Severe Dry Eye Syndrome After Radiotherapy for Head-and-Neck Tumors
8
CLINICAL INVESTIGATION Head and Neck Cancer SEVERE DRY EYE SYNDROME AFTER RADIOTHERAPY FOR HEAD-AND-NECK TUMORS NIRANJAN BHANDARE, M.S.,* VITALI MOISEENKO,PH.D., y WILLIAM Y. SONG,PH.D., z CHRISTOPHER G. MORRIS, M.S.,* M. T ARIQ BHATTI, M.D., x AND WILLIAM M. MENDENHALL, M.D.* *Department of Radiation Oncology, University of Florida College of Medicine, Gainesville, FL; y Vancouver Cancer Centre, Vancouver, BC, Canada; z University of California, San Diego, San Diego, CA; x Department of Ophthalmology and Medicine (Division of Neurology), Duke University Medical Center, Durham, NC Purpose: To investigate the incidence of severe dry eye syndrome (DES) after external beam radiotherapy for head-and-neck cancer and its dependence on the parameters relevant to external beam radiotherapy. Methods and Materials: The present retrospective study included 78 patients treated for primary extracranial head-and-neck tumors between 1965 and 2000, whose lacrimal apparatus/entire globe was exposed to fractionated external beam radiotherapy. The dose received by the major lacrimal gland was used for analysis. The end point of the present study was the ophthalmologic diagnosis of severe DES leading to vision compromise. Results: Of the 78 patients, 40 developed severe DES leading to visual compromise. The incidence of DES increased steadily from 6% at 35–39.99 Gy to 50% at 45–49.99 Gy and 90% at 60–64.99 Gy. With a mean of 0.9 years (range, 1 month to 3 years), the latency of DES was observed to be a function of the total dose and the dose per fraction. On univariate and multivariate analysis, the total dose (p < .0001 and p < .0001, respectively) and dose per fraction (p # .0001 and p = .0044, respectively) were significant. However, age, gender, and the use of chemoradiotherapy were not. The actuarial analysis indicated a 5-year probability of freedom from DES of 93% for doses <45 Gy, 29% for 45–59.9 Gy, and 3% doses $60 Gy. A logistic normal tissue complication probability model fit to our data obtained a dose of 34 and 38 Gy corresponding to a 5% and 10% incidence of DES. Conclusion: With a dose of 34 Gy corresponding to a 5% incidence of DES, the risk of severe DES increased, and the latency decreased with an increase in the total dose and dose per fraction to the lacrimal gland. The effect of chemo- radiotherapy and hyperfractionation on the risk of DES needs additional investigation. Ó 2012 Elsevier Inc. Dry-eye syndrome, Radiotherapy, Head-and-neck tumors. INTRODUCTION Dry eye syndrome (DES) is a disorder that results from deficiencies or defects in the components of lubrication that can lead to structural and functional abnormalities of the ocular surface. In 2007, the International Dry Eye Workshop defined DES as ‘‘a disease of tears and ocular surface that results in symptoms of discomfort, visual disturbance, and tear film instability with potential damage to ocular surface. It is accom- panied by increased osmolarity of tear film and inflammation of the ocular surface’’ (1). External beam radiotherapy (EBRT) for head-and-neck tumors involving the orbit and the tissues adjacent to the orbit often delivers high radiation doses to the eye, including the adnexa; the lacrimal system, including the major and accessory lacrimal glands, lacrimal canaliculi, lacrimal sac, and nasolacrimal duct; the ocular surface, including the cornea and conjunctiva; the eyelids; the meibomian glands; and associated sensory and motor nerves. Radiation damage to the lacrimal system can lead to corneal abnormalities and ocular dysfunction. Although direct radiation damage to the corneal epithelium and endothelium (2) can be associated with an acute reaction, delayed DES, resulting from disordered ocular lubrication due to damage to the lacrimal glands, has been reported in patients who were persistently symptomatic after subsidence of the acute radiation reactions (3, 4). Although mild to moderate DES is often successfully manageable with supportive therapy, severe DES can result in ulceration and/or infection of the cornea, thickening of the corneal surface, corneal erosion, punctate keratopathy, epithelial defects, corneal abrasions, ulceration, neovascula- rization, scarring, thinning, perforation, and corneal necrosis, leading to irreversible corneal opacity with compromised vision, severe pain, and eye loss. Severe DES after EBRT for head-and-neck cancer is a sparsely reported ocular Reprint requests to: Niranjan Bhandare, M.S., Department of Radiation Oncology, University of Florida Health Science Center, P.O. Box 100385, 2000 SW Archer Rd., Gainesville, FL, 32610- 0385. Tel: (352) 265-8217; Fax: (352) 265-8417; E-mail: bhandn@ shands.ufl.edu Conflict of interest: none. Received Nov 8, 2010, and in revised form April 28, 2011. Accepted for publication May 16, 2011. 1501 Int. J. Radiation Oncology Biol. Phys., Vol. 82, No. 4, pp. 1501–1508, 2012 Copyright Ó 2012 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/$ - see front matter doi:10.1016/j.ijrobp.2011.05.026
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Severe Dry Eye Syndrome After Radiotherapy for Head-and-Neck Tumors

Int. J. Radiation Oncology Biol. Phys., Vol. 82, No. 4, pp. 1501–1508, 2012Copyright � 2012 Elsevier Inc.
