 53, 403–415.

expression rate of MMP-7 and TIMP-1 than pure DCIS(P = 0.008 and P = 0.029 respectively), as well as ahigher expression rate of MMP-9 and TIMP-3 than inthe DCIS component of mixed cases (P = 0.004 andP < 0.001, respectively), whereas pure DCIS showed ahigher expression rate of MMP-9 (P < 0.001) and -11(P = 0.026), and TIMP-3 (P = 0.003) than in the DCIScomponent of mixed cases. On the other hand, we alsofound significant differences in MMP ⁄ TIMP expressionin neoplastic cells between both the DCIS and IDCcomponent of mixed cases. Thus, the IDC componentshowed higher expression of MMP-9 (P = 0.004) and-13 (P = 0.002) than the corresponding DCIS com-ponents. In contrast, our results demonstrated thatMMP-1 expression was significantly higher in the DCIScomponent than in the invasive component of mixedcases (P = 0.002).
Our results also showed wide variability in theintensity and percentage of positive neoplastic areas,between pure DCIS and the DCIS component of mixedcases. Therefore, immunohistochemistry results werecategorized using a score based on the intensity ofreactivity and a specific software program that calcu-
lated the percentage of immunoreactive areas auto-matically. As can be seen in Table 2, the DCIScomponent of mixed cases showed a higher score forMMP-7 immunoreactivity compared with pure DCIScases (P < 0.002), whereas scores for MMP-9, -11,and TIMP-3 were significantly higher in pure DCIS(P < 0.001 for each of these comparisons). Table 2also shows the scores for each protein in the IDCcomponent of mixed cases. It is of note that scores inDCIS lesions are related to malignant cells in neoplasticducts, whereas in IDC of mixed cases they correspondto neoplastic cells and stromal cells [fibroblasts andmononuclear inflammatory cells (MIC)]. Because ofthis, the scores of DCIS and IDC are not entirelycomparable. Nevertheless, we investigated for possiblestatistical correlations between both paired DCIS andIDC lesions in mixed cases. Our results showed signi-ficant but low correlation between both DCIS and theinvasive components of mixed cases for MMP-2(r = 0.36, P = 0.021). However, our results did notshow significant correlations for the other MMPs andTIMPs between either paired sets of lesions in mixedcases (data not shown).
Table 2. MMP and TIMPscores in pure DCIS and inDCIS component of mixedcases
Factors Pure DCIS P*
Mixed cases
DCIS Adjacent IDC
MMP-1 82 (0–255.9) NS 144.3 (0–247.2) 92 (0–250)
MMP-2 0 (0–223.7) NS 0 (0–178.5) 46 (0–207)
MMP-7 45.2 (0–128.4) 0.002 69.6 (0–245.8) 135 (25–270)
MMP-9 76.1 (0–276.6) 0.0001 0 (0–133.1) 80 (0–264)
MMP-11 146.3 (0–278.4) 0.0001 43.4 (0–255) 160 (50–269)
MMP-13 48.7 (0–141.4) 0.01 0 (0–161.8) 62 (0–180)
MMP-14 54.2 (0–251.5) NS 43.6 (0–149.4) 80 (0–261)
TIMP-1 57 (0–271.6) NS 59.8 (0–145.8) 145 (0–285)
TIMP-2 66.6 (0–221) 0.02 49 (0–195.8) 129 (0–243)
TIMP-3 57 (0–266.5) 0.0001 0 (0–91.7) 115 (0–280)
Samples of tissue sections were either insufficient or lost in pure DCIS cases for analysis in fivecases for MMP-1, three cases for MMP-7, MMP-9, MMP-13 and TIMP-3, two cases forMMP-11 and TIMP-1, one case for TIMP-2. The values shown correspond to the total of casesanalysed for each protein. For DCIS component of mixed cases, samples of tissue sectionswere either insufficient or lost for analysis in three cases for MMP-9, two cases for MMP-1,MMP-7 and MMP-14, one for MMP-11. The values shown correspond to the total of casesanalysed for each protein.
DCIS, Ductal carcinoma in situ; IDC, invasive ductal carcinoma; TIMP, tissue inhibitor ofmetalloproteinase; MMP, matrix metalloproteinase.
*P-value, pure DCIS versus DCIS of mixed cases.
408 L O Gonzalez et al.
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd, Histopathology, 53, 403–415.
Tab
le3.
Rel
atio
nsh
ipbet
wee
nM
MPs
and
TIM
Ps
expre
ssio
nsc
ore
san
dcl
inic
opat
holo
gic
alan
dbio
logic
alch
arac
terist
ics
in56
case
sof
DC
ISof
the
bre
ast
