SEASONAL APPLICATION ...
48
* e Human Resources Department City of Milford 70 West River Street Milford, CT 06460 (203) 783-3239 An Equal Oppor(uni(y Employer l SEASONAL APPLICATION RECREATION SEASONAL Position applying for PLEASE TYPE OR PRINT CLEARLY IN BLACK INK. Ail blanks must be completed in order for application to be considered. PERSONAL INFORMATION I ooo- Othernamesbywhichyouhavebeenknown -Last6digi(sofsoc.sec.No? How Iong at this address? Yesrs/Mon(hs Zip Code Last Name Present Address: No. and S)ree! Ci(y Sta}e Zip Code Mailing address (if different from residenceaddress) No. and Stree! Home Telephone Cellular In case of emergency, notify: Name Rela(ionship List any relatives or members of your household who are employed by the City of Milford Name(s) JobTitle l EMPLOYMENT I Can you perform the essential functions of the job for which you are applying, with or without a reasonable accommodation? r?es Jo If no, please explain: Haveyoueverbeendischargedoraskedtoresign? ?Yesl? Ihir:xcvslaaevavnla:r- '--' lfyes, pleaseexplain: No l RELEVENT WORK EXPERIENCE r Next to each work area, please indicate your experience in this field. It is important that you be specific and provide as much information as possible. Include the amount of time you spent doing this type of work and for whom. How many years/months? /f this was part of your job, what percentage of your time was spent doing it? /f selected your starting rate of pay will be commensurate with your experience as notes in this application. Employer Your 3ob title r TRUCK DRIVINF/PLOWING or ROAD CONSTRUCTION/MAINTENANCE: l First Name M.I. City Email S}a}e Telephone Number Department % TOTAL TIME l l TO l Hours per week Page I of3 DO NOT WRITE IN THIS SPACE €Q Rev, by: €NQ €Educ €exp €uotcityee €other
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of SEASONAL APPLICATION ...

*
eHuman Resources DepartmentCity of Milford70 West River Street
Milford, CT 06460
(203) 783-3239
An Equal Oppor(uni(y Employer
l
SEASONAL APPLICATION
RECREATION SEASONAL
Position applying for
PLEASE TYPE OR PRINT CLEARLY IN BLACK INK.Ail blanks must be completed in order for application to be considered.
PERSONAL INFORMATION I
ooo-
Othernamesbywhichyouhavebeenknown -Last6digi(sofsoc.sec.No?
How Iong at this address?Yesrs/Mon(hs
Zip Code
Last Name
Present Address:
No. and S)ree! Ci(y Sta}e Zip Code
Mailing address (if different from residenceaddress)No. and Stree!
Home Telephone Cellular
In case of emergency, notify:
Name Rela(ionship
List any relatives or members of your household who are employed by the City of MilfordName(s) JobTitle
l EMPLOYMENT I
Can you perform the essential functions of the job for which you are applying, with or without a reasonable accommodation? r?es JoIf no, please explain:
Haveyoueverbeendischargedoraskedtoresign? ?Yesl?Ihir:xcvslaaevavnla:r- '--'lfyes, pleaseexplain:
No
l RELEVENT WORK EXPERIENCE r
Next to each work area, please indicate your experience in this field. It is important that you be specific and provide as muchinformation as possible. Include the amount of time you spent doing this type of work and for whom. How manyyears/months? /f this was part of your job, what percentage of your time was spent doing it? /f selected your starting rate ofpay will be commensurate with your experience as notes in this application.
EmployerYour 3ob title
r TRUCK DRIVINF/PLOWING or ROAD CONSTRUCTION/MAINTENANCE: l
First Name M.I.
City
S}a}e
Telephone Number
Department
% TOTAL TIMEll
TO
lHours per week
Page I of3
DO NOT WRITE IN THIS SPACE
€Q Rev, by:€NQ€Educ
€exp€uotcityee€other
ppiscitelli
Typewritten Text
Circle Selection(s) Camp Happiness Counselor / Lifeguard / Playground Counselor
cschull
Rec Logo

*
Light Equipment:What best describes your skill Ievel with a payloader?What best describes your skill Ievel with a backhoe?What best describes your skill Ievel with a small €ractor?Heavy Equipment:What best describes your skill level with a grader?What best describes your skill Ievel with a Cat225 excavator?What best describes your skill Ievel with a bulldozer?
g Excellent[] Excellent[] Excellent
g Excellent[] Excellentg Excellent
0 Very good[] Very good0 Very good
0 Very good0 Very good€ Very good
g Good[1 GoodgGood
g Good€GoodgGood
gFair€ Fairg Fair
gFair[lFair[]Fair
[] Never Used[] Never Usedg Never Used
g Never Usedg Never Used€ Never Used
i OTHER TRAINING, SKILLS, AND/OR LICENSES r
Page2of3
Employer FROM I TO l TOTALTIMEYour job title
Hours per weekOTHER WORK:
"!g'("3A
*
l DRIVER'S LICENSE i
DRIVER'S LICENSE: If the position for which you are applying will require you to operate a vehicle:(1 ) You must possess a valid driver's license,(2) Any special endorsements must be current and valid,(3) If you are offered employment by the City of Milford, and if your driver's license is from another state, you will be required as a
condition of employment to obtain a valid Connecticut Driver's License before you can beginwork.
Do you have a valid driver's Iicense: Yes @ -€Classification
State
Expiration Date License #
Endorsements:
l
FINALISTS WILL BE REQUIRED, UPON NOTIF?CATION, TO SUBMIT A COPY OF THEIR DRMNG ABSTRACT. Note: Drivingabstracts may be obtained at any Connecticut Department of Motor Vehicles office. This fee is at the finalist's expense.
l
SIGNATURE ofAPPLlCANT DATE
Page 3 of 3

INV?TATION TO SELF-IDENTIFYill
Ea!::
City of Milford Recreation Seasonal
Position applying for(use the ti}Ie that appears on the job announcement)
l SECTION 1: CANDIDATE INFORMAT?ONIt is the policy of the City of Milford to recruit, hire, and promote qualified people in all job classifications regardless of age, race, gender, color,religion, creed, national origin, marital or veteran status, sexual orientation, gender identity or expression, disability ot any other legally protectedstatus, unless they are bona-fide occupational qualifications.
i
The following information is needed for compliance with governmental reporting requirements. While completion of this sec(ion is voluntary, allapplicants are strongly urged to complete this as part of the pre-employment process. Applicants so choosing, may identify on the form that they havechosen not to provide the City of Milford with the requested information by checking the appropriate box in Section 4. This infomiation will not affect inany way your employment opportuni(ies. The information obtained will be kept confidential and may only be used in accordance with the provisions ofapplicable federal laws, executive orders, and regulations, including those which require the information to be summarized and reported to theFederal Government for civil rights enforcement purposes.
l (SECTION 2: GENERAL INFORMATION
Name Date
r
1Social Security Number 000 (Last six di[its ONLY)
l }SECTION 3: STATlSTICALiNFORMATION I
PLEASE ANSWER THE FOLLOWING QUESTION:
What is your race/ethnicity? (Please mark the ? that describes the race/ethnicity category with which you primarily identify.)Race/Ethnic Identification
[?](No} Hispanic or Laffno) All persons having origins in any of The original peoples of Nor}h and Souffi America (including Cen(ral America), andwho main!ains tribal affiliation or commuruty auachmen}.
€(No( Hispanic or LaUno) All persons having origins in any of Uie original peoples of The Fat Eas(, Sou(heas( Asia, or the Indian Subconffnen}?ding, for example, Cambodia. China, India, Japan, Korea, Malaysia, Pakis!an, The Phillipine Islands, Thailand, and Vietnam.
(No! Hispanic or LaUno) All persons having origins in any of the black tacial groups of Africa.
All persons of Cuban, Mexican, Puetto Rican, Cen!ral or South America, or oTher Spanish culire or origin, regardless of race.
(No! Hispanic or LaUno) All persons having origins in any ol ffie original peoples of Hawaii, Guam, Samoa, or Pacific Islands.
American Indian or
Alaska Native
Asian
Black or African American
Hispanic or LatinoNative Hawaiian or Other
Pacific IslanderWhite
Two or more races
€Male
€(Noi of Hispanic or LaUno origin.) All persons having origins in any of the original peoples of Eutope. The Middle Easl or NorTh Africa.€A person who primanly idenbfies wi!h two or more of the above race/e}hnicity ca!egories.[lFemaleGender
l :SECTION 4: :NON-PARTIC?PATION
I have read the above statement and have chosen not to complete this form.
Please check box if applicable
a
i
]
Page 1 of 1
JT(I J('] m FN E'! (4 i{! kJ IN (] l NT!] N ITrhSl ('> NHow did you hear about this job? (Please check one.) " -a '-'a '- " '[]Milford Mirror []Human Resources or Department Bulletin Board[lOther newspaper (give name): Community Agency (give name):
[lCity Websiie [lProfessional Joi.irnal (give name):[llnternet (Iist site): [lOther (please specify):l]City Employee
APPLICANT DISCLOSURE FORM
City of Milford
l CR?MINAI CONViCnON INFORMATIONHave you ever been oonvicted of any offenses other }hari juvenile, youthful ofiender, or a minor {raTfic viola!ion?
Have you ever been disqualiiied for a position with the City of Milford due lo a criminal conviclion or failure todisclose a criminal oonviction remrd? If yes, list the job Utle and date of disqualifica(ion;Job Tiue' Date of Disqualitication:
W+l NOTE:
THIS INFORMATION WILL BE REVIEWED ONLY BY MEMBERS OF THEHUMAN RESOURCES DEPARTMENT AND HIRING I?ANAGERS.
Yes No
YesJ[] NoJ[]
i
Applicants are required to disclose the existence of any criminal convic(ion, regardless of the nalure, dace or Iocation thereof, with the exception ofminor traffic violations or an arrest, criminal charge, or convic}ion lhat has been erased. The types of records subjec} to erasure under Conneciiai(law are as follows: (a) a finding of delinquenq or that a child was a member of a family wi(h service needs; (b) a sentence as a youthful offender; (c)a criminal charge that was dismissed or onolled;' (d) a criminal charge for which the person was found nor guilty; or (e) a convic!:on for which theperson received an absolu}e pardon.
The information provided below is subject to the (erms of the 'Pre-Employment Statement" on Page s of this application. A criminal conviction will no(necessarily resul! in the reiection of this application, bu} will be considered as it rela(es to the nature of the position sought, and in light of anyapplicable s(ate and federal law
Name (Prin0 Title of Posi(ion Sought
Applicant's Signatute Da}e
DATE OF CONVICTION OFFENSE DATE OF ARRESTPLACE OF ARREST
(Ciiy/Staie)SENTENCE

o is%r..tz*al ?7
Name:
Departmem; Recreation
(::ity of ')VLilford
Emergency Contacts Form
PositionTitle: Seasonal Temporary
In the event of an emergency, please notify:
Employee Signature Date
Note: /t is the employee's responsibility to update the Human Resources Department with anychanges to the information provided on this form.
1.
RelationshipName
Address Home Number Mobile Number Work Number
2.
Name Relationship
Address Home Number Mobile Number Work Number

*
FormW-4
Depar}ment oj the TreasmlIntemal Revenue Service
Employee's Withholding Certificatek Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay.
r Give Form W-4 to your employer.k Your withholding is subject to review by the IRS.
IOMB No. 1545-0074
2O20
Step1:
Personal
Information l
Enter
iocial security number
38 your name match theon your social securi'by
' If not, to ensure you getfor your earriinqs, 'contactit 8el0-772-121'3 or go tossa.gov.
(c)-g Single or Married filing separatelygMarried filing jointly (or Qualifying widow(er))gHead of household (Check only if yovlre unmarried and pay more than half the costs of keeping up a home for yourself and a qualifying individual.)
Complete Steps 2-4 oNLY if they apply to you; otherwise, skip to Step s. See page 2 for more information on each step, who canclaim exemption from withholding, when to use the online estimator, and privacy.
Step 2: Complete this step if you (1) hold more than one job at a time, or (2) are married filing jointly and your spouseMultiple Jobs also works. The correct amount of withholding depends on income earned from all of these jobs.or Spouse Do only one of the following.Works (a) Use the estimator at www.irs.govlW4App for most accurate withholding for this step (and Steps 3-4); or
(b) Use the Multiple Jobs Worksheet on page 3 and enter the result in Step 4(c) below for roughly accurate withholding; or(c) If there are only two jobs total, you may check this box. Do the same on Form W-4 for the other job. This option
is accurate for jobs with similar pay; otherwise, more tax than necessary may be withheld . . . . . k 0
TIP: To be accurate, submit a 2020 Form W-4 for all other jobs. If you (or your spouse) have self-employmentincome, including as an independent contractor, use the estimator.
Complete Steps 3-4(b) on Form W-4 for only ONE of these jobs. Leave those steps blank for the other jobs. (Your withholding willbe most accurate if you complete Steps 3-4(b) on the Form W-4 for the highest paying job.)
Step 3: If your income will be $200,000 or less ($400,000 or less if married filing jointly):Claim
Dependents Multiply the number of qualifying children under age 17 by $2,000 r $
Multiply the number of other dependents by $500 )$
Add the amounts above and enter the total here
(a) Other income (not from jobs). If you want tax withheld for other income you expectthis year that won't have withholding, enter the amount of other income here. This mayinclude interest, dividends, and retirement income .
Step 4(optional):
Other
Adjustments(b) Deductions. If you expect to claim deductions other than the standard deduction
and want to reduce your withholding, use the Deductions Worksheet on page 3 andenter the result here
Step s:
SignHere
Under penalties of perjury, l aeclare that this certificate, to the best of my knowledge and belief, is true, correct, and complete.
>Employee's signature (T his form is not valid unless you sign it.)
Employers iOnly
>Date
Employer identificationnumber (EIN)
For Privacy Act and Paperwork Reduction Act Notice, see page 3. Cat. No. 10220Q Form W-4 (2020)
la) Firs} name and middle ini}ial Castname'- - '
Address
City or town, state, and ZIP code
3l
[M
Employer's name and address First date of
employment

