Massage for Mechanical Neck Disorders - A Systematic Review
10
SPINE Volume 32, Number 3, pp 353–362 ©2007, Lippincott Williams & Wilkins, Inc. Massage for Mechanical Neck Disorders A Systematic Review Jeanette Ezzo, PhD, CMT,* Bodhi G. Haraldsson, RMT,† Anita R. Gross, MSc,‡ Cynthia D. Myers, PhD, LMT,§ Annie Morien, PhD, PA-C, LMT, Charlie H. Goldsmith, PhD,¶ Gert Bronfort, PhD, DC,# Paul M. Peloso, MD, MSc,** and the Cervical Overview Group Study Design. Systematic review. Objective. To assess the effects of massage on pain, function, patient satisfaction, cost of care, and adverse events in adults with neck pain. Summary of Background Data. Neck pain is common, disabling, and costly. Massage is a commonly used mo- dality for the treatment of neck pain. Methods. We searched several databases without lan- guage restriction from their inception to September 2004. We included randomized and quasirandomized trials. Two reviewers independently identified studies, abstracted data, and assessed quality. We calculated the relative risks and standardized mean differences on primary outcomes. Trials could not be statistically pooled because of heterogeneity in treatment and control groups. Therefore, a levels-of-evi- dence approach was used to synthesize results. Results. Overall, 19 trials were included, with 12/19 receiving low-quality scores. Descriptions of the massage intervention, massage professional’s credentials, or expe- rience were frequently missing. Six trials examined mas- sage as a stand-alone treatment. The results were incon- clusive. Results were also inconclusive in 14 trials that used massage as part of a multimodal intervention be- cause none were designed such that the relative contri- bution of massage could be ascertained. Conclusions. No recommendations for practice can be made at this time because the effectiveness of massage for neck pain remains uncertain. Pilot studies are needed to characterize massage treatment (frequency, duration, number of sessions, and massage technique) and estab- lish the optimal treatment to be used in subsequent larger trials that examine the effect of massage as either a stand- alone treatment or part of a multimodal intervention. For multimodal interventions, factorial designs are needed to determine the relative contribution of massage. Future reports of trials should improve reporting of the conceal ment of allocation, blinding of outcome assessor, adverse events, and massage characteristics. Standards of reporting for massage interventions, similar to Consolidated Stan- dards of Reporting Trials, are needed. Both short and long-term follow-up are needed. Key words: neck pain, cervical dysfunction, cervico- genic headache, mechanical neck disorders, massage, manual therapy, whiplash, chronic pain. Spine 2007;32: 353–362 Neck disorders are common, and can be severely dis- abling and costly. 1–6 According to the 2003 US National Health Interview Survey, 15% of adults age 18 years and older reported that in the past 3 months, they had expe- rienced neck pain that had lasted 1 day or more. Of these, 15% experienced migraine or severe headache lasting 1 day or more. 7 Neck pain frequently becomes chronic, and 10% of males and 17% of females have reported neck pain that has lasted longer than 6 months. 8 Motor vehicle crashes leave 24% to 50% of subjects with persistent symptoms at 12 months. 9 Mas- sage is commonly used to treat persistent neck pain. However, studies of its effectiveness on neck pain have been inconclusive. 10 –15 The objectives of this review were: (1) to assess the efficacy and effectiveness of massage. either alone or in combination with other treatments on pain, function/ disability, patient satisfaction, and global perceived ef- fect in adults with mechanical neck disorders; (2) to as- sess the secondary outcomes of adverse events and cost of care; and (3) where appropriate, to conduct sensitivity analysis to assess the influence of study methodological quality, symptom duration, and subtypes of neck disor- der on the magnitude of treatment effects. Materials and Methods Inclusion Criteria. Any published or unpublished random- ized controlled trial (RCT) or quasi-RCT, either in full text or abstract form, was included. The participants were adults who suffered from acute (less than 30 days), subacute (30–90 days), or chronic (greater than 90 days) neck disorders. Neck disor- ders were categorized as: (1) mechanical neck disorders, includ- ing whiplash-associated disorders category I and II, 16,17 myo- fascial neck pain, and degenerative changes 18 ; (2) neck disorder with headache 19 –21 ; and 3 neck disorders with radicular find- ings, including whiplash-associated disorders category III. 16,17 Studies were excluded if they investigated neck disorders with: (1) definite or possible long tract signs (e.g., myelopa- thies); (2) neck pain caused by other pathologic entities (e.g., rheumatoid arthritis, ankylosing spondylitis, spasmodic torti- collis, fractures, and dislocations) 18 ; (3) headache not of cervi- From *JPS Enterprises, Baltimore, MD; †West Coast College of Mas- sage Therapy, Massage Therapy Association of British Columbia, Van- couver, British Columbia, Canada; ‡McMaster University, Hamilton, Ontario, Canada; §Integrative Medicine Program, H. Lee Moffitt Can- cer Center and Research Institute, Tampa, FL; Dermatology and Skin Cancer Clinic, Gainesville, FL; ¶Department of Clinical Epidemiology & Biostatistics, McMaster University, and Father Sean O’Sullivan Re- search Centre, St. Joseph’s Healthcare, Hamilton, Ontario, Canada; #Northwestern Health Sciences University, Bloomington, MN; and **Product Benefit Risk Assessment and Management, Amgen Inc., Thousand Oaks, CA. The manuscript submitted does not contain information about medical device(s)/drug(s). Institutional and Professional Organizational funds were received in support of this work. No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this manuscript. Address correspondence and reprint requests to Jeanette Ezzo, PhD, CMT, 1905 West Rogers Avenue, Baltimore, MD 21209; E-mail: [email protected] 353
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Massage for Mechanical Neck Disorders - A Systematic Review

SPINE Volume 32, Number 3, pp 353–362©2007, Lippincott Williams & Wilkins, Inc.
Massage for Mechanical Neck DisordersA Systematic Review
Jeanette Ezzo, PhD, CMT,* Bodhi G. Haraldsson, RMT,† Anita R. Gross, MSc,‡Cynthia D. Myers, PhD, LMT,§ Annie Morien, PhD, PA-C, LMT,� Charlie H. Goldsmith, PhD,¶Gert Bronfort, PhD, DC,# Paul M. Peloso, MD, MSc,** and the Cervical Overview Group
Study Design. Systematic review.Objective. To assess the effects of massage on pain,
function, patient satisfaction, cost of care, and adverseevents in adults with neck pain.
Summary of Background Data. Neck pain is common,disabling, and costly. Massage is a commonly used mo-dality for the treatment of neck pain.
Methods. We searched several databases without lan-guage restriction from their inception to September 2004.We included randomized and quasirandomized trials. Tworeviewers independently identified studies, abstracted data,and assessed quality. We calculated the relative risks andstandardized mean differences on primary outcomes. Trialscould not be statistically pooled because of heterogeneity intreatment and control groups. Therefore, a levels-of-evi-dence approach was used to synthesize results.
Results. Overall, 19 trials were included, with 12/19receiving low-quality scores. Descriptions of the massageintervention, massage professional’s credentials, or expe-rience were frequently missing. Six trials examined mas-sage as a stand-alone treatment. The results were incon-clusive. Results were also inconclusive in 14 trials thatused massage as part of a multimodal intervention be-cause none were designed such that the relative contri-bution of massage could be ascertained.
