Stockholm Convention on Persistent Organic Pollutants
31
K1172149 290611 SC UNITED NATIONS UNEP/POPS/COP.5/INF/13/Rev.1 Stockholm Convention on Persistent Organic Pollutants Distr.: General 29 June 2011 English only Conference of the Parties to the Stockholm Convention on Persistent Organic Pollutants Fifth meeting Geneva, 25–29 April 2011 Item 4 (a) (ii) of the provisional agenda* Matters related to the implementation of the Convention: measures to reduce or eliminate releases from intentional production and use: exemptions Additional information to supplement the report on the development of reporting and reviewing requirements for the use of lindane Note by the Secretariat 1. As referred to in paragraph 3 of document UNEP/POPS/COP.5/18, the Secretariat of the Stockholm Convention on Persistent Organic Pollutants, in collaboration with the World Health Organization, conducted a preliminary evaluation of the use of lindane based on information received from parties by 31 December 2010. The information was submitted in response to a questionnaire on the use of the substance, which is intended to support the establishment of reporting and reviewing requirements for such use in accordance with the specific exemption. 2. The annex to the present note contains additional information to supplement the report. It has not been formally edited. * UNEP/POPS/COP.5/1.
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Stockholm Convention on Persistent Organic Pollutants

K1172149 290611
SCUNITED NATIONS
UNEP/POPS/COP.5/INF/13/Rev.1
Stockholm Convention on Persistent Organic Pollutants
Distr.: General 29 June 2011 English only
Conference of the Parties to the Stockholm Convention on Persistent Organic Pollutants Fifth meeting Geneva, 25–29 April 2011 Item 4 (a) (ii) of the provisional agenda* Matters related to the implementation of the Convention: measures to reduce or eliminate releases from intentional production and use: exemptions
Additional information to supplement the report on the development of reporting and reviewing requirements for the use of lindane
Note by the Secretariat
1. As referred to in paragraph 3 of document UNEP/POPS/COP.5/18, the Secretariat of the Stockholm Convention on Persistent Organic Pollutants, in collaboration with the World Health Organization, conducted a preliminary evaluation of the use of lindane based on information received from parties by 31 December 2010. The information was submitted in response to a questionnaire on the use of the substance, which is intended to support the establishment of reporting and reviewing requirements for such use in accordance with the specific exemption.
2. The annex to the present note contains additional information to supplement the report. It has not been formally edited.
* UNEP/POPS/COP.5/1.

UNEP/POPS/COP.5/INF/13/Rev.1
2
Annex
Additional information to the report on the development of reporting and reviewing requirements for the use of lindane March 2011
Table of contents 1 Introduction..............................................................................................................................3
2 Situation analysis of the use of lindane............................................................................3
2.1 Summary of responses to the Secretariat’s questionnaire ...............................3 2.2 Country specific information available from other sources............................4
3 Regulations, initiatives, and regimes for the control of lindane ...............................5
4 Information on alternatives to lindane .............................................................................6
5 Example of guidelines for the safe use of lindane........................................................7
Appendix 1: Questionnaire on lindane sent to all Parties ....................................................11
Appendix 2: World Health Organization’s reports on head lice........................................12
Appendix 3: Information on the control of head lice ............................................................13
Appendix 4: Information on the control of scabies ...............................................................16
Appendix 5: Outreach by the North American Regional Action Plan (NARAP) on Lindane and other Hexachlorocyclohexane (HCH) Isomers...................................19
Appendix 6: Articles related to scabies.....................................................................................21
UNEP/POPS/COP.5/INF/13/Rev.1
3
Introduction 1. By its decision SC-4/15, the Conference of the Parties to the Stockholm Convention on Persistent Organic
Pollutants amended part I of Annex A to the Convention to list lindane therein with a specific exemption for the use of lindane as a human health pharmaceutical for the control of head lice and scabies as a second line treatment.
2. In paragraph 2 of the same decision, the Conference of the Parties requested the Secretariat to cooperate with the World Health Organization (WHO) in developing reporting and reviewing requirements for the use of lindane in accordance with the exemption for the substance, taking into consideration the concluding statement in the Persistent Organic Pollutants Review Committee’s risk management evaluation on the chemical (UNEP/POPS/POPRC.3/20/Add.4), and to report on that cooperation to the Conference of the Parties at its fifth meeting.
3. In response the Secretariat, in collaboration with WHO, developed a questionnaire and conducted a survey on the use of lindane to support the establishment of reporting and reviewing requirements for the use of lindane in accordance with the specific exemption for the substance. The questionnaire was sent to the official contact points and national focal points of the Stockholm Convention and the representatives of permanent missions to the United Nations Office at Geneva in September 2010. Based on the information received from parties by 31 December 2010, the Secretariat, in collaboration with WHO, has conducted a preliminary evaluation of the use of lindane.
4. The present report summarizes key findings and potential gaps identifies in the information submitted and in other relevant sources, including scientific literatures.
Situation analysis of the use of lindane
Summary of responses to the Secretariat’s questionnaire 5. The Secretariat has received the information from the following 43 parties The response rate to the questionnaire
from parties was 24 %:
(a) African region: Central African Republic, Madagascar, Malawi, Mali, Nigeria, Sudan, Uganda and Zambia.
(b) Asian region: Bahrain, China, Iran, Japan, Kuwait, Qatar, Sri Lanka, Tajikistan, Turkey, and Vietnam
(c) Central and Eastern European region: Croatia, Czech Republic, Armenia, Bosnia and Herzegovina, Bulgaria, Moldova, Republic of Macedonia, Romania,
(d) Latin American and Caribbean region: Honduras, Mexico, Panama, Trinidad and Tobago Uruguay and Venezuela.
(e) Western Europe and other region: Austria, Canada, European Commission, Germany, Liechtenstein, Lithuania, Netherlands, New Zealand, Norway and Portugal.
6. Listed below is a summary of information submitted.
(a) Production, use, import and export of lindane:
i) Production: China reported the production of lindane has been stopped but existing stocks of the technical grade lindane is used for the production of lindane cream, as a treatment of head lice.
ii) Use: 10 countries (23% of the responses) reported the use of lindane for pharmaceutical use. Two countries reported use in agriculture. Central Africa reported use in wood treatment and Japan reported the use of lindane for research and experiments. Two countries reported the use of lindane for first-line treatment of head lice and/or scabies. Rest of the countries reported that the uses of lindane are limited to second-line treatments of head lice and scabies.
iii) Export: Canada, EU and Germany reported the export of lindane. Germany reported an export of 300 kg to Venezuela in 2008, but no export in 2009, and an export of 50 kg to Pakistan in 2010. Central African Republic reported no export of lindane. However, it states in the remarks that small quantities are being exported.
iv) Import: 7 countries (16% of the responses) reported the import of lindane. Germany reported import from India in 2008 and from Great Britain in 2010. Zambia reported that registration holders import from India. Nigeria reported illegal import and use of lindane.

UNEP/POPS/COP.5/INF/13/Rev.1
4
v) Stockpiles: 4 countries reported the presence of stockpiles, though the question was not included in the questionnaire.
vi) 24(67% of the responses) countries reported no production, export, import or use of lindane.
(b) National policy and regulations on lindane:
i) Five countries reported that they had no regulation on the size of retail packages.
ii) Two countries reported that they had no regulatory actions that ensure protection of vulnerable groups. One country reported that it has no regulation on contents of labels.
(c) Availability of non-chemical and chemical alternatives to lindane:
i) Three countries reported to have initiatives to promote alternative products, methods and strategies to the use of lindane.
(d) Public awareness and outreach programmes for lindane:
i) Canada reported the presence of outreach and awareness programmes on the proper use of lindane.
