
Clinical results after different operative treatment methods of radial head and neck fractures
11
Clinical results after different operative treatment methods of radial head and neck fractures A systematic review and meta-analysis of clinical outcome J. Zwingmann *, M. Welzel, D. Dovi-Akue, H. Schmal, N.P. Su ¨ dkamp, P.C. Strohm Department of Orthopaedic and Trauma Surgery, University of Freiburg Medical Center, Hugstetter Straße 55, 79106 Freiburg, Germany Introduction Radial head fractures are common injuries of the elbow joint, with an incidence from 25 to 30 per 100,000 adults. 1,2 Severe fractures may result in major disability. 3 These fractures often occur secondary to an indirect axial force, such as that involved in motor vehicle accidents or falling on an outstretched hand. Studies and follow-up results are difficult to interpret because 30% of patients with a radial head fracture have associated injuries of the elbow. 4 The Mason classification is widely used to describe the radial head and neck fracture 5 and was modified by Broberg and Morrey 6 with type II fractures that have more than 2 mm of displacement, involving at least 30% of the radial head. Type III fractures are significantly comminuted. Johnston added a type IV fracture to the classification, which is a radial head or neck fracture associated with an elbow dislocation. 3 There is no consensus on the best treatment therapy for Mason– Johnston Classification types II–IV fractures. Therefore, the aim of this systematic review was evaluate the best available evidence on this topic. Conservative management of displaced intra-articular fractures of the radial head could lead to loss of function from immobilization of the elbow joint or from malunion. Moreover a post-traumatic arthritis could be developed. It is generally agreed that fractures with no relevant displacement (Mason Type I) should be treated conservatively. 7 For type II fractures, there is no general agreement in the literature on the superiority of surgical or conservative treatment. Type III fractures are commonly treated with surgery. Several surgical treamtent options are described as follows: ORIF (open reduction and internal fixation) with screws, plates, k-wires or biodegradable (polylactide) pins, implantation of a prosthesis or resection of the radial head. Injury, Int. J. Care Injured xxx (2013) xxx–xxx A R T I C L E I N F O Article history: Accepted 1 April 2013 Keywords: Radial head fracture Radial neck fracture Meta-analysis Systematic review Mason classification A B S T R A C T Introduction: There is no consensus on optimal treatment strategy for Mason type II–IV fractures. Most recommendations are based upon experts’ opinion. Methods: An OVID-based literature search were performed to identify studies on surgical treatment of radial head and neck fracture. Specific focus was placed on extracting data describing clinical efficacy and outcome by using the Mason classification and including elbow function scores. A total of 841 clinical studies were identified describing in total the clinical follow-up of 1264 patients. Results: For type II radial head and neck fractures the significant best treatment option seems to be ORIF with an overall success rate of 98% by using screws or biodegradable (polylactide) pins. ORIF with a success rate of 92% shows the best results in the treatment of type III fractures and seem to be better than resection and implantation of a prosthesis. For this fracture type the ORIF with screws (96%), biodegradable (polylactide) pins (88%) and plates (83%) showed the best results. In the treatment of type IV fractures similar results could be found with a tendency of the best results after ORIF followed by resection and implantation of a prosthesis. If a prosthesis was implanted, the primary implantation seems to be associated with a better outcome after type III (87%) and IV (82%) fractures compared to the results after a secondary implantation. Discussion: Recommendations for surgical treatment of radial head and neck fractures according to the Mason classification can now be given with the best available evidence. Level of evidence: IV ß 2013 Elsevier Ltd. All rights reserved. * Corresponding author. Tel.: +49 761 270 63670; fax: +49 761 270 63680. E-mail addresses: [email protected] (J. Zwingmann), [email protected] (M. Welzel), [email protected] (D. Dovi-Akue), [email protected] (H. Schmal), [email protected] (N.P. Su ¨ dkamp), [email protected] (P.C. Strohm). G Model JINJ-5353; No. of Pages 11 Please cite this article in press as: Zwingmann J, et al. Clinical results after different operative treatment methods of radial head and neck fractures. Injury (2013), http://dx.doi.org/10.1016/j.injury.2013.04.003 Contents lists available at SciVerse ScienceDirect Injury jo ur n al ho m epag e: ww w.els evier .c om /lo cat e/inju r y 0020–1383/$ – see front matter ß 2013 Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.injury.2013.04.003
-
Upload
southerndenmark -
Category
Documents
-
view
0 -
download
0
Transcript of Clinical results after different operative treatment methods of radial head and neck fractures
Injury, Int. J. Care Injured xxx (2013) xxx–xxx
G Model
JINJ-5353; No. of Pages 11
Clinical results after different operative treatment methods of radialhead and neck fracturesA systematic review and meta-analysis of clinical outcome
J. Zwingmann *, M. Welzel, D. Dovi-Akue, H. Schmal, N.P. Sudkamp, P.C. Strohm
Department of Orthopaedic and Trauma Surgery, University of Freiburg Medical Center, Hugstetter Straße 55, 79106 Freiburg, Germany
A R T I C L E I N F O
Article history:
Accepted 1 April 2013
Keywords:
Radial head fracture
Radial neck fracture
Meta-analysis
Systematic review
Mason classification
A B S T R A C T
Introduction: There is no consensus on optimal treatment strategy for Mason type II–IV fractures. Most
recommendations are based upon experts’ opinion.
Methods: An OVID-based literature search were performed to identify studies on surgical treatment of
radial head and neck fracture. Specific focus was placed on extracting data describing clinical efficacy
and outcome by using the Mason classification and including elbow function scores.
A total of 841 clinical studies were identified describing in total the clinical follow-up of 1264
patients.
Results: For type II radial head and neck fractures the significant best treatment option seems to be ORIF
with an overall success rate of 98% by using screws or biodegradable (polylactide) pins.
ORIF with a success rate of 92% shows the best results in the treatment of type III fractures and seem
to be better than resection and implantation of a prosthesis. For this fracture type the ORIF with screws
(96%), biodegradable (polylactide) pins (88%) and plates (83%) showed the best results.
