
Edge profile of commercially available square-edged intraocular lenses
sio
s
2tbgctitwMp
ig1mw
9
Prophylactic Selective Laser Trabeculoplasty in thePrevention of Intraocular Pressure Elevation After
Intravitreal Triamcinolone Acetonide Injection
ERCUMENT BOZKURT, NECIP KARA, AHMET TAYLAN YAZICI, KEMAL YUKSEL, AHMET DEMIROK,
OMER FARUK YILMAZ, AND SERIF DEMIRI
mids
awsaitiev
sfl
● PURPOSE: To evaluate the prophylactic efficacy ofelective laser trabeculoplasty for preventing an increasen intraocular pressure (IOP) after intravitreal triamcin-lone acetonide injection.
● DESIGN: Prospective, comparative, interventional caseeries.
● METHODS: We studied 31 eyes with a baseline IOP of1 mm Hg or more of 31 patients for which intravitrealriamcinolone acetonide injection was planned for dia-etic macular edema. The patients were divided into 2roups, a study group and control group. The study groupomprised 15 eyes of 15 patients that underwent selec-ive laser trabeculoplasty a mean of 8.3 � 4.1 days beforentravitreal triamcinolone acetonide injection. The con-rol group comprised 16 eyes of 16 patients who under-ent only intravitreal triamcinolone acetonide injection.ain outcomes measures were mean IOP and number of
atients requiring antiglaucomatous therapy.● RESULTS: Mean baseline IOP was 21.6 � 0.9 mm Hgn the study group and 21.5 � 0.8 mm Hg in the controlroup (P � .98). Mean IOP at 1 day after injection was7.0 � 2.0 mm Hg in the study group and 19.5 � 4.3m Hg in the control group (P � .23). Mean IOP at 1eek after injection was 16.9 � 1.7 mm Hg and 18.4 �
4.0 mm Hg, respectively (P � .49); mean IOP at 1month after injection was 16.4 � 1.5 mm Hg and 20.8 �5.6 mm Hg, respectively (P � .003); mean IOP at 3months after injection was 15.8 � 2.5 mm Hg and18.3 � 5.5 mm Hg, respectively (P � .01); and meanIOP at 6 months after injection was 15.7 � 1.4 mm Hgand 17.1 � 1.5 mm Hg, respectively (P � .03). Thenumber of patients requiring antiglaucomatous therapyduring follow-up was 0 of 15 eyes in the study group and8 of 16 eyes in the control group (P � .001).● CONCLUSIONS: The IOP elevation after intravitrealtriamcinolone acetonide injection may be prevented byperforming selective laser trabeculoplasty before intrav-itreal triamcinolone acetonide injection, especially in
Accepted for publication May 26, 2011.From the Beyoglu Eye Research and Education Hospital, Istanbul,
Turkey (E.B., N.K., A.T.Y., K.Y., A.D., O.F.Y); and the Department ofPhysiology, School of Medicine, Duzce University, Duzce, Turkey (S.D.).
Inquiries to Necip Kara, Kartaltepe Mahallesi, Akin Sokak, AkinApartmani. No. 8/14, Bakirkoy/Istanbul, Turkey; e-mail: dr.necipkara@
ogmail.com
© 2011 BY ELSEVIER INC. A76
cases with a baseline IOP of 21 mm Hg or more. (AmJ Ophthalmol 2011;152:976–981. © 2011 by ElsevierInc. All rights reserved.)
