![Pyrazolo[3,4- d ]pyrimidines as Potent Antiproliferative and Proapoptotic Agents toward A431 and 8701-BC Cells in Culture via Inhibition of c-Src Phosphorylation](https://static.fdokumen.com/doc/165x107/63334468a290d455630a0f86/pyrazolo34-d-pyrimidines-as-potent-antiproliferative-and-proapoptotic-agents.jpg)
Serum From Patients With Severe Heart Failure Downregulates eNOS and Is Proapoptotic Role of Tumor...
10
Grigolato and Roberto Ferrari Comini, Maurizio Volterrani, Paolo Bonetti, Giovanni Parrinello, Moris Cadei, Pier Giovanni Laura Agnoletti, Salvatore Curello, Tiziana Bachetti, Fabio Malacarne, Giuseppina Gaia, Laura α Proapoptotic: Role of Tumor Necrosis Factor- Serum From Patients With Severe Heart Failure Downregulates eNOS and Is Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1999 American Heart Association, Inc. All rights reserved. is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Circulation doi: 10.1161/01.CIR.100.19.1983 1999;100:1983-1991 Circulation. http://circ.ahajournals.org/content/100/19/1983 World Wide Web at: The online version of this article, along with updated information and services, is located on the http://circ.ahajournals.org//subscriptions/ is online at: Circulation Information about subscribing to Subscriptions: http://www.lww.com/reprints Information about reprints can be found online at: Reprints: document. Permissions and Rights Question and Answer this process is available in the click Request Permissions in the middle column of the Web page under Services. Further information about Office. Once the online version of the published article for which permission is being requested is located, can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Circulation in Requests for permissions to reproduce figures, tables, or portions of articles originally published Permissions: by guest on February 3, 2014 http://circ.ahajournals.org/ Downloaded from by guest on February 3, 2014 http://circ.ahajournals.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Serum From Patients With Severe Heart Failure Downregulates eNOS and Is Proapoptotic Role of Tumor...

Grigolato and Roberto FerrariComini, Maurizio Volterrani, Paolo Bonetti, Giovanni Parrinello, Moris Cadei, Pier Giovanni
Laura Agnoletti, Salvatore Curello, Tiziana Bachetti, Fabio Malacarne, Giuseppina Gaia, LauraαProapoptotic: Role of Tumor Necrosis Factor-
Serum From Patients With Severe Heart Failure Downregulates eNOS and Is
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1999 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.100.19.1983
1999;100:1983-1991Circulation.
http://circ.ahajournals.org/content/100/19/1983World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on February 3, 2014http://circ.ahajournals.org/Downloaded from by guest on February 3, 2014http://circ.ahajournals.org/Downloaded from

Serum From Patients With Severe Heart FailureDownregulates eNOS and Is Proapoptotic
Role of Tumor Necrosis Factor-a
Laura Agnoletti, MSc; Salvatore Curello, MD; Tiziana Bachetti, MSc; Fabio Malacarne, MSc;Giuseppina Gaia, MSc; Laura Comini, MSc, PhD; Maurizio Volterrani, MSc, PhD; Paolo Bonetti, MD;
Giovanni Parrinello, PhD; Moris Cadei; Pier Giovanni Grigolato, MD; Roberto Ferrari, MD, PhD
Background—Cytokine activation and endothelial dysfunction are typical phenomena of congestive heart failure (CHF).We tested the hypothesis that incubating human umbilical vein endothelial cells with serum from patients with CHF willdownregulate endothelial constitutive nitric oxide synthase (eNOS) and induce apoptosis.
Methods and Results—We studied 21 patients with severe CHF. Levels of tumor necrosis factor-a (TNF-a) and severalneuroendocrine parameters were assessed. eNOS was measured by Western Blot analysis and apoptosis by opticalmicroscopy and flow cytometry. We observed (1) eNOS downregulation (difference versus healthy subjects at 24 hours[P,0.05] and 48 hours [P,0.001]), (2) nuclear morphological changes typical of apoptosis; and (3) a high apoptoticrate with propidium iodide (increasing from 2.160.4% to 11.361.2% at 48 hours;P,0.001 versus healthy subjects) andannexin V. An anti-human TNF-a antibody did not completely counteract these effects. A strong correlation existedbetween eNOS downregulation and apoptosis (r520.89; P,0.001).
Conclusions—Serum from patients with severe CHF downregulates eNOS expression and increases apoptosis. High levelsof TNF-a likely play a role, but they cannot be the only factor responsible.(Circulation. 1999;100:1983-1991.)
Key Words: heart failuren tumor necrosis factorn endotheliumn nitric oxide synthasen apoptosis
Congestive heart failure (CHF) is a syndrome character-ized by neuroendocrine and cytokine activation.1,2
Among cytokines, tumor necrosis factor-a (TNF-a) and itssoluble receptors I (sTNF-RI) and II (sTNF-RII) are in-creased in patients with severe CHF.3–6
In in vitro experiments, high doses of TNF-a induceendothelial dysfunction as a result of the downregulation ofendothelial constitutive nitric oxide synthase (eNOS)7 expres-sion and the increase of apoptosis, a mechanism of physio-logical cell death. Whether or not the negative effects ofTNF-a on eNOS and apoptosis also occur in CHF is notknown. However, endothelial dysfunction does occur in CHF,as demonstrated in studies in dogs and humans.8,9 This maybe due to the activation of several circulating neurohor-mones.9 Because of the poor correlation between neurohor-mones and systemic vascular resistances,10 other systems arenecessarily involved in this pathological process.11
To evaluate the potential role of TNF-a in endothelialdysfunction, we studied the protein expression of eNOS andthe rate of apoptosis of human umbilical vein endothelialcells (HUVECs) after incubation for#48 hours with serum
from patients with CHF in New York Heart Association(NYHA) class IV. eNOS was evaluated by Western blotanalysis and apoptosis by both optical microscopy and flowcytometry.