Conclusions. No recommendations for practice can bemade at this time because the effectiveness of massagefor neck pain remains uncertain. Pilot studies are neededto characterize massage treatment (frequency, duration,number of sessions, and massage technique) and estab-lish the optimal treatment to be used in subsequent largertrials that examine the effect of massage as either a stand-alone treatment or part of a multimodal intervention. Formultimodal interventions, factorial designs are needed todetermine the relative contribution of massage. Futurereports of trials should improve reporting of the conceal
ment of allocation, blinding of outcome assessor, adverseevents, and massage characteristics. Standards of reportingfor massage interventions, similar to Consolidated Stan-dards of Reporting Trials, are needed. Both short andlong-term follow-up are needed.
Key words: neck pain, cervical dysfunction, cervico-genic headache, mechanical neck disorders, massage,manual therapy, whiplash, chronic pain. Spine 2007;32:
353–362
Neck disorders are common, and can be severely dis-abling and costly.1–6 According to the 2003 US NationalHealth Interview Survey, 15% of adults age 18 years andolder reported that in the past 3 months, they had expe-rienced neck pain that had lasted 1 day or more. Ofthese, 15% experienced migraine or severe headachelasting 1 day or more.7 Neck pain frequently becomeschronic, and 10% of males and 17% of females havereported neck pain that has lasted longer than 6months.8 Motor vehicle crashes leave 24% to 50% ofsubjects with persistent symptoms at 12 months.9 Mas-sage is commonly used to treat persistent neck pain.However, studies of its effectiveness on neck pain havebeen inconclusive.10–15
The objectives of this review were: (1) to assess theefficacy and effectiveness of massage. either alone or incombination with other treatments on pain, function/disability, patient satisfaction, and global perceived ef-fect in adults with mechanical neck disorders; (2) to as-sess the secondary outcomes of adverse events and costof care; and (3) where appropriate, to conduct sensitivityanalysis to assess the influence of study methodologicalquality, symptom duration, and subtypes of neck disor-der on the magnitude of treatment effects.
Materials and Methods
Inclusion Criteria. Any published or unpublished random-ized controlled trial (RCT) or quasi-RCT, either in full text orabstract form, was included. The participants were adults whosuffered from acute (less than 30 days), subacute (30–90 days),or chronic (greater than 90 days) neck disorders. Neck disor-ders were categorized as: (1) mechanical neck disorders, includ-ing whiplash-associated disorders category I and II,16,17 myo-fascial neck pain, and degenerative changes18; (2) neck disorderwith headache19–21; and3 neck disorders with radicular find-ings, including whiplash-associated disorders category III.16,17
Studies were excluded if they investigated neck disorderswith: (1) definite or possible long tract signs (e.g., myelopa-thies); (2) neck pain caused by other pathologic entities (e.g.,rheumatoid arthritis, ankylosing spondylitis, spasmodic torti-collis, fractures, and dislocations)18; (3) headache not of cervi-
From *JPS Enterprises, Baltimore, MD; †West Coast College of Mas-sage Therapy, Massage Therapy Association of British Columbia, Van-couver, British Columbia, Canada; ‡McMaster University, Hamilton,Ontario, Canada; §Integrative Medicine Program, H. Lee Moffitt Can-cer Center and Research Institute, Tampa, FL; �Dermatology and SkinCancer Clinic, Gainesville, FL; ¶Department of Clinical Epidemiology& Biostatistics, McMaster University, and Father Sean O’Sullivan Re-search Centre, St. Joseph’s Healthcare, Hamilton, Ontario, Canada;#Northwestern Health Sciences University, Bloomington, MN; and**Product Benefit Risk Assessment and Management, Amgen Inc.,Thousand Oaks, CA.The manuscript submitted does not contain information about medicaldevice(s)/drug(s).Institutional and Professional Organizational funds were received insupport of this work. No benefits in any form have been or will bereceived from a commercial party related directly or indirectly to thesubject of this manuscript.Address correspondence and reprint requests to Jeanette Ezzo, PhD,CMT, 1905 West Rogers Avenue, Baltimore, MD 21209; E-mail:[email protected]
353

cal origin but associated with the neck; or (4) coexisting head-ache when either neck pain was not dominant or the headachewas not provoked by neck movements or sustained neck pos-tures, or “mixed” headache.
Studies using massage alone or combined with other thera-pies were included. Massage was defined as contact with ormanipulation of the soft tissues of the human body with thehand, foot, arm, or elbow on the structures of the neck. Mas-sage techniques included Swedish techniques, fascial or connec-tive tissue release techniques, cross fiber friction, and myofas-cial trigger point techniques. Techniques based on subtleenergy manipulation or noncontact (Reiki, Polarity) were ex-cluded.
The comparison groups could either be a control or othertreatment. A control could be: (1) sham or placebo; (2) notreatment control; (3) active treatment control (i.e., massage �ultrasound vs. ultrasound); and (4) inactive treatment control(i.e., massage � sham ultrasound vs. sham ultrasound). Othertreatments could be: (1) one active treatment versus anothervery different active treatment (i.e., massage vs. exercise); (2)one type of treatment (i.e., Chinese massage) versus anothertype of a similar treatment (i.e., Western massage); and (3) onedosage of a treatment versus another dosage of the same treat-ment (i.e., 3 weeks 9 sessions of Chinese massage vs. 3 weeks 3sessions of Chinese massage).
The primary outcomes were pain relief, disability/function,patient satisfaction, and global perceived effect. Secondary out-comes were adverse events and cost. Follow-up definitionswere: (1) immediately posttreatment, less than or equal to 1day; (2) short-term follow-up, greater than 1 day, but less than3 months; (3) intermediate-term follow-up, 3 months to lessthan a year; and (4) long-term follow-up, 1 year or longer.Unless otherwise specified, the longest follow-up period is re-ported in Table 1.
Search Strategy. A research librarian searched the followingdatabases without language restriction from root up to Septem-ber 2004: MEDLINE (January 1966 to September 2004),EMBASE (January 1980 to September 2004), Manual Alterna-tive and Natural Therapy (1985 to September 2004), Cumula-tive Index to Nursing and Allied Health Literature (January1982 to March 2004), Index to Chiropractic Literature (1980to September 2004), and CENTRAL (The Cochrane LibrarySeptember 2004). Terms were consistent with the CochraneBack Group and have been published elsewhere.41,42 We alsoscreened references, communicated with the Cochrane BackGroup and other experts, and searched our own personal files.
Pairs of independent reviewers identified citations and se-lected studies. At least 2 independent reviewers abstracted datausing a standardized abstraction form. We contacted primaryauthors if data were not reported on primary outcomes. Whenthe author could not be contacted or data were not available,values were imputed using previously published imputationrules.43,44 When data could not be retrieved from the author,the author’s report of significance was reported in tabularform. Two independent reviewers assessed methodologicalquality using the 11-item Cochrane Back Pain scale with dis-agreement resolved by consensus. A high-quality score wasgreater than 5 criteria met (Table 2).42
Clinical applicability addresses whether the results are under-standable and usable by clinicians applying the interventions. Toassess clinical applicability, we developed a 6-item checklist usingthe criteria from a number of sources (Table 3).41,52–54 The check-
list included questions about completeness of reporting on impor-tant clinical applicability items (items 1, 2, 3, and part of 5) as wellas on questions asking whether specific items had been satisfacto-rily performed (items 4, 6, and part of 5). Pairs of independentreviewers assessed each study, and discussion resolved disagree-ments.
