
Microsatellite instability analysis of sinonasal carcinomas
7
http://oto.sagepub.com/ Otolaryngology -- Head and Neck Surgery http://oto.sagepub.com/content/140/1/55 The online version of this article can be found at: DOI: 10.1016/j.otohns.2008.10.038 2009 140: 55 Otolaryngology -- Head and Neck Surgery Llorente and Mario A. Hermsen Jorge García Martínez, Jhudit Pérez-Escuredo, Fernando López, Carlos Suárez, César Álvarez-Marcos, José Luis Microsatellite instability analysis of sinonasal carcinomas Published by: http://www.sagepublications.com On behalf of: American Academy of Otolaryngology- Head and Neck Surgery can be found at: Otolaryngology -- Head and Neck Surgery Additional services and information for http://oto.sagepub.com/cgi/alerts Email Alerts: http://oto.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: What is This? - Jan 1, 2009 Version of Record >> at University of Groningen on August 26, 2014 oto.sagepub.com Downloaded from at University of Groningen on August 26, 2014 oto.sagepub.com Downloaded from
Transcript of Microsatellite instability analysis of sinonasal carcinomas

http://oto.sagepub.com/Otolaryngology -- Head and Neck Surgery
http://oto.sagepub.com/content/140/1/55The online version of this article can be found at:
DOI: 10.1016/j.otohns.2008.10.038
2009 140: 55Otolaryngology -- Head and Neck SurgeryLlorente and Mario A. Hermsen
Jorge García Martínez, Jhudit Pérez-Escuredo, Fernando López, Carlos Suárez, César Álvarez-Marcos, José LuisMicrosatellite instability analysis of sinonasal carcinomas
Published by:
http://www.sagepublications.com
On behalf of:
American Academy of Otolaryngology- Head and Neck Surgery
can be found at:Otolaryngology -- Head and Neck SurgeryAdditional services and information for
http://oto.sagepub.com/cgi/alertsEmail Alerts:
http://oto.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Jan 1, 2009Version of Record >>
at University of Groningen on August 26, 2014oto.sagepub.comDownloaded from at University of Groningen on August 26, 2014oto.sagepub.comDownloaded from

Otolaryngology–Head and Neck Surgery (2009) 140, 55-60
ORIGINAL RESEARCH–SINONASAL DISORDERS
Microsatellite instability analysis of
sinonasal carcinomas
Jorge García Martínez, MSc, Jhudit Pérez-Escuredo, MSc,Fernando López, MD, Carlos Suárez, MD, PhD,César Álvarez-Marcos, MD, PhD, José Luis Llorente, MD, PhD, and
Mario A. Hermsen, PhD, Oviedo, Asturias, SpainOBJECTIVES: Intestinal-type sinonasal adenocarcinoma (ITAC)and squamous cell carcinoma of the nasal cavity (SCCNC) arehistopathologically but not etiologically similar to colorectal ade-nocarcinoma or to laryngeal squamous cell carcinoma, respec-tively. Microsatellite instability (MSI) is involved in both tumors.The aim of this study was to investigate a possible role for MSI inthe pathogenesis of two types of nasal carcinoma.MATERIAL AND METHODS: DNA obtained from frozen tu-mor samples of 41 ITACs and 24 SCCNCs was analyzed for shiftsin five mononucleotide microsatellite loci by multiplex PCR.RESULTS: The allelic patterns of one ITAC (2%) and fiveSCCNCs (21%) revealed an allelic shift for at least one of the fiveloci, indicating microsatellite instability.CONCLUSION: MSI may be involved in squamous cell carci-noma, but not in adenocarcinoma of the nasal cavities.© 2009 American Academy of Otolaryngology–Head and NeckSurgery Foundation. All rights reserved.
