
Update on neuroendocrine tumors - OncologyPRO
48
GASTROENTEROPANCREATIC NEUROENDOCRINE TUMORS Update on neuroendocrine tumors Nicola Fazio, M.D., Ph. D. Division of Gastrointestinal Medical Oncology and Neuroendocrine Tumors European Institute of Oncology Milan, Italy 3rd ESO-ESMO-RCE Preceptorships & Clinical Update on Rare Adult Solid Cancers Do not duplicate or distribute without permission from author and ESO
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Update on neuroendocrine tumors - OncologyPRO
GASTROENTEROPANCREATIC NEUROENDOCRINE
TUMORS
Update on neuroendocrine tumors
Nicola Fazio, M.D., Ph. D.
Division of Gastrointestinal Medical Oncology
and Neuroendocrine Tumors
European Institute of Oncology
Milan, Italy
3rd ESO-ESMO-RCE Preceptorships & Clinical Update on Rare Adult SolidCancers
01.12.2018 - 03.12.2018
Milan, Italy
ADVANCED COURSES & SEMINARS
Rare genito-urinary cancers, Rare gynaecological cancers, Rare head and neck cancers, Rare
tumors, Sarcoma
* Third party registration should be used if you are requesting an individual registration for
someone who is not you.
Please note that website registration under your name will be needed before registering
someone else to this event.
Programme
PRECEPTORSHIPS ON RARE ADULT SOLID CANCERS
1 December8:30 Registration and coffee entry
8:50 Welcome
P.G. Casali, IT
INTRODUCTION (plenary)
9:00 Epidemiology and rare cancer networking
A. Trama, IT
9:30 The pathologic diagnosis
A.P. Dei Tos, IT
10:00 Clinical decision making in RC
3rd ESO-ESMO-RCE Preceptorships & Clinical Update on Rare Adult SolidCancers
01.12.2018 - 03.12.2018
Milan, Italy
ADVANCED COURSES & SEMINARS
Rare genito-urinary cancers, Rare gynaecological cancers, Rare head and neck cancers, Rare
tumors, Sarcoma
* Third party registration should be used if you are requesting an individual registration for
someone who is not you.
Please note that website registration under your name will be needed before registering
someone else to this event.
Programme
PRECEPTORSHIPS ON RARE ADULT SOLID CANCERS
1 December8:30 Registration and coffee entry
8:50 Welcome
P.G. Casali, IT
INTRODUCTION (plenary)
9:00 Epidemiology and rare cancer networking
A. Trama, IT
9:30 The pathologic diagnosis
A.P. Dei Tos, IT
10:00 Clinical decision making in RC
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
DISCLOSURE
◆ Personal financial interests:
Novartis, Ipsen, Pfizer, Merck Serono, Advanced Accelerator Applications, MSD
◆ Institutional financial interests:
Novartis, Ipsen, Merck Serono, MSD, Pharmacyclics, Incyte, Halozyme, Roche,
Astellas, Pfizer
◆ Non-financial interests:
• ESMO Coordinator of the Neuroendocrine, Endocrine neoplasms and CUP Faculty
• ENETS (European Society of Neuroendocrine Tumors) advisory board member
• AIOM coordinator for neuroendocrine neoplasms guidelines
• ITANET Scientific committee member, Member of the task force for interaction with
patients associationsDo not duplica
te or distr
ibute without
permiss
ion from author a
nd ESO

OBJECTIVES
❖ To describe epidemiology and clinical
characteristics of GEP NEN
❖ To review the management of patients with
advanced disease
❖ To summarize the main recent new insights
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
OBJECTIVES
❖ To describe epidemiology and clinical
characteristics of GEP NEN
❖ To review the management of patients with
advanced disease
❖ To summarize the main recent new insights
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

Nicola Fazio, M.D., Ph.D. IEO, European Institute of Oncology, IRCCS, Milan
GEP NENs: European epidemiological data
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

G1
(Ki-67 < 2% and/or MI < 2)
G2
(Ki-67 3-20% and/or MI 2-20)
G3
(Ki-67 > 20% and/or MI > 20)
WHO 2010 GI NEN classification
NET
(Tumours)
NEC
(Carcinomas)
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

G1
(Ki-67 < 2% and/or MI < 2)
G2
(Ki-67 3-20% and/or MI 2-20)
G3
(Ki-67 > 20% and/or MI > 20)
WHO 2017 Pancreatic NEN classification
G3
(Ki-67 > 20% and/or MI > 20)
NET
(Tumours)
NEC
(Carcinomas)Do not duplica
te or distr
ibute without
permiss
ion from author a
nd ESO
Survival is related to the
stage, grade and primary site.
Dasari, JAMA Oncol 2017
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
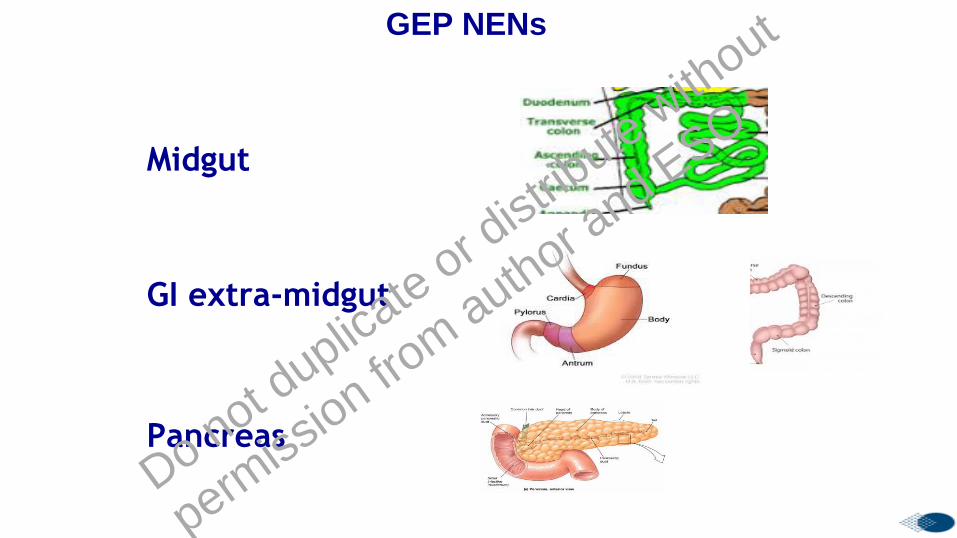
Midgut
GI extra-midgut
Pancreas
GEP NENs
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

