The use of the rib grafts in head and neck reconstruction
10
ORIGINAL ARTICLE The use of the rib grafts in head and neck reconstruction Alaa Kamel Abdel-Haleem a, * , Radwan Nouby b , Mohammed Taghian b a ENT Department, Assiut University Hospital, Assiut, Egypt b Department of Neurosurgery, Assiut University Hospital, Assiut, Egypt Received 5 June 2011; accepted 3 August 2011 Available online 16 September 2011 KEYWORDS Rib; Defects; Reconstruction Abstract Background: Many grafting materials are available for reconstructing variable defects of the head and neck. Objective: The aim is to describe the advantages and disadvantages of the rib grafts in head and neck reconstruction. Patients and methods: The rib grafts were used to reconstruct variable deformities and/or defects in the mandible (12 patients), nose (13 patients), skull and cranial base (six patients), maxilla (five patients), trachea (three patients), and auricle (one patient). Results: All patients showed good healing at the recipient site with successful reconstruction of the structural deformity and accepted esthetic and functional results indicating survival and take of the grafts except in one patient (2.5%) where graft necrosis occurred because of infection. Wound dehiscence and graft exposure were not reported. At the donor site, mild wound infection occurred in two patients (5%) which was controlled by conservative measures with no reports of dehiscence or pneumothorax. Conclusion: The rib provides reliable abundant grafting materials sufficient to successfully recon- struct variable defects in the head and neck region. ª 2011 Egyptian Society of Ear, Nose, Throat and Allied Sciences. Production and hosting by Elsevier B.V. All rights reserved. 1. Introduction Reconstruction of different kinds of defects or deformities of congenital or acquired etiology is a fundamental and frequent practice in head and neck surgery. The use of different types of autogenous grafting and alloplastic materials has minimized the resultant functional and cosmetic problems associated with such defects and deformities. 1 Alloplasts have the following advantages: unlimited availability, lack of donor site morbid- ity, ease of contouring, maintenance of shape and volume over time and relative simplicity of insertion. Although they have achieved widespread success, alloplasts have potentially serious complications of infection, aggressive foreign body 2090-0740 ª 2011 Egyptian Society of Ear, Nose, Throat and Allied Sciences. Production and hosting by Elsevier B.V. All rights reserved. Peer review under responsibility of Egyptian Society of Ear, Nose, Throat and Allied Sciences. doi:10.1016/j.ejenta.2011.08.004 Production and hosting by Elsevier * Corresponding author. Tel.: +20 088 236 1250, mobile: +20 010 553 4200. E-mail address: [email protected] (A. K. Abdel-Haleem). Egyptian Journal of Ear, Nose, Throat and Allied Sciences (2011) 12, 89–98 Egyptian Society of Ear, Nose, Throat and Allied Sciences Egyptian Journal of Ear, Nose, Throat and Allied Sciences www.esentas.org
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of The use of the rib grafts in head and neck reconstruction

Egyptian Journal of Ear, Nose, Throat and Allied Sciences (2011) 12, 89–98
Egyptian Society of Ear, Nose, Throat and Allied Sciences
Egyptian Journal of Ear, Nose, Throat and Allied
Sciences
www.esentas.org
ORIGINAL ARTICLE
The use of the rib grafts in head and neck reconstruction
Alaa Kamel Abdel-Haleem a,*, Radwan Nouby b, Mohammed Taghian b
a ENT Department, Assiut University Hospital, Assiut, Egyptb Department of Neurosurgery, Assiut University Hospital, Assiut, Egypt
Received 5 June 2011; accepted 3 August 2011Available online 16 September 2011
20
Sc
Pe
Th
do
*
55
E
KEYWORDS
Rib;
Defects;
Reconstruction
90-0740 ª 2011 Egyptian So
iences. Production and hosti
er review under responsibili
roat and Allied Sciences.
i:10.1016/j.ejenta.2011.08.004
Production and h
Corresponding author. Tel
3 4200.
-mail address: alaakamelent
ciety of
ng by Els
ty of Eg
osting by E
.: +20 08
@yahoo.
Abstract Background: Many grafting materials are available for reconstructing variable defects of
the head and neck.
Objective: The aim is to describe the advantages and disadvantages of the rib grafts in head and
neck reconstruction.
Patients and methods: The rib grafts were used to reconstruct variable deformities and/or defects in
the mandible (12 patients), nose (13 patients), skull and cranial base (six patients), maxilla (five
patients), trachea (three patients), and auricle (one patient).
Results: All patients showed good healing at the recipient site with successful reconstruction of the
structural deformity and accepted esthetic and functional results indicating survival and take of the
grafts except in one patient (2.5%) where graft necrosis occurred because of infection. Wound
dehiscence and graft exposure were not reported. At the donor site, mild wound infection occurred
in two patients (5%) which was controlled by conservative measures with no reports of dehiscence
or pneumothorax.
Conclusion: The rib provides reliable abundant grafting materials sufficient to successfully recon-
struct variable defects in the head and neck region.ª 2011 Egyptian Society of Ear, Nose, Throat and Allied Sciences.
Production and hosting by Elsevier B.V. All rights reserved.
Ear, Nose, Throat and Allied
evier B.V. All rights reserved.
yptian Society of Ear, Nose,
lsevier
8 236 1250, mobile: +20 010
com (A. K. Abdel-Haleem).
1. Introduction
Reconstruction of different kinds of defects or deformities ofcongenital or acquired etiology is a fundamental and frequentpractice in head and neck surgery. The use of different types of
autogenous grafting and alloplastic materials has minimizedthe resultant functional and cosmetic problems associated withsuch defects and deformities.1 Alloplasts have the following
advantages: unlimited availability, lack of donor site morbid-ity, ease of contouring, maintenance of shape and volume overtime and relative simplicity of insertion. Although they have
achieved widespread success, alloplasts have potentiallyserious complications of infection, aggressive foreign body

90 A.K. Abdel-Haleem et al.
reaction, extrusion and damage to the soft tissue and skin cov-ering.2 Among sources of non-vascularized autografts, the ribis unique in providing cartilage, bone, and combination of
both. The use of different rib components in grafting is anestablished and basic modality in nasal,3,4 auricular,5,6 crico-tracheal,7,8 cranial9,10 and mandibular reconstruction.11
The aim of this study is to describe the advantages and dis-advantages of the rib grafts in head and neck reconstruction.