NTRAVITREAL TRIAMCINOLONE ACETONIDE INJECTION
has become an important therapeutic method for sev-eral retinal diseases, including diabetic macular edema,
age-related macular, degeneration, proliferative diabeticretinopathy, retinal vein occlusions, and noninfectiousposterior uveitis.1,2 Several side effects of intravitrealcorticosteroids have been reported, such as endophthalmi-tis, increased intraocular pressure (IOP), cataract forma-tion, vitreous hemorrhage, retinal detachment, and centralserous chorioretinopathy.3–7 Elevated IOP, however, is the
ost common side effect of intravitreal triamcinolonenjection.2 The reported prevalence of IOP elevation afterifferent doses of intravitreal triamcinolone varies amongtudies, ranging from 40% to 77%.1,2,8
Among the risk factors for steroid-induced glaucoma,a history of pre-existing glaucoma, high baseline IOP,younger age, history of IOP elevation after previousintravitreal triamcinolone injections, and first-degreerelatives with primary open-angle glaucoma have beenreported.1,9 –12 The IOP elevation after intravitreal tri-mcinolone injection usually can be treated medicallyith either monotherapy or combination therapy. In
ome cases, however, IOP elevation is not controlleddequately with medical therapy, or the patients may bentolerant to the ocular and systemic adverse effects ofhese drugs. Some patients require surgical intervention,ncluding surgical removal of the corticosteroid, trab-culectomy, Ahmed valve placement, or pars planaitrectomy.1,4,13,14
Since 2002, selective laser trabeculoplasty (SLT) hasbecome available for the treatment of glaucoma. SLT is aneffective treatment method for lowering IOP in patientswith open-angle glaucoma such as primary open-angleglaucoma, pigmentary glaucoma, pseudoexfoliation glau-coma, and normal-tension glaucoma.15–17 The aim of thistudy was to assess the effect of preinjection SLT treatmentor preventing IOP elevation after intravitreal triamcino-one injection in patients with a baseline IOP of 21 mm Hg
r more.LL RIGHTS RESERVED. 0002-9394/$36.00doi:10.1016/j.ajo.2011.05.027
rRRbwappgbprgoaetvat
METHODS
● STUDY POPULATION AND DESIGN: This prospective,andomized study was performed at the Beyoglu Eyeesearch and Training Hospital in the Glaucoma andetina Departments. The study included patients with aaseline IOP of at least 21 mm Hg for whom treatmentith an intravitreal injection of 4 mg triamcinolonecetonide was planned for diabetic macular edema. Allatients were in a nonproliferative diabetic retinopathyhase. The patients were divided into 2 groups. The studyroup comprised consecutive patients who underwent SLTefore the intravitreal injection. The control group com-rised consecutive patients who underwent only intravit-eal triamcinolone injection. Patients with a history oflaucoma, those with first-degree relatives with primarypen-angle glaucoma, those with gonioscopically occlud-ble angles, and those with previous ocular surgery werexcluded. Also, patients with a follow-up period of lesshan 6 months were excluded from the analysis. Botherbal and written informed consent were obtained fromll patients for both the intravitreal triamcinolone injec-ion and SLT procedures.
● SELECTIVE LASER TRABECULOPLASTY PROCEDURE:
All SLT procedures were performed by the 2 physicians(E.B., N.K.). All of the patients were administered 1 dropof topical proparacaine (Alcaine; Alcon, Fort Worth,Texas, USA) and a Latina SLT lens (Ocular Instruments,Bellevue, Washington, USA) was used to visualize theangle. The laser beam was focused on the trabecularmeshwork. The initial energy setting was 0.7 mJ and wasincreased or decreased by 0.1 mJ until intermittent smallcavitation bubbles were visible. The inferior or nasal 180
TABLE. Comparison of the Mean Intraocular Pressure BaAcetonide in Patients Who Underwent Selective Laser Trab
Patients Who Only Underwent Intravitr
Group Baseline After SLTa 1 Day
Study group
Mean � SD 21.7 � 0.9 16.6 � 2.1 17.1 � 2.0
Range 21 to 24 15 to 21 14 to 22
Control group
Mean � SD 21.6 � 0.9 — 19.5 � 4.3
Range 21 to 24 — 16 to 30
P valueb .90 — .095
IOP � intraocular pressure; IVTA � intravitreal triamcinolone ace
deviation.aPerformed a mean 8.3 days after SLT.bMann–Whitney U test.
degrees were treated with contiguous laser spots. A mean
PROPHYLACTIC LASER THERAPY FORVOL. 152, NO. 6
of 54.4 � 5.6 SLT spots were applied. One drop ofbrimonidine 0.2% was administered immediately after thelaser procedure. Floromethalon (Flarex; Alcon Laborato-ries, Inc) eye drops were administered 4 times daily for 1week.