Data Analysis. For continuous data, standardized mean differ-ences (95% confidence interval) were calculated using a random-effects model. Relative risks were calculated for dichotomous out-comes. The number needed to treat and treatment-advantagecalculations were calculated when a clear positive effect was seen.Our calculations appear after the reported results in Table 1.
To reach final conclusions, we used the levels-of-evidenceapproach.42,55 Strong evidence denoted consistent findings inmultiple high-quality RCTs. Moderate evidence denoted find-ings in a single, high-quality RCT or consistent findings inmultiple low-quality trials. Limited evidence indicated a singlelow-quality RCT. Conflicting evidence denoted inconsistent re-sults in multiple RCT. No evidence meant no studies wereidentified. Consistent was defined as at least two thirds of thetrials showing the same results.
Results
From 538 postings, 19 trials were selected.22–40 Of these,8 had more than 1 publication.34,46–49,56–58 One ap-peared only as an abstract.39 Four were in non-Englishlanguages and required translation.22,25,35,40
Six trials assessed multiple disorders.23,25,30,33,38,40
Thirteen studied mechanical neck disorder.23,25–33,36,38,40
Seven studied headache of cervical origin.22,25,33,37–39
Three evaluated neck disorder with some radicular signsand symptoms.23,35,45
Of the 19 trials, 12 received a low-quality score (Table2). Few trials described or used appropriate concealmentof allocation (5/19) avoided or controlled for cointerven-tions (6/19). Slightly more than half (10/19) reportedblinding the outcome assessor.
On the clinical applicability scale, the characteristicsof the study participants (i.e., gender, age) were wellreported. The characteristics of the massage were ade-quately reported in less than half the trials (8/19), and11/19 trials reported enough detail to determine whodelivered the intervention. Statistical results were seldomreported according to Consolidated Standards of Re-porting Trials (CONSORT)51 guidelines. The main out-come was rated as being client centered in all trials (19/19), and the timing of evaluation of outcome was ratedas sensible in most (17/19) trials. In all, 2/19 trials wererated as having adequately balanced efficacy with safety,primarily because few reported adverse events at all, andfew reported efficacy statistics adequately.
Trials were small, with a median of 20 per group(mode � 15; minimum to maximum � 8–87). We werenot able to pool trials or conduct sensitivity analysis dueto substantial heterogeneity in the massage treatment,the treatment combinations, and control groups.
Six studies24,27–29,31,37 examined massage alone as atreatment group. Four of these compared massage to a
354 Spine • Volume 32 • Number 3 • 2007

Table 1. Interventions and Outcomes
Author (y), Participants Intervention Outcome
Ammer and Rathkolb22 (1990) G3: massage, munaripack Pain intensity (5-point scale):n(A/R): 45/45 G2: ultra, direct gal, ultraviolet light Reported results: NSAcute/subacute/chronic NDH G1: manip, pulsed gal
Patient perceived effect (5-point scale):Treatment schedule: 2 w, 10 s Reported results: NRDuration of follow-up: immediate
Calculated results: data insufficientBrodin23 (1985) G3: massage, heat, mob, trac, edu, analg G2: mock therapy
(massage, trac, es), edu, analgPain intensity (9-point scale transformed to
dichotomous outcomes)n(A/R): 63/71 G1: analg Reported results: sig favoring G3 vs. 1;
G3 vs. 2Chronic MND (25% with radicular
findings or lower cervicaldegenerative changes)
Treatment schedule: 3 w, 9 s Calculated results:Duration of follow-up: 1 w RR (G3 vs. 1): 0.44 (95% CI 0.16–1.24)
RR (G3 vs. 2): 0.42 (95% CI 0.15–1.21)NNT (G3 vs. 1): 4Adverse events: 10 patients from G1; mock
therapy (G2) reported slight discomfortCen et al 24 (2003) Group A: traditional Chinese massage group C: no
treatmentn(A/R): 28/31 Group B: ex Function (Northwick Park Pain
Questionnaire; score 0–100):Chronic MND Reported results: sig favoring A vs. B, A vs. C
Treatment schedule: group A � 6 w, 18 sessions; groupB � 1 initial visit, 5 telephone follow-ups
Duration of follow-up: immediate Calculated results:SMD (A vs. C): �1.75 (95% CI �2.82
to �0.68)*SMD (A vs. B): �0.55 (95% CI �1.53 to 0.42)
Fialka et al 25 (1989) Group 3: massage trac, ex Pain:n(A/R): 60/60 Group 1: stereodynamic interferential current Neck pain and headache (present
or absent)Acute MND, NDH Group 2: iontophoresis Reported results: not clear
Group 4: no treatmentCalculated results:
Treatment schedule: 2 times per w for 5 w RR (3 vs. 4): 0.33 (95% CI 0.11, 0.99)*Duration of follow-up: immediate RR (3 vs. 1): 0.22 (95% CI 0.04–1.11)
RR (3 vs. 2): 0.17 (95% CI 0.03–0.85)*Gam et al 26 (1998) Group A: massage, ultra, ex Pain at rest (VAS 10 cm):n(A/R): 58/67 Group B: massage, sham ultra, ex group C: no treatment Reported results: NS10% Chronic MND
Treatment schedule: 4 w, total 8 s Calculated results:Duration of follow-up: 6 m SMD (Ga vs. Gc): �0.75 (95% CI �1.4
to �0.10)*SMD (Gb vs. Gc): �0.27 (95% CI �0.90,
to 0.35)Pain on function (VAS 0–10 cm)Reported results: NSCalculated results:SMD (Ga vs. Gc): �0.07 (95% CI �0.69
to 0.56)SMD (Gb vs. Gc): �0.00 (95% CI �0.62
to 0.62)Hanten et al 27 (1997) Group 1: occipital release† Pain pressure thresholdn(A/R): 60/60 Group 2: McKenzie neck exercises group 3: no treatment Reported results: NSPain duration: NR Treatment schedule: 1 s Calculated results:
Duration of follow-up: immediate SMD (1 vs. 3): �0.07 (95% CI �0.69 to 0.55)SMD (1 vs. 2): �0.24 (95% CI �0.87 to 0.38)
Hanten et al 28 (2000) Group 1: self-ischemic compressions† Pain (VAS 100 mm, mean over 24 hours)n(A/R): 40/40 Group 2: active neck movements Reported results: sig favoring group 1
(ANCOVA P � 0.043)MND without radicular symptomsPain duration: NR Treatment schedule: 5 d Calculated results:
Duration of follow-up: 3 d SMD: �0.61 (95% CI �1.24 to 0.03)Hou et al 29 (2002) B2: ischemic compression† heat, rom Pain (VAS 100 mm)
B3: ischemic compression, TENS, heat, rom(Continued)
355Massage for Mechanical Neck Disorders • Ezzo et al
Table 1. Continued
Author (y), Participants Intervention Outcome
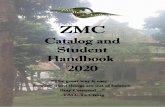
