
Cerebral glycolysis: a century of persistent misunderstanding ...
Upload
independentCategory
view
0download
0
Persistent effects of cognitive-behavioral stressmanagement on cortisol responses to acute stressin healthy subjects—A randomized controlled trial
K. Hammerfald, C. Eberle, M. Grau, A. Kinsperger, A. Zimmermann,U. Ehlert, J. Gaab*
Clinical Psychology and Psychotherapy, Institute of Psychology, University of Zurich,University of Zurich, Zurichbergstr. 43, CH-8044 Zurich, Switzerland
Received 13 June 2005; received in revised form 15 August 2005; accepted 17 August 2005
KEYWORDSCortisol;Cognitive-behavioralstress managementtraining;Psychosocial stress
Summary Psychosocial stress leads to a release of cortisol. While thispsychoneuroendocrine response helps to maintain physiological as well aspsychological equilibrium under stress, exaggerated secretion of cortisol has beenshown to have negative effects on somatic health and cognitive functioning. Thestudy set out to examine the long-term effects of cognitive-behavioral stressmanagement training on cortisol stress responses in healthy men and women.Eighty-three healthy subjects were randomly assigned to cognitive-behavioral
stress management (CBSM) training or a control condition. Four months after theCBSM, 76 subjects underwent a standardized psychosocial stress test. Salivarycortisol responses were assessed repeatedly before and after the stress test.Subjects in the CBSM group showed significantly reduced cortisol stress responses.
With regard to gender, this effect was observed in both men and women. However,the magnitude of the CBSM effect on cortisol responses was smaller in women than inmen. Use of oral contraceptives in women influenced the cortisol response, but didnot have an impact on the CBSM effect on cortisol.The results show that the previously reported attenuation of cortisol stress
responses through CBSM persists and are observable in both men and women. Sincestress-induced alterations of hypothalamus pituitary adrenal axis functioning arediscussed to be involved in the onset and maintenance of both somatic andpsychiatric conditions, similar interventions could be used for prevention andtherapy of these detrimental stress effects.Q 2005 Elsevier Ltd. All rights reserved.
1. Introduction
In terms of its ubiquitous effects on importantphysiological systems, the hypothalamus–pituitary–adrenal (HPA) axis has been proposed as a major
Psychoneuroendocrinology (2006) 31, 333–339
www.elsevier.com/locate/psyneuen
0306-4530/$ - see front matter Q 2005 Elsevier Ltd. All rights reserved.doi:10.1016/j.psyneuen.2005.08.007
* Corresponding author. Tel.: C41 1 6343096; fax: C41 16343696.
E-mail address: [email protected] (J. Gaab).
pathway linking psychosocial stress to its negativeconsequences on somatic and psychological wellbeing (McEwen, 1998). There is accumulatingevidence supporting a causal relation betweenincreased activity and reactivity of HPA axishormones and negative health outcomes.
For example, acute HPA axis responses to labora-tory stressors have been shown tobe linked to the riskforupper respiratory tract infection that isassociatedwith stressors in the natural environment (Cohenet al., 2002). With respect to possible long-termeffects, an abnormal cortisol patternwas shown tobeprospectively associated with increased incidence ofcardiovascular-related events and type 2 diabetes inmen (Rosmond et al., 2003). Furthermore, resultsfrom the ‘MacArthur studies of successful aging’provideevidence for long-termdetrimentaleffects ofelevated cortisol levels in the elderly, with higherbaseline urinary free cortisol levels being related todeclines in memory performance in women (Seemanet al., 1997) or higher incidence of fractures in menand women (Greendale et al., 1999).
In addition, cortisol is a primary mediator ofallostatic load (representing the cumulative phys-iological burden exacted on the body throughattempts to adapt to life’s demands), which hasbeen associated with significantly increased risk for7-year mortality as well as declines in cognitive andphysical functioning in the elderly (Seeman et al.,2001). Also, administration of cortisol beforeretrieval leads to a decrease in memory perform-ance (Het et al., 2005).
The release of cortisol has been shown to berelated to the experience or anticipation of stress(Smyth et al., 1998; Dickerson and Kemeny, 2004;Gaab et al., 2005). Therefore, interventions aimingto modulate the perception and appraisal as well asto improve stress-related coping strategies arepossible means with which to modulate cortisollevels as a consequence of stressful experiences. Ina randomized controlled trial study, our groupreported attenuated cortisol responses to a stan-dardized psychosocial stress test in healthy malesubjects two weeks after a short, group-basedcognitive-behavioral stress management training(CBSM) (Gaab et al., 2003). The current study setout to examine the stability over time and thegeneralizability with regard to gender of theseendocrine effects of CBSM in healthy subjects.