In the respiratory epithelium of the nasal cavity and para-nasal sinuses, two tumor types predominantly occur: ad-
enocarcinoma and squamous cell carcinoma. Both tumortypes are relatively infrequent, representing 0.5 percent ofall malignant neoplasms and 3 percent of head and neckcancers with an age of onset of 55 to 65 years.1 Adenocar-cinomas are named intestinal-type sinonasal carcinoma(ITAC) because of their histopathological resemblance tocolorectal adenocarcinoma. Squamous cell carcinomas ofthe nasal cavities (SCCNC) are similar to other squamouscell carcinomas of the upper aerodigestive tract. However,both ITAC and SCCNC are quite different with respect totheir etiology. Unlike colorectal adenocarcinoma, ITAC isstrongly associated with professional exposure to wood dustparticles, whereas tobacco, a strong etiological factor forhead and neck squamous cell carcinoma, does not seem toplay an important role in SCCNC. For both tumors, standardtherapeutic modalities include surgery followed by radio-therapy in advanced stages, sometimes with chemotherapy
Received September 5, 2008; revised October 20, 2008; accepted
October 27, 2008.0194-5998/$36.00 © 2009 American Academy of Otolaryngology–Head and Necdoi:10.1016/j.otohns.2008.10.038
at Universitoto.sagepub.comDownloaded from
treatment. Distant and lymph node metastases are excep-tional (5%-10%). The overall 5-year survival is 40 percentfor ITAC and 60 percent for SCCNC with local recurrence(30%-60%) as the main cause of death.2,3
ITAC is located most frequently (85%) in the ethmoidsinus and the upper part of the nasal cavity. It only excep-tionally arises in the other sites of the nasal cavity (maxil-lary sinus in 10%); these cases are usually not related towood dust exposure.4 Five histopathological types of si-nonasal ITAC are distinguished: papillary or PTCC-I (Pap-illary Tubular Cylinder Cell I), colonic (PTCC-II), solid(PTCC-III), mucinous (alveolar goblet and signet ring), andmixed (transitional). The most frequent type is colonic(40%), followed by solid (20%), papillary (18%), and mu-cinous and mixed type (22% combined). ITACs are notknown to arise from a clearly defined precursor lesion;however, squamous metaplasia and dysplasia in the vicinityof the tumor have been described.2 The strong relation ofITAC to exposure to wood dust makes it a disease almostexclusive to carpenters and furniture makers. Despite thisclear etiology, it is still unknown by what molecular mecha-nism sinonasal adenocarcinomas develop. Because wood dustdoes not have mutagenic properties, it is hypothesized thatprolonged exposure to and irritation by wood dust particlesstimulates cellular turnover by inflammatory pathways.4
SCCNC arises mostly in the maxillary sinus (60%-70%),followed by the ethmoid sinus (12%-25%), the nasal cavity(10%-15%), and occasionally in the sphenoidal and frontalsinus (1%). The most important histopathological types arekeratinizing and nonkeratinizing SCCNCs; they are furtherclassified according to their grade of differentiation. SCC-NCs are preceded by metaplasia, and some reports claimthat inverted papilloma may be a precursor lesion. Etiolog-ical factors may be exposure to nickel, chlorophenol, andtextile dust, but probably not tobacco.3
In this paper we wanted to explore the possibility ofmicrosatellite instability (MSI) as a mechanism involved in
k Surgery Foundation. All rights reserved.
y of Groningen on August 26, 2014

56 Otolaryngology–Head and Neck Surgery, Vol 140, No 1, January 2009
the development of ITAC and SCCNC. First, because intumors histopathologically similar to ITAC and SCCNC(colorectal adenocarcinoma and head and neck squamouscell carcinoma, respectively), MSI has been found in ap-proximately 20 to 30 percent of cases.5,6 Second, a propor-tion of ITACs and SCCNCs are DNA diploid carrying verylittle DNA copy number changes, which is a characteristicfrequently observed in MSI-positive tumors.7
MATERIALS AND METHODS
Tumor Samples
Tumor samples of 41 ITAC and 24 SCCNC patients wereobtained from surgical resection specimens; necrotic areaswere avoided and specimens were stored in liquid nitrogen.Two ITAC patients received previous radiotherapy. In-formed consent was obtained from all patients, and thestudy was approved by the ethical committee of our insti-tute. All patients underwent radical surgery and, in all cases,resection margins were free of tumor.
