
Development and Implantation of a Minimally Invasive Wireless Subretinal Neurostimulator
Upload
independentCategory
view
0download
0
Quality of Vision after Bilateral MultifocalIntraocular Lens ImplantationA Randomized Trial e AT LISA 809M versus AcrySofReSTOR SN6AD1
Vincenzo Maurino, MD, BQOphth,1 Bruce D. Allan, MD, FRCOphth,1,3 Gary S. Rubin, PhD,2,3
Catey Bunce, DSc,1 Wen Xing, MSc,1 Oliver Findl, MD,1,4 for the Moorfields IOL Study Group*
Purpose: To compare postoperative visual symptoms and spectacle freedom after bilateral implantation ofthe AT LISA 809M (Carl Zeiss Meditec, Jena, Germany) versus the AcrySof ReSTOR SN6AD1 (Alcon Laboratories,Irvine, CA) multifocal intraocular lens (IOL).
Design: Double-masked, prospective, randomized, controlled clinical trial.Participants: A total of 188 patients undergoing bilateral sequential cataract surgery or bilateral refractive
lens exchange.Methods: Patients were preoperatively randomized (allocation ratio 1:1) to bilateral implantation with the AT
LISA 809M IOL or ReSTOR SN6AD1 IOL. Postoperative outcomes were assessed 4 to 8 months after second eyesurgery.
Main Outcome Measures: The primary outcome was visual symptoms evaluated with the Quality of Vision(QoV) questionnaire. Secondary outcomes included other questionnaire data (CatQuest-9SF, spectacle inde-pendence, vision satisfaction, and dysphotopsia) and visual function measures (near, intermediate, and distancevisual acuity, binocular reading speed [International Reading Speed Texts], contrast sensitivity, and forward lightscatter). Adverse events, including intraoperative and postoperative complications, also were evaluated.
Results: There was no significant difference between IOL groups in Rasch-adjusted QoV scores for fre-quency (P ¼ 0.95), severity (P ¼ 0.56), and bothersomeness (P ¼ 0.34) of visual symptoms; median (interquartile)scores for these QoV subscales were 29 (15e37), 22 (13e27), and 14 (0e29) for the AT LISA 809M IOL group,respectively, and 32 (15e37), 22 (13e30), and 14 (0e29) for the ReSTOR SN6AD1 IOL group, respectively. Halowas the most prominent dysphotopsia symptom, with 6% in both IOL groups reporting halo symptoms as verybothersome. Complete spectacle independence was achieved in 69 of 84 (82.1%) AT LISA 809M recipients and66 of 85 (77.6%) ReSTOR SN6AD1 recipients (P ¼ 0.57). Preferred reading distance was slightly nearer for the ATLISA 809M IOL. There were no statistically significant differences in any of the other secondary outcomemeasures.
Conclusions: Visual symptoms were similar after bilateral implantation of the AT LISA 809M and ReSTORSN6AD1 IOLs. Both these diffractive bifocal IOLs produce high levels of spectacle independence and patientsatisfaction. However, a small but clinically significant minority of patients remained symptomatic and dissatisfiedwith visual results 4 to 8 months after surgery. Ophthalmology 2015;-:1e11 ª 2015 by the American Academy ofOphthalmology.
Spectacle independence is a central aim in modern cataractsurgery. Although bilateral monofocal intraocular lens(IOL) implantation leads to high levels of patient satisfac-tion, most patients still require spectacles for at least someactivities after surgery.1,2 Flexible haptic monofocal IOLshave delivered only limited gains in near vision over con-ventional monofocal IOLs, and these diminish with time.3
Multifocal IOLs with diffractive or refractive opticsdesigned to deliver more than 1 point of optimum focushave been more successful, delivering unaided distancevision at the same level as monofocal IOLs with
� 2015 by the American Academy of OphthalmologyPublished by Elsevier Inc.
significantly better unaided near vision and complete spec-tacle independence in a high proportion of patients,2,4,5 butthe tradeoff between gains in spectacle freedom and opticalside effects for multifocal IOLs is widely recognized.4,5
Research has focused on optic design improvementsaiming to optimize spectacle freedom while minimizingvisual symptoms. Designs based on diffractive optics haveproduced superior near vision and greater spectacle inde-pendence than refractive multifocal IOLs, with similar levelsof visual symptoms.6,7 A reduced near focus addition8 and,more recently, trifocal optics6,9,10 have been introduced to
1http://dx.doi.org/10.1016/j.ophtha.2014.10.002ISSN 0161-6420/14

Table 1. Inclusion and Exclusion Criteria
Inclusion criteria Sequential bilateral cataract surgery or refractive lens exchangeMotivation for spectacle independenceAge �21 yrs
Exclusion criteria Ocular comorbidity (amblyopia, retina, or optic nerve pathology) that may reduce postoperative CDVAReduced zonular/capsular stabilityCorneal astigmatism >1.50 DIOLMaster (Carl Zeiss Meditec, Jena, Germany) biometry not possibleIOL power <10 or >30 DProfessional night drivers, pilots, and other occupations for which induced dysphotopsia could threaten careerVulnerable groups, including patients in residential care or with learning difficulties or severe psychiatric disordersPoor mobilityPoor comprehension of written English
CDVA ¼ corrected distance visual acuity; D ¼ diopters; IOL ¼ intraocular lens.
Ophthalmology Volume -, Number -, Month 2015
enhance the intermediate range. Further optical modifica-tions, including variations in asphericity and diffractive stepprofile variations, have been developed to improve thequality of vision. We compare 2 market-leading diffractivebifocal IOLs, the AT LISA 809M (Carl Zeiss Meditec, Jena,Germany) and the AcrySof ReSTOR SN6AD1 (AlconLaboratories, Irvine, CA), each featuring diffractive stepprofile variations designed to minimize visual symptomsafter implantation,6,8,9,11e13 in a double-masked, prospec-tive, randomized, controlled trial using a validated dys-photopsia questionnaire14 as the main outcome measure.