MethodsPopulations StudiedThis study was performed at the Cardiology Departments of theUniversities of Brescia and Ferrara and at the Heart Failure Unit ofthe Salvatore Maugeri Foundation, Gussago, Brescia, Italy. A total of21 male patients with severe CHF (NYHA class IV) and 21 healthysubjects (normal controls) participated in the study. All gave in-formed consent, and local Ethics Committee approval was obtained.The Table shows the clinical characteristics of the populationsstudied.
The average age of the patients was 5669 years. The causes ofCHF were coronary artery disease (n514), idiopathic dilated cardio-myopathy (n55), or valvular disease (n52). The mean left ventric-ular ejection fraction, as assessed by 2D echocardiogram, was2165%. Hemodynamic parameters were measured in the postab-sorptive state with a Swan-Ganz catheter. Cardiac output wasdetermined by thermodilution with a Gould cardiac output computer(model SP 1445). All patients were treated with angiotensin-
Received February 18, 1999; revision received June 15, 1999; accepted July 8, 1999.From the Salvatore Maugeri Foundation, Institute for Care and Research, Cardiovascular Pathophysiology Research Centre (L.A., T.B., G.G., L.C.),
and the Departments of Cardiology (S.C., P.B.), Statistics (G.P.), and Pathologic Anatomy (M.C., P.G.G.), University of Brescia; the ImmunologyDepartment, Spedali Civili, Brescia (F.M.); the Cardiology Department, Gussago, Brescia (M.V.); and the Department of Cardiology, University ofFerrara (R.F.), Italy.
Correspondence to Prof Roberto Ferrari, Cardiovascular Pathophysiology Research Center, Salvatore Maugeri Foundation, Via Pinidolo, 23, 25064Gussago, Brescia, Italy. E-mail [email protected]
© 1999 American Heart Association, Inc.
Circulation is available at http://www.circulationaha.org
1983 by guest on February 3, 2014http://circ.ahajournals.org/Downloaded from
converting enzyme inhibitors, diuretics, and digoxin; some were alsotaking vasodilators, low-doseb-blockers, and positive inotropicagents. Thirteen patients were receiving hepatic hydroxymethylglu-taryl coenzyme A reductase inhibitors. Anti-inflammatory drugswere not allowed during the 2 weeks preceding the study. Exclusioncriteria included infections; renal failure; pulmonary, thyroid, andcollagen vascular diseases; and malignancy.
The normal control group was sex- (male) and age-matched(5764 years) to the patients. No subjects in this group had anyclinical sign of acute or chronic illnesses or any symptoms related tothe cardiovascular system.
Blood ProcessingAfter 30 minutes of supine rest, peripheral venous blood was takenand centrifuged within 1 hour to measure serum electrolytes,norepinephrine (NE), aldosterone, plasma renin activity (RA), atrialnatriuretic peptide (ANP), TNF-a, sTNF-RI, and sTNF-RII. Allserum samples were stored at280°C.
Plasma HormonesPlasma NE levels were measured by high-performance liquid chro-matography with electrochemical detection.4,12 Levels of RA, aldo-sterone, and ANP were measured by radioimmunoassay (DiaSorin,Radim).
TNF-a ImmunoactivityAntigenic TNF-a was determined by a sandwich ELISA with acommercially available kit (Medgenix Diagnostic). The mixture ofmonoclonal antibodies used does not neutralize TNF-a, whichallows the measurement of total circulating TNF-a, even if bound tosoluble TNF receptors. The sensitivity of the assay is 3 pg/mL.
sTNF-RI and sTNF-RIISerum sTNF-RI and sTNF-RII levels were assessed by a sandwichELISA with a commercially available kit (Amersham). The mini-mum detectable doses for sTNF-RI and sTNF-RII were 2.5 and 5pg/mL, respectively.
Cell CultureHUVECs were isolated from umbilical cords using the method ofJaffe et al.13 No additional growth factor was added to propagate thecultures. HUVECs were characterized by immunofluorescence forvon Willebrand factor and by microscope observation of typicalcobblestone morphology.
Between splits 2 and 4, the cells were treated with 40 ng/mLTNF-a (13108 units/mg) for 6, 12, 24, and 48 hours to establish apositive control group. Moreover, HUVECs were incubated for thesame times with 20% serum from either the normal controls orpatients with CHF. To test the specific role of TNF-a, we used 1mg/mL monoclonal anti-human TNF-a antibody (Genzyme).
Nitric Oxide Synthase AnalysiseNOS immunoblotting was performed as previously described.14
Mouse monoclonal anti-human eNOS (Affiniti) and peroxidase-conjugated rabbit anti-mouse IgG (Dako) were used as primary andsecondary antibodies, respectively. The specific signal was detectedwith an enhanced chemiluminescence system (ECL, Amersham) andquantified by densitometry. Each sample was processed 3 times.
Qualitative Assessment of Apoptosis byOptical MicroscopyOptical microscopy assessment was performed by the ApopTag-peroxidase kit and by hematoxylin-eosin and Feulgen staining.
