Proceedings - Fetch dvm360
530
Proceedings Fetch Virtual, a dvm360 ® Conference November 12-14, 2020 Fetch dvm360® conference brought to you by The best read veterinary team journal. Bam.
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Proceedings - Fetch dvm360

ProceedingsFetch Virtual, a dvm360® Conference
November 12-14, 2020
Fetch dvm360® conference brought to you by
The best read veterinary team journal. Bam.

Health care information changes rapidly and thus the materials herein presented should not be relied upon to be fully comprehensive or error free. The ideas, content, and conclusions presented in the 2020 Fetch dvm360®
Conference proceedings and herein, in whole or part, are those of the speakers and do not necessarily represent the viewpoint, position, or endorsement of
Fetch dvm360® or Multimedia Animal Care, LLC. The information is for general information only and without warranties of any kind.
ISBN# 978-1-60759-324-9
Our faculty are the best around
Darby Affeldt, DVM, RCIP
Rachael Allbaugh, DVM, MS, DACVO
Mary Kate Anderson, DVM
Michael A. Azzarello, MBA, BS
Liz Bales, VMD
Mike Barletta, DVM, MS, PhD, DACVAA
Marty Becker, DVM
Todd Behre, DVM, PMP
Jan Bellows, DVM, DAVDC, ABVP
John Berg, DVM, DACVS
Mary Berg, BS, LATG, RVT, VTS (Dentistry)
Kim Bishop, DVM
Dawn Boothe, DVM, MS, PhD, DACVIM, DACVCP
Harry W. Boothe, DVM, MS, DACVS
Ashley Bourgeois, DVM, DACVD
Antonio Bowens, DVM
Priscilla Bowens, DVM, JD, MPH
Michele Broadhurst, DC, ICCSP, FIAMA, IVCA, CCRP
Walter Brown, BS, RVTg
Matthew Brunke, DVM, DACVSMR, CCRP, CVPP, CVA
Courtney Campbell, DVM, DACVS-SA
Anthony P. Carr, Dr. med. vet., DACVIM
Mia Cary, DVM
Betsy Charles, DVM, MA
Jenifer Chatfield, DVM, DACZM, DACVPM
Stephen Cital, RVT, SRA, RLAT, VCC, CVPP, VTS-LAM (Res Anesthesia)
Elizabeth Colleran, DVM, MS, DABVP feline specialist
Don Costlow, DVM
Dennis Tim Crowe Jr., DVM, DACVS-Emeritus,
Charter DACVECC, FCCM NRAEMT, CFF
Steve Dale, CABC
Ethan Dawe
Victoria Deamer-Smith, RVN
Lauren Demos, BVMS, HonsBSc, DABVP (Feline)
Caitlin DeWilde, DVM
Robin Downing, DVM, MS, DAAPM, DACVSMR, CVPP, CCRP
Michele Drake, DVM
David Dycus, DVM, MS, CCRP, DACVS-SA
Amanda Dykstra, DVM, MPH, DABVP
Ryane Englar, DVM, DABVP
Sue Ettinger, DVM, DACVIM (Oncology)
Alec Failor
Thomas C. Favale, Jr., DVM, LMSW
Mariacamila Garcia Estrella, BS
Jordan Gesimondo, DVM
David Hall
Lindsay Hallman, CVT
Bash Halow, LVT, CVPM
Natalie Hoepp, DVM, MS, DACVP
Stephanie Hickey, DVM
Liz Hughston, MEd, RVT, CVT, LVT, VTS (SAIM, ECC)
Alex Hynes, BVSc, MVS, MANZCVS
Michael H. Jaffe, DVM, MS, CCRP, DACVS
Kimberly Johnson Hatchett, MD
Chand Khanna, DVMP, PhD DACVIM (Oncology)
Kristin Kirkby Shaw, DVM, PhD, DACVS, DACVSMR
Erika Krick, DVM, ACVIM (Oncology)
Heather Kvitko-White, DVM, DACVIM
Michael Lappin, DVM, PhD, DACVIM (SAIM)
Lisa Lippman, DVM
Mary Lopez
Lydia Love, DVM, DACVAA
Mike Lucroy, DVM, MS, DACVIM
Patrick Mahaney, VMD, CVA, CVJ
Lisa Mausbach, DVM, MSOL-LM-PLM, SHRM-CP
Brennan McGoldrick, DVM, MBA
Charles McMillan, DVM
Shawn McVey, MA, MSW
Kristen Messenger, DVM, PhD, DACVAA, DACVCP
Shawn Messonnier, DVM
John Meyer, PhD
Jeff Nichol, DVM
Christopher Pachel, DVM, DACVB, CABC
Mariana Pardo, MV, BVSc, DACVECC
Valerie Parker, DVM, DACVIM, DACVN
Michael Petty, DVM, CVPP, CVMA, CCRT, CAAPM
Dan Phillips, DVM
Gerardo Poli, BVSc, MVS, MANZCVS
Kathryn Primm, DVM, CVPM
Serena Pudelski, RVT
Jennifer Quammen, DVM, MPH
Narda Robinson, DO, DVM, MS, FAAMA
Rebecca Robinson-Davis, CBI
Denise Rollings, CVT, VTS (Dentistry)
Robin Saar, RVT, VTS (Nutrition)
Tracy Sands, DVM
Allen M. Schoen, DVM, PhD (hon), MS
Judy Seltzer, BVetMed, MRCVS, DACVD
Carolyn Shadle, PhD
Melissa Shapiro, DVM
Tracy Sheffield, BS, LVT, CVPM
Tim Shu, DVM
Robert J. Silver, DVM, MS
Aaron Smiley, DVM
Adam Smith, DVM
Emily Stein, PhD
Jennifer Steinberg, DVM, DACVP
Debbie Stoewen, DVM, MSW, RSW, PhD
Melissa Supernor, LVT, CVT, VTS, CFE, CCFP
Karen Trainor, DVM, MS, DACVP
Christina V. Tran, DVM (Multicultural VMA president)
Josh Vaisman, CCFP, MAPPCP (PgD)
Jessica Vogelsang, DVM
Aaron Wallace, DVM, MS, MBA
Courtney Waxman, CVT, RVT, VTS (ECC)
Kristin Welch, DVM, DACVECC
Brandon Werber
Jeff Werber, DVM
Fred Wininger, VMD, MS, DACVIM (Neurology)
Jan Woods
Nate Zhang
Joanne Zimmermann, BS, CVT, VTS (Anesthesia & Analgesia)
Anesthesiology Mike Barletta, DVM, MS, PhD, DACVAA,
Anesthesia for the animal with gastrointestinal and hepatic disease .......................................................1
Lydia Love, DVM DACVAA and Joanne Zimmerman CVT, VTS (Anesthesia & Analgesia)
The anesthesia checklist you need .............................. 4
Behavior Jeff Nichol, DVMBang! Pop! Fire in the Sky: Misery Worsens with Repeated Storms ....................................................... 16
Christopher Pachel, DVM, DACVB, CABC
Do you see what I see? Medical conditions masquerading as aggression problems ..................21
Incorporating behavior strategies into patient care: Practical solutions for daily situations .......... 23
More than just a naughty cat: Understanding feline nuisance behaviors ........................................... 25
Multi-cat households: identifying and addressing problems before the fur starts flying ..................... 27
Prescribing for separation anxiety: How do you decide? ................................................... 30
Room for one more! Introducing a new cat or dog to the household ............................................. 32
C.A.L.MAllen Schoen, DVM, PhD (hon), MSIntegrating CALM (c) to co-create a more expansive approach to veterinary medicine ..........34
Career Development Lisa Mausbach, DVM, MSOL-LM-PLM, SHRM-CP
Kaleidoscope Veterinarian Careers ........................... 39
Serena Pudelski, RVTBeing a solo RVT and business coach- serving outside of a clinical setting ...................................... 50
Clinical Pharmacology Dawn Boothe, DVM, MS, PhD, DACVIM, DACVCP
Clinical use of glucocorticoids .................................... 52Non-glucocorticoid immunomodulators ..................63Therapeutic drug monitoring: A case based approach .............................................. 74
Compounding Michael A. Azzarello, MBA, BSUnderstanding compounding medications .............82
Controlled Drug Substance Jan WoodsCONTROLLED SUBSTANCES 101: How and Why You Must Comply! .......................................................87
Dentistry Jan Bellows, DVM, DAVDC, ABVP 20+ dental hacks for your dental practice ............. 107Feline stomatitis where do you begin? ...................108Easy steps to extract those nasty teeth .................115
Table of Contents

Dermatology Ashley Bourgeois, DVM, DACVD Calling all vets and vet techs —how to speak derm successfully! ......................................................119
Tackling the itchy cat challenge ............................... 123
Diversity Mariacamila Garcia Estrella, BS Building cultural competence and improving Spanish communication with Latinx clients ....... 128
Emergency Medicine and Critical Care
Jennifer Chatfield, DVM, DACZM, DACVPM
Disaster response made easy: infectious diseases .....................................................131
Dennis Tim Crowe Jr., DVM, DACVS-Emeritus, Charter DACVECC, FCCM NRAEMT, CFF
Emergency tracheotomy: The surgical parachute that saves lives .......................................................... 133
Kristin Kirkby Shaw, DVM, PhD, DACVS, DACVSMR
Vacuum assisted wound closure for traumatic wounds ......................................................141
Feline Medicine Elizabeth Colleran, DVM, MS, DABVP feline specialist
How chronic disease affects pain perception & management .......................................................... 143
Lauren Demos, BVMS, HonsBSc, DABVP (Feline)
Feline examination: streamline the exam and maximize your findings .................................... 148
Financial Health Darby Affeldt, DVM, RICPWalk your talk: Client procrastination harms your patients & your procrastination could be hurting your financial goals ................................................... 149
Infectious Diseases Jennifer Chatfield, DVM, DACZM, DACVPM
What we know about SARS-CoV-2…and what it means for practitioners ............................................151
Integrative Medicine Matthew Brunke, DVM, DACVSMR, CCRP, CVPP, CVA & Michele Broadhurst DC, ICCSP, FIAMA, IVCA, CCRP
An integrative approach to complementary care in veterinary practice ................................................ 154
Internal Medicine Anthony Carr, Dr. med. vet., DACVIM ECG basics ................................................................... 163EPI in dogs .................................................................... 170IMHA: Bad blood ......................................................... 174Practical management of renal failure .................. 178The cutting edge medicine ........................................ 183
International Health Certificate
Amanda Dysktra, DVM, MPH, DABVP Interstate and international transport: Concerns for the general practitioner ....................................188
Neurology Antonio L. Bowens, DVM Management of seizures in the canine and feline patient .......................................................191
Vestibular Disease ...................................................... 193
Fred Wininger, VMD, MS, DACVIM (Neurology)
Neuro–what they never taught in vet school ........ 196Vision and Pupils.......................................................... 198
Nutrition Robin Saar RVT, VTS (Nutrition)How to effectively utilize nutrition technicians: how to utilize staff, & encourage effective communication with clients about nutrition .......201
Oncology Chand Khanna, DVMP, PhD DACVIM (Oncology)
Delivering hope to canine hemangiosarcoma ..... 205
Michael D. Lucroy, DVM, MS, DACVIM
Cancer Immunotherapy — An inside job ............... 209
Sue Ettinger, DVM, DACVIM (Oncology)
Osteosarcoma review and what’s new 2020 ....... 212What’s new in cancer 2020 ...................................... 218What’s new in mast cell tumor treatments ..........224Urine liquid biopsy: The New for bladder cancer in dogs .........................................................................229
Ophthalmology Rachel A. Allbaugh, DVM, MS, DACVO
Feline Ophthalmology – Practical tips for diagnosing and treating common cat conditions ...........................................234
OrthopedicsCourtney Campbell, DVM, DACVS-SA
Top 5 orthopedic pearls you need to know ............ 237
David Dycus, DVM, MS, CCRP, DACVS-SA
Distal extremity injuries – sprain or worse of the achilles complex? ....................................................... 251
It’s a puppy, what could possibly go wrong? Developmental orthopedic conditions .................255
Hip Dysplasia: Conservative and rehabilitation management .................................... 261
Kristin Kirkby Shaw, DVM, PhD, DACVS, DACVSMR
Elbow disorders in dogs and cats: Methods of treatment .............................................270
The 3 R’s of CCL: Repair, rehab and research ....... 274The not-so-magic eight ball: Predicting OA by early diagnosis of eight developmental orthopedic diseases...................... 276
Pain Management Michael C Petty, DVM, CVPP, CVMA, CCRT, CAAPM
Monoclonal antibodies for pain................................278I know that dog has chronic pain: convincing the owner ................................................286
Parasitology Jennifer Chatfield, DVM, DACZM, DACVPM
Fun with felines…and fleas? ......................................292
Michael W. Dryden, DVM, PhD, DACVM-Parasit
Dog parks and parasite risk ......................................295
Pet Disability Melissa Shapiro, DVM A veterinarian’s guide to pets with disabilities and special needs ......................................................299
Pet Insurance Shawn Messonnier, DVM CEF’s-Retirement Investing .....................................301
Pet insurance to achieve better medicine, better business ............................................306
Practice Management Carolyn C. Shadle, Ph.D. and John L. Meyer, Ph.D.
Care for a lifetime .......................................................310
Mia Cary, DVM Caregivers burden-how to help our clients and ourselves.............................................................. 313
Caitlin DeWilde, DVM Social Media and marketing for technicians ......... 317
Bash Hallow, LVT, CVPMCan I vent? The negative effects of blowing off steam ................................................................... 320
What’s the Buzz? ........................................................323
Naphia ....................................................................326
Dan Phillips, DVM Master the interview for mentorship and career success ............................................. 334
Kathryn Primm, DVM, CVPMBreaking down the P&L: The star chart to your galaxy ..................................................................335
Carolyn C. Shadle, Ph.D. and John L. Meyer, Ph.D.
Getting to win-win when there’s a conflict among team members ..........................................................344
Tracy Sheffield, BS, LVT, CVPMDealing with difficult clients .................................... 348One good new idea: Practice management tips and techniques...........................................................354
Work Environment: The Overlooked Profit Center ................................359
Shelter Medicine Amanda Dykstra, DVM, MPH, DABVP
Tips and tricks: Helpful advice for those new to shelter medicine ........................................................369
Spay/neuter surgical techniques to improve outcomes and efficiency in general practice...... 370
Soft Tissue Harry W. Boothe, DVM, MS, DACVS
Exploratory laparotomy with biopsy techniques ...................................................... 372
Thoracic surgery: Focus on approaches and closure ......................... 376
TechnologyJessica Vogelsang, DVMVeterinary telehealth: 5 effective strategies ........379The ROI of virtual care ...............................................382
Lisa Lippman, DVM Use of wearable “smart” collars for clinical assessment ...................................................385
Jeff Werber, DVM and Brandon Werber
Like it or not, telemedicine is now mainstream: How to prepare for what’s ahead ........................ 388
ToxicologyLiz Hughston, MEd, RVT, CVT, LVT, VTS (SAIM, ECC)
The solution to pollution: Top toxicity tips ............. 391
Veterinary TechnicianWalter Brown Jr., RVTgHey Doc, we’re in the RED! A review of distributive/vasodilatory shock ..............................396
Fluids: “I like the way you move”: A review of fluid balance .........................................401
Ryane E. Englar, DVM, DABVPCommunication challenges at teaching hospitals: The veterinary technician’s perspective .............. 405
Liz Hughston MEd, RVT, CVT, LVT, VTS (SAIM, ECC)
PICC lines and jug caths and io’s oh my! Advanced vascular access techniques for veterinary technicians ..............................................410
Git `er down: Nursing care for the megaesophagus patient ......................................... 415
Every patient, every time: Kirby’s rule of 20.......... 419
Rachel Lees RVT, KPA CTP, VTS (Behavior)
As Seen on T.V? Understanding and Discussing Dominance Theory and Punishment with Clients and Veterinary Professionals ..................................428
So, You Want to be a Veterinary Behavior Technician? The role of Veterinary Technicians in behavior ..................................................................432
Courtney Waxman, CVT, RVT, VTS (ECC)
Sepsis survival guide ...................................................437Tech tools: Multi-parameter monitoring ................444 The vet techs critical patient checklist ...................449
Veterinary Technician Dentistry
Denise Rollings CVT, VTS (Dentistry)
Dental and Oral Abnormalities ............................... 458Feline dentistry ............................................................462 From the exam room to the dental table ..............466
Virtual Day CareColoring Book For Children! .................................472Children’s Coloring Book Pages (Banfield) ............ 481The Science of Loving Pets ....................................... 491
Well Being Debbie L Stoewen, DVM, MSW, RSW, PhD
Veterinary happiness: from the personal to the professional ....................................................510
Wellness at work: Everyone has a role, and every role is critical ............................................................... 516

Anesthesia for the animal with gastrointestinal and hepatic disease
Patients with gastrointestinal and hepatic diseases have an increased anesthetic risk. It is important to know if the disease is treated and under control before anesthetizing these patients.
By Michele Barletta, DVM, MS, PhD, DACVAA, University of Georgia, College of Veterinary Medicine, Department of Large Animal Medicine, Athens GA
Ideally these animals should be stabilized before the procedure whenever possible. Fluid, electrolyte, and acid-base disturbances should be corrected prior to anesthesia. As in all patients, a thorough physical examination is paramount. A complete blood work including cell blood count, serum chemistry and electrolytes, and urine analysis are recommended. Abdominal radiographs and ultrasound should also be evaluated before anesthesia.
Acute GI Diseases:
Pathophysiology These patients can present obstructions (foreign bodies, masses, intussusception) or a perforation of the GI tract. Nausea and vomiting can be present and can lead to dehydration, electrolyte abnormalities, acid-base imbalance. Loss of GI vascular and mucosal integrity can lead to leakage of toxic substances and sepsis. These patients are susceptible to bacteremia, endotoxemia, sepsis, hypotension, and arrhythmias. If abdominal distension is present, the animal can show signs of respiratory distress, poor tissue perfusion, and pain.
Preanesthetic preparation Evaluate the hydration of the patient and treat shock if present. Aggressive fluid therapy may be necessary before anesthesia. Electrolytes and acid-base abnormalities should be evaluated and treated. Abdominal distension and pain need to be addressed as soon as possible. A large needle can be used as a trocar to decompress the stomach. Alternatively, a gastric tube can be used as soon as the animal is induced. Antiemetic drugs, such as metoclopramide and maropitant, can be administered in the pre-anesthetic period (avoid metoclopramide if a GI obstruction is suspected). Endotracheal intubation and protection of the airway should be established quickly to prevent aspiration in case of vomiting/regurgitation. Antimicrobial therapy should be administered in septic patients. Before induction of general anesthesia, preoxygenate the patient, evaluate the ECG and treat arrhythmias if present.
Drug considerations In ill patients, opioids and benzodiazepines can provide analgesia and sedation with minimal effects on the cardiovascular system. In severely compromised patients combinations of these drugs can be sufficient to place an endotracheal tube. Acepromazine can cause hypotension, has a long duration, and provides no analgesia. For sick patients it is best to avoid this drug. Alpha-2 agonists should also be avoided due to depression of the cardiovascular system. Ketamine can be used in combination with benzodiazepines to induce general anesthesia.
1
Alternatively, propofol can be administered. Propofol can cause hypotension (administer slowly to decrease this risk), has short duration, does not provide analgesia, and causes respiratory depression. Isoflurane and sevoflurane can be used to maintain general anesthesia. However, they can cause hypotension. Use injectable drugs (i.e. opioids, lidocaine, ketamine) administered as CRI to decrease the amount of inhalant required.
Intraoperative and post-operative monitoring/support Mechanical ventilation can improve O2 delivery, however it can also decrease venous return to the heart (positive intrathoracic pressure during inspiration) and decrease cardiac output, blood pressure, and tissue perfusion. Minimize inhalant concentration by using drugs such opioids and ketamine, since high levels of inhalant can lead to hypotension. In most cases an arterial catheter should be placed to allow for invasive blood pressure and arterial blood gas monitoring. Positive inotropes may be needed before, during, and after the anesthetic episode. An ECG should be constantly evaluated for arrhythmias. Packed cell volume, total protein, glucose, and blood gas values should be checked regularly during anesthesia. Fluid therapy may include crystalloids, colloids, and blood products. Analgesic drugs should be administered before, during, and after the anesthetic episode. Monitor and maintain a normal body temperature throughout the procedure. Oxygen supplementation may be required in recovery.
Chronic GI diseases:
Pathophysiology Chronic GI diseases usually cause a decreased in nutrient availability with consequent weight loss, malabsorption and hypoproteinemia. Special attention should be given to the albumin level and glucose. Animals with chronic GI disease may need plasma or a synthetic colloid such as hetastarch prior to anesthesia if the protein level is less than 4.0 g/dl or the albumin is less than 1.5 g/dl since proteins are necessary to maintain a normal oncotic pressure. Most anesthetic drugs are protein-bound and a decrease in albumin causes and increase in free drug in the plasma. It may be important to consider decreasing the dose of drugs that are highly protein bound.
Hepatic disease The liver plays an important role in the synthesis and homeostasis of several products, including glucose, plasma proteins (including albumin), clotting factors V, VII, IX, XI, XII, XIII, fibrinogen, prothrombin, prekallikrein, plasminogen, alpha2-antiplasmin, antithrombin and others. The liver is also responsible for the biotransformation and elimination of many drugs. Hepatic enzyme activity is not indicative of hepatic function. Pre-and postprandial bile acids and ammonia are used to assess hepatic function.
Precautions for anesthesia in the patient with liver disease 1. Avoid drugs requiring extensive hepatic metabolism or excretion. If this is necessary,
decrease the dose if possible.2. Maintain adequate cardiac output and blood pressure to prevent poor hepatic flow.3. Avoid hypoxemia as it can lead to hepatic hypoxia.
2
4. Check the coagulation status of the patient and be prepared to treat. Be prepared for a blood transfusion if clotting times are abnormal.
5. Monitor and treat hypoproteinemia and hypoglycemia before and during the anesthetic event.
Drug considerations an anesthetic management The use of short acting and reversible drugs is recommended. Phenothiazines (acepromazine) require extensive hepatic metabolism and can cause hypotension. In patients with hepatic disfunction these drugs can prolong the recovery time. Alpha-2 agonists cause depression of the cardiovascular system leading to decreased splanchnic blood flow and potential hypoperfusion and tissue hypoxia. They provide sedation and analgesia and can be reversed. Most opioids are metabolized in the liver, however hepatic blood flow is more important that the enzymatic activity for their biotransformation. They provide analgesia and are reversible. Benzodiazepines have a wide safety margin, are reversible, are metabolized in the liver and do not provide analgesia. Propofol undergo hepatic and extra-hepatic metabolism, has a short duration of action, and does not provide analgesia. Isoflurane and sevoflurane can be used to maintain general anesthesia. Patients with hepatic disease may need intravenous colloids due to decreased oncotic pressure. If hypotension is present, inotropic therapy should also be considered. Monitor blood glucose and supplement with 1-5% dextrose if necessary. Patients with portosystemic shunt can present with hypoglycemia, coagulopathies, hypoalbuminemia, abnormal response to drugs metabolized in the liver, and neurologic signs such as hepatic encephalopathy and seizures. Prior to and during anesthesia check plasma protein levels, glucose, and acid-base status. These patients often need colloids, glucose supplementation and correction of metabolic acidosis.
3
The anesthesia checklist you need
By Lydia Love DVM DACVAA & Joanne Zimmerman CVT, VTS (Anesthesia & Analgesia)
The practice of anesthesia requires constant vigilance. But human beings, even highly qualified clinicians with years of experience, make mistakes. Human error is inevitable, and during the conduct of general anesthesia, the consequences of error can be devastating. It has been estimated that preventable anesthetic-related mortality may be as high as 1 in 13,000 human anesthetic events, across all ASA physical status subdivisions (Lagasse 2002). Although large prospective studies have determined perianesthetic mortality rates in a variety of species treated by veterinarians, no data exist concerning mortality specifically related to error in veterinary anesthetic practice.
Error can be defined as an act that through ignorance or accident leads to the "failure of a planned action to be completed as intended or the use of a wrong plan to achieve an aim."
(Lagasse 2002; Kohn et al 2000). Human and system factors play a role in the perpetration of perianesthetic error. Poor communication and overly strict hierarchical behavior are responsible for a portion of error whereas fatigue, the repetitive nature of the task, and work-related or personal stress can impair cognitive function and contribute to mistakes in perioperative decision-making. Table 1 lists human and system factors that may contribute to error.
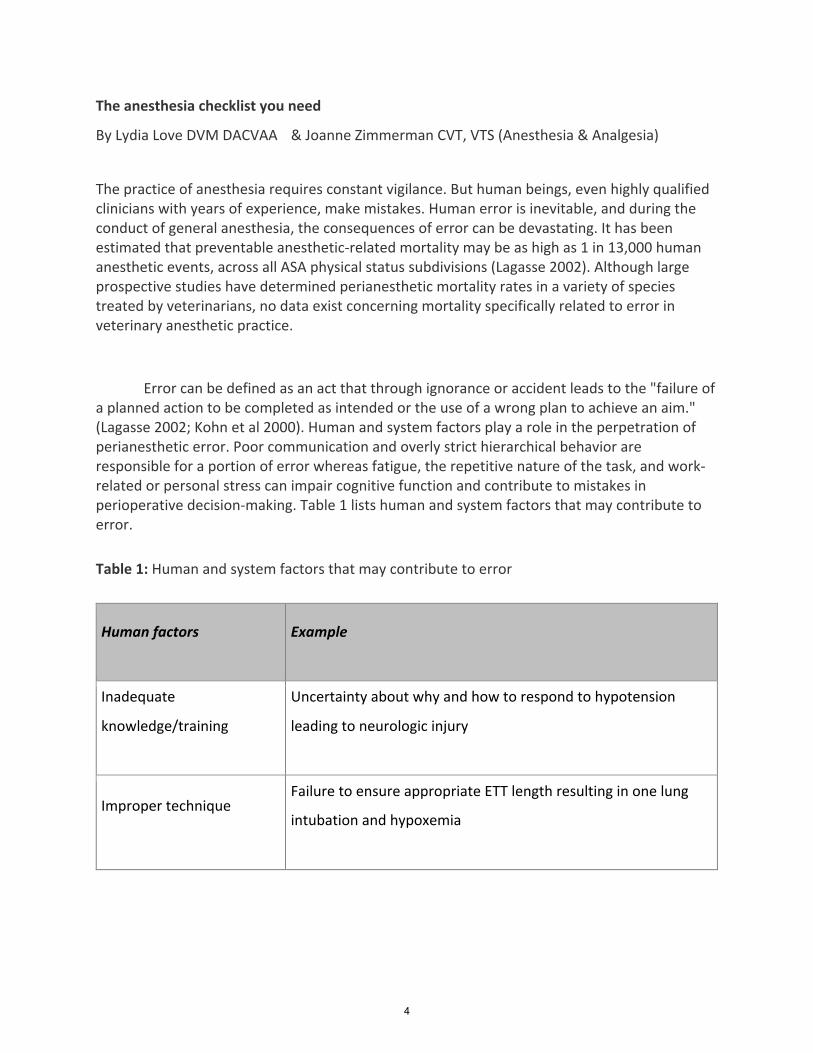
Table 1: Human and system factors that may contribute to error
Human factors Example
Inadequate
knowledge/training
Uncertainty about why and how to respond to hypotension
leading to neurologic injury
Improper technique Failure to ensure appropriate ETT length resulting in one lung
intubation and hypoxemia
4
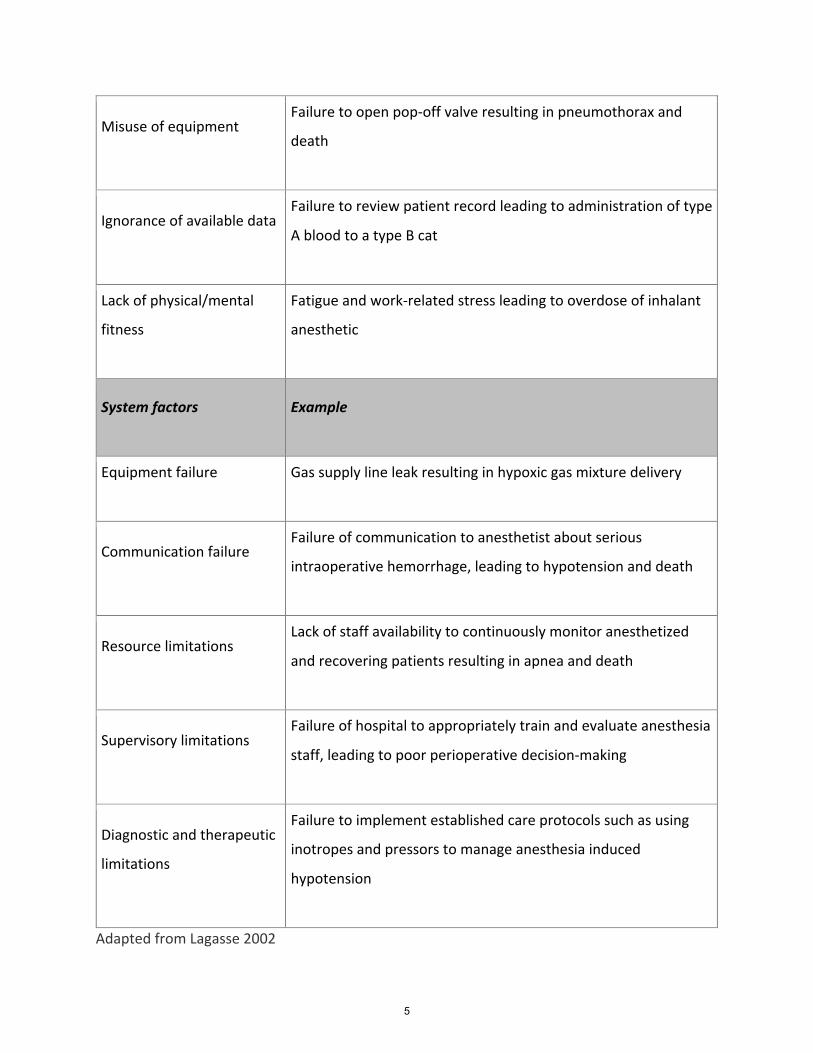
Misuse of equipment Failure to open pop-off valve resulting in pneumothorax and
death
Ignorance of available data Failure to review patient record leading to administration of type
A blood to a type B cat
Lack of physical/mental
fitness
Fatigue and work-related stress leading to overdose of inhalant
anesthetic
System factors Example
Equipment failure Gas supply line leak resulting in hypoxic gas mixture delivery
Communication failure Failure of communication to anesthetist about serious
intraoperative hemorrhage, leading to hypotension and death
Resource limitations Lack of staff availability to continuously monitor anesthetized
and recovering patients resulting in apnea and death
Supervisory limitations Failure of hospital to appropriately train and evaluate anesthesia
staff, leading to poor perioperative decision-making
Diagnostic and therapeutic
limitations
Failure to implement established care protocols such as using
inotropes and pressors to manage anesthesia induced
hypotension
Adapted from Lagasse 2002
5

The traditional approach to medical error tends to be focused on the individual and identifies
an individual's carelessness, distractedness, or failure to remember as the underlying cause. It is
unwise, however, to blame individual shortcomings for lapses in anesthetic care as human error
is inevitable and personal condemnation does little to improve care on an institutional level.
The question to ask when reviewing an anesthetic error is not "Who is to blame?" but "How
and why did the safeguards fail?"
Charles Perrow (1999) in discussing the aviation and nuclear industries first introduced the
concepts of complexity and tight-coupling as applied to high risk processes. A complex system is
one in which there are many parts that interact with each other as well as with external factors
in many different ways, some of which may be unpredictable. The parts of a tightly-coupled
system have significant and quickly developing effects on each other. It is easy to see how these
concepts can be translated to anesthetic care. Moreover, Perrow makes the argument that
when most accidents in an industry are due to operator error, it should be considered that the
required task is set up in an impossible manner, that the system itself is actually to blame.
Reduction of anesthesia-related error is contingent upon developing effective systems
of error-trapping. Improved quality of care is achieved not through enhanced individual
endeavors alone but by improving supporting processes and establishing stable systems that
make it harder for mistakes to occur. Perioperative routines that acknowledge the complexity
of the task at hand while enhancing transmission of information and empowering all
anesthesia team members can help to lessen anesthesia errors. Such supporting systems need
to be developed to identify errors before they occur and prevent them. Checklists have a long
history in complex and tightly coupled professions such as the aviation industry. Adopted
following the fatal introduction of a substantially more technically demanding aircraft in the
mid-1930s, checklists have become a standard in aviation. Over the past decade, checklists
have emerged in human healthcare settings in an attempt to improve patient safety.
6
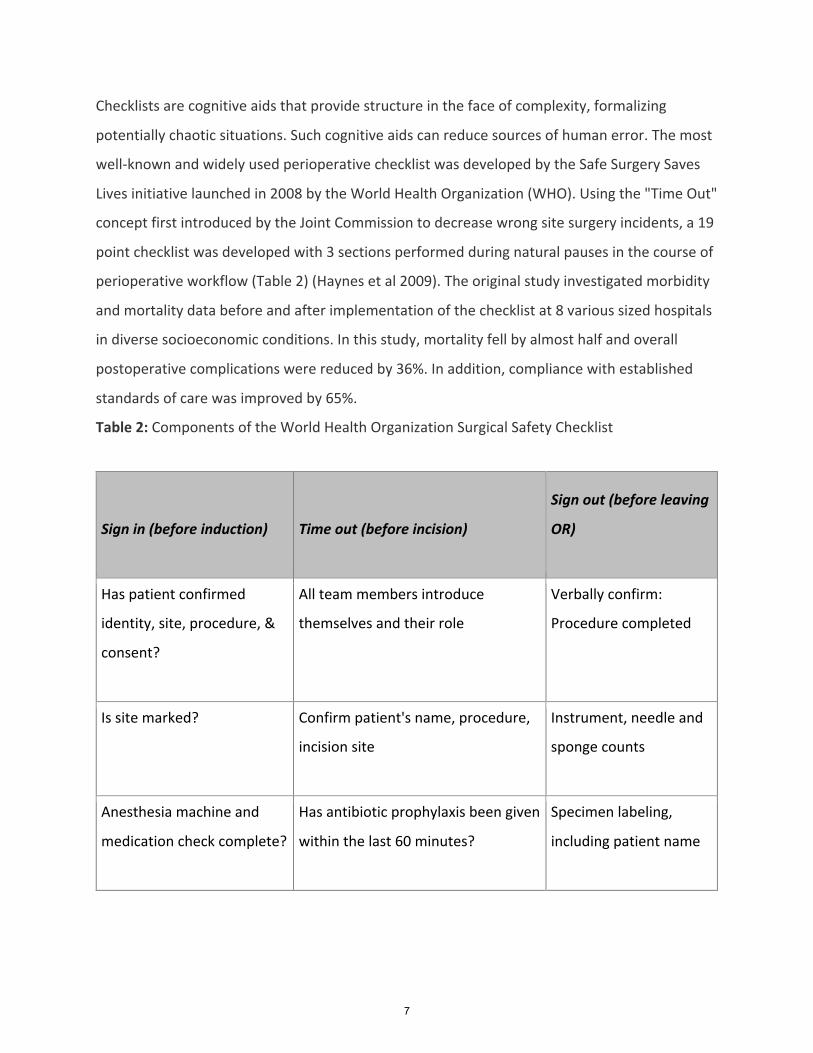
Checklists are cognitive aids that provide structure in the face of complexity, formalizing
potentially chaotic situations. Such cognitive aids can reduce sources of human error. The most
well-known and widely used perioperative checklist was developed by the Safe Surgery Saves
Lives initiative launched in 2008 by the World Health Organization (WHO). Using the "Time Out"
concept first introduced by the Joint Commission to decrease wrong site surgery incidents, a 19
point checklist was developed with 3 sections performed during natural pauses in the course of
perioperative workflow (Table 2) (Haynes et al 2009). The original study investigated morbidity
and mortality data before and after implementation of the checklist at 8 various sized hospitals
in diverse socioeconomic conditions. In this study, mortality fell by almost half and overall
postoperative complications were reduced by 36%. In addition, compliance with established
standards of care was improved by 65%.
Table 2: Components of the World Health Organization Surgical Safety Checklist
Sign in (before induction) Time out (before incision)
Sign out (before leaving
OR)
Has patient confirmed
identity, site, procedure, &
consent?
All team members introduce
themselves and their role
Verbally confirm:
Procedure completed
Is site marked? Confirm patient's name, procedure,
incision site
Instrument, needle and
sponge counts
Anesthesia machine and
medication check complete?
Has antibiotic prophylaxis been given
within the last 60 minutes?
Specimen labeling,
including patient name
7
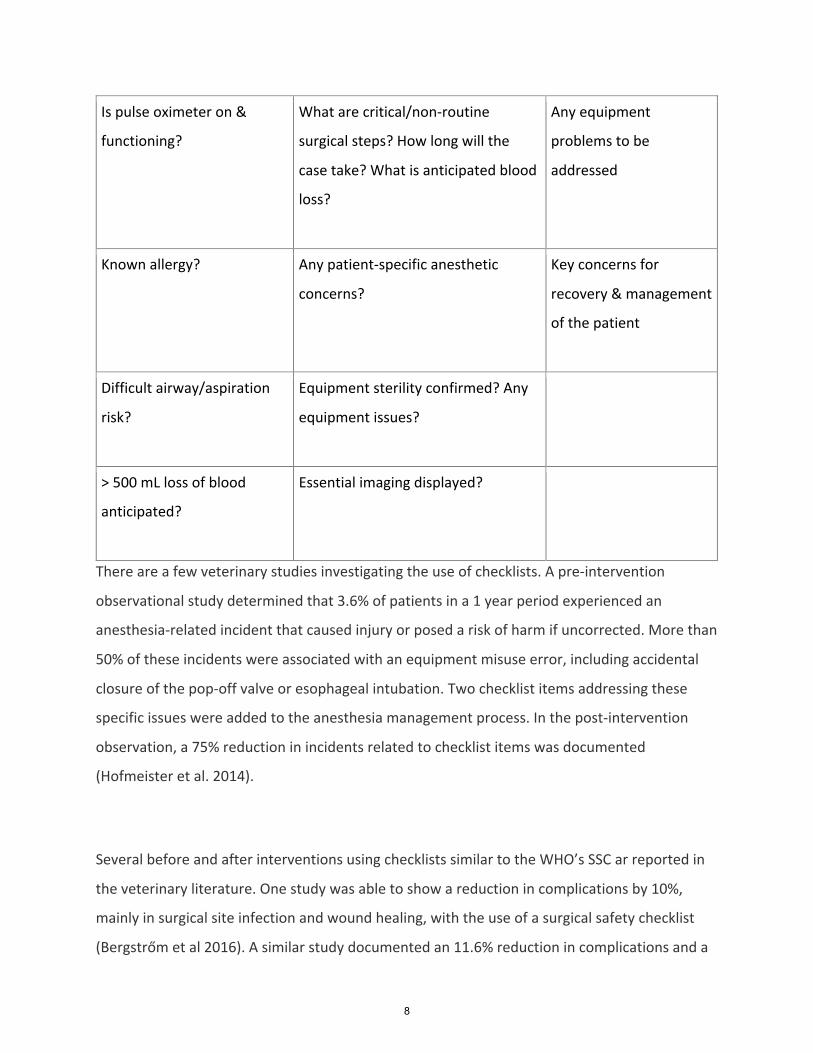
Is pulse oximeter on &
functioning?
What are critical/non-routine
surgical steps? How long will the
case take? What is anticipated blood
loss?
Any equipment
problems to be
addressed
Known allergy? Any patient-specific anesthetic
concerns?
Key concerns for
recovery & management
of the patient
Difficult airway/aspiration
risk?
Equipment sterility confirmed? Any
equipment issues?
> 500 mL loss of blood
anticipated?
Essential imaging displayed?
There are a few veterinary studies investigating the use of checklists. A pre-intervention
observational study determined that 3.6% of patients in a 1 year period experienced an
anesthesia-related incident that caused injury or posed a risk of harm if uncorrected. More than
50% of these incidents were associated with an equipment misuse error, including accidental
closure of the pop-off valve or esophageal intubation. Two checklist items addressing these
specific issues were added to the anesthesia management process. In the post-intervention
observation, a 75% reduction in incidents related to checklist items was documented
(Hofmeister et al. 2014).
Several before and after interventions using checklists similar to the WHO’s SSC ar reported in
the veterinary literature. One study was able to show a reduction in complications by 10%,
mainly in surgical site infection and wound healing, with the use of a surgical safety checklist
(Bergstrőm et al 2016). A similar study documented an 11.6% reduction in complications and a
8
reduced incidence of severe complications when the SSC checklist was used (Cray et al. 2018).
Finally, the use of a checklist specific to interventional veterinary cardiology procedures was
able to reduce complications by 13.4% (Ward et al. 2018).
To date, no negative effects on patient safety have been reported with the use of checklists.
However, some studies investigating perianesthetic efficiency have yielded equivocal evidence.
In addition, one large study reporting the experience following the government mandated
adoption of the WHO SSC in Ontario, was unable to demonstrate any positive effect of checklist
use on morbidity or mortality.14 These results have generated a fair amount of conflict and
critics have argued that compliance with the checklist was not actually measured, no data to
assess adherence to established standards of care was reported, the majority of procedures
were outpatient and very low risk, and that the 3 month follow-up period was too short.
(Urbach et al 2014) It should be noted that all evidence for and against checklist use is so far
observational in nature and no randomized controlled prospective studies have been
completed.
While on the surface, checklists ensure completion of critical tasks, capture near-misses, and
encourage identification of and planning for critical events, the most important result of
checklist use may be promotion of interdisciplinary and post-hierarchical communication.
Appropriately used checklists allow participants to articulate a coherent perioperative strategy,
creating a "team" out a "group" of personnel. The point is to ensure the entire healthcare team
is knowledgeable, on the same page, & that appropriate evidence-based measures have been
completed. The consistent use of checklists can promote patient safety and, at the same time,
generate an overarching culture of safety.
Checklists can be of the "challenge-response" or the "read-do" format. In general, "challenge-
response" checklists are used when participants have experience with the process, whereas
9
"read-do" checklists are used in situations that are relatively unusual. For example, a team
preparing a patient for a surgical procedure should normally be able to perform the steps from
memory and the checklist should merely confirm that they have indeed been completed.
However, a "read-do" checklist may be useful in crisis situation where the time demands and
possibly unfamiliar actions required may best be organized by a real time cognitive aid.
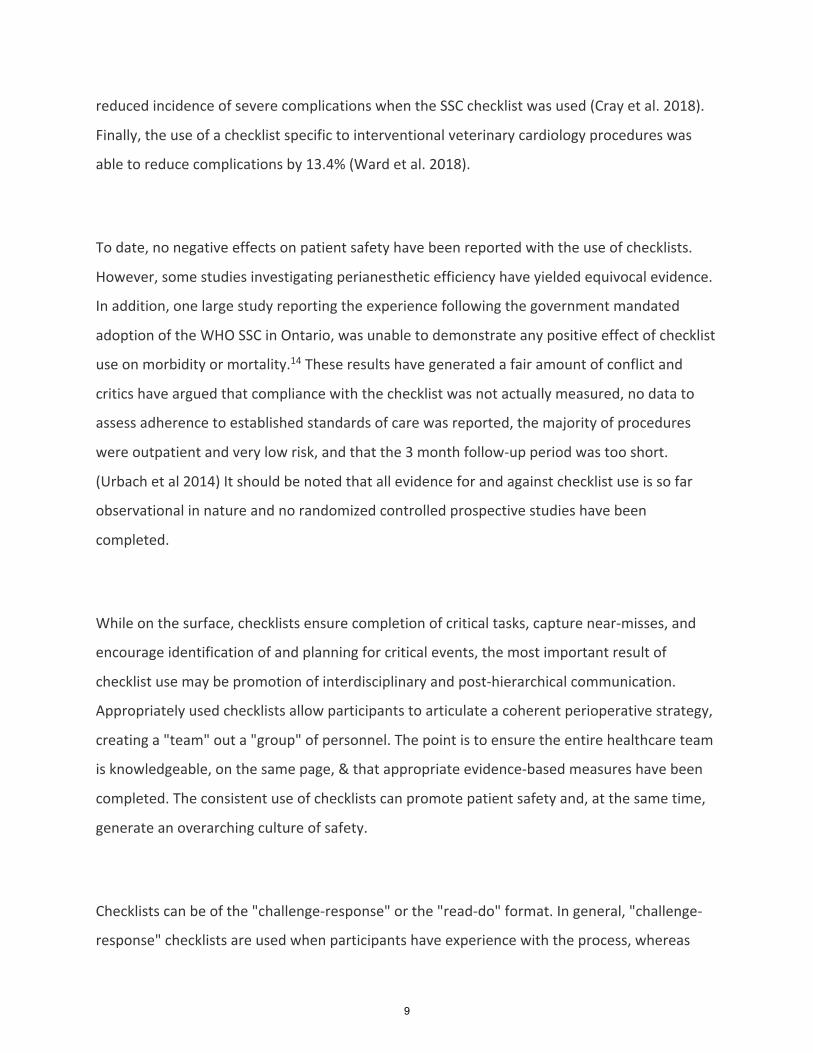
A good checklist is one that is comprehensive yet brief! It should be simple, clear, and
focused on patient safety. The items on the checklist should be actionable and targeted to
critical steps. The font and language should be straightforward, and items should not take up
more than one standard page. Generally, the checklist should take less than 1 minute to
complete, and care should be taken to minimize workflow disruptions. Natural pauses before
an irreversible step in a process should be identified in which to perform the checklist. As
encouraged by WHO, checklists should be tailored to the circumstances and resources at hand.
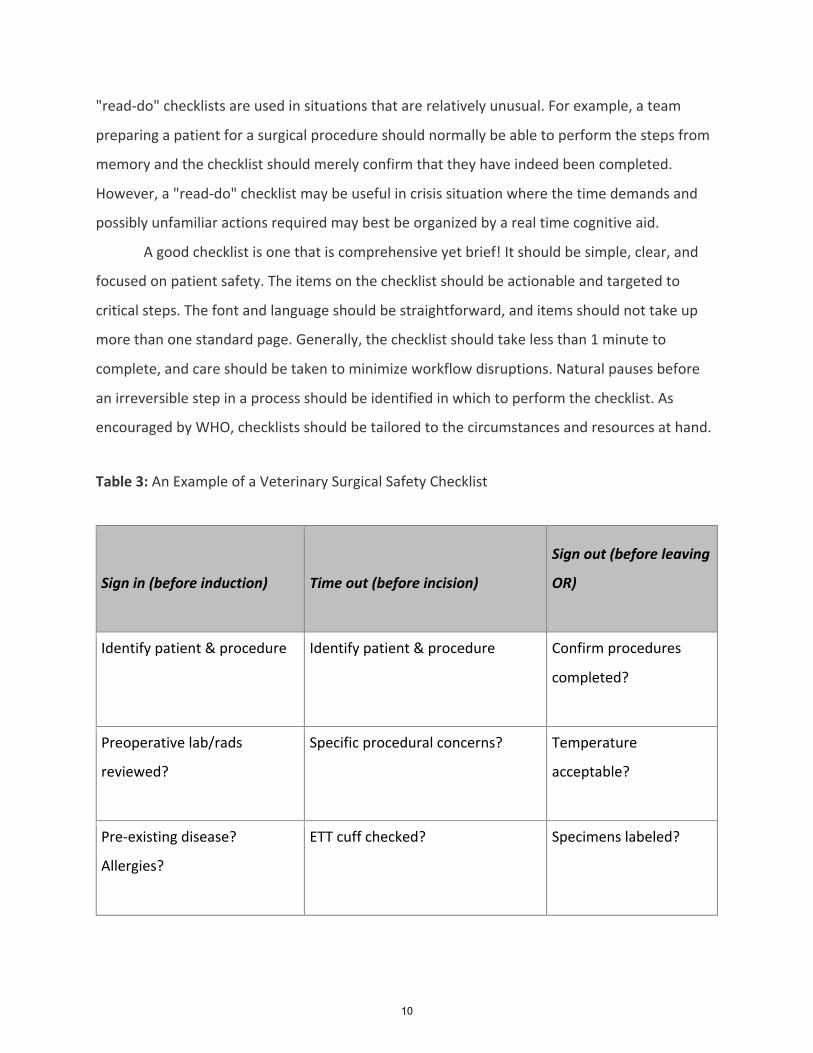
Table 3: An Example of a Veterinary Surgical Safety Checklist
Sign in (before induction) Time out (before incision)
Sign out (before leaving
OR)
Identify patient & procedure Identify patient & procedure
Confirm procedures
completed?
Preoperative lab/rads
reviewed?
Specific procedural concerns? Temperature
acceptable?
Pre-existing disease?
Allergies?
ETT cuff checked? Specimens labeled?
10
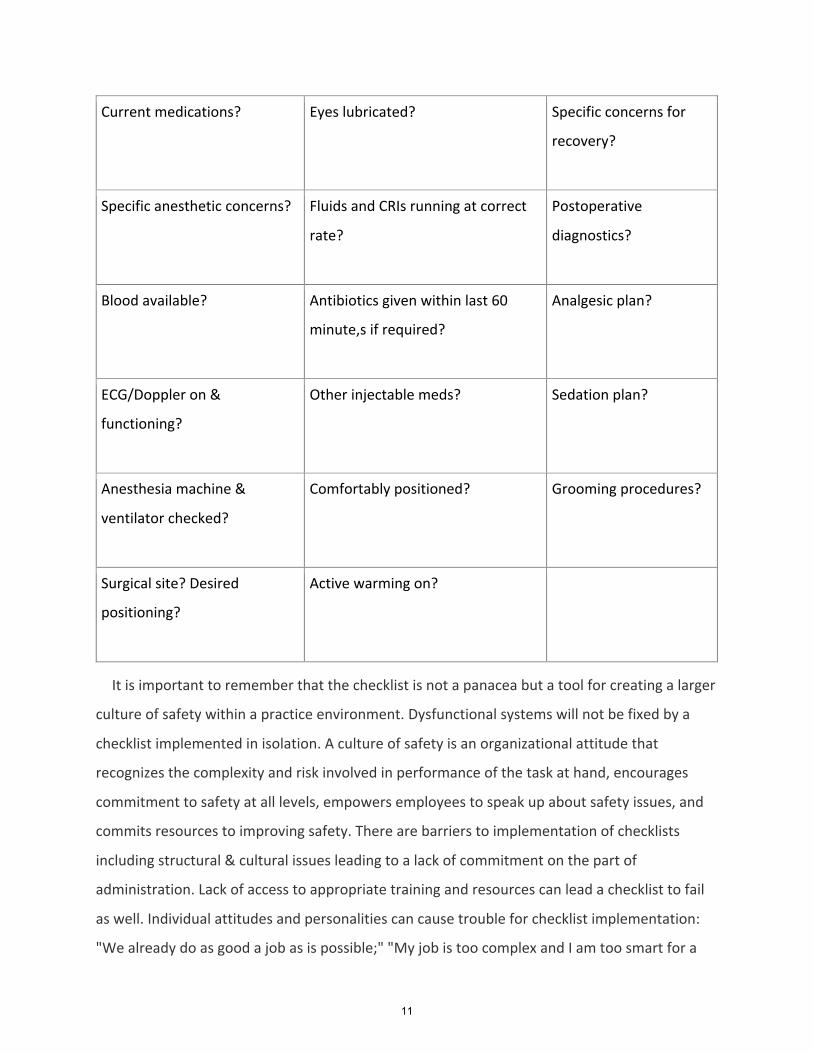
Current medications? Eyes lubricated? Specific concerns for
recovery?
Specific anesthetic concerns? Fluids and CRIs running at correct
rate?
Postoperative
diagnostics?
Blood available? Antibiotics given within last 60
minute,s if required?
Analgesic plan?
ECG/Doppler on &
functioning?
Other injectable meds? Sedation plan?
Anesthesia machine &
ventilator checked?
Comfortably positioned? Grooming procedures?
Surgical site? Desired
positioning?
Active warming on?
It is important to remember that the checklist is not a panacea but a tool for creating a larger
culture of safety within a practice environment. Dysfunctional systems will not be fixed by a
checklist implemented in isolation. A culture of safety is an organizational attitude that
recognizes the complexity and risk involved in performance of the task at hand, encourages
commitment to safety at all levels, empowers employees to speak up about safety issues, and
commits resources to improving safety. There are barriers to implementation of checklists
including structural & cultural issues leading to a lack of commitment on the part of
administration. Lack of access to appropriate training and resources can lead a checklist to fail
as well. Individual attitudes and personalities can cause trouble for checklist implementation:
"We already do as good a job as is possible;" "My job is too complex and I am too smart for a
11
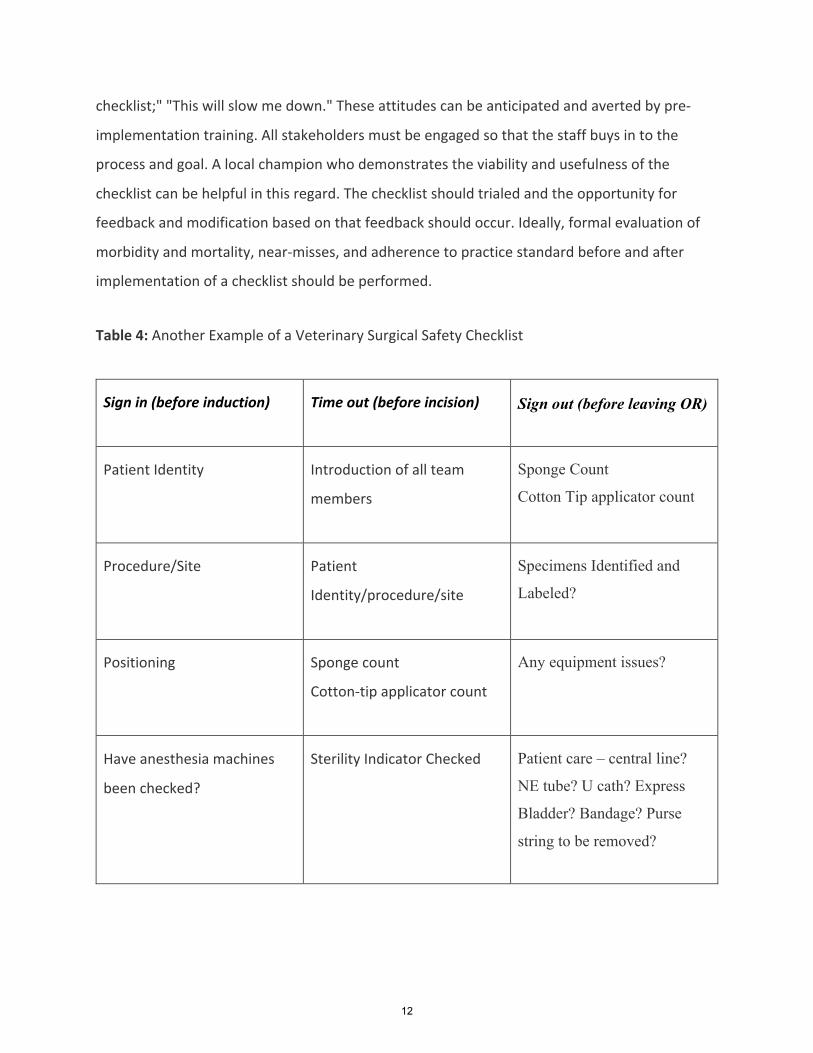
checklist;" "This will slow me down." These attitudes can be anticipated and averted by pre-
implementation training. All stakeholders must be engaged so that the staff buys in to the
process and goal. A local champion who demonstrates the viability and usefulness of the
checklist can be helpful in this regard. The checklist should trialed and the opportunity for
feedback and modification based on that feedback should occur. Ideally, formal evaluation of
morbidity and mortality, near-misses, and adherence to practice standard before and after
implementation of a checklist should be performed.
Table 4: Another Example of a Veterinary Surgical Safety Checklist
Sign in (before induction) Time out (before incision) Sign out (before leaving OR)
Patient Identity Introduction of all team
members
Sponge Count
Cotton Tip applicator count
Procedure/Site Patient
Identity/procedure/site
Specimens Identified and
Labeled?
Positioning Sponge count
Cotton-tip applicator count
Any equipment issues?
Have anesthesia machines
been checked?
Sterility Indicator Checked Patient care – central line?
NE tube? U cath? Express
Bladder? Bandage? Purse
string to be removed?
12
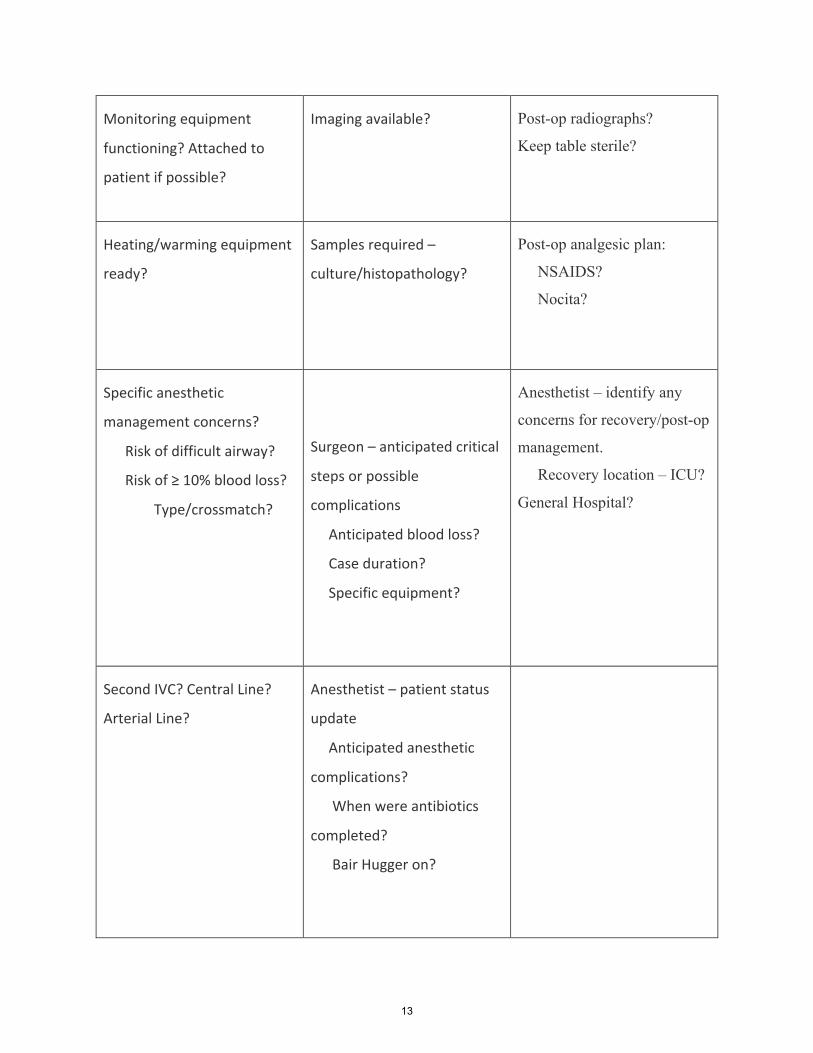
Monitoring equipment
functioning? Attached to
patient if possible?
Imaging available? Post-op radiographs?
Keep table sterile?
Heating/warming equipment
ready?
Samples required –
culture/histopathology?
Post-op analgesic plan:
NSAIDS?
Nocita?
Specific anesthetic
management concerns?
Risk of difficult airway?
Risk of ≥ 10% blood loss?
Type/crossmatch?
Surgeon – anticipated critical
steps or possible
complications
Anticipated blood loss?
Case duration?
Specific equipment?
Anesthetist – identify any
concerns for recovery/post-op
management.
Recovery location – ICU?
General Hospital?
Second IVC? Central Line?
Arterial Line?
Anesthetist – patient status
update
Anticipated anesthetic
complications?
When were antibiotics
completed?
Bair Hugger on?
13
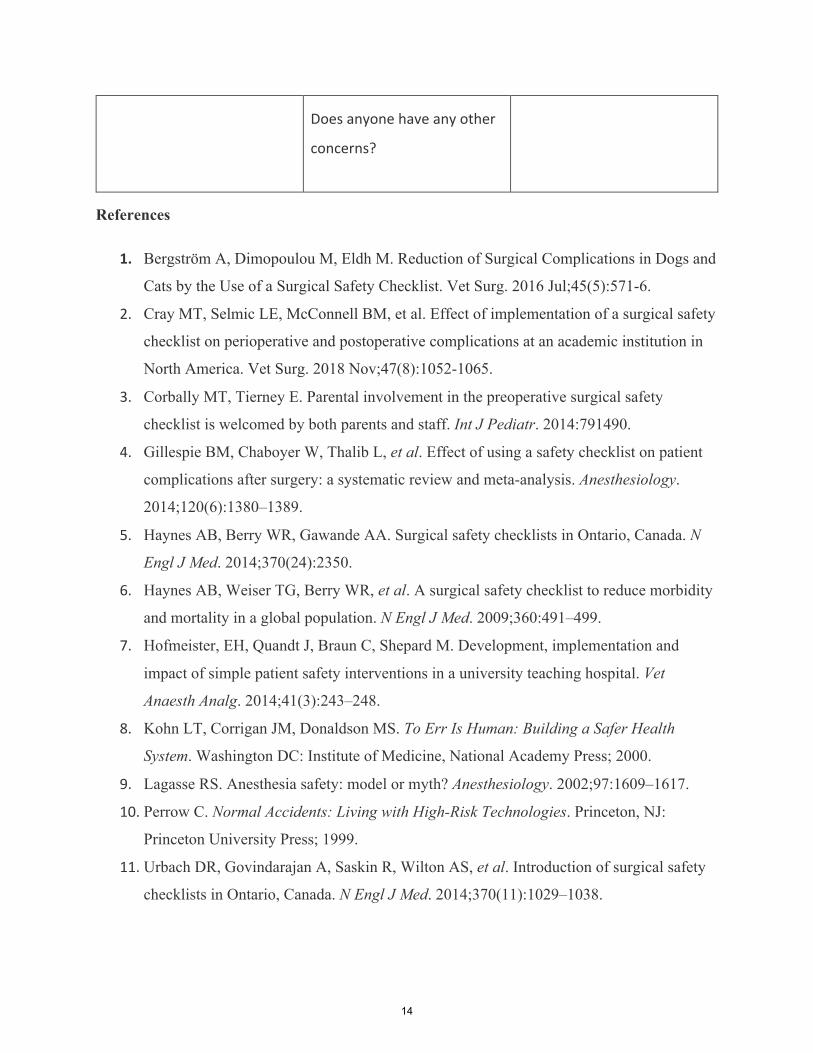
Does anyone have any other
concerns?
References
1. Bergström A, Dimopoulou M, Eldh M. Reduction of Surgical Complications in Dogs and
Cats by the Use of a Surgical Safety Checklist. Vet Surg. 2016 Jul;45(5):571-6.
2. Cray MT, Selmic LE, McConnell BM, et al. Effect of implementation of a surgical safety
checklist on perioperative and postoperative complications at an academic institution in
North America. Vet Surg. 2018 Nov;47(8):1052-1065.
3. Corbally MT, Tierney E. Parental involvement in the preoperative surgical safety
checklist is welcomed by both parents and staff. Int J Pediatr. 2014:791490.
4. Gillespie BM, Chaboyer W, Thalib L, et al. Effect of using a safety checklist on patient
complications after surgery: a systematic review and meta-analysis. Anesthesiology.
2014;120(6):1380–1389.
5. Haynes AB, Berry WR, Gawande AA. Surgical safety checklists in Ontario, Canada. N
Engl J Med. 2014;370(24):2350.
6. Haynes AB, Weiser TG, Berry WR, et al. A surgical safety checklist to reduce morbidity
and mortality in a global population. N Engl J Med. 2009;360:491–499.
7. Hofmeister, EH, Quandt J, Braun C, Shepard M. Development, implementation and
impact of simple patient safety interventions in a university teaching hospital. Vet
Anaesth Analg. 2014;41(3):243–248.
8. Kohn LT, Corrigan JM, Donaldson MS. To Err Is Human: Building a Safer Health
System. Washington DC: Institute of Medicine, National Academy Press; 2000.
9. Lagasse RS. Anesthesia safety: model or myth? Anesthesiology. 2002;97:1609–1617.
10. Perrow C. Normal Accidents: Living with High-Risk Technologies. Princeton, NJ:
Princeton University Press; 1999.
11. Urbach DR, Govindarajan A, Saskin R, Wilton AS, et al. Introduction of surgical safety
checklists in Ontario, Canada. N Engl J Med. 2014;370(11):1029–1038.
14

1. Ward J, McLaughlin A, Burzette R, et al. The effect of a surgical safety checklist on
complication rates associated with permanent transvenous pacemaker implantation in
dogs. J Vet Cardiol. 2018 Dec 5.
15
Bang! Pop! Fire in the Sky: Misery Worsens with Repeated Storms Jeff Nichol, DVM, IAABC Noise reactivity is a major source of distress for pets and their families.
• Phobia: Persistent and excessive fear of some stimulus that is out of proportion to the threat it may present.
• Each event is worse • Pet parents expect us to be ready to help. • “Noise reactivity is a common problem for dogs and may progress to true
phobia. Survey studies report that some type of noise reaction occurs in up to half of all pet dogs throughout their lifetimes, indicating that noise reactivity and/or phobia is a welfare issue.”
Phenotypic determination of noise reactivity in 3 breeds of working dogs: A cautionary tale of age, breed, behavioral assessment, and genetics Journal of Veterinary Behavior Volume 16, Karen L. Overall, Arthur E. Dunham, Soraya V. Juarbe-Diaz
Activation of sympathetic pathways
• Epinephrine release from the adrenals • Fight or flight • “Affected dogs show a range of signs of distress including trembling, freezing,
panting, social withdrawal, pacing, salivating, and escape behaviors. Is noise reactivity reflected in auditory response variables, including those that measure cognition, in dogs? Initial findings Journal of Veterinary BehaviorVolume 16November–December 2016Pages 65-75 Peter M. Scheifele, Kristine E. Sonstrom, Arthur E. Dunham, Karen L. Overall
• Hypervigilance, avoidance, and if highly agitated: aggression when handled or restrained
• High individual variability Multi-systemic involvement
• Tachycardia • Inappetence, vomiting, diarrhea, hypersalivation • Dilated pupils • Tachypnea • Excessive hair shedding, self-mutilation • Activation of HPA, glucocorticoid release • Reduced BDNF, hippocampal atrophy
Comparison of serum brain-derived neurotrophic factor in dogs with and without separation anxiety
16
Alexandra Moesta, Gahee Kim, Christina R. Wilson-Frank, Hsin-Yi Weng, Niwako Ogata
History
• Fearful or anxious in other contexts? With other triggers? • Diagnose and manage all behavior disorders affecting the pet. • Whether the individual gets highly active or becomes passive, phobias result in
sudden and profound changes. • The individual’s responses will allow custom-tailored treatment • Video from home: How severe is the fear or phobia?
o Excessive fear? o Manic? Stuporous? Pacing?
• Ask pet parents how they respond so we can explain what not to do. “Noise reactivity and phobia have been shown to be comorbid conditions, and their presence may increase the risk and severity of other anxiety-related conditions. Anxiety disorders may interfere with dogs' abilities to perform problem-solving tasks or to interpret information that could be useful in such tasks, including tasks involving or affected by noise.”, Peter M. Scheifele, Kristine E. Sonstrom, Arthur E. Dunham, Karen L. Overall
Behavioral comorbidities
• Just as important as identifying noise phobia itself • “High comorbidity was observed between different anxieties: fearful dogs had a
significantly higher noise sensitivity and separation compared with nonfearful dogs. Fearful dogs were also more aggressive compared with nonfearful dogs.”
• “Fearful personality may predispose to specific anxieties such as noise sensitivity or separation anxiety.”
Prevalence, comorbidity, and behavioral variation in canine anxiety Author links open overlay panel Katriina Tiiraab SiniSulkamaabHannesLohiab
• Assisi Calmer Canine quiz database (about 14,000) 36% of dogs with separation anxiety also have anxiety associated with fireworks specifically 40% have anxiety related to other noises. The brain is not alone
• Thorough physical exam + neurologic exam if indicated • Rule-out involvement of metabolic causes • Chemistry, CBC, thyroid screen • Chronic or intermittent soft stool, urine or fecal soiling, inappetence
o Find all factors. o Treat everything.
17
Etiopathogenesis • Neurochemical and structural abnormalities in the pet’s brain
o Heredity, genetic mapping, herding breeds o Structural brain abnormalities have been discovered in standard poodles
& Irish soft coated wheaten terriers* o Classical conditioning from past storms
• Empathic pet parents - What they can do o “Being petted and talked to is associated with lower physiological and
behavioral stress.” ** o Reprimands and punishment exacerbate fear
• Restraint of a frantic pet worsens panic, can trigger defensive aggression *Handegard, et al **Effectiveness of treatments for fireworks fears in dogs Reimer, Journal of Veterinary Behavior, vol 37 Genetics
• “Familial aggregations of affected dogs have been reported, and increased prevalence in certain breeds has been suggested.”
Karen L. Overall, Arthur E. Dunham, Soraya V. Juarbe-Diaz • Herding dogs may be over-represented • Adolescent and geriatric dogs may be at greater risk • The prevalence estimate for noise sensitivity was 39.2 %, 26.2% for general
fearfulness, and 17.2% for separation anxiety. The owner reported the median onset age for noise sensitivity to be 2 years and varied between 8 weeks and 10 years (N = 407).
Avoidance
• Mutt Muffs • Closet with no exterior walls • Light flashes ramp-up the fear
o Close the blinds o Thunder Cap
• Loud fan • Avoid crating unless pet voluntarily enters • Do not latch the door
Pet Parent involvement
• Empathy • Kindness • Comforting an anxious dog may validate its unhealthy emotional state • Reprimands and punishment exacerbate fear • Explain the origins to clients
18
o Neurochemical and structural abnormalities in their pet’s brain (hippocampus, amygdala, locus ceruleus
o Genetic predisposition for anxiety-related behavior disorders o Classical conditioning
• Be nearby as a source of security • Restraining a frantic pet: worsens panic, can trigger defensive aggression
Preempt Fear
• Noise phobias infrequent; may also occur with thunderstorms, gun shots • Board pet • Co-morbid separation anxiety almost daily damage to welfare • Dogs with other anxiety-related behavior disorders • Calmer Canine
Relaxation exercises
• A special bed • T Touch • Earned reinforcers
Reduce fear/phobia • Frightened dogs may seek plumbing behind toilet • Metal bathtub or feeding trough • Storm season may require long term anxiolytic medication. Start 4-6 weeks ahead.
Desensitization & counterconditioning, carefully and consistently applied, enhance the bond and reduce anxiety. • Strong pet parent commitment • Can regress if fear stimuli are not avoided • Not a replacement for drugs or tPEMF Counterconditioning • Give a treat or play when a loud bang is heard.
• 70% dog parents reported improvement • Relaxation exercises - similar effectiveness
• Sounds Scary CD • Play it quietly in the next room. • Follow each sound with a party • 55% reported it as effective
• Pressure vests (Thunder Shirt) • 44% reported effectiveness
• Prescription medication • 70% reported effectiveness
19
Drugs • Benzodiazepines
o Quick acting, 2-4 hour duration o Dogs
§ Diazepam § Alprazolam § Clorazepate
o Cats § Lorazepam
• SSRIs o 3-4 weeks to effect o Fluoxetine, paroxetine, sertraline
• Dexmedetomidine o Sileo – oral transmucosal o 20 minutes to onset; 2 hour duration
• Pheromones • Avoid acepromazine
Prognosis • Fair - good in many cases
o Genetic factors o Environmental influences
• Pet parent involvement essential to optimal improvement o Commitment to pet’s welfare o Willingness to change or adjust treatment
• Client follow-up/video monitoring Expect relapses
• If pet has anxiety-related behavioral comorbidities it may need long term anxiolytic medication.
• Repeat Calmer Canine treatment courses as-needed. • Desensitization and counterconditioning methods, carefully and consistently
applied, enhance the bond and reduce anxiety.
20
Do you see what I see? Medical conditions masquerading as aggression problems
By Christopher Pachel, DVM, DACVB, CABC Animal Behavior Clinic, Portland, OR Pet owners report a wide variety of concerns to veterinary staff members, including changes in elimination patterns, changes in energy level or eating patterns, or concerns about changes in the way a pet is moving or ambulating. In most instances, what the owners are reporting are behavior changes, which makes it incredibly important that veterinary staff members have the knowledge to differentiate medical causes from primary behavioral concerns and to advise regarding diagnostic testing and appropriate therapies for the pet owner’s concerns. While not all behavioral changes occur due to an underlying medical issue, some of them do! And it is our opportunity as medical professionals to know how to gather information and identify which cases will benefit from additional diagnostics or treatment, while keeping in mind that many of the potential medical concerns that may underlie aggression problems may not be apparent on routine physical examination. Before considering specific medical diagnoses, it may be helpful to consider that many of the underlying conditions that manifest as aggression are those that are associated with pain, discomfort, irritability, or distress for the animal. The impact of the medical problem may alter the animal’s threshold for response or may result in fundamental behavioral changes. Observing the animal and asking specific questions of the caregiver(s) may reveal information about the animal’s response to handling, attention that is being paid to a specific area of the body, or perhaps changes in mobility or activity. These signs can be highly variable from one animal to the next, which means that the clinical team must remain curious and open to considering all aspects of the information that is both observed and is shared with them by clients. Musculoskeletal causes of behavior change may include osteoarthritis, tumors or cancerous growths, or may be due to traumatic injuries or ligament tears. Neurological causes might include intervertebral disc disease or spinal trauma, or might occur secondarily to metabolic conditions (e.g. portosystemic shunt leading to hepatic encephalopathy). Other causes might include hormonal problems such as hyper- or hypothyroidism, Cushing’s disease, Addison’s disease, or changes occurring secondary to spay or neuter surgery. Gastrointestinal causes of behavior change may include malabsorption or maldigestion, insufficient caloric intake, nausea, food hypersensitivity, dental disease, or any condition causing abdominal pain. Hormonal causes as listed previously, or any source of discomfort can also affect appetite and other aspects of behavior in a variety of ways. Although clients do commonly report changes in behavior as being “unprovoked”, this is rarely a true assessment of the situation and a comprehensive history is often required to identify the underlying pattern. Medical problems such as seizure or neurological problems, hormonal
21

changes (acute or chronic), or anything causing irritability or resulting in “trigger stacking” should be considered. Behavioral problems that more commonly fit into this category may include resource guarding or conflict related aggression, fear/anxiety issues, or animals with reactive behavior patterns. An underlying factor of insufficient owner knowledge or awareness should also be considered as there is often a discrepancy between the owner’s perception and what actually occurs during an incident. When behaviors occur in a pattern that is unexpected to either other owner or the clinician, there should be a higher index of suspicion of medical causes, especially for pediatric or geriatric patients in which dramatic changes in behavior are not expected. In these cases, the list of medical conditions that may cause behavior changes can be extensive, and clinical signs will vary based on the underlying cause. In some cases the behavior change is actually normal (change in tolerance of puppy’s behavior by adult household dog as pup reaches early social maturity, etc.) and treatment of the problem may require understanding of normal behavior and subsequent education for the pet owner.
22
Incorporating behavior strategies into patient care: Practical solutions for daily situations By Christopher L. Pachel, DVM, DACVB, CABC Animal Behavior Clinic, Portland, OR Even before we put hands on a dog or cat for a physical exam, we can use body language cues to understand their level of comfort, arousal, fear, etc. For example, twitching of the tail in a cat is often a sign of increased arousal, especially in combination with dilated pupils. On the other hand, resting in a sternal position with hips in lateral recumbency, with the tail stretched out behind, is an indication of a relaxed demeanor in that moment for both dogs and cats. For dogs, tail position over the horizontal, or stiff posture/movement may indicate an increase in arousal, whereas a crouched posture while avoiding eye contact is more likely to indicate fear or anxiety. Additional visual examples and discussion will be provided within the session. It is important both for patient comfort as well as for staff safety that we remain aware of those body language signals and treat them as “words” in a conversation. The signals that an animal gives will change over the course of an exam, an appointment, or a hospital stay, and that is valuable information to consider! The signals that we give with our own body language will affect the “conversation” as well and have the potential to be misinterpreted by other species. For example, direct approach with sustained eye contact may indicate focus, attentiveness, or interest when we are speaking to another person. However, approaching a dog or cat in the same manner may be perceived as an overt threat, and may elicit a vastly different reaction from what was intended! The majority of problems that we encounter during exams of intolerant animals are fear based, and we run the risk of creating or exacerbating fear related problems (defensive aggression, etc.) unless we factor in the animal’s emotional state into our approach and our procedures. Strategies for reducing patient stress begin even before the patient enters the exam room, and may include things such as managing the traffic flow within the reception area, providing visual barriers to block line of sight of other animals, or allowing clients to check in by phone from the parking lot to avoid bringing stressed animals into the clinic before staff is ready for them. Speaking with a calm, quiet voice, and allowing the animal to “warm up” to social interaction can be helpful for animals that may be on the fearful or stressed end of the spectrum. It may be possible to use food reinforcement in an intentional way to help the animal acclimate to the clinic environment more quickly, although this isn’t possible for all patients or all situations. Providing for patient comfort can be done by ensuring secure footing on all exam surfaces, making specific carrier recommendations to owners of cats and small dogs, and by making a point to create positive emotional experiences for our patients before we start to see signs of stress. Video and photo examples of potential strategies will be reviewed during this session.
23
It is also possible to incorporate classical and operant training strategies into our routines in such a way that we can leverage food and other reinforcement to improve patient comfort and facilitate “procedures” such as stepping on the scale in the lobby. Video examples, and details of how/when to reach for each strategy will be covered. We can also improve safety and patient comfort by using tools such as body wraps, head collars, proactive leash handling, and effective use of basket muzzles (generally preferred over other muzzle types). Continuing the awareness of the physical environment through the examination room and into the treatment and hospitalization areas of the clinic can reduce patient stress as well. Minimizing offensive odors, reducing unnecessary noise, allowing for visual separation between patients of different species, and using environmental treatments such as pheromones or calming music can provide measurable benefit. Practicing techniques such as towel wrapping of cats, physical position changes (standing to lateral, etc.), and low stress restraint methods are incredibly helpful when it comes to facilitating procedures such as venipuncture, radiographs, or transport through the clinic. Strategies and methods will be discussed and shown. Taking a detailed history and troubleshooting potential complications can help greatly in reducing the potential for treatment failure after a patient is discharged from the clinic. Taking a moment to ask pointed questions such as “does your home have stairs?” or “will your dog eliminate when on leash?” can identify obstacles for post-orthopedic procedure patients, for example. Developing a plan that is specific for the individual patient can be accomplished quickly and efficiently with just a bit of pre-planning. That history information will also allow you to identify training strategies that may be of benefit for patients, especially when procedures have a flexible or elective timeline. Teaching a patient to eliminate on leash, improving confinement or separation tolerance, practicing polite greetings without jumping up, and auditioning puzzle toys for mental enrichment can all help to prevent specific problems during the recovery period.
24
More than just a naughty cat: Understanding feline nuisance behaviors
By Christopher Pachel, DVM, DACVB, CABC Animal Behavior Clinic, Portland, OR Nuisance behaviors are generally considered to be normal behaviors that occur in problematic ways. They have the potential for annoying people and may sometimes pose danger to the animal himself or to other individuals in the household. Although they certainly can create frustration and difficulties within the household, they are not generally “expressions of dominance”, or occurring due to vengeance or spite, as they sometimes are attributed to by owners or perhaps even individuals within the veterinary or training communities. It can be helpful to start with a few questions before jumping in with recommendations for how to address these issues. • Is the behavior normal for the animal or species? • What interventions have been attempted to address the problem so far? • What is reinforcing the behavior such that it continues or gets stronger? • Does the owner have realistic expectations for improvement? • Does the owner understand normal feline behavior? • Does the owner have a basic understanding of learning theory and how to appropriately
guide the process of behavior change? • Does the owner or household have the ability to implement the necessary management and
training plan? The answers to these and other questions they directly affect your assessment as well as the recommendations that you provide. Fantastic resources exist to help owners determine whether they are providing an appropriate level of enrichment as well as an environment that meets the needs of their animal. https://www.catvets.com/public/PDFs/PracticeGuidelines/EnvironmentalNeedsGLS.pdf this document outlines the five pillars of healthy feline environment, including: • Provide your cat with a safe place • Provide your cat with multiple and separated key resources • Provide your cat with the opportunity for play and predatory behavior • Provide your cat with positive, consistent, and protectable social interactions • Provide your cat with an environment that respects the importance of his sense of smell Translating these and other guidelines into practical recommendations generally involves first ensuring that the animal’s biological and behavioral needs have been met. From there, implanting management strategies and arranging the daily living environment in such a way that reduces or eliminates the animal’s ability to rehearse the unwanted behavior. Followed by implementation of treatment strategies such as teaching incompatible behaviors or providing feedback that renders the undesired behavior irrelevant or unproductive.
25
When choosing intervention options, practitioners should make a point to refer to the humane hierarchy of behavior change procedures (image provided within presentation). This hierarchy first emphasizes health, nutrition, and the physical setting, followed by antecedent arrangements and positive reinforcement, all of which should be considered prior to differential reinforcement of alternate behaviors or potentially aversive strategies such as extinction, negative reinforcement, negative punishment, and certainly positive punishment. Several of the more common “nuisance behaviors” for cats are scratching of furniture, climbing on counters, pouncing upon owners or family members, perceived hyperactivity, chewing and other destructive behaviors, excessive nocturnal activity, and vocalization or other attention seeking behaviors. Each of these patterns will be discussed in detail throughout the presentation, with an emphasis on understanding how to determine whether the behaviors are normal and appropriate for the animal, as well as discussion of appropriate and inappropriate intervention options.
26

Multi-cat households: identifying and addressing problems before the fur starts flying By Christopher Pachel, DVM, DACVB, CABC Animal Behavior Clinic, Portland, OR
Social structure The social structure of the free-living domestic cat colony is matrilineal, and colonies are formed when there are sufficient food resources to support a group. Colony members recognize other group members and engage in a variety of social behaviors including allorubbing, allogrooming, approaching with an elevated tail and resting in close physical proximity to one another. Similar interactions are typically observed between cats living together within a home; those behaviors may help to maintain a friendly, social group dynamic between the cats. When cats live together in a home at higher densities than what might be observed in a free-living colony, “time-sharing” of specific locations may be observed in addition to space sharing or resting in close proximity to all other household members. However, not all cats live together amicably, and it is possible to have varying levels of tension ranging from avoidance to overt aggression. Recognizing and dealing with some of the early warning signs may help to prevent further break down of the relationship or higher levels of aggression. Problem identification: Early warning signs may be as subtle as a lack of direct interaction between the cats and this may go unnoticed by many owners. In more obvious cases, the owners may describe spatial segregation with the cats avoiding each other or spending more time in parts of the home away from the other cat. The owners may also see active displacement of one cat from favorite resting locations by the other, or they may see one of the cats resting in such a way that they block the other cat’s access to food, water or litter box locations. Owners often interpret the lack of overt fighting as evidence that the cats are still getting along normally when that may not be the case. Behaviors such as autogrooming, oral behavior, scratching and shaking of the head may be significantly elevated above baseline in the minute following a conflict with another household cat and these behaviors may be noted by observant owners. Normal play in cats includes mutual interaction from each of the cats and can be very active with intense physical contact. However, if all of the physical interactions are characterized by one cat chasing or stalking the other or if the “target” shows frequent hissing, swatting or avoidance behaviors, the relationship may not be as friendly as it first appeared. Owners may also describe periods of tension after situations such as one of the cats returning from a veterinary appointment or after seeing an outdoor cat through one of the home windows. It may be necessary to ask specifically about these issues in multi-cat households during routine examinations rather than waiting for clients to self-report the problem. Intervention strategies:
27
When tension is suspected or observed, clinicians should recommend early intervention rather than taking the more passive approach of waiting to see whether the problem intensifies or resolves itself. Providing cats with increased availability of resources such as food stations (not necessarily more food), water sources, litter boxes (distributed throughout the living space) or 3-dimensional resting places can all help to decrease the social pressure and decrease resource based competition between the cats. It is also important to be sure that young, active cats have access to appropriate outlets for predatory and play behaviors to reduce the likelihood of those behavior being redirected to housemates. Using active toys, increasing the number of owner-initiated play sessions, feeding with food dispensing toys and providing supervised outdoor access can all help to lessen tension between the cats. In households with a more assertive cat, putting a belled collar on the “aggressor” may help provide the other cat with an advance warning system that allows for easier conflict avoidance. Other tools such as a “cat bib” can help to inhibit behaviors such as stalking or pouncing by some cats. In households where the tension between the cats is already more intense, it may be helpful to physically separate the cats until they can be gradually reintroduced to each other with rotational access to a shared living space, scent transfer, or desensitization and counterconditioning sessions. Pheromone therapy such as Feliway™ can also help to reduce tension between the cats and may encourage affiliative behaviors such as bunting or facial marking. Prevention: The primary socialization window for cats is earlier than in dogs and only lasts from 2-7 weeks. Even so, continuing to expose older kittens to other unfamiliar cats in socialization classes can help to build normal social skills and reduce the potential for later intercat aggression issues. Kittens may have an easier time adapting to a new household and may be better tolerated by adult resident cats. In one study of paired indoor cats, there were no observed differences in affiliative or aggressive behaviors based on gender. However, females were never observed to allorub other females and male/male pairs spent more time in close proximity to one another. The length of time the cats lived together was negatively correlated with the amount of observed aggression but size of the house and the weight difference between the cats was not correlated with aggression rate. Acquiring littermate kittens may not completely prevent future issues but it does allow the kittens to acclimate to each other at a young age and may be more successful than introducing adult cats to one another. In households where a new cat was introduced to a resident cat, approximately ½ of households reported putting the cats together without an introduction period and ½ of the households also reported fighting between the cats during the
28
introduction. Current fighting at the time of study was associated with behaviors such as scratching and biting during initial introduction, outdoor access and the owner’s perception of the first meeting as unfriendly or aggressive. In another study, aggression between housemate cats was more likely to be initiated by male than female cats although the aggression was equally likely towards other males or towards females. 30 out of 48 cases were rated as “cured” although there was not a significant difference in the number of treatment cures based on the gender of cats involved. Clients should be advised to introduce unfamiliar cats to one another slowly using methods such as segregation, scent transfer, allowing cats to interact through a screen door or introducing the cats with the help of confinement tools such as kennels or harness/leash combinations. In free-living environments, outsiders are generally accepted to the group after a period of time on the periphery of the group. Arranging the physical environment or household routines to accommodate this pattern may be helpful for some cats.
29
Prescribing for separation anxiety: How do you decide? Christopher Pachel, DVM, DACVB, CABC Animal Behavior Clinic, Portland, OR Canine separation anxiety is characterized by signs such as destructiveness, inappropriate elimination and distress vocalizations that occur in the actual or virtual absence of the owner or caregiver. Other behavioral signs exhibited by the dog may include hypersalivation, anxiety in response to pre-departure cues, rearranging of household items or hyperattachment behaviors during interactions with the owner. Standard treatment for separation anxiety may include safe management, avoidance of departures/isolation, providing sufficient exercise prior to owner departure, as well as behavior modification strategies focusing on independence training and conditioning a positive emotional response to separation/isolation. These plans are often augmented or supplemented with either situational or maintenance medications, or both. It is important to confirm the diagnosis prior to initiating treatment because other conditions can have similar presenting signs. Differential diagnoses for destructive behavior can include play behavior, environmental exploration, noise phobia, territorial aggression or under stimulation. Similarly, differential diagnoses for inappropriate elimination may include incomplete housetraining, urinary tract infection or other urinary tract conditions, conditions resulting in polyuria such as diabetes or hyperadrenocorticism, marking behavior or lack of sufficient outdoor access for normal elimination. Specifically for separation anxiety, it can be helpful to consider how the animal responds when the owner or caregiver is present, how the animal responds to that individual’s departure routine, behavior observed while the dog is separated/alone, and how the dog engages with the caregiver at the time of their return. This information is useful for establishing a pre-treatment baseline, measuring progress through treatment, and also for targeting medication choices specific to this animal’s needs. When considering whether to prescribe psychotropic medication for a patient for any behavioral condition, including separation anxiety, I start with three questions. 1. Is this a patient likely to benefit from the inclusion of medication within the treatment plan? 2. Which approach to medication use is indicated by the clinical history? (maintenance/daily,
situational/event, combination) 3. Which specific neurotransmitter or treatment effect is desired? Behavior patterns such as fear/anxiety, impulsivity/arousal, aggression of varying types, compulsive disorder, and urine marking are examples of diagnoses that may fall into the category of “yes” for the first question. Of course, it should be noted that behavioral medications should always be prescribed within a treatment plan that includes safety/management recommendations as well as behavior modification strategies.
30

Maintenance medication use is more likely to be appropriate when triggers are difficult to identify or avoid, when they may occur unpredictably or with high frequency, or when multiple triggers are present. Onset of action is variable, but typically within the range of 3-6 weeks before full effect of medication can be evaluated, while recognizing that side effects may occur prior to onset of treatment effects. Situational medications may be more appropriate when triggers of undesired behavior are easily identifiable, predictable, and/or infrequent. Medication is likely to be used as adjunctive support, and clients should be advised of the likely onset of action. One advantage is the ability to adjust doses to desired effect within a short trial period rather than requiring multiple weeks of sustained treatment prior to assessment of impact. Most options have a short duration of action that makes sustaining a consistent blood level of medication somewhat challenging. This presentation will include a short list of specific details about each of the following medications that will influence your decision of when/if to prescribe them for your patients, with examples specific to the condition of separation anxiety provided throughout. MAINTENANCE MEDICATIONS:
• Fluoxetine • Paroxetine • Sertraline • Clomipramine
SITUATIONAL MEDICATIONS:
• Trazodone • Clonidine • Benzodiazepines (5) • Acepromazine
ADJUNCTIVE MEDICATIONS:
• Gabapentin • Buspirone • Amitriptyline
31
Room for one more! Introducing a new cat or dog to the household By Christopher Pachel, DVM, DACVB, CABC Animal Behavior Clinic, Portland, OR Introducing new pets to an existing pet household can be a daunting or intimidating task for dog and cat owners, and problems associated with these introductions are easier to avoid than they are to solve once they’ve occurred. Knowing how to guide your clients through this process will decrease the risk of conflicts and increase the integration success rate for your patients. There are a few general principles that should be followed, regardless of the animal species that are being introduced to one another. The first is, “go as slow as is needed”. While it may be possible to work through the introduction and integration steps quickly, clients should be prepared to assess how the animals are responding along the way, and be prepared to advance through the steps as slowly as is required for each animal to be comfortable. It is a natural tendency to rush, but this is much more likely to lead to problems if either animal should become overwhelmed or defensive. The second is, “plan ahead”. If the client has a choice about which animal to bring into the home, it makes sense to choose wisely. This may include making informed decisions about the gender of the new pet, the age of the pet, or perhaps the temperament or play style. If it isn’t an option to choose based on these details, it may still be helpful to adjust the speed or the process of introductions based on that information. The third is, “set up for success”. This may involve exercising the animals prior to introduction, or perhaps letting stressed cats fully recover after a car ride before starting the process. It also helps to have at least one person available per animal when possible. That way, if emergency separation is required, this is more likely to be accomplished quickly and easily. If multiple people aren’t available, the steps may need to be adjusted to include more significant management and proactive control. Clients should be advised of the body language cues that might signal stress, arousal, tension, or overt aggression. This allows clients to take a break or perhaps stop the introduction process entirely until they can seek additional guidance. When multiple introductions are required, clients should make an active decision about whether to proceed with individual introductions first, or to make the introduction “en masse”. Past experience with the individual animals or perhaps information about their temperaments will help in making this decision. Clients should be advised to not assume that a particular pet will accept a newcomer, even if previous introductions have gone smoothly – it is impossible to fully predict the way a new relationship will develop.
32
Most introductions benefit from the proactive use of safety tools such as a leash (useful both for dogs and for cats), using a collar or harness that is appropriate for the pet, or using physical barrier options such as a baby gate, screen door, crate, tether, or confinement space. When interaction is allowed, leaving a light weight drag leash attached to each animal can be useful if separation is required. Some animals respond well to body pressure and are more relaxed while wearing a body wrap or other pressure device. When introducing unfamiliar dogs to one another, a variety of strategies can be used including: introducing the dogs in an unfamiliar location (minimizes territorial behavior), allowing them to interact off leash (not always appropriate but avoids leash tension), avoiding resources such as food/toys or owner attention during the initial interaction, and remaining aware of body language cues throughout the interaction. Some dogs respond well to structured interactions and others respond better to casual, low pressure interactions. When in doubt about what is likely to work well, it may be an option to gradually introduce the dogs to one another by walking in parallel and slowly moving them closer together as they are able to relax or settle. This last technique can be accomplished in casual or very structured ways depending on what the situation calls for. When introducing unfamiliar cats to one another, it is very helpful to understand the normal routine for integration of a cat into an existing colony. This generally includes a period of “life on the periphery” followed by a slow/gradual integration into the social interactions and physical environment. It can be helpful to work through steps such as: scent transfer, rotational access to common space, proactive use of a confinement space (crate, cat tent, etc.), use of harness/leash to control distance, or allowing the cats to interact through a gate or screen door. Care should also be taken to ensure that the environment provides sufficient resources such as food stations, water sources, litter boxes, and resting/hiding places. The recommendations outlined for introduction of single-species pairs can also be followed when introducing a dog to a cat or vice versa. In addition, it is important to prevent either animal from chasing the other during the initial interaction; this can be a difficult pattern to overcome once it has started! Cats typically respond better, especially if they have limited familiarity to dogs, when elevated resting places are provided throughout the space. If problems are encountered, clients should seek additional advice from you or from a skilled behavior professional with experience and extensive knowledge of how to work through these steps and troubleshoot existing problems as they arise.
33
Integrating CALM (c) to co-create a more expansive approach to veterinary medicine By Allen Schoen, MS, DVM, PhD (hon.), CVA,
Center for Integrative Animal Health, Saltspring Island, B.C., Canada
A human being is part of a whole, called by us the ‘Universe,’ a part limited in time and space. He experiences himself, his thoughts and feelings, as something separated from the rest—a kind of optical delusion of his consciousness. This delusion is a kind of prison for us, restricting us to our personal desires and to affection for a few persons nearest us. Our task must be to free ourselves from this prison by widening our circles of compassion to embrace all living creatures and the whole of nature in its beauty—Albert Einstein
This presentation is an invitation to veterinarians to explore the possibility of creating a more expansive approach to veterinary medicine based on this quote by Albert Einstein. This new approach to animal health care is now unfolding through the integration of CALM ©. CALM is the acronym for the “Conscious Animal Loves Movement. CALM is based on my vision that through the harnessing of the healing power of the love of animals and uniting conscious animal lovers throughout the world we may be able to help co-create a healthier, happier, more harmonious society. What I have seen during my forty years of pioneering holistic integrative veterinary medicine in practice, research, academia and being an author or editor of seven books, is that there is a subset of conscious animal lovers who are aware of a deeper connection to animals and are actually searching for ways to expand those connections in their lives. Many of these animal lovers are looking for places where they can connect with other kindred spirits who share a similar yearning. These conscious animal lovers include veterinarians, our family, our staff and many of our clients. Perhaps, we as veterinarians can help co-create more expansive healing centers, environments to create healthier, happier, more harmonious communities. I have come to appreciate that this trans-disciplinary, more global perspective to healing our society, based on the scientific principles of CALM is possible. There are countless transformative experiences that can possibly unfold through CALM.
This is the vision of CALM. It is based on what I call “The Seven Pillars of CALM, which are introduced in this presentation. CALM is based on the integration of the latest research in HeartMath, Mind/Body Medicine, quantum physics, the new biology, the science of compassion and other approaches into a new vision for animal health care.
It seems that the human race is going through some major shifts in consciousness at the moment, with some polarization at each extreme. There appears to be some cognitive dissonance in the collective field. I sense that the human race is in the process of waking
34
up to a number of different realities, simultaneously. As a result, the way we perceive and observe the world around us on a larger scale is starting to drastically change. So if you want to help change the world, change the way you look at things, and the things you look at will change.
We can do this in our veterinary practices. It begins with our own thoughts and emotions and radiates out from there to how we choose to be in this world, in our veterinary practices, to our staff, clients, patients, colleagues and our community. We may do it quite well, subconsciously by simply being a compassionate, caring veterinarian. If we wish to go beyond that and envision co-creating a healthier, more harmonious world through a different perspective on One Health, a trans-disciplinary approach has unfolded for me through years of study. The integration of this “trans-disciplinary” approach has evolved into CALM ©. CALM can be integrated into your veterinary practice, career and life in numerous ways to improve your life overall. The CALM approach is based on what I call “The Seven Pillars” of CALM. These include seven scientifically based perspectives:
1. Heart Coherence 2. Mind/Body Medicine Coherence 3. Human Animal Bond Neuroscience Coherence 4. Trans-species and Unified Field Coherence 5. Planetary Environmental Coherence 6. Compassionate Action Coherence 7. CALM Ambassadorship
Essentially Heart Coherence is based on research from the HeartMath Institute on the interconnectedness of all beings and the planet. They have developed approaches for heart coherence between humans and between humans and animals such as dogs and horses. They discovered that the largest electromagnetic field emanating from animals/humans is from the heart. This measurable electromagnetic heart field radiates out for at least 3 feet from human hearts, depending on our state of mind and heart mind. This field interacts with the fields of other living beings. They have also found that there is a “heartmind” of cardio neurons and now there is a whole new field of cardioneurology.
The second pillar is Mind/Body Medicine Coherence. It is based on research from Harvard Medical School’s Department of Mind/Body Medicine, The Center for Investigating Healthy Minds at the U. of Wisconsin as well as Mindfulness Based Stress Reduction (MBSR) approaches developed by Jon Cabot Zinn. The practice of “The Relaxation Response” and variations on the theme will be introduced. These are all part of a mind/body/spirit self care approach for ourselves, our family, staff, patients, colleagues, clients and our community
The physical body component of the third pillar includes compassionate self-care based
35
on physical exercise approaches from conventional exercise programs to dance therapy as well as eastern approaches such as Tai Chi, Qi Gong and others.
The third pillar is based on integrating the latest studies in neuroscience from researchers like Dr. Bruce Lipton, Dr. Joe Dispenza as well as others into a trans-species neuroscience approach.
The fourth pillar is based on the latest research in quantum physics on the Unified Field Theory, quantum entanglement and my own theories called “The Trans-species Field” and “Compassionate Field” theories.
The fifth pillar, planetary environment coherence is based on HeartMath planetary coherence, unified planetary field theory, traditional indigenous knowledge, environmental interconnectedness and sustainable living.
The sixth pillar, Compassionate Action Coherence is based on Dr. Karen Armstrong’s Charter For Compassion, The Compassionate Cities program and the Blue Ribbon Project in addition to other charitable action approaches to create a more harmonious world.
These six pillars are the foundation for the seventh pillar, CALM Ambassadorship. After taking training and studying the scientific foundations of the six pillars, a CALM ambassador puts it all together and submits a paper sharing how the pillars have changed their personal and or professional life’s journey, how they plan to share that with the world and help co-create a healthier, happier, more harmonious world. If one chooses to become a CALM ambassador, a CALM ambassador integrates these six pillars into a new way of seeing the world, being in the world and helping to co-create a more harmonious world. This can begin within your own personal life, your veterinary practice, your community and radiate out from there in virtually endless ways to be of benefit to all beings.
This is how we can use the healing power of the love of animals to be a channel for healing our world. This is how CALM and the seven pillars of CALM can transform your veterinary practice and your life.
Veterinarians throughout the world are just beginning to integrate these approaches into a more expansive vision of what animal health and healing can be. Perhaps as veterinarians, we can actually be “healers of the world” heart by heart, mind by mind, creating a new vision of animal hospitals as animal healing centers and even more expansive as community healing centers. Perhaps we can go beyond limiting ourselves to necessary pharmaceuticals and surgical procedures and create more holistic, integrative practices that can help heal all beings in many more ways than we ever imagined, through the healing power of the love of animals and the human animal bond.
As the world-famous psychotherapist, Carl Jung said “your visions will become clear only
36
when you can look into your own heart. Who looks outside, dreams, who looks inside, awakes.”
Based on this foundational awareness that your consciousness creates your reality, that you become familiar with through CALM one can now appreciate how the latest in neuroscience and quantum physics validates many ancient philosophical and spiritual teachings on the universal interconnectedness of all life. Hopefully this may stimulate
thoughts and ideas within each of you on how this relates to creating a 21st
century integrative veterinary practice. Perhaps it is limitless on how one can use the knowledge presented in CALM to create the practice of your hearts’ desire, your dream practice, your very own unique approach to creating a healing practice for animals, their human family and all beings.
It is a joy to share the insights of CALM and a new vision of creating 21st century holistic
integrative veterinary practices with you.
If you are interested in studying CALM and becoming an ambassador of CALM, please contact me at [email protected] or through my website, www.drschoen.com .
I look forward to hearing how these insights impact you on creating the next steps on your own veterinary and personal life journeys. Thank you so much being here and for being you!
Go forth and do good!
References
1. Schoen, A., Creating a 21st Century Integrative Acupuncture Practice Based on 35 Years of Practice, Research and Academic Experience: From Neuroscience to Quantum Physics, IVAS/AVAG Joint Congress on Veterinary Acupuncture Proceedings. IVAS. 44-70. 2017.
2. HeartMath Institute, Heartmath.org 3. Dr. Davidsons Center for Investigating Healthy Minds,
www.investigatinghealthyminds.org/cihm 4. Resonance Science.org. 5. Rauscher, E., “The Mental Universe”; Nature 436:29,2005.38. Harrimein, N.,
The Resonance Foundation, http://resonance.is.39. Harrimein, N., The Resonance Foundation, The Connected Universe video: https://www.youtube.com/user/ResonanceIS
6. Schoen, A, & Gordon, S, The Compassionate Equestrian, 25 Principles to Live By When Caring for and Working With Horses, Trafalgar Square, North Pomfret, VT. 2015.
7. Henneman, K, Quantum Acupuncture: The Theories of Everything Part 4: The Practitioner and The Patient—Coherent Non-Locality, Intentional Consciousness
37

and Implicate Entanglements, IVAS Proceedings, Ft. Collins CO, 2015. 8. The Charter for Compassion Institute, charterforcompassion.org9. www.drschoen.com, CALM Pillars on Awakening With Your Animal Family,
Awaketvnetwork.live. 2020.
38
Kaleidoscope Veterinarian Careers By Lisa Mausbach, DVM, MSOL-LM-PLM, SHRM-CP Compassion Fatigue vs Burnout Compassion Fatigue –the work you do • Emotional & physical burden created by helping others in distress (pets, clients, other
staff members...) • Vicarious or secondary traumatic stress • Causes a decreased ability for empathy toward suffering in the future (“empty bucket”) • Cannot be fixed by changing jobs –profession change may be necessary
Burnout –where you work Can have similar signs & triggers as compassion fatigue Burnout can be prevented/treated Individually • Set boundaries • Change work position/job • Leave job –find a new place to work
Organizationally Fix the work environment Work Culture Available Resources Book: Standing @ the Edge –Joan Halifax • Altruism (selfless acts) →pathologic altruism • Empathy (sense suffering) →empathic distress • Integrity (strong sense of moral principles) →moral suffering • Respect (hold beings & things in high regard) →disrespect • Engagement →Burnout spectrum
Veterinary Well-being 2018 Merck Veterinary Well-being Study Wellbeing examines how satisfied one is with their life & how they believe their life compares to the best possible or worst possible life for them Who is doing well?? • Male • Older (>55 yrs) • In a relationship (married) • Higher income • Working less hours • Low/no student debt • Practice owners • Limited/no evening hours • Food-animal practitioners • Veterinarians NOT in clinical practice
39
Who is in trouble? • **Associates in clinical practice** -~60% SA. Private Practice • ER/Urgent Care doctors –evening shits/long hours • Equine • Rural • Female veterinarians; veterinarians < 55 years old • Women
o 61.7% (AVMA, 2018) • < 55 years old
o 83.9% < 75 yrs (AVMA, 2018) o 39% millennials
In UK: 7-year limit for veterinarians in clinical practice (Limb, 2018) Attitude toward the profession % recommending profession –41%• • Avg. US adults –71%/Human Physicians 51% % NOT recommending profession –33% / % UNSURE –26% • Avg US adults –13%/Human 41% (unsure not an option) • 59%!!!
Reasons for NOT recommending the veterinary profession low income (54%) high student debt (53%) **personal toll the profession takes on a person’s life (44%)** Key important issues facing our profession **By Levels of Importance** High Student Debt (67%) Stress Level of Veterinarians** (53%) • Veterinary Suicide Rate (52%) • Ability to retire comfortably (48%) • Finding financially rewarding jobs (28%) •Declining Willingness/Ability** of clients to
pay (27%) • Rx drugs OTC 24%
REMEMBER.... “Burnout is primarily a SYSTEMLEVEL PROBLEM driven by excess job demands and inadequate resources and support, NOT AN INDIVIDUAL PROBLEM triggered by personal limitations.” --Tait D Shanafelt, Joel Goh, & Christine A. Sinsky Challenges ahead....barriers to effective change Facts: Nationally –people/public/pet parents • America’s middle class is shrinking. COVID will make this worse
40
• “middle-income” Americans are adults whose annual household income is 2/3rds to double the national median, after incomes have been adjusted for household size.
• Wider gap of income disparity btw upper middle class/higher income Americans & blue collar or the working poor
• Recognition of the human-animal bond is greater in our times vs every in history –do we “REALLY” feel that only the “haves” should own pets and the “have nots” shouldn’t? ie: the old, the sick, the poor?
Industry-wide • How to practice medicine & what is considered “quality of practice” has changed • Price of vet care is going up –value is being placed on the wrong commodities ($50
HWT’s) • Most practices / consultants are geared for the upper middle class & above • Avg stay in clinical practice is 7 yrs or less...why?? • People want Ritz Carlton service when they have a budget for Motel 6 –concierge style
medicine. o This will NEVER work without burning out the veterinarians & staff members on
the clinic floor Changing (reversing) the income pyramid within the industry Let’s try to place more of the income in the hands of the veterinarians/care providers on the clinic floor. • The industry is dependent on making money off veterinarians & veterinary clinics • Consultants • Business platforms –software, telemedicine, inventory handling, operations
management • Look outside the industry (to business to human medicine) for business “hacks” to lower
operating expenses • Why is it that folks who often only have a bachelor’s degree in business are at the top of
the food chain (both in salary/compensation AND leadership) vs. the highly skilled folks “in the trenches” actually “doing the work” with the pets
o Walmart, Thrive, Mars, Vetco, most consolidators o Non-profit & shelter executive directors o The essentials of running a business nowadays can be learned online “for free” o “Why”? Because the “80/20” belief of a veterinarians “worth” is still the norm &
the skilled talent is leaving the clinic floor Group-think • “The boiling frog story is often used as a metaphor for people’s inability to react to
gradual/incremental but significant changes or to events which have become commonplace”
• Neither organizations nor doctors are not truly valuing A DOCTOR’S contribution to the industry...how can we expect pet owners or the public at large to value our contribution?!? Free office visits/consults and engagement time with a doctor...
41
• About clinical medicine, the definition of INSANITY is....doing the same thing over & over but expecting different results
Clinical practice • A need for specific-service focused clinics (HVHQSN, urgent care, ER/critical/overnight
care, outpatient surgery centers, dental centers, wellness clinics primarily run by clinic staff –ie: no DVM exam)
• Utilizing pre-existing clinic equipment/space to its fullest potential (co-shared clinic space / leasing space or equipment)
• Physician pay structure –moving away from production-based pay to value/merit-based pay structures
• Placing more accountability on pet owners –signing waivers/” care-giver” bill of rights • Remember...every clinic NEEDS a veterinarian for their license & DEA to
operate...PERIOD • With respect to liability.... there is not another individual within the organization who is
(medically) responsible for anything and everything happening to the pet while under a doctor’s care, EVEN as an associate.
o A doctor risks their livelihood every day when allowing other people to administer care/advice under the umbrella of THEIR license
When a doctor complains about their job we hear.... • “Our thoughts and prayers” are given vs “Doing something” • “Benign Neglect” ...a policy in which hopes that ignoring a problem is the best solution • “This is what you signed up for” • “Since I had to suffer so will you” →Initiation, Indoctrination, Hazing of interns &
“green” doctors • “That’s the way we have always done it” • “We have already tried that” • The problem is YOU–you are a “trouble-maker,” pot-stirrer, not a team-player, etc.
And therefore, we are losing experienced clinical veterinarians by the hundreds and maybe even thousands to industry, academia or other “non-clinical” jobs Do not be our own worst enemy • Let us get out of our own way!
o As doctors, often we are the WORST critics, the most cynical, the least flexible, & the most egotistical
o Suspicion of other colleagues, competition for clients/patients, ego’s o Perfectionism –underutilizing staff o Barriers to patient care
§ Pricing structures -$30-50 HWT § Technician PE’s/[Wellness] exams § Refilling prescriptions –requiring labwork/recheck
42
o Shrink the wage gap between upper level leadership/management vs the working professionals “in the trenches”
• Increased compensation, perks, benefits for additional skillsets that keep doctors practicing in clinics
• Have all leadership positions spend time working on the floor from time to time at least 1-full day/month with primary care duties
• “Call truth to BS –be civil” Brene Brown o For many (most?) working DIRECTLY with the public at large can be the
hardest/most stressful part of the job o AND working with animals by nature can be very challenging, unpredictable, and
dangerous o Evaluate the “why” an individual is seeking a position off the clinic floor o Give ALL clinicians time “away” from direct client interactions –mentoring o Place more incentive/reward on the client facing portion of a doctor’s job duties
The dark side –work as a calling Learning to watch out for your “Blind Spots” Job Idolization–an unhealthy/unrealistic view of one’s work as being of ultimate importance in the context of life. Work becomes so important that other roles/responsibilities are neglected/abandoned Workaholism–the compulsion or the uncontrollable need to work incessantly. An addiction. Unable to psychologically detach from work. • Feeling compelled to work because of internal pressures. • Having persistent thoughts about work when not working. • Working beyond what is reasonably expected of the worker (as established by the
requirements of the job or basic economic needs) despite the potential for negative consequences (e.g., marital issues).
• Not a behavior –it is a mentality • Not synonymous with work engagement*
Exploitation • Individual –Emotional Blackmail • Organizational commodification of a calling; not being paid for the “actual” time spent
working on job-related tasks • Asking [passionate] workers to do more work is exploitative • A myth/fallacy that people who heed a higher calling can be satisfied intrinsically & can
be manipulated to get people to downplay practical needs or concerns. “TAKE THE REINS” & CONTROL YOUR CALLING Where do we start?
43
• Don’t be OK with thinking...I just want to “do my job” & all I want to do is “practice medicine.”
• Once you believe that medicine is your only role...you have given up you “seat at the table”
• “Get a bigger table, you are going to need more seats...” • “If they don’t give you a seat at the table, bring a folding chair” –Shirley Chisholm
“You are not powerless” Remember.... • It’s OK if your job is just your job –where you go to make a living to pay your bills and
provide for you & your family.... • It is also OK to love what you do for work –just remember your job IS NOT a hobby or
volunteer position. You deserve to be valued AND compensated for ALL time spent on work-related tasks...
• Work “smarter not harder or longer” –allowing personal reserves to enjoy your passion or live your calling OUTSIDE of work...
HAVE COURAGE!! Brene Brown –braving the wilderness • Be willing to standalone for what you believe in
Resilience Definition: ability to persevere, capacity to rebound (recover) & adapt • Resiliency depends on many factors, some of which include social support, exercise and
health, moral compass, mindfulness, optimism, cognitive flexibility, enjoyment, resilient role models, religion and spirituality, purpose, and growth.
• Physicians who care for themselves do a better job of caring for others and are less likely to commit errors, be impaired, or leave practice, all of which are costly to the health care system.
Let us start holding our industry & organizational leaders accountable • Demand systems that are organized to care for the care giver & not only appeal to the
pet owning community • Focus needs to be on ORGANIZATIONAL ways to help build individual
resilience*Personal Training Approaches for Resilience • Set healthy work boundaries around your time!!•Learn to SAY NO! • Let your job be “JUST A JOB” • If you get knocked down, get back up again! • Relaxation Techniques, Exercise, Life Skills (Coping with work-related & personal
stressors), CBT • Get sleep, exercise, self-care
Workload and interpersonal issues have been identified as the two largest job stressors. This finding led to the development of interventions that target an employee’s skills in time management, goal setting, delegation, negotiation, and confrontation.
44
• Strategies for Challenging Negative Thoughts o Reality testing, looking for alternative explanations, putting it in perspective,
Using goal-directed thinking 7-Factors of Resilience
1. Emotion control: The ability to control feelings amid adversity. 2. Impulse control: The ability to shut out distraction and urges and to restrain reaction. 3. Problem-solving: The ability to identify the causes of a problem and what can or can’t be
controlled. 4. Realistic optimism: The belief that things can change for the better, that you can control
your life’s direction while being aware of the challenges. 5. Self-confidence: A sense of mastery and belief in one’s abilities. 6. Empathy: The ability to read and react to others’ social and emotional cues. 7. Reaching out: The ability to seek out new challenges and relationships.
Resilience tools-7 Skills to boost your resilience Learning Your ABCs: When confronted with adversity, listen to your thoughts, identify what you say to yourself when faced with a challenge, and understand how your thoughts affect your feelings and behavior. Avoiding Thinking Traps: Don’t make mistakes that undermine resilience. Detecting Icebergs: Identify your deep, maybe hidden beliefs and determine when they help and hurt you. Challenging Beliefs: Find new problem solving/thinking strategies to not pursue the wrong solutions. Putting It in Perspective: Stop thinking about “what if” and perceiving every failure as a catastrophe. Calming and Focusing: Stay calm and focused when overwhelmed by stress or emotion. Real-time Resilience: Change your counterproductive thoughts into more resilient ones. WHAT ARE YOU WORTH?!? • # of years in practice • Type of practice • Internship trained? • Specialty CE courses/certifications • UTD on latest recommendations? • Skillsets –dentistry, surgery, HVHQSN, telehealth, communication courses, business
degree o Benefits –what is nice vs what do you need?
• •What can you provide to yourself ON YOUR OWN that is much more economical & can be a tax ride off?
How much should a business profit on the knowledge, expertise, & skillsets of associates?... Why is a doctor’s (associate’s) worth determined by a productivity #? And why are associates only worth 20%?
45
DID YOU KNOW?: Hairdressers who booth rent keep at least 40-60% of the revenue they generate Consolidators, Big Corporations, Venture Capitalists are entering the animal health care industry for because there is A LOT money to be made –PERIOD. • Well managed practices 16-20% ROI • The clinical landscape of veterinary medicine today is vastly different than it has been in
the past • People seeing pets as people, pets seen as family members, telemedicine, e-commerce,
corporatization of practice & services (vaccine clinics) The salaries of health system executives are an increasing source of frustration for physicians. Many physicians feel that they are working harder and contributing more than the hospital CEO, whose salary is widely known because it is published in the media every year. Independent contractor vs employee?!? Associate employee PROS: • Job Stability • Benefits • Collaborative environment • Sense of belonging
CONS: Must follow a schedule • You are not the boss • Organizational politics • Power dynamics • Less autonomy / control
Freelance contractor or consultant PROS: • Flexibility • Independence • Benefits of business ownership • Increased profitability for your time • Better pay
*CONS: • Avoid office politics / power dynamics • Higher tax rate →Self-employment • No company benefits • Less stability / consistency • More traveling
YOU DO YOU!!! –Dr. Mia Cary What do YOU want out of your veterinary career? • If you still love medicine & taking care of patients, do it on YOUR OWN TERMS!
The freelance veterinarian Take the Reins & Control Your Career [Calling]!
46
Innovative Alternatives to Life as an Associate Veterinarian –Kaleidoscope Careers YOU are VALUABLE (and in high demand!) • Relief / Locum Work
o Covering open shifts o Telehealth o Expanded service offerings (behavior, nutrition, rehab, surgery, dentistry) o Integrate new services –mobile/house-call/euthanasia o Research new products/servicesConsulting services
• Contract work o Vaccination Clinics o Wellness Clinics o Private Practice o Non-Profit
• Utilize large veterinary corporations -Capitalize on Available Resources/Opportunities • Shelters & Non-Profits
o HVHQSN • Co-Shared Clinic Space • Mobile Practice • Home Hospice / Euthanasia • Telemedicine / Teletriage
o VCPR / State Laws • Expert witness • Case Reviews • Consulting expert –companies • Service ConsultingVCPR / State Laws
o Mary Jane / Pain Mgmt / Behavior / Husbandry / Nutrition / HVHQSN • Speaking • Writing
WAVE OF THE FUTURE?!? “Think Outside the Box” Hybrid-Careers Service-Specific Clinics Co-Shared Clinic Spaces What if you can come back & practice clinical medicine and MINIMIZING one of the parts that causes so much stress –the client interactions?!?....I think I have found a way! ACTION STEPS for a career ON YOUR OWN TERMS! • NETWORK NETWORK NETWORK !!
o Facebook / Twitter / Instagram o Linked In / NextDoor o Podcasts / Blogging / Crowdfunding sites (Patreon/Ko-Fi) / Online & Digital
Content Platforms to sell information o Groups / Organizations
47
o In / Out of Vet Med • Get comfortable with technology
o Vet Apps / SoftwareBusiness Apps / Software • Load up on CE
o Free, online, local, conferences • Start your own business / brandLLC, S-Corp, etc
o Merchant provider accounts • Outsource where possible • Virtual Assistants / Receptionist • HR • Telehealth/Teletriage • Capitalize on Available Resources/Opportunities
o For-profit clinic corporations o Pharma & other corporate entities
“JUST DO IT!!!”BE BRAVE! • Stop giving your time & energy away for someone else to realize their dreams &
financial success from YOUR knowledge, skillsets, expertise & hard work You Deserve It! References
1. Ariely, D., & Lanier, W. L. (2015). Disturbing Trends in Physician Burnout and Satisfaction With Work-Life Balance: Dealing With Malady Among the Nation’s Healers. Mayo Clinic Proceedings, 90(12), 1593-1596.
2. Brown, B. (2015). Brown, B. (2015). Rising strong. Random House.Random House. 3. Brown, B. (2017). Braving the wilderness: The quest for true belonging and the courage
to stand alone.Random House. 4. DeChant, P., & Shannon, D. W. (2016). Preventing physician burnout: Curing the chaos
and returning joy to the practice of medicine.CreateSpace Indepedent Publishing Platform.
5. d'Ettorre, G., & Greco, M. (2015). Healthcare Work and Organizational Interventions to Prevent Work-related Stress in Brindisi, Italy. Safety and Health at Work, 35-38.
6. Duffy, R., Dik, B., Douglass, R., & Valdez, B. (2018). Work as a Calling: A TheoreticalModel. Journal of Counseling Psychology, Vol. 65(4), 423–439. doi:http://dx.doi.org/10.1037/cou0000276
7. Epstein, R., & Krasner, M. (2013). Physician resilience: what it means, why it matters, and how to promote it. Academic Medicine, 88(3), 301-303. doi:doi: 10.1097/ACM.0b013e318280cff0
8. Hauser, W., & Furman, J. (2018, October/November). A Prescription for Change. Today's Veterinary Business.
9. Holowaychuk, M. K. (2017). Strategies for fostering resilience as veterinary care providers. The Canadian VeterinaryJournal, 58(10), 1113.
10. Ipsen*, C., & Jensen, P. L. (2012). Organizational options for preventing work-related stress in knowledge work. International Journal of Industrial Ergonomics, 325-334.
48
11. Kim, J., Campbell, T. S., & Kay, A. C. (2020). Understanding Contemporary Forms of Exploitation: Attributions of Passion Serve to Legitimize the Poor Treatment of Workers. Journal of Personality and Social Psychology: Interpersonal Relations and Group Processes, 118(1), 121–148. doi:http://dx.doi.org/10.1037/pspi0000190
12. Kulkarni, S., Holly Bell, H., Hartman, J. L., & Herman-Smith, R. L. (2013). Exploring Individual and Organizational Factors Contributing to Compassion Satisfaction, Secondary Traumatic Stress, and Burnout in Domestic Violence Service Providers. Journalof the Society for Social Work and Research, 4(2), 114-130.
13. Leiter, M. P., & Maslach, C. (2003). Areas of worklife: an organizational approach to organizational predictors of job burnout. Emotional and Physiological Processes and Positive Intervention Strategies, 91-134. doi:10.1016/S1479-3555(03)03003-8
14. Limb, M. (.-y. (2018). Limb, M. (2018). Seven-year limit for vets in clinical practice. Veterinary Record. doi:http://dx.doi.org/10.1136/vr.k1970Linzer, M., Levine, R., Meltzer, D., Poplau, S., Warde, C.,& West, C. P. (2014). 10 bold steps to prevent burnout in general internal medicine.
15. Linzer, M., Levine, R., Meltzer, D., Poplau, S., WardeJournal of general internal medicine, 29(1), 18-20., 29(1), 18-20. doi:DOI: 10.1007/s11606-013-2597-8
16. Moffett, J.,Matthew, S., & Fawcett, A. (2015). Building Career Resilience. In Practice, 37(1), 38-41. doi:dx.doi.org/10.1136/inp.g3958
17. Oswald, A. J., Proto, E., & Sgroi, D. (2015). Happiness and productivity. Journal of Labor Economics, 789-822.
18. Revesencio, J. (2015,July 22). Why happy employees are 12% more productive.Retrieved December 1, 2017, from FastCompany: https://www.fastcompany.com/3048751/happy-employees-are-12-more-productive-at-work
19. Shanafelt, T. D., & Noseworthy, J. H. (2016). Executive Leadership and Physician Well-being: Nine Organizational Strategies to Promote Engagement and Reduce Burnout. Mayo Clinic Proceedings, 129-149.
20. Shanafelt, T. D., Gorringe, G., Menaker, R., A., S., Reeves, D., Buskirk, S. J., . . . 21. Swensen, S. J. (2015). Impact of Organizational Leadership on Physician Burnout and
Satisfaction. Mayo Clinic Proceedings, 90(4), 432-440.Swensen, S. J., & Shanafelt, T. (2017). An Organizational Framework to Reduce Professional Burnout and Bring Back Joy in Practice. The Joint Commission Journal on Quality and Patient Safety 2017, 43(6), 308-313. doi:https://doi.org/10.1016/j.jcjq.2017.01.007
22. Volk, J. O., Schimmack, U., Strand, E. B., Lord, L. K., & Colin W. Siren, C. W. (2018). Executive Summary of the Merck Animal Health Veterinary Well-being Study. JAVMA, 252(10), 1231-1238.
23. West, C. P., Dyrbye, L. N., Erwin, P. J., & Shanafelt, T. D. (2016). Interventions to prevent and reduce physician burnout: a systematic review and meta-analysis. The Lancet, 388(10057), 2272-2281. doi:doi: 10.1016/S0140-6736(16)31279-X
49
Being a solo RVT and business coach- serving outside of a clinical setting By Serena Pudelski, RVT (Small Animal) In veterinary medicine there is this universal mentality that an RVT cannot work outside of a Veterinary Clinic. For many reasons this is a legitimate concern, however I have found a way to practice as an RVT in a legal, fun, and interactive way. In most veterinary practices, a registered technician only makes on average $13-$25/hour.1Which can put a strain on someone, even if they are married, or make it very difficult to live on your own, barely making on average $30,000/year. The boundaries for an RVT are as follows: they cannot diagnose. Cannot Prescribe medications. Cannot perform surgery. This is the standard in the United States. The copious amounts of services we can provide if we really write it down, and home in on the skills we have, can really benefit not just an RVT but pet parents as well. Our knowledge is impeccable and can be utilized out of a clinic to impact lives. Being a Solo RVT can add a valuable component to someone’s life in a few ways. Make them more independent, open up streams of income, learn how to make their own rates, and be in charge of a business they can control, change and evolve into. Not to say every technician should leave the clinical setting, but in my experience, it was the only option I had when I left my clinic. But for so many, after about 5 years, they leave the profession for higher paying jobs, or have multiple side hustles to make ends meet. Not because they don’t love the profession, but they hate the pay. The hours. The drama. The lack of freedom of calling the shots in their own lives. What does being a solo RVT mean? It means I have a legal LLC, and run a business around routine care, pet sitting, administering medications, fluids, and pet strategy. Each day is different, but that is part of the fun! I track all the expenses, run reports, track my income, marketing, networking, and client education. I have also invested in business classes, and coaches too. Services we can offer as RVT’s: anything we can train an owner how to do for themselves. Nail trims, ear cleaning, anal gland expression, wing trims, teeth trims for pocket pets, walking dogs, medically necessary grooming (not the fufu kind), coat care, pet transportation, and pet strategy calls. My kit I carry has all the essentials, and a fully stocked first aid kit. Why do people need this service? Because they are scared to injure themselves, or their pets. I feel like it’s my duty to share my skills with whoever needs it. I have heard over and over what a convenient, efficient, and helpful business I run. Many of my clients ask for referrals for their families in other states! They want this service. It’s easy for them and saves them time. Why stress animals out in the car, and carriers? By the time they get to the clinic, the owners are exhausted, and the pets are stressed. I have also offered Strategy Sessions for my clients as well. They have questions, so why can’t an educated professional answer them? So, I started doing it. I triage their concerns, give advice based on the chief complaint, and make recommendations based on a detailed history. If a vet needs to get involved, I make it known
50
that I do not replace a DVM but act more like a partner in health. I have clients all over the states, thankfully to the digital age of the internet and social media. With their questions, also comes new pet questions. Many of my clients want to get a pet but are unsure how or what pet is a good fit for their lifestyle. I come alongside them and explain the basic care needed for many species, husbandry costs, veterinary needs, dietary needs, among other things. I also record the sessions and give helpful PDf’s and checklists, so they feel confident getting into something new. As an RVT the client education over the last few months has been essential. I have been getting so many questions that I have built out digital pet care for my clients as well. Video trainings on an array of topics, and many being built out over the remainder of this year. If I can automate a majority of the trainings, but still be there to answer their questions, they can really have the best of both worlds. With curbside appointments, they may forget to ask questions, get meds refilled, or forget the names of their regular prescriptions. With digital training, they can take the time at home, prior to their appointment, and really get their issues down on paper. One of the ways I wish to change veterinary medicine is to show RVT’s a couple things: how to build their own successful house call businesses if they want to, and to show them how to build digital pet care courses. We need to be heard, and this is a fun way to get our skills, knowledge and love of animals into the world. There are so many ways to impact the lives of pet owners, and pets, and these are just a few different avenues. My business was a side hustle for 2 years. It caught on quickly, and I was able to triple my income. I want others to experience the joy that I have found. The freedom and remember why they went into veterinary medicine in the first place. My course is called The Vet Tech Society, and my program is all inclusive. I take those with nonbusiness knowledge and walk them through step by step how to do it. What equipment is needed. What software to use. How to get paid. ALL THE THINGS. My goal is to change the world. Let’s do this. References:
1. https://www.payscale.com/research/US/Job=Registered_Veterinary_Technician_(RVT)/Hourly_Rate
51

Clinical use of glucocorticoids By Dawn Merton Boothe, DVM, PhD, DACVIM, DACVCP Auburn University, AL
For good reasons, glucocorticoids (GLs) have been the cornerstone of immunosuppressive therapy in humans and animals. Their impact on immunomodulation reflects inhibition at every stage of the immune response, including both innate and acquired, and cell- mediated responses; the humoral response, however, is minimally directly affected. However, understanding their safe and effective use is complicated by their complex physiologic effects. They are among the most important hormones in the body, responsible for normal support and support during times of stress.
Molecular mechanism of action In the future, new glucocorticoids are apt to be “designer” drugs. The design reflects changes in drug structure that will cause them to be more selective in their directing effects. An understanding of the current mechanism of action is necessary to appreciate potential changes. The effects of GLs are generally recognized to be dose dependent. GLs must pass through target cell membranes where they bind to intracellular receptors which are also complexed with heat shock proteins in the cytoplasm of the target cell. Binding of the GL to the receptors causes the receptor to dissociate from the heat shock protein; the GL and receptor then move into the nucleus where the GL binds to specific DNA sequences or receptors called GL responsive elements (GRE). The GL can now influence gene expression. Binding to GRE in the promoter regions of GL-regulated genes (positive GRE) facilitates gene expression (transactivation) whereas binding negative GRE (nGRE) represses genes and their expression (referred to as transrepression). The GL receptor (GR) generally has a lower affinity for nGRE compared to pGRE. Transactivation generally involves binding to specific DNA recognition leading to direct transcription; accordingly, these activities are also referred to as cis. This is in contrast to repressive activities which tend to involve (indirect) protein-protein couplings that then modulate other transcription factors (eg, NFk-B, AP-1, STAT-5or NF-AT) such that their activity is modified; these activities are referred to as trans. The largely undesirable metabolic effects associated with long-term GLC therapy appear to be mediated by transactivation or cis activities, whereas desirable anti-inflammatory and immunomodulatory effects appear to reflect transrepression or trans activities through n-GREs. Because GL-nGRE interactions appear to occur at lower concentrations compared to p-GRE effects, limiting GL use to lower doses should decease undesirable side effects. Alternative pathways increasing can be expected to be specifically targeted by “designer or dissociative GLC” that are more potent for trans repression rather than other actions. Dexamethasone and prednisolone are examples of a “symmetrical” GLC, characterized by equal binding affinity for both cis and transactions (or trans repression and activation). In contrast, medroxyprogesterone acetate is predominately transrepressive.
Glucocorticoid resistance
52
GLC resistance can be congenital (gene mutation) or acquired. Pharmacokinetic causes include poor compliance and poor bioavailability. Pharmacodynamic resistance includes reduction in functional GR number/ location, binding, and transactivation ability. Mutations/polymorphisms contribute to much of this. Selected diseases may be associated with lowered sensitivity to GLC; variability among patients has led to the development of diagnostic tools that can assess GLC responsiveness. Resistance may reflect decreased receptor number (eg, down regulation) or affinity. Reversible down-regulation is a documented sequela of GL treatment (demonstrated in T-lymphocytes of humans receiving GL to treat host-versus graft rejection). This type of resistance might be avoided by higher doses of GL, including pulse dosing. A relative imbalance of GL receptor isoforms may also be responsible: the α isoform binds to GLs, DNA and transcription factors, thus modulating transcription, whereas the β isoform binds to DNA, but not other ligands and fails to activate transcription, thus potentially interfering α isoform actions. Some human patients with severe IBD that fail to respond to high doses of GLs have poor antiproliferative response by blood T-lymphocytes whereas responder completely inhibit. A similar situation has been demonstrated for other chronic allergy-based diseases, such as asthma or rheumatoid arthritis, and renal allograft rejection. Other factors that may contribute to poor response to GLC include overexpression of the multidrug resistance gene (MDR1 polymorphism) which might be reversible by co administration of cyclosporine, an inhibitor of P-glycoprotein. Stress is another example of variability in GRa expression with variability in receptor expression reflecting duration of the stress, indivisual differences and other factors. Decreased receptors are associated with higher circulating GLC. Interestingly, depression may be associated with a depletion of the GR pool.
Physiologic effects of glucocorticoids. Glucocorticoids support the body in times of stress (think flight or fight). The metabolic effects of glucocorticoids are particularly profound and help explain the typical presentation of a patient with spontaneous or iatrogenic hyperadrenocorticism. The goal of corticosteroids in general is to maintain the body for stress, including fight of flight. For glucocorticoids, a major role is maintaining plasma glucose to assure that the brain receives the energy it needs to function. The CNS is the only organ that does not require insulin for glucose to enter the cell. As such, the body, through glucocorticoids, make sure the CNS is fed. Protein will be broken down (a peripheral catabolic effect). Muscle atrophy, the skin becomes thin and wounds do not heal. However, in the liver, the deaminated protein will be converted to glucose (which is released) and glycogen (which is stored for later release). As such, glucocorticoids are anabolic in the liver. Carbohydrate formation (glucose) increases while tissue utilization of glucose is impair (an antiinsulin effect). Hyperglycemia and glycogen storage in the liver occur. Lipids are also impacted: although not directly converted to glucose, they are used to generate energy. They also are redistributed: animals often have fat pads develop on their hind end; the pendulous abdomen reflects not only weakened abdominal muscles, but also accumulation of belly fat. Triglycerides and cholesterol may be increased. Contributing to flight of fight is an
53
increased red blood cell mass. This reflects increased production as well as a decrease in rbc phagocytosis (part of the normal life span of the red blood cell; inhibiting this effect is particularly important in patients with immune-mediated hemolytic anemia). Typical of glucocorticoids, whether endogenous or exogenous, is the stress leukogram: neutrophilia which reflects demargination of neutrophils into the blood, and redistribution of lymphocytes and eosinophils out of the circulating blood.
Critically important to the flight or fight response are the permissive effects of glucocorticoids which occur as physiologic (as well as pharmacologic) doses. A physiologic dose is low and is more likely to mimic endogenous secretions. The permissive effects of glucocorticoids largely reflect the ability to facilitate the response of the body to adrenergic signals. These include alpha mediated peripheral vaso constriction which maintains vascular tone (while distributing blood to skeletal muscles in anticipation of flight), increasing cardiac output through increased heart rate and contractility (beta one effects) and increase oxygenation of tissues by assuring bronchodilation (beta 2 effects). These effects do not relay on synthesis of effect proteins and as such occur rapidly. These effects, for example are the reason that asthmatic cats should be treated with glucocorticoids simultaneously with bronchodilators and why patients with hypadrenocorticism, or relative adrenal insufficiency (ie, critical care patients) must receive physiologic concentrations of glucocorticoids to avoid cardiovasacular collapse. Other organs impacted particularly by glucocorticoids are the respiratory tract, with the permissive effects on bronchodilation critical. The impact of glucocorticoids on normal cardiovascular physiology is just as important as the impact of mineralocorticoids on sodium and water retention. In the face of deficiency, the loss of vascular tone will result in cardiovascular collapse which will be exacerbated by loss of cardiac efficiency in terms of rate and contractility. An important side effect of glucocorticoids reflects their permissive effects combined with mineralocorticoid effects: patients with early congestive heart failure may develop clinical failure, or their disease may worsen due to increased afterload (vasoconstriction) and, if mineralocorticoid effects, increased sodium and water retention. The latter might be offset by using an aldosterone antagonist (ie, spironolactone) diuretic and the use of Angiotensin converting enzyme inhibitors might be indicated. A potentially under recognized impact of glucocorticoids is on thrombosis. Dexamethasone may have less risk of cardiac abnormalities because it does not cause sodium retention. As a specific Cox-2 inhibitor, glucocorticoids will inhibit prostacyclin, which otherwise would offset the thrombogenic effects of Cox-1 mediated thromboxane. In the presence of high glucocorticoids, prostacyclin is maximally inhibited, which may allow thromboxane mediated platelet aggregation to go unchecked, leading to thrombosis. The effects of glucocorticoids on bone include direct chondrocyte death and can lead to cartilage destruction particularly with long term use. The effects of glucocorticoids on blood glucose and CSF production were discussed. However, an important CNS effect not previously mentioned is the euphoric effect that is evident when glucocorticoids are administered. The euphoria is associated with increased appetite (which is among the reasons they have been used in “ADR” patients). These responses, however, can mask clinical signs of disease,
54

misleading the owner into thinking the patient is doing well. In the gastrointestinal tract, glucocorticoids by virtue of their effect on cyclooxygenase, can increase the risk of gi ulceration. This is more likely to occur in patients that already are at risk or in patients that have had a spinal injury that results in altered blood flow to the gi tract. However, glucocorticoids are not as ulcerogenic as NSAIDs. The impact of glucocorticoids on calcium and sodium/chloride in the gi tract were previously discussed. In the reproductive tract, glucocorticoids induce partuition or cause abortion in a variety of species, particularly cows and horses, and as such, should be avoided in pregnant animals. Endocrine Glucocorticoids are antiinsulin. Patients in a state of hyperadrenocorticism are more apt to develop diabetes mellitus (which may not resolve with discontinuation of therapy), are largely resistant to insulin treatment, and will disrupt diabetic control in previously controlled patients.
Electrolytes Glucocorticoids cause loss of water. This reflects an anti-antidiuretic hormone effect at the level of the collecting tubule, but also centrally. Part of this latter effect reflects centrally mediated increased water consumption. If the glucocorticoid has mineralocorticoid effects, sodium and water retention will occur in the kidney, ileum and ciliary body of the eye and probably CSF. Serum calcium also is impacted by glucocorticoids which act to deplete the body of calcium by preventing its absorption, mobilizing it from bone and increasing urine excretion. This can cause osteoporosis (a primary human problem because of the long time it takes to develop) but can be of therapeutic benefit in states of life-threatening hypercalcemia, such as might accompany a secondary hyperparathyroidism state accompanying some neoplasias.
Inflammation and immunomodulation: For lymphocytes, GLs cause up or down regulation of up to 2000 genes involved in the regulation of the immune response targeting both early and late phases of inflammation. GLs 1. reduce circulating lymphocytes; 2. alter lymphocyte response to mitogens and antigens (T lymphocytes are inhibited to a greater degree than B lymphocytes); 3. alter white blood cell function; 4. inhibit edema, fibrin deposition, leukocyte migration, phagocytic activity, collagen deposition, and capillary and fibroblast proliferation (generally through inhibition of lymphokines and other soluble mediators of inflammation); 5. induce annexin I, which inhibits phospholipase 2, thus blocking the release of arachidonic acid and its subsequent conversion to eicosanoids (i.e., prostaglandins, thromboxanes, prostacyclins, and leukotrienes); 6. preferentially inhibit transcription of cyclooxygenase 2, the inducible form of cyclooxygenase, thus decreasing the risk of toxicity. 7. induce protein MAPK phosphatase 1, which, through various actions inactivates a number of proteins important in the signaling of cytokines; 8. inhibit transcription of NF-k-B. Effect on immune cells: GL 9. inhibit release of tumor necrosis factor and interleukin-2 (IL-2) from activated macrophages. 10. Inhibit release of platelet-activating factor from leukocytes and mast cells; 11. Inhibit macrophage migration-inhibition factor, (macrophages migrate away from the affected area); 12. Block IFN-released from activated T cells (needed to facilitate antigen
55
processing by macrophages). 13. inhibit synthesis and release of IL-1 by macrophages thus, suppressing activation of T cells, and IL-2 synthesis by activated T cells. 14. Inhibit bactericidal and fungicidal actions of macrophages.15. Alter synthesis of and biologic response to collagenase, lipase, and plasminogen activator. 16. Inhibit the inducible form of nitric oxide synthase (iNOS). Interestingly, despite their effective immunosuppressant effects, gluocorticoids have been associated with allergic reactions, including type I acute anaphylaxis. Central Nervous System: GL: 1. Maintain adequate plasma concentrations of glucose for cerebral functions, maintain cerebral blood flow, and influence electrolyte balance; 2. Decrease formation of cerebrospinal fluid; 3. influence mood (including "euphoria"), behavior, and brain excitability.4. regulate neuronal excitation; 5. induce glutamine synthetase in both the central and peripheral nervous systems. Increased glutamate has been associated with CNS pathology. 6. Among the effects of some glucocorticoids in the CNS is a protective effect against oxygen radical formation that commonly accompanies CNS trauma or hypoxia. This reflects the ability of selected drugs to insert themselves in the lipid component of the cell membrane, thus stabilizing it when the membrane is damaged. Damage puts into play a cascade of mechanisms that generates the oxygen radicals. Methyl-prednisolone may be more able than other steroids to decrease the negative impact of CNS damage on oxygen radical formation.
Glucocorticoid Preparations Close to 50 different generic corticosteroid products are approved for human use and several for (small) animal use. They differ in their routes of delivery, but also in their duration of action, mineralocorticoid activity, and anti-inflammatory potency. As the anti-inflammatory potency of a particular agent increases, its biologic half-life and duration of action also increase. For example, dexamethasone is 30 X and prednisolone 4 X as potent as hydrocortisone in impairing glucose metabolism. However, this comparative potency is based on inflammation, and in rats, with little evidence of its applicability to all other species. Nonetheless, it is the basis of different dosing regimens. With current drugs, anti-inflammatory properties parallel the effects on carbohydrate and protein metabolism, but
56
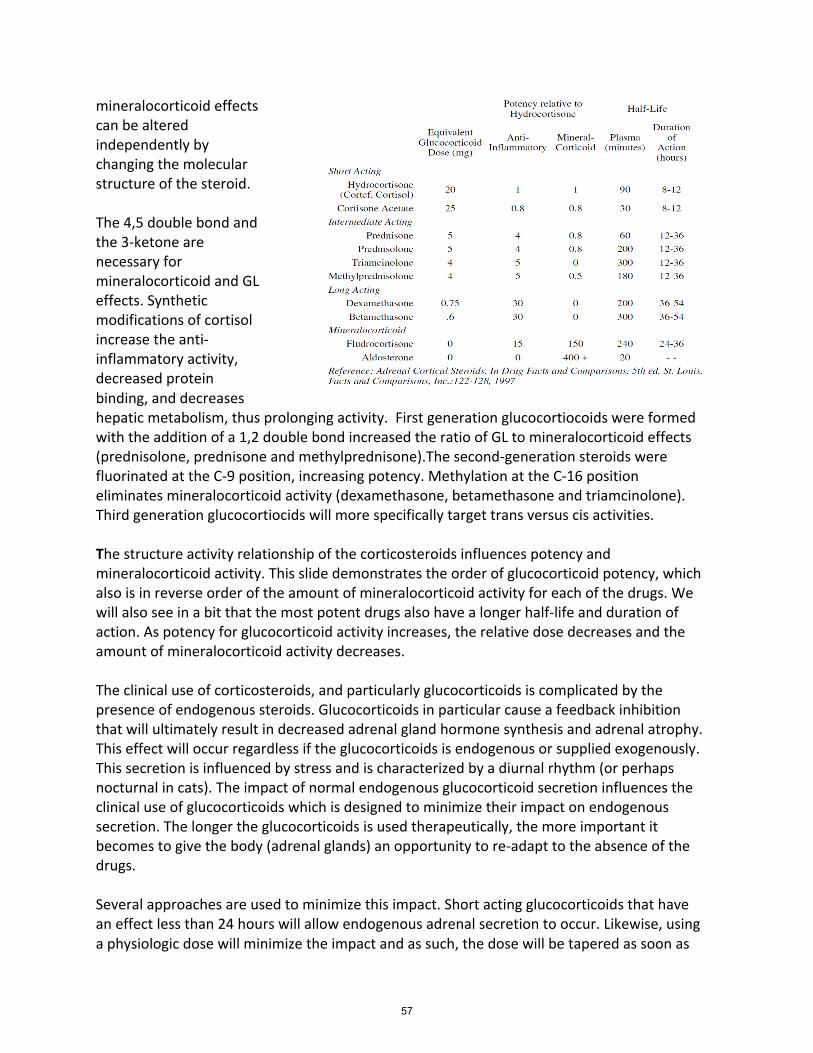
mineralocorticoid effects can be altered independently by changing the molecular structure of the steroid. The 4,5 double bond and the 3-ketone are necessary for mineralocorticoid and GL effects. Synthetic modifications of cortisol increase the anti-inflammatory activity, decreased protein binding, and decreases hepatic metabolism, thus prolonging activity. First generation glucocortiocoids were formed with the addition of a 1,2 double bond increased the ratio of GL to mineralocorticoid effects (prednisolone, prednisone and methylprednisone).The second-generation steroids were fluorinated at the C-9 position, increasing potency. Methylation at the C-16 position eliminates mineralocorticoid activity (dexamethasone, betamethasone and triamcinolone). Third generation glucocortiocids will more specifically target trans versus cis activities.
The structure activity relationship of the corticosteroids influences potency and mineralocorticoid activity. This slide demonstrates the order of glucocorticoid potency, which also is in reverse order of the amount of mineralocorticoid activity for each of the drugs. We will also see in a bit that the most potent drugs also have a longer half-life and duration of action. As potency for glucocorticoid activity increases, the relative dose decreases and the amount of mineralocorticoid activity decreases.
The clinical use of corticosteroids, and particularly glucocorticoids is complicated by the presence of endogenous steroids. Glucocorticoids in particular cause a feedback inhibition that will ultimately result in decreased adrenal gland hormone synthesis and adrenal atrophy. This effect will occur regardless if the glucocorticoids is endogenous or supplied exogenously. This secretion is influenced by stress and is characterized by a diurnal rhythm (or perhaps nocturnal in cats). The impact of normal endogenous glucocorticoid secretion influences the clinical use of glucocorticoids which is designed to minimize their impact on endogenous secretion. The longer the glucocorticoids is used therapeutically, the more important it becomes to give the body (adrenal glands) an opportunity to re-adapt to the absence of the drugs. Several approaches are used to minimize this impact. Short acting glucocorticoids that have an effect less than 24 hours will allow endogenous adrenal secretion to occur. Likewise, using a physiologic dose will minimize the impact and as such, the dose will be tapered as soon as
57
possible to alternate day use. Morning administration will more likely mimic normal secretion in the dog. Finally, as the drug is finally discontinued, the dose will be gradually tapered to allow the body to adjust to the declining presence of the drug. The duration of the taper should reflect the duration of therapy.
Disposition The disposition of glucocorticoids contributes to clinical differences in response. Those available for oral administration are well absorbed orally in some but not all species. Cats and horses do not appear to absorb prednisone well; indeed, some dogs may absorb less prednisone compared to prednisolone, warranting use of the later drug in non-responders. Prednisone and its ketone hydroxylated active metabolite, prednisolone, are not truly equivalent in cats: both area under the curve (AUC) and maximum drug concentration (Cmax), parameters that measure oral bioavailability, are decreased substantially (by more than 75%) for prednisone when the same dose is given compared to prednisolone. This probably reflects oral absorption rather than metabolism because prednisone also does not show up on the blood of cats when given prednisone orally. Absorption of parenteral glucocorticoids is manipulated through the addition of R groups. Esters must be hydrolyzed by esterases in the muscle (or plasma) and the rate of hydrolysis is impacted by the specific esterase. Succinate esters are very rapidly released (including in the plasma) versus acetates which are very slowly release. Acetate products thus are “depo” preparations and even if an “intermediate” or “short” acting glucocorticoid active pharmaceutical ingredient is administered, if the ester is only very slowly released, the drug is not short acting. Further, if a drug with a depo ester is administered IV, embolization of this drug in the lungs can be lethal. If it is white, do not give IV. Pivalate is added to desoxycorticosterone, rendering it a slow release mineralocorticoid that might be given monthly. Glucocorticoids might also be given topically to minimize systemic exposure and subsequent suppression of the hypothalamic pituitary adrenal axis (HPAA). However, do NOT assume that sufficient drug will not be absorbed: studies have demonstrated sufficient absorption, particularly when applied to inflamed skin, or joints, etc such that the HPAA axis is impacted.
In an attempt to minimize the systemic effects of glucocorticoids applied topically in humans, manufacturers have again manipulated drugs. The term “soft” glucocorticoids have been applied to those administered locally with the intent to avoid systemic side effects. These include ocular, inhalant and gastrointestinal. Such drugs must be potent, which precludes the systemic drugs. Inhalant drugs may still be orally absorbed as they travel up the mucociliary tract and drugs in the GI tract may be absorbed orally. One manipulation that has minimized systemic side effects of such drugs is first pass metabolism. Examples include beclamethasone, fluticasone (commonly used in asthematic cats) available in metered device inhalers (MDA), and budesonide, available in oral capsules. However, studies have demonstrated that in animals, the drugs must not be entirely metabolized with first pass because side effects may occur. Interestingly, demodectic mange of the muzzle has been reported in cats receiving inhalant glucocorticoids. Likewise, topical effects of budesonide
58
(because of its potency) in the gi tract may increase the risk of GI ulceration which might not have occurred with other systemic glucocorticoids. As a reminder, based on duration of action, drugs can be divided into short acting, generally less than 12 hrs, intermediate, generally 12 to 36 hrs (including prednisolone) and long acting, generally greater than 36 hrs, represented by dexamethasone. The intermediate acting, particularly the preds, may be short acting enough that once daily therapy (and especially alternate day therapy) is sufficient to minimize suppression of the HPAA axis. As a reminder, as duration of action increases, so does potency, anti-inflammatory effects, and side effects. Most patients for which glucocorticoid therapy is implemented will require prolonged therapy. Ideally, because of their side effects, use will be limited to life or organ threatening diseases. It is important to start with a high enough dose and to maintain it long enough to avoid resistance. Once remission is achieved, the dose should then be tapered to a minimum effective dose. Morning dosing with a short acting drug, going to alternate day therapy, and tapering withdrawal have been discussed. The dose as indicated before varies with the potency, but also with the intent: ideally ultimate doses will be physiologic but as disease is forced into remission, the highest dose might be a “shock dose” (which is rarely indicated), followed by an immunosuppressive dose, followed by an anti-inflammatory dose. Drugs Room precludes describing all GL sed in dogs or cats; discussion will be limited to important points. Prednisolone versus Prednisone: Prednisone is rapidly metabolized by the liver to prednisolone (C-11 ketol reduction). Prednisone and prednisolone generally are (inappropriately) considered equivalent in terms of therapeutic use in veterinary medicine; veterinary dosing formularies generally make no distraction between the two. Yet, in the cat, the AUC for prednisolone was 3230.55 ng/mL/h and Cmax of 1400.81 ng/mL with a half -life for excretion of 1 h. This compares to a prednisolone AUC of 672.63 ng/mL/h and Cmax of 122.18 ng/mL following oral administration of prednisone; interestingly, a portion of the AUC reflected a half-life which was much longer at 2.46 h. In cats, a 3 to 5-fold dose should be given; in dogs, a 2-fold increase should be sufficient. Methylprednisolone has greater antioxidant activity that has been shown to be beneficial in the treatment of experimental spinal cord trauma in cats and experimentally induced E. coli bacteremia. Dexamethasone phosphate was developed for humans in order to reduce the volume of the drug that needed to be given. The phosphate salt is more soluble in water and thus allows for a higher concentration. It is not more likely (indeed may be less lipid soluble) to move into cells faster because it will be dephosphorylated in the liver prior to penetrating the cell.
Inhalant glucocorticoids Generally inhalant glucocorticoids are delivered by metered device inhalers which are intended to deliver high concentrations locally, that is, at the site of action. For asthma, the preferred route in humans with mild disease is low-dose inhaled glucocorticoids.
59
Beclomethasone was among the first aerosol glucocorticoids developed for inhalant therapy. Examples of corticoisteroids marketed as inhalant metered devices (MDIs; see later discussion) in the United States include beclomethasone dipropionate (Beclovent), triamcinolone acetonide (Azmacort), flunisolide (Aerobid), budesonide (Pulmicort), fluticasone propionate (Flovent), and mometasone (Asmanex). Corticosteroid delivery of MDIs has been improved by the advent of hydrocarbon fluoroalkyl (HFA)–propelled MDI. Beclomethasone dipropionate delivery to peripheral airways increases from 5% to 15% for the chlorofluorocarbon -propelled preparation to 50% to 60% with the HFA propellant.91 Not only is total lung delivery increased, but the depth of penetration also is enhanced which is critical to successful therapy. Although side effects are minimized compared to systemic delivery using MDI, up to 90% of an inhaled dose is still deposited on the oral mucosa or pharynx and swallowed in humans. Because animals cannot be directed to inhale, a similar or greater proportion of drug deposition might be anticipated in animals. Multiple methods have emerged to reduce adversities associated with glucocorticoids administered by MDI without decreasing efficacy. Differences in pharmaceutical (delivery) and pharmacokinetic properties largely determine variable responses to inhaled glucocorticoids. Characteristics that can be manipulated to influence efficacy or safety include potency (the amount of drug or number of molecules that impart a target response), thus allow use in a MDI; retention at the site of action, thus prolonging local effect, and rapid metabolism, thus decreasing systemic effects. Corticosteroids marketed in MDI vary up to fivefold or more in potency. The relative potency of drugs marketed as MDI roughly follows the following order: monmetasone, which exceeds both fluticasone and budesonide, which, in turn, are 2 to 3 times more potent than beclomethasone; triamcinolone is the least potent of these drugs. While potency does allow administration of a small dose, it does not predict clinical efficacy of inhaled glucocorticoids.91 Despite sixfold differences in potencies among inhaled glucocorticoids, comparative clinical trials in humans have failed to demonstrate differences in efficacy when drugs are administered at equipotent dosages.91 Further, dose response curves for inhaled glucocorticoids tend to be flat, indicating that increasing doses is not likely to enhance efficacy. Among the mechanisms whereby undesirable side effects of GLCs can be minimized is topical administration of drugs that are potent for the glucocorticoid receptor (GR) but also rapidly metabolized should the drug be absorbed into systemic circulation via the oral route. These efforts generally reflect manipulation of chemical groups on the D ring of the GLC. The term “soft glucocorticoids” has been used to refer to these drugs. Examples include beclomethasone, budesonide, and fluticasone propionate, steroids designed specifically for use in inhalant metered doses. Their potency when inhaled varies in clinical trials, with fluticasone propionate being most potent and budesonide and beclomethasone dipropionate approximately equipotent. Time of onset in humans to budesonide is approximately 10 hours based on evidence of clinical improvement at that time. Improvement can be expected over the next 1 to 2 days, with maximum effects potentially
60
not being evident until 2 weeks after therapy has begun. Drugs have been manipulated to prolong local presence. Inhaled corticosteroids generally are delivered as microcrystals, which must dissolve in the epithelial mucosal fluid. Crystals must be water soluble to ensure local delivery before the mucociliary tract removes the drug. However, alteration of dissolution times may also affect local delivery and thus local effects. For example, the dissolution time for budesonide is 6 minutes compared with beclomethasone dipropionate (5 hours) and fluticasone (8 hours). Lipophilicity of the drug enhances uptake and the duration of local effects. The addition of a halogen increases tissue retention compared with nonhalogenated drugs. Lipophilicity is greatest for beclomethasone and fluticasone followed by budesonide, with triamcinolone followed by dexamethasone and, finally, prednisolone as the least liphophilic. Not surprisingly, the most lipophilic of the drugs also is associated with the greatest number of side effects, including suppression of the hypothalamic pituitary adrenal axis. In humans, fluticasone is both the most potent and most lipophilic glucocorticoid. As such, it is characterized by the greatest evidence of systemic side effects. Recommendations for humans are that high-dose fluticasone propionate (>500 mg twice daily) be used only on the order of a physician and that the dose be titrated down to the lowest effective dose. Budesonide offers an example of a different type of manipulation that may allow longer dosing intervals while minimizing side effects. Because of its structure (a free C21 hydroxyl group), excess intracellular budesonide complexes with long chain fatty acids. The complex is inactive but probably allows persistence of the drug at the site, much as a depot form would, with reversible esterification occuring as receptors are depleted of active drugs. Other drugs with a free C21 hydroxyl include triamcinolone, flunisolide, and ciclesonide, although long-chain fatty acid esterification has not been determined for them. Neither fluticasone, nor beclomethasone dipropionate, and probably mometasone, form fatty acid esters.9
Therapeutic Considerations: Unless one is administering GLs for replacement therapy in a deficiency state (i.e., hypoadrenocorticism or relative hypoadrenocortical deficiency), GL therapy is not directed at the inciting agent. GL therapy is intended to reduce the physiologic processes that are activated in response to the disease. Despite the adverse events associated with their use, GCL continue to be heavily used in veterinary medicine, and potentially at doses that exceed that recommended. Indeed, in human medicine, the use of GLC clearly exceeds that recommended in textbooks and review papers. The advantages of low versus high doses have been previously discussed and are addressed again in Adverse Reactions. In general, an anti-inflammatory dose is considered to be 10 times the "physiologic" dose, and immunosuppressive doses are twice the anti-inflammatory dose. Shock doses of GLs have been reported at 5 to 10 times the immunosuppressive dose; however, the disadvantages of this high dose and the advantages of low dose therapy in shock patients are discussed below. When treating a patient for an immediately life-threatening condition such as immune-mediated hemolytic anemia, therapy should be aggressive, with a minimum effective dose determined after response has been achieved. Because high doses of GLs are often required to adequately treat immune-mediated diseases, adverse effects are likely to occur and should
61
be anticipated. Tapering of doses not only helps avoid side effects associated with long term therapy but may also avoid antibody rebound that has been associated with abrupt withdrawal of gluccorticoids in human patients treated for prevention of graft versus host transplant rejection. Dose reduction in patients with autoimmune diseases should be conducted gradually. The reduced dose should be continued for at least 2 weeks before the next attempted dose reduction, and the actual dose should be decreased by no more than half. It is essential to assess the patient's status frequently for recurrence of clinical signs. Concurrent administration of additional immunosuppressive (azathioprine, cyclophosphamide, chlorambucil) or anti-inflammatory drugs antihistamines, omega fatty acids, pentoxyfylline, leukotriene receptor antagonists) may allow the GL dose to be decreased (“dose sparing” effect). High-dose pulse therapy has been reported in human patients with acute relapse of chronic graft-versus-host disease. Using an open design, patients either receiving no immunsuppressive therapy or patients which failed (a median of 2 failures) current therapy (mean prednisolone dose of 0.2 mg/kg/day, range of 0-2.5 mg/kg/day) were treated with methyprednisolone at 10 mg/kg IV or PO for 4 days. The rationale behind the high dose is based on the lympholytic properties of this dose, thus causing destruction of lymphcytes that otherwise would cause irreversible organ damage. The high dose is assumed to target the (non-genomic) metabolic processes necessary for sustained activity of lymphocytes, as opposed to the low (genomic) doses which target lympyocyte replication. Additionally, the high dose is considered to overcome GL receptor saturation associated with GL therapy, causing significant GL down regulation. Induction of T- lymphocyte apoptosis may also occur. Antiviral and antimicrobial therapy (sulfanomides) accompanied high dose GL therapy. During a 2-year follow-up, patients tolerated the therapy well, with no major life-threatening effects occurring in the first 3 post treatment months. However, three patients developed infections after completion of the therapy, suggesting profound immunosuppression. Yet, the median time to progression of disease was 2 years after treatment, leading the authors to conclude that high-dose pulse steroid therapy is an effective and well tolerated treatment for progressive graft-versu-host disease. Side effects of GLs can occur if withdrawal of a GL occurs too rapidly. In human patients receiving GLs, the most frequent problem encountered with rapid withdrawals is recrudescence of the underlying condition for which the GL was indicated.
Side effects/adverse effects Glucocorticoids can influence clinical pathology results. The stress leukogram was previously discussed. Hypeglycemia and increased BUN reflect the formation of glucose from protein and increased cholesterol and triglycerides their impact on lipid mobilization and metabolism. Increases in hepatic transaminases (SALT, SAST) might reflect a glycogen storage type of response or direct effect, but this is should not generally be considered a hepatopathy. Likewise, glucocorticoids are potent inducers of serum alkaline phosphatase and a history of glucocorticoid therapy should be sought in patients with high SALKP and no other indicators of disease. The PU/PD effects (central and renal) cause hyposthenuria (dilute urine), which contributes to poor immune function in the urine. As such, it is not unusual for patients to have bacteria; this may not represent true infection and may not necessarily need treating. Finally, if the HPAA axis is negatively impacted, the thyroid axis also might be inhibited. The
62

side effects of glucocorticoids should largely be predictable based on their physiologic effects. Note that the euphoria can be profound. Immunosuppression cannot be avoided by use of anti-(Lu et al., 2020; Nixon et al., 2013; Okano, 2009; Petta et al., 2016; Sebaldt et al., 1990; Singh et al., 2020; Wilkinson et al., 2018)infectious drugs: these should not be used to “cover” a patient receiving glucocorticoids. Note that while iatrogenic hypoadrenocorticism is unusual (because of proper dose tapering), iatrogenic hyperadrenocorticism is not, although it may not be severe. Among the possible side effects of glucocorticoids in horses is laminitis, perhaps because of glucocorticoid induced vasoconstriction and altered blood supply to the hoof. As such, inhalant drugs might be better for treatment of chronic respiratory disease. Fat redistribution is not a serious side effect. The risk of GI ulcers is greater with potent, “topical” drugs compared to less potent systemically intended drugs; and of course, in patients receiving NSAIDs. The hepatopathy associated with glycogen storage generally does not present a risk to the patient. The risk of pulmonary thromboembolism may be a reason to avoid using these drugs in patients at risk for thromboembolic events or with bleeding disorders. Several contraindications exist for glucocorticoids. Again, understanding their physiologic effects allows most of these to be predicted. Their impact in pancreatitis is not really understood. Renal disease may be worsened if the poorly compensated kidneys are subsequently exposed to larger amounts of blood urea nitrogen. With chronic therapy, glucocorticoids may lower seizure threshold, increasing the risk of epilepsy. References:
1. Lu, S., Zhou, Q., Huang, L., Shi, Q., Zhao, S., Wang, Z., Li, W., Tang, Y., Ma, Y., Luo,
X., Fukuoka, T., Ahn, H.S., Lee, M.S., Luo, Z., Liu, E., Chen, Y., Zhou, C., Peng, D., 2020. Effectiveness and safety of glucocorticoids to treat COVID-19: a rapid review and meta-analysis. Ann Transl Med 8, 627-627.
Nixon, M., Andrew, R., Chapman, K.E., 2013. It takes two to tango: Dimerisation of glucocorticoid receptor and its anti-inflammatory functions. Steroids 78, 59-68.
Okano, M., 2009. Mechanisms and clinical implications of glucocorticosteroids in the treatment of allergic rhinitis. Clin Exp Immunol 158, 164-173.
Petta, I., Dejager, L., Ballegeer, M., Lievens, S., Tavernier, J., De Bosscher, K., Libert, C., 2016. The Interactome of the Glucocorticoid Receptor and Its Influence on the Actions of Glucocorticoids in Combatting Inflammatory and Infectious Diseases. Microbiology and Molecular Biology Reviews 80, 495-522.
Sebaldt, R.J., Sheller, J.R., Oates, J.A., Roberts, L.J., 2nd, FitzGerald, G.A., 1990. Inhibition of eicosanoid biosynthesis by glucocorticoids in humans. Proceedings of the National Academy of Sciences of the United States of America 87, 6974-6978.
Singh, A.K., Majumdar, S., Singh, R., Misra, A., 2020. Role of corticosteroid in the management of COVID-19: A systemic review and a Clinician's perspective. Diabetes Metab Syndr 14, 971-978.
Wilkinson, L., Verhoog, N.J.D., Louw, A., 2018. Disease- and treatment-associated acquired glucocorticoid resistance. Endocr Connect 7, R328-R349.
63