GEP NET: clinical presentation
At diagnosis mainly:
✓ Advanced (mostly liver)
✓ Non functioning (no clinical syndrome)
✓ Sporadic
✓ SSTR-2 positive (at 68Ga-DOTA-peptide-PET/CT)
Cives et al., CA Cancer J Clin 2018
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
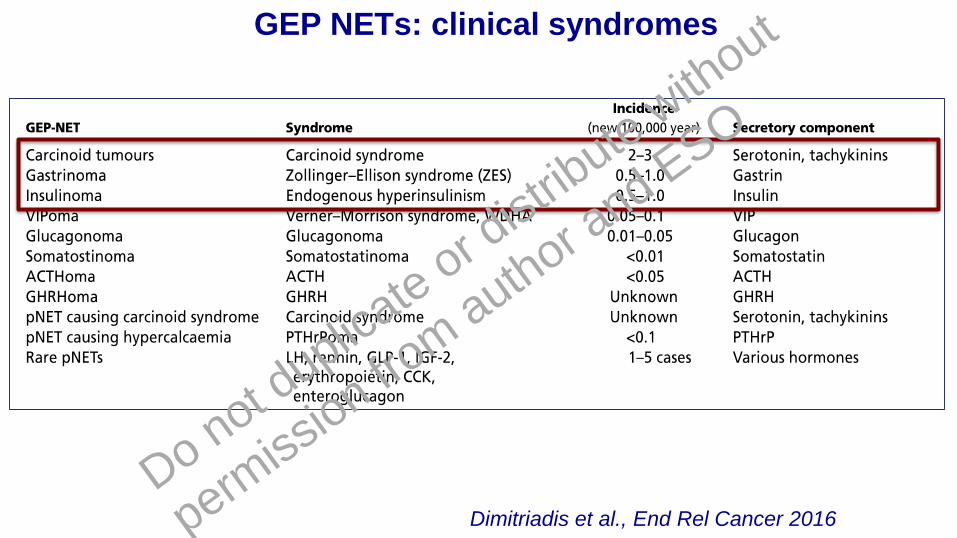
GEP NETs: clinical syndromes
Dimitriadis et al., End Rel Cancer 2016
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
OBJECTIVES
❖ To describe epidemiology and clinical
characteristics of GEP NEN
❖ To review the management of patients with
advanced disease
❖ To summarize the main recent new insights
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
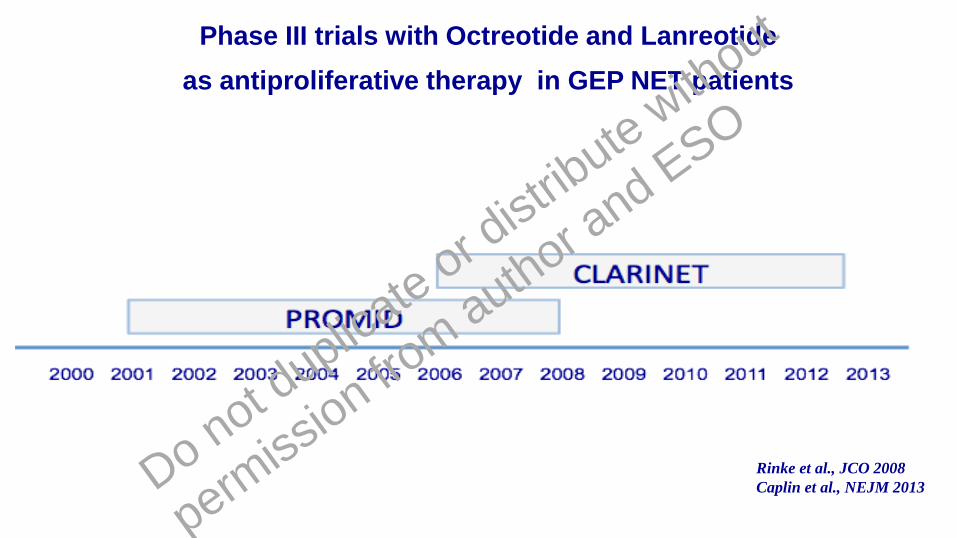
Phase III trials with Octreotide and Lanreotide
as antiproliferative therapy in GEP NET patients
Rinke et al., JCO 2008
Caplin et al., NEJM 2013Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
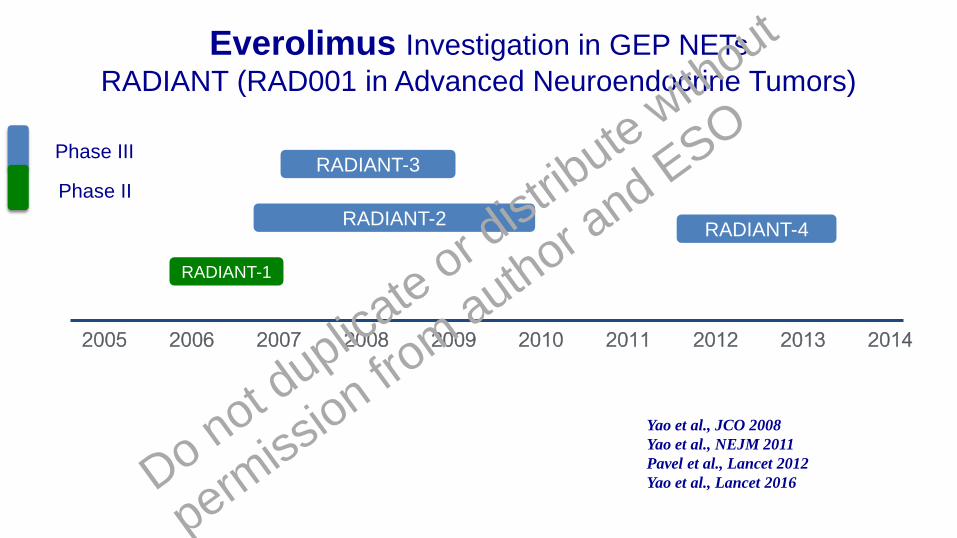
Everolimus Investigation in GEP NETs
RADIANT (RAD001 in Advanced Neuroendocrine Tumors)
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
RADIANT-3
RADIANT-2
RADIANT-1
RADIANT-4
Phase III
Phase II
Yao et al., JCO 2008
Yao et al., NEJM 2011
Pavel et al., Lancet 2012
Yao et al., Lancet 2016Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
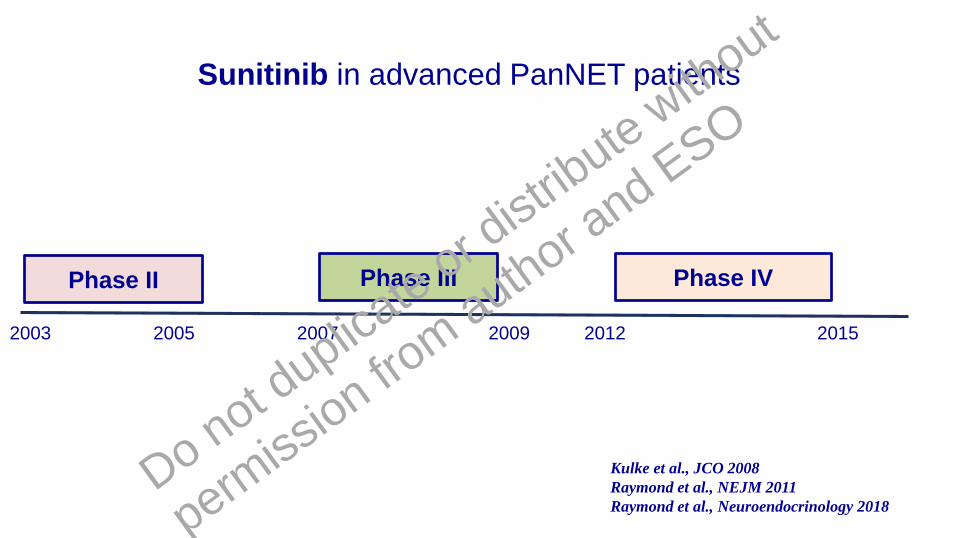
Phase III Phase IV
Sunitinib in advanced PanNET patients
Phase II
2003 2005 2007 2009 2012 2015
Kulke et al., JCO 2008
Raymond et al., NEJM 2011
Raymond et al., Neuroendocrinology 2018
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
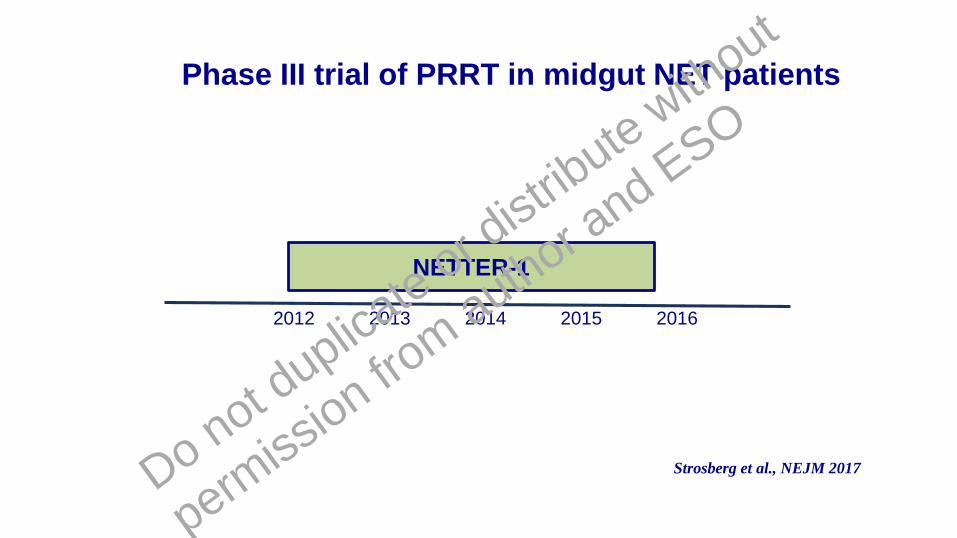
NETTER-1
Phase III trial of PRRT in midgut NET patients
2012 2013 2014 2015 2016
Strosberg et al., NEJM 2017Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