ApopTag-Peroxidase KitCytological samples, fixed in 95% alcohol, were stained with theApopTag-peroxidase kit (Oncor): the reaction is referred to asTUNEL detection. In this process, residues of digoxigenin nucleotideare catalytically added to DNA by terminal deoxinucleotidaltransferase.15
Hematoxylin-Eosin StainingThe cytological slides were placed in Harris hematoxylin (Bio-Optica) for 1 minute and contrasted in bidistilled water. They were
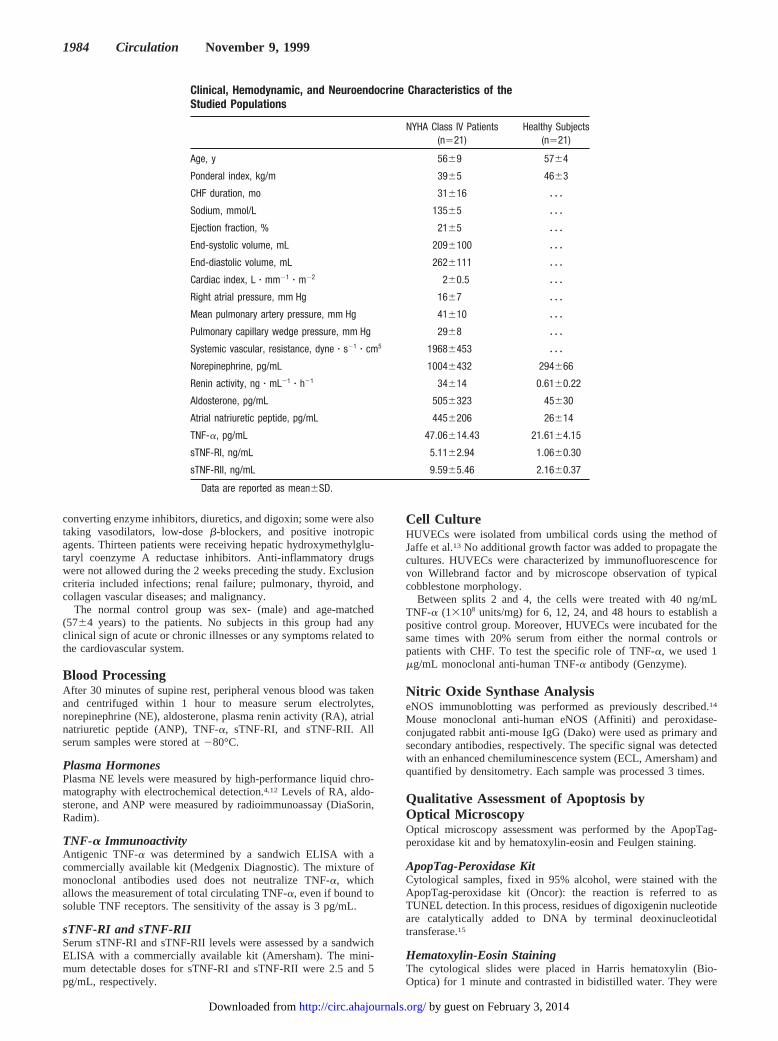
Clinical, Hemodynamic, and Neuroendocrine Characteristics of theStudied Populations
NYHA Class IV Patients(n521)
Healthy Subjects(n521)
Age, y 5669 5764
Ponderal index, kg/m 3965 4663
CHF duration, mo 31616 z z z
Sodium, mmol/L 13565 z z z
Ejection fraction, % 2165 z z z
End-systolic volume, mL 2096100 z z z
End-diastolic volume, mL 2626111 z z z
Cardiac index, L z mm21 z m22 260.5 z z z
Right atrial pressure, mm Hg 1667 z z z
Mean pulmonary artery pressure, mm Hg 41610 z z z
Pulmonary capillary wedge pressure, mm Hg 2968 z z z
Systemic vascular, resistance, dyne z s21 z cm5 19686453 z z z
Norepinephrine, pg/mL 10046432 294666
Renin activity, ng z mL21 z h21 34614 0.6160.22
Aldosterone, pg/mL 5056323 45630
Atrial natriuretic peptide, pg/mL 4456206 26614
TNF-a, pg/mL 47.06614.43 21.6164.15
sTNF-RI, ng/mL 5.1162.94 1.0660.30
sTNF-RII, ng/mL 9.5965.46 2.1660.37
Data are reported as mean6SD.
1984 Circulation November 9, 1999
by guest on February 3, 2014http://circ.ahajournals.org/Downloaded from

dehydrated through the increasing alcohol scale and fixed by xylenewith Eukitt balsam.16
Feulgen StainingThe cytological slides were treated with HCl at 60°C for 7 to 10minutes and then placed in Schiff reactive medium (Sigma) for 45minutes at room temperature, washed in tap water, dehydratedthrough the decreasing alcohol scale, and fixed by xylene with Eukittbalsam.17
Quantitative Assessment of Apoptosis by Flow CytometryApoptosis was quantified by flow cytometry using a slightly modi-fied version of the method of Nicoletti et al.18 Endothelial cells fixedin 1 mL of cold 70% ethanol were then incubated with a solution of100 mg/mL propidium iodide (PI) and immediately analyzed. Thecorrect threshold was selected using the apoptotic model in murinethymocytes after 72 hours of culture with dexamethasone 1027
mol/L. Apoptotic cell nuclei, which were easily distinguishable fromdebris by the condensation of nuclear chromatin, emitted redfluorescence in red rodamine fluorescence channels 46 to 146. Thesubdiploid population was detected using the fluorescein isothiocya-nate (FITC)–annexin V/PI double-staining method of Vermes et al19;it was then analyzed with a flow cytometer (Cytoron Absolute;Ortho) using ABS software. Dead cells were excluded by setting anappropriate threshold trigger on the low forward light scatterparameter, and nonspecific staining was assessed using FITC-conjugated nonimmune mouse IgG (Coulter).