Methods
Study Design
This study was conducted at 5 sites in 2 hospitals: Moorfields EyeHospital, London (4 sites), and King’s College Hospital, London(1 site). The protocol was approved by the U.K. CollaborativeResearch Ethics Committee. The principles of Good ClinicalPractice were adhered to throughout in accordance with theDeclaration of Helsinki. The study was a prospective, randomized,controlled clinical trial, registered at www.controlled-trials.com/ISRCTN64155646.
Enrollment of Participants
This trial included patients undergoing sequential bilateral cataractsurgery or refractive lens exchange. Inclusion and exclusioncriteria are detailed in Table 1. Eligible patients were identified byparticipating surgeons at their preoperative assessment, given anexplanation of the trial and its aims, and sent home with detailedtrial information designed to be readily comprehensible to anonexpert reader. After a minimum cooling-off period of 24 hours,provisional consent to participate in the trial was obtained bytelephone after further counseling with trial coordinators. Confir-mation of willingness to participate in the trial was obtained 5 to 10days before surgery. Participants were then registered in the trialand received a randomization number. Written confirmation ofconsent to participate in the trial was obtained by participatingsurgeons upon admission for first eye surgery.
Randomization and Treatment Allocation
Study patients were randomized by a medical statistician to bilateralimplantation of the AT LISA 809M or the ReSTOR SN6AD1multifocal IOL using a 1:1 treatment allocation ratio. Minimizationwas used to help distribute this 1:1 allocation ratio evenly
2
throughout participating sites and recruitment settings (NationalHealth Service or private practice). Minim software (http://www-users.york.ac.uk/wmb55/guide/minim.htm) was used for random-ization sequence generation, allocation concealment, treatmentallocation, and minimization.
Trial Intraocular Lenses
The AT LISA 809M (near addition þ3.75 diopters [D]) and theReSTOR SN6AD1 (near addition þ3.00 D) are both bifocal dif-fractive IOLs. Both have modifications to the diffractive stepprofile designed to increase light distribution to the distance focusand reduce light scatter, aiming to improve subjective visualquality while preserving good unaided near visual function.
The ReSTOR SN6AD1 IOL is distance dominant but pupil sizedependent, with a graded reduction of diffractive step height(apodization) toward the periphery of the central diffractive zone.Discounting scattered light, the ReSTOR SN6AD1 IOL has a 50/50 distance to near focus light distribution in the central 2 mm ofthe optic, which transitions to 100% distribution to the distancefocus outside the 3.6-mm-diameter diffractive zone.
The AT LISA 809M IOL has a wider-angle step transition withalternate refractive and diffractive zones across the full width of theoptic. A 65/35 distance-to-near focus light distribution ratio ismaintained at all pupil diameters.
Treatment and Surgical Technique
IOLMaster (Carl Zeiss Meditec) optical biometry was usedthroughout. Intraocular lens dioptric power was selected targetingemmetropia, using the IOL power corresponding to the negative(myopic) predicted refractive outcome closest to zero. Biometryprintouts were configured using optimized calculation constantspublished by the User Group for Laser Interferometric Biometry(http://www.augenklinik.uni-wuerzburg.de/ulib/c1.htm). TheSRKT biometry formula was used in IOL power calculations for alleyes with an axial length �22 mm. The Hoffer Q biometry formulawas used for all other eyes.
Phacoemulsification and IOL implantation were performed by12 consultant ophthalmic surgeons in the Moorfields IOL StudyGroup through a 2.4-mm limbal or clear corneal incision. Limbalrelaxing incisions (http://www.lricalculator.com) were used in eyeswith 1.00- to 1.50-D keratometric astigmatism (all eyes had a�1.50-D keratometric astigmatism) (Table 1). The IOLs wereimplanted in the capsular bag using the manufacturers’ recom-mended IOL loading and injection technique. The interval betweenthe first and second eye surgery was 1 to 4 weeks. Remedial laserrefractive surgery was offered to all patients with symptomaticrefractive errors after completion of the trial assessment.

Did not meet
Analyzed Analyzed
Figure 1. CONSORT trial flow diagram. IOL ¼ intraocular lens.
Maurino et al � RCT: AT LISA 809M vs. ReSTOR SN6AD1
Outcomes and Assessment
All patients were reviewed 3 weeks after the second eye surgery inaccordance with routine clinical care policies for patients under-going cataract surgery at participating sites.
Primary and secondary trial outcomes were assessed by aresearch-trained optometrist at a single visit 6 months (4e8months) after the surgery in the second eye using standard oper-ating procedures for data acquisition and archiving.
The primary outcome measure was the Quality of Vision (QoV)questionnaire score.14 The QoV is a validated, Rasch-adjustedquestionnaire in which patients are asked to rate 10 dysphotopsiaitems illustrated by standard photographs, scoring each item (0, 1,2, 3) in relation to how frequent, severe, and bothersome theirsymptoms are (30 items in total).
Secondary outcomes included additional vision-related ques-tionnaire items, binocular and uniocular measures of visual func-tion, eye examination findings, and surgical complication rates.
Questionnaires were completed at the trial assessment visit withguidance, when necessary, from the optometrist performing thetrial assessment. Additional questionnaire items were the Catquest9-SF cataract visual disability questionnaire,15 spectacle depen-dence questionnaire items, an overall satisfaction with vision rat-ing, and additional dysphotopsia items.16 The Catquest 9-SF is aRasch-adjusted cataract visual disability questionnaire that askspatients to rate difficulty with a range of vision-related daily ac-tivities. Spectacle dependence was examined by asking patients torate how often (always, sometimes, or never) they used spectaclesfor any purpose, for distance vision (driving, reading text ontelevision), intermediate vision (computer work, working with
3

Table 2. Baseline Characteristics
AT LISA 809MIOL
(n [ 94)
ReSTOR SN6AD1IOL
(n [ 94)
Mean age, yrs (SD) 67 (9.1) 68 (9.5)Gender, n (%)Female 57 (60.6) 48 (51.1)Male 37 (39.4) 46 (48.9)
Ethnicity, n (%)White 60 (63.8) 59 (62.8)Asian 14 (14.9) 14 (14.9)Black 4 (4.3) 9 (9.6)Other 2 (2.1) 2 (2.1)Unknown 14 (14.9) 10 (10.6)
Recruitment setting, n (%)NHS 80 (85.1) 79 (84.0)Private practice 14 (14.9) 15 (16.0)
Center, n (%)*Moorfields Eye Hospital 83 (88.3) 84 (89.4)Kings College Hospital 11 (11.7) 10 (10.6)
NHS ¼ National Health Service; SD ¼ standard deviation.*Patient recruitment and surgery were performed at 4 sites within Moor-fields Eye Hospital NHS Foundation Trust and at Kings College Hospital.