lorm W-4 (2020) Page 2
General Instructions
Future DevelopmentsFor the Iatest information about developments related toForm W-4, such as Iegislation enacted affer it was published,go to www.irs.gov/FormW4.
Purpose of FormComplete Form W-4 so that your employer can withhold therorrect federal income tax from your pay. If too Iittle isviithheld, you will generally owe tax when you file your taxraturn and may owe a penalty. If too much is withheld, you willcenerally be di.ie a refund. Complete a new Form W-4 whenchanges to your personal or financial situation would changethe entries on the form. For more information on withholdingand when you must furnish a new Form W-4, see Pub. 505.Exemption from withholding. You may claim exemption fromwithholding for 2020 if you meet both of the followingconditions: you had no federal income tax Iiability in 2019 andyou expect to have no federal income tax Iiability in 2020. YouSad no federal income tax Iiability in 2019 if (1 ) your total tax onIine 16 on your 2019 Form 1040 or 1 040-SR is zero (or lessthan the sum of Iines 1 8a, 1 8b, and 1 8c), or (2) you were notrequired to file a return because your income wels below thefiling threshold 'ior your correct filing status. If you claimexemption, you will have no income tax withheld from yourpaycheck and may owe taxes and penalties when you file your:?020 tax return. To claim exemption from withholding, cerkifythat you meet both of the conditions above by writing "Exempt"on Form W-4 in the space below Step 4(c). Then, completeSteps 1 a, 1 b, and s. [)o not complete any other steps. You willneed to submit a new Form W-4 by February 16, 2021.Your privacy. If you preler to Iimit information provided inSteps 2 through 4, use the online estimator, which will alsoincrease accuracy.
As an alternative to the estimator: if you have concernswith Step 2(c), you may choose Step 2(b); if you haveconcerns with Step 4(a), you may enter an additional amountyou want withheld per pay perioa in Step 4(c). If this is theonly job in your household, you may instead check the boxin Step 2(c), which will increase yoor withholding andsignificantly reduce your paycheck (often by thousands ofdollars over the year).
When to use the estimator. Consider using the estimator atwww.irs.gov/W4App if you:
1 . Expect to work only part of the year;
2. Have dividend or capital gain income, or are subject toadditional taxes, such as the additional Medicare tax;
3. Have self-employment income (see below); or4. Prefer the most accurate withholding for multiple jobsituations.
Self-employment. Gerierally, you will owe both income andself-employment taxes on any self-employment income youreceive separate from the wages you receive as anemployee. If you want to pay these taxes throughwithholding from your wages, use the estimator atwww.irs.gov/W4App to figure the amount to have withheld.Nonresident alien. If you're a nonresident alien, see Notice1392, Supplemental F'orm W-4 Instruetianf for NonresidentAliens, be4ore completing this form. a' -?
Specific InstructionsStep 1 (c). Check your anticipated filing status. This willdetermine the standard deduction and tax rates used tocompute your withholding.
Step 2. Use this step if you (1 ) have more than one job at thesame time, or (2) are married filing jointly and you and yourspouse both work.
Option (a) most accurately calculates the additional taxyou need to have withheld, while option (b) does so with aIittle Iess accuracy.
If you (and your spouse) have a total of only two jobs, youmay-instead check the box in option (c). The box must also bechecked on the Form W-4 for the other job. If the box ischecked, the standard deduction and tax brackets will be cutin half for each job to calculate withholding. This option isroughly accurate for jobs with similar pay; otherwise, more taxthan necessary may be withheld, and this extra amount will beIarger the gea{er the difference in pay is between the two jobs.
[Q Multiple jobs, Complete Steps 3 through 4(b) on onlyone Form W-4. Withholding will be most accurate ifyou do this on the Form W-4 for the highest paying job.
Step 3. Step 3 of Form W-4 provides instructions fordetermining the amount of the child tax credit and the creditfor other dependents that you may be able to claim whenyou file your tax return. To qualify for the child tax credit, thechild must be under age 17 as of December 31 , must beyour dependent who generally Iives with you for more thanSalf the year, and must have the required social securitynumber. You may be able to claim a credit for otherdependents for whom a child tax credit can't be claimed,such as an older child or a qualifying relative. For additionaleligibility requirements for these creaits, see Pub. 972, ChildTax Credit and Credit for Other Dependents. You can alsoinclude other tax credits in this step, such as education taxcredits and the foreign tax credit. To do so, add an estimateof the amount for the year to your credits for dependentsand enter the total amount in Step 3. Including these creditswill increase your paycheck and reduce the amount of anyrefund you may receive when you file your tax return.Step 4 (optional).
Step 4(a). Enter in this step the total of your otherestimated income for the year, if any. You shouldn't includeincome from any jobs or self-employment. If you completeStep 4(a), you Iikely won't have to make estimated taxpayments for that income. If you prefer to pay estimated taxrather than having tax on other income withheld 1rom yourpaycheck, see Form 1 040-ES, Estimated Tax for Individuals.
Step 4(b). Enter in this step the amount from the DeductionsWorksheet, Iine s, if you expect to claim deductions other thanthe basic standard d-eduction on your 2020 tax return andwant to reduce your withholding to account for thesedeductions. This includes both itemized deductions and otherdeductions such as for student Ioan interest and IRAs.
Step 4(c). Enter in this step any additional tax you wantwithheld from your pay each pay period, including anyamounts from the Multiple Jobs Worksheet, Iine 4. Entering anamount here will reduce your paycheck and will either increaseyour refund or reduce any amount of tax that you owe.

'orm 'N-4 (2020)
Step 2(b) - Multiple Jobs Worksheet (Keep for your records.)
Page 3
W you choose the option in Step 2(b) on Form W-4, complete this worksheet (which calculates the total extra tax for all jobs) on only ONEForm W-4. Withholding will be most accurate if you complete the worksheet and enter the result on the Form W-4 for the highest paying job.klote: If more than one job has annual wages of more than $120,000 or there are more than three jobs, see Pub. 505 for additionalhbles; or, you can use the online withholding estimator at www.irs.gov/W4App.
1 Two jobs. If you have two jobs or yov're married filing jointly and you and your spouse each have onejob, find the amount from the appropriate table on page 4. Using the "Higher Paying Job" row and the"Lower Paying Job" column, find the value at the intersection of the two household salaries and enterthatvalueonlinel.Then,skiptoline3 . . . . . . . . . . . . . . . . . . . . . 1 $
2 Three jobs. If you and/or your spouse have three jobs at the same time, complete Iines 2a, 2b, and2c below. Otherwise, skip to line 3.
a Find the amount from the appropriate table on page 4 using the annual wages from the highestpaying job in the "Higher Paying Job" row and the annual wages for your next highest paying jobin the "Lower Paying Job" column. Find the value at the intersection of the two household salariesand enter that value on Iine 2a . 2a $
b Add the annual wages of the two highest paying jobs from Iine 2a together and use the total as thewages in the "Higher Paying Job" row and use the annual wages for your third job in the "LowerPaying Job" column to find the amount from the appropriate table on page 4 and enter this amounton Iine 2b 2b $
c Add the amounts from Iines 2a and 2b and enter the result on Iine 2c . 2c $
3 Enter the number of pay periods per year for the highest paying job. For example, if that job paysweekly, enter 52; if it pays every other week, enter 26; if it pays monthly, enter 12, etc. 3
4 Divide the annual amount on line 1 or line 2c by the number of pay periods on Iine 3. Enter thisamount here and in Step 4(c) of Form W-4 for the highest paying job (along with any other additionalamount you want withheld)
Step 4(b) - Deductions Worksheet (Keep for your records.)
4$
Ia'yl1 Enter an estimate of your 2020 itemized deductions (from Schedule A (Form 1040 or 1 040-SR)). Such
deductions may include qualifying home mortgage interest, charitable contributions, state and localtaxes (up to $1 o,ooo), and medical expenses in excess of 1 0% of your income . 1$
* $24,800 if you're married filing jointly or qualifying widow(er)(2 Enter: < * $18,650 if you're head of household* $12,400 if you're single or married filing separately
) 2$
3 If Iine 1 is greater than Iine 2, subtract Iine 2 from Iine 1 . If Iine 2 is greater than Iine 1 , enter "-0-" 3$
4 Enter an estimate of your student Ioan interest, deductible IRA contributions, and certain otheradjustments (from Schedule 1 (Form 1040 or 1 040-SR)). See Pub. 505 for more information 4$
s Add lines 3 and 4. Enter the result here and in Step 4(b) of Form W-4 . 5$
Privacy Act and Paperwork Reduction Act Notice. We ask for the informationon this form to carry out the Internal Fleveriue laws of the United States. InternalRevenue Code sections 3402(f)(2) and 6109 and their regulations require you toprovide this information? your 6mployer uses it to determine your federal rncomerax withholding. Failure to provide a -properly completed form will result in yourbeing treated as a single person with no other entries on the form; providingfraudulent information may subject you to penalties. Routine vses of thisinformation include giving it to the Department of Justice for civil and criminallitigation; to cities, s;ates, the Distri?i 'of Columbia, and u.s. pommonwealths andpossessions for use in administering their tax laws; and to the Deparkment ofHealth and Human Services for use in the National Direc4tory of New Hires. Wemay also disclose this information to other countries under a tax treaty, to federalana state agencies to enforce lederal nontax criminal laws, or to federal lawenforcement and intelligence agencies to combat terrorism.
You are not required to provide the information reques{ed on a form that issubiect to the Paperwork Reduction Act unless the <orm displays a valid OMBcontrol number. Books or records relating to a form or its instructions must beretained as long as their contents may become material in the administration ofany Internal Revenue law. Generally, tax returns and return information areconfidential, as required by Code section 61 03.
The averaqe time and expenses required to complete and file this form will varydepending o-n individual circumstances. For estimated averages, see theinstructions for your income tax return.
If you have suggestions ior making this form simpler, we would be happy to t'iearfrom you. See the instructions for your income tax return.

Form W-4 (2020) Page 4
Higher PayinmAnnual Taxable
Wage & Salary
$0- 9,999
$io,ooo- 1giggg
$20,000- 29,999
$30,000- 39,999
$40,000- 49,999
$50,000- 59,999
$eo,ooo- 69,999
$70,000- '79,999
$80,000- 99,999
$100,000 - 149,999
$t 50,000 - 239,999
$240,000 - 259,999
$260,000 - 279,999
$280,000 - 299,999
$300,000 - 319,999
$320,000 - 364,999
$365,000 - 524,999
$525,000 and over
Higher Paying JobjAnnual Taxable
Wage & Salary
$0- 9,999
$10,000- 19,999
$20,000- 29,999
$30,000- 39,999
$40,000- 59,999
$60,000- 79,999
$80,000- 99,999
$t oo,ooo-124,999
$t 25,000 - 149,999
$t 50,000 - 174,999
$t 75,000 - 199,999
$200,000 - 249,999
$250,000 - 399,999
$400,000 - 449,999
$450,000 and over
Higher Pa)/ing JoblAnnual Taxable
Wage & Salary
so- g,ggg
$io,ooo- 1g,ggg
$20,000- 29,999
$30,000- 39,999
$40,000- 59,999
$60,000- 79,999
$80,000- 99,999
$i oo,ooo - 124,999
$125,000 - 14giggg
$i 50,000 - 174,999
$i 75,000 - 199,999
$200,000 - 249,999
$250,000 - 349,999
$350,000 - 449,999
$450,000 and over
Married Filing Jointly or Qualifying Widow(er)Lower Paying Job Annual Taxable Wage & Salary
i$110,000-l 120',000i $1,870I 4,070l 5,900l 7,100l 8,220i 9,220i 10,220l 11,240i 13,460i 15,180l 16,250i 18,170l 19,770
21,370
22,970
26,840
29,280
31 ,650
Single or Married Filing SeparatelyLower Paying Job Annual Taxable Wage & Salary
i$11o,ooo -i 120,000i $2,040l 3,830i 5,110i 6,310i s,osoi 10,060l 12,060l 14,620i 17,370l 20,120
21 ,230
21,930
21,930
22,540
24,300
Head of Household
lower Paying Job Annual Taxable Wage & Salary
i$ii o,ooo -i 120:000il 4,440i 5,850i 7,140l 9,360i 12,380i 14,380l 16,870i 19,620l 22,370l 23;980
l
? 24,870' 24,870
25,200
27,240
$0-9,999
$10,000 -i giggg
$20,000 -29,999
$30,000 -39,999
$40,000 -4g,ggg
$50,000 -59,999
$60,000 -69,999
$70,000 -79,999
$80,000 -89,999
$90,000 -gg,ggg
$100,000 -i og,ggg
$0
220
850
$220
1 ,220
1 ,900
$850
1 ,900
2,730
$900
2,100
2,930
$i ,020
2,220
3,050
$1 ,020
2,220
3,050
$1 ,020
2,220
3,050
$i ,020
2,220
3,240
$1,020
2,410
4,240
$1,210
3,410
5,240
$1 ,870
4,070
5,900900
1,020
1 ,020
2,100
2,220
2,220
2,930
3,050
3,050
3,130
3,250
3,250
3,250
3,370
3,570
3,250
3,570
4,570
3,440
4,570
5,570
4,440
5,570
6,570
5,440
6,570
7,570
8,440
7,570
8,570
7,100
8,220
9,220
1 ,020
1 ,020
1,060
2,220
2,220
3,260
3,050
3,240
5,090
3,440
4,440
6,290
4,570
5,570
7,420
5,570
6,570
8,420
6,570
7,570
9,420
7,570
8,570
10,420
8,570
9,570
11 ,420
9,570
10,570
12,420
10,220
11 ,220
13,260
1 ,870
2,040
2,040
4,070
4,440
4,440
5,900
6,470
6,470
7,100
1870
7,870
8,220
9,190
9,190
9,320
10,390
10,390
10,520
11 ,590
11 ,590
11 ,720
12,790
12,790
12,920
13,990
13,990
14,120
15,190
15,520
14,980
16,050
17,170
2,040
2,040
2,040
4,440
4,440
4,440
6,470
6,470
6,470
7,870
7,870
8,200
9,190
g,tgo
10,320
10,390
10,720
12,320
11 ,590
12,720
14,320
13,120
14,720
16,320
15,120
16,720
18,320
17,120
18,720
20,320
1 B,770
20,370
21 ,970
2,720
2,970
3,140
5,920
6,470
6,840
8,750
9,600
10,170
10,950
12,100
12,870
13,070
14,530
15,500
15,070
16,830
18,000
1 7,070
19,130
20,500
19,070
21 ,430
23,000
21 ,290
23,730
25,500
23,590
26,030
28,000
25,540
27,980
30,150
$0-9,999
$1 0,000 -* giggg
$20,000 -29,999
$30,000 -39,999
$40,000 -49,999
$50,000 -59,999
$60,000 -69,999
$70,000 -79,999
$80,000 -89,999
$90,000 -99,999
$100,000 -109,999
$460
940
1,020
$940
1 ,530
1,610
$1,020
1,610
2,130
$1,020
2,060
3,130
$1 ,470
3,060
4,130
$1 ,870
3,460
4,540
$1 ,870
3,460
4,540
$1 ,870
3,460
4,720
$1 ,870
3,640
4,920
$2,040
3,830
5,110
$2,040
3,830
5,110
1 ,020
1 ,870
1 ,870
2,060
3,460
3,460
3,130
4,540
4,690
4,130
5,540
5,890
5,130
6,690
7,090
5,540
7,290
7,690
5,720
7,490
7,890
5,920
7,690
8,090
6,120
7,890
8,290
6,310
8,080
8,480
6,310
8,080
9,260
2,020
2,040
2,040
3,810
3,830
3,830
5,090
5,110
5,110
6,290
6,310
7,030
7,490
7,510
9,030
8,090
8,430
10,430
8,290
9,430
11 ,430
8,490
10,430
12,580
9,470
11 ,430
13,880
10,460
12,420
15,170
11 ,260
13,520
16,270
2,360
2,720
2,970
4,950
5,310
5,860
7,030
7,540
8,240
9,030
9,840
10,540
11 ,030
12,140
12,840
12,730
13,840
14,540
14,030
15,140
15,840
15,330
16,440
17,140
16,630
1 1740
18,440
17,920
19,030
19,730
19,020
20,130
20,830
2,970
2,970
3,140
5,860
5,860
6,230
8,240
8,240
8,810
10,540
10,540
11,310
12,840
12,840
13,810
14,540
14,540
15,710
15,840
15,840
17,210
17,140
17,140
18,710
18,440
18,450
20,210
19,730
19,940
21 ,700
20,830
21,240
23,000
$0-giggg
$10,000 -19,999
$20,000 -29,999
$30,000 -39,999
$40,000 -4giggg
$50,000 -59,999
$60,000 -69,999
$70,000 -79,999
$80,000 -89,999
$90,000 -ggiggg
$ioo,ooo -i og,ggg
$0
830
930
$830
1 ,920
2,130
$930
2,130
2,350
$1 ,020
2,220
2,430
$1,020
2,220
2,900
$1 ,020
2,680
3,900
$1 ,480
3,680
4,900
$1 ,870
4,070
5,340
$1 ,870
4,130
5,540
$1 ,930
4,330
5,740
$2,040
4,440
5,850
1,020
1,020
1 ,870
2,220
2,530
4,070
2,430
3,750
5,310
2,980
4,830
6,600
3,980
5,860
7,800
4,980
7,060
g,ooo
6,040
8,260
10,200
6,630
8,850
10,780
6,830
9,050
10,980
7,030
9,250
11,180
7,140
9,360
11 ,580
1 ,900
2,040
2,040
4,300
4,440
4,440
5,710
5,850
5,850
7,000
7,140
7,360
8,200
8,340
9,360
9,400
9,540
11 ,360
t O,600
11 ,360
13,360
11,180
12,750
14,750
11 ,670
13,750
16,010
12,670
1 4,750
17,310
13,580
1 5,770
18,520
2,040
2,720
2,970
5,060
- 5,920
6,470
7,280
8,130
8,990
9,360
10,480
11 ,370
11 ,360
12,780
13,670
13,480
15,080
15,970
15,780
17,380
18,270
1 7,460
19,070
19,960
18,760
20,370
21 ,260
20,060
21 ,670
22,560
21 ,270
22,880
23,770
2,970
2,970
3,140
6,470
6,470
6,840
8,990
s,ggo
9,560
11 ,370
11 ,370
12,140
13,670
13,670
14,640
15,970
15,970
17,140
18,270
18,270
19,640
19,960
19,960
21,530
21 ,260
21 ,260
23,030
22,560
22,560
24,530
23,770
23,900
25,940