All 41 ITAC patients were male and 35 had professionalexposure to wood dust. All 41 ITACs were located in theethmoid sinus. The mean age was 64 years (range 48-84years). Eleven tumors were stage I, six stage II, 13 stage III,eight stage IVa, and three stage IVb. No patient had metas-tases at the time of diagnosis. According to the WorldHealth Organization histological classification (WHO-CAN), our series comprised six papillary type or PTCC-I(Papillary Tubular Cylinder Cell-I), 17 colonic (PTCC-II),eight solid (PTCC-III), and 10 mucinous type tumors. Fol-low-up information was available with a median of 14months (range 1-97 months). The median survival was 34months (range 1-97 months). Twenty-six patients receivedradiotherapy after surgery. Seven patients developed metas-tases in the brain and nine had local recurrence.
Of 24 SCCNC patients, 15 were male and nine werefemale. Four tumors were located in the ethmoid sinus and20 in the maxillary sinus. The mean age was 58 years (range47-85 years). Three tumors were stage II, seven stage III, sixstage IVa, and eight stage IVb. No patient had metastases atthe time of diagnosis. Nine tumors were well-differentiated,five moderately, and 10 poorly. Follow-up information wasavailable with a median of 15 months (range 1-211 months).The median survival was 27 months (range 1-211 months).Seventeen patients received radiotherapy after surgery. Onepatient developed a metastasis in the brain and 14 had localrecurrence.
A complete listing of clinical data is presented in Tables 1and 2.
Microsatellite Instability Analysis
Tumor DNA was extracted with Qiagen extraction kits
(Qiagen GmbH, Hilden, Germany). Approximately 2 ng ofat Universitoto.sagepub.comDownloaded from
tumor DNA was amplified according to the manufacturer’srecommendations in a multiplex PCR using a MSI analysiskit (Promega Biotech Iberica, Barcelona, Spain) consistingof primers for five nearly monomorphic mononucleotidemarkers: BAT-25, BAT-26, NR-21, NR-24, and MONO-27(Table 3), buffers, and reagents.
The PCR reaction mix contained 17 �L nuclease freewater, 2.5 �L GoldST_R 10� Buffer, 2.5 �L10� multiplexprimer mix, 0.5 �L AmpliTaq Gold DNA Polymerase at 5units/L, and 2.5 Ml NA at 0.8 ng/�L. Amplification tookplace according to the following cycling profile: 1 cycle95°C for 11 minutes; 1 cycle 96°C for 1 minute; 10 cycles94°C for 30 seconds, ramp for 68 seconds to 56°C, hold for30 seconds, ramp 50 seconds to 70°C, hold for 45 seconds;20 cycles at 90°C for 30 seconds, ramp for 60 seconds to56°C, hold for 30 seconds, ramp 50 seconds to 70°C, holdfor 45 seconds; 60°C for 30 minutes final extension; 4°Chold. The PCR products were analyzed by capillary elec-trophoresis with an ABI 3100 Genetic Analyzer (AppliedBiosystems, Warrington, UK). Data analysis was done byGeneScan software (Applied Biosystems). A shift in allelesize of three or more base pairs of one or more of the fivemarkers was scored as MSI-positive. A negative controlDNA sample was provided in the Promega kit, and weperformed a positive control experiment using DNA froman MSI-positive colorectal cancer patient that showed ashift of all five mononucleotide markers (Fig 1).
