Interventional procedure overview of endoscopic ablation for ...
Primary Treatment of Acute Dacryocystitisby Endoscopic Dacryocystorhinostomy withSilicone Intubation Guided by a Soft Probe
Wencan Wu, MD, PhD,1 Wentao Yan, BS,1 Julia K. MacCallum, BS,2 Yunhai Tu, MS,1 Alice C. Jiang,2
Yuan Yang, MS,1 Tianlin Xiao, MD, PhD,1 Jin Li, MD, PhD,1 Qinmei Wang, BS,1 Jia Qu, MS1
Purpose: To investigate the suitability of cold steel endonasal endoscopic dacryocystorhinostomy (EES-DCR) with circular bicanalicular intubation with silicone tubes (CBIST) guided by a soft probe for the primarytreatment of acute purulent dacryocystitis (APD).
Design: Prospective, randomized, interventional case series.Participants: Seventy-two patients (59 females, 13 males) with a median presenting age of 55�12 years
(range, 28–71 years).Methods: Eighty-four patients with unilateral APD were equally and randomly divided into 2 groups. Cold
steel EES-DCR was performed after the lacrimal abscess formation, and external dacryocystorhinostomy(E-DCR) was performed 1 to 2 weeks after resolution of the acute inflammation. In both groups, CBIST guidedby a soft probe was performed and the silicone tubes were kept in the lacrimal passages for 3 months.Postoperative follow-up ranged from 12 to 24 months. Outcomes were compared between both groups,considering resolution time for external acute inflammation, success rate of free lacrimal passage reconstruction,and lack of complications as indicators of treatment suitability.
Main Outcome Measures: Time for resolution of the external acute inflammation, success rate of freelacrimal passage reconstruction, and complications.
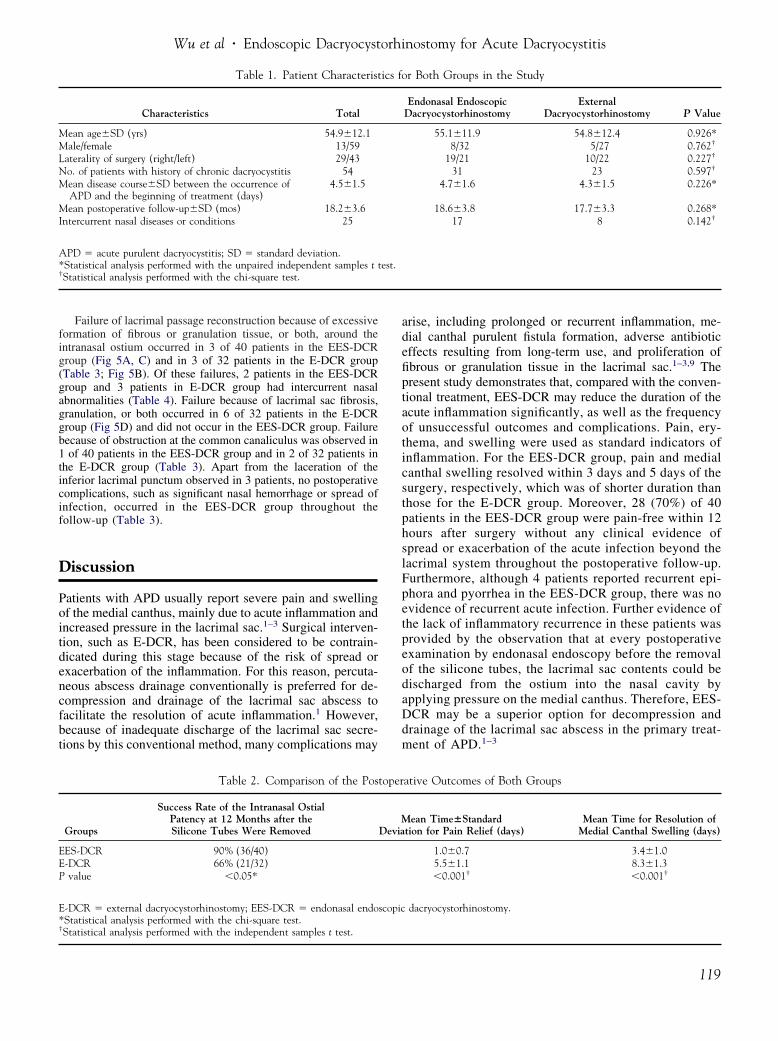
Results: In this study, complete postoperative data were acquired from 40 patients in the EES-DCRgroup and from 32 patients in the E-DCR group, and the outcomes were compared. Acute inflammationresolved more quickly in the EES-DCR group than in the E-DCR group (P�0.05). Ostium patency at 12months after silicone tube removal was achieved in significantly more patients in the EES-DCR group (36/40[90%]) than in the E-DCR group (21/32 [65.7%]; P�0.01). In the EES-DCR group, lacrimal passagereconstruction failed because of intranasal ostial closure in 3 patients and because of common canaliculusobstruction in 1 patient. In the E-DCR group, lacrimal passage reconstruction failed because of intranasalostial closure in 3 patients, lacrimal sac fibrosis, granulation, or both in 6 patients, and common canaliculusobstruction in 2 patients. Other than the slight laceration of the inferior puncta, no significant complicationsarose from the treatments.