2. Methods
2.1. Subjects and design
Three hundred and fifteen subjects (all 2nd-yearpsychology students of the University of Zurich in
2002) were invited to participate in the studythrough a letter to all 2nd-year psychology studentsof the University of Zurich. Recruitment wasrestricted to this population to reduce interintervi-dual differences in the frequencies and extent ofexternal academic stressors. Interested subjectshad the opportunity to enroll online. They thenreceived a screening questionnaire, containingexclusion criteria (any acute or chronic somatic orpsychiatric disorder) and a complete description ofthe study. One hundred and two students enrolledonline and 96 returned the screening questionnaire.Thirteen interested subjects had to be excluded,and 83 subjects, therefore participated in thestudy.
Upon return of all screening questionnaires andinformed consent, all subjects fulfilling the selec-tion criteria were randomly assigned to eight groups(four treatment and four control groups). In orderto allow CBSM group sessions, group size wasrestricted to maximum NZ12. Allocation conceal-ment was achieved through the use of sequentiallynumbered, opaque and sealed envelopes. Ran-domization resulted in eight groups (four CBSMgroups: NZ42, four control groups: NZ41; with 10or 11 subjects in each group). Since treatmentgroups 1–4 and waiting control groups 5–8 did notdiffer significantly in terms of demographic vari-ables (age, gender, habitual smoking, use of oralcontraceptives and body mass index, data notshown), they were joined to form one treatmentgroup and one control group. Subjects in thetreatment and control group did not differ signifi-cantly with regard to the distribution of gender,smoking and use of oral contraceptives (seeTable 1).
Four months after the termination of the CBSMfor the treatment group, all subjects underwent astandardized psychosocial stress test (Trier SocialStress Test, TSST, Kirschbaum et al., 1993).Subjects of the CBSM group performed the TSSTwithin a 2-week period, whereas controls per-formed the TSST in a 4-week period. To rule outmajor differences of external factors, such as
Table 1 Demographic variables.
CBSMgroup
Controlgroup
Gender (male/female)
11/31 13/28 c2Z0.31;PZ0.58
Smoking (yes/no) 13/29 6/35 c2Z3.13;PZ0.08
Oral contracep-tives (yes/no)
17/14 12/15 c2Z0.62;PZ0.43
K. Hammerfald et al.334
season and external stressors, all subjects per-formed the TSST with the same four weeks. Not allparticipants underwent the TSST. Reasons fordropout were: Refusal to further participate inthe study (NZ1) and inability to keep the TSSTappointment within the TSST testing period (NZ6).Subjects not performing the TSST did not differ inbaseline variables from TSST performers (age,gender, habitual smoking, use of oral contra-ceptives and body mass index, data not shown).Thirty-nine subjects of the CBSM and 37 subjects ofthe control group performed the TSST. After thetermination of the study, all controls received CBSMtraining.
2.2. Psychosocial stress test
The Trier Social Stress Test (TSST) has repeatedlybeen found to induce profound endocrine responsesin 70–80% of the subjects tested (Kirschbaum et al.,1993). Subjects were briefly introduced to the TSST(2 min) and then returned to a different room,where they had 10 min to prepare and to completea questionnaire designed to assess cognitiveappraisal processes (PASA) of the anticipated stresssituation. Afterwards, subjects were taken backinto the TSST room, where they underwenta simulated job interview (5 min) followed by amental arithmetic task (5 min) in front of acommittee of two people. Saliva samples wereobtained immediately before, and one, 10, 20, 30,45, and 60 min after the TSST. To control forvariations of cortisol levels over the circadianrhythm, the TSST was performed from 14.00 to18.00 h. The TSST committee and the studypersonnel were blind to group assignment. TheTSST was performed in different rooms than theCBSM.
2.3. Psychometric measures
Anticipatory cognitive appraisal processes in theTSST were assessed with the Primary AppraisalSecondary Appraisal Scale (PASA). The PASA com-prises 16 situation-specific items, forming fourprimary (Challenge, Threat, Self-Concept of OwnCompetence and Control Expectancy) and twosecondary scales (Primary AppraisalZ(ChallengeCThreat)/2 and Secondary AppraisalZ(Self-Conceptof Own CompetenceCControl Expectancy)/2). Pri-mary scales can be summed up to a general stressindex (Stress IndexZ(Primary AppraisalKSecond-ary Appraisal), representing the sum of primary andsecondary appraisal. The reliability and factorial
validity of the PASA has been shown to be good(Gaab et al., 2005).
