
When education seeps into 'free play' : How preschool children accomplish multilingual education

Endoscopic Papillectomy: When and How?
José Celso Ardengh MD, PhD, FASGELivre-docente de Gastroenterologia e Cirurgia HCFMRP-USP
www.cebed.com.br / [email protected]

Introduction
�Ampullary neoplasia
�Rare and often malignant
�Prognosis
�Generally better
�Than for other digestive malignancies
�Detection of small lesions
�Proper staging are therefore important
Gan SI et al. Gastrointest Endosc. 2007;66:425–434.

Definition
�Periampullary region
�Papilla of Vater and the two centimeters surrounding it
Gan SI et al. Gastrointest Endosc. 2007;66:425–434
Albores-Saavedra J et al. J Surg Oncol.2009;100:598

Histologically
�Originate in the epithelium
�Duodenal wall
�Pancreatic tissue
�Bile duct or the structures of the ampullarycomplex
Gan SI et al. Gastrointest Endosc. 2007;66:425–434
Albores-Saavedra J et al. J Surg Oncol.2009;100:598
Epidemiology
�Infrequent
�Malignancy rate of more than 90%
�Periampullary tumors
5% of malignant gastrointestinal tumors
�Ampullary tumors
Less than 1%
Scarpa A et al. Am J Path 1993
Albores-Saavedra J et al. J Surg Oncol.2009;100:598.
Sarmiento JM et al. Surg Clin North Am. 2001;81:543–555

Overall Resection Rate
�Peri and ampullary cancers 50%-70%
�Pancreatic cancer 15%-25%
�Biliary cancer 10%
�Duodenal cancer 10%
Sarmiento JM et al. Surg Clin North Am. 2001;81:543–555
O’Connell JB et al. Ann Surg Oncol.2008;15:1820–1817
Prognosis and Survival
�Depends
�Tissue of origin and the tumor stage
�Survival
�Ampullary and duodenal tumors 4 to 5 y
�Bile duct tumors 3 y
�Pancreatic tumors < 1 y
Sarmiento JM et al. Surg Clin North Am. 2001;81:543–555
O’Connell JB et al. Ann Surg Oncol.2008;15:1820–1817

5-year survival rates
GB, Cancer of the gallbladder, BD, cancer of the bile duct; PV, cancer of the papilla of Vater

Etiology
�Villous adenomas
�Tubulo-villousadenomas
�Hemangiomas
�Leiomyomas
�Leiomyofibromas
�Lipomas
�Lymphangiomas
�Neuroendocrinetumors

Neuroendocrine Tumor

Clinical Presentation
�Often asymptomatic
�Incidentally discovered
�Symptoms related to obstruction
�Jaundice and cholangitis
�Acute recurrent pancreatitis
�Significant weight loss = invasive process
Bertoni G et al. Endoscopy.1997;29:685–688.

Diagnosis
�Endoscopic appearance and histology
�Side-view endoscopy
�Confirmation with forceps biopsy
� Accuracy has been questioned
� May not take a representative sample
� Accuracy rates of 62% to 85%Bellizzi AM et al. Am J Clin Pathol. 2009;132:506–513
Roggin KK et al. Ann Surg Oncol.2005;12:971–980
Eswaran SL et al. Gastrointest Endosc. 2006;64:925–932

Management Decisions
�Staging is necessary
�Modalities
�Trans-abdominal ultrasound (US)
�Computed tomography (CT)
Provide valuable information� Identifying lymphadenopathy
� Metastatic lesions
�Magnetic ResonanceCholangiopancreatography
Do not adequately visualize the ampullary area

Modalites for Staging
�Endoscopic retrograde cholangiopancreatography
�Endoscopic Ultrasound (EUS)
�Intraductal US (IDUS)
EUS Staging
�Useful
�Investigation of ampullary tumors
�Identify and staging small lesions better than others imaging methods
�Considered
�One of the optimal indications for evaluating the papilla
Adler DG et al. Gastrointest Endosc. 2006;64:849–854.
Trede M et al.Surg Clin North Am. 2001;81:595–610

