
Melanoma of the head and neck
6
Melanoma of the Head and Neck MATTHEW N. HARRIS, M.D., DANIEL F. ROSES, M.D., ALFRED T. CULLIFORD, M.D., STEPHEN L. GUMPORT, M.D. A series of 94 patients with cutaneous malignant melanoma of the head and neck region has been studied. Fifty-three of the patients had regional lymph node dissections performed and the results in 37 performed more than 5 years ago are presented. The policy of elective lymph node dissection for invasive melanoma of the head and neck is strongly endorsed, although not proven by the data presented in this limited series. Whenever possible, a total exci- sional biopsy should be performed to establish the diagnosis. It is recommended that all melanomas be classified by the method of Clark and Mihm and that the level of invasion also be deter- mined. There is an appreciable error in the clinical evaluation of lymph nodes for metastases. In general, it is suggested that elective regional lymph node dissections be performed for in- vasive melanoma (levels III, IV and V). The literature per- taining to cutaneous melanoma of the head and neck has been reviewed and surgical and pathological problems peculiar to lesions of this region are emphasized. HE HEAD and neck region has been reported to be the most common anatomic site for cutaneous malignant melanoma.19 It would seem that lesions in an area so readily visible would be detected at an early stage and therefore have a more favorable prognosis. However, melanomas of the head and neck remain as difficult to treat as those found at other sites. Five year survival figures have ranged between 30% and 45% according to several collected series.1'3'49'32'34 A rationale for effective treatment has eluded most investigators to the present time. The recent interest in uniform clinical and his- tologic classification maiy offer criteria for delineating appropriate therapy in individual cases. We have re- viewed our experience with cutaneous melanoma of the head and neck with particular reference to such clinical and histologic classification and have reviewed the ex- perience of others. Submitted for publication February 12, 1975. This study was supported by the Sylvia and Mortimer Hyams Memo- rial Fund. Reprint requests: Matthew N. Harris, M.D., New York University Medical Center, 566 First Avenue, New York, N.Y., 10016. From the Tumor Service, Department of Surgery, New York University Medical Center, New York, New York Methods In 1949 a study of malignant melanoma was initiated on the Tumor Service of the Department of Surgery at the New York University Medical Center. From 1949 to August, 1974 the authors have personally treated 94 pa- tients with cutaneous melanoma of the head and neck. Lesions of the eye and mucous membranes were not included in this review. Patients with lentigo maligna (freckle of Hutchinson) were excluded as well. Only pa- tients whose therapy was instituted for potential cure were included. All patients were followed by the operat- ing surgeon, after surgical therapy. Forty-nine of these patients have been treated in the last 5 years and are not entered in 5-year survival statistics, but are included in the total series. The following general principles were used for therapy: 1) A total excisional biopsy of the melanoma was done wherever feasible. Larger lesions, particularly those clin- ically suspicious for lentigo maligna and lentigo maligna melanoma were diagnosed by a representative incisional biopsy.8'15 2) After the diagnosis of melanoma was confirmed, a wide and deep re-excision of the biopsy site was per- formed. In most instances, closure of the site of re- excision was achieved with the use of a split thickness or full thickness skin graft. 3) Regional lymph node dissections, "in continuity" with the primary lesion when possible, were done for invasive melanoma. Dissections were done not only when the nodes appeared to be positive by clinical evalu- ation, but for clinically uninvolved nodes as well. The contra-indications to elective regional lymph node dissection in this series of patients were: 1) The melanoma which was classified as superficial 86
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Melanoma of the head and neck

Melanoma of the Head and Neck
MATTHEW N. HARRIS, M.D., DANIEL F. ROSES, M.D., ALFRED T. CULLIFORD, M.D., STEPHEN L. GUMPORT, M.D.
A series of 94 patients with cutaneous malignant melanoma of thehead and neck region has been studied. Fifty-three of the patientshad regional lymph node dissections performed and the results in37 performed more than 5 years ago are presented. The policy ofelective lymph node dissection for invasive melanoma of the headand neck is strongly endorsed, although not proven by the datapresented in this limited series. Whenever possible, a total exci-sional biopsy should be performed to establish the diagnosis. It isrecommended that all melanomas be classified by the method ofClark and Mihm and that the level of invasion also be deter-mined. There is an appreciable error in the clinical evaluationof lymph nodes for metastases. In general, it is suggested thatelective regional lymph node dissections be performed for in-vasive melanoma (levels III, IV and V). The literature per-taining to cutaneous melanoma of the head and neck has beenreviewed and surgical and pathological problems peculiar tolesions of this region are emphasized.