Printed in the USA. All rights reserved0360-3016/$ - see front matter
jrobp.2011.05.026
doi:10.1016/j.iCLINICAL INVESTIGATION Head and Neck Cancer
SEVERE DRY EYE SYNDROME AFTER RADIOTHERAPYFOR HEAD-AND-NECK TUMORS
NIRANJAN BHANDARE, M.S.,* VITALI MOISEENKO, PH.D.,y WILLIAM Y. SONG, PH.D.,z
CHRISTOPHER G. MORRIS, M.S.,* M. TARIQ BHATTI, M.D.,x AND WILLIAM M. MENDENHALL, M.D.*
*Department of Radiation Oncology, University of Florida College of Medicine, Gainesville, FL; yVancouver Cancer Centre,Vancouver, BC, Canada; zUniversity of California, San Diego, San Diego, CA; xDepartment of Ophthalmology andMedicine (Division
of Neurology), Duke University Medical Center, Durham, NC
ReprintRadiationP.O. Box0385. Telshands.ufl
Purpose: To investigate the incidence of severe dry eye syndrome (DES) after external beam radiotherapy forhead-and-neck cancer and its dependence on the parameters relevant to external beam radiotherapy.Methods and Materials: The present retrospective study included 78 patients treated for primary extracranialhead-and-neck tumors between 1965 and 2000, whose lacrimal apparatus/entire globe was exposed to fractionatedexternal beam radiotherapy. The dose received by the major lacrimal gland was used for analysis. The end point ofthe present study was the ophthalmologic diagnosis of severe DES leading to vision compromise.Results: Of the 78 patients, 40 developed severe DES leading to visual compromise. The incidence of DES increasedsteadily from 6% at 35–39.99 Gy to 50% at 45–49.99 Gy and 90% at 60–64.99 Gy.With a mean of 0.9 years (range,1 month to 3 years), the latency of DES was observed to be a function of the total dose and the dose per fraction. Onunivariate andmultivariate analysis, the total dose (p < .0001 and p < .0001, respectively) and dose per fraction (p#.0001 and p = .0044, respectively) were significant. However, age, gender, and the use of chemoradiotherapy werenot. The actuarial analysis indicated a 5-year probability of freedom from DES of 93% for doses <45 Gy, 29% for45–59.9 Gy, and 3% doses$60 Gy. A logistic normal tissue complication probability model fit to our data obtaineda dose of 34 and 38 Gy corresponding to a 5% and 10% incidence of DES.Conclusion:With a dose of 34Gy corresponding to a 5% incidence of DES, the risk of severeDES increased, and thelatency decreasedwith an increase in the total dose and dose per fraction to the lacrimal gland. The effect of chemo-radiotherapy and hyperfractionation on the risk of DES needs additional investigation. � 2012 Elsevier Inc.
Dry-eye syndrome, Radiotherapy, Head-and-neck tumors.
INTRODUCTION
Dry eye syndrome (DES) is a disorder that results fromdeficiencies or defects in the components of lubrication thatcan lead to structural and functional abnormalities of the ocularsurface. In 2007, the International Dry EyeWorkshop definedDES as ‘‘a disease of tears and ocular surface that results insymptoms of discomfort, visual disturbance, and tear filminstabilitywith potential damage to ocular surface. It is accom-panied by increased osmolarity of tear film and inflammationof the ocular surface’’ (1). External beam radiotherapy(EBRT) for head-and-neck tumors involving the orbit andthe tissues adjacent to the orbit often delivers high radiationdoses to the eye, including the adnexa; the lacrimal system,including the major and accessory lacrimal glands, lacrimalcanaliculi, lacrimal sac, and nasolacrimal duct; the ocularsurface, including the cornea and conjunctiva; the eyelids;the meibomian glands; and associated sensory and motor
requests to: Niranjan Bhandare, M.S., Department ofOncology, University of Florida Health Science Center,100385, 2000 SW Archer Rd., Gainesville, FL, 32610-: (352) 265-8217; Fax: (352) 265-8417; E-mail: [email protected]
1501
nerves. Radiation damage to the lacrimal system can lead tocorneal abnormalities and ocular dysfunction. Although directradiation damage to the corneal epithelium and endothelium(2) can be associated with an acute reaction, delayed DES,resulting from disordered ocular lubrication due to damageto the lacrimal glands, has been reported in patients whowere persistently symptomatic after subsidence of the acuteradiation reactions (3, 4).
Although mild to moderate DES is often successfullymanageable with supportive therapy, severe DES can resultin ulceration and/or infection of the cornea, thickening ofthe corneal surface, corneal erosion, punctate keratopathy,epithelial defects, corneal abrasions, ulceration, neovascula-rization, scarring, thinning, perforation, and corneal necrosis,leading to irreversible corneal opacity with compromisedvision, severe pain, and eye loss. Severe DES after EBRTfor head-and-neck cancer is a sparsely reported ocular
Conflict of interest: none.Received Nov 8, 2010, and in revised form April 28, 2011.
Accepted for publication May 16, 2011.

Table 2. Treatment characteristics
Treatment characteristic Patients (n)
FractionationOnce daily
1.36–2.0 Gy/fraction 64 (82)<150 36$150 42<180 60$180 18
Twice daily1.1 or 1.2 Gy/fraction 14 (18)
Chemoradiotherapy 13 (17)Treatment planningCT or CT-MR based 54Phantom CT based 24
Treatment techniqueAppositional anterior field 2Anterior and lateral (wedged) 42Bilateral (wedge pair) 30Multiple fields (>3 fields) 3
Patient distribution by dose decile (Gy)$70 11$60–69.99 19$50–59.99 11$40–49.99 9$30–39.99 23$20–29.99 5
Abbreviations: CT = computed tomography; MR = magneticresonance.Data in parentheses are percentages.
1502 I. J. Radiation Oncology d Biology d Physics Volume 82, Number 4, 2012
morbidity but can severely affect a patient’s quality of life.The purpose of the present study was to evaluate the inci-dence of DES by updating the University of Florida studyby Parsons et al. (3) using a relatively larger data set extend-ing over a range of doses from 20 to 75 Gy to the lacrimalgland and to analyze it further using both statistical andmod-eling techniques.