2. Patients and methods
The rib grafts were used in reconstructing deformities ordefects in the craniomaxillofacial skeleton and trachea in 40
consecutive patients in the departments of ENT and neurosur-gery, Assiut University Hospital during the period fromMarch1999 to December 2009. They were 21 female and 19 male,
with an age range of 8–61 years. According to the site neededto be reconstructed, they were categorized into patients indi-cated for mandibular, nasal, cranial, maxillary, tracheal, andauricular reconstruction (Tables 1 and 2).
The preoperative clinical data of concern included the etiol-ogy, duration, site, and description of the structural, func-tional, and esthetic consequences of the deformity or the
defect.The radiologic investigations included plain chest X-ray,
orthopandentogram (panorama) in patients with mandibular
deformities, and CT and occasionally MRI before and aftercontrast administration in patients with tracheal stenosis andcranial and maxillary tumors.
Flexible fiberoptic laryngoscopy and rigid bronchoscopy
were done in patients with tracheal stenosis.
2.1. Graft harvesting, set, and fixation
The right sixth rib was harvested, osseous only or chondro-osseous (costochondral), for mandibular, maxillary and cra-nial reconstruction. An inframammary skin incision was done
down to the muscles that were split and retracted to expose therib. The periostium was sharply incised along the anterior sur-face of the rib and carefully dissected in a circumferential man-
ner from both surfaces by curved and Doyn elevators takingcare not to injure the underlying pleura. The bone was sharplyseparated from the chondral junction and cut posteriorly withbone cutting forceps. When a costochondral graft (CCG) was
desired for reconstructing the mandibular ramus, the perichon-drium on the anterior surface was preserved in continuity with
Table 1 Type of the rib grafts used in patients with mandibular, n
Diagnosis
Mandibular defects:
Unilateral temporomandibular joint ankylosis
Bilateral temporomandibular joint ankylosis
Flat body
Segmental post ablative defect
Nasal dorsal saddling
Tracheal stenosis
Cauliflower auricular deformity
a small strip of periostium. If another graft was desired thefourth one was harvested.
The right ninth costal cartilage was the source of cartilage
grafts used in reconstructing nasal dorsal saddling, trachealstenosis, and auricular deformities. A subcostal skin incisionwas used and dissection was continued as previously described
strictly in a circumferential subperichondrial fashion. Theanterior perichondrium was preserved in the cases of trachealreconstruction.
During harvesting, continuous palpation of the underlyingrib is essential to avoid pleural injury. Pneumothorax was ex-cluded by the absence of air leakage after filling the woundwith saline solution while the anesthetist was applying positive
pressure into the lungs. The wound was then infiltrated with5–10 ml of 2% xylocaine and closed in layers after applicationof a suction drain. The rib grafts used to reconstruct the man-
dible (split rib, onlay whole rib, CCGs) were fixed by 0.5 mmstainless steel wire or 13 mm long titanium self tabbing mini-screws preceded by maxillomandibular fixation that was re-
leased 1–3 weeks postoperatively (except in the patient wherethe rib was used as an onlay graft). For nasal reconstruction,an endonasal approach consisting of a transfixion septal inci-
sion and bilateral intercartilagenous incisions was used to cre-ate the dorsal and columellar pockets. The dorsal cartilagestrut was fixed to the upper lateral cartilage by a 4/0 polyglac-tin 910 transverse stitch on both sides. The columellar strut
was fixed to the anterior nasal spine and the medial crura ofthe lower lateral cartilage by 4/0 polyglactin 910 stitches. Incranioplasty, the rib bone was split, contoured by bone bend-
ing forceps, and fixed by stainless steel wires to the edges of theskull defect and by 2/0 polyglactin 910 stitches to the pericra-nium. The split ribs were fixed by 0.5 mm stainless steel wires
or to previously contoured titanium 2 mm thickness miniplatesthat were fixed to the remaining nasal, zygomatic and maxil-lary alveolar bones in mid face reconstruction. In tracheal
reconstruction, the trachea was exposed, tracheostome wasrefashioned, the stenotic area above the tracheostome was slitopened till the lumen was reached, a silicone tracheal T tubewas inserted and the rib cartilage was carved to reconstruct
the anterior tracheal wall with perichondrium facing mucosal.It was fixed to the trachea using 3/0 prolene stitches. The fol-lowing additive surgical procedures were done:
� Temporalis muscle flaps were used in patients with tempo-romandibular joint (TMJ) ankylosis (10 patients) and with
maxillary defects (five patients).
asal, tracheal, and auricular reconstruction.
Type of graft N
12
Unilateral costochondral graft 6
Bilateral costochondral graft 4
Onlay rib bone 1
Split rib bone 1
13
Dorsal and columellar cartilage struts 9
Dorsal cartilage strut 4
Costal cartilage 3
Costal cartilage 1

Table 2 The cause and the site of defects in patients subjected to cranioplasty and maxillary reconstruction.
Diagnosis Reconstructed defect N
Frontal osteoma Frontal bone 4–5 · 10 cm 2
Frontoethmoidal fibrous dysplasia Anterior cranial base: 2 · 5 cm 1
Medial wall of the orbit
Nasomaxillary buttress
Bifrontal interosseous meningioma Anterior cranial base: 4 · 10 cm 1
Bifrontal 9 · 20 cm
Frontal mucocoele Anterior cranial base 4 · 5 cm 1
Squamous cell carcinoma of the temporal bone Temporal bone 4 · 8 cm 1
Pleomorphic adenoma of palate Bilateral pterygomaxillary buttresses 2
Recurrent maxillary myxoma Pterygomaxillary buttress 1
Zygomaticomaxillary buttress
Orbital floor
Recurrent adenoid cystic carcinoma of the maxilla Pterygomaxillary buttress 1
Zygomaticomaxillary buttress
Osteomyelitis of the maxilla Pterygomaxillary buttress 1
Zygomaticomaxillary buttress
The use of the rib grafts in head and neck reconstruction 91
� Nasal osteotomies were done in three patients with saddlingand significant septal deviations were corrected in anotherthree patients.