HE HEAD and neck region has been reported to be themost common anatomic site for cutaneous malignant
melanoma.19 It would seem that lesions in an area soreadily visible would be detected at an early stage andtherefore have a more favorable prognosis. However,melanomas of the head and neck remain as difficult totreat as those found at other sites. Five year survivalfigures have ranged between 30% and 45% according toseveral collected series.1'3'49'32'34 A rationale for effectivetreatment has eluded most investigators to the presenttime. The recent interest in uniform clinical and his-tologic classification maiy offer criteria for delineatingappropriate therapy in individual cases. We have re-viewed our experience with cutaneous melanoma of thehead and neck with particular reference to such clinicaland histologic classification and have reviewed the ex-perience of others.
Submitted for publication February 12, 1975.This study was supported by the Sylvia and Mortimer Hyams Memo-
rial Fund.Reprint requests: Matthew N. Harris, M.D., New York University
Medical Center, 566 First Avenue, New York, N.Y., 10016.
From the Tumor Service, Department of Surgery, New YorkUniversity Medical Center, New York, New York
MethodsIn 1949 a study of malignant melanoma was initiated on
the Tumor Service of the Department of Surgery at theNew York University Medical Center. From 1949 toAugust, 1974 the authors have personally treated 94 pa-tients with cutaneous melanoma of the head and neck.Lesions of the eye and mucous membranes were notincluded in this review. Patients with lentigo maligna(freckle of Hutchinson) were excluded as well. Only pa-tients whose therapy was instituted for potential curewere included. All patients were followed by the operat-ing surgeon, after surgical therapy. Forty-nine of thesepatients have been treated in the last 5 years and are notentered in 5-year survival statistics, but are included inthe total series.The following general principles were used for therapy:1) A total excisional biopsy of the melanoma was done
wherever feasible. Larger lesions, particularly those clin-ically suspicious for lentigo maligna and lentigo malignamelanoma were diagnosed by a representative incisionalbiopsy.8'15
2) After the diagnosis of melanoma was confirmed, awide and deep re-excision of the biopsy site was per-formed. In most instances, closure of the site of re-excision was achieved with the use of a split thickness orfull thickness skin graft.
3) Regional lymph node dissections, "in continuity"with the primary lesion when possible, were done forinvasive melanoma. Dissections were done not onlywhen the nodes appeared to be positive by clinical evalu-ation, but for clinically uninvolved nodes as well.The contra-indications to elective regional lymph node
dissection in this series of patients were:1) The melanoma which was classified as superficial
86

MELANOMA OF THE HEAD AND NECK
(now defined as levels I & II). 2) The melanoma arising ina lentigo maligna (Freckle of Hutchinson) unless thelymph nodes were clinically positive. 3) A primary site sosituated that the lymphatic drainage might be to severaldifferent groups of regional lymph nodes. 4) The pres-ence of serious intercurrent disease. 5) The elderly pa-tient (70 years of age or over). 6) The presence of distantmetastases.
Fifty-three patients had regional lymph nodes dissec-tions performed. Thirty-eight patients had elective opera-tions (clinically negative nodes) and 15 had therapeuticprocedures (clinically positive nodes). There were nooperative mortalities.
In developing guidelines for the surgical treatment ofmelanoma, we are now using the clinical and histologicclassification of the disease as described by Clark, Mihmand associates.62627 Statistics regarding the success ofvarious therapeutic approaches would be meaninglesswithout a standard reference for pathologic classifica-tion. When considering melanoma of the head and neckparticularly, an increase in the frequency of lentigomaligna melanoma in any series will alter the resultsfavorably.
Clark has defined three types of malignant melanoma:1) Lentigo maligna melanoma (LMM) 2) Superficialspreading melanoma (SSM) 3) Nodular melanoma(NMM). Lentigo maligna melanoma and superficialspreading melanoma evolve through a long, relativelysuperficial phase which has been referred to as the cen-trifugal growth phase. During this phase, which can varyfrom one to 40 years, the tumors have a distinctive clini-cal appearance and, if removed at this time, a greaterthan 95% cure of affected patients may result. Nodularmelanoma has no such radial growth phase but starts itsgrowth directly in a vertical fashion.