Non-glucocorticoid immunomodulators Dawn M Boothe, D.V.M., M.S., P.H.D., Diplomate, ACVIM, ACVCP Department of Anatomy Physiology and Pharmacology College of Veterinary Medicine, Auburn University Pathophysiology Treatment of immune mediated diseases includes those directed toward self (eg, auto-immune diseaseas) or those associated with a chronic allergic/inflammatory response. Both are impacted by T-lymphocytes, but the latter is largely associated with an imbalance toward TH2 helper cells and the former TH1 helper cells. As such, a focus on the role of T cells in the immune reponse is appropriate. T lymphocytes provide the primary regulation of the immune response. T cell activity begins with specific antigen recognition by a receptor on the surface of the cell.4 T cells are further subdivided into several populations of cells depending on their role in immunoregulation. Helper cell (CD4 T cells; Th cells) receptors recognize and bind to the peptide–MHC class II complex of APC cells. In response to IL-1, CD4 cells consequently proliferate and become primed as either Th1 or Th2 CD4cells, which modulate further responses in both the cell-mediated and humoral arms. Migration of activated lymphocytes from lymph nodes to tissues is facilitated by adhesion molecules expressed by endothelial cells in tissues. For chronic inflammatory allergic diseases, this migration is enhanced by permeability in the epithelial cells of the target tissue (ie, lungs, gastrointestinal tract, skin). Whether a T cell becomes Th1 or Th2 reflects the stimulating cytokine: IL-12 activates signal transducer and activator of transcription 4 (STAT-4), which regulates Th1 differentiation, whereas IL-4 activates STAT-6 and Th2 differentiation.5 The Th1 subsets of CD4 produce primarily proinflammatory cytokines such as IFN-γ (IFN-γ) and tumor necrosis factor-alpha (TNF-α) (cachexin). As such, Th1 cells regulate signals that promote cell-mediated immunity and control intracellular pathogens. Th1 response is paramount to successful resistance to most microbial pathogens, including bacteria, intracellular protozoa, and fungal organisms. Additionally, Th1 cells mediate organ-specific autoimmunity and as such are crucial to the pathogenesis of autoimmune diseases. In contrast to immune-mediated diseases, in which Th1 cells play key roles, key effector cells in all chronic allergic diseases include eosinophils, basophils, and Th2 cells. Their involvement occurs through release of preformed, or formed insitu, granule proteins and cytokines.7 Cysteinyl-leukotrienes appear to have an important role in the regulation of human eosinophil hematopoiesis, recruitment, and activation. Eosinophils are generated from CD34+ progenitors in the bone marrow upon stimulation by cytokines such as IL-5. Cys-leukotrienes (LTs) may also play a role in eosinophil regulation. Eosinophil–basophil colony-forming units increase in number, adhesion, and function, including production of IL-4 when exposed in vitro in the presence of LTD4. These responses are blocked by the presence of cysLT1 antagonists. Th2 cells also secrete antiinflammatory cytokines (IL-4, IL-5, IL-9, IL-10, IL-13) and support the humoral immune response, including host defense against intestinal helminths. Because of their
64

antiinflammatory effects, Th2 cytokines can decrease autoimmune diseases associated with cell-mediated immunity; however, an imbalance toward Th2 cells have been implicated in the pathogenesis of asthma and allergy. Cytokines that promote immune and inflammatory responses (e.g., IL-6, IFN-γ, IL-12, and IL-18) as well as those that suppress the immune response (e.g., IL-4, IL-10, IL-13) mediate cellular responses through the JAK –STAT signaling pathway, a rapidly acting, major signaling pathway. The pathway is initiated by cytokines (eg, IL, IFNs, selected peptide hormones) which bind to receptors (generally transmembrane) activating a JAK tyrosine kinase. Activation of the kinases results in phosphorylation of the receptor which attracts the STAT protein which also is then activated by phosphorylation. The activated STAT protein translocates to the nucleus, where it binds to the DNA, causing transcription. Immune cell proliferation and differentiation is initiated. Up to 4 JAK (“Just Another Kinase” or Janus activated; JAK1-3, plus one)and seven STAT (transcription proteins, including STAT-1 through -4, 5a and 5b, and STAT-6) proteins have been identifi ed in mammals, each with a specifi c function in the immune response that modulates either proinfl ammatory or antiinfl amatory. Fro example, JAK1 is a tyrosine kinase that signals selected transmembrane cytokine receptors that stimulate responses from IL-2, IL-4 and IL-10 receptor families as well as a number of other signals, including interferons. STAT-3, activated by IL-6 in acute inflammation, appears to play a role in chronic inflammation. Dysregulation of the influence of STAT-4 and STAT-6—which have contrary effects—has been associated with immune-mediated diseases. Drugs Cyclosporine is a T-cell specific immuomodulator approved for use in humans for immune suppression of graft vs host transplant rejection, autoimmune disorders, red cell aplasias and, increasing IBD. The standard preparation is very lipophilic and as such must be prepared in oil and oral absorption is bile acid dependent; oral bioavailability ranges from 20 to 50%. Newer microemulsion preparations (Atopica® or Neoral®) is not as dependent on bile acids for oral absorption and is more bioavailable. Bioavailability of orally administered cyclosporine approximates 25-30% following multiple oral administration in cats (n=6), Food may impair the aborption of CsA. The drug is not absorbed topically following transdermal administration. The drug accumulates in erythrocytes (accounting for 50% or more of the drug in humans), and leukocytes (accounting for 10 to 20% of circulating drug in humans) As such, monitoring of whole blood rather than plasma or serum is recommended. Remaining circulating drug is bound to plasma lipoproteins. Further, concentrations in skin are up to 10-fold higher than blood, although this is based on homogenate data In contrast, largely due to the influence of ATP-binding transporters P-glycoproteins, especially the B1 cassette (PgP, MDR1 gene product), little CsA crosses the blood brain barrier. The drug is metabolized by the liver to a large number of metabolites, which are likely to vary among animals. The drug is metabolized predominantly by the liver, although sufficient metabolism occurs by intestinal enterocytes that oral bioavailability is impacted. Liver disease will decrease clearance of CsA substantially. Monitoring is recommended in the presence of hepatic or gastrointestinal disease. Cytochrome 3A4 (commonly associated with P-glycoprotein or other efflux pumps) plays a major role in
65

metabolism; many of the drug interactions involving CsA also involve CYP3A4 or associated glycoprotein. Over 25 to 30 metabolites have been documented in humans. In cats, elimination half-life of CsA is 8 hrs which was similar to that following IV administration. Ocular administration might serve as an alternative route for systemic delivery of CsA in cats. Following administration of either an oral preparation or an ocular preparation of CsA in olive oil, peak concentrations ranged from 450 to 1033 ng/ml and 288 to 648 ng/ml, respectively, with an absorption lag time ranging from 0 to 1.34 hr for the oral solution, and 0.27 to 1.2 hr for ocular preparation. The elimination half-life ranged from 2.41 to 10.04 hr, and 3.09 to 15.75 hr, respectively. Blood concentrations were sufficient to inhibit lymphocyte activity as measured in vitro, leading the authors to conclude that ocular administration of CsA in an olive oil vehicle might be a reasonable alternative to oral, or even IV, administration in cats intolerate to the latter. Side Effects: Cyclosporine appears to be much safer in animals compared to human for which it is haracterized by a narrow therapeutic index with renal toxicity the primary adverse effect. Renal tubular cells develop hyperuricemia (worsened by diuretics) and hyperkalemia (a renal tubular and erythrocyte ion channel effect) (Kahan, 1993). Hepatic injury also occurs. Although less common than renal dysfunction, the risk of severe hepatic damage is markedly increased when cyclosporine is used in combination with cytotoxic drugs. Cyclosporine also increases the incidence of gallstones in human patients. The risk of renal and hepatic toxicities does not appear to be as great in small animals. The risk of renal damage is, however, likely to be enhanced with concurrent administration of several other drugs, including other nephrotoxic drugs, and may be of greater risk in animals undergoing renal transplantation. Hyperlipidemia also has been reported in humans, particularly in patients receiving glucocorticoids. Other side effects reported in humans include hepatotoxicity, neurotoxicity, diabetes, gastrointestinal upset, and hypertension. Development of B-cell lymphoma also has been reported. Side effects in dogs reflect gastrointestinal upset and dermatologic or mucosal abnormalities. Vomiting may occur in put to 40% of dogs, although it may be intermittent and short I duration. Diarrhea occurs less commonly (16-18%). Cyclosporin apparently inhibits insulin secretion in a dose-dependent manner. Rare neurotoxocity, characterizied by reversible cortical blindness has been reported in human patients receiving CsA following bone marrow transplantation. Monitoring Cyclosporine concentrations should be monitored as a guide to effective yet safe dosing regimens. Guidelines offered in human medicine have served as targets for veterinary patients although the appropriateness of extrapolation has not been addressed. Plasma or blood concentration of cyclosporine is the predominant determinant of drug effect although an active metabolite may contribute up to 10% of activity in humans not receiving ketoconazole. Several methods are available for measuring cyclosporine concentrations, including high-performance liquid chromatography (HPLC), which generally detects only the parent compound, , and immunoassays based on monoclonal antibodies (eg, FIPA by Abbott TdX)which are less likely to detect metabolites compared to polyclonal based assays. Each assay appears to be clinically
66

useful, although the target concentrations will vary with the methodology, the sample collected (eg, whole blood, plasma or serum) and the timing of the sample (eg, peak or trough). For example, because much of CsA in whole blood is located in red blood cells, concentrations based on whole blood (WB) will be higher than that measured in serum or plasma or serum (PS) as will concentrations of parent and metabolite (antibody based assays, particularly polyclonal) compared to parent compound only (HPLC). In humans, recommended trough (before next dose) CsA concentrations (ng/ml) are for HPLC, 100 to 300 (WB); RIA, monoclonal antibody methodology: 150 to 400 (WB) or 50 to 125 (PS); RIA, polyclonal antibody methodology: 200 to 800; fluorescent polarized immunoassay: 250 to 1000. In dogs, blood concentrations measured by TDx assay are 1.8 times higher than those measured with HPLC assay. For IBD, concentrations fo 250 ng/ml are recommended. The laboratory to be used for monitoring purposes must be contacted before collection of samples for CsA monitoring. The dosing regimen recommended for treatment of atopy. Should not be assumed to be effective for treatment of immune mediated diseases. In humans, cyclosporine is usually administered by mouth every 12 hof 4500 to 5500 ng/ml are recommended. The risk of graft versus host rejection was markedly reduced when CsA dosing was based on peak rather than through concentrations in humans. However, the use of this parameter as a predicator of CsA exposure is based on a 12-hour dosing interval. Monitoring is recommended at least monthly for the first several months of therapy and preferably weekly for the first month of therapy, or until concentrations are stable. With the advent of renal transplantation availability at several facilities, CsA is increasingly being used to prevent graft-host rejections. Cats respond better than dogs, with renal allografts being maintained at 7.5 mg/kg every 12 hours coupled with prednisolone (0.125 to 0.25 mg/kg every 12 hours). Trough concentrations of whole blood should be maintained at 750ng/mL (HPLC) the first month after transplantation but can be reduced to 500-250 ng/mL thereafter. Other potential indications for cyclosporine warrant further investigation. Cats suffering from Ascaris suum–induced airway reactivity had decreased reactivity and remodeling after receiving cyclosporine; differences were noted with 24 hours of therapy. Note that the immunomodulatory effects generally will necessitate twice daily dosing (5 mg/kg twice daily) because of the short half-life of the drug in cats (5to 9 hrs). With the exception of atopy (as per approval data), once daily dosing of cyclosporine is not likely to be preferred. In humans, peak concentrations are more predictive of area under the curve; a target of 4500-5000 ng/ml is recommended. Note that often a more cost-effective approach for reaching target concentrations is decreasing the interval rather than increasing the dose. Doubling concentrations will require doubling the dose, but tripling concentrations will require a 4-fold dose increase, and quadrupling the drug concentrations will require an 8 fold dose increase. Mycophenolate mofetilMycophenolate mofetil (MMF) is the morpholinoethyl ester pro-drug of mycophenolic acid (MPA) is a product of several Penicillium species that possesses antibacterial, antifungal, antiviral, antitumor, and immunosuppressive properties. MPA is a potent, selective, non-competetive yet reversible inhibitor of inosine monophosphate dehydrogenase (IMPDH). This enzyme is critical for the production of the guanine triphosphate
67

precursor guanine monophosphate, which in turn is necessary for the de novo synthesis of purine nucleotides. As such, the drug is an antimetabolite. Two isoforms of human inosine monophosphate dehydrogenase (IMPDH) exist. Type I is expressed constitutively expressed in normal, non-replicating cells, and while type II is upregulated in replicating (including neoplastic) cells to the point that it is the predominating isoform. As IMPDH is inhibited, GTP is depleted; failure to make mRNA precludes synthesis of proteins, including cytokines, necessary for cell proliferation. Unlike other anticancer antimetabolites, MMF and its active metabolite MPA are relatively selective for lymphocytes because they are solely dependent on de novo synthesis of purines for DNA synthesis. Mycophenolate mofetil is the first drug since cyclosporine to be approved in the United States for prevention of renal allograft rejection; it has proven useful for treatment of steroid—resistant acute liver rejection (Pfitzmann 2003). In addition to its antiproliferative properties towards lymphocytes, MPA also impairs proliferation in non-immune cells, including. smooth muscle cells, renal tubular cells and mesangial cells, and dermal fibroblasts. As such, MMF might be indicated for non-immune mediated diseases associated with fibrosis. The primary side effects in human patients receiving the drug for allograft rejection are leukopenia, gastrointestinal upset, and cytomegalovirus disease. The incidence is, however, small. Gastrointestinal upset is characterized by nausea, diarrhea, vomiting, and abdominal cramping. Gastrointestinal toxicity (and bone marrow suppression) may reflect the need for IMDPH II because of the normally replicating nature of these tissues (Neerman 2003).Oral bioavailability of MMF is poor, but extensive first pass metabolism to MPA yields a reasonably orally bioactive compound in humans and dogs.Thus far, no information is available for mycophenolate in cats. Because it is a prodrug, and will not be effective unless activated, this drug should be used cautiously if at all in cats. “ “Soft” glucocorticoids Although glucocorticoids, among the mechanisms to minimize systemic response to glucocorticoids is to use them locally. The term “soft glucocorticoids” has been used to refer to drugs that are potent for the glucocorticoid receptor (GR) but also rapidly metabolized should the drug be absorbed into systemic circulation via the oral route. These efforts generally reflect manipulation of chemical groups on the D ring of the GLC. Examples include beclomethasone, budesonide, and fluticasone propionate, steroids designed specifically for use in inhalant metered doses. Their potency when inhaled varies in clinical trials, with fluticasone propionate being most potent and budesonide and beclomethasone dipropionate approximately equipotent. They are applied topically in the respiratory tract (with local effects) in order to avoid side effects associated with consumption. Soft GLs are potent for glucocorticoid receptors but also rapidly metabolized by the liver (ie, undergo 1st pass metabolism) should the drug be absorbed into systemic circulation. Examples include beclamethasone, budesonide and fluticasone proprionate, steroids designed specifically for use in inhalant metered doses. Their inhalant potency varies, with fluticasone propionate being most potent and budesonide and beclomethasone dipropionate approximately equipotent. Time of onset in humans to budesonide is approximately 10 hrs based on evidence of clinical improvement at that time. Improvement can be expected over the next 1-2 days, with maximum effects potentially not
68

being evident until 2 weeks after therapy has begun. In humans,budesonide is rapidly metabolized in the liver by CYP3A4 with affinity of metabolites of the GCR being less than 1% of the parent. Yet, 100% of topically (inhalant) administered drug in humans appears as metabolites in the urine, indicating that systemic absorption of the drug does occur, with as much as 25% circumventing hepatic metabolism before entering systemic circulation. Budesonide is particularly interesting because it binds locally to the receptor in the lungs, more so than receptors in peripheral tissues. Inside the cell, the drug is esterified and is released only with de-esterification. As such, the drug is stored locally and slowly released. The ability to esterify varies among tissues, with pulmonary tissue apparently having a much higher capacity compared to other tissues, leading to greater storage in airways compared to peripheral tissues. Drugs which impair CYP3A4 may increase the plasma drug concentration of budesonide over 7-fold. In the gastrointestinal tract, budesonide appears to be sufficiently orally absorbed in dogs that the hypothalamic-pituitary –adrenal –axis will be suppressed. The extent that budesonide will be removed by first pass metabolism following oral administration in cats is not known, but it is possible metabolism will be incomplete.
Despite their apparent popularity, only a small amount of evidence supports the clinical efficacy of inhalant glucocorticoids. An MDI has been demonstrated to effectively deliver drug to the peripheral airways of cats. Inhaled glucocorticoids have been recommended for use in cats with asthma if they cannot be effectively dosed orally, although few studies have provided guidance. One abstract has reported a beneficial effect of flunisolide (250 μg/puff) but not zafirlukast (10 mg orally every 12 hours) in cats with experimental feline asthma. Reinero and coworkers compared the impact of inhaled flunisolide (250 μg puff twice daily) to that of oral prednisone (10 mg/day orally) and placebo on indices of inflammation and adrenal gland suppression in healthy cats (n = 6). Mean eosinophil count was decreased by both compared to placebo. No treatment effect was apparent with regard to serum immunoglobulin or cytokine activity. The inhaled glucocorticoid was associated with lower baseline cortisol compared with placebo and lower cortisol after adrenocorticotropic hormone stimulation compared with oral and placebo therapy. A limitation of the study may have been the use of prednisone rather than prednisolone as is suggested by impact on cortisol concentrations, although oral therapy did impact both T and B cells. This study supports the potentially inappropriate use of prednisone in cats and suggests that topical flunisolide therapy may suppress the hypothalamic pituitary adrenal axis in cats with flunisolide. Note that clinical signs may not be a sufficient indicator of resolution of peripheral airway inflammation as was demonstrated in cats receiving oral prednisolone for 3 weeks. Despite clinical response, 7/10 cats still had inflammation in the peripheral airways. In cats, facial demodecosis has been reported in the muzzle area after mask delivery of fluticasone.
Other Steroids Danazol (5 mg/kg 2-3 times daily orally) is classified as an androgen but is characterized by weak androgenic activity. In human patients, danazol has proved effective in stimulating increased concentrations of complement inhibitor and thus is indicated for treatment of angioneurotic edema (Wilson, 1995). Danazol also has immunomodulatory effects that are of
69
benefit in type II immune complex diseases. Danazol apparently decreases the expression of or blocks Fc receptors on macrophages; initial displacement of glucocorticoids due to competition of binding sites is less likely to be effective as glucocorticoid clearance increases. (Ward, 1995; Stadtmauer et al., 1991; Choudhry et al., 1995; Schreiber et al., 1987). The drug has proved useful in a number of type II immune-mediated diseases, including immune-mediated hemolytic anemia (autoimmune hemolytic anemia) and immune-mediated thrombocytopenia (Gorman, 1995; Ward, 1996; Bloom et al., 1989; Holloway et al., 1990). Medroxyprogesterone acetate has been used for treatment of selected immune-mediated diseases in lieu of glucocorticoids, or in patients that have not responded to glucocorticoids. Medroxyprogesterone exhibits glucocorticoid-like effects, which reflect, in part, actions at the level of DNA-transcription. The impact of gluocorticoids on DNA transcription was reviewed (Chapter 17); those glucocorticoids which target trans (rather than cis) repression (rather than activation) are directed toward desirable effects, avoiding many undesireable metabolic effects. Medroxyprogesterone appears to potentially focus on undesirable effects, being characterized by a preponderance of transrepression activity rather than transactivation or cis activity (Shulz 2004).Chlorambucil: Chlorambucil is an alkylating anticancer drug used for immunosuppression in diseases associated with marked lymphcytic infiltration. It often is used (0.1 mg/kg orally every 48 hours) used in lieu of cyclophosphamide. As with cyclophosphamide, leukopenia and thrombocytopenia are potential side effects of this drug. Pemphigus foliaceus in cats can be treated with chlorambucil as the first choice (Rhodes, 1995). Daily therapy (0.1 to 0.2 mg/kg/day) should be continued until lesions have markedly reduced, which may take 4 to 8 weeks. Alternate-day therapy should be implemented when approximately 75% improvement occurs and continued for several weeks. Complete blood counts should be monitored every 2 weeks of chlorambucil therapy (Rhodes, 1995). Leukotrienereceptor antagonists Leukotrienes are very potent causes of marked edema, inflammation, and bronchoconstriction (Funk 2001). Their inhibition by glucocortiocids may be limited, leaving a void in therapy (Currie 2005). The approval of drugs that specifically inhibit the formation of LTs or their actions have offered a new avenue of control of respiratory inflammatory disease (e.g., asthma) in human medicine. Two classes of drugs have focused on their impact on leukotrienes: leukotriene synthesis (5-lipoxygenase) inhibitors (zileuton) and leukotriene-receptor antagonists (LRA). The latter class has proven to be more effective. Currently, two LRA are approved in the United States: zafirulokast, administered twice daily, and montelukast, administered once daily. The disposition of neither drug has been studied in dogs or cats; in humans, the dosing intervals reflect a half-life of 5 and 10 hr respectively, for the two drugs. In human clinical trials, LRA inhibit early and late phase bronchoconstrictionand increased bronchial hyperresponsiveness in response to allergens, accumulation of inflammatory cells and mediators in bronchial lavage fluid, and acute bronchospasms stimulated by exercise, cold air and aspirin. Their bronchodilatory effects are less than that of long acting β-adrenergics whereas the anti-inflammatory effects are less than that of glucocorticoids (Currie 2005). However, response does occur to single doses. In contrast to β-adrenergics, tolerancedoes not
70
develop toward LAR effects. Their use has been associated with improvement of asthma either as sole therapy (in lieu of low dose inhaled glucocorticoids) in mild to moderate asthma, or as add-on therapy regardless of diseases severity in glucocorticoids non-responders. The LAR are well tolerated, particularly when compared to glucocorticoids. A subset of asthmatics treated with LAR have developed Churg-Strauss syndrome (CSS), a state of systemic hypereosinophilia. However, its emergence may reflect decreased doses of glucocorticoids permitted once LAR are begun, rather than a toxic effect of LAR. Recommendations regarding the role of LAR in treatment of human asthma are dynamic. Currently, because they are less effective than glucocorticoids, their role as monotherapy should be avoided, even with mild disease. In contrast, LRA have proven effective as monotherapy for treatment of allergic rhinitis in humans. For asthma, because of their unique mechanism of action, LAR have been combined with a number of other drugs used to treat asthma. For example, Glucocorticoids minimally impact cys-LT; as such, combination with LAR would be expected to have an additive effect as has been demonstrated when combined with inhaled glucocortiocids. The combinationof LAR and glucocortiocoids generally is as effective as glucocorticoids combined with β-adrenergic agonists. The use of LRA as part of triple therapy, ie,with corticosteroids, β-adrenergics is a reasonable, albeit, understudied therapeutic approach in patients not responding to dual therapy. Finally, LRA also have been recommended in the treatment of aspirin-sensitive asthma (see below). The role of LAR in the treatment of feline asthma has had little scientific support, although this should not preclude their use, particularly in animals that have not sufficiently responded to, or cannot tolerate (eg, diabetics) corticosteroids. Receptors for leukotrienes have yet to be identified in the smooth muscle of airways in cats; further, LTs have not been identified in the urine or plasma of cats with experimentally –induced asthma (Norris 2003). However, LTs were associated with experimentally induced heartworm disease in cats (Boothe 2006). The recent approach to asthma as a systemic response mediated atthe level of the bone marrow, warrants consideration of the use of LRA for treatment of feline asthma, particularly in non-responders or patients that cannot tolerate glucocorticoids. Other potential indications would include control of inflammation in dogs in which glucocorticoids are contraindicated, or pulmonary diseases characterized by eosinophilic infiltrate. Anecdotally, LAR appear to be safe in both dogs and cats, although no study has validated safety. Pentoxyfylline is a methylxanthine derivitive (similar to theophylline) with minimal respiratory or cardiac effects. Its ability to change rheological properties (perhaps by changing red blood cell deformability, or blood viscosity) and potential anti-inflammatory effects (including potential antiplatelet aggregation) has led to its use in dermatomyositis, atopy, and pruritis associated with atopy in dogs. It decreases synthesis of mRNA for TNFα, which may be its primary mechanism of action. It also has been used for treatment of immune-mediated diseases of the skin. Metabolites of the compound contribute a large component of pharmacologic activity. It has been studied in dogs, but not cats, but appears to be very safe. 10-15 mg/kg orally twice daily, for 2 to 6 weeks).
71

Small drug molecules are those that are sufficiently small to enter a cell and reach targeted intracellular targets. Tyrosine Kinase Inhibitors (TKI): Tyrosine kinases are molecules responsible for cellular signal transduction. By transferring a phosphate group from ATP to a tyrosine molecule target protein, the serve as “on-off” switches for signals that communicate cell functions. For example, cancer growth may become unregulated if a protein kinase fails to switch off, as may occur with mutations, thus causing the cell to respond constitutively, rather than in response to signals. Serine and threonine do the same function for their respective proteins. Over 90 tyrosine kinases have been found in the human genome. Tyrosine kinases can be activated by molecules located at two sites. Examples of cell membrane receptors activating tyrosine kinases involved with cancer include growth factors (epidermal growth factors [EGFR], platelet derived growth factor (PDGFR], vascular endothelial growth factor [VEGFR:HER2/neu]); these enzymes have an identified role in breast, gastrointestinal, non-small-cell lung and panctreatic cancer. A number of tyrosine kinase inhibitors have been developed in human medicine to treat a variety of cancers: imatinib (gastrointestinal stromal tumors or hronic myleoblastic leukemias), nilotinib (chronic myelogenous leukemia, targeting Abl), sunitinib (VEGFR, PDGFR and others), and gefitinib (EGRF). Tyrosine kinase inhibitors (TKI) are designed to compete with target substrates for tyrosine kinase activity. The more specific the drug for its target molecule, the less the toxicity. Potential toxicities include myocardial damage and protein loss (renal?), the latter monitored at least biweekly for the first 3 months of therapy and then monthly thereafter (treatment is discontinued until resolved and then re-instituted at a reduced manner). In veterinary medicine, two tyrosine kinase inhibitors (TKI) have been approved for treatment mast cell disease in dogs in the USA. Toceranib (Palladia®; a “sister” to sunitinib), is a receptor TKI that targets over 50 tyrosine kinases; its major targets are KIT, PDGFR and VEGFR2 and Flt-3. Palladia® is marketed as an anti-angiogenic, antiproliferative therapy. The package insert indicates a 59% response rate (complete remission to no progression of disase) at 3.25 m g/kg/every other day. Among the side effects are vascular disorders, including severe diarrhea (> 1/100) thromboembolism (COX-2 specific NSAIDs might need to be avoided), gastrointestinal bleeding, “penias” (neutropenia [> 1/100], anemia, thrombocytopenia), hypoalbuminemia (> 1/10) hepatotoxicity or nephrotoxicity. Masitinib (Kinavet®/Masivet®) has been designed to be more selective than imatinib, targeting KIT, PDGFR and Lyn. Presumably, it is less likely toinhibit tyrosine kinases that result in toxicity, thus allowing higher doses. Based on studies in Europe and the USA, mastitinib has increased survival rates in dogs with non-resectable tumors, allowing “curative” therapy in some dogs. Most TKI in humans are transported by multiple transporters, including P-glycoprotein in portals of entry and sanctuaries, as well as tumor cells. metabolized by major CYP enzymes. The package insert for masitinib does indicate that the activity of a number of CYP enyzmes (including 2C9, 2D6, 3A4 and 3A5) are inhibited by masitinib, suggesting care should be taken with combination with other drugs. For Palladia®, no CYP enzymes are cited in regards to potential inhibition by the drug, although enzyme inhibition will increase Palladia® concentrations. Non-cancer potential indications for masitinib include atopic dermatitis (particularly dogs not responsive to cyclosporine, glucocorticoids or dogs with severe pruritus; clinical trial ongoing), inflammatory bowel disease, arthritis and feline asthma.
72
Oclacitinib (Apoquel®) Among the approaches to control selected cytokine or inflammatory signal-based disease are drugs which target specific molecules. These include drugs which inhibit tyrosine kinases(TK) including JAK. Among the newest drugs to be approved in veterinary medicine is oclacitinib (Apoquel®). It is particularly potent for JAK 1, which in combination with JAK2 and another tyrosine kinase, increase the presence of a number of interleukins, including IL-31, an important mediator of the inflammatory response in atopic animals. Unlike many other tyrosine kinase inhibitors, which are often associated with adverse effects because of the inhibition of growth factors, oclacitinib appears to be well tolerated. It has proven a rapid, effective treatment for atopy. Its role in other chronic inflammatory diseases remains to be demonstrated, in part because its potency for JAK 1 as opposed to other JAKS may limit application. Feline asthma is among the conditions for which some information is emerging. (Gonzales et al., 2014) Cytopoint is a monoclonal antibody directed toward IL-31. As such, its application to other chronic inflammatory diseases may be limited. An advantage is its long duration of action. A potential disadvantage is that as a protein, its impact on chronic allergies may need to be explored. Note also, since it is a biologic agent, it is approved through the United States Department of Agriculture and as such, data supporting efficacy and safety may not be as robust as would be expected for a drug approved by the Food and Drug Administration. (Chan et al., 2019; Galli et al., 2008; Mohajeri et al., 2018)
1. Archer, T.M., Boothe, D.M., Langston, V.C., Fellman, C.L., Lunsford, K.V., Mackin, A.J., 2014. Oral cyclosporine treatment in dogs: a review of the literature. J Vet Intern Med28, 1-20.
2. Chan, B.C.L., Lam, C.W.K., Tam, L.-S., Wong, C.K., 2019. IL33: Roles in Allergic Inflammation and Therapeutic Perspectives. Frontiers in Immunology10.
3. Galli, S.J., Tsai, M., Piliponsky, A.M., 2008. The development of allergic inflammation. Nature454, 445-454.
4. Gonzales, A.J., Bowman, J.W., Fici, G.J., Zhang, M., Mann, D.W., Mitton-Fry, M., 2014. Oclacitinib (APOQUEL(®)) is a novel Janus kinase inhibitor with activity against cytokines involved in allergy. J Vet Pharmacol Ther37, 317-324.
5. Mohajeri, M.H., Brummer, R.J.M., Rastall, R.A., Weersma, R.K., Harmsen, H.J.M., Faas, M., Eggersdorfer, M., 2018. The role of the microbiome for human health: from basic science to clinical applications. Eur J Nutr57, 1-14. (Archer et al., 2014)
73
Therapeutic drug monitoring: A case base approach
By Dawn Merton Boothe, DVM, PhD, DACVIM, DACVCP Auburn University
IntroductionThe success of any fixed dosing regimen most often is based on the patient's clinical response to the
drug. Fixed dosing regimens are designed to generate plasma drug concentrations (PDC) within a therapeutic range, ie, achieve the desired effect while avoiding toxicity. However, a therapeutic range (Cmin and Cmax ) is a population parameter that describes the range between which 95% of the animals might respond. Response below the therapeutic range does not necessarily indicate therapy is not needed; likewise, failure should not be considered only if the drug is above the maximum range. For some patients, the maximum range will need to be exceeded and should be considered if the drug is safe and respon. Thus, the absence of seizures in a dog with subtherapeutic concentrations is not justification for discontinuing the drug. On the other hand, a very small proportion of animals respond at concentrations higher than the recommended maximum and risk-benefit considerations should determine the need to add a second drug.
Marked inter-individual variability in physiology, response to disease and response to drugs results in variability in dose-response relationships. The most recent examples are Collie breeds with the MDR gene mutation, and drug interactions involving CYP3A4 or P-glycoprotein. Changes in drug metabolism and excretion induced by age, sex, disease or drug interactions are among the more important factors which can cause PDC to become higher or lower than expected. Therapeutic drug monitoring replaces the trial and error approach to dosing regimen designs that may prove costly both financially and to patient health. Monitoring is indicated in clinical situations in which an expected therapeutic effect of a drug has not been observed, or in cases where drug toxicity related due to high toxic PDC is suspected. In addition, TDM can be used to establish whether or not optimum therapeutic drug concentrations have been achieved for drugs characterized by a response that is difficult to detect or in which the manifestations of disease are life threatening and the trial and error approach to modification of dosing regimen is unacceptable. In situations in which chronic drug administration is expected, TDM can be used to define the effective target PDC in the patient. The target PDC can then be used if pharmacokinetics change in the patient over the course of chronic drug administration due to disease, environmental changes, age or drug [or diet] interactions. Drug monitoring has also been useful in identifying owner noncompliance as a cause of therapeutic failure or adverse reactions.
Drugs for which TDM is most useful are characterized by one or more of the following: 1) serious toxicity coupled with a poorly defined or difficult to detect clinical endpoint (eg, antibimicrobials, anticonvulsants and cyclosporine); 2) a steep dose-response curve for which a small increase in dose can result in a marked increase in desired or undesired response (eg, theophylline; [TPH], or phenobarbital [PB] in cats); 3) a narrow therapeutic range (eg, digoxin); 4) marked inter-individual pharmacokinetic variability which increases the variability in the relationship between dose and PDC (eg, PB); 5) non-linear pharmacokinetics which may lead to rapid accumulation of drugs to toxic concentrations (eg, phenytoin or, in cats, PB); and an unexpected toxicity due to drug interactions (eg, enrofloxacin induced TPH toxicity or chloramphenicol or clorazepate induced PB toxicity). In addition, TDM is indicated when a drug is used chronically, and thus is more likely to induce toxicity or changes in pharmacokinetics (ie, anticonvulsants), or in life-threatening situations in which a timely response is
74
critical to the patient (eg, epilepsy or bacterial sepsis). Drugs for which TDM might not be indicated include those characterized by a wide therapeutic index which are seldom toxic even if PDC are higher than recommended, or those for which response can be easily monitored by clinical signs.
Not all drugs can be monitored by TDM; certain criteria must be met. Patient response to the drug must correlate with (ie, parallel) PDC. Drugs whose metabolites (eg, diazepam) or for which one of two enantiomers comprise a large proportion of the desired pharmacologic response cannot be as effectively monitored by measuring the parent drug. Rather, all active metabolites and/or the parent drug should be measured. For cyclosporine (CsA), for which parent and some metabolites are active, HPLC measures only the parent whereas immunoassays measure parent and some metabolites. For many drugs, recommended therapeutic ranges in animals have been extrapolated from those determined in humans, but care must be taken for this approach (eg, bromide and procainamide). The drug must be detectable in a relatively small serum sample size, and analytical methods must be available to rapidly and accurately detect the drug in plasma. Cost of the analytical method must be reasonable.
Implementation and response to TDM requires an understanding of the relationships between PDC, interval (T) and drug elimination half-life [t½]. In general, TDM should not be implemented until PDC have reached steady state in the patient. Steady-state PDC occur at the point when drug input and drug elimination (ie, distribution, metabolism and/or excretion) are equilibrated. Although PDC change to some degree during the dosing interval, they remain constant between intervals at steady-state (note that “steady-state is not actually reached with drugs whose half-life [ t½] is substantially shorter than the dosing interval). With multiple drug dosing at the same regimen, PDC will reach 50, 75 and 87.5% of steady-state concentration at one, two or three half-lives, respectively (and so on) regardless of the drug. The same time period (ie, 3-5 drug half-lives) must elapse prior to monitoring if any portion of the original dosing range (ie, dose, frequency or route) is changed. For drugs with a long t½, compared to the dosing interval, drug accumulation can be very dramatic (ie, the drug concentrations following the first dose (PDCfirst ) are much lower than drug concentrations at steady state (PDCss). The dosing regimen of such drugs is designed such that drug concentrations will be in the therapeutic range, but only when steady state concentrations have been achieved. The amount that the drug accumulates depends on how much shorter the interval is compared to the t½ (ratio of T: t½). For drugs characterized by a long t½, TDM can be implemented by measuring concentrations at approximately one drug t½ at which time PDC will be approximately 50% of PDCss. A third alternative to proactive monitoring is available for patients for whom steady-state concentrations must be reached immediately. A loading dose can be administered to rapidly achieve therapeutic PDC. After a loading dose is administered, the maintenance dose should be “just right” to maintain PDC achieved after loading. If not, a problem may not become obvious until steady-state occurs (ie, 3 to 5 t½; for bromide, this would be 3 months). However, monitoring can be used to pro-actively evaluate the proper maintenance dose. When using a loading dose, TDM might be performed three times. Using bromide as an example, the first time is after oral absorption of the last dose of the loading dose is complete to establish a baseline (eg, day 6). The second time would be one drug t½ later (eg, 21 days), to assure that the maintenance dose is able to maintain concentrations achieved by loading. One drug t½ later is recommended because most of the change in drug concentrations that will occur if the maintenance dose is not correct will be present at this time. If the second sample (collected at one drug t½) does not approximate the first (collected immediately after the load), the maintenance dose can be modified at this time rather than waiting for steady state and the risk of therapeutic failure or toxicity. In general, monitoring of a drug
75
with a long half-life requires only one sample. Generally, for consistency’s sake, we suggest collection of a trough (before the next dose).
Many drugs are characterized by half-lives that are much shorter than the dosing interval. For these drugs, no to little accumulation occurs, the concept of "steady-state" is perhaps irrelevant, and response can be evaluated with the first dose (or as soon as the disease has had time to respond). The amount PDC declines during a dosing interval, that is, the fluctuation between Cmax/Cmin) depends, again on the relationship between t½ and interval. If the interval is 1, 2, 3, or 4 times the t½, PDC will decrease 50, 75 and 87.5%, respectively during the dosing interval . This fluctuation may be unacceptable (eg, antiepilpetics, some cardiac drugs, potentially cyclosporine) or acceptable (eg, aminoglycoside drugs which act irreversibly). Detection of this fluctuation will require collection of both a peak and trough sample. The peak PDC (Cmax ) is the maximum concentration achieved after a dose is administered and presumably it should not exceed the recommended Cmax if the drug is not safe. Timing of peak sample collection can be difficult to predict; ideally, absorption and distribution should be complete. The route of drug administration can influence the time at which peak PDC occur, which will vary among drugs. For orally administered drugs, absorption is slower (1-2 hours) and distribution is often complete by the time peak PDC have been achieved. However, the absorption rate can vary widely due to factors such as product preparation, the effect of food or patient variability. Because food can slow the absorption of many drugs, fasting is generally indicated (if safe) prior to therapeutic drug monitoring; however exceptions are noted for some drugss (ie, imadazole antifungals). Generally, peak PDC occur 2-4 hours after oral administration. Some drugs are simply absorbed more slowly than others (eg, PB) and the time of peak PDC sample collection is longer (eg, 2 to 5 hours for PB). For drugs administered intravenously, absorption is not a concern but distribution is. For some IM and SC administrations, absorption occurs rapidly (ie, 30-60 minutes), but, again, drug distribution may take longer. Thus, PDC generally are measured 1-2 hours after administration after parenteral drug administration. Exceptions must be made for drugs, such as digoxin, for which distribution may take 6-8 hours. Samples should not be collected for these drugs until distribution is complete (Table 1).
Collection of peak and trough sample is particularly important for drugs characterized by a narrow therapeutic range and a short half-life. For such drugs, calculating the t½ might be useful for determined an appropriate dosing interval, although both a peak and trough sample should be collected (t½ =0.693/
kel, where kel = LN(C1/C2]/t2-t1, where C and t are the concentration and time point of the 1st (peak)
and 2nd (trough) sample, respectively (Table 1). This can be easily calculated using Microsoft Excel). In contrast to drugs with a short t½, peak and trough concentrations will not differ substantially for drugs whose t½ is much longer than the dosing interval (eg, bromide, and for some patients, PB) and a single sample is generally sufficient for such drugs. Single samples might also be indicated for slow release products (eg, TPH) since constant drug absorption mitigates a detectable difference between peak and trough concentrations. If the question to be answered by TDM is one of toxicity, a single peak sample (eg, digoxin or PB), or trough sample (AMG) may answer the question; if efficacy, a single trough sample, for example for antiepileptics. The impact of drug interactions (eg, induction [eg PB] or inhibition [eg, cyclosporine and ketoconazole]), or disease [eg, cardiac disease an beta blockers or digoxin] on drug clearance may cause a drug to shift from a short half-life to a long half-life or vice versa. For example, we have measured half-lives as short as 12 hrs for PB and 9 hrs for digoxin, or as long as 150 hrs for cyclosporine. For such drugs, a prudent approach would be monitoring at baseline
76
and then at proposed steady-state once the second drug has begun, or the disease changes. Peak and trough samples might be collected before and after the change has been implemented such that time to steady-state might actually be predicted based on half-life (eg, if ketoconazole is added to cyclosporine). Peak and trough samples might be collected in any patient that is not responding well to therapy with any drug which may have a short t½ compared to the dosing interval. For example, peak and trough digoxin should be collected when disease is stable and decompensates, and should be considered when drug therapy is changed, particularly if the patient responds: as renal clearance changes, so will digoxin concentrations. If a kinetic profile of a patient is the reason for TDM, the two samples preferably are collected at the peak and trough times unless the interval is so long that drug may not be detectable at the trough time (ie, AMG administered at 12 or 24 hour dosing intervals). The most accurate kinetic information is generated from patients receiving an IV dose since the volume of distribution can be estimated along with drug elimination t½. For oral doses, only the rate of elimination and drug t½ can be obtained.
We have used monitoring of amikacin as a means of monitoring the impact of aminoglycoside therapy on renal function. (See Table for 3 yr old 40 kg canine cross with deep pyoderma associated with methicillin resistant Staph intermedius whose MIC for amikacin was less than 4 mcg/ml. Rifampin (7.5 mg/kg bid po) was added to therapy and peak and trough amikacin concentrations were measured sequentially across time after IV administration such that clearance could be calculated (amikacin dosed at 15 mg/kg IV once daily).
The minimum information necessary for interpretation of PDCs includes the following: 1) The total daily dose of drug which will be correlated with the patient's measured PDC. 2) Time intervals of drug administration are particularly important for drugs with short half-lives (eg, AMG). Provision of this information assures the clinical pharmacologist that blood samples contain the actual trough and/or peak drug concentrations. From this data, a drug t½ can be calculated and a proper dosing interval can be determined. 3) The patient's clinical status is important because both acute and chronic diseases can dramatically alter drug disposition patterns. This is particularly true for patients with renal, liver or cardiac disease. If this information is lacking, disease-induced changes in drug disposition cannot be distinguished from other causes such as non-compliance or drug interactions. 4) Concurrently administered drugs may alter drug disposition patterns and thus contribute to individual differences in drug disposition. Frequency, dose, amount and the actual times of all drugs given to the patient must be known in order to recognize or predict potential drug interactions. 5) Physiologic characteristics such as patient species, breed and age are often important to the interpretation of PDC because known or predictable differences they may induce drug disposition, or because of known differences in pharmacodynamic responses. Weight must be provided in order to determine Vd. 6) The reason for TDM should be given, ie, has the patient failed therapy or is the patient exhibiting signs of toxicity?
Once results are received, either the dose or interval of a drug might be modified (or if all is well, left alone) If patient PDC is to high or low, and particularly if the t½ is long, then the dose can be change in proportion to the desired change in PDC. Thus, if the PB is 20 µg/ml and the target is 25 µg/ml, then the old dose should be increased (or decreased) by 25-20/20 or 25%. This approach can be repeated until the maximum (or minimum) end of the therapeutic range is reached. If the t½ is short, decreasing the dosing interval may be more cost effective. Note that for each t½ to be added to the dose interval, the dose must be doubled (to add 2 t½, the dose must be quadrupled, for 3- t½, the dose must be increased 8 fold, etc).
77
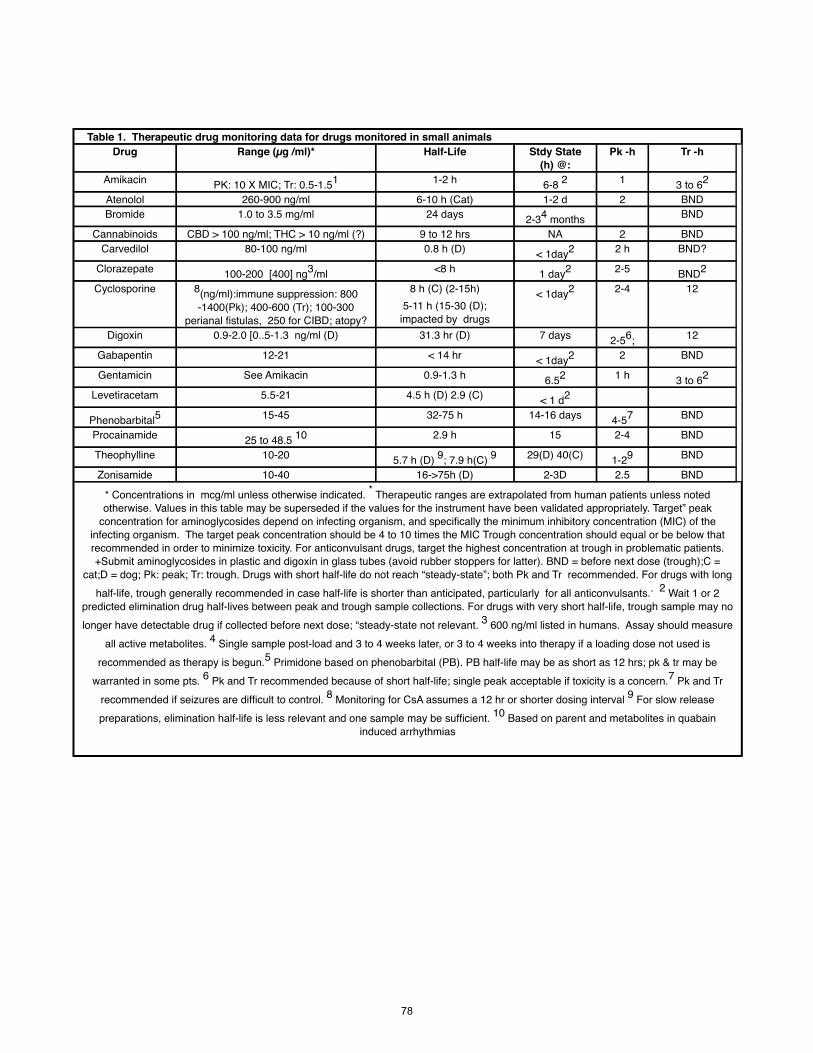
Table 1. Therapeutic drug monitoring data for drugs monitored in small animalsDrug Range (µg /ml)* Half-Life Stdy State
(h) @:Pk -h Tr -h
Amikacin PK: 10 X MIC; Tr: 0.5-1.51 1-2 h 6-8 2 1 3 to 62
Atenolol 260-900 ng/ml 6-10 h (Cat) 1-2 d 2 BNDBromide 1.0 to 3.5 mg/ml 24 days 2-34 months BND
Cannabinoids CBD > 100 ng/ml; THC > 10 ng/ml (?) 9 to 12 hrs NA 2 BNDCarvedilol 80-100 ng/ml 0.8 h (D) < 1day2 2 h BND?
Clorazepate 100-200 [400] ng3/ml <8 h 1 day2 2-5 BND2
Cyclosporine 8(ng/ml):immune suppression: 800 -1400(Pk); 400-600 (Tr); 100-300
perianal fistulas, 250 for CIBD; atopy?
8 h (C) (2-15h) 5-11 h (15-30 (D);
impacted by drugs
< 1day2 2-4 12
Digoxin 0.9-2.0 [0..5-1.3 ng/ml (D) 31.3 hr (D) 7 days 2-56; 12
Gabapentin 12-21 < 14 hr < 1day2 2 BND
Gentamicin See Amikacin 0.9-1.3 h 6.52 1 h 3 to 62
Levetiracetam 5.5-21 4.5 h (D) 2.9 (C) < 1 d2
Phenobarbital5 15-45 32-75 h 14-16 days 4-57 BND
Procainamide 25 to 48.5 10 2.9 h 15 2-4 BND
Theophylline 10-20 5.7 h (D) 9; 7.9 h(C) 9 29(D) 40(C) 1-29 BND
Zonisamide 10-40 16->75h (D) 2-3D 2.5 BND
* Concentrations in mcg/ml unless otherwise indicated. * Therapeutic ranges are extrapolated from human patients unless noted otherwise. Values in this table may be superseded if the values for the instrument have been validated appropriately. Target” peak
concentration for aminoglycosides depend on infecting organism, and specifically the minimum inhibitory concentration (MIC) of the infecting organism. The target peak concentration should be 4 to 10 times the MIC Trough concentration should equal or be below that recommended in order to minimize toxicity. For anticonvulsant drugs, target the highest concentration at trough in problematic patients. +Submit aminoglycosides in plastic and digoxin in glass tubes (avoid rubber stoppers for latter). BND = before next dose (trough);C =
cat;D = dog; Pk: peak; Tr: trough. Drugs with short half-life do not reach “steady-state”; both Pk and Tr recommended. For drugs with long half-life, trough generally recommended in case half-life is shorter than anticipated, particularly for all anticonvulsants.. 2 Wait 1 or 2
predicted elimination drug half-lives between peak and trough sample collections. For drugs with very short half-life, trough sample may no longer have detectable drug if collected before next dose; “steady-state not relevant. 3 600 ng/ml listed in humans. Assay should measure
all active metabolites. 4 Single sample post-load and 3 to 4 weeks later, or 3 to 4 weeks into therapy if a loading dose not used is recommended as therapy is begun.5 Primidone based on phenobarbital (PB). PB half-life may be as short as 12 hrs; pk & tr may be
warranted in some pts. 6 Pk and Tr recommended because of short half-life; single peak acceptable if toxicity is a concern.7 Pk and Tr recommended if seizures are difficult to control. 8 Monitoring for CsA assumes a 12 hr or shorter dosing interval 9 For slow release preparations, elimination half-life is less relevant and one sample may be sufficient. 10 Based on parent and metabolites in quabain
induced arrhythmias
78
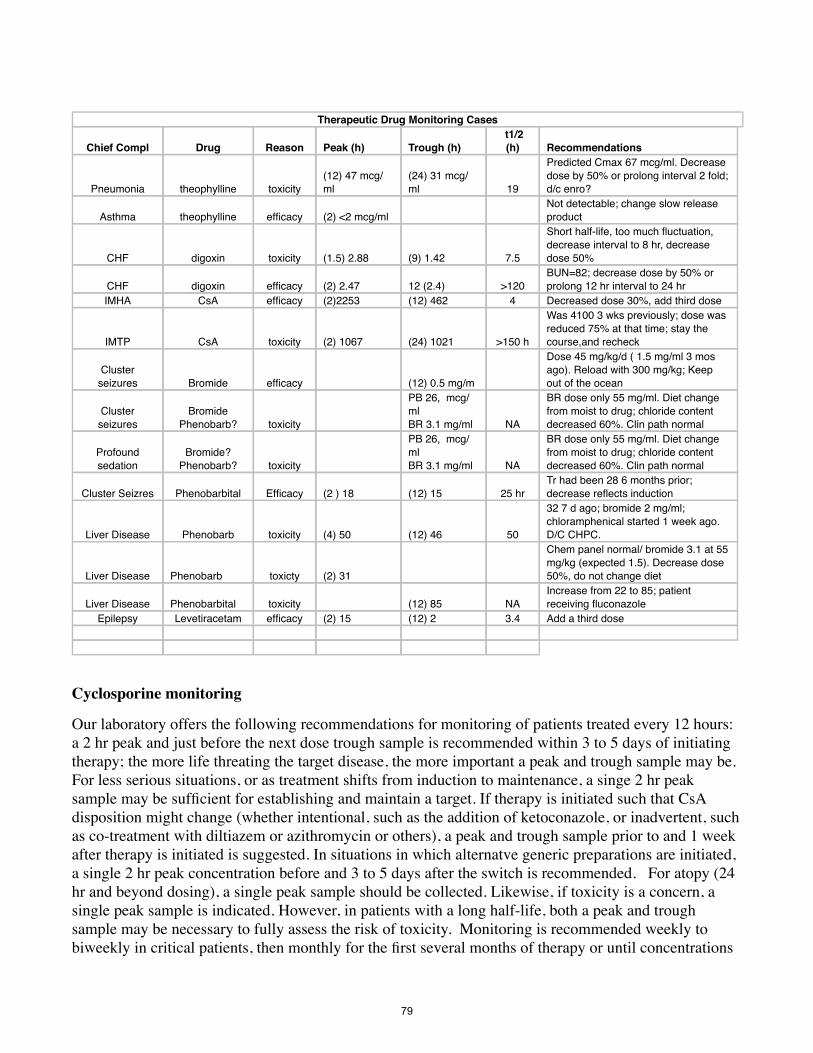
Therapeutic Drug Monitoring Cases
Chief Compl Drug Reason Peak (h) Trough (h) t1/2 (h) Recommendations
Pneumonia theophylline toxicity(12) 47 mcg/ml
(24) 31 mcg/ml 19
Predicted Cmax 67 mcg/ml. Decrease dose by 50% or prolong interval 2 fold; d/c enro?
Asthma theophylline efficacy (2) <2 mcg/ml Not detectable; change slow release product
CHF digoxin toxicity (1.5) 2.88 (9) 1.42 7.5
Short half-life, too much fluctuation, decrease interval to 8 hr, decrease dose 50%
CHF digoxin efficacy (2) 2.47 12 (2.4) >120BUN=82; decrease dose by 50% or prolong 12 hr interval to 24 hr
IMHA CsA efficacy (2)2253 (12) 462 4 Decreased dose 30%, add third dose
IMTP CsA toxicity (2) 1067 (24) 1021 >150 h
Was 4100 3 wks previously; dose was reduced 75% at that time; stay the course,and recheck
Cluster seizures Bromide efficacy (12) 0.5 mg/m
Dose 45 mg/kg/d ( 1.5 mg/ml 3 mos ago). Reload with 300 mg/kg; Keep out of the ocean
Cluster seizures
Bromide Phenobarb? toxicity
PB 26, mcg/mlBR 3.1 mg/ml NA
BR dose only 55 mg/ml. Diet change from moist to drug; chloride content decreased 60%. Clin path normal
Profound sedation
Bromide? Phenobarb? toxicity
PB 26, mcg/mlBR 3.1 mg/ml NA
BR dose only 55 mg/ml. Diet change from moist to drug; chloride content decreased 60%. Clin path normal
Cluster Seizres Phenobarbital Efficacy (2 ) 18 (12) 15 25 hrTr had been 28 6 months prior; decrease reflects induction
Liver Disease Phenobarb toxicity (4) 50 (12) 46 50
32 7 d ago; bromide 2 mg/ml; chloramphenical started 1 week ago. D/C CHPC.
Liver Disease Phenobarb toxicty (2) 31
Chem panel normal/ bromide 3.1 at 55 mg/kg (expected 1.5). Decrease dose 50%, do not change diet
Liver Disease Phenobarbital toxicity (12) 85 NAIncrease from 22 to 85; patient receiving fluconazole
Epilepsy Levetiracetam efficacy (2) 15 (12) 2 3.4 Add a third dose
Cyclosporine monitoring
Our laboratory offers the following recommendations for monitoring of patients treated every 12 hours: a 2 hr peak and just before the next dose trough sample is recommended within 3 to 5 days of initiating therapy; the more life threating the target disease, the more important a peak and trough sample may be. For less serious situations, or as treatment shifts from induction to maintenance, a singe 2 hr peak sample may be sufficient for establishing and maintain a target. If therapy is initiated such that CsA disposition might change (whether intentional, such as the addition of ketoconazole, or inadvertent, such as co-treatment with diltiazem or azithromycin or others), a peak and trough sample prior to and 1 week after therapy is initiated is suggested. In situations in which alternatve generic preparations are initiated, a single 2 hr peak concentration before and 3 to 5 days after the switch is recommended. For atopy (24 hr and beyond dosing), a single peak sample should be collected. Likewise, if toxicity is a concern, a single peak sample is indicated. However, in patients with a long half-life, both a peak and trough sample may be necessary to fully assess the risk of toxicity. Monitoring is recommended weekly to biweekly in critical patients, then monthly for the first several months of therapy or until concentrations
79
are stable. For long term maintenance, the frequency of samply may vary with the stability of the patient but should range from 3 to 6 months. Target concentrations vary with the condition but generally, based on a 12 hr dosing interval (using FPIA), a peak concentration of 800 to 1400 ng/ml and a trough concentration of 400 to 600 ng/ml (monoclonal based assay) is recommended for immune mediated diseases. For renal transplantation, trough concentrations of 750 ng/ml are suggested for the first month and 350 to 400 ng/ml, thereafter. For chronic allergic inflammatory disorders, lower concentrations are recommended: 250 ng/ml trough concentrations for chronic inflammatory bowel disorders, and for perianal fistulae, 12 hour trough concentrations at 100 to 600 ng/ml (the higher for induction, the lower for maintenance).
Anticonvulsant therapeutic drug monitoring
Phenobarbital Generally, a single trough sample should be sufficient for TDM. However, if induction of drug-metabolizing enzymes has occurred, the elimination half-life may be sufficiently short to allow excessive fluctuation in PDC during the dosing interval. This short half-life can be detected only if both peak and trough samples are measured. In a phenobarbital-naïve dog, or when phenobarbital doses are changed, baseline samples should be determined at steady state, 9 to 14 days after beginning therapy. A recheck trough sample 1 to 3 months later would be prudent to detect induction. Many of our patients respond to phenobarbital at concentrations below the minimum therapeutic range of 15 g/mL, which suggests that a lower therapeutic range may be indicated in dogs.
BromideBecause the elimination half-life of bromide is so long, manipulating the dose before steady state is reached may be necessary for some patients. Collection of a sample at one half-life after the start of therapy (i.e., 3-4 weeks) can be performed to proactively assess the dose; doubling the 3 weeks concentration should approximate the steady state concentration. Baseline should be established at 2.5 to 3 months. If the patient is loaded, a sample should be collected the day after loading is complete, and then at one half-life. The former sample is indicated to determine what the loading dose achieved and the latter to ensure that the maintenance dose is maintaining what the loading dose has achieved; the two samples should be within 15% of each other. If not, the maintenance dose can be adjusted proportionately. Note that a 3-week sample in a patient that received a loading dose is minimally useful without the post-load monitoring sample for comparison: concentrations may increase or decrease depending on the accuracy of the maintenance dosed. In all patients, regardless of the method of dosing, a final sample should be collected at steady state to establish baseline. Finally, if the maintenance dose is altered, a concentration might be measured at one half-life to proactively assess the impact of the change, but the minimum re-assessment should occur at the new steady state (i.e., 2.5 to 3 months after the dose change). Additionally, bromide might also be checked before and after any change in diet or medication that impacts chloride excretion has occurred.
ZonisamideThe half-life of zonisamide is generally longer than 24 hours; therefore concentrations should not fluctuate sufficiently during a 12-hour dosing interval to routinely justify a peak and trough sample. Because toxicity is not likely to be as great a concern as therapeutic failure, a trough sample is recommended for routine monitoring. In problematic patients a peak and a trough may be justified to rule out a short half-life as a contributing cause of difficult control. Currently, zonisamide is among the
80

drugs for which the maximum therapeutic range, which has been established in humans, can be exceeded with minimal adverse effects in dogs.
Levetiracetam The half-life of levetiracetam (standard release) can be as short as 1 to 2 hours. However, the half-life can be also longer than 8 to 10 hours; longer half-lives should be anticipated if the slow release preparation is used. Because the duration of the half-life is not known, peak and trough samples are recommended at the beginning of therapy to determine the half-life in patients. Control is much more likely to be accomplished with an 8-hour dosing interval in a patient with a longer half-life. Once the half-life is established, a trough sample is recommended if only single samples are to be collected. A mid-sample concentration has little to offer, particularly given that drug concentrations may drop 50% or more from mid-interval concentrations. Thus it is prudent to identify the lowest concentration possible during the interval. The recommended therapeutic range should be targeted by trough, rather than peak, concentration. Note that in a drug with a very short half-life (e.g., 2 hours), peak concentrations in a patient may be as much as 8 times as high as trough concentrations. Levetiracetam is sufficiently safe that a high peak concentration is likely to be tolerated. Because drug concentrations do not accumulate with drugs administered at an interval substantially longer than the half-life, steady state does not occur. Therefore levetiracetam (or another drug with a short half-life) might be monitored in the first 3 to 5 days of therapy. Waiting one seizure interval to ensure that seizures are adequately controlled is reasonable. The approach for monitoring levetiracetam can be followed with other anticonvulsants associated with a short half-life compared to the dosing interval (e.g., gabapentin), unless the drugs is potentially toxic. In such situations, monitoring peak and trough concentrations routinely may be prudent.
GabapentinThe half-life of gabapentin also is short suggesting that both peak and trough samples be collected.
Recommendations for collection are similar to those for levetiracetam.
81
Understanding compounding medications
By Michael A. Azzarello MBA, BS, LVT, CVT Freehold, NJ Introduction With recent attempts by the Federal Drug Administration to restrict aspects of veterinary compounding medications, compounding preparations have received increased attention over the last year. As veterinarians and veterinary technicians, we understand there are many FDA-approved medications available to use when treating a patient. However, what about when we come across a medication that is on backorder or no longer manufactured. Additionally, some medications aren’t available in the milligram that we may need or a flavor your patient may want to take. We all know how hard it can be to pill a cat, compounding improves the chance of compliance sometimes reducing the number of pills, tablets, capsules etc. a patient may have to take. It is these times that we may look to compounded medications. History of Compounded Medication: It is difficult to pinpoint the ancestries of compounding as the process of combining different agents began in a basic form before the term compounding ever existed. However, the art of compounding medications can be linked to the origins of pharmacy itself and the first documented chemical processes can be traced as far back as the time of the Egyptians (Pharmacy Compounding - History and Evolution). Historically, compounding has been an integral part of the pharmaceutical process; in fact, there was a time when all medicines were compounded. But since the advent of high-volume pharmaceutical manufacturing, most people today are familiar only with manufactured medicines. The result was a decline in the need or reimbursement for compounding, and large chain pharmacies of today became the new normal. As long as animals continue to have unique needs for custom medications, or medications become commercially unavailable, there always will be a need for compounding. Guidelines and Agencies That Regulate Compounding: United States Pharmacopeia Chapters
General Compounding (Non-Sterile)-USP795 United States Pharmacopeia develops standards for compounding nonsterile medications to help ensure patient benefit and reduce risks such as contamination, infection, or incorrect dosing. (USP General Chapter Pharmaceutical Compounding – Nonsterile Preparations)
Sterile Compounding- USP 797
United States Pharmacopeia develops standards for preparing compounded sterile medications to help ensure patient benefit and reduce risks such as
82
contamination, infection, or incorrect dosing. (USP General Chapter Pharmaceutical Compounding –Sterile Preparations)
State Board of Pharmacies
Every state has a pharmacy board or similar regulatory authority. Any practitioner who uses their own compounded preparations or prescribes compounded preparations in their practice should familiarize themselves with the applicable state pharmacy requirements.
DEA
Monitor compounding of controlled substances National Association of Board of Pharmacies
Founded in 1904, the National Association of Boards of Pharmacy (NABP) aims to ensure the public’s health and safety through its pharmacist license transfer and pharmacist competence assessment programs, as well as through its Digital Pharmacy, formerly known as Verified Internet Pharmacy Practice Sites® (VIPPS®), Drug Distributor formerly known as Verified-Accredited Wholesale Distributor® (VAWD®), and DMEPOS Pharmacy accreditation programs. (About: National Association of Board of Pharmacies 2020)
Pharmacy Compounding Accreditation Board (PCAB)
PCAB is a nonprofit organization that provides a voluntary accreditation program for compounding pharmacies nationwide. PCAB assesses pharmacies that compound medications whether in the retail, hospital, mail order, or closed-door setting. This includes the combining, mixing, or altering of drug ingredients to create a medication pursuant to a prescription order for an individually identified patient. An extensive on-site survey conducted by an independent expert and annual verification ensures compliance with the non-sterile and sterile pharmacy compounding process defined by USP <795> and USP <797>. (PCAB Compounding Pharmacy Accreditation) PCAB assesses those pharmacies that voluntarily apply, and awards the PCAB Seal of Accreditation to those pharmacies that accept the PCAB requirements, meet the criteria, and comply with the Rules and Terms of the PCAB program, including adherence to the PCAB Standards.
Does the FDA Regulate Veterinary Compounding?
The Federal Food, Drug, and Cosmetic Act (FD&C Act) permits compounding of animal drugs when the source of the active ingredient is a finished FDA-approved drug and not a bulk drug substance.
83
Animal drugs compounded from bulk drug substances are not FDA-approved and have not been reviewed by the FDA for evidence that they are safe, effective, properly manufactured, accurately labeled, and adequately packaged. In 2015 and again in 2018, the FDA drafted guidance (GFI 256) to state their enforcement priorities related to drugs compounded from bulk drug substance and to clarify for veterinarians, pharmacists, and others concerned with treating sick animals the circumstances in which they do not intend to take action against drugs compounded from bulk drug substance. (video-FDA Drafts Guidance To Restrict Type of Pet Medication https://www.mymedsmatter.com/video-fda-drafts-guidance-restrict-type-pet-medication)
Who Can Legally Compound Veterinary Preparations?
• A licensed veterinarian within the context of a VCPR. • A licensed pharmacist on the order (prescription) of a licensed veterinarian.
Liability Using Compounded Medications
The AVMA has guidelines for use of compounded preparations that can be obtained through their website. All in all, though the liability falls on the prescribing veterinarian and thus you should always be sure to be using a reputable pharmacy. Clients should always be made of the risks associated with the use of compounded preparations and all communication should be documented within the patient’s record.
Choosing a Compounding Pharmacy
Video- https://www.yahoo.com/entertainment/checking-compounding-pharmacy-making-drugs-100128144.html
Much like shopping for other important professional services and products, references from respected colleagues should be considered. You can also check with your state pharmacy board to see if any complaints have been lodged against a particular pharmacy. The FDA has a Web site where any warning letters to a particular pharmacy or manufacturer are posted (www.fda.gov/ICECI/EnforcementActions/WarningLetters/default.htm) and can be reviewed.
• Is your pharmacy accredited by PCAB? • Is your pharmacy licensed with my state board of pharmacy to fill prescriptions? • How long will it take for you to produce the preparation I need? • How does your pharmacy determine beyond-use dating for your compounded
preparations? • Is there a process for preparations recalls? • How does the pharmacy record adverse events? • Does the pharmacy have a quality assurance program?
84
• Where is the pharmacy obtaining its bulk drug substances; is it FDA approved? • What type of sterility testing completed?
When to Consider Compounding Veterinarians often prescribe compounded medications to help owners with compliance. When a patient cannot utilize the medication in its commercial form, a pharmacist can prepare the medication in a topical, liquid, or small size for that specific patient to easily take. Veterinary patients could have unique allergies or toxicities to commercially available medications. Sometimes this has to do with the preservatives, dyes, or binders that the medication produced with. As we can imagine, manufacturers do not have the ability to make a medication that is conducive to every size of animal we care for. There is no one size fits all, as we have in some of our over the counter medications you are commonly familiar with. Treatment in our profession sometimes requires a tailored dosage-strength for patients with unique needs. Flavoring advancements have enhanced patient compliance drastically over the years. We now have the ability to tailor a medication to the flavor that would be more compatible with food that a patient would normally eat. This allows owners to have an easier time administering the medication, sometimes allowing it to be offered as a treat. Finally, as our patient’s age, owners can become responsible for giving multiple medications on a daily period. This obviously could become problematic if owners aren’t home or causing stress by having to capture the pet each time the pet needs medication. Pharmacists can combine several medications to enhance the chances the patient will take the proper medications daily. Closing Remarks/Summary: Veterinarians and veterinary technicians should always try and utilize a manufactured drug whenever possible. However, our review of pharmaceutical compounding demonstrates alternatives when there may be a patient that may require an alteration of the manufactured product. We also know that some medications will go on backorder and to continue medication continuity for our patients we turn to a compounded formulation. Veterinary technicians need to be on the frontline of deciding on a compounding pharmacy that veterinarians can trust and the liability and consequences of picking a pharmacy that may not have a quality assurance program in place. In the end, it is the patient's health and safety that needs to be kept in the forefront when deciding to use a compounding medication. References
85
About: National Association of Board of Pharmacies. (2020, May 01). Retrieved September 15, 2020, from https://nabp.pharmacy/about/
February 28: Pharmacy Fun Fact. (n.d.). Retrieved September 24, 2020, from https://www.pharmacytimes.com/news/february-28-pharmacy-fun-fact
Global, R. (2018, December 07). Part 2: To regulate or not to regulate. Retrieved September 24, 2020, from https://medium.com/@rayy.global/part-2-to-regulate-or-not-to-regulate-78957caf5446
NABP. (2020, April 01). Retrieved September 24, 2020, from https://nabp.pharmacy/
PCAB Compounding Pharmacy Accreditation. (n.d.). Retrieved September 15, 2020, from https://www.achc.org/compounding-pharmacy.html
Pharmacy Compounding - History and Evolution. (n.d.). Retrieved September 10, 2020, from https://www.medisca.com/compounding/history-and-evolution
Should You Be Checking Which Compounding Pharmacy Is Making Your Drugs? (2020, September 10). Retrieved September 15, 2020, from https://www.yahoo.com/entertainment/checking-compounding-pharmacy-making-drugs-100128144.html
USP 42 - NF 37 The United States Pharmacopeia and National Formulary 2019 - Shop: Deutscher Apotheker Verlag. (n.d.). Retrieved September 24, 2020, from https://www.deutscher-apotheker-verlag.de/shop/produkt/9783769273304/usp-42-nf-37-the-united-states-pharmacopeia-and-national-formulary-2019
USP General Chapter Pharmaceutical Compounding – Nonsterile Preparations. (n.d.). Retrieved September 15, 2020, from https://www.usp.org/compounding/general-chapter-795
USP General Chapter Pharmaceutical Compounding – Sterile Preparations. (n.d.). Retrieved September 15, 2020, from https://www.usp.org/compounding/general-chapter-797
Video: FDA drafts guidance to restrict type of pet medication. (n.d.). Retrieved September 15, 2020, from https://www.mymedsmatter.com/video-fda-drafts-guidance-restrict-type-pet-medication
86
1
CONTROLLED SUBSTANCES 101: How and Why You Must Comply!
Presented By Jan WoodsPrevious Practice Owner & Co-Founder of Ask Jan For Help!Regulatory and Operational ConsultantEmail: [email protected]: 913-302-4999
Sponsored by Epicur PharmaThis presentation is approved by AAVSB for 3 hours of continuing education credit in jurisdictions that recognize RACE approval
Please note: The governm ent changes laws frequently. As of Novem ber 2020 the inform ation contained in this presentation is current. Rem em ber to check w ith the various governm ental agencies or your attorney for changes that m ay affect yourhospital/clin ic
Prepared Especially for Veterinary Practices A Federal Presentation in 3 Parts-Part 1
© Copyright 2019
12
MY DOGS
2
3
WHO IS JAN WOODS?
• Veterinary Practice Owner
• Hospital Administrator
• Consulted with Attorneys and DVMs who werecited by the DEA
• V.P. of Operations & Development- Human Healthcare
• Industry consultant
• Key Opinion Leader, Zoetis Animal Health
• Nationally Recognized Public Speaker
• Veterinary Practice News Contributor
• Director of Education & Regulatory Affairs, Cubex, LLC
• Regulatory & Operational Consultant at VeterinaryBusiness Advisors
• Co-Founder of Ask Jan For Help, LLC
34
If you have any regulatory or practice management questions, please feel free to contact me anytime:
Jan Woods, Co-Founder of Ask Jan For Help, LLCØ Email: [email protected]Ø Cell/Text: 913-302-4999
Epicur PharmaIf you have any questions for Epicur Pharma Pharma, want to open an account, place an order, or ask questions, please contact:
Ø Branson Bruce: 856-818-8625Ø Sam Newton: 856-242-4705Ø Jon Michailides: 856-816-5781
Ask Jan For Help!
QUESTIONS?
4
5
HOW TO PROTECT YOUR PEOPLE, YOUR PRACTICE AND YOUR PROFIT
ü Learn how to minimize your risk by instituting effective controlled substance systems.
ü Learn what’s really required by the DEA for controlled substance compliance in your practice.
ü Learn how the DEA’s controlled substance regulations affect your practice.
ü Learn why you should follow the DEA’s controlled substance regulations, when you feel that nobody else does.
ü Learn how to effectively and efficiently manage your controlled substances, according to regulations and best practice suggestions.
ü Learn how to make your controlled substance inventories easier and more accurate.
ü Learn about staff and patient theft.ü Learn how to think like an auditor.ü Learn how to minimize your risk.
What Will I Learn Today?
56
SNAP QUIZ
1. Who takes precedence, the State or Federal government, State Pharmacy Board or the Veterinary Board when setting the DEA controlled substancelaws that impact your practice?
2. Are DVMs, RVTs, CVTs & LVTs obligated to follow the same regulations as MDs, DOs, Oral Surgeons, PAs, RNs, etc.?
3. What is a Controlled Substance, What is an OTC? What is a Legend Drug? How Can You Tell The Difference in Your Pharmacy?
4. Can Legend Drugs & Controlled Substances be Returned?
5. Are Prescription Diets Really a Prescription?
6. How much revenue (in dollars) does the average primary care veterinarian lose each year in missed charges- (includes pharmacy and professional treatment charges)?
7. What’s the number one reason why a DEA Agent or government auditor would show up at your clinic/hospital?
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. Copyright 2019
TIME TO TEST YOUR KNOWLEDGE
6
87
7
Can Legend & Controlled Substances Be Returned?
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your practice. Copyright 2019
Due to State and Federal law, prescriptions are NON-returnable items.
Please verify the medications you are picking up before leaving the pharmacy.
We apologize for any inconvenience.
Thank you, Walgreens’ Staff.
Signs Posted at Walgreens’ Pharmacies
78
Client Resources for Prescription Drug Disposal
8
9
üVeterinarians around the country are receiving phone calls claiming to be board inspectors or DEA agents
üCalling about investigation matters
üUsing fake names such as Peter Williams
üDEA will never ask for any form of payment by telephone
Be Aware! DEA Auditor Fraud Calls Are Occurring
910
• Incomplete or Inferior Record Keeping
• Lack of Security
• Failure to Prevent DrugTheft/Diversion
• DEA Registration & Licensing Issues
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic.© Copyright 2019
MOST COMMON VIOLATIONS CITED BY THE DEA
10
11
1. Prescribing outside the scope of practice
2. Failing to maintain required documents
3. Failing to dispose of controlled substancesaccording to regulations
4. Failing to maintain inventory records according to State & Federal regulations
5. Prescribing without a documented establishedVeterinary Client & Patient Relationship
6. Failing to maintain up-to-date registration documentation
1-7 per Dr. M ichael O ’Neil Professor and Vice-Chair Departm ent of Pharm acy
Practice Drug D iversion, Substance Abuse & Pain M anagem ent Consultant
CONTROLLED SUBSTANCE REGULATIONS OFTEN VIOLATED BY
PRACTITIONERS
1112
• “Don’t get caught in the crossfire”.
• “On October 1, 2019, the Drug Enforcement Administration (DEA) released its 2020 fiscal year work plan to its diversion investigators. The plan outlines increased enforcement efforts and administrative resources dedicated to the identification and investigation of prescribers (including veterinarians) that are dispensingdisproportionately large amounts of controlled substances”.
•“Boom—instant audit. And once they’re in, it can be tough getting them out.”
Source: Titan Group, LLC & AAHA NewsStat
Written by Tony McReynolds, Oct 11, 2019
DEA ISSUES NEW MARCHING ORDERS IN THE WAR AGAINST OPIOID ADDICITION
12
88
13
According to the government, Dr. _______, over multiple years of practicing as a veterinarian and while running an active animal hospital, failed to properly inventory, track, and maintain control over controlled substances,including thousands of units of opioids such as fentanyl, hydromorphone, and morphine.
By not properly inventorying, tracking, and maintaining control over the controlled substances, he violated the Controlled Substances Act.
These violations were discovered by DEA investigators during an on-site inspection of Dr. _________ veterinary hospital, which included an audit of his drug control practices.
DEA investigators found CSA violations with respect to all twelve of the twelve controlled substances audited. DEA also found failures to properly destroy controlled substances.
This matter was investigated by the U.S. Drug Enforcement Administration, Diversion Control Division, in conjunction with the United States Attorney’s Office.The statements in this release are only allegations. In entering into a civil settlement, Dr. _______ did not admit to liability, and the agreement indicates that the parties entered into the settlement to avoid the uncertainty and expense of further litigation. Assistant U.S. Attorney Jacob Licht and Deputy Civil Chief Amanda Rocquehandled this matter on behalf of the United States Government.
VETERINARIAN PAYS $226,000 AND SURRENDERS LICENSE TO RESOLVE
ALLEGATIONS THAT HE FAILED TO PROPERLY TRACK AND CONTROL OPIOIDS!
1314
•Do the DVMs working at your hospital or clinic have to have his/her own DEAnumber?
•What About Part Time & Relief Vets?
WHO CAN ADMINISTER, DISPENSE & PRESCRIBE CONTROLLED SUBSTANCES (AKA NARCOTICS)?
Reference: Page 7 of the DEA’s Practitioner’s ManualPlease note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic.. © Copyright 2019
14
15
Ø “Under the CSA, the term “practitioner” is defined as a physician, dentist, veterinarian, scientific investigator,pharmacy, hospital, or other person licensed, registered, or otherwise permitted, by the United States or the jurisdiction in which the practitioner practices or performs research, to distribute, dispense, conduct research with respect to,administer, or use in teaching or chemical analysis, acontrolled substance in the course of professionalpractice or research. EVERY person or entity that handlescontrolled substances MUST be registered with the DEA or beexempt by regulation from registration.”
Ø What does the Federal DEA say about DEA registration?
Ø Exemption! What exemption?
Ø Source: Page 7 of the DEA’s Practitioner’s Manual
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. © Copyright 2019
DEA PRACTITIONER’S MANUAL SAYS:
1516
“Registration Requirements Once a substance is brought within the scope of the CSA, almost any person or organization that handles that substance, except for the end user, becomes subject to a comprehensive system of regulatory requirements. (111) The goal of the regulatory scheme is to create a “closed system” of distribution in which only authorized handlers may distribute controlled substances. (112) Central to the closed system of distribution is the requirement that individuals or entities that work with controlled substances register with DEA.
Exemption! What exemption? Risk, What Risk?
WHAT DOES THE FEDERAL DEA PRACTITIONER’S MANUAL SAY ABOUT A DEA REGISTRATION? Source: The Controlled Substances Act (CSA): A Legal Overview for the 116th Congress October 9, 2019
Please note: The governm ent changes laws frequently. As of Novem ber 2020 the inform ation contained in this presentation is current. Rem em ber to check w ith the various governm ental agencies or your attorney for changes that m ay affect your hospital/clinic. © Copyright 2019
16
17
Exemption? What Exemption? Practitioner’s Use of DEA Number
MANUFACTURERS, DISTRIBUTORS, AND DISPENSERS OF CONTROLLED SUBSTANCES EXCEPTIONS TO REGISTRATION AND FEES Source: §1301.22 Exemption of agents and employees; affiliated practitioners.
(a) “The requirement of registration is waived for any agent or employee of a person who is registered to engage in any group of independent activities, if such agent or employee is acting in the usual course of his/her business or employment”.
(b) “An individual practitioner who is an agent or employee of another practitioner (other than a mid-level practitioner) registered to dispense controlled substances may, when acting in the normal course of business or employment, administer or dispense (other than byissuance of prescription) controlled substances if and to the extent that such individual practitioner is authorized or permitted to do so by the jurisdiction in which he or she practices, under the registration of theemployer or principal practitioner in lieu of being registered him/herself”.
(c) “An individual practitioner who is an agent or employee of a hospital or other institution may, when acting in the normal course of business or employment, administer, dispense, or prescribe controlled substancesunder the registration of the hospital or other institution which isregistered in lieu of being registered him/herself, provided that:
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. © Copyright 2019
1718
(1) Such dispensing, administering or prescribing is done in the usual course of his/her professional practice;
(2) Such individual practitioner is authorized or permitted to do so by the jurisdiction in which he/she is practicing;
(3) The hospital or other institution by whom he/she is employed has verified that the individual practitioner is so permitted to dispense, administer, or prescribe drugs within the jurisdiction;
(4) Such individual practitioner is acting only within the scope of his/her employment in the hospital or institution;”
“(5) The hospital or other institution authorizes the individual practitioner to administer, dispense or prescribe under the hospital registration and designates a specific internal code number for each individual practitioner so authorized. The code number shall consist of numbers, letters, or a combination thereof and shall be a suffix to the institution's DEA registration number, preceded by a hyphen (e.g., APO123456-10 or APO123456-A12); and
(6) A current list of internal codes and the corresponding individual practitioners is kept by the hospital or other institution and is made available at all times to other registrants and law enforcement agencies upon request for the purpose of verifying the authority of the prescribing individual practitioner.” Source: [62 FR 13950, Mar. 24, 1997]
Exemption? What Exemption? Practitioner’s Use of DEA Number
Federal law requires that practitioners maintain a DEA number in order to write prescriptions for controlled substances.
Under federal law, a DEA number is not technically required to write prescriptions for non-controlled medications such as antibiotics.
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. © Copyright 2019
18
89
19
1. Remember the Regulations
2. Is the DEA Registrant DVM out of the practice for lunch, out sick, hasa day off or on vacation?
3. Direct, Immediate & IndirectSupervision
4. Required controlled substance documentation in a Closed System
5. Valid VCPRPlease note: The government changes laws frequently. As of November 2020 the information contained in this presentationis current. Remember to check with the various governmental agencies or your attorney for changes that may affect yourpractice. ©Copyright 2019
Is My Practice At Risk When My Associates Practice Without a DEA Number?
1920
Answer: The Controlled Substances Act requires a separate registration for each principal place of business or professional practice where controlled substances are manufactured, distributed, or dispensed as set forth in 21 U.S.C. § 822(e). The DEA issues a registration based, in part, upon the authority to handle controlled substances granted by the state in which a practitioner practices, as set forth in 21 U.S.C. § 823(f).
Title 21 C.F.R. § 1301.12(a) states, “A separate registration is required for each principal place of business or professional practice at one general physical location where controlled substances are manufactured, distributed, imported, exported, or dispensed by a person.”
Title 21 U.S.C. § 802(10) defines the word “dispense.” The term “dispense” means “to deliver a controlled substance to an ultimate user or research subject by, or pursuant to the lawful order of, a practitioner, including the prescribing and administering of a controlled substance . . .”
DEA has provided a limited exception to this requirement in that practitioners who register at one location in a state, but practice at other locations within the same state, are not required to register with DEA at any other location in that state at which they only prescribe controlled substances. 21 C.F.R. § 1301.12(b)(3). If they maintain supplies of controlled substances, administer, or directly dispense controlled substances at a location, practitioners must register that location. 21 U.S.C. § 823(f).
Check to see if your state requires a separate State DEA number for each location where you practice veterinary medicinePlease note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
Question: What is the DEA’s Policy Concerning Locum Tenens (aka Relief Vets)
20
21
This information is addressed in more detail by DEA in the Final Rule, Clarification of Registration Requirements for Individual Practitioners, which DEA published in the Federal Register on December 1, 2006. Please be aware that practitioners who wish to administer, dispense, or prescribe controlled substances in multiple states have the following options regarding a DEA registration: Practitioners will need to obtain a separate DEA registration in each state where they plan to administer, dispense, or prescribe controlled substances. If the practitioners will be working solely in a hospital/clinic setting, they may use the hospital's DEA registration instead of registering independently with DEA if the hospital agrees and the situation warrants. 21 C.F.R. §1301.22(c).
Alternately, under 21 C.F.R. § 1301.51, practitioners may transfer their existing DEA registration from one state to another as needed by contacting DEA's Registration and Program Support Section at 1-800-882-9539 or request the change online at www.DEAdiversion.usdoj.gov. DEA will investigate each modification of registration as if it was a new application. DEA will issue a new DEA certificate with the appropriate changes if DEA approves the modification.
DEA has provided a limited exception to this requirement in that practitioners who register at one location in a state, but practice at other locations within the same state, are not required to register with DEA at any other location in that state at which they only prescribe controlled substances. 21 CFR § 1301.12(b)(3).
As a first step in the regulatory drafting process, on October 28, 2009, the DEA published in the Federal Register an Advanced Notice of Proposed Rulemaking titled, Registration Requirements for Individual Practitioners operating in a "Locum Tenens" Capacity. Any changes that DEA proposes regarding Locum Tenens will first be published in the Federal Register and will be open to public comment. o:032409, u:091310
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
Question: What is the DEA’s Policy Concerning Locum Tenens (aka Relief Vets)
2122
Ø If you are ordering controlled substances for your use, they must be sent directly to the location where they will be used, and thatlocation must correspond to the address listed on your DEA registration. (i.e. Your Home)
Ø Black Bagging: The DEA does not permit any licensed practitioner to transport controlled substances away from the location to which they were delivered, to another location where a different DEAregistration is in force.
Ø DEA-registered veterinarians are permitted to transport controlled substances to an unregistered location, such as a client’s home or another location where animals need attention, to dispensecontrolled substances on an "as-needed and random basis,” provided the veterinarian does not maintain a principal place of professional business at any of these other locations.
Ø Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
Relief Veterinarian DEA License Clarification
22
23
Per the Controlled Substances Act (CSA), the Drug Enforcement Administration (DEA) was created in 1973. Created the compliance program in 1971
The CSA set forth federal laws around illicit and pharmaceutical controlled substances
The DEA is responsible for ensuring that all controlled substance transactions occur within a CLOSED SYSTEM from manufacturer to the ultimate end user, (aka the pet or pet parent ).
Additional Source: HTTP://www.deadiversion.usdoj.gov/pubs/manuals/pract/index.htmlPlease note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your practice. ©Copyright 2019
Why Do I Have To Follow The Rules? No One Else Does.......Do They?
“Ultimate user” mean a person who lawfully obtained, and who possesses a controlled substance for his own use, or for the use of a member of his household, or for an animal owned by him or a member of his household.” Source: CFR 21 USC 802 (27)
(111) The goal of the regulatory scheme is to create a “closed system” of distribution in which only authorized handlers may distribute controlled substances. (112) Central to the closed system of distribution is the requirementthat individuals or entities that work with controlled substances register withDEA. Source: The Controlled Substances Act (CSA): A Legal Overview for the 116thCongress October 9, 2019
2324
• § 1301.76 Other security controls for practitioners.
• (a) The registrant shall not employ, as an agent or employee who has access to controlled substances, any person who has been convicted of a felony offense relating to controlled substances or who, at any time, had an application for registration with the DEA denied, had a DEA registration revoked or has surrendered a DEA registration for cause.
• For purposes of this subsection, the term ‘‘for cause’’ means a surrender in lieu of, or as a consequence of, any federal or state administrative, civil or criminal action resulting from an investigation of the individual’s handling of controlled substances.
• Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
WHAT DOES THE DEA SAY ABOUT BACKGROUND CHECKS?
24
90
25
CSA § 1301.90 Employee Screening Procedures.
“It is the position of DEA that the obtaining of certain information by non practitioners is vital to fairly assess the likelihood of an employee committing a drug security breach”.
“It is, therefore, assumed that the following questions will become a part of an employer’s comprehensive employee screening program:
Ø Question: Within the past five years, have you been convicted of afelony, or within the past two years, of any misdemeanor or are you presently formally charged with committing a criminal offense? (Do not include any traffic violations, juvenile offenses or military convictions, except by general court-martial.) If the answer is yes, furnish details of conviction, offense, location, date and sentence.
Ø Question: In the past three years, have you ever knowingly used any narcotics, amphetamines or barbiturates, other than those prescribed to you by a physician? If the answer is yes, furnish details”.
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember tocheck with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
WHAT DOES THE DEA SAY ABOUT BACKGROUND CHECKS? (cont.)
2526
q HR Law suggests that you must extend a conditional job offer 1st, before runningbackground check.
qq Tell the applicant during your interview that if they
are offered a job, it will be a conditional, based on findings of the background check. Reiterate this when you are offering a conditional job offer to a potential new hire.
q I use a company called Backgrounds Plus, LLC. And my contact is Brooks Rentrop. Hisphone number is 816-896-3204.
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
HR Law and Background Checks
26
27
• When audited, you may be asked for a copy ofyour controlled substance policy
• Why? It shows the DEA agent who and how yourpractice handles controlled substances from ordering to administration and/or dispensing
• If you would like a policy or have any controlledsubstance question, please feel free to contact me via email at [email protected] or call me at 913-302-4999. I am always happy to help.
Reference: Title 21 Code of Federal Regulations. PART 1304 — RECORDS AND REPORTS OF REGISTRANTS. GENERAL INFORM ATION §1304.04 M aintenance of records and inventories
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with thevariousgovernmental agenciesor your attorney for changes that mayaffect your practice. ©Copyright 2019
CONTROLLED SUBSTANCE POLICIES & PROCEDURES MANUAL
2728
• Schedule II Controlled Substances must be orderedon a 222 Form
• The DEA can be reached by calling 800-882-9539 orthrough the web at ww.deadiversion.usdoj.gov
• 222 forms must be ordered directly from the DEA• Keep a permanent copy of all your order sheets
• You can order your 222 forms and your narcoticson line through the government’s e-commerce program entitled, Controlled Substance Ordering System (CSOS).
THE NEW 222 FORM HAS ARRIVED!When is a Power of Attorney required?
Reference: 21 CFR 21, 1305, 1311, 1305.13 Procedure for filling DEA Forms 222, Sec.1305.12 Procedure for executing DEA Forms 222.
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic.. ©Copyright 2019
ORDERING CONTROLLED SUBSTANCES
28
29
CSOS Controlled Substance Ordering Systemhttps://www.deaecom.gov/applycert.html
2930
POWER OF ATTORNEY FOR 222 FORM & CSOSSOURCE: CODE FEDERAL REGULATIONS TITLE 21SA SEC. 1305.05 POWER OF ATTORNEY.
Power of Attorney for DEA Forms 222 and Electronic Orders______________________________________________________________(Name of registrant)______________________________________________________________(Address of registrant)______________________________________________________________(DEA registration number)I, ____ (name of person granting power), the undersigned, who am authorized to sign the current application for registration of the above-named registrant under the Controlled Substances Act or Controlled Substances Import and Export Act, have made, constituted, and appointed, and by these presents, do make, constitute, and appoint ____ (name of attorney-in-fact), my true andlawful attorney for me in my name, place, and stead, to execute applications for Forms 222 and to sign orders for Schedule I and II controlled substances, whether these orders be on Form 222 or electronic, in accordance with 21 U.S.C. 828 and Part 1305 of Title 21 of the Code of Federal Regulations. I hereby ratify and confirm all that said attorney must lawfully do or cause to be done by virtue hereof.______________________________________________________________(Signature of person granting power)I, ____ (name of attorney-in-fact), hereby affirm that I am the person named herein as attorney-in-fact and that the signature affixed hereto is my signature.(signature of attorney-in-fact)Witnesses:1. ______2. ______Signed and dated on the ____ day of ____, (year), at ____ .
30
91
31
POWER OF ATTORNEY REVOCATION FOR 222 FORM & CSOS FORM
Notice of RevocationThe foregoing power of attorney is hereby revoked by the undersigned, who is authorized to sign the current application for registration of the above-named registrant under the Controlled Substances Act or the Controlled Substances Import and Export Act. Written notice of this revocation has been given to the attorney-in-fact ____ this same day.______________________________________________________________(Signature of person revoking power)Witnesses:1. ______2. ______Signed and dated on the ____ day of ____, (year), at ____.(d) A power of attorney must be executed by the person who signed the most recent application for DEA registration or reregistration; the person to whom the power of attorney is being granted; and twowitnesses.(e) A power of attorney must be revoked by the person who signed the most recent application for DEA registration or reregistration, and two witnesses.
Source: Source: Code Federal Regulations Title 21SA Sec. 1305.05 Power of attorney.
3132
Ø Drugs and other substances considered controlled substancesunder CSA are divided into five classes
Ø Based on accepted medical use and likelihood of causingdependence and abuse
Ø Each class may have different rules around the prescribing,administering or dispensing
Ø States may place controlled substances on different schedulesthan federally recommended. For example, Tramadol, Gabapentin, etc.
Ø Some states have six & seven controlled substance schedules(i.e. legalized recreational marijuana)
Ø You are required to know when legend drugs becomecontrolled substances and vice versa
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic.
©Copyright 2019
SCHEDULES OF CONTROLLED SUBSTANCES
Watch your State regulations to determine if all of your controlled substances are placed in the right schedule
32
33
CONTROLLED SUBSTANCES SHIPMENT ARRIVAL
REGULATIONS & BEST PRACTICE SUGGESTIONS:
The employee unpacking the narcotics should be registered in the front of
your controlled substance log(s)
The employee should notate on the third, (3rd) page of the 222 order
form the following receipt information;
All invoices, packing slips and 222 Forms should be
kept in their corresponding controlled substance logs or in a locked file cabinet
by schedule.
Best Practice: All narcotics should be
immediately entered into your inventory log(s). Reference: 21 CFR 21,
1305, 1311
Time, date, quantity and initials of who received the
drug should be on the invoice and stapled to the
222 or invoice or both if it’s a Schedule II
3334
“Due to staffing limitations, in clinic settings without automated drug storage there is often a single person, typically a nurse, who oversees drug ordering, receives the drugs, and stocks them.
However, separation of ordering, receiving, and stocking duties is considered a best practice to prevent diversion during the procurement process.
Having a separate person witness each stage of procurement or independently verify ordering and stocking records may be a solution if complete separation is not feasible”.
BEST PRACTICE:SEPARATION OF DUTIESBY KIMBERLY NEW, JD, BSN, RN
Ø The person who orders and purchases the drugs should be a different person from the person who receives the controlled substances, checks them in, logs them and adds them to either the closed or open inventory
Ø Ideally this should not be the person who pays your bills Ø Separation of duties for ordering, receiving and paying invoices is
a Best Practice recommendation and one that the DEA is paying close attention to currently
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
34
35
REGULATORY & BEST PRACTICE SUGGESTIONS: Let’s Talk Drug Scheduling and Recordkeeping Compliance
• Follow all Federal, State, Veterinary Board & Pharmacy Board controlled substance regulations
• You should be familiar with all controlled substance regulations. You should never state; “I didn’t know” if audited!• Keep Your Doctor’s In Compliance:
• Controlled Substances should be entered by drug name, size and strength
• Federal law requires Schedule II C.S. logs be kept separate from Schedule III, IV and V controlled substances logs.
• Suggest keeping your Schedule III, IV & V logs separate also to reduce human error
• Includes 222 forms, CSOS forms, etc.
• Keep a new page for each drug by using a numerical & lettering system per bottle/box, per distributor, etc.
• Different manufacturer, different distributor, different strength, different content count, i.e. (100 vs. 500 count bottle), different lot numbers, different expiration numbers– they should be entered on separate page in your logbook.
Sources include CFR Title 21:Sec. 1304.04, Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
Source: CFR, Title 21: §1304.04 Maintenance of records and inventories.
(f) Each registered manufacturer, distributor, importer, exporter, narcotic treatment program and compounder for narcotic treatment program shall maintaininventories and records of controlled substances as follows:
(1) Inventories and records of controlled substances listed in Schedules I and II shall be maintained separately from all of the records of the registrant; and(2) Inventories and records of controlled substances listed in Schedules III, IV, and V shall be maintained either separately from all other records of the registrant or in such formthat the information required is readily retrievable fromthe ordinary business records of the registrant.
(g) Each registered individual practitioner required to keep records and institutional practitioner shall maintain inventories and records of controlled substances in the manner prescribed in paragraph (f) of this section.
3536
BEST PRACTICE & REGULATORY REQUIREMENTS:KEEP LOGS CURRENT, COMPLETE & ACCURATE
• Date• Number assigned to each box/container (each numbered
sequentially).• Drug name, size, strength• Manufacturer AND Distributor• Lot number AND Invoice number• Date dispensed or transferred from closed to open• Transferred from Closed to Open (specific department)• If the reconciliation was taken at the opening of business (am)
or the close of business (pm) • Balance on hand• DVM and employee’s initials
All from Closed PLUS:• Date Dispensed
• Owner’s name & address
• Species• Patient’s name• Drug amount used• Diagnosis (aka Reason)
Enter new, unopened stock here.
Reference: Title 21 CFR 1304.06 &§1304.21Reference: 21 CFR 21, 1305, 1311Reference 16 CCR 2032.3(a)(8,12)
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
36
92
37
CONTROLLED SUBSTANCES 101: How and Why You Must Comply!
Presented By Jan WoodsPrevious Practice Owner & Co-Founder of Ask Jan For Help!Regulatory and Operational ConsultantEmail: [email protected]: 913-302-4999
Sponsored by Epicur PharmaThis presentation is approved by AAVSB for 3 hours of continuing education credit in jurisdictions that recognize RACE approval
Please note: The governm ent changes laws frequently. As of Novem ber 2020 the inform ation contained in this presentation is current. Rem em ber to check w ith the various governm ental agencies or your attorney for changes that m ay affect yourhospital/clin ic
Prepared Especially for Veterinary Practices A Federal Presentation in 3 Parts- Part 2
© Copyright 2019
3738
If you have any regulatory or practice management questions, please feel free to contact me anytime:
Jan Woods, Co-Founder of Ask Jan For Help, LLCØ Email: [email protected]Ø Cell/Text: 913-302-4999
Epicur PharmaIf you have any questions for Epicur Pharma Pharma, want to open an account, place an order, or ask questions, please contact:
Ø Branson Bruce: 856-818-8625Ø Sam Newton: 856-242-4705Ø Jon Michailides: 856-816-5781
Ask Jan For Help!
QUESTIONS?
38
39
SAMPLE DISPENSING &
RECONCILIATION LOGSOBLIGATIONS OF REGISTRANTS - RECORD KEEPING & REPORTING
“THE CSA AND ITS IMPLEMENTING REGULATIONS IMPOSE MULTIPLE RECORDKEEPING AND REPORTING REQUIREMENTS ON REGISTRANTS. REGISTRANTS MUST UNDERTAKE A BIENNIAL INVENTORY OF ALL STOCKS OF CONTROLLED SUBSTANCES THEY HAVE ON HAND, AND MAINTAIN RECORDS OF EACH CONTROLLED SUBSTANCE
THEY MANUFACTURE, RECEIVE, SELL, DELIVER, OR OTHERW ISE DISPOSE OF. (130) IN ADDITION, CONTROLLED SUBSTANCES IN SCHEDULES I AND II MAY ONLY BE DISTRIBUTED PURSUANT TO A W RITTEN ORDER. (131) COPIES OF
EACH ORDER FORM MUST BE TRANSMITTED TO DEA. (132) RECORDS OF ORDERS MUST BE PRESERVED FOR TW O YEARS AND MADE AVAILABLE FOR GOVERNMENT REVIEW UPON REQUEST. (133)” SOURCE: THE CONTROLLED SUBSTANCES ACT
(CSA): A LEGAL OVERVIEW FOR THE 116TH CONGRESS OCTOBER 9, 2019
3940
RECORDING NEWLY RECEIVED CONTROLLED SUBSTANCES
1. Unopened (newly received) controlled substances should be entered into the CLOSED (aka unopened or backstock) section of your logbooks, by SCHEDULE
2. Exception: Immediate Use
3. As unopened narcotics are opened for use they should be transferred from your Closed Reconciliation Logs to your Open Reconciliation Logs
4. You should notate in your log books WHEN you transfer narcotics from unopened to opened
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic.©Copyright 2019
40
41
RECONCILIATION- EXAMPLE- CLOSED CONTAINERSCONTROLLED SUBSTANCE RECONCILIATION LOG – CLOSED CONTAINER
Drug Nam e:______________________________ Size:______________ Strength:_______________ Distributor:______________________
M fg:_______________________________ Bottle or Box #________________________________ Date Received:_______________
DATE INVOICE# BOTTLE or Box # LOT# EXPIRY DATETRANSFERRED FROM UNOPENED TO OPEN BALANCE INITIALS INITIALS
4142
DISPENSING & RECONCILIATION- EXAMPLEDRUG NAME: SIZE: STRENGTH: DATE RCV'D: ____________
BOTTLE # INVOICE# LOT# DATE OPENED:
Date Case Label orOwner & Patient Demographic Information
Diagnosis/ Notes
Initial Balance
Amount Dispensed or Administered
Remaining Balance
Ordered By
AuthorizedStaff Initials Doctor Initials
Controlled Substance Reconciliation Log - OPENED CONTAINER- LIQUID
42
93
43
•For Manual LoggingWeigh Your Controlled Substances
•Ohaus Scout Pro Portable Electronic Balance, 200g Capacity, 0.01g Readability
•DVM Suggestion: “We switched to hublesssyringes for small doses of drugs like as Bup.”
BEST PRACTICE SUGGESTION:
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
4344
Concerned about hub loss? Epicur has an answer! •The accuracy of volumetric measuring is dependent on many factors, including temperature, pressure, andmechanism of extraction
•Measuring by weight eliminates these factors and relies only on product density which results in greateraccuracy in the filling process at Epicur and your office!
•At Epicur all product density is fixed, and all units are weighed throughout the manufacturing process toensure consistent fill volume
•In addition to accuracy of fill volume and consistency between batches, this also allows for a better traceability of controlled substances.
•Solution? Order From Epicur and use a weigh scale!
EPICUR PHARMA
44
45
Drug Name:_________________________ Size: __________________ Strength:__________________________________
Date Received:_______________Manufacturer:_________________Disrtributer:______________Amt Rcv'd:________________
Bottle #:_________ Invoice #: ______________ Lot #:_________ Expiry Date: ________________Date Opened:_______________
Date Client Name & AddressDiagnosis/
Notes
Pills Beginning
Balance
Pills Amount
Used
Pills Balance on
Hand Ordered
By
Authorized Staff
InitialsDoctor Initials
Controlled Substance Reconciliation Log - Opened Container --PILLS
DISPENSING & RECONCILIATION- EXAMPLE
4546
Drug Name:_________________________ Size: __________________ Strength:__________________________________
Date Received:_______________Manufacturer:_________________Distributor:________________Amt Rcv'd:________________
Box #:_________ Invoice #: ______________ Lot #:_________ Expiry Date: ________________Date Opened_______________
Date Client Name & AddressDiagnosis/No
tesPatches On
Hand# of Patches
Used
Balance of Patches
RemainingOrdered
By
Authorized Staff
InitialsDoctor Initials
Controlled Substance Reconciliation Log - Opened Container --- PATCHES
DISPENSING & RECONCILIATION- EXAMPLE
46
47
As you reconcile your controlled substance reconciliation logs, you may discover a discrepancy!
If a discrepancy occurs, it should be entered on the Controlled Substance Discrepancy Log- OR- add a column to your controlled substance logs showing the discrepancy.
DISCREPANCY LOG
Reference: Title 21 CFR §1301.74 & 1301.76
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic.©Copyright 2019
4748
DISCREPANCY LOG EXAMPLEControlled Substance Discrepancy Log
Year
InventoryDate Item Discrepanc
y
Repeated loss ofsame substance or
same type of substance?
Potential for association with
individual or activity?
(List Activity)
Pattern of loss(Type of substance or association with
individual or activity)?
Insignificant (I) or
Reported to DEA ( R )
Review completed (Initial & Date)
48
94
49
1. Controlled Substances that are drawn up and not used dueto a change in the patient’s condition, or treatment change should be entered in your Controlled Substance Open Reconciliation Log as wasted and also entered into your Administration Waste Log.
2. -OR- have a separate column in your daily controlled substance reconciliation logs showing the waste.
3. If you have a separate administration waste log, it shouldcontain the following information:
Reference: Title 21 CFR §1301.76 other security controls for practitioners Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
ADMINISTRATION WASTE LOG
4950
ADMINISTRATION WASTE LOG EXAMPLE
CONTROLLED SUBSTANCE ADMINISTRATION WASTE LOG
Page #________________ Year____________
DATE Client Nam e Patient Nam e Address Drug Nam e, Strength & Am ount Dispensed Am ount Given To Patient Am ount W asted DV M Sig W itness Sig R equired
50
51
How To Stay DEA Compliant When Wasting A Controlled Substance AKA MEDICAL WASTE
Title 21 Code of Federal Regulations PART 1304 — RECORDS AND REPORTS OF REGISTRANTSCONTINUING RECORDS §1304.21 General requirements for continuing records.Ø e) Record of destruction. In addition to any other recordkeeping requirements, any registered person that
destroys a controlled substance pursuant to §1317.95(d) or causes the destruction of a controlledsubstance pursuant to §1317.95(c), shall maintain a record of destruction on a DEA Form 41. The recordsshall be complete and accurate and include the name and signature of the two employees who witnessedthe destruction. Except, destruction of a controlled substance dispensed by a practitioner for immediate administration at the practitioner's registered location, when the substance is not fully exhausted (e.g., some of the substance remains in a vial, tube, or syringe after administration but cannot or may not be further utilized), shall be properly recorded in accordance with §1304.22(c), and such record need not be maintained on a DEA Form 41.
Ø US Bio Clean States: “Although the DEA states that it seeks to determine a variety of destruction methods, the onlyacceptable method of destruction for pharmaceutical wastage (i.e., drugs dispensed to a patient and not fully used,such as a single syringe with remaining controlled substance) at this time is incineration.
Ø Therefore, the only method that currently meets the DEA requirement for both the non-retrievable and destructionstandards involves a two-part process:• Wasting the medication into a suitable neutralizing media, such as a Cactus Smart Sink or an Rx Destroyer. A
solidifier can also be used for liquid only waste.• Placing the neutralized container into a non-hazardous pharmaceutical waste container that will be sent out
for incineration”.Ø Check with your State Vet Board, VMA, DEA and/or the Pharmacy Board to see if they wiIl accept this method of
controlled substance waste destruction
Ø Medical waste only destruction https://usbioclean.com/how-to-dispose-of-controlled-substances/
EXPIRED controlled substances require the use of a reverse distributor. More later…..P le a s e n o te : T h e g o v e r n m e n t c h a n g e s la w s f r e q u e n t ly . A s o f N o v e m b e r 2 0 2 0 th e in fo r m a t io n c o n ta in e d in th is p r e s e n ta t io n is c u r r e n t . R e m e m b e r to c h e c k w i th th e v a r io u s g o v e r n m e n ta l a g e n c ie s o r y o u r a t to r n e y fo r c h a n g e s th a t m a y a f fe c t y o u r p r a c t ic e . © C o p y r ig h t 2 0 1 9
5152
DAILY RECONCILIATION OF YOUR BACKSTOCK AND OPEN CONTROLLED SUBSTANCES?
BEST PRACTICE SUGGESTION:
What? Why? How?• The Word Current: Every registrant required to
keep records pursuant to §1304.03 shall maintain,on a current basis, a complete and accurate record of each substance
• Best Practice: Controlled Substance Reconciliation Manual logs should be reconciledonce a day for a day practice and at every shift change for a 24x7 practice.
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your practice.©Copyright 2019
This Photo by Unknown Author is licensed under CC BY52
53
1. An anesthesia log should be maintained. Note: If youhave an anesthesia monitoring sheet, then this may suffice versus a separate log.
2. When controlled substances are removed for use with a patient, they should be logged into both your controlled substance reconciliation log and your anesthesia log or monitoring sheet.
ANESTHESIA LOG OR ANESTHESIA MONITORING SHEET
BEST PRACTICE SUGGESTION:
Please note: The government changes laws frequently. As of August 2019 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
5354
1. An annual reconciliation inventory of all your scheduled drugs, (I-IV), should be taken on or about December 31st of each calendar year
2. The date the reconciliation inventory was taken should be written on your annual inventory form
3. The annual reconciliation inventory form should state if it was taken at the opening or closing of the day
4. The past year’s-controlled substance books should be permanently closed and retained
5. All controlled substances should be transferred into the new year’s controlled substance reconciliation logs by schedule
6. Federal regs require a complete inventory biennially (2 years). 7. State Regulations may differ from the federal requirement!
CLOSE AND OPEN YOUR LOGS ANNUALLY
BEST PRACTICE & REGULATORY SUGGESTIONS:
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your practice. ©Copyright 2019
54
95
55
SAMPLE: DOCUMENTATION REQUIRED FOR ANNUAL CLOSE & INVENTORY
Schedule II ___________ Open Year Ending:_____________________
Date of Inventory:______________________________________________________________________________
Complete exactly as it appears in the DEA Certificate:________________________________________________
Name of Registrant:____________________________________________________________________________
Name of Practice:______________________________________________________________________________
Address:______________________________________________________________________________________
City, State, Zip_________________________________________________________________________________
DEA Registration Number:_______________________________________________________________________
Date Issued:___________________________________________________________________________________
Date Expires:__________________________________________________________________________________
This inventory valid for Closing on Dec _____ 20_______ & Opening/Transfer Dec _____, 20_____ for 20_____ Substance Unit Manufacturer Quantity
55
Veterinarians have traditionally been exempt from state-run PMP programs.
Not anymore.
More and more states are removing PMP exemptions, meaning hours of additional administrative burden placed on practice staff, and a whole new area of legal risk.
Note: PMP is being discussed by most Vet Boards and Board of Pharmacy across the United States
PrescriptionMonitoring
Program
56
57
1. All current controlled substance logs should be kept in a locked cabinet
2. All outdated controlled substance logs should be kept indefinitely, in a locked cabinet and be readily retrievable to any government official who can produce proper ID when he/she asks to see them.
3. DEA Regulation 21 CFR 1304-04(a) requires: All controlled substance records are required to be maintained for two (2) years
4. Know your State Regulations5. Consider Longer! Why?
.
STORING & RETAINING YOUR CONTROLLED SUBSTANCE LOGS
5758
1. DEA Regulations state that all Controlled Substances shouldbe kept in a securely locked cabinet that is permanently adhered to the wall or floor
2. A double locked cabinet is frequently used, but not required byDEA regulations. Check you State Regs!
3. If you have a double locked cabinet, you should:a). Limit access to a few trusted nurses; b). Control and account for the keys at all times; c). Two separate locks should be equipped with two differentkeys (or combinations) to access the drug cabinet.
4. The front door of your hospital should not be considered as one of the two locks.
5. Let’s see what your state says about security………………..
STORAGE OF CONTROLLED SUBSTANCES
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic.
©Copyright 2019
58
59
WOULD YOU RATHER PRACTICE MEDICINE OR DO REGULATORY PAPERWORK?
5960
CHARGE APPROPRIATELY
• Admin time (logs & reports)
• Security & storage requirements• Regulatory risk
SHOULD YOU REALLY BE CHARGING THE SAME DISPENSING FEE FOR BOTH?
1.Add a separate controlled substance handling fee
2.Increase your existing dispensing, administration and/orinjection fee codes
3.Increase the mark-up on your controlled substances
4.Consider an automateddispensing cabinet
FOUR WAYS TO COVER YOUR COSTS
60
96
61
• Digital narcotics logs reduce human error and savesignificant time
• Captures charges electronically for greater security.
• Fingerprint access is more secure and faster than keys
BENEFITS of an Automated Dispensing System
FOR EASE OF OPERATION CONSIDER AN AUTOMATED DISPENSING SYSTEM
6162
ü Each dispensing log should maintain the writtenstandard
ü The automated system maintains the information required in 21 CFR 1304.24(a),
ü The automated system has the capability of producing a hard copy printout of the programsdispensing records,
ü The automated system must be approved by theDEA
WHAT THE DEA SAYS. . .
CONSIDER AN AUTOMATED DISPENSING SYSTEM
62
63
Refills and new Rx’s that are telephoned into a pharmacy should be written in the patient’s chart.
The script and the reason for the legend/controlled substance prescribed should be written clearly in the patient’s medical record Does not matter if you are dispensing or prescribing. Don’t forget your refill notation (if allowed).
If you are dispensing directly to the patient/end user, it should also be written in the pharmacy section of the patient’s chart. The medical record and pharmacy section must match your controlled substance logs!
The patient’s chart should contain the following information:Ø DateØ Patient’s name & sexØ AddressØ Owner’s nameØ Drug nameØ Drug strengthØ QuantityØ LimitsØ Refills (if any)Ø Name of firm requesting authorizationØ Name of employee/DVM transmitting approval.
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current.Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright2019
PRESCRIPTIONS: BEST PRACTICE SUGGESTION AND/OR REGULATION:
6364
The DEA states this “is an Area of Great Confusion!”Did you know that the EPA can fine you up to $37,500 per violation, per day for disposing of your pharmaceutical waste incorrectly? That’s in addition to a DEA citation!
1. All outdated drugs removed from your closed/open inventory should be noted in your reconciliation logs as outdated and shipped immediately to a reverse distributor with date of shipment
2. Follow the reverse distributor’s return directions completely
3. The destruction list should identify all the drugs you surrendered by dateof surrender, drug name & strength, lot number and original invoicenumber
4. The reverse distributor should send you a manifest stating receipt bydrug name, strength, lot number and date of destruction
5. Your list of surrendered drugs and the reverse distributor’s manifest should be permanently kept with your controlled substance logs, or inyour file cabinet by date and invoice number
EXPIRED OR UNWANTED CONTROLLED SUBSTANCE DESTRUCTION
Reference: Title 21 CFR PART 1317(a)-Disposal of Controlled Substances by RegistrantsPlease note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
64
65
REVERSE DISTRIBUTORSPharmaceutical Credit Corp Franklin, TN (800) 487-4308 www.pcccredit.com
Return Logistics CorpSavannah, GA (912) 748-5100 www.returnlogistics.com
Chesapeake Waste SolutionsManheim, PA (717) 653-8882 www.cwsva.com
Guaranteed Returns Holbrook, NY (800) 473-2138 www.guaranteedreturns.com
Return Solutions Knoxville, TN 800-579-4804 www.drugreturns.com
EXP Pharma Svcs CorpUnion City, CA (800) 350-0397 www.expworld.com
Far West ReturnsSacramento, CA (916) 524-6465-Mike www.farwestreturns.com
P.S. IndustriesSeattle, WA (206) 749-0739 www.psireturns.com
EZ Pharmacy ReturnsAnoka, MN(800) 440-0613 www.ezpharmacyreturns.com
Drug & Laboratory DisposalPlainwell, MI (800) 685-9824 www.dld-nc.com
Pharma LogisticsMundelein, IL (888) 729.7427 www.pharmalogistics.com
Pharmaceutical Returns SvcNorth Aurora, IL (800) 215-5878 www.pharmreturns.net
Rx Reverse Distributors, IncSebastian, FL (866) 388-7973 www.rxrd.com
PharmaLinkLargo, FL (800) 257-3527 www.pharmalinkinc.com
Clean HarborsNorwell, MA (800) 282-0058 www.cleanharbors.com
United Rx SolutionsBohemia, NY 11716844-741-9718Van Schuette, VP, ext #102UnitedRxSolutions.com
6566
1. Remember: Controlled Substances are a “ClosedSystem”
2. Registrants address are specific to location3. Controlled Substances belong to the person
(Registrant) who has a DEA # and who signed the 222order form
4. Controlled Substances should not be “loaned”, “borrowed’, “given” or “sold” to another DVM or hospital
5. You may “borrow” from the same owned satellite hospital, if you closely follow the DEA’s regulationsand use the DEA’s required forms
6. The 5% Rule: No more than 5% of your annual CSinventory may be transferred between registrants
7. COVID 19 changes to 5% Rule.
IS LOANING, BORROWING OR SELLING BETWEEN REGISTRANTS OKAY?DEA’S 5% RULE
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
66
97
Why you should not draw up or dispense controlled substances until you are ready to use them…….
Different bottles or vials of controlled substances should not be mixed in advance
Why?
• Different lot numbers• Expiration dates vary
• Different manufacturers• Potential errors & theft• Cannot guarantee the strength
• Not an FDA/DEA approved drug
PRE-MIXING OF CONTROLLED SUBSTANCES
Reference: Title 21 CFR 1304.06 &§1304.21Reference: 21 CFR 21, 1305, 1311
Please note: The governm ent changes laws frequently. As of Novem ber 2020 the inform ation contained in this presentation is current. Rem em ber to check w ith the various governm ental agencies or your attorney for changes that m ay affect your hospital/clinic. ©Copyright 2019
6768
THE OPIOID CRISIS DOESN’T APPLY TO ME! DOES IT?
If an airplane went down every week, would you notice?
The same number of people are dying every week from painkiller overdoses!
68
69
The Social and Economic Impact of the Opioid Crisis
6970
• The Centers for Disease Control and Prevention states “Drug overdose deaths continue to increase in the United States.
• From 1999 to 2017, more than 700,000 people have died from adrug overdose.
• Around 68% of the more than 70,200 drug overdose deaths in2017 involved an opioid.
• In 2017, the number of overdose deaths involving opioids (including prescription opioids and illegal opioids like heroin and illicitly manufactured fentanyl) was 6 times higher than in1999.
• On average, 130 Americans die every day from an opioid overdose”.
• An article published by AAHA.net in 2013 stated that “overone-half of AAHA members surveyed said they have worked with a veterinary professional that had an addiction problem”.
SOBERING STATISTICS
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
70
71
In some states 36% of all arrests are Health Care Professionals!
• Easy Access to Controlled Substances• Theft/Attempted Theft• Conspiracy• Unlawful Distribution• Record Keeping• Doctor Shopping• Trafficking
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
IS THERE AN OPIOID PROBLEM IN VETERINARY MEDICINE?
7172
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
72
98
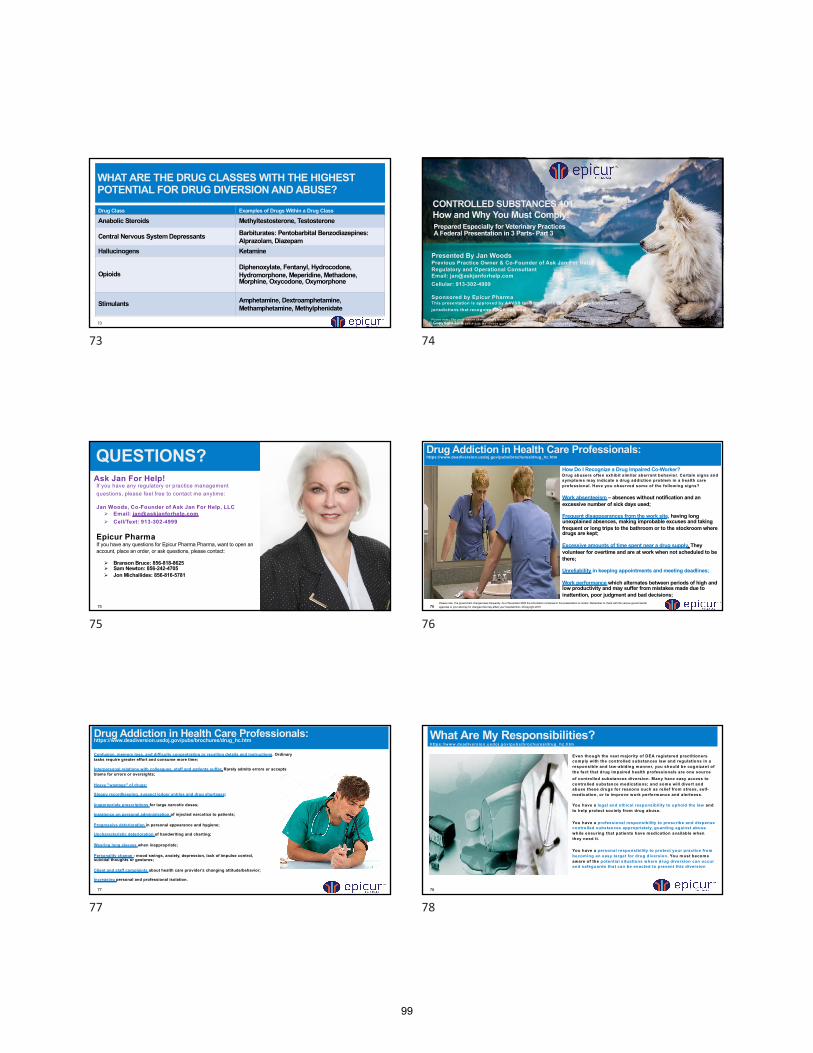
73
WHAT ARE THE DRUG CLASSES WITH THE HIGHEST POTENTIAL FOR DRUG DIVERSION AND ABUSE?
Drug Class Examples of Drugs Within a Drug Class
Anabolic Steroids Methyltestosterone, Testosterone
Central Nervous System Depressants Barbiturates: Pentobarbital Benzodiazepines: Alprazolam, Diazepam
Hallucinogens Ketamine
OpioidsDiphenoxylate, Fentanyl, Hydrocodone, Hydromorphone, Meperidine, Methadone, Morphine, Oxycodone, Oxymorphone
Stimulants Amphetamine, Dextroamphetamine, Methamphetamine, Methylphenidate
7374
CONTROLLED SUBSTANCES 101: How and Why You Must Comply!
Presented By Jan WoodsPrevious Practice Owner & Co-Founder of Ask Jan For Help!Regulatory and Operational ConsultantEmail: [email protected]: 913-302-4999
Sponsored by Epicur PharmaThis presentation is approved by AAVSB for 3 hours of continuing education credit in jurisdictions that recognize RACE approval
Please note: The governm ent changes laws frequently. As of Novem ber 2020 the inform ation contained in this presentation is current. Rem em ber to check w ith the various governm ental agencies or your attorney for changes that m ay affect yourhospital/clin ic
Prepared Especially for Veterinary Practices A Federal Presentation in 3 Parts- Part 3
© Copyright 2019
74
75
If you have any regulatory or practice management questions, please feel free to contact me anytime:
Jan Woods, Co-Founder of Ask Jan For Help, LLCØ Email: [email protected]Ø Cell/Text: 913-302-4999
Epicur PharmaIf you have any questions for Epicur Pharma Pharma, want to open an account, place an order, or ask questions, please contact:
Ø Branson Bruce: 856-818-8625Ø Sam Newton: 856-242-4705Ø Jon Michailides: 856-816-5781
Ask Jan For Help!
QUESTIONS?
7576
How Do I Recognize a Drug Impaired Co-Worker?Drug abusers often exhibit sim ilar aberrant behavior. Certain signs and symptoms may indicate a drug addiction problem in a health care professional. Have you observed some of the following signs?
Work absenteeism – absences without notification and an excessive number of sick days used;
Frequent disappearances from the work site, having long unexplained absences, making improbable excuses and taking frequent or long trips to the bathroom or to the stockroom where drugs are kept;
Excessive amounts of time spent near a drug supply. They volunteer for overtime and are at work when not scheduled to be there;
Unreliability in keeping appointments and meeting deadlines;
Work performance which alternates between periods of high and low productivity and may suffer from mistakes made due to inattention, poor judgment and bad decisions;
Drug Addiction in Health Care Professionals:https://www.deadiversion.usdoj.gov/pubs/brochures/drug_hc.htm
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
76
77
Confusion, memory loss, and difficulty concentrating or recalling details and instructions. Ordinary tasks require greater effort and consume more time;
Interpersonal relations with colleagues, staff and patients suffer. Rarely admits errors or accepts blame for errors or oversights;
Heavy "wastage" of drugs;
Sloppy recordkeeping, suspect ledger entries and drug shortages;
Inappropriate prescriptions for large narcotic doses;
Insistence on personal administration of injected narcotics to patients;
Progressive deterioration in personal appearance and hygiene;
Uncharacteristic deterioration of handwriting and charting;
Wearing long sleeves when inappropriate;
Personality change - mood swings, anxiety, depression, lack of impulse control, suicidal thoughts or gestures;
Client and staff complaints about health care provider's changing attitude/behavior;
Increasing personal and professional isolation.
Drug Addiction in Health Care Professionals:https://www.deadiversion.usdoj.gov/pubs/brochures/drug_hc.htm
7778
Even though the vast majority of DEA registered practitioners comply with the controlled substances law and regulations in a responsible and law-abiding manner, you should be cognizant of the fact that drug impaired health professionals are one source of controlled substances diversion. Many have easy access to controlled substance medications; and some will divert and abuse these drugs for reasons such as relief from stress, self-medication, or to improve work performance and alertness.
You have a legal and ethical responsibility to uphold the law and to help protect society from drug abuse.
You have a professional responsibility to prescribe and dispense controlled substances appropriately, guarding against abusewhile ensuring that patients have medication available when they need it.
You have a personal responsibility to protect your practice from becoming an easy target for drug diversion. You must become aware of the potential situations where drug diversion can occur and safeguards that can be enacted to prevent this diversion
What Are My Responsibilities?https://www.deadiversion.usdoj.gov/pubs/brochures/drug_hc.htm
78
99
79
Health care professionals often avoid dealing with drug impairment in their colleagues. There is a natural reluctance to approach a co-worker suspected of drug addiction. There is the fear that speaking out could anger the co-worker, resulting in retribution, or could result in a colleague's loss of professional practice.
Many employers or co-workers end up being "enablers" of health care practitioners whose professional competence has been impaired by drug abuse. Addicted colleagues are often given lighter work schedules, and excuses are made for their poor job performance. Excessive absences from the work site are often overlooked. Drug impaired co-workers are protected from the consequences of their behavior. This allows them to rationalize their addictive behavior or continue their denial that a problem even exists.
If you recognize the aforementioned signs or symptoms in a co-worker, it's time to demonstrate concern. You may jeopardize a person's future if you cover up or don't report your concerns. Many well-educated, highly trained, and experienced health care practitioners lose their families, careers, and futures to substance abuse. Tragically, some health care workers have even lost their lives to their drug addiction because the people who saw the signs and symptoms of their drug use refused to get involved.
By becoming involved, you cannot only help someone who may be doing something illegal, but more importantly, your action could affect the safety and welfare of your addicted employee or coworker AND those patients or the public who may come in contact with him or her.
Should I Become Involved?https://www.deadiversion.usdoj.gov/pubs/brochures/drug_hc.htm
7980
“Drug abuse and drug dealing are serious problems that should be handled by qualified professionals. If you suspect that a drug deal is in progress, do not intervene on your own. Contact security or notify the police”.
“If you are a DEA registrant and become aware of a theft or significant loss involving controlled substances, you must immediately report the theft or loss to the nearest DEA office, as well as your local police department”.
Should I Become Involved?https://www.deadiversion.usdoj.gov/pubs/brochures/drug_hc.htm
80
81
It is time for veterinary medicine to take up a “4-eyes” system to control drugs that are commonly used in suicide attempts. This means that, in every clinic possible, it should require two people to access these drugs. Noone should be able to get to themalone”.
“There are a number of ways to create a 4-eyes system, and some practices already have it inplace. For example, I knowof a clinic inWashington that has two locks ontheir controlledsubstance safe. The doctors have keys that fit one and the technicians andmanager have keys that fit the other. This simple systemwas put inplace as a safeguardagainst opioidabuse. It’s nowdoingdouble duty as a suicide prevention strategy”.
“Alternatively, all drug management systems from Cubex (a company that provides automated medication and supply management to the veterinary, dental and healthcare industries) comes equippedwith their Witness feature. This systemrequires thumbprint recognition fromtwoapprovedpeople before allowingaccess tocontrolleddrugs. The company focuses onDEA-compliance andoperates ona subscriptionbasis. Their most popular product for veterinary clinics is the Cubex Mini.
“We need to install 4-eyes systems across our profession, and we need to educate our staff about why we are doingso. Preventingsuicide seemsdifficult, but with this approach, I think we can make important headway. We can take the most available, accessible andcommonmethodof suicide inour profession and lock it up —sothat noone canget to it alone ina matter of moments”.
“We’re talking about our friends, colleagues and employees. If we can save even 1% of those we are currently losing to suicide, isn’t it worth it?”
What do we do about suicide? It’s Time To Limit ACCESS TO Means By Dr. Andy Roark
8182
AN INEXPENSIVE & VALUABLE RESOURCE
82
83
1. Exercising caution with clients who request combination of controlled substances;2. Determine the medical necessity of controlled substances for your patients;3. Documenting thoroughly when prescribing narcotics or why choosing not to prescribe;4. Protecting access to prescription pads;5. Keeping a DEA or license number confidential, unless disclosure is required by State law;6. Ensuring that prescriptions are written clearly to minimize the potential for forgery;7. Moving to electronic prescribing so that paper prescriptions are not required;8. Adhering to strict refill policies and educating you staff why;9. Using State Prescription Drug Monitoring Programs where required, to monitor patient prescribing before refilling or adding new medications;10. Referring patients with extensive pain management or prescription-controlled medication needs to specialized veterinarians;11.Communicating & collaborating with pharmacists or police when
suspicious behaviors are observed
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. © Copyright 2019
Suggested Precautions to Avoid Being Taken Advantage of by Drug-Seeking Clients:
8384
84
100
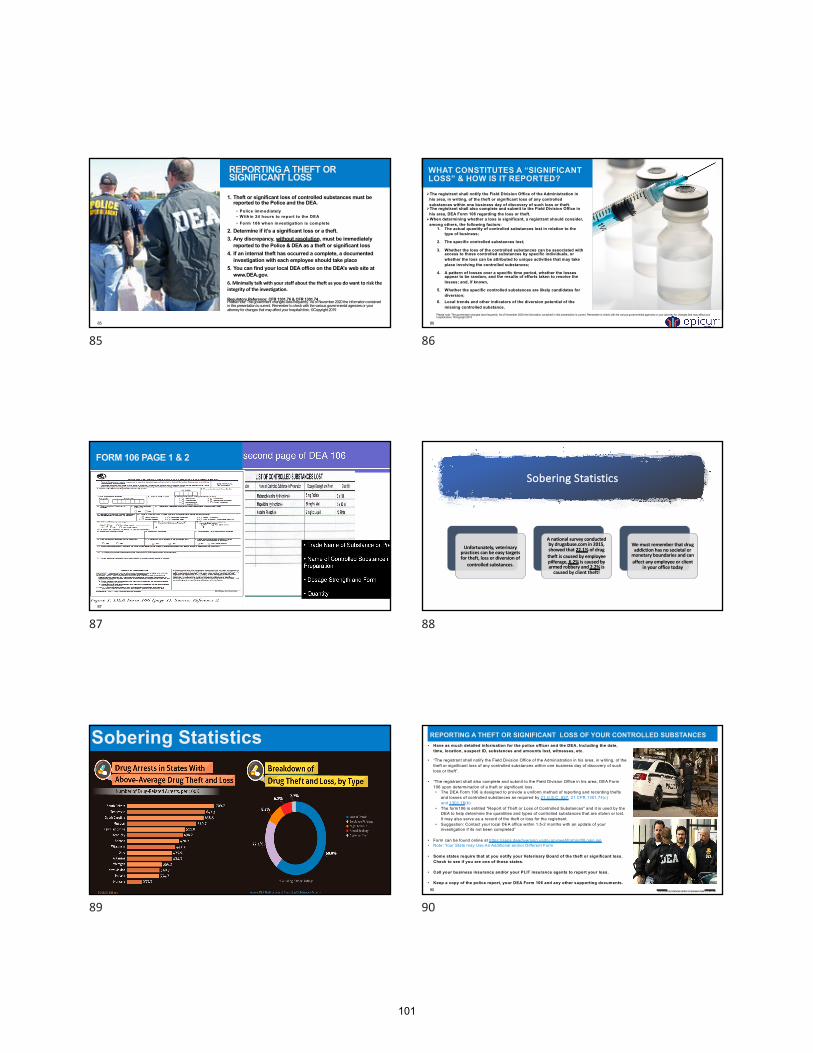
85
1. Theft or significant loss of controlled substances must be reported to the Police and the DEA.
• Police immediately• W ithin 24 hours to report to the DEA• Form 106 when investigation is complete
2. Determine if it’s a significant loss or a theft.3. Any discrepancy, without resolution, must be immediately
reported to the Police & DEA as a theft or significant loss4. If an internal theft has occurred a complete, a documented
investigation with each employee should take place 5. You can find your local DEA office on the DEA’s web site at
www.DEA.gov.6. Minimally talk with your staff about the theft as you do want to risk the integrity of the investigation.
Regulatory Reference: CFR 1301.76 & CFR 1301.74
REPORTING A THEFT OR SIGNIFICANT LOSS
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
8586
ØThe registrant shall notify the Field Division Office of the Administration in his area, in writing, of the theft or significant loss of any controlled substances within one business day of discovery of such loss or theft.
ØThe registrant shall also complete and submit to the Field Division Office in his area, DEA Form 106 regarding the loss or theft.
ØWhen determining whether a loss is significant, a registrant should consider, among others, the following factors:
1. The actual quantity of controlled substances lost in relation to thetype of business;
2. The specific controlled substances lost;
3. Whether the loss of the controlled substances can be associated withaccess to those controlled substances by specific individuals, orwhether the loss can be attributed to unique activities that may take place involving the controlled substances;
4. A pattern of losses over a specific time period, whether the losses appear to be random, and the results of efforts taken to resolve the losses; and, if known,
5. Whether the specific controlled substances are likely candidates fordiversion;
6. Local trends and other indicators of the diversion potential of themissing controlled substance.
WHAT CONSTITUTES A “SIGNIFICANT LOSS” & HOW IS IT REPORTED?
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
86
87
FORM 106 PAGE 1 & 2
87
Sobering Statistics
Unfortunately, veterinary practices can be easy targets for theft, loss or diversion of
controlled substances.
A national survey conducted by drugabuse.com in 2015, showed that 22.1% of drug theft is caused by employee pilferage, 6.2% is caused by armed robbery and 2.2% is
caused by client theft!
We must remember that drug addiction has no societal or
monetary boundaries and can affect any employee or client
in your office today
88
89
Sobering Statistics
8990
• Have as much detailed information for the police officer and the DEA. Including the date,time, location, suspect ID, substances and amounts lost, witnesses, etc.
• “The registrant shall notify the Field Division Office of the Administration in his area, in writing, of thetheft or significant loss of any controlled substances within one business day of discovery of such loss or theft”.
• “The registrant shall also complete and submit to the Field Division Office in his area, DEA Form106 upon determination of a theft or significant loss. • The DEA Form 106 is designed to provide a uniform method of reporting and recording thefts
and losses of controlled substances as required by 21 U.S.C. 827, 21 CFR 1301.74(c) and 1301.76(b).
• The form106 is entitled "Report of Theft or Loss of Controlled Substances" and it is used by theDEA to help determine the quantities and types of controlled substances that are stolen or lost.It may also serve as a record of the theft or loss for the registrant.
• Suggestion: Contact your local DEA office within 1.5-2 months with an update of yourinvestigation if its not been completed”
• Form can be found online at https://apps.deadiversion.usdoj.gov/webforms/dtlLogin.jsp• Note: Your State may Use An Additional and/or Different Form
• Some states require that at you notify your Veterinary Board of the theft or significant loss.Check to see if you are one of those states.
• Call your business insurance and/or your PLIT insurance agents to report your loss.
• Keep a copy of the police report, your DEA Form 106 and any other supporting documents.
REPORTING A THEFT OR SIGNIFICANT LOSS OF YOUR CONTROLLED SUBSTANCES
This Photoby Unknown Author is licensed under CC BY-NC
90
101
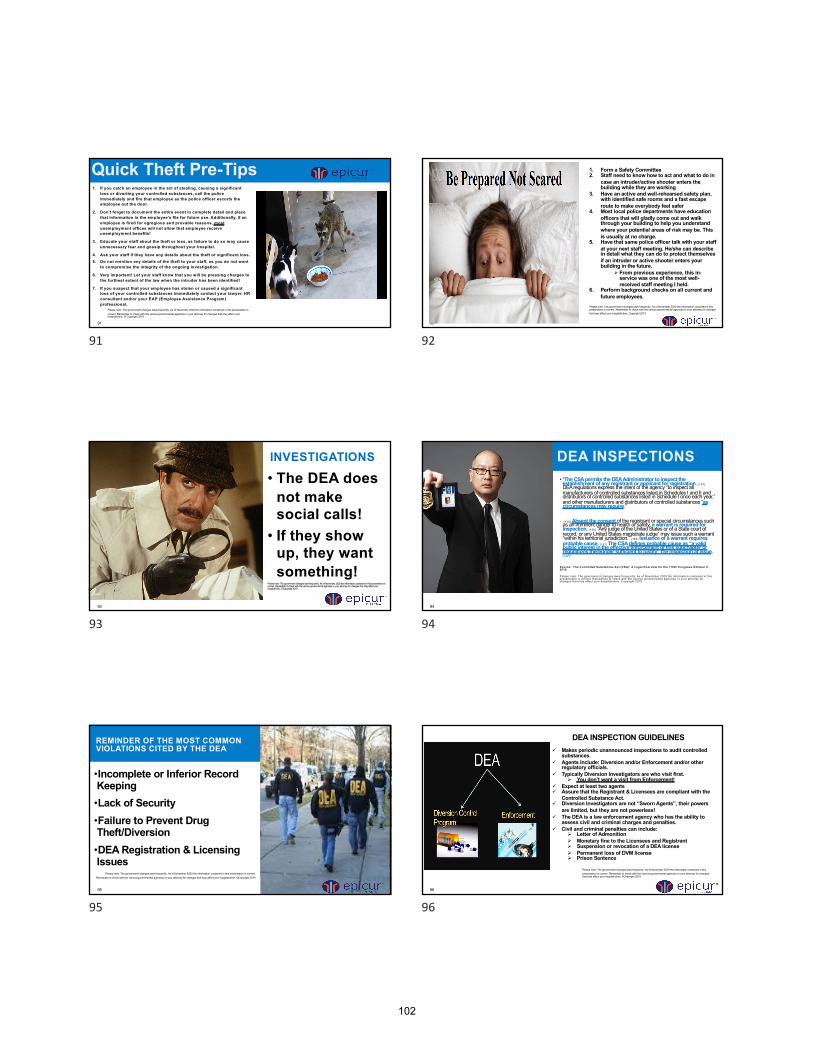
91
1. If you catch an employee in the act of stealing, causing a significantloss or diverting your controlled substances, call the policeimmediately and fire that employee as the police officer escorts the employee out the door.
2. Don’t forget to document the entire event in complete detail and place that information in the employee’s file for future use. Additionally, if anemployee is fired for egregious and provable reasons, mostunemployment offices will not allow that employee receiveunemployment benefits!
3. Educate your staff about the theft or loss, as failure to do so may causeunnecessary fear and gossip throughout your hospital.
4. Ask your staff if they have any details about the theft or significant loss.5. Do not mention any details of the theft to your staff, as you do not want
to compromise the integrity of the ongoing investigation.
6. Very important! Let your staff know that you will be pressing charges tothe furthest extent of the law when the intruder has been identified!
7. If you suspect that your employee has stolen or caused a significant loss of your controlled substances immediately contact your lawyer, HRconsultant and/or your EAP (Employee Assistance Program)professional.
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. © Copyright 2019
Quick Theft Pre-Tips
9192
Quick Prevention Tips:
1. Form a Safety Committee2. Staff need to know how to act and what to do in
case an intruder/active shooter enters the building while they are working
3. Have an active and well-rehearsed safety plan, with identified safe rooms and a fast escaperoute to make everybody feel safer
4. Most local police departments have education officers that will gladly come out and walk through your building to help you understand where your potential areas of risk may be. This is usually at no charge.
5. Have that same police officer talk with your staff at your next staff meeting. He/she can describe in detail what they can do to protect themselvesif an intruder or active shooter enters your building in the future.
Ø From previous experience, this in-service was one of the most well-received staff meeting I held.
6. Perform background checks on all current and future employees.
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. Copyright 2019
92
93
INVESTIGATIONS
• The DEA doesnot makesocial calls!
• If they showup, they wantsomething!
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
9394
• “The CSA permits the DEA Administrator to inspect the establishment of any registrant or applicant for registration. (137) DEA regulations express the intent of the agency “to inspect all manufacturers of controlled substances listed in Schedules I and II and distributors of controlled substances listed in Schedule I once each year,” and other manufacturers and distributors of controlled substances “as circumstances may require.”
• “(138) Absent the consent of the registrant or special circumstances such as an imminent danger to health or safety, a warrant is required for inspection. (139) “Any judge of the United States or of a State court of record, or any United States magistrate judge” may issue such a warrant “within his territorial jurisdiction.” (140) Issuance of a warrant requires probable cause. (141) The CSA defines probable cause as “a valid public interest in the effective enforcement of this subchapter or regulations thereunder sufficient to justify” the inspection at issue. (142)”
Source: The Controlled Substances Act (CSA): A Legal Overview for the 116th Congress October 9, 2019
Please note: The governm ent changes laws frequently. As of Novem ber 2020 the inform ation contained in this presentation is current. Rem em ber to check w ith the various governm ental agencies or your attorney for changes that m ay affect your hospital/clinic. Copyright 2019
DEA INSPECTIONS
94
95
•Incomplete or Inferior Record Keeping•Lack of Security•Failure to Prevent Drug Theft/Diversion•DEA Registration & Licensing Issues
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
•
REMINDER OF THE MOST COMMON VIOLATIONS CITED BY THE DEA
9596
DEA INSPECTION GUIDELINESü Makes periodic unannounced inspections to audit controlled
substances.ü Agents Include: Diversion and/or Enforcement and/or other
regulatory officials.ü Typically Diversion Investigators are who visit first.
Ø You don’t want a visit from Enforcement! ü Expect at least two agents ü Assure that the Registrant & Licensees are compliant with the
Controlled Substance Act.ü Diversion Investigators are not “Sworn Agents”, their powers
are limited, but they are not powerless!ü The DEA is a law enforcement agency who has the ability to
assess civil and criminal charges and penalties.ü Civil and criminal penalties can include:
Ø Letter of AdmonitionØ Monetary fine to the Licensees and RegistrantØ Suspension or revocation of a DEA licenseØ Permanent loss of DVM licenseØ Prison Sentence
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
96
102
97
BE PREPARED•DEA inspections can occur at anytime of the day•Have your attorney on speed dial and call immediately!•All staff must be knowledgeable and well rehearsed with all Federal, State and Veterinary Board Regulations so they can handle an audit or answer an agent’s questions.
•Staff should know your practice’s controlled substances:Ø Policies and ProceduresØ SecurityØ OrderingØ StorageØ LoggingØ AdministrationØ Record RetrievalØ Controlled Substance Retrieval
Always Remember It’s a Closed SystemPlease note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. © Copyright 2019
9798
DEA Registration Note: this should also be posted in a visible place in your office
• State pharmacy practitioner license. Check your State RegsNote: this should also be posted in a visible place in your office
• Your most recent biennial(or annual) inventory. Check your state regs• DEA form 222 records or CSOS for Schedule II substances
Your Purchasing Records • Invoices for Schedule III, IV, and V substances
Your purchasing records • Receiving logs/records • Inventory logs/records • Administration and dispensing logs/records • DEA form 106 records
Report of Theft or Loss of Controlled Substances • DEA form 41 records
Registrant Record of Controlled Substances Destroyed • Disposal & Waste logs/records • Other records you keep that document accounting of controlled substances Additional documents that may be applicable: • Training records for your staff who have been trained on the DEA’s Practitioner’s Manual and/or Controlled Substance Policy • Home State Controlled Substance license (Note: this should also be posted in a visible place in your office)• Power of Attorney
CREATE A DEA AUDIT READINESS FILE
SOURCE: OMS CONSULTING FIRM
98
99
BE PREPARED TO PROVIDE ANY OR ALL OF THE FOLLOWING TO THE DEA AGENT(S)
BUT ONLY WHEN ASKED & BE SPECIFIC…..
Show DVM licensure and DEA Certificate of Registrations of all
your Doctors
A list of all personnel with access to controlled substances, this includes
name, addressBackground checks
Policy & Procedures Last Complete Inventory (Biannual) Current Usage Logs that are Current, Accurate & Complete
Disposal RecordsPurchasing Records Invoices, Packing Slips & 222 forms. Make sure that your Schedule I & II records are Separate from your lll’s, IV & V’s.
Waste or breakage spillage reports
Theft/Significant loss Reports Access to Controlled Substances
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. © Copyright 2019
99100
1. Ask the reason for the inspection 2. Review the agent’s credentials3. Ask for a photo ID4. Ask for their contact information5. Ask for their business card(s)6. You have the right to decline their visit.
But if you do, be prepared for a warrant the next business day
7. Take the agents to a private conference room so they have room to work
8. Ask for an opening conference9. Sign the Notice of Inspection (DEA Form 82).
FYI: This form grants the DEA agents “informed consent” from the Registrant and Licensee permission to search yourproperty/practice.
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
What To Do When The DEA Arrives…..
100
101
WHAT IS THE DEA REALLY LOOKING FOR WHEN THEY AUDIT A VETERINARY PRACTICE?Applicable Regulations Can Be Found In Sections of the 21 CFR, Section # 1300
DVM RegistrationRegulations Found in Part # 1301
Practice Security, Which Includes Theft and Theft Prevention
Regulations found in Part #1301.7 - 1301.76Employee Screening (aka Background Checks)
Regulations found in Part #1301.90 – 1301.93Labeling and Packaging
Regulations found in Part #1302 Records and Recordkeeping
Regulations can be found in Part #1304
Applicable Regulations Can Be Found In Sections of the 21 CFR, Section # 1300Order Forms
Regulations can be found in Part #1305Prescriptions
Regulations can be found in Part #1306Destruction and/or Disposal
Regulations can be found in Part #1307Schedules of Controlled Substances & List I & II Chemicals
Regulations can be found in Parts #1308 & 1310Miscellaneous:
TrainingPolicies & ProceduresSOP’sLoss and Diversion
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
101102
ü You should expect the agents to walk around your practice for aphysical inspections.
ü Make sure that you go everywhere with them and take copiousnotes.
ü The Agent(s) may audit controlled substances to track your usagefrom the last annual and/or biannual inventory and/or purchaseorders.
ü Expect the DEA agent to ask to see your controlled substance logs& ordering/storing/dispensing/administration/prescribing systems
ü They may ask the Registrant/Licensees to physically count, weigh or inventory the controlled substances.
ü They may copy any records
ü If original records or controlled substances are taken off site, the DEA Agent(s) must provide you a receipt. This is called a DEA Form12
ü Make sure you keep copies of any records removed from yourpractice and a list (perhaps pictures too) of all controlled substances removed from your practice.
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
Throughout The Inspection
102
103
103
Most Importantly:üTake notes of all recommendations & observations üBe courteous, polite and cordialüDon’t argue or debate with the Agent(s)üAsk questions regarding the DEA’s findings, so corrective actions can be be takenüAnswer all questions honestly and concisely as possibleüBe truthful & don’t speculateüAsk for clarification if you do not understand a questionüDo not admit guilt üDo not offer your opinion or volunteer informationüDo not talk about past audits, accidents or incidentsüWalk around with the auditor during the inspection üIf you don’t have the answer, tell the agent you will find someone who doesüAsk for a closing conference so you can learn how to “think like an auditor” in the future!
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. © Copyright 2019
Throughout The Inspection
103
103104
q “List of up to three individuals for whom the Inspector should ask for upon arrival at thefacility” “Primary Contact, Secondary Contact & Tertiary Contact. Information required: Name, Title, E-mail, Phone
q State Registration History: “Date registered with city, county, state, name, addresses, if moved, all owners by %, etc”.
q Does the Registrant currently possess any controlled substances?
q What is the current status of the Registrant's DEA Registration? (Valid, Name, Number, etc.)
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
INSPECTORS MAY ALSO REQUIRE:
104
105
q Who is responsible for controlled substances? (Nameor Names)
q Has the Registrant granted Power of Attorney to any individuals for ordering controlled substances? (Nameor Names)
q Is each DVM registered with the DEA? (Y or N) If no, how do non-registered DVMs prescribe controlled substances?
q Does the registrant currently possess any controlledsubstance samples? Y or N
q Primary and Secondary Supplier of ControlledSubstances
q Storage and Security. How Stored and How Accessed,etc.
q How are the prescription pads stored?
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
INSPECTORS MAY ALSO REQUIRE:
105106
q How are unexecuted controlled substances order formsstored? (222’s)
q Does the facility take possession of patients’ personalcontrolled substances? If so, describe how patient’s personal controlled substances are stored and the records are maintained.
q Inventory Dates and system of maintenance. How recorded? Include receipts, 222s, invoices and other documents acknowledging receipt of controlled substance II’s.
q Describe the system of ordering and receiving Schedules II, III, IV & V controlled substances. Provideforms, receipts, ho maintained and logged, etc.
q Describe the procedure for dispensing controlled substances. How are the records maintained? How are the logs maintained? How are the automated dispensing technology reports retrieved, etc.?
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
INSPECTORS MAY ALSO REQUIRE:
106
107
q Describe how the records are maintained for the administration of controlled substances? How are the logs maintained?
q How are the automated dispensing technology reportsretrieved, etc.?
q Describe effective security measures to maintaineffective control for the prevention of controlled substance theft and diversion”.
q Suggestion: A CONTROLLED SUBSTANCE POLICYthat covers the above information
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. ©Copyright 2019
Note: Inspectors May Also Require slides were extracted from North Carolina Clinic Application for Renewal DHHS 226-D. and are a good resource for everyone
INSPECTORS MAY ALSO REQUIRE
107108
WHAT TO DO IF A PLAN OF CORRECTION (POC) IS REQUIRED BY THE DEA!
q You will receive a letter of findingsq The letter is from the government and requires your
immediate attentionq You can expect to provide a very comprehensive
written, Plan of Correction, (aka POC)q Link each correction in your POC to the actual
citation/reg quoted in your letter q You must assure that all identified areas are
corrected precisely and conciselyq Meet or beat all required time framesq Keep all copiesq Follow-Up, follow-up with the Agent
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. Copyright 2019
108
104
109
QUICK CONTROLLED SUBSTANCE COMPLIANCE REMINDERS
109110
VETERINARIANS GUIDE TO LIMIT LIABILITY SOURCE JACKSON LLP, HEALTHCARE LAWYERS
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. Copyright 2019
110
111
According to federal regulations, all Drug Enforcement Administration (DEA) applicants and registrants shall meet the following record keeping requirements:
1. Your records must show the flow of controlled substance into and out of the practice – includingany time a controlled substance is acquired, dispensed, administered, distributed, stolen, lost, disposed of and inventoried;
2. You must keep two physically separate files – one for Schedules I & II substances, and one forSchedule III-V substances;
3. Your controlled substance records must be readily retrievable;
4. You must store all copies of DEA Form 222 * (the form used for ordering Schedule II controlled substances) in a substantially constructed, securely locked cabinet and you must immediately report to the DEA any change in a copy (or copies) of the form’s status (used/unused, lost, stolen);
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. © Copyright 2019
Quick Controlled Substances Compliance Reminders:
111112
5. You may issue prescriptions for controlled substances in writing, verbally, or electronically whenavailable (using systems meeting DEA criteria), or by fax (note that a paper prescription is needed before any pharmacy can dispense a Schedule II substance).
Prescriptions must include the following: Ø Date;Ø Signature of registrant;Ø DEA registration number;Ø Patient’s name/address;Ø Practitioner’s name/address;Ø Drug name, strength, dosage form and quantity;Ø Directions for use (frequency and route of administration); andØ Number (if any) of refills authorized
Ø Note that Schedule II drugs cannot be refilled.Ø Note that state law may restrict the ability to refill or the number of refills.
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. © Copyright 2019
Quick Controlled Substances Compliance Reminders:
112
113
6. You may transfer controlled substances to another DEA registrant, but all transfers must be recorded and cannot comprise more than 5% of all the dosage units you distribute and dispense;
7. You must report thefts or significant losses within one business day to the DEA, the state-controlled substance authority, and local police. The occurrence must be recorded on DEA Form 106;
Ø Find your local DEA officeØ Find your State’s controlled substance authority
8. You must record controlled substance spills on DEA Form 41 and keep the form on file at yourfacility;
9. Federal regulations require that the records be kept for at least two years.
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. © Copyright 2019
Quick Controlled Substances Compliance Reminders:
113114
10. Per DEA rules, an inventory of all controlled substances must be maintained separately and taken biennially on May 1st, or two (2) years from the day of the last inventory, of every odd-numbered year.The written inventory record must include the following:
Ø Date;Ø Time of day the inventory was performed;Ø Each finished form (e.g., 100-milligram tablet);Ø Number of dosage units for each finished form. An exact count of Schedule II drugs is required; an
estimate is generally satisfactory for Schedule III-V (unless the container holds >1000 dosage units);Ø Number of bottles;Ø Disposition of the controlled substances.
Remember: Check Your State Regulations! Always follow the most stringent regulation.
For More Information:Section IV – Recordkeeping requirements; https://www.deadiversion.usdoj.gov/pubs/manuals/pract/section4.htm Practitioner’s Manual; https://www.deadiversion.usdoj.gov/pubs/manuals/pract/pract_manual012508.pdfDEA Office of Diversion Control, The Controlled Substances Act (CSA): A Legal Overview for the 116th Congress October 9, 2019
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. © Copyright 2019
Quick Controlled Substances Compliance Reminders:
114
105