Statistical AnalysisThe significant difference in means of the studied variables wastested by Student’st test. The correlation between variables wastested by Spearman’s rank or Pearson’s correlation methods, depend-ing on the type of distribution of each variable. Multiple linearregression analysis was used to study the possible associationbetween apoptosis and eNOS with TNF-a and hormones. Thecorrelation between variables and the multiple linear regressionanalysis were performed only on data from patients with CHF. Thecomparison between patients with CHF and normal controls wasanalyzed by the linear mixed effects model, with adjustment formultiple comparisons. The tests were considered statistically signif-icant atP,0.05.
ResultsThe Table shows the clinical characteristics, plasma hor-mones, and TNF-a data of the populations studied. In patientswith CHF, the cardiac index was severely reduced (260.5 L zmin21 z (m2)21), the right atrial and pulmonary pressures werehigh (1667 and 41610 mm Hg, respectively), and thesystemic vascular resistances (19686453 dynez s21 z cm5)and serum levels of sodium were lowered (13565 mmol/L).Mean values for RA and aldosterone were 34614 ngz mL21 zh21 and 5056323 pg/mL, respectively. Plasma concentrationsof NE and ANP were 3.4 and 17 times greater, respectively,than those of the normal controls. The mean values ofantigenic TNF-a in patients with CHF and in normal controlswere 47.1614.4 and 21.664.1 pg/mL, respectively(P,0.001). The same patterns were recorded for the solublereceptors of the cytokine (P,0.001 for both sTNF-RI andsTNF-RII versus normal controls).
eNOSFigures 1 and 2, respectively, show a representative Westernblot of eNOS and the mean data for each group obtained afterincubation with exogenous TNF-a 40 ng/mL (positive con-trol) and serum from normal controls and patients with CHF,both with and without the anti-human TNF-a antibody. As
expected, the incubation of the HUVECs with TNF-a re-sulted in a downregulation of eNOS expression: after 6 hours,a 23% reduction versus normal control was observed(P,0.05), which reached 85% after 48 hours (P,0.001). Theaddition of the anti-human TNF-a antibody completely coun-teracted this decrease.
In normal controls, the incubation of HUVECs had noeffect on eNOS, whereas in patients with CHF, it resulted ina time-dependent downregulation of the protein expression(P,0.05 andP,0.001 versus normal controls after 24 and 48hours, respectively). The TNF-a antibody partially counter-acted the inhibitory effect of the serum from patients withCHF.
Multiple linear regression analysis was performed with thevariables from patients with CHF that significantly correlatedwith eNOS expression. After step-wise selection, TNF-alevels showed a mild correlation to the reduction of eNOSexpression (r50.51;P,0.05).
Qualitative Assessment of Apoptosis byOptical MicroscopyThe apoptotic pattern, as observed with optical microscopy, isshown in Figure 3. HUVECs from normal controls did notundergo relevant changes (A through C), whereas those frompatients with CHF showed changes in nuclear profile andalterations of chromatin structure (D through F). The immu-nocytochemical ApopTag-peroxidase staining (brown posi-tive nuclei) showed the increase of the DNA 39OH terminalsthat was generated by the internucleosomic rupture, whichprecedes the detachment of the apoptotic bodies. With thismethod, in the normal controls, a positive nucleus could be
Figure 1. Western blot of eNOS. Representative Western blot ofresults reported as means in Figure 2.
Agnoletti et al TNF-a Downregulates eNOS and Is Proapoptotic 1985
by guest on February 3, 2014http://circ.ahajournals.org/Downloaded from

occasionally detected in some fields; conversely, in patientswith CHF, $1 positive nucleus was detectable in each field(D). This finding was also confirmed by the hematoxylin-eosin and Feulgen stains (E and F). The most frequentalteration was nuclear membrane expansion (sometimes ovoi-dal), which was associated with hyperchromatic zones; thesenuclei appeared as pyknotic nuclei later evolving in apoptoticbodies.
Quantitative Assessment of Apoptosis byFlow CytometryFigure 4 shows apoptosis over 6, 12, 24, and 48 hours asmeasured by flow cytometry using a solution of PI as thefluorochrome after membrane ethanol permeabilization. Thetop panels show representative cytofluorometric recordingsof HUVECs in positive and normal controls and patients withCHF. As expected, a proportional induction of apoptosisoccurred over time, which reached a maximum of 33.762.6%at 48 hours. Obviously, the induced apoptosis was completelycounteracted by adding the anti-human TNF-a antibody(P,0.001) (Figure 4, lower left). The lower right panels showthe mean data obtained from the incubation of HUVECs with
the serum from either normal controls or patients with CHF,with and without the anti-human TNF-a antibody. Over 48hours, the percentage of apoptotic cells in normal controlsincreased from 1.860.8% to 4.260.5%. In patients withCHF, a higher rate of apoptosis existed when compared withnormal controls; this higher rate could be seen at 6 hours, andit increased from 2.160.4% to 11.361.2% at 48 hours(P,0.001 at both 24 and 48 hours). The addition of theanti-human TNF-a antibody to the serum from patients withCHF reduced, but did not counteract, its apoptotic effect(P,0.001 at both 24 and 48 hours versus CHF withoutantibody).
