
Prophylactic Endoscopic Coagulation to Prevent Bleeding After Wide-Field Endoscopic Mucosal...
9
Prophylactic Endoscopic Coagulation to Prevent Bleeding After Wide-Field Endoscopic Mucosal Resection of Large Sessile Colon Polyps Farzan F. Bahin, * ,‡ Mahendra Naidoo, * Stephen J. Williams, * Luke F. Hourigan, § Donald G. Ormonde, k Spiro C. Raftopoulos, k Bronte A. Holt, * Rebecca Sonson, * and Michael J. Bourke* ,‡ *Department of Gastroenterology and Hepatology, Westmead Hospital, Sydney, New South Wales, Australia; ‡ Westmead Clinical School, University of Sydney, Sydney, New South Wales, Australia; § Department of Gastroenterology and Hepatology, Princess Alexandra Hospital, Brisbane, Queensland, Australia; k Department of Gastroenterology and Hepatology, Sir Charles Gairdner Hospital, Perth, Western Australia, Australia BACKGROUND & AIMS: Clinically significant postendoscopic mucosal resection bleeding (CSPEB) is the most frequent significant complication of wide-field endoscopic mucosal resection (WF-EMR) of advanced mucosal neoplasia (sessile or laterally spreading colorectal lesions > 20 mm). CSPEB requires resource-intensive management and there is no strategy for preventing it. We investigated whether prophylactic endoscopic coagulation (PEC) reduces the incidence of CSPEB. METHODS: We performed a prospective randomized controlled trial of 347 patients (mean age, 67.1 y; 55.3% with proximal colonic lesions) undergoing WF-EMR for advanced mucosal neoplasia at 3 Australian tertiary referral centers. Patients were assigned randomly (1:1) to groups receiving PEC (n [ 172) or no additional therapy (n [ 175, controls). PEC was performed with coagu- lating forceps, applying low-power coagulation to nonbleeding vessels in the resection defect. CSPEB was defined as bleeding requiring admission to the hospital. The primary end point was the proportion of CSPEB. RESULTS: Patients in each group were similar at baseline. CSPEB occurred in 9 patients receiving PEC (5.2%) and 14 controls (8.0%; P [ .30). CSPEB was associated significantly with proximal colonic location on multivariate analysis (odds ratio, 3.08; P [ .03). Compared with the proximal colon, there was a significantly greater number (3.8 vs 2.1; P [ .002) and mean size (0.5–1 vs 0.3–0.5 mm; P [ .04) of visible vessels in the distal colon. CONCLUSIONS: PEC does not significantly decrease the incidence of CSPEB after WF-EMR. There were signifi- cantly more and larger vessels in the WF-EMR mucosal defect of distal colonic lesions, yet CSPEB was more frequent with proximal colonic lesions. ClinicalTrials.gov NCT01368731. Keywords: Colonoscopy; Colonic Polyps; Postpolypectomy; Prevention. L arge laterally spreading and sessile colonic lesions 20 mm or larger (advanced mucosal neoplasia [AMN]) are precursors to invasive colorectal cancer, a leading cause of cancer-related morbidity and mortality worldwide. 1 As a safe and cost-effective ambulatory day-only procedure, wide-field endoscopic mucosal resection (WF-EMR) progressively is replacing surgery as the preferred treatment for these lesions. 2,3 Postpro- cedure bleeding is the most common significant compli- cation of WF-EMR. Clinically significant post-EMR bleeding (CSPEB) is defined as any bleeding occurring after the completion of the procedure necessitating emergency room presentation, hospitalization, or re- intervention (either repeat endoscopy, angiography, or surgery). 4 The rate of CSPEB after an uneventful WF- EMR of AMN is 7% overall, 5–7 and approaches 12% in the proximal colon. 4,6 CSPEB may be life-threatening and requires resource-intensive management. 8 Establish- ing an effective, safe, and cost-effective intervention to reduce CSPEB is an important milestone in improving Abbreviations used in this paper: AMN, advanced mucosal neoplasia; CSPEB, clinically significant postendoscopic mucosal resection bleeding; PEC, prophylactic endoscopic coagulation; WF-EMR, wide-field endo- scopic mucosal resection. © 2015 by the AGA Institute 1542-3565/$36.00 http://dx.doi.org/10.1016/j.cgh.2014.07.063 Clinical Gastroenterology and Hepatology 2015;13:724–730
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Prophylactic Endoscopic Coagulation to Prevent Bleeding After Wide-Field Endoscopic Mucosal...
Prophylactic Endoscopic Coagulation to Prevent Bleeding AfterWide-Field Endoscopic Mucosal Resection of Large SessileColon PolypsFarzan F. Bahin,*,‡ Mahendra Naidoo,* Stephen J. Williams,* Luke F. Hourigan,§
Donald G. Ormonde,k Spiro C. Raftopoulos,k Bronte A. Holt,* Rebecca Sonson,*and Michael J. Bourke*,‡
*Department of Gastroenterology and Hepatology, Westmead Hospital, Sydney, New South Wales, Australia; ‡WestmeadClinical School, University of Sydney, Sydney, New South Wales, Australia; §Department of Gastroenterology and Hepatology,Princess Alexandra Hospital, Brisbane, Queensland, Australia; kDepartment of Gastroenterology and Hepatology, Sir CharlesGairdner Hospital, Perth, Western Australia, Australia
BACKGROUND & AIMS: Clinically significant postendoscopic mucosal resection bleeding (CSPEB) is the most frequentsignificant complication of wide-field endoscopic mucosal resection (WF-EMR) of advancedmucosal neoplasia (sessile or laterally spreading colorectal lesions > 20 mm). CSPEB requiresresource-intensive management and there is no strategy for preventing it. We investigatedwhether prophylactic endoscopic coagulation (PEC) reduces the incidence of CSPEB.