Clinical and pathologic studies have indicated thatmalignant melanoma can be further classified accordingto levels of invasion. Five levels of invasion have beendescribed, ranging from level I where all the tumor cellsare above the base membrane (in situ melanoma) to levelV where the subcutaneous tissues are invaded. Experi-ence has shown a very low incidence of metastatic dis-ease in lentigo maligna melanoma and melanoma con-fined to the dermal-epidermal junction or papillary dermis(level I and level II).37 We have used levels of depth ofinvasion as one of our indications as to whether electiveregional lymph node dissections are performed. We donot do elective lymph node dissections for level I or levelII lesions but favor them for level III or deeperlesions. 11,13,14
Combination of classification type and level of inva-sion permits some precision in predicting the subsequentbehavior of a given group of malignant melanomas. Forexample: malignant melanoma of the superficial spread-
87
ing type at level II invasion, produces metastases inabout 8% of patients, while malignant melanoma of thenodular type at level V invasion probably causes death ingreater than 80o of the patients.35We perform radical neck dissection for invasive
melanoma (level III, IV, and V) whether or not regionalnodes are clinically involved. Microscopic deposits ofmetastatic disease in regional lymph nodes are not palpa-ble. When the pathologist reports the nodes to be nega-tive on random study of a so-called "prophylactic orelective lymph node dissection", serial sections may stillfind the nodes to be positive.23
Excisions in the head and neck region must be con-sidered differently than those on the trunk or extremities.In areas other than the head and neck we usually recom-mend a 3-5 cm margin from the tumor site for excisionwith inclusion of the underlying muscle fascia. On theface, there are several additional factors to be consid-ered: 1) Disfigurement with wide excision. 2) The pres-ence of the facial nerve on deeper dissection. 3) Thelymphatic drainage, especially in the parotid region. 4)The rich lymphatic and vascular network on the scalpand forehead. 5) The necessity for grafting on periosteumor even bare bone. In general, for wide excisions on theface a margin of 2-3 cm is used except on the scalp wherea margin of 5-6 cm is suggested.4 There is no one standardoperation for melanoma of the head and neck. Thetechnique for radical neck dissection has been well de-scribed in the literature.24'25'30 In addition, the surgeonmust be thoroughly familiar with the lymphatic drainageof the head and neck to adapt the operation for eachindividual location. Careful followup is essential to detectpossible reappearance of the melanoma, occurrence of asecond primary and the possibility of another, but differ-ent, neoplasm.
ResultsDuring the study a total of 94 patients with cutaneous
malignant melanoma of the head and neck were treatedsurgically. Fifty-three of these patients had a radical neckdissection for invasive melanoma. Thirty-seven of theneck dissections were performed more than 5 years ago.There was a 90% followup of these patients and all pa-tients dead from causes other than melanoma or lost tofollowup were counted as if they died from melanoma.An analysis of radical neck dissection for invasive
melanoma performed on 37 patients more than 5 yearsago is presented in Table 1. The following results areemphasized:
1) When the surgeon believed the regional lymphnodes to be negative clinically and after removal theywere reported by the pathologist on random sections tobe negative as well, 61% of these patients were alive andwell 5 years or more after their treatment.
2) Death of two patients in the category where the
Vol. 182 No. I

Ann. Surg. - July 1975HARRIS AND OTHERS
LaW L WITH RECUR. LOST DEAD TOTALNODES CLIN. E) 14 (61 %) 1( 4%) 2 ( 9%) 6 (26%) 23
MICROSCOPICALLYNEGATIVE CLIN. 0 0 0 1 (50%) 1 (50%) 2
TABLE 1. Results of Radi-cal Neck Dissection for In-vasive Melanoma (Opera-tions Over 5 Years Ago)
NODESMICROSCOPICALLY
POSITIVE
CLIN. e o
CLIN. @ 1 (17%)
DEATH FROM ALL CAUSES
0 0
0 0
40% OVER-ALL LaW
6 (100%) 6
5 (83%) 6
37
surgeon believed the regional lymph nodes to be positiveclinically, but after removal they were reported to benegative microscopically.
3) There were 6 patients in the group in which thesurgeon believed the regional lymph nodes to be negativeclinically but were reported as being microscopicallypositive. All are dead.
4) In the group in which the surgeon believed the re-
gional nodes to be clinically positive and were reported as
being microscopically positive as well, 17% of this smallseries were alive and well 5 years or more after thedefinitive surgery.Of the total number of patients who had a radical neck
dissection done more than 5 years ago, 40% are alive andwell. It is much too early to properly include the resultsin the 16 additional patients who had this procedure per-formed more recently.
Table 2 presents our errors in clinically assessing theinvolvement of lymph nodes in the neck with metastaticmelanoma. Of 34 patients in whom the nodes were ni-croscopically negative, two were considered positiveclinically, an error of 6%. Of 32 patients in whom thenodes were clinically negative, 6 were microscopicallypositive, an error of 19%.