METHODS AND MATERIALS
The present retrospective study reviewed themedical records of 78adult patients who underwent EBRT for selected extracranial head-and-neck malignancies between 1965 and 2000 at the Universityof Florida. These 78 patients had no pre-existing ocular morbiditiesand their entire globe, including the lacrimal apparatus, had beenexposed to radiation. The treatment techniques varied significantlyowing to the heterogeneity of the treatment sites, histologic features,and duration. Tables 1 and 2 present the patient and treatmentcharacteristics, respectively.
Dose estimationBecause of the relatively small thickness of the cornea (average
thickness, 0.6 mm; range, 0.52–0.67) and the shallow depth of thelacrimal glands of Krause and Wolfring located in conjunctival for-nices, an accurate estimation of the radiation dose received by theorgans (5) is difficult and unreliable. Therefore, in the present study,we analyzed the dose to the major lacrimal gland, which offeredconsistency for comparison with previous studies (3, 6). Locatedin the supratemporal orbit at an approximate depth of 1.0 cm (3),the major lacrimal gland is composed of two lobes—the orbitallobe and the much smaller palpebral lobe—and its volume variesfor males (0.06–0.5 cm3) and females (0.01–0.54 cm3) (7). Theradiation doses to the major lacrimal gland were estimated frompatient-specific treatment plans using computed tomography scansor computed tomography–magnetic resonance imaging fusion,
Table 1. Patient characteristics (n = 78)
Patient characteristics Patients (%)
GenderMale 55 (70)Female 23 (30)
RaceWhite 67 (86)Black 9 (12)Hispanic 1 (�1)Asian 1 (�1)
Histologic typeSquamous cell carcinoma 22Lymphoma 28Esthesioneuroblastoma 8Adenoid cystic carcinoma 7Adenocarcinoma 4Orbital pseudotumor 4Juvenile angiofibroma 2Malignant melanoma 3
Primary siteOrbit 33Maxillary sinus 26Nasal cavity 10Ethmoid sinus 5Skin 4
Data in parentheses are percentages.
when available. For the patientswhowere treated earlier in the seriesand did not have three-dimensional plans, we used scaled computedtomography scans of a RANDO Phantom (Phantom Laboratory,Salem, NY), with appropriate patient-specific scaling correctionfactors.
Ophthalmologic assessmentAfter 1976, irrespective of their visual status, baseline pre-RT
evaluations were obtained for all patients whose optical apparatuswas in the vicinity of the treatment volume. Post-RTophthalmologyevaluations were available for all the patients in the present study.Severe DES was recorded when a patient persistently exhibitedsymptoms after subsidence of an acute radiation reaction thatultimately resulted in compromised vision (Radiation TherapyOncology Group Acute Radiation Morbidity Scoring CriteriaGrade 3 and 4 toxicity and National Cancer Institute’s CommonTerminology for Adverse Advents for DES Grade 2 and 3).Although severe DES can be diagnosed from the symptoms alone,all patients in our review underwent one or more tests. These testsincluded slit-lamp biomicroscopy to assess the changes in the tearfilm, cornea, or lens; Schirmer’s test I to measure the amount of tearfilm; Schirmer’s test II to measure reflex secretion; a tear breakuptime test to gauge the tear film instability; tear protein analysis tomeasure the lysozyme levels in tears; a lactoferrin assay to assessthe lacrimal gland function; and conjunctival and corneal stainingto evaluate the ocular surface damage.
Statistical analysisSAS and JMP software (SAS Institute, Cary, NC) were used for
all statistical analyses. The Kaplan-Meier product-limit methodprovided estimates of freedom from DES (8). The log-rank test
Dry eye syndrome after RT for head-and-neck tumors d N. BHANDARE et al. 1503
provided evidence of statistical significance of the following poten-tial prognostic factors: total dose received by the major lacrimalgland, fractionation schedule, chemoradiotherapy, age at treatment,and gender. Multivariate analysis of these same variables wasaccomplished with Cox regression analysis, and backward selec-tion provided the most parsimonious final model (9). To assesslatency, the Wilcoxon signed rank test was applied to the subsetof patients who experienced DES. The univariate prognostic factorswere dose, dose/fraction, and years to DES.
Radiobiologic modelingA logistic function was used to describe the dose response for
DES (10):
P ¼ 1
1þ exp
�� 4g50
�D
D50
� 1
�� (1)
where P is the probability of DES, D50 is the dose at which 50% ofthe patients develop DES; and g50 is the normalized slope at D50.The logistic function was separately fitted to once-daily fraction-
ation and combined the once- and twice-daily fractionation patientdata. The maximum likelihood method, as described by Thameset al. (11), was used to obtain the parameter estimates. In brief,the model parameter values were obtained by maximizing the log-arithm of maximum likelihood, M:
ln M ¼X
fri ln PðD50;g50;DiÞþ
ðni � riÞ ln ð1� PðD50;g50;DiÞÞg (2)
where Di is the dose, ni is the number of patients receiving the doseDi; ri is the number of patients who received the dose Di and devel-oped DES. Confidence intervals for the model parameters D50 andg50 were calculated using the profile-likelihood method (12, 13).To calculate the 95% confidence interval, the cutoff value was setto the maximal value minus c2/2 with 1 degree of freedom anda significance level of 0.05. Fitting was performed using individualdata (i.e., the patients were entered in Eq. 2 individually). Clinicallysignificant dosimetric predictors, specifically the doses correspond-ing to a 5% and 10% incidence of DES and the normal tissue compli-cation probability at a dose of 45, 50, 55, and 60 Gy, were calculatedusing the best-fit-model parameters. Bootstrap resampling was usedto simulate the data sets for model fitting (14). Sampling wasrepeated 10,000 times to establish the confidence intervals.