7. Brazil, China, Mauritius, South Africa, Switzerland, Thailand and Zambia indicated that they have taken steps to control and reduce release of lindane.
8. Canada, the United States, the Czech Republic, the Republic of Zambia and Brazil have mechanisms to monitor and control lindane. Other countries also have programs to share information concerning the uses, alternatives and regulations of lindane.
9. Majority of the lindane users are from developing countries. Most of them reported that lindane is used only as second-line treatment for head lice and scabies. However there is still a lack of information on the countries that are using lindane. The stockpiles of lindane could be traded. There is a lack of information on the presence of lindane stockpiles and its influence on present use of lindane.
10. National policies for regulation of lindane range considerably, from no regulatory control to full prohibition of use of lindane to controlling packaging and labeling requirements. There is also lack of information on adequacy of national policies to ensure effective regulation of lindane for its intended use and to promote the use of alternatives and to assure protection of vulnerable groups.
11. Public awareness and outreach programmes including initiatives to promote alternative products, methods and strategies to the use of lindane do not exist in many countries.
Country specific information available from other sources Australia:
12. In January 2010, following discussions with the Australian Pesticides and Veterinary Medicines Authority (APVMA) and the Department of Agriculture, Fisheries and Forestry about the future of lindane, the sole registrant advised that the importation of lindane active constituent had ceased in 2009 and indicated that it wished to withdraw the registration of the product. The processes to cancel the sole remaining lindane product registration and remove the label from Public Chemical Registration Information System of the Australian Pesticides and Veterinary Medicines Authority (PubCRIS) were completed on 7th June 2010. Since there was no longer any need to review lindane, the APVMA removed it from the Priority Candidate Review List of the Australian Pesticides and Veterinary Medicines Authority1.
Czech Republic: 13. The Czech Republic has an education and awareness POPs campaign for the Stockholm Convention and the
United Nations Economic Commission for Europe’s Convention on Long-range Transboundary Air Pollution) based on the Czech National Implementation Plan which includes aspects related to lindane as a POP.
European Union: 14. Persistent organic pollutant emissions assessment was published by the EU in October 20102. One of the
conclusions was that HCH emissions in the 32 countries of the European Economic Area have fallen by 86% from 1990 to 2008. However, six countries have reported increases in emissions (Estonia, Germany, Hungary, Italy, Latvia and Romania). Of this overall decrease in emissions, 44% may be accounted for by decreased emissions from the ‘Agriculture’ sector, 29% from ‘Non-road transport’, and 21% from ‘Waste’. In 2008, 99% of emissions of HCH were from ‘Industrial process’ sources.
1 http://www.apvma.gov.au/products/review/a_z_reviews.php 2 http://www.eea.europa.eu/data-and-maps/indicators/eea32-persistent-organic-pollutant-pop-emissions-1/assessment

UNEP/POPS/COP.5/INF/13/Rev.1
5
Mexico 15. Mexico developed and published a National Diagnostic Report on lindane in 2004. The report includes
information on production, imports, exports, commercial names, prices, selling patterns, quantities used and possible alternatives which can be found at the website of the National Institute of Ecology.
Sweden 16. Sweden has extensive information on treatment regimes for all available drugs against scabies and lice may be
found on the Swedish Medical Products Agency or in the list of pharmaceutical products in Sweden.
United States: 17. Use of lindane products in agriculture was allowed until 1 October 2009, in order to minimize costs associated
with disposal of unusable stocks. From that date and onwards no lindane has been used in agriculture.
18. Unites State Environmental Protection Agency (USEPA) Office of Pesticide Program maintains a website with recent regulatory decisions on lindane. The Food and Drug Administration (USFDA) has a website for safety alerts for primary care providers, pharmacists and consumers.
Regulations, initiatives, and regimes for the control of lindane 19. According to the risk management evaluation on lindane, the control measures for lindane are currently
implemented in several countries including banning of production, use, sale and imports, cancellation of registration, clean-up of contaminated sites, and public health advisories and hazard warnings for pharmaceutical uses. A thorough review of existing control measures that have already been implemented in several countries, shows that risks from exposure of humans and the environment to lindane can be reduced significantly.
20. Some countries that have already prohibited or restricted the use of lindane, consider the use of existing stockpiles for a limited time period as feasible, leaving a limited amount of waste for disposal. Contaminated sites of former lindane producers, old storages and dumps have to be addressed by several countries. Further consideration may be given to control measures regarding the production such as prevention and sound management of generated waste.
21. There are two major regional initiatives, the European Union and the Commission for Environmental Cooperation with USA, Canada and Mexico cooperating via the joining of forces, have a strong capacity to deal with lindane and with other POPs issues.
European Union: 22. A total ban of the export of lindane is foreseen as for April 2011 on the basis of an amendment of the EU
regulation 689/2008 concerning the export and import of dangerous chemicals. Until 31 December 2007, the use of lindane was allowed for public health and veterinary topical insecticide. EU has established an extensive system where all EU Member countries periodically meet and use standard reporting on all obligations for the Stockholm Convention and are all lindane issues automatically covered.
23. The main issues the EU Commission reports on the application of the POPs Regulation (including lindane) are: control of production, placing on the market and use, stockpiles, emissions, waste management, implementation plans, monitoring, information exchange, technical assistance, reporting, and penalties.
24. The EU uses the website called Communication and Information Resource Center Administrator (CIRCA) which is a collaborative workspace with partners of the European Institutions where a large number of interest groups exchange their information. The Persistent Organic Pollutants Interest Group consists of the Competent Authorities for the implementation of Regulation (EC) Nr 850/2004 on POPs of the EU Member States. These competent authorities report and meet periodically on their obligations and all related documents are available. The EU Commission, Directorate-General Environment Directorate D - Water, Chemicals and Biotechnology ENV.D.3 – Chemicals and Nanomaterials is the organizer. CIRCA Interest Group has a library with all data and reports submitted, however till present there is no free access to the network and the information, but interested parties can apply for membership of the Persistent Organic Pollutants Interest Group and then could get access codes and then make use of the available information.
North American Regional Action Plan on lindane and Other Hexachlorocyclohexane (HCH) Isomers: 25. Similar initiatives are in place for USA, Canada and Mexico. Spearheaded by the Commission for Environmental
Cooperation (CEC), these three countries have produced “The North American Regional Action Plan (NARAP) on lindane and Other Hexachlorocyclohexane (HCH) Isomers” in November 2006. The NARAP is a continental strategy for the governments of Canada, Mexico and the United States to address exposure risks through a variety of national regulatory and management actions, outreach and education efforts, science and research, capacity building, and collaborative cross-border activities.
UNEP/POPS/COP.5/INF/13/Rev.1
6
26. Lindane ban in California shows that it can be realized within the existing public health system transfer3. Apart from lindane, the the CEC has made NARAPs for chlordane, DDT, Mercury, PCBs, Dioxins, Furans and Hexachlorobenzene, Poly Brominated Diphenyl Ethers (PBDE) as well as on Environmental Monitoring and Assessment.4 This shows that the CEC is a good regional initiative to deal with issues like lindane, and that such initiatives are well able to deal with POPs issues in total.
27. Since California banned lindane, four scabies outbreaks were reported by four counties to the California Department of Health Services (CDHS) Surveillance and Statistics Section. Prior to the ban, CDHS issued guidelines to all physicians to use Malathion instead of lindane to control head lice. For scabies outbreaks CDHS developed and distributed to healthcare facilities a guideline where CDHS recommends the use of Ivermectin to treat patients with severe scabies. Although Ivermectin has not been approved by the FDA for use for scabies and it is not recommended by CDHS for typical scabies or prophylaxis, Ivermectin has been used in outbreaks in California for treatment of symptomatic cases and for mass prophylaxis because of its ease of use and probable greater compliance and efficacy compared to Permethrin.