RESULTS
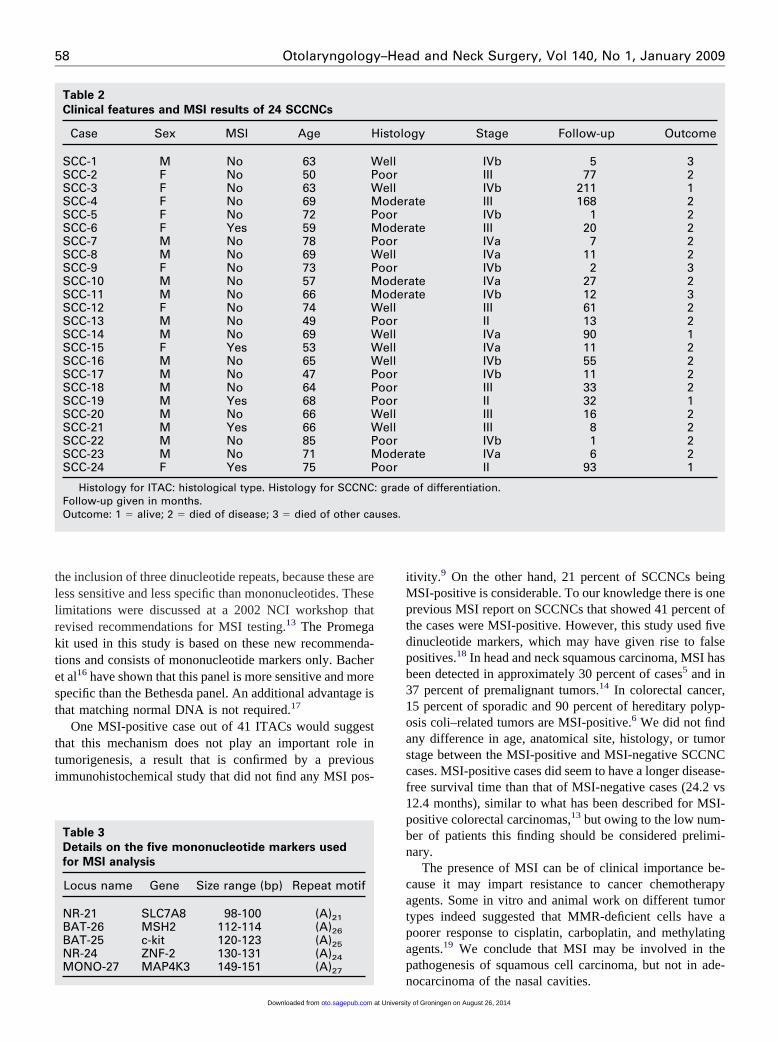
All tumors gave interpretable PCR products and their sizeswere within the range indicated by the manufacturers. Oneof 41 (2.4%) ITACs and five of 24 (21%) SCCNCs werefound to be MSI-positive. An example of an MSI-positiveSCCNC case is given in Figure 1. Two cases showed adisplacement of BAT-26, two cases showed a displacementof NR-21, and one case had displacement of BAT-25 andBAT-26.
DISCUSSION
To date little is known of the genetic changes involved inthe development of ITAC and even less is known aboutSCCNC. Because of the histopathological resemblance ofITAC to colorectal adenocarcinoma, studies on ITAC so farhave focussed on expression patterns of a limited number ofproteins known to be involved in colorectal adenocarci-noma, such as p53, b-catenin, and K-ras.8-10 Other studiesapplied genome-wide screening techniques as chromosomeCGH or microarray CGH7.7,11,12 The overall conclusion ofthese studies seems to be that the pattern of gains and lossesis rather unique and only partially resembles colorectal
adenocarcinoma.y of Groningen on August 26, 2014

57Martínez et al Microsatellite instability analysis of . . .
In this study we investigated the possibility that MSIplays a role in the development of ITAC and SCCNC. MSIis well studied in colorectal tumors, where it was firstdiscovered in familial tumors, but later, in sporadic colo-rectal tumors.13 MSI has also been demonstrated in othercancers, such as breast, ovarian, and head and neck can-cer.5,14,15 Tumorigenesis may be driven through the inacti-vation of tumor suppressor genes caused by replicationerrors in short repetitive sequences present within a gene orregulatory sequences of a gene. Examples are TGF-�RIIand BAX in colorectal cancer.16 In a way this mechanism is
Table 1
Clinical features and MSI results of 41 ITACs
Case Sex MSI Age H
ITAC-1 M No 51 SITAC-2 M No 70 CITAC-3 M No 57 MITAC-4 M No 61 MITAC-5 M No 66 CITAC-6 M No 73 MITAC-7 M No 71 CITAC-8 M No 65 CITAC-9 M No 49 CITAC-10 M No 61 MITAC-11 M No 52 PITAC-12 M No 69 CITAC-13 M No 52 CITAC-14 M No 72 CITAC-15 M Yes 62 MITAC-16 M No 82 SITAC-17 M No 58 MITAC-18 M No 78 PITAC-19 M No 53 PITAC-20 M No 58 CITAC-21 M No 49 MITAC-22 M No 73 CITAC-23 M No 63 SITAC-24 M No 51 CITAC-25 M No 65 CITAC-26 M No 68 MITAC-27 M No 69 PITAC-28 M No 66 SITAC-29 M No 56 SITAC-30 M No 54 CITAC-31 M No 58 SITAC-32 M No 84 SITAC-33 M No 81 MITAC-34 M No 68 PITAC-35 M No 66 MITAC-36 M No 72 SITAC-37 M No 92 CITAC-38 M No 66 CITAC-39 M No 48 CITAC-40 M No 59 PITAC-41 M No 50 C
Histology for ITAC: histological type. Histology for SCCNCFollow-up given in months.Outcome: 1 � alive; 2 � died of disease; 3 � died of other ca
no different from mutagen-driven tumorigenesis, in which
at Universitoto.sagepub.comDownloaded from
genes are chemically altered by an external factor such astobacco, or from chronic inflammation–related cancer inwhich it is thought that inflammatory cells produce muta-genic oxygen radicals that damage DNA.