� The pericranium was used to reconstruct the anterior cra-nial base with the split rib bone grafts in three patients.
Patients were followed up during a period that ranged fromsix months to six years.
3. Results
3.1. Patients with mandibular defects or deformities (Table 1)
All the patients with TMJ ankylosis (10 subjects) were suffer-ing from limitation of mouth opening, chewing difficulties,
multiple caries, and dental malocclusions following traumain the form of a fall on the chin dating back to a period of4–20 years. When such trauma was in the childhood period,the patients acquire facial deformity in the form of retrogna-
thia with symmetric face in bilateral ankylosis and asymmetryin the form of deviation of the chin to the affected side in uni-lateral cases. Such patients suffer from snoring and possible
sleep apnea.In these 10 patients the CCGs were used to reconstruct the
ramus after condylectomy and coronoidectomy. This was fol-
lowed by restoration of mouth opening as measured by a max-imal interincisal distance of more than 35 mm maintained bymouth training exercises for a period not less than 6 months.
Improvement of the esthetic deformity (retrognathia and facialasymmetry) was noted in all patients especially in youngpatients with unilateral ankylosis in the form of correction ofretrognathia and chin deviation except in a single patient (with
unilateral TMJ ankylosis) because of infection of the graft.Another patient needed to trim a projecting edge of the appliedCCG that was causing a prominent angle.
In another patient the use of the rib bone as an onlay graftwas followed by a satisfactory esthetic result in camouflagingthe post traumatic flattened right mandibular body deformity
(Fig. 1).The split rib bones were used to successfully reconstruct a
segmental mandibular body defect of 5 cm length followingexcision of an adenocarcinoma of the submandibular gland
with good healing and prevention of the post mandibulectomy
esthetic deformity.
3.2. Patients with nasal dorsal saddling (Table 1)
The cause of saddling in these patients was a neglected facialtrauma (10 patients) and previous submucous resection ofthe nasal septum (three patients). None had previous attempts
of surgical correction of saddling. Preoperatively, all thepatients were found to have variable degrees of broadeningand saddling of the nasal dorsum, shortening of the columella,rounded nostrils and tip deformity in the form of low projec-
tion and downward rotation (Fig. 2a). Three patients sufferedfrom nasal obstruction due to significantly deviated septum.Postoperatively all the patients reported satisfactory esthetic
results (Fig. 2b). None of the grafts was extruded. Woundshealed without reported infections. Minor degree of dorsalgraft wrapping was noted in a single patient.
3.3. Patients with cranial and skull base defects
The split rib bone grafts were used to primarily reconstruct
defects in the frontal (Figs. 3 and 4a) and temporal bones ofa size that ranges from 32 cm2 to 180 cm2 and in the anteriorcranial base with a size of 10–40 cm2 (Table 2). The ribs werecompletely filling the whole defect with rib to rib contact in all
the cranial defects except in the patient with the interosseousmeningioma where the defect consisted of both frontal bones(Fig. 4a). In all patients wound healing was reported without
infection, dehiscence or graft exposure. Good esthetic resultwas obtained in these patients with prevention of the sinkingskin flap syndrome with no reports of pulsating exophthalmos
or enophthalmos. A less satisfactory result, albeit accepted bythe patient, was noted in the patient with the bifrontal menin-gioma. CSF leaks were not reported.
3.4. Patients with maxillary defects
Together with the temporalis myofascial flaps, the split ribbone grafts fixed by plates and screws or wires were used in pri-
mary (four patients) (Fig. 4b) and secondary (one patient)
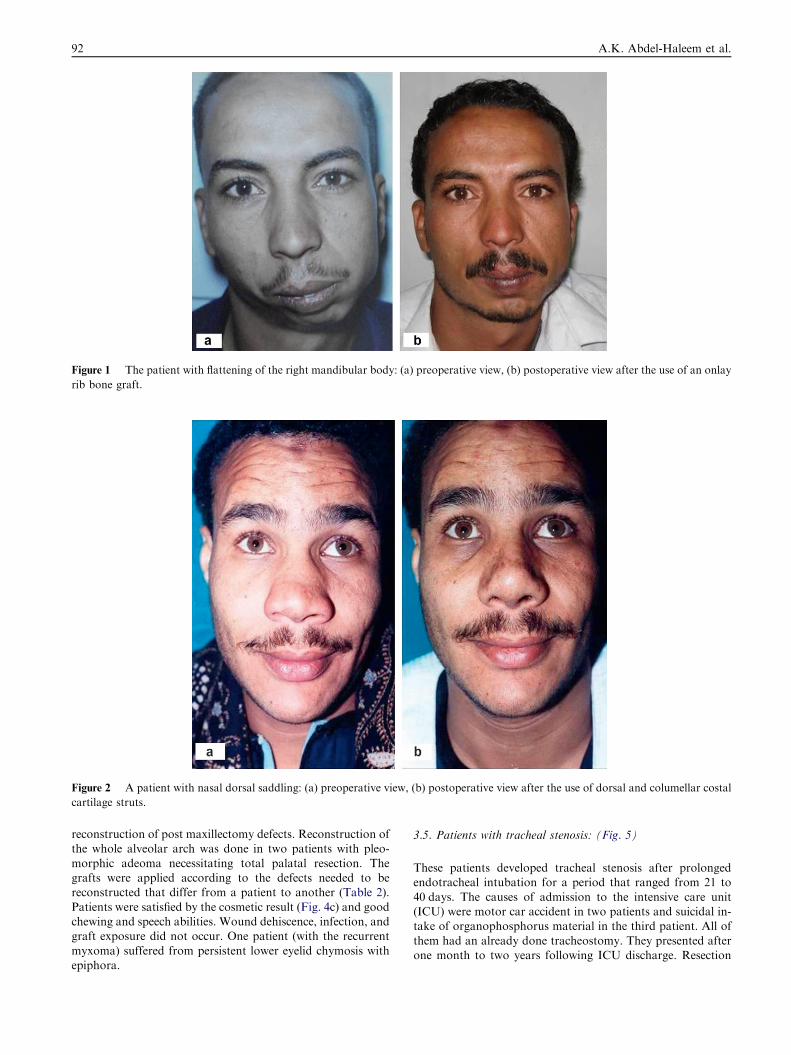
Figure 1 The patient with flattening of the right mandibular body: (a) preoperative view, (b) postoperative view after the use of an onlay
rib bone graft.