Ophthalmology Volume -, Number -, Month 2015
hands), and near vision (reading, fine near work). Overall satis-faction with vision after surgery was examined by asking patientsto rate whether they were very satisfied, satisfied, neither satisfiednor unsatisfied, unsatisfied, or very unsatisfied. The 4 additionaldysphotopsia questions16 were as follows: “Since your surgery,have you noticed any” halo, glare or dazzle, unwanted images, orshadows? Patients were asked to respond by indicating whetherthey had not experienced these symptoms at all (“none”) or foundthem “barely noticeable,” “annoying,” or “debilitating.”
Distance visual acuity (VA) was tested at 4 m using the backlitPrecision Vision EDTRS Distance Acuity Chart 2000 (PrecisionVision, LaSalle, IL) in standard office lighting conditions. Near VAwas tested at the preferred reading distance using the Precision
Table 3. Quality of Vision Questionnaire Scores
AT LISA809MIOL
(n [ 84)
ReSTORSN6AD1
IOL(n [ 84) P Value
Nonparametric analysisFrequency 29 (15e37) 32 (15e37) 0.954*Severity 22 (13e27) 22 (13e30) 0.596*Bothersome 14 (0e29) 14 (0e29) 0.341*
Parametric analysisFrequency 27 (15.4) 28 (16.7) 0.867y
Severity 21 (14.4) 22 (14.4) 0.622y
Bothersome 16 (17.0) 19 (18.0) 0.326y
Data are Rasch-adjusted Quality of Vision (QoV) subscale scores.Nonparametric data are median (interquartile range) and parametric dataare mean (standard deviation).TheQoV questionnaire scores were the primary outcomemeasure. Althoughcontinuous data, Rasch-adjusted QoV scores were highly skewed towardlower values (better visual quality). Nonparametric and nonparametric an-alyses were similar, showing no difference between intraocular lens (IOL)groups.*ManneWhitney U test.yt Test.
4
Vision Reduced EDTRS Near Acuity Chart 2000 designed for useat 40 cm. The same chart was used at 70 cm to measure intermediateVA. Letter counting (total number of letters correctly read) wasused to score VA throughout. Twenty letters were added to inter-mediate VA scores to correct for the alteration in viewing distanceusing the near acuity chart. Reference tables calibrated by chart andviewing distance were used to convert letter counts to the logarithmof the minimum angle of resolution and Snellen equivalents fordescriptive data presentation. Binocular VA data were usedthroughout with measurement of unaided (uncorrected distance,uncorrected intermediate, and uncorrected near VA) and distancespectacle-corrected (corrected distance, distance-corrected inter-mediate, and distance-corrected near VA) distance, intermediate,and near VA.
Binocular reading speed at the preferred reading distance wastested using standard International Reading Speed Texts.17
Reading speed (words per minute) was calculated using the for-mula reading speed ¼ number of words read correctly/time inseconds to read text�60. Binocular contrast sensitivity wasmeasured in standard office lighting conditions using Pel-lieRobson charts with a viewing distance of 1 m.
Retinal stray light was measured using the C-Quant forwardlight scatter test (Oculus Optikgerate, Wetzlar-Dutenhofen, Ger-many).18 Infrared photography using an AMO WaveScan aberr-ometer (Abbott Medical Optics, Santa Ana, CA) was used tomeasure mesopic pupil diameter, and slit-lamp examination wasused to grade IOL decentration in approximate 0.5-mm steps(0e0.5, 0.5e1, 1e1.5, and >1.5 mm) with reference to the non-dilated pupil centroid using a fine 1-mm slit beam and the centralpoint of the diffractive rings, easily visible on the IOL surface, tofacilitate estimation. Intraoperative and postoperative complicationswere recorded prospectively on clinical record forms.
Masking
This trial was double masked. Patients were not told which of thetrial lenses were implanted until all data had been collected andrecorded at the outcome assessment. Optometrists performingoutcome assessments were also masked to the identity of the lensimplanted. Slit-lamp examinations were performed after recordingall other data to minimize any risk of bias attributable to lensidentification during examination. Statisticians were masked to thelens identity until after analysis of the primary outcome data.
Sample Size
Our study was powered to have an 80% chance of detecting a 50%reduction in the number of patients reporting glare or dazzlesymptoms after bilateral multifocal IOL implantation using a 2-tailed Wilcoxon rank-sum test with a significance threshold set atP � 0.05. The null hypothesis was that dysphotopsia symptomswould be similar for IOLs tested in both arms of the trial. Byallowing for 10% patient dropout, a recruitment target of 94 pa-tients per arm or 188 patients in total was set.
This power analysis is based on background data from a non-validated single dysphotopsia question rating glare or dazzle on a4-point scale16 used in an earlier multifocal lens trial performed byour group,2 and predates the availability of the QoV instrument,14
which was subsequently adopted as the main outcome measure in aprotocol modification before commencement of the trial. The QoVquestionnaire also uses a 4-point scale for patient-reporteddysphotopsia symptoms, including glare, but is a validated, Rasch-weighted instrument. Because no prior QoV data were available formultifocal IOL recipients, all analyses performed in this studyshould be regarded as exploratory.