‘70 ’80 ’90 2011
STZ in
panNET
Octreotide
IFN in carcinoid
syndrome
Lanreotide
in carcinoid
syndrome
Sunitinib
Everolimus
in panNET
PRRT in
GEP NET
FDA/EMA approved therapies for patients with advanced GEP NETs
2015
Lanreotide in
GEP
Octreotide in
midgut
2016
Everolimus in
non functioning
Lung and GI
Telotristatin refractory
carcinoid syndrome
diarrhea
2017
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
No validated predictive biomarker for sunitinib and everolimus
Martins et al., Targeted Oncol 2017
REVIEW ARTICLE
Predictive Markers of Response to Everolimus and Sunitinibin Neuroendocrine Tumors
Diana Martins1&Francesca Spada1
&Ioana Lambrescu1&Manila Rubino1
&
Chiara Cella1&Bianca Gibelli 2 &Chiara Grana3
&Dario Ribero4&Emilio Bertani 4 &
DavideRavizza5&Guido Bonomo6
&Luigi Funicelli 7&Eleonora Pisa8
&Dario Zerini 9 &
Nicola Fazio1&IEO ENETS Center of Excellence for GEP NETs
# Springer International Publishing Switzerland 2017
Abstract Neuroendocrine tumors (NETs) represent a large
and heterogeneous group of malignancies with various bio-
logical and clinical characteristics, depending on the site of
origin and the grade of tumor proliferation. In NETs, as in
other cancer types, molecularly targeted therapies have radi-
cally changed the therapeutic landscape. Recently two
targeted agents, the mammalian target of rapamycin inhibitor
everolimus and the tyrosine kinase inhibitor sunitinib, have
both demonstrated significantly prolonged progression free
survival in patients with advanced pancreatic NETs. Despite
these important therapeutic developments, there are still sig-
nificant limitationsto theuseof theseagentsdueto thelack of
accuratebiomarkers for predicting tumor responseand effica-
cy of therapy. In this review, we provide an overview of the
current clinical data for theevaluation of predictive factorsof
response to/efficacy of everolimus and sunitinib in advanced
pancreatic NETs. Surrogate indicators discussed include cir-
culating and tissue markers, as well as non-invasive imaging
techniques.
Key Points
Everolimus and sunitinib are widely investigated
targeted cancer therapies, and they are both globally
approved by regulatory authorities for the treatment of
pancreatic NETs.
The establishment of predictive markers of response to
everolimus and sunitinib in NETs is of extreme importance
for their efficient use.
Most efforts to define predictive biomarkers have failed,
with the exception of chromogranin-A and neuron-specific
enolase for advanced pancreatic NETs treated with
everolimus.
1 Introduction
Neuroendocrine tumors (NETs) comprise a heterogeneous
group of malignanciesoriginating from the diffuseendocrine
system. Even though NETsareconsidered a raremalignancy,
representing about two new cases per 100.000 persons per
year, their incidenceand prevalenceseem to berising steadily
[1]. Someof thepossible reasons for the increasing incidence
* Nicola Fazio
1 Unit of Gastrointestinal Medical Oncology and Neuroendocrine
Tumors, European Instituteof Oncology, IEO, 20141 viaRipamonti,
435 Milan, Italy
2 Division of Otolaryngology-Head and Neck Surgery, European
Instituteof Oncology, IEO, Milan, Italy
3 Division of Nuclear Medicine, European Instituteof Oncology, IEO,
Milan, Italy
4 Division of Hepatobiliopancreatic Surgery, European Instituteof
Oncology, IEO, Milan, Italy
5 Division of Endoscopy, European Instituteof Oncology, IEO,
Milan, Italy
6 Division of Interventional Radiology, European Instituteof
Oncology, IEO, Milan, Italy
7 Division of Radiology, European Instituteof Oncology, IEO,
Milan, Italy
8 Division of Pathology, European Institute of Oncology, IEO,
Milan, Italy
9 Division of Radiotherapy, European Instituteof Oncology, IEO,
Milan, Italy
Targ Oncol
DOI 10.1007/s11523-017-0506-5
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
In patients with advanced GEP NET
there is no absolute evidence about
a specific sequence or integration of
therapies
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

