Effect of in-the-bag intraocular lens fixation on the prevention of posterior capsule opacification
8
Effect of in-the-bag intraocular lens fixation on the prevention of posterior capsule opacification Jagat Ram, MD, Suresh K. Pandey, MD, David J. Apple, MD, Liliana Werner, MD, PhD, Gagandeep S. Brar, MD, Ramandeep Singh, MD, Kulbhushan P. Chaudhary, MD, Amod Gupta, MD ABSTRACT Purpose: To compare the incidence of posterior capsule opacification (PCO) after extra- capsular cataract extraction (ECCE) and phacoemulsification and to evaluate the role of posterior chamber intraocular lens (PC IOL) haptic fixation and biomaterial/design in reducing the incidence. Setting: Postgraduate Institute of Medical Education and Research, Chandigarh, India; Center for Research on Ocular Therapeutics and Biodevices, Storm Eye Institute, Medical University of South Carolina, Charleston, South Carolina, USA. Methods: This study comprised 278 eyes of 263 patients having ECCE and 318 eyes of 297 patients having phacoemulsification with PC IOL implantation. Posterior capsule opacification leading to a decrease in Snellen visual acuity of 2 or more lines was considered visually significant. The presence of PCO and IOL haptic fixation were evaluated postoperatively using slitlamp biomicroscopy. Haptic position was noted as in-the-bag (B–B), 1 haptic in the bag and 1 in the sulcus (bag–sulcus [B–S]), or both haptics out of the bag (sulcus–sulcus [S–S]). In addition, the rate of visually significant PCO was compared among 3 IOL biomaterials: poly(methyl methacrylate), silicone, and hydrophobic acrylic. Results: Visually significant PCO occurred in 42.45% of eyes having ECCE and 19.18% of eyes having phacoemulsification (P , .001, chi-square test) after a mean follow-up of 2.4 years 6 0.7 (SD). In both groups, visually significant PCO was significantly less in eyes with B–B fixation than in those with B–S or S–S fixation (P , .001). The rate of visually significant PCO in all eyes in the phacoemulsification group with B–B fixation was low (11.90%) and was significantly lower in eyes with a hydrophobic acrylic IOL (2.22%; P , .05, chi-square test). Conclusions: In-the-bag PC IOL fixation is required to consistently reduce the incidence of PCO. Thorough removal of lens substance, including hydrodissection-assisted cor- tical cleanup, and in-the-bag PC IOL fixation seem to be the most important factors in reducing PCO, regardless of surgical procedure or IOL type used. Intraocular lens biomaterial and design also help prevent PCO. J Cataract Refract Surg 2001; 27: 1039 –1046 © 2001 ASCRS and ESCRS © 2001 ASCRS and ESCRS 0886-3350/01/$–see front matter Published by Elsevier Science Inc. PII S0886-3350(00)00841-5
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Effect of in-the-bag intraocular lens fixation on the prevention of posterior capsule opacification

Effect of in-the-bag intraocular lensfixation on the prevention of posteriorcapsule opacification
Jagat Ram, MD, Suresh K. Pandey, MD, David J. Apple, MD,Liliana Werner, MD, PhD, Gagandeep S. Brar, MD,Ramandeep Singh, MD, Kulbhushan P. Chaudhary, MD,Amod Gupta, MD
ABSTRACT
Purpose: To compare the incidence of posterior capsule opacification (PCO) after extra-capsular cataract extraction (ECCE) and phacoemulsification and to evaluate the role ofposterior chamber intraocular lens (PC IOL) haptic fixation and biomaterial/design inreducing the incidence.
Setting: Postgraduate Institute of Medical Education and Research, Chandigarh, India;Center for Research on Ocular Therapeutics and Biodevices, Storm Eye Institute,Medical University of South Carolina, Charleston, South Carolina, USA.
Methods: This study comprised 278 eyes of 263 patients having ECCE and 318 eyes of297 patients having phacoemulsification with PC IOL implantation. Posterior capsuleopacification leading to a decrease in Snellen visual acuity of 2 or more lines wasconsidered visually significant. The presence of PCO and IOL haptic fixation wereevaluated postoperatively using slitlamp biomicroscopy. Haptic position was noted asin-the-bag (B–B), 1 haptic in the bag and 1 in the sulcus (bag–sulcus [B–S]), or bothhaptics out of the bag (sulcus–sulcus [S–S]). In addition, the rate of visually significantPCO was compared among 3 IOL biomaterials: poly(methyl methacrylate), silicone, andhydrophobic acrylic.
Results: Visually significant PCO occurred in 42.45% of eyes having ECCE and 19.18% ofeyes having phacoemulsification (P , .001, chi-square test) after a mean follow-up of2.4 years 6 0.7 (SD). In both groups, visually significant PCO was significantly less ineyes with B–B fixation than in those with B–S or S–S fixation (P , .001). The rate ofvisually significant PCO in all eyes in the phacoemulsification group with B–B fixationwas low (11.90%) and was significantly lower in eyes with a hydrophobic acrylic IOL(2.22%; P , .05, chi-square test).