Information on alternatives to lindane 28. According to the risk management evaluation by the POPs review committee, alternatives to agricultural
application of lindane are available, efficient, technically feasible and accessible. Guidance and support should be provided to countries with difficulty in replacing lindane for agricultural use. However, failures have been reported for scabies and lice treatments.
29. Some countries are concerned about the availability and efficacy of alternatives for certain pharmaceutical and agricultural uses. For these particular cases, it has been proposed to give incentives to find more environmental and health friendly alternatives. Issuing public health advisories would also be recommended to control lindane use patterns and reduce risks associated.
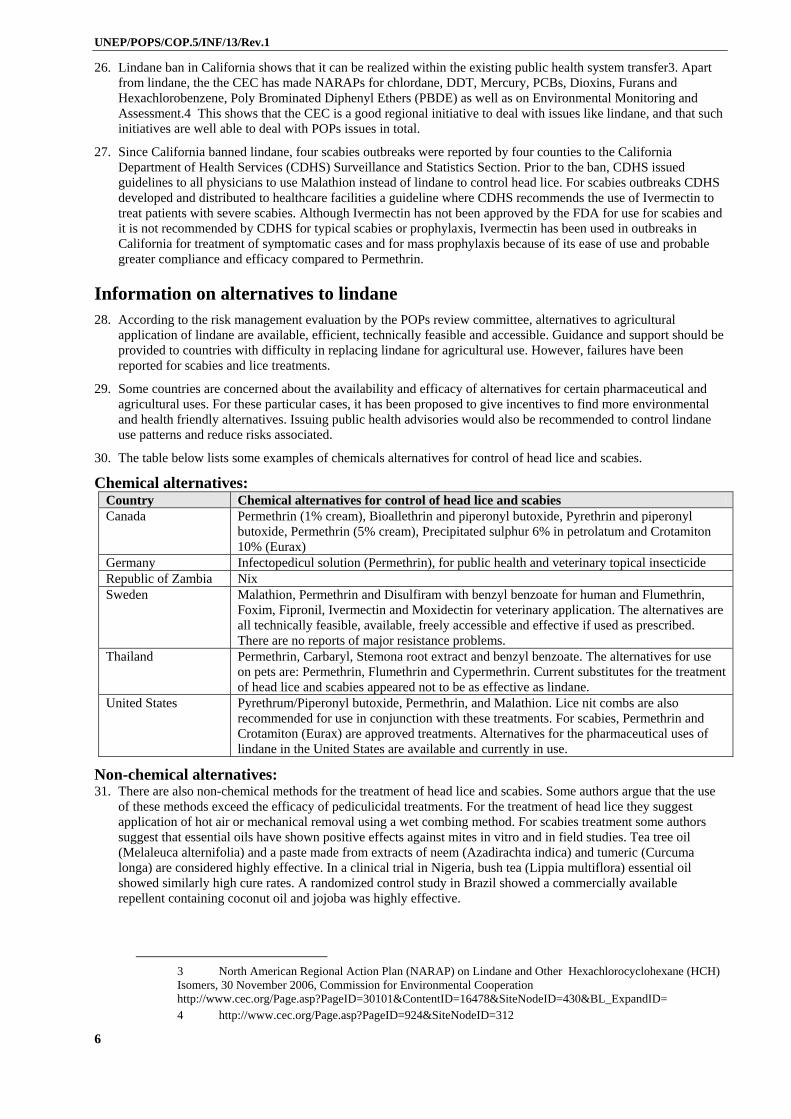
30. The table below lists some examples of chemicals alternatives for control of head lice and scabies.
Chemical alternatives: Country Chemical alternatives for control of head lice and scabies Canada Permethrin (1% cream), Bioallethrin and piperonyl butoxide, Pyrethrin and piperonyl
butoxide, Permethrin (5% cream), Precipitated sulphur 6% in petrolatum and Crotamiton 10% (Eurax)
Germany Infectopedicul solution (Permethrin), for public health and veterinary topical insecticide Republic of Zambia Nix Sweden Malathion, Permethrin and Disulfiram with benzyl benzoate for human and Flumethrin,
Foxim, Fipronil, Ivermectin and Moxidectin for veterinary application. The alternatives are all technically feasible, available, freely accessible and effective if used as prescribed. There are no reports of major resistance problems.
Thailand Permethrin, Carbaryl, Stemona root extract and benzyl benzoate. The alternatives for use on pets are: Permethrin, Flumethrin and Cypermethrin. Current substitutes for the treatment of head lice and scabies appeared not to be as effective as lindane.
United States Pyrethrum/Piperonyl butoxide, Permethrin, and Malathion. Lice nit combs are also recommended for use in conjunction with these treatments. For scabies, Permethrin and Crotamiton (Eurax) are approved treatments. Alternatives for the pharmaceutical uses of lindane in the United States are available and currently in use.
Non-chemical alternatives: 31. There are also non-chemical methods for the treatment of head lice and scabies. Some authors argue that the use
of these methods exceed the efficacy of pediculicidal treatments. For the treatment of head lice they suggest application of hot air or mechanical removal using a wet combing method. For scabies treatment some authors suggest that essential oils have shown positive effects against mites in vitro and in field studies. Tea tree oil (Melaleuca alternifolia) and a paste made from extracts of neem (Azadirachta indica) and tumeric (Curcuma longa) are considered highly effective. In a clinical trial in Nigeria, bush tea (Lippia multiflora) essential oil showed similarly high cure rates. A randomized control study in Brazil showed a commercially available repellent containing coconut oil and jojoba was highly effective.
3 North American Regional Action Plan (NARAP) on Lindane and Other Hexachlorocyclohexane (HCH) Isomers, 30 November 2006, Commission for Environmental Cooperation http://www.cec.org/Page.asp?PageID=30101&ContentID=16478&SiteNodeID=430&BL_ExpandID= 4 http://www.cec.org/Page.asp?PageID=924&SiteNodeID=312

UNEP/POPS/COP.5/INF/13/Rev.1
7
32. The report by International POPs Elimination Network (IPEN) entitled “Lindane: Pharmaceutical and Agricultural Alternatives”5 has collected experiences on non-chemical head lice and scabies. The use of lindane as a treatment for lice and scabies is outmoded due to increasing resistance, lack of efficacy, and its toxicity. The authors have presented a variety of viable alternatives to replace the use of lindane for pharmaceutical purposes in the treatment of lice, but it is found that there is still a lack of non-chemical alternatives for treatment of scabies. The report is summarized in the table below:
Non-chemical alternatives for Head lice 33. The application of hot air was found to be an effective, safe treatment and unlikely to evolve resistance without
any adverse effects of treatment. 34. Mechanical removal using a wet combing method and specialized LiceMeister™ comb, as well as a removal
method using the so-called “Bug Buster” kit (a prescribed mechanical measure). A prescribed mechanical method of treatment was four times more effective than current over-the counter pediculicides for eliminating head lice.
35. Dimethicone lotion was shown to be more effective than malathion and permethrin treatments. 36. The use of Cetaphil cleanser was 96% effective and had a 94% long-term cure rate with no toxicity. Cetaphil
cleanser was found to have cure rates exceeding those of permethrin, malathion, “Bug Busting” (particular type of mechanical removal used in the UK), and dimethicone.
37. It was also stated that even without full effective treatments, the management of headlice can be much improved by attention to diagnosis, contact management, and outcome of treatment.