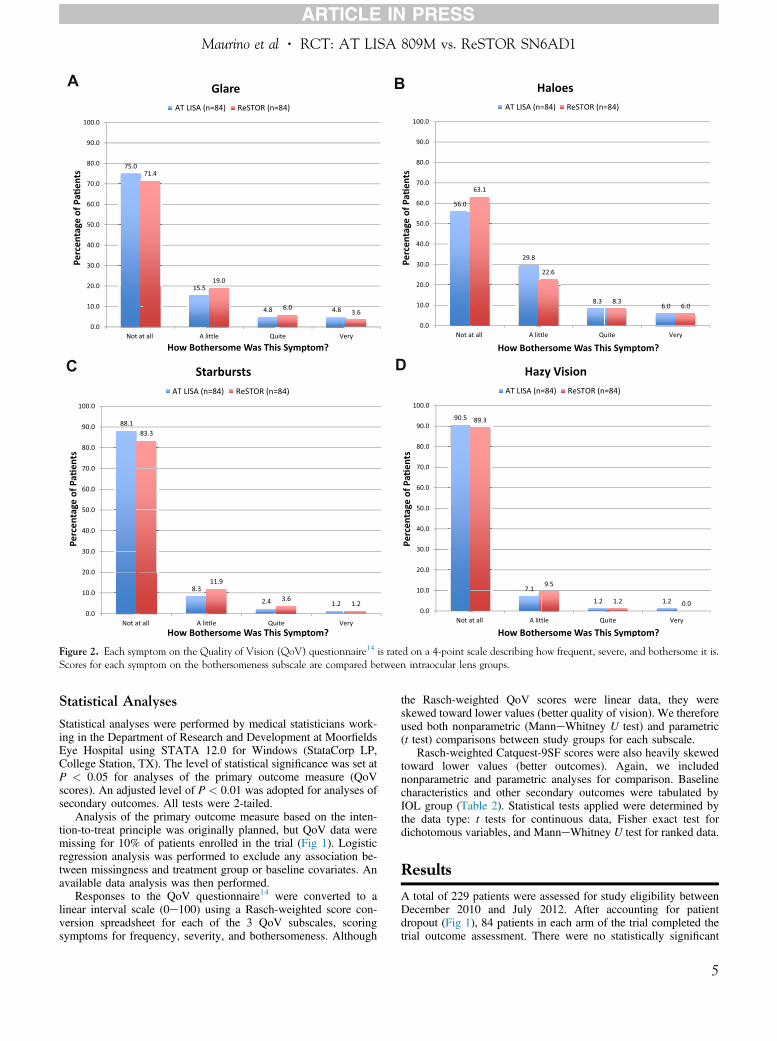
Figure 2. Each symptom on the Quality of Vision (QoV) questionnaire14 is rated on a 4-point scale describing how frequent, severe, and bothersome it is.Scores for each symptom on the bothersomeness subscale are compared between intraocular lens groups.
Maurino et al � RCT: AT LISA 809M vs. ReSTOR SN6AD1
Statistical Analyses
Statistical analyses were performed by medical statisticians work-ing in the Department of Research and Development at MoorfieldsEye Hospital using STATA 12.0 for Windows (StataCorp LP,College Station, TX). The level of statistical significance was set atP < 0.05 for analyses of the primary outcome measure (QoVscores). An adjusted level of P < 0.01 was adopted for analyses ofsecondary outcomes. All tests were 2-tailed.
Analysis of the primary outcome measure based on the inten-tion-to-treat principle was originally planned, but QoV data weremissing for 10% of patients enrolled in the trial (Fig 1). Logisticregression analysis was performed to exclude any association be-tween missingness and treatment group or baseline covariates. Anavailable data analysis was then performed.
Responses to the QoV questionnaire14 were converted to alinear interval scale (0e100) using a Rasch-weighted score con-version spreadsheet for each of the 3 QoV subscales, scoringsymptoms for frequency, severity, and bothersomeness. Although
the Rasch-weighted QoV scores were linear data, they wereskewed toward lower values (better quality of vision). We thereforeused both nonparametric (ManneWhitney U test) and parametric(t test) comparisons between study groups for each subscale.
Rasch-weighted Catquest-9SF scores were also heavily skewedtoward lower values (better outcomes). Again, we includednonparametric and parametric analyses for comparison. Baselinecharacteristics and other secondary outcomes were tabulated byIOL group (Table 2). Statistical tests applied were determined bythe data type: t tests for continuous data, Fisher exact test fordichotomous variables, and ManneWhitney U test for ranked data.
Results
A total of 229 patients were assessed for study eligibility betweenDecember 2010 and July 2012. After accounting for patientdropout (Fig 1), 84 patients in each arm of the trial completed thetrial outcome assessment. There were no statistically significant
5

Figure 2. (continued).
Ophthalmology Volume -, Number -, Month 2015
6

Maurino et al � RCT: AT LISA 809M vs. ReSTOR SN6AD1
differences in baseline characteristics for patients (n ¼ 94) assignedto either arm of the trial (Table 2) or in the age or gender of patientscompleting the study versus dropping out. All 29 patients recruitedin private practice completed the study after randomization,whereas 12% of patients (19/159) recruited in National HealthService clinics dropped out.
Primary Outcome Measure
Four to 8 months after second eye surgery, there was no statisti-cally significant difference in the severity, frequency, or bother-someness of dysphotopsia symptoms between AT LISA 809M andReSTOR SN6AD1 IOL recipients (Table 3), regardless of whethera nonparametric or parametric analysis was performed. Scores ineach of the QoV subscales were highly correlated. The distributionof symptom scores for each item in the bothersomeness subscalewas similar for both the trial lenses (Fig 2AeH). Halo was the mostprominent visual symptom (Fig 2B), with 8.3% and 6% patients inboth groups finding halo symptoms “quite” or “very” bothersome,respectively.
Secondary Outcome Measures
Results for secondary outcome measures were similar in bothgroups (Table 4); 82.1% of AT LISA 809M IOL recipients and77.4% of ReSTOR SN6AD1 IOL recipients were completelyspectacle independent after surgery (P ¼ 0.565, ManneWhitney Utest). The preferred reading distance was slightly closer for the ATLISA 809M IOL (Table 4). A nonsignificant trend toward greaterpostoperative astigmatism in right eye data (Table 4) was absent inleft eye data. Right and left eye data were similar for all otheruniocular outcome measures.