In the treatment of type IV fractures similar results could be found with a tendency of the best results
after ORIF followed by resection and implantation of a prosthesis.
If a prosthesis was implanted, the primary implantation seems to be associated with a better outcome
after type III (87%) and IV (82%) fractures compared to the results after a secondary implantation.
Discussion: Recommendations for surgical treatment of radial head and neck fractures according to the
Mason classification can now be given with the best available evidence.
Level of evidence: IV
� 2013 Elsevier Ltd. All rights reserved.
Contents lists available at SciVerse ScienceDirect
Injury
jo ur n al ho m epag e: ww w.els evier . c om / lo cat e/ in ju r y
Introduction
Radial head fractures are common injuries of the elbow joint,with an incidence from 25 to 30 per 100,000 adults.1,2 Severefractures may result in major disability.3 These fractures often occursecondary to an indirect axial force, such as that involved in motorvehicle accidents or falling on an outstretched hand. Studies andfollow-up results are difficult to interpret because 30% of patientswith a radial head fracture have associated injuries of the elbow.4
The Mason classification is widely used to describe the radialhead and neck fracture5 and was modified by Broberg and Morrey6
with type II fractures that have more than 2 mm of displacement,
* Corresponding author. Tel.: +49 761 270 63670; fax: +49 761 270 63680.
E-mail addresses: [email protected] (J. Zwingmann),
[email protected] (M. Welzel), [email protected]
(D. Dovi-Akue), [email protected] (H. Schmal),
[email protected] (N.P. Sudkamp),
[email protected] (P.C. Strohm).
Please cite this article in press as: Zwingmann J, et al. Clinical results affractures. Injury (2013), http://dx.doi.org/10.1016/j.injury.2013.04.0
0020–1383/$ – see front matter � 2013 Elsevier Ltd. All rights reserved.
http://dx.doi.org/10.1016/j.injury.2013.04.003
involving at least 30% of the radial head. Type III fractures aresignificantly comminuted. Johnston added a type IV fracture to theclassification, which is a radial head or neck fracture associatedwith an elbow dislocation.3
There is no consensus on the best treatment therapy for Mason–Johnston Classification types II–IV fractures. Therefore, the aim ofthis systematic review was evaluate the best available evidence onthis topic. Conservative management of displaced intra-articularfractures of the radial head could lead to loss of function fromimmobilization of the elbow joint or from malunion. Moreover apost-traumatic arthritis could be developed. It is generally agreedthat fractures with no relevant displacement (Mason Type I)should be treated conservatively.7 For type II fractures, there is nogeneral agreement in the literature on the superiority of surgical orconservative treatment. Type III fractures are commonly treatedwith surgery. Several surgical treamtent options are described asfollows: ORIF (open reduction and internal fixation) with screws,plates, k-wires or biodegradable (polylactide) pins, implantation ofa prosthesis or resection of the radial head.
ter different operative treatment methods of radial head and neck03

J. Zwingmann et al. / Injury, Int. J. Care Injured xxx (2013) xxx–xxx2
G Model
JINJ-5353; No. of Pages 11
Very little is known about the clinical outcomes after differenttreatment methods, and the number of patients included in eachstudy are quite small. Moreover, the optimal type of surgery is notyet identified.6,8–10 ORIF of radial head fractures is believed to besuperior to radial head resection for the treatment of unstable,displaced fractures of the radial head (in terms of strength), theinitial stability of the forearm and elbow, and the later develop-ment of arthritis.11–15 The absence of radiocapitellar contact hasbeen associated with the development of ulnohumeral arthrosis inlong-term retrospective case series.16,17 However, without com-parative concurrent prospective controls treated with ORIF orprosthetic arthroplasty, the influence of radiocapitellar contact isstill debatable.
Nevertheless, scientific evidence seems limited. Most recom-mendations are based upon expert opinions. This presentsystematic review and meta-analysis was conducted to evaluatethe best available evidence for surgical treatment of radial headand neck fractures using the Mason–Johnston Classification forclinical practice.
Materials and methods
This systematic review and meta-analysis was based on anOVID-based literature search. Here all published clinical studies onthe surgical treatment of radial head and neck fractures were foundin the following databases: MEDLINE, MEDLINE preprints,EMBASE, CINAHL, Life Science Citations, the British NationalLibrary of Health, and the Cochrane Central Register of ControlledTrials (CENTRAL). The time period for the search was from January1st, 1948 to February 1st, 2011. The literature searching wasperformed on February 21st, 2011 and the following systematicstrategy was used:
(1) Radius fractures; (2) (radial adj3 head).mp.; (3) (radial adj3neck).mp.; (4) (radius adj3 head).mp.; (5) (radius adj3 neck).mp.;(6) 2 or 3 or 4 or 5; (7) 1 and 6; (8) (radial adj3 head adj3fracture*).mp.; (9) (radius adj3 head adj3 fracture*).mp.; (10)(radial adj3 neck adj3 fracture*).mp.; (11) (radius adj3 neck adj3fracture*).mp.; (12) 8 or 9 or 10 or 11; (13) 12 not 7; (14) 7 or 13.
Methods of the analysis and the inclusion criteria werespecified in advance and documented in a protocol. Any studyreporting clinical information on operative treatment of radialhead and neck fractures was considered potentially relevant andselected for primary review.
A total of 841 clinical studies on the operative treatment ofradial head and neck fractures were identified. Abstracts for all841 studies were evaluated in a primary screening by 2independent reviewers using the inclusion and exclusion criteriapresented in Table 1. Afterwards, 2 independent reviewerssystemically recorded data from 231 studies on the characteristicsand design, level of evidence, demographic parameters, fractureclassification, surgical technique and rehabilitation protocol,associated operative procedures, clinical follow-up, and treat-ment outcome scores. A specific analysis was performed onextracting data describing clinical efficacy after radial head andneck fractures using the Mason–Johnston Classification andincluding elbow function scores. The level of evidence wasclassified according to the definition given by the Oxford Centrefor Evidence-based Medicine.18 All prospective, randomised,controlled studies (Levels I and II) and all prospective orretrospective studies with or without control groups (Levels IIIand IV) were accepted for inclusion into the study if they providedclinical outcome measures of the elbow with a follow-up of morethan 1 year after surgery. Studies with follow-up rates less than70% were excluded to reduce transfer and exclusion bias.