● INTRAVITREAL TRIAMCINOLONE INJECTION PROCE-
DURE: All injections were performed by the same vitreo-retinal surgeon (A.T.Y.). The intravitreal triamcinolonewas administered with topical anesthesia using propara-caine HCl 0.5% (Alcaine). After sterilization of the ocularsurface and periocular area with 10% povidone iodine, 4mg triamcinolone acetonide (0.1 mL of 40 mg/1.0 mLsuspension; Kenacort [Bristol-Myers Squibb, Istanbul, Tur-key]) was injected with a 30-gauge needle at the inferona-
0
5
10
15
20
25
Baseline postop 1 day
postop 1 week
postop 1 month
postop 3 month
postop 6 month
Mea
n IO
P, m
mH
g
study groupcontrol group
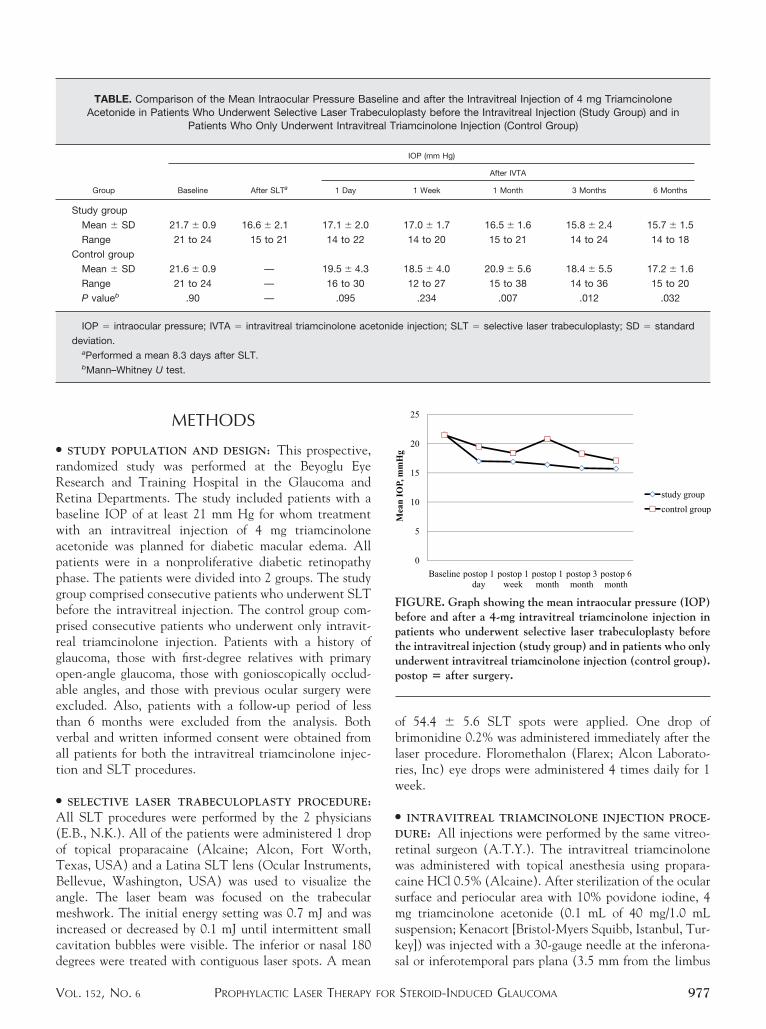
FIGURE. Graph showing the mean intraocular pressure (IOP)before and after a 4-mg intravitreal triamcinolone injection inpatients who underwent selective laser trabeculoplasty beforethe intravitreal injection (study group) and in patients who onlyunderwent intravitreal triamcinolone injection (control group).postop � after surgery.
and after the Intravitreal Injection of 4 mg Triamcinoloneplasty before the Intravitreal Injection (Study Group) and inriamcinolone Injection (Control Group)
IOP (mm Hg)
After IVTA
1 Week 1 Month 3 Months 6 Months
17.0 � 1.7 16.5 � 1.6 15.8 � 2.4 15.7 � 1.5
14 to 20 15 to 21 14 to 24 14 to 18
18.5 � 4.0 20.9 � 5.6 18.4 � 5.5 17.2 � 1.6
12 to 27 15 to 38 14 to 36 15 to 20
.234 .007 .012 .032
e injection; SLT � selective laser trabeculoplasty; SD � standard
selineeculoeal T
tonid
sal or inferotemporal pars plana (3.5 mm from the limbus
STEROID-INDUCED GLAUCOMA 977

fl
ata
apmw
mwip(ia
dtle
ct
in phakic eyes, 3.0 mm in pseudophakic eyes). Paracentesiswas not performed in any patient. After the procedure, atopical antimicrobial agent was administered to allpatients.