Oncological scientific societes NEN scientific societes
Italian NEN guidelines
NET guidelinesfrom several different scientific societes
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
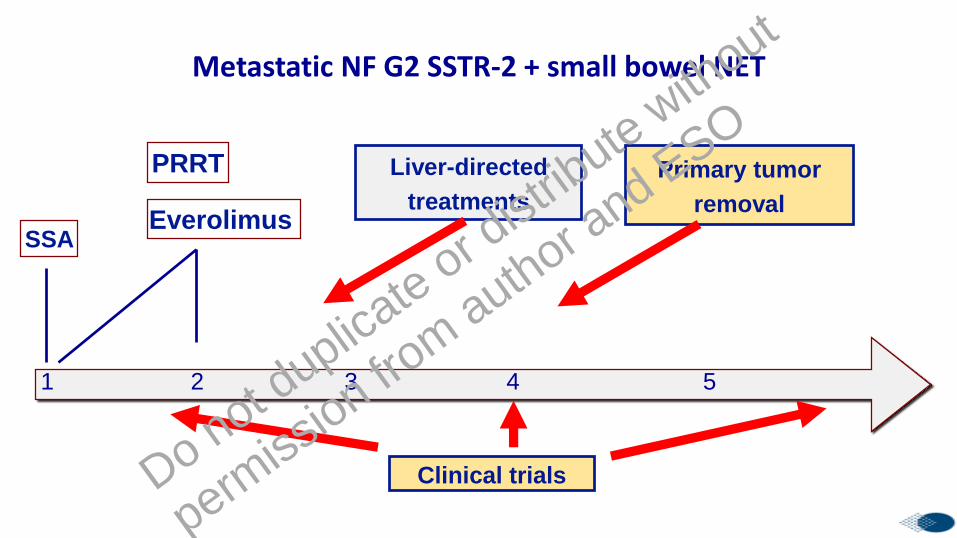
SSA
1 2 4 53
Clinical trials
Liver-directed
treatments
Primary tumor
removal
Metastatic NF G2 SSTR-2 + small bowel NET
Everolimus
PRRT
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
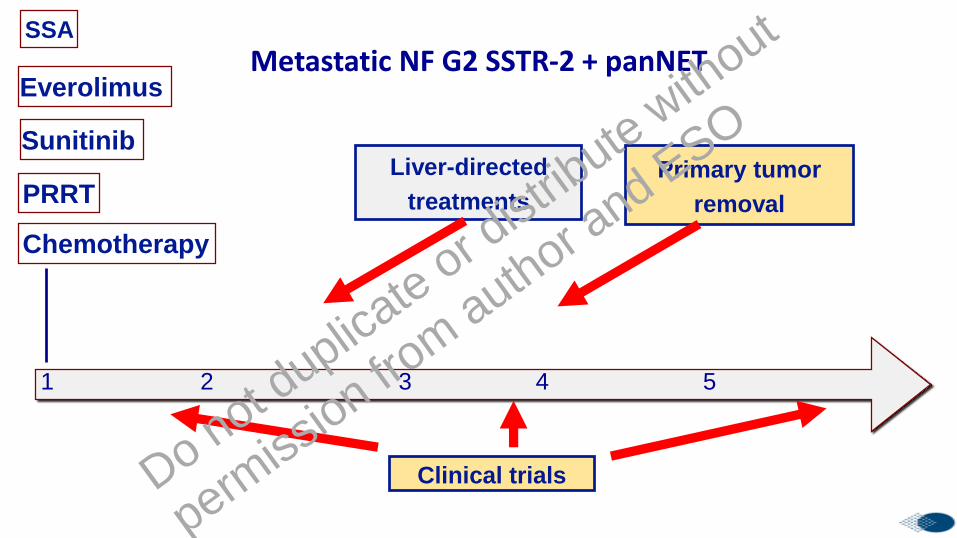
PRRT
Chemotherapy
Everolimus
Sunitinib
SSA
1 2 4 53
Clinical trials
Liver-directed
treatments
Primary tumor
removal
Metastatic NF G2 SSTR-2 + panNET
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
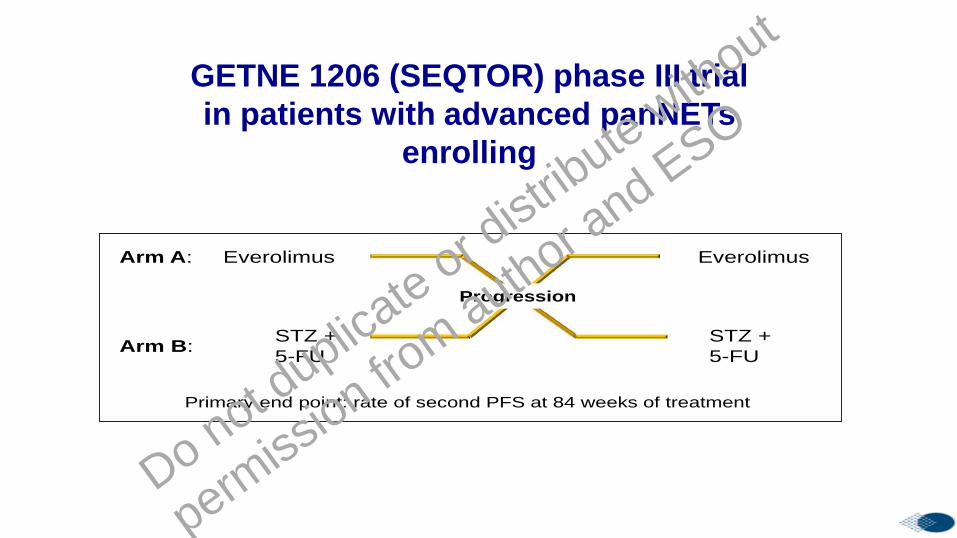
GETNE-1206 (SEQTOR): Phase III Study in Patients With
Advanced pNET
Unpublished data. Clinicaltrials.gov ID, NCT02246127.
Primary end point: rate of second PFS at 84 weeks of treatment
Progression
Everolimus
STZ +
5-FU
Everolimus
STZ +
5-FU
Arm A:
Arm B:
Compare efficacy and safety of everolimus followed by chemotherapy with
STZ + 5-FU upon progression, or the reverse sequence (chemotherapy with
STZ + 5-FU followed by everolimus upon progression)
26
GETNE 1206 (SEQTOR) phase III trial
in patients with advanced panNETs
enrolling
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

177Lu-edotreotide
Everolimus
Rand. 2:1
Phase III
G1-G2 SSTR-2 +++, advanced progressive GEP NET
COMPETE trial
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