A total of 58 clinical studies were identified and were evaluatedin a primary screening by 2 independent medical investigators,
Please cite this article in press as: Zwingmann J, et al. Clinical results affractures. Injury (2013), http://dx.doi.org/10.1016/j.injury.2013.04.0
who systemically extracted data on study characteristics anddesign, level of evidence, demographic parameters, fractureclassification, surgical technique and rehabilitation protocol,associated surgical procedures, clinical follow-up, and treatmentoutcomes. Specific focus was placed on extracting data describingthe clinical efficacy of operative treatment, including elbowfunction scores. All participants had to be >14 years of age, andonly studies reporting on operative treatment were included.
To assess the methodological quality, the modified ColemanMethodology Scores and subscales were determined for eachincluded study19,20 with the assigning subscores to 10 specificcriteria. Studies were analysed by assigning a score for eachcriterion, with a score between 0 and 100. A score of 100 indicatesthe highest study quality. The modified Coleman MethodologyScore has been used previously to analyse methodological qualityin other published studies.21,22
In total, 12 different outcome parameters have been used in theincluded studies. Functional outcome measures implicated in thereviewed studies included the following scores, which were allvalidated:
16� Mayo Elbow Performance Score (MEPS),23 15� Broberg andMorrey Index (BMI),16 4� Score by Radin Riseborough (RR),24 3�Morrey Score,23 3� modifications of the Morrey Score,25,26 1�Radin Riseborough Score modified by Mackay et al.,27 1� ScoringSystem of Mikic et al.,28 1� Elbow Function Assessment Scale(EFA),29 1� E.S.S.S.E Score,30 1� Score by Steinberg et al.,31 1�Score by Harrington et al.,32 1� Score by Steinhauser et al.33
In each individual score, ‘‘good’’ and ‘‘excellent’’ results wereidentified according to the recommendations given by the authors ofthe individual score. The percentage of ‘‘good’’ and ‘‘excellent’’results was considered the ‘‘success rate’’ and was reported as such.
Outcomes in the present systematic review were analyseddepending on the fracture type according to the Mason–JohnstonClassification as well as depending on the surgical techniqueapplied. Because various modifications of surgical principles wereperformed in the studies included in the present article, thesurgical techniques were categorised into major treatment sub-groups based on different therapeutic approaches: ‘‘Conservativetreatment, resection, ORIF (open reduction internal fixation), andradial head prosthesis’’. Additionally, the ORIF and prosthesisgroups were split into subgroups based on the specific treatment(e.g., ORIF with screws only). Specific meta-analyses wereperformed in these subgroups.
The data were independently checked against the originalpapers in an unblended, standardised manner by 2 reviewersusing a standard quality-control procedure. Any differences ofopinion between the original reviewer and the quality controlreviewer were resolved by discussion and reference to the studypaper and a consensus was achieved. The data were analysedusing established statistical software (SPSS software Version 17.0,R-Project 2.15.0, package ‘meta’ by G. Schwarzer). The analysedstandard deviations were computed for the reported means perpaper. This analysis took possible study effects into account, and arandom-effects model was used for statistical analysis. For allmeta-analyses, tests for differences between subgroups wereperformed. The results are given as p-values. Significant p-valuesindicate an existing difference in the summary interventioneffects between subgroups. Furthermore, taking the quantity ofstatistical heterogeneity between studies into account, values of I2
were calculated for each subgroup.
Results
All inclusion and exclusion criteria were set a priori (Table 1).According to the above criteria, 610 of the 841 studies wereexcluded from the present systematic review, leading to a total of
ter different operative treatment methods of radial head and neck03

Table 1Reasons for drop out and number of remaining studies for further analysis.
841 clinical studies were identified after the search strategy for medical databases
Primary screening by 2 independent reviewers
Inclusion criteria: All clinical studies about treatment and outcome of radial head and radial neck fractures.
Exclusion criteria: Reviews, Case Reports, epidemiological studies, radiological studies, biomechanical/cadaveric studies, studies about operative technique
231 studies met primary inclusion criteria
Secondary screening by 2 independent reviewers with full-text articles
Number of studies and reasons for drop out:
39 Children <14
29 No sub-divison of outcomes after treatment and fracture classification
18 No Mason-Johnston modification applied or appliable
16 Children and Adults not subdivided
13 Language other than English or German
11 No specific outcome
8 Classification unclear
7 Surgical technique
6 Review articles
5 Case report
5 Conflicting data
4 No fracture
4 Age not reported
4 No Outcome, just recommendations
3 Follow-up time ≤ 12 months
1 Presentation
58 remaining studies for further analysis
The reasons for dropout and the number of remaining studies for further analysis after the primary and secondary screening processes.
J. Zwingmann et al. / Injury, Int. J. Care Injured xxx (2013) xxx–xxx 3
G Model
JINJ-5353; No. of Pages 11
231 studies for further evaluation. After secondary review of thefull text, an additional 173 studies were excluded for reasons givenin Table 1. The remaining 58 studies were included in the presentanalysis.