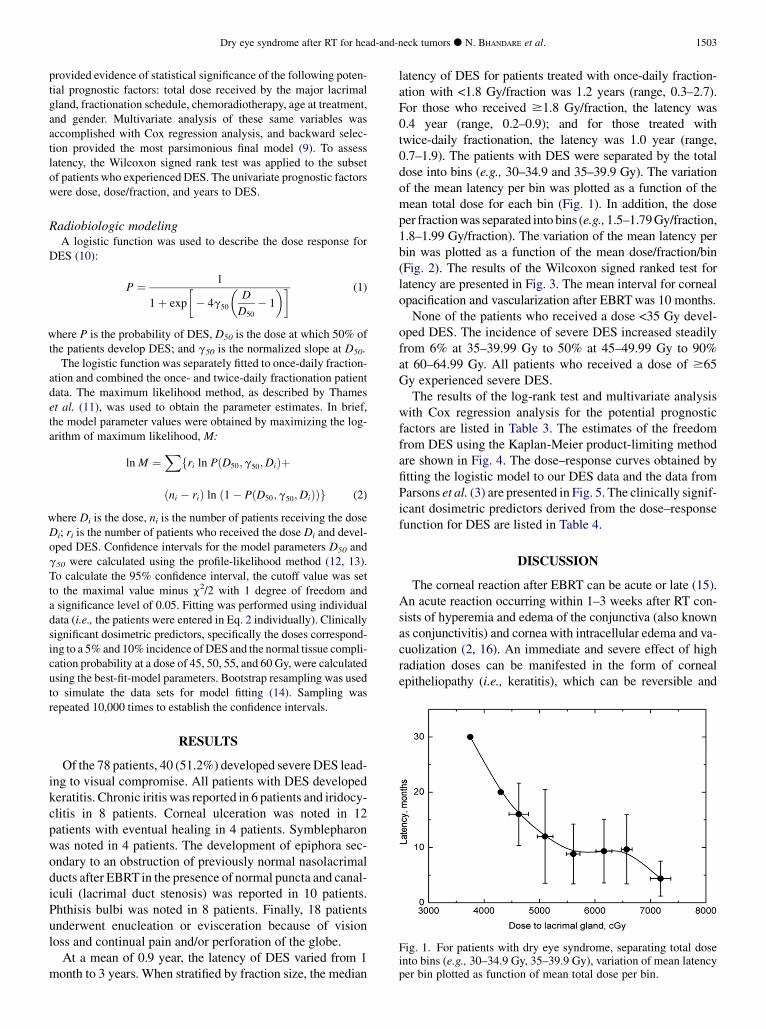
Fig. 1. For patients with dry eye syndrome, separating total doseinto bins (e.g., 30–34.9 Gy, 35–39.9 Gy), variation of mean latencyper bin plotted as function of mean total dose per bin.
RESULTS
Of the 78 patients, 40 (51.2%) developed severeDES lead-ing to visual compromise. All patients with DES developedkeratitis. Chronic iritis was reported in 6 patients and iridocy-clitis in 8 patients. Corneal ulceration was noted in 12patients with eventual healing in 4 patients. Symblepharonwas noted in 4 patients. The development of epiphora sec-ondary to an obstruction of previously normal nasolacrimalducts after EBRT in the presence of normal puncta and canal-iculi (lacrimal duct stenosis) was reported in 10 patients.Phthisis bulbi was noted in 8 patients. Finally, 18 patientsunderwent enucleation or evisceration because of visionloss and continual pain and/or perforation of the globe.
At a mean of 0.9 year, the latency of DES varied from 1month to 3 years. When stratified by fraction size, the median
latency of DES for patients treated with once-daily fraction-ation with <1.8 Gy/fraction was 1.2 years (range, 0.3–2.7).For those who received $1.8 Gy/fraction, the latency was0.4 year (range, 0.2–0.9); and for those treated withtwice-daily fractionation, the latency was 1.0 year (range,0.7–1.9). The patients with DES were separated by the totaldose into bins (e.g., 30–34.9 and 35–39.9 Gy). The variationof the mean latency per bin was plotted as a function of themean total dose for each bin (Fig. 1). In addition, the doseper fractionwas separated into bins (e.g.,1.5–1.79Gy/fraction,1.8–1.99 Gy/fraction). The variation of the mean latency perbin was plotted as a function of the mean dose/fraction/bin(Fig. 2). The results of the Wilcoxon signed ranked test forlatency are presented in Fig. 3. The mean interval for cornealopacification and vascularization after EBRTwas 10 months.
None of the patients who received a dose <35 Gy devel-oped DES. The incidence of severe DES increased steadilyfrom 6% at 35–39.99 Gy to 50% at 45–49.99 Gy to 90%at 60–64.99 Gy. All patients who received a dose of $65Gy experienced severe DES.
The results of the log-rank test and multivariate analysiswith Cox regression analysis for the potential prognosticfactors are listed in Table 3. The estimates of the freedomfrom DES using the Kaplan-Meier product-limiting methodare shown in Fig. 4. The dose–response curves obtained byfitting the logistic model to our DES data and the data fromParsons et al. (3) are presented in Fig. 5. The clinically signif-icant dosimetric predictors derived from the dose–responsefunction for DES are listed in Table 4.
