
Implementation of endoscopic ultrasound for lung cancer staging

EXTENDED ENDOSCOPIC TRANSSPHENOIDALAPPROACH FOR EXTRASELLARCRANIOPHARYNGIOMAS
OBJECTIVE: Suprasellar craniopharyngiomas have been classically removed using avariety of transcranial approaches. Historically, the transsphenoidal route was reservedfor intrasellar-infradiaphragmatic, and preferably cystic, lesions. With the advent ofthe endoscope in transsphenoidal surgery, its obvious advantages combined with neu-rosurgeons’ increasing interest in extended transsphenoidal approaches made suprasel-lar and even intraventricular craniopharyngiomas accessible for removal via such alow route.PATIENTS AND METHODS: Between January of 2004 and April of 2006, six men andfour women (mean age, 57.2 yr; range, 26–70 yr) underwent surgery for craniopharyn-gioma, including two intrasuprasellar, one suprasellar, six suprasellar-intraventricular,and one that was purely intraventricular. Three patients had undergone a previous tran-scranial surgery via the pterional approach, whereas one patient had undergone atranssphenoidal microsurgical approach. The surgical method consisted of an extendedendoscopic transsphenoidal approach with removal of the upper half of the sella, thetuberculum sellae, and the posterior part of the planum sphenoidale, using a “three-four hands” technique.RESULTS: Total craniopharyngioma removal was achieved for seven patients, subtotalremoval was possible for two patients, and one patient had a partial removal. Twopatients developed a postoperative cerebrospinal fluid leak that required a successfulendoscopic revision of the cranial base reconstruction. One patient died 5 weeks laterbecause of hypothalamic dysfunction. All patients with visual field and/or visual acu-ity defect improved except one patient, in which we observed a slight worsening ofvisual acuity in one eye. Preoperative pituitary dysfunction did not improve in anypatient. In three patients, we observed the new occurrence of permanent diabetesinsipidus. One patient developed a sphenoid sinus mycosis, which was treated withantimycotic therapy. We did not observe carotid injury, epistaxis from the sphenopala-tine artery, or airway difficulties.CONCLUSION: For selected patients, the extended endoscopic endonasal approach forremoval of suprasellar craniopharyngioma seems to provide a valid alternative to tran-scranial approaches.
KEY WORDS: Cranial base, Craniopharyngioma, Endoscope, Endoscopic transsphenoidal surgery,Suprasellar lesions
Neurosurgery 61[ONS Suppl 2]:ONS219–ONS228, 2007 DOI: 10.1227/01.NEU.0000280113.98151.24
NEUROSURGERY VOLUME 61 | OPERATIVE NEUROSURGERY 2 | NOVEMBER 2007 | ONS219
Enrico de Divitiis, M.D.Department of Neurological Sciences,Division of Neurosurgery,Università degli Studi di NapoliFederico II,Naples, Italy
Paolo Cappabianca, M.D.Department of Neurological Sciences,Division of Neurosurgery,Università degli Studi di NapoliFederico II,Naples, Italy
Luigi M. Cavallo, M.D., Ph.D.Department of Neurological Sciences,Division of Neurosurgery,Università degli Studi di NapoliFederico II,Naples, Italy
Felice Esposito, M.D., Ph.D.Department of Neurological Sciences,Division of Neurosurgery,Università degli Studi di NapoliFederico II,Naples, Italy
Oreste de Divitiis, M.D.Department of Neurological Sciences,Division of Neurosurgery,Università degli Studi di NapoliFederico II,Naples, Italy
Andrea Messina, M.D.Department of Neurological Sciences,Division of Neurosurgery,Università degli Studi di NapoliFederico II,Naples, Italy
Reprint requests:Enrico de Divitiis, M.D.,Department of Neurological Sciences,Division of Neurosurgery,Università degli Studi di NapoliFederico II,Via S. Pansini, 5,80131 Naples, Italy.Email: [email protected]
Received, November 30, 2006.Accepted, March 16, 2007.
Surgical management of craniopharyn-gioma still represents a challenge for allneurosurgeons. Despite the fact that such
lesions have benign histological features, fromthe surgeon’s perspective, they are among themost complex pathologies in neurosurgery.This can be attributed to their deep location,
their proximity to important neurovascularstructures, their different relationships withthe brain (2) and the pial and subarachnoidspaces (9), and their tendency to recur, evenafter gross total removal.
A certain agreement has existed regardingthe choice of using the transcranial approach
TUMORSurgical Technique

for surgical treatment of suprasellar and ventricular cranio-pharyngiomas, and limiting the transsphenoidal approach forintrasellar or intrasuprasellar infradiaphragmatic lesions (19,23, 32, 33).
Weiss (37) first reported good results with the surgicalremoval of supradiaphragmatic craniopharyngiomas oncejudged amenable only to transcranial surgery, using a trans-nasal transsphenoidal microscopic approach extended fromthe sella to the posterior portion of the planum. In subse-quent years, several other authors used such a modifiedtranssphenoidal approach to successfully treat patients withsupradiaphragmatic craniopharyngioma (11, 17, 26, 28, 31,34, 35).
The recent and rapid diffusion of endoscopy into transsphe-noidal surgery (3, 4, 6, 12, 24) has led some authors, alreadyexperienced in endoscopic pituitary surgery, to perform sur-gical removal of suprasellar lesions through a pure, fullyendoscopic, extended transnasal transsphenoidal approach(5, 14, 21, 25).
We report our experience in treating 10 consecutive patientswho underwent this technique for removal of several types ofcraniopharyngioma. The aim of this work is to describe thesurgical technique and the clinical outcome of our patientseries. We emphasize the flexibility of this approach for access-ing different types of craniopharyngioma, as well as the advan-tages and limits as compared with transcranial and transsphe-noidal microscopic approaches.