2.4. Cognitive-behavioral stressmanagement (CBSM)
All subjects attended group-based cognitive-beha-vioral stress management training described else-where (Gaab et al., 2003). Groups met on twoalternate Saturdays or Sundays, respectively.Groups of up to 11 subjects received a total of10 h of CBSM. The sessions were conducted by twoclinical psychologists (JG and KH), according to astandardized training manual. The CBSM focused onfour cognitive-behavioral stress-reducing tech-niques (cognitive restructuring, problem-solving,self-instruction, progressive muscle relaxation). Allparticipants received a training manual containing asummary of theoretical models and stress-reducingtechniques as well as a set of flash cards (size: 10!7 cm), which briefly described each CBSM tech-nique. Exercises and role-plays used in the grouptherapy sessions did not resemble the situation usedin the TSST. The CBSM training employed wassimilar to the training used in an earlier publication(Gaab et al., 2003).
2.5. Sampling methods and biochemicalanalyses
Saliva was collected with Salivette (Sarstedt,Rommelsdorf, Germany) collection devices.Samples were stored at K20 8C until biochemicalanalysis took place. Salivary free cortisol wasanalyzed by using a commercial chemilumines-cence immunoassay (IBL Hamburg, Germany).Inter- and intraassay coefficients of variation werebelow 10%. To reduce error variance caused byimprecision of the intraassay, all samples of onesubject were analyzed in the same run.