115
CHANGES, THOUGHTS & SUGGESTIONS
This presentation included both Federal Regulation Requirements, as well as Best Practice Suggestions to help you minimize your risk
Due to the opioid crisis, there have been more changes and new regulations added in the last 1 to 2 years
Gabapentin is expected to become a controlled substance nationally very soon.
Rumor: Morphine is being considered for a Schedule I Classification
Chain of Custody laws went into effect on Dec 31, 2006
Continually watch the DEA, your State Regulations & your Veterinary Board’s website for regulatory changes and announcements.
Read all articles about controlled substances, reguatory updates and changes.
If you are audited, do not claim, I didn’t know - or- Why Should I have To Do This, Nobody Else Has To?
Remember: A DEA agent can just drop by for any reason, so know your rights
The DEA is rumored to have hired over 300 DEA agents nationally specifically for veterinary healthcare
Please Note: The government changes law frequently. As of November 2020 the information contained in this presentation is current.
115116
QUESTIONS?JUST ASK JAN
FOR HELP!913-302-4999
WWW.ASKJANFORHELP.COM
by Unknown Author is licensed under CC BY-NC
116
117
If you have any regulatory or practice management questions, please feel free to contact me anytime:
Jan Woods, Co-Founder of Ask Jan For HelpØ Email: [email protected]Ø Cell/Text: 913-302-4999
Epicur PharmaIf you have any questions for Epicur Pharma Pharma, want to open an account, place an order, or ask questions, please contact:
Ø Branson Bruce: 856-818-8625Ø Sam Newton: 856-242-4705Ø Jon Michailides: 856-816-5781
Ask Jan For Help!
1. ALWAYS REMEMBER THE DEA’S CLOSED SYSTEM
2. ALWAYS STAY CURRENT, COMPLETE AND ACCURATE WITH YOUR RECONCILIATION LOGS AND RECORDKEEPING
117118
• The Federal Controlled Substances Act: Title 2I CFR 1308 to end• CFR: http://gpoaccess.gov/cfr/index/html• The Federal Register: http://www.gpoaccess.gov/fr/index.html• The Controlled Substances Act (CSA), Title II of the Comprehensive
Drug Abuse Prevention and Control Act of 1970• Code of Federal Regulations, Section 1304.11 Inventory Requirements • DEA clarifies reporting of controlled substance loss. Federal Register:
July 8, 2003 (Volume 68, Number 130)][Proposed Rules] [Page 40576-40579]From the Federal Register Online via GPO Access [wais.access.gpo.gov][DOCID:fr08jy03-20] DEPARTMENT OF JUSTICE Drug Enforcement Administration21 CFR Part 1301[Docket No. DEA-196P]RIN 1117-AA73
• Practitioner’s Manual, can be found on the internet at DEA’s Web Site (under “publications” www.DEAdiversion.usdoj.gov)
• Please feel free to call me anytime at 913-302-4999, email me at [email protected] or go online to my website at www.askjanforhelp.com
Please note: The government changes laws frequently. As of November 2020 the information contained in this presentation is current. Remember to check with the various governmental agencies or your attorney for changes that may affect your hospital/clinic. Copyright 2019
Federal Regulatory Requirements & Resources
118
106
20+ dental hacks for your dental practice
Jan Bellows, DVM, Dipl. AVDC, ABVP (canine and feline)
ALL PETS DENTAL Weston, Florida
A Hack is any trick, shortcut, skill, or novelty method that increases productivity and efficiency, in all walks of life. The term was primarily used by computer experts who suffer from information overload or those with a playful curiosity in the ways they can accelerate their workflow in ways other than programming:
1. Take cell phone dental images to email and print 2. Four/six-handed dentistry 3. Dental charting-paper (vin/aaha), electronic –vetdentalchart.com 4. Dental cytology 5. #11 vs. #15 blade 6. Periosteotome 7. Thin wing tipped elevators 8. Sharpen with every extraction 9. Rongeurs vs. Extraction forceps 10. Steris feline and canine extraction sets 11. Football diamond burs for alveolarplasty 12. Vet-tome- im3 13. Hemablock 14. Vetcorder after extubation monitor 15. Deciduous teeth extractions 16. Maxillary canine extraction 17. Gingival recession treatment 18. Molar extraction closure 19. Symphyseal separation repair –suture/composite 20. Caudal mandible fracture repair with buttons 21. Alveolar bone expansion removal 22. Type two resorption/crown reduction gingival closure 23. Co2 laser treatment for refractory caudal mucositis 24. Therapy laser post-extraction 25. Flap hooks made from needles 26. The 9:00 PM phone call
107
Feline stomatitis where do you begin?
By Jan Bellows, DVM, Dipl. AVDC, ABVP (Canine and Feline Specialties)
ALL PETS DENTAL
Start with the Basics
What is stomatitis?
A cat’s mouth is constantly exposed to bacteria, viruses, and other agents of disease. In a healthy mouth, there is a balance between disease, the patient and the immune response. When an imbalance occurs, a cat’s inadequate or exaggerated response to plaque leads to marked inflammation of the gums and mucous membranes. Historically, virtually any significant inflammation of a cat’s mouth was incorrectly called stomatitis or faucitis. Stomatitis is still used, but only to describe wide-spread inflammation inside the mouth compared to the inflammation located only on the gums.
Many causes of stomatitis are suspected, including genetic predisposition, environmental stress, diet, viruses (calici, herpes) and bacterial infection (Bartonella spp.) infection. Only calici virus is seen in cats affected by chronic oropharyngeal (mouth and throat) inflammation (97%) compared to a controlled group of cats (25%). Although some cats who have stomatitis are positive for Bartonella spp., cause and effect has not been proven.
History and clinical signs
The median age of affected cats is seven. Affected cats have often had signs such as difficulty swallowing, lack of appetite that causes weight loss, excessive saliva, grinding of teeth, and face pawing. The cat may not want to open the mouth when eating. The cat’s hair coat is often unkempt because grooming is too painful with such a sore mouth. Bad breath and bleeding inside the mouth are common.
In some cats, inflammation is apparent only around the back teeth. Other cats show marked inflammation on the gums (gingivitis) and the periodontitis that follows untreated gingivitis.
Gingivitis is a medical term that refers to inflammation of the gums. Gingivitis is the earliest phase of periodontal disease. Stomatitis refers to a more generalized inflammation of the mucous membranes within the mouth, and may involve the gums, tongue, inner surfaces of the lips, and/or the floor and roof of the mouth. Feline chronic gingivostomatitis (FCGS) is the generally accepted umbrella term however the American Veterinary Dental College approved terms for inflammation in the mouth.
x Gingivitis: inflammation of gingiva x Periodontitis: inflammation of non-gingival periodontal tissues (i.e. the periodontal ligament and alveolar
bone) x Alveolar mucositis: inflammation of alveolar mucosa (i.e., mucosa overlying the alveolar process and
extending from the mucogingival junction without obvious demarcation to the vestibular sulcus and to the floor of the mouth)
x Sublingual mucositis: inflammation of mucosa on the floor of the mouth x Labial/buccal mucositis: inflammation of lip/cheek mucosa x Caudal mucositis: inflammation of mucosa of the caudal oral cavity, bordered medially by the palatoglossal
folds and fauces, dorsally by the hard and soft palate, and rostrally by alveolar and buccal mucosa
108
x Stomatitis: inflammation of the mucous lining of any of the structures in the mouth; in clinical use the term
should be reserved to describe wide-spread oral inflammation (beyond gingivitis and periodontitis) that may also extend into submucosal tissues (e.g., marked caudal mucositis extending into submucosal tissues may be termed caudal stomatitis. Note: The fauces are defined as the lateral walls of the oropharynx that are located medial to the palatoglossal folds. The areas lateral to the palatoglossal fold, commonly involved in feline stomatitis, are not the fauces.
x Contact mucositis and contact mucosal ulceration: lesions in susceptible individuals that are secondary to mucosal contact with a tooth surface bearing the responsible irritant, allergen, or antigen. They have also been called “contact ulcers” and “kissing ulcers”.
x Palatitis: inflammation of mucosa covering the hard and/or soft palate x Glossitis: inflammation of mucosa of the dorsal and/or ventral tongue surface
What causes feline stomatitis?
A multifactorial etiology is suspected, including genetic predisposition, environmental stress, diet, and viral and bacterial infection. Only calici virus has shown significant presence in those cats affected by chronic oropharyngeal inflammation (97%) compared to a controlled group of cats (25%) in one study. Herpes virus is not thought to be involved. Pasteurella multocida subsp. multocida is a predominant bacterial species found in FCGS. This species is associated with the normal feline flora but a large increase in its prevalence in FCGS suggests that it may be an important etiological agent of this disease although there is no evidence showing a cause‐and‐effect relationship. When specific pathogen‐ free cats were inoculated with serum from positive feline chronic oropharyngeal inflammation cats, those inoculated developed oral signs of ulceration but did not develop FCGS. In a study of nearly 9,000 cats affected with oral lesions, greater than 20% of animals with chronic stomatitis were retrovirus (feline leukemia virus [FeLV] and/or feline immunodeficiency virus [FIV]) positive. In another study of 60 cats with caudal stomatitis, 7% were positive for FeLV and 8% positive for FIV. None were positive for both FeLV and FIV.
Diagnostics and treatment workflow
Initial care for mild cases of non-caudal stomatitis includes teeth cleaning with ultrasonic and hand instruments above and below the gingival margin, followed by a tooth-by-tooth clinical examination and full-mouth intraoral radiography. All abnormalities are charted, including probing depths. Those teeth affected with greater than stage 1 periodontal disease should be extracted.
Home plaque control includes daily application of OraVet® plaque barrier gel and antimicrobial mouth rinses containing chlorhexidine gluconate (Oral Hygiene Rinse-Virbac, Fort Worth, TX) to help decrease the oral bacterial load. Daily rubbing with a Q-tip applicator dipped in water-packed tuna juice (for taste) to the free gingival margin to remove plaque may also be helpful. A hypoallergenic diet (Hills® z/d, Waltham-Royal Canin® HP23) and feeding from ceramic or glass dishes (not plastic ones) may also be beneficial.
Nonsurgical management of FCGS may initially appear to be effective in some cases as evidenced by clinical resolution of inflammation. Unfortunately, the response appears to be short term and in direct response to the actions of antimicrobials, anti‐inflammatories, and immunosuppressive medications that may decrease inflammation but does not alter the etiology nor long‐ term outcome.
109
Antimicrobials
Antimicrobials are recommended only when used in conjunction with surgery and then sparingly. An antibiotic that affects both gram‐positive and gram‐negative organisms is recommended. Both clindamycin and amoxicillin potassium clavulanate are approved by the FDA to be used to treat dental infections. Although not approved specifically for dental infections, metronidazole may be beneficial in treating this disease due to its antibacterial activity and anti‐inflammatory action. Sample doses are:
x Clindamycin 5–10 mg/kg BID for 10 days x Amoxicillin/clavulanate potassium 10–20 mg/kg BID for 7–10 days x Metronidazole at 11–22 mg/kg in divided dose twice daily for 7–10 days. In addition to its antibacterial
activity, metronidazole has some anti-inflammatory action, which may be beneficial in treating this disease
Anti-Inflammatory Medication
Corticosteroids
Repeated repositol corticosteroid injections usually provide clinical improvement initially, but eventually they decrease the body’s ability to resist the inflammatory process and predispose cats to diabetes mellitus. Prednisone (2 mg/kg orally) initially daily, followed by every other day may be helpful to control inflammation but should not be regarded as a preferred form of therapy. Intralesional triamcinolone, although temporarily effective in controlling inflammation, is not considered a viable long-term therapy. Meloxicam Nonsteroidal anti‐inflammatories (NSAIDs) have a place in the management of FCGS post surgically. Short‐term meloxicam is the nonsteroidal of choice by this author. Note, repeated use of meloxicam in cats has been associated with acute renal failure and death. Cyclosporine
Cyclosporine is a potent immunosuppressive agent that inhibits T‐cell activation by blocking the transcription of genes coded for specific pro‐inflammatory cytokines (IL‐2 and IL‐4). If this positive feedback loop of activation of T‐cells by IL‐2 is suppressed, the inflammatory process can be minimized. Cyclosporine can be used to decrease inflammation in refractory cases once all the teeth have been extracted. Side effects from the use of cyclosporine include hepatic dysfunction, impaired renal function, and anemia. There have been anecdotal reports of neoplasia emergence in some of the cats treated. Outdoor cats or cats eating a raw diet should be tested for Toxoplasma gondii prior to cyclosporine therapy. Additionally, cyclosporine should only be administered to indoor cats because outdoor cats are at higher risk of infection (especially toxoplasmosis) due to immunosuppression and impaired ability to fight infection adequately. Side‐effect risk rises with increasing dose and duration of cyclosporine therapy. Informed consent of the usage of cyclosporine is important. Cyclosporine takes time to be effective with improvement often seen by four weeks and the maximum benefit by eight weeks. The absorption rates will also vary with the form of medication. It is recommended that treated patients have blood levels evaluated to avoid toxicity from high levels and to ensure an adequate amount of medication is being administered. Trough whole‐blood cyclosporine levels (attained 12 hours after last dosage given) should be taken monthly if there is no clinical improvement. The goal of > 300 ng/ml should be attained, and if values are lower, treatment dosage is increased accordingly. Sandimmune® and Neoral® are not bioequivalent and cannot be used interchangeably. Sandimune (Novartis) has an expected absorption rate on oral administration of about 30% and Neoral (Novartis) about 60%. Recommended dosage is 2 mg/kg PO BID (Neoral) and up to 7.5– 15 mg/kg PO BID (Sandimune). Adjunct therapy with corticosteroids is recommended in some patients.
110
A blinded study of 16 cats showed significant clinical improvement using a microemulsified suspension of cyclosporine. The product was compounded to 60 mls using 2.5 mg/kg in a cod liver oil base with tuna flavoring added. After compounding, this medication was administered at 1.0 mls PO BID. Establishing trough whole‐ blood cyclosporine levels > 300 ng/ml showed the most significant improvement clinically (72%).
Modified cyclosporine is now available for cats (Atopica – Elanco Animal Health). The dosage for that product is 7.5–10.0 mg/kg daily, given at higher dosage than microemulsified cyclosporine to achieve adequate blood levels. Transient vomiting and diarrhea are the most common side effects of this medication. A notable outcome of this study using Atopica revealed more favorable clinical success with patients that have not received previous corticosteroids (69% vs. 45%). Interferon
Interferon omega (Virbagen; Virbac) has also been used successfully, off‐label, managing refractory cases of FCGS both orally and intralesionally due to antiviral, immunomodulatory, and anti‐proliferative effects. It is important that other causes of dental disease/oral inflammation, which may also be contributing factors to FCGS (e.g. periodontitis, tooth resorption), are investigated and eliminated prior to using interferon. This may involve removal of all the teeth or only the teeth caudal to the canines.
Interferon is a glycoprotein, which is destroyed in the stomach. Transmucosal (topical) administration requires much lower dosage than systemic administration. Normally, owners will report that their cat begins to eat and feel better within a few weeks, but it may take three months or longer before the visible lesions resolve especially if corticosteroids were administered in the past. If there is no apparent improvement in wellbeing within three weeks, the cat should be further investigated to check for other factors such as retained tooth roots or bacterial infection. Supportive therapy with pain relief, appropriate short‐term antibiotic therapy, and oral hygiene for any teeth remaining are also recommended. Mesenchymal adipose-derived stem cell therapy inhibits activated T lymphocyte proliferation. Autologous or allogenic cell infusion given twice (a month apart) appeared to decrease the degree of inflammation and effect a cure in over 60% of refractory cases in one published study. Surgical Management of FCGS
Extraction of Selective Teeth / Full-Mouth Extraction
Laboratory evaluation in cases of FCGS should include CBC, serum profile, bleeding time, thyroid (T4), urinalysis, and tests for FeLV and FIV. A majority of the cases will have elevated globulin levels and will be negative for FeLV and FIV. The purpose of the workup is not to reach a diagnosis, but rather an attempt to identify possible underlying causes and to provide information for safe anesthesia. Testing for calicivirus and Bartonella is not recommended in that the results do not change therapy. Pre‐extraction intraoral radiographs are important to evaluate root anatomy pathology. For those cases of unilateral presentation, histopathology is recommended to rule out malignancy.
Supragingival and subgingival plaque appears to be one of the multifactorial initiating sources of oropharyngeal inflammation. The only treatment thus far shown to have long-term positive results without the need for further medication in a majority of affected cats is tooth extraction to remove plaque retentive surfaces. Removing teeth decreases the plaque burden. The decision whether all teeth are extracted or only the premolars and molars is based on examination findings. If marked inflammation, periodontal pockets or tooth resorption are noted around the canines and/or incisors, those teeth are also extracted.
When caudal stomatitis or marked vestibular mucositis is present and there is no visible inflammation surrounding the canines and incisors, and when radiographic changes are not evident surrounding the canines or incisors, extraction of all teeth and root fragments caudal to the canine teeth is the treatment of choice. When the gingiva surrounding the canines or incisors are inflamed or abnormal on radiographs, they also should be extracted.
111
If available, carbon dioxide laser rastering of inflamed and proliferative tissue in the caudal oral cavity is performed after extractions to remove surface area for plaque to accumulate.
Antibiotics approved to treat dental infections are administered for two weeks postoperatively. Daily prednisolone (0.5mg/kg) is also prescribed for one week after surgery. Pain management in surgical patients is accomplished with pre-anesthetic opioid administration (buprenorphine), intraoperative local anesthetics (bupivacaine), and postoperative opioids given orally for five to seven days.
To evaluate response to extraction in cases of chronic caudal stomatitis, a retrospective study of dental extractions in sixty calicivirus-positive cats was conducted. In that study 50% of the cases resolved without the need for further treatment, 37% significantly improved requiring less medication to control the stomatitis than before the extractions, 13% improved but required similar amounts of continuing anti-inflammatory treatment, and 7% did not improve from medical or surgical care.
For those patients with anorexia prior to presentation that present in poor condition, nutritional support via pharyngostomy or gastrostomy tube is indicated pre-and/or postoperatively until eating returns to normal.
Presurgical radiographs are important to evaluate root anatomy and pathology. Teeth with tooth resorption lesions are often undergoing root replacement resorption, making luxation and elevation difficult. Pulverizing or atomizing the root within the alveolus with a water-cooled high-speed handpiece and dental bur may result in removing excess supporting bone, removing too little tooth, or causing trauma to adjacent anatomy, and should be avoided.
Postoperative examination is performed two weeks after surgery. If any teeth are left, application of a plaque preventative is recommended, and the client is shown how to control plaque daily with Q-tips, OraVet®, and 0.12% chorhexidine gluconate irrigation.
Dental Extractions
Dental extractions are the most commonly performed surgical procedures in general dental practice. The objectives of extractions are to remove the tooth with minimal trauma to the alveolar bone and surrounding soft tissues eliminating periodontal and periapical disease.
x All incisors, canines, and maxillary second premolars have one root. x The maxillary third premolars and all mandibular pre- molars and molar have two roots. x The maxillary fourth premolar has three roots. x The maxillary molar may have one to three roots. Bone overlying the maxillary teeth is thinner com- pared
to bone around the mandibular teeth.
There are variations concerning the number of roots the maxillary third premolar and molar has. In approximately 10 % of cats this tooth is three‐rooted. A preoperative radiograph should be evaluated before extraction.
Pre/Post-Extraction Radiographs
Dental radiographs obtained before extraction provide information regarding shape, number, position of roots, degree of bony anchorage, and can be used as an education tool to review with clients. Post‐extraction radio‐ graphs also supply documentation for the medical record to confirm complete tooth extraction.
Equipment for Extractions
112
x Gauze sponges x Suction tip, if suction available
x Scalpel handle with Nos. 11 and 15 scalpel blades Thumb forceps x Iris scissors Bone curette x 4‐0 and 5‐0 absorbable suture with curved cutting needle Dental elevators – Freer, Molt 2/4,
periosteotome Wing‐tipped elevator set x Root tip pick x Small‐breed extraction forceps or rongeurs Needle holder x Suture scissors x Mouth props or lap sponges to keep the patient’s mouth open while dental extractions are being
performed x Sharpening kit
Flap Design, Procedure, and Closure
Surgical tooth extraction involves removing several millimeters of the coronal buccal or labial alveolar bone underlying the attached gingiva to facilitate creating a bony trough along the root, which provides a purchase point for an elevator to rotate the tooth from the alveolus. This is accomplished by raising a periodontal flap that exposes the alveolar bone and underlying root surface, preserves attached gingiva, and allows suturing without tension. The base through which the attachment and circulation is maintained is called the pedicle. Flap Closure
Surgical closure of extraction defects helps ensure food and oral debris do not enter the extraction site. Closure also minimizes the risk of clot dislodgement resulting in alveolar osteitis (dry socket), which is known to be painful in humans. Absorbable 3‐0–5‐0 suture material should be used to close exposure flaps. Monocryl® (Ethicon, Inc.) is a synthetic, monofilament suture material that combines absorption with the strength and smoothness of nylon suture. Cat gut can also be effective for closing flaps. A swaged‐on 3/8‐circle, reverse‐cutting needle (FS‐2 or P‐3, Ethicon, Inc.) is preferred. The suture needle should be held anterior to the curvature but not at the tip. If the needle is held too close to the tip of the needle holder, the veterinarian will not be able to pass the suture as far as needed through the tissues. Sutures should be placed from movable to non‐movable tissue when possible and the knots should not lie on the incision line. The sutured flap should be tension free. A continuous suture pattern should be considered, because it reduces the number of knots. Inverted knots are preferred, minimizing plaque retention. The surgical knots should include three to five throws (depending on suture type) to prevent loosening.
References
x Arzi, B., Ko, E.M., Verstrate, F.M. et al. (2016 January). Therapeutic efficacy of fresh, autologous mesenchymal stem cells for severe refractory gingivostomatitis in cats. Stem Cells Transl. Med. 5 (1): 75–86.
x Belgard, S., Truyen, U., Thibault, J.C. et al. (2010). Relevance of feline calicivirus, feline immunodeficiency virus, feline leukemia virus, feline herpesvirus and Bartonella henselae in cats with chronic gingivostomatitis. Berl. Munch.
x Bellei, E., Dalla, F., Masetti, L. et al. (2008). Surgical therapy in chronic feline gingivostomatitis (FCGS). Vet. Res.
x Commun. 32: 231–234. x Corbee, R.J., Booij‐Vrieling, H.E., van de Lest, C.H.A. et al. (2012). Inflammation and wound healing in cats
with chronic gingivitis/stomatitis after extraction of all premolars and molars were not affected by feeding of two diets with different omega‐6/omega‐3 polyunsaturated fatty acid ratios. J. Anim. Physiol. Anim. Nutr. 96: 671–680.
113

x Farcas, N., Lommer, M.J., Kass, P.H., and Verstraete, F.J.M. (2014). Dental radiographic findings in cats with chronic gingivostomatitis (2002–2012). J. Am. Vet. Med. Assoc. 244: 339–345.
x Harley, R., Gruffydd‐Jones, T.J., and Day, M.J. (2011). Immunohistochemical characterization of oral mucosal lesions in cats with chronic gingivostomatitis. J. Comp. Pathol. 144: 239–250.
x Lommer, M. (2013). Efficacy of cyclosporine for chronic, refractory stomatitis in cats: a randomized, placebo‐ controlled, double‐blinded clinical study. J. Vet. Dent. 30: 8–17.
x Southerden, P. and Gorrel, C. (2007). Treatment of a case of refractory feline chronic oropharangyeal inflammation with feline recombinant interferon omega.
114
Easy steps to extract those nasty teeth
By Jan Bellows, DVM, Dipl. AVDC, ABVP (canine and feline specialties) ALL PETS DENTAL Weston, Florida
First do no harm… Second figure out which teeth need to be extracted
While the goal in veterinary dentistry is to save teeth, it sometimes becomes necessary to extract them. Indications are fractured teeth, periodontal disease that is not treatable, orthodontic disease, dental crowding, and chronic ulcerative conditions. In addition to additional fees, clients may be come emotionally disturbed over the loss of teeth. The doctor should advise his or her clients of alternative types of therapy prior to treatment if any, for once the tooth is extracted, it is final.
The most common indication for extraction is moderate to advanced periodontal disease. Periodontal disease is progressive and can be painful. If there is evidence of greater than 25% support loss of a tooth extraction be considered.
Instrumentation Elevators: Because there are a variety of sizes of teeth, one needs a variety of sizes of dental elevators. Generally, select the elevator that best fits the contour of the tooth to be extracted. 301ss elevators are even smaller. The 301 series also have been modified by notching the back side of the instrument, creating a fork to assist in preventing the instrument from sliding off alveolar crests. The 301ss would be effective in elevating incisors. The 301s would be effective in elevating incisors, small canines and premolars. While the 301 would be effective in elevating cat canine teeth. The 301, 301s and 301ss elevators are small, delicate elevators. The 301s is especially useful in extracting feline teeth and the
The Heidbrink root tip pick, HB10/11, and Miltex 76 are root tip picks useful in elevation and for extracting retained root tips. They also can be used to cut the gingival attachment off of the tooth prior to displacement with dental elevators.
Extraction Forceps: Smaller extraction forceps have been designed for cat teeth. They have more parallel jaws, increasing the surface contact and are much more effective than the human incisor forceps formerly used in veterinary dentistry. It is best to use spring-loaded forceps.
Magnification & Lighting: One frustrating aspect of the extraction of roots is the limited access and poor visibility. These problems may be decreased by the use of magnification (3 power) and head lamps.
Sterilization of Equipment: Since extraction is a surgical procedure and the instrument penetrates tissue sterile instruments should be used. While it is true that the tissue surrounding the tooth is already infected, it is inappropriate to add different species of bacteria to the infection. Chemical disinfectants may be effective, but they take time to work, and must be thoroughly washed off prior to use. Sharp instruments may become dull by chemical sterilization. Some metals will weaken. Gas sterilization techniques are less hazardous to the instrument. Autoclaving techniques
115
use a combination pressure and steam heat to sterilize instruments. Sterilization must be monitored, either by the use of chemical strips that turn colors when the proper sterile conditions have been achieved or by biological monitors which check for bacterial growth after sterilization. Extraction Technique There are three ways of removing a tooth from its socket-force, elevation and surgical techniques. The force technique fractures bone (and tooth root) and causes more trauma than necessary and is discouraged. Elevation stretches and tears the periodontal ligament fibers by insertion of the elevator into the alveolus and using it as a wedge. Rotational motions rather than “teeter-totter” motions should be used. The tooth is eased out of the socket rather than using brute strength. The key to this approach is to be patient. All of the root should be removed, except in the rare circumstance where more damage would be the result of root retrieval. The surgical technique creates a flap, removes the buccal plate of bone and removes the root through the opening created in the buccal wall. Step-by step Single root teeth in dogs are the incisors, canines, and first premolar, in cats the incisors and canines. The first step in tooth extraction is to sever the gingival attachment. A # 11 scalpel blade, root tip pick or dental elevator is most commonly used. Patiently work all the way around the tooth. Occasionally it may be helpful to use a round or pear-shaped bur on a high-speed handpiece to separate the ligament. Be sure to use plenty of water to keep the tissues cool, otherwise, bone necrosis may occur, secondary to thermal injury. Vertical rotation force occurs when the elevator is used parallel to the root. After the sulcular gingival attachment has been severed, begin to work an elevator, whose curve approximates that of the tooth, into the space between the tooth and the alveolus. It is helpful to place a slow, gentle, steady pressure on the tooth rather than quick, rocking motions. The slow steady pressure (holding the pressure on each side 5 - 15 seconds) will break down the periodontal ligament so that the tooth exfoliates easily. Placing the elevator perpendicular to the crown and tooth root in the interproximal space employs the horizontal extraction position. Pressure is placed on the tooth to be extracted by a coronal rotation of the instrument. Care should be taken not to luxate the tooth that is acting as a fulcrum. When the periodontal ligament breaks down, hold onto the tooth with extraction forceps for easy removal. To increase the speed of healing, the socket and associated gingiva should be disinfected by curettage and irrigation. Finally, the gingiva is sutured using 4-0 suture material (catgut, Monocryl). Section multi-root teeth before extracting them. Once the crown has been sectioned, each individual root is treated like a separate single rooted tooth and extracted. The only difference in this technique is that adjoining roots may be used as a fulcrum for the extraction before and after the root has been elevated. A high-speed handpiece with a 701 bur works best. First expose the furcation and start sectioning the tooth from the furcation towards the crown. The incision through the crown can go directly up from the furcation, splitting the crown in half or thirds. Alternatively, the incision can be angled toward a crown developmental fissure, sectioning the crown unequally.
116
In the dog, all premolars except the first premolar (1 root) and the maxillary fourth premolar (3 roots), should be sectioned by using a high-speed bur to cut between the tip of the crown and the furcation. The maxillary fourth premolar should be separated between the furcations and the crown of each of the three roots. This will create three separate tooth segments that can be elevated one at a time. Flaps Surgical extractions are performed by making releasing incisions on the mesiobuccal and distobuccal line angles between adjacent teeth. These releasing incisions are joined by an intrasulcular incision that follows the gingival margin. The periosteum and gingiva are elevated off the bone with a periosteal elevator, to create a full-thickness gingival flap. The buccal plate of bone over the tooth is removed with a water-cooled high-speed bur. The root is removed, and the flap is closed without tension over the alveolar socket. Post op Radiographs taken postoperatively allow the practitioner to verify that the entire tooth has been extracted. Radiographs create a permanent record of the procedure. The trauma and possible pain to the patient caused by the disease condition or the procedure creates the need for the consideration of pain medication administered by the injection of a local anesthetic, parenteral injection, oral medication, and skin patch when indicated. Complications
• Tooth roots may become separated during the extraction procedure creating non-extracted root fragments. The preferred treatment in this situation is to create a buccal flap over the fragment for removal.
• Collateral damage to other oral or extra oral structures including perforation and orbital contusion of the eye with sharp dental instruments.
Using proper instrumentation and extraction technique makes the extraction simpler, safer and easier on the patient and practitioner. Multirooted teeth should always be sectioned prior to extraction to prevent the likely hood of fractured root segments. Difficult extractions can be accomplished by gingival flap surgery to facilitate atraumatic elevation of the root in a buccal direction. Pre and postoperative radiographs and pain control help document what has been done and provide the patient with a relatively painless procedure. References
1. DeBowes LJ. Simple and surgical exodontia. Vet Clin Small Anim 2005; 35:963–984. 2. Gunew M, Marshall R, Lui M, Astley C. Fatal venous air embolism in a cat undergoing dental extractions. J
Small Anim Pract2008; 49, 601–604. 3. Holmstrom SE, Frost, P, Eisner ER. Exodontics. In: Veterinary Dental Techniques for the Small Animal
Practitioner. 3rd ed. Philadelphia: Saunders, 2004, pp. 291–338. 4. Kapatkin AS, Manfra Marretta S, Schloss AJ. Problems associated with basic oral surgical techniques.
In: Problems in Veterinary Medicine. Dentistry. Manfra Marretta S ed., 1990; 2: 85–109. 5. Reiter AM, Brady CA, Harvey CE. Local and systemic complications in a cat after poorly performed dental
extractions. J Vet Dent 2004;21: 215–221. 6. Reiter AM. Dental surgical procedures. In: BSAVA Manual of Canine and Feline Dentistry. Eds. C. Tutt, J.
Deeprose, D. Crossley. BSAVA, Gloucester (UK), 2007, pp. 178– 195. 7. Scheels JL, Howard PE. Principles of dental extraction. Sem Vet Med Surg 1993; 8:146–154.
117
8. Smith MM, Smith EM, La Croix N, et al. Orbital penetration associated with tooth extraction. J Vet Dent 2003;20:8–17.
9. Van Foreest A: Exodontia (tooth extraction in dogs). EJCAP 1993; 3:35–42. 10. Verstraete FJM. Exodontics. In: Textbook of Small Animal Surgery. Philadelphia: WB Saunders, 2003; 2696–
2709.
118
Calling all vets and vet techs- how to speak derm successfully! Ashley Bourgeois DVM, Dip ACVD Animal Dermatology Clinic Portland, OR Caregiver burden
Pruritus can dramatically affect patient and owner quality of life. Pet owners have reported that, as the level of itch goes up in their pet, their pet’s quality of life goes down. Market research has shown most (75%) of owners with pruritic dogs are concerned for their pet’s well-being. Emotions expressed by owners of these itchy dogs were sadness (46%), frustration (44%), and helplessness (43%).1 Studies have shown an inverse relationship between QoL (quality of life) and pruritus.2,3
Caregiver burden is defined as encountering a range of problems while providing informal care to a loved one with an illness. One study has suggested that, by the time owners bring their dog to a dermatology service, they have a higher caregiver burden than that of the typical dog owner.4 In addition, when the skin disease was well controlled, caregiver burden was equivalent to a normal dog with no disease.4 There are many issues that can lead to the frustration of owners of allergic pets. These can include odor, appearance of lesions, time spent at appointments, finances, failed treatments, and encountering mixed messages between different sources. Considering the complexity of allergic itch, it may be easy for owners to feel uncertain, disappointed, irritated, and even angry. Good client communication and empathy can help. The impact of allergic itch on patient and owner quality of life, as well as the potential for client frustration, highlights the importance of a consistent, thorough team approach to diagnosing and treating patients with allergic pruritus. Plant the seed early
Allergies are not cured, but managed. In most cases, there will not be a one-time treatment that will provide a dog or cat a cure that lasts forever, so owners should know that up front. Continued therapy and an ongoing veterinary relationship will be required the rest of the pet’s life. It is important for owners to realize that from the first appointment. A plan will be formulated that works for that particular patient and owner, but frequent check-ins and therapies will be required to keep the pet comfortable. Your client understanding that from the beginning can save a lot of frustration in the future. Infections are a secondary issue related to allergies. It can be confusing for an owner to realize allergies and infections are different issues but impact one another. When owners understand this relationship, they are often more willing to commit to multimodal therapy, including frequent bathing and ear flushes. Even with the first ear infection, let the owner know it can be an early sign of allergies. Give owners signs to watch for at home such as paw chewing, scratching, rubbing, etc. This prevents owners from being surprised when there is another infection or symptoms progress.
119
Address the short-term and long-term concerns of the owner. Assure them that their pet’s current pruritus will be relieved immediately with an antipruritic. But, to prevent recurrences and infection chronically, the root cause needs to be worked up which takes time. Be proactive about flares
Even well-controlled allergic pets experience flares. For example, seasons change, food gets dropped, and flea control gets missed. Owners should be educated to understand that flares happen and what that looks like. Routine recalls should be established to check in so the owner feels supported. In addition, providing different methods of contact such as phone, email, text messaging, and communication apps can help the owner feel at ease in a communication method that best works for them. Flares happen. Owners should be guided to monitor for the various signs of flare-ups, even if their pet is currently doing well. Having a proactive mentality should be encouraged. Do what is possible
Figuring out the owner’s main goal is essential when starting a diagnostic investigation for allergic disease. Every client has a different priority or definition of success for their pet.
o Do they want their pet to stop itching today? o Do they care most about getting rid of the odor? o Are they proactive owners who want to avoid chronic medications? o Will they bathe daily if it avoids systemic antibiotics?
The best plan is the one that can get done. If you have an elderly, arthritic client, daily baths for a Great Dane might not be possible. If a pet is fearful of veterinary visits, maybe we should rely on oral medications given at home rather than injections given within the clinic. It is essential to see if the plan you develop is a realistic one for the owner. Home care instructions could be clear and explain what is going on besides what medications to give. Veterinary visits can be overwhelming, and owners can easily forget what was discussed. Even just a sentence or two can help an owner understand the steps moving forward. Empathize and relate
Remember, skin issues are generally a visual ailment. Your client sees physical changes happening with their pet’s skin, and they want to take care of them. Clients can come in with many different expectations and emotions. Each client needs to be handled a different way regarding how to present information such as diagnostics and treatment. It takes practice, but you’ll learn to pick up on subtleties that reveal the needs of each individual client. Some clients want lots of information, and will want to understand the reasoning behind every diagnostic test, treatment, and long-term outlook. These clients will ask lots of questions and be very engaged (direct eye contact, head nodding, etc.). If your client is disengaged during an appointment
120
(blank stare, looking around the room, fidgeting, etc.), it may be due to information overload. Some clients just want you to give clear home care instructions without the details. If you aren’t sure what they need, take a step back and check in with the client. Pause partway through and ask, “What questions do you have?”. Empathy for frustrated clients is a skill that will ultimately lead to relief for their pets. When we can relate to them and recognize their goals, we have the best opportunity to make progress with a treatment plan and become a part of that pet’s team. Relate it to humans
People tend to understand things better if they know a human who has gone through something similar. For example, if an owner has a child with allergies causing sneezing and conjunctivitis, you can explain how their dog’s ear infection is similar to summer causing their child’s symptoms to progress. Other examples (though not exactly the same immunologically) can be food allergies or ectoparasite/insect hypersensitivity. Peanut allergy is prevalent among people, so it is an easy thing for owners to understand. When explaining why it is important to use a prescription food for a diet trial rather than an over-the-counter diet, relate this to how sensitive peanut allergic children are to products just made in a facility with peanuts. Most of us are familiar with the warnings on various food products - "Manufactured on equipment that processes products containing peanuts". Prescription diets take various precautions such as testing for common allergenic proteins and strict cleaning/processing procedures to avoid residue from being present in a pet food, even if it is not listed on the ingredient list. This is why it is extremely important to use prescription or home-cooked foods for a diet trial, and not an over-the-counter diet. Some owners are hesitant to use flea prevention since they don’t visualize fleas in their environment. You can compare the different immunological reaction a person with a bee allergy has compared to a non-allergic individual when exposed. It takes minimal exposure for some flea allergic pets to have a tremendous pruritic response. These are just simple concepts that can provide a clearer picture for owners regarding your recommendations for the allergic workup. Don’t forget referral!
Referral to a board-certified dermatologist should be considered early in allergic patients. Even if symptoms and infections are not severe, a dermatologist can intervene with safe therapies to prevent progression. The veterinary team should be proactive and let owners know the option is available. Develop a relationship with your local dermatologist because many cases need to be co-managed. Also, you can discuss cases before referring them to maximize diagnostic results upon initial examination. If you don’t have a dermatologist in your area there are telemedicine companies available that provide consultation options regardless of your location. References 1. Pruritus: Insight into the dog and dog owner’s journey - Quantitative Report. Prepared for Zoetis, May 2013
121
2. Noli, C. Assessing quality of life for pets with dermatologic disease and their owners. Vet Clin North Am Small Anim Pract. 2019; 49(1): 83-93. 3. Favrot C, Linek M, Mueller R, et al. Development of a questionairre to assess the impact of atopic dermatitis on health-related quality of life of affected dogs and their owners. Vet Dermatol 2010; 21(1): 64-70. 4. Spitznagel M, Solc M, Chapman K, et al. Caregiver burden in the veterinary dermatology client: comparison to healthy controls and relationship to quality of life. Vet Dermatol 2019;30(1):3-e2.
122
Tackling the itchy cat challengeAshley S. Bourgeois, DVM, Dip ACVDAnimal Dermatology Clinic Portland, OR
IntroductionIdentifying pruritus in cats can be difficult due to their independent nature. Owner assessment can be influenced by the amount of time the owner spends with the cat and how the owner defines itchiness. Overgrooming is often overlooked as being a sign of “itch”. A trichogram can be very informative to help determine if a cat is licking excessively. Hairs may be plucked from regions of hypotrichosis and microscopically evaluated for signs of trauma. Hairs with tapered ends are normal. Broken and blunted follicular tips suggest overgrooming.
Diagnostic testing for a pruritic cat can include skin scraping, flea combing, cytology, dermatophyte culture, Wood’s light examination, and skin biopsies. Finally, if all other pruritic disorders have been ruled out, appropriate work-up for allergic skin disease should be pursued.
It’s important to remember multiple causes of pruritus can be present in the same patient and pruritic effect can be additive. For example, a food allergic cat infested with fleas will be more pruritic than a cat with only one of those conditions. In order to achieve maximum comfort, all possible causes of pruritus must be managed.
Collecting historyHistory is one of the most valuable diagnostic tools in dermatology. Sometimes it provides greater diagnostic significance than the physical/dermatologic exam because no lesion pattern in cats is pathognomonic for any specific diagnosis. Taking the time to record and evaluate a thorough history helps you make the diagnosis more quickly and accurately. Signalment, seasonality, travel history, pruritus level, and response to previous medications can provide significant diagnostic information. An important component to proper history taking is to ask open ended questions. History questionnaires can be a time effective way to collect important information prior to the appointment.
The dermatologic examinationClinicians can gain critical diagnostic information without expensive and/or invasive tests, just by looking at the skin. The type and distribution of lesions provide valuable etiologic information. When pruritus is demonstrated in the exam room, the clinician can gain a clearer understanding of the severity of this patient's condition. Keeping records on size of lesions such as eosinophilic plaques and areas of self-induced alopecia can help assess the response to therapy on recheck.
Secondary infectionsSuperficial bacterial pyoderma is underdiagnosed in cats. Crusted papular eruptions or miliary dermatitis are the most common presentation of folliculitis in the cat. However, large areas of erythematous and erosive dermatoses can also be associated with large numbers of bacterial organisms. Bacterial infections are generally considered a secondary complication of underlying disease, but management of the bacterial component can be a critical factor in achieving control and remission of the primary disease. It is essential that cutaneous cytology is routinely performed on skin lesions to appropriately diagnose and treat the pyoderma while working up the underlying primary cause.
Case presentation #1- Bald belly cat
Hints in the history: In young cats, ectoparasites (such as Ctenocephalides felis) are usually at the top of the differential list. It is important to ask about parasiticides used on the presenting cat AND all of the other animals at home. Don’t assume a client is administering parasiticides just because they have purchased them in the past. Travel, seasonality, gastrointestinal signs, and dietary history can provide useful clues to decipher between food allergy, flea allergy, and atopy.
123
Paraneoplastic alopecia may be a higher consideration in older cats. Has the cat ever had skin issues prior to this? How is the cat systemically feeling? Psychogenic alopecia is far less common than hypersensitivity dermatitis, but since these conditions may be clinically indistinguishable information about the cat's anxiety level and behavior may aid in the diagnosis.
Exam tips: It is important to differentiate between hair falling out and hair being pulled out. As discussed above, a trichogram can help differentiate. Pruritic diseases such as hypersensitivity disorders cause self-induced alopecia (pulled out). Regions such as the caudal abdomen are easily accessible to the cat's mouth, thus alopecia at these regions may be more commonly self-induced.
Cats with lesions also affecting the rump or tail and with miliary dermatitis are more likely to be flea allergic. Look for evidence of fleas and flea dirt. However, these do not have to be identified for a flea allergy to be the cause of pruritus.
For paraneoplastic alopecia, the lesions are typically bilaterally symmetrical and the skin appears shiny. The cat will also systemically not feel well.
The workup: Diagnosing a hypersensitivity disorder can often occur with history alone. But identifying the exact type of hypersensitivity disorder can be difficult, especially when more than one allergy is present. Keep in mind that atopic dermatitis is typically a diagnosis of exclusion.
Besides cytology to identify secondary infection, a parasiticide trial with a quality product is very important and often the first step in pruritic rule outs. Ingredients such as spinosad (Comfortis®; Elanco), selamectin (Revolution®; Zoetis) and dinotefuran (Vectra® (with pyriproxifen); Ceva) can provide great speed of kill for fleas. However, the new class isoxazolines have been beneficial since they are also effective against several types of lice and mites. This is very helpful during the work up of a pruritic cat. Commercially available isoxazolines labeled for cats in the United States include sarolaner (Revolution Plus® (with selamectin); Zoetis) and fluralaner (Bravecto® and Bravecto Plus® (with moxidectin); Merck).
Case presentation #2 Facial excoriations/ulceration
Hints in the history: Several types of feline parasitic diseases including feline scabies (Notoedres cati), ear mites (Otodectes cynotis), and feline demodicosis (Demodex cati and Demodex gatoi) can present as pruritic facial dermatitis. If humans or other cats in the home have also experienced pruritus it is important to pursue a parasiticidal trial first.
Cutaneous adverse food reactions (CAFR) often present as head and neck pruritus in the cat. Although the cat is presenting for skin disease, don't forget to ask about gastrointestinal upset. Cats with CAFR present significantly more often with digestive signs compared with those affected by other types of hypersensitivity dermatitis.
History of any exacerbation of symptoms caused by stress and/or glucocorticoid administration can be helpful in assessing the possibility of viral infections such as feline rhinotracheitis (feline α-herpesvirus-1). Upper respiratory symptoms including sneezing and conjunctivitis may also be present.
Exam tips: No lesion pattern is pathognomonic for any specific diagnosis in the cat. However, one multicenter study out of Europe found that cats with food allergy presented significantly more frequently with lesions affecting the head and neck (Hobi et al 2011). Look for clinical signs such as excoriations and from secondary infection. Otoscopic examination should be performed routinely to evaluate for signs of otitis which is common in food allergic cats.
124
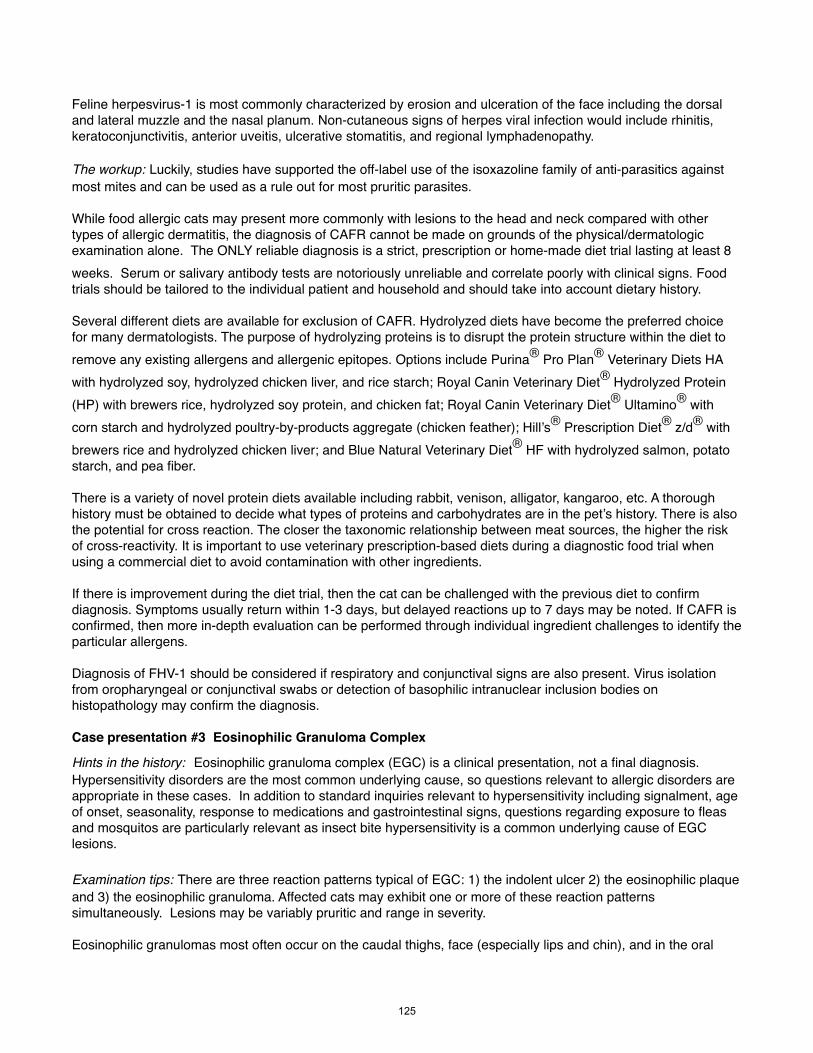
Feline herpesvirus-1 is most commonly characterized by erosion and ulceration of the face including the dorsal and lateral muzzle and the nasal planum. Non-cutaneous signs of herpes viral infection would include rhinitis, keratoconjunctivitis, anterior uveitis, ulcerative stomatitis, and regional lymphadenopathy.
The workup: Luckily, studies have supported the off-label use of the isoxazoline family of anti-parasitics against most mites and can be used as a rule out for most pruritic parasites.
While food allergic cats may present more commonly with lesions to the head and neck compared with other types of allergic dermatitis, the diagnosis of CAFR cannot be made on grounds of the physical/dermatologic examination alone. The ONLY reliable diagnosis is a strict, prescription or home-made diet trial lasting at least 8 weeks. Serum or salivary antibody tests are notoriously unreliable and correlate poorly with clinical signs. Food trials should be tailored to the individual patient and household and should take into account dietary history.
Several different diets are available for exclusion of CAFR. Hydrolyzed diets have become the preferred choice for many dermatologists. The purpose of hydrolyzing proteins is to disrupt the protein structure within the diet to remove any existing allergens and allergenic epitopes. Options include Purina® Pro Plan® Veterinary Diets HA with hydrolyzed soy, hydrolyzed chicken liver, and rice starch; Royal Canin Veterinary Diet® Hydrolyzed Protein (HP) with brewers rice, hydrolyzed soy protein, and chicken fat; Royal Canin Veterinary Diet® Ultamino® with corn starch and hydrolyzed poultry-by-products aggregate (chicken feather); Hill’s® Prescription Diet® z/d® with brewers rice and hydrolyzed chicken liver; and Blue Natural Veterinary Diet® HF with hydrolyzed salmon, potato starch, and pea fiber.
There is a variety of novel protein diets available including rabbit, venison, alligator, kangaroo, etc. A thorough history must be obtained to decide what types of proteins and carbohydrates are in the pet’s history. There is also the potential for cross reaction. The closer the taxonomic relationship between meat sources, the higher the risk of cross-reactivity. It is important to use veterinary prescription-based diets during a diagnostic food trial when using a commercial diet to avoid contamination with other ingredients.
If there is improvement during the diet trial, then the cat can be challenged with the previous diet to confirm diagnosis. Symptoms usually return within 1-3 days, but delayed reactions up to 7 days may be noted. If CAFR is confirmed, then more in-depth evaluation can be performed through individual ingredient challenges to identify the particular allergens.
Diagnosis of FHV-1 should be considered if respiratory and conjunctival signs are also present. Virus isolation from oropharyngeal or conjunctival swabs or detection of basophilic intranuclear inclusion bodies on histopathology may confirm the diagnosis.
Case presentation #3 Eosinophilic Granuloma Complex
Hints in the history: Eosinophilic granuloma complex (EGC) is a clinical presentation, not a final diagnosis. Hypersensitivity disorders are the most common underlying cause, so questions relevant to allergic disorders are appropriate in these cases. In addition to standard inquiries relevant to hypersensitivity including signalment, age of onset, seasonality, response to medications and gastrointestinal signs, questions regarding exposure to fleas and mosquitos are particularly relevant as insect bite hypersensitivity is a common underlying cause of EGC lesions.
Examination tips: There are three reaction patterns typical of EGC: 1) the indolent ulcer 2) the eosinophilic plaque and 3) the eosinophilic granuloma. Affected cats may exhibit one or more of these reaction patterns simultaneously. Lesions may be variably pruritic and range in severity.
Eosinophilic granulomas most often occur on the caudal thighs, face (especially lips and chin), and in the oral
125
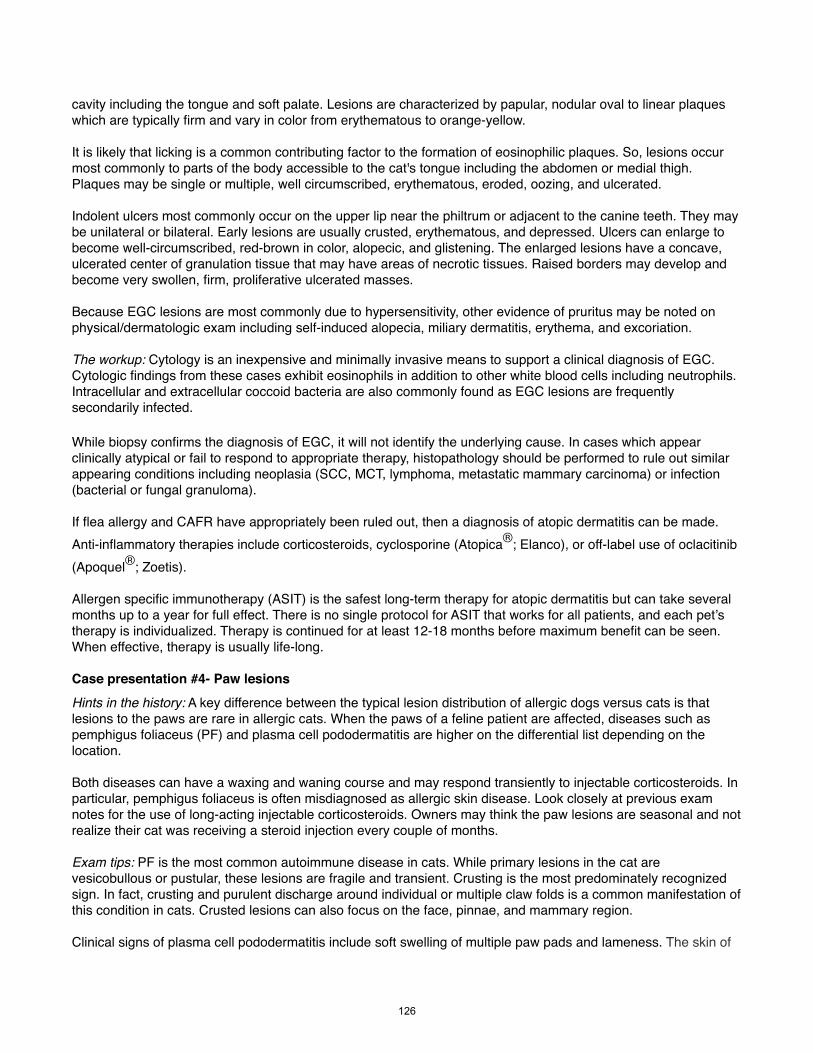
cavity including the tongue and soft palate. Lesions are characterized by papular, nodular oval to linear plaques which are typically firm and vary in color from erythematous to orange-yellow.
It is likely that licking is a common contributing factor to the formation of eosinophilic plaques. So, lesions occur most commonly to parts of the body accessible to the cat's tongue including the abdomen or medial thigh. Plaques may be single or multiple, well circumscribed, erythematous, eroded, oozing, and ulcerated.
Indolent ulcers most commonly occur on the upper lip near the philtrum or adjacent to the canine teeth. They may be unilateral or bilateral. Early lesions are usually crusted, erythematous, and depressed. Ulcers can enlarge to become well-circumscribed, red-brown in color, alopecic, and glistening. The enlarged lesions have a concave, ulcerated center of granulation tissue that may have areas of necrotic tissues. Raised borders may develop and become very swollen, firm, proliferative ulcerated masses.
Because EGC lesions are most commonly due to hypersensitivity, other evidence of pruritus may be noted on physical/dermatologic exam including self-induced alopecia, miliary dermatitis, erythema, and excoriation. The workup: Cytology is an inexpensive and minimally invasive means to support a clinical diagnosis of EGC. Cytologic findings from these cases exhibit eosinophils in addition to other white blood cells including neutrophils. Intracellular and extracellular coccoid bacteria are also commonly found as EGC lesions are frequently secondarily infected.
While biopsy confirms the diagnosis of EGC, it will not identify the underlying cause. In cases which appear clinically atypical or fail to respond to appropriate therapy, histopathology should be performed to rule out similar appearing conditions including neoplasia (SCC, MCT, lymphoma, metastatic mammary carcinoma) or infection (bacterial or fungal granuloma).
If flea allergy and CAFR have appropriately been ruled out, then a diagnosis of atopic dermatitis can be made. Anti-inflammatory therapies include corticosteroids, cyclosporine (Atopica®; Elanco), or off-label use of oclacitinib (Apoquel®; Zoetis).
Allergen specific immunotherapy (ASIT) is the safest long-term therapy for atopic dermatitis but can take several months up to a year for full effect. There is no single protocol for ASIT that works for all patients, and each pet’s therapy is individualized. Therapy is continued for at least 12-18 months before maximum benefit can be seen. When effective, therapy is usually life-long.
Case presentation #4- Paw lesionsHints in the history: A key difference between the typical lesion distribution of allergic dogs versus cats is that lesions to the paws are rare in allergic cats. When the paws of a feline patient are affected, diseases such as pemphigus foliaceus (PF) and plasma cell pododermatitis are higher on the differential list depending on the location.
Both diseases can have a waxing and waning course and may respond transiently to injectable corticosteroids. In particular, pemphigus foliaceus is often misdiagnosed as allergic skin disease. Look closely at previous exam notes for the use of long-acting injectable corticosteroids. Owners may think the paw lesions are seasonal and not realize their cat was receiving a steroid injection every couple of months.
Exam tips: PF is the most common autoimmune disease in cats. While primary lesions in the cat are vesicobullous or pustular, these lesions are fragile and transient. Crusting is the most predominately recognized sign. In fact, crusting and purulent discharge around individual or multiple claw folds is a common manifestation of this condition in cats. Crusted lesions can also focus on the face, pinnae, and mammary region.
Clinical signs of plasma cell pododermatitis include soft swelling of multiple paw pads and lameness. The skin of
126

the pad may develop a purplish hue and may even ulcerate. The central metacarpal or metatarsal pads are usually affected. However, all pads may be involved.
The workup: Cytology can be suggestive of PF with the finding of acantholytic keratinocytes, however histopathology is needed for definitive diagnosis in most cases. Acantholytic cells in the cat can be challenging to isolate on cytology or histopathology and evaluation of multiple sectioning samples may need to be requested. Focusing on lesions with heavy crusting can increase the diagnosis yield. Treatment with corticosteroids, cyclosporine, or chlorambucil is the most commonly used therapy for this condition. Prognosis is generally good although some cases can be challenging to achieve remission.
To diagnose plasma cell pododermatitis, fine needle aspirate of predominantly plasma cells and clinical presentation may be enough. However, histopathology may be needed for definitive diagnosis. Treatment options include doxycycline (which should be given with water or in a liquid form with cats), corticosteroids, cyclosporine, or surgical excision.
References
1. Ravens P, Xu B, et al. Feline atopic dermatitis: a retrospective study of 45 cases (2001-2012). Vet Dermatol 2014. 25: 95-e28.
2. Yang C, Huang H. Evidence-based veterinary dermatology: a review of published studies of treatments for Otodectes cynotis (ear mite) infestation in cats. Vet Dermatol 2016. 27: 221-e56.
3. Guaguere E, Muller A, et al. Feline demodicosis: a retrospective study of 12 cases. Vet Dermatol 2004. 15: 34.
4. Yu H, Vogelnest L. Feline superficial pyoderma: a retrospective study of 52 cases (2001-2011). Vet Dermatol 2012. 23: 448-e86.
5. Moriello K, Coyner K, et al. Diagnosis and treatment of dermatophytosis in dogs and cats. Vet Dermatol 2017. 28. 266-e68.
6. Simpson D, Burton G. Use of prednisolone as a monotherapy in the treatment of feline pemphigus foliaceus: a retrospective study of 37 cats. Vet Dermatol. 24: 598-e144.
7. Caporali C, Albanese F, et al. Two cases of feline paraneoplastic alopecia associated with a neuroendocrine pancreatic neoplasia and a hepatosplenic plasma cell tumour. Vet Dermatol 2016. 27: 508-e137.
8. Woolley KL, Kelly RF, Fazakerley J et al. Reduced in vitro adherence of Staphylococcus species to feline corneocytes compared to canine and human corneocytes. Vet Dermatol 2008; 19: 1–6.
9. Bryan J, Frank L. Food allergy in the cat: a diagnosis by elimination. Journal of Feline Medicine and Surgery 2010; 12: 861-866.
10. Hobi S, et al. Clinical characteristics and causes of pruritus in cats: a multicenter study on feline hypersensitivity-associated dermatoses. Vet Dermatol. 2011;22(5):406-413.
127
Building cultural competence and improving spanish communication with latinx clients
By Mariacamila Garcia Estrella DVM/MPH Candidate, Cornell CVM 2023 [email protected] Abstract: This presentation is aimed at increasing awareness and understanding of Latinx culture among veterinarians and how they can better connect and communicate with Latinx clients. It aims to do this via personal anecdotes from the author, statistics regarding the lack of diversity in the profession and by providing an overview of Latinx culture in the United States in the context of veterinary medicine. The presentation also provides advise on how to build rapport with Latinx clients and increase support for Latinx veterinary staff and pre-veterinary/veterinary students Keywords: Diversity, Inclusion, Latinx, Cultural Competence, Latinx Culture Introduction The author describes her personal immigration story, the difficulties of growing up as a first generation Colombian-American, explains naming conventions in Latinx countries, the difficulties of becoming a U.S citizen, and her personal journey to veterinary school. She also discusses how she first realized the importance of being bilingual and bicultural in veterinary medicine. Building an understanding of latinx culture in the context of veterinary medicine In this section the author explains cultural competence, defines the differences between Hispanic, Latino(a), Latinx and Spanish, provides an overview of the lack of diversity of Latinx and other BIPOC people enrolled in veterinary school as well as those that are practicing veterinarians. She discusses the importance of representation in veterinary medicine and describes the average Latinx pet owner in the U.S. She goes on to emphasize the rapid growth of the Latinx population and why veterinarians should care about this. The author also describes the factors affecting pet ownership among Latinx people, how acculturation highly influences views towards animals, and describes key features of Latinx culture. She also discusses the importance of migrant farmworkers and why production animal veterinarians should be more aware of their struggle. Building rapport with latinx clients In this section the author provides a list of suggestions on how to interact with Latinx clients in order to improve veterinarian-client relations. Supporting latinx veterinarians, veterinary students, and veterinary technicians In this part of the presentation the author provides suggestions for improving inclusivity and equity of Latinx people and other BIPOCs in veterinary medicine. She also introduces the work of the Latinx Veterinary Medical Association, a new affinity group dedicated to improving the
128
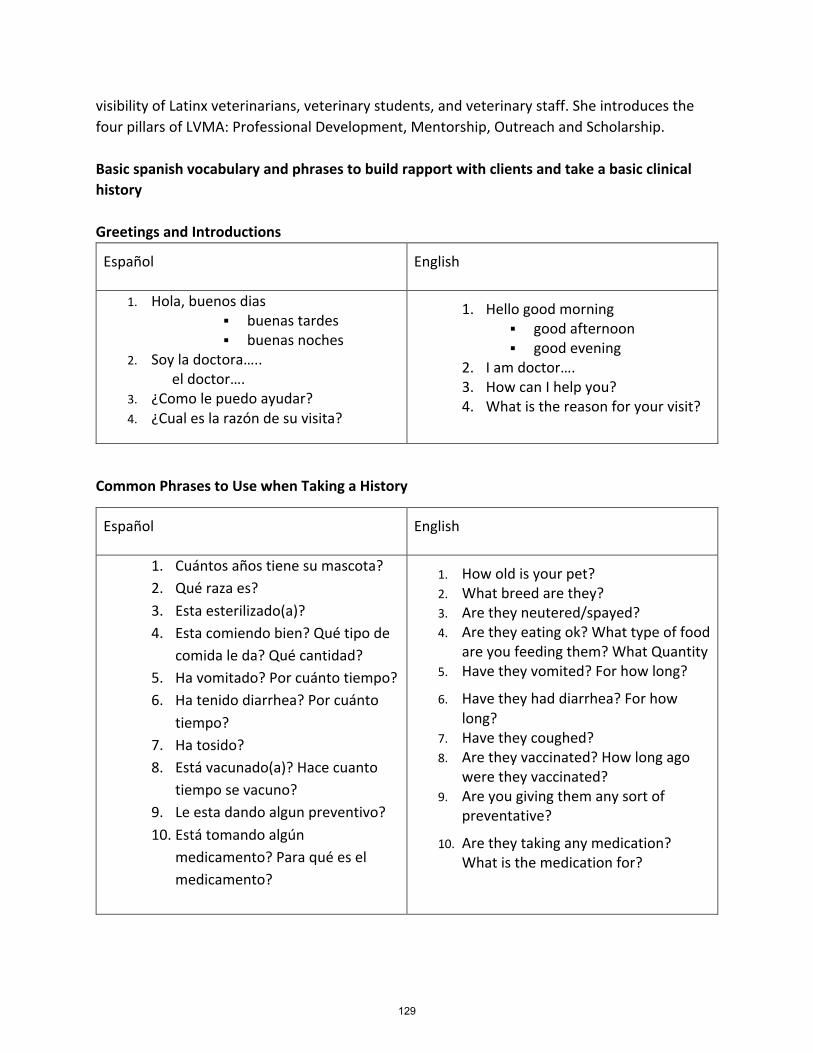
visibility of Latinx veterinarians, veterinary students, and veterinary staff. She introduces the four pillars of LVMA: Professional Development, Mentorship, Outreach and Scholarship. Basic spanish vocabulary and phrases to build rapport with clients and take a basic clinical history Greetings and Introductions
Español
English
1. Hola, buenos dias § buenas tardes § buenas noches
2. Soy la doctora….. el doctor….
3. ¿Como le puedo ayudar? 4. ¿Cual es la razón de su visita?
1. Hello good morning § good afternoon § good evening
2. I am doctor…. 3. How can I help you? 4. What is the reason for your visit?
Common Phrases to Use when Taking a History
Español
English
1. Cuántos años tiene su mascota? 2. Qué raza es? 3. Esta esterilizado(a)? 4. Esta comiendo bien? Qué tipo de
comida le da? Qué cantidad? 5. Ha vomitado? Por cuánto tiempo? 6. Ha tenido diarrhea? Por cuánto
tiempo? 7. Ha tosido? 8. Está vacunado(a)? Hace cuanto
tiempo se vacuno? 9. Le esta dando algun preventivo? 10. Está tomando algún
medicamento? Para qué es el medicamento?
1. How old is your pet? 2. What breed are they? 3. Are they neutered/spayed? 4. Are they eating ok? What type of food
are you feeding them? What Quantity 5. Have they vomited? For how long?
6. Have they had diarrhea? For how long?
7. Have they coughed? 8. Are they vaccinated? How long ago
were they vaccinated? 9. Are you giving them any sort of
preventative?
10. Are they taking any medication? What is the medication for?
129

References:
1. Western. What does it mean to be culturally competent? http://makeitourbusiness.ca/blog/what-does-it-mean-be-culturally-competent#:~:text=Cultural%20competence%20is%20the%20ability,cultural%20practices%20and%20world%20views
2. Pawsibilities. Background. Accessed Septermber 30,2020. https://pawsibilitiesvetmed.com/1931-2/
3. AAVMC. Annual Data Report. doi:10.1017/CBO9781107415324.004 4. Research and Markets Adds Report: Hispanics as Pet Market Consumers.
Manufacturing Close-Up. 2017. Accessed September 29, 2020 https://search-ebscohostcom.proxy.library.cornell.edu/login.aspx?direct=true&db=edsgbe&AN=edsgcl.515780488&site=eds-live&scope=site
5. Landau RE. Assessing the preparedness of the veterinary profession to communicate with limited English proficient Spanish-speaking pet owners. Diss Abstr Int Sect B Sci Eng. 2015;AAI3613172. https://search.proquest.com/docview/1648596449?accountid=14874%0Ahttp://whel-primo.hosted.exlibrisgroup.com/openurl/44WHELF_BANG/44WHELF_BANG_services_page?genre=dissertations+%26+theses&issn=&title=Assessing+the+preparedness+of+the+veterinary+profession+.
130
Disaster response made easy: Infectious diseases By Jenifer Chatfield, DVM, DACZM, DACVPM DrJenTheVet.com Dade City, Florida Disaster response in the face of disease outbreaks is typically complex, however infectious diseases present special considerations in their response. Infectious disease response ranges from containment to eradication and may include containment measures such as quarantine and isolation. The principles on which these decisions are made are based in science and medicine. Containment measures in disaster response are not novel concepts and are, in fact, used fairly routinely by public health officials. Unfortunately, most of the general public is unaware of these measures taken to safeguard the public health. How do we know when to respond? Recognizing when to respond can be as important as understanding how to respond. Initially, the index case of any outbreak is identified as a “suspect clinical case.” Then, a presumptive test is performed and if positive, then the case is termed a presumptive positive case. This initial screening test is typically performed by a local or state lab and will be relied upon for negative results that are truly negative. Following a presumptive positive result, a conformational test will be performed at a federally accredited lab. A diagnostic test performed for this purpose will ideally have a very low false positive rate. This final confirmation will most often be performed at NVSL (animal/agriculture samples) or at the CDC (human samples and some animal samples), but not exclusively. Only after the results are confirmed at a federally accredited lab will the full response to a foreign pathogen outbreak be initiated. Tools of the Response Whether an agriculture or public health led response, the tools available for disease containment and eradication remain the same, except for one – depopulation or euthanasia is a tool unique to the agriculture field. With that single exception, the tools available include:
• Quarantine – separation of those individuals who may have been exposed to the pathogen but are currently deemed not infected.
• Isolation – separation of those individuals currently confirmed to be infected • Cordon Sanitaire – quarantine of a geographic area to prevent the exit of anyone or any
creature from the area and contain the infection until the disease has “burned out” in the population. Typically, border is attended by military forces. This tool is RARELY used.
Take home points • Disaster Response follows the same incident command structure, no matter the hazard. • Infectious disease response can complex due to the need for containment measures. • Veterinarians are uniquely positioned to contribute significantly to efficient response to
infectious diseases. • The public health structure in the US relies on response partners, including veterinarians, to
successfully respond to infectious disease outbreaks.
131
• In today’s global health community, it is important for all healthcare professionals (includingveterinarians!) engage in infectious disease prevention and response.
References 1. Nightingale SL, Prasher JM, Simonson S. Emergency Use Authorization (EUA) to enable use of
needed products in civilian and military emergencies, United States. Emerg Infect Dis. 2007 Jul.Available from http://wwwnc.cdc.gov/eid/article/13/7/06-1188.
2. Smith RD. Responding to global infectious disease outbreaks: lessons from SARS on the role of riskperception, communication and management. Soc Sci Med. 2006 Dec;63(12):3113-23. Epub 2006Sep 15.
132

Emergency tracheotomy: The surgical parachute that saves lives
Dennis Tim Crowe, Jr., DVM, DACVS-Emeritus, Charter DACVECC, FCCM, NRAEMT, CFF
Mobile Veterinary Surgery of Georgia; Veterinary Surgery, Emergency and Critical Care Consulting, Bogart, GA, and VCA Regional Institute for Veterinary Emergencies and Referrals, Chattanooga, TN
Of all the emergency procedures I have done as a veterinarian over the last 48 years it without a doubt that there is no other that has made such a profound impact on saving the patient’s life than emergency tracheotomy (ET). Although not commonly needed the procedure of emergency tracheotomy is truly a surgical parachute. Like a parachute on a light aircraft, when it is needed, nothing else will take its place. Its lifesaving, simple to perform, practical and necessary if a patient arrives at the hospital or clinic without a patent airway and common tracheal intubation cannot be performed. There is no time to refer these patients so every clinician must be able to perform it. As I look back on the tracheotomy procedures I have done, I am reminded that these are probably not commonly taught in veterinary school. Even as a surgical resident I cannot remember it being taught either. Yet there is need. Therefore, I am providing a nutshell “need to know” presentation that will provide the following:
1. An overview of emergency care readiness (as this is critical in ET as every second counts). 2. A review of the ABCDE guidelines for the priorities in emergency care. Note A is airway. 3. A review of the indications for ET based on my experience (estimated to have done 40-50). 4. A review of the various ways to perform the procedures that I have found the best. 5. A review of tracheotomy care, particularly important, as without good care death can occur. 6. A review of complications that can occur with the procedure or following its use.
Readiness Just like the boy scout whose motto of “being prepared” is stived for in every situation, so should each veterinarian and the practices that they are in also strive for this. This is particularly important when it comes to being able to perform lifesaving procures like ET. One should examine the facility and see if it is in a state of readiness. An easy way to decide this is to pretend you are the patient and you are losing your patent airway and walk from the parking lot into the lobby and imagine all the areas involved that must be ready to have your life saved. The following areas are involved: Facility in general – Have a “ready area” designated where the emergency patient would be taken to for immediate assessment and treatment. Best to be an “open concept” set up that would have all items and supplies easily obtained without opening drawers or cabinets. A gurney- rolling exam table; crash cart, suction; oxygen, anesthetic machine preferably with a volume cycled and pressure limited ventilator attached; oxygen arranged to be able to provide jet-blow-by oxygen; Staff – at least 1-2 immediately available; Doctors (with staff) to do emergency techniques recommended to be practiced are venous cutdowns and ET; Supplies – sterile clear ET tubes arranged with ties already in them and syringes attached and have the amount of air needed to inflate the endotracheal tube (ET) tube cuff. Ambu bag valve mask system. PEEP valve. Might have to improvise; Must be bold at times as procedures done may not be commonly done (ET and IV cutdowns or IO canula
133
placement); Training and practice includes sessions using a mannequin (really a pet-akin) or a cadaver (owner donated) using these to perform the various techniques, invaluable. Anything that can be done to shorten the procedure time should be done. This includes “tabbing the tape” and using preloaded syringes on ET tubes; Digital radiography and “bedside” ultrasound are examples of helping being in a” state of readiness” including both hand operated suction and the set up with a suction drain: Airway, Breathing, Bleeding, Cardiovascular, Disability and Everything else is a handy mnemonic that can be used effectively to guide and prevent areas being ignored. Tracheotomy indications Two sayings I have in emergency surgery are the following:
1. “Never let the skin come between you and the vein, referring to the placement of a vascular access catheter, either by doing a ‘facilitative maneuver’ or a more formal ‘cutdown’ to provide for IV administration of drugs, fluids and blood products.
2. “Never let the skin come between you and the airway, referring to an emergency tracheotomy (ET).
When I was a scout the technique of ET was in the 1954 Boy Scout Manual: Handbook for Boys. The procedure was outlined step-by-step to be used to save a life if the obstructed airway was not able to be opened with standard non-invasive methods. This is the principle reason for this presentation: To present a safe and effective means of providing an open airway to our four legged patients should they have an obstructed airway that cannot be opened sufficiently using commonly used less invasive procedures. The technique in animals is like that outlined in the BSA Scout Manual that I referred to earlier. Training can be done using a mannequin, commercial “petakin” or a stuffed animal with a trachea made of a piece of corrugated anesthetic tubing inserted into its neck, or a cadaver that owners have donated for use to help teach with. Specific indications for ET: • Rapidly occurring obstruction - Some examples of causes include:
• Food that cannot be dislodged • Trauma – laryngeal, pharyngeal, glossal
• Swelling – snake bite • Hematoma formation – rodenticide, other bleeding abnormalities • Laryngeal mass with hemorrhage • Unknown – infection – caustic agents
• Laryngeal dysfunction not responding to sedation, nasotracheal cannula oxygen, corticosteroids, tPEMF therapy, nasopharyngeal, nasal, collar, boat, or cage supplied oxygen
• Postoperative airway obstruction – Some examples of causes include: • Edema from surgical procedures • Post airway procedures • Post palatal procedures • Post maxillary procedures
134
• Post dental procedures • Post tongue and tonsil procedures
• For airway access to treat pneumonia and severe pulmonary edema • To provide suctioning, PPV-PEEP • To provide lung recruitment.
Example of an emergency tracheotomy that saved a patient’s life
Sarah is a middle-aged Golden Retriever that was brought in by the owner at 7 PM. The dog is unconscious and bleeding profusely from a hole in the top of her head. She is also breathing through this hole and blood is spewing into the air with every breath she takes. The owner said he was walking the dog and she stepped out in front of car. An ET was completed immediately as there was so much blood coming into the patient’s airway. A venous cutdown was also needed to gain vascular access. She was placed on a ventilator and the head prepped and draped for surgery. Multiple pieces of bone and a ruptured left eye were removed, and bleeding temporarily controlled by packing. Irrigation and electrosurgery was used to definitively control the bleeding vessels and the hole in the nasal-frontal region was closed with a sliding skin flap. Over the course of several days Sarah gradually improved and the tracheotomy tube was able to be removed. She was able to be discharged and received follow-up rechecks for several weeks. Other than a missing eye she made a complete recovery. The tracheotomy site granulated shut and healed with barely a scar.
Pre-emptive procedures
As a patient presents with a partially to fully obstructed airway the following may be helpful in preventing the need for emergency tracheotomy:
• Targeted Pulsed Electromagnetic Field Therapy. This decreases inflammatory cytokines and increases anti-inflammatory cytokines. Is a LOOP (Assisi Animal Health) that is an antenna and the generator attached to it. It generates a very specific short wave radio signal that penetrates into tissues at least 70 cm. It causes an increase in cNO which increases capillary blood flow and decreases swelling and this begins to occur within microseconds. Its FDA approved for pain and edema. It is turned on, laid over the affected area and runs for 15 minutes. Treatments can be done every 2-4 hours for acute conditions such as swelling around an airway caused by trauma.
• Jet Blow by oxygen and other supplemental oxygen techniques. Here oxygen tubing is attached to a an oxygen source and the other end fitted with a 14 g IV catheter or small nozzle and when the oxygen is administered it jets out and can be directed into the mouth and larynx of the patient and assist in providing critical amounts of oxygen on inhalation.
• Sedation (often especially important) to quiet the patient, to the point of deep sedation to allow for a oral, pharyngeal, and laryngeal examination and this also decreases oxygen need and often allows placement of such supportive oxygen catheters as nasopharyngeal, nasotracheal or transtracheal.
135
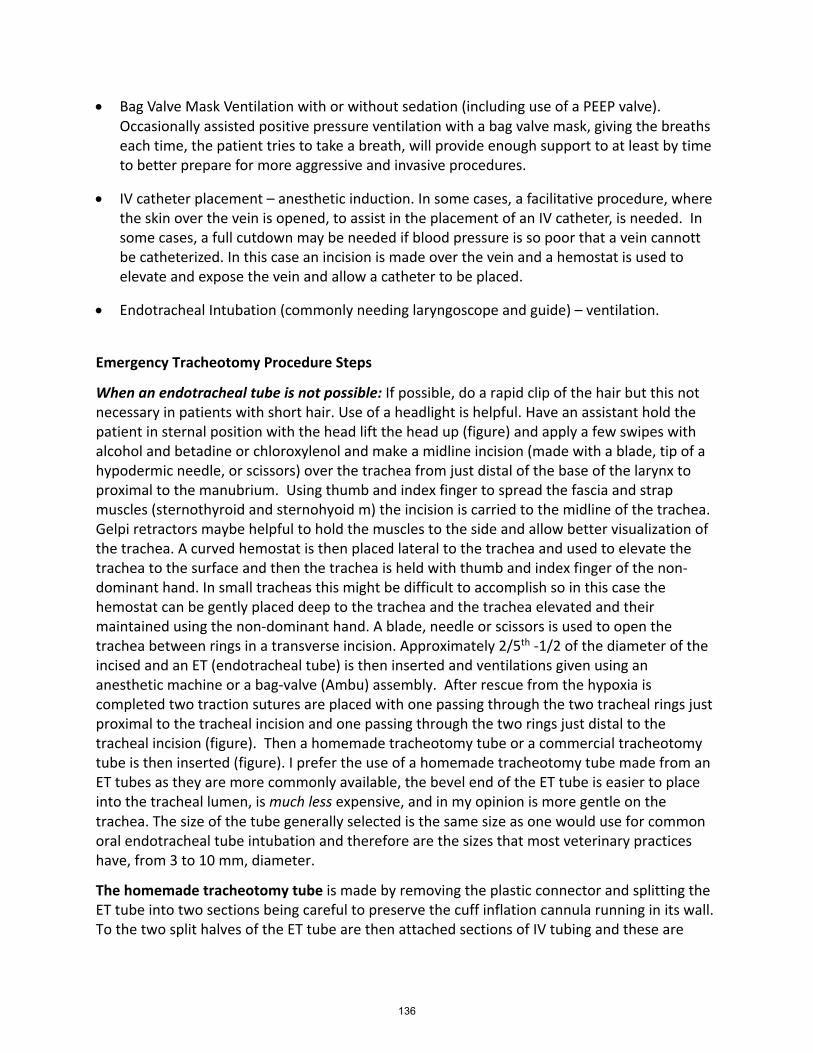
• Bag Valve Mask Ventilation with or without sedation (including use of a PEEP valve). Occasionally assisted positive pressure ventilation with a bag valve mask, giving the breaths each time, the patient tries to take a breath, will provide enough support to at least by time to better prepare for more aggressive and invasive procedures.
• IV catheter placement – anesthetic induction. In some cases, a facilitative procedure, where the skin over the vein is opened, to assist in the placement of an IV catheter, is needed. In some cases, a full cutdown may be needed if blood pressure is so poor that a vein cannott be catheterized. In this case an incision is made over the vein and a hemostat is used to elevate and expose the vein and allow a catheter to be placed.
• Endotracheal Intubation (commonly needing laryngoscope and guide) – ventilation.
Emergency Tracheotomy Procedure Steps
When an endotracheal tube is not possible: If possible, do a rapid clip of the hair but this not necessary in patients with short hair. Use of a headlight is helpful. Have an assistant hold the patient in sternal position with the head lift the head up (figure) and apply a few swipes with alcohol and betadine or chloroxylenol and make a midline incision (made with a blade, tip of a hypodermic needle, or scissors) over the trachea from just distal of the base of the larynx to proximal to the manubrium. Using thumb and index finger to spread the fascia and strap muscles (sternothyroid and sternohyoid m) the incision is carried to the midline of the trachea. Gelpi retractors maybe helpful to hold the muscles to the side and allow better visualization of the trachea. A curved hemostat is then placed lateral to the trachea and used to elevate the trachea to the surface and then the trachea is held with thumb and index finger of the non-dominant hand. In small tracheas this might be difficult to accomplish so in this case the hemostat can be gently placed deep to the trachea and the trachea elevated and their maintained using the non-dominant hand. A blade, needle or scissors is used to open the trachea between rings in a transverse incision. Approximately 2/5th -1/2 of the diameter of the incised and an ET (endotracheal tube) is then inserted and ventilations given using an anesthetic machine or a bag-valve (Ambu) assembly. After rescue from the hypoxia is completed two traction sutures are placed with one passing through the two tracheal rings just proximal to the tracheal incision and one passing through the two rings just distal to the tracheal incision (figure). Then a homemade tracheotomy tube or a commercial tracheotomy tube is then inserted (figure). I prefer the use of a homemade tracheotomy tube made from an ET tubes as they are more commonly available, the bevel end of the ET tube is easier to place into the tracheal lumen, is much less expensive, and in my opinion is more gentle on the trachea. The size of the tube generally selected is the same size as one would use for common oral endotracheal tube intubation and therefore are the sizes that most veterinary practices have, from 3 to 10 mm, diameter.
The homemade tracheotomy tube is made by removing the plastic connector and splitting the ET tube into two sections being careful to preserve the cuff inflation cannula running in its wall. To the two split halves of the ET tube are then attached sections of IV tubing and these are
136

used to hold the tube in place and the plastic connector is re-inserted (figure). A section of IV tubing is then tied around the connector and around the ET tube at the end of the split to hold the connector in place well. This holds the connector in place well, allowing an Ambu bag or breathing circuit to be able to be attached.
After the tracheotomy tube is inserted through the tracheal incision it is held in place by carrying the ends of the IV tubing around the patient’s neck and tying tight enough to keep the tracheotomy tube snug against the neck but not so snug that is causes undue pressure (figure). By using this method of anchoring the tube in place it can be removed rapidly should a sudden occlusion of the lumen of the tube occur due to a coughing up of exudate or a clot. A plastic angled connector is also helpful to use to prevent the ventral aspect of the patient’s head from occluding the tube (figure).
When an endotracheal tube is already present The patient is placed in dorsal recumbency and the neck is hyperextended using a bag of fluids or a tightly rolled towel under the neck and duct tape or other tape is used to hold the patient in position with the head extended (figure). After prepping and draping (which is optional), an incision is made in the midline over the trachea in a longitudinal fashion extending from a few tracheal rings caudal to the larynx to a few tracheal rings cranial to the manubrium. The strap muscles are separated with the thumb and index finger or with one or two curved hemostats and the trachea exposed. Using thumb and index finger or a curved hemostat the trachea is elevated (figure) and a transverse incision is made between two tracheal rings extending on its ventral aspect approximately 2/5 to ½ the diameter (figure). Two traction sutures are placed in the two tracheal rings immediately proximal and distal to the tracheotomy (figure). A homemade (preferred) or commercial tracheotomy tube is then inserted and as the ET tube is withdrawn from the patient’s airway (figure). The tracheotomy tube is connected to the anesthetic circuit, a dressing is applied (a 4x4 gauze sponge folded into a “pair of pants” that fit around the neck of the tracheotomy tube as it exits the neck, and two sections of IV tubing attached to the wings of the tracheotomy tube are then tied around the patient’s neck to prevent the tracheotomy tube from coming out.
Tracheotomy tube care
First and foremost, the most important task in the care of a tracheotomy tube is its constant observation. NO patient with a tracheotomy tube in place can ever be left unattended. This is because all it takes is a minute for a patient to become unconscious and with hypoxia should a sample of thick sputum, a clot, or a thick section of exudate coughed up into the lumen of the tracheotomy tube causing its complete obstruction and this then causing life-threatening asphyxia. Should this go unwitnessed this can quickly lead to death of the patient. If sudden tracheal occlusion does occur and witnessed, the tube is quickly removed, and a clean tube inserted.
As a routine, it is recommended that the tracheotomy tube be removed and a clean one inserted every 8-12 hours regardless of whether there are any indications that some lumen compromise has occurred. Invariably there is always some build up for exudate that happens and causes some partial tube occlusion. This occurs both inside the lumen of the tracheotomy tube and the space between the tube and the tracheal lumen as well. Therefore, the best policy
137
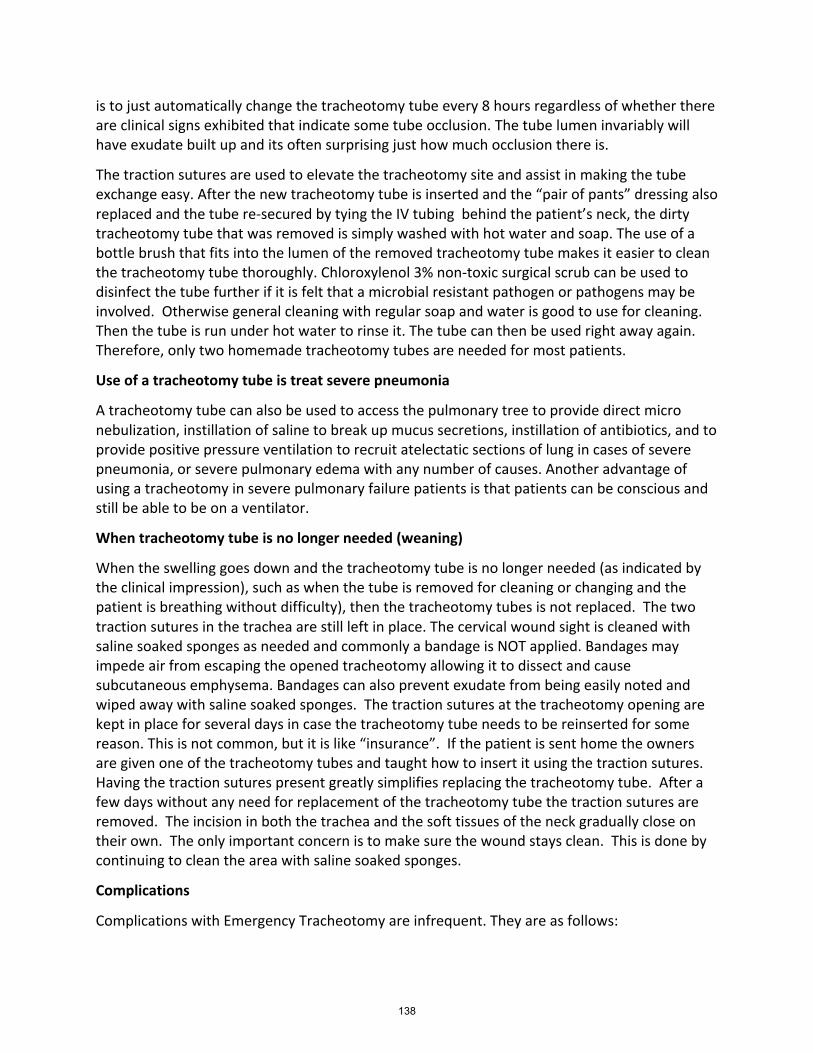
is to just automatically change the tracheotomy tube every 8 hours regardless of whether there are clinical signs exhibited that indicate some tube occlusion. The tube lumen invariably will have exudate built up and its often surprising just how much occlusion there is.
The traction sutures are used to elevate the tracheotomy site and assist in making the tube exchange easy. After the new tracheotomy tube is inserted and the “pair of pants” dressing also replaced and the tube re-secured by tying the IV tubing behind the patient’s neck, the dirty tracheotomy tube that was removed is simply washed with hot water and soap. The use of a bottle brush that fits into the lumen of the removed tracheotomy tube makes it easier to clean the tracheotomy tube thoroughly. Chloroxylenol 3% non-toxic surgical scrub can be used to disinfect the tube further if it is felt that a microbial resistant pathogen or pathogens may be involved. Otherwise general cleaning with regular soap and water is good to use for cleaning. Then the tube is run under hot water to rinse it. The tube can then be used right away again. Therefore, only two homemade tracheotomy tubes are needed for most patients.
Use of a tracheotomy tube is treat severe pneumonia
A tracheotomy tube can also be used to access the pulmonary tree to provide direct micro nebulization, instillation of saline to break up mucus secretions, instillation of antibiotics, and to provide positive pressure ventilation to recruit atelectatic sections of lung in cases of severe pneumonia, or severe pulmonary edema with any number of causes. Another advantage of using a tracheotomy in severe pulmonary failure patients is that patients can be conscious and still be able to be on a ventilator.
When tracheotomy tube is no longer needed (weaning)
When the swelling goes down and the tracheotomy tube is no longer needed (as indicated by the clinical impression), such as when the tube is removed for cleaning or changing and the patient is breathing without difficulty), then the tracheotomy tubes is not replaced. The two traction sutures in the trachea are still left in place. The cervical wound sight is cleaned with saline soaked sponges as needed and commonly a bandage is NOT applied. Bandages may impede air from escaping the opened tracheotomy allowing it to dissect and cause subcutaneous emphysema. Bandages can also prevent exudate from being easily noted and wiped away with saline soaked sponges. The traction sutures at the tracheotomy opening are kept in place for several days in case the tracheotomy tube needs to be reinserted for some reason. This is not common, but it is like “insurance”. If the patient is sent home the owners are given one of the tracheotomy tubes and taught how to insert it using the traction sutures. Having the traction sutures present greatly simplifies replacing the tracheotomy tube. After a few days without any need for replacement of the tracheotomy tube the traction sutures are removed. The incision in both the trachea and the soft tissues of the neck gradually close on their own. The only important concern is to make sure the wound stays clean. This is done by continuing to clean the area with saline soaked sponges.
Complications
Complications with Emergency Tracheotomy are infrequent. They are as follows:
138
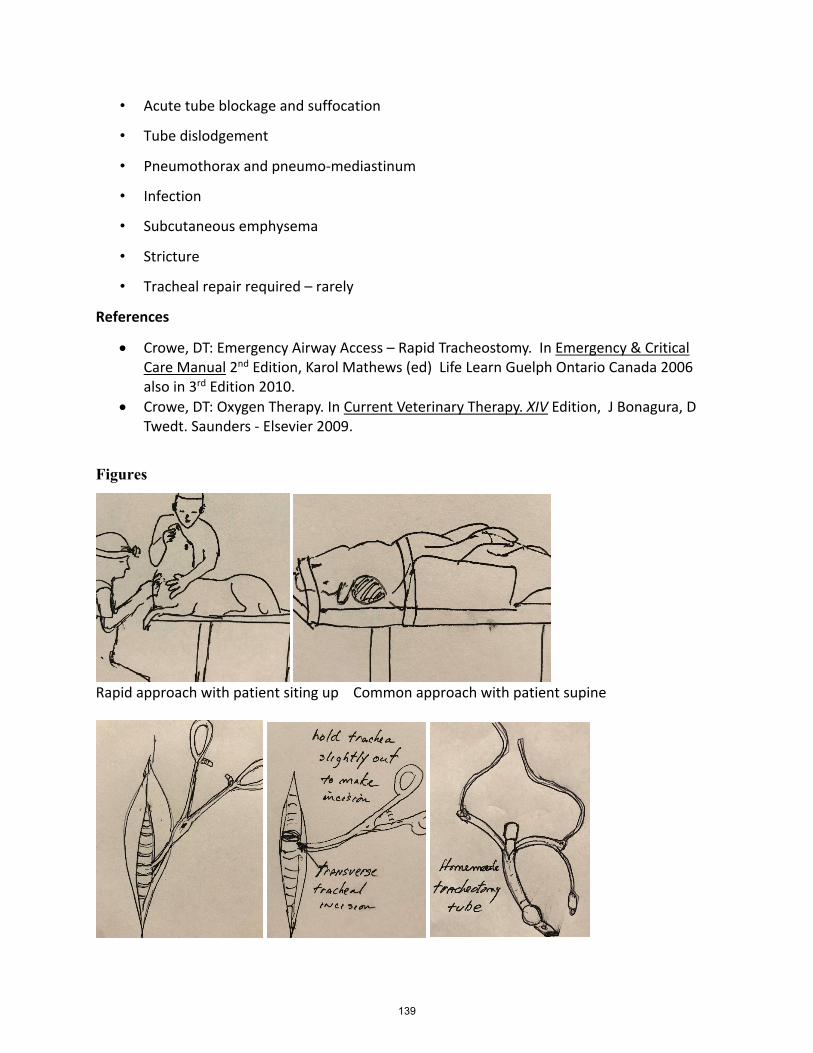
• Acute tube blockage and suffocation
• Tube dislodgement
• Pneumothorax and pneumo-mediastinum
• Infection
• Subcutaneous emphysema
• Stricture
• Tracheal repair required – rarely
References
• Crowe, DT: Emergency Airway Access – Rapid Tracheostomy. In Emergency & Critical Care Manual 2nd Edition, Karol Mathews (ed) Life Learn Guelph Ontario Canada 2006 also in 3rd Edition 2010.
• Crowe, DT: Oxygen Therapy. In Current Veterinary Therapy. XIV Edition, J Bonagura, D Twedt. Saunders - Elsevier 2009.
Figures
Rapid approach with patient siting up Common approach with patient supine
139
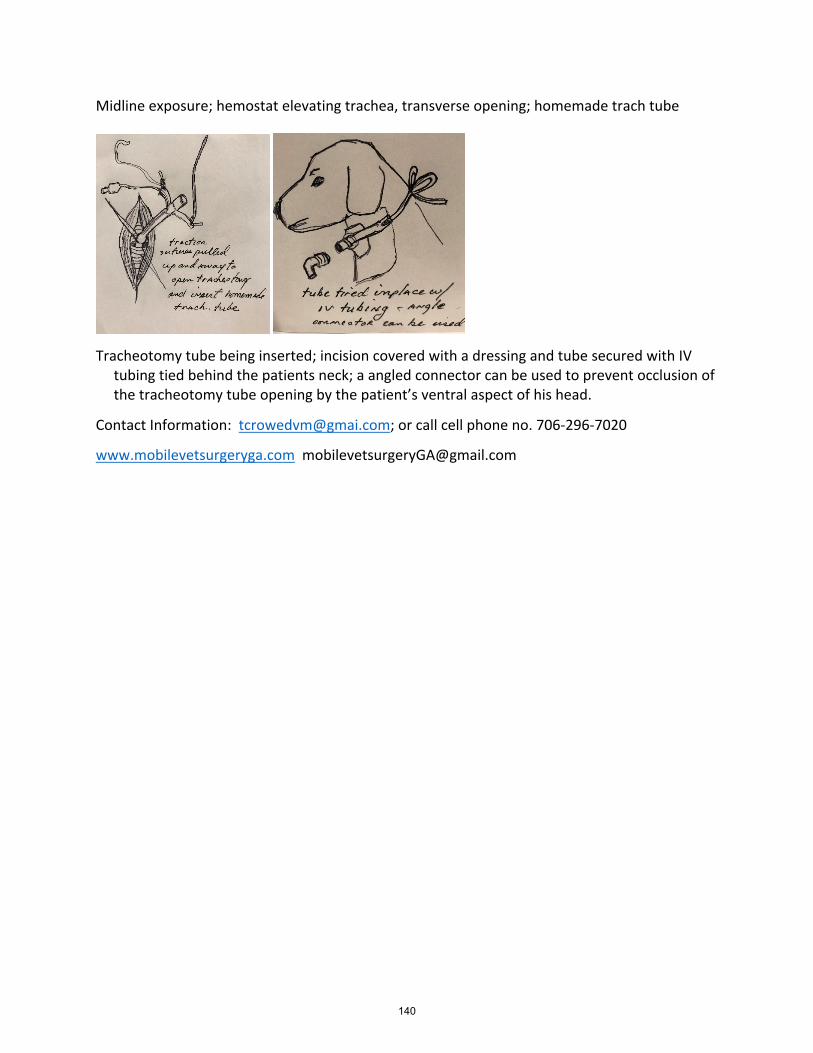
Midline exposure; hemostat elevating trachea, transverse opening; homemade trach tube
Tracheotomy tube being inserted; incision covered with a dressing and tube secured with IV
tubing tied behind the patients neck; a angled connector can be used to prevent occlusion of the tracheotomy tube opening by the patient’s ventral aspect of his head.
Contact Information: [email protected]; or call cell phone no. 706-296-7020
www.mobilevetsurgeryga.com [email protected]
140
Vacuum assisted wound closure for traumatic wounds
By Kristin Kirkby Shaw, DVM, MS, PhD, CCRT, DACVS-SA, DACVSMR Animal Surgical and Orthopedic Center &SOUND Veterinary Rehabilitation Center, Seattle WA CARE: Canine Arthritis Resources & Education www.caninearthritis.org Wound management is commonly performed in small animal practice for a wide range of traumatic wounds. One technique that has become standard of care for wound management in human medicine is negative pressure wound therapy (NPWT), also known as vacuum-assisted closure. NPWT was first introduced in human traumatology in the 1990’s and since that time, over 8 million human patients have benefited from the technique. The first case report in the veterinary field was in 2007 and involved a tiger cub that had multiple open wounds. NPWT was successfully used in this case to assist wound closure and prepare the cub for reconstructive surgery. Since then, at least 10 scientific reports of NPWT in veterinary patients have been published, with likely thousands of patients having been treated. The benefits of NPWT include increasing blood flow, removing extravascular fluid, increasing granulation tissue, speeding wound closure, increasing bacterial clearance, and enhancing skin flap or graft survival. NPWT is particularly useful for large wounds with loss of skin or deep pocketing, such as are common following vehicular trauma or bite wounds. Additional indications include surgical dehiscence, chronic non-healing wounds, skin grafts and flaps (bed and over graft/flap), prevention of post-operative edema (applied over a closed incision), management of open abdomen, and compartment syndrome. The mechanism of action of NPWT is similar to other surgical techniques that take advantage of tissue adaptation to applied tensile forces, such as distraction osteogenesis or skin stretching. The subatmospheric pressure applied by the device alters the cytoskeleton of cells, disrupts integrin binding, leading to increased intracellular 2nd messengers and stimulation of cell proliferation. It is crucial to note that NPWT does not debride the wound bed, so basic first-principle wound care is essential prior to using NPWT. The hair around the wound should be clipped very wide, ideally using a razor. The wound is copiously lavaged and any necrotic tissue and gross contamination is excised. In some cases, wet-to-dry bandage changes are needed to prepare the wound bed prior to NPWT. There are at least 2 commercially available NPWT devices, with one device specifically marketed for veterinary use: Kinetic Concepts Inc (KCI) V.A.C. KCI was the company that developed the first Vacuum Assisted Closure (V.A.C.) pump in the 1990s, and the device has been modified since that time. The equipment that is needed to apply NPWT includes sterile open cell foam, drainage catheter and egress tubing, adhesive dressing, and a suction device. KCI V.A.C. provides a kit that includes this equipment. Additional equipment that is considered helpful includes skin staples, adhesive stoma paste and adhesive spray. If one does not have access to the KCI V.A.C., it is possible to use commercially available open cell polyurethane
141
foam with pore size 400-600 m, a large bore red rubber catheter (10- 14 Fr), Christmas tree adapter, suction tubing, collection reservoir, and an adjustable suction pump capable of intermittent or continuous negative pressure between -50 to -150 mmHg. The basic principles of applying and using NPWT include maintenance of an air-tight seal, setting the pressure to -125 mmHg for open wounds and -50 to -75 mmHg over an incision, monitoring hemodynamic status if large volume of fluid is drained, and changing the bandage every 48-36 hours. This last point highlights one of the primary advantages of NPWT compared to traditional dressing changes in that it allows less frequent bandage changes, particularly for highly exudative wounds. This author recommends that patients remain hospitalized while receiving NPWT; however, the KCI V.A.C. FreedomTM is designed to be portable and potentially allow outpatient dressing changes. The greatest risk with allowing patients to leave the hospital with this bandage in place is loss of air-tight seal and need for trouble shooting of the device. This lecture will describe application of NPWT using commercial devices as well as “DIY.” For additional details, readers are referred to two review articles: Kirkby KA, et al. Compendium 2009 and Stanly BJ. Vet Clin North Am 2017. References 1. Argenta LC, Morykwas MJ. Vacuum-assisted closure: a new method for wound control and treatment: clinical experience. Ann Plast Surg 1997;38(6):563-577. 2. Morykwas MJ, Argenta LC, Shelton-Brown EI, et al. Vacuum-assisted closure: a new method for wound control and treatment: animal studies and basic foundation. Ann Plast Surg 1997;38(6):553-562. 3. Venturi ML, Attinger CE, Mesbahi AN, et al. Mechanisms and clinical applications of the vacuum-assisted closure (VAC) device. Am J Clin Dermatol 2005;6(3):185-194. 4. Lafortune M, Fleming GJ, Wheeler JL, et al. Wound management in a juvenile tiger (Panthera tigris) with vacuum-assisted closure (V.A.C. therapy). J Zoo Wildlife Med, 2007. 5. Kirkby KA, Wheeler JL, Farese JP, et al. Vacuum-assisted wound closure therapy: Application and mechanism of action. Compendium Clin Ed Vet. 2009. 6. Stanley BJ. Negative pressure wound therapy. Vet Clin North Am 2017.
142
How chronic disease affects pain perception & management By Elizabeth Colleran, DVM, MS, DABVP (Feline) Frailty In human medicine, there is accumulating evidence that frailty is becoming one of the world’s most serious health issues.i Given the longevity that companion cats are experiencing, at least in North America, it could be reasoned that an understanding of frailty and its constituent parts would be useful toward an understanding of the differences that occur in cats as they experience the many physical manifestations of disease. This understanding will provide a platform toward a clearer picture of planning interventions and management strategies for cats with comorbidities. Frailty is a geriatric condition characterized by an increased vulnerability to external stressors. It is strongly linked to adverse outcomes. Frailty is different from aging, disability and co-morbidity although it is distinctly related to these factors. For example, although frailty prevalence increases with age, it occurs independently of chronological age. Frailty does not yet have an internationally recognized standard definition, although the general premise is that frailty may be considered to be a geriatric syndrome reflecting multi-system dysfunction and in which individuals are able to dynamically transition between severity states. Multiple reasons exist as to why it is so difficult to define frailty, including: its complex etiology, the often independent work of frailty researchers and the inherent difficulty in distinguishing frailty from both aging and disability. Frailty has a strong biological component and it is thought to result from cumulative cellular damage over the lifetime. The specific pathophysiological pathways underpinning frailty are not yet clearly known al though there is evidence that both malnutrition and sarcopenia may have similar causal pathways. Inflammation is one such pathway and is well-established as a causal factor in frailty. Pro-inflammatory cytokines can influence frailty either directly, for example by promoting protein degradation or indirectly by altering metabolic processes.ii The biological causative mechanisms of frailty are different than those causing aging. Frailty occurs when not one, but multiple physiological processes decline. The more systems that are in a diminished state, the greater the likelihood of frailty. While physiological systems do lose some of their homeostatic reserve at advanced ages, there is an inherent reserve or buffer, suggested in humans to be about 30% which an individual can lose and still function well. Frailty is thought result when this threshold is surpassed in multiple physiological systems – so much so that repair mechanisms cannot maintain system homeostasis.iii Pre-frailty (latent) frailty is thought to be the silent precursor to frailty, manifesting as frailty when external stressors, such as acute illness, injury or psychological stress occur.iii All of this has yet to be studied, described or quantified in cats, despite the importance of separating illness and degenerative conditions from frailty and chronological age. Aging refers to the natural and progressive series of life stages. Although it is often misunderstand to be a pathologic process, it is the normal time dependent changes that occur in the life of every organism. Disease must be distinguished from aging as conditions for which interventions are possible and desirable. Frailty must be distinguished from disease, chronological aging and disability in order to plan interventions that address the loss of reserves that define it. Pain
143
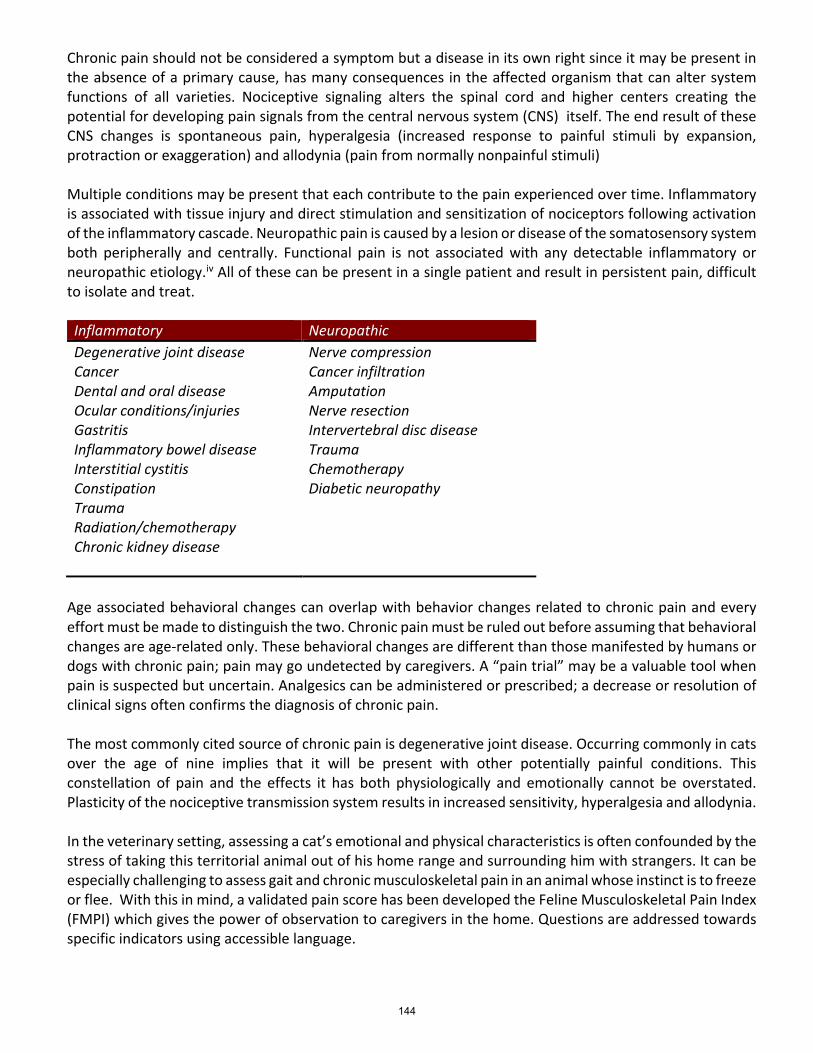
Chronic pain should not be considered a symptom but a disease in its own right since it may be present in the absence of a primary cause, has many consequences in the affected organism that can alter system functions of all varieties. Nociceptive signaling alters the spinal cord and higher centers creating the potential for developing pain signals from the central nervous system (CNS) itself. The end result of these CNS changes is spontaneous pain, hyperalgesia (increased response to painful stimuli by expansion, protraction or exaggeration) and allodynia (pain from normally nonpainful stimuli) Multiple conditions may be present that each contribute to the pain experienced over time. Inflammatory is associated with tissue injury and direct stimulation and sensitization of nociceptors following activation of the inflammatory cascade. Neuropathic pain is caused by a lesion or disease of the somatosensory system both peripherally and centrally. Functional pain is not associated with any detectable inflammatory or neuropathic etiology.iv All of these can be present in a single patient and result in persistent pain, difficult to isolate and treat. Inflammatory Neuropathic Degenerative joint disease Nerve compression Cancer Cancer infiltration Dental and oral disease Amputation Ocular conditions/injuries Nerve resection Gastritis Intervertebral disc disease Inflammatory bowel disease Trauma Interstitial cystitis Chemotherapy Constipation Diabetic neuropathy Trauma Radiation/chemotherapy
Chronic kidney disease
Age associated behavioral changes can overlap with behavior changes related to chronic pain and every effort must be made to distinguish the two. Chronic pain must be ruled out before assuming that behavioral changes are age-related only. These behavioral changes are different than those manifested by humans or dogs with chronic pain; pain may go undetected by caregivers. A “pain trial” may be a valuable tool when pain is suspected but uncertain. Analgesics can be administered or prescribed; a decrease or resolution of clinical signs often confirms the diagnosis of chronic pain. The most commonly cited source of chronic pain is degenerative joint disease. Occurring commonly in cats over the age of nine implies that it will be present with other potentially painful conditions. This constellation of pain and the effects it has both physiologically and emotionally cannot be overstated. Plasticity of the nociceptive transmission system results in increased sensitivity, hyperalgesia and allodynia. In the veterinary setting, assessing a cat’s emotional and physical characteristics is often confounded by the stress of taking this territorial animal out of his home range and surrounding him with strangers. It can be especially challenging to assess gait and chronic musculoskeletal pain in an animal whose instinct is to freeze or flee. With this in mind, a validated pain score has been developed the Feline Musculoskeletal Pain Index (FMPI) which gives the power of observation to caregivers in the home. Questions are addressed towards specific indicators using accessible language.
144
Another validated method designed for feline caregivers Subjective Nighttime Restlessness Evaluation (SNORE). Its purpose is to measure the pet owner’s assessment of the severity of disturbed sleep due to chronic. pain: The SNoRE is a questionnaire with appropriate readability and proven discriminatory ability. Full validity testing is continuing, and further versions of the SNoRE may well take place in the future. (table) Client Specific Outcome Measures (CSOMf) is also a caregiver assessment tool for pain whose purpose is to measure the pet owner’s assessment of how difficult it is for their cat to perform certain specific activities. It has been used to evaluate the impact of osteoarthritis or degenerative joint disease associated pain in cats. The Client Specific Outcome Measure was originally developed for use in dogs where it was adapted from the Cincinatti Orthopedic Disability Index (Gingerich & Strobel 2003) and then further adapted for use in cats (Lascelles et al. 2010). Its appeal is that the activities followed are individualized for each individual animal in their own environment, making it potentially more relevant than set questions on a questionnaire. It allows owners, working with a trained clinician, to select a set number of activities that their cat is impaired in performing, rate the amount of difficultly the cat has in performing those activities (currently recommended scale from 5=impossible to 1=no problem). The CSOM, once constructed, is used to follow this set of activities over time. Change from baseline in total score (the sum of scores across the 3 activities) is used as the outcome of interest to monitor the progression of impairment, or response to therapy. (table and document). Facial expressions of pain in cats: the development and validation of a Feline Grimace Scale was recently published. This study reported the development and validation of the FGS in the clinical setting using image assessment. A diverse sample of cats was included, with cats presenting pain from different sources and intensities. The FGS was developed by comparing the facial features of control and painful cats, then its validity and reliability were tested using images obtained from the video-recordings. Two distinct populations of cats (healthy control cats and client-owned painful cats) of various breeds were studied. There were more females than males in the control group, but both genders were equally represented within the client-owned group, besides, there was no effect of sex on FGS scores. Sex and strain differences in laboratory animals have been previously reported in pain research, hence the importance of including both sexes in the development of a pain scale. Although different breeds were represented within the client-owned population, most of the cats were domestic short-haired. Brachycephalic breeds were not included. Other causes of pain included cancer pain which is caused by several mechanism, some or all within the individual patient. Inflammatory pain is caused by tumor growth and destruction of adjacent tissues and structures. Visceral pain can be caused by distension; neuropathic pain by nerve compression or a primary tumor of the nervous system. Cancer treatment including surgery, chemotherapy and radiation therapy are common causes of pain. Periodontal disease is another common comorbidity particularly in older cats. If there is inflammation in the oral cavity there is pain present. Dysphagia, pawing at the mouth during or after eating and other less obvious signs – food preference changes, eating behavior, avoidance and reluctance to be petted around the head – are all indicators that pain is present. v Any chronic condition affecting the gastrointestinal system and causing visceral distension such as megacolon or constipation is painful. Inflammatory bowel disease is chronic intestinal inflammation often
145
occur concomitantly with pancreatitis or cholangitis. These inflammatory conditions should all be considered chronic abdominal pain sources. Treatment Appropriate assessment of chronic pain is critical to successful treatment in the cat with one or more comorbidities. Identification of a primary cause will facilitate treatment only if all of the other potential sources of pain have been included in the assessment. The relationship of the owner to the cat must remain a paramount consideration when planning therapy. Preservation of the powerful bond between a caregiver and beloved cat is crucial to the well-being of everyone involved. Understanding the pathophysiology of the painful condition is required to make a plan for long term therapy. A questionnaire like FMPI or one that is arrived at in consultation with the owner that assesses behavior changes can be repeated over time to assess whether or not the pain management modalities chosen for the patient are working. Each “score” is compared to previous ones to visualize trends, identify patterns of behavior and improve outcomes. This information is used to make adjustments, or provide evidence that the plan is improving the life of the patient. Pain management plans tend to have several components, including pharmaceuticals (e.g. NSAIDs, analgesics), nonpharmaceutical anti-inflammatory devices (e.g. laser therapy, Assisi Loop) and nonpharmaceutical additions (e.g. heat, furniture adjustment, ramps), so a reliable, verifiable and validated survey for judging which combination of multimodal pain management is best for this patient is required. Error! Bookmark not defined. . Challenges in the treatment of chronic pain in cats :
• Difficulty recognizing and assessing resulting in ineffective treatment • Fear of adverse effects • Lack of cat-specific data on pharmaco-kinetics and –dynamics • Individual variability in response • Failing to implement multi-modal approach • Cost • Caregiver compliance, time commitment and expectationsvi
Case examples will be discussed.
i Dent, E, Kowal, P. at al. Frailty measurement in research and clinical practice: A review. 2016 European Journal of Internal Medicine 2016; 31, 3-10. ii Cesari m, Landi F, et al. Sarcopenia and physical frailty: two sides of the same coin. Front Aging neuroscience 2014; 6:192. iii Lang PO, Michel JP, et al. Frailty syndrome: a transitional state in a dynamic process. Gerontology 2009; 55 (5): 539-49. iv Monteiro, B. Lascelles,D . Assessment and recognition of chronic maladaptive pain in Feline Anesthesia and Pain Management first edition ed: Steagall, Robertson, Taylor. John Wiley & sons, 2018, 241-242. v Bellow, J. Center S. et al. Aging in Cats: Common physical and functional changes. Journal of Feline Medicine and Surgery. (2016) 18, 533-550.
146

vi Monteiro, B Trancy E. Treatment of Chronic (Maladaptive) Pain. Feline Anesthesia and Pain Management first edition ed: Steagall, Robertson, Taylor.JohnWiley&sons.2018,257-279.
147
Feline examination: streamline the exam and maximize your findings Lauren Demos BVMS Hons DABVP (Feline) The overall purpose of physical examination is to determine the health status of a patient. Ideally, this will equate to diagnosing illness prior to overt clinical signs; in sick patients, the examination will be to guide a diagnostic plan. Human circles have coined the phrase periodic health examination, to replace the term physical exam. Generally, physical examination should follow an established pattern, meaning the examiner is less likely to forget any portion of the exam. Each organ system should be examined at every visit, though exceptions might be made for patients who have recently been seen and are following up on items of specific concern. Variations to the examination process will also occur based on patients themselves. For instance, in a senior cat, you may want to delay examination until a blood pressure is obtained. Or, in a fractious patient, you may elect to do a TPR after the physical examination, in in conjunction with, to minimize handling of the patient. Components of the examination process:
1. Pre-examination -Presenting complaint(s) -Diet and meds -Changes in patient/household since last visit -Update chronic concerns
2. TPR(BP) 3. Examination
a. Occult i. Behavior, appearance, gait, mentation, vision, hearing, odors, etc.
b. Physical i. Methodical examination of all organ systems
ii. Repeat palpation/examination of any areas of concern 4. Post-examination
- Upon completion of the initial physical examination, findings should be documented as soon as possible. If diagnostics are warranted, they should be performed and/or scheduled. If diagnostics are not warranted, the date and purpose of the next visit should be determined and scheduled.
148
Walk your talk: Client procrastination harms your patients & your procrastination could be hurting your financial goals
By Darby Affeldt, DVM, RICP, Financial Advisor & Associate Partner – North Star Resource Group
Have you ever said to your veterinary client that their animal needs some care, now (or yesterday)? Of course, silly question, right? Yet, we all know that people procrastinate, and there are many reasons for this, it’s not always about money. Thinking along these lines, it’s not a surprise that people procrastinate, and in all kinds of areas of their own lives – not just with the care of their animals. “Thank you Captain Obvious” you might be thinking…but you might ask yourself if there is any part of you procrastinating when it comes to your own financial life? And if so, why? Some of the reasons people procrastinate are:
- Money - Uncertainty - Inconvenience - Fear of Failure OR Fear of Success - Aversion to discomfort - Overextended - Fear of the Unknown - Perfectionism - There are many more…
In this session, we will explore how if we are telling our veterinary clients that their procrastination – for whatever reason – is harming their animal, then it’s important we self-reflect and understand that our own financial procrastination, no matter to what degree, is possibly harming our own goals, success, future.
Financial procrastination can make it very difficult to navigate the risks in retirement. Here are some:
1. Waiting to invest. If we wanted to reach a certain financial goal in retirement, i.e. $1M (though we don’t to use general rules of thumb), the less years we have until retirement the more we’d have to put away monthly. This may not be feasible at certain ages, i.e. when our kids are in college, etc.
2. Longevity. With advances in medicine, we are living longer and healthier lives. Yet this can mean we outlive our savings. Starting early with good savings habits can make all the difference.
3. Market Volatility. Early and careful portfolio strategies will help navigate the expected ups and downs of the financial markets.
4. Rising Health care costs. The cost of health care is going up, and Medicare doesn’t cover it all. Medicare also doesn’t cover long-term care costs for those who have assets – there are rules.
5. Taxes. These may go up, it’s important to start saving early and looking to specific strategies to navigate this possibility.
6. Inflation 7. When and how much to Withdraw in retirement. Using rules of thumb can present problems
since no two financial situations are alike!
149

8. Sequence of Returns Risk. Bull and Bear markets can make a significant difference to portfolios when drawing assets in retirement. Early and careful planning is key to navigate these up down markets and the timing of our retirement decumulation strategies.
9. Carrying Debt into retirement. This can work out but really depends on so many other factors; it is important to work towards becoming debt free if possible.
Attendees should come away with a good understanding that their success very much depends on their own financial habits, and hopefully inspired to Walk their Talk and address their financial lives or get a second set of eyes on their planning (or lack thereof), as soon as possible.
150

What we know about SARS-CoV-2…and what it means for practitioners By Jenifer Chatfield, DVM, DACZM, DACVPM DrJenTheVet.com Dade City, Florida As the country continues to reopen following the unprecedented and somewhat clumsy shutdown that swept the country (except for 5 states that remained fully open), it seems like a good time to update what we know about SARS-CoV-2, COVID-19, the disease it causes, and animals. To date, no evidence exists that pets (or other animals) are a threat for disease transmission to humans. However, it is clear that some animals (dogs, cats – even big ones, ferrets, and mink) can contract the disease from significant and persistent contact with infected humans. To date, reports of likely infection in animals include 2 domestic cats, multiple dogs, ferrets in a lab setting, farmed mink, and apparent infection of multiple big cats in a single zoo (2 lions, 2 amur leopards, 2 Malayan tigers). The majority of these animals had no clinical signs but were PCR positive and had a history of contact with confirmed positive humans. In fact, the dog that was first presumptive positive for COVID-19 in the USA (the pug in NC), turned out to be negative after all. Are animals playing a role in maintaining community transmission of SARS-CoV-2? SARS-CoV-2 in animals A recent non-peer-reviewed report from an online microbiology conference seems to prevent evidence that cats and dogs are more commonly infected with SARS-CoV-2 than has been previously known. However, caution is advised when interpreting the results of this data as the population sampled was quite small (17 cats, 18 dogs, 1 ferret for PCR and only 8 cats and 10 dogs for serology) and the exact interpretation of serological positive results remains unknown. What is known is that the sample population in this study was from households where owners were confirmed SARS-CoV-2 positive and that all 4 cats that were serologically positive and 1 cat with an indeterminate PCR test, were exhibiting respiratory signs or other signs of illness as reported BY THE OWNER. Again, caution should be exercised when interpreting any data that has not yet been peer-reviewed, has a small sample population, and where owner reporting of non-specific clinical signs are involved. For practitioners in the US, the process for investigating the SaRS-CoV-2 status of patients remains unchanged. Initially, other more common differentials for respiratory or other signs should be ruled out, if possible. Then, if owner history indicates confirmed COVID-19 infection and persistent close contact with the pet, practitioners should contact their State Public Health Veterinarian (PHV). Then, the State PHV will determine is testing is warranted and what procedures are to be employed. As with all respiratory illness, animal owners should be directed to avoid contact with their animals. If owners do not have alternate options for animal care, practitioners can offer boarding the pet until public health officials determine the owner is no longer infectious. People remain the main source of infection with SARS-CoV-2 for other people. But how infectious are they? And when? While we do not know exactly when infected people stop shedding, it does appear from current data that most infected people begin shedding the virus prior to the onset of clinical symptoms and that the peak of shedding occurs sometime early during the course of illness. All of this
151
information should be cautiously interpreted though as the data on which these statements are based utilizes PCR testing results and we all know that PCR does not assess pathogen viability, only the presence of genetic material. Antibody titers have become the latest and greatest method for assessing one’s risk of infection; however, an elevated titer does not necessarily demonstrate immunity and lack of an elevated titer does not necessarily imply susceptibility to infection. Recent studies have identified SARS-CoV-2 specific T-cells indicating that antibodies may not be the only mechanism by which a person may be protected from infection.
The mask Finally, we come to the newest hippest fashion accessory – the mask. While all the cool kids seem to be sporting them (with personalized patterns, etc.), unfortunately, the efficacy of masks in containing this virus is unknown. In fact, per the CDC, “A cloth face covering may not protect the wearer, but it may keep the wearer from spreading the virus to others.” Please note the use of the operative word, “may.” The CDC recommends that everyone wear masks in public settings around people who don’t live in your household and when you can’t stay 6 feet away from others. If maintaining reasonable physical distance from others especially while remaining in open air (outside) spaces is possible, then masks are not necessary. Furthermore, when considering types of face coverings to prevent transmission in public spaces, what about those face shields? As of the end of September 2020, the CDC does not recommend the use of gaiters or face shields as, “evaluation of these face covers is on-going, but effectiveness is unknown at this time.”
Transmission…in need of repair? Just like the six other coronaviruses that can infect humans, SARS-CoV-2 is spread through viral particles in respiratory droplets. The virus does not exist in the air independent of the droplets as far as we know and that would be unlikely anyhow. Many different ways for stating this route of transmission exist and when the CDC recently changed their webpage to reflect a different way to say the same thing, the collective global head exploded. Then, the CDC removed the newly rephrased information and – you guessed it – another explosion. Despite all explosive activity, the fact remains that human-to-human direct spread of the virus through respiratory secretions (droplets) continues to be the major culprit for transmission of SARS-CoV-2. Contact with fomites and asymptomatic (or pre-symptomatic) people remain insignificant sources of infection at this time.
Take home points 1. Pet owners should ALWAYS be directed to avoid contact with animals when either are exhibiting
clinical disease of any kind, but most especially when the respiratory system is involved.2. Caution is appropriate and necessary when interpreting early data relating to an emerging
pathogen.3. Common sense and understanding of the application of the route of transmission is best strategy
to prevent infection with an emerging pathogen.4. SARS-CoV-2 is transmitted via contact with respiratory droplets that must make contact with mucus
membranes or a break in the skin – the pathogen cannot penetrate intact skin, fabric, Kleenex, etc.
152
5. SARS-CoV-2 is not the first emerging pathogen or even the first emerging coronavirus in ourlifetimes and it will not be the last – so take a breath and this too shall pass.
References 1. https://eurekalert.org/pub_releases/2020-09/esoc-sss091720.php2. https://www.cdc.gov/coronavirus/2019-ncov/community/veterinarians.html#testing-animals
153
An integrative approach to complementary care in veterinary practice
Matthew Brunke, DVM, CCRP, CVPP, CVA Diplomate, American College of Veterinary Sports Medicine and Rehabilitation Medical Director, Veterinary Surgical Centers Rehabilitation, Vienna, VA
Michele Broadhurst, DC, CCRP, FIAMA, CVC IVCA, CCSP, Mtech chiro
Within veterinary medicine there is a growing trend for alternative and adjunct therapies for pain control and improvement of mobility. This presentation will cover the fundamentals of four areas that have evidence-based medicine to support their use in veterinary medicine. They are Traditional Chinese Veterinary Medicine (TCVM), massage therapy, chiropractic care and myofascial release and dry needling
Traditional Chinese Veterinary Medicine (TCVM), although relatively new to the Western world, is a medical system that has been used in China to treat animals for thousands of years. It is an adaptation and extension of Traditional Chinese Medicine (TCM) used to treat humans. Speaking broadly, Chinese Medicine is a complete body of thought and practice grounded in Chinese Daoist philosophy. Though it can be traced back over two millennia in recorded history, it, like any medical system, continues to evolve today, and current research on acupuncture and herbal medicine is beginning to shed light on its mechanism of action.
Chinese Medicine Theory Chinese Medicine is based on the Daoist worldview that the body is a microcosm of the larger, surrounding universe. As such, the cosmic laws and forces that govern the external world also govern the body’s internal environment. Just as life-energy or “Qi” is an innate force of the universe, it too is a fundamental force of the body, driving its every action and transformation. Yin-Yang theory, which is central to Daoist philosophy, also features prominently in Chinese Medicine. This theory describes how opposing forces of the universe - light and dark, hot and cold, etc,- mutually create and transform each other, and play a key role in the characterization of physiological function and disease.
Disharmony and Disease In Chinese Medicine theory, disease is understood as an imbalance in the body, and diagnosis proceeds through identifying the underlying “pattern” of disharmony. Pattern diagnosis differs from conventional Western medical diagnosis in that it takes into account not only disease signs but how these signs relate to the individual patient. Thus, TCVM practitioners will consider the temperament, sex, age, activity, and environment of an animal along with the animal’s particular disease signs. This approach stems from the belief that the body is as an interconnected system of forces and functions so that disease and disharmony must be examined with respect to the whole patient. For this reason, Chinese Medicine is often regarded as more holistic than conventional Western Medicine.
154
The Four Branches of TCVM Once a particular type of disharmony or disease pattern is identified, treatment often proceeds through a combination of treatment modalities. Though the terms Chinese Medicine and acupuncture are often used interchangeably in the West, acupuncture is actually only one modality or “branch” of TCM and TCVM. There are actually four branches of TCVM – Acupuncture, Herbal Medicine, Food Therapy and Tui-na (Qi-gong, a form of Chinese meditative exercise, is a fifth branch of TCM that is excluded from TCVM because it cannot be performed by animals).
1. Acupuncture is a treatment that involves the stimulation of points, typically achievedthrough the insertion of specialized needles into the body. Acupuncture points typicallylie along the body’s Meridian Channels along which Qi flows. Most veterinaryacupuncture points and Meridian lines are transposed to animals from humans, thoughknowledge of some “classical points” defined on particular species have been retainedand are used to this day.
2. Herbal Medicine utilizes herbal ingredients listed within the Chinese Herbal MateriaMedica in particular combinations or formulas to treat particular disease patterns.Herbal formulas are administered orally and are typically given in powder form tohorses and other large animals and in tea pill or capsule form to cats and dogs.
3. Food Therapy is the use of diet to treat and prevent imbalance within the body. Itutilizes knowledge of the energetics of food ingredients to tailor diets for individualanimals.
4. Tui-na is a form of Chinese medical massage in which different manipulations areapplied to acupoints and Meridians to promote the circulation of Qi and correctimbalances within the organ systems.
Reasons for Massage Massage is defined as the systematic, therapeutic, and functional stroking and kneading of the body. Pain and physical exertion often result in considerable muscle tension. Contraction of the muscles reduces local blood flow in the affected region. This, in turn, reduces the oxygen supply to the affected muscles and reduces the removal of metabolic waste products from the muscles. This inevitably leads to a vicious circle of pain, muscle tension and more pain.
Effects of massage Various massage techniques are used to locally increase the blood flow, which is often seen as a visible reddening of the skin in the treatment area (hyperemia). The increased blood flow results in improved oxygen supply and removal of waste products and helps to accelerate muscle recovery, accelerated remove of the so-called algogenic substances from body tissues, an increase in tissue temperature and elasticity, and increased nutrients (via blood flow) to an area. Massage increases venous and lymphatic return and is useful in mobilizing adhesions. Massage may stimulate the release of endorphins, endogenous substances that bring about
155
further pain relief. Neurological effects such as improved sensory input and change muscle tone (stimulate poor muscles, relax tense ones) may be seen.
Benefits of Massage Massage should be used as a multimodal approach to pain management and rehabilitation.
• Massage can be used to reduce swelling and edema; reduce muscle, joint, andconnective tissue (fascia) pain.
• It can be beneficial in the reduction of inflammation of skeletal muscle that has beenacutely damaged by exercise
• Massage has been shown to improve functional recovery and decrease delayed onsetmuscle soreness (DOMS)
• The attentive care of a therapist and the owner has a positive effect on the patient,though this has not yet been substantiated by scientific studies. Massage helps theowners bond with their pets because it requires mutual trust. In addition to itstherapeutic effects, massage also has a positive effect on the healing process
• This prolonged physical contact with the patient also allows for further diagnosis.Repeated palpation of an area gives a practitioner a better understanding of soft tissueproblems of the patient. This can be reassessed at future visits, allowing them to see ifthe therapy is working and the patient is improving
Indications Massage can be used to treat a variety of conditions. The main indications for massage therapy are logical consequences of the above-mentioned effects.
• The indication for massage is muscle tension secondary to spinal and joint disease.Segmental nerve irritation, physical overexertion, gait anomalies and guarding oftenlead to severe muscle tension. Naturally, this tension not only affects the tissues in theimmediate surroundings, but also in more distant parts of the body. For this and otherreasons, the physiotherapist must always remember to view each case holistically.
• By increasing blood flow in the treated area, massage not only increases the elasticity oftendons and ligaments, but also improves joint and muscle function.
• Early massage therapy after trauma and/or surgery helps prevent or improve congestionin the affected area and prevents adhesions.
• In neurological patients with paresis and paralysis, massage is used to improve muscletone and sensory awareness.
• Mainly in sports medicine but also in therapeutic indications, massage is used toprepare the muscles and connective tissues for training; in the cool-down phase aftertraining, massage accelerates muscle recovery.
156
Contraindications • Local skin infection • Systemic infection • Hypotension • Shock • Infected skin, open wounds • Vasculitis • Deep vein thrombosis • Embolism • Bleeding disorders • Bruising secondary to diseases such as autoimmune hemolytic anemia, immune mediated
thrombocytopenia • Hyperthermia, fever • Cancer – use professional judgement in benign vs. malignant
Precautions • Osteopenia, osteomyelitis • Causes pain • Brachycephalic breeds (caution around airway, heavy pressure on thorax can cause
respiratory issues) • Atlanto-axial luxation, Wobbler’s, IVDD (acute, painful, unstable) • Young patient – immature skeleton, open growth plates • Excessive massage could lead to discomfort • Unknown growth (cancer?) • If you or the patient are not comfortable with the situation
Massage Techniques Effleurage (gliding, stroking) Effects Effleurage is a superficial tissue manipulation technique that increases blood flow, counteracts venous stasis and promotes the flow of lymph fluid. It also serves as a means of initial contact with the patient in preparation for further tissue manipulation. Procedure:
• As a rule, gliding movements are made in the direction of hair growth. • Stand beside or behind the patient and place the open hands flat on the muscles,
starting from the neck.
157
• Stroke the muscles gently and not too rapidly, proceeding from the neck, down the back and to the croup and hind legs.
• Encircle each leg – or as much as you can grasp – in one hand and glide the hands downward. After reaching the feet, start stroking again from neck to feet.
• Note: It is important to maintain physical contact with the animal when moving from one part of the body (e.g. the feet) to another (e.g. the neck). Therefore, leave one hand on one leg while placing the other on the neck, then move the second hand to the neck.
• Now used both hands to stroke from the neck to the shoulder blades and down the front legs, which can also be encircled in the hands.
• Next, treat the lateral chest and abdominal muscles by stroking column-wise down the chest and abdominal wall in as many columns as necessary to cover the entire area.
• The hand pressure can be cautiously increased the second time around. • Stroking is normally carried out with the animal standing but can also be used in a
recumbent patient. • Repeat the stroking procedure as often as necessary until the animal relaxes.
When to Use: Stroking should always be performed at the beginning of a massage session. Stroking also serves to relax the patient between deep tissue manipulation and at the end of a massage session. Pétrissage (kneading) Effects: Petrissage can be applied superficially or deeply. Muscle tone is decreased by kneading superficially and increased by kneading deeply. Procedure: Various kneading techniques can be used. When kneading superficially, a roll of skin and subcutaneous tissue is gently grasped, thereby raising it from the lower tissue structures.
• Kneading gently stretches and mobilizes the skin. After grasping the roll of skin, release and slide the hands forward to the next segment, then grasp another roll of skin.
• Proceed from tail to head when treating the back, and from distal to proximal when treating the limbs.
• Kneading should proceed in the direction of the muscle fibers, but can also be diagonal or perpendicular to them.
158
Kneading deeply comprises a direct muscle treatment. • Grasp an individual muscle group in one or both hands and knead as described below. • Place the thumbs on one side of the muscles and the fingers on the other. Now,
alternately open and close the hands, kneading the muscles between the thumbs and fingers.
• You can start kneading gently and gradually increase the pressure. • To treat the back, place one hand on either side of the back or place both hands on the
same side. Knead in the direction of the muscle fibers in the first case, and opposite to the fiber direction in the second.
Note: Especially when manipulating deeper tissues, kneading can induce pain. Therefore, always increase the pressure gradually while carefully monitoring the patient's response. When to Use: Do not start kneading unless the patient is relaxed. Always loosen the tissues by stroking or shaking between each round of kneading. Animal Chiropractic is a field of animal health care that focuses on the preservation and health of the neuro-musculo-skeletal system. Nerves control everything that happens in animals. Anything adversely affecting the nervous system will have detrimental effects that will resonate throughout the entire body. The command centers of the nervous system are the brain and spinal cord which are protected by the spine. The spine is a complex framework of bones (vertebra), ligaments, muscles and nerves. If the movement and biomechanics of the vertebra become dysfunctional, they can interfere with the performance of the nerves that are branching off of the spinal cord and going to all of the muscles and organs. As this occurs, your animal can lose normal mobility, resulting in stiffness, tension, pain and even organ dysfunction. Additionally, when normal movement is affected, and left unattended, it will ultimately impact your animal’s entire wellbeing and quality of life.
The nervous system also coordinates the body’s ability to heal and regulate itself. Trauma, overuse, or underuse may cause the vertebra of the spine to become hypomobile, and the surrounding muscles and ligaments may become compromised and inflamed. Nerves could become trapped in these damaged tissues, or in the passages they use to exit the spine. Their signals become unable to adequately reach their destinations. When they don’t, these impaired structures lose their ability to heal. This can directly and dramatically impact your animal’s health. Symptoms of spinal fixation are vast, and may include pain, spasm, sensitivity to touch, lameness, gait abnormalities and postural compromise. These are the symptoms that are the easiest to detect. It may take a trained doctor to distinguish some of the more subtle changes that occur when organs begin to malfunction.
The goal of an animal chiropractor is to restore function and mobility to the compromised vertebra in an effort to re-establish neurologic transmissions. This allows the body to perform at its optimum potential. These doctors use their hands to identify areas of restriction; and
159
once identified, the animal chiropractor applies a precise thrust on the immobile anatomical structures. This treatment restores the normal motion of the vertebra thus removing neurological interference. When the nerves can efficiently communicate with all the structures in your animals’ bodies, they will begin to heal from within. Animal Chiropractic is not meant to replace traditional veterinary care. It is not an alternative treatment, but rather an integrative method that when used in conjunction with good traditional veterinary care, will provide years of happy and healthy living. This is the beginning of a more modern, comprehensive approach to your animal’s healthcare. It is an effective and valuable means of restoring and maintaining their strength, vigor and well-being. And by exploring and treating the root causes of your animal’s aches, pains and illnesses, will ensure maximum improvement, top performance and an exceptional quality of life for the animal companions we love.
Animal Chiropractic is a developing area of expertise in animal healthcare.
Today, more people recognize that loving and caring for their pets extends beyond providing food and shelter. Quality pet healthcare is no longer limited to spaying and immunizations. With the emerging field of Animal Chiropractic, people are appreciating new ways for their pets to achieve and maintain optimal health. Animal Chiropractic offers non-surgical, drug-free options for correcting bone, disc, and soft-tissue disorders related to improper spinal configuration and movement. When vertebrae become immovable through trauma, injury or degenerative wear and tear, the joints between them become jammed, often affecting the nerves that are in these congested areas. Because the nerves are the communication links from these joints to the brain and spinal cord, messages to the rest of the body become interrupted, leading to pain and loss of function. Animal Chiropractic focuses on the restoration and preservation of heath by removing communication barriers and restoring normal function. This therapy is not limited to an injured or sick pet. Healthy and athletic animals are ideal candidates for chiropractic examination and care.
Maintaining proper structural alignment permits optimal function of the muscles, nerves and tissues supporting the joints, resulting in improved movement, stance and flexibility. This alignment promotes increased agility, endurance, and overall performance. Broader benefits include superior immune function, healthier metabolism and a vibrant nervous system, facilitating your animal’s natural ability to heal. Chiropractic can enhance the quality of your pet’s life, ensuring active and healthy years. More and more often veterinarians are utilizing animal chiropractors in their offices. They do so because animal chiropractors examine and treat areas of biomechanics and the functional nervous system that often go unnoticed by traditional veterinary care. By working in conjunction with veterinarians, animal chiropractors aid in restoring your pet’s optimal health by treating the whole patient. Animal Chiropractic is “NOT” intended to assume the primary health care responsibility of animals or replace veterinary medicine.
Chiropractic care for animals is one of the fastest growing and most valuable occupations available in animal healthcare today.
Doctors certified in Animal Chiropractic are widely recognized and available throughout the United States, Canada, and some other countries around the world. These practitioners are
160
licensed chiropractors and/or veterinarians who have attended and graduated from an accredited animal chiropractic school; many of them successfully completing certifying exams from either the American Veterinary Chiropractic Association (AVCA) or the International Veterinary Chiropractic Association (IVCA). These certified professionals are trained and experienced in attending to your pet’s neuromusculoskeletal challenges and needs. Animal chiropractic unifies two professions which provide a combination of skills uniquely proficient at caring for you animals. It combines science, mechanics and a caring compassion to provide results that improve the quality of life of your pet. Animal Chiropractic has been beneficial for performance animals, injured animals, athletes, show animals, and family pets. Whether to enhance performance address injury or illness or simply for preventative care, Animal Chiropractic can make a positive difference in any animal’s life.
Myofascial pain In dogs, skeletal muscle makes up approximately 44% of live body weight in mixed breed and pure-bred dogs. In greyhounds, muscle to live weight is approximately 57% (6). Yet, there continues to be a deficiency in both veterinary education and veterinary literature about skeletal muscle and its role in pain and dysfunction. Muscle pain or myalgia is described as an aching, cramping pain that is difficult to localize and can refer to deep somatic tissues. Myalgia activates cortical structures and is inhibited by descending pain-modulating pathways.
Muscular injury can occur from trauma or biomechanical overloading. Injured muscles are shortened, with increased tone and tension due to varied states of over contraction and contracture (7). In people, myofascial pain, characterized by the presence of myofascial trigger points (MFTPs), is estimated to account for 85% of muscle pain (myalgia) due to injury (8). Myofascial pain and MFTPs are now being recognized as clinical entities in veterinary patients; however, minimal literature exists (9) so it is often ignored. We will be addressing the importance of treating myofascial pain in practice, the functional and structural changes that can result and different treatment options. Selected References
1. Millis D, Levine D, Canine Rehabilitation and Physical Therapy, 2nd edition, Elseveir, Philadelphia, 2014.
2. Bockstahler B, Levine D, Millis D, Essential Factos of Physiotherapy in Dogs and Cats: Rehabilitation and Pain Management, 2nd edition, BE VetVerlag, Germany, 2019
3. Broadhurst M A clinicians guide to myofascial pain in the canine patient. 2020 4. Traditional Chinese Veterinary Medicine: Fundamental Principles, 2nd Edition. Huisheng
Xie, DVM PhD, Vanessa Preast, DVM PhD Published by: Chi Institute Press.
5. Dr. Xie’s Veterinary Acupuncture. Huisheng Xie, DVM PhD Vanessa Preast, DVM PhD. Published by: Blackwell Publishing.
161
6. Evans HE, de Lahunta A: Miller’s Anatomy of the Dog, 4th Edition. Elsevier Saunders, 2013, St. Louis, Missouri
7. Lee JC, Lin DT, Hong C: The effectiveness of simultaneous thermotherapy with ultrasound and electrotherapy with combined AC and DC current on the immediate pain relief of myofascial trigger points. Journal of Musculoskeletal Pain 1997 5:81-90
8. Simons DG, Stolov WC: Microscopic Features of Transient Contraction of Palpable Bands in Canine Muscle. Am J of Physical Med 1776; 55(2):65-88
9. Simons DG, Stolov WC: Microscopic Features of Transient Contraction of Palpable Bands in Canine Muscle. Am J of Physical Med 1776; 55(2):65-88
162
ECG BASICS By Anthony Carr, Dr. med. vet., DACVIM (internal medicine) Western College of Veterinary Medicine University of Saskatchewan, Saskatoon, Saskatchewan, Canada
Electrocardiography is an integral part of the cardiological exam. It is the only way to determine heart rhythm accurately and to determine if there are any conduction abnormalities. This is also the most useful part of an ECG. ECGs can do other things however, these are not nearly as important. An ECG is a recording of the electrical activity of the heart recorded on the surface of the body (or from the esophagus). Standard lead systems have been developed, these help determine the orientation of the depolarizing forces, an indirect indicator of the position of the heart in the chest cavity. These lead systems are however not needed to determine rhythm, you could in theory record the ECG from the fingertips if you have to. Some of the images used in these notes are from Tilley’s Essentials of Canine and Feline Electrocardiography. I. ECG basics
1. How can an ECG be recorded: A standard lead system can be used an electrodes attached to the limbs. This does require that the patient be in right lateral recumbency. This must be done if amplitude measurements are to be made (only in lead II). Alternatively a direct chest lead system can be used for rhythm diagnosis. Telemetry, holter monitors (24 hour ambulatory ECG) and cardiac event recorders (push a button and it records ECG immediately before and after the button is pushed) are other specialized ECG forms.
2. What can an ECG do extremely well: Only the ECG can determine rhythm or conduction abnormalities.
3. What can an ECG do well: The ECG can be helpful in evaluating for heart enlargement. These changes are however not specific nor sensitive. It is more sensitive in cats because there are less confounding breed differences. The ECG is also more helpful with certain congenital heart diseases. It can be helpful for diagnosing pericardial effusion and hyperkalemia.
4. What can an ECG not do: It cannot give a definitive answer regarding heart size, imaging studies are needed. ECGs also do not reflect the mechanical strength of the heart, an ECG can be normal and no pulse may be present.
5. What are the indications for an ECG: arrhythmia on auscultation, syncope, heart murmur, pre-, intra- and postop monitoring, dyspnea, cyanosis, drug monitoring (digoxin, beta blocker, tricyclic antidepressants), emergency cases (trauma, GDV, urethral obstruction, hyperkalemia suspect), periocardiocentesis (VPCs indicate the needle is tickling the heart), certain breeds (doberman, boxer), unexplained brady- or tachycardia.
163
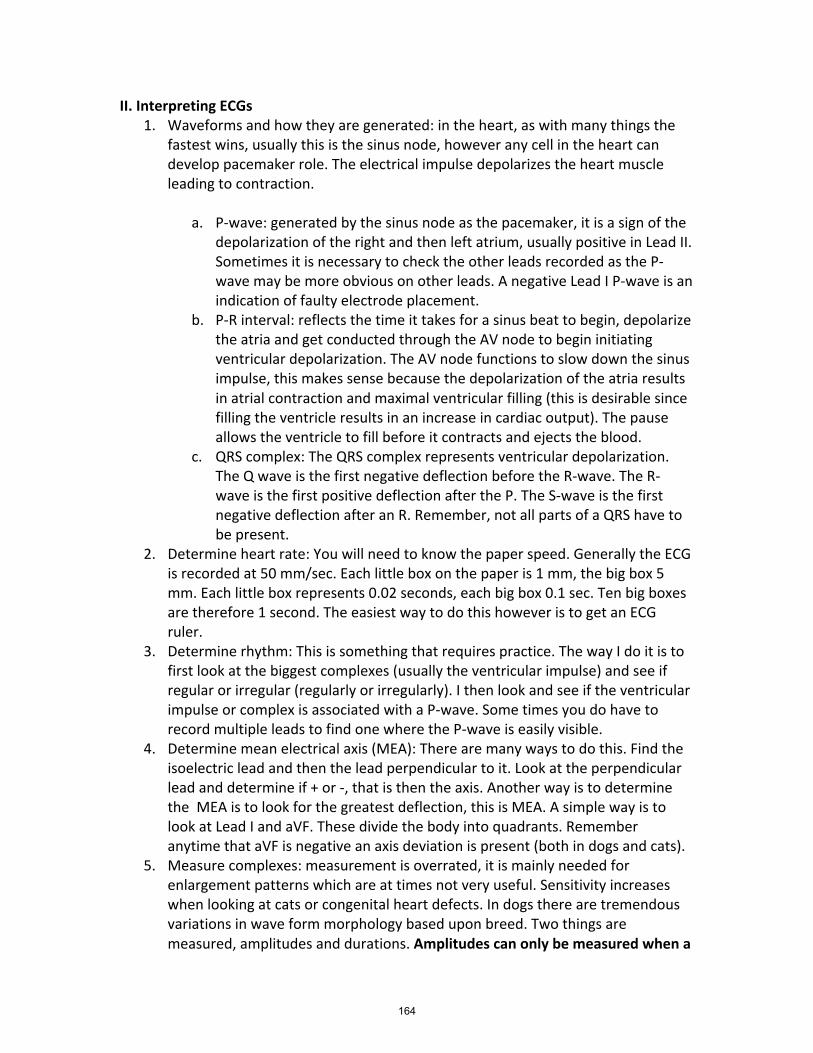
II. Interpreting ECGs 1. Waveforms and how they are generated: in the heart, as with many things the
fastest wins, usually this is the sinus node, however any cell in the heart can develop pacemaker role. The electrical impulse depolarizes the heart muscle leading to contraction.
a. P-wave: generated by the sinus node as the pacemaker, it is a sign of the
depolarization of the right and then left atrium, usually positive in Lead II. Sometimes it is necessary to check the other leads recorded as the P-wave may be more obvious on other leads. A negative Lead I P-wave is an indication of faulty electrode placement.
b. P-R interval: reflects the time it takes for a sinus beat to begin, depolarize the atria and get conducted through the AV node to begin initiating ventricular depolarization. The AV node functions to slow down the sinus impulse, this makes sense because the depolarization of the atria results in atrial contraction and maximal ventricular filling (this is desirable since filling the ventricle results in an increase in cardiac output). The pause allows the ventricle to fill before it contracts and ejects the blood.
c. QRS complex: The QRS complex represents ventricular depolarization. The Q wave is the first negative deflection before the R-wave. The R-wave is the first positive deflection after the P. The S-wave is the first negative deflection after an R. Remember, not all parts of a QRS have to be present.
2. Determine heart rate: You will need to know the paper speed. Generally the ECG is recorded at 50 mm/sec. Each little box on the paper is 1 mm, the big box 5 mm. Each little box represents 0.02 seconds, each big box 0.1 sec. Ten big boxes are therefore 1 second. The easiest way to do this however is to get an ECG ruler.
3. Determine rhythm: This is something that requires practice. The way I do it is to first look at the biggest complexes (usually the ventricular impulse) and see if regular or irregular (regularly or irregularly). I then look and see if the ventricular impulse or complex is associated with a P-wave. Some times you do have to record multiple leads to find one where the P-wave is easily visible.
4. Determine mean electrical axis (MEA): There are many ways to do this. Find the isoelectric lead and then the lead perpendicular to it. Look at the perpendicular lead and determine if + or -, that is then the axis. Another way is to determine the MEA is to look for the greatest deflection, this is MEA. A simple way is to look at Lead I and aVF. These divide the body into quadrants. Remember anytime that aVF is negative an axis deviation is present (both in dogs and cats).
5. Measure complexes: measurement is overrated, it is mainly needed for enlargement patterns which are at times not very useful. Sensitivity increases when looking at cats or congenital heart defects. In dogs there are tremendous variations in wave form morphology based upon breed. Two things are measured, amplitudes and durations. Amplitudes can only be measured when a
164
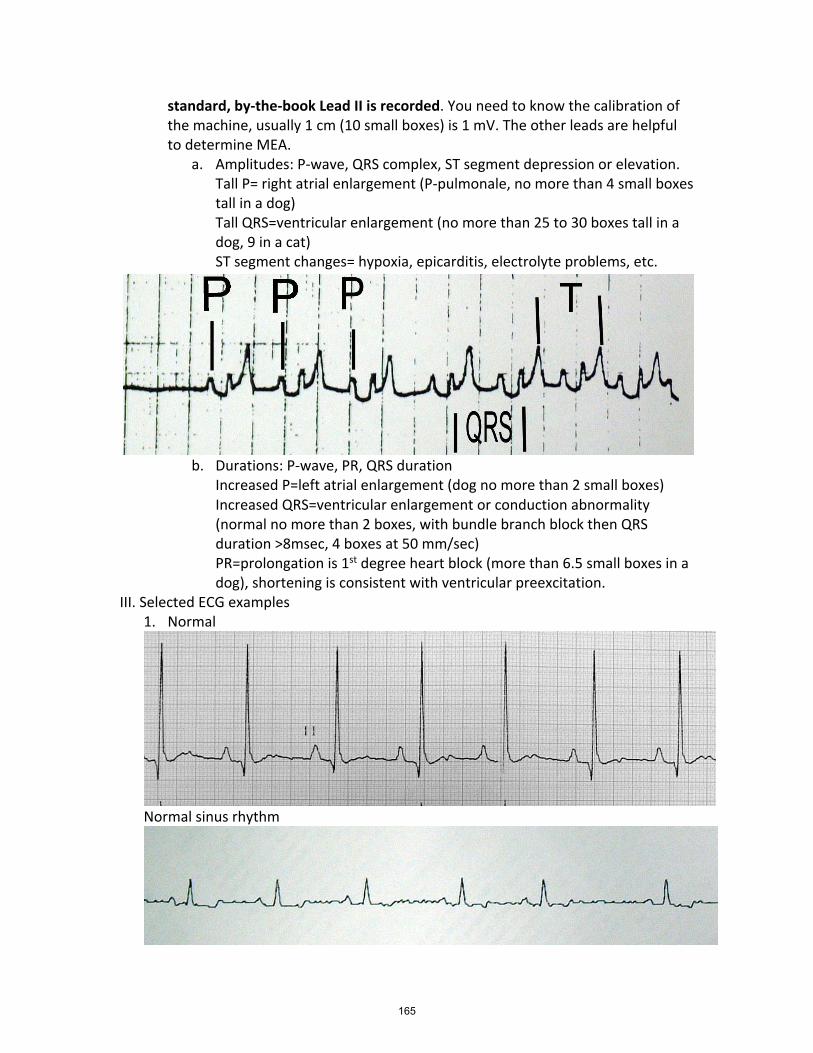
standard, by-the-book Lead II is recorded. You need to know the calibration of the machine, usually 1 cm (10 small boxes) is 1 mV. The other leads are helpful to determine MEA.
a. Amplitudes: P-wave, QRS complex, ST segment depression or elevation. Tall P= right atrial enlargement (P-pulmonale, no more than 4 small boxes tall in a dog) Tall QRS=ventricular enlargement (no more than 25 to 30 boxes tall in a dog, 9 in a cat) ST segment changes= hypoxia, epicarditis, electrolyte problems, etc.
b. Durations: P-wave, PR, QRS duration
Increased P=left atrial enlargement (dog no more than 2 small boxes) Increased QRS=ventricular enlargement or conduction abnormality (normal no more than 2 boxes, with bundle branch block then QRS duration >8msec, 4 boxes at 50 mm/sec) PR=prolongation is 1st degree heart block (more than 6.5 small boxes in a dog), shortening is consistent with ventricular preexcitation.
III. Selected ECG examples 1. Normal
Normal sinus rhythm
165
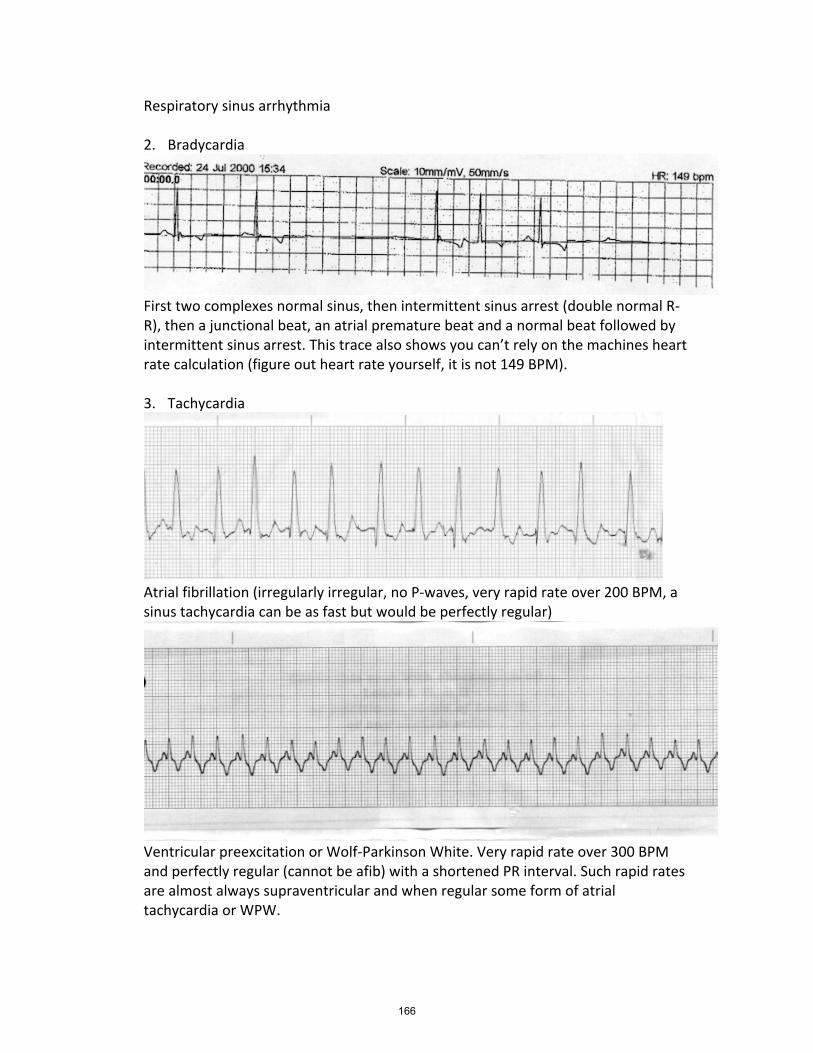
Respiratory sinus arrhythmia 2. Bradycardia
First two complexes normal sinus, then intermittent sinus arrest (double normal R-R), then a junctional beat, an atrial premature beat and a normal beat followed by intermittent sinus arrest. This trace also shows you can’t rely on the machines heart rate calculation (figure out heart rate yourself, it is not 149 BPM). 3. Tachycardia
Atrial fibrillation (irregularly irregular, no P-waves, very rapid rate over 200 BPM, a sinus tachycardia can be as fast but would be perfectly regular)
Ventricular preexcitation or Wolf-Parkinson White. Very rapid rate over 300 BPM and perfectly regular (cannot be afib) with a shortened PR interval. Such rapid rates are almost always supraventricular and when regular some form of atrial tachycardia or WPW.
166
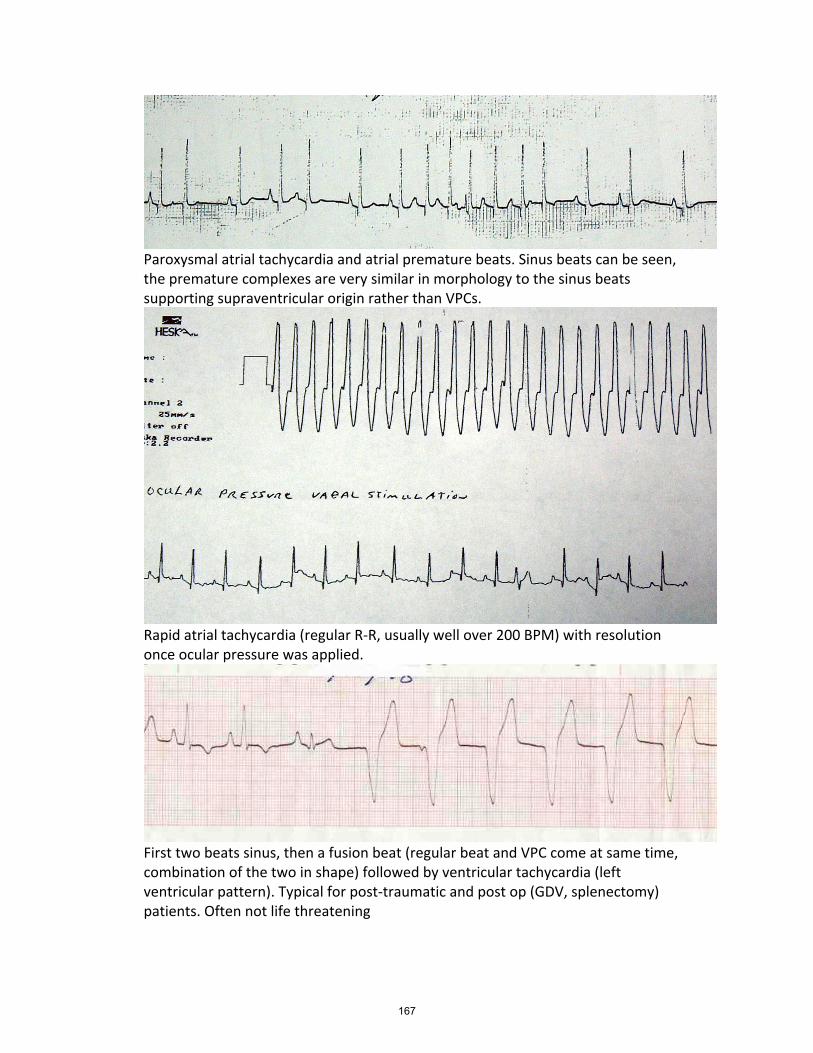
Paroxysmal atrial tachycardia and atrial premature beats. Sinus beats can be seen, the premature complexes are very similar in morphology to the sinus beats supporting supraventricular origin rather than VPCs.
Rapid atrial tachycardia (regular R-R, usually well over 200 BPM) with resolution once ocular pressure was applied.
First two beats sinus, then a fusion beat (regular beat and VPC come at same time, combination of the two in shape) followed by ventricular tachycardia (left ventricular pattern). Typical for post-traumatic and post op (GDV, splenectomy) patients. Often not life threatening
167
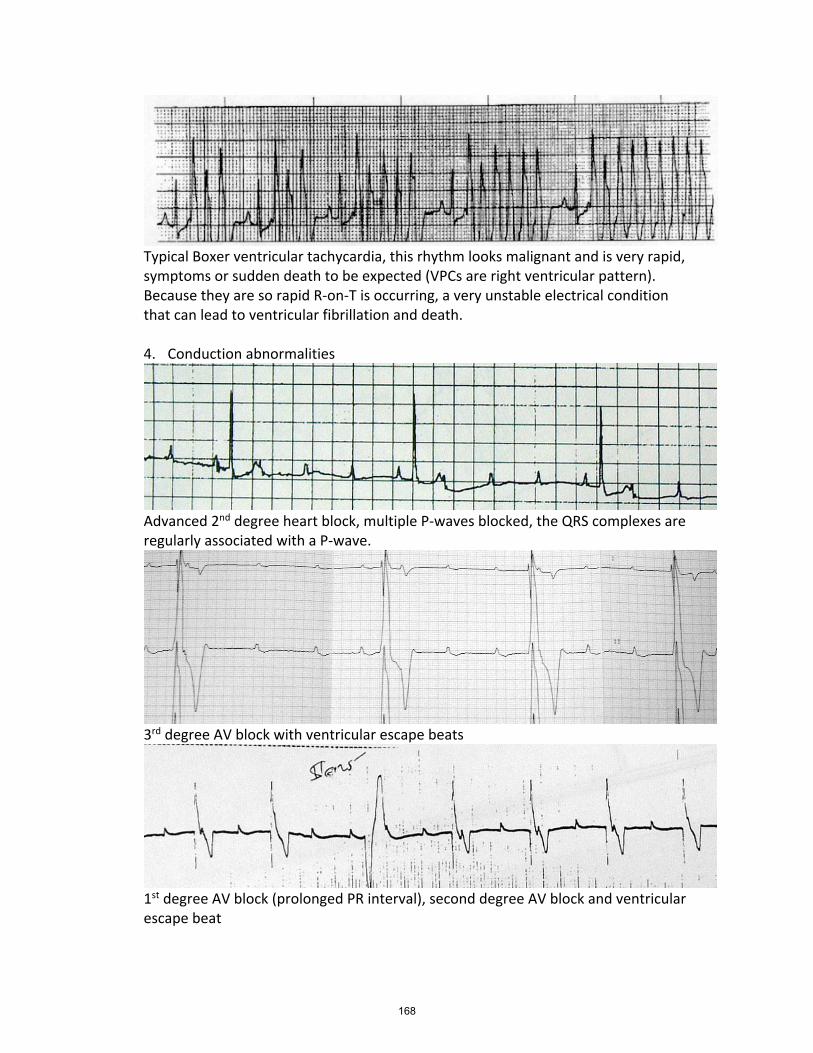
Typical Boxer ventricular tachycardia, this rhythm looks malignant and is very rapid, symptoms or sudden death to be expected (VPCs are right ventricular pattern). Because they are so rapid R-on-T is occurring, a very unstable electrical condition that can lead to ventricular fibrillation and death. 4. Conduction abnormalities
Advanced 2nd degree heart block, multiple P-waves blocked, the QRS complexes are regularly associated with a P-wave.
3rd degree AV block with ventricular escape beats
1st degree AV block (prolonged PR interval), second degree AV block and ventricular escape beat
168
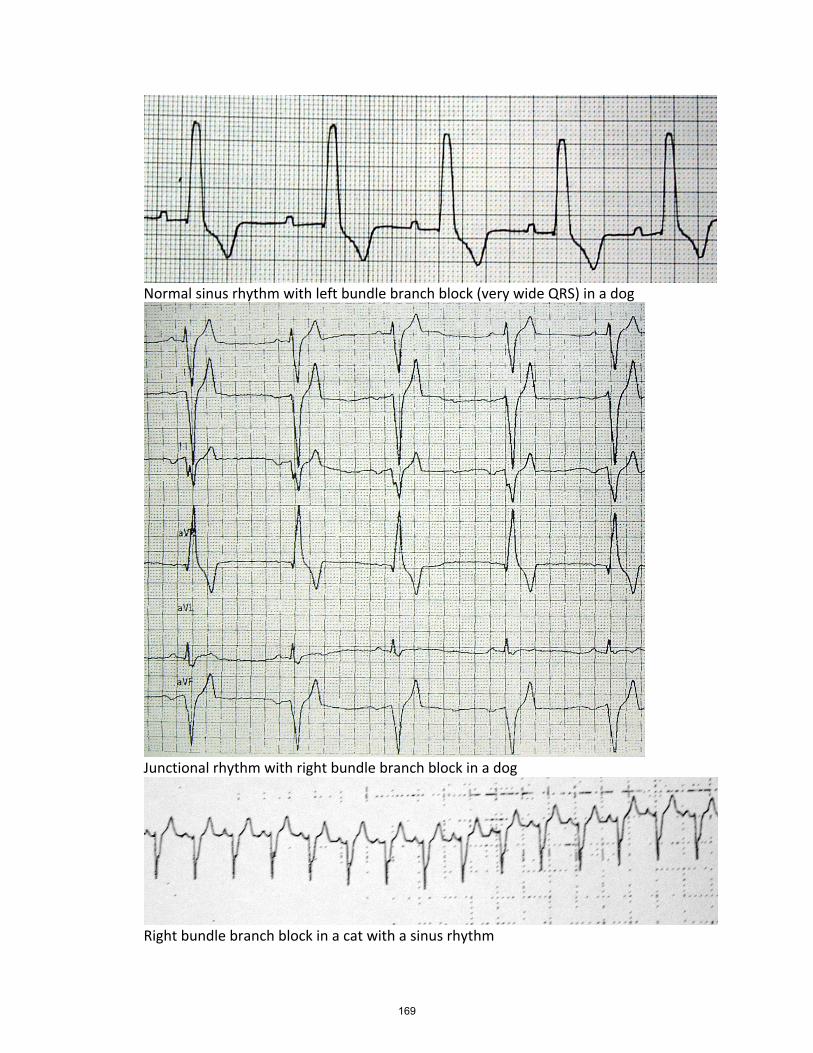
Normal sinus rhythm with left bundle branch block (very wide QRS) in a dog
Junctional rhythm with right bundle branch block in a dog
Right bundle branch block in a cat with a sinus rhythm
169