The patients were followed up for 6 months after theintravitreal triamcinolone injection. Additional data werecollected, including age, treated eye, and sex. IOP mea-surements before and at 1 day, 1 week, 1 month, 3 months,and 6 months after intravitreal injection were recorded.The IOP was measured by the same investigator with samecalibrated Goldman applanation tonometer. He wasmasked when measuring the IOP at each visit. Threemeasurements were obtained from each eye. The mean ofthe 3 measurements was used in the statistical analyses.When IOP after injection exceeded 24 mm Hg, anantiglaucomatous drug was administered. The patientswho had received antiglaucomatous medication were fol-lowed up for glaucomatous damage.
● STATISTICAL ANALYSIS: All statistical tests were per-formed using SPSS software version 16 (SPSS, Inc, Chi-cago, Illinois, USA). The independent-samples t test,Mann–Whitney U test, and Fisher exact test were per-ormed for statistical analysis. Differences with a P value ofess than .05 were considered significant.
RESULTS
THE STUDY INCLUDED 31 EYES OF 31 PATIENTS. ALL PA-
tients completed the 6-month follow-up period. The studygroup comprised 15 eyes of 15 patients (6 men, 9 women;mean age, 60.1 years). The control group comprised 16eyes of 16 patients (9 men, 7 women; mean age, 58.5years). There was no statistically significant differencebetween the 2 groups with regard to sex or age (P � .47nd P � .57, respectively). The mean central cornealhickness in the study and control group was 544.4 � 13.5nd 546.6 � 11.5, respectively (P � .61). The baseline
cup-to-disc ratio was 0.42 � 0.10 and 0.39 � 0.08 in thestudy and control groups, respectively (P � .458).
The indication for intravitreal triamcinolone injectionwas macular edema secondary to diabetes mellitus in all ofthe patients. In the study group, the mean period betweenthe SLT and intravitreal injection was 8.3 � 4.1 days(range, 7 to 20 days). IOP measurement after SLT wasperformed a mean of 8 days after SLT in the study group.The mean number of previous intravitreal triamcinoloneinjections was 0.85 � 0.9 (range, 0 to 2) in the study groupand 0.71 � 1.1 (range, 0 to 3) in the control group and didnot differ significantly between groups (P � .51).
The Table presents the mean IOP values of the 2 groupst baseline and during the follow-up period. Only 2atients in the study group had IOP values of more than 21m Hg after intravitreal injection. These 2 IOP values
ere 22 mm Hg and 24 mm Hg, observed at 1 day and 3AMERICAN JOURNAL OF978
onths after injection, respectively. The IOPs decreasedithout antiglaucomatous therapy. Mean IOP values after
ntravitreal injection were lower in the study group com-ared with the control group at all of the follow-up visitsFigure). Except for at day 1 and week 1 after intravitrealnjection, the differences between groups were significantt each follow-up visit.
None of the patients required antiglaucomatous eyerops during the 6-month follow-up after intravitrealriamcinolone injection in the study group, but IOP-owering medications were required in 8 (50%) of the 16yes in the control group (P � .001). In the control group,
an antiglaucomatous eye drop was required in 4 patients at1 day after injection, in 4 patients at 1 week after injection,in 7 patients at 1 month after injection, in 6 patients at 3months after injection, and in 6 patients at 6 months afterinjection. The number of antiglaucomatous drops variedfrom 1 to 3 for patients who required antiglaucomatousmedication in the control group. No further interventions,such as glaucoma surgery, were required.
In the control group, 8 of 16 patients (50%) who hadreceived antiglaucomatous medications underwent opticnerve head examination, visual field test with Goldmanperimetry, and peripapillary nerve fiber layer measurementwith Stratus optic coherence tomography (Carl Zeiss Med-itec, Dublin, California, USA). There were no glaucomatouschanges such as glaucomatous cupping, glaucomatous visualfield defects, and thinning of the peripapillary retinal nervefiber.