Conclusions: In-the-bag PC IOL fixation is required to consistently reduce the incidenceof PCO. Thorough removal of lens substance, including hydrodissection-assisted cor-tical cleanup, and in-the-bag PC IOL fixation seem to be the most important factors inreducing PCO, regardless of surgical procedure or IOL type used. Intraocular lensbiomaterial and design also help prevent PCO. J Cataract Refract Surg 2001; 27:1039–1046 © 2001 ASCRS and ESCRS
© 2001 ASCRS and ESCRS 0886-3350/01/$–see front matterPublished by Elsevier Science Inc. PII S0886-3350(00)00841-5

Reducing the incidence of posterior capsule opacifi-cation (PCO), the most common complication of
primary extracapsular cataract extraction (ECCE) andphacoemulsification, is a major concern.1–13 From the1980s to the early 1990s, PCO rates ranged from 30%to 50% in most practices. Considering the large numberof cataract surgeries performed worldwide each year, thiscomplication has important medical, social, and eco-nomic implications.
Although in most cases of PCO the visual axis maybe cleared by a neodymium:YAG (Nd:YAG) laser pos-terior capsulotomy, the procedure can lead to severalmedical and nonmedical complications. It is expensive,costing the Medicare system in the United States up toan estimated $250 million per year during the 1990s.5
Use of the Nd:YAG laser in rural areas of developingcountries is financially prohibitive. The lack of availabil-ity of this equipment often limits widespread applica-tion of ECCE and intraocular lens (IOL) implantationin these areas.
The main reasons for in-the-bag (capsular) implan-tation of posterior capsule IOLs (PC IOLs) are that itleads to good lens centration, sequesters the IOL fromadjacent uveal tissue, and places the lens at a maximumdistance from the cornea.1,2,14 As early as 1984, Apple etal.1,2 postulated that capsular fixation may reduce theoccurrence of PCO; however, this has not been verifiedby clinical or experimental studies.
This study was performed in a clinical setting inwhich both standard ECCE and phacoemulsification
are used with clinical expertise, allowing side-by-sidecomparison of the 2 procedures. The effect of surgery,IOL fixation, and IOL biomaterial/design on the rate ofPCO was evaluated.
Patients and MethodsThe clinical results of patients having cataract sur-
gery by the same surgeon (J.R.) from 1990 to 1996 at amajor referral tertiary care center in North India wereevaluated. Patients having ECCE or phacoemulsifica-tion with implantation of a PC IOL for age-related cat-aract were included in the study.
In most cases, an ECCE was performed beforephacoemulsification equipment became available at thecenter in 1995. After 1995, most cataract surgeries wereperformed using phacoemulsification. An ECCE wasusually done in patients with a hard cataract, small pu-pil, or shallow anterior chamber or when the phaco-emulsification equipment was not functional.
The following patient data were evaluated: age atsurgery, date and type of cataract surgery, type of IOLimplanted, surgical complications, underlying ocular orsystemic health problems that might affect the eye, andpostoperative (Snellen) best corrected visual acuity(BCVA). The presence of clinically visually significantPCO, IOL fixation, and the date of Nd:YAG laser pos-terior capsulotomy (if performed) were also noted.
Patients were excluded if they had cataract associ-ated with systemic disease such as diabetes mellitus orwith ocular disease such as uveitis, glaucoma, pseudoex-foliation syndrome, retinal morbidity, or ocular trauma.Patients who had intraoperative complications such asposterior capsule tears with or without vitreous loss andthose with poor pupil dilation (,6.0 mm) were alsoexcluded.
All surgeries were performed using local (peribulbaror retrobulbar) anesthesia. In patients having ECCE, alimbal incision was made and an anterior capsulotomyperformed using the envelope technique. In more recentcases, a continuous curvilinear capsulorhexis (CCC)technique was also used. Cortical cleaving hydrodissec-tion was performed followed by nucleus expression. Ifthe nucleus was too large to deliver through a relativelysmall CCC, 2 radial incisions were made on the CCCmargin at the 10 and 2 o’clock positions to aid nuclearexpression. Cortical cleanup was performed using a 20
Accepted for publication November 9, 2000.
From the Department of Ophthalmology, Postgraduate Institute of Med-ical Education and Research, Chandigarh (Ram, Brar, Singh, Gupta),and Indira Gandhi Medical College Shimla, Shimla (Chaudhary), In-dia; The Center for Research on Ocular Therapeutics and Biodevices,Storm Eye Institute, Medical University of South Carolina, Charleston,South Carolina, USA (Pandey, Apple, Werner).
Presented in part at the 56th All India Ophthalmological Society Con-ference, Guwahati, India, February 1998.
Supported in part by an unrestricted grant from Research to PreventBlindness, Inc., New York, New York, USA.
None of the authors has a financial or proprietary interest in any materialor method mentioned.