EPI in dogs Anthony P. Carr, DACVIM Professor, Small Animal Clinical Sciences WCVM, Saskatoon, Canada What is exocrine pancreatic insufficiency? Exocrine pancreatic insufficiency (EPI) is a condition where the pancreas no longer produces adequate amounts of digestive enzymes. Clinical signs usually will not occur until over 90% of the exocrine pancreas has become non-functional. The majority of cases in dogs are caused by pancreatic acinar atrophy, though some may also develop because of chronic pancreatitis. Clinical signs develop because digestion no longer occurs properly leading to malabsorption with weight loss and diarrhea. Maldigestion and malabsorption does not just result from the enzyme deficiency. The disease also leads to changes in small intestinal digestive processes. Small intestinal bacterial overgrowth (SIBO) is also frequently seen and can contribute to the diarrhea seen. Low cobalamin levels are also seen which may play a role with small intestinal disease in these dogs. What is pancreatic acinar atrophy? Pancreatic acinar atrophy (PAA) is a condition where a normal pancreas undergoes atrophy. A familial predisposition in German Shepherds and rough-coated collies has been established. It can however occur in any breed with large breed dogs being more commonly affected. What is a typical signalment for EPI? Since PAA is the most common cause of EPI many of the patients are German Shepherds. They tend to be young animals, usually under 2 years of age. What are the clinical signs of EPI? Signs of EPI are relatively typical, though they can be caused by other diseases as well. Dogs with EPI can have profuse diarrhea. The bowel movements are often malodorous. Borborygmus and flatulence are common. These patients will have a ravenous appetite yet continue to lose weight. Poor hair coat is common because of the malnourishment present. On occasion other signs such as vomiting, coprophagia, pica and anorexia can be seen. Routine clinical pathologic tests rarely document abnormalities. Folate levels may be elevated and cobalamin concentration decreased in dogs with EPI. This may be from SIBO, however the cobalamin deficiency may also occur because the pancreas produces a factor needed for cobalamin absorption that can be lacking in dogs with EPI.
170

How is EPI diagnosed? EPI is generally diagnosed with pancreatic function tests. Canine TLI is currently the preferred test for EPI. The animal should be fasted 12 hours to collecting serum for analysis. Low TLI concentration in patients with typical clinical signs are considered highly diagnostic. Low TLI values can be found in dogs without clinical signs. Many other tests have been tried but none are superior to TLI. How is EPI treated? Treatment of EPI hinges on enzyme replacement and nutritional intervention. Powdered pancreatic enzymes work best and are used at 1 to 2 teaspoons per meal. There is no need to pre-incubate the food. Alternatively, fresh pancreas (50-100g/meal) can be used. The majority of the enzymes are destroyed in the stomach so some dose titration may be needed. Although raw pancreas results in higher GI lipase activity, response rates between powdered enzymes and raw pancreas were comparable. In these patients it is vital to manage their diet carefully. Initial management can be with a high-quality maintenance diet. Fat restriction should not be attempted initially, in fact fat supplemented diets may be a consideration if body condition cannot be improved. If this results in persistent diarrhea, a fat restricted, highly digestible diet should be tried. Cobalamin injections can be given (250-500 μg, repeat as indicated by serum levels), especially to those patients that are responding poorly to therapy. Cobalamin concentration can be determined via a blood test. Vitamin absorption may generally be inadequate in these patients so that use of vitamin supplements is prudent. Antibiotics are indicated if SIBO is suspected to be contributing to poor therapeutic response. Metronidazole, tylosin and tetracyclines are all good options for this. Tylosin may be preferable as it seems to be very good at treating chronic diarrhea in dogs. What is the Prognosis for EPI? Generally, the prognosis is good, especially if the initial response to therapy is good. Around 60% of dogs will do very well, 10% get better and 20% do poorly. With a poor initial response overall survival seems shortened. Cobalamin deficiency has been the only factor that seemed to correlate with how well the initial response was. Factors that did not have an effect were the type of supplement used, additional drugs used, or diet used. EPI in Cats The diagnosis of EPI in dogs and cats has become more common as the assay for feline trypsin-like immunoreactivity (fTLI) became available. The test is considered diagnostic for EPI if a concentration of < 8 μg/L is found. Previous to this diagnosis was complicated based upon clinical signs and a variety of fecal digestion assays. There is relatively little information on EPI in cats that has been published. There have been individual case reports as well as 3 case series that included 41 cases.1-3 These case series showed that weight loss was the most common clinical sign of EPI in cats. Diarrhea was common, but
171
not present in all cats and often not like the "typical" feces noted in dogs (voluminous, malodorous, steatorrhea). Polyphagia was uncommon. Age range was quite broad from 3 months to 16 years with the majority being middle aged. Although these case series are interesting they only provide information on a small number of patients, considering that in 2010 there 775 samples submitted to the Gastrointestinal Laboratory at Texas A&M University with fTLI concentrations consistent with a diagnosis of feline EPI.4 At the 2011 ACVIM Forum in New Orleans a research abstract was presented by researchers from the GI Laboratory and Department of Clinical Sciences at Texas A&M.5 The researchers searched their database for cats with a TLI concentration below 8 μg/L found over a 15-month period. Questionnaires were sent to the veterinarians that had submitted the samples, with 150 surveys being returned. There were many breeds involved and it did not seem that there was a clear breed predilection, though this could not be definitively determined with this type of study. Mean age of the cats was 8.1 years ± 4 with 41% being female and 59% male. Body condition was poor with a median of 3/9. Of the cats that had cobalamin determined, 77% were deficient with many of them having undetectable concentrations. Folate was increased in 47% of the cats where it was determined. The most common clinical sign in this study was weight loss which was seen in 91% of the cats. The amount of weight loss varied widely from 40 grams to 6.82 kg with a median of 1.4 kg. Loose stools were seen in only 62% of the affected cats. Other clinical signs included poor haircoat (50%), anorexia (45%), increased appetite (42%), depression (40%), watery diarrhea (28%), and vomiting (19%). Concurrent diseases were also quite commonly reported (58%). The most common ones were inflammatory bowel disease (IBD, 21%), diabetes (14%), pancreatitis (11%) and hepatic lipidosis (6%). Of the affected cats 68% were treated with pancreatic enzyme supplementation with a good response in 66%, partial response in 24% and poor response in 10%. This study is interesting on many levels. It is the largest study to date, so the clinical information is very valuable. There are of course potential methodological issues with survey studies that introduce bias depending on high the response rate, though in this case they do not detract from the clinical relevance of the data. EPI in cats is certainly not as rare as we once thought it was. The clinical presentation deviates significantly from the typical presentation in a dog. Weight loss is certainly common in both dogs and cats and can be quite pronounced, however in cat's diarrhea is clearly not a consistent finding. The diarrhea also appears to be much less severe when it is seen and often does not have the characteristics, we expect to see such as large volume, highly fluid and greasy appearing stools. Polyphagia does occur in some cats, however almost half the cats were reported to have a decreased appetite. A variety of concurrent diseases were found, most of them are not surprising. The etiology of EPI in cats in most cases probably relates to chronic pancreatitis and easily
172

explains the 11% of cats that were thought to have pancreatitis in this study.1-4 In dogs it usually is related to pancreatic acinar atrophy which may also be the cause of EPI in very young cats.4 With chronic pancreatitis you can also see the development of endocrine pancreatic insufficiency, e.g. diabetes. Hepatic lipidosis has also been linked with pancreatitis. IBD was reported in 21% of the cats with EPI which may well have to do with what is termed triad disease or triaditis. In cats it has been shown that there is a statistical association between IBD, pancreatitis and cholangiohepatitis. Treatment for EPI with pancreatic enzyme supplementation was successful in a significant percentage of the cases. The cats with EPI also had other issues that might have impacted management. Most of the cats had low cobalamin concentrations. It has been previously shown that in cats with hypocobalaminemia supplementation of parenteral cobalamin is often needed to resolve GI signs (250 μg subcutaneously weekly for 6 weeks, then once monthly with periodic checks of serum concentration). In addition, the presence of EPI may be associated with small intestinal dysbiosis (formerly termed small intestinal bacterial overgrowth). The low cobalamin and high folate would certainly point toward this diagnosis. If pancreatic enzyme supplementation and cobalamine injection do not resolve signs, consideration should be given to antibiotic therapy. Dietary therapy is also very important, though to date there are no studies that tell us which diets to preferentially use. This study does point out that EPI is not as rare as we thought and it would seem prudent to test for fTLI concentration in cats with unexplained weight loss or chronic diarrhea, even if they are very young. The presence of hypocobalaminemia should also increase the suspicion that EPI is present. It should also be considered in those cats with diabetes that appear to have good glycemic control but consistent weight loss or diarrhea. In the unexplained weight loss cases where blood work, T4, thoracic radiographs and abdominal ultrasound did not establish a diagnosis, I would often perform endoscopy to determine if occult neoplasia or some form of IBD was present. Based on this study, I will certainly have fTLI, cobalamin and folate determined prior to this more expensive and invasive diagnostic procedure. References 1. Steiner JM, Williams DA. Serum feline trypsin-like immunoreactivity in cats with exocrine pancreatic insufficiency. J Vet Intern Med 2000;14:627-629 2. Kook PH, Zerbe P, Reusch CE. Exokrine Pankreasinsuffizienz bei der Katze. Schweiz Arch Tierheilk 2011;153:19-25. 3. Thompson KA, Parnell NK, et al. Feline exocrine pancreatic insufficiency: 16 cases (1992-2007). J Feline Med Surg 2009;11:935-940. 4. Steiner JM. Exocrine pancreatic insufficiency in the cat. Topics in Compan An Med 2012;27:113-116. 5. Xenoulis PG, Wooff P, et al. Feline exocrine pancreatic insufficiency: 150 cases. J Vet Intern Med 2012;26:765.
173

IMHA: Bad blood By Anthony Carr, Dr. med. vet., DACVIM (internal medicine) Western College of Veterinary Medicine University of Saskatchewan, Saskatoon, Saskatchewan, Canada Immune-mediated hemolytic anemia Etiology and pathophysiology: The cause of IMHA has been discussed at length. Genetics are involved as there are breed predispositions such as the Cocker Spaniel. In addition gender may also play a role. The reason why a predisposition exists are to date unclear, though they may have something to do with red blood cell antigens or the way the immune system works. Various triggers are also thought to play a role. Vaccination has also been incriminated. In one paper 25% of dogs had been vaccinated within the last month before presentation. In several other papers an association has not been seen. Certainly in my research such a link could not be made. Drug administration and infections may also play a role. The majority of cases are idiopathic. Once the process has been initiated, red cells are tagged for destruction by the binding of immunoglobulins or complement. Depending upon how tagged, the RBCs will be destroyed either intravascularly or extravascularly. The sites of red cell removal include liver, spleen and bone marrow. The autoantibodies can be directed at very early RBCs such as reticulocytes causing an anemia that appears non-regenerative as the precursors are removed first. Diagnosis Diagnosis with IMHA can proceed along the name of the disease. All components of the name, that is "immune-mediated" "hemolytic" and "anemia" need to be satisfied for a definitive diagnosis. Anemia is usually the easiest part to determine. At times one or the other areas will be present without being able to satisfy the others. This is the case when a positive Coombs test is present in an animal without anemia. This does not diagnose IMHA, in fact it may be a marker for neoplasia. There are a variety of ways to determine that an anemia is immune-mediated. One way is a positive Coombs test, unfortunately both false positive and false negative results occur. The Coombs test identifies bound immunoglobulins or complement on the RBCs. Some types of antibodies will be picked up better than others and at times processing of the RBCs wash the antibodies off. Overall it still is a very good test. The presence of autoagglutination is definitive for IMHA. It must be differentiated from Rouleaux formation by diluting 1 drop of blood with several drops of saline. If gross agglutination is not seen, look at the slide under a microscope for aggregates of clumped RBCs. The
174

presence of a large number of spherocytes is also a strong indicator of IMHA (pieces of the RBC membrane have been removed, leaving more hemoglobin behind in a smaller RBC). Hemolysis must also be present to confirm IMHA. Spherocytes are a sign of both immune-mediated destruction as well as hemolysis. Icterus is if present can indicate hemolysis, though the degree of jaundice will depend upon the rapidity of hemolysis as well as possible damage to the liver (hypoxia through anemia, thrombi). Hemoglobinuria is also a strong indicator of hemolysis if urinary tract disease has been ruled out. Hemolysis determined on a blood draw is however very easy to induce, even in normal animals so it has be interpreted carefully. It is important to remember that all the various areas must be present to have a definitive diagnosis of IMHA. Hemolysis can occur through mechanisms that are not immune mediated. Anemia can be caused by many problems. Unfortunately in some cases all the pieces of the puzzle will not fit together and the diagnosis will merely be presumptive. A definitive diagnosis does allow a very aggressive treatment approach. If not definitive, frequent reassessment is indicated to make sure another disease process has not been overlooked. Clinical findings Clinical signs will depend predominantly on how anemic the animal is and how rapidly it got to the reduced PCV. If given time, animals can adapt to relatively severe anemias, on the other hand rapid progression usually makes the animal more symptomatic. Because a large part of the body is being attacked a very vigorous immune response is occurring with the liberation of many cytokines and inflammatory mediators. These cause many of the severe systemic signs seen with IMHA such as dever, lethargy, and anorexia.In most cases the mucous membranes will be pale and jaundiced. Often liver and splenic enlargement is palpated in these patients. Concurrent ITP (IMHA and ITP together are called Evan's Syndrome) can also contribute clinical signs such as petechia, melena and hematuria. Discoloration of the urine is common either through blood, hemoglobin or bilirubin. Therapy Many things have been tried to treat IMHA, whether they work or not has been definitively determined. Most of the preferences listed are individual opinions, though there has been interest in generating data in this regard recently. Though many things have changed in veterinary medicine, the cornerstone of IMHA therapy still are corticosteroids. These usually are given at immune-suppressive dosages (2mg/kg of prednisone BID or equivalent dosages of other glucocorticoids). This dose is then very gradually tapered over months. The corticosteroids cause side-effects frequently,
175
fortunately they are rarely life threatening. Many other immune suppressives have been used. Unfortunately there is no hard clinical evidence to guide the clinician in the choice of therapy to use. Cyclophosphamide (200 mg/m2 given once i.v. or p.o.) has been a drug commonly used in severe cases of IMHA. Concern has been raised whether this medication may actually have a negative effect. Overall I have not been impressed by its efficacy and generally no longer use this medication in IMHA. Certainly bone marrow suppression can occur which would tend to interfere with a proper and vigorous regenerative response. Azathioprine has also been used, I routinely start this medication concurrently to the corticosteroids. This will allow me to taper the corticosteroids more rapidly, improving the owners perception of the quality of life. It is thought that this drug takes 3 to 4 weeks before becoming effective, though this has been questioned as well. It is unlikely that it works very rapidly however. Danazol (5 mg/kg BID) has also been used, though recent work does raise the question whether it has any benefit and the costs are quite high. Certainly it also is not a fast acting agent. Cyclosporine has relatively immediate effects. In a small study it did show some efficacy, and I have the impression it is a useful therapy to help to get a more rapid response to therapy. It is relatively expensive, though this disease generally is rarely cheap to treat. We compared a group of dogs receiving prednisone and azathioprine to a group getting these two drugs as well as cyclosporine. Outcomes were essentially similar. There was wide variation in the blood levels achieved so that therapeutic monitoring of cyclosporine therapy is recommended. Another treatment modality is the infusion of human intravenous IgG which was the most expensive. Though a promising treatment it can be difficult to impossible to get the medication. We have seen adverse effects in one dog that became extremely pruritic. Though the medication worked fast, in a small study mortality remained unchanged, apparently because the animals still thrombosed. Besides immune suppression, supportive care is vital in these patients. Fluid therapy is almost always indicated. This may help to prevent sludging (promotes thrombosis) as well as helping the kidneys deal with hemoglobin (can cause acute renal damage). Some people are worried about further diluting the PCV, but it is important to remember that fluids do not decrease the overall body's red blood cell mass. Fluid therapy counters the decrease in PCV from dilution by increasing perfusion. If the PCV is low enough (usually a clinical judgement, certainly most cases in the single digits qualify) a transfusion is indicated. In fact we may be letting the PCV drop too low in these patients. The presence of hepatic necrosis in these cases is not rare and probably relates to hypoxia. This may play a central role in promoting clotting. As such we probably should be aiming for higher PCVs than we previously have, although there is no objective data to support
176

this contention. This can be blood or blood substitutes (whereby substitutes have only a 24 to 48 hour half life). With blood transfusions it is likely that the transfused blood will be destroyed as rapidly as the patient's own blood. There was some concern raised that transfusions may worsen prognosis (adding fuel to a fire), but this has not been backed up by most recent studies. It is likely that this initial finding was because those dogs more seriously effected needed more blood and had a worse outcome because of the more severe disease they had rather than because of the transfusions per se. Heparin has been given (50-75 units/kg s.q. TID) to possibly reduce thrombotic problems, though to date information is not available if this truly is efficacious. The main concern is that we focus on immune suppression, however most cases die within the first week of presentation, where immune suppression is not yet likely to have occurred. We need focus more on preventing thrombi and providing optimal supportive care rather than playing with newer and more potent immune suppressives. Recent studies have suggested that low dose aspirin (0.5-2 mg/kg/day) may be helpful as well. Another alternative is plavix (clopidogrel) which I tend to use routinely. References: Available upon request from the author.
177

Practical management of renal failure By Anthony P. Carr, Dr. med. vet., DACVIM Western College of Veterinary Medicine University of Saskatchewan, Saskatoon, Canada Hypertension and CRF It is known that high blood pressure is associated with renal disease in many species including cats and dogs. That this is important is known from many studies including ones involving dogs. A study from the University of Minnesota looked at 45 dogs with spontaneous renal disease.1 They divided the dogs into a high (systolic 161-201 mmHg) intermediate (144-160 mmHg) and low (107-143) blood pressure group. The dogs were in mild to moderate renal failure (BUN around 70 + 30 mg/dL or 25 + 11 nmol/L; creatinine 3.5 + 1.5 mg/dL or 300 + 130 µmol/L) and all groups were similar in this manner. The high blood pressure group was more likely to die and took less time to develop a uremic crisis (clinical signs with at least a 20% rise in BUN in comparison to previous visit where signs were absent). In fact the high blood pressure group had half the life expectancy of the other groups (300 vs. 600 days). The dogs in the high blood pressure group were also the only ones to have retinal changes (3 of 14). Some dogs were treated with antihypertensive medications if systolic blood pressure was greater than 180 mmHg two consecutive visits or if retinal lesions were seen. This resulted in 11 dogs being treated (amlodipine, diltiazem, enalapril alone or in combination), though only 1 dog responded. One reason why hypertension is associated with progressive renal damage is the loss of autoregulatory ability by the diseased kidney. Autoregulation allows the kidney to maintain relatively constant renal blood flow and glomerular filtration rate even if mean arterial pressure varies from 70 to 150 mmHg.2 This is one reason why hypertension alone in animals is unlikely to cause renal problems since autoregulation protects the glomerulus from increased systemic blood pressure. Autoregulation has been shown in various rodent models and has also been clearly demonstrated in dogs. In dogs that underwent partial nephrectomy the ability to autoregulate was severely impaired when a 7/8 nephrectomy was carried out, whereas those dogs with ¾ nephrectomy were less compromised.3 Autoregulation at both low and higher pressures was impaired. This means that dogs with renal failure are more likely to have hypoperfusion of the kidney at mean arterial pressures that are usually considered adequate (loss of autoregulation at 100 mmHg MAP). These dogs also are more likely to also pass on elevated systemic blood pressures to the glomerulus, leading to progressive renal function loss. In the 7/8 nephrectomy dogs GFR increased almost linearly with increased MAP. Based upon the association of hypertension with progressive decline of renal function it is vital that blood pressure be measured routinely and repeatedly on all patients with chronic renal disease. Once blood pressures are elevated (on repeated measurement
178
sessions or if ocular lesions are present) it is imperative that appropriate antihypertensive therapy be instituted. Based upon the scientific literature systolic pressures greater than 160 mmHg and diastolic pressures greater than 100 mmHg in patients with renal disease warrant therapy. This is considered a category with moderate risk of target organ damage as determined by the group of clinicians involved with producing a consensus statement on hypertension for the ACVIM. The reported percentages of dogs and cats that are hypertensive varies from study to study. Percentages greater than 50% have been reported in some studies. Lower percentages have also been seen, in one study of 103 cats with CRF only 20% were hypertensive at initial presentation.4 Hypertension in this study was defined as a systolic blood pressure >175 mmHg (Doppler determination) with ocular lesions or having this degree of elevation at a subsequent visit. The presence of hypertension did not relate to the severity of azotemia, though it was related to lower potassium concentrations. The hypertensive cats in this study were more likely to have cardiovascular abnormalities (gallops, murmurs, arrhythmias) and 70% of the cats had ocular lesions. Of course this study only looked at blood pressure one time, not repeatedly. It is still unknown what percentage of cats will go on to develop hypertension during the time they are in CRF. In dogs the situation is confusing. One study showed that few dogs with renal insufficiency or failure were hypertensive. 5 This study however used an upper normal value for systolic of 175 mmHg and for diastolic of 111 mmHg. These values are considered hypertensive by many. At the ECVIM meeting in 2004 a presentation was given that presented data on 519 dogs with renal disease. Of these dogs 60% had a systolic pressure > 150 mmHg and 70% a diastolic pressure > 95 mmHg. 6 Experimental models of renal failure in dogs support the concept that CRF leads to elevations in blood pressure in this species as well and that this elevation correlates with poorer outcome.7 Blood pressures increased around 20 mmHg for MAP, DAP and SAP in the more severely affected dogs, in the less affected dogs it was only approximately a 10 mmHg increase. This translated however to a significantly greater loss of renal function (creatinine around 1/3 higher in these dogs). Dogs with surgery and higher blood pressures also tended to be more proteinuric than the lower pressure groups, though the degree of proteinuria was mild (UP:UC of around 2). Appropriate management of hypertension depends upon a variety of pharmacologic products. In cats with marked hypertension, amlodipine is the drug of choice. This medication has been shown to be effective in both spontaneous and experimental renal disease. The magnitude of decrease in blood pressure has been shown to be approximately 30 mmHg when given at 0.25 mg/kg in cats.8 ACE inhibitors can also be used for hypertension, however blood pressure reduction is usually modest, approximately 5 to 20 mmHg.9,10 The use of ACE inhibitors is however correlated with improved outcome. In cats with induced renal insufficiency benazapril resulted in higher GFR values and lower blood pressures than cats given placebo.9 This study also
179

demonstrated that there is no need for dosage adjustment with benazapril in renal failure/insufficiency. Benazapril has also been shown to reduce glomerular capillary pressure and systemic blood pressure in cats with induced renal insufficiency.11 In an experimental model in dogs use of an ACE inhibitor also reduced blood pressure mildly and glomerular capillary pressure which should aid in limiting progressive renal injury.12 CRF and diet Diets have been a mainstay of treating chronic renal failure for decades. There has been considerable research done on trying to ascertain what dietary factors influence renal disease. Restricting dietary protein has been a cornerstone of renal diets. This is based upon the marked exacerbation of signs of uremia associated with feeding high protein diets. It needs to be remembered that certain species, especially cats, are obligate carnivores and require higher protein diets. Significant protein restriction can result in protein-calorie malnutrition. There are many other potential positive effects of renal diets including increased potassium concentrations, decreased phosphate levels, decreased sodium and improved acid-base status. Scientific publications support the positive effects of dietary management of CRF in dogs and cats with spontaneous renal disease. In one study 50 cats were enrolled. Of these 29 were fed a veterinary renal diet whereas 21 were not because of lack of compliance (by cat or owner). The veterinary diet led to lower phosphate, urea and PTH concentrations as well as more than doubling the lifespan of the patients.13 A retrospective study compared 175 cats on maintenance diets to 146 cats on various renal diets. Survival time was 7 months for the convential diets and 16 months for the renal diets.14 A randomized clinical trial in dogs showed similar results. Dogs fed a renal diet took longer to develop a uremic crisis, had less azotemia, and had a longer lifespan.15 Renal secondary hyperparathyroidism With renal disease, hyperparathyroidism develops. Initially the kidney is not able to excrete phosphorus which results in increased PTH secretion. PTH decreases reabsorption of phosphate by the kidney. In addition the kidney is responsible for the final step that produces active vitamin D. Since vitamin D levels are low, less calcium is absorbed. Usually vitamin D and calcium have a negative feedback effect on the parathyroid gland. The increase in PTH concentration has several effects. PTH liberates calcium from the bone, however it also liberates more phosphate as well. In humans this is well recognized as metabolic bone disease, a painful and debilitating consequence of chronic renal disease. Increased PTH also leads to mineralization of the kidneys and other soft tissues and plays a role in the progressive renal injury. There has been much interest in blunting secondary hyperparathyroidism. One approach is to use calcitriol, or active vitamin D. This is meant to provide negative feedback on the parathyroid gland and thereby blunt the spike in PTH concentrations. This can only be done in early renal disease however as it will increase phosphate and calcium concentrations. In many clinical cases phosphate concentrations are too high to
180
allow the safe use of calcitriol without risking increased soft tissue mineralization. The other approach is to feed a diet low in phosphorus. This has resulted in lower phosphate concentrations and a decrease in PTH concentration.13 In addition to using diets, aggressive use of phosphate binders can also be beneficial. These substances bind phosphorus in the food so that it will pass through the GI tract without being absorbed. In most instances aluminum salts have been used, though calcium containing products are also available. The predominant drawback to these products is that they reduce the palatability of the diet. In addition, recently aluminum toxicity was reported in 2 dogs on aluminum containing phosphate binders. Recent work with a chitosan and calcium product has shown promise. A significant decrease in phosphate concentration occurred as well as a decrease in urea concentration. This could of course be because of decreased food intake, though in healthy cats given the product food intake remained fairly constant. It may in fact be because chitosan causes reduced ammonia absorption and protein digestibility. Chitosan chewing gum has been found to be effective in reducing phosphorus levels in humans with hyperphosphatemia resistant to diet and oral phosphate binders. In addition recent studies suggest that renal secondary hyperparathyroidism is evident even before phosphorus concentrations rise. References
1. Jacob F, Polzin DJ, et al. Association between initial systolic blood pressure and risk of developing a uremic crisis or of dying in dogs with chronic renal failure. JAVMA 2003;222:322-329.
2. Navar L. Renal autoregulation: perspectives from whole kidney and single nephron studies. Am J Physiol 1978;234: F357-F370.
3. Brown SA, Finco DR. Navar LG. Impaired renal autoregulatory ability in dogs with reduced renal mass. J Am Soc Nephrol 1995;5:1768-1774.
4. Syme HM, Barber PJ, Markwell PJ, Elliot J. Prevalence of systolic hypertension in cats with chronic renal failure at initial evaluation. JAVMA 2002;220:1799-1804.
5. Michell AR, Bodey AR, Gleadhill A. Absence of hypertension in dogs with renal insufficiency. Renal Failure 1997;19:61-68.
6. Cowgill LD. Systemic hypertension in dogs with renal failure. 14th ECVIM Congress, Barcelona, 2004.
7. Finco DR. Association of systemic hypertension with renal injury in dogs with induced renal failure. JVIM 2004;18:289-294.
8. Mathur S, Syme H, et al. Effects of the calcium channel antagonist amlodipine in cats with surgically induced hypertensive renal insufficiency. AJVR 2002;63:833-839.
9. King JN, Strehlau G, Wernsing J, Brown SA. Effect of renal insufficiency on the pharmacokinetics and pharmacodynamics of benazapril in cats. J Vet Pharmacol Therap 2002;25;371-378.
181
10. Miller RH, Lehmkuhl LB, et al. Effect of enalapril on blood pressure, renal function, and the renin-angiotensin-aldosterone system in cats with autosomal dominant polycystic kidney disease. AJVR 1999;60:1516-1525.
11. Brown SA, Brown CA, et al. Effects of the angiotensin converting enzyme inhibitor benazapril in cats with induced renal insufficiency. AJVR 2001;62:375-383.
12. Brown SA, Finco DR, et al. Evaluation of the effects of inhibition of angiotensin converting enzyme with enalapril in dogs with induced renal insufficiency. AJVR 2003;64:321-327.
13. Elliott J, Rawlings JM, et al. Survival of cats with naturally occurring chronic renal failure: effect of dietary management. J Sm Anim Pract 2000;41:235-242.
14. Plantinga EA, Everts H, et al. Retrospective study of the survival of cats with acquired chronic renal insufficiency offered different commercial diets. Veterinary Record 2005;157:185-187.
15. Jacob F, Polzin DJ, et al. Clinical evaluation of dietary modification for treatment of spontaneous chronic renal failure in dogs. JAVMA 2002;220:1163-1170.
16. Wagner E, Schwendenwein I, Zentek J. Effects of a dietary chitosan and calcium supplement on Ca and P metabolism in cats. Berl Münch Tierärzt Wschr 2004;117:310-315.
182
The cutting edge medicine By Anthony P. Carr, Dr. med. vet., DACVIM, Professor WCVM, Small Animal Clinical Sciences, Saskatoon, Canada
Probiotics
What makes it a probiotic
• Gets through GI tract (resistant to stomach acid) • Colonizes GI tract • Has a health impact • Many probiotics do not meet these criteria
Probiotic: Sivoy (VSL3 for pets, now Visbiome) Rossi et al, ACVIM Forum 2015
• 10 cats with history of constipation, refractory to medical treatment, 3 diagnosed as megacolon, 7 as chronic constipation
• No antibiotics for 1 month • Probiotics are promising in humans with constipation • Cats were given 200 billion bacteria orally for 90 days • Clinical, endoscopic and histopathologic exam at T=0 and after treatment • Histologically fewer interstitial cells of Cajal found vs. normal cats • After treatment considerable improvement in the Feline Chronic Enteropathy Activity
Index (what’s that??) FCEAI • Combination of gastrointestinal signs, endoscopic abnormalities, serum total protein,
serum alanine transaminase/alkaline phosphatase activity, and serum phosphorous concentration
• Histology improved • ICC cells increased as well
VSL3 in dogs Study by Rossi et al in PLOS One 2014
• 10 dogs given VSL 3 • 10 dogs given prednisolone and metronidazole (had somewhat worse disease, even
though randomized) • 10 control dogs for microbiota • Decreased clinical signs • canine IBD activity based on attitude/activity, appetite, vomiting, stool consistency,
stool frequency, and weight loss, scored 0-3, • add scores and rank as clinically insignificant (score 0–3), mild (score 4–5), moderate
(score 6–8) or severe (score 9 or greater) • Increased markers of regulatory T cell function (TGF beta, Fox P3+ cells)
183
• Increased citrulin is suggestive of re-established gut barrier as marker of enterocyte mass
• Took longer for VSL3 to work (median 10 days vs. 5 days with pred and metronidazole ) with regard to vomiting and diarrhea resolving
SF68 (Enterococcus faecium, Fortiflora) and Amoxi-Clav in Cats ACVIM Abstract 2015 Forum
• Camille Torres-Henderson et al. • With amoxicillin-clavanulate it is not uncommon to see vomiting, diarrhea and
inappetance in cats • Double blind, placebo controlled trial • 34 cats enrolled (research cats) • Initial monitoring period to exclude stress diarrhea cats • All got amoxi-clav BID for 7 days • Each day appetite, attitude, hydration, vomiting, and consistency of feces was monitored • Cats got either Fortiflora or the palability enhancer in the product • No vomiting during acclimation • With antibiotics 7 of the Fortiflora and 6 of the placebo cats vomited at least once • No difference between groups • Soft pile stools in 11 of the Fortiflora and 12 placebo cats • In the Fortiflora cats 61% had non-formed or puddle feces, whereas 86% of placebo had
that • Only placebo cats had worst scores possible • 68% of placebo stools were soft piles or worse vs. 44% on probiotic Proviable Multiple ingredients “Synbiotic” are pre- and probiotics administered together to be “synergistic” • Capsule contains 5 billion bacteria as well as 2 prebiotics • Formulation is proprietary • Hart et al., JFMS 2012 • Open label study • All treatments remained the same but the cats got 21 days of Proviable • Looked at fecal scores and owner perception of diarrhea • Owner survey before start of treatment, looked at 30 days before start • Fecal score on last day of treatment • 52 cats completed the study • Fecal score 6.0 ± 1.0 to 4.4 ± 1.6 • Thirty-eight owners (72%) reported that their cat’s diarrhea ‘improved’ with
supplementation, while 13 (24%) owners reported ‘no change’ and two owners (4%) reported that their cat’s diarrhea ‘got worse’.
Cobalamin
184
Known to be associated with chronic GI problems, EPI, chronic enteropathies, dysbiosis • Recent survey showed 36% of dogs chronic GI disease had a low cobalamin • In a large survey of cats with GI disease (261 cats) over 40% were cobalamin deficient • Vital role in a variety of metabolic processes • Deficiency can result in neuropathies and immunodeficiency • More important is associated with villus atrophy and malabsorption • Clinically weight loss, lethargy and continued GI signs have been considered signs of
deficiency • May need to supplement, generally give by injection: 250 ug s.q. (cats, or 250-1000 ug in
dogs) weekly for 6 weeks, if signs are good no need for additional administration What About Oral Cobalamin? Toresson et al, ACIVM Abstract 2014
• Treated dogs with chronic enteropathy and low cobalamin with tablets (1 mg cobalamin per tablet)
• dogs < 20 kg = ¼ tablet/10 kg dog • dogs ≥ 20 kg 1 tablet/day) • 39 dogs included • Follow up 20 to 195 days • Cobalamin increased in all dogs, from 54 to 1,305 pmol/L (median: 534 pmol/L). • Median concentration 178 (117-199) pmol/L before and 713 (224-1,476) pmol/L after • Cutoff for normal is 173
Cobalamin and Feline Intestinal Disease Torreson et al, JFMS, 2017
• Retrospective study • Had signs of an enteropathy (lymphoma, EPI, IBD, many not diagnosed definitively) • Cobalamin below 250 pmol/L • Treated with oral tablet (0.25 mg/day) • Total of 25 cats included • Tablets were given for a variable amount of time • Cobalamin concentration rechecked between 27 and 94 days of treatment • Initial concentration128 pmol/l (111–250 pmol/l) • After treatment 2701 pmol/l (738–16,359 pmol/l) • Two of the cats had been previously supplemented and then supplementation had
stopped • Makes it clear that with oral supplementation that it needs to be continuous to work • Unknown but likely that frequency or dosage can be reduced • Interesting that the EPI cats also increased • Cobalamin absorption needs intrinsic factor produced by pancreas • In humans a intrinsic factor independent absorption pathway has been found • Appears possible in cats and dogs too
185
CKD and stomach ulcers • Common sense thing, right? • Increased stomach acid leads to stomach ulcers • Really??, maybe GERDS, maybe with mast cell tumors • Gastrin controls stomach acid • Proven • Gastrin is excreted by kidney so gastrin concentration goes up • Proven • Therefore ipso facto CKD leads to hyperacidity, stomach ulcers and we need to reduce
acid production • Proven???? • Ulcers seem appropriate given GI clinical signs with CKD not uncommon • Vomiting • Inappetance • Upper GI bleeding • What about the science (we should try to be evidence based)?? • Study from 1979 looked at 4 dogs • Ulcers not found • Mineralization and edema found, atrophy of gastric glands (so how is acid produced??)
as well as a vasculopathy • Peters et al, JVIM 2005 • 28 dogs that went to necropsy with a diagnosis of CKD at Cornell • 7 control dogs without CKD or GI problems • 9 known to be chronic, others less clear if chronic or not • Vasculopathy and mineralization were inversely related • In dogs renal disease commonly has GI pathology however not ulcers, mainly it is a
vasculopathy • Even though vasculopathy, necrosis with ulceration uncommon (1 dog) • Gland atrophy common so unsure if stomach acid can be produced
Conclusion In dogs signs of uremic gastropathy can occur, however ulcers do not occur often. Routine use of stomach acid suppressants is not indicated, use only if signs of upper GI bleeding or esophagitis What about in cats? Case series of 8 cats with ulcers, none had CKD (Liptak, JFMS, 2002)
• 2008 Cianciolo et al, JAVMA • 70 cats with renal failure from melamine contaminated food • 14 died or were euthanized • 3 had gastric mineralization • Involved 37 CKD cats, 12 controls
186
• Looked at necropsy information • Cats were grouped based on severity of azotemia: mild (SCr: 1.6–2.8 mg/dL), moderate
(SCr: 2.9–5.0 mg/dL), and severe (SCr: >5.0 mg/dL • 9 mild, 9 moderate, 18 severely azotemic • The higher that calcium phosphorus product the more likely mineralization was present • Edema and inflammation were not present which is different from humans and dogs • GI signs seen do not seem to be related directly to GI pathology • In this study 84% had a history of inappetance and 45% of vomiting • Conclusion in cats • CKD is commonly associated with GI signs
These signs are not linked to ulcers in almost all cases, therefore the routine use of anti-ulcer medications is not indicated. Treatment for GI signs should address symptoms present, i.e. vomiting, nausea, inappetance which may be central in origin
187

Interstate and international transport: Concerns for the general practitioner
By Amanda Dykstra, DVM, MPH, DABVP (Shelter Medicine Practice)
Companion animals are transported across state and federal borders primarily by owners relocating with their pets, organizations attempting to improve animal welfare, breeders and individuals hoping for commercial gain, and by those assisting with disaster response efforts. From a superficial view, many would see transport as an overall positive venture that helps even out the oversupply and undersupply of adoptable pets and improve animal welfare. The CDC’s suspension of dogs entering the US from Egypt in May 2019 due to three rabid dogs being imported from that country along with a recent article describing illegal puppy imports at JFK airport have shed light once again on the dangers of animal transport.1,2
Some veterinarians are concerned that transport may be good for individual animals but detrimental for ‘dogkind’. Regulations and guidance for animal movement exist, including a USDA requirement that dogs entering the country from areas with a high rabies risk must be over 4 months old and vaccinated for rabies. Dogs entering the country for sale are supposed to be 6 months old.1,3 Unfortunately, transport guidelines are generally considered recommendations, and enforcement of regulatory measures is not a priority.
Importers have used many tactics to illegally get animals into the country.1 Some break rules for emotional reasons, others for monetary gain. Flight parent is a term used for people that think they are doing a good deed by transporting a rescue dog when they are actually providing a means for commercial breeders to get dogs into the US. In 2017 one of these flight parents was bit by a rabid chihuahua with a fake rabies certificate. Importers also claim their dogs are rescues without a monetary value, transport pregnant bitches so pups will be born in the US, and have been known to sell animals on social media, with partners in the US acting as individual breeders. Those involved with animal welfare have also been accused of falsifying paperwork or using other means to get animals into the US where they can be adopted.
International transport has introduced a new strain of Canine Distemper Virus to North America.4 The canine influenza outbreak that started in the Chicago area in 2015 has also been linked directly to dogs rescued from Asia.4 The University of Wisconsin Shelter Medicine Program recently assisted with the response to dogs transported from Korea that were identified has having brucellosis.5 There are also concerns about pathogens being introduced that we haven’t yet directly linked to transport, including antibiotic-resistant bacteria.4 The dangers go beyond companion animals. Public health officials are concerned about the potential introduction of zoonotic agents and the impact on wildlife populations that are naïve to foreign disease.
There are similar concerns about interstate transport. The spread of vector-borne diseases like Lyme6 and heartworm disease to non-endemic areas have many root causes, but some veterinarians are concerned that transporting animals from endemic to non-endemic areas may be one of those causes.
188
Interstate transport does increase live release rates and decrease overcrowding in shelters. It may also decrease the amount of people turning to commercial breeders when shelters do not have adoptable puppies. It also allows people to feel like they are doing something to help and provides feelings of goodwill for those involved. During times of natural disaster, emptying shelters allow for emergency housing for animals in the disaster area. Risks of interstate transport include the misdiagnosis of transported animals due to veterinarians not realizing their patients came to the area from regions where locally rare diseases are more common. The spread of infectious disease, including introducing new strains to naïve populations and the spread of vectors is possible. There has also been concern that transport may be leading to an increased resistance to antiparasiticides. Sporadic transfer makes it more difficult to find lost animals, especially following a natural disaster. Also, moving animals that are not behaviorally sound may put themselves and the humans involved at risk for injury. As with international transport, there is also risk about the transmission of zoonotic disease and the potential misdiagnosis of disease that is not endemic for areas the person has lived or traveled.
There are ways to decrease the risks, including procedures and protocols at the source and destination shelters that set standards for vaccine requirements, testing for vector-borne disease, administration of anti-parasitics prior to movement, and quarantine periods at the destination shelter. General care requirements, such as proper identification, behavior evaluation, and thorough physical exams at both the source and destination also help decrease risk. Practitioners that are accustomed to educating those looking for a new pet about how to avoid puppy mills and catteries may want to also consider discussing how and why to avoid buying an animal transported from other countries. And many are calling for tougher regulations for importing dogs and cats into the US from abroad.
Transporting companion animals across state and federal borders has become a controversial issue in veterinary medicine. Many views it as a life-saving measure that is worth the risk, while others have grave concerns about the impacts from a One Health perspective. These concerns have been quietly discussed in the veterinary community for many years. As those discussions become louder and make their way into news headlines, we will be called upon to work with public health officials to find solutions that allow for life-saving transports but decrease the risks to the community.
References
1. Houle MK, Centers for Disease Control and Prevention. Perspective From the Field: Illegal Puppy Imports Uncovered at JFK Airport. Available at: https://www.cdc.gov/importation/bringing-an-animal-into-the-united-states/operation-dog-catcher.html. Accessed Jul 17, 2019.
2. Centers for Disease Control and Prevention. Notice of Temporary Suspension of Dogs Entering the United States from Egypt. Available at: https://www.cdc.gov/importation/bringing-an-animal-into-the-united-states/Egypt-dogs-temp-suspension.html. Accessed Jul 19, 2019.
189
3. Animal and Plant Health Inspection Service. Animal Welfare Act and Animal Welfare Regulations. Available at: https://www.aphis.usda.gov/animal_welfare/downloads/AC_BlueBook_AWA_FINAL_2017_508comp.pdf. Accessed Jul 19, 2019.
4. Waldron, P, Cornell University. New Strain of Canine Distemper Virus Arrives in North America. Available at: https://news.cornell.edu/stories/2019/03/new-strain-canine-distemper-virus-arrives-north-america. Accessed Jul 20, 2019.
5. University of Wisconsin Shelter Medicine Program. UW Shelter Medicine Program Assists Wisconsin Animal Shelters with Canine Brucellosis Response. Available at: https://www.uwsheltermedicine.com/news/2019/3/uw-shelter-medicine-program-assists-wisconsin-animal-shelters-with-canine-brucellosis-response. Accessed Aug 10, 2019.
6. Self SCW, McMahan CS, Brown DA, et al. A large-scale spatio-temporal binomial regression model for estimating seroprevalence trends. Environmetrics 2018;29: e2538.
Other Resources Available:
• Canadian Veterinary Medical Association. Importation of Dogs into Canada. Available at: https://www.canadianveterinarians.net/importation-of-dogs-into-canada?fbclid=IwAR0h9gsehaa7FmM2uP9v5fn879OLYvxMXmpdf3OMs4kZ9b81d6H5z1ErcNY. Accessed Aug 2, 2019.
• American Veterinary Medical Association. Animal Travel and Transport. Available at: https://www.avma.org/public/petcare/cvi/pages/default.aspx. Accessed Jul 29, 2019.
• Association of Shelter Veterinarians. Guidelines for Standards of Care in Animal Shelters. Available at: https://www.sheltervet.org/assets/docs/shelter-standards-oct2011-wforward.pdf. Accessed Aug 1, 2019.
190

Management of seizures in the canine and feline patient
By Antonio L. Bowens, DVM
Seizures are one of the most common neurological problems seen in companion animals, especially in dogs. Although there are various causes of seizures, the most common cause is idiopathic epilepsy. The term “idiopathic” refers to the fact that there is no known or identifiable cause for the seizures. Other possible causes include congenital abnormalities of the brain (i.e. hydrocephalus, cysts, etc.), metabolic diseases (i.e. portosystemic shunts, hypoglycemia, etc.), inflammatory/infectious diseases (i.e. primary or secondary: encephalitis), head trauma, a cerebrovascular event, or brain tumors. In order to identify the underlying neuropathological cause(s) for seizures, typically further diagnostic testing is recommended: complete blood work, urinalysis, pre & post bile acids, resting ammonium levels, thoracic & abdominal radiographs, abdominal ultrasound, EEG, a CT scan or MRI (MRI is considered the best diagnostic modality), CSF analysis, and serology titers (to rule-out infectious agents).
In almost all cases of epilepsy, seizures progressively worsen if gone untreated. There is usually a relatively slow increase in the duration, frequency, and/or severity of seizures as the patient gets older. For this reason, it is generally good practice to begin anticonvulsant medication early in the seizure disorder. Thus, by giving the medication, we hope it will slow the progression of seizures. In an ideal world, administering anticonvulsant medication would completely stop all seizure activity; however, this is rarely possible. The goal of treatment is to decrease the seizure duration, frequency, and severity, so that the patient may have a good quality of life.
In about 70% of cases, we can achieve good seizure control; meanwhile 30% of canines treated for idiopathic epilepsy do not improve with one or two anticonvulsant drugs. These patients are referred to as refractory idiopathic epilepsy patients. They require a third or fourth medication, in order to get better control of their seizures.
Numerous anticonvulsant drugs are available to people and companion animals with seizure disorders. The majority of these drugs are metabolized by the liver and eliminated via the urogenital system. Unlike phenobarbital, the newer/alternative anticonvulsant drugs are minimally metabolized by the liver and have lesser known side effects. These drugs include:
• Levetiracetam • Gabapentin, • Zonisamide • Pregabalin • Topirmate.
191

Patients that are receiving anticonvulsant medication require regularly scheduled examinations and blood level monitoring. It is especially important to weigh your patient periodically, because any weight gain or loss may affect the dose of medication the patient needs. Every 3 – 6 months, depending on how many medications the patient is on and if you are frequently changing the dosages, blood levels should be re-evaluated, even if the seizure activity is well controlled.
As mentioned earlier all anticonvulsant medications have side effects. Once again, our aim is to try to obtain good control of the patient’s seizure episodes, duration, and frequency with minimal side effects. Make sure you are aware of the possible side effects of the medication that you choose for your patient.
References
• Glass, E. and de Lahunta, A. Veterinary Neuroanatomy and Clinical Neurology. Philadelphia: W.B. Sauders Company, (3rd edition) 2009; chapter 18.
• Dewey, C. A Practical Guide to Canine/Feline Neurology (2nd edition). 2008. Iowa State. chapter 7.
• March, Philip A. Saunders Manual of Small Animal Practice. 2006 : 1249–1276. • Szelecsenyi, U. Giger, L. Golini, I. Mothersill, P. R. Torgerson, F. Steffen.
Survival in 76 cats with epilepsy of unknown cause: a retrospective study Vet Rec. 2017 Nov; 181(18): 479. doi: 10.1136/vr.104281
• Tsz Hong Law, Emma S. S. Davies, Yuanlong Pan, Brian Zanghi, Elizabeth Want, Holger A. Volk. A randomized trial of a medium-chain TAG diet as treatment for dogs with idiopathic epilepsy Br J Nutr. 2016 May; 115(9): 1696.
• M. Podell, H.A. Volk, M. Berendt, W. Löscher, K. Muñana, E.E. Patterson, S.R. Platt. 2015 ACVIM Small Animal Consensus Statement on Seizure Management in Dogs. J Vet Intern Med. 2016 Mar-Apr; 30(2): 477–490.
• A. Pakozdy, P. Halasz, A. Klang. Epilepsy in Cats: Theory and Practice. J Vet Intern Med. 2015 Jan-Feb; 29(1): 485.
• Moore, Sarah A. Seizures and epilepsy in cats. Vet Med (Auckl) 2014; 5: 41–47.
192

Vestibular Disease
Antonio L. Bowens, DVM
The vestibular system is one of the primary structural components of the nervous system in dogs and cats responsible for balance and body posture. Cranial nerve eight, the vestibulocochlear nerve, is the major cranial nerve intimately associated with the vestibular system. The vestibular apparatus houses the first order of neurons that allow the canine and feline to functionally move without having to consciously equilibrate each voluntary movement. This system closely interacts with the cerebellum. The cerebellum’s sole function is coordination. Combined, these two systems permit the body to move in fine synchronous motion with relation to gravity. If any pathological agent disturbs the vestibular system the animal’s equilibrium can be altered. The principal clinical signs associated with vestibular dysfunction are ataxia, head tilt, ipsilateral circling (usually tight), and nystagmus. The vestibular system has been divided into two major anatomical/functional entities. They are the central vestibular system and the peripheral vestibular system.
The central component is identified as the portion of the vestibular system within the brain stem. The primary characteristics of a unilateral central vestibular dysfunction are ataxia, either an ipsilateral or contralateral head tilt, falling or rolling, tight circling, ipsilateral postural reaction deficits, altered mental status, multiple cranial nerve deficits, a resting or positional vertical nystagmus, or a nystagmus that changes with position. The “hallmark” clinical features of central vestibular involvement are thought to be postural reaction deficits and/or a vertical nystagmus. These clinical findings will not be observed in a patient with bilateral or unilateral peripheral vestibular disease. Therefore, assessing proprioceptive positioning/placement is an excellent neurologic parameter that can be utilized for differentiating between central and peripheral vestibular disease. Sometimes cranial nerves V, VI, VII, IX, or X may be affected if the causative lesion extends to other adjacent areas of the brainstem.
Other possible differentials that can mimic central vestibular dysfunction are disease processes or lesions impeding/involving the cerebellum. The clinical presentation of a patient that has a cerebellar dysfunction, secondary to neuropathology affecting neuroanatomical structures of the caudal cerebellar peduncle and/or the floccculonodular lobe, are hypermetria, ataxia, and fine intention tremors (H.A.T) along with an absent menace response. Also, clinical signs of neuropathology affecting the cerebellum may be seen in association with patients that have a paradoxical vestibular syndrome (which is also a central vestibular problem). Although this may appear similar to vestibular disease, its clinical presentation is easily identified by the presence of a contralateral head tilt, nystagmus (fast phase toward the side of the lesion), falling, hypermetric gate, ipsilateral proprioceptive deficits, and an ipsilateral menace deficit.
The peripheral component of the vestibular system is recognized as the outer area of the brain stem. The common clinical signs associated with unilateral peripheral vestibular dysfunction include: ataxia (with no postural/CP deficits), ipsilateral head tilt, tight ipsilateral circling, +/- vomiting, and +/- resting or positional horizontal or rotary nystagmus (with the fast phase away from the side of the lesion). The clinical signs associated with a bilateral peripheral vestibular
193

disease include ataxia, (+/- truncal swaying), swaying of the head, lack of a physiological nystagmus, head tilt, or righting response. These patients typically do not have the presence of a pathological nystagmus, head tilt, postural reaction deficits, or conscious proprioceptive deficits. With time, the patient may adapt to these deficits and appear to “improve.” However, blindfolding the patient will expose the clinical signs as well as make them more obvious. Patients with peripheral vestibular disease do not have postural reaction or conscious proprioceptive deficits. NOTE: unilateral vestibular disease is thought to be more common than bilateral vestibular disease. Lastly, peripheral vestibular disease is more commonly seen in a clinical setting in comparison to central vestibular disease.
The presence of a pathologic process involving the inner and middle ear can result in a Horner’s syndrome, vestibular disturbance, and facial paresis/palsy. The clinical signs of Horner’s syndrome result from a lesion involving the post-ganglionic sympathetic pathways to the iris and consist of miosis, ptosis, third eyelid prolapse, and enophthalmos. Facial paresis/palsy occurs secondary to a lesion of cranial nerve VII as it passes through the middle ear and is characterized by facial deficits including blink, menace, and palpebral response.
The importance of the clinician gaining a good history as well as performing a complete and thorough physical as well as a neurological examination is key to a successful localization and diagnosis. There are many cases that may have obvious diagnoses based on the history alone; however, it is important to perform a thorough neurological examination, as additional information may be collected. Once the physical and neurological exams have been performed, the clinician is in a more suitable position to start developing a list of differentials as well as choosing the best diagnostic test available. Clinically, it is very important to develop a list of differential diagnoses (via the D.A.M.N.I.T scheme) as well as performing the appropriate diagnostic test in order to accurately treat the disease process involved. Furthermore, the extent of the neuropathology will ultimately determine the prognosis.
References
• Bowens, A., & Gordon, P. Equilibrium Loss and Head Tilt in a Dog. Compendium on Continuing for the Practicing Veterinarian: A Clinical Snapshot February 2004.
• Glass, E. and de Lahunta, A. Veterinary Neuroanatomy and Clinical Neurology. Philadelphia: W.B. Sauders Company, (3rd edition) 2009; chapter 12.
• Dewey, C. A Practical Guide to Canine/Feline Neurology (2nd edition). 2008. Iowa State. chapter 8.
• March, Philip A. Saunders Manual of Small Animal Practice. 2006 : 1249–1276. • Radulescu, S. Humm, K., Eramanis, L., Volk,H. Church, D. Brodbelt, D.
O'Neill, D. Vestibular disease in dogs under UK primary veterinary care: Epidemiology and clinical management. J Vet Intern Med. 2020 Sep; 34(5): 1993–2004.
• Platt, S. Vestibular Disorders. Consultations in Feline Internal Medicine. 2006 : 527–545.
• Orlandi, R. Gutierrez-Quintana, R. Carletti, B. Cooper, C. Brocal, J. Silva, S. Gonçalves, R. Clinical signs, MRI findings and outcome in dogs with
194
peripheral vestibular disease: a retrospective study. BMC Vet Res. 2020; 16: 159.
195
Neuro –what they never taught in vet school By Fred Wininger, VMD, MS, DACVIM(Neurology) Chiari-like Malformation and Syringomyelia There are several names for this condition, such as caudal occipital malformation syndrome (COMS), but the consensus from the working group is that Chiari-like malformation should be used. It is an extremely common condition in Cavalier King Charles Spaniels and other small and toy breed dogs. It has been reported rarely in cats. It is a congenital malformation of the occipital bone of the skull with overcrowding of the caudal fossa. More than 50% of dogs with CM develop syringomyelia. Dogs are typically young adults when clinical signs develop but we are starting to diagnose patients sooner likely due to more awareness of this condition. The most common clinical signs are episodic scratching of the head, neck and ears or phantom scratching. Neck pain, vestibular dysfunction, seizures also can be seen, and some patients can develop lower motor neuron signs, such as a root signature. On MRI there is a poor correlation between the severity of clinical signs and the severity of the changes on MRI. A recent study found that signs of pain are common with Chiari-like malformation but not depending on the presence of syringomyelia. Otitis media with effusion (OME, sometimes called primary secretory otitis media (PSOM)) can also be seen in brachycephalic dogs and is likely due to poor drainage of the middle ear. OME can cause ear discomfort but was not significantly associated with head or ear rubbing in dogs with CM/SM. Medical therapy for dogs with CM/SM includes medications to alleviate pain and medications to decrease CSF production. Prednisone can be used for reduction of CSF production and to inhibit inflammatory mediators. Omeprazole has been shows to decrease CSF production with IV or intraventricular injection, but we don’t know if oral omeprazole has the same effect. However, it can reduce the oral bioavailability of gabapentin if given within 2 hours of each other. Acupuncture can also be considered for pain management. Surgical therapy can be considered if medical management fails. The goal of surgery is to decompress the structures at the foramen magnum. Recurrence due to fibrous tissue can recur following surgery. Infarction On the human side, someone in the US has a stroke every 40 seconds. Every year more than 795,000 people in the US have a stroke. 87% of strokes in people are ischemic strokes. It was once thought that strokes were rare in veterinary patients, however, ischemic and hemorrhagic infarcts can occur. With ischemic infarcts there is a transient lack of oxygen to the brain which damages the tissue. In hemorrhage infarcts, extravasation of blood
196
occurs in the brain tissue. Territorial infarcts affect large arteries and therefore larger areas of the brain. The two most common larger arteries affected are the middle cerebral artery and the rostral cerebellar artery. The penumbra is the area of brain tissue around the stroke that is ischemic, but not infarcted (necrotic). It is at a high risk of further damage unless delivery of oxygen is rapidly restored. In human medicine, minimizing the area of the penumbra that changes to an infarcted area is key. In veterinary medicine, we need to support the patients and protect the penumbra via oxygen therapy, maintenance of perfusion with IV fluids, and maintenance of blood pressure. Clinical signs of a stroke are typically peracute or acute in onset and can progress for the first 24 hours. If patients are progressing beyond 24 hours, causes other than strokes should be investigated. The clinical signs associated with the stroke are based on the area of the brain affected. Thalamic infarcts can cause a mix of clinical signs that can make the lesion seem multifocal or can be silent infarcts. An underlying cause of infarction is not identified in 40% of cases in human medicine and that number may be similar in veterinary medicine. Causes that can predispose our patients to infarction include Cushing’s disease, hypertension, cardiac disease, kidney disease, hypothyroidism, hyperlipidemia, protein-losing nephropathy, and Chiari-like malformation. Routine lab work, thoracic radiographs, and blood pressure measurement should be performed. Treatment of strokes is mainly supportive care. Mannitol or hypertonic saline can be given if there are signs of increased intracranial pressure, and the head and neck should be elevated. If systemic hypertension is identified, then treatment should be started. For patients with ischemic infarcts, prevention of future strokes with clopidogrel or aspirin can be considered.
197
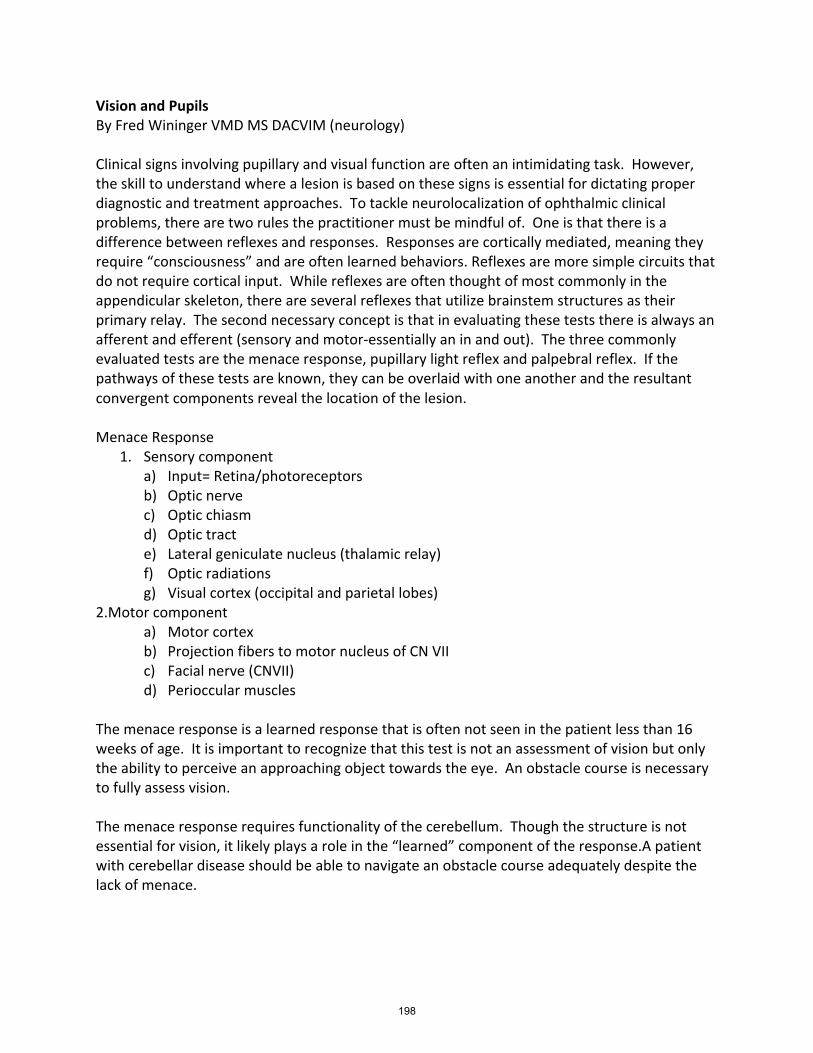
Vision and Pupils By Fred Wininger VMD MS DACVIM (neurology) Clinical signs involving pupillary and visual function are often an intimidating task. However, the skill to understand where a lesion is based on these signs is essential for dictating proper diagnostic and treatment approaches. To tackle neurolocalization of ophthalmic clinical problems, there are two rules the practitioner must be mindful of. One is that there is a difference between reflexes and responses. Responses are cortically mediated, meaning they require “consciousness” and are often learned behaviors. Reflexes are more simple circuits that do not require cortical input. While reflexes are often thought of most commonly in the appendicular skeleton, there are several reflexes that utilize brainstem structures as their primary relay. The second necessary concept is that in evaluating these tests there is always an afferent and efferent (sensory and motor-essentially an in and out). The three commonly evaluated tests are the menace response, pupillary light reflex and palpebral reflex. If the pathways of these tests are known, they can be overlaid with one another and the resultant convergent components reveal the location of the lesion. Menace Response
1. Sensory component a) Input= Retina/photoreceptors b) Optic nerve c) Optic chiasm d) Optic tract e) Lateral geniculate nucleus (thalamic relay) f) Optic radiations g) Visual cortex (occipital and parietal lobes)
2.Motor component a) Motor cortex b) Projection fibers to motor nucleus of CN VII c) Facial nerve (CNVII) d) Perioccular muscles
The menace response is a learned response that is often not seen in the patient less than 16 weeks of age. It is important to recognize that this test is not an assessment of vision but only the ability to perceive an approaching object towards the eye. An obstacle course is necessary to fully assess vision. The menace response requires functionality of the cerebellum. Though the structure is not essential for vision, it likely plays a role in the “learned” component of the response.A patient with cerebellar disease should be able to navigate an obstacle course adequately despite the lack of menace.
198
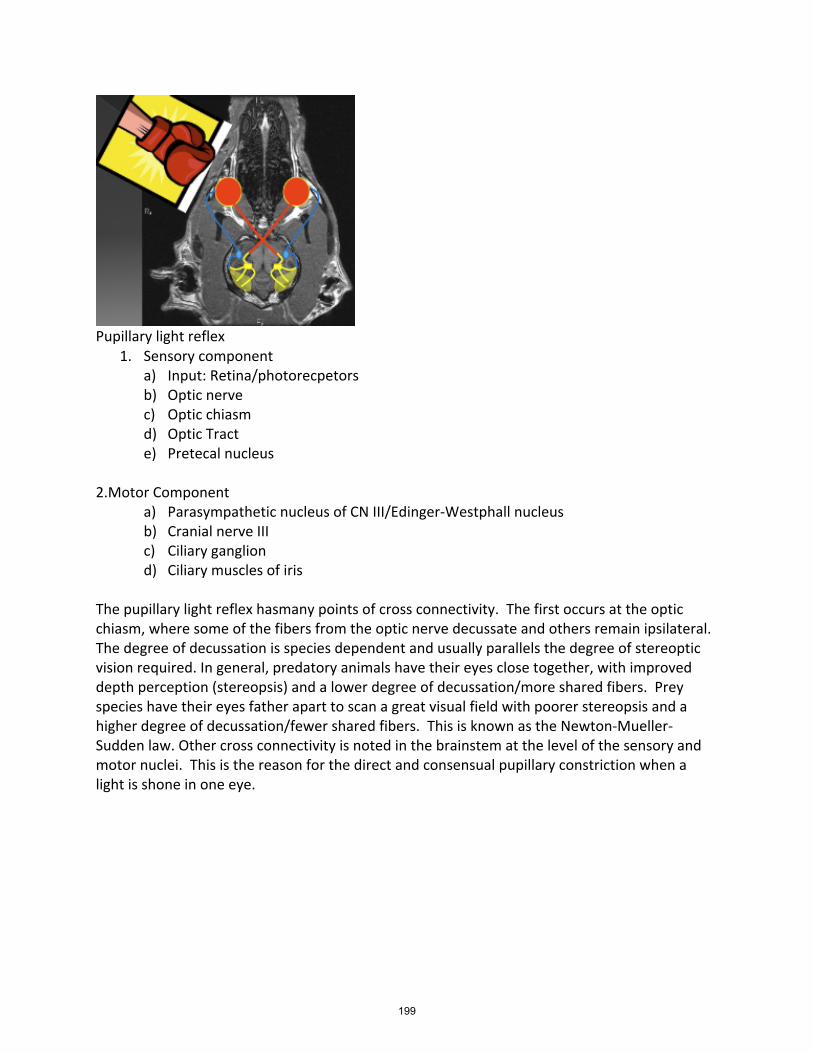
Pupillary light reflex
1. Sensory component a) Input: Retina/photorecpetors b) Optic nerve c) Optic chiasm d) Optic Tract e) Pretecal nucleus
2.Motor Component
a) Parasympathetic nucleus of CN III/Edinger-Westphall nucleus b) Cranial nerve III c) Ciliary ganglion d) Ciliary muscles of iris
The pupillary light reflex hasmany points of cross connectivity. The first occurs at the optic chiasm, where some of the fibers from the optic nerve decussate and others remain ipsilateral. The degree of decussation is species dependent and usually parallels the degree of stereoptic vision required. In general, predatory animals have their eyes close together, with improved depth perception (stereopsis) and a lower degree of decussation/more shared fibers. Prey species have their eyes father apart to scan a great visual field with poorer stereopsis and a higher degree of decussation/fewer shared fibers. This is known as the Newton-Mueller-Sudden law. Other cross connectivity is noted in the brainstem at the level of the sensory and motor nuclei. This is the reason for the direct and consensual pupillary constriction when a light is shone in one eye.
199
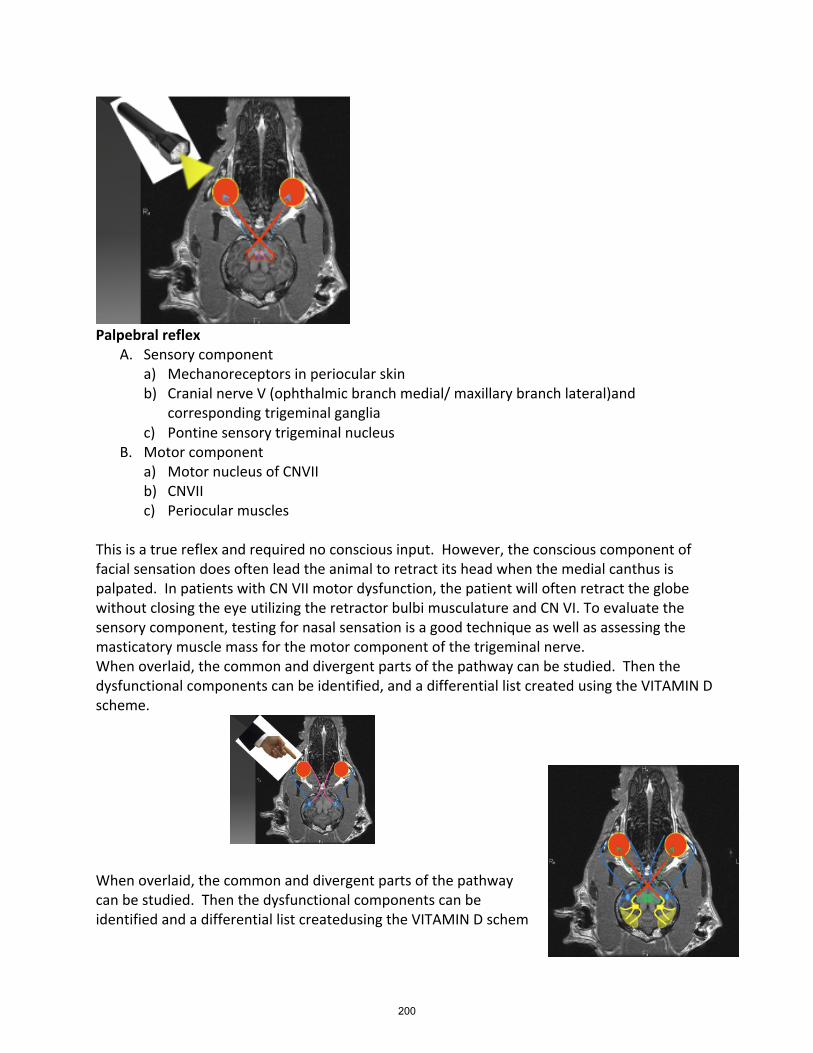
Palpebral reflex
A. Sensory component a) Mechanoreceptors in periocular skin b) Cranial nerve V (ophthalmic branch medial/ maxillary branch lateral)and
corresponding trigeminal ganglia c) Pontine sensory trigeminal nucleus
B. Motor component a) Motor nucleus of CNVII b) CNVII c) Periocular muscles
This is a true reflex and required no conscious input. However, the conscious component of facial sensation does often lead the animal to retract its head when the medial canthus is palpated. In patients with CN VII motor dysfunction, the patient will often retract the globe without closing the eye utilizing the retractor bulbi musculature and CN VI. To evaluate the sensory component, testing for nasal sensation is a good technique as well as assessing the masticatory muscle mass for the motor component of the trigeminal nerve. When overlaid, the common and divergent parts of the pathway can be studied. Then the dysfunctional components can be identified, and a differential list created using the VITAMIN D scheme. When overlaid, the common and divergent parts of the pathway can be studied. Then the dysfunctional components can be identified and a differential list createdusing the VITAMIN D schem
200
Howtoeffectivelyutilizenutritiontechnicians: howtoutilizestaff,&encourageeffectivecommunicationwithclientsaboutnutrition ByRobinSaarRVT,VTS(Nutrition)RanchDocsVeterinaryServices,Lethbridge,Alberta,Canada Nutritionisacomponentofeverypet’sdailyrequirements.Howdoesyourclinicconveyinformationaboutits’patientsdailyneeds?Doesyourclinichaveanutritionadvocate,orisallthestafftrainedtodiscussnutritionalneeds?Veterinarytechsandnursesarewelleducatedandareagreattooltoaidveterinariansincommunicatingtheirrecommendationstoclients. InitialConsiderationsWhenDevelopingaNutritionDepartment Createaclinicphilosophy:Wheninitiallydevelopingadepartmentinyourclinic,itisimportanttocreateaclinicphilosophy.Whatisthemissionstatementforyourclinic?Whattypeofclientsdoesyourclinicattract?Whattypeofclientdoyouwanttoattract?
Revenueconsiderations:Oncethephilosophyisestablished,youcanassesshowthecliniccanincreaserevenuesellingpetfood?Therearedifferentwaystoestablishwhatareasonablemark-upisforyourarea.Whatwillthemarketbear?Onewaytoassessthisistoseewhatthepetstoresareselling“specialty”or“limitedingredient”dietsfor. Next,addresshowyourcliniccanbecompetitivewithotherclinicsinyourarea?Byofferingadiscountonedaypermonth,youcanportraytoclientsthatyouappreciatethevalueoftheirmoneywithoutoverlycompromisingyourprofits.DuringtheCOVIDpandemic,theworldrespondedwithincreasingon-lineordering.2Byallowingclientstoorderfromtheconvenienceoftheirhomesyoumayseeanincreaseinimpulsebuyssuchastreatsandtoys,aswellasrepeatpurchases.Offercomplimentarynutritionconsults.Haveadesignatedtechnicianthatofferscomplimentaryconsultstoprovidespecificinformationandcalculationsforpatients.Clientsappreciatethespecializedservice,andareeagerforrecommendations.Considerhowthisprocessincreasestrustandsecuresreturnvisitsandsales.Finally,beindividualinacompetitivemarket.Howcanyourclinicstandoutfromtheotherclinics?Canyoucarryanutritionbrandthatmaynotbeavailableatneighbouringclinics,orofferspecializedserviceslikehomedelivery? Productdisplays:Howyoudisplayproductsiscrucialwhenestablishingyournutritiondepartment.Dietsshouldbeseparatedbyspecies,andbearrangedinanorderlymanner.Thisincludeshavingconsistencyinhowyoudisplayproducts,andkeepingtheareapleasingtothesenses;theyshouldbevisuallypleasing,haveanon-overwhelmingandcomfortingscent,bepeaceful,andallowforclientstohandletheproducts.Ifyouhaveasmallreceptionareadisplayproductsthatmayenticeclients,orareappropriateforawiderangeofclients. Havingproductpricespostedonorneartheproductsallowsclientstimetoprocessthenumericalvalueoftheproduct.Clientsmayhavemisconceptionsthatthedietsare“expensive”,andbynotknowingwhatthenumericalvalueistheymayhave
201
misconceptionsregardingthecost.Postingpricesgivesclientstimetoevaluateiftheycanafford,orwhatsizeofbagtheycanaffordofadietyouhaverecommended. It’salwaysaboutgoodcommunication Mostveterinariansandtechniciansdon’tgointoveterinarymedicinebecausetheylovesales.Welovescience,animals,andarenotusuallygoodatselfpromotionor“pushing”productsonclients.Themisconceptionliesinthedefinitionofsales.Salesinvolvepeoplewhoareexcellentcommunicatorswhocanreadclients,andgivecompellinginformationaboutproducts.3Therearemanysituationswherewefeeljustifiedinusing“sales”:pre-anestheticbloodwork,vaccinationprotocols,ordiagnostictestingarejustsomeexamplesofareasthatclinicsfeelcomfortableadvisingthepurchaseoftheirrecommendations.Weunderstandtheimportanceoftheseproducts,andseevalueincommunicatingtoclientswhywerecommendthem.Nutrientsarerequiredbypetseveryday. Communicationintheteam:Todevelopastrongteamandconveysolidaritytoclients,itisimperativethattheentireteamsaythesamemessage.Muchlikeclinicalprotocols,theteammustgivethesameadvicetoclientsinregardstonutrition.Ifonepersongivescontraindicatingadviceyoumaylosetrustinthatclient.Theyfeelpressureanddistrustfromthosegivingtherecommendation,andhaveconcerntowardsthestaffmemberwhogivesconflictingadvice. Allowyourteamtobeapartofdiscussingtheclinicphilosophy;howtheyseeitbenefitingtheclient,andwhattheycandotoparticipateintheprocess.Givetechniciansresponsibilitytobeinvolvedinareasoftheclinic,allowingthemtodevelopprideinwheretheywork.Havethemaidinthedevelopmentorcontributiontoanewsletter,socialmediapage,orprovidein-clinicseminars.Supportingtheteamenablesthemtocontribute,andempowerthembysettingexpectations.Byearningteamtrust,havingtheentireteamsaythesamemessage,andhelpingtheteamgrowanddevelopconfidencewillgivethemtheconfidencetospeakwithclients. Developingandtransferringtrust:Tohaveclientshearandfollowtheteams’recommendations,weneedtodeveloptrust.Weknowthatintoday’ssocietypeoplewanttotrust,butdotheyalwaystrustthebestsource?Thelevelofconfidencethatapersondisplaysmaycreateafalsesenseoftrust.Bysupportingourteamwewillhaveconfidentspeakerswhoknowtheclinicphilosophy,whatinformationwewanttoshareandhowtoshareit.Theycanspeakknowingthattheirvetssupportthem,andtheywon’tbecontraindicated. Anotherformoftrustbuildingissharingstories.Clientswanttoknowthattheyarenottheguineapigstryingthisproduct,orthatyouareinit“forthemoney”.Sharepersonalstoriesfrompersonal,teamorpatients’experienceswiththenutritionalproductyouarerecommending.Createabondwiththeclientsbysharingsomethingpersonal. Haveyoueverheardaclientstatethatthey“lovethereceptionteamanddon'tcarewhatvettheyhave”,orpraisesonevetbutisalwayscondescendingtothereceptionandtechnicianteam?Theseclinicsmaynotbetransferringtrustproperly.Transferringtrust
202
involvesensuringthateveryoneontheteamshares,andtransfersinformationtothenextteammember.Thisinformationincludesgivingtheclientdirectionstowhattheyshoulddo,andwhat’shappeningnext.Bycreatingapositiveflowthroughtheclinicduringappointmentsorproceduresthecliniccangaintheclient’strustbyshowingcontrol,anduniformityduringthatsituation. HowCanTechniciansBeUtilizedInANutritionDepartment? Technicianshavemanyrolesinaclinicalsituation.Inregardstonutritiontherearemanypartsofanutritionconsultthatatechscantaketheleadon: 1.Gettingahistory-“HowmuchfooddoyouputinFluffy’smouthfromthesecondshewakesuptillshegoestosleep?”.Techsarealreadytrainedtogetcompletehistoriesandknowhowtoaskopenendedquestions. 2.Calculations-Techsareknowledgeableincompletingcomplexmathematicalequations.Therearefewsimplemathematicalequationsthattheyshouldbedoinginyournutritiondepartmenteveryday:A.Calculatingenergyrequirements:CalculatingRestingEnergyRequirements(RER),MaintenanceEnergyRequirements(MER),Dailyenergyrequirements(DER),requirementswhilepregnantornursing,andrequirementsforthoseinanegativeenergybalanceorstarvation.5B.Calculatingkcal/cuporcanfromenergyrequirement.Bytakingtheenergyrequirements,anddividingthembythekcal/cup(orcan)wecaneasilycalculatehowmuchofthatdietapatientneedsperday.5C.%BodyWeightLoss-Apatientthatlosesmorethan5%bodyweightinashortperiodoftimeshouldindicatetoveterinarystaffapossiblehealthconcern.7Generalguidelinesforinitiatingnutritionalsupportincludetheloss,oranticipatedlossof10%bodyweight.4Withoutcalculatingthisamount,especiallyinacatorsmallbreeddogtheweightlossmaynotbeasapparent.Forexample,acatthatweighed4.5kg(9.9lbs)onemonthagohasacurrentweightof4.2kg(9.24)equalsa6.7%weightloss.Hadthiscalculationnotbeencompleteditmaynotbeobviousthatthepetislosingasignificantamountofweight.5 3.Dealingwithconflict-Techsareverycapableofdealingwithclientswhoaremisinformedandneedclarificationtoremoveconflict.Byteachingyourteamtoacknowledgewhattheclienthassaid,removingtheword“But”or“actually”fortheword“AND”,andsharingstoriescanhelpdeflectconflict. 4.Givingnutritionalinformationandrecommendationsincases-dependingonthelevelofeducationofyourtech,youcanutilizeyourtechtoeitherprovideyourdietaryrecommendations,orallowthemtoshareinformationtheyhavereceivedintrainingsuchasspecializedcontinuingeducation,certification,oracompletionofaveterinarytechnicianspecialty. Growthtakestime,patience,andencouragementtomeetourexpectations Byestablishingaclinicphilosophy,creatingaclientfriendlynutritionarea,supportingyourteam,anddevelopingtrustyoucanaidinthegrowthofyournutritiondepartment.Techsareinvaluableinaidinginthisgrowthandshouldbedirectedtobeleadersinthisdepartment.“Nutritionisapartofeverypet,everysingledayoftheirlife”.
203
References:
1. https://www.ovma.org/pet-owners/choosing-a-pet/2. https://www.bigcommerce.com/blog/covid-19-ecommerce/#understanding-panic-
buying-and-coronavirus3. https://todaysveterinarybusiness.com/defens-sales-rep/4. https://www.navta.net/page/specialties5. A.Fascettietal:AppliedVeterinaryClinicalNutrition;Wiley,20166. A.Wortingeretal;NutritionandDiseaseManagementforVeterinaryTechnicians
andNurses2ndEdition;Wiley;20177. Handetal:SmallAnimalClinicalNutrition5thEdition;MarkMorrisInst.,2010
204
Delivering hope to canine hemangiosarcoma By Chand Khanna, DVM, PhD, DACVIM (Onc), DACVP (Hon) Ethos Discovery and EthosVeterinary Health
Where our attack on canine hemangiosarcoma began? Ethos Discovery began its attack on hemangiosarcoma through the first-ever, prospective, nationwide, multicenter study of canine hemangiosarcoma (CHAMP Study; Stewart et al, JVCO May 2020). This taught us that hemangiosarcoma is not a single cancer, but rather at least four cancers, characterized by specific genomic alterations. From our unique perspective as cancer biologists and veterinary oncologists, we have viewed these distinct cancer entities through the optics of novel therapeutics that may be reasonably applied to the identified disease subsets. Additionally, our preliminary data has demonstrated the presence of mutated cancer DNA in the blood of dogs with these cancers (i.e. liquid biopsy; Favaro et al, sub. Bioarchive/10.1101/2020.08.20.260349, Aug 2020), which provides unique and additional opportunities to improve outcomes for patients. Our experience with this and other prospective studies has provided a new Perspective on Hope for our patients and has fueled our launch of the largest prospective study of this disease ever. Indeed, this highly advanced clinical trial of 400 dogs with hemangiosarcoma in the field of precision medicine through an umbrella study design (Ethos PUSH; Precision Medicine Umbrella Study for Hemangiosarcoma) now seeks curative outcomes for dogs with this disease. An umbrella study segments patients with a given cancer (such as hemangiosarcoma) into molecular subsets (planned post hoc for this study), with specific therapeutics that target genomic alterations of that patient subset. Collectively, this approach to cancer therapy is referred to as Precision Medicine (PMED). The success of PMED in the field of oncology has been shown to require an understanding of a drug and its interaction with a molecular target in the disease of interest (referred to as “molecular context”) and is best delivered within a specific cancer rather than in its application to any cancer, where this understanding of molecular context is not as possible and these challenges may explain some of the recent failures to demonstrate therapeutic value of PMED, most noteworthy in large human studies. Our studies with novel drugs and a focus on a single cancer provides an opportunity to understand context in hemangiosarcoma, and now allows this molecularly-informed cancer PMED trial to seek curative outcomes for dogs with this disease. What I thought I knew about Canine Splenic Hemangiosarcoma? Despite my training as a practicing veterinary oncologists and cancer biologist, I previously developed a very traditional perspective on canine hemangiosarcoma, characterized by the following:
• This is a cancer derived from canine vascular endothelial cells; • In the typical older large breed dogs presenting with hemoabdomen, a very small
proport (<4%) of tumors are benign.
205
• These dogs have a high risk for surgical complications resulting in a guarded prognosis related to splenectomy. These surgical risks include bleeding, reperfusion injury, cardiac events and others;
• The long-term outcomes for dogs following surgery and chemotherapy are predictably poor and best described by the median survival of 6 months.
What I now believe about Canine Splenic Hemangiosarcoma? Any reasonable assessment of the body of evidence in veterinary oncology recognizes that most of our evidence comes from the relatively lower hierarchies of evidence, most characterized by retrospective studies, single arm anecdotes and the absence of controlled studies. Despite my awareness of these shortcomings, over the last 24 months of detailed re-assessment of past studies and our new prospective and unpublished data, my perceptions have changed, and I have new optimism for patients, characterized by the following:
• This is not a single cancer but at least four distinct cancer subtypes that likely have distinct prognoses and optimal therapy;
• In the typical older large breed dogs presenting with hemoabdomen, approximately 40% of tumors are benign and cured with surgery alone.
• In the setting of state-of-the-art veterinary ER and ICU services, the risks of mortality associated with splenectomy have been effectively managed, such that >95% of dogs walk out of the hospital in < 40 hours.
• The long-term outcomes for dogs following surgery and chemotherapy are highly varied. Identification of the most aggressive subset of dogs who will recur within 30 days of surgery. Providing alternative treatment options to this subset of dogs with the most aggressive disease will lead to a 12-month survival of 37.5% in the remaining population using existing therapy alone.
Canine hemangiosarcoma unmet needs.
• A presurgical point-of-care (POC) diagnostic to distinguish benign from malignant disease is needed for our patients.
• A blood test that can define burden of disease, prognosis and response to therapy is needed.
• Better treatments given after surgery for dogs with hemangiosarcoma are needed. We are actively developing solutions for all of these unmet needs as a means to deliver hope to hemangiosarcoma patients. Canine hemangiosarcoma molecular profiling (CHAMP) study. Our first ever nation-wide, multicenter, prospective study of dogs with hemoabdomen launched over 4 years ago. Data from this study has been published with several new manuscripts on their way:
206
• Stewart et al., JVCO May 2020: In this prospective description of the clinical cohort we
learned that many more splenic tumors were benign than expected from past retrospective data, and that the vast majority of dogs now recover favorably from surgery.
• Favaro et al., Bioarchive Aug 2020. This manuscript describes our analysis of cell free tumor DNA as a liquid biopsy approach to deliver on the unmet needs of this disease in dogs (described above). Briefly, we can distinguish benign and malignant tumors of the spleen through a blood test at presentation and this approach may allow assessment of cancer burden in dogs.
• Hendricks et al sub. Sub. Cancer Research Priority reports. Sept 2020. This manuscript summarizes our assessment of the genomic landscape of hemangiosarcoma, with an emphasis on the lens of a scientific rationale for new therapeutics and more broadly the opportunity to study and understand the heterogeneity of this cancer in humans and dogs.
A summary of Delivering Hope to Hemangiosarcoma. As a result of careful re-analysis of existing data, new prospective research, and over two decades of clinical experience we are liberated and optimistic about new Hope that can be delivered to hemangiosarcoma patients and their families, that collectively aspire for curative outcomes for this highly aggressive canine cancer. The new perspective on Hope includes, but is not limited to the following:
• A greater proportion of older large breed dogs who present with hemoabdomen from presumed rupture of splenic tumors have benign tumors than predicted from past primarily retrospective studies. These tumors are cured with surgery and more owners should be counseled to consider surgery in the acute management of hemoabdomen
• With the existing state-of-the art in veterinary ER and critical care medicine, the vast majority of dogs undergoing splenectomy will survive surgery and will be discharged in less than 40 hours with limited morbidity. Accordingly, owners should not be unduly concerned over short-term surgical risk as they consider the options for surgery in the acute management of hemoabdomen
• Routine pre-surgery abdominal ultrasounds are important to define cause of hemoabdomen but may not be sufficiently informative as staging tests for dogs. Accordingly, abdominal ultrasound results alone should not be used to communicate prognosis for hemangiosarcoma.
• A holistic assessment of outcome data for this disease using conventional treatment approaches reveals strategies to select and identify dogs with the greatest chance of curative outcomes today.
• Novel liquid biopsy approaches for this disease will further simplify pre-operative decision-making for families considering surgery in the acute management of hemoabdomen. These liquid biopsy approaches may also lend value to pre and post-operative prognostication and therapeutic tailoring
207
• At the intersection of our new understanding of the canine hemangiosarcoma genome and cancer therapeutics, several new options for the treatment of hemangiosarcoma have emerged.
• A nation-wide 5-year, 400 dog prospective study of hemangiosarcoma has been launched to deliver curative outcomes for dogs with this disease.
208
Cancer Immunotherapy – An inside job By Michael D. Lucroy, DVM, MS, DACVIM (Oncology) Torigen Pharmaceuticals, Inc., Farmington, CT Introduction Cancer immunotherapy represents a diverse group of treatment strategies designed to enhance the host’s immune response to cancer by increasing immunosurveillance, increasing cytotoxic cell activity, and decreasing immunosuppressive signaling. In human medicine, immuno-oncology is developing into a subspecialty – the so-called fourth pillar of cancer treatment. In veterinary medicine, the progression of cancer immunotherapy has been slower due to lack of reagents to monitor specific immune responses, and challenges in the regulatory landscape that slow bringing products to market. Here we review a few immunotherapy strategies and current options available for veterinary cancer patients. Overcoming immunosuppression By avoiding detection or destruction by the immune system, cancer cells are able to grow and spread. The tumor microenvironment plays an active role in the recruitment and proliferation of T regulatory cells (Tregs), resulting in secretion of immunosuppressive factors leading to local immunosuppression within tumor tissue. Another way that tumors thwart the immune system is by exploiting immune checkpoints. Programmed cell death 1 (PD-1) receptors are highly expressed on tumor invading lymphocytes and programmed cell death ligand (PD-L1) is constitutively expressed on many types of tumor cells. Activation of PD-1/PD-L1 signaling negatively regulates T cell-mediated immune response, including decreasing INF-γ, TNF-α, and IL-2, and depressing lytic activity. It may also promote Treg activity. Metronomic chemotherapy (i.e., daily low doses of chemotherapy, typically an oral alkylating agent like cyclophosphamide or chlorambucil) is purported to selectively deplete immunosuppressive Tregs and improve the potency of tumor-non-specific effector T cells (Teffs),1 and currently represents the only option for addressing tumor immunosuppression in veterinary medicine. Immune checkpoint inhibitors (monoclonal antibodies directed against PD-1 or PD-L1) have been shown to enhance antitumor immunity and produce durable clinical responses with an increase in patient survival in human oncology,2 and would be predicted to provide similar benefits for veterinary patients at such time as they become available. Non-specific immunomodulators As the name suggests, non-specific immunomodulators cause general stimulation the immune system with the goal of promoting antitumor immunity. Examples include interferons, interleukins, and Mycobacterium bovis Bacillus Calmette-Guérin (BCG). Immunocidin® is a veterinary preparation of a mycobacterial cell wall extract approved by the USDA for intratumoral injections into canine mammary tumors and equine sarcoids. There is little in the published literature about its use in dogs, and the complete response rate for sarcoids was just over 50%.3
Monoclonal antibodies Monoclonal antibodies, such as rituximab, have been highly successful in prolonging the life of people with diffuse large B cell non-Hodgkin’s lymphoma. Monoclonal antibodies bind to a specific target and may fix complement or lead to antibody-dependent cell-mediated cytotoxicity (ADCC) resulting in cancer cell death. Recently two monoclonal antibodies were under development for canine B cell and T cell lymphoma. Although they gained regulatory approval, neither were found to be efficacious and were removed from the market. Currently there are no commercially available monoclonal antibodies for veterinary cancer treatment. T cell therapy
209
CAR-T therapy consists of giving patients an infusion of their own T cells that have been genetically modified ex vivo to recognize a specific cancer target. This has been referred to as a living drug. Currently CAR-T is not available for veterinary patients, but Elias Animal Health is developing a combination of an autologous cancer vaccine (see below) with a form of T-cell therapy. After dogs have been given an autologous cancer vaccine, they undergo apheresis (via jugular catheter under sedation or general anesthesia) to collect T-cells for ex vivo expansion. Those cells are then returned to the patient. Cancer vaccines Cancer vaccines may be broadly divided into preventive and therapeutic vaccines. In human medicine, immunizations against diseases like hepatitis B and human papilloma virus greatly decrease the risk for hepatocellular carcinoma and cervical cancer, respectively and can be considered preventive. In veterinary medicine, the available cancer vaccines are therapeutic and aimed at slowing cancer progression and delaying onset of metastatic disease. Canine Melanoma Vaccine The Oncept® Canine Melanoma Vaccine consists of a DNA plasmid that encodes for human recombinant tyrosinase. The dog’s immune system develops a response against this human protein which may result in a directed response against tyrosinase found in canine melanoma.4 Currently Oncept® is the only USDA approved therapeutic cancer vaccine for veterinary use. Canine Osteosarcoma Vaccine A genetically modified Listeria expressing Her2/neu was in development for the treatment of canine osteosarcoma. Although early studies were promising5, the vaccine is not currently available. This is a clever strategy for directing an immune response against a specific cancer target. Autologous Cancer Vaccines Autologous cancer vaccines are a form of active cancer immunotherapy whereby the antigenic material is derived from the patient’s own tumor. Tumor cells are processed ex vivo and returned to the patient with the goal of stimulating both a humoral and cell-mediated immune response against multiple known and unknown tumor-associated antigens, rather than relying on a single antigen or exogenous monoclonal antibody. Various methods of tumor processing have been used to create autologous tumor vaccines, including whole cell vaccines, tumor cell lysates, isolation of specific intracellular components (e.g., heat shock proteins), and transfection of cells to induce novel antigen presentation. Cancer cells are inactivated before being administered to the patient by lysing, chemical fixation, or irradiation. The dosing of autologous tumor vaccines is variable and intramuscular, subcutaneous, and intradermal administration have been described. Autologous tumor vaccines have several potential advantages over conventional cancer therapy. First, they have been associated with fewer, and less severe adverse events in veterinary patients. Second, the course of therapy may be shorter than a protracted chemotherapy or radiation therapy protocol. The cost for treatment is often less, particularly when considering the attendant costs of managing adverse events with chemotherapy or radiation therapy. Lastly, autologous tumor vaccines are cancer-type agnostic and may be useful against a wide variety of solid tumors in any species. Safety Evidence for that autologous cancer vaccines is safe for of immunotherapy for dogs comes from two recently published studies. The first report, from a group in Australia, described the outcome following 150 intramuscular injections of an adjuvanted autologous tumor lysate preparation to a population of 28 cancer-bearing dogs.14 No significant adverse events were reported. The second report, from Torigen, described the outcomes from 93 cancer-bearing dogs treated with the prescribed series of 3 subcutaneous injections of an
210
adjuvanted whole-cell autologous tumor cell vaccine produced by mechanical tumor cell dissociation.15 Approximately 10% of the treated dogs developed mild adverse events after vaccine administration. All of the described adverse events were characterized as grade I on the VCOG scale, and included redness or discomfort at the injection site, mild lethargy, transient decrease in appetite, or low-grade fever. None of the described adverse events required medical intervention and all resolved spontaneously. Options for veterinary patients Torigen Pharmaceuticals offers a commercially available autologous tumor vaccine preparation for use in veterinary patients that is an investigational treatment under the auspices of the USDA. This is an adjuvanted whole-cell vaccine created by mechanical dissociation and chemical fixation, which is created quickly because there are no in vitro cell expansion or transfection steps. Future directions As the tools to quantify the immune response in companion animals continue to evolve, we can expect immunotherapy to become the fourth pillar of animal cancer treatment as it has in human oncology. Work is needed to define efficacy of various immunotherapy approaches, and how they can best be combined with surgery, chemotherapy and radiotherapy for maximum patient benefit. References 1. Gaspar TB, et al; The use of low-dose metronomic chemotherapy in dogs-insight into a modern cancer
field; Vet Comp Oncol 2018; 16(1):2. 2. Akinleye A, Rasool, Z. Immune checkpoint inhibitors of PD-L1 as cancer therapeutics. J Hematol Oncol
2019; 12(92). https://doi.org/10.1186/s13045-019-0779-5 3. Caston SS, et al; Evaluation of locally injected mycobacterium cell wall fraction in horses with sarcoids. J
Equine Vet Sci 2020; 90. https://doi.org/10.1016/j.jevs.2020.103102 4. Grosenbaugh DA, et al; Safety and efficacy of a xenogeneic DNA vaccine encoding for human tyrosinase as
adjunctive treatment for oral malignant melanoma in dogs following surgical excision of the primary tumor. Am J Vet Res 2011; 72(12):1631-1638.
5. Mason NJ, et al; Immunotherapy with a HER2-Targeting Listeria Induces HER2-Specific Immunity and Demonstrates Potential Therapeutic Effects in a Phase I Trial in Canine Osteosarcoma. Clin Cancer Res 2016; 22(17):4380-4390.
6. Aswaq M, et al; Immunologic response to autologous tumor vaccine; Arch Surg 1964;89(3):485. 7. Peters LC, et al; Preparation of immunotherapeutic autologous tumor cell vaccines from solid tumors;
Cancer Res 1979; 39(4):1353. 8. Berd D, et al; Treatment of metastatic melanoma with an autologous tumor-cell vaccine: clinical and
immunologic results in 64 patients; J Clin Oncol 1990; 8(11):1858. 9. Berd D, et al; Immunization with haptenized, autologous tumor cells induces inflammation of human
melanoma metastases; Cancer Res 1991; 51(10):2731. 10. Karcher J, et al; Antitumor vaccination in patients with head and neck squamous cell carcinoma with
autologous virus-modified tumor cells; Cancer Res 2004; 64(21):8057. 11. Teng MW, et al; Classifying cancers based on T-cell Infiltration and PD-L1. Cancer Res 2015; 75:2139. 12. Nemunaitis J, et al; Tumor vaccines and cellular immunotherapies; Ann Transl Med 2016; 4(S1):S24. 13. National Institutes of Health 2020; Accessed 13 February 2020 https://clinicaltrials.gov 14. Weir C, et al; The safety of an autologous cancer vaccine platform in canine cancer patients; Vet Sci 2018;
5(4):87. 15. Crossley RA, et al; Safety evaluation of autologous tissue vaccine cancer immunotherapy in a canine
model; Anticancer Res 2019; 39(4):1699.
211
Osteosarcoma review and what’s new 2020 By Sue Ettinger, DVM, DACVIM (Oncology) Dr Sue Cancer Vet PLLC, Tarrytown, NY USA
Key points:
• Osteosarcoma (OSA) is the most common primary canine bone cancer in dogs, and it is locally aggressive and highly metastatic.
• The majority of dogs with appendicular osteosarcoma have no evidence of metastasis at diagnosis, but most will likely succumb to metastasis.
• Early diagnostics are key. If you are presented with a large- or giant-breed dog that is lame and has swelling at metaphyseal site, it is osteosarcoma until proven otherwise. Recommend and take radiographs promptly.
• To determine the best treatment plan for a patient and owners, it is important to understand efficacy of the various protocols, the potential toxicities, and prognostic factors.
• Dogs treated with local therapy and chemotherapy live significantly longer than dogs without treatment and with local therapy only, and chemotherapy is generally well-tolerated in most dogs. Only a minority develop significant toxicity.
Who, what, where, why? What - Osteosarcoma is the most common primary bone cancer, accounting for 85% of all skeletal cancers and 5% of all neoplasia. Osteosarcoma is a malignant mesenchymal tumor of primitive bone cells that produce extracellular matrix of osteoid. The biologic behavior is aggressive locally and highly metastatic. At the primary site, there may be bone lysis or bone production or both, soft tissue swelling, and pathologic fracture (not negative prognostic). While OSA is highly metastatic, <10-15% have detectable metastasis at diagnosis, but 90% die within 1 year with amputation alone due to metastasis
Who - Osteosarcoma is estimated to occur in > 10,000 dogs per year, but this is likely an underestimate. It typically occurs in middle aged and older dogs, but there is a small peak at 1.5 to 2 years old. Rib osteosarcoma occurs in younger adults (5 years old). OSA is common in large and giant breeds with increasing weight and height. In the U.S., breeds most at risk are St Bernard, Great Dane, Irish Setter, GSD, Rottweilers, Dobermans, and Golden Retrievers. The dog SIZE is more important than breed. The risk of osteosarcoma is 60 times higher in dogs weighing > 30 kg, and 8 times higher in dogs weighing 20-30 kg. Appendicular osteosarcoma accounts for 95% of all cases in dogs >40 kg but only 40-80% of all cases <15 kg. Axial osteosarcoma can occur in any breed and at any location.
Why - Large and giant-breed dogs are predisposed. Body size (increasing weight and more specifically height) appears to be most predictive factors for osteosarcoma, and it is more important than breed. Hereditary basis is suspected based on the large breed prevalence. The most thoroughly described mutation that contributes to formation and/or progression is p53. Additional genetic factors studied are RB and PTEN tumor suppressor genes. Osteosarcoma is more prevalent in males than females, but in the St Bernard, Great Dane, and Rottweilers, females outnumber the males, and females more affected by axial (except rib and spine). Sex hormones also appear to have a protective role. In Rottweilers neutered before 1 year of age, 1 in 4 developed osteosarcoma and more likely than intact
212
dogs. OSA has also been associated with fractures, metallic implants, chronic osteomyelitis and ionizing radiation.
Where-75% of osteosarcoma is appendicular, and 25% is in axial bones. It typically occurs in the metaphyseal region of long bones, towards the knee and away from the elbow, front limbs are two times more affected than hind limbs. The most common sites are the distal radius and proximal humerus, while in the hind limbs, osteosarcoma lesions are evenly distributed among the distal femur, distal tibia, and proximal tibia. The proximal femur less common, and osteosarcoma distal to carpus and hock is rare. In the axial location: 27% mandible, 22% maxilla, 15% spine, 14% cranium, 10% ribs, 9% sinonasal, and 6% pelvis. Multicentric is uncommon reported in <10% cases. Extraskeletal osteosarcoma is rare, and some reported sites include mammary, subcutaneous, spleen, GIT, eye, and kidney.
What do we see? Most dogs appear in pain, and many are presented with progressive lameness. Palpable swelling may or may not be present. Acute severe swelling is typical with pathologic fracture, but only 3% pathologic fractures due to osteosarcoma. If you are presented with a large- or giant-breed dog that is lame and has swelling at metaphyseal site, it is osteosarcoma until proven otherwise and do radiographs promptly. Diagnostic work up A presumptive diagnosis is based on signalment, history, physical examination, and radiographs. Differentials include other primary bone neoplasia (chondrosarcoma, fibrosarcoma, hemangiosarcoma, histiocytic sarcoma), metastatic bone cancer (usually diaphyseal), multiple myeloma or lymphoma of bone, systemic mycosis, bacterial osteomyelitis, bone cysts, and healing bone injury. When taking radiographs, take good quality lateral and craniocaudal views. The abnormalities vary from mostly lysis to mostly osteoblastic. Common features include cortical lysis, soft tissue extension and swelling, new bone extension in sunburst pattern, Codman’s triangle deposition of new bone on cortex at periphery. While osteosarcoma does not cross joint, it can invade adjacent bones. Radiographic changes can be similar to fungal osteomyelitis.
Preliminary Diagnosis: Cytology While cytology is not definitive, it is supportive and can distinguish malignant vs non-malignant with an accuracy of 70-85%. In diagnostic samples, ALP staining can differentiate osteosarcoma from other sarcomas. Ultrasound-guidance can be helpful to aid sample collection. Pre-op biopsy Pre-operative biopsy is not required in cases with classic signalment, history, PE/location, and radiographic appearance, and there is little possibility of fungal or bacterial osteomyelitis. On the other hand, biopsy is recommended if there is non-diagnostic or atypical cytology (carcinoma), the owner wants confirmation, or it is not a classic case. Always submit larger specimen at surgery to confirm. When doing pre-op biopsy, plan carefully if limb spare is option so contaminated tissue is removed. There is also 10-20% false negatives rate. The open incisional approach collects a large sample but post-surgical complications include hematoma, seeding, infection, fracture, and wound breakdown. The
213
trephine technique is 94% diagnostic but increases the fracture risk. Closed needle biopsy can be done with a Jamshidi and is 92% accurate for tumor diagnosis and 83% accurate for tumor subtype, but accuracy is dependent on experience and comfort level. In some case, repeated attempts may yield “reactive bone”. Biopsy at CENTER of lesion, and incision and biopsy tract should be planned that will be removed a definitive surgery. Fluoroscopy or CT-guided biopsy can be useful. Samples collected from the peripheral bone lesion are more likely to be non-diagnostic and contain reactive bone. Staging Staging includes minimum database, local lymph node fine needle aspirate, orthopedic exam for bone metastasis, 3-view chest radiographs or chest CT scan. Treatment recommendations and prognosis are based on plain radiographs, not advanced imaging. Less than 5% of dogs have lymph node metastasis but it is a negative prognostic factor. Bone survey radiographs are not typically recommended unless there are suspicious or painful lesions. It involves taking a lateral of all bone and VD of the pelvis and can be considered to rule out bone metastasis and 6% of dogs have bone metastasis detected (vs 4% chest). Bone scans have conflicting reports of usefulness. Abdominal ultrasound is not recommended for osteosarcoma staging but can be considered if determining is the bone lesion is a metastatic lesion or there are abnormalities on the chemistry panel. CT scan is recommended for axial tumors. Prognostic factors For appendicular osteosarcoma, the median survival time (MST) with surgery alone is 4 to 5 months. Well-established negative predictors include young age (<5 years old), large tumor size, humerus location, and high histologic grade. Other factors include small body size, larger tumors, extraskeletal tumors, percent bone necrosis, mitotic index, and overt metastasis (lungs, LN)
For non-appendicular, the head locations (mandible, maxilla, skull) are locally aggressive but have a lower metastatic rate (37%). With skull surgery alone, the MST is longer than limb at 7 months. The 1-year survival with mandibulectomy is 71%, but the MST is 5 months for maxillectomy. Following rib resection, the MST is 3 month, and 8 months for surgery and chemo. Stage III dogs with measurable metastasis have a worse prognosis with a MST of 2 months. Dogs with bone metastasis do better than lung (4 months vs 2 months), and lymph node metastasis is a negative prognostic factor (2 months vs 8 months). Dogs with elevated ALP have shorter disease free interval (DFI) and survival time (ST). Remember, prognostic factors cannot predict an individual’s response. Treatment modalities Treatment pearls Treatment for osteosarcoma is ideally both local and systemic. Since chemotherapy significantly improves the median survival time (MST), it is considered part of the standard of care. The majority of dogs tolerates chemotherapy quite well and will maintain a good to excellent quality of life even during chemotherapy. Treatment: Surgery Surgical options include amputation or limb spare techniques to address the primary tumor. Amputation is the standard treatment for appendicular osteosarcoma. Alone, it is palliative and a very effective way to remove the source of pain. Amputation alone does not increase survival (other than
214
preventing pain-related death) and most dogs succumb to metastasis. While we as veterinarians know that amputation is well-tolerated, many owners are shocked by the procedure and often reluctant to consider the radical procedure. It is important to screen the patient well and rule out concurrent musculoskeletal and neurologic abnormalities. Even middle-aged and older large-breed dogs with moderate arthritis are typically candidates. Owner satisfaction is typically excellent post-operatively, and most dogs compensate well. Alternatives to amputation includes limb spare techniques and stereotactic radiation. Surgical limb-spare procedures allow the preservation of limb function and are an alternative when amputation is not physically an option or is declined by the owner. Limb-spare procedures do not increase survival times and systemic therapy is still recommended after the delay metastasis. There are various limb-spare procedures described but the techniques involve surgical resection of the effected bone and replacement with a bone implant, bone plating and arthrodesis to stabilize the joint. Since residual disease likely remains, the region is treated with radiation, IA cisplatin or chemotherapy impregnated beads. Distal radius and ulnar lesions are most amenable, and the tumor should involve less than 50% of the bone with minimal soft tissue extension. These techniques have similar survival times but have much higher complication rates due to infection, implant failure and local tumor recurrence. For axial osteosarcoma, wide surgical excision is recommended but can be challenging due to the proximity of adjacent vital structures. If margins are incomplete, post-operative radiation is recommended to prevent local recurrence. Treatment: Radiation Like surgery, radiation is a local treatment option. Stereotactic radiation therapy (SRT) is an alternative limb-spare technique for local control. SRT delivers extremely precise high dose radiation with multiple beams within precision accuracy. Less normal tissue that surrounds the tumor is irradiated, so there are fewer radiation side effects, higher dose to tumor, and fewer treatments (typically 1 to 3). Unlike conventional RT, there are similar survival times with stereotactic radiation therapy combined with chemotherapy compared to amputation and chemotherapy. However, there is still the risk of pathologic fracture after treatment, and some dogs will have too much osteolysis at presentation to be candidates. CT-based prognostic factors can help predict the likelihood of fracture. SRT is also an option for non-resectable axial tumors. Palliative radiation can be very effective for bone tumors, and is a good option if amputation is declined. Most dogs (75 to 90%) respond favorably, and analgesia is improved. There is variation with duration of analgesia and most typically lasts 4 to 6 months, but it can be durable for greater than 1 year, and palliative radiation can be combined with adjuvant IV chemotherapy. Treatment: Chemotherapy The goal of chemotherapy is to achieve is to delay the metastatic disease that develops quickly after amputation or limb-spare procedure. Most studies have evaluated doxorubicin, cisplatin, or carboplatin in varying combinations. The most commonly used chemotherapy drug is carboplatin based on a large study comparing doxorubicin, carboplatin, and alternating. Choice of protocol (single vs combination) did not result in significant differences in DFI or ST, but the carboplatin protocol resulted in a lower
215
proportion of dogs experiencing side effects, and helpful in maintaining high quality of life during treatment. I recommend 6 treatments after local therapy. Unfortunately, 95% of dogs will eventually succumb to metastasis and additional therapy is needed. Palladia can be beneficial is some dogs with gross pulmonary metastasis. Other treatment options Pain control Pain control for the patient is a priority. Multimodality therapy is more effective. For pain medications, I recommend an NSAID and then adding other analgesics such as gabapentin, amantadine, Tramadol, and acetaminophen with codeine. Palliative radiation can be very helpful for appendicular and axial cases (see above). Bisphosphonates are osteoclast inhibitors than inhibit bone resorption and are used in human patients with diffuse skeletal metastasis. Approximately 30% dogs have decreased pain. Direct cytotoxicity to has also been reported suggesting interaction with radiation therapy and/or chemotherapy. I recommend zoledronate @ 0.1 mg/kg IV every 4 weeks. This must be diluted in 60 ml 0.9 % NaCl and Immunotherapy: Canine Osteosarcoma Vaccine (COV) A canine osteosarcoma vaccine (COV) was being developed by Aratana, which was acquired by Elanco in the Spring of 2019. This is a recombinant HER2/neu expressing Listeria therapeutic vaccine being studied at UPenn by Dr Mason. Listeria monocytogenes is a gram-positive, intracellular bacteria that is capable of inducing potent innate and adaptive immune responses. The Listeria causes the induction of CD8+ cytotoxic T-cell responses against the target antigen. The use of a highly-attenuated form of L. monocytogenes has been proven effective to introduce target antigens into antigen-presenting cells (monocytes, macrophages and dendritic cells). It is a highly attenuated strain of L. monocytogenes that has a chimeric human HER2/neu antigen. In mouse models, this has been shown to break tolerance and induce potent CD4+ and CD8+ T-cell responses against HER2/neu. In the first small study, 18 dogs with appendicular osteosarcoma (OSA) treated first with amputation and chemotherapy (i.e., 4 doses of carboplatin) received one of four doses of ADXS31-164 intravenously every 3 weeks for 3 administrations. There was a decrease in the incidence of metastatic disease and significantly increased survival time (1, 2 and 3-year survival rates vs. historical control group). The median survival time of 11 historical control dogs was 316 days vs. 8 of the treated dogs with grade I disease, that achieved a median survival time of 956 days (p<0.0001). 11 of the 18 treated dogs have surpassed the median survival time (MST) of the control group. Adverse events were mild to moderate and primarily consisted of fever, lethargy, and nausea/vomiting. Aratana had conditional licensure for this product in the USA and a larger safety study was completed in 2019. As of January 2020, Elanco will no longer pursue this specific canine osteosarcoma vaccine for licensure (conditional or full licensure) after careful evaluation of the risks and probability of future study success. The decision was made due to factors related to safety and low probability of success for licensure, including the frequency of adverse events, including isolation of Listeria monocytogenes from 5 treated dogs. The COV vials that are still in clinics do not need to be returned, but people should be aware that the vaccine is no longer conditionally licensed and no further product
216
will be available. To return unused vials, please call Elanco Customer Service: 1-800-782-8977. Elanco is continuing to pursue additional platforms/molecules for cancer treatment. Summary & prognosis Osteosarcoma is the most common primary bone tumor is dogs. The biologic behavior is aggressive locally and highly metastatic. Less than 10-15% of dogs have detectable metastasis at diagnosis, but 90% die within 1 year with amputation alone due to metastasis. Definitive therapy requires both local and systemic treatments. For appendicular osteosarcoma, amputation addresses the local disease and is palliative. The MST with surgery alone is 4 to 5 months, with 90 to 100% mortality rate in one year. Other palliative approaches include palliative radiation, pain medications, and bisphosphonate. Surgical limb spare and SRT offer alternative options to amputation for local control. The ability to control the progression of osteosarcoma metastasis remains the challenge for our patients, and systemic chemotherapy is the backbone for therapy after achieving local control. With chemotherapy, the 1-year survival rate is 40-50% and 20-25% of dogs are alive at two years. The immunotherapy looks promising but is still in development. Well-established prognostic factors include adjuvant chemotherapy, low grade (rare for osteosarcoma), and normal total and bone ALP. Dogs treated with chemotherapy live significantly longer than dogs only treated with local therapy, and chemotherapy is generally well-tolerated in most dogs. YOUTUBE RESOURCES (feel free to share) Amputation - What Every Pet Owner Needs to Know: VLOG 67 https://youtu.be/9nM1gN5iChY Bone Cancer in Dogs What You Need to Know About Osteosarcoma (part 1) VLOG 71 https://youtu.be/D61VsYJeDjE Bone Cancer in Dogs What You Need to Know About Osteosarcoma (part 2) VLOG 72 https://youtu.be/hdlVxXMa7FQ References
1. Ehrhart BP, Christensen NI, Fan TM. Tumors of the Skeletal System. In: Small Animal Clinical Oncology. 6th ed. St. Louis Missouri: Elsevier Saunders; 2020: 524-564.
2. Bailey DB. Osteosarcoma. In Clinical Veterinary Advisor Dogs and Cats. 3rd edition. St. Louis Missouri: Elsevier Mosby; 2015: 740-742
3. Ruslander D. Tumors of the Musculoskeletal System. In Cancer Management in Small Animal Practice. Saunders 2010. 333-342
4. Selmic LE et al. Comparison of carboplatin and doxorubicin-based chemotherapy protocols in 470 dogs after amputation for treatment of appendicular osteosarcoma. J Vet Intern Med. 2014 Mar-Apr ;28(2):554-63. doi: 10.1111/jvim.12313. Epub 2014 Feb 10
217
What’s new in cancer 2020 By Sue Ettinger, DVM, DACVIM (Oncology) Dr Sue Cancer Vet PLLC, Tarrytown, NY, USA It’s an exciting time in the world of veterinary oncology. We are making continual strides with therapies and diagnostics in an effort to help not only diagnose cancers earlier but offer novel therapies to owners. Please note these proceeding may not reflect all topics discussed as I am going to update this based on current research and topics. Tigilanol tiglate for mast cell tumors Tigilanol tiglate (TT) is a novel small molecule drug that is delivered by intratumoral injection and is currently under development to provide a new and alternative treatment for canine cutaneous or subcutaneous mast cell tumors (MCT). Tigilanol tiglate was discovered and is being developed by the Qbiotics Group. Tigilanol tiglate is isolated form the Australian rainforest plant Fontainea picrosperma. TT is a diterpene ester and functions as an anti-tumor drug via various processes part of which includes activation of protein kinase C (PKC). (In oncology, taxanes are an example of diterpenes in widespread clinical use.) It causes a rapid localized inflammatory response, disrupts tumor vasculature and tumor cell death by oncolysis. This leads to hemorrhagic necrosis and destruction of the tumor with usually within 4 to 7 days of treatment with enhanced wound healing of the treatment site. Tigilanol tiglate stimulates healing of the tumor deficit or 'wound' that remains after the tumor has been destroyed. STELFONTA® (tigilanol tiglate) is currently available in Europe and the UK. It was approved by the European Medicines Agency (EMA) in January 2020, making it the first pharmaceutical treatment available for all grades of canine non-resectable, non-metastatic MCT. It is also approved by the UK Veterinary Medicines Directorate (VMD) and Swissmedic. On September 21, 2020, the US Food and Drug Administration Center for Veterinary Medicine (FDA-CVM) concluded that all technical sections for the STELFONTA (tigilanol tiglate) application for marketing authorization are complete. The final stage of administrative review has commenced, with formal registration as a veterinary pharmaceutical expected mid-November 2020 pending approval. Applications for marketing authorization are currently under late-stage review in Australia as well. The dose was characterized in a study published in 2019. It has since been evaluated in 123 dogs with cutaneous or lower limb subcutaneous mast cell tumors (MCT) confirmed by fine needle aspiration cytology. This study was part of the subsequent approval by the EMA for tigilanol tiglate. Dogs were randomized 2:1 to treatment with a single intratumoral injection of tigilanol tiglate or to sham treatment (untreated controls) in an investigator- and owner-masked multicenter study. The primary efficacy outcome was complete response (CR) or disappearance of the target lesion at day 28, according to RECIST (Response Evaluation Criteria in Solid Tumors) guidelines as determined by the Veterinary Cooperative Oncology Group (VCOG).
218
118 dogs were evaluated. 60 of the 80 dogs (75%) randomized treatment with TT achieve complete remission after single injection compared with two of the 38 dogs (5.3%) by day 28. 18 of 20 treated dogs not achieving a complete remission received a second injection. 88% (70/80 evaluable) of the dogs achieved complete remission within the possible 2-dose treatment strategy. Wound development is anticipated pathology associated with the mechanism of action of the drug. The most frequent adverse events were transient reactions at the treatment site. Owners indicated that overall health related quality of life of treated is similar to that of untreated dogs. The disease-free interval at the tigilanol tiglate treatment site for patients treated in clinical trials is 90% at one year. The disease-free interval was assessed for those patients treated in the US clinical trial that achieved a complete response at four weeks following a single tigilanol tiglate treatment. There were 74 dogs available for assessment at 12 months following initial complete remission to tigilanol tiglate. Sixty-five dogs (88%) had no evidence of local MCT recurrence. In summary, 75% of MCT achieved a complete response after a single tigilanol tiglate treatment (intratumoral injection) and 88% following a second treatment. The disease-free interval at the tigilanol tiglate treatment site for patients treated in clinical trials is 90% at one year. Tigilanol tiglate (TT) was highly effective for treatment and was well tolerated with manageable side effects. Tigilanol tiglate has the potential to provide another local treatment option for dogs with MCT. Additional updates will be provided. Canine lymphoma Tanovea CA-1™ Tanovea™ (rabacfosadine) is the first FDA conditionally approved drug for the treatment of lymphoma in dogs.and licensed to VetDC (previously known as VDC-1101). It designed to preferentially target and attack cancer cells implicated in lymphoma. The data from studies totaling well over 330 patients have shown Tanovea™ to be highly effective against lymphoma (LSA) with a 60-80% overall response rate. Not surprisingly, responses are higher in naïve LSA vs relapse and in dogs with a B-cell phenotype. Data suggests Tanovea™ is well-tolerated with a similar side effect profile as other commonly used agents. The drug is given via the intravenous route at 1mg/kg every 3 weeks. The FDA has recently given Conditional Approval and the drug is NOT restricted to only oncologists. While the first study looked at its use as a single agent, a recent study looked at the use in combination with doxorubicin in naïve lymphoma patients, alternating for a total of 6 doses. The overall response rate was improved to 84% (68% CR, 16% PR) and a progression free interval of 6.5 months. In a new study of 52 dogs with relapsed lymphoma treated with at least one doxorubicin protocol, they evaluated L-asparaginase given with rabacfosadine (RAB), Dogs were treated with RAB at 1.0 mg/kg IV every 21 days for up to a total of 5 doses. L-asparaginase was administered at 400 IU/kg SQ concurrently with the first 2 treatments of RAB. The overall response rate (ORR) for all dogs was 67%, with 19 dogs (41%) achieving a complete response (CR). The median progression-free survival time (MPFS) was 63 days (range 5-428 days). Dogs experiencing a CR as their best response had an MPFS of 144 days (range 44-428 days). Adverse events were similar to previous studies evaluating single agent
219
RAB. Failure to achieve a CR and having previously received L-ASP were negative prognostic factors on multivariate analysis.
Although the majority of side effects associated with this agent are similar to those of most chemotherapeutics, two unique side effects (and one that is not unusual) occur, that clinicians need to recognize and know how to treat.
• Pulmonary fibrosis: this was recorded in a small percentage of the patients treated and the mechanism is unknown. As this was fatal in some cases, screening with thoracic films and exclusion of patients with pre-existing pulmonary issues, or particular breeds at risk of pulmonary fibrosis, is warranted.
• Dermatopathy occurred in a minority of patients and often appears along the pinna and chest. Per VetDC, resolution of the side effects occurs once discontinuing the protocol.
• Anorexia: Although the data provided by VetDC suggests that this is not dissimilar to other agents, the anorexia appears more prolonged than that commonly seen with other agents. I recommend being very proactive with anti-nausea medications and appetite stimulants, using them as preventatives over waiting for anorexia, nausea, and vomiting to occur. To prevent delay chemotherapy induced nausea and vomiting (CINV), I recommend being very proactive with oral nausea/anti-emetic drugs and appetite stimulants given at home in the days following chemotherapy. I always recommend oral Cerenia and Entyce for 7 days following administration
This represents the first lymphoma specific drug to add to our arsenal in a long time. It will likely be added to a multidrug protocol and the data will suggest where this agent best fits. One option that seems quite interesting based upon the presented data is the combination with doxorubicin, which is a less costly and time efficient protocol compared with standard CHOP. Prednisone vs. no prednisone Recent studies suggest there is no survival benefit of prednisone in a multi-agent protocol. We have certain patients when prednisone therapy maybe contraindicated, such as a dog with diabetes mellitus or nonregulated hyperadrenocorticism. Two recent randomized trials looked at dogs that received a vincristine-cyclophosphamide-doxorubicin based protocol with and without prednisone and found no difference in any measure of outcome. In my opinion, I still include prednisone in the multi-agent protocol, but I will eliminate it if there’s a medical reason, or I will taper it more quickly (and discontinue if needed) if the patient is having moderate to severe side effects. Should dogs with t-cell lymphoma be treated differently than dogs with b-cell lymphoma? Phenotype is the best independent prognostic factor; prognosis is worse with T-cell than B-cell, with the exception of low-grade/indolent subtypes. While it is known that dogs with T-cell lymphoma generally do worse when treated with CHOP based chemotherapy compared to B-cell dogs, the question remains how and if to change the protocol for dogs with high grade T-cell lymphoma. We will discuss some of the alternative protocols that are “alkylator rich”, as it is possible, they may result in improved outcomes for dogs with non-indolent T-cell lymphoma. A retrospective study was published evaluating a mechlorethamine-vincristine-procarbazine-prednisone (MOPP) based protocol in dogs with T-cell lymphoma. An overall response rate
220
(ORR) of 98% (78% complete remission), a median progression free survival (PFS) of 189 days, and a MST of 270 days was reported. (Note a study documented a similar overall response rate, MST, and PFS with CHOP in dogs with T-cell lymphoma.) More recently, additional reports have described outcomes including LOPP (Lomustine-vincristine-procarbazine-prednisone) or VELCAP-TSC (asparaginase-vincristine-CYC-DOX-actinomycin D-procarbazine-lomustine). In these reports, overall response rates ranged from 73% to 97% (64–90% CR), median PFS was 175 – 431 days and MST was 237 to 507 days. I have personally also modified the CHOP protocol as well to replace Lomustine for doxorubicin (unpublished). Osteosarcoma & immunotherapy A canine osteosarcoma vaccine (COV) was being developed by Aratana, which was acquired by Elanco in the Spring of 2019. This is a recombinant HER2/neu expressing Listeria therapeutic vaccine being studied at UPenn by Dr Mason. Listeria monocytogenes is a gram-positive, intracellular bacteria that is capable of inducing potent innate and adaptive immune responses. The Listeria causes the induction of CD8+ cytotoxic T-cell responses against the target antigen. The use of a highly-attenuated form of L. monocytogenes has been proven effective to introduce target antigens into antigen-presenting cells (monocytes, macrophages and dendritic cells). It is a highly attenuated strain of L. monocytogenes that has a chimeric human HER2/neu antigen. In mouse models, this has been shown to break tolerance and induce potent CD4+ and CD8+ T-cell responses against HER2/neu. In the first small study, 18 dogs with appendicular osteosarcoma (OSA) treated first with amputation and chemotherapy (i.e., 4 doses of carboplatin) received one of four doses of ADXS31-164 intravenously every 3 weeks for 3 administrations. There was a decrease in the incidence of metastatic disease and significantly increased survival time (1, 2 and 3-year survival rates vs. historical control group). The median survival time of 11 historical control dogs was 316 days vs. 8 of the treated dogs with grade I disease, that achieved a median survival time of 956 days (p<0.0001). 11 of the 18 treated dogs have surpassed the median survival time (MST) of the control group. Adverse events were mild to moderate and primarily consisted of fever, lethargy, and nausea/vomiting. Aratana had conditional licensure for this product in the USA and a larger safety study was completed in 2019. As of January 2020, Elanco will no longer pursue this specific canine osteosarcoma vaccine for licensure (conditional or full licensure) after careful evaluation of the risks and probability of future study success. The decision was made due to factors related to safety and low probability of success for licensure, including the frequency of adverse events, including isolation of Listeria monocytogenes from 5 treated dogs. The COV vials that are still in clinics do not need to be returned, but people should be aware that the vaccine is no longer conditionally licensed and no further product will be available. To return unused vials, please call Elanco Customer Service: 1-800-782-8977. Elanco is continuing to pursue additional platforms/molecules for cancer treatment. The cadet braf/plus test for canine urothelial carcinomas Urothelial carcinomas (UC) includes tumors of the lower urinary tract and prostatic carcinoma (PC). These are aggressive genitourinary cancers in dogs, characterized by invasion to surrounding tissues and high metastatic potential. Urothelial carcinoma affects the bladder, urethra and kidneys of male
221
and female dogs and also the prostate of males. Diagnosis is often based upon signalment, ultrasound, traumatic catheterization, urine cytology, but definitive diagnosis is limited to histopathology via cystoscopy or surgical exploratory, requiring an invasive and costly biopsy. There has definitely been a need for a non-invasive test for UC. The CADET® BRAF Assay can be used for diagnosis and monitoring of UC including canine transitional cell carcinoma (TCC) and prostatic carcinoma (PC). This test offers a less invasive way to diagnose these cancers. Recent studies identified a mutation (V595E) in the canine b-raf gene in a large proportion of canine urothelial carcinoma (UC), which include TCC and prostatic carcinoma (PC). In assessing various cancers including epithelial, mesenchymal, and hematopoietic, the V595E mutation was identified in canine UC with the highest penetrance rates of up to 87%. Knowing bladder and prostatic cancers shed tumor cells into urine, the presence of the V595E mutation in urine appeared to be an excellent molecular diagnostic marker. The polymerase chain reaction (PCR) assay of urine tests for a common mutant gene in UC cancers. The test is 85% sensitive and 100% specific for canine urothelial carcinoma and prostate carcinoma patients. (Mochizuki)
The assay has since been validated in hundreds of clinical cases, demonstrating the mutation is not present in the urine of healthy dogs, or from dogs that have benign bladder diseases (bladder polyps, inflammation or chronic cystitis). In cases in which a biopsy of a mass was performed, there was concordance between BRAF mutation-positive in free-catch urine and pathology-based confirmation of a bladder/prostatic carcinoma. As such, the presence of the mutation in canine urine is therefore a highly specific indicator of the presence of a UC. In addition, the CADET® BRAF-PLUS assay was launched commercially in July 2018 and will be run on every BRAF mutation undetected case automatically. This assay detects copy number variations associated with TCC/UC in more than two-thirds of BRAF mutation negative patients. The new test increases overall sensitivity to detect a TCC/UC from 87% to >95%. This translates to only 5% false negatives. The Cadet BRAF test is exclusively available through Antech Diagnostics. https://www.antechdiagnostics.com/about/news/cadet-braf-and-braf-plus-now-available-exclusively-through-antech-diagnostics Potential advantages of the assay:
• The free-catch urine system is fully non-invasive. Urine sample can be collected while the patient is at the clinic or by the owner at home.
• The assay permits detection for earliest detection of emerging UC, including TCC – even before overt signs of the cancer become evident.
• With the add on Cadet BRAF Plus test, there is only 5% false negatives • 0% false positives • Timely detection of UC allows owners to direct their resources toward effective treatment
of the cancer itself, rather than the non-specific clinical signs. • Unlike prior bladder cancer tests, the test is not affected by the presence of blood, protein,
glucose, or bacteria in the urine. How can we use the test in practice knowing early detection & diagnosis are important for UC?
222
• I am currently using the CADET® BRAF test as a diagnostic for UC. A positive BRAF testing can substitute for tissue diagnosis (histology, cytology). If the BRAF mutation is not detected, the urine specimen is then assessed by the lab using a proprietary algorithm to determine whether it meets the criteria for analysis with CADET® BRAF-PLUS. No additional urine is required.
• I am also using serial CADET® BRAF/PLUS tests to monitor during chemotherapy to assess response to treatment, often in conjunction with bladder ultrasound. This provides an objective response to see how an individual patient’s tumor is responding to chemotherapy.
• Educate our clients about high risk breeds. But remember other breeds & mixed breeds can sadly be diagnosed too. If a client has a high-risk breed, consider screening with the CADET® BRAF test. I consider screening at-risk breeds every 4 to 6 months with this easy-to-collect urine test.
• If a patient, especially over the age of 6, has lower urinary tract clinical signs or multiple UTI, I recommend additional tests (abdominal ultrasound, BRAF urine test, cytology or biopsy) - it will depend on the case. Consider referral to a specialist.
Advanced diagnostics are most useful early. Clinical signs for UC are often subtle, nonspecific and confused for other lower urinary tract diseases. The CADET® BRAF test provides a non-invasive, easy-to-collect urine test for earliest detection of emerging UC – even before overt signs of the cancer become evident. Timely detection of UC allows owners to direct their resources toward effective treatment of the cancer itself, rather than the non-specific clinical signs. If your patient is diagnosed with TCC or PC, there are treatment options. The most common ones are chemotherapy, NSAIDs, and sometimes surgery but there are others, so consider referral or consultation with an oncologist. Treatment is well tolerated, and treated dogs typically live longer than untreated dogs. REFERENCES:
1. Miller J, Campbell J, Blum A, et al. Dose Characterization of the Investigational Anticancer Drug Tigilanol Tiglate (EBC-46) in the Local Treatment of Canine Mast Cell Tumors. Front Vet Sci. 2019;6:106. Published 2019 Apr 9. doi:10.3389/fvets.2019.00106
2. Johannes CM Abstract, 2019 ACVIM Forum; Phoenix AZ 3. De Ridder T, et al. Journal of Veterinary Internal Medicine 2020; doi 10.1111/jvim.15806 4. Campbell J, et al. Veterinary Cancer Society Annual Conference 2019 5. Thamm DH, et al. BMC Veterinary Research 2014;10:30-34. 6. Vail DM, et al. Clin Cancer Res 2009;15:3503-3510 7. Thamm DH, et al. J Vet Intern Med 2017;31:872–878 8. Brodsky EM, et al. Asparaginase and MOPP treatment of dogs with lymphoma. JVIM
2009;23:578. 9. Fulkerson CM, Knapp D. Tumors of the Urinary System. In: Small Animal Clinical Oncology St.
Louis: Elsevier–Saunders; 2020. p. 645-656. 10. Bryan JN. Transitional Cell Carcinoma in Clinical Veterinary Advisor Dogs and Cats. 4th edition.
St. Louis Missouri: Elsevier Mosby; 2020: 991-992. 11. Mochizuki H, et al. PLoS One. 2015;10(12):e0144170. doi: 10.1371/journal.pone.0144170. 12. Fulkerson CM, Knapp DW. Management of transitional cell carcinoma of the urinary bladder in
dogs: a review. Vet J. 2015 Aug;205(2):217-25. 13. Cawley JR, et al. J Vet Intern Med. 2020 Mar;34(2):882-889. doi: 10.1111/jvim.15723.
223
What’s new in mast cell tumor treatments By Sue Ettinger, DVM, DACVIM (Oncology) Dr Sue Cancer Vet PLLC, Tarrytown, NY, USA Mast cell tumors (MCT) are the most common cutaneous tumor in dogs, accounting for 16 to 21% of skin tumors. Early detection and aspirates before surgical removal are important for successful outcomes. One size does not fit all, and MCT are treatable. While some low and intermediate grade MCT can be cured with an adequate surgery, some high grade MCT are more aggressive with survival times of less than 3 to 6 months without treatment. Still dogs even high grade ones with metastasis are treatable. But improved survival has been reported with aggressive local and systemic therapy for dogs with high grade MCT and high mitotic index MCT. Prognostic factors: Treatment decisions are based on the presence or absence of negative prognostic factors and the clinical stage of disease. There are many prognostic factors, but the more significant predictors include:
• Histologic grade • Stage • Mitotic index: Mitotic Index is an indirect measure of cell proliferation based on number of mitotic
figures and is a strong prognostic factor. It can be performed during routine histology. Look for this on your biopsy report. MI has been associated with metastasis and survival (but not recurrence)
• C-kit mutation • MCT panel score which includes other proliferation markers that require additional
immunohistochemical staining such as AgNOR and Ki-67. • Others include size, location, recurrence, clinical signs
Remember, prognostic factors cannot predict an individual’s response. Treatment Treatment of MCT can vary from simple and straightforward to complicated and controversial. Treatment decisions are often based in the clinical stage (presence of regional and/or distant metastasis) and the presence of prognostic factors. Surgical resection with clean and wide margins is recommended, but questions often arise in determining which dogs need chemotherapy post-operatively. Should chemotherapy protocol be different for dogs with or without the c-kit mutation? And what to do with dogs with multiple MCT? Dogs with low grade/grade 1 MCT or that have low proliferation scores and are c-kit negative can typically be managed with local therapy (surgery and/or radiation). Surgery Surgery is the ideal treatment in areas amenable to wide resection. The recommendations for margins have historically been 3 cm but this was largely anecdotal. More recently, surgical margins have been evaluated for MCT < 5 cm. Two cm lateral margins may be adequate for most small and lower grade (grade 1 and grade 2) MCT with 1 fascial plane deep. The majority of naïve dermal MCT are intermediate or low grade and will be cured with surgery alone, provided site is amenable. In some locations, wide margins are often not possible, such as the distal limb. In my opinion, amputation is probably too aggressive. But further therapy will likely be needed after surgery. For incomplete margins post-operative options include external beam radiation therapy, scar revision (second surgery), and chemotherapy. This emphasizes the need for early detection and identification of
224
what the mass is prior to resection, so the first surgery can be curative intent surgery. Radiation therapy (RT) Radiation is recommended when wide surgical excision is not feasible. MCT are responsive to radiation. Monotherapy has varying control rates with reported 1-year control rates of 50%. However, a better approach is often surgery with adjuvant radiation. First surgery is performed to achieve microscopic disease (clinical stage 0) followed by full course radiation therapy. A typical course of radiation is 15 treatments over 3 weeks and has high control rates of 85-95% 2-year control rates for grade 1 and 2 MCT. For macroscopic MCT, the combination of steroids with palliative radiation has been reported to have an improved overall response rate (ORR) of 75%. Palliative radiation is typically weekly radiation for 4 weeks. Alternative local therapies Intralesional therapies such as deionized water or corticosteroids may provide temporary shrinkage but unfortunately are rarely effective for long-term tumor control. Electrochemotherapy, cryotherapy, and photodynamic therapy are also reported. Tigilanol tiglate Tigilanol tiglate (TT) is a novel small molecule drug that is delivered by intratumoral injection and is currently under development to provide a new and alternative treatment for canine cutaneous or subcutaneous mast cell tumors (MCT). Tigilanol tiglate was discovered and is being developed by the Qbiotics Group. Tigilanol tiglate is isolated form the Australian rainforest plant Fontainea picrosperma. TT is a diterpene ester and functions as an anti-tumor drug via various processes part of which includes activation of protein kinase C (PKC). (In oncology, taxanes are an example of diterpenes in widespread clinical use.) It causes a rapid localized inflammatory response, disrupts tumor vasculature and tumor cell death by oncolysis. This leads to hemorrhagic necrosis and destruction of the tumor with usually within 4 to 7 days of treatment with enhanced wound healing of the treatment site. Tigilanol tiglate stimulates healing of the tumor deficit or 'wound' that remains after the tumor has been destroyed. STELFONTA® (tigilanol tiglate) is currently available in Europe and the UK. It was approved by the European Medicines Agency (EMA) in January 2020, making it the first pharmaceutical treatment available for all grades of canine non-resectable, non-metastatic MCT. It is also approved by the UK Veterinary Medicines Directorate (VMD) and Swissmedic. On September 21, 2020, the US Food and Drug Administration Center for Veterinary Medicine (FDA-CVM) concluded that all technical sections for the STELFONTA (tigilanol tiglate) application for marketing authorization are complete. The final stage of administrative review has commenced, with formal registration as a veterinary pharmaceutical expected mid-November 2020 pending approval. Applications for marketing authorization are currently under late-stage review in Australia as well. The dose was characterized in a study published in 2019. It has since been evaluated in 123 dogs with cutaneous or lower limb subcutaneous mast cell tumors (MCT) confirmed by fine needle aspiration cytology. This study was part of the subsequent approval by the EMA for tigilanol tiglate. Dogs were randomized 2:1 to treatment with a single intratumoral injection of tigilanol tiglate or to sham treatment (untreated controls) in an investigator- and owner-masked multicenter study. The primary efficacy outcome was complete response (CR) or disappearance of the target lesion at day 28, according to RECIST (Response Evaluation Criteria in Solid Tumors) guidelines as determined by the Veterinary Cooperative Oncology Group (VCOG). Other outcome measures included wound healing, tolerability and safety and health-related quality of life.
225
Treated dogs with less than complete remission could receive a second injection into the tumor on day 30, and untreated dogs to be crossed over to the treatment on day 30. 118 dogs were evaluated. 60 of the 80 dogs (75%) randomized treatment with TT achieve complete remission after single injection compared with two of the 38 dogs (5.3%) by day 28. 18 of 20 treated dogs not achieving a complete remission received a second injection. 88% (70/80 evaluable) of the dogs achieved complete remission within the possible 2-dose treatment strategy. 96% (55/57) achieved complete remission after the first injection remained tumor free at post treatment day 84. Of the 38 dogs in the untreated control group, 33 were crossed over to the TT treatment group and 62.5% achieve complete remission by day 28, and 44.4% of those remaining tumor-free posttreatment day 84. Wounds developed in 95% (111/117) of the dogs treated and healed rapidly following tumor slough. Wound development is anticipated pathology associated with the mechanism of action of the drug. The most frequent adverse events were transient reactions at the treatment site. Owners indicated that overall health related quality of life of treated is similar to that of untreated dogs. The disease-free interval at the tigilanol tiglate treatment site for patients treated in clinical trials is 90% at one year. The disease-free interval was assessed for those patients treated in the US clinical trial that achieved a complete response at four weeks following a single tigilanol tiglate treatment. There were 74 dogs available for assessment at 12 months following initial complete remission to tigilanol tiglate. Sixty-five dogs (88%) had no evidence of local MCT recurrence. In summary, 75% of MCT achieved a complete response after a single tigilanol tiglate treatment (intratumoral injection) and 88% following a second treatment. The disease-free interval at the tigilanol tiglate treatment site for patients treated in clinical trials is 90% at one year. Tigilanol tiglate (TT) was highly effective for treatment and was well tolerated with manageable side effects. Tigilanol tiglate has the potential to provide another local treatment option for dogs with MCT. Additional updates will be provided. Supportive medications Any dog that has grossly detectable tumor should have supportive medications, including H1 blocker (diphenhydramine) and a proton pump blocker (omeprazole) or H2 blocker (famotidine). Anti-emetics and appetite stimulants are often recommended. Chemotherapy Poorly differentiated and metastatic MCT will typically progress to kill the dog and chemotherapy is recommended. The goal of systemic adjuvant chemotherapy is to decrease the likelihood of metastasis and improve disease free intervals. Patients to be considered for chemotherapy are the high risk patients, based on prognostic factors such as biopsy or special stains (including increased mitotic index > 5 per 10 HPF and c-kit mutation positive). A recent study showed that dogs with low-grade MCT that underwent surgical excision of the primary tumor and elective lymphadenectomy of the regional LN have a good prognosis. The use of adjuvant medical treatment in that study dogs does not seem to provide any benefit in terms of progression and survival. Drugs used are vinblastine, Lomustine, Palladia, cyclophosphamide, hydroxyurea, and chlorambucil. Dogs with multiple MCT in a short time period may also be considered for chemotherapy, as well as for non resectable MCT in the neo-adjuvant setting (prior to surgery). Chemotherapy for non-resectable MCT is considered palliative. For dogs with measurable tumors, chemotherapy has variable response rates, and responses tend to be short-lived. Response rates of up
226
to 64% have been reported, but studies have shown that combination therapies offer improved efficacy over single agent protocols. I prefer the combination of vinblastine and prednisone, which has reported efficacy for gross disease of 47%. For high grade MCT and high mitotic index MCT, survival times vary due to recurrence and/or metastasis, but improved survival has been reported with aggressive local and systemic therapy, including vinblastine and prednisone, vinblastine and prednisone with Lomustine or cyclophosphamide. MST in the various studies range from 11 months to over 5 years. How to treat c-kit positive vs negative mct? It is important to note that dogs with both C-kit positive and negative tumors demonstrated a positive response to Palladia therapy in the pivotal clinical trial. C-kit mutation status testing is not required prior to initiation of therapy. Knowing the C-kit mutation status, however, may help guide therapy in some cases as long-term treatment with Palladia can be expensive (depending on size of dog). In cases of macroscopic, high grade, c-kit positive MCT, I will typically start with vinblastine and prednisone to more gradually reduce tumor burden prior to starting longer-term Palladia therapy. This more measured, gradual treatment approach has been better tolerated with improved overall clinical outcomes. Steroids Steroids can have an anti-cancer effect and also decreased peritumoral edema and inflammation. As a single agent in grade 2 and grade 3 MCT, the overall response rate (ORR) was 20% (5 of 25). But when steroids were given orally prior to radiation for non-resectable grade 1 to 3 MCT, the ORR was higher at 75% (18/24). When given prior to surgery (neo-adjuvant) for grade 1-3 MCT, the ORR was 70%. Prognosis Mast cell tumors are treatable, but there can be a wide range of outcomes for patients. Early detection and identification with aspirates before surgery will help improve treatment outcomes. The most significant prognostic factor is tumor grade. For dogs with completely excised low-grade MCT, the prognosis is excellent. Approximately only 5% of these will recur or metastasize. For dogs with incompletely excised low and intermediate grade MCT, additional surgery or radiation is recommended. The prognosis can still be good for long term tumor control with 80-90% 2 to 5 year control rates. For high grade MCT and high mitotic index MCT, survival times vary due to recurrence and/or metastasis, but improved survival has been reported with aggressive local and systemic therapy. About 10 to 40% of dogs develop additional lesions (especially Pugs and boxers) so routine monitoring at home is so important. I recommend owners do this monthly and show them how in my YouTube video. https://youtu.be/1fHwHAUFgC8 I also recommend pet owners keep track with skin maps available on my website. https://drsuecancervet.com/skin-maps/ Youtube resources on mct & stelfonta (feel free to share)
• And Promising New Cancer Treatment For Pets Vlog 107 https://youtu.be/ybBv9Iyjvqc • Exciting New Mast Cell Tumor Treatment for Dogs: VLOG 108https://youtu.be/HM1XgCmtJPE • Your Dog has a Mast Cell Tumor, Now What, Part One: Vlog
63 https://youtu.be/3pmq05E8hZg • Mast Cell Tumors In Dogs Treatment Options, Now What, Part 2 Vlog 64
https://youtu.be/IFuqwtSTR7Mo
227
REFERENCES: 1. London CA, Thamm DH. Mast Cell Tumors. In: Small Animal Clinical Oncology. 6th ed. St. Louis Missouri: Elsevier Saunders; 2020: 382-403. 2. Geiger T. Mast Cell Tumors, Dog. In Clinical Veterinary Advisor Dogs and Cats. 4th edition. St. Louis Missouri: Elsevier Mosby; 2020: 634-636. 3. McCaw DL. Mast Cell Tumors. In Cancer Management in Small Animal Practice. Saunders 2010. 317-321 4. Kuipel. M, et al Proposal of a 2-tier histologic grading system for canine cutaneous mast cell tumors to more accurately predict biological behavior. Vet Path 48(1) 147-155. 2011. 5. Miller J, Campbell J, Blum A, et al. Dose Characterization of the Investigational Anticancer Drug
Tigilanol Tiglate (EBC-46) in the Local Treatment of Canine Mast Cell Tumors. Front Vet Sci. 2019;6:106. Published 2019 Apr 9. doi:10.3389/fvets.2019.00106
6. Johannes CM Abstract, 2019 ACVIM Forum; Phoenix AZ 7. De Ridder T, et al. Journal of Veterinary Internal Medicine 2020; doi 10.1111/jvim.15806 8. Campbell J, et al. Veterinary Cancer Society Annual Conference 2019 9. Marconato L, et a. Vet Comp Oncol. 2020; doi: 10.1111/vco.12566
228
Urine liquid biopsy: The new for bladder cancer in dogs This session will focus on the new non-invasive free-catch urine test from Antech Diagnostics that detects the b-raf mutation found in bladder and prostate cancer, or urothelial carcinoma. It will cover early detection in dogs with abnormal urinary signs as well as high risk breeds, early diagnosis, monitoring and prevention. We will discuss how best to use this test in your practice to manage and monitor these patients. By Sue Ettinger, DVM, DACVIM (Oncology) Dr Sue Cancer Vet PLLC, Tarrytown, NY, USA Canine transitional cell carcinoma (TCC) is unfortunately often found late as the clinical signs mimic a urinary tract infection (UTI), with hematuria, stranguria, incontinence, and pollakiuria. Additionally, many dogs also have a concurrent UTI, so the clinical signs temporarily improve when treated with antibiotics. Urothelial carcinomas (UC) includes tumors of the lower urinary tract and prostatic carcinoma (PC). These are aggressive genitourinary cancers in dogs, characterized by invasion to surrounding tissues and high metastatic potential. Urothelial carcinoma affects the bladder, urethra and kidneys of male and female dogs and also the prostate of males. Lower urinary tract tumors are relatively rare in dogs, estimated to be less than 2% of reported tumors. The majority of lower urinary tract tumors are malignant, with transitional cell carcinoma (TCC) the most common. TCC is most commonly located in the trigone area, and 50% of dogs will have urethral involvement from extension of the primary bladder mass. (Knapp) There are many challenges with canine bladder cancer. Many patients have clinical signs that are mimic a UTI, and there is a temporary resolution with antibiotics and/or anti-inflammatories. Patients are often misdiagnosed with a resistant UTI or cystitis. Generally, TCC is not diagnosed early but only after it has invaded into the bladder wall, at which point most treatment options are palliative at best. Physical examination can be normal, but abnormalities may include tenderness on abdominal palpation, palpable caudal abdominal mass, distended urinary bladder, and urethral mass and or prostatic involvement on rectal exam. (Knapp, Bryan) Common sites of metastasis include lymph node, liver, lung, and other site have been reported including kidney, spleen, uterus, GI tract, bone, muscle and cystocentesis needle tracts. At presentation, 15% have local lymph node metastasis, and distant metastasis is present in about 20% of cases. Distant metastasis is present in about 50% of cases at death and the cancer can lead to urinary tract obstruction. (Knapp, Bryan) Treatment In general, surgery is considered palliative due to high metastatic rates and normal tissue often contains neoplastic or pre-neoplastic tissue. Since the trigone lesion is most common, complete surgical excision is unlikely, while apex lesions can be operable. Visual assessment at the time of cystectomy is often inaccurate for achieving tumor-free margins. Wide surgical excision is
229
imperative. Even with complete resections, surgery is rarely curative, and recurrence is likely, either due to microscopic cells at the margins or development of de novo tumors. Surgery reduces clinical signs but may not extend survival. (Knapp, Bryan) Medical management is the mainstay for TCC therapy. Although TCC is typically not curable, treatment is often well-tolerated, so treated dogs live longer and live well. Approximately 75% of dogs respond favorably to treatment and can enjoy several months to a year or more of good quality life. Several drug combinations and protocols have been evaluated. Mitoxantrone and NSAID therapy is well tolerated and can cause reduction in tumor size, palliation and improvement of clinical signs, and increased survival times. Other drugs evaluated include vinblastine, doxorubicin, and metronomic oral chlorambucil. Vinorelbine has also been evaluated as rescue therapy. (Allstadt, Arnold, Fulkerson, Kaye, McMillan, Pippy, Schrempp) Detection and diagnosis Early detection of bladder cancer is important in dogs especially the high risk breeds. Overall, there is a higher incidence of bladder cancer in 14 popular breeds of dogs: American Eskimo Dog, Australian Cattle Dog, Australian Shepherd, Beagle, Bichon Frise, Border Collie, Parson Russell Terrier, Lhasa Apso, Rat Terrier, Russell Terrier, Scottish Terrier, Shetland Sheepdog, West Highland White Terrier, and Wire Fox Terrier. These 14 breeds account for 23% of all cases, indicating that mixed breed dogs account for the majority (77%) of TCC/UC. In the non-high risk group, 69% or more than 2 out of 3 cases are detected in mixed breed dogs. Diagnosis is often based upon signalment, ultrasound, traumatic catheterization, and urine cytology. Cytology is limiting as tumor cells may be identified in urine sediment in one-third of dogs with TCC, and reactive transitional cells may look like TCC cells. Cystocentesis has been associated with needle-tract implantation of neoplastic cells in some cases and should be avoided, though controversial. Currently a reliable test for definitive diagnosis is limited to histopathology via cystoscopy or surgical exploratory, requiring an invasive and costly biopsy. In addition, cystoscopy can be limited by the size and gender of affected patient, in addition to the necessary skills and equipment to do cystoscopy. It is clearly a challenge for veterinarians to get an early diagnosis of urothelial cancers, potentially delaying the start of appropriate therapy. There has definitely been a need for a non-invasive test for UC. The CADET® BRAF ASsay The CADET® BRAF Assay can be used for diagnosis and monitoring of UC including canine transitional cell carcinoma (TCC) and prostatic carcinoma (PC). This test offers a less invasive way to diagnose these cancers.
Recent studies identified a mutation (V595E) in the canine b-raf gene in a large proportion of canine urothelial carcinoma (UC), which include TCC and prostatic carcinoma (PC). In assessing various cancers including epithelial, mesenchymal, and hematopoietic, the V595E mutation was identified in canine UC with the highest penetrance rates of up to 87%. Knowing bladder and
230
prostatic cancers shed tumor cells into urine, the presence of the V595E mutation in urine appeared to be an excellent molecular diagnostic marker. The polymerase chain reaction (PCR) assay of urine tests for a common mutant gene in UC cancers. The test is 85% sensitive and 100% specific for canine urothelial carcinoma and prostate carcinoma patients. (Mochizuki)
The assay has since been validated in hundreds of clinical cases, demonstrating the mutation is not present in the urine of healthy dogs, or from dogs that have benign bladder diseases (bladder polyps, inflammation or chronic cystitis). In cases in which a biopsy of a mass was performed, there was concordance between BRAF mutation-positive in free-catch urine and pathology-based confirmation of a bladder/prostatic carcinoma. As such, the presence of the mutation in canine urine is therefore a highly specific indicator of the presence of a UC. In addition, the CADET® BRAF-PLUS assay was launched commercially in July 2018 and will be run on every BRAF mutation undetected case automatically. This assay detects copy number variations associated with TCC/UC in more than two-thirds of BRAF mutation negative patients. The new test increases overall sensitivity to detect a TCC/UC from 87% to >95%. This translates to only 5% false negatives. This is in contrast to the previously available Veterinary Bladder Tumor Antigen test (VBTA), which is 85% sensitive for TCC but only 45% specific in the presence of other urinary tract disease (hematuria, pyuria). The urine for the patient must be inactive, limiting its usefulness in dogs with abnormal urinalyses. VBTA can be used as a screening test, and a negative result is 85% reliable. However, a positive result does NOT confirm TCC, and additional diagnostics such as the CADET® BRAF test are warranted to confirm a diagnosis. The Cadet BRAF test is exclusively available through Antech Diagnostics. https://www.antechdiagnostics.com/about/news/cadet-braf-and-braf-plus-now-available-exclusively-through-antech-diagnostics Potential advantages of the assay:
• The free-catch urine system is fully non-invasive. Urine sample can be collected while the patient is at the clinic or by the owner at home.
• The assay permits detection for earliest detection of emerging UC, including TCC – even before overt signs of the cancer become evident.
• With the add on Cadet BRAF Plus test only 5% false negatives • 0% false positive. • Timely detection of UC allows owners to direct their resources toward effective
treatment of the cancer itself, rather than the non-specific clinical signs. • Unlike prior bladder cancer tests, the test is not affected by the presence of blood,
protein, glucose, or bacteria in the urine. How am I using this test? How can we use the test in practice knowing early detection & diagnosis are important for UC?
231
I am currently using the CADET® BRAF test as a diagnostic for UC. A positive BRAF testing can substitute for tissue diagnosis (histology, cytology). If the BRAF mutation is not detected, the urine specimen is then assessed by the lab using a proprietary algorithm to determine whether it meets the criteria for analysis with CADET® BRAF-PLUS. No additional urine is required. I am also using serial CADET® BRAF tests to monitor during chemotherapy to assess response to treatment, often in conjunction with bladder ultrasound. This provides an objective response to see how an individual patient’s tumor is responding to chemotherapy. Educate our clients about high risk breeds. But remember other breeds & mixed breeds can sadly be diagnosed too. If a client has a high-risk breed, consider screening with the CADET® BRAF test. I consider screening at-risk breeds every 4 to 6 months with this easy-to-collect urine test. If a patient, especially over the age of 6, has lower urinary tract clinical signs or multiple UTI, I recommend additional tests (abdominal ultrasound, BRAF urine test, cytology or biopsy) - it will depend on the case. Consider referral to a specialist. If your patient is diagnosed with TCC or PC, there are treatment options. The most common ones are chemotherapy, NSAIDs, and sometimes surgery but there are others, and treatment is well tolerated. Consider referral to an oncologist. Advanced diagnostics are most useful early. Clinical signs for UC are often subtle, nonspecific and confused for other lower urinary tract diseases. The CADET® BRAF test provides a non-invasive, easy-to-collect urine test for earliest detection of emerging UC – even before overt signs of the cancer become evident. Timely detection of UC allows owners to direct their resources toward effective treatment of the cancer itself, rather than the non-specific clinical signs. If your patient is diagnosed with TCC or PC, there are treatment options. The most common ones are chemotherapy, NSAIDs, and sometimes surgery but there are others, so consider referral or consultation with an oncologist. Treatment is well tolerated, and treated dogs typically live longer than untreated dogs. Youtube resources on uc & cadet braf/plus test (feel free to share)
• Symptoms of Bladder Cancer in Pets, How to Catch this Early: Vlog 109 https://youtu.be/Cctg3u1WB_w
• Does This Urine Test Replace Invasive Biopsy For Transitional Cell Carcinoma In Dogs? Vlog 110 https://youtu.be/L2_B66ZXH28
• Dog Bladder Cancer Treatment Options: Vlog 111 https://youtu.be/_doiK2wSeRQ References
• Knapp D, McMillan S. Tumors of the urinary system. In: Withrow SJ VD, editor. Withrow and MacEwen’s Small Animal Clinical Oncology St. Louis: Elsevier–Saunders; 2013. p. 572-82.
• Bryan JN. Transitional Cell Carcinoma in Clinical Veterinary Advisor Dogs and Cats. 4th edition. St. Louis Missouri: Elsevier Mosby; 2020: 991-992.
• Mochizuki H, et al. PLoS One. 2015;10(12):e0144170. doi: 10.1371/journal.pone.0144170.
232
• Allstadt SD, et al, J Vet Intern Med. 2015 Jan;29(1):261-7. • Arnold EJ, et al. J Vet Intern Med. 2011 Nov-Dec;25(6):1385-90. • Fulkerson CM, Knapp DW. Vet J. 2015 Aug;205(2):217-25. • Kaye ME, et al. Vet Comp Oncol. 2015 Dec;13(4):443-51. • McMillan SK, et al.. J Am Vet Med Assoc. 2011 Oct 15;239(8):1084-9. • Rippy SB, et al. BMC Vet Res. 2016 Nov 17;12(1):257. • Schrempp DR, et al.. J Am Vet Med Assoc. 2013 Jun 1;242(11):1534-8.
233