TEM alone or CAP-TEM in PanNET?
Kunz, ASCO 2018 oral presentationDo not duplicate or d
istribute without
permiss
ion from author a
nd ESO
Original Paper
Neuroendocrinology
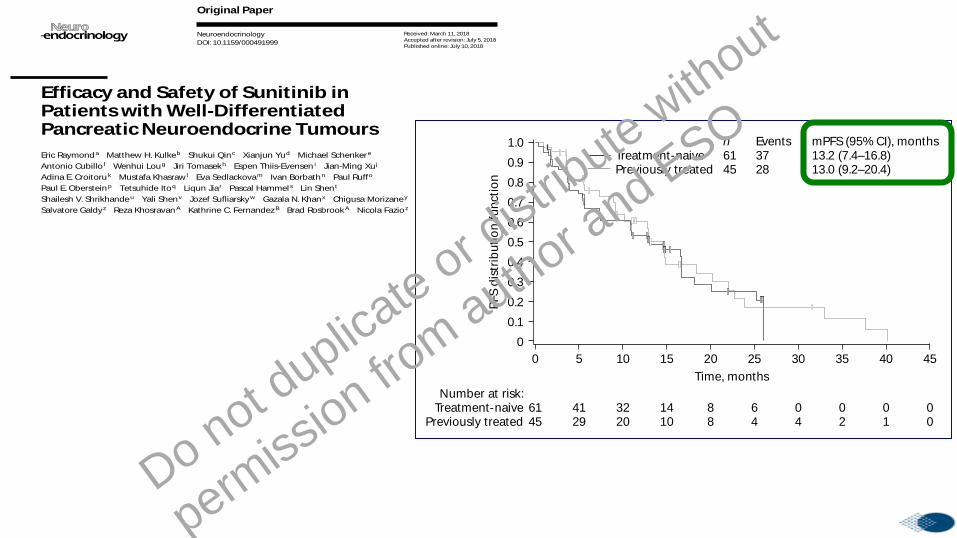
Efficacy and Safety of Sunitinib in Patients with Well-Differentiated Pancreatic Neuroendocrine Tumours
Eric Raymond
a Matthew H. Kulke
b Shukui Qin
c Xianjun Yu
d Michael Schenker
e
Antonio Cubillo
f Wenhui Lou
g Jiri Tomasek
h Espen Thiis-Evensen
i Jian-Ming Xu
j
Adina E. Croitoru
k Mustafa Khasraw
l Eva Sedlackova
m Ivan Borbath
n Paul Ruff
o
Paul E. Oberstein
p Tetsuhide Ito
q Liqun Jia
r Pascal Hammel
s Lin Shen
t
Shailesh V. Shrikhande
u Yali Shen
v Jozef Sufliarsky
w Gazala N. Khan
x Chigusa Morizane
y
Salvatore Galdy
z Reza Khosravan
A Kathrine C. Fernandez
B Brad Rosbrook
A Nicola Fazio
z
a Department of Medical Oncology, Paris Saint-Joseph Hospital Group, Paris, France; b
Program in Neuroendocrine
and Carcinoid Tumors, Dana-Farber Cancer Institute, Boston, MA, USA; c PLA Cancer Center, Nanjing Bayi Hospital,
Nanjing, China; d Pancreatic and Hepatobiliary Surgery, Fudan University Shanghai Cancer Center, Shanghai,
China; e Centrul de Oncologie Sf. Nectarie, Oncologie Medicala, Craiova, Romania; f Hospital Universitario Madrid
Sanchinarro, Centro Integral Oncológico Clara Campal, Madrid, Spain; g Zhongshan Hospital, Fudan University,
Shanghai, China; h Faculty of Medicine, Masaryk Memorial Cancer Institute, Masaryk University, Brno, Czech
Republic; i Department of Gastroenterology, Oslo University Hospital, Rikshospitalet, Oslo, Norway; j No. 307
Hospital, Academy of Military Medical Sciences, Beijing, China; k Department of Medical Oncology, Fundeni Clinical
Institute, Bucharest, Romania; l Andrew Love Cancer Center, Geelong Hospital, Victoria, VIC, Australia; m
Všeobecné
Fakultní Nemocnice v Praze Onkologická Klinika, Prague, Czech Republic; n Hepato-Gastroenterology Department,
Cliniques Universitaires Saint-Luc, Brussels, Belgium; o Faculty of Health Sciences, University of the Witwatersrand,
Johannesburg, South Africa; p Division of Hematology/Oncology, Columbia University Medical Center, New York,
NY, USA; q Department of Medicine and Bioregulatory Science, Graduate School of Medical Sciences, Kyushu
University, Fukuoka, Japan; r China-Japan Friendship Hospital, Beijing, China; s
Service d’Oncologie Digestive, Hôpital
Beaujon, Clichy, France; t Key Laboratory of Carcinogenesis and Translational Research (Ministry of Education),
Department of GI Oncology, Peking University Cancer Hospital and Institute, Beijing, China; u GI and HPB Surgical
Oncology, Tata Memorial Hospital, Mumbai, India; v West China Hospital of Sichuan University, Chengdu, China;
w 2nd Department of Oncology, Faculty of Medicine, Comenius University, Bratislava, Slovakia; x
Henry Ford Health
System, Detroit, MI, USA; y National Cancer Center, Tokyo, Japan; z
Division of Gastrointestinal Medical Oncology and
Neuroendocrine Tumors, European Institute of Oncology, IEO, Milan, Italy; A Pfizer Oncology, Pfizer Inc., San Diego,
CA, USA; B Pfizer Oncology, Pfizer Inc., Cambridge, MA, USA
Received: March 11, 2018
Accepted after revision: July 5, 2018
Published online: July 10, 2018
Nicola FazioDivision of Gastrointestinal Medical Oncology and Neuroendocrine TumorsEuropean Institute of Oncology, IEOVia Ripamonti 435, IT–20143 Milan (Italy)E-Mail nicola.fazio @ ieo.it
© 2018 S. Karger AG, Basel
E-Mail [email protected]
www.karger.com/nen
DOI: 10.1159/000491999
Keywords
Pancreatic neuroendocrine tumour · Progression-free
survival · Overall survival · Safety · Sunitinib
Abstract
Background: In a phase III study, sunitinib led to a significant
increase in progression-free survival (PFS) versus placebo
in patients with pancreatic neuroendocrine tumours (pan-
NETs). This study was a post-marketing commitment to sup-
Dow
nloa
ded
by:
Ist.E
uro
peo
di O
ncol
ogia
193.
204.
98.2
10 -
10/
10/2
018
7:45
:11
PM
Raymond et al.Neuroendocrinology4DOI: 10.1159/000491999
PFS d
istr
ibu
tio
n f
un
cti
on
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0
0 10 15 20 25
Time, months
6145
4129
3220
1410
88
64
04
02
01
00
30 35 40 45
Number at risk:Treatment-naive
Previously treated
a
n Events mPFS (95% CI), monthsTreatment-naive 61 37 13.2 (7.4–16.8)Previously treated 45 28 13.0 (9.2–20.4)
5
PFS d
istr
ibu
tio
n f
un
cti
on
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0
0 10 15 20 25
Time, months
6145
2925
2217
1111
68
45
14
02
00
00
30 35 40 45
Number at risk:Treatment-naive
Previously treated
c
n Events mPFS (95% CI), monthsTreatment-naive 61 25 18.7 (5.6–NE)Previously treated 45 24 16.5 (7.4–22.9)
5
PFS d
istr
ibu
tio
n f
un
ctio
n
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0
0 10 15 20 25
Time, months
6145
3026
2215
99
37
15
04
02
00
––
30 35 40 45
Number at risk:Treatment-naive
Previously treated
b
n Events mPFS (95% CI), monthsTreatment-naive 61 31 11.1 (5.5–16.7)Previously treated 45 26 9.5 (7.4–18.4)
5
Fig. 1. Kaplan-Meier estimates of progres-sion-free survival in treatment-naive and previously treated patients with panNETs (full analysis set). a Assessed by investiga-tors. b Assessed by independent third-par-ty radiology according to RECIST v1.0. c Assessed by independent third-party radi-ology according to Choi criteria. CI, confi-dence interval; mPFS, median progression-free survival; NE, not estimable; panNET, pancreatic neuroendocrine tumour; RE-CIST, Response Evaluation Criteria in Sol-id Tumours.
Do
wn
loa
de
d b
y:
Ist.
Eu
rop
eo
di O
nco
log
ia
19
3.2
04
.98
.21
0 -
10
/10
/20
18
7:4
5:1
1 P
M
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
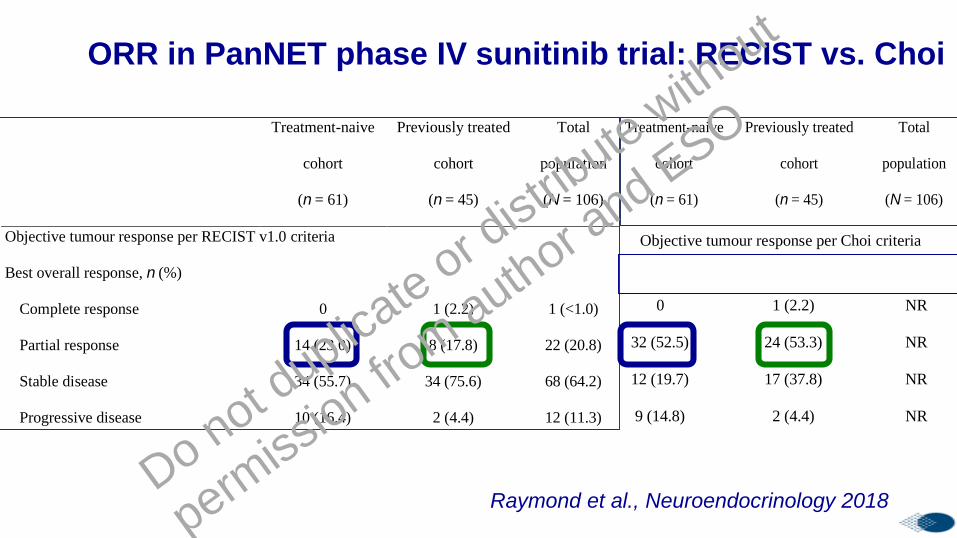
ORR in PanNET phase IV sunitinib trial: RECIST vs. ChoiSupplementary Table S2. Summary of efficacy measures according to independent
radiologic review (full analysis set)
Treatment-naive
cohort
(n = 61)
Previously treated
cohort
(n = 45)
Total
population
(N = 106)
Objective tumour response per RECIST v1.0 criteria
Best overall response, n (%)
Complete response 0 1 (2.2) 1 (<1.0)
Partial response 14 (23.0) 8 (17.8) 22 (20.8)
Stable disease 34 (55.7) 34 (75.6) 68 (64.2)
Progressive disease 10 (16.4) 2 (4.4) 12 (11.3)
Missing 3 (4.9) 0 3 ( 2.8)
Objective response rate 14 (23.0) 9 (20.0) 23 (21.7)
95% exact CIa 13.2–35.5 9.6–34.6 14.3–30.8
Objective tumour response per Choi criteria
Best overall response, n (%)
Complete response 0 1 (2.2) NR
Partial response 32 (52.5) 24 (53.3) NR
Stable disease 12 (19.7) 17 (37.8) NR
Progressive disease 9 (14.8) 2 (4.4) NR
Missing 8 (13.1) 1 (2.2) NR
Objective response rate 32 (52.5) 25 (55.6) NR
95% exact CIa 39.3–65.4 40.0–70.4 NR
Time to tumour progression per Choi criteria
Median (95% CI)b time to progression, 18.7 (5.6–NE) 16.7 (7.4–30.9) NR
Supplementary Table S2. Summary of efficacy measures according to independent
radiologic review (full analysis set)
Treatment-naive
cohort
(n = 61)
Previously treated
cohort
(n = 45)
Total
population
(N = 106)
Objective tumour response per RECIST v1.0 criteria
Best overall response, n (%)
Complete response 0 1 (2.2) 1 (<1.0)
Partial response 14 (23.0) 8 (17.8) 22 (20.8)
Stable disease 34 (55.7) 34 (75.6) 68 (64.2)
Progressive disease 10 (16.4) 2 (4.4) 12 (11.3)
Missing 3 (4.9) 0 3 ( 2.8)
Objective response rate 14 (23.0) 9 (20.0) 23 (21.7)
95% exact CIa 13.2–35.5 9.6–34.6 14.3–30.8
Objective tumour response per Choi criteria
Best overall response, n (%)
Complete response 0 1 (2.2) NR
Partial response 32 (52.5) 24 (53.3) NR
Stable disease 12 (19.7) 17 (37.8) NR
Progressive disease 9 (14.8) 2 (4.4) NR
Missing 8 (13.1) 1 (2.2) NR
Objective response rate 32 (52.5) 25 (55.6) NR
95% exact CIa 39.3–65.4 40.0–70.4 NR
Time to tumour progression per Choi criteria
Median (95% CI)b time to progression, 18.7 (5.6–NE) 16.7 (7.4–30.9) NR
Supplementary Table S2. Summary of efficacy measures according to independent
radiologic review (full analysis set)
Treatment-naive
cohort
(n = 61)
Previously treated
cohort
(n = 45)
Total
population
(N = 106)
Objective tumour response per RECIST v1.0 criteria
Best overall response, n (%)
Complete response 0 1 (2.2) 1 (<1.0)
Partial response 14 (23.0) 8 (17.8) 22 (20.8)
Stable disease 34 (55.7) 34 (75.6) 68 (64.2)
Progressive disease 10 (16.4) 2 (4.4) 12 (11.3)
Missing 3 (4.9) 0 3 ( 2.8)
Objective response rate 14 (23.0) 9 (20.0) 23 (21.7)
95% exact CIa 13.2–35.5 9.6–34.6 14.3–30.8
Objective tumour response per Choi criteria
Best overall response, n (%)
Complete response 0 1 (2.2) NR
Partial response 32 (52.5) 24 (53.3) NR
Stable disease 12 (19.7) 17 (37.8) NR
Progressive disease 9 (14.8) 2 (4.4) NR
Missing 8 (13.1) 1 (2.2) NR
Objective response rate 32 (52.5) 25 (55.6) NR
95% exact CIa 39.3–65.4 40.0–70.4 NR
Time to tumour progression per Choi criteria
Median (95% CI)b time to progression, 18.7 (5.6–NE) 16.7 (7.4–30.9) NR
Supplementary Table S2. Summary of efficacy measures according to independent
radiologic review (full analysis set)
Treatment-naive
cohort
(n = 61)
Previously treated
cohort
(n = 45)
Total
population
(N = 106)
Objective tumour response per RECIST v1.0 criteria
Best overall response, n (%)
Complete response 0 1 (2.2) 1 (<1.0)
Partial response 14 (23.0) 8 (17.8) 22 (20.8)
Stable disease 34 (55.7) 34 (75.6) 68 (64.2)
Progressive disease 10 (16.4) 2 (4.4) 12 (11.3)
Missing 3 (4.9) 0 3 ( 2.8)
Objective response rate 14 (23.0) 9 (20.0) 23 (21.7)
95% exact CIa 13.2–35.5 9.6–34.6 14.3–30.8
Objective tumour response per Choi criteria
Best overall response, n (%)
Complete response 0 1 (2.2) NR
Partial response 32 (52.5) 24 (53.3) NR
Stable disease 12 (19.7) 17 (37.8) NR
Progressive disease 9 (14.8) 2 (4.4) NR
Missing 8 (13.1) 1 (2.2) NR
Objective response rate 32 (52.5) 25 (55.6) NR
95% exact CIa 39.3–65.4 40.0–70.4 NR
Time to tumour progression per Choi criteria
Median (95% CI)b time to progression, 18.7 (5.6–NE) 16.7 (7.4–30.9) NR
Raymond et al., Neuroendocrinology 2018Do not duplica
te or distr
ibute without
permiss
ion from author a
nd ESO