Characteristics of included patients
A total of 58 studies, split into 144 study-subgroups, wereincluded in this systematic review. In total, the studies describedthe clinical follow-up of 1264 patients. The average postoperative
Please cite this article in press as: Zwingmann J, et al. Clinical results affractures. Injury (2013), http://dx.doi.org/10.1016/j.injury.2013.04.0
follow-up was 67.5 months (range 12.5–408). The mean number ofstudy-subgroup subjects was 8.8 � 9.0 (range 1–62 patients). Theaverage age of the individuals ranged from 14 to 84 years of age(mean 40.5 � 8.5 years). In 97 study-subgroups (n = 709), the genderdistribution was reported, with a total of 384 men (54.2%) and 325female (45.8%). In total, 845 surgically treated radial head and neckfractures could be evaluated in the meta-analysis. The Mason–Johnston Classification was used for all 1264 cases with the followingnumbers for each type: I = 169 (13.4%), II = 338 (26.7%), III = 373(29.5%) and IV = 384 (30.4%).
ter different operative treatment methods of radial head and neck03
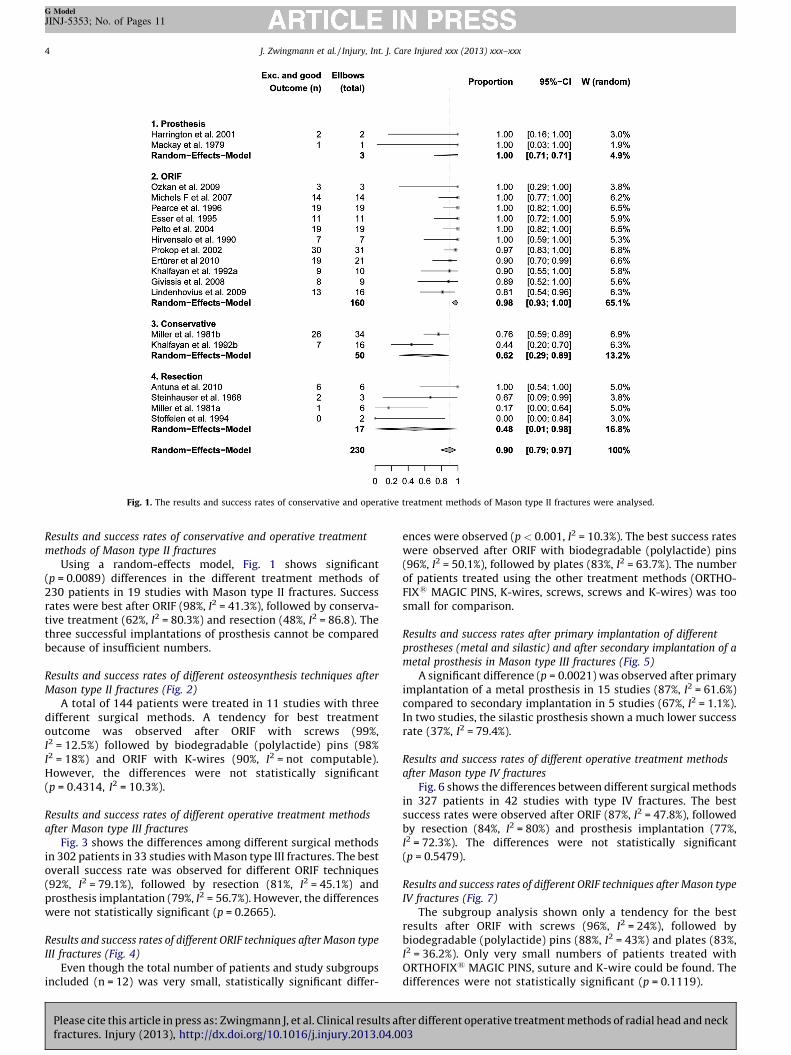
Fig. 1. The results and success rates of conservative and operative treatment methods of Mason type II fractures were analysed.
J. Zwingmann et al. / Injury, Int. J. Care Injured xxx (2013) xxx–xxx4
G Model
JINJ-5353; No. of Pages 11
Results and success rates of conservative and operative treatment
methods of Mason type II fractures
Using a random-effects model, Fig. 1 shows significant(p = 0.0089) differences in the different treatment methods of230 patients in 19 studies with Mason type II fractures. Successrates were best after ORIF (98%, I2 = 41.3%), followed by conserva-tive treatment (62%, I2 = 80.3%) and resection (48%, I2 = 86.8). Thethree successful implantations of prosthesis cannot be comparedbecause of insufficient numbers.
Results and success rates of different osteosynthesis techniques after
Mason type II fractures (Fig. 2)
A total of 144 patients were treated in 11 studies with threedifferent surgical methods. A tendency for best treatmentoutcome was observed after ORIF with screws (99%,I2 = 12.5%) followed by biodegradable (polylactide) pins (98%I2 = 18%) and ORIF with K-wires (90%, I2 = not computable).However, the differences were not statistically significant(p = 0.4314, I2 = 10.3%).
Results and success rates of different operative treatment methods
after Mason type III fractures
Fig. 3 shows the differences among different surgical methodsin 302 patients in 33 studies with Mason type III fractures. The bestoverall success rate was observed for different ORIF techniques(92%, I2 = 79.1%), followed by resection (81%, I2 = 45.1%) andprosthesis implantation (79%, I2 = 56.7%). However, the differenceswere not statistically significant (p = 0.2665).
Results and success rates of different ORIF techniques after Mason type
III fractures (Fig. 4)
Even though the total number of patients and study subgroupsincluded (n = 12) was very small, statistically significant differ-
Please cite this article in press as: Zwingmann J, et al. Clinical results affractures. Injury (2013), http://dx.doi.org/10.1016/j.injury.2013.04.0
ences were observed (p < 0.001, I2 = 10.3%). The best success rateswere observed after ORIF with biodegradable (polylactide) pins(96%, I2 = 50.1%), followed by plates (83%, I2 = 63.7%). The numberof patients treated using the other treatment methods (ORTHO-FIX1 MAGIC PINS, K-wires, screws, screws and K-wires) was toosmall for comparison.
Results and success rates after primary implantation of different
prostheses (metal and silastic) and after secondary implantation of a
metal prosthesis in Mason type III fractures (Fig. 5)
A significant difference (p = 0.0021) was observed after primaryimplantation of a metal prosthesis in 15 studies (87%, I2 = 61.6%)compared to secondary implantation in 5 studies (67%, I2 = 1.1%).In two studies, the silastic prosthesis shown a much lower successrate (37%, I2 = 79.4%).