38. The results of two case studies involving large institutional settings indicate that treatments for head lice and scabies effective without the use of lindane products (before the lindane ban) have been listed under this section and under chemical alternatives for scabies in the following part.
39. The California Department of Corrections, with a population of over 150,000 inmates per year has treated head lice and scabies without lindane, instituting alternative treatments two years prior to the ban on the use of pharmaceutical lindane enacted by the California legislature in 2002. The corrections system has effectively treated both lice and scabies through the use of Elimite cream (5% permethrin) for scabies and several non-lindane products for head lice. The Department of Corrections recommends the use of combs to treat head lice.
40. A second case study of the Sutter Delta Medical Center in Antioch California demonstrates effective treatment of lice and scabies without the use of lindane. A 1% permethrin compound is used for head lice treatment and scabies is treated with a 5% permethrin cream. Both alternative treatments have been successful with no problems reported. The U.S. Centers for Disease Control and the American Social Health Association consider a 5% permethrin cream or lotion to be the most effective treatment for scabies.
41. Non-chemical alternatives for Scabies
42. Scabies is a major parasitic disease public health problem in many resource-poor regions. It causes substantial morbidity from secondary infections and post-infective complications such as acute post-streptococcal glomerulonephritis. Scabies is strongly associated with poverty and overcrowding.
43. Due to adverse events during use and the toxic effects of lindane and other scabicides, viable less toxic alternatives for the treatment of scabies have been developed and the following alternatives have been documented (Note that a part of this information has been forwarded in 2007. See chapter 2.3 under non-chemical alternatives):
44. Essential oils have shown an impressive effect against mites in vitro as well as in field studies. Tea tree oil (Melaleuca alternifolia) is highly successful against mites in vitro. In a clinical trial in Nigeria, bush tea (Lippia multiflora) essential oil resulted in similar high cure rates.
45. A paste made from neem extracts (Azadirachta indica) and tumeric (Curcuma longa) cured 97% of patients with scabies with no adverse reactions.
46. A randomized control study in Brazil demonstrated that a commercially available repellent containing coconut oil and jojoba was highly effective.
47. A 5% solution of tea tree oil (Melaleuca alternafolia) with the active component terpinen-4-ol was found highly effective in treating scabies. Australian researchers compared the survival time of scabies mites exposed to 5% tea tree oil with those exposed to ivermectin and permethrin and found that tea tree oil was more effective than the other treatments. However, caution should be exercised with the topical use of tea tree oil because it may cause contact dermatitis in some individuals.
Example of guidelines for the safe use of lindane
5 IPEN, International POPs Elimination Network, Lindane: Pharmaceutical and Agricultural Alternatives, April 2009 www.ipen.org

UNEP/POPS/COP.5/INF/13/Rev.1
8
48. Some countries such as Australia, Canada, the United Kingdom and the United States reported policies and guidelines on lindane. For example, the Food and Drug Administration (USFDA) issued Public Health Advisory (PHA) entitled “Safety of Topical Lindane Products for the Treatment of Scabies and Lice”. The PHA provides use of topical formulations of lindane lotion and lindane shampoo for the treatment of scabies and lice.
49. In addition, the boxed warning on the package emphasizes that it is a second-line treatment, updates information about its potential risks especially in children and adults weighing less than 110 pounds, and reminds practitioners that reapplication of lindane lotion or lindane shampoo is not the appropriate treatment, if itching continues after the single treatment.
50. Lindane product package sizes are limited to one and two ounces in order to minimize the potential for patients to apply the product in excess and to minimize reapplication of lindane. Pharmacists should dispense a quantity sufficient for a single treatment, not to exceed two fluid ounces.
51. Also, a medication guide, designed to inform patients of the risks of lindane products and provide instructions for appropriate use of the drugs, must be dispensed by the pharmacist with each new prescription.
52. Lindane is approved for topical treatment of pediculosis and scabies in patients "who have either failed to respond to adequate doses, or are intolerant of, other approved therapies." Lindane has been on the market since 1951, but was labeled as second-line therapy in 1995 because there are safer alternative treatments that should be used first. Second-line therapy is used when the patient cannot tolerate the first-line drug of choice or the patient has used the first-line drug of choice as instructed and the treatment has failed.
53. Examples of other medications approved to treat scabies and lice include the following:
permethrin cream 5% (Acticine, Elimite, Nix) Scabies:
crotamiton cream (Eurax)
malathion lotion 0.5% (Ovide, prescription only)
pyrethrum 0.33% with piperonyl butoxide shampoo and cream rinse
Lice:
permethrin cream rinse 1% (Nix and Rid)
Current Issues: 54. FDA has determined that lindane products have benefits that outweigh risks when used as directed. Most serious
adverse events reported in association with lindane products have been due to misuse.
55. However, there have been rare case reports of serious reactions with apparently normal use. These reports highlight the need to emphasize the potential toxicity of lindane in the product labels and educate healthcare providers and patients about the risks and how to minimize them, as well as to develop mechanisms to facilitate safe use, once the drug is dispensed to patients. These mechanisms include having lindane products available only in small packaged amounts to avoid excess application and requiring that the Medication Guide be given to the patient by the pharmacist with each new prescription.
Current Safety Information: 56. Safety information for lindane comes from FDA’s Adverse Event Reporting System (AERS), which is derived
from spontaneous adverse event reports through FDA’s MedWatch Program and literature reports submitted to the Agency. Rates of adverse events cannot be calculated from this system and underreporting is presumed, especially for older products like lindane lotion and shampoo.
57. The adverse events of concern for lindane are systemic events due to absorption of this lipophilic drug following topical application. The majority of events occurred in patients with contraindications to the use of lindane, in patients who used the medication in excessive amounts, or in those who misused the lindane product. Of the adverse event cases in the FDA database with a serious outcome (hospitalization, disability or death), only 20% used lindane according to the directions in the label. All other patients did not use lindane according to directions in the label. Most commonly, patients often reapplied lindane because of continued itching after the treatment, either on their own volition or at their doctor’s recommendation.
Deaths: 58. Three deaths due to lindane use have been confirmed, although 17 deaths have been reported associated with
lindane use. The three confirmed deaths all included use of lindane not in accordance with the label, including multiple topical applications or oral ingestion. Lindane toxicity was confirmed by autopsy in a child, and was diagnosed in an adult. The third death occurred in an adult who ingested lindane for suicide purposes.
59. Of the remaining 14 deaths associated with lindane, but not confirmed, there were 4 children, 9 adults and 1 patient of unknown age. All of these deaths occurred when lindane was applied topically. In 9 cases, use was not
UNEP/POPS/COP.5/INF/13/Rev.1
9
in accordance with the label (exceeded label use - 7, oral administration – 1, use was contraindicated - 2). Scabies and head and/or pubic lice were the predominant indications for use.
Neurologic Risks: 60. The risk of neurologic side effects associated with lindane is known from clinical trials, spontaneous post-
marketing reporting data and literature reports. These side effects have ranged from dizziness to seizures. In post-marketing reports, neurologic side effects occurred in patients who misused lindane, as well as in patients who used lindane according to labeled instructions. Among the adverse event reports in the FDA database, 70% reported neurologic events including seizure, dizziness, headache and paresthesia.
Increased Risk in Younger and/or Smaller Patients and the Elderly: 61. Lindane is contraindicated for use in neonates and should be used with extreme caution in children and in
individuals weighing less than 50 kg (110 lbs). Among adverse event reports in which the outcome was serious (resulted in hospitalization, disability or death), the very young and the elderly appeared to be more susceptible to lindane’s adverse effects and had worse outcomes.