Clin
icopat
holo
gic
alan
dbio
logic
alch
arac
terist
ics
nM
MP-1
MM
P-2
MM
P-7
MM
P-9
MM
P-1
1M
MP-1
3M
MP-1
4TIM
P-1
TIM
P-2
TIM
P-3
Tota
lca
ses
56
82
(0–2
55.9
)0
(0–2
23.7
)45.2
(0–1
28.4
)76.1
(0–2
76.6
)146.3
(0–2
78.4
)48.7
(0–1
41.4
)54.2
(0–2
51.5
)57
(0–2
71.6
)66.6
(0–2
21)
57
(0–2
66.5
)
Age
(yea
rs)
£55
32
81.1
(0–2
27)
0(0
–223.7
)38.3
(0–1
17.6
)63.2
(0–2
64)
144.5
(0–2
72.8
)48.3
(0–1
41.4
)48.9
(0–2
16.6
)58
(0–2
71.6
)56.8
(0–1
97.4
)43.4
(0–2
66.5
)
>55
24
82
(0–2
55.9
)0
(0–1
95)
56.1
(0–1
28.4
)87.3
(0–2
76.6
)151.1
(0–2
78.4
)52
(0–1
11.8
)56.4
(0–2
51.5
)56.1
(0–2
53)
102.8
(0–2
21)
62.7
(0–2
51.6
)
Men
opau
salst
atus
Pre
men
opau
sal
19
77
(0–1
47.1
)0
(0–2
23.7
)37.9
(0–1
09.8
)64.8
(0–2
64)
139.2
(0–2
72.8
)49
(0–7
3.9
)44.4
(0–2
16.6
)48.5
(0–2
71.6
)52.8
(0–1
88.1
)42.4
(0–2
66.5
)
Post
men
opau
sal
37
82.3
(0–2
55.9
)0
(0–2
08.3
)52
(0–1
28.4
)80.1
(0–2
76.6
)151.1
(0–2
78.4
)47.6
(0–1
41.4
)54.9
(0–2
51.5
)59.7
(0–2
53)
95.2
(0–2
21)
60.8
(0–2
61.1
)
Arc
hitec
tura
lsu
bty
pes
Mic
ropap
illar
y7
69.1
(0–8
3.8
)0
(0–1
26.4
)50.3
(0–9
8.8
)105.2
(0–1
57)
140.6
(120.7
–272.8
)0
(0–6
3.6
)56.6
(44.4
–134.6
)64.7
(0–1
47.9
)107.5
(0–2
11.7
)60.4
(0–1
61.9
)
Cribiform
8147.3
(0–2
55.9
)0
(0–1
95)
61.4
(38.5
–116.8
)64.2
(0–2
76.6
)152.8
(42–2
77.8
)52.8
(0–6
3)
56.2
(0–2
51.5
)45.2
(0–2
53)
136.5
(43.6
–221)
116.4
(42.4
–251.6
)
Solid
16
128.1
(0–2
27.4
)0
(0–7
1.6
)49.6
(0–1
20.1
)74.3
(0–1
70.2
)151
(56.4
–278.4
)48.9
(0–1
01.5
)49
(0–2
16.6
)59
(0–2
71.6
)72.2
(38.9
–188.1
)37.5
(0–2
37)
Com
edo
7121.2
(0–2
54.4
)0
(0–1
33.2
)38.1
(0–6
1.6
)96
(0–1
68.6
)92.9
(0–1
62.1
)24.3
(0–1
41.4
)22.7
(0–1
40)
60.8
(0–2
09.2
)88
(0–1
20.3
)115
(36.8
–261.1
)
Mix
ed18
74.5
(0–2
50.5
)0
(0–2
23.7
)37.3
(0–1
28.4
)62.8
(0–2
64)
151.5
(0–2
67)
49
(0–1
11.8
)55.8
(0–1
67.4
)48.5
(0–1
49.2
)52.3
(0–2
11)
38.2
(0–2
66.5
)
His
tolo
gic
algra
de
G-1
23
129.2
(0–2
55.9
)0
(0–1
95)
54.3
(0–1
20.1
)64.2
(0–2
76.6
)151.1
(0–2
78.4
)50.9
(0–1
01.5
)59.1
(0–2
51.5
)60
(0–2
53)
84.7
(0–2
21)
62.7
(0–2
51.6
)
G-2
764.4
(49.3
–121.2
)0
(0–3
1.1
)23.8
(0–1
28.4
)67.5
(0–1
68.6
)144.3
(0–2
01.4
)47
(0–1
41.4
)42.3
(0–1
40)
49.6
(0–1
20.3
)77.8
(0–1
33.2
)37.7
(0–1
51.5
)
G-3
26
81.1
(0–2
54.4
)0
(0–2
23.7
)38.1
(0–1
09.8
)99.6
(0–2
64)
143.4
(0–2
72.8
)45.4
(0–7
3.9
)53.8
(0–2
16.6
)56.1
(0–2
71.6
)60.6
(0–2
11.7
)58.7
(0–2
66.5
)
Per
iduct
alin
flam
mat
ory
infiltra
te*
***
**
No
37
82.3
(0–2
54.4
)0
(0–2
23.7
)51.7
(0–1
28.4
)71.8
(0–2
57.1
)144.3
(0–2
53.3
)48.3
(0–1
41.4
)44.4
(0–1
52.4
)49.6
(0–1
49.2
)63.6
(0–2
11.7
)43.4
(0–2
44.1
)
Yes
19
77
(0–2
55.9
)0
(0–1
95)
40.1
(0–7
2.4
)135.5
(0–2
76.6
)152.8
(0–2
78.4
)49.1
(0–7
3.9
)71.9
(0–2
51.5
)63.9
(0–2
71.6
)107.5
(0–2
21)
92.7
(0–2
66.5
)
Oes
trogen
rece
pto
rs*
Neg
ativ
e14
61.5
(0–7
9.9
)0
(0–1
26.4
)19.3
(0–7
8.2
)77.1
(0–1
68.6
)146.7
(0–2
72.8
)53.3
(0–1
41.4
)64.3
(0–2
51.5
)64.1
(0–2
53)
66.6
(0–2
00.4
)66.9
(0–1
54.2
)
Posi
tive
42
121.2
(0–2
55.9
)0
(0–2
23.7
)51.6
(0–1
28.4
)74.3
(0–2
76.6
)146.3
(0–2
78.4
)48.7
(0–1
11.8
)51.4
(0–2
16.6
)52.1
(0–2
71.6
)71.1
(0–2
21.1
)42.4
(0–2
66.5
)
Pro
ges
tero
ne
rece
pto
rs**
Neg
ativ
e23
73.1
(0–2
54.4
)0
(0–1
26.4
)51.6
(0–1
16.8
)63.7
(0–1
63.8
)139.1
(0–2
72.8
)38.5
(0–7
0.6
)53.6
(0–2
51.5
)49.5
(0–2
53)
59.2
(0–2
00.4
)52.2
(0–1
54.2
)
Posi
tive
33
120.6
(0–2
55.9
)0
(0–2
23.7
)38.5
(0–1
28.4
)97.3
(0–2
76.6
)151
(0–2
78.4
)50.9
(0–1
41.4
)55.8
(0–2
16.6
)60
(0–2
71.6
)102.4
(0–2
21)
62.7
(0–2
66.5
)
Val
ues
are
repre
sente
das
med
ian
(ran
ge)
.Sa
mple
sof
tiss
ue
sect
ions
wer
eei
ther
insu
ffici
ent
or
lost
for
anal
ysis
infive
case
sfo
rM
MP-1
,fo
ur
case
sfo
rM
MP-7
,th
ree
for
MM
P-9
,M
MP-1
3an
dTIM
P-3
,tw
ofo
rM
MP-1
1an
dTIM
P-1
,one
for
TIM
P-2
.The
valu
essh
ow
nco
rres
pond
toth
eto
talof
case
san
alys
edfo
rea
chpro
tein
.
TIM
P,
Tis
sue
inhib
itor
of
met
allo
pro
tein
ase;
MM
P,
mat
rix
met
allo
pro
tein
ase.
*P
=0.0
1;
**P
=0.0
4;
***P
=0.0
03.