Advanced 2016 ENETs guidelines
“Patients with 5–20% Ki-67 pNET can be treated
with chemotherapy”
“Factors that favour chemotherapy compared with targeted therapies:
✓ Bulky disease;
✓ Symptomatic patient;
✓ Rapid tumour progression in ≤ 6–12 months;
✓ Patients with a possible chance of achieving a response to
allow for surgery (neoadjuvant option)”
Pavel M, et al. Neuroendocrinology 2016
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
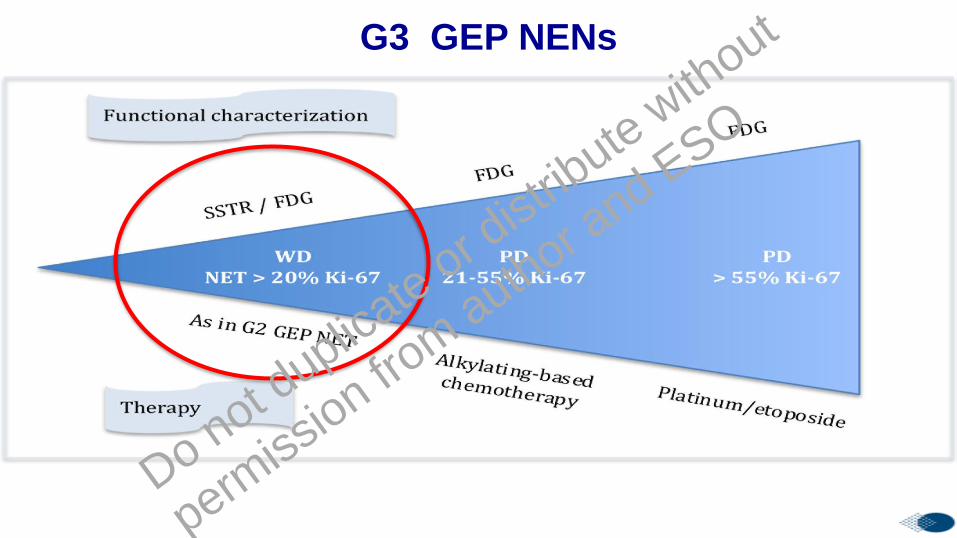
G3 GEP NENs
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
In NET G3 biological therapies,
PRRT and liver-directed
treatments should be considered
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
OBJECTIVES
❖ To describe epidemiology and clinical
characteristics of GEP NEN
❖ To review the management of patients with
advanced disease
❖ To summarize the main recent new insights
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