METHODS: We performed a prospective randomized controlled trial of 347 patients (mean age, 67.1 y;55.3% with proximal colonic lesions) undergoing WF-EMR for advanced mucosal neoplasia at 3Australian tertiary referral centers. Patients were assigned randomly (1:1) to groups receivingPEC (n [ 172) or no additional therapy (n [ 175, controls). PEC was performed with coagu-lating forceps, applying low-power coagulation to nonbleeding vessels in the resection defect.CSPEB was defined as bleeding requiring admission to the hospital. The primary end point wasthe proportion of CSPEB.
RESULTS: Patients in each group were similar at baseline. CSPEB occurred in 9 patients receiving PEC(5.2%) and 14 controls (8.0%; P [ .30). CSPEB was associated significantly with proximalcolonic location on multivariate analysis (odds ratio, 3.08; P [ .03). Compared with theproximal colon, there was a significantly greater number (3.8 vs 2.1; P [ .002) and mean size(0.5–1 vs 0.3–0.5 mm; P [ .04) of visible vessels in the distal colon.
CONCLUSIONS: PEC does not significantly decrease the incidence of CSPEB after WF-EMR. There were signifi-cantly more and larger vessels in the WF-EMR mucosal defect of distal colonic lesions, yetCSPEB was more frequent with proximal colonic lesions. ClinicalTrials.gov NCT01368731.
Keywords: Colonoscopy; Colonic Polyps; Postpolypectomy; Prevention.
Large laterally spreading and sessile colonic lesions20 mm or larger (advanced mucosal neoplasia
[AMN]) are precursors to invasive colorectal cancer, aleading cause of cancer-related morbidity and mortalityworldwide.1 As a safe and cost-effective ambulatoryday-only procedure, wide-field endoscopic mucosalresection (WF-EMR) progressively is replacing surgeryas the preferred treatment for these lesions.2,3 Postpro-cedure bleeding is the most common significant compli-cation of WF-EMR. Clinically significant post-EMRbleeding (CSPEB) is defined as any bleeding occurringafter the completion of the procedure necessitatingemergency room presentation, hospitalization, or re-intervention (either repeat endoscopy, angiography, or
surgery).4 The rate of CSPEB after an uneventful WF-EMR of AMN is 7% overall,5–7 and approaches 12% inthe proximal colon.4,6 CSPEB may be life-threateningand requires resource-intensive management.8 Establish-ing an effective, safe, and cost-effective intervention toreduce CSPEB is an important milestone in improving
Abbreviations used in this paper: AMN, advanced mucosal neoplasia;CSPEB, clinically significant postendoscopic mucosal resection bleeding;PEC, prophylactic endoscopic coagulation; WF-EMR, wide-field endo-scopic mucosal resection.
© 2015 by the AGA Institute1542-3565/$36.00
http://dx.doi.org/10.1016/j.cgh.2014.07.063
Clinical Gastroenterology and Hepatology 2015;13:724–730

the safety outcomes of WF-EMR. In addition, because ofthe emergence of colorectal cancer screening programs,AMN is being detected more frequently and thus WF-EMR is becoming more commonplace. Currently, thereis no proven effective therapy in the prevention of CSPEBafter WF-EMR.
The WF-EMR resection defect often containsnumerous blood vessels of various sizes that logically arepresumed to cause or contribute to subsequent CSPEB.Observational data have shown that prophylactic endo-scopic coagulation (PEC) is effective in preventingbleeding after endoscopic resection of superficialneoplastic lesions in the upper gastrointestinal tract9 andthe technique thus has become a fundamental compo-nent of the treatment procedure. We performed a pro-spective randomized controlled trial to evaluate thesafety and efficacy of PEC in the prevention of CSPEBafter WF-EMR for colorectal AMN.
Methods
Trial Design
This was a prospective multicenter study withbalanced randomization (1:1) conducted at 3 Australiantertiary referral centers. The study had institutionalethics board approval (HREC2010/11/4.12(3155) AURED) and was registered (ClinicalTrials.gov NumberNCT01368731). It was investigator-initiated and receivedno external funding. All authors had access to the studydata and reviewed and approved the final manuscript.
Participants
Patients referred for WF-EMR of AMN (colorectalsessile or laterally spreading lesions ! 20 mm) wereenrolled. Written informed consent was obtained fromeach patient on the day of the procedure.
Study Setting and Conduct
Patients were asked to cease antiplatelet agents 7 daysbefore, and recommence them 5 days after, the procedure.Management of anticoagulant therapy was standardized
in accordance with current guidelines,10 with patientsadvised to cease warfarin 4 doses before WF-EMR.Warfarin was recommenced on the day after WF-EMR.
The following exclusion criteria applied at the time ofcolonoscopy: lesion size less than 20 mm, Paris classifi-cation 0-Ip appearance, suspected invasive disease,WF-EMR of multiple lesions in 1 session, incompletelyresected lesion, or muscularis propria injury (suspectedor confirmed). Patients with the uncommon occurrence ofmajor intraprocedural bleeding also were excludedbecause other interventions for hemostasis are required(clips, epinephrine injection) and may act as confounders.Patients with a bleeding diathesis or those taking warfarinwithin 4 doses of the procedure also were excluded.