Figure 2 A patient with nasal dorsal saddling: (a) preoperative view, (b) postoperative view after the use of dorsal and columellar costal
cartilage struts.
92 A.K. Abdel-Haleem et al.
reconstruction of post maxillectomy defects. Reconstruction ofthe whole alveolar arch was done in two patients with pleo-
morphic adeoma necessitating total palatal resection. Thegrafts were applied according to the defects needed to bereconstructed that differ from a patient to another (Table 2).
Patients were satisfied by the cosmetic result (Fig. 4c) and goodchewing and speech abilities. Wound dehiscence, infection, andgraft exposure did not occur. One patient (with the recurrent
myxoma) suffered from persistent lower eyelid chymosis withepiphora.
3.5. Patients with tracheal stenosis: (Fig. 5)
These patients developed tracheal stenosis after prolongedendotracheal intubation for a period that ranged from 21 to
40 days. The causes of admission to the intensive care unit(ICU) were motor car accident in two patients and suicidal in-take of organophosphorus material in the third patient. All of
them had an already done tracheostomy. They presented afterone month to two years following ICU discharge. Resection
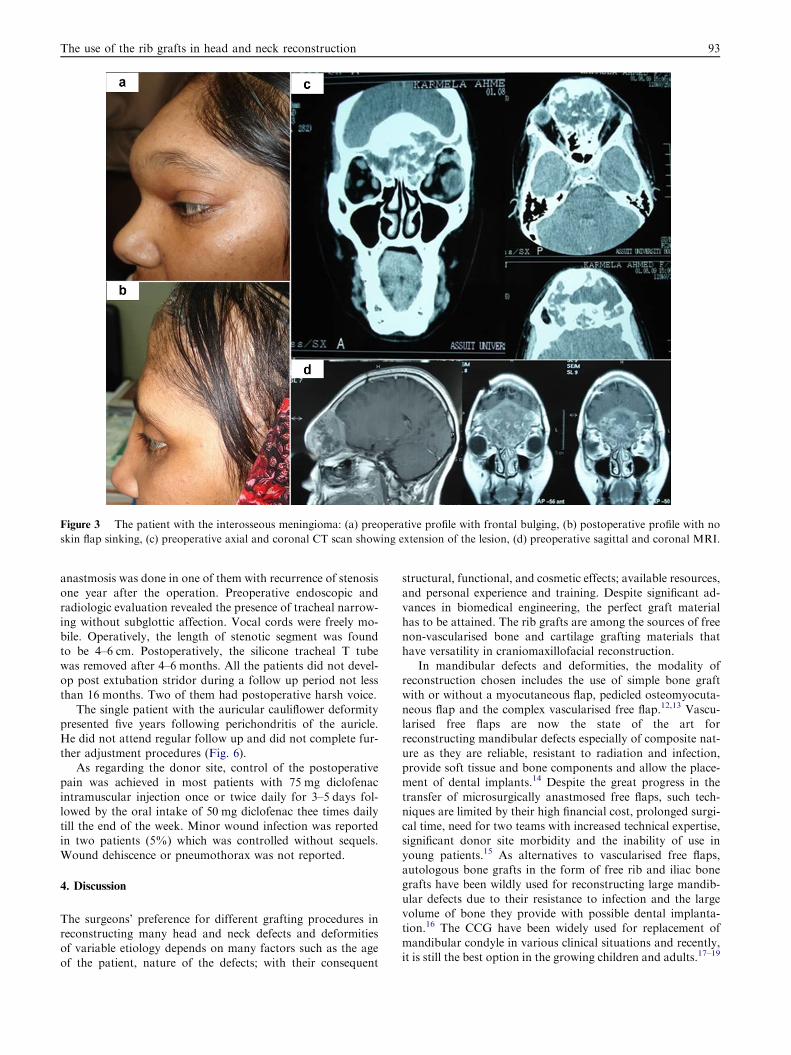
Figure 3 The patient with the interosseous meningioma: (a) preoperative profile with frontal bulging, (b) postoperative profile with no
skin flap sinking, (c) preoperative axial and coronal CT scan showing extension of the lesion, (d) preoperative sagittal and coronal MRI.
The use of the rib grafts in head and neck reconstruction 93
anastmosis was done in one of them with recurrence of stenosisone year after the operation. Preoperative endoscopic and
radiologic evaluation revealed the presence of tracheal narrow-ing without subglottic affection. Vocal cords were freely mo-bile. Operatively, the length of stenotic segment was foundto be 4–6 cm. Postoperatively, the silicone tracheal T tube
was removed after 4–6 months. All the patients did not devel-op post extubation stridor during a follow up period not lessthan 16 months. Two of them had postoperative harsh voice.
The single patient with the auricular cauliflower deformitypresented five years following perichondritis of the auricle.He did not attend regular follow up and did not complete fur-
ther adjustment procedures (Fig. 6).As regarding the donor site, control of the postoperative
pain was achieved in most patients with 75 mg diclofenac
intramuscular injection once or twice daily for 3–5 days fol-lowed by the oral intake of 50 mg diclofenac thee times dailytill the end of the week. Minor wound infection was reportedin two patients (5%) which was controlled without sequels.
Wound dehiscence or pneumothorax was not reported.
4. Discussion
The surgeons’ preference for different grafting procedures inreconstructing many head and neck defects and deformitiesof variable etiology depends on many factors such as the age
of the patient, nature of the defects; with their consequent
structural, functional, and cosmetic effects; available resources,and personal experience and training. Despite significant ad-
vances in biomedical engineering, the perfect graft materialhas to be attained. The rib grafts are among the sources of freenon-vascularised bone and cartilage grafting materials thathave versatility in craniomaxillofacial reconstruction.