DISCUSSION
The corneal reaction after EBRT can be acute or late (15).An acute reaction occurring within 1–3 weeks after RT con-sists of hyperemia and edema of the conjunctiva (also knownas conjunctivitis) and cornea with intracellular edema and va-cuolization (2, 16). An immediate and severe effect of highradiation doses can be manifested in the form of cornealepitheliopathy (i.e., keratitis), which can be reversible and
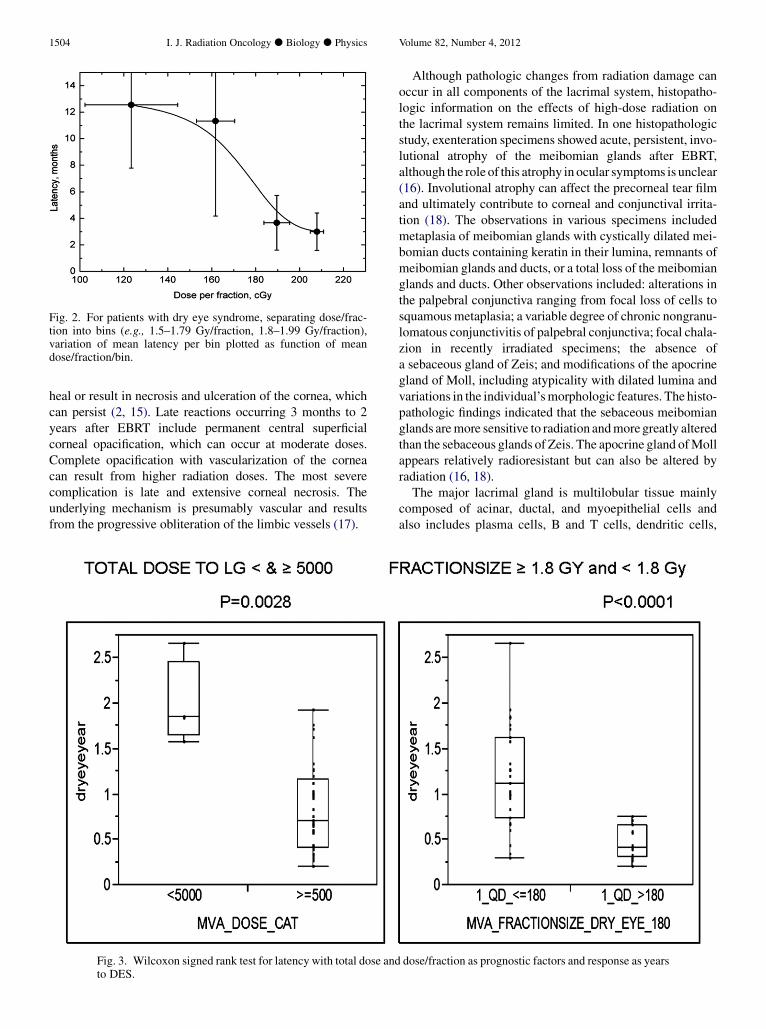
Fig. 2. For patients with dry eye syndrome, separating dose/frac-tion into bins (e.g., 1.5–1.79 Gy/fraction, 1.8–1.99 Gy/fraction),variation of mean latency per bin plotted as function of meandose/fraction/bin.
1504 I. J. Radiation Oncology d Biology d Physics Volume 82, Number 4, 2012
heal or result in necrosis and ulceration of the cornea, whichcan persist (2, 15). Late reactions occurring 3 months to 2years after EBRT include permanent central superficialcorneal opacification, which can occur at moderate doses.Complete opacification with vascularization of the corneacan result from higher radiation doses. The most severecomplication is late and extensive corneal necrosis. Theunderlying mechanism is presumably vascular and resultsfrom the progressive obliteration of the limbic vessels (17).
Fig. 3. Wilcoxon signed rank test for latency with total dose andto DES.
Although pathologic changes from radiation damage canoccur in all components of the lacrimal system, histopatho-logic information on the effects of high-dose radiation onthe lacrimal system remains limited. In one histopathologicstudy, exenteration specimens showed acute, persistent, invo-lutional atrophy of the meibomian glands after EBRT,although the role of this atrophy in ocular symptoms is unclear(16). Involutional atrophy can affect the precorneal tear filmand ultimately contribute to corneal and conjunctival irrita-tion (18). The observations in various specimens includedmetaplasia of meibomian glands with cystically dilated mei-bomian ducts containing keratin in their lumina, remnants ofmeibomian glands and ducts, or a total loss of the meibomianglands and ducts. Other observations included: alterations inthe palpebral conjunctiva ranging from focal loss of cells tosquamousmetaplasia; a variable degree of chronic nongranu-lomatous conjunctivitis of palpebral conjunctiva; focal chala-zion in recently irradiated specimens; the absence ofa sebaceous gland of Zeis; and modifications of the apocrinegland of Moll, including atypicality with dilated lumina andvariations in the individual’smorphologic features. The histo-pathologic findings indicated that the sebaceous meibomianglands aremore sensitive to radiation andmoregreatly alteredthan the sebaceous glands of Zeis. The apocrine gland ofMollappears relatively radioresistant but can also be altered byradiation (16, 18).
The major lacrimal gland is multilobular tissue mainlycomposed of acinar, ductal, and myoepithelial cells andalso includes plasma cells, B and T cells, dendritic cells,
dose/fraction as prognostic factors and response as years

Table 3. Risk of developing severe dry eye syndrome afterexternal beam radiotherapy
Parameter
p
Univariateanalysis
Multivariateanalysis
Total dose (Gy)<40 <.0001 *$40<45 <.0001$45<50 <.0001 <.0001$50
Age (y)#56 (median) .577 .371>56
SexMale .7881 .719Female
ChemoradiotherapyYes .0583 .0526No
FractionationOnce daily .256 .314Twice daily
Fraction size (Gy)<1.8 <.0001 .0044$1.8<1.5 .0001 y
$1.5
* Only 1 dose stratification tested.y Only 1 fraction size tested.
Fig. 5. Logistic normal tissue complication probability model fit.
Dry eye syndrome after RT for head-and-neck tumors d N. BHANDARE et al. 1505
macrophages, monocytes, and mast cells (19). The acinarcells, the most significant component of the lacrimal gland,synthesize, store, and secrete proteins, many of which haveantibacterial or growth factor properties and are essential forthe health of the ocular surface (19, 20). Ductal cells modifythe primary fluids secreted by the acinar cells and secretewater and electrolytes. The myoepthelial cells containmultiple processes and a- smooth muscle actin and arethought to contract and force fluid out of the ducts ontothe ocular surface (20). Radiation damage to the constituent
Fig. 4. Estimates of freedom from severe dry eye syndrome usingKaplan-Meier product-limiting method.
secretory cells of the major lacrimal gland can lead to atro-phy, cell death, apoptosis, functional compromise, andsecretory abnormalities (17).