Conclusions: Cold steel EES-DCR with CBIST guided by a soft probe is a promising alternative for theprimary treatment of APD with abscess formation.
Financial Disclosure(s): The authors have no proprietary or commercial interest in any materials discussed
in this article. Ophthalmology 2009;116:116–122 © 2009 by the American Academy of Ophthalmology.The standard practice for the treatment of acute purulentdacryocystitis (APD) has not included surgical interventionbecause of concerns about the risks of exacerbation andspread of infection. For this reason, external dacryocysto-rhinostomy (E-DCR) usually is performed after the resolu-tion of acute infection through the use of warm compresses,systemic antibiotics, and percutaneous abscess drainage.1
This treatment plan, however, may result in several com-plications, such as prolonged or recurrent infection, ad-verse antibiotic effects because of long-term use, cuta-neous scar or fistula formation, and failure of lacrimalsystem reconstruction because of scarring or granulomaformation in the lacrimal sac.
Recently, a few authors have reported that laser-assisted
endonasal endoscopic dacryocystorhinostomy (EES-DCR),116 © 2009 by the American Academy of OphthalmologyPublished by Elsevier Inc.
also known as hot steel EES-DCR, may be an alternative forthe primary treatment of APD because of decreased mor-bidity and a shortened duration of required antibiotic treat-ment in comparison with conventional therapies.2,3 How-ever, the efficacy of this intervention varies widely, andwhether it has the same success rate of the lacrimal passagereconstruction as the conventional therapy by E-DCR isuncertain.2,3 Meanwhile, laser-assisted EES-DCR seems tobe less effective than cold steel EES-DCR for the treatmentof chronic dacryocystitis because of the small size of theostia created and the ostial fibrosis and stenosis resultingfrom the heat generated by bone and mucosa ablation witha holmium:yttrium aluminum garnet (holmium:YAG) andpotassium titanyl phosphate (KTP) laser.4–6 The present
study was a first attempt to address the need for prospective,ISSN 0161-6420/09/$–see front matterdoi:10.1016/j.ophtha.2008.09.041

Wu et al � Endoscopic Dacryocystorhinostomy for Acute Dacryocystitis
randomized studies of cold steel EES-DCR versus the con-ventional management of APD by E-DCR.
Patients and Methods
Overview
The present study was performed at the Eye Hospital of WenzhouMedical College between January 2003 and December 2007, incompliance with the guidelines of the Declaration of Helsinkiissued by the World Medical Association. Eighty-four patientswere diagnosed with unilateral APD based on their medical his-tories and the observation of lacrimal sac abscess formation onphysical examination. Intercurrent nasal diseases and conditionswere diagnosed by a senior otorhinolaryngologist. This study wasapproved by the institutional review board, and informed consentwas obtained from all participants.
The 84 patients were divided equally and randomly into 2 groups,and all patients were treated before surgery with intravenous antibi-otics. Cold steel EES-DCR was performed after the lacrimal abscessformation in the EES-DCR group, whereas E-DCR was performed 1to 2 weeks after resolution of the acute inflammation by percutaneousabscess drainage in the E-DCR group. In both groups, circular bi-canalicular intubation with a silicone tube (CBIST) guided by a softprobe was performed, and the silicone tubes were kept in the lacrimalpassages for 3 months. Postoperative follow-up ranged from 12 to 24months. At follow-up, the patients’ interim medical histories wererecorded and endonasal endoscopic examinations of intranasal ostiumpatency and lacrimal irrigation were performed. Ostial patency wasdefined as the absence of epiphora by history and examination,free-flowing irrigation through the lacrimal system, and normal-appearing mucosa covering the intranasal ostium.
Prepared Soft Probe and the Silicone Tube
The soft probe is softer than conventional stainless steel probes. Itconsists of a segmental epidural catheter with a smooth and bluntblind tip and a stainless steel acupuncture needle. The acupunctureneedle is inserted through the lumen of the proximal end into theepidural catheter to increase its rigidity (Fig 1). The silicone tubeapparatus is comprised of a silicone tube, a silicone fuse, and asilicone loop. The silicone fuse and loop are tied tightly to the endof the silicone tube (Fig 1).