2.6. Statistical analyses
Repeated measures ANOVAs and ANCOVAs testedfor significant condition!time interactions onsalivary cortisol responses. All reported resultswere corrected by the Greenhouse-Geisser pro-cedure, where appropriate (violation of sphericityassumption). Pairwise comparisons were performedfor each cortisol sample. For cortisol parameters,areas under the response curve were calculatedwith respect to increase from increase (AUCi) usingthe trapezoidal method as an indicator for theintegrated cortisol response in the TSST (Pruessneret al., 2003). In line with previous observations
Persistent Effects of CBSM on cortisol stress responses 335
(Gaab et al., 2003), we expected a multivariateeffect size of f2Z0.20 (representing a medium tolarge effect size). Based on 0.8 power to detect asignificant difference of this effect size and a 5%significance level, 80 subjects were required.Unless indicated, all results shown are meansGstandard error of means (SEM). When appropriate,effect size parameters are shown (effect sizeconventions: f2: 0.02Zsmall, 0.15Zmedium,0.35Zlarge; d: 0.20Zsmall, 0.50Zmedium,0.80Zlarge).
3. Results
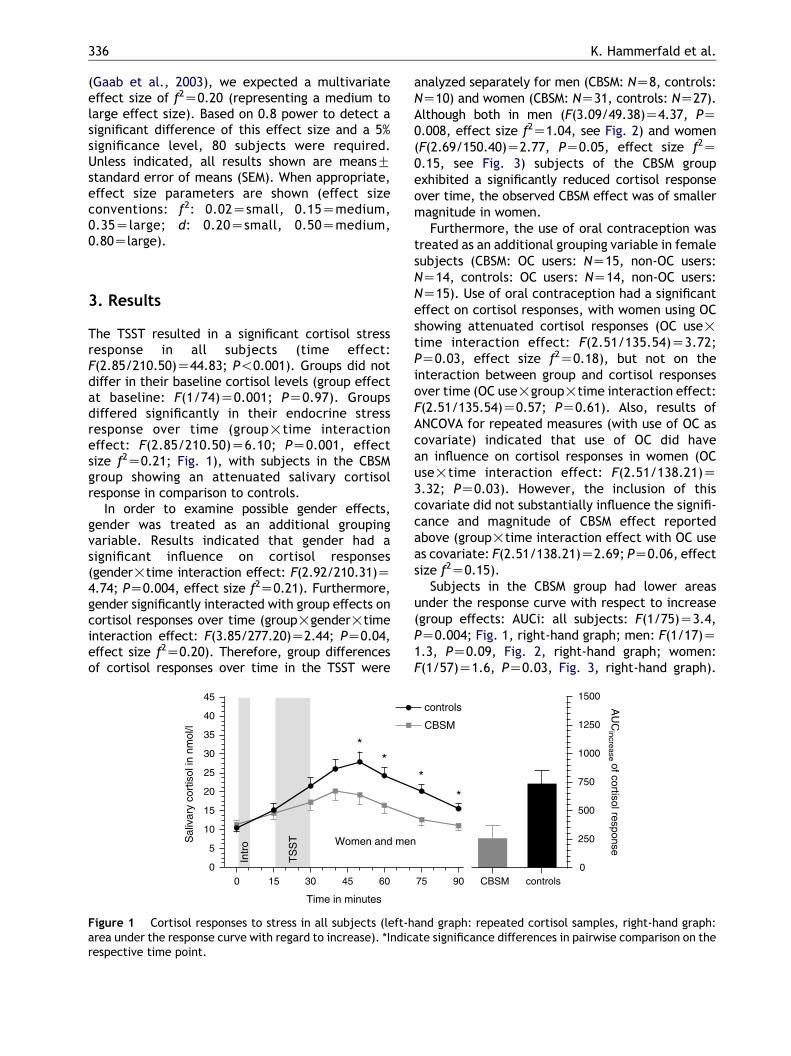