All WF-EMR procedures were performed by a studyinvestigator or a senior therapeutic endoscopy fellowunder their direct supervision. All consultant endo-scopists have extensive tertiary-level WF-EMR experi-ence. They had performed PEC routinely before the studyon an ad hoc basis for lesions thought to be at high risk ofCSPEB. Colonoscopy was performed using a high-definition Olympus 180 or 190 series variable-stiffnesscolonoscope (Q180/190 PCF/CF; Olympus, Tokyo,Japan). The lesion assessment and WF-EMR techniquewas standardized across the 3 centers and has beendescribed previously in detail.11,12 The injection solutionconsisted of 1 mL of methylene blue or 0.4% indigocarmine and 1 mL of 1:10,000 epinephrine combinedwith 8 mL of succinylated gelatin (Gelofusine; B. Braun,Bella Vista, Australia) solution.13,14
In all cases the lesion was removed usingmicroprocessor-controlled current (VIO 300D Endocut QEffect 3; ERBE Electromedizin, Tübingen, Germany).Standardized assessment of the resection defect includedevaluation of the number, size, and presence of hernia-tion of blood vessels, as well as fibrosis in the resectiondefect. Assessment of vessel and lesion size was esti-mated against the known diameter of snares used duringthe procedure (Figure 1A). Herniation of vessels wasdefined as a vertical protrusion of the vessel above thesubmucosal connective tissue within the resection defect,without overlying connective tissue (Figure 1B).
Persistent intraprocedural bleeding (significantoozing or pulsatile bleeding for >60 seconds despite
Figure 1. (A) Assessmentof vessel and lesion sizewas estimated against theknown diameter of snaresused during the proce-dure. (B) Herniation ofvessels: this was definedas a vertical protrusion ofthe vessel above the sub-mucosal connective tissuewithin the resection defect.
April 2015 PEC to Prevent Bleeding After WF-EMR 725
water jet irrigation) was treated with snare-tip softcoagulation (SOFT COAG at 80 W Effect 4; ERBEElectromedizin).15
All patients in the study underwent a structured tele-phone interview at 14 days. Any postprocedure bleedingand timing in relation to the index procedure was recor-ded. Data were collected on the following: need for repeatcolonoscopy, endoscopic intervention, angiographicembolization or surgery, hospitalization, and mortality.Any further postprocedural adverse events beyond14 days also were identified when patients presented fortheir 4-month scheduled endoscopic review.
Intervention
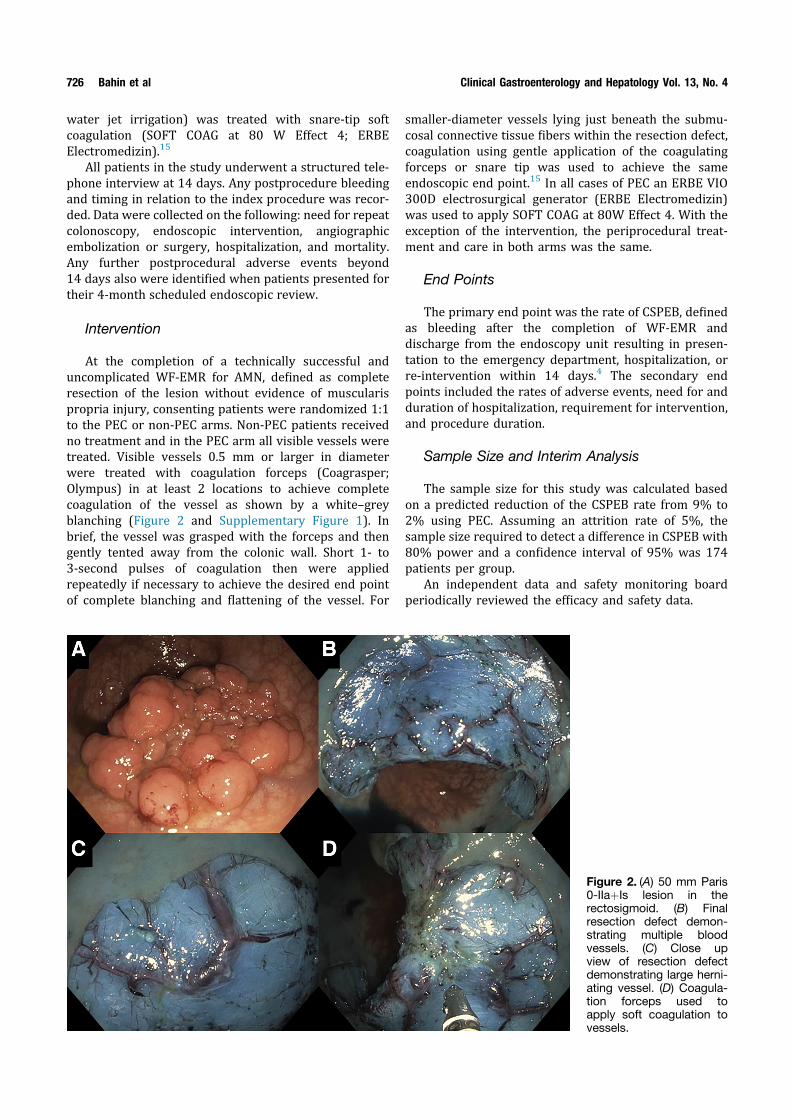
At the completion of a technically successful anduncomplicated WF-EMR for AMN, defined as completeresection of the lesion without evidence of muscularispropria injury, consenting patients were randomized 1:1to the PEC or non-PEC arms. Non-PEC patients receivedno treatment and in the PEC arm all visible vessels weretreated. Visible vessels 0.5 mm or larger in diameterwere treated with coagulation forceps (Coagrasper;Olympus) in at least 2 locations to achieve completecoagulation of the vessel as shown by a white–greyblanching (Figure 2 and Supplementary Figure 1). Inbrief, the vessel was grasped with the forceps and thengently tented away from the colonic wall. Short 1- to3-second pulses of coagulation then were appliedrepeatedly if necessary to achieve the desired end pointof complete blanching and flattening of the vessel. For
smaller-diameter vessels lying just beneath the submu-cosal connective tissue fibers within the resection defect,coagulation using gentle application of the coagulatingforceps or snare tip was used to achieve the sameendoscopic end point.15 In all cases of PEC an ERBE VIO300D electrosurgical generator (ERBE Electromedizin)was used to apply SOFT COAG at 80W Effect 4. With theexception of the intervention, the periprocedural treat-ment and care in both arms was the same.