n(A/R): 19/19 B6: interferential current, myofascial release technique*heat, rom
Reported results: sig favoring B6 vs. B1, B3vs. B1, NS for B2 vs. B1
MND B1: heat, romPain duration: NR Calculated results:
SMD (B2 vs.B1): �0.54 (95% CI �125 to 0.16)Treatment schedule: 1 s SMD (B3 vs. B1): �1.07 (95% CI �1.91
to �0.24)*Duration of follow-up: immediate SMD (B6 vs. B1): �1.20 (95% CI �2.05
to �0.36)*Hoving et al 30 (2002) (PT): massage, ex, rom, trac, es, heat Pain (NRS, 0–10)n(A/R): 178/183 (MT): mob, coordination and stabilization techniques; rom Reported results: sig favoring MT over PTAcute, subacute, chronic MND
with and without radicularfindings, NDH
(GP): general practitioner care
Calculated results:Treatment schedule: 6 w, 6 s SMD (PT vs. MT): 0.41 (95% CI 0.04–0.78)‡Duration of follow-up: 52 w SMD (PT vs. GP): 0.34 (95% CI �0.02 to 0.70)
Function (Neck Disability Index, 0–50)Reported results: sig favoring MT over PTCalculated results:SMD (PT vs. MT): 0.12 (95% CI �0.25 to 0.48)SMD (PT vs. GP): 0.28 (95% CI �0.08 to 0.64)Global perceived effect (perceived
recovery, %)Reported results: sig favoring MT over PTCalculated results:RR (PT vs. MT): 1.32 (95% CI 0.78–2.22)RR (PT vs. GP): 0.85 (95% CI 0.55–1.31)Adverse events: benign and transientCost of care: favors MTTotal costsReported results: NSCalculated results:SMD (MT vs. PT): �0.34 (95% CI �0.70 to 0.02)SMD (PT vs. GP): �0.02 (95% CI �0.38 to 0.33)Total direct costsReported results: sig favoring MT vs. PTCalculated results:SMD (MT vs. PT): �0.49 (95% CI �0.85 to
�0.17)‡SMD (PT vs. GP): 0.21 (95% CI �0.15 to 0.56)Total indirect costsReported results: NS PT vs. MTCalculated results:SMD (MT vs. PT): �0.28 (95% CI �0.64 to 0.08)SMD (PT vs. GP): �0.07 (95% CI �0.43 to 0.28)Duration off workReported results: NS PT vs. MTCalculated results:SMD (MT vs. PT): �0.29 (95%vCI �0.71 to 0.12)SMD (PT vs. GP): �0.10 (95% CI �0.51 to 0.32)
Irnich et al 31 (2001) (M): conventional Western massage Pain (VAS 100 mm)n(A/R): 165/177 (A): acupuncture Reported results: sig favoring A vs. M
(P � 0.0052) at 1 w; NS at 3 mSubacute MND without radicular
symptoms(S): sham laser
Calculated results:Treatment schedule: 3 times a w for total of 5 s SMD (M vs. S): �0.01 (95% CI �0.38 to 0.36)Duration of follow-up: 3 m SMD (M vs. A): 6.49 (95% CI �3.42 to 16.40)
Adverse events: slight pain or loweredblood pressure reported by 4 patients inmassage group, 17 patients in theacupuncture group, 12 patients in shamacupuncture group
Jordan et al 32 (1998) (PT): massage, heat, ultra, mob, trac, pnf, ed Pain (3, 11-point box scales)n(A/R): 102/119 (CH): manip, trac, soft tissues treatments, ed Reported results: NS
(Continued)
356 Spine • Volume 32 • Number 3 • 2007

Table 1. Continued
Author (y), Participants Intervention Outcome
Chronic MND (INT): intensive trainingCalculated results:
Treatment schedule: 6 w, 12 s SMD (PT vs. CH): 0.00 (95% CI �0.48 to 0.48)Duration of follow-up: 52 w SMD (PT vs. INT): 0.00 (95% CI �0.47 to 0.47)
Function: (self-report disability index, 30-point scale)
Reported results (PT vs. Int): NSCalculated results:SMD (PT vs. CH): 0.00 (95% CI �0.48 to 0.48)SMD (PT vs. INT): �0.25 (95% CI �0.73 to 0.22)Patient perceived effect (6-point scale)Reported results: NSAdverse events: NR. One patient in the
manipulation group was excludedbecause 1 chiropractic treatmentresulted in persistent acute pain
Karlberg et al 33 (1996) (G1): massage, mob, ex, relaxation, analg, ed Pain (VAS; 100 mm)n(A/R): 17/17 (G2): wait list Reported results: sig favoring G1MND, NDH“recent onset,” suspect
“subacute”Follow-up: immediate Calculated results:
SMD: �1.47 (95% CI �2.58 to �0.36)*NNT: 2Treatment advantage: 40.8%
Koes34 (1992) (PT): massage, ex, heat, es Severity of main complaint (10-point scale)n(A/R): 58/64 (GP) general practitioner Reported results: NSSubacute and chronic MND (MT): manip, mob
(PL) placebo ultra Calculated results:SMD (PT vs. PL): 0.79 (95% CI 0.04–1.53)‡
Treatment schedule: 9 w SMD (PT vs. GP): 0.00 (95% CI �0.70 to 0.69)Duration of follow-up: 3, 6, and 12 w months (were not
used due to significant loss of follow-up and cross over)SMD (PT vs. MT): 0.64 (95% CI �0.08 to 1.35)
Function: (10-point scale)Reported results: NSCalculated results:SMD (PT vs. PL): 0.73 (95% CI �0.02 to 1.48)SMD (PT vs. GP): �0.16 (95% CI �0.86 to
0.55)SMD (PT vs. MT): 0.75 (95% CI 0.00–1.50)
Kogstad et al 35 (1978) (MT): massage, heat, manip Global perceived effect (objective andsubjective findings)
n(A/R): 50/50 (CT): massage, heat, isometric ex, trac (PL): placebotablets
Reported results: sig at immediate follow-upfavoring MT vs. PL, CT vs. PL. NSat 18 m
MND with radicular symptomsPain duration: NR Treatment schedule: 5 w, 8 s for MT; 12 s for CT Calculated results:
RR (MT vs. PL) 0.77 (95% CI 0.16–3.61)Duration of follow-up: 18 m RR (MT vs. CT) 0.33 (95% CI 0.08–1.32)
Levoska et al 36 (1993) (PE): passive exercise: heat, massage, stretches, ex Pain (occurrence of pain symptoms inhead, neck, or shoulder)
n(A/R):44/47 (AE): active exercise Reported results: sig (P � 0.01) favoringactive exercise immediatelyposttreatment; NS at 1 y
MNDPain duration: NR Treatment schedule: 5 w, 3 times per w Calculated results:
RR: 0.50 (95% CI 0.18–1.42)Duration of follow-up: 1 y
Nilsson et al 37 (1997) (ST): massage, sham laser Headache intensity per episode (VAS scale)n(A/R): 53/54 (Manip): manipulation Reported results: sig favoring manipChronic NDH
Treatment schedule: 3 w Calculated results:Follow-up: 1 w SMD: 0.45 (95% CI �0.10 to 0.99)
Provinciali et al 38 (1996) Group A: massage, mob, ex, ed Pain (VAS: 0–10):n(A/R): 60/60 Group B: ultra, TENS, es Reported results: NS at immediate follow-up;
sig favoring group A at 6 m(Continued)
357Massage for Mechanical Neck Disorders • Ezzo et al

control group for pain. They showed limited evidence ofno benefit for pain relief when compared to various con-trol conditions. One trial24 assessed function and re-ported 18 sessions of traditional Chinese massage(TuiNa) to be significantly better than no treatment forchronic mechanical neck disorders. Three trials com-pared massage to another active treatment: acupunc-ture,31 exercise,27 or manipulation37 (Table 1). Resultswere mixed.