PATIENTS AND METHODS
Between January of 2004 and April of 2006, in the Department ofNeurosurgery of the Università degli Studi di Napoli Federico II, sixmen and four women (mean age, 57.2 yr; range, 26–70 yr) underwentan extended endoscopic transsphenoidal approach for treatment ofcraniopharyngioma by the senior author (EdD) and his coauthor(LMC). The series includes two intrasuprasellar, one suprasellar, sixsuprasellar-intraventricular, and one purely intraventricular cranio-pharyngiomas (Tables 1 and 2). Three patients had undergone a previ-ous transcranial surgery via the pterional approach, and one patienthad undergone a transsphenoidal microsurgical approach. At theiradmission, four patients presented with pan-hypopituitarism, andthree patients had diabetes insipidus. All but two patients harboredvariable degrees of visual field and/or visual acuity defect. Onewoman (Patient 8) with an intra/extraventricular craniopharyngiomapresented with hydrocephalus and progressive worsening of her cog-nitive and neurological functions. None of the patients had previouslyreceived radiation therapy. All patients underwent an endocrinologicalevaluation preoperatively, 1 month after surgery, and every 6 monthsthereafter. All patients underwent formal visual-field and visual-acuityevaluation pre- and postoperatively. Neuroradiological evaluationincluded brain and sellar magnetic resonance imaging, before and afterintravenous paramagnetic contrast agent (gadolinium-labeled diethyl-enetriamine pentaacetic acid) administration. Computed tomographicscans of the craniofacial bones and the sellar area provided the defini-tion of and relationships between the sphenoid, sella, and other bonestructures involved in the procedure.
On postoperative Day 4 and after 1 month, we performed endo-scopic exploration of the nasal cavity of each patient, to ascertain the
effectiveness of the cranial base reconstruction. An early postoperativeneuroradiological evaluation via magnetic resonance imaging wasscheduled for 7 days after surgery, and a subsequent magnetic reso-nance imaging study was performed 3 months later.
The Surgical TechniqueThe technique was extensively described by our group in a recent
publication (15). Nevertheless, some steps of the surgical approach arepeculiar and therefore warrant a brief description here.
In contrast with our standard approach, whereby the endoscope isfixed to an autostatic holder to allow one surgeon to bimanually per-form the surgery, preferably via one of the patient’s nostrils, theextended approach is performed by two surgeons through both nos-trils, thereby enabling the surgeons to use two or three surgical instru-ments in addition to the endoscope. This provides the surgeons with adeep perspective and a closer view during the intradural maneuvers.For a successful approach, the two surgeons must respect some rules.The endoscope is moved freehand in and around the surgical field toprovide visual information about the relationships between the tumorand the various neurovascular structures. This is the “dynamic” aspectof the technique; the endoscope constantly follows the fine in-and-outmovements of the instruments in the surgical field during the dissec-tion of the lesion, thereby minimizing the risk of injury to the nearbyneurovascular structures. This “three-four hands technique” (two orthree instruments plus the endoscope inserted through both nostrils) asdescribed by some authors (7, 27) is the result of such cooperationbetween the two surgeons that in some way they share the same role,care, and responsibilities.
The anterior intercavernous sinus should be managed before thedura is opened. The sinus runs within the dura of the upper part of thesella, and is almost always present; however, sometimes, instead of asingle channel, it is made up of a fine, rich plexus that covers most ofthe dura of the sella turcica. This situation may present with profusebleeding, forcing the surgeon to abort the procedure (34). The sinus iscoagulated and cut. The lateral edges of the sinus are gently coagulatedto enable retraction and to gain more room. Such coagulation shouldnot be extended too far laterally because of the proximity of the intra-cavernous carotid arteries. Our policy is to not use miniclips too closethe sinus, because their presence can restrict the surgeon’s view of theintradural space.
The osteodural opening created to reach the lesion should be aswide as the classical opening of the lamina terminalis (average area,52.84 mm2 [16]), to enable control of the entire ventricular chamber.
After the dura overlaying the planum has been opened, the pituitarygland is gently pushed downward. This allows for a supraglandularroute (20, 35) and avoids the necessity of cutting the gland.
When working on suprasellar prechiasmatic craniopharyngiomas,the tumor can be seen immediately after the dural opening, anterior tothe chiasm and in front of the stalk. The opposite is true with respectto intraventricular craniopharyngiomas: the tumor is not readily visi-ble, because it is located behind the stalk and the chiasm, and it mustbe approached by passing laterally to the stalk.
Tumor removal is performed by fine and meticulous dissection fromthe chiasm, the stalk, and the superior hypophyseal arteries. The ante-rior communicating artery complex, located above the chiasm, is pro-tected by an arachnoidal sheet.
At the end of the tumor resection, the surgical cavity is inspectedwith 0- and 30-degree endoscopes to check the entirety of the removaland to control any bleeding. A meticulous hemostasis is achieved.Careful reconstruction of the cranial base defect is performed in accor-dance with our previously described policy (15). A balloon stent is
ONS220 | VOLUME 61 | OPERATIVE NEUROSURGERY 2 | NOVEMBER 2007 www.neurosurgery-online.com
DE DIVITIIS ET AL.

introduced through one nostril, inflated in the sphenoid cavity, and leftin place for 5 days to support the graft material (27). We use no pack-ing in the nose at the end of the procedure.
RESULTS AND COMPLICATIONS
Total lesion removal was achieved in seven patients. In twopatients, a subtotal removal was possible; for one patient, thiswas because a calcified fragment adhered to the left posterior
cerebral artery, and in the other, the thin tumor capsule adheredto the right optic nerve.