Reprint requests to Jagat Ram, MD, Department of Ophthalmology,Postgraduate Institute of Medical Education and Research, Chandigarh,160012, India. E-mails: [email protected]; [email protected]; [email protected].
IN-THE-BAG IOL FIXATION TO PREVENT PCO
J CATARACT REFRACT SURG—VOL 27, JULY 20011040
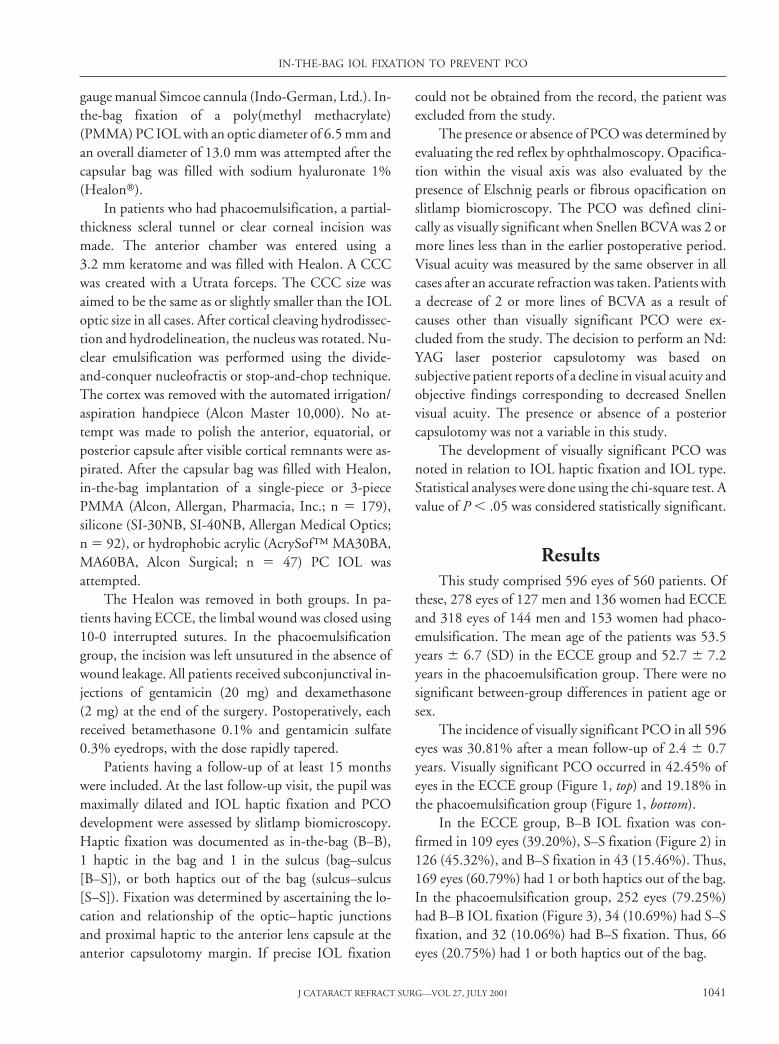
gauge manual Simcoe cannula (Indo-German, Ltd.). In-the-bag fixation of a poly(methyl methacrylate)(PMMA) PC IOL with an optic diameter of 6.5 mm andan overall diameter of 13.0 mm was attempted after thecapsular bag was filled with sodium hyaluronate 1%(Healont).
In patients who had phacoemulsification, a partial-thickness scleral tunnel or clear corneal incision wasmade. The anterior chamber was entered using a3.2 mm keratome and was filled with Healon. A CCCwas created with a Utrata forceps. The CCC size wasaimed to be the same as or slightly smaller than the IOLoptic size in all cases. After cortical cleaving hydrodissec-tion and hydrodelineation, the nucleus was rotated. Nu-clear emulsification was performed using the divide-and-conquer nucleofractis or stop-and-chop technique.The cortex was removed with the automated irrigation/aspiration handpiece (Alcon Master 10,000). No at-tempt was made to polish the anterior, equatorial, orposterior capsule after visible cortical remnants were as-pirated. After the capsular bag was filled with Healon,in-the-bag implantation of a single-piece or 3-piecePMMA (Alcon, Allergan, Pharmacia, Inc.; n 5 179),silicone (SI-30NB, SI-40NB, Allergan Medical Optics;n 5 92), or hydrophobic acrylic (AcrySof™ MA30BA,MA60BA, Alcon Surgical; n 5 47) PC IOL wasattempted.
The Healon was removed in both groups. In pa-tients having ECCE, the limbal wound was closed using10-0 interrupted sutures. In the phacoemulsificationgroup, the incision was left unsutured in the absence ofwound leakage. All patients received subconjunctival in-jections of gentamicin (20 mg) and dexamethasone(2 mg) at the end of the surgery. Postoperatively, eachreceived betamethasone 0.1% and gentamicin sulfate0.3% eyedrops, with the dose rapidly tapered.
