
Illusory perception of gratings stimulating a small number of neurones
Upload
independentCategory
view
1download
0
Meta-analysis: Effect of Prophylactic HematopoieticColony-Stimulating Factors on Mortality and Outcomes of InfectionLillian Sung, MD, PhD; Paul C. Nathan, MD, MSc; Shabbir M.H. Alibhai, MD, MSc; George A. Tomlinson, PhD; and Joseph Beyene, PhD
Background: Benefits of prophylactic hematopoietic colony-stimu-lating factors (CSFs) in adults and children receiving cancer chemo-therapy or undergoing stem-cell transplantation (SCT) are unclear.
Purpose: To determine whether prophylactic CSFs decrease mor-tality, infections, and febrile neutropenia more than does placebo orno therapy in patients with cancer and in patients undergoing SCT.
Data Sources: Electronic searches of Ovid MEDLINE and EMBASEfrom inception until April 2007 and of the Cochrane Central Reg-ister of Controlled Trials until the second quarter of 2006.
Study Selection: We selected 148 trials that were reported in anylanguage that randomly assigned patients to CSFs or to eitherplacebo or no therapy. Prophylactic CSFs were given concurrentlywith or after initiation of chemotherapy.
Data Extraction: Two reviewers independently extracted data ontostandardized forms.
Data Synthesis: Short-term all-cause mortality appeared to be sim-ilar between the prophylactic CSF and the control groups (7.6% vs.
8.0%; relative risk, 0.95 [95% CI, 0.84 to 1.08]; absolute riskreduction, 0.4% [CI, �0.5% to 1.4%]). Risks for infection-relateddeath with CSFs and placebo or no therapy were 3.1% and 3.8%,respectively (relative risk, 0.82 [CI, 0.66 to 1.02]; absolute riskreduction, 0.8% [CI, 0.0% to 1.5%]). Use of CSFs reduced thefollowing more than did placebo or no therapy: documented infec-tions (median rate, 38.9% vs. 43.1%; rate ratio, 0.85 [CI, 0.79 to0.92]), microbiologically documented infections (median rate,23.5% vs. 28.6%; rate ratio, 0.86 [CI, 0.77 to 0.96]), and episodesof febrile neutropenia (median rate, 25.3% vs. 44.2%; rate ratio,0.71 [CI, 0.63 to 0.80]).
Limitations: Trial designs, including assessments of infections, andparticipants were heterogeneous. Estimates of mortality effectswere imprecise.
Conclusions: Prophylactic CSFs may have little or no effect onmortality but do decrease rates of infection in patients receivingcancer chemotherapy or those undergoing SCT.
Ann Intern Med. 2007;147:400-411. www.annals.orgFor author affiliations, see end of text.
Granulocyte colony-stimulating factor (G-CSF) andgranulocyte-macrophage colony-stimulating factor
(GM-CSF) are hematopoietic colony-stimulating factors(CSFs) that decrease the duration and severity of neutro-penia in adults and children receiving chemotherapy forcancer and those undergoing stem-cell transplantation(SCT) (1, 2). Several systematic reviews have examinedwhether CSFs affect other outcomes of patients with can-cer in different prophylactic settings (3–9). These reviews,which summarized data from 6 to 34 studies, usuallyfound that CSFs reduced febrile neutropenia and docu-mented infections. None found statistically significant re-ductions in infection-related mortality and all-cause mor-tality, although CIs around such estimates were wide giventhe rarity of these outcomes.
Although no single trial or previous systematic reviewhad sufficient power to exclude a clinically significant ben-efit of prophylactic CSFs on short-term all-cause mortality,we hypothesized that combining all available data fromrandomized trials in patients with cancer and in the SCT
setting would improve the ability to determine whetherCSFs influence this outcome. Thus, we sought to deter-mine whether prophylactic CSFs decrease all-cause and in-fection-related mortality, as well as infections and febrileneutropenia, more than do placebo or no therapy in pa-tients with cancer and patients undergoing SCT. We alsoperformed stratified analyses and meta-regression to ex-plore whether effects differed among certain subgroups ofpatients.
METHODS
Data Sources and SearchesWe developed a protocol for the review and followed
standard Quality of Reporting of Meta-Analyses(QUOROM) guidelines (10). We performed electronicsearches of Ovid MEDLINE from 1966 to 24 April 2007,of EMBASE from 1980 to 26 April 2007, and of the Coch-rane Central Register of Controlled Trials until the secondquarter of 2006. The search strategy included the followingMedical Subject Heading terms and text words: granulocytecolony-stimulating factor, granulocyte-macrophage colony-stimulating factor, neoplasms, stem cell transplant, and bonemarrow transplant. We also used abbreviated, generic, andtrade names for all available G-CSFs and GM-CSFs, in-cluding pegfilgrastim. The search was limited to random-ized, controlled trials. We also contacted the pharmaceuti-cal manufacturers of G-CSFs and GM-CSFs.
See also:
Web-OnlyAppendix TablesAppendix FiguresConversion of graphics into slides
Annals of Internal MedicineReview
400 © 2007 American College of Physicians

Study SelectionWe defined inclusion and exclusion criteria a priori.
Studies were included if 1) patients were randomly as-signed to CSFs or to placebo or no therapy, 2) CSFs weregiven concurrently with or after initiation of chemotherapyor conditioning for SCT but before neutropenia devel-oped, and 3) chemotherapy or conditioning regimens orother supportive care was not planned to systematicallydiffer between study groups. We described reasons for ex-cluding studies by using a hierarchical system that rankedreasons for exclusion in the following order: 1) absence ofplacebo or no-treatment group; 2) allocation not randomlyassigned; 3) intervention not administered concurrentlywith or after initiation of chemotherapy, or SCT condi-tioning (we excluded studies of priming in which CSFtherapy was initiated before chemotherapy) or administra-tion not prophylactic; 4) systematically different chemo-therapy or conditioning regimens; 5) systematically differ-ent supportive care; and 6) duplicate publication. Studiesincluded in the meta-analysis were not restricted by lan-guage or publication status.
Two reviewers independently evaluated the titles andabstracts of publications identified by the search strategy,and any publication thought to be potentially relevant byeither reviewer was retrieved in full. The reviewers were notblinded to study authors or outcomes. Final inclusion ofstudies in the meta-analysis was determined by agreementof both reviewers. Agreement between reviewers was eval-uated by using a � statistic. Strength of agreement as eval-uated by the � statistic was defined as slight (� � 0.00 to0.20), fair (� � 0.21 to 0.40), moderate (� � 0.41 to
0.60), substantial (� � 0.61 to 0.80), or almost perfect(� � 0.81 to 1.00) (11).
Data Extraction and Quality AssessmentThe primary outcome measure was short-term all-
cause mortality. Wherever possible, we assessed this out-come at 1 month after the initiation of use of the studydrug. If data at 1 month were not available, we used theclosest data between 3 and 6 weeks for chemotherapy re-cipients and up to 100 days or survival to discharge forpatients undergoing SCT. Secondary outcomes were infec-tion-related mortality, documented infections, microbio-logically documented infections, and febrile neutropenia.Other outcomes of interest were those related to other in-fections (sterile-site bacterial infections, documented fun-gal infections, and clinically documented infections), fe-brile neutropenia (durations of febrile neutropenia, fever,and neutropenia), and resource utilization (antibacterialand antifungal administration and duration of hospitaliza-tion). In principle, documented infections were composedof microbiologically and clinically documented infections;however, if detailed descriptions were not provided, werelied on the authors’ categorization of infectious out-comes. Two reviewers extracted data. We attempted tocontact all authors to obtain information not available inthe retrieved reports; 29 responded, and 4 provided addi-tional data.
We assessed study quality by using elements of theJadad scale (12), which examines adequacy of randomiza-tion, double-blinding, and description of withdrawals anddropouts. The primary purpose of the Jadad scale is to
Figure 1. Flow diagram of trial identification and selection.
Excluded ( n = 139) Absence of placebo/no-treatment group: 26Allocation not randomized: 30 Intervention not administered concurrently with or
following initiation of chemotherapy or conditioning for SC T, or in the prophylactic setting: 17
Systematically dif ferent chemotherapy or conditioning regimen: 6
Systematically dif ferent supportive care: 4 Duplicate publication or interim analysis: 54 Administration of CSFs other than G-CSF or GM-CSF: 2
Potentially relevant references identified and screened
( n = 4205)
Full articles retrieved for detailed evaluation
( n = 287)
Excluded by review of abstract: did not fulfill inclusion/exclusion criteria ( n = 3918)
Studies included in meta-analysis
( n = 148)
CSF � colony-stimulating factor; G-CSF � granulocyte colony-stimulating factor; GM-CSF � granulocyte-macrophage colony-stimulating factor;SCT � stem-cell transplantation.
ReviewProphylactic Colony-Stimulating Factors
www.annals.org 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 401

examine elements that may affect bias. We performed strat-ified analyses by elements that we felt to be the greatestthreats to validity, namely double-blinding and concealedallocation (inability to determine which treatment the nextparticipant will receive in the trial). However, for the pur-pose of describing the included studies, we also present thesummary Jadad scale, which ranges from 0 to 5 and inwhich a higher score is associated with higher quality. Weused the � statistic to assess agreement in study quality asextracted by the two reviewers.
Data Synthesis and AnalysisThis meta-analysis combined data at the study level
and not at the individual-patient level. For all-cause andinfection-related mortality, data were synthesized by usingrelative risk as the effect measure; a relative risk less than 1suggests that CSFs are associated with a reduction in thatoutcome. For all-cause mortality, we also present the abso-lute risk reduction associated with CSF prophylaxis. Be-cause several of the trials applied the assigned interventionafter a single randomization to multiple cycles of chemo-therapy and the results were presented in aggregate form, adifferent analytic approach was used for the nonsurvivalcategorical outcomes. When categorical data from multiple
cycles or therapeutic groups (for example, different doses ofCSFs) were available, events were aggregated and assumedto follow a Poisson distribution and are presented per cyclefor the overall analyses. The outcome was expressed as thenatural logarithm of the rate ratio, with the variance of therate ratio determined by using the delta method (13). Forcontinuous outcomes, we made the following assumptionsto facilitate data synthesis: The mean can be approximatedby the median; the range contains 6 SDs, the 95% CIcontains 4 SEs, and the interquartile range contains 1.35SDs. Continuous outcome variables were expressed as themean difference, which represents the overall difference be-tween CSF and placebo or no-therapy strategies. For ex-ample, the mean difference for fever duration is the overalldifference in days of fever between CSF and placebo or notherapy, with negative numbers indicating that durationwas shorter with CSFs. Effect sizes were weighted by theirinverse variance.
Because we anticipated heterogeneity between studies,we used a random-effects model (14) for all analyses. Weexplored the potential sources of heterogeneity with strati-fied analyses and random-effects meta-regression for theprimary and secondary outcomes. We present stratifiedanalyses by age group (pediatric, adult, or older patients),diagnosis (leukemia, solid tumor/lymphoma, or SCT),whether the primary study mandated the use of antibacte-rial prophylaxis (yes or no), CSF type (G-CSF or GM-CSF), timing of CSF administration (concurrent with che-motherapy or following completion of the chemotherapycycle), concealed allocation (yes or no), and double-blinded design (yes or no). To examine the association ofstudy-level characteristics and treatment effect, we fittedrandom-effects meta-regression models to the natural log-arithm of the relative risks or rate ratios by using thePROC MIXED procedure in SAS statistical software, ver-sion 9.1 (SAS Institute, Cary, North Carolina). The natu-ral logarithm of the relative risk or rate ratio was assumedto have a normal distribution, and a maximum likelihoodmethod was used to estimate model variables. The ran-dom-effects meta-regression model included fixed effectsfor the covariates, and a random intercept term was speci-fied to model residual heterogeneity not accounted for bythe covariates. For the stratified analyses and meta-regressions, only studies that reported on a single stratumwere included, to avoid double-counting. For example,studies that included both pediatric and adult patients butdid not report data separately by age group were excludedfrom the stratified analysis and meta-regression for age. Weexplored the possibility of publication bias by examiningfunnel plots (15).
The meta-analysis was performed by using ReviewManager, version 4.2 (The Cochrane Collaboration, Ox-ford, United Kingdom). Meta-regression was performed byusing SAS software. All tests of significance were 2-sided,and statistical significance was defined as a P value less than0.05.
Table 1. Characteristics of Included Studies*
Characteristic Studies Presenting Data(n � 148), n (%)
Age group 91†Pediatric (�18 y) 18 (19.8)Adult (18–65 y) 60 (65.9)Older (�65 y) 13 (14.3)
Diagnosis 143†Leukemia 40 (28.0)Solid tumor or lymphoma 78 (54.5)SCT 25 (17.5)
Type of CSF 144†G-CSF 83 (57.6)GM-CSF 61 (42.4)
Study-mandated antibiotic prophylaxis 147†Yes 27 (18.4)No 120 (81.6)
Concurrent administration of chemotherapy 146†Yes 27 (18.5)No 119 (81.5)
Concealed allocationAdequate 37 (25.0)Unclear 111 (75.0)
Double-blind designYes 54 (36.5)No 94 (63.5)
* CSF � colony-stimulating factor; G-CSF � granulocyte colony-stimulating fac-tor; GM-CSF � granulocyte-macrophage colony-stimulating factor; SCT � stem-cell transplantation.† Number of studies that consisted exclusively of 1 stratum or had data available toevaluate the characteristic.
Review Prophylactic Colony-Stimulating Factors
402 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 www.annals.org

