
The use of prophylactic antibiotics for caesarean section
78
1 EDITORIAL The use of prophylactic antibiotics for caesarean section – what is the most appropriate regimen for Nepal ? Not surprisingly, there are many differences in clinical practice in Nepal from those in a more developed country. One of the most notable differences is that surrounding the use of antibiotics. In any surgical specialty anywhere in the world, strenuous efforts are made to minimise post-operative infection. The precise details of the measures taken, quite rightly, vary from place to place depending on a number of local factors, including the availability and cost of antibiotics, the nature of aseptic and antiseptic procedures in both the operating theatre and the wards as well as the population’s general level of nutrition and personal hygiene. At BPKIHS (BP Koirala Institute of Health Science) in Eastern Nepal the approach in recent years has been to give a full therapeutic course of a combination of antibiotics deemed likely to be effective against relevant pathogens. This usually consists of ampicillin (500 mg 6-hourly intravenously for two days, then 500 mg 6-hourly orally for another five days) and metronidazole (500 mg 8-hourly intravenously, then 400 mg 8-hourly orally for another five days). As well as the cost implications, such widespread and prolonged use of these drugs provokes concern regarding the emergence of antimicrobial resistance. In Western settings, there is consensus nowadays that, for any abdominal surgery, prophylactic antibiotics are a highly cost-effective measure and they are widely prescribed in this context. Their use at caesarean section has been shown clearly to reduce morbidity. 1 To summarise the current W estern evidence-based approach 1, 2, 4 to the usage of prophylactic antibiotics for caesarean section: Antibiotic prophylaxis has been shown to reduce the risk of febrile morbidity, endometritis, wound infection, urinary tract infection and other serious post- operative complications (including septic shock, pelvic abscess, and septic pelvic vein thrombophlebitis). Reduction in post-operative morbidity leads to reduction in length of hospital stay and less use of other costly resources in the treatment of this morbidity as well as a reduction in patient suffering. It has been demonstrated that there is a reduction in the relative risk of endometritis and wound infection for women having elective (planned) Caesarean section as well as those having emergency procedures. It is not clear which particular agent is the drug of choice. Both ampicillin and first generation cephalosporins appear to represent good choices for prophylaxis in women undergoing caesarean section. Clindamycin is an appropriate alternate choice for penicillin-allergic women. More costly extended-spectrum penicillins, second or third-generation cephalosporins and combination regimens have not been demonstrated to be more effective. It appears to be unnecessary to administer antibiotics likely to be active against every potential pathogen. Systemic administration of these agents is recommended. There is no evidence to suggest that a multiple dose regimen is of greater benefit to the woman than a single-dose regimen. Furthermore, single dose regimens are likely to be less expensive. It is unnecessary to give any further antibiotics post- operatively except in cases of established infection. There is currently insufficient evidence upon which to base a recommendation regarding the optimal timing of antibiotic administration (preoperative versus after cord clamping). The use of prophylactic antibiotics in no way diminishes the importance of established aseptic and antiseptic measures. Likewise, good surgical technique, especially in minimising tissue damage and ensuring meticulous haemostasis, remains extremely important. There is no shortage of publications on the subject but nearly all the research has taken place in western hospitals where conditions are often very different from those pertaining in developing countries. In the important Cochrane Review looking at different antibiotic regimens, “… all fifty-one trials included in the review were conducted in industrialized countries (United States, Canada, Israel, Italy, Switzerland or Netherlands).” 1 Norman Morris Department of Obstetrics and Gynaecology BPKIHS, Dharan, Nepal N. J. Obstet. Gynaecol Vol. 1, No. 1, p. 1 - 3 May 2006
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of The use of prophylactic antibiotics for caesarean section

1
E D I T O R I A L
The use of prophylactic antibiotics for caesarean section –what is the most appropriate regimen for Nepal ?
Not surprisingly, there are many differences in clinical practicein Nepal from those in a more developed country. One of themost notable differences is that surrounding the use ofantibiotics.
In any surgical specialty anywhere in the world, strenuousefforts are made to minimise post-operative infection. Theprecise details of the measures taken, quite rightly, vary fromplace to place depending on a number of local factors,including the availability and cost of antibiotics, the natureof aseptic and antiseptic procedures in both the operatingtheatre and the wards as well as the population’s generallevel of nutrition and personal hygiene.
At BPKIHS (BP Koirala Institute of Health Science) inEastern Nepal the approach in recent years has been to givea full therapeutic course of a combination of antibioticsdeemed likely to be effective against relevant pathogens. Thisusually consists of ampicillin (500 mg 6-hourlyintravenously for two days, then 500 mg 6-hourly orally foranother five days) and metronidazole (500 mg 8-hourlyintravenously, then 400 mg 8-hourly orally for another fivedays). As well as the cost implications, such widespreadand prolonged use of these drugs provokes concern regardingthe emergence of antimicrobial resistance.
In Western settings, there is consensus nowadaysthat, for any abdominal surgery, prophylactic antibiotics area highly cost-effective measure and they are widely prescribedin this context. Their use at caesarean section has been shownclearly to reduce morbidity. 1
To summarise the current Western evidence-based approach1,
2, 4 to the usage of prophylactic antibiotics for caesarean section:
� Antibiotic prophylaxis has been shown to reducethe risk of febrile morbidity, endometritis, woundinfection, urinary tract infection and other serious post-operative complications (including septic shock, pelvicabscess, and septic pelvic vein thrombophlebitis).
� Reduction in post-operative morbidity leads toreduction in length of hospital stay and less use ofother costly resources in the treatment of thismorbidity as well as a reduction in patient suffering.
� It has been demonstrated that there is a reduction inthe relative risk of endometritis and wound infectionfor women having elective (planned) Caesareansection as well as those having emergencyprocedures.
� It is not clear which particular agent is the drug ofchoice. Both ampicillin and first generationcephalosporins appear to represent good choices forprophylaxis in women undergoing caesarean section.Clindamycin is an appropriate alternate choice forpenicillin-allergic women.
� More costly extended-spectrum penicillins, secondor third-generation cephalosporins andcombination regimens have not beendemonstrated to be more effective.
� It appears to be unnecessary to administer antibioticslikely to be active against every potential pathogen.
� Systemic administration of these agents isrecommended.
� There is no evidence to suggest that a multiple doseregimen is of greater benefit to the woman than asingle-dose regimen. Furthermore, single doseregimens are likely to be less expensive. It isunnecessary to give any further antibiotics post-operatively except in cases of established infection.
� There is currently insufficient evidence upon which tobase a recommendation regarding the optimal timingof antibiotic administration (preoperative versus aftercord clamping).
� The use of prophylactic antibiotics in no waydiminishes the importance of established aseptic andantiseptic measures. Likewise, good surgicaltechnique, especially in minimising tissue damage andensuring meticulous haemostasis, remains extremelyimportant.
There is no shortage of publications on the subject but nearlyall the research has taken place in western hospitals whereconditions are often very different from those pertaining indeveloping countries. In the important Cochrane Reviewlooking at different antibiotic regimens, “… all fifty-one trialsincluded in the review were conducted in industrializedcountries (United States, Canada, Israel, Italy, Switzerlandor Netherlands).” 1
Norman MorrisDepartment of Obstetrics and Gynaecology
BPKIHS, Dharan, Nepal
N. J. Obstet. Gynaecol Vol. 1, No. 1, p. 1 - 3 May 2006

2
There is very little evidence available as to whether thewestern experience can be extrapolated to Nepal, although inthe WHO Reproductive Health Library, the conclusions ofthe Cochrane Review are considered applicable.
2.3. Applicability of the results of the
Cochrane Review
The results of this review are applicable to under-resourcedsettings, especially those where caesarean section rates arehigh. Although the review includes a dozen studies fromthe developing countries data from these studies have notbeen analysed separately. If this were done results mayshow not only similar results but also a higher effect in thesame direction (i.e. of reducing infectious puerperalmorbidity). Even considering some differences and difficultiesin diagnostic criteria, the high prevalence of poor social andeconomic conditions, anaemia, blood loss, vaginalexaminations, prelabour rupture of membranes and otherpathological conditions could account for a strongerprotective effect of antibiotic prophylaxis.
The recommendation to use ampicillin or first generationcephalosporin for the purpose of caesarean section antibioticprophylaxis makes this task easier. These antibiotics are infact the most common drugs that have been used in the pastdecades in developing countries.3
The author strongly supported a post-graduate thesis onthis subject in 2004-2005. Consensus within the Departmentof Obstetrics and Gynaecology at BPKIHS led to a studycomparing two regimens of antibiotic prophylaxis. Thethesis, by Dr Rishi Ram Tiwari, was entitled “A comparativestudy of prophylactic antibiotics versus standard post-operative treatment for control of infection in caesareansections”. I was involved as Dr Rishi’s guide.
The patients in Prophylaxis Group A were given a single 2Gdose of cephazolin intravenously at the time of anaestheticinduction; those in Prophylaxis Group B were given thestandard double antibiotic regimen described above. Twohundred consecutive patients were randomly allocated tothe two groups. Post-operative morbidity and costs associatedwith the two regimens were compared.
It would have been theoretically desirable to include a controlgroup receiving no prophylactic antibiotics at all; however,the weight of evidence in the existing literature would makethis ethically unacceptable.
The results of this study have been accepted forpresentation at the Ninth Conference of the Nepal Societyof Obstetricians and Gynaecologists, now planned forApril –May 2006.
Out of the 200 women in the study, 183 were available foranalysis: 92 in ‘Prophylaxis group A’ and 91 in ‘Prophylaxisgroup B’.
Only 9 out of the 92 women in Group A developed a woundinfection compared with 19 out of the 91 in Group B. Thiswas statistically significant (p=0.038). Only 3 of theinfections in Group A were regarded as “severe” (usuallywound dehiscence requiring secondary resuturing) whereas8 in Group B were “severe”. This did not achieve statisticalsignificance (p= 0.116) although the trend seems clear.
When cost was considered, it was seen that themedian total cost of treatment was 2550 rupees (range 2475– 4832) for women in Group A and 3252 rupees (range 2550-6976) for those in Group B. This difference is highlysignificant statistically (p < 0.0001).
The main component in the cost difference was the cost ofthe antibiotics themselves, but there were also statisticallysignificant differences in laboratory costs and hospital bedcharges (related to increased length of stay).
In summary, the results obtained from this non-blindedrandomised controlled trial showed that a pre-caesarean singleintravenous dose of a broad-spectrum first generationcephalosporin significantly more effective in the preventionof post-operative wound infection than a much moreexpensive post-operative regimen of two antibiotics, givenover seven days. The cephalosporin used was cephazolinand the post-operative regimen comprised the use of bothampicillin and metronidazole.
Sadly, the wound infection rate in BPKIHS at the time of thestudy was alarmingly high. In our study, wound infectionwas not only the most common post-operative complicationbut also it was the only clinically significant post-operativecomplication.
The antibiotic regimen in group B was five times the cost ofthe single dose of cephazolin.
Although prophylactic antibiotics have been shown to reducethe risk of post-operative wound infection, they will notconceal other deficiencies in peri-operative care. They cannever be a substitute for meticulous surgical technique andconstant vigilance regarding operating theatre conditions andpost-operative wound care.
It is the author’s hope that further, more detailed studies,perhaps in several developing country locations, should becarried out, in order to verify the above results. The findingsmight be different in terms of prevention of wound infection;they might also be different in terms of cost-effectiveness,depending on the availability and cost of antibiotics. Forexample, the relative cost of ampicillin and cephazolin maydiffer markedly in different settings.
It would also be of great interest to survey the medicalcommunity of Nepal to ascertain current practice in thisarea. Ideally this should include not only NESOG members,but all medical practitioners in Nepal who perform caesareansections on a regular basis.
Norman Morris

3
About the author:Graduated from the University of Melbourne, Australia, postgraduate training in the UK beforereturning to Melbourne to work at Queen Victoria Medical Centre, Monash Medical Centre and inprivate practice for 17 years.
For seven years he worked in northern Australia as a Staff Specialist / Senior Staff Specialist atCairns Base Hospital with teaching responsibilities in the University of Queensland and JamesCook University.
An Additional Professor in the Department of Obstetrics and Gynaecology at BPKIHS in Dharansince November 2003.
correspondence:Norman Morris, Department of Obstetrics and Gynaecology BPKIHS, Dharan, Nepalemail : [email protected]
References
1. Smaill F, Hofmeyr GJ. Antibiotic prophylaxis forcesarean section (Cochrane Review). In: The CochraneLibrary, Issue 4, 2003. Chichester, UK: John Wiley &Sons, Ltd
2. Hopkins L, Smaill F. Antibiotic prophylaxis regimensand drugs for cesarean section (Cochrane Review). In:
The Cochrane Library, Issue 4, 2003. Chichester, UK:John Wiley & Sons, Ltd.
3. Cecatti JG. Antibiotic prophylaxis for caesareansection: RHL commentary (last revised: 11 November1999). The WHO Reproductive Health Library, No 7,Update Software Ltd, Oxford, 2004.
4. Therapeutic Guidelines: Antibiotic. 10th edition March1998 (Therapeutic Guidelines Limited, NorthMelbourne, Australia)
The use of prophylactic antibiotics for caesarean section
4
Current trends in the management ofectopic pregnancy
Introduction
Ectopic pregnancy is implantation of the fertilized ovumoutside the uterine cavity. The incidence of ectopic pregnancyhas been rising steadily in the last four decades. In the USA,it has steadily increased from 4.5/1000 in the 1970s to nearly20/1000 pregnancy in the 1990s.1 In the UK also, the incidenceof ectopic pregnancy has been reported to rise 3.8 fold from1966 to 1996. This is partly due to improved diagnosis.2
Incidence in India is reported 1 in 300 by ICMR in 1989.Hospital admissions due to ectopic pregnancy also increasedfour-fold from the early 1970s to the late 80s, but the late1990s saw a decline in admissions due to changes in practicebrought about by early diagnosis hence medical andconservative management without admission.3 Thus, despitean increasing incidence, both hospital admissions and maternaldeaths due to ectopic pregnancy are declining. Neverthelessit still remains a leading cause of maternal death in the firsttrimester.4 First successful surgical treatment of ectopicpregnancy was described by Tail in 1883. He performedsalpingectomy in 4 cases and all survived. In 1940 bloodbank facility developed and prognosis became better for thesecases. Availability of pregnancy test in 1960 and ultrasoundscan in 1970 were significant advances for early diagnosis ofectopic pregnancy.
With advent of serum βHCG measurement as marker forectopic pregnancy early and accurate diagnosis is possibleand it is the key for medical management of ectopicpregnancy.
Risk factors of tubal pregnancy
Various factors that increase the risk of ectopic pregnancyinclude tubal factors, zygote abnormalities, ovarian factors,intrauterine devices (IUDs), etc. Among tubal factors,salpingitis increases the risk of ectopic pregnancy 2-4fold,5 tubal ligation and recanalization by 9-10 fold6 andprevious tubal surgery by 20 fold.7 In a woman who hasalready had one tubal pregnancy the risk of havingrepeat ectopic pregnancy is 7 to 13 times greater than overallrisk.8
Infertility increases the risk of ectopic pregnancy moderately,mainly because of tubal factors. This is particularly true forpregnancies that occur during infertility treatment.In multiparas with a history of infertility for 14 years
there is a 2-3 fold increased risk of ectopic pregnancy. Theincidence of ectopic pregnancy following in vitro fertilization(IVF) procedures is reported in up to 28% of cases, i.e.,a six-fold risk.9 Some studies have reported increasedectopic pregnancy rates with use of clomiphene citrate too,probably due to altered tubal function from hormonefluctuations.10 Intrauterine devices prevent intrauterinepregnancy more effectively than tubal pregnancy and,therefore, if pregnancy occurs with an IUD in situ, it is morelikely to be ectopic.11 A higher proportion of ovarian ectopicpregnancies has been seen in IUD users (5.5% vs 0% innonusers).12,13
Natural history of tubal pregnancy
Spontaneous resolution, either by regression or tubal abortion,is expected in up to 60% of cases.14 Tubal abortion is commonwhen the ectopic pregnancy is situated at the ampullary orfimbrial region. Choriodecidual haemorrhage separates theovum from tube and thereafter one of the four things mayhappen. It may resolve completely, present withhaematosalpinx, or may keep trickling, resulting in persistentpain and the formation of a pelvic hematocele. Rarely, tubalabortion may result in secondary abdominal pregnancy. Acutetubal rupture is the classical course, which occurs morecommonly at the isthmic site. The patient develops acuteabdomen and hypovolaemia. Sometimes tubal rupture canhave a chronic course if bleeding at the site is not acute orsevere.
Clinical features
There is a wide spectrum of symptoms and signs, rangingfrom asymptomatic to the haemodynamically unstable. Earlyectopic pregnancy may be entirely asymptomatic. The most
Nutan Agarwal, Vidushi Kulshrestha, Alka KriplaniDepartment of Obstetrics and Gynaecology, AIIMS,
New Delhi, India
I N V I T E D A R T I C L E
Table 1. Symptoms and signs of ectopic pregnancy16
Symptoms and signs Approximate percentage
Abdominal pain 95%Amenorrhoea 85%Vaginal bleeding 75%Dizziness, fainting 25%Passage of tissues 10%Adnexal tenderness 80%Adnexal mass 50%Uterine enlargement 25%
correspondence:Prof. Alka Kriplani, Department of Obstetrics and Gynaecology, AIIMS, New Delhi, India,email: [email protected]
N. J. Obstet. Gynaecol Vol. 1, No. 1, p. 4 - 12 May 2006

5
commonly reported symptoms are lower abdominal pain,amenorrhoea and vaginal bleeding. The classical symptomsof ectopic pregnancy are found in 30% of cases and usuallypresent between 5-9 weeks of amenorrhoea.15
Abdominal pain has a wide spectrum ranging from mild tosevere, lower to upper abdomen, unilateral or bilateral,localized or generalized, continuous or intermittent. Half ofthe cases presenting with amenorrhoea may experiencespotting per vaginum at the time of the expected period.Vaginal bleeding occurs due to inadequate endocrine function.The failing trophoblast may lead to involution of the deciduaand occasionally the entire decidua is sequestrated or expelledthrough the cervical canal (decidual cast), mimicking passageof products of conception.
On examination, ipsilateral adnexal tenderness is frequentlyfound. Cervical excitation, i.e., tenderness on movement ofthe cervix, may be present in about two-thirds of cases. Anadnexal mass may be palpable if it is > 3cm in size.17 Caremust be taken while performing bimanual examination asvigorous manipulation may expedite rupture of the ectopicgestational mass. The patient may present with tachycardia,hypotension, abdominal distension, marked reboundtenderness and shoulder tip pain in cases of acute ruptured ectopic.
Early diagnosis
Nowadays, a larger number of pregnancies, especially thosereceiving infertility treatment, are monitored early and thediagnosis of ectopic pregnancy can be established before anysymptoms manifest. Early diagnosis is essential to preventmaternal mortality and preserve future fertility. To achievethis, it is important to ‘think’ ectopic. The diagnosis of ectopicpregnancy should be suspected in any sexually active womanof reproductive age who presents with symptoms of lowerabdominal pain and delayed menstruation, until provenotherwise. All women with a history of any of thepredisposing factors such as infertility, pelvic inflammatorydisease, previous ectopic pregnancy, tubal surgery, IUD use,or use of assisted reproductive techniques (ART) must bescreened for ectopic. This is done by a urine pregnancy test,ultrasound and follow up with serum β-hCG, if required.Screening has been shown to reduce the risk of rupture from2.1% to 0.6%.18
Diagnosis
The importance of symptoms and signs should not beunderestimated despite the powerful diagnosticarmamentarium. They not only help in diagnosing thecondition, but also influence the choice of treatment.A good history and physical examination can diagnoseectopic pregnancy with 60% accuracy.19 However, varioustests have become available over the last decade that haverevolutionized the diagnosis of ectopic pregnancy. Of these,serum β-hCG and ultrasound are the most important.
Diagnostic tests
1. Serum β-hCG2. Transabdominal and transvaginal ultrasound3. Uterine curettage
4. Serum progesterone5. Doppler6. Culdocentesis7. Laparoscopy
Serum β-hCG
Serum β-hCG is the principal endocrine marker of pregnancy.It can be detected in maternal serum as early as 10 days afterfertilization. β-hCG is positive in virtually all ectopicpregnancies. On very rare occasions ectopic pregnancy maybe found where β−hCG cannot be detected in serum. It maybe due to very small volume of trophoblastic tissue whichmay be progressively degenerating. As the β-hCG levels varyin pregnancy, a single measurement cannot distinguishbetween an ectopic and intrauterine pregnancy, but repeatingthe measurement within 48-72 hours is useful. This is thenormal doubling time of β-hCGin normal pregnancy. In 85%of normal intrauterine pregnancies, the β-hCG rises by 66%in 48 hours and 114% in 72 hours. In ectopic pregnancies onthe other hand, 85% of ectopic pregnancies have no or lessthan 66% rise in 48 hours and their doubling time is usually> 7 days.20
Drawbacks of β-hCG testing: β-hCG alone is unreliable forthe following reasons:1. In 15% of intrauterine pregnancies the rise is
subnormal, whereas in 15% of ectopic pregnanciesthere is a normal rise of serum β-hCG.
2. An abnormal pattern of serum β-hCG levels in ectopicpregnancy cannot be distinguished from the oneobserved in a failing intrauterine pregnancy.
3. Serum β-hCG levels cannot correlate with the size orsite of the ectopic.
Ultrasound
The introduction of ultrasonography has revolutionized thediagnosis and management of ectopic pregnancy. It can beused to evaluate the contents of endometrial cavity, identifyan adnexal mass as small as 10 mm and assess the amount offree peritoneal fluid.
Both transvaginal and transabdominal ultrasound are used toestablish the diagnosis of ectopic pregnancy. Usingtransvaginal ultrasound the diagnosis can be made one weekearlier, with better visualization and assessment of the fluidin Pouch of Douglas, whereas the transabdominal scanprovides a broader view of the pelvis, detection of unusualsites and assessment of peritoneal fluid.
The ultrasound picture can be very variable in ectopicpregnancy and correlation with clinical findings andserum β-hCG level is required to establish the correctdiagnosis.
1. Definite intrauterine pregnancy
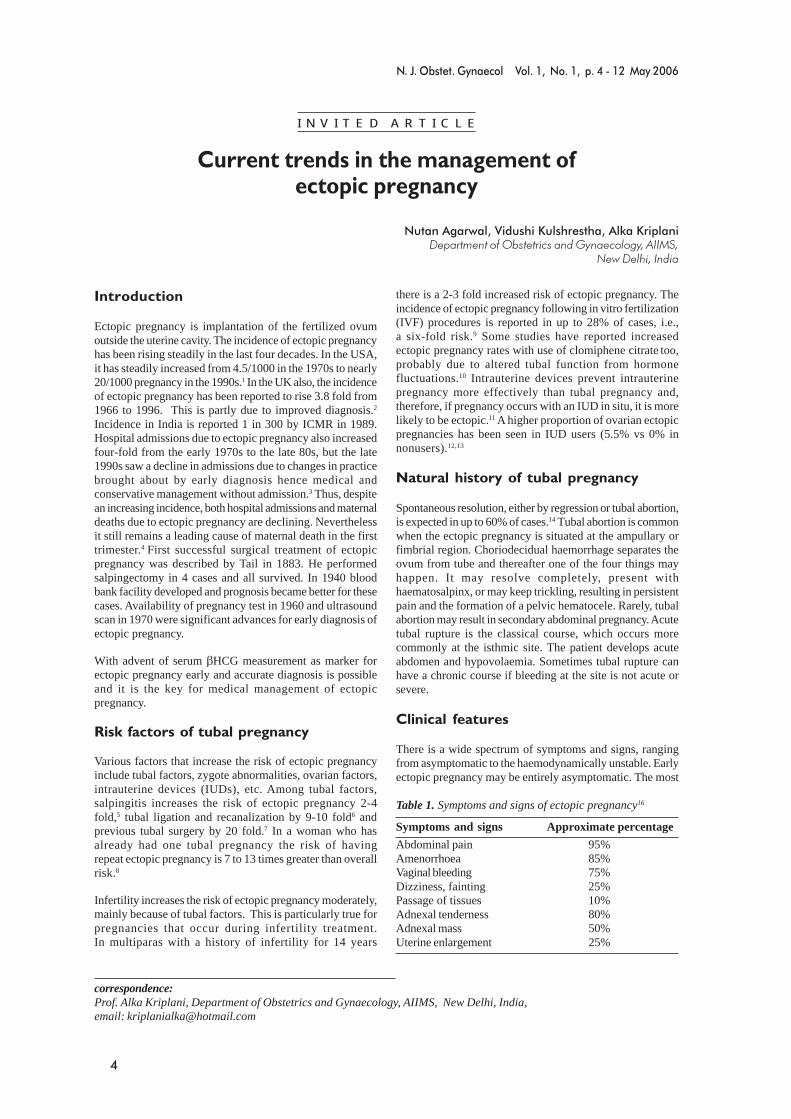
If a definite intrauterine pregnancy is seen, the likelihood ofa coexisting ectopic pregnancy is extremely low. Thepossibility of heterotopic pregnancy should be kept in mindin pregnancy after IVF. An intrauterine gestation sac is locatedeccentrically in the intrauterine cavity with a double decidualsac sign (DDSS) (Fig.1).
Current trends in the management of ectopic pregnancy
6
Figure 1:Intrauterine gestational sac showing doubledecidual sac sign (DDSS)
3. Abnormal intrauterine pregnancy
Various ultrasound features that can be seen at different stagesof decay of the embryo include: gestation sac with no fetalpole, no cardiac activity in the fetal pole, irregular crenatedborder of the gestation sac, larger sac with no DDSS or large,thin-walled yolk sac.
4. Probable ectopic
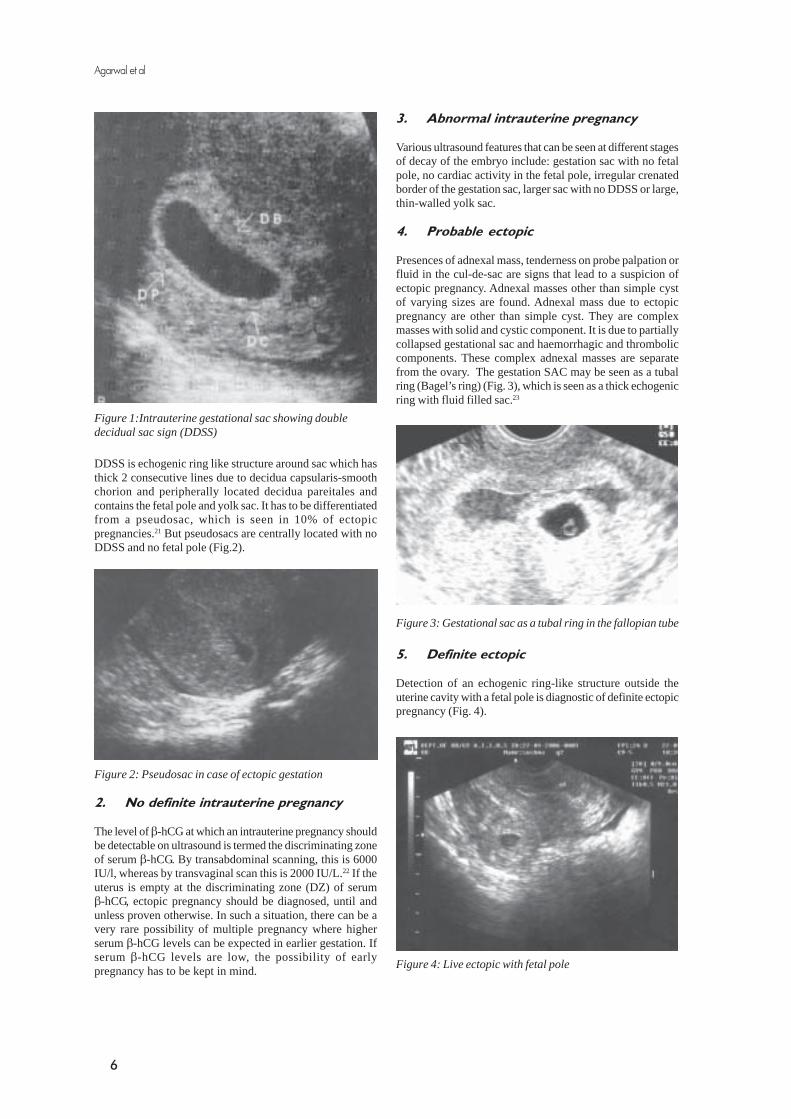
Presences of adnexal mass, tenderness on probe palpation orfluid in the cul-de-sac are signs that lead to a suspicion ofectopic pregnancy. Adnexal masses other than simple cystof varying sizes are found. Adnexal mass due to ectopicpregnancy are other than simple cyst. They are complexmasses with solid and cystic component. It is due to partiallycollapsed gestational sac and haemorrhagic and thromboliccomponents. These complex adnexal masses are separatefrom the ovary. The gestation SAC may be seen as a tubalring (Bagel’s ring) (Fig. 3), which is seen as a thick echogenicring with fluid filled sac.23
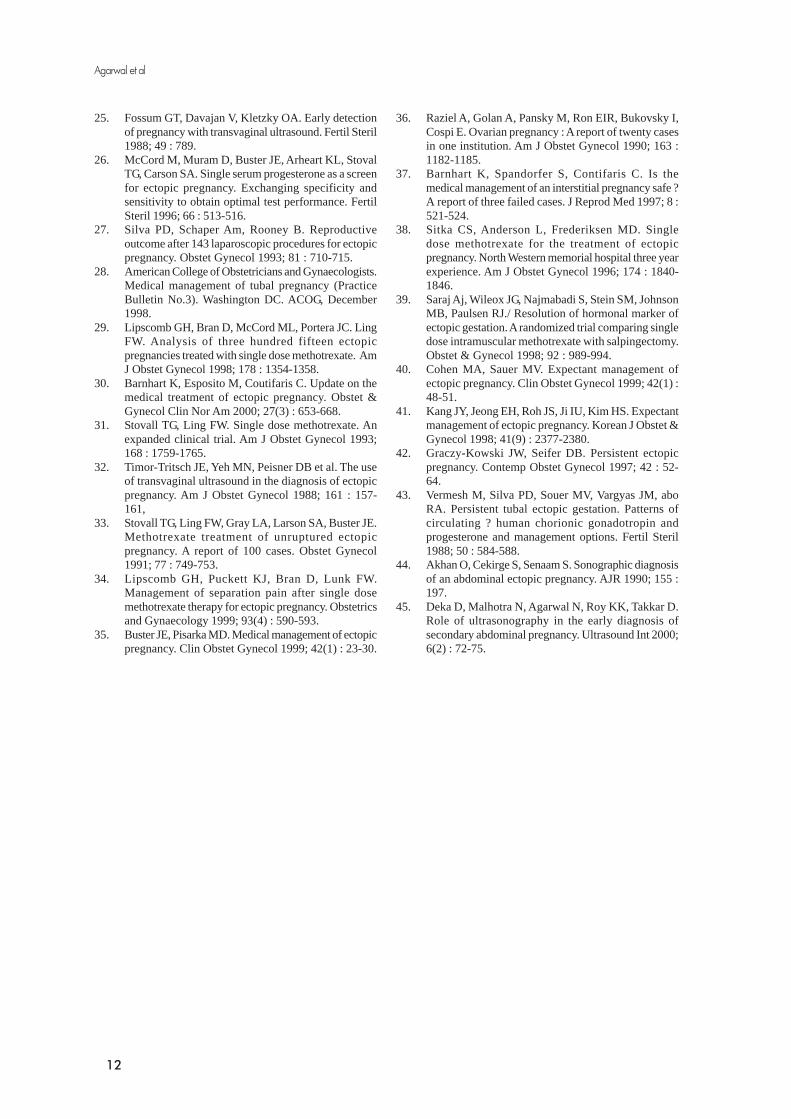
Figure 2: Pseudosac in case of ectopic gestation
DDSS is echogenic ring like structure around sac which hasthick 2 consecutive lines due to decidua capsularis-smoothchorion and peripherally located decidua pareitales andcontains the fetal pole and yolk sac. It has to be differentiatedfrom a pseudosac, which is seen in 10% of ectopicpregnancies.21 But pseudosacs are centrally located with noDDSS and no fetal pole (Fig.2).
Figure 3: Gestational sac as a tubal ring in the fallopian tube
5. Definite ectopic
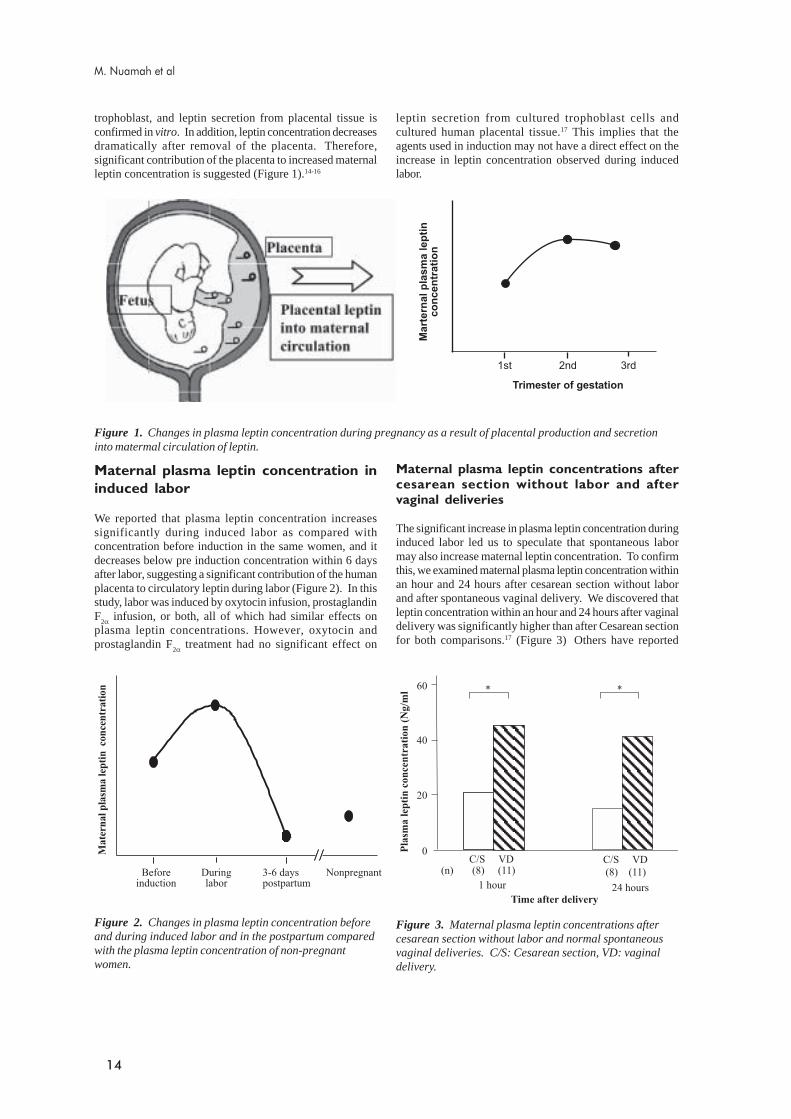
Detection of an echogenic ring-like structure outside theuterine cavity with a fetal pole is diagnostic of definite ectopicpregnancy (Fig. 4).
2. No definite intrauterine pregnancy
The level of β-hCG at which an intrauterine pregnancy shouldbe detectable on ultrasound is termed the discriminating zoneof serum β-hCG. By transabdominal scanning, this is 6000IU/l, whereas by transvaginal scan this is 2000 IU/L.22 If theuterus is empty at the discriminating zone (DZ) of serumβ-hCG, ectopic pregnancy should be diagnosed, until andunless proven otherwise. In such a situation, there can be avery rare possibility of multiple pregnancy where higherserum β-hCG levels can be expected in earlier gestation. Ifserum β-hCG levels are low, the possibility of earlypregnancy has to be kept in mind.
Figure 4: Live ectopic with fetal pole
Agarwal et al

7
Drawbacks of ultrasonography: Diagnosis byultrasonography may be difficult in the following situations:1. Differentiation between a pseudosac and a true
intrauterine gestation sac may be difficult.2. In the absence of an intrauterine pregnancy with low
serum b-hCG levels, the possibility of very early viableintrauterine pregnancy has to be kept in mind.
3. The absence of intrauterine pregnancy above DZ serumb-hCG level does not rule out abortion.
4. There is a remote possibility of heterotopic pregnancy,especially after ART.
5. Other adnexal masses and corpus luteum can bemisdiagnosed as ectopic.
Correlation with Serum βββββ-hCG andultrasonography
Proper evaluation, follow up ultrasonography and serum β-hCG may be required in certain situations to establish thediagnosis and plan the choice of treatment. If β-hCG levels arebelow the discriminating zone and no intrauterine sac is seen,follow up is required after 48 hours to assess rise in β-hCG aswell as appearance of a gestational sac once the DZ is reached.The DZ is considered 6000 IU for trans-abdominal and 2000IU for trans-vaginal ultrasound, but with the availability ofhigh resolution scanners, it is reported to be as low as 3000 IU/L for trans-abdominal and 1000 IU/l for trans-vaginalultrasound.24 An average gestational sac is detectable at 35days at β-hCG level of 1000 IU/L, the fetal poleis visible at40 days at β-hCG level of 3000 IU/L and cardiac activity isseen at 47 days at β-CG level of 3000 IU/ml.25
Other diagnostic modalities
Doppler ultrasound can be helpful to differentiate betweena true and pseudo-gestational sac. High velocity flow is seenin developing placentation, so it is seen at endometrium innormal or abnormal intrauterine pregnancy but not in ectopicpregnancy.
Dilatation and curettage (D&C) can differentiate ectopicfrom non-viable intrauterine pregnancy. Villi can be checkedimmediately in normal saline after curettage. Chorionic villifloat, dediduas settles. Histological findings consistent withpregnancy confirm the clinical diagnosis. This can be furtherfollowed up with bhCG, a fall of > 50% in 24 hours indicatingabortion. Caution should be taken to avoid disruption of anearly viable intrauterine pregnancy and D&C should beavoided as far as possible.
Serum progesterone testing takes only 2-3 hours and asingle measurement may be helpful in identifying normaldeveloping pregnancy. A level exceeding 25 ng/ml is associatedwith intrauterine viable pregnancy whereas a value <5 ng/mlis highly suggestive of non-viable pregnancy. However, levelsbetween 5-25 ng are inconclusive, so it has limited value.26
Culdocentesis : A significant amount of non-clotted blood isindicative of haemoperitoneum. In case of haemoperitoneumwith positive pregnancy test, ectopic pregnancy is thecommonest cause. Serous fluid or pus is a sign negative forectopic pregnancy. Dry tap is inconclusive. In cases of ectopicpregnancy with little or no intra-abdominal bleeding ororganized pelvic hematocele culdocentesis may be falsely
negative. Because of the widespread availability of sonography,it is rarely indicated nowadays.
Differential diagnosis of early tubalpregnancy
There are various conditions which can be confused withectopic pregnancy1. Abortion: Abortion also presents with amenorrhoea
and uterine bleeding. Pain may be accompanied butpain is not associated with fainting attacks. Adnexaltenderness is not a feature unless there is associatedsalpingitis.
2. Acute or subacute salpingitis – there may be irregularuterine bleeding with occurrence of lower abdominalpain. Amenorrhoea may not be there but patients havetenderness with or without adnexal mass, it is usuallya bilateral condition.
3. Early pregnancy with corpus luteum – sometimes apatient in early pregnancy may present with abdominalpain. If a corpus luteum is felt in adnexa. It can beconfined as adnexal mass due to ectopic pregnancy.But tenderness will be definitely less in such cases.
4. Torsion or rupture of ovarian cyst with sudden onsetof pain and fainting attack or collapse with findings ofadnexal mass may be confusing.
Treatment
Treatment options for ectopic pregnancy are surgery, medicalmanagement or expectant. Previously surgery was regardedmandatory because of risk of rupture of ectopic pregnancy.Now, with early diagnosis, medical management or expectantmanagement is also possible. Choice of treatment in theindividual case depends on the characteristics of the patient,desire for future fertility, facilities and expertise available atthe center, compliance, socioeconomic status and preferenceof the patient.
Surgery
Surgery is the mainstay of treatment. It is the preferred modeif the fallopian tube is already ruptured, pain is persisting for>24 hours or the patient is not suitable for medical management.Surgery may be conservative or radical. Conservative surgery,i.e., salpingostomy or fimbrial expression is the logical optionfor women who wish to preserve their fertility. The subsequentintrauterine pregnancy rate is greater but there is also a higherrecurrence risk of ectopic pregnancy.27 Radical surgery, i.e.,salpingectomy, is indicated in cases of ruptured ectopic,uncontrolled bleeding, extensive tubal damage, large tubalpregnancy (> 5 cm), recurrent ectopic on the same side orprevious reconstructive surgery.
Laparotomy is done for haemodynamically unstable patientswith a frank haemoperitoneum. Such patients are bestwheeled directly to the theatre without further ado. A wide-bore intravenous cannula is inserted and a sample obtained atthe same time so that adequate blood can be cross-matchedand obtained immediately. If there is any doubt about thesource of the bleeding, the abdomen is opened through avertical incision that can be extended as required, but if thereis no doubt about the diagnosis a Pfannenstiel incision may
Current trends in the management of ectopic pregnancy