EUS/uTNM Classification
uT Classification Neoplastic tissue invasion
uT1 Tu limited to the ampullary region
uT2 Tu invades duodenal wall
uT3 Tu invades the pancreas to 2.0 cm
uT4 Tu invades the pancreas more than 2.0 cm
uN Classification Presence Lymph Node
uN0 Free lymph nodes
uN1 With suspected lymph nodes metastasis

Accuracy
�Conventional EUS
�EUS > CT = MRI > US
�IDUS
�Higher resolution than EUS
�High frequency waves (20-30 MHz)
IDUS > EUS
Chen CH et al. J Clin Ultrasound.2001;29:313–321
Cannon ME et al. Gastrointest Endosc. 1999;50:27–33
Chen CH et al. Hepatogastroenterology. 2001;48:1750–1753
Itoh A et al. Gastrointest Endosc. 1997;45:251–260
Ito K et al. Gastrointest Endosc. 2007;66:740–747
Menzel J et al. Gastrointest Endosc. 1999;49:349–357
Menzel J Am J Gastroenterol. 2000;95:605–616

EUS Technique

uT1N0

uT1N0
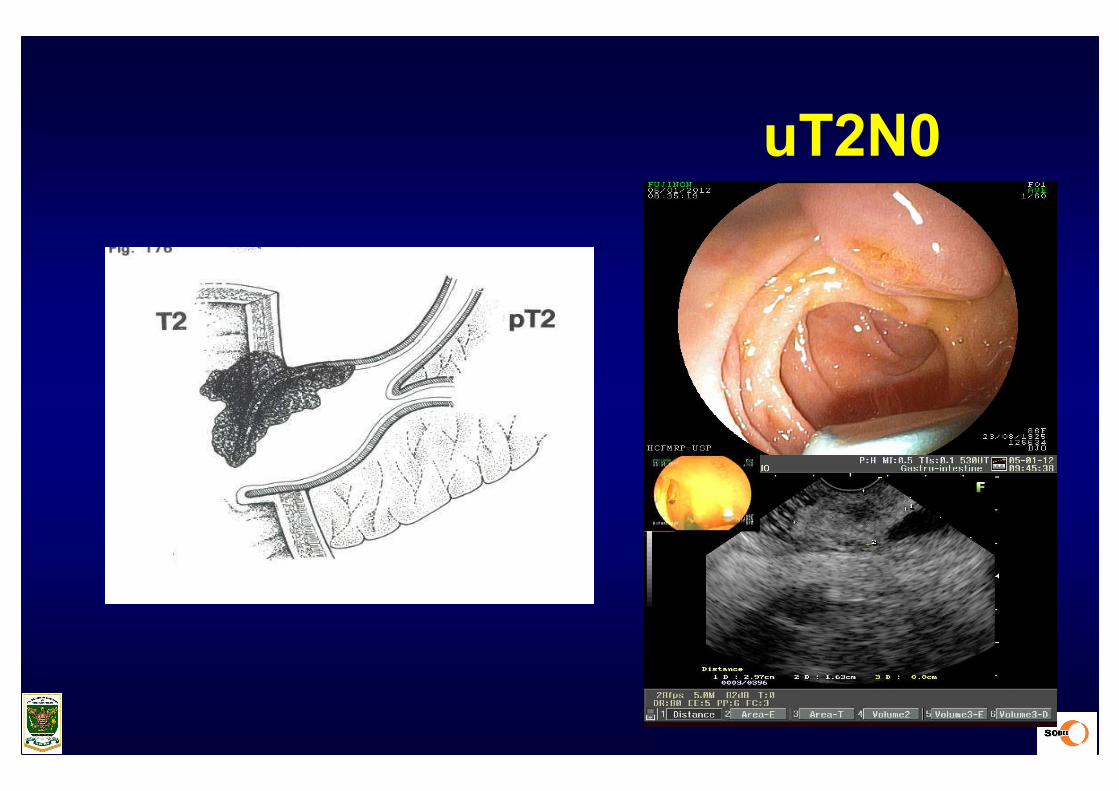
uT2N0

uT3N0

uT4N0

uT1N0

MRI/MRCP
�Reserved
�Patients with bile duct abnormalities
� Previously identified on CT or US
� That need further clarification prior to more invasive
investigative studies