The TSST resulted in a significant cortisol stressresponse in all subjects (time effect:F(2.85/210.50)Z44.83; P!0.001). Groups did notdiffer in their baseline cortisol levels (group effectat baseline: F(1/74)Z0.001; PZ0.97). Groupsdiffered significantly in their endocrine stressresponse over time (group!time interactioneffect: F(2.85/210.50)Z6.10; PZ0.001, effectsize f2Z0.21; Fig. 1), with subjects in the CBSMgroup showing an attenuated salivary cortisolresponse in comparison to controls.
In order to examine possible gender effects,gender was treated as an additional groupingvariable. Results indicated that gender had asignificant influence on cortisol responses(gender!time interaction effect: F(2.92/210.31)Z4.74; PZ0.004, effect size f2Z0.21). Furthermore,gender significantly interacted with group effects oncortisol responses over time (group!gender!timeinteraction effect: F(3.85/277.20)Z2.44; PZ0.04,effect size f2Z0.20). Therefore, group differencesof cortisol responses over time in the TSST were
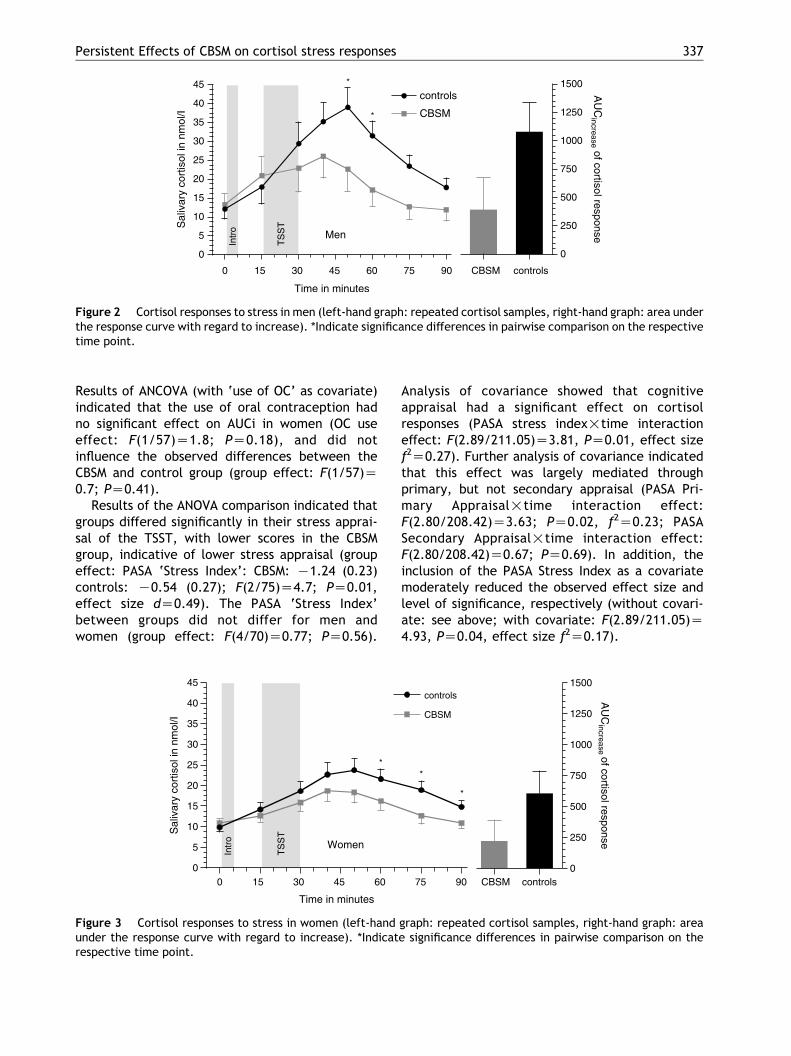
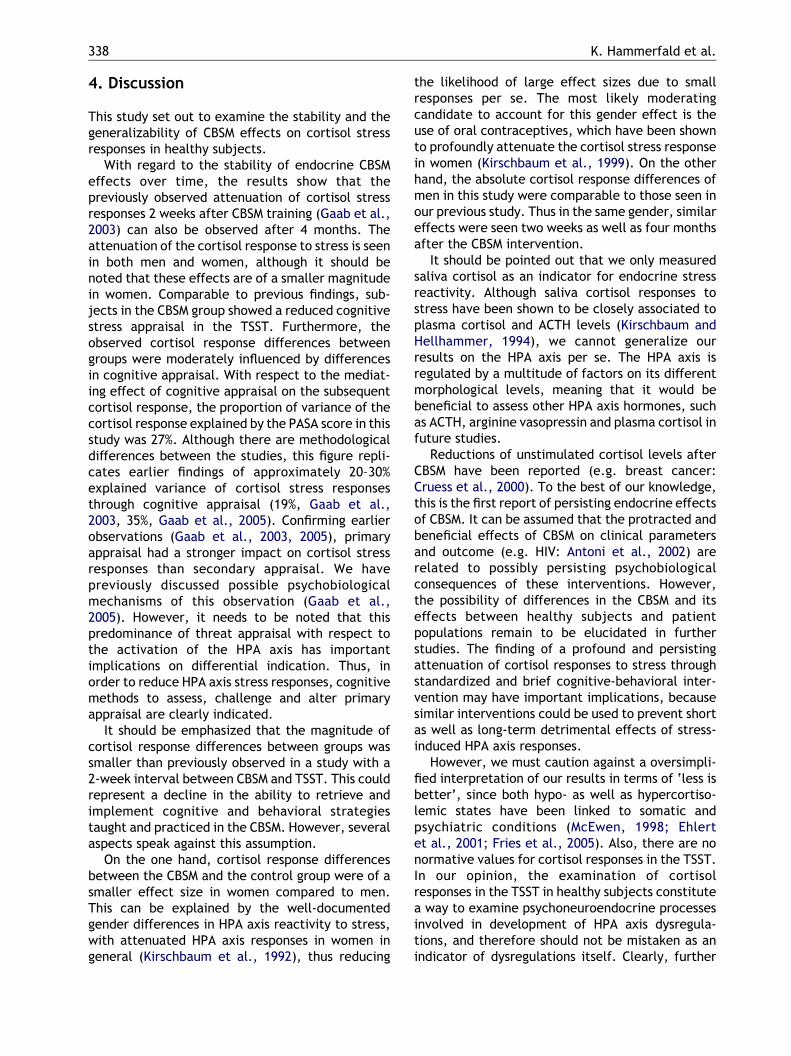
analyzed separately for men (CBSM: NZ8, controls:NZ10) and women (CBSM: NZ31, controls: NZ27).Although both in men (F(3.09/49.38)Z4.37, PZ0.008, effect size f2Z1.04, see Fig. 2) and women(F(2.69/150.40)Z2.77, PZ0.05, effect size f2Z0.15, see Fig. 3) subjects of the CBSM groupexhibited a significantly reduced cortisol responseover time, the observed CBSM effect was of smallermagnitude in women.