Adverse events after SLT included a mild transientanterior chamber reaction in 2 patients (13%) and tran-sient ocular discomfort in 3 patients (20%). During thefollow-up period, no severe complications, such as endo-phthalmitis, retinal detachment, or vitreous hemorrhage,occurred.
DISCUSSION
IN THE PAST DECADE, INTRAVITREAL TRIAMCINOLONE ACE-
tonide injection has gained popularity as a treatment optionfor diabetic macular edema. The treatment effect is transient,however, and often requires repeated injections.18
Although the precise mechanism of IOP elevation afterintravitreal triamcinolone injection is not understoodcompletely, steroid-associated IOP elevation has beenassociated with a reduction in aqueous outflow.19,20 A highoncentration of corticosteroid receptors has been de-ected in the trabecular and anterior uveal meshwork.21
Intravitreal triamcinolone injection may lead to an accu-mulation of glycosaminoglycans in the extracellular matrixof the trabecular meshwork, a decrease in the phagocyticactivity of the trabecular endothelial cells, and a decreasein prostaglandins that regulate outflow.12,22–25 Corticoste-roids also impair outflow by increasing the tight junctions
between trabecular meshwork endothelial cells.26 Addi-OPHTHALMOLOGY DECEMBER 2011

mepestaiigptci
tionally, intravitreal triamcinolone may cause acute IOPelevation as a result of mechanical obstruction of thetrabecular meshwork by the triamcinolone particles or itsvehicle.27 Beer and associates suggested that measurableconcentrations of triamcinolone would be expected to lastfor approximately 3 months.28
SLT is an effective and safe treatment method forlowering IOP in cases with open-angle glaucoma. SLT hasa pulse duration of 3 nanoseconds and a default spotdiameter of 400 �m. The standard treatment protocol is totreat 180 degrees of trabecular meshwork with 50 spots at0.6 to 1.0 mJ.29 The SLT laser causes selective photother-
olysis of pigmented trabecular cells without any collat-ral structural damage to the trabecular meshwork. Theigment molecule is targeted selectively, resulting in itsxpansion and subsequent cellular damage. Biologic theoryuggests that SLT treatment induces a proliferation ofrabecular and endothelial cells and a release of chemot-ctic and vasoactive agents, such as interleukin-1alpha,nterleukin-1beta, and tumor necrosis factor �, withoutnducing coagulative damage. These cytokines stimulateelatinases and the accumulation of macrophages. Macro-hage recruitment and changes in cytokines also stimulatehe matrix metalloproteinase pathway, resulting in phago-ytosis and extracellular matrix remodeling, which leads toncreased aqueous outflow.30 SLT also may improve out-
flow by decreasing the number of tight junctions betweentrabecular endothelial cells.29
As mentioned above, SLT and corticosteroids haveopposite effects on the trabecular meshwork. The effect ofcorticosteroids on the trabecular meshwork may be pre-vented using SLT, and aqueous outflow may be improved.We hypothesized that steroid-induced IOP elevation canbe prevented by injecting intravitreal triamcinolone beforeSLT in cases with a baseline IOP of more than 21 mm Hg.There are only a few reports in the literature on the use oflaser trabeculoplasty for increased IOP secondary to intra-vitreal triamcinolone. Previously, SLT for elevated IOPafter intravitreal injection was reported to be a safe andeffective treatment for IOP elevation.30–33
The rate of IOP elevation after a 4-mg intravitrealtriamcinolone injection ranges from 40% to 50%.2,9,10,34
A high baseline IOP is a risk factor for IOP elevation afterintravitreal triamcinolone injection.2,9,34 Patients with abaseline IOP of more than 15 mm Hg have a 60% chanceof an IOP of 24 mm Hg or higher developing after a 4-mgintravitreal triamcinolone injection.9
In the present study, 8 (50%) of 16 patients demon-
strated a pressure elevation of more than 21 mm Hg in thePROPHYLACTIC LASER THERAPY FORVOL. 152, NO. 6
control group and 8 patients required antiglaucomatouseye drops. Successful results were obtained with injectionof intravitreal triamcinolone before SLT treatment. In thestudy group, a mean 5-mm Hg (23%) IOP reduction wasachieved with SLT before intravitreal injection. MeanIOP values after intravitreal injection were lower in thestudy group at all of the follow-up visits. In the study group,only 2 patients had an IOP exceeding 21 mm Hg, andnone of the patients required treatment with an antiglau-comatous agent.