In mandibular defects and deformities, the modality ofreconstruction chosen includes the use of simple bone graftwith or without a myocutaneous flap, pedicled osteomyocuta-
neous flap and the complex vascularised free flap.12,13 Vascu-larised free flaps are now the state of the art forreconstructing mandibular defects especially of composite nat-
ure as they are reliable, resistant to radiation and infection,provide soft tissue and bone components and allow the place-ment of dental implants.14 Despite the great progress in the
transfer of microsurgically anastmosed free flaps, such tech-niques are limited by their high financial cost, prolonged surgi-cal time, need for two teams with increased technical expertise,significant donor site morbidity and the inability of use in
young patients.15 As alternatives to vascularised free flaps,autologous bone grafts in the form of free rib and iliac bonegrafts have been wildly used for reconstructing large mandib-
ular defects due to their resistance to infection and the largevolume of bone they provide with possible dental implanta-tion.16 The CCG have been widely used for replacement of
mandibular condyle in various clinical situations and recently,it is still the best option in the growing children and adults.17–19

Figure 4 (a) Operative view showing the split rib grafts reconstructing the bifrontal defect in the patient with the interosseous
meningioma; (b) operative view of the split rib graft reconstructing the zygomaticomaxillary and pterygomaxillary buttresses; (c)
postoperative view of a patient after maxillary reconstruction with an accepted esthetic appearance; (d) postoperative 3DCT scan of the
patient in (c) showing the survived bone grafts.
94 A.K. Abdel-Haleem et al.
In this study 14 CCGs were used to reconstruct the mandibularramus after condylectomy in 10 patients with TMJ ankylosis
(four bilateral and six unilateral). In such cases the graft wasproved to have the advantages of restoring the shortened pos-terior face height, correcting the facial disfigurement in the
form of symmetric and non-symmetric retrognathia, prevent-ing recurrence of the ankylosis, and providing a potential forgrowth in children.20 Graft loss because of infection seems tobe the major disadvantage of the use of CCG. The periopera-
tive administration of systemic antibiotics and the temporarystorage of the graft in an antibiotic/saline solution are consid-ered to limit the incidence of such infection.18 This complica-
tion was reported in a single out of 10 patients with relapseof retrognathia that is planned to be corrected by mandibularadvancement using distraction osteogenesis. Although there
are reports of CCG overgrowth,21 such phenomenon was notreported in this study possibly because of the limited numberof patients. Based on a histological study, the asymmetric mas-ticatory movement and the uneven loading of the recon-
structed condyle were suggested to interpret overgrowth ofCCG.22
In the remaining two patients, where the significant bone
defect or deformity requires large volume of bone, the prefer-able grafting material would be either the rib or the ilium asalternatives to the vasularized bone transfer. Although the iliac
bone graft is preferred by some authors in reconstructing seg-mental mandibular defects because of providing bone of favor-
able thickness in accepting implants and restoring alveolarcrest,16 it was not used in the patient with the postablative de-
fect because of her refusal. In the patient with flattening of themandibular body, the rib was a more favorable choice becauseof its shape similarity, suitable thickness and pliability in con-
touring than the iliac bone. Still the problem of resorption islimiting the use of autologous bone grafting. Recently, theaddition of bone inducing factors as Recombinant Bone Mor-phogenetic Proteins as an osteoinductive material to the con-
ventional osteoconductive graft scaffolds, was tried withsuccessful results in achieving predictable reconstruction andpreventing graft resorption.13 Another point of importance
in preventing graft resorption, is stabilization of the graftedbone by maxillomandibular fixation and proper rigid fixationof the graft to the recipient site allowing bone to bone
contact.12,18,23
Several grafting and alloplastic materials are described incorrection and augmentation of the nasal saddling deformitythat results from reduced structural support secondary to sur-
gery, trauma or infection.2 Although alloplasts have multipleadvantages, many experts believe that they should not be thefirst choice particularly in rhinoplastic procedures as they have
increased risk of extrusion because of three reasons; first, thenose being of prominent location is commonly traumatizedwith an increased risk of trauma-associated displacement and
extrusion, second, the thin skin soft tissue envelope providinglittle cushioning for the alloplast, and third, mobility of the
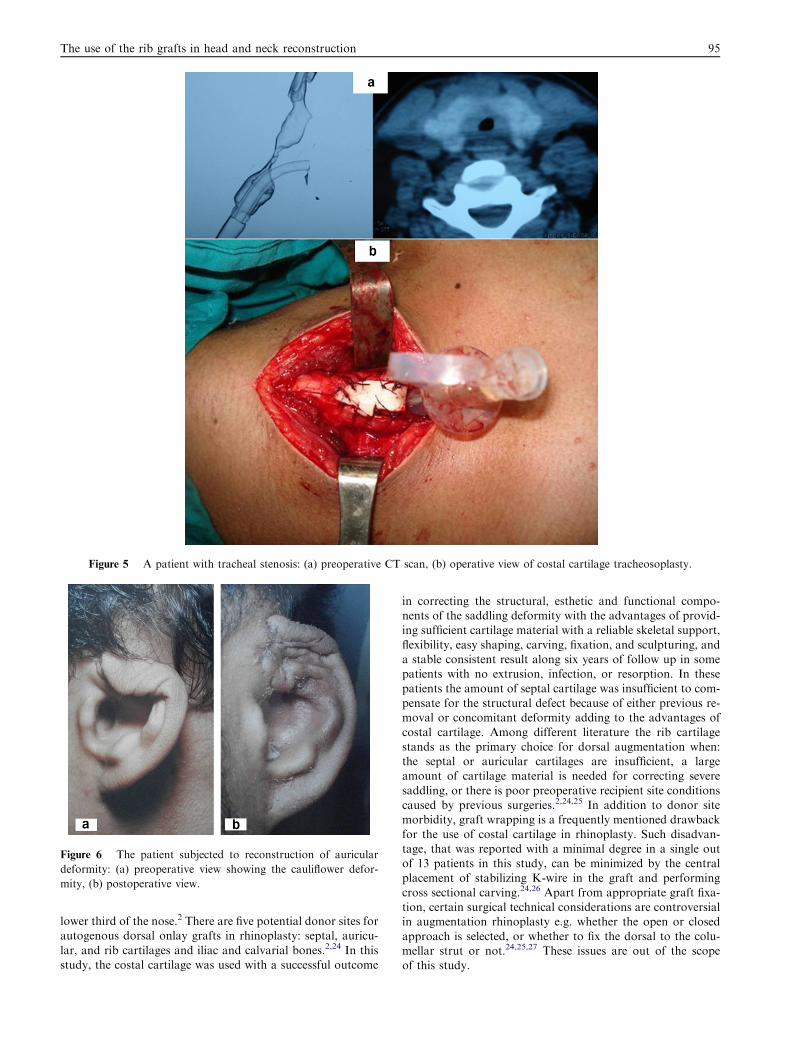
Figure 5 A patient with tracheal stenosis: (a) preoperative CT scan, (b) operative view of costal cartilage tracheosoplasty.