ERCP
Key points
�Ampullary lesion
� Into the biliary or pancreatic duct
�Therapeutic intervention
�Usually performed immediately preceding
�Cholangiopancreatoscopy
� Has also been described
Hopper AD et al. Gastrointest Endosc. 2010;71:967–975
Judah JR & Draganov PV. World J Gastroenterol. 2008;14:3129–3136

Treatment Options
�Optimal treatment
�No established
�Surgical excision
�Endoscopic ablation
�Endoscopic therapy
Binmoeller KF et al., Gastrointest Endosc 1993
Martin JA et al., Gastrointest Endosc 1997
Greenspan AB et al., Gastrointest Endosc 1997

Endoscopic Therapy
�Snare excision (1993)
�Small amount of literature reports
�Complications
�Severe acute pancreatitis
Plastic stents (MPD)??
�Periodic control
Local endoscopic biopsies
Binmoeller KF et al., Gastrointest Endosc 1993
Martin JA et al., Gastrointest Endosc 1997
Greenspan AB et al., Gastrointest Endosc 1997

Resection Technique
�Papillectomy and ampullectomy
�Frequently used interchangeably
�Papillectomy for endoscopic resection
�Ampullectomy for surgical resection
Han J, Kim MH. Gastrointest Endosc. 2006;63:292–301
Resection Technique
�“en bloc” resection
�Advantage
�Shortened procedure time
�Reduced use of electrocautery
�Complete tissue specimen
�Piece meal ressection

Materials
�Endoscopic polypectomy snares
�Fine wire snares designed for ampullaryresection
�Electrocautery
Norton ID et al. Gastrointest Endosc. 2002;56:239–243

Submucosal Injection
�Prior
�May be performed?!?!
�Lift sign negative
Associated with malignancy
Contraindication at complete endoscopic removal
Yamao T, et al. Surg Endosc. 2010;24:119–124
Boix J et al. Surg Endosc. 2009;23:45–49

Submucosal Injection
�Injection of
�Saline and epinephrine
�Decrease the risk of bleeding
�Most commonly injected fluids include
Methylene blue, hydroxypropylmethylcellulose and sodium hyaluronate
Kahaleh M et al. Am J Gastroenterol. 2004;99:2335–2339
Desilets DJ et al.Gastrointest Endosc. 2001;54:202–208

Submucosal Injection
�No
�Injection may
�Distort the ampullary anatomy
�Create a “dome” effect
Make effective snare placement for en
bloc resection more difficult
Yamao T, et al. Surg Endosc. 2010;24:119–124
Boix J et al. Surg Endosc. 2009;23:45–49

Endoscopic Papillectomy

Ablative Therapies
�Following snare resection
�Destroy any remaining tissue
�Argon plasma coagulation (APC)
Most frequently used
�Laser
�Bipolar electrocautery
Hopper AD, et al. Gastrointest Endosc. 2010;71:967–975

Sphincterotomy
�Often performed
�Improving pancreaticobiliary drainage
�Complications of papillectomy
�Pancreatitis
�Placement of a pancreatic duct stent following ampullary adenoma resection
Singh P et al. Gastrointest Endosc. 2004;60:544–550

Neuroendocrine Tumor

Impact of Technical Modification of EUS-guided Endoscopic Papillectomyfor Ampullary Neoplasm on the rate of post-resection acute pancreatitis
�Indications for EP – 41 patients
�T1 tumor without tumor spread into the bile/pancreatic duct
�EUS MPD diameter before
�Two groups
Group A (25)PD stent was placed in patients without MPD dilatation (30 and 35 mm)
Group B (16)Underwent EP with insertion of a PD stent.
� Occurrence of adverse events (AEs) was compared between the groups in relation to the MPD diameter as determined by EUS
Ardengh et al. Gastrointest Endosc. DDW 2013;Su 1579