End Points
The primary end point was the rate of CSPEB, definedas bleeding after the completion of WF-EMR anddischarge from the endoscopy unit resulting in presen-tation to the emergency department, hospitalization, orre-intervention within 14 days.4 The secondary endpoints included the rates of adverse events, need for andduration of hospitalization, requirement for intervention,and procedure duration.
Sample Size and Interim Analysis
The sample size for this study was calculated basedon a predicted reduction of the CSPEB rate from 9% to2% using PEC. Assuming an attrition rate of 5%, thesample size required to detect a difference in CSPEB with80% power and a confidence interval of 95% was 174patients per group.
An independent data and safety monitoring boardperiodically reviewed the efficacy and safety data.
Figure 2. (A) 50 mm Paris0-IIaþIs lesion in therectosigmoid. (B) Finalresection defect demon-strating multiple bloodvessels. (C) Close upview of resection defectdemonstrating large herni-ating vessel. (D) Coagula-tion forceps used toapply soft coagulation tovessels.
726 Bahin et al Clinical Gastroenterology and Hepatology Vol. 13, No. 4

Randomization
The allocation sequence was prepared by a non-procedural research nurse using a computer-generatedrandom numbers table. Participants were assignedrandomly to 1 of 2 treatment groups in a 1:1 fashion. Nostratification according to participating site was per-formed. The sequence was inside a locked cupboard inthe procedure room, which only the research nurse couldaccess. The schedule was consulted by the researchnurse at the time of randomization during each proce-dure. Patients were blinded to the intervention received.
Statistical Methods
Demographic and baseline characteristics were sum-marized using descriptive statistics. Categoric variableswere described using frequencies and percentages. Theirdistributions were compared between treatment groupswith the chi-square test or the Fisher exact test whennecessary. Continuous variables were summarized usingthe mean, median, and interquartile range. Their distribu-tions were compared between treatment groups with theMann–Whitney test. The significance threshold was 0.05for all analyses. All analyses were exploratory and noadjustment was made for multiple comparisons. Multiplelogistic regression with backward stepwise variable se-lection was used to identify the independent predictors ofoutcomes of interest. Candidate variables for inclusion in amodel includedanyvariable significant at aPvalueof 0.1orless on univariable analysis. If more than 1 lesion meetinginclusion criteria was resected during the study period,only 1 lesionwas included in the analysis. SPSS20 software(SPSS, Inc, Chicago, IL) was used for statistical analyses.
Results
The flow of patients through each stage of the study isdetailed in Supplementary Figure 2.
Recruitment and Patient Flow
Over 25 months to June 2013, there were 680 pa-tients undergoing WF-EMR who were assessed foreligibility for study inclusion and invited to participate.Of the 384 patients who consented to participate in thestudy, 37 were excluded for the following reasons: anysuspicion of muscularis propria injury (13 patients),incomplete resection (6 patients), multiple EMRs in 1session (5 patients), no resection performed because ofsuspicion of carcinoma (4 patients), lesion size less than20 mm (4 patients), Paris Ip appearance (2 patients), andmajor intraprocedural bleeding (2 patients). Theremaining 347 patients (mean age, 67.1 y; 51.3% men,55.3% proximal colonic lesion) were randomized. Nopatients dropped out of the study.
Baseline Information
Patient groups were similar at baseline (Table 1).
Outcomes
The results for the primary and secondary end pointsare detailed in Table 2. PEC was applied effectively to allallocated patients. The rate of CSPEB was 5.2% in the PECarm and 8% in the conventional arm (relative risk, 0.65;P¼ .30). Therewas no significant difference in the rates ofhospitalization, inpatient nights, or need for CSPEB inter-vention between the 2 groups. The procedure durationalso was not significantly different between the 2 groups.Other than bleeding there were no procedure-relatedadverse events in either group. The time of CSPEB pre-sentation was not influenced by PEC. PEC did not reduceCSPEB in proximal colonic lesions (hepatic flexure andproximally) or in patients taking antiplatelet agents lessthan 7 days before WF-EMR. When excluding the 15 pa-tients (PEC: aspirin, 3 patients; clopidogrel, 1 patient; non-PEC: aspirin, 10 patients; clopidogrel, 1 patient) who had
Table 1. Baseline Characteristics
N ¼ 347WF-EMR þ PEC
(n ¼ 172)WF-EMR(n ¼ 175) P value
Median age (IQR), y 66.0 (16) 70.0 (15) .45Men 47.7% 54.9% .18American Society
of Anesthesiologistsgrade
.01
I 56.4% 41.7%II 38.4% 46.3%III 5.2% 10.3%IV 0% 1.1%
Antiplatelet use inpast 7 days
2.3% 6.3% .07
Mean lesion size(IQR), mm
39.5 (25) 39.8 (21) .85
Mean procedure time(IQR), min
24 (20) 26 (22) .41
Paris classification .330-Is 8.7% 14.3%0-IIa 47.1% 45.7%0-IIaþIs 34.3% 29.1%0-IIb 4.1% 4.5%0-IIc, 0-IIbþc, 0-IIaþc 4.1% 4.6%
En bloc resection 12.9% 16.1% .41Proximal colon location 54.7% 56.3% .18Intraprocedural bleeding 27.3% 34.9% .13Submucosal fibrosis 21.5% 28.2% .15Visible vessels 69.8% 67.4% .89Mean number of
vessels (IQR), mm4.6 (4) 4.3 (3) .45
Median size oflargest vessel, mm
0.3–0.5 0.3–0.5 .77
Vessel herniation 32.0% 22.3% .10Fibrosis in resection
defect13.3% 15.4% .63
IQR, interquartile range.