In one patient only a partial removal was possible becausethe cleavage plane between the tumor fragment and the wall ofthe third ventricle was not well defined. Two patients devel-oped a postoperative cerebrospinal fluid leak, which requiredus to perform an early (and successful) endoscopic revision ofthe cranial base graft. Patient 8 died 5 weeks after surgery as aresult of a brainstem hemorrhage that induced hypothalamic
NEUROSURGERY VOLUME 61 | OPERATIVE NEUROSURGERY 2 | NOVEMBER 2007 | ONS221
EXTENDED ENDOSCOPIC TRANSSPHENOIDAL APPROACH
TABLE 1. Clinical findings and surgical outcomes of 10 patients treated for craniopharyngioma using an extended endoscopic transsphenoidalapproach
Preoperative Preoperative Previous Tumor Postoperative Postoper-Patient Age/endocrinologi- visual surgical removal endocrinolo- ative visual Complicationsno. sexcal symptoms symptoms procedures (extent) gical outcome outcome
1 70/F Bitemporal Transcranial Total Improvedhemianopia approach
2 58/M Panhypopituit- Bitemporal hemianopia; Transsphenoi- Subtotal Unchanged Improved Cerebrospinalarism, diabetes visual acuity: dal approach fluid leakinsipidus right, 1/200; left, 1/20
3 68/M Superior bitemporal Total Panhypop- Improvedquadrantopia ituitarism
4 63/M Bitemporal hemianopia Transcranial Subtotal Improvedvisual acuity: right, 1/30 approach
5 58/M Panhypopituitarism, Transcranial Total Unchangeddiabetes insipidus approach
6 57/M Panhypopituitarism Bitemporal hemianopia; Total Unchanged Improved Cerebrospinal fluidvisual acuity: left, 1/30 leak, diabetes insipidus
7 47/F Diabetes visual acuity: Partial Unchanged Improved on right,insipidus right, 1/30; left, 2/10 worsened on left
8 57/F Total Brainstem hemorrhage
9 68/M Panhy- Bitemporal hemia- Total Unchanged Improved Diabetes insipidus,popituitarism nopia visual acuity: chronic subdural
right, 6/10; left, 3/10 hematoma
10 26/F Hyperprolactinemia Total Unchanged Diabetes insipidus
TABLE 2. Surgical findings of 10 patients treated for craniopharyngioma using an extended endoscopic transsphenoidal approach
Patient Age/ Sella Tumor Relationship of lesion Pial Tumorno. sex size location with chiasm invasion characteristics
1 70/F Normal Infra- and suprasellar Retrochiasmatic No Cystic
2 58/M Enlarged Infra- and suprasellar Prechiasmatic No Solid
3 68/M Normal Intra- and extraventricular Retrochiasmatic No Solid
4 63/M Reduced Suprasellar Retrochiasmatic No Cystic and solid
5 58/M Normal Intra- and extraventricular Retrochiasmatic Yes Cystic and solid
6 57/M Normal Intraventricular Retrochiasmatic No Solid
7 47/F Normal Intra- and extraventricular Retrochiasmatic Yes Cystic and solid
8 57/F Normal Intra- and extraventricular Retrochiasmatic No Cystic and solidwith hydrocephalus
9 68/M Normal Intra- and extraventricular Prechiasmatic No Cystic and solid
10 26/F Normal Intra- and extraventricular Retrochiasmatic No Cystic and solid

dysfunction with irreversible disturbance of fluid and elec-trolyte balance.
All patients with visual field and/or visual acuity defectsimproved, except one patient, whom we observed experi-enced worsening of visual acuity in one eye and improve-ment in the other. Preoperative pituitary dysfunction did notimprove in any patient. In three patients, we observed thenew occurrence of permanent diabetes insipidus. One patientdeveloped a sphenoid sinus mycosis that was successfullytreated with antimycotic therapy. We did not observe carotidinjury, epistaxis from the sphenopalatine artery, or airway dif-ficulties in any patients.
For almost all patients, we identified intracranial air on theearly postoperative images. This was caused by copious intra-operative cerebrospinal fluid release. No case of symptomatichypertensive pneumocephalus occurred. One patient devel-oped a bilateral chronic subdural hematoma 3 weeks after theoperation. Once this patient was treated with evacuation on thesubdural collections, there were no additional problems.
DISCUSSION
A transcranial microscopic approach has traditionally beenpreferred for removal of tumors located entirely within thethird ventricle or extending upward out of a normal or smallsella. The transsphenoidal approach, either microscopic orendoscopic, has been restricted to intrasellar subdiaphrag-matic tumors that extend upward from an enlarged sella tur-cica, and only partially involve the anteroinferior part of thethird ventricle, according to Grades I and II of Samii’s classifi-cation (36). This dogmatic statement can be considered ques-tionable after the introduction of the extended transsphenoidalapproach for treatment of suprasellar supradiaphragmaticcraniopharyngioma, as it provides additional bone removalfrom the anterior cranial base.
The site of origin, path of growth, location of the tumor, andsite of invasion of the third ventricle play important roles in thechoice of the proper approach.
Transcranial versus Transsphenoidal ApproachComparison of the transcranial approach versus the
transsphenoidal route for management of extrasellar supradi-aphragmatic craniopharyngioma is made primarily on thebasis of operative nuances. Our personal series and the seriesof others working with the extended transsphenoidal approach(1, 11, 17, 20, 21, 26, 29, 31, 35) involve patient populations thatare too small to allow conclusions to be made regarding clini-cal results and outcomes.
Several transcranial approaches have been advocated for theresection of craniopharyngiomas, and each has both advan-tages and limits.
Although each surgeon uses his or her most familiar tech-nique, the pterional approach seems to have several advan-tages over other craniotomies (39). Nevertheless, a single routefor craniotomy has proven insufficient in many cases, as high-lighted by Fahlbusch et al. (20) in a recent comprehensive study
of a large patient series. Furthermore, once the intradural spacehas been reached, various surgical corridors are presently usedto access the areas where the tumor is localized. As a matter offact, Yasargil (38) described seven different intradural corridorsto manage all the different extensions of the craniopharyn-
ONS222 | VOLUME 61 | OPERATIVE NEUROSURGERY 2 | NOVEMBER 2007 www.neurosurgery-online.com
DE DIVITIIS ET AL.
FIGURE 1. Anatomical figures showing the suprasel-lar prechiasmatic area used for the transsphenoidalremoval of extraventricular craniopharyngioma.AComA, anterior communicating artery complex;ON, optic nerve; Ch, chiasm; Ps, pituitary stalk; sha,superior hypophyseal artery.