Role of the Funding SourceThe funding source had no role in the design, con-
duct, or reporting of this analysis or in the decision tosubmit the manuscript for publication.
DATA SYNTHESIS
Figure 1 shows trial identification and selection. Atotal of 4205 titles and abstracts were reviewed, and 287full articles were retrieved. Of these, 148 satisfied pre-defined inclusion criteria and were included in the finalmeta-analysis. The reviewers had almost perfect agreementon articles for inclusion (� � 0.91 [95% CI, 0.86 to0.96]).
Table 1 summarizes the characteristics of the 148 in-cluded studies. Appendix Table 1 (available at www.annals.org) describes each study and associated references. The148 studies included 16 839 participants or cycles; 8474were randomly assigned to CSF and 8365 to placebo or notreatment. The median Jadad score for study quality was 2(range, 0 to 5), with substantial interrater agreement(weighted � � 0.73 [CI, 0.66 to 0.80]). We found noevidence of possible publication bias for either primary orsecondary outcomes (funnel plots not shown).
The median overall all-cause mortality rate in the pla-cebo or no-treatment groups was 4.9% (interquartilerange, 2.6% to 12.2%). Table 2 and Figure 2 (16–95)demonstrate that short-term all-cause mortality appearedto be similar between the prophylactic CSF groups and the
control groups (7.6% vs. 8.0%; relative risk, 0.95 [CI, 0.84to 1.08]; absolute risk reduction, 0.4% [CI, �0.5% to1.4%]). Risks for infection-related death with CSFs andplacebo or no therapy were 3.1% and 3.8%, respectively(relative risk, 0.82 [CI, 0.66 to 1.02]; absolute risk reduc-tion, 0.8% [CI, 0.0% to 1.5%]).
Appendix Table 2 (available at www.annals.org)shows the number of episodes and number of cycles at riskfor documented infections, microbiologically documentedinfections, and febrile neutropenia. The use of CSFs re-duced the following more than did placebo or no therapy:documented infections (median rate, 38.9% vs. 43.1%;rate ratio, 0.85 [CI, 0.79 to 0.92]), microbiologically doc-umented infections (median rate, 23.5% vs. 28.6%; rateratio, 0.86 [CI, 0.77 to 0.96]), and episodes of febrile neu-tropenia (median rate, 25.3% vs. 44.2%; rate ratio, 0.71[CI, 0.63 to 0.80]) (Table 2).
Table 2 also illustrates that CSFs were associated witha 17% reduction in the rate of sterile-site bacterial infec-tions, although this reduction was not statistically signifi-cant (P � 0.069). In contrast, the 25% decrease in the rateof clinically documented infections was statistically signif-icant (P � 0.005). Prophylactic CSFs did not affect therate of fungal infections. As expected, prophylactic CSFsreduced the duration of febrile neutropenia by a little morethan 1 day and reduced the time of recovery to an absoluteneutrophil count of 0.5 � 109 cells/L or greater by almost4 days. Resource utilization, measured by days of paren-
Table 2. Outcomes with Prophylactic Colony-Stimulating Factors versus Placebo or No Treatment*
Outcome Studies, n Effect (95% CI)† P Value
MortalityAll-cause mortality 80 Relative risk, 0.95 (0.84 to 1.08) 0.4
Risk reduction, 0.4% (�0.5% to 1.4%) 0.5Infection-related mortality 67 Relative risk, 0.82 (0.66 to 1.02) 0.070
Risk reduction, 0.8% (0.0% to 1.5%) 0.055Infections
All documented 60 Rate ratio, 0.85 (0.79 to 0.92) �0.001Microbiologically documented 41 Rate ratio, 0.86 (0.77 to 0.96) 0.006Sterile site bacterial 24 Rate ratio, 0.83 (0.68 to 1.01) 0.069Documented fungal 21 Rate ratio, 0.98 (0.70 to 1.37) 0.9Clinically documented 23 Rate ratio, 0.75 (0.62 to 0.92) 0.005
Fever and neutropeniaFebrile neutropenia 49 Rate ratio, 0.71 (0.63 to 0.80) �0.001Duration of febrile neutropenia 13 Mean difference, �1.38 d (�2.21 to �0.56 d) 0.001Duration of fever 34 Mean difference, �0.45 d (�0.87 to �0.04 d) 0.030Time to ANC �0.5 � 109 cells/L 53 Mean difference, �3.79 d (�4.28 to �3.29 d) �0.001Time to ANC �1.0 �109 cells/L 37 Mean difference, �5.03 d (�5.78 to �4.28 d) �0.001
Resource utilizationDuration of parenteral antibiotic therapy‡ 25 Mean difference, �1.81 d (�2.52 to �1.11 d) �0.001Administration of systemic antifungal agents 7 Rate ratio, 0.81 (0.64 to 1.01) 0.061Duration of antifungal therapy 8 Mean difference, �1.03 d (�2.38 to 0.32 d) 0.134Duration of hospitalization 43 Mean difference, �2.41 d (�3.13 to �1.70 d) �0.001
* ANC � absolute neutrophil count.† All analyses used a random-effects model. A relative risk and rate ratio less than 1 and a mean difference less than 0 suggest that colony-stimulating factor is better thanplacebo or no therapy.‡ Only duration of parenteral antibiotic administration, but not total antibiotic administration (including oral antibiotics), could be examined because very few of the studiesexplicitly described administration of oral antibiotics to treat febrile neutropenia or infections.
ReviewProphylactic Colony-Stimulating Factors
www.annals.org 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 403

teral antibiotic therapy and duration of hospitalization,also was reduced with prophylactic CSFs.
Figure 3 illustrates the stratified analyses by age groupand diagnosis. There was no interaction between age orpopulation diagnosis group and CSF effect, indicating thatthe effect of CSFs does not differ between subgroups.Studies that mandated antibacterial prophylaxis demon-strated a significantly greater beneficial effect of CSFs oninfection-related mortality (P � 0.010) compared withstudies that did not mandate antibacterial prophylaxis.Otherwise, mandating prophylaxis was not associated withdifferent CSF effects compared with studies that did notmandate prophylaxis (Appendix Figure 1, available at www.annals.org). Appendix Figures 2 to 7 (available at www.annals.org) present forest plots for all-cause mortality and
infection-related mortality by age group, diagnosis, andmandated antibacterial prophylaxis.
Appendix Tables 3 to 6 (available at www.annals.org)present additional stratified analyses and meta-regressions.The use of G-CSFs had a greater effect than use of GM-CSFs on reducing documented infections and febrile neu-tropenia, but all-cause mortality and infection-related mor-tality did not differ (Appendix Table 3). Concurrentadministration of CSF did not worsen all-cause mortalityor infection-related mortality compared with CSF admin-istered after chemotherapy (Appendix Table 4). Neitherconcealed allocation nor double-blinding affected the pri-mary or secondary outcomes (Appendix Tables 5 and 6).
As previously mentioned, the median rate of febrileneutropenia in the placebo groups was 44.2%. We dichot-
Figure 2. Forest plot of all-cause mortality associated with colony-stimulating factors.
Review Prophylactic Colony-Stimulating Factors
404 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 www.annals.org

omized studies into those with a baseline rate of febrileneutropenia of 20% or less than or greater than 20%. Ad-ministration of CSF did not result in greater reductions infebrile neutropenia or infection-related mortality rates instudies with a higher baseline rate of febrile neutropenia.The rate ratios for CSF effect on febrile neutropenia were0.62 (CI, 0.29 to 1.29; n � 10) in studies with a rate offebrile neutropenia of 20% or less and 0.71 (CI, 0.63 to0.80; n � 39) in studies with a rate of febrile neutropeniagreater than 20% (P for interaction � 0.2). The relativerisks for CSF effect on infection-related mortality were0.67 (CI, 0.24 to 1.90; n � 6) in patients with a lower rateof febrile neutropenia and 0.72 (CI, 0.46 to 1.14; n � 26)(P for interaction � 0.4) in patients with a higher rate offebrile neutropenia. Correspondingly, meta-regression also
demonstrated that there was no interaction between therate of febrile neutropenia (as a continuous variable) andCSF effect on infection-related mortality (P � 0.2).
DISCUSSION
In this meta-analysis of 148 randomized trials, wefound that prophylactic CSFs had small or no effects onshort-term all-cause mortality in patients with cancer re-ceiving chemotherapy or undergoing SCT. The lack of asubstantial effect on all-cause mortality was consistentacross patient populations and across CSF type and timingof administration. The 0.4% observed reduction in all-cause mortality was not statistically significant and proba-bly is too small to be clinically meaningful even if this
Figure 2—Continued
Squares represent the point estimate of the outcome of each included study. Squares to the left of the vertical line indicate that colony-stimulating factorreduces mortality compared with placebo or no treatment. Horizontal lines around the squares represent 95% CIs. The size of the squares reflects eachstudy’s relative weight, and the diamond represents the aggregate risk ratio (RR) and 95% CI.
ReviewProphylactic Colony-Stimulating Factors
www.annals.org 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 405

Figure 3. Primary and secondary outcomes associated with colony-stimulating factors, by patient characteristics.
Top. Stratified analyses by age of patient population. Bottom. Stratified analyses by underlying diagnosis of patient population. Squares represent thepoint estimate of the outcome for that stratum. Squares to the left of the vertical line indicate that colony-stimulating factor administration reduces thatoutcome. Horizontal lines around the squares represent 95% CIs. The effect measures are relative risks for all-cause mortality and infection-relatedmortality and rate ratios for infections and febrile neutropenia. The P values for interaction refer to an interaction between colony-stimulating factoreffect and strata and were derived from meta-regression. All analyses used a random-effects model. SCT � stem-cell transplantation; ST � solid tumor.
Review Prophylactic Colony-Stimulating Factors
406 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 www.annals.org

reduction were true. However, it also is important to notethat the 95% CI around the estimate (�0.5% to 1.4%)does not exclude the possibility of either a small harmful orbeneficial effect on mortality.
We failed to demonstrate a significant reduction inall-cause mortality, but we noted a 0.8% reduction in in-fection-related mortality from a baseline risk of 3.8% inthe control groups (although this reduction did not satisfyconventional definitions of statistical significance). Thereare 3 plausible explanations for this observed discrepancybetween the impact of CSFs on all-cause mortality andinfection-related mortality. First, the apparent reduction ininfection-related mortality may be a chance finding. Sec-ond, CSFs may reduce infection-related mortality but con-currently increase mortality from other causes. Several non-randomized studies have found that CSFs are associatedwith increased rate of graft-versus-host disease and treat-ment-related mortality after allogeneic SCT (96–98).However, a recent meta-analysis of randomized trials inSCT recipients failed to show that CSFs were associatedwith graft-versus-host disease or treatment-related death(9). Third, infection-related mortality is more difficult toascertain than overall mortality because it requires subjec-tive decision making regarding the cause of death. In manysettings, particularly in patients undergoing SCT, infec-tion-related mortality is susceptible to classification bias,whereas all-cause mortality is not. Thus, this difference inall-cause mortality and infection-related mortality may berelated to biased ascertainment in the latter outcome.
Two perspectives on these findings are possible. Thefirst is that regardless of the explanation, a reduction ininfection-related mortality is not clinically important if it isnot associated with a reduction in all-cause mortality. Con-versely, infection-related deaths may be a minor compo-nent of overall deaths, and, therefore, any beneficial effectof CSFs may be obscured when all deaths are examined.
Although we failed to demonstrate a benefit of CSFson all-cause mortality or infection-related mortality, CSFsdo affect other clinically important outcomes, includingfebrile neutropenia, documented infections, and microbio-logically documented infections. These findings, in addi-tion to a reduction in clinically documented infections,duration of febrile neutropenia, and duration of neutrope-nia, might be expected to be associated with improvedquality of life or reduced costs. The potential impact ofCSF use on costs is highlighted by the reduction in days ofparenteral antibiotic therapy and duration of hospitaliza-tion. Consequently, a final determination of whether CSFsare beneficial will depend on a multidimensional outcomethat incorporates survival, costs, patient preferences, andquality of life associated with different treatment options.Whereas little research has focused on the impact of pro-phylactic CSFs on quality of life or preferences, severalcost-effectiveness analyses have been published. These anal-yses have demonstrated little consistency in the direction ofcosts, irrespective of the underlying patient population—
some studies have found cost liability, whereas others havedemonstrated cost savings (7, 9, 99). Future researchaimed at guiding clinical decision making should focus onexpected differences in quality of life associated with CSFadministration; preferences of health care professionals, pa-tients, and family; and more precise estimation of costs indifferent clinical scenarios.
This meta-analysis complements a recent systematicreview of the administration of prophylactic antimicrobialagents in patients receiving chemotherapy (100). In thatanalysis of 95 studies, the authors found that antibioticprophylaxis decreased the risk for death from any cause bythe end of follow-up (as defined by each study), with arelative risk of 0.67 (CI, 0.55 to 0.81). They did not findthat the underlying diagnosis or undergoing SCT ex-plained heterogeneity in the effect. In our systematic re-view, the effect of prophylactic CSFs on infection-relatedmortality was greater in studies that mandated antibacterialprophylaxis. It is important to recognize that this analysisdemonstrates the effect of mandating, rather than receiv-ing, antibacterial prophylaxis, because most studies thatdid not mandate prophylaxis did not describe the numberof patients who actually received such an intervention. Al-though these results are provocative and suggest that the 2interventions may be synergistic, caution is needed becausethe studies that mandate prophylaxis might be systemati-cally different in some way, which may explain this effect.
The most recent recommendations from the AmericanSociety of Clinical Oncology suggest that primary prophy-laxis with CSFs should be implemented when the antici-pated risk for febrile neutropenia is greater than 20%(101). Our meta-analysis suggests that, on average, febrileneutropenia is reduced by 30%. However, in contrast tothe American Society of Clinical Oncology guidelines, wefound no difference in the effect of CSFs on febrile neu-tropenia according to whether the risk for febrile neutro-penia was greater or less than 20%. Qualitatively, the effectof CSFs was greater in patients with a risk for febrile neu-tropenia of 20% or less (although the interaction term wasnot significant). The rate of febrile neutropenia in the con-trol group also did not influence the CSF effect on infec-tion-related mortality, which is arguably a more importantend point than febrile neutropenia. Consequently, we sug-gest that the threshold for using CSFs should be influencedby quality of life, costs, and patient preferences, rather thanby the risk for febrile neutropenia alone. More detailedanalyses of different thresholds could be accomplished byusing a cost-effectiveness approach that incorporates qual-ity of life.
A potential limitation of this meta-analysis is that weincluded studies with a wide variety of patient characteris-tics and trial designs (although all were randomized). How-ever, the absence of heterogeneity in the primary outcome(all-cause mortality) and most secondary outcomes sup-ports the decision to include these different populationsand studies. Indeed, this larger sample size greatly increases
ReviewProphylactic Colony-Stimulating Factors
www.annals.org 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 407