Fourteen trials22,23,25,26,29,30,32,33,35,36,38–40,45 incor-porated massage as 1 component of a multimodal inter-vention (Table 1). However, none of the trials were de-signed such that the relative contribution of massagecould be ascertained. Therefore, the evidence remainsunclear about the benefit of massage in multimodal in-terventions.
Three studies reported adverse events.23,30,31Adverseevents, when reported, were rare, short lived, and be-nign, mostly pertaining to transient discomfort aftertreatment.
One study examined cost of care.30 This trial com-pared physical therapy methods of massage, manualtraction, exercise, interferential, and heat (PT) to mobi-
lization and stabilization techniques (MT). There was nosignificant difference between the PT and MT groups fortotal costs or total indirect costs. However, there was asignificant difference favoring the MT group for totaldirect costs (Table 1).
Discussion
Although there has been a marked increase in the num-ber of publications that incorporate massage since thelast Cochrane systematic review a decade ago,11 the con-tribution of massage to managing cervical pain remainsunclear. This review did not find a strong or moderatelevel of evidence for massage alone relative to a control.Six studies in our review were assessed as stand-alonemassage treatments; however, each study used a differentform of “massage” (e.g., 1-finger Chinese meditationmassage, ischemic compression, conventional Westernmassage and occipital release). Of these, 2 gave 1 treat-ment, and 1 gave self-administered massage, practicesthat are uncommon and, perhaps, suboptimal in the clin-ical setting. Furthermore, it is likely that the small samplesizes and inability to pool data made it difficult to findany statistically significant effect.
Table 1. Continued
Author (y), Participants Intervention Outcome
Acute/subacute MND, WAD,NDH, CES
Treatment schedule: 2 w, 10 1-h s Calculated results:Duration of follow-up: 6 m SMD �0.79 (95% CI �1.32, �0.26)*
NNT: 6 favoring group ATreatment advantage: 36.9% favoring
group AFunction: return to work (d)Reported results: sig favoring group ACalculated results:SMD: �1.05 (95% CI �1.59 to �0.51)*Self-assessment of outcome (ordinal scale:
�3 to � 3):Reported results: NS
Reginiussen et al 39 (2000) (MT): massage, mob, manip, stretch (PT): ex, diathermy Pain (headache and neck pain intensity)n(A/R): ?/63 Reported results: sig favoring MT at 1 w
and 3 mNDH Treatment schedule: 3 w/6 sPain duration: NR Duration of follow-up: 12 w Function (Neck Disability Index, 0–50)
Reported results: sig favoring MT at 1 w;NS at 3 m
Schnabel et al 40 (2002) (PT): massage, lymph drainage, heat, ex Pain intensity (NRS 0–10)n(A/R): 124/168 (SC): soft collar Reported resultsAcute WAD, NDH (ST): soft collar, analg
Calculated results:Treatment schedule: 14 d SMD �0.51 (95% CI �0.84 to �0.18)*Duration of follow-up: 4 w
Function: (NRS 0–10)Reported results: sig (P � 0.01) favoring PTCalculated results:SMD �0.47 (95% CI �0.79 to �0.14)*
*Significant favoring massage treatment.†Technique counted as massage treatment.‡Significant favoring nonmassage treatment.analg indicates analgesic medications; ANCOVA, analysis of covariance; CES, cephalgic; Cgal, galvanic current; CI, confidence interval; ed, education; es, electricalstimulation; ex, exercise; f, frequency per week; manip, manipulation; m, month(s); MND, mechanical neck disorder; mob, mobilization; n(A/R), No. analyzed/randomized; NDH, neck disorder with headache; NNT, No. needed to treat; NR, not reported; NRS, nominal rating scale; NS, not significant; pnf, proprioceptiveneuromuscular facilitation; rom, range of motion; RR, relative risk; s, sessions; sig, significant; SMD, standardized mean difference; trac, traction; ultra, ultrasound;w, week(s); WAD, whiplash-associated disorder.
358 Spine • Volume 32 • Number 3 • 2007

Likewise, our review did not find a strong or moderatelevel of evidence for or against massage in studies thatcombined massage with other methods. Several difficul-ties undermined our understanding of the contribution
of massage to the overall effect. Primarily, the designswere such that the relative contribution of massage couldnot be ascertained apart from other therapies with whichit was combined. Factorial designs would be needed to
Table 2. Methodological Quality Assessment
Author (y)
Questions
Total/11 Low/HighA B C D E F G H I J K
Ammer and Rathkolb22 (1990) 0 1 0 0 0 1 0 1 0 0 1 4 LBrodin23 (1985) 1 1 0 0 0 0 0 1 0 1 1 5 LCen et al 24 (2003) 0 1 1 0 0 0 0 1 1 0 1 5 LFialka et al 25 (1989) 0 1 0 0 0 1 0 1 1 0 1 5 LGam et al 26 (1998) 1 1 1 1 1 0 0 0 1 1 1 8 HHanten et al 27 (1997) 0 1 1 0 1 1 1 0 0 0 1 6 HHanten et al 28 (2000) 0 0 0 0 1 1 1 1 0 0 1 5 LHou et al 29 (2002) 0 1 0 0 0 1 0 1 0 0 1 4 LHoving et al 30 (2002) 1 1 1 0 1 1 1 1 0 1 1 9 HIrnich et al 31 (2001) 0 1 1 0 1 1 0 1 0 0 1 6 HJordan et al 32 (1998) 1 1 1 0 0 0 1 1 0 1 1 7 HKarlberg et al 33 (1996) 0 1 0 0 0 1 0 1 0 0 0 3 LKoes et al 34,45–49 (1991–1992) 1 1 0 0 1 1 0 1 0 1 1 7 HKogstad et al 35 (1978) 0 0 0 0 0 0 0 0 0 0 0 0 LLevoska et al 36 (1993) 0 1 0 0 0 0 0 1 0 0 1 3 LNilsson et al 37,50,51 (1995–1997) 0 1 0 0 0 1 0 1 0 0 1 5 LProvinciali et al 38 (1996) 0 1 0 0 0 1 0 1 0 0 1 5 LReginiussen et al 39 (2000) 0 1 0 0 0 0 0 1 0 0 1 3 LSchnabel et al 40 (2002) 0 1 0 1 1 1 1 1 0 0 1 7 HTotal/19 5 17 6 1 7 12 5 16 3 5 17
For all questions, 1 � yes.Question: A, Was the treatment allocation concealed?; B, Was the drop-out rate described and acceptable?; C, Were cointerventions avoided or similar?; D, Wasthe patient blinded to the intervention?; E, Was the outcome assessor blinded to the intervention?; F, Did the analysis include an intention-to-treat analysis?; G,Was the compliance acceptable in all groups?; H, Were the groups similar at baseline regarding the most important prognostic indicators?; I, Was the care providerblinded to the intervention?; J, Was the method of randomization adequate?; K, Was the timing of the outcome assessment in all groups similar?