Study of MMPs and their tissue inhibitors in DCIS 409
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd, Histopathology, 53, 403–415.

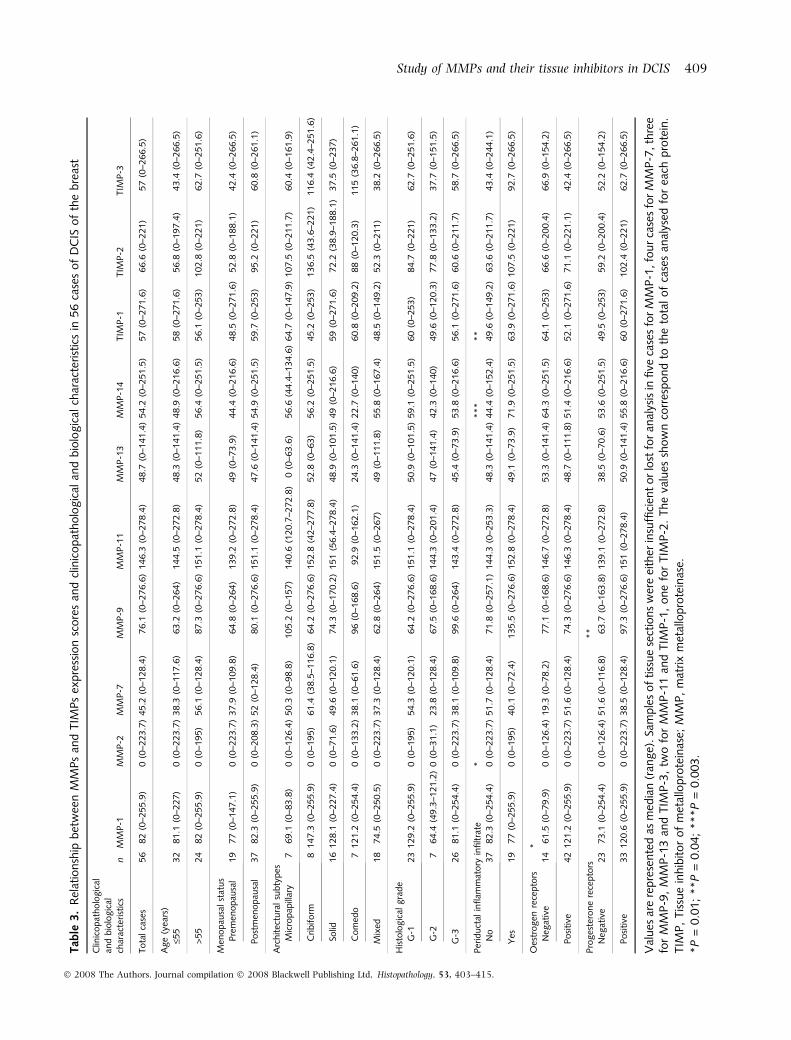
Table 3 shows the relationship between the totalimmunohistochemical scores for several proteins inneoplastic ducts of 56 pure DCIS and clinicopatholog-ical parameters, including the age and menopausalstatus of the patients, architectural subtype, histolog-ical grade and ER and PR status, and periductalinflammatory infiltrate. Immunoreactivity values forMMP-1 were significantly higher in DCIS with ER+status (P = 0.01); whereas reactivity values for MMP-9were significantly higher in DCIS with PR+ status(P = 0.04). It is of note that we chose a value of 4 asthe cut-off for hormone receptor positivity, which iscurrently used in our Institution in a clinical context.Nevertheless, when a cut-off point of 3 was used, nosignificant changes were seen. On the other hand, DCISwith periductal inflammatory infiltrate showed signifi-cant higher MMP-2 (P = 0.01) and -14 (P = 0.003),and TIMP-1 (P = 0.04). However, for the DCIS com-ponent of mixed cases, no significant associations were
found between MMP ⁄ TIMP expression and the clini-copathological parameters (data not shown).
To identify specific groups of tumours with distinctMMP ⁄ TIMP immunohistochemical expression profilesin cases of pure DCIS, the data were analysed byunsupervised hierarchical cluster analysis. The algo-rithm orders proteins on the horizontal axis andsamples on the vertical axis based on similarity oftheir expression profiles. This analysis was performedwith the score values that were reformatted (positive–negative) choosing the median as the cut-off value.Thus, the dendogram shows a first-order division ofthe tumours into two distinct MMP ⁄ TIMP molecularprofiles (Figure 2A). MMP-1, -9, and MMP-11, -13 and-14, TIMP-1, -2 and -3 were identified as showingsignificantly high expression in group 2 (n = 30)compared with group 1 (n = 26) (Table 4).
As regards the recognized importance of the stroma inthe biology of malignancies, in the present study we also
MM
P_2
A B C
MM
P_9
MM
P_1
1M
T1_
MM
PT
IMP
_3T
IMP
_1M
MP
_13
TIM
P_2
MM
P_1
MM
P_7
MM
P_9
MM
P_1
3M
MP
_7T
IMP
_1M
MP
_2T
IMP
_3M
MP
_11
MM
P_1
MT
1_M
MP
TIM
P_2
MM
P_9
MM
P_2
MM
P_7
MM
P_1
3T
IMP
_1T
IMP
_3M
T1_
MM
PM
MP
_11
MM
P_1
TIM
P_2
Figure 2. Hierarchical cluster analysis of global MMPs ⁄ TIMPs expression in the different cell types of breast cancer as measured by
immunohistochemistry on TMA. Graphical representation of hierarchical clustering results according to score values in neoplastic cells A, crude
values in fibroblasts B, and mononucelar inflammatory cells C, around the neoplastic ducts. Rows, neoplastic tumour samples; columns,
MMPs ⁄ TIMPs. Protein expression is depicted according to a colour scale: red, positive staining; green, negative staining; grey, missing data.
No major clustering of tumours is shown according to crude values for neoplastic cells or mononucelar inflammatory cells. Two major
clusterings of tumours (1 and 2) are shown for score values in neoplastic cells and for crude values for fibroblasts or mononuclear
inflammatory cells around the neoplastic ducts.
410 L O Gonzalez et al.
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd, Histopathology, 53, 403–415.