Discussion
Although we believe that a wide and deep excision of amelanoma of the head and neck combined with radicallymph node dissection may control local disease andlymphatic spread there is no known control for thehematogenous spread of melanoma that has proven effec-tive. In this regard, one might speculate that local controlusing a rather extensive operative procedure in the headand neck region is not justified. It must be kept in mindthat recurrent disease in this area is particularly disablingand disfiguring. Several of our patients developed distantmetastases without evidence of local reappearance. Thequality of survival may be markedly improved if an
adequate local operation has been performed.We have reviewed the recent literature concerning the
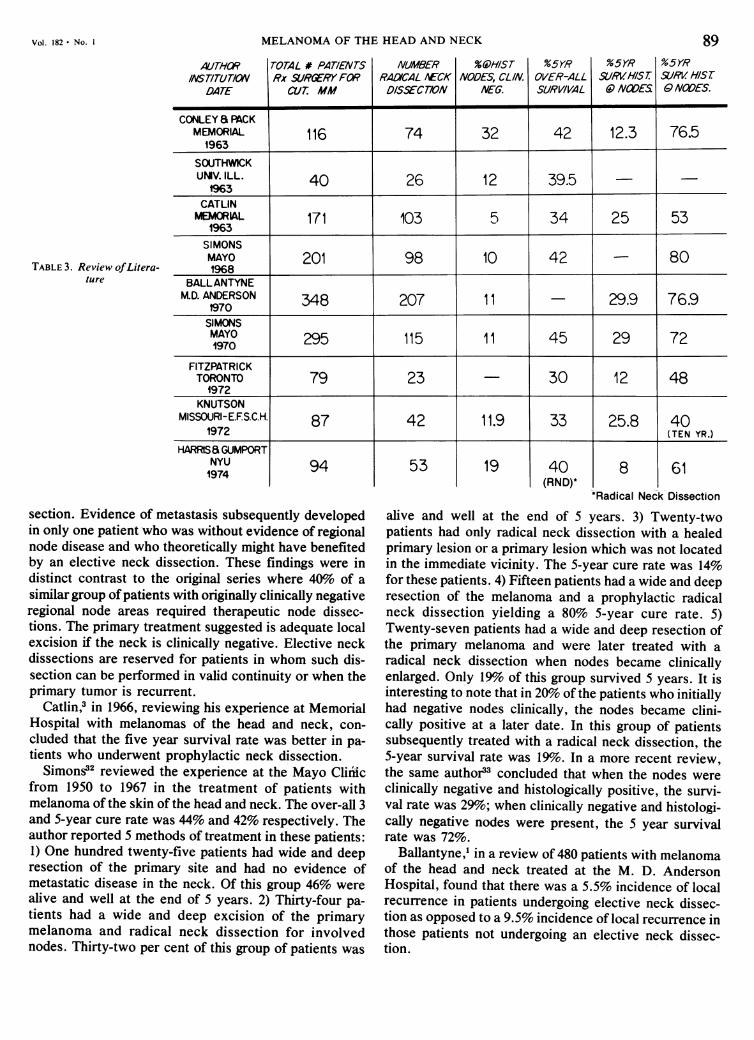
treatment of melanoma of the head and neck region andour results are not dissimilar to those of others (Table 3).
Kragh and Erich reporting on the Mayo Clinic ex-
perience22 in 1960 found that of the 63 patients who hadwide local excisions without neck dissection, 11 de-veloped local lymphatic metastases.Conley and Pack4 in 1963 reported an over-all 5-year
cure rate of 42%. Twenty-five per cent of their patientshad evidence of local recurrence because of inadequateprimary excision; 9.5% of the patients developed satel-litosis. On admission 48% had evidence of regionalmetastases on physical examination. The authors notedthat primary melanomas of the scalp area had the highestincidence of regional metastases (76%). Local recurrence
was highest in lesions of the scalp. The authors, there-fore, recommended a 5-6 cm margin for adequate primaryexcision in this area and stressed that all primary exci-sions should be accompanied by skin grafts. Eighteen per
cent of the patients developed systemic metastasis with-out evidence of regional involvement. A total of 74 radi-cal neck dissections were done. Forty-eight patients un-
derwent radical neck dissection for Stage II disease; thesurvival for this group of patients was 14 to 25%.