Patients having a follow-up of at least 15 monthswere included. At the last follow-up visit, the pupil wasmaximally dilated and IOL haptic fixation and PCOdevelopment were assessed by slitlamp biomicroscopy.Haptic fixation was documented as in-the-bag (B–B),1 haptic in the bag and 1 in the sulcus (bag–sulcus[B–S]), or both haptics out of the bag (sulcus–sulcus[S–S]). Fixation was determined by ascertaining the lo-cation and relationship of the optic–haptic junctionsand proximal haptic to the anterior lens capsule at theanterior capsulotomy margin. If precise IOL fixation
could not be obtained from the record, the patient wasexcluded from the study.
The presence or absence of PCO was determined byevaluating the red reflex by ophthalmoscopy. Opacifica-tion within the visual axis was also evaluated by thepresence of Elschnig pearls or fibrous opacification onslitlamp biomicroscopy. The PCO was defined clini-cally as visually significant when Snellen BCVA was 2 ormore lines less than in the earlier postoperative period.Visual acuity was measured by the same observer in allcases after an accurate refraction was taken. Patients witha decrease of 2 or more lines of BCVA as a result ofcauses other than visually significant PCO were ex-cluded from the study. The decision to perform an Nd:YAG laser posterior capsulotomy was based onsubjective patient reports of a decline in visual acuity andobjective findings corresponding to decreased Snellenvisual acuity. The presence or absence of a posteriorcapsulotomy was not a variable in this study.
The development of visually significant PCO wasnoted in relation to IOL haptic fixation and IOL type.Statistical analyses were done using the chi-square test. Avalue of P , .05 was considered statistically significant.
ResultsThis study comprised 596 eyes of 560 patients. Of
these, 278 eyes of 127 men and 136 women had ECCEand 318 eyes of 144 men and 153 women had phaco-emulsification. The mean age of the patients was 53.5years 6 6.7 (SD) in the ECCE group and 52.7 6 7.2years in the phacoemulsification group. There were nosignificant between-group differences in patient age orsex.
The incidence of visually significant PCO in all 596eyes was 30.81% after a mean follow-up of 2.4 6 0.7years. Visually significant PCO occurred in 42.45% ofeyes in the ECCE group (Figure 1, top) and 19.18% inthe phacoemulsification group (Figure 1, bottom).
In the ECCE group, B–B IOL fixation was con-firmed in 109 eyes (39.20%), S–S fixation (Figure 2) in126 (45.32%), and B–S fixation in 43 (15.46%). Thus,169 eyes (60.79%) had 1 or both haptics out of the bag.In the phacoemulsification group, 252 eyes (79.25%)had B–B IOL fixation (Figure 3), 34 (10.69%) had S–Sfixation, and 32 (10.06%) had B–S fixation. Thus, 66eyes (20.75%) had 1 or both haptics out of the bag.
IN-THE-BAG IOL FIXATION TO PREVENT PCO
J CATARACT REFRACT SURG—VOL 27, JULY 2001 1041

Table 1 shows the rate of visually significant PCO inall eyes by group according to IOL fixation. In theECCE group, the rate of visually significant PCO wassignificantly less in eyes with B–B IOL fixation than in
those with S–S or B–S fixation (P , .001). There was nosignificant difference in PCO rates between the S–S andB–S subgroups. In the phacoemulsification group, PCOrates were significantly less in eyes with B–B fixation
Figure 1. (Ram) Diagrams comparing the incidence of PCO afterECCE (top) with that after phacoemulsification (bottom) with IOL im-plantation emphasize the importance of surgical factors, especiallyin-the-bag fixation, in reducing PCO.
Figure 2. (Ram) Slitlamp photograph of the right eye of a 63-year-old woman 2 years after ECCE with S–S fixation of a single-piecePMMA IOL shows visually significant PCO (Elschnig pearls).
Figure 3. (Ram) Clinical photographs of 3 cases after phacoemul-sification and in-the-bag IOL fixation. Note the CCC with slight anteriorcapsule opacification. There is no PCO. A: a 65-year-old man with aB–B fixated 3-piece PMMA IOL. B: A 55-year-old man with a B–Bfixated silicone IOL with polypropylene haptics (SI-30NB). C: A 52-year-old man with a B–B fixated hydrophobic acrylic IOL (AcrySof).
IN-THE-BAG IOL FIXATION TO PREVENT PCO
J CATARACT REFRACT SURG—VOL 27, JULY 20011042

than in those with S–S or B–S fixation. There was nosignificant difference in PCO rates between the B–S andthe S–S subgroups.
Table 2 shows the PCO rates in the phacoemulsifi-cation group according to IOL type. Overall PCO rateswere significantly less in eyes with a hydrophobic acrylicIOL than in those with a silicone or PMMA IOL (P ,.05). There was no significant difference in PCO ratesbetween the PMMA and silicone IOL subgroups.