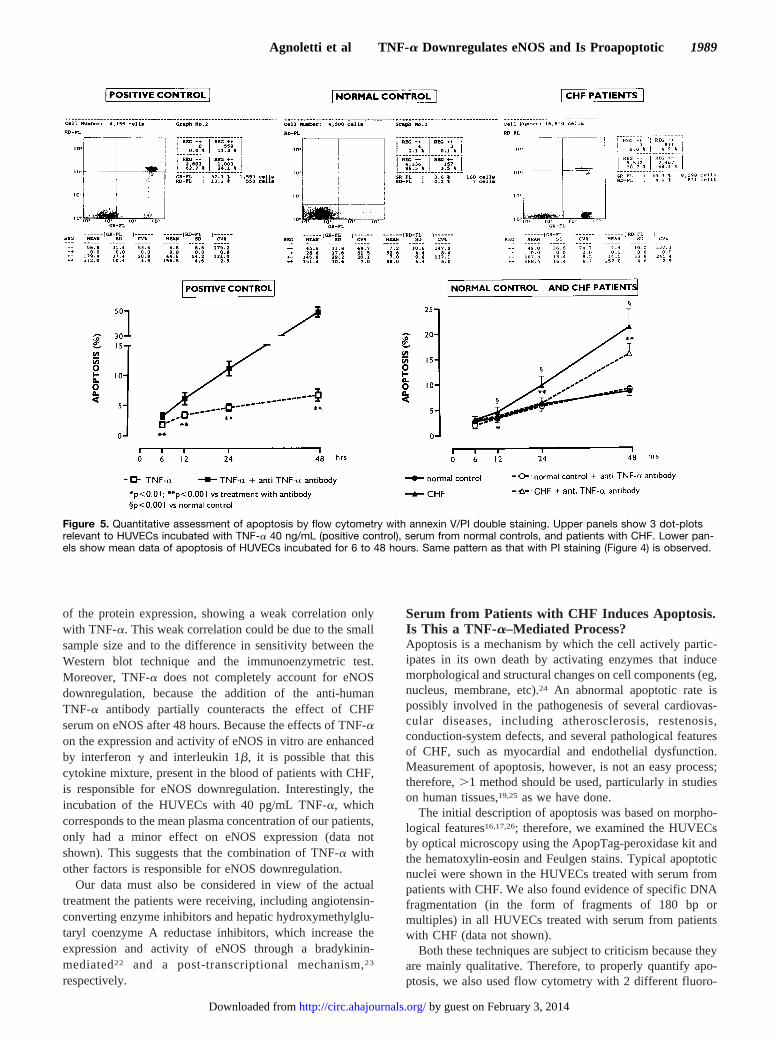
To better quantify apoptosis, we also performed flowcytometry using annexin V/PI double staining (Figure 5).Annexin V binds with a high affinity to phosphatidylserine,which is normally located in the inner part of the cellmembrane. In the early apoptotic states, phosphatidylserinetranslocates from the inner to the outer layer of the cellmembrane, thus allowing its binding to annexin V. PI usedwithout ethanol acts as a cellular viability marker. Therefore,annexin V reveals the early apoptotic processes of still-viablecells, whereas PI, which binds to DNA as a consequence
Figure 2. Analysis of eNOS. A, eNOS protein expression inHUVECs incubated for 6 to 48 hours with serum from nor-mal controls. TNF-a 40 ng/mL was positive control, andTNF-a plus anti-human TNF-a antibody was also used. B,eNOS protein expression in HUVECs incubated for 6 to 48hours with serum from normal controls, from patients withCHF, and from patients with CHF plus anti-human TNF-aantibody. Incubation of HUVECs with serum from patientswith CHF downregulates eNOS expression in comparisonto normal controls at 24 and 48 hours. TNF-a antibody onlypartially counteracts this effect. In positive controls, cleartime-dependent eNOS downregulation exists.
1986 Circulation November 9, 1999
by guest on February 3, 2014http://circ.ahajournals.org/Downloaded from

of end-stage apoptosis or ongoing necrosis, reveals signs ofmembrane permeability impairment. The upper panel ofFigure 5 shows 3 dot-plots of HUVECs relevant to positivecontrols, normal controls, and patients with CHF. The dot-plot of the positive controls clearly identified 3 differentclusters of cells: (1) viable ones that were not stained byeither of the 2 markers, (2) apoptotic ones that were positivelystained only by annexin V, and (3) end-stage apoptotic ornecrotic cells that were stained by both markers. The dot-plotfrom the normal controls did not show relevant positivity toannexin V or PI, whereas incubation with serum from patientswith CHF showed a similar cell distribution to that of thepositive controls. The mean data are shown in the lowerpanels and resemble the data presented in Figure 4, althoughannexin V revealed higher apoptosis than PI at each evalua-tion time.
Correlation AnalysesA strong negative correlation exited between the downregulationof eNOS expression and apoptosis (r520.89;P,0.001), sug-gesting a link between the 2 phenomena. In addition, multiplelinear regression analysis performed on patients with CHF,including all the parameters studied, showed significant corre-lation with apoptosis. After step-wise selection, only TNF-ablood levels were significantly related to apoptosis (r50.56;P,0.05). A strong correlation also existed between TNF-a andits receptors (r50.76;P,0.05 for both sTNF-RI and sTNF-RII)and between the 2 receptors (r50.87;P,0.01). Conversely, nocorrelation was found among apoptosis, neurohormones, or anyof the clinical parameters measured.