decided to investigate the MMP ⁄ TIMP molecular profileby the main stromal cellular types around the neoplasticmammary ducts in pure DCIS. Figure 1B shows exam-ples of TMAs with immunoreactivity in fibroblastic cellsand MICs in the stroma around the neoplastic mam-mary ducts. Table 5 shows the percentage of cases ofpure DCIS with immunopositivity for each protein inthese stromal cells. The percentage of positive cells foreach protein was always >80% in positives cases foreach type of cell. No significant relationship was foundbetween the expression of MMPs or TIMPs by MICs orfibroblasts and the several clinicopathological parame-ters considered in this study (data not shown). Never-theless, it is remarkable that unsupervised hierarchicalcluster analysis defined, in fibroblast cells as in MICs,two distinct MMP ⁄ TIMP molecular profiles (Figure 2Band C respectively). MMP-1, -2, -9, -13 and 14, andTIMP-1, -2 and -3 showed a significantly higherpercentage of expression in fibroblast cell group 2(n = 13) compared with fibroblast cell group 1(n = 43), whereas MMP-9, -11 and -14, and TIMP-2and -3 showed a significantly higher percentage ofexpression in MIC group 2 (n = 16) compared with MIC
group 1 (n = 40) (Table 5). In summary, it is remark-able that MMP-9 and -14, and TIMP-2 and -3 werecommonly expressed in the corresponding clustergroups of neoplastic and stromal cells having a highMMP ⁄ TIMP molecular profile.
Discussion
MMP expressions may serve as a survival signalcreating an invasive phenotype and may be an earlyrequirement in breast tumorigenesis. However, MMPand TIMP expression in non-invasive breast carcinomahas not been closely examined to date. In the presentwork, we have demonstrated that these factors may beexpressed at an early stage of tumour development, asalso reported by other authors for MMP-2, -3, -9, -13,-14 and 26, and TIMP-1 and -2.50,56–61 In addition, wehave also found variability in expression of thesespecific biological factors in DCIS, which may be ofpotential clinical interest to define prognosis of theseearly neoplastic lesions.
Although a score based on the intensity of reactivityand the percentage of the immunoreactive area is amore precise method for a more complete evaluation ofexpression of factors by neoplastic cells, the resultsof this method differ between DCIS and IDC. This isbecause, whereas DCIS is composed exclusively ofneoplastic epithelial cells, in IDC it represents a mix-ture of both neoplastic and stromal cells. Likewise,we consider that stromal cells around the neoplasticmammary ducts of the DCIS component from mixedcases may be biologically influenced by stromal cellsfrom the adjacent invasive component. For thesereasons, in the present study we have compared onlythe crude expression of MMPs and TIMPs in neoplasticcells, between pure DCIS or the DCIS component ofmixed cases with T1 IDC. These latter two groups wereincluded because these tumours seem to represent thestages of development following DCIS. Thus, it wasremarkable that MMP-7 and TIMP-1 expression wassignificantly higher in IDC than in pure DCIS. MMP-7(matrilysin 1) is a stromelysin that degrades type IVcollagen, fibronectin and laminin. It has been shownthat MMP-7 is aberrantly expressed in human breasttumours and that elimination of MMP-7 is associatedwith low invasiveness and slow tumour growth.62 Ithas also been recently reported that MMP-7 over-expression in breast cancer (MCF-7) cells enhancescellular invasiveness and activation of proMMP-2 andMMP-9.63 Thus, our data seem to emphasize the role ofMMP-7 in invasion in breast cancer. With regard toTIMP-1, if TIMPs inhibit MMPs in vivo, it would beexpected that high levels of these inhibitors would
Table 4. Expression of MMP and TIMP in two groups byhierarchical clustering of pure DCIS according to score
Factors
Group 1,n = 26(score value)
Group 2,n = 30(score value) P
MMP-1 62.9 (0–254.4) 129.9 (0–255.9) 0.01
MMP-2 0 (0–223.7) 0 (0–208.3) NS
MMP-7 47.7 (0–117.6) 38.1 (0–128.4) NS
MMP-9 43.2 (0–105.2) 147.9 (0–276.6) 0.0001
MMP-11 138.9 (0–234.6) 157.8 (0–278.4) 0.01
MMP-13 37.8 (0–53.5) 62 (0–141.5) 0.0001
MMP-14 35.3 (0–130.4) 64.6 (0–251.5) 0.0001
TIMP-1 39.8 (0–144.9) 66.2 (0–271.6) 0.0001
TIMP-2 44.1 (0–133.2) 120.1 (0–221) 0.0001
TIMP-3 0 (0–120.5) 120.4 (0–266.5) 0.0001
Values are represented as median (range). Samples of tissuesections were either insufficient or lost for analysis in fivecases for MMP-1, four cases for MMP-7, three for MMP-9,MMP-13 and TIMP-3, two for MMP-11 and TIMP-1, andone for TIMP-2. The values shown correspond to the total ofcases analysed for each protein.
DCIS, Ductal carcinoma in situ; TIMP, tissue inhibitor ofmetalloproteinase; MMP, matrix metalloproteinase.
Study of MMPs and their tissue inhibitors in DCIS 411
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd, Histopathology, 53, 403–415.

prevent tumour progression and thus be less expressedin invasive breast carcinoma. However, TIMPs aremultifunctional proteins that, in addition to theirMMP-inhibitory effect, also demonstrate distincttumour-stimulatory functions, such as stimulation ofcell proliferation.10 Likewise, a number of studies havedemonstrated an association between high TIMP-1expression and poor prognosis of breast cancerpatients.13,38
In the present study, we have also found significantdifferences in MMP ⁄ TIMP expression between pureDCIS and the DCIS component of mixed cases. Un-expectedly, pure DCIS showed high levels of MMP-9and -11 compared with the DCIS component of mixedcases. These differences in MMP expression may be dueto the different stages of neoplastic development. Otherauthors have also reported high MMP-9 expression inpure DCIS 61 and it is suggested that levels of MMP-9expression may play a role in the very early stages ofDCIS development, but once the BM has been breached,cancer cells become less dependent on the activity ofMMP-9.61 On the other hand, our data show higherTIMP-3 expression in pure DCIS compared with the
DCIS component of mixed cases. We consider thatthis finding is relevant considering the putative roleof TIMP-3 in tumour growth inhibition. Thus, it hasbeen shown that TIMP-3 antagonizes primary tumourgrowth, angiogenesis, apoptosis, tumour invasion andthe development of metastasis.11,64–67 In addition,recent studies on methylation-associated silencing ofTIMP-3 have also suggested a tumour suppressor rolefor several tumour types.68–72 This tumour suppressorfunction of TIMP-3 might not be directly related to itseffect as an MMP inhibitor: TIMP-3 overexpressioninduces apoptosis in several cell types.11,65,73–75 Inaddition, TIMP-3 is unique, in that it binds to theextracellular matrix after secretion, in contrast toTIMP-1 and TIMP-2. Due to this confined localization,TIMP-3 could be involved in specific local inhibition ofMMPs, similar to the membrane-anchored metallopro-teinase inhibitor RECK.76 Therefore, on the basis of allof these data, our results suggest that the lack ofTIMP-3 expression in pure DCIS may be a potentialmarker of invasive growth.