8
be preferable. On opening the rectus sheath, the peritoneumis seen bulging with bluish colour reflected through from thehaemoperitoneum. The peritoneal cavity is opened and, whilethe assistant suctions off the collected blood, the surgeonimmediately plunges a hand into the pelvis and feels for theuterine fundus and pulls it out of the collected pool. Pullingup the uterus immediately decreases the amount of bleeding.The tubes are rapidly inspected and the site of bleedingidentified and clamped. If the tube is grossly damaged, partialsalpingectomy is the treatment of choice. A series of clampsis applied at the base of the tube and ligated with 1-0 chromiccatgut or Vicryl. It used to be the practice to cover the stumpof the tube by the round ligament using the modified Coffeysuture but this practice has now been abandoned. If futurefertility is not desired, the contra-lateral tube is ligated byPomeroy’s technique. The peritoneal cavity is lavaged wellto wash out all collected blood.
Laparoscopic surgery is preferable in haemodynamically stablepatients as it is minimally invasive. Relative contraindicationincludes previous surgery, extensive pelvic adhesions, largeblood clots, insufficient laparoscopic facilities or inexperienceof the surgeon.
Linear salpingostomy
Linear salpingostomy is standard conservative surgery forectopic pregnancy. Ectopic pregnancy is identified and tubeis immobilized. A linear incision is made on the antimesosalpinxwall of the tube at the point where it is maximally distended.Incision is made by unipolar electro-cautery or laser. Theproducts of conception are flushed out with irrigating solutionat high pressure. A combination of blunt and hydrodissectionshould be used. Specimen is grasped with claw forceps andremoved. One should try to avoid removing the productspiecemeal. Bleeding points can be coagulated. Tube is irrigatedcarefully and inspection should be done for haemostasis underwater. The tubal incision is left open to heal by secondaryintention.
Fimbrial expression by “milking” the tube may be appropriatein cases of ampullary pregnancy if the pregnancy is aborting,trophoblastic tissues are expressed out by compressing thetube from proximal to distal side and further tube can bewashed with irrigating solution. Thin suction cannula can beinserted from fimbrial side and solution can be flushed inunder pressure. Tube should be thoroughly inspected forany retained products. Care should be taken by wash of allbits of trophoblastic tissue from the tube. Milking can leadto damage to the cilia. If there are large blood clots minilaparotomy is often indicated in such cases.
In cases of chronic ectopic, if there is hematocele it is suckedout cleared. Trophoblastic tissue may be in the pelvis andadhered to other organs like intestine. Trophoblastic tissuesas much as possible are removed. Badly adherent bits can beleft as there is risk of bleeding or injury to organs.Salpingectomy has to be done if there is badly rupturedfallopian tube and it is unrepairable condition or the futurefertility is not required. Pelvis and abdominal cavity isthoroughly irrigated.
Medical management
Where facilities for β-hCG estimation and ultrasound exist,there is timely diagnosis of ectopic pregnancy and the needfor surgical visualization is eliminated in many cases. Hencemedical treatment is effective and safe in carefully selectedcases, provided a definite diagnosis of ectopic pregnancy canbe made. The patient must be willing and eligible for medicalmanagement. All contraindications should be ruled out. Usingthe following criteria, about 40% of ectopic pregnancies arefound to be appropriate for medical management:28
Eligibility criteria for medical management
� Haemodynamically stable patient� Unruptured ectopic� Reliable and compliant patient, can return for follow
up� Ectopic pregnancy < 4 cm in size� No contraindication for methotrexate� Normal blood counts, liver and kidney function� No suspected heterotopic pregnancy� No history of prolonged pain (>24 hours)� Desirous of future fertility
Presence of cardiac activity in the ectopic embryo and serumβ-hCG levels >10000 mIU/ml are relative contraindicationsfor medical management, although reports have shownsuccessful outcome in such cases also.29 We have also usedmethotrexate successfully in 2 cases of live ectopic and in 2cases with the high β-hCG lvel of 28000 and 40,000 mIU/mlrespectively. But close supervision in hospital is essential inthese cases.
Treatment regimen
Methotrexate is the drug of choice. Both single and multipledose regimens have been described. In the multidose regimen,methotrexate is given in a dose of 1mg/kg IV or IM followedby leucovorin 0.1mg/kg orally 24 hours later and the doserepeated every alternate day up to a maximum of 4 dosesuntil bhCG level declines by 15%. Serum bhCG should beassessed at day 0, 3, 5 and 7 until hCG declines 15% fromprevious value.30 Not all patients need four doses. The second,third or fourth dose is administered only if the bhCG valuedoes not show response. After response is achieved, thepatient is monitored with weekly bhCG levels until these areundetectable. If there is no response even after 4 doses, thepatient is maintained drug-free for a week to decrease therisk of side effects.31
The single dose regimen is more commonly used as it haslesser side effects. Methotrexate is given in a dose of 50mg/m2 IV or IM. bhCG is measured on Day 0, 4 and 7. Thereshould be a fall of 15% between Day 4 and 7. A rise in levelis often seen on day 4 and does not indicate failure of response.In fact, an initial rise is sometimes caused by the release oftrophoblastic tissues into circulation. If the bhCG levels areincreased or plateau between day 4 and 7, a second weeklydose can be given.32 Although most of the reports showsadministration by methotrexate by intramuscular route, we
Agarwal et al

9
personally feel intravernous route is a better option. In ourexperience in 2 cases where patient did not respond to IMinjection responded to intravenous injections. In one casewho received first intramuscular injection at nearly 10,000bhCG did not respond and β-hCG level raised upto 40,000at D7 and surprisingly responded to second intravenousinjection and did not require any surgery. Her β-hCG becamenegative in 10 weeks.
Monitoring and follow up
Most patients can be managed on an outpatient basis. Whilereceiving methotrexate, the patient should be instructed not totake folic acid, salicylates or alcohol, and should avoid exposureto sun and maintain abstinence. She should be observed forheavy bleeding, pain, especially severe and persistent (>12hours), any sign of rupture and haematocrit. The most difficultaspect is to distinguish between transient pain due to successof therapy from that of tubal rupture. Transient abdominalpain after 3 days for 4-12 hours is presumably due to tubalabortion.33 About 80% of cases who have pain after medicalmanagement do not require surgery.34 The patient can beadmitted if required. Ultrasonography is not of much help.35
The patient is followed with weekly β-hCG monitoring tilllevels are undetectable. Resolution usually takes 5 weeks anda maximum of 7 weeks.36 Medical management is notconsidered successful until β-hCG is no longer detectable inthe serum. There are cases of treatment failure even withβ-hCG value as low as < 50mIU/ml.37
Surgical intervention
Surgical intervention may be necessary if there is orthostatichypotension, decreasing haematocrit, persistent or severepain, any sign of tubal rupture or impending tubal rupture.Surgery is indicated if the patient no longer wants to continuewith medical therapy or if medical therapy fails.
Risk of tubal rupture
The risk of tubal rupture is greater with high levels of serumβ-hCG. The presence of cardiac activity is associated withhigher failure rate 14% vs 4.7% when cardiac activity isabsent.29 The tube is unlikely to rupture if the mass is < 2 cmand β-hCG is < 2000 mIU/ml, although cases of rupturehave been reported even with β-hCG of < 5 mIU/ml.38
Success rate
In review of 26 studies the overall success rate with themultiple dose regimen is greater than with the single doseregimen (95% vs 90%).39 In the single dose regimen, 15% ofcases need more than one dose. Multidose is less convenientand associated with more side effects 48% vs 29% in singledose. Comparison of medical management and conservativesurgery has shown that success rate and patency is the samein both, whereas resolution is faster with salpingostomy.40
Expectant management
The fact that some patients of ectopic pregnancy havespontaneous resolution, either through regression or throughtubal abortion, is the basis of expectant management of ectopicpregnancy. Selection of patients for expectant managementdepends on the initial serum β-hCG levels and size of theectopic gestation. It is a reasonable option in very carefullyselected patients. Stringent inclusion criteria include: ectopicmass < 3 cm, β-hCG < 1000mIU/ml and absence of cardiacactivity. Approximately 15-20% cases of ectopic pregnancymay be appropriate for expectant management. The patientis closely monitored with clinical symptoms, haematocritand weekly β-hCG till undetectable. Transvaginalultrasonography is performed if required. The overall successis approximately 70%. Complete resolution may take 4weeks. Patients with persistent or increasing β-hCG levelsshould be treated with medical or surgical therapy. The riskof tubal rupture on expectant management is reported to beabout 2.5%.41
Surgically assisted medical management
Patients diagnosed before tubal rupture can be treatedwith alternative treatment options. Besides systemicmedical management local injections of tropholytic agentsmay be alternative options. These local injections may beinjected either by ultrasound guidance or by laparoscopicguidance. Laparoscopically guided local injection does notseem to be logical option as once patient is exposed tolaparoscopy, it is ideal to remove the ectopic gestation at thesame sitting.
However, ultrasound guided salpingocentesis can be aoption in certain cases of unruptured ectopic pregnancy toavoid the side effects of systemic drug. It is limited tothose patients in whom ultrasound positively localizes atubal mass. Needle injection should be precisely and safelyguided into exact gestational target site. The most reliableultrasound finding for ectopic pregnancy is observationof live embryo outside of the uterus. Tubal ring is anotherhighly specific sonographic appearance. Salpingocentesis canbe performed in those patients with these specific findingsonly.
Variety of the treatment agents including methotrexate 10mg,hyperosmolar glucose and potassium chloride are used. Thereis lack of widespread acceptance of this technique. There aresome distinct potential advantages. One is avoidance of riskof laparoscopic surgery and secondly, its lack of systemictoxicity of methotrexate. There is delivery of high localconcentration of methotrexate with reduced incidence ofsystemic side effects. But, efficacy is considered same as IMinjection, there is need for experienced practitioner to performthis procedure. Other risks are infection, haemorrhage, tubaldamage at the site of injection. We gave KCl along with IVmethotrexate in two live ectopics and both responded to thetreatment.
Current trends in the management of ectopic pregnancy

10
Persistent ectopic pregnancy
Conservative surgical management of ectopic pregnancy aswell as medical therapy may not entirely eradicate thetrophoblastic tissue. The remaining trophoblast may remainviable and continue to grow, leading to persistent ectopicpregnancy. The incidence of persistent ectopic has beenreported to vary from 2 to 20%,42 although in our practice itis very low.
Persistent ectopic pregnancy may result in sudden tubalrupture and haemorrhage. The diagnosis should be suspectedin a woman who has abdominal pain after conservativesurgical management. Sonographic identification of apersistent ectopic mass may not always be possible due tosmall size.
bhCG levels decrease rapidly after salpingostomy. Onpostoperative day 12, the level declines to less than 10% ofthe preoperative value.Increasing or plateauing bhCG levelsare obvious indications of persistent ectopic pregnancy.
Predictors of persistent ectopic
The fall in serum bhCG level on day 1 can be a predictor ofpersistent ectopic. More than 85% cases where there is a fallof > 50% in the bhCG level on the first postoperative daywill not develop a persistent ectopic, whereas if the fall is >75% on day 1, the risk is almost nil.43 An increased risk ofpersistent ectopic is seen in cases where the ectopic is smaller< 2 cm in diameter, bhCG is high > 3000 mIU/ml and rapidlyrising, the implantation site is medial to the salpingostomyincision or removal is done piecemeal. Weekly follow upwith bhCG is recommended following conservativesurgery.
Treatment of persistent ectopic
The treatment of persistent ectopic pregnancy is single dosemethotrexate. The role of prophylactic methotrexate toprevent persistent ectopic following conservative surgeryhas not yet been determined.
The pregnancy rate does not seem to decrease after persistentectopic and chances of recurrent ectopic are also not high.
Abdominal pregnancy
Abdominal pregnancy occurs in 1 in 8000 pregnancies andthe mortality is 8 times higher than other ectopics. Abdominalpregnancy can be primary or secondary. Primary abdominalpregnancy is implanted in peritoneal cavityitself. Diagnosisof primary abdominal ectopic pregnancy is made byStuddiford criteria which include :1. The presence of normal tube and ovary2. The absence of placental fistula3. Presence of pregnancy related to peritoneal surface.
Secondary abdominal pregnancy is more common. Herethe pregnancy is initially implanted in the ampullary or
fimbrial part of tube. It may be expelled from the tube andmay then get re-implanted onto any peritoneal area in theabdomen. The placenta grows anywhere in the abdominalcavity.
Medical management may be of little value in abdominalpregnancy. Advanced abdominal pregnancy is managed bylaparotomy. Preoperative diagnosis of abdominal pregnancyis difficult. The sonographic features as suggestive ofabdominal pregnancy are described as visualization of fetusas a part separate from the uterus, failure to visualize theuterine wall between the fetus and the urinary bladder, closeapproximation to the abdominal wall and visualization ofextra-uterine placental tissue.44 Diagnosis is often missed onultrasound. We also reported a case where diagnosis wasmissed on first ultrasound.45 When ultrasound findings areequivocal or inconclusive, magnetic resonance imaging shouldbe performed.
Surgery is indicated whenever the diagnosis is established.Intraoperative decision regarding removal or non-manipulation of placenta is an important management issue.In early abdominal pregnancy it may be possible to removeplacenta completely but in advanced cases it may be quitedifficult. In such circumstances, management includes ligationof umbilical cord close to the placenta and leaving it in situ. Itmay be followed up by ultrasound and bhCG for placentalinvolution. Methotrexate may be indicated in certain caseswith persistent bhCG level.
Interstitial pregnancy
The incidence of interstitial pregnancy is 1 in 5000pregnancies. Rupture is usually delayed to 9-12 weeksgestation because of myometrial distensibility. Previoussalpingectomy is a unique risk factor for interstitial pregnancyand is seen in 25% of cases. The diagnosis is made byultrasound. The gestation sac is located within themyometrium towards the site of the fallopian tube butdetached from the endometrial echo. A myometrium mantle,i.e., at least 5 mm myometrium between the gestation sacand endometrium, is seen. Traditionally, the treatment iscornual resection or hysterectomy. However, in cases wherean early diagnosis of interstitial pregnancy can be established,systemic or local methotrexate can be attempted first.
Ovarian pregnancy
The incidence of ovarian pregnancy is 1 in 40,000 pregnancies.The clinical features are the same as in ectopic tubalpregnancy, but 30% of cases are haemodynamically unstable.There is a high association with IUD use. Ovarian pregnanciesare mistaken for ruptured corpus luteum.
The diagnosis of ovarian pregnancy is made by Spiegelberg’scriteria1. Intact fallopian tubes2. Ovarian tissue in sac wall3. Ovarian connection to uterus with ligament4. Fetal sac in position of ovary.
Agarwal et al

11
Both diagnosis and treatment can be done by laparoscopy.Removal of ectopic gestation, ovarian wedge resection oroophorectomy can be performed.
Cervical pregnancy
It occurs in 1 in 1200 pregnancies. As implantation occurs inthe cervical canal, it can be confused with partially expelledspontaneous abortion of an intrauterine pregnancy. Onultrasound, the gestation sac is seen below the level of theinternal os and located within the limits of the cervix, deeplypenetrating into one of the cervical walls. If the diagnosis isnot confirmed, CT or MRI may be valuable. Predisposingfactors include preexisting cervical pathology, cervical surgeryand Asherman’s syndrome.Treatment modalities include systemic or local methotrexate,arterial embolization, cervical curettage followed by balloontamponade, cervical curettage and, lastly, hysterectomy iffuture fertility is not a concern.
Heterotopic pregnancy
Heterotopic pregnancy, where pregnancy occurssimultaneously in intrauterine as well as at an ectopic site,has been reported in 1 in 30,000 pregnancies. It occurs in upto 1% of pregnancies after assisted reproductive techniques(ART). It should be suspected in a patient who has undergonecontrolled ovarian hyperstimulation, with or without ART.
There are several diagnostic pitfalls. Serial bhCG may not beuseful because of the concomittant intrauterine pregnancy.
There is no role of medical management in these cases. Surgicalmanagement is required to treat this type of ectopicpregnancy.
References
1. Ectopic pregnancy – United States. 1990-1992. JAMA1995; 273 : 533.
2. Rajkhowa M, Glass MR, Rutherford AJ, Balen AH,Sharma V, Cuckle HS. Trends in the incidence of ectopicpregnancy in England and Wales from 1966 to 1996.Br J Obstet Gynecol 2000; 107 : 369-374.
3. Ectopic pregnancy in William Obstetrics. 21st Ed.McGraw Hill, 883-919.
4. Grimes DA. The morbidity and mortality of pregnancy: still risky business. Am J Obstet Gynecol 1995; 170: 1489-1494.
5. Chow W, Daling JR, Cates W, Greenberg RS.Epidemiology of ectopic pregnancy. Epidemiol Rev1987; 9 : 70-94.
6. World Health Organization. Task force on intrauterinedevices for fertility regulation. A multinational casecontrol study of ectopic pregnancy. Clin Reprod Fertil1985; 3 : 131-143.
7. Ankum WM, Bol BWJ, Vander Veen F, BossyutPMM. Risk factors for ectopic pregnancy. A meta-analysis. Fertil Steril 1996; 65 : 1093-1099.
8. Revised by Neerja Bhatia, Ectopic pregnancy. InJeffcoate’s Principle of gynaecology Internationaledition, 6th edn. Arnold publisher,2001.
9. Marcus SF, Brinsden PR. Analysis of the incidenceand risk factors associated with ectopic pregnancyfollowing in vitro fertilization and embryo transfer.Hum Reprod 1995; 10 : 199-203.
10. Karande VC, Flood JT, Heard N, Veeck L, MousherSJ. Analysis of ectopic pregnancies resulting from invitro fertilization and embryo transfer. Hum Reprod1991; 6 : 446-449.
11. Mol BWJ, Ankum WM, Bossyut PMM, VanderVeen F. Contraception and the risk of ectopicpregnancy. A meta-analysis. Contraception 1995; 52 :337-341.
12. Raziel A, Golan A, Pansky M, Ron EIR, Bukovsky I,Cospi E. Ovarian pregnancy : A report of twenty casesin one institution. Am J Obstet Gynecol 1990; 163 :1182-1185.
13. Breen JL. A 21 year survey of 654 ectopic pregnancies.Am J Obstet Gynecol 1970; 106 : 1004.
14. Ylostalo P, Cacciatore B, Sjoberg J, Kaariainen M,Tenhunen A, Stenman UH. Expectant management ofectopic pregnancy. Obstet Gynecol 1992; 80 : 345-348.
15. Tay JI, Moore J, Walker JJ. Ectopic pregnancy. BMJ2000; 320 : 916-919.
16. Pisarska MD, Carson SA, Buster JE. Ectopicpregnancy. Lancet 1999; 351 : 115-1120.
17. Graezykowski JW, Seifer DB. Diagnosis of acute andpersistent ectopic. Clin Obstet Gynecol 1999; 42(1) :9-22.
18. Mole BMJ, Vander Veen F, Bossuyt PMM. Symptomfree women at increased risk of ectopic pregnancy.Should we screen ? Acta Obstet Gynecol Scand 2002;81 : 661-672.
19. Barhhart KT, Katz I, Hummel A, Gracia Cr. Presumeddiagnosis of ectopic pregnancy. Obstet Gynecol 2002;100(3) : 505-510.
20. Romero R, Kadar H, Castro D. The value of serialhuman chorionic gonadotropin testing as a diagnostictool in ectopic pregnancy. Am J Obstet & Gynecol1986; 155 : 392.
21. Maccato ML, Estrada R, Faro S. Ectopic pregnancywith undetectable serum and urine ?hCG levels anddetection of ?hCG in the ectopic trophoblast byimmunocytochemical evaluation. Obstet Gynecol 1993;81 : 878-880.
22. Sadek AL, Schiotz HA. Transvaginal sonography inthe management of ectopic pregnancy. Acta ObstetGynecol Scand 1995; 74 : 293-296.
23. Kadar N, Bohrer M, Kemmann E, Shelden R. Thediscriminatory human chorionic gonadotrophin zonefor endovaginal sonography. A prospective,randomized study. Fertil Steril 1994; 61 : 1018.
24. Cacciatore B, Stenma U, Ylostalo P. Diagnosis ofectopic pregnancy by vaginal ultrasonography incombination with discriminatory serum hCG level of1000 IU/L (IRP). Br J Obstet Gynecol 1990; 97 : 904-908.
Current trends in the management of ectopic pregnancy
12
25. Fossum GT, Davajan V, Kletzky OA. Early detectionof pregnancy with transvaginal ultrasound. Fertil Steril1988; 49 : 789.
26. McCord M, Muram D, Buster JE, Arheart KL, StovalTG, Carson SA. Single serum progesterone as a screenfor ectopic pregnancy. Exchanging specificity andsensitivity to obtain optimal test performance. FertilSteril 1996; 66 : 513-516.
27. Silva PD, Schaper Am, Rooney B. Reproductiveoutcome after 143 laparoscopic procedures for ectopicpregnancy. Obstet Gynecol 1993; 81 : 710-715.
28. American College of Obstetricians and Gynaecologists.Medical management of tubal pregnancy (PracticeBulletin No.3). Washington DC. ACOG, December1998.
29. Lipscomb GH, Bran D, McCord ML, Portera JC. LingFW. Analysis of three hundred fifteen ectopicpregnancies treated with single dose methotrexate. AmJ Obstet Gynecol 1998; 178 : 1354-1358.
30. Barnhart K, Esposito M, Coutifaris C. Update on themedical treatment of ectopic pregnancy. Obstet &Gynecol Clin Nor Am 2000; 27(3) : 653-668.
31. Stovall TG, Ling FW. Single dose methotrexate. Anexpanded clinical trial. Am J Obstet Gynecol 1993;168 : 1759-1765.
32. Timor-Tritsch JE, Yeh MN, Peisner DB et al. The useof transvaginal ultrasound in the diagnosis of ectopicpregnancy. Am J Obstet Gynecol 1988; 161 : 157-161,
33. Stovall TG, Ling FW, Gray LA, Larson SA, Buster JE.Methotrexate treatment of unruptured ectopicpregnancy. A report of 100 cases. Obstet Gynecol1991; 77 : 749-753.
34. Lipscomb GH, Puckett KJ, Bran D, Lunk FW.Management of separation pain after single dosemethotrexate therapy for ectopic pregnancy. Obstetricsand Gynaecology 1999; 93(4) : 590-593.
35. Buster JE, Pisarka MD. Medical management of ectopicpregnancy. Clin Obstet Gynecol 1999; 42(1) : 23-30.
36. Raziel A, Golan A, Pansky M, Ron EIR, Bukovsky I,Cospi E. Ovarian pregnancy : A report of twenty casesin one institution. Am J Obstet Gynecol 1990; 163 :1182-1185.
37. Barnhart K, Spandorfer S, Contifaris C. Is themedical management of an interstitial pregnancy safe ?A report of three failed cases. J Reprod Med 1997; 8 :521-524.
38. Sitka CS, Anderson L, Frederiksen MD. Singledose methotrexate for the treatment of ectopicpregnancy. North Western memorial hospital three yearexperience. Am J Obstet Gynecol 1996; 174 : 1840-1846.
39. Saraj Aj, Wileox JG, Najmabadi S, Stein SM, JohnsonMB, Paulsen RJ./ Resolution of hormonal marker ofectopic gestation. A randomized trial comparing singledose intramuscular methotrexate with salpingectomy.Obstet & Gynecol 1998; 92 : 989-994.
40. Cohen MA, Sauer MV. Expectant management ofectopic pregnancy. Clin Obstet Gynecol 1999; 42(1) :48-51.
41. Kang JY, Jeong EH, Roh JS, Ji IU, Kim HS. Expectantmanagement of ectopic pregnancy. Korean J Obstet &Gynecol 1998; 41(9) : 2377-2380.
42. Graczy-Kowski JW, Seifer DB. Persistent ectopicpregnancy. Contemp Obstet Gynecol 1997; 42 : 52-64.
43. Vermesh M, Silva PD, Souer MV, Vargyas JM, aboRA. Persistent tubal ectopic gestation. Patterns ofcirculating ? human chorionic gonadotropin andprogesterone and management options. Fertil Steril1988; 50 : 584-588.
44. Akhan O, Cekirge S, Senaam S. Sonographic diagnosisof an abdominal ectopic pregnancy. AJR 1990; 155 :197.
45. Deka D, Malhotra N, Agarwal N, Roy KK, Takkar D.Role of ultrasonography in the early diagnosis ofsecondary abdominal pregnancy. Ultrasound Int 2000;6(2) : 72-75.
Agarwal et al

13
Differences in maternal plasma leptin concentrationduring human pregnancy, induced labor, after cesarean
section without labor and vaginal deliveries:A review
Abstract:Leptin plays important role in energy metabolism. Human placenta produces leptin contributing to an increase inmaternal plasma leptin concentration during pregnancy. Recently we reported subsequent increase in maternal plasmaleptin concentration during labor. Plasma leptin concentration of pregnant women fell to the level of non pregnantwomen with the same BMI within a few days postpartum. Leptin mRNA expression (leptin/GAPDH) in placental tissuesobtained after spontaneous vaginal deliveries was greater than that in placental tissues obtained after cesarean sectionwithout labor. These findings indicate that labor increases placental leptin production. During labor, maternal energyrequirement increases during active uterine contraction. Fetal energy metabolism may also be influenced by labor.Therefore, we speculate a physiological significance of placental leptin in maternal and fetal energy metabolism duringpregnancy and during labor.
Key words: leptin, labor, cesarean section, placenta
Introduction
Leptin, the obese (ob) gene product, is a 16 kD peptidehormone produced abundantly in adipose tissue. It stimulatesenergy expenditure and reduces appetite leading to decreasein body weight.1,2 Leptin plays important roles in energymetabolism and in reproduction. For instance, micewith mutation in the ob gene exhibit reduced activity,metabolism, and body temperature, which are restored withdaily injection of recombinant leptin.3 Fertility defect inhomozygous obese female mice (ob/ob mice) is treated withrecombinant leptin.4 In addition, our laboratory recentlyreported that female transgenic skinny mice over expressingleptin, exhibit accelerated puberty and intact fertilityat a younger age.5 Other studies have also shown thatleptin has other pleiotrophic peripheral actions such asneovascularization, wound healing and immunomodulationas well as initiation of pregnancy. However, the ability tostimulate energy metabolism is thought to be the centralfunction of leptin.6-10
Maternal energy requirement increases during pregnancy andduring labor. Thus, it is plausible that leptin may play someroles in the energy metabolism of both mother and fetus.However, studies on leptin in pregnancy as well as in laborare limited.11-13
We have demonstrated placental production of leptin duringhuman pregnancy. The purpose of this manuscript is tosummarize our recent advances in the study of leptin inpregnancy and labor and to show the effect of labor on leptinproduction and secretion from the human placenta. We alsobriefly review the biological significance of placental leptinin gestation.
LEPTIN CONCENTRATION DURING
PREGNANCY AND LABOR
Maternal plasma leptin concentration in
pregnancy
We have reported that leptin is also produced by humanplacental trophoblasts and secreted into maternal andfetal circulations.14,15 Leptin concentration in pregnant womenis higher than that in age and BMI matched non-pregnantwomen. Moreover, plasma leptin concentration increasessignificantly during pregnancy as masses of adiposetissue and placenta increase. Although plasma leptinconcentration shows a positive correlation with BMI innon-pregnant women, plasma leptin concentration in pregnantwomen does not show any correlation with BMI. On theother hand, leptin mRNA expression is observed in placental
Mercy A Nuamah, Shigeo Yura, Norimasa Sagawa*, Hiroaki Itoh, Shingo Fujii Department of Gynecology and Obstetrics, Kyoto University,
54 Shogoin Kawahara-cho, Sakyo-ku, Kyoto 606-8507, Japan *Department of Obstetrics and Gynecology, Mie University Faculty of Medicine
2-174 Edobashi, Tsu, Mie 514-8507 Japan
correspondence:Mercy A Nuamah, Department of Gynecology and Obstetrics, Kyoto University, 54 Shogoin Kawahara-cho,Sakyo-ku, Kyoto 606-8507, Japan email: [email protected],ac.jp
N. J. Obstet. Gynaecol Vol. 1, No. 1, p. 13 - 17 May 2006
A R E V I E W
14
trophoblast, and leptin secretion from placental tissue isconfirmed in vitro. In addition, leptin concentration decreasesdramatically after removal of the placenta. Therefore,significant contribution of the placenta to increased maternalleptin concentration is suggested (Figure 1).14-16
Figure 2. Changes in plasma leptin concentration beforeand during induced labor and in the postpartum comparedwith the plasma leptin concentration of non-pregnantwomen.
Figure 3. Maternal plasma leptin concentrations aftercesarean section without labor and normal spontaneousvaginal deliveries. C/S: Cesarean section, VD: vaginaldelivery.
M. Nuamah et al
�
��
��
��
������������� ������ ��������
���������� ��������� ��������
����������������������
� �
���������� ������� ��������
Figure 1. Changes in plasma leptin concentration during pregnancy as a result of placental production and secretioninto matermal circulation of leptin.
Maternal plasma leptin concentration in
induced labor
We reported that plasma leptin concentration increasessignificantly during induced labor as compared withconcentration before induction in the same women, and itdecreases below pre induction concentration within 6 daysafter labor, suggesting a significant contribution of the humanplacenta to circulatory leptin during labor (Figure 2). In thisstudy, labor was induced by oxytocin infusion, prostaglandinF
2α infusion, or both, all of which had similar effects onplasma leptin concentrations. However, oxytocin andprostaglandin F
2α treatment had no significant effect on
leptin secretion from cultured trophoblast cells andcultured human placental tissue.17 This implies that theagents used in induction may not have a direct effect on theincrease in leptin concentration observed during inducedlabor.
Maternal plasma leptin concentrations aftercesarean section without labor and aftervaginal deliveries
The significant increase in plasma leptin concentration duringinduced labor led us to speculate that spontaneous labormay also increase maternal leptin concentration. To confirmthis, we examined maternal plasma leptin concentration withinan hour and 24 hours after cesarean section without laborand after spontaneous vaginal delivery. We discovered thatleptin concentration within an hour and 24 hours after vaginaldelivery was significantly higher than after Cesarean sectionfor both comparisons.17 (Figure 3) Others have reported
���������������������� ������ �
���������������
������� ��
!"����#�$���$����%
&��$�������
��� ��� ���
������������������
���
���
����
����
����
���
�
��
��
���
15
augmented placental leptin release during advanced laborbased on higher umbilical venous and arterial blood leptinconcentrations in the vaginal delivery group compared withthe Cesarean group.18 Although leptin secretion into umbilicalcirculation accounts for only a small percentage of leptinproduced in the placenta,18 this finding supports thepossibility that placental leptin production increases duringlabor.
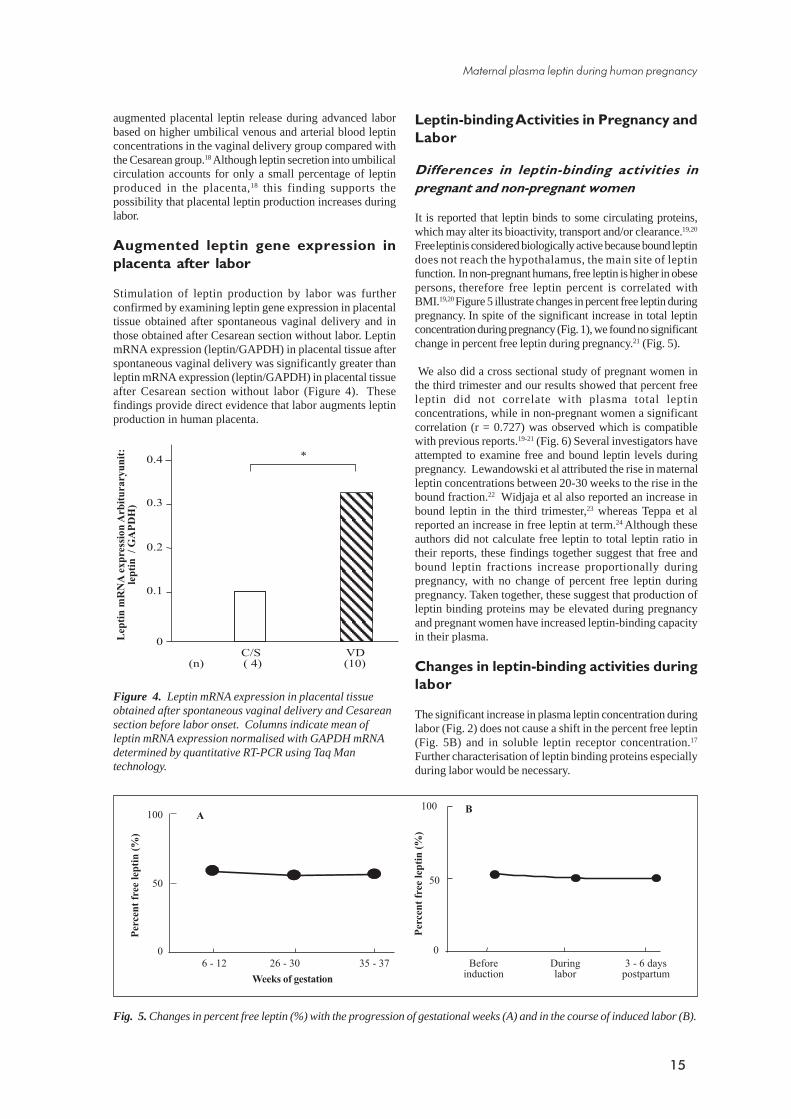
Augmented leptin gene expression in
placenta after labor
Stimulation of leptin production by labor was furtherconfirmed by examining leptin gene expression in placentaltissue obtained after spontaneous vaginal delivery and inthose obtained after Cesarean section without labor. LeptinmRNA expression (leptin/GAPDH) in placental tissue afterspontaneous vaginal delivery was significantly greater thanleptin mRNA expression (leptin/GAPDH) in placental tissueafter Cesarean section without labor (Figure 4). Thesefindings provide direct evidence that labor augments leptinproduction in human placenta.
Leptin-binding Activities in Pregnancy and
Labor
Differences in leptin-binding activities in
pregnant and non-pregnant women
It is reported that leptin binds to some circulating proteins,which may alter its bioactivity, transport and/or clearance.19,20
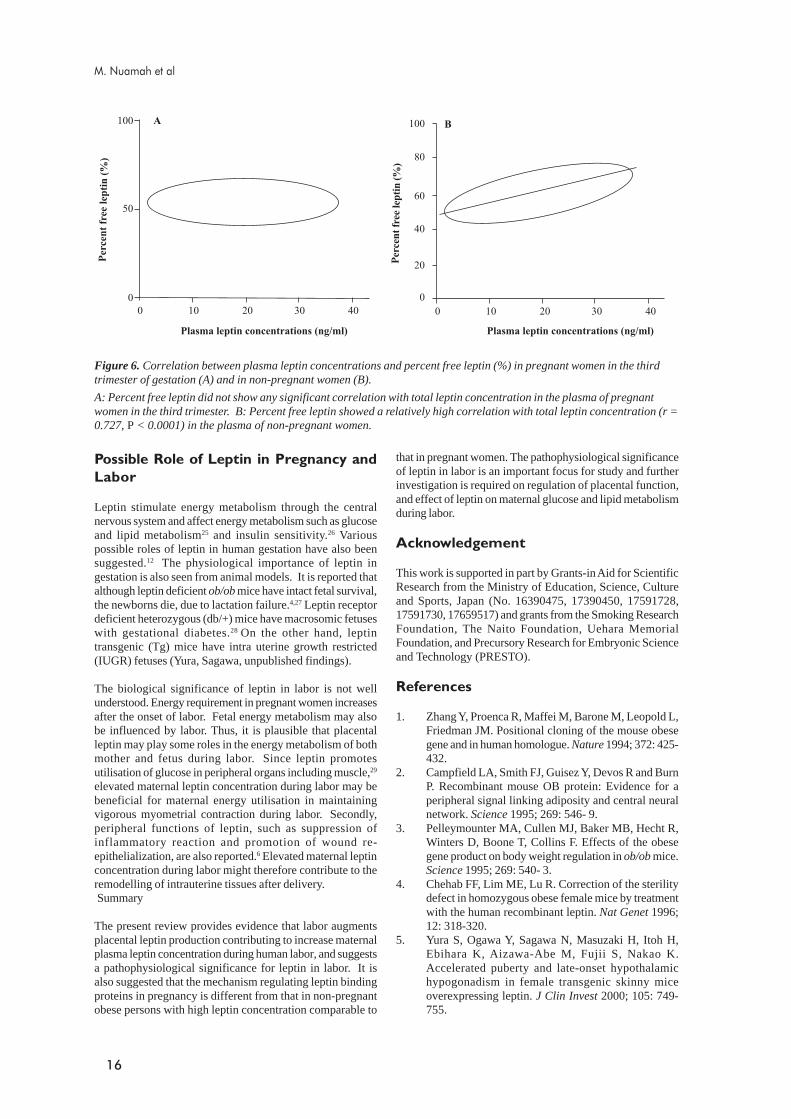
Free leptin is considered biologically active because bound leptindoes not reach the hypothalamus, the main site of leptinfunction. In non-pregnant humans, free leptin is higher in obesepersons, therefore free leptin percent is correlated withBMI.19,20 Figure 5 illustrate changes in percent free leptin duringpregnancy. In spite of the significant increase in total leptinconcentration during pregnancy (Fig. 1), we found no significantchange in percent free leptin during pregnancy.21 (Fig. 5).
We also did a cross sectional study of pregnant women inthe third trimester and our results showed that percent freeleptin did not correlate with plasma total leptinconcentrations, while in non-pregnant women a significantcorrelation (r = 0.727) was observed which is compatiblewith previous reports.19-21 (Fig. 6) Several investigators haveattempted to examine free and bound leptin levels duringpregnancy. Lewandowski et al attributed the rise in maternalleptin concentrations between 20-30 weeks to the rise in thebound fraction.22 Widjaja et al also reported an increase inbound leptin in the third trimester,23 whereas Teppa et alreported an increase in free leptin at term.24 Although theseauthors did not calculate free leptin to total leptin ratio intheir reports, these findings together suggest that free andbound leptin fractions increase proportionally duringpregnancy, with no change of percent free leptin duringpregnancy. Taken together, these suggest that production ofleptin binding proteins may be elevated during pregnancyand pregnant women have increased leptin-binding capacityin their plasma.
Changes in leptin-binding activities during
labor
The significant increase in plasma leptin concentration duringlabor (Fig. 2) does not cause a shift in the percent free leptin(Fig. 5B) and in soluble leptin receptor concentration.17
Further characterisation of leptin binding proteins especiallyduring labor would be necessary.
Figure 4. Leptin mRNA expression in placental tissueobtained after spontaneous vaginal delivery and Cesareansection before labor onset. Columns indicate mean ofleptin mRNA expression normalised with GAPDH mRNAdetermined by quantitative RT-PCR using Taq Mantechnology.
�
�'�
�'�
�'!
����������������� �������������
�������� ��!"#
����������������������������������������������� ��������������� ����������������������������
��'�
Fig. 5. Changes in percent free leptin (%) with the progression of gestational weeks (A) and in the course of induced labor (B).
�
������������������$
#
�
(�
���
��"��� ���"�!� !(�"�!)%��&�� ������ �
���������������
������������������$
#
�
(�
���
!�"�����#�$���$����%
������� ��
'
Maternal plasma leptin during human pregnancy
16
Possible Role of Leptin in Pregnancy and
Labor
Leptin stimulate energy metabolism through the centralnervous system and affect energy metabolism such as glucoseand lipid metabolism25 and insulin sensitivity.26 Variouspossible roles of leptin in human gestation have also beensuggested.12 The physiological importance of leptin ingestation is also seen from animal models. It is reported thatalthough leptin deficient ob/ob mice have intact fetal survival,the newborns die, due to lactation failure.4,27 Leptin receptordeficient heterozygous (db/+) mice have macrosomic fetuseswith gestational diabetes.28 On the other hand, leptintransgenic (Tg) mice have intra uterine growth restricted(IUGR) fetuses (Yura, Sagawa, unpublished findings).
The biological significance of leptin in labor is not wellunderstood. Energy requirement in pregnant women increasesafter the onset of labor. Fetal energy metabolism may alsobe influenced by labor. Thus, it is plausible that placentalleptin may play some roles in the energy metabolism of bothmother and fetus during labor. Since leptin promotesutilisation of glucose in peripheral organs including muscle,29
elevated maternal leptin concentration during labor may bebeneficial for maternal energy utilisation in maintainingvigorous myometrial contraction during labor. Secondly,peripheral functions of leptin, such as suppression ofinflammatory reaction and promotion of wound re-epithelialization, are also reported.6 Elevated maternal leptinconcentration during labor might therefore contribute to theremodelling of intrauterine tissues after delivery. Summary
The present review provides evidence that labor augmentsplacental leptin production contributing to increase maternalplasma leptin concentration during human labor, and suggestsa pathophysiological significance for leptin in labor. It isalso suggested that the mechanism regulating leptin bindingproteins in pregnancy is different from that in non-pregnantobese persons with high leptin concentration comparable to
that in pregnant women. The pathophysiological significanceof leptin in labor is an important focus for study and furtherinvestigation is required on regulation of placental function,and effect of leptin on maternal glucose and lipid metabolismduring labor.
Acknowledgement
This work is supported in part by Grants-in Aid for ScientificResearch from the Ministry of Education, Science, Cultureand Sports, Japan (No. 16390475, 17390450, 17591728,17591730, 17659517) and grants from the Smoking ResearchFoundation, The Naito Foundation, Uehara MemorialFoundation, and Precursory Research for Embryonic Scienceand Technology (PRESTO).
References
1. Zhang Y, Proenca R, Maffei M, Barone M, Leopold L,Friedman JM. Positional cloning of the mouse obesegene and in human homologue. Nature 1994; 372: 425-432.
2. Campfield LA, Smith FJ, Guisez Y, Devos R and BurnP. Recombinant mouse OB protein: Evidence for aperipheral signal linking adiposity and central neuralnetwork. Science 1995; 269: 546- 9.
3. Pelleymounter MA, Cullen MJ, Baker MB, Hecht R,Winters D, Boone T, Collins F. Effects of the obesegene product on body weight regulation in ob/ob mice.Science 1995; 269: 540- 3.
4. Chehab FF, Lim ME, Lu R. Correction of the sterilitydefect in homozygous obese female mice by treatmentwith the human recombinant leptin. Nat Genet 1996;12: 318-320.
5. Yura S, Ogawa Y, Sagawa N, Masuzaki H, Itoh H,Ebihara K, Aizawa-Abe M, Fujii S, Nakao K.Accelerated puberty and late-onset hypothalamichypogonadism in female transgenic skinny miceoverexpressing leptin. J Clin Invest 2000; 105: 749-755.
Figure 6. Correlation between plasma leptin concentrations and percent free leptin (%) in pregnant women in the thirdtrimester of gestation (A) and in non-pregnant women (B).
A: Percent free leptin did not show any significant correlation with total leptin concentration in the plasma of pregnantwomen in the third trimester. B: Percent free leptin showed a relatively high correlation with total leptin concentration (r =0.727, P < 0.0001) in the plasma of non-pregnant women.
'�
������������� ������ ���������#
�
(�
���
� �� �� !� ��
������������� ������ ���������#
������������������$
#
�
��
��
��
��
���
� �� �� !� ��
������������������$#
M. Nuamah et al