Variável Grupo Média IC 95% Diferença (IC95%) Valor-p
Tamanho da lesão
Com prótese 1,67 (a) (1,44 ; 1,95)
0,38 (0,33 ; 0,43) 0,04 (b)
Sem prótese 1,29 (a) (1,06 ; 1,57)
Diâmetro colédoco
Com prótese 1,06 (0,64 ; 1,08)
0,19 (-0,10 ; 0,48) 0,19 (c)
Sem prótese 0,87 (0,88 ; 1,22)
Diâmetro DPP
Sem prótese 0,45 (0,38 ; 0,50)
0,08 (-0,01 ; 0,18) 0,11 (c)Com prótese 0,37 (0,29 ; 0,44)
(a) Médias geométricas
( b) Ajustado por sexo e idade, segundo modelo de regressão linear
( c) Ajustado por sexo, idade e tamanho da lesão, segundo modelo de regressão linear
Analysis of variables in 41 patients with neoplasia
Ardengh et al. Gastrointest Endosc. DDW 2013;Su 1579

Comparison between the groups with and without denture prosthesis pancreatic
No stent StentP value (a)
n (%) n (%)
Type of lesion 0.49
Adenoma 10 (40.0) 8 (50.0)
Adenocarcinoma 9 (36.0) 3 (18.8)
Hiperplasia 2 (8.0) 2 (12.5)
Carcinoide 2 (8.0) 1 (6.2)
Lipoma 2 (8.0) 0 -
GIST 0 - 1 (6.2)
Hamartoma 0 - 1 (6.2)
Complications
Acute pancreatitis 2 (8.0) 8 (50.0) <0.01
Bleeding 5 (20.0) 1 (6.2) 0.38
Cholangigitis 1 (4.0) 0 - 1.00
Cholecystitis 1 (4.0) 0 - 1.00
Amilase 0.76
≤ 330 14 (56.0) 8 (50.0)
> 330 11 (44.0) 8 (50.0)
AP Surgery 0.27
UT1N0 22 (88.0) 16 (100.0)
pt3n1b 3 (12.0) 0 -
Ardengh et al. Gastrointest Endosc. DDW 2013;Su 1579

Outcomes
�Success rates
�Papillectomy range from 46% to 92%
�Recurrence range from 0% to 33%
�Large retrospective series
�102 patients
�Underwent endoscopic resection
�Success rate of 84%
Han J, Kim MH.Gastrointest Endosc. 2006;63:292–301
Irani S et al. Gastrointest Endosc. 2009;70:923–932

Complications
�Morbidity rate (range 10-58%) 23%
�Pancreatitis 25%
�Bleeding 25%
�Perforation
�Cholangitis
�Papillary stenosis
�Mortality rate (range 0%-7%) 0.4%
Han J, Kim MH.Gastrointest Endosc. 2006;63:292–301

Perforation

Papillectomy Complications

Surveillance
�No consensus
�Initial surveillance endoscopy is generally performed at 1 mo to 6 mo
�Follow with endoscopy every 3 mo to 12 mo for the next 2 years
�Side-viewing endoscope
�FAP patients
Duodenal polyps with the use of chromoendoscopy
Dekker E, et al. Endoscopy. 2009;41:666–669

Conclusions
�Endoscopic advances
�Expanded
�Endoscopy in the therapeutic management
�Staging modalities available
�Clinicians should utilize in order to make the most appropriate management decision for these patients

Conclusions
�Surgery �Treatment of choice
� Ampullary adenocarcinoma and adenomas with extensive intraductal growth
�Treatment and Surveillance�Definitive guidelines
� More further studies
Copyright © 2022 FDOKUMEN




