62. Animal studies have demonstrated that younger animals are more susceptible to the neurologic side effects seen with lindane use. In addition, smaller children have a larger body surface to volume ratio that may result in proportionately larger risk of systemic exposure. For this reason, lindane has long been contraindicated for use in neonates. It is not known whether the developing nervous system of children also increases their susceptibility to neurologic toxicity.
Other Populations with Increased Risk: 63. Patients who have conditions, such as HIV infection, or take certain medications that may lower the seizure
threshold should be prescribed lindane with caution. They may be at greater risk for serious adverse events. The new lindane label lists examples of some of these conditions and medications. The label also highlights special precautions for use of lindane in women who are breastfeeding infants.
64. There are case reports of neurologic adverse events in nursing home patients treated with lindane. Factors that may have increased their susceptibility to these adverse events include concomitant medications, underlying medical conditions, and advanced age. Special consideration should be given prior to treating this population with lindane, even if they are greater than 50 kg.
Summary: 65. Lindane products should be prescribed carefully, and quantities prescribed should be limited to amounts for a
single application. Patients are at risk for serious neurologic adverse events, and even death, particularly with early retreatment. It is not known how soon after administering one dose of lindane that a second dose can be safely administered. Post-treatment itching is common, especially in the treatment of scabies and does not necessarily indicate treatment failure.
66. The instructions for lindane use have been clarified in the products’ professional labels and in the Medication Guides, which by law must be dispensed with all prescriptions of lindane. Because most of the serious adverse events reported have been because of misuse of lindane lotion and lindane shampoo, it is very important that patients understand the importance of using this medication in a manner consistent with product labeling.
67. The FDA wants healthcare providers to be aware of this new safety information and the changes that have occurred in the label for topical lindane lotion and lindane shampoo prescribed for the treatment of scabies and lice (both head and pubic lice), respectively. Healthcare providers should consider this new safety information when deciding whether to prescribe lindane lotion or lindane shampoo for patients who may be at risk for serious adverse drug sequelae.
68. The following items of particular concern to parents of children with special needs are excerpted from an FDA FAQ on lindane:
(a) Serious side effects including seizures and deaths have been reported to the FDA in patients who use too much lindane or after a second treatment with lindane.
(b) Seizures can happen in some patients even if they use lindane as directed.
(c) Certain people are at higher risk to develop seizures and death from lindane. This includes: babies and children, and people weighing less than 110 pounds.

UNEP/POPS/COP.5/INF/13/Rev.1
10
(d) You should not use lindane shampoo or lindane lotion if you: have a seizure disorder (convulsions, fits) or have ever had a seizure, especially seizures that have been hard to control; have open sores or crusted (scabby) sores on the skin around your head and neck, or lots of broken skin in the treatment area; have other skin conditions such as psoriasis or atopic dermatitis.
(e) It is difficult to know who may experience side effects, however, tell your health care provider if you: have HIV or AIDS; have diabetes; have had a head trauma, seizures, or a brain tumor; have liver disease; take any medications, including prescription and non-prescription medications, vitamins and supplements.
(f) Some medications can increase your chances of having a seizure, such as: Antidepressants, Chlorpromazine (Thorazine) and other antipsychotics, Chloroquine, Ciprofloxacin (Cipro) or penicillins, Methocarbamol (Robaxin), Pemoline (Cylert), Promethazine (Phenergan), Theophylline, Corticosteroids.
(g) There is increasing concern that patients weighing less than 110 pounds, the elderly and babies may be more susceptible to side effects. Babies, because of their size and thin skin may absorb more lindane shampoo or lindane lotion and may be more at risk for serious side effects.
(h) Lindane may cause serious side effects such as seizures (convulsions, fits) or death. Lindane can also make you feel sleepy, dizzy, or can cause body shaking that you cannot control. The most common side effects of lindane are: itching skin, burning skin, dry skin, or a skin rash.
(i) To report serious side effects, visit www.fda.gov/medwatch and click on "Submit Report" in the blue sidebar, or call 1-800-FDA-1088.
Lindane shampoo and lindane lotion for the treatment of scabies and lice:
69. Listed below are FDA’s updates to the labeling of lindane shampoo and lindane lotion for the treatment of scabies and lice6. Lindane products can cause serious side effects for many reasons, even when used as directed. It is important for patients and caregivers to understand how to properly use these products. Lindane products should be prescribed carefully, and quantities prescribed should be limited to amounts for a single application.
(a) Revised Lindane shampoo Label [PDF]7 (b) Medication Guide for Lindane Shampoo [PDF]8 (c) Revised Lindane lotion Label [PDF]9 (d) Medication Guide for Lindane Lotion [PDF]10 (e) Public Health Advisory on Lindane (f) Questions and Answers for Lindane (g) Warning on Lindane for Scabies and Lice - Video presentation and text from FDA Patient Safety News (h) FDA versus EPA Exposure Chart [PDF] (i) Assessment [PDF] (j) Post Marketing Safety Review [PDF]
6 http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm110452.htm 7 http://www.accessdata.fda.gov/drugsatfda_docs/label/2003/006309shampoolbl.pdf 8 http://www.fda.gov/downloads/Drugs/DrugSafety/UCM133688.pdf 9 http://www.accessdata.fda.gov/drugsatfda_docs/label/2003/006309lotionlbl.pdf 10 http://www.fda.gov/downloads/Drugs/DrugSafety/UCM133687.pdf

UNEP/POPS/COP.5/INF/13/Rev.1
11
Appendix 1: Questionnaire on lindane sent to all Parties
The Secretariat, in collaboration with WHO, developed a questionnaire on the use of lindane to support the establishment of reporting and reviewing requirements for the use of lindane in accordance with the specific exemption for the substance. The questionnaire is reproduced below:
UNEP/POPS/COP.5/INF/13/Rev.1
12
Appendix 2: World Health Organization’s reports on head lice
In 1992, the WHO Expert Committee11 confirmed the deletion of lindane from the WHO Model List of Essential Medicines and stated that for scabies and pediculicides “Lindane is deleted since it is toxic to the environment and humans, and safer alternatives are available.”
In 1997, WHO published a report on Human Lice which reviews a status from 1985 to 1997.12 The report contains prevalence of human lice infestations in seven regions (Americas, Central and Eastern Europe, Middle East, Africa, Southeast Asia and Western Pacific), the control of human lice infestations, chemical and non-chemical strategies of control. Below is a summary of the report.
Chemicals in use: Lindane: It was already reported that due to toxicological concerned and the spread of insecticide resistance, that the use of lindane for lice control was expected to decline, especially where alternative compounds were available.
Malathion: Head lice resistance was reported in France and UK, but it is still effective against head lice in most areas and considered safe to use.
Carbaryl: Considered as reasonably effective, but there exists some concerns from UK Ministry of Health led to availability only on prescription.
Permethrin: Its use was threatened due to increasing permethrin/pyrethroid resistance, as reported from Czech Republic (144), France (44), Israel (119) and UK (26).
Phenothrin: Similar results on resistance as permithrin, and expected limit in its use as well as for other pyrethroids.
Benzyl benzoate: It has been widely used for treatment of Pediculosis and scabies, but is not always an effective ovicide. Occurrence of skin irritation is common. It is extensively used in Russia, and is no longer registered for lice control in USA, and only available on prescription in Canada.
Ivermectin: Widely used throughout western Africa to control transmission of human nematode Oncherca Volvulus. It was also thought to have the potential to be the drug of choice against mites and human lice. It has not yet been registered for control of human lice. The necessity of a second treatment to ensure control of infestations and occurrence of relatively mild but frequent side effects among treated people may, however, limit the use of it for human control. At present time, there is no systemic insecticide registered for human lice control.