Figure 6 The patient subjected to reconstruction of auricular
deformity: (a) preoperative view showing the cauliflower defor-
mity, (b) postoperative view.
The use of the rib grafts in head and neck reconstruction 95
lower third of the nose.2 There are five potential donor sites forautogenous dorsal onlay grafts in rhinoplasty: septal, auricu-
lar, and rib cartilages and iliac and calvarial bones.2,24 In thisstudy, the costal cartilage was used with a successful outcome
in correcting the structural, esthetic and functional compo-nents of the saddling deformity with the advantages of provid-ing sufficient cartilage material with a reliable skeletal support,
flexibility, easy shaping, carving, fixation, and sculpturing, anda stable consistent result along six years of follow up in somepatients with no extrusion, infection, or resorption. In these
patients the amount of septal cartilage was insufficient to com-pensate for the structural defect because of either previous re-moval or concomitant deformity adding to the advantages of
costal cartilage. Among different literature the rib cartilagestands as the primary choice for dorsal augmentation when:the septal or auricular cartilages are insufficient, a largeamount of cartilage material is needed for correcting severe
saddling, or there is poor preoperative recipient site conditionscaused by previous surgeries.2,24,25 In addition to donor sitemorbidity, graft wrapping is a frequently mentioned drawback
for the use of costal cartilage in rhinoplasty. Such disadvan-tage, that was reported with a minimal degree in a single outof 13 patients in this study, can be minimized by the central
placement of stabilizing K-wire in the graft and performingcross sectional carving.24,26 Apart from appropriate graft fixa-tion, certain surgical technical considerations are controversialin augmentation rhinoplasty e.g. whether the open or closed
approach is selected, or whether to fix the dorsal to the colu-mellar strut or not.24,25,27 These issues are out of the scopeof this study.

96 A.K. Abdel-Haleem et al.
The surgical repair of large skull defects is still a challengefor the craniofacial surgeon. In addition to the cosmetic consid-erations, these defects when large leave a significant area of the
brain unprotected and are known to be associated with chronicheadache, developmental delay in young children, and the syn-drome termed sinking-skin-flap syndrome.10,28,29 Alloplasts
and autologous grafts are the options for cranioplasty. Amongalloplasts titanium has been used extensively in the last 20 yearsdue to its malleability, lightweight, and bioinert and non-mag-
netic properties.10,30 Others include polymethylmethacrylate,31
hydroxyapatite32 and more recently bioceramics.33 Because ofthe increased rate of infection, extrusion, and intense foreignbody reaction associated with the use of alloplasts, cranioplasty
using autologous split rib and calvarium has been universallyaccepted as the preferred option in adults and pediatric pa-tients.33–35 In this study the split rib was preferred than the split
calvarium although the latter is easier to harvest during crani-oplasty without the need for an extracranial operation. Splitcalvarium is harder, stiffer, and difficult to shape and bend than
the rib graft. Moreover, it is limited by the individually variableskull thickness and cannot provide large amount of bone toreconstruct big cranial defects. Follow up of the patients in this
study proved the ability of the rib graft to not only preventproblems of cranial defects but also successfully reconstructskull base defects avoiding their drastic complications. Theuse of split rib grafts placed across each other arranged in a
fashion mimicking the baseball catcher’s mask is a recentlyintroduced novel surgical solution to solve the problem of hugedefects with minimal grafting material.36,37
Different techniques are readily available to reconstruct par-tial maxillectomy defects with a considerable success. A pros-thetic obturator is a simple solution for a small defect after
inferior maxillectomy.38 A clasp retained obturator can laterbe substituted by a more stable one based on bone anchored im-plants. In edentulous patients with poor prosthetic stability or
in large inferior maxillectomy defects, the temporalis muscleflap is an easy, simple, and reliable method of reconstruction.39
However, reconstruction of extensive post maxillectomy de-fects is among the most difficult surgical tasks because of their
complex nature involving soft tissue and bone components, theresultant esthetic grotesque deformity and the associated func-tional disability in eating, and speaking. With the development
of vascularized composite tissue transfer using microsurgicaltechniques, reconstruction of such maxillary defects has beenachieved to a high level of functional and esthetic results.40
Limitations to such techniques were previously mentioned.As an alternative to the vascularised composite flaps the splitrib grafts fixed to previously contoured miniplates supportedby the temporalis myofascial flap were used in reconstructing
partial as well as total maxillary defects in the patients of thepresent study whether primary or secondary. Following thistechnique, considerably accepted esthetic and functional results
were obtained with a clinical and radiological evidence of a reli-able skeletal support without noticeable resorption for at leasttwo years (Fig. 4c and d). The important role of buttress recon-
struction in the surgical management of maxillary skeletal de-fects has been addressed.41 The split rib grafts were fixed byinterosseous wires or miniplates in a manner affording restora-
tion of the pterygomaxillary and/or the zygomaticomaxillarybuttresses which is an important approach to obtain the mosteffective reconstruction of complex maxillectomy defects.40
Several therapeutic procedures are described for managingtracheal stenosis including observation, tracheostomy, balloondilatation, laser and a variety of open surgical procedures.42
Laser vaporization proved disappointing results in circumfer-ential scarring of segments more than 1 cm.43 Various stentsto enlarge the stenotic part of the trachea have been used,
but the indications for their use are not clear. The choice ofthe open surgical procedures depends on the length of the ste-notic segment. Segmental tracheal resection with an end to end
anastmosis became the best method but only for short stenoticsegment without involvement of the upper part of the subglot-tis. For patients with medium length stenosis, the slide trache-oplasty has become a preferred method that doubles the
circumference of the trachea. In long segment tracheal steno-sis, tracheal reconstruction with a variety of grafting materialshas been the surgical treatment of choice.42 The costal cartilage
has been useful in this study as a grafting material in tracheo-plasty as preferred by many studies.44,45 The abundance of car-tilage material sufficient to reconstruct long tracheal segment,
stability, strength, absence of resorption and ease of shapingand fixation resemble the advantages of the costal cartilagein tracheoplasty. In general tracheoplasty is considered suc-
cessful if the patient is decannulated with an adequate com-fortable breathing without the need for reintubation over along period of follow up. The three patients suffering frompostintubtion tracheal stenosis presented in this study were
successfully decannulated and practiced a normal physicalactivity without respiratory difficulty along a period of followup not less than 16 months.