our study’s power compared with previously publishedmeta-analyses. A second limitation is that none of our out-comes was reported by every study. This raises the possi-bility of selective reporting of outcomes and the potentialfor bias. Finally, although this meta-analysis included16 839 participants or cycles, it was underpowered to dem-onstrate very small differences in mortality. However,whether such small reductions in short-term mortality areclinically meaningful in this setting is uncertain.
In summary, we failed to demonstrate that prophylac-tic CSFs are associated with a statistically significantchange in all-cause mortality. Use of CSFs may reduceinfection-related mortality by a small amount. However,CSFs do reduce infections, infection-related morbidity,and resource use. Decision making about this interventionshould be based on further exploration of costs, patientpreferences, and quality of life.
From the University of Toronto, The Hospital for Sick Children, andUniversity Health Network, Toronto, Ontario, Canada.
Grant Support: In part by a career development award with the Cana-dian Child Health Clinician Scientist Training Program, a strategic pro-gram with the Canadian Institutes of Health Research (Dr. Sung).
Potential Financial Conflicts of Interest: None disclosed.
Requests for Single Reprints: Lillian Sung, MD, PhD, Division ofHaematology/Oncology, The Hospital for Sick Children, 555 UniversityAvenue, Toronto, Ontario M5G 1X8, Canada; e-mail, [email protected].
Current author addresses are available at www.annals.org.
References1. Lehrnbecher T, Welte K. Haematopoietic growth factors in children withneutropenia. Br J Haematol. 2002;116:28-56. [PMID: 11841397]2. American Society of Clinical Oncology. Recommendations for the use ofhematopoietic colony-stimulating factors: evidence-based, clinical practice guide-lines. J Clin Oncol. 1994;12:2471-508. [PMID: 7964965]3. Lyman GH, Kuderer NM, Djulbegovic B. Prophylactic granulocyte colony-stimulating factor in patients receiving dose-intensive cancer chemotherapy: ameta-analysis. Am J Med. 2002;112:406-11. [PMID: 11904116]4. Bohlius J, Reiser M, Schwarzer G, Engert A. Impact of granulocyte colony-stimulating factor (CSF) and granulocyte-macrophage CSF in patients with ma-lignant lymphoma: a systematic review. Br J Haematol. 2003;122:413-23.[PMID: 12877668]5. Bohlius J, Reiser M, Schwarzer G, Engert A. Granulopoiesis-stimulatingfactors to prevent adverse effects in the treatment of malignant lymphoma.Cochrane Database Syst Rev. 2004:CD003189. [PMID: 15266474]6. Berghmans T, Paesmans M, Lafitte JJ, Mascaux C, Meert AP, Sculier JP.Role of granulocyte and granulocyte-macrophage colony-stimulating factors inthe treatment of small-cell lung cancer: a systematic review of the literature withmethodological assessment and meta-analysis. Lung Cancer. 2002;37:115-23.[PMID: 12140132]7. Sung L, Nathan PC, Lange B, Beyene J, Buchanan GR. Prophylactic gran-ulocyte colony-stimulating factor and granulocyte-macrophage colony-stimulat-ing factor decrease febrile neutropenia after chemotherapy in children with can-cer: a meta-analysis of randomized controlled trials. J Clin Oncol. 2004;22:3350-6. [PMID: 15310780]8. Sasse EC, Sasse AD, Brandalise S, Clark OA, Richards S. Colony stimulatingfactors for prevention of myelosupressive therapy induced febrile neutropenia in
children with acute lymphoblastic leukaemia. Cochrane Database Syst Rev. 2005:CD004139. [PMID: 16034921]9. Dekker A, Bulley S, Beyene J, Dupuis LL, Doyle JJ, Sung L. Meta-analysis ofrandomized controlled trials of prophylactic granulocyte colony-stimulating fac-tor and granulocyte-macrophage colony-stimulating factor after autologous andallogeneic stem cell transplantation. J Clin Oncol. 2006;24:5207-15. [PMID:17114653]10. Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF. Improv-ing the quality of reports of meta-analyses of randomised controlled trials: theQUOROM statement. Quality of Reporting of Meta-analyses. Lancet. 1999;354:1896-900. [PMID: 10584742]11. Landis JR, Koch GG. The measurement of observer agreement for categor-ical data. Biometrics. 1977;33:159-74. [PMID: 843571]12. Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ,et al. Assessing the quality of reports of randomized clinical trials: is blindingnecessary? Control Clin Trials. 1996;17:1-12. [PMID: 8721797]13. Bieler GS, Williams RL. Ratio estimates, the delta method, and quantalresponse tests for increased carcinogenicity. Biometrics. 1993;49:793-801.[PMID: 8241374]14. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials.1986;7:177-88. [PMID: 3802833]15. Sutton AJ, Duval SJ, Tweedie RL, Abrams KR, Jones DR. Empirical as-sessment of effect of publication bias on meta-analyses. BMJ. 2000;320:1574-7.[PMID: 10845965]16. Ohno R, Tomonaga M, Kobayashi T, Kanamaru A, Shirakawa S, MasaokaT, et al. Effect of granulocyte colony-stimulating factor after intensive inductiontherapy in relapsed or refractory acute leukemia. N Engl J Med. 1990;323:871-7.[PMID: 1697646]17. Crawford J, Ozer H, Stoller R, Johnson D, Lyman G, Tabbara I, et al.Reduction by granulocyte colony-stimulating factor of fever and neutropeniainduced by chemotherapy in patients with small-cell lung cancer. N Engl J Med.1991;325:164-70. [PMID: 1711156]18. Kaplan LD, Kahn JO, Crowe S, Northfelt D, Neville P, Grossberg H, et al.Clinical and virologic effects of recombinant human granulocyte-macrophagecolony-stimulating factor in patients receiving chemotherapy for human immu-nodeficiency virus-associated non-Hodgkin’s lymphoma: results of a randomizedtrial. J Clin Oncol. 1991;9:929-40. [PMID: 2033429]19. Nemunaitis J, Rabinowe SN, Singer JW, Bierman PJ, Vose JM, FreedmanAS, et al. Recombinant granulocyte-macrophage colony-stimulating factor afterautologous bone marrow transplantation for lymphoid cancer. N Engl J Med.1991;324:1773-8. [PMID: 1903847]20. De Witte T, Gratwohl A, Van Der Lely N, Bacigalupo A, Stern AC, SpeckB, et al. Recombinant human granulocyte-macrophage colony-stimulating factoraccelerates neutrophil and monocyte recovery after allogeneic T-cell-depletedbone marrow transplantation. Blood. 1992;79:1359-65. [PMID: 1536959]21. Gorin NC, Coiffier B, Hayat M, Fouillard L, Kuentz M, Flesch M, et al.Recombinant human granulocyte-macrophage colony-stimulating factor afterhigh-dose chemotherapy and autologous bone marrow transplantation with un-purged and purged marrow in non-Hodgkin’s lymphoma: a double-blind place-bo-controlled trial. Blood. 1992;80:1149-57. [PMID: 1515637]22. Gulati SC, Bennett CL. Granulocyte-macrophage colony-stimulating factor(GM-CSF) as adjunct therapy in relapsed Hodgkin disease. Ann Intern Med.1992;116:177-82. [PMID: 1728202]23. Khwaja A, Linch DC, Goldstone AH, Chopra R, Marcus RE, WimperisJZ, et al. Recombinant human granulocyte-macrophage colony-stimulating fac-tor after autologous bone marrow transplantation for malignant lymphoma: aBritish National Lymphoma Investigation double-blind, placebo-controlled trial.Br J Haematol. 1992;82:317-23. [PMID: 1419813]24. Link H, Boogaerts MA, Carella AM, Ferrant A, Gadner H, Gorin NC,et al. A controlled trial of recombinant human granulocyte-macrophage colony-stimulating factor after total body irradiation, high-dose chemotherapy, and au-tologous bone marrow transplantation for acute lymphoblastic leukemia or ma-lignant lymphoma. Blood. 1992;80:2188-95. [PMID: 1421390]25. Pettengell R, Gurney H, Radford JA, Deakin DP, James R, Wilkinson PM,et al. Granulocyte colony-stimulating factor to prevent dose-limiting neutropeniain non-Hodgkin’s lymphoma: a randomized controlled trial. Blood. 1992;80:1430-6. [PMID: 1381626]26. De Witte T, Vreugdenhil G, Schattenberg A. Prolonged administration ofrecombinant granulocyte-macrophage colony-stimulating factor (GM-CSF) afterT-cell-depleted allogeneic bone marrow transplantation. Transplant Proc. 1993;
Review Prophylactic Colony-Stimulating Factors
408 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 www.annals.org

25:57-60. [PMID: 8351721]27. Gerhartz HH, Engelhard M, Meusers P, Brittinger G, Wilmanns W, Schli-mok G, et al. Randomized, double-blind, placebo-controlled, phase III study ofrecombinant human granulocyte-macrophage colony-stimulating factor as ad-junct to induction treatment of high-grade malignant non-Hodgkin’s lympho-mas. Blood. 1993;82:2329-39. [PMID: 7691256]28. Linch DC, Scarffe H, Proctor S, Chopra R, Taylor PR, Morgenstern G,et al. Randomised vehicle-controlled dose-finding study of glycosylated recombi-nant human granulocyte colony-stimulating factor after bone marrow transplan-tation. Bone Marrow Transplant. 1993;11:307-11. [PMID: 7683552]29. Shaffer DW, Smith LS, Burris HA, Clark GM, Eckardt JR, Fields SM,et al. A randomized phase I trial of chronic oral etoposide with or withoutgranulocyte-macrophage colony-stimulating factor in patients with advanced ma-lignancies. Cancer Res. 1993;53:5929-33. [PMID: 8261405]30. Aviles A, Dıaz-Maqueo JC, Talavera A, Nambo MJ, Garcıa EL. Effect ofgranulocyte colony-stimulating factor in patients with diffuse large cell lymphomatreated with intensive chemotherapy. Leuk Lymphoma. 1994;15:153-7. [PMID:7532056]31. Calderwood S, Romeyer F, Blanchette V, Chan H, Doyle J, Greenberg M,et al. Concurrent RhGM-CSF does not offset myelosuppression from intensivechemotherapy: randomized placebo-controlled study in childhood acute lympho-blastic leukemia. Am J Hematol. 1994;47:27-32. [PMID: 8042612]32. Gisselbrecht C, Prentice HG, Bacigalupo A, Biron P, Milpied N, Rubie H,et al. Placebo-controlled phase III trial of lenograstim in bone-marrow transplan-tation. Lancet. 1994;343:696-700. [PMID: 7510813]33. Miles DW, Fogarty O, Ash CM, Rudd RM, Trask CW, Spiro SG, et al.Received dose-intensity: a randomized trial of weekly chemotherapy with andwithout granulocyte colony-stimulating factor in small-cell lung cancer. J ClinOncol. 1994;12:77-82. [PMID: 7505809]34. Stahel RA, Jost LM, Cerny T, Pichert G, Honegger H, Tobler A, et al.Randomized study of recombinant human granulocyte colony-stimulating factorafter high-dose chemotherapy and autologous bone marrow transplantation forhigh-risk lymphoid malignancies. J Clin Oncol. 1994;12:1931-8. [PMID:7521907]35. Bajorin DF, Nichols CR, Schmoll HJ, Kantoff PW, Bokemeyer C, Dem-etri GD, et al. Recombinant human granulocyte-macrophage colony-stimulatingfactor as an adjunct to conventional-dose ifosfamide-based chemotherapy for pa-tients with advanced or relapsed germ cell tumors: a randomized trial. J ClinOncol. 1995;13:79-86. [PMID: 7799046]36. Bui BN, Chevallier B, Chevreau C, Krakowski I, Peny AM, Thyss A, et al.Efficacy of lenograstim on hematologic tolerance to MAID chemotherapy inpatients with advanced soft tissue sarcoma and consequences on treatment dose-intensity. J Clin Oncol. 1995;13:2629-36. [PMID: 7595717]37. Bunn PA Jr, Crowley J, Kelly K, Hazuka MB, Beasley K, Upchurch C,et al. Chemoradiotherapy with or without granulocyte-macrophage colony-stim-ulating factor in the treatment of limited-stage small-cell lung cancer: a prospec-tive phase III randomized study of the Southwest Oncology Group. J Clin On-col. 1995;13:1632-41. [PMID: 7602352]38. Dombret H, Chastang C, Fenaux P, Reiffers J, Bordessoule D, Bouabdal-lah R, et al. A controlled study of recombinant human granulocyte colony-stimulating factor in elderly patients after treatment for acute myelogenous leu-kemia. AML Cooperative Study Group. N Engl J Med. 1995;332:1678-83.[PMID: 7539109]39. Klumpp TR, Mangan KF, Goldberg SL, Pearlman ES, Macdonald JS.Granulocyte colony-stimulating factor accelerates neutrophil engraftment follow-ing peripheral-blood stem-cell transplantation: a prospective, randomized trial. JClin Oncol. 1995;13:1323-7. [PMID: 7538555]40. Nemunaitis J, Rosenfeld CS, Ash R, Freedman MH, Deeg HJ, AppelbaumF, et al. Phase III randomized, double-blind placebo-controlled trial of rhGM-CSF following allogeneic bone marrow transplantation. Bone Marrow Trans-plant. 1995;15:949-54. [PMID: 7581096]41. Ottmann OG, Hoelzer D, Gracien E, Ganser A, Kelly K, Reutzel R, et al.Concomitant granulocyte colony-stimulating factor and induction chemoradio-therapy in adult acute lymphoblastic leukemia: a randomized phase III trial.Blood. 1995;86:444-50. [PMID: 7541660]42. Riikonen P, Rahiala J, Salonvaara M, Perkkio M. Prophylactic administra-tion of granulocyte colony-stimulating factor (filgrastim) after conventional che-motherapy in children with cancer. Stem Cells. 1995;13:289-94. [PMID:7542114]43. Rowe JM, Andersen JW, Mazza JJ, Bennett JM, Paietta E, Hayes FA, et al.
A randomized placebo-controlled phase III study of granulocyte-macrophage col-ony-stimulating factor in adult patients (� 55 to 70 years of age) with acutemyelogenous leukemia: a study of the Eastern Cooperative Oncology Group(E1490). Blood. 1995;86:457-62. [PMID: 7605984]44. Schmitz N, Dreger P, Zander AR, Ehninger G, Wandt H, Fauser AA, et al.Results of a randomised, controlled, multicentre study of recombinant humangranulocyte colony-stimulating factor (filgrastim) in patients with Hodgkin’s dis-ease and non-Hodgkin’s lymphoma undergoing autologous bone marrow trans-plantation. Bone Marrow Transplant. 1995;15:261-6. [PMID: 7539668]45. Seymour AM, de Campos E, Thatcher N, De Greve J, Cunningham D,Howell A, et al. A single-blind, randomised, vehicle-controlled dose-findingstudy of recombinant human granulocyte colony-stimulating factor (lenograstim)in patients undergoing chemotherapy for solid cancers and lymphoma. Eur JCancer. 1995;31A:2157-63. [PMID: 8652235]46. Stone RM, Berg DT, George SL, Dodge RK, Paciucci PA, Schulman P,et al. Granulocyte-macrophage colony-stimulating factor after initial chemother-apy for elderly patients with primary acute myelogenous leukemia. Cancer andLeukemia Group B. N Engl J Med. 1995;332:1671-7. [PMID: 7760868]47. Takeshita A, Ohno R, Hirashima K, Toyama K, Okuma M, Saito H, et al.[A randomized double-blind controlled study of recombinant human granulocytecolony-stimulating factor in patients with neutropenia induced by consolidationchemotherapy for acute myeloid leukemia. (rG.CSF clinical study group)]. Rin-sho Ketsueki. 1995;36:606-14. [PMID: 7543956]48. Woll PJ, Hodgetts J, Lomax L, Bildet F, Cour-Chabernaud V, Thatcher N.Can cytotoxic dose-intensity be increased by using granulocyte colony-stimulat-ing factor? A randomized controlled trial of lenograstim in small-cell lung cancer.J Clin Oncol. 1995;13:652-9. [PMID: 7533825]49. Greenberg P, Advani R, Keating A, Gulati SC, Nimer S, Champlin R, et al.GM-CSF accelerates neutrophil recovery after autologous hematopoietic stem celltransplantation. Bone Marrow Transplant. 1996;18:1057-64. [PMID: 8971373]50. Jones SE, Schottstaedt MW, Duncan LA, Kirby RL, Good RH, MennelRG, et al. Randomized double-blind prospective trial to evaluate the effects ofsargramostim versus placebo in a moderate-dose fluorouracil, doxorubicin, andcyclophosphamide adjuvant chemotherapy program for stage II and III breastcancer. J Clin Oncol. 1996;14:2976-83. [PMID: 8918495]51. Weiss GR, Shaffer DW, DeMoor C, Rinaldi DA, Rodriguez GI, EckardtJR, et al. A randomized phase I study of oral etoposide with or without granu-locyte-macrophage colony-stimulating factor for the treatment of patients withadvanced cancer. Anticancer Drugs. 1996;7:402-9. [PMID: 8826608]52. Wexler LH, Weaver-McClure L, Steinberg SM, Jacobson J, Jarosinski P,Avila N, et al. Randomized trial of recombinant human granulocyte-macrophagecolony-stimulating factor in pediatric patients receiving intensive myelosuppres-sive chemotherapy. J Clin Oncol. 1996;14:901-10. [PMID: 8622038]53. Yau JC, Neidhart JA, Triozzi P, Verma S, Nemunaitis J, Quick DP, et al.Randomized placebo-controlled trial of granulocyte-macrophage colony-stimulat-ing-factor support for dose-intensive cyclophosphamide, etoposide, and cisplatin.Am J Hematol. 1996;51:289-95. [PMID: 8602629]54. Zittoun R, Suciu S, Mandelli F, de Witte T, Thaler J, Stryckmans P, et al.Granulocyte-macrophage colony-stimulating factor associated with inductiontreatment of acute myelogenous leukemia: a randomized trial by the EuropeanOrganization for Research and Treatment of Cancer Leukemia CooperativeGroup. J Clin Oncol. 1996;14:2150-9. [PMID: 8683249]55. Fridrik MA, Greil R, Hausmaninger H, Krieger O, Oppitz P, Stoger M,et al. Randomized open label phase III trial of CEOP/IMVP-Dexa alternatingchemotherapy and filgrastim versus CEOP/IMVP-Dexa alternating chemother-apy for aggressive non-Hodgkin’s lymphoma (NHL). A multicenter trial by theAustrian Working Group for Medical Tumor Therapy. Ann Hematol. 1997;75:135-40. [PMID: 9402845]56. Fukuoka M, Masuda N, Negoro S, Matsui K, Yana T, Kudoh S, et al.CODE chemotherapy with and without granulocyte colony-stimulating factor insmall-cell lung cancer. Br J Cancer. 1997;75:306-9. [PMID: 9010043]57. Geissler K, Koller E, Hubmann E, Niederwieser D, Hinterberger W, Geiss-ler D, et al. Granulocyte colony-stimulating factor as an adjunct to inductionchemotherapy for adult acute lymphoblastic leukemia—a randomized phase-IIIstudy. Blood. 1997;90:590-6. [PMID: 9226158]58. Gisselbrecht C, Haioun C, Lepage E, Bastion Y, Tilly H, Bosly A, et al.Placebo-controlled phase III study of lenograstim (glycosylated recombinanthuman granulocyte colony-stimulating factor) in aggressive non-Hodgkin’slymphoma: factors influencing chemotherapy administration. Groupe d’Etudedes Lymphomes de l’Adulte. Leuk Lymphoma. 1997;25:289-300. [PMID:
ReviewProphylactic Colony-Stimulating Factors
www.annals.org 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 409