17
6. Cui JZ, Hornan D, Potter MJ, Greve MD, Hinz BJ,Samad A, Matsubara JA. The role of leptin in choroidalneovascularization. Am J Ophthalmol 2001; 132: 792-4.
7. Frank S, Stallmeyer B, Kampfer H, Kolb N,Pfeilschifter. Leptin enhances wound re-epithelialization and constitutes a direct function ofleptin in skin repair. J Clin Invest 2000; 106: 501- 9.
8. Sagawa N, Yura S, Itoh H, Kakui K, Takemura M,Nuamah MA, Ogawa Y, Masuzaki H, Nakao K, FujiiS. Possible role of placental leptin in PregnancyEndocrine 2002; 19: 65-71.
9. Masuzaki H, Ogawa Y, Aizawa-Abe M, Nakao K.Transgenic approach toward leptin biology: the clinicalimplications of leptin for the treatment of obesity-associated diabetes and obesity-related hypertension.Endocr J 2002; 49: 109-119.
10. Lage M, Garcia-Mayor RV, Tome MA, Cordido F,Valle-Inclan F, Considine RV, Caro JF, Dieguez C,Casanueva FF. Serum leptin levels in womenthroughout pregnancy and the postpartum period andin women suffering spontaneous abortion. ClinEndocrinol (Oxf) 1999; 50: 211- 16.
11. Anim-Nyame N, Sooranna SR, Steer PJ, Johnson MR.Longitudinal analysis of maternal plasma leptinconcentrations during normal pregnancy and pre-eclampsia. Hum Reprod 2000; 15: 2033- 6.
12. Ashworth CJ, Hoggard N, Thomas L, Mercer JG,Wallace JM, Lea RG Placental leptin. Rev Reprod 2000;5: 18-24.
13. Yoshimitsu N, Douchi T, Kamio M, Nagata Y.Differences in umbilical venous and arterial leptin levelsby mode of delivery. Obstet Gynecol 2000; 96: 342-5.
14. Masuzaki H, Ogawa Y, Sagawa N, Hosoda K,Matsumoto T, Mise H, Nishimura H, Yoshimasa Y,Tanaka I, Mori T, Nakao K. Nonadipose tissueproduction of leptin: leptin as a novel placenta-derived hormone in humans. Nature Med 1997; 3: 1029-1033.
15. Yura S, Sagawa N, Ogawa Y, Masuzaki H, Mise H,Matsumoto T, Ebihara K, Fuji H, Nakao K.Augmentation of leptin synthesis and secretionthrough activation of protein kinase A and C in culturedhuman trophoblastic cells. J Clini Endocrinol Metab1998; 83: 3609-3614.
16. Sagawa N, Yura S, Itoh H, Kakui K, Takemura M,Nuamah MA, Ogawa Y, Masuzaki H, Nakao K, FujiiS. Leptin as a novel placenta-derieved hormone inhumans. Trophoblast Research 1999; 13: 25-34
17. Nuamah MA, Yura S, Sagawa N, Itoh H, Mise H,Korita D, Kakui K, Takemura M, Ogawa Y, Nakao Kand Fujii S. Significant Increase in Maternal PlasmaLeptin Concentration in Induced Delivery: A PossibleContribution of Pro-inflammatory Cytokines to
Placental Leptin Secretion. Endocrine J 2004; 51: 177-187.
18. Linnemann K, Malek A, Sager R, Blum WF, SchneiderH, Fusch C. Leptin production and release in the duallyin vitro perfused human placenta. J Clin EndocrinolMetab 2000; 85: 4298-4301.
19. Houseknecht KL, Mantzoros CS, Kuliawat R, HadroE, Flier JS, Kahn BB. Evidence for leptin binding tothe proteins in serum of rodents and humans:modulation with obesity. Diabetes 1996; 45: 1638-1643.
20. Sinha MK, Opentanova I, Ohannesian JP, KolaczynskiJW, Heiman ML, Hale J, Becker CW, Bowsher RR,Stephens TW, Caro JF. Evidence of free and boundleptin in human circulation. Studies in lean and obesesubjects and during short-term fasting. J Clin Invest1996; 98: 1277-1282.
21. Nuamah MA, Sagawa N, Yura S, Mise H, Itoh H,Ogawa Y, Nakao K and Fujii. S Free-to-total leptinratio in maternal plasma is constant throughout humanpregnancy. Endocrine J 2003; 50: 421-428.
22. Lewandowski K, Horn R, O’Callaghan CJ, Dunlop D,Medley GF, O’Hare P, Brabant G Free leptin, boundleptin, and soluble leptin receptor in normal anddiabetic pregnancies. J Clin Endocrinol Metab 1999;84: 300-306.
23. Widjaja A, Hofmann R, Bruhn J, Muhlen A, BrabantG. Free and bound leptin levels during human pregnancy.Gynecol Endocrinol 2000; 14: 264-269.
24. Teppa RJ, Ness RB, Crombleholme WR, Roberts JM.Free leptin is increased in normal pregnancy and furtherincreased in preeclampsia. Metabolism 2000; 49: 1043-1048.
25. Frederich RC, Hamann A, Anderson S, Lollmann B,Lowell BB, Flier JS Leptin levels reflect body lipidcontent in mice: evidence for diet-induced resistanceto leptin action. Nat Med 1995; 1: 1311-1314.
26. Cohen B, Novick D, Rubinstein M. Modulation ofInsulin Activities by Leptin. Science 1996; 274: 1185-1188.
27. Mounzih K, Qiu J, Ewart-Toland A and Chehab FF.Leptin Is Not Necessary for Gestation and ParturitionBut Regulates Maternal Nutrition via a LeptinResistance State. Endocrinology 1998; 139: 5259-5262.
28. Yamashita H, Shao J, Ishizuka T, Klepcyk PJ,Muhlenkamp P, Qiao L, Hoggard N, Friedman JE.Leptin Administration Prevents SpontaneousGestational Diabetes in Heterozygous Leprdb/+ Mice:Effects on Placental Leptin and Fetal Growth.Endocrinology 2001; 142: 2888-2897
29. Burcelin R, Brunner H, Seydoux J, Thorensa B,Pedrazzini T. Increased insulin concentrations andglucose storage in neuropeptide Y Y1 receptor-deficient mice. Peptides 2001; 22: 421-427.
Maternal plasma leptin during human pregnancy
18
Introduction:
Deep transverse arrest (DTA) is defined as non descendand arrest of fetal head in transvesrse position at transischial diameter “0” station for half to one hour despite ofgood uterine contractions. It is unclear how commonthis problem is, but delivery in this position is not affectedunless the arrest is released. Earlier mid-pelvic operativevaginal delivery were in use to a larger extent and sometimesthis was performed in an operating theatre with full preparationto proceed for caesarean section, achieving fair amount ofsuccess with the use of manual rotation forceps extraction,non-rotational forceps, rotational Kjelland’s forceps andvacuum.1-6 As of current practice patterns majority ofrespondents have abandoned mid cavity vaginal delivery infavor of caesarean in view of both maternal and fetal benefitwith an operative mid cavity vaginal delivery rate of nomore than 15%.
Deep transverse arrest: Cent percent advocacy ofcaesarean yet without morbidity.
Ashma Rana, Archana Amatya, Geeta Gurung, Najindra Maharjan, Yogya R. ShakyaDepartment of Obstetrics and Gynaecology, TU Teaching Hospital Kathmandu Nepal
AbstractsAims: To study morbidity associated with second stage caesarean in deep transverse arrest (DTA) with regards tointervention within or after 2 hours of cervical dilatation.
Method: Retrospective study of deep transverse arrest (DTA) was carried for 5 years counting back from 2006 April, TUTeaching Hospital, Nepal. Process: emergency caesarean (Em.CS) in second stage with cephalic presentation for non-progress/obstructed labor and DTA were collected from labor room delivery record from Dept of Obs/Gyn and medicalrecord section.
Results: DTA (28) with unduly prolonged second stage of labor over 2hours (9) or falling within 2 hours (19) wereanalyzed dropping off 7/35 cases not meeting the criteria of DTA. Majority (23) were nullipara, rest 5 being Para 1-2;all at term pregnancy with few beyond term 27 [37 -40 (19); > 40 -42 weeks (8)] (1) at 43 weeks. Labor had beeninduced in 8; some for pre-labor rupture of the membrane (6), wherein meconium stained liquor was evidenced in 4.Inverted T incision (5) was given over the uterus to facilitate delivery of babies, 3 as reverse breech achieved without anyintraoperative complication. Whereas failed planned VBAC in a post caesarean pregnancy with spontaneous initiationof labor, while extracting an average size (3150gm) baby did cause an extension which during the reparative processinadvertently included a bite on the left ureter resulting in ureterovaginal fistula. The median birth weight was 3250Gms; a single baby that contributed to obstructed labor weighed 2700 gms, having low Apgar at one minute. All babieswere alive at birth, neonates seeking special care for glial haematoma (1) and 2 for RDS. Hospitalization was extendedto 17-22 days in 4 cases, 3 for maternal indication; for chest and wound infections (1) relaparotomy for haemoperitoneumdue to oozes from uterine wound (1) abdominal wound infection and resuture (1)
Conclusions: DTA were encountered rather fewer than feared and were confronted with maternal and neonatalmorbidity although total avoidance of instrumental intervention was advocated with cent percent exercise of caesarean.We conclude that answer to DTA is not just only a caesaren but a careful caesarean.
Key words: Deep transverse Arrest, obstructed labor, Second stage caesarean,
In our institution caesarean section rate has doubled from itsincidence of 9% 10 years ago and caesarean is ideally used todeliver head in transverse arrest, when there is non descendof head in transverse position at “O” station half to onehour, in presence of good uterine contractions. This studyaims to find out overall maternal and neonatal gain withapplication of caesarean section with respect to prolongedsecond stage, taken as 2h for primigravidas.
Material and Method:
Retrospective analysis of all the caesarean in the past 5 yearscounting back from April 2006 for DTA was studied from theDept of Obs/Gyn TU Teaching Hospital, Kathmandu, Nepal.Data source was labour room delivery record book, from whichall the second stage CS for cephalic presentations were collectedand those which had DTA as an indication were further verifiedfrom Medical Record Section and analyzed.
correspondence:Prof. Ashma Rana, Department of Obstetrics and Gynaecology, TU Teaching Hospital Kathmandu Nepal,email: [email protected]
N. J. Obstet. Gynaecol Vol. 1, No. 1, p. 18 - 22 May 2006
O R I G I N A L A R T I C L E S

19
Results:
During this 5 years study period; second stage caesareansection in cephalic presentation for DTA were recorded in 35cases out of which only 28 cases were studied excluding 7cases which did not meet the definition of DTA. Two casesdocumented as DTA were transverse position in first stageof labor with cervical dilatation of 4 and 7 cms respectively.In rest of the 5 cases the operative note indicated occipitoposterior (2), occipito anterior (2) and in one case fetalposition was not mentioned, hence these 7 cases werededucted.
DTA as an obstetric problem was much more magnified thanreal, as it was far less than presumed representing negligible(< 1%) percentage of total caesarean, surprisingly being nilin one of the years.
It occurred mostly in nullipara 23{P0 (21) P
0 +A
1 (2)}; and
P1: 5 {P
1 (3), P
1+A
1 (1) & P
2 (1)}. Mean age of these women
were 25.2 years; and average age ranged from 20-37. Theperiod of gestation ranged from 37-43 weeks, meangestational age being 40 weeks [ 15 (37-40); 12 (>40-42 ); 1(> 42)] (Table 1).
minute Apgar score and weighing 2700gms, all the otherwomen were allowed for vaginal delivery as their pelvis werefound to be adequate at admission. Of the 4 multipara withsingle parity, only one case had a caesarean deliverypreviously (birth weight of 3000 Gms) 10 years back forfetal distress and had been planned for vaginal birth aftercaesarean (VBAC); spontaneous labor at 40 weeks. In thiscase, the first stage of labor progressed very well beinginterrupted by DTA (ROT) and underwent C/Section after 2h and 5 min of second stage with the delivery of 3100 gmsbaby complicated by deep vaginal extension of uterine incisionof 4 cm; leading to uretero-vaginal fistula unfortunately as asequel to left ureteric ligation, which had been inadvertentlycaught during difficult repair (Fig 1).
In all these 28 women labor was spontaneous in 17(augmented 2); induced 10 and not recorded in one. Therewas history of premature rupture of membrane (PROM) in10: [within 12 hours in (9) after 72 hours in another onecase]. Since routine partographic labor management wasstarted from the last 3 years onwards; the partographicassessment was not incorporated in the study visualizinggap of sufficient information over the past preceding 2 years.
Duration of second stage was not known exactly for a casethat was brought from mountainous region with obstructedlabour for 2 days, excluding this; the second stage of labourwas within 2 hours (h) in 18 and beyond 2 h in 9 cases (3 ofthe 9 cases being 3 h and more). Delivery by caesarean wasaccomplished duly within 2 hours in 12: [1h in (7); > 1h but> 2 h in (5 )]; more than 2 h in 15:[ >2 h (6 ), > 2h but < 3 h(6), 3 h in (1) & > 3 hours in (2).] Deep transverse arrest wasquickly managed within one hour (adhering to definition ofarrest as ½hr) in 7 cases even before one could label prolongedsecond stage of labour.
All these were delivered primarily by caesarean without anytrial of instrumental delivery. And in most cases operationwere performed under spinal anesthesia. Abdomen wasopened either vertically or by transverse or Misgav approach.And the uterus was opened by transverse incision in thelower uterine segment with vertical extension making aninverted T in 5 cases, which almost appeared as classicalcaesarean in one case with cephalad extension (fig. 2). Uterineincision expansion was bluntly done in most of the cases.Meconium stained liquor was seen in 5 cases which werefound to be thick in 2 cases. Baby was found to be lying inright occipito transverse (ROT) in 12 and Left occipitotransverse (LOT) in 11 of the 23 cases. In 5 cases of transversearrest, position either ROT/LOT was not mentioned. InvertedT was applied in all 3 cases where the baby was delivered asreverse breech in addition to 2 other cases. Babies weredelivered as cephalic in rest of all the other 23 cases. Therewas no mention of push from below unlike pull from abovein the form of reverse breech extraction as mentioned in the3 cases.
Intraoperative complication was uterine incision extensionin 2 cases, one where inverted T incision was given and in theother where it was not given.
Clinical pelvimetry had been recorded in 14 /23 primigravidasand in a case of second gravida with non recurrent cause forprevious caesarean delivery done for non arrest disorder (fetaldistress) at 36 completed weeks, although our hospital policyis to assess pelvis during antenatal check up routinely. Thisis because many women discontinued the antenatal care visitsat or around this period of gestation, turning up in establishedlabor. In all these cases of pelvic assessment, pelvis wasfound to be adequate except in one case where it had beendocumented as borderline with a note for reassessment to bemade in labor.
Besides one woman chartered from Solukhumbu, one ofthe remote mountainous areas, with obstructed labor andsecond stage documented of 12 h who underwent immediatecaesarean delivery resulting in a live baby with poor one
Factors ≤2h (N=19) >2 hours (n=9)
G* age > 40 weeks 8 4
PROM for 12h 4 2
Induced labor 5 4
MSL 2 2
Baby delivered as 4 1inverted T (⊥) (r** breech 2) (r breech)
Uterine incision 1 1extension at CS (relaparotomy) (UVF)***
Birth weight >3.5 kg 7 3
Table 1. DTA factors
*Gestational, ** Reverse Breech ***Uretero-vaginal fistula,
DTA and morbidity

20
There was prolonged hospitalization for more than theaverage of 3-6 days in 9 cases, 5 cases stayed for 9-14days and 4 cases for 17- 22 longest stays. The over staywas for chest/wound infection (1), relaparotomy (1)resuture for (1), and reason was for baby in neonatal careunit (1)
Next extension was down in the vagina, this important casewas the one, planned for VBAC; was not without significantmorbidity; where ureteric ligation occurred while repairingthe deep vaginal extensions of uterine incision of 4 cms,ureteovaginal fistula being detected when the woman retunedafter being discharged with the history of urinary leakage,substantiated by intravenous urogram (IVU) and cystoscopicexamination on 10th post operative day.
All the babies had good 5 min Apgar. Baby weighed from2700 (1) gms to 4000 gms and the mean and median birthweight was 3300gms & 3250gms respectively weighing 2700-2900 gms ( 2 ); 3100 -3400 ( 16 ); 3600-3900 ( 9 ) and 4000(1). Only few babies acquired neonatal admission,one with glial haematoma and other 2 were admitted forrespiratory distress syndrome (RDS). One baby stayed for22 days because of respiratory distress, this was one bornby caesarean after a spontaneous labor in post datedpregnancy with history of PROM 2½ h and good Apgar(Table 2 b).
There were 3 cases of wound infection but none withburst abdomen, 2 of them required higher antibiotics and
Second stage Low NICU Neonatalduration Apgar Admission stay
in NICU
< 2 h - 3 1 (22days)- MAS*
- RDS**
- Glial
- injury
> 2 h 1
*MAS, meconium aspiration syndrome.**RDS, respiratory distress syndrome.
Table 2 b. Neonatal morbidity
Rana et al
Fig. 1 IVU: left ureteric ligation Fig. 2 Upward extension of inverted T incision
Table 2 a Maternal morbidity
Duration of Post operative Foley’s Catheter Wound Hospital stay2nd stage complications kept for > 1 week Infection > 7 days
< 2 hours Relaparotomy 1 1 6 (17-22 D=3)
> 2 hours UV Fistula 2 resuture (2) 4 (17D=1)
The first extension resembled like a classical caesarean withvertical T (Fig. 2) requiring relaparotomy within 8 hourspostoperatively for hemoperitoneum immediately becauseof oozing from the contractile portion of the upper segment.She was taken to intensive care unit (ICU) and was transfusedwith blood, platelet rich plasma with an extendedhospitalization for 19 days (Table 2 a).
resuture as their wound had grown E. coli and Proteus.Retrospectively neither of them had PROM nor inducedlabor. Labor had started off spontaneously and augmentedfurther which was intervened only within 2 -3 hours bycaesarean when labor was at standstill with pfannenstielincision in one of them. There was thick MSL in both thecases.

21
Discussion
Many obstetricians currently like to play safe obstetricpractice opting rather for a simple procedure like caesareanas compared to challenging obstetrics intervention in face ofDTA where 100% success is not guaranteed.1-6 It is alsobecause, given choices, only few laboring women would agreeto go on trial for instrumental delivery, even though fewfailures (<10% ) have been reported or less morbidities areassociated when instrumental deliveries were performed inthe background of full operative preparedness.5,6 And ourinstitution being a newly established since the last 2 decades,operative vaginal delivery has never been a policy for midcavity obstruction. Kjelland forceps is like a museum pieceand manual rotation forceps extraction is never practiced orpopular. Hence caesarean section was performed invariablyin all mid cavity arrest of labor in DTA.
What took us by surprise are the fetal weight and the pelvicadequacy. Pelvis assessed at the time of labor was found to beadequate and the average weight of the baby was only 3250gms,yet the desired forward rotation was not obliging even in theabsence of dry labor in most of these cases. There was no firststage abnormality, which is usually viewed to precede all thesecond stage dystocia demanding caesarean delivery.7
Surprisingly all the second stage caesarean were operatedunder spinal anesthesia and we personally feel, generalanesthesia would have been better option in cases of DTAunless contraindicated. Also abdominal opening by verticallower midline incision would have been a better alternativethan pfannenstiel incision practiced in most of the cases,including both the complicated cases, one of them with uretericdamage and other one with upper uterine segment extensionsof incision needing reopening for hemoperitoneum.
There are reports of second stage prolongation beyond 4hours giving satisfactory neonatal outcome at vaginal deliveryindicating that the intervention should be based on the rate ofprogress rather than the elapsed time since full cervicaldilatation when maternal and fetal conditions are satisfactory.8
And in our study second stage was extensively prolonged,projected as 12h in 1 of the 28 cases with full blown signs ofobstructed labour. The quick decision for caesarean was madealmost after half an hour from the occurrence of DTA affectingthe birth by or around one hour of full cervical dilatation (7/28; 25%), second stage d” 2h or >2 hours being prevalent in19 and 9 cases respectively.
Fetal transverse positions has been associated withprolonged second stage of labor comparable to occipitoposterior (3.6:3.8 h) ending in vaginal delivery andquiet unclear of the fact whether some of them representedDTA.9 But these cross limit beyond 2 h were adoptedfor second stage dystocia and not for DTA. In our study too,all the 4 babies delivered beyond 3 h, with birth weight of2700, 3000, 3100 and 3600gms had no neonatal problem,although mother acquired wound infection in 2 cases andresuture in one case.
None of the women were managed by epidural analgesia andso this did not affect the second stage in any way.10
There was no marked difference in morbidity betweencaesarean undertaken at and before or after 2 hours of secondstage. In maternal condition, extension of the uterine incisionwere evident in both the groups, but more serious morbiditylike ureteric ligation was evident in one where second stagewas more than 2 hours. All the neonatal complications weremet in caesarean performed before 2h, though one baby hadApgar score of 3/10 at 1 min at birth in case of obstructedlabour. There was no birth asphyxia from caesarean as hasbeen reported.1 The baby fared well there after (table1, 2)Caesarean at full cervical dilatation has always meant fearfrom unintended uterine incision extension and intraoperativetrauma, which occurred in 2 of our cases.10 One of the caseshad previous caesarean for fetal distress and based on thesuccess rate of VBAC for antecedent primary caesarean fornon-arrest disorder, she was allowed to proceed from activestage of spontaneous labour at term until intervention bycaesaren was required because of prolonged second stage of2h and 5 min; where baby extracted as cephalic (not reversebreech) complicated in vaginal extension.11 A favorableoutcome has been foreseen by pullingout the baby as reversebreech and which was applied for the extraction of 3 babiesthat were found to weigh 2700, 3400, 3500 gms respectively.12
but this either could not amend possible complication ofextension of incision, in a nullipara with the baby weighed of3500 gms, nearly producing a classical CS like incision withrelaparatomy and extended hospitalization.
With regards to serious morbidities from urinarycomplications that followed complicated caesarean orcaesarean hysterectomy, 18 cases of obstetric ureterovaginalfistula in to to was retrieved from index medicus, one beingsimilar to our case where the ureter had been included whilerepairing deep cervical tear and was diagnosedpostoperatively like ours.13-14 but in our case, there was nopost partum haemorrhage or excessive bleeding from theuterine incision site that could have attributed uretericligation.
We must emphasize on proper expansion of uterine incisionbecause unintended extension at second stage caesarean hasbeen reported to be up to 35%.15, 16 The next step to rememberis giving of a low vertical uterine incision whenever difficultyin delivering the baby is anticipated.17 This lower verticaluterine incision is also applied if, access to the lower uterinesegment is limited by prematurity, an obstructing lesion, atransverse lie, or if the presenting part is high. Cesareanbreech extraction has been lately applying this lowervertical incision with some trials without promisingoutcome.18
We had a case of primary intraperitoneal hemorrhage frombleeding that occurred mainly from vertical end of the invertedT incison that occupied upper uterine segment. Such anaccount of haemoperitoneum from bleeding uterine incisonhas not been reported except for a bladder flap haematoma asa complication arising at uterine incision site.19,20 The postoperative complications depended on the incison site andclosure technique, closure by single layer has been morebeneficial over the interrupted suture, which we are practicingat our institution. Abdominal wound infection was another
DTA and morbidity

22
morbidity factor which contributed 10% in study, in additionto mal union from uterine incision resulting in post partumhaemorrhage. 19-21
Conclusion
We noted that even caesarean section was not without seriouscomplication in view of ureteric ligation and post operativebleeding from uterine incision extension while dealing withDTA; that perhaps could have been avoided possibly by fullanticipation and proper attention at surgery. The morbidityrelated to duration of caesarean at second stage before orbeyond 2 h being comparable, the former having more ofneonatal and latter more of the maternal morbiditiesrespectively. We conclude by repeating that answer to DTAis not only a caesaren but a careful caesarean.
Reference
1. Jain V, Guleria K, Gopalan S, Narang A. Mode ofdelivery in deep transverse arrest. Int J GynaecolObstet 1993; 43(2):129-35
2. Schiff E, Friedman SA, Zolti M, Avraham A, KayamZ, Mashiach S, Carp H. A matched controlled studyof Kielland’s forceps for transverse arrest of the fetalvertex 2001; 21(6):576
3. Lacreta O. : More on the Kielland forceps. ZentralblGynakol 1986; 108(2):104-11.
4. Herabutya Y, O-Prasertsawat P, Boonrangsimant P.Br J Obstet Gynaecol. Kielland’s forceps or ventouse-a comparison. 1988 May; 95(5):483-7.
5. Bofill JA, Rust OA, Perry KG, Roberts WE, MartinRW, Morrison JC. Operative vaginal delivery: a surveyof fellows of ACOG. Obstet Gynecol. 1996 Dec;88(6):1007-10.
6. Lowe B. Fear of failure: a place for the trial ofinstrumental delivery. Br J Obstet Gynaecol 1987;94(1):60-6
7. Garrett K, Butler A, Cohen WR. Cesarean deliveryduring second-stage labor: characteristics and diagnosticaccuracy. J Matern Fetal Neonatal Med 2005 Jan;7(1):49-53.
8. Janni W, Schiessl B, Peschers U, Huber S, Strobl B,Hantschmann P, Uhlmann N, Dimpfl T, Rammel G,Kainer F. The prognostic impact of a prolonged secondstage of labor on maternal and fetal outcome. ActaObstet Gynecol Scand 2002. Mar; 81(3):214-21
9. Senecal J, Xiong X, Fraser WD; Pushing Early OrPushing Late with Epidural study group. 1: Effect offetal position on second-stage duration and laboroutcome. Obstet Gynecol. 2005 Apr; 105(4):763-72.
10. Paterson CM, Saunders NS, Wadsworth J. Thecharacteristics of the second stage of labour in 25,069singleton deliveries in the North West Thames Health
Region, 1988. Br J Obstet Gynaecol 1992 May;99(5): 377-80.
11. Allen VM, O’Connell CM, Baskett TF. Maternal andperinatal morbidity of caesarean delivery at full cervicaldilatation compared with caesarean delivery in the firststage of labour. BJOG. 2005 Jul; 112(7):986-90
12. Onifade RA, Omigbodun AO. Impact of maximalcervical dilatation at primary caesarean delivery onmode of delivery in the following pregnancy. NigerPostgrad Med J. 2003 Sep; 10(3): 173-6.
13. Fasubaa OB, Ezechi OC, Orji EO, Ogunniyi SO,Akindele ST, Loto OM, Okogbo FO. Delivery of theimpacted head of the fetus at caesarean section afterprolonged obstructed labour: a randomised comparativestudy of two methods. J Obstet Gynaecol 2002 Jul;22(4): 375-8.
14. Onuora VC, al Ariyan R, Koko AH, Abdelwahab AS,al Jawini N.Major injuries to the urinary tract inassociation with childbirth. East Afr Med J. 1997 Aug;74(8):523-6
15. Bazeed M, Nabeeh A, el-Kenawy M, AshamallahA.Urovaginal fistulae: 20 years’ experience. Eur Urol.1995; 27(1):34-8.
16. Yeong CT, Lim TL, Tan KH. Ureteral injuries in anObstetric and Gynaecology Teaching Hospital. Med JMalaysia 1998 Mar; 53(1): 51-8.
15. Rodriguez AI, Porter KB, O’Brien WF. Blunt versussharp expansion of the uterine incision in low-segmenttransverse cesarean section. Am J Obstet Gynecol 1994Oct; 171(4): 1022-5.
16. Hameed N, Ali MA.Maternal blood loss by expansionof uterine incision at caesarean section—a comparisonbetween sharp and blunt techniques. J Ayub Med CollAbbottabad. 2004 Jul-Sep; 16(3):47-50.
17. St George L, Kuah KB. Low vertical uterine incisionin caesarean section. Aust N Z J Obstet Gynaecol1987 Feb; 27(1):10-3.
18. Schutterman EB, Grimes DA.Comparative safety ofthe low transverse versus the low vertical uterineincision for cesarean delivery of breech infants. ObstetGynecol. 1983 May; 61(5): 593-7.
19. Baker ME, Bowie JD, Killam AP. Sonography of post-cesarean-section bladder-flap hematoma. AJR Am JRoentgenol. 1985 Apr; 144(4): 757-9.
20. Hohlagschwandtner M, Chalubinski K, Nather A,Husslein P, Joura EA.Continuous vs interruptedsutures for single-layer closure of uterine incision atcesarean section. Arch Gynecol Obstet. 2003 Apr;268(1):26-8. Epub 2002 May 7.
21. Griffiths J, Demianczuk N, Cordoviz M, Joffe AM.Surgical site infection following elective Caesariansection: a case-control study of post dischargesurveillance. J Obstet Gynaecol Can 2005 Apr;27(4):340-4.
Rana et al

23
Puspha Chaudhary Maternity Hospital, Thapathali, Kathmandu
Why do women come late in labor leadingto accidental – out – of hospital delivery ?
A hospital based study
Introduction
Accidental - out of - hospital deliveries are AOH reported tobe associated with high rates of perinatal morbidity andmortality. Delivery en-route to the hospital when womenenter the active stage of labor so rapidly that results inaccidental - out - of hospital delivery. Such deliveries carrysignificant risk to the mother and the baby as well. Babiesborn before arrival {BBA} rate of an area serves as an indexof the accessibility of perinatal care.1 A survey report byDuvekot et al (1994) showed that there were differences inpostnatal complications like postpartum hemorrhage {16%Vs 4.3%}, retained placenta {21% Vs 1.3%} and puerperalsepsis {18% Vs 3.4%} between accidental - out - of hospitaldeliveries and hospital deliveries. They also reporteddifferences in stillbirth rate {10.5% Vs 2.3%} and neonataldeath rate {4% Vs 2.5%} among A-O-H deliveries and healthcenter deliveries.2
In Kathmandu valley, the health care facilities are relativelywell run and transport facilities are widely available. In spiteof that, unfortunately, reporting late in labor is surprisinglynot uncommon. In fact, many women are so late that theydeliver either in the taxi on the way to the hospital or withinthe hospital premises. Adequate counseling andcommunication during antenatal visits regarding symptomsand signs of the onset of labor help the women decide place
of birth and understand birth preparedness. Unfortunately,only a small proportion of pregnant women have regularantenatal care in Nepal (11%).3
We conducted this study to determine the prevalence ofaccidental - out - of hospital deliveries at Maternity Hospitaland to find out reasons behind this delay in arrival to thehospital.
Methodology
This was a hospital based cross sectional descriptive studyat Maternity Hospital, Kathmandu. Forty-five women whodelivered on the way to the Maternity Hospital during thetime period of 060/09/01 to 060/12/31 were interviewed usinga structured questionnaire. Women referred from other healthfacility or women who developed complications at homebirth and decided to come to the hospital were excluded fromthe study.
The variables recorded were as follow: age, marital status,education of husband and wife, parity, area of residence,socio-economic class, religion, caste and ethnicity, antenatalvisits, counseling during ANC visits regarding signs andsymptoms of labor pain, pre-planning about place of birth,home to hospital distance, availability of transport and onsetof labor to delivery interval.
AbstractObjective: To find out the prevalence of accidental - out - of hospital delivery and determine reasons for delay inarrival to Maternity hospital leading to accidental - out - of hospital delivery.
Methodology: This was a hospital based cross sectional descriptive study conducted at Maternity Hospital, Kathmandu.Women who delivered on the way to the Maternity Hospital during the time period of 060/09/01 to 060/12/31 (4months) were interviewed using a structured questionnaire.
Results: The prevalence of such accidental - out - of hospital deliveries was 45 out of 5703 deliveries i.e. 0.78%.Almost half of them felt that they were unable to understand that labor has already started (48.88%) though most of themhad regular ANC visits at Maternity Hospital (73.33%). Thirteen of them said that there was nobody to accompany themat home (28.88%). Eight of them felt that labor will not happen so soon and ignored symptoms of onset of labor pain(17.77%). Eight of them were late due to delay in getting transport (17.77%), whereas 5 patients were late due todisturbed / diverted traffic (11.11%). In three cases, transport was not available due to Nepal Band and delay was dueto arranging ambulance (6.66%). Decision to go to hospital was delayed by family members in four cases (8.88%).Almost half of patients had more than one reason for delay in arrival (44.44%).
Conclusion: It appears that inadequate counseling during ANC visits about signs and symptoms of labor pain, lack ofpre-planning regarding place of birth, inability to get transport in time and unavailability of family members to accompanythe women when labor pain started were main reasons behind delay in arrival to the hospital leading to accidental - out- of hospital delivery unfortunately.
Key words: accidental - out - of hospital delivery, ANC visits, reason for delay
correspondence:Dr. Pushpa Chaudhary, Postal address: GPO- 8975, EPC- 5110, Kathmandu, Nepal, E-mail : [email protected]
N. J. Obstet. Gynaecol Vol. 1, No. 1, p. 23 - 25 May 2006

24
The reasons behind delay were recorded as direct questioningand recorded in structured questionnaire. Pre testing ofquestionnaire was done for 5 cases of accidental - out of -hospital deliveries at Maternity Hospital. Data analysis wasdone by simple manual descriptive analysis using frequencyand percentage.
Results
The prevalence of accidental – out - of hospital deliverieswas 45 out of 5703 deliveries i.e. 0.78%. There were 8 womenin age group of 19 years or less (17.77 %), 23 women in agegroup of 20-24 years (51.11 %), 11 women in age group of25-30 years (24.44 %) and 3 women in age group of 30years or more (6.66%).
The level of education among patients themselves wasclassified as illiterate - 16 (35.55%), primary level – 15(33.33%), secondary level – 11 (24.44%), higher secondary-3 (6.66%).
Majority of women (n= 37) who had accidental - out - ofhospital delivery were of parity 1 or 2 (82.22%), whereas 2of them were primigravida (4.44%) and 6 of them were ofparity 3 or 4 (13.33%).
There were 27 patients from urban area (60.00%), whereas18 patients belonged to rural area (40.00%). Majority ofwomen (n= 29) belonged to middle class group (64.44%),whereas 16 of them were of lower class group (35.55%).More than half of patients (n =27) were Hindus (60.00%),13 of them were Buddhists (28.88%), whereas 5 of thembelonged to other religion (11.11%).
(17.7%) whereas one of them came all the way from Dhadingdistrict i.e. outside the Kathmandu valley (2.22%).
Majority of women (n=38) came for antenatal visits (84.44%),whereas 6 of them had no antenatal care (13.33%). Majorityof women (n=33) came to maternity hospital for antenatalvisits (73.33%). Three of them had antenatal care at healthpost (6.66%), 2 at other hospital (4.44%) whereas 1 at privateclinic (2.22%).
Discussion
Prevalence of A-O-H was found to be 0.78% in this study.During this study period, there were many strikes and so-called Band not only from Maoists but also from otherpolitical parties and it is probable that many such deliverieswent unreported. Shailesh Core et al (2001) from Mumbai,India reported the incidence of such deliveries to be 0.20 %,4
whereas it was reported to be as high as 5.3% from TygerbergHospital by Bester M F et al (1994).5 Similarly Vanessa ARodie et al (2001) reported the incidence of such deliveriesto be as 0.6%.6 On the other hand, incidence of A-O-H wasfound to be as high as 2% by Sheiner E et al (2002).7
Almost half of these women (n= 22) felt that they wereunable to understand that labor has already started (48.88%).It was surprising to believe as majority of them were multipara(n= 37 i.e. 82.22%). It could be possible that they ignoredsymptoms and signs of labor pain. Duration of labor inmultiparas are shorter compared to primigravida and mightresult in unexpected - out - of hospital delivery. Multiparityis reported to be a risk factor of A-O-H by Sheiner E et al(2002)7, Vanessa A Rodie et al (2001)6, Spillane H et al (1996)8,
Main reason for delay No. of patients %
Unable to understand that labor has started 22 48.88
Nobody at home was available to accompany 13 28.88
Felt that labor will not happen so soon 8 17.77
Decision to go to hospital was delayed by family members 4 8.88
Home delivery was initial plan 1 2.22
Engagement in other work/harvesting 1 2.22
Difficulty in Arranging money 1 2.22
Inability to get transport 8 17.77
Disturbed/diverted traffic 5 11.11
Transport not available due to strike/holiday/nighttime 3 6.66
More than 1 reason 20 44.44
Table 1: Main reasons for accidental - out - of hospital delivery (AOH)
Caste and ethnicity wise distribution of patients showed 9Brahmin (20%), 9 Chhetri (20%), 1 Rai (2.22%), 1 Limbu(2.22%), 7 Lama (15.55%), 9 Newar (20%), and 9 others(20%).
Majority of women (n=22) lived within the ring road ofKathmandu valley (48.8%), 14 of them lived outside the ringroad but within municipality area (31.1%), 8 of them livedoutside the municipality area but within the Kathmandu valley
Bester M F et al (1994).5 Additional inquiry revealed thatthough most of these women came for antenatal visits atMaternity Hospital but they were not counseled well aboutsymptoms and signs of labor pain. These findings suggestthat inadequate counseling made these women unable tounderstand the need to reach Hospital in time.
Another major reason identified was that there was nobodyto accompany them at home when labor pain started and
P. Chaudhary

25
Recommendations
1. Birth preparedness including plan for place of deliveryshould be encouraged during antenatal visits. Clientsshould be clearly explained about symptoms and signsof onset of labor and need for quick arrival to thehospital.
2. Clients should be made aware of A-O-H during antenatalvisits
3. Women and their family should be explained aboutneed for arrangement for transport, ambulancefacility, and arrangement of money in emergencysituation and important telephone numbers duringantenatal visits.
4. Routine history taking should be targeted to find outhistory of precipitate labor and proper arrangementshould be made for these clients.
References
1. Potter P C, Pelteret R, Reynolds L, Motala A, KibelM A. Born before arrival. A study at the new Somersethospital, Cape Town. S Afr Med j. 1984 Sept8;66(10):377-80
2. Duvekot E, Winjen M. A comparison between healthcenter deliveries and deliveries born before arrival inthe Aitape district. P N G Med J. 1994 Sep; 37(3):173-7.
3. Family health division, Ministry of Nepal (1996):Making safe motherhood work in Nepal: programmaticand elements of challenges. JNMA, 1996 vol 34,No118, 119:180-184.
4. Kore S, Rao S, Toke A, Gupta G, Badhwar V R.Delivery on wheels. Journal of Obst &Gyn of India.Issue nov- V R Dec 2001
5. Bester M E, Van Rensburg MJ. Nursing study on theoccurrence of unplanned home births in Tygerberghospital Curationis 1994 Aug; 17(3): 20-3
6. Vanessa A. Rodie, Andrew J. Thomson and Jane E.Norman. Accidental out - of - hospital delivery: Anobstetric and neonatal case control study ActaObstetricia ET Gynecologia Scandinavica Vol 81 issue1 page 50 January 2002
7. Sheiner E, Shoha Vardi I, Hadar A, HershkovitzR, Sheiner EK, Mazor M. Accidental out - of - hospitaldelivery as an independent risk factor forperinatal mortality. J Reprod Med 2002 Aug; 47(8):625-30
8. Spillane H, Khalil G, Turner M. Babies born beforearrival at the Coombe women’s hospital, Dublin. IrMed J 1996 Mar – Apr; 89(2): 59-9
9. Baseline survey report on birth preparedness at Sirahadistrict, Nepal by Save the Children Sept, 2002 p-6-7 (unpublished).
arrival was late because they waited for somebody toaccompany them (n=13 i.e.28.88%). Inability tocommunicate to family members away from home may havecontributed to this situation.
Eight of them felt that labor will not happen so soon andignored symptoms of labor pain (17.77%).These includethose five cases where delivery was very quick suggestive ofprecipitate labor. It is hard to predict precipitate labor duringantenatal period but prior history of undue short labor shouldwarn the clinician about recurrence of problem in subsequentdelivery.
Transport factor was responsible for many A-O-H. Eight ofthem were late due to delay in getting transport (17.77%),whereas 5 patients were late due to disturbed / diverted traffic(11.11%). Three of them said that transport was not availabledue to Nepal Band and delay was due to time taken forarranging ambulance (6.66%). Many of them said thattransport was available easily only during day time (n=27i.e.60%). Delay in getting access to transport at night,particularly on holidays, could contribute to delay in arrivalas reported by Shailesh Core et al (2001)4. Similarly, lack oftransport was reported to be a causative factor of A-O-H byBester M F et al (1994).5
Availability of transport is one of them most important factorinfluencing delay in arrival to the hospital. In Nepal, so-called Band was so common during the study period thattransport was not easily available. Political parties’processions results in diverted traffic causing unnecessarydelay in arrival to the hospital.
Four patients said that decision to go to hospital was delayedby family members (8.88%). Timely decision to go to hospitalmay have avoided the delivery on the way to hospital.Further inquiry revealed that majority of women (n= 28) didnot have any discussion about place of birth during ANCvisits (73.68%). In fact, 14 of them had no discussion even inthe family (36.84%) about place of birth. These findingsagain highlight the fact that birth preparedness was inadequatein these women and birth preparedness was not encouragedduring ANC visits. A survey report on birth preparedness inSiraha district showed that place of birth was planned by63.2% of women.9 Almost half of patients had more thanone reason for delay in arrival (44.44%). As for example; fewwomen waited for somebody to accompany them and couldnot get transport in time when family members were at home.
Conclusion
Women’s economic empowerment is the answer to timelyhealth seeking tendency coupled by improvement in law andorder; a step forward to many setback in our society.
Accidental – out – of hospital delivery?