Cold Steel Endonasal EndoscopicDacryocystorhinostomy Surgical Technique
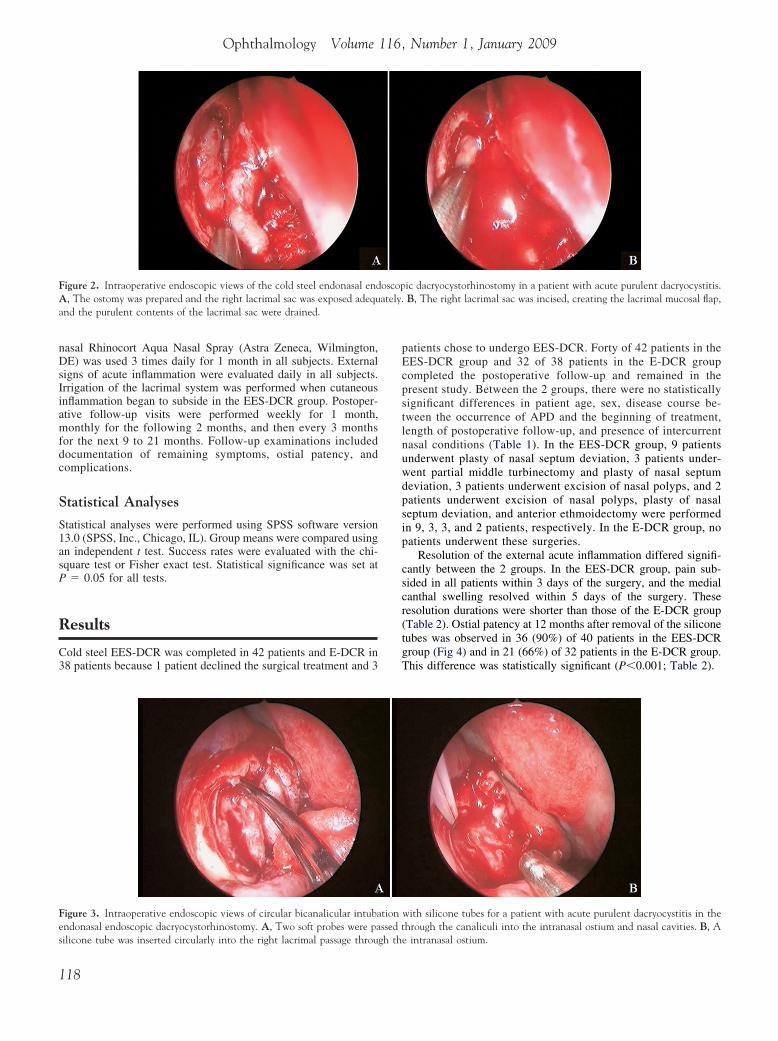
Cold steel EES-DCR was performed as described by Wormald.7 Thepatient was placed in a supine position. Except when intercurrentnasal conditions were being corrected simultaneously under generalanesthesia, EES-DCR with CBIST generally was performed underlocal anesthesia. After infiltrating a mixture of 2 ml 2% lidocaine andepinephrine (1:100 000) into the lateral nasal wall, an external anteriorethmoidal nerve block and an infraorbital nerve block were per-formed. Under direct visualization with a 45° 4-mm endonasal endo-scope (Karl Storz, Tuttlingen, Germany), the lateral nasal mucosa wasincised in the area of the lacrimal sac fossa with a no. 15 scalpel andremoved. Either a Hajek-Koffler forward-biting punch or an angled(15°) coarse diamond burr attached to a microdebrider (XPS3000;Medtronic Xomed, Minneapolis, MN) was used to remove the lacri-mal bone, as well as the frontal process of the maxillary bone at thenasal wall of the lacrimal sac fossa. This maneuver created an osteot-omy approximately 8 mm in diameter and 10 mm in length (Fig 2A).
Next, the blind tip of the soft probe was inserted through the superiorpunctum and was rotated carefully into the lacrimal sac to tent itsmedial wall, incising it anteriorly as far as possible with a sickle knife(Medtronic Xomed) to release purulent material from the abscessedlacrimal sac (Fig 2B). After extracting the soft probe, the lacrimalpassage was irrigated with a combination antibiotic-corticosteroidsolution (80 mg tobramycin sulfate with 2 mg dexamethasone sodiumphosphate in 3 ml normal saline solution), and the posterior lacrimalsac flap was stretched adequately. After CBIST was performed guidedby the soft probe (Fig 3A, B), the lacrimal sac flap was flattenedposteriorly and a piece of MeroGel (Medtronic Xomed, Jacksonville,FL) was placed to stabilize the flap during initial healing. Whenoperations for intercurrent nasal diseases or conditions were per-formed simultaneously, the nasal cavity was packed with Merocel8-cm packs (Medtronic Xomed) to minimize postoperative bleeding;otherwise, no packs were used. When used, the nasal packs wereremoved 3 to 5 days after surgery.