Adverse Events
Intraoperative and postoperative complications are detailed inTable 5. A trend toward more frequent IOL damage (P ¼ 0.03,Fisher exact test) during injection was observed for the AT LISA809M IOL, with 12 of 185 recipients (6.8%) having a split in thehaptic or optic, typically close to the haptic/optic junction. Im-mediate IOL exchange was required in 5 of 185 recipients (2.7%)because the IOL damage was judged sufficient to constitute a riskto optical performance or IOL centration by the operating surgeon.No patient elected to exchange lenses because of intolerable visualsymptoms. No yttriumealuminumegarnet (YAG) laser capsulot-omies were performed between the second eye surgery and the trialassessment.
Discussion
These data demonstrate no clinically significant differencein visual symptoms, spectacle independence, or overallsatisfaction with vision 4 to 8 months after bilateral im-plantation of 2 widely used contemporary diffractivemultifocal IOLs: the AT LISA 809M or the ReSTORSN6AD1.
This is the first study to quantify visual symptoms aftermultifocal IOL implantation using the QoV questionnaire.14
The QoV questionnaire has some important advantages overprevious nonvalidated, patient-reported measures of visualsymptoms used in multifocal IOL trials. Standard photo-graphs are used to illustrate each symptom. These illustra-tions help to promote good item separation and greaterconsistency of understanding between respondents for the
individual dysphotopsia items scored. The QoV question-naire was also developed using Rasch analysis. Briefly,Rasch analysis can be used to determine whether all ques-tionnaire items are examining the same latent trait and toconvert ordinal data into a linear interval scale. Eachresponse is weighted appropriately with respect to the traitbeing examined (quality of vision for the QoV question-naire) rather than assuming that each increment is equallyweighted for all the items scored.19
We adopted the QoV questionnaire as our main outcomemeasure in a protocol change after the initial planning andfunding of the trial because of the advantages cited earlier.No prior QoV data for multifocal IOL recipients wereavailable to guide a power calculation. Therefore, the ana-lyses we present are exploratory. For the nonvalidated 4-point scale rating glare or dazzle16 and used as the mainoutcome in the original power calculation, there was nosignificant difference between IOL groups (Table 6).
Mean QoV scores for frequency, severity, and bother-someness subscales for the AT LISA 809M and theReSTOR SN6AD1 IOLs were 27, 21, and 16, respectively,and 28, 22, and 19, respectively. Comparison with pub-lished mean QoV scores on the same subscales from patientsbefore (7, 6, and 5) and 3 months after (3, 2, and 1) myopicor hyperopic LASEK20 suggests that, for either of thecontemporary diffractive multifocal IOLs studied, visualsymptoms remain relatively prominent 4 to 8 months aftersecond eye surgery.
A sample size of 172 in each arm of an expanded trialwould have 85% power to detect a difference in mean QoVscores of 5 units on Rasch-adjusted subscales, assuming acommon standard deviation of 15.4 (Table 3) and using a 2-group t test with a 0.05 2-sided significance level. On the basisof the same conditions, the sample size reported was poweredto detect a difference in meanQoV scores of 7 units. To detecta 50%decrease inmeanQoV scores, theminimum required toapproach parity with results from monofocal IOL implanta-tion,21 only 23 patients per arm are required.
A total of 5 of 94 (5.3%) Tecnis ZM900 IOLs (AbbottMedical Optics) were exchanged within 1 year of surgery inan earlier randomized trial performed by the Moorfields IOLStudy Group because of dissatisfaction with image quality.2
None of the patients participating in the trial we reportelected to exchange the IOL for this or any other indicationwithin 1 year of second eye surgery. Two patients in the ATLISA 809M group reporting they were “very unsatisfied”(Table 4) with vision overall also reported that they were“very satisfied” in response to a similar item in the Catquest9-SF questionnaire, indicating problems with data recordingor response accuracy in satisfaction ratings for these pa-tients. Nonetheless, some patients in both IOL groupsclearly remained unsatisfied or very unsatisfied with overallvisual results at the 4- to 8-month postoperative trialassessment (Table 4). Although visual symptoms tend toimprove with time after multifocal IOL implantation5 anddissatisfaction often relates to factors independent of theIOL design (residual refractive error and posterior capsularopacification),22,23 these data underline the importance ofcontinued development in the optical design of multifocalIOLs and further clinical research aiming to quantify the
7
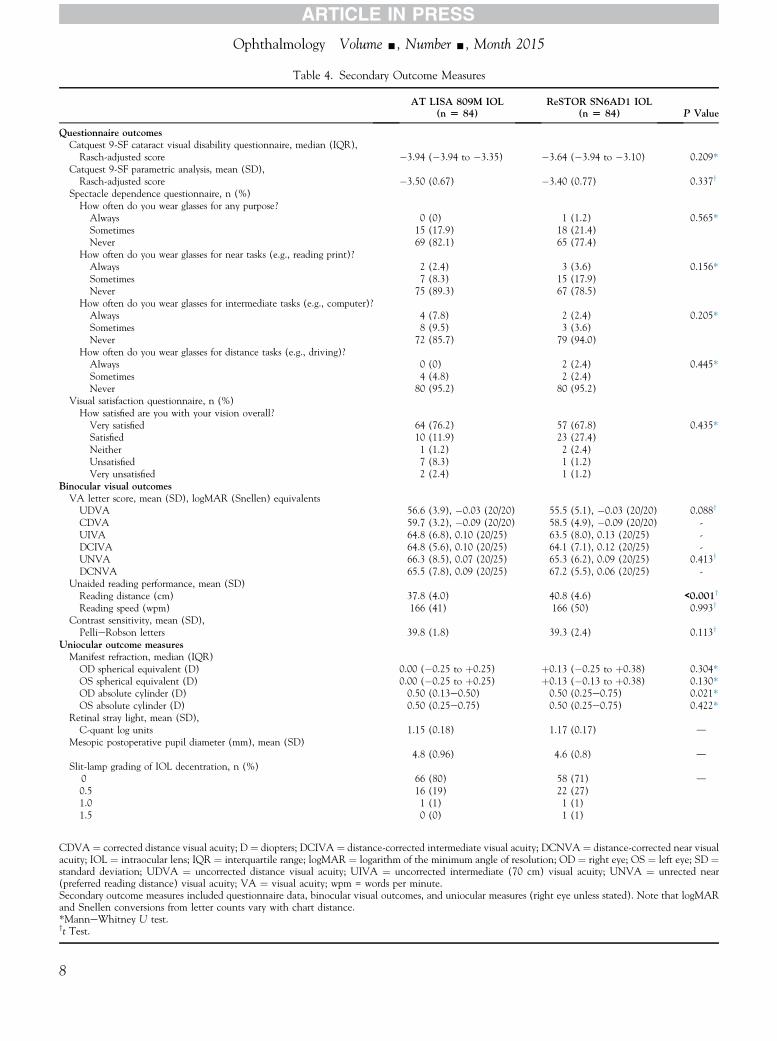
Table 4. Secondary Outcome Measures
AT LISA 809M IOL(n [ 84)
ReSTOR SN6AD1 IOL(n [ 84) P Value
Questionnaire outcomesCatquest 9-SF cataract visual disability questionnaire, median (IQR),Rasch-adjusted score �3.94 (�3.94 to �3.35) �3.64 (�3.94 to �3.10) 0.209*
Catquest 9-SF parametric analysis, mean (SD),Rasch-adjusted score �3.50 (0.67) �3.40 (0.77) 0.337y
Spectacle dependence questionnaire, n (%)How often do you wear glasses for any purpose?