*
Department of Revenue ServicesState of Connecticut
(Rev. 1 2/1 9)
Employee Instructions
- Read the instructions on Page 2 before completing this form. - Choose the statement that best describes your gross income.a Select the filing status you expect to report on your Connecticut - Enter the Withholding Code on Line 1 below.
income tax return. See instructions.
' If you are claiming the Military Spouses Residency Relief Act (MSRRA) exemption, see instructions on Page 2.
Employees: See Employee General Instructions on Page 2. Sign and return Form CT-W4 to your employer. Keep a copy for your records.1 . Withholding Code: Enter Wrthholding Code Ie(ter chosen from above. ....................... 1 .
2. Additional withholding amount per pay period: If any, see instructions. . ..................... 2. $
(] Check if you are claiming+ho All(-DDA 6 -e-'- -+i - -the MSRRA exemptionand enter state of legalresidence/domicile:
3. Reduced withholding amount per pay period: If any, see instructions. ........................ 3. $
Form CT-W4Employee's Withholding Certificate
Complete this form in blue or black ink only.
Effective Januaiy 1, 2020
Declaration: I declare under penalty of Iaw that l have examined this certificate and, to the best of my knowledge and belief, it is true, complete, andcorrect. l understand the penalty for reporting false information is a fine of not more than $5,000, imprisonment-for not more than five years, or both.
Employers: See Employer Instructions, on Page 2.
Is this a new or rehired employee? 0 No 0 Yes Enter date hired:mm/dd/yyyy
Married Filing Jointly Wi}hholdingCode
Our expected combined annual gross income is less than orequal to $24,000 or I am claiming exemption under the MilitarySpouses Residency Relief Act (MSRRA)' and no withholdingis necessary.
E
My spouse is employed and our expecled combined annualgross income is greater than $24.000 and Iess than or equalto $100,500. See Certain Mamed IndMduals, Page 2.
A
My spouse is not employed and our expected combinedannual gross income is greater than $24,000.
c
My spouse is employed and our expected combinedannual gross income is greater than $1 oo,soo.
D
l have significan} nonwage income and wish to avoid havingtoo Iittle tax withheld.
D
I am a nonresident of Connecticut with substantial other income D
Qualifying Widow(er) WilhhOldin(1Code
My expected annual gross income is less than or equal to$24,000 or I am claiming exemption under the MSRRA" andno withholding is necessary.
E
My expec{ed annual gross income is greater than $24,000. c
I have significant nonwage income and wish to avoid having tooIittle tax withheld. D
I am a nonresident of Connedicut with substantial other income. D
Married Filing Separately Wi}hholdin@Codh
My expected annual gross income is less than or equal to$12,000 or I am claiming exemption under the MSRRA" andno withholding is necessary.
E
My expected annual gross income is greater than $12,000. A
I have significant nonwage income and wish to avoid havingtoo Iittle tax withheld.
D
l am a nonresident of Connecticut with substantial other income. D
l Single WithholdingCoda
My expected annual gross income is less than or equal to$15,000 and no withholding is necessary.
E
My expected annual gross income is greater than $15,000. F
I have significant nonwage income and wish to avoid havingtoo Iittle tax withheld.
D
l am a nonresident of Connecticut with substantial other income. D
Head of Household Vlli}hholdingCode
My expected annual gross income is less than or equal to$19,000 and no withholding is necessary.
E
My expected annual gross income is greater than $1 g,ooo. B
I have significant nonwage income and wish (o avoid havingtoo Iittle tax withheld.
D
I am a nonresident of Connecticut with substantial other income. D
Firstname MI Lastname Social Security Number
Home address (number and street, apartment number, suite number, PO Box)
City/town State ZlPcode
Employee's signature Date
Employer's business nameCity of Milford
Federal Employer Identification Number06-6002037
Employer'sbusinessaddress -
Parsons Complex, 70 West River StreetCity/town Stare ZlPcode Milford CT 06460-3317
Contact personMarianne Klinga, Treasurer
Telephone'number '203- 783 -3230

Form CT-W4 Instructions
Employee General InstructionsForm CT-W4, Employee's Withholding Certificate, provides youremployer with the necessary information to withhold the correctamount of Connecticut income tax from your wages to ensure thatyou will not be underwithheld or overwithheld.
You are required to pay Connecticut income tax as income is earnedor received during the year. You should complete a new Form CT-W4at least once a year or if your tax situation changes.
If your circumstances change, such as you receive a bonus or yourfiling status changes, you must furnish your employer with a newForm CT-W4 within ten days of the change.Gross Income
For Form CT-W4 purposes, gross income means all income fromall sources, whether received in the form of money, goods, property,or services, not exempt from Tederal income tax, and includes anyadditions to income from Schedule 1 of Form CT-1040, ConnecticutResident Income Tax Return or Form CT-1040NR/PY, ConnecticutNonresident and Part-Year Resident Income Tax Return.
Filing StatusGenerally, the filing status you expect to report on your Connecticutincome tax return is the same as the filing status you expect to reporton your federal income tax return. However, special rules apply tomarried individuals who file a joint federal return but have a differentresidency status. Nonresidents and part-year residents should seethe instructions to Form CT-1040NR/PY.
Check Your WithholdingYou may be underwithheld if any of the following apply:
You have more than one job;You qualify under Certain Married lndividuals', orYou have substantial nonwage income.
If you are underwithheld, you should consider adjusting yourwithholding or making estimated payments using Form CT-1040ES,Estimated Connecticut Income Tax Payment Coupon for Individuals.You may also select Withholding Code ?D? to elect the highest Ievelof withholding.
If you owe $1 ,000 or more, after subtracting from your Connecticutincome tax the amount withheld from your income for the prior taxableyear, and any PE Tax Credit, you may be subject to interest on theunderpayment at the rate of 1 % per month or fraction of a month.
To help determine if your withholding is correct, see InformationalPublication 2020(7), Is My Connecticut Withholding Correct?Certain Married Individuals
If you are a married individual filing jointly and you and your spouseboth select Withholding Code"A," you may have too much or tooIittle Connecticut income tax withheld from your pay. This is becausethe phase-out of the personal exemption and credit is based on yourcombined incomes. The withholding tables cannot reflect your exactwithholding requirement without considering the income of your spouse.To minimize this problem, and determine if you need to adjust yourwithholding using Line 2 or Line 3, see IP 2020(7).
Nonresident Employees Working Partly Within and PartlyOutside of Connecticut
If you work partly within and partly outside of Connecticut forthe same employer, you should also complete Form CT-W4NA,Employee's Withholding or Exemption Certificate - NonresidentApportionment, and provide it to your employer. The information onForm CT-W4NA and Form CT-W4 will help your employer determinehow much to withhold from your wages for services performed withinConnecticut. For Convenience of the Employer Test information, seeForm CT-W4NA. To obtain Form CT-W4NA, visit the Department ofRevenue Services (DRS) website at portal.ct.gov/DRS or requestthe form from your employer. Any nonresident who expects to have noConnecticutincome tax Iiability should choose Withholding Code ?E.?
Form CT-W4 (Rev. 1 2/1 9)
Armed Forces Personnel and Veterans
If you are a Connecticut resident, your armed forces pay is subjectto Connecticut income tax withholding unless you qualify as anonresident for Connecticut income tax purposes. If you qualify asa nonresident, you may request that no Connecticut income tax bewithheld from your armed forces pay by entering Withholding Code ?E?on Line 1.
Military Spouses Residency Relief Act (MSRRA)If you are claiming an exemption from Connecticut income tax underthe MSRRA, you must provide your employer with a copy of yourmilitary spouse's Leave and Earnings Statement (LES) and a copyof your military dependent ID card.
See Informational Publication 2019(5), Connecticut Income TaxInformation for Armed Forces Personnel and Veterans.
Employer InstructionsFor any employee who does not complete Fomi CT-W4, you are requiredto withhold at the highest marginal rate of 6.99% wi(hout allowancefor exemption. You are required to keep Form CT-W4 in your files foreach employee. See Informational Publication 2020(1), ConnecticutEmployer's Tax Guide, Circular CT, for complete instructions.
Report Certain Employees Claiming Exemption From Withholdingto DRS
Employers are required to file copies of Form CT-W4 with DRS forcertain employees claiming ?E" (no withholding is necessary). SeeIP 2020(1 ). Mail copies of Forms CT-W4 meeting the conditions listedin IP 2020(1 ) under Reporting Certain Employees to.'
Department of Revenue ServicesPO Box 2931
Hartford CT 06104-2931
Report New and Rehired Employees to the Department of LaborNew employees are workers not previously employed by yourbusiness, or workers rehired after having been sepatated from yourbusiness for more than sixty consecutive days.
Employers with offices in Connecticut or transacting business inConnecticut are required to report new hires to the Department ofLabor (DOL) within 20 days of the date of hire.
New hires can be reported by:Using the Connecticut New Hire Reporting website atwww.ctnewhires.com:
Faxing copies of completed Forms CT-W4 to 800-816-1108: or
Mailing copies of completed Forms CT-W4 to:
Connecticut Department of LaborOffice of Research, CT-W4200 Folly Brook BlvdWethersfield CT 06109
For more information on DOL requirements or for alternative reportingoptions, visit the DOL website at www.ctdol.state.ct.us or call DOLat 860-263-6310.
For More Information
Call DRS during business hours, Monday through Friday:800-382-9463 (Connecticut calls outside the Greater Hartfordcalling area only); or860-297-5962 (from anywhere).
TTY, TDD, and Text Telephone users only may transmit inquiriesanytime by calling 860-297-4911 . Taxpayers may also call 711 forrelay services. A taxpayer must tell the 71 1 operator the number he orshe wishes to call. The relay operator will dial it and then communicateusing a TTY with the taxpayer.
Forms and Publications
Visit the DRS website at portal.ct.gov/DRS to download and printConnecticut tax forms and publications. Page 2 of 2

*
@I
Employment Eligibility Verification
Department of Homeland SecurityU.S. Citizenship and Immigration Services
USCIS
Form I-9
OMB No. 1615-0047
Expires 08/31/2019
I am aware that federal law provides for imprisonment and/or fines for false statements or use of false documents inconnection with the completion of this form.
l attest, under penalty of perjury, that l am (check one of the following boxes):
r START HERE: Read instructions carefully before completing this form. The instructtons must be available, either in paper or electronically,during completion of this form. Employers are liable for errors in the completion of this form.
ANTI-D?SCRIMINAT?ON NOTICE: It is illegal to discriminate against work-authorized individuals. Employers CANNOT specify whichdocument(s) an employee may present to establish employment authorization and identity. The refusal to hire or continue to employan individual because the documentation presented has a future expiration date may also constitute illegal discrimination.
I attest, under penalty of perjury, that l tiave assisted in the completion of Section 1 of this form and that to the best of myknowledge the information is true and correct.
@ Emplo.s'er ( 'rinrplele.'< .Vv-xI l'uge (!>Form I-9 07/17/17 N Page l of 3
Section 1. Empl0yee lnformation and Atteitation (Employees must cornplete and sign Sgictron 1 of Form /-9 no laterthan the flrst dey of employment. but no{ before acc*pting a y& offer )
Last Name (Famrly Name) First Name (Given Name) Middle Initial
Address (Street Number and Name) Apt. Number City or Town State ZIP Code
Date of Birth (mm/dd/yyyy) u.s. Social Security Number
ffl D []Employee's E-mail Address Employee's Telephone Number
@1 . A citizen of the United States
02. A noncitizen national of the United States (See instructrons)
g3. A lawful permanent resident (Alien Registration Number/USCIS Number):
04. An alien authorized to work until (expiration date,if applicable, mm/dd/yyyy):Some aliens may write N/A in the expiration date field. (See instructions)
Aliens authorized to work must provide only one of the following document numbers to complete Form l-9.'An Alien Registration Number/USCIS Number OR Form l-94 Admrssion Number OR Foreign Passporf Number.
l.Alien Registration Number/USCIS Number:
OR
2. Form l-94 Admission Number:
OR
3. Foreign Passport Number:
Country of Issuance:
QR Code - Section j
Do Not Write ln This Space
Signature of Employee Today's Date (mm/dd/yyyy)
Preparer and/or Trans4ator Certification (check one):01 di4 riot use a preperer or translator. [1 A preparer(s) and/or (ranslator(s) aggis(ed the employee in cornple.ting Section 1 .(Fi*kls b*low must be completed and srjgned when prepamrs and/or translators assist ari employee in completrng Section 1. )
Signature of Preparer or Translator Today's Date (mm/dd/yyyy)
Last Name (Famrly Name) First Name (Given Name)
Address (Street Number and Name) City or Town State ZIP Code

@ Employment Eligibility Verification
Department of Homeland SecurityU.S. Citizenship and Immigration Services
l
lListA OR List B List C
Identity and Employment Authorization Identity Employment Authorization
Certification: l attest, under penalty of perjury, that (1) l have examined the document(s) presented by the above-named employee,(2) the above-listed document(s) appear to be genuine and to relate to the employee named, and (3) to the best of my knowledge theemployee is authorized to work in the United States.
The employee's first day of employment (mm/dd/yyyy): (See instructions for exemptions)
l attest, under penalty of periury, that to the best of my knowledge, this employee is authorized to work in the United States, and ifthe employee presented document(s), the document(s) l have examined appear to be genuine and to relate to the individual.
USCIS
Form I-9
OMB No. 1615-0047
Expires 08/31/2CH9
AND
Forml-9 07/17/17 N Page 2 of 3
Section 2. Employer or Authorized Representative Revmw and Verification(Employers or therr authonzed nbpresb*ntative must compWe and sngn Se.ctron 2 withyn 3 business da ys of the empkoyee's first day of employment. Yournust ph yscally exama'e one docurnent korn Lrs( A OR a combtnahon of one doctrmenl from Lrsl B and one dum*nt fmm List C as lrst*d ori the listsof AcceptabJe Documerits.':)
Employee lnfo from Section 1Last Name (Family Name) First Name (Given Name) M.I. Citizenship/lmmigration Status
Document Title DocumentTitle DocumentTitle
lssuingAuthority IssuingAuthority
Documen(Number DocumentNumber
Expiration Date (if any)(mm/dd/yyyy) Expiration Date (if any)(mm/dd/yyyy)
Issuing Authority
Document Number
Expiration Date (if any)(mm/dd/yyyy)
Document'Title '
Additional Information QR Code - Sec}ions 2 & 3
Do Not Wri}e ln This Spacelssuing Authority
Document Number
Expiration Date (if any)(mm/dd/yyyy)
Document Title
lssuing Authority
Document Number
Expiration Date (if any)(mm/dd/yyyy)
Signature of Employer or Authorized Representative Today's Date (mm/dd/yyyy) Title of Employer or Authorized Representative
Last Name of Employer or Authorized Representa}ive First Name of Employer or Au(horized Representative Employer's Business or Organization Name
City of Milford
Employer's Business or Organization Address (Street Number and Name)Parsons Complex, 70 West River Street
City or Town
Milford
State
CT
ZIP Code
06460-3317
Sectmn 3. Reverification and Rehires ( TO be comphbeo aiio signeri by emphyer or authorizaa representative )A. New Name 0f applicable) B. Da}e of Rehire (if applrcable)
Last Name (Family Name) First Name (Grven Name) Middle lnitial Date (mm/dd/yyyy)
C. lf }he employee's prevrous grant of employmeni authorization has expsred. provide the informaiion for the document or receipl }hat establishescontinuing employmen! authoriza}ion in the space provided below
Document Title Document Number Expiration Date (if any) (mm/dd/yyyy)
Signature of Employer or Authorized Representative Today's Date (mm/dd/yyyy) Name of Employer or Authorized Representative