Feline Ophthalmology – Practical tips for diagnosing and treating common cat conditions By Rachel A. Allbaugh, DVM, MS, Diplomate ACVO Iowa State University Department of Veterinary Clinical Sciences, Ames, IA
Though cats may get many of the same eye problems as other species it is important to remember that they are not small dogs and that some of their ocular issues require different management strategies or that simply they can get diseases that other species do not get. Awareness of these considerations and knowledge of certain feline ophthalmic issues is important in small animal practice.
Conjunctivitis
Conjunctivitis is a common ophthalmic problem in feline patients and a frequent cause for presentation to veterinarians. Clinical signs include blepharospasm, epiphora or discolored ocular discharge, conjunctival hyperemia and possibly chemosis. Infectious etiologies are the most common cause of conjunctivitis in cats, including Feline Herpesvirus-1 (FHV-1), Chlamydophila felis, Mycoplasma spp., and calicivirus. The specific agent may be difficult to identify so empiric therapy is commonly used to treat patients while avoiding drugs that may suppress the immune system or worsen clinical signs. Antibiotic agents used include topical erythromycin, oxytetracycline, or chloramphenicol ointment TID-QID and/or systemic doxycycline 10 mg/kg PO daily to address possible bacterial agents. Antiviral therapy (famcyclovir 90 mg/kg PO BID and/or compounded ophthalmic cidofovir 0.5% BID), +/- adjunctive therapy with L-lysine or other supplements, is commonly used to manage FHV-1. Antibiotic and/or antiviral therapy is typically continued for 2 weeks past the resolution of clinical signs.
Corneal Ulceration
Corneal ulcers in cats may be most commonly caused by FHV-1 or trauma, but eyelid or eyelash abnormalities can also cause ulcers. Dendritic ulcers are pathognomonic for FHV-1 infection; however superficial geographic ulcers are a more common presentation. Bacterial organisms are typically secondary invaders which complicate compromised corneas. Simple, uncomplicated ulcers should be managed in a way that prevents infection/complication, reduces pain and aids healing (which should occur in a matter of days) while not impeding it (e.g. with topical steroids/nonsteroidals/anesthetics). Therapy includes a topical ophthalmic antibiotic TID-QID, such as tetracycline, erythromycin, chloramphenicol, tobramycin or a fluoroquinolone. Antibiotics containing neomycin and polymyxin are not recommended in cats due to potential topical hypersensitivity and rare anaphylactic reaction risk. If discomfort is noted with ulceration then ophthalmic atropine SID-BID +/- a pain-relieving drug can be used for a few days. A recheck is warranted in 3-5 days to ensure ulcer healing without complication. Any nonhealing feline superficial ulcer with no other obvious cause should be treated as a herpetic ulcer with an antiviral +/- lysine, in addition to a topical antibiotic to prevent secondary bacterial infection. Ulcers with loose epithelial lips that are superficial are also likely due to FHV-1 and may require sterile cotton-tip applicator debridement or other therapies to encourage healing (e.g. diamond burr or superficial keratectomy). Grid keratotomy should NOT be performed given the risk of causing a corneal sequestrum.
234
Complicated, melting and/or infected ulcers require more aggressive management with culture and cytology helpful to guide therapy. Treatment may include topical ophthalmic antibiotics every 1-4 hours, plasma/serum every 1-4 hours, atropine BID, a pain-relieving drug, and a systemic antibiotic. An E-collar may be needed to prevent injury of a fragile eye. Eyes should be rechecked in 36-48 hours to assess patient comfort and ensure the eye is not worse. Ulcers 50% deep or greater are candidates for surgery as well as those that worsen or fail to improve with appropriate medical therapy. Ruptured corneal ulcers may be able to seal and heal on their own with aggressive medical therapy but surgery is usually recommended. Surgical options for complicated ulcers include a conjunctival graft, corneoconjunctival transposition, corneal transplant, collagen or amnion graft.
Corneal Sequestrum
Sequestra may form in the corneas of cats due to chronic irritation (e.g. exposure, entropion, grid keratotomy) or due to FHV-1 infection. They may develop at the site of chronic corneal ulcers as well. Brown to black discoloration is present representing necrotic collagen. Though lesions may slough on their own, surgical removal via a superficial keratectomy is recommended to prevent inadvertent globe rupture. Use of topical lubricants long term may minimize the risk of recurrence or development in the opposite eye in predisposed cats.
Eosinophilic Keratitis
Eosinophilic keratitis is an immune-mediated disease which manifests as a pinkish-white superficial or proliferative lesion of the feline cornea due to blood vessel ingrowth and inflammatory cell infiltration. Lesions commonly start near the lateral or medial limbus but can progress to involve the entire cornea and cause blindness. It is typically nonpainful and may be unilateral or bilateral. Diagnosis is made by consistent clinical appearance and surface cytology, which shows eosinophils among other inflammatory cells. Treatment with topical ophthalmic dexamethasone sodium phosphate or prednisolone acetate QID followed by gradual decreasing and/or immunomodulating drugs (e.g. cyclosporine or tacrolimus) BID is generally effective at managing the disease, though long term low dose therapy may be needed to maintain control. For cats with corneal ulceration or steroid-induced FHV-1 issues, topical ophthalmic compounded megestrol acetate 0.5% can be used. Oral lysine 500 mg PO BID is a beneficial adjunctive therapy given the common association with FHV-1, and if recrudescence is noted during steroid therapy an antiviral should be used as well.
Uveitis
Intraocular inflammation in cats may manifest as anterior uveitis, chorioretinitis, or both (panuveitis). Causes include infectious diseases (FeLV, FIV, FIP, Toxoplasmosis, Cryptococcosis, Blastomycosis, Histoplasmosis, Bartonella, others?), immune mediated diseases (lymphocytic plasmacyctic uveitis, autoimmune diseases), neoplasia (lymphosarcoma, other ocular tumors), trauma, and other issues. Patients presenting with uveitis should have a complete ocular examination done to identify all abnormalities and help plan therapy. A complete physical exam and baseline labwork should be done to assess general health status and direct further testing. Specific etiologic agents can be tested for and additional diagnostic studies can be performed (lymph node aspirate with cytology, radiographs, ultrasound). Empiric therapy of the ocular disease includes topical ophthalmic prednisolone acetate QID, topical ophthalmic atropine
235

ointment SID-BID if appropriate, and systemic therapy which may include meloxicam, prednisolone, doxycycline, clindamycin, or antifungal therapy. Following clinical improvement, the topical steroid should be gradually decreased (e.g. every 1-2 weeks) but not discontinued completely until 2-4 weeks past the resolution of clinical signs.
Iris Melanoma
Diffuse iris melanoma is a potentially malignant ocular tumor in cats. Darkly pigmented spots that form on a cat’s iris should be monitored for progression to help distinguish between freckles, benign melanosis, and neoplasia. Early lesions may be treated with a diode laser to hopefully maintain a visual eye, but extensive change that is accompanied by a thick “dusted” iris surface, free pigment cells in the anterior chamber, impaired pupil shape/function, or secondary glaucoma warrants enucleation with the eye submitted for ocular histopathology.
Hypertensive Retinopathy
Systemic hypertension commonly affects older cats and ocular changes may be noted on fundic examination. Minor changes include a mottled cobblestone tapetal appearance, tortuous retinal blood vessels or small retinal hemorrhages while more severe changes include bullous retinal detachments and extensive intraocular hemorrhage. Clinical signs recognized by owners may include acute blindness and dilated pupils. Testing should be done to look for an underlying cause of the hypertension and to help guide therapy, but generally amlodipine 0.625 mg PO SID is used and increased as needed +/- other medications are added to achieve blood pressure control while monitoring renal values. If caught early and treated adequately detached retinas can reattach and cats can regain vision, but some degree of retinal degeneration will remain. Unfortunately, if chronic the prognosis for vision is guarded.
Toxic Retinal Degeneration
Enrofloxacin has been shown at high doses to cause acute retinal degeneration in cats. Doses less than 5 mg/kg/day are generally safe but owners of cats undergoing treatment should still monitor for dilated pupils or signs of vision loss and discontinue use immediately if noted. Recommended Veterinary Ophthalmology Textbooks:
• Slatter’s Fundamentals of Veterinary Ophthalmology, 6th edition. David J Maggs, Paul E Miller and Ron Ofri. Elsevier. 2017
236
Top 5 orthopedic pearls you need to know
By Courtney Campbell, DVM, DACVS-SA, VetSurg
The objectives of this lecture are to review less commonly discussed topics in clinical orthopedics. The focus of the lecture will include only a few key points on each topic. A full and comprehensive review of a basic orthopedic exam and orthopedic principles is beyond the scope of this lecture. The presentation will highlight and illustrate important points using a combination of photos and videos. The proceeding notes include only a few key points that will be discussed in more detail in the lecture #1 Neuropathic Exam Description: The presence of neuropathic pain is a common and often undiagnosed cause of lameness and pain in small animal patients. The recognition of radial and sciatic nerve pain syndromes is currently poor in clinical practice but continues to progress and evolve. The underlying causes, examination techniques, classic examination findings, diagnostic options and treatment protocols will be discussed with case examples. Introduction Neuropathic pain is poorly understood in human medicine and is grossly under recognized in veterinary medicine. This is an emerging field in both human and animals. To improve our recognition, study, and knowledge of this condition, evaluating for neuropathic pain syndromes has been standardized and consistently evaluated in all of our orthopedic exams at VetSurg. Neuropathic pain is defined as pain caused by a lesion or disease of the somatosensory system. This definition is deliberately broad because it represents a broad category of pain syndromes. The pain syndromes may encompass a wide variety of peripheral and central disorders. Clinically, neuropathic pain syndromes are characterized by the combination of positive and negative clinical findings. The positive clinical findings include pain, paresthesia, and dysesthesia. (e.g., tingling, numbness, pins and needles, ). Negative clinical findings may include neurological sensory deficits in the painful area. Dogs and cats may present with various combinations of symptoms including spontaneous pain, continuous or paroxysmal, and inappropriate evoked pain. (i.e. allodynia). The appropriate terminology to utilize when describing nerve dysfunction has been documented in canines and is helpful when learning about neuropathic syndromes and communicating clinical findings (Appendix 1, Moore 2016). The classic presentation of peripheral neuropathic pain in our practice includes painful peripheral neuropathies of the sciatic and radial nerve. However, lumbar or cervical foraminal radiculopathies, can also be relatively frequent causes of neuropathic pain It can be frustrating to evaluate a patient for pain and lameness, only to have an otherwise normal orthopedic exam. To help avoid overlooking the possibility of neuropathic pain, is important to evaluate every animal for the presence of paraspinal, sciatic and radial hyperpathia. It is important to understand that in cases of neuropathic pain, the nerve is hypersensitive to
237

palpation, can induce inappropriate neuromuscular activity, including painful muscle spasm, but the underlying cause of the nerve hypersensitivity development is frequently not primary nerve pathology. Nerve pain syndromes are often secondary to intervertebral disc disease, static and dynamic nerve foramen impingement, vertebral instability, recent surgery, trauma, abnormal conformation, abnormal gait and chronic joint pain. Sciatic Nerve Pain Syndrome (NPS): The sciatic nerve is the largest nerve in the pelvic limb, is responsible for flexing the stifle and extending the hock and is derived from the L5-S1 spinal nerves. The fibers unite to form a single nerve. The nerve travels along the medial aspect of the ilial shaft inside the pelvis and crosses over the ischium shaft caudal to the hip joint. The nerve travels down the posterior thigh between the hamstring muscles to the popliteal fossa directly caudal and slightly proximal to the stifle joint. The nerve divides at this point tinto the tibial nerve which innervates muscular structures caudal to the stifle and tibia and the peroneal nerve which innervates lateral and cranial to the stifle and tibia. To evaluate for sciatic pain/hypersensitivity of the right pelvic limb, place the left hand under the abdomen to support and help restrain the animal while standing. The patient’s right rear foot should have light contact with the floor but not be weight-bearing. This allows the hamstring muscles to relax and the sciatic tract to be more easily localized. The right hand is placed on the lateral thigh and the thumb is used to place pressure on the sciatic nerve tract. To place pressure directly on the nerve, the thumb must go between (and deep to) the biceps femoris and the semitendinosus muscle. Normal dogs will not react to the stimulus. Dogs who are hypersensitive to the nerves will react. The degree of response is subjectively assessed and documented as equivocal (+/-), mild (+), moderate (2+) or severe (3+). Radial Nerve Pain Syndrome (NPS): The radial nerve is the largest nerve in the thoracic limb, is responsible for extending the elbow, wrist and toes and is derived from the C6-T2 spinal nerves. Severe radial nerve damage is most frequently present when an animal appears significantly lame and is often dragging the front paw on the ground. However, the radial nerve can be affected by neuropathic syndromes as well. To evaluate for radial nerve hyperpathia, stand behind the animal and place the right hand on the right tricep. Palpate the long and lateral head of the triceps muscle and at the level of the greater tubercle palpate between the tricep muscle bellies directly behind the shoulder joint. You will use your thumb to apply moderate direct and continuous pressure to the nerve tract at this site. Normal animals do not react. Animals with radial nerve hypersensitivity will react sharply. The degree of response is subjectively assessed and documented as equivocal (+/-), mild (+), moderate (2+) or severe (3+). The cause of radial NPS varies from primary nerve pathology due to peripheral nerve sheath tumor, foraminal impingement due to chronic IVDD, chronic or acute cervical hypermobility, caudal cervical canal and foramen stenosis and secondary due to chronic pain and dysfunction of a thoracic limb anatomic area or joint (ex chronic elbow OA/DJD). Axial Skeleton Although it is difficult to distinguish the neuropathic pain component from vertebral articular joint degenerative disease pain, disc-related spinal pain and paraspinous muscle spasm it is highly
238
likely that there are components of neuropathic hypersensitivity present when examining the vertebral column. During pelvic limb exam it is wise to palpate the lumbar, lumbo-sacral and tail base area carefully for discomfort and pain. Digital pressure of the musculature on either side of the vertebral column, the vertebral column itself and some assessment of lumbar mobility can be helpful. Combining the findings of the lumbar exam with the sciatic nerve tract palpation allows a balanced assessment of spinal and nerve tract disorders. Although not prioritized in the examination for neuropathic pain it is important for the clinician to observe for the presence of ataxia on initial gait exam and test the patient’s conscious proprioception. If there are abnormalities in either of these areas a more complete neurological examination is warranted and recommended.
The cervical region can be evaluated for pain by taking the cervical spine through a range of motion and by applying direct digital pressure to the region. Palpation and mobilization of both the C1 and C6 vertebra is possible by utilizing the transverse processes of the individual vertebrae. The presence of pain when manipulating these vertebrae may be due to vertebral pathology, intervertebral disc disease or the presence of neuropathic pain.
Recording carefully the presence of vertebral pain, spinal muscle spasm and neuropathic tract pain allows an accurate medical record, provides a baseline and progressive assessment to be built with which to determine treatment efficacy and allows classification of a nerve pain syndrome (NPS) into a resolving, static or progressive disorder. The formulation of a examination, medication and rehabilitation program is essential to achieve success in managing neuropathic syndromes (Appendix 2, Holsworth 2019). The choice of medication, the dosage and frequency of medication vary (Appendix 3, Moore 2016) but good guidelines have been established (Moore SA, 2016) and with the addition of appropriate imaging and the use of corticoid epidurals in more severely or persistent sciatic NPS cases it is possible to treat and resolve many of the affected patients. In cases that are progressive, show significant neurological abnormalities or are refractory it will be necessary to consult a veterinary neurologist and often entertain the use of advanced cross-sectional imaging (contrast CT and/or MRI). Appendix 1, Moore 2016
239
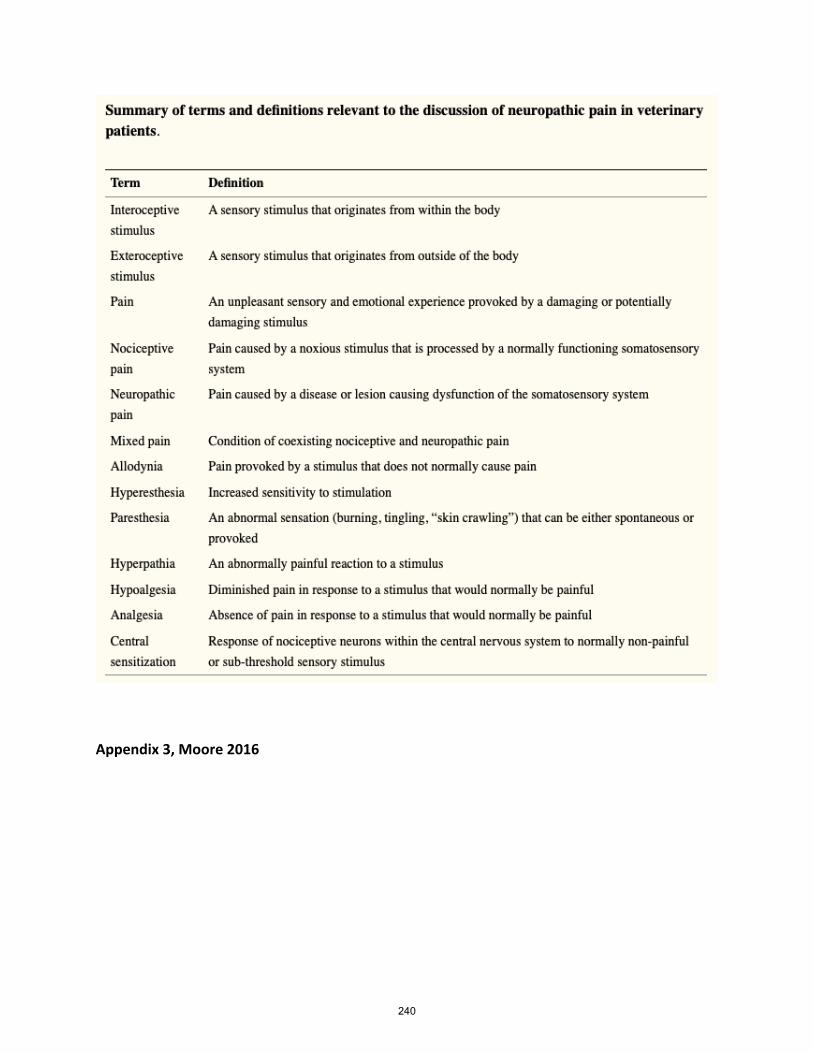
Appendix 3, Moore 2016
240
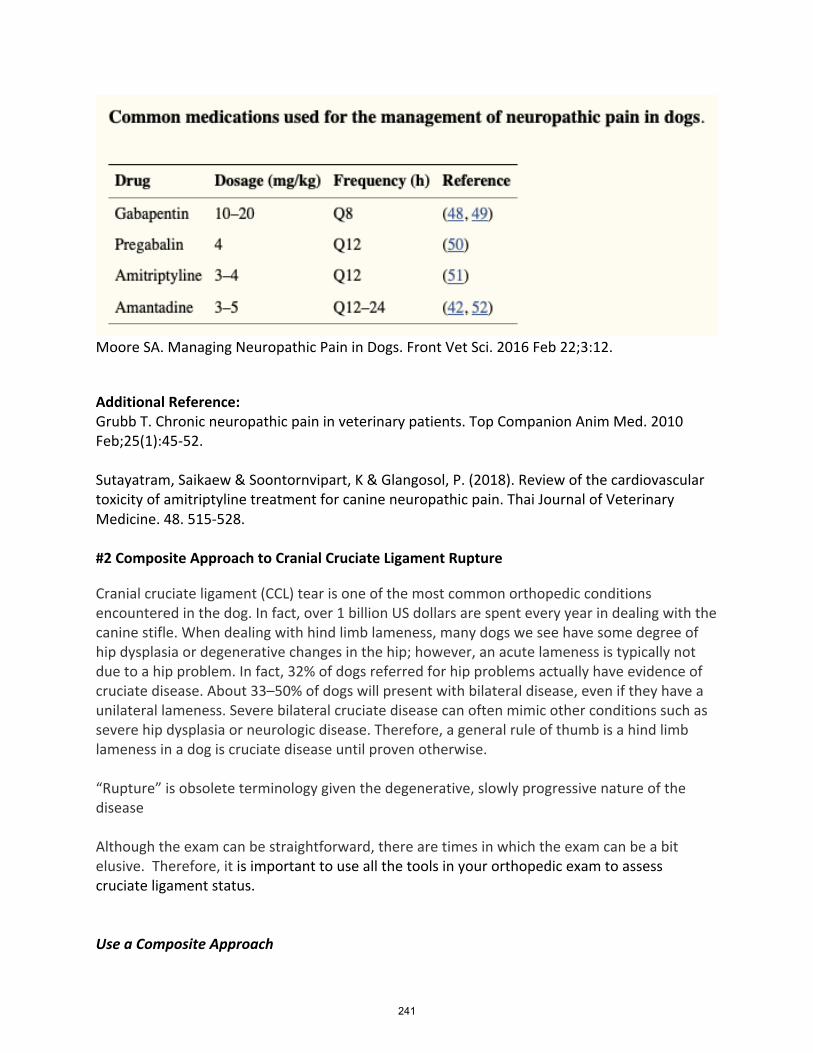
Moore SA. Managing Neuropathic Pain in Dogs. Front Vet Sci. 2016 Feb 22;3:12.
Additional Reference: Grubb T. Chronic neuropathic pain in veterinary patients. Top Companion Anim Med. 2010 Feb;25(1):45-52. Sutayatram, Saikaew & Soontornvipart, K & Glangosol, P. (2018). Review of the cardiovascular toxicity of amitriptyline treatment for canine neuropathic pain. Thai Journal of Veterinary Medicine. 48. 515-528. #2 Composite Approach to Cranial Cruciate Ligament Rupture
Cranial cruciate ligament (CCL) tear is one of the most common orthopedic conditions encountered in the dog. In fact, over 1 billion US dollars are spent every year in dealing with the canine stifle. When dealing with hind limb lameness, many dogs we see have some degree of hip dysplasia or degenerative changes in the hip; however, an acute lameness is typically not due to a hip problem. In fact, 32% of dogs referred for hip problems actually have evidence of cruciate disease. About 33–50% of dogs will present with bilateral disease, even if they have a unilateral lameness. Severe bilateral cruciate disease can often mimic other conditions such as severe hip dysplasia or neurologic disease. Therefore, a general rule of thumb is a hind limb lameness in a dog is cruciate disease until proven otherwise. “Rupture” is obsolete terminology given the degenerative, slowly progressive nature of the disease Although the exam can be straightforward, there are times in which the exam can be a bit elusive. Therefore, it is important to use all the tools in your orthopedic exam to assess cruciate ligament status. Use a Composite Approach
241
History: Usually a Pelvic Limb Lameness Effusion: Parapatellar Palpation (CCL rupture, septic arthritis, tick-borne disease, or immune-mediated arthritis, neoplasia) Cranial Drawer Test: Palpate in both Flexion and Extension.
The CCL has two bands, the craniomedial, which remains taut in both flexion and extension and the caudolateral, which is taut in extension but lax in flexion. For example, if the craniomedial band is torn and the caudolateral band is intact, cranial drawer is only present in flexion because in extension the caudolateral band is taut. If the caudolateral band is torn and the craniomedial band is intact, no cranial drawer is present because the craniomedial band is taut in both flexion and extension.
Positive Sit Test: Yes or No
Talar OCD These dogs may also display a positive “sit-test,” making talar OCD a differential diagnosis for cranial cruciate ligament disease
Crepitus: Typical with Chronic Tears. May see medial buttress Tibial Compression Test
Cranial tibial thrust is a test meant to mimic active weight bearing. The goal is to hold the stifle at a standing angle (approximately 135 degrees) and while holding the stifle still flex the hock. If the CCL is ruptured there should be a cranial displacement of the tibia. As with cranial drawers, tibial thrust should be checked in both flexion and extension.
Hyperextension Pain - The forgotten test
Pain on hyperextension is usually the forgotten test but is very reliable. Most affected dogs will exhibit some degree of pain.
Other Tests:
• Internal Rotation: o Although the rotational motion about the medial-lateral axis far exceeds the o motion about the other two axes, approximately 20° of varus valgus and
internal-external rotation occurs over an entire walking-gait cycle in normal dogs.
• Talar Hyperextension: o Additionally, tarsal hyperextension on the stance phase may be due to painful
conditions more proximal in the limb, such as cranial cruciate ligament rupture, hip dysplasia, or lumbosacral stenosis
Pitfalls in Diagnosis Cranial Drawer
• Bent wrists • Less assertive • Sliding skin
242
• Internal rotation • Failure to assess in range of motion
#3 The Benefit of Comparison Radiographs Radiographs of the axial and appendicular skeleton are frequently performed, and interpretation is often complicated by anatomic norm-variations as well as incidental findings that, in the majority of cases, are clinically insignificant. While cats are relatively standard, dogs come in all shapes and sizes with inherent variations that can be misinterpreted as disease unless recognized as normal. Additionally, variation in radiographic positioning leads to countless variations in the appearance of normal structures. Determining normal from abnormal is one of the most difficult, if not the most difficult, part of the radiographic interpretative process. Many dogs and cats have congenital, developmental, and degenerative changes that are insignificant clinically but apparent radiographically. Commonly, these variations or disorders are the result of the breeding selection of the past decades. This morphologic diversity in our companion animals has been commonly accepted as normal. Examples Demonstrating the Need for Comparison Radiographs
1. Growth Plate Evaluation Tibial Crest Avulsion Injuries
• Proximal tibial physis: The proximal tibial physis has several stages of ossification. For a relative long period of this ossification process, the tibial tuberosity will be isolated by growth cartilage from the proximal tibia. This finding should not be over interpreted as an avulsion fragment.
• In juvenile animals with open physes, it is important to give the contralateral (both views of both limbs), and always do individual images of each side, as identically positioned as possible and with the area of interest centered on the plate. If you can identify swelling or a focus of pain, indicate that and center on that location.
HOD vs Panosteitis • Hypertrophic osteodystrophy is a developmental, auto-
inflammatory disease of the bones that is usually first seen between the age of 3- 8 months; the condition becomes more infrequent after 5 months. Breed predilection is large breed dogs. There is no clear breed predilection and the true cause is unknown. Possible theories include abnormalities related to Vitamin D, calcium, and phosphorus metabolism. Vitamin C deficiency has also been theorized.
• Most lesion usually are located in the distal aspect of the radius, ulna and tibia but also seen in the proximal metaphyseal regions of these bones.
• Condition is usually bilaterally symmetrical. • History: painful walking or reluctance to move.
243
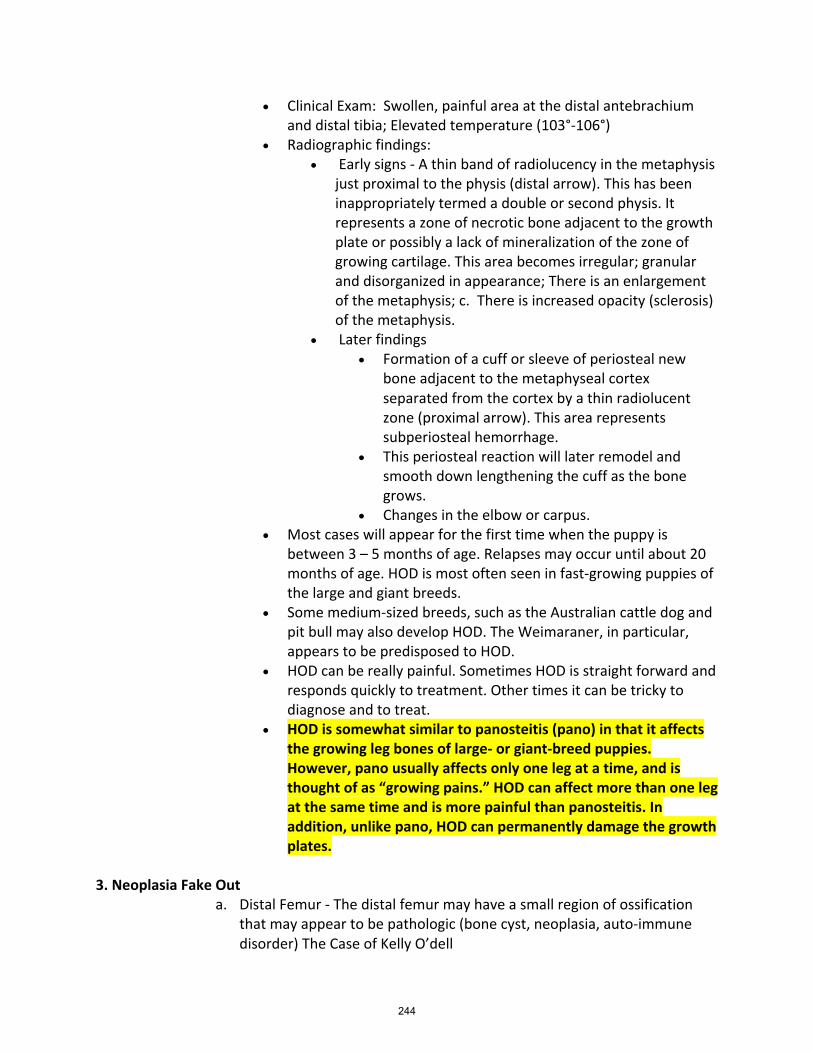
• Clinical Exam: Swollen, painful area at the distal antebrachium and distal tibia; Elevated temperature (103°-106°)
• Radiographic findings: • Early signs - A thin band of radiolucency in the metaphysis
just proximal to the physis (distal arrow). This has been inappropriately termed a double or second physis. It represents a zone of necrotic bone adjacent to the growth plate or possibly a lack of mineralization of the zone of growing cartilage. This area becomes irregular; granular and disorganized in appearance; There is an enlargement of the metaphysis; c. There is increased opacity (sclerosis) of the metaphysis.
• Later findings • Formation of a cuff or sleeve of periosteal new
bone adjacent to the metaphyseal cortex separated from the cortex by a thin radiolucent zone (proximal arrow). This area represents subperiosteal hemorrhage.
• This periosteal reaction will later remodel and smooth down lengthening the cuff as the bone grows.
• Changes in the elbow or carpus. • Most cases will appear for the first time when the puppy is
between 3 – 5 months of age. Relapses may occur until about 20 months of age. HOD is most often seen in fast-growing puppies of the large and giant breeds.
• Some medium-sized breeds, such as the Australian cattle dog and pit bull may also develop HOD. The Weimaraner, in particular, appears to be predisposed to HOD.
• HOD can be really painful. Sometimes HOD is straight forward and responds quickly to treatment. Other times it can be tricky to diagnose and to treat.
• HOD is somewhat similar to panosteitis (pano) in that it affects the growing leg bones of large- or giant-breed puppies. However, pano usually affects only one leg at a time, and is thought of as “growing pains.” HOD can affect more than one leg at the same time and is more painful than panosteitis. In addition, unlike pano, HOD can permanently damage the growth plates.
3. Neoplasia Fake Out
a. Distal Femur - The distal femur may have a small region of ossification that may appear to be pathologic (bone cyst, neoplasia, auto-immune disorder) The Case of Kelly O’dell
244
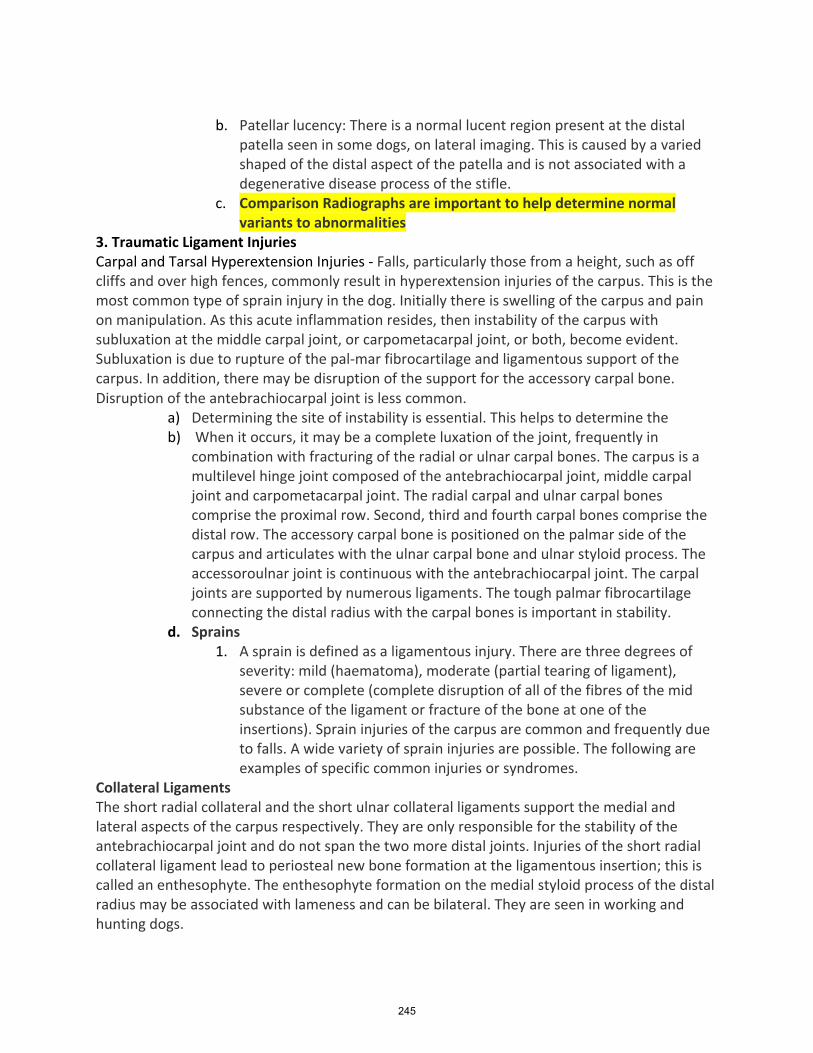
b. Patellar lucency: There is a normal lucent region present at the distal
patella seen in some dogs, on lateral imaging. This is caused by a varied shaped of the distal aspect of the patella and is not associated with a degenerative disease process of the stifle.
c. Comparison Radiographs are important to help determine normal variants to abnormalities
3. Traumatic Ligament Injuries Carpal and Tarsal Hyperextension Injuries - Falls, particularly those from a height, such as off cliffs and over high fences, commonly result in hyperextension injuries of the carpus. This is the most common type of sprain injury in the dog. Initially there is swelling of the carpus and pain on manipulation. As this acute inflammation resides, then instability of the carpus with subluxation at the middle carpal joint, or carpometacarpal joint, or both, become evident. Subluxation is due to rupture of the pal-mar fibrocartilage and ligamentous support of the carpus. In addition, there may be disruption of the support for the accessory carpal bone. Disruption of the antebrachiocarpal joint is less common.
a) Determining the site of instability is essential. This helps to determine the b) When it occurs, it may be a complete luxation of the joint, frequently in
combination with fracturing of the radial or ulnar carpal bones. The carpus is a multilevel hinge joint composed of the antebrachiocarpal joint, middle carpal joint and carpometacarpal joint. The radial carpal and ulnar carpal bones comprise the proximal row. Second, third and fourth carpal bones comprise the distal row. The accessory carpal bone is positioned on the palmar side of the carpus and articulates with the ulnar carpal bone and ulnar styloid process. The accessoroulnar joint is continuous with the antebrachiocarpal joint. The carpal joints are supported by numerous ligaments. The tough palmar fibrocartilage connecting the distal radius with the carpal bones is important in stability.
d. Sprains 1. A sprain is defined as a ligamentous injury. There are three degrees of
severity: mild (haematoma), moderate (partial tearing of ligament), severe or complete (complete disruption of all of the fibres of the mid substance of the ligament or fracture of the bone at one of the insertions). Sprain injuries of the carpus are common and frequently due to falls. A wide variety of sprain injuries are possible. The following are examples of specific common injuries or syndromes.
Collateral Ligaments The short radial collateral and the short ulnar collateral ligaments support the medial and lateral aspects of the carpus respectively. They are only responsible for the stability of the antebrachiocarpal joint and do not span the two more distal joints. Injuries of the short radial collateral ligament lead to periosteal new bone formation at the ligamentous insertion; this is called an enthesophyte. The enthesophyte formation on the medial styloid process of the distal radius may be associated with lameness and can be bilateral. They are seen in working and hunting dogs.
245
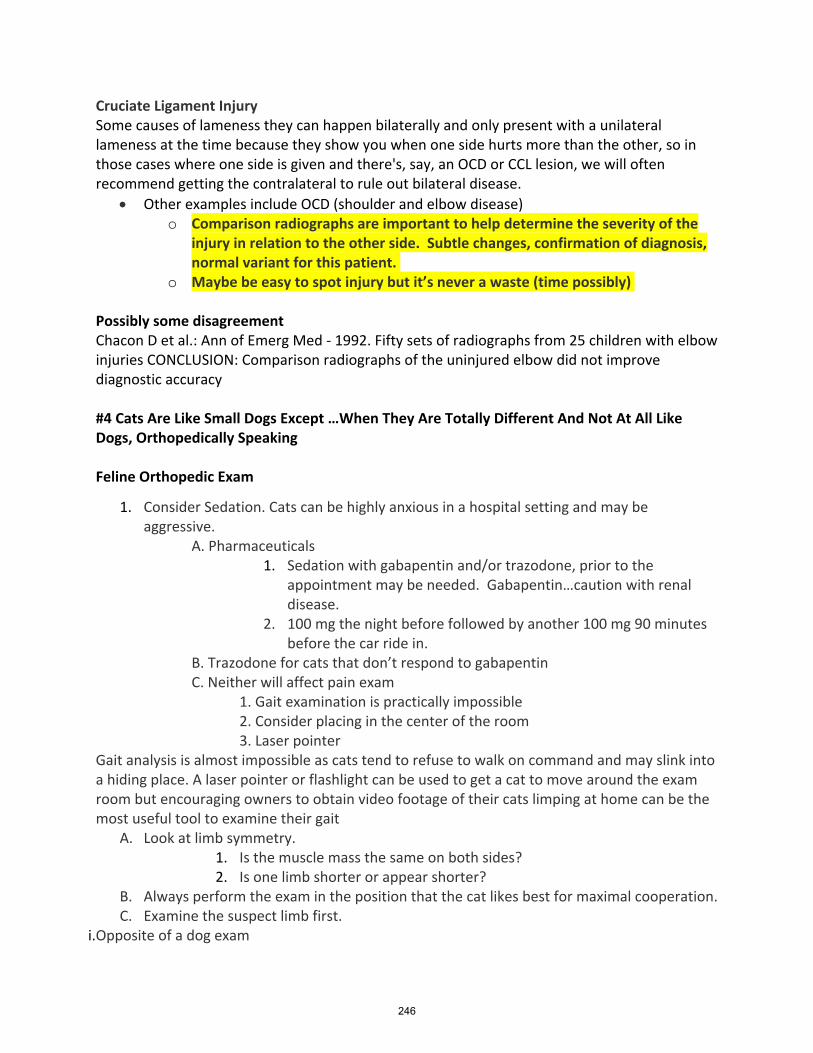
Cruciate Ligament Injury Some causes of lameness they can happen bilaterally and only present with a unilateral lameness at the time because they show you when one side hurts more than the other, so in those cases where one side is given and there's, say, an OCD or CCL lesion, we will often recommend getting the contralateral to rule out bilateral disease.
• Other examples include OCD (shoulder and elbow disease) o Comparison radiographs are important to help determine the severity of the
injury in relation to the other side. Subtle changes, confirmation of diagnosis, normal variant for this patient.
o Maybe be easy to spot injury but it’s never a waste (time possibly) Possibly some disagreement Chacon D et al.: Ann of Emerg Med - 1992. Fifty sets of radiographs from 25 children with elbow injuries CONCLUSION: Comparison radiographs of the uninjured elbow did not improve diagnostic accuracy #4 Cats Are Like Small Dogs Except …When They Are Totally Different And Not At All Like Dogs, Orthopedically Speaking Feline Orthopedic Exam
1. Consider Sedation. Cats can be highly anxious in a hospital setting and may be aggressive.
A. Pharmaceuticals 1. Sedation with gabapentin and/or trazodone, prior to the
appointment may be needed. Gabapentin…caution with renal disease.
2. 100 mg the night before followed by another 100 mg 90 minutes before the car ride in.
B. Trazodone for cats that don’t respond to gabapentin C. Neither will affect pain exam
1. Gait examination is practically impossible 2. Consider placing in the center of the room 3. Laser pointer
Gait analysis is almost impossible as cats tend to refuse to walk on command and may slink into a hiding place. A laser pointer or flashlight can be used to get a cat to move around the exam room but encouraging owners to obtain video footage of their cats limping at home can be the most useful tool to examine their gait
A. Look at limb symmetry. 1. Is the muscle mass the same on both sides? 2. Is one limb shorter or appear shorter?
B. Always perform the exam in the position that the cat likes best for maximal cooperation. C. Examine the suspect limb first.
i.Opposite of a dog exam
246
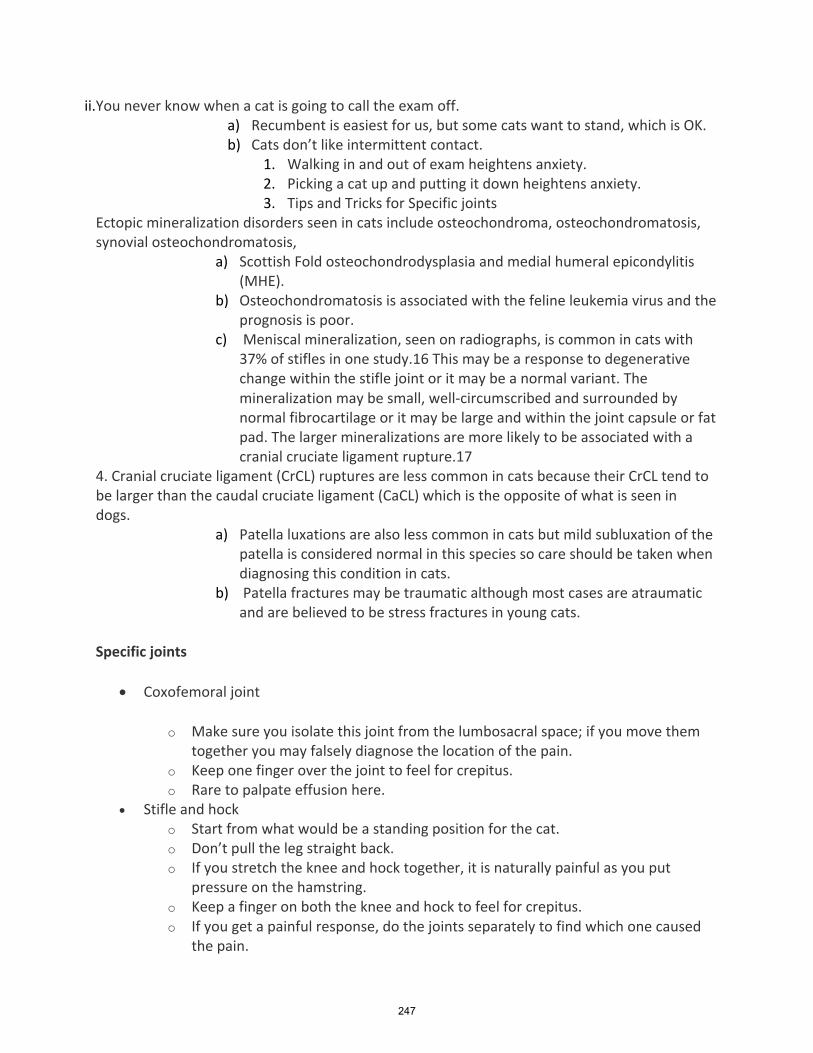
ii.You never know when a cat is going to call the exam off. a) Recumbent is easiest for us, but some cats want to stand, which is OK. b) Cats don’t like intermittent contact.
1. Walking in and out of exam heightens anxiety. 2. Picking a cat up and putting it down heightens anxiety. 3. Tips and Tricks for Specific joints
Ectopic mineralization disorders seen in cats include osteochondroma, osteochondromatosis, synovial osteochondromatosis,
a) Scottish Fold osteochondrodysplasia and medial humeral epicondylitis (MHE).
b) Osteochondromatosis is associated with the feline leukemia virus and the prognosis is poor.
c) Meniscal mineralization, seen on radiographs, is common in cats with 37% of stifles in one study.16 This may be a response to degenerative change within the stifle joint or it may be a normal variant. The mineralization may be small, well-circumscribed and surrounded by normal fibrocartilage or it may be large and within the joint capsule or fat pad. The larger mineralizations are more likely to be associated with a cranial cruciate ligament rupture.17
4. Cranial cruciate ligament (CrCL) ruptures are less common in cats because their CrCL tend to be larger than the caudal cruciate ligament (CaCL) which is the opposite of what is seen in dogs.
a) Patella luxations are also less common in cats but mild subluxation of the patella is considered normal in this species so care should be taken when diagnosing this condition in cats.
b) Patella fractures may be traumatic although most cases are atraumatic and are believed to be stress fractures in young cats.
Specific joints
• Coxofemoral joint
o Make sure you isolate this joint from the lumbosacral space; if you move them together you may falsely diagnose the location of the pain.
o Keep one finger over the joint to feel for crepitus. o Rare to palpate effusion here.
• Stifle and hock o Start from what would be a standing position for the cat. o Don’t pull the leg straight back. o If you stretch the knee and hock together, it is naturally painful as you put
pressure on the hamstring. o Keep a finger on both the knee and hock to feel for crepitus. o If you get a painful response, do the joints separately to find which one caused
the pain.
247
• Elbow o Refresh your memory on normal elbow anatomy as it can be a bit confusing;
many veterinarians just put their hands on the condyles instead of the joint as they manipulate it.
o Palpate for effusion, usually on the medial side. o Look at a lot of normal elbows so you know effusion when you feel it. o Keep the carpus flexed for maximum extension of the elbow. o Feel for crepitus. o Look for limited flexion, which is common in elbow OA. In normal cats or with
mild OA, you should not be able to get your finger between the brachium and antebrachium when flexed. OA cats may not have complete flexion and your finger will fit in.
• Shoulder o Confusing to locate in obese cats o Many times, we think we are extending the shoulder, but we are just mostly
moving the scapula around. o Isolate the scapula by holding it on its cranial edge while moving the shoulder.
• Lumbosacral space o Easiest to do with cat standing. o Don’t push on the space, all cats will move away from the pressure. o Pick up back legs/pelvis. o Flex with back legs off of table.
• Other joints o These were special tips for the major joints. o Look at the rest of spine; carpal, tarsal and toe joints; mandibular pain; tail pain.
#5 Can I Splint That? The Five Type of Fractures that You Don’t Want to Splint Introduction External coaptation (casts and splints) can be used successfully to treat some fractures. Case selection is of primary importance and indiscriminate use of external coaptation can lead to poorly healing fractures. After the appropriate case has been selected then there are the technical aspects of splint and cast application that are equally as important. The technique needs to be exact and the casts should be meticulously managed. The technical aspects of cast management are beyond the scope of this discussion but today I would like to talk about case selection. Can I splint that fracture is a question that is commonly pondered in veterinary hospitals when considering conservative treatment for fracture repair? Fractures amenable to an external coaptation and those who will have the highest success may be different. A clinician should select cases with a very high probability of achieving union in a relatively short period of time. One does not want to select cases that have a low probability of achieving union for obvious reasons including cast or splint morbidity, time, pain, delayed healing, nonunion, cost, among
248
other factors. Further, when using external coaptation for managing fractures there is essentially a race between achieving union and suffering a complication associated with the use of external coaptation. Hence, ideal cases are those in which union can be achieved before complications arise. In addition, there are consequences to prolonged immobilization of joints, making external coaptation undesirable in cases in which fracture stabilization would be needed for a long time. In trying to select optimal cases I recommend considering 3 general factors:
D. Patient characteristics E. Fracture characteristics F. Owner characteristics
Fracture Characteristics Several fracture characteristics have to be considered.
G. Anatomic location: Basic guidelines for managing fractures with external coaptation dictate that the joint proximal to and distal to the fracture need to be stabilized. Therefore, in all practicality the only long-bone fractures that are readily managed with external coaptation are below the elbow and below the stifle. Fractures of the humerus and femur should not be managed with external coaptation because it is extremely difficult to adequately immobilize the shoulder or hip joint with spica splints.
H. Energy associated with the fracture and the degree of soft tissue damage: Fractures that have occurred secondary to low energy trauma tend to have less soft tissue injury and heal more rapidly. An example might be a spiral tibial fracture suffered when a dog had its limb caught in a fence. Conversely, fractures associated with high energy trauma and with extensive soft tissue trauma, such as injuries suffered with vehicular trauma, tend to heal more slowly and are less suitable to management with external coaptation.
I. Fracture stability: Fractures with poor inherent stability are clearly poor choices for management with external coaptation. Examples of such fractures include highly comminuted fractures in which the fracture gap may collapse. Interestingly, and counterintuitively, perfectly clean transverse fractures can also be mechanically unstable in terms of rotational forces. Since external coaptation cannot counteract rotation these fractures are better stabilized with surgery. The exception to this is if there are interdigitating fragments at the fracture line that can 'lock' into one another and prevent rotation of the fracture segments inside the cast. On the opposite end of the spectrum are fractures that have good inherent stability. One relatively obvious example includes fractures in which just one cortex of a bone is fractured. These can include greenstick fractures and can also occasionally include skeletally mature animals. Similarly, the minimally displaced spiral tibia fracture discussed above can be relatively stable, particularly if the fibula remains intact and provides an additional mechanical support. Lastly, if just one bone in a limb segment that has multiple bones is fractured (e.g., the ulna but the radius is intact, the tibia but the fibula is intact, one metacarpal) these cases are amenable to external coaptation.
249
J. Degree of fracture reduction and load sharing: Fractures in which the two fracture segments are greatly displaced, and alignment and/or apposition is poor and cannot be made acceptable should be treated with surgery. This is because the fracture needs to be appropriately reduced so that a malunion is avoided. In addition, if a fracture is not reduced such that load can be transmitted effectively across the fracture line the fracture gap may collapse.
K. Skin integrity: If there is sufficient trauma to the skin such that bandaging and wound care is needed then external coaptation is not desirable. When one removes the splint or cast to treat the skin or wounds the fracture is unsupported. Fracture alignment and apposition can change while the fracture is unsupported. It is more desirable to stabilize such fractures surgically in a way that facilitates wound management.
L. Location within the bone: Because of the way external coaptation functions to provide stability, external coaptation cannot provide much stability to small fracture segments. Accordingly, fractures that are mid-diaphyseal are more amenable to casting than fractures that are closer to a joint. For example, proximal tibial metaphyseal fractures are not a good choice for fracture management because the small proximal fracture segment is not well stabilized.
Special Types of Fractures
• Juxta-articular Fractures • Ulnar Styloid process - • Radius/Ulna Fractures - high rate of nonunion with external coaptaton • Articular Fractures - Require meticulous anatomic reconstruction • Chrondrodystrophic Legs - Confirmation makes splinting difficult.
6 Types of fractures that might be amenable to closed fixation
o Greenstick o Longbone fractures o Impaction fractures o Closed fractures below elbow/stifle o Type A or B Fractures o Rapidly healing fractures o Minimally displaced fractures with the adjacent bone remaining intact
§ (i.e. spiral tibia fracture discussed above can be relatively stable, if the fibula remains intact and provides additional mechanical support)
§ Just one bone in a limb segment that has multiple bones is fractured (e.g., the ulna but the radius is intact, the tibia but the fibula is intact, one metacarpal) these cases are amenable to external coaptation.
250
Distal extremity injuries – sprain or worse of the achilles complex? David Dycus, DVM, MS, CCRP, DACVS-SA Chief of Orthopedic Surgery,Nexus Veterinary Bone & Joint Center Medical Director, Nexus Veterinary Specialists Learner Objectives: -Recognize how to approach patients with distal extremity injuries -Define how to determine the difference between a partial or complete Achilles injury as well as SDF luxations -Appreciate new diagnostic modalities and treatment options for patients with distal extremity injuries Distal extremity injuries (distal to the stifle) can be a common source of hind limb lameness. In the canine Achilles injuries, superficial digital flexor tendon luxation, and collateral ligament injuries are the most common, while in the feline collateral ligament injuries occur more frequently. Part of the problem with some of these injuries is defining the extent of damage to the tissues as well as deciding if conservative or surgical management is needed for optimal outcome. Superficial digital flexor tendon luxation (SDF): The superficial digital flexor (SDF) tendon is a portion of the common calcanean tendon (Achilles tendon). It originates on the lateral supracondylar tuberosity of the femur and inserts onto the lateral and medial surfaces of the calcaneus; it then continues on to the phalanges to allow for digital flexion. There is a bursa (calcaneal bursa) that lies deep to the SDF at the level of the tuber calcaneus as well as a retinaculum on both the medial and lateral aspects. SDF luxation is associated with vigorous activity and may be caused by rotational forces directly to the tendon where it is crossing the calcaneus. Such rotational forces are noted during agility training and competing as well as during backyard activities for the companion. This can result in disruption to the retinaculum leading to either a lateral or medial luxation; with a lateral luxation being the most common (likely due to the under development of the medial retinaculum). Once luxated, the tearing and fibrosis of the retinaculum can lead to a secondary bursitis. In addition to rotational forces leading to an SDF luxation, certain breeds such as Shelties and Collies are commonly affected, which suggest a possible hereditary basis. Obesity and confirmation have been noted to be contributing factors as well. Patients presenting with an SDF luxation may have an intermittent to continuous low-grade limp. In some situations, the lameness may have been extreme at the onset of the injury, and then may have improved to only stiffness or soreness especially in the canine athlete or working dog. SDF luxation is commonly noted in younger dogs (less than 1.5 years); however, I have seen this injury in older dogs. Upon examination there may be a
251
“popping” sensation noted as the hock is placed through range of motion (ROM), especially during flexion with either internal or external rotation. There may be swelling noted on either side of the calcaneus with discomfort on palpation. In cases where there is a bursitis there may be a large soft swelling noted over the tuber calcaneus. The diagnosis can further be aided by radiographs, which may show swelling in the region of the calcaneus. I find that radiographs may help rule out other conditions but are not very helpful in diagnosing an SDF luxation. Diagnostic musculoskeletal ultrasound (MSK US) can be an asset in diagnosing an SDF luxation. MSK US will allow the identification of the direction of the luxation as well as if the retinaculum is torn or severely stretched. True SDF luxations are a surgical disease with a very good prognosis. The torn retinaculum is identified, and then large non-absorbable suture is used to repair the retinaculum. Following this the hock is immobilized for a period of about 2-4 weeks. Once the hock is no longer immobilized formal rehabilitation therapy is instituted with a focus on improving ROM as well as static and dynamic therapeutic exercises to regain strength in the operated limb. A 6% recurrence rate has been reported. Achilles tendon injuries: An Achilles tendon injury can be a catastrophic career ending injury in both the canine athlete and working dog. In the companion it can result in a decreased quality of life. The Achilles tendon (Common Calcaneal tendon) is made up of three components: the gastrocnemius tendon, common tendon (combined tendons of the biceps femoris, gracilis, and semitendinosus), and the SDF tendon. The blood flow varies throughout the tendon; however, the mid-body has the poorest blood supply. In addition, there are five avascular fibrocartilaginous zones in the distal tendon. Injuries can occur from lacerations to the tendon even without any overt skin trauma. However, more commonly avulsion of the gastrocnemius and/or common tendon from its insertion is seen. The injury is noted after heavy activity in mature dogs (Labrador Retrievers and Doberman Pinschers are noted to be overrepresented). While a degenerative process is suspected, there is no definitive proof that this is the cause. The damage tends to occur in the area of the fibrocartilaginous zones (i.e. in the distal portion) where there is thought to be increased areas of loading and stress. Patients with an Achilles tendon injury may present with an acute non-weight bearing lameness if the injury is acute. In more chronic presentations patients may be weight bearing lame and plantigrade at the stance. If the SDF is intact there will be flexion of the digits associated with the plantigrade stance. Most cases will present with swelling/thickening of the Achilles complex. There is excessive hock flexion with the stifle extended upon palpation. Manipulation of the hock and Achilles tendon may or may not result in pain or discomfort. Radiographs much like with an SDF luxation can help to rule out other disease conditions; however, radiographs are not very helpful in identifying the degree of injury. There may be soft tissue swelling with calcification and periosteal reaction to the calcaneus. MRI can be used to aid in the diagnosis; however, I
252
find that MSK US is helpful in identifying the degree of injury (complete versus partial tear), where the tendon(s) is torn, and the degree of fibrous tissue. Personally, I think that MSK US is more sensitive and specific than our orthopedic examination in differentiating complete from partial tears. The findings on MSK US can help dictate treatment options. Acute lacerations of the Achilles tendon should be surgically repaired by debriding the torn ends and primarily suturing the ends back to together. This is then followed up with immobilization of the hock in a relative extended position. For “degenerative” tears I will base my decision making on the MSK US. For grade 1 strains (stretched fibers with an inflammatory response but no evidence of tearing) I will immobilize the hock with a semi-custom tarsal wrap (DogLeggs, www.dogleggs.com) with or without the addition of thermoplast. The period of immobilization will be for about 6-8 weeks. During this period patients undergo formal rehabilitation therapy. For grade 2 strains (damaged fibers with evidence of partial tearing) I will immobilize the hock with either a semi-custom tarsal wrap with thermoplast or a custom tarsal brace (available through many different manufacturers) in addition to formal rehabilitation therapy. To help with augmenting the healing response regenerative medicine (platelet rich plasma and/or stem cell) can be considered. This is performed by injections via ultrasound guidance into the damaged portion of the tendon. Grade 3 strains (complete fiber disruption) likely need surgical intervention for the best chance of success. Conservative management of a grade 3 Achiles injury will result in lifelong need of some form of support (tarsal wrap or tarsal brace). There are numerous surgical techniques described such as removal of fibrous tissue and attempting to suture the primary ends together or using suture patterns to imbricate the tendon and fibrous tissue. In cases with more than 1 cm of fibrous tissue this proves challenging. Alternatively, I prefer to use fresh frozen canine allografts to provide scaffolding over the fibrous tissue or over the primary repair as an on-lay graft. This is then augmented with platelet rich plasma (PRP). Following surgical intervention the hock is rigidly immobilization (brace, splint, cast, or trans-articular external skeletal fixator) for approximately 6-8 weeks. After this 6-8 week period I then allow slight loading of the tendon with either a custom controlled range of motion brace or a hinged trans-articular external skeletal fixator or a tarsal wrap with thermoplast. The goal is to allow slow loading and range of motion over time to stimulate healing of the tendon, but not so much stress that it causes damage to the surgical repair. A formal rehabilitation program is essential to promote tendon healing and allow slowly progressive loading. The recovery time is generally very long and I would expect the entire healing process to be successful to take 6 months to 1 year. The prognosis can be good despite the lack of normal tendon architecture. References -Dyce KM, Sack WO, Wensing CJG. The locomotor apparatus. In: Textbook of Veterinary Anatomy, 2nd ed. Philadelphia, PA: WB Saunders; 31-98, 1996.
253
-Lotsikas PJ, Lotsikas FM, Hummel D, et al. Disorders of the pelvic limb: diagnosis and treatment. In: Canine Sports Medicine and Rehabilitation, 2nd ed. Hoboken NJ: Wiley Blackwell; 353-388, 2018. -Gamble LJ, Canapp DA, Canapp SO. Evaluation of Achilles tendon injuries with findings from diagnostic musculoskeletal ultrasound in canines: 43 cases. Veterinary Evidence, doi: http://dx.doi.org/10.18849/ve.v2i3.92, 2017.
254
It’s a puppy, what could possibly go wrong? Developmental orthopedic conditions By David Dycus, DVM, MS, CCRP, DACVS-SA Chief of Orthopedic Surgery, Nexus Veterinary Bone & Joint Center Medical Director, Nexus Veterinary Specialists Learning Objectives: -Recognize how to approach developing dogs with developmental orthopedic problems -Define the different developmental orthopedic problems -Recognize the differences between the developmental orthopedic problems -Understand the diagnostic and treatment approaches to patients with developmental orthopedic problems Developmental orthopedic diseases (DOD) are those, which are identified during postnatal skeletal growth. The common DOD discussed here are hypertrophic osteodystrophy (HOD), panosteitis, craniomandibular osteopathy, retained ulnar cartilaginous cores, Legg-Calve-Perthes disease, and osteochondrosis/osteochondritis dessecans (OCD). While elbow dysplasia and hip dysplasia are a type of DOD disease they are covered elsewhere. Hypertrophic Osteodystrophy (HOD) A DOD in young, rapidly growing dogs also referred to as metaphyseal osteopathy, skeletal scurvy, juvenile scurvy, infantile scurvy, Moller Barlow’s disease, and osteodystrophy II. The incidence is roughly 2.8/100,000 with patients presenting between 2 and 6 months of age. HOD is predominantly seen in large and giant breed dogs. Great Danes, Chesapeake Bay Retrievers, Irish Setters, Boxers, German Shepherd, Golden Retrievers, Labrador Retrievers, and Weimaraners are at an increased risk with males 2.3 times more likely to develop HOD than females. There are numerous proposed causes such as vitamin C deficiency, over nutrition, heritability, infections, and vaccines; however, no single cause has been determined. More recent studies have refuted the vitamin C and over nutrition theories. Heritability has been suggested for at risk breeds and has been shown in a family of Weimaraners. Infection is thought because many of the patients have a history of systemic illness with the addition of leukocytosis, although in most studies an infectious process has not been identified. One study did document an association with HOD and canine distemper virus; however, a large multi-institutional study did not support a link between HOD and canine distemper. Diagnosis of HOD is based on signalment, history, clinical signs, and radiographs. The distal radius, ulna, and tibia are the most commonly affected bones. Clinical signs include swelling of the metaphyseal region of the bone and the lesions are often bilateral. The swelling may be warm upon palpation with varying degrees of pain and lameness (from mildly lame to a having a reluctance to want to walk. Some patients may
255

exhibit systemic signs of illness such as hyperthermia, depression, inappetence, anorexia, and diarrhea. The pathognomonic radiographic sign is a lucent line in the metaphysis parallel to a narrow zone of increased radiodensity just adjacent to the physis (the so called “double physeal line”). There can be varying degrees of periosteal and endosteal proliferation. Differential diagnosis includes secondary nutritional hyperparathyroidism, septic polyarthritis, retained cartilaginous cores, and hypertrophic osteopathy. In the majority of cases HOD is self-limiting within days to weeks but can persist for months. The prognosis is typically good to excellent; however, in very severe cases death has been reported. For mild cases, analgesics along with a balanced diet should be provided. In more severe cases supportive treatment may be needed especially if the patient is reluctant to eat. Furthermore, owners should be warned about the possibly of angular limb deformity in severe cases. In Weimaraners specifically with severe HOD without bacteremia may respond better to corticosteroids than to NSAIDS.1 Panosteitis Panosteitis is a self-limiting inflammatory disease of the bone marrow of long bones. It is sometimes referred to as enostosis, eosinophilic panosteitis, and shifting leg lameness with an incidence of about 2.6/1000 patients. Breeds that are at an increased risk or Airedale Terriers, Irish Setters, German Shorthair Pointers, Doberman Pinschers, Afghans, Great Danes, Saint Bernard’s, Bernese Mountain Dogs, Newfoundland’s, Mastiffs, Bassett Hounds, Rottweiler’s, Cocker Spaniels, Golden Retrievers, Labrador Retrievers, and German Shepherds. Given the list of pre-disposed breeds panosteitis is primarily a disease of large to giant breed dogs; however, it has been reported in small breed dogs. Age at presentation is typically between 5-12 months of age but up to 2 years of age has been noted. Males are affected more than females with a ratio of 4:1. Histologically, the first changes noted consist of empty spaces in the adipose bone marrow, vascular proliferation with local bone formation around the nutrient foramen. These changes are thought to lead to vascular congestion and secondary increases in intraosseous pressure. The exact origin and etiology is still unknown. Much like HOD the diagnosis is derived from the signalment, history, and clinical signs along with radiographs. The hallmark clinical sign is a shifting leg lameness with pain on palpation of affected long bones. The degree of the lameness and pain can be variable from mild to inability to walk. Typically, the owner will report an acute lameness with no history of trauma. The most commonly affected bone is the ulna (42%), followed by the radius (25%), humerus (14%), femur (11%), and tibia (8%). Radiographs are helpful to differentiate panosteitis from other conditions (such as HOD, OCD, etc.). The appearance on radiographs will depend on the stage of the disease. In the early stage of disease radiographs may be normal or have a decrease in radiodensity in the medullary cavity near the nutrient foramen. As the disease progresses, the increase in medullary opacity will develop a granular pattern with loss of normal trabecular pattern. Other
256

findings include periosteal bone formation. After 4-6 weeks the densities will regress leaving a trabecular pattern that is coarser than normal. Treatment consists of rest and analgesics; however, treatment does not influence the outcome. Recurrence is possible, but the severity will decrease over time as the dog matures. Craniomandibular Osteopathy Craniomandibular Osteopathy is also known as craniomandibular osteoarthropathy, craniomandibular osteodystrophy, mandibular periostitis, lion jaw, Westie jaw, and Scotty jaw with an incidence reported as 1.4/100,000 cases. There is no reported sex predisposition; however, puppies less than 6 months of age are at the highest risk. The incidence is reported to decrease with age. West Highland White Terriers and Scottish Terriers are at an increased risk; other breeds reported to be affected are Boxers, Labrador Retrievers, Great Danes, Boston Terriers, Great Danes, and German Shepherd’s. Given the strong breed predisposition in West Highland White Terriers, a heritable etiology has been suggested, and an autosomal recessive mode of inheritance has been demonstrated in this breed. The disease is characterized by either unilateral or bilateral symmetric irregular osseous proliferations of mainly the mandible, but the tympanic bullae can also be affected. Osteoclastic resorption of lamellar bone occurs, which is followed by the presence of primitive bone that will expand beyond the periosteum. The bone is replaced by a fibrous-type stroma and inflammatory cells invade the border of the lesion destroying adjacent connective tissue and muscle. Clinical signs will vary from minor difficulty eating and chewing to complete inability to open the mouth and thus the inability to eat or drink. Because of the lack of nutrition additional clinical signs include weight loss, salivation, depression, and pain while eating. Physical examination will reveal enlargement or irregularity of the mandibles. The patient’s mouth may be able to be opened only partially or not at all, and the teeth are unaffected. Often times blood work and urinalysis are unremarkable. Radiographs will demonstrate bony proliferation of the mandible and/or bullae. CT can be useful to identify lesions and to better delineate the areas affected. It can be self-limiting when the dog is 11-13 months of age; however, patients may need varying levels of supportive care such as feeding soft food/gruel, syringe feeding, or placing a feeding tube. Nutrition and hydration are key parameters to monitor. Given the pain involved with trying to open or close the mouth analgesics are indicated. Over time the bony proliferations will regress completely or partially. Surgical excision of the proliferation is not recommended due to the recurrence within 3 weeks. Rostral hemimandibulectomy has been reported for a severe case that facilitated lapping of food.2 Euthanasia has been performed for patients with uncontrollable discomfort or with lesions that do not resolve and affect quality of life.
257
Retained Ulnar Cartilaginous Cores Also known as retained endochondrial cartilage cores, this is a cone of growth plate cartilage that projects from the distal ulnar growth plate into the distal metaphysis. Histologically, the retained cartilaginous core consists of viable hypertrophic chondrocytes. It is essentially failure of the growth plate cartilage to convert to metaphyseal bone, while some consider it a growth plate manifestation of osteochondrosis. Like most DOD it occurs predominately in large to giant breed dogs. If the retained ulnar cartilaginous core is associated with reduced ulnar length then changes similar to premature closure of the distal ulnar growth plate are noted. These changes consist of cranial bowing of the radius, external rotation, and valgus deviation of the paw; additional subluxation of the carpus and elbow may be seen. Radiographs are mainstay for the diagnosis, where a radiolucent core (typically triangle in shape) of cartilage is noted in the distal ulnar metaphysis. There may be an area of sclerosis surrounding the area. The core may extend up to 3-4 mm into the metaphysis. This must be differentiated from premature closure of the distal ulnar growth plate. No correlation has been noted between the size of the lesion, histopathology and severity of deformity. Treatment is based off the degree of deformity. If no deformity is noted then no treatment is recommended, and the core may disappear spontaneously. In these cases, it is recommended to closely monitor patients for the development of deformities, especially of the carpus and elbow. In cases with moderate to marked deformity the surgical correction of the deformity may be required. Legg-Calve Perthes Disease Avascular necrosis of the femoral head is noted as a noninflammatory localized ischemia of the femoral head and neck, which results in deformation of the femoral head and neck leading to a pelvic limb lameness. It has also been referred to as aseptic necrosis of the femoral head, coxa plana, osteochondrosis, and osteochondritis coxae juvenilis. Small breed dogs are the most commonly affected with toy breeds and Terriers predisposed. Initially, the disease is histologically characterized by necrosis of the trabeculae of the femoral head, followed next by the fragmentation phase where loading of the affected hip causes collapse of the epiphysis and secondary thickening and cleft formation of the articular surface. Osteochondrosis/osteochondritis Dessecans (OCD) In short OCD is a disturbance of endochondrial ossification. There is failure of the cartilage matrix calcification and vascular ingrowth, which results in cartilage retention. The cartilage retention results in thickening of the articular epiphyseal cartilage. There are two distinct areas of osteochondrosis: the growth plate-epiphyseal complex (GEC), and the articular-epiphyseal complex (AEC). Proposed causes of osteochondrosis include
258
genetics (especially with large and giant breed dogs), rapid growth, calcium supplementation, hormonal influences, ischemia and trauma. The incidence of AEC osteochondrosis is 8.1/1000 patients with male dogs more affected than female dogs with a typical age at presentation of 4-9 months. Proposed mechanisms for the pathogenesis of AEC osteochondrosis is it is a result of generalized disease; however, this does not adequately address the species and site-specific nature of osteochondrosis. The other proposed mechanism is it starts as a focal disease from vascular trauma and subsequent necrosis of the subchondral bone or necrosis of the epiphyseal cartilage canals. This necrosis may possibly lead to cartilage ischemia and necrosis. The necrosis may occur at a development stage when the vessels from the perichondrium are being replaced by vessels from the adjacent epiphyseal bone marrow. As this is occurring the vessels are susceptible to damage by conformational forces and/or microtrauma. If the vessels become damaged and thus necrotic then a cartilaginous infarct develops, which prevents endochondrial ossification. Osteochondrosis latens is used to describe the initial cartilage necrosis, at this stage the disease process can be resolved or progress to osteochondrosis manifesta where larger areas of necrotic cartilage resists vascular invasion. This will then persist during growth and can be detectable. If the overlying articular cartilage fissures or fractures (thus developing a flap) then the commonly known osteochondrosis/osteochondritis dissecans (OCD) lesion develops. The most commonly affected joint is the shoulder, followed by the elbow, tarsus, and stifle. The caudocentral or caudomedial aspect of the shoulder is affected the most commonly and it is bilateral in 27-68% patients, while the lesions of the medial aspect of the humeral condyle are common areas affected in the humerus; 96% of lesions in the stifle affect the medial femoral condyle, and in the talus the medial or lateral trochlear ridge is affected. Clinical signs associated with osteochondrosis typically become apparent when a cartilage flap (OCD) develops. One theory is the motion between the flap and the subchondral bone, or the altered loading may provoke pain. If the flap detaches it can become what is known as a “joint mouse”, which may further contribute to synovitis and OA progression. Patients tend to present from 4-9 months of age with a compliant of lameness or exercise intolerance. Many cases will show signs of a unilateral lameness; however, the disease is commonly noted bilaterally so careful examination of the contralateral joint in warranted. Once a patient presents with clinical signs of a lameness the OCD lesion is considered chronic and a defect in the subchondral bone is well developed. Radiographs are a sensitive diagnostic method that may demonstrate disruption of the subchondral bone with flattening or concavity of the normal contour. Sclerotic margins may be seen around the defect. Contrast arthrograms can be used to demonstrate unmineralized cartilage flaps and joint mice, effusion, and new bone
259

formation. CT is also useful in demonstrating an OCD lesion. Arthroscopy is useful as both a diagnostic and therapeutic modality. Aims of treatment need to include elimination of pain and lameness, restoration of the cartilage surface with tissue of similar nature to the native tissue, normalization of joint biomechanics, and prevention of further joint degeneration. Conservative management may be recommended with small subchondral lesions and when the patient is mildly lame or asymptomatic. This form of treatment is only recommended for dogs younger than 6 months of age. Conservative management consists of NSAIDS, exercise restriction, chondroproctants, rehabilitation therapy, and weight control. Persistence of clinical signs suggests the patient should be treated with a surgical approach. Surgical management consists of either an arthrotomy or arthroscopy (the authors preferred method). Surgical treatment consists of flap excision and joint mouse removal. Additional treatment may consist of removing peripheral cartilage that is not firmly adhered and stimulation of fibrocartilage to the underlying subchondral bed. OCD of the shoulder usually carries a good to excellent prognosis; however, other joints affected with OCD carry a guarded prognosis with continued progression of OA and an intermittent lameness. References: 1. Abeles V, Harrus S, Angles JM, et al: Hypertrophic osteodystrophy in six Weimaraner puppies associated with systemic signs. Vet Rec 145:130, 1999. 2. Watson AJ, Adams WM, Thomas CB: Craniomandibular osteopathy in dogs. Compend Contin Educ 17:911, 1995.
260

Hip Dysplasia: Conservative and rehabilitation management By David Dycus, DVM, MS, CCRP, DACVS-SA Chief of Orthopedic Surgery, Nexus Bone & Joint Center Medical Director, Nexus Veterinary Specialists Key Points: - Hip Dysplasia has a complex pathophysiology with the predominant feature of laxity - The conservative management of hip dysplasia is considered to be palliative - The goals of conservative management are to reduce clinical signs of pain, improve hip range of motion, improve strength, maintain muscle mass, and slow the progression of OA Hip dysplasia (HD) has become one of the most common orthopedic conditions that leads to joint inflammation and secondary osteoarthritis. Medical/conservative management is an option in patients with HD. It is important to understand that conservative management is considered a palliative approach rather than a definitive approach in both the immature and mature dog. Since the conservative approach to HD is considered palliative the approach should be multimodal. The goals are to reduce the clinical signs of pain, improve hip range of motion (ROM), improve hip strength, maintain muscle mass, and slow down or minimize progression of OA in the immature dog. In the mature dog the goals are similar to management of osteoarthritis (OA) in any joint.1 To appropriately achieve the goals there needs to be a focus in weight reduction, strength, and fitness. To be able to even focus on these areas the patients have to be comfortable so minimizing joint pain is paramount. This can be accomplished with the use of pharmaceuticals or disease modifying OA agents (DMOAs). In addition to assist not only with pain management but on strength and fitness then formal rehabilitation can be considered through the use of manual therapies, therapeutic exercises, and physical modalities.1 Weight Reduction, Strength, and Fitness: From a weight reduction standpoint, a higher plane of nutrition or anything that leads to rapid growth has been shown to lead to a higher incidence of HD. Earlier fusion of acetabular growth plates has been thought to lead to dysplastic hips. Increased bodyweight is an influential environmental factor. Increased bodyweight alone does not cause HD but it plays an instrumental role in the manifestation of the disease phenotype. Furthermore, weight reduction has been accepted as a highly effective preventive strategy for delaying or preventing the onset of OA in susceptible dogs. In Gail Smiths lifespan study of Labs2, it was reported that heavier dogs developed radiographic OA on an average of 6 years earlier than the restricted fed group. Heavier dogs required long-term treatment for OA on average 3 years earlier, which was reported by Kealy et al.3,4
261

To achieve weight reduction the goal is for 10% reduction. This is derived from humans where losing 10% of body weight improved comfort in patients with OA. For this to be done safely I shoot for 1-2% weekly. From a diet standpoint this is established by feeding 60% of the calories needed to maintain the current body weight. Unfortunately, diet alone is rarely successful for long-term weight management. The other important consideration is a controlled low impact exercise program. Daily exercise can only occur in the presence of a pain free joint; therefore, minimizing joint pain is paramount. Daily exercise can consist of leash walking, waking in water, and swimming. When performed on a daily basis exercise can help to maintain strength and range of motion. In humans with OA it is reported that muscle strength decreases due to disuse and reflex inhibitions due to the contractions of muscles adjacent to arthritic joints. The loss of strength can be measured both quantitative (due to a loss of muscle mass) and qualitative (due to a loss of muscle performance). At this time there is nothing in the literature reported on the loss of strength in dogs. This is likely because it would be hard to actually quantify. However, loss of muscle mass is reported commonly in dogs with hip dysplasia and we assume this is due to disuse. From this we can suspect that loss of muscle mass may be correlated with loss of muscle strength. Daily exercise helps maintain fitness and endurance. To achieve this it requires repeated motion over a given period of time. In dogs this will not be achieved through self-driven activities in the back yard, but rather is achieved with the compliant owner that is willing to perform daily activities with their dog. Again, daily exercise at the very basic needs to consist of long leash walks. Achieving daily exercise requires that the patient is comfortable and pain is minimized. Minimizing Joint Pain Minimizing Joint pain is the absolute most important factor when it comes to the conservative management of hip dysplasia. This is achieved through multiple routes such as optimizing the living conditions or in other words making lifestyle changes, tailoring activities, encouraging weight loss, pharmaceuticals, and disease DMOAs. From an optimization of living conditions in the dog little is actually known. From an OA standpoint clinical signs include periods of calmness (the so called “status quo”) and periods of exacerbation of signs known as flare-ups. Over time these flare-ups will become more frequent, severe, and last longer. Commonly, flare-ups result from excessive activity in unfit dog or the so-called “weekend warriors”. Flare-ups may last several hours to several weeks. Determining if a flare-up is present is critical. In most mature dogs that present to you for a “hip consult” they are in the middle of a flare-up; otherwise, why would the owner have elected to come see you? If there is a history of a sudden loss of performance, or inability to climb stairs or exercise intolerance then this could indicate a flare-up. Making irreversible decisions such as surgery or euthanasia during a flare-up should be avoided. During a flare-up the focus should be on rest and pain management to get the patient back to status quo. The goal
262
is to avoid strenuous activities such as jumping up, chasing, retrieving, or playing with other dogs. Unfortunately, owners like these activities because dogs love them, they are easy to do, and require minimal to no owner participation. Once the flare-up is under control then the patient can go back to their status quo with a focus on daily exercise to maintain muscle strength and range of motion as well as work to maximize the duration between flare-ups. By far and large the biggest aspect of conservative management is controlling joint pain with pharmaceuticals because without proper pain relief nothing else matters. We will not be able to successfully achieve strengthening, maintenance of muscle mass or ROM. To adequately control pain we must be able to interfere with both the peripheral (inflammation and damage) and central (neuropathic) aspects of pain. The goal of addressing the peripheral component is decreasing the transduction and transmission of noxious stimuli. Non-steroidal anti-inflammatories (NSAIDs), and piprants (GalliprantÒ) seem to be at the center of this in both human and veterinary medicine. In the dog NSAIDs have been shown to improve both peak vertical force and vertical impulse.5 In addition they have a positive impact on comfort and mobility. NSAIDs can have infrequent but potentially serious side effects and should be used cautiously in dogs, especially in patients with compromised liver or renal function or gastrointestinal disease. This becomes relevant since many older dogs with OA secondary to hip dysplasia are older when disease conditions are more likely to be present. Periodic enzymatic and liver function screening is recommended in dogs receiving NSAIDs. While, there is no consensus on the frequency of these screenings, it seems reasonable to perform them before the administration of NSAIDs, after a few weeks of administration, and when clinical signs arise. The central component of minimizing joint pain is to manage the peripheral sensitization and spinal cord “wind-up”. For this to occur there has to be a multimodal approach with the use of analgesics adjunctive or as an alternative to NSAIDs From a central component there are various medications that can be used. One big question that is becoming discussed more and more is the use of tramadol in dogs. From a pharmacokinetic standpoint we know there are big differences between the dog and humans. Interestingly, Steven Budsberg6 presented data from a 3-year project that was a double blind, placebo controlled crossover study that used both positive and negative controls. They found that tramadol was no different than using a placebo when it came to objectively measuring pain and that the positive control revealed that the dogs did indeed objectively improve proving that their model worked. Tramadol may act as a good selective serotonin reuptake inhibitor (SSIR). In some dogs it can act as a good sedative and dogs tend to become “spacy” on it. I suspect this is what people perceive as it being effective. In addition the metabolism is rapid and variable in dogs. When combined with other SSIRs it can increase the likelihood of serotonin sickness. Other analgesic options include the use of codeine (1-1.5 mg/kg q8h), which is my preferred choice of opioid. Amantadine (3-5 mg/kg q24h) is actually the only drug that has been studied to manage canine OA. It can act as an NMDA inhibitor and when combined with
263
other analgesic’s can provide good pain relief. Gabapentin (5-10 mg/kg q8-12h) has become a commonly used medication in the management of OA for central wind-up pain. It acts as a calcium channel blocker; however, some of the mechanism of action is unknown. It should be noted that we have no data supporting its use in OA management. Amitriptyline (0.5-1.0 mg/kg q12-24h) is another medication that can be used. It is a selective serotonin reuptake inhibitor so caution must be used when combining it with tramadol. One of my biggest soapboxes is this current thought that using tramadol and an NSAID is appropriate for long-term management of painful conditions. Opioids are not designed to be used for everyday management of pain associated with OA. Why do you think we have a current opioid crisis in the US?? They are designed to be used short-term and only as needed. They are beneficial during periods of flare-ups. I would love to see everyone move away from the NSAID/tramadol approach and stating, “that’s all we can do” theory. In addition to the other aspects of minimizing joint pain, DMOAs can be considered. In humans over 30 compounds have been shown to provide some degree of pain relief when analyzed prospectively. There is a lack of data in veterinary medicine, but it does exist. In dogs we tend to focus on glucosamine/chondroitin sulphate, polyunsaturated (omega-3) fatty acids, and polysulfated glycosaminoglycans. In general, the world of joint supplements can be deep and dark, if you only recommend a joint supplement to an owner, they are going to buy the cheapest they can find; however, they need to be told that not all are created equal. The FDA has no regulations on nutraceuticals therefore anyone can start a nutraceutical company. No company has to meet label claim and in fact 93% of companies fail to meet label claim. The source, purity, ethical issues, safety, and good manufacturing protocols (GMP) all have to be considered when choosing a company. What has also been shown is we need a product that has both glucosamine/chondroitin sulfate given that the chondroitin sulfate has such poor bioavailability alone. Also, a synergistic effect has been shown with both a glucosamine/chondroitin sulfate product. Remember that source plays a huge role in this so just because a product has both does not mean it will be synergistic. Furthermore, Sherman Canapp demonstrated not only efficacy but also a projective effect justifying the use before injury or evidence of radiographic OA.7 Omega 3 fatty acids are important for managing inflammation. Essentially, omega-3 fatty acids reduce levels of arachadonic acid in the cell membrane, which lowers the production of certain prostaglandins, which in turn reduces inflammation. Interestingly, canine chondrocytes store EPA, which is a type of omega-3 fatty acid. This helps decrease aggrecan degradation and turns off the signaling responsible for making degradative enzymes. Inflammation begins with chondrocyte damage leading to the release of arachadonic acid from the cell membrane phospholipid. As the inflammatory cascade continues lipoxygenase is released causing the release of leukotrienes. Furthermore cyclooxygenase is released from arachadonic acid leading the production of prostaglandins. Both leukotriene’s and prostaglandins cause continued inflammation
264
and tissue damage. Omega-3 fatty acids replace the omega-6 fatty acids and help inhibit the production of lipoxygenase and cyclooxygenase. The dose of omega-3 FA for OA management is much higher than for other conditions, the current recommendation is for 150-175 mg/kg of DHA/EPA. Polysulfated glycosaminoglycans are the only other class of drugs approved by the FDA to treat OA in the dog. These are considered disease modifying osteoarthritis drugs and are also approved for use in horses. Polysulfated glycosaminoglycans are water-based, for intramuscular Injection at a dosage of 2 mg/lb. body weight, IM, twice weekly for up to 4 weeks with a maximum of 8 injections). The specific MOA is not known, however in vitro studies show inhibition of serine proteinases PGE2 synthesis metalloproteases hyaluronidases and others as well as increased synthesis of protein, collagen, proteoglycans, and hyaluronic acid. Anecdotally “maintenance” injections monthly are considered helpful. The label is designed for IM usage; however, SQ usage is considered acceptable, but it should be known that it is off-label. Formal Rehabilitation Rehabilitation can play a huge role in achieving our goals of conservative management of HD. The definition of rehabilitation is the treatment or management of physical disability, malfunction, or pain using physical agent. There are various methods to achieve this such as physical modalities like therapeutic ultrasound, neuromuscular electrical stimulation (NEMS), trans-cutaneous electrical, stimulation (TENS), therapeutic laser, magnetic field therapy, shock wave therapy, manual therapies and therapeutic exercise. The goals of rehabilitation are to maintain muscle mass, build muscle support around joint, reduce pain, and weight loss. The basics of manual therapy include cold/warm therapy in addition to massage, acupuncture, and electro-acupuncture. It should be noted that cold therapy and massage should always be performed after exercise, not before. Cold therapy should be applied for 10-20 minutes 2-3 times daily. It will decrease nerve conduction and edema so it can be very useful for the management of central pain management. It is also helpful during flare-ups. Low-level warm packs in addition to acupuncture or electro-acupuncture can help with decreasing myofascial pain and tension. They help by stimulating the Aβ sensory fibers while sparring the Aδ and C fibers. Low-level heat allows for vasodilation and normalization of blood flow; it should be applied for 10 minutes 2-3 times daily. Little is known about the impact of OA on joint motion; however, in patients with hip dysplasia we know that they lose hip extension, not flexion. Normal hip extension is approximately 160°; interestingly a loss of less than 10° is probably not clinically relevant. Because it is easier to maintain motion rather than to regain it when it is lost assessing joint motion through goniometry is vital. ROM and stretching are typically incorporated early in the course of rehabilitation to increase flexibility, prevent adhesions, remodel periarticular fibrosis, and improve extensibility. This is accomplished
265
with 10-30 reps 2-4 times daily for range of motion and 20-40 second holds for stretching. Technically, range of motion is completed without muscle contraction while moving the joint through its full range of motion. Any force applied at the end of ROM is considered stretching. Both range of motion and stretching are more effective when tissues are heated. In addition, ROM/stretching can be incorporated into part of the daily exercise program to maintain mobility, enhance blood/lymphatic flow, and improve synovial fluid production. Therapeutic exercises are really the occupational aspect of rehabilitation. While little is known about the proprioception in dogs with OA or in immature dogs with hip laxity it is logical to assume that some sensory deficits are present. The focus of therapeutic exercises should be on balance and proprioception. This can be accomplished with lots of different things such as weight shifting (15-25 repitions 2-4 times daily), 3-legged standing (10-20 repitions 2-4 times daily) to more advanced exercises using balance boards, wobble boards, or exercise balls. Patients can also walked on uneven surfaces such as air mattresses, foam rubber, sand, etc. The overall goal is to do things that promote extension of the hip. Probably the most effective and simplest form of therapeutic exercise out there is controlled leash walking. However, when we discus this approach in patients with hip dysplasia it is important to consider what we are trying to achieve and how walking will affect this. For example walking on level ground will generate 35° of motion in the hip. Simply walking on an inclined treadmill will increase hip extension by 3°. Interestingly, trotting does not seem to increase ROM anymore than walking. Walking up stairs can increase hip extension by 10° while walking up an incline does not help in increasing hip extension. My plan is to start and build up to level ground walking for 20 minutes 2-3 times daily and slowly continue to add time to get to 45 minutes. Once at 20 minutes comfortably then inclined walking with stair ascent and decent should be added. Lastly, adding declined slopes and uneven terrain. Some simple therapeutic exercises that can be taught to owners to do at home are Cavalettis, sit-to-stand, and dancing exercises. Cavalettis will improve total hip ROM. Increasing the height of the bars will result in further increasing total hip ROM. Sit-to-stands are excellent to improve total hip ROM. It won’t directly lead to increased hip extension; however, it is excellent to use in the early phases when hip extension is painful. Dancing exercises are some of my favorite. Some consideration has to be made regarding the direction that dogs are being asked to dance. Forward dancing results in less hip extension and therefore is probably safer and more comfortable in the early phases. Once the dog’s hip extension is improved or more comfortable then walking backwards can be incorporated as walking backwards puts more stress on hip extension. If I were asked to provide my basic at home exercise plan for both the immature dog for hip dysplasia management or the older dog with OA I would start with a 5-10 minute warm up followed by walking. The goal is to get to 20 minutes on flat ground before adding in inclines, stair ascent/decent and finally declined slope and uneven terrain. Once returned from walking I then have the owners perform 10-20 repitions of sit-to-stand exercises along with 10 repitions of dancing exercises. The dancing is initially
266

performed forward, and once comfortable performed backwards. Following the exercises I have the owners perform 10-20 repitions of ROM along with 20-40 second holds for stretching. Lastly, the dogs are allowed 5-10 minutes of a cool down. All of this is performed 2-3 times daily. The goal of physical modalities in formal rehabilitation is to augment therapeutic exercises as well as help with tissue healing. Various modalities such as therapeutic ultrasound, electrical stimulation, shock wave, therapeutic laser, and hydrotherapy can all be included. Therapeutic ultrasound (US) can be beneficial in patients with hip dysplasia to aid improving ROM and decreasing pain and muscle spasm. It allows heating of the deeper tissues than what can be achieved with hot packing alone. The thermal effect of therapeutic US may increase collagen extensibility, blood flow, and pain threshold. To achieve the maximum benefit an intensity of 1.0-2.0 W/cm2 is used for a treatment time of about 8-10 minutes. Since the thermal effects of therapeutic US are short-lived ROM and stretching exercises are commonly performed during the US session. Electrical stimulation is useful for increasing muscle strength, ROM, and muscle tone. In addition it can improve pain control, decrease edema and muscle spasm. There are 2 types of electrical stimulation; neuromuscular electrical stimulation (NMES) is helpful for muscle re-education, prevention of muscle atrophy, and enhanced joint movement. Transcutaneous electrical stimulation (TENS) is helpful for pain control. In patients with hip dysplasia with long standing muscle atrophy NMES can be used twice weekly for 10-20 minutes; alternatively in pains with hip dysplasia and pain then TENS can be used 2-3 times weekly for 30 minutes. Laser therapy is gaining in popularity for various disease conditions. It can be useful to relieve pain, reduce inflammation, and increase microcirculation through the concept of photobiomodulation. My biggest thing is that laser therapy is used as part of rehabilitation, not as standalone rehabilitation. For patients with hip dysplasia and secondary OA I typically recommend 8-10 J/cm2. A generalized protocol is to start with 6 treatments over a 3-week period followed by maintenance treatments every 3-4 weeks. Regardless of the treatment protocol, the treatment should be designed to achieve the appropriate dose, number of treatments, and interval between treatments for the best outcome. Also, as a side note please ensure to wear goggles (both the 2 and 4 legged individuals). Extracorporeal shockwave therapy (ESWT) uses shock waves to target tissue to cause a release of energy. This release creates a biologic response to promote analgesia and decreases inflammatory mediators. The full analgesic effect is unknown, but thought to be due to the release of cytokines and growth factors centered around decreasing inflammation and swelling. One study showed that 4 weeks of treatment can improve ground reaction forces (GRF) in dogs for 3 months. Commonly sedation or anesthesia is needed to deliver 500-1,000 shocks at mJ/mm2 and 180 pulses/min. Ideally, there are 2 treatments spaced 3-4 weeks apart. Hydrotherapy is commonly recommended as part of the conservative management of hip dysplasia. We typically consider underwater treadmill therapy (UWTM) more beneficial than swimming. The changes in joint flexion are improved with both UWTM
267

and swimming; however, almost near normal joint extension is noted in UWTM compared to swimming where hip joint extension is limited. In addition, the UWTM encourages a more normal gait pattern than what is achieved with swimming. The benefits of UWTM are the benefit of buoyancy, which allows active muscle contraction with decreased weight bearing, the hydrostatic pressure that reduces edema and decreases pain and the resistance that helps strengthen muscles, and improves endurance. In general UWTM will improve ROM and comfort while increasing muscular fatigue and building endurance. Initially, most patients should be started at 2-5 minutes 1-2 times weekly with the goal to work up to 10-20 minutes with as few of breaks as possible. When choosing a treatment program it comes down to what stage of hip dysplasia is the patient in. In young immature dogs with hip laxity there should be a focus on daily exercise and weight management. However, it is important not to push aggressive exercise till after maturity. I will also add in DMOAs around 6 months of age. Also, to help promote hip extension I will have the owners incorporate ROM, sit-to-stands and dancing exercises. In addition daily play is very important. In mature dogs with OA and minor locomotion problems there should be a focus on decreasing pain, maintaining limb and core strength, maintain flexibility and stimulating proprioception. Simple pharmacologic steps are usually adequate such as using an NSAID at the lowest dose possible as infrequently as possible in addition to DMOAs. These patient should begin and remain on a long-term daily exercise plan with lots and lots of walking in addition to the ROM/stretching, sit-to-stand, dancing, and walking over/around obstacles. In mature dogs with moderate to severe OA the first step is pain control. This is accomplished through a multimodal pharmaceutical approach, as well as incorporating ice/heat, massage, acupuncture, TENs, and rest. Once pain is under control then the goal is to initiate a conservative and lightly progressive exercise program. This typically includes formal rehabilitation for 4-6 weeks along with daily walking and a home exercise plan. The absolute overall goal is to improve the patient’s mobility, strength, and proprioception so we can give them the best quality of life as possible. In summary our overall goals are to reduce the clinical signs of pain, improve hip ROM, improve hip strength, maintain muscle mass, and slow down or minimize progression of OA. To appropriately achieve the goals there needs to be a focus in weight reduction, strength, and fitness. To be able to even focus on these areas the patients have to be comfortable so minimizing joint pain is paramount. This can be accomplished with the use of pharmaceuticals or disease modifying OA agents (DMOAs). The “meats and potatoes” of the long-term home exercise plan is daily walking and therapeutic exercises such as sit-to-stands and dancing exercises. Also, the addition of ROM/massage/stretching can be beneficial in maintaining hip ROM. To assist not only with pain management but also on strength and fitness then formal rehabilitation can be considered through the use of manual therapies, therapeutic exercises, and physical modalities. A patient centered approach should be undertaken to improve the quality of
268

life. If the conservative approach does not lead to an improvement in quality of life then surgical intervention should be considered. References 1. Dycus DL, Levine D, Marcellin-Little DJ. Physical rehabilitation for the management of canine hip dysplasia. Vet Clin Small Anim 47:823, 2017. 2. Smith GK, Paster ER, Powers MY, et al: Lifelong diet restriction and radiographic evidence of osteoarthritis of the hip joint in dogs. J Am Vet Med Assoc 229:690, 2006. 3. Kealy RD, Lawler DF, Ballam JM, et al. Five-year longitudinal study on limited food consumption and development of osteoarthritis in coxofemoral joints in dogs. J Am Vet Med Assoc 210:222, 1997. 4. Kealy RD, Lawler DF, Ballam JM, et al. Effects of diet restriction on life span and age-related changes in dogs. J Am Vet Med Asssoc 220:1315, 2002. 5. Aragon CL, Hofmeister EH, Budsberg SC. Systematic review of clinical trials of treatments for osteoarthritis in dogs. J Am Vet Med Assoc 230;514, 2007. 6. Budsberg SC. Efficacy of tramadol in dogs with osteoarthritis. Abstract, ACVS 2017. 7. Canapp SO, McLaughlin RM, Hoskinson JJ, et al. Scintigraphic evaluation of dogs with acute synovitis after treatment with glucosamine hydrochloride and chondroitin sulfate. Am J Vet Res 60:1552, 1999.
269

Elbow disorders in dogs and cats: Methods of treatment
By Kristin Kirkby Shaw, DVM, MS, PhD, CCRT, DACVS-SA, DACVSMR Animal Surgical and Orthopedic Center & SOUND Veterinary Rehabilitation Center, Seattle WA.CARE: Canine Arthritis Resources & Education www.caninearthritis.org
Elbow dysplasia is a developmental orthopedic disease and common cause of lameness in dogs. The word “dysplasia” means abnormal growth and development. Elbow dysplasia is condition that dogs are born with and will eventually lead to arthritis. Genetics, trauma, and dietary factors may play a role in elbow dysplasia. There are three different conditions that fall under the umbrella of elbow dysplasia. All forms of elbow dysplasia will result in osteoarthritis (OA), even with early surgical intervention. However, early diagnosis and development of a pro-active arthritis plan will offer the best opportunity for managing the patient’s pain and lifestyle long term. Fragmented medial coronoid process (FMCP) FMCP is the most common type of elbow dysplasia. The medial coronoid process is a small tip of the ulna that should normally articulate perfectly with the radial head and medial humeral condyle. FMCP means that there is a fissure or complete separation of the medial coronoid process from the ulna. This may result from abnormal stresses placed on the coronoid process during growth and development. Common clinical signs of FMCP begin between 5-8 months of age and include acute or chronic intermittent limping, stiffness, and choppy gait. Lameness is usually made worse by exercise, and is prominent after resting. In some cases, lameness is not apparent until later in life. Many dogs will stand with their leg externally rotated to decrease pressure on the coronoid process. Palpation of joint effusion may be present deep to the anconeus muscle. Older dogs may have decreased range of motion of the joint. The clinical signs of FMCP are very similar to those of OCD, and it is likely that the two coexist in a third of cases. Most of the time FMCP is present in both elbows, but clinical signs may be worse on one side. Radiographs should be taken of any dog with suspected elbow dysplasia, however, they may be inconclusive. Radiographic changes consistent with FMCP include sclerosis of the ulnar notch and osteophyte formation on the radial head and olecranon. In older dogs, degenerative joint disease will be apparent. It is difficult to visualize the coronoid process on radiographs, and FMCP is rarely diagnosed on radiographs alone. Definitive diagnosis requires either surgical joint exploration, typically with arthroscopy, or CT scan. Treatment of FMCP requires a multi-modal approach. Surgery (typically arthroscopic) is usually recommended in order to remove the abnormal osteochondral fragment; however it is important to recognize that this does not leave behind a normal elbow joint and OA will progress and require non-surgical management. There are numerous other surgical procedures proposed to change the biomechanics of the elbow or partially or completely replace the joint. At this time, none of these procedures have gained wide spread acceptance due to lack of consistently positive outcomes.
270
Osteochondritis Dessicans (OCD) Osteochondrosis is a defect in bone growth that results in an area of cartilage not forming properly and not being held tightly down to the underlying bone. Over time, this abnormal area of cartilage may partially split away, forming a cartilage flap which causes pain when it moves in the joint space. This condition is termed osteochondritis dissecans (OCD). Once formed, this cartilage flap cannot heal back down to the underlying bone. Instead, it will either continue to degenerate in place, or may break free and migrate to another area of the joint (these free pieces are known as “joint mice”). In either case, the presence of the flap will cause pain and inflammation within the joint. OCD can occur in the elbow as well as other joints including the shoulder, stifle and tarsus. Clinical signs of OCD begin between 5-8 months of age and include acute or chronic intermittent limping, stiffness, and choppy gait. Lameness is usually worse after exercise, and is prominent after resting. In some cases, lameness does not show up until later in life when arthritis has set in. The history and clinical findings with OC/OCD are identical to FMCP and advanced diagnostic imaging is needed to establish a diagnosis. Treatment for OCD consists of surgical removal of the cartilage flap. There are procedures that replace the osteochondral defect with an autogenous, allogenic or synthetic osteochondral graft. However, it is important to realize that while surgery often provides improvement in lameness, this will not be a curative surgery and long term management of OA will be required. Ununited Anconeal Process (UAP) The anconeal process is the large upper tip of the ulna that articulates with the humerus. There is normally a physis in this part of the bone. UAP develops when this physis doesn’t close, resulting in a partially attached anconeal process. This leads to instability or detachment of the process and OA of the elbow. UAP is most commonly diagnosed in German Shepherds. Clinical signs are usually not seen before 5-8 months of age. Occasionally, lameness is not observed until the dog is several years old. In the earliest stages, the only clinical signs may be a slight limp, swelling on the lateral aspect of the elbow (often confused with a hygroma) and standing or walking with the paw externally rotated. Palpation of the joint in older dogs may reveal swelling and crepitus within the joint. A preliminary diagnosis may be made based on clinical signs, age and breed. The diagnosis will be confirmed by flexed lateral view. There are several surgical options that may be considered for young dogs diagnosed with UAP. These include: arthroscopy to evaluate the entire joint, reattaching the anconeal process with a screw, ulnar osteotomy to relieve tension on the UAP so that it may fuse, or excision of the anconeal process. Like other components of elbow dysplasia, UAP will result in some degree of long-term OA.
OA management
271
While cats can also develop some forms of elbow dysplasia, they may likely develop primary arthritis due to aging changes rather than secondary OA as occurs in dogs. Long term OA management is required for all forms of elbow dysplasia and OA in both species. Management of OA requires development of a plan that is thorough and tailored to the individual patient and client. The Comprehensive Care Quad was developed by this author to ensure a systematic approach to developing an OA treatment plan for patients. Not every treatment strategy will be employed, but each category must be addressed in order to offer the wide range of management techniques available at this time.
1. Pain Management • The foundation of pain management is use of a non-steroidal anti-
inflammatory (NSAID), including cox-inhibiting products or Galliprant. These medications have proven efficacy, and when used appropriately, have a strong safety profile. Dogs should not be denied proven analgesia based on age (too young or too old). If traditional cox-inhibiting NSAIDs are contra-indicated, most dogs are able to tolerate Galliprant. While Onsior is not labeled for long-term use in cats in the US, it is approved for long term use in cats in many other countries. This author frequently prescribes Onsior (off label) for long term use in cats with OA, so long as clients are well educated on ensuring their cat is maintaining hydration. When NSAIDs are insufficiently managing pain, other medications such as amantadine, gabapentin, acetaminophen (DOGS ONLY!), methocarbamol and codeine may be added.
• Needles: There are currently 3 common pain management techniques for OA administered by injection:
i. Adequan- this is an FDA approved product that is labeled as a disease modifying osteoarthritic drug for use in dogs and horses. It is most effective at preserving articular cartilage when used early in the OA disease process. Its mechanism of action also provides pain relief through decreasing inflammation in a mechanism distinct from NSAIDs. It is administered intra-muscularly or subcutaneously (NOT intra-articularly). This author recommends Adequan (off-label) subcutaneously in cats
ii. Intra-articular therapy- this includes administration of steroids, hyaluronic acid, platelet rich plasma, and/or stem cell therapy directly into the effected joint. There is research to support each of these techniques, and intra-articular therapy should be a routine part of managing OA in dogs and possibly cats. Novel intra-articular therapies are currently being developed, including radioactive tin (Tin 117m), which may offer long-term pain relief.
iii. Acupuncture- this is a non-pharmaceutical technique that may offer adjunctive pain relief for many animals.
• Surgery: As discussed above, surgery is often part of treating elbow disorders, but will not provide successful long term management alone.
272
2. Nutritional Management • Weight management is the single most important aspect of managing OA.
Clients should be counseled early in the pet’s life about the importance of their dog or cat maintaining a lean body condition (4.5/9). Veterinarians should be prepared to make specific diet recommendations, including caloric requirements for weight loss and maintenance.
• Nutritional supplements: these include omega 3 fatty acids, cannabis, and many other products that may help support joint health. Veterinarians should be prepared to have an evidence-based discussion with pet owners on the value of nutritional supplements. While the research is somewhat limited in this category, the majority of pet owners will use a joint supplement, even if not prescribed by the veterinarian. Therefore, this author urges veterinarians to make specific recommendations for products that they know and trust.
3. Lifestyle Management • Activity modification- Animals with OA should engage in regular, low impact
exercise such as walking (ideally 20-60 minutes per day), swimming and scent detection such as “Noseworks.” High impact activity such as running, jumping, and ball-play should be avoided.
• Home environment- The animal’s home environment needs to be modified to accommodate their needs, including ensuring non-slip flooring, including on stairs, and using ramps and steps if needed. Litter boxes should be modified for cats to allow easy entry and exit. Adequate bedding is essential. Other modifications may including raising the food bowl or limiting access to certain areas of the house that are “OA friendly.”
• Assistive devices- Harnesses, slings, support wraps and orthotics may all have a place in management of OA.
4. Rehabilitation Techniques • Formal physical rehabilitation can be very helpful for dogs and cats with OA.
Consultation with a veterinarian or physical therapist certified in canine rehabilitation (CCRT, CCRP) is strongly recommended. Rehabilitation techniques that are helpful for animals with elbow OA include targeted therapeutic exercise, manual therapy and therapeutic modalities such as cold/compression, PEMF and photobiomodulation.
For more information on these treatment options and associated references see www.caninearthritis.org.
273
The 3 R’s of CCL: Repair, rehab and research
By Kristin Kirkby Shaw, DVM, MS, PhD, CCRT, DACVS-SA, DACVSMR Animal Surgical and Orthopedic Center & SOUND Veterinary Rehabilitation Center, Seattle WA. CARE: Canine Arthritis Resources & Education www.caninearthritis.org
Several reports indicate that dogs participating in post-operative rehabilitation following CCL surgery have superior short-term outcomes compared to dogs that do not participate in formal rehabilitation. While the initial data is supportive, there is significant need for larger studies investigating the role of rehabilitation following CCL surgery. Furthermore, in order for long-term, multi-center, prospective studies to identify predictors of successful outcome following CCL surgery, a standardized approach to post-operative rehabilitation in dogs should be adopted. As a primary step toward developing rehabilitation protocols to test in multi-center clinical trials, review of the fundamental principles of physical rehabilitation as they apply to tissue healing following CCL surgery is necessary.
A multi-disciplinary group including veterinary rehabilitation specialists, physical therapist, and veterinary surgeons have convened to eventually develop guidelines for physical rehabilitation post-CCL surgery. In order to develop these guidelines, we have outlined 4 initial steps:
1. Conduct surveys of veterinary surgeons and rehabilitation practitioners to understand current recommendations for rehabilitation post-CCL surgery. The results of one of these surveys was published in Vet Surg in 2020 (Eiermann J et al.)
2. Review the currently available evidence for rehabilitation post-CCL surgery. This systematic review is currently in preparation for submission to Vet Surg.
3. Review the physiologic principles of physical rehabilitation, including: tissue healing, goals of therapy throughout stages of healing, progression of therapy, and objective and functional assessment of outcomes. This manuscript was published in Vet Surg in 2020 (Shaw KK et al.)
4. Develop and test several post-CCL rehabilitation protocols in multi-center, prospective clinical trials. These protocols will be developed based on best available evidence combined with clinical experience. One trial was initiated prior to COVID and is currently on hold.
The results of the surveys outlined above indicate that over 90% of veterinarians surveyed would welcome evidence-based guidelines for post CCL rehabilitation. Until these guidelines become available, post-operative rehabilitation programs should be designed such that patients progress based on individual assessment according to the degree of tissue healing, strength and achievement of functional goals. Therapists must fully understand phases of tissue healing, re-assess the patient frequently, use clinical reasoning skills to progress treatment appropriately for the individual patient. Goals of rehabilitation include: decrease pain, soft tissue swelling and joint effusion; facilitate tissue healing; restore normal arthrokinematics and osteokinematic motion; promote weight bearing to initiate muscle contractions for dynamic stabilization of the stifle joint; normalize proprioception; restore normal neuromuscular patterning (functional movements); normalize muscle function, strength, endurance and mass in the operated limb; improve health of the post-
274

operative joint; weight loss, if indicated; address and resolve compensatory issues in other limbs that may be causing pain and gait dysfunction; decrease probability of further injury; hasten return to normal activity/ full function. Physical rehabilitation should begin immediately post-operatively and continue ideally until the patient has returned to full activity. Rehabilitation techniques include manual therapy, therapeutic exercise, and therapeutic modalities. Hydrotherapy is not required in order to provide comprehensive and high-quality therapy, so long as the individual providing therapy is trained in manual therapy, therapeutic modalities and therapeutic exercise progression. Cryotherapy, particularly with cold/compression, should be used in the immediate post-operative treatment following CCL surgery. Therapeutic modalities such laser, extracorporeal shock wave therapy (ESWT), neuromuscular electrical stimulation (NMES), and pulsed electromagnetic field therapy (PEMF) have limited evidence to support their use and are considered to be supplementary equipment that, when used safely, may potentially provide therapeutic benefits. There are general differences in expectations for recovery and slight modifications in rehabilitation therapy depending on the type of surgery performed (extra-capsular vs. osteotomy).
References
• Shaw KK, Alvarez L, Foster SA, Tomlinson JE, Shaw AJ, Pozzi A. Fundamental Principles of Rehabilitation and Musculoskeletal Tissue Healing. Vet Surg 49(1):22-32, 2020.
• Eiermann J, Shaw KK, Evans R, Kowaleski M, Schmierer P, Bergh MS, Cuddy L, Bleedhorn J, Kieves N, Lotsikas P, Pozzi A. Postoperative rehabilitation protocols following cranial cruciate ligament surgery in dogs: A 2017 survey of veterinary practitioners. Accepted to Vet Surg 49(1):80-87, 2020.
• Baltzer WI, Smith-Ostrin S, Ruaux CG. Evaluation of the clinical effects of diet and physical rehabilitation in dogs following tibial plateau leveling osteotomy. J Am Vet Med Assoc 2018; 252:686-700.
• Romano LS, Cook JL. Safety and functional outcomes associated with short-term rehabilitation therapy in the post-operative management of tibial plateau leveling osteotomy. 2015 Can Vet J 56:942-946.
• Drygas KA, McClure SR, Goring RL, Pozzi A, Robertson SA, Wang C. Effect of cold compression therapy on postoperative pain, swelling, range of motion, and lameness after tibial plateau leveling osteotomy in dogs. J Am Vet Med Assoc 2011;238(10):1284-1291.
Additional references available upon request
275
The not-so-magic eight ball: Predicting OA by early diagnosis of eight developmental orthopedic diseases By Kristin Kirkby Shaw, DVM, MS, PhD, CCRT, DACVS-SA, DACVSMR Animal Surgical and Orthopedic Center & SOUND Veterinary Rehabilitation Center, Seattle WA. CARE: Canine Arthritis Resources & Education www.caninearthritis.org
Osteoarthritis (OA) effects an estimated 20% of dogs and is the leading cause of chronic pain in canine patients. There is widespread misconception among veterinarians and pet owners that OA is a condition that only effects older dogs. In fact, at least half of cases of canine OA are diagnosed in dogs over the age of 8 years of age. Yet another staggering statistic is that 50% of cases of OA go undiagnosed. This may be due to a combination of pet owners and veterinarians not being aware of the early signs of OA, and importantly, understanding what causes OA in dogs. Humans (and potentially cats) develop primary OA; this is a degenerative condition of joints that results due to “normal wear and tear,” which develops as we age. Dogs most often develop secondary OA, due to an underlying developmental or traumatic injury to the joint. The most common cause of OA in dogs is Developmental Orthopedic Disease (DOD), including hip dysplasia, elbow dysplasia and medial patella luxation. By definition, DODs are present in juvenile dogs. Identifying these dogs at risk of OA early in life offers the best opportunity for pro-active care. There are at least 8 common DODs that lead to OA in dogs:
1. Hip Dysplasia (HD) Hip dysplasia can be diagnosed in very young dogs. This author suggests that all puppies, particularly those breeds at risk of HD, should be tested for an Ortolani sign when they are 16 weeks of age. If the Ortolani exam is positive, this indicates hip laxity, i.e., the dog has hip dysplasia. A PennHip radiographic exam can be performed at this age as well, which provides an objective measurement of hip laxity and can compare the severity of laxity to other dogs of the same breed. There are 2 surgical procedures that can only be performed in juvenile dogs with HD: juvenile pubic symphisiodesis (JPS) and triple (or double) pelvic osteotomy (T/DPO). Clients of dogs with HD should be counseled on weight management, activity recommendations, optimal age for spay/ neutering, and pain management.
2. Fragmented medial coronoid process (FMCP, a form of elbow dysplasia) FMCP is the most common form of elbow dysplasia. Dogs with this condition typically present between 6-9 months of age with unilateral or bilateral forelimb lameness. CT or arthroscopy is usually needed to confirm the diagnosis. Consultation with a surgeon is recommended at this time to discuss potential surgical interventions. However, no matter what surgery is performed, long term OA management will be needed. 3. Ununited anconeal process (UAP, a form of elbow dysplasia) UAP is a relatively infrequent form of elbow dysplasia but can easily be diagnosed based on a flexed lateral radiograph in dogs over the age of 5-6 months. Consultation with a surgeon is
276
recommended at the time of diagnosis to discuss potential surgical interventions. However, no matter what surgery is performed, long term OA management will be needed. 4. Osteochondrosis (OC/OCD) of the elbow Like other forms of elbow dysplasia, OC/OCD typically presents in dogs between 6-9 months of age. Consultation with a surgeon is recommended at the time of diagnosis to discuss potential surgical interventions. However, no matter what surgery is performed, long term OA management will be needed. 5. Osteochondrosis of the shoulder OC/OCD of the shoulder presents very similarly to elbow dysplasia. A single lateral radiograph of the shoulder is typically sufficient to diagnosis the condition. Consultation with a surgeon is recommended at the time of diagnosis to discuss surgical interventions. Typically, surgical treatment results in an excellent long-term prognosis. However, the patient should be monitored closely long term as OA will develop but may not become clinically significant. 6. Osteochondrosis of the tarsus Like other DODs, this condition typically presents in dogs under 1 year of age. The OC/OCD lesion is typically present on the medial trochlear ridge, and firm swelling of the medial tarsus can often be palpated. Radiographs are often sufficient for diagnosis, though CT may be needed in some cases to confirm a diagnosis. While surgery can potentially be pursued, it does not offer an excellent prognosis and long-term management of OA is essential. 7. Medial patella luxation (MPL; or lateral patella luxation, LPL) Patella luxation is typically due to congenital malalignment of the quadriceps mechanism and abnormal biomechanical forces acting on the patella and femoral trochlea. Patella luxation is graded 1-4 based on the severity of luxation, and many cases can progress in severity. MPL has been shown to lead to OA of the stifle and is also a predisposing cause for cranial cruciate ligament rupture, which will lead to significant OA if not treated surgically. Not all cases of M/LPL will require surgery, but discussion of comprehensive management of OA and at least semi-annual monitoring is recommended.
8. Avascular necrosis of the femora head (Legg-Calve Perthes Disease) This condition typically develops in miniature and small breed dogs. A disruption in blood supply to the femoral neck and head leads to irregular growth of the hip joint, which will result in OA. The condition is typically painful, leading to significant lameness and discomfort with manipulation of the hip. Radiographs are sufficient for diagnosis, and femoral head and neck ostectomy (FHO) offers an excellent prognosis.
For more information on these conditions, including diagnosis, treatment, and references see www.caninearthritis.org.
277
Monoclonal antibodies for painBy Michael C Petty, DVMArbor Pointe Veterinary HospitalCanton, Michigan, USA
Overview of the Issue: New therapies are on the horizon for the treatment of painObjectives of the Presentation:
1. What is pain?
2. What happens when Pain is uncontrolled
3. Understanding OA in cats
4. Understanding OA in dogs
5. Understanding what a monoclonal antibody is.
6. Understanding the role that Nerve Growth Factor (NGF) plays in pain
7. Clinical relationship between NGF and inflammation
Summary including 5 KEY “TAKE HOME” POINTS1. Uncontrolled pain can lead to serious complications and advanced pain states2. Pain in cats is often diagnosed by behavioral changes3. Pain in dogs is often diagnosed by a combination of client observation of both
behavior and physical issues4. Anti-NGF monoclonal antibodies treat both pain and inflammation5. Anti-NGF Monoclonal Antibodies are an emerging new way to treat pain
PROCEEDINGS1. What is Pain?
a. Definitions:i. An unpleasant sensory or emotional experience associated with
actual or potential damage, or described in terms of such damageii.The biology of pain is never straightforward, even when it appears
to be. b. Pain is a multidimensional and is a uniquely individual experience
involving many factorsi. Behavioral
1. Physical activity2. Medicaitons3. Pain behaviors4. Sleep
ii.Sociocultural1. Environment2. Family
iii.Physiologic
278
1. Location2. Onset3. Duration4. Etiology
iv.Sensory1. Intensity2. Quality3. Pattern
v.Emotional1. Mood2. Anxiety3. Well-being
vi. Cognitive1. Coping
c. Pain definitionsi. Analgesia: Absence of pain in response to stimulation that normally
is painfulii.Hyperalgesia: An exaggerated and prolonged response to noxious
stimulusiii.Allodynia: Pain elicited by non-noxious stimuli (light touch pain)iv.Neuropathic pain: Pain caused or initiated by a primary lesion,
injury or dysfunction in the PNS or CNSv.Sensitization: The process where action potential threshold is
shifted toward less intensive stimuli in either the CNS or PNSd. Nociception
i. From Latin “to hurt”ii.Nociceptors are a specialized subset of sensory neurons that are
activated by painful stimuli…the first responders when there is injury or damage
iii.Two types of nociceptors1. A-delta fibers that are responsible for fast/lancing pain
a. mechanical2. C-fibers that mediate slow and poorly localized pain
a. Thermalb. Chemical
e. Complexity of peripheral pain receptor signalingi. Immune Cells are activated
1. Mast Cells2. Neutrophils3. Macrophages4. Th17 Cells5. Gamma delta T cells
ii.Activation of the immune cells cause a release of different types of mediators and cytokines, depending on the cell that is stimulated
1. Common ones are histamine, NGF and Prostaglandin among others
279
iii. These mediators and cytokines then attach to different receptors on the nociceptor neuron.
1. For example: Macrophages release PGE2 which then bind to the EP1-4 receptors on the nociceptor
f. Chronic Paini. Not just lingering acute painii.Acute pain is
1. Purposeful2. Short duration3. Causes temporary changes4. Pain resolves as injury resolves
iii. Chronic pain is1. Non-purposeful2. Long-standing3. Involves modification of a pain pathway4. Pain does not resolve when the injury resolves
g. Pain pathway:i. Transduction (point of pain event)ii.Transmission through the nerve pathwayiii.Spinal Modulation by the things like the dorsal root ganglion and
the NMDA pathwayiv.Perception by the conscious area of the brain
2. What happens when pain is uncontrolleda. Centralization or hypersensitization, sometimes known as wind-up pain
i. A form of neuroplasticity wherein the neurons change form and function in response to changes in their environment
ii.Leads to a state of induced pain hypersensitivityiii.Pain that persists beyond the normal healing time or where healing
will not occurb. Risk of delaying pain management
i. Preemptive and preventive analgesia has been shown to control pain most effectively
ii.But by the time we see clinical signs, the initial injury has likely become chronic
3. Current OA toolboxa. NSAIDsb. Platelet Rich Plasmac. Stem Cellsd. Nutraceuticalse. Joint dietsf. Rehabilitationg. Acupunctureh. Gabapentinoidsi. Ketaminej. TCA’sk. Alpha-2 Agonists
280
l. Opioids4. What does this mean for chronic pain patients?
a. Catsi. Cats have behaviors and interactions that are based on keeping
them safe1. Avoidance and evasion2. Hiding outside signs of weakness, pain or illness
ii.Cats live in a vertical world1. Cats feel safest in an elevated location
iii. Prevalence of feline OA1. OA is the most common cause of chronic pain in all species2. Prevalence in cats
a. Depending on study 61% to 91% of all cats3. OA may be present in the absence of obvious radiographic
changes, but radiographic chances do not always correlate with clinical signs nor the degree of pain suffered.
iv. Risk factors1. Primary: No clear underlying cause2. Secondary
a. Congenitalb. Infectiousc. Developmentald. Prior trauma
3. Obesity? May play a role in young catsv.Why do we miss signs of Feline OA?
1. Most cats don’t limp2. Cats can compensate for severe disease because they are
small and agile3. Radiographic changes are variable4. Cause is usually unknown v. congenital deformities5. Many cats with OA are actually underweight6. Commonly affected joints are elbow hips and stifle
vi. Identifying Chronic Pain1. Behavioral changes are the most common sighs of OA pain
in catsa. Client input is crucial…signs are often dismissed as
normal aging b. Without intervention, the cat’s vertical world becomes
more horizontal2. Owner observed Behavioral changes
a. Active Signsi. Hesitation jumpingii.Climbing a few stairs at a timeiii.Eliminating outside the litter boxiv.Increase sleeping, less awakev.Decrease in play
281
b. Inactive signsi. Grump moodsii.Less interactioniii.Less happyiv.Unkempt haircoatv.Overgrown claws
c. Handouts and interactive website checklistsi. Zoetis
1. Cat OA pain checklist2. Interactive cartoons of cats showing
normal v. abnormal activityvii. Diagnosis of Feline OA
1. Cat behavior…already discussed2. Orthopedic exam
a. Patient and gentleb. Look for swollen or enlarged jointsc. Crepitus, joint thickening and effusiond. Pain
3. Radiographsa. Periarticular osteophytesb. OA may be present in the absence of obvious
radiographic changesc. Radiographic changes may not correlate with clinical
signs of OA and degree of painb. Dogs
i. About OA in dogs1. Population affected
a. OA affects 1 in 5 dogs over 1 year of age in the usb. #1 cause of pain
2. Conformational in origin for many dogsa. Chondrodysplasiab. Hip dysplasiac. OCDd. Elbow dysplasiae. Luxating patellaf. Cruciate disease
ii.Diagnosing OA in dogs1. Canine OA Staging tool (COAST)
a. Improves and standardizes approach to diagnosis and monitoring of canine OA over time
b. For primary care practicesc. Proactive and multidisciplinary team approachd. https://www.galliprantvet.com/us/en/coast-tools
5. Treatment and Management a. Primary Goal is to restore quality of life
i. Lifestyle changes
282
ii.Pharmacologic interventioniii. Nonpharmacological intervention
b. Lifestyle changesi. Environmental modification
1. Steps and ramps2. Additional litterboxes for cats3. Easy access to food and water (no stairs, etc)
ii.Supportive Management1. Weight loss2. Controlled exercise3. Grooming
c. Pharmacologic Interventioni. NSAIDS
1. Many for dogs2. Cats?
ii.Gabapentiniii.Amantadine
d. Nonpharmacological interventioni. Rehabii.Nutraceuticalsiii.Dietiv.Weight lossv.Acupuncture!vi.Laservii.Surgeryviii.PRP
6. Anti-NGF Monoclonal antibodiesa. What is on the Horizon?
i. NGF is a neuromediator that plays a major role in acute and chronic pain signaling in animals
1. Inflammation2. Neuropathic pain
ii.Pro-inflammatory cytokines stimulate the release of pain mediators such as NGF from immune cells
1. Increased levels can cause hyperalgesia2. Sensitizes nerves to other factors so they respond more
greatly to other stimuliiii. Long-acting, injectable monoclonal antibodies are being
studied1. * In September 2020 the European Medicines Agency gave
a “Positive opinion” on a caninized anti-NGF monoclonal antibody called bedinvetmab
2. Look it up at https://www.ema.europa.eu/en/medicines/veterinary/
b. Future Toolbox targeting NGFi. NGF has emerged as a very important target for OA pain control
283
ii.Currently the most promising method to target NGF is through monoclonal antibodies (MAbs)
iii.Inhibition of NGF function via anti-NGF antibodies markedly reduces hyperalgesia and behavioral indicators of pain in various animal models of inflammatory OA
References• McGuire DB, Comprehensive and multidimensional assessment and
measurement of pain. J Pain Symptom Manage 1992(5):312-319• Redi, Danielle, “An introduction to Pain Pathways and Mechanisms.” British
Journal of Hospital Medicine, vol 74, no. Sup12, 2013 pp C188-C191• Brodin E, Ernberg M, Olgart L, Nor Tannelegforeening Tid, 2016; 126: 28-33
Neurobiology: General considerations from acute to chronic pain• Woolf C, Moving from Symptom Control toward Mechanism-Specific
Pharmacologic Management, Pain 2004• J.H Kaas, in International Encyclopedia of the Social and Behavioral Sciences,
2001• Woolf C, 2011 Central sensitization: Implications for the diagnosis and treatment
of pain. Pain 152:S2-S15• Williams MD et al. Feasibility and repeatability of thermal quantitative sensory
testing in normal dogs and dogs with hind limb osteoarthritis associated pain, The Vet Journal. 199(1):63-67 2014
• Woolf C, Moving from Symptom Control toward Mechanism Specific Pharmacologic Management, Pain 2004
• Johnston, SA Osteoarthritis: joint anatomy, physiology and pathobiology. Vet Clin N Am Small Anim Pract 27: 699-723; 1997
• Muir WW, Choosing and administering the right analgesia therapy. Veterinary Pain Management, Mosby, Columbus 2003
• Journal of Feline Medicine and Surgery (2013) 15, 219-230 AAFP and ISFM Feline Environmental Needs Guidelines https://www.catbehaviorassociates.com/increase-your-cats-vertical-territory/
• Handbook of Small Animal Anesthesia and pain Mgt (2nd edition) page 393• Slingerland LI et al, Cross-sectional study of the prevalence and clinical features
of osteoarthritis in 100 cats, Vet J 2011 Mar;187(3):304-9• Lascelles BD, Henry JB, Brown J, et alCross-sectional study evaluating the
prevalence of radiographic degenerative joint disease in domesticated cats, Vet Surg
• Hardie EM, Roe SC, Martin FR: Radiographic evidence of degenerative joint disease in geriatric cats: 100 cases (1994-1997) J Am VetMed Assoc 2002; 220:628-632
• American Veterinary Medical Association (2018) US pet ownership and demographics sourcebook. Shaumburg, Ill: Center for information management, AVMA
• Robertson, S (2008, November 1) Osteoarthritis in cats: What we now know about recognition and treatment. Retrieved March 14, 2018 from Veterinary
284
Medicine• Bennet, D, et al Osteoarthritis in the Cat: How common is it and how easy to
recognize, J Fel Med & Surg, 2012, (14) 65-75• Godfrey DR, Osteoarthritis in cats: a retrospective radiological study. J Small
Anim Pract 2005 46(9); 425-429• EpsteinM, et al, 2015 AAHA/AAFP Pain Management Guidelines for Dogs and
Cats• Merola I, Mills,DS, Behavioural signs of pain in cats: an expert consensus PLoS
One 2016• Klinch MP et al Owner-perceived signs and veterinary diagnosis in 50 cases of
feline osteoarthritis, Can Vet J 2012; 53:1181-6• Bennett D et al, A study of owner observed behavioural and lifestyle changes in
cats with musculoskeletal disease before and after analgesic therapy, J Feline Med Surg; 200911:997-1004
• Lascelles. BD. Et al, Relationship of orthopedic examination, goniometric measurements, and radiographic signs of degenerative joint disease in cats, BMC Vet Res 2012
• Fox S and Millis D, In: Multimodal Management of Canine Osteoarthritis, 2010 p. 24
• Sparkes, AH et al. ISFM and AAFP consensus guidelines: long-term use of NSAIDS in cats, J. Feline Med Surg, 12(7) 2010 pp 521-38
• Marino CL, Lascelles BDX, et al. 2014 Prevalence and classification of chronic kidney disease in cats randomly selected from four age groups and in cats recruited for degenerative joint disease studies. Journal of Feline Medicine and surgery 16, 465-472
• Isola M, et al, Nerve growth factor concentrations in the synovial fluid from healthy dogs and dogs with secondary osteoarthritis, Vet Comp Orthop Tramatol. 2011
• Watson JJ, et al, Targeting nerve growth factor in pain: what is the therapeutic potential? BioDrugs 2008
285
I know that dog has chronic pain: Convincing the OwnerBy Michael C Petty, DVMArbor Pointe Veterinary Hospital
Overview of the Issue: Allowing the owner to understand signs of pain in their dogObjectives of the Presentation:
1. Understanding and explaining the disconnect between signs of pain that you may see and what the owner sees.
2. Understanding how behavioral changes are the best way for the owner to understand signs of chronic pain
3. Looking at signs of pain in the dog by distant observation
4. Understanding what a pain exam comprises
5. Clinical metrology for diagnosing pain
6. Learning how to implement the Canine Osteoarthritis Staging Tool in practice
Summary including 5 KEY “TAKE HOME” POINTS1. Key point 1 Many owners see signs of pain but misinterpret them as aging or
something else2. Key point 2 A complete pain exam involves giving the owner a pain survey,
distant observation by the veterinary team and a physical exam3. Key point 3 Choose a pain assessment tool for the owner. The author prefers the
Canine Brief Pain Inventory4. Key point 4 The Canine Osteoarthritis Staging Tool is important for both the
diagnosis and treatment of chronic OA pain5. Key point 5 Osteoarthritis is the leading cause of euthanasia. Early diagnosis
and therapy can lead to longer and happier lives in dogs
SummaryToo often we see patients in our practice that would benefit from management of the chronic pain associated with osteoarthritis. Yet convincing the owners that there is a problem that needs therapy can be a challenge; many owners feel that a common behavioral change, such as reluctance to walk on slippery floors as one example, has nothing to do with the pain of OA. This lecture discusses how to approach the diagnosis of pain including discussions with the owner, using validated pain scoring systems, and incorporating the Canine Osteoarthritis Staging tool into your practice. References/Suggested Reading
1. Epstein ME. Today’s Veterinary Practice. Nov/Dec 2013
Cachon, T et al. Vet J. 2018; 235: 1-8
286
Sharon Kerwin. ORTHOPEDIC EXAMINATION IN THE CAT Clinical tips for ruling in/out common musculoskeletal disease, Journal of Feline Medicine and Surgery (2012) 14, 6–12James Grierson. Dealing with pelvic fractures in cats, In Practice, April 2019, Volume 41, 106-114Shannon Kerrigan, and Duane Robinson. Juvenile Orthopedic Disease in Dogs & Cats Part 2: Congenital & Neonatal Orthopedic Diseases; Today’s Veterinary Practice, September/October 2016, 24-31Ingrid Balsa, and Duane Robinson. Juvenile Orthopedic Disease in Dogs & Cats Part 1: Musculoskeletal Development & Pediatric Bone Diseases, Today’s Veterinary Practice, May/June 2016, 38-45Duane A. Robinson. Orthopedic Follow-Up Evaluations: Identifying Complications, Today’s Veterinary Practice, September/October 2014, 71-79Deborah E. Linder. Physical Activity Programs for Cats. http://www.cliniciansbrief.com/, April 2019, 27-31David Bennett, Siti Mariam bt Zainal Ariffin and Pamela Johnston. Osteoarthritis in the cat: 1. How common is it and how easy to recognise?, Journal of Feline Medicine and Surgery 2012 14: 65David Bennett, Siti Mariam bt Zainal Ariffin and Pamela Johnston. Osteoarthritis in the cat: 2. How should it be managed and treated? Journal of Feline Medicine and Surgery 2012 14: 76Sorrel Langley-Hobbs. Musculoskeletal oddities in the cat: An overview of some curious causes of lameness, Journal of Feline Medicine and Surgery 2012 14: 31.Mary Ellen Goldberg. Feline Physical Rehabilitation and the Veterinary Technician/Nurse, Proceedings AVMA 2018, Denver, CO, July 13-17Sharp B. FELINE PHYSIOTHERAPY AND REHABILITATION 1. Principles and potential. Journal of Feline Medicine and Surgery (2012) 14, 622–632Goldberg and Tomlinson. Physical Rehabilitation for Veterinary Technicians and Nurses, 2018, Wiley/Blackwell, Hoboken, NJ ISBN 9781119017356Face Validity of a proposed tool for staging canine osteoarthritis: Canine OsteoArthritis Staging Tool (COAST) The veterinary Journal 235 (2018) 1-8
Additional COAST tools can be found at: https://www.galliprantfordogs.com/vet/coast courtesy of Elanco
1. There is often a “disconnect” between what we see in our patients and how the owners see their pets.
a. It is often expressed as functional and behavioral issues but the owner does not see these things as signs of pain
i. Issues using stairs
ii.Trouble getting into or out of cars and other vehicles
iii. Reluctance to play
287
iv. Fear of slippery surfaces
v.Even limping might be viewed as a non-painful issue.
b. They may even bring these things to your attention, but then say, “thankfully, he/she is not in pain”
2. The pain exam starts with distant observation.
a. These observations may be from
i. The receptionist
ii.The veterinary nurse
iii.The veterinarian
iv.Any staff member
b. Things to look out for
i. Scuffing of feet, sometimes accompanied by a click as the nails hit the floor
ii.Urination posture is often compromised with hip and knee pain
1. An incomplete squat, compared to almost touching the ground with a dog not in pain
iii. A slow walk into the clinic
iv. And of course, any gait abnormality
c. The pain exam continues in the exam room with closer observation
i. Scuffed or worn nails, especially the central nails
ii.Standing up front legs first
1. Dogs normally stand rear legs first or all four legs simultaneously
iii. A hip dysplasia stance
1. A normal dog will stand in such a way that you can draw a straight line from the shoulder, to the elbow and the back of the foot. Rear legs are usually stretched out behind them
2. A dog with hip dysplasia shifts their weight forward. This results in a line dropped from the shoulder completely missing the shoulder joint and landing at the toes. The rear legs are generally directly under the hips.
3. The Physical exam
a. Best done on the floor with all but the smallest of dogs
288
b. It should start with casual petting and touching.
i. This can be your preliminary exam
ii.Look for areas of heat, muscle fasciculation and sensitivity to touch
c. Methodically go through each limb.
i. I usually save the suspect limb for last
ii.Flex and extend each limb, comparing degree of flexion and extension, something called the range of motion, of one side to the other. Flexion should usually end in a soft feel, extension should be more abrupt but without pain.
d. Difficult patients
i. Some dogs are impossible to assess
1. Aggression
2. Stoicism
ii. It is OK to send the dog home to return later in the day or another day with an anti-anxiety medication like trazodone on board
iii. It is also OK to sedate for exam and radiographs
4. Chronic pain surveys
a. It is important to ask:
i. It may not be obvious to the owner
ii. It may not be obvious to you
iii. It is always obvious to the dog in pain, however you have to know how to ask about it
b. The survey
i. Best to use validated surveys
ii.Chronic pain only. Acute pain requires a separate survey
iii.Must be for dogs, not for cats
iv.Try to pick one that is short and thus more likely to be administered by your staff and completed by your client.
c. My favorites are the Canine Brief Pain Inventory-Abbreviated version (CBPI) and the Liverpool Osteoarthritis in Dogs (LOAD)
i. Both have links to download in the resources
289
d. Pain Interference Section of the CBPI
i. Middle section
ii.Asks six performance questions
1. Owner rates from 1 (no problem) to 10 (impossible)
iii. Questions
1. General activity
2. Enjoyment of life
3. Ability to rise to standing from lying down
4. Ability to walk
5. Ability to Run
6. Ability to climb stairs, curbs, doorsteps, etc.
iv. Scoring
1. “0” no pain
2. <2.5 Mild
3. 2.5-6 Moderate
4. 6.1-9 Severe
5. > 9 Extreme
v.Treatments
1. Any score other than zero must be suspect…sometimes owners under report to what they want the dog to be, not how they are.
2. Every score of 2.5 or higher should be offered pain treatments
a. Treatments vary
i. Degree of pain
ii.Owner’s capabilities
1. Administration
2. Time
3. Money
iii. Your own skill set
5. The Canine Osteoarthritis Staging Tool (COAST)
290
a. Why?
i. Proposal to improve and standardize the approach to diagnosis and monitoring of canine OA over time
ii.Developed by 9 international specialists
iii. Designed for use in primary care practices
Encompasses early detection and discussion of “at risk” patientsi. Is proactive, multidisciplinary team approach
b. COAST Publication: See resource page for link to publication and link to resource tools
c. Two focuses: preclinical and clinical
i. Preclinical risk factors
1. Genetic
2. Intense Activity
3. Joint Injury
4. Joint Surgery
5. Excess Body Weight
6. Age
ii.Clinical factors based on
1. CBPI or LOAD
2. Observations
3. Pain exam
d. Key steps of COAST (this is best looked at by going to https://www.galliprantfordogs.com/vet/coast)
i. Grade the Dog and Grade the Joint
1. Then stage the OA
2. Treat and repeat
ii.Convert the CBPI or LOAD to a COAST conversion by downloading tools from above link.
291