26
Post Partum Haemorrhage in a Teaching Hospital
Introduction
The International Federation of Gynaecology and Obstetrics(FIGO) and the international confederation of midwives(ICM) have launched a major international initiative in Sept.2003 to prevent post partum hemorrhage (PPH) as well asto propose new ideas in the treatment of PPH, where a jointstatement on the active management of the third stage oflabour was agreed upon by all organizations to prevent PPH.As it has been recognized that blood loss of 1000 ml occursin 1% when active management of third stage of labor isundertaken compared to 3% in expectant management.1-2
Post Partum Haemorrhage (PPH) is one of the major causesof maternal death worldwide with a reported incidence of 5 -18% of all deliveries depending upon the use of prophylacticuterotonic drugs.3-6 And PPH accounts for 25 % of all maternalmortality and could be as high as 55% in underdevelopedcountries.7
Globally when we look at PPH, two third of women withPPH have no identifiable risks factors and in vast majority ofcases (90%) PPH is due to uterine atony brought about bygrandmultiparity, prolonged 2nd stage of labour, precipitatelabour and polyhydramnios. Adaptation of advancedtechnology/techniques from newer researches have helpedus to reduce blood loss equal or more than 500ml whichforms the quantitive definations of PPH. Prostaglandins(carboprost and misoprostol) known to potentiate the action
Pramila Pradhan, Suman Thapamagar, Sushmita Lama Department of Obstetrics and Gynaecology, Nepal Medical College, Attorkhel, Jorpati
Abstract:Objective: To review the incidence, demographic features, morbidity and mortality of post partum hemorrhage.
Study Design: A retrospective study of subjects with post partum hemorrhage managed at Nepal Medical CollegeTeaching Hospital during the period Jan, 2003 – Dec, 2005.
Methods and Materials: The subjects with post partum hemorrhage were identified from hospital records. PPHcases were reviewed and analyzed using SPSS (version 10) software. Outcome measures: morbidity and mortality.
Results: The incidence of PPH was 5.54 cases per 1000 deliveries. The mean age of the study population was 24.6 yrs.Primiparity was at 54.5% while grand multiparity 2.9%. Among ethnic groups, Mongols were 48% and Aryan and others52%. Most of the patients had antenatal checkup 89. 6%. Deliveries were at full term in 83.0% while preterm and postterm were 14.1% and 2.9% respectively. Spontaneous onset of labour was seen in 85.7% with augmentation in 31.4%.Induction of labour was required in 5.7% of cases. Vaginal deliveries were recorded in 88.6% including a breechdelivery and delivery of a set of twin. The mean blood loss was 827.14 ml with maximum up to 2.5L. Traumatic PPH werefound in 54.3%, atonic uterus in 37.1% and retained 23%. Traumatic cases (perineal, vaginal, cervical tear) wererepaired. Uterine atony was managed by uterotonic drugs, uterine massage and uterine packing. Massive PPH incaesarean delivery needed internal iliac artery ligation in one and internal iliac artery ligation with hysterectomy in othercase. Blood transfusion was required 48.6% of PPH. There was a case who was revived from PPH in a case of liverdisease but died of hepatic encephalopathy.
Conclusion: As most of the PPH is unpredictable occurring without warning, one need to carry out appropriatemeasures swiftly, in a stepwise manner without wasting time.
Key words: Post partum hemorrhage, genital trauma, uterine atony, hysterectomy.
of oxytocin do have important role.8-11 Tamponade bymechanical measures like uterine packing with 4 inches gaugeand inflating a Sangstaken- Blakemore tube inside the uterushave been successful in stopping PPH.12 Uterine compressionsutures (B-Lynch Brace or one of the modifications),stepwise devascularisation of uterine blood supply (uterine,branches of ovarian arteries and internal iliac artery ligation)are other techniques. With internal iliac artery ligation,extensive collateral circulation is established in pelvis andwith such a procedure hysterectomy can be avoided in 50%.7
Such emergency hysterectomies (subtotal or total) that couldbe appropriately performed to arrest hemorrhage 25% cases.Angiographic arterial embolisation is also helpful in manyinstances.
Methods and Materials
This is a retrospective study of postpartum hemorrhagemanaged at Nepal Medical College Teaching Hospital duringthe period of three years (Jan, 2003 – Dec, 2005). Thecenter is fully equipped with emergency operation facilitywhich includes round the clock anesthetists, operation theatrefacilities. A full laboratory with blood transfusion facilities isavailable at all the time. Information on the total number ofmaternities (live and stillborn) was obtained from the obstetricward, operation theatre and intensive care unit records. Thecases who had blood loss 500 ml or more during vaginaldelivery and 1000ml or more during Lower segment caesareansection (LSCS) were identified and a detailed review of their
corresspondence:Pramila Pradhan, Prof. & Head of Department, Nepal Medical College, Attorkhel, Jorpati,Email: [email protected]
N. J. Obstet. Gynaecol Vol. 1, No. 1, p. 26 - 29 May 2006
27
medical record was carried out using a standard format. Datawere recorded regarding patients’ age, race, parity, gestationalage, antenatal care, identifiable risk factors, and mode ofdelivery, amount of blood loss, attributable causes of PPH,resuscitation and treatment methods of PPH.
The obstetric service providers team; consisted of staff nurses,house officers, middle grade obstetricians (registrars, lecturers,assistant professors) and the senior consultants (Professorsand Associate professors). The team also included interndoctors who acquire training under the supervision of seniors.Normal deliveries are conducted by house officers or interndoctors under direct supervision. Instrumental/operativedeliveries are conducted by middle grade obstetricians and/orsenior consultants. All complications are immediatelyattended and managed by the middle grade obstetrician andsenior consultants.
The main outcome measures used for the analysis wereamount of blood loss, causes of PPH, treatment methods,associated morbidities and mortality. The data collected wereanalyzed using data analysis computer software SPSS(version 10).
Results
In our study, we identified 35 cases of primary post partumhemorrhage among 2106 deliveries during the study periodof 3 years which gives the incidence of PPH to be 5.54 casesper 1000 deliveries. The mean age of study populationwas 24.66 yrs (SD 4.51 yrs) with the range of 17 – 39 yrs(Table 1). Nineteen cases (54.5%) were primipara whileonly one case was grand multipara. Thirty one cases (89.6%)had antenatal checkup while four cases (11.4%) neverattended antenatal clinic.Twenty nine cases (83.0%) were full term deliveries while
28
6
1
0
5
10
15
20
25
30
ml
500 - 1000 1100 - 2000 2100 +
PPH - Blood loss
Figure 1: Amount of Blood loss
(Table 2), ten cases (37%) had cervical tear, 6 cases of PPHhad retained placenta (Table 3).
The traumatic cases were dealt by repairing of the tear ofgenital tract. Most of the atonic causes responded toconventional method of uterotonic drugs (oxytocin andergometrine) and uterine massage and/or bimanualcompression of uterus.
In 2 cases of caesarean delivery internal iliac artery ligationalone or in combination with hysterectomy was needed inorder to control the bleeding. Retained placenta were removedmanually under anaesthesia in 5 cases (Table 4 ).
Blood transfusion was required in 23 (48.6%) cases. Meanblood volume transfused was 2.42 pints (SD 1.12) of wholeblood. One case required 5 pints of whole blood transfusion.
There was one maternal death (2.9%) which was aconsequence to hepatic encephalopathy and PPH.
Vaginal Instrumental Caesarean Section Total
ND Abn vag del Forceps Vacuum Emerg. Elect.
29 2 1 (2.9%) 1 (2.9%) 1 (2.9%) 1 (2.9%) 35 (100%)
Twin (1)* Prolonged Previous cs,
Breech (1)† second stage now CPD
Table 1. Mode of delivery
preterm and post term were 14.1% and 2.9% respectively(Table 1). Nineteen (85.7%) cases of PPH had spontaneousonset of labour and 31.4% of the cases had augmentation oflabour due to slow progress. Two were cases of inducedlabour. Four cases were brought after delivery at home.Majority had vaginal delivery (88%) including one breechdelivery and a set of twin delivery. PPH occurred in 2 casesof instrumental and 2 cases of cesarean deliveries. The meanblood loss was 827.14 ml (SD 458.79) with the range of 500– 2500 ml. One case of Emergency LSCS had blood loss of2.5 L. (Fig 1 ).
Genital tract trauma was found in 28 (54.3%) cases, whereasatony of the uterus was the main cause in 12 (37.1%) andretained placenta or bits of placenta was found in nine (23%)cases of PPH. Most of the cases had more than one causes
Discussion
The incidence of PPH in this study is 5.54 cases per 1000deliveries, which is similar to other studies 2-4 The Mongolrace ( lama, Sherpa, Rai, Magar, Gurung, Tamang) are thecommon inhabitants around this institution and had highpercent of PPH. Further study in this group would beinteresting.
This agreeable incidence is so, because of the routine practiceof active management of 3 rd stage of labour in our hospital.It’s also because of anticipation of PPH and quick action linetaken as in cases of induction of labour, prolonged secondstage, advanced maternal age, grand multiparity, operativedeliveries etc. Counseling women with high risk for PPH(previous history of PPH or retained placenta and third stage
NB: twin – (1) *); † Breech delivery (1) were among the 4 home delivery
PPH in a Teaching Hospital
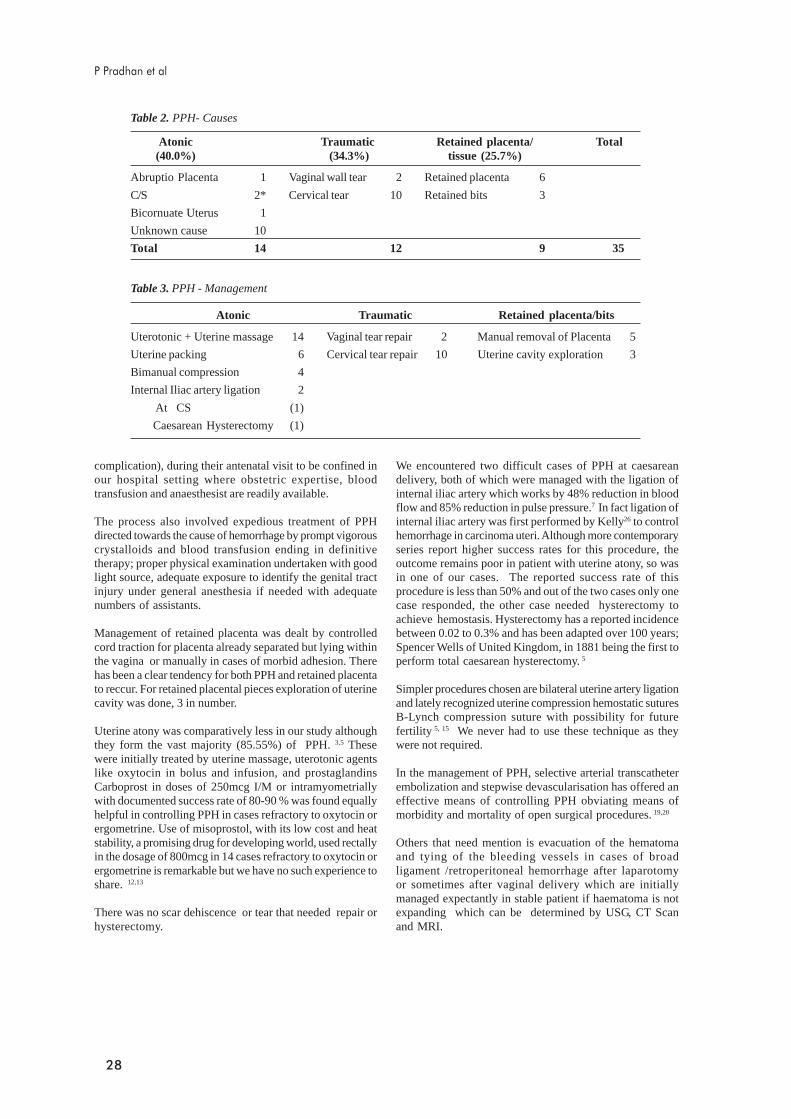
28
complication), during their antenatal visit to be confined inour hospital setting where obstetric expertise, bloodtransfusion and anaesthesist are readily available.
The process also involved expedious treatment of PPHdirected towards the cause of hemorrhage by prompt vigorouscrystalloids and blood transfusion ending in definitivetherapy; proper physical examination undertaken with goodlight source, adequate exposure to identify the genital tractinjury under general anesthesia if needed with adequatenumbers of assistants.
Management of retained placenta was dealt by controlledcord traction for placenta already separated but lying withinthe vagina or manually in cases of morbid adhesion. Therehas been a clear tendency for both PPH and retained placentato reccur. For retained placental pieces exploration of uterinecavity was done, 3 in number.
Uterine atony was comparatively less in our study althoughthey form the vast majority (85.55%) of PPH. 3,5 Thesewere initially treated by uterine massage, uterotonic agentslike oxytocin in bolus and infusion, and prostaglandinsCarboprost in doses of 250mcg I/M or intramyometriallywith documented success rate of 80-90 % was found equallyhelpful in controlling PPH in cases refractory to oxytocin orergometrine. Use of misoprostol, with its low cost and heatstability, a promising drug for developing world, used rectallyin the dosage of 800mcg in 14 cases refractory to oxytocin orergometrine is remarkable but we have no such experience toshare. 12,13
There was no scar dehiscence or tear that needed repair orhysterectomy.
We encountered two difficult cases of PPH at caesareandelivery, both of which were managed with the ligation ofinternal iliac artery which works by 48% reduction in bloodflow and 85% reduction in pulse pressure.7 In fact ligation ofinternal iliac artery was first performed by Kelly26 to controlhemorrhage in carcinoma uteri. Although more contemporaryseries report higher success rates for this procedure, theoutcome remains poor in patient with uterine atony, so wasin one of our cases. The reported success rate of thisprocedure is less than 50% and out of the two cases only onecase responded, the other case needed hysterectomy toachieve hemostasis. Hysterectomy has a reported incidencebetween 0.02 to 0.3% and has been adapted over 100 years;Spencer Wells of United Kingdom, in 1881 being the first toperform total caesarean hysterectomy. 5
Simpler procedures chosen are bilateral uterine artery ligationand lately recognized uterine compression hemostatic suturesB-Lynch compression suture with possibility for futurefertility 5, 15 We never had to use these technique as theywere not required.
In the management of PPH, selective arterial transcatheterembolization and stepwise devascularisation has offered aneffective means of controlling PPH obviating means ofmorbidity and mortality of open surgical procedures. 19,20
Others that need mention is evacuation of the hematomaand tying of the bleeding vessels in cases of broadligament /retroperitoneal hemorrhage after laparotomyor sometimes after vaginal delivery which are initiallymanaged expectantly in stable patient if haematoma is notexpanding which can be determined by USG, CT Scanand MRI.
Atonic Traumatic Retained placenta/bits
Uterotonic + Uterine massage 14 Vaginal tear repair 2 Manual removal of Placenta 5
Uterine packing 6 Cervical tear repair 10 Uterine cavity exploration 3
Bimanual compression 4
Internal Iliac artery ligation 2
At CS (1)
Caesarean Hysterectomy (1)
Atonic Traumatic Retained placenta/ Total(40.0%) (34.3%) tissue (25.7%)
Abruptio Placenta 1 Vaginal wall tear 2 Retained placenta 6
C/S 2* Cervical tear 10 Retained bits 3
Bicornuate Uterus 1
Unknown cause 10
Total 14 12 9 35
Table 2. PPH- Causes
Table 3. PPH - Management
P Pradhan et al

29
Overall the women who suffered PPH improved dramaticallywith unfortunate death of a woman who died because of acomplication of hepatic encephalopathy.
Conclusion
As PPH is unpredictable mostly occurring without warning,one need to carry out appropriate measures swiftly, in astepwise manner to control obstetric hemorrhage withoutwasting time, aiming first for a conservative approach beforeemergency obstetric hysterectomy, a potentially life-savingprocedure is considered at unavoidable catastrophe; leavingthe type of surgical approaches best to obstetrician’sexperience.
References:
1. Prediv0lleWJ, ElbourneD,McdonaldS et al. Activemanagement of 3rd stage of labour versus expectant
2. RogersJ,WoodJ,McCandlishRet al. Active vsexpectant management of 3rd stage of labour; Hinchinabrooke randomized controlled trial. Lancet1998;351:693-99 management. Cochrane Database systemrevision 2000; 2i CDooooo7.
3. Gilbert L, Porter W, Brown VA Post partumhaemorrhage : a continuing problem Br J obstetgynaecol 1987; 94 : 67-71
4. N singh,V singh. Methylergometrine and carboprosttromethamine prophylaxis for post partumhaemorrhage. J Obstet gynaecol India 2005 ; 55: 4:325-32
5. CunninghamFG,GrantNF, Levenok J et al.(edn)William’s Obstetric 21st ed. USA,MCgrawhill.2001;619-70
6. Pritchard JA,Baldwin RM, Dickey JC, Wiggins KM.Blood volume changes in pregnancy and thepuerperium. Red blood cell loss and changes inapparent blood volume during and following vaginaldelivery, Caesarean section and total hysterectomy.Am J Obstet gynaecol 1962 ; 84: 1271
7. Drife J. Management of primary post partumhaemorrahge. Br J obstet gynaecol 1997 ; 104: 275-77
8. O’BrianP,El-Refach-GordonA et al.Rectallyadministered misoprostal for the treatment of PPHunresponsive to oxytocin and ergometrine: adescriptive study. Obstet Gynaecol 1998;92(2):212-14
9. LokugamageAV,SullivanKR,NikuLI et al. A randomizedstudy comparing rectally administered misoprostolvs syntrometrine infusion for the cessation ofprimary PPH. Acta Obstet Gynaecol Scand2001;80(9):835-39
10. Hoj A, Cardoso P, Nielson BB. Effect of sublingualmisoprostol on severe post partum haemorrhage in aprimary health centre in guinea-Bissau: randomizeddouble blind clinical trial. Br Med J 2005; 331
11. Hofmegr GJ, Walravan G, Gulmezoglu et at:Misoprostol to treat post partum haemorrhage: asystemic review, BJ OG 2005; 112: 547-53.
12. MaierRC. Control of post partum haemorrhage withuterine packing. Am J Obstet Gynaecol1993;169:317-21: Discussion 321-23
13. Kaunitz AM, Hughes JM, Grimes DA et al. Causes ofmaternal mortality in the United States. ObstetGynaecol 1985; 65 : 605-12
14. MukhopadhayP,NaskarT,HazreS, Bhattacharya D.Emergency internal iliac artery ligation - Still a lifesaving procedure. Jr obstet gynaecol India2005;55:2:144-45.
15. Mukherjee P,DacC, MukherjeeG et al. Emergencyinternal iliac artery ligation in obstetrical andGynaecological haemorrhag .Jr obstet Gynaecol India2002; 52:147- 49
16. Agarwal V. Kriplani A. Post partum haemorrhage(flow chart) Asian J obstet Gynaecol practice 2002;6:49
17. Deux JF, Bazot M. Le Blanche AF et al. Is selectiveembolization of uterine arteries a safe alternative tohysterectomy in patients with post partumhaemorrhage AJR 2001; 177: 145-149.
18. B-lynchC,Cokar A, Lawal AH, Abu J, Cowen MJ.The B-Lynch surgical technique for the control ofmassive post partum haemorrhage. An alternative tohysterectomy? five cases reported . Br J obstetgynaecol 1997; 104:372-75
19. Pal M, Biswas AK, Bhattacharya SM.B-Lynch Bracesuturing in primary post partum haemorrhage duringcasaerean section. Jr obstet Gynaecol research 2003;29:5:317-19
20. In Bonnar J(ed) Recent advances in obstetrics andgynaecology Vol.20 London. Churchil Livingstone1998; 141-152.
21. Badawy SZA, Etman A,Singh M,Murphy K,MayelliT,Philadelphia M Uterine artery embolization.The rolein obstetric and gynaecology.J clin Imaging.2001;25:288-95.
PPH in a Teaching Hospital

30
Introduction
The uterine rupture is one of the dreaded catastrophes inobstetric practices. In developing country like Nepal 85 to92 % deliveries take place at home. Ignorance, poverty, lackof education and lack of health service-facilities lead toobstetrical complications leading to the maternal morbidityand mortality in child-bearing age of the women in developingcountries.
This study was aimed to compare the scenarios of the casesof the rupture of the pregnant uterus (RU) at an interval ofseven and half years in the same hospital. Cases of RUadmitted in the busiest maternity hospital of Kathmanduwhere every year 16000 deliveries occur with Caesareansection rate of 11% were studied.
Materials and methods
Information about the cases of RU after 28 weeks ofpregnancy were collected from the admission charts of theMaternity Hospital. Sixty-five cases were in group A andthe study period was for 8 ½ years (1985 mid April- 1993November), which were published in the Journal of Instituteof Medicine (IOM) in 1993.3 Sixty-seven cases in group Bwere admitted during the period of 4 years (2002 mid April-2005 mid April).
Changing scenario of cases of uterine rupture
Saraswati M. PadhyeDepartment of Obstetrics & Gynaecology,
Kathmandu Medical College Teaching Hospital,Kathmandu, Nepal
AbstractAim: To compare the scenarios of ruptured uterus admitted in one of the busiest Maternity Hospital, Kathmandu Nepalwith delivery rate of 16000 births/year; during 2 different periods; 1985 mid April - 1993 November (8 ½ years) groupA & 2002 -2005 mid April (4 years) group) Grp B
Method: One hundred and thirty two cases of the ruptured uterus (RU) after 28 weeks of pregnancy were included inthe study. A comparative study of 65 cases (Group A) and 67 cases (Group B) was undertaken for the study by analyzingthe case records of the hospital. The incidence of ruptured uterus cases referred from outside the valley, antenatal care(ANC) clinic attendance, age, parity, etiology and pathology of rupture, mode of surgical treatment, maternal mortalityand fetal outcome were analyzed.
Results: The incidence of RU in A and B was 1:1536 and 1:984 respectively. 5 cases were referred from outside thevalley health care centres in group B. Antenatal attendance was increased in group B. Ages of the patients were inbetween 25-34yrs in both the groups. Para 4 in group A and para 1 & 2 in group B were present. Spontaneous rupturewas almost one & half times more in group B, scar rupture was doubled in group B and iatrogenic (Traumatic) rupturewas same in both groups. Mainly lower segment was involved in both groups. Laparotomy, repair & bilateral tuballigation were main surgical treatment provided to both the groups. Maternal deaths due to RU ware 11(17%)in group A& only one (0.1.5%) in group B. Perinatal mortality was 90% in group A & 83% in group B.
Conclusion: More standard ANC care and parturition by trained health worker will help to reduce RU cases.
Key words: antenatal care, maternal death, perinatal mortality, ruptured uterus, trained health worker
Result
The total number of cases of RU were 132 [ groupA (65 ) +group B (67)]. There were no referred cases from outsideValley in group A, but in group B, 5 cases were referred fromvery far off district hospital / health posts.
There were a total of hundred thousands (100,000) live birth(LB) deliveries during the study period of group A. Caesareansection (CS) rate was 7%, maternal mortality in the studyperiod was 117 (0.12%) with an incidence of RU to be 1:1538(0.065%) (Table 1.).
In group B, there were 65921 LB, CS rate of 11%, maternalmortality 31(0.045%) with the incidence of RU 1: 984(0.1%). In both groups the maximum number of women was25 to 34 years old. It was 58% (No.38/65) in group A and 46% (No.31/67) in group B. In group A, 28% (No.18/65) werePara 3, whereas in group B 25% were para 1 and 2 (17/67each). ANC attendance was 23% (No 15/65) in group A andwas 39% (No.26/67) in group B. Spontaneous rupture was65% (No.42/65) in group A. It was 0.042% in relation to theLB of that period. In group B, it was 63% (No.42/67) and0.064% in relation to the LB which was about 1.5 timeshigher than group A. The scar rupture was 22% (No.14/65)in group A which was 0.014% in relation to the LB, whereasit was 28% (No.19/67) in group B. Also it was 0.029% in
Correspondence :Prof. Saraswati M. Padhye, Department of Obstetrics & Gynaecology, Kathmandu Medical College Teaching Hospital,Sinamangal, Kathmandu, E-mail:- [email protected]
N. J. Obstet. Gynaecol Vol. 1, No. 1, p. 30 - 33 May 2006

31
relation to the LB, which was double than in group A.Similarly, the traumatic (Iatrogenic) rupture remained stablein studies, i.e.14% (No.9/65) in group A and 9%, (6/67) ingroup B corresponding to 0.009% in relation to the LB inboth groups (Table 2-4).
The perinatal mortality in the study period was 4.8% ingroup A and 3.3% in group B in the hospital. There wasperinatal mortality of 91% in group A and it was 88% ingroup B in cases of RU. Fetal abnormality likeHydrocephalus which was the cause of the RU due toobstructed labour11 was in 11% in group A (No. 7) and it was4.5% (No. 3) in group B in RU cases. However, the incidenceof hydrocephalus seems to be reduced in group B which maybe due to early diagnosis of such abnormality by earlydetection with Ultrasonography.
Discussion
The incidence of RU has been increased during the studyperiod of group B (1:984 live births) compared to studyperiod of group A (1: 1538 live births). This may be due toincreased awareness among the people in the later years,which brought them to the hospital, though late. The otherreason could be the improvement in transport facility in thelater years, which helped them to reach the higher centers.1
Moreover the health personnel who provide service at theperiphery must have got training regarding the referralmechanism, so they could refer the patient in time to thetertiary centers with a referral letter. This is seen in thisstudy as in group B there were 5 cases referred from outsidewhile no cases had been referred during the study periodgroup A. Schrinsky (1978) in his review article had found the
Group A B
No. of cases 65 67
Period of study 8.5 yrs 4 yrs(1985 mid April to Nov. 1993) (2002 mid April to 2005 mid April)
Place of study Maternity Hospital, Kathmandu Maternity Hospital, Kathmandu
Referred case 0 5
Incidence of uterine rupture 1:1538 (0.065%) 1:984 (0.1%)
Total no. of live birth(LB) 1000,00 65921
Caesarean section rate 7% 11%
Maternal mortality rate 117 (0.12%) 31 (0.045%)
Maternal mortality rate due to RU 11 (0.011%) 1 (0.0015%)
Age of maximum number of patients 25-34 years (58%) 25-34 years (46%)
Parity (number of patients) 3 (28%) 1 & 2 (25%)
Grand multipara 16 (25%) 15 (22%)
ANC attendance 23% 39%
Group A B
Spontaneous rupture 42 (65%) (0.042%)* 42(63%) (0.064)*
Scar rupture 14 (22%) (0.014%)* 19 (28%) (0.029%)*
Traumatic (Iatrogenic) 9 (14%) (0.009%)* 6 (9%) (0.009%)*
Aetiology
* In relation to LB
Group Lower segment (LS) Upper segment (US) US+LS. Others Total.
A 43(66%) 12(18.5%) 10(15.4%) 0 65
B 34(51%) 3(4.5%) 27(40%) 3(4.5%)* 67
Table 1. Ruptured uterus in two setting influenced by various factors
Table 2. On set of rupture-uterus in relation to livebirth (LB)
Table 4. Types of uterine rupture
Table 3. Sites of rupture (Pathology)
Group Complete rupture Incomplete rupture Unknown Total
A 45(69%) 19(29%) 1(1.5) 65
B 50(75%) 14(21%) 3(4.5%) 67
*Site not mentioned in 3, one had inverted T.
Changing scenario in uterine rupture
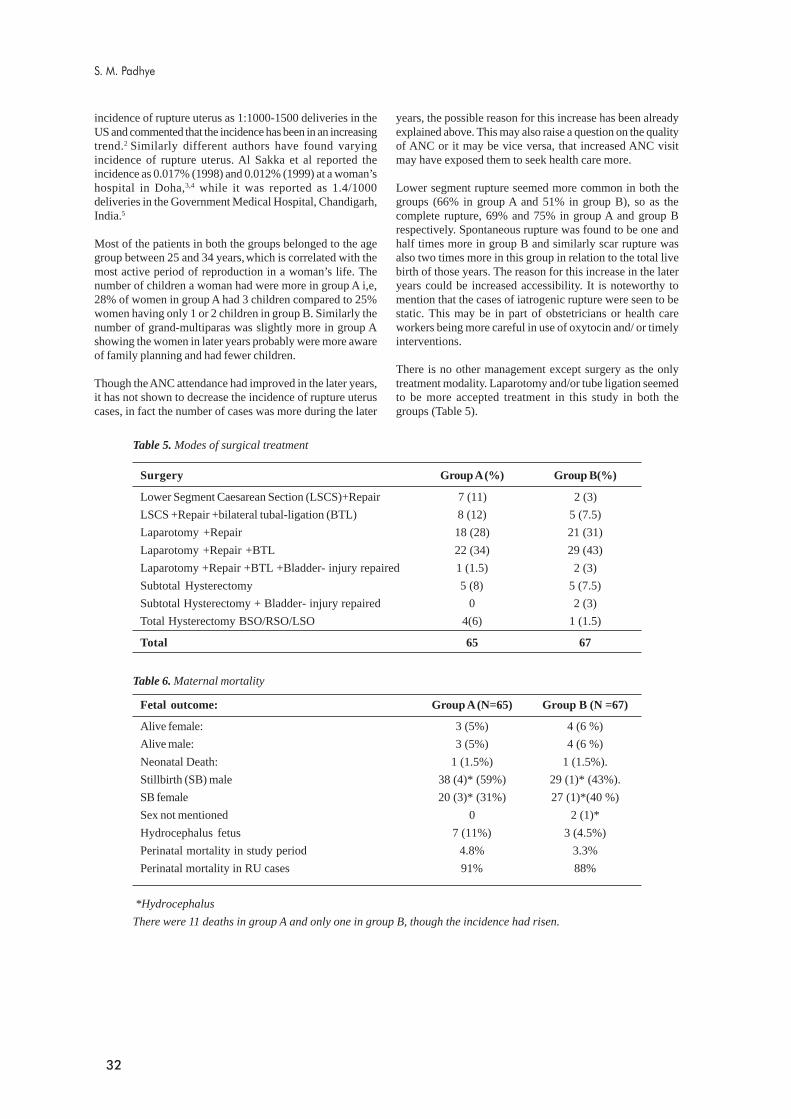
32
incidence of rupture uterus as 1:1000-1500 deliveries in theUS and commented that the incidence has been in an increasingtrend.2 Similarly different authors have found varyingincidence of rupture uterus. Al Sakka et al reported theincidence as 0.017% (1998) and 0.012% (1999) at a woman’shospital in Doha,3,4 while it was reported as 1.4/1000deliveries in the Government Medical Hospital, Chandigarh,India.5
Most of the patients in both the groups belonged to the agegroup between 25 and 34 years, which is correlated with themost active period of reproduction in a woman’s life. Thenumber of children a woman had were more in group A i,e,28% of women in group A had 3 children compared to 25%women having only 1 or 2 children in group B. Similarly thenumber of grand-multiparas was slightly more in group Ashowing the women in later years probably were more awareof family planning and had fewer children.
Though the ANC attendance had improved in the later years,it has not shown to decrease the incidence of rupture uteruscases, in fact the number of cases was more during the later
years, the possible reason for this increase has been alreadyexplained above. This may also raise a question on the qualityof ANC or it may be vice versa, that increased ANC visitmay have exposed them to seek health care more.
Lower segment rupture seemed more common in both thegroups (66% in group A and 51% in group B), so as thecomplete rupture, 69% and 75% in group A and group Brespectively. Spontaneous rupture was found to be one andhalf times more in group B and similarly scar rupture wasalso two times more in this group in relation to the total livebirth of those years. The reason for this increase in the lateryears could be increased accessibility. It is noteworthy tomention that the cases of iatrogenic rupture were seen to bestatic. This may be in part of obstetricians or health careworkers being more careful in use of oxytocin and/ or timelyinterventions.
There is no other management except surgery as the onlytreatment modality. Laparotomy and/or tube ligation seemedto be more accepted treatment in this study in both thegroups (Table 5).
S. M. Padhye
Surgery Group A (%) Group B(%)
Lower Segment Caesarean Section (LSCS)+Repair 7 (11) 2 (3)
LSCS +Repair +bilateral tubal-ligation (BTL) 8 (12) 5 (7.5)
Laparotomy +Repair 18 (28) 21 (31)
Laparotomy +Repair +BTL 22 (34) 29 (43)
Laparotomy +Repair +BTL +Bladder- injury repaired 1 (1.5) 2 (3)
Subtotal Hysterectomy 5 (8) 5 (7.5)
Subtotal Hysterectomy + Bladder- injury repaired 0 2 (3)
Total Hysterectomy BSO/RSO/LSO 4(6) 1 (1.5)
Total 65 67
*Hydrocephalus
There were 11 deaths in group A and only one in group B, though the incidence had risen.
Table 5. Modes of surgical treatment
Table 6. Maternal mortality
Fetal outcome: Group A (N=65) Group B (N =67)
Alive female: 3 (5%) 4 (6 %)
Alive male: 3 (5%) 4 (6 %)
Neonatal Death: 1 (1.5%) 1 (1.5%).
Stillbirth (SB) male 38 (4)* (59%) 29 (1)* (43%).
SB female 20 (3)* (31%) 27 (1)*(40 %)
Sex not mentioned 0 2 (1)*
Hydrocephalus fetus 7 (11%) 3 (4.5%)
Perinatal mortality in study period 4.8% 3.3%
Perinatal mortality in RU cases 91% 88%

33
Maternal mortality due to RU had reduced markedly in thespan of years reflecting the improvement in the standard ofmanagement in the Maternity Hospital (Table 6). Doctorswere more able to think and suspect about the case of ruptureuterus and could diagnose it immediately. The governmenton their part had helped in purchasing more sophisticatedanesthetic and other necessary equipments.
Although perinatal mortality had reduced from 91% in groupA to 88% in group B, the mortality is very high as expectedin such cases. The number of hydrocephalus cases hadbeen found to be reduced in the later period, which could bedue to routine use of ultrasound, at least in the urban areas,detecting the abnormality earlier leading to termination ofpregnancy.
Conclusion
More standard antenatal care and care during labor/deliveryby trained health worker will help to reduce ruptured uterus.
Recommendation
We have to continue our efforts to reach the goal set by theHis Majesty’s Government to reduce the maternal mortalityby providing the service to the hospitals of periphery bydeputing trained birth attendants for the delivery.
Acknowledgement
I am grateful to the Director and Mrs. Shanti Baidya, themedical recordist of Maternity Hospital, Prof. Kanti Giriand Mr. Ranjit Singh Thapa (KMC) for their help to preparethispaper.
References
1. Padhye SM, Rupture of the Pregnant Uterus – A 20Years Review. Original article, Kathmandu UniversityMedical Journal (2005) Vol 3, No. 3, Issue 11, 234 –238
2. D. C. Schrinsky, R. C. Benson, a review. Journal ObstetGynecol suv, 1978 Apr;33(4):2 17-32
3. Al Sakka M, A. hansho and L. Khan, Rupture of thepregnant uterus – a 21 year review: Internation Journalof Gynaecology & Obstetrics Volume 63, Issue 2, 1November 1998, page 105-108.
4. Al Sakka M, Danleh W, Al Hassani S:Case series of uterine rupture ansd subsequentpregnancy outcome, Int J Fertil Womens Med. 1999Nov-Dec; 44(6): 297-300
5. Kumari I, Goel P, Sehgal A, Devi K: Rupture of GravidUterus: Experience at an Urban Medical Centre in Northern India,J Obst Gynecol Ind Vol. 53, No. 6 : Nov/Dec 2003 pg 558-562
Changing scenario in uterine rupture

34
Emergency obstetric hysterectomy: Experience atBP Koirala Institute of Health Sciences
The aim of the present study was to analyze the prevalence,indications, contributory factors and outcomes of Emergencyobstetric hysterectomy in a tertiary care centre (BP KoiralaInstitute of Health Sciences, Dharan)
Materials and methods
A retrospective analysis of the entire 102 cases of Emergencyobstetric hysterectomies done over a period of five years(January 2001- December 2005) at BP Koirala Institute ofHealth Sciences, Dharan was carried out. Relevant data wereextracted using a pre-designed form. Case histories, operativereports, postoperative care and perinatal outcomes of thepatients and babies were analyzed. The study also includedhysterectomies done for complications following pregnancytermination such as perforation and sepsis.
Results
Altogether 102 patients underwent Emergency obstetrichysterectomy among a total of 20,701 deliveries during thestudy period yielding an Emergency obstetrical hysterectomy/all delivery ratio of 1:200 (prevalence: 4.9 per 1000).
Introduction
Emergency obstetrical hysterectomy can be performed inconjunction with caesarean delivery or can be performedafter a vaginal delivery for complications such as postpartumhemorrhage.
In no other gynecological or obstetrical surgery is the surgeonin much a dilemma as when deciding to resort to an emergencyhysterectomy. On one hand, it is the last resort to save amother’s life, and on the other hand, the mother’s reproductivecapability is sacrificed. Many times it is a very difficultdecision and requires critical clinical judgment. Proper timingand meticulous care may reduce or prevent maternalcomplications.1
In modern obstetrics, the overall prevalence of Emergencyobstetrical hysterectomy is 0.05%,2 but there are considerabledifferences in its prevalence in different parts of the worlddepending upon modern obstetrical services, standard andawareness of antenatal care and effectiveness of familyplanning activities (table 5). It is as diverse as 1 in 349 inNigeria to 1.3/1000 births in South California.3
Hanoon P Pokharel *, Asima Mukhopadhyay **, Abhinav Vaidya ***,Dawa J Lama *, Basudev Banerjee *, Paras K Pokharel ***
* Department of Obstetrics and Gynaecology, BPKIHS,Dharan, Nepal
** Department of Obstetrics and Gynaecology, University of Sheiffield, UK*** Department of Community Medicine, BPKIHS,
Dharan, Nepal
AbstractObjectiveObjectiveObjectiveObjectiveObjective.To study prevalence, indications, contributory factors and outcomes of Emergency obstetric hysterectomyat Teaching Hospital, BP Koirala Institute of Health Sciences, Dharan.
MethodsMethodsMethodsMethodsMethods. A retrospective analysis of the cases of emergency obstetric hysterectomy performed over a period offive years from January 2001- December 2005 was done. Maternal characteristics, operative reports, postoperativecare and perinatal outcomes were studied in detail.
ResultsResultsResultsResultsResults.There were 102 cases of Emergency obstetric hysterectomies among a total of 20,701 deliveries,representing a prevalence of 1 in 200 deliveries (prevalence: 4.9 per 1000). Majority of the cases wereunbooked (98%). The mean age of the patients was 30.07 years. It was more common in multipara (53.9%).The most common indication was uterine rupture (41.1%). Subtotal abdominal hysterectomies were done in55(53.9%) and total abdominal hysterectomies in the rest. The proportions of maternal mortality were 30(29.4%).Perinatal mortality and neonatal death were 44 (43.1%) and 4(3.9%) respectively.
ConclusionConclusionConclusionConclusionConclusion. Emergency obstetric hysterectomy is a life saving procedure. The high prevalence of obstetricalhysterectomies indicates the negligence and lack of knowledge among population about pregnancy andchildbirth. Adequate reproductive health education to primary health care providers, traditional birth attendantsand early referral are essential to reduce this condition.
KKKKKeywords: eywords: eywords: eywords: eywords: Emergency obstetrical hysterectomy, perinatal outcome, subtotal hysterectomy
Correspondence:Dr.(Mrs.) Hanoon P. Pokharel Assistant Professor, Department of Obstetrics & GynaecologyBP Koirala Institute of Health Sciences Dharan, Sunsari 56701, Nepal. Phone: +977-25-530033 (R)Fax: +977-25-520251 (O) [email protected] URL:www.bpkihs.edu
N. J. Obstet. Gynaecol Vol. 1, No. 1, p. 34 - 37 May 2006
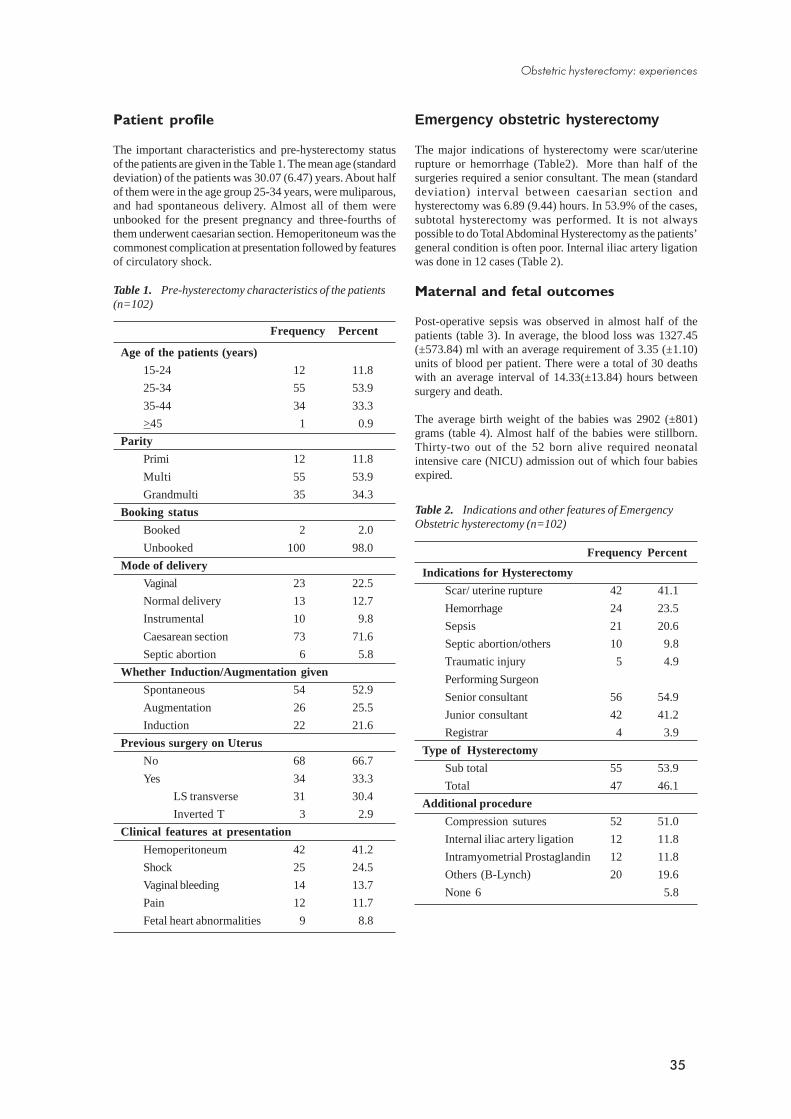
35
Emergency obstetric hysterectomy
The major indications of hysterectomy were scar/uterinerupture or hemorrhage (Table2). More than half of thesurgeries required a senior consultant. The mean (standarddeviation) interval between caesarian section andhysterectomy was 6.89 (9.44) hours. In 53.9% of the cases,subtotal hysterectomy was performed. It is not alwayspossible to do Total Abdominal Hysterectomy as the patients’general condition is often poor. Internal iliac artery ligationwas done in 12 cases (Table 2).
Maternal and fetal outcomes
Post-operative sepsis was observed in almost half of thepatients (table 3). In average, the blood loss was 1327.45(±573.84) ml with an average requirement of 3.35 (±1.10)units of blood per patient. There were a total of 30 deathswith an average interval of 14.33(±13.84) hours betweensurgery and death.
The average birth weight of the babies was 2902 (±801)grams (table 4). Almost half of the babies were stillborn.Thirty-two out of the 52 born alive required neonatalintensive care (NICU) admission out of which four babiesexpired.
Frequency Percent
Age of the patients (years)
15-24 12 11.8
25-34 55 53.9
35-44 34 33.3
>45 1 0.9
Parity
Primi 12 11.8
Multi 55 53.9
Grandmulti 35 34.3
Booking status
Booked 2 2.0
Unbooked 100 98.0
Mode of delivery
Vaginal 23 22.5
Normal delivery 13 12.7
Instrumental 10 9.8
Caesarean section 73 71.6
Septic abortion 6 5.8
Whether Induction/Augmentation given
Spontaneous 54 52.9
Augmentation 26 25.5
Induction 22 21.6
Previous surgery on Uterus
No 68 66.7
Yes 34 33.3
LS transverse 31 30.4
Inverted T 3 2.9
Clinical features at presentation
Hemoperitoneum 42 41.2
Shock 25 24.5
Vaginal bleeding 14 13.7
Pain 12 11.7
Fetal heart abnormalities 9 8.8
Table 1. Pre-hysterectomy characteristics of the patients(n=102)
Patient profile
The important characteristics and pre-hysterectomy statusof the patients are given in the Table 1. The mean age (standarddeviation) of the patients was 30.07 (6.47) years. About halfof them were in the age group 25-34 years, were muliparous,and had spontaneous delivery. Almost all of them wereunbooked for the present pregnancy and three-fourths ofthem underwent caesarian section. Hemoperitoneum was thecommonest complication at presentation followed by featuresof circulatory shock.
Table 2. Indications and other features of EmergencyObstetric hysterectomy (n=102)
Frequency Percent
Indications for Hysterectomy
Scar/ uterine rupture 42 41.1
Hemorrhage 24 23.5
Sepsis 21 20.6
Septic abortion/others 10 9.8
Traumatic injury 5 4.9
Performing Surgeon
Senior consultant 56 54.9
Junior consultant 42 41.2
Registrar 4 3.9
Type of Hysterectomy
Sub total 55 53.9
Total 47 46.1
Additional procedure
Compression sutures 52 51.0
Internal iliac artery ligation 12 11.8
Intramyometrial Prostaglandin 12 11.8
Others (B-Lynch) 20 19.6
None 6 5.8
Obstetric hysterectomy: experiences
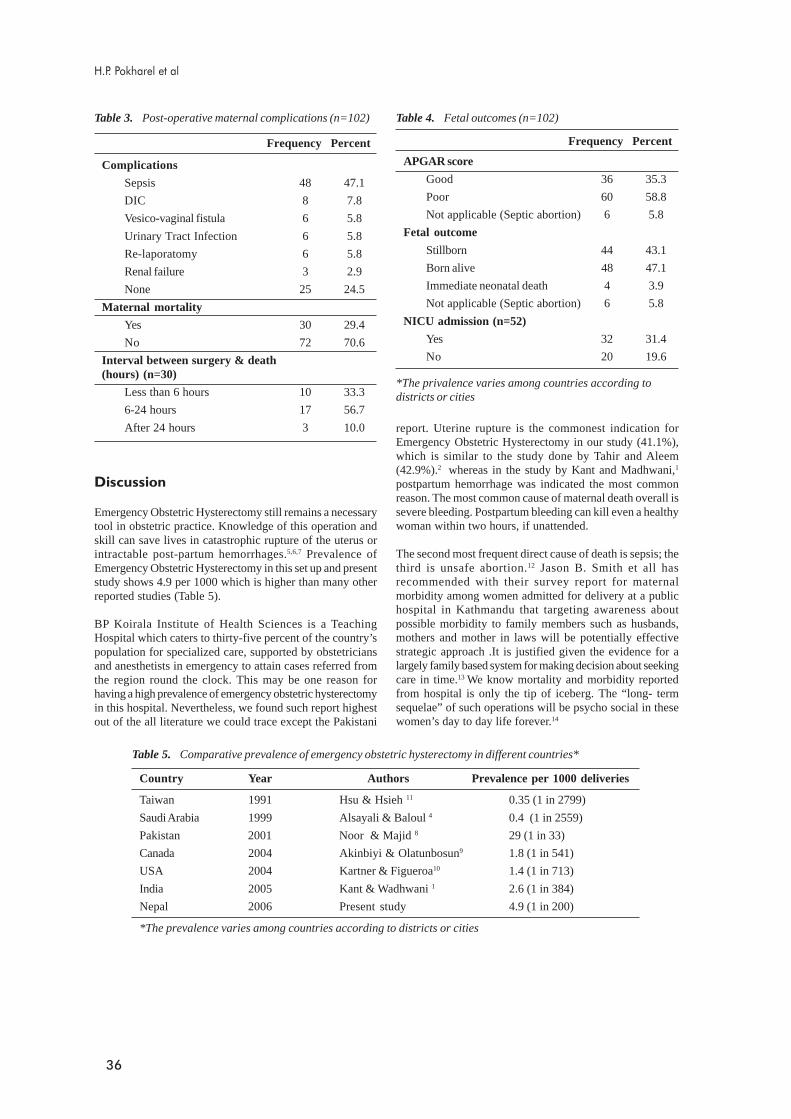
36
Complications
Sepsis 48 47.1
DIC 8 7.8
Vesico-vaginal fistula 6 5.8
Urinary Tract Infection 6 5.8
Re-laporatomy 6 5.8
Renal failure 3 2.9
None 25 24.5
Maternal mortality
Yes 30 29.4
No 72 70.6
Interval between surgery & death(hours) (n=30)
Less than 6 hours 10 33.3
6-24 hours 17 56.7
After 24 hours 3 10.0
Frequency Percent
Table 3. Post-operative maternal complications (n=102)
report. Uterine rupture is the commonest indication forEmergency Obstetric Hysterectomy in our study (41.1%),which is similar to the study done by Tahir and Aleem(42.9%).2 whereas in the study by Kant and Madhwani,1
postpartum hemorrhage was indicated the most commonreason. The most common cause of maternal death overall issevere bleeding. Postpartum bleeding can kill even a healthywoman within two hours, if unattended.
The second most frequent direct cause of death is sepsis; thethird is unsafe abortion.12 Jason B. Smith et all hasrecommended with their survey report for maternalmorbidity among women admitted for delivery at a publichospital in Kathmandu that targeting awareness aboutpossible morbidity to family members such as husbands,mothers and mother in laws will be potentially effectivestrategic approach .It is justified given the evidence for alargely family based system for making decision about seekingcare in time.13 We know mortality and morbidity reportedfrom hospital is only the tip of iceberg. The “long- termsequelae” of such operations will be psycho social in thesewomen’s day to day life forever.14
Table 4. Fetal outcomes (n=102)
*The privalence varies among countries according todistricts or cities
APGAR score
Good 36 35.3
Poor 60 58.8
Not applicable (Septic abortion) 6 5.8
Fetal outcome
Stillborn 44 43.1
Born alive 48 47.1
Immediate neonatal death 4 3.9
Not applicable (Septic abortion) 6 5.8
NICU admission (n=52)
Yes 32 31.4
No 20 19.6
Frequency Percent
Country Year Authors Prevalence per 1000 deliveries
Taiwan 1991 Hsu & Hsieh 11 0.35 (1 in 2799)
Saudi Arabia 1999 Alsayali & Baloul 4 0.4 (1 in 2559)
Pakistan 2001 Noor & Majid 8 29 (1 in 33)
Canada 2004 Akinbiyi & Olatunbosun9 1.8 (1 in 541)
USA 2004 Kartner & Figueroa10 1.4 (1 in 713)
India 2005 Kant & Wadhwani 1 2.6 (1 in 384)
Nepal 2006 Present study 4.9 (1 in 200)
*The prevalence varies among countries according to districts or cities
Table 5. Comparative prevalence of emergency obstetric hysterectomy in different countries*
H.P. Pokharel et al
Discussion
Emergency Obstetric Hysterectomy still remains a necessarytool in obstetric practice. Knowledge of this operation andskill can save lives in catastrophic rupture of the uterus orintractable post-partum hemorrhages.5,6,7 Prevalence ofEmergency Obstetric Hysterectomy in this set up and presentstudy shows 4.9 per 1000 which is higher than many otherreported studies (Table 5).
BP Koirala Institute of Health Sciences is a TeachingHospital which caters to thirty-five percent of the country’spopulation for specialized care, supported by obstetriciansand anesthetists in emergency to attain cases referred fromthe region round the clock. This may be one reason forhaving a high prevalence of emergency obstetric hysterectomyin this hospital. Nevertheless, we found such report highestout of the all literature we could trace except the Pakistani