Table 3. Clinical Applicability Assessment
Author (y)
Questions
Total/61 2 3 4 5 6
Ammer and Rathkolb22 (1990) 1 1 1 1 0 1 5Brodin23 (1985) 1 0 1 1 0 1 4Cen et al 24 (2003) 0 1 1 1 0 1 4Fialka et al 25 (1989) 1 0 1 1 0 1 4Gam et al 26 (1998) 1 0 1 1 0 1 4Hanten et al 27 (1997) 0 1 1 1 0 1 4Hanten et al 28 (2000) 0 1 1 1 0 1 4Hou et al 29 (2002) 0 1 1 1 0 1 4Hoving et al 30 (2002) 1 0 1 1 1 1 5Irnich et al 31 (2001) 0 1 1 1 1 1 5Jordan et al 32 (1998) 1 0 1 1 0 1 4Karlberg et al 33 (1996) 1 1 1 1 0 1 5Koes34 (1992) 1 0 1 1 0 1 4Kogstad et al 35 (1978) 0 0 1 1 0 0 2Levoska et al 36 (1993) 1 0 1 1 0 1 4Nilsson et al 37 (1997) 1 1 1 1 0 1 5Provinciali et al 38 (1996) 0 0 1 1 0 1 3Reginiussen et al 39 (2000) 0 0 0 1 0 1 2Schnabel et al 40 (2002) 1 0 1 1 0 1 4Total/19 11 8 18 19 2 18
For all questions, 1 � yes and 0 � no.Question: 1, For the index and control interventions, was enough detail given about who delivered the intervention? (a. professional, b. referral source, c. treatmentsetting); 2, For the index and control interventions, was enough detail given about their method of delivery to permit replication? (a. dose, b. frequency, c. duration,d. technique); 3, Was enough information provided about the characteristics of the study patients to permit us to relate them to the spectrum of patients withthis problem? (a. gender, b. age, c. comorbidities, d. disorder); 4, Was the main outcome(s) client centered? (a. pain, b. function, c. satisfaction/global perceivedeffect); 5, Based on the presented evidence, do authors balance efficacy and safety? (a. compliant with CONSORT, b. intergroup difference significant, c. adverseeffects reported and minimal); and 6, Was the timing of evaluation of the intervention sensible, given the mechanisms of action of the effect?Note: For a question to score a “yes,” all the lettered items after it had to be sufficiently reported and score a “yes” to meet applicability criteria.
359Massage for Mechanical Neck Disorders • Ezzo et al

tease out the contribution of massage from other thera-pies, and these were not done. In the absence of factorialdesigns, we aimed to find a superior multimodal treat-ment in general, but such a pattern did not emerge.
Several methodological or reporting problems werenoted related to the massage intervention. Most studieslacked a definition, description, or rationale for massage,or massage technique selected. There are numerous mas-sage techniques, and these techniques can have differentphysiologic effects. Massage research would benefit froma massage taxonomy59 with standardized vocabulary,definitions, and known mechanisms of action of variousmassage techniques. Such a standardized referencewould greatly assist researchers in selecting appropriatetechniques and also assist in interpreting the results ofexisting massage studies.
In most trials in this review, researchers did not justifythe other dosing parameters such as frequency (numberof MT sessions per week), duration (length of time ofeach massage session), and depth/pressure and durationof application of depth. Massage pilot studies are neededthat establish an optimal or at least adequate treatmentby exploring dosing variables. These studies should beconducted before doing a larger trial. This would be sim-ilar to the small dose-finding studies conducted in phar-maceutical trials in order to establish a minimally effec-tive or biologically active dose.
Observational data presented in a massage meta-analysis60 suggest the total number of massage sessionsmay influence the pain outcomes noting no pain reduc-tion immediately after a single massage, but significantpain reduction days to weeks after multiple massages.Although they did not find a similar pattern for the timeduration of a session, they note that little is known aboutthe variables for massage for pain relief, including theoptimal frequency, optimal duration of session, and the“decay” time in analgesic effect.
Furthermore, many of the trials in this review did notreport sufficient details on the massage characteristics topermit replication. Reporting conventions such as thoseproposed in the CONSORT statement52 for clinical tri-als generally, or the STRICTA61 statement for clinicaltrials of acupuncture specifically, are needed for massagetrials to report the massage parameters in a transparentand standardized way.
The qualifications or experience of the persons per-forming massage were also frequently missing from thereports, and this may reflect researchers’ lack of consid-eration given to this issue. Persons who do massage varyfrom those with no formal training to those with doc-toral degrees in massage therapy, and potential variabil-ity in outcomes may be associated with the level of ex-perience or training of the persons performing massage.Future trials need to provide justification for the thera-pist(s) selected to perform the intervention. To ensure thecompetence of the massage professional(s) being used ina trial, investigators may wish to require specific creden-tials, experience, and even a working interview, which
includes receiving a massage from the massage thera-pist.62
From the trials reporting adverse effects, adverse ef-fects of massage appear to be minimal and transient.However, the majority of trials did not mention adverseevents. It was not clear from those reports whether ad-verse effects had not been measured or had been mea-sured, but none occurred. To achieve a balanced discus-sion between efficacy and harm, trials need to documentall adverse events, measure and report side effects in astandardized format, and, equally important, to docu-ment if none occur.
In our review, no trials met the criteria of doubleblinding (blinded patients and care providers). This isbecause in massage studies, blinding patients can be dif-ficult, and blinding care providers is impossible. Otherdesign features, therefore, must attempt to compensatefor the lack of blinding. For example, it is important toensure that treatments are equally credible and accept-able to patients to minimize placebo effects and highdropout rates. It is also important to collect and reportinformation on patients’ previous experience with mas-sage, or their expectations of massage, to assess the im-pact of expectations. Finally, although it is difficult toblind the patients and therapists, the outcomes assessorand statistician can and should always be blinded.
The outcome measures in the studies described in ourreview were diverse, and several were not validated. Theuse of reliable and valid outcome measures is essential toreduce bias, provide standardized and precise measures,and allow for comparisons across trials. Disability ori-ented outcomes such as “return to work,” “activities ofdaily living,” and “function” were rarely reported. Wesuggest that these be included in future studies as thesecapture a dimension of patients’ experiences that are notnecessarily captured by pain outcomes.
Our approach to summarizing the literature has sev-eral strengths. We conducted a comprehensive, librarian-assisted search of multiple databases. A minimum of 2people extracted data, and the principal investigator(A.R.G.) verified data entry. In addition, we used a groupconsensus approach coupled with the Sackett55 and vanTulder42 hierarchy on the strength of the evidence tominimize bias.