Non-insecticidal methods of control: Various types of combs have been used since antiquity. It is stated that careful grooming with various types of combs would either remove lice or nits and combing would injure adult lice resulting in their death. It refers also to the Burgess (1995) report reviewing literature on head lice control on grooming that the number of head lice either increased or were undiminished. It also emphasizes that body louse eggs are attached to clothes rather than hairs of the body, and that suitable laundering of clothes of infested individuals is an essential part of the body-louse control programme. It also states that necessary means for laundering clothes are inadequate in places such as refugee camps and other areas of civil unrest, where body lice control is most needed, under which conditions one still will have to rely on insecticide treatment. It advices on launder beddings of kids infested, as nits may survive on beddings. Also that combs and hair brushes should be washed in hot water with strong soap.
11 The Use of Essential Drugs, Model List of Essential Drugs (seventh List), Page 51, Fifth Report of the WHO Expert Committee, WHO Expert Report Series 825, 1992 12 Gratz NG. Human lice: Their prevalence, control and resistance to insecticides: A review 1985-1997. Geneva: World Health Organization, 1997. <whqlibdoc.who.int/hq/1997/WHO_CTD_WHOPES_97.8.pdf
UNEP/POPS/COP.5/INF/13/Rev.1
13
Appendix 3: Information on the control of head lice In the United States, approximately 6-12 million infestations occur each year mostly among children from ages 6-12 of all socioeconomic groups.13 A 1997 report estimated that approximately 6 to 12 million infestations occur each year in the United States, but this number was based on sales of pediculicides and is most likely an overestimation. Anecdotal reports from the 1990s estimated annual direct and indirect total cost of $367 million, including remedies and other consumer costs, lost wages, and school system expenses. More recently, treatment costs have been estimated at $1 billion.14 USA FDA15, Information on the current status was summarized as follows: Pharmaceutical use of lindane in the United States has continued to decline each year. In 2009, usage of lindane for lice and scabies in the United States was less than 5% (less than 85 kg) of that used in 1998.
Benzyl alcohol lotion (5%) is a new alternative, now approved by the FDA for lice, and a half dozen other drugs are in the pipeline for lice treatment. Oral ivermectin is not approved for use for scabies.
California Ban on Pharmaceutical lindane16 provides also a number of outcomes that could be used when implementing bans in other regions or countries:
“Response to lindane" ban: More than one-half (61%) of pediatricians reported to have used lindane before the ban, and the vast majority (81%) were aware of the ban. Of the providers who reported using lindane prior to the ban, virtually all (94%) reported changing their prescribing practices as a result of the ban.
Most respondents (78%) did not notice any difficulties after the lindane ban. However, 30 providers did report difficulties after the ban. Of these, most used lindane before the ban (26 of 30; 87%) and only 4 of 30 did not report prior lindane use. Those providers who reported that they had used lindane pre-ban and noticed difficulties after the ban were far more likely to be in solo private practice (35% vs. 7%) and to have been in practice > 15 years (58% vs. 44%). Providers reporting difficulty after the ban cited resistant lice as the main reason (97%); however, overall reports of resistant scabies were minimal (5%), as were increased cases of lice (7%) or scabies (1%). There were no significant differences among volume of head lice or scabies cases seen in the previous 3 months between providers who reported difficulties and those who did not.
Treatment preferences: The majority of respondents (69%) stated their first-line treatment preference for head lice was 1% permethrin, followed by 5% permethrin (9%) and other over-the-counter (OTC) methods including pyrethrum (8%). Respondent preference for second-line head lice treatment was malathion (51%), followed by 5% permethrin (19%). For scabies treatment, the majority (92%) of respondents expressed preference for 5% permethrin (92%), followed by crotamiton (5%). Second-line treatment preference for scabies included crotamiton (32%), followed by 5% permethrin (25%), malathion (21%), and others (22%).”
Chemical alternatives for head lice US FDA states examples of other medications approved to treat lice include the following:
a) malathion lotion 0.5% (Ovide, prescription only)
b) pyrethrum 0.33% with piperonyl butoxide shampoo and cream rinse
c) permethrin cream rinse 1% (Nix and Rid)17
d) Ulesfia (Benzyl Alcohol Lotion 5% for Topical Use)
e) Natroba (Spinosad 9%) which is ovicidal18.
13 Frankowski, B.L. et al. 2002. American Academy of Pediatrics Clinical Report on Head Lice. Pediatrics 110 (3):638-643 14 Barbara L. Frankowski, Joseph A. Bocchini, Jr and Council on School Health and Committee on Infectious Diseases, Head Lice, Pediatrics 2010;126;392-403; originally published online Jul 26, 2010; DOI: 10.1542/peds.2010-1308. http://www.pediatrics.org/cgi/content/full/126/2/392 15 Personal communication Abigail Jacobs, FDA, 12 December 2010 16 Elizabeth H. Humphreys,1 Sarah Janssen,2,3 Ann Heil,4 Patricia Hiatt,5,6Gina Solomon,2,3,6 and Mark D. Miller3,6,7 Outcomes of the California Ban on Pharmaceutical Lindane: Clinical and Ecologic Impacts. Environmental Health Perspectives. 2008;116(3):297-302. © 2008 National Institute of Environmental Health Sciences 17 FDA Public Health Advisory: Safety of Topical Lindane Products for the Treatment of Scabies and Lice http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm110845.htm 18 On January 18, 2011, the U.S. Food and Drug Administration approved Natroba (spinosad) Topical Suspension 0.9%, a pediculicide, for the treatment of head lice infestation in patients ages 4 years and older. The safety and effectiveness of Natroba Topical Suspension 0.9%, have been established in two multicenter, randomized, active-

UNEP/POPS/COP.5/INF/13/Rev.1
14
It should be noted that Crotamiton is not currently approved by the FDA for use as a pediculicide19 The International League of Dermatological Societies (ILDS), (A non-Governmental Organization in official Relations with the World Health Organization) states20: In conclusion, the ILDS group has not found evidence that rates the use of lindane for the treatment of head lice as more effective than comparators. In all studies, it showed a record low level of efficacy compared with alternative antiparasitics. Published evidence shows that it is also less effective than Permethrin in scabies infestations. There is insufficient evidence to compare its effectiveness with other agents such as benzyl benzoate or sulphur containing preparations. It is important that more than one treatment is available for both human parasitic infestations in view of the growing problem of resistance to antiparasitic agents. However there are alternatives to lindane for topical application such as benzyl benzoate or sulphurs for scabies and malathion and carbaryl for head lice which show either equivalent or superior efficacy. ILDS states in another publication21: There are two systematic reviews. Permethrin and malathion are effective against head lice when resistance is not present. There is limited evidence for the efficacy of other insecticides such as d-phenotrin. Resistance to pyrethroids may occur. In a RCT (Randomized Controlled Trial) (253 people), dimeticone lotion was compared with d-phenotrin; no significant difference was found in the number of individuals free of lice at 14 days. Dimeticone may represent a treatment option when other modalities have failed. Oral cotrimoxazole should not be used because there is both little evidence of efficacy and a risk of severe cutaneous drug reaction. There is insufficient evidence for combing and wet combing with conditioner (i.e., bug-busting). Analysis of a trial using oral ivermectin is in process. In the case of body lice, apart from treatment with oral antibiotics indicated because of associated bacterial infection, washing clothes may be sufficient. Non-chemical alternatives for head lice A non-chemical approach is strongly pushed by a large number of concerned non-governmental organizations (numerous websites mainly in the United States and the United Kingdom) and governments (the United Kingdom government) based on a trend of increase in head lice cases due to increasing resistance to chemical treatment.