FIGURE 2 A–C, preoperativemagnetic resonance images reveala prechiasmatic suprasellar-intra-ventricular craniopharyngioma(Patient 9). D and E, postoperativemagnetic resonance images showthe gross total removal of the lesion.

giomas in his series. The tumor can be removed by extra-axialdissection in the parachiasmatic area, such as the prechiasmaticspace, the opticocarotid triangle, and the superior carotid bifur-cation triangle. These structures can be only mobilized for afew millimeters; therefore, the tumor is often dissected andremoved without direct visual control. Furthermore, in partic-ularly complex situations, combined approaches have beenproposed to perform gross total lesion removal, such as prechi-asmatic translamina terminalis for suprasellar craniopharyn-giomas that occupy the anterior portion of the third ventricle;and transcallosal-translamina terminalis for craniopharyn-giomas that extend within the third ventricle, to control theintraventricular part of the lesion via the transcallosal route,and the parachiasmal area through the opening of the laminaterminalis. These routes have been realized either through twosmall craniotomies (38) or one large craniotomy (30).
Finally, the importance of a prefixed chiasm and the lowposition of the anterior communicating artery complex shouldnot be underestimated. These conditions may lead to a very dif-ficult tumor resection in all types of basal approaches.
Using the extended transsphenoidal route permits the sur-geon to reach from below the various types of craniopharyn-giomas and perform the dissection under direct visual control.Using the same surgical corridor, depending on the site ofthe lesion, the surgeon can work either below or above the
NEUROSURGERY VOLUME 61 | OPERATIVE NEUROSURGERY 2 | NOVEMBER 2007 | ONS223
EXTENDED ENDOSCOPIC TRANSSPHENOIDAL APPROACH
FIGURE 3. Intraoperative images of Patient 9. A, iso-lation of the superior intercavernous sinus (sis). B,after the section of the superior intercavernous sinusand the opening of the dura, the craniopharyngiomapromptly becomes visible. T, tumor; CP, carotid protu-berance; S, sella; C, clivus.
A
B
FIGURE 4. Intraoperative images of Patient 9. Thecystic part of the tumor is opened (A) and dissected allaround from the neurovascular structures (B and C).T, tumor; ON, optic nerve; ICA, internal carotidartery; DS, dorsum sellae; Ps, pituitary stalk; Pg, pitu-itary gland; A2, second tract of the anterior cerebralartery; AcoA, anterior communicating artery; A1,first tract of the anterior cerebral artery; msa, medialstriate arteries.
A
B
C

optic chiasm and throughboth sides of the stalk, tomanage both the suprasellarprechiasmatic and the intra-ventricular craniopharyn-giomas.
Suprasellar extraventricu-lar craniopharyngiomas arevisualized in a surgical areawhere they have relationshipswith the underside of theoptic apparatus, laterally withthe internal carotid arteries,posteriorly with the pituitarystalk, and lateral to the stalk,the superior hypophysealarteries (15). Small vesselsarising from the internalcarotid artery and the supe-rior hypophyseal arteries thatprovide a vascular supply tothe inferior surface of theoptic apparatus and to thestalk are often visualized andshould be preserved. In suchsituations, the optic chiasm islocalized over the tumor,while the anterior communi-cating artery, protected by thearachnoid over the chiasm, isusually not involved in thetumor dissection maneuvers(Figs. 1–5).
Intraventricular cranio-pharyngiomas are visualized
in a surgical area where they have relationships with the pos-terior aspect of the stalk and the inferoposterior aspect of theoptic apparatus. Working alternatively from both sides of thestalk, the floor of the third ventricle is reached but it is oftenunrecognizable, because it may have been disrupted by thetumor growth. In some cases, because it is more important toradically remove the craniopharyngioma, the pituitary stalkmight be cut to facilitate the surgical maneuvers. The trajectoryafforded by the transsphenoidal approach permits the neuro-surgeon to work along the same axis of the path of growth ofthis type of craniopharyngioma. In such a way, the suprasellar,purely intraventricular masses that are associated with a smallor normal sella, which traditionally are considered unsuitablefor treatment via the transsphenoidal route (8, 11), can be suc-cessfully removed using this technique (Figs. 6–9). However,not every patient with a craniopharyngioma is a suitable can-didate for such extended approaches.
The degree of pneumatization of the sphenoid sinus isimportant. Presellar or conchal-type sinuses represent a relativecontraindication to the extended approach. The main land-marks within the sphenoid sinus are not easily recognizable,
ONS224 | VOLUME 61 | OPERATIVE NEUROSURGERY 2 | NOVEMBER 2007 www.neurosurgery-online.com
DE DIVITIIS ET AL.
C
A B
D
FIGURE 5. Intraoperative images of Patient 9. A–C, the intraventricular component of the tumor is removedthrough the enlarged pituitary stalk (Ps). D, after lesion removal, the endoscopic exploration with a 30-degree angledendoscope allows better visualization of the course of both frontopolar arteries (FP). ON, optic nerve; Ch, optic chi-asm; T, tumor; PG, pituitary gland; A2, second tract of the anterior cerebral artery; AcoA, anterior communicatingartery; msa, medial striate arteries; A1, first tract of the anterior cerebral artery.
FIGURE 6. Anatomical figures showing the subchi-asmatic route used for transsphenoidal removal ofintraventricular craniopharyngioma. ON, opticnerve; Ch, chiasm; ICA, internal carotid artery; OT,optic tract; sha, superior hypophyseal artery; ps,pituitary stalk; BA, basilar artery.

thus the risk of injury to the intracavernous internal carotidarteries and the optic nerves is increased. The presence of ahigh dorsum can increase the difficulty of the procedure, espe-cially in patients who have retrosellar extension of the lesion.The anterior intercavernous sinus can influence the bone resec-tion because of its sometimes profuse bleeding.