Furthermore, the use of oral contraception wastreated as an additional grouping variable in femalesubjects (CBSM: OC users: NZ15, non-OC users:NZ14, controls: OC users: NZ14, non-OC users:NZ15). Use of oral contraception had a significanteffect on cortisol responses, with women using OCshowing attenuated cortisol responses (OC use!time interaction effect: F(2.51/135.54)Z3.72;PZ0.03, effect size f2Z0.18), but not on theinteraction between group and cortisol responsesover time (OC use!group!time interaction effect:F(2.51/135.54)Z0.57; PZ0.61). Also, results ofANCOVA for repeated measures (with use of OC ascovariate) indicated that use of OC did havean influence on cortisol responses in women (OCuse!time interaction effect: F(2.51/138.21)Z3.32; PZ0.03). However, the inclusion of thiscovariate did not substantially influence the signifi-cance and magnitude of CBSM effect reportedabove (group!time interaction effect with OC useas covariate: F(2.51/138.21)Z2.69; PZ0.06, effectsize f2Z0.15).
Subjects in the CBSM group had lower areasunder the response curve with respect to increase(group effects: AUCi: all subjects: F(1/75)Z3.4,PZ0.004; Fig. 1, right-hand graph; men: F(1/17)Z1.3, PZ0.09, Fig. 2, right-hand graph; women:F(1/57)Z1.6, PZ0.03, Fig. 3, right-hand graph).
Figure 1 Cortisol responses to stress in all subjects (left-hand graph: repeated cortisol samples, right-hand graph:area under the response curve with regard to increase). *Indicate significance differences in pairwise comparison on therespective time point.
K. Hammerfald et al.336
Results of ANCOVA (with ‘use of OC’ as covariate)indicated that the use of oral contraception hadno significant effect on AUCi in women (OC useeffect: F(1/57)Z1.8; PZ0.18), and did notinfluence the observed differences between theCBSM and control group (group effect: F(1/57)Z0.7; PZ0.41).
Results of the ANOVA comparison indicated thatgroups differed significantly in their stress apprai-sal of the TSST, with lower scores in the CBSMgroup, indicative of lower stress appraisal (groupeffect: PASA ‘Stress Index’: CBSM: K1.24 (0.23)controls: K0.54 (0.27); F(2/75)Z4.7; PZ0.01,effect size dZ0.49). The PASA ‘Stress Index’between groups did not differ for men andwomen (group effect: F(4/70)Z0.77; PZ0.56).
Analysis of covariance showed that cognitiveappraisal had a significant effect on cortisolresponses (PASA stress index!time interactioneffect: F(2.89/211.05)Z3.81, PZ0.01, effect sizef2Z0.27). Further analysis of covariance indicatedthat this effect was largely mediated throughprimary, but not secondary appraisal (PASA Pri-mary Appraisal!time interaction effect:F(2.80/208.42)Z3.63; PZ0.02, f2Z0.23; PASASecondary Appraisal!time interaction effect:F(2.80/208.42)Z0.67; PZ0.69). In addition, theinclusion of the PASA Stress Index as a covariatemoderately reduced the observed effect size andlevel of significance, respectively (without covari-ate: see above; with covariate: F(2.89/211.05)Z4.93, PZ0.04, effect size f2Z0.17).
Figure 2 Cortisol responses to stress in men (left-hand graph: repeated cortisol samples, right-hand graph: area underthe response curve with regard to increase). *Indicate significance differences in pairwise comparison on the respectivetime point.
Figure 3 Cortisol responses to stress in women (left-hand graph: repeated cortisol samples, right-hand graph: areaunder the response curve with regard to increase). *Indicate significance differences in pairwise comparison on therespective time point.
Persistent Effects of CBSM on cortisol stress responses 337
4. Discussion
This study set out to examine the stability and thegeneralizability of CBSM effects on cortisol stressresponses in healthy subjects.
With regard to the stability of endocrine CBSMeffects over time, the results show that thepreviously observed attenuation of cortisol stressresponses 2 weeks after CBSM training (Gaab et al.,2003) can also be observed after 4 months. Theattenuation of the cortisol response to stress is seenin both men and women, although it should benoted that these effects are of a smaller magnitudein women. Comparable to previous findings, sub-jects in the CBSM group showed a reduced cognitivestress appraisal in the TSST. Furthermore, theobserved cortisol response differences betweengroups were moderately influenced by differencesin cognitive appraisal. With respect to the mediat-ing effect of cognitive appraisal on the subsequentcortisol response, the proportion of variance of thecortisol response explained by the PASA score in thisstudy was 27%. Although there are methodologicaldifferences between the studies, this figure repli-cates earlier findings of approximately 20–30%explained variance of cortisol stress responsesthrough cognitive appraisal (19%, Gaab et al.,2003, 35%, Gaab et al., 2005). Confirming earlierobservations (Gaab et al., 2003, 2005), primaryappraisal had a stronger impact on cortisol stressresponses than secondary appraisal. We havepreviously discussed possible psychobiologicalmechanisms of this observation (Gaab et al.,2005). However, it needs to be noted that thispredominance of threat appraisal with respect tothe activation of the HPA axis has importantimplications on differential indication. Thus, inorder to reduce HPA axis stress responses, cognitivemethods to assess, challenge and alter primaryappraisal are clearly indicated.