Non-chemical approaches are strongly related to large-scale community programmes like in the United Kingdom (bug busting initiatives) and in the United States, where the organizational aspects play an important role.
A number of Bug busting initiatives22 reported: Chester (the United Kingdom) saw a 24 percent reduction in prescribing costs for lice medication (April 2004 - March 2005) and local healthcare staff reported to have spent less time advising parents.In the Ghent (Belgium) study, 677 children from three schools took part, with active infestation rates in the schools from 13 to 20 per cent. By involving the whole school community in a bug busting approach – including children, parents and school, health and community staff –infestations were reduced by two-thirds.
In 2010, Australian scientists reported that both topical treatment with dimeticone and wet combing is shown to be viable treatment options. Both methods have a high level of parental acceptance and practically no potential side effects. The use of topical, plant-based compounds, although clinical efficacy data are still relatively limited, was also reported23as another promising option.
On April 9, 2009, FDA approved a new prescription medication for the treatment of head lice. Ulesfia (benzyl alcohol) lotion, 5%24, is approved for use in children 6 months of age and older. This new drug is the first FDA-approved head lice product with benzyl alcohol as the active ingredient. The safety and effectiveness of Ulesfia lotion, 5%, were shown in two studies of more than 600 people with active head lice infestation. The study participants received two, ten minute treatments with either Ulesfia lotion or a topical inactive substance (placebo), one week apart. More than 75 percent of the participants who received Ulesfia lotion were lice-free 14 days after the final treatment, compared to 26 percent who received the placebo. The lotion kills lice but not nits, so the second
controlled studies. A total of 552 subjects received a 10-minute treatment with Natroba. If live lice were seen a week later, a second treatment was applied. The proportion of subjects who were lice-free fourteen days after the final treatment of Natroba was approximately 86 percent compared to 44 percent of the control group. Common adverse events reported include redness or irritation of the eyes and skin. 19 IPEN, International POPs Elimination Network, Lindane: Pharmaceutical and Agricultural Alternatives, April 2009 www.ipen.org 20 Effectiveness of Lindane in scabies and head lice infestations, Sent on behalf of the ILDS Group by RJ Hay, O. Chosidow and A Mahé 21 International League of Dermatological Societies working group: Antoine Mahé, Olivier Chosidow, Luigi Naldi, Rod Hay, & Jean-Hilaire Saurat, Proposals for the revision of the WHO essential drugs list concerning drugs that are used to treat skin diseases 22 Multi-country review shows that Bug Buster Kits reduce head lice and social stigma, Journal of Clinical Nursing, PRESS RELEASE, Monday 1 October 2007b 23 Marc Tebruegge, Anastasia Pantazidou and Nigel Curtis What's bugging you? An update on the treatment of head lice infestation, Arch Dis Child Educ Pract Ed published online August 5, 2010, doi: 10.1136/adc.2009.178038 (Australian scientists) 24 Treating Head Lice FDA Consumer Health Information / U.S. Food and Drug Administration, July 2009

UNEP/POPS/COP.5/INF/13/Rev.1
15
treatment is needed to kill lice that have hatched since the first treatment. Common side effects of the medication include irritation of the skin, scalp, and eyes, and numbness of the scalp where the product is applied. The product is not approved for use in children younger than 6 months, and premature infants could be at risk for developing serious side effects such as seizure, coma, and death.
Standard Nurse Protocols for Registered Professional Nurses for 2010 of the Division of Public Health, 25 states that treatment emphasis should be on Non-Pharmacologic methods especially manual removal of nits, as resistance to pediculocides is increasing. Additionally, it is mentioned that in a recent study, these products were found in the urine of school children in Georgia, and the long term effects of exposure to pediculocides is unknown. It is recommended to remove nits with nit comb working through very small sections of hair at a time. Fine toothed metal combs specifically made for removing nits work better for most persons. Combing should be repeated every 3-4 days for two weeks. To aid removal, hair should be soaked with 1:1 white vinegar: water solution.
The Canadian Paediatric Society (CPS)26 reports that Health Canada has recently approved the use of a new noninsecticidal product containing isopropyl myristate 50% and ST-cyclomethicone 50% (Resultz, Nycomed Canada Inc) for the treatment of head lice in children of four years of age and older. The agent works by dissolving the waxy exoskeleton of the louse, leading to dehydration and death. The product is applied to a dry scalp, and rinsed off in ten minutes. This product is not ovicidal, and thus a second application within one week is recommended. Several small phase II trials (200 to 300 participants only) have demonstrated efficacy with minimal side effects.Most common side effects are mild erythema and pruritis of the scalp (26-29). Phase III trials are ongoing.
In Germany, head lice products that are listed as medical products are biocides, which have to be registered or approved, according to EU Biocide Directive 98/8/EC concerning the placing of biocides products on the market. As this directive is not yet completely implemented, there are at present only very few biocide products that are approved. At present only two out of around 20,000 products are approved in Germany and one is in the process of approval.
An up-to-date state of the art on head lice experiences is given by Frankowski et al, in 2010. A summary of nine key points is given below:
a) No healthy child should be excluded from or allowed to miss school time because of head lice. No-nit policies for return to school should be abandoned.
b) Pediatricians should be knowledgeable about head lice infestations and treatments; they should take an active role as information resources for families, schools, and other community agencies.
c) Unless resistance to these products has been proven in the community, 1% permethrin or pyrethrins can be used for treatment of active infestations.
d) Instructions on the proper use of products should be carefully communicated. Because current products are not completely ovicidal, applying the product at least twice, at proper intervals, is recommended if permethrin or pyrethrin products are used or if live lice are seen after malathion therapy. Manual removal of nits immediately after treatment with a pediculicide is not necessary to prevent spread. In the school setting, nit removal may be considered to decrease diagnostic confusion.
e) If resistance to available over-the-counter products has been proven in the community, if the patient is too young, or if parents do not wish to use a pediculicide, consider recommending “wet-combing” or an occlusive method (such as petroleum jelly or Cetaphil), with emphasis on careful technique, and repeating for at least two weekly cycles.
f) Benzyl alcohol 5% can be used for children older than 6 months, or malathion 0.5% can be used for children of two years or older, in areas where resistance to permethrin or pyrethrins has been demonstrated, or can be used topatients with documented infestation that has failed to respond to appropriately administered therapy with permethrin or pyrethrins.
g) New products should be evaluated of their safety and effectiveness.
h) School personnel involved in detection of head lice infestation should be appropriately trained. The importance and difficulty of correctly diagnosing an active head lice infestation should be emphasized. Schools should examinetheir lice-related policies with this in mind.
i) Head lice screening programs have not been proven to have a significant effect over time on the incidence of head lice in the school setting and are not cost-effective. Parent education programs may be helpful in the management of head lice in the school setting.
25 http://health.state.ga.us/pdfs/nursing/Protocol%20Manual/2010/9.0%20Child%20Health.pdf 26 Head lice infestations: A clinical update. Infectious Diseases and Immunization Committee, Canadian Paediatric Society (CPS). Paediatr Child Health 2008;13(8):692-6. Reference No. ID 2008-06. At http://www.cps.ca/english/statements/id/id08-06.htm
UNEP/POPS/COP.5/INF/13/Rev.1
16
Appendix 4: Information on the control of scabies Scabies is a neglected parasitic disease that is a major public health problem in many resource-poor regions. It causes substantial morbidity from secondary infections and post-infective complications such as acute post-streptococcal glomerulonephritis. The disease is strongly associated with poverty and overcrowding, and the associated stigma can ostracise affected individuals. Treatment of scabies in poor countries needs integration of drug treatment programmes with efforts to improve the socioeconomic conditions and education programmes to reduce stigma27.