The tumor’s consistency, blood supply, and adherences tothe surrounding neurovascular structures can present obsta-cles for the approach. In our experience, the time required foran extended approach is still superior to that required for atranscranial approach, although in others’ hands (10), it couldbe considered an attractive alternative to other techniques inthe event that one prefers to avoid prolonged surgery.
Transsphenoidal Endoscopy versus MicroscopyThe main differences between the endoscopic procedure and
the microsurgical technique are related to the properties of the
NEUROSURGERY VOLUME 61 | OPERATIVE NEUROSURGERY 2 | NOVEMBER 2007 | ONS225
EXTENDED ENDOSCOPIC TRANSSPHENOIDAL APPROACH
FIGURE 7. A and B, preoperative magnetic resonance images from Patient6 reveal a pure intraventricular craniopharyngioma. C and D, early (24-hpostoperative) computed tomographic scan. Note the small blood clot on theright wall of the third ventricle (C) and the cranial base defect reconstructionwith correct position of the sheet of Lactosorb (Lorenz Surgical, Inc.,Jacksonville, FL) synthetic bone substitute (D). E and F, postoperative (3 mo)magnetic resonance images show complete lesion removal.
FIGURE 8. Intraoperative images of Patient 6. Thetumor was gradually dissected from the chiasm (A),the stalk (B), and the third ventricular cavity walls(C). Ch, optic chiasm; T, tumor; Ps, pituitary stalk;Pg, pituitary gland; ON, optic nerve.
absent when the “endonasal”technique is used either endo-scopically or microscopically.Furthermore, when the endo-nasal approach is used, nasalpacking is not required. Thishelps to minimize patients’breathing difficulties, headache,and dryness of the oral mucosaand is associated with excellentpatient compliance (18).
Aside from these benefits, thelimitations of endoscopy shouldbe considered. The present endo-scopic technology yields a bidi-mensional computer-processedimage on the video monitor,which is lacking in the depth per-spective that is provided by thesuperior binocular stereoscopicvision of the operating micro-scopes. Moreover, the endoscope
lens produces images with maximal magnification at its centerand contraction at its periphery (a barrel effect), and the nearestimages are disproportionally enlarged, while remote images arefalsely miniaturized. This limit can be overcome with continu-ous in-and-out movements of the endoscope.
Handling dedicated endoscopic instruments and the associ-ated different and variably angled tips is challenging whenworking in the tight corners that the angled endoscopes aredesigned to expose (13).
Finally, in contrast with the microsurgical technique, whereone surgeon alone can accomplish the procedure, our personalendoscopic technique requires two surgeons with previousextensive experience with the use of the endoscope in stan-dard transsphenoidal surgery.
CONCLUSIONS
Using the extended endoscopic endonasal approach forsuprasellar craniopharyngiomas allows the surgeon to avoidbrain retraction, permits early exposure of the lesion, providesgood visualization of the pituitary gland, stalk, and main vas-cular structures, and minimizes optic apparatus manipulation.The procedure can be accomplished regardless of the chiasmposition, often enabling a gross total removal of the lesion withcomparable outcomes and complication rates that are achievedwith other current techniques.
Despite encouraging recent preliminary reports on a series ofseveral patients operated on with this technique, conclusiveresults in terms of completeness of lesion removal, adequate fol-low-up, recurrence rate, and endocrinological results are not yetavailable, thereby delaying a truly objective judgment.Additional experience with this kind of technique is required forus to determine the overall efficacy of such a new approach.Limitations still exist concerning the size of the tumor, the oper-
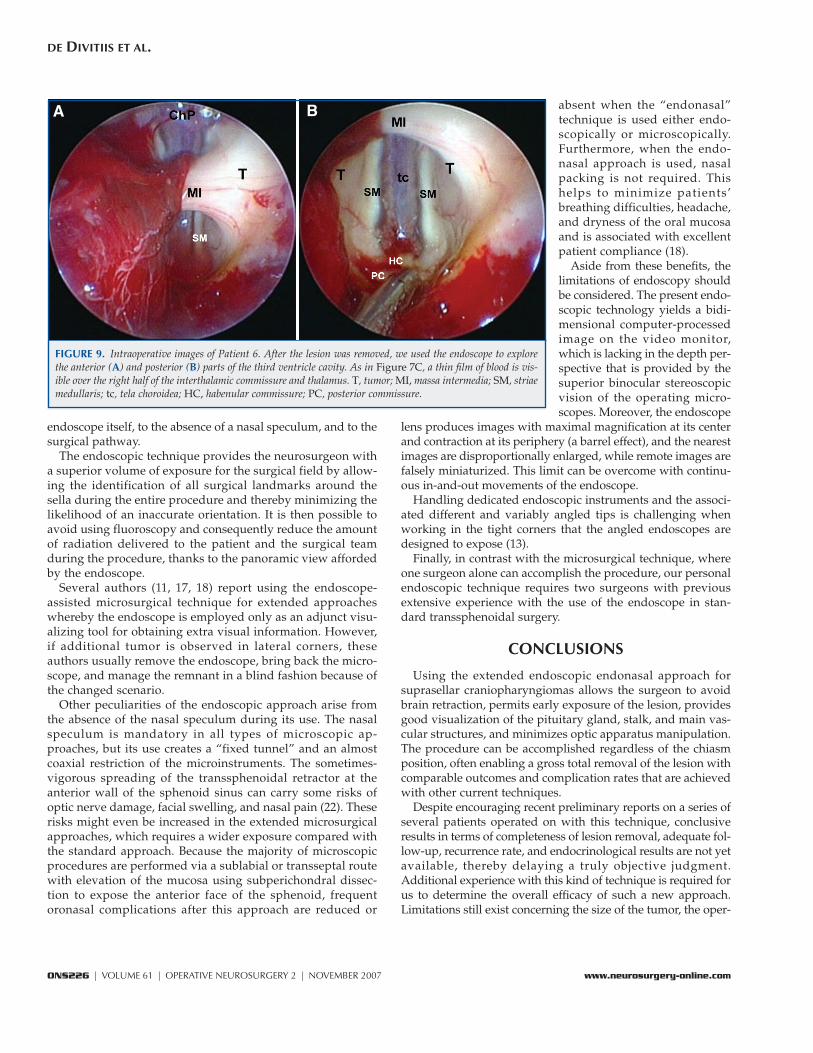
FIGURE 9. Intraoperative images of Patient 6. After the lesion was removed, we used the endoscope to explorethe anterior (A) and posterior (B) parts of the third ventricle cavity. As in Figure 7C, a thin film of blood is vis-ible over the right half of the interthalamic commissure and thalamus. T, tumor; MI, massa intermedia; SM, striaemedullaris; tc, tela choroidea; HC, habenular commissure; PC, posterior commissure.
endoscope itself, to the absence of a nasal speculum, and to thesurgical pathway.