April 2015 PEC to Prevent Bleeding After WF-EMR 727

taken antiplatelet agents within 7 days of WF-EMR, therates of CSPEBwere similar between the PEC and non-PECarms (5.4% vs 6.7%; P ¼ .61).
CSPEB occurred in 23 patients (6.6%) and occurredwithin 24 hours in 14 patients (60.9%), within 24 to 48hours in 6 patients (26.1%), within 2 to 7 days in 2patients (8.7%), and within 8 to 14 days in 1 patient(4.3%). The median CSPEB presentation time was lessthan 24 hours (range, <24 h to 12 d).
The factors associated with CSPEB are listed inTable 3. On univariate analysis CSPEB was associatedsignificantly with proximal colonic lesion location (P ¼.02) and antiplatelet use in the past 7 days (P ¼ .03). Onmultivariate analysis CSPEB was associated significantlywith proximal colonic lesion location (P ¼ .03; odds ratio,3.1; 95% confidence interval, 1.1–8.5), and there was atrend with antiplatelet use in the past 7 days (P ¼ .05;odds ratio, 3.8; confidence interval, 0.97–14.99). Vesselcharacteristics were not associated significantly withCSPEB, or was the presence of intraprocedural bleeding.
Influence of Lesion Location on VesselCharacteristics and Clinically SignificantPostendoscopic Mucosal Resection Bleeding
When the lesions were separated into proximal anddistal locations, the distal colon had a significantly greatermean number (3.8 vs 2.1; P¼ .002), median size (0.5–1 vs0.3–0.5 mm; P¼ .04), and prevalence of vessel herniation
(33.8% vs 21.9%; P ¼ .02) (Supplementary Table 1 ).CSPEB occurred significantly more often in the proximalcolon (9.4% vs 3.2%; P¼ .02). The rates of CSPEB was notsignificantly different across the three study sites(Supplementary Table 2).
Discussion
This was a prospective randomized controlled trial toexamine the effectiveness of endoscopic coagulation inthe prevention of CSPEB, the most frequent majorcomplication of colonic WF-EMR. CSPEB may be associ-ated with significant patient morbidity and managementis resource intensive. A recent large multicenter pro-spective study found that CSPEB occurs in 6.0% of pa-tients.8 Most patients presented within 48 hours afterthe procedure (66%), 21% had hemodynamic instability,26% received a blood transfusion, and 42% underwentcolonoscopy, of whom 81% required endoscopic inter-vention. The median inpatient stays were 1 and 3 daysfor patients with “mild” and “moderate/severe” ASGEadverse outcomes, respectively.16
Effective, readily applicable, and safe prevention ofCSPEB has emerged as a key aspect to improve patientoutcomes after WF-EMR. There is limited literatureregarding effective prevention of CSPEB pertaining toAMN. Because of the low bleeding rate of conventionalpolypectomy few studies have been able to achieve suf-ficient power to report statistically meaningful resultsfor any prophylactic intervention.17–19 Because the
Table 2. Outcomes of Patients With and Without ProphylacticEndoscopic Coagulation
N ¼ 347WF-EMR þ PEC
(n ¼ 172)WF-EMR(n ¼ 175) P value
CSPEB (6.6%)Total 9 (5.2%) 14 (8.0%) .30<24 h 5 (55.6%) 9 (64.3%)24–48 h 3 (33.3%) 3 (21.4%)3–7 d 1 (11.1%) 1 (7.1%)8–14 d 0 (0%) 1 (7.1%)
CSPEB proximalcolonic lesions
7 (4.1%) 11 (6.3%) .37
CSPEB distalcolonic lesions
2 (1.2%) 3 (1.7%) .68
CSPEB antiplateletagents past 7 days
0 (0%) 3 (1.7%) .52
Median procedureduration (IQR), min
35 (35) 30 (22) .69
Hospitalization 10 (5.8%) 14 (8.0%) .42Median inpatient
nights (IQR), d2 (2) 2 (1) .59
Need for intervention 5 (2.9%) 5 (2.9%) .36Colonoscopy 3 (60.0%) 4 (80.0%)Angiography/
embolization1 (20.0%) 1 (20.0%)
Transfusion 4 (80.0%) 1 (20.0%)Perforation 0 0 N/ADeath 0 0 N/A
IQR, interquartile range.
Table 3. Factors Associated With Clinically SignificantPost–WF-EMR Bleeding
Factors
Univariate analysis
Pvalue
Multivariate analysis
VariablesP
valueOdds ratio(95% CI)
Patient Age .67Sex .73American Society
of Anesthesiologistsgrade
.36
Antiplatelet uselast 7 days
.03 .05 3.8 (0.97–14.99)
Anticoagulant uselast 4 doses
.60
Lesion Mean lesion size .21Paris classification .74Proximal colonic
location.02 .03 3.1 (1.1–8.5)
Vessels Visible vessels .26Number of vessels .42Size of largest vessel .71Vessel herniation .92
Defect Intraproceduralbleeding
.94
Fibrosis .89
CI, confidence interval.