Southwick and associates34 in 1963 reviewed the ex-
perience at the University of Illinois with cutaneousmelanoma of the head and neck. No patient who had a
recurrent lesion and clinical evidence of regional nodedisease was without tumor for 5 years. Four of 9 patientswith metastatic disease and primary control survived.The prognosis for this group of patients was not signifi-cantly different from those who had an elective neck dis-
TABLE 2. Evaluation of Nodes in 53 Radical Neck Dissections
NODES-CLINICAL IMPRESSION
NODES- +
MICROSCOPIC
l9o of clinically negative nodes were microscopically positive.
13 6
2 32t
88
Vol. 182 No. I
AL/THORANSTITUTICN
DATE
TABLE 3. Review ofLitera-ture
MELANOMA OF THE HEAD AND NECK
TOTAL # PATIENTS NUMBER %WHISTRx SURIRY FOR RACVCAL AECK NODES, CL/N.
CUT. MM DISSECT/ON NEG.
%5YROVER-ALLSURVIVAL
5YRSURVHIST.0 NODES
89%5YRS-/V HISI6) NODES.
CONLEY a PACKMEMORIAL 116 74 32 42 12.3 76.5
'1963
SOUTHWICKUMV. ILL. 40 26 12 39.5 - -
1963
CATLINMEMORAL3 171 103 5 34 25 53
1963SIMONSMAYO 201 98 10 42 - 80
BALLANTYNEM.D. ANDERSON 348 207 11 - 29.9 76.9
1970SIMONSMAYO 295 115 11 45 29 721970
FITZPATRICKTORONTO 79 23 - 30 12 48
1972KNUTSON
1972OURI-E.S.C.H 87 42 11.9 33 25.8 401972 (TEN YR.)
HARRISa GUMPORTNYU1974 94
section. Evidence of metastasis subsequently developedin only one patient who was without evidence of regionalnode disease and who theoretically might have benefitedby an elective neck dissection. These findings were indistinct contrast to the original series where 40% of asimilar group ofpatients with originally clinically negativeregional node areas required therapeutic node dissec-tions. The primary treatment suggested is adequate localexcision if the neck is clinically negative. Elective neckdissections are reserved for patients in whom such dis-section can be performed in valid continuity or when theprimary tumor is recurrent.
Catlin,3 in 1966, reviewing his experience at MemorialHospital with melanomas of the head and neck, con-cluded that the five year survival rate was better in pa-tients who underwent prophylactic neck dissection.
Simons32 reviewed the experience at the Mayo Cliiiicfrom 1950 to 1967 in the treatment of patients withmelanoma of the skin of the head and neck. The over-all 3and 5-year cure rate was 44% and 42% respectively. Theauthor reported 5 methods of treatment in these patients:1) One hundred twenty-five patients had wide and deepresection of the primary site and had no evidence ofmetastatic disease in the neck. Of this group 46% werealive and well at the end of 5 years. 2) Thirty-four pa-tients had a wide and deep excision of the primarymelanoma and radical neck dissection for involvednodes. Thirty-two per cent of this group of patients was
53 19 40(RND)*
alive and well at the end of 5
8 61*Radical Neck Dissection
years. 3) Twenty-twopatients had only radical neck dissection with a healedprimary lesion or a primary lesion which was not locatedin the immediate vicinity. The 5-year cure rate was 14%for these patients. 4) Fifteen patients had a wide and deepresection of the melanoma and a prophylactic radicalneck dissection yielding a 80% 5-year cure rate. 5)Twenty-seven patients had a wide and deep resection ofthe primary melanoma and were later treated with aradical neck dissection when nodes became clinicallyenlarged. Only l9o of this group survived 5 years. It isinteresting to note that in 20% of the patients who initiallyhad negative nodes clinically, the nodes became clini-cally positive at a later date. In this group of patientssubsequently treated with a radical neck dissection, the5-year survival rate was 19%o. In a more recent review,the same author33 concluded that when the nodes wereclinically negative and histologically positive, the survi-val rate was 29%; when clinically negative and histologi-cally negative nodes were present, the 5 year survivalrate was 72%.
Ballantyne,1 in a review of 480 patients with melanomaof the head and neck treated at the M. D. AndersonHospital, found that there was a 5.5% incidence of localrecurrence in patients undergoing elective neck dissec-tion as opposed to a 9.5% incidence of local recurrence inthose patients not undergoing an elective neck dissec-tion.