Results and success rates of different operative treatment methods
after Mason type IV fractures
Fig. 6 shows the differences between different surgical methodsin 327 patients in 42 studies with type IV fractures. The bestsuccess rates were observed after ORIF (87%, I2 = 47.8%), followedby resection (84%, I2 = 80%) and prosthesis implantation (77%,I2 = 72.3%). The differences were not statistically significant(p = 0.5479).
Results and success rates of different ORIF techniques after Mason type
IV fractures (Fig. 7)
The subgroup analysis shown only a tendency for the bestresults after ORIF with screws (96%, I2 = 24%), followed bybiodegradable (polylactide) pins (88%, I2 = 43%) and plates (83%,I2 = 36.2%). Only very small numbers of patients treated withORTHOFIX1 MAGIC PINS, suture and K-wire could be found. Thedifferences were not statistically significant (p = 0.1119).
ter different operative treatment methods of radial head and neck03

Fig. 2. The results and success rates of different osteosynthesis techniques after Mason type II fractures were analysed.
Fig. 3. The results and success rates of different operative treatment methods after Mason type III fractures were analysed.
J. Zwingmann et al. / Injury, Int. J. Care Injured xxx (2013) xxx–xxx 5
G Model
JINJ-5353; No. of Pages 11
Please cite this article in press as: Zwingmann J, et al. Clinical results after different operative treatment methods of radial head and neckfractures. Injury (2013), http://dx.doi.org/10.1016/j.injury.2013.04.003

Fig. 4. The results and success rates of different ORIF techniques after Mason type III fractures were analysed.
Fig. 5. The results and success rates after primary implantation of different prostheses (metal and silastic) and after secondary implantation of metal prostheses in Mason type
III fractures were analysed.
J. Zwingmann et al. / Injury, Int. J. Care Injured xxx (2013) xxx–xxx6
G Model
JINJ-5353; No. of Pages 11
Please cite this article in press as: Zwingmann J, et al. Clinical results after different operative treatment methods of radial head and neckfractures. Injury (2013), http://dx.doi.org/10.1016/j.injury.2013.04.003

Fig. 6. The results and success rates of different operative treatment methods after Mason type IV fractures were analysed.
J. Zwingmann et al. / Injury, Int. J. Care Injured xxx (2013) xxx–xxx 7
G Model
JINJ-5353; No. of Pages 11
Results and success rates of primary implantation of different
prostheses (metal and silastic) and secondary implantation of metal
prosthesis after Mason type IV fractures (Fig. 8)
The primary implantation of a metal prosthesis seems tobe associated with a better outcome in 18 studies (82%,I2 = 55.1%) compared to outcomes in 5 studies after secondaryimplantation (76%, I2 = 56.4%) (p = 0.217). A lower success ratewas observed in three studies with the silastic prosthesis (28%,I2 = 89.2%).
Results of the Coleman Methodology Score for the 58 included studies
Table 2
.
Summary
For type II radial head and neck fractures, ORIF seems to be thebest treatment option, with an overall success rate of 98% usingscrews or biodegradable (polylactide) pins.
Please cite this article in press as: Zwingmann J, et al. Clinical results affractures. Injury (2013), http://dx.doi.org/10.1016/j.injury.2013.04.0
Moreover, ORIF, with a success rate of 92%, demonstrates thebest results for the treatment of type III fractures and seems to besuperior to resection and prosthesis implantation. In this group,ORIF with screws (96%), biodegradable (polylactide) pins (88%) andplates (83%) had the best results.
In the treatment of type IV fractures, similar results wereobserved with a tendency of the best results after ORIF, followed byresection and prosthesis.
For prosthesis implantation, primary implantation seems to beassociated with a better outcome after type III (87%) and IV (82%)fractures compared to the results after secondary implantation.
Discussion
The purpose of this study was to evaluate the best availableevidence for the stage-dependent treatment of radial head andneck fractures according to the Mason–Johnston classification. Themost important finding was that although various algorithms aresuggested by different experts for the stage-dependent treatment
ter different operative treatment methods of radial head and neck03

Fig. 7. The results and success rates of different ORIF techniques after Mason type IV fractures were analysed.
Fig. 8. The results and success rates of primary implantation of different prostheses (metal and silastic) and secondary implantation of metal prostheses after Mason type IV
fractures were analysed.
J. Zwingmann et al. / Injury, Int. J. Care Injured xxx (2013) xxx–xxx8
G Model
JINJ-5353; No. of Pages 11
Please cite this article in press as: Zwingmann J, et al. Clinical results after different operative treatment methods of radial head and neckfractures. Injury (2013), http://dx.doi.org/10.1016/j.injury.2013.04.003

Table 2Results of the Coleman Methodology Score (CMS).
Max
CMS
Mean
score
SD Range
Part A 60 26.5 7.4 13–15
(1) Study size 10 1.9 2.6 0–10
(2) Follow up 5 4.6 1.2 0–5
(3) Surgical procedures (n) 10 8.2 3.7 0–10
(4) Type of study 15 1.3 3.6 0–15
(5) Diagnostic certainty 5 5.0 0 5–5
(6) Description of surgical technique 5 4.5 1.2 3–10
(7) Description of post-op
rehabilitation
10 1.1 3.1 0–10
Part B 40 18.4 2.8 12–24
(1) Outcome criteria 10 6.1 1.8 0–7
(2) Procedure for assessing outcome 15 5.6 1.5 4–9
(3) Despriction of subject
selection process
15 12.2 3.7 5–15
Coleman Methodology Score (parts A + B) 100 44.8 8.5 30–70
Table shows the overall Coleman Methodology Score of the 58 included studies.
J. Zwingmann et al. / Injury, Int. J. Care Injured xxx (2013) xxx–xxx 9
G Model
JINJ-5353; No. of Pages 11
of radial head and neck fractures, there is a lack of scientificevidence for surgical treatment of these radial fractures.