External Dacryocystorhinostomy TechniqueThe E-DCR procedures were performed in the conventional man-ner.8 After making an approximately 1.5-cm incision in themedial canthus, the fibers of the orbicularis oculi muscle wereseparated using blunt dissection to expose the periosteum over-lying and medial to the anterior lacrimal crest. After incision ofthe periosteum, an osteotomy approximately 10 mm in diameterwas prepared. The lacrimal sac and nasal mucosa were openedlongitudinally to form anterior and posterior flaps. The posteriorflaps were sutured together with 2 or 3 5-0 Dexon sutures(Davis-Geck, Wayne, NJ), and CBIST was performed guidedby the soft probe. The anterior flaps also were sutured togetherwith 5-0 Dexon sutures. The periosteum, orbicularis oculi mus-cle, and skin were closed in separate layers in the standardmanner. Nasal packing was not performed.
Postoperative Care and Follow-upAfter surgery, combination antibiotic-corticosteroid eye drops and
Figure 1. Image depicting the soft probe and the silicone tubes. The softprobe (narrow black arrow) consists of a segmental epidural catheter (largewhite arrow) with a smooth, blunt, blind tip and a stainless steel acupunctureneedle (narrow white arrow). The acupuncture needle is inserted into theepidural catheter through the lumen of the proximal end to increase itsrigidity. The silicone tube apparatus (large black arrow) is comprised of asilicone tube, a silicone fuse, and a silicone loop, which are tied tightly to theend of the silicone tube.
systemic antibiotics were administered for 5 to 7 days, and intra-
117
Ophthalmology Volume 116, Number 1, January 2009
nasal Rhinocort Aqua Nasal Spray (Astra Zeneca, Wilmington,DE) was used 3 times daily for 1 month in all subjects. Externalsigns of acute inflammation were evaluated daily in all subjects.Irrigation of the lacrimal system was performed when cutaneousinflammation began to subside in the EES-DCR group. Postoper-ative follow-up visits were performed weekly for 1 month,monthly for the following 2 months, and then every 3 monthsfor the next 9 to 21 months. Follow-up examinations includeddocumentation of remaining symptoms, ostial patency, andcomplications.
Statistical Analyses
Statistical analyses were performed using SPSS software version13.0 (SPSS, Inc., Chicago, IL). Group means were compared usingan independent t test. Success rates were evaluated with the chi-square test or Fisher exact test. Statistical significance was set atP � 0.05 for all tests.
Results
Cold steel EES-DCR was completed in 42 patients and E-DCR in38 patients because 1 patient declined the surgical treatment and 3
Figure 2. Intraoperative endoscopic views of the cold steel endonasal endA, The ostomy was prepared and the right lacrimal sac was exposed adequand the purulent contents of the lacrimal sac were drained.
Figure 3. Intraoperative endoscopic views of circular bicanalicular intubaendonasal endoscopic dacryocystorhinostomy. A, Two soft probes were pa
silicone tube was inserted circularly into the right lacrimal passage through th118
patients chose to undergo EES-DCR. Forty of 42 patients in theEES-DCR group and 32 of 38 patients in the E-DCR groupcompleted the postoperative follow-up and remained in thepresent study. Between the 2 groups, there were no statisticallysignificant differences in patient age, sex, disease course be-tween the occurrence of APD and the beginning of treatment,length of postoperative follow-up, and presence of intercurrentnasal conditions (Table 1). In the EES-DCR group, 9 patientsunderwent plasty of nasal septum deviation, 3 patients under-went partial middle turbinectomy and plasty of nasal septumdeviation, 3 patients underwent excision of nasal polyps, and 2patients underwent excision of nasal polyps, plasty of nasalseptum deviation, and anterior ethmoidectomy were performedin 9, 3, 3, and 2 patients, respectively. In the E-DCR group, nopatients underwent these surgeries.
Resolution of the external acute inflammation differed signifi-cantly between the 2 groups. In the EES-DCR group, pain sub-sided in all patients within 3 days of the surgery, and the medialcanthal swelling resolved within 5 days of the surgery. Theseresolution durations were shorter than those of the E-DCR group(Table 2). Ostial patency at 12 months after removal of the siliconetubes was observed in 36 (90%) of 40 patients in the EES-DCRgroup (Fig 4) and in 21 (66%) of 32 patients in the E-DCR group.This difference was statistically significant (P�0.001; Table 2).
ic dacryocystorhinostomy in a patient with acute purulent dacryocystitis.B, The right lacrimal sac was incised, creating the lacrimal mucosal flap,
with silicone tubes for a patient with acute purulent dacryocystitis in thehrough the canaliculi into the intranasal ostium and nasal cavities. B, A
oscopately.
tionssed t
e intranasal ostium.