DiscussionWe investigated some aspects of the endothelial function ofpatients with CHF by applying an original experimental
Figure 3. Qualitative assessment of apoptosis by optical microscopy. Cytological smears of untreated and treated HUVECs were used.Apoptotic morphology is indicated by arrow. Normal control: nuclei with normal chromatin structure stained by Feulgen (A), hematoxylin(B), and ApopTag (C) reaction. Patients with CHF: morphological aspects of nuclear apoptotic regression consisting of buddings andchromatic condensation zones (D) that evolve in apoptotic bodies (E). Immunocytochemical ApopTag staining: brown positive nuclei (F).
Agnoletti et al TNF-a Downregulates eNOS and Is Proapoptotic 1987
by guest on February 3, 2014http://circ.ahajournals.org/Downloaded from

approach. We tested the serum of patients with CHF on the invitro function of HUVECs. Because we used the serum ofpatients as the “real” clinical mean, we avoided the artificialuse of single or multiple exogenous inducers of endothelialdysfunction, as occurs in the classical in vitro/ex vivoexperiments. Moreover, by determining HUVEC eNOS ex-pression and apoptosis, we overcame the limitations of theindirect evaluation of endothelial dysfunction that are typicalof clinical studies. HUVECs (human origin) resemble ahomologous milieu, although they are not strictly indicativeof endothelial cells in other systemic blood vessels.
Our data show that serum from patients with severe CHFdownregulates eNOS expression and increases apoptosis,indirectly suggesting endothelial dysfunction. Because nocorrelation existed between neurohormones and the 2 endpoints relevant to the endothelial function measured in thecurrent study, we anticipate a possible role of another system:the system of cytokines and, in particular, TNF-a. Althoughour findings cannot be fully extrapolated to in vivo clinicalconditions, they do represent the consequences of abnormalinteraction between the bloodstream of patients with CHFand human endothelium. Obviously, our data cannot demon-strate any organ/tissue dysfunction because endothelium isonly 1 of the involved components.
Serum from Patients With CHF Downregulatesthe Expression of eNOS. Is This aTNF-a–Mediated Process?The endothelium regulates vascular tone by producing vaso-dilating and vasoconstrictive substances.20 In normal vessels,acetylcholine induces NO synthesis by activating eNOS.20
Conversely, in patients with CHF, acetylcholine results in ablunted vasodilating response, whereas nitric oxide–donoradministration exerts a vasodilating response similar to thatobserved in normal controls, suggesting the integrity of thevascular muscle cell. One explanation for this apparentparadox is that eNOS expression is impaired in CHF. Arecent study in dogs with severe CHF indicates that theimpaired response to acetylcholine is due to reduced eNOSexpression, confirming that the 2 phenomena are closelylinked.8
Cytokines, when used in vitro, inhibit eNOS expression.21
Our data, which were obtained by directly administering TNF-ato HUVECs expressing TNF receptors, confirm this finding.Thus, the direct administration of TNF-a to HUVECs can bereferred to as an alternative cytotoxicity assay because it resem-bles the physiopathological conditions.
The incubation of the HUVECs with serum from patientswith CHF also resulted in a time-dependent downregulation
Figure 4. Quantitative assessment of apoptosis by flow cytometry with PI. Upper panels show representative cytofluorimetric record-ings relevant to HUVECs incubated with TNF-a 40 ng/mL (positive control), serum from normal controls, and patients with CHF. Lowerpanels show mean data of apoptosis of HUVECs incubated for 6 to 48 hours. Incubation of HUVECs with serum from patients withCHF results in higher rate of apoptosis in comparison with normal controls at 24 and 48 hours (lower right panel). TNF-a antibody onlypartially counteracts this effect. In positive controls, proportional induction of apoptosis occurs over time (lower left panel).
1988 Circulation November 9, 1999
by guest on February 3, 2014http://circ.ahajournals.org/Downloaded from
of the protein expression, showing a weak correlation onlywith TNF-a. This weak correlation could be due to the smallsample size and to the difference in sensitivity between theWestern blot technique and the immunoenzymetric test.Moreover, TNF-a does not completely account for eNOSdownregulation, because the addition of the anti-humanTNF-a antibody partially counteracts the effect of CHFserum on eNOS after 48 hours. Because the effects of TNF-a
on the expression and activity of eNOS in vitro are enhancedby interferong and interleukin 1b, it is possible that thiscytokine mixture, present in the blood of patients with CHF,is responsible for eNOS downregulation. Interestingly, theincubation of the HUVECs with 40 pg/mL TNF-a, whichcorresponds to the mean plasma concentration of our patients,only had a minor effect on eNOS expression (data notshown). This suggests that the combination of TNF-a withother factors is responsible for eNOS downregulation.
Our data must also be considered in view of the actualtreatment the patients were receiving, including angiotensin-converting enzyme inhibitors and hepatic hydroxymethylglu-taryl coenzyme A reductase inhibitors, which increase theexpression and activity of eNOS through a bradykinin-mediated22 and a post-transcriptional mechanism,23
respectively.
Serum from Patients with CHF Induces Apoptosis.Is This a TNF-a–Mediated Process?Apoptosis is a mechanism by which the cell actively partic-ipates in its own death by activating enzymes that inducemorphological and structural changes on cell components (eg,nucleus, membrane, etc).24 An abnormal apoptotic rate ispossibly involved in the pathogenesis of several cardiovas-cular diseases, including atherosclerosis, restenosis,conduction-system defects, and several pathological featuresof CHF, such as myocardial and endothelial dysfunction.Measurement of apoptosis, however, is not an easy process;therefore,.1 method should be used, particularly in studieson human tissues,19,25 as we have done.