HARRIS AND OTHERS
Fitzpatrick and associates,9 in 1972, reported their ex-perience in treating 79 patients with melanoma of thehead and neck. The authors found that survival corre-lated well with level of penetration, intensity of lym-phocytic reaction and presence or absence of marginalspread. The authors felt that except for well-lateralizedtumors, prophylactic neck dissection is unlikely to berewarding.
Knutson and associates,20 in 1972, reviewed their ex-
perience treating 87 patients with melanoma of the headand neck at the Ellis Fischel State Cancer Hospital. Theauthors felt that by statistical analysis there was a 40%chance that differences observed in survival at 5 years
among patients undergoing elective radical neck dissec-tion would not be reproducible and would be caused bychance. The propensity for superficial and invasivemelanomas to recur following local excision was
analyzed and the authors noted that the mean durationbetween diagnosis and recurrence for the superficialmelanomas was 33 months as compared to 12.3 months inthe invasive group.
Wayte and Helwig37 reviewed the Armed Forces Insti-tute of Pathology experience with 85 patients with a
melanotic freckle of Hutchinson. Most of these lesionswere between 1 and 3 cm in size and the authors corre-
lated larger lesions with the higher likelihood of discover-ing malignant melanoma (when the lesions were over 5cm in size there was a 75% chance of discoveringmelanoma in the lesion). The chance of a melanoticfreckle containing malignant melanoma is greatest whenthe lesion is located on the torso and least when it islocated in the head and neck region. Metastases do occur
with melanomas arising from such freckles and 4 patientsof 85 did develop metastatic disease. This low incidenceof metastatic disease with lentigo maligna melanoma ap-
pears to justify our conservative attitude in treating theselesions. In their series, fifty-three per cent of the melan-otic freckles did contain malignant melanoma. In thosepatients with melanoma arising from such freckles, the2-year survival was 85.7% and the 5-year survival was
73% when adequate followup was possible.Conley and associates,5 in 1971, described a variant of
malignant melanoma, the desmoplastic type. They de-scribed the initial lesion as an inconspicuous superficialpigmented lesion usually located in the head and neckregion. This was followed by a deep infiltrating tumefac-tion of fibrous consistency. The appearance of the infil-trating mass from the pigmented skin lesion was usuallybetween 6 months and 2 years. In most instances thisinfiltrating tumefaction was initially thought to representfibromatosis or fibrosarcoma histologically. The true na-
ture of the lesion was frequently revealed by examiningthe regional lymph nodes which were taken in a coinci-dental biopsy. Recurrent disease was usually manifestedby a local appearance of a large subcutaneous firm mass.
entity when a surgeon is confronted with a patient with astubbornly recurrent "fibroma" or "fibromatosis"which is associated with an antecedant inconspicuouspigmented lesion of the overlying skin. Use of electron-microscopy is suggested for accurate diagnosis. We havehad 5 such cases in our experience and confirm the find-ings of Conley.Pack and associates28 in 1970 reviewed 42 cases of
melanoma of the external ear comprising 14% of themelanomas of the head and neck area in their series.Thirty-three per cent had regional lymph node metas-tases when first seen.
Ward and Acquarelly of Los Angeles36 also reviewedtheir experience in treating malignant melanoma of theexternal ear. They reported that the ear is the site ofmalignant melanoma in approximately 1-10% of the re-ported cases of melanoma of the head and neck. The5-year survival for melanoma of the external ear is ap-proximately 22%. Melanomas in this site, as in other sitesof the body, cannot be diagnosed by their appearance.Expert dermatologists were screened in this regard andtheir diagnostic accuracy was only 48% in 169 cases. Theauthors felt that 10% disseminate by the hematogenousroute and an additional 17% disseminate by lymphaticand hematogenous routes in combination. They believedthat a 3-5 cm margin must be removed for adequateexcision in this location. It should be noted that in theirfour cases, the external auricle was totally removed totreat the primary lesion. They cited their preference forroutine treatment of melanomas in this location by radi-cal neck dissection because of the frequent involvementof regional lymph nodes and the fact that while correla-tion between clinically palpable nodes and histologic evi-dence of melanoma in the lymphatics is high, 16 to 50% ofclinically negative nodes contain microscopic malignan-cies. In addition, the true incidence of microscopicallypositive nodes may be underestimated since few speci-mens are submitted for thorough serial sections.Huvos and associates18 in 1973 reported on prognostic
factors in a retrospective study of 119 patients seen at theMemorial Cancer Center with cutaneous malignantmelanoma of the head and neck. The authors emphasizedthat ulceration of the surface of malignant melanoma isan ominous sign indicating that the melanoma cells haveactively penetrated the underlying dermis. Cellular typesshowed no prognostic significance in this study. Em-phasis was given to the need for establishing the depth ofinvasion of the lesion into the dermis and subcutaneoustissue in determining prognosis.A recent paper by Hanson and McCarten16 suggests
that the prognosis in malignant melanoma correlates wellwith the thickness of the lesion and the degree of lym-phocytic infiltration. The authors feel that for all Stage Ilesions less than 1.5 mm in vertical thickness, the mosteffective treatment could be local excision. For Stage I
The author stressed the importance of awareness of this
90 Ann. Surg. July 1975
lesions 1.5 mm or greater in thickness, the addition of

Vol. 182 * No. I MELANOMA OF THE HEAD AND NECK 91
elective node dissection offers significantly improvedsurvival; however, the most dramatic improvement oc-curred in those cases with minimal lymphocytic infiltra-tion. ConclusionsThe results of the surgical management of cutaneous
melanoma of the head and neck are far from satisfactory.The first line of defense is the detection and adequatetreatment of early lesions. In general, physicians, ancil-lary help and the public at large are unaware of thecharacteristic appearance of these tumors during theearly curable phase of the disease. It is believed thateducation of physicians and of the public could result in amarked reduction of mortality due to malignant melano-ma.