Wu et al � Endoscopic Dacryocystorhinostomy for Acute Dacryocystitis
Failure of lacrimal passage reconstruction because of excessiveformation of fibrous or granulation tissue, or both, around theintranasal ostium occurred in 3 of 40 patients in the EES-DCRgroup (Fig 5A, C) and in 3 of 32 patients in the E-DCR group(Table 3; Fig 5B). Of these failures, 2 patients in the EES-DCRgroup and 3 patients in E-DCR group had intercurrent nasalabnormalities (Table 4). Failure because of lacrimal sac fibrosis,granulation, or both occurred in 6 of 32 patients in the E-DCRgroup (Fig 5D) and did not occur in the EES-DCR group. Failurebecause of obstruction at the common canaliculus was observed in1 of 40 patients in the EES-DCR group and in 2 of 32 patients inthe E-DCR group (Table 3). Apart from the laceration of theinferior lacrimal punctum observed in 3 patients, no postoperativecomplications, such as significant nasal hemorrhage or spread ofinfection, occurred in the EES-DCR group throughout thefollow-up (Table 3).
Discussion
Patients with APD usually report severe pain and swellingof the medial canthus, mainly due to acute inflammation andincreased pressure in the lacrimal sac.1–3 Surgical interven-tion, such as E-DCR, has been considered to be contrain-dicated during this stage because of the risk of spread orexacerbation of the inflammation. For this reason, percuta-neous abscess drainage conventionally is preferred for de-compression and drainage of the lacrimal sac abscess tofacilitate the resolution of acute inflammation.1 However,because of inadequate discharge of the lacrimal sac secre-tions by this conventional method, many complications may
Table 1. Patient Characterist
Characteristics Total
Mean age�SD (yrs) 54.9�12.1Male/female 13/59Laterality of surgery (right/left) 29/43No. of patients with history of chronic dacryocystitis 54Mean disease course�SD between the occurrence of
APD and the beginning of treatment (days)4.5�1.5
Mean postoperative follow-up�SD (mos) 18.2�3.6Intercurrent nasal diseases or conditions 25
APD � acute purulent dacryocystitis; SD � standard deviation.*Statistical analysis performed with the unpaired independent samples t†Statistical analysis performed with the chi-square test.
Table 2. Comparison of the Pos
Groups
Success Rate of the Intranasal OstialPatency at 12 Months after theSilicone Tubes Were Removed
EES-DCR 90% (36/40)E-DCR 66% (21/32)P value �0.05*
E-DCR � external dacryocystorhinostomy; EES-DCR � endonasal endo*Statistical analysis performed with the chi-square test.†
Statistical analysis performed with the independent samples t test.arise, including prolonged or recurrent inflammation, me-dial canthal purulent fistula formation, adverse antibioticeffects resulting from long-term use, and proliferation offibrous or granulation tissue in the lacrimal sac.1–3,9 Thepresent study demonstrates that, compared with the conven-tional treatment, EES-DCR may reduce the duration of theacute inflammation significantly, as well as the frequencyof unsuccessful outcomes and complications. Pain, ery-thema, and swelling were used as standard indicators ofinflammation. For the EES-DCR group, pain and medialcanthal swelling resolved within 3 days and 5 days of thesurgery, respectively, which was of shorter duration thanthose for the E-DCR group. Moreover, 28 (70%) of 40patients in the EES-DCR group were pain-free within 12hours after surgery without any clinical evidence ofspread or exacerbation of the acute infection beyond thelacrimal system throughout the postoperative follow-up.Furthermore, although 4 patients reported recurrent epi-phora and pyorrhea in the EES-DCR group, there was noevidence of recurrent acute infection. Further evidence ofthe lack of inflammatory recurrence in these patients wasprovided by the observation that at every postoperativeexamination by endonasal endoscopy before the removalof the silicone tubes, the lacrimal sac contents could bedischarged from the ostium into the nasal cavity byapplying pressure on the medial canthus. Therefore, EES-DCR may be a superior option for decompression anddrainage of the lacrimal sac abscess in the primary treat-ment of APD.1–3
r Both Groups in the Study
Endonasal EndoscopicDacryocystorhinostomy
ExternalDacryocystorhinostomy P Value
55.1�11.9 54.8�12.4 0.926*8/32 5/27 0.762†
19/21 10/22 0.227†
31 23 0.597†
4.7�1.6 4.3�1.5 0.226*
18.6�3.8 17.7�3.3 0.268*17 8 0.142†
ative Outcomes of Both Groups
ean Time�Standardtion for Pain Relief (days)
Mean Time for Resolution ofMedial Canthal Swelling (days)
1.0�0.7 3.4�1.05.5�1.1 8.3�1.3�0.001† �0.001†
dacryocystorhinostomy.