l
LISTS OF ACCEPTABLE DOCUMENTS
All documents must be UNEXPIRED
Employees may present one selection from List Aor a combination of one selection from List B and one selection from List C.
Examples of many of these documents appear in Part 13 of the Handbook for Employers (M-274).
Refer to the instructions for more information about acceptable receipts.
Fon'nl-9 07/17/17 N Page 3 of 3
LISTA LISTB LISTC
Documents that Establish Documents that Establish Documents that Establish
Bothldentityand Identity EmploymentAuthorizationEmploymentAuthorization OR AND
1. u.s. Passport or u.s. Passport Card 1. Driver's Iicense or ID card issued by aState or outlying possession of theUnited States provided it contains aphotograph or information such asname, date of birth, gender, height, eyecolor, and address
1. ASocialSecurityAccountNumbercard, unless the card includes one of
the following restrictions:
(1) NOTVALID FOR EMPLOYMENT
(2) VALID FOR WORK ONLY WITHINS AUTHORIZATION
(3) VALID FOR WORK ONLY WITHDHS AUTHORIZATION
2. Permanent Resident Card or Alien
Registration Receipt Card (Form I-551 )
3. Foreign passport that contains atemporary I-551 stamp or temporaryI-551 printed notation on a machine-readable immigrant visa
2. ID card issued by federal, state or Iocalgovernment agencies or entities,provided it contains a photograph orinformation such as name, date of birth,gender, height, eye color, and address
4. Employment Authorization Documentthat contains a photograph (FormI-766)
2. Certification of report of birth issuedby the Department of State (FormsDS-1350, FS-545, FS-240)
3. School ID card with a photograph5. For a nonimmigrant alien authorized
to work for a specific employerbecause of his or her status:
a. Foreign passporI and
b. Form I-94 or Form I-94A that has
the following:
(1 ) The same name as the passportand
(2) An endorsement of the alien'snonimmigrant status as long asthat period of endorsement hasnot yet expired and theproposed employment is not inconflict with any restrictions orIimitations identified on the form.
3. Original or certified copy of birthcertificate issued by a State,county, municipal authority, orterritory of the United Statesbearing an official seal
4. Voter's registration card
5. u.s. Military card or draft record
6. Military dependent's ID card
4. Native American tribal document7. u.s. Coast Guard Merchant Mariner
Card5. u.s. Citizen ID Card (Form I-197)
8. Native American tribal document6. ldentification Card for Use of
Resident Citizen in the United
States (Form I-1 79)9. Driver's license issued by a Canadian
government authority
For persons under age 18 who areunable to present a document
Iisted above:
7. Employment authorizationdocument issued by theDepartment of Homeland Security
6. Passpork from the Federated States ofMicronesia (FSM) or the Republic ofthe Marshall Islands (RMI) with Forml-94 or Form I-94A indicatingnonimmigrant admission under theCompact of Free Association Betweenthe United States and the FSM or RMI
10. School record or report card
11. Clinic, doctor, or hospital record
12. Day-care or nursery school record

City of Milford
Direct Deposit Policy
Direct Deposit occurs when The City of Milford electronically transmits yo?ir net pay into abank acco?mt(s) of yo?ir choice each payday. As part of the direct deposit process, an einailnotification will prompt yo?i each pay period to view yo?ir electronic Direct Deposit Advicethro?igh the Employee Self Service ("ESS?) portal. Each employee participating in the directdeposit program will have an acco?int established on the ESS with a secure password to accesshis/her paycheck details. Employees will also have the ability to view accrued vacation, sicktime, and other benefit infori'nation as well as print their paycheck detai)s, if desired. Payrollfunds are transmitted to be available at 9:00 a.m. on each payday. The actual availability oftJiese funds is determined by your bank or credit ?inion.
Employee Eligibility/Requirement: Active, permanent employees are eligible and required toreceive their pay via direct deposit. Seasonal and part-time employees are also eligible andreq?iired to receive their pay via direct deposit. Bxceptions for seasonal and part-time employeesmay be made on a case-by-case basis as determined by the Finance Depaiti'i'ient.
Account Eligibility: With the new MUNIS system, rmiltiple bank acco?ints (checking orsavings) can be set up using direct deposit once a Direct Deposit Enrolli'nent Form is completedfor each bank/credit union account. Initially, when the payroll system is converted, all employeepay will be deposited into the single direct deposit bank acco?mt currently established for eachemployee. Once the system conversion is completed, the Finance Department will anno?incewhen additional bank accounts can be added for direct deposit payments.
Enrollment: New hires rmist sign up for direct deposit by completing the Direct DepositEnrollment Forin (copy attached), which is typically distributed in their orientation packets.Bank acco?int testing will begin when the new hires begin working. All other eligible employeescan sign up for additional direct deposit acco?mts by completing the Direct Deposit EnrollmentForm and submitting it to the Payroll Office. A voided check (for a checking acco?int) or aletter/direct deposit form from yo?ir financial institution (for a savings account) must be attachedto the Direct Deposit Enrollment Form. Please note that the start-up implementation usuallytakes at least two payroll periods to go into effect. The first week a test transmission (no fiindstransferred) is cond?icted with the employee's bank, and the second week (assuming that the testtransmission was successful) yo?ir net pay will be deposited electronically.
Changes/Cancellation: Direct deposit can be changed at any time with written notificationsubmitted to the Payroll Supervisor and/or Payroll Specialist in Finance using the Direct DepositEnrollment Form. Changes regarding your direct deposit (new bank, new acco?int number, etc)take at least two payroll weeks to be processed. Please note: employees are respomible fornotifying the Payroll Supervisor and/ or Payroll Specialist of any bank changes that wouldaffect their direct deposit (i.e.: closed accoxmt, txew account, new barik name, new bankrouting/aba number, etc). Changes should be communicated to the Payroll Office as soon aspossible.
Types of payments: special payments (such as longevity pay, retro pays, advance vacation pay,education bonus etc.) will continue to be separate transactions and are included in the directdeposit. For example, an employee enrolled in direct deposit receiving regular pay and longevitypay in the same pay period, will see two separate deposits into his/her account.

Multiple Direct Deposits: Beginning August s, 2019, ei'nployees will have the ability to deposittheir earnings at m?iltiple banks and/or credit ?inions. Up to four (4) deposits can be set-up as flatamo?ints and one (l) account cast be set-up as a percentage of the gross earnings in that payperiod. The deposits will be made in the following order: First flat amount, then second flatamount arid so on; once the flat amounts have been deducted, any selected percentage will bedeposited into the chosen acco?int; fiiially, any remaining net pay will be deducted into theemployee's primary bank account. If in a given week, there are not sufficient fiinds to cover thepercentage amo?int, the system WILL NOT make that percentage deposit and any balance offunds will be deposited as net pay into the employee's primary bank account
Thanksgiving week: During the week of the Thanksgiving holiday, direct deposited funds maynot be available ?intil the Friday after Thanksgiving, when funds are normally available.

City of MilfordDirect Deposit Enrollment/Authorization Form
To enroll in or change a Direct Deposit, complete this 'form and return to the Payroll Office along with aVOIDED CHECK or BANK LETTER/BANK FORM
NAME: DEPT: "'re"' - 4520 JOB TITLE, Seasonal TemPorarY
NETDirectDeposit DNEW OCHANGEName of Eank or Credit Union:Account #.a
9-Digit Romiiig #:
xmount: OnaianceolpayADDITIONALFLATAMOUNTDirectDeposit DNEWName of Bank or Credit Union:Account #:
9-Digit Routing #;Amount: € $
ADDITIONAL FLA T AMOUNT Direct Deposit [7 NE FName of Bank or Credit Union:Account #.a
9-Digit Routing # a
Amount: [] $
ADDITIONALFLATAMOUNTDirectDeposit DNEWName of Bank or Credit Union:Account #:
9-Digit Routing # 'Amount: € $
ADDITIONALPERCENTAGEDirectDeposit DNEWName ofBank or Credit Union.'Account #:
9-Digit Routing # aAmount: €
TypeofAccoumJJChecking DSaving)OFFfCE USE ONL Y: MUNIS Code !!!!?
DCHANGE DCANCEL
rypeo(iiccount:Dchecicing DsavingsOFFICE USE ONIY: AfUNlS Code
[]CHANGE DCANCEL
rypeo(iiccount:Dcheching DsavingsOFFICE USE ONL Y: MUNIS Code
D c+r,aw:;g D cmcgr,
Type ofAccount: D Checking D SavingsOFFICE USE ONL Y: MUN?S Code
D cnmcp O ciiucpr,
rypeo(,account:DChecking DSavingsOFF]CE USE ONLY: MUNIS Cnde%
The City of Milford is hereby authorized to directly deposit my pay to the account(s) listed above. Thisauthorization will remain in effect until l modify or cancel it in writing. In the event that my employer depositsfunds erroiieo?isly into my account, I autl'iorize my employer to debit my acco?mt for an amo?int not to exceed theoriginal amount of credit. I have read the Direct Deposit Policies and understand the content.
Employee's Signature:
Print Name
Rev. 04/09/20 19
Date :

*
SEASONAL/TEMPORARY EMPLOYEE NEW HIRE/REHIRE
NAME:
DEPARTMENT:
DATE:
Recreation Department
Please initial indicating receipt and/orSubmission of applicable documents
1. Americans with Disabilities Act (ADA)
2. Electronic Monitoring Notice
3. Insurance Marketplace Coverage Options
4. Paid Sick Leave Notice
s. Sexual Harassment Policy
6. Zero Tolerance Workplace Violence Policy
7. Public Records Policy 05: Disposition of Public Records
8. Workers' Compensation Medical Care Plan
9. Drug/Alcohol Abuse Policy
10. Direct deposit form. (Complete if working more than 90 days)
11 . Public Works-if employee hold CDL license please submit a copy to Human Resources.
NA
Human Resources DepartmentJuly 2019

cjTY OF MILFORD - AMERICANS WITH DISABILITIES ACT
POLICY AND GRIEVANCE PROCEDURE
It is the policy of the City of Milford to make the use of all public facilities and services, as well as allemployment opportunities with the City of Milford, fully compliant with the Americans with Disabilities Actof 1 990. To that end, the following grievance procedure shall be implemented effective immediately:
1. Any person may submit either in person or in writing, a complaint regarding inadequate access oralleged discrimination to the Assistant to the Mayor. (ADA designee) A record of the complaint
' - -----'-an-d-actiorr-will-be-maintairie?d.Adn5isi5nbyftie-ADA-dgsigneeshaJl5eTeri-dere'd-wiffiinfifteen(15) working days of receipt of the complaint.
2. If the complaint is not resolved to the satisfaction of the complainant by the ADA designee, thecomplainant may forward the complaint within ten (10) working days of receipt of the ADAdesignee's decision to an ADA compliance committee. The committee shall be composed of tworepresentatives from the Board of Aldermen, two representatives from the disabled community,one representative from the business or non-profit sectors, one representative from educationand one representative from the health/medical profession. The committee will be appointed bythe Chairman of the Board of Aldermen,
3. The committee shall be charged to establish ground rules or procedures for hearing complaints,requests or suggestions from disabled persons regarding access to and participation in publicfacilities, services, activities and functions in the community. Further, the committee shall bedirected to hear such complaints in public, affer adequate public notice is given. If, however, thecomplainant wishes to be heard in closed session, the Committee may honor that request. Thecommittee shall issue a decision within thirty (30) working days of hearing the complaint. Recordsof meetings of the Committee shall be maintained in accordance with State law.
4. If the complaint is not resolved to the complainant's satisfaction by the committee, complainantmay forward it to the Board of Aldermen within ten (10) working days of receipt of the committee'sdecision. An open, public meeting of the Board will precede the vote. A determination must bemade within thirty (30) working days of the hearing. The decision of the Board of Aldermen isfinal.
s. A record of action taken on each request or complaint must be maintained as a part of therecords or minutes at each Ievel of the grievance process.
6. The individual's right to prompt and equitable resolution of the complaint shall not be impaired byhis/her pursuit of other remedies, such as the filing of a complaint with the u.s. Department ofJustice or any other appropriate federal agency. Furthermore, the filing of a lawsuit in state orfederal district court may occur at any time. The use of this grievance procedure is not aprerequisite to the pursuit of other remedies.
re-typed 04-21 -'I 0

CITY OF MILFORD
ELECTRONIC MONITORING NOTICE
Pursuaxit to the requirements of Public Act 98-142, ?An Act Requiring Notice toEmployees of Electronic Monitoring by En'iployers," City employees shouldrecognize that their work activities and communications may be subject toelectronic monitoring.
?Electronic monitoring? is defined by tbe Act as G'the collection of information on anemployer's premises concerning employees' activities or eommunications by anymeans other than direct observation, including the use of a computer, telephone,wire, radio, camera, electromagnetic, photoelectronic or photo-optical systems, butnot including the collection of information for security purposes in common areas ofthe employer's premises which are held out for use by the public, or which isprohibited under state or federal law."
Employees may be subject to electronic monitoring or recording (including sound,voice or video devices) while in City facilities and other locations where Citybusiness is conducted, except that employees will not be subject to any suchmonitoring or recording in areas designed for the health or personal comfort of theemployees or for safeguarding of their possessions, such as rest rooms, Iocker roomsor lounges.
Employees should understand that their activities involving City computerequipment and computer and/or electronie documents, data and communications,including e-mail and internet usage, are subject to being monitored, recorded andreviewed. Employees should be aware that the fact that a document, data orcommunication has been ?deleted? by the employee does not mean that the itemcannot be monitored or retrieved and reviewed.
Employees will not be subject to electronic monitoring or recording of the content oftheir direct telephone conversations, except as may be permitted under state andfederal law.
THIS NOTICE SHALL BE POSTED IN A CONSPICUOUS PLACE WHICH IS
READILY AVAILABLE FOR VIEWING BY EMPLOYEES.

Form
OMB No. 1Approo210-Oa
?ved
149
(expires s-31-2020)
s@PART A: General lnfo Q l?
nrormaxlon
When key parts of the health care Iaw take el1ect in 2014, tl?iere will be a new way to buy health insurance: the Health
Insurance Marketplace. To assist you as you evaluate options for you and your family, this notice provides some basic
information about the new Marketplace and employment-based health coverag)e ollered by your errployer.
What is the Health lnaurance Marketplace?
The Marketplace is designed to help you find health insurance that meets your needs and fits your budget. The
Marketplace offers ?one-stop shopping? to find and corrupare private health insurance options. You may also be eligible
for a new kind of tax credit that Iovvers your monthly premium right away. Open enrollment for health insurance
covera@e through the Marketplace begins in October 2013 for coverage starting as early as January 1 , 2014.
Can l Save Money on my Health Insurance Prem}ums }n the Marketplace?
You may qualify to save money and lovver your monthly premium , but only if your employer does not oTfer coverage, or
ollers coverage that doesn't meet certain standards. The savings on your premium that you're eligible for depends on
your household income.
Does Employer Health Coverage Affect El}g}b}lity for Premium Savings through the Marketplace?Yes. If you have an ofler of health coverage from your employer that meets certain standards, you will not be eligible
for a tax credit through the Marketplace and may wish to enroll in your employer's health plan. t-lowever, you may be
eligible for a tax credit that Iowers your monthly premium , or a reduction in certain cost-sharing if your employer does
not offer coverage to you at all or does not oller coverage that meets certain standards. If the cost of a plan from your
employer that would cover you (and not any other members of your family) is more than 9.5% of your household
income for the year, or if the coverage your employer provides does not meet the ?minimum value? standard set by the
Alfordable Care Act, you may be eligible for a tax credit.'
Note: If you purchase a health plan through the Marketplace instead of accepting health coverage offered by your
employer, then you may lose the employer contribution (if any) to the employer-offered coverage. Also, this employer
contribution -as well as your employee contribution to employer-o11ered coverage - is often excluded from income for
Feaeral and State income tax purposes. Your payments for covera@e through the Marketplace are made on an after -
tax basis.
How Can I Get More Information?
For more information about your coverage offered by your employer, please check your summary plan description or
contact Benefits & Pension Coordinator- 203-783-3224
The Marketplace can help you evaluate your coverage options, including your eligibility for coverage through the
Marketplace and its cost, Please visit HealthCare.gov for more information, including an online application for health
insurance coverage and contact information for a Health Irisurarice Marketplace in your area.
' An em'L:}lo'ler s4onsored heal}h plan meels llje ?m:n:mum value sfandard? il lhe plan's shaTe 01 the folal allowed bene{i{ costs COVeLedby the plan is no less than 60 percent oj such costs.