Criteria for clinical and histologic classification arenow available to help the surgeon select an appropriateoperation for each individual patient so as to achieve themaximum benefit with the least amount of "radical"surgery. The policy of elective lymph node dissection forinvasive superficial spreading and nodular melanoma ofthe head and neck (levels III, IV and V) is stronglyendorsed, although not proven by the data presented inthis limited series. However, our previous analysis of theresults of regional lymph node dissection for melanomaof all regions suggests that there is benefit to be obtainedfrom elective regional lymph node dissections performedselectively."1
In the years to come, surgery may evolve as a methodfor the prevention of local recurrence and the reductionof total tumor volume so that other agents may beemployed effectively as definitive therapy. Certainly theproblem of hematogenous dissemination is not solved.Reports concerning the use of immunotherapy2 7.1O021,29,31and chemotherapyl21 7 are encouraging. Adjuvanttherapy or postoperative therapy using one or both ofthese modalities in patients with "high-risk primaries"and Stage II disease may prove to be particularly impor-tant. Cooperative effort is needed since the treatment ofmelanoma may serve as a model for the treatment ofmany other neoplastic diseases.
References1. Ballantyne, A. J.: Malignant Melanoma of the Skin of the Head and
Neck. Am. J. Surg., 120:425, 1970.2. Bast, R. C. Jr., Zbar, B., Borsos, T., and Rapp, H. J.: BCG and
Cancer. N. Engl. J. Med., 290:1413 and 1458, 1974.3. Catlin, D.: Cutaneous Melanoma of the Head and Neck. Am. J.
Surg., 112:512, 1966.4. Clark. W. H., Jr., Lynn, F., Bernardino, E. A., and Mihm. M. C.:
The Histogenesis and Biologic Behavior of Primary HumanMalignant Melanomas of the Skin. Canc. Res., 29:705, 1969.
5. Conley, J. and Pack, G. T.: Melanoma of the Head and Neck. Surg.Gynecol. Obstet., 116:15, 1963.
6. Conley, J., Lattes, R. and Orr, W.: Desmoplastic MalignantMelanoma (A Rare Variant of Spindle Cell Melanoma). Cancer,28:914, 1971.
7. Einhorn, L. H., Burgess, M. A., Vallejos, C., et al.: PrognosticCorrelations and Response to Treatment in Advanced MetastaticMalignant Melanoma. Canc. Res., 34:1995, 1974.
8. Epstein, E., Bragg, K. and Linden, G.: Biopsy and Prognosis ofMalignant Melanoma. JAMA, 208:1369, 1969.
9. Fitzpatrick, P. J., Brown, T. C. and Reid, J.: Malignant Melanomaof the Head and Neck: a Clinicopathological Study. Can. J.Surg., 15:90, 1972.
10. Fudenberg, H. H., Levin, A. S., Spitler, L. E., et al.: TheTherapeutic Uses of Transfer Factor. Hosp. Prac., Jan: 95, 1974.
11. Gumport, S. L. and Harris, M. N.: Results of Regional LymphNode Dissection for Melanoma. Ann. Surg., 179:105, 1974.
12. Gutterman, J. V., Mavligit, G., Gottlieb, J. A., et al.: Chemoim-munotherapy of Disseminated Malignant Melanoma with Di-methyl Triazeno Imidazole Carboxamide and BacillusCalmette-Guerin. N. Engl. J. Med., 291:592, 1974.