ics fo
test.
toper
MDevia
scopic
119
Ophthalmology Volume 116, Number 1, January 2009
Another major goal of treatment in APD is to reconstructa free-flowing lacrimal system. External dacryocystorhinos-tomy is an effective conventional method for lacrimal pas-sage reconstruction after the acute inflammation has sub-
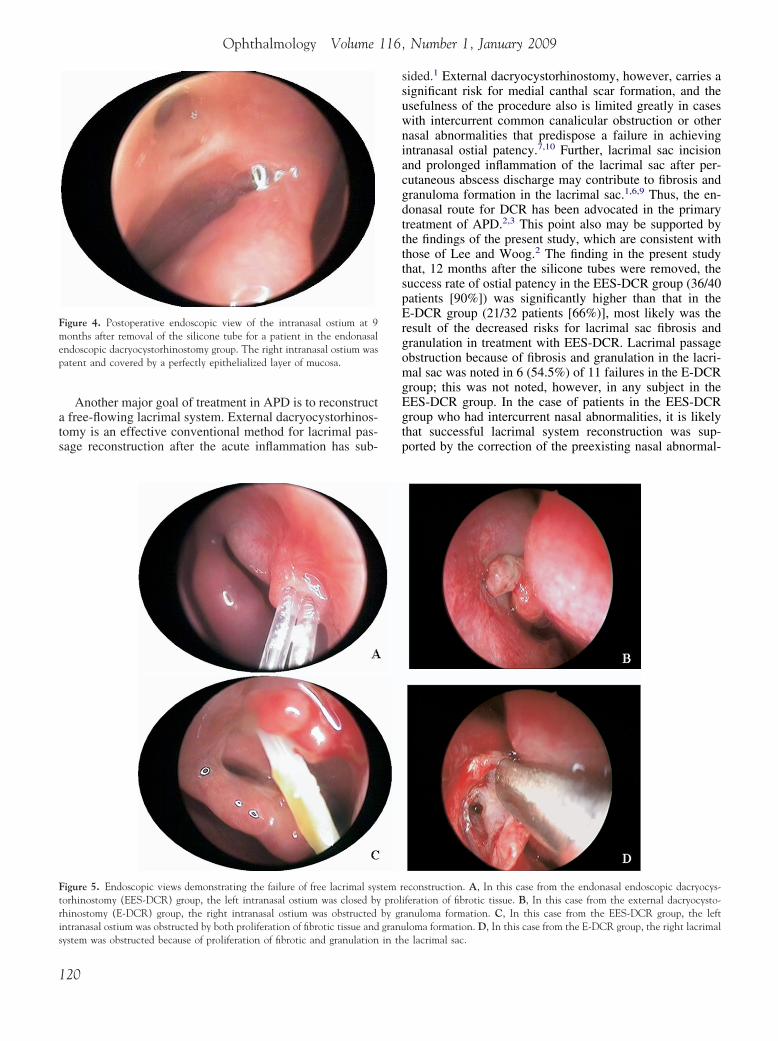
Figure 4. Postoperative endoscopic view of the intranasal ostium at 9months after removal of the silicone tube for a patient in the endonasalendoscopic dacryocystorhinostomy group. The right intranasal ostium waspatent and covered by a perfectly epithelialized layer of mucosa.