PART B: Information About Health Coverage Offered by Your EmployerThis section contains information about any health covera@e offerea by your employer. If you decide to complete anapplication for coverage in the Marketplace, you will be asked to provide this information. This information is numberedto conespond to the Marketplace application.
3. Employer name
City of Milfords. Employer address
70 West River St
7. City
Milford
10. Who can we contact about employee health coverage at this job?Benefits & Pension Coordinator
11. Phone number (if different from above) r 12. Email address
i 4. Employer Identification Number (EIN)
I 6. Employer phone number203-783-3224
1 8. State
CT r 9. ZIP code
06460
Here is some basic information about health coverage offered by this employer:*As your employer, we offer a health plan to:
[] All employees. Eligible employees are:
EI Some employees. Eligible employees are:
i+With respect to dependents:
[x We do oNer coveraqe. Eligible dependents are:
€ We do not oNer coVeraQe.
[x If checked, this covera@e meets the minimum value standard, and the cost of this covera@e to you is intendedto be affordable, based on employee wages.
** Even if your employer intends your coverage to be affordable, you may still be eligible for a premiumdiscount through the Marketplace. The Marketplace will use your household income, along with other lactors,to determine wl'ieAher you may be eligible for a premium discount. If, for example, your wages vary fromweek to week (perhaps you are an hourly employee or you work on a commission basis), if you are newlyemployed mid-year, or if you have o{her income losses, you may still qualify for a premium discount.
If you decide to shop for coverage in the Marketplace, HealthCare.gov will guide you through the process. Here's theemployer information you'll enter when you visit HealthCare.gov to find out if you can get a tax credit to lower yourmonthly premiums.

The information below corresponds to the Marketplace Employer Coverage Tool. Completing this section is optional foremployers, but will help ensure employees understand their coverage choices.
13. Is the employee currently eligible for coverage offered by this employer, or will the employee be eligible inthe next 3 months?
[1 Yes (Continue)13a. If the employee is not eligible today, including as a result of a waiting or probationary period, when is the
employee eligible for coverage? (mm/dd/yyyy) (Continue)No (STOP and return this form to employee)(Ul
14. Does the employer offer a health plan that meets the minimum value standard?"?0yes (GO to'question 15) g 'No (STOP and return rorm to employee)
15. For the lowest-cost plan that meets the minimum value standard" offered only to the employee (don't includefamily plans): If the employer has wellness programs, provide the premium that the employee would pay if he/ shereceived the maximum discount for any tobacco cessation programs, and didn't receive any other discounts based onwellness programs.a. How much would the employee have to pay in premiums for this plan? $iloyee
[lEvib.Howoften?[]Weekly [lEvery2weeks ' 0Twiceamonth 0Monthly []Quarterly @Yearly
If the plan year will end soon and you know that the health plans olfered will change, go to question 16. If you don'tknow, STOP and return form to employee.
16. What change will the employer make for the new plan year?€ Employer won't offer health coveraqe€ Employer will start offering health coverage to employees or change the premium for the Iowest-cost plan
available only to the employee that meets the minimum value standard." (Premium should reflect thediscount for wellness programs. See question 15.)
a. How much would the employee have to pay in premiums for this plan? $b.Howoften??Weekly ?Every2weeks ' ?Twiceamonth '0Monthly []Quarterly ?Yearly
a An employer-sponsored health plan meets the ?minimum value siandard? if the plan's share ol the total allowed benefit cos}s coveted bythe plan is no less than 60 petcerit of such costs (Section 36B(cX2)(CXii) of the Internal F3evenue Code ol 1986)

I
NOTICE
l
PUBLIC ACT 11-52-AN ACT MANDATING EMPLOYERS PROVIDE
PAID SICK LEAVE TO EMPLOYEES.
Each employer with 50 or more employees shall provide paid sick leave annually to each of its service workers in the state.The paid sick leave shall accrue beginning January 1, 2012 for current employees, or for a service viorker hired after January 1,2012, beginning on the service worker's date of employment.
Accrual
The accrual is at a rate of one hour of paid sick Ieave for each 40hours vvorked by a service vvorker up to a maximum of 40 hours percalendar year.
* No service worker shall be entitled to use more than the
maximum number of accrued hours.
Carry OverEach service worker shall be entitled to carry over up to 40 unusedaccrued hours of paid sick Ieave from the current calendar year tothefollowingcalendaryear.
Use of Paid Sick Leave
A service vvorker shall be entitled to the use of accrued paid sickIeave upon the completion of the service worker's 680'h hour ofemployment
* from January 1, 2012, for current service workers, orh if hired after January 1, 2012, upon the completion of the
service worker's 680'h hour of employment from the dateof hre, unless the employer agrees to an earlier date.
A service vvorker shall not be entitled to the use of accrued paid sickleave if such service worker did not work ari average of 10 or morehours a week for the employer in the most recent complete calendarquarter.
PayEach employer shall pay each service worker for paid sick leave at apay rate equal to the greater of either
* thenormalhourlywageforthatserviceworker,or* the minimum fair wage rate under secuon 31-58 of the
general statutes in effect for the pay period during whichthe employee used paid sick Ieave.
Reasons for Use of Leave
A service worker may use paid sick leave for his or her own:* illness, injury or health condition;* the medical diagnosis, care or treatment of ms or her
mental illness or physical illness, injury or health condiUon;or
* preventative medical care.
A service vvorker may use patd sick leave for a child's or spouse's:* illness, iniury or health condition; the medical diagnosis,* care or treatment of a mental or physical illness, injury or
health condition; or
ii preventative medical care
A service viorker may use paid sick Ieave if the service worker is avictim of family violence or sexual assault:
* for medical care or psychological or other counseling forphysical or psychological injury or disability;
i+ to obtain services from a victim services organization;* torelocateduetosuchfamilyviolenceorsexualassault;
* to par)icipate in any civil or criminal proceedings related to orresulting from such family violence or sexual assault.
Notice
If Ieave is foreseeable, the employer may require advance notice.If leave is unforeseeable, the employer may require notice as soon aspracticable.
Reasonable Documentation
Documentation for paid sick Ieave of 3 or more consecutive work daysmay be required
ii documentation signed by a health care provider who istreating the servtce viorker or the senAce worker's child orspouse indicating the need for the number of days of suchIeave shall be considered reasonable documentation.
* a court record or documentation signed by a service workeror volunteer working for a victim services organization, anattorney, a police ofFicer or other counselor involved with theservice vvorker shall be considered reasonable documentation
for a victim of family violence or sexual assault.
Prohibition of Retaliation or Discriminatfon
No employer shall take retaliatory personnel action or discriminateagainst an employee because the employee:
* requests or uses paid sick leave either in accordance with theact; or
* in accordance with the employer's own paid sick leave policy,as the case may be; or
* files a complaint with the Labor Commissioner alleging theemployer's violation of the act
Collective BargaintngNothing in the act shall diminish any rights provided to any employee orsersAce worker under a collective bargaining agreement, or preempt oroverride the terms of any collective bargaining agreement effectivepriortoJanuaryl,2012.
Complaint ProcessAny employee aggrieved by a violation of the provisions of the act mayfile a complaint with the Labor Commissioner. Upon receipt of any suchcomplaint, said Commissioner may hold a hearing. After a hearing, theCommissioner may assess a civil penalty or award other relief.
This is not the complete Paid Sick Leave law. Please contactyour Human Resources offlce for additional information.
Effective 1/1/12

CITY OF MILFORDSEXUAL HARASSMENT POLICY
Pursuant to Section 46a-60 et seq. of the Connecticut General Statutes, it is the policy of the City of Milfordthat sexuaf harassment in the workplace is unacceptable and will not be tolerated. All employees of theCity of Milford, whether management personnel or non-management personnel, are expected to avoid anybehavior or conduct toward any other employee that could be interpreted as sexual harassment.
Sexual tiarassment is defined generally as "unwelcome sexual advances, requests for sexual f:avors andother verbal or physical conduct of a sexual nature." Thus, no employee should be subjected to unsolicitedand-unwelcome-sexual-overtures-or-conduct, either-verbal-or-physical,-or be-jed-to -believe .that-an.- .- -- ???emptoyment opportunity or benefit will in any way depend upon "cooperation" of a sexual nature- Further,no employee should be subjected to unwanted exposure to sexually explicit materials of any type in theworkplace.
Conduct is improper if.
. (a) submission to the conduct is either art explicit or implicit term or condition ofempJoyment;
(b) submission to or rejecUon of the conduct is used as a basis for employmentdecisions affecUng the person involved; or
(c) the conduct has the purpose or effect of interfering with an individual's workpeformance or environment.
Sexual harassment does not refer to occasional compliments of a socially acceptable nature. It refers tobehavior which is not welcome, which is personally intimidating, hostiie, or offensive which debilitatesmorale, and therefore interferes with work effecUveness.
Appropriate management and/or supervisory personnel shall promptly investigate all complaints of sexualharassment, including interviewing the complainant and the person(s) alleged to have engaged in sexualharassment. If, as a result of the investigation, it is found that the complaint has merit, the appropriatemanagement and supervisory personnel shall take prompt corrective acUon. Such action may includediscipline up to aand including termination of the offending employee or employees.
Any employee of the City of Milford who feels that he or she has been the victim of sexual harassmentshould nofify his or her supervisor, department head, and/or the Personnel Director at the very earliestopportunity. If the complaint is found to have merk, corred3ve action will be implemented. If the comp)aintis found to be of insufficient merit, all involved parties will be so notified.
Reporting Procedure
Within ten (10) workir'ig days of any incident which an employee believes constitutes unwelcome conductof a sexually harassing nature, the employee shall:
1. Reducetheallegationtowriting,ifpossible.
2. Notifythedepartmenthead,orifthedepartmentheadisthepersonwhoseconductis the subject of the complaint, notify the Personnel Director.
3. Cooperate in the investigation of the charge.

CITY OF MILFORDZERO TOLERANCE WORKPLACE VIOLENCE POLICY*
!NTRODUCTION
The City of Milford is committed to preventing workplace violence and to providing a safe, healthyworkplace, free from violent, threatening or harassing behavior that affects its employees, officialsand members of the public. The City does not and will not tolerate threats, threatening behavior,acts of violence, or any related conduct that disrupts another's work performance or the City'sability to conduct business. Furthermore, the City will not tolerate any acts of violence committedby or against its employees, officials or members of the pub?ic, whi?e on or off City property,performing City of Milford business or at any City-sponsored event.
This Policy shall apply to all City buildings, facilities and workplaces including, but not limited to,offices, vehicles, work sites and any other location where City business and /or City-sponsoredevents are conducted.
In furtherance of this commitment, the City of Milford adopts this "ZERO TOLERANCEWORKPLACE VIOLENCE POLICY" for its employees and officials to address intimidation,harassment, coercion, violence or threats of violence that may occur while on or off City property,performing City of Milford business or at any City-sponsored event.
OBTECTIiVE
The objectives of this policy are to achieve the following:
1. Reduce the potential for violence in and around the workplace;
2. Encourage and foster a work environment characterized by respect and healthy conflictresolution;
3. Promote the safety and well-being of all people in our workplace; and
4. Mitigate the negative consequences for employees who experience or encounter violence intheir work lives.
DEFiN{TiON OF WORKPLACE VIOLENCE
For purposes of this policy, "Workplace Violence" means an act or behavior, verba} or nonverbalcommunication, or expression, whether direct or through the use of City of Milford's property,facilities or resources, which:
cityofMilford 1
Zero Tolerance Workplace Violence PolicyAdopted December 2016* Thfs policy excluded City of Milford Police Officers, they are covered by the established departmental policy.

')> Is violent;
> Threatens, harasses, intimidates or coerces another employee, officials, vendors, membersof the public;
> Can reasonably be interpreted as an intent to cause harm;
)- Is physically assaultive;> Utilizes City resources to threaten, stalk or harass anyone at the workplace or outside of
the workplace;> A reasonable person would perceive as menacing;)> Involves carrying or displaying weapons or other dangerous instrument, except as
otherwise required in the course of their employment with the City;> Involves the destruction of property or throwing objects in a manner reasonably perceived
to be threatening; or> Consists of a communicated or reasonably perceived threat to harm another individual(s)
or in any way endanger the safety of an individual(s).
The following list of behaviors, while not inclusive, provides examples of conduct prohibited bythis Policy.
> Causing physical injury or trauma to another person, including but not limited to beating,stabbing, shooting and sexual assault;
> Making harassing threatening remarks, telephone calls, letters, or other forms of written orelectronic communication;
> Aggressive or hostile behavior that creates a reasonable fear of injury to another person(s)or subjects another individual(s) to emotional distress;
> Intentionally damaging Ctty of Milford property or property of another employee(s);> Possession of a weapon while on City property or while on City business, except as
otherwise required in the course of their employment with the City;> Committing acts motivated by, or related to, sexual harassment or domestic violence;> Hitting or shoving an individual(s);> Harassing surveillance, also known as "stalking," the willful, malicious and repeated
following of another person(s);> Psychological traumas such as threats, obscene phone calls, e-mails, texts or posts on social
media;> Intimidating or attempting to coerce an employee to do wrongful acts that would adversely
affect the interests of the City of Milford or cause harm to other individual(s); or> Any other behavior that causes others to feel unsafe (i.e. bullying)
REPORTING PROCEDURES
In a true emergency, employees should not hesitate to call 9-1-1. Any dangerous or potentiallydangerous situations shall be reported immediately to a supervisor and/or the Human ResourcesDepartment. Reports may be made anonymously. All reported incidents will be promptly
CityofMilford 2Zero Tolerance Workplace Violence PolicyAdopted December 2016* This policy excluded City of Milford Police Officers, they are covered by the established departmental policy.

dinvestigated. Reports or incidents warranting confidentia)ity will be handled appropriately aninformation will be disclosed to others only on a need-to-know basis. All parties involved in asituation will be counseled and the results of investigations will be discussed with them. The Citywill actively intervene at any indication of a possibly hostile or violent situation.
The City will not retaliate against employees making good-faith reports of violence, threats orsuspicious individuals or activities. Any weapon or dangerous instrument in the possession of anemployee who is not otherwise authorized to carry same in the course of or as a condition of theiremployment with the City will be confiscated. There is no expectation of privacy with respect tosuch items in the workplace. In order to maintain workplace safety and the integrity of itsinvestigation, the City of Milford may suspend employees suspected of workplace violence orthreats of violence, either with or without pay, pending investigation.
Any employee who has obtained a protective or restraining order against another individual,which restricts the behavior of the individual such that the he/she would be in violation of saidorder by coming near the employee, must provide a copy of said order to their supervisor and/orthe department head. The City of Milford is committed to supporting victims of domestic violenceby providing referrals to EAP and community resources and providing time off for reasons relatedto domestic violence.
RISK REDUCTION MEASURES
? The Human Resources Department takes reasonable measures to conduct backgroundinvestigations to review candidates' backgrounds and reduce the risk of hiring individuals with ahistory of violent behavior and/or past convictions for violent crimes.
Individual Situations: While we do not expect employees to be skilled at identifying potentiallydangerous pe'i-sons, employees are expected to exercise good judgment and to inform the HumanResources Department and his/her immediate supervisor if any employee exhibits behaviorwhich could be a sign of a potentially dangerous situation. Such behavior includes, but is notlimited to:
> Bringing or discussing bringing weapons or other dangerous instruments to theworkplace;
> Displaying overt signs of extreme stress, resentment, hostility, or anger;> Makingthreateningremarksorhomicidal/suicidalcomments;> Sudden or signtficant deterioration of performance;> Increased belligerence;> Hypersensitivit37 to criticism;> Apparent obsession with a supervisor or coworker or employee grievance;> Preoccupation with violent themes;> Obsessive interest in recently publicized violent events;
3city of MilfordZero Tolerance Workplace Violence PolicyAdopted December 2016* This policy excluded City of Mflford Poljce Officers, they are covered by the established departmental policy.

>
>
>
Outbursts of anger;Extreme disorganization; orDisplaying irrational or inappropriate behavior.
Employee Assistance Program (EAP): Employees are encouraged to utilize the EmployeeAssistance Program to address any concerns or issues the employee may have in an effort to
prevent any potential acts of violence.
DANGEROUS/EMERGENCY SITUATIONS
In the event of an emergency where the situation involves imminent danger, the employee shouldimmediately call 9-1-1 and take the appropriate steps as directed by law enforcement officials.Employees who confront or encounter an armed or dangerous person should not attempt tochallenge or disarm the individual. Employees should remain calm, make constant eye contact andtalk to the individual. If a supervisor can be safely notified of the need for assistance withoutendangering the safety of the employee or others, such notice should be given. Otherwise,cooperate and follow the instructions given.
ENFORCEMENT
Threats, threatening conduct, or any other acts of aggression or violence in the workplace will notbe tolerated. Any employee determined to have committed such acts will be subject to disciplinaryaction, up to and including termination of employment. Any individual(s) engaged in a violent actwill be reported to the proper authorities. The City will work together with law enforcementofficials to aid in the investigation and prosecution of anyone who commits violent acts inviolation of this Policy.
g,?.,, (1/ - ?;bK - ZDl&
Mayor Benjamin G. Blake Date
cityofMilford 4Zero Tolerance Workplace Violence PolicyAdopted December 2016* This policy excluded City of Milford Police Officers, they are covered by the established departmental poficy.
CITY OF MILFORDZERO TOLERANCE WORKPLACE VIOLENCE POLICY*
Employee Acknowledgement Form
} acknowledge that l have received and read a copy of: "The City of Milford Zero ToleranceWorkplace Violence Polig". l understand it is my responstbility to read, understand, andcomp}y with this policy. By my signature below, } agree to comply with said policy andunderstan.d that violation(s) of the policy may result in discipltnary action, up to andincluding termination of employment, in accordance with the terms set forth in a collectivebargaini'ng agreement and/or the Municipal Employee Relations Act (MERA), whereapplicable.
Employee Name (print):
Employee Signature:
Date:
Acknowledgement Form revised: 02/15/17

!!,Office of the Public Records Administrator
Connecticut State LibraryState of Connecticut
Public Records Policy 05: Disposition of Public Records
Date Issued: November 28, 2011
Supersedes: General Letter #5: Destruction of Public Records (revised 07/25/1995), Disposition of LocalGovernment Records (1999), and Disposition of Education Records (1999).
1. Scope and Authority
Scope
This policy provides guidance for the disposition of public records, including destruction or transfer. Itapplies to all employees of state agencies within the executive department, towns, cities, boroughs,districts, and other political subdivisions of the state.
AuthorityThe Office of the Public Records Administrator is authorized to approve disposition of public records, underthe authority granted by §11-8, §11-8a, §11-8b, and §7-109 of the General Statutes of Connecticut (CGS).
Definitions
"Agency" means a state agency, municipality, or political subdivision falling under the authority of therecords management program administered by the Connecticut State Library as referred to in CGS §11-8.
"Public record" means any recorded data or information relating to the conduct of the public's businessprepared, owned, used, received or retained by a public agency, or to which a public agency is entitled toreceive a copy by law or contract under section 1-218, whether such data or information be handwritten,typed, tape-recorded, printed, photostated, photographed or recorded by any other method. [Source: CGS§1-200(5).?
"Official record copy" means the original or official copy of a record that is retained for legal, operational, orhistorical purposes. For example, if records are kept in both electronic and hard copy format, the agencymust identify the official record copy. [Source: ARMA International. Glossary of Records and InformationManagement Terms, 3'd ed. Lenexa, KS: ARMA International, 2007.]
"Non-record" means any item that is not usually included within the scope of official records. Examples ofnon-records are extra (duplicate) copies kept only for convenience, reference materials, and blank forms.[Source: ARMA, Glossary.]
11. Policies
Agency ResponsibilityAgencies are responsible for providing all employees with a copy of this policy, obtaining a signedacknowledgment of receipt from each employee, and keeping the signed acknowledgment on file.

Public Records Policy 05: Disposition of Public RecordsPage 2 of s
Retention of Records
Records must be retained for the established retention periods as listed on published records retentionschedules, available at http://ctstatelibrary.org/publicrecords/. Retention requirements apply only to theofficial record copy.
Disposition of RecordsDisposition of records refers to either destruction of records or transfer of records to the custody of anotherentity. Records may not be destroyed or transferred until the Office of the Public Records Administrator hasreturned a signed Records Disposition Authorization form to the requester. If a record does not appear on arecords retention schedule, it does not mean that an agency may dispose of the record without permissionfrom this office. Please contact this office for guidance.
Legal FrameworkPursuant to CGS §11-8b and §7-109, records shall not be removed, destroyed, mutilated, transferred orotherwise damaged or disposed of, in whole or in part, except as provided by law or under the rulesestablished by the Office of the Public Records Administrator. F'ursuant to CGS §1-240 and §53-153,unauthorized removal or destruction of records is a misdemeanor or felony offense and is punishable by fineor imprisonment. In addition, the destruction of records is an illegal subject of collective bargaining pursuantto Lieberman v. Board of Labor Relations [216 Conn. 25 (1990)]. Therefore, a union agreement that involvesthe destruction of public records prior to the retention period established by this office would conflict withthe relevant provisions of the General Statutes of Connecticut.
Destruction Holds
No record may be destroyed if there are pending or active litigation; investigations; audits; Freedom ofInformation Act (FOIA) requests; or other cases, claims, or actions. If there is a destruction hold placed on arecord, the retention period does not change, but is suspended until the action is resolved and the hold isIifted. Once the hold is lifted, the record may be destroyed after the Office of the Public RecordsAdministrator has returned a signed Records Disposition Authorization form to the requester.
Removal of Personal Data
Pursuant to CGS §4-193(e), an agency shall maintain information about a person which is relevant andnecessary to accomplish the lawful purposes of the agency. To obtain permission to destroy or removerecords classified as "irrelevant" and "unnecessary" under these provisions, agencies may submit a Requestfor Removal of Public Records Personal Data Files (Form RC-076 or Form RC-077).
111. Procedures
A. Destruction of Records
Approval ProcessOnce records have met the retention period, agencies should submit the appropriate Records DispositionAuthorization form to this office at least thirty days prior to the proposed date of destruction. The PublicRecords Administrator and the State Archivist will review the form to ensure the records have fulfilled the
retention requirements and that no record of enduring historical value will be destroyed. This office willreturn the form to the agency indicating approval or denial. This form serves as evidence of authorized legaldestruction if the records are audited, investigated, or subpoenaed as evidence.
Method of Destruction

Public Records Policy 05: Disposition of Public RecordsPage 3 of s
The records may be destroyed after receipt of the signed disposition form. This office recommends amethod that ensures the total destruction of the record. The format of the record dictates the method bywhich it should be destroyed:
wi Hard copy formats, such as paper, microfilm, microfiche, and x-rays, should be shredded with across cut shredder and recycled.Electronic media, such as floppy disks, Compact Disks, VHS tapes, audiocassettes, hard drives, andrewritable disks, should be degaussed, overwritten, or erased. Agencies should be aware of specialconditions associated with confidential or sensitive electronic records as erasure does not alwaysensure data destruction. Physical destruction of the media may be the only secure way to destroydata permanently.
s
At the time of disposal, the agency should record the actual date of destruction on the Records DispositionAuthorization form and attach any supporting documentation, such as a Certificate of Destruction. Pleasenote that if the organization contracts with a commercial vendor, the vendor should provide a Certificate ofDestruction attesting to the actual destruction of the records. Retain these records for the retention periodfor Records Disposition Authorization records.
B. Transfer of Records
Approval Process
Agencies should submit the appropriate Records Disposition Authorization form to this office at least thirtydays prior to the proposed date of transfer. The Public Records Administrator and the State Archivist willreview the form to ensure the records are eligible for transfer and that the new custodian is approved fortransfer. This office will return the form to the agency indicating approval or denial. This form serves asevidence of authorized transfer of Iegal custody of records if the records are audited, investigated, orsubpoenaed as evidence.
Transfer to Archival Repository
For records that have a retention period of "permanent/archival," the agency should transfer the records tothe Connecticut State Archives or another approved archival repository. All agencies should use the
appropriate Records Disposition Authorization form, as well as the State Archives' Memorandum of Transferor an equivalent form from an archival repository. For transfer to the State Archives, refer to Transfer ofRecords to the State Archives and Collection Policy for the State Archives, available athttp:7ctstatelibrary.org/state-archives/.
Transfer to Another EntityMany agencies have faced or will face consolidation, relocation, or reorganization. Agencies must considerhow records will be handled and plan accordingly. Pursuant to CGS §11-8b, "Public records shall bedelivered by outgoing officials and employees to their successors and shall not be otherwise removed,transferred, or destroyed unlawfully.?
State agencies should reTer to Public Records Policy 06: Retention of Records for Agency Closures, Mergers,and Consolidations. Pursuant to CGS §4-38d(f), "Unless otherwise expressly provided by law, the head of adepartment, institution or agency, the functions, powers or duties of which are so assigned or transferred,shall deliver to the department, institution, agency or authority to which such assignment or transfer ismade all contracts, books, maps, plans, papers, records and property pertaining to or used in connectionwith the functions, powers or duties so assigned or transferred."

Public Records Policy 05: Disposition of Public RecordsPage 4 of s
Records should be organized for transfer to the successor agency or program. Agencies should utilize theRecords Disposition Authorization form to request transfer of records to another entity (e.g., from oneagency to another). Agencies may choose to establish a written agreement, such as a Memorandum ofU nderstanding, and should include a copy of any agreement when submitting the Records DispositionAuthorization form.
C. Disposition of Education Records
Educational institutions must comply with additional records maintenance requirements of applicableFederal laws, such as the Family Educational Rights and Privacy Act (FERPA) and the Individuals withDisabilities Education Act (IDEA). Educational institutions are defined as "federally funded educationalagencies or institutions.? Education records are defined as "records that are (1) directly related to a studentand (2) maintained by an educational agency or institution or by a party acting for the agency or institution"[20 USC §1232(g) and 34 CFR §99].
Retention requirements for education records are listed on the Municipal Records Retention Schedule Ma:
Education Records a nd the State of Connecticut Records Retention Schedule ss: Higher Education Records.The State of Connecticut considers records to be no longer needed to provide educational services to a childwhen the retention requirement is fulfilled. If a student moves from one educational institution toanother, the agency should maintain a copy of the student's education record and send the original to thereceiving school district (the record follows the student). Both educational institutions should retain theircopy of the student's education record for the retention period.
Special Education RecordsPursuant to 34 CFR §300.573(al "The public agency shall inform parents when personally identifiableinformation collected, maintained, or used under this part is no longer needed to provide educationalservices to the child" and (b) "The information must be destroyed at the request of the parents. Howeve5 apermanent record of a student's name, address, and phone number, his or her grades, attendance record,classes attended, grade level completed, and year completed may be maintained without time limitation."The agency shall only destroy these records after they have met the retention period. Before executing adirective to destroy records, the agency should inform parents / adult students, in record destructionnotices, that the parent or student may need these records in the future for Social Security benefits or otherpurposes.
APSEP and RESC Education Records
Records of students placed by local or regional boards of education or other state agencies in regionaleducation service centers (RESCs) or approved private special education programs (APSEPs) are educationrecords (including, but not limited to, medical records). In accordance with Section E of the Principles,Procedures and Standards for the Approval of Private Special Education Program (06/1998),"when a copy ofa student"s education record is maintained by the facility, the facility must inform the parents/guardiansthat a copy of their student's records is maintained within the agency and must provide theparents/guardians access to the copy. The private facility must also inform the local education agency thatthey are maintaining a copy of the student's record." In addition, "when children placed by a local schooldistrict or other public agency are discharged from a private facility, that facility shall ensure that all recordsare Torwarded to that public agency.?
Please note that RESC-operated magnet schools, unlike APSEPs, maintain the responsibility to collect andretain student records as any other local education agency. The magnet school is responsible for maintaining

Public Records Policy 05: Disposition of Public RecordsPage s of s
the records, destroying such records with approval of the Office of the Public Records Administrator, and fortransferring records to another school in which the child enrolls.
If you have any questions regarding this policy, please contact this office at (860) 757-6540.
Approved by
z*t4w:tS 'ss.oLeAnn R. Power, CRM
Public Records Administrator
November 28, 2011
Date

*
',...?>';?
STATE OF CONNECTICUT
Records Retention and DQsposition Policy
Acknowledgment of Receipt
Pursuant to §1-240 and §53-153 of the General Statutes of Connecticut, unauthorized removalor destruction of public records, as defined in §1-200(5), is a misdemeanor or a felony offenseand is punishable by fine or imprisonment.
1,lType or print full name)
, have received a copy of the State of Connecticut Public
Records Policy os: Disposition of Public Records.
Signature Date
Records Retention and Disposith>n Policy Acknowledgement of Receipt (Form RC-001) issued by the Connecticut State Library, Office of the Public RecordsAdministrator (revised 12/2013)

The MCMC CareSysWorkers' Compensation Medical Care Pian
City of Milford
Eppncriw: DATE OF PLAN 'xs :
OCTOBER 8, 2013
REVISED DATE:
OCTOBER 1, 2016JANUARY 1, 2017
'l'i 'l'l lt'l ill} }
Prepnrea for:
PMA Management Corp. of New England101 Barnes Road
Suite 300
' Wautngford,CTO6492l
City of lVJilfordMedical Care Plan
To All Bmployees:
City of Milford has elected to become a participating employer in an F,mployers Medical Care Plan filedwith the Connecticut Workers' Compensation Commission- The Employer Medical Care Plan allowsCity of Milford to direct employees to a list of medical providers for treatment of work-related injuriesand illnesses. Employees are obliged to obtain treatment from providers in the approved plan;failure to do so may suspend an employees= right to receive workers' compensation benefits, subjectto the order of a Worker's Compensation Commiss;ioner. The City of Milford Employer Medical CarePlan is part of The MCMC CareSys Medical Care Plan, of P?MA Management Corp. of New England,the employer's risk management firm. The effective date of the Employers Medical Care Plan isOctober 8, 2013- The revised date is effective January 1, 2017.
As an employee of City of Milford, you must report a work-related injury or illness to your supervisor,who will complete a First Report of ?njury Form before the end of the shift. If you require medicalintervention or evaluation for your injury, you will be directed to your choice from an occupational healthcenter to receive treatment. :[f you require further medical treattnent, contact your program coordinator. Ifyou have a medical emergency, go to the nearest emergency department.
You may obtain follow-up medical care from providers listed on The MCMC CareSys Medical Caxe Plandirectory, which is available through your progrmn coordinator. Should your injury require specialtytreatment not available in The MCMC CaxeSys Medical Care Plan, a consultant from an approved listestablished by the Workers' Compensation Cornrnission may be chosen for your treatment.
Please review the medical care plan guide, and sign the Employee Acknowledgment, recognizing yourunderstanding and that 'you have read and understand the process for treatment of work-related injuries orilloesses.
'1 %1 11 }}
If you are out of work as a result of your work-related injury, you win be contacted regularly by yourprogram coordinator and/or the ?PMA Management Corp. of New England Claims Coordinator todetermine. that your medical needs are met. Each of you is an important member of the City of Milfordand the purpose of this program is to ensure you receive appropriate medical treatment in a timely mannerto facilitate recovery.
The City of Milford Medical Care Plan includes a utilization review company which is available to youshould there be any questions or disputes about the level and/or quality of care.
The Management staffs at City of Milford, PMA Mana7ement Corp- of New England, and MCMCCareSys Ilc are available to assist you frorri the time of your injury tbrough recovery and return to work.
1%

TWBLVE QUESTIONS
You Ask About Workers' Compensation Protection.
1. WhatisWorkers'Compensation?
The purpose of Workers' Compensation is to provide injured workers and those who dependupon them with a means of support when they are unabie to work because of a work-relatedd sability. Its purpose also is Fo bring about a prompt recovery. Workers' compensation isbasically a no-fault system with benefits paid, no rriatter who is responsible.
2. What is a "Work-Related ][n3ury or Illness?"
The term "Work-Related ][njury or mness" is used to describe any injury or disease whichresults from work or working conditions and which occurs during the employee's service tothe employer.
3. WhohandlesaWorkers'Compensationclaim?PMA Management Corp. cf :Thle.vt Briglarid is the claims administrator for City of Milford.They administer all compensation benefits an injured worker is entitled to receive. If youhave any questions about workers' compensation, contact your program coordinator or PA/!AManagement Corp. of New Bngland.
4. How do you get benefits?
Report the injury to your supervisor irnmediately! Just specify what, where, when and how itour supi'onJlati0happened, enough information so that he/she can complete the First Report of Jnjury form.
Prompt reporting is the key. Benefits are automatic for work-related injuries or illnesses-But, notMng can happen until your employer knows about the injury, no matter how slight.tll 70ur employer k
.abling if an infectiiEven a cut finger cm'i be disabung if an in'fection develops.
s. 'What if you need prescription dmgs?li I}? 11 11 11 'l 11 li
All prescriptions needed because of a workers' compensation illness or injury are reimbursed.criptii:ers' c*by vvorkers' compensation insurance.
6. What is the compensation for total disability?Compensation for Total Disability is money that you receive if the Medical Provider certifiesthat your illness or injury causes you to lose more than three (3) days of work. You canexpect that tHe amount wiu be 75% <yf your net earnings, subject to a minimum andmaximum determined by law-
City of Milford and PMA Management Corp.Provider. When the Medical Provider releast
. of New England work closely with the MedicalProvider. When the 'Qedical Provider releases you to return to full duty, 1!6e. temporarydisability wage support stops.
7. What if the doctor releases you to modified work?Bring your physician's written instructions to your program coordinator immediately. City of
duty port( positio
Milford wilt try to provide you with a temporary modified duty position to meet your doctor'sspecified resttictions. Tf the pay rate for your modified duty posrtion is less than tbe pay ratespeciiied resttictions. li' the pay rate for your modi'ixed duty position is less than ffie pay rafor your regular position, your weekly compensation will be 75%, of the difference in theafter tax earning's between the two positions.

?l
I
tiJ.
8. What is permanent disability?1.
1.I
1.
Permanentldisability is a term, whi{;h describes the lastinj'effect of an on-the-job injury orillness. Tf you have s permanent physical limitation from 'your injuty or illness, PMAManagement Corp. of"New Englana provid;s yoY ;ith -a:dditron'ar payment.- As you would
:nt depiensatio
expect, the mnount of payment depends upon the effect of the injury. The State ofConnecticut Workers' Compensation law -establishes a schedulefor payment of permanentxle for pi
ability, :disability injuries or illnesses based on your percentage of disability-, as detemnined by yourphysician and your salary at the time or the injury.
9- Where do you obtain medical treatment?
Prompt medical care is a key element to a fast recovery from an injury or illness. Emergencymedical care and medical follow-up treatment can often mean the difrerence betweencomplete recovery from an jnjury or lasting physical disability. H you become injured attg physical disability.
CARE nVIMED?A'lwork:, GET EMER GENCY ?DICAL CAm nVIMEDNATErY FROM THE'HBA.REST EMERG.ENCY DEPARTMENT OR MEDICAL CARE PLAN MEDICALCENTER.
If you are injured during regular working hours, you should report your injury to yomsupervisor and proceed to a plan primmy care center. ff you b'icome injtired when the centersare closed, you should go to-the nearest emergency department.
10- What if you need continuing medical treatment?
In the event an employee's injury requires additional medical care beyond the initial visit tothe emergency deparhnent, a-choice-of a p'x'mary care physician will -continue to providenecessmy treatment and referrals to specralists when neeaed.
Should your injury require specialty treatment not available in The MCMC CareSys MedicalCare Plan, a consultant from an approved Iist established by the Workers' CompensationCommission may be chosen for your treatment
Employees. ,are required to obtaiq. .,treatment from provjders in the approved ,plan.nmptoyees.pre required to obtai?Failure to do 80 may suspend an Wmployee's right to re€eive workersf-compefsationbenefits, subject to the order of a WorMers' Compensation Commissioner.-
11. What if you have further questions?
If you have further question.s regarding your workers' compensation benefits, contact youru you nave mrtner questions regaraing your worKers' compensiprogram coordinator or PMA Management Corp. of New Bnglitgland Claims Manager art 203-
- 679H3900 or 1-800-379-0276.
12. What if you question your medical treatment?
MCMC CareSys can review the medical care and services being provided to you. They canbe contacted at 1-800-992-5531 ext 7257.
l
?ll
1,11
City of Milrord4
EffectiveDate: 10/8/2013
Rev2sed Date: 10/1/2016RevisedDate: 1/l/2017

, Modified Duty Procedure ,
PoJicyCity of Milford will provide modified duty whenever possible to all employees who have. areduced work capacity as a result of an occupational injury/inness.
PurposeTo permit the injured employee to remain in the work environment and to affect an expedientreturn to hislher regular job.
The designated Workers' Compensation Coordinator for City of Milford win initiate andmaintain contact with both the employee and his/her supervisor following a work relatedm.iury-
1.
11 l*
t!J 11
s.
The physician will be asked to assess the employee's ability to return to duty in either afull or modified capacity, based on a description of the employee's regular work. Thephysicimi must specify in writing the type and duration of any restriction.
3. The designated Workers' Compensation Coordinator will inform the departmentsupervisor of the employee's readiness to return to work, identifying full or limited workcapacity.
4. Based on the physician's determination of the employee's work capacity, the supervisormust decide if the employee's job may be modified by temporarily:
Eliminating or modifying specific tasks;Reducing the work hours and/or days;Reass:iping the employee to,a more appropriate position,sxpmg
'7sl 1l % 11 !I, 11 'l it
:[f the unit or department is unable to place the employee in a suitable position, theadministrator will try to locate an appropriate position in another unit or department.
6. The employee vvin be reevaluated at the end of each restriction period and the positionwill be modified according to the ennployee's progress. Both the employee anddepartment supervisor will be informed of what should be expected of the employee ateach stage.
7- At the end of eight weeks, the employee will be evaluated as to the need to extendmodified duty, resume fun duties, be permanently reassigned to a more appropriateposition or be directed to a retr?ing program offered by the State of Connecticut.
2.
(a)(b)(C)
'I,.1

AIOZ/[/[ :Qig(lpaspiaH
910Z/(/02 :alt!?p:isHha'H
ElO'tl910t :oit'aahp:iaB9
pxoiiiruio Ao
ale(1
rli
g.xn)'eu%v s,aaAoldtuH
agtut) Km lw Kdos g lsgnbg.x uga 1 pugls.xgpun 1 -amp s4q'4 lz (€saa2a.tag p>qpaH Jo noymqp.too3aq3 aao.iduq 01 saqlap2nB iapptoi,( lnr4paH pun mKv,y, Q'Q) )o Adoa'B palsanbgx )ou ahz'q 1
apnaH piam)mdaq .zolpuv .ia2mivH '.tos7a.tadn5,s,aadoldzua pa.tqruy aq;) auw4 alqvl7vm s3 3uauinaop spp casyauaqlO alsa#bat -uodn aaKoldma Kw o3pap7tto.td aq lytit? Kdoa y osaaKoldma Kq 2qaa7a .xo/ alq'ulyvm s2 t(gaayia5; ln:4paH Jo noym4p.zoo3-, aql pao.zdml <4 sazqlap3tzB .4ap3ao.xHlri:4paH puv .toKv,y, luattxnaop uogesugdmo3 ,sxa:qxoq aq,I,i, s-*,1,i, 'llii,li lilri.i. i,i,;,i, ii!i
9)B([
'G)i-n)B'[I% aaaa-ii{o{d'-"2EF
QtuB% lupd
o.rguo7ss'rmtnoa 'uo2)esuadtnoa ,sxa4xom 'B JO .rgp.xogq) of laa[qns slHgugq uo4lqsuadmos ,s.xg:q.xom ahHgag?z o) s)qfip Km puadsns K'am s)ugtugxHnbg?t
siupld a'q) mollol o) amlp,) )vql ptrelsxgpun I osluamax4riba'21 ug?,I axr,) 'yeaHpgH yaAo?dtnHp.xol'BH JO K:443 a'q'i JO Adoa B pamgrhgx 9AB! 'p.xoll;H JO Q43 )o ggAoldtug pgu$.xgpun gq) 'I
P"JIT.TA1 JO A)k)

Employees: See Employee General Instructions on Page 2. Sign and return Form CT-W4 to your employer. Keep a copy for your records.1. Withholding Code: Enter Withholding Code letter chosen from above. ....................... 1.
2. Additional withholding amount per pay period: If any, see instructions. . ..................... 2. $
3. Reduced withholding amount per pay period: If any, see instructions. ........................ 3. $
Form CT-W4Employee’s Withholding Certificate
Department of Revenue Services State of Connecticut(Rev. 12/20)
Effective January 1, 2021
Employee Instructions• Read the instructions on Page 2 before completing this form.• Select the filing status you expect to report on your Connecticut
income tax return. See instructions.
• Choose the statement that best describes your gross income. • Enter the Withholding Code on Line 1 below.
Check if you are claiming the MSRRA exemption and enter state of legal residence/domicile:_____________________
Employers: See Employer Instructions, on Page 2.
Complete this form in blue or black ink only.
Declaration: I declare under penalty of law that I have examined this certificate and, to the best of my knowledge and belief, it is true, complete, and correct. I understand the penalty for reporting false information is a fine of not more than $5,000, imprisonment for not more than five years, or both.
Is this a new or rehired employee? No Yes Enter date hired:mm/dd/yyyy
* If you are claiming the Military Spouses Residency Relief Act (MSRRA) exemption, see instructions on Page 2.
Our expected combined annual gross income is less than or equal to $24,000 or I am claiming exemption under the Military E Spouses Residency Relief Act (MSRRA)* and no withholding is necessary.My spouse is employed and our expected combined annual gross income is greater than $24,000 and less than or equal A to $100,500. See Certain Married Individuals, Page 2.
My spouse is not employed and our expected combined C annual gross income is greater than $24,000.
My spouse is employed and our expected combined D annual gross income is greater than $100,500.
I have significant nonwage income and wish to avoid having D too little tax withheld.
I am a nonresident of Connecticut with substantial other income. D
Withholding Code
My expected annual gross income is less than or equal to $24,000 or I am claiming exemption under the MSRRA* and E no withholding is necessary.My expected annual gross income is greater than $24,000. CI have significant nonwage income and wish to avoid having too D little tax withheld.
I am a nonresident of Connecticut with substantial other income. D
Withholding CodeQualifying Widow(er)
Married Filing Jointly My expected annual gross income is less than or equal to $12,000 or I am claiming exemption under the MSRRA* and E no withholding is necessary.My expected annual gross income is greater than $12,000. AI have significant nonwage income and wish to avoid having D too little tax withheld.
I am a nonresident of Connecticut with substantial other income. D
Withholding Code
My expected annual gross income is less than or equal to E $15,000 and no withholding is necessary.My expected annual gross income is greater than $15,000. FI have significant nonwage income and wish to avoid having D too little tax withheld.
I am a nonresident of Connecticut with substantial other income. D
Withholding Code
My expected annual gross income is less than or equal to E $19,000 and no withholding is necessary.My expected annual gross income is greater than $19,000. BI have significant nonwage income and wish to avoid having D too little tax withheld.
I am a nonresident of Connecticut with substantial other income. D
Withholding Code
Married Filing Separately
Single
Head of Household
First name Ml Last name Social Security Number
Home address (number and street, apartment number, suite number, PO Box)
City/town State ZIP code
Employee’s signature Date
Employer’s business name Federal Employer Identification Number
Employer’s business address
City/town State ZIP code
Contact person Telephone number – –