Table 3 shows the PCO rates in the phacoemulsifi-cation group according to IOL fixation. In eyes withB–B fixation, the rate of visually significant PCO wassignificantly less in those with an acrylic IOL than inthose with a silicone IOL (P , .05). The PCO rate waslower in eyes with B–B fixation of acrylic lenses than ineyes with B–B fixation of PMMA lenses; the differencewas not statistically significant using the chi-square test(P 5 .0749). However, the Fisher exact test showed astatistically significant difference between the acrylicand PMMA groups (P 5 .0452). No significant differ-ence was found in visually significant PCO between eyeswith B–B fixated PMMA IOLs and those with B–Bfixated silicone IOLs.
Discussion
Posterior capsule opacification is the most commoncomplication of ECCE and phacoemulsification leadingto decreased visual acuity.1–13 Early studies of ECCEand phacoemulsification found PCO rates as high as30% to 50%. A 1998 metaanalysis of published articleson PCO noted an incidence by the mid-1990s of 25%over 5 years.15 A recent series of papers and several clin-icopathological studies4,9,11,16–19 identify 6 factors thatprevent PCO (Table 4). When these factors are appliedto the surgical procedure, the incidence of PCO maydrop into the single digits.11 The present study con-firmed that one factor, consistent IOL fixation, preventsPCO. The rate of visually significant PCO was signifi-cantly less in eyes with in-the-bag fixation than in thosein which 1 or both haptics were out of the bag, regardlessof surgical technique (ECCE or phacoemulsification) orIOL type.
Over a follow-up of at least 15 months, the overallincidence of visually significant PCO in all eyes in ourstudy was 30.81%. The incidence was 42.45% in theECCE group and 19.18% in the phacoemulsificationgroup. These rates are in accordance with the results ofseveral clinical studies with long-term follow-ups. Al-though primary in-the-bag fixation was attempted in allcases, most IOLs implanted in the ECCE group(60.79%) had 1 or both haptics out of the bag, probablybecause an envelope capsulotomy was required for nu-clear removal in most cases. This result is similar to thosein the era of can-opener and envelope techniques.20,21
In contrast, in the phacoemulsification group, in whicha CCC was used in all cases, 79.25% of IOLs had in-the-bag haptic fixation at the last examination.
Table 1. Posterior capsule opacification rates by IOL fixation.
Fixation
ECCE (n 5 278) Phacoemulsification (n 5 318)
Numberof Eyes
VS PCONo
VS PCONumberof Eyes
VS PCONo
VS PCO
n (%) n (%) n (%) n (%)
B–B 109 16 (14.67) 93 (85.32) 252 30 (11.90) 222 (88.09)
B–S 126 80 (63.49) 46 (36.51) 34 15 (44.12) 19 (55.88)
S–S 43 22 (51.16) 21 (48.84) 32 16 (50.00) 16 (50.00)
ECCE 5 extracapsular cataract extraction; VS PCO 5 visually significant PCO; B–B 5 bag–bag; B–S 5 bag–sulcus; S–S 5 sulcus–sulcus
Table 2. Posterior capsule opacification rates in the eyes havingphacoemulsification (n 5 318) according to IOL type.
PCO
IOL Type, n (%)
PMMA(n 5 179)
Silicone(n 5 92)
Acrylic(n 5 47)
Visually significant 36 (20.11) 22 (23.91) 3 (6.38)
None 143 (79.89) 70 (76.09) 44 (93.62)
PMMA 5 poly(methyl methacrylate); PCO 5 posterior capsuleopacification
IN-THE-BAG IOL FIXATION TO PREVENT PCO
J CATARACT REFRACT SURG—VOL 27, JULY 2001 1043

Aqueous fluorometric and clinicopathological stud-ies have shown that capsular bag placement of a PC IOLis preferable to B–S or S–S fixation.1,2,5,14 However, todate, few clinical reports have focused on the type ofhaptic fixation. This is because it is difficult to preciselyidentify the position of IOL haptics in living postoper-ative eyes. Although PC IOL fixation can be assessed inliving eyes postoperatively using cycloscopy,22 this is notpossible in cases in which pupil dilation is poor. Purelyclinical studies that correlate IOL biomaterial and de-sign with the development of PCO have one potentialweakness; that is, it may be difficult to discern whetherthe IOL haptics are in the bag. In our study, the type offixation could be determined by biomicroscopy undermaximum pupil dilation; the examiner was able to notethe position of each proximal haptic near the optic–haptic junction in relation to the margin (torn edge) ofthe anterior capsulotomy and classify fixation as B–B,B–S, or S–S.
The incidence of PCO was high (60.35%) in eyeshaving ECCE when the IOL was fixated out of the bag.The rate was significantly lower (14.67%) when capsu-lar bag fixation was achieved and even lower (11.90%)
in eyes having phacoemulsification and in-the-bag IOLfixation.
The results of this study correlate well with those ofclinicopathological studies of postmortem humanglobes,1–4,8,9 which also found that B–B fixation of PCIOLs achieves good IOL centration and minimizesPCO formation. In a prospective analysis of 3493 post-mortem eyes with PC IOLs,9 the incidences of centralPCO and Nd:YAG laser capsulotomy were consistentlyinfluenced by IOL fixation. Eyes with B–B fixation of anAcrySof or 1 of 3 silicone IOLs had less central PCO anda lower posterior capsulotomy rate than eyes with aPMMA IOL. However, the high capsulotomy rate withPMMA IOLs was related not only to biomaterial butalso to a high incidence of out-of-the-bag fixation after acan-opener or envelope anterior capsulotomy with ra-dial tears in the anterior capsule.