Always 0 (0) 1 (1.2) 0.565*Sometimes 15 (17.9) 18 (21.4)Never 69 (82.1) 65 (77.4)
How often do you wear glasses for near tasks (e.g., reading print)?Always 2 (2.4) 3 (3.6) 0.156*Sometimes 7 (8.3) 15 (17.9)Never 75 (89.3) 67 (78.5)
How often do you wear glasses for intermediate tasks (e.g., computer)?Always 4 (7.8) 2 (2.4) 0.205*Sometimes 8 (9.5) 3 (3.6)Never 72 (85.7) 79 (94.0)
How often do you wear glasses for distance tasks (e.g., driving)?Always 0 (0) 2 (2.4) 0.445*Sometimes 4 (4.8) 2 (2.4)Never 80 (95.2) 80 (95.2)
Visual satisfaction questionnaire, n (%)How satisfied are you with your vision overall?
Very satisfied 64 (76.2) 57 (67.8) 0.435*Satisfied 10 (11.9) 23 (27.4)Neither 1 (1.2) 2 (2.4)Unsatisfied 7 (8.3) 1 (1.2)Very unsatisfied 2 (2.4) 1 (1.2)
Binocular visual outcomesVA letter score, mean (SD), logMAR (Snellen) equivalentsUDVA 56.6 (3.9), �0.03 (20/20) 55.5 (5.1), �0.03 (20/20) 0.088y
CDVA 59.7 (3.2), �0.09 (20/20) 58.5 (4.9), �0.09 (20/20) -UIVA 64.8 (6.8), 0.10 (20/25) 63.5 (8.0), 0.13 (20/25) -DCIVA 64.8 (5.6), 0.10 (20/25) 64.1 (7.1), 0.12 (20/25) -UNVA 66.3 (8.5), 0.07 (20/25) 65.3 (6.2), 0.09 (20/25) 0.413y
DCNVA 65.5 (7.8), 0.09 (20/25) 67.2 (5.5), 0.06 (20/25) -Unaided reading performance, mean (SD)Reading distance (cm) 37.8 (4.0) 40.8 (4.6) <0.001y
Reading speed (wpm) 166 (41) 166 (50) 0.993y
Contrast sensitivity, mean (SD),PellieRobson letters 39.8 (1.8) 39.3 (2.4) 0.113y
Uniocular outcome measuresManifest refraction, median (IQR)OD spherical equivalent (D) 0.00 (�0.25 to þ0.25) þ0.13 (�0.25 to þ0.38) 0.304*OS spherical equivalent (D) 0.00 (�0.25 to þ0.25) þ0.13 (�0.13 to þ0.38) 0.130*OD absolute cylinder (D) 0.50 (0.13e0.50) 0.50 (0.25e0.75) 0.021*OS absolute cylinder (D) 0.50 (0.25e0.75) 0.50 (0.25e0.75) 0.422*
Retinal stray light, mean (SD),C-quant log units 1.15 (0.18) 1.17 (0.17) d
Mesopic postoperative pupil diameter (mm), mean (SD)4.8 (0.96) 4.6 (0.8) d
Slit-lamp grading of IOL decentration, n (%)0 66 (80) 58 (71) d0.5 16 (19) 22 (27)1.0 1 (1) 1 (1)1.5 0 (0) 1 (1)
CDVA ¼ corrected distance visual acuity; D ¼ diopters; DCIVA ¼ distance-corrected intermediate visual acuity; DCNVA ¼ distance-corrected near visualacuity; IOL ¼ intraocular lens; IQR ¼ interquartile range; logMAR ¼ logarithm of the minimum angle of resolution; OD ¼ right eye; OS ¼ left eye; SD ¼standard deviation; UDVA ¼ uncorrected distance visual acuity; UIVA ¼ uncorrected intermediate (70 cm) visual acuity; UNVA ¼ unrected near(preferred reading distance) visual acuity; VA ¼ visual acuity; wpm = words per minute.Secondary outcome measures included questionnaire data, binocular visual outcomes, and uniocular measures (right eye unless stated). Note that logMARand Snellen conversions from letter counts vary with chart distance.*ManneWhitney U test.yt Test.