The endoscopic technique provides the neurosurgeon witha superior volume of exposure for the surgical field by allow-ing the identification of all surgical landmarks around thesella during the entire procedure and thereby minimizing thelikelihood of an inaccurate orientation. It is then possible toavoid using fluoroscopy and consequently reduce the amountof radiation delivered to the patient and the surgical teamduring the procedure, thanks to the panoramic view affordedby the endoscope.
Several authors (11, 17, 18) report using the endoscope-assisted microsurgical technique for extended approacheswhereby the endoscope is employed only as an adjunct visu-alizing tool for obtaining extra visual information. However,if additional tumor is observed in lateral corners, theseauthors usually remove the endoscope, bring back the micro-scope, and manage the remnant in a blind fashion because ofthe changed scenario.
Other peculiarities of the endoscopic approach arise fromthe absence of the nasal speculum during its use. The nasalspeculum is mandatory in all types of microscopic ap-proaches, but its use creates a “fixed tunnel” and an almostcoaxial restriction of the microinstruments. The sometimes-vigorous spreading of the transsphenoidal retractor at theanterior wall of the sphenoid sinus can carry some risks ofoptic nerve damage, facial swelling, and nasal pain (22). Theserisks might even be increased in the extended microsurgicalapproaches, which requires a wider exposure compared withthe standard approach. Because the majority of microscopicprocedures are performed via a sublabial or transseptal routewith elevation of the mucosa using subperichondral dissec-tion to expose the anterior face of the sphenoid, frequentoronasal complications after this approach are reduced or
ONS226 | VOLUME 61 | OPERATIVE NEUROSURGERY 2 | NOVEMBER 2007 www.neurosurgery-online.com
DE DIVITIIS ET AL.
A B

ative field depth, hemorrhage management, osteodural defectreconstruction, the steep learning curve, and securing adequatelydedicated instruments. Additional progress is obviouslyexpected in terms of technological development, such as theadvent of high-definition monitors and video cameras, improve-ment of illumination and image quality, dedicated low-profileinstruments, improvement of chip-stick technology, and others.
Provided that the transcranial microscopic approach repre-sents the first option for treatment of supradiaphragmaticcraniopharyngioma today, our belief is that this technique, inappropriately selected patients, could substitute for the time-honored classical techniques and allow safe and effectivemanagement of not only craniopharyngioma, but also othermasses located in the suprasellar area, without great risk tothe integrity of the optic apparatus, neurovascular structures,and hypothalamus.
REFERENCES
1. Abe T, Ludecke DK: Transnasal surgery for infradiaphragmatic craniopharyn-giomas in pediatric patients. Neurosurgery 44:957–966, 1999.
2. Adamson TE, Wiestler OD, Kleihues P, Yasargil MG: Correlation of clinicaland pathological features in surgically treated craniopharyngiomas.J Neurosurg 73:12–17, 1990.
3. Cappabianca P, Alfieri A, de Divitiis E: Endoscopic endonasal transsphe-noidal approach to the sella: Towards functional endoscopic pituitary surgery(FEPS). Minim Invasive Neurosurg 41:66–73, 1998.
4. Cappabianca P, Cavallo LM, Colao A, Del Basso De Caro M, Esposito F,Cirillo S, Lombardi G, de Divitiis E: Endoscopic endonasal transsphenoidalapproach: Outcome analysis of 100 consecutive procedures. Minim InvasiveNeurosurg 45:193–200, 2002.
5. Cappabianca P, Frank G, Pasquini E, de Divitiis O, Calbucci F: Extended endo-scopic endonasal transsphenoidal approaches to the suprasellar region, planumsphenoidale and clivus, in de Divitiis E, Cappabianca P (eds): EndoscopicEndonasal Transsphenoidal Surgery. Wien, Springer-Verlag, 2003, pp 176–187.
6. Carrau RL, Jho HD, Ko Y: Transnasal-transsphenoidal endoscopic surgery ofthe pituitary gland. Laryngoscope 106:914–918, 1996.
7. Castelnuovo P, Pistochini A, Locatelli D: Different surgical approaches to thesellar region: Focusing on the “two nostrils four hands technique.” Rhinology44:2–7, 2006.
8. Ciric I: Variations on the standard transsphenoidal approach to the sellarregion, with emphasis on the extended approaches and parasellarapproaches: Surgical experience in 105 cases. Neurosurgery 55:551, 2004(comment).
9. Ciric IS, Cozzens JW: Craniopharyngiomas: Transsphenoidal method ofapproach-for the virtuoso only? Clin Neurosurg 27:169–187, 1980.
10. Couldwell WT: Extended transsphenoidal craniotomy: Experience in 104cases (abstract). Presented at American Association of Neurological Surgeons,Orlando, Florida, 2004.
11. Couldwell WT, Weiss MH, Rabb C, Liu JK, Apfelbaum RI, Fukushima T:Variations on the standard transsphenoidal approach to the sellar region,with emphasis on the extended approaches and parasellar approaches:Surgical experience in 105 cases. Neurosurgery 55:539–550, 2004.
12. de Divitiis E: Endoscopic transsphenoidal surgery: Stone-in-the-pond effect.Neurosurgery 59:512–520, 2006.