A total of 58 studies reporting clinical outcomes of 1264patients were included. The mean follow up for the entirepopulation reported in this review was 67.5 months (range12.5–408). Patient characteristics seem to be representative ofradial head and neck fractures.
Although all studies included reported clinical outcomesfollowing surgical treatment can be considered ‘‘interventional’’studies, the vast majority of the studies identified are ‘‘caseseries’’ without control groups. Therefore, the studies representan evidence level of IV. There was only one randomised andcontrolled trial,34 one retrospective prognostic study with a levelof evidence of II35 and five case-control studies with a level of III.This left 51 case-series (7 prospective, 44 retrospective) withlevel IV, which demonstrates the low overall evidence grade.Thus, concerning the overall quality of the present meta-analysis,the quality of the investigated published data was poor. With theinclusion criteria of a follow-up �1year and follow-up rates�70%, most of the 841 studies initially found had to be excluded.Of the remaining 231 studies, sufficient evidence could only befound in 58 (Table 1).
As a result of our method of splitting the data into studysubgroups according to the Mason–Johnston Classification andspecific therapy, the number of treated patients for each studybecame very small. In the investigated study subgroups, theaverage number of patients included was only 8.8 (�9), with amaximum of 62 patients. The variety of scoring systems used (intotal, 12 different scoring systems for patient evaluation) furtherdemonstrates that in the functional assessment of the elbow jointthere are no standardised scores that are routinely used by themajority of the authors. The average Coleman Methodology Score ofthe studies included in the present review was 44.8 (�8.5) points.The highest subscores were found for surgical technique, diagnosticcertainty, patient selection process, follow-up and concomitantsurgical procedures, while the lowest subscores were evaluated forstudy size and study design.
The purpose of this study was to describe the availableliterature on clinical outcomes following surgical treatment ofradial head and neck fractures and to draw the best possibleconclusion based upon the best evidence available. Therefore, theprimary outcome parameter of the present review was defined asthe clinical outcome and success rate of the individual surgicaltechnique applied. ‘‘Success’’ has been defined as a ‘‘good’’ or‘‘excellent’’ outcome according to the individual scoring systemused in the present study. This approach has been chosen because a
Please cite this article in press as: Zwingmann J, et al. Clinical results affractures. Injury (2013), http://dx.doi.org/10.1016/j.injury.2013.04.0
great variety of different scoring systems have been used in theincluded studies. The methodology is similar to recently publishedmeta-analysis on related subjects.20,22 This methodology and thevariety of surgical techniques described, along with differentstages of the Mason–Johnston Classification, make a quantitativecomparison of different approaches difficult. To achieve thehighest quality in our analysis of the data, the authors usedthe random-effects model. In contrast to the fixed-effects model,the random-effects model incorporates heterogeneity. This modeltakes into account that intervention effects across studies naturallydiverge, but follow some distribution. If this variance exceedsnatural heterogeneity, statistical heterogeneity is present. Thismay due to the mostly inevitable methodological and clinicaldifferences between studies. To incorporate this problem, wecomputed values of I2. Nevertheless, there is no consensus aboutwhen statistical heterogeneity is too grave to pool together theintervention effects across studies.36
When treatment of radial head and neck fractures is analysed,different associated injuries should also be taken into accountbecause it seems likely that these elbow fractures (of the humerus,the ulna and/or radius) also influences surgical outcome. Further-more, this might also overlay outcome of different surgicaltechniques as described in the present meta-analysis as alimitation of this study. Details on surgical approaches dependingon treatment outcome are not described carefully in the vastmajority of the studies included. The principal goal of treatment isto maintain good elbow function and, thus, to retain adequatemotion and joint stability. In general, the treatment of radial headfractures is based on the fracture type and the presence of anyassociated injury.23 There is no doubt that radial head fractureswith no or minimal displacement should be treated conservatively.
Mason type II fractures
Early studies advocated either conservative management orresection of the radial head as the standard treatments for type IIfractures.23,37 As knowledge was growing, the understanding ofthe functional importance of the radial head as a secondarystabilizer to valgus stress and, as an axial weight-bearing structure,led to the better understanding of its biomechanics and dictatedtreatment options. Currently, several techniques have beenintroduced based on the specific type (degree of displacement)of fracture being treated, but the optimal choice of treatment andsurgery is still today controversial.7 ORIF could a choice of surgicaltreatment when a mechanical block of motion exist or the radialhead fracture led to a destruction of more than 1/3 of the articularsurface. Moreover the fracture displacement of �2 mm or arelevant depression of the articular surface, a huge lesion of thecartilage, an additional proximal ulnar fracture, an additionalrupture of the ulnar collateral ligament or an injury of the distalradioulnar joint could be an indication for ORIF.7
Currently internal fixation has become popular becausecontemporary techniques have improved surgical outcomes andAO mini-screws and mini-plates, (Synthes, Paoli, PA), Herbertscrews (Zimmer, Warsaw, Ind.), and biodegradable (polylactide)pins are used for the restoration of the fractured radial head andneck.38–41 This systematic review underlines with best availableevidence the good outcomes after ORIF with screws andbiodegradable (polylactide) pins for type II radial head and neckfractures, with an overall success rate of 98% (I2 = 41.3).
Mason type III fractures
Comminuted fractures are mostly high-energy injuries andare currently treated by early complete resection of the radialhead or radial head replacement.23,37 Partial resection is not
ter different operative treatment methods of radial head and neck03

J. Zwingmann et al. / Injury, Int. J. Care Injured xxx (2013) xxx–xxx10
G Model
JINJ-5353; No. of Pages 11
recommended.42 Internal fixation techniques are demandingand time-consuming in the presence of multiple fragments.These fractures are very difficult to fix due to poor bone qualityand/or inadequate fixation of very small fragments. Conse-quently, secondary complications including pseudarthrosis andfragment dislocation must be mentioned. Therefore, an intra-operative decision should always be made for an adequateanatomic reduction and stable internal fixation.39,40 One the onehand the resection of the radial head is not a challengingsurgery, but on the other hand it is very often associated withdifferent kinds of complications.7 However, in this review, witha success rate of 92% (I2 = 79.1%), ORIF has the best results in thetreatment of type III fractures and seems to be better thanresection and implantation of a prosthesis. Here, ORIF withbiodegradable (polylactide) pins (96%, I2 = 50.1%) and plates(83%, I2 = 67.3%) had the best results.