37
Conclusion
Emergency obstetric hysterectomy remains an essentiallife saving procedure. The high prevalence of obstetricalhysterectomies indicates the negligence and lack of knowledgeamong population about pregnancy and childbirth. Effectiveantenatal care, identification of patients at risk, enhancementof blood transfusion facilities, together with improvement ofsurgical skills are important to reduce the morbidity andmortality associated with the operation. Adequatereproductive health education to primary health careproviders, traditional birth attendants and early referral areessential to reduce this condition. Attempts to reduce theprimary caesarean section rate should be helpful in reducingthe relative risk of hysterectomy.
References
1. Kant Anita, Wadhwani Kavita, Emergency Obstetricshysterectomy Obstet Gynecol India vol. 55, No. 2:2005, 132-134.
2. Tahir S, Aleem M, Akram S. Indication and maternaloutcome of emergency Peripartum Hysterectomy. PakJ Med Sci 2003; 19 (3): 182-186.
3. Edward H, Park Benjamin P. Sachs .PostpartumHaemorrhage and other problems of third stage. InHigh Risk pregnancy, management options 2nd ed.Philadelphia: W B Saunders, 1999:1231-1246
4. Sturdee DW, Rushton DL. Cesarean and postpartumhysterectomy.Br J Obstet. Gynecol 1986; 93: 270-4.
5. Sinha H, Mishra M. Hysterectomy for Obstetricemergency. J Obstet Gynecol India.2001:51:111-4.
6. Thonet RGN. Obstetric hysterectomy: an 11-yearexperience.Br J Obstet Gynecol.1986; 93:794-8.
7. Deborah A. et al, Emergency obstetric hysterectomy—an increasing incidence, Vol.19, 1999, 580-83.
8. Noor S, Majid S, Ruby N. An audit of obstetricalhysterectomy. J coll Physician Surg Pak 2001:11(10):642-5.
9. Akinbiyi A.A, Olatunbosun O.A. Emergencyobstetrical hysterectomies.(how many are Potentiallypreventable?):A 28-years experience in Saskatoon.JGyn. surg, 2004;20(3):81-87.
10. Kastner ES, Figueroa R et al. Emergency PeripartumHysterectomy: Experience at a CommunityTeaching Hospital. OBstete & Gynecol 2002; 99:971-975.
11. Hsu TY, Hsieh CC, Lo LM, Soong YK. EmergencyObstetric hysterectomy: report of fifteen cases.Changgeng Yi Xue Za Zhi. 1991; 14(2): 111-6.
12. Notes and news: The Global Picture. Regional HealthForum, Vol.9,No1,2005.
13. Jason B. Smith et all: Maternal morbidities amongwomen admitted for delivery at a public hospital inKathmandu.JNMA 1996; Vol.34, No118 &119:132-140.
14. Stef Anie A Schwartz PhD and Donald E Williams:Psychological aspects of gynecologic Surgery.Pub.Med http://www.cme.hu/dlObject.php?aid=345&/268-279.PDF.
Obstetric hysterectomy: experiences

38
Four-year service experience of a birthingcenter in an urban Nepal
AbstractAim: This paper presents findings based on the Birthing Center’s four-year service experience, the first midwife-run(BC) in a community hospital in the capital of Nepal established in 1995.
Method: Patan hospital records, unpublished assessment reports, feedback from the staff (managers, midwives,obstetricians and pediatricians) during an in-house review symposium four years period (1995-1999)Results: During the four years that the BC has operated, 28% of all deliveries (including those in the consultant-ledMaternity Unit) at the hospital took place at the BC. About three-fourths of all admissions at the BC were deliveredwithin the BC itself, while the remaining were referred to the hospital’s Maternity Unit [Overall, 25.4% Antenataltransfers (22.9%) were done mainly due to slow progress and postnatal transfers (2.5%) were done mainly due toretained placenta and hypertension]. Of the patients transferred out, 15% required pediatric care and 3% requiredadmittance to the special-care nursery. Examination of the Maternity Unit records showed that 47% of the women whodelivered in the Maternity Unit could have been admitted to the BC.
Conclusions: Several strategies undertaken to improve triaging of patients would allow more efficient utilization ofthe BC resources with further more reduction in cost, both to the patients and the hospital.
Key words: birthing centre, cost reduction, maternity unit, transfer
Introduction
Birthing centers are increasingly accepted worldwideas an alternative low cost place of birth. The concept isespecially relevant for developing countries withlimited resources and constraints regarding availability ofhospital beds and specialists. The birthing centers havetaken on various models, including in-hospital centersand free standing.1,2,3 The standard of care and safety ofbirthing centers have been analyzed.1,3-11 These variousstudies have concluded that when proper risk analysesare conducted and referral rules followed, there is noevidence of increased maternal or perinatal risk at thebirthing center compared to standard hospital deliveries. Theexistence of facilities for transferring patients and linkingwith a referral hospital is essential for the successfulfunctioning of a birthing center.
In Nepal, the first birthing center within a communityhospital in the capital was established in 1995. In thispaper, we present a four-year service experience of thebirthing center in Nepal. More specifically, we presentfindings on the proportion of cases cared for at the birthingcenter to total deliveries at the hospital. We examine thepatterns of ante-and postnatal referrals and reasonsfor referral. Finally, we also discuss strategies beingundertaken to make the birthing center more efficient andmore effective.
Patan Hospital Birthing Center
In response to the increasing demand for antenatal careand safe deliveries in the Kathmandu Valley, Patan Hospitalintroduced the concept of a birthing center in its premises inJanuary 1995.12 Patan Hospital is run by a board representingvarious sectors of the community. It also receives a fixedamount of financial support from the government.
The birthing center was established with the followingobjectives: to provide safe childbirth care with limited use oftechnology and minimal duration of hospitalization (bydischarging within twenty-four hours after birth) for pregnantwomen at low risk, with provision of prompt referral ofmother or baby in case of any problem; to lessen the caseload at the hospital’s Maternity Unit, and at the same timegive priority to women at high risk; to use knowledge andskills of nurse midwives and auxiliary nurse midwives(ANMs) to provide appropriate, friendly, low-cost care withminimum bureaucratic procedures in a safe environment; andto provide a training site for relevant categories of healthpersonnel in the country.
The criteria for admittance to the BC were clearly defined.The exclusion criteria included both past and antenatalhistories. A pregnant woman with any of the followinghistories was not eligible for admittance to the birthing center:previous caesarian section, operations on the uterus (including
Kundu Yangzom*, Neelam Adhikari**, Ram Shova Risal**** Department of Obstetrics and Gynaecology, Patan Hospital
** Department of Pediatrics, Patan Hospital*** Patan Hospital
Correspondence:Dr. Kundu Yangzom, Former Head Department of Obstetrics and Gynaecology, Director Patan Hospital,E-mail: [email protected]
N. J. Obstet. Gynaecol Vol. 1, No. 1, p. 38 - 41 May 2006
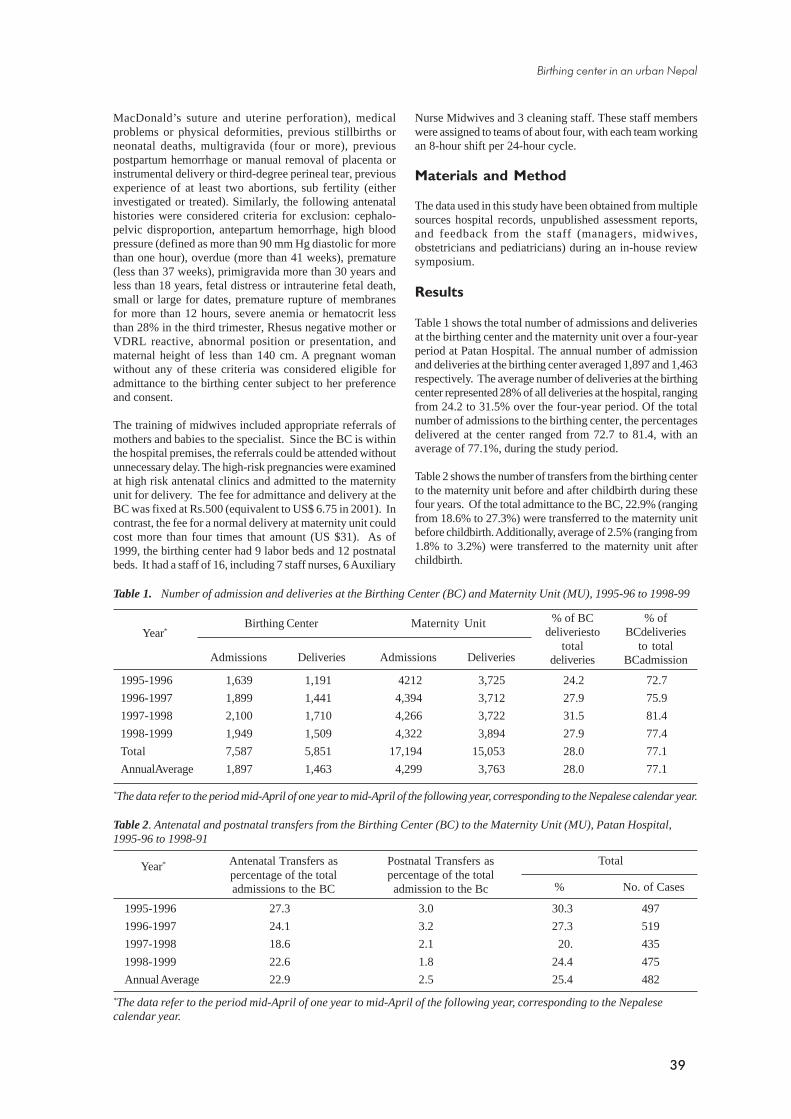
39
1995-1996 27.3 3.0 30.3 497
1996-1997 24.1 3.2 27.3 519
1997-1998 18.6 2.1 20. 435
1998-1999 22.6 1.8 24.4 475
Annual Average 22.9 2.5 25.4 482
*The data refer to the period mid-April of one year to mid-April of the following year, corresponding to the Nepalesecalendar year.
Table 2. Antenatal and postnatal transfers from the Birthing Center (BC) to the Maternity Unit (MU), Patan Hospital,1995-96 to 1998-91
Year* Antenatal Transfers aspercentage of the totaladmissions to the BC
Postnatal Transfers aspercentage of the total
admission to the Bc % No. of Cases
Total
Table 1. Number of admission and deliveries at the Birthing Center (BC) and Maternity Unit (MU), 1995-96 to 1998-99
*The data refer to the period mid-April of one year to mid-April of the following year, corresponding to the Nepalese calendar year.
1995-1996 1,639 1,191 4212 3,725 24.2 72.7
1996-1997 1,899 1,441 4,394 3,712 27.9 75.9
1997-1998 2,100 1,710 4,266 3,722 31.5 81.4
1998-1999 1,949 1,509 4,322 3,894 27.9 77.4
Total 7,587 5,851 17,194 15,053 28.0 77.1
AnnualAverage 1,897 1,463 4,299 3,763 28.0 77.1
Admissions Deliveries Admissions Deliveries
% ofBCdeliveries
to totalBCadmission
Maternity UnitBirthing CenterYear*
MacDonald’s suture and uterine perforation), medicalproblems or physical deformities, previous stillbirths orneonatal deaths, multigravida (four or more), previouspostpartum hemorrhage or manual removal of placenta orinstrumental delivery or third-degree perineal tear, previousexperience of at least two abortions, sub fertility (eitherinvestigated or treated). Similarly, the following antenatalhistories were considered criteria for exclusion: cephalo-pelvic disproportion, antepartum hemorrhage, high bloodpressure (defined as more than 90 mm Hg diastolic for morethan one hour), overdue (more than 41 weeks), premature(less than 37 weeks), primigravida more than 30 years andless than 18 years, fetal distress or intrauterine fetal death,small or large for dates, premature rupture of membranesfor more than 12 hours, severe anemia or hematocrit lessthan 28% in the third trimester, Rhesus negative mother orVDRL reactive, abnormal position or presentation, andmaternal height of less than 140 cm. A pregnant womanwithout any of these criteria was considered eligible foradmittance to the birthing center subject to her preferenceand consent.
The training of midwives included appropriate referrals ofmothers and babies to the specialist. Since the BC is withinthe hospital premises, the referrals could be attended withoutunnecessary delay. The high-risk pregnancies were examinedat high risk antenatal clinics and admitted to the maternityunit for delivery. The fee for admittance and delivery at theBC was fixed at Rs.500 (equivalent to US$ 6.75 in 2001). Incontrast, the fee for a normal delivery at maternity unit couldcost more than four times that amount (US $31). As of1999, the birthing center had 9 labor beds and 12 postnatalbeds. It had a staff of 16, including 7 staff nurses, 6 Auxiliary
Nurse Midwives and 3 cleaning staff. These staff memberswere assigned to teams of about four, with each team workingan 8-hour shift per 24-hour cycle.
Materials and Method
The data used in this study have been obtained from multiplesources hospital records, unpublished assessment reports,and feedback from the staff (managers, midwives,obstetricians and pediatricians) during an in-house reviewsymposium.
Results
Table 1 shows the total number of admissions and deliveriesat the birthing center and the maternity unit over a four-yearperiod at Patan Hospital. The annual number of admissionand deliveries at the birthing center averaged 1,897 and 1,463respectively. The average number of deliveries at the birthingcenter represented 28% of all deliveries at the hospital, rangingfrom 24.2 to 31.5% over the four-year period. Of the totalnumber of admissions to the birthing center, the percentagesdelivered at the center ranged from 72.7 to 81.4, with anaverage of 77.1%, during the study period.
Table 2 shows the number of transfers from the birthing centerto the maternity unit before and after childbirth during thesefour years. Of the total admittance to the BC, 22.9% (rangingfrom 18.6% to 27.3%) were transferred to the maternity unitbefore childbirth. Additionally, average of 2.5% (ranging from1.8% to 3.2%) were transferred to the maternity unit afterchildbirth.
% of BCdeliveriesto
totaldeliveries
Birthing center in an urban Nepal

40
Reason % (n=96)
Retained placenta / ragged membranes 20.6
Postnatal hypertension 16.3
Postpartum tubectomy 14.3
Rhesus incompatibility 12.4
Postpartum fever 11.6
Hematoma 9.9
Postpartum hemorrhage 8.1
Extensive vaginal tear 4.0
Other 2.8
Table 4: Reasons for transfers after childbirth from theBirthing Center to the Maternity Unit, 1996-97 and1998-99*
Table 3: Reasons for transfer of the patients (before childbirth) from the Birthing Center to the Maternity 1996-1999*
Reason % (n=898)
Slow progress 44.1
Meconium stained liquor 13.4
Fetal distress 8.3
Other medical problems in mother 7.2
Malpresentations 5.0
Bad obstetric history 3.0
Spontaneous rupture of membranes
(>12 hrs, not in labor) 2.6
Prolonged second stage 2.2
Patient’s request 2.0
Other 12.2
*The data refer to the period mid-April of one year to mid-April of the following year, corresponding to the Nepalesecalendar year.
*The data refer to the period mid-April of one year to mid-April of the following year, corresponding to the Nepalesecalendar year.
The reasons for transfer of the patients to the maternity unitbefore and after childbirth were analyzed for two years, 1996-1997 and 1998-1999 (Tables 3 and 4). About 44% of the caseswere transferred before childbirth due to slow progress. Asecond important reason for the transfer was meconium stainedliquor. Just over 8% of the cases were transferred due to fetaldistress. The most important reason for the transfer afterchildbirth was retained placenta or ragged membranes (20.6%).The other reasons were hypertension, postpartum tubectomy,Rh - incompatibility and postpartum fever.
In the year 1998-1999, 440 patients were transferred tomaternity unit. The outcome of those patients transferred tomaternity unit in 1998-1999 was analyzed. 71.4% had vaginaldelivery after augmentation with syntocinon drip, 17.8%had LSCS, and the rest 11.8% were delivered by vacuumextraction or forceps. Thus, training of midwives at thebirthing center for starting the syntocinon drip in suitablecases was seen as a step towards reducing the transfers tomaternity unit. The use of partograph was found also to beuseful as a more objective assessment towards earlyrecognition of any possible complications.
The possibility of midwives doing uterine exploration forretained placenta and ragged membrane in the birthing centeritself was discussed but ruled out by the obstetricians. 14.3%of post child birth transfers were for postpartum tubectomy.It was decided to transfer these patients back to the birthingcenter rather than the maternity unit, even though they wouldstay in hospital for more than twenty-four hours. This wasin accordance with the objectives of the B.C.
The midwives at the BC have been trained to resuscitatepatients, examine newborns, detect any abnormalities, andrefer accordingly. About 14 to 16% of the babies born at thebirthing center required consultation of a pediatrician duringthe four-year period. The consultations were done at thebirthing center itself. Most of these cases required a fewhours extra observation. Only 2.5-4% of all the babies bornduring the four-year period at the birthing center needed tobe transferred and admitted to special care nursery (data notshown in a table).
Table 5. Reasons for pediatric consultations forbabies born at the Birthing Center, 1995-96 and 1998-99*
Reason % (n=396)
Meconium stained liquor 58.9
Low Birth Weight (IUGR) 8.8
Prematurity 5.4
Low apgar 5.1
Poor sucking 7.0
Respiratory distress 4.8
Congenital anomalies 4.2
Fever 2.0
Spontaneous rupture ofMembrances (>24 hrs) 1.8
Other
*The data refer to the period mid-April of one year to mid-April of the following year, corresponding to the Nepalesecalendar year.
The reasons for the pediatrician consultation were alsoanalyzed for the periods 1995-1996 and 1998-1999 in orderto assess the appropriateness of consultations and identifyareas in which further training for midwives could benecessary (Table 5). The most important reason forconsultation was meconium stained liquor (representing about
60% of the cases). The second most important reason waslow birth weight. Both were felt appropriate reasons forpediatric consultation.
In order to assess the proportion of the patients whodelivered at the maternity unit eligible for admittance to thebirthing center, we reviewed the records of the patientsdelivered at the maternity unit for one year (mid-April 1998to mid-April 1999). We predetermined to systematically pickup about 50 cases from each of the four months (to take intoaccount seasonal variations, if any). Accordingly, every sixthcase from each of the four months was reviewed. Just over47% of the cases delivered at the maternity unit during thatyear could have been admitted to the birthing center (Table6). As noted by reviewing the admittance cases, but not the
K. Yangzom et al

41
deliveries, the percentage eligible might be slightly lower. Inthis sense, 47% should be considered as an upper boundestimate of potential clients for the birthing center. Thesedata clearly indicate the considerably more patients couldhave been handled by the birthing center. A more carefultriaging of the patients could have lessened the burden on thematernity unit.
and scope of the birthing center, and provision of bettercounseling especially for low-risk patients about the optionsavailable within the hospital. The importance of revision ofthe exclusion criteria was also discussed. It was alsorecommended that controlled syntocinon drips may beinitiated at birthing center under the supervision of anobstetrician and that over time midwives themselves couldfeel confident to handle this. It was also recommended thatthe birthing center patients who had postpartum tubectomyat the hospital could be transferred back to the birthing centerrather than to the maternity unit. These patients could stayat the birthing center for more than twenty-four hours butwould require minimal care. These recommendations are beingimplemented and are expected to result in more efficient andeffective functioning of the birthing center at the hospital.
References
1. Waldenstorm U, Nilsson CA. A randomized controlledstudy of birth center care versus standard maternitycare: effects on women’s health. Birth 1997; 24(1):17-26.
2. Alisjahbana A, Williams C, Dharmayanti R, HermawanD Kwast BE, Koblinky M. An integrated villagematernity service to improve referral pattern in a ruralarea in West-Java. Int J Gynaecal Obstet 1995; 48Suppl: S83-94.
3. Garite TJ, Snell BJ, Walker DL, Darrow VC.Development and experience of a university based,freestanding birthing center. Obstet Gynecol 1995;86(3):411-6.
4. Adhikari N, Shah S, Amataya A, Perinatal mortality –a hospital based study. Nepas Journal, 1995;15(1):21-29.
5. Waldenstrom U, Nilsson CA, Winbladh B. TheStockholm birth center trial: maternal and infantoutcome. Br J Obstet Gynaecol 1997;104(4):410-8.
6. David M, Von Schwarzenfeld HK, Dimer JA,Kentenich H. Perinatal outcome in hospital and birthcenter obstetric care. Int J Gynaecal Obstet 1999;65(2):149-56.
7. Campbell R. Review and assessment of selectioncriteria used when booking pregnant women at differentplaces of birth. Br J Obstet Gnaecol 1999; 106(6):550-6.
8. Harrington LC, Miller DA, McClain CJ, Paul RH.Vaginal birth after cesarean in a hospital-based birthcenter staffed by certified nurse midwives. J NurseMidwifery 1997;42(4): 304-7.
9. Fullerton JT, Jackson D, Snell BJ, Besser M, DickinsonC, Garite T. Transfer rates from freestanding birthcenters: a comparison with the national birth centerstudy. J Nurse Midwifery 1997;42 (1):9-16.
10. Waldenstrom U, Lawson J. Birth centre practices inAustralia. Aust N Z J Obstet Gynaecol 1998; 38(1):42-50.
11. Curtin SC. Recent changes in birth attendant, place ofbirth, and the use of obstetric interventions, UnitedStates, 1989-1997. J Nurse Midwifery 1999;44(4):349-54.
12. Mona Bomgaars. The birth of a birthing centre atPatan Hospital. J Nepal Medical Association1996:34(118-119): 165-167.
Discussion and Conclusion
The results reviewed here suggest that triaging of low riskpatients to a birthing center is a viable strategy, especially ina resource-poor country like Nepal. This provides thenecessary services at less cost to the patients and lessens theburden on the maternity unit. During the four years that theBC has operated, 28% of all deliveries (including those in thematernity unit) at the hospital took place at the BC.
About three-fourths (77%) of all admissions at the BC weredelivered within the BC itself, while the remaining 23% wasreferred to the hospital’s maternity unit. Overall, 25.4% ofall admissions to the BC were transferred to the maternityunit. Antenatal transfers (22.9%) were done mainly due toslow progress. Postnatal transfers (2.5%) were done mainlydue to retained placenta and hypertension. Of the patientstransferred out, 15% required pediatric care and 3% requiredadmittance to the special-care nursery. Further examinationof the records showed that 47% of the patients who deliveredat the maternity unit could have been admitted to the BC.This would have resulted in a more efficient utilization of theBC resources and also reduction in cost both to the patientsand the hospital.
In mid-1999, the experience of the birthing center wasreviewed by the hospital administrators, physicians andnurses of the Patan Hospital. It was recognized that thebirthing center could play larger role in meeting the needs ofthe expectant mothers. For this, several steps needed to beundertaken, including better coordination between the birthingcenter and maternity unit, provision of information to theexpectant mothers (and their husbands) about on the role
Table 6. Percentage of patients delivered at the MaternityUnit who could have been eligible to be admitted to theBirthing Center, 1998-1999*
Month Eligible Not Eligible(%) n=95 (%) n=106
Mid-April to mid-May 62.0 38.0
Mid-July to mid-Aug. 44.0 56.0
Mid- Oct. to mid-Nov. 47.1 52.9
Mid-Jan. to mid-Feb. 36.0 64.0
All 47.3 52.7
Total no. cases 95 106
*The data refer to the period mid-April of one year to mid-April of the following year, corresponding to the Nepalesecalendar
Note: The exclusion criteria for admittance to the BirthingCenter are discussed in the text.
Birthing center in an urban Nepal

42
Two years experience of neonatal services in KathmanduUniversity Teaching Hospital,
B&B hospital
Introduction
Kathmandu University Teaching Hospital (KUTH), B&B isa tertiary level referral hospital for different specialties inNepal. After the establishment of KUTH, Department ofPaediatrics was established and different Paediatrics servicesalong with Neonatal services have been started since January2004. However, KUTH B&B is one of the few institutionswhere conduct of all deliveries and attendance are providedby specialists. Specialists care facilities for Nepal’s annualbirths are not only limited but also are beyond the reach asabout 90% of babies are born at home.
The Department of Paediatrics has now the experiences ofmore than 2 years. In the background of this, the presentstudy was undertaken to know the profile of newborns andalso birth outcome and its association in this newly builtpublic-private partnership teaching hospital.
Materials and methods
The study included 227 women who gave birth during 1/1/04to 31/12/06. All deliveries were conducted by specialistObstetrician and Gynaecologist were attended by Pediatrician.Maternal and Neonatal data were recorded on the standardproforma meticulously with their consent. Birth weight was
taken at birth without clothes on using calibrated electronicweighing machine. The standard intrauterine growth chartwas used for classifying babies for low birth weight andsmall for gestational age.
Results
The study consisted of 227 women who gave birth to 110(48%) males and 117 (52%) females. Majority (90%) of thebabies were weighing equal to or more than 2500 grams(Fig 1). Low birth weight was seen in 21 (9%) babies andmost of them were born at term. There were 210 (92%) fullterm babies, 10 (5%) pre-term babies and 7 (3%) post- termbabies. Small for gestation (SGA) was found in 9 (4%) babiesand all were Full-term small for gestation (FT, SGA). Themean birth weight was 3 kg.
All the mothers had antenatal checkups (ANC). 220 (97%)mothers had more than 4 ANC visits and 7 (3%) mothershad 2 ANC visits only. Majority (187=83%) of the motherswere in the age group between 20-30 years. There were120 (53%) normal vaginal deliveries, 92 (40%) caesareansections and 15 (7%) forceps delivery as shown in thefigure 2. 215 (95%) and 12 (5%) babies were born by vertexpresentation and breech presentation. There were108(47.5%) primiparous, 109(48%) multiparous and10(4.5%) grandmultiparous women.
Rajesh L Gurubacharya*, Chanda Karki***Department of Pediatrics, **Department of Obstetrics & Gynaecology,
Kathmandu University Teaching Hospital
AbstractObjective: To know the profile of newborns and to study the association between services provided by the specialistsand the birth outcome.
Methods: The study included 227 women who gave birth during 1/1/04 to 31/12/06. All deliveries were conductedand attended by Obstetrician and Gynaecologist and Pediatrician respectively. Maternal and Neonatal data wererecorded on the standard proforma.
Results: There were 227 babies during the study period. Mean birth weight was 3 kg. Low birth weight (LBW) wasfound in 9% of the babies only and most of them were born at term. There were 5% preterm, 4% small for gestation(SGA) and 7% large for gestation (LGA) babies. 8% meconium-stained babies were uneventful. All the mothers hadantenatal checkups (ANC) and their education was above secondary education and college graduate. The socio-economic background was quite good. 97% of mothers had more than 4 antenatal checkup visits. There were 60% ofhigh-risk cases. There were 53% normal vaginal deliveries, 40% caesarean sections and 7% forceps deliveries. Therewere two neonatal deaths.
Conclusions: The mean birth weight is good and the LBW rate is also very low in the study. This reflects better health,nutritional, educational status of pregnant women and antenatal care they received during the pregnancy. There wereonly two neonatal deaths, which may correlate with better specialist’s care being provided. This study contributes to theunderstanding of the constant growth of caesarean section and more studies are recommended for future benefits andindications of caesarean procedures.
Keywords: New born, birth weight, delivery, specialist, record keeping
Correspondence:Dr. Rajesh L Gurubacharya, Department of Pediatrics, Kathmandu University Teaching Hospital, Sinamangle,Kathmandu, Email: [email protected]
N. J. Obstet. Gynaecol Vol. 1, No. 1, p. 42 - 44 May 2006

43
Six (3%) babies had mild perinatal asphyxia and haduneventful recovery. There were 2 babies born with cleft lipand palate. One baby was born with left sided deformed earwith absent external auditory meatus and anotia. There wereonly 2 neonatal deaths. One little baby died of fulminantneonatal sepsis and the other died due to consequences ofcongenital hydrocephalus; both of them were prematureand LBW. There was one case of infant of diabetic mother.19 (8%) babies born with meconium stained liquor werevigorous and none of them developed meconium aspirationsyndrome.
Discussion
The study was undertaken to give a glimpse of neonatalservice in a newly built public-private partnership teachingHospital where all deliveries were attended by specialistpediatrician. Though small sample size was the limitation ofthe study, certain inferences can be drawn.
Low birth weight defined as a birth weight less than 2500gmremains a significant public health problem in many partsof the world and is associated with range of both shortand long term adverse consequences. In the study, the LBWrate is low (9%) and most of them were born at term. Thiscorrelates well with the mother’s health, nutrition, bettereducational status of pregnant women, antenatal carethey received during the pregnancy and their socioeconomicstatus.
Tracy and associates1 found that lower hospital volume isnot associated with adverse birth outcomes. Similar is theexperience of our study where there were only two neonataldeaths because of congenital hydrocephalus and fulminantneonatal sepsis. Our study reveals comparatively highcaesarean rate. This high rate may draw concern; however,this rate of caesarian section is justified as fetal distress,malpresentations, big baby, placenta praevia and pregnancywith two previous caesarean sections were the mainindications in our study. High proportion of high risk cases(60%) coming to this hospital for safe delivery by theobstetricians of choice may be the main reason of high ratesof caesarian section.
Parazzini and associates2 found caesarean section rates rosesteadily with maternal age, being about three times higher inwomen aged 40 years or more than in teen-agers. Maternaleducation was directly associated with caesarean sectionrates: Compared with women with only primary schooleducation, those with college education reported about 40%higher rate of caesarean section. This determinant is alsofound in our study where majority of our motherswere college educated and from good socioeconomicbackground.
Hanvoravongchai and associates6 found certain other factorsinvolved in an increasing caesarean section rate, like: Maternalage, multiparty, previous caesarean section, patient choice(e.g. for fear of vaginal delivery).
Conclusion
The mean birth weight is good and the LBW rate is also verylow in the study. This reflects better health, nutritional,educational status of pregnant women and antenatal care
Figure 1: Birth weight of the babies
Figure 2: Types of deliveries
���
����
���
���� ������� ���������
������ ����� ����
�����
�
��
��
��
��
�
�
��
�
�
�
�
�
(!*
)*
��*
&��%���+�����������+��# ,����$������+��#�����������������
Neonatal services in KU Teaching Hospital

44
they received during the pregnancy. Also there were onlytwo neonatal deaths, which may correlate with betterspecialist’s care being provided. However, despite thelimitation of the study being a small sample size, it emphasizesthe importance of good and genuine record keeping that wouldprovide insight to neonatal and obstetrics services. This studycontributes to the understanding of the constant growth ofcaesarean section and would lead us to investigate caesareansection in different hospitals in Nepal. Thus more studiesare recommended, not only from medical but multi-disciplinary perspectives, for e.g.: social, anthropological,legal and ethical studies are required for future benefits andindications of caesarean procedures.
Keeping meticulous records of patients attending the hospitalis the effective way of documenting services provided by thedoctors and the hospital.
Acknowledgement
The authors would like to acknowledge all the motherswho kindly consented to be enrolled in this study. Our sincerethanks to Obstetric and Gynaecology Departmentwithout them, we might not be able to shed light into thisarea. The authors would like to acknowledge the generouscontributions of Dr. Simmi Misra Gurubacharya and DevAshish Malakar.
References
1. Tracy S k, Sullivan E, Dahlen H, et al. Does size matter?A population- based study of birth in lower volumematernity hospitals for low risk women. BJOG: AnInternational Journal of Obstetrics & Gynaecology2006; 113(1): 86-96.
2. Parazzini F, Pirotta N, Vecchia C, et al. Determinantsof Caesarean section rates in Italy. BJOG: AnInternational Journal of Obstetrics & Gynaecology1992; 99(3): 203-206.
3. Tangcharoensathien V, Chantarasatit N, Sittitoon C, etal. Pattern of hospital deliveryin Thailand. 1990-1996.Nonthaburi: Health System Research Institute, 1998.
4. Agarwal S, Agarwal A, Bansal A K, et al. Birth weightpatterns in Rural Undernourished Pregnant Women.Indian Pediatr 2002; 39:244-253.
5. Mathai M, Jacob S, Karthikeyan N G. Birth weightstandards for south Indian babies. Indian Pediatr 1996;33:203-209.
6. Hanvoravonghai P, Letiendumrong J, TeerawattananonY,et al. Implications of Private Practice in PublicHospitals on the Cesarean Section Rate inThailand.1998. Health System Research Institute,1998
R. Gurubacharya & C. Karki

45
Adolescent girls’ perspectives on sexual and reproductivehealth illnesses and their care seeking behavior
in rural Nepal
Introduction
The adolescent period is a time in which individuals exploreand develop their sexuality, gender and sex role. These factorshave a profound influence on a young person’s current andfuture health, most directly through exposure to safe or unsafesexual practices but also through the propensity of youngpeople to be perpetrators or victim of violence or abuse. Formany years, the health of young people has been neglectedas they are less vulnerable to disease than children or thevery old.1 Sources of information and contraceptive adviceare rarely available or accessible to them.2
Illnesses relating to sexual and reproductive health mattersmay receive inadequate attention as these problems areshrouded in a culture of silence, embarrassment and shame.3
When young people lack guidance, information and measuresto prevent exposure are inadequate, they will be less likelyto seek timely professional medical help and more likely toundertake dangerous self-treatment. This may lead topermanent impairment of health, infertility, psychologicaldamage and even death, which may affect not only theirfamilies but also society as a whole.2
Adolescents learn about reproductive health and sexualmatters by observing the behavior of the adults around them,by listening to peers and older siblings, through the media inall its forms and by acquiring the knowledge of parents orother trusted mentors. Such information, however, is limited
Anand Tamang, Jyotsna Tamang, Binod Nepal, Ramesh AdhikariCentre for Research on Environment Health and Population Activities,
Kathmandu, Nepal
and sometimes even erroneous. Unprotected premaritalsexual relations are taking place at earlier ages giving rise notonly to problems of early pregnancy and childbearing, butalso to induced abortion in hazardous circumstances, tosexually transmitted diseases including humanimmunodeficiency virus infection leading to AIDS.
A study conducted in India among married adolescent girlsshowed that general illnesses were quickly addressed, whilereproductive health problems were usually not addressed. Itwas also seen that husbands played a major role in addressingthe reproductive health needs of these adolescent women;the decision on whether women should seek treatment forillness rested largely with their husbands.3
A study in Nigeria reports that adolescents had someknowledge on STDs although they knew more about HIVand AIDS than about other STDs. Although treatment seekingbehaviours varied, the majority of adolescents reportedthat they would disclose their symptoms to their friends. Infocus group discussions, most participants agreed thatadolescents with a STD symptom would seek care from atraditional faith healer, followed by patent medicine dealers,private doctors and hospitals; not mentioned were publicdoctors or other sources available in the area.4 A second studyamong Nigerian adolescents suggested that while knowledgeof several aspects of reproductive health was widespread,few adolescents were correctly able to identify the monthlyfertile period of a woman, suggesting knowledge remainedincomplete and superficial.5
AbstractAim: To study the knowledge and health seeking behavior of the adolescent on the sexual and reproductive health.
Methods: Unmarried adolescent girls aged 14-19 years representing four major ethnic communities of Nepal werecovered in the study using both qualitative (focused ethnographic study) and quantitative (sample survey) methodologies.
Results: The results showed that the adolescent girls, irrespective of ethnic group, were poorly informed aboutreproductive health issues and held a range of misperceptions about their etiology. They are familiar with a range ofmenstrual problems, as well as symptoms of reproductive and urinary tract infections. The preferred sources of careamong the adolescent girls tend to exclude the formal health system. Adolescent girls were more likely to prefer homeremedies and traditional faith healers if action was sought.
Conclusion: The findings of this study, while exploratory in nature, are useful in designing culturally appropriatehealth intervention packages and adolescent friendly health services aimed at minimizing the risk of health complicationsassociated with the experience of menstrual, reproductive and urinary tract problems.
Key words: adolescent girls, menstrual problems, reproductive health, urinary tract infection, white discharge
The study on which this paper is based received funding support from the Special Programme of Research, Developmentand Research Training in Human Reproduction of the World Health Organization, Geneva. The authors are affiliated toCenter for Research on Environment Health and Population Activities (CREHPA), Kathmandu, Nepal.
correspondence:Anand Tamang, Director, CREHPA, Kathmandu, Nepal, email: [email protected]
N. J. Obstet. Gynaecol Vol. 1, No. 1, p. 45 - 51 May 2006