We have also found several aspects of biologicalinterest related to MMP expression in pure DCIS. Thus,
Table 5. Expression of MMP and TIMP in two groups by hierarchical clustering of DCIS with distinct MMP ⁄ TIMP molecularprofile in neoplastic, fibroblasts and mononuclear inflammatory cells of the stroma around the neoplastic ducts
Factor
Fibroblast cells
P
MIC
P
Cluster group 1(n = 43)Positive cases,n (%)
Cluster group 2(n = 13)Positive cases,n (%)
Cluster group 1(n = 40)Positive cases,n (%)
Cluster group 2(n = 16)Positive cases,n (%)
MMP-1 11 (27.5) 8 (72.7) 0.01 14 (37.8) 10 (71.4) NS
MMP-2 3 (7) 8 (61.5) 0.0001 0 (0) 0 (0) NS
MMP-7 2 (4.9) 2 (18.2) NS 3 (7.9) 1 (7.1) NS
MMP-9 2 (5) 12 (92.3) 0.0001 5 (13.5) 11 (68.8) 0.0001
MMP-11 25 (61) 12 (92.3) NS 22 (57.9) 15 (93.8) 0.02
MMP-13 3 (7.3) 5 (41.7) 0.01 7 (18.9) 6 (37.5) NS
MMP-14 7 (16.3) 10 (76.9) 0.0001 8 (20) 13 (81.3) 0.0001
TIMP-1 1 (2.4) 4 (30.8) 0.01 10 (26.3) 5 (31.3) NS
TIMP-2 19 (45.2) 13 (100) 0.001 21 (53.8) 16 (100) 0.003
TIMP-3 4 (9.8) 11 (91.7) 0.0001 3 (8.1) 13 (81.3) 0.0001
Samples of tissue sections were either insufficient or lost for analysis in five cases for MMP-1, four cases for MMP-7, three forMMP-9, MMP-13 and TIMP-3, two for MMP-11 and TIMP-1, one case for TIMP-2. The values shown correspond to the totalof cases analysed for each protein.
MIC, Mononuclear inflammatory cells; DCIS, ductal carcinoma in situ; IDC, invasive ductal carcinoma; TIMP, tissue inhibitor ofmetalloproteinase; MMP, matrix metalloproteinase.
412 L O Gonzalez et al.
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd, Histopathology, 53, 403–415.

inmunoreactivity values for MMP-1 expression weresignificantaly higher in DCIS with ER+ status, whereasMMP-9 expression was significantly higher in DCISwith PR+ status. Likewise, there is evidence thatoestrogens may regulate the expression of MMP-9 inbreast cancer cells.77,78 However, to our knowledge,the association of higher MMP-1 expression and ER+tumours is new. This may be related to possiblehormone regulation of these factors in the early phaseof tumour development. Also noteworthy was theexistence of a positive and significant associationbetween periductal inflammatory infiltrate and MMP-2, -14 or TIMP-1 scores in pure DCIS. These associa-tions may be of biological interest considering thatthese factors may simulate periductal angiogenesis andtherefore B and T cells may be recruited through highendothelial venules induced by the DCIS. In addition,the inflammatory infiltrate could also influence angio-genesis by releasing angiogenic factors.79
Of note, we also analysed the possible relationshipbetween MMP ⁄ TIMP expression in both DCIS and IDCcomponents of mixed cases. Our data revealed onlya significant but low correlation of MMP-2 scoresbetween the two lesions. In addition, we found signifi-cant differences between the two paired sets of lesionsfor the expression by neoplastic cells of MMP-1, -9 and-13, perhaps indicating that the step of DCIS to invasivephenotype implicates some significant changes in theexpression of MMP ⁄ TIMP. Nevertheless, further studiesare necessary for a better assessment of this transfor-mation, as well as its possible clinical significance.
Although the consideration of single MMPs or TIMPsseems to have biological importance in DCIS, we alsodecided to investigate the possible existence of distinctphenotypes of potential clinical interest in the expres-sion of MMP ⁄ TIMP in pure DCIS. When median scorevalues are considered, we found two defined subsets ofpure DCIS. One of these (n = 30) showed greaterexpression of MMP-1, -9, -11, -13 and -14, TIMP-1,-2 and -3. Likewise, considering the putative relevanceof stromal cells in the biological behaviour of breastcancer, we also decided to analyse the expression ofMMPs and TIMPs by two important populations ofstromal cells around the neoplastic mammary ducts:fibroblasts and MICs. Our results indicate the expres-sion of those proteins by these stromal cells in pureDCIS. Also remarkable, in fibroblasts as well as in MICs,was the finding of two distinct MMP ⁄ TIMP molecularprofiles. In addition, it was of note that MMP-9 and-14, and TIMP-2 and -3, were commonly expressed inthe corresponding cluster groups of neoplastic andstromal cells, which have a high MMP ⁄ TIMP mole-cular profile. Nevertheless, it should be borne in mind
that these latter subgroups also showed low levelsof MMP-7, which was expressed at higher levels ininvasive breast carcinomas and that, in contrast, theyshowed higher levels of TIMP-3 compared with theDCIS component of mixed cases. Therefore, furtherprospective studies will be necessary to assess which ofthese subgroups of pure DCIS might be more associatedwith the progression from preinvasive to invasivetumours and whether one of these two may have arole in predicting recurrence in DCIS.
In conclusion, our results indicate the existence ofvariability in MMP ⁄ TIMP expression by DCIS, which isof potential biological and clinical interest in breastcancer. Therefore, we consider that there is a need for astudy of a large number of DCIS cases with long termfollow-up, focused on invasive recurrence to evaluatethe predictive and prognostic value of these biochem-ical markers. The identification of a molecular profileassociated with tumour recurrence after breast conser-vative surgery (BCS), would be highly beneficial tofacilitate slection of the majority of DCIS patients with avery low risk of developing invasive recurrence who donot need radiotherapy after BCS.