Ophthalmology Volume -, Number -, Month 2015
8

Table 5. Adverse Events
Outcome Measure AT LISA 809M IOL (Eyes Operated [ 185) ReSTOR SN6AD1 IOL (Eyes Operated [ 187)
Intraoperative complicationsPosterior capsule tear 1 4IOL damage not requiring lens exchange 7 1IOL damage requiring lens exchange 5 2Other 1 (iris prolapse) 1 (wrong IOL implanted*)
Postoperative complicationsRefractive surprise 2y 0Other 1 (CME 1; iritis 1) 5 (CME 4; iritis 1)
CME ¼ cystoid macular edema; IOL ¼ intraocular lens.Intraocular lens damage during injection was observed in both arms of the trial. Cystoid macular edema required drug treatment.*A reserve lens for the contralateral eye was implanted and immediately exchanged for the correct lens during surgery in 1 case.yTwo cases had LASIK treatment for a surprise refractive result (�1-diopter postoperative spherical equivalent refractive error) after the postoperativeassessment.
Maurino et al � RCT: AT LISA 809M vs. ReSTOR SN6AD1
inherent tradeoff between relative spectacle freedom andvisual symptoms.
Promising results recently have been reported for bothnewer refractive multifocal IOLs24 and trifocal, diffractive,multifocal IOLs.10 Wider adoption of the QoV questionnaireshould help clinicians to more accurately evaluate visualsymptoms after multifocal IOL implantation and facilitatedata comparison between trials. Current problems includevariations in data display, with publications showing QoVscores and analyses in parametric20 or nonparametric21
formats. We used both formats and found no difference inanalyses (Table 3). Patient fatigue during assessment, andthe potential deleterious effect on concentration, responses,and data quality, also may affect the utility of longerquestionnaire instruments, such as the 30-item QoV ques-tionnaire. We found scores for the 3 subscales to be highlycorrelated and are currently examining whether a shortened10-item QoV questionnaire based on the severity or
Table 6. Additional Dyspho
AT LISA 809M IOL (n [ 84)
Since your surgery, have you noticedany glare or dazzle?
None 21 (25.0)Barely noticeable 40 (47.6)Annoying 21 (25.0)Debilitating 2 (2.4)
Since your surgery, have you noticedany unwanted images?
None 71 (84.5)Barely noticeable 10 (11.9)Annoying 3 (3.6)Debilitating 0 (0)
Since your surgery, have you noticedany unwanted shadows?
None 78 (92.8)Barely noticeable 5 (6.0)Annoying 0 (0)Debilitating 1 (1.2)
Dysphotopsia questions adapted with permission from Tester et al.16
Data are no. (%).*ManneWhitney U test.
bothersomeness subscale alone might quantify visualsymptoms with equal accuracy.
The Catquest 9-SF questionnaire15 is a Rasch-analyzedinstrument designed to quantify visual disability or howmuch difficulty patients have with a range of activitiesbecause of their vision. The Catquest 9-SF recently has beenshown to be more responsive to cataract surgery than arange of alternative Rasch-scaled questionnaire in-struments.25 Catquest 9-SF scores in the current study(Table 4) were similar to published postoperative scores forcataract surgery with monofocal lenses,26 whereas QoVscores were worse.21 This suggests that visual symptomsassociated with the multifocal IOLs used in this trial werenot, in general, functionally disabling.
To help examine visual performance alongside ques-tionnaire data, we used binocular measures throughout, andnear vision was measured at the preferred reading distance,which was slightly closer for the AT LISA 809M IOL
topsia Assessment Items
ReSTOR SN6AD1 IOL (n [ 84) P Value*
39 (46.4) 0.77226 (31.0)18 (21.4)1 (1.2)
77 (91.7) d5 (5.9)2 (2.4)0 (0)
76 (90.5) d6 (7.1)2 (2.4)0 (0)
9

Ophthalmology Volume -, Number -, Month 2015
(Table 4). No other statistically significant differences wereobserved for secondary outcome measures.
Patients choosing multifocal lenses are motivated byspectacle freedom and do not normally wear spectacles tocorrect low-grade residual refractive error.5 To maximizeexternal validity for our data, any spectacle correction forresidual refractive error before the trial assessment wasentirely elective and driven by visual comfort. Biometry andsurgical technique were standardized, and both residualrefractive error and uncorrected binocular VA measureswere similar in both arms of the trial (Table 4). Although therelationship between IOL optic performance and visualsymptoms could have been examined in a pure context bysystematically correcting all residual refractive error, thiswould not reflect IOL performance in the real world.
In conclusion, overall, both the IOLs examined in thistrial, the AT LISA 809M and the ReSTOR SN6AD1, per-formed well. Approximately 4 of 5 patients were completelyspectacle free after surgery, and levels of overall satisfactionwere generally high. But visual symptoms 4 to 8 monthsafter surgery, and halo in particular, were more bothersomefor recipients of these contemporary diffractive multifocallenses than for monofocal IOL recipients. There is a tradeoffbetween visual symptoms and spectacle freedom for patientsreceiving multifocal IOL implantation.4,5
References
1. Moorfields IOLSG, Allan B. Binocular implantation of theTecnis Z9000 or AcrySof MA60AC intraocular lens in routinecataract surgery: prospective randomized controlled trialcomparing VF-14 scores. J Cataract Refract Surg 2007;33:1559–64.
2. Wilkins MR, Allan BD, Rubin GS, et al. Randomized trial ofmultifocal intraocular lenses versus monovision after bilateralcataract surgery. Ophthalmology 2013;120:2449–2455 e1.
3. Ong HS, Evans JR, Allan BD. Accommodative intraocularlens versus standard monofocal intraocular lens implantationin cataract surgery. Cochrane Database Syst Rev 2014;5:CD009667.
4. Leyland M, Pringle E. Multifocal versus monofocal intraocularlenses after cataract extraction. Cochrane Database Syst Rev2006;(4):CD003169.
5. de Vries NE, Nuijts RM. Multifocal intraocular lenses incataract surgery: literature review of benefits and side effects.J Cataract Refract Surg 2013;39:268–78.
6. Gatinel D, Houbrechts Y. Comparison of bifocal and trifocaldiffractive and refractive intraocular lenses using an opticalbench. J Cataract Refract Surg 2013;39:1093–9.
7. Cochener B, Lafuma A, Khoshnood B, et al. Comparison ofoutcomes with multifocal intraocular lenses: a meta-analysis.Clin Ophthalmol 2011;5:45–56.