Several methods have been used in MSI screening. Ini-tially, various microsatellite markers were used, includingmono- and dinucleotides and other markers. In 1997, anNCI workshop recommended a panel of five microsatellitemarkers consisting of two mononucleotide markers (BAT-25and BAT-26) and three dinucleotide repeats (D2S123,D5S346, and D17S250), known as the Bethesda panel. This
gy Stage Follow-up Outcome
III 7 2c II 38 1ous IVb 2 2ous III 68 1c III 34 2ous IVa 6 2c II 48 1c I 5 1c III 72 1ous IVb 9 2ry III 80 1c I 36 2c III 55 2c II 20 1ous IVa 12 1
III 17 2ous I 32 2ry II 28 1ry II 82 1c I 97 1ous I 84 2c III 21 2
III 8 2c IVa 1 3c III 12 1ous IVa 14 2ry II 12 1
IVa 7 2IVb 12 2
c I 14 1IVa 13 2I 24 2
ous IVa 1 2ry III 15 2ous III 20 1
III 22 1c I 0 3c I 13 1c I 6 1ry IVa 6 1c I 6 1
of differentiation.
istolo
olidoloniucinucinoloniucinoloniolonioloniucin
apillaoloniolonioloniucinoliducin
apillaapillaoloniucinoloniolidolonioloniucin
apillaolidolidoloniolidoliducin
apillaucinolidoloniolonioloniapillaoloni
: grade
uses.
panel of markers did, however, have limitations owing to
y of Groningen on August 26, 2014
58 Otolaryngology–Head and Neck Surgery, Vol 140, No 1, January 2009
the inclusion of three dinucleotide repeats, because these areless sensitive and less specific than mononucleotides. Theselimitations were discussed at a 2002 NCI workshop thatrevised recommendations for MSI testing.13 The Promegakit used in this study is based on these new recommenda-tions and consists of mononucleotide markers only. Bacheret al16 have shown that this panel is more sensitive and morespecific than the Bethesda panel. An additional advantage isthat matching normal DNA is not required.17
One MSI-positive case out of 41 ITACs would suggestthat this mechanism does not play an important role intumorigenesis, a result that is confirmed by a previousimmunohistochemical study that did not find any MSI pos-
Table 2
Clinical features and MSI results of 24 SCCNCs
Case Sex MSI Age H
SCC-1 M No 63 WSCC-2 F No 50 PSCC-3 F No 63 WSCC-4 F No 69 MSCC-5 F No 72 PSCC-6 F Yes 59 MSCC-7 M No 78 PSCC-8 M No 69 WSCC-9 F No 73 PSCC-10 M No 57 MSCC-11 M No 66 MSCC-12 F No 74 WSCC-13 M No 49 PSCC-14 M No 69 WSCC-15 F Yes 53 WSCC-16 M No 65 WSCC-17 M No 47 PSCC-18 M No 64 PSCC-19 M Yes 68 PSCC-20 M No 66 WSCC-21 M Yes 66 WSCC-22 M No 85 PSCC-23 M No 71 MSCC-24 F Yes 75 P
Histology for ITAC: histological type. Histology for SCCNCFollow-up given in months.Outcome: 1 � alive; 2 � died of disease; 3 � died of other ca
Table 3
Details on the five mononucleotide markers used
for MSI analysis
Locus name Gene Size range (bp) Repeat motif
NR-21 SLC7A8 98-100 (A)21BAT-26 MSH2 112-114 (A)26BAT-25 c-kit 120-123 (A)25NR-24 ZNF-2 130-131 (A)24MONO-27 MAP4K3 149-151 (A)
27at Universitoto.sagepub.comDownloaded from