The initial description of apoptosis was based on morpho-logical features16,17,26; therefore, we examined the HUVECsby optical microscopy using the ApopTag-peroxidase kit andthe hematoxylin-eosin and Feulgen stains. Typical apoptoticnuclei were shown in the HUVECs treated with serum frompatients with CHF. We also found evidence of specific DNAfragmentation (in the form of fragments of 180 bp ormultiples) in all HUVECs treated with serum from patientswith CHF (data not shown).
Both these techniques are subject to criticism because theyare mainly qualitative. Therefore, to properly quantify apo-ptosis, we also used flow cytometry with 2 different fluoro-
Figure 5. Quantitative assessment of apoptosis by flow cytometry with annexin V/PI double staining. Upper panels show 3 dot-plotsrelevant to HUVECs incubated with TNF-a 40 ng/mL (positive control), serum from normal controls, and patients with CHF. Lower pan-els show mean data of apoptosis of HUVECs incubated for 6 to 48 hours. Same pattern as that with PI staining (Figure 4) is observed.
Agnoletti et al TNF-a Downregulates eNOS and Is Proapoptotic 1989
by guest on February 3, 2014http://circ.ahajournals.org/Downloaded from

chromes: PI and annexin V-FITC. Flow cytometry allows thedetection of events occurring in thousands of cells whencompared with microscopy, which can only explore limitedfields. Because PI detects apoptosis only in the advancedstages, when the loss of fragmented DNA is already anongoing process, we also used annexin V to quantify the earlyphases of apoptosis. In addition, we combined annexin Vwith PI but without ethanol, thus using PI as a dye-exclusiontest to establish the integrity of cell membranes. The calcu-lation of the percentage of apoptosis did not include the cellswith marked membrane alterations because, at end-stageapoptosis, membrane permeability changes in apoptotic andnecrotic cells are indistinguishable.
Our data confirm that, in vitro, the endothelium has aphysiological rate of apoptosis that is not influenced bycytokines; they also show that serum from patients with CHFis proapoptotic. More than 30 inducers of apoptosis have beenidentified, including neurohormones, cytokines, and newlydiscovered genes and second messengers,27–29thus making itdifficult to identify the primum movens.
We tested the hypothesis that TNF-a plays a crucial role inthe complex biochemistry of apoptosis signaling.30 Thiscytokine induces its cytotoxic effects by binding to specificreceptors present in almost all cells.31 TNF-RI has a cytoplas-mic signaling motif called the death domain,30 which inducescaspases activation, resulting in inactivation of several pro-teins controlling different functions.32 All these changesinduce the morphological characteristics that differentiateapoptosis from necrosis. Interestingly, we found a 5-foldincrease in sTNF-RI, suggesting that TNF-a interacted withthis receptor.
TNF-a may increase the inducible type of nitric oxidesynthase (iNOS) expression, and the resulting peroxinitritewould induce apoptosis. However, this sequence of eventsis expected in bovine aortic endothelial cells but not inHUVECs.33 We did not observe any induction of iNOS (datanot shown), thus ruling out the possibility of TNF-a–induced,high-output nitric oxide production in human endothelialcells.
Although TNF-a is one of the main regulators of endothe-lial cell life/death equilibrium, other factors may play a majorrole in the maintenance of this ratio. Among these, NFkB,whose activation can be stimulated by TNF-a itself underspecific conditions, increases the resistance to the apoptoticstimuli; angiotensin II, by a different modulation of thereceptors AT1 and AT2, can have a pro- or antiapoptoticeffect; and Bcl-2 family members can also promote or inhibitapoptosis induced by certain triggers.
ConclusionsOur results support the hypothesis that the circulatingblood of patients with CHF causes endothelial dysfunction.TNF-a likely plays a role, but it is not the only responsiblefactor.
AcknowledgmentsThis work was supported by the National Research Council targetedproject 9100156 PF41, “Prevention and Control of Disease Factors”;by the European Commission project PL 950838 “The New Ischemic
Syndromes”; and by the Local Grant for Scientific Research “TNF-ain Endothelial Dysfunction in Patients With Severe Heart Failure,”which was issued by the University of Ferrara. The authors thankMichela Palmieri and Daniela Bastianon for technical assistance,Alessandro Bettini for editing the text, and Roberta Bonetti forsecretarial assistance.
References1. Levine B, Kalman J, Mayer L, Fillit HM, Packer M. Elevated circulating
levels of tumor necrosis factor in severe chronic heart failure.N EnglJ Med. 1990;323:236–241.
2. Mann DL, Young JB. Basic mechanisms in congestive heart failure:recognizing the role of proinflammatory cytokines.Chest. 1994;105:897–904.
3. Torre-Amione G, Kapadia S, Lee J, Durand JB, Bies RD, Young JB,Mann DL. Tumor necrosis factor-a and tumor necrosis factor receptors inthe failing human heart.Circulation. 1996;92:1479–1486.
4. Ferrari R, Bachetti T, Confortini R, Opasich C, Febo O, Corti A, CassaniG, Visioli O. Tumor necrosis factor soluble receptors in patients withvarious degrees of congestive heart failure.Circulation. 1995;92:1479–1486.
5. Shan K, Kurrelmeyer K, Seta Y, Wang F, Dibbs Z, Deswal A, Lee-Jackson D, Mann DL. The role of cytokines in disease progression inheart failure.Curr Opin Cardiol. 1997;12:218–223.
6. Oral H, Kapadia S, Nakano M, Torre-Amione G, Lee J, Lee-Jackson D,Young JB, Mann DL. Tumor necrosis factor-alpha and the failing humanheart.Clin Cardiol. 1995;18:IV20–IV27.