The weakness of this paper rests with limitations ofthe primary studies. We were unable to make any firmstatements about the strength of the evidence due to 4major limitations of the studies: (1) the majority of stud-ies were of low methodological quality; (2) the majorityof studies used massage as 1 component in a multimodaltreatment but did not use a research design such as afactorial design that could ascertain the relative contri-bution of massage; (3) no study provided pilot data jus-tifying the minimal effective “amount” of massage (fre-quency, duration, dose, technique), thus we could notassess whether adequate doses of massage had beengiven; and (4) many studies were underpowered butcould not be pooled due to heterogeneous populations,
360 Spine • Volume 32 • Number 3 • 2007

massage techniques, treatment combinations, and con-trol groups.
Conclusions
Implications for PracticeNo firm statement can be made about the efficacy ofmassage for neck pain due to the limitations of existingstudies.
Implications for ResearchFor trials using massage as a stand-alone treatment or amultimodal intervention, pilot studies of various mas-sage treatments are needed to ascertain an optimal mas-sage treatment (frequency, duration, number of sessions,and massage technique) that can then be used in a sub-sequent larger trial. For multimodal interventions, facto-rial designs are needed to determine the relative contri-bution of massage. Adverse effects in massage trialsshould be assessed and reported consistently. Addition-ally, future trials should improve reporting of the con-cealment of allocation, blinding of outcome assessor andsubject, and massage characteristics. Standards of re-porting for massage interventions, similar to CONSORTare needed. Both short and long-term follow-up areneeded. Future metaanalyses need to consider prognosticfactors (e.g., psychological factors, central sensitization)during sensitivity analysis. For this to occur, trials needto assess these items during the conduct of the trial.
Key Points
● This review examined 19 trials for neck pain anddysfunction; 12/19 received low-quality scores.● Six trials examined massage as a stand-alonetreatment; 14 examined massage as part of a mul-timodal intervention.● Results are inconclusive due to methodologicallimitations of the studies.● Future research should ascertain an optimal mas-sage treatment (frequency, duration, number ofsessions, and massage technique) ahead of doing alarge trial.● When using multimodal interventions, future re-search should use factorial designs so that the rel-ative contribution of massage can be determined.
AcknowledgmentsThis review was adapted from Haraldsson BG, GrossAR, Myers CD, Ezzo JM, Morien A, Goldsmith C, Pe-loso PM, Bronfort G, Cervical Overview Group. Mas-sage for mechanical neck disorders. The Cochrane Data-base of Systematic Reviews Submitted for publication inIssue 3, 2006. Copyright Cochrane Library, reproducedwith permission.
References
1. Cote P, Cassidy D, Corroll L. The Saskatchewan health and back pain sur-vey. The prevalence of neck pain and related disability in Saskatchewanadults. Spine 1998;23:1689–98.
2. Makela M, Heliovaara M, Sievers K, et al. Prevalence determinants andconsequences of chronic neck pain in Finland. Am J Epidemiol 1991;134:1356–67.
3. Rajala U, Keinanen-Kiukanniemi S, Uusimaki A, et al. Musculoskeletal painsand depression in a middle-aged Finnish population. Pain 1995;61:451–7.
4. Takala J, Sievers K, Klaukka T. Rheumatic symptoms in the middle-agedpopulation in southwestern Finland. Scand J Rheumatol 1982;47:15–29.
5. Westerling D, Jonsson BG. Pain from the neck-shoulder region and sickleave. Scand J Soc Med 1980:8131–36.
6. Linton SJ, Hellsing AL, Hallden K. A population-based study of spinal painamong 35–45 year old individuals. Prevalence, sick leave and health care use.Spine 1998;23:1457–63.
7. -Lethbridge-Cejku M, Schiller JS, et al. Summary health statistics for U.S.adults: National Health Interview Survey, 2002. Vital Health Stat 10 2004;222:1–151.
8. Bovim G, Schrader, Sand T. Neck pain in the general population. Spine1994;19:1307–9.
9. Cassidy JD, Carroll LJ, Cote P, et al. A. Effect of eliminating compensationfor pain and suffering on the outcome of insurance claims for whiplashinjury. N Engl J Med 2000;342:1179–86.
10. Bodgduk N. Whiplash: why pay for what does not work? J MusculoskeletalPain 2001;8:29–53.
11. Aker PD, Gross AR, Goldsmith CH, et al. Conservative management ofmechanical neck pain: systematic overview and meta-analysis. BMJ 1996;313:1291–6.
12. Gross AR, Kay T, Hondras M, et al. Manual therapy for mechanical neckdisorders: a systematic review. Man Ther 2002;7:131–49.
13. Hoving JL, Gross AR, Gasner D, et al. A critical appraisal of review articleson the effectiveness of conservative treatment of neck pain. Spine 2001;26:196–205.
14. Peeters GGM, Verhagen AP, deBie RA, et al. The efficacy of conservativetreatment in patients with whiplash injury. Spine 2001;26:E64–73.
15. Kjellman GV, Skargren EI, Oberg BE. A critical analysis of randomisedclinical trials on neck pain and treatment efficacy. A review of the literature.Scand J Rehabil Med 1999;31:139–52.
16. Spitzer WO, Leblanc FE, Dupuis M. Scientific approach to the assessmentand management of activity related spinal disorders. Spine 1987;7:S1–59.
17. Spitzer WO, Skovron ML, Salmi LR, et al. Scientific monograph of theQuebec Task Force on Whiplash-Associated Disorders: redefining “whip-lash” and its management. Spine 1995;20:1S–73S.
18. Schumacher HR, Klippel JH, Koopman WJ, eds. Primer on the RheumaticDiseases. 10th ed. Atlanta, GA: Arthritis Foundation; 1993.
19. Classification and diagnostic criteria for headache disorders, cranial neural-gias and facial pain. Headache Classification Committee of the InternationalHeadache Society. Cephalalgia 1988;8(suppl 7):1–96.
20. Olesen J, Gobel H. ICD-10 Guide for Headaches. Guide to the classification,diagnosis and assessment of headaches in accordance with the tenth revisionof the International Classification of Diseases and related health problemsand its application to neurology. Cephalalgia 1997;(suppl 17)19:29–30.
21. Sjaastad O, Fredriksen TA, Pfaffenrath V. Cervicogenic headache: diagnosticcriteria. Headache 1990;30:725–6.
22. Ammer K, Rathkolb O. Physical therapy in occipital headaches. ManualMedizin 1990;28:65–8.
23. Brodin H. Cervical pain and mobilization. Man Med 1985;2:18–22.24. Cen SY, Loy SF, Sletten EG, et al. The effect of traditional Chinese therapeu-
tic massage on individuals with neck pain. Clin Acupunct Orient Med 2003;4:88–93.
25. Fialka V, Preisinger E, Bohler A. Physical diagnosis and physical therapy ofwhiplash injury [in German]. Phys Med Saln Med Klim 1989;18:390–7.
26. Gam AN, Warming S, Larsen LH. Treatment of myofascial trigger-pointswith ultrasound combined with massage and exercise–A randomised trial.Pain 1998;73–9.
27. Hanten WP, Barret M, Gillespie-Plesko M. Effects of active head retractionwith retraction/extension and occipital release on pressure pain threshold ofcervical and scapular trigger points. Physiother Theory Pract 1997;285–91.