9168439]59. Heil G, Hoelzer D, Sanz MA, Lechner K, Liu Yin JA, Papa G, et al. Arandomized, double-blind, placebo-controlled, phase III study of filgrastim inremission induction and consolidation therapy for adults with de novo acutemyeloid leukemia. The International Acute Myeloid Leukemia Study Group.Blood. 1997;90:4710-8. [PMID: 9389686]60. Legros M, Fleury J, Bay JO, Choufi B, Basile M, Condat P, et al. rhGM-CSF vs placebo following rhGM-CSF-mobilized PBPC transplantation: a phaseIII double-blind randomized trial. Bone Marrow Transplant. 1997;19:209-13.[PMID: 9028547]61. Linch DC, Milligan DW, Winfield DA, Kelsey SM, Johnson SA, Little-wood TJ, et al. G-CSF after peripheral blood stem cell transplantation in lym-phoma patients significantly accelerated neutrophil recovery and shortened timein hospital: results of a randomized BNLI trial. Br J Haematol. 1997;99:933-8.[PMID: 9432046]62. Lowenberg B, Boogaerts MA, Daenen SM, Verhoef GE, Hagenbeek A,Vellenga E, et al. Value of different modalities of granulocyte-macrophage colo-ny-stimulating factor applied during or after induction therapy of acute myeloidleukemia. J Clin Oncol. 1997;15:3496-506. [PMID: 9396403]63. Moreau P, Fiere D, Bezwoda WR, Facon T, Attal M, Laporte JP, et al.Prospective randomized placebo-controlled study of granulocyte-macrophage col-ony-stimulating factor without stem-cell transplantation after high-dose melpha-lan in patients with multiple myeloma. J Clin Oncol. 1997;15:660-6. [PMID:9053491]64. Pui CH, Boyett JM, Hughes WT, Rivera GK, Hancock ML, Sandlund JT,et al. Human granulocyte colony-stimulating factor after induction chemother-apy in children with acute lymphoblastic leukemia. N Engl J Med. 1997;336:1781-7. [PMID: 9187068]65. Bernasconi C, Alessandrino EP, Bernasconi P, Bonfichi M, Lazzarino M,Canevari A, et al. Randomized clinical study comparing aggressive chemotherapywith or without G-CSF support for high-risk myelodysplastic syndromes or sec-ondary acute myeloid leukaemia evolving from MDS. Br J Haematol. 1998;102:678-83. [PMID: 9722293]66. Fosså SD, Kaye SB, Mead GM, Cullen M, de Wit R, Bodrogi I, et al.Filgrastim during combination chemotherapy of patients with poor-prognosismetastatic germ cell malignancy. European Organization for Research and Treat-ment of Cancer, Genito-Urinary Group, and the Medical Research Council Tes-ticular Cancer Working Party, Cambridge, United Kingdom. J Clin Oncol.1998;16:716-24. [PMID: 9469362]67. Godwin JE, Kopecky KJ, Head DR, Willman CL, Leith CP, Hynes HE,et al. A double-blind placebo-controlled trial of granulocyte colony-stimulatingfactor in elderly patients with previously untreated acute myeloid leukemia: aSouthwest oncology group study (9031). Blood. 1998;91:3607-15. [PMID:9572995]68. Hidalgo M, Mendiola C, Lopez-Vega JM, Castellano D, Mendez M, Ba-tiste-Alenton E, et al. A multicenter randomized Phase II trial of granulocyte-colony stimulating factor-supported, platinum-based chemotherapy with flexiblemidcycle cisplatin administration in patients with advanced ovarian carcinoma.PSAMOMA Cooperative Group, Spain. Cancer. 1998;83:719-25. [PMID:9708936]69. Larson RA, Dodge RK, Linker CA, Stone RM, Powell BL, Lee EJ, et al. Arandomized controlled trial of filgrastim during remission induction and consol-idation chemotherapy for adults with acute lymphoblastic leukemia: CALGBstudy 9111. Blood. 1998;92:1556-64. [PMID: 9716583]70. Michon JM, Hartmann O, Bouffet E, Meresse V, Coze C, Rubie H, et al.An open-label, multicentre, randomised phase 2 study of recombinant humangranulocyte colony-stimulating factor (filgrastim) as an adjunct to combinationchemotherapy in paediatric patients with metastatic neuroblastoma. Eur J Can-cer. 1998;34:1063-9. [PMID: 9849455]71. Steward WP, von Pawel J, Gatzemeier U, Woll P, Thatcher N, Koschel G,et al. Effects of granulocyte-macrophage colony-stimulating factor and dose in-tensification of V-ICE chemotherapy in small-cell lung cancer: a prospective ran-domized study of 300 patients. J Clin Oncol. 1998;16:642-50. [PMID:9469353]72. Witz F, Sadoun A, Perrin MC, Berthou C, Briere J, Cahn JY, et al. Aplacebo-controlled study of recombinant human granulocyte-macrophage colo-ny-stimulating factor administered during and after induction treatment for denovo acute myelogenous leukemia in elderly patients. Groupe Ouest Est Leuce-mies Aigues Myeloblastiques (GOELAM). Blood. 1998;91:2722-30. [PMID:9531581]
73. Clarke V, Dunstan FD, Webb DK. Granulocyte colony-stimulating factorameliorates toxicity of intensification chemotherapy for acute lymphoblastic leu-kemia. Med Pediatr Oncol. 1999;32:331-5. [PMID: 10219333]74. Ifrah N, Witz F, Jouet JP, Francois S, Lamy T, Linassier C, et al. Intensiveshort term therapy with granulocyte-macrophage-colony stimulating factor sup-port, similar to therapy for acute myeloblastic leukemia, does not improve overallresults for adults with acute lymphoblastic leukemia. GOELAMS Group. Cancer.1999;86:1496-505. [PMID: 10526278]75. Ohno R, Mizoguchi H, Tomonaga M, Aoki N, Takaku F. A randomized,controlled study of rhG-CSF (KW-2228) in patients with neutropenia inducedby chemotherapy in acute leukemia. Biotherapy. 1999;13:701-9.76. Ojeda E, Garcia-Bustos J, Aguado M, Arrieta R, Quevedo E, Yuste VJ,et al. A prospective randomized trial of granulocyte colony-stimulating factortherapy after autologous blood stem cell transplantation in adults. Bone MarrowTransplant. 1999;24:601-7. [PMID: 10490724]77. Thomas X, Fenaux P, Dombret H, Delair S, Dreyfus F, Tilly H, et al.Granulocyte-macrophage colony-stimulating factor (GM-CSF) to increase effi-cacy of intensive sequential chemotherapy with etoposide, mitoxantrone and cyt-arabine (EMA) in previously treated acute myeloid leukemia: a multicenter ran-domized placebo-controlled trial (EMA91 Trial). Leukemia. 1999;13:1214-20.[PMID: 10450749]78. Bishop MR, Tarantolo SR, Geller RB, Lynch JC, Bierman PJ, Pavletic ZS,et al. A randomized, double-blind trial of filgrastim (granulocyte colony-stimu-lating factor) versus placebo following allogeneic blood stem cell transplantation.Blood. 2000;96:80-5. [PMID: 10891434]79. Harousseau JL, Witz B, Lioure B, Hunault-Berger M, Desablens B, DelainM, et al. Granulocyte colony-stimulating factor after intensive consolidation che-motherapy in acute myeloid leukemia: results of a randomized trial of the GroupeOuest-Est Leucemies Aigues Myeloblastiques. J Clin Oncol. 2000;18:780-7.[PMID: 10673519]80. Michel G, Landman-Parker J, Auclerc MF, Mathey C, Leblanc T, Legall E,et al. Use of recombinant human granulocyte colony-stimulating factor to in-crease chemotherapy dose-intensity: a randomized trial in very high-risk child-hood acute lymphoblastic leukemia. J Clin Oncol. 2000;18:1517-24. [PMID:10735900]81. Pfreundschuh M, Hasenclever D, Loeffler M, Ehninger G, Schmitz N,Kirchner H, et al; German Hodgkin’s Lymphoma Study Group. Dose escala-tion of cytotoxic drugs using haematopoietic growth factors: a randomized trial todetermine the magnitude of increase provided by GM-CSF. Ann Oncol. 2001;12:471-7. [PMID: 11398878]82. Przepiorka D, Smith TL, Folloder J, Anderlini P, Chan KW, Korbling M,et al. Controlled trial of filgrastim for acceleration of neutrophil recovery afterallogeneic blood stem cell transplantation from human leukocyte antigen-matched related donors. Blood. 2001;97:3405-10. [PMID: 11369630]83. Channa J, Hashmi KZ. Role of recombinant granulocyte-macrophage colo-ny-stimulating factors in reducing the duration of neutropenia. J College PhysSurg Pakistan. 2002;12:538-41.84. Dallorso S, Rondelli R, Messina C, Pession A, Giorgiani G, Fagioli F, et al.Clinical benefits of granulocyte colony-stimulating factor therapy after hemato-poietic stem cell transplant in children: results of a prospective randomized trial.Haematologica. 2002;87:1274-80. [PMID: 12495901]85. Hołowiecki J, Giebel S, Krzemien S, Krawczyk-Kulis M, Jagoda K, KoperaM, et al. G-CSF administered in time-sequenced setting during remission induc-tion and consolidation therapy of adult acute lymphoblastic leukemia has bene-ficial influence on early recovery and possibly improves long-term outcome: arandomized multicenter study. Leuk Lymphoma. 2002;43:315-25. [PMID:11999563]86. Usuki K, Urabe A, Masaoka T, Ohno R, Mizoguchi H, Hamajima N, et al;Gran AML Study Group. Efficacy of granulocyte colony-stimulating factor inthe treatment of acute myelogenous leukaemia: a multicentre randomized study.Br J Haematol. 2002;116:103-12. [PMID: 11841402]87. Doorduijn JK, van der Holt B, van Imhoff GW, van der Hem KG, KramerMH, van Oers MH, et al. CHOP compared with CHOP plus granulocytecolony-stimulating factor in elderly patients with aggressive non-Hodgkin’s lym-phoma. J Clin Oncol. 2003;21:3041-50. [PMID: 12915593]88. Schmitz N, Ljungman P, Cordonnier C, Kempf C, Linkesch W, Alegre A,et al. Lenograstim after autologous peripheral blood progenitor cell transplanta-tion: results of a double-blind, randomized trial. Bone Marrow Transplant. 2004;34:955-62. [PMID: 15489865]89. Thomas X, Boiron JM, Huguet F, Reman O, Sutton L, Turlure P, et al;
Review Prophylactic Colony-Stimulating Factors
410 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 www.annals.org

Groupe d’Etude et de Traitement de la Leucemie Aigue Lymphoblastique del’Adulte (GET-LALA Group). Efficacy of granulocyte and granulocyte-macroph-age colony-stimulating factors in the induction treatment of adult acute lympho-blastic leukemia: a multicenter randomized study. Hematol J. 2004;5:384-94.[PMID: 15448664]90. Amadori S, Suciu S, Jehn U, Stasi R, Thomas X, Marie JP, et al; EORTC/GIMEMA Leukemia Group. Use of glycosylated recombinant human G-CSF(lenograstim) during and/or after induction chemotherapy in patients 61 years ofage and older with acute myeloid leukemia: final results of AML-13, a random-ized phase-3 study. Blood. 2005;106:27-34. [PMID: 15761020]91. Vogel CL, Wojtukiewicz MZ, Carroll RR, Tjulandin SA, Barajas-FigueroaLJ, Wiens BL, et al. First and subsequent cycle use of pegfilgrastim preventsfebrile neutropenia in patients with breast cancer: a multicenter, double-blind,placebo-controlled phase III study. J Clin Oncol. 2005;23:1178-84. [PMID:15718314]92. Zwierzina H, Suciu S, Loeffler-Ragg J, Neuwirtova R, Fenaux P, Beksac M,et al; EORTC Leukemia Cooperative Group. Low-dose cytosine arabinoside(LD-AraC) vs LD-AraC plus granulocyte/macrophage colony stimulating factorvs LD-AraC plus Interleukin-3 for myelodysplastic syndrome patients with a highrisk of developing acute leukemia: final results of a randomized phase III study(06903) of the EORTC Leukemia Cooperative Group. Leukemia. 2005;19:1929-33. [PMID: 16151466]93. Burton C, Linch D, Hoskin P, Milligan D, Dyer MJ, Hancock B, et al. Aphase III trial comparing CHOP to PMitCEBO with or without G-CSF inpatients aged 60 plus with aggressive non-Hodgkin’s lymphoma. Br J Cancer.2006;94:806-13. [PMID: 16508640]94. Milligan DW, Wheatley K, Littlewood T, Craig JI, Burnett AK; NCRIHaematological Oncology Clinical Studies Group. Fludarabine and cytosine areless effective than standard ADE chemotherapy in high-risk acute myeloid leuke-mia, and addition of G-CSF and ATRA are not beneficial: results of the MRCAML-HR randomized trial. Blood. 2006;107:4614-22. [PMID: 16484584]
95. Thomas X, Raffoux E, Botton S, Pautas C, Arnaud P, de Revel T, et al.Effect of priming with granulocyte-macrophage colony-stimulating factor inyounger adults with newly diagnosed acute myeloid leukemia: a trial by the AcuteLeukemia French Association (ALFA) Group. Leukemia. 2007;21:453-61.[PMID: 17252021]96. Ringden O, Labopin M, Gorin NC, Le Blanc K, Rocha V, Gluckman E,et al. Treatment with granulocyte colony-stimulating factor after allogeneic bonemarrow transplantation for acute leukemia increases the risk of graft-versus-hostdisease and death: a study from the Acute Leukemia Working Party of the Eu-ropean Group for Blood and Marrow Transplantation. J Clin Oncol. 2004;22:416-23. [PMID: 14691124]97. Remberger M, Naseh N, Aschan J, Barkholt L, LeBlanc K, Svennberg P,et al. G-CSF given after haematopoietic stem cell transplantation using HLA-identical sibling donors is associated to a higher incidence of acute GVHD II-IV.Bone Marrow Transplant. 2003;32:217-23. [PMID: 12838288]98. Eapen M, Horowitz MM, Klein JP, Champlin RE, Loberiza FR Jr, Ring-den O, et al. Higher mortality after allogeneic peripheral-blood transplantationcompared with bone marrow in children and adolescents: the Histocompatibilityand Alternate Stem Cell Source Working Committee of the InternationalBone Marrow Transplant Registry. J Clin Oncol. 2004;22:4872-80. [PMID:15520055]99. Adams JR, Lyman GH, Djubegovic B, Feinglass J, Bennett CL. G-CSF asprophylaxis of febrile neutropenia in SCLC. Expert Opin Pharmacother. 2002;3:1273-81. [PMID: 12186620]100. Gafter-Gvili A, Fraser A, Paul M, Leibovici L. Meta-analysis: antibioticprophylaxis reduces mortality in neutropenic patients. Ann Intern Med. 2005;142:979-95. [PMID: 15968013]101. Smith TJ, Khatcheressian J, Lyman GH, Ozer H, Armitage JO, BalducciL, et al. 2006 update of recommendations for the use of white blood cell growthfactors: an evidence-based clinical practice guideline. J Clin Oncol. 2006;24:3187-205. [PMID: 16682719]
NEW PEER REVIEWERS
Sign up to become a peer reviewer for Annals of Internal Medicine bygoing to www.annals.org and selecting “Information for: Authors/Reviewers.” Then select “Reviewer Information” and register as a newreviewer. Note that Annals reviewers whose reviews are returned on timeand are judged satisfactory by the Editors may receive up to 3 Category1 CME credits per review (maximum, 15 credits in a calendar year).
ReviewProphylactic Colony-Stimulating Factors
www.annals.org 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 411