It should be emphasized that the magnitude ofcortisol response differences between groups wassmaller than previously observed in a study with a2-week interval between CBSM and TSST. This couldrepresent a decline in the ability to retrieve andimplement cognitive and behavioral strategiestaught and practiced in the CBSM. However, severalaspects speak against this assumption.
On the one hand, cortisol response differencesbetween the CBSM and the control group were of asmaller effect size in women compared to men.This can be explained by the well-documentedgender differences in HPA axis reactivity to stress,with attenuated HPA axis responses in women ingeneral (Kirschbaum et al., 1992), thus reducing
the likelihood of large effect sizes due to smallresponses per se. The most likely moderatingcandidate to account for this gender effect is theuse of oral contraceptives, which have been shownto profoundly attenuate the cortisol stress responsein women (Kirschbaum et al., 1999). On the otherhand, the absolute cortisol response differences ofmen in this study were comparable to those seen inour previous study. Thus in the same gender, similareffects were seen two weeks as well as four monthsafter the CBSM intervention.
It should be pointed out that we only measuredsaliva cortisol as an indicator for endocrine stressreactivity. Although saliva cortisol responses tostress have been shown to be closely associated toplasma cortisol and ACTH levels (Kirschbaum andHellhammer, 1994), we cannot generalize ourresults on the HPA axis per se. The HPA axis isregulated by a multitude of factors on its differentmorphological levels, meaning that it would bebeneficial to assess other HPA axis hormones, suchas ACTH, arginine vasopressin and plasma cortisol infuture studies.
Reductions of unstimulated cortisol levels afterCBSM have been reported (e.g. breast cancer:Cruess et al., 2000). To the best of our knowledge,this is the first report of persisting endocrine effectsof CBSM. It can be assumed that the protracted andbeneficial effects of CBSM on clinical parametersand outcome (e.g. HIV: Antoni et al., 2002) arerelated to possibly persisting psychobiologicalconsequences of these interventions. However,the possibility of differences in the CBSM and itseffects between healthy subjects and patientpopulations remain to be elucidated in furtherstudies. The finding of a profound and persistingattenuation of cortisol responses to stress throughstandardized and brief cognitive-behavioral inter-vention may have important implications, becausesimilar interventions could be used to prevent shortas well as long-term detrimental effects of stress-induced HPA axis responses.
However, we must caution against a oversimpli-fied interpretation of our results in terms of ‘less isbetter’, since both hypo- as well as hypercortiso-lemic states have been linked to somatic andpsychiatric conditions (McEwen, 1998; Ehlertet al., 2001; Fries et al., 2005). Also, there are nonormative values for cortisol responses in the TSST.In our opinion, the examination of cortisolresponses in the TSST in healthy subjects constitutea way to examine psychoneuroendocrine processesinvolved in development of HPA axis dysregula-tions, and therefore should not be mistaken as anindicator of dysregulations itself. Clearly, further
K. Hammerfald et al.338

studies, preferably in high-risk populations, areneeded.
Acknowledgements
This work was supported by Fonds zur Forderung desAkademischen Nachwuchses des Zurcher Universi-tatsvereins to Jens Gaab
References
Antoni, M.H., Cruess, D.G., Klimas, N., Maher, K., Cruess, S.,Kumar, M., Lutgendorf, S., Ironson, G., Schneiderman, N.,Fletcher, M.A., 2002. Stress management and immune systemreconstitution in symptomatic HIV- infected gay men overtime: effects on transitional naive T cells (CD4(C)CD45RA(C)CD29(C)). Am. J. Psychiatry 159, 143–145.
Cohen, S., Hamrick, N., Rodriguez, M.S., Feldman, P.J., Rabin,B.S., Manuck, S.B., 2002. Reactivity and vulnerability tostress-associated risk for upper respiratory illness. Psycho-som. Med. 64, 302–310.