13. Harris, M. N., Gumport, S. L. and Maiwandi, H.: Axillary LymphNode Dissection for Melanoma. Surg. Gynecol. Obstet.,135:936, 1972.
14. Harris, M. N., Gumport, S. L., Berman, I. R. and Bernard, R. W.:Ilioinguinal Lymph Node Dissection for Melanoma. Surg.Gynecol. Obstet., 136:33, 1973.
15. Harris, M. N. and Gumport, S. L.: Total Excision Biopsy forPrimary Malignant Melanoma. JAMA, 226:354, 1973.
16. Hansen, Mulloy G., McCarten and Alan D.: Tumor Thickness andLymphocytic Infiltration in Malignant Melanoma of the Headand Neck. Am. J. Surg., 128:557, 1974.
17. Hill, G. J., Ruess, R., Berris, R., et al.: Chemotherapy of MalignantMelanoma with DTIC and Nitrosurea Derivatives (BCNU,CCNU). Ann. Surg., 180:167, 1974.
18. Huvos, A. G., Mike, V., Donnellan, M. J., Seemayer, J., Strong,E. W.: Prognostic Factors in Cutaneous Melanoma of the Headand Neck. Am. J. Pathol., 71:33, 1973.
19. Knutson, C. O., Hori, J. M., Spratt, J. S., Jr.: Melanoma. CurrentProblems in Surgery, Year Book Medical Publishers, Inc., 1971.
20. Knutson, C. O., Hori, J. M. and Watson, F. R.: Melanoma of theHead and Neck. Am. J. Surg., 124:543, 1972.
21. Kragh, L. V. and Erich, J. B.: Malignant Melanomas of the Headand Neck. Ann'. Surg., 151:91, t960.
22. Krementz, E. T., Mansell, P. W. A., Horning, M. D., et al.:Immunotherapy of Malignant Disease: The Use of Viable Sen-sitized Lymphocytes or Transfer Factor Prepared from Sen-sitized Lymphocytes. Cancer, 33:394, 1974.
23. Lane, N., Lattes, R. and Malm, J.: Clinicopathological Correlationin a Series of One Hundred Seventeen Malignant Melanomas ofthe Skin of- Adults. Cancer, 11: 1025, 1958.
24. MacFee, W. F.: Transverse Incisions for Neck Dissection. Ann.Surg., 151:280, 1960.
25. Martin, H., DelValle, B., Ehrlich, H. and Cahan, W. G.: NeckDissection. Cancer, 4:441, 1951.
26. McGovern, V. J., Mihm, M. C. Jr., Bailly, C., et al.: The Classifi-cation of Malignant Melanoma and Its Histologic Reporting.Cancer, 32:1446, 1973.
27. Mihm, M. C., Clark, W. H., Jr. and From, L.: This Clinical Diag-nosis Classifications and Histogenic Concept of the Early Statusof Cutaneous Malignant Melanomas. N. EngI. J. Med., 284:1078,1971.
28. Pack, G. T., Conley, J. and Oropeza, R.: Melanoma of the ExternalEar. Arch. Otolaryng., 92:106, 1970.
29. Roenigk, H. H.: Immunotherapy of Malignant Melanoma. Derm.Digest, July 9, 1974.
30. Rush, B. F., Jr.: A Standard Technique for in Continuity Incisionsof the Head and Neck. Surg. Gynecol Obstet., 121:353, 1965.
31. Seigler, H. F., Shingleton, W. W., Metzgar, R. S., et al.: Im-munotherapy in Patients with Melanoma. Ann. Surg., 178:352,1973.
32. Simons, J. N.: Malignant Melanoma of the Head and Neck. Am. J.Surg., 116:494, 1968.
33. Simons, J. N.: Malignant Melanoma of the Head and Neck. Am. J.Surg., 124:485, 1972.
34. Southwick, H. W., Slaughter, D. P. and Hinkamp, J. F.: MalignantMelanomas of the Skin of the Head and Neck. Am. J. Surg.,106:852, 1963.
35. Unpublished data, Malignant Melanoma Cooperative Group, Au-gust, 1974.
36. Ward, N. 0. and Acquarelli, M. J.: Malignant Melanoma of theExternal Ear. Cancer, 21:226, 1968.
37. Wayte, D. M. and Helwig, E. B.: Melanotic Freckle of Hutchinson.Cancer. 21:893, 1968.




