13. de Divitiis E, Cappabianca P: Endoscopic Pituitary Surgery: Anatomy andSurgery of the Transsphenoidal Approach to the Sellar Region. Tuttlingen, Endo-Press, 2004.
14. de Divitiis E, Cappabianca P, Cavallo LM: Endoscopic transsphenoidalapproach: Adaptability of the procedure to different sellar lesions.Neurosurgery 51:699–707, 2002.
15. de Divitiis E, Cavallo LM, Cappabianca P, Esposito F: Extended endoscopicendonasal transsphenoidal approach for the removal of suprasellar tumors:Part 2. Neurosurgery 60:46–59, 2007.
16. de Divitiis O, Angileri FF, d’Avella D, Tschabitscher M, Tomasello F:Microsurgical anatomic features of the lamina terminalis. Neurosurgery50:563–570, 2002.
17. Dusick JR, Esposito F, Kelly DF, Cohan P, DeSalles A, Becker DP, Martin NA:The extended direct endonasal transsphenoidal approach for nonadenoma-tous suprasellar tumors. J Neurosurg 102:832–841, 2005.
18. Dusick JR, Esposito F, Mattozo CA, Chaloner C, McArthur DL, Kelly DF:Endonasal transsphenoidal surgery: The patient’s perspective-survey resultsfrom 259 patients. Surg Neurol 65:332–342, 2006.
19. Fahlbusch R, Honneger J, Buchfelder M: Transsphenoidal microsurgery forcraniopharyngiomas, in Schmidek HH (ed): Shmidek and Sweet OperativeNeurosurgical Techniques: Indications, Methods and Results. Philadelphia, W.B.Saunders, 2000, pp 503–511.
20. Fahlbusch R, Honegger J, Paulus W, Huk W, Buchfelder M: Surgical treatmentof craniopharyngiomas: Experience with 168 patients. J Neurosurg90:237–250, 1999.
21. Frank G, Pasquini E, Doglietto F, Mazzatenta D, Sciaretta V, Farneti G,Calbucci F: The endoscopic extended transsphenoidal approach for cranio-pharyngiomas. Oper Neurosurg 59:75–83, 2006.
22. Garcia AS, Rhoton AL Jr: Speculum opening in transsphenoidal surgery.Neurosurgery 59 [Suppl 1]:ONS35–40, 2006.
23. Honegger J, Buchfelder M, Fahlbusch R, Daubler B, Dorr HG: Trans-sphenoidal microsurgery for craniopharyngioma. Surg Neurol 37:189–196,1992.
24. Jho HD, Carrau RL: Endoscopic endonasal transsphenoidal surgery:Experience with 50 patients. J Neurosurg 87:44–51, 1997.
25. Jho HD, Ha HG: Endoscopic endonasal skull base surgery: Part 1—The mid-line anterior fossa skull base. Minim Invasive Neurosurg 47:1–8, 2004.
26. Kaptain GJ, Vincent DA, Sheehan JP, Laws ER Jr: Transsphenoidal approachesfor the extracapsular resection of midline suprasellar and anterior cranialbase lesions. Neurosurgery 49:94–101, 2001.
27. Kassam AB, Snyderman C, Gardner P, Carrau R, Spiro R: The expandedendonasal approach: A fully endoscopic transnasal approach and resection of theodontoid process: Technical case report. Neurosurgery 57 [Suppl 1]:E213, 2005.
28. Kato T, Sawamura Y, Abe H, Nagashima M: Transsphenoidal-transtubercu-lum sellae approach for supradiaphragmatic tumours. Technical note. ActaNeurochir (Wien) 140:715–719, 1998.
29. Kitano M, Taneda M: Extended transsphenoidal approach with submucosalposterior ethmoidectomy for parasellar tumors. Technical note. J Neurosurg94:999–1004, 2001.
30. Konovalov AN: Microsurgery of craniopharyngiomas, in Rand RW (ed):Microneurosurgery. Toronto, Mosby, 1985, pp 196–213.
31. Kouri JG, Chen MY, Watson JC, Oldfield EH: Resection of suprasellar tumorsby using a modified transsphenoidal approach. Report of four cases. J Neurosurg 92:1028–1035, 2000.
32. Laws ER Jr: Transsphenoidal microsurgery in the management of cranio-pharyngioma. J Neurosurg 52:661–666, 1980.
33. Laws ER: Transsphenoidal surgery, in Apuzzo MLJ (ed): Brain Surgery:Complications Avoidance and Management. New York, Churchill Livingstone,1993, pp 357–362.
34. Laws ER, Kanter AS, Jane JA Jr, Dumont AS: Extended transsphenoidalapproach. J Neurosurg 102:825–828, 2005.
35. Maira G, Anile C, Albanese A, Cabezas D, Pardi F, Vignati A: The role oftranssphenoidal surgery in the treatment of craniopharyngiomas. J Neurosurg 100:445–451, 2004.
36. Samii M, Samii A: Surgical management of craniopharyngiomas, in SchmidekHH (ed): Schmidek and Sweet: Operative Neurosurgical Techniques: Indications,Methods and Results. Philadelphia, W.B. Saunders, 2000, pp 489–502.
37. Weiss M: The transnasal transsphenoidal approach, in Apuzzo MLJ (ed):Surgery of the Third Ventricle. Baltimore, Williams & Wilkins, 1987, pp 476–494.
38. Yasargil MG: Craniopharyngiomas, in Yasargil MG (ed): Microneurosurgery ofCNS Tumors. Stuttgart, Georg Thieme-Verlag, 1996, pp 205–223.
39. Yasargil MG, Curcic M, Kis M, Siegenthaler G, Teddy PJ, Roth P: Totalremoval of craniopharyngiomas. Approaches and long-term results in 144patients. J Neurosurg 73:3–11, 1990.