728 Bahin et al Clinical Gastroenterology and Hepatology Vol. 13, No. 4

bleeding rate is higher in the WF-EMR setting, insightsgained from this more extreme environment may beapplicable to conventional polypectomy.
Endoscopic options for the prevention of post-polypectomy bleeding and CSPEB include injection(submucosal epinephrine), hemostatic spray or gel, me-chanical methods (endoscopic clips and detachablesnares), and coagulation therapy (argon plasma and softcoagulation).7,17–24 Randomized controlled trials havefailed to show a significant reduction in postpolypectomybleeding with prophylactic clip placement to close themucosal defect and argon plasma coagulation in colonicpolyps with a mean size of less than 1 cm.23,25 However,a recent meta-analysis suggested a beneficial prophy-lactic effect with epinephrine and mechanical hemostasisfor polyps greater than 10 mm.26 A retrospective anal-ysis of prophylactic clip placement to close the endo-scopic resection defect involving 524 colonic lesionsgreater than 20 mm over 12 years suggested a statisti-cally significant benefit.7 The delayed bleeding rate was9.7% in the unclipped group vs 1.8% in the fully clippedgroup. On multivariate analysis the association of notclipping and delayed bleeding had an odds ratio of 6.Apart from the inherent limitations of a retrospectivedesign there may have been a bias toward the clippedcohort because lesions that could be closed are likely tobe smaller and thus potentially may have a lower rate ofCSPEB. Furthermore, it is technically challenging toproperly close very large defects with clips. The meanlesion size in our study approached 40 mm, comparedwith 31 mm in the earlier-described study.
Exposed vessels within the EMR defect seem a logicaltherapeutic target to prevent CSPEB. A previous obser-vational study evaluating endoscopic submucosal dis-section of early gastric cancers (1083 lesions; mean size,44 mm) suggested that PEC was effective in reducingpostresection bleeding.9 A similar outcome was plausiblewith PEC to prevent colonic CSPEB. Furthermore, PEC iseasy to use, inexpensive, and widely applicable. It can beapplied to defects of any size, unlike endoscopic clipping.As shown here, PEC with soft coagulation is also verysafe. It is underpinned by sound electrophysiologicalprinciples. Peak voltage is capped at 190 V, resulting inever-increasing resistance to current flow during tissuedesiccation. This acts as a built-in safety mechanism thatprevents deep thermal injury.15
In our study, PEC to visible vessels in the resectiondefect did not result in a statistically significant benefit.The rates of CSPEB were 5.2% and 8.0% in the PEC andnon-PEC arms, respectively. PEC did not significantlyreduce secondary outcomes such as the need for inter-vention for CSPEB, hospitalization, or length of hospitalstay. Although not effective in CSPEB prevention, PECwas safe, easy to apply, and did not result in periproce-dural complications, hospitalization, or increased proce-dure duration.
The factors significantly associated with CSPEB onunivariate analysis were proximal colonic lesion
location and antiplatelet agent use in the past 7 days. Onmultivariate analysis, proximal colonic lesion locationwas the only significant factor. These findings areconsistent with previously published literature.4,6,7
Upon stratification of CSPEB based on lesion locationand use of antiplatelet agents in the past 7 days, nosignificant differences were noted with PEC. Vesselcharacteristics and the presence of intraproceduralbleeding did not predict CSPEB.
A novel finding of the study was that although themajority of CSPEB occurred in WF-EMR of proximalcolonic lesions, the distal colonic resection defects had agreater number, size, and presence of vessel herniation.This finding challenges the hypothesis that the stigmatathat are presumed to be predictive of bleeding (such asnonbleeding vessels in the resection defect) are thesource of subsequent CSPEB. Our study has shown thattreating such stigmata did not result in a significantreduction in CSPEB. Because PEC was applied effectivelyto all lesions in the resection defect, there may be otherfactors relating to the connective tissue support struc-ture around the vessels within the resection defect orlocal blood supply that drive CSPEB. A greater under-standing of the pathophysiological mechanisms of CSPEBis required to develop more targeted prophylacticinterventions.
A limitation of the trial is that the sample size wasinsufficient to show a more modest statistically signifi-cant reduction in CSPEB. If a statistically significant trendreflecting the risk reduction seen in our study was tocontinue, a randomized controlled trial with 1305 pa-tients per arm would be needed. At that level 36 lesionsneed to be treated with PEC to prevent 1 CSPEB event.For this end point it is doubtful whether such a finding isclinically meaningful.
We have included patients using antiplatelet agentswithin 7 days in the analysis to reflect real-life practice.Such patients were numerically greater in the non-PECgroup and may have increased the rates of CSPEB ratein this group. When excluding patients using antiplateletagents the rates of CSPEB were 5.4% and 6.7% in thePEC and non-PEC arms, respectively (P ¼ .61). Even if avery large trial was performed to show such a riskreduction with statistical significance, the actual clinicalbenefit of PEC is weak at best.
In summary, although PEC is safe, it is not signifi-cantly effective in the prevention of CSPEB and relatedend points. Further research efforts need to be dedicatedto determine efficacious prophylactic therapies thatreduce CSPEB.
Supplementary Material
Note: To access the supplementary material accom-panying this article, visit the online version of ClinicalGastroenterology and Hepatology at www.cghjournal.org,and at http://dx.doi.org/10.1016/j.cgh.2014.07.063.
April 2015 PEC to Prevent Bleeding After WF-EMR 729
References1. Gellad ZF, Provenzale D. Colorectal cancer: national and inter-
national perspective on the burden of disease and public healthimpact. Gastroenterology 2010;138:2177–2190.