Current Author Addresses: Drs. Sung and Nathan: Division of Haema-tology/Oncology, The Hospital for Sick Children, 555 University Ave-nue, Toronto, Ontario M5G 1X8, Canada.Dr. Alibhai: Toronto General Hospital, Room EN 14-214, 200 Eliza-beth Street, Toronto, Ontario M5G 2C4, Canada.Dr. Tomlinson: Toronto General Hospital, Eaton Building East, Room238, 13th Floor, 200 Elizabeth Street, Ontario M5G 2C4, Canada.Dr. Beyene: Child Health Evaluative Sciences, Research Institute of TheHospital for Sick Children, Room 1206, 123 Edward Street, Toronto,Ontario M5G 1E2, Canada.
102. Lehrnbecher T, Zimmermann M, Reinhardt D, Dworzak M, Stary J,Creutzig U. Prophylactic human granulocyte colony-stimulating factor after in-duction therapy in pediatric acute myeloid leukemia. Blood. 2007;109:936-43.[PMID: 17008536]103. Creutzig U, Zimmermann M, Lehrnbecher T, Graf N, Hermann J,Niemeyer CM, et al. Less toxicity by optimizing chemotherapy, but not byaddition of granulocyte colony-stimulating factor in children and adolescentswith acute myeloid leukemia: results of AML-BFM 98. J Clin Oncol. 2006;24:4499-506. [PMID: 16983120]104. Faber E, Pytlık R, Slaby J, Zapletalova J, Kozak T, Raida L, et al. Indi-vidually determined dosing of filgrastim after autologous peripheral stem celltransplantation in patients with malignant lymphoma—results of a prospectivemulticentre controlled trial. Eur J Haematol. 2006;77:493-500. [PMID:17042769]105. Kuzhan O, Arpaci F, Ozet A, Ozturk B, Komurcu S. Delayed molgramos-tim administration after autologous peripheral blood stem cell transplantationdoes not add any benefit regarding hematologic engraftment and supportive ther-apy requirements: A prospective randomized trial. Turkish J Cancer. 2006;36:57-63.106. Rao R, Shammo JM, Enschede SH, Porter C, Adler SS, Venugopal P,et al. The combination of fludarabine, cyclophosphamide, and granulocyte-macrophage colony-stimulating factor in the treatment of patients with relapsedchronic lymphocytic leukemia and low-grade non-Hodgkin’s lymphoma. ClinLymphoma. 2005;6:26-30. [PMID: 15989703]107. Timmer-Bonte JN, de Boo TM, Smit HJ, Biesma B, Wilschut FA,Cheragwandi SA, et al. Prevention of chemotherapy-induced febrile neutropeniaby prophylactic antibiotics plus or minus granulocyte colony-stimulating factor insmall-cell lung cancer: a Dutch randomized phase III study. J Clin Oncol. 2005;23:7974-84. [PMID: 16258098]108. Valteau-Couanet D, Faucher C, Auperin A, Michon J, Milpied N, BoironJM, et al. Cost effectiveness of day 5 G-CSF (lenograstim) administration afterPBSC transplantation: results of a SFGM-TC randomised trial. Bone MarrowTransplant. 2005;36:547-52. [PMID: 16007101]109. Gonzalez-Vicent M, Madero L, Sevilla J, Ramirez M, Dıaz MA. A pro-spective randomized study of clinical and economic consequences of using G-CSF following autologous peripheral blood progenitor cell (PBPC) trans-plantation in children. Bone Marrow Transplant. 2004;34:1077-81. [PMID:15516942]110. Wang TJ, Liu LL, Cheng GH, Liu XL, Qu YQ, Wu ZF, et al. [A briefreport on effect of rhG-CSF in treating leukopenia after radio-and chemo-therapyof patients with breast cancer]. Zhongguo Shi Yan Xue Ye Xue Za Zhi. 2004;12:381-2. [PMID: 15228673]111. Grigg A, Solal-Celigny P, Hoskin P, Taylor K, McMillan A, Forstpoint-ner R, et al; International Study Group. Open-label, randomized study of peg-filgrastim vs. daily filgrastim as an adjunct to chemotherapy in elderly patientswith non-Hodgkin’s lymphoma. Leuk Lymphoma. 2003;44:1503-8. [PMID:14565651]112. Heath JA, Steinherz PG, Altman A, Sather H, Jhanwar S, Halpern S, et al;Children’s Cancer Group. Human granulocyte colony-stimulating factor in chil-dren with high-risk acute lymphoblastic leukemia: a Children’s Cancer GroupStudy. J Clin Oncol. 2003;21:1612-7. [PMID: 12697887]113. Papaldo P, Lopez M, Cortesi E, Cammilluzzi E, Antimi M, Terzoli E,et al. Addition of either lonidamine or granulocyte colony-stimulating factor doesnot improve survival in early breast cancer patients treated with high-doseepirubicin and cyclophosphamide. J Clin Oncol. 2003;21:3462-8. [PMID:12972521]114. Hornedo J, Sola C, Solano C, Lopez JJ, Alonso S, Lluch A, et al; SOLTIGroup. The role of granulocyte colony-stimulating factor (G-CSF) in the post-
transplant period. Bone Marrow Transplant. 2002;29:737-43. [PMID:12040470]115. Little MA, Morland B, Chisholm J, Hole A, Shankar A, Devine T, et al.A randomised study of prophylactic G-CSF following MRC UKALL XI inten-sification regimen in childhood ALL and T-NHL. Med Pediatr Oncol. 2002;38:98-103. [PMID: 11813173]116. Long HJ 3rd, Rayson S, Podratz KC, Abu-Ghazaleh S, Suman V, Hart-mann LC, et al. Long-term survival of patients with advanced/recurrent carci-noma of cervix and vagina after neoadjuvant treatment with methotrexate, vin-blastine, doxorubicin, and cisplatin with or without the addition ofmolgramostim, and review of the literature. Am J Clin Oncol. 2002;25:547-51.[PMID: 12477995]117. Osby E, Bjorkholm M, Lundahl J, Forslid J. Granulocyte function inelderly patients receiving chemotherapy for aggressive non-Hodgkin’s lymphoma.Effect of granulocyte colony-stimulating factor. Eur J Intern Med. 2002;13:448.[PMID: 12384135]118. Patte C, Laplanche A, Bertozzi AI, Baruchel A, Frappaz D, Schmitt C,et al. Granulocyte colony-stimulating factor in induction treatment of childrenwith non-Hodgkin’s lymphoma: a randomized study of the French Society ofPediatric Oncology. J Clin Oncol. 2002;20:441-8. [PMID: 11786572]119. Bradstock K, Matthews J, Young G, Lowenthal R, Baxter H, Arthur C,et al; Australian Leukaemia Study Group. Effects of glycosylated recombinanthuman granulocyte colony-stimulating factor after high-dose cytarabine-basedinduction chemotherapy for adult acute myeloid leukaemia. Leukemia. 2001;15:1331-8. [PMID: 11516093]120. Goldstone AH, Burnett AK, Wheatley K, Smith AG, Hutchinson RM,Clark RE; Medical Research Council Adult Leukemia Working Party. Attemptsto improve treatment outcomes in acute myeloid leukemia (AML) in older pa-tients: the results of the United Kingdom Medical Research Council AML11trial. Blood. 2001;98:1302-11. [PMID: 11520775]121. Trigg ME, Peters C, Zimmerman MB. Administration of recombinanthuman granulocyte-macrophage colony-stimulating factor to children undergo-ing allogeneic marrow transplantation: a prospective, randomized, double-masked, placebo-controlled trial. Pediatr Transplant. 2000;4:123-31. [PMID:11272605]122. Usuki K, Urabe A. Safety of G-CSF in remission induction therapy in adultde novo acute myelogenous leukemia (a randomized study). Biotherapy. 2000;14:563-5.123. Piccirillo N, Sica S, Laurenti L, Chiusolo P, La Barbera EO, Sora F, et al.Optimal timing of G-CSF administration after CD34� immunoselected periph-eral blood progenitor cell transplantation. Bone Marrow Transplant. 1999;23:1245-50. [PMID: 10414910]124. Dunlop DJ, Eatock MM, Paul J, Anderson S, Reed NS, Soukop M, et al.Randomized multicentre trial of filgrastim as an adjunct to combination chemo-therapy for Hodgkin’s disease. West of Scotland Lymphoma Group. Clin Oncol(R Coll Radiol). 1998;10:107-14. [PMID: 9610900]125. Feng F, Zhou L. [Randomized controlled study of leucomax (recombinanthuman granulocyte-macrophage colony stimulating factor, rhGM-CSF) in thetreatment of cancer chemotherapy-induced leucopenia]. Zhonghua Zhong LiuZa Zhi. 1998;20:451-3. [PMID: 10920943]126. Kawano Y, Takaue Y, Mimaya J, Horikoshi Y, Watanabe T, Abe T, et al.Marginal benefit/disadvantage of granulocyte colony-stimulating factor therapyafter autologous blood stem cell transplantation in children: results of a prospec-tive randomized trial. The Japanese Cooperative Study Group of PBSCT. Blood.1998;92:4040-6. [PMID: 9834207]127. Laver J, Amylon M, Desai S, Link M, Schwenn M, Mahmoud H, et al.Randomized trial of r-metHu granulocyte colony-stimulating factor in an inten-sive treatment for T-cell leukemia and advanced-stage lymphoblastic lymphomaof childhood: a Pediatric Oncology Group pilot study. J Clin Oncol. 1998;16:522-6. [PMID: 9469336]128. Lee SM, Radford JA, Dobson L, Huq T, Ryder WD, Pettengell R, et al.Recombinant human granulocyte colony-stimulating factor (filgrastim) followinghigh-dose chemotherapy and peripheral blood progenitor cell rescue in high-grade non-Hodgkin’s lymphoma: clinical benefits at no extra cost. Br J Cancer.1998;77:1294-9. [PMID: 9579836]129. Stoger H, Samonigg H, Krainer M, Ploszczynski M, Nirnberger G, MacaS, et al. Dose intensification of epidoxorubicin and cyclophosphamide in meta-static breast cancer: a randomised study with two schedules of granulocyte-mac-rophage colony stimulating factor. Eur J Cancer. 1998;34:482-8. [PMID:9713297]
Annals of Internal Medicine
W-78 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 www.annals.org