28. Hanten WP, Olson SL, Butts NI, et al. Effectiveness of a home program ofischemic pressure followed by sustained stretch for treatment of myofascialtrigger points. Physiother Theory Pract 2000;80:997–1003.
29. Hou C-R, Tsai L-C, Cheng K-F. Immediate effects of various physical ther-apeutic modalities on cervical myofascial pain and trigger-point sensitivity.Arch Phys Med Rehabil 2002;83:1406–14.
30. Hoving JL, Koes BW, de Vet HC, et al. Manual therapy, physical therapy, orcontinued care by a general practitioner for patients with neck pain. A ran-domized, controlled trial. Ann Intern Med 2002;136:713–22.
31. Irnich D, Behrens N, Molzen H. Randomized trial of acupuncture comparedwith conventional massage and “sham” laser acupuncture for treatment ofchronic neck pain. BMJ 2001;322:1574–8.
361Massage for Mechanical Neck Disorders • Ezzo et al

32. Jordan A, Bendix T, Nielsen H, et al. Intensive training, physiotherapy, ormanipulation for patients with chronic neck pain: a prospective single-blindrandomized clinical trial. Spine 1998;23:311–9.
33. Karlberg M, Magnusson M, Eva-Maj M. Postural and symptomatic im-provement after physiotherapy in patients with dizziness of suspected cervi-cal origin. Arch Phys Med Rehabil 1996;77:874–82.
34. Koes BW. Efficacy of Manual Therapy and Physiotherapy for Back and NeckComplaints [thesis]. den Haag: Cip-Gegevens Koninklijke Bibliotheek;1992.
35. Kogstad, OA, Karterud S, Gudmundsen J. Cervicobrachialgia. A controlledtrial with conventional therapy and manipulation [in Norwegian]. TidsskrNor Laegeforen 1978;98:845–8.
36. Levoska S, Keinanen-Kiukaanneimi S. Active or passive physiotherapy foroccupational cervicobrachial disorders? A comparison of two treatmentmethods with a 1-year follow-up. Arch Phys Med Rehabil 1993;74:425–30.
37. Nilsson N, Christensen HW, Hartvigsen J. The effect of spinal manipulationin the treatment of cervicogenic headache. J Manipulative Physiol Ther1997;20:326–30.
38. Provinciali L, Baroni M, Illuminati L, et al. Multimodal treatment to preventthe late whiplash syndrome. Scand J Rehabil Med 1996;28:105–11.
39. Reginiussen T, Johnsen R, Torstensen TA. Efficiency of manual therapy onpatients with cervicogenic headache: a randomized single blinded controlledtrial. In: Singer KP, ed. International Federation of Manipulation Therapy,7th Scientific Conference; November 2000; Perth, Western Australia. Ab-stract 105.
40. Schnabel M, Vassiliou T, Schmidt TH, et al. Results of early mobilisation ofacute whiplash injuries [in German]. Schmerz 2002;16:15–21.
41. Clarke M, Oxman AD. Cochrane Reviewers’ Handbook 4.1.5. Oxford:Update Software; 2002.
42. van Tulder M, Furlan A, Bombardier C, et al. Updated method guidelines forsystematic reviews in the cochrane collaboration back review group. Spine2003;28:1290–9.
43. Sutton AJ, Abrahams KR, Jones DR, et al. Chapter 13. In : Methods forMeta-Analysis in Medical Research: Missing Data. Toronto, Canada: JohnWiley and Sons; 2002.
44. Little RJU, Ruben DV. Statistical Analysis with Missing Data. Toronto,Canada: John Wiley and Sons; 1987.
45. Koes B, Boutter LM, Knipshild PG. The effectiveness of manual therapy,physiotherapy and continued treatment by general practitioner for chronicnonspecific back and neck complaints. J Manipulative Physiol Ther 1991;14:498–502.
46. Koes BW, Bouter LM, van Mameren H, et al. Randomised clinical trial ofmanipulative therapy and physiotherapy for persistent back and neck com-plaints: results of one year follow up. BMJ 1992;304:601–5.
47. Koes BW, Bouter LM, van Mameren H, et al. The effectiveness of manual
therapy, physiotherapy, and treatment by the general practitioner for non-specific back and neck complaints. Spine 1992;17:28–35.
48. Koes BW, Bouter LM, van Mameren H, et al. Randomized clinical trial ofmanual therapy and physiotherapy for persistent back and neck complaints.Manual Therapy in the Netherlands 1992;1:7–12.
49. Koes BW, Bouter LM, van Mameren H, et al. A blinded randomized clinicaltrial of manual therapy and physiotherapy for chronic back and neck com-plaints: physical outcome measures. J Manipulative Physiol Ther 1992;15:16–23.
50. Nilsson N, Christensen HW, Hartvigsen J. Lasting changes in passive rangeof motion after spinal manipulation: A randomized, blind, controlledtrial. J Manipulative Physiol Ther 1996;19:165– 8.
51. Nilsson N. A randomized controlled trial of the effect of spinal manipulationin the treatment of cervicogenic headache. J Manipulative Physiol Ther1995;18:435–40.
52. Altman DG, Schulz KF, Moher D, et al. CONSORT Group (ConsolidatedStandards of Reporting Trials). The revised CONSORT statement for re-porting randomized trials: explanation and elaboration. Ann Intern Med2001;134:663–94.
53. Guyatt GH, Sackett DL, Cook DJ. Users guides to medical literature. II. Howto use an article about therapy or prevention. B. What were the results andwill they help me caring for my patient? JAMA 1994;271:59–63.
54. Shekelle PG, Andersson G, Bombardier C, et al. A brief introduction to thecritical reading of clinical literature. Spine 1994;19:2028S–31S.
55. Sackett DL, Straus SE, Richardson WS, et al. Evidence-Based Medicine: Howto Practice and Teach EBM. 2nd ed. Edinburg: Churchill Livingstone; 2000.
56. Brodin H. Cervical pain and mobilization. Int J Rehabil Res 1984;7:190–1.57. Jordan A, Bendix T, Nielsen H, et al. A. Intensive training, physiotherapy, or
manipulation for patients with chronic neck pain. A prospective single-blindrandomized clinical trial. In: Proceedings of the 1996 International Con-ference on Spinal Manipulation; October 18 –19, 1996; Bournemouth,England.
58. Koes B. A randomized clinical trial of manual therapy and physiotherapy forpersistent back and neck complaints. Subgroup analysis and relationshipbetween outcomes measure. J Manipulative Physiol Ther 1993;16:211–9.
59. Sherman KJ, Dixon MW, Thompson D, et al. Development of a taxonomy todescribe massage treatments for musculoskeletal pain. BMC ComplementAltern Med 2006;6:24.
60. Moyer CA, Rounds J, Hannum JW. A meta-analysis of massage therapyresearch. Psychol Bull 2004;130:3–18.
61. MacPherson H, White A, Cummings M, et al. STRICTA Group. Standardsfor reporting interventions in controlled trials of acupuncture: the STRICTArecommendations. J Altern Complement Med 2002;8:85–9.
62. Eisenberg DM, Cohen MH, Hrbek A, et al. Credentialing complementaryand alternative medical providers. Ann Intern Med 2002;137:965–73.
362 Spine • Volume 32 • Number 3 • 2007