These findings suggest that there may be advantages toinjecting intravitreal triamcinolone before SLT in patientswith a baseline IOP of at least 21 mm Hg and plannedtreatment with a 4-mg intravitreal triamcinolone injectionfor diabetic macular edema. First, an IOP elevation afterintravitreal injection may occur between office visits and itmay be prevented by injecting intravitreal triamcinolonebefore SLT. Second, this procedure is especially importantwhen patients are unable to come in for IOP measurementsafter intravitreal injection. Also, noncompliance with anti-glaucomatous therapy is a common concern for glaucomapatients. Some factors such as adverse effects, treatment cost,number of instilled doses, number of prescribed eye drops, andcoexisting illnesses account for the poor compliance. Inject-ing intravitreal triamcinolone before SLT may eliminate theneed for antiglaucomatous eye drops and their side effects.Thus, patient quality of life is preserved.
Although SLT is reported to be a safe procedure, some sideeffects, such as intraocular pressure spikes, iritis, transientocular pain, and peripheral anterior synechiae, can occur.35,36
As an adverse effect after SLT in the present study, a mildtransient anterior chamber reaction was observed in only 2cases, and 3 patients noted ocular discomfort.
In conclusion, IOP elevation is a common side effectafter intravitreal triamcinolone injection, and its rateincreases in cases with higher baseline IOP. Although IOPelevation usually responds to topical glaucoma medication,in some cases, it is not very well controlled despite fullglaucoma medication, and surgical intervention is re-quired. The findings of the present study indicate that IOPelevation after intravitreal injection can be prevented withSLT when performed before injection in patients with arisk factor for steroid-induced glaucoma. As a risk factor,we investigated only cases with a higher baseline IOP.Future studies to evaluate the effect of SLT when per-formed before injection in cases with other risk factors forIOP elevation after intravitreal triamcinolone injection,such as pre-existing glaucoma or a family history of
glaucoma, are necessary.ALL AUTHORS HAVE COMPLETED AND SUBMITTED THE ICMJE FORM FOR DISCLOSURE OF POTENTIAL CONFLICTS OFInterest, and none were reported. Involved in conduct and design of study (E.B., N.K., A.T.Y.); Collection, analysis, and interpretation of data andwriting of article (E.B., N.K., A.T.Y., K.Y.); and Review and approval of manuscript (E.B., N.K., A.T.Y., K.Y., A.D., O.F.Y., S.D.). Verbal and writteninformed consent were obtained from all patients for the procedures in accordance with the Declaration of Helsinki, and the Ethics Committee of DuzceUniversity, Duzce, Turkey, approved the study.
STEROID-INDUCED GLAUCOMA 979
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
REFERENCES
1. Roth DB, Verma V, Realini T, Prenner JL, Feuer WJ,Fechtner RD. Long-term incidence and timing of intraocularhypertension after intravitreal triamcinolone acetonide in-jection. Ophthalmology 2009;116(3):455–460.
2. Rhee DJ, Peck RE, Belmont J, et al. Intraocular pressurealterations following intravitreal triamcinolone acetonide.Br J Ophthalmol 2006;90(8):999–1003.
3. Nelson ML, Tennant MT, Sivalingam A, Regillo CD,Belmont JB, Martidis A. Infectious and presumed noninfec-tious endophthalmitis after intravitreal triamcinolone ace-tonide injection. Retina 2003;23(5):686–691.
4. Kaushik S, Gupta V, Gupta A, Dogra MR, Singh R.Intractable glaucoma following intravitreal triamcinolone incentral retinal vein occlusion. Am J Ophthalmol 2004;137(4):758–760.
5. Jonas JB, Degenring RF, Kamppeter BA. Outcome of eyesundergoing trabeculectomy after intravitreal injections oftriamcinolone acetonide. J Glaucoma 2004;13(3):261.