46
In Nepal in contrast, studies suggest considerable gaps inyoung people’s knowledge of reproductive health. A studyconducted in Makwanpur district has shown widespreadlack of awareness among adolescent girls about genital hygieneand safe sanitation practices during menstruation.6 Over twothirds of these adolescent girls faced some menstruationrelated health problems immediately before or at the time oftheir menstrual period. A majority reported the experience ofsymptoms of urinary tract infections. Another study carriedout on adolescent girls in a rural district situated on theoutskirts of Kathmandu Valley has shown that althoughadolescent girls lacked information on physiology andsexuality, they displayed considerable knowledge andawareness of changes during puberty, menstruation andpregnancy, reproductive functions and family planningmethods.7
In Nepal, adolescents comprise more than one-fifth (22percent) of the total population. Owing to high fertility andyoung age distribution of population, the proportion ofadolescents in the total population is likely to increase in thecoming years.8 However, information is lacking on the waysin which unmarried adolescent girls perceive health problemsincluding sexual and reproductive health problems, their feltneeds and patterns of health seeking behavior, and constraintsto health care utilization. This gap in knowledge poses anobstacle to the design of appropriate and youth friendlyprogramme strategies and interventions that meet theirneeds. The present paper is aimed at fulfilling theseinformation gaps.
Methodology and Data Source
This paper reports on data drawn from a descriptive studyentitled “Adolescent health maintenance behavior in Nepal:A focussed ethnographic study” conducted by the authorswith support from WHO. The study integrates qualitativeand quantitative research designs. Focussed ethnographicstudy (FES) methodology was employed to solicit qualitativeinformation on illnesses including sexual and reproductivehealth illnesses as perceived by the adolescent girls, theirtreatment seeking behaviour and constraints to utilisation ofhealth care facilities. FES is a rapid assessment procedurewhich is best suited to construct explanatory models of ahealth problem or illness.1
The study covered four major ethnic communities of Nepal –two from the hilly region (Gurung and Tamang) and two fromthe terai region (Rajbanshi and Tharu). These ethniccommunities were drawn from six districts. Unmarriedadolescent girls aged 13-19 years from both rural and urbanareas constituted the sample. FES tools such as Freelists, FreePilesorts, Severity Rating and Matrix were employed among20-25 adolescents in each ethnic community. Ethnographicdata were analyzed using ANTHROPAC software packages.The survey data analysed in the present paper refer to 1092unmarried rural adolescent girls aged 14-19 from the four ethniccommunities – Gurung (262), Rajbansi (281), Tamang (271)and Tharu (278). A multi-staged sampling technique wasemployed for the selection of villages in the districts inhabitedby these ethnic communities. Bivariate analyses are performedto study the influence of selected demographic and socialvariables such as age, education, ethnicity, work status andfamily structure on prevalence of specific SRH and their careseeking behavior.
Results from the focus ethnographic study
Types of Sexual and Reproductive HealthProblems Identified
Rural adolescent girls identified as many as 78 healthproblems faced by adolescent females in the Freelistingexercises (Table 1) Problems reported included headache,fever, various problems associated with menstruation, aswell as cancer, leprosy and AIDS. Of the 78 problems, fourproblems were most frequently identified: headache(70 responses), lower abdomen pain during menstruation(66 responses), fever (41 responses) and cough and cold(40 responses). One-fourth of the problems mentioned bythe adolescent girls (25 problems) were sexual andreproductive health (SRH) related problems, including urinarytract infection (UTI) related problems. Interestingly, themajority of the SRH problems (16 out of 25 problems) wererelated to menstruation. Most common menstruation relatedproblems mentioned were: lower abdomen pain duringmenstruation, irregular menstruation, backache duringmenstruation and excess menstrual bleeding.
SRH problems by ethnic groups
Comparatively, Tharu girls have cited larger number of SRHproblem (16) than the rest of the ethnic groups. Gurung girlshave cited 13, Tamang 11 and Rajbanshi 9. Five menstrualproblems and one urinary tract problem were cited byadolescent girls from all the four ethnic groups. Thecommonly cited problems are: lower abdomen pain duringmenses, irregular menses, and backache during menses, excessbleeding during menses, lumpy discharge during menses andburning urination. Comparatively, the problem of ‘lowerabdomen pain during menstruation’ has the highest salienceas most adolescent girls from all the four ethnic groups havementioned this problem (66 girls in all). ‘Irregularmenstruation’ was cited by a considerable number of Gurunggirls (10 out of 25 girls) and ‘backache during menstruation’by Tharu girls (8/20 girls). Among the urinary tract problems,‘burning urination’ was mentioned most frequently byGurung girls (6/25 girls) and followed by the Tamang girls (4/16). Among the reproductive tract problems, white dischargeand vaginal itching was frequently reported by the Tamanggirls (4/16 and 4/7 respectively). The number of responsesfor rest of the SRH problems is low; 5 and below (Table 1).
Perceived Etiology of SRH Problems
Most SRH problems experienced by adolescents relate largelyto menstruation, although urinary tract disorders and dischargeand itching are also reported. In order to explore perceivedetiology of each set of problems described and assesssimilarities and differences in such explanations across ethnicgroups, we present below the explanations offered byadolescents about the five leading menstruation related problemsas well as one each from the two remaining sets of problemsdescribed, namely, burning urination and white discharge.
By and large etiological explanations given by adolescentgirls centre around two main factors and these are commonacross all ethnic groups, particularly with reference tomenstrual problems (lower abdominal pain duringmenstruation, irregular menstruation) and burning urination:
A. Tamang et al

47
Table 1. Free-listing of sexual and reproductive health related problems of rural adolescent girls by ethnic group*
S.N. Problems Rajbansi Tharu Gurung Tamang Totaln=20 n=20 n=25 n=20 n=85
A Menstrual problems1. Lower abdomen pain during menstruation 15 16 18 17 662. Irregular menstruation 3 6 10 4 233. Backache during menstruation 1 8 5 4 184. Excess bleeding during menstruation 2 5 3 5 155. Fever during menstruation - 4 - 2 66. Lumpy discharge during menstruation 3 1 1 1 67. Scanty bleeding during menstruation 2 2 - - 48. Diarrhoea during menstruation - 2 - - 29. Giddiness/dizziness/headache during menstruation - 4 - - 410. Scars/sores around cleavage/genital area - 1 1 - 2
during menstruation11. Thin white discharge accompanying - - 1 - 1
menstruation bleeding12. Breast pain during menstruation - - 1 - 113. Loss of appetite during menstruation - - 2 - 2
B Urinary tract problems14. Burning urination 3 3 6 4 1615. Urine blockage/urine retention - 1 4 2 716. Red coloured urination 1 - - 1 2
C Discharge/itching/ulcer17. White discharge - 1 2 4 718. Vaginal itching - 1 - 4 519 Ulcer in the Uterus - 1 - - 120. Ulcer around genital area - - 1 - 1
21. AIDS 1 1 2
* Certain similar responses in the Freelists are clubbed in the present table
intakes of certain food items (sour and/or hot foods) andbeliefs about witchcraft (bad spell of witch). Burning urinationwas commonly associated, moreover, with the perceivedcondition of the body (body heat). Only one group, Tamanggirls, related the occurrence of white discharge with sexualintercourse.
Perceived Severity
The severity ranking exercise conducted among adolescents ofeach ethnic group (20-21 per group). A total of nine problemswere included in the exercise. The number of problems ratedas “severe” by 50 percent or more adolescent girls of GurungClearly, reproductive health problems were not perceived assevere in most cases. For example, four conditions were ratedsevere by 50% or more respondents in the group in twocommunities: Gurung and Tamang; two conditions were ratedsevere by Rajbanshi girls and just one by Tharu girls. Whatwas consistent however was that in all four ethnic communities,excess bleeding during menses was reported as a severeproblem. Lumpy discharge during menses was rated severe byover 50 percent of all girls in three of the four groups (exceptingTharu girls among who 50% or more have rated only oneproblem as severe).
Scores were attributed to responses on severity of eachcondition, (if the condition was perceived as mild, 0, 1 ifintermediate and 2 if severe). Aggregating these scores it
becomes clear again that excessive bleeding duringmenstruation ranks as most severe among three ethniccommunities (Tharu, Gurung and Rajbanshi) and second byTamang girls who ranked white discharge as most severe.
Health Care Seeking Pattern
Most adolescent girls, irrespective of the type and nature ofthe SRH problem, do not generally seek medical attentionfrom a health facility. Problems related to menstruation andwhite discharge are considered “normal” or conditions that“happen to girls” and are “due to weakness” (especiallyamong the Rajbanshi and Tharu girls). As a consequence, noaction is taken, and if the problem persists, they rely uponhome remedies, and subsequently upon traditional faithhealers. It is only if these actions prove ineffective and theproblem is unbearable that a health post/sub-health post,hospital or private doctor or private medicine shops areconsulted (Table 2).
Corresponding to perceptions of witchcraft as underlyingmenstrual problems, reliance on traditional faith healers fortreatment is quite widespread among all the ethniccommunities under study. Normally, the village faith healeris rarely bypassed even if alternative sources of treatmentare sought, since these communities maintain that modernmedicines will be ineffective unless the patient is first seenby a faith healer. Among the four groups, Gurung girls are
Adolescent girls’ perspectives on SRH
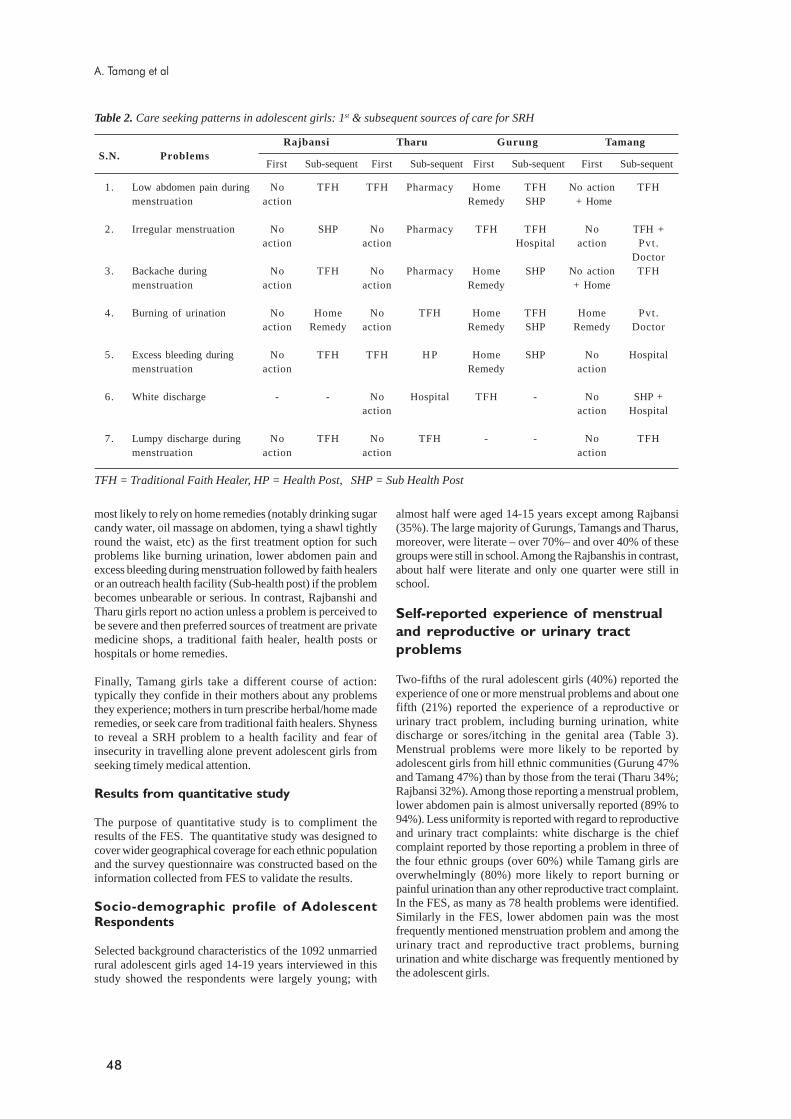
48
1. Low abdomen pain during No TFH TFH Pharmacy Home TFH No action TFHmenstruation action Remedy SHP + Home
2. Irregular menstruation No SHP No Pharmacy TFH TFH No TFH +action action Hospital action Pvt .
Doctor3. Backache during No TFH No Pharmacy Home SHP No action TFH
menstruation action action Remedy + Home
4. Burning of urination No Home No TFH Home TFH Home Pvt.action Remedy action Remedy SHP Remedy Doctor
5. Excess bleeding during No TFH TFH H P Home SHP No Hospitalmenstruation action Remedy action
6. White discharge - - No Hospital TFH - No SHP +action action Hospital
7. Lumpy discharge during No TFH No TFH - - No TFHmenstruation action action action
TFH = Traditional Faith Healer, HP = Health Post, SHP = Sub Health Post
Table 2. Care seeking patterns in adolescent girls: 1st & subsequent sources of care for SRH
First Sub-sequentS.N. Problems
TamangGurungTharuRajbansi
First Sub-sequent First Sub-sequent First Sub-sequent
most likely to rely on home remedies (notably drinking sugarcandy water, oil massage on abdomen, tying a shawl tightlyround the waist, etc) as the first treatment option for suchproblems like burning urination, lower abdomen pain andexcess bleeding during menstruation followed by faith healersor an outreach health facility (Sub-health post) if the problembecomes unbearable or serious. In contrast, Rajbanshi andTharu girls report no action unless a problem is perceived tobe severe and then preferred sources of treatment are privatemedicine shops, a traditional faith healer, health posts orhospitals or home remedies.
Finally, Tamang girls take a different course of action:typically they confide in their mothers about any problemsthey experience; mothers in turn prescribe herbal/home maderemedies, or seek care from traditional faith healers. Shynessto reveal a SRH problem to a health facility and fear ofinsecurity in travelling alone prevent adolescent girls fromseeking timely medical attention.
Results from quantitative study
The purpose of quantitative study is to compliment theresults of the FES. The quantitative study was designed tocover wider geographical coverage for each ethnic populationand the survey questionnaire was constructed based on theinformation collected from FES to validate the results.
Socio-demographic profile of AdolescentRespondents
Selected background characteristics of the 1092 unmarriedrural adolescent girls aged 14-19 years interviewed in thisstudy showed the respondents were largely young; with
almost half were aged 14-15 years except among Rajbansi(35%). The large majority of Gurungs, Tamangs and Tharus,moreover, were literate – over 70%– and over 40% of thesegroups were still in school. Among the Rajbanshis in contrast,about half were literate and only one quarter were still inschool.
Self-reported experience of menstrual
and reproductive or urinary tract
problems
Two-fifths of the rural adolescent girls (40%) reported theexperience of one or more menstrual problems and about onefifth (21%) reported the experience of a reproductive orurinary tract problem, including burning urination, whitedischarge or sores/itching in the genital area (Table 3).Menstrual problems were more likely to be reported byadolescent girls from hill ethnic communities (Gurung 47%and Tamang 47%) than by those from the terai (Tharu 34%;Rajbansi 32%). Among those reporting a menstrual problem,lower abdomen pain is almost universally reported (89% to94%). Less uniformity is reported with regard to reproductiveand urinary tract complaints: white discharge is the chiefcomplaint reported by those reporting a problem in three ofthe four ethnic groups (over 60%) while Tamang girls areoverwhelmingly (80%) more likely to report burning orpainful urination than any other reproductive tract complaint.In the FES, as many as 78 health problems were identified.Similarly in the FES, lower abdomen pain was the mostfrequently mentioned menstruation problem and among theurinary tract and reproductive tract problems, burningurination and white discharge was frequently mentioned bythe adolescent girls.
A. Tamang et al
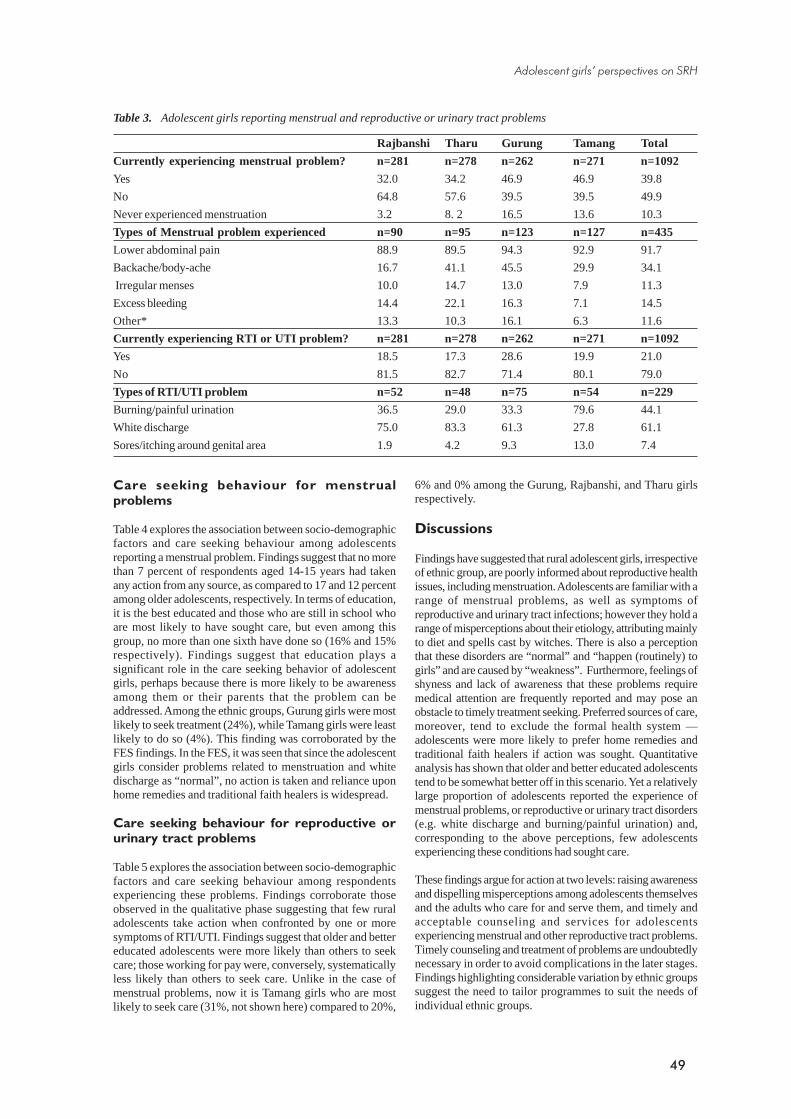
49
6% and 0% among the Gurung, Rajbanshi, and Tharu girlsrespectively.
Discussions
Findings have suggested that rural adolescent girls, irrespectiveof ethnic group, are poorly informed about reproductive healthissues, including menstruation. Adolescents are familiar with arange of menstrual problems, as well as symptoms ofreproductive and urinary tract infections; however they hold arange of misperceptions about their etiology, attributing mainlyto diet and spells cast by witches. There is also a perceptionthat these disorders are “normal” and “happen (routinely) togirls” and are caused by “weakness”. Furthermore, feelings ofshyness and lack of awareness that these problems requiremedical attention are frequently reported and may pose anobstacle to timely treatment seeking. Preferred sources of care,moreover, tend to exclude the formal health system —adolescents were more likely to prefer home remedies andtraditional faith healers if action was sought. Quantitativeanalysis has shown that older and better educated adolescentstend to be somewhat better off in this scenario. Yet a relativelylarge proportion of adolescents reported the experience ofmenstrual problems, or reproductive or urinary tract disorders(e.g. white discharge and burning/painful urination) and,corresponding to the above perceptions, few adolescentsexperiencing these conditions had sought care.
These findings argue for action at two levels: raising awarenessand dispelling misperceptions among adolescents themselvesand the adults who care for and serve them, and timely andacceptable counseling and services for adolescentsexperiencing menstrual and other reproductive tract problems.Timely counseling and treatment of problems are undoubtedlynecessary in order to avoid complications in the later stages.Findings highlighting considerable variation by ethnic groupssuggest the need to tailor programmes to suit the needs ofindividual ethnic groups.
Care seeking behaviour for menstrualproblems
Table 4 explores the association between socio-demographicfactors and care seeking behaviour among adolescentsreporting a menstrual problem. Findings suggest that no morethan 7 percent of respondents aged 14-15 years had takenany action from any source, as compared to 17 and 12 percentamong older adolescents, respectively. In terms of education,it is the best educated and those who are still in school whoare most likely to have sought care, but even among thisgroup, no more than one sixth have done so (16% and 15%respectively). Findings suggest that education plays asignificant role in the care seeking behavior of adolescentgirls, perhaps because there is more likely to be awarenessamong them or their parents that the problem can beaddressed. Among the ethnic groups, Gurung girls were mostlikely to seek treatment (24%), while Tamang girls were leastlikely to do so (4%). This finding was corroborated by theFES findings. In the FES, it was seen that since the adolescentgirls consider problems related to menstruation and whitedischarge as “normal”, no action is taken and reliance uponhome remedies and traditional faith healers is widespread.
Care seeking behaviour for reproductive orurinary tract problems
Table 5 explores the association between socio-demographicfactors and care seeking behaviour among respondentsexperiencing these problems. Findings corroborate thoseobserved in the qualitative phase suggesting that few ruraladolescents take action when confronted by one or moresymptoms of RTI/UTI. Findings suggest that older and bettereducated adolescents were more likely than others to seekcare; those working for pay were, conversely, systematicallyless likely than others to seek care. Unlike in the case ofmenstrual problems, now it is Tamang girls who are mostlikely to seek care (31%, not shown here) compared to 20%,
Table 3. Adolescent girls reporting menstrual and reproductive or urinary tract problems
Rajbanshi Tharu Gurung Tamang Total
Currently experiencing menstrual problem? n=281 n=278 n=262 n=271 n=1092
Yes 32.0 34.2 46.9 46.9 39.8
No 64.8 57.6 39.5 39.5 49.9
Never experienced menstruation 3.2 8. 2 16.5 13.6 10.3
Types of Menstrual problem experienced n=90 n=95 n=123 n=127 n=435
Lower abdominal pain 88.9 89.5 94.3 92.9 91.7
Backache/body-ache 16.7 41.1 45.5 29.9 34.1
Irregular menses 10.0 14.7 13.0 7.9 11.3
Excess bleeding 14.4 22.1 16.3 7.1 14.5
Other* 13.3 10.3 16.1 6.3 11.6
Currently experiencing RTI or UTI problem? n=281 n=278 n=262 n=271 n=1092
Yes 18.5 17.3 28.6 19.9 21.0
No 81.5 82.7 71.4 80.1 79.0
Types of RTI/UTI problem n=52 n=48 n=75 n=54 n=229
Burning/painful urination 36.5 29.0 33.3 79.6 44.1
White discharge 75.0 83.3 61.3 27.8 61.1
Sores/itching around genital area 1.9 4.2 9.3 13.0 7.4
Adolescent girls’ perspectives on SRH
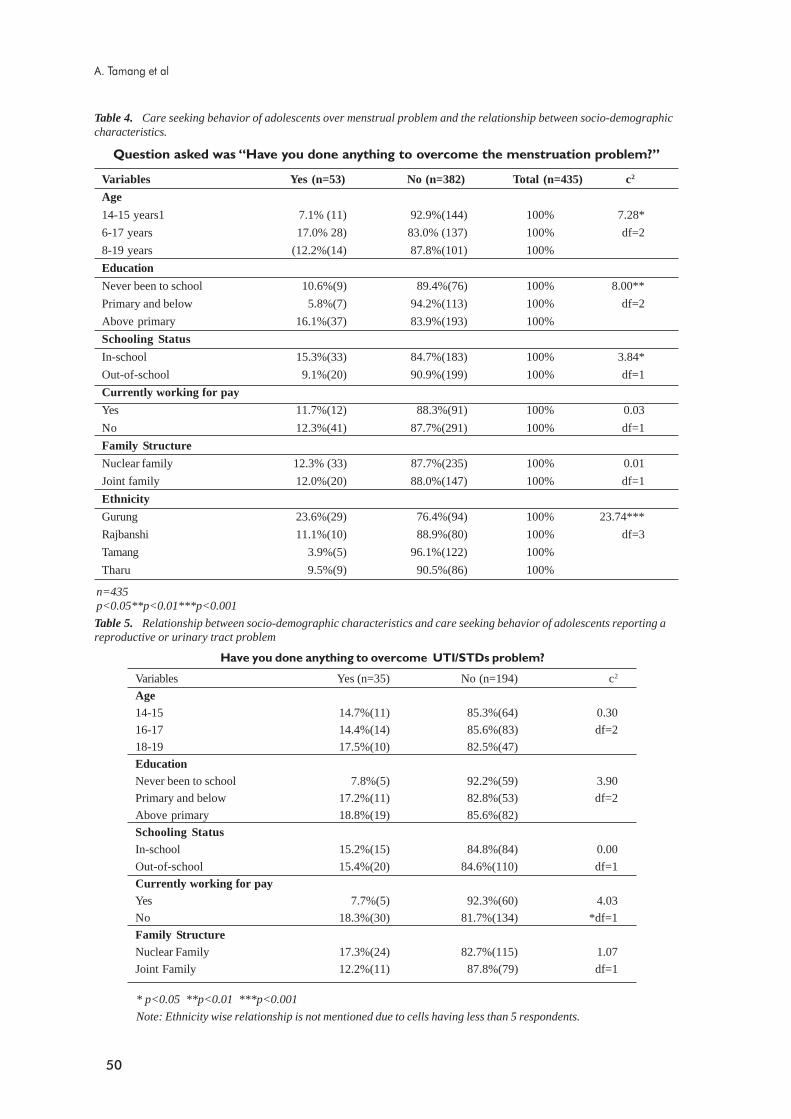
50
Question asked was “Have you done anything to overcome the menstruation problem?”
Table 4. Care seeking behavior of adolescents over menstrual problem and the relationship between socio-demographiccharacteristics.
Variables Yes (n=53) No (n=382) Total (n=435) c2
Age
14-15 years1 7.1% (11) 92.9%(144) 100% 7.28*
6-17 years 17.0% 28) 83.0% (137) 100% df=2
8-19 years (12.2%(14) 87.8%(101) 100%
Education
Never been to school 10.6%(9) 89.4%(76) 100% 8.00**
Primary and below 5.8%(7) 94.2%(113) 100% df=2
Above primary 16.1%(37) 83.9%(193) 100%
Schooling Status
In-school 15.3%(33) 84.7%(183) 100% 3.84*
Out-of-school 9.1%(20) 90.9%(199) 100% df=1
Currently working for pay
Yes 11.7%(12) 88.3%(91) 100% 0.03
No 12.3%(41) 87.7%(291) 100% df=1
Family Structure
Nuclear family 12.3% (33) 87.7%(235) 100% 0.01
Joint family 12.0%(20) 88.0%(147) 100% df=1
Ethnicity
Gurung 23.6%(29) 76.4%(94) 100% 23.74***
Rajbanshi 11.1%(10) 88.9%(80) 100% df=3
Tamang 3.9%(5) 96.1%(122) 100%
Tharu 9.5%(9) 90.5%(86) 100%
n=435p<0.05**p<0.01***p<0.001
Table 5. Relationship between socio-demographic characteristics and care seeking behavior of adolescents reporting areproductive or urinary tract problem
Have you done anything to overcome UTI/STDs problem?
Variables Yes (n=35) No (n=194) c2
Age14-15 14.7%(11) 85.3%(64) 0.30
16-17 14.4%(14) 85.6%(83) df=2
18-19 17.5%(10) 82.5%(47)
EducationNever been to school 7.8%(5) 92.2%(59) 3.90
Primary and below 17.2%(11) 82.8%(53) df=2
Above primary 18.8%(19) 85.6%(82)
Schooling StatusIn-school 15.2%(15) 84.8%(84) 0.00
Out-of-school 15.4%(20) 84.6%(110) df=1
Currently working for payYes 7.7%(5) 92.3%(60) 4.03
No 18.3%(30) 81.7%(134) *df=1
Family StructureNuclear Family 17.3%(24) 82.7%(115) 1.07
Joint Family 12.2%(11) 87.8%(79) df=1
* p<0.05 **p<0.01 ***p<0.001
Note: Ethnicity wise relationship is not mentioned due to cells having less than 5 respondents.
A. Tamang et al

51
Conclusions
The findings of this study, while exploratory in nature, areuseful in designing culturally appropriate health interventionpackages or services aimed at minimizing the risk ofhealth complications associated with the experience ofmenstrual, reproductive and urinary tract problems amongadolescent girls in rural areas of Nepal.
References
1. Alan Guttmacher Institute. Into a New World: YoungWomen’s Sexual and Reproductive Lives. The AlanGuttmacher Institute, New York. 1998.
2. Barua A. and Kurz K. Reproductive Health-Seekingby Married Adolescent Girls in Maharashtra, India.Reproductive Health Matters 2001; 9(11): 53-62.
3. Central Bureau of Statistics. Population Monographof Nepal. CBS, Kathmandu. 1995.
4. CREHPA.. Reproductive Health Care: Knowledge,Attitude and Practice among Adolescents in ProgramAreas of PLAN Makwanpur. Makwanpur. 1996.
5. Harlow, SD. and Campbell O. Menstrual Dysfunction:A Missed Opportunity for Improving ReproductiveHealth in Developing Countries. Reproductive HealthMatters 2001; 9(11): 142-147.
6. Harlow SD, Ephross SA. Epidemiology ofMenstruation and it Relevance to Women’s Health.Epidemiologic Reviews. 17:265-86. In: Harlow SD andCampbell O 2001. Menstrual Dysfunction: A Missed
Opportunity for Improving Reproductive Health inDeveloping Countries. Reproductive Health Matters.1995. 9(11) p. 142-147.
7. Mathur S., Malhotra A., Mehta M. AdolescentGirls’ Life Aspirations and Reproductive Health inNepal. Reproductive Health Matters 2001. 9(17):91-9.
8. Nichols D., Lapido OA., Paxman JM., Otolorin EO..Sexual Behavior, Contraceptive Practice, andReproductive Health among Nigerian Adolescents.Studies in Family Planning 1986. 17(2): 100-106.
9. Temin MJ., Okonofua FE., Omorodion FO., RenneEP., Coplan P., Heggenougan HK., Kaufman J.Perceptions of Sexual Behavior and Knowledge aboutSexually Transmitted Diseases among Adolescents inBenin City, Nigeria. International Family PlanningPerspectives 1999. 25(4): 186-190.
10. Vicdan K., Kukner S., Dabakoglu T. Demographicand Epidemiologic Features of Female Adolescents inTurkey. Journal of Adolescent Health. 18:54-58 (inHarlow, SD. and Campbell, O. 2001. MenstrualDysfunction: A Missed Opportunity for ImprovingReproductive Health in Developing Countries.Reproductive Health Matters.1996.9(11): 142-147.
11. World Health Organization. The Health of YoungPeople: A Challenge and a Promise. World HealthOrganization, Geneva. 1993.
12. World Health Organization. The Reproductive ofAdolescents: A Strategy for Action. A Joint WHO/UNFPA/UNICEF Statement. World HealthOrganization, Geneva. 1989.
Adolescent girls’ perspectives on SRH

52
Introduction
Since Marshall, Marchetti and Krantz introduced theapplication of retropubic urethrovesical suspension in 1949,trans-abdominal procedures have been used with increasingfrequency and with higher success rates to correct urinaryincontinence. Although numerous technologies and variationof retropubic repairs have been described, the basic conceptremains the same; to suspend and to stabilize the bladderneck and proximal urethra in a retropubic position to preventtheir descent outside the sphere of abdominal pressuretransmission during raised intra-abdominal pressure. I havebeen using new MMK operation for female incontinencesince 1997, whenever indicated. Here is an analysis anddiscussion of my experience.
New technique of MMK operation
The method of the original MMK operation has beenmodified. After the usual retropubic dissection, three suturesare placed on either side of urethrovesical junction using No.1 vicryl. The most medial stitch is placed 1cm lateral to theurethrovesical junction (as delineated by inflated Foley’sbulb), the intermittent stitch 2cm and lateral most 3cm lateralto the bladder neck ensuring a good thickness of paraurethraltissue excluding vaginal mucosa. After taking each bite onparacolpos, the needle is passed through the periosteum ofpubic symphysis just below the Cooper’s ligament at similardistances. Sutures are tied only after taking all bitessuccessively on either side.
This modification differs from the original MMK in the sensethat exclusive midline sutures on cartilage of symphysis
Retropubic surgery for female stress incontinence
Chendra Dev ChawlaDepartment of Obstetrics and Gynaecolgy, Kathmandu University Medical School,
Dhulikhel, Nepal
AbstractObjective : To compare the results of this modified Marshall Marchetti Krantz (MMK) operation with vaginal repair infemale incontinence and to study the prognostic variables that determine the success.
Methods : Urinary stress incontinence was treated by modified MMK operation in 59 and by Kelly’s vaginal repair in42 women. All were assessed preoperatively by detailed history, clinical examination. Sophisticated urodynamic studieswere not done. Follow up was done initially at 3 months, then at 6 and 12 months
Results : Better results were obtained with this modified MMK operation (88%) compared to vaginal repair (68%).Results were excellent in type I incontinence and in the absence of pelvic floor relaxation. Hysterectomy did not seem toimprove the results. Complication rates were acceptable with modified MMK operation
Conclusion : I recommend this modified MMK operation as a primary surgery for female urinary stress incontinenceto obtain higher cure rates and to minimize the incidence of recurrent urinary stress incontinence following repair.
Key Words: Stress incontinence, Kelly’s repair, modified MMK operation
pubis is avoided and it differs from Burch colposuspensionbecause Cooper’s ligaments are avoided, and as the suturesare placed relatively high in Burch colposuspension, the extrapull while tying the knots which may cut through theparavaginal tissues is avoided.
Patients and methods
Between 1998 and 2005, a total of 93 cases of stressincontinence were done and they were divided into:
Group 1a: includes those with 1st and 2nd degree uterovaginaldescent who underwent abdominal hysterectomy withChawla’s sling operation and modified MMK operation(n=19).
Correspondence :Prof. Dr. Chander Dev Chawla, Prof. and Head of Department of Obstetrics and Gynaecolgy,Kathmandu University Medical School, Dhulikhel, Kavre, Nepal, email : rita [email protected]
Figure 1: Adopted (new) modification of MMK operation
N. J. Obstet. Gynaecol Vol. 1, No. 1, p. 52 - 55 May 2006
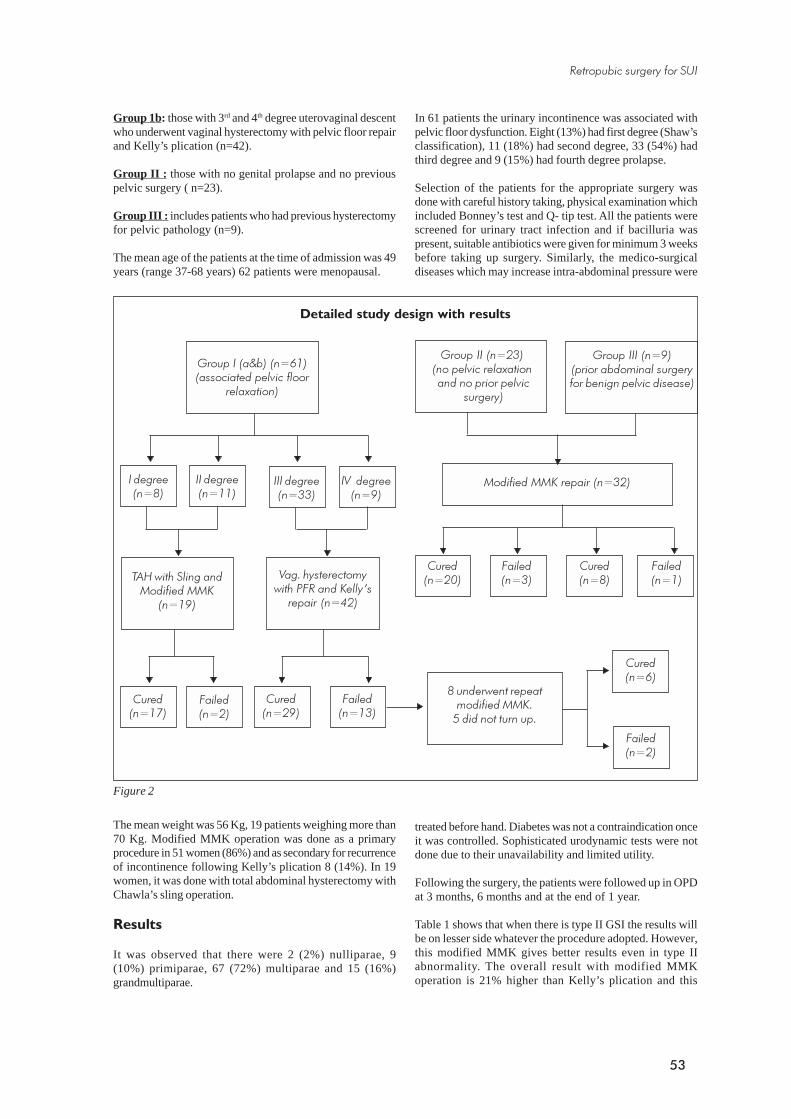
53
Group 1b: those with 3rd and 4th degree uterovaginal descentwho underwent vaginal hysterectomy with pelvic floor repairand Kelly’s plication (n=42).
Group II : those with no genital prolapse and no previouspelvic surgery ( n=23).
Group III : includes patients who had previous hysterectomyfor pelvic pathology (n=9).
The mean age of the patients at the time of admission was 49years (range 37-68 years) 62 patients were menopausal.
In 61 patients the urinary incontinence was associated withpelvic floor dysfunction. Eight (13%) had first degree (Shaw’sclassification), 11 (18%) had second degree, 33 (54%) hadthird degree and 9 (15%) had fourth degree prolapse.
Selection of the patients for the appropriate surgery wasdone with careful history taking, physical examination whichincluded Bonney’s test and Q- tip test. All the patients werescreened for urinary tract infection and if bacilluria waspresent, suitable antibiotics were given for minimum 3 weeksbefore taking up surgery. Similarly, the medico-surgicaldiseases which may increase intra-abdominal pressure were
Group I (a&b) (n=61)(associated pelvic floor
relaxation)
I degree(n=8)
II degree(n=11)
III degree(n=33)
IV degree(n=9)
TAH with Sling andModified MMK
(n=19)
Vag. hysterectomywith PFR and Kelly’s
repair (n=42)
Cured(n=17)
Failed(n=2)
Cured(n=29)
Failed(n=13)
Detailed study design with results
Figure 2
Group II (n=23)(no pelvic relaxation and no prior pelvic
surgery)
Modified MMK repair (n=32)
Cured(n=20)
Failed(n=3)
8 underwent repeatmodified MMK.
5 did not turn up.
Cured(n=8)
Group III (n=9)(prior abdominal surgeryfor benign pelvic disease)
Failed(n=1)
Cured(n=6)
Failed(n=2)
The mean weight was 56 Kg, 19 patients weighing more than70 Kg. Modified MMK operation was done as a primaryprocedure in 51 women (86%) and as secondary for recurrenceof incontinence following Kelly’s plication 8 (14%). In 19women, it was done with total abdominal hysterectomy withChawla’s sling operation.
Results
It was observed that there were 2 (2%) nulliparae, 9(10%) primiparae, 67 (72%) multiparae and 15 (16%)grandmultiparae.
treated before hand. Diabetes was not a contraindication onceit was controlled. Sophisticated urodynamic tests were notdone due to their unavailability and limited utility.
Following the surgery, the patients were followed up in OPDat 3 months, 6 months and at the end of 1 year.
Table 1 shows that when there is type II GSI the results willbe on lesser side whatever the procedure adopted. However,this modified MMK gives better results even in type IIabnormality. The overall result with modified MMKoperation is 21% higher than Kelly’s plication and this
Retropubic surgery for SUI
54
Complications No.
Sutures through bladder resulting in hematuria 4
Bladder tears -
Need for blood transfusion 5
Wound hematoma 1
Wound infection 3
Osteitis pubis 2
Thrombophlebitis 1
Urinary tract infection 2
Urethral occlusion -
Postoperative urinary retention 10
Fistula -
difference is statistically significant (chi square test, x2=6.59,p<0.01). The average operating time exclusively for modifiedMMK operation was 34 minutes. When anterior abdominalwall was opened for the first time, the incision could belimited to 4cm in majority of the cases. However, in thepresence of previous scar the incision was increased to 6-8cm, anticipating bladder injury due to fibrosis.
used preoperative diagnostic urodynamic tests. Of 2712 cases,2334 (86.1%) succeeded, 73 (2.7%) improved and 305(11.2%) failed. The success rate of primary surgery was92.1%; the success rate was 84.5% when used for recurrenturinary incontinence following failed vaginal procedure. Mystudy supports the same findings.
The complication rates were acceptable. All the patients whounderwent modified MMK operation were on catheterdrainage for minimum of seven days. The residual urinevolume ranged between 65-150 ml (mean 78 ml) on the dayof catheter removal.
In 10 patients recatheterization was done as 6 of them couldnot void at all and in 4 it was considered because the residualurine exceeded 100 ml. However all of them could voidspontaneously after some days of catheterization and bladderdrill.
In my series of patients who underwent modifiedMMK operation, two had osteitis pubis, as evidenced bysevere suprapubic pain radiating to thighs, marked tendernessand swelling over the pubic symphysis developing inthird week of surgery. None of them had radiological featuresof bone destruction. Both responded to antibioticsand NSAIDs. Whenever the space of Retzius had thetendency to ooze at the end of procedure, romavac suctiondrain for retropubic space was used. Five patients weretransferred in post operative ward as drainage of urineexceeded 400 ml. None of them needed more than one pint ofblood.
Table 1. Results of surgery according to the type ofincontinence
Kelly’s Modified MMK
n Cure % n cure %
Type I 12 9 75% 24 22 91.7%
Type II 30 20 66.7% 27 24 88.9%
Total 42 29 69% 51 46 90.1%
Table 2. Results of modified MMK Operation
Procedure Total no Success
N= 59 rate
No %
Done as a primary procedure 51 (46/51) 90.1
Done as a secondary procedure 8 (6/8) 75
for failed Kelly’s plication
without abdominal hysterectomy (21/23) 89.5
with abdominal hysterectomy (17/19) 89.5
Type I incontinence (22/24) 91.7
Type II incontinence (24/27) 88.9
Overall success rate (52/59) 88.1
Table 3: Complications of modified MMK operation
Discussion
In this series, 69% of those who had Kelly’s repair and88.1% of those who had modified MMK operation werecured. Rotational descent of urethra (Type II incontinence)and pelvic floor relaxation were adverse prognostic factors.Though there are contradicting reports regarding success rateaccording to the type of urinary stress incontinence, in thisseries better results were obtained in patients with type Iincontinence. Combining hysterectomy did not seem toimprove the overall results.
Mainprize and Drutz summarized 56 articles reporting theresults of MMK procedures. Only few of these researches
C.D. Chawla