Figure 5. Endoscopic views demonstrating the failure of free lacrimal systorhinostomy (EES-DCR) group, the left intranasal ostium was closed byrhinostomy (E-DCR) group, the right intranasal ostium was obstructedintranasal ostium was obstructed by both proliferation of fibrotic tissue and
system was obstructed because of proliferation of fibrotic and granulation in th120
sided.1 External dacryocystorhinostomy, however, carries asignificant risk for medial canthal scar formation, and theusefulness of the procedure also is limited greatly in caseswith intercurrent common canalicular obstruction or othernasal abnormalities that predispose a failure in achievingintranasal ostial patency.7,10 Further, lacrimal sac incisionand prolonged inflammation of the lacrimal sac after per-cutaneous abscess discharge may contribute to fibrosis andgranuloma formation in the lacrimal sac.1,6,9 Thus, the en-donasal route for DCR has been advocated in the primarytreatment of APD.2,3 This point also may be supported bythe findings of the present study, which are consistent withthose of Lee and Woog.2 The finding in the present studythat, 12 months after the silicone tubes were removed, thesuccess rate of ostial patency in the EES-DCR group (36/40patients [90%]) was significantly higher than that in theE-DCR group (21/32 patients [66%)], most likely was theresult of the decreased risks for lacrimal sac fibrosis andgranulation in treatment with EES-DCR. Lacrimal passageobstruction because of fibrosis and granulation in the lacri-mal sac was noted in 6 (54.5%) of 11 failures in the E-DCRgroup; this was not noted, however, in any subject in theEES-DCR group. In the case of patients in the EES-DCRgroup who had intercurrent nasal abnormalities, it is likelythat successful lacrimal system reconstruction was sup-ported by the correction of the preexisting nasal abnormal-
econstruction. A, In this case from the endonasal endoscopic dacryocys-iferation of fibrotic tissue. B, In this case from the external dacryocysto-anuloma formation. C, In this case from the EES-DCR group, the leftloma formation. D, In this case from the E-DCR group, the right lacrimal
tem rprol
by grgranu
e lacrimal sac.

Wu et al � Endoscopic Dacryocystorhinostomy for Acute Dacryocystitis
ities during surgery, although there was no significant sta-tistical difference between the 2 groups. In the EES-DCRgroup, intranasal ostial patency was not achieved in only 3(17.6%) of 17 patients with preexisting nasal abnormalities.In contrast, intranasal ostial patency was not achieved be-cause of the development of fibrosis, granulation tissue, orboth around the ostium in 3 (37.5%) of 8 patients withpreexisting nasal abnormalities in the E-DCR group.
The highly edematous mucosa of the lacrimal systemresulting from acute inflammation and preexistent stenosisof the common canaliculus add challenges to a successfullacrimal sac reconstruction for APD.1 Failure of lacrimalpassage reconstruction 12 months after removal of the sil-icone tubes because of obstruction at the inferior or com-mon canaliculus occurred in only 3 (4.2%) of 72 patients inthe present study, lower than that reported by Lee andWoog2 and Morgan et al.3 This may be associated with theuse of the soft probe during operations and during CBIST,although there is lack of adequate clinical evidence tosupport this. Compared with the use of a rigid optic fiber asdescribed in the laser-assisted EES-DCR,2,3,6 the softprobe’s smooth, blunt, rounded, and blind tip can, to a largeextent, decrease the risk of injuries to the canaliculus innermucosa, formation of a sinus tract or false fistula because ofhigh swelling of the medial canthus in APD, or both. Inaddition, after extracting the inner needle and cutting off itsblind tip, it becomes very easy to perform CBIST. However,even when great care is taken, injuries to the canaliculuscannot always be prevented because of the highly edema-tous mucosa of canaliculi. Further, stenosis or obstruction ofcanaliculus in APD may be not identified readily when thepatient first seeks care.1–3 Therefore, it is necessary toperform CBIST. Findings of the present study demonstrate
Table 3. Surgical Complications and Cause
Groups
Ostial ClosureBecause of
Fibrotic Tissue
Ostial ObstructionBecause of
Granulation Tissue
Lacrimal Passage OBecause of Fibro
Granulation Tin the Lacrim
EES-DCR 2 1 0E-DCR 1 2 6
E-DCR � external dacryocystorhinostomy; EES-DCR � endonasal endoPosition of the lacrimal passage obstruction was determined by irrigation anthe second surgery of cold steel EES-DCR.
Table 4. Success Rate of Free Lacrimal Passage Reconstrucin Bo
Groups Total
Success Rateof Lacrimal
Passage ReconstructionNasal Sept
Deviation
EES-DCR 17 82.4% (14/17) 9E-DCR 8 62.5% (5/8) 5P value 0.274*
E-DCR � external dacryocystorhinostomy; EES-DCR � endonasal endoIn the EES-DCR group, surgery of the intercurrent nasal diseases was perf
*Statistical analysis performed with the Fisher exact probability test.that it can be performed safely. In the present study, thetubes were retained in the canaliculi for 3 months aftersurgery in all 72 patients. Apart from the observation oflaceration of the inferior punctum in 7 patients (9.7%), therewere no other complications associated with CBIST.
Currently, 2 techniques are used to perform EES-DCR:the laser-assisted method and the cold steel method.4,5,7,10
The cold steel method used in the present study was usedmainly to create a larger bony ostium and a more substantialopening of the lacrimal sac, to minimize the risks of fibrosisand stenosis from heat generation during bony and mucosalablation with the holmium:yttrium aluminum garnet (hol-mium:YAG) and potassium titanyl phosphate (KTP) laser,and to facilitate the intranasal ostial patency.4–6 In theauthors’ experience, nasal mucosal flaps were advocatedto be removed during surgery to increase the ease ofsurgical manipulation and to decrease tissue trauma.Without excision of the flaps, surgical manipulation oftenis hindered by significant hemorrhage from acutely in-flamed tissues. Excision of the flaps in patients simulta-neously undergoing correction of nasal abnormalitiesalso eliminates the risks of ostial closure resulting fromdislocation of the flaps during nasal packing.