Mason type IV fractures
According to Morrey, radial head fractures with a posteriordislocation of the elbow are classified as complicated injuries.23
An elbow dislocation is often associated with injuries of themedial ligaments, which are the primary stabilizers to valgusstress at the elbow. For such cases, the preservation of the radialhead is of paramount importance in maintaining elbow stabili-ty.42 If the radial head cannot be preserved, torn ligaments mustbe repaired and radial head prosthesis is considered. Harringtonand Tountas32 have reported radial head replacement withoutligamentous reconstruction with satisfactory results. Unfortu-nately, poor results are associated with this type of fracture. Lossof elbow flexion and an average of 208 forearm rotation areusually observed. A higher incidence of heterotopic ossification isalso observed.43
In the treatment of type IV fractures, similar results could befound. There was a tendency for the best results after ORIF,followed by resection and implantation of a prosthesis.
Radial head prosthesis
Especially in patients with unreconstructable radial headfractures, the radial head arthroplasty is used in an attempt tominimise the complications of radial head resection. Its use may beindicated in comminuted fractures of the radial head occurring incombination with tears of the interosseous ligament of the forearmor complex instability after elbow injuries {23;harpe F, 2001#135;de Boer, 1999 #111;}.
Silicone implants have an overall increase in failure ratecompared with metallic implants, including reactive synovitis,inflammatory arthritis, fractures of silastic implants, and aquestionable amount of supporting axial stability.10,25
If a prosthesis was implanted, primary implantation seems tobe associated with a better outcome after type III (87%, I2 = 61.1%)and IV (82%, I2 = 56.4) fractures compared to the results after asecondary implantation.
After analyzing the results of the reviewed literature, theauthors suggest for the operative treatment of radial head fracturesan osteosynthesis with a sense of proportion. Head-preservingtechniques should not be performed at all costs. That means that,for example, an intraoperative complete resection of the radialhead for reconstruction purposes on the OR table should beavoided with the risk of necrosis in the near future. Moreover, nosignificant intraarticular steps or defects should be toleratedbecause the risk of developing an arthritic joint in a short time isrelatively high. In these cases, the authors recommend primaryimplantation of a prosthesis, which is associated with a better longterm outcome for the treated patient. With this algorithm, the
Please cite this article in press as: Zwingmann J, et al. Clinical results affractures. Injury (2013), http://dx.doi.org/10.1016/j.injury.2013.04.0
secondary implantation of a prosthesis and the associated worseoutcome should be reduced. A resection is a possible treatmentoption but should mainly be performed in older patients.
Conclusion
For type II fractures, the best treatment options seem to be ORIFusing screws or biodegradable (polylactide) pins. Moreover, ORIFhas the highest success rate in the treatment of type III fracturesand seems to be better than resection and implantation of aprosthesis. Here, the ORIF with screws, biodegradable (polylactide)pins and plates had the best results. In the treatment of type IVfractures, similar results could be found with a tendency for thebest results to occur after ORIF, followed by resection andimplantation of a prosthesis.
If there is a need for implantation of a prosthesis, primaryimplantation seems to be associated with a better outcome aftertypes III and IV fractures compared to the results after a secondaryimplantation.
Role of the funding source
There were no sources of funding and no involvement of studysponsors in the study design; collection, analysis and interpreta-tion of data; the writing of the manuscript; the decision to submitthe manuscript for publication.
Conflict of interest
All authors disclose any financial and personal relationshipswith other people or organisations that could inappropriatelyinfluence (bias) their work.
Ethical approval
There is no ethical committee needed for this type of study.
References
1. Kaas L, van Riet RP, Vroemen JP, Eygendaal D. The epidemiology of radial headfractures. J Shoulder Elb Surg 2010;19:520–3.
2. Kaas L, van Riet RP, Vroemen JP, Eygendaal D. The incidence of associatedfractures of the upper limb in fractures of the radial head. Strateg Trauma LimbReconstr 2008;3:71–4.
3. Johnston GW. A follow-up of one hundred cases of fracture of the head of theradius with a review of the literature. Ulster Med J 1962;31:51–6.
4. Schofer MD, Peterlein CD, Kortmann HR. Radial head prosthesis – treatment ofcomminuted radial head fractures combined with elbow instability. Z OrthopUnfall 2008;146:760–7.
5. Mason ML. Some observations on fractures of the head of the radius with areview of one hundred cases. Br J Surg 1954;42:123–32.
6. Broberg MA, Morrey BF. Results of treatment of fracture-dislocations of theelbow. Clinical orthopaedics and related research 1987;216:109–19.
7. Roidis NT, Papadakis SA, Rigopoulos N, Basdekis G, Poultsides L, Karachalios T,et al. Current concepts and controversies in the management of radial headfractures. Orthopedics 2006;29:904–16. quiz 917–908.
8. Geel CW, Palmer AK, Ruedi T, Leutenegger AF. Internal fixation of proximalradial head fractures. J Orthop Trauma 1990;4:270–4.
9. King GJ, Evans DC, Kellam JF. Open reduction and internal fixation of radial headfractures. J Orthop Trauma 1991;5:21–8.
10. Knight DJ, Rymaszewski LA, Amis AA, Miller JH. Primary replacement of thefractured radial head with a metal prosthesis. J Bone Joint Surg Br 1993;75:572–6.
11. Ring D. Open reduction and internal fixation of fractures of the radial head.Hand Clin 2004;20:415–27. vi.
12. Ikeda M, Sugiyama K, Kang C, Takagaki T, Oka Y. Comminuted fractures of theradial head. Comparison of resection and internal fixation. J Bone Joint Surg Am2005;87:76–84.