Although used in a single patient, the use of rib graft is anestablished modality in auricular reconstruction.46 Because ofthe complexity of the auricular structure, the tedious process
of harvesting rib cartilage, the difficulty of achieving an esthet-ically satisfactory result, the multiplicity of the surgical stagestill an end result is obtained with the possible need for revision
and skin expansion, some prefer the use of other reconstructivemethods as the porous polyethylene implants or osseointegrat-ed prosthesis.46,47 From the result shown in the single patientof this study, advantages of the costal cartilage grafts in auric-
ular reconstruction could not be stated with the need of morepatients compliant for follow up.
The post operative pain and the threat of pneumothorax
present the major rib graft donor site morbidities. The formerwas reduced by performing muscle ‘‘split’’ rather than ‘‘cut’’during flap harvest, infiltration of the wound with xylocaine
at the end of the procedure, and the use of post operative anal-gesia. Pneumothorax was prevented by strict preservation ofthe posterior periosteum.
In this study, the rib showed the potential to supply the
reconstructive surgeon with cartilage and/or bone of abundantamount that provide suitable grafting materials in many headand neck defects and/or deformities that are easily shaped,
bent, sculptured, and fixed with bone of good osteoconductiveproperty and a fair degree of resorption resistance. The ampleblood supply of the head and neck region which is assumed to
inhibit bone graft resorption36 may explain the high rate of ribgraft take in this study with a single case of graft loss (2.5%)because of infection. The good osteoconductivity of the split
rib graft refers to its high content of progenitor cells which willinitiate the bone formation at a short span of time13. However,stating particular advantages of the rib grafts in each defect
The use of the rib grafts in head and neck reconstruction 97
requires further studies including large number of patientsamong each category of defects with a longer follow up.
5. Conclusions
� The rib provides reliable abundant grafting materials suffi-cient to successfully reconstruct variable defects in the headand neck region.
� The best use of the rib cartilage is in dorsal augmentation ofthe nasal saddling deformity and in tracheoplasty.� The costochondral graft is the modality of choice in recon-
structing the mandibular ramus.� The split rib bones are reliable grafts in cranioplasty.� The rib bone can be an alternative to composite vascular-
ised flaps in maxillary and mandibular reconstruction.
References
1. Gurtner GC, Evans GR. Advances in head and neck reconstruc-
tion. Plast Reconstr Surg. 2000;106:672–682.
2. Ansari K, Asaria J, Hilger P, Adamson PA. Grafts and implants in
rhinoplasty-Techniques and long-term results. Operat Tech Otolar-
yngol. 2008;19:42–58.
3. Daniel RK. Rhinoplasty and rib grafts: evolving a flexible operative
technique. Plast Reconstr Surg. 1994;94:597–609.
4. Cakmak O, Ergin T. The versatile autogenous costal cartilage graft
in septorhinoplasty. Arch Facial Plast Surg. 2002;4:172–176.
5. Brent B. The correction of microtia with autogenous cartilage
grafts: II. Atypical and complex deformities. Plast Reconstr Surg.
1980;66:13–21.
6. Thorne CH, Brecht LE, Bradley JP, et al. Auricular reconstruction:
indications for autogenous and prosthetic techniques. Plast Recon-
str Surg. 2001;107:1241–1252.
7. Zalzal GH. Rib cartilage grafts for the treatment of posterior glottic
and subglottic stenosis in children. Ann Otol Rhinol Laryngol.
1988;97:506–511.
8. Zalzal GH. Treatment of laryngotracheal stenosis with anterior and
posterior cartilage grafts: a report of 41 children. Arch Otolaryngol
Head Neck Surg. 1993;119:82–86.
9. Taggard DA, Menezes AH. Successful use of rib grafts for
cranioplasty in children. Pediatr Neurosurg. 2001;34:149–155.
10. Josan VA, Sgouros S, Walsh AR, Dover MS, Nishikawa H,
Hockley AD. Cranioplasty in children. Childs Nerv Sust.
2005;21:200–204.
11. Wersall J, Bergstedt H, Korlof B, Lind MG. Split-rib graft for
reconstruction of the mandible. Otolaryngol Head Neck Surg.
1984;92:270–276.
12. Banerjee AR, Westmore GA. Free rib graft reconstruction of the
mandible: a forgotten option? Ann R Coll Surg Engl.
1995;77:278–282.
13. Balaji SM. Mandibular cystic defect: A composite approach with
rhBMP-2 and rib graft. J Maxillofac Oral Surg. 2009;8:27–30.
14. Mehta R, Deschler DG. Mandibular reconstruction in 2004: An
analysis of different techniques. Curr Opin Otolaryngol Head Neck
Surg. 2004;12:288–293.
15. Stosic S. Mandibular reconstruction state-of-the-art and perspec-
tives. Vojnosanit Pergl. 2008;65:397–403.
16. Guven O. Rehabilitation of severely atrophied mandible using iliac
crest bone grafts and dental implants: report of two cases. J Oral
Implatol. 2007;33:122–126.