Information on the effects of radiation on the nasolacrimaldrainage system remains limited, because ductal patency isnot routinely evaluated after high-dose EBRT. After highradiation doses, desquamation of the epithelial lining of thenasolacrimal duct and sac and associated inflammation canlead to duct obstruction (21). The development of epiphorasecondary to the obstruction of previously normal nasolacri-mal ducts after radiation in the presence of normal puncta andcanaliculi have been reported (22), although the possibility oftumor invasion in such cases should be eliminated.
Signs, symptoms, and diagnosis of DESThe common symptoms of severe DES include dryness,
stinging, burning, irritation, itching, scratchy eye, tired eye,photophobia, pain, redness, a foreign body sensation, mucousdischarge, excessive tearing (which can paradoxically becauseof corneal irritation with reflex tearing), blurry vision related totear film irregularity, and vision loss in advanced stages. Thesigns of DES include bulbar conjunctival vascular dilation, de-creased tear meniscus, irregular corneal surface, decreased tearbreakup time, punctuate epithelial keratopathy, cornealfilaments, increased debris in the tear film, conjunctival pleat-ing, superficial punctuate keratitis with positive fluoresceinstaining, and corneal edema. The signs of advanced DESinclude ulceration, vascularization, opacification, and perfora-tion. For classification of DES according to the severity, the In-ternationalDryEyeWorkshopadopted andmodified theDelphiPanel Report (23, 24), which presents four levels of severity asmild, moderate, severe, and severe and/or disabling (Table 5).Using these guidelines, post-RT DES can be classified accord-ing to its severity. At present, no uniform criterion is availablefor the diagnosis of DES. AlthoughDES can be clinically diag-nosed in most cases, the combination of information, includingsigns and symptoms from the patient history and examination,along with one or more tests, offers objectivity to the diagnosisby determining both the quantity and quality of the tears (25).

Table 4. Risk of developing severe dry eye syndrome: Analysis of logistic normal tissue complication probability model fitting
Investigator Fractionation D5 (Gy) D10 (Gy) NTCP45 (%) NTCP50 (%) NTCP55 (%) NTCP60 (%) D50 (Gy) g50
Present study Once daily 34.6(28.5–42.5)
38.0(33.0–44.6)
34.1(11.3–60.9)
60.8(36.9–91.3)
82.4(64.5–99.0)
93.3(82.1–99.9)
48.0(44.0–52.0)
2.64(1.64–4.07)
Once andtwice daily
36(30.5–44.2)
39.3(34.6–45.3)
29.4(9.2–51.9)
56.9(33.5–85.1)
80.7(63.2–97.7)
93(82.6–99.7)
48.8(45.1–52.5)
2.81(1.83–4.22)
Parsonset al (3)
Once andtwice daily
28.9 32.2 75.7 93.1 97.2 99.2 40.3(34.7–48.9)
2.44(1.00–6.20)
Abbreviations:D = total dose to lacrimal gland; NTCP = normal tissue complication probability; D5, D10, D50 = dose corresponding to 5%,10%, and 50% complication rate; NTCP45, NTCP50, NTCP55, NTCP60 = normal tissue complication probability at 45, 50, 55, and 60 Gy; g50 =normalized slope at D50.Data in parentheses are 95% confidence intervals.
1506 I. J. Radiation Oncology d Biology d Physics Volume 82, Number 4, 2012
Treatment- and patient-related factorsTotal dose. A few studies have reported the incidence of
DES in relation to the total radiation dose (Fig. 6) (3, 4, 26).Many of these data sets were limited by their small patientcohorts. A steep increase in the incidence of severe DES ata dose >30 Gy was reported in 2 studies (3, 4). In contrast,the development of DES at doses <30 Gy was not observed.Bessell et al. (4) observed an increase in DES from 4.5%for doses of 30–39 Gy to 23% for doses of 40–49 Gy. Parsonset al. (3) reported a 25% incidence of DES for doses of 30–40Gy, 50% for doses 40–45 Gy, and 100% for doses >57 Gy. Inour data set, the incidence increased from 6.7% for doses of35–40 Gy to 25% for 40–45 Gy, 50% for 45–50 Gy, and90% for doses >60 Gy. On both univariate (p < .0001) andmultivariate (p< .0001) analyses, the total dose to the lacrimalgland was statistically significant for the incidence of DES.Kaplan-Meier analysis showed a significant decrease in thefreedom from DES from 93% for doses <45 Gy to 29% fordoses $45–59.9 Gy and 3% for doses $60 Gy. The logistic
Table 5. Dry ey
Symptoms 1 2
Discomfort, severity,and frequency
Mild and/or episodic Moderate episodic orchronic, stressor no stress
Visual symptoms None or episodic,mild fatigue
Annoying and/oractivity- limiting,episodic
Conjunctival injection None to mild None to mildConjunctival staining None to mild VariableCorneal staining(severity/location)
None to mild Variable
Corneal/tear signs None to mild Mild debris, decreasedmeniscus
Lid/meibomianglands
MGD variablypresent
MGD variably present
TBUT (s) Variable #10Schirmer score(mm/5 min)
Variable #10
Abbreviations: MGD = meibomian gland dysfunction; TBUT = tear b* Must have signs and symptoms.y Data in Table 5 came from Behrens et al (24) and Perry (25).
normal tissue complication probability model fit to our dataobtained a 5% incidence for a dose of 34 Gy and 10% inci-dence for a dose of 38Gy. The results of thismodel fit are con-sistent with those from Bessell et al. (4). In contrast, Parsonset al. (3) observed only 2 cases at doses of 30–40Gy; however,their rate was high (25%) owing to the relatively smaller dataset (8 patients) in that dose bin. This relatively greater esti-mated incidence owing to the relatively smaller dose bins inthe study by Parsons et al. (3) is also reflected in the upwardshift seen in Fig. 6. These data clearly show an associationbetween the total dose received by the lacrimal gland andthe incidence of DES.