NEUROSURGERY VOLUME 61 | OPERATIVE NEUROSURGERY 2 | NOVEMBER 2007 | ONS227
EXTENDED ENDOSCOPIC TRANSSPHENOIDAL APPROACH

COMMENTS
In this article, de Divitiis et al. describe the pure endoscopic extendedtranssphenoidal approach to resection of craniopharyngiomas involv-
ing the suprasellar region. This series, although small, clearly demon-strates that the purely endoscopic extended transsphenoidal approachis a possible alternative to either the extended microscopic transsphe-noidal or the microscopic transcranial approaches to these challenginglesions. The authors point out the limitations and relative advantagesand disadvantages of this approach. The follow-up is relatively shortand the series is small, so a longer range of experience is necessary tofully delineate the efficacy of this approach and whether it should berecommended over other approaches. There is no question that the roleof the endoscope in neurosurgery will continue to expand in responseto improved instrumentation, surgical experience, and surgeon educa-tion. The authors are part of one of the leading groups responsible forpushing the field forward in this arena. Over the course of years, theNaples group has produced an excellent body of work. This article addsto the growing supportive evidence for the feasibility and efficacy ofpurely endoscopic surgery for sella and parasellar lesions.
Charles Y. Liu Los Angeles, California
This is an excellent article that discusses the extended transsphe-noidal approach to craniopharyngiomas in the suprasellar space.
This is a benign tumor situated in a very difficult space for access froma craniotomy approach. I believe the relatively recent report fromFahlbusch et al. (1) best summarizes the craniotomy approach, results,and limitations. Attempts to be overly aggressive, as have been sug-gested in earlier literature, have led to significant patient injury.Adjunctive therapy is often used now after surgery.
With the extended transsphenoidal approach, it may be possible toachieve a higher degree of removal and perhaps total removal in somecases. Very long-term follow-up will truly be necessary to knowwhether total removal has been achieved. Nevertheless, this approachmay give the best and safest exposure of this deep region. The authorshave shown some success, although still with 10% mortality, 10%visual decline, and 20% incidence of cerebrospinal fluid leak, and thisis with an experienced team of endoscopic surgeons. They wiselypoint out the experience needed and the degree of difficulty associatedwith this procedure. With future advances in endoscopic technologyand well-designed instruments, I believe this will be our best avenuefor access to the craniopharyngioma. Even with this more direct andextensive view, the adherences to surrounding vital structures may bethe limiting factor.
Kalmon D. Post New York, New York
1. Fahlbusch R, Honegger J, Paulus W, Huk W, Buchfelder M: Surgical treat-ment of craniopharyngiomas: Experience with 168 patients. J Neurosurg90:237–250, 1999.
de Divitiis et al. present their preliminary experience in the treatmentof extrasellar craniopharyngiomas using an extended endoscopic
transsphenoidal approach. This approach was originally and still con-tinues to be performed with the microscope. The advent of the endo-scope has enabled it now to also be performed using this equipment.
I am convinced that in selected cases, the extended transsphenoidalapproach offers great advantages with respect to the craniotomyapproach, principally in retrochiasmatic craniopharyngiomas associ-ated or not with a prefixed chiasm. In these circumstances, the cran-iotomy approach is very difficult; conversely, the transsphenoidalapproach is direct, avoids brain retraction and chiasm manipulation,yields an excellent view of the operatory field, and allows the surgeonto work in the trajectory of the tumor growth. The main disadvantagesinvolve poor vascular control if a hemorrhage occurs and difficultyobtaining watertight repair at the end of the procedure. The key toforeseeing tumor removal is in identifying the location of the tumorwith respect to the meningeal membranes. Only extrapial tumors areremovable; unfortunately, magnetic resonance imaging is unable toconvey similar information at this time. The article by de Divitiis et al.is an important contribution that confirms the fact that selected cases ofextrasellar craniopharyngioma can be removed using an extendedendoscopic transsphenoidal approach. To know the safest and mosteffective technique to use in different situations, a larger series is nec-essary to allow comparison between the extended transsphenoidalapproach, performed either with the microscopic technique or withthe endoscopic technique, and the craniotomy approaches.
Giorgio FrankBologna, Italy
The authors expand upon their previously reported experience withthe endoscopic transsphenoidal approach in this retrospective
analysis of 10 patients with primarily suprasellar craniopharyngiomas.Although the sizes and locations of these lesions are not delineated, themajority of patients had visual compromise and/or endocrine dys-function, and four patients had undergone previous craniotomy. Muchof the report describes important operative nuances that the authorshave gleaned from their experience with a variety of sellar and parasel-lar lesions using this approach.
The anatomic results of this surgical series are impressive in thatnear-total removal was achieved in 9 of 10 patients, although long-term follow-up for late recurrence and detailed endocrinological out-come are not provided. The morbidity of this approach, however, wassubstantial, including mortality (10%), cerebrospinal fluid leak (20%),new visual deficit (10%), new permanent diabetes insipidus (30%), anddelayed subdural hematoma (10%). I agree with the authors that thetranssphenoidal trajectory provides a potentially superior access com-pared with craniotomy approaches for many craniopharyngiomas, asit allows access between anterior communicating arteries, chiasm andfrontobasal perforators cranially, and midbrain structures caudally.Nevertheless, there is substantial benefit with craniotomies in visualiz-ing critical structures before resection and the ability to change theangle of attack beyond the relative limitations of the transsphenoidalapproach. Increased familiarity with the transsphenoidal approach,improvements in instrumentation, and augmentation of intraoperativeimaging (1) will undoubtedly lead to additional enhancements of thetechnique that the authors have described in this pioneering article.
Marc R. MaybergSeattle, Washington
1. Mayberg MR, Cunningham EJ, LaPresto E: Image-guided endoscopy:Description of technique and potential applications. Neurosurg Focus 19:E10,2005.
ONS228 | VOLUME 61 | OPERATIVE NEUROSURGERY 2 | NOVEMBER 2007 www.neurosurgery-online.com
DE DIVITIIS ET AL.
Copyright © 2022 FDOKUMEN




