17. MacIntosch RB. Current spectrum of costochondral and dermal
grafting. In: Bell WH, editor. Modern practice in orthognathic and
reconstructive surgery, vol. 2. Philadelphia: WB Saunders;
1992:872–949.
18. Donkor P, Bankas DO, Boakey G, Ansah S, Acheampong AO.
The use of autogenous rib grafts in maxillofacial reconstruction.
Ghana Med J. 2006;40:127–131.
19. Ahmed J, Chuckwulobelu R, Sebire NJ, Hartely REJ, Dunaway
DJ. Hemimandibulectomy and autologous costochondral rib graft
reconstruction for a case of melanotic neuroectodemal tumour of
infancy arising within the mandible. Int J Ped Otolarhinolaryngol
Extra. 2007;2:189–193.
20. El Sheikh MM, Medra AM. Management of unilateral temporo-
mandibular joint ankylosis associated with facial asymmetry. J
Craniomaxillofac Surg. 1997;25:109–115.
21. Samman N, Cheung LK, Tideman H. Overgrowth of a costo-
chondral graft in an adult male. Int J Oral Maxillofac Surg.
1995;24:333–335.
22. Peltomaki T, Quevedo LA, Jeldes G, Ronning O. Histology of
surgically removed overgrown osteochondral rib grafts. J Cranio-
maxillofac Surg. 2002;30:355–360.
23. Collyer J, McKenzie J, Sneddon KJ. Screw and ‘‘washer’’ fixation
for onlay rib grafts to the mandible. Br J Oral Maxillofac Surg.
2008;46:609.
24. Gunter JP, Cochran CS, Marin VP. Dorsal augmentation with rib
cartilage. Semin Plast Surg. 2008;22:74–89.
25. Riechelman H, Rettinger G. Three-step reconstruction of complex
saddle nose deformities. Arch Otolaryngol Head Neck Surg.
2004;130:334–338.
26. Adams WP, Rohrich RJ, Gunter JP, et al.. The rate of wrapping
in irradiated and non irradiated homograft rib cartilage: A
controlled comparison and clinical implications. Plast Reconstr
Surg. 1999;103:265–270.
27. Constantian MB. Rhinoplasty in graft-depleted patient. Oper Tech
Plast Reconstr Surg. 1995;2:67–81.
28. Schwabeggwr AH, Rainer C, Laimer I, Huemer GM. Hemispheric
brain volume replacement with free latissimus dorsi flap as first
step in skull reconstruction. Microsurgery. 2005;25:325–328.
29. Stula D. The problem of the ‘‘sinking skin-flap syndrome’’ in
cranioplasty. J Maxillofac Surg. 1982;10:142–145.
30. Ducic Y. Titanium mesh and hydroxyapatite cement cranioplasty:
a report of 20 cases. J Oral Maxillofac Surg. 2002;60:272–276.
31. Eppley BL. Biomechanical testing of alloplastic PMMA cranio-
plasty materials. J Craniofac Surg. 2005;16:140–143.
32. Durham SR, McComb JG, Levy ML. Correction of large
(>25 cm2) cranial defects with ‘‘reinforced’’ hydroxyapatite
cement: technique and complications. Neurosurgery.
2003;52:842–845.
33. de Oliveira RS, Brigato R, Madureira JFG, et al. Reconstruction
of a large complex skull defect in a child: a case report and
literature review. Childs Nerv Syst. 2007;23:1097–1102.
34. Matsuno A, Tanaka H, Iwamuro H, et al.. Analyses of the factors
influencing bone graft infection after delayed cranioplasty. Acta
Neurochir (Wien). 2006;148:535–540.
35. Moreira-Gonzalez A, Jackson IT, Miyawaki T, Barakat K,
DiNick V. Clinical outcome in cranioplasty: critical review in
long-term follow up. J Craniofac Surg. 2003;14:144–153.
36. Takumi I, Akimoto M. Catcher’s mask cranioplasty for extensive
cranial defects in children with an open head trauma: a novel
application of partial cranioplasty. Childs Nerv Syst.
2008;24:927–932.
37. Takumi I, Akimoto M. Advantage of the Catcher’s mask
cranioplasty for post-surgical infectious skin trouble. Childs Nerv
Syst. 2009;25:493–495.
38. Aramany MA, Meyrs EN. Prosthetic reconstruction following
resection of the hard and soft palate. J Prosthetic Dent.
1978;16:174–178.
39. Dallan I, Lenzi R, Sellari-Franceschini S, Tschabitscher M,
Muscatello L. Temporalis myofacial flap in maxillofacial recon-
struction: anatomical study and clinical application. J Cranio-
Maxillofac Surg. 2009;37:96–101.

98 A.K. Abdel-Haleem et al.
40. Yamamto Y. Mid-face reconstruction after maxillectomy. Int J
Clin Oncol.. 2005;10:218–222.
41. Yamamto Y, Kawashima K, Sugihara T, et al. Surgical manage-
ment of maxillectomy defects based on the concept of buttress
reconstruction. Head Neck. 2004;26:147–256.
42. Phipps LM, Raymond JA, Angeletti TM. Congenital tracheal
stenosis. Crit Care Nurse. 2006;26:60–69.
43. Duncavage JA, Ossoff RH, Toohill RJ. Carbon dioxide laser
management of laryngeal stenosis. Ann Otol Rhinol Laryngol.
1985;94:565–569.
44. Younis RT, Lazar RH, Astor F. Posterior cartilage graft in a
single-stage laryngotracheal reconstruction. Otolaryngol Head
Neck Surg. 2003;129:168–175.
45. Pradhan T, Kapil S, Thakar A. Posterior cricoid split with costal
cartilage augmentation for high subglottic stenosis. Indian J
Otolaryngol Head Neck Surg. 2008;60:147–151.
46. Dashan Y, Haiyue J, Qinghua Y, et al. Technical innovations in
ear reconstruction using a skin expander with autogenous cartilage
grafts. J Plast Reconstr Aesthet Surg. 2008;61:559–569.
47. Lee TS, Lim SY, Pyon JK, Mun GH, Bang SI, Oh KS. Secondary
revisions due to unfavourable results after microtia reconstruction.
J Plast Reconstr Aesthet Surg. 2010;63:940–946.