Implantation of PC IOLs may delay PCO becauseof a barrier effect created by the IOL optic.1–4,6,19 Thisbarrier reduces the migration of lens epithelial cells(LECs) from the equatorial zone onto the central poste-rior capsule (Figure 4). The greater the contact betweenthe posterior surface of the IOL and the anterior surface
Table 3. Posterior capsule opacification rates in the eyes having phacoemulsification (n 5 318) according to IOL type and fixation.
Fixation
IOL Type
PMMA Silicone Acrylic
VS PCONo
VS PCO VS PCONo
VS PCO VS PCONo
VS PCO
n (%) n (%) n (%) n (%) n (%) n (%)
B–B 17 (13.07) 113 (86.92) 12 (15.58) 65 (84.41) 1 (2.22) 44 (97.77)
B–S 10 (35.71) 18 (64.28) 4 (80.00) 1 (20.00) 1 (100) 0
S–S 9 (42.85) 12 (57.14) 6 (60.00) 4 (40.00) 1 (100) 0
PMMA 5 poly(methyl methacrylate); VS PCO 5 visually significant posterior capsule opacification; B–B 5 bag–bag; B–S 5 bag–sulcus; S–S 5
sulcus–sulcus
Table 4. Factors that reduce PCO.
Surgery-Related Factors(Capsular Surgery) IOL-Related Factors (Ideal IOL)
1. Hydrodissection-enhanced cortical cleanup 1. Biocompatible IOL to reduce stimulation of cell proliferation
2. In-the-bag fixation 2. Maximal IOL optic–posterior capsule contact; angulated haptic;bioadhesive biomaterial to create a shrink-wrap3. CCC diameter slightly smaller than that of IOL
optic, placing CCC edge on the anteriorsurface of the optic, helping sequester thecapsular bag, and shrink-wrapping thecapsule around the IOL optic
3. IOL optic geometry: square, truncated edge
IN-THE-BAG IOL FIXATION TO PREVENT PCO
J CATARACT REFRACT SURG—VOL 27, JULY 20011044
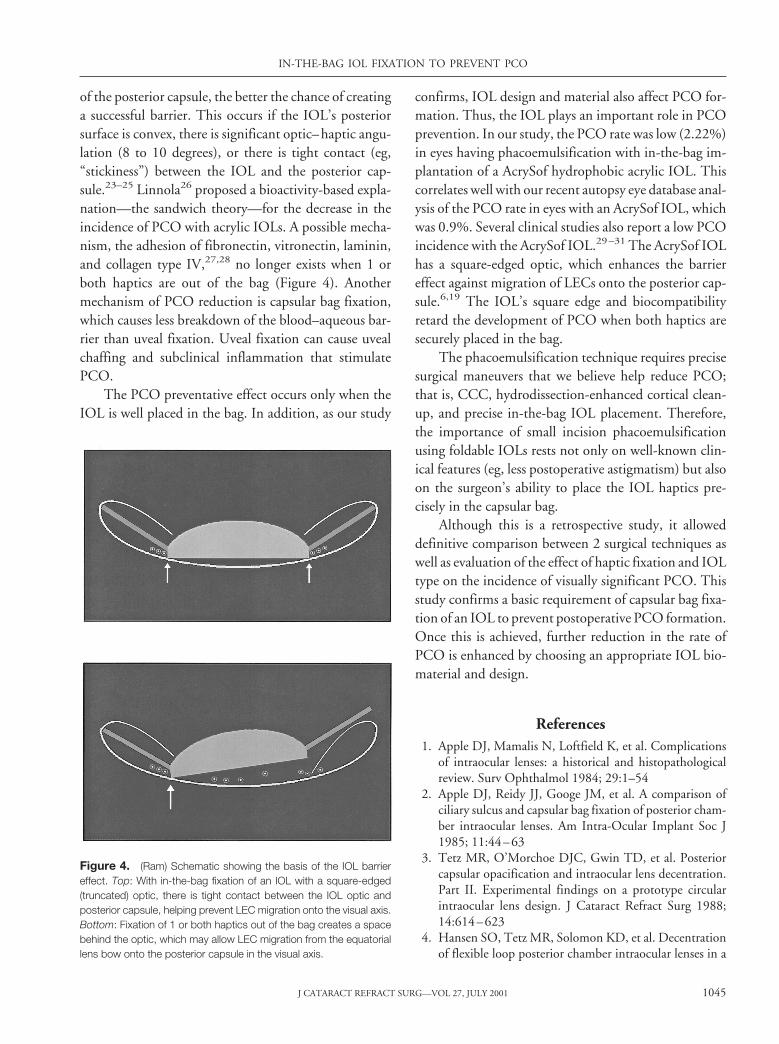
of the posterior capsule, the better the chance of creatinga successful barrier. This occurs if the IOL’s posteriorsurface is convex, there is significant optic–haptic angu-lation (8 to 10 degrees), or there is tight contact (eg,“stickiness”) between the IOL and the posterior cap-sule.23–25 Linnola26 proposed a bioactivity-based expla-nation—the sandwich theory—for the decrease in theincidence of PCO with acrylic IOLs. A possible mecha-nism, the adhesion of fibronectin, vitronectin, laminin,and collagen type IV,27,28 no longer exists when 1 orboth haptics are out of the bag (Figure 4). Anothermechanism of PCO reduction is capsular bag fixation,which causes less breakdown of the blood–aqueous bar-rier than uveal fixation. Uveal fixation can cause uvealchaffing and subclinical inflammation that stimulatePCO.