Cruess, D.G., Antoni, M.H., McGregor, B.A., Kilbourn, K.M.,Boyers, A.E., Alferi, S.M., Carver, C.S., Kumar, M., 2000.Cognitive-behavioral stress management reduces serumcortisol by enhancing benefit finding among women beingtreated for early stage breast cancer. Psychosom. Med. 62,304–308.
Dickerson, S.S., Kemeny, M.E., 2004. Acute stressors and cortisolresponses: a theoretical integration and synthesis of labora-tory research. Psychol. Bull. 130, 355–391.
Ehlert, U., Gaab, J., Heinrichs, M., 2001. Psychoneuroendocri-nological contributions to the etiology of depression,posttraumatic stress disorder, and stress-related bodilydisorders: the role of the hypothalamus-pituitary-adrenalaxis. Biol. Psychol. 57, 141–152.
Fries, E., Hesse, J., Hellhammer, J., Hellhammer, D.H., 2005. Anew view on hypocortisolism. Psychoneuroendocrinology 30,1010–1016.
Gaab, J., Blattler, N., Menzi, T., Pabst, B., Stoyer, S., Ehlert, U.,2003. Randomized controlled evaluation of the effects ofcognitive-behavioral stress management on cortisolresponses to acute stress in healthy subjects. Psychoneur-oendocrinology 28, 767–779.
Gaab, J., Rohleder, N., Nater, U.M., Ehlert, U., 2005.Psychological determinants of the cortisol stress response:the role of anticipatory cognitive appraisal. Psychoneuroen-docrinology 30, 599–610.
Greendale, G.A., Unger, J.B., Rowe, J.W., Seeman, T.E., 1999.The relation between cortisol excretion and fractures inhealthy older people: results from the MacArthur studies-Mac. J. Am. Geriatr. Soc. 47, 799–803.
Het, S., Ramlow, G., Wolf, O.T., 2005. A meta-analytic review ofthe effects of acute cortisol administration on humanmemory. Psychoneuroendocrinology 30, 771–784.
Kirschbaum, C., Hellhammer, D.H., 1994. Salivary cortisol inpsychoneuroendocrine research: recent developments andapplications. Psychoneuroendocrinology 19, 313–333.
Kirschbaum, C., Wust, S., Hellhammer, D., 1992. Consistent sexdifferences in cortisol responses to psychological stress.Psychosom. Med. 54, 648–657.
Kirschbaum, C., Pirke, K.M., Hellhammer, D.H., 1993. The ’TrierSocial Stress Test’–a tool for investigating psychobiologicalstress responses in a laboratory setting. Neuropsychobiology28, 76–81.
Kirschbaum, C., Kudielka, B.M., Gaab, J., Schommer, N.C.,Hellhammer, D.H., 1999. Impact of gender, menstrual cyclephase, and oral contraceptives on the activity of thehypothalamus-pituitary-adrenal axis. Psychosom. Med. 61,154–162.
McEwen, B.S., 1998. Protective and damaging effects of stressmediators. N. Engl. J. Med. 338, 171–179.
Pruessner, J.C., Kirschbaum, C., Meinlschmid, G., Hellhammer,D.H., 2003. Two formulas for computation of the area underthe curve represent measures of total hormone concentrationversus time-dependent change. Psychoneuroendocrinology28, 916–931.
Rosmond, R., Wallerius, S., Wanger, P., Martin, L., Holm, G.,Bjorntorp, P., 2003. A 5-year follow-up study of diseaseincidence in men with an abnormal hormone pattern.J. Intern. Med. 254, 386–390.
Seeman, T.E., McEwen, B.S., Singer, B.H., Albert, M.S., Rowe,J.W., 1997. Increase in urinary cortisol excretion and memorydeclines: MacArthur studies of successful aging. J. Clin.Endocrinol. Metab. 82, 2458–2465.
Seeman, T.E., McEwen, B.S., Rowe, J.W., Singer, B.H., 2001.Allostatic load as a marker of cumulative biological risk:MacArthur studies of successful aging. Proc. Natl. Acad. Sci.USA 98, 4770–4775.
Smyth, J., Ockenfels, M.C., Porter, L., Kirschbaum, C.,Hellhammer, D.H., Stone, A.A., 1998. Stressors and moodmeasured on a momentary basis are associated with salivarycortisol secretion. Psychoneuroendocrinology 23, 353–370.
Persistent Effects of CBSM on cortisol stress responses 339
Copyright © 2022 FDOKUMEN




