13. Edwards Jr GS, Jupiter JB. Radial head fractures with acute distal radioulnardislocation. 506 Essex-Lopresti revisited Clin Orthop 1988;234:61–9.
14. Sanchez-Sotelo J, Romanillos O, Garay EG. Results of acute excision of theradial head in elbow radial head fracture-dislocations. J Orthop Trauma2000;14:354–8.
ter different operative treatment methods of radial head and neck03

J. Zwingmann et al. / Injury, Int. J. Care Injured xxx (2013) xxx–xxx 11
G Model
JINJ-5353; No. of Pages 11
15. Esser RD, Davis S, Taavao T. Fractures of the radial head treated by internalfixation: late results in 26 cases. J Orthop Trauma 1995;9:318–23.
16. Broberg MA, Morrey BF. Results of delayed excision of the radial head afterfracture. J Bone Joint Surg Am 1986;68:669–74.
17. Goldberg I, Peylan J, Yosipovitch Z. Late results of excision of the radial head foran isolated closed fracture. J Bone Joint Surg Am 1986;68:675–9.
18. Hanzlik S, Mahabir RC, Baynosa RC, Khiabani KT. Levels of evidence in researchpublished in the journal of bone and joint surgery (American volume) over thelast thirty years. J Bone Joint Surg Am 2009;91:425–8.
19. Coleman BD, Khan KM, Maffulli N, Cook JL, Wark JD. Studies of surgical outcomeafter patellar tendinopathy: clinical significance of methodological deficienciesand guidelines for future studies. Victorian Institute of Sport Tendon StudyGroup. Scand J Med Sci Sports 2000;10:2–11.
20. Jakobsen RB, Engebretsen L, Slauterbeck JR. An analysis of the quality ofcartilage repair studies. J Bone Joint Surg Am 2005;87:2232–9.
21. Mithoefer K, McAdams T, Williams RJ, Kreuz PC, Mandelbaum BR. Clinicalefficacy of the microfracture technique for articular cartilage repair in the knee:an evidence-based systematic analysis. Am J Sports Med 2009;37:2053–63.
22. Zwingmann J, Sudkamp NP, Schmal H, Niemeyer P. Surgical treatment ofosteochondritis dissecans of the talus: a systematic review. Arch Orthop TraumaSurg 2012;132:1241–50.
23. Morrey BF. The elbow and its disorders. 3rd ed. Philadelphia: WB Saunders; 2009.24. Radin EL, Riseborough EJ. Fractures of the radial head. A review of eighty-eight
cases and analysis of the indications for excision of the radial head and non-operative treatment. J Bone Joint Surg Am 1966;48:1055–64.
25. Khalfayan EE, Culp RW, Alexander AH. Mason type II radial head fractures:operative versus nonoperative treatment. J Orthop Trauma 1992;6:283–9.
26. Geel CW, Palmer AK. Radial head fractures and their effect on the distalradioulnar joint. A rationale for treatment. Clin Orthop 1992;275:79–84.
27. Mackay I, Fitzgerald B, Miller JH. Silastic replacement of the head of the radiusin trauma. J Bone Joint Surg Br 1979;61-B:494–7.
28. Mikic ZD, Vukadinovic SM. Late results in fractures of the radial head treated byexcision. Clin Orthop 1983;181:220–8.
Please cite this article in press as: Zwingmann J, et al. Clinical results affractures. Injury (2013), http://dx.doi.org/10.1016/j.injury.2013.04.0
29. de Boer YA, van den Ende CH, Eygendaal D, Jolie IM, Hazes JM, Rozing PM.Clinical reliability and validity of elbow functional assessment in rheumatoidarthritis. J Rheumatol 1999;26:1909–17.
30. Loreto CA, Rollo G, Comitini V, Rotini R. The metal prosthesis in radial headfracture: indications and preliminary results. La Chirurgia degli organi di movi-mento 2005;90:253–70.
31. Steinberg EL, Golomb D, Salama R, Wientroub S. Radial head and neck fracturesin children. J Pediatr Orthop 1988;8:35–40.
32. Harrington IJ, Tountas AA. Replacement of the radial head in the treatment ofunstable elbow fractures. Injury 1981;12:405–12.
33. Steinhauser J. Total resection of the radius head in fractures at the upper spikeend. Arch Orthop Unfallchir 1968;63:162–75.
34. Ruan HJ, Fan CY, Liu JJ, Zeng BF. A comparative study of internal fixation andprosthesis replacement for radial head fractures of Mason type III. Int Orthop2009;33:249–53.
35. Nalbantoglu U, Kocaoglu B, Gereli A, Aktas S, Guven O. Open reduction andinternal fixation of Mason type III radial head fractures with and without anassociated elbow dislocation. J Hand Surg 2007;32:1560–8.
36. Higgins JPT GS. Cochrane Handbook for Systematic Reviews of InterventionsVersion 5.1.0 The Cochrane Coll*aboration, 2011; 2011.
37. McKee, Skeletal trauma. 2nd ed. Philadelphia, WB Saunders; 1998.38. Routt Jr MLN, Mills WJ. Percutaneous fixation of pelvic ring disruptions. Clin
Orthop 2000;375:15–29.39. Ring D, Quintero J, Jupiter JB. Open reduction and internal fixation of fractures of
the radial head. J Bone Joint Surg Am 2002;84-A:1811–5.40. McArthur RA. Herbert screw fixation of fracture of the head of the radius. Clin
Orthop 1987;224:79–87.41. Furry KL, Clinkscales CM. Comminuted fractures of the radial head. Arthroplasty
versus internal fixation Clin Orthop 1998;353:40–52.42. Sharpe FKS. Operative treatment of elbow injuries. New York: Springer-Verlag
Inc.; 2001.43. Davidson PA, Moseley Jr JB, Tullos HS. Radial head fracture. A potentially
complex injury. Clin Orthop 1993;297:224–30.
ter different operative treatment methods of radial head and neck03




