The PCO preventative effect occurs only when theIOL is well placed in the bag. In addition, as our study
confirms, IOL design and material also affect PCO for-mation. Thus, the IOL plays an important role in PCOprevention. In our study, the PCO rate was low (2.22%)in eyes having phacoemulsification with in-the-bag im-plantation of a AcrySof hydrophobic acrylic IOL. Thiscorrelates well with our recent autopsy eye database anal-ysis of the PCO rate in eyes with an AcrySof IOL, whichwas 0.9%. Several clinical studies also report a low PCOincidence with the AcrySof IOL.29–31 The AcrySof IOLhas a square-edged optic, which enhances the barriereffect against migration of LECs onto the posterior cap-sule.6,19 The IOL’s square edge and biocompatibilityretard the development of PCO when both haptics aresecurely placed in the bag.
The phacoemulsification technique requires precisesurgical maneuvers that we believe help reduce PCO;that is, CCC, hydrodissection-enhanced cortical clean-up, and precise in-the-bag IOL placement. Therefore,the importance of small incision phacoemulsificationusing foldable IOLs rests not only on well-known clin-ical features (eg, less postoperative astigmatism) but alsoon the surgeon’s ability to place the IOL haptics pre-cisely in the capsular bag.
Although this is a retrospective study, it alloweddefinitive comparison between 2 surgical techniques aswell as evaluation of the effect of haptic fixation and IOLtype on the incidence of visually significant PCO. Thisstudy confirms a basic requirement of capsular bag fixa-tion of an IOL to prevent postoperative PCO formation.Once this is achieved, further reduction in the rate ofPCO is enhanced by choosing an appropriate IOL bio-material and design.
References1. Apple DJ, Mamalis N, Loftfield K, et al. Complications
of intraocular lenses: a historical and histopathologicalreview. Surv Ophthalmol 1984; 29:1–54
2. Apple DJ, Reidy JJ, Googe JM, et al. A comparison ofciliary sulcus and capsular bag fixation of posterior cham-ber intraocular lenses. Am Intra-Ocular Implant Soc J1985; 11:44–63
3. Tetz MR, O’Morchoe DJC, Gwin TD, et al. Posteriorcapsular opacification and intraocular lens decentration.Part II. Experimental findings on a prototype circularintraocular lens design. J Cataract Refract Surg 1988;14:614–623
4. Hansen SO, Tetz MR, Solomon KD, et al. Decentrationof flexible loop posterior chamber intraocular lenses in a
Figure 4. (Ram) Schematic showing the basis of the IOL barriereffect. Top: With in-the-bag fixation of an IOL with a square-edged(truncated) optic, there is tight contact between the IOL optic andposterior capsule, helping prevent LEC migration onto the visual axis.Bottom: Fixation of 1 or both haptics out of the bag creates a spacebehind the optic, which may allow LEC migration from the equatoriallens bow onto the posterior capsule in the visual axis.