Scabies can be a serious problem in long-term care facilities, crowded living environments and economically poor conditions in general. Scabies may be complicated by secondary bacterial infections of the lesions, and scabies has been identified as a risk factor for development of post-streptococcal glomerulonephritis. In the United States, children cannot return to school with untreated lice or scabies.
Unlike in industrialized countries, scabies is a major public health threat in the developing world. Scabies is common in resource-poor urban and rural communities, with prevalence reaching up to 10% in the general population and 50% in children. In an urban slum in Bangladesh, the incidence in children younger than 6 years was 952 per 1000 per year, which means nearly all children had at least one scabies infection per year.28
The global prevalence of scabies is estimated at 300 million cases, but the level of infection varies between countries and communities29.
It is very common in tropical developing countries, with a total annual number of cases in the world that has been grossly estimated as 50 to 300 million30.
“Outbreaks of scabies in healthcare facilities, particularly acute care hospitals, are not uncommon in California, and can last for months if not promptly recognized and managed aggressively. To address this problem, the California Department of Health Services developed and distributed to healthcare facilities a guideline for the management of scabies outbreaks31 and a recommendation for the prevention and control of scabies in California long-term care facilities32
In Brazil, programs to control ectoparasites are non-existent in the country’s public health system. Due to neglecting of these diseases by the population itself and health care professionals, the diseases’ highly contagious characteristics and lack of effective treatment and/or presence of animal reservoirs together with a complex life cycle, effective control of ectoparasites is an enormous public health challenge.33
Alternative treatments for scabies No new practices could be found on non-chemical treatments for scabies in the literature. Two systematic reviews are available in the reports of International League of Dermatological Societies (ILDS)34, mainly focusing on treatment strategies to control disease in individual patients and looking at short term results. The evidence indicates that permethrin is more effective than crotamiton, lindane and malathion, and that it is associated with fewer side effects than lindane. Lindane has been withdrawn from some markets as it has the potential to cause neurotoxicity where it has been used incorrectly. 12-25% benzyl benzoate is also widely used, but there is lack of data on its efficacy compared with other scabicides, although there is global agreement that it is equivalent to, or slightly less efficacious than, permethrin. Limited data are available concerning the use of oral ivermectin, especially in children; it is contra-indicated during pregnancy.
27 http://www.cdc.gov/parasites/scabies/health_professionals/meds.html 28 http://www.cdc.gov/parasites/scabies/health_professionals/meds.html 29 Bachewar NP, Thawani VR, Mali SN, Gharpure KJ, Shingade VP, Dakhale GN, Comparison of safety, efficacy, and cost effectiveness of benzyl benzoate, permethrin, and ivermectin in patients of scabies, JMF's ACPM Med. College, Dhule, India. Indian J Pharmacol 2009 Feb; 41(1):9-14bb 30 Effectiveness of Lindane in scabies and head lice infestations, Sent on behalf of the ILDS Group by RJ Hay, O. Chosidow and A Mahé 31 http://www.cdph.ca.gov/pubsforms/Guidelines/Documents/MgmntofScabiesOutbreaks.pdf 32 http://www.cdph.ca.gov/pubsforms/Guidelines/Documents/PrevConofScabies.pdf 33 Jörg Heukelbach 1 Fabíola Araújo Sales de Oliveira 1 Hermann Feldmeier 2. Ectoparasitoses e saúde pública no Brasil: desafios para controle. Ecoparasitoses and public health in Brazil: challenges for control 1 Fundação Mandacaru. Rua José Vilar de Andrade 257, Fortaleza, CE 60833-830, Brasil. [email protected]. 2 Institute of International Health, Center for Humanities and Health Sciences, Faculty of Medicine, Free University of Berlin. Fabeckstrasse 60-62, 12203,Berlin, Germany. [email protected] OPINIÃO OPINION 34 Effectiveness of Lindane in scabies and head lice infestations, Sent on behalf of the ILDS Group by RJ Hay, O. Chosidow and A Mahé

UNEP/POPS/COP.5/INF/13/Rev.1
17
Oral ivermectin has not yet been widely licensed for use against scabies, except in France. In a RCT (85 people), topical permethrin was more effective than oral ivermectin at 14 days, but a second dosage at day 14 showed a 95% efficacy at day 28; in another RCT (181 people), ivermectin was less effective than 12.5% benzyl benzoate at 14 and 28 day. While the level of efficacy of oral ivermectin compared to topical scabicides in individual cases are insufficiently documented, nor has the optimal dose regimen been established (1 or 2), it wasshown to be very useful in the control of epidemics in small closed communities. There is also evidence that oral ivermectin given to treat scabies in an epidemic context may reduce the occurrence of glomerulonephritis. There are limited data concerning strategies to control dissemination in the Community.
A programme to control scabies among the whole Kuna Indian population in the small San Blas islands of the Republic of Panama documented that simultaneous treatment of the whole population with permethrin 5% cream caused the prevalence to fall from 33% to less than 1%; as long as continued surveillance and treatment of newly introduced cases was maintained, prevalence of scabies remained below 1.5% for over 3 years.
US FDA states examples of other medications approved to treat scabies include the following:
a) permethrin cream 5% (Acticine, Elimite, Nix)
b) crotamiton cream (Eurax)35
California Department of Public Health (CPDH) recommends the use of ivermectin to treat patients with severe (e.g. keratotic) scabies that are likely to be refractory to cutaneous medication, and that are the source for outbreaks in healthcare facilities. Although not recommended by CPDH for typical scabies or prophylaxis, ivermectin has also been used in outbreaks for treatment of symptomatic cases and for mass prophylaxis because of its ease in application and probable greater compliance and efficacy compared to permethrin. It should be noted that ivermectin has not been approved by the FDA for use for scabies. Institution of mass prophylaxis has always been successful in terminating the outbreak. CPDH has received no reports of adverse effects from any of these uses. However, it is not known how adverse effects were monitored for and controlled studies have not been conducted.”36
The United Kingdom 37 summarizes treatment as follows:
(a) Treatment: Two topical treatments are recommended in the United Kingdom. Benzyl benzoate is regarded as too irritant, and crotamiton is ineffective compared to other recommended options.
(b) Recommended Regimens:
i) Permethrin 5% cream (Level of evidence Ib, Grade of recommendation A)
ii) Malathion 0.5% aqueous lotion (Level of evidence IV, Grade of recommendation C)
(a) Allergy: Treatments to which there is known hypersensitivity should be avoided.
(b) Pregnancy and Breastfeeding: Permethrin is safe during pregnancy or breast-feeding.
Qualifying Statements:
(a) Drugs considered were ivermectin, permethrin, crotamiton and benzyl benzoate. Ivermectin is not licensed as a treatment for scabies in the United Kingdom. There were no randomized controlled trials (RCTs) found involving malathion. Lindane is no longer available in the United Kingdom because of its toxicity. There were no controlled studies found of treatments for crusted (Norwegian) scabies.
(b) The recommendations in this guideline may not be appropriate for use in all clinical situations. Decisions to follow these recommendations must be based on the professional judgment of the clinician and consideration of individual patient circumstances.
(c) All possible care has been undertaken to ensure the publication of the correct dosage of medication and route of
(d) A variety of safe, effective alternatives to the use of lindane for treatment of scabies, including sulphur in petrolatum, permethrin, oral ivermectin in combination with topical permethrin and kerotlytic therapy, as well as certain medicinal oils have been reported38.
(e) Researchers cited data from several clinical trials and concluded that oral ivermectin is as effective as topical lindane for the treatment of human scabies39.
35 FDA Public Health Advisory: Safety of topical Lindane Products for the Treatment of Scabies and Lice http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm