Rhabdomyosarcoma of the head and neck in children
10
RHABDOMYOSARCOMA OF HEAD AND NECK IN CHILDREN Corn bination Treatment by Surgery, Irradiation, and Chernotlrcrapy SARAH S. DONALDSON, MD,* JOSEPH R. CASTRO, MD,+ JORDAN R. WILBUR, MD,~ AND RICHARD H. JESSE, JR., MD~ Combined systematic therapy offers the best chance of cure for children with rhabdomyosarcoma originating in the head and neck. Recommended therapy includes: 1. local excision or biopsy; 2. radiation therapy with doses of 6,000 rads/6 weeks, and 3. multi-drug chemotherapy, i.e., vincristine sulfate, acti- nomycin D, and cyclophosphamide. Severe ocular, dental, soft tissue, and possibly bone complications may be encountered. Provision for prompt medical and nursing support must be available for possible associated morbidity. Of 19 patients treated, minimum 2-year survival is 74%, and local control 89%. Late recurrences or complications require further follow-up. HABDOMYSARCOMA IS A DIAGNOSTIC AND R therapeutic problem in the management of pediatric tumors, representing the most common soft tissue sarcoma of childhood.12 Those tumors originating in the head and neck area may be considered separately from other rhabdomyosarcomas, as they create spe- cific problems and have a distinct prognosis. Children with rhabdomyosarcoma originating in the head and neck can be effectively treated Presented at the First Joint Meeting of the James Ewine Societv. the Societv of Head and Neck SurEeons. and ;he Arneiican Radi;m Society, Boca Raton, Fla.; May 14-19, 1972. From the Departments of Radiotherapy, Pediatrics, and Surgery, M.D. Anderson Hospital and Tumor In- stitute, Houston, Tex. Supported by Grants CA-08122, CA-03713, and CA. 06294, from the National Cancer Institute, National In- stitutes of Health, United States Public Health Service, and the Russell G. Adderley Research Fund. Fellow, Department of Radiology, Division of Ra- diation Therapy, Stanford University School of Medi- cine, Stanford, Calif. + Chief, Department of Radiotherapy, Mt. Zion Hos- pital and Medical Center, San Francisco, Calif. t Head, Department of Pediatrics, M.D. Anderson Hospital and Tumor Institute, Houston, Tex. gChief, Head and Neck Service, Department of Sur- gery, M.D. Anderson Hospital and Tumor Institute, Houston, Tex. Address for reprints: Sarah S. Donaldson, MD, De. partment of Radiology, Division of Radiation Therapy, Stanford University School of Medicine, Stanford, Calif. 94305. The authors wish to thank Edward Maxwell, MD, Head of Department of Radiology, St. Joseph’s Infir- mary, Louisville, Ky. for the use of the diagnostic radi- ograph (Fig. 7). Received for publication September 11, 1972. by combined surgery, radical radiation ther- apy, and aggressive chemotherapy.16J8 Our previous experience in the evolution of these treatment techniques has been reported.11 Our purpose here is to update these results in a group of patients treated with systematic combined therapy (surgery, irradiation, and chemotherapy) . MATERIALS AND METHODS Twenty-five children with a diagnosis of rhabdomyosarcoma, primary in the head and neck area, presented at the University of Texas, M.D. Anderson Hospital at Houston, between July 1965 and June 1970. Of these 25 pediatric patients (16 years and under), three had initial therapy at other institutions, two were found to have distant metastasis, and one was initially given single drug chemother- apy, rather than combination chemotherapy. The responses to combined therapy of the remaining 19 patients form the basis of this report. All were found free of widespread disease and treated with curative intent. A minimum follow-up period of 2 years is avail- able on these patients which previously has been adequate for evaluation of treatment techniques since most primary recurrences and distant metastases occur within this time.ll The age at diagnosis was 2 to 15 years, with an average age 8x2 years and a median of 7 years. The sex distribution revealed 8 males 26
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Rhabdomyosarcoma of the head and neck in children

RHABDOMYOSARCOMA OF HEAD AND NECK IN CHILDREN
Corn bination T r e a t m e n t by Surgery, Irradiation, and Chernotlrcrapy
SARAH S. DONALDSON, MD,* JOSEPH R. CASTRO, MD,+ JORDAN R. W I L B U R , M D , ~
AND RICHARD H. JESSE, J R . , M D ~
Combined systematic therapy offers the best chance of cure for children with rhabdomyosarcoma originating in the head a n d neck. Recommended therapy includes: 1. local excision or biopsy; 2. radiation therapy with doses of 6,000 rads/6 weeks, a n d 3. multi-drug chemotherapy, i.e., vincristine sulfate, acti- nomycin D, and cyclophosphamide. Severe ocular, dental , soft tissue, a n d possibly bone complications may be encountered. Provision for p rompt medical a n d nursing support must be available for possible associated morbidity. Of 19 patients treated, minimum 2-year survival is 74%, and local control 89%. Late recurrences or complications require fur ther follow-up.
HABDOMYSARCOMA IS A DIAGNOSTIC AND R therapeutic problem in the management of pediatric tumors, representing the most common soft tissue sarcoma of childhood.12 Those tumors originating in the head and neck area may be considered separately from other rhabdomyosarcomas, as they create spe- cific problems and have a distinct prognosis. Children with rhabdomyosarcoma originating in the head and neck can be effectively treated
Presented at the First Joint Meeting of the James Ewine Societv. the Societv of Head and Neck SurEeons. and ;he Arneiican Radi;m Society, Boca Raton, Fla.; May 14-19, 1972.
From the Departments of Radiotherapy, Pediatrics, and Surgery, M.D. Anderson Hospital and Tumor In- stitute, Houston, Tex.
Supported by Grants CA-08122, CA-03713, and CA. 06294, from the National Cancer Institute, National In- stitutes of Health, United States Public Health Service, and the Russell G. Adderley Research Fund.
Fellow, Department of Radiology, Division of Ra- diation Therapy, Stanford University School of Medi- cine, Stanford, Calif.
+ Chief, Department of Radiotherapy, Mt. Zion Hos- pital and Medical Center, San Francisco, Calif.
t Head, Department of Pediatrics, M.D. Anderson Hospital and Tumor Institute, Houston, Tex.
gChief, Head and Neck Service, Department of Sur- gery, M.D. Anderson Hospital and Tumor Institute, Houston, Tex.
Address for reprints: Sarah S. Donaldson, MD, De. partment of Radiology, Division of Radiation Therapy, Stanford University School of Medicine, Stanford, Calif. 94305.
The authors wish to thank Edward Maxwell, MD, Head of Department of Radiology, St. Joseph’s Infir- mary, Louisville, Ky. for the use of the diagnostic radi- ograph (Fig. 7).
Received for publication September 11, 1972.
by combined surgery, radical radiation ther- apy, and aggressive chemotherapy.16J8 Our previous experience in the evolution of these treatment techniques has been reported.11 Our purpose here is to update these results in a group of patients treated with systematic combined therapy (surgery, irradiation, and chemotherapy) .
MATERIALS AND METHODS
Twenty-five children with a diagnosis of rhabdomyosarcoma, primary in the head and neck area, presented at the University of Texas, M.D. Anderson Hospital at Houston, between July 1965 and June 1970. Of these 25 pediatric patients (16 years and under), three had initial therapy at other institutions, two were found to have distant metastasis, and one was initially given single drug chemother- apy, rather than combination chemotherapy. T h e responses to combined therapy of the remaining 19 patients form the basis of this report. All were found free of widespread disease and treated with curative intent. A minimum follow-up period of 2 years is avail- able on these patients which previously has been adequate for evaluation of treatment techniques since most primary recurrences and distant metastases occur within this time.ll
The age at diagnosis was 2 to 15 years, with an average age 8x2 years and a median of 7 years. The sex distribution revealed 8 males
26

No. 1 RHABDOMYOSARCOMA OF HEAD AND NECK IN CHILDREN Donaldson et al. 27
TABLE 1. Sites of Primarv Tumor
Nasophary nx
canal Nasal cavity Orbit Cheek (boccinator muscle and masseter
Maxillary antrum Retromolar trigone area Tonsilar area Scalp. Temporal muscle
nasopharynx and/or external auditory
muscle)
TOTAL
5
1 2 2
1 3 1 1 2 1
19
and 11 females. One patient was Negro, the other 18 were Caucasians.
The sites of the primary tumor are listed in Table 1. Eight of 19 tumors originated in the nasopharynx or nasal cavity. In only two cases in this series was the site of origin in the orbit; in six patients, the primary'site was in the cheek or adjacent area, i.e., tonsil, retro- molar trigone, or maxillary antrum.
All patients had histologic confirmation of their tumor by the Department of Pathology, M.D. Anderson Hospital. Tumors were cate- gorized according to the Horn and Enterline classification.G Table 2 shows the histoclassi- fication; most patients had embryonal rhab- domyosarcoma.
CLINICAL STAGING
A proposed clinical staging is shown in Table 3, a modification of the American Joint Com- mittee for Cancer Staging, and the U.I.C.C. classification for head and neck tumors. Clini- cal work-up was individualized depending on the site of the primary lesion. Routine studies in all patients included: chest x-ray, complete blood count, platelet count, liver function tests, and bone marrow aspirate. Most patients had, in addition, skeletal survey, skull and sinus films. Selected patients had brain scan, liver scan, bone scan, EEG, lumbar puncture, radiographic tomograms, arteriograms, and lymphangiogram. The importance of com- plete work-up is reflected in the fact that while some patients had localized disease, 10 were staged as T,3 after extensive evaluation because of the tendency of rhabdomyosarcoma to invade diffusely in soft tissues or bone.
* V.A.C.-vincristine sulfate, actinomycin D, and cy- clophosphamide.
TABLE 2. Histology
Embryonal 13 Botryoid 0 Alveolar 4 Unclassified 2 Pleomorphic 0
TOTAL 19
TREATMENT TECHNIQUES
Systematic combined therapy consisted of surgery, radiation therapy, and V.A.C." chem- otherapy (Fig. 1).
Surgery A complete excision of the primary was pos-
sible in only 3 of 19 patients. All were staged as TI, although one patient had an orbital primary treated by exenteration; the other two patients had scalp primaries. In two additional cases, incomplete excision was per- formed initially, because of extensive soft tis- sue and periosteal invasion. Of the 14 remain- ing patients, the initial surgical approach was biopsy only.
Three patients had surgical procedures later in the course of their therapy. One patient re- quired an orbital exenteration for radiation keratitis and iritis. An additional patient re- quired an orbital exenteration and later a bi- frontal craniotomy for local control of invasive
TABLE 3.
N-0 N-1 N-2 N-3 Total - T- 1 4 1* - 5
T-2 - 1 1 2 T-3 10 1 1 - 12
14 3 1 1 19
-
Staging+ T- 1
T-2
T-3
N-0 N-1
N-2
N-3
Tumor localized to one region or site, i.e., orbit, scalp. Tumor extension to neighboring structures or two or more sites, i.e., cheek + tonsillar area, nasopharynx, soft palate. Radiographic evidence of bone destruction, or cranial nerve involvement. No clinical evidence of lymph node metastasis. Single clinically positive lymph node less than 3 cm in diameter. Single lymph node over 3 cm in diameter, or multiple ipsilateral palpable nodes. Fixed lymph nodes or bilateral palpable nodes.
* Presented to M.D. Anderson Hospital with lymph
+ Modification of American Joint Committee for node metastasis after excision of primary.
Cancer Staging, and the U.I.C.C. classification.

28 CANCER January 1973 Vol. 31
I
FIG. 1. Schedule for combination therapy: surgery, irradiation, and chemotherapy.
tumor. One patient had a maxillary antro- tomy after 2 years because of the radiographic suspicion of infection vs. tumor.
Radiation Therapy High-dose irradiation was given at tumor
doses of 5,000 rads/5 weeks to 6,500 rads/8 weeks to the primary tumor. Eleven patients were treated with cobalt60 teletherapy, five pa-
tients with electron beam, energies ranging from 6-18 MeV, and three patients with combi- nation of both modalities.
Three patients with primary tumors were treated in planned split course fashion with 3,000-3,500 rads/3-4 weeks, a 2- to 4-week split in therapy followed by 2,000-3,000 rads/3 weeks. Treatment ports and isodose dis- tributions were individualized for each patient. In general, the portals included the primary tumor with wide margins, and the adjacent lymph node stations, ranging in size from 6 x 5 cm to 12 x 9 cm. Wedged fields were fre- quently utilized to localize the high dose area and protect normal structures. Additional shielding was used where possible for protec- tion, such as intra-oral stents to move the tongue out of the radiation field, etc. In select cases, modified weighting of 2: 1 was used for unilateral disease. Prophylatic neck irradia- tion was not administered in No cases. T h e high neck nodes generally were included in the primary treatment field, with low neck nodes included only if clinically positive nodes were present in the upper neck. When neck treat- ment was given, doses utilized were 4,000
FIG. 2 (left). Treatment portals in a patient with a T,N, nasopharynx primary. FIG. 3 (right). Radiographic localization films in same patient, T,N, nasopharynx primary.

No. 1 RHABDOMYOSARCOMA OF HEAD AND NECK IN CHILDREN Donaldson et al. 29
rads/4 weeks to 6,000 rads/6 weeks. Only 6 of the 19 patients required neck treatment.
An example of treatment portals and radi- ographic localization films in a patient with a T3N2 tumor of nasopharynx primary is shown in Figs. 2 and 3.
Radiographs and isodose distribution in a patient with a T,N,, tumor arising in the left maxillary antrum and extending to the floor of the orbit, zygoma, and mandible with bony erosion are shown in Figs. 4 and 5. Two 45" wedged fields were utiliLed to include a gener- ous target volume within 100% isodose curve,
Chemotherapy The same plan of chemotherapy was initi-
ated in each case but was modified individu- ally depending on the patient's tolerance. Early in the study, in some patients with small primary tumors, adequacy of drug therapy was considered at a slightly lower drug dose, if they had complete surgical removal and high- dose postoperative irradiation. The plan of chemotherapy was to achieve maximal drug response, within acceptable limits of toxicity.
Vincristine sulfate: A dose of 2 mg/mz I.V., weekly for 12 weeks (maximum dose 2 mg) was completed by 16 of 19 patients. One pa- tient received only six injections and did not complete the course following hospital dis- charge, and one patient had only five injec- tions. Selected patients had modified dosages depending on their tolerance. In no patient was vincristine therapy discontinued because of toxicity. One patient has had a supplemen- tal vincristine course consisting of 12 initial injections, followed by every 3 months rein- forcement of every week x 4, repeated for 5 cycles, due to inability to tolerate further actinomycin D.
Actinomycin D: A dose of .075 mg/kg I.V. (maximum 0.5 mg/day) given over 5- to %day period with courses repeated every 3 months x 5. Repeated courses were given depending on the patient's tolerance. Early in the study, in selected cases of Stage I disease, it was not felt necessary to give repeated courses of drug.
Cyclophospharnide: Chemotherapy includes long-term cyclophosphamide treatment given orally for 2 years at doses of 2.5 mg/kg daily. In the first patients with T, tumors treated in this group, cyclophosphamide was omitted it they were felt to be cured by initial treatment. More recently, all patients received cyclophos- phamide.
Other agents: Three of 19 patients failed in-
FIG. 4. Localization radiograph in a patient with T,N, tumor of left maxillary antrum, extending to floor of orbit, zygoma, and mandible.
itial chemotherapy and were given trials with a variety of other agents which were unsuc- cessful.
lo I 4 C060 D fUsed 8 xBI 45" Wedge
80 crn SSD
Left
FIG. 5. Isodose distribution in same patient using two 45O wedged fields.
30 CANCER January 1973 Vol. 3 1
KWOl pot,cnrs 4 5 (19) Tunc ycoi-s
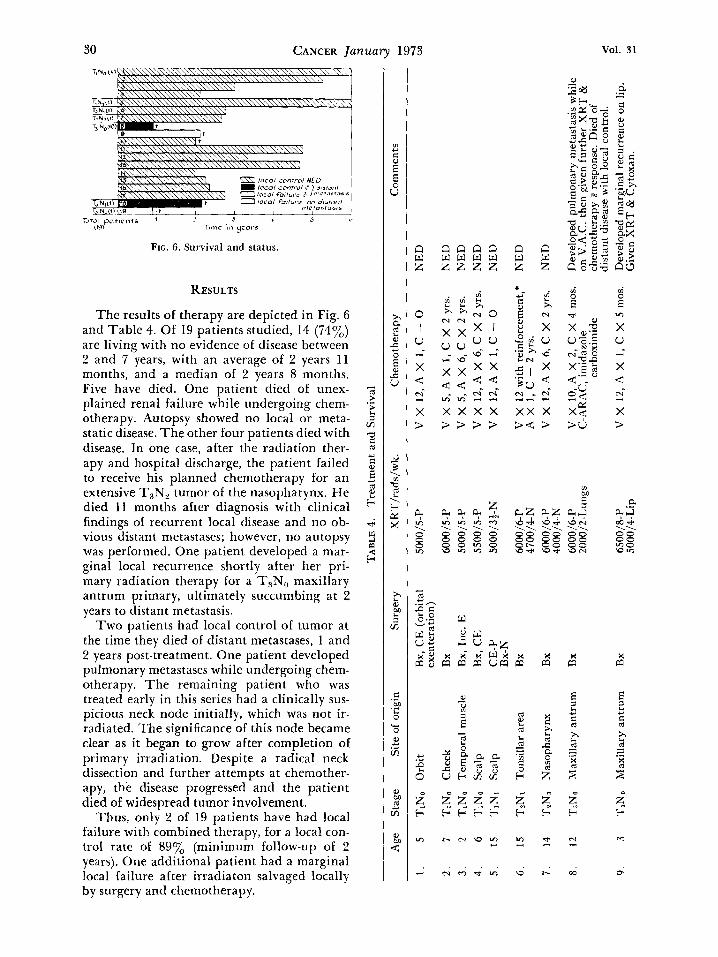
FIG. 6. Survival and status.
RESULTS
The results of therapy are depicted in Fig. 6 and Table 4. Of 19 patients studied, 14 (74y0) are living with no evidence of disease between 2 and 7 years, with an average of 2 years 11 months, and a median of 2 years 8 months. Five have died. One patient died of unex- plained renal failure while undergoing chem- otherapy. Autopsy showed no local or meta- static disease. The other four patients died with disease. In one case, after the radiation ther- apy and hospital discharge, the patient failed to receive his planned chemotherapy for an extensive T,N, tumor of the nasopharynx. He died 11 months after diagnosis with clinical findings of recurrent local disease and no ob- vious distant metastases; however, no autopsy was performed. One patient developed a mar- ginal local recurrence shortly after her pri- mary radiation therapy for a T,N, maxillary antrum primary, ultimately succumbing at 2 years to distant metastasis.
Two patients had local control of tumor at the time they died of distant metastases, 1 and 2 years post-treatment. One patient developed pulmonary metastases while undergoing chem- otherapy. The remaining patient who was treated early in this series had a clinically sus- picious neck node initially, which was not ir- radiated. The significance of this node became clear as i t began to grow after completion of primary irradiation. Despite a radical neck dissection and further attempts at chemother- apy, the disease progressed and the patient died of widespread tumor involvement.
Thus, only 2 of 19 patients have had local failure with combined therapy, for a local con- trol rate of 89% (minimum follow-up of 2 years). One additional patient had a marginal local failure after irradiaton salvaged locally by surgery and chemotherapy.
n w z
0 I u
X d m-
3
3
n n a a w w w w z z z z n w z
al zc?l

z ?
10.
11
T3N
o O
rbit
4500
/3-N
A
dditi
onal
XR
T to
m
edia
stin
um t
ibia
, ab
dom
en
Bx,
Inc
. E
x 2
6000
/6-P
(o
rbit
al e
xent
erat
ion
& c
rani
otom
y)
Dev
elop
ed n
eck
node
s. X
RT
to n
eck
node
s. D
evel
oped
dis
tant
met
asta
sis
&
died
with
loc
al a
nd d
ista
nt d
isea
se.
Req
uire
d or
bita
l ex
ente
rati
on f
or
blin
dnes
s w
hile
on
V.A
.C.
Loca
l re
curr
ent
tum
or I
nc. E
X 2
. A
bon
e m
arro
w w
as f
, an
d ch
emo-
th
erap
y re
star
ted.
Sh
e di
ed o
f re
nal
faii
ure
and
NE
D io
cai
or m
etas
tati
c at
aut
opsy
. 11
. 8
T3N
o N
asop
hary
nx
Bx
5500
/5&
P V
X 1
2, A
X 1
, C X
2 y
rs.
NE
D
NE
D
V.A
.C.
X 6
mos
.
V X
12,
A X
1, C
X 5
mos
.
Mit
omyc
in C
X 7
Aza
picy
l X
I
V X
12,
A X
5, C
X 2
yrs
. 3
wk.
spl
it
P 30
00/3
V
X 6
, A X
3, C
X 2
yrs
. R
eexp
lore
d at
2 y
ears
-NE
D
1 1 1
12.
7 T3
No
Nas
opha
rynx
and
/or
Bx
3000
/2
13.
11
T3N
o N
asop
hary
nx
Bx
5OoO
/5-P
ear
Ree
xplo
rati
on
14.
10
T3N
o N
asal
cav
ity
Bx
5800
/S-P
V
X 1
2, A
X 6
, C X
2 y
rs.
NE
D
NE
D
15.
3 T
3No
Nas
opha
rynx
Bx
3000
/3
V X
12,
A X
5, C
X 2
yrs
. 3
wk.
spl
it
P 22
00/2
V
X 1
2, A
X 6
, C X
2 y
rs.
V X
12,
A X
5, C
X 2
yrs
.
Req
uire
d or
bita
l ex
ente
rati
on f
or
XR
T co
mpl
icat
ion
wit
h N
ED
. N
ED
16.
5 T
3N0
Max
illa
ryan
trum
Bx
6000/6-P
(orb
ital
exe
nter
atio
n)
4 w
k. s
plit
P
3OoO
/3
V X
12,
A X
2,
C X
2 m
os.
A q
uest
iona
bly
clin
ical
ly +
node
not
R
x'd.
ini
tial
ly g
rew
, req
uiri
ng
L. r
ad.
neck
dis
sect
ion.
Cyt
oxan
then
st
arte
d.
3OoO
/3-s
pine
D
auno
myc
in, V
AM
P D
ista
nt e
xtra
dura
l & t
high
dis
ease
re
quir
ed f
urth
er X
RT
and
che
mo-
th
erap
y.
Pati
ent
died
of
dist
ant
met
asta
sis,
w
ith
loca
l co
ntro
l.
17.
7 T
,No
Ret
rom
olar
tri
gone
Bx
3.50
014
area
18.
9 T
3N1
Nas
alca
vity
Bx, I
nc.
E
6100
/6-P
L.
rad.
nec
k di
ssec
tion
2700
/2-t
high
19.
8 T
3N2
Nas
opha
rynx
Bx
5600
/7-P
V
X 6
, A X
1, C
X 0
Pa
tien
t los
t to
follo
w-u
p w
ith
inco
mpl
ete
6000
/6-L
nec
k ch
emot
hera
py t
reat
men
t.
5000
/5-R
nec
k D
ied
wit
h lo
cal
fail
ure,
but
no
dist
ant
dise
ase.
Bx =
Bio
psyo
nly
CE
= C
ompl
ete
exci
sion
In
c. E
= I
ncom
plet
e ex
cisi
on
P =
Pri
mar
y N
= N
eck
* =
Wit
h q
wk.
X 4 in
ject
ions
rep
eate
d 3
mon
ths
X 5
cyc
les
C-A
RA
C =
Cyt
oxan
-Cyt
osin
e A
rabi
nosi
de
VA
MP
= V
incr
istin
e, A
min
opht
heri
ne,
6-M
erca
ptop
urin
e, P
redn
ison
e N
ED
= N
o ev
iden
ce o
f di
seas
e V
x #
inj
ecti
ons
= (
Vin
cris
tine
) A
X #
.cou
rses
= (
Act
inom
ycin
D)
C x
tim
e =
(C
yclo
phos
phar
nide
)
> 3 z M n E

52 CANCER January 1973 Vol. 31
COMPLICATIONS OF TREATMENT
Eye: Seven of the 19 patients had tumor in- volving the eye or orbit which necessitated therapy to the eye; two had primary orbital tumors, and five had orbital extension from another primary. One of the seven patients was treated by orbital exenteration primarily. Only one of the remaining six patients has re- quired orbital enucleation for radiation kera- titis, iritis, and conjunctivitis, 8 months after therapy. However, one patient has an asymp- tomatic radiation-induced cataract occurring 27 months after therapy, and one patient has mild superficial keratitis with early corneal stippling one year post-therapy. Two patients who had the eye included in the radiation field had no ocular difficulties, but one died 11 months after treatment with local control of tumor but widespread metastasis, and the second had a corneal shield utilized through- out the radiation therapy. The sixth patient required exenteration for residual orbital tumor after irradiation. Further ocular com- plications may be encountered as late antici- pated sequelae.
Oral: Fifteen of the 19 patients had tumor involving the oral cavi ty-oropharynx, naso- pharynx, or paranasal sinus regions -requiring that the primay irradiation field include a portion of the oral cavity. The addi- tive effect of actinomycin D and irradiation demonstrated the most severe morbidity in terms of mucositis, dysphagia, glossitis, phar- yngitis, esophagitis, gingivitis, and erythema. This reaction correlated with the size and pos- tion of the irradiation field. Mucositis was fre- quently severe and confluent, and, in some pa- tients, necessitated nasogastric tube feeding for adequate nutrition as well as intravenous fluids for hydration. Two patients have devel- oped post-irradiation trismus, a sequela of the large volume of tissue treated. X-rays of one patient show lytic defects suggestive of osteo- radionecrosis of the mandible after 20 months. To date, 2 of the 15 patients have had severe dental problems as a sequelae of irradiation to the teeth and gums. In both, there is dental decay, and, in one, there is also atrophy of the zygoma and an abnormal occlusion within the irradiated field. Xerostomia is an anticipated complication in this group of patients.
Infection: Localized infection has occurred on seven occasions in 5 of the 19 patients. There were three instances of ear infections, one which required simple mastoidectomy
after 2 years of recurrent infections. Cellulitis in the irradiated cheek and facial tissue has occurred in two cases-in one 18 months after irradiation and in one 3 months after irradia- tion, in association with administration of ac- tinomycin D. T ~ L I S , reactivation of latent ra- diation effects in irradiated tissues which have returned to normal in appearance is referred to as the recall phenomena.
There have been two episodes of infection after enucleation. One patient developed a Pseudomonas infection in the graft after or- bital exenteration; another developed celluli- tis around the prosthetic retainer after enu- cleation.
Skin: T h e anticipated skin changes of irra- diation have included erythema, desquama- tion, and tanning. These reactions have been exaggerated by the concomitant use of actino- mycin D but have created no long-term effects, to date. Subsequent courses of actinomycin D intensified the erythema, oral ulceration, and mucositis, as recall phenomena.
Drugrelated: Vincristine therapy was asso- ciated with alopecia, neurotoxicity, and con- stipation. Peripheral neurotoxicity was often marked, but not severe enough to require cessa- tion of drug. A cyclophosphamide-related hemorrhagic cystitis was observed in 2 of 16 cases, and confirmed at cystoscopy in one pa- tient.
Bone marrow suppression-leukopenia, thrombocytopenia, and anemia-was fre- quently observed related to both actinomycin D and cyclophosphamide. Adjustments in the schedule of cyclophosphamide were made if the total neutrophil count was less than 1,000 cells/mms.
DISCUSSION
There has been no widely accepted staging system for rhabdomyosarcoma, as has been ob- served for other childhood tumors such as Wilms’ tumor, neuroblastoma, or lymphomas. The proposed staging system (Table 3) dem- onstrates that: 1. rhabdomyosarcoma extend- ing beyond a local region, i.e., beyond TI, is often shown by careful evaluation to be asso- ciated with bone destruction or cranial nerve involvement (TR) in 12/14 (86y0) of patients, and 2. the presence of lymph node metastases does not correlate directly with size or extent of primary tumor. Only 5/19 (Zf3yo) patients have clinically apparent nodal disease, which includes only 2/12 (18%) patients with T, neoplasms.

No. 1 RHAUDOMYOSARCOMA OF HEAD A N D NECK I N CHILDREN * Donnldson et al. 33
In other large series including head and neck primaries, the orbit is a frequent primary site and associated with a good prognosis.19-22 Probably this is related to the paucity of lym- phatics in the orbit and i t s bony confines, which makes wide invasion of tumor less likely and earlier diagnosis more probable. In coti- trast to the good prognosis of orbital lesions, tumors located in the nasal cavity-nasopliar- ynx and maxillary antrum have previously had a poor prognosis11 presumably because of abundant lymphatics, ease of extension to neighboring structures, and lack of anatomical confines to tlie tumor. Seventy-four per cent of tlie patients in the present series had such le- sions: 8/19 (429/0) tumors arose in the nasal cavity-nasopharynx, and 6/19 (32Yu) in the cheek or neighboring area. Yet this group, with a previously poor outlook, had a local control rate of 14/16 (86Yu) with a follow-up period ranging frotn 11-63 months.
Nonembryonal forms of rhabdomyosar- coma, i.e., alveolar or pleomorphic forms; have also been associated with a poor prognosis.”zz T o date, no difference in prog nosis has been noted in our patients with the nonembryonal form of rhabdomyosarcoma.
Early and aggressive therapy is essential in obtaining a cure. Only 1 of the 3 patients with less aggressive treatment elsewhere, referred to tlie M.D. Anderson Hospital after local fail- ure, was salvaged. T w o patients who pre- sented with metastatic disease are dead from disease, local and distant. One patient treated with single agent chemotherapy only, in addi- tion to irradiation, died of widespread meta- static disease, with local control.
A radical surgical approach with exentera- tion is still recommended by somes.9 as the treatment of choice for obital primaries. How- ever, the sites of origin in head and neck pri- maries often preclude curative excision, or re- quire a severely mutilating or unacceptably deforming 0pera t ion .4~7~~~ The present series denionstrates that biopsy alone, followed by aggressive irradiation and chemotherapy has been beneficial in treating these primaries. Such an approach offers the child maximum therapy to a wide field and, in a high percent- age of patients, prevents the need for further s u rg i c a 1 procedures .
Rhabdomyosarcoma has been shown to be radiosensitivelOJ5 and radiocurable in select cases.l.19 However, local failure with irradia- tion alone has led to suggestions for such combinations as preoperative irradiation fol-
lowed by radical excision,13 or irradiation with attempt to potentiation by c l i e m ~ t l i e r a p y . ~ J ~ ~ ~ Our own experience has led us to attempt a systematic, aggressive combination approach to treatment.?l
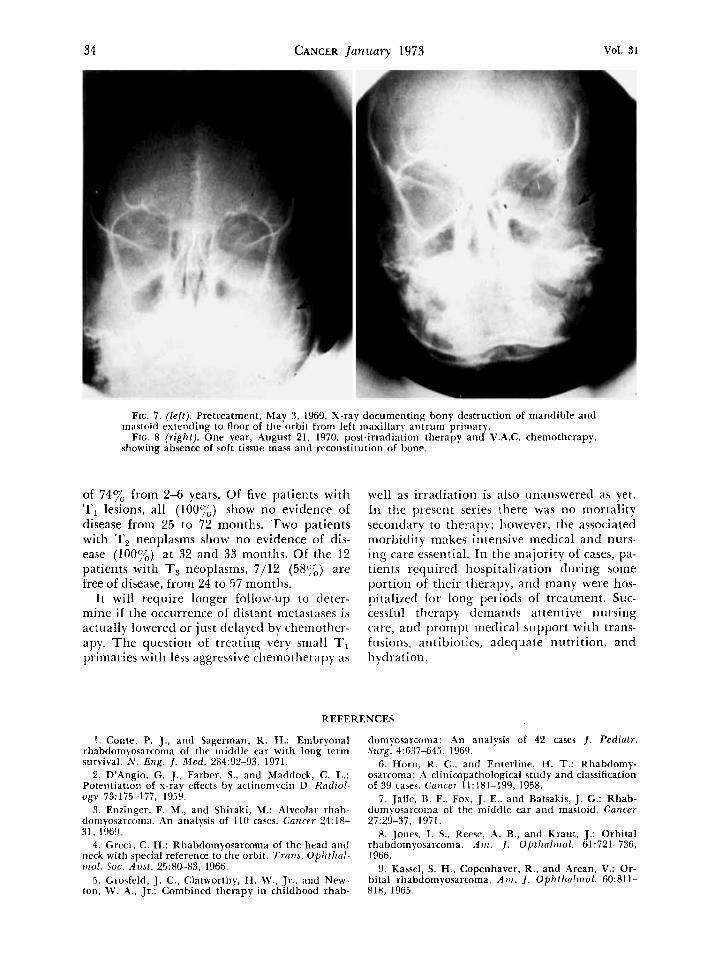
Altliougli i t has been suggested that bone involvement by tumor is beyond tlie control of irradiation alone,l7 we have seen instances where pretreatment bone destruction healed under the effect of irradiation and cliemotlier- apy. Figures 7 arid 8 exemplify a case of tlocu- merited bony destruction of the mandible and mastoid extending to tlie floor of the orbit from a primary rliabdomyosarcoma of tlie left maxillary antrum. One year following radia- tion therapy, 6,000 rads/6 weeks and V.A.C. chemotherapy, follow-up x-rays show absence of soft tissue mass and reconstitution of bone.
Adequate radiation therapy requires wide fields and large volumes of tissue to be irra- diated. Clinically suspicious lymph node in- volvement should be surgically confirmed or included in the radiation field. One must be willing to accept sequelae of irradiation, i.e., expected eye complications, arrest in bone growth, and oral problems, if approaching a patient with curative intent. The reactions from irradiation are severe, particularly with addition of actinomycin D.2.23 Split course therapy may be useful in allowing time for subsidence of tissue reactions and possibly re- ducing the volume of tissue to be irradiated in the second course of treatment. Intense local therapy and support including meticulous oral hygiene and nutritional support is re- quired to decrease local reactions. Prompt in- tensive antibiotic therapy at the first sign of infection is also vital.
Two failures in the T3 group were second- ary to inadequate coverage of tlie primary tumor by the initial radiation portals with rapid marginal recurrence and eventual dis- seminated disease. Caution must be taken to ensure wide coverage since rhabdomyosarcoma locally invades widely. In one patient with ex- tensive cranial nerve involvement, i t was nec- essary to use large fields encompassing the base of the skull.
A review of the literature reveals that the overall survival of rhabdomyosarcoma of head and neck has ranged between 10-3070 in large series. More recently, the use of adjuvant chemotherapy in addition to irradiation and surgery has been suggested as a possible ap- proach to improving survival statistics.20s22 The present series shows an overall survival
34 CANCER January 1973 Vol. 31
FIG. 7. (left). Pretreatment, May 3 , 1969. X-ray documenting bony destruction of mandible and
FIG. 8 (right). One year, August 21, 1970, post-irradiation therapy and V.A.C. chemotherapy, mastoid extending to floor of the orbit from left maxillary antrum primary.
showing absence of soft tissue mass and reconstitution of bone.
of 74% from 2-6 years. Of five patients with TI lesions, all ( l O O ~ o ) show no evidence of disease from 25 to 72 months. Two patients with T, neoplasms show no evidence of dis- ease (100%) at 32 and 33 months. Of the 12 patients with T, neoplasms, 7/12 (5875) are free of disease, from 24 to 57 months.
I t will require longer follow-up to cleter- mine if the occiirrence of distant meta5tases is actually lowered or just delayed by chemother- apy. The question of treating very small TI primaries with less aggressive chemotherapy as
well as irradiation is also unanswered as yet. In the piesetit series there was no mortality secondary to therapy; however, the associated morbidity makes intensive meclical and nurs- ing care essential. In the tnajority of cases, pa- tients required IiospitaliLation during some portion of their therapy, and many were hos- pitalized for long periods of treatment. Suc- cessful therapy demands attentive nursing care, and prompt medical support with trans- fusions, antibiotics, adequate nutrition, and hydration.
REFERENCES
1 . Conte, P. J., and Sagerman. R. H.: Embryonal rhabdomyosarcoma of the middle ear with long term survival. N . Eng. J . Med. 284:92-93, 1971.
2. D'Angio. G. J., Farber, S.. and Maddock, C. L.: Potentiation of x-ray effects by actinomycin D. Radiol- ogy 73:175-377, 1959.
3. Enzinger, F. M., and Shiraki, M.: Alveolar rhab- doniyosarcoma. An analysis of 110 cases. Cancer 24:18- 31, 1969.
4. Greer. C. H.: Rhabdomyosarcoma of the head and neck with special reference to the orbit. Trans. Ophthn l - viol. SOC. A t ~ s t . 25:80-83, 1966.
5. Grosfeld, J . C.. Clatworthy, H . W., Jr.. and New- ton, W . A , . Jr.: Combined therapy in childhood rhab-
domyosarcoma: .4n analysis of 42 cases J . Pediatr. Szirg. 4:G37-645. 1969.
6. Horn, R. C.. and Enterline, H. T.: Rhabdomy- osarcoma: A clinicopathological study and classification of 39 cases. Cancer ll:l81-199, 1958.
7. Ja tk , B. F., Fox, J. E.. and Batsakis, J. C.: Rhab- tlomyosarcon~a of the middle ear and mastoid. Cancer 27:29-37, 1971.
8. Jones. I . S., Reesr, ,4. B., and Kraut. J.: Orbital rhabdomyosarcoma. A m . J . Optlialmol. 61 :721-736, 1966.
9. Kassel, S. H., Copenhaver, R., and Arean, V.: Or- bital rhabdomyosarcoma. A m . J. Ophtholmol . 60:811- 818, 1965.

No. 1 KHAUDOMYOSARCOMA OF HEAD AND NECK IN CHILDREN * Donnldson et al. 35
10. Lederman, M.: Radiotherapy in the treatment of orbital tuinours. Nr. J. Ophtltalmol. 40592-610, 1956.
11. Litidberg, R. D.: Rliabdomyosarconia in chil- tlrcn: Treatment and Icsults. Neoplasia in childhood. The University of Texas M.D. Anderson Hospital and Tuiiior Institute. Chicago, Ill., Year Book Medical Pub- lishers, Iiic.; pp. 209-217, 1969.
12. Maliour, G. H., Soule, E . H., Mills, S. D., and Lynn, H . U.: Rhabdomyosarcoma in infants and chil- dren: A clinicopathologic study of 75 cases. J . Pediutr.
13. McNeer, G. P., Cantin, J., Chu, F., and Nickson, J. J . : Effectiveness of radiation therapy in the manage- ment' of sarcoma of the soft somatic tissues. Cancer
14. Nelson, A . J.: Embryonal rhabdomyosarcoma. Report of 24 cases and study of the effectiveness of ra- diation therapy upon the primary tumor. Cnncer 22:64-68, 1968.
15. Perez-Tamayo, R.., and Kramer, S.: Rhabdomy- osarconia of the head and neck in children: Place of radiotherapy. Ruriiol. C l i n . Nor th ,4m. 33:307-318, 1964.
16. Pinkel, D., and Pickren, J.: Rhabdomyosarcoma in children. J A M A 175.293-298, 1961.
Si0.g. 2:402-409, 1967.
22:391-397, 1968.
17. Potter, G. D.: Embryonal rhabodmyosarcoma of the middle ear in children. Cancer 19:?21-226, 1966.
18. Pratt, C . B., Hustu, H. O., Fleming, I. D., and Pinkel, D.: Coordinated treatment of childhood rhab- doinyosarcoma with surgery, radiotherapy and combi- nation chemotherapy. Cuncer Res. 32:6&610, 1972.
1Y. Sagerman, R. H., Trettcr, P., and Ellsworth, R. M.: The treatment of orbital rhabdomyosarcoma of children with primary radiation therapy. A m . J . Iioentgenol. 114:31-34, 1972.
20. Santamaria, J . N., Colebatch, J . H., and Canip- bell, P. E . : Rhabdomyosarcoma. A study of 27 cases. Royal Children's Hospital, Melbourne 1954-1968. A v s - tmlas . Radiol. 14:438-442, 1970.
21. Sutow, W. W.: Chemotherapeutic management of childhood rhabdomyosarcoma. Ncoplasia in childhood. The University of Texas M.D. Anderson Hospital and Tumor Institute. Chicago, Ill., Year Book Medical Pub- lishers, Inc., 1969; pp. 201-208.
22. Sutow, W. W., Sullivan, M. P., Reid, H. L., Tay- lor, H. G., and Griffith, K . M.: Prognosis in childhood rhabdomyosarcoma. cancer 25: 1384-1390, 1970.
23. Tan, C. T. C., Dargeon, H. W., and Burchenal, J. H.: T h e effect of actinoniycin D on cancer in child- hood. Pediotrrics 24:544-561, 1959.