itivity.9 On the other hand, 21 percent of SCCNCs beingMSI-positive is considerable. To our knowledge there is oneprevious MSI report on SCCNCs that showed 41 percent ofthe cases were MSI-positive. However, this study used fivedinucleotide markers, which may have given rise to falsepositives.18 In head and neck squamous carcinoma, MSI hasbeen detected in approximately 30 percent of cases5 and in37 percent of premalignant tumors.14 In colorectal cancer,15 percent of sporadic and 90 percent of hereditary polyp-osis coli–related tumors are MSI-positive.6 We did not findany difference in age, anatomical site, histology, or tumorstage between the MSI-positive and MSI-negative SCCNCcases. MSI-positive cases did seem to have a longer disease-free survival time than that of MSI-negative cases (24.2 vs12.4 months), similar to what has been described for MSI-positive colorectal carcinomas,13 but owing to the low num-ber of patients this finding should be considered prelimi-nary.
The presence of MSI can be of clinical importance be-cause it may impart resistance to cancer chemotherapyagents. Some in vitro and animal work on different tumortypes indeed suggested that MMR-deficient cells have apoorer response to cisplatin, carboplatin, and methylatingagents.19 We conclude that MSI may be involved in thepathogenesis of squamous cell carcinoma, but not in ade-
gy Stage Follow-up Outcome
IVb 5 3III 77 2IVb 211 1
ate III 168 2IVb 1 2
ate III 20 2IVa 7 2IVa 11 2IVb 2 3
ate IVa 27 2ate IVb 12 3
III 61 2II 13 2IVa 90 1IVa 11 2IVb 55 2IVb 11 2III 33 2II 32 1III 16 2III 8 2IVb 1 2
ate IVa 6 2II 93 1
of differentiation.
istolo
elloorelloder
ooroder
oorell
ooroderoderell
oorellellell
oorooroorellell
ooroder
oor
: grade
uses.
nocarcinoma of the nasal cavities.
y of Groningen on August 26, 2014

59Martínez et al Microsatellite instability analysis of . . .
Figure 1 Results of three MSI analyses by multiplex PCR. A, Negative control DNA with one peak for all five markers. B, Positivecontrol DNA from a known MSI-positive colorectal adenocarcinoma patient having extra peaks for all five markers. C, Example of case
SCC-24 showing an extra peak for marker NR-21 (arrow).at University of Groningen on August 26, 2014oto.sagepub.comDownloaded from
60 Otolaryngology–Head and Neck Surgery, Vol 140, No 1, January 2009
ACKNOWLEDGEMENTS
Drs Aurora Astudillo-González and Blanca Vivanco Allende, Departmentof Pathology, Hospital Universitario Central de Asturias: histopathologicalclassifications.
AUTHOR INFORMATION
From the Department of Otorhinolaryngology, IUOPA, Hospital Univer-sitario Central de Asturias.
Corresponding author: Mario A. Hermsen, Dept Otorrinolaringología In-stituto Universitario de Oncología del Principado de Asturias (IUOPA),Edificio H Covadonga 1a Planta Centro, Lab 2, Hospital UniversitarioCentral de Asturias, Celestino Villamil s/n, 33006 Oviedo.
E-mail address: [email protected].
AUTHOR CONTRIBUTIONS
Mario A. Hermsen: study design, writer; Jorge García Martínez: studyplanning, genetic data collection, writer; Jhudit Pérez-Escuredo: geneticdata collection; Fernando López: clinical data collection; Carlos Suárez:samples and clinical data collection; César Álvarez-Marcos: samples andclinical data collection; José Luis Llorente: samples and clinical datacollection.
FINANCIAL DISCLOSURE
This study was supported by grant PI05-1387 of Fondos de InvestigaciónSanitaria (FIS), Spain.