New TKIs
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

Novel TKIs in GEP NETs
Phase III
Phase III
Phase III
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
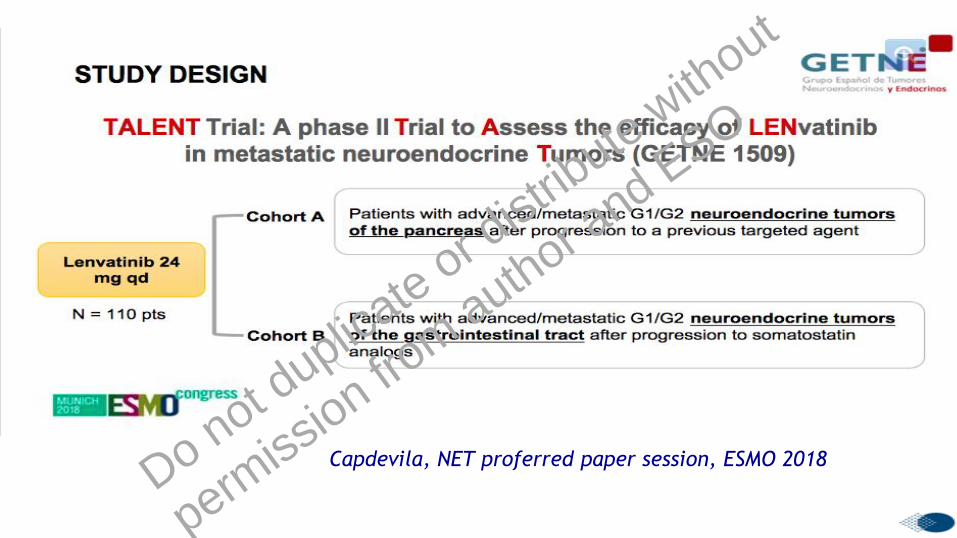
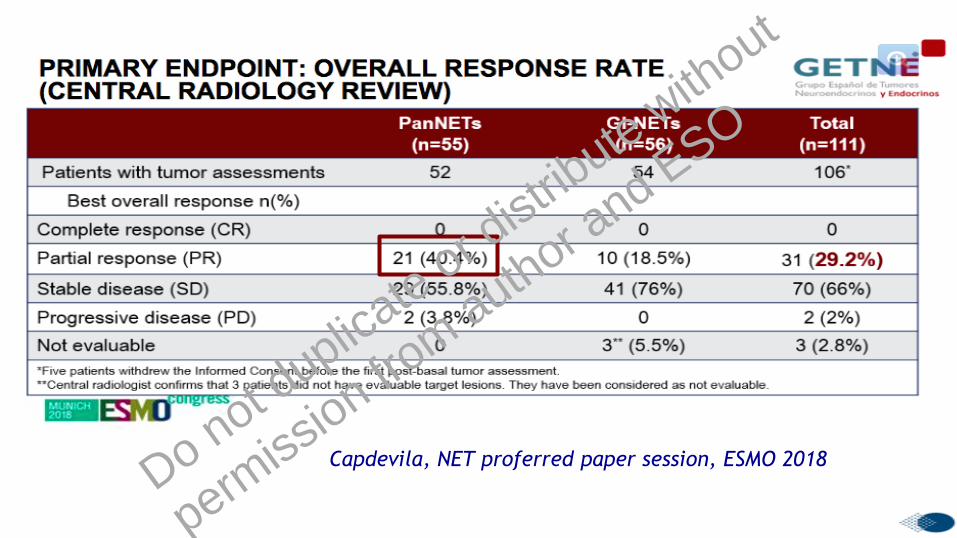
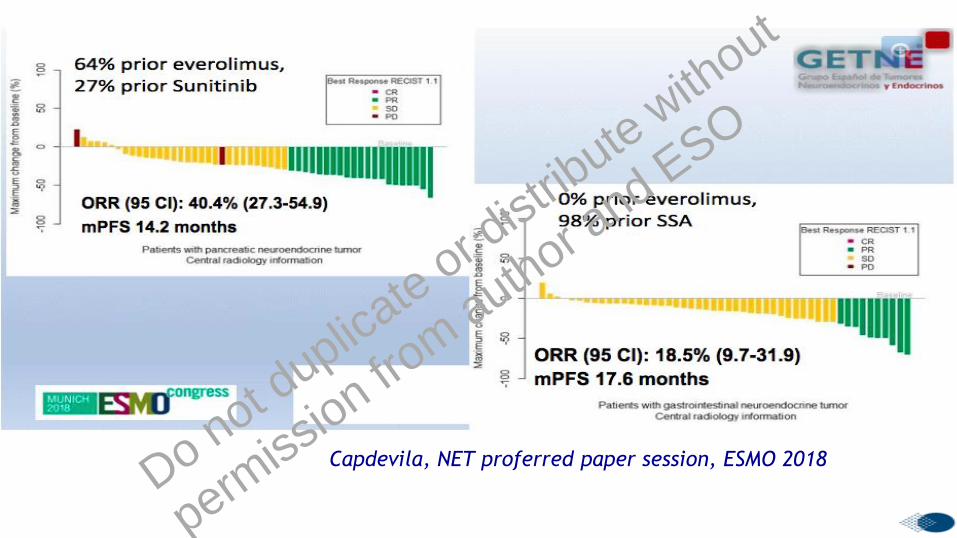
Capdevila, NET proferred paper session, ESMO 2018Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
Capdevila, NET proferred paper session, ESMO 2018Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
Capdevila, NET proferred paper session, ESMO 2018Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