Acknowledgements
We thank to Dr Antonio Merino for his collaboration inhistopathological evaluation of tumours. This workwas supported by a grant from FIS-PI040137 Fondo deinversion Sanitaria del Instituto Carlos III (FIS-Spain)and Obra Social Cajastur.
References
1. Ernster VL, Ballard-Barbash R, Barlow WE et al. Detection of
ductal carcinoma in situ in women undergoing screening
mammography. J. Natl Cancer Inst. 2002; 94; 1546–1554.
2. Bijker N, Rutgers EJ, Peterse JL et al. Variations in diagnostic and
therapeutic procedures in a multicentre, randomized clinical trial
(EORTC 10853) investigating breast-conserving treatment for
DCIS. Eur. J. Surg. Oncol. 2001; 27; 135–140.
3. Fisher B, Bauer M, Margolese R et al. Five-year results of a
randomized clinical trial comparing total mastectomy and
segmental mastectomy with or without radiation in the treat-
ment of breast cancer. N. Engl. J. Med. 1985; 312; 665–673.
4. Houghton J, George WD, Cuzick J et al. Radiotherapy and
tamoxifen in women with completely excised ductal carcinoma
in situ of the breast in the UK, Australia, and New Zealand:
randomised controlled trial. Lancet 2003; 362; 95–102.
5. Julien JP, Bijker N, Fentiman IS et al. Radiotherapy in breast-
conserving treatment for ductal carcinoma in situ: first results of
the EORTC randomised phase III trial 10853. EORTC Breast
Cancer Cooperative Group and EORTC Radiotherapy Group.
Lancet 2000; 355; 528–533.
6. Fisher B, Dignam J, Wolmark N et al. Lumpectomy and radiation
therapy for the treatment of intraductal breast cancer: findings
Study of MMPs and their tissue inhibitors in DCIS 413
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd, Histopathology, 53, 403–415.

from National Surgical Adjuvant Breast and Bowel Project B-17.
J. Clin. Oncol. 1998; 16; 441–452.
7. Adeyinka A, Emberley E, Niu Y et al. Analysis of gene expression
in ductal carcinoma in situ of the breast. Clin. Cancer Res. 2002;
8; 3788–3795.
8. Nofech-Mozes S, Spayne J, Rakovitch E, Hanna W. Prognostic
and predictive molecular markers in DCIS: a review. Adv. Anat.
Pathol. 2005; 12; 256–264.
9. Nelson AR, Fingleton B, Rothenberg ML, Matrisian LM. Matrix
metalloproteinases: biologic activity and clinical implications.
J. Clin. Oncol. 2000; 18; 1135–1149.
10. Jiang Y, Goldberg ID, Shi YE. Complex roles of tissue inhibitors of
metalloproteinases in cancer. Oncogene 2002; 21; 2245–2252.
11. Baker AH, George SJ, Zaltsman AB, Murphy G, Newby AC.
Inhibition of invasion and induction of apoptotic cell death of
cancer cell lines by overexpression of TIMP-3. Br. J. Cancer 1999;
79; 1347–1355.
12. Guedez L, McMarlin AJ, Kingma DW et al. Tissue inhibitor of
metalloproteinase-1 alters the tumorigenicity of Burkitt’s lym-
phoma via divergent effects on tumor growth and angiogenesis.
Am. J. Pathol. 2001; 158; 1207–1215.
13. Wurtz SO, Schrohl AS, Sorensen NM et al. Tissue inhibitor of
metalloproteinases-1 in breast cancer. Endocr. Relat. Cancer
2005; 12; 215–227.
14. Hagedorn HG, Bachmeier BE, Nerlich AG. Synthesis and degra-
dation of basement membranes and extracellular matrix and
their regulation by TGF-beta in invasive carcinomas (Review).
Int. J. Oncol. 2001; 18; 669–681.
15. Bachmeier BE, Iancu CM, Jochum M, Nerlich AG. Matrix
metalloproteinases in cancer: comparison of known and novel
aspects of their inhibition as a therapeutic approach. Expert Rev.
Anticancer Ther. 2005; 5; 149–163.
16. Sternlicht MD, Werb Z. How matrix metalloproteinases regulate
cell behavior. Annu. Rev. Cell Dev. Biol. 2001; 17; 463–516.
17. Egeblad M, Werb Z. New functions for the matrix metalloprotein-
ases in cancer progression. Nat. Rev. Cancer 2002; 2; 161–174.
18. Turk V, Kos J, Turk B. Cysteine cathepsins (proteases) – on the
main stage of cancer? Cancer Cell 2004; 5; 409–410.
19. Rifkin DB, Mazzieri R, Munger JS, Noguera I, Sung J. Proteo-
lytic control of growth factor availability. APMIS 1999; 107;
80–85.
20. Manes S, Llorente M, Lacalle RA et al. The matrix metallopro-
teinase-9 regulates the insulin-like growth factor-triggered
autocrine response in DU-145 carcinoma cells. J. Biol. Chem.
1999; 274; 6935–6945.
21. Noe V, Fingleton B, Jacobs K et al. Release of an invasion
promoter E-cadherin fragment by matrilysin and stromelysin-1.
J. Cell Sci. 2001; 114; 111–118.
22. Fingleton B, Vargo-Gogola T, Crawford HC, Matrisian LM.
Matrilysin [MMP-7] expression selects for cells with reduced
sensitivity to apoptosis. Neoplasia 2001; 3; 459–468.
23. Yu Q, Stamenkovic I. Cell surface-localized matrix metallopro-
teinase-9 proteolytically activates TGF-beta and promotes tumor
invasion and angiogenesis. Genes Dev. 2000; 14; 163–176.
24. Stetler-Stevenson WG. Matrix metalloproteinases in angiogene-
sis: a moving target for therapeutic intervention. J. Clin. Invest.
1999; 103; 1237–1241.
25. Dong Z, Kumar R, Yang X, Fidler IJ. Macrophage-derived
metalloelastase is responsible for the generation of angiostatin
in Lewis lung carcinoma. Cell 1997; 88; 801–810.
26. Cornelius LA, Nehring LC, Harding E et al. Matrix metallo-
proteinases generate angiostatin: effects on neovascularization.
J. Immunol. 1998; 161; 6845–6852.
27. Ferreras M, Felbor U, Lenhard T, Olsen BR, Delaisse J. Generation
and degradation of human endostatin proteins by various
proteinases. FEBS Lett. 2000; 486; 247–251.