Fun with felines…and fleas? By Jenifer Chatfield, DVM, DACZM, DACVPM DrJenTheVet.com What do you think of when someone says “fleas?” What about if they say cats? What if someone says cat fleas? It is a near certainty that no one thinks of “fun!” If you are not appropriately repulsed at the thought of fleas in cats…in the carpet…in the bed…uh, you get the idea, then let’s discuss a bit of flea history, flea-associated zoonotic diseases, and flea prevention in cats…even those super special “indoor only” cats. A bit of history The oldest known species of fleas have been found in Baltic amber dating back nearly 35 to 50 million years ago. In fact, the color puce was so named in France in the summer of 1775, with the queen being dressed in a brown lutestring (silk), the king good humoredly observed, it was “couleur de puce”, the color of fleas. I am sure that ruined the evening! Fleas permeated nearly every part of society – not just the poorest populations. When something permeates every class and division of society, people tend to focus on it, hence drawings of the flea from egg to adult, as well as more famous pieces of art included the reflection of fleas among the populace. A German doctor named Franz Ernst Brückmann (1697-1753) designed the first flea trap in the early 1700s and they were popular for a short period. The flea-trap became something of a popular fashion accessory as it could be worn on a ribbon as a necklace, hanging down inside a dress. It consisted of a hollow fenestrated tube, sometimes ornately carved and made of silver or ivory, inside which would be a small rod, tuft of fur or a piece of cloth. This would be smeared with a few drops of blood, to attract the fleas, and also fat, honey resin, designed to make the fleas stick fast to it as they crawled inside, and which was removed as necessary to get rid of them. It could also be placed in a bed to address an infestation. Flea biology The most common flea is the cat flea, Ctenocephalides felis. Adult cat fleas do not willingly leave their hosts, and inter-animal transfer of adult fleas is rare except in animals that share sleeping quarters. Many animals have their own species of flea. Fleas have a four-part life cycle consisting of eggs, larvae, pupae, and adults. The primary hosts for C. felis and C. canis are cats and dogs, respectively, although other mammals, including humans, may be fed upon. The average life cycle duration in households is 3-8 weeks, but can be 12-14 days or 350 days depending on temperature and humidity (colder and drier = longer). No stage is cold-resistant (<37.4F) so survive in North as adults on hosts. Disease issues in cats with fleas Fleas can cause a number of pathological conditions in cats including:
• Flea Anemia • Bartonella, Bartonella henselae, in both dogs and cats • Tapeworms • Feline Miliary Dermatitis
292
Zoonotic disease concerns with feline fleas • Cat scratch disease = Bartonella henselae• Murine typhus/feline typhus = Rickettsia typhi• Plague = Yersinia pestis
Based upon evolving evidence, B. henselae appears to fulfill all criteria for a stealth, intravascular, and endotheliotropic pathogen that can induce chronic neurological symptoms.
Flea prevention options Many methods of flea prevention are utilized by clients – we have all heard them! However, treating the cat’s environment is not effective flea control and prevention. The pet is the source of the ongoing infestation and should be treated safely and appropriately. Clients listen to their veterinarians. Have the conversation with clients and provide specific and direct recommendations. The threat of disease for both the cat (even indoor only cats) and their owners is real and significant – continue to bang the drum with cat owners to help them, and their cats, live happier, healthier, flea-free lives.
“Take Home” Points 1. Indoor only cats get fleas and should be on prevention2. Fleas do present a disease risk to owners and cats3. All pets in the household must be treated for and provided with prevention for fleas4. Continue to have the conversation with cat owners and where possible make specific and direct
recommendations to increase compliance
References 1. https://www.epa.gov/pets/controlling-fleas-and-ticks-around-your-home2. https://www.sciencedirect.com/topics/veterinary-science-and-veterinary-medicine/oriental-rat-
flea3. https://www.cdc.gov/plague/faq/index.html#how4. Case study mentioned in lecture:
https://parasitesandvectors.biomedcentral.com/articles/10.1186/s13071-016-1547-95. https://www.cdc.gov/bartonella/cat-scratch/index.html6. Pathogens in fleas collected from cats and dogs: distribution and prevalence in the UK. Abdullah,
Swaid et al. “Pathogens in fleas collected from cats and dogs: distribution and prevalence in theUK.” Parasites & Vectors (2019).
7. Feline Miliary Dermatitis BRITISH SMALL ANIMAL VETERINARY CONGRESS 2008 Ralf S. Mueller,MAVSc, DACVD, FACVSc, DECVD, DrMedVet, DrHabil, FAAAAI. Ludwig Maximilian UniversityMunich, Germany.
8. https://www.cdc.gov/bartonella/veterinarians/index.html9. Essential Oils ref: DE S. O. BATISTA, L., CID, Y., DE ALMEIDA, A., PRUDÊNCIO, E., RIGER, C., DE
SOUZA, M., . . . CHAVES, D. (2016). In vitro efficacy of essential oils and extracts of Schinus molle L.against Ctenocephalides felis felis. Parasitology, 143(5), 627-638.
10. Grooming and control of fleas in cats. Robert A. Eckstein and Benjamin L. Hart. In Applied AnimalBehaviour Science. 68(2):10 May 2000, Pp.141-150.
293
11. Marie-Christine Cadiergues and Charline Pressanti. Efficacy of Spinosad Tablets Administered to aColony of 15 Indoor Cats Naturally Infested with Fleas. ISRN Veterinary Science. Volume 2014,Article ID 484308, 4 pages.
294

Dog parks and parasite risk Michael W. Dryden, DVM, PhD, DACVM-Parasit University Distinguished Professor (Emeritus) College of Veterinary Medicine, Kansas State University In today’s society dogs are extremely mobile. Many dog owners take their pets when traveling by car or plane and numerous hotels and restaurants are “pet-friendly”. Increasingly many municipalities have established “dog-parks”, where dogs and their owners can interact often without leash restrictions.1 While all this travel and dog interaction is beneficial to the human-animal bond, it does pose certain risks. One of which is parasite contamination of areas in which these dogs have access.2-5
The most recent study of dog parks and parasitism5 was conducted between July – August 2019. Investigators visited 288 dog parks in 30 metropolitan areas in the United States. Cites included in the study included Atlanta, Boston, Chicago, Albuquerque, Austin, New York City, Cleveland, Bakersfield, Charlotte, Philadelphia, Detroit, Boise, Houston, Washington DC, Indianapolis, Denver, Miami/Ft Lauderdale, Kansas City, Los Angeles, Nashville, Minneapolis, Phoenix, New Orleans, St Louis, Portland, Oklahoma City/Tulsa, Sacramento, Raleigh/Durham, Seattle and Tampa. At each park they collected 10 freshly deposited canine samples provided by the dog’s owners. At each park owners completed brief questionnaires and only one dog sampled per household was collected. Fecal examinations were conducted with both centrifugal flotation and antigen testing (Fecal Dx® + Giardia).5
Samples were examined from 3006 dogs. At least one intestinal parasite was detected in 622 (20.7%) samples, nematodes in 263 (8.8%), with hookworms, whipworms and ascarids in 7.1, 1.9 and 0.6% of samples, respectively. A sample positive for one or more intestinal parasites was found in 245 (85.1%) parks, with nematodes found in 143 (49.7%). Combined, CAI and CF detected 78.4% more intestinal nematode infections than CF alone. Hookworm and whipworm infections were detected in all age groups, but ascarids were only detected in dogs less than 4 years-old. Approximately 42% of dogs aged less than 1 year were positive for nematodes or Giardia. The hookworm results are interesting and concerning. Hookworms, almost exclusively Ancylostoma caninum, were found in 214 (7.1%) of the dogs but in a staggering 43.4% of the dog parks. Hookworms were found most commonly in the southeast region (15.3% of dogs and 72% of dog parks) and lowest in the west (1.5% of dogs and 17% of dog parks). Ancylostoma caninum is a highly pathogenic blood sucking parasite that can produce anemia and death in dogs. It is also a zoonotic threat producing cutaneous larva migrans, pneumonitis and rarely eosinophilic enteritis6 While there have been a number of products historically available that could effectively treat and prevent hookworms in dogs, the recent emergence of multiple-drug resistant (MDR) Ancylostoma7 is causing considerable concern within the profession. While initially
295
documented in greyhounds, MDR Ancylostoma has now been documented in numerous other breeds. Chronic hookworms in dogs is not an uncommon problem. But determining the cause of the chronic cases and proving resistance is difficult. Reinfection from contaminated yards or other areas outdoors these dogs have access. Remember that A. caninum has a development or prepatent period as short as 2 – 3 weeks. Therefore, a dog can be infected and shed eggs in as little as 2 to 3 weeks. Therefore, the finding of a positive fecal between monthly dosing of broad-spectrum heartworm preventives may occur and is not indicative of product failure. What this is indicating is that the dog is experiencing exposure to infective larvae and is at risk of hookworm infection and disease. Clearly such dogs are greatly benefiting from the regular administration of the broad-spectrum heartworm preventive. A fecal positive for hookworm eggs between monthly dosing of the product is strong reinforcement to continue its administration! In some retired greyhounds (and other breeds) these dogs do appear to be chronically infected and the problem may be attributed to “leak-back”, also called “larval leak”. These dogs have large somatic (tissue) larvae burdens. Infective larvae are acquired throughout their lives while being raised and housed in sand runs and pens. Many of these larvae undergo somatic migration and become encysted in various tissues in the dog. At various times during the dog’s life some of the larvae may be “reactivated” and migrate back to small intestine, where they mature. Finally, true anthelmintic resistance has now been documented in Ancylostoma caninum in greyhounds and other breeds of dogs that likely have had contact with environments greyhounds have frequented.7-10 Some of these nematodes appear to be multi-drug resistant. Resistance can be assessed by conducting a quantitative fecal exam (EPG), administering the correct dose of milbemycin oxime, pyrantel or fenbendazole and rechecking a quantitative fecal exam in 7 to 10 days. If the worms are susceptible the fecal should be negative or egg numbers should be reduced by >90%. The other nematode parasite of considerable pathogenic importance that was recovered was Trichuris vulpis. It was found in 58 (1.9%) dogs but in 18.1% of all dog parks. Interestingly it was found in 9% of dog parks in the west, 18% of dog parks in the east and Midwest and 26% of dog parks in the south. This is a parasite that is often underdiagnosed and underappreciated in may practices. It has been well documented that classic passive flotation fecal procedures are markedly inferior to centrifugation procedures in their ability to recover the heavy bi-polar plugged eggs of Trichuris vulpis.11 In particular study a passive flotation technique recovered T. vulpis eggs in only 37.7% of 239 positive samples.12 Veterinarians often do not appreciate the pathogenesis of this parasite. Larvae and adults have a “mouth spear”. Tip of spear cuts and shreds tissue and blood vessels allowing the worm to feed.13 Clinical signs are dependent on worm numbers, extent of gut penetration, and reaction of the host. Worms may be found deeper in the gut wall through the muscular mucosa in lymphoid follicles which become necrotic. Cause of necrosis may be whipworms secretions and/or secondary bacterial infection. Clinical signs are variable and range from mild to severe
296
and include anorexia, weight loss, mucoid or bloody diarrhea, vomiting and even death.13,14 Use of appropriate preventive medications are important, because not all broad-spectrum heartworm preventives are effective in eliminating T. vulpis.
Clearly the most common parasite recovered in this study was Giardia. Giardia was detected in 13% (391) of all dogs in in a staggering 74.0% of dog parks. I think that veterinarians are increasingly coming to recognize just how common Giardia occurs in our pet dog population and this study further reinforces that prevalence. But the significance that high infection rate is still not clearly understood. Most adult dogs with Giardia are asymptomatic and the zoonotic implications are not understood. Most of the Giardia isolates recovered from dogs are not the same genetic isolates that we recover from humans. Recently in a 40-year retrospective study conducted by the CDC they did not find a single giardia outbreak (an outbreak was defined as two or more cases of giardiasis that were epidemiologically linked by time or location of exposure to a common source) linked to a dog or cat. On the Companion Animal Parasite Council web site it states “Human infection from a dog or cat source has not been conclusively demonstrated in North America.” Canine strains of G. duodenalis are not known to be infective to immunocompetent human hosts. However, people with increased susceptibility to infection due to underlying disease should consider limiting their exposure to Giardia-infected pets. https://capcvet.org/guidelines/giardia/. This does not mean that no human is not going to get Giardia from a dog or cat, it just means that it is extremely unlikely. Giardia has also been difficult to accurately diagnose. Given the poor sensitivity of direct smears (≈32%)17 and unreliability of cyst identification by veterinary technicians utilizing passive fecal techniques (18%) or even centrifugation techniques (22% - 64%)18, fecal antigen assays have been increasing utilized in private practices. When diagnosing and treating giardiasis it is important to remember that the prepatent period of tis protozoan can be as short as 6 days. Therefore, a positive test 2 to 3 weeks following treatment does not necessarily indicate a treatment failure, it just as likely indicates reinfection. Retesting 5 days post-treatment is a much better indicator of success or failure or treatment. References
1. The Trust for Public Land. Dog park rankings for the 100 largest U.S. cities, 2019. https ://www.tpl.org/sites /defau lt/files /City%20Par k%20Fac ts%20Dog %20Par ks%20201 9_R5_0.pdf. Accessed 11 Feb 2020.
2. Smith AF, Semeniuk CAD, Kutz SJ, Massolo A. Dog-walking behaviors affect gastrointestinal parasitism in park-attending dogs. Parasit Vectors. 2014;7:429.
3. Duncan KT, Koons NR, Litherland MA, Little SE, Nagamori Y. Prevalence of intestinal parasites in fecal samples and estimation of parasite contamination from dog parks in central Oklahoma. Vet Parasitol Reg Stud Reports. 2020;19:100362.
4. Savadelis MD, Evans CC, Mabry KH, LeFavi LN, Klink BD, von Simson C, et al. Canine gastrointestinal nematode transmission potential inmunicipal dog parks in the southeast United States. Vet Parasitol Reg Stud Reports. 2019;18:100324.
297
5. Stafford K, Kollasch TM, Duncan KT, Horr S, Goddu T, Heinz-Loomer C,. Rumschlag AJ, Ryan WG, Sweet S, Little SE. Detection of gastrointestinal parasitism at recreational canine sites in the USA: the DOGPARCS study. Parasit Vectors. 2020 Jun 01; 13(1):275.
6. Bowman DD, Montgomery SP, Zajac AM, Eberhard ML, Kazacos KR. Hookworms of dogs and cats as agents of cutaneous larva migrans. Bowman et al. Trends Parasitol. 2010 Apr;26(4):162-7.
7. Castro J, Howell SB, Schaefer JJ, Avramenko RW, Gilleard JS, Kaplan RM. Multiple drug resistance in the canine hookworm Ancylostoma caninum: an emerging threat? Parasit Vectors. 2019 Dec 9;12(1):576.
8. Kitchen S, Ratnappan R, Han S, Leasure C, Grill E, Iqbal Z, Granger O, O'Halloran DM, Hawdon JM. Isolation and characterization of a naturally occurring multidrug-resistant strain of the canine hookworm, Ancylostoma caninum. Int J Parasitol. 2019 Apr;49(5):397-406.
9. Hess LB, Millward LM, Rudinsky A, Vincent E, Marsh A. Combination Anthelmintic Treatment for Persistent Ancylostoma caninum Ova Shedding in Greyhounds. J Am Anim Hosp Assoc. 2019 May/Jun;55(3):160-166.
10. Castro J, Mansour A, Charles S, Hostetler J, Settje T, Kulke D, Kaplan RM. Efficacy evaluation of anthelmintic products against an infection with the canine hookworm (Ancylostoma caninum) isolate Worthy 4.1F3P in dogs. Int J Parasitol Drugs Drug Resist. 2020 Aug;13:22-27.
11. Dryden MW, Payne PA, Ridley R, Smith V. Gastrointestinal Parasites: the practice guide to accurate diagnosis and treatment. Supplement to Compendium: Continuing Education for Veterinarians. 28 (8A): 3 -13, 2006.
12. Dryden MW, Herrin BH, Payne PA, Smith V, Ritchie D, Hegarty E. Further comparison of centrifugation versus passive fecal flotation for the recovery of Toxocara canis, Trichuris vulpis and Ancylostoma caninum eggs. Joint meeting Am. Assoc. Vet. Parasitol. 62nd Annual Meeting, WAAVP 27th Conference. 7 – 11 Jul Madison, WI.
13. HendrixCM, BlagburnBL, Lindsay DS: Whipworms and intestinal threadworms. In GrieveRB (Ed.): Parasitic Infections. Vet Clin NA Sm Animal Practice 17(6): 1355-1366, Philadelphia, Saunders, 1987.
14. DrydenMW, GaafarSM: Whipworm infection in small animals. Comp An Pract 2(5): 17-22, 1988.
15. Ballweber LR, Xiao L, Bowman DD, Kahn G, Cama VA. Giardiasis in dogs and cats: update on epidemiology and public health significance. Trends Parasitol. 2010 Apr;26(4):180-189.
16. Adam EA, Yoder JS, Gould LH, Hlavsa MC, Gargano JW. Giardiasis outbreaks in the United States, 1971–2011. Epidemiol Infect 144(13): 2790-2801, 2016.
17. Olson ME, Leonard NJ, Strout J. Prevalence and diagnosis of Giardia infection in dogs and cats using a fecal antigen test and fecal smear. Can Vet J. 2010 Jun;51(6):640-2.
18. Dryden MW, Payne PA, Smith V. Accurate diagnosis of Giardia spp. and proper fecal examination procedures. Vet. Therapeutics 7(1), 4 – 14, 2006
298
A veterinarian’s guide to pets with disabilities and special needs By Melissa Shapiro, DVM Visiting Vet Service, Piglet, the deaf blind pink puppy Pets with disabilities and special needs are not new or rare in veterinary medicine. Some animals are born with congenital defects which affect hearing and vision, the respiratory tract, and limbs. Other animals are affected by metabolic diseases that are not immediately recognized at birth but manifest over their first few years of life. And when animals live long enough, most will inevitably develop disabilities and special needs in the form of chronic mobility issues, diabetes, cancer, or other organ failure. The increased use of social media platforms has helped normalize pets with disabilities and special needs. Through social media pages and featured viral videos, disabled pets have been given an opportunity to serve as ambassadors for other pets and people with special needs. Many of these pets are the focus of educational programs, rescue groups, and nonprofit organizations that teach positive attitude, inclusion, empathy, and kindness. While this group of animals indicates immensely positive shifts towards awareness and normalization of disabilities, it is important to remember that not all pets with disabilities and special needs are celebrities. Many pets with disabilities and special needs find themselves in shelters or abandoned on the streets, while others, sometimes due to a lack of understanding, follow a path towards euthanasia. Despite so many easily accessible resources, when presented with pets with disabilities or special needs, often at the request of breeders, it is still common for veterinarians to agree to or recommend euthanasia, even in the case of minor congenital defects. While euthanasia is the kindest option for some, many of these animals have the potential to live good quality, productive lives despite their disabilities. Agreeing to euthanasia is not a requirement, especially when there are viable alternatives. Fortunately, many pets with disabilities live in loving homes with devoted, caring families. Their people spare no cost in time, energy, or money to ensure optimal medical care and quality of life. Even though some of these animals are destined to have significantly shortened lifespans, their people understand and commit to loving and caring for them for as long as possible. It is critical then that veterinarians are well equipped with the tools and resources to support these families, especially given that these special needs pets often require frequent veterinary hospital visits. So, what is a veterinarian’s role in the care of a pet with disabilities and special needs? Veterinarians are trained to treat urinary tract infections and pressure sores commonly found in paralyzed animals. They can diagnose and treat uveitis or glaucoma in a double merle Australian Shepherds and diagnose diabetes and teach clients how to give insulin to their pets. But caring for pets with disabilities and special needs requires veterinarians to have a much deeper involvement and understanding beyond just the specific diagnosis and standard
299
treatment. It requires developing thoughtful and close partnerships with special needs pet-parents and can be extremely rewarding for many veterinarians. Providing this kind of individualized veterinary care goes beyond just supporting the client with medical advice. It often involves pointing the client towards additional resources as they navigate the world of caring for a disabled pet. There is an extensive network of special needs pet parents who are knowledgeable about the ins and outs of supplies (wheels, diapers, slings, ramps), protocols, and even treatment options. Some are current clients willing to advise and guide others with newly acquired disabled pets. Social media support groups and rescue groups can also be a great supplement to veterinary care for special needs pets. Beyond taking care of disabled pets in their own practice, vets can take an active role in helping pets with disabilities more broadly. Using their status as a medical professional, vets can take the opportunity to educate, advocate, and even help arrange optimal placement of disabled and special needs dogs, cats, and other pets. Awareness of the resources to help in these situations can make this active role second nature. Rescue organizations have readily available websites and social media pages dedicated to disabled and special needs pets that clients find helpful. Vets can easily partner with these groups to streamline protocols and recommendations for disabled animals that deserve a second chance. While many disabled pets live relatively normal lives despite minor challenges, profoundly disabled animals might not be able to participate in what most would consider “normal” daily routines and activities. This does not mean that they can’t live happy, active, and meaningful lives. It is very important for veterinarians to understand the potential for these animals to become loving family members, therapy pets, educators, advocates, and influencers. Veterinarians play a critical role in working with caring clients who devote tremendous amounts of time, energy, and money into ensuring their disabled pets have a good quality, happy life.
300
CEF’s-Retirement Investing
By Shawn Messonnier, DVM
Abstract
• Saving vs Investing-
• Saving-Short-term goals (less than 5 years,) Emergency Fund (6-12 months of living expenses.) Keeps principal safe, hopefully some yield.
• Investing-Long-term goals, NOT Emergency Fund! Principal at risk but potential for growth (capital gains) AND/OR income (income more important in retirement, gains more important earlier in life.
• Need BOTH savings and Investing…never too late to start.
• Younger investors invest for growth where income is not important. Older investors near or in retirement still need a growth component (inflation) but need cash flow/income.
Options
• Options for Savings-CD’s, Money Mkt Funds, Savings Acct.
• Pros/Cons each.
• Main Options for Investing- Open End Mutual Funds (“mutual funds,”) Closed End Mutual Funds (CEF’s,) Individual Stocks (dividend paying.)
• Pros/Cons each.
Rule of 72
• Rule of 72-Very Important! Use to determine length of time for your money to double or % return when money doubles.
• The Formula for the Rule of 72 Is
• Years to Double=72/Interest Rate (Yield)
OR
Yield=72/Years to Double
Example-If an investment promises an 8% annual compounded rate of return, it will take approximately (72 / 8) = 9 years to double the invested money.
• The rule assumes continuous compounding and not removing extra money nor adding extra money.
301
Budgeting
• Used for monthly expenses-make budgeting easy
• Categories up to you, but typically groceries, entertainment, utilities, gas, charities, miscellaneous.
• KISS-don’t need too many envelopes!
Bucket system
• Harold Evensky-creator
• Cash flow in retirement
3 buckets-#1-short term ongoing cash needs (1-3 years living expenses)..#2-bonds/balanced funds/CEF’s/dividend stocks…#3 growth bucket-stocks and stock mutual funds/ETF’s
Portfolios can be conservative/intermediate/aggressive
Buckets refilled/adjusted annually
• Reference-Morningstar
4% rule
• The Four Percent Rule states that you can withdraw 4% of your portfolio each year in retirement for a comfortable life without depleting your principal for a period of 33 years.
• It was created using historical data on stock and bond returns over a 50-year period.
• May not be realistic…also concerns about inflation.
• One common misconception is that the 4% rule dictates that retirees withdraw 4% of their portfolio’s value each year during retirement. The 4% applies only in year one of retirement. After that inflation dictates the amount withdrawn. The goal is to maintain the purchasing power of the 4% withdrawn in the first year of retirement.
• William Bengen adopted the assumption that a retiree’s portfolio would be invested 50% in stocks (the S&P 500) and 50% in bonds (intermediate term Treasuries) … Bengen assumed a 10.3% return on stocks and a 5.2% return on bonds. Using this asset allocation, he tested a range of first-year withdrawal rates:
• 3% withdrawal rate: All portfolios lasted 50 years.
302
• 4% withdrawal rate: Most portfolios lasted 50 years. Retirements started in 10 of the 50 years examined fell short of this mark, although they all lasted about 35 years or longer.
• 5% withdrawal rate: More than half of the portfolios were exhausted in less than 50 years, with the worst portfolios lasting no more than about 20 years.
• 6% withdrawal rate: Only seven portfolios lasted 50 years, with about 10 lasting fewer than 20 years.
My accounts
• Emergency Fund-Cash/MMF
• Vacation/Travel-1/2 cash, ½ CEF’s.
• ¼ Mutual Funds-growth with minimal yield
• ¾ dividend stocks (including MLPS/REITS,) CEF’s (bonds, muni bonds, stocks.)-yield with some growth
• 1 year before retirement-cash (stop reinvesting) =1 year of expenses
Cash flow-dividend stocks
• Individual Stocks vs Dividend Stock Mutual Funds
• Picking stocks can be timely and is often hit-or-miss even by experts. Increasing the number of dividend stocks to between 50-100 different stocks in a variety of industries/sectors minimizes risk of loss of principal (the amount of money you invest) and the chance that too many of your stocks will suffer dividend cuts or suspensions (can you say COVID-19?!)
• There are no guarantees in cash flow, but dividend stocks tend to bring greater cash flow than cash, CD’s, or bonds (although bonds/bond funds can also provide cash flow and help balance the risk of a retirement portfolio.)
• Bonds-taxable vs tax-free.
CEF’S
• CEFs are mutual funds actively managed by a fund manager, like many mutual funds, but do not issue or redeem shares daily as is the case with mutual funds. A CEF portfolio is typically focused on a narrower subset of securities, such as a specific industry or market sector, which makes them more subject to volatility. Unlike “open” mutual funds, CEF’s are considered "closed" because they raise capital only one time, at an initial public offering, before being closed to any additional share offerings.
303
• A CEF trades like a stock—on a stock exchange or over the counter—while an open-end mutual fund is bought and sold directly with the fund company or a brokerage firm.
• Unlike open ended mutual funds, CEF’s trade at a discount (usually) or premium to the value of the assets in the fund (called the NAV.) In general, investors try to buy CEF’s when the discount to the NAV is larger than average, and extra money is made as the discount narrows and the share price increases (this gain is only realized if shares are sold as their value increases, similar to an open-end mutual fund or individual stock; investors can buy and hold and never sell and simply get the monthly or quarterly cash flow.)
• A second feature of CEF’s is debt, as many CEFs borrow money to buy holdings in the fund (debt is called leverage, which averages around 33%.) That can boost yield by adding to the number of holdings in a CEF that are paying dividends, interest or capital-gain income. But it can also magnify losses as securities can lose value if interest rates rise (especially in interest rate sensitive securities like bonds.)
• One final feature to remember is that some of the income of some CEFs consists of “return of principal (capital)” rather than from earnings. A CEF may return principal if, for example, it is unable to meet periodic distribution levels that shareholders have come to expect. Depleting capital can erode the CEF's share price over time. This is usually not a problem for well-run funds and can be advantageous when taxes are due.
CEF’S-Cash Flow
• Cash is given to the investor of CEF’s in 2 ways-cash flow (represented as yield on the fund, paid monthly, quarterly, biannually, annually,) and growth of the share price (capital gains similar to stocks and mutual funds.) The yield/cash flow is what makes these funds so appealing to (retirement) investors and averages 6.73%, quite a bit higher than the S&P 500. This means for every $100,000 invested you would get $6730 cash flow annually. In general, CEF’s are chosen as investments by those who want regular (but not guaranteed) cash flow, such as retirees.
• Average cash flow varies with type of CEF (bond vs stock.)
• Tax-free bonds average 4.5-5% (22% tax rate=6%, 40.8%=8%.)
• Stock CEF’s average-7-8% (varies with type of fund.)
• MUCH better cash flow than many other investments, but don’t forget potential risks.
References
304
• cefa.com
• Morningstar.com
• Cefconnect.com
• Suredividend.com
• Simplysafedividends.com
305
Pet insurance to achieve better medicine, better business By Shawn Messonnier, DVM History of Pet Insurance Surprise! Pet health insurance is over 100 years old. The first policy was written in 1890 by Claes Virgin, founder of Länsförsäkrings Alliance, a Swedish insurance company still around today. The original policies extended to horses and livestock; and by 1947, the first pet insurance policy was sold in Britain. By 2009, Britain had the second highest level of pet insurance in the world followed by Sweden. 1890– The first pet insurance policy is written by Claes Virgin, founder of Länsförsäkrings Alliance. 1924– The first dog receives insurance coverage in Sweden. 1947 – Britain starts issuing pet insurance policies. 1980 – Veterinary Pet Insurance (VPI) was the first company to offer pet health insurance in North America (Nationwide was VPI’s underwriter since it was founded and acquires the company outright in 2009). 1982– Lassie receives the first pet insurance policy in the United States, issued by Veterinary Pet Insurance (VPI). 1989– Pet health insurance is introduced to Canada by Petplan, MediPet and Petsure. 2007– The North American Pet Health Insurance Association (NAPHIA) is founded to establish and maintain standards for the pet health insurance industry. 2010 – Healthy Paws Pet Insurance enrolled its first pet in February 2010. 2014 – Dr. Jack Stephens, founder and president of PetsBest Insurance and the man credited with starting pet insurance in North America, retires. North American Pet Health Insurance Market Surpassed $1.71B (USD) in 2019 The North American Pet Health Insurance Association (NAPHIA) is comprised of reputable pet health insurance (PHI) organizations from across Canada and the United States. In 2019, over 2.81 million pets were insured across North America, which represents a 16% increase over 2018 U.S. $1.56 billion USD – total premium volume 2,517,122 – total number of pets insured 83% of insured pets were dogs versus 17% cats The average accident and illness premium for dogs was $585.40/year or $48.78/month (figures
306
in USD) The average accident and illness premium for cats was $349.93/year or $29.16/month (figures in USD) Canada $159 million USD – total premium volume ($208.6 million CAD) 302,424 – total number of pets insured 78% of insured pets were dogs versus 22% cats Why pet owners want insurance? What you’re finding is that pets have really changed their place in the family hierarchy…some studies have said that anywhere from 95% to 98% of pet owners say their pet is part of the family. Pet owners are now called “pet parents” and some groups fight for equal rights for pets (interesting, in France there is a political party for pets!) Sarah Wooten, DVM, CVJ, Fetch dvm360 conference speaker, agrees, adding that younger pet owners are demanding more than the basic care expected by previous generations. “They want holistic, integrative options. Wellness to them is not just about vaccines and heartworm prevention. It’s also mental, emotional and environmental,” Dr. Wooten says. “They want wellness in all of those aspects. So, if you provide those services, it is so valuable.” Over the past five or so years, the market for pet insurance has grown younger. The 25- to 44-year age group is now the primary market for pet insurance, with 28% of pet owners 25 to 34 years old and 20% of 35- to 44-year-old pet owners purchasing pet insurance. One possible explanation for the growth in these markets is an increase in employer-backed pet insurance (not always the best option as the employer offers 1 plan) has evolved as a product, further contributing to an increase in popularity. Once seen mostly as coverage for emergencies and accidents, wellness is the new trend (not all companies cover wellness and the definition of “wellness care” varies among companies). Pros Client
• (Usually) takes the objection of costs/expenses off of the table. • Allows client to say YES rather than NO to care pet needs. Can take advantage of expensive technology/treatments. • Pet gets healthier quicker. Improves pet-parent bond. • Pet lives longer. Improves bond. • Prevents euthanasia (unless prognosis is grave.) Improves bond. • Bonds to practice-more, regular visits. • Note-Insurance combined with 3rd party payments can reduce need for upfront payment as “loan” paid off with arrival of insurance check.
Pet • Gets better quicker! • Gets care it needs/deserves rather than simply what the owner can afford at the time of illness.
307
• Gets diagnosis/care earlier in the course of the disease. • Gets more frequent care; regular follow-up visits and wellness visits (if wellness covered.) • Avoids euthanasia most of the time. • Lives healthier life. • Lives longer life. • Increases bond to owner and practice.
If wellness is part of insurance package, pet gets regular wellness care. This avoids skipping essential services (vaccines or titers, dental care, HW preventive, routine lab tests, etc.) Essential services vital to disease prevention and early diagnosis of more serious medical issues. If wellness care is included, often gets earlier diagnosis of serious, even fatal diseases. This helps the client (pet is saved,) pet (early diagnosis=life or at least comfort care for remainder of life,) and practice (ongoing treatment and repeated visits/testing/care=steady/greater revenue). Practice
• Get to practice more (and BETTER) medicine (you get to be a doctor more often than simply doing vaccines/spays/neuters, etc.) • You get to do more testing/use more advanced treatments/technologies. • Better results, fewer deaths/euthanasia. • Bonds clients and pets to practice (and maybe staff through less euthanasia and higher tech “stuff.”) • Increased practice revenue from clients saying YES to needed care rather than NO, MAYBE, or PLAN B (cheaper care that may be less effective.)
Cons
• YOU (and staff) have to “sell”/encourage clients to sign up. Many clients don’t think the pet “needs” insurance until pet is sick/injured. • Takes time and education of staff (handouts from company, practice-specific handouts, etc.) • Takes time to help file claims for visit (we usually file the claim for client but some practices have clients file their own claims. What’s the difference?) • Clients may not understand how insurance works (do I pay you at the time of the visits??) and have unrealistic expectations of what will/won’t be covered or when payment is made. • YOU/STAFF are NOT selling insurance-this is illegal. Therefore, client needs to do her own homework by getting online and also asking company representative questions. • A real pain in the rear IF you go with the wrong company!!
Marketing Insurance • Handouts-show examples of several companies, handouts supplied by companies (lunch and learn with company reps) • Social media-examples from my practice
308
• New client kit/folder • Doctor AND staff talk with client • Ask client if she will be using pet insurance to pay for today’s visit.
STAFF should get AND USE the insurance-they can more easily “sell” the insurance if they are using it and are satisfied (and this means their pet care is FREE!!!!) Some companies offer a discount for staff (I believe they should give it away to staff.) In my practice I spend a few minutes at the start of the visit for new clients asking them if they have insurance I then discuss several options and show them the handouts in their new client kits. I let them know the cost of care especially more expensive procedures like cancer treatment and specific breed issues/costs. I encourage them to get it ASAP BEFORE any problems arise. This is especially true for puppies and kittens. Most owners don’t think young pets will get sick, poisoned, or injured but I point out it happens all the time, and then you can still get insurance, but it won’t cover pre-existing problems that may be lifelong. Ask the insurance company for ideas/help/brochures, etc. for marketing support; lunch n learn. How to choose the “right”/” best” insurance company for your clients/practice-IMPT! Remember-you are NOT a licensed agent, so you don’t “sell” insurance. You can recommend, promote, endorse insurance. Talk with several companies to learn which companies may fit the needs of your practice/clients. My practice is holistic/functional medicine and not every company covers these therapies. Is wellness coverage important to you/your clients? Not all policies cover this. ALWAYS remind your clients that you don’t sell insurance and THEY need to follow-up on any information you give them by contacting the recommended companies and asking questions-you don’t want to be held accountable for any misinformation! The “right”/” best” insurance is the one your clients will use, and which is most generously and easily reimbursed! Various options-deductibles, percentage coverage/co-pay, wellness (what is wellness??) or illness/injury only, “holistic” (what does this mean?,) annual deductible vs per incident, dog/cat or exotics too, ease of filing claims/appeals, waiting period before coverage starts and before payment made to client, etc.
309
Care for a lifetime By Carolyn C. Shadle, Ph.D. and John L. Meyer, Ph.D.
Your veterinary practice has the opportunity to serve clients and their pets from the time they adopt their pets until the end of the pets’ lives. With such a long relationship, you may even be able to help your clients when they are ready to select a new pet. You help new pet owners learn about the care they will provide at home – feeding, training and exercising their pets. As the pet grows, you help the client with wellness visits and intervene when there is a health problem, including the inevitable issues senior pets face.
Finally, when the pets’ lives are ending, you are an important friend and veterinarian offering skillful and caring euthanasia service and appropriate support for owners who grieve the loss of their pets.
Advantage of lifetime care The obvious advantage of serving clients and their pets for the lifetime of the pets is the health of the pets. Because you know the pets’ histories and the care that the owners provide, you know when and how to advise them.
There have been many changes in the veterinary field, including improved and sophisticated healthcare opportunities and a major realignment of veterinary practices. We have seen corporations purchasing independent practices to create “chains,” providing a complete line of veterinary services. We have seen “big box” pet stores emerge. They sell products for pets but also provide many of the services - including vaccination clinics - that veterinarians have traditionally provided –and usually at a lower cost. Internet pharmacies now make veterinary prescriptions available 24/7/365, often at a lower cost.
These changes present major competition for independently-owner veterinary practices, so that attracting and maintaining clients for the life of their pets has become a major challenge – and opportunity.
How to establish a lifetime care practice We’ll address three areas which help practices compete, maintain their clients, and watch their patients thrive and grow.
Engaging with and retaining clients The most important area is establishing a trusting relationship with the clients – from day one. It turns out that in addition to the continuity of care benefiting the health of the pets, retaining clients makes economic sense. Research suggests that it costs seven times more to acquire a new client than it does to retain a client.
Why do clients leave? Well, of course, some move out of the area. But research indicates that the average business loses around 20% of its clients each year by failing to focus on the existing client relationship.
310
Preventive care Many practices focus on their existing clients stressing the importance of preventive care. They prefer to have their patients stay well than to see only sick pets. To make this economic for both the practice and the client, many practices are offering wellness plans. Such plans give clients assurance of what their annual veterinary wellness costs will be , and they provide the practice with an assurance of ongoing revenue.
You may want to bundle services in a number of different plans to address different client needs and preferences. Developing these plans takes time and thought so be sure to reach out for help. One resource that can help you through the process is the book written by Debbie Boone, CVPM and Wendy Hauser, DVM. The Veterinarian’s Guide to Healthy Pet Plans.
Reminders Preventive care requires your clients to visit your practice even when their pet is well. Whether your clients have purchased a wellness plan or not, they may need reminders to return for regular preventive care. You may be using email, texts, phone calls or post cards, or you may have starting using one of the tech services. A resource you might check out is Partners for Healthy Pets. Among other things in its “Toolbox” it provides help with “forward booking” and a reminder program for inactive clients. Partners also helps with building wellness plans. What is unique about its reminder service is that it targets patients based on the client’s visitation history (and not a timetable for a specific service). Also, it offers an empathetic message. Instead of shaming clients for falling behind on visits, it recognizes that the clinic knows that the client has the pet’s optimum health in mind but, as a busy person, may need a reminder of the importance of regular checkups.
Adopt telemedicine If you hadn’t secured a telemedicine platform prior to the outbreak of the COVID-19, the challenge of serving during this pandemic may have got you thinking. Clearly, the time has come to extend this opportunity to your clients. Even in healthy times, telemedicine provides a convenience to your clients – less travel, less waiting, less uncertainty around what might be an emergency. This service, whether used only during your operating hours or to extend service to 24/7, will also free up exam rooms.
An increasing number of software providers are available to help you get started, to show you how to monetize your time giving advice remotely, and how to link your telemedicine service with your Electronic Medical Records.
A new organization, The Veterinarian Virtual Care Association, was founded in May and stands ready to assist you in finding a provider and networking with users.
Relationship selling Engaging with clients entails learning the difference between relationship selling and traditional or transactional selling. In the former, you endeavor to get to know the client before doing “a
311
sell.” In the latter, you respond to a client purchase request but omit any conversation that shows you care about the client and the client’s pet.
Listening skills, including the show of empathy, are particularly important when engaging with your clients. It is wise to spend some “lunch ‘n’ learn” time being sure everyone on the team is enhancing their listening skills and appreciating the power of empathy.
Client education Another reason your clients will want to stay with you is because they know they can get the information they need to care for their pet. They’ll be directed to help with training and behavior issues. They’ll come to appreciate the health benefits of owning and bonding with a pet. And they will get trusted information on how to proceed with medical conditions or end-of-life decisions.
One source of useful educational material is The Pet Effect, a campaign led by the Human-Animal Bond Research Institute. Check them out for their flyers, posters and videos. These materials are both educational and entertaining. They are a useful resource to provide to clients who need to wait for their appointment.
Products and services The final area to consider in maintain your client for the lifetime of the pet is related to the products and services you can provide your clients. The more convenient you will make it for them to maintain a healthy pet, the more likely they are to look to you to fulfill their needs for medication, pet food and supplies and stay with you.
Online veterinary pharmacies are available 24/7/365. You can link up with a provider and provide the same convenience with the added benefit to your client of dependable advice. The profit margin is very small, but it may be worth it to maintain your clients – and maintain control over what they learn and what they purchase.
In the end, trust and convenience are the most important elements – aside from your excellent medical care – that will keep your clients with you for the lifetime of their pet.
Resources: Debbie Boone, CVPM and Wendy Hauser, DVM: The Veterinarians Guide to Healthy Pet Plans: http://www.theveterinariansguidetohealthypetplans.com Partners for Healthy Pets: http://www.partnersforhealthypets.org/inactive_client_program.aspx The Pet Effect campaign: https://habri.org/the-pet-effect/ Veterinarian Virtual Care Association: VVCA.org
312
Caregiver burden -how to help our clients and ourselves By Mia Cary, DVM Cary Consulting Greensboro, NC Untangling the Terminology
• Burnout -a cumulative process marked by emotional exhaustion and withdrawal associated with increased workload and institutional stress, NOT trauma-related.
• Caregiver Burden -the strain or load borne by a person who cares for a chronically ill, disabled, or elderly family member or pet.
Clients and Caregiver Burden Several recent studies, including the work of Dr. Mary Beth Spitznagel published in the January 2019 issue of JAVMA, point to the fact that client-based factors can contribute to occupational stress in veterinary medicine. Clients providing care for their pets with chronic or prolonged illnesses can suffer from caregiver burden. Accompanying caregiver burden is often a reduction in the ability to engage in relationships, such as with their veterinarian, in healthy ways. This can in turn result in increased stress for the veterinary team. Compassion Fatigue-a secondary traumatic stress disorder that results from exposure to another person’s/patient’s traumatic experience(s) and creates high levels of emotional stress. It can occur due to exposure from one patient or can be due to a cumulative level of trauma. Compassion fatigue is also called “vicarious traumatization” or secondary traumatization. Compassion fatigue differs from burnout, but both conditions can co-exist. Compassion Satisfaction-a joy or sense of achievement found in helping and caring for others. How Compassion Fatigue and Caregiving Burden Differ While there are many similarities between compassion fatigue in veterinarians and caregiver burden in people, the latter often do not have access to the same preventive measures that many employers offer such as professional counseling and mental health days. Caregivers typically forego breaks and help from others in order to provide the care their pet or family member needs. They can feel they are the only ones that can provide the support their loved one needs. How Compassion Fatigue and Caregiver Burden Differ from Burnout A major distinction between both compassion fatigue and caregiver burden versus burnout, is that both professional and family caregivers, when pushed to their limit, can experience a weakened sense of empathy for those in their care. Actions, such as yelling or hitting, that are not characteristic of the caregiver’s typical behavior could result. When one reaches a level of insensitivity or indifference for a family member or patient in their care, it’s important to step back from the caregiving role in order to recalibrate and recharge. Another difference is that there can be a more rapid onset and a more rapid recovery from compassion fatigue versus burnout.
313
The oxygen mask rule is legit It’s true what the flight attendants tell us. If there is an emergency while in flight, we should put the oxygen mask that drops down on ourselves first, before we try to put it on our child or whomever is occupying the seat next to us. Why? Because we are better equipped to help others when we take care of ourselves first. This is practicing self-care. As with everything, this is easier to own on the good days then it is on the days that we are having a rough time. Most of us need a tipping point of some sort that forces us to finally accept this guiding principle to be true. My tipping point was in my early days with Boehringer Ingelheim (BI). During the industry phase of my career I was able to conduct an annual, anonymous 360º feedback survey for myself and my direct reports (which I highly recommend looking into if you have not been involved in one!). This particular year I opened my 360º feedback report to see lots of green (strengths), a little yellow (areas that need attention), and a big band of red (red flag –this area needs immediate attention). Nearly every team member had marked me extremely low on work-life balance. As I read their comments, I realized that they knew my intentions were good when I emphasized the importance of their home-life and that their families came first, but I wasn’t walking the talk and it made the working environment uncomfortable. I’m so grateful to that team for their radical candor and willingness to call me on what I needed to be called on. Thanks to their feedback I modified my routine and made more time in my schedule for myself and my family members. I now know that the better I take care of myself then the better equipped I am to take care of and serve others. And that I must walk the talk. We all need that tipping point to help us own the idea that self-care is the right thing to do, hopefully for you it’s something as benign as candid feedback from respected colleagues. Own this principle and start acting accordingly before you’re too burnt out to care. Put that oxygen mask on and remember that self-care is not selfish, it’s foundational for everything else in our lives! Help Ourselves, Help Our Clients The Nine Dimensions of Wellbeing As the oxygen mask principle tells us, we must first stabilize our own base before we can be consistently empathetic with our clients. The best way to stabilize our base is making time to consider each of the 9 dimensions of wellbeing listed just below. Rate yourself on a scale of 1 to 5 -are you thriving (i.e. 5), surviving (i.e. 3) or are you completely burnt out (ie 0)? Know where you are today, decide where you want to be tomorrow, and make a plan that puts you on that path.
• Work/Career Dimension • Emotional Dimension • Spiritual Dimension • Social Dimension • Creativity & Diversity Dimension • Environmental Dimension • Intellectual Dimension
314
• Financial Dimension • Physical Dimension
Client Support Supporting our clients as they deal with their own caregiver burden is one of the greatest gifts that veterinary professionals can provide. One way we can support our clients is by being aware of the following three common caregiver self-defeating habits, and helping our clients understand how to prevent or overcome them.
1. Resisting painful emotions: Resisting painful emotions is often likened to holding a beachball under the water. We can do it, but the effort can deplete us. Instead of resisting emotional pain we can encourage our clients by letting them know what they are feeling is natural, that it’s okay to feel sad when a pet’s health is deteriorating. By stepping back we can be with our upsets instead of being our upset. If they need to cry, let them cry. If laughter helps a client to relieve stress, let them laugh.
2. Brooding: One way we attempt to control our feelings is by focusing on the facts with our thinking mind. Inadvertently this can lead to overthinking potential worse case scenarios and a downward spiral can become overwhelming and even derail caregiving. This is a good time to invest in mindfulness. Being in the present moment and engaging in positive, absorbing activities can help us change how we feel by changing what we do. Encourage owners of chronically ill patients to invest in their favorite activities in order to maintain perspective and recharge their batteries. it can be as simple as going for a walk-in a nearby park or immersing in a mystery novel.
3. Scolding ourselves: Caregivers are often their own harshest critic and constantly question themselves if they are doing enough for their loved one. We can support them with encouraging words, as veterinary professionals we can empathize from our experiences as caregivers and also as fellow human beings.
Radical Candor Kim Scott defines radical candor as the communication approach that relies on caring deeply and speaking directly. Scott’s work originated with leading others however it can also apply to self-awareness and being honest with ourselves.In the context of supporting our clients, it’s about being direct and doing so because we authentically care for them as well as our patients. Now What Take a moment to consider what resonates with you the most.Decide what will work for you and your practice and which key points discussed today you wish to utilize to create a roadmap for supporting yourself, your team, and your clients.One ThingWhat one thing are you going to do first? What one thing will have the biggest impact for you? It might be reading one of the resources listed below in the next 24 hours or sharing the concept of radical candor with colleagues in your practice next week.Make sure your one thing is SMART -specific, measureable, attainable, relevant, and time-bound. What are you doing to do when? And remember, #youdoyou.
315
Resources Assessment of Caregiver Burden American Institute of Stress AVMA Wellbeing Resources Caregiver Burden Caregiver Burden in Owners of Sick Companion Animals Caring for Yourself While Caring for Another Compassion Fatigue vs Caregiver Burnout Compassion Fatigue: When Caregivers go Beyond Burnout Elderly Care Plan 101 Helping Clients Face the Caregiver's Dilemma Personal Care Plans: The Secret to Confident Caregiving Radical Candor Journal Scan -Caregiver Burden of Owners with Very Ill Pets
316
10/16/20
2
Where can vet techs work on social media and marketing?
5
When &Where
6
Why are vet techs well suited for marketing?
7
Why Technicians
CLIENT RELATIONSHIP
EDUCATION EXPERIENCE PROXIMITY
AWARENESS
8
10/16/20
1
#VETTECHLIFESOCIALMEDIAANDMARKETING
FORTECHNICIANS
CAITLIN DEWILDE,DVM
1
Who
326K Posts # VETTECHLIFE
2
What kind of social media and marketing can vet techs do?
3
IN CLINICMATERIALS
COMMUNITYEVENTS
What:
SOCIALMEDIA GOOGLE WEBSITE CONTENT
EMAILNEWSLETTER APPCOMMUNICATION REVIEW SITES
4
10/16/20
1
#VETTECHLIFESOCIALMEDIAANDMARKETING
FORTECHNICIANS
CAITLIN DEWILDE,DVM
1
Who
326K Posts # VETTECHLIFE
2
What kind of social media and marketing can vet techs do?
3
IN CLINICMATERIALS
COMMUNITYEVENTS
What:
SOCIALMEDIA GOOGLE WEBSITE CONTENT
EMAILNEWSLETTER APPCOMMUNICATION REVIEW SITES
4
317
10/16/20
2
Where can vet techs work on social media and marketing?
5
When &Where
6
Why are vet techs well suited for marketing?
7
Why Technicians
CLIENT RELATIONSHIP
EDUCATION EXPERIENCE PROXIMITY
AWARENESS
8
10/16/20
3
How Can Vet Techs Use Social Media for the Practice?
9
How
CREATE PUBLISH RESPOND MONITOR
REPORT PROMOTE COLLABORATE
How To Get The Job
10
How To Get The Job
CE/TRAINING POLICY TRIAL PROOF OFROI
11
A little more about ROI.....
Technicians are in a unique position to:
Track social media analytics
Send clients to the right links
Integrate with appointment
booking systems
Work with PMS and client forms
Understand driving value to the
right products/services and when
12
10/16/20
3
How Can Vet Techs Use Social Media for the Practice?
9
How
CREATE PUBLISH RESPOND MONITOR
REPORT PROMOTE COLLABORATE
How To Get The Job
10
How To Get The Job
CE/TRAINING POLICY TRIAL PROOF OFROI
11
A little more about ROI.....
Technicians are in a unique position to:
Track social media analytics
Send clients to the right links
Integrate with appointment
booking systems
Work with PMS and client forms
Understand driving value to the
right products/services and when
12
318
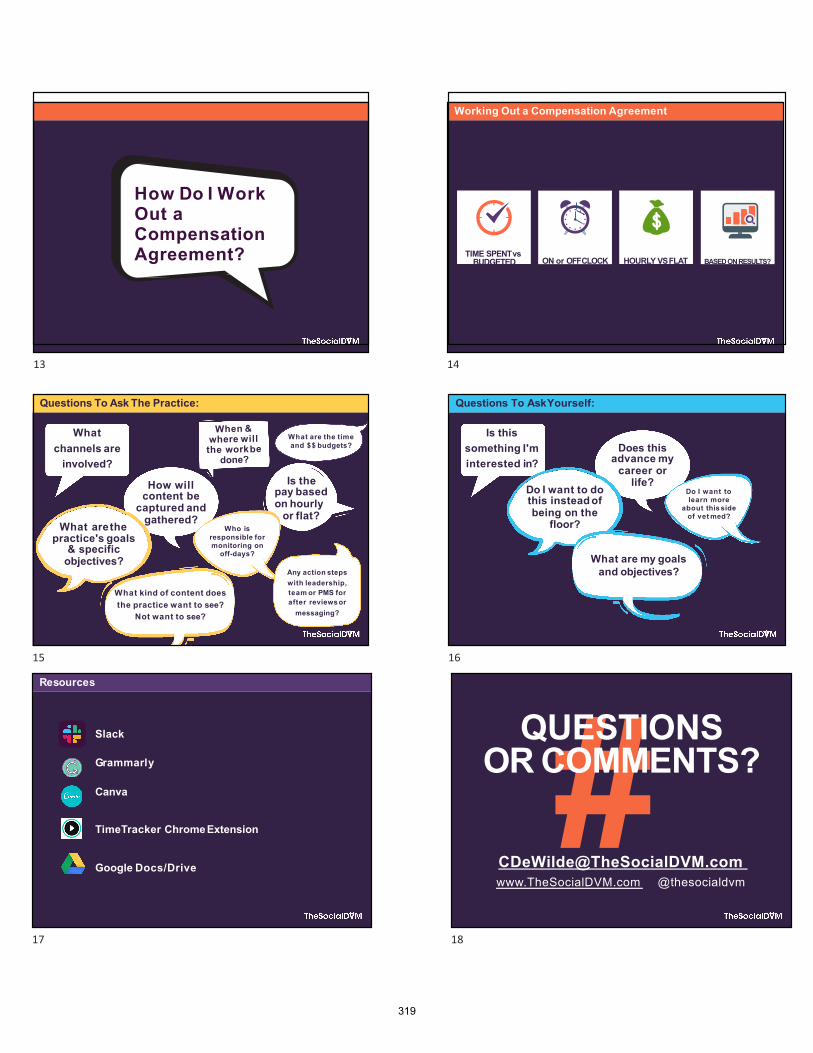
10/16/20
4
How Do I Work Out a Compensation Agreement?
13
Working Out a Compensation Agreement
TIME SPENTvs BUDGETED ON or OFFCLOCK HOURLY VSFLAT BASED ONRESULTS?
14
Questions To Ask The Practice:
What channels are
involved?
How will content be
captured and gathered?
When &where willthe workbe
done?
Is the pay based on hourly
or flat?What arethe
practice's goals & specific
objectives?
Who is responsible for monitoring on
off-days?
Any action steps with leadership, team or PMS for after reviews or
messaging?
What kind of content does the practice want to see?
Not want to see?
What are the time and $$ budgets?
15
Questions To AskYourself:
Is this something I'm interested in?
Does this advance my
career or life?Do I want to do
this instead of being on the
floor?
Do I want to learn more
about this side of vet med?
What are my goals and objectives?
16
10/16/20
4
How Do I Work Out a Compensation Agreement?
13
Working Out a Compensation Agreement
TIME SPENTvs BUDGETED ON or OFFCLOCK HOURLY VSFLAT BASED ONRESULTS?
14
Questions To Ask The Practice:
What channels are
involved?
How will content be
captured and gathered?
When &where willthe workbe
done?
Is the pay based on hourly
or flat?What arethe
practice's goals & specific
objectives?
Who is responsible for monitoring on
off-days?
Any action steps with leadership, team or PMS for after reviews or
messaging?
What kind of content does the practice want to see?
Not want to see?
What are the time and $$ budgets?
15
Questions To AskYourself:
Is this something I'm interested in?
Does this advance my
career or life?Do I want to do
this instead of being on the
floor?
Do I want to learn more
about this side of vet med?
What are my goals and objectives?
16
10/16/20
5
Resources
Slack
Grammarly
Canva
TimeTracker ChromeExtension
Google Docs/Drive
17
#QUESTIONS
OR COMMENTS?
www.TheSocialDVM.com @thesocialdvm
18
319
Can I vent? The negative effects of blowing off steam
By Bash Halow, CVPM, LVT
For some time, veterinary professionals have been hooked on venting, the process of blowing off steam to a coworker. But venting is counterproductive, habit-forming, and revealing of much deeper personal and professional issues that should command your attention. Here are some things to consider the next time you want to gas up your workplace with a rant.
You don’t want to vent, you want to feel valued
Though venters usually sound entitled, powerful and in control, they are really afraid, insecure, and…don’t vomit in your mouths… in need of a hug. The urge to vent is a cry for love, reassurance, and praise. If you’re going to vent to someone, make sure it’s someone who genuinely cares and is ready to make you feel valued when you’re done with your fuming.
It’s usually based on fiction
The things that work us into a lather are often all inside our head. The printer goes down, Joanne your coworker goes MIA, three clients stack up at the desk, and all lights on the phone start to blink at once. You need to vent, not because you have failed, but because you feel as though you will fail. But that’s all just defeatist’s talk bottled up in your head. This scenario is every bit as much a chance to prove your fabulousness, as it is a chance to be revealed a flop. Venting, in this case, isn’t alleviating you of anything; it’s just supporting a fake narrative that will bomb. If you must vent in cases like these, choose a person that will reassure you that you will triumph, not tank.
Vent for help and perspective
You may need to vent because you find yourself in an honest-to-goodness pickle and you don’t know what to do. In this case, don’t seek out someone that is going to agree with you that the world is conspiring to make your life miserable. Look for someone that can bring perspective and problem solving to the situation. Use venting as a pathway to a solution, not just a chance to smolder.
It may be a sign of laziness
Many of us need to vent because the system in which we work is broken. Again and again, it sets us up for failure and we feel like we need to fly off the handle. But venting about such a predicament may be just your way of sidestepping your responsibility to step up, step in, and fix things on a more global scale.
320
It can backfire Those that don’t care about you don’t want to hear you complain. They want to watch you work, preferably with your mouth closed. Venting to people that don’t care about what you’re going through can leave you feeling more alienated and alone than when you started. It can make things worse What if you actually have the courage to vent to the person that’s the source of your frustration? “Do you have to be such a jerk all the time, Dr. Gibbons, or do you just save it up for when I’m on the schedule?” If Dr. Gibbons is sitting on his own powder keg of anxiety, venting to Dr. Gibbons isn’t going to make you feel better; it’s going to make you unemployed. It’s probably a warning sign you need help You’re not really crying about the latest callout, the nasty look that Dr. Watson gave you in treatment, or what your supervisor said to you in the break room. You were ready to cry long before you set foot in this nuthouse. In fact, you might not be here in the first place if you weren’t already on the verge of tears. Get help. You are thinking, acting, feeling, and responding based on all kinds of subconscious urges and neuroses. We all are! Explore what they are with an experienced therapist, sort through them, and take responsibility for your happiness. If we’re going to cry, let’s make it tears of happiness. insightful leadership can help Most of us don’t work at our jobs, we work at trying to make our jobs work. That is to say the workflow, tools, team members (sometimes), facility, schedule and process by which we try to get the already-nearly-impossible job of veterinary medicine done are a hindrance, not a help. Leaders should recognize that one reason why employees are so often ready to blow is because how we’re asking them to work also blows. Veterinary practice teams can usually be put into two silos: those that focus on client and patient care, and those that focus on how to care for clients and patients. Protocols, paperwork, chart audits, and sign offs have their place in safe, great medicine, but when paperwork starts to supersede patient care, we risk disengagement, cheat our team members of work that’s more fulfilling, and prime them for the need to vent. There is empirical evidence that team members who are allowed to care directly for clients and patients are happier, turn over less, are more successful at their jobs, earn their employers more money, have better health, and have higher job security. Yes, venting, when done right, can have a positive impact on your life, but there are richer
321

ores to be mined in reducing roadblocks to great patient care, to healthy team member interaction, and to one’s own personal responsibility for good mental health.
322
What’s the buzz? By Bash Halow, CVPM, LVT Consolidation Consolidation in the veterinary space, a normal phenomenon that occurs in all industries, continues to heat up. According to experts, we are in stage 2-3 of a four-part process in which smaller companies merge to create larger, more efficient enterprises. These companies then form strategic alliances with others to create industry giants whose products, sales, and influence can span the globe. Consolidation is driving historic sales prices. In the past, veterinary practices were often sold for a 4-6 multiple of their adjusted net earnings (EBITDA). Today, some companies are paying 8-11 times EBITDA for single or small groups of practices with large groups of practices being sold for as much as 13-19 times their EBITDA. Consolidation puts a significant amount of pressure on older veterinarians to sell and tends to keep private practitioners shut out of a bidding war that they cannot afford. Additionally, consolidation is having these effects on our industry: • It is driving up the wages of doctors and credentialed technicians. • It is improving the work life balance of veterinarians and some lay staff. • It is providing more upward mobility to support staff members, former practice owners,
and managers as opportunities inside groups that own 300-1000 veterinary practices grow.
• It is drawing some pharma funding and support away from private practices. • It is putting pressure on smaller suppliers as wholesale deals lower the profit margin on
products. • It is making website visibility more difficult for private, smaller practices as larger
corporations flex their expertise and wealth to optimally advertise online. • It forces veterinary associations, at every level, to reevaluate the needs of their
membership and to decide whether to emphasize the needs of the consolidated groups or the private practices that they have traditionally served.
• It reduces the need for independent continuing education events as corporations provide more internal learning opportunities.
• It draws outside investors into the marketplace whose sole interest is to capitalize on the consolidation trend by buying practices, packaging them, and then reselling them at a higher multiple to larger entities.
Data mining and ownership There is a growing concern that many of the companies that have access to client data through veterinarians’ POS software are selling that data to third parties who can then turn around and use that same data to compete with the private practices from where it was obtained. The Association of Veterinary Informatics (AVI) is a not-for-profit group of veterinary professionals that explores, encourages, and assists private practices with understanding and leveraging data. As concern about data mining and ownership mounts, interest in the AVI grows. Their annual conference is held in conjunction with all three Fetch conferences, so be sure to attend.
323
Integration Companies like Idexx and Henry Schein are working hard to integrate their software with all other aspects of their business. Veterinary practices that partner with these two industry giants will have access to more detailed reportage and more client follow-through capability. The ability of Avimark’s Rapport to now allow clients to schedule their own appointments will undoubtedly be leveraged by the software’s corporate accounts to streamline new client acquisition. Payment options Companies like Vetbilling.com now offer Pet Health Savings Accounts and Wellness Plans. They are also beta testing an app that can efficiently assist the practice with writing payment plans for clients. The app: • Allows practices to quickly gather client data; • Runs a soft (doesn’t affect the client’s credit score) credit check (with the client’s
permission of course); • Allows the client to provide verified approval for the credit check via their cell phone • Provides immediate recommendations to the practice for the terms of the payment plan • Is free to the practice, provided that the client agrees to the plan.
The company has seen dramatic success with its product at some veterinary hospitals. In one case, a practice increased revenue by 400K in one year! The explosion of CBD products for pets The decriminalization of CBD in many states has waves of pet owners looking for sources of CBD for their pets. Veterinarycannabis.org, led by Dr. Casara Andre, aims to teach veterinary professionals how to safely and legally educate pet owners about CBD in pets. Erosion of food, pharmacy and OTC sales Online pharmacies and giants like Amazon, CVS, Wal-Mart, and Chewies continue to flex their marketing prowess and online ubiquity to capture new clients and lock them into to sales. Pharmacy sales at many practices have dropped by 5% and it’s likely that both food and pharmacy sales will rapidly decline as the above-mentioned companies and others use online tracking to understand the buying habits of pet owners and to market to them with increased effectiveness. Additionally, allotting more and more time for our professional team to research, approve, and communicate online pharmacy requests means that we are paying our employees to work for another company’s profit. The pet experience Petco is following the lead of companies like Whole Foods and Apple Computer and creating retail experiences for pet owners. The model continues to evolve. To date, PetCoach, as the venture is called has experimented with pet food cooking stations, on demand veterinary professional advice through a monthly subscription service, telemedicine, grooming, and pet training. These stores are tracking the movement of clients through the store, taking note of what clients are finding interest in and what they are not, and making adjustments accordingly.
324

Higher wages and a shortage of veterinary professionals It was mentioned above, but it merits reemphasizing: the current growth in our industry, the changing demographics, and competition by veterinary corporations is creating a shortage of veterinarians and veterinary technicians. Some veterinary practices have been searching for associate veterinarians for more than a year without a single applicant. As ownership opportunities decrease, it is likely that fewer students will opt for a career in veterinary medicine that comes with an MD-sized debt without the MD-sized salary. Already many hospitals are searching for foreign trained veterinarians to close their ranks. Telemedicine Despite the smoke, telemedicine has yet to catch fire. Still, some practices are exploring free telephone consults with veterinarians as a way to introduce new clients to the practice and to try to drive sales. Practices that have wellness plans are using telemedicine to connect licensed veterinary technicians with plan holders that have had a recent visit to the vet. Instead of coming into the practice, the plan holder can call a veterinary professional and consult with him or her over the phone. Under the direction of the veterinarian, advice or medicine can be dispensed, provided that the client patient relationship is still in good standing. The practice can then take advantage of the appointment slot that would have otherwise been filled to provide service to a new client or one that is not on the plan. Since the plan holders are paying a monthly fee for the service, there is no drop-in revenue. At the time of this writing, there are other new trends and products, but we’ll discuss these at the meetings in Kansas and San Diego
325

STATE OF THE INDUSTRY
2019
naphia.org326
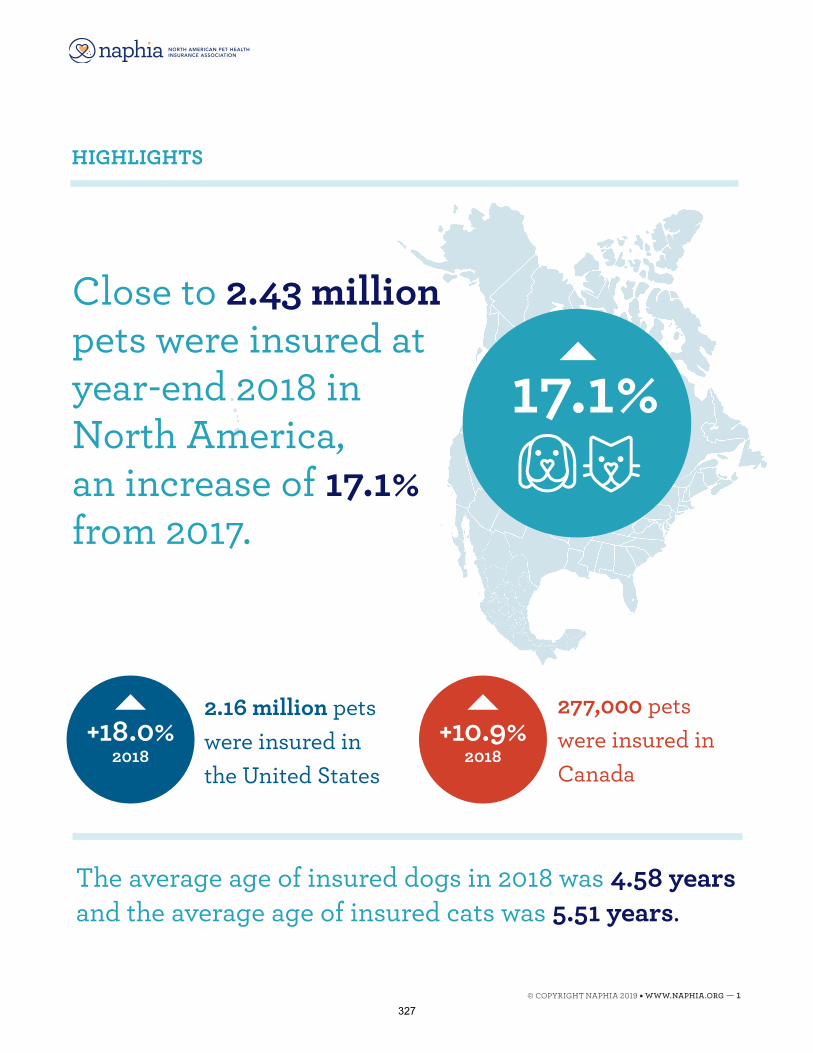
HIGHLIGHTS
2.16 million pets were insured in the United States
+18.0% 2018
277,000 pets were insured in Canada
+10.9% 2018
The average age of insured dogs in 2018 was 4.58 years and the average age of insured cats was 5.51 years.
17.1%
Close to 2.43 million pets were insured at year-end 2018 in North America, an increase of 17.1% from 2017.
© COPYRIGHT NAPHIA 2019 • WWW.NAPHIA.ORG — 1327
© COPYRIGHT NAPHIA 2019 • WWW.NAPHIA.ORG — 2
All dollar amounts in this report are expressed in the country’s currency (U.S. and Canada) from 2014 to 2018.
Accident & Illness/Insurance with Embedded Wellness represented 93.1% of total Gross Written Premium in 2018 in North America.
In total, across North America, dogs represented approximately 88.9% of In-Force Gross Written Premium in 2018, for a total of $1.26 billion USD.
GROSS WRITTEN PREMIUM
328
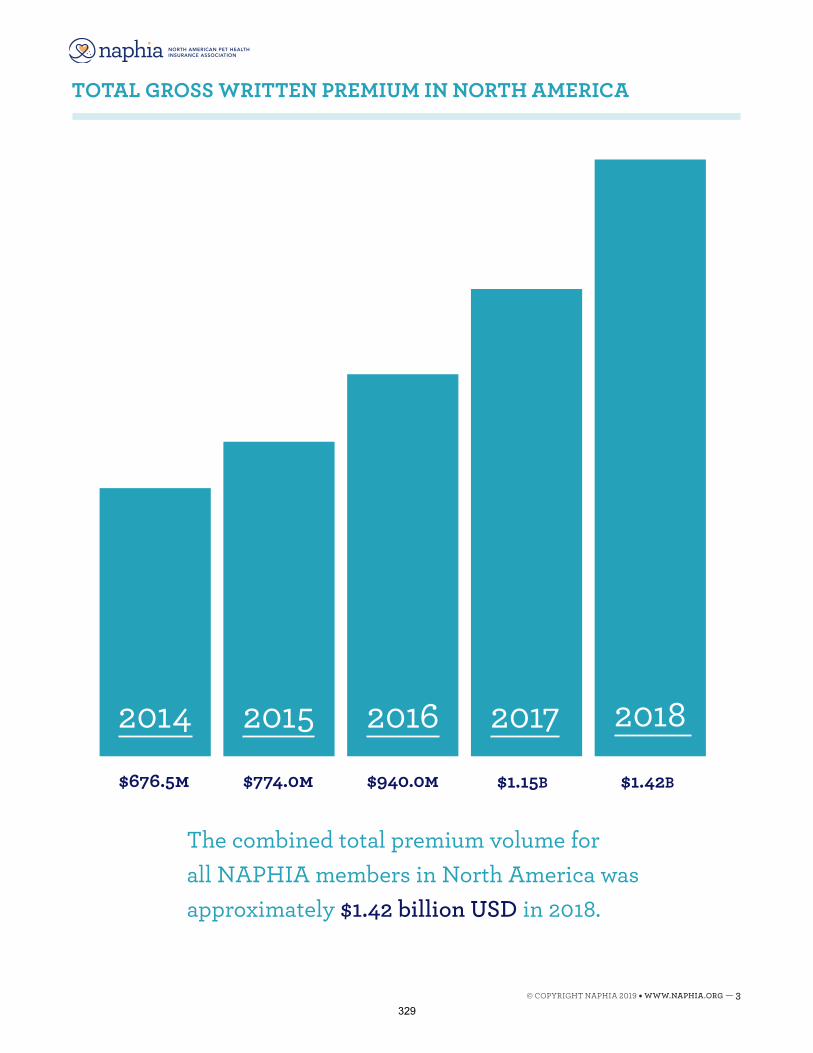
2014$676.5m
TOTAL GROSS WRITTEN PREMIUM IN NORTH AMERICA
The combined total premium volume for all NAPHIA members in North America was approximately $1.42 billion USD in 2018.
2015$774.0m
2016$940.0m
2017$1.15B
2018
$1.42B
© COPYRIGHT NAPHIA 2019 • WWW.NAPHIA.ORG — 3329
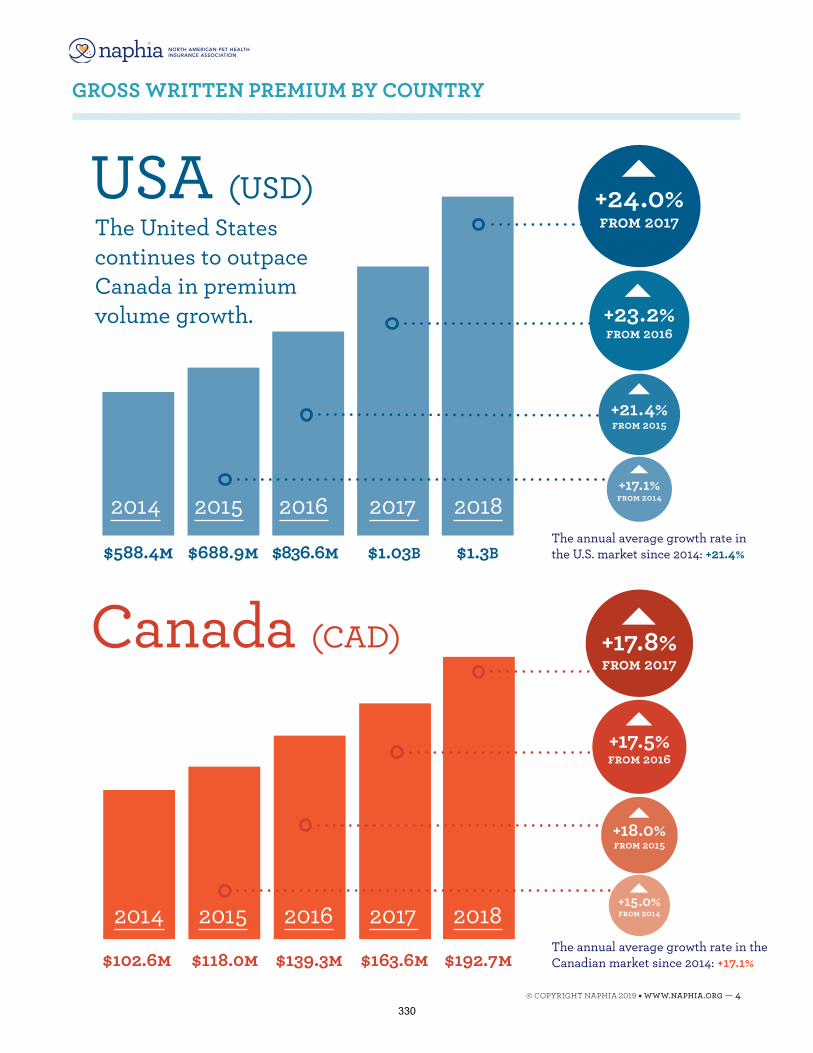
2014
$102.6m
2014
$588.4mThe annual average growth rate in the U.S. market since 2014: +21.4%
USA (USD)
2015
$688.9m
2016
$836.6m
2017
$1.03B
2018
$1.3B
+21.4% from 2015
+23.2% from 2016
+24.0% from 2017
+17.1% from 2014
The annual average growth rate in the Canadian market since 2014: +17.1%
Canada (CAD)
2015
$118.0m
2016
$139.3m
2017
$163.6m
2018
$192.7m
The United States continues to outpace Canada in premium volume growth.
+17.5% from 2016
+18.0% from 2015
+15.0% from 2014
+17.8% from 2017
GROSS WRITTEN PREMIUM BY COUNTRY
© COPYRIGHT NAPHIA 2019 • WWW.NAPHIA.ORG — 4330
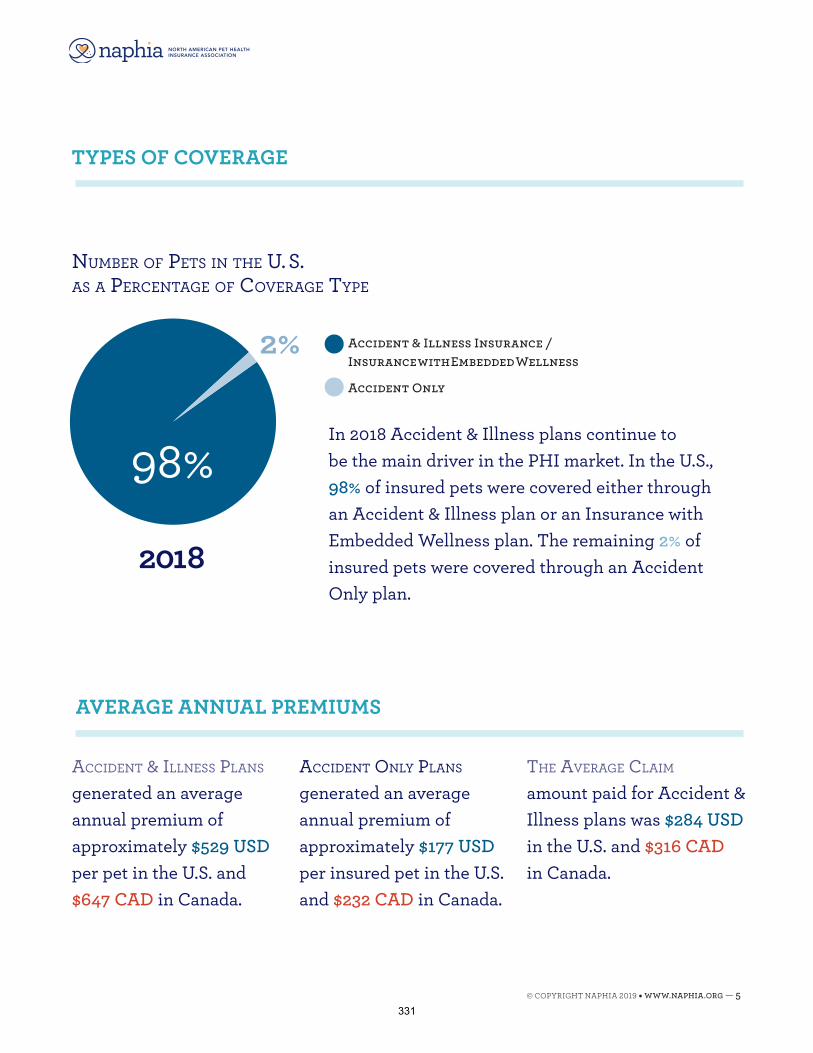
TYPES OF COVERAGE
AVERAGE ANNUAL PREMIUMS
Accident & illness PlAns generated an average annual premium of approximately $529 USD per pet in the U.S. and $647 CAD in Canada.
Accident Only PlAns generated an average annual premium of approximately $177 USD per insured pet in the U.S. and $232 CAD in Canada.
the AverAge clAim amount paid for Accident & Illness plans was $284 USD in the U.S. and $316 CAD in Canada.
In 2018 Accident & Illness plans continue to be the main driver in the PHI market. In the U.S., 98% of insured pets were covered either through an Accident & Illness plan or an Insurance with Embedded Wellness plan. The remaining 2% of insured pets were covered through an Accident Only plan.
98%
number Of Pets in the u. s. As A PercentAge Of cOverAge tyPe
Accident & Illness Insurance / Insurance with Embedded Wellness
Accident Only
2018
2%
© COPYRIGHT NAPHIA 2019 • WWW.NAPHIA.ORG — 5331
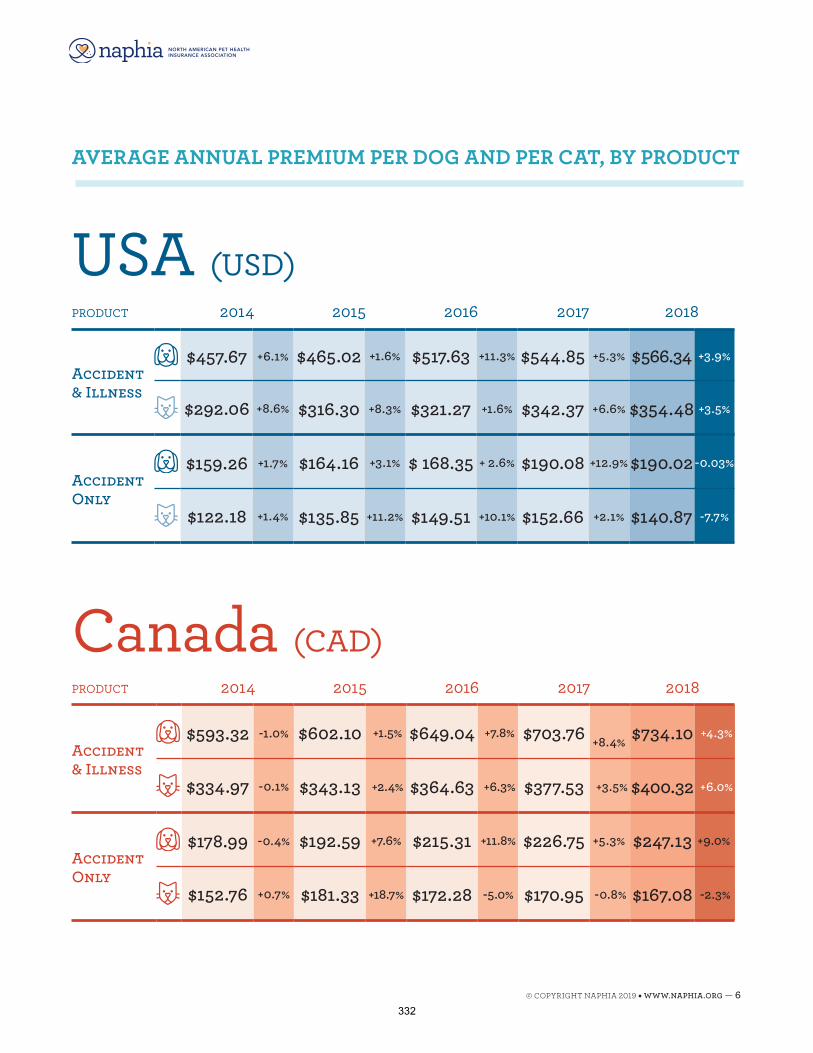
PrOduct 2014 2015 2016 2017 2018
Accident & Illness
$457.67 +6.1% $465.02 +1.6% $517.63 +11.3% $544.85 +5.3% $566.34 +3.9%
$292.06 +8.6% $316.30 +8.3% $321.27 +1.6% $342.37 +6.6% $354.48 +3.5%
Accident Only
$159.26 +1.7% $164.16 +3.1% $ 168.35 + 2.6% $190.08 +12.9% $190.02 -0.03%
$122.18 +1.4% $135.85 +11.2% $149.51 +10.1% $152.66 +2.1% $140.87 -7.7%
USA (USD)
AVERAGE ANNUAL PREMIUM PER DOG AND PER CAT, BY PRODUCT
Canada (CAD)PrOduct 2014 2015 2016 2017 2018
Accident & Illness
$593.32 -1.0% $602.10 +1.5% $649.04 +7.8% $703.76 +8.4% $734.10 +4.3%
$334.97 -0.1% $343.13 +2.4% $364.63 +6.3% $377.53 +3.5% $400.32 +6.0%
Accident Only
$178.99 -0.4% $192.59 +7.6% $215.31 +11.8% $226.75 +5.3% $247.13 +9.0%
$152.76 +0.7% $181.33 +18.7% $172.28 -5.0% $170.95 -0.8% $167.08 -2.3%
© COPYRIGHT NAPHIA 2019 • WWW.NAPHIA.ORG — 6332
All statistics and figures presented in this report are based on the data submitted to Willis Towers Watson by the participating companies. The data was collected by means of a survey questionnaire/data call, completed by the following companies (and their related entities/brands):
Crum & Forster Pet Insurance Group ASPCA Pet Health Insurance, Hartville Pet
Insurance, PetPremium Pet Health Insurance, Prudent Pet
Embrace Pet Insurance Embrace, USAA, Geico, AllState, Bolt Agency,
American Family, American Modern, Nationstar Mortgage, SWBC, Armed Forces, Leasing Desk
FIGO Pet InsuranceHealthy Paws Pet Insurance & FoundationNationwidePetFirst Pet InsurancePetHealth Inc. 24PetWatch, Ontario SPCA Pet
Insurance Programs, Petango, PetCare, PTZ Insurance Services Ltd.
Petline Insurance*
Petsecure, Desjardins, HBC, CAA, The Personal, OVMA Pet Health Insurance, Peppermint
PetPartners PetPartners, AKC Pet Insurance
and CFA Pet Insurance
Petplan Pet InsurancePets Best Insurance Pets Best Insurance, Farmers Insurance,
Progressive Insurance, BB&T Insurance Services
Pets Plus UsTrupanion
MEET THE PARTICIPANTS
*Note: Not a NAPHIA member company.
Willis Towers Watson (NASDAQ: WLTW) is a leading global advisory, brokering and solutions company that helps clients around the world. With over 45,000 employees in more than 140 different countries, they provide solutions to individuals and institutions that manage risk, optimize benefits, cultivate talent and expand the power of capital.
Recognized as experts in travel insurance, credit card insurance, creditor/debtor insurance and other niche insurance markets, Willis Towers Watson provides these industries with unique market intelligence (through market surveys and varied consulting services). Willis Towers Watson monitors these markets, including various industry events, developments and innovations affecting insurance and brings this knowledge to bear across a variety of disciplines to provide best-in-class support for product development, underwriting and actuarial support, and assistance with third party provider relationships.
ABOUT WILLIS TOWERS WATSON
© COPYRIGHT NAPHIA 2019 • WWW.NAPHIA.ORG — 7333
Master the interview for mentorship and career success
By Dan Phillips, DVM
CEO Vet Mentor Solutions, LLC.
Today’s interview process reflects an inherently broken system. Finding and hiring the right employee to fill any role is critical in business. The hiring process is even more important when it comes to clinicians in the classic veterinary small business setting. Similarly, identifying the right practice, the right employer, and the right culture is a must for any employee looking for a long-term relationship and commitment with an organization.
Yet the hiring and interview process often boils down to a 1-2-hour interview or half day shadowing event to help make these critical decisions. Crazy!?
Assuming that we can’t re-invent the entire HR and interview process, what are things that we can do maximize this time to help align practices and veterinarians more effectively?
In this lecture we will work to maximize the interview process in several ways:
- We’ll define the components of a successful interview from BOTH the employer and employee perspective
- Discuss critical steps for prospective employees to take to effectively prepare for an interview to ensure their needs are met.
- Review the questions every employee MUST get answered during an interview. Especially new associate veterinarians to ensure they will get the mentorship they need and desire.
- Highlight common mistakes made by veterinarians everyday during the interview process leading them to accepting the wrong position.
334
Breaking Down the P&L: The Star Chart to your Galaxy
By Kathryn Primm, DVM, CVPM
Owner/manager since 1998, www.applebrookanimal.com [email protected] Host of Nine Lives with Dr. Kat and Dr. Kat Gone to the Dogs on PetLife Radio
My name is Kathryn Primm DVM, CVPM and I founded and run my own small animal practice. I also administrate several Facebook groups for veterinary professionals, and I noticed that there were questions about the P&L statement. I had assumed that those who owned (or planned to own) a practice were already well versed in this form of accounting, but apparently that is not the case and I want to help. I learned how to first set up my hospital and my accounting software from my parents and from independent study, reading Veterinary Economics ,and following big names in Practice Management, like Karen Felsted, Fritz Woods, and Denise Tumblin. Practice Management was a very cursory one hour class when I was in vet school, so I had to teach myself along the way and learn by doing. I think this needs to be better and this lecture is my contribution. There is more than one way to manage a practice and I will show you the general ways to generate the reports, but then I will share what works for me in my small practice. I feel like the concepts are important in any size practice and they are and have been working for me. However, managing a practice is like any endeavor- there is always room for growth and I miss being able to talk to you face to face because each time I lecture, I find that my own ideas are stimulated and I can look for better ways to grow and change. I hope that my ideas can help stimulate you. Do not restrict yourself to only doing exactly what I explain. I am going to endeavor to teach you methods to measure your own achievements. What is the P&L?
Also known as the income statement, the profit and loss statement (P&L) is the summary of revenues and expenses over a period of time.
A veterinary hospital is a business, just like Walmart or McDonalds. We provide products and services to the public in exchange for money. Profit is not a dirty word and you deserve to work hard and be paid well. We are in business to be paid, otherwise it would be a charity and we would have to find another way to feed ourselves. **Sustainable businesses must show a reasonable profit in order for the owners to spend their time and investments there. Someday your practice will need to be sold and the owners move on and you need to be able to demonstrate profitability to maximize the investment. Why should you look at the p&l? Veterinarians are notorious martyrs. This is a great place for a manager to step in and keep the focus on business. Control freaks like me need metrics, both to encourage me when things are going well and to galvanize a plan to improve things when they aren’t.
335
Define goals- If you do not know what your metrics have been historically, you can’t know where you want them to go. Just like managing obesity in pets, you need to know the starting weight before you know if the weight loss program is being effective. Bonuses and rewards- I like rewarding my team. It makes me feel good to help them and it makes them feel inspired that they are appreciated. You can identify trends that the hospital can improve on to provide better care for all patients and better customer service for your clients to uphold your mission. Something that is not where you want it to be is merely an opportunity to grow and improve. If you are monitoring the metrics and you can show improvement over each year, then your business is more valuable to an onlooker or potential buyer. You can see that there is value in looking at your Profit and Loss Statement. Who needs to see the P&L?
Depending on your practice hierarchy and structure, sometimes the practice manager knows first and knows more often and the owner wants to only be given occasional updates. I did a lecture with Debbie Hill (a fellow CVPM) at a conference early this year about who makes decisions-owner or manager, and she told me that she has been a manager for her owner for so long and she manages three practices for him. She said that he trusts her and really just wants a basic update of how things are going and doesn’t want to be involved in the nuts and bolts of the management of the practices. So, she is the one that monitors the P&L and she reports the metrics to him in a meeting occasionally. On the other hand, I own and manage my practice, so I am the one that monitors. You will have to find your “happy place” with your owner or management style. I like metrics and I like looking at the statement and coming up with plans, so I am the one that looks and reports the findings to my office manager and team. You will find your balance as you go with this. But it is important that the manager and the owner (and their accountant) see and understand the income statement. The team needs to be aware of the overall nuts and bolts of profitability in order to understand their roles in the success of the business. They need to understand that in order to be there to have jobs and help pets, we cannot operate in an environment of nonprofit.
Why does the team need to know about profit?
You do not need to share your complete P&L with your entire team. It is more important that they are aware of how their work impacts the KPI (key practice indicators). In my opinion, your team needs updates and ways that they can impact the numbers. In other words, they need attainable goals defined for them. Your P&L goes hand in hand with your KPI when you are making goals.
• PCT (per client transaction)
336
• Patient visits • New client numbers • Overall Profit • Profit Sharing
The list shows that values that I think are important for team members to understand. PCT (Per Client Transaction) is how much each client spends at a visit. This value tells you if you and your team are offering all the services and products that are appropriate for each patient. New client numbers show you if you want to change your external marketing. This value can be impacted by your appointment scheduling protocols, for example. Patient visits are the number of pets that walk through your door and it can be influenced heavily by your internal marketing, like scheduling rechecks, follow up communication and reminder systems. Overall profitability comes from your income statement. It is not necessary that you share the actual statement with your entire team because just like Debbie Hill’s owner, they want you to assess the numbers and tell them the bottom line and what you want them to do to impact it. Odds are your whole team is not as excited by metrics as I am. Now profit-sharing programs get the team a little more excited. Our profit sharing is based on gross revenue for simplicity. Since we want to grow a minimum of 6% per year, our Tier 1 goal must be higher than that. We also have a Tier 2 goal which is very lofty and we were well on target early in the year and then COVID hit. The end of the target period for us was end of June, so we will see how it goes for the second half. I think we will make the Tier 2 goal. \ Any time period as long as you set an analogous time period to compare. You might choose to look at some basics every day. I do not look at our full income statement every day, but I do look at our bottom line (gross revenue) each day because I have already calculated a break-even point and I like to know that we are covering our overhead costs every day. This year has been different with COVID and PPP and we did not know how the pandemic would affect us, so I certainly check my P&L at least monthly and compare it to pre COVID. Also because of PPP and some of the criteria around staffing and time off, I have kept an eye on things. Monthly- I think monthly is reasonable. You are probably doing other monthly reports anyway. I know in Tennessee, we have sales tax reports and payroll tax reports, so Period Totals from my PMS and my P&L are a part of the monthly cycle. Quarterly- As a sole proprietor, I am required to make Quarterly Estimate payments, so I also generate some quarterly reports and send them to my accountant. Yearly- Certainly at year end, you will need to generate a P&L for planning and tax purposes. How do I get this report?
337
Let’s briefly go over HOW to generate this report. When I lecture in person and I survey the audience, there are always those that are considering buying a practice or opening a practice and they need to know more of the basics. And then there are practice managers at every level of experience, so I want to touch on this so no one is left behind, but not spend a long time on it. Across the top menu in Quickbooks are many different options. This one is in the Reports menu. Scroll down to Company and Financial and then choose Profit & Loss Prev Year Comparison. I like to compare to the previous year and sometimes even further back. At the top of the report, there is an area where you can customize the report for any date range that you want. But for the sake of this talk (and even to simplify my own work, so I do not run off down a rabbit hole), I usually choose the prev year comparison. This will open up a long report, so I am going to try to simplify it for the sake of the slides. Once the report opens, I think that it is important that you customize the report so that the values that are the most meaningful to you are present. Again, these reports are so customizable that it is easy to go chasing after a value that might be less meaningful. You will want to customize for % income. Click customize report in the upper left of the menu at the top, check the box next to % Income and then click ok. The customize report window will then close and you will be looking at your P&L. Hit enter or click somewhere on the P&L itself to be sure that it makes the customizations and recognizes the date range that you have selected. The reason that I think it is important to choose % income is because it is a standardization that allows you to compare your own practice to other practices, regardless of the specifics of those practices. The actual report is too long for a single image on a slide, so I broke it into sections to help you understand. At the very top, you will see what I have cropped out for this slide. At the left is the Accounting method. Accounting method is decided before your first tax return for income tax purposes so if you are looking at a statement, it is already decided. I am not a CPA so be sure to consult your own accountant. On the right is the date range you have chosen. (Here you want to check that the report does actually show the dates you picked because sometimes if you did not click or hit enter, the report will not apply your changes and the numbers will not be what you thought they were). Again, I think that Previous year comparison is valuable because of the seasonal component to vet med and I want to have an accurate “apples to apples” comparison. Obviously, if you compared July to December, the comparison would be less valuable. Beneath the heading (accrual method and date), you will see the report begin.
338
Any P &L will present with four basic sections, 1. Income 2. Costs 3. Expenses 4. Net income. I am going to break down each of these sections and streamline where I think your attention should be. The first section is income. Obviously, income is money coming in. When you set up your QB program, you need to have assigned accounts to your income centers before your P&L is maximally useful. If you have not assigned accounts to your income, this part of your P&L may be a little less valuable to you, but obviously, you must be generating an income and it is nice to know the places that income can be coming from. We are going to talk a little more about assigning accounts in the next slide. This section of your P&L however is about gross revenue and you want to see positive revenue and increased income over the previous year. Once you have the categories defined, you can scan down the right side where % income is and rapidly see if there is a big change since last year. Big changes may indicate errors in entry. In the last slide, I briefly touched on assigning accounts to income. This allows you see growth opportunities or recognize changes to your business model…What about leveraging vendor rebates? Maybe your boarding income completely dissolved because of a pandemic??? It might stimulate you to ask tough questions and be able to find the answers, like “Should we have grooming?” But remember, income is only half the story! Just because something appears to be bringing in a lot of income does not mean that it should be your focus. For example, if you see that grooming is bringing in a large income, but the costs of the groomer and all the supplies is very high, you may want to reconsider. In my hospital, our largest income is from patient fees. We do not offer grooming any longer. If you want to track a profit center and set up a team wide initiative, like a dental month or a microchip push, you would want to set up income categories for those, but remember, each days deposits, all the income will have to be broken out and put into the QB category. For me, this is very time consuming, so we have only a few income accounts. The more detailed you can get about entering and categorizing the data entry, the more meaningful these numbers will be, sometimes, you have to weigh out the time on data entry versus the value you get from these particular entries. A quick word about How to enter these items specifically. On your home screen/dashboard, there is an icon that says Record Deposits clicking it will open this window. Your accountant or consultant can help you with the initial set up of these accounts and AAHA is a good source as well. In this area, I have simplified the input at my hospital to basics, like patient fees and vendor rebates to save time on entry, but you can certainly drill down more to specific areas if you choose because, again, the more detail you have in your data entry, the more valuable the report is.
339
The bubble points to where you put where the account the income is attributed to, like patient fees. So, you would click on the dropdown and scroll through your predetermined accounts as you enter the deposits. The next section is Cost of Goods Sold or COGS. COGS tells you where your money is going. Here, in my opinion, the account categories are even more critical!
1. Define the accounts for all of your inventory items 2. When orders are placed, a Purchase Order should be used. When the order arrives, the
items are checked into the computer and manually checked into inventory. It is a good idea if the person ordering is not the same person who checks the items in and have all involved initial the packing slip, etc, so there is accountability when needed.
3. When the invoice/statement arrives, break it apart and assign accounts for the items. (Next slide shows exactly how to input these when paying bills)
This is a more time-consuming task, but it is so important! Let’s talk about where you would input the account so that your income statement can tell you the right numbers. Control A opens up your Chart of Accounts menu and you can add/remove edit these as you choose. In 2016, we added an account for Fear Free because we wanted to see how much the extra things, we were doing actually cost to help us maintain profitability and guide our efforts on pricing moving forward. Then when you go to pay the bills, the window looks like this and the dropdown menu allows you to select the account specific to the expense. For example, you can order Flea, tick and HW products from BI, but you can also order vaccines. If you place an order with BI, you must either place two separate orders, one for vaccines only and one for HW or you will need to break apart the invoice for the costs of each category so you can enter them correctly. It is not the end of the world if an expense is attributed to the wrong account, because this categorization is for your internal use, but accuracy can help you trust your reports and of course, your chart of accounts would have to include separate accounts for HW prevention and for vaccines. The more detailed your data entry is, the more valuable your reports will be. My husband is National Director for Data Acquisition for a large hospital consulting firm on the human side. Our dinner time conversations frequently involve the way that hospital staff input things that renders the data less useful. To me, his job seems insurmountable because of the sheer numbers of people that handle data all over the nation and the room for error overwhelms me, but in many animal hospitals, the team members responsible for inventory and accounts payable are somewhat smaller. This is something that is individual to your
340
hospital. You define which categories mean something to you. Every animal hospital will have RX, OTC, medical supplies, but some may not handle pet food or carry flea and tick products. I could tell you how we specifically do it at Applebrook, but it will not directly apply to your hospital. But as you saw on a previous slide, we have the things that we want to watch set up as categories in our Chart of Accounts, like Rx, Fear Free, OTC, Flea/tick/HW, Radiology expense, etc. The next big section is expenses. We have talked about COGS, cost of goods sold and now we are talking about expenses. They seem like the same thing, but for the purpose of your P&L, there is a difference. Cost is an amount that has to be paid or spent to buy or obtain something, like an item or a product.The definition of expense an amount of money that must be spent (especially regularly) to pay for something. An expense is an ongoing payment, like utilities, rent, payroll, and marketing. We can call these “operational expenses”. The same ideas apply to these more fixed expenses. You still have to attach them to an account when paying the bills so you can track where your money is going, and these categories allow your P&L to be more meaningful. Again % income can allow you to see big changes over the same time the previous year to help you see red flags. Any big change must be investigated. It does not mean that there is theft or an error, but you need to know why there is a big change. One year, our water bill was rapidly higher. We investigated for a leak and did not find one. We started locking up our hose under the building because it looked like long-haul truckers who were parking on the vacant lot next door may have been washing their rigs with it. We noted a big change, investigated and implemented a strategy and the change leveled out. Such an example illustrates this process working well. Another very significant expense is Employee costs. This is an operational expense because it is ongoing, paid regularly and does not purchase an item or product. You are in control somewhat of these costs, however, I am of the strong opinion that you get what you pay for so I strive to pay my team very well and I expect a very strong work ethic. You are not in charge of the payroll taxes you must pay, as these are defined by government. Remember to account for these extra employee costs when you calculate your % for benchmark comparisons. The Well-Managed Practice Benchmarks Study (2017) % of gross income for paraprofessional staff:
• 22.5% (wages only) • 0.6% (retirement) • 1.4% (payroll taxes) • 24.5% (total cost)
I have found that CE and uniforms are also important investments I can make in my team. My team takes their CE requirements very seriously. We require CE for every employee down to the kennel staff. A CE requirement helps solidify your commitment to having a high performing
341
team with veterinary careers and not just a job. Our company invests in an Employee IRA match program. It is another benefit to help the team know that we value them, and we see employment with Applebrook Animal Hospital as a career and not just a job. We want long term employees who are high performers since we know that staff turnover negatively impacts all aspects of the business. This part of your P&L will tell you your exact percent for any time period and the numbers fill in automatically each time you process payroll. Remember there is no asset associated with expenses (versus cost) so administrative expenses fall into the expense portion of your P&L. Administrative expenses are necessary costs that are associated with the management, administrative, clerical, and general functions within an organization. In the case of Applebrook Animal Hospital, we have these broken out in the categories shown the slide. I know it may be hard to see the entries on the slide, but I have selected out the ones that I think are the most critical:
• Professional Dues (AVMA, AAHA, etc) • Taxes and licenses (In my state, I pay a “professional tax” because my profession has
been deemed especially taxable, for whatever reason. But so has my accountant’s profession, so she and I complain together)
• Credit card processing can be a real expense. You want to be watching for better deals, but remember, there is a hassle factor associated with making a change that must be accounted for in the cost of your time.
• Accounting, consulting and legal fees must be accounted for. Our accountant is an indispensable asset to my team.
Miscellaneous expenses Try to avoid using this blanket category. If you can make the expense fit accurately into a more specific group, it is a great idea. Office supplies should be logged as such so that you can see if there is a sudden unexplained change and investigate it. My friend who owns a practice in CA had a PM who was ordering personal supplies on the clinic Staples account and had my friend not been looking at her P&L, this PM would still be employed there slowly embezzling.
Advertising and marketing
To me, this is the fun part. I like keeping my clients and team engaged. I believe that fun is the missing component in workplace success. Some people say that your advertising budget should be 8-10% of your gross. Mine does not fall in this benchmark now (mostly because of COVID), but I do notice that the more I invest in Client Communications and marketing both internal and external, the more the practice grows. Expenses can be a Black Hole where your money goes, never to be seen or heard from again. Your P & L is the way to keep your money from being sucked into the black hole.
342
Net Income The 4th section is net income. In this section, the program computes your gross revenue minus your expenses to tell you the net income. Obviously, you want this to be a positive number and you would like it to be a higher number than the years before it.
According to VHMA reports, veterinary hospitals average around 6% growth year over year before 2020. January thru Feb 2020 started strongly with an overall growth of 7.6%, but COVID declines in March thru May have brought the overall average down to 2.3%. June and July both showed significant growth, so we are making up for lost ground now. So if improving net income is one of your goals, how can your P&L help with that? This is the fun part, so let’s get to it! Plotting a course with your P&L
We talked about checking your income statement to see trends, watch for changes that might identify errors or theft, give yourself a sense of control over the function of your hospital and help you know if you can bonus or raise yourself or your team, but how do you further use the P&L to your advantage? The same menu along the top that you used to customize and select your % income, also has an Excel feature. You can export the report into an Excel spreadsheet where you can play with it and test theories and ideas to see what the impact might be. Here is how: From your Reports menu, Company and Financial and then Profit and Loss Statement Prev Year Comparison (don’t forget to set the dates you want to account for the current deposit etc.) The beauty of excel is that it has the formulas embedded in it, so you can enter in any number you want to project and see the impact on your bottom line… IF YOU ARE ENTERING YOUR DATA CORRECTLY. In this example, this practice has shown 11.29% growth over the previous year. This makes us happy! Use your P&L to make your team excited about small goals and to feel that your collective passion is paying off. You can start with simple changes like the small fee, but you can also look at anything…reducing your expenses, making sure every patient gets a fecal exam…literally anything and with some simple math and plugging the values in at the right place will give you the results of the change. You can use these at team meetings to inspire others. You can know what reward program you could afford to offer. (even better, get your vendors in on the reward programs!)
I hope that this summary helps you understand and utilize your P&L statement to make your practice grow and to make you and your team feel like your work is successful.
343
Getting to win-win when there’s a conflict among team members
By Carolyn C. Shadle, Ph.D. and John L. Meyer, Ph.D.
Even among friends and good colleagues some conversations are difficult. Let’s face it, while the vast majority of conversations we have are pleasant and enjoyable, you know that a few are not. They are the ones that are long remembered, like old scars. They are ones that can lead to strained relationships over time.
When you find yourself in conflict, your goal is to resolve it so that each party gets what is needed and you can call it a “win-win.”
Any conversation requires each of the parties to listen and share. In a conflict, sometimes you find it difficult to share your views. Maybe the other person has great power and authority, is not a good listener, or wants to avoid the subject.
In spite of this, you want to share your view and speak up.
Speaking up can be difficult Why do you hold back? What makes it difficult for you to speak up?
First, you may feel that what you did or how you feel is right and the other person is wrong. This is where you often begin thinking you must score points. Second, you have feelings about it, some of which you may be totally unaware – like anger, resentment, embarrassment or fear. Negating those feelings is as if scanning the newspaper. The receiver gets the headline but not the story. And you may fear that your strong feelings will spill out and appear as an attack.
And finally, your self-identity is on the line. You may want to be judged as one who is competent, friendly, easy-to-know, responsible or fair. You may wonder if your sense of yourself will be altered if you confront your colleague.
Being aware of these three elements can help your participation more effectively in difficult conversations.
You believe you are right Let’s take the first point: you believe you are right. Indeed, an independent judge might agree that you ARE right. The problem is that when we approach a confrontation with such assurance we immediately threaten our colleagues. Consider shifting your purpose. Instead of entering the conversation with the intent to prove that you are right, consider viewing the conversation as a learning experience, as one scouting for information and understanding. What can you learn about the thoughts, needs, motivations or intents of your colleague?
You have feelings
344
The second point is addressing that undercurrent of feelings that bubbles along – sometimes erupting but often quiet and unnoticed. Before you approach your colleague, ask yourself what feeling is stirring within you. Are you angry? If so, what is behind the anger? Maybe the primary feeling is fear of not performing effectively. In a difficult conversation there is usually a lot that is not said. It may be that parties are not saying what they are thinking or feeling because the problem is blinding them from such awareness. Or, they think it wisest to leave some things unsaid. Your task is to listen for the feelings behind the words – both yours and those of your colleague, watch the body language, and think about the person with whom you are conversing. What can you understand that may be true but is not uttered?
You care about your self-image Sensitivity to your self-image and that of your colleague, the third point, will also enable you to be more empathetic and probably more humane. It is not likely that you want to destroy your colleague’s sense of self. You just want to get the problem solved! Think about your own sense of self, too. You will probably want to maintain a professional image and not that of one who “flies off the handle.”
Alternatives So, let’s put these principles to work. What alternatives do you have to ensure that David appreciates your concern about putting the employee manual online instead of in a print copy.
You could enlist his help by saying, "Help me understand more fully what your vision is for this manual.” David would appreciate that and it’s highly appropriate. But eventually you can’t ignore your own feelings
You could continue to swallow it, but in that case, too, you are negating your own feelings and needs. What happens the next time when you are pressed and have to ignore your viewpoint for his?
You could insult him. “You know, you’re being old fashioned ignoring the importance of documents being online.” But he may feel threatened and this is not likely to advance the conversation.
Notice that in all these cases you are missing the opportunity for a learning conversation. What is behind David’s resistance? What don’t you know?
A learning conversation To move to a learning conversation, you might try using an I-statement. You may be familiar with this format. It enables you to take charge of your needs (rather than be passive) and identify and share your feelings. Doing so often results in your colleague recognizing you as a person with honest feelings and needs. The I-statement also enables you to outline how the situation affects you (which is your contribution to a learning conversation).
345
You could say, for example, “I feel strongly about embracing technology and making it easy to keep this manual updated.”
Your colleague may inform you that he is mistrusting of technology, has had experience “losing” documents in cyberspace. Or you might learn that he fears that competitors might get into the system and read the manual.
If he is defensive, this is your chance to ensure him that you are on a learning path – not a path to prove him wrong or score points – and that you will listen for what is NOT said. How is he feeling? What does he think about your confrontation? How is he feeling about himself?
The power of the i-message This is a statement about where YOU are coming from – now thoughts about him. It is a statement of how you feel. For example, “I feel anxious about our practice embracing technology.” This is an expression of how you feel. You own it. Other people cannot deny how you feel. “ In some cases, you “could say, “I need….” Or “I want…” In any case, the focus is on yourself: “I….”
Many of us are not accustomed to sharing our feelings, so it may be a challenge to identify your feelings. It’s powerful, however, when you can. Look for a useful inventory of feeling words for help.
Listen Sometimes, when you confront others with an I-message, they will react and be defensive. Now what?
Now it is time to switch gears and, instead of confronting again, pause to listen to the defense. Such a response confirms that you are listening to the other person. “You’ve had some bad experiences with online documents.” Or “You think I’m being difficult you, but that’s not my intent. I want to find a solution that will work for both of us.”
Context Difficult conversations are often the result of a problem that has been present for a while. Conflict over the publication of the employee manual may not be the first time there has been a difference of opinion about the use of technology. This may be an on-going issue. Your goal is to leave the conversation with a win for each party, if possible, and surely to maintain a good relationship in order to continue the dialogue.
A number of difficult conversations may be required before you come to a mutual understanding. Just remember, make them learning conversations.
References • Douglas Stone, Bruce Patton and Sheila Heen of the Harvard Negotiation Project, Difficult
Conversations, published by Penguin Books, 2000.
346

• Carolyn C. Shadle and John L Meyer, Communication Case Studies: Building Interpersonal Skillsin the Veterinary Practice, published by the American Animal Hospital Association, 2011.
• Carolyn C. Shadle and John L. Meyer, Positive People Experiences, La Jolla, CA ICS, Inc., 2016.
347
Dealing with difficult clients By Tracy Sheffield, VPM
Difficult client behaviors can occur for many reasons. Uncovering the root cause and using effective tools to manage these behaviors can yield positive results. There are many types of difficult clients. Angry, traumatized, entitled, scared are just some of the emotions a client can bring to the practice that can create a difficult situation.
Unhappy clients can be broadly categorized into two groups. There are clients who are angry or unhappy due to outside causes, in other words, nothing that happened in the practice. The other group are the clients that are upset due to things that occurred within the practice. In truly difficult cases, a client could belong to both groups.
There are basic techniques applicable to both groups and techniques to remediate situations that have occurred in the practice. In dealing with a difficult client, the first step is to decide to which group the client belongs and assists in deciding how to approach the situation.
Steps with angry or upset clients The first step in dealing with any upset or angry client is listening to them. It is not just sitting idly by while they rant, it requires empathetic listening. This is a skill that the entire team of a veterinary practice would do well to learn.
Empathetic listening means paying attention to another person, identifying their emotions, and responding with compassion and without judgment. The basic principle behind empathetic listening is to first try to understand the other person’s perspective and then try to have your own point of view understood. This sounds easy but in the heat of the moment, it can be difficult to do. It means setting aside your own emotions and listening with openness. Neurologically speaking, it means tamping down your own amygdala-driven threat sensors while listening to the other person. Nothing productive comes of speaking when two people are in “the red zone”. This is a zone of mutual threat and fear where defensiveness is activated, and no one listens. It is most helpful when the upset person knows they can talk without fear of interruption. With no interruptions, high emotions tend to deescalate and hearing the whole perspective is often enlightening. Empathetic listening makes it possible to connect with someone on both an emotional and cognitive level. 1
Before responding and summing up the issues the client has laid out, pay particular attention to the tone of voice used. There is a study in human medicine that underscores the extreme importance of vocal tone. Audiotapes of surgeons communicating with patients were filtered so that only the volume, pace and rhythm of their conversations were audible. These recordings were then played for a group of volunteers. The volunteers that listened to the tapes were able to determine from tone of voice by itself, which of the surgeons had a history of malpractice claims filed against them and which did not. A tone of voice that suggests dominance and a lack of concern was found to be the most damaging.2Get feedback and
348
practice talking paying attention to tone of voice. It is a skill that can be learned and will assist greatly in creating good results with an upset client. Sum up with the client their list of complaints and concerns. Allow the client to add and edit the list until they feel the staff member has a full grasp of the issues. This summation should be interspersed with empathetic comments to demonstrate to the client that the issue has been truly understood. 3 Justify the anger. A good outcome is far less likely when there is no justification for the client’s anger. This is particularly true if the client is in error. If the client is in error, tact and care are necessary to prevent the client from any deep embarrassment. A deeply embarrassed client may feel so ashamed of their behavior that they will choose to take their business elsewhere rather than go to a place where they feel like they made a fool of themselves. Reassure the errant client that anyone would feel the way they did based on the information they had at the time. Let them know that you appreciate their effort to listen and get all the facts. Reiterate that their anger at the time was completely reasonable. Thank them for taking the time to get all the facts and let them know they should always feel free to contact the practice when something doesn’t seem right. Handled this way, the client is much more likely to remain a client of the practice. If the client has a legitimate complaint, validate it. Don’t try to make excuses. Own the error. “Yes, a mistake was made on your bill.” will do a lot more to calm a client down rather than nebulous excuses such as “We get really busy and someone new must have done this.” Apologize where applicable. “I am very sorry this billing error occurred.” Let the client know how the issue will be addressed. “At our next staff meeting we will review the procedure that allowed this error to happen so it will not happen again.”Offer remediation. “We will credit this immediately. Would you like a credit issued to your credit card or would you like a credit on your account?” If you are not sure what would be appropriate remediation, ask the client what they would like.4 Use of loyalty programs in these situations can be very helpful. Putting points on their program does much more for the practice and the client rather than discounting services. In summation for the angry or upset client listen, reiterate, justify, remediate. Traumatized Clients These clients have either just witnessed or been a part of a traumatic event. They may burst into the reception area, perhaps screaming, perhaps incoherent and sometimes covered in blood. They may have a blood covered pet with then. These situations often involved a pet that has been attacked either by another animal or sometimes a person. It can be that the owner unintentionally injured their own pet. For example, they may have backed over their dog with a car. Fortunately, events of this type are relatively rare, but they do happen. Staff should be trained to react to these situations immediately. The pet should be immediately taken to the treatment area and the upset client moved to a private location such as an
349
available exam room or office. Ask the client what happened. During the account of the incident, reassure the client that they handled the situation correctly wherever possible. This is extremely important to calm the client down and relieve the emotional stress of the event. What happens in the immediate aftermath of a traumatic event is how the event is solidified in the person’s mind. By giving positive reinforcement during the recounting of the incident you relieve much of the future stress when the recall the incident. 5
Be aware that emotional trauma can cause low blood sugar. Low blood sugar can cause additional emotional distress and mood instability. 6 Have available water and a snack and encourage the client to take a sip of water and a bite of the snack. Even a small bite can help with the stress induced hypoglycemia. Determine the needs of the client. If they need to clean up, provide the supplies to do so. If they have injuries, offer first aid supplies to the client. Do not assist the client with treating any injuries to themselves. Encourage them to seek medical attention. Attend to any telephone calls that should be made in relation to the incident. These may include calls to local law enforcement, EMS, and animal control. It may also be necessary to call someone to assist with transportation if the client is unfit to drive. While caring for the needs of the client do not overlook keeping them updated on the condition of their pet. Not knowing the status of a loved one is a huge emotional stressor.7 Following these procedures should quickly allow the client to relax to a more emotionally stable state .All staff should be trained in these steps so when a traumatic incident occurs, it will be dealt with in a way that yields the best outcome for both the client and the patient. Entitled Clients These clients may be very long-term clients and expect a certain series of events with each visit. If things do not go as expected, they can become quite upset. Also included in this group are the ultra-wealthy. The lives of the ultra-wealthy run far differently than those of the middle class which makes up the bulk of veterinary clientele. When the long-term client does not have their expectations met, the situation should be handled much the same way the angry client is handled. Listen to and recount the complaint and justify the anger. In this case the remediation will include a list of steps that will be taken to meet the client’s needs. Such as chart will be marked ‘morning appointments only’ or client needs to see Dr. Smith whenever possible and needs clear notification on the occasions that Dr. Smith is unavailable to see them. The upper class tend to have greater self-absorption and reduced sensitivity to others’ suffering. 8 This can yield situations where the wealthy client loudly demands immediate care for her sneezing cat and cannot understand why the doctor won’t leave the hit-by-car dog currently needing the staff’s attention. This socially entrenched narcissistic viewpoint is not
350
easily altered. Understand and accept that is unlikely that they will easily be brought to an understanding of why their perceived needs are unmet. Clients with Financial Issues Anger can be the mask that covers a sense of shame. When a client is unable to pay for what they know their pet needs, they can become angry that the cost of care is a barrier to the treatment they want for their pet. There are a couple of possible solutions to help these people. There are a wide variety of third-party payment options available to veterinary practices. Additionally, through the American Veterinary Medical Fund it is possible to set up a charitable fund to help these clients. Well Informed Clients Internet informed clients can present unique challenges to veterinarians. They may be so convinced that they know all the issues of their pet’s condition that they are unwilling or unable to listen to any other viewpoint. They may argue the recommendations regarding a treatment plan. When getting someone to change their mind, the general tactic employed is usually pushing. Presenting additional reasons for the person to change their mind does not often yield the desired results. Examples of this kind of push back include phrases like “The breeder said this puppy doesn’t need any more vaccinations” or “Why would I do blood work?” Explaining the benefits of the needed services doesn’t do a particularly good job of getting people to change their minds. There are five recurring barriers to change, but each can be overcome with the right strategy. 9
1. Reduce Reactance People like to feel that they are in control. They have an innate negative reaction to persuasion and will deploy countermeasures against it. When you try to get someone to do something, they feel disempowered. Rather than feeling like they made the choice, they feel as if it were made for them. So, they say no or do something else, even when they might have originally been happy to go along. Psychologists call this negative response, “reactance.” If you present just one solution, the client will spend their time shooting holes in it. Instead present a variety of options. This puts them back in control as they are selecting what they want instead of being told what to do. To avoid reactance, gently guide the person down the path but make sure they feel in control. One way to do this is to highlight what they would do for themselves and what they would recommend to others. Ask them, if they had a friend with an aging pet, how would they explain the value of blood work after they had heard the values of it. 2. Ease Endowment This could also be phrased as happiness with the status quo. People tend to stick with what they are familiar with and what they know. This could appear in the exam room with a phrase
351
like “We’ve never done blood work before.” The challenge here is that generally, the status quo isn’t that bad, so why do something differently? The technique to consider here is to inform the client of the hidden costs of inaction. Point out that a disease process such as diabetes is much easier to manage and less expensive to manage if caught early. 3. Shrink Distance People want information that compares favorably to their existing views. Psychological experiments going back 50 years have found a “zone of acceptance,” an area close enough to people’s existing beliefs that they will consider the new information. Using the blood work example, pointing out that a human doctor needs to see blood work to have a fully picture of the person’s complete health, it is even more important in animals as they cannot tell us if they are feeling slightly unwell. 4. Alleviate Uncertainty Any change yields uncertainty. “Do I need to do the blood work? Does my dog really need to eat that special food?” To ease uncertainty, lower the barrier to trial. For example, if blood has already been drawn for, say a heartworm test, pointing out that we don’t have to do anything more to the animal to do the blood work often overcomes client resistance. Similarly, with food, a small trial size will allow the client to try the product without having to make full commitment. 5. Find Corroborating Evidence For big changes, sometimes hearing from one person is not enough. There is strength in numbers. Hearing from multiple people often provides enough proof to drive action. Bring in a technician who had a dog diagnosed with diabetes and it was only found through blood work. Use social media to refer the client to case studies you have posted. Understanding that others have been happy taking the action can induce the reluctant client to take action as well. To get people to change their minds, it’s not about pushing harder or expending more energy. It is about reducing barriers to action. Once you understand that, you can change anything. 10
Human interactions are fraught with challenges. The mood and mindset of all individuals involved determine the outcome. Understanding and using the techniques to manage difficult situations will not only create positive results but it will lower the stress levels of the people involved in coming to resolutions in difficult situations. References 1. Riess MD, Helen The Empathy Effect, Sounds True Boulder Colorado 2018 2. Amdady, Nalini, Debi LaPlante, Thai Nguyen et al. Surgeons tone of voice: a clue to malpractice history “Surgery” 132, no 1 (July 2002) 3. Gerber, Michael, Peter Weinstein DVM The E-Myth Veterinarian Prodigy Business Books 2015
352

4. Ibid 5. Shalev MD, Arieh Treating Survivors in the Acute Aftermath of Traumatic Events traumacenter.org 6. Korn PhD, Leslie Eliminating Functional Hypoglycemia to Stabilize Mood Psychology Today,Online Format April 4, 2016 7. Shalev MD, Arieh Treating Survivors in the Acute Aftermath of Traumatic Events traumacenter.org 8. Piff, Paul K. Wealth and the Inflated Self: Class, Entitlement, and Narcissism Personality and Social Psychology Bulletin 2014, Vol 40 9. Berger PhD, Jonah The Catalyst: How to Change Anyone’s Mind Simon & Schuster March 2020 10. Ibid
353
One good new idea: Practice management tips and techniques By Tracy L. Sheffield, BS, LVT, CVPM Introduction Effective practice management covers a broad array of topics. It can be difficult to find new ideas to improve the business let alone the daunting task implementing these new ideas. The purpose of this presentation is to introduce information in the areas of marketing, human resources, operations and finance that are easy to apply and will improve business operations and profitability. Marketing Mostly Outside the Digital Box As the world is so digitized now, it is often easy to forget there are unique and effective marketing techniques that do not involve Google or the internet. There is already much information on web presence and social media and how to use them. There is one virtual area, however that is often overlooked, voice assistants. Alexa, Siri, Cortana and Google assistant should all be talking about your practice. In order for these voice assistants to do so, you must claim your business listings on the following sites: Google, Bing,Apple maps and Yelp. Alexa also receives information from Yext so using Yext (formerly Local Vets) will help in voice assistant recommendations. Do you like to talk? If you have a local low power radio station, consider pitching a show idea to them. Shows can be recorded in advance so they can be taped at your convenience. Alternatively, some practices like to produce a podcast. Podcasting kits can be purchased, often for less than $100. Decide what you want your radio show or podcast to be. Do you want to interview people who do interesting things with animals, do you want to celebrate the human animal bond, your show is only limited by your imagination? Both of these ideas require a time commitment but can yield new clients at low cost. Hosting events is a great way for potential new clients to find your practice. Events are limited only by your imagination. A big one can be holding an open house. A well-done open house requires advance planning. Doing and open house to coincide with an anniversary of some sort gives some meaning to the event. One-year anniversary at our new location,25 years in business, Dr. Smith’s five-year celebration with our practice. All of these are reasons to hold an open house. Decide on your traffic flow through the building. Create a one-way traffic pattern with stations along the way. Think about making the stations child friendly. The first station might be in an exam room. Have a stuffed animal patient that you have put a small ball into and have the children palpate to see if they can find the lump.
354
The next station might be in the lab and they can look into the microscope. Have a slide of parasite eggs ready and an ID chart so they can have fun identifying what they see in the microscope. Of course, live ear mites would be exciting as well. Another station might be radiology and there can be a variety of interesting radiographs to look at. The activity might include counting how many puppies there are if an appropriate radiograph is available. The final station is the refreshment station along with a technician or doctor there to answer questions. Preparation is the key to success for an open house. Start planning two months in advance in order to have time to advertise the event and plan for every station. It should go without saying that a deep cleaning of the facility should happen before any open house. Does your practice find itself doing unpaid charitable work? Change this up and get paid for it. How? Implement an AVMF fund. It is very easy to set up, all donations to it are tax deductible for the giver and it gives you a pool of money to tap into when there are charity cases that need help. It is the responsibility of the practice to fund it. AVMF will provide the needed materials for a donate button on the website. Putting on fundraisers is a great way to get both community attention and raise money for the fund. Some successful fund raisers might be holding a pet portrait painting party or having a Halloween costume contest for pets. All donations to your fund are tax deductible and the AVMF takes care of all the paperwork. For more information on how to set up an AVMF fund go to AVMF.org You can create a “Paint your pet’s portrait party”. This can be done with any of the painting for fun chains around the country. These chains will supply everything you need, art supplies, music and teachers. Participants pay a fee and that money covers the cost of the painting team and the remainder goes to your charitable fund. At Halloween consider a costume contest for pets. Holding an event like this at the local nursing home or veteran’s home yields wonderful PR and a great sense of having done a nice thing for a lot of people as well as raising money for your charitable fund. There are a lot of other ideas to consider for events, have a professional photographer come and do portraits of pets, for equine practices organize a trail ride. Events are only limited by your creativity. When considering an idea for an event, consider if it sounds fun to you. If the answer is yes, then go ahead with it. Be thoughtful on how you spend your marketing dollars. Print is not dead; it just needs to be used thoughtfully. There are companies such as Homeowner Data Services that can provide mailing lists of homes purchased in the last 30 days. If you have new subdivisions popping up in your area, explore the use of EDDM. Every door direct mail. Make the envelope interesting enough to open. For example, address it to “the pet lover who lives here.” Using print in a targeted manner can yield a profitable return on investment.
355
Create a targeted plan for lapsing clients. These are the clients that have not been to the practice in the last 12-18 months. Research shows these clients are at high risk of becoming inactive clients. Choose a service, for example feline rabies. Create a letter that explains the importance of the service and close the letter with a promise to follow up with a phone call to answer any questions the client may have and book an appointment. When the phone call is made the client is expecting it and there is much less client resistance. A good return it 10-15% appointments booked from letters sent and phone calls made. Keeping clients active is easier than attracting new clients. Does your community have any sort of local magazine? If you like to write this is a great way to reach people. A solid formula for these types of articles is a humorous or provocative introductory paragraph, then provide information about your topic and explain why it is important for pet owners to know about it and then finish with a call to action. Operations Complete telephone training is often overlooked. Yet this is one of the most important parts of keeping the business side of a practice up and running. Everyone should know how to answer the phone, engage the client and book the appointment. Training should include pre-surgical protocols as well as providing estimates for common procedures. Phrases like “I don’t know” and “We can’t...” should not occur in any phone conversation. Two-way texting has revolutionized client communications. It saves much time by eliminating phone calls while keeping clients fully informed. Additionally, you have a complete record of information given to the client. Texting can be a form of telemedicine with video and photos. It is excellent for surgical updates to clients. Looking for a high return on investment? Take a look at in house sharps disposal. Medical Innovations makes a device that melts all sharps into a “hockey puck” which can then legally be discarded with the regular trash. The machine pays for itself in approximately 18 months to 2 years in money saved overusing a commercial medical waste pick up company. With this system you also get rid of the boxes of sharps laying around the practice waiting for pick up making this a safer and more sanitary system of sharps disposal. The company will help you in compliance for all medical waste disposal. Here's an inventory quick fix. Take the Mark Opperman red dot challenge. Pick a week to put a red sticky dot on every inventory item in the practice. Then check at 30, 60 and 90 days to see what still is sitting on the shelf with a red dot. This will help you decide par levels and decide what items do not need to be on your shelf or should only be special order items. There is a platform to make inventory easier. Vetcove is free and allows you to price out shopping lists quickly and efficiently. You simply type in an item and Vetcove will show a list of all distributors that carry this item and the price. You can select the best price and it will go into that distributors shopping cart. When ordering through Vetcove you can see when the last time you ordered the item was and how many were ordered. Careful use of Vetcove will allow
356
the user to purchase inventory at the best prices and adjust the order to have the most items delivered in the fewest number of boxes. Client retention and compliance are always issues that directly impact practice profitability. Preventive medicine and preventive care plans are the buzzwords in this area but outside of large corporate veterinary clinics they aren't gaining much traction. Why is this? There are several reasons why 75%of veterinary practices do not pursue preventive care plans. First preventive care does not resonate with the public. If their pet is already healthy, why do they need care? Second there is the issue of collecting and keeping track of payments. Third there is the issue of the client understanding what they are purchasing. Clients often confuse a preventive or wellness package with insurance. They think they are making monthly payments that will cover all veterinary care for the year. When they bring a sick pet in and find out that the costs aren't covered by their plan, the client can be justifiably upset. There is an easier, less complicated way to accomplish the same thing using a loyalty program. A well thought out loyalty program answers the needs of client retention, assists in compliance and is easy to administer. There are many options for loyalty programs. There are stand-alone platforms and there are loyalty programs tied to various veterinary apps. Investigate each type to see which is best suited to your practice. It is a lot of time and money to get a new client to walk in the door. Once they come in a loyalty program will help keep them as a client. Neglecting employee safety can be very costly. Tune up your safety procedures. An easy way to do this is to contact local law enforcement, sheriff or police and ask if they will do an outreach program at your next staff meeting. This is a free service that they offer, and they are happy to do it. They will look over your facility and identify areas that need improvement, for example more lights in the parking area. They will go over with you what kind of issues should be reported to law enforcement and what actions the staff should take if it appears that a client may be tilting towards violence. An OSHA check up can bring your practice into compliance. There are a variety of ways to get your practice to OSHA compliance. Some of the options are free. You can go to your state On-SiteConsultation Directory/Occupational Safety and Health Administration and arrange for an inspector to go over your practice and let you know what you need to do to become compliant. There are also many services that do this for a fee. Getting paid is always important. There are a wide variety of payment tools available to the veterinary practice. Care credit, Scratchpay and Vet Billing are just some of the examples of third-party payment options. Each of these are different in what they do and how they work, and each meets a different need. Having multiple options allows a practice to meet the needs of a larger number of clients. Have links to payment options on your website. Are missed charges a problem in your practice? Get team members on board to prevent them and catch them. A bounty program can help with this. Reward team members when they are meticulous about recording treatments, recommendations and procedures they can be paid a
357
bounty when they have done an exceptional job with a complex invoice. Pay a bounty when a team member catches a missed charge. Paying a bounty is far less expensive than missing a charge. The take home here is, make your staff excited about accurate entries on procedures and catching missed charges. Are you making the most of your credit card rewards? Bills that are regularly paid in full every month can be run through a rewards card for travel points and other rewards. This will allow a practice to rapidly accumulate points that can be used to benefit the practice, for example sending more team members to conferences. Points can cover the cost of airfare and hotel bills. Perhaps you feel need onsite help. Where do you go to find a consultant with the expertise you need? VetPartners.org has a list of consultants. You can search by geographic region or by expertise. It is a great place to start the search for individualized help. Insurance, perhaps the one area of practice management that no one gets too excited about, but it is terribly important for financial safety. Any risk you do not insurance against is a risk that you are willing to accept yourself. A major point to consider. If you have an employ drive a vehicle for you, they vehicle needs to be titled in the name of the practice. If you want to lose everything you own, allow an employee to drive your personal vehicle. This is a risk you should be unwilling to accept on your own. Another important point in insurance to consider is the scheduling of expensive breakable equipment. Things like the capture plate on any of your digital x-ray systems, a cold therapeutic laser should be scheduled individually on your inland marine policy. Equipment like this can have a high probably of breakage and is expensive to replace. Scheduling these items cover them against breakage. If you need the answer to an obscure or unique practice management question? Consider joining the Veterinary Hospital Mangers Association. The VHMA has a library of documents that covers almost any need. Even better, they have an open forum which is like VIN for hospital management. If you are having a human resources issue or an inventory issue, post it on the open forum and someone has likely already dealt with the problem and will have an answer for you. You do not have to reinvent the wheel.
358
Work Environment: The Overlooked Profit Center Tracy Sheffield, BS, LVT, CVPM A workplace free of damaging behaviors has consistently been shown to increase workforce productivity, reduce on-the-job errors, reduce employee turnover, and create happier clients. Unaddressed workplace issues are a major reason for associate veterinarians to consider finding another position. Introduction The veterinary workplace environment is overlooked at the peril of business profitability. Practice owners want to focus on veterinary medicine, not business management. Neglecting business management, specifically issues related to the workplace environment, has hidden costs to the business. A lack of understanding of the true costs of an un-managed work environment leads practice owners to choose inaction as the most expedient answer to difficult workplace situations. Inaction can be the worst response when faced with a workplace issue. Inaction can frustrate associates to the point that they leave a practice where they enjoyed practicing quality medicine but found the work environment too toxic to tolerate any longer. Adopting and enforcing behavior expectations for all staff members and creating a civil, professional, and safe work environment improves the bottom line in any business setting. Veterinarians seeking associate positions would be well advised to evaluate the workplace environment before deciding to accept a position. A toxic work environment leads many associates to leave a position even though they appreciate other facets of their employment. A survey of workplace environment issues found that the veterinary profession has much room for improvement. Changes to improve a work environment are reasonably easy to implement, do not require an outlay of cash, and have a direct impact on improving volume and quality of work produced. Methods and Materials Participants Responses came from 205 veterinarians. 87.8% (n=180) were female and 12.2% (n=25) were male. Of these 205, 191 completed the full survey. 33.51% (n=64) have been in practice less than two years; 45.03% (n=86) have been in practice two to five years; 13.09% (n=25) have been in practice six to fifteen years; and 8.38% (n=16) have been in practice greater than 15 years. Survey A nine-question, anonymous survey was made available on various veterinary-only social media platforms and by direct e-mail to Texas Veterinary Medical Association members. The direct e-mail recipients received selection bias based on the year graduated. Part of the purpose of the survey was to determine management response to issues. As recent graduates and relatively new hires are more likely to be subordinate to management rather than in management themselves, this puts them in the position to evaluate management rather than evaluating their own management skills.
359
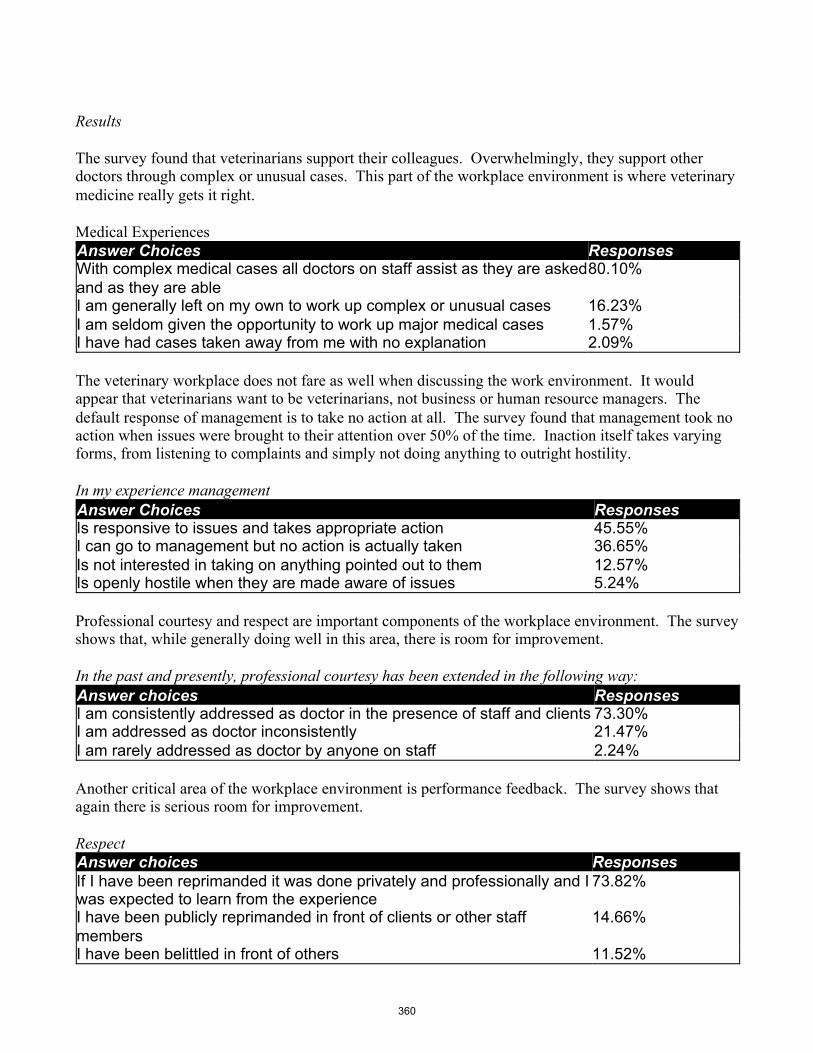
Results The survey found that veterinarians support their colleagues. Overwhelmingly, they support other doctors through complex or unusual cases. This part of the workplace environment is where veterinary medicine really gets it right. Medical Experiences Answer Choices Responses With complex medical cases all doctors on staff assist as they are asked and as they are able
80.10%
I am generally left on my own to work up complex or unusual cases 16.23% I am seldom given the opportunity to work up major medical cases 1.57% I have had cases taken away from me with no explanation 2.09% The veterinary workplace does not fare as well when discussing the work environment. It would appear that veterinarians want to be veterinarians, not business or human resource managers. The default response of management is to take no action at all. The survey found that management took no action when issues were brought to their attention over 50% of the time. Inaction itself takes varying forms, from listening to complaints and simply not doing anything to outright hostility. In my experience management Answer Choices Responses Is responsive to issues and takes appropriate action 45.55% I can go to management but no action is actually taken 36.65% Is not interested in taking on anything pointed out to them 12.57% Is openly hostile when they are made aware of issues 5.24% Professional courtesy and respect are important components of the workplace environment. The survey shows that, while generally doing well in this area, there is room for improvement. In the past and presently, professional courtesy has been extended in the following way: Answer choices Responses I am consistently addressed as doctor in the presence of staff and clients 73.30% I am addressed as doctor inconsistently 21.47% I am rarely addressed as doctor by anyone on staff 2.24% Another critical area of the workplace environment is performance feedback. The survey shows that again there is serious room for improvement. Respect Answer choices Responses If I have been reprimanded it was done privately and professionally and I was expected to learn from the experience
73.82%
I have been publicly reprimanded in front of clients or other staff members
14.66%
I have been belittled in front of others 11.52%
360
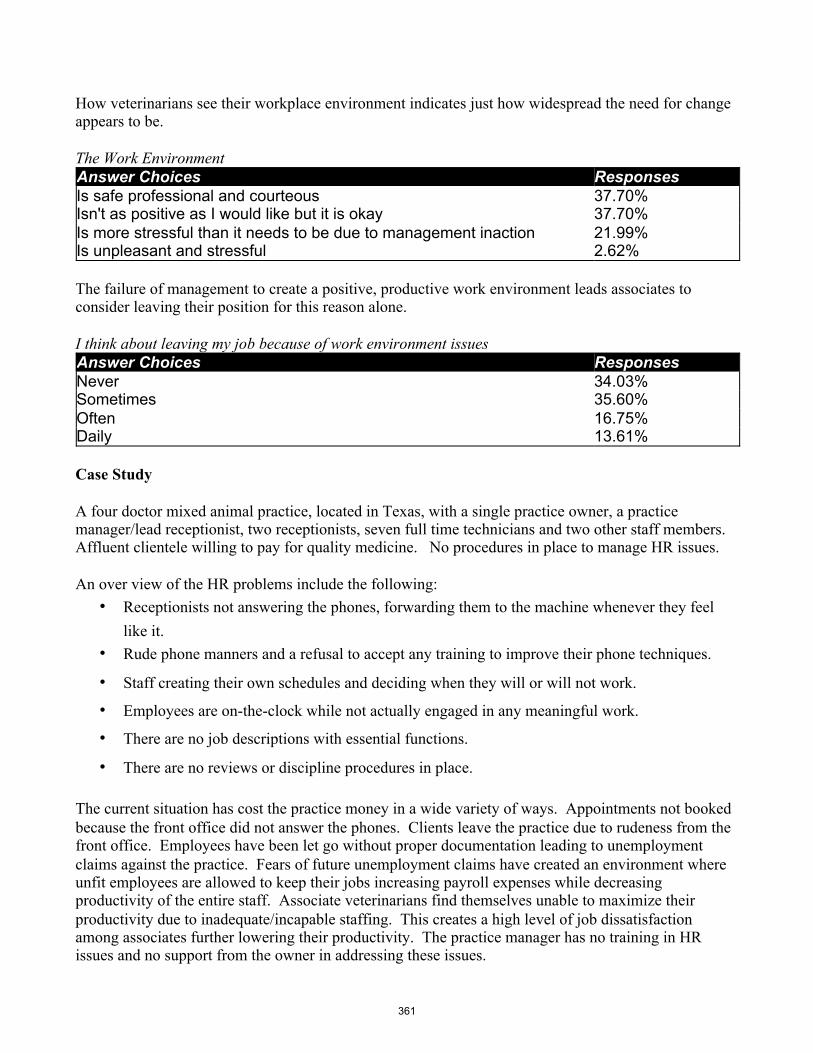
How veterinarians see their workplace environment indicates just how widespread the need for change appears to be. The Work Environment Answer Choices Responses Is safe professional and courteous 37.70% Isn't as positive as I would like but it is okay 37.70% Is more stressful than it needs to be due to management inaction 21.99% Is unpleasant and stressful 2.62% The failure of management to create a positive, productive work environment leads associates to consider leaving their position for this reason alone. I think about leaving my job because of work environment issues Answer Choices Responses Never 34.03% Sometimes 35.60% Often 16.75% Daily 13.61% Case Study A four doctor mixed animal practice, located in Texas, with a single practice owner, a practice manager/lead receptionist, two receptionists, seven full time technicians and two other staff members. Affluent clientele willing to pay for quality medicine. No procedures in place to manage HR issues. An over view of the HR problems include the following:
• Receptionists not answering the phones, forwarding them to the machine whenever they feel like it.
• Rude phone manners and a refusal to accept any training to improve their phone techniques.
• Staff creating their own schedules and deciding when they will or will not work.
• Employees are on-the-clock while not actually engaged in any meaningful work.
• There are no job descriptions with essential functions.
• There are no reviews or discipline procedures in place. The current situation has cost the practice money in a wide variety of ways. Appointments not booked because the front office did not answer the phones. Clients leave the practice due to rudeness from the front office. Employees have been let go without proper documentation leading to unemployment claims against the practice. Fears of future unemployment claims have created an environment where unfit employees are allowed to keep their jobs increasing payroll expenses while decreasing productivity of the entire staff. Associate veterinarians find themselves unable to maximize their productivity due to inadequate/incapable staffing. This creates a high level of job dissatisfaction among associates further lowering their productivity. The practice manager has no training in HR issues and no support from the owner in addressing these issues.
361
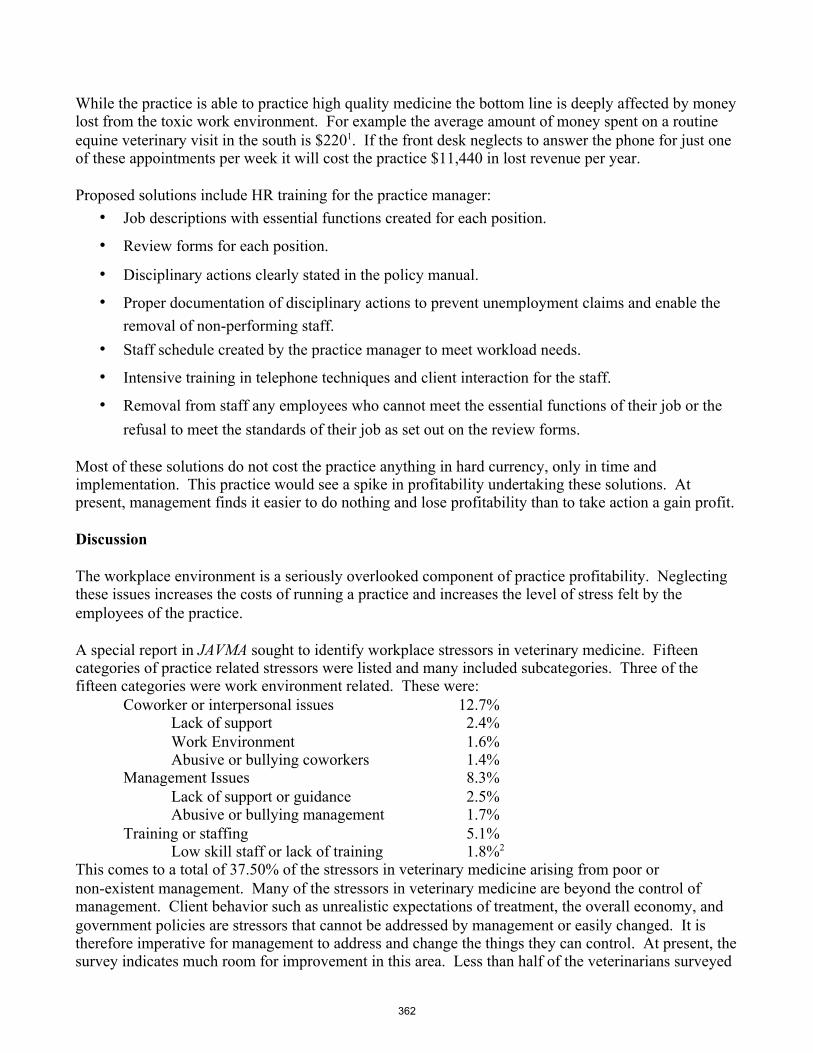
While the practice is able to practice high quality medicine the bottom line is deeply affected by money lost from the toxic work environment. For example the average amount of money spent on a routine equine veterinary visit in the south is $2201. If the front desk neglects to answer the phone for just one of these appointments per week it will cost the practice $11,440 in lost revenue per year. Proposed solutions include HR training for the practice manager:
• Job descriptions with essential functions created for each position.
• Review forms for each position.
• Disciplinary actions clearly stated in the policy manual.
• Proper documentation of disciplinary actions to prevent unemployment claims and enable the removal of non-performing staff.
• Staff schedule created by the practice manager to meet workload needs.
• Intensive training in telephone techniques and client interaction for the staff.
• Removal from staff any employees who cannot meet the essential functions of their job or the refusal to meet the standards of their job as set out on the review forms.
Most of these solutions do not cost the practice anything in hard currency, only in time and implementation. This practice would see a spike in profitability undertaking these solutions. At present, management finds it easier to do nothing and lose profitability than to take action a gain profit. Discussion The workplace environment is a seriously overlooked component of practice profitability. Neglecting these issues increases the costs of running a practice and increases the level of stress felt by the employees of the practice. A special report in JAVMA sought to identify workplace stressors in veterinary medicine. Fifteen categories of practice related stressors were listed and many included subcategories. Three of the fifteen categories were work environment related. These were:
Coworker or interpersonal issues 12.7% Lack of support 2.4% Work Environment 1.6% Abusive or bullying coworkers 1.4%
Management Issues 8.3% Lack of support or guidance 2.5% Abusive or bullying management 1.7%
Training or staffing 5.1% Low skill staff or lack of training 1.8%2
This comes to a total of 37.50% of the stressors in veterinary medicine arising from poor or non-existent management. Many of the stressors in veterinary medicine are beyond the control of management. Client behavior such as unrealistic expectations of treatment, the overall economy, and government policies are stressors that cannot be addressed by management or easily changed. It is therefore imperative for management to address and change the things they can control. At present, the survey indicates much room for improvement in this area. Less than half of the veterinarians surveyed
362
indicated that management took action on workplace issues. Failure to take action may indicate a lack of management training on how and what kind of action is appropriate and a lack of knowledge on how to execute the action. Inaction can also be seen as a failure of leadership. While it is easier to “hope the problem will go away” this is an unrealistic, damaging, and ultimately costly approach. Proactive behavior is always more effective than reactive behavior. Setting standards of behavior will curtail future workplace issues. Addressing all veterinarians on staff as doctor at all times is not only a professional courtesy, it also reminds clients what they are paying for. They are paying for the professional care of a well-educated and well-trained doctor to care for their animal's health care needs. Failure to address the veterinarians on staff as doctor warrants disciplinary action by management. A verbal warning the first time and a write up the second time. If management takes this seriously, the staff will as well. The extent to which civility and kindness can improve the bottom line is often overlooked. Civility is a key component of the work environment. Civility is how someone feels about how they are treated. It is the viewpoint of the recipient that in a large part defines civility. Lack of civility often stems from lack of awareness on the part of the person engaging in uncivil behavior. Employees should be trained and supervisory staff should model the behavior expected for all employees. Due to the nature of veterinary medicine, the work environment can be stressful due to life-and-death situations. Exacerbating the stress by un-empathetic leadership will cause the quality and quantity of work performed to drop. This in turn will affect cash flow. Workplace performance is based on feedback. Without feedback, employees are in the dark about their performance and how they could be improving. However, feedback given incorrectly is, arguably, even worse. How criticisms are given and received goes a long way in determining how satisfied people are with their work, with those they work with, and with those to whom they are responsible. 3 The survey found that 25% of veterinarians have been criticized inappropriately. These types of behaviors by management are among the most damaging to the workplace environment. They leave both the recipient and anyone who witnessed it less effective in their jobs because of time spent dwelling on the incident. This type of incivility must be eliminated from the workplace by management becoming aware of what they are doing when giving employees performance feedback. The temptation to “let an employee have it” after an error is made can be very strong indeed. This is the very situation where management must take a step back and frame the feedback in such a way that both the employee and therefore the business will benefit. The artful critique is the formula that can be applied in these situations. This critique technique is made up of four areas, each that need to be utilized for successful management of a problem that will yield an employee motivated to learn from the mistake and not repeat it. Be specific. Pick a significant incident, an event that illustrates a key problem that needs changing or a pattern of deficiency, such as the inability to demonstrate proficiency at a particular task. It demoralizes people just to hear that they are doing “something” wrong without knowing specifics. Focus on the specifics, what was done well and what was done poorly, and how it could be changed.
363
Offer a solution. For example, a doctor who is inconsistent about making follow up calls may benefit from communication training and the front desk providing a daily list of cases seen with phone numbers and a place for notes that can then be put in the record by the front desk. Be present. Face to face is the most effective way to communicate and a memo or e-mail is not the way to deal with any personnel issues. Be sensitive. Reviews and criticism call for empathy. Be direct but be kind. Remember you are wanting to inspire, not demoralize. The goal here is to see the criticism as valuable information about how to do better and not as a personal attack. 4
Mistakes by employees can be a major reason for management to react in an uncivil manner. This is not the only reason for this type of behavior in the workplace. Studies on the subject came up with a wide variety of reasons. More than half claimed they were overloaded and more than 40% said they had 'no time to be nice'. 25% said they were rude because their leaders were disrespectful. Another quarter said that their companies lacked guidelines or training about how to treat people.5 The costs of incivility are immense. A look at what incivility does to the productivity of workers: • 48% intentionally decreased work effort.
• 47% intentionally decreased their time spent at work.
• 38% intentionally decreased the quality of their work.
• 80% lost work time worrying about the incident.
• 63% lost work time avoiding the offender.
• 66% said that their performance declined.
• 78% said that their commitment to the organization declined.
• 12% said that they left their job because of the uncivil treatment.
• 25% admitted to taking their frustration out on customers.6
In a veterinary setting the costs of rude behavior can be even higher: it can lead to medical errors and cause patient death. People on the receiving end of rude behavior have their thoughts hijacked by the incident. The mind tends to dwell on the insult, not on the task at hand. This can have disastrous results in medicine. In a study of 4500 medical doctors and nurses, 71% tied disruptive behavior (defined as “abusive personal conduct,” including condescending, insulting or rude behavior) to
364
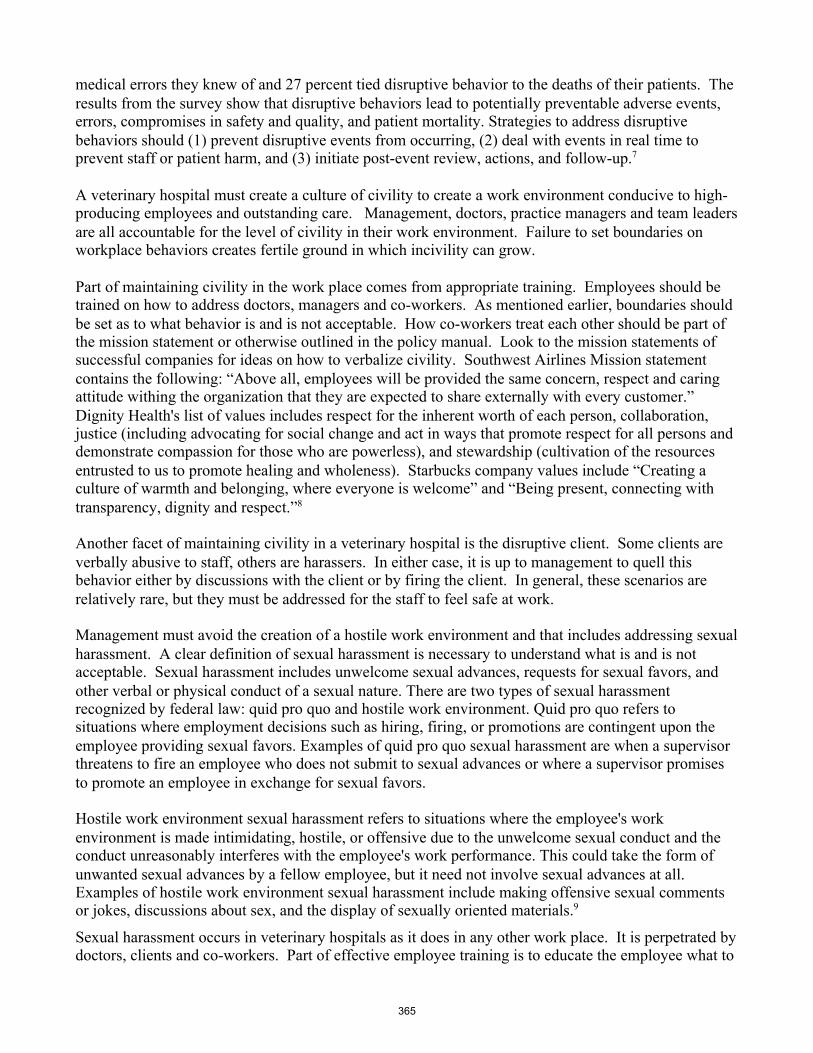
medical errors they knew of and 27 percent tied disruptive behavior to the deaths of their patients. The results from the survey show that disruptive behaviors lead to potentially preventable adverse events, errors, compromises in safety and quality, and patient mortality. Strategies to address disruptive behaviors should (1) prevent disruptive events from occurring, (2) deal with events in real time to prevent staff or patient harm, and (3) initiate post-event review, actions, and follow-up.7 A veterinary hospital must create a culture of civility to create a work environment conducive to high- producing employees and outstanding care. Management, doctors, practice managers and team leaders are all accountable for the level of civility in their work environment. Failure to set boundaries on workplace behaviors creates fertile ground in which incivility can grow. Part of maintaining civility in the work place comes from appropriate training. Employees should be trained on how to address doctors, managers and co-workers. As mentioned earlier, boundaries should be set as to what behavior is and is not acceptable. How co-workers treat each other should be part of the mission statement or otherwise outlined in the policy manual. Look to the mission statements of successful companies for ideas on how to verbalize civility. Southwest Airlines Mission statement contains the following: “Above all, employees will be provided the same concern, respect and caring attitude withing the organization that they are expected to share externally with every customer.” Dignity Health's list of values includes respect for the inherent worth of each person, collaboration, justice (including advocating for social change and act in ways that promote respect for all persons and demonstrate compassion for those who are powerless), and stewardship (cultivation of the resources entrusted to us to promote healing and wholeness). Starbucks company values include “Creating a culture of warmth and belonging, where everyone is welcome” and “Being present, connecting with transparency, dignity and respect.”8 Another facet of maintaining civility in a veterinary hospital is the disruptive client. Some clients are verbally abusive to staff, others are harassers. In either case, it is up to management to quell this behavior either by discussions with the client or by firing the client. In general, these scenarios are relatively rare, but they must be addressed for the staff to feel safe at work. Management must avoid the creation of a hostile work environment and that includes addressing sexual harassment. A clear definition of sexual harassment is necessary to understand what is and is not acceptable. Sexual harassment includes unwelcome sexual advances, requests for sexual favors, and other verbal or physical conduct of a sexual nature. There are two types of sexual harassment recognized by federal law: quid pro quo and hostile work environment. Quid pro quo refers to situations where employment decisions such as hiring, firing, or promotions are contingent upon the employee providing sexual favors. Examples of quid pro quo sexual harassment are when a supervisor threatens to fire an employee who does not submit to sexual advances or where a supervisor promises to promote an employee in exchange for sexual favors. Hostile work environment sexual harassment refers to situations where the employee's work environment is made intimidating, hostile, or offensive due to the unwelcome sexual conduct and the conduct unreasonably interferes with the employee's work performance. This could take the form of unwanted sexual advances by a fellow employee, but it need not involve sexual advances at all. Examples of hostile work environment sexual harassment include making offensive sexual comments or jokes, discussions about sex, and the display of sexually oriented materials.9
Sexual harassment occurs in veterinary hospitals as it does in any other work place. It is perpetrated by doctors, clients and co-workers. Part of effective employee training is to educate the employee what to
365
do and who to report to if harassment is occurring. It is then up to management to investigate and act appropriately. Failure to do so not only creates a work environment where employees feel unsafe, it leaves the practice open to legal action.
To create a safe work environment, violence and the potential for violence in the workplace must be addressed. Workplace violence occurs in the veterinary workplace as it does in any segment of business. According to the FBI, the perpetrators of workplace violence can be broken into four types.
Type of Act Description of Act Type I Offender has no relationship with the victim or workplace establishment.
In these incidents, the motive most often is robbery or another type of crime
Type II Offender currently receives services from the workplace, often as a customer, client, patient student, or other type of consumer.
Type III Offender is either a current or former employee who is acting out toward coworkers, managers or supervisors.
Type IV Offender is not employed at the workplace, but has a personal relationship with an employee. Often these incidents are due to domestic disagreements between an employee and the offender.
Figure 1 – Classification of Workplace Violence Acts10
The first strategy employed to combat workplace violence should be prevention. This falls under the heading of “know your employee”. When employee behavior changes it should be reviewed to determine if it is a behavior of concern. Behaviors of concern can help workers recognize potential problems with fellow employees. If a coworker begins acting differently, determining the frequency, duration, and intensity of the new, and possibly troubling, behavior can prove helpful. Specific behaviors of concern that should increase vigilance for coworkers and supervisors include sadness, depression, threats, menacing or erratic behavior, aggressive outbursts, references to weaponry, verbal abuse, inability to handle criticism, hypersensitivity to perceived slights, and offensive commentary or jokes referring to violence. These behaviors—when observed in clusters and coupled with diminished work performance (as manifested by increased tardiness or absences, poor coworker relations, and decreased productivity)—may suggest a heightened violence potential. It must be pointed out, however, that no single behavior is more suggestive of violence than another. All actions have to be judged in the proper context and in totality to determine the potential for violence. Not surprisingly, relationship problems (e.g., emotional/psychological or physical abuse, separation, or divorce) can carry over from home to the work setting. Certain signs that may help determine if a coworker is experiencing such difficulties include disruptive phone calls and e-mails, anxiety, poor concentration, unexplained bruises or injuries, frequent absences and tardiness, use of unplanned personal time, and disruptive visits from current or former partners. Care must be taken when dealing with what can be highly charged situations. Companies may lack the expertise to handle these on their own and may have to consult with experienced professionals. Finally, all incidents are different and must be viewed on their own individual merits. Experience has shown that no “one size fits all” strategy exists. 11
366