REFERENCES
1. Bhattacharyya N. Cancer of the nasal cavity: survival and factorsinfluencing prognosis. Arch Otolaryngol Head Neck Surg 2002;128:1079–83.
2. Franchi A, Santucci M, Weing B. Adenocarcinomas. In: Barnes L,Evenson JW, Reichart P, et al, editors. World health organizationclassification of tumours. Pathology and genetics of head and necktumours. Lyon: IARC; 2005. p. 20–3.
3. Pilch BZ, Bouquot J, Thompson LDR. Squamous cell carcinoma. In:Barnes L, Evenson JW, Reichart P et al, editors. World health orga-nization classification of tumours. Pathology and genetics of head and
neck tumours. Lyon: IARC; 2005. p. 15-7.at Universitoto.sagepub.comDownloaded from
4. Llorente JL, Pérez Escuredo J, Alvarez-Marcos C, et al. Genetic andclinical aspects of wood dust related intestinal-type sinonasal adeno-carcinoma. Eur Arch Otorhinolaryngol. 2008 Jun 17 [Epub ahead ofprint].
5. El-Naggar AK, Hurr K, Huff V, et al. Microsatellite instability inpreinvasive and invasive head and neck squamous carcinoma. Am JPathol 1996;148:2067–72.
6. Aaltonen LA, Peltomäki P, Leach FS, et al. Clues to the pathogenesisof familial colorectal cancer. Science 1993;260:812–6.
7. Hermsen MAJA, Llorente Pendás JL, Pérez Escuredo J, et al. Highresolution genome-wide oligonucleotide microarray CGH analysis ofDNA copy number changes in sinonasal adenocarcinoma. Head Neck.In press.
8. Perez P, Dominguez O, Gonzalez S, et al. K-ras gene mutations inethmoid sinus adenocarcinoma: prognostic implications. Cancer 1999;86:255–64.
9. Perez-Ordonez B, Huynh NN, Berean KW, et al. Expression of mis-match repair proteins, beta catenin, and E cadherin in intestinal-typesinonasal adenocarcinoma. J Clin Pathol 2004;57:1080–3.
10. Saber AT, Nielsen LR, Dictor M, et al. K-ras mutations in sinonasaladenocarcinomas in patients occupationally exposed to wood orleather dust. Cancer Lett 1998;126:59–65.
11. Korinth D, Pacyna-Gengelbach M, Deutschmann N, et al. Chromo-somal imbalances in wood dust-related adenocarcinomas of the innernose and their associations with pathological parameters. J Pathol2005;207:207–15.
12. Ariza M, Llorente JL, Alvarez-Marcos C, et al. Comparative genomichybridization in primary sinonasal adenocarcinomas. Cancer 2004;100:335–41.
13. Laghi L, Bianchi P, Malesci A. Differences and evolution of themethods for the assessment of microsatellite instability. Oncogene2008;27:6313–21.
14. Sardi I, Franchi A, De Campora L et al. Microsatellite instability as anindicator of malignant progression in laryngeal premalignancy. HeadNeck 2006;28:730–9.
15. Halford SE, Sawyer EJ, Lambros MB, et al. MSI-low, a real phenom-enon which varies in frequency among cancer types. J Pathol 2003;201:389–94.
16. Bacher JW, Flanagan LA, Smalley RL, et al. Development of afluorescent multiplex assay for detection of MSI-High tumors. DisMarkers 2004;20:237–50.
17. Ebinger M, Sotlar K, Weber A, et al. Simplified detection of micro-satellite instability in colorectal cancer without the need for corre-sponding germline DNA analysis. J Clin Pathol 2006;59:1114–5.
18. Uryu H, Oda Y, Shiratsuchi H, et al. Microsatellite instability andproliferating activity in sinonasal carcinoma: molecular genetic andimmunohistochemical comparison with oral squamous cell carcinoma.Oncol Rep 2005;14:1133–42.
19. Papouli E, Cejka P, Jiricny J. Dependence of the cytotoxicity ofDNA-damaging agents on the mismatch repair status of human cells.
Cancer Res 2004;64:3391–4.y of Groningen on August 26, 2014




