7. Yoshizumi M, Perrella MA, Burnett JC, Lee ME. Tumor necrosis factordownregulates an endothelial nitric oxide synthase mRNA by shorteningits half-life. Circ Res. 1993;73:205–209.
8. Smith CG, Sun D, Hoegler C, Roth BS, Zhang X, Zhao G, Xu X-B,Kobary Y, Pritchard K Jr, Sessa WC, Hintze TH. Reduced geneexpression of vascular endothelial NO synthase and cyclooxygenase-1 inheart failure.Circ Res. 1996;78:58–64.
9. Katz SD. Mechanisms and implications of endothelial dysfunction incongestive heart failure.Curr Opin Cardiol. 1997;12:259–264.
10. Packer M. Is tumor necrosis factor an important neurohormonalmechanism in chronic heart failure?Circulation. 1995;92:1379–1382.
11. Katz SD, Rao R, Berman JW, Schwarz M, Demopoulos L, Bijou R,LeJemtel TH. Pathophysiological correlates of increased serum tumornecrosis factor in patients with congestive heart failure.Circulation.1994;90:12–16.
12. Ceconi C, Condorelli E, Quinzanini M, Rodella A, Ferrari R, Harris P.Noradrenaline, atrial natriuretic peptide, bombesin and neurotensin inmyocardium and blood of rats in congestive cardiac failure.CardiovascRes. 1989;23:674–682.
13. Jaffe EA, Nachman L, Becker CG, Minick CR. Culture of human endo-thelial cells derived from umbilical veins.J Clin Invest. 1973;52:2745–2756.
14. Bachetti T, Comini L, Agnoletti L, Pedersini P, Gaia G, Cargnoni A,Bellet M, Curello S, Ferrari R. Effects of chronic noradrenaline on thenitric oxide pathway in human endothelial cells.Basic Res Cardiol.1998;93:250–256.
15. Sharov VG, Sabbah HN, Shymoyama H, Goussev A, Lesch M, GoldsteinS. Evidence of cardiocyte apoptosis in myocardium of dogs with chronicheart failure.Am J Pathol. 1996;148:141–149.
16. Bancroft JD, Stevens A, eds.Theory and Practice of Histological Tech-niques.Edinburgh: Churchill Livingstone; 1990:109–118.
17. Schulte E, Wittekind D. Standardization of Feulgen-Schiff technique.Histochemistry. 1989;91:321–333.
18. Nicoletti I, Migliorati G, Pagliacci MC, Grignani F, Riccardi C. A rapidand simple method for measuring thymocyte apoptosis by propidiumiodide staining and flow cytometry.J Immunol Methods. 1991;139:271–279.
19. Vermes I, Haanen C, Steffens-Nakken H, Reutelingsperger C. A novelassay for apoptosis flow cytometry detection of phosphatidylserineexpression on early apoptotic cells using fluorescein labeled annexin V.J Immunol Methods. 1995;184:39–51.
20. Ryan US, Rubanyi GM, eds.Endothelial Regulation of Vascular Tone.New York: Marcel Dekker Inc; 1992.
21. Rosenkranz-Weiss P, Sessa WC, Milstien S, Kaufman S, Watson CA,Pober JS. Regulation of nitric oxide synthesis by proinflammatory cyto-
1990 Circulation November 9, 1999
by guest on February 3, 2014http://circ.ahajournals.org/Downloaded from

kines in umbilical vein endothelial cells.J Clin Invest. 1994;93:2236–2243.
22. Hornig B, Kohler C, Drexler H. Role of bradykinin in mediating vasculareffects of angiotensin-converting enzyme inhibitors in humans.Circu-lation. 1997;95:1115–1118.
23. Laufs U, La Fata V, Plutzky J, Liao JK. Upregulation of endothelial nitricoxide synthase by HMG CoA reductase inhibitors.Circulation. 1998;97:1129–1135.
24. Sen S. Programmed cell death: concept, mechanism and control.Biol Rev.1992;67:287–319.
25. MacLellan WR, Schneider MD. Death by design: programmed cell deathin cardiovascular biology and disease.Circ Res. 1997;81:137–144.
26. Gold R, Schmied M, Giegerich G, Breitschopf H, Hartung HP, ToykaKV, Lassmann H. Differentiation between cellular apoptosis and necrosisby the combined use ofin situ tailing and nick translation techniques.LabInvest. 1994;71:219–225.
27. Kroemer G, Petit P, Zamzami N, Vayssiere JL, Mignotte B. The bio-chemistry of programmed cell death.FASEB J. 1995;9:1277–1287.
28. Nagata S. Apoptosis by death factor.Cell. 1997;88:355–365.29. Osborne BA, Schwartz LM. Essential genes that regulate apoptosis.
Trends Cell Biol. 1994;4:394–403.30. Schultze-Osthoff K, Krammer PH, Droge W. Divergent signaling via
APO-1/Fas and the TNF receptor, two homologous molecules involved inphysiological cell death.EMBO J. 1994;13:4587–4596.
31. Tartaglia LA, Goeddel DV. Two TNF receptors.Immunol Today1992;13:151–153.
32. Tan X, Wang YJ. The caspase-RB connection in cell death.Trends CellBiol. 1998;8:116–120.
33. Linscheid P, Schaffner A, Blau N, Schoedon G. Regulation of6-pyruvoyltetrahydropterin synthase activity and messenger RNAabundance in human vascular endothelial cells.Circulation. 1998;98:1703–1706.
Agnoletti et al TNF-a Downregulates eNOS and Is Proapoptotic 1991
by guest on February 3, 2014http://circ.ahajournals.org/Downloaded from




