Fraction size and fractionation. The effect of fractionsize and fractionation on the development of DES has notbeen evaluated in published studies. Parsons et al. (3)reported three injuries that occurred at the lowest doseswhen 2 of the 3 patients received a dose/fraction of $2 Gy(32 Gy/16 fractions, 35 Gy/20 fractions, and 45 Gy/21 frac-tions). In some studies, all the patients diagnosed with DES
e severityy
Level
3 4*
Severe frequent orconstant without stress
Severe and/or disablingand constant
Annoying, chronic and/orconstant, limiting activity
Constant and/orpossibly disabling
+/� +/++Moderate to marked MarkedMarked central Severe punctuate erosions
Filamentary keratitis, mucousclumping, increasedtear debris
Filamentary keratitis, mucousclumping, increased teardebris, ulceration
Frequent Trichiasis, keratinization,symblepharon
#5 Immediate#5 #2
reakup time.

Fig. 6. Incidence of severe dry eye syndrome after external beamradiotherapy. Curves shown in plot for present study and study byParsons et al. (3) are logistic model fit to data. Curves for Bessellet al. (4), Letschert et al. (26), Morita et al. (18), and Jiang et al.(6) are simple interpolations or connected points (if only 2 wereavailable).
Dry eye syndrome after RT for head-and-neck tumors d N. BHANDARE et al. 1507
(4, 18, 26) received doses close to or >2 Gy/fraction. Fittingthe Cox proportional hazards model with a forward inclusionvariable, Jiang et al. (6) found that the total dose times thedose per fraction and the overall treatment time were signif-icantly related to differences in the latency of visual impair-ment. Univariate (p < .0001) and multivariate (p = 0.0044)analysis of our data showed that a fraction size of $1.80Gywas significant for the incidence of DES. Further support-ing these results, our data showed that the mean incidence forpatients with DES in each dose/fraction bin increased with anincrease in the mean dose/fraction (Fig. 7), indicating theeffect of fraction size on the incidence of DES. Althoughthe fraction size was significant in our analysis, fractionation(once or twice daily) was not significant on univariate (p =.256) or multivariate (p = .314) analysis. However, in ourdata set, only 7 of the 14 patients who received twice-dailyfractionation received doses >39 Gy to the major lacrimal
Fig. 7. For patientswith dry eye syndrome, separating dose/fractioninto bins (e.g., 1.5–1.79 Gy/fraction, 1.8–1.99 Gy/fraction),variation in incidence per bin plotted as function of mean dose/frac-tion/bin.
gland, limiting the significance of the conclusions drawnfrom the univariate and multivariate analyses.
Chemoradiotherapy. The data on the synergistic effects ofchemotherapy delivered with EBRT in the development ofDES remains anecdotal and sparse. Parsons et al. (3)observed that 2 of the 3 patients who developed DES afterrelatively low radiation doses (32–45 Gy) and long latencyhad also received chemotherapy. Jiang et al. (6) reportedthat chemoradiotherapy significantly affected the likelihoodof corneal injury at doses of $56 Gy and related the receiptof chemoradiotherapy to differences in latency. However,the incidence of DES was reported to be 100% for doses>57 Gy in the study by Parsons et al. (3) and was 90% fordoses >60 Gy in our study, making such an analysis difficult.In our data analysis, adjuvant chemotherapy was not signifi-cant on univariate (p = .058) or multivariate (p = .052) anal-ysis. In our data set, only 7 of the 13 patients who receivedchemotherapy had received doses >39 Gy to the major lacri-mal gland, limiting the significance of the conclusions ofunivariate or multivariate analysis in regard to the synergisticeffects of radiotherapy and chemotherapy. The data onwhether adjuvant chemotherapy contributes to an increasedincidence of post-RT DES remain conflicting and need addi-tional examination.
Age and gender. The information on the significance ofage or gender on post-RTDES remains sparse in the publishedstudies. Although the incidence of idiopathic DES is morecommon in populations aged $40 years, post-RT DES doesnot exhibit age dependence. Parsons et al. (3) analyzed theincidence of severe DES according to patient age and totaldose. They found that the incidence of injury was not affectedby patient age within each dose range. Our data analysesshowed that age (univariate, p = .57; multivariate, p = .96)and gender (univariate, p = .78; multivariate, p = .96) werenot statistically significant variables.
Latency. Parsons et al. (3) reported that most patients whoreceived >45 Gy and developed DES were symptomaticwithin 1 month after RT, and corneal opacification and vascu-larization were pronounced 9–10 months later. Severe DESwas observed 1–2 months after RT in patients who receiveddoses >57 Gy and was frequently followed by corneal opaci-fication within 1 year. Three cases of DES (32 Gy in 16 frac-tions within 22 days, 35.5 Gy in 20 fractions within 32 days,and 45 Gy in 21 fractions within 29 days) showed slow devel-opment of corneal vascularization and opacification within 4,8, and 11 years, respectively. Jiang et al. (6) observed themedian interval to the manifestation of corneal injury to be9 months (range, 1–31) for doses of 41.8–74.7 Gy to the lac-rimal gland delivered at 1.02–3.72 Gy/fraction. Reportingthat doses >60 Gy were associated with a latency of <1 year,Morita and Kawabe (18) suggested that the latency of cornealulceration was a function of the total radiation dose receivedby the cornea. In our data set, the mean latency of 0.9 yearvaried from 0.2 to 3.0 years. Our data showed that the meanlatency for patientswithDES in each bin decreasedwith a cor-responding increase in the mean total dose for the bin as wellas with an increase in the mean dose/fraction for the bin (Figs.