Staff should be made aware if a client exhibits these behaviors of concern in response to a poor outcome. Any threat of violence made by a client should be reported to local law enforcement. Recognition of the potential for workplace violence and what to do in the case of workplace violence should be a part of staff training. Local law enforcement is generally available to conduct seminars on the subject of workplace violence and this resource should be utilized. All members of staff will feel safer and more confident if they are educated on workplace violence. Only 35.48% of surveyed veterinarians rated their workplace as safe, professional and courteous. This indicates much more needs to be done by practice owners and management to improve their workplace. Practice owners should consider professional management of their practice if they are not interested in the management aspect of their business. As it has been outlined here, failure to manage is too costly to ignore. The acquisition of a practice manager or hospital administrator will free up the owner/veterinarian to focus on the practice of medicine and limit their administrative time to major issues and then delegate the resolution of them to the practice manager. This improves practice profitability two ways, the owner/veterinarian has more time to practice and the workplace environment issues are addressed and resolved.
To determine to what extent the workplace environment affects job satisfaction the survey asked how often participants considered leaving their job due to work environment issues. The responses indicate only one third of veterinarians never thought about leaving their jobs because of workplace issues. Fully two thirds of the respondents gave some thought about leaving their positions and half of those thought about it often or daily. Replacing departing associates is time consuming and expensive.
Conclusion
The costs to a veterinary practice from failure to manage the work environment are steep. Costs can arise from decreased employee productivity, employee turnover, unemployment claims, lost clients, medical mistakes and lawsuits.
Staff must be properly trained, evaluated and motivated to yield productive, profitable performance. Top tier performance can only occur when the work environment is safe and civil. Creating and supporting this type of work environment will increase practice profitability through outstanding workplace performance and dedication. Veterinarians must consider the workplace environment as well as the quality of medicine practiced when considering a position. Practice owners and/or management must improve and be willing to make the changes necessary for creating a positive workplace environment. These steps include managing the behavior of support staff and clients, setting the standard of behavior for associates veterinarians as well. A system of regular evaluation and feed back for all employees needs to be in place. Practices should have a process for employees to bring issues to management. This process should include reporting back to the person who made the complaint on what if any action was taken and the reasons for the course of action. Failure to follow these steps increases the costs of running a practice and decreases profits and decreases the workplace satisfaction of all employees and the practice owner. References
1. DVM360.com staff, The Data: A close look at the veterinary equine clients habits and spending. http://veterinarybusiness.dvm360.com/data-close-look-veterinary-equine-clients-habits-and-spending?pageID=2
367
2. Vande Griek O, Clark M, Witte T, et al Development of a Taxonomy of Practice-Related Stressors Experienced by Veterinarians in the United States. JAVMA January 15, 2018 Volume 252 Number 2
3. Goleman D, Emotional Intelligence, Why it can matter more than IQ. Bantam Books 1995 4. Ibid 5. Porath C, Mastering Civility, A Manifesto for the Workplace. Grand Central Publishing 2016 6. Porath C, Pearson C. The Price of Incivility. Harvard Business Review Jan-Feb 2013 7. Rosenstein AH, O'Daniel M. A Survey of the Impact of Disruptive Behaviors and
Communication Defects on Patient Safety. Joint Commission Journal on Quality and Patient Safety 34, no. 8 (2008)
8. Porath C, Mastering Civility, A Manifesto for the Workplace. Grand Central Publishing 2016 9. Berlin R, Sexual Harassment in the Workplace Defined.
http://www.alllaw.com/articles/employment/article37.asp 10. Romano S, Levi-Minzi M, Rugala E, et al, Workplace Violence Prevention, Readiness and
Response. FBI Law Enforcement Bulletin January 2011 11. Ibid.
368
Tips and tricks: Helpful advice for those new to shelter medicine
By Amanda Dykstra, DVM, MPH, DABVP (Shelter Medicine Practice)
Not long ago, shelter medicine was thought of as something that veterinarians went into when they had failed elsewhere. This misconception still exists as does the prevalent belief that shelter medicine is simply the practice of small animal medicine with less resources and less concern for practicing quality medicine. As the practice has evolved, shelter medicine has been recognized as a specialty all its own with boarded specialists practicing around the world and a plethora of research focused on the advancement of shelter medicine practice.
Unfortunately, education in shelter medicine is still lacking in many university programs and many of those with shelter programs still focus primarily on spay/neuter surgery and neglect to teach students about the important concepts involved with managing a population in a shelter setting. This is not true for all university programs, however, as a handful of innovative programs have led the way in shelter medicine education and research.
My presentation will go over many of the things that are helpful to those new the shelter medicine practice, but I wanted to include what is often the most useful knowledge in the proceedings. The following references will help anyone as they enter the field: (References are in random order).
https://www.aspcapro.org/
https://www.maddiesfund.org/index.htm
https://www.sheltermedicine.com/
https://www.sheltermedicine.com/
https://www.aspca.org/humane-alliance
• Merck, M. (Ed.). (2012). Veterinary forensics: animal cruelty investigations. John Wiley & Sons.
• Rochlitz, I. (Ed.). (2005). The welfare of cats (Vol. 3). Dordrecht: Springer. • Miller, L., & Hurley, K. (Eds.). (2009). Infectious disease management in animal shelters.
John Wiley & Sons. • Yin, S. A. (2009). Low stress handling, restraint and behavior modification of dogs & cats:
techniques for developing patients who love their visits. CattleDog Pub.. • Weiss, E., Mohan-Gibbons, H., & Zawistowski, S. (Eds.). (2015). Animal behavior for
shelter veterinarians and staff. John Wiley & Sons. • Miller, L., & Zawistowski, S. (Eds.). (2012). Shelter medicine for veterinarians and staff.
John Wiley & Sons. • White, S. (Ed.). (2020). High-quality, High-volume Spay and Neuter and Other Shelter
Surgeries. John Wiley & Sons.
369
Spay/neuter surgical techniques to improve outcomes and efficiency in general practice
By Amanda Dykstra DVM, MPH, DABVP (Shelter Medicine Practice)
Elective gonadectomy is one of the most common veterinary procedures performed in the United States.1 For years, veterinarians have debated the preferred methods for “desexing” dogs and cats. One issue that repeatedly comes up during this argument is whether the more efficient methods standardized in high volume spay/neuter clinics are “shortcuts” that are taken at the expense of patient care. The argument could be made, however, that efficiency in itself is a valuable means of decreasing adverse post-operative outcomes.
In both the human and veterinary medical fields, there has been a movement towards less invasive surgical techniques.2 Scrotal castrations are less invasive than prescrotal castrations, have smaller incisions, and require less surgical time,3 benefitting both the patient and surgeon. In general, efficient techniques with smaller incisions reduce anesthetic time, decrease healing time, decrease wound dehiscence, and decrease post-operative pain.3,4
Studies dealing with post-surgical complication rates should be interpreted with the understanding that it is somewhat difficult to assess post-surgical complication rates. Follow up protocols vary, the clinical interpretation of “complication” varies, and record keeping is often not ideal.5 In one review of medical records, the frequency of post-operative complications in dogs is approximately 6.1%.6 One study at a veterinary school revealed that 14.2% of dogs spayed by fourth year veterinary students had postoperative complications.7 Complications commonly seen in castrated dogs include inflammation or infection of the surgery site, excessive patient attention to the surgical site, scrotal hematoma, abscess, and dehiscence.5 Older animals appear to have more complications than younger animals.5,6 Increased surgical time also appears to be associated with increased complications overall.7 As body weight increases, surgical time also increases; animals with high body weights, therefore, also tend to have higher complication rates.7 When considering only postoperative infection rates, the risk is associated with the duration of surgery, the number of people in the operating room, and the cleanliness of the surgical site.8 When inflammation is considered, the same three factors apply, as does the patient’s weight.8 One retrospective study of wound infections following clean-contaminated sites found that the only factors that were statistically significant were surgical and anesthetic time, neuter status, and concurrent endocrinopathy.9 Because sterilization is always performed on intact dogs and is generally performed on healthy animals without pre-existing endocrinopathy, the factors relevant to this discussion are surgical and anesthetic time.
While the scientific evidence is somewhat limited, one could conclude from available studies that surgical efficiency should be an important goal of surgical training in order to decrease unwanted outcomes. This presentation will focus on some of the simple changes veterinarians can make that can improve their efficiency and patient outcomes.
References
370
1. Greenfield CL, Johnson AL, Schaeffer DJ. Perspectives in professional education: frequency of use of various procedures, skills, and areas of knowledge among veterinarians in private small animal exclusive or predominant practice and proficiency expected of new veterinary school graduates. J Am Vet Med Assoc 2004;224:1780-1787.
2. Parkinson T. Progress towards less invasive veterinary surgery. Vet Rec 2012;171:67-68. 3. Bushby PA. Surgical techniques for spay/neuter In: Miller L,Zawistowski S, eds. Shelter
Medicine for Veterinarians and Staff. Second ed. Ames, Iowa: Wiley-Blackwell, 2013;625-647.
4. Looney AL, Bohling MW, Bushby PA, et al. The Association of Shelter Veterinarians veterinary medical care guidelines for spay-neuter programs. J Am Vet Med Assoc 2008;233:74-86.
5. Pollari FL, Bonnett BN. Evaluation of postoperative complications following elective surgeries of dogs and cats at private practices using computer records. Can Vet J 1996;37:672-678.
6. Pollari FL, Bonnett BN, Bamsey SC, et al. Postoperative complications of elective surgeries in dogs and cats determined by examining electronic and paper medical records. J Am Vet Med Assoc 1996;208:1882-1886.
7. Burrow R, Batchelor D, Cripps P. Complications observed during and after ovariohysterectomy of 142 bitches at a veterinary teaching hospital. Vet Rec 2005;157:829.
8. Eugster S, Schawalder P, Gaschen F, et al. A prospective study of postoperative surgical site infections in dogs and cats. Vet Surg 2004;33:542-550.
9. Nicholson M, Beal M, Shofer F, et al. Epidemiologic evaluation of postoperative wound infection in clean-contaminated wounds: a retrospective study of 239 dogs and cats. Vet Surg 2002;31:577-581.
371

Exploratory laparotomy with biopsy techniques By Harry W. Boothe, DVM, MS, DACVS Exploratory laparotomy (celiotomy) is often indicated when a disease process involving a structure within the peritoneal cavity requires diagnosis, prognosis, or therapy. Ideally, exploratory laparotomy provides an opportunity for both a definitive diagnosis and therapeutic intervention. Similar to performing a physical examination, one should be thorough, efficient, and consistent when performing an exploratory laparotomy.1-2 Biopsy with histologic examination should be a part of essentially every exploratory laparotomy in which a direct surgical diagnosis (e.g., enteric foreign body, intussusception) is not achieved. Basingan interpretation on gross evaluation alone during an exploratory celiotomy assures that an accurate definitive diagnosis will not be reached in too many instances. Tissues biopsied at laparotomy often include liver, intestine, lymph node, kidney, prostate, stomach, spleen, and pancreas. Less commonly biopsied tissues are urinary bladder and greater omentum. Liver biopsy One of the simplest methods is the suture fracture of guillotine technique. This method is limited in that only the periphery of a liver lobe may be sampled, although variably sized samples may be obtained. Use a loop of suture material (e.g., 2-0 polydioxanone) to strangulate liver tissue proximal to the proposed biopsy site. Sharply divide the liver tissue distal to the ligature. Use a wedge resection technique to remove larger biopsy samples. Place two rows of overlapping, full-thickness horizontal mattress sutures through the liver. Excise the specimen distal to the sutures. After either of the above methods, cover the incised edge of liver with greater omentum. Another versatile method of liver biopsy involves use of a skin biopsy puncha. Any portion of the liver may be sampled using this method; however, smaller, partial thickness samples are obtained. Drill the biopsy punch into the hepatic tissue and twist it to obtain the specimen. Avoid excessively deep penetration into the hepatic tissue to avoid larger vessels. Insert either a topical hemostatic agent (e.g., absorbable gelatin sponge) or omentum into the defect. Intestinal biopsy Principles of intestinal biopsy acquisition include the need to perform multiple biopsies along the length of the small intestine, obtain full-thickness samples, and protect the properly closed biopsy site. Technical considerations include size of the biopsy specimen to acquire, closure technique, and method of protection of the enteric incision. Intestinal biopsies are efficiently obtained using a skin biopsy puncha. Use a 6 mm biopsy punch in dogs and a 4 mm biopsy puncha in cats. Position the biopsy punch at the antimesenteric aspect and exert rotary forces, taking care to avoid trauma to the opposite (mesenteric) aspect of the intestine. Complete the transection by using Metzenbaum scissors at the base. Close the defect transversely in a single layer using a full-thickness appositional suture pattern (e.g., simple interrupted) of synthetic absorbable suture (e.g., 4-0 polydioxanone).3A wedge resection technique, with the wedge centered on the antimesenteric aspect and oriented transversely, yields larger samples. Techniques for visceral wound protection include use of greater omentum ora serosal patch. Use greater omental coverage of the properly closed biopsy site when uncomplicated wound
372

healing is expected. Place a serosal patchin situations of potential delayed wound healing (e.g.,peritonitis or possibly hypoproteinemia). Lymph node biopsy Abdominal lymph nodes frequently sampled by the author include one or more from the following lymph centers: celiac lymph center (pancreaticoduodenal), cranial mesenteric lymph center (left colic), and iliosacral lymph center (medial iliac). Excisional or incisional biopsies are preferred to simple aspiration o provide morphologic interpretation. Preserve regional blood supply to adjacent tissue during excisional or incisional biopsies. For excisional biopsies, interrupt the blood supply to the lymph node with sutures or electrosurgery, and carefully dissect the lymph node from surrounding tissues. Minimize trauma to avoid tissue distortion. Kidney biopsy Kidney biopsies provide both diagnostic and prognostic information. Biopsy may be achieved using either a needle biopsy technique or a wedge resection technique. For a needle biopsy, insert the needleb through the renal capsule at the caudal aspect of the kidney and direct it within the cortex toward the cranial pole. Exert digital pressure to achieve hemostasis at the needle exit site. Wedge resection biopsies yield larger, more reliable biopsy specimens, yet have a higher risk of hemorrhage during and following biopsy. Incise the renal capsule and excise a wedge-shaped segment of renal cortex using a #15scalpel blade. Close the defect using mattress sutures placed through the renal capsule and parenchyma. Hemostasis may be enhanced by incorporating greater omentum into the closure. Prostatic biopsy Prostatic biopsies may be performed by either needle biopsy or wedge resection (incisional) techniques. Exposure of the prostate gland is aided by exteriorizing and applying cranial traction on the urinary bladder with a stay suture. Incisional biopsies provide more tissue for interpretation; however, they have more potential for complications, such as hemorrhage, infection, or urine leakage. Techniques of needle and incisional biopsy of the prostate gland are similar to those used for the kidney. Take care to avoid penetrating the prostatic urethra during biopsy. Gastric biopsy Gastric biopsies are usually performed in association with gastrotomy. Obtain the specimen by excising an elliptical section of full-thickness gastric wall from one side of the gastrotomy wound edge. Close the stomach wall in two layers (mucosa/submucosa and seromuscular) using a simple continuous pattern of synthetic absorbable suture material(e.g., 3-0 polydioxanone). Splenic biopsy One technique for splenic biopsy is the wedge resection technique. After placement of a row of overlapping, full-thickness horizontal mattress sutures, excise the specimen by sharp dissection distal to the sutures. Oversew the edges with a simple continuous pattern of synthetic absorbable suture material (e.g., 4-0 poliglecaprone 25). Greater omentum also may be
373
incorporated. Alternatively, a biopsy punch may be used to obtain splenic tissue. Larger splenic samples may be obtained by performing a partial splenectomy. Pancreatic biopsy A partial pancreatectomy is used to perform a pancreatic biopsy. Carefully bluntly dissect the pancreatic parenchyma near the end of one lobe of the pancreas to expose pancreatic ducts and blood vessels. Doubly ligate vessels and ducts with monofilament synthetic absorbable (e.g., 4-0 polydixanone) or nonabsorbable (e.g., 4-0 polypropylene) sutures and transect the tissue distal to the ligatures. Biopsy of other tissues Urinary bladder biopsies are usually taken at the time of cystotomy. Obtain an elliptical shaped full-thickness specimen from one edge of the cystotomy wound margin. Microbiologic sampling of a part of the excised tissue may be indicated. Close the cystotomy incision in one (normal bladder wall thickness) or two (thickened bladder wall) appositional suture lines using synthetic absorbable suture material (e.g., 4-0 polydioxanaone). Greater omental biopsies are achieved by excising a section of omentum isolated by sutures. Preserve the greater omentum whenever possible, as its functions benefit the healing of visceral wounds. Wound closure considerations Sutures in the body wall should incorporate the linea alba and external fascial sheath of the rectus abdominis muscle only, being placed to incorporate6to 8mm of fascia on each aspect of the incision. Closure of a paramedian body wall incision is accomplished by suturing the external fascial sheath only. Peritoneum, muscle, and internal fascial sheath are not sutured, as fewer complications result. Achieve apposition of wound edges. Either continuous or interrupted suture patterns using either synthetic absorbable (e.g., polydioxanone) or nonabsorbable (e.g., polypropylene) suture material is acceptable. Close the subcutaneous tissue and skin routinely. Summary Biopsy of abdominal tissues is an important part of an exploratory laparotomy whenever a direct surgical diagnosis is not achieved. Efficient and effective methods for sampling most abdominal tissues are available. Goals of biopsy include obtaining representative sample(s), maximizing information to the veterinary pathologist, and minimizing patient morbidity.
a) Baker's biopsy punch, Baker Cummings, Key Pharmaceuticals, Miami, FL 33169. b) Tru-Cut® disposable biopsy needle, Travenol Laboratories, Inc., Deerfield, IL 60015.
Reference sand Suggested Reading
1. Pastore GE, Lamb, CR, Lipscomb V.Comparison of the results of abdominalultrasonography and exploratory laparotomy in the dog and cat.J Am Anim Hosp Assoc2007;43: 264.
2. Boothe HW, Slater MR, Hobson HP, et al. Exploratory celiotomy in 200 nontraumatized dogs and cats. Vet Surg1992;21:452.
374

3. Matz BM, Boothe HW, Wright JC, et al. Effect of enteric biopsy closure orientation on enteric circumference and volume of saline needed for leak testing. Can Vet J2013;55:1255.
375

Thoracic surgery: focus on approaches and closure By Harry W. Boothe, D.V.M., M.S., D.A.C.V.S. Surgical Approaches1 The choice of surgical approach depends largely on the type of access needed for the thoracic surgery. Intercostal (lateral) thoracotomy and median sternotomy are the two most commonly performed thoracic approaches in small animals. Be certain to clip and prepare a sufficient area to anticipate placement of a thoracostomy tube and the potential need to extend the incision. Intercostal (lateral) Thoracotomy Use this approach to expose a specific region of a hemithorax. Intercostal thoracotomy provides good access to the heart, pulmonary hilus, and mediastinum. Intercostal spaces 4 through 6 are entered most frequently. Use the lateral thoracic radiograph to identify he affected lung lobe. When performing a lung lobectomy, center the approach over the hilus of the affected lung lobe, not over the lesion (cranial lobe -4th or 5th, middlelobe -5th, caudalor accessory lobe -6th intercostal space). Use a 4th intercostal thoracotomy incision (5th in the cat) to expose the heart in the dog. Use the 8th intercostal space to expose the caudal esophagus. Incise the skin parallel to the ribs extending from just ventral to the costovertebral junction to just dorsal to the sternum. Incise the latissimus dorsi muscle with scissors parallel to the skin incision. Verify intercostal space identification by counting caudally from the first rib. Incise the serratus ventralis muscleparallel to its fibers. Incise the intercostal muscles midway between ribs, and bluntly penetrate the pleura to allow the lungs to fall away from the lateral thoracic wall before extending the intercostal incision. Insert rib retractorsaover laparotomy sponges to protect skin and muscle. Place a thoracostomy tube as described below.b,c Close the intercostal space by placing 2-0 to 1 absorbable sutures circumcostally to appose the ribs. Pre-place these sutures to help avoid traumatizing adjacent structuresor lung tissue. Traction exerted by an assistant placed on untied sutures aids closure. Close the serratus ventralis and scalenus muscles as a separate layer. Close the latissimus dorsi muscle separately with a simple continuous pattern of absorbable material incorporating the fascia. Close the subcutaneous tissue and cutaneous trunci muscle together. Close the skin in routine fashion. Median Sternotomy Use this approach to access the entire thoracic cavity. It is indicated when exploration of both sides of the thoracic cavity is necessary. Structures in the dorsal thoracic cavity (e.g., pulmonary hilus) are more difficult to access through this approach. Exposing cranial or caudal mediastinal tissue and performing a more complete subtotal pericardiectomy is facilitated through a median sternotomy. Avoid incising the entire length of the sternum, as postoperative sternal instability and pain are minimized by having one intact sternebra. Incise the skin, subcutaneous tissues, and muscle over the sternum with a scalpel. Cut the sternum on midline with an oscillating saw, taking care to limit penetration of the saw blade. Protect underlying tissues once the thoracic cavity is entered. Protect the tissues with moistened laparotomy sponges, and position retractorsa to achieve adequate visibility. Place a thoracostomy tube prior to closing the incision. Close the sternal incision by placing stainless steel wire (24 to 20 gauge) in a figure-eight pattern to appose each incised sternebra. Pre-place these sutures to aid visibility.
376
Close the pectoral muscles and subcutaneous tissues in separate layers, usually in a simple continuous pattern of synthetic absorbable suture (e.g., 4-0 poliglecaprone 25). Close the skin routinely. Thoracostomy Tube Placement2 A thoracostomy tube may be placed either at the time of thoracotomy or as a separate procedure. Guidelines for tube selection suggest that cats will usually accept a 14 to 16 F tube. Dogs accept tubes ranging from 14 to 16 F (< 7 kg body weight), 18 to 22 F (7 to 15 kg body weight), 22 to 28 F (16 to 30 kg body weight), and 28 to 36 F (> 30 kg body weight). Placement Technique at the Time of Thoracotomy Place a thoracostomy tube such that its skin exit point and thoracic wall entry point are offset. Do not position the thoracostomy tube in the primary incision. Match the size of the tube to the patient size and its intended use. During a lateral thoracotomy, plan to have the tube enter the thoracic wall two intercostal spaces caudal to the primary thoracotomy incision. During a median sternotomy, place the tube parasternally. Position the fenestrated end of the thoracostomy tube near the ventral aspect of the thoracic cavity. Connect the exterior of the thoracostomy tube to a three-way stopcock (requires an adaptor). Use a friction suture pattern to secure the tube to the skin. Position a C-clamp on the tube below the three-way stopcock for added safety. Cover the thoracostomy tube with a bandage. Placement Technique as a Separate Procedure Use a thoracostomy tube when there is sufficient accumulation of air or fluid to warrant repeated pleural evacuation. A single thoracostomy tube is usually sufficient to control the pleural cavity in most dogs and cats. Some commercially available chest tubes have a metal stylet.b Others are inserted via a guidewire utilizing the modified Seldinger/catheter-over-guidewire technique.c Risk of injury to underlying tissues may be increased when placing trocar-type thoracostomy tubes as a separate procedure. Create a small skin incision just larger than the tube diameter at the dorsal aspect of the caudal thorax. Advance the tip of the tube subcutaneously about two intercostal spaces before inserting the tube into the pleural cavity with a controlled thrust. Remove the trocar, and advance the tube such that all fenestrations are within the pleural cavity. Quickly insert an appropriately-sized adaptor and 3-way stopcock,place a friction suture, and evacuate the pleural cavity. Bandage the thoracostomy tube in place. Thoracic Wall Trauma1,3 Rib fractures occur relatively commonly in small animals, particularly after blunt trauma. Many rib fractures are treated non-surgically with analgesics and bandage application. Penetrating thoracic wounds often result from dog fights. The concept of hidden trauma is common in small animals with penetrating thoracic wounds. Surgical exploration of penetrating thoracic wounds may be indicated after attempted non-surgical treatment. Flail chest occurs when several adjacent ribs are fractured in at least two places, and a segment of chest wall is unstable. Stabilization of the affected portion of chest wall may be necessary to improve ventilation. Place sutures around
377

the affected ribs and attach them to an external fixation device that spans the traumatized portion of chest wall. Thoracic Wall Neoplasia1 Most thoracic wall tumors present as a localized swelling of the thoracic wall, although pleural effusion may be present. Tumor staging is important in the preoperative planning process. Thoracic radiography helps determine bone involvement, pleural effusion, and pulmonary metastasis. Computerized tomography may be especially useful in planning surgical removal of soft tissue sarcomas. Surgical resection with wide margins of grossly normal tissue is usually the treatment of choice. Full thickness resection of multiple ribs may require surgical reconstruction of the thoracic/abdominal wall by using synthetic material (polypropylene meshd). With tumors of the caudal thoracic wall, cranial advancement of the diaphragm may be a closure option. Position an appropriately-sized (slightly larger than the defect) and shaped piece of polypropylene mesh to cover the defect. Suture the mesh to the edges of the defect, taking care to draw the mesh tightly across the defect. Appropriately place a thoracostomy tube and cover the mesh with either thoracic wall musculature or an omental pedicle flap. Close the subcutaneous tissue and skin in a routine fashion.
a) Finochietto rib retractor, Codman, Raynham, MA 02767 b) Trocar catheter, Deknatel, Inc., Fall River, MA 02720 c) Guidewire inserted chest tube, Mila International, Inc., Florence, KY 41042 d) Polypropylene mesh, C. R. Bard, Inc., Cranston, RI 02920
References and Suggested Reading
1. Hunt GB. Thoracic wall. InJohnston SA and Tobias KM (eds): Veterinary Surgery: Small Animal, 2nded. Elsevier, Inc., St. Louis, 2018, p 2001.
2. Tobias KM, Darrow BG, Radlinsky MG. Thoracic cavity. InJohnston SA and Tobias KM (eds): Veterinary Surgery: Small Animal, 2nded. Elsevier, Inc., St. Louis, 2018, p 2019.
3. Kolata RJ. Management of thoracic trauma. Vet Clin North AmSmall Anim Pract1981;11: 103.
378
Veterinary telehealth: 5 effective strategies By Jessica Vogelsang, DVM, CVJ Pawcurious Media San Diego, CA Back in 2018, I started a Facebook group for veterinarians interested in telemedicine. It had two members. For the next two years, it continued to have two members- until March of 2020. Within a month, we passed the 3,000-member mark. Like many things in life, telemedicine fell into the category of “not necessary until it is.” The adoption of telehealth has been nothing short of stratospheric. For many veterinarians, they had to implement entire strategies on the fly due to lack of information, guidance, and help. In many cases, fearing the worst with lockdowns and not knowing how critical these platforms might become, veterinarians signed up with a video platform and watched it sit there unused as they found themselves unexpectedly busier than ever with curbside appointments. Six months in, we have a much better appreciation for the incredible opportunities virtual care technologies bring to the table, as well as some clear examples of the most useful ways one can implement these tools to make life better right now, while preparing for the future. Let’s break this down into five clear steps to get you on the right path.
1. Understand that telehealth is much bigger than telemedicine Many of the fears surrounding telemedicine can be alleviated when you take the time to really understand the difference between telehealth and telemedicine. Although most of the conversations with regards to regulations and things that might go wrong center around telemedicine, the truth is, most of what you will be using falls under the greater umbrella of virtual care. Telemedicine is the use of remote tools to diagnose, prescribe, or prognose. As this is the practice of medicine, it requires a VCPR. Whether or not one can establish a VCPR using telemedicine is changing daily, as states continue to make rapid changes to the practice act. Telehealth is a much, much bigger bucket. Telehealth involves the use of remote tools to share any sort of health information. In addition to telemedicine, it includes interactions Ebetween staff and the clients. It also includes any sort of educational tools found online such as webinars, blogs, and videos. Virtual care is somewhere in between and generally involves a veterinary professional’s use of remote tools to interact with a client. Beyond telemedicine, this can mean things like a technician doing triage, bringing in a remote consultant specialist, or sending radiographs out for interpretation.
379
2. Start with the immediate problems The reason many people struggled to make virtual care a success during COVID is they assumed a problem that didn’t wind up existing. We thought that, like we saw in human medicine, there would be a big push to keep patients out of the exam rooms. As it turns out, our patients weren’t the problem- just the owners. On the other hand, phone lines are jammed, exams are booked out for weeks, and ERs are dealing with waits over 6-8 hours in many cases. Those same tools and technologies that make telemedicine possible can be used to ease those bottlenecks that are your most immediate problem. So, start there by helping your staff work more efficiently and scale the service you can provide to pet owners.
3. Begin with the easiest tasks
On the scale of difficulty, telehealth strategy goes as follows:
• Using the phone for everything • Optimizing the self-service aspects of your website • Automating tasks like appointment reminders • Mastering virtual care basics • Beginning Telemedicine • Advanced Telemedicine • Futurist Telemedicine
If you skip ahead in this process, you’re quickly going to find you’re getting bogged down in the step prior. Don’t skip to video visits for dermatology if your staff doesn’t know how to triage. It won’t stick.
4. Focus on Asynchronous communication first
Many people assume telemedicine is dominated by live video. But that’s not how things have played out. Technology allows us to divide the way we communicate into two buckets: Synchronous: Live communication like phone calls, IMs, and video chats
Asynchronous: Anything that involves a message that’s stored until the other person is ready to deal with it. This includes emails, text messages, and voicemail.
The practices that have had the most success in virtual care started by using asynchronous messaging to deal with their immediate bottlenecks. As clients and staff became more used to interacting with them using these tools, they gradually expanded
380
the scope of services they were able to offer. Without taking these steps, both clients and staff were too overwhelmed to figure out how to make virtual care happen.
5. Stay in your comfort zone You don’t hear that every day with regards to telemedicine, right? Many people assume embarking on a telehealth journey will push them past their comfort zones and that makes it not worth the effort. But that’s not how it works.
• Virtual care basics: These are things you are already doing; you just leave them to the end of the day because they take up valuable time, or leave until tomorrow, or leave to your staff to handle. We’re talking prescription refills, “is this normal” puppy questions, lab results, inpatient updates, and triage. These are some of the most basic communications we do that rarely require a patient to come in, shouldn’t need a VCPR, and cause a lot of logjams on the phone.
• Beginner telemedicine. If you’ve mastered all the ways your staff can use virtual care to improve client communication, you can move onto beginner telemedicine. These are problems that are rarely urgent, the patients are stable, and you already have a VCPR with the client. We’re talking wellness appointment client education, behavior, post op follow ups, adjusting medications for stable chronic patients, quality of life evaluations. Many of these interactions take place for free on the phone already. Virtual care tools allow you to monetize this.
• Advanced telemedicine. Honestly, many clinics never even get to this point and are happily moving along with the first two categories. But if you’re ready for dealing with acute illnesses, you are now in advanced telemedicine. Depending on your state, this may be a current or a new client. While your judgment as a clinician allows you to handle anything you deem appropriate, the most commonly utilized use cases here are GI issues and dermatology.
Remember, as in human medicine, you always reserve the right to refuse to do a telemedicine appointment if you feel the patient needs to come in. This means your staff needs to be trained well enough in triage to correctly route cases to the ER or in house, and away from the telemedicine doctor.
381
The ROI of virtual care By Jessica Vogelsang, DVM, CVJ Pawcurious Media, San Diego, CA Like many of you, I spend way too many times answering text messages from friends, family, and vaguely acquainted neighbors with questions about their pets. I try to set boundaries, and I’m occasionally successful, but the truth is it is really hard for me to ignore something that’s right in front of my face, especially when I am worried that a pet needs care. We joke a lot about sending someone a link to our Venmo account first. Then we laugh because of course, these people who are imposing upon us with messages would never pay for our advice, right? Except they do. Time and again, veterinarians who have a structured way to both offer and charge for virtual care say the same thing: Clients pay. Sure, some may gripe- what else is new- but the majority of them are so happy that they were able to access their trusted care provider instead of taking their chances on the internet. The clients you want to keep and grow your practice with are the same ones who value access to you, your time, and will compensate you for it. This mental hurdle leaves many veterinarians hesitant to even start the process of onboarding telemedicine, but once the decision has been made it’s important to realize much of the value in virtual care lays not only with the veterinarian, but with the team. When it comes to monetizing virtual care, it can be helpful to begin by using currently available telehealth technologies to improve staff efficiency and scale access to care. At its core, the value in virtual care is allowing teams to function more effectively both in and out of the hospital environment, allowing staff inside the clinic walls to focus on the activities that generate the highest production and require the physical presence of both pet and veterinarian. And who is the biggest key to your success? Your technicians. Outlining Duties In a traditional model, we’ve never had to consider which tasks could be performed virtually. People function in set routines that are often inefficient but struggle to determine workflows that might ease some of this burden. That’s where virtual care technologies can come in. If the only thing you do is take some of the front desk burden off the CSRs by re-routing some of the most common, non-urgent questions to technicians, you’ll find these virtual tools already paying dividends in terms of time saved:
• Triage • Prescription refills • Follow up questions
382
• Need records • General health advice
Eliminating these bottlenecks improves workflow, allows CSRs more time to focus on the in-house patients, and allows technicians to be more directly involved in some of the patient care communications that get handed off to the doctors. Doctor duties Sitting on the phone is one of the least effective uses of a doctor’s time. Yet it’s something veterinarians find themselves doing every day, usually without compensation, under the assumption that is it both expected and unchangeable. If you break down the daily duties of both doctors and the technicians, and remove the hands-on tasks that must be performed in hospital, you are left with a series of communication tasks that, while often performed by the doctor, are usually well within a trained technician’s skillset to handle.
• Lab results • General client education • Estimates • Follow up questions
How to transition to paid virtual care There is no one-size fits all approach to asking people to pay you for your time, but the consensus from clinics is, the decision needs to apply to all the doctors equally, and the CSRs need to be trained to make virtual care the default offer in the appropriate uses cases. “I need to talk to the doctor” Choice 1 (Live): a technician can speak with you, or you can schedule a video call with Dr. Smith. She is available at these times and a 15-minute call is $XX. Choice 2 (Asynchronous): Would you like to leave a message using our app/ messaging feature? A doctor who may get sidetracked for 20 minutes on the phone can answer texts in a few minutes. This is a route chosen by many who still want to be the point of contact with the patient or is following up on an issue and does not want to charge, but also wants to safeguard their time. If the message describes a new issue that should be addressed by the doctor, you can then offer an in-person visit, an e-consult (visit through messaging), or a live video visit. How Much to Charge?
383
Again, hospitals have taken different approaches to charging depending on whether the team is production vs salary and whether or not the telemedicine doctor will be seeing the patient when they come in. Most clinics charge between 75-100% of the cost of an in-person visit. This gives you leeway in determining whether or not a client will be charged an additional fee if they are examined at the hospital. Things that increase the perception of value:
• Scheduling a visit. Having a set time with the doctor indicates that this is an actual visit and will be charged as such.
• Naming the communication something new. An e-consult carries a different weight than saying “We’re now charging for phone calls.”
• Convenience. When clinics are backed up for days or weeks, using telemedicine visits allows non-urgent cases to be seen more quickly. If they do need to come in, their time in the clinic is shortened and may only require a technician visit.
384
Use of wearable “smart” collars for clinical assessment
By Lisa Lippman, DVM
WHAT: Wearable smart collars enable clinicians and pet owners to monitor aspects of a dog’s behavior when they are unsupervised. Data from the sensor is collected and analyzed through a mobile phone app.
HOW: With the continuously improving biometric technology, wearable technology is proving to be a popular and useful tool for both practitioners and owners. Combined with regular veterinary visits, they represent a new form of continuous care that can help owners aggregate data that, with veterinary supervision, can be used to monitor overall health and wellness and potentially identify issues.
Wearable smart monitors can help both veterinarians and pet owners. They can:
• Aid in the early detection of diseases, representing an unprecedented level of preventive medicine and continuity of care.
• Improve the management of existing medical conditions, allowing caretakers and practitioners to monitor the animal in a more natural, less stressful setting (the home).
• Pioneer an age of truly personalized pet medicine, helping veterinarians and their owners craft solutions tailored to the needs and condition of each specific patient.
• Support the discovery of important data about health and behavior through applying analytics on data from a large number of pets that can be translated into novel treatments and solutions.
• Help to oversee and treat common canine ailments and health concerns, such as skin issues and weight management.
• Alert the owner to any changes to the animals behavior that may have otherwise gone unnoticed without the use of continuous monitoring (changes in sleep patterns, exercise habits, caloric intake, etc.)
Technology of wearables
• RFID sensors (radiofrequency identification) • GPS trackers • Motion sensors • Bluetooth • Accelerometor sensors • Cameras
385
• Lights
What They Track
• Daily activity – trends • Rest patterns • Distance traveled • Nutrition • Calories burned • Licking and scrarching behavior • GPS coordinates • HR & Other Vital Signs
Major brands: Animo by SurePetCare Tracks, analyzes patterns, and alerts to any drastic changes in:
• Activity • Rest • Sleep • Nutrition (calories) • Behavior (barking, scratching, shaking)
Whistle GO by Whistle:
Tracks, analyzes patterns, and alerts to any drastic changes in: • Activity • Sleep • Behavior (scratching, licking) • Nutrition (food calculator)
Also contains access to televet care, health goal tracking, and GPS tracking.
A note on Smart Feeders: Along with the advancing technology of wearable collars, companies like SurePetCare are introducing lines of “smart feeders”, bowls that help track, monitor, and control a pets food and caloric intake (as well as helping with common feeding-related behavioral issues in multi-pet households, such as one animal monopolizing the food of the other).
386
Conclusion:
Improved quality of data and growing interest in the usage of “smart” wearables in the pet health industry (following that of the human world) is expected to eventually make these products more viable and widespread.
It’s the valuable data that is being supplied to veterinarians combined with the peace of mind wearables can give pet owners that makes the technology likely to progress in both utility and popularity.
Sources
https://bigdata-madesimple.com/pet-wearables-the-next-billion-dollar-market/
https://www.prudentpet.com/blog/tech-pet-wearables/
https://vetrax.com/vetrax-now-available-to-veterinary-practices/
https://www.surepetcare.com/en-us/animo
https://www.grandviewresearch.com/industry-analysis/pet-wearable-market
https://www.aspcapetinsurance.com/resources/pets-and-wearable-tech/
https://www.nationalgeographic.com/animals/2020/03/cat-tracker-shows-where-pets-go/
387
Like it or not, telemedicine is now mainstream: How to prepare for what’s ahead Dr. Jeff Werber and Brandon Werber Old dog, new tricks A rose by any other name • Telemedicine is nothing new • You’ve been doing it every day • Texts, calls, emails...all Telemedicine • Being done in the worst way
Human medicine is leading, but we’re catching up fast! • Nearly 100% of hospitals offer Telemedicine • Most have done a virtual visit in the last 3 months • Expectations are being set here for access to and continuity of care • Employee benefits programs integrating (Disney, Facebook, Starbucks...)
Who’s using telemedicine? • EVERYBODY
Breaking it down • Millennials (largest, fastest-growing, highest spending) • Boomers • COVID broadened the net • High risk, older demos climbing our engagement graphs
We’re Evolving • Our clients’ expectations have forced an evolution
Hello, I’m Dr. Google I’m your new pet care expert • 3 out of 4 pet parents go to Google or social for answers, before even trying to talk to a
vet • 76% of all pet owners said they’d do a virtual visit • 34% of pet parents will switch to a vet who offers remote care
We’ve Been Losing the Relationship That Makes Us Special We Were Trending in the Wrong Direction • 16 mins a year face to face with our vet (Pre-COVID) • ~50% of pets won’t be seen by a vet this year • 50% of pet parents say they don’t have a primary vet • 8/10 clients can’t remember their own vet’s name
... but now we’re getting back to prioritizing what matters!
388
The impact of COVID-19 • 2% to 32% of hospital adoption of telemedicine overnight • Massive burst in adoption by veterinarians and pet parents globally • New workflows implemented (i.e. curbside) • Sentiment feel more transactional than ever • Clinics booked out 4-8 weeks • Staff is exhausted and stressed • No time for anything • Lots of new pet parents (potential clients)
Telemedicine is the solution already in front of you • Daytime Triage
o 40% of visits and 80% of rechecks could be virtual o Lightens workload o Stop turning away and booking out clients 4+ weeks o Exam rooms stay open for those that need o Save time and reduce stress
• Curbside Efficiency & Client experience • Better access to care = stronger client retention & engagement
Biggest myths What’s stopping those from joining the (r)evolution? • A. There’s no time
o (ask yourself why) • B. Burned out staff
o (see A.) • C. Not tech-savvy vets/clients
o (you don’t need to be Elon Musk) • D. My clients don’t want it
o (most do or will after trying it) • E. Cannibalization of office visits
o (it’s actually driving more of them) • F. It’s going to add too much to my plate
o (It will help take things off your plate) o
OK I’M IN Now what? How to Choose the Right Platform for YOU Telemedicine is not a one-size-fits-all • Understand and prioritize your goals (save time? Increase $? Workflow efficiency? Tak
load off staff?) • What are your must-haves?
389
o After-hours triage to promote work/life balance o Mobile & desktop versions o Single-use or full platform o Video, chat (synchronous and asynchronous), phone o Embedded payments o Self serve or full support team
5 keys to success How to Be Successful Using Telemedicine
1. It’s not all or nothing - start small if you need to (find your champions) 2. Workflow integration is EVERYTHING 3. Isolate and prioritize use cases (re-checks, curbside, triage, etc.) 4. Track and analyze: results will inspire the team (map back to core objectives) 5. First 30 days are critical. Regular team check-ins and goals6.Bonus - Make is fun (fun
fund) THANK YOU!Reach out to [email protected]
390
The solution to pollution: Top toxicity tips By Liz Hughston, MEd., RVT, CVT, LVT, VTS (SAIM)(ECC) VetTechXpert Poison control expertsConsultation with an animal poison control center is recommended when dealing with any toxicity in your clinic or hospital. These centers are open 24/7 and staffed with specialists in Toxicology with an encyclopedic knowledge of toxicants and their treatment in many veterinary species. Consultations with these services are very reasonable, and one fee provides you with unlimited follow-up as needed while treating that patient.
ASPCA Animal Poison Control Center: 1-888-4ANI-HELP (1-888-426-4435) • www.aspca.org/pet-care/animal-poison-control • $65 consultation fee
Pet Poison Helpline: 1-855-764-7661
• www.petpoisonhelpline.com • $59 consultation fee
Many toxic product manufacturers may also cover the cost of consultation with poison control centers, or may have treatment information for exposure to veterinary species. Having the owner call the manufacturer may be helpful in many cases. Basics of treating toxicities As in any emergency presentation, the first priority must be ensuring that the patient is stable by performing a thorough primary survey, starting with the ABCs: Airway, Breathing, and Circulation. If a patient presents seizing or in shock, these life-threatening conditions must be ameliorated prior to instituting treatment for the specific toxicant. While the patient is being stabilized, a history can be obtained from the owner, including the specifics of the toxicant involved. When gathering this information, it is critical to obtain as much information about the toxicant as possible. Ideally the owner will bring any packaging or bottles along with the pet at presentation. If not, web searches can be helpful for identification of active ingredients and contents of the product if the owner knows the brand name. Other important history information to gather includes the length of time the animal has been exposed to the toxicant (i.e. how long since ingestion or application), the route of exposure (i.e. topical, ingestion, inhalation), and how much of the toxicant the pet was exposed to. Decontamination Once the patient is stable, the toxicant has been identified, and the details of the exposure are known, measures should be taken to prevent further absorption of the toxicant. Different decontamination methods are employed depending on the method of exposure and the patient’s status at presentation. External decontamination: In cases of topical exposure (i.e. alkali cleaning agents, chemicals, pyretherins in cats), thorough bathing in tepid or room temperature water with degreasing dish soap (such as Dawn®) is indicated with copious rinsing to be sure that the agent is completely washed away.
391
Rinsing of the affected area should continue for a minimum of 10 minutes, and longer if signs persist. Extra care must be taken when bathing patients who are recumbent or with reduced responsiveness or reflexes to avoid aspiration while bathing. Ensure that the patient is thoroughly dried after rinsing and check core body temperature frequently to avoid hypothermia, especially in pediatric, geriatric, or debilitated patients. Patients exposed to chemical agents, particularly alkali agents, will likely need extensive wound care in the post-decontamination period. Those patients exposed to alkali agents require longer rinsing periods to help remove and dilute as much of the agent as possible and prevent it from penetrating more deeply in the patient’s tissues. Internal decontamination: In cases where a toxicant was ingested, there are several methods we can employ to prevent absorption from the GI tract: Emesis induction In many cases, inducing emesis is the first step in GI decontamination, which – if successful – will remove between 40 and 80% of stomach contents. If a patient has altered mentation, is recumbent, or lacks a gag reflex, emesis is contraindicated. Emesis is also contraindicated in the ingestion of agents that are corrosive, alkali, acidic, or hydrocarbons. Inducing emesis should ideally be done in the controlled environment of the animal hospital, under supervision of trained veterinary staff. Emesis induction is far from a benign procedure and can lead to dangerous sequelae, including aspiration pneumonia, which can be a life-threatening complication. In dogs, the pharmaceutical agent of choice for inducing emesis is apomorphine (aka “apo”). Apo binds to dopamine receptors in the chemoreceptor trigger zone (CRTZ), the area of the brain responsible for inducing nausea. Apo comes in pill form, which can be crushed and placed in the conjunctival sac; vomiting usually begins within five to ten minutes. While relatively effective at inducing emesis, administering apo in this manner can lead to conjunctival irritation, as well as corneal damage. Apo is compounded into an injectable agent by several compounding pharmacies and can be administered IV; vomiting usually begins two to three minutes after administration. Most patients vomit four or five times, but nausea may persist after the stomach is “emptied” so administration of an anti-emetic such as maropitant is indicated, particularly if the clinician wishes to administer agents orally to further decontaminate the gastrointestinal tract (see below). Because apo is a derivative of morphine, it can cause sedation, particularly if multiple doses are administered. Dogs should be monitored closely to ensure they maintain their gag and swallow reflexes. While apo is very effective in dogs it is not an effective emetic agent in cats because cats don’t have as many dopamine receptors. Alpha-2 agonists such as xylazine or dexmedetomidine are better choices, though cats are notoriously difficult patients in which to induce vomiting. Dosing for apo, xylazine, and dexmedetomidine can be found in veterinary formularies. Hydrogen peroxide at a concentration of 3% is often recommended to induce emesis at home. While I prefer to have patients in the controlled environment of the animal hospital for emesis induction, if clients live far away, or the agent is particularly lethal, reducing absorption as much as possible before presentation to the animal hospital may be indicated. Hydrogen peroxide must be used with caution as its method of inducing vomiting is from direct irritation of the stomach lining. It is a caustic substance, with a pH of around 4 or 5 and aspiration leads to a vicious pneumonia and chemical pneumonitis. A study published in the Journal of Veterinary Emergency and Critical Care this year
392

found “[s]ignificant visual and histopathologic gastric lesions” after administration of two doses of 3% hydrogen peroxide. No lesions were found in dogs who were administered apo in the conjunctival sac. It may be prudent for these patients to receive gastric protectants upon presentation to your hospital. Agents such as salt or mustard powder or other substances are not recommended for emesis induction. Dilution: Induction of emesis is contraindicated in the case of ingestion of caustic or corrosive agents that may cause damage to the physical structure of the GI tract or hydrocarbons that can be quite dangerous if aspirated. In case of digestion of these types of toxicants, dilution with milk or GI-coating agents (e.g. milk of magnesia) is indicated, potentially followed by a cathartic agent. If a lethal amount of toxicant is ingested – or the toxicant is especially dangerous – gastric lavage may be employed to empty the stomach (see below). Adsorptive agents: Activated charcoal can be administered in many toxicity cases to prevent absorption from the GI tract. The charcoal will adsorb certain toxic agents and facilitate excretion with the feces. Often a cathartic agent such as sorbitol is added to the charcoal to speed emptying of the GI tract (see below). Not all toxicants bind to activated charcoal so consultation with a trusted toxicology reference or an animal poison control center is warranted prior to administration. Cathartic agents: Sorbitol, lactulose, magnesium salts, or bulk fiber can be used to speed transit of a toxicant through the intestinal tract. The increased speed decreases chances of absorption from both the large and small intestine. These agents are especially effective when combined with an adsorptive agent, such as activated charcoal. Gastric lavage: Ingestions of hydrocarbons, caustic substances, bulky (e.g. bread dough), or very lethal toxicants may require gastric lavage. Gastric lavage requires general anesthesia and must always proceed with a cuffed endotracheal tube in place to protect the patient’s airway from both lavage fluid and stomach contents. Thorough lavage can achieve 80-90% emptying of the stomach contents. Surgical removal: If the toxicant is solid (i.e. intact batteries, pennies), endoscopic or surgical removal is the most effective method to prevent toxicant absorption. In cases where absorption has already occurred such as ingestion of xylitol, alcohol, or if presentation to the animal hospital is delayed, it may be possible and necessary to decontaminate the patient’s bloodstream. A mainstay of treatment is dilution using IV fluids. IV fluid administration will help to dilute any toxicant absorbed, as well as increasing renal blood flow, which may increase excretion of toxin while also providing supportive care for the patient. There are agents available to practitioners to help clear toxins from the blood stream. Intralipid Emulsion Therapy: Intralipid emulsion (ILE) is the fat portion of partial or total parenteral nutrition solutions. The use of ILE for intoxications began with the study of the treatment of local anesthetic overdoses in the 1990’s. Since then, ILE has been viewed as the “holy grail” of blood stream decontamination in cases of lipophilic toxicants. The more lipophilic the toxin, the more likely it is that ILE could be used as a treatment. Lipophilicity is described using a log P value. If the toxin’s log P value
393
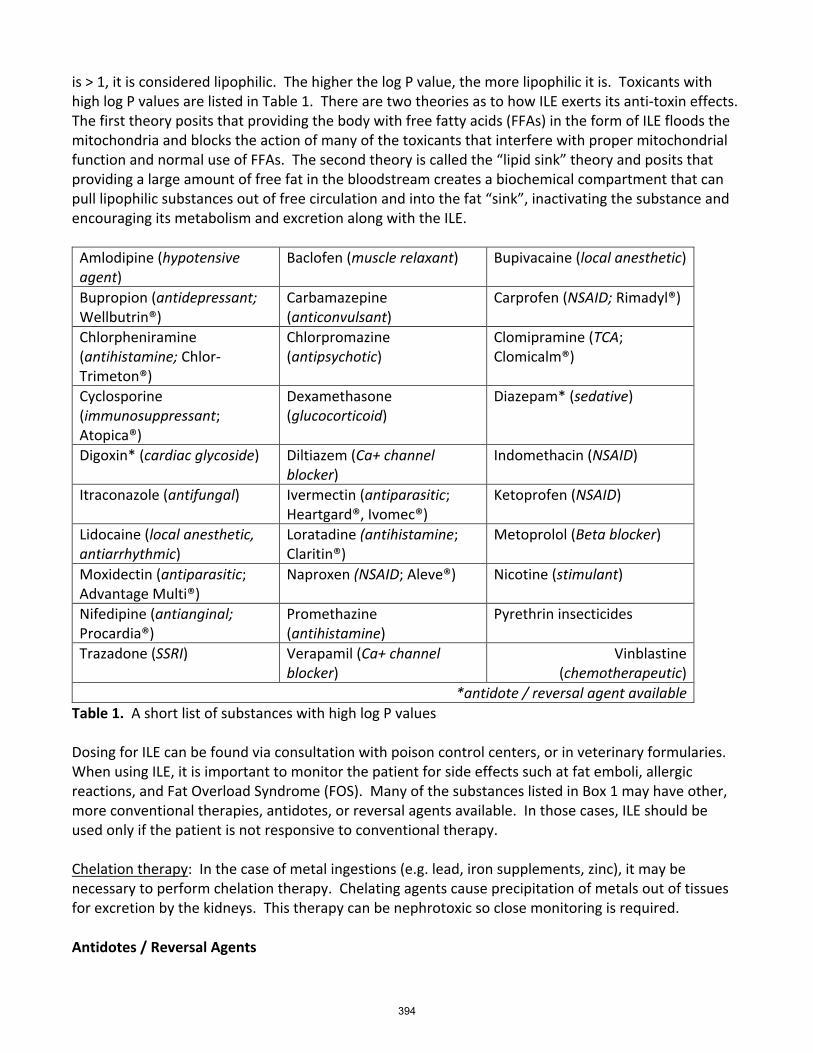
is > 1, it is considered lipophilic. The higher the log P value, the more lipophilic it is. Toxicants with high log P values are listed in Table 1. There are two theories as to how ILE exerts its anti-toxin effects. The first theory posits that providing the body with free fatty acids (FFAs) in the form of ILE floods the mitochondria and blocks the action of many of the toxicants that interfere with proper mitochondrial function and normal use of FFAs. The second theory is called the “lipid sink” theory and posits that providing a large amount of free fat in the bloodstream creates a biochemical compartment that can pull lipophilic substances out of free circulation and into the fat “sink”, inactivating the substance and encouraging its metabolism and excretion along with the ILE.
Amlodipine (hypotensive agent)
Baclofen (muscle relaxant) Bupivacaine (local anesthetic)
Bupropion (antidepressant; Wellbutrin®)
Carbamazepine (anticonvulsant)
Carprofen (NSAID; Rimadyl®)
Chlorpheniramine (antihistamine; Chlor-Trimeton®)
Chlorpromazine (antipsychotic)
Clomipramine (TCA; Clomicalm®)
Cyclosporine (immunosuppressant; Atopica®)
Dexamethasone (glucocorticoid)
Diazepam* (sedative)
Digoxin* (cardiac glycoside) Diltiazem (Ca+ channel blocker)
Indomethacin (NSAID)
Itraconazole (antifungal) Ivermectin (antiparasitic; Heartgard®, Ivomec®)
Ketoprofen (NSAID)
Lidocaine (local anesthetic, antiarrhythmic)
Loratadine (antihistamine; Claritin®)
Metoprolol (Beta blocker)
Moxidectin (antiparasitic; Advantage Multi®)
Naproxen (NSAID; Aleve®) Nicotine (stimulant)
Nifedipine (antianginal; Procardia®)
Promethazine (antihistamine)
Pyrethrin insecticides
Trazadone (SSRI) Verapamil (Ca+ channel blocker)
Vinblastine (chemotherapeutic)
*antidote / reversal agent available Table 1. A short list of substances with high log P values Dosing for ILE can be found via consultation with poison control centers, or in veterinary formularies. When using ILE, it is important to monitor the patient for side effects such at fat emboli, allergic reactions, and Fat Overload Syndrome (FOS). Many of the substances listed in Box 1 may have other, more conventional therapies, antidotes, or reversal agents available. In those cases, ILE should be used only if the patient is not responsive to conventional therapy. Chelation therapy: In the case of metal ingestions (e.g. lead, iron supplements, zinc), it may be necessary to perform chelation therapy. Chelating agents cause precipitation of metals out of tissues for excretion by the kidneys. This therapy can be nephrotoxic so close monitoring is required. Antidotes / Reversal Agents
394

In cases where an antidote or reversal agent is available it should be administered as early as possible, while also pursuing stabilization, decontamination, and supportive care efforts. Nursing and Supportive Care Regardless of the toxicant the patient is exposed to, supportive care is key to good patient outcomes. Most patients will require IV fluid therapy and, in some cases, intensive nursing care and monitoring. Veterinary technicians who are familiar with toxicology concepts and treatment modalities are central to ensuring that patients recover with minimal long-lasting effects.
395
Hey Doc, we’re in the RED! A review of distributive/vasodilatory shock By Walter L. Brown, Jr. , RVTg Red mucous membranes are sometimes encountered on physical examination of patients in shock. There is a relatively short list of differentials for red mucous membranes. It is important to consider the possibilities for red mucous membranes since many of the differentials are life threatening What are the differentials for red mucous membranes? Most commonly, red mucous membranes are the result of vasodilation or increased blood oxyhemoglobin content. Vasodilation: Vasodilation is the active dilation of blood vessels, which occurs in response to circulating cytokines and other inflammatory mediators or as a result of active cooling mechanisms in an overheated patient.
• Sepsis is the systemic response to infection. That is, infection leads to systemic release of cytokines and inflammatory mediators (such as nitric oxide and prostacyclin), which cause dilation of blood vessels and red mucous membranes in the dog.
• Anaphylaxis (or anaphylactic shock) is a hypersensitivity to an allergen such as a protein, drug, or venom that results in rapid systemic release of histamine. High circulating histamine levels cause vasodilation which decreases resistances to blood flow, thus causing more blood to flow into the capillaries causing mucous membranes to become red.
• Mast cell tumors can also cause vasodilation due to histamine release. Mast cell tumors are most commonly found in the skin but can also occur in spleen, liver, and various tissues of the body. When a large mast cell tumor is stimulated or traumatized, such as via fine needle aspiration, a massive release of histamine (degranulation) can occur leading to systemic vasodilation. .
• Heat Stroke is elevation of body temperature above normal by increased heat production or environmental exposure that exceeds the body’s ability to lose heat. Vasodilation is the body’s compensation mechanism in attempt to cool itself. Blood from the core is pumped out to dilated vessels in the periphery and skin where the greater exposure of the dilated blood vessels facilitates loss of heat to the environment.
Increased oxygen content in the blood Toxins that bind in place of oxygen or prevent unloading of oxygen into the periphery can make mucous membranes appear red. Such toxins include carbon monoxide, arsenic, and cyanide. Carbon monoxide binds more tightly to hemoglobin than oxygen and causes the cells to appear red as if carrying oxygen. Cyanide and arsenic both prevent cells from taking oxygen from the red blood cells by uncoupling oxidative phosphorylation (the cellular energy making process
396
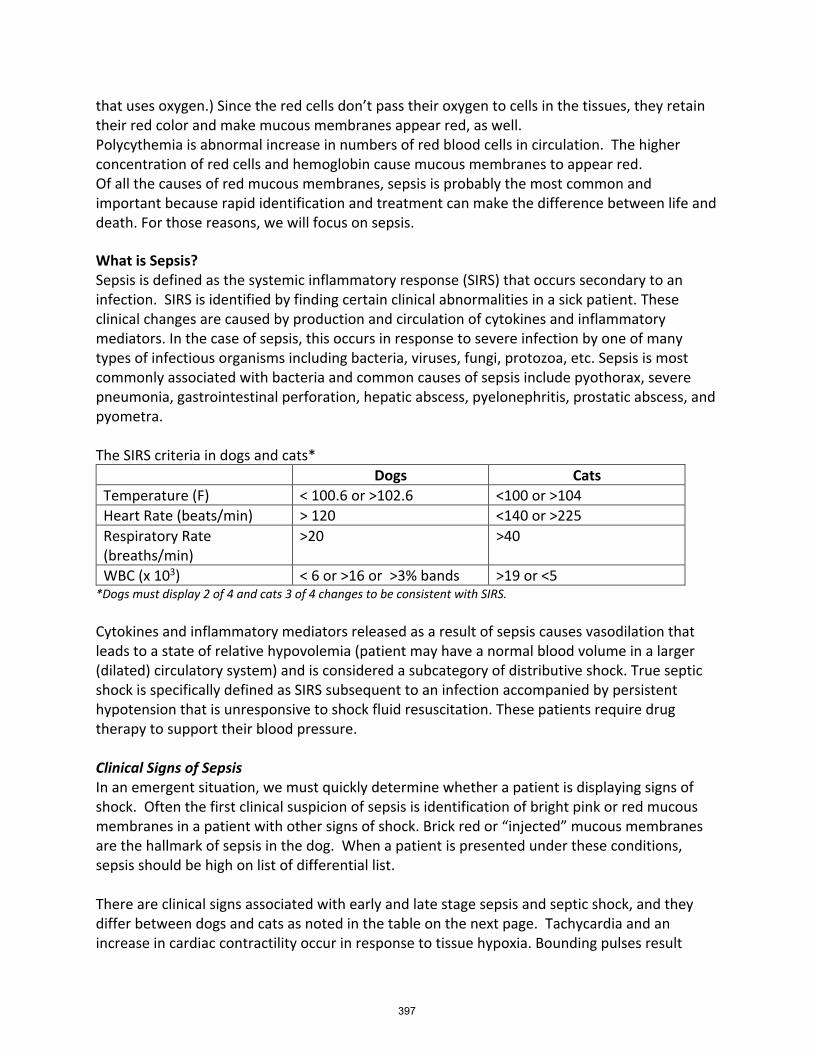
that uses oxygen.) Since the red cells don’t pass their oxygen to cells in the tissues, they retain their red color and make mucous membranes appear red, as well. Polycythemia is abnormal increase in numbers of red blood cells in circulation. The higher concentration of red cells and hemoglobin cause mucous membranes to appear red. Of all the causes of red mucous membranes, sepsis is probably the most common and important because rapid identification and treatment can make the difference between life and death. For those reasons, we will focus on sepsis. What is Sepsis? Sepsis is defined as the systemic inflammatory response (SIRS) that occurs secondary to an infection. SIRS is identified by finding certain clinical abnormalities in a sick patient. These clinical changes are caused by production and circulation of cytokines and inflammatory mediators. In the case of sepsis, this occurs in response to severe infection by one of many types of infectious organisms including bacteria, viruses, fungi, protozoa, etc. Sepsis is most commonly associated with bacteria and common causes of sepsis include pyothorax, severe pneumonia, gastrointestinal perforation, hepatic abscess, pyelonephritis, prostatic abscess, and pyometra. The SIRS criteria in dogs and cats*
Dogs Cats Temperature (F) < 100.6 or >102.6 <100 or >104 Heart Rate (beats/min) > 120 <140 or >225 Respiratory Rate (breaths/min)
>20 >40
WBC (x 103) < 6 or >16 or >3% bands >19 or <5 *Dogs must display 2 of 4 and cats 3 of 4 changes to be consistent with SIRS. Cytokines and inflammatory mediators released as a result of sepsis causes vasodilation that leads to a state of relative hypovolemia (patient may have a normal blood volume in a larger (dilated) circulatory system) and is considered a subcategory of distributive shock. True septic shock is specifically defined as SIRS subsequent to an infection accompanied by persistent hypotension that is unresponsive to shock fluid resuscitation. These patients require drug therapy to support their blood pressure. Clinical Signs of Sepsis In an emergent situation, we must quickly determine whether a patient is displaying signs of shock. Often the first clinical suspicion of sepsis is identification of bright pink or red mucous membranes in a patient with other signs of shock. Brick red or “injected” mucous membranes are the hallmark of sepsis in the dog. When a patient is presented under these conditions, sepsis should be high on list of differential list. There are clinical signs associated with early and late stage sepsis and septic shock, and they differ between dogs and cats as noted in the table on the next page. Tachycardia and an increase in cardiac contractility occur in response to tissue hypoxia. Bounding pulses result
397
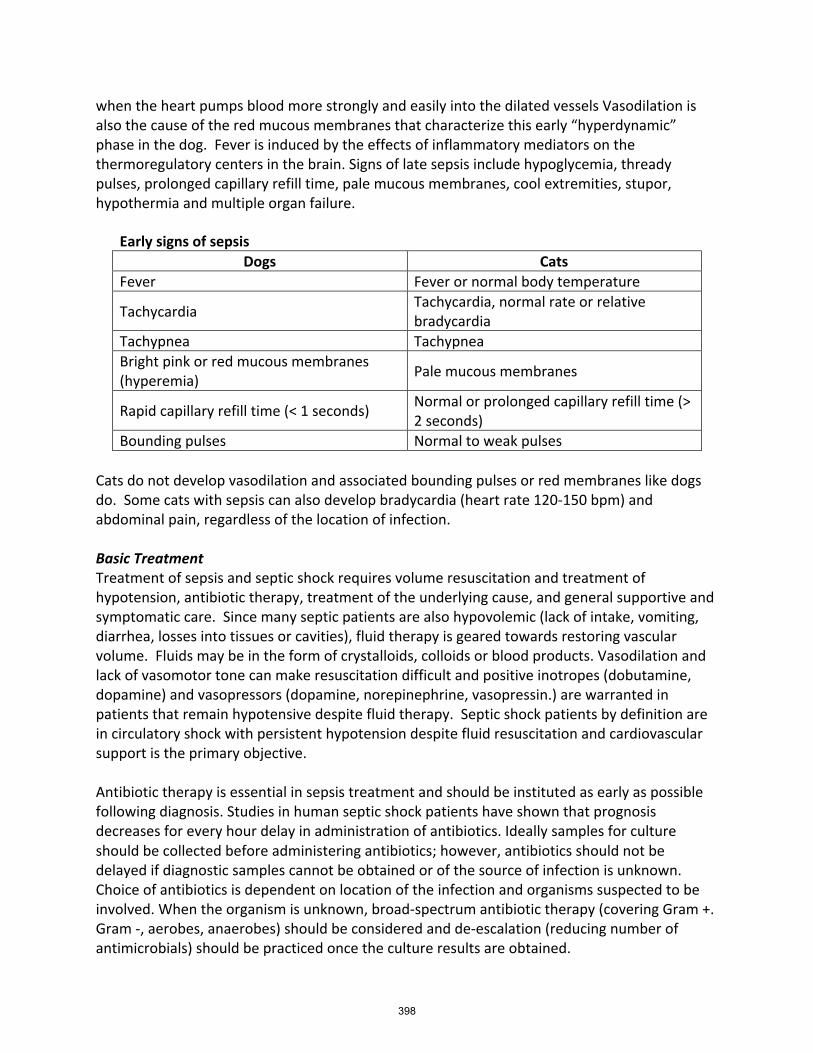
when the heart pumps blood more strongly and easily into the dilated vessels Vasodilation is also the cause of the red mucous membranes that characterize this early “hyperdynamic” phase in the dog. Fever is induced by the effects of inflammatory mediators on the thermoregulatory centers in the brain. Signs of late sepsis include hypoglycemia, thready pulses, prolonged capillary refill time, pale mucous membranes, cool extremities, stupor, hypothermia and multiple organ failure.
Cats do not develop vasodilation and associated bounding pulses or red membranes like dogs do. Some cats with sepsis can also develop bradycardia (heart rate 120-150 bpm) and abdominal pain, regardless of the location of infection. Basic Treatment Treatment of sepsis and septic shock requires volume resuscitation and treatment of hypotension, antibiotic therapy, treatment of the underlying cause, and general supportive and symptomatic care. Since many septic patients are also hypovolemic (lack of intake, vomiting, diarrhea, losses into tissues or cavities), fluid therapy is geared towards restoring vascular volume. Fluids may be in the form of crystalloids, colloids or blood products. Vasodilation and lack of vasomotor tone can make resuscitation difficult and positive inotropes (dobutamine, dopamine) and vasopressors (dopamine, norepinephrine, vasopressin.) are warranted in patients that remain hypotensive despite fluid therapy. Septic shock patients by definition are in circulatory shock with persistent hypotension despite fluid resuscitation and cardiovascular support is the primary objective. Antibiotic therapy is essential in sepsis treatment and should be instituted as early as possible following diagnosis. Studies in human septic shock patients have shown that prognosis decreases for every hour delay in administration of antibiotics. Ideally samples for culture should be collected before administering antibiotics; however, antibiotics should not be delayed if diagnostic samples cannot be obtained or of the source of infection is unknown. Choice of antibiotics is dependent on location of the infection and organisms suspected to be involved. When the organism is unknown, broad-spectrum antibiotic therapy (covering Gram +. Gram -, aerobes, anaerobes) should be considered and de-escalation (reducing number of antimicrobials) should be practiced once the culture results are obtained.
Early signs of sepsis Dogs Cats
Fever Fever or normal body temperature
Tachycardia Tachycardia, normal rate or relative bradycardia
Tachypnea Tachypnea Bright pink or red mucous membranes (hyperemia) Pale mucous membranes
Rapid capillary refill time (< 1 seconds) Normal or prolonged capillary refill time (> 2 seconds)
Bounding pulses Normal to weak pulses
398
Source control, or the removal or repair of diseased tissue or organs, should be performed as soon as possible after the patient is stabilized. Examples include thoracostomy tube placement and pleural space lavage to treat pyothorax, spay of an animal with pyometra, abdominal exploratory and repair of perforated bowel or drainage of hepatic abscesses. Nursing Care and Monitoring Excellent nursing care can make the difference in the outcome of patients being treated for sepsis. Special attention must be given to these patients as their status can change rapidly. It is imperative that oxygenation status, blood pressure and cardiac function are monitored. It takes a skilled and attentive technician to recognize and address subtle changes in patient status. Blood pressure provides information on how well blood is being pumped throughout the body. Doppler and oscillometric methods are most commonly used to measure blood pressure. Each has pros and cons. Dopplers are often preferred if patients are very tachycardic, bradycardic, or arrhythmogenic since the oscillometric method has a hard time accurately reading under those circumstances. A decreasing blood pressure may be one of the early signs that a patient is deteriorating. Blood pressure should be measured at least 3-4 times daily in a stable septic patient. Unstable or hypotensive patients may have BP measured hourly or multiple times per hour during resuscitation. Pulse oximetry is the most practical and noninvasive way of measuring oxygenation status. A normal SpO2 ranges from 94-100% and a SpO2 less than 90% is consistent with oxygen dependency. Oxygen therapy is also indicated for patients with evidence of hypoxemia. Any patient with evidence of hypoxemia (PaO2 <60 mmHg or SpO2 < 90%) should receive supplemental oxygen. Nutritional support is important to patients recovering from sepsis. Nutrition aids in tissue healing, maintain protein levels, and provide substrates for energy production. Patients that aren’t eating on their own can be provided enteral nutrition via nasoesophageal, esophagostomy, gastrostomy, or jejunostomy tubes. In patients that cannot tolerate enteral feedings, intravenous total parenteral nutrition (TPN) is also an option. Septic patients are often weak or hypotensive, and are unable to stand or rotate themselves thus requiring padded bedding, frequent cleaning of soiled bedding and re-positioning. Supportive care may include rotating of the patient from side to side; passive range of motion (PROM) exercises, intravenous catheter care, changing soiled bedding, etc. Use of intermittent warming methods may also be required. Since multi-organ failure is a possible consequence of sepsis, it is also a good idea to periodically check bloodwork on septic patients. Of particular interest are the PCV/TP and blood glucose measurements. Serial PCV monitoring can help with ensure adequate fluid balance. Variable changes in blood glucose have been reported in dog suffering from sepsis.
399

Hyperglycemia is sometimes seen in early sepsis due to stress. Hypoglycemia is seen in advanced stages of sepsis and treatment requires supplementation with dextrose in fluids. Prognosis Shock is a dynamic and complex syndrome. Despite aggressive therapy, mortality rates range from 20% - 68%. Human studies have shown that early interventions can improve prognosis. The ability to intervene early is directly related to recognizing the shock syndrome. The index of suspicion must be heightened in patients with compatible history or clinical signs, such as red mucous membranes. It is also important to recognize that there are species-specific differences in sepsis
400

Fluids: “I like the way you move”: A review of fluid balance By Walter L. Brown, Jr. RVTg Fluid balance is an important aspect of veterinary medicine. Understanding fluid balance and how it effects the body is vital in preparation and guidance of fluid therapy plans. Fluid therapy should be considered in patients that are at risk of fluid imbalances. It is important that we learn how these fluids move and are managed in the body in order to maintain homeostasis. Fluids help maintain body temperature and cell structure, and aid in transport of nutrients, gases and waste. Total Body Water (TBW) The body mass of an average healthy animal is approximately 60% water (0.6L/kg; total body water, or TBW). This percentage may vary with age and fat content. Neonates and animals less than six months of age may have a higher water content (70-80%) compared to a geriatric patient (35-45%). Fat content also impact the body’s water percentage. Animals with higher fat content often have reduced total body water. These fatty tissues decrease the compartment size in which these bodily fluids are normally contained. Fluid Compartments The two primary compartments of water storage are intracellular fluid (ICF) and extracellular fluid (ECF). The two compartments are separated by capillary walls and cell membranes. Intracellular fluid is found inside the cells and extracellular fluid (ECF) is found outside the cells. The ECF is further subdivided into intravascular fluid (in the vessels) and interstitial fluid (in the tissues). The body also contains transcellular fluids which cause little change in total body water. These fluids are found in cerebrospinal column, pleural cavity, lymph system, joints and eyes. The ICF contains approximately 66% of the TBW (0.4L/kg) whereas the ECF contains 33% (0.2L/kg). Within the ECF compartment, 75% of the fluid is interstitial whereas the remaining 25% resides as plasma water within the vascular system. Fluid Movement Fluids are allowed to move between compartment through semipermeable membranes. Semipermeable membranes allow some substances to pass through it while limiting movement of others. Water passes through these membranes easily. Fluids pass through these membranes constantly in an attempt to maintain proper fluid balance. Solutes and solvents move through cell membranes and capillaries in various ways:
• Osmosis is defined as the passive movement of water from an area with more water to an area with less water. Areas with more water have relatively fewer solutes than an area with less water. Osmosis stops when the water to solute concentration equalizes on both sides of the membrane.
• Diffusion is defined as the movement of solutes from an area of higher concentration to an area of lower concentration. These solutes that are allowed to cross the membrane use passive transport. Passive transport requires no energy to cross the membrane.
401
There are times when solutes may require energy to move across the cellular membrane. This is called active transport.
• Active transport uses ATP to move solutes from areas of lowers concentration to areas of higher concentration. Sodium and potassium frequently move across the cell membrane using ATP in a mechanism called the sodium potassium pump. There are also other solutes including calcium, hydrogen, sugars and amino acids that rely on active transport to move across the membranes. Osmosis and diffusion are the two methods of fluid and solute movement at the cellular level.
Hydrostatic Pressure Fluid and solute movement in the vascular are affected by capillary pressure. Capillaries are the only vessels in the vascular system with walls thin enough to allow the movement of solutes across them. This movement within the capillaries is vital in maintain proper fluid balance. Fluids move through the capillaries through a process called capillary filtration. The movement of blood through these capillaries exert pressure called hydrostatic pressure. When the pressure inside the vascular is greater than the pressure in the surrounding interstitial tissue, fluids and solutes inside the capillaries are forced out into the interstitial space. When the hydrostatic pressure in the capillaries are less than that outside of it, fluids and solutes move back inside the capillaries. An example of this constant movement is seen with capillary filtration at the arteriole end containing higher pressure than at the venule in containing lower pressures. Albumin & Colloid Osmotic Pressure Reabsorption is also an important process that is used to prevent too much fluid from leaving the vasculature in spite of hydrostatic pressure. The protein albumin plays a major role in reabsorption in the vascular system. Albumin is a large protein and colloid made by the liver that does not readily cross the capillary walls. Albumin causes an osmotic effect that helps with reabsorption in the vascular system. The osmotic pull into the vascular is known as colloid osmotic pressure (COP). The average COP is approximately 25mmHg. Hydrostatic pressure and COP have an inverse relationship which allows the constant movement of fluid in and out of the vascular system. When hydrostatic pressure exceeded the COP, water and solutes can move into the interstitial tissues. When the hydrostatic pressure falls below the COP water and solute move back into the vascular system. An example of this fluctuation of pressure difference can be seen in capillary arterioles where hydrostatic pressure is increased moving water out in spite of COP, and reabsorption at the venules where COP exceed hydrostatic pressure pulling water into the vascular system. Fluid Types Fluid in the body is are found in three types of solutions; isotonic, hypotonic and hypertonic. Each solution has a difference in osmolarity compared to another. Osmolarity is the concentration of solutes in a solution and impact the tonicity. Tonicity describes the osmotic effect of extracellular solutions on cells. This impacts the number of solutes and fluids that move across the cell membrane in order to maintain proper cell balance.
402
• An isotonic solution is defined as those that have the same osmolarity as another solution. When isotonic fluids are separated by a semipermeable membrane, the fluids are considered balanced and no solute nor fluid movement occurs across the membrane. A number of isotonic fluids are used in veterinary medicine to restore or maintain proper fluid balance (ie. 0.9% saline, Lactated Ringer Solution, Plasmalyte A). These fluids have comparative osmolarity to blood and are considered isotonic.
• A hypotonic solution is defined as fluids that have a lower osmolarity compared to another. When hypotonic and isotonic solutions are separated by a semibearable membrane a net imbalance occurs. The difference in osmolarity cause fluids to shift across the membrane from an area with more water and a relatively less solute concentration (Hypotonic), to an area with less water and higher solute concentration. Movement across the membranes occur until both areas equilibrate and are isotonic in comparison. This also occurs when comparing a hypotonic solution to a hypertonic solution. Two commonly used hypotonic solutions used in veterinary medicine fluid therapies are 0.45% saline and 5% dextrose in water (D5W). Caution must be used when using hypotonic fluids. Hypotonic fluids increase the amount of plasma water in blood compared to the cellular water, promoting rapid fluid shifts in the cell causing cell swelling.
• Hypertonic solutions are defined as those that have a higher osmolarity compared to another solutions. When hypertonic and isotonic solutions are separated by a semipermeable membrane a fluid shift occurs due to a difference in osmolarities. Fluid will move from the area with more water (isotonic) and fewer solutes to the area with less water (hypertonic) and more solutes. This movement occurs until both compartments area equilibrate. 7.4% saline or hypertonic saline is the most commonly used hypertonic solution used in veterinary medicine. Normal saline (0.9% saline) with 5% dextrose added can also be considered a hypertonic solution when comparing it with blood.
Fluid Maintenance Proper fluid balance is maintained through a number of mechanisms in the body. The kidneys are one of the primary organs responsible for fluid maintenance. The nephrons are functional units of the kidney and is where fluid regulations occur. The average dog filters approximately 60 liters of plasma water over the course of a day through the kidneys and approximately 99% of this fluid is reabsorbed. The waste eliminated during this filtration is moves to the bladder in the form of urine. If the body losses even the smallest percentage of water, the kidneys take compensatory steps in order to conserve water. This conservation of water contributes to a more concentrated urine. When the rate of filtration, called the glomerulus filtration rate (GFR), increase or decrease from normal levels the kidneys respond by conserving or excreting fluid producing either a concentrated or diluted urine. There are a number of hormones that impact fluid balance. Antidiuretic hormone (ADH) is produced in the hypothalamus and stored in the posterior pituitary gland. ADH restores fluid volume by reducing diuresis and increasing water retention. The entire mechanism of ADH actions goes beyond the scope of this lecture and more information can be found in reference
403
reading. Increases in serum osmolarity or a decrease in blood volume stimulate the release of ADH from the posterior pituitary gland. This constant cycle of ADH release keeps fluid levels balanced through the day. The renin-angiotensin-aldosterone system (RAAS) helps maintain proper fluid balance. Through a complex mechanism the RAAS stimulates the adrenal glands to produce aldosterone. Aldosterone is a mineralocorticoid hormone that promotes sodium conservation in the kidneys. This conservation of sodium promotes the conservation of water increasing blood pressure and fluid retention. Atrial natriuretic peptide (ANP) is also a hormone that plays a vital role in maintaining proper fluid balance. This hormone is secreted by cells in the atria. ANP counteracts the effects of the RAAS by reducing the blood pressure and intravascular volume. ANP has the ability to decrease ADH release, promote vasodilation, increase GFR, and suppress renin levels that trigger the RAAS. Disease processes such as renal and heart failure may impact the amount of ANP released by atrial cells. Conditions that cause atrial stretching also lead ANP release and include atrial tachycardia, increase sodium intake, drug therapies and vasoconstriction. Thirst is the simplest but most effective form of the bodies attempt to balance water. Thirst is stimulated when there are fluid losses or when eating salty foods. This promotes an increase in serum osmolality that trigger the thirst center in the hypothalamus that tells the animal to drink water. This water is absorbed by the intestines into the blood stream where it is distributed throughout the various compartments. The constant shifting of fluids, nutrients and waste between the bodies compartments is vital in proper fluid balance. A change in one compartment can easily impact fluids in another. As technicians it is important that we are able to recognize and are knowledgeable of these potential changes. These fluid shifts can have major implications in patient care. Having a basic knowledge in fluid balance is the foundation for administering and monitoring patients that may be receiving aggressive fluid therapies. This knowledge along with stellar physical examination and history taking skill makes the difference in recognizing early signs of fluid imbalance that could be deferential to a patient’s health.
404
Communication challenges at teaching hospitals: The veterinary technician’s perspective By Ryane E. Englar, DVM, DABVP (Canine and Feline Practice) Associate Professor and Director, Veterinary Clinical Skills University of Arizona College of Veterinary Medicine Oro Valley, Arizona, USA Objectives:
• Recognize that poor communication is a barrier to human and veterinary healthcare and a common denominator in malpractice litigation. Corrosion of the veterinarian-client-patient relationship (VCPR) may adversely impact patient care
• Understand that communication challenges in clinical practice are not unique to veterinarians; veterinary students also contribute to these through interactions with clients at university teaching hospitals. Team members, particularly veterinary technicians, witness these challenges when they are paired with students during patient intake, history-taking, physical exam, review of estimates, discussions about procedures and procedural risks, and at times of discharge.
• Introduce survey that launched in March 2019 to elicit licensed veterinary technicians’ perspectives concerning student-client communication breakdowns within the Veterinary Health Center (VHC) at Kansas State University College of Veterinary Medicine
• Identify common communication challenges that veterinary technicians observed in student-client interactions
• Strategize solutions for reducing communication challenges between students and clients at university teaching hospitals by improving communication training in veterinary education
Communication is the backbone of human healthcare Although the delivery of high-quality human healthcare requires clinicians to be well versed in medical knowledge, clinicians must also be able to effectively communicate and collaborate with patients in order to succeed at case management. Clinical reasoning in isolation achieves nothing. At its core, relationship-centered care requires connectivity between providers and their patients. In fact, it is the perception that authentic partnership exists between the provider and the patient that in many ways influences the consumer’s satisfaction with healthcare. The common denominator is effective communication.
Effective communication in clinical practice improves: (1-9)
• Rapport and trust between provider and patient • Diagnostic accuracy • Patient adherence • Patient compliance
405
• Patient coping skills • Patient outcomes
o Physical, emotional, and mental health o Return to function o Symptom resolution
• Patient satisfaction with care • Physician satisfaction with their career
By contrast, ineffective communication splinters working relationships between providers and their patients: (2, 10-13)
• Patients do not feel heard • Patients that do not feel heard are more likely to disagree with providers’
recommendations • Patients that disagree with providers’ recommendations are less likely to comply • Noncompliance is costly and misunderstandings arise because communication is
unclear • New patient concerns arise late in the consultation and may not be acknowledged or
addressed Communication is equally valuable to veterinary practice Effective communication also strengthens the veterinarian-client-patient relationship (VCPR) by establishing and maintaining trust.(14) Trust is a practice-builder:
• Clients are more likely to return to the practice for follow-up care • Clients are more likely to refer others to the practice
Any breach in trust leads to client dissatisfaction. A dissatisfied client is more likely to pursue legal action, particularly if they feel that they (or their pet) were wronged. Poor communication is a frequent cause of board complaints.(14-17) What do veterinary clients perceive as being poor communication? Historically, veterinary clients have perceived that communication is poor when:
• Veterinary team members are judgmental about client’s choices concerning patient care • Veterinary team members are unclear about patient care instructions • Veterinary team members give mixed messages • Veterinary team members display inappropriate non-verbal cues • Veterinary team members relay conflicting pieces of information • Veterinary team members withhold key information from them about physical exam
findings, patient diagnosis, patient prognosis, procedural risks, and/or treatment options.
•
406
Most research that explores communication preferences (and complaints!) in veterinary medicine concentrates on client experiences in private practice.
Yet communication mishaps predate graduation.
As a veterinary educator who is passionate about developing pre-clinical communication training for students, I want to consider communication challenges that take place in our own backyard, that is, within the university teaching hospital. If our graduates are to succeed in clinical practice, then we must ensure that communication challenges that take place in the teaching hospital are identified and addressed as opportunity areas for growth. If we can acknowledge these problem areas while students are still under our wing, then we can potentially lessen the chance that students will take bad habits with them into clinical practice.
Oversight of communication within the teaching hospital Other than clinicians, who among the veterinary team is tasked with overseeing most client interactions? Who is out there on the frontlines seeing it all?
Veterinary technicians are an amazing resource in teaching hospitals (as well as clinical practice). In many ways, they are the glue that hold the veterinary profession together.
They serve on the front lines and behind the scenes, advocating for and maintaining patient care
In teaching hospitals, they are indispensable. They are often the silent observers who see it all – at intake, in the exam room, in the treatment area, in the ICU, and at time of discharge.
Our veterinary technicians are therefore perhaps the best equipped to tell us what goes on behind the scenes when we clinicians aren’t present. What goes right? Or perhaps, better put, what goes wrong --- and why?
Surveying technicians at the veterinary teaching hospital at kansas state university college of veterinary medicine To answer these questions, my colleagues and I launched a survey in March 2019 that invited licensed veterinary technicians who were employed by the Veterinary Teaching Hospital at Kansas State University College of Veterinary Medicine to share firsthand observations of communication challenges between students and clients. Participation in the survey was voluntary. No financial (or other) incentives were associated with participation.
The objective of this research was to bring to light communication challenges that students may consistently struggle with.
If these communication challenges can be identified and subsequently incorporated into the pre-clinical curriculum, then students can potentially learn from past experiences so that communication challenges do not continue to occur at the same frequency or follow graduates into clinical practice.
In total, 16 veterinary technicians participated:
407
• 15 identified as female; 1 identified as male
• Age range varied from 18-25 (N=2), 26-35 (N=4), 36-45 (N=8), and 46-55 (N=2)
• 11/16 had 5+ years of vet tech experience; 3/16 had 3-5 years of experience; 2/16 had 1-2 years
• 15/16 had worked previously as a vet tech; that is, this was not their first job as a licensed tech
• 5/16 had worked at other teaching hospitals; that is, K-State was not their first vet school job
• Respondents represented Pet Health (Primary Care), Dermatology, Small Animal Internal Medicine, Small Animal Surgery, Food Animal Medicine, Equine Medicine, Large Animal Surgery, Exotic Animal and Wildlife, Dentistry, and Large Animal Overnight/ICU
Admittedly, the sample size is small; however, given that this is the first study of its kind to consider the veterinary technician’s perspective concerning communication challenges at teaching hospitals, my research team and I saw this as a valuable starting point to open the door to conversation.
This presentation will present survey results using the following content areas as an outline:
• What are common causes of miscommunication at the university teaching hospital? • What escalates communication challenges • What do clients want? • What can students do better? • What do we need to teach students about clinical communication to support their
growth?
References
1. Stein TS, Nagy VT, Jacobs L. Caring for patients one conversation at a time: Musings from the interregional clinician patient communication leadership group. Permanente J. 1998;2(4):62-8.
2. Beckman HB, Frankel RM. The effect of physician behavior on the collection of data. Ann Intern Med. 1984;101(5):692-6.
3. Becker MH. Patient adherence to prescribed therapies. Med Care. 1985;23(5):539-55. 4. Coleman VR. Physician behaviour and compliance. J Hypertens Suppl. 1985;3(1):S69-71. 5. Garrity TF. Medical compliance and the clinician-patient relationship: a review. Soc Sci
Med E. 1981;15(3):215-22. 6. Stewart MA. Effective physician-patient communication and health outcomes: a review.
CMAJ. 1995;152(9):1423-33. 7. Travaline JM, Ruchinskas R, D'Alonzo GE, Jr. Patient-physician communication: why and
how. J Am Osteopath Assoc. 2005;105(1):13-8.
408
8. Matthews DA, Suchman AL, Branch WT, Jr. Making "connexions": enhancing the therapeutic potential of patient-clinician relationships. Ann Intern Med. 1993;118(12):973-7.
9. Suchman AL, Matthews DA. What makes the patient-doctor relationship therapeutic? Exploring the connexional dimension of medical care. Ann Intern Med. 1988;108(1):125-30.
10. Englar RE, Williams M, Weingand K. Applicability of the Calgary-Cambridge Guide to Dog and Cat Owners for Teaching Veterinary Clinical Communications. J Vet Med Educ. 2016;43(2):143-69.
11. Berg JS, Dischler J, Wagner DJ, Raia JJ, Palmer-Shevlin N. Medication compliance: a healthcare problem. Ann Pharmacother. 1993;27(9 Suppl):S1-24.
12. Joos SK, Hickam DH, Gordon GH, Baker LH. Effects of a physician communication intervention on patient care outcomes. J Gen Intern Med. 1996;11(3):147-55.
13. Levinson W, Gorawara-Bhat R, Lamb J. A study of patient clues and physician responses in primary care and surgical settings. JAMA. 2000;284(8):1021-7.
14. Show A, Englar RE. Evaluating Dog and Cat Owner Preferences for Calgary-Cambridge Communication Skills: Results of a Questionnaire. J Vet Med Educ. 2018:1-10.
15. Martin EA. Managing client communication for effective practice: what skills should veterinary graduates have acquired for success? J Vet Med Educ. 2006;33(1):45-9.
16. Radford AD, Stockley P, Taylor IR, Turner R, Gaskell CJ, Kaney S, et al. Use of simulated clients in training veterinary undergraduates in communication skills. Vet Rec. 2003;152(14):422-7.
17. Robinson R. College of Veterinarians of Ontario (CVO); 2005.
409
PICC lines and jug caths and io’s oh my! Advanced vascular access techniques for veterinary technicians By Liz Hughston, MEd., RVT, CVT, LVT, VTS (SAIM)(ECC) VetTechXpert, San Jose, CA Types of vascular access Peripheral venous access: This is the most common type, typically achieved with an over-the-needle, short catheter (2.5 – 5cm), placed in a peripheral vein. Common sites are the cephalic veins, lateral saphenous veins, medial saphenous veins, or pedal veins. Used for fluid therapy and medication administration. Intraosseus access: A needle placed into the intramedullary cavity, which is highly vascularized. Used for emergency vascular access. Appropriate for short-term (24-48 hours maximum) fluid therapy and medication administration. IO catheters are indicated in cases of severe hypotension (e.g. cardiopulmonary arrest, shock), severe dehydration, extremely small body size, or inaccessible IV access (due to: edema, burns, thrombosis, obesity, etc.). Central venous access: These catheters are either single lumen or multi-lumen and are long enough to reach the central venous circulation. Central lines can be placed in the jugular vein, or peripherally in the lateral saphenous vein (in dogs) or the medial saphenous vein (in cats). Single-lumen central lines may be placed through-the-needle and are excellent for sampling, sparing the patient multiple punctures over the course of their hospitalization. Fluids and medications may be administered via these catheters as well. Multi-lumen central lines are indicated for the administration of total parenteral nutrition (TPN), hyperosmolar fluids, or simultaneous administration of incompatible medications or fluids. Multi-lumen central lines may be placed via a peel-away introducer or via an over-the-wire (aka Seldinger) technique. These lines may also be used for sampling. Multi-lumen central lines may be placed in the jugular vein or peripherally (PICC). Peripherally Inserted Central Catheters (aka PICC lines) are generally placed in the lateral saphenous vein in dogs and the medial femoral vein in cats. Depending on the size of the patient and the length of the catheter, the tip may be anywhere from the entry to the right atrium to the abdominal vena cava. If a jugular central line is to be used to measure central venous pressure (CVP), it should be measured so that the tip of the catheter sits in the vena cava just cranial to the right atrium. This is the optimum site for measurement of CVP. Maintaining vascular access Peripheral IV catheters should be checked at least once every 24 hours for patency and signs of infection. It is advisable to untape (or unwrap) the IV catheter completely so that the insertion site can be visualized for signs of inflammation or infection. Patency may be checked by flushing the catheter and palpating for the pulse of fluid in the proximal vein; generally speaking, there is no need to regularly flush a catheter that is being used for IV fluid administration. Alternatively, a technician may be able to draw blood back from the catheter to confirm patency. The areas both distal and proximal to the IV catheter should be checked for swelling frequently. If the catheter slips, extravasation of fluid may occur causing pain, swelling, and the potential for tissue damage if certain drugs (e.g.
410
chemotherapy) or fluids (e.g. dextrose solutions) are leaked into the interstitium. If an IV catheter site appears red, inflamed, or infected, or if there is evidence of catheter slippage the peripheral catheter should be removed and replaced immediately. Most peripheral catheters may remain in place as long as they are patent with no signs of infection, though some sources indicate replacing peripheral catheters every 72-96 hours. Central venous catheters should also be checked once a day for signs of infection or inflammation. Because of the length of these catheters, extravasation can be more difficult to detect in central catheters: for jugular central lines, palpate the mediastinum and inspect for swelling or signs of inflammation. For central lines placed peripherally (PICC), the proximal limb should be inspected for swelling. Any central line showing signs of infection at the insertion site should be removed to avoid giving the infection access to the central circulation. Intraosseous catheters should only remain in place until vascular access can be achieved. Once a patent intravenous catheter is in place, the IO catheter should be removed.
Complications of Vascular Access While most of us obtain vascular access every day, it is important to remember that it is not a completely benign procedure and many complications exist. Some are minor such as bruising or bleeding at the catheter site. But more serious, life-threatening complications can occur including catheter embolization, air embolization, thrombosis, or catheter site infections. These are particularly dangerous when they occur in central catheters. Jugular central line placement – seldinger technique
Supplies needed: • At least one assistant + two restrainers • Clippers • Surgical scrub • Sterile gloves • Sterile drapes • Large-bore (18 or 20 gauge), short over-the-needle catheter • Guide-wire catheter kit
o Guide-wire o Dilator o Catheter (single or multi-lumen) o Plastic catheter holders o Caps
• T-port(s) if no needless ports are supplied with the catheter kit • Sterile gauze • Heparanized saline • Suture (3-0 or 2-0 on a cutting needle) • Needle holders • Thumb forceps • Ioban™ or Tegaderm™ square • Bandage material
411
• Bandage scissors
Procedure: 1. Collect all supplies. 2. Sedate patient, if necessary. The patient should remain as still as possible during the course
of the placement of the catheter. 3. The patient may be placed in either lateral or dorsal recumbency. It is helpful to have two
people restraining the patient: one to hold the head and occlude the vessel and one to pull the thoracic limbs caudally and restrain the caudal end of the patient. In lateral recumbency, a rolled towel under the neck can help make the jugular vein more visible.
4. Clip a wide area to avoid contamination of the site and to allow the Ioban™ or Tegaderm™ to stick to the skin.
5. Aseptically prepare the site, using a surgical scrub technique (alternating scrub and alcohol). 6. Wash hands and don sterile gloves. 7. Perform final scrub of site and maintain a sterile field. 8. Drape the area using either a fenestrated drape or two sterile drapes: one cranial and one
caudal to the insertion site. 9. Using sterile technique, measure from the insertion site to the third intercostal space. Do
not allow the tip of the guidewire to go beyond the fourth intercostal space. 10. Using sterile technique, measure the catheter from the insertion site to the third intercostal
space. 11. Place the large-bore IVC into the jugular vein, inserting toward the heart. 12. Insert the guidewire into the vessel through the IVC to the premeasured length. 13. Without letting go of the guidewire, remove the IVC. Be sure to keep all parts of the
guidewire sterile and ensure that it does not slip. 14. Insert the dilator over the wire into the vessel. Often it is helpful to tent the skin over the
wire during insertion, and rotate the dilator into the vessel. Hold the dilator in place for a few seconds, and then remove it without moving the wire. Expect bleeding during this phase of placement.
15. Insert the catheter over the wire into the vessel. If you are placing a multi-lumen catheter, the wire will exit from the distal port – be sure there is no cap on the end of the distal port. Insert the catheter to the premeasured length.
16. Remove the wire, leaving the catheter in place. 17. Aspirate all ports of the catheter to ensure good blood flow. Aspiration prior to flushing
ensures that you will not embolize your patient with air. 18. Flush all ports with sterile saline and attach caps or T-ports. 19. Many times, the entire length of the catheter is not used. Excess catheter length may be
secured with the plastic catheter holders provided in the kit. 20. Secure the catheter holder to the catheter using suture material. The catheter holder has a
groove so that a circumferential suture may be used to hold the catheter in place. 21. Suture the catheter to the skin through the holes provided in the catheter holder. 22. Place Ioban™ or Tegaderm™ over the insertion site. If those materials are not available, a
sterile dressing may be applied. 23. Apply a loose neck wrap to cover and protect the site. 24. Aspirate and flush all ports to confirm patency.
412
25. Check the position of the catheter via lateral thoracic radiograph. The tip should rest just cranial to the right atrium, particularly if the catheter will be used to measure CVP.
Intraosseous catheters Intraosseus (IO) catheters are an excellent choice for providing drugs and fluids to those patients in which intravenous access is difficult – if not impossible – to obtain in a timely fashion. The materials are readily available in most veterinary practices and can mean the difference between life and death in patients presenting in cardiovascular collapse in which IV access is not easily obtainable. The IO route has been proven to provide access to the central circulation comparable to the access provided by central venous catheterization, making it the first choice for administration of drugs and fluids when IV access cannot be achieved. It is especially useful in neonatal, pediatric, exotic, and obese patients, as well as those patients with peripheral edema or trauma that precludes access to traditional IV catheter sites. IO catheters are contraindicated if peripheral or central IV access can be obtained, in case of fractures or other skeletal abnormalities at insertion sites, and they cannot be placed in pneumatic bones in avian species.
Placement Sites • Trochanteric fossa of the femur • Proximal humerus • Tibial tuberosity • Proximal ulna (avian species primarily) • Wing of the ilium • Proximal tibia on the flat, medial surface • Ischium • Greater tubercle of the humerus
Supplies needed
• Clippers • Surgical scrub • 1% lidocaine for infusion of the periosteum • Sterile gloves • Needle:
o Dogs, cats: 16- to 20-gauge bone marrow needle OR commercial IO needle (EZ-IO, Jamshidi, B.I.G., etc.)
o Young dogs, cats: 18- to 22-gauge spinal needle o Neonates, exotics: 18- to 25-gauge hypodermic needle
• T-port (primed with heparinized flush) • Heparinized flush • Tape • Suture
Procedure
1. Select appropriate insertion site and palpate anatomical landmarks. 2. If time allows, clip and aseptically prep the area of insertion.
413
3. If your patient is conscious, instill lidocaine to the level of the periosteum. 4. Place your finger along the long axis of the selected bone as a guide. 5. Insert and twist the needle into the bone along the long axis.
a. Insert and twist along a single line – avoid movement in the third dimension. b. You will feel resistance as you penetrate the cortex.
6. Continue to apply gentle pressure and rotation as you insert the needle into the medullary cavity of the selected bone.
7. Confirm proper placement BEFORE administering fluids or drugs (see below) 8. Attach the T-port and fluid line. 9. Secure the catheter
a. Tape butterfly around the needle hub, sutured or stapled to the skin b. Some IO catheters come with their own butterflies for attachment
Confirming placement It is very important to confirm proper placement of the IO catheter prior to administering fluids or drugs. There are several methods available:
• Gently flick the hub of the needle/catheter: it should not wiggle, but be firmly held by the bone
• Move the limb: the needle/catheter should move in-line with the bone in which it is inserted
• Flush the catheter: you should feel little to no resistance, and there should be no evidence of swelling of the limb during instillation of the flush solution.
• In young animals, you may be able to aspirate marrow from the medulla. • If time allows, a radiograph offers definitive proof of proper placement.
Potential complications (and how to avoid them):
Osteomyelitis • Adhere to strict aseptic technique during placement
• Remove the IO catheter as soon as IV access can be obtained
Compartment Syndrome (fluid accumulating in the muscle causing increased pressure, pain, and potentially necrosis)
• Ensure proper placement within the medullary cavity before fluid administration
Iatrogenic fracture • Restrict movement along the long axis of the bone
• Avoid excessive pressure Pain on infusion • Instill 2% lidocaine before bolusing fluid
References Available upon request
414
Git `er down: Nursing care for the megaesophagus patient By Liz Hughston, MEd., RVT, CVT, LVT, VTS (SAIM)(ECC) VetTechXpert, Megaesophagus is a condition characterized by the loss of muscular tone in and subsequent dilation of the esophagus. The primary clinical sign is regurgitation, but may also include weight loss, loss of body condition (secondary to malnutrition), respiratory distress (secondary to aspiration pneumonia), muscle pain, stiff gait, and generalized weakness (secondary to various neuromuscular diseases – most commonly myasthenia gravis). Definitive diagnosis of megaesophagus is accomplished via radiography. In some cases, if the condition is suspected based on history and other clinical signs but not obvious on radiographs, a barium swallow procedure may be completed. If megaesophagus is present, the barium will be seen to pool in the dilated section of the esophagus, without completing passage into the stomach. History provided by the owner of the dog is also an important component in the diagnosis of megaesophagus. Regurgitation is a hallmark of megaesophagus and must be differentiated from both vomiting and dysphagia (Table 1). The differentiation can be made when the nurse obtains the history from the client: regurgitation has no prodromal nausea, no retching, nor any bile produced. Additionally, if the patient produces fluid in the exam room, the nurse can test it with litmus paper: the pH of regurgitated fluid is normally ≥ 7, while the pH of vomited fluid is either ≤ 5 or ≥ 8. This difference in acidity is indicative of where the fluid originated from in the gastrointestinal tract, with stomach contents usually containing more acid. In cases of dysphagia, dogs have difficulty picking up and/or holding food in their mouth, leading to malnutrition because they are unable to move food from the plate or bowl into the digestive system. Dysphagia can be confused with regurgitation due to the lack of nausea and retching and the apparent production of undigested food from the patient’s mouth seen in both conditions. Careful observation of the patient during feeding is required to differentiate between dysphagia and regurgitation.
REGURGITATION VOMITING No nausea Prodromal nausea No retching Retching prior to production of fluid No bile in fluid May have bile (depending on duration of
vomiting and liver function) pH of fluid ≥ 7 pH of fluid ≥ 8 or ≤ 5 Passive process Active process Table 1: Differentiating regurgitation from vomiting.
Megaesophagus can be either a congenital condition or an acquired condition. Congenital megaesophagus is rare, with reported predisposition in Miniature Schnauzers, Great Danes, Dalmations, Irish Setters, German Shepherd Dogs, Labrador Retrievers, Chinese Shar-Peis, Newfoundlands, and Fox Terrier breeds. Congenital megaesophagus usually manifests at weaning, when puppies begin eating solid food. Clinical signs include regurgitation, coughing, fever, and – in some cases – weight loss. Congential megaesophagus is thought to be due to incomplete nervous
415
system development in the esophagus meaning that there is some chance that esophageal function may improve over time as the dog ages and the nervous system continues to mature. Most commonly, megaesophagus is an idiopathic acquired condition, occurring in dogs eight years old or older (also known as adult-onset primary megaesophagus). However, there are also several underlying conditions that can induce megaesophagus. The most common underlying condition – responsible for approximately 25% of acquired secondary megaesophagus cases – is myasthenia gravis (MG). In MG, autoantibodies act against the nicotinic acetylcholine receptor in the motor end plate of the neuromuscular junction resulting in an approximately 80% reduction in the number of available receptors. Acetylcholine is responsible for stimulating muscle contraction and destruction of its receptors leads to generalized muscle weakness, including both smooth and voluntary muscle groups. Other causes of acquired megaesophagus include neuromuscular and autoimmune diseases such as lupus, polymyositis/polymyopathy, dermatomyositis, dysautonomia, distemper, and tetanus. Lead and organophosphate toxicities can also lead to megaesophagus, along with several other miscellaneous conditions including hypoadrenocorticism, hiatal hernia, esophagitis, and thymoma. Conditions such as esophageal stricture and persistent right aortic arch have signs that are similar to megaesophagus including regurgitation. However, in these cases, the musculature of the esophagus is functioning properly, but a physical narrowing causes esophageal dilation and subsequent regurgitation. Esophageal stricture may be corrected surgically or endoscopically via balloon dilation of the narrowed area of the esophagus. A persistent right aortic arch requires surgical repair and ligature of the aortic remnant. Esophageal function usually returns to normal after repair or removal of the stricture. In those cases where an underlying cause can be identified, treatment focuses on correcting the underlying condition, which will often resolve the megaesophagus. In cases of MG, either neostigmine or pyridostigmine are generally prescribed. Both drugs are acetylcholinesterase inhibitors, which can improve muscular function by letting acetylcholine persist in the neuromuscular junction, allowing for more saturation of the available receptors. Some cases may also benefit from immunosuppressive drug therapy, as the destruction of the receptors is caused by autoantibodies. According to the UC Davis Neurology Department, up to 87% of cases diagnosed with MG will go into spontaneous remission within 4 months of diagnosis; if remission occurs, there is the possibility for resolution of megaesophagus. In those forms of megaesophagus where an underlying cause cannot be identified, treatment focuses on attaining and maintaining adequate nutritional intake and carefully managing feeding, as well as supportive care for complications that may arise subsequent to megaesophagus. The most serious complication – and the one most often responsible for mortality in these cases – is aspiration pneumonia. Patients with megaesophagus suffer from aspiration pneumonia at a high rate due to the frequency of regurgitation, and the inability to clear material from the esophagus effectively – particularly during and/or after meals. To help minimize the chances of aspiration, patients should be fed in an elevated position and the position should be maintained for 15-30 minutes after feeding to ensure that all food moves into the stomach with the assistance of gravity. This can be achieved by placing food bowls on a stepladder or staircase, holding the dog’s front feet in your lap while sitting in a chair during feeding, or using a “Bailey Chair”. The Bailey Chair was developed by Joe and Donna Koch for their megaesophagus dog, Bailey. The chair is designed to hold a dog in an upright – or “begging” – position during meals so gravity works to move food out of the hypomotile and dilated
416
esophagus and into the stomach. Ideally, dogs with megaesophagus should be fed small meals 4-6 times a day, and must sit upright both during feeding and for a period of time afterward so the chairs are well-padded for comfort. In addition to upright or elevated feedings, the consistency of the food offered to megaesophagus dogs is important. Some dogs have an easier time moving food that is blended to a gruel-like consistency, while some are more tolerant of food portioned into meatballs. The dog’s caloric intake should be carefully monitored to ensure that he is getting the proper nutrition. To calculate a dog’s caloric needs, the formula for Resting Energy Requirement is used: BWkg
0.75 x 70 = number of calories required for 24 hours There are a variety of calculators available online (http://www.dogfoodadvisor.com/dog-feeding-tips/dog-food-calculator/), some of which include caloric content of specific diets. If an owner is unable to maintain the dog’s nutritional requirements with elevated feedings (due to regurgitation), a gastric feeding tube (“g-tube”) may be placed. Placement requires anesthesia and surgery but, once in place, g-tubes can be maintained for long periods of time and allow for nutrition to be provided to the patient by avoiding the dilated esophagus altogether. In addition to monitoring caloric intake, owners must carefully monitor their dog’s hydration status. Dogs with megaesophagus often have trouble drinking and holding down water because of its thin consistency. Many owners will use thickening agents such as gelatin, gluten, or other agents as an additive to water to increase its consistency, making it less likely to be regurgitated and aspirated. If thickening does not work, many owners will provide fluid supplementation via the subcutaneous route. As was previously mentioned, the most serious and life-threatening complication of megaesophagus is aspiration pneumonia. Many dogs with megaesophagus suffer aspiration because of regurgitation, generally because they have accessed water and/or food when not in an elevated position. Owners should be instructed to monitor their dogs closely and present them for evaluation and treatment at the first sign of cough or illness, as outcomes may be improved with prompt treatment. Treatment of aspiration pneumonia may entail hospitalization, IV fluid therapy, antibiotic therapy, supplemental oxygen, or even mechanical ventilation. Aspiration pneumonia is the most frequent cause of death in dogs with megaesophagus. Another common complication of megaesophagus is esophagitis – which can also worsen megaesophagus through the formation of scar tissue, which may cause strictures in the lower esophagus. Esophagitis is believed to be caused by backflow of gastric acid from the stomach into the esophagus via the lower esophageal sphincter. Food material retained in the dilated esophagus can also contribute to esophageal inflammation and irritation. This inflammation and irritation can lead to stricture formation within 1-3 weeks. While elevated feedings go a long way towards minimizing the risks associated with megaesophagus, there are also pharmaceutical interventions that can be added to a dog’s regimen to help minimize complications. In those cases where an underlying cause of megaesophagus can be identified, such as MG, medication to treat the underlying disorder may improve or reverse the megaesophagus. Traditional gastrointestinal mobility agents such as cisapride and metoclopramide are not currently recommended in the treatment of canine megaesophagus because they have been shown to increase tone in the lower esophageal sphincter, thereby slowing esophageal emptying, leading to worsening dilation of the esophagus and a greater risk for regurgitation. Proton pump inhibitors (e.g.
417

omeprazole), H2-blockers (e.g. famotidine), and antacids (e.g. calcium carbonate), reduce stomach acid, making any leakage from the stomach into the esophagus less irritating, reducing esophagitis. Sucralfate binds to eroded areas of mucosa and may be used to help heal ulcers caused by esophagitis. Bethanechol, a cholinergic agent, may help improve esophageal function. Bethanechol stimulates muscarinic receptors in the sympathetic nervous system, thereby increasing gastric motility and may have a positive impact on peristalsis throughout the gastrointestinal system, including improvements in esophageal tone. Studies are ongoing, but anecdotal evidence for the usefulness of bethanechol is positive at this time. A study published in April 2017 in The Veterinary Record (doi: 10.1136/vr.103832) investigated the use of sildenafil as a treatment for congenital megaesophagus and found improvements in esophageal dilation on radiographs, as well as more weight gain in the puppies in the treatment group. In vitro, sildenafil decreased tone of the lower esophageal sphincter, With careful management and monitoring, most megaesophagus dogs can do well. Minimizing the risk of aspiration pneumonia is paramount, as is maintaining adequate caloric intake to maintain proper nutrition. Constant vigilance for complications is an important point for owner education, as prompt treatment will lead to better outcomes.
418
Every patient, every time: Kirby’s rule of 20 By Liz Hughston, MEd., RVT, CVT, LVT, VTS (SAIM)(ECC) VetTechXpert, San Jose, CA Patients presenting to the veterinary hospital can appear relatively stable, but their conditions can change very quickly, depending on disease process. This can surprise technicians who are not expecting a sudden change in their patient’s status, or who are not monitoring the patient closely. In my own nursing practice, I refer to Kirby’s Rule of Twenty to evaluate patients under my care and these proceedings will use the Rule of Twenty as an outline and guide for helping technicians learn fundamental nursing techniques to take back to their own practices. Monitoring parameters: The rule of twenty Developed by Dr. Rebecca Kirby – a founding member of ACVECC – the checklist is a guide for monitoring organ systems in critical patients. Originally intended for septic patients, use of the checklist has expanded to cover any critically ill patients that require intense monitoring, including those in which Systemic Inflammatory Response Syndrome (SIRS), Acute Respiratory Distress Syndrome (ARDS), or Multiple Organ Dysfunction Syndrome (MODS) are of concern. Over the years since its development, advances in technology have updated the list to include things like ultrasound examinations and other advanced monitoring techniques. Future developments may also warrant updates to this list, and emphasizes the dynamic nature of the instrument and veterinary medicine. While this checklist was developed for critical patients, its principles can be applied when treating patients we see every day. It is, however, most useful in an in-patient environment. The checklist should be reviewed at least once a day by the clinician, with adjustments to the treatment plan as warranted. For the veterinary technician, this list serves as a guide to the systematic review of a patient’s body systems, and can lead us to bring concerns to the clinician that have arisen between examinations. The condition of a patient can change from minute-to-minute, and the veterinary technician is ideally positioned to note changes, as he or she is at the cage-side, monitoring the patient closely. This list is not static, and does not need to follow in a set order for each patient. Every disease process is different and every patient will present in different ways, with individual needs and concerns. Using a checklist such as The Rule of Twenty ensures that every body system is monitored and appropriate support provided when needed. There is some overlap between the parameters, and none can be used in isolation from the others. #1 Fluid balance Fluid balance is one of the most important parameters to monitor in our patients. There are two components to overall fluid balance: intravascular volume (perfusion) and interstitial volume (hydration) and both are important to the overall function of the body’s systems. Too little intravascular volume and your patient does not perfuse, leading to hypotension, lactatemia, low cardiac output, and the potential for several electrolyte derangements. Too much intravascular volume may cause your patient to become fluid overloaded leading to edema, effusions, and cardiac dysfunction. If your patient is dehydrated, their cells are losing both fluid and their ability to perform their normal functions. It is important to note that a patient can be volume-depleted and not
419

dehydrated and vice versa. Recognizing which fluid compartment requires help balancing is key in determining the therapy required. Intravascular volume can be measured in many different ways by the veterinary technician. The easiest, and least equipment intensive method, is by tracking the forward perfusion parameters of heart rate, mucous membrane color, capillary refill time, mentation, pulse quality, and temperature. With a few pieces of equipment common to most veterinary practices, further perfusion parameters such as blood pressure, urine output, lactate measurements, and central venous pressure can also be indicative of intravascular volume status. Checking skin turgor or mucous membrane moistness can assess hydration, and serial body weight measurements can be an indicator of whether a patient is achieving and/or maintaining adequate hydration. However, patients who are third-spacing fluids – moving volume into non-physiologically active spaces such as the abdomen, thorax, or interstitium – will maintain body weight while their perfusion parameters worsen. And don’t underestimate your own eyes and ears! Overhydrated patients will have changes in lung auscultation indicating congestion, along with nasal discharge, and chemosis (swelling of the conjunctiva). Tachycardia, pale mucous membranes, prolonged CRT, dull mentation, weak pulses, and low body temperature are all indicators of poor perfusion and an increase in intravascular volume is warranted. If these signs are seen, veterinary technicians should bring concerns to the clinician and perhaps suggest adjustments to IV fluid therapy, or administration of boluses of crystalloid fluids. In general, perfusion problems can and should be corrected quickly through rapid recognition and administration of IV volume. Dry mucous membranes, or decreased skin turgor should also be brought to the clinician’s attention, as they are indicative of dehydration. In general in cases of dehydration, correction should be made more slowly – usually over the course of 24 hours. It is important to also factor ongoing losses in the form of urine, diarrhea, or vomiting in your calculations in order to bring your patients fluid status into balance. To determine how much fluid your patient will need to correct its dehydration, use the following formula:
BWkg x % dehydration x 1000 = total mLs needed to correct dehydration To determine your patient’s maintenance fluid needs, the following formula may be used:
Dogs: BWkg0.75 x 132 = 24 hour fluid requirement
Cats: BWkg0.75 x 80 = 24 hour fluid requirement
Take the two numbers and add them together to calculate the 24-hour fluid requirement for your patient to correct current dehydration and replace ongoing losses. Divide the number by 24 and you have the hourly rate to deliver to your patient over the first 24 hours. The fluid plan should be evaluated and adjusted as needed to avoid fluid overload or overhydration. In cases of fluid overload, diuretics can help increase urine output and remove excess fluid from the vascular space. Fluid can then shift from the interstitial space to maintain volume and perfusion in normal ranges.
#2 Oncotic pull
420
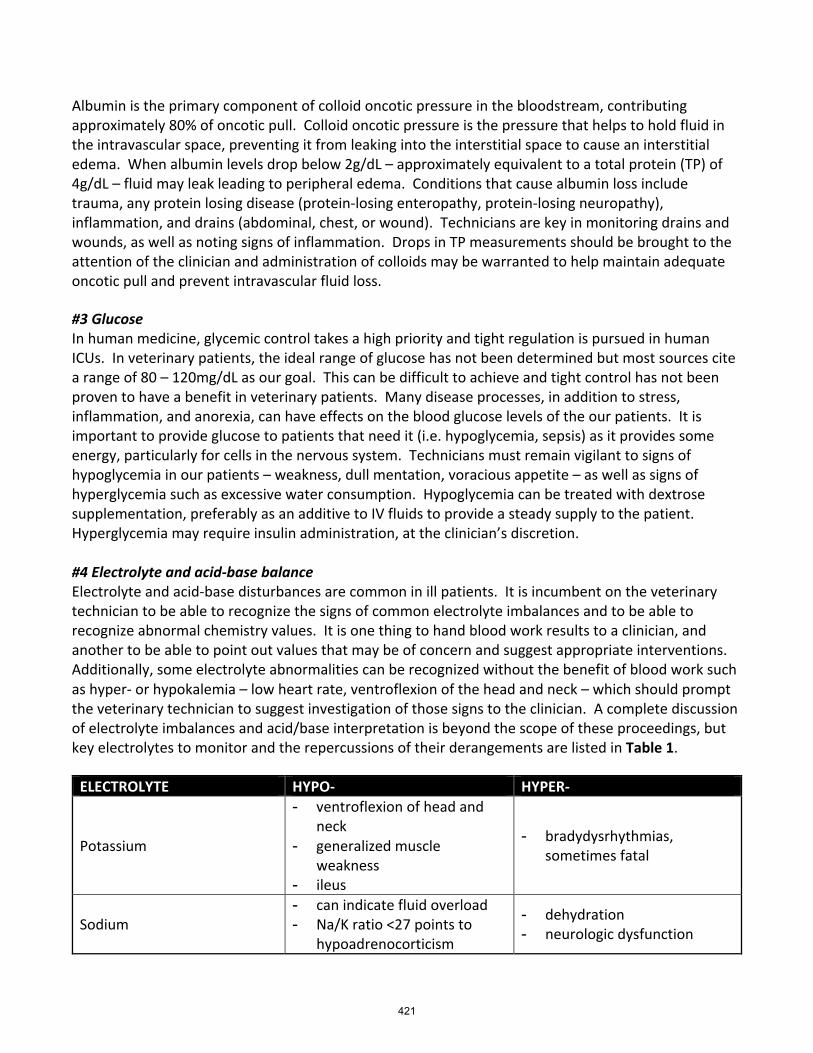
Albumin is the primary component of colloid oncotic pressure in the bloodstream, contributing approximately 80% of oncotic pull. Colloid oncotic pressure is the pressure that helps to hold fluid in the intravascular space, preventing it from leaking into the interstitial space to cause an interstitial edema. When albumin levels drop below 2g/dL – approximately equivalent to a total protein (TP) of 4g/dL – fluid may leak leading to peripheral edema. Conditions that cause albumin loss include trauma, any protein losing disease (protein-losing enteropathy, protein-losing neuropathy), inflammation, and drains (abdominal, chest, or wound). Technicians are key in monitoring drains and wounds, as well as noting signs of inflammation. Drops in TP measurements should be brought to the attention of the clinician and administration of colloids may be warranted to help maintain adequate oncotic pull and prevent intravascular fluid loss. #3 Glucose In human medicine, glycemic control takes a high priority and tight regulation is pursued in human ICUs. In veterinary patients, the ideal range of glucose has not been determined but most sources cite a range of 80 – 120mg/dL as our goal. This can be difficult to achieve and tight control has not been proven to have a benefit in veterinary patients. Many disease processes, in addition to stress, inflammation, and anorexia, can have effects on the blood glucose levels of the our patients. It is important to provide glucose to patients that need it (i.e. hypoglycemia, sepsis) as it provides some energy, particularly for cells in the nervous system. Technicians must remain vigilant to signs of hypoglycemia in our patients – weakness, dull mentation, voracious appetite – as well as signs of hyperglycemia such as excessive water consumption. Hypoglycemia can be treated with dextrose supplementation, preferably as an additive to IV fluids to provide a steady supply to the patient. Hyperglycemia may require insulin administration, at the clinician’s discretion. #4 Electrolyte and acid-base balance Electrolyte and acid-base disturbances are common in ill patients. It is incumbent on the veterinary technician to be able to recognize the signs of common electrolyte imbalances and to be able to recognize abnormal chemistry values. It is one thing to hand blood work results to a clinician, and another to be able to point out values that may be of concern and suggest appropriate interventions. Additionally, some electrolyte abnormalities can be recognized without the benefit of blood work such as hyper- or hypokalemia – low heart rate, ventroflexion of the head and neck – which should prompt the veterinary technician to suggest investigation of those signs to the clinician. A complete discussion of electrolyte imbalances and acid/base interpretation is beyond the scope of these proceedings, but key electrolytes to monitor and the repercussions of their derangements are listed in Table 1.
ELECTROLYTE HYPO- HYPER-
Potassium
- ventroflexion of head and neck
- generalized muscle weakness
- ileus
- bradydysrhythmias, sometimes fatal
Sodium - can indicate fluid overload - Na/K ratio <27 points to
hypoadrenocorticism
- dehydration - neurologic dysfunction
421
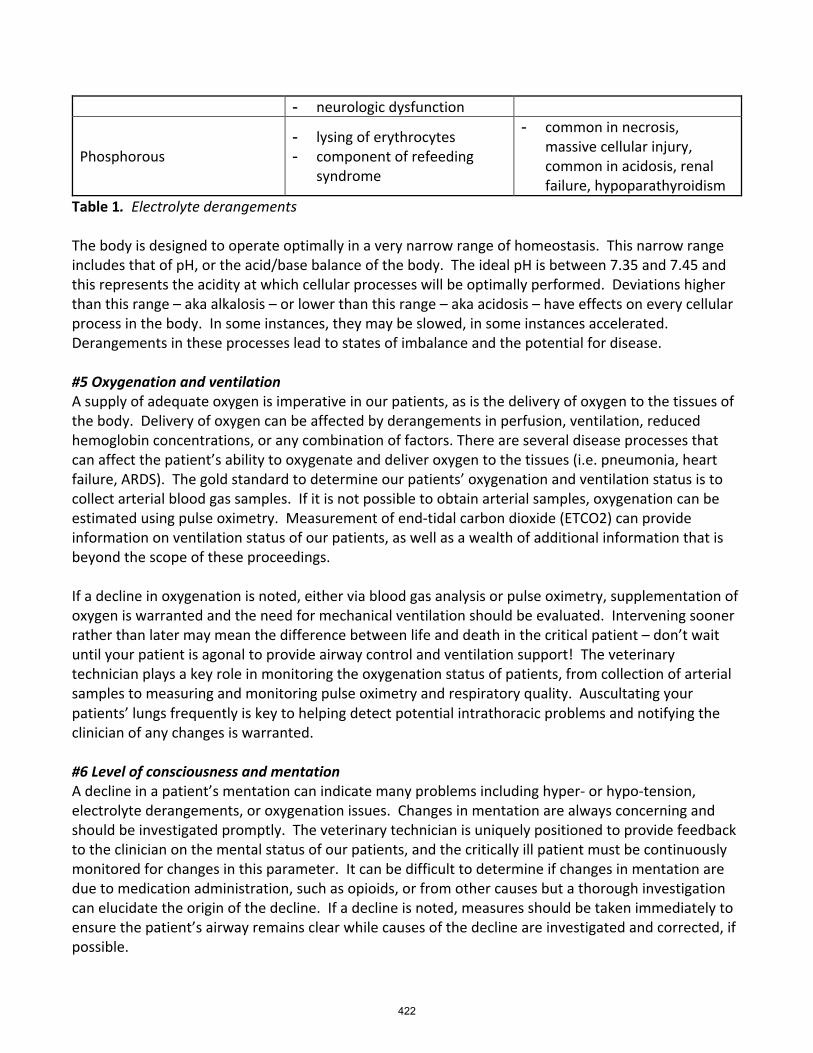
- neurologic dysfunction
Phosphorous - lysing of erythrocytes - component of refeeding
syndrome
- common in necrosis, massive cellular injury, common in acidosis, renal failure, hypoparathyroidism
Table 1. Electrolyte derangements The body is designed to operate optimally in a very narrow range of homeostasis. This narrow range includes that of pH, or the acid/base balance of the body. The ideal pH is between 7.35 and 7.45 and this represents the acidity at which cellular processes will be optimally performed. Deviations higher than this range – aka alkalosis – or lower than this range – aka acidosis – have effects on every cellular process in the body. In some instances, they may be slowed, in some instances accelerated. Derangements in these processes lead to states of imbalance and the potential for disease. #5 Oxygenation and ventilation A supply of adequate oxygen is imperative in our patients, as is the delivery of oxygen to the tissues of the body. Delivery of oxygen can be affected by derangements in perfusion, ventilation, reduced hemoglobin concentrations, or any combination of factors. There are several disease processes that can affect the patient’s ability to oxygenate and deliver oxygen to the tissues (i.e. pneumonia, heart failure, ARDS). The gold standard to determine our patients’ oxygenation and ventilation status is to collect arterial blood gas samples. If it is not possible to obtain arterial samples, oxygenation can be estimated using pulse oximetry. Measurement of end-tidal carbon dioxide (ETCO2) can provide information on ventilation status of our patients, as well as a wealth of additional information that is beyond the scope of these proceedings. If a decline in oxygenation is noted, either via blood gas analysis or pulse oximetry, supplementation of oxygen is warranted and the need for mechanical ventilation should be evaluated. Intervening sooner rather than later may mean the difference between life and death in the critical patient – don’t wait until your patient is agonal to provide airway control and ventilation support! The veterinary technician plays a key role in monitoring the oxygenation status of patients, from collection of arterial samples to measuring and monitoring pulse oximetry and respiratory quality. Auscultating your patients’ lungs frequently is key to helping detect potential intrathoracic problems and notifying the clinician of any changes is warranted. #6 Level of consciousness and mentation A decline in a patient’s mentation can indicate many problems including hyper- or hypo-tension, electrolyte derangements, or oxygenation issues. Changes in mentation are always concerning and should be investigated promptly. The veterinary technician is uniquely positioned to provide feedback to the clinician on the mental status of our patients, and the critically ill patient must be continuously monitored for changes in this parameter. It can be difficult to determine if changes in mentation are due to medication administration, such as opioids, or from other causes but a thorough investigation can elucidate the origin of the decline. If a decline is noted, measures should be taken immediately to ensure the patient’s airway remains clear while causes of the decline are investigated and corrected, if possible.
422
#7 Blood Pressure Blood pressure can be monitored via indirect or direct (arterial) methods. In either case, the goal is to maintain Mean Arterial Pressure at or above 60mmHg in order to maintain adequate levels of organ perfusion. Systemic blood pressure is the product of cardiac output and systemic vascular resistance and alterations to either variable – increased/decreased pre-load, increased/decreased heart rate, vasodilation or constriction – will lead to increases or decreases in blood pressure. The veterinary care team can use medications and fluids to affect the variables and, consequently, blood pressure. Sudden changes in blood pressure are cause for concern and should be brought to the attention of the clinician for investigation. #8 HEart rate, rhythm, and contractility Veterinary technicians must auscult their patients regularly and listening to the heart sounds carefully can give an indication of problems with rate or rhythm that should be brought to the attention of the clinician. Some disease processes can cause changes in heart rate and rhythm, as previously discussed in these proceedings. If possible, electrocardiographic (ECG) monitoring is warranted in any patient with ausculted arrhythmias. Some arrhythmias may require treatment with anti-arrhythmic medications; many respond to fluid therapy and oxygen supplementation. Checking pulse quality and pressure frequently can provide an idea of the heart’s contractility and changes may necessitate performance of an echocardiogram to better evaluate contractility. If contractility is decreased, inotropic support may be warranted and the veterinary technician is key in administering and monitoring these medications. #9 Albumin We discussed albumin briefly in conjunction with #2 ONCOTIC PULL but albumin is also key for the proper functioning of many medications. Low albumin levels may necessitate a decrease in dosages of certain drugs, particularly those that are highly protein bound as an excess of free and active drug can have adverse effects on the patient. Supplementation of albumin remains a controversial topic. If serial measurements of albumin or TP are not possible, technicians can monitor the body condition of their patients and watch for peripheral edema, which can indicate leakage from the intravascular space. #10 Coagulation Patients’ clotting ability should be monitored closely: check every venipuncture site, monitor IV catheter sites, check for cavitary bleeds, monitor for petechia or ecchymoses. Early signs can be very subtle and many only be detected by the most observant among us. If a coagulopathy is suspected, serial platelet counts can be performed to determine a patient’s response to therapy. Treatment of the underlying inciting cause is key to treating any coagulopathy. Depending on the underlying cause, transfusion of Fresh Whole Blood or Fresh Frozen Plasma may be warranted. #11 Red Blood Cell / Hemoglobin Concentration Hemoglobin in erythrocytes is key to delivering oxygen to the tissues of the body. Veterinary technicians must be able to recognize signs of low hemoglobin concentration – decreased SpO2, coupled with tachycardia, increased respiratory rate, and lethargy – and bring them to the attention of the clinician. In some cases, transfusion of blood products may be warranted to increase the oxygen
423
carrying capacity of the blood. While low hemoglobin concentrations are a more common concern in veterinary medicine, high concentrations can lead to blood with a high viscosity, decreasing microvascular blood flow and predisposing the patient to thrombus formation. Veterinary technicians must also be cognizant of inadvertently causing anemia via sampling, particularly in small or pediatric patients. Only enough blood required to run the ordered test should be drawn to avoid iatrogenic anemia.
#12 Renal Function Any systemic disease – particularly shock and inflammatory disease processes – can lead to kidney dysfunction. There are also several medications we use regularly in critically ill or septic patients that can cause nephrotoxicity (amikacin, gentamycin, etc). Checking the patient’s blood urea nitrogen (BUN) and creatinine concentrations can inform the veterinary care team about the patient’s renal function, particularly in conjunction with measurements of urinary output (UOP) and urine specific gravity (USG). High chemistry values and/or low urine output warrant appropriate IV fluid therapy, as ordered by the veterinarian and administered and monitored by the veterinary technician. If the USG does not change in the face of fluid therapy, adjustments in the fluid therapy plan may be indicated. Normal urine output, for a normovolemic patient, should be 1-2ml/kg/hr which can be measured via indwelling urinary catheters, or weighing bedding or pee pads. #13 Immune Status / Antibiotic Dosages It is important for the veterinary technician to avoid causing harm to our patients, and that includes exposing them to infections. White blood cell counts can give the veterinary care team an idea of the patient’s immune status, as well as regular temperature checks. If a patient spikes a fever while in the hospital, immediate investigation into catheter sites must take place. Any indwelling devices with evidence of bacterial infection should be removed and cultured so appropriate antibiotic therapy can be instituted. Veterinary technicians are responsible for calculating, administering and monitoring the therapeutic effect of medications, and can serve as a final check-and-balance on medications ordered by the veterinarian. #14 GI Motility and Mucosal Integrity Noting the frequency and quality of stool production gives the veterinary technician a window into the motility of the patient’s GI tract, as does listening to gut sounds. It is very important to maintain the integrity of the gut mucosa to prevent gut-derived sepsis (previously known as bacterial translocation) by providing support to enterocytes – either with enteral or parenteral nutrition – and assisting motility when possible. Ulcerations may be evident in the oral cavity (as is the case in some cats in kidney failure), or evidence of GI ulceration may present as bloody or tarry stools or vomit. #15 Drug Dosages and Metabolism Veterinary technicians are responsible for administering and monitoring many medications in the ICU and can serve as the final check-and-balance for any medication ordered by the clinician. Checking to be sure that the dosage is appropriate for the patient, and knowing the purpose of medications being administered, is an important component in critically thinking about each patient’s care. Concerns about dosages or the patient’s response to medication due to metabolic derangements should be discussed with the clinician.
424
#16 Nutrition Preserving gut function and health, increasing protein levels (including albumin), improving immune function: all depend on nutrition. Dogs and cats that have not eaten in three days begin to slow down their metabolism and go into a state of starvation. It is imperative that proper nutrition be provided to patients as soon as is feasible and the veterinary technician must advocate for proper nutrition for their patients. Enteral feeding is the preferred method (“If the gut works, use it!”) and helps to preserve enterocytes and protect the integrity of the GI mucosa, lessening the chances of gut-derived sepsis. If it is not possible to use the gut, parenteral feeding methods should be pursued and require hospitalization. Feeding tubes that can be used on an outpatient basis are also helpful. #17 Pain control The veterinary technician is the primary advocate for pain control for their patients and any patient in pain or discomfort should be provided with appropriate analgesia in a timely fashion. Pain causes a stress response and release of catecholamines that are detrimental to healing and contribute to both morbidity and mortality. In most patients, the best analgesic will be one of the pure-mu agonist opioid pain medications (morphine, fentanyl, etc.) due to their cardiovascular sparing properties and the ability to reverse them if necessary. Consider the use of regional and local blocks when possible. In the otherwise healthy patient, NSAIDs are another analgesic option. Veterinary technicians can also use adjunct pain relief methods such as massage, passive range of motion (PROM), heat or ice packs (as appropriate), or laser therapy to control patients’ pain. #18 Nursing care In addition to what has already been discussed in these proceedings, this also includes physical therapy, ensuring that patients are well padded, checking for skin integrity, and maintaining all catheters and tubes and other attachments to the patient. Don’t underestimate the power of clean, dry bedding, or a walk outside in the sunshine! Even if your patient isn’t ambulatory, just being out of the hospital for a short time can improve their wellbeing. As Dr. Kirby herself said, “The veterinarian is only as good as the supporting staff.” #19 Wound and bandage care Bandages must be checked daily to ensure they are clean and dry, with no strikethrough or swelling of the limb either distal or proximal to the bandage. The veterinary technician should also check to make sure the bandage hasn’t slipped and isn’t pinching or causing other discomfort to the patient. Depending on the purpose of the bandage, and the condition being treated, bandage changes may also be performed by the technician, according to the veterinarian’s wound care plan. #20 Tender loving care One of the most important things we do, as veterinary technicians, is provide attention and TLC to our patients. Gentle petting, a calm tone of voice, massage: all fall into this category. Try to put yourself in your patient’s paws and think what you would like if you were in the hospital. Offer tasty food, turn off the lights at night to allow restful sleep, and allow owners to visit (if it doesn’t cause more anxiety in your patient).
425
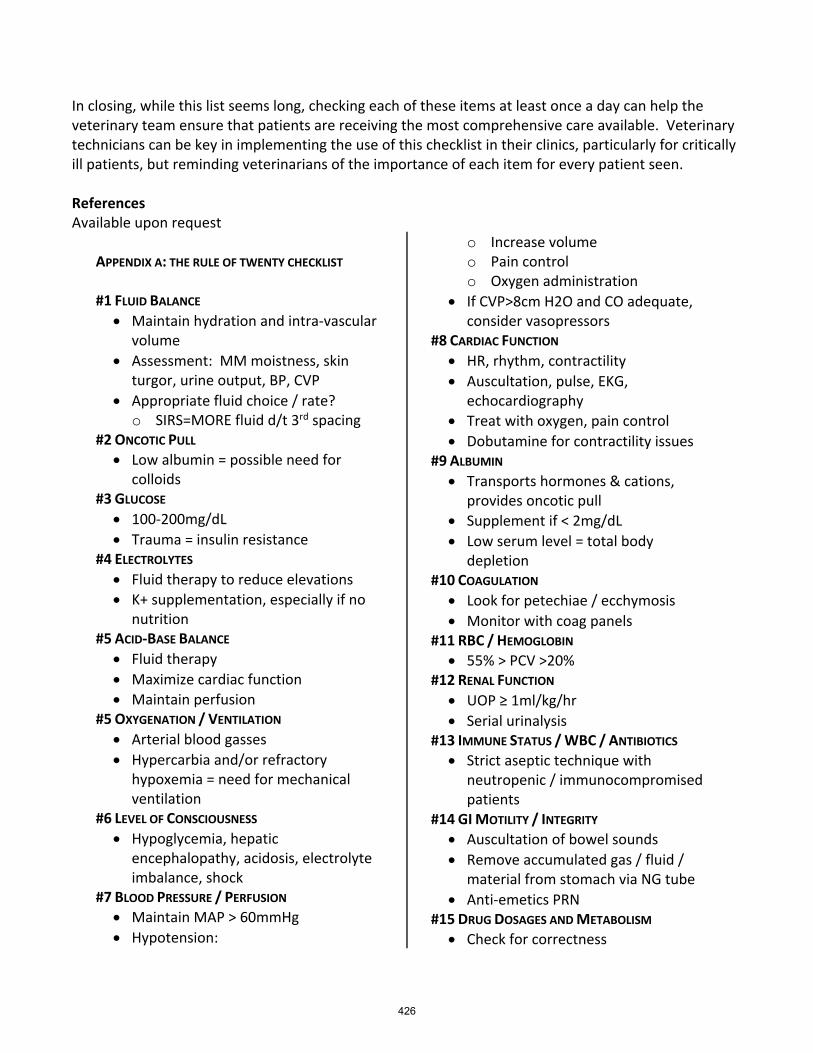
In closing, while this list seems long, checking each of these items at least once a day can help the veterinary team ensure that patients are receiving the most comprehensive care available. Veterinary technicians can be key in implementing the use of this checklist in their clinics, particularly for critically ill patients, but reminding veterinarians of the importance of each item for every patient seen. References Available upon request
APPENDIX A: THE RULE OF TWENTY CHECKLIST
#1 FLUID BALANCE • Maintain hydration and intra-vascular
volume • Assessment: MM moistness, skin
turgor, urine output, BP, CVP • Appropriate fluid choice / rate? o SIRS=MORE fluid d/t 3rd spacing
#2 ONCOTIC PULL • Low albumin = possible need for
colloids #3 GLUCOSE • 100-200mg/dL • Trauma = insulin resistance
#4 ELECTROLYTES • Fluid therapy to reduce elevations • K+ supplementation, especially if no
nutrition #5 ACID-BASE BALANCE • Fluid therapy • Maximize cardiac function • Maintain perfusion
#5 OXYGENATION / VENTILATION • Arterial blood gasses • Hypercarbia and/or refractory
hypoxemia = need for mechanical ventilation
#6 LEVEL OF CONSCIOUSNESS • Hypoglycemia, hepatic
encephalopathy, acidosis, electrolyte imbalance, shock
#7 BLOOD PRESSURE / PERFUSION • Maintain MAP > 60mmHg • Hypotension:
o Increase volume o Pain control o Oxygen administration
• If CVP>8cm H2O and CO adequate, consider vasopressors
#8 CARDIAC FUNCTION • HR, rhythm, contractility • Auscultation, pulse, EKG,
echocardiography • Treat with oxygen, pain control • Dobutamine for contractility issues
#9 ALBUMIN • Transports hormones & cations,
provides oncotic pull • Supplement if < 2mg/dL • Low serum level = total body
depletion #10 COAGULATION • Look for petechiae / ecchymosis • Monitor with coag panels
#11 RBC / HEMOGLOBIN • 55% > PCV >20%
#12 RENAL FUNCTION • UOP ≥ 1ml/kg/hr • Serial urinalysis
#13 IMMUNE STATUS / WBC / ANTIBIOTICS • Strict aseptic technique with
neutropenic / immunocompromised patients
#14 GI MOTILITY / INTEGRITY • Auscultation of bowel sounds • Remove accumulated gas / fluid /
material from stomach via NG tube • Anti-emetics PRN
#15 DRUG DOSAGES AND METABOLISM • Check for correctness
426
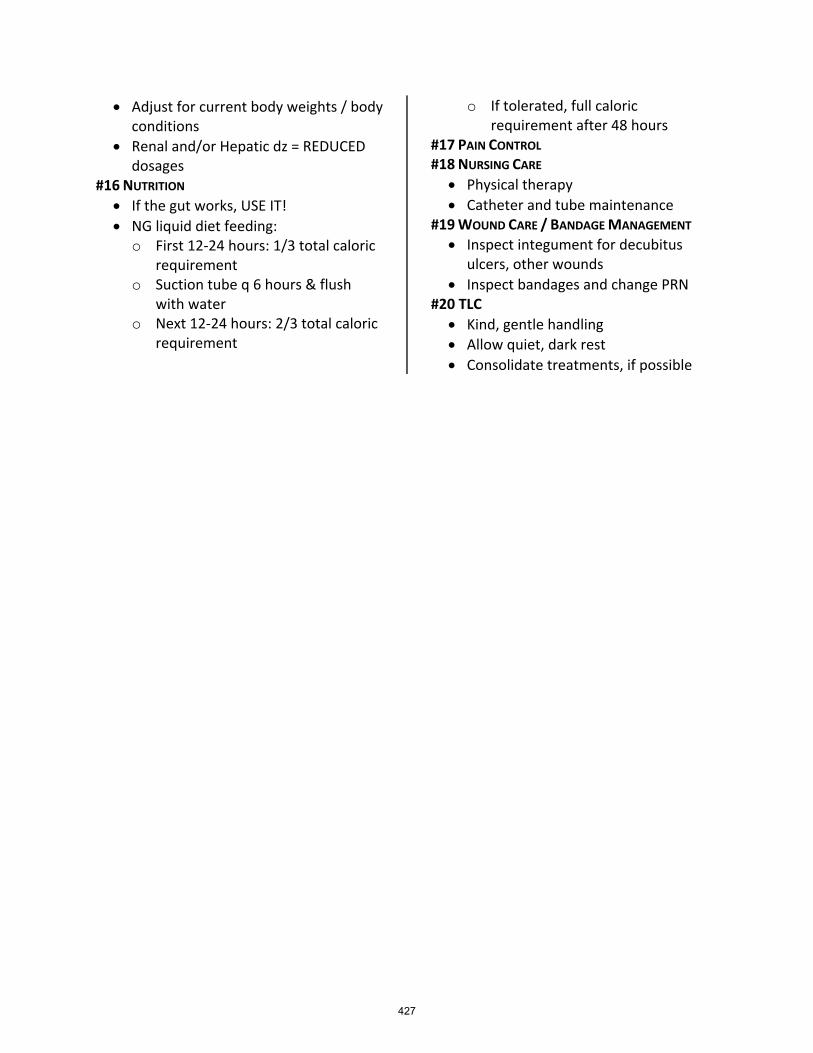
• Adjust for current body weights / body conditions
• Renal and/or Hepatic dz = REDUCED dosages
#16 NUTRITION • If the gut works, USE IT! • NG liquid diet feeding: o First 12-24 hours: 1/3 total caloric
requirement o Suction tube q 6 hours & flush
with water o Next 12-24 hours: 2/3 total caloric
requirement
o If tolerated, full caloric requirement after 48 hours
#17 PAIN CONTROL #18 NURSING CARE • Physical therapy • Catheter and tube maintenance
#19 WOUND CARE / BANDAGE MANAGEMENT • Inspect integument for decubitus
ulcers, other wounds • Inspect bandages and change PRN
#20 TLC • Kind, gentle handling • Allow quiet, dark rest • Consolidate treatments, if possible
427
As Seen on T.V? Understanding and Discussing Dominance Theory and Punishment with Clients and Veterinary Professionals Rachel Lees RVT, KPA CTP, VTS (Behavior) The Behavior Clinic, Olmsted Falls, Ohio Objectives of this Lecture:
• Understand the Four Quadrants of Learning o Pro’s and Con’s
• Criteria involved when using Punishment • Comprehend Dominance Theory and the associated flaws in this training philosophy • Grasp Scientific Theories of Learning in Dogs
o Understand the importance of positive reinforcement and why it is the current recommended training philosophy in veterinary behavior.
Classical Conditioning vs. Operant Conditioning:
• Classical Conditioning: Associative learning in which an animal associates a novel stimulus with another stimulus that already causes a reaction.
o Pavlov Experiments in the early 1900’s • Operant Conditioning: Learning in which a behavior is affected by its consequences.
o B.F Skinner o When a behavior is followed by something the animal wants, the behavior will
strengthen. o When a behavior is followed by something the animal dislikes or fears, the behavior will
weaken. Understanding the Four Quadrants of Operant Conditioning:
• Positive Reinforcement: Adding a stimulus to increase or strengthen the behavior • Positive Punishment: Adding a stimulus to decrease or weaken the likelihood of the behavior • Negative Reinforcement: Eliminating a stimulus to increase or strengthen the behavior • Negative Punishment: Eliminating a stimulus to decrease or weaken the behavior
Break Down the Definition to Prevention Confusion:
o Positive = Adding a stimulus to the situation (+) o Negative = Taking something away from the situation (-) o Reinforcement = Strengthens the behavior o Punishment = Weakens the behavior
Positive Reinforcement and Reinforcers:
• Forms of Reinforcement: o Treats o Human Food o Play o Petting o Praise
428
o Scent • Example: During puppy training, the puppy should be taken out on leash to eliminate. When
the puppy eliminates outside, we then give a treat during the last drop of urine or stool. o The behavior of eliminating outside has been positively reinforced as we added food to
increase the likelihood of the puppy repeating the behavior of voiding outside.
** When used the reinforcement must be reinforcing to the learner. Find what the learner enjoys! ** Positive Punishment and Punishers:
• Forms of Punishment: o Shock o Tug of Collar o Squirts of Water o Citronella Spray o Yelling/Screaming o Physical Manipulation (hitting)
• Example: A dog barks at people passing by the home. The owner purchased a citronella collar to spray every time the dog barks. The dog is fearful of the sound and dislikes the smell of the citronella being sprayed.
o The behavior of barking has been positively punished as the citronella spray is emitted when the dog barks, decreasing the likelihood of the barking behavior.
**If used the punishment must be strongly disliked to the animal to decrease the likelihood of the
behavior being repeated. ** Negative reinforcement:
• Example: o A dog or horse wears a head collar. When the animal chooses to pull forward and start
moving the nose loop tightens around the snout causing discomfort. When they settle and walk with the handler, the nose loop loosens reinforcing the behavior of walking next to the handler.
§ The behavior of walking next to the handler was negatively reinforced by eliminating the discomfort around the snout.
Negative punishment:
• Example: o When an owner comes home, their dog is over the moon excited and begins to jump
and lick their face. The handler turns his back when the dog jumps up taking away the social interaction the dog is looking for.
§ The behavior of jumping is being negatively punished by removing the attention of the handler to decrease the likelihood of the jumping behavior.
Criteria for punishment to be successful:
• The animal’s motivation strength is not too high
429
o The stronger the motivation to perform the behavior, the less likely punishment will work.
o Example: A dog runs through the invisible fence to chase a rabbit because of a strong innate motivation.
• Occurs every time the behavior occurs and should be associated with the behavior and not other people or animals.
• Occurs within seconds of the behavior occurring EVERYTIME it occurs • Proper Intensity
o Must be high enough to interrupt the behavior immediately after application o A higher motivation requires a higher level of punishment
§ Humane or Inhumane? • Timing
o Within 0.5 seconds of the undesired behavior occurring ** These techniques are typically very confrontational and can cause increased stress and anxiety for the pet and the owner. These techniques are not recommended and can be counterproductive to any
behavioral treatment plan. ** Why should we use positive reinforcement techniques?
• Will enhance the human animal bond • Foster a healthy and non-stressful relationship with the handler/owner • Increases confidence in both the owner and learner
o Team Sport o Be the Leader in this Dance!
• Low potential for adverse effects • Improved retention time • Hands off and nonthreatening • Anyone can train the pet
Dominance theory: Is my dog alpha? Dominance theory is one giant misunderstanding. The original idea of dominance theory was the result from studies were conducted in the 1940’s with captive unrelated wolves by David Mech. These studies concluded that dogs have social hierarchies comparable to wolves. Over time the adaptive concept went as far as to assume that the human family can replace the dog pack. It was then suspected that a dog will try to gain the top position over human family members and may become aggressive to lower ranking “members of the pack”. The misunderstanding starts with the original research. These initial studies were short term and only focused on 1% of a wolf’s life. Within the research, it was stated that the notion of “alpha wolf” and the struggle to be the “alpha of the pack” were based on observations of captive groups of unrelated wolves. These were artificial social groups and bear little resemblance to a pack of free-living wolves that are all related to one another. In 2008, David Mech stated that the idea that individuals in a family of volves are engaged in constant daily struggles to battles to one up each other at that dogs are the same with us is simply untrue.
430
After this original research was released the animal world began making conclusions and relating all of these “wolf” studies to domestic dogs and then generalized the information to relate to dogs and humans. Unfortunately, when these conclusions were made, we had ignored 15,000 years of domestication between the wolf and the domestic dog. Dr. Ian Dunbar made the comment that trying to understand dogs better by studying wolves is comparable to humans attempting to improve parenting skills by studying primates! Finally, when the researchers were observing the wolves within the original study, they had misinterpreted specific pieces of body language and behavior into forcible dominance displays. Some of these behaviors include “pinning” a subordinate wolf to the ground. After years of continued research, we found that these displays were ritualistic appeasement behaviors to avoid conflict. Therefore, in the above example, the “subordinate” wolf is not forced on the ground but voluntarily performs this behavior to eliminate conflict. These techniques have been proven to increase stress and anxiety in both the animal and the owner. These theories are counterproductive in any behavioral treatment plan. These methods can also damage the human animal bond and therefore lead the animal to be rehomed or euthanized. Educating clients is especially important as there is large amount of conflicting information written in books, on television, and on the internet. Be sure to discuss your clinic’s recommendations on animal training during the pet’s first appointment so the owner and pet have the best chance at strengthening and enhancing the human animal bond instead of damaging it. The truth about punishment and dominance theory: Meghan Herron, DVM, DACVB, at The Ohio State University, published research concluding that use of forceful techniques can increase the likelihood of aggression toward owners. Unfortunately, the conflict inherent in the alpha-dog theory makes for appealing television, so the idea has been widely disseminated. Veterinary behavior professionals are now working to teach updated concepts that will enhance the bond between humans and dogs instead of putting a barrier between them. The study released the following pieces of information:
• Confrontational methods applied by dog owners before their pets were presented for behavior consultation were associated with aggressive responses form the owner.
• Confrontational methods such as hitting or kicking the dog, alpha roll, dominance down, growling at the dog, etc. had elicited increased aggression to the owner
References
1. Herron, Meghan E. Shofer, Frances. Reisner, Illana R. 2009. Survey of the use and outcome of confrontational and non-confrontational training methods in client-owned dogs showing undesired behaviors. Applied Animal Behaviour Science. 117. 1-2. 47-54. https://doi.org/10.1016/j.applanim.2008.12.011
2. Shaw, Julie K. Martin, Debbie. Canine and Feline Behavior for Veterinary Technicians and Nurses. John Wiley & Sons, Inc. 2015.
431
So, You Want to be a Veterinary Behavior Technician? The role of Veterinary Technicians in behavior By Rachel Lees RVT, KPA CTP, VTS (Behavior) The Behavior Clinic, Olmsted Falls, Ohio Veterinary Technician’s Oath: “I solemnly dedicate myself to aiding animals and society by providing excellent care and services for animals, by alleviating animal suffering, and promoting public health. I accept my obligations to practice my profession’s Code of Ethics, and furthering my knowledge and competence thought a commitment to lifelong learning” This oath is strategically placed at the beginning of this lecture as a reminder. Whatever specialty you may be working toward, it is important to remember that we are Veterinary Technicians first. There are a large amount of job opportunities after you obtain your VTS (Behavior) but remember that as a technician you are valued in the veterinary profession and your skills are needed in veterinary practices all over the country. Whether you stay at your practice and educate the everyday pet owner, start your own training business, or work solely in a research facility our skills and education as a veterinary technician are invaluable. Criteria that create a successful veterinary behavior
• Leadership within the practice and the profession • Strong Knowledge and Training Skill Set
• Learning Theory Knowledge • Clicker and Positive Reinforcement Trainer
• Observational Skills • Understanding of Normal vs. Abnormal behavior of ALL species • Strong Communication and Coaching Skills • Non- Judgmental and supportive Attitude • Compassion and Empathy
What does a Veterinary Behavior Technician do?
• Speak our patient's language and educate the client on what their animal is trying to say • Assist and educate the veterinary community with cooperative veterinary care techniques and
give our patients a voice during these stressful scenarios • Coach and support owners through the treatment and behavior therapy plan • Lead puppy and kitten kindergarten classes • Enhance and strengthen the human animal bond • Educate veterinary teams, animal training professionals, and the public on humane and science-
based training techniques
432