130. McQuaker IG, Hunter AE, Pacey S, Haynes AP, Iqbal A, Russell NH.Low-dose filgrastim significantly enhances neutrophil recovery following autolo-gous peripheral-blood stem-cell transplantation in patients with lymphoprolifera-tive disorders: evidence for clinical and economic benefit. J Clin Oncol. 1997;15:451-7. [PMID: 9053465]131. van Pelt LJ, de Craen AJ, Langeveld NE, Weening RS. Granulocyte-macrophage colony-stimulating factor (GM-CSF) ameliorates chemotherapy-induced neutropenia in children with solid tumors. Pediatr Hematol Oncol.1997;14:539-45. [PMID: 9383806]132. Zinzani PL, Pavone E, Storti S, Moretti L, Fattori PP, Guardigni L, et al.Randomized trial with or without granulocyte colony-stimulating factor as ad-junct to induction VNCOP-B treatment of elderly high-grade non-Hodgkin’slymphoma. Blood. 1997;89:3974-9. [PMID: 9166835]133. Magrath I, Adde M, Shad A, Venzon D, Seibel N, Gootenberg J, et al.Adults and children with small non-cleaved-cell lymphoma have a similar excel-lent outcome when treated with the same chemotherapy regimen. J Clin Oncol.1996;14:925-34. [PMID: 8622041]134. Muhonen T, Jantunen I, Pertovaara H, Voutilainen L, Maiche A,Blomqvist C, et al. Prophylactic filgrastim (G-CSF) during mitomycin-C, mi-toxantrone, and methotrexate (MMM) treatment for metastatic breast cancer. Arandomized study. Am J Clin Oncol. 1996;19:232-4. [PMID: 8638531]135. Paterakis GS, Tsavaris N, Loukopoulos D. The effect of GM-CSF onreticulocytes, haemoglobin and haematocrit in patients receiving chemotherapyfor solid tumours. Clin Lab Haematol. 1996;18:7-12. [PMID: 9118614]136. Shi YK, He XH, Wang ZP. Clinical study of low dose granocyte (recom-binant human granulocyte colony-stimulating factor, rhG-CSF, Lenograstim) onneutropenia induced by chemotherapy with CD regimen on lung cancer patients.Chinese Journal of Clinical Oncology. 1996;23:873-6.137. Vannucchi AM, Bosi A, Ieri A, Guidi S, Saccardi R, Lombardini L, et al.Combination therapy with G-CSF and erythropoietin after autologous bonemarrow transplantation for lymphoid malignancies: a randomized trial. BoneMarrow Transplant. 1996;17:527-31. [PMID: 8722349]138. Welte K, Reiter A, Mempel K, Pfetsch M, Schwab G, Schrappe M, et al.A randomized phase-III study of the efficacy of granulocyte colony-stimulatingfactor in children with high-risk acute lymphoblastic leukemia. Berlin-Frankfurt-Munster Study Group. Blood. 1996;87:3143-50. [PMID: 8605328]139. Bergmann L, Karakas T, Knuth A, Lautenschlager G, Mitrou PS, HoelzerD. Recombinant human granulocyte-macrophage colony-stimulating factor aftercombined chemotherapy in high-grade non-Hodgkin’s lymphoma—a random-ised pilot study. Eur J Cancer. 1995;31A:2164-8. [PMID: 8652236]140. Burdach SE, Muschenich M, Josephs W, Frisch J, Schulz G, Jurgens H,et al. Granulocyte-macrophage-colony stimulating factor for prevention of neu-tropenia and infections in children and adolescents with solid tumors. Results ofa prospective randomized study. Cancer. 1995;76:510-6. [PMID: 8625134]141. Chevallier B, Chollet P, Merrouche Y, Roche H, Fumoleau P, Kerbrat P,et al. Lenograstim prevents morbidity from intensive induction chemotherapy inthe treatment of inflammatory breast cancer. J Clin Oncol. 1995;13:1564-71.[PMID: 7541448]142. Chi KH, Chen CH, Chan WK, Chow KC, Chen SY, Yen SH, et al. Effectof granulocyte-macrophage colony-stimulating factor on oral mucositis in headand neck cancer patients after cisplatin, fluorouracil, and leucovorin chemother-apy. J Clin Oncol. 1995;13:2620-8. [PMID: 7595716]143. Dibenedetto SP, Ragusa R, Ippolito AM, Lo Nigro L, Di Cataldo A,D’Amico S, et al. Assessment of the value of treatment with granulocyte colony-stimulating factor in children with acute lymphoblastic leukemia: a randomizedclinical trial. Eur J Haematol. 1995;55:93-6. [PMID: 7543060]144. Hansen F, Stenbygaard L, Skovsgaard T. Effect of granulocyte-macrophagecolony-stimulating factor (GM-CSF) on hematologic toxicity induced by high-dose chemotherapy in patients with metastatic breast cancer. Acta Oncol. 1995;34:919-24. [PMID: 7492381]145. Katano M, Nakamura M, Matsuo T, Iyama A, Hisatsugu T. Effect ofgranulocyte colony-stimulating factor (G-CSF) on chemotherapy-induced oralmucositis. Surg Today. 1995;25:202-6. [PMID: 7543781]146. Logothetis CJ, Finn LD, Smith T, Kilbourn RG, Ellerhorst JA, ZukiwskiAA, et al. Escalated MVAC with or without recombinant human granulocyte-macrophage colony-stimulating factor for the initial treatment of advanced ma-lignant urothelial tumors: results of a randomized trial. J Clin Oncol. 1995;13:2272-7. [PMID: 7666085]147. Ardizzoni A, Venturini M, Sertoli MR, Giannessi PG, Brema F, DanovaM, et al. Granulocyte-macrophage colony-stimulating factor (GM-CSF) allows
acceleration and dose intensity increase of CEF chemotherapy: a randomisedstudy in patients with advanced breast cancer. Br J Cancer. 1994;69:385-91.[PMID: 8297739]148. Eguchi K, Kabe J, Kudo S, Mano K, Morinari H, Nakada K, et al. Efficacyof recombinant human granulocyte-macrophage colony-stimulating factor forchemotherapy-induced leukopenia in patients with non-small-cell lung cancer.Cancer Chemother Pharmacol. 1994;34:37-43. [PMID: 8174201]149. Eguchi K, Etou H, Miyachi S, Morinari H, Nakada K, Noda K, et al. Astudy of dose escalation of teniposide (VM-26) plus cisplatin (CDDP) with re-combinant human granulocyte colony-stimulating factor (rhG-CSF) in patientswith advanced small cell lung cancer. Eur J Cancer. 1994;30A:188-94. [PMID:7512356]150. Engelhard M, Gerhartz H, Brittinger G, Engert A, Fuchs R, Geiseler B,et al. Cytokine efficiency in the treatment of high-grade malignant non-Hodgkin’s lymphomas: results of a randomized double-blind placebo-controlledstudy with intensified COP-BLAM �/- rhGM-CSF. Ann Oncol. 1994;5 Suppl2:123-5. [PMID: 7515644]151. Gebbia V, Valenza R, Testa A, Cannata G, Borsellino N, Gebbia N. Aprospective randomized trial of thymopentin versus granulocyte—colony stimu-lating factor with or without thymopentin in the prevention of febrile episodes incancer patients undergoing highly cytotoxic chemotherapy. Anticancer Res.1994;14:731-4. [PMID: 7516641]152. Hamm J, Schiller JH, Cuffie C, Oken M, Fisher RI, Shepherd F, et al.Dose-ranging study of recombinant human granulocyte-macrophage colony-stimulating factor in small-cell lung carcinoma. J Clin Oncol. 1994;12:2667-76.[PMID: 7989942]153. Hiraoka A, Masaoka T, Mizoguchi H, Asano S, Kodera Y, Kitamura K,et al. Recombinant human non-glycosylated granulocyte-macrophage colony-stimulating factor in allogeneic bone marrow transplantation: double-blind pla-cebo-controlled phase III clinical trial. Jpn J Clin Oncol. 1994;24:205-11.[PMID: 8072199]154. Rampling R, Steward W, Paul J, Macham MA, Harvey E, Eckley D.rhGM-CSF ameliorates neutropenia in patients with malignant glioma treatedwith BCNU. Br J Cancer. 1994;69:541-5. [PMID: 8123485]155. Shi YK, Sun Y, Su M. Clinical study of recombinant human granulocyte-macrophage colony-stimulating factor on chemotherapy-induced leukopenia.Chinese Journal of Clinical Oncology. 1994;9:356-9.156. Shi YK, Feng FY, Sun Y. Clinical study of recombinant human granulocytecolony-stimulating factor (rhG-CSF) on leucopenia induced by chemotherapywith CE regimen on lung cancer patients. Chinese Journal of Clinical Oncology.1994;33:739-42.157. Spitzer G, Adkins DR, Spencer V, Dunphy FR, Petruska PJ, VelasquezWS, et al. Randomized study of growth factors post-peripheral-blood stem-celltransplant: neutrophil recovery is improved with modest clinical benefit. J ClinOncol. 1994;12:661-70. [PMID: 7512124]158. Gebbia V, Testa A, Valenza R, Borsellino N, Cipolla C, Cannata G, et al.A prospective evaluation of the activity of human granulocyte-colony stimulatingfactor on the prevention of chemotherapy-related neutropenia in patients withadvanced carcinoma. J Chemother. 1993;5:186-90. [PMID: 7690396]159. Kaku K, Takahashi M, Moriyama Y, Nakahata T, Masaoka T, Yoshida Y,et al. Recombinant human granulocyte-macrophage colony-stimulating factor(rhGM-CSF) after chemotherapy in patients with non-Hodgkin’s lymphoma; aplacebo-controlled double blind phase III trial. Leuk Lymphoma. 1993;11:229-38. [PMID: 8260897]160. Ohno R, Tomonaga M, Ohshima T, Masaoka T, Asou N, Oh H, et al. Arandomized controlled study of granulocyte colony stimulating factor after inten-sive induction and consolidation therapy in patients with acute lymphoblasticleukemia. Japan Adult Leukemia Study Group. Int J Hematol. 1993;58:73-81.[PMID: 7693029]161. Trillet-Lenoir V, Green J, Manegold C, Von Pawel J, Gatzemeier U,Lebeau B, et al. Recombinant granulocyte colony stimulating factor reduces theinfectious complications of cytotoxic chemotherapy. Eur J Cancer. 1993;29A:319-24. [PMID: 7691119]162. Anderson H, Gurney H, Thatcher N, Swindell R, Scarffe JH, Weiner J.Recombinant human GM-CSF in small cell lung cancer: a phase I/II study.Recent Results Cancer Res. 1991;121:155-61. [PMID: 1650015]163. de Vries EG, Biesma B, Willemse PH, Mulder NH, Stern AC, Aalders JG,et al. A double-blind placebo-controlled study with granulocyte-macrophage col-ony-stimulating factor during chemotherapy for ovarian carcinoma. Cancer Res.1991;51:116-22. [PMID: 1988077]
www.annals.org 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 W-79

164. Havemann K, Klausmann M, Wolf M, Fischer JR, Drings P, Oster W.Effect of rhGM-CSF on haematopoietic reconstitution after chemotherapy insmall-cell lung cancer. J Cancer Res Clin Oncol. 1991;117 Suppl 4:S203-7.[PMID: 1665493]165. Kotake T, Miki T, Akaza H, Kubota Y, Nishio Y, Matsumura Y, et al.Effect of recombinant granulocyte colony-stimulating factor (rG-CSF) on che-motherapy-induced neutropenia in patients with urogenital cancer. Cancer Che-mother Pharmacol. 1991;27:253-7. [PMID: 1705488]166. Liberati AM, Cinieri S, Schippa M, Di Clemente F, Filippo S, Grignani F.GM-CSF: clinical trials in non-Hodgkin’s lymphoma patients with chemother-apy induced leucopenia. Leukemia. 1991;5 Suppl 1:119-22. [PMID: 1890860]167. Jost LM, Pichert G, Stahel RA. Placebo controlled phase I/II study ofsubcutaneous GM-CSF in patients with germ cell tumors undergoing chemo-therapy. Ann Oncol. 1990;1:439-42. [PMID: 1707298]168. Oyama A, Ota K, Asano S, Takaku F, Yoshida Y, Uzuka Y, et al. [Adouble-blind, cross-over clinical trial of recombinant human G-CSF on neutro-penia induced by chemotherapy for non-Hodgkin’s lymphoma]. Nippon GanChiryo Gakkai Shi. 1990;25:2533-48. [PMID: 1702132]169. Powles R, Smith C, Milan S, Treleaven J, Millar J, McElwain T, et al.Human recombinant GM-CSF in allogeneic bone-marrow transplantation forleukaemia: double-blind, placebo-controlled trial. Lancet. 1990;336:1417-20.[PMID: 1978880]
W-80 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 www.annals.org

Appendix Table 1. Characteristics of Included Studies*
Study, Year (Reference) CSFGroup,n
ControlGroup,n
Population CSF Type Diagnosis AntibioticProphylaxis
ConcealedAllocation
Double-Blinding
Lehrnbecher et al., 2007 (102) 161 156 Pediatric G-CSF Leukemia No Unclear NoThomas et al., 2007 (95) 124 135 Adult GM-CSF Leukemia No Unclear NoBurton et al., 2006 (93) 387 397 Elderly G-CSF Lymphoma/
solid tumorYes Unclear No
Creutzig et al., 2006 (103) 134 138 Pediatric G-CSF Leukemia No Adequate NoFaber et al., 2006 (104) 40 31 Adult G-CSF SCT Yes Adequate YesKuzhan et al., 2006 (105) 16 15 Pediatric, adult GM-CSF SCT No Unclear NoMilligan et al., 2006 (94) 178 178 Adult, elderly G-CSF Leukemia No Adequate NoAmadori et al., 2005 (90) 360 362 Elderly G-CSF Leukemia No Adequate NoRao et al., 2005 (106) 22 12 Adult, elderly GM-CSF Leukemia, lymphoma/
solid tumorNo Unclear No
Timmer-Bonte et al., 2005 (107) 90 85 Adult G-CSF Lymphoma/solidtumor
Yes Unclear No
Valteau-Couanet et al.,2005 (108)
80 79 Pediatric, adult G-CSF SCT No Adequate No
Vogel et al., 2005 (91) 463 465 Adult, elderly PEG Lymphoma/solidtumor
No Adequate Yes
Zwierzina et al., 2005 (92) 59 59 Adult, elderly GM-CSF Leukemia No Adequate NoGonzalez-Vicent et al., 2004 (109) 51 66 Pediatric G-CSF SCT Yes Unclear NoSchmitz et al., 2004 (88) 98 94 Adult G-CSF SCT No Adequate YesThomas et al., 2004 (89) 95 74 Adult G-CSF Leukemia No Adequate NoWang et al., 2004 (110) 50 50 Adult G-CSF Lymphoma/solid
tumorNo Unclear No
Doorduijn et al., 2003 (87) 197 192 Elderly G-CSF Lymphoma/solidtumor
No Unclear No
Grigg et al., 2003 (111) NA NA Elderly G-CSF,PEG
Lymphoma/solidtumor
No Unclear No
Heath et al., 2003 (112) 130 129 Pediatric G-CSF Leukemia Yes Unclear NoPapaldo et al., 2003 (113) 254 243 Adult G-CSF Lymphoma/solid
tumorNo Unclear No
Channa and Hashmi, 2002 (83) 10 5 Pediatric, adult GM-CSF Leukemia No Unclear YesDallorso et al., 2002 (84) 110 111 Pediatric G-CSF SCT No Unclear NoHolowiecki et al., 2002 (85) 33 31 Adult G-CSF Leukemia No Unclear NoHornedo et al., 2002 (114) 29 20 Adult G-CSF SCT No Unclear NoLittle et al., 2002 (115) 46 46 Pediatric G-CSF Leukemia, lymphoma/
solid tumorYes Unclear No
Long et al., 2002 (116) 18 18 Adult, elderly GM-CSF Lymphoma/solidtumor
No Adequate No
Osby et al., 2002 (117) 8 6 Elderly G-CSF Lymphoma/solidtumor
No Unclear No
Patte et al., 2002 (118) 75 73 Pediatric G-CSF Lymphoma/solidtumor
Yes Unclear No
Usuki et al., 2002 (86) 120 125 Adult, elderly G-CSF Leukemia No Adequate NoBradstock et al., 2001 (119) 54 58 Adult G-CSF Leukemia No Adequate NoGoldstone et al., 2001 (120) NA NA Elderly G-CSF Leukemia No Unclear YesPfreundschuh et al., 2001 (81) 30 30 Adult GM-CSF Lymphoma/solid
tumorNo Unclear Yes
Przepiorka et al., 2001 (82) 21 21 Adult G-CSF SCT Yes Unclear NoBishop et al., 2000 (78) 26 24 Adult G-CSF SCT No Adequate YesHarousseau et al., 2000 (79) 100 94 Adult G-CSF Leukemia No Adequate NoMichel et al., 2000 (80) 34 33 Pediatric G-CSF Leukemia No Unclear NoTrigg et al., 2000 (121) 17 18 Pediatric GM-CSF SCT No Adequate YesUsuki and Urabe, 2000 (122) 15 13 Adult, elderly G-CSF Leukemia NoClarke et al., 1999 (73) 17 17 Pediatric G-CSF Leukemia, lymphoma/
solid tumorYes Unclear No
Ifrah et al., 1999 (74) 35 29 Adult GM-CSF Leukemia, SCT No Adequate YesOhno et al., 1999 (75) 21 18 Adult G-CSF Leukemia No Unclear NoOjeda et al., 1999 (76) 30 32 Adult G-CSF SCT Yes Unclear NoPiccirillo et al., 1999 (123) 6 6 Adult G-CSF SCT Yes Unclear NoThomas et al., 1999 (77) 95 97 Adult GM-CSF Leukemia No Unclear YesBernasconi et al., 1998 (65) 53 52 Adult, elderly G-CSF Leukemia No Unclear NoDunlop et al., 1998 (124) 25 22 Adult G-CSF Lymphoma/solid
tumorNo Adequate No
Feng and Zhou, 1998 (125) 55 55 Adult GM-CSF Lymphoma/solidtumor
No Unclear No
Continued on following page
www.annals.org 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 W-81