6. Savage H, Roh M. Safety and efficacy of intravitreal triam-cinolone. Arch Ophthalmol 2004;122(7):1083.
7. Thompson JT. Cataract formation and other complicationsof intravitreal triamcinolone for macular edema. Am JOphthalmol 2006:141(4):629–637.
8. Yamashita T, Uemura A, Kita H, Sakamoto T. Intraocularpressure after intravitreal injection of triamcinolone ace-tonide following vitrectomy for macular edema. J Glaucoma2007;16(2):220–224.
9. Smithen LM, Ober MD, Maranan L, Spaide RF. Intravitrealtriamcinolone acetonide and intraocular pressure. Am JOphthalmol 2004;138(5):740–743.
10. Park HY, Yi K, Kim HK. Intraocular pressure elevation afterintravitreal triamcinolone acetonide injection. Korean JOphthalmol 2005;19(2):122–127.
11. Jonas JB, Degenring RF, Kreissig I, Akkoyun I, KamppeterBA. Intraocular pressure elevation after intravitreal triam-cinolone acetonide injection. Ophthalmology 2005;112(4):593–598.
12. Jones R 3rd, Rhee DJ. Corticosteroid-induced ocular hyper-tension and glaucoma: a brief review and update of theliterature. Curr Opin Ophthalmol 2006;17(2):163–167.
13. Jonas J, Kreissig I, Degenring R. Secondary chronic open-angle glaucoma after intravitreal triamcinolone acetonide.Arch Ophthalmol 2003;121(5):729–730.
14. Agrawal S, Agrawal J, Agrawal TP. Vitrectomy as a treat-ment for elevated intraocular pressure following intravitrealinjection of triamcinolone acetonide. Am J Ophthalmol2004;138(4):679–680.
15. Latina MA, Sibayan SA, Shin DH, Noecker RJ, MarcellinoG. Q-switched 532-nm Nd:YAG laser trabeculoplasty (selec-tive laser trabeculoplasty): a multicenter, pilot, clinical study.Ophthalmology 1998;105(11):2082–2088.
16. Damji KF, Shah KC, Rock WJ, Bains HS, Hodge WG.Selective laser trabeculoplasty vs argon laser trabeculoplasty:a prospective randomized clinical trial. Br J Ophthalmol1999;83(6):718–722.
17. Melamed S, Simon GB, Levkovitch-Verbin H. Selectivelaser trabeculoplasty as a primary treatment for open-angle
glaucoma. Arch Ophthalmol 2003;121(7):957–960.AMERICAN JOURNAL OF980
8. Avitabile T, Longo A, Reibaldi A. Intravitreal triamcino-lone compared with macular laser grid photocoagulation forthe treatment of cystoid macular edema. Am J Ophthalmol2005;140(4):695–702.
9. Armaly MF. Effect of corticosteroids on intraocular pressureand fluid dynamics. II. The effect of dexamethasone in theglaucomatous eye. Arch Ophthalmol 1963;70:492–499.
0. Mccarty GR, Schwartz B. Increased concentration ofglucocorticoid receptors in rabbit iris-ciliary body com-pared to rabbit liver. Invest Ophthalmol Vis Sci 1982;23(4):525–528.
1. Southern AL, Gordon GG, L’hommedieu D, Ravikumar S,Dunn MW, Weinstein BI. 5 beta-Dihydrocortisol: possiblemediator of the ocular hypertension in glaucoma. InvestOphthalmol Vis Sci 1985;26(3):393–395.
2. Rubin B, Taglienti A, Rothman RF, Marcus CH, Serle JB.The effect of selective laser trabeculoplasty on intraocularpressure in patients with intravitreal steroid-induced ele-vated intraocular pressure. J Glaucoma 2008;17(4):287–292.
3. Spaeth GL, Rodrigues MM, Weinreb S. Steroid-inducedglaucoma: A. Persistent elevation of intraocular pressure. B.Histopathologic aspects. Trans Am Ophthalmol Soc 1977;75:353–381.
4. Johnson DH, Bradley JMB, Accott TS. The effect of dexa-methasone on glycosaminoglycans of human trabecularmeshwork in perfusion organ culture. Invest Ophthalmol VisSci 1990;31(12):2568–2571.