Capdevila, NET proferred paper session, ESMO 2018Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

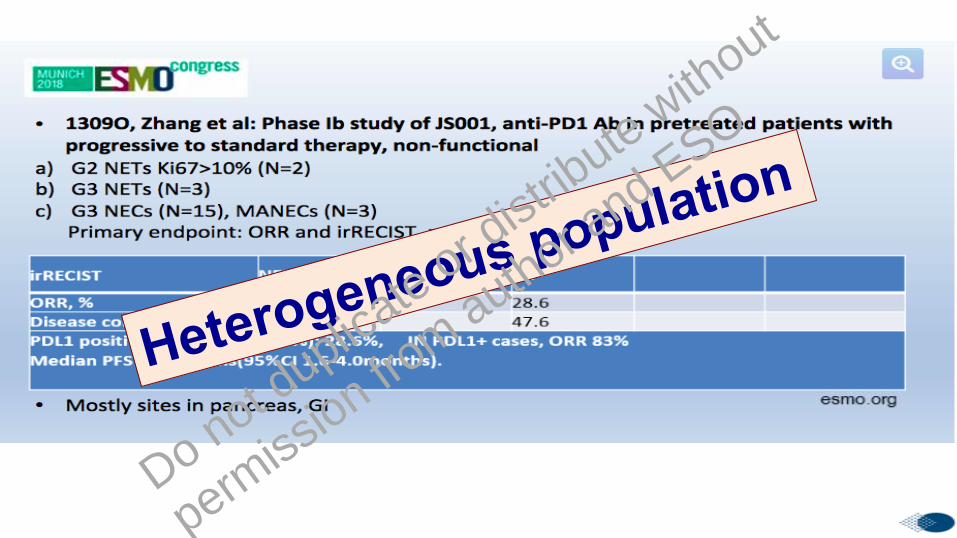
Immune checkpoint inhibitors
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

PDR001 in GEP and Lung NET/NEC
Phase II multi-cohort international study
PDR001 binds to PD-1 so blocking
both PD-L1 and PD-L2▪ Well differentiated:
▪ GI cohort (n=30)
▪ Pancreatic cohort (n=30)
▪ Thoracic cohort (n=30)
▪ Poorly differentiated:
▪ GEP cohort (n=20)
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

Statistical assumption: at least 10% PR
Yao, ESMO 2018 NET Proferred Paper SessionDo not duplica
te or distr
ibute without
permiss
ion from author a
nd ESO

Yao, NET proferred paper session, ESMO 2018Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

Pentheroudakis, ESMO 2018 NET Highlights
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

1
Pembrolizumab for Patients With PD-L1–Positive Advanced Carcinoid or Pancreatic Neuroendocrine Tumors: Results From the KEYNOTE-028 StudyJanice M. Mehnert,1 Emily Bergsland,2 Bert H. O’Neil,3 Armando Santoro,4 Jan H. M. Schellens,5 Roger B. Cohen,6
Toshihiko Doi,7 Patrick A. Ott,8 Michael J. Pishvaian,9 Igor Puzanov,10 Kyaw L. Aung,11 Chiun Hsu,12
Christophe Le Tourneau,13 Jean-Charles Soria,14 Elena Élez,15 Kenji Tamura,16 Marlena Gould,17 Guoqing Zhao,17
Karen Stein,17 Sarina A. Piha-Paul18
1Rutgers Cancer Institute of New Jersey, New Brunswick, NJ, USA; 2University of California San Francisco, San Francisco, CA, USA; 3Indiana University,
Simon Cancer Center, Indianapolis, IN, USA; 4Humanitas Research Hospital-Humanitas Cancer Center, Rozzano-Milano, Italy; 5Netherlands Cancer
Institute, Amsterdam, Netherlands; 6University of Pennsylvania, Philadelphia, PA, USA; 7National Cancer Center Hospital East, Chiba, Japan; 8Dana-
Farber Cancer Institute, Boston, MA, USA; 9Lombardi Comprehensive Cancer Center, Georgetown University, Washington, DC, USA; 10Roswell Park
Cancer Institute, Buffalo, NY, USA; 11Princess Margaret Cancer Centre, Toronto, ON, Canada; 12National Taiwan University Hospital, Taipei, Taiwan; 13Institut Curie, Paris, France; 14Institut Gustave Roussy Cancer Center, Villejuif, France; 15Vall d'Hebron University Hospital and Vall d'Hebron Institute of
Oncology (VHIO), Barcelona, Spain; 16National Cancer Center Hospital, Tokyo, Japan; 17Merck and Co., Inc., Kenilworth, NJ, USA; 18The University of
Texas MD Anderson Cancer Center, Houston, TX, USA
*Response assessment: Every 8 weeks for first 6 months; every 12 weeks thereafter
Primary endpoints: ORR per RECIST v1.1 (investigator review)
Secondary endpoints: PFS, OS, duration of response, and safety
KEYNOTE-028 (NCT02054806): Phase 1b Multicohort Study of Pembrolizumab for PD-L1+ Advanced Solid Tumors
Response
Assessment*
Pembrolizumab
10 mg/kg IV
Q2W
CR, PR, or SD
Treat for 24 months
or until
progressionb or
intolerable toxicity
Confirmed PDb or
unacceptable
toxicity
Discontinue
pembrolizumab
Patients
• Carcinoid tumors or
well or moderately
differentiated pNETs
• Failure of or inability to
receive standard
therapy
• ECOG PS 0 or 1
• ≥1 meas◆rable lesion
• PD-L1 positivitya
• No autoimmune
disease or interstitial
lung disease
aAt least 1% modified proportion score or interface pattern (QualTek IHC using 22C3 antibody clone).bIf SD or better when pembrolizumab discontin◆ed and s◆bseq◆ently ha❖e PD, patients may be eligible to res◆me pembroliz◆mab for ≥1 year.cIf clinically stable, patients are to remain on pembrolizumab until progressive disease is confirmed on a second scan performed ≥4 weeks later.
Mehnert J, ESMO 2017
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
ASCO 2018 Poster session: Vijayvergia et al.
Pembrolizumab monotherapy in patients with previously
treated metastatic high grade neuroendocrine neoplasms
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

CLOSING REMARKS
• Although many different treatments are available no
therapeutic sequence or integration has been validated so far
for tumor growth control
• Therefore GEP NET patients should be preferably managed
involving a NEN referral Centers with a NEN-dedicated MDT
• Predictive factors of response/efficacy are a urgent unmet
need
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

European Institute of Oncology, IEO, Milan, Italy
ENETS Center of Excellence for GEP NETs
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO




