2. Moss A, Bourke MJ, Williams SJ, et al. Endoscopic mucosalresection outcomes and prediction of submucosal cancer fromadvanced colonic mucosal neoplasia. Gastroenterology 2011;140:1909–1918.
3. Swan MP, Bourke MJ, Alexander S, et al. Large refractorycolonic polyps: is it time to change our practice? A prospectivestudy of the clinical and economic impact of a tertiary referralcolonic mucosal resection and polypectomy service (withvideos). Gastrointest Endosc 2009;70:1128–1136.
4. Metz AJ, Bourke MJ, Moss A, et al. Factors that predict bleedingfollowing endoscopic mucosal resection of large colonic lesions.Endoscopy 2011;43:506–511.
5. Buchner AM, Guarner-Argente C, Ginsberg GG. Outcomes ofEMR of defiant colorectal lesions directed to an endoscopyreferral center. Gastrointest Endosc 2012;76:255–263.
6. Burgess NG, Metz AJ, Williams SJ, et al. Risk factors for intra-procedural and clinically significant delayed bleeding after wide-field endoscopic mucosal resection of large colonic lesions. ClinGastroenterol Hepatol 2014;12:651–661. e1–3.
7. Liaquat H, Rohn E, Rex DK. Prophylactic clip closure reducedthe risk of delayed postpolypectomy hemorrhage: experience in277 clipped large sessile or flat colorectal lesions and 247control lesions. Gastrointest Endosc 2013;77:401–407.
8. Burgess NG, Williams SJ, Hourigan LF, et al. A managementalgorithm based on outcomes of clinically significant delayedbleeding after wide-field endoscopic mucosal resection of largecolonic lesions. Clin Gastroenterol Hepatol 2014;12:1525–1533.
9. Takizawa K, Oda I, Gotoda T, et al. Routine coagulation ofvisible vessels may prevent delayed bleeding after endoscopicsubmucosal dissection–an analysis of risk factors. Endoscopy2008;40:179–183.
10. Anderson MA, Ben-Menachem T, Gan SI, et al. Management ofantithrombotic agents for endoscopic procedures. GastrointestEndosc 2009;70:1060–1070.
11. Bourke M. Endoscopic mucosal resection in the colon: a prac-tical guide. Tech Gastrointest Endosc 2011;13:35–49.
12. Holt BA, Bourke MJ. Wide field endoscopic resection foradvanced colonic mucosal neoplasia: current status and futuredirections. Clin Gastroenterol Hepatol 2012;10:969–979.
13. Moss A, Bourke MJ, Metz AJ. A randomized, double-blind trialof succinylated gelatin submucosal injection for endoscopicresection of large sessile polyps of the colon. Am J Gastro-enterol 2010;105:2375–2382.
14. Moss A, Bourke MJ, Kwan V, et al. Succinylated gelatin sub-stantially increases en bloc resection size in colonic EMR: arandomized, blinded trial in a porcine model. GastrointestEndosc 2010;71:589–595.
15. Fahrtash-Bahin F, Holt BA, Jayasekeran V, et al. Snare tip softcoagulation achieves effective and safe endoscopic hemostasisduring wide-field endoscopic resection of large colonic lesions(with videos). Gastrointest Endosc 2013;78:158–163.e1.
16. Cotton PB, Eisen G, Romagnuolo J, et al. Grading thecomplexity of endoscopic procedures: results of an ASGEworking party. Gastrointest Endosc 2011;73:868–874.
17. Dobrowolski S, Dobosz M, Babicki A, et al. Prophylactic sub-mucosal saline-adrenaline injection in colonoscopic poly-pectomy: prospective randomized study. Surg Endosc 2004;18:990–993.
18. Lee SH, Chung IK, Kim SJ, et al. Comparison of post-polypectomy bleeding between epinephrine and saline submu-cosal injection for large colon polyps by conventionalpolypectomy: a prospective randomized, multicenter study.World J Gastroenterol 2007;13:2973–2977.
19. Paspatis GA, Paraskeva K, Theodoropoulou A, et al.A prospective, randomized comparison of adrenaline injection incombination with detachable snare versus adrenaline injectionalone in the prevention of postpolypectomy bleeding in largecolonic polyps. Am J Gastroenterol 2006;101:2805; quiz 913.
20. Choi KD, Jung HY, Lee GH, et al. Application of metal hemoclipsfor closure of endoscopic mucosal resection-induced ulcers ofthe stomach to prevent delayed bleeding. Surg Endosc 2008;22:1882–1886.
21. Iishi H, Tatsuta M, Narahara H, et al. Endoscopic resection oflarge pedunculated colorectal polyps using a detachable snare.Gastrointest Endosc 1996;44:594–597.
22. Kouklakis G, Mpoumponaris A, Gatopoulou A, et al. Endoscopicresection of large pedunculated colonic polyps and risk ofpostpolypectomy bleeding with adrenaline injection versusendoloop and hemoclip: a prospective, randomized study. SurgEndosc 2009;23:2732–2737.
23. Lee CK, Lee SH, Park JY, et al. Prophylactic argon plasmacoagulation ablation does not decrease delayed post-polypectomy bleeding. Gastrointest Endosc 2009;70:353–361.
24. Quintanilla E, Castro JL, Rabago LR, et al. Is the use of pro-phylactic hemoclips in the endoscopic resection of largepedunculated polyps useful? A prospective and randomizedstudy. J Interv Gastroenterol 2012;2:99–104.
25. Shioji K, Suzuki Y, Kobayashi M, et al. Prophylactic clip appli-cation does not decrease delayed bleeding after colonoscopicpolypectomy. Gastrointest Endosc 2003;57:691–694.