Form CT-W4 (Rev. 12/20) Page 2 of 2
Form CT-W4 Instructions Employee General Instructions
Form CT-W4, Employee’s Withholding Certificate, provides your employer with the necessary information to withhold the correct amount of Connecticut income tax from your wages to ensure that you will not be underwithheld or overwithheld.You are required to pay Connecticut income tax as income is earned or received during the year. You should complete a new Form CT-W4 at least once a year or if your tax situation changes.If your circumstances change, such as you receive a bonus or your filing status changes, you must furnish your employer with a new Form CT-W4 within ten days of the change.Gross IncomeFor Form CT-W4 purposes, gross income means all income from all sources, whether received in the form of money, goods, property, or services, not exempt from federal income tax, and includes any additions to income from Schedule 1 of Form CT-1040, Connecticut Resident Income Tax Return or Form CT-1040NR/PY, Connecticut Nonresident and Part‑Year Resident Income Tax Return.Filing StatusGenerally, the filing status you expect to report on your Connecticut income tax return is the same as the filing status you expect to report on your federal income tax return. However, special rules apply to married individuals who file a joint federal return but have a different residency status. Nonresidents and part-year residents should see the instructions to Form CT-1040NR/PY. Check Your WithholdingYou may be underwithheld if any of the following apply:• You have more than one job;• You qualify under Certain Married Individuals; or• You have substantial nonwage income.If you are underwithheld, you should consider adjusting your withholding or making estimated payments using Form CT-1040ES, Estimated Connecticut Income Tax Payment Coupon for Individuals. You may also select Withholding Code “D” to elect the highest level of withholding.If you owe $1,000 or more, after subtracting from your Connecticut income tax the amount withheld from your income for the prior taxable year, and any PE Tax Credit, you may be subject to interest on the underpayment at the rate of 1% per month or fraction of a month. To help determine if your withholding is correct, see Informational Publication 2021(7), Is My Connecticut Withholding Correct?Certain Married IndividualsIf you are a married individual filing jointly and you and your spouse both select Withholding Code “A,” you may have too much or too little Connecticut income tax withheld from your pay. This is because the phase-out of the personal exemption and credit is based on your combined incomes. The withholding tables cannot reflect your exact withholding requirement without considering the income of your spouse. To minimize this problem, and determine if you need to adjust your withholding using Line 2 or Line 3, see IP 2021(7).Nonresident Employees Working Partly Within and Partly Outside of ConnecticutIf you work partly within and partly outside of Connecticut for the same employer, you should also complete Form CT-W4NA, Employee’s Withholding or Exemption Certificate - Nonresident Apportionment, and provide it to your employer. The information on Form CT-W4NA and Form CT-W4 will help your employer determine how much to withhold from your wages for services performed within Connecticut. For Convenience of the Employer Test information, see Form CT-W4NA. To obtain Form CT-W4NA, visit the Department of Revenue Services (DRS) website at portal.ct.gov/DRS or request the form from your employer. Any nonresident who expects to have no Connecticut income tax liability should choose Withholding Code “E.”
Armed Forces Personnel and VeteransIf you are a Connecticut resident, your armed forces pay is subject to Connecticut income tax withholding unless you qualify as a nonresident for Connecticut income tax purposes. If you qualify as a nonresident, you may request that no Connecticut income tax be withheld from your armed forces pay by entering Withholding Code “E” on Line 1.Military Spouses Residency Relief Act (MSRRA)If you are claiming an exemption from Connecticut income tax under the MSRRA, you must provide your employer with a copy of your military spouse’s Leave and Earnings Statement (LES) and a copy of your military dependent ID card.See Informational Publication 2019(5), Connecticut Income Tax Information for Armed Forces Personnel and Veterans.
Employer InstructionsFor any employee who does not complete Form CT-W4, you are required to withhold at the highest marginal rate of 6.99% without allowance for exemption. You are required to keep Form CT-W4 in your files for each employee. See Informational Publication 2021(1), Connecticut Employer’s Tax Guide, Circular CT, for complete instructions.Report Certain Employees Claiming Exemption From Withholding to DRSEmployers are required to file copies of Form CT-W4 with DRS for certain employees claiming “E” (no withholding is necessary). See IP 2021(1). Mail copies of Forms CT-W4 meeting the conditions listed in IP 2021(1) under Reporting Certain Employees to: Department of Revenue Services PO Box 2931 Hartford CT 06104-2931Report New and Rehired Employees to the Department of Labor New employees are workers not previously employed by your business, or workers rehired after having been separated from your business for more than sixty consecutive days.Employers with offices in Connecticut or transacting business in Connecticut are required to report new hires to the Department of Labor (DOL) within 20 days of the date of hire. New hires can be reported by:• Using the Connecticut New Hire Reporting website at
www.ctnewhires.com;• Faxing copies of completed Forms CT-W4 to 800-816-1108; or • Mailing copies of completed Forms CT-W4 to: Connecticut Department of Labor Office of Research, CT-W4 200 Folly Brook Blvd Wethersfield CT 06109For more information on DOL requirements or for alternative reporting options, visit the DOL website at www.ctdol.state.ct.us or call DOL at 860-263-6310.For More InformationCall DRS Monday through Friday, 8:30 a.m. to 4:30 p.m. at:• 800-382-9463 (Connecticut calls outside the Greater Hartford
calling area only); or • 860-297-5962 (from anywhere).TTY, TDD, and Text Telephone users only may transmit inquiries anytime by calling 860-297-4911. Taxpayers may also call 711 for relay services. A taxpayer must tell the 711 operator the number he or she wishes to call. The relay operator will dial it and then communicate using a TTY with the taxpayer.Forms and PublicationsVisit the DRS website at portal.ct.gov/DRS to download and print Connecticut tax forms and publications.
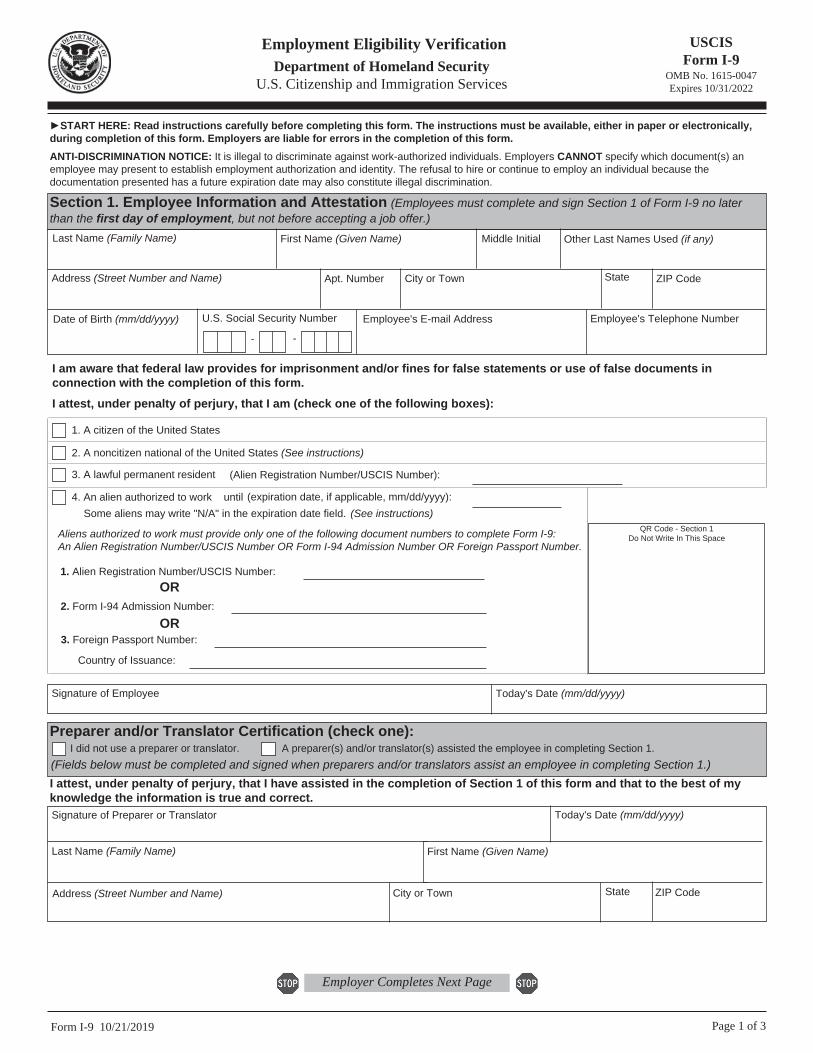
USCIS Form I-9
OMB No. 1615-0047 Expires 10/31/2022
Employment Eligibility Verification Department of Homeland Security
U.S. Citizenship and Immigration Services
Form I-9 10/21/2019 Page 1 of 3
►START HERE: Read instructions carefully before completing this form. The instructions must be available, either in paper or electronically, during completion of this form. Employers are liable for errors in the completion of this form. ANTI-DISCRIMINATION NOTICE: It is illegal to discriminate against work-authorized individuals. Employers CANNOT specify which document(s) an employee may present to establish employment authorization and identity. The refusal to hire or continue to employ an individual because the documentation presented has a future expiration date may also constitute illegal discrimination.
Section 1. Employee Information and Attestation (Employees must complete and sign Section 1 of Form I-9 no later than the first day of employment, but not before accepting a job offer.)Last Name (Family Name) First Name (Given Name) Middle Initial Other Last Names Used (if any)
Address (Street Number and Name) Apt. Number City or Town State ZIP Code
Date of Birth (mm/dd/yyyy)
- -
Employee's E-mail Address Employee's Telephone Number U.S. Social Security Number
1. A citizen of the United States
2. A noncitizen national of the United States (See instructions)
3. A lawful permanent resident
4. An alien authorized to work until (See instructions)
(expiration date, if applicable, mm/dd/yyyy):
(Alien Registration Number/USCIS Number):
Some aliens may write "N/A" in the expiration date field.
I am aware that federal law provides for imprisonment and/or fines for false statements or use of false documents in connection with the completion of this form.
I attest, under penalty of perjury, that I am (check one of the following boxes):
Aliens authorized to work must provide only one of the following document numbers to complete Form I-9: An Alien Registration Number/USCIS Number OR Form I-94 Admission Number OR Foreign Passport Number.
1. Alien Registration Number/USCIS Number:
2. Form I-94 Admission Number:
3. Foreign Passport Number:
Country of Issuance:
OR
OR
QR Code - Section 1 Do Not Write In This Space
Signature of Employee Today's Date (mm/dd/yyyy)
Preparer and/or Translator Certification (check one): I did not use a preparer or translator. A preparer(s) and/or translator(s) assisted the employee in completing Section 1.(Fields below must be completed and signed when preparers and/or translators assist an employee in completing Section 1.)I attest, under penalty of perjury, that I have assisted in the completion of Section 1 of this form and that to the best of my knowledge the information is true and correct.Signature of Preparer or Translator Today's Date (mm/dd/yyyy)
Last Name (Family Name) First Name (Given Name)
Address (Street Number and Name) City or Town State ZIP Code
Employer Completes Next Page

Form I-9 10/21/2019 Page 2 of 3
USCIS Form I-9
OMB No. 1615-0047 Expires 10/31/2022
Employment Eligibility Verification Department of Homeland Security
U.S. Citizenship and Immigration Services
Section 2. Employer or Authorized Representative Review and Verification (Employers or their authorized representative must complete and sign Section 2 within 3 business days of the employee's first day of employment. You must physically examine one document from List A OR a combination of one document from List B and one document from List C as listed on the "Lists of Acceptable Documents.")
Last Name (Family Name) M.I.First Name (Given Name)Employee Info from Section 1
Citizenship/Immigration Status
List AIdentity and Employment Authorization Identity Employment Authorization
OR List B AND List C
Additional Information QR Code - Sections 2 & 3 Do Not Write In This Space
Document Title
Issuing Authority
Document Number
Expiration Date (if any) (mm/dd/yyyy)
Document Title
Issuing Authority
Document Number
Expiration Date (if any) (mm/dd/yyyy)
Document Title
Issuing Authority
Document Number
Expiration Date (if any) (mm/dd/yyyy)
Document Title
Issuing Authority
Document Number
Expiration Date (if any) (mm/dd/yyyy)
Document Title
Issuing Authority
Document Number
Expiration Date (if any) (mm/dd/yyyy)
Certification: I attest, under penalty of perjury, that (1) I have examined the document(s) presented by the above-named employee, (2) the above-listed document(s) appear to be genuine and to relate to the employee named, and (3) to the best of my knowledge the employee is authorized to work in the United States. The employee's first day of employment (mm/dd/yyyy): (See instructions for exemptions)
Today's Date (mm/dd/yyyy)Signature of Employer or Authorized Representative Title of Employer or Authorized Representative
Last Name of Employer or Authorized Representative First Name of Employer or Authorized Representative Employer's Business or Organization Name
Employer's Business or Organization Address (Street Number and Name) City or Town State ZIP Code
Section 3. Reverification and Rehires (To be completed and signed by employer or authorized representative.)A. New Name (if applicable)Last Name (Family Name) First Name (Given Name) Middle Initial
B. Date of Rehire (if applicable)Date (mm/dd/yyyy)
Document Title Document Number Expiration Date (if any) (mm/dd/yyyy)
C. If the employee's previous grant of employment authorization has expired, provide the information for the document or receipt that establishes continuing employment authorization in the space provided below.
I attest, under penalty of perjury, that to the best of my knowledge, this employee is authorized to work in the United States, and if the employee presented document(s), the document(s) I have examined appear to be genuine and to relate to the individual. Signature of Employer or Authorized Representative Today's Date (mm/dd/yyyy) Name of Employer or Authorized Representative
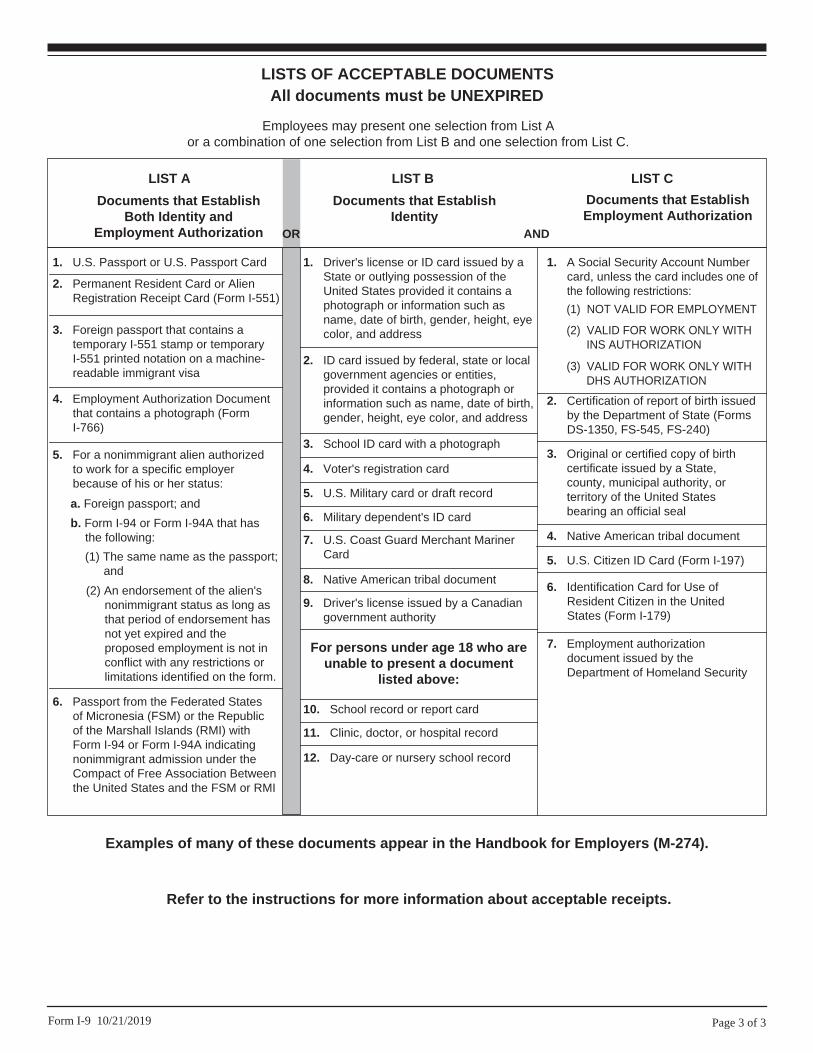
LISTS OF ACCEPTABLE DOCUMENTSAll documents must be UNEXPIRED
Employees may present one selection from List A or a combination of one selection from List B and one selection from List C.
LIST A
2. Permanent Resident Card or Alien Registration Receipt Card (Form I-551)
1. U.S. Passport or U.S. Passport Card
3. Foreign passport that contains a temporary I-551 stamp or temporary I-551 printed notation on a machine-readable immigrant visa
4. Employment Authorization Document that contains a photograph (Form I-766)
5. For a nonimmigrant alien authorized to work for a specific employer because of his or her status:
Documents that Establish Both Identity and
Employment Authorization
6. Passport from the Federated States of Micronesia (FSM) or the Republic of the Marshall Islands (RMI) with Form I-94 or Form I-94A indicating nonimmigrant admission under the Compact of Free Association Between the United States and the FSM or RMI
b. Form I-94 or Form I-94A that has the following:(1) The same name as the passport;
and(2) An endorsement of the alien's
nonimmigrant status as long as that period of endorsement has not yet expired and the proposed employment is not in conflict with any restrictions or limitations identified on the form.
a. Foreign passport; and
For persons under age 18 who are unable to present a document
listed above:
1. Driver's license or ID card issued by a State or outlying possession of the United States provided it contains a photograph or information such as name, date of birth, gender, height, eye color, and address
9. Driver's license issued by a Canadian government authority
3. School ID card with a photograph
6. Military dependent's ID card
7. U.S. Coast Guard Merchant Mariner Card
8. Native American tribal document
10. School record or report card
11. Clinic, doctor, or hospital record
12. Day-care or nursery school record
2. ID card issued by federal, state or local government agencies or entities, provided it contains a photograph or information such as name, date of birth, gender, height, eye color, and address
4. Voter's registration card
5. U.S. Military card or draft record
Documents that Establish Identity
LIST B
OR AND
LIST C
7. Employment authorization document issued by the Department of Homeland Security
1. A Social Security Account Number card, unless the card includes one of the following restrictions:
2. Certification of report of birth issued by the Department of State (Forms DS-1350, FS-545, FS-240)
3. Original or certified copy of birth certificate issued by a State, county, municipal authority, or territory of the United States bearing an official seal
4. Native American tribal document
6. Identification Card for Use of Resident Citizen in the United States (Form I-179)
Documents that Establish Employment Authorization
5. U.S. Citizen ID Card (Form I-197)
(2) VALID FOR WORK ONLY WITH INS AUTHORIZATION
(3) VALID FOR WORK ONLY WITH DHS AUTHORIZATION
(1) NOT VALID FOR EMPLOYMENT
Page 3 of 3Form I-9 10/21/2019
Examples of many of these documents appear in the Handbook for Employers (M-274).
Refer to the instructions for more information about acceptable receipts.