In summary, the outcomes of EES-DCR with CBISTguided by a soft probe with the conventional treatment forAPD were compared. This approach for APD seems toyield a higher success rate with minimal tissue invasionand minimal trauma to the lacrimal system with fewercomplications. By allowing for adequate drainage of thelacrimal sac abscess, providing simultaneous correctionof nasal abnormalities that predispose the failure of in-tranasal ostial patency, and protecting the lacrimal sys-tem mucosa from injury, the rapid resolution of acute
ostoperative Lacrimal Passage Obstruction
ctiond/ors
Lacrimal PassageObstruction at the
Common CanaliculusLaceration of theInferior Punctum
MedialCanthal PurulentFistula Formation
1 3 02 4 3
dacryocystorhinostomy.bing of the lacrimal passage and also by what the endoscope showed during
in Patients with Intercurrent Nasal Diseases or Conditionsroups
Nasal Septal Deviationand Middle Turbinate
HypertrophyNasalPolyps
Nasal Septal Deviationand Nasal Polyp andChronic Ethmoiditis
3 3 23 0 0
dacryocystorhinostomy.simultaneously, whereas in the E-DCR group, no surgery was performed.
s of P
bstrutic anissueal Sac
scopicd pro
tionth G
al
scopicormed
121

Ophthalmology Volume 116, Number 1, January 2009
infection likely contributes to the higher success rate ofthis approach. Thus, the technique of cold steel EES-DCR with CBIST guided by a soft probe is a promisingalternative for the conventional treatment of APD with alacrimal sac abscess.
References
1. Cahill KV, Burns JA. Management of acute dacryocystitisin adults. Ophthal Plast Reconstr Surg 1993;9:38 – 41;discussion 42.
2. Lee TS, Woog JJ. Endonasal dacryocystorhinostomy in theprimary treatment of acute dacryocystitis with abscess forma-tion. Ophthal Plast Reconstr Surg 2001;17:180–3.
3. Morgan S, Austin M, Whittet H. The treatment of acutedacryocystitis using laser assisted endonasal dacryocystorhi-
nostomy. Br J Ophthalmol 2004;88:139–41.ison, Wisconsin.
122
4. Metson R, Woog JJ, Puliafito CA. Endoscopic laser dacryo-cystorhinostomy. Laryngoscope 1994;104:269–74.
5. Hehar SS, Jones NS, Sadiq A, Downes RN. Endoscopicholmium: YAG laser dacryocystorhinostomy—safe and effectiveas a day-case procedure. J Laryngol Otol 1997;111:1056–9.
6. Hartikainen J, Grenman R, Puukka P, Seppa H. Prospectiverandomized comparison of external dacryocystorhinostomyand endonasal laser dacryocystorhinostomy. Ophthalmology1998;105:1106–13.
7. Wormald PJ. Powered endoscopic dacryocystorhinostomy.Laryngoscope 2002;112:69–72.
8. Sodhi PK, Pandey RM, Malik KP. Experience with bicanal-icular intubation of the lacrimal drainage apparatus combinedwith conventional external dacryocystorhinostomy. J Crani-omaxillofac Surg 2003;31:187–90.
9. Walland MJ, Rose GE. Factors affecting the success rate ofopen lacrimal surgery. Br J Ophthalmol 1994;78:888–91.
10. Sprekelsen MM, Barberan MT. Endoscopic dacryocystorhinos-tomy: surgical technique and results. Laryngoscope 1996;106:
187–9.Footnotes and Financial Disclosures
Originally received: February 5, 2008.Final revision: September 21, 2008.Accepted: September 24, 2008. Manuscript no. 2008-173.
1 Eye Hospital of Wenzhou Medical College, Wenzhou, Peoples’ Republicof China.
2 Department of Surgery, University of Wisconsin Medical School, Mad-
Financial Disclosure(s):The author(s) have no proprietary or commercial interest in any materialsdiscussed in this article.
Supported by the Foundation of the Health Department in the Zhejiangprovince of China (2007A144).
Correspondence:Wencan Wu, Eye Hospital of Wenzhou Medical College, No. 270, Xu-eyuan Xi Road, Wenzhou City 325027, Peoples’ Republic of China.
E-mail: [email protected].Copyright © 2022 FDOKUMEN