26. Corte C, Burger D, Horgan G, et al. Postpolypectomy haemor-rhage following removal of large polyps using mechanical he-mostasis or epinephrine: a meta-analysis. United EuropeanGastroenterol J 2014;1:1–9.
Reprint requestsAddress requests for reprints to: Michael J. Bourke, MBBS, FRACP, Director ofEndoscopy, Department of Gastroenterology and Hepatology, WestmeadHospital, c/o Suite 106a, 151-155 Hawkesbury Road, Westmead, Sydney, NewSouth Wales 2145, Australia. e-mail: [email protected]; fax:(þ612) 9633-3958.
AcknowledgmentsThe authors would like to acknowledge the work of Dr Karen Byth Wilson(University of Sydney), who assisted with the statistical analysis of the study.
Conflicts of interestThe authors disclose no conflicts.
FundingFarzan Bahin was supported by a grant from the National Health and MedicalResearch Council of Australia. The Cancer Institute New South Wales providedfunding for a research nurse and data manager to assist with the administrationof the study. There was no influence from the National Health and MedicalResearch Council or the Cancer Institute on study design or conduct, datacollection and management, analysis, interpretation, preparation and review, orapproval of the manuscript.
730 Bahin et al Clinical Gastroenterology and Hepatology Vol. 13, No. 4

SupplementaryFigure 1. (A) 60 mm Paris0-IIaþIs lesion in thetransverse colon. (B) Largevessel in the resectiondefect (> 2 mm diameter)during WF-EMR. (C) Multi-ple vessels noted in thefinal WF-EMR defect. (D)Coagulation forceps graspthe vessel. (E) Soft coagu-lation is applied using thecoagulating forceps. (F)Final resection defectfollowing PEC.
SupplementaryFigure 2. Study flowchart.
April 2015 PEC to Prevent Bleeding After WF-EMR 730.e1
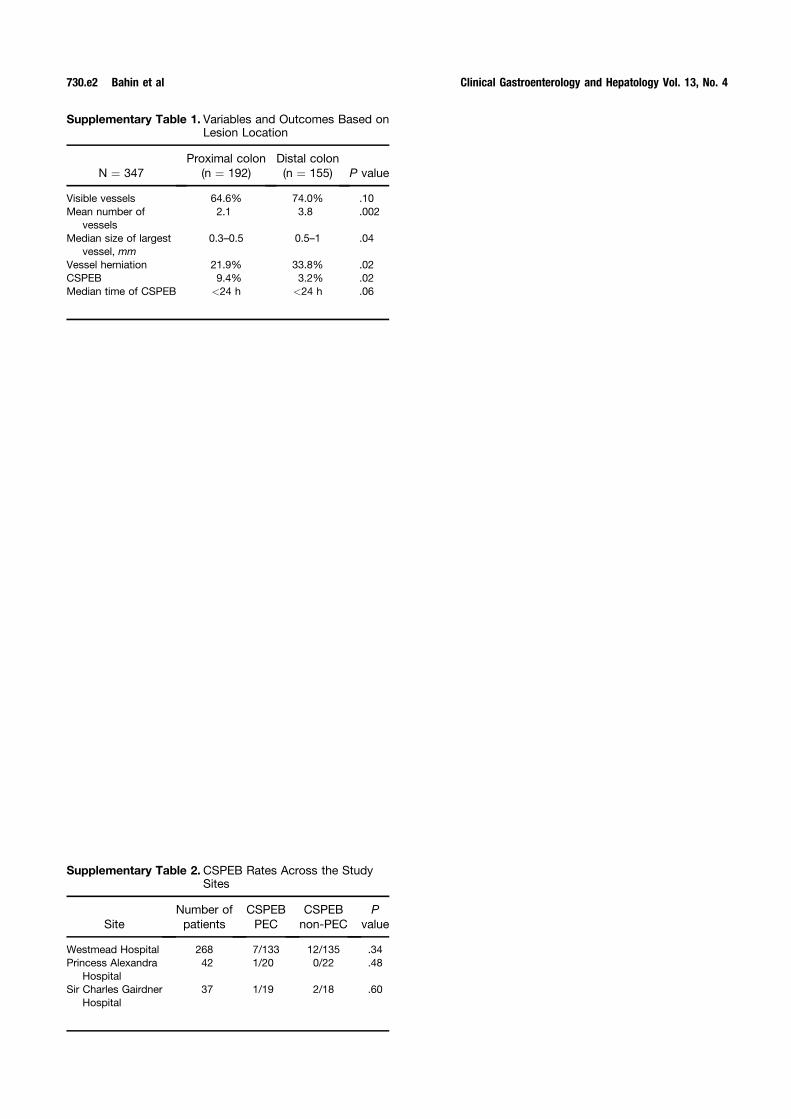
Supplementary Table 1. Variables and Outcomes Based onLesion Location
N ¼ 347Proximal colon
(n ¼ 192)Distal colon(n ¼ 155) P value
Visible vessels 64.6% 74.0% .10Mean number of
vessels2.1 3.8 .002
Median size of largestvessel, mm
0.3–0.5 0.5–1 .04
Vessel herniation 21.9% 33.8% .02CSPEB 9.4% 3.2% .02Median time of CSPEB <24 h <24 h .06
Supplementary Table 2. CSPEB Rates Across the StudySites
SiteNumber ofpatients
CSPEBPEC
CSPEBnon-PEC
Pvalue
Westmead Hospital 268 7/133 12/135 .34Princess Alexandra
Hospital42 1/20 0/22 .48
Sir Charles GairdnerHospital
37 1/19 2/18 .60
730.e2 Bahin et al Clinical Gastroenterology and Hepatology Vol. 13, No. 4




