The role of the Veterinary Behavior Technician in general practice:
• Triaging Behavioral Issues o Medical vs. Behavioral vs. Training o Understand when a diagnosis is needed
• Assisting the veterinarian or veterinary behaviorist as needed with patient care • Treatment and Behavioral Modification Appointments
o After diagnosis is given o If offered, can increase revenue in the practice
• Preventative Care/Classes o Puppy Classes o Kitten Kindergarten o Obedience Classes
• Pet Selection Counseling o Sessions are done BEFORE the animal is in the “family” o The goal of these sessions are to educate the client about normal canine/feline
behavior, breed selection, prepare the client for the new arrival, promote positive reinforcement training, and finally promoting the hospital’s services.
Triaging behavioral issues: When a client calls with a behavioral concern, the veterinary technician must feel comfortable to triage the issue to set up the best appointment for the client and patient. It is important to keep in mind that medical conditions can increase a patient’s irritability and make a behavioral problem worse. Physical pain and sensory perception changes can alter behavior and increase stress, anxiety, aggression, or elimination issues. If there is any sudden change in behavior a technician should always recommend that the client is evaluated by the veterinarian for a diagnosis. In my practice, we also disclose if an animal has done harm to themselves (separation related issues), placed their teeth on a human or other dog, has a large aggressive display, or is showing severe panic and anxiety that they should always be scheduled for a consultation with the veterinarian. If a client calls with a training related problem such as jumping or potty training a diagnosis from the veterinarian may not be needed. Our clinic would recommend an appointment with the Veterinary Behavior Technician so we can evaluate the patient and find if there is stress and anxiety present or if there is just a lack of training. Role of the Veterinary Behavior Technician in the consultation:
• Be the Host of the Consultation with nonthreatening body language • For the patient and the client
• Assess the patients learning, skill set, response to cued behaviors, and log behavioral observations
• Assist with examination and lab work collection PRN using low stress and fear free techniques • Introduce and begin training with tools that may be part of the RX plan
• Head collars • Basket Muzzles
433
• Harnesses • Coach and educate owners on prescribed behavioral therapy
• TAG Teach Certification • Clarify, problem solve, and discuss ways to make the treatment plan fit into their lifestyle
The goals of the veterinary technician in the consultation appointment are to bond with the client, patient, and gain the client’s trust. Obtaining that trust is crucial to the success of the treatment plan so the veterinary behavior team can get information from the client easily and create an open relationship to increase client compliance. The veterinary behavior technician’s overall goals are to encompass client communication, including education, awareness, and prevention before, during, and after the consultation. The technician can also assist the veterinarian with the clinical behavioral consultation. Utilizing a veterinary technician for behavior cases provides for a more comprehensive and successful behavior service for the hospital and client/patient. The Process of becoming a VTS (Behavior) Technician: Go to the AVBT website:
• www.avbt.net • How to Become a Specialist tab
Memberships and Candidate Packet:
• Download and Read the Candidate Letter • Become a Member of NAVTA • Become a Member of SVBT • Recommended Reading List
• https://avbt.net/recommended-reading Curriculum Vitae
• Use template found on www.avbt.net Letters of Recommendation
• Two Letters required (any combination) o VTS (Behavior) o ACVB diplomate o Supporting veterinarian
Skills Assessment List:
• Each skill must have a date and initial next to it o SAS are encouraged to make notes in the notes section.
• Choose a primary skills assessment supervisor to assess your skills. o This person should be a licensed veterinarian or credentialed veterinary technician and
will be contacted if questions arise during the packet evaluation process.
434
o People other than credentialed veterinary personnel can be used as SASs, but they must be approved by the AVBT Regents ([email protected])
o You may use more than one person as your SAS Time Sheets:
• Three (3) years minimum work experience in animal behavior with a minimum of 4000 hours or its equivalent in the field of animal behavior: clinical or research based.
• All experience must be completed within five (5) years prior to your application. • Applicable time is not required to be under the supervision of a veterinarian if it can be proven
preventative (puppy, kitten classes, assessments, etc.). • Submit two sheets: one preventative (75% or 3000 hours) and one treatment (25% or 1000
hours). • These sheets must have the times totaled at end of each sheet.
Prevention Hour Examples: teaching puppy and kitten classes, teaching obedience classes, triaging phone calls, preventative appointments (jumping, mouthing, etc) Intervention/Treatment Hour Examples: consultation with the veterinarian, recheck appointments with the veterinarian, technician appointments working with the behavioral therapy prescribed, happy visits (after a diagnosis has been given). **All hours must be achieved when coaching or interacting with the client and patient. Working solely with Fear Free or Low Stress Techniques during an appointment do NOT count as hours** Continuing Education:
• A minimum of forty (40) continuing education hours related to veterinary behavior or behavioral research.
• Accepted CE must be acquired within the last five (5) years prior to submitting the application. • Continuing education must be received from an accredited veterinary technician school, school
of veterinary medicine or national, regional, or state veterinary recognized conference. • Accepted CE includes but is not limited to APDT, Clicker Expo and other state, regional and
national conferences. Case Logs:
• Submit a minimum of fifty (50) cases occurring within one (1) calendar year within the three (3) years before application.
• No more than twenty five percent (25%) can be of a preventative nature, not requiring a veterinary diagnosis.
• Submit two logs: one for prevention (25% or 12 cases) and one for treatment (75% or 38 cases) Case Reports:
• Case reports should come from your case log. • Case reports must be the original work of the applicant.
435
• A minimum of three (3) case reports must have a veterinarian’s diagnosis. • A minimum of two (2) species must be represented. • A maximum of one (1) case report could be a problem prevention case not requiring a
veterinarian’s diagnosis. • A maximum of one (1) case report could be a pet selection counseling report not requiring a
veterinarian’s diagnosis. •
Peer Reviewed Article: • Include a copy or link to your article • Potential publications could include but are not limited to the NAVTA journal, ILAR journal, Lab
Animal journal, SVBT newsletter, AVSAB newsletter, Journal of Veterinary Behavior, or other scientific journals.
• Peer reviewed articles are read and approved by knowledgeable peers in the field. They must contain citations of scientific references. They should contain an appendix of client handouts for treatment options.
• CONFIRM THAT THE PUBLICATION WILL BE PEER REVIEWED • Client information is confidential and should not be included in published articles.
References:
o Shaw, Julie K. Martin, Debbie. Canine and Feline Behavior for Veterinary Technicians and Nurses. John Wiley & Sons, Inc. 2015.
o www.avbt.net
436

Sepsis survival guide By Courtney Waxman, MS, CVT, RVT, VTS (ECC) Purdue University Veterinary Nursing Program, West Lafayette, IN USA Overview Sepsis and septic shock are true life-threatening emergencies that affect our veterinary patients. Since 2004, the Surviving Sepsis Campaign has been publishing international guidelines for the management and resuscitation of patients with sepsis or septic shock. Members of this Campaign are considered experts in the field of veterinary emergency and critical care and have worked together to create evidence-based guidelines, providing updates every four years (the most recent guidelines published in 2016). Early recognition and prompt emergency care is crucial to having a successful patient outcome. Sepsis The term sepsis is derived from the Greek word meaning sepo, or “decomposition of animal or vegetable organic matter in the presence of bacteria.” Sepsis is a common finding in the veterinary emergency and critical care setting and causes high mortality rates in our patients (30-50%). According to the 2016 Surviving Sepsis Campaign (SSC), sepsis is defined as “life-threatening organ dysfunction caused by a dysregulated host response to infection.” Septic shock is defined as “a subset of sepsis in which underlying circulatory and cellular/metabolic abnormalities are profound enough to substantially increase mortality.” The definitions and research surrounding sepsis are continuously evolving as our understanding of the disease process progresses. Despite a continuum of updated terminology, sepsis remains a broad term that’s applied to an incompletely understood disease process. This challenge must be met by a knowledgeable and skilled veterinary team in order to have the best chances of positive patient outcome. Pathophysiology Sepsis is a clinical syndrome that results from an infection that can be bacterial, fungal, protozoal, or viral in origin. For sepsis to develop, a complex pathway derived from systemic inflammatory response syndrome (SIRS) in response to an infection must occur. SIRS is the clinical manifestation of systemic inflammation in response to infectious or noninfectious causes. The infectious pathogen is recognized by pathogen-associated molecular patterns (PAMPs) and microbial-associated molecular patterns (MAMPs), which stimulates the immune response. PAMP and MAMP activation leads to a massive cytokine release (exotoxins act as “super-antigens” to induce widespread T cell activation) and macrophage activation (initiative tumor necrosis factor release), further propagating the inflammatory cascade. Neutrophils respond to the cytokine release by producing reactive oxygen series and nitrous oxide (NO2), resulting in host tissue damage due alterations to systemic vascular resistance (SVR). This excessive inflammatory response results from disproportionate activation of proinflammatory mediators and/or lack of regulatory counterparts.
437

The pathophysiology of sepsis is complex, but the major homeostatic changes include loss of vasomotor tone, injury to the endothelial cell layer, and dysregulation of inflammation and coagulation. Vasomotor tone is lost due to the overproduction of NO2, which causes systemic vasodilation and leads to a distributive shock state. Distributive shock occurs when there is ineffective or inappropriate circulation and distribution of blood volume. This leads to a maldistribution of blood flow, in which vessels dilate and create peripheral blood pooling. During vasodilation, the vessels expand, making the normal blood volume insufficient and causing the blood to be displaced away from the heart and central circulation. Endothelial injury occurs from microcirculatory derangements that increase vascular permeability. This leads to vascular fluid shifts, bacterial translocation (i.e. GI tract) and impaired oxygen delivery to tissues. Dysregulation of the inflammatory response occurs due to cytokine release, which upregulates tissue factor levels to initiate the coagulation cascade. The normal coagulation cascade involves activation of the platelet plug and anticoagulant pathways to maintain hemostasis; during sepsis, these process are inhibited due to downregulation (decreased levels) of antithrombin. This leads to the hemostatic balance favoring a procoagulant state, increasing the patient’s risk of disseminated intravascular coagulopathy (DIC). When the patient becomes affected by SIRS, multi-organ dysfunction syndrome (MODS) can occur. MODS is the physiologic derangements of major body systems (i.e. cardiovascular, respiratory, neurological, renal, hepatic, GI) associated with the progression of uncontrolled sepsis and SIRS. Causes Common causes of sepsis include abdominal disease (i.e. penetrating trauma, pancreatic abscess, hepatic abscess), GI disease (i.e. ulceration/perforation from long-term NSAID usage, foreign body, gallbladder rupture), surgical site dehiscence, cardiac disease (i.e. endocarditis), pulmonary/pleural space disease (i.e. pneumonia, lung abscess, pyothorax), renal disease (i.e. pyelonephritis, cystitis, renal abscess uroabdomen), reproductive disease (i.e. pyometra, mastitis, prostatitis), and injured soft tissue (i.e. traumatic wounds, osteomyelitis, infectious joint effusions). In the author’s experience, the most common cause of sepsis is septic peritonitis from GI disease. Clinical signs Patients who present with sepsis often have a non-specific or vague history. Clinical signs include lethargy, weakness, hyporexia/anorexia, abdominal discomfort, vomiting, diarrhea, increased respiratory rate/effort, feeling warm to the touch, having reddened skin, swelling of extremities/joints (+/- limping), or infected looking/odorous wounds. Patients who develop sepsis within the hospital setting generally is discovered either through the diagnostic workup (i.e. blood work, imaging), following a procedure (i.e. thoracocentesis, ultrasound, joint taps), or post-operatively from laparotomy (patients are most at risk from GI dehiscence 3-5 days following surgery).
438
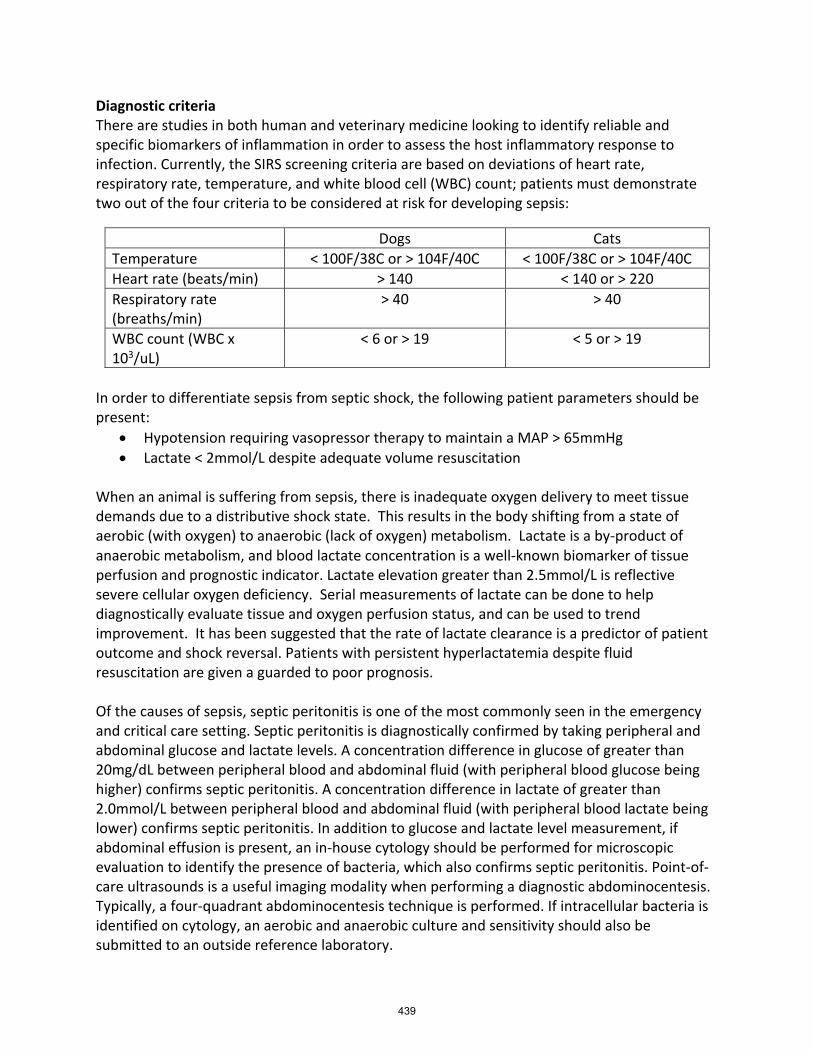
Diagnostic criteria There are studies in both human and veterinary medicine looking to identify reliable and specific biomarkers of inflammation in order to assess the host inflammatory response to infection. Currently, the SIRS screening criteria are based on deviations of heart rate, respiratory rate, temperature, and white blood cell (WBC) count; patients must demonstrate two out of the four criteria to be considered at risk for developing sepsis:
Dogs Cats Temperature < 100F/38C or > 104F/40C < 100F/38C or > 104F/40C Heart rate (beats/min) > 140 < 140 or > 220 Respiratory rate (breaths/min)
> 40 > 40
WBC count (WBC x 103/uL)
< 6 or > 19 < 5 or > 19
In order to differentiate sepsis from septic shock, the following patient parameters should be present:
• Hypotension requiring vasopressor therapy to maintain a MAP > 65mmHg • Lactate < 2mmol/L despite adequate volume resuscitation
When an animal is suffering from sepsis, there is inadequate oxygen delivery to meet tissue demands due to a distributive shock state. This results in the body shifting from a state of aerobic (with oxygen) to anaerobic (lack of oxygen) metabolism. Lactate is a by-product of anaerobic metabolism, and blood lactate concentration is a well-known biomarker of tissue perfusion and prognostic indicator. Lactate elevation greater than 2.5mmol/L is reflective severe cellular oxygen deficiency. Serial measurements of lactate can be done to help diagnostically evaluate tissue and oxygen perfusion status, and can be used to trend improvement. It has been suggested that the rate of lactate clearance is a predictor of patient outcome and shock reversal. Patients with persistent hyperlactatemia despite fluid resuscitation are given a guarded to poor prognosis. Of the causes of sepsis, septic peritonitis is one of the most commonly seen in the emergency and critical care setting. Septic peritonitis is diagnostically confirmed by taking peripheral and abdominal glucose and lactate levels. A concentration difference in glucose of greater than 20mg/dL between peripheral blood and abdominal fluid (with peripheral blood glucose being higher) confirms septic peritonitis. A concentration difference in lactate of greater than 2.0mmol/L between peripheral blood and abdominal fluid (with peripheral blood lactate being lower) confirms septic peritonitis. In addition to glucose and lactate level measurement, if abdominal effusion is present, an in-house cytology should be performed for microscopic evaluation to identify the presence of bacteria, which also confirms septic peritonitis. Point-of-care ultrasounds is a useful imaging modality when performing a diagnostic abdominocentesis. Typically, a four-quadrant abdominocentesis technique is performed. If intracellular bacteria is identified on cytology, an aerobic and anaerobic culture and sensitivity should also be submitted to an outside reference laboratory.
439

Treatment Management of a septic patient is centered on fluid therapy, antibiotic therapy, infectious source control, and overall supportive care. The first step is obtaining venous access. Venous access in a septic patient can sometimes be difficult to obtain due to compromised perfusion from cardiovascular compromise (i.e. vasodilation, hypotension). It’s most ideal to place a large gauge, short length IV catheter in the cephalic vein. IV catheter size is preferably 18-gauge in medium to large sized dogs and 20-gauge in small dogs and cats. Smaller gauge IV catheters create increased resistance to fluid flow, which is counterproductive as fluid resuscitation involves providing rapid, large volume therapy. The cephalic vein is preferred as it allows for easier access, reduces the likelihood of contamination from GI or urinary losses, allows for better visualization as the vessel is closer to the heart, and reduces potential issues with patient mal-positioning or occlusion. Aggressive fluid therapy is necessary to maintain circulatory status. Intravenous isotonic crystalloids are the mainstay fluid type, as they have the most similar composition to patient’s extracellular fluid compartment. Crystalloid solutions include 0.9% NaCl, Lactated Ringer’s (LRS), Normosol-R and Plasmalyte-A. Since septic patients suffer from a distributive shock state, shock volumes of fluids need to be initiated. The shock volume of crystalloid solutions is equal to an animal’s blood volume, and vary slightly depending on the reference source and species. In canines, the shock dose of IV crystalloids is 60 to 90ml/kg. In felines, the shock dose of IV crystalloids is 45 to 60ml/kg. When delivering shock doses of crystalloids, you should start with aliquots, such as ¼ or 1/2 the full shock dose, and then reassess the patient. Ideally, shock doses of IV crystalloids should be administered rapidly, over 10-15 minutes. It is often necessary to implement a pressure bag rather than the typical fluid pump. Synthetic colloids are also a fluid option during fluid resuscitation. Colloid solutions contain large molecules suspended in crystalloid solutions that help maintain intravascular volume because they don’t as readily cross the blood vessel barrier. Because molecules in colloids are bigger, they tend to remain within the intravascular space longer, thus better sustaining intravascular volume. The most commonly available synthetic colloids are derivatives of hydroxyethyl starches. Synthetic colloids can be given as a bolus at 5-10ml/kg IV. They can also be used as a CRI so long as the dose doesn’t exceed 20ml/kg within 24 hours. In recent years, there has been controversy and debate about the use of synthetic colloids in fluid resuscitation. There has been more recent research and evidence in the human field about the adverse effects of synthetic colloid use. The main concerns of colloid use in human medicine is they may cause acute kidney injury and coagulation derangements. While there is currently no veterinary evidence regarding the adverse effects of colloid use, many clinicians are giving more patient consideration prior to implementing colloid use. The use of hypertonic solutions can also be life-saving in the emergency setting. Hypertonic saline is an excellent choice for rapid, small-volume resuscitation. The most commonly used hypertonic solution is 7-7.5% hypertonic saline. Hypertonic saline is dosed at 3-5ml/kg and
440
given IV over 10-15 minutes. Although short-lived (typically 30 minutes), the transient cardiovascular effects of administration may provide enough time for other therapies, such as crystalloids, to take full effect. Use of hypertonic saline is also desirable as you can deliver a much smaller volume to obtain the wanted restoration of intravascular volume effect. Hypertonic saline is often and ideally given in combination with isotonic crystalloids. Vasopressors (i.e. norepinephrine, dopamine) may be indicated if there’s no cardiovascular improvement with fluid resuscitation. Vasopressors are potent vasoconstrictors used to redirect blood flow from the peripheral to central circulation, with the goal of increasing blood pressure. It’s important to note that vasopressors should be considered after the patient has been fully fluid resuscitated (received their full shock dose of IV crystalloids). Evaluation of resuscitation endpoints (early goal-directed therapy) can help determine when a patient has been adequately volume resuscitated and stabilized. Traditional endpoints that should be routinely assessed include improvement in mentation, heart rate, mucous membrane color, capillary refill time, and pulse quality. The parameters for these endpoints vary slightly based on the severity of the patient’s status. The resuscitation endpoint of blood pressure is specific for the septic patient; fluid resuscitation should continue until mean arterial blood pressure (MAP) remains above 65mmHg. Administration of IV antibiotic therapy should be initiated as soon as possible after recognition of sepsis. The rapidity of getting antibiotics onboard has been associated with mortality rates, with human studies showing that starting antibiotics within one hour is crucial. Human studies also show that there is no correlation between choosing the wrong antibiotic and increased mortality; ideally, a broad-spectrum antibiotic should be initially administered, and then antibiotic therapy should be tailored to the patient based on culture and sensitivity results. Finding the source of infection is critical to patient outcome. Of the infectious causes, bacterial infection is by far the most commonly seen. Identifying the source of infection often involves surgical intervention and correction. If the source of infection is surgical in nature (i.e. penetrating trauma, pancreatic/hepatic abscess, GI ulceration/perforation, foreign body, gallbladder rupture, previous surgical site dehiscence), there are specific anesthetic considerations to keep in mind. Patients with sepsis or septic shock are considered high risk anesthesia candidates (ASA IV/V). Opioids and benzodiazepines are considered effective adjuncts. Ketamine and alfaxalone are preferred anesthetic drugs of choice due to their cardiopulmonary-sparing effects. Propofol should be avoided due to its cardiopulmonary side effects. Other supportive care measures include central venous access, gastrointestinal (GI) support, early nutritional intervention, and patient comfort. Sepsis treatment requires high fluid volumes and often multiple fluid and medication types. In order to better facilitate delivery of fluids and drugs, central venous access is beneficial. Strict sterile technique should be followed when placing a central line (either jugular or peripherally inserted central catheter [PICC]). As the GI tract is a major source of sepsis, pharmacological support should include antiemetics,
441

antacids, and prokinetics. Providing nutritional intervention early in a critical patient has been shown to decrease hospital stays and decrease morbidity/mortality. The preferred method of providing nutrition in the hospital setting is enteral nutrition. Enteral nutrition is when nutrition is delivered via the GI tract. There is a saying amongst criticalists and nutritionists alike, “If the gut works, use it!” Enteral nutrition is the most physiologically appropriate method of feeding, as doing so helps maintain GI mucosa, helps prevents bacterial translocation from the gut, and increases wound healing and the immune response. Lastly, ensuring patient comfort while in the hospital setting is important for patient wellbeing and recovery. The use of steroids in septic patients is still considered controversial. In human studies, steroid use in septic patients with adrenal insufficiency has decreased the amount of vasopressors needed. However, patients who are already challenged with systemic infection can become further immunocompromised with steroid use, which can exacerbate their illness. Patients can also experience GI ulceration and thrombotic events following steroid administration. Therefore, due to lack of studies in veterinary medicine supporting steroid administration, their use for septic patients has fallen out of favor. Nursing care Septic patients present in an unstable condition, and the importance of the role of the veterinary technician cannot be overstated. Dedicated nursing care and close monitoring are essential during the stabilization and hospitalization periods of a septic patient. Special care should be taken when handling patients with either confirmed of suspected sepsis in order to avoid worsening of the sepsis clinical syndrome. Proper handling includes wearing gloves during every patient interaction, changing gloves frequently, following sterile catheter placement techniques (i.e. IV, arterial, urinary), providing wound care and management (i.e. drains, incisions), and keeping patients clean and dry, and providing wound care and management. Monitoring often involves one-on-one care for several hours during initial stabilization and throughout hospitalization. During stabilization therapies, it is primarily the veterinary technician assessing the patient and recording vital signs. A full set of vital signs should initially be taken every 10-30 minutes, depending on the severity of the patient’s condition. Focus should be around the six perfusion parameters (mentation, heart rate, pulse quality, mucous membrane color, CRT and extremity temperature), but should also include the frequent auscultation, use of blood pressure measurement (invasive or noninvasive), and ECG monitoring. As the patient becomes less critical, vital sign recordings, blood pressure and/or ECG monitoring can decrease in frequency to every one to four hours. Additional monitoring should include careful assessment of ins/outs (i.e. fluid volume in, urine output out), signs of fluid overload (i.e. clear nasal discharge, chemosis, cough), pain assessment using pain scoring systems, and recumbent care if the patient is non-ambulatory. Nursing care also includes administration of numerous medications, which means it’s essential that veterinary technicians understand drug pharmacokinetics/pharmacodynamics, incompatibilities, side effects, and contraindications.
442

Often times there are advanced skills associated with septic patient care. These include central venous access, arterial catherization, urinary catheterization, nasal feeding tube placement, and closed-suction drain management. If the infectious source of sepsis is respiratory, advanced skills could also include nasal oxygen placement/care and thoracostomy tube care. It is also important to note the importance of communication. Clear communication with fellow nursing staff and doctors will help to ensure continuity of care. This includes reporting changes in patient status, requiring written versus verbal orders, verifying treatment orders, accurate documentation in the medical record (i.e. treatment sheet, nursing notes, client communications), and thorough patient rounds during shift changes. Human nursing studies have shown the increases in patient mortality when nursing staff does not follow a structured systematic approach to rounding on coming staff. Conclusion Sepsis is one of the most severe critical illness facing companion animals, with survival rates ranging from 30-50%. The SSC guidelines regarding sepsis is making is easier to recognize, diagnose, and successfully treat our patients. Veterinary technicians and nurses should understand the pathophysiology of sepsis in order to help with earlier recognition, initiation of emergent therapies, and critical nursing case of a septic patient. References
1. Silverstein DC. Small animal critical care medicine. St. Louis, MO: Elsevier, Saunders; 2015.
2. Scalf R. Study guide to the AVECCT examination. San Antonio, TX: AVECCT; 2014 3. Battaglia AM, Steele AM, Battaglia AM. Small animal emergency and critical care for
veterinary technicians. St. Louis, MO: Elsevier; 2016. 4. Norkus, C. L. (2019). Veterinary technicians manual for small animal emergency and
critical care. Hoboken, NJ: Wiley. 5. Dellinger, R. P., Levy, M. M., Rhodes, A., Annane, D., Gerlach, H., Opal, S. M., Moreno, R.
(2016). Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock, 2015. Intensive Care Medicine,39(2), 165-228. doi:10.1007/s00134-012-2769-8
443
Tech tools: Multi-parameter monitoring By Courtney Waxman, MS, CVT, RVT, VTS (ECC) Purdue University Veterinary Nursing Program
Overview In the critical care setting, there are a variety of machines, equipment, and tools to use at our disposal in order to better monitor our patients. Often, critically ill patients require more advanced monitoring than just assessing the standard vital parameters. In the emergency room, these tools include electrocardiogram, blood pressure measurement, pulse oximetry, capnography,venous blood gas analysis, central venous pressure, and urine output. Electrocardiogram Assessment of heart function involves both a mechanical and electrical evaluation. Auscultation of heart rate and evaluation of electrocardiogram (ECG) tracings can be used as indicators of the heart’s ability to appropriately pump blood and provide systemic perfusion. Heart rate is usually the first cardiovascular parameter you perform when going through your initial assessment. Tachycardia is generally accepted as a heart rate greater than 160-180bpm in dogs and greater than 200bpm in cats. Bradycardia is generally accepted as a heart rate less than 80-100bpm in dogs and less than 150-160bpm in cats. Tachycardia could be indicative of fear, excitement, anxiety, pain, or shock (hypovolemia, hypotension). Bradycardia could be indicative of conduction disturbances, decreased cardiac output, poor perfusion, neurologic disease (i.e. increased intracranial pressure), hypothermia, increased vagal tone, drug overdose, or severe electrolyte disturbances. In addition to noting the auscultated HR, it should also be noted if there are any irregularities. Use of an ECG machine enables evaluation of the heart’s electrical components and is helpful in determining if an arrhythmia is present. Being familiar with what a normal ECG rhythm looks like is important to be able to recognize when an abnormal ECG rhythm occurs. Arrhythmias may result from a variety of conditions, including underlying cardiac disease, anesthesia, trauma, electrolyte disturbances, and ischemia. Common arrhythmias seen in emergency and critical care are divided into tachyarrhythmias and bradyarrhythmias. Basics of ECG Interpretation A normal ECG rhythm is divided into 5 parts: P, Q, R, S, and T waves. The P wave begins the complex and represents atrial depolarization. The QRS complex represents ventricular depolarization. The T wave represents atrial repolarization and completes the complex. The ECG reflects the electrical stimulus for contraction, not the actual mechanical activity of the heart. When interpreting an ECG, it’s helpful to go in a stepwise approach:
1. Determine the rate 2. Identify the P wave 3. Identify the QRS complex 4. Identify the T wave 5. Determine if it is regular or irregular (look at R-R interval)
444
Tachyarrhythmias Sinus tachycardia is a regular, sinus rhythm at a fast rate. This can be secondary to pain, fear, anxiety/stress, exercise, hypotension, anemia, shock states, and sepsis. Ventricular premature contractions (VPCs) occur when the impulse of contraction is initiated by the ventricles rather than the atrium. ECG features absent P waves and a wide, bizarre QRS complex. Ventricular tachycardia (V-tach) is composed of continuous VPCs with a HR exceeding 180bpm. ECG features runs of VPCs and is considered a life-threatening rhythm as it can progress into ventricular fibrillation. Accelerated Idioventricular Rhythm (AIVR) is composed of frequent VPCs with a HR less than 180bpm. It is typically secondary to non-cardiac diseases, such as neoplasia, GDV, pain, trauma, sepsis, and end-stage organ failure. This arrhythmia is commonly mistaken for V-tach. Supraventricular tachycardia (SVT) is an arrhythmia that originates in the atrium. SVT results in development of systolic dysfunction and congestive heart failure (CHF). ECG features of SVT are narrow appears QRS complexes, absent or abnormal, or buried P waves, and a HR exceeding 220bpm. SVT usually occurs from cardiac diseases that cause atrial enlargement (i.e. DCM). Atrial fibrillation (A-fib) is an arrhythmia that is irregular. ECG features absent P waves, possible F (fibrillation) waves, an irregularly irregular R-R interval, and a high rate. A-fib is typically indicative of primary heart disease. Bradyarrhythmias Sinus bradycardia is a regular, sinus rhythm at a slow rate. This can be secondary to increased vagal tone, increased intracranial pressure, hypothermia, renal disease, severe shock, or drug side effects. Atrioventricular (AV) block occurs when there’s impaired conduction from the atrium to the ventricles (may be partial or complete). The different degrees of AV block are classified according to the level of conduction impairment. Each arrhythmia has P waves with no associated QRS complexes. Atrial standstill is an arrhythmia that originates in the atrium and occurs when the atrium is unable to conduct the electrical pulse to complete the cardiac cycle. ECG features absence of P waves preceding any of the QRS complexes. The most common cause for this arrhythmia is hyperkalemia from urethral obstruction. Sick sinus syndrome (SSS) is a syndrome caused by malfunction of the entire conduction system. It’s characterized by periods of tachycardia followed by sinus bradycardia and/or sinus arrest (failure of SA node to depolarize). ECG features prolonged periods of no P waves or QRS complexes (asystole). This arrhythmia is intermittent and may have a normal rhythm between episodes. The prolonged periods of sinus arrest is what causes syncope.
445
Electrical alternans are a phenomenon in which P waves are present and QRS complexes appear normal, however the height of each QRS complex alternates and is uneven. This rhythm occurs when there is pericardial effusion; the heart “swings” within the fluid each beat. Other arrhythmias to be familiar with include the three most common cardiopulmonary arrest rhythms; pulseless electrical activity (PEA), ventricular fibrillation (V-fib), asystole. PEA occurs when the electrical system continues to function, but mechanical activity ceases. V-fib occurs when there is aberrant, uncoordinated activity of the muscle cells in the ventricles leading to a “quivering” mechanical activity. Asystole occurs when there is complete cessation of electrical and mechanical heart activity. Blood Pressure Arterial blood pressure monitoring can be very useful in critical care cases as another means of assessing cardiovascular function. Blood pressure (BP) is reflective of appropriate cardiac output and perfusion. Blood pressure is the by-product of cardiac output (CO) and systemic vascular resistance (SVR). CO is the amount of blood pumped by the heart and SVR is the amount of resistance of blood as it moves from the central to peripheral circulation.
BP = CO x SVR
Factors such as varying shock states, hypovolemia, cardiac disease, and renal disease can affect adequate perfusion. BP is further broken down into three measurements, systolic, diastolic, and mean. Systolic BP is the maximum arterial pressure during cardiac contraction. Diastolic BP is the arterial pressure during cardiac relaxation. Mean BP (MAP) is the combined result of systolic and diastolic. Each measurement is in millimeters of Mercury (mmHg).
MAP = [(2 x diastolic0 + systolic)]
3
Maintaining a systolic BP > 90mmHg or mean BP > 60mmHg is essential for maintaining organ perfusion. Blood pressure is measured via non-invasive, indirect methods, such as oscillometric or Doppler technique, and via invasive, direct methods, such as arterial catheterization. Oscillometric technique uses an oscilloscope and utilize an automatic pressure system to inflate and deflate the cuff. The system picks up oscillations beneath the cuff to generate an electronic reading of systolic, diastolic, and MAP. Doppler technique uses ultrasound waves from the artery that are transmitted to a speaker via a crystal. The crystal is placed over the artery (pulse) to generate an audible sound of the patient’s blood flow. The cuff is inflated using a sphygmomanometer bulb until the audible sound is no longer heard, then the bulb is slowly released (deflating the cuff) while watching the sphygmomanometer gauge until audible blood flow is heard again. Doppler only generates a systolic reading. For either indirect technique, it’s important to use the appropriate cuff size (approximately 40% of the limb circumference) as well as use the same limb for each measurement to ensure consistency and accuracy of results. Using too big a cuff results in a falsely low reading while using too small a cuff results in a falsely high reading. It’s also important to note that trends in blood pressure readings are more important than a one-time measurement. Arterial catheterization is an advanced skill and allows for second-by-second measurement of BP. Direct measurement shows a continuous waveform that reflects each phase of the
446
patient’s blood pressure. The most common site for catheterization is in the dorsal pedal artery. After performing a sterile prep, it’s best for the catheter to be held as if it were a pencil, inserting where you feel the pulse throbbing beneath your finger. It is common for the arterial blood to “pulse” backwards into the stylet. Advance and secure the arterial catheter as you would an IV catheter. It is imperative that the arterial catheter be labeled as such so as not to accidentally infusion fluids or medications. Arterial catheters must be maintained by very frequent used of heparinized saline flush for patency. Pulse oximetry The pulse oximeter gives insight into respiratory function, specifically oxygenation. Oxygenation refers to how well oxygen is diffused from the alveoli, bound to hemoglobin, and dissolved and delivered to bodily tissues. Pulse oximetry is an easy, noninvasive means to measure the oxygen saturation of hemoglobin (SpO2). Arterial blood gas monitoring is the gold standard for assessing oxygenation and ventilation status. Hypoxemia is defined as a low oxygen level in the blood (SpO2 < 95%). Causes of hypoxemia include low inspired oxygen concentration (low FiO2), hypoventilation, ventilation-perfusion mismatch, and diffusion impairment. For patients who are not oxygenating well (i.e. SpO2 < 95%), supplemental oxygen therapy may be necessary. Oxygen supplementation can be provided via flow-by, face mask, oxygen hood, oxygen cage, nasal cannulas, or intubation. Another tool worth mentioning is the oxyhemoglobin dissociation curve. The curve depicts the relationship between oxygen hemoglobin saturation and partial pressures of oxygen. The curve is determined by hemoglobin’s affinity for oxygen (how readily hemoglobin acquires and releases oxygen molecules). The relationship is sigmoid in shape, and factors such as temperature, PCO2 and pH affect the curve. The curve shows that small changes in hemoglobin saturation (SpO2) correlate with large changes (roughly 4x lower value) in PaO2. Capnography The capnograph gives insight into respiratory function, specifically ventilation. Ventilation is the process of appropriate gas exchange within the alveoli; oxygen is inhaled, and carbon dioxide is exhaled. The capnograph measures end-tidal carbon dioxide (ETCO2), which is a by-product of cellular metabolism. Capnography is a comprehensive measurement device that displays each phase of the ETCO2 waveform. Arterial blood gas monitoring is the gold standard for assessing oxygenation and ventilation status. ETCO2 is reflective of partial pressure of CO2 (PaCO2) under ideal situations, and a gradient exists between the two. There are four phases to a normal capnogram. Phase I represents the inspiratory baseline and should be at zero. Phase II represents the expiratory upstroke and is made up of alveolar gas and dead space. Phase III is the alveolar plateau, the end of which represents the maximum CO2 exhaled from the patient from where the EtCO2 reading is taken. Phase IV represents inspiration, where the level of CO2 passing through the sensor drops to and stays at zero. A normal capnogram results in an identical shape, and any variation requires analysis to determine the cause.
447
In critical care, hypoventilation is more common than hyperventilation. Hypoventilation (hypercapnia) is defined as alveolar ventilation lower than that required to maintain normal CO2 (CO2 > 60mmHg). Causes of hypoventilation include neuromuscular disease, chest wall trauma, drugs or toxins, brainstem disease, or airway obstruction. If we don’t intervene, consequences of hypoventilation include respiratory acidosis, myocardial depression, vasodilation, increased intracranial pressure, and hypoxemia. For patients who are not ventilating well, intubation and manual/mechanical ventilation may be necessary. Central venous pressure Central venous pressure (CVP) is the measurement of the hydrostatic pressure in the vena cava. Measuring CVP provides an estimation of blood pressure within the right atrium as an indicator for vascular volume. Normal CVP is between 8-10cmH20. CVP is sued to provide information about intravascular blood volume, cardiac function, efficacy of fluid therapy, and risk of volume overload. The use CVP monitoring has fallen out of favor over recent years. Urine output Urine output (UOP) should be closely monitored in the critically ill, as it is reflective of appropriate renal function. The function of the nephron is to remove body waste, conserve solutes and produce urine; urine is the end-product. Urine production is dependent on proper nephron function, appropriate blood supply to the glomerulus, and patency of the urinary tract. In a euvolemic patient, normal urine output in dogs and cats is 1-2ml/kg/hr. Change in any of the factors indicates impaired renal function, resulting in abnormal urine output. The three most common kinds of abnormal urine output are polyuria (UOP > 1-2ml/kg/hr), oliguria (UOP < 1ml/kg/hr), and anuria (lack of urine). Causes of decreased UOP include dehydration, hypoperfusion, prolonged hypotension, trauma to the urinary system (i.e. urethral, ureteral, bladder rupture). Causes of increased UOP include over-hydration (i.e. fluid overload), endocrine disease (i.e. diabetes mellitus), or post-obstructive diuresis. During states of abnormal UOP, urinary catheters should be placed using sterile technique and maintained for more accurate assessment of UOP. UOP should be measured every 2-4 hours and urinary catheter care should be performed every 6-8 hours. UOP, in addition to other renal parameters (body weight, bloodwork), is used to help guide fluid therapy. Conclusion As veterinary technicians, we should be comfortable and familiar with what additional monitoring tools we can use on our patients in order to have the highest standard of patient care and monitoring. References
1. Silverstein DC. Small animal critical care medicine. St. Louis, MO: Elsevier, Saunders; 2015. 2. Scalf R. Study guide to the AVECCT examination. San Antonio, TX: AVECCT; 2014 3. Battaglia AM, Steele AM, Battaglia AM. Small animal emergency and critical care for veterinary
technicians. St. Louis, MO: Elsevier; 2016. 4. Creedon JMB, Davis H. Advanced monitoring and procedures for small animal emergency and
critical care. Chichester, West Sussex: Wiley-Blackwell; 2012. 5. Norkus, C. Veterinary technician’s manual for small animal emergency and critical care.
Hoboken, NJ: Wiley-Blackwell; 2013.
448

The vet techs critical patient checklist By Courtney Waxman, MS, CVT, RVT, VTS (ECC) Purdue University Veterinary Nursing Program, West Lafayette, IN USA Overview As veterinary medicine is continuously evolving, so are pet owner expectations for the level of care their pets receive. Using Kirby’s Rule allows veterinary technicians to look at the overall clinical picture of the patient and implement critical thinking skills. Kirby’s Rule of 20 was created by Rebecca Kirby, DVM, DACVIM, DACVECC, and is a checklist of 20 parameters that should be evaluated daily in critically ill patients. Kirby’s Rule of 20 is used as a tool/reference to ensure quality patient care in critical patients are being monitored. The parameters on the checklist are:
1. Fluid balance 11. Coagulation 2. Albumin/oncotic pull 12. Renal function 3. Mentation 13. GI motility & integrity 4. Heart rate, contractility, rhythm 14. Nutrition 5. Blood pressure 15. Immune status (antibiotics) 6. Oxygenation & ventilation 16. Drug dosage & metabolism 7. Body temperature 17. Wound care & bandages 8. Electrolytes & acid-base 18. Pain control 9. Glucose 19. Nursing care 10. RBCs & hemoglobin 20. Tender loving care
Fluid balance Physiologically speaking, the body’s fluid compartments are divided between intracellular (ICF), or within the cell, and extracellular (ECF), or the intravascular and interstitial, compartments. Fluid imbalances occur from any condition(s) that alters a patient’s ability to adequately compensate and restore its own fluid requirements, thus requiring medical intervention. Intravenous fluids are used in the critically ill to maintain intravascular volume and adequate perfusion. To develop a fluid therapy plan, things like hydration status and ongoing losses are considerations that should be included in determining maintenance and replacement fluid therapy. When it comes to monitoring fluid therapy, a variety of parameters are assessed. First, assess the patient; this is done by evaluating physical parameters (heart rate, pulse quality, mm color/moisture, CRT, extremity temperature, attitude/mentation, blood pressure, skin turgor). Next, assess ongoing losses, which can include vomiting, diarrhea, polyuria, third spacing, or wound loss. Then, assess the patient’s inputs versus outputs, which can be done by evaluating urine output and serial body weights. Additionally, lab values, such as PCV/TP, lactate levels and acid-base status, can give insight on a patient’s fluid status. Fluid therapy should also be monitored for signs of fluid overload, or overhydration; sings include serous nasal discharge, chemosis, subcutaneous edema, ascites, increased respiratory rate, coughing, and restlessness. Overall, knowing a patient’s disease process (i.e. renal failure, CHF, SIRS, pediatric) also allows for a better understanding of the patient’s fluid requirements.
449
Albumin/oncotic pull Albumin is the predominant protein within the intravascular space and is responsible for maintaining vascular integrity and colloid oncotic pressure (COP). Oncotic pull is what keeps fluids within the vascular space; without albumin, there would be increased intravascular permeability, resulting in fluids leaving the intravascular space and causing third spacing and edema. Critical patients often suffer from hypoalbuminemia, which can result in hypotension or interstitial or pulmonary edema. Nutritional support, synthetic colloids and intravenous albumin are therapies that can be used to raise albumin levels. It should be noted that using plasma to raise albumin is not considered an appropriate therapy, as it requires a significant amount of plasma to do so (it takes 40-50ml/kg FFP to raise albumin by 1g/dL). Mentation Assessment of the patient’s neurologic status should be performed in every critical patient, not only in those with a primary neurological disorder. These parameters include level of consciousness (LOC), breathing pattern, pupillary light reflexes (PLR), pupil size and location, posture, reflexes, and the use of coma scale evaluation. The frequency of neurologic assessment will depend on the patient’s stability. Evaluation of a patient’s LOC can be classified as normal/alert, dull/depressed/obtunded (slowed/inappropriate response to sensory stimuli), stuporous (unconscious but rousable to noxious stimuli) or comatose (unconscious and unresponsive). Changes in LOC can be indicative of decreased cerebral function (i.e. lack of oxygen supply, change in cerebral perfusion) and should be addressed quickly to prevent further deterioration. One of the most commonly used coma scales is the Modified Glascow Coma Scale (MGCS). The MGCS can be used to record progression or regression of the TBI patient over a period of time. The MGCS involves three separate categories, including assessment of LOC, motor activity, and brainstem reflexes. A score is given for each of these categories based on the patient’s clinical findings; a higher score will correlate with a better prognosis while a lower score will correlate with a poorer prognosis. This scaling system is beneficial because of it allows for an objective evaluation of the patient that can be used to monitor progression or deterioration of their neurological state. Any change in mentation (positive or negative) should be reported to the clinician and warrants intervention. Heart rate, contractility, rhythm Assessment of heart function involves both a mechanical and electrical evaluation. Frequent auscultation of heart rate, palpation of pulse quality, blood pressure measurement and evaluation of mucous membrane color can all be used as indicators of the heart’s ability to appropriately pump blood and provide systemic perfusion. Heart rate is usually the first cardiovascular parameter you perform when going through your initial assessment. Tachycardia is generally accepted as a heart rate greater than 160-180bpm in dogs and greater than 200bpm in cats. Bradycardia is generally accepted as a heart rate less than 80-100bpm in dogs and less than 150-160bpm in cats. Tachycardia could be indicative of fear, excitement, anxiety, pain, or shock (hypovolemia, hypotension). Bradycardia could be indicative of conduction disturbances, decreased cardiac output, poor perfusion, neurologic disease (i.e. increased intracranial pressure), hypothermia, increased vagal
450

tone, drug overdose, or severe electrolyte disturbances. Pulse rate and quality should be taken in conjunction with HR auscultation. Pulse rate is reflective of systemic perfusion, and should match the auscultated HR. Pulse quality is reflective of the amount of blood that is pumped through the body with each heartbeat, which is known as stroke volume. An animal’s pulse quality can be described as normal (a steady pulsation against your finger that is synchronous with the heart rate), weak (a lighter than normal pulsation against your finger), bounding (a harder than normal pulsation against your finger), or absent (lack of pulsation against your finger). A normal pulse is indicative of normal stroke volume. Weak pulses are concerning for decreased stroke volume, poor contractility, or peripheral vasoconstriction. It should also be noted whether or not pulse deficits (absent pulses during cardiac contraction) are present, as they are also an indicator of inadequate stroke volume. Bounding pulses are reflective of systolic-diastolic difference in arterial blood pressure, which is concerning for increased stroke volume and vasodilation. Absent pulses indicate a failure in appropriate peripheral perfusion. Contractility refers to the strength of contraction of each heart eat. In addition to noting the HR during auscultation, it should also be noted if there are any irregularities, which can indicate an arrhythmia and would warrant performing further diagnostics, such as an electrocardiogram (ECG). Use of an electrocardiogram (ECG) enables an evaluation of the heart’s electrical components and is helpful in determining if an arrhythmia is present. Being familiar with what a normal ECG rhythm looks like is important to be able to recognize when an abnormal ECG rhythm occurs. Common arrhythmias seen in critical care include tachyarrhythmias (sinus tachycardia, VPCs, ventricular tachycardia, SVT, atrial fibrillation) and bradyarrhythmias (sinus bradycardia, AV blocks, atrial standstill, sick sinus syndrome, bundle branch blocks). Blood pressure Arterial blood pressure monitoring can be very useful in critical care cases. Blood pressure (BP) is reflective of appropriate cardiac output and perfusion; maintaining a systolic BP > 90mmHg or mean BP > 60mmHg is essential for maintaining organ perfusion. Blood pressure is most easily measured via non-invasive indirect methods, such as oscillometric or Doppler technique. It is important to use the appropriate cuff size (approximately 40% of the limb circumference) as well as use the same limb for each measurement to ensure consistency and accuracy of results. In critically ill patients, hypotension is more common than hypertension. Hypotension is caused by decreased cardiac preload or decreased venous return. Examples of disease processes that can cause hypotension include hypovolemia, GDV, anaphylaxis, sepsis, SIRS, pleural space disease and heart disease. Trends in blood pressure readings are more important than a one-time measurement. Other methods of monitoring perfusion besides BP include mentation, heart rate, pulse quality, mucous membrane color, capillary refill time, and extremity temperature. Oxygenation and ventilation Pulmonary function can be compromised in critically ill patients for a variety of reasons, and assessing respiratory parameters is vital. Ventilation is the process of appropriate gas exchange within the alveoli; oxygen is inhaled, and carbon dioxide is exhaled. Oxygenation refers to how well oxygen is diffused from the alveoli, bound to hemoglobin, and dissolved and delivered to bodily
451
tissues. The “gold standard” for measuring oxygenation and ventilation status is through arterial blood gas; however, this is not always a feasible option. Alternatively, parameters such as respiratory rate, respiratory effort, respiratory character, lung auscultation, pulse oximetry and venous blood gas can be used. Pulse oximetry (SpO2) is an easy, noninvasive means to measure the oxygen saturation of hemoglobin. A venous blood gas allows for measurement of CO2, which is the parameter that indicates appropriate ventilation. For patients who are not oxygenating well (i.e. SpO2 < 95%), supplemental oxygen therapy may be necessary. For patients who are not ventilating well (i.e. CO2 > 60mmHg), intubation and manual/mechanical ventilation may be necessary. Another tool worth mentioning is the oxyhemoglobin dissociation curve. The curve depicts the relationship between oxygen hemoglobin saturation and partial pressures of oxygen. The curve is determined by hemoglobin’s affinity for oxygen (how readily hemoglobin acquires and releases oxygen molecules). The relationship is sigmoid in shape, and factors such as temperature, PCO2 and pH affect the curve. The curve shows that small changes in hemoglobin saturation (SpO2) correlate with large changes (roughly 4x lower value) in PaO2. Body temperature Body temperature is part of the initial clinical examination and should be measured regularly in every critically ill patient. Temperature is most accurately measured via rectal thermometer, and fluctuations should be reported to the clinician. Animals maintain their temperature within a range called the "set-point." The set-point is determined by the thermoregulatory center in the hypothalamus. When an animal's temperature rises or falls out of this range, the body reacts by increasing or decreasing the core temperature in an attempt to return to the set point. Hyperthermia can be attributed to environmental exposure (i.e. heatstroke), infectious sources, inflammatory sources, or neoplastic diseases. Hypothermia can be attributed to anesthetic recovery or systemic disease processes (i.e. cardiovascular disorders, shock). Permissive hypothermia is sometimes tolerated in cases of traumatic brain injury or head trauma, as lower temperatures decrease metabolic demands. Electrolytes and acid-base Electrolyte abnormalities are a common finding on lab work and can have harmful consequences if not identified and corrected. Sodium, potassium, chloride, and calcium should all be monitored and maintained within their normal ranges. They are critical for cell function, cardiac performance, vascular tone, brain function, neuromuscular activity, and fluid balance. Other electrolytes that should be monitored, if possible, are phosphorus and magnesium. Changes in electrolytes can manifest as changes in mentation (sodium), ECG rhythms (potassium, calcium), and acid-base status (chloride). Assessment of acid-base status gives insight into three physiologic processes: alveolar ventilation (venous), acid-base (venous or arterial), and oxygenation (arterial). Venous blood gas (VBG) analysis is arguably one of the most routinely used point of care tests done in the critical care setting. A VBG is performed when there is a need to know what a patient’s acid-base or ventilation status is. The results of a VBG gives the veterinary team more information about the severity of a critical patient’s disease, so that appropriate interventions (i.e. fluid therapy, electrolyte supplementation,
452
oxygen support) can be provided. When evaluating a patient’s VBG result, the values needed for interpretation are pH, PCO2, and HCO3. The pH is a measurement of acidity or alkalinity of the blood (how many hydrogen molecules are present in the blood). An excess of hydrogen ions causes a decrease in pH (acidosis), while a shortage of hydrogen ions causes an increase in pH (alkalosis). The PCO2 is a measurement of the partial pressure of carbon dioxide in the blood. PCO2 is an indicator of the respiratory component of a blood gas analysis. An excess of CO2 causes an acidosis, while a shortage of CO2 causes an alkalosis. The HCO3 is a measurement of bicarbonate (bicarb) in the body. Bicarb is a major buffer and represents the metabolic component of blood gas analysis. Acid-base disturbances in critically ill animals include metabolic acidosis, metabolic alkalosis, respiratory acidosis and respiratory alkalosis. Metabolic acidosis is the most common acid-base derangement in critically ill animals. Glucose Glucose is considered the body’s primary energy source and is utilized by every cell. Glucose is stored in the liver in the form of glycogen. Ideally, blood glucose levels should be maintained between 65-120mg/dL. Alterations in blood glucose (BG) can occur from many disease states/processes. Hypoglycemia can be caused by excess insulin (i.e. overdose, insulinoma), toxins (i.e xylitol), hepatic disease, metabolic disease (i.e. hypoadrenocorticism, Fanconi syndrome), or sepsis. Hyperglycemia can be caused by lack of insulin (i.e. diabetes mellitus, DKA), neurological disorders, or renal disease. In critical illness, hypoglycemia is more common than hyperglycemia. Depending on the disease state, frequent blood glucose monitoring may be necessary, in which case placement of a sampling catheter may be worthwhile. RBCs and hemoglobin Red blood cells (RBCs) contain hemoglobin and are therefore responsible for carrying and transporting oxygen molecules throughout the circulatory system; each hemoglobin molecule can carry four oxygen molecules. Maintaining adequate hemoglobin levels is therefore essential to maintaining adequate oxygen delivery. Measuring packed cell volume (PCV) is a quick and easy test to measure the concentration of RBCs. In critical patients, a decrease in RBCs can become life-threatening due to impaired perfusion and lead to multiorgan dysfunction. The kidneys respond to decreased oxygen delivery from anemia by releasing erythropoietin, a hormone which stimulates production of RBCs by the bone marrow. The spleen is responsible for storage and removal of old or damaged red blood cells. If anemia is present and associated with clinical signs (tachycardia, tachypnea, lethargy, altered mentation), administration of blood component therapy (i.e. whole blood, packed red blood cells) may be warranted. Administering blood products is not a benign therapy; it requires blood typing and cross-matching to limit the chance of a reaction, as well as frequent monitoring during a transfusion for signs of a reaction. Coagulation Coagulation is the process of clot formation within the vasculature. Coagulation abnormalities occur in the critically ill due to diseases processes affecting hemostasis. These include thrombocytopenia, von Willebrand’s, hemophilia, hepatic disease, rodenticide toxicity, or hypercoagulable states (i.e. Cushing’s, IMHA, sepsis). Evaluation of clotting times (PT, aPTT)
453
requires specific blood draw techniques to ensure accuracy. It is also necessary to monitor for signs hemorrhage, which include petechia, ecchymoses, hematuria, or bleeding from incisions and wounds. In cases of severe coagulopathy, it may be indicated to implement blood component therapy (i.e. fresh frozen plasma). Another concern in the critically ill is the development of disseminated intravascular coagulopathy (DIC). DIC is a systemic activation of coagulation that leads to widespread microvascular thrombosis. Renal function The kidneys are vital to life and are responsible for many functions that help maintain overall homeostasis. Their functions include fluid regulation, hormone production, and excretion of metabolic waste products. They maintain the volume and composition of body fluids (water and electrolyte balance), they absorb solutes (proteins, amino acids, glucose), and they remove metabolic waste from the body (urea, uric acid, creatinine). The kidneys receive approximately 20-25% of overall cardiac output and help maintain arterial blood pressure, and therefore are susceptible to damage/injury during periods of poor perfusion. When any of the kidney’s functions become disrupted, there can be systemic consequences. A common disease process in critically ill patients is acute kidney injury (AKI). Acute kidney injury (AKI) is a clinical syndrome, defined as a rapid deterioration in kidney function resulting from injury. Azotemia is recognized by abnormally high concentrations of body waste compounds within the blood, primarily blood urea nitrogen (BUN) and creatinine. Azotemia from AKI can further be grouped as prerenal, intrinsic renal, and postrenal, and is reflective of the type of AKI a patient is experiencing. Prerenal refers to “before” the kidney, meaning injury is caused by other physiological factors in which renal ischemia results (i.e. hypovolemia, dehydration, cardiac compromise, vasodilatory diseases). Intrinsic renal refers to direct damage to the renal parenchyma (i.e. toxins, infectious insult, neoplasia). Postrenal refers to “after” the kidney, meaning there is an obstruction or impediment in the outflow of urine that prevents urine from being eliminated from the body (i.e. urethral obstruction, urolithiasis, trauma). Urine output (UOP) should be closely monitored in the critically ill, as decreased urine output can also be indicative of impaired renal function. Normal UOP in a well-perfused, hydrated animal should be between 1-2ml/kg/hr. During states of abnormal UOP (i.e. polyuria, oliguria), urinary catheters should be placed and maintained to obtain a more accurate assessment of UOP. Other renal parameters to monitor include serial body weights, auscultation, and bloodwork to evaluate renal values. GI Motility & Integrity It is not uncommon for critically ill patients to initially present in a state of shock. Shock states result in perfusion priority being given to vital organ systems (brain, heart, lungs), which means other organ systems like the GI tract suffer. Hypoperfusion to the GI tract can contribute to increased intestinal permeability, which can lead to bacterial translocation and potentially sepsis. Common diseases associated with gastrointestinal dysfunction are parvovirus, hemorrhagic gastroenteritis, ileus, foreign body obstruction, gastric ulceration, gastric atony, IBD, PLE, and secondary disease states (i.e. pancreatitis, cholangiohepatitis, hepatic lipidosis). The use of prokinetics, such as
454

metoclopramide, can help enhance motility. Gastroprotectants, such as famotidine, pantoprazole, ondansetron, and sucralfate, can all be used to decrease acid secretions and limit the likelihood of ulceration. Antiemetics, such as maropitant, should be used to curb nausea. Nutrition Nutrition is probably the most overlooked aspect of caring and managing critically ill patients. As veterinary medicine has advanced, so has the outlook on providing nutritional support to our patients. Nutrition should be provided to every patient, every time, as it is necessary for recovery from all disease processes. The methods of providing nutrition in a hospital setting include enteral and parenteral nutrition. Enteral nutrition is when nutrition is provided via the GI tract. The use of nasoesophageal and nasogastric feeding tubes are minimally invasive, relatively short-term methods of providing nutritional support; bolus feeding or trickle feeding options are available. Additionally, esophagostomy tubes can be surgically placed for more long-term nutritional support. For enteral nutrition, the patient’s resting energy requirement (RER) should be calculated and feedings should be started at ¼ to 1/3 RER. One potential complication of enteral nutrition is refeeding syndrome, which is a potentially life-threatening catabolic state in which there’s a rapid shift of intracellular electrolytes, causing hypokalemia, hypophosphatemia, and hypomagnesemia. Parenteral nutrition is when nutrition is provided intravenously. Parenteral nutrition can further be divided into partial parenteral nutrition (PPN) or total parenteral nutrition (TPN). Strict sterile technique is required when placing IV access for parenteral nutrition. One advantage to PPN/TPN is that the nutritional formulation can be custom made (dextrose, lipids, amino acids, electrolytes, vitamins) based on the patient’s specific needs. Immune status The function of the immune system is to protect the body from invasion of foreign microorganisms. The immune system of the critical patient can be affected by patient factors, disease factors, and environmental factors. These factors include immunosuppression (i.e. leukopenia, undergoing chemotherapy), GI dysfunction (risk for bacterial translocation, aspiration, malnutrition), drug suppression, autoimmune disease processes, wound contamination, indwelling catheters/tubes/drains, infectious agents (i.e. zoonotic diseases), and nosocomial infections. Monitoring should include evaluation of white blood cells (i.e. daily CBC, daily blood smear), submission of culture and susceptibility, body temperature (monitor for fever), and daily assessment of wounds and/or insertion sites (i.e. incisions, IV catheter insertion sites) for signs of infection (discharge, odor, heat). Ideally, gloves should be worn with every patient and changed between patients. Use of antibiotics should be carefully chosen so as not to contribute to antibiotic resistance. Drug dosage and metabolism Pharmacokinetics is a branch of pharmacology that’s concerned with how drugs move within the body; the processes include absorption, distribution, metabolism and excretion. The medications of each patient should be reviewed daily to assess drug doses, dose frequency, and drug interactions. Medical calculations should also be double checked prior to administering medications to prevent over/under-dosing, especially as patient weights can change while hospitalized. Patient
455

considerations should also be reviewed, such as patients with renal/hepatic disease that may have altered metabolisms or determining if a patient still requires a medication. Wound care and bandages Wound care involves not only wounds or bandages from incisions or lacerations, but also insertion sites. Any incision should be inspected daily for signs of infection or dehiscence; any dressings over an incision should be changed when soiled. Any wounds that have bandages should also be inspected and changed daily. IV catheter sites should be broken down, inspected and re-taped daily; any sign of infection, loss of patency or inflammation and the insertion site should be removed and replaced. Any tube insertion sites (i.e. feeding tubes, chest tubes, penrose drains, etc.) should be inspected for patency and gently cared for. During handling of any wound or bandage, gloves should be worn always. Pain control Being able recognize, evaluate and alleviate pain is integral in the well-being of our patients. Over the last several years, the concepts of pain and pain management have become more prevalent within the veterinary field. Within emergency and critical care, the physiology, recognition, and management of pain has been given more research and attention. The International Association for the Study of Pain defines pain as, “an unpleasant sensory and emotional experience associated with actual or potential tissue damage”. Nociceptors (pain receptors) are present in the nervous system and become stimulated by a noxious stimulus (stimulation of a nerve ending). Nociception is the sensory process that involves a series of electrical events that start at the site of tissue injury, convey signals to the central nervous system, and result in the perception of pain. Nociception is essentially the pain pathway and can be broken down into four processes: transduction, transmission, modulation and perception. A noxious stimulus occurs at the site of tissue damage, which initiates the transduction process the pain pathway. Transduction is the conversion of physical energy into electrical energy by the nociceptor. The electrical energy then becomes a nerve impulse that can travel in the pain pathway along the nervous system. Transmission is propagation of the electrical nerve impulses in the nervous system. This moves the nerve impulse from the site of tissue damage to the spinal cord. Modulation is amplification, inhibition or suppression of nerve pain signals within the spinal cord. Perception is the integration, processing and recognition of nerve signals in the brain. Perception is how the animal feels pain and is a subjective experience. Signs of pain can be classified as either behavioral (i.e. vocalizations, inability to rest, agitation, change in temperament, drop in activity level, insomnia, inappetence, immobility) or physiological (i.e. tachycardia, tachypnea, hypertension, hyperthermia, increased metabolic rate, decreased GI blood flow, immune-suppression). Pain assessments should be included in the physical assessment of a patient. Monitoring for changes in pain using pain scoring systems is a great way to determine if pain is being managed appropriately or if additional pain relief therapies are needed. Pain, if left unidentified/untreated, leads to greater morbidity, mortality, and suffering. Nursing care & tender loving care
456

Providing nursing care to the critically ill involves a skilled, knowledgeable, attentive and trained nursing staff. Nursing care are all the things that go above and beyond and that might not explicitly be listed on the treatment sheet. Things like giving soft/plush bedding, physical therapy for recumbent patients, warming up food, providing urinary catheter care, ensuring cleanliness/baths, giving “privacy screens” for timid patients, applying eye lubrication for patients in oxygen kennels, flushing IV catheters to ensure patency when not on IV fluids, evaluating pain scores, etc. It is our job to care for our patients and be their advocate. All patients should be handled and spoken to kindly in order to help minimize stress and anxiety that can develop in a hospital setting. Taking the extra time to love and snuggle on your patients gives us a mental break and helps patients feel better. References
1. Silverstein DC. Small animal critical care medicine. St. Louis, MO: Elsevier, Saunders; 2015. 2. Scalf R. Study guide to the AVECCT examination. San Antonio, TX: AVECCT; 2014 3. Battaglia AM, Steele AM, Battaglia AM. Small animal emergency and critical care for
veterinary technicians. St. Louis, MO: Elsevier; 2016. 4. Norkus, C. Veterinary technician’s manual for small animal emergency and critical care.
Hoboken, NJ: Wiley-Blackwell; 2013. 5. Creedon, J. M., & Davis, H. (2012). Advanced monitoring and procedures for small animal
emergency and critical care. Oxford: Wiley-Blackwell.
457

Dental and oral abnormalities By Denise S. Rollings, CVT, VTS (Dentistry) Pet Dental Education, LLC. Even though as technicians we are not allowed to diagnose disease, we certainly should be able to recognize it. No one is perfect and the more eyes, the better! The doctor may actually miss something or depend on the technician to point out abnormalities. Recognizing oral pathology is essential in order to perform proper dental charting. Abrasion (AB): wear of a tooth caused by an external source such as a tennis ball, dermatitis wear or cage chewing. Over time, this behavior may cause the teeth to wear completely down to the gingiva. Attrition (AT): wear of a tooth caused by tooth to tooth contact. This is usually seen when there is some type of malocclusion. In both situations, if this occurs slowly, reparative dentin will form, protecting the pulp. This feels smooth when an explorer is run across it. However, if the damage occurs faster than reparative dentin can form, the result is pulp exposure and repair, or removal of the tooth is necessary. Fractured Teeth: The severity of tooth fractures ranges from an Enamel Fracture (T/FX/EF); Uncomplicated Crown Fracture (T/FX/UCF): involves the dentin but not the pulp canal; Complicated Crown Fracture (T/FX/CCF): involves the pulp canal; Uncomplicated Crown Root Fracture (T/FX/UCRF): fractures involving the crown and root but not the pulp canal; Complicated Crown Root Fracture (T/FX/CCRF): fracture of the crown and root involving the pulp canal; Root Fracture (T/FX/RF): fracture of the root; Any fracture that involves pulp exposure is painful and can be a source of infection. These teeth need to be repaired for removed! Non-Vital Teeth (T/NV): this is sometimes also referred to as pulpitis; appears gray, pink or purple and may even turn tan or brown in color; it is a result of pulpal hemorrhage caused by some type of trauma. Carious Lesion (CA): is sometimes referred to as a cavity; It is the result of tooth decay from the acid produced by the plaque bacteria fermenting carbohydrates; usually brown in color and an explorer will stick. These are often found on the occlusal surface of the maxillary first premolar in dogs although it can occur on any surface. If it is caught early enough it can be repaired with a filling similar to a humans or if it’s into the pulp canal the tooth must be extracted. Missing Teeth: may actually be missing, previously extracted, unerupted, fractured off crown or may have fallen out. All missing teeth must be radiographed to determine if there are retained tooth roots, an impacted or embedded tooth or a dentigerous cyst. A dentigerous cyst can cause bone destruction and must be completely removed.
458

Crowded (CWD) or Rotated (ROT) Teeth: very common in brachycephalic breeds; these teeth can cause periodontal disease. Strict home care is necessary or selective extraction of these teeth should be considered. Supernumerary Teeth (SN): extra teeth; if they are causing crowding they should be removed. Persistent Deciduous Teeth (DT/P): may also be referred to as retained; may cause malocclusions or crowding. A radiograph must be taken to determine if there is an adult tooth that hasn’t erupted yet. If so, the RD must be removed. Oronasal Fistulas (ONF): Occurs when periodontal disease erodes the bone separating the oral cavity from the nasal cavity. This can happen with any tooth in the maxilla but is most common with the maxillary canine teeth and may result in sneezing or nasal discharge. Probe all the way around to tooth as these most often occur on the palatal aspect. Removal of the diseased teeth and a tension free closure of the site is necessary. ONF is very common in dachshunds. Tooth Resorption (TR): previously called FORL, neck lesion, cervical line lesion, cat cavity. Tooth resorption can occur in any mammal however we see most often in cats. The cause is unknown. It is the destruction of mineralized tissue, including the enamel, dentin and cementum. All or part of the tooth may be destroyed. An explorer is run along the tooth and it will catch in the defect. Intra oral radiographs are necessary to determine the proper treatment which may be extraction or crown amputation. Tooth resorption is painful. Do not leave these teeth to deteriorate. There are 5 stages and 3 types of tooth resorption and will be discussed in detail in another lecture. Canine tooth resorption is a bit different than feline tooth resorption. It is usually caused by excessive force applied to the periodontal ligament such as hard chewing, malocclusion, or trauma. It is thought to be non-painful unless it occurs in the crown or the gumline, or if the dog appears painful, then the tooth should be extracted. Stomatitis (Caudal Mucositis): The cause is unknown. Signs include halitosis, not eating or grooming or appearing painful while eating or grooming, drooling, or screaming when yawning. This condition is very painful. Full mouth extractions often are necessary even when medical management has been attempted and continued after extractions. Often time the canines and incisors are left and may need to be extracted in the future. Some cases do not respond to any treatment and we have to try to control the pain as best as we can. Steroids or laser therapy may also be attempted. Chronic Ulcerative Paradental Stomatitis (CUPS): also known as Buccal Mucositis. Occurs most often in dogs. It is caused by an immune response to the plaque bacteria on the teeth. Any paradental surface that touches the crowns of the teeth becomes inflamed, ulcerated and painful. There is often severe, necrotic smelling halitosis. Plaque control is essential in controlling the process and often full mouth extractions are necessary and curative. Furcation Exposure (F 1-3): The horizontal bone loss in between the roots of a multirooted tooth. F1: the probe goes less than halfway through the furcation F2: the probe goes halfway
459

through the furcation F3: the probe goes all the way through the furcation. F1 and F2 can be salvaged with curettage. Daily brushing in essential in saving these teeth. The owner needs to be aware of the commitment and instructed on proper brushing. F3 needs to be extracted. Mobility (M 1-3): Mobility is measured in mm by how much the tooth moves from its axis. Use the probe to rock the tooth to check for mobility. M1: is movement less than 0.5mm. M2: is movement 0.5mm to 1.0mm M3: is tooth movement greater than 1.0mm and these teeth need to be extracted. Periodontal Pocket (PP): Every single tooth in the mouth should be treated a separate patient. There are 42 patients in the dog mouth and 30 patients in the cat mouth. Use a periodontal probe to walk around the entire tooth. The normal gingival sulcus in a dog is 3mm or 5mm in a giant breed and any pocket in a cat is pathological. Any abnormal depth should be documented in the dental record. Closed root planning should be performed on pocket depths less than 5mm and open root planning should be performed on pocket depths greater than 5mm. The owner must provide daily home care to help prevent periodontal disease from getting worse. Malocclusion (MAL): MAL/1 is when the jaws are in normal relation to each other but one or more teeth are out of alignment. Basenarrow canines are a condition where the mandibular canines are lingually displaced and hit the hard palate. The treatment is extraction, crown reduction with vital pulp therapy or orthodontic movement. This is a painful condition and should not be left untreated. Every pet should have a comfortable bite. Other MAL/1 are base-wide canines leading to lip trapping; Lance tooth: in which a tooth is mesio or retro versed and may be contacting other teeth as seen commonly in the sheltie. Orthodontic movement or extraction of these teeth should be performed is there is contact with other teeth causing pain; Rostral crossbite: incisors touch end to end or are labio or palatally versed; Caudal crossbite: The maxillary fourth premolar is lingual to the mandibular first molar. This is common in collies and sight hounds.
• MAL/2: The lower jaw is short in relation to the upper jaw and teeth may be malpositioned • MAL/3: The lower jaw is long in relation to the upper jaw as is commonly seen in brachycephalic breeds. The maxillary incisors may be contacting the gingiva lingual to the mandibular incisors causing trauma and pain. The treatment for any malocclusion causing trauma is extraction, crown reduction with vital pulp therapy or orthodontic movement. The recovery time, commitment of the owner to bring the pet back for multiple visits and ability to do home care should be considered when deciding the treatment plan.
Oral Mass (OM): Any abnormal tissue in the mouth should be biopsied and sent out for histopath. We cannot determine what the tissue is without it as our eyes are not microscopes! Some common benign oral masses seen in our pets include: Acanthomatous Ameloblastoma: originate from the odontogenic tissue and is locally invasive and rarely metastasize. They are usually firm, smooth and located rostrally on the mandible and maxilla. The mass should be excised including any teeth contacting the mass. Gingival Hyperplasia (GH): an overgrowth or
460
enlargement of the gingiva, commonly seen in boxers, bulldogs, pugs and Boston terriers. Some medications such as cyclosporine may promote the growth of GH. Gingival hyperplasia forms psuedopockets entrapping plaque bacteria and debris promoting periodontal disease. It should be excised to decrease pocket depth and diligent home care is a must. Papilloma: benign and viral in origin. They are contagious between dogs and commonly seen in younger dogs. Papillomas may resolve spontaneously and may reoccur. They should be removed if there is bleeding or cause difficulty eating. Malignant oral tumors are invasive and may metastasize. A veterinary dentist and oncologist should be considered for treatment that may include surgery removal, chemotherapy or radiation. Fibrosarcoma: slow growing, firm, flat and locally invasive. Usually occur on the maxilla. Malignant melanoma: usually pigmented but may be amelanotic and therefore are pink or red and occur on the gingiva and buccal or labial mucosa. They are highly invasive and commonly metastasize. Squamous cell carcinoma: ulcerative and red in appearance. Most common oral tumor in cats and can be found anywhere in the mouth. Always check under the tongue to check for abnormal tissue. SCC is locally invasive and rapidly growth. Prognosis is poor. Enamel Hypoplasia (EH): hypo mineralization of the enamel that occurs usually during the first few weeks of life when the animal has a high fever. The enamel producing cells are damaged by the fever. It can affect one or all teeth. Avulsed or partially avulsed tooth: The tooth is completely or partially out the socket. This is a dental emergency and may possibly be salvaged with trip to a veterinary dentist ASAP for treatment. References
• Blackwell’s Five-Minute Veterinary Consult Clinical Companion Small Animal Dentistry. Lobprise, Blackwell Publishing; Ames; 2007
• Small Animal Dental Procedures for Veterinary Technicians and Nurses. Perrone; Wiley-Blackwell; Ames; 2013
• Veterinary Dentistry for the Small Animal Technician. Kesel, Blackwell Publishing Company, Ames; 2000
• Veterinary Dentistry for the Technician and Office Staff. Holstrom; Saunders: Philadelphia; 2000
461
Feline dentistry By Denise S. Rollings, CVT, VTS (Dentistry) Pet Dental Education, LLC. General anatomy The juvenile feline dentition is as follows:2 x (3/3 i, 1/1 c, 3/2 pm) = 26 teeth. Notice there are no molars in the young feline patient. The permanent adult feline dentition is as follows:2 x (3/3 I, 1/1 C, 3/2 PM, 1/1 M) = 30 teeth. The adult feline naturally is missing the 1stmaxillary premolar, and the mandibular 1stand 2ndpremolars. This is recognized in the Triadan numbering system therefore 105, 205, 305, 306, 405 and 406 are missing. The jaws should be of equal length with teeth that interdigitate into a normal scissor bite. Any deviation from this is considered a malocclusion. A class 3 malocclusion is commonly seen in Persian cats where the lower jaw is long in relation to the upper jaw causing crowded and rotated teeth. Feline tooth resorption Tooth resorption has had many names over the years including cervical neck lesion, cervical line lesion, feline odontoclastic resorptive lesion (FORL). It is now officially called tooth resorption as many species develop tooth resorption, not just the feline. Tooth resorption is the destruction (resorption) of the hard-dental tissue by odontclasts. There have been many, various studies on this topic and the etiology of tooth resorption is still not known definitively. Tooth resorption can be seen in cats of any age however it’s usually not seen before the age of 2 years and the number of lesions increase with age. Since there has been an increase of incidence of tooth resorption since the 1970’s, it is thought that changes in diet, introducing commercial foods, indoor lifestyle, and other factors may have an influence. While any tooth can develop tooth resorption there seems to be an increased predilection of teeth 307 and 407 to develop tooth resorption first. There is no way to predict which teeth will develop tooth resorption or predict how fast it will progress. This can cause a lot of frustration for the pet parent so it’s important to explain the disease process, the treatment and the prognosis the best way we can. Tooth resorption is painful because the exposed dentinal tubules and pulp, plain and simple, it’s painful. Signs include jaw chattering, head shaking, dropping food, oral bleeding or less commonly, anorexia. Clients may notice missing teeth since as the disease progresses, the tooth is destroyed, and granulation tissue fills the defect in. There are five stages of tooth resorption as defined by the American Veterinary Dental College. Stage 1 (TR 1): Mild dental hard tissue loss of the enamel and/or cementum. This is the hardest stage to identify and may be visual but may only be tactile by running an explorer along the tooth. Stage 2 (TR 2) Moderate dental hard tissue loss of the enamel and dentin or the cementum and dentin but not extending into the pulp. Stage 3 (TR 3): Deep dental hard tissue loss with loss of the enamel or cementum and dentin and extending into the pulp chamber or canal. Most of the tooth retains its integrity. Stage 4 (TR 4): Extensive hard dental tissue loss extending into the pulp. Most of the tooth has lost its integrity. This stage is divided into substages.TR 4a: Crown and root are equally affected. TR 4b: Crown is more affected than the root. TR 4c: Root is more affected than the crown. Stage 5 (TR 5): The crown is no longer visible
462
and there is no recognizable tooth structure remaining of the crown or root. There may be hard bump of tissue still present. Tooth resorption is further divided into three types based on radiographic appearance:
• Type 1: The appearance of the tooth is relatively normal radiopacity and a normal periodontal ligament space with either a focal or multifocal radiolucency.
• Type 2: The appearance of the tooth has either focal or multifocal radiolucency within the tooth and a loss or narrowing of the periodontal ligament space.
• Type 3: This includes both Type 1 and Type 2 and is only seen in multi-rooted teeth. There will be areas of normal and narrowed periodontal ligament space with either focal or multifocal radiolucency. In order to diagnose tooth resorption, a complete oral exam including the use of a dental explorer with the patient under anesthesia needs to be performed and full mouth intraoral dental radiographs need to be obtained. The plaque and calculus should first be scaled off. The explorer should be run along the tooth with the most likely area for tooth resorption being the cementoenamel junction. The explorer will “stick” in the lesion and check any areas of granulation tissue as well. The recommended treatment and standard of care is that any affected tooth be extracted if there is a complete periodontal ligament and intact root. The roots should not be drilled out as this does not completely remove the root and can damage the bone and nerves. A crown amputation with intentional root retention can be performed with Type 2 tooth resorption when there is no visible periodontal ligament on the radiographs. This treatment is less invasive and can only be performed if there is no periodontal disease, endodontic disease or mucositis (stomatitis). In the case of Stage 5 tooth resorption, if there are no root remnants and the gingiva has healed over and is smooth, no further treatment is needed. Gingivostomatitis Gingivostomatitis is the inflammation of the gingiva and oral mucosa with ulcerative or proliferative lesions. These lesions can occur on the lateral aspects of the tongue, pharyngeal walls, palatal glossal folds, buccal mucosa, lips and gingiva. It’s very painful and debilitating. As with tooth resorption, there is no known cause. One theory is that it’s caused by a hyperimmune response to the plaque bacteria in the oral cavity. Viral etiologies such as calcivirus, herpes virus, feline leukemia, feline immunodeficiency virus, and feline infectious peritonitis along with Bartonella henselae infection, have been suspected although a cat with gingivostomatitis does not mean it has one of these viruses. The most common signs we see in our patients with gingivostomatitis are severe halitosis, blood tinged saliva, screaming while eating or yawning, running away from the food bowl, drooling, or weight loss. The affected tissue is red, swollen, and ulcerated. To properly diagnose gingivostomatitis, a complete oral exam and biopsy of the affected tissue should be obtained and sent out for histopath to rule out other diseases such as squamous cell carcinoma, severe periodontal disease or eosinophilicgranuloma. In addition, full mouth radiographs and blood work including viral screening are recommended. Gingivostomatitis is difficult and complicated to treat. The goal is to reduce or remove the plaque in the mouth. Often times a combination of treatment is necessary to control the disease. Medical management does not cure the disease. It’s an attempt to control pain and inflammation. Analgesics, anti-inflammatories, antibacterials,
463

immunosuppressants, antivirals and steroids are often used. Cats have a high sensitivity to NSAIDS so extreme caution must be used especially with long term use. Fentanyl and buprenorphine are relatively easy to give transmucosally or transdermally. Antivirals may help if herpes is the known cause. The body can begin to destroy its own tissues, creating significant inflammation, when the immune system is activated, therefore, immunosuppressives such as prednisolone or cyclosporine, may help provide relief. Antibiotics such as Doxycycline can help decrease the bacterial load in the mouth. Home care includes daily tooth brushing, which may be very difficult in an extremely painful cat. Surgical treatment is the most common treatment. Often the cat owner is hesitant to have the teeth extracted. It’s important that we stress to the owner that cats do just fine and eat well without any teeth and will indeed feel better without any teeth. Surgical extractions of all the teeth and roots and any retained tooth roots is ideal. The patient can have up to an80%cure rate. The earlier on in the disease the extractions are performed, the better the resolution. Some veterinarians prefer to extract all cheek teeth and try to leave the canines and incisors, knowing the remaining teeth may need to be extracted in the future. Daily brushing to control the plaque on the remaining canines and incisors is essential. It is also important to inform the owner of the possibly to need further extraction and the commitment to daily home care. Other veterinarians prefer to do full mouth extractions and not take the chance of leaving the canines and incisors. In either case, medical management may still be needed. It can take 3-6 week to see resolution of the inflamed tissue following extractions so multiple recheck appointments are a must to make sure the cat is responding and comfortable. Another option for treatment is laser therapy to help reduce the proliferative inflamed tissue therefore decreasing the bacterial holding surfaces. Medical management and extraction may still be needed. Early diagnosis and treatment is imperative for the best outcome for the patient. Squamous cell carcinoma Squamous cell carcinoma is the most common oral tumor that occurs in cats. It occurs most often in the premolar and molar region of the maxilla and the premolar area of the mandible along with the sublingual region. The lips, buccal mucosa, tongue, oropharynx and tonsillar region are also common. There does not appear to be a sex predilection. SCC is highly malignant and locally aggressive. Treatment for SCC is surgical excision with 1-2 cm margins from radiographic evidence of the mass involvement. Due to the already small size of the cats’ oral cavity and depending on the location and size of the tumor, this can be difficult. Radiation therapy for palliative treatment is an option or in combination with surgery. Chemotherapy agents do not appear to be effective in treatment SCC. Regardless of any or all treatments, SCC has a very poor prognosis. References
• Blackwell’s Five-Minute Veterinary Consult Clinical Companion SmallAnimal Dentistry. Lobprise, Blackwell Publishing; Ames; 2007
• Small Animal Dental, Oral & Maxillofacial Disease. Niemiec,Manson Publishing; London; 2010
464

• Small Animal Dental Procedures for Veterinary Technicians and Nurses. Perrone, Wiley-Blackwell; Iowa; 2013
465

From the exam room to the dental table By Denise S. Rollings, CVT, VTS (Dentistry) Pet Dental Education, LLC. Veterinary dentistry isn’t just about cleaning teeth or getting rid of bad breath. A dental procedure is an anesthetized procedure that requires trained and educated veterinarians and veterinary technicians. Dentistry should be treated like every other anesthetized procedure that takes place in the veterinary hospital. Only veterinarians can diagnose disease, but the veterinary technician plays a major role in assisting the veterinarian. The veterinary technician assists by obtaining an accurate history, recognizing pathology and bringing it to the doctors’ attention. The veterinary technician can be trained to perform a proper and thorough dental cleaning and obtain diagnostic dental radiographs. Periodontal disease is the top disease diagnosed in dogs and cats with 80% of all dogs and cats over the age of 3 having some stage of periodontal disease. Every patient should be receiving routine dental care. The following outlines the steps of the dental procedure day. The pre-anesthetic exam Oral history and oral exam: Look for and ask the owner about: bad breath, swollen, red, or bleeding gums, excessive drooling, changes in eating or chewing habits including dropping food, going to the food but not eating, vocalizing while eating, tooth loss, and disinterest in toys. Often times, pets show no signs of pain. Find out what the pet chews on and any and all home dental care. A patient may avoid a toy or a particular food due to pain and the owner may perceive it as the pet not liking that item anymore. Blood work: A lot of our patients are geriatric, and we need to make sure there isn’t underlying disease. Age is not a disease. Age can predispose our patients to having coexisting disease. Ideally lab work should be done before the day of the procedure in case there are abnormalities found. Having the lab work completed ahead of time will prevent a procedure from being cancelled the day of the procedure due to abnormalities. It will also allow the patient to be treated for the abnormalities ahead of time and also allows that patients’ protocol to be tailored to their needs. A chemistry panel, complete blood count, +/- coagulation panel, urinalysis, chest radiographs, echocardiogram, ECG, and blood pressure should be considered for evaluation. Client communication: It takes a person three times to hear something before it sinks in. The doctor discusses it, the technician goes over it with paperwork and the client service representative mentions it again and offers to schedule the appointment. Handout a dental report card, pamphlet, and/or treatment plan. Greenies and Virbac have premade report cards so you don’t even have to make your own. If you are ready to take on making your own, use what’s available. Don’t reinvent the wheel. The day of the procedure Perform another physical exam upon admission including a TPR and hydration status. Make sure you get and all phone numbers and emergency numbers. Tell the owners they must be able to be reached and have someone else as back up to make decisions on their behalf. Know the owners wishes and have it in writing in case of an emergency. The technician should review the treatment plan, estimate, and consent forms again with the client. The treatment plan should be as accurate as possible, and the technician should go through it with the client line by
466

line. One can use pictures, models, skulls, videos, and charts to explain procedure, pathology, and importance of the treatment. There should be a low and high-end range on the estimate as a worst-case scenario. This will help prevent stress to the client and the staff over unexpected expenses. Take a deposit for the low end of the estimate in the morning and take care of the difference at discharge. The doctor and technician should review the history and lab results. An American Society of Anesthesiologist (ASA) Physical Status Scale should be assigned to each patient: Class I Normal healthy patient, no underlying disease, minimal risk. Class II Mild systemic disease, animal able to compensate, slight risk. Class III Obvious disease present, moderate systemic disease, moderate risk Class IV Significantly compromised by disease, severe systemic disease, high risk. Class V Moribund, life threatening systemic disease, extreme risk. An anesthesia plan including PAIN CONTROL should be tailored for each and every patient based on that particular patients needs and health status. Anesthesia should not be “cookie cutter”. Pre, intra, post, and at home pain medication equals a multimodal approach to pain management. Premedicants can be a sedative that will help reduce stress in the fearful patient. During the procedure, opioids allow for lower inhalant anesthesia because of the analgesic properties. Protocols should be based on patient’s information, PE, workup status and temperament, preexisting conditions. As mentioned earlier, age is not a disease. An Induction agent should be selected as well because all our patients need to be intubated. Nerve blocks can be used intraoperatively to help reduce the amount of inhaled gas anesthesia used and help our patients have a smoother anesthetic procedure and recovery. Nonsteroidal anti-inflammatory can be considered on an individual basis. Protecting yourself Personal Protection Equipment (PPE): Wear eye protection! Goggles, loupes, or a visor should be worn by everyone in the operatory area as pieces of calculus, tooth, bone, blood, saliva, and even broken burs become airborne and can cause an eye injury or infection. Surgical face mask that covers mouth and nose should be worn. Anti-fog masks are helpful in preventing protective eye wear from fogging up. Appropriately fitted gloves and protective clothing such as a gown or lab coat and surgical caps should be worn to prevent bacterial contamination of clothing and hair. Consider hearing protection if the noise of the dental unit running is bothersome. Ergonomics is an applied science concerned with designing and arranging the things people use so that it is efficient and safe. Dentistry is a lot of small, repetitive, movements that can strain our muscles, tendons, and ligaments. In order to protect ourselves from fatigue and short- or long-term injury, we should practice the best ergonomics possible. Lift tables adjust to an individual, so arms are parallel with the table. A dental saddle seat allows one to sit it with back straight, thighs slightly angled to the floor, and gaze looking down; not bending over. Utilizing a modified pen grasp when holding instruments reduces strain of repetitive movements. Fatigue mats can be used if one is standing for long periods of time Patient monitoring
467
Nothing replaces a qualified person who can access values, interpret changes and intervene when needed. Several parameters should be monitored; however, the equipment should never be a substitute for hands-on human monitoring. Heart Rate: Use a stethoscope to auscult the heart sound and the pulses should be checked manually. Pay attention and make note of the strength of the pulse. Quality is as important as quantity. Respiration: Evaluate both quantity and quality. Respiratory failure can lead to cardiovascular failure. Check mucous membrane color and capillary refill time. Increased respiratory rate could mean light anesthetic depth and decreased respirations could mean a deep anesthetic plane. Measures should be taken to correct both of these. Blood Pressure: Hypotension is a very common complication of anesthesia but that doesn’t mean it’s okay. Hypotension needs to be addressed and corrected as needed. Blood pressure can change due to depth of anesthesia, shock, strength of cardiac contraction, and blood volume. Systolic pressure should stay about 80-90mmHg and mean arterial pressure should stay above 60mmHg to make sure the vital organs receive adequate profusion. Intravenous fluids and decreasing anesthetic depth can help perfusion. End Tidal Carbon Dioxide: A capnograph measures the end tidal (ET) CO2 level in the patient. It allows for assessment of ventilation over time using a graphic display. The end tidal CO2 should be between 35-45mmHg. Common problems are: improper placement of the endotracheal tube, a leaking cuff of an endotracheal tube, or apnea to name a few. Electrocardiogram: ECG should be continuously monitored so any changes or abnormalities in the electrical changes or heart rate can be recognized early. Pulse Oximetry: Measures the arterial oxyhemoglobin saturation. Oxygen saturation should be between 98-100%. Causes of saturation of 90% or less include hypovolemia, anemia, shock, probe becoming dislodged, low respirations, or poor ventilation. Temperature: Keep patients warm. Our patients become very wet during a dental procedure and therefore are at risk of hypothermia. Monitor temperature throughout the entire procedure. It is easier to maintain temperature than try to warm them up once they are cold. Cold pets become hypotensive, bradycardic, develop arrhythmias, and hypothermia can decrease kidney function, prolong recovery and prolong healing. Use warm air heaters, circulating water blankets, wrap feet, and keep the pet as dry as possible. Check the temperature of the warming devices as well. Do not allow for thermal burns and do not leave an unconscious animal on heat without being monitored. Intravenous fluids: Keep patients on an IV fluid pump to ensure they are receiving the proper amount of fluids and to help prevent accidental fluid overload. Monitor fluid rate and change as needed. Use an appropriate rate of 2-10ml/kg/hr based on health, hydration, and blood loss of the patient. Decrease the fluid rate for patients with cardiac disease.
468
Steps to the complete dental procedure There should be a qualified technician monitoring anesthesia and a qualified technician performing the dental procedure. It is not safe for one technician to be doing both. Neither job cannot be performed correctly or safely if one person is doing both. Start with a pre-intubation exam. Check the occlusion of the patient before intubation. Once the patient is intubated, the endotracheal tube will prevent the mouth from closing. Take pictures of the occlusion so there’s reference to look at if attrition is found on the complete oral exam. Note asymmetry of the head and muscles, look for draining tracts, check lymph nodes and skin around mouth. Open the mouth to check the range of motion before induction. Once the pet is under anesthesia, obtain photos before cleaning the teeth. Check all surfaces of the teeth and note calculus, plaque, and missing teeth. Check the buccal mucosa, tongue, and palate for any abnormalities including granulomas, chewing lesions, lacerations, ulcerations, or oral masses. Rinse the oral cavity with 0.12% chlorhexidine solution. This reduces the number of bacteria the staff and patient are exposed to during the procedure. Leave on for a few minutes or even brush the teeth with it before starting. Remove supragingival plaque and calculus. This is most important to the owner because it is what they see, however it’s the least important to the patient. Use the powered (ultrasonic, magnetorestrictive, or piezo) scaler to begin with. Do not spend more than ten seconds on a tooth at a time and be sure you are using enough water to cool and irrigate the tooth. Remove subgingival plaque and calculus with a curette or perio tip. This is the least visible to the owner but the most important to the patient. Plaque bacteria is the cause of periodontal disease, not calculus. The plaque must be removed from any subgingival space. Check your work. Use the air water syringe to rinse the mouth of calculus and blood and then to dry the teeth. Look for the chalky white residue that remains on the teeth. That’s the calculus that has been missed. Remove what is left with a hand scaler and/or curette. Polish the teeth using fine or flour grade paste above and below the gum line. Flare the polishing cup under the gingival sulcus. Use a light touch and spend only five to ten seconds or less per tooth. Polishing smooths the tooth surface and removes irregularities created by scaling. This decreases the surface area for plaque bacteria to stick to. Once all of the calculus and plaque have been removed and teeth polished, rinse the tooth surface and sulcus to remove debris, and paste. At this point, some like to apply fluoride. Fluoride can decrease sensitivity. Do not use in renal patients because fluoride is excreted through the kidneys and our patients cannot spit it out. Obtain full mouth radiographs! Radiographs are a must and are part of comprehensive oral exam. We can see the crown and determine periodontal pockets, but we can’t see what’s there. Radiographs tell us if a tooth can be repaired or if it needs to be removed. This is an extra diagnostic tool. The majority of pathology is below the gum line. 80% of the dental anatomy is not visible. Radiographs must be obtained post extractions as well. Charting: Use four handed dentistry. The doctor performs a complete oral exam using probe/explorer and technician documents the findings. A technician can be trained to perform
469
a complete oral exam; however, a veterinarian must diagnose pathology. Probe every single tooth. Walk the probe around the entire tooth measure pocket depth. The explorer is run along the gum line and occlusal surfaces to check for imperfections. It’s very tactile and one will feel the “ping” or sticky. Note all furcation exposure, mobility, gingival recession, enamel defects, fractures, tooth resorption, oral masses and caries. A treatment plan should be customized for each tooth in every patient based on the complete oral exam, probing, and intraoral radiographs. Surgery, extractions, and advanced dental procedures must be performed by a veterinarian. Take post procedure photographs of both sides and cover the endotracheal tube with the tongue so it doesn’t look to scary to the owner in the picture. During anesthetic recovery, check temperature, blood pressure, heart rate, and respiratory rate post operatively. Most of our dental patients are not young spay and neuter patients, they are geriatric and may be compromised. Watch them closely. Clean their faces! Do not send a wet, bloody faced pet home. Rinse the face and dry thoroughly. Keep them comfortable. Do not let them sit in urine or feces. Return them to their owner in almost the same condition (or better) they came in as. Enter charges for the procedures performed. Charge for your and the doctors time. Transfer the pre and post pictures and radiographs to be printed or emailed to the owner. Discharge instructions Personalize the instructions based on the individual’s condition. Include feeding instructions, medications and recheck dates. Have the directions and instructions for medications to go home in writing for the owner. It should include when the owner should start the medications, how often to give them, how many to give, what the medication is for, and for how many days. If oral surgery was performed, the pet’s needs to be rechecked to make sure all sites are healed anytime between 7-14 days post operatively. They should also come back in 3, 6, 9 or 12 months for an oral exam and this is determined by the extent of periodontal disease present and the breed. Toy breeds are more predisposed to have periodontal disease than large or giant breed dogs. Discuss this with the owner. Put reminders in the computer to generate a reminder for future appointments. Discuss home care with the owner when they bring the pet back for the follow up exam. They are usually overwhelmed at the time of surgery and may not comprehend the conversation. Send a packet home with samples of all of the products you carry that may be appropriate for that patient. Explain what they are and how they work. Now that the teeth are nice and clean, we need to keep them that way. Don’t pat yourself on the back yet. Bacteria are already multiplying as they are walking out the door. Educate the client on the importance of home care to help protect their investment. Proper dentistry takes a team but can be achieved so we can improve the lives of pets, one tooth at a time.
470

References • Blackwell’s Five Minute Veterinary Consult Clinical Companion Small Animal Dentistry.
Lobprise, Blackwell Publishing; Ames; 2007 • Small Animal Dental Procedures for Veterinary Technicians and Nurses. Perrone; Wiley-
Blackwell; Ames; 2013 • Veterinary Dentistry for the Small Animal Technician. Kesel, Blackwell Publishing
Company, Ames; 2000 • Veterinary Dentistry for the Technician and Office Staff. Holstrom; Saunders:
Philadelphia; 2000
471
What I learned on my trip to Mount Laurel Animal
Hospital and Farm
472
ChickensFun Facts:• There are more chickens living on earth than people.• Chickens can run at a speed of 9 mph.• Girl Chickens are hens and boy chickens are roosters.• A hen can lay about 300 eggs each year.
ROOSTER
HEN
CHICK
473
DogsFun Facts:
• Dogs pant when they are hot because they have no sweat glands on their body except at their paws.
• Despite their breed or size, all dogs have 42 teeth and 321 bones-all breeds.• A dog’s heart beats at 120 times/minute; compared to the human heart which
beats at 80 times/minute.
Things that are toxic and can hurt dogs 1. Chocolate2. Sugarless gum or candy3. Grapes or Raisins
shiba inu
basset hound
Pit Bull Terrier
474
CatsFun Facts:
• A cat’s sense of hearing is over three times stronger than humans • A cat’s sense of smell is over 13 times stronger than humans.• Cats sleep 16 hours or more every 24 hours.• A cat’s eyes reflect light enabling them to see in the dark.
Domestc Long Hair
Domestc Short Hair
Tabbysphynx
475
TurtlesFun Facts:
• Though turtles are very slow on land (0.1 - 0.5 mph), many can swim much faster (5 - 20mph)
• A turtle shell (made up of 60 bones) is attached to its spine - This is the reason why turtles can feel pain through their shell.
• Turtles do not have external ears to hear - they only feel vibrations. However, their sense of smell is strong.
Eastern box turtle
red-eared slider
476
GoatsFun Facts:
• Young goats are called kids• Goats communicate with each other by bleating• Goats are very intelligent and curious animals. • Goats have excellent coordination. They have great balance and are
thus able to survive living on mountains. They can even climb trees and some species can jump over 5 feet high.
477
SheepFun Facts:
• Some Sheep have horns and some do not• Sheep have wool for hair and is used for making clothing and blankets• Many sheep are born as Twins• Sometimes the milk from sheep is made into Feta cheese
478

EmuFun Facts:
• Emus are birds but they can’t fly.• They are the second largest birds in the world. The largest is the Ostrich.• They can run at 30 miles per hour. • Emus can swim • An emu can grow to between 5 to 6.5 feet in height and can weigh up to 130 lbs. • Emus lay large blue/green eggs. The eggs are bigger than a softball.
479
VeterinarianWhat is this job like?If you like animals and science, you might want to be a veterinarian. Veterinarians are animal doctors and take care of sick and injured animals. They perform surgery and give medicine.When an animal is sick, vets examine it to find out why. They look for clues in the way an animal looks, acts, and smells. For example, if a dog is walking in a strange way, that might be because it hurt its leg. Vets need to look carefully because animals can’t say what is wrong. Vets also give blood tests, x-rays, and other tests, looking for clues about an animal’s illness. Then, vets decide what kind of medicine the animal needs. Vets prevent problems by giving vaccinations and check-ups and fixing teeth. They also teach owners how to feed and train their animals.Vets use special tools to perform surgeries. They fix broken bones, take out tumors, replace knees and hips, and more. Vets also treat and cover wounds. They need to be ready to see blood, organs, and bones.Most vets treat small pets, including dogs, cats, and gerbils. But a few focus on large animals, such as sheep, cows, and horses. Large-animal vets usually drive to ranches and stables where their patients live. They check for infections in the animals and give advice to the animals’ owners. Often, they help when the animals give birth. A few vets work in zoos and aquariums. They care for zebras, sharks, and other wild crea-tures.In addition to helping sick animals, vets can work as animal inspectors, checking to make sure that farm animals are healthy and that their living spaces are clean. Another option for vets is doing scientific research. They try to make new medicines.Vets work in many different places. Vets who do research work in laboratories. Most vets who take care of animals work in small clinics and hospitals. But some work in large hospitals with the most advanced equipment. Many vets supervise technicians and assistants. And many own their own business and are their own boss.Because animals can get sick at anytime, vets often work long hours. Those in group practices may take turns working weekends or evenings and dealing with emergen-cies. Many vets like their work because they can be with animals every day. But because some animals are scared or hurt, they sometimes try to bite, kick, or scratch their vets.
Being a veterinarian is a fun but challenging profession.480
Pets are awesome!They’re also a big responsibility! Just like you,
pets need to be cared for and loved.
CAPTAINNOODLES
481
ms_57223
Stamp
12
6
9 3
CAPTAINNOODLES
A pet doctor is called a veterinarian.
Pets need to visit the doctor for
regular checkups.
482
CAPTAINNOODLES
Help your pet stay healthy. Don’t feed them food o your plate or too many treats!
Pets need fresh water & healthy food.
Did you know a dog’s nose print is just as unique as your ngerprint?
What if you had a nose like a dog?
INSTRUCTIONS: Color and cut out the image above. Use string to place the nose over your own!
484
INSTRUCTIONS: Help Captain Noodles nd his way back home.
CAPTAINNOODLES
Pets need proper identification. An ID tag and microchip can help get
pets home if they are ever lost.
485
CAPTAINNOODLES
People toothpaste is not good for pets and can make them sick. Use only toothpaste made for pets!
Pets need their teeth cleaned regularly!
PETBEDCAT
IDTAGRABBIT
DOG
VETERINARIANCLEANTEETH
LOVESNAKEMEOW
A L B A I J L Y W L S N C V P
F O N D P F T V D K A D O T I
R E T E V A Q Y C I X F D A S
W A J A C M K H R L S B H W U
G O B M C L E A N T E E T H O
V T E B D E N M K M V H T S B
O N A M I I M O S C O N Z N X
F L Y M R T N S N P L T J A R
D O G E A B B F Y C T Z H K N
P N T A P U S A B H W X H E Y
A E J R S F M H L R L R K K Q
V F U S S G L S A W E X L U X
K G O R E T A W F C K R J E V
Q E Y G N M T D E P H Y S I E
K D U Q K D B O X G K T Z I J
W X A P E T B E D C I R V Q B
Pets need a warm, safe place to sleep.
WATER
INSTRUCTIONS: Find all words listed above in the word search.
Zzzz...
CAPTAINNOODLES
487

Pets need exercise.
CAPTAINNOODLES
INSTRUCTIONS: Circle 5 things dierent between each pet set.
CAPTAINNOODLES
488
INSTRUCTIONS: Draw a picture of you and your pet in the heart above!
Pets need lots and lots of love!
489
I promise to care for my pet and provide:
Regular visits to the veterinarian
Healthy pet food and water
Proper identication
A warm, safe place to sleep
Lots of exercise
Lots of love and aection
Your name
My Pet Promise.
Your pet's name
490
the science of loving pets
491
Dear Students,
When you love pets, it’s only natural to want to learn as much as you can about them and even think about having a job with animals in the future. At Banfield Pet Hospital, we know all about this because we love pets too! In this edition of Banfield Pet Academy, you are going to practice working with dogs and cats using our favorite subject — science — and experience what it is like to examine, diagnose and treat pets in your very own hospital. Using advice from our veterinarians and veterinary technicians, we’ll provide insight into how you can pursue a veterinary career.
Whether you are a pet owner, pet lover or future veterinary professional, we hope Banfield Pet Academy will show you the rewards that come with helping pets live happy and healthy lives!
Sincerely,
Your friends at Banfield Pet Hospital
492

Types of Veterinarians Small animal: Most veterinarians are small animal veterinarians, providing preventive care, treating and diagnosing illnesses, performing surgeries and delivering other routine care for cats, dogs and pocket pets, such as hamsters and guinea pigs. Some small animal veterinarians specialize in emergency care and certain diseases, like cancer.
Shelter: These veterinarians rescue and treat animals living in shelters, ensuring they are healthy and ready to be adopted into new homes.
Large animal: Large animal veterinarians specialize in livestock and large animals such as horses, cows, goats and pigs. Like small animal veterinarians, they provide exams, give vaccinations and perform surgeries, but travel to farms and ranches to provide services.
Government: Veterinarians can also work for the government in wildlife and conservation, public health, environmental health and even with the Food and Drug Administration to ensure food and drugs are safe for animals.
Zoo: These veterinarians help exotic animals in zoos and other wildlife habitats. They provide veterinary care for animals ranging from parrots to elephants and help with breeding programs, behavior management and nutrition.
493
Additional Hospital Roles Credentialed Veterinary Technician
Credentialed veterinary technicians complete their education and pass an exam certifying them to work alongside veterinarians caring for pets, assisting in surgeries, maintaining medical records and educating clients.
Veterinary Assistant
Veterinary assistants support veterinarians and credentialed veterinary technicians. They maintain the safety of pets and clients, help to provide quality veterinary care in the hospital, as well as feed and walk animals.
Hospital Receptionist
Receptionists greet and welcome pets and their owners, schedule appointments, provide home care instructions, let the medical team know of incoming emergencies and keep exam rooms clean and ready for the next patient.
494
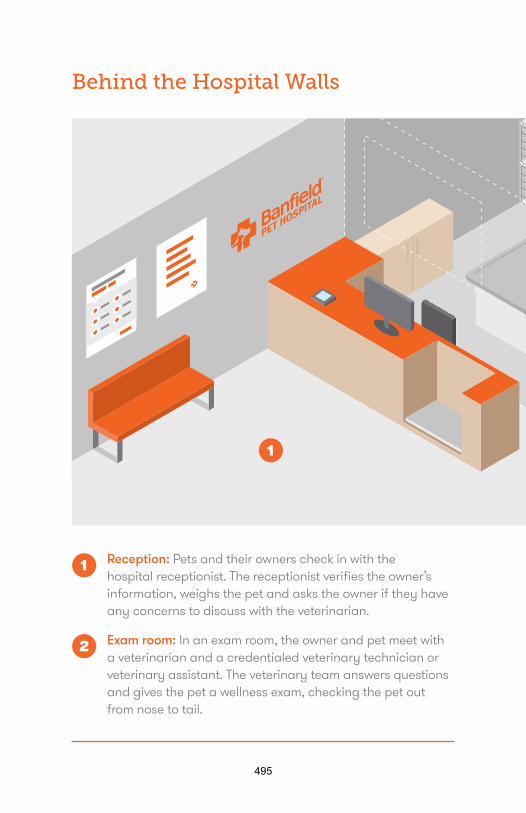
Reception: Pets and their owners check in with the hospital receptionist. The receptionist verifies the owner’s information, weighs the pet and asks the owner if they have any concerns to discuss with the veterinarian.
Exam room: In an exam room, the owner and pet meet with a veterinarian and a credentialed veterinary technician or veterinary assistant. The veterinary team answers questions and gives the pet a wellness exam, checking the pet out from nose to tail.
Behind the Hospital Walls
1
1
2
495
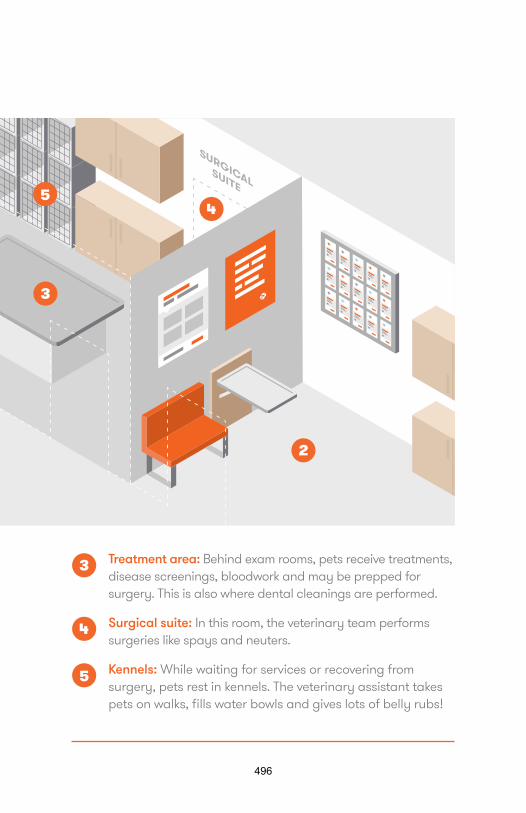
Treatment area: Behind exam rooms, pets receive treatments, disease screenings, bloodwork and may be prepped for surgery. This is also where dental cleanings are performed.
Surgical suite: In this room, the veterinary team performs surgeries like spays and neuters.
Kennels: While waiting for services or recovering from surgery, pets rest in kennels. The veterinary assistant takes pets on walks, fills water bowls and gives lots of belly rubs!
2
3
3
4
4
5
5
496
Ask-A-Veterinarian
Q: How long did it take you to become a veterinarian?
A: Programs can vary, but typically veterinarians need a four-year undergraduate degree, followed by a four-year graduate degree at a veterinary school.
Q: What’s the difference between a veterinarian and a credentialed veterinary technician?
A: A veterinarian is a doctor who diagnoses illnesses, performs surgeries and prescribes medications for pets. Credentialed veterinary technicians, like a registered nurse for humans, assist in surgical procedures and administer medication and vaccines for pets.
497
Q: What’s the best part of working in a pet hospital?
A: Every veterinary professional has a different opinion, but many would probably tell you they love making pets happy and healthy. From performing surgery, to helping pets with itchy skin, to preventing harmful diseases by giving vaccinations, the connection and bond between people and pets in undeniable!
Q: What subjects did you study in college to help prepare you for veterinary school?
A: Veterinary schools like candidates that are strong in science and mathematics. Some schools even look at your GPA in advanced science classes in undergraduate study, such as physics and organic chemistry, as a consideration in your application. It is also important to take a variety of classes and participate in diverse activities to differentiate yourself from other students who are applying.
Q: What surprised you most about this career?
A: It’s different for everyone, but it can often be surprising the level of connection and bond you make with your patients. You love them like your own pets!
498
Case Study #1 PREVENTIVE CARE IS THE BEST CARE
SCENARIO:Bella comes to your hospital twice a year for comprehensive exams. These regular visits are called preventive care because they are opportunities for the veterinarian to catch any potential problems early and give Bella vaccines to protect her from diseases. It’s also a time when Bella’s owner can ask questions and get advice from the veterinary team.
STEPS OF A WELLNESS EXAM:• First check the TPR – otherwise known as temperature,
pulse and respiratory rate• Examine the teeth and mouth• Look at the eyes and ears• Check the coat and skin• Feel the belly• Manipulate the legs
499
Preventive care is important because it can help the veterinary team detect a problem early and ensure a better prognosis, simpler treatment and an earlier recovery.
Question 1: What issues can a veterinarian detect early by examining a pet’s teeth?
Question 2: What is a veterinarian looking for when they check the coat and skin?
Question 3: Why is it important for the veterinarian to check a pet’s weight?
Question 4: What concerns might the veterinarian be looking for when moving a dog’s legs during an exam?
ANSWER: 1: Plaque and tarter build up. Dental disease in dogs and cats is very common and if untreated, can be dangerous. Annual cleaning and brushing your pets’ teeth at home can help prevent dental issues. 2: Veterinarians are looking for lumps, bumps, fleas and ticks and signs of allergies. 3: When pets are overweight it can add pressure on their joints, which can be painful to walk and play. The added weight can also increase the risk of diabetes. 4: Veterinarians look at an animal’s flexibility and feel for signs of arthritis while moving their limbs during an exam.
500
Case Study #2 BAILEY’S LIMP
SCENARIO:Bailey was playing fetch with his owner when she noticed he started to limp. Bailey came into your hospital and now you are part of the provider team. It’s time to help Bailey!
What should the veterinarian do first?
During the exam we found Bailey is limping on his back right leg. When we felt the leg, he yelped and there is some visible swelling. What should we do next?
501
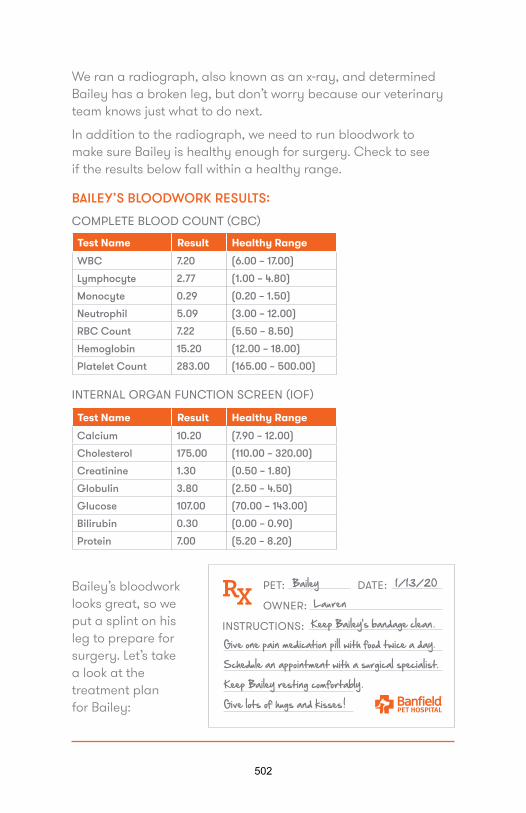
We ran a radiograph, also known as an x-ray, and determined Bailey has a broken leg, but don’t worry because our veterinary team knows just what to do next.
In addition to the radiograph, we need to run bloodwork to make sure Bailey is healthy enough for surgery. Check to see if the results below fall within a healthy range.
BAILEY’S BLOODWORK RESULTS:
Test Name Result Healthy Range
WBC 7.20 (6.00 – 17.00)
Lymphocyte 2.77 (1.00 – 4.80)
Monocyte 0.29 (0.20 – 1.50)
Neutrophil 5.09 (3.00 – 12.00)
RBC Count 7.22 (5.50 – 8.50)
Hemoglobin 15.20 (12.00 – 18.00)
Platelet Count 283.00 (165.00 – 500.00)
COMPLETE BLOOD COUNT (CBC)
Test Name Result Healthy Range
Calcium 10.20 (7.90 – 12.00)
Cholesterol 175.00 (110.00 – 320.00)
Creatinine 1.30 (0.50 – 1.80)
Globulin 3.80 (2.50 – 4.50)
Glucose 107.00 (70.00 – 143.00)
Bilirubin 0.30 (0.00 – 0.90)
Protein 7.00 (5.20 – 8.20)
INTERNAL ORGAN FUNCTION SCREEN (IOF)
Bailey’s bloodwork looks great, so we put a splint on his leg to prepare for surgery. Let’s take a look at the treatment plan for Bailey:
502

Case Study #3 MAX’S MOUTH
SCENARIO:Max isn’t feeling well. His owner says he hasn’t been eating much, his face looks a little different and his breath smells bad. He just hasn’t been acting himself. You’re the provider team and you need to help Max feel better.
What should the veterinarian do first? What questions should the veterinary team ask the owner?
During the exam we found that Max has a chipped tooth and the gums are red and swollen. What should we do next?
A. Put the pet under anesthesia and take a digital radiographof the teeth
B. Have the owner keep an eye on Max and call if it gets worseC. Prep Max for emergency dental surgeryD. Prescribe a softer food for Max to eat and see if the tooth
heals on its own
ANSWER: A
503
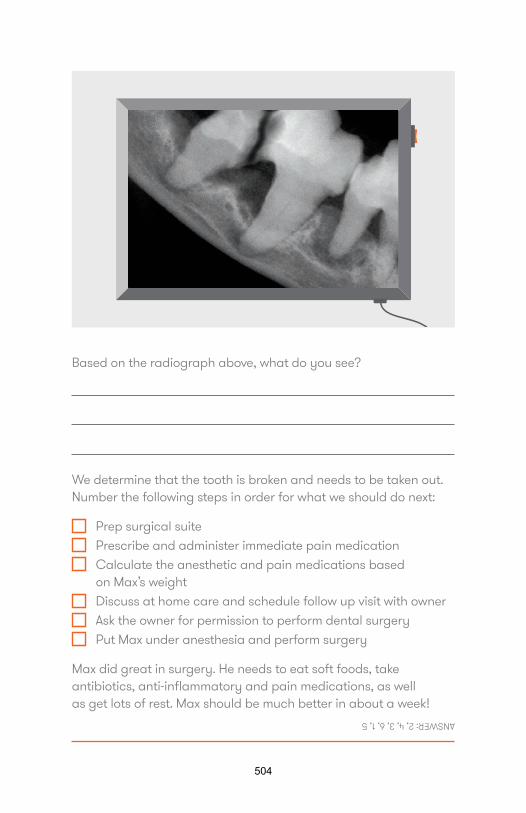
Based on the radiograph above, what do you see?
We determine that the tooth is broken and needs to be taken out. Number the following steps in order for what we should do next:
Prep surgical suite Prescribe and administer immediate pain medication Calculate the anesthetic and pain medications based
on Max’s weight Discuss at home care and schedule follow up visit with owner Ask the owner for permission to perform dental surgery Put Max under anesthesia and perform surgery
Max did great in surgery. He needs to eat soft foods, take antibiotics, anti-inflammatory and pain medications, as well as get lots of rest. Max should be much better in about a week!
ANSWER: 2, 4, 3, 6, 1, 5
504

Microscope Slides
Malassezia pachydermatis (Yeast): a microorganism that plays a major role in ear infections for dogs and cats.
Canine eosinophil: an increased number of cells found in dogs with allergies, causing rashes or itchy skin, shown in purple above. The surrounding, smaller cells are normal red blood cells.
Veterinarians often examine a pet’s blood under a microscope to help with a diagnosis. Here are a few examples of things they see frequently.
505
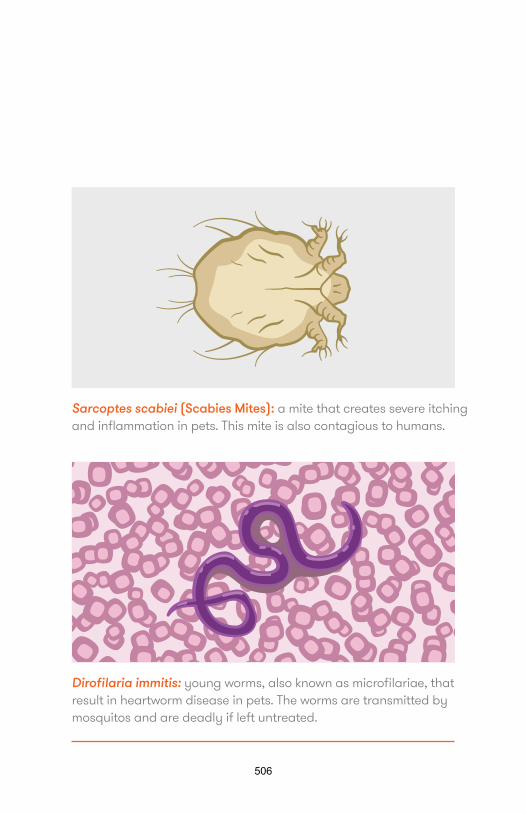
Sarcoptes scabiei (Scabies Mites): a mite that creates severe itching and inflammation in pets. This mite is also contagious to humans.
Dirofilaria immitis: young worms, also known as microfilariae, that result in heartworm disease in pets. The worms are transmitted by mosquitos and are deadly if left untreated.
506
Veterinary Medicine Glossary
American Veterinary Medical Association (AVMA) – an organization representing veterinarians and providing resources and educational opportunities.
Canine Parvovirus – a highly contagious disease that attacks the stomach and intestines but can be prevented by vaccinating your dog.
Caudal – a direction indicating toward the tail of the pet.
Cranial – a direction indicating toward the head of the pet.
Cranial cavity – the space formed inside the skull, including the brain.
Dermatophytosis – also known as ringworm, these are organisms found in the soil and show up as skin lesions on pets.
Diabetes Mellitus – a serious medical condition where your pet cannot control blood sugar levels due to problems with insulin production or function.
Dorsal – a direction indicating toward the back or top of the body, opposite of ventral.
Osteoarthritis – a form of arthritis and chronic disease caused by inflammation and damage to bone and joint tissue.
Rabies – a potentially fatal viral infection that can affect all mammals, but can be easily prevented in cats and dogs by a vaccine.
Thoracic cavity – the chamber of the body that includes the lungs and heart within the ribs.
Ventral – a direction indicating toward the belly or underside of the body, opposite of dorsal.
507
How Can You Learn More?
• Volunteer at a local animal shelter
• Take math and science classes in high school andcollege, including:– Biology– Chemistry– Physics– Anatomy– Physiology– Calculus– Statistics
• Find your closest veterinary schools and veterinarytechnician schools
• Conduct interviews of veterinary professionals
508

©Banfield 2019.11
509

Veterinary happiness: from the personal to the professional By Debbie L Stoewen DVM, MSW, RSW, PhD
Since the dawn of written history, happiness has attracted the attention of great philosophers, including Confucius, Buddha, Socrates, and Aristotle1,2 has been variously conceptualized and defined throughout history, influenced by the thinking of the times. Today it has come to be recognized as, “the experience of joy, contentment, or positive well-being, combined with a sense that one’s life is good, meaningful, and worthwhile”.3 This definition of happiness encompasses two distinct components: eudaimonic happiness, which comes from meaningful pursuits and is associated with life satisfaction, and hedonic happiness, which comes from pleasure or goal fulfilment and is associated with positive affect.4 Perhaps because it sounds more precise or scientific, researchers often refer to happiness as “subjective well-being.”
Subjective well-being is typically assessed by measuring both components, life satisfaction and positive affect.3 Interestingly, the emerging scholarship of happiness extends beyond the study of individual happiness to embody group and organizational happiness, and even the happiness of entire societies and countries, measuring perceptions of life satisfaction and affective states as reported by the citizenry.5 One country has gone so far as to prioritize “Gross National Happiness” over “Gross National Product” believing, “if the Government cannot create happiness for its people, there is no purpose for the Government to exist.”5 Bhutan has gained global attention for its national policy and development plans to bring about a society-wide rise in happiness.
The question as to what makes people happy (and why some are happier than others) is an important one.6 One of the primary goals of scientific enquiry in this area has been to identify the main predictors of human happiness.7 The focus has been on “chronic” happiness, the enduring level of happiness over a particular period of life, not the ups and downs of momentary or daily happiness.8 Substantial research has grown around three primary types of factors that are believed to causally affect chronic happiness, namely, the set point, life circumstances, and intentional activity.8
There's a growing body of literature that proposes that happiness is heritable, that we are born with what's called a "set point" for happiness.8 About 50% of happiness is thought to be “set” (i.e. genetically determined), and in this way, is fixed, stable over time, and immune to influence or control. As Lyubomirsky and colleagues (2005) forward, “The set point probably reflects relatively immutable intrapersonal, temperamental, and affective personality traits, such as extraversion, arousability, and negative affectivity, that are rooted in neurobiology, are highly heritable, and change little over the life span.” (p. 117) It seems we have an inborn predisposition to be happy or unhappy related to person-specific neurological differences.9
Beyond a hereditary predisposition to happiness, about 10% of happiness is thought to be related to circumstantial factors, that is, the incidental but relatively stable aspects of an individual’s life.8
Such factors include demographic variables such as the individual’s age, gender, and ethnicity; personal history variables (i.e. life events that may affect happiness); life status variables,
510
including marital status, occupational status, job security, income, health, and religious affiliation; and location variables, including the national, geographical, and cultural aspects of where the individual resides.8 In her 2010 review on happiness, Fisher states, “There is evidence that subjective well-being is on average higher among those who are married, embedded in supportive social networks, employed, participate in religious and leisure activities, earn more money, are of higher social and occupational status, believe they are healthy, and live in prosperous, democratic and individualistic countries as opposed to poorer collectivist countries.”(p. 392) Importantly, you’ll be happy to know that the remaining 40% of happiness is thought to be related to engaging in intentional activities, including regularly exercising, nurturing social relationships, choosing and pursuing authentic goals, seeking opportunities to experience flow, meditating, and practicing gratitude, kindness, forgiveness and spirituality.8 Unlike trying to increase one’s set point or changing one’s life circumstances, both arguably often difficult to impossible, these happiness-enhancing activities and practices are considered fruitful avenues to sustainable increases in chronic happiness.8 Thus, 40% of happiness lies within personal control. As almost everyone wants to be happy, and “the happy life” is the preferred life10, knowing that there are ways to increase happiness is encouraging. Increasing happiness, however, is not necessarily as straightforward as one might think because of an evolutionary aspect of human nature called hedonic adaptation (or the hedonic treadmill). As described by Frederick and Loewenstein (1999), hedonic adaptation is the psychological process by which people become accustomed to a positive or negative stimulus, such that the emotional effects of that stimulus are attenuated over time.11 What this means is that, despite major positive or negative events or life changes, we tend to continually adapt and return to a relatively stable baseline of happiness. Through declines in positive emotions and rises in aspirations – the two ways in which adaptation occurs – we return to the original set point.12 The good news, however, is that the adaptation effect has been found to be weaker with intentional activities than life circumstances, enabling the potential to increase happiness over time.8 The benefits of happiness are multifold. Based on 225 research studies, happy people are more successful across multiple life domains.10 Happy people are more creative; are better leaders and negotiators; are more helpful and philanthropic; have superior jobs and make more money; are more productive at work; have more friends and social support; are more likely to marry and have fulfilling marriages (and less likely to divorce); cope better with stress and trauma; and health-wise, have stronger immune systems, are physically healthier, and live longer. Research findings point towards a bidirectional link between happiness and success: not only does success make people happy, but positive affect – the hallmark of happiness – engenders success.10
With the virtually universal desire to be happy, live the happy life, and be successful, the question of happiness in the workplace is compelling. The average person spends more time working than any other daily activity of life and, over a lifetime, an average of 90,000 hours on the job.13,14 With that much time spent in the workplace, happiness at work cannot but contribute to a substantial share of overall happiness. Although happiness is not a term that has been widely used in the
511
study of employee experiences, organizational researchers have studied a number of person-level constructs that seem to have considerable overlap with the broad concept of happiness.6 These include job satisfaction (the most central and frequently used construct), organizational commitment, job involvement, engagement, thriving and vigor, flow and intrinsic motivation, and affect at work. When contemplating the question of happiness in the veterinary workplace, the closest data to answer this may be found in veterinary career and job satisfaction surveys, veterinary wellness surveys, and an occasional peer-reviewed article on the topic of job satisfaction.15-18
Keeping in mind that happiness can only be partly assessed based on career and job satisfaction studies (as job satisfaction is only a related construct to estimate workplace happiness), based on these studies, the following broad strokes may be forwarded. It appears, based on global questions of career and job satisfaction, that the majority, 70-80%, of veterinarians are happy. At the same time, it appears that happiness may be on the decline, as fewer veterinarians consider themselves “more happy,” and more consider themselves “less happy,” than 5 years ago; fewer veterinarians consider themselves physically, mentally, and emotionally healthy as compared to a decade ago; and fewer veterinarians seem to be recommending veterinary medicine as a career. Sources of dissatisfaction include the on-the-job amount of stress (with time management, clients’ inability to pay for services, and difficult client and coworker relationships), the amount of money earned, the chances for promotion, and the amount of recognition received. Sources of satisfaction include challenging work and keeping up with advances, good client and coworker relationships, and helping clients and animals.
In truth, these studies tell us very little about veterinary happiness. The study of happiness falls under the auspices of positive psychology, a relatively new field of study that examines healthy states, such as happiness, strength of character, and optimism.19 Psychology has traditionally focused on dysfunction (mental illness and other psychological problems) and how to treat it, however positive psychology, founded by Dr. Martin Seligman at the turn of the century, focuses on how ordinary people can become happier and more fulfilled. 21,22 It proposes that “people want to lead meaningful and fulfilling lives, to cultivate what is best within themselves, and to enhance their experiences of love, work, and play.”22
Scientific research on happiness in the field of veterinary medicine has not yet begun. Although this is similar to what’s (not) happening in human medicine, there is early evidence of research efforts in nursing.23-26 It is not surprising that there is so little research in the health care professions – positive psychology is an emerging field of research. As the scholarship expands and establishes a stronger foothold in the arena of scientific enquiry, this will change. There is a call for research on happiness in the health care professions, most notably from leaders in medicine and nursing.23, 25, 27 As Kerfoot states, “We now have the opportunity to learn from the research and embed happiness and well-being in our organizations.”
Although we don’t really know how happy veterinarians are or what particular aspects of their daily endeavours make them happy, for the time being we can draw on the research findings in
512
the broad study of organizational happiness. According to Warr, and referenced by Bartram and Boniwell, the following factors are considered fundamental to happiness in the workplace:
1. Positive contact with other people 2. Supportive and considerate supervision 3. The freedom to voice ideas and be heard 4. A sense of involvement in change 5. Recognition of achievements 6. The belief that you are doing something worthwhile 7. A reasonably clear role 8. Some personal control (discretion and decision latitude) 9. Variety in tasks, skills, or location 10. The opportunity to use and acquire personal skills 11. A manageable workload and goals 12. Equity (shared expectations, fairness, absence of discrimination) 13. A sense of job security 14. Safe and comfortable surroundings 15. Doing a job that is valued by the organization and society
If we render these factors into the context of veterinary medicine, what might this mean for us in our places of work when envisioning happy veterinarians and teams working in happy practices? It means, first and foremost, that there needs to be open communication. We need to flatten the traditional hierarchical system of management and encourage participative management.29 We need to cultivate personable environments where it is safe to speak up and express feelings. We need to value and take genuine interest in our colleagues, not only to discover their unique strengths and interests, but to provide the platform to enable them to build those strengths and pursue those interests. We need to embrace a workplace culture that practices kindness, gratitude, optimism, curiosity, playfulness, humor, open-mindedness, and hope, for these are the character virtues that facilitate happiness.30 We need to coach, guide, acknowledge, and appreciate, igniting not just the spark, but the torchbearer within each of us. We need to balance support with challenge, stability with variety and new opportunities, and ensure that workloads are shared and demands are reasonable. We need to trust and respect one another, and lastly, we need to remember that what we do does make a difference. Aristotle, one of the greatest thinkers in the history of western science and philosophy, stated, “Happiness is the meaning and purpose of life, the whole aim and end of human existence.” If this is true, which I believe it is, it is time for us to join the call for research on happiness in health care. Echoing Kerfoot, let us take the opportunity to learn from the research so we can embed happiness and well-being in our organizations – from primary care practices to university-based tertiary care centres. Echoing Kerfoot, “When can we get started?” References
1. McMahon DM. Happiness: A History. New York: Atlantic Monthly Press, 2006.
513
2. The Pursuit of Happiness, Available from: http://www.pursuit-of-happiness.org/science-of-happiness/ Last accessed September 3, 2020.
3. Lyubomirsky S. The How of Happiness: A New Approach to Getting the Life You Want. New York, NY: Penguin Books, 2007.
4. Ryan RM, Deci EL. On happiness and human potentials: A review of research on hedonic and eudaimonic well-being. Annu Rev Psychol 2001;52:141-166.
5. World Happiness Report, Available from: http://worldhappiness.report/ Last accessed April 15, 2019.
6. Fisher CD. Happiness at work. Int J Manag Rev. 2010;12:384–412. 7. Galinha I, Pais-Ribeiro JL. Cognitive, affective and contextual predictors of subjective
wellbeing. International Journal of Wellbeing 2011;2(1):34-53. 8. Lyubomirsky S, Sheldon KM, Schkade D. Pursuing happiness: The architecture of
sustainable change. Review of General Psychology 2005a;9:111-131. 9. Diener E, Suh EM, Lucas RE, Smith HL. Subjective well-being: Three decades of progress.
Psychological Bulletin 1999;125(2):276-302. 10. Lyubomirsky S, King LA, Diener E. The benefits of frequent positive affect: Does
happiness lead to success? Psychological Bulletin 2005b;131:803-855. 11. Frederick S, Loewenstein G. Hedonic adaptation. In Kahneman D, Diener E, Schwarz N,
Eds, Well-being: The foundations of hedonic psychology. New York: Russell Sage Foundation, 1999.
12. Sheldon KM, Lyubomirsky S. The Challenge of Staying Happier: Testing the Hedonic Adaptation Prevention Model. Pers Soc Psychol Bull 2012;38:670-680.
13. Bureau of Labour Statistics: American Time Use Survey. United States Department of Labour, Available from: http://www.bls.gov/tus/charts/ Last accessed September 3, 2020.
14. Pryce-Jones J. Happiness at work: Maximizing your psychological capital for success. West Sussex, UK: Wiley-Blackwell, 2010.
15. 2004 & 2015 OVMA Veterinary Career Satisfaction Surveys. Contact the OVMA at https://www.ovma.org/.
16. 2005 & 2015 dvm360 Job Satisfaction Surveys, Available from: http://veterinarynews.dvm360.com/2015-dvm360-job-satisfaction-survey?pageID=1 Last accessed September 3, 2020.
17. 2015 Veterinary Economics Career and Family Survey, Available from: http://veterinarybusiness.dvm360.com/are-you-happy Last accessed September 3, 2020.
18. Moore IC, Coe JB, Adams CL, Conlon PD, Sargeant JM. The role of veterinary team effectiveness in job satisfaction and burnout in companion animal veterinary clinics. JAVMA 2014;245(5):513-524.
19. Seligman MEP, TED Talk, Available from: https://www.ted.com/speakers/martin_seligman Last accessed September 3, 2020.
20. Seligman MEP, Csikszentmihalyi M. Positive psychology: An introduction. American Psychologist 2000;55:5-14.
21. Psychology Today, Available from: https://www.psychologytoday.com/basics/positive-psychology Last accessed September 3, 2020.
514
22. Positive Psychology Center, Available from: http://www.positivepsychology.org/ Lastaccessed September 3, 2020.
23. Angood PB. We Know About Physician Burnout; What About Physician Happiness?Physician Executive Journal 2013;39(4):4-5.
24. Appel L, Labhart L, Balczo P, McCleary N, Raley M, Winsett RP. A comparative study of ahappiness intervention in medical-surgical nurses. Medsurg Nursing 2013;22(5):319-324.
25. Ozkara San E. Concept Analysis of Nurses’ Happiness. Nursing Forum 2015;50(1):55-62.26. Boonyarak K. Factors predicting the work happiness of professional nurses. Available
from: http://hdl.handle.net/10755/202260 Last accessed September 14, 2020.27. Kerfoot KM. The pursuit of happiness, science, and effective staffing: the leader's
challenge. Nursing Economics 2012;30(5):305-306, 260.28. Warr P. Work, Happiness and Unhappiness. London, UK: Psychology Press, 2007.29. Bartram D, Boniwell I. The science of happiness: achieving sustained psychological well-
being. In Practice 2007;29:478-482.30. Seligman MEP. Authentic Happiness: Using the New Positive Psychology to Realize Your
Potential for Lasting Fulfillment. New York: Free Press, 2002.
515
Wellness at work: Everyone has a role, and every role is critical By Debbie L Stoewen DVM, MSW, RSW, PhD
Wellness is “the active process of becoming aware of and making choices toward a successful existence both as individuals within society and within the work environment.”1Wellness enhances physical, mental, and social well-being, and in one word, “health.” In recent years, wellness has moved into the workplace as enterprises – meaning both for-profit and nonprofit companies, businesses, firms, institutions and organizations designed to provide goods and/or services – have recognized the role that the workplace can play in supporting worker health. While enterprises have the responsibility to provide safe and hazard-free work environments, they also have the opportunity to promote worker health and foster healthy workplaces.2 The average person spends more time working than any other daily activity of life,3 and, over a lifetime, an average of 90,000 hours on the job.4 The workplace, therefore, is an important setting, not only for health protection – to prevent occupational injury – but also health promotion – to improve overall health and well-being.2,5
Worker health, safety and well-being not only benefits workers and their families. It has substantial implications for the productivity, competitiveness and sustainability of enterprises.5 As recognized by the World Health Organization (WHO), “The wealth of business depends on the health of workers.6”
Accordingly, to support workers is to support the enterprise. There is a strong imperative to build healthy workplaces as the two are inextricably intertwined.
The healthy workplace
The concept of the healthy workplace is not new, but it has indeed changed, evolving from a nearly exclusive focus on occupational health and safety (managing physical, chemical, biological and ergonomic hazards), to include work organization, workplace culture, lifestyle, and the community, all of which can profoundly influence worker health.6 Today’s healthy workplace includes both health protection and promotion.6 In short, it includes wellness.
The WHO has captured these elements in its definition of the healthy workplace. Based on a systematic literature and expert review, WHO proposes the following definition of a healthy workplace: A healthy workplace is one in which workers and managers collaborate to use a continual improvement process to protect and promote the health, safety and well-being of all workers and the sustainability of the workplace by considering the following, based on identified needs: 5, 6
• Health and safety concerns in the physical work environment;• Health, safety and well-being concerns in the psychosocial work environment,
including organization of work and workplace culture;• Personal health resources in the workplace; and• Ways of participating in the community to improve the health of workers, their
families and other members of the community.
Based on this definition, healthy workplace initiatives can be cultivated in four spheres6: • Physical work environment• Psychosocial work environment• Personal health resources
516
• Community involvement Physical work environment There are many kinds of physical hazards that can threaten the health and safety of workers. Examples of such hazards include electrical dangers; ergonomic-related risks (e.g. repetitive motion, awkward posture, or excessive force); radiation exposure, machine-related injuries; and the risk of a work-related motor vehicle crash. These hazards need to be recognized, assessed, minimized, eliminated, or controlled.6,7
Psychosocial work environment There are also “psychosocial hazards” that can threaten the health and safety of workers. These are better known as work stressors and are related to the psychological and social conditions of the workplace, including the organizational culture as well as attitudes, values, beliefs and daily practices, rather than the physical conditions.6 They can be harmful to the mental and physical health of workers, with evidence of two to three times greater risk of mental illness, injuries, back pain, and workplace conflict and violence.6 As derived directly from the WHO Healthy Workplace Framework and Model (Burton, 2010):
Examples of psychosocial hazards include but are not limited to: • Poor work organization (problems with work demands, time pressure, decision latitude,
reward and recognition, support from supervisors, job clarity, job design, poor communication)
• Organizational culture (lack of policies and practice related to dignity or respect for all workers, harassment and bullying, gender discrimination, intolerance for ethnic or religious diversity, lack of support for healthy lifestyles)
• Command and control management style (lack of consultation, negotiation, two-way communication, constructive feedback, and respectful performance management)
• Lack of support for work-life balance Ways to influence the psychosocial work environment:
• Reallocate work to reduce workload, remove supervisors or retrain them in communication and leadership skills, enforce zero tolerance for workplace harassment and discrimination
• Allow flexibility to deal with work-life conflict situations; provide supervisory and co-worker support (resources and emotional support); allow flexibility in the location and timing of work; and provide timely, open and honest communication
• Protect workers by raising awareness and providing training to workers, for example regarding conflict prevention or harassment situations
Personal health resources The provision of personal health resources in the workplace can support or motivate worker efforts to improve or maintain their personal health practices or lifestyle, as well as monitor and support their physical and mental health.6,7 Such resources include health services, information, opportunities, and flexibility. Although work can get in the way of making healthy lifestyle choices, motivated and innovative employers do what they can to remove the barriers and support the personal health goals of their employees.
517
As derived directly from the WHO Healthy Workplace Framework and Model (Burton, 2010): Examples of personal health resource issues in the workplace:
Employment conditions or lack of knowledge may make it difficult for workers to adopt healthy lifestyles or remain healthy. For example: • Physical inactivity may result from long work hours, cost of fitness facilities or equipment,
and lack of flexibility in when and how long breaks can be taken • Poor diet may result from lack of access to healthy snacks or meals at work, lack of time to
take breaks for meals, lack of refrigeration to store healthy foods, or lack of knowledge
Examples of ways to enhance workplace personal health resources: These may include medical services, information, training, financial support, facilities, policy support, flexibility, and promotional programs to enable and encourage workers to develop healthy lifestyle practices.
Involvement in the community Community involvement refers to the ways in which a workplace goes above and beyond to involve itself within the community in which it operates, offering expertise and resources (beyond its day-to-day offerings) to support the social and physical wellbeing of the community (6). Activities that positively influence the physical and mental health, safety and well-being of workers and their families offer the greatest advantage. Examples include spearheading a community project and volunteering in community initiatives to benefit those in need. Those in veterinary medicine might ask, “But how does all of this apply to me in the veterinary workplace? Why would I want to think beyond the necessities of occupational health and safety when there’s already more than enough to think about – and do – with running a practice?” These are valid questions, and the answers are just as important as the questions. Why build a healthy workplace? First, it is the right thing to do. Ensuring employee health and safety follows one of the most basic of universally accepted ethical principles, “do no harm.6” There is a moral imperative to create healthy veterinary workplaces that do not harm the mental or physical health, safety, or well-being of its employees.6 Second, it is the smart thing to do. There is a wealth of data demonstrating that in the long term, businesses that protect and promote employee health tend to be the most successful and competitive.6 They have the most physically and mentally healthy and satisfied employees; less sick leave, disability, and turnover; and higher productivity and quality of products and services.6,7Businesses that do not protect and promote employee health incur significant costs on multiple levels. To clarify, it’s not that work is generally regarded as bad for physical and mental health and well-being. On the contrary, when compared to worklessness or unemployment, work is good for physical and mental health and well-being.8 Work is usually the main source of income to make a living and fully participate in society, and it is strongly connected to individual identity and social status.8 However, it can have harmful as well as beneficial effects on health and well-being depending on the workplace. There are costs in all directions – for workers, the workplace, the community, and beyond – if worker health and wellness and the imperative to create healthy workplaces are disregarded.
518
Build a healthy practice: your wellness program Wellness needs to be rooted in your past and tied to your hopes for your future. This means your program begins with where you are now, and moves forward with the question, “What steps can we take to promote even more wellness?” Developing a wellness program builds on what you’re already doing right! When considering your workplace facilities, make sure the ergonomics meet workers’ needs. What ways can you make the physical work easier? The AVMA offers guidelines for ergonomics in the veterinary workplace as well as practical ideas for setting up a workplace wellness program.10-12 Take a look at your break room. Could a spruce-up turn it into a better stress-relief space? Is there an area that could be used for stretching, light exercise, meditation or yoga? Could a temporary partition be used to separate some space from the rest of the room? Can you create a “work-free zone” at your hospital, a space where no “shop talk” is allowed? What about the aesthetics at your hospital? Is there room for some inspirational artwork? Are there ways to “green” your hospital with plants, even if it requires changes in lighting? Consider “catifying” your hospital if you don’t already have a clinic cat. In the moments when most needed, a clinic cat can be a real comfort. Consider walking meetings – or even a walking club! Walking is not only great for exercise, but also creative thinking. Can lunches or breaks be coordinated so walking/workout buddies can get regular exercise time together? Can stretch exercises be performed at work areas? What about organizing a sports team to represent your practice in a local league or tournament? It’s not only great for exercise, but also team-building. Develop a “Wellness Board” and encourage each other to share information about local clubs, events, and opportunities. Encourage healthy snacks, prepare healthy meals for office meetings and potlucks, and share healthy recipes. Encourage nutrition challenges (e.g. 7 days sugar-free). The challenge itself can bring a new kind of dialogue and playfulness to your hospital. Are other challenges possible? What about walking, biking, or running challenges? What about sleeping challenges, like aiming for 7 hours of sleep/day? Sleep is restorative, and in this way, benefits health and well-being. Provide adequate and coordinated staffing and resources to promote efficient client and patient care. Invite everyone’s ideas as to how to work smarter to better manage the workload.13 Ensure that people have the time to take breaks and get lunch. Place limits on overtime, provide adequate vacation, and promote work-life balance. Minimize work-home interference by allowing flexibility in scheduling and enabling ready coverage for important life events (births, funerals, illness, and family emergencies). Cultivate a collegial work environment. Embrace a participatory management style. What kinds of communication would this necessitate? How would an inclusive, empowering approach with decision-making, and making decision-making processes more overt, support health and well-being? Talk with one another about how you can tailor your jobs to best suit individual strengths, interests, and aptitudes. Then tailor-away! Provide opportunities for training and development. Life-long learning rekindles passion and growth.13 Can you cover the costs (or part thereof) of continuing education? Can you allow paid time off? What about opportunities to learn about coping with stress, compassion fatigue, burnout,
519
conflict resolution, and managing difficult conversations to sustain resilience? Workshops, classes, and online options are available.
How can you better coach, guide, acknowledge, and appreciate one another? How can you encourage a culture where people can be genuine and express feelings? Can you debrief as a team at the end of each day/shift? Emotional support is vital to sustaining resilience. Close relationships are a powerful means for promoting positive emotions and effective recovery.13 Retreats, team-building exercises, and holiday parties are great ways to foster close relationships.
How can you contribute to your community? Perhaps you could participate in an Adopt-a-family program during the holidays, organize a beach or park clean-up, or take on a community beautification project. What about partnering with a civic organization, church, or charity to help those in need? These activities not only “give back” to the community, but cultivate camaraderie and teamwork, necessary to resilience.
Wellness is the process of becoming aware of, and making choices toward, a successful existence, as individuals within society – and the work environment. You can create a culture of wellness by establishing a supportive work environment that encourages everyone to make health and well-being a priority. Increasingly, enterprises large and small, and from all sectors, are bringing wellness into the workplace. The workplace has a role to play in promoting health and well-being, to the benefit of both workers and the productivity, competitiveness and sustainability of the workplace. It’s time we pause to consider what we’re doing in our esteemed profession to promote health and well-being and foster healthy veterinary workplaces, and ask ourselves “What else can we be doing?” Wellness is a process, rooted in our past and tied to our hopes for the future. What do we want for our future? It’s ours to create. Let’s go do it!
Selected References
1. American Veterinary Medical Association: Guiding Principles for State Veterinary WellnessPrograms. Available from: https://www.avma.org/resources/wellbeing/guiding-principles-state-veterinary-wellness-programs Last accessed January 4, 2020.
3. Bureau of Labour Statistics: American Time Use Survey. United States Department of Labour,Available from: http://www.bls.gov/tus/charts/ Last accessed January 4, 2020.
4. Pryce-Jones J. Happiness at work: Maximizing your psychological capital for success. West Sussex,UK: Wiley-Blackwell, 2010.
5. Healthy workplaces: a model for action. World Health Organization. Available from:http://www.who.int/occupational_health/publications/healthy_workplaces_model.pdf Lastaccessed January 4, 2020.
6. Burton, J. WHO Healthy Workplace Framework and Model: Background and Supporting Literatureand Practices. 2010. Available from:http://www.who.int/occupational_health/healthy_workplace_framework.pdf Last accessedJanuary 4, 2020.
8. Waddell G and Burton AK. Is work good for your health and well-being? Department of Work andPensions, UK. 2006. Available from:
520
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/214326/hwwb-is-work-good-for-you.pdf Last accessed January 4, 2020.
9. Six Dimensions of Wellness. Available from:http://www.nationalwellness.org/?page=six_dimensions Last accessed January 4, 2020.
10. Veterinary Ergonomic Guidelines. Available from: https://www.avma.org/policies/veterinary-ergonomic-guidelines Last accessed January 4, 2020.
11. Setting Up a Workplace Wellbeing Program. Available from:https://www.avma.org/resources/wellbeing/setting-workplace-wellbeing-program Last accessedJanuary 4, 2020.
12. Healthy Behaviors Shape Your Practice Wellness Program. Available from:https://www.avma.org/resources/wellbeing/setting-workplace-wellbeing-program/healthy-behaviors-shape-your-practice-wellness-program Last accessed January 4, 2020.
13. Krall EJ. Ten commandments of physician wellness. Clinical Medicine & Research 2014;12(1-2):6-9.
– Complete List Available Upon Request –
521