Appendix Table 1—Continued
Study, Year (Reference) CSFGroup,n
ControlGroup,n
Population CSF Type Diagnosis AntibioticProphylaxis
ConcealedAllocation
Double-Blinding
Fosså et al., 1998 (66) 128 129 Adult G-CSF Lymphoma/solidtumor
No Unclear No
Godwin et al., 1998 (67) 103 104 Elderly G-CSF Leukemia No Unclear YesHidalgo et al., 1998 (68) 40 40 Adult, elderly G-CSF Lymphoma/solid
tumorNo Adequate No
Kawano et al., 1998 (126) 30 28 Pediatric G-CSF SCT No Unclear NoLarson et al., 1998 (69) 102 93 Adult, elderly G-CSF Leukemia No Adequate NoLaver et al., 1998 (127) 45 43 Pediatric G-CSF Leukemia, lymphoma/
solid tumorNo Unclear No
Lee et al., 1998 (128) 11 12 Adult G-CSF SCT Yes Unclear NoMichon et al., 1998 (70) 31 28 Pediatric G-CSF Lymphoma/solid
tumorNo Unclear No
Steward et al., 1998 (71) 150 150 Adult GM-CSF Lymphoma/solidtumor
No Adequate Yes
Stoger et al., 1998 (129) 24 24 Adult GM-CSF Lymphoma/solidtumor
No Adequate No
Witz et al., 1998 (72) 110 122 Elderly GM-CSF Leukemia No Unclear YesFridrik et al., 1997 (55) 38 36 Adult, elderly G-CSF Lymphoma/solid
tumorNo Unclear No
Fukuoka et al., 1997 (56) 32 31 Adult, elderly G-CSF Lymphoma/solidtumor
No Unclear No
Geissler et al., 1997 (57) 25 26 Adult, elderly G-CSF Leukemia Yes Unclear NoGisselbrecht et al., 1997 (58) 80 80 Adult G-CSF Lymphoma/solid
tumorNo Unclear Yes
Heil et al., 1997 (59) 259 262 Adult, elderly G-CSF Leukemia Yes Adequate YesLegros et al., 1997 (60) 25 25 Adult GM-CSF SCT No Unclear YesLinch et al., 1997 (61) 34 28 Adult G-CSF SCT No Adequate NoLowenberg et al., 1997 (62) 60 63 Adult GM-CSF Leukemia No Unclear NoMcQuaker et al., 1997 (130) 19 19 Adult G-CSF SCT Yes Unclear YesMoreau et al., 1997 (63) 56 31 Adult GM-CSF Leukemia No Unclear YesPui et al., 1997 (64) 73 75 Pediatric G-CSF Leukemia Yes Unclear Yesvan Pelt et al., 1997 (131) 14 14 Pediatric GM-CSF Lymphoma/solid
tumorNo Unclear No
Zinzani et al., 1997 (132) 77 72 Elderly G-CSF Lymphoma/solidtumor
Yes Unclear No
Greenberg et al., 1996 (49) 204 199 Adult GM-CSF SCT No Unclear YesJones et al., 1996 (50) 70 72 Adult GM-CSF Lymphoma/solid
tumorYes Unclear Yes
Magrath et al., 1996 (133) 18 16 Pediatric, adult GM-CSF Lymphoma/solidtumor
No Unclear No
Muhonen et al., 1996 (134) 16 15 Adult G-CSF Lymphoma/solidtumor
No Unclear No
Paterakis et al., 1996 (135) 17 16 Adult, elderly GM-CSF Lymphoma/solidtumor
No Unclear No
Shi et al., 1996 (136) 22 22 Adult G-CSF Lymphoma/solidtumor
No Unclear No
Vannucchi et al., 1996 (137) 10 10 NA G-CSF SCT No Unclear NoWeiss et al., 1996 (51) 16 7 Adult, elderly GM-CSF Lymphoma/solid
tumorNo Unclear No
Welte et al., 1996 (138) 17 17 Pediatric G-CSF Leukemia Yes Unclear NoWexler et al., 1996 (52) 18 18 Pediatric, adult GM-CSF Lymphoma/solid
tumorNo Unclear No
Yau et al., 1996 (53) 28 28 Adult GM-CSF Lymphoma/solidtumor
Yes Unclear Yes
Zittoun et al., 1996 (54) 27 26 Adult GM-CSF Leukemia No Adequate NoBajorin et al., 1995 (35) 55 49 Adult GM-CSF Lymphoma/solid
tumorNo Unclear No
Bergmann et al., 1995 (139) 17 17 Adult, elderly GM-CSF Lymphoma/solidtumor
No Unclear Yes
Bui et al., 1995 (36) 22 26 Adult, elderly G-CSF Lymphoma/solidtumor
No Adequate Yes
Bunn et al., 1995 (37) 107 108 Adult, elderly GM-CSF Lymphoma/solidtumor
No Adequate No
Burdach et al., 1995 (140) 42 42 Pediatric GM-CSF Lymphoma/solidtumor
No Unclear No
Chevallier et al., 1995 (141) 61 59 Adult G-CSF Lymphoma/solidtumor
No Unclear Yes
W-82 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 www.annals.org

Appendix Table 1—Continued
Study, Year (Reference) CSFGroup,n
ControlGroup,n
Population CSF Type Diagnosis AntibioticProphylaxis
ConcealedAllocation
Double-Blinding
Chi et al., 1995 (142) 20 20 Adult GM-CSF Lymphoma/solidtumor
No Unclear No
Dibenedetto et al., 1995 (143) 14 18 Pediatric G-CSF Leukemia No Unclear NoDombret et al., 1995 (38) 88 85 Elderly G-CSF Leukemia No Unclear YesHansen et al., 1995 (144) 11 9 Adult GM-CSF Lymphoma/solid
tumorNo Unclear No
Katano et al., 1995 (145) 4 7 Adult G-CSF Lymphoma/solidtumor
No Unclear No
Klumpp et al., 1995 (39) 22 19 Adult G-CSF SCT Yes Adequate NoLogothetis et al., 1995 (146) 25 23 Adult, elderly GM-CSF Lymphoma/solid
tumorNo Unclear No
Nemunaitis et al., 1995 (40) 53 56 Pediatric, adult GM-CSF SCT Adequate YesOttmann et al., 1995 (41) 37 38 Adult G-CSF Leukemia Yes Unclear NoRiikonen et al., 1995 (42) 20 20 Pediatric G-CSF Leukemia, lymphoma/
solid tumorNo Unclear No
Rowe et al., 1995 (43) 60 57 Elderly GM-CSF Leukemia No Unclear YesSchmitz et al., 1995 (44) 15 14 Adult G-CSF SCT No Unclear NoSeymour et al., 1995 (45) 12 13 Adult, elderly G-CSF Lymphoma/solid
tumorNo Unclear Yes
Stone et al., 1995 (46) 193 195 Elderly GM-CSF Leukemia No Adequate YesTakeshita et al., 1995 (47) 57 64 Adult, elderly G-CSF Leukemia No Unclear YesWoll et al., 1995 (48) 34 31 Adult, elderly G-CSF Lymphoma/solid
tumorNo Unclear No
Ardizzoni et al., 1994 (147) 32 30 Adult GM-CSF Lymphoma/solidtumor
Yes Adequate No
Aviles et al., 1994 (30) 20 22 Adult G-CSF Lymphoma/solidtumor
No Unclear No
Calderwood et al., 1994 (31) 16 19 Pediatric GM-CSF Leukemia No Unclear YesEguchi et al., 1994 (148) 22 23 Adult, elderly GM-CSF Lymphoma/solid
tumorNo Unclear Yes
Eguchi et al., 1994 (149) 5 5 Adult, elderly G-CSF Lymphoma/solidtumor
No Unclear No
Engelhard et al., 1994 (150) 87 85 Adult, elderly GM-CSF Lymphoma/solidtumor
No Unclear Yes
Gebbia et al., 1994 (151) 23 28 Adult, elderly G-CSF Lymphoma/solidtumor
No Unclear Yes
Gisselbrecht et al., 1994 (32) 163 152 Pediatric, adult G-CSF SCT No Adequate YesHamm et al., 1994 (152) 83 75 Adult, elderly GM-CSF Lymphoma/solid
tumorNo Unclear No
Hiraoka et al., 1994 (153) 28 25 Pediatric, adult GM-CSF SCT No Unclear YesMiles et al., 1994 (33) 23 17 Adult, elderly G-CSF Lymphoma/solid
tumorYes Unclear No
Rampling et al., 1994 (154) 13 13 Adult GM-CSF Lymphoma/solidtumor
No Unclear No
Shi et al., 1994 (155) 21 21 Adult, elderly GM-CSF Lymphoma/solidtumor
No Unclear No
Shi et al., 1994 (156) 22 22 Adult G-CSF Lymphoma/solidtumor
No Unclear No
Spitzer et al., 1994 (157) 19 18 Adult G-CSF,GM-CSF
SCT Yes Unclear No
Stahel et al., 1994 (34) 29 14 Adult G-CSF SCT No Unclear NoDe Witte et al., 1993 (26) NA NA NA GM-CSF SCT No Unclear YesGebbia et al., 1993 (158) 43 43 Adult G-CSF Lymphoma/solid
tumorNo Unclear Yes
Gerhartz et al., 1993 (27) 59 66 Adult, elderly GM-CSF Lymphoma/solidtumor
No Adequate Yes
Kaku et al., 1993 (159) 29 30 Adult, elderly GM-CSF Lymphoma/solidtumor
No Unclear Yes
Linch et al., 1993 (28) 23 25 Adult G-CSF SCT No Unclear NoOhno et al., 1993 (160) 27 28 Adult G-CSF Leukemia No Adequate NoShaffer et al., 1993 (29) 9 9 Adult, elderly GM-CSF Lymphoma/solid
tumorNo Unclear No
Trillet-Lenoir et al., 1993 (161) 65 64 Adult, elderly G-CSF Lymphoma/solidtumor
No Unclear Yes
De Witte et al., 1992 (20) 29 28 Adult GM-CSF SCT No Unclear YesGorin et al., 1992 (21) 41 47 Pediatric, adult GM-CSF SCT No Unclear Yes
Continued on following page
www.annals.org 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 W-83

Appendix Table 1—Continued
Study, Year (Reference) CSFGroup,n
ControlGroup,n
Population CSF Type Diagnosis AntibioticProphylaxis
ConcealedAllocation
Double-Blinding
Gulati and Bennett, 1992 (22) 12 12 Adult GM-CSF SCT Yes Adequate YesKhwaja et al., 1992 (23) 29 29 Adult GM-CSF SCT No Adequate YesLink et al., 1992 (24) 39 40 Pediatric, adult GM-CSF SCT No Adequate YesPettengell et al., 1992 (25) 41 39 Adult, elderly G-CSF Lymphoma/solid
tumorYes Unclear No
Anderson et al., 1991 (162) 26 30 Adult, elderly GM-CSF Lymphoma/solidtumor
No Unclear No
Crawford et al., 1991 (17) 101 110 Adult, elderly G-CSF Lymphoma/solidtumor
No Unclear Yes
de Vries et al., 1991 (163) 18 28 Adult, elderly GM-CSF Lymphoma/solidtumor
No Unclear Yes
Havemann et al., 1991 (164) Adult, elderly GM-CSF Lymphoma/solidtumor
No Unclear No
Kaplan et al., 1991 (18) 16 10 Adult GM-CSF Lymphoma/solidtumor
No Unclear No
Kotake et al., 1991 (165) 32 38 Adult, elderly G-CSF Lymphoma/solidtumor
No Unclear No
Liberati et al., 1991 (166) Adult GM-CSF Lymphoma/solidtumor
No Unclear Yes
Nemunaitis et al., 1991 (19) 65 63 Pediatric, adult GM-CSF SCT No Unclear YesJost et al., 1990 (167) 10 4 Adult, elderly GM-CSF Lymphoma/solid
tumorNo Unclear Yes
Ohno et al., 1990 (16) 48 50 Pediatric, adult G-CSF Leukemia No Adequate NoOyama et al., 1990 (168) 16 18 Adult, elderly G-CSF Lymphoma/solid
tumorNo Unclear Yes
Powles et al., 1990 (169) 20 20 Adult GM-CSF SCT No Unclear Yes
* CSF � colony-stimulating factor; G-CSF � granulocyte colony-stimulating factor; GM-CSF � granulocyte-macrophage colony-stimulating factor; NA � not available;PEG � pegfilgrastim; SCT � stem-cell transplantation.
W-84 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 www.annals.org

Appendix Table 2. Events and Number at Risk for Nonmortality Outcomes*
Study, Year (Reference) Febrile Neutropenia Documented Infections Microbiologically DocumentedInfections
CSF Group Control Group CSF Group Control Group CSF Group Control Group
Events Cycles Events Cycles Events Cycles Events Cycles Events Cycles Events Cycles
Lernbecher et al., 2007 (102) 115 322 108 312 55 322 52 312Thomas et al., 2007 (95) 24 124 26 135Creutzig et al., 2006 (103) 46 122 51 124Faber et al., 2006 (104) 22 40 18 31Amadori et al., 2005 (90) 99 350 105 350 223 350 211 350Rao et al., 2005 (106) 3 22 1 12Timmer-Bonte et al., 2005 (107) 21 368 39 353 50 368 73 353 3 368 14 353Valteau-Couanet et al., 2005 (108) 31 160 18 79 27 160 16 79Vogel et al., 2005 (91) 6 463 78 465Zwierzina et al., 2005 (92) 8 59 2 59Schmitz et al., 2004 (88) 66 98 86 94 23 98 49 94Thomas et al., 2004 (89) 26 162 18 74Wang et al., 2004 (110) 0.5 50.5 2.5 50.5Doorduijn et al., 2003 (87) 72 197 86 192 135 1191 180 1195Heath et al., 2003 (cohort 1) (112) 44 68 43 61 21 68 26 61 19 68 22 61Heath et al., 2003 (cohort 2) (112) 50 60 52 65 23 60 28 65 20 60 22 65Papaldo et al., 2003 (113) 3 254 16 243Holowiecki et al., 2002 (85) 27 64 25 58 15 64 16 58Little et al., 2002 (115) 34 46 42 46Osby et al., 2002 (117) 2 8 2 6Patte et al., 2002 (118) 133 150 131 145 18 150 17 145Usuki et al., 2002 (86) 100 120 114 125Bradstock et al., 2001 (119) 36 54 40 58Przepiorka et al., 2001 (82) 10 21 10 21 9 21 10 21Harrousseau et al., 2000 (79) 89 184 107 175Michel et al., 2000 (80) 8 202 22 198Trigg et al., 2000 (121) 10 17 10 18Ohno et al., 1999 (75) 15 46 8 21 29 46 15 21Piccirillo et al., 1999 (123) 4 15 4 6Dunlop et al., 1998 (cohort 1) (124) 1 12 4 11 7 13 8 12Dunlop et al., 1998 (cohort 2) (124) 6 11 5 10 9 12 7 10Fosså et al., 1998 (66) 25 128 38 129 8 128 10 129Godwin et al., 1998 (67) 75 104 66 103 50 104 45 103Hidalgo et al., 1998 (68) 6 220 10 202Larson et al., 1998 (69) 78 100 81 93Lee et al., 1998 (128) 3 11 6 12Michon et al., 1998 (70) 27 123 43 110Steward et al., 1998 (71) 81 150 80 150Stoger et al., 1998 (129) 5 24 3 24Witz et al., 1998 (72) 74 110 88 122 24 110 34 122Fridrik et al., 1997 (55) 16 38 21 36 14 38 19 36Fukuoka et al., 1997 (56) 14 32 24 31Geissler et al., 1997 (57) 3 25 11 26 10 25 20 26 8 25 16 26Gisselbrecht et al., 1997 (58) 52 82 62 80 21 26 33 41 21 26 33 41Heil et al., 1997 (59) 96 259 94 262Legros et al., 1997 (60) 13 25 7 25Linch et al., 1997 (61) 34 34 25 28 16 34 14 28Lowenberg et al., 1997 (62) 46 60 49 63 10 60 6 63Pui et al., 1997 (64) 42 73 51 75 12 73 27 75 2 73 5 75Zinzani et al., 1997 (132) 4 77 15 72Jones et al., 1996 (50) 6 262 8 281Magrath et al., 1996 (133) 31 72 37 64 13 72 19 64Muhonen et al., 1996 (134) 6 16 7 15Weiss et al., 1996 (51) 2 16 1 7Welte et al., 1996 (138) 21 121 55 137 10 121 21 137Wexler et al., 1996 (52) 67 167 134 303 38 167 71 303 23 167 21 303Yau et al., 1996 (53) 32 64 32 57Zittoun et al., 1996 (54) 22 27 19 26Bajorin et al., 1995 (35) 19 103 32 92Bui et al., 1995 (36) 5 22 15 26 3 22 1 26Chevallier et al., 1995 (141) 47 61 53 59 8 61 16 59Dombret et al., 1995 (38) 32 88 32 85 15 88 13 85Hansen et al., 1995 (144) 8 39 10 31 0.5 39.5 0.5 31.5
Continued on following page
www.annals.org 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 W-85