28. Jones JL, Glynn P, Walker RA. Expression of MMP-2 and MMP-9,
their inhibitors, and the activator MT1-MMP in primary breast
carcinomas. J. Pathol. 1999; 189; 161–168.
29. Duffy MJ, Maguire TM, Hill A, McDermott E, O’Higgins N.
Metalloproteinases: role in breast carcinogenesis, invasion and
metastasis. Breast Cancer Res. 2000; 2; 252–257.
30. Talvensaari-Mattila A, Paakko P, Blanco-Sequeiros G, Turpeen-
niemi-Hujanen T. Matrix metalloproteinase-2 (MMP-2) is asso-
ciated with the risk for a relapse in postmenopausal patients with
node-positive breast carcinoma treated with antiestrogen adju-
vant therapy. Breast Cancer Res. Treat. 2001; 65; 55–61.
31. Baker EA, Stephenson TJ, Reed MW, Brown NJ. Expression of
proteinases and inhibitors in human breast cancer progression
and survival. Mol. Pathol. 2002; 55; 300–304.
32. Talvensaari-Mattila A, Paakko P, Turpeenniemi-Hujanen T.
Matrix metalloproteinase-2 (MMP-2) is associated with survival
in breast carcinoma. Br. J. Cancer 2003; 89; 1270–1275.
33. Grieu F, Li WQ, Iacopetta B. Genetic polymorphisms in the
MMP-2 and MMP-9 genes and breast cancer phenotype. Breast
Cancer Res. Treat. 2004; 88; 197–204.
34. Li HC, Cao DC, Liu Y et al. Prognostic value of matrix
metalloproteinases (MMP-2 and MMP-9) in patients with lymph
node-negative breast carcinoma. Breast Cancer Res. Treat. 2004;
88; 75–85.
35. Sivula A, Talvensaari-Mattila A, Lundin J et al. Association of
cyclooxygenase-2 and matrix metalloproteinase-2 expression in
human breast cancer. Breast Cancer Res. Treat. 2005; 89; 215–220.
36. Chantrain CF, Shimada H, Jodele S et al. Stromal matrix
metalloproteinase-9 regulates the vascular architecture in neuro-
blastoma by promoting pericyte recruitment. Cancer Res. 2004;
64; 1675–1686.
37. Pellikainen JM, Ropponen KM, Kataja VV et al. Expression of
matrix metalloproteinase (MMP)-2 and MMP-9 in breast cancer
with a special reference to activator protein-2, HER2, and
prognosis. Clin. Cancer Res. 2004; 10; 7621–7628.
38. Vizoso FJ, Gonzalez LO, Corte MD et al. Study of matrix
metalloproteinases and their inhibitors in breast cancer. Br. J.
Cancer 2007; 96; 903–911.
39. Mimori K, Ueo H, Shirasaka C, Mori M. Clinical significance of
MT1-MMP mRNA expression in breast cancer. Oncol. Rep. 2001;
8; 401–403.
40. Nielsen BS, Rank F, Lopez JM et al. Collagenase-3 expression in
breast myofibroblasts as a molecular marker of transition of
ductal carcinoma in situ lesions to invasive ductal carcinomas.
Cancer Res. 2001; 61; 7091–7100.
41. Ree AH, Florenes VA, Berg JP et al. High levels of messenger
RNAs for tissue inhibitors of metalloproteinases (TIMP-1 and
TIMP-2) in primary breast carcinomas are associated with
development of distant metastases. Clin. Cancer Res. 1997; 3;
1623–1628.
42. McCarthy K, Maguire T, McGreal G et al. High levels of tissue
inhibitor of metalloproteinase-1 predict poor outcome in patients
with breast cancer. Int. J. Cancer 1999; 84; 44–48.
43. Nakopoulou L, Giannopoulou I, Stefanaki K et al. Enhanced
mRNA expression of tissue inhibitor of metalloproteinase-1
(TIMP-1) in breast carcinomas is correlated with adverse
prognosis. J. Pathol. 2002; 197; 307–313.
44. Schrohl AS, Christensen IJ, Pedersen AN et al. Tumor tissue
concentrations of the proteinase inhibitors tissue inhibitor of
metalloproteinases-1 (TIMP-1) and plasminogen activator
414 L O Gonzalez et al.
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd, Histopathology, 53, 403–415.

inhibitor type 1 (PAI-1) are complementary in determining
prognosis in primary breast cancer. Mol. Cell Proteomics 2003;
2; 164–172.
45. Schrohl AS, Holten-Andersen MN, Peters HA et al. Tumor tissue
levels of tissue inhibitor of metalloproteinase-1 as a prognostic
marker in primary breast cancer. Clin. Cancer Res. 2004; 10;
2289–2298.
46. Visscher DW, Hoyhtya M, Ottosen SK et al. Enhanced expression
of tissue inhibitor of metalloproteinase-2 (TIMP-2) in the stroma
of breast carcinomas correlates with tumor recurrence. Int. J.
Cancer 1994; 59; 339–344.
47. Remacle A, McCarthy K, Noel A et al. High levels of TIMP-2
correlate with adverse prognosis in breast cancer. Int. J. Cancer
2000; 89; 118–121.
48. Polette M, Clavel C, Cockett M et al. Detection and localization of
mRNAs encoding matrix metalloproteinases and their tissue
inhibitor in human breast pathology. Invasion Metastasis 1993;
13; 31–37.
49. Lebeau A, Nerlich AG, Sauer U, Lichtinghagen R, Lohrs U. Tissue
distribution of major matrix metalloproteinases and their tran-
scripts in human breast carcinomas. Anticancer Res. 1999; 19;
4257–4264.
50. Kim HJ, Park CI, Park BW, Lee HD, Jung WH. Expression of MT-1
MMP, MMP2, MMP9 and TIMP2 mRNAs in ductal carcinoma
in situ and invasive ductal carcinoma of the breast. Yonsei Med. J.
2006; 47; 333–342.
51. Consensus conference on the classification of ductal carcinoma
in situ. Hum. Pathol. 1997; 28; 1221–1225.
52. Silverstein MJ, Poller DN, Waisman JR et al. Prognostic classifi-
cation of breast ductal carcinoma-in-situ. Lancet 1995; 345;
1154–1157.