5. Seftor REB, Stamer WD, Seftor EA, Snyder RW. Dexameth-asone decreases tissue plasminogen activator activity intrabecular meshwork organ and cell cultures. J Glaucoma1994;3(4):323–328.
6. Underwood JL, Murphy CG, Chen J, et al. Glucocorticoidsregulate transendothelial fluid flow resistance and formationof intercellular junctions. Am J Physiol Cell Physiol 1999;277(2):330–342.
7. Singh IP, Ahmad SI, Yeh D, et al. Early rapid rise inintraocular pressure after intravitreal triamcinolone ace-tonide injection. Am J Ophthalmol 2004;138(2):286 –287.
8. Beer PM, Bakri SJ, Singh RJ, Liu W, Peters GB 3rd, MillerM. Intraocular concentration and pharmacokinetics of tri-amcinolone acetonide after a single intravitreal injection.Ophthalmology 2003;110(4):681–686.
9. Alvarado JA, Betanzos A, Franse-Carman L, Chen J,González-Mariscal L. Endothelia of Schlemm’s canal andtrabecular meshwork: distinct molecular, functional, andanatomic features. Am J Physiol Cell Physiol 2004;286(3):621–634.
0. Pizzimenti JJ, Nickerson MM, Pizzimenti CE, Kasten-AkerAG. Selective laser trabeculoplasty for intraocular pressureelevation after intravitreal triamcinolone acetonide injec-tion. Optom Vis Sci 2006;83(7):421–425.
1. Baser E, Seymenoglu R. Selective laser trabeculoplasty for thetreatment of intraocular pressure elevation after intravitreal triam-cinolone injection. Can J Ophthalmol 2009;44(3):e21.
2. Rubin B, Taglienti A, Rothman RF, Marcus CH, Serle JB.The effect of selective laser trabeculoplasty on intraocularpressure in patients with intravitreal steroid-induced ele-
vated intraocular pressure. J Glaucoma 2008;17(4):287–292.OPHTHALMOLOGY DECEMBER 2011

3
3
33. Yuki K, Inoue M, Shiba D, Kawamura R, Ishida S, Ohtake Y.Selective laser trabeculoplasty for elevated intraocular pres-sure following subtenon injection of triamcinolone ace-tonide. Clin Ophthalmol 2010;26(4):247–249.
34. Vasconcelos-Santos DV, Nehemy PG, Schachat AP, Ne-hemy MB. Secondary ocular hypertension after intravitrealinjection of 4 mg of triamcinolone acetonide: incidence and
risk factors. Retina 2008;28(4):573–580.PROPHYLACTIC LASER THERAPY FORVOL. 152, NO. 6
5. Melamed S, Ben Simon GJ, Levkovitch-Verbin H. Selectivelaser trabeculoplasty as primary treatment for open-angleglaucoma: a prospective, nonrandomized pilot study. ArchOphthalmol 2003;121(7):957–960.
6. Tang M, Fu Y, Fu MS, et al. The efficacy of low-energyselective laser trabeculoplasty. Ophthalmic Surg Lasers Im-
aging 2011;42(1):59–63.STEROID-INDUCED GLAUCOMA 981
Biosketch
Ercument Bozkurt, MD, was born in 1969 in Izmir, Turkey. He graduated from Aegean Medical Faculty and specialisedin ophthalmology in Saint-Pierre Hospital branch of Free University of Brussels, Belgium. Dr Bozkurt is assistant directorin Beyoglu Eye Training and Research Hospital, Istanbul, Turkey. His main area of interest is anterior segment surgery andglaucoma.
PROPHYLACTIC LASER THERAPY FOR STEROID-INDUCED GLAUCOMAVOL. 152, NO. 6 981.e1
Biosketch
Necip Kara, MD, received a medical degree from Meram Medical Faculty of Selcuk University in Konya, Turkey andspecialized in Ophthalmology in the Beyoglu Eye Training and Research Hospital, Istanbul, Turkey. His main researchinterests include ophthalmic lasers, cataract and refractive surgery.
AMERICAN JOURNAL OF OPHTHALMOLOGY981.e2 DECEMBER 2011
Copyright © 2022 FDOKUMEN




