55
Few surgeons suggest that the patient should complete herchildbearing before surgical correction of incontinence isattempted. In literature, only 8 pregnancies have been reportedafter MMK operation, 7 of them delivered vaginally. In thisseries there were four (1 nullipara and 3 primiparae) patientswho underwent modified MMK operation with uterineconservation. No pregnancies were reported in follow upperiod so far.
Comments
Surgical correction of stress incontinence in women remainsa complex and distressing situation. We continue to favourthe less complex Kelly’s plication combined with vaginalhysterectomy with pelvic floor repair (Mayo-Ward) for theusual patient with minimal moderate stress incontinenceand associated pelvic floor relaxation. However, abdominalprocedure should be considered for those with severe urinaryincontinence (perhaps aggravated by a medical disease suchas COPD or by obesity); those with apparently goodvesical support (e.g., a snug vagina with minimal anteriorrotational descent of urethrovesical junction) and thoseassociated with intra-abdominal disease that requiressuprapubic incision. The primary retropubic suspension,which relies more on substantial tissues, would appear toprovide more permanent urethral support and everlasting
control of symptoms in patients with complex and severedegree of urinary incontinence. It will also eliminate thedistressing incident of recurrent stress incontinence associatedwith vaginal repair.
References1. Marshal VF, Marchetti AA, Krantz KE: The correction
of stress incontinence by simple vesicourethralsuspension. Surg. Gynecol. Obst 1949; 88:509,
2. Parnel JP, Marshal VF, Vaughan ED Jr.: Primarymanagement of urinary stress incontinence by theMarshal-Marchetti- Krantz vesicourethropexy. J Urol1982; 127: 679
3. Chawla CD, Synopsis of Clinical Obstetrics. NewDelhi. BI Churchill Livingstone Pvt. Ltd. 2001.Chapter 20:179-182
4. Park GS, Miller EJ. Surgical treatment of stress urinaryincontinence: a comparison of the Kelly’s placation,Marshal-Marchetti- Krantz, and Pereyra procedures.Obstet gynecol 1988; 71: 575-579
5. Green. TH, Development of a plan for diagnosis andtreatment of urinary stress incontinence. Am J ObstetGynecol 1962; 83:632
6. Mainprize TC, Drutz HP. The Marshal- Marchetti-Krantz procedure: a critical review. Obstet GynecolSurv 1988; 43:724-729
Retropubic surgery for SUI

56
Introduction
In Latin, “Prolapsus” means a slipping forth. It means thefalling or slipping out of the place of a part or viscus1. GenitalProlapse is a condition in which the female reproductiveorgans descend down the birth canal.2 Prolapse may bedefined as the downward displacement of one of the pelvicorgans from its normal location in females which is oftenaccompanied by urinary, bowel, sexual or local symptoms.3
Symptoms common to all type of prolapse is feeling ofdragging, loop in the vagina or something coming down.1-4 Inthe uterine prolapse, there is always some associated descentof the anterior vaginal wall. Uterine descent can be graded asfirst degree when the cervix descends but lies above theintroitus, second degree, where the cervix descends to thelevel of introitus. In third degree the uterus lies outside thevaginal opening.
Objective of the study
To study the laboratory profile of preoperative patientsplanned for surgical treatment with special interests focussedon urine analysis and findings of pus cell in different degree ofgenital prolapse so as to find out the incidence of UTI.
Pratap Shahi,* Ganesh Dangal,** Ranga Bahadur Basnet,** Basudha Shrestha** Sanjit Shrestha**
*Tribhuvan University Teaching Hospital, Maharajgung, Kathmandu, Nepal.**Department of Obstetrics and Gynaecology, Kathmandu Model Hospital,
Exhibition Road, Kathmandu, Nepal
Genital prolapse and possible urinary tract infection:findings from preoperative work up
in the community set up.
Correspondence:Dr. Ganesh Dangal, MBBS, MD (OB/GYN),Consultant GynaecologistDepartment of Obstetrics and Gynaecology, Kathmandu Model HospitalGPO Box 12887, Kathmandu, Nepal, E-mail: [email protected], Phone: 00977-1-5555802
AbstractAim: To find out the incidence of urinary tract infection in relation to various degree of uterovaginal prolapse by simpleurine analysis.
Methodology: 100 women with different degrees of genital prolapse were investigated preoperatively before thesurgical treatment in the Gauri Shankar General Hospital in Dolakha in 2005. The incidence of urinary tract infection(UTI) based on the urine analysis showing more than 5 pus cells per high power field (HPF) in different degrees of UVPwas studied.
Results: First, second and third degrees of UVP were found to be 7%, 59 % and 34% respectively. The resultsof various investigations are as follows; haemoglobin level was found between 9 - 17 gm%, similarly blood sugar levelwas found between 3- 5 mmol/L and blood urea level was found between 3-8mmol/L. Pyuria was found in 15.2% ofsecond degree prolapse followed by 14.2% of first degree and 11.7% of third degree prolaspe.
Conclusion: The study showed that urinary tract infection was present in significant numbers (14%) of genital prolapsepatients being slightly high in the case of second degree without any marked difference implying that the cause of UTImust be primarily due to prolapse of the bladder, cystocele rather than the degrees of UVP.
Key words: Genital Prolapse /uterovaginal prolapse, Urinary tract infection (UTI), pus cells
Methods and materials
This study was done in the Gaurishankar General Hospital,Dolakha, at the time of free Surgical Camp of Uterovaginalprolapse (genital prolapse), which was organized by theKathmandu Model Hospital from April 19th - 27th 2005.
100 women with genital prolapse from 30 different VDC ofDolakha district and nearby districts were taken as studysubjects.
Urine collected by clean catch mid-stream urine were subjectedmicroscopic studies. Urine examination was done by taking5ml of urine, which was centrifuged for 5 minutes and depositwas examined by the binocular microscope in high powerfield. There was no facilities for urine culture and sensitivity.
Blood sample for haemoglobin, blood sugar and ureaestimation were collected by standard technique; veinpuncture and analysed in a way given below.4-6
Urine examination by microscopic examination in HPF.Glucose estimation by glucose oxidase peroxidase method.Urea estimation by enzymatic method.Haemoglobin estimation by cyanmethemoglobin.
N. J. Obstet. Gynaecol Vol. 1, No. 1, p. 56 - 58 May 2006

57
Materials
Microscope Urine containerColorimeter UristicksCentrifuge Cover slipsTest tube CalculatorSlides Water bath Normal SalinePencilDistilled water CuvetteRack Pipette
Chemicals
Glucose reagent (Glucozyme)Urea standardUrea reagent (Ureazyme)Haemoglobin standardHaemoglobin reagent (Drabkin’s solution)Glucose standard
Result
Among 100 genital prolapse patients 7% had first degreeprolapse, 59 % had second degree prolapse and 34% hadthird degree genital prolapse. According to the age-wisedistribution of genital prolapse patients, highest percentageof genital prolapse patients (51 %) were found in theage group 40-59 followed by the age group 60-79(Fig 1).
Haemoglobin level >12gm% was seen in 39 cases, followedby those with haemoglobin of 11- 12 gm% (15+34= 49),haemoglobin 9-10 gm% in 12 cases (Table 1).
Similarly blood urea level of the genital prolapse patientranged from 3 to 8 mmol/1. Among them 4% genital prolapsepatient had 8 mmol/1 urea level and 26% genital prolapsepatient had 3 mmol/1 urea levels. Maximum number of genitalprolapse patient had 4 mmol/1 urea levels.
Among the total 100 genital prolapse patients, 39% of thegenital prolapse patient had 4 mmol/l blood glucose level and34%, 21%, 5% and 1% genital prolapse patient had bloodglucose level of 15, 3, 6, and 7 mmol/1 respectively.
Discussion
The genital prolapse is the major problem in the countrysideof Nepal, where women do not have access to adequatemedical services. Many women are suffering from theuterovaginal prolapse associated with urethrocele, cystocele,rectocele, enterocele.
Dolkha being the mountainous region, anaemia is lesscommon, with preponderance of high percentages of womenwith haemoglobin observed above 12gm%.
It is learnt from this study that highest percentage of thepyuria was found in the second degree genital prolapse patient(15.2%) followed by first degree (14.2%) genital prolapsepatient. This is because the residual urine remains in theurinary bladder in cystocele, associated in these cases ofUVP resulting incomplete voiding and retention of urinecontributing to bacterial infection. Most urinary tract infectionare ascending infections to urethra, bladder, ureters and kidney.If UTI can be defined as significant pyuria (a non-timedvoided urine sample showing more than 5 -10 pus cells/ HPFexamined from the urine sediment), in the presence ofurinary symptoms then 41% women suffered UTI. It hasbeen noted that about 4-6% of female of childbearing agewill have UTI at any surgery and 10-20% of female willexperience a UTI in their lifetime.7,8 This study could notfind marked difference in pus cell count in different degreesof the prolapse.
���������������� �� ���������� ������������
��"!- ��"(-
��")- ��"--
������� �������
� �� �
���(
(
�(��
�
�
(
��
�(
!�
!(
�� �����
!�
�
�(
��
./ ../ .../
�
���������������������������������� ��������� ������������
&�'����0
�����������*
!�"�(�10, 2�(�10,0�����������������
�*��*��*!�*��*(�*��*)�*��*-�*
��"�!�10,
///
�(')�*
�)'��*
)�'��*
�*
��'-)*
��'-�*
��'��*
�('��*
��')�*
In this study 5% third degree genital prolapse patients werein the age group (20-39) and 15% were in the age group 40-59. Similarly 12 % and 2% third degree genital prolapsepatient were in the age group 60-79 and 80-99 respectively.This result showed that the percentage of the prolapseincreases with the age.
Highest percentage of the pus cell, more than 5 pus cells/HPF was found in the second degree genital prolapse patient(15.2%) followed by first degree genital prolapse patients(14.2 %) and third degree genital prolapse patients (11.7 %)(Fig 2).
Investigating genital prolapse in the community
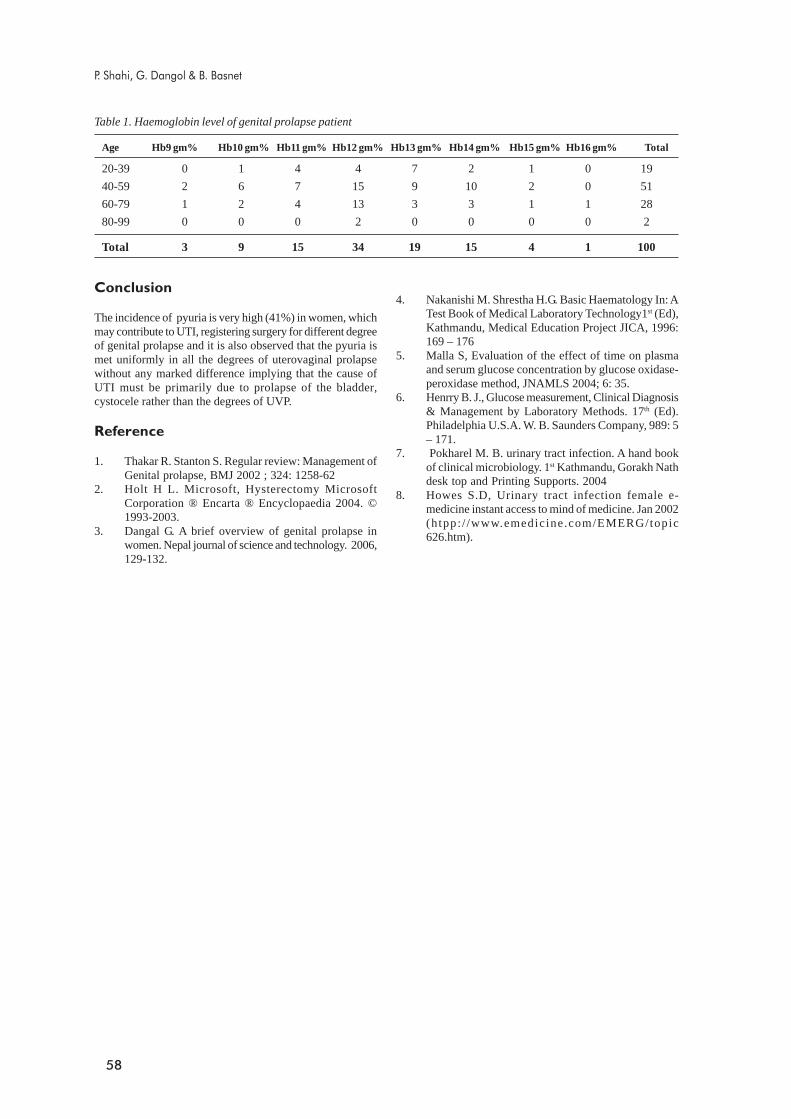
58
Age Hb9 gm% Hb10 gm% Hb11 gm% Hb12 gm% Hb13 gm% Hb14 gm% Hb15 gm% Hb16 gm% Total
20-39 0 1 4 4 7 2 1 0 19
40-59 2 6 7 15 9 10 2 0 51
60-79 1 2 4 13 3 3 1 1 28
80-99 0 0 0 2 0 0 0 0 2
Total 3 9 15 34 19 15 4 1 100
Conclusion
The incidence of pyuria is very high (41%) in women, whichmay contribute to UTI, registering surgery for different degreeof genital prolapse and it is also observed that the pyuria ismet uniformly in all the degrees of uterovaginal prolapsewithout any marked difference implying that the cause ofUTI must be primarily due to prolapse of the bladder,cystocele rather than the degrees of UVP.
Reference
1. Thakar R. Stanton S. Regular review: Management ofGenital prolapse, BMJ 2002 ; 324: 1258-62
2. Holt H L. Microsoft, Hysterectomy MicrosoftCorporation ® Encarta ® Encyclopaedia 2004. ©1993-2003.
3. Dangal G. A brief overview of genital prolapse inwomen. Nepal journal of science and technology. 2006,129-132.
Table 1. Haemoglobin level of genital prolapse patient
4. Nakanishi M. Shrestha H.G. Basic Haematology In: ATest Book of Medical Laboratory Technology1st (Ed),Kathmandu, Medical Education Project JICA, 1996:169 – 176
5. Malla S, Evaluation of the effect of time on plasmaand serum glucose concentration by glucose oxidase-peroxidase method, JNAMLS 2004; 6: 35.
6. Henrry B. J., Glucose measurement, Clinical Diagnosis& Management by Laboratory Methods. 17th (Ed).Philadelphia U.S.A. W. B. Saunders Company, 989: 5– 171.
7. Pokharel M. B. urinary tract infection. A hand bookof clinical microbiology. 1st Kathmandu, Gorakh Nathdesk top and Printing Supports. 2004
8. Howes S.D, Urinary tract infection female e-medicine instant access to mind of medicine. Jan 2002(htpp: / /www.emedicine.com/EMERG/topic626.htm).
P. Shahi, G. Dangol & B. Basnet

59
Introduction
Heterotopic pregnancy is the coexistence of intrauterine andextra-uterine pregnancies. Naturally occurring heterotopicpregnancy is very rare, being said to occur once in every4000 to 30,000 pregnancies. It was first described byDuverney in 1708 during an autopsy.2 Almost certainly theincidence has increased in recent years, in parallel with theincreasing incidence of tubal pregnancies generally. This isattributed to the increased use of assisted reproductivetechnology and the increased incidence of tubal damage frompelvic inflammatory disease and tubal surgery, both forinfertility and for sterilization. Earlier and more precisediagnosis of ectopic pregnancies also adds to the number ofthese diagnoses.
Case report
A 29 years old multigravida was admitted to the gynaecologyward at BPKIHS, Dharan, on 28.1.04 with a one-day historyof abdominal pain and vomiting. There was no vaginal bleeding.Her last menstrual period had begun on 15.12.03, i.e., she hadhad 6 weeks and 2 days amenorrhoea. There was no significantpast medical or surgical history. On examination she wasfound to be extremely pale and had tachycardia. The abdomenwas distended and there was marked generalized tenderness.On vaginal examination, cervical excitation pain and generalizedpelvic tenderness were present. The uterine contour could notbe defined. Urinary pregnancy test was positive. The clinicaldiagnosis was clearly that of a ruptured ectopic pregnancyand an emergency laparotomy was performed.
At operation massive haemoperitoneum was found, togetherwith a ruptured right ampullary pregnancy. The uterus wasbulky and the left tube normal. Both ovaries were normal.Right salpingectomy was carried out and a three-unit blood
transfusion was given. The woman’s post-operative recoverywas uneventful. Histopathological examination of the excisedtube confirmed the presence of chorionic villi.
On 23.5.04 (four months after the laparotomy) the womanpresented to the gynaecology out-patients departmentcomplaining of an abdominal mass. She was otherwise welland had not menstruated since the laparotomy. On abdominalexamination she appeared to be about 24 weeks pregnant.An ultrasound examination revealed a normal singleintrauterine pregnancy, with biometry suggesting 22 weeksand 4 days gestation. (This corresponded almost exactlywith the calculated 22 weeks and 6 days from her LMP). Inother words, the uterine pregnancy would have been a littlemore than six weeks gestation at the time that her tubalpregnancy was diagnosed and treated.
Regular antenatal care was uneventful. On 9.9.04, after 38weeks and 3 days amenorrhoea, the woman went intospontaneous labor and proceeded to the normal delivery of ahealthy female baby, weighing 3.1 kg.
Comment
Heterotopic pregnancy is rare. Usually a pregnancy isdiagnosed and is assumed to be intra-uterine (even afterultrasound examination) until clinical features of an ectopicpregnancy manifest themselves, often with an unexpected(and potentially fatal) intra-abdominal haemorrhage. Thediagnosis is therefore often late. Earlier diagnosis depends onthe clinician having a high suspicion. Quantitativemeasurements of serum beta-HCG levels are of no use, becausethe intra-uterine pregnancy will be producing normal andrising levels. Ultrasonography has the most valuablecontribution in the diagnosis of ectopic pregnancy. Becauseof the dire emergency, as the patient had presented in shock,
Spontaneous heterotopic pregnancy – not so rare?A case report
Sangeeta Mishra, Norman MorrisDepartment of Obstetricts and Gynecology,
B P Koirala Institute of Health Sciences,Dharan, Nepal
AbstractA 29-year old multigravida presented with a ruptured tubal pregnancy and underwent right salpingectomy. Four monthslater she presented with an abdominal mass and an intra-uterine pregnancy was confirmed. The ultrasound datingindicated that the intra-uterine conception had occurred before the tubal pregnancy was diagnosed. She subsequentlydelivered a healthy baby at term; an example of heterotypic pregnancy.
Key words: ruptured tubal pregnancy, heterotopic /heterotypic pregnancy,
Correspondence:Sangeeta Mishra, MD. Department of Obstetricts and Gynecology, B P Koirala Institute of Health Sciences,Dharan, Nepalmail: [email protected]
C A S E R E P O R T
N. J. Obstet. Gynaecol Vol. 1, No. 1, p. 59 - 60 May 2006

60
laparotomy was performed immediately. If ultrasound hadbeen done in this case at the time of presentation, heterotopicpregnancy would have been diagnosed there and then. Despitethe surgery and exposure to general anaesthesia in earlypregnancy, it is surprising that the pregnancy advanced tosix months when the patient became aware hereself and camefor antenatal visit.
These days heterotypic pregnancy is not so surprising dueto artificial reproductive technology and embryo transferand these goes well detected.1-3 Spontaneous progression ofundetected intrauterine pregnancy from the time of surgicalmanagement of acute or subacute ruptured ectopic pregnancyon post operative follow up is rare but rarer must be thisone, where patient herself self reported the pregnancy at midtrimester. On the contrary, spontaneous abortion of anintrauterine pregnancy has followed ectopic rupture.4
Sometime in these rare cases of heterotypic pregnancy intra-uterine pregnancy is assumed on the basis of ultrasounddiagnosis until clinical features of an ectopic pregnancymanifest themselves, often with an unexpected (andpotentially fatal) intra-abdominal haemorrhage. The diagnosisof heterotypic pregnancy being therefore late.
Earlier diagnosis depends on the clinician having a high indexof suspicion. Quantitative measurements of serum beta-HCG levels are of no use, because the intra-uterine pregnancywill be producing normal and rising levels serum beta-HCG.Pregnant women with risk factors for ectopic pregnancy
require particularly careful assessment. Risk factors includea history of tubal pregnancies, pelvic inflammatory disease,tubal sterilization and tubal infertility (especially those whohave undergone tubal reconstructive surgery or used artificialreproductive technology (including ovulation induction andin vitro fertilization).3 Other women at risk include thosewho conceive despite the use of an intra-uterine contraceptivedevice or progestogen –only contraceptive pills.
Conclusion
Spontaneous heterotypic pregnancy is rare and hence maygo undiagnosed when faced with surgical emergencies likeruptured ectopic where one hurries for quick management ofthe condition after a clinical diagnosis.
References
1. Aneziokoro EA. Heterotropic pregnancy with livetwins. African J Reprod Health, 2002 Dec; 6 (3): 117-119
2. Harrington JC, Lyons EA. Heterotopic pregnancy.Available from: http://www.thefetus.net
3. Gruber I, Lahodny J, Illmensee K, Losch A.Heterotopic pregnancy: report of three cases. WienKlin Wochenschr. 2002 Mar 28;114(5-6):229-32.
4. Sisa CM. Double (uterine and ectopic) pregnancy of apatient using an intrauterine contraceptive device. AmJ Obstet Gynecol 1984 Aug 15; 149(8): 912.
S. Mishra & N. Morris

61
Introduction
Postpartum hemorrhage is the major cause of maternalmortality and morbidity in developing world1. Postpartumhemorrhage (PPH) is defined as a blood loss of more than500 ml after vaginal delivery and more than 1000 ml aftercaesarean delivery 2. There are several causes of PPH most ofwhich are unpredictable. However few conditions likeplacenta previa, abruptio placentae, prolonged labor andmultiple pregnancy increases the risk of PPH. When the riskof hemorrhage is anticipated one should be prepared tomanage such situation promptly and efficiently. Bleedingfrom placental site in placenta previa sometimes can be verydifficult to manage. Several measures can be used to controlthe bleeding from placental site in placenta previa duringcaesarean section like uterotonics, direct pressure with warmpacks, sewing placental bed with figure of 8 stitches,continuous locking sutures, ligation of uterine arteries andultimately hysterectomy when all measures fail. Several newertechniques are also coming in practice like pelvic arteryembolisation and application of isthmic-cervical appositionsuture. Isthmic-cervical apposition sutures arrests bleedingfrom lower segment by occluding placental bed vessels bythe apposition of the anterior and posterior walls3.
Case report
A 25 years primi gravida at 40 weeks 4 days of pregnancypresented to emergency room with pain lower abdomen forthree hours. She had regular antenatal periods that had beenuneventful. Obstetric scan, done at 22 weeks showedposterior placenta away from lower uterine segment. Onexamination during admission her vitals were normal, heruterus was of term size, cephalic presentation, 2/5 palpable,fetal heart sound 140/ min and mild contraction. On vaginal
Isthmic-cervical apposition suture for postpartumhemorrhage during caesarean section
for placenta previa:A case report
Nira Singh Shrestha, Meena ThapaDepartment of Obstetrics & Gynecology,
Kathmandu Medical College Teaching Hospital,Sinamangal, Kathmandu.
AbstractExcessive hemorrhage due to bleeding from placental bed in placenta previa is one of the difficult situation obstetriciansface every now and then. Several measures are there for managing bleeding from placental bed in placenta previa likeuterotonics, manual compression, undersewing placental bed, uterine artery ligation, internal iliac ligation and evenhysterectomy in severe intractable hemorrhage. We report a case of excessive bleeding from placental bed in placentaprevia during cesarean section managed successfully by isthmic- cervical apposition suture when measures like uterotonicsand undersewing placental bed failed to control the bleeding.
Key words: Placenta previa, Post partum hemorrhage, isthmic-cervical apposition suture.
examination; cervix was 30 % effaced, Os 1.5 cm dilated,head at “-1 station”, membrane intact and pelvis adequate.About six hours after admission, there was vaginal bleedingslightly more than show, but stopped on its own after fewminutes. Patient was kept under close observation andbleeding per vagina restarted again about 2 hours later. Therewere no signs of abruptio placentae. Emergency lowersegment cesarean section was done for
antepartum hemorrhage not being sure whether it was placentaprevia based on the ultra sonogram done at 22 weeks withfinding of placenta away from lower segment. At surgeryType II posterior placenta previa was found with generalizedoozing from placental bed. Uterotonics (oxytocin, methergin)and several figures of eight stitches were taken at placentalbed, but bleeding continued despite all the measures taken.Isthmic-cervical apposition suture was given with chromiccatgut no.2. Bleeding was completely controlled. Uterus wasthen closed in 2 layers, abdomen closed by usual method.Total blood loss was 700 ml. Postoperative period wasuneventful and the patient was discharged on 6th postoperativeday. Follow up at 2 weeks and 6 weeks detected noabnormality.
Comment
B-lynch et al4 described the technique of uterine compressionsuture in patient with intractable postpartum hemorrhage.This technique achieved complete hemostasis and avoideddifficult pelvic surgery while preserving patient’s uterus andfertility. But its complex sequence of suturing is hard toremember during emergency. Mukhopadhyay andArulkumaran3 modified B-lynch suture to make it simplerand have also described isthmic-cervical apposition sutureto stop persistent bleeding coming from the lower uterinesegment due to placenta previa during cesarean section.
Correspondence:Nira Singh Shrestha, KMC, Sinamangal, Kathmandu, email: [email protected]
N. J. Obstet. Gynaecol Vol. 1, No. 1, p. 61 - 62 May 2006
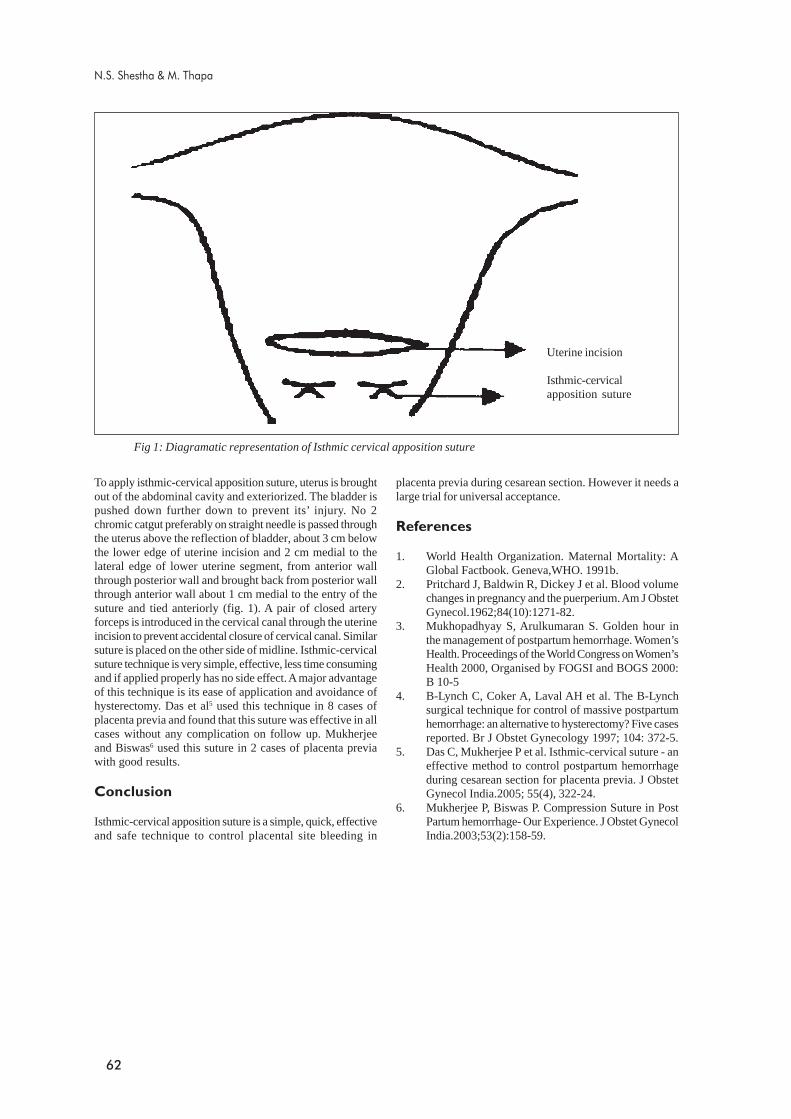
62
placenta previa during cesarean section. However it needs alarge trial for universal acceptance.
References
1. World Health Organization. Maternal Mortality: AGlobal Factbook. Geneva,WHO. 1991b.
2. Pritchard J, Baldwin R, Dickey J et al. Blood volumechanges in pregnancy and the puerperium. Am J ObstetGynecol.1962;84(10):1271-82.
3. Mukhopadhyay S, Arulkumaran S. Golden hour inthe management of postpartum hemorrhage. Women’sHealth. Proceedings of the World Congress on Women’sHealth 2000, Organised by FOGSI and BOGS 2000:B 10-5
4. B-Lynch C, Coker A, Laval AH et al. The B-Lynchsurgical technique for control of massive postpartumhemorrhage: an alternative to hysterectomy? Five casesreported. Br J Obstet Gynecology 1997; 104: 372-5.
5. Das C, Mukherjee P et al. Isthmic-cervical suture - aneffective method to control postpartum hemorrhageduring cesarean section for placenta previa. J ObstetGynecol India.2005; 55(4), 322-24.
6. Mukherjee P, Biswas P. Compression Suture in PostPartum hemorrhage- Our Experience. J Obstet GynecolIndia.2003;53(2):158-59.
To apply isthmic-cervical apposition suture, uterus is broughtout of the abdominal cavity and exteriorized. The bladder ispushed down further down to prevent its’ injury. No 2chromic catgut preferably on straight needle is passed throughthe uterus above the reflection of bladder, about 3 cm belowthe lower edge of uterine incision and 2 cm medial to thelateral edge of lower uterine segment, from anterior wallthrough posterior wall and brought back from posterior wallthrough anterior wall about 1 cm medial to the entry of thesuture and tied anteriorly (fig. 1). A pair of closed arteryforceps is introduced in the cervical canal through the uterineincision to prevent accidental closure of cervical canal. Similarsuture is placed on the other side of midline. Isthmic-cervicalsuture technique is very simple, effective, less time consumingand if applied properly has no side effect. A major advantageof this technique is its ease of application and avoidance ofhysterectomy. Das et al5 used this technique in 8 cases ofplacenta previa and found that this suture was effective in allcases without any complication on follow up. Mukherjeeand Biswas6 used this suture in 2 cases of placenta previawith good results.
Conclusion
Isthmic-cervical apposition suture is a simple, quick, effectiveand safe technique to control placental site bleeding in
Fig 1: Diagramatic representation of Isthmic cervical apposition suture
N.S. Shestha & M. Thapa
Uterine incision
Isthmic-cervicalapposition suture

63
Introduction
Failure of development of vagina (agenesis) affects one in 4to 5 thousand female births.1 Imperforate vagina is causedby the failure of cells to degenerate in the center of the vaginalplate and by the failure of the vaginal canal to open into theurogenital sinus while an imperforate hymen is caused bythe failure of cells to degenerate in the lower part of thevaginal plate and the wall of the urogenital sinus.2
The three main types of congenital vaginal occlusions thatlead to hydrometrocolpos include imperforate hymen,transverse vaginal septum and segmental vaginal atresia. Inthe rare segmental atresia, there is a thick fibrous tissueobliterating a segment of vagina while in transverse vaginalseptum, a fibroepithelial membrane is present most often inthe mid-portion of the vagina. We describe a case report.
Case report
Twenty-one years old (Gravida 1, Parity 0) underwentroutine obstetrical ultrasound at 34 weeks of gestation.Sonogram revealed a large cystic mass of approximately 5.7x 5.2 cm in dimension occupying the fetal pelvis and thelower abdomen, displacing the urinary bladderanterosuperiorly. The mass showed low-level internal echoesand peripheral, lobulated and echogenic component. Bothkidneys were normal and there was no hydro-ureteronephrosis. Provisional diagnosis of dermoid cyst wasmade ultrasonographically (Fig.1). Review of prior routinescreening scan performed at 18th weeks of gestation showednormal anatomy of the fetus.
Congenital vaginal obstruction withintrauterine hydrometrocolpos:
A case report
Ghanshyam Gurung, Ram K Ghimire, Benu Lohani, Laxman R PokharelDepartment of Radiology and Imaging, TU Teaching Hospital Institute of Medicine,
Kathmandu, Nepal
AbstractIntrauterine hydrometrocolpos is a rare condition caused by congenital vaginal obstruction. Imperforate hymen is themost common cause and manifests as a huge abdominopelvic mass. Ultrasonography is an invaluable tool in screeningand evaluation of fetal intra-abdominal mass but even with serial ultrasonography it may be very difficult to delineate theexact site of origin and come to a diagnosis. MRI is the most reliable and sensitive modality to evaluate complexmalformations/ masses. In a female child born with cystic abdominopelvic mass a thorough neonatal examination afterbirth focusing on the urogenital system and the extremities will give a significant clue in diagnosis and subsequentmanagement of hydrometrocolpos. Here we present a case of intrauterine hydrometrocolpos which remained indiagnostic dilemma until the postnatal period.
Key words: complex malformations, congenital vaginal obstruction, hydrometrocolpos
Correspondence:Ghanshyam Gurung, Department of Radiology and Imaging, TU Teaching Hospital Institute of Medicine,Kathmandu, Nepal, email: [email protected] Tel. no.: 4243327; Mobile: 9851035217
A repeat sonogram was performed a week later to reevaluatethe fetus and to review the diagnosis. Though a detailedevaluation of the urinary bladder was difficult it appeared tobe flattened and displaced anteriorly. A large smooth tubular/cystic mass extending from pelvis to the upper abdomenwas noted with mild wall thickening, suggesting bowel originof the mass. Thus a diagnosis of dilated rectum with co-existent ano-rectal malformation was made. Scanning of therest of the fetal parts revealed no abnormality .
Labor was induced at 35+2 days of gestation and a normalvaginal delivery with episiotomy was possible with undesiredmild intrapartum eclampsia that complicated the event. Alive, female baby of 2 kgs, with an Apgar score of 2/10, 8/10was delivered. CNS reflexes were intact and normal. Local
Figure 1
Fig.1 Transverse and sagittal antenatal ultrasound scansat 34 weeks of gestation showing a complex cystic mass infetal pelvis. A diagnosis of dermoid cyst was given.
N. J. Obstet. Gynaecol Vol. 1, No. 1, p. 63 - 65 May 2006

64
examination revealed a large and compressible, cystic massin the perineal region increasing in size during bouts of cry.Anal opening was intact. Laboratory parameters were withinnormal range except for mild hyperbilirubinemia.
Ultrasound scanning of the neonatal abdomen was carriedout immediately after delivery. A large cystic abdominopelvicmass without clear delineation of its origin was re-noted.MRI was then considered for further evaluation. A large,pear shaped, cystic abdominopelvic mass with low signalintensity in T1WI and high signal intensity in T2WI wasseen to be extending inferiorly into the perineal region. Urinarybladder was separately identified anterior to the cystic mass.Lumbar and sacral spines were normal and rectum wasidentified between the cystic mass and sacrum. Diagnosis ofhydrometrocolpos was suggested (Fig. 2). A detailed physicalexamination was then carried out by the neonatologist, whichclarified the abnormality.
Comment
Imperforate hymen is the simplest of these lesions.2 It maymanifest as a huge abdominopelvic mass due to retained fluidand mucus. Vaginal obstructions are usually diagnosed in thenew born as intrapelvic mass lesions, hydrocolpos in thenewborn and haematocolpos at puberty.1
In some cases, fetal urination into the uterus and vagina occurswhich causes their dilatation. This is because of a commonurogenital sinus. The result may be proximal urinary tractdilatation due to pressure effect. Sometimes, there may be arectovaginal communication on the dorsal wall of the lowervagina above the urogenital sinus, allowing meconium to mixwith urine. If there is communication between rectum anduterus/vagina, the malformation is then referred to as thecloacal form of imperforated anus.2
Fig. 3 Sagittal ultrasound scan of the neonatal uterus afterdrainage
Gurung et al
Fig.2 T1 and T2 weighted Sagittal MRI Scan of theneonate showing a large fluid filled uterus and vagina.
The baby became febrile after few days of conservativeobservation. Staphylococcus aureus was isolated in bloodculture. Pediatric surgeons were then called in for surgicalintervention. Approximately, 1500 ml thin fluid, mixed withpus, gushed out in pressure after a small incision was placedin the hymen. A drain tube of 7 Fr was then kept in situ forthe subsequent drainage.
Cytology report from the fluid sample revealed plenty ofinflammatory cells ruling out the possibility of dermoid cyst.Culture and sensitivity of the same fluid didn’t show anygrowth within 24 hours. A week post- drainage, rescanningwas done which revealed slightly bulky but normal uteruswith the drain tube inside the uterine cavity. The cystic masshad completely disappeared (Fig 3).
When a large cystic abdominopelvic mass is noted in thefetus during ultrasonography, one should not be confusedwith uterine – vaginal swelling, a self-limiting conditionreceding rapidly after birth attributed to maternal estrogenstimulation. McKusick – Kaufman syndrome (MKKS) andBardet Biedl syndrome (BBS) are associated with congenitalhydrometrocolpos. Some affected infants may have fingerand toe anomalies as part of a genetically determinedsyndrome. MKKS is a rare, recessively inherited condition,reported mainly in young children characterized by vaginalatresia with hydrometrocolpos, postaxial polydactyly andcongenital heart defects.3 MKKS was first delineated byMcKusick et al in 1964 in two Amish siblings and rapidlyconfirmed over 60 cases have now been reported andautosomal recessive inheritance is clearly established.4
Cardinal features of MKKS are hydrometrocolpos andpolydactyly and it is often reported as the “hydro-metrocolpos polydactyly syndrome.5,6

65
BBS is another recognized but heterogeneous group ofautosomal recessive disorder characterized by retinaldystrophy or retinitis pigmentosa (appearing usually between10 and 20 years age), post axial polydactyly, obesity,nephropathy, mental disturbances or occasionally mentalretardation.7,8
In our case, there was no evidence of upper urinary tractdilation, anal opening was patent and the extremities includingthe finger and toes were normal. This ruled out the possibilityof syndromes associated with hydrometrocolpos.
Conclusion
Ultrasonography is an invaluable tool in screening andevaluation of fetal intra-abdominal mass, however; exactdelineation of its origin may be difficult even in the postnatalperiod. Currently, MRI is the most reliable and sensitivemodality to evaluate complex neonatal intra-abdominalmalformations/ masses and determine their site of origin.Suspicion of hydrometrocolpos should be made when a largecystic abdominopelvic mass is noted in the fetus duringultrasonography and the scan should be directed to detectany associated fetal congenital anomaly, especially of thegenitourinary system, extremities, and the heart. Appropriateantenatal delivery and intervention protocols should then beformulated for a desired fetal outcome.
In a developing nation like Nepal where antenatal ultrasoundis not widely available, a thorough neonatal examination afterbirth focusing on the external genitalia may provide asignificant clue in diagnosing and subsequent management
of hydrometrocolpos in any female child born withabdominopelvic lump.
References
1. Caffey John. Caffey’s Pediatric X-ray Diagnosis:Disorder of Genital Tract, 1985; vol-2, 8:1909
2. Richard S. Snell, M. D. Ph.D .Clinical Embryology formedical students: The Genital system, 3:237
3. Albert David, Pierre Bitoun, Didier Lacombe et al;.Hydrometrocolpos and polydactyly: a commonneonatal presentation of Bardet-Biedl and Mc Kusick-Kaufman syndromes. J med Genet 1999; 36:599-603(August)
4. McKusick V, Bauer BL, Koop CE, Scott RB.Hydrometrocolpos as a simply inherited malformation.JAMA 1964; 189:813-816.
5. Cantani A, Tacconi ML, Benincori N, et al. Raresyndromes. The Kaufman –McKusick syndrome. Areview of the 44 cases reported in the literature. AnnGenet 1987; 30:70-74 (medline)
6. Chitayat D, Hahm SY, Marion RW, et al. Furtherdelineation of the McKusick-Kaufmanhydrometrocolpos-polydactyly syndrome. Am J DisChild 1987; 141:1133-1136
7. Schachat AP, Maumenee IH. The Bardet-Biedlsyndrome and related disorders. Arch Ophthalmol1982; 100: 285 -288.
8. Green JS, Parfrey PS,Harnett JD, et al. The cardinalmanifestations of Bardet-Biedl syndrome, a form ofLaurence-Moon-Biedl syndrome. N Engl J Med 1989;321:1002-1009
Intrauterine hydrometrocolpos