1508 I. J. Radiation Oncology d Biology d Physics Volume 82, Number 4, 2012
1 and 2). The Wilcoxon signed ranked test showed that thelatency is related to the dose (p < .0028) and dose/fraction(p = .0001). These results indicate that the total dose andfraction size influences the latency of DES.
Although several treatment options might provide relieffrom mild to moderate DES, severe DES remains a chronicproblem that can significantly affect a patient’s quality oflife. Severe DES can be caused by radiation injury to severalocular structures, including the major lacrimal gland, con-junctival goblet cells, accessory lacrimal glands, and meibo-mian glands. Often the radiation damage occurs to more thanone of these structures; thus, the exclusion or reduction ofthe dose to the major lacrimal glands from EBRT mightnot be sufficient to avoid DES. Irrespective of the age and
chemotherapy status of the patient, reducing the total doseand fraction size to all the components of the lacrimal systemmight be necessary to reduce the incidence of delayed severeDES.
CONCLUSION
With a 5% incidence of DES at a dose of 34 Gy, the inci-dence of post-RT severe DES increases significantly, and itslatency decreases with a corresponding increase in the totaldose and dose/fraction to the major lacrimal glands. Theeffects of chemoradiotherapy and hyperfractionation onthe incidence of post-RT severe DES needs additionalexamination.
REFERENCES
1. The definition and classification of dry eye disease: Reportof the Definition and Classification Subcommittee of the In-ternational Dry Eye WorkShop (2007). Ocul Surf 2007;5:75–92.
2. Fujishima H, Shimazaki J, Tsubota K. Temporary corneal stemcell dysfunction after radiation therapy. Br J Ophthalmol 1996;80:911–914.
3. Parsons JT, Bova FJ, Fitzgerald CR, et al. Severe dry-eyesyndrome following external beam irradiation. Int J RadiatOncol Biol Phys 1994;30:775–780.
4. Bessell EM, Henk JM, Whitelocke RA, et al. Ocular morbidityafter radiotherapy of orbital and conjunctival lymphoma. Eye1987;1:90–96.
5. Hogan MJ, Alvarado JA, Weddell JC. Histology of human eye.Philadelphia: WB Saunders; 1971. pp. 55–100.
6. Jiang GL, Tucker SL, Guttenberger R, et al. Radiation-in-duced injury to the visual pathway. Radiother Oncol 1994;30:17–25.
7. Koutrouza-Tavlaridis N, Elzarka A. Lacrimal gland ultra-sound. Accessed November 6, 2003. Available from: http://www.medicalultrasound.org/open/bulletin/full_articles/v6_n4_Lacrimal.pdf.
8. Kaplan EL, Meier P. Nonparametric estimation from incom-plete observations. J Am Stat Assoc 1958;53:457–481.
9. Cox DR. Regression models and life tables—Series B (method-ological). J R Stat Soc 1972;34:187–220.
10. Bentzen SM, Tucker SL. Quantifying the position and steep-ness of radiation dose-response curves. Int J Radiat Biol1997;71:531–542.
11. Thames HD Jr., Rozell ME, Tucker SL, et al. Direct analysis ofquantal radiation response data. Int J Radiat Biol Relat StudPhys Chem Med 1986;49:999–1009.
12. Roberts SA, Hendry JH. The delay before onset of acceleratedtumour cell repopulation during radiotherapy: A directmaximum-likelihood analysis of a collection of worldwidetumour-control data. Radiother Oncol 1993;29:69–74.
13. Cox DR. The analysis of binary data. 1st ed. London: Methuen;1977.
14. Iwi G, Millard RK, Palmer AM, et al. Bootstrap resam-pling: A powerful method of assessing confidence intervalsfor doses from experimental data. Phys Med Biol 1999;44:N55–N62.
15. Chaques VM, Saornil MA, Herreras JM. Corneal perforationdue to late radiation therapy-induced corneal necrosis—Clini-copathological correlation. Ocul Immunol Inflamm 2000;8:67–71.
16. Kadota Y, Okisaka S, Mizukawa A, et al. A case of corneal per-foration and retinopathy followed by external radiotherapy formaxillary carcinoma.FoliaOphthamol Jpn 1988;39:2466–2471.
17. Stephens LC, Schultheiss TE, Price RE, et al. Radiation apo-ptosis of serous acinar cells of salivary and lacrimal glands.Cancer 1991;67:1539–1543.
18. Morita K, Kawabe Y. Late effects on the eye of conformationradiotherapy for carcinoma of the paranasal sinuses and nasalcavity. Radiology 1979;130:227–232.
19. Dartt DA. Regulation of tear secretion.Adv ExpMed Biol 1994;350:1–9.
20. Zoukhri D. Effect of inflammation on lacrimal gland function.Exp Eye Res 2006;82:885–898.
21. Nakissa N, Rubin P, Strohl R, et al. Ocular and orbital compli-cations following radiation therapy of paranasal sinus malig-nancies and review of literature [Review]. Cancer 1983;51:980–986.
22. Peral A, Carracedo G, Acosta MC, et al. Increased levels ofdiadenosine polyphosphates in dry eye. Invest OphthalmolVis Sci 2006;47:4053–4058.
23. 2007 Report of the Dry Eye WorkShop (DEWS). Ocul Surf2007;5:63–204.
24. Behrens A, Doyle JJ, Stern L, et al. Dysfunctional tear syn-drome: A Delphi approach to treatment recommendations.Cornea 2006;25:900–907.
25. Perry HD. Dry eye disease: Pathophysiology, classification,and diagnosis. Am J Manag Care 2008;14:S79–S87.
26. Letschert JG, Gonzalez-Gonzalez D, Oskam J, et al. Results ofradiotherapy in patients with stage I orbital non-Hodgkin’slymphoma. Radiother Oncol 1991;22:36–44.