53. Allred DC, Harvey JM, Berardo M, Clark GM. Prognostic and
predictive factors in breast cancer by immunohistochemical
analysis. Mod. Pathol. 1998; 11; 155–168.
54. Parker RL, Huntsman DG, Lesack DW et al. Assessment of
interlaboratory variation in the immunohistochemical deter-
mination of estrogen receptor status using a breast cancer
tissue microarray. Am. J. Clin. Pathol. 2002; 117; 723–
728.
55. Eisen MB, Spellman PT, Brown PO, Botstein D. Cluster analysis
and display of genome-wide expression patterns. Proc. Natl Acad.
Sci. U.S.A. 1998; 95; 14863–14868.
56. Scorilas A, Karameris A, Arnogiannaki N et al. Overexpression of
matrix-metalloproteinase-9 in human breast cancer: a potential
favourable indicator in node-negative patients. Br. J. Cancer
2001; 84; 1488–1496.
57. Soini Y, Hurskainen T, Hoyhtya M, Oikarinen A. Autio-Harmai-
nen H. 72 KD and 92 KD type IV collagenase, type IV collagen,
and laminin mRNAs in breast cancer: a study by in situ
hybridization. J. Histochem. Cytochem. 1994; 42; 945–951.
58. Nielsen BS, Sehested M, Kjeldsen L et al. Expression of matrix
metalloprotease-9 in vascular pericytes in human breast cancer.
Lab. Invest. 1997; 77; 345–355.
59. Ponder BA. Cancer genetics. Nature 2001; 411; 336–341.
60. Shekhar MP, Werdell J, Santner SJ, Pauley RJ, Tait L. Breast
stroma plays a dominant regulatory role in breast epithelial
growth and differentiation: implications for tumor development
and progression. Cancer Res. 2001; 61; 1320–1326.
61. Zhao YG, Xiao AZ, Park HI et al. Endometase ⁄ matrilysin-2 in
human breast ductal carcinoma in situ and its inhibition by
tissue inhibitors of metalloproteinases-2 and -4: a putative role in
the initiation of breast cancer invasion. Cancer Res. 2004; 64;
590–598.
62. Jiang WG, Davies G, Martin TA et al. Targeting matrilysin and its
impact on tumor growth in vivo: the potential implications in
breast cancer therapy. Clin. Cancer Res. 2005; 11; 6012–6019.
63. Wang F, Reierstad S, Fishman DA. Matrilysin over-expression in
MCF-7 cells enhances cellular invasiveness and pro-gelatinase
activation. Cancer Lett. 2006; 236; 292–301.
64. Chambers AF, Matrisian LM. Changing views of the role of
matrix metalloproteinases in metastasis. J. Natl. Cancer Inst.
1997; 89; 1260–1270.
65. Ahonen M, Baker AH, Kahari VM. Adenovirus-mediated gene
delivery of tissue inhibitor of metalloproteinases-3 inhibits
invasion and induces apoptosis in melanoma cells. Cancer Res.
1998; 58; 2310–2315.
66. Spurbeck WW, Ng CY, Strom TS, Vanin EF, Davidoff AM.
Enforced expression of tissue inhibitor of matrix metalloprotein-
ase-3 affects functional capillary morphogenesis and inhibits
tumor growth in a murine tumor model. Blood 2002; 100;
3361–3368.
67. Collen A, Hanemaaijer R, Lupu F et al. Membrane-type matrix
metalloproteinase-mediated angiogenesis in a fibrin–collagen
matrix. Blood 2003; 101; 1810–1817.
68. Bachman KE, Herman JG, Corn PG et al. Methylation-associated
silencing of the tissue inhibitor of metalloproteinase-3 gene
suggests a suppressor role in kidney, brain, and other human
cancers. Cancer Res. 1999; 59; 798–802.
69. Zochbauer-Muller S, Fong KM, Virmani AK et al. Aberrant
promoter methylation of multiple genes in non-small cell lung
cancers. Cancer Res. 2001; 61; 249–255.
70. Kang SH, Choi HH, Kim SG et al. Transcriptional inactivation of
the tissue inhibitor of metalloproteinase-3 gene by DNA hyper-
methylation of the 5¢-CpG island in human gastric cancer cell
lines. Int. J. Cancer 2000; 86; 632–635.
71. Ueki T, Toyota M, Sohn T et al. Hypermethylation of multiple
genes in pancreatic adenocarcinoma. Cancer Res. 2000; 60;
1835–1839.
72. Wild A, Ramaswamy A, Langer P et al. Frequent methylation-
associated silencing of the tissue inhibitor of metalloproteinase-3
gene in pancreatic endocrine tumors. J. Clin. Endocrinol. Metab.
2003; 88; 1367–1373.
73. Ahonen M, Ala-Aho R, Baker AH et al. Antitumor activity and
bystander effect of adenovirally delivered tissue inhibitor of
metalloproteinases-3. Mol. Ther. 2002; 5; 705–715.
74. Baker AH, Zaltsman AB, George SJ, Newby AC. Divergent effects
of tissue inhibitor of metalloproteinase-1, -2, or -3 overexpression
on rat vascular smooth muscle cell invasion, proliferation, and
death in vitro. TIMP-3 promotes apoptosis. J. Clin. Invest. 1998;
101; 1478–1487.
75. Smith MR, Kung H, Durum SK, Colburn NH, Sun Y. TIMP-3
induces cell death by stabilizing TNF-alpha receptors on the
surface of human colon carcinoma cells. Cytokine 1997; 9; 770–
780.
76. Brew K, Dinakarpandian D, Nagase H. Tissue inhibitors of
metalloproteinases: evolution, structure and function. Biochim.
Biophys. Acta 2000; 1477; 267–283.
77. Paquette B, Bisson M, Therriault H et al. Activation of matrix
metalloproteinase-2 and -9 by 2- and 4-hydroxyestradiol.
J. Steroid Biochem. Mol. Biol. 2003; 87; 65–73.
78. Di GH, Lu JS, Song CG et al. Over expression of aromatase protein
is highly related to MMPs levels in human breast carcinomas.
J. Exp. Clin. Cancer Res. 2005; 24; 601–607.
79. Lee AH, Happerfield LC, Bobrow LG, Millis RR. Angiogenesis and
inflammation in ductal carcinoma in situ of the breast. J. Pathol.
1997; 181; 200–206.
Study of MMPs and their tissue inhibitors in DCIS 415
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd, Histopathology, 53, 403–415.




