IN-THE-BAG IOL FIXATION TO PREVENT PCO
J CATARACT REFRACT SURG—VOL 27, JULY 2001 1045

series of 222 postmortem eyes. Ophthalmology 1988;95:344–349
5. Apple DJ, Solomon KD, Tetz MR, et al. Posterior cap-sule opacification. Surv Ophthalmol 1992; 37:73–116
6. Nishi O. Posterior capsule opacification. Part 1: experi-mental investigations. J Cataract Refract Surg 1999; 25:106–117
7. Tetz MR, Nimsgern C. Posterior capsule opacification.Part 2: clinical findings. J Cataract Refract Surg 1999;25:1662–1674
8. Ram J, Apple DJ, Peng Q, et al. Update on fixation ofrigid and foldable posterior chamber intraocular lenses.Part I. Elimination of fixation-induced decentration toachieve precise optical correction and visual rehabilita-tion. Ophthalmology 1999; 106:883–890
9. Ram J, Apple DJ, Peng Q, et al. Update on fixation ofrigid and foldable posterior chamber intraocular lenses.Part II. Choosing the correct haptic fixation and intraoc-ular lens design to help eradicate posterior capsule opaci-fication. Ophthalmology 1999; 106:891–900
10. Apple DJ, Peng Q, Visessook N, et al. Surgical preven-tion of posterior capsule opacification. Part I. Progress ineliminating this complication of cataract surgery. J Cat-aract Refract Surg 2000; 26:180–187
11. Apple DJ, Peng Q, Visessook N, et al. Eradication ofposterior capsule opacification: documentation of amarked decrease in Nd:YAG laser posterior capsulotomyrates noted in an analysis of 5416 pseudophakic humaneyes obtained postmortem. Ophthalmology 2001; 108:505–518
12. Apple DJ, Auffarth GU, Peng Q, Visessook N. FoldableIntraocular Lenses. Evolution, Clinicopathologic Corre-lations, and Complications. Thorofare, NJ, Slack, Inc;2000
13. Apple DJ, Ram J, Foster A, Peng Q. Elimination of cat-aract blindness: a global perspective entering the new mil-lennium. Surv Ophthalmol 2000; 45(suppl 1):451–455
14. Miyake K, Asakura M, Kobayashi H. Effect of intraocu-lar lens fixation on the blood-aqueous barrier. Am J Oph-thalmol 1984; 98:451–455
15. Schaumberg DA, Dana MR, Christen WG, Glynn RJ. Asystematic overview of the incidence of posterior capsuleopacification. Ophthalmology 1998; 105:1213–1221
16. Werner L, Apple DJ, Pandey SK. Postoperative prolifer-ation of anterior and equatorial lens epithelial cells. In:Buratto L, Osher RH, Masket S, eds, Cataract Surgery inComplicated Cases. Thorofare, NJ, Slack, 2000; 399–417
17. Apple DJ, Peng Q, Ram J. The 50th anniversary of theintraocular lens and a quiet revolution (editorial). Oph-thalmology 1999; 106:1861–1862
18. Peng Q, Apple DJ, Visessook N, et al. Surgical preven-tion of posterior capsule opacification. Part 2: enhance-
ment of cortical cleanup by focusing on hydrodissection.J Cataract Refract Surg 2000; 26:188–197
19. Peng Q, Visessook N, Apple DJ, et al. Surgical preven-tion of posterior capsule opacification. Part 3: intraocularlens optic barrier effect as a second line of defense.J Cataract Refract Surg 2000; 26:198–213
20. Apple DJ, Park SB, Merkley KH, et al. Posterior chamberintraocular lenses in a series of 75 autopsy eyes. Part I:loop location. J Cataract Refract Surg 1986; 12:358–362
21. Park SB, Brems RN, Parsons MR, et al. Posterior cham-ber intraocular lenses in a series of 75 autopsy eyes. PartII: postimplantation loop configuration. J Cataract Re-fract Surg 1986; 12:363–366
22. Miyake K. Observing posterior capsule lens haptics inliving postoperative eyes. Ophthalmic Surg 1984; 15:658–660
23. Nagata T, Minakata A, Watanabe I. Adhesiveness ofAcrySof to a collagen film. J Cataract Refract Surg 1998;24:367–370
24. Oshika T, Nagata T, Ishii Y. Adhesion of lens capsule tointraocular lenses of polymethylmethacrylate, silicone,and acrylic foldable materials: an experimental study. Br JOphthalmol 1998; 82:549–553
25. Oshika T, Suzuki Y, Kizaki H, Yaguchi S. Two yearclinical study of a soft acrylic intraocular lens. J CataractRefract Surg 1996; 22:104–109
26. Linnola RJ. Sandwich theory: bioactivity-based explana-tion for posterior capsule opacification. J Cataract RefractSurg 1997; 23:527–535
27. Linnola RJ, Werner L, Pandey SK, et al. Adhesion offibronectin, vitronectin, laminin, and collagen type IV tointraocular lens materials in pseudophakic human au-topsy eyes. Part I: histological sections. J Cataract RefractSurg 2000; 26:1792–1806
28. Linnola RJ, Werner L, Pandey SK, et al. Adhesion offibronectin, vitronectin, laminin and collagen type IV tointraocular lens materials in pseudophakic human au-topsy eyes. Part II: explanted IOLs. J Cataract RefractSurg 2000; 26:1087–1818
29. Hayashi H, Hayashi K, Nakao F, Hayashi F. Quantita-tive comparison of posterior capsule opacification afterpolymethylmethacrylate, silicone, and soft acrylic in-traocular lens implantation. Arch Ophthalmol 1998;116:1579–1582
30. Hollick EJ, Spalton DJ, Ursell PG, et al. The effect ofpolymethylmethacrylate, silicone, and polyacrylic in-traocular lenses on posterior capsular opacification 3years after cataract surgery. Ophthalmology 1999; 106:49–54
31. Ursell PG, Spalton DJ, Pande MV, et al. Relationshipbetween intraocular lens biomaterials and posterior cap-sule opacification. J Cataract Refract Surg 1998; 24:352–360
IN-THE-BAG IOL FIXATION TO PREVENT PCO
J CATARACT REFRACT SURG—VOL 27, JULY 20011046