8. Maxwell WA, Cionni RJ, Lehmann RP, Modi SS. Functionaloutcomes after bilateral implantation of apodized diffractiveaspheric acrylic intraocular lenses with a þ3.0 or þ4.0 diopteraddition power Randomized multicenter clinical study.J Cataract Refract Surg 2009;35:2054–61.
10
9. Madrid-Costa D, Ruiz-Alcocer J, Ferrer-Blasco T, et al. Op-tical quality differences between three multifocal intraocularlenses: bifocal low add, bifocal moderate add, and trifocal.J Refract Surg 2013;29:749–54.
10. Mojzis P, Pena-Garcia P, Liehneova I, et al. Outcomes of anew diffractive trifocal intraocular lens. J Cataract RefractSurg 2014;40:60–9.
11. Alio JL, Elkady B, Ortiz D, Bernabeu G. Clinical outcomesand intraocular optical quality of a diffractive multifocalintraocular lens with asymmetrical light distribution. J CataractRefract Surg 2008;34:942–8.
12. Alio JL, Plaza-Puche AB, Pinero DP, et al. Optical analysis,reading performance, and quality-of-life evaluation after im-plantation of a diffractive multifocal intraocular lens.J Cataract Refract Surg 2011;37:27–37.
13. Cillino G, Casuccio A, Pasti M, et al. Working-age cataractpatients: visual results, reading performance, and quality of lifewith three diffractive multifocal intraocular lenses. Ophthal-mology 2014;121:34–44.
14. McAlinden C, Pesudovs K, Moore JE. The development of aninstrument to measure quality of vision: the Quality of Vision(QoV) questionnaire. Invest Ophthalmol Vis Sci 2010;51:5537–45.
15. Lundstrom M, Pesudovs K. Catquest-9SF patient outcomesquestionnaire: nine-item short-form Rasch-scaled revision ofthe Catquest questionnaire. J Cataract Refract Surg 2009;35:504–13.
16. Tester R, Pace NL, Samore M, Olson RJ. Dysphotopsia inphakic and pseudophakic patients: incidence and relation tointraocular lens type(2). J Cataract Refract Surg 2000;26:810–6.
17. Trauzettel-Klosinski S, Dietz K, Group IRS. Standardizedassessment of reading performance: the New InternationalReading Speed Texts IReST. Invest Ophthalmol Vis Sci2012;53:5452–61.
18. Franssen L, Coppens JE, van den Berg TJ. Compensationcomparison method for assessment of retinal straylight. InvestOphthalmol Vis Sci 2006;47:768–76.
19. Massof RW, Rubin GS. Visual function assessment ques-tionnaires. Surv Ophthalmol 2001;45:531–48.
20. McAlinden C, Skiadaresi E, Pesudovs K, Moore JE. Quality ofvision after myopic and hyperopic laser-assisted subepithelialkeratectomy. J Cataract Refract Surg 2011;37:1097–100.
21. Skiadaresi E, McAlinden C, Pesudovs K, et al. Subjectivequality of vision before and after cataract surgery. ArchOphthalmol 2012;130:1377–82.
22. de Vries NE, Webers CA, Touwslager WR, et al. Dissatis-faction after implantation of multifocal intraocular lenses.J Cataract Refract Surg 2011;37:859–65.
23. Woodward MA, Randleman JB, Stulting RD. Dissatisfactionafter multifocal intraocular lens implantation. J CataractRefract Surg 2009;35:992–7.
24. Venter JA, Pelouskova M, Collins BM, et al. Visual outcomesand patient satisfaction in 9366 eyes using a refractivesegmented multifocal intraocular lens. J Cataract Refract Surg2013;39:1477–84.
25. McAlinden C, Gothwal VK, Khadka J, et al. A head to headcomparison of 16 cataract surgery outcome questionnaires.Ophthalmology 2011;118:2374–81.
26. Lundstrom M, Behndig A, Kugelberg M, et al. The outcome ofcataract surgery measured with the Catquest-9SF. Acta Oph-thalmologica 2011;89:718–23.

Maurino et al � RCT: AT LISA 809M vs. ReSTOR SN6AD1
Footnotes and Financial Disclosures
Originally received: July 17, 2014.Final revision: September 7, 2014.Accepted: October 3, 2014.Available online: ---. Manuscript no. 2014-1111.1 Moorfields Eye Hospital, London, United Kingdom.2 University College London, Institute of Ophthalmology, London, UnitedKingdom.3 NIHR Biomedical Research Centre based at Moorfields Eye HospitalNHS Foundation Trust and UCL Institute of Ophthalmology, London,United Kingdom.4 Vienna Institute for Research in Ocular Surgery, Vienna, Austria.
Data from this trial were presented in part at: the European Society ofCataract and Refractive Surgeons Annual Scientific Congress, October5e9, 2013, Amsterdam, The Netherlands.
*Moorfields IOL Study Group: Bruce Allan, Catey Bunce, Oliver Findl,Emma Hollick, Alex Ionides, Brian Little, Vincenzo Maurino, VictoriaMcCudden, Miriam Minahan, Con Petsoglu, Gary Rubin, George Saleh,Wen Xing, Seema Verma, and Mark Wilkins.
Financial Disclosure(s):The author(s) have no proprietary or commercial interest in any materialsdiscussed in this article.
Funded by an unrestricted grant from Carl Zeiss Meditec and the Depart-ment of Health’s NIHR Biomedical Research Centre for Ophthalmology atMoorfields Eye Hospital and the UCL Institute of Ophthalmology. Theviews expressed in the publication are those of the authors and notnecessarily those of the Department of Health funding organizations, whichhad no role in the design or conduct of this research.
Abbreviations and Acronyms:D ¼ diopter; IOL ¼ intraocular lens; QoV ¼ Quality of Vision;VA ¼ visual acuity.
Correspondence:Bruce D. Allan, MD, FRCOphth, Moorfields Eye Hospital, 162 CityRoad, London EC1V 2PD, United Kingodm. E-mail: [email protected].
11
Copyright © 2022 FDOKUMEN




