Appendix Table 2—Continued
Study, Year (Reference) Febrile Neutropenia Documented Infections Microbiologically DocumentedInfections
CSF Group Control Group CSF Group Control Group CSF Group Control Group
Events Cycles Events Cycles Events Cycles Events Cycles Events Cycles Events Cycles
Logothetis et al., 1995 (146) 11 72 5 64 33 70 25 64Nemunaitis et al., 1995 (40) 34 53 51 56Ottmann et al., 1995 (41) 16 37 22 39Riikonen et al., 1995 (42) 2 20 10 20Rowe et al., 1995 (43) 27 52 33 47Schmitz et al., 1995 (44) 13 33 6 14 11 33 5 14Stone et al., 1995 (46) 112 179 118 184Takeshita et al., 1995 (47) 33 57 53 64Woll et al., 1995 (48) 22 34 21 31Aviles et al., 1994 (30) 7 172 41 168Calderwood et al., 1994 (31) 6 16 9 19 7 16 6 16 2 16 2 19Eguchi et al., 1994 (148) 3 22 3 23Gebbia et al., 1994 (151) 5 23 18 28Gisselbrecht et al., 1994 (32) 101 152 102 146 142 152 136 146 68 152 66 146Rampling et al., 1994 (154) 5 16 2 34Spitzer et al., 1994 (157) 2 19 1 18Stahel et al., 1994 (34) 22 29 13 14 25 29 14 14 7 29 4 14Gebbia et al., 1993 (158) 5 43 14 43Gerhartz et al., 1993 (27) 19 59 51 66 5 59 13 66Kaku et al., 1993 (159) 4 29 8 30Linch et al., 1993 (28) 78 96 22 25Ohno et al., 1993 (160) 20 79 9 28 15 79 8 28Shaffer et al., 1993 (29) 2.5 10.5 0.5 11.5Trillet-Lenoir et al., 1993 (161) 17 65 34 64 25 65 21 64De Witte et al., 1992 (20) 13 29 15 28Gorin et al., 1992 (21) 16 41 22 47Gulati and Bennett, 1992 (22) 12 12 12 12Link et al., 1992 (24) 18 39 28 40Pettengell et al., 1992 (25) 9 41 17 39 7 41 5 39Anderson et al., 1991 (162) 1 26 2 30Crawford et al., 1991 (17) 26 92 58 102 23 352 33 248de Vries et al., 1991 (163) 0.5 18.5 1.5 28.5Kaplan et al., 1991 (18) 22 58 28 42Jost et al., 1990 (167) 2 10 1 4Ohno et al., 1990 (16) 5 48 15 50 3 48 7 50Oyama et al., 1990 (168) 6 45 12 45
* Values are the numbers of events and cycles at risk. CSF � colony-stimulating factor.
W-86 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 www.annals.org

Appendix Figure 1. Stratified analyses by studies that mandated antibacterial prophylaxis in the study design.
Squares represent the point estimate of the outcome for that stratum. Squares to the left of the vertical line indicate that the colony-stimulating factorintervention reduces that outcome. Horizontal lines around the squares represent 95% CIs. The effect measures are relative risks for all-cause mortalityand infection-related mortality and rate ratios for infections and febrile neutropenia. The P values for interaction refer to an interaction betweencolony-stimulating factor effect and strata and were derived from meta-regression. All analyses used a random-effects model.
www.annals.org 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 W-87

Appendix Figure 2. Forest plot of all-cause mortality associated with colony-stimulating factors, by age group.
W-88 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 www.annals.org
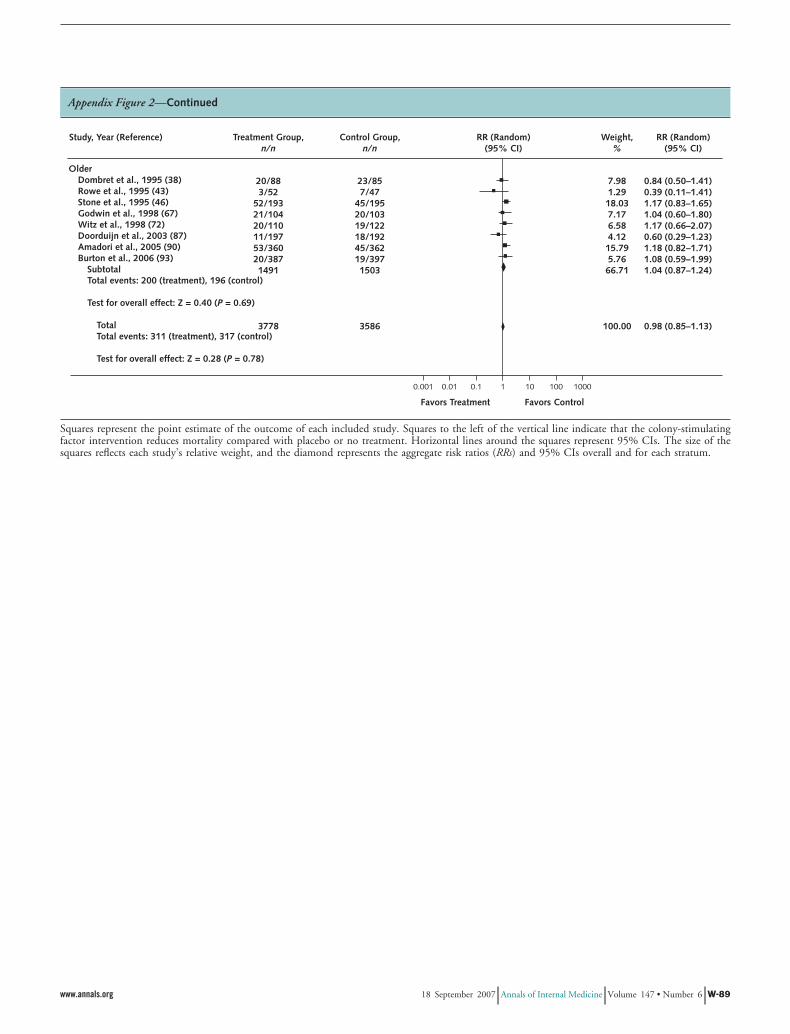
Appendix Figure 2—Continued
Squares represent the point estimate of the outcome of each included study. Squares to the left of the vertical line indicate that the colony-stimulatingfactor intervention reduces mortality compared with placebo or no treatment. Horizontal lines around the squares represent 95% CIs. The size of thesquares reflects each study’s relative weight, and the diamond represents the aggregate risk ratios (RRs) and 95% CIs overall and for each stratum.
www.annals.org 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 W-89

Appendix Figure 3. Forest plot of all-cause mortality associated with colony-stimulating factors, by diagnosis.
W-90 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 www.annals.org
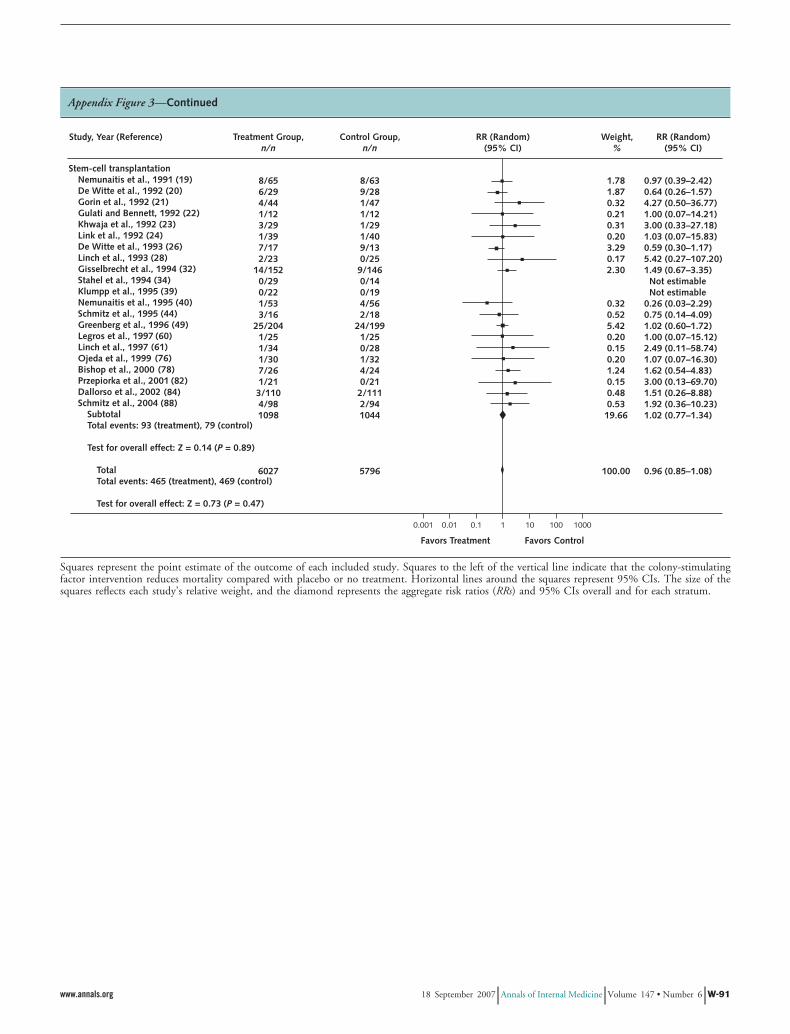
Appendix Figure 3—Continued
Squares represent the point estimate of the outcome of each included study. Squares to the left of the vertical line indicate that the colony-stimulatingfactor intervention reduces mortality compared with placebo or no treatment. Horizontal lines around the squares represent 95% CIs. The size of thesquares reflects each study’s relative weight, and the diamond represents the aggregate risk ratios (RRs) and 95% CIs overall and for each stratum.
www.annals.org 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 W-91

Appendix Figure 4. Forest plot of all-cause mortality associated with colony-stimulating factors, by studies that mandatedantibacterial prophylaxis.
W-92 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 www.annals.org

Appendix Figure 4—Continued
Squares represent the point estimate of the outcome of each included study. Squares to the left of the vertical line indicate that the colony-stimulatingfactor intervention reduces mortality compared with placebo or no treatment. Horizontal lines around the squares represent 95% CIs. The size of thesquares reflects each study’s relative weight, and the diamond represents the aggregate risk ratios (RRs) and 95% CIs overall and for each stratum.
www.annals.org 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 W-93

Appendix Figure 5. Forest plot of infection-related mortality associated with colony-stimulating factors, by age group.
´
˚
Squares represent the point estimate of the outcome of each included study. Squares to the left of the vertical line indicate that the colony-stimulatingfactor intervention reduces mortality compared with placebo or no treatment. Horizontal lines around the squares represent 95% CIs. The size of thesquares reflects each study’s relative weight, and the diamond represents the aggregate risk ratios (RRs) and 95% CIs overall and for each stratum.
W-94 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 www.annals.org

Appendix Figure 6. Forest plot of infection-related mortality associated with colony-stimulating factors, by diagnosis.
www.annals.org 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 W-95

Appendix Figure 6—Continued
Squares represent the point estimate of the outcome of each included study. Squares to the left of the vertical line indicate that the colony-stimulatingfactor intervention reduces mortality compared with placebo or no treatment. Horizontal lines around the squares represent 95% CIs. The size of thesquares reflects each study’s relative weight, and the diamond represents the aggregate risk ratios (RRs) and 95% CIs overall and for each stratum.
W-96 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 www.annals.org

Appendix Figure 7. Forest plot of infection-related mortality associated with colony-stimulating factors, by studies that mandatedantibacterial prophylaxis.
www.annals.org 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 W-97

Appendix Table 3. Subgroup Analysis, by Type of Colony-Stimulating Factor*
Outcome G-CSF GM-CSF P Value forInteraction‡
Studies,n
Effect (95% CI)† Studies,n
Effect (95% CI)†
All-cause mortality 45 Relative risk, 0.98 (0.83–1.15) 34 Relative risk, 0.95 (0.84–1.08) 0.3Infection-related mortality 42 Relative risk, 0.84 (0.66–1.06) 24 Relative risk, 0.82 (0.49–1.38) 0.6Documented infections 41 Rate ratio, 0.83 (0.76–0.91) 17 Rate ratio, 0.92 (0.78–1.07) 0.034Microbiologically documented infection 29 Rate ratio, 0.85 (0.76–0.96) 12 Rate ratio, 0.90 (0.68–1.19) 0.7Febrile neutropenia 33 Rate ratio, 0.72 (0.64–0.81) 15 Rate ratio, 0.88 (0.75–1.03) 0.001
* G-CSF � granulocyte colony-stimulating factor; GM-CSF � granulocyte-macrophage colony-stimulating factor.† All analyses used a random-effects model. A relative risk or rate ratio less than 1 suggests that colony-stimulating factor is better than placebo or no therapy.‡ P values were derived from meta-regression.
Appendix Figure 7—Continued
Squares represent the point estimate of the outcome of each included study. Squares to the left of the vertical line indicate that the colony-stimulatingfactor intervention reduces mortality compared with placebo or no treatment. Horizontal lines around the squares represent 95% CIs. The size of thesquares reflects each study’s relative weight, and the diamond represents the aggregate risk ratios (RRs) and 95% CIs overall and for each stratum.
W-98 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 www.annals.org

Appendix Table 4. Subgroup Analysis, by Concurrent Administration of Chemotherapy
Outcome Yes No P Value forInteraction†
Studies,n
Effect (95% CI)* Studies,n
Effect (95% CI)*
All-cause mortality 13 Relative risk, 0.89 (0.64–1.23) 69 Relative risk, 0.96 (0.85–1.09) 0.5Infection-related mortality 7 Relative risk, 0.62 (0.19–2.03) 60 Relative risk, 0.83 (0.66–1.03) 0.031Documented infections 11 Rate ratio, 0.78 (0.56–1.08) 49 Rate ratio, 0.86 (0.80–0.93) 0.136Microbiologically documented infection 3 Rate ratio, 0.72 (0.47–1.11) 38 Rate ratio, 0.86 (0.77–0.97) 0.8Febrile neutropenia 8 Rate ratio, 0.62 (0.42–0.93) 41 Rate ratio, 0.71 (0.63–0.81) 0.077
* All analyses used a random-effects model. A relative risk or rate ratio less than 1 suggests that colony-stimulating factor is better than placebo or no therapy.† P values were derived from meta-regression.
Appendix Table 5. Subgroup Analysis, by Concealed Allocation
Outcome Yes No P Value forInteraction†
Studies,n
Effect (95% CI)* Studies,n
Effect (95% CI)*
All-cause mortality 25 Relative risk, 1.08 (0.90–1.30) 49 Relative risk, 0.84 (0.70–1.00) 0.2Infection-related mortality 18 Relative risk, 0.97 (0.67–1.42) 46 Relative risk, 0.77 (0.58–1.03) 0.4Documented infections 20 Rate ratio, 0.90 (0.82–0.98) 41 Rate ratio, 0.83 (0.74–0.92) 0.3Microbiologically documented infection 10 Rate ratio, 0.79 (0.65–0.96) 30 Rate ratio, 0.87 (0.75–1.02) 0.5Febrile neutropenia 9 Rate ratio, 0.64 (0.38–1.05) 37 Rate ratio, 0.73 (0.65–0.82) 0.4
* All analyses used a random-effects model. A relative risk or rate ratio less than 1 suggests that colony-stimulating factor is better than placebo or no therapy.† P values were derived from meta-regression.
Appendix Table 6. Subgroup Analysis, by Double-Blinding
Outcome Yes No P Value forInteraction†
Studies,n
Effect (95% CI)* Studies,n
Effect (95% CI)*
All-cause mortality 32 Relative risk, 0.96 (0.82–1.13) 41 Relative risk, 0.92 (0.75–1.13) 0.9Infection-related mortality 26 Relative risk, 0.88 (0.63–1.24) 37 Relative risk, 0.80 (0.59–1.08) 0.2Documented infections 21 Rate ratio, 0.83 (0.72–0.96) 38 Rate ratio, 0.84 (0.76–0.92) 0.9Microbiologically documented infections 18 Rate ratio, 0.80 (0.68–0.95) 23 Rate ratio, 0.89 (0.77–1.04) 0.9Febrile neutropenia 15 Rate ratio, 0.62 (0.47–0.82) 31 Rate ratio, 0.71 (0.66–0.86) 0.2
* All analyses used a random-effects model. A relative risk or rate ratio less than 1 suggests that colony-stimulating factor is better than placebo or no therapy.† P values were derived from meta-regression.
www.annals.org 18 September 2007 Annals of Internal Medicine Volume 147 • Number 6 W-99
Copyright © 2022 FDOKUMEN




