66
Introduction
Cervical intraepithelial neoplasia (CIN) is an establishedprecursor of invasive cervical cancer which does not alwaysneed radical surgery (hysterectomy). Excision proceduressuch as cold knife, electro diathermy or laser conization ofthe cervix are major surgical modalities of CIN though it isnot practiced frequently in Nepal due to many reasons.Traditional cold knife conization has been used successfullyfor generations to excise the lesion extending into theendocervical canal. Although Laser conization and LEEP hasbeen replacing cold knife conization because of theiradvantages over it, it is still the time-honored technique,which continues to be used in most part of developingcountries, although not without complications as is describedin this case.
Case report
A 38 years old lady, P2+0
was admitted in the departmentof Obs/Gyn on 2nd March 2006 (18/11/ 062)withthe complaint of lower abdominal pain for seven dayswhich had increased in intensity for the last three days,such that none of the analgesics taken could relieve thisunbearable pain.
She had undergone cold knife cervical conization (Fig 1) forCIN III which was picked up by cervical cytology andconfirmed by colposcopy directed biopsy one year back on23rd Feb 2005 (11/11/061) in our setup. Following conizationthere was amenorrhoea of 2 months but Transvaginalsonography (TVS) then revealed normal pelvic findings. Onthe third month of conization, the cervical cytology revealed adisease free condition. Subsequently she had regular periodsbut the flow decreased in amount in the successive menstrualcycles but with the increasing dysmenorrhoea. In the last 2cycles prior to the admission, (11 months of conization) therewas decreased menstrual flow (spotting) and severedysmenorrhoea, which she self medicated with the intake ofanalgesics; the next menstruation; judged was without any
Complete cervical stenosis resulting hematometrafollowing cold knife conization for CIN III:
A case report
Geeta Gurung, Ashma Rana, Archana Amatya, Shilu AdhikariDepartment of Obstetrics and Gynaecology, TU Teaching Hospital, Kathmandu
AbstractAmong the several recognized complications of cervical conization for pre-invasive carcinoma of cervix, stenosis is theone. We have encountered a case of cervical stenosis in a 38 years old multiparous lady, who had presented withspotting and severe dysmenorrhoea after conization for cervical intraepithelial neoplasia (CIN) III, which is reportedhere with.
Key words: cervical intraepithelial neoplasia (CIN) III, cervical conization, cervical stenosis, hematometra
Figure 1 cervical conization
spotting; accompanied by severe abdominal pain, ?premenstrual pain; not relieved with analgesics, seekinghospitalization. Her bladder and bowel habits were unchanged.On pelvic examination, ballooning up of lower uterine partwas identified; a small puckered dimple was seen in thejunction between the posterior vaginal wall and the balloonedup lower uterine part. TVS showed fluid filled ballooned uplower part of uterus whereas the upper uterine part lookednormal, with small amount of fluid collection in the cavity(Fig 2).
With the diagnosis of hematometra due to cervical stenosisfollowing cervical conization, dilatation and drainage was
correspondence:Dr. Geeta Gurung, DGO, FCPS, Associate Professor, Department of obstetrics and gynaecology TU Teaching hospitalKathmandu, email: [email protected]
N. J. Obstet. Gynaecol Vol. 1, No. 1, p. 66 - 67 May 2006
sureshh

67
attempted. The dilatation could not be done simply by dilatorsdue to dense fibrosis and was initiated by making an incisionwith 16 gauze needle in the puckered area. This allowedvisualization of the cervical os which was successively dilated
up to 12 Hegar. About 70 ml of thick chocolate fluid wasdrained (Fig 3). Two days after the dilatation and drainageTVS was repeated which showed the disappearance of thelower ballooned up area (cervicometra) hence she wasdischarged.
Comment
It is well understood from this case, how necessary counselingis, with regards to the type of menstruation, that one certainlywould be enabled to make early detection of cervical stenosisand its consequences postoperatively.
Regular follow up for repeat cervical smear at three monthlyintervals is also equally mandatory.
Cervical stenosis, one of the documented late complicationsof conizaton seen in this woman after one year of theprocedure was indicated by spotting and dysmenorrhoea.Cervical stenosis is defined as cervical narrowing that preventsinsertion of 2.5 mm Hegar dilator1 with regards to which thiscase can be labeled as complete cervical stenosis. The risk ofpostoperative cervical stenosis is higher in wider excision ofcervix beyond 20 mm of height for extensive endocervicallesion.2 The parity, age, previous treatment for CIN,satisfactory colposcopy, size of lesion, its histological typeand the extent of excision do not increase the risk of cervicalstenosis. A study done by Mathevet P and colleagues showed4 out of 28 patients who developed cervical stenosis in 3years duration following cold knife conization.3 Similar studyshowed the incidence of cervical stenosis of 11.8% in 212patients following cold knife conization in comparison with1.6 % of 439 Patients following laser conization.2
Conclusion
Following conization, the possible complication of cervicalstenosis and hematometra must be born in mind that couldexpress as decreased menstrual flow (spotting) and increasingdysmenorrhoea.
References
1. Baldauff JJ, Dreyfus M, Ritter J, Mayer P, PhilippeE. Risk of cervical stenosis after large loop excision orlaser conization. Obstet Gynecol 1996; (6): 933
2. Nordland K, Skjeldestad FE Hagen B. Treatment ofcervical intraepithelial neoplasia before and afterintroduction of laser conization. Tidsskr NorLaegeforen. 2005;125 (2):167-9.
3. Mathevet P, Chemali, Roy M, Dargent D. Long termoutcome of randomized study comparing threetechniques of conization: cold knife, laser and LEEP.Eur J Obstet Gynecol Reprod Biol 2003; 10: 106.
Figure 3. Drainage of chocolate colored tarry blood
Hematometra following cold knife conization
Figure 2 Hematometra following cervical stenosis (TVS)

68
Fig.1: A male with Klinefelter syndrome (47 XXY). Statureincreased, body shape somewhat feminine, small penis withatrophied testes.
Introduction
Before the chromosomal abnormalities were understood thesyndrome that was described in 1942 by Harry Klinefelterwas named after him as Klinefelter syndrome. It is one of themost common sex chromosome aneuploidy with incidenceof 1 in 300 to 1 in 1000 male births in all racial groups.Though phenotype is less striking it is one of the commoncauses of hypogonadism in male. Klinefelter males are tallerthan average with disproportionately long arms and legs,gynaecomastia, spermatogenesis with legdigism andhypergonadotrophy. They also have lower level oftestosterone that puts them into the risk of osteoporosis andhigh risk of neoplasia of germ cells and breast1. They aresterile due to atrophy of seminiferous tubules. About 16-30% show gynaecomastia2. Although not mentally retarded,they have IQ 10-15 points below normal3.
Klinefelters have 47 XXY karyotypes, though 15% aremosaic i.e. they have both cell lines 47 XXY and 46 XY.
About 50% of XXY conceptus are aborted spontaneously.Even individuals with 48 XXXY and 49 XXXXY karyotypeshave been reported4. Presence of Y chromosome gives themmale phenotype, however increase in number of extra Xchromosome increases their mental retardedness and otherphysical abnoramalities5.
Case report
A 24 years old male presented to the surgery OPD unit 2 atBPKIHS, Dharan, Nepal with complaints of absence of pubichair and underdeveloped genital organs.
On examination he was found to have small penis with scrotumhaving atrophied testes of the size of a peanut, femininevoice, gynaecomastia and absence of axillary hair. He wastaller than average. He was suspected of a case of testicularfeminization and was referred to biochemistry laboratoryfor hormonal and cytogenetics laboratory for chromosomalanalysis. (Fig 1)
Sex chromosome aneuploidy (Klinefelter syndrome)analyzed by cytogenetic test:
A case report
Monika Thapa*, Chandra B Jha*, Akshay Pratap**, Guna B Thapa***
*Cytogenetics laboratory, Department of Anatomy, BPKIHS, Dharan, Nepal**Department of Surgery, BPKIHS, Dharan, Nepal
***Department of Radiology, BPKIHS, Dharan, Nepal.
AbstractA 24 years old male suspected of a case of testicular feminization was referred to cytogenetics laboratory for chromosomalanalysis. He had 47 XXY cell line. It was a case of Klinefelter syndrome, confirmed by karyotyping test. He was referredto the endocrinologist for further management.
Key words: chromosomal analysis, cytogenetics, endocrinologist, Klinefelter syndrome, testicular feminization
correspondence:Dr. Monika Thapa, Cytogenetics Laboratory, Department of Anatomy, BPKIHS, Dharan, NepalEmail: [email protected] Phone: 00977-25-525555 extn. 2443(off), 2477(Lab.)
N. J. Obstet. Gynaecol Vol. 1, No. 1, p. 68 - 69 May 2006

69
Comment
His pedigree was analyzed for three generations. Hisgrandparents and parents are normal. There was no historyof consanguineous marriage between the parents and at thetime of pregnancy of index case the mother was below thirty.His two other siblings are normal, married and have normalchildren. His chromosomal analysis showed presence of 47XXY cell line in all the fifty metaphase spreads examined(Fig.2). There was no major structural abnormality found inhis chromosomes.
Fig.2: Karyogram showing chromosomes chromosomes47 XXY.
As reported earlier, extra X chromosome is contributed inabout 56% of cases by mother than father, which can becorrelated with non-disjunction of the sex chromosomesduring the first and second meiotic division of gametogenesisof both parent6.
His hormonal assay shows very high level of FSH 25.91(Normal 1-1.4 MIU/ml) and LH 14.56 (Normal 0.7-7.4 MIU/ml). Estradiol level was 15.0pg/ml (Normal 7.63-42.6pg/ml).However testosterone level was 0.49ng/ml which was farbelow the normal range found in male (2.8-8.0ng/ml).Ultrasonography report showed bilateral testicular atrophy.
The only treatment for Klinefelter’s is supplementation oftestosterone that has been found to support androgendependent processes like facial and body hair, muscle massdevelopment, libido etc. Cholesterol level is also recommendedto be monitored with testosterone. In addition regular self-examination of breast for the risk of breast cancer isrecommended. The index case has been advised to see theendocrinologist for the treatment.
References
1. Horowitz M, Wishart JM,O’Loughlin PD et al.Osteoporosis and Klinefelter’s syndrome. ClinEndocrin. 1992; 36:113-118.
2. Paulsen CA, Plymate SR. Klinefelter’s syndrome. InKing RA, Rotter J, Motulsky AH (eds): The Geneticbasis of common Diseases. Oxford University Press,New York, 1992: 876-894.
3. Jorde LB, Carey JC, Bamshad MJ, White RL. MedicalGenetics 2nd ed. Mosby Publishers, 1999.
4. MacDonald M, Harsold T, Harvey J, Wang LH,Morton NE, Jacobs P. The origin of 47,XXY and47,XXX aneuploidy: Heterogenous mechanisms androle of aberrant recombination. Hum. Molec. Genet.1994; 3: 1365-1371.
5. David LR, Rimoin J, Michael C, Reed EP, Bruce RK.Principles and practice of Medical Genetics, 4th ed.,Vol. 1, Churchill-Livingstone, 2002.
6. Harvey J, Jacobs PA, Hassold T, Pettay D. Thepaternal origin of 47,XXY males. Birth Defects OriginalArticle Series 1990; 26: 289-296.
Klinefelter syndrome analyzed by cytogenetic test

70
Introduction
Dysgenesis is the defective embryonic development of anorgan. Ovarian dysgenesis is an abnormal ovariandevelopment leading to rudimentary gonadal developmentand failure of ovarian hormone secretion. Because of thegonadal failure, patients with dysgenetic gonads will havestreak ovaries and primary amenorrhoea due to lack of ovarianhormones.
Case report
A 24 years unmarried lady presented with complaints ofpain lower abdomen for 4 days, which was intermittent innature, was mild to severe in intensity. There ware noaggravating or relieving factors. She also had weakness, hadnever attained menarche and never sought medical advice.
On examination, she was comfortable, average built with heightof 142 cm. Her secondary sexual characters were not developed.Per abdominal examination showed an oval mass of 8x6 cm inthe right lumbar region which was slightly tender on palpation.Per vaginal examination was not done as patient was virgin.On digital rectal examination, uterus was not appreciated.
Ultrasonography of the abdomen and pelvis revealed acomplex mass in right adnexia of 11.2 x 10.8 x 8.1 cm, withhigh diastolic flow suggesting malignancy. Ovaries were notvisualized; uterus was small measuring 5x1.4x1 cm only.There were mild right sided hydronephrosis and small amountof ascites.
All the investigations including tumor markers Serum βhCG,CA 125 and α feto protein were within normal limits. Follicularstimulating hormone level estimation could not be done atthat time.
Laparotomy was done suspecting ovarian malignancy andon opening the abdomen there was hemorrhagic ascites of
Ovarian dysgenesis and dysgerminoma:A case report
Paban K. Sharma, Isha Shrestha, Meera HadaDepartment of Obstetrics and Gynaecology,
Patan Hospital, Lalitpur, Nepal
AbstractA case of a 24 year lady had presented to us with sexual infantilism, primary amenorrhoea and pain abdomen hadlaparotomy finding of an ovarian tumor which histologically confirmed to be dysgerminoma. In a patient with primaryamenorrhoea and sexual infantilism, possibility of ovarian dysgenesis with high probability of gonadal malignancyshould be kept in mind.
Key words: Dysgerminoma, Gonadal dysgenesis, ovarian dysgenesis and primary amenorrhoea
about 500 ml, a right ovarian tumor of 12 x 10 cm size, whichwas friable and ruptured during surgery (fig 1). Uterus &other ovary were rudimentary. Other areas including liver,omentum and bowel were free of deposits and no lymphnodes were palpable. A total hysterectomy with bilateralsalphingo-oopherectomy was done and surgical staging of Icwas made.
Ascitic fluid cytology came out to be negative for malignantcells but Histopathology report was suggestive ofDysgerminoma. Other ovary, uterus and omentum were freeof microscopic deposits.
With all above findings a final diagnosis of ovariandysgerminoma in a dysgenetic gonad was made and patientwas referred to cancer hospital for radiotherapy.
Comment
There is a risk of development of gonadal tumor in a dysgeneticgonad. The most important part of gonadal dysgenesis is thegenesis of gonadoblastoma in the presence of the Y-chromosome.1 It appears that, in the X linked form, XYgonadal dysgenesis may be caused by a point deletion ormutation of a gene on the X- chromosome, which controlsthe gonad specific receptor for the H-Y antigen.2 The absenceof Sertoli cells in these patients, causing lack of androgenbinding protein with deficient local concentration of androgensand consequent failure of maturation of spermatogonia, maylead to unregulated proliferation of germ cells, and henceexplain the frequency of gonadal neoplasia in the 46XYfemale.3 In a patient with 46XX karyotype, the malignantpotential is probably less. In any female with gonadaldysgenesis and a Y chromosome in her karyotype, there is aneed for a diligent search for the gonadectomy as soon aspossible to avoid the risk of gonadal neoplasia, whether benignor malignant.3-7 If the possibility of a Y chromosome cannotbe excluded, gonadectomy should be performed because ofthe risk of malignancy.5
Correspondence:Dr. Paban Sharma, ConsultantDepartment of OBGYN, Patan Hospital, GPO 252, Kathmandu, Nepalemail: [email protected] Phone: 9851097844
N. J. Obstet. Gynaecol Vol. 1, No. 1, p. 70 -71 May 2006

71
The high prevalence of gonadal tumors in children with mixedand pure gonadal dysgenesis warrants consideration of early,bilateral, prophylactic gonadectomy once the diagnosis isestablished with certainty.8,9 In all patients with 45X/46XYgonadal dysgenesis and a male phenotype, gonadal biopsiesshould be considered as soon as the syndrome is diagnosed.10
Although girls with Turner’s syndrome (45X) are not at riskfor malignancy, patients with feminizing testicular syndromewith XY chromosomes and patients with “mixed gonadaldysgenesis” are at risk for malignancy, and bilateralgonadectomy should be performed.
Conclusion
Dysgerminoma in dysgenetic gonad is uncommon whichfurther can be reduced by gonadectomy in cases of sexualinfantilism with demonstrable Y chromosome sequences, thathas higher propensity for malignancy.
References
1. Lukusa T, Fryns JP, Kleczkowska A, Van den BergheH. Centre for Human Genetics, University of Leuven,Belgium.
2. Mann JR, Corkery JJ, Fisher HJ, Cameron AH,Mayerova A, Wolf U, Kennaugh AA, Woolley V. TheX linked recessive form of XY gonadal dysgenesiswith a high incidence of gonadal germ cell tumours:
clinical and genetic studies. J Med Genet. 1983 Aug;20(4):264-70.
3. Kaplan E.S: Gonadal dysgenesis in a phenotypic femalewith an XY chromosomal constitution. Afr Med J.1978 Apr 8; 53(14):552-3.
4. MacMahon RA, Cussen LJ, Walters WA. Importanceof early diagnosis and gonadectomy in 46, XY females.J Pediatr Surg. 1980 Oct; 15(5):642-5.
5. Krasna IH, Lee ML, Smilow P, Sciorra L, Eierman L.Risk of malignancy in bilateral streak gonads: the roleof the Y chromosome. J Pediatr Surg. 1992 Nov;27(11):1376-80.
6. Ranjan V, Jandial V, Dean JC.Turner’s syndrome withsex chromosome mosaicism.Eur J Obstet GynecolReprod Biol. 1995 Mar;59(1):109-10.
7. Ashby WB. Swyer syndrome with gonadoblastoma.Int J Gynaecol Obstet. 1981 Mar; 19(1):73-7.
8. Gourlay WA, Johnson HW, Pantzar JT, McGillivrayB, Crawford R, Nielsen WR. Gonadal tumors indisorders of sexual differentiation. Urology. 1994Apr;43(4):537-40.
9. Isurugi K, Aso Y, Ishida H, Suzuki T, Kakizoe T, MotegiT, Nishi T, Aoki H. Prepubertal XY gonadal dysgenesisPediatrics. 1977 Apr; 59(4):569-73.
10. Muller J, Skakkebaek NE, Ritzen M, Ploen L, PetersenKE. Carcinoma in situ of the testis in children with45,X/46,XY gonadal dysgenesis. J Pediatr. 1985 Mar;106(3):431-6.
Uterus
L Ovary
R ovarian tumor mass
Figure 1: Right ovarian tumor with rudimentary uterus and left ovary
Ovarian dysgenesis and dysgerminoma

72
What is unmet need?
As defined by the Demographic and Health Surveys, theunmet need group includes all fecund women who are marriedor living in union, and thus presumed to be sexually active,who either do not want any more children or who wish topostpone the birth of their next child for at least two moreyears but are not using any method of contraception. Unmetneed is a current-status measure and not a lifetimemeasure.
What is the magnitude of the problem?
In developing countries millions of women have unmet need,estimated by Population Reports in 1996 at about 100million, or about one married woman in every five. In Indiathis figure is 31 million, in Pakistan and Bangladesh it is 5.7million and 4.4 million, respectively 1. Twenty eight percentof currently married women in Nepal have an unmet need forfamily planning services, of which 11 percent have a need forspacing and 16 percent have a need for limiting.2. In a Hospitalbased study conducted in Maternity hospital, Kathmandushowed that 69% of patients attending the pregnancyconfirmation clinic had planned (wanted) pregnancy and 31%had unplanned pregnancy. 67.7% of women among thosewho did not want pregnancy had never used contraceptives21.3% of those with unplanned pregnancy requested fortermination. 29% had used but discontinued, the main reasonsfor doing so was fear of side effects.3
How to address the unmet need?
To develop an unmet need strategy1, programs need to1. Understand the various reasons for unmet need, based
on qualitative research and survey data.2. Determine the size and composition of the unmet need
subgroups by analyzing survey findings and other data.3. Identify high-priority subgroups that the program will
be best able to reach.4. Design and deliver information and services to meet
the specific needs of each selected subgroup.
Reasons for unmet need4,5
� Difficulties with access� Poor quality of family planning supplies and services� Health concerns about contraceptives and side effects
Male involvement in unmet need forfamily planning
Sudha SharmaMaternity Hospital, Thapathali, Kathmandu, Nepal
� Lack of information� Opposition from husbands, families, and communities� Little perceived risk of pregnancy: infrequent sexual
activity and old age
Women often may not reveal the real reasons because ofembarrassment, politeness, or other cultural constraints andinstead substitute what they regard as more acceptableresponses.
The strategies to address the unmet need are� Maximizing access to good-quality health and family
planning services� Emphasizing on communication.� Collaborating with other services for new mothers and
young children.� Focusing on men as well as women
Why men involvement?
Men have traditionally borne a great share of responsibilityfor family planning among couples. Natural methods ofcontraception like the withdrawal method have been a widelyaccepted method, and safe periods, periodic abstinence andother natural methods have been practiced by the couplesfrom time immemorial. Condoms have become a popularmethod for contraception as well as prevention of sexuallytransmitted infection. Although less common than femalesterilization, vasectomy is widely practiced. Other methodsof contraceptives for men are also being researched. Additionalmeasures are required for increasing the involvement ofmen in family planning. The ICPD Programme of Action,noting that “men exercise preponderant power in nearly everysphere of life,” called for more male participation andsharing of responsibility in family planning6. It has been saidthat a woman may have unmet need for family planningbecause of the high “social cost of challenging the oppositionfrom her spouse or any one else in her social influence group”7
It was noted from the NDHS conducted in Nepal2 thatdiscussion of family planning between the spouses isuncommon and only two in five women and one in two menwho know of a contraceptive method said they have discussedfamily planning with their spouses in the year before thesurvey. Other studies from Nepal8, 9 had also indicatedopposition from the husband as reason for the unmetneed. One report10 indicates that in seven sub-Saharancountries contraceptive use among women whose husbandsdisapprove of family planning averages only one-third
B R I E F C O M M U N I C A T I O N
Correspondence:Prof. Sudha Sharma, NAMS, Maternity Hospital, Thapathali, Kathmandu, Nepal email: [email protected]
N. J. Obstet. Gynaecol Vol. 1, No. 1, p. 72 - 73 May 2006

73
as much as among women whose husbands approve of it. InKenya, among women who had stopped using contraceptionfor reasons other than having another child, 12% had stoppedbecause their husbands wanted another child or had forcedthem to discontinue for another reason. The same reportoutlines the following reasons for men opposing familyplanning
� Want more children� Worry that their wives might be unfaithful if protected
from pregnancy� Not approving male physicians to examine their wives� Have religious objections� Fear the side effects of contraception� Wish to control wives’ behavior
It was also noted that husbands’ attitudes might affect notonly whether or not wives use contraception but also thechoice of a method and how long it is used. Analysis ofwomen’s perception of opposition from husband indicatesthat in Botswana only 47% of women with an unmet needthink that their husbands approve of family planningcompared with 82% of contraceptive users. In Pakistan thedifference is even more striking, 32% compared with 83%.Spousal communication regarding family planning was alsonoted to be low in Ghana- only 44% of women with unmetneed had discussed family planning with their husbands inthe preceding year compared with 72% of contraceptive users.The same report indicated that in India the level of unmetneed for limiting births was significantly lower among coupleswho had discussed family planning than among those whohad not, but discussion made little difference to unmet needfor spacing. Consequences of husband’s disapproval wasnoted11 to manifest as abstinence under one pretext or anotherand if the woman was pregnant, she was found to resort toback street abortion rather than face disapproval anddiscredit.
Conclusions
Reasons for unmet need vary among and within countries; it isdifficult to generalize about the determinants of unmet need.Nevertheless, a common observation is that couples would bemotivated to use contraception if they want to prevent thebirth of a next child and/or if they perceive the woman to be atrisk of becoming pregnant. Health professionals should involvethe husbands as much as possible when counseling women forfamily planning. In Antenatal and gynecology out patient clinicsopportunities of discussions on family planning should becreated and offered to the couples.
References
1. Population Reports Volume XXIV, Number 1,September, 1996.
2. Nepal Demographic and Health Survey. Ministry ofHealth, New ERA, ORC MacroS, 2001.
3. Sharma S. and Shrestha U., NESOG Souvenir 2000.4. Bongaarts, J. and Bruce, J. The causes of unmet need
for contraception and the social content of services.Studies in Family Planning 26(2): 57-75. Mar.-Apr. 1995.
5. NAG, M. Some cultural factors affecting costs offertility regulation. Population Bulletin of the UnitedNations 17: 17-38. 1984.
6. Report of the ICPD (94/10/18).7. STASH, S. Reasons for unmet need in Nepal: An attempt
to pick up where fertility surveys leave off. [1995]8. Shrestha, A., Stoeckel, J., and Tuladhar, J.M. Factors
related to non-use of contraception among coupleswith an unmet need for family planning in Nepal.Kathmandu, Nepal, New Era, 1988. 81 p.
9. Indu Bhushan JHSPH Center for communicationprograms , Nov 1997.
10. Ravindran, T.K.S. Users’ perspectives on fertilityregulation methods. Economic and Political Weekly,Nov. 13-20, 1993. p. 2508-2512.
Male involvement in family planning
74
℘ Good evening Madam.� Good evening Ashma.
℘ How do you describe your life?� Good. A beautiful journey from 1961 onwards. It
was an eventful excursion and I am thankful toGod who gave me courage to cross over all thehurdles.
℘ How do you see your long journey in this profession,now that you are the first lady Dean of Nepal Academyof Medical (NAMS) science, do you feel like your goalmet?
� So long so good. I hardly plan thing. I go onworking. I was asked to shoulder the responsibilityfor this good work. For me work is necessary andimportant, not always the placement. I will take itas it comes.
℘ How do you see the future of Obstetrics andGynaecology in Nepal?
� Definitely great. It is the circumstances that askfor a change and its’ time that dictates everychanges. We have seen vast expansion of obstetricsand gynaecology services in Nepal. Right now thetime has come for us to expand in sub specialties.This helps us to take the social responsibility ofour profession.
℘ Is NAMS in the direction towards subspecialty?What is the subject you are thinking to bring intoaction?
� Yes, our first work up is on GyaecologicalOncology.
℘ When was your first involvement with Institute ofmedicine (IOM)?
� From it’s establishment in 1979.
℘ What stopped you from being a part of IOM, since youhave been coordinating most of the educationalactivities, for long; for eg, MBBS, DGO and MD Gyne/Obs?
� Glad to hear that I have been a part of IOM. Icontributed what I could afford to and for meposition is not the prime thing. It is just importantthat I have been kept occupied and had somethingto give right from the inception. It does not matterto me how and where I am. I have tried to beconstantly involved with academic exercise. I havealso been involved as the organizer of Royalcollege of Obstricians and Gynaecologistsexaminations from 1987-2000. Now I am enjoyingworking for MD/MS and Fellowship program ofNAMS.
℘ Yes your book has been very much appreciated in mostof medical college in Nepal.
� The book, Essentials Obstetric Functions waspublished by Health learning Material Centre,Maharajgunj in 1995 for the benefit of student’slearning basic and comprehensive obstetric care.
℘ How do you see the Department of OBS/GYN at T.Teaching Hospital?
� I am fully satisfied with the accomplishmentof the department in TUTH; now that there are 3professors; the output is still going to be better.
An evening with D. S. Malla.
S P E C I A L A R T I C L E
N. J. Obstet. Gynaecol Vol. 1, No. 1, p. 74 -75 May 2006

75
℘ Who is more important for you: patient or student, mebeing one of your students?
� Medical students cannot be students if thereare no patients. Patients in the medicalinstitutions get evidence based and improved carebecause of academic atmosphere and questioningby the students. So both are equally importantfor me.
℘ What would make differences in our MD education?� The involvement of students and teacher is most
important and basically a better supervision couldmake a difference.
℘ Has any of your dream come true?� One of them is the formation of the Maternal
Mortality and Morbidity Review Committee inFHD of Department of Health, Ministry ofHealth and Population. In the presentation ofstudy result of Maternal Mortality and Morbidityin different hospitals of Nepal in Geneva 1990,such committee was recommended for ourcountry to reduce very high maternal mortalityratio in Nepal. After 15 years it’s being exercisednow.
℘ What is the most important aspect of your life?� Work well done and duty attended. In profession
listen to the patient patiently, accommodate theirpreferences and choices in their care.
℘ Your secret to success?� Work is worship. I try to be a positive thinker.
Someone has to say that you are successful notyourself. This is the secret.
℘ Who has impressed you the most and how?� My teachers. One of them has been so kind and
polite, she never got angry and scolded anyone,whatever the context was. Whenever I am a bitrough to my students, I remember her verymuch.
I am what I am today because the principal of thecollege who accepted me as a science student onhis own responsibility in spite of me being a nonscience student in SLC board. I bow to thepeople who are considerate in difficultcircumstances.
℘ What has been your inspiration?� The source of inspiration has been people and
events. My mother and her determination to makea girl child educated was my first inspiration. Myhusband, who is so considerate and loving. Icouldn’t have achieved anything without hisconstant support and affection.
℘ What is your hobby?� To have long walks and house keeping.
℘ What is your favorite past time?� Reading biograhies.
℘ Your passion?� Do the given task well.
℘ What is your best music?� Folk music and bhajan. I also love bhajan by Indian
singer.
℘ How do you keep yourself so fit physically?� I do minimal exercise, could not be a disciplined
person in diet and exercises, eat as much as I likewhenever I get. Let me tell you I enjoy eatingpotatoes in any form.
℘ Everyone speaks that you look so dignified!� Thank you for your compliment.
℘ Any particular incidence that has shaken you?� Ten years ago, there was a 24 years woman who
was brought in shock after a clandestine abortion.We were shocked at laprotomy to find uterusseverely lacerated, missing chunks of left ureterupto renal pelvis and sigmoid colon. There weremany holes in small intestine. Left nephrectomyand colostomy was done after the repair of theinjury in the uterus and bowel. She recovered andleft home in three weeks.
℘ Inspiring words for our Journal?� My best wishes for Nepal Journal of Obstetrics
and Gynaecology.
℘ What will help in making this Journal a mark?� It depends on the reviewer’s credential and
author’s responsibility on report writing. One hasto develop the specialty of the writing skills.
About Prof. D.S Malla
Prof. Dibyashree Malla, FRCOG is currently the Dean of Nepal Academy of Medical Sceince (NAMS)corresspondence: [email protected]
An evening with D. S. Malla.

76
Introduction
Nepal Society of Obstetricians and Gynaecologists (NESOG)is a professional organization of obstetricians andgynaecologists established in 1988 A.D.
The idea of formation of society of obstetricians andgynaecologists was conceived way back in 1974 when Dr.Savitri Gurung and Dr. Sanu Maiyan Dali attended aconference on “Asian Regional Conference on Familyplanning” held in Manila, Philippines, in January 6-11, 1974.
This conference was inaugurated by Mrs. Imelda Marcos,the first lady and was attended by 10,000 women medicaldoctors .The theme of the conference was “How to mobilizemedical women in Family planning”. Dr. Gurung and Iwere astonished to see so many women doctors in one hall.It was beyond our imagination. During the meeting, wewere asked by our international colleagues whether we had asociety of obstetricians and gynaecologists. We quietly saidno. It just remained a dream at that time as we were onlyabout ten obstetricians and gynaecologists in the wholecountry.
Fourteen years later in May 1988, the author had gone toJapan to present a paper on “Family Planning in Nepal” inSixth Annual Meeting of Society for Advancement ofContraception”. There Emeritus Prof. Hiroaki Somaintroduced the author to two eminent people: Late Prof.Mijuno, and Late Emeritus Prof. Shan S. Ratnam, thesecretary general of Asia Oceania Federation of Obstetricsand Gynaecology (AOFOG). On that occasion, theyhighlighted the importance of the society and showed theirkeen willingness to help Nepal in this regard. On her return,the author narrated the joyful events with Dr. Bhola Rijal,then, the Associate Professor, Department of Obstetrics andGynaecology, Tribhuvan University Teaching Hospital. Wehad a couple of in - house meeting. Then finally, we called Dr.Dibya Shree Malla of Maternity Hospital and discussed thepossibility of the formation of Nepal Society of Obstericiansand Gynaecologists in a couple of meetings.
Eventually, the dream became a reality in November 1988.With the encouragement of Emeritus Prof. Hiroaki Soma(Visiting Consultant at Prasuti Griha and visiting Professorat Institute of Medicine), Prof. Sanu Maiyan Dali, Dr. DibyaShree Malla and Dr. Bhola Rijal discussed and called a meetingto establish the Nepal Society of Obstetricians &
Sanu Maiya DaliDepartment of Obstetrics and Gynaecology, Nepal Medical college, Jorpati, Kathmandu , Nepal
Nepal Society of Obstetricians andGynaecologists (NESOG):
Tracing it’s history
Gynaecologists at the Superintendent Quarter of ParopakarShree Panch Indra Rajya Laxmi Devi Prasuti Griha (MaternityHospital). Finally, NESOG was born in November 1988 at avery prestigious place, Paropakar Shree Panch Indra RajyaLaxmi Devi, Prasuti Griha.
This first formal meeting was attended by the followingfounder members.Dr. Dibya Shree MallaDr. Sanu Maiya DaliDr. Bhola RijalDr. Annapurna ShresthaDr. Junu ThapaDr. Mahodadhi ShresthaDr. Swaraj Rajbhandari
Objectives of NESOG
The objective of NESOG is to serve the people by renderingfully educational, scientific and public health oriented servicesof high standard in the field of obstetrics and gynaecologicaldiseases in Nepal.
NESOG’s Adhoc Committee
NESOG’s Adhoc Committee was formed in November 1988and the executive members were as follows:President : Dr. Dibya Shree MallaVice President : Dr. Sanu Maiya DaliGen Secretary : Dr. Bhola RijalTreasurer : Dr.Saraswati M PadhyeJt. Treasurer : Dr. Junu ThapaSecretary : Dr. Mahodadhi Shrestha
Socio Cultural Sub-committee
Secretary : Dr. Swaraj RajbhandariMembers : Dr. Neelam Pradhan
: Dr. Kundu Yangzom: Dr. Kasturi Malla: Dr. Achala Vaidhya: Dr. Yamuna Suwal
NESOG office
-One room was provided for NESOG office by Dr. DibyaShree Malla, the Superintendent of Maternity Hospital.
correspondence:Prof. Sanu Maiya Dali, MD. FRCOG Nepal Medical college, Jorpati, email: [email protected]
N. J. Obstet. Gynaecol Vol. 1, No. 1, p. 82 - 82 May 2006

77
International meeting
NESOG had the opportunity to organize First Internationalmeeting on 28th January, 1989 with Emeritus Prof. H. Somaand the Japanese colleagues. Emeritus Prof. H. Soma,Emeritus Prof. Shan S. Ratnam and Late Prof. Mijuno helpedNESOG to receive sister affiliation with AOFOG.
Academic activities
NESOG started its academic activities by holding workshopsin collaboration with AOFOG and scientific meetings withFamily Health International.
The well wishers of NESOG, AOFOG members like LateEmeritus Prof. Shan. S. Ratnam from Singapore, Prof. PeterElliot from Australia, Emeritus Prof. H. Soma from Japan,Prof. Rohit Bhatt from India and Dr. Kanti Giri from WHO,SEARO had helped to hold its first workshop on Maternal& Perinatal Health and Family Planning in 16-17 March,1990 (3rd & 4th Chaitra, 2046).
NESOG had financial constraints in receiving the AOFOGJournals. Emeritus Prof. Hiroaki Soma had been kind enoughto support NESOG financially each year. He has beensupporting AOFOG Journal shipping charge with JapaneseYen 25000 every year since 1990.
NESOG had its first election on 29th March, 1991 (15 Chaitra,2047) at Maternity Hospital, Thapathali. The following officebearers were elected for the following post for the year 1991-1993.
President : Dr. Bhola RijalVice – President : Dr. Mahodadhi ShresthaGeneral Secretary : Dr. Bimala LakheyTreasurer : Dr. Ganga ShakyaJoint Secretary : Dr. Pramila PradhanJoint Treasurer : Dr. Neelam Pradhan
Socio Cultural Subcommittee
Secretary : Dr. Sushila ShresthaMembers : Dr. Lata Bajracharya
: Dr. Rita Manandhar: Dr. Rekha Hamal: Dr. Amita Thapa
The second workshop on maternal and perinatal health andfamily planning organized by NESOG and AOFOG washeld on 19-20 Nov, 1991 (3rd and 4th Mangsir, 2048). AOFOGMembers like Prof. Peter Elliot from Australia, Prof. R. Samilfrom Indonesia, Prof. P. Tiwari from India and Prof. S. Khatunfrom Bangladesh came to attend the workshop fordisseminatating information and discuss the strategies forthe reduction of maternal and perinatal mortality.
Since then NESOG had been involved in various activities ofSafe Motherhood and reproductive health program of HMG,MOH.
In 1991, the author was awarded with AOFOG youngGynaecologist award. Since then many NESOG Membershad been the recipients of AOFOG Young Gynaecologist
Award. The author had the pleasure of serving NESOG asthe fourth President in the year 1995-1997.
AOFOG Council meeting: Historical
Landmark
November 7-8, 1997 had been another landmark in the historyof NESOG. NESOG had the pleasure of hosting 5th councilmeeting. The unique thing about this council meeting wasthat after the council meeting was over, all AOFOG Councilmembers, the outstanding Professors of Asia Oceania Regionwere busy updating the NESOG members, Medical Officersand Post graduate Students of M.D. in Obstetrics &Gynaecology in continuing Medical Education (CME)programs held at Maternity Hospital, Kathmandu andPokhara Manipal College of Medical Sciences. The Presidentof AOFOG and other AOFOG Council members were busyin National Level Workshops held in Bhaktapur and Pokharato educate the health workers on Reproductive healthincluding Safe Motherhood for dissemination at the grassroot level.
NESOG is holding regular CME Programs, publishingNewsletters and organizing free clinic at Kakani Village andBanepa to promote its academic activities.
Important events
Ten years later, two important events took place.
Dr June Thapa Oration
Dr. June Thapa Oration was established on 16 August, 1998by Dr. Loke Bikram Thapa and family to deliver the Orationby Eminent Gynaecologists and Obstetricians in every twoyears in the International Conference organized byNESOG.
Shri Hira Nanda Vaidya Memorial Oration
Shri Hira Nanda Vaidya memorial medical trust wasestablished on 29 December, 1998 by Professor Sanu MaiyanDali and family members of Late Hira Nanda Vaidya tohonour Eminent International and National Obstetriciansand Gynaecologist during National and InternationalConferences organized by NESOG every year.
On 21-22, February, 1999, the Tenth Happy BirthAnniversary of NESOG was celebrated by two importantevents: The First NESOG/ June Thapa Oration was deliveredby Emeritus Prof. Shan S. Ratnam. The First NESOG/Hirananda Vaidya Memorial Oration was delivered by Prof.S. Das Gupta.
Soma Award
Emeritus Prof. H. Soma, the honorary member of NESOGhas set up Soma Award in the National Conference of NESOGin the year 2000 for the best paper.
NESOG Award
NESOG Award was established by the society in the year2000 to encourage young gynaecologists for their academicexcellence.
NESOG history

78
NESOG is a member of� South Asian Federation of Obstetrics and Gynaecology
(SAFOG)� Asia Oceanea Federation of Obstetrics and Gynecology
(AOFOG).� International Federation of Obstetrics and Gynecology
(FIGO)� Safe Motherhood Network.To meet the increasing demands in our speciality for takingup a leadership role in the National priority areas, NESOGhas established a few sub committees like Safe MotherhoodCommittee, Adolescent Health and Development Committeeand Oncology Committee.
Partnership
To achieve its goal NESOG has been working very closelywith the Ministry of Health, HMG of Nepal and otherdevelopment partners like WHO, UNICEF, SSMP (NSMP),NFHP (Engender Health and JHPIEGO) and had developeda training manual for adolescent health and developmentprogram for doctors, nurses and counselors and the Nepaliversion of the manual with the support from FHD/MOH/WHO. Both the manuals address adolescent health anddevelopment in a holistic way and provide coverage of awide range of adolescent health and development issues,including counseling.
NESOG worked with NSMP/ WRLHP/ FHD to establishan EOC monitoring system in Nepal. Following legalizationof abortion in Nepal NESOG has participated in the taskforce developed by FHD/MOH for policy formulation, andsubsequently in the technical Committee for implementationof comprehensive abortion services (TCIC), and hascontributed in various areas.
The society is also an affiliate institution with Nepal HealthResearch Council and has contributed to obtaining theRockefellar Foundation Award.
NESOG’s greatest achievement in 2005
NESOG had started working towards fulfilling its dream ofconstructing its own building. NESOG is working very hardto have its own building for fostering teaching learningactivities, training programs and research activities. Buildingconstruction fund was established with generous contributionof all NESOG members. Thanks to the president of NESOGDr. Chanda Karki and executive committee members whoseuntiring efforts helped NESOG to be owner of 171/2 annas ofland at Nilbarahi, Sanothimi in 2005. Soon NESOG plans tohave its own building.
Donations
On 22-27th April, 2002, well wishers of NESOG and AOFOGmembers like Prof. Kim and Prof. S.N Bae from Korea andProf Peter Elliot, Prof. Bob Osborne and Prof. Bowditchfrom Australia worked hard to make colposcopy and cytologyworkshop a grand success.
Prof. Elliot has donated 4 microscopes with two teaching
aids, two cervical biopsy forceps and few speculums to thesociety. Prof. Kim has donated a cervicogram. Dr. LaniAckermann American Academy of Family Physician donateda colposcopy machine.NESOG has been organising National conference annuallyand International Conferences every two years. NESOG hadthe pleasure of hosting 5th SAFOG Conference in Nepal inthe year 2005. The Author had the honor and pleasure ofdelivering SAFOG Oration “Making Pregnancy Safer: ACommunity Perspective.”
17 yrs later, NESOG formed the Education Committee andJournal Committee on 20 Shrawan, 2062 (4, August, 2005)and appointed Prof. Sanu Maiya Dali as Chief of the EducationCommittee and Dr. Asma Rana as the chairperson of theJournal Committee respectively.
It has been a dream since the establishment of NESOG to seeNESOG growing as an Institution like the Royal College ofobstetricians and Gynaecologists of London, Royal Collegeof Obstetricians and Gynaecologists of Australia,Sri Lankan College of Obstetricians and Gynaecologists andmany more like this in other countries.
Formation of the Education Committee is the milestone inthe direction of establishment of NESOG as an Institution.With the dedicated efforts of NESOG members, one day itwill be a reality. NESOG members will be working togetherin setting standards to improve women’s health as done bythe Royal College of Ostetricians & Gynaecologists inLondon. The education Committee will be working in liaisonwith all member countries to fulfill its necessities toachieve our mission.
NESOG Education Committee successfully performed Deskreview of the sectoral policies, strategies and plans, assessingthe human and financial resources in the process of revisingnational safe motherhood long term plan 2002-2017, alongwith support to Safe Motherhood Programs (SSMP) andFHD. The gaps, deficiencies and discrepancies in the planhad been identified and suggested key areas, issues, concernsand approaches that need to be incorporated in the plan.
Late Emeritus Prof. Shan Ratnam, Secretary General ofAOFOG had helped the society since its inception and hisphilosophy was “to accept responsibility for women’s healthby looking beyond the hospital walls”. NESOG membershad done so by reaching to grass root level healthcareproviders and training them on active management of thirdstage of labour. NESOG feels proud to work with NursingAssociation of Nepal (NAN) in training grass root levelhealthcare providers on active management of third stage oflabour at 4 developmental regions of Nepal.
Thus NESOG has come a long way with various activities inthe process of developing into an Institution. NESOG hasworked with FHD/MOH in formulating national policy,strategy and plan related to maternal and neonatal health andlooks forward to participating actively in the educationalactivities at the national level in future as well.
Long Live NESOG !
S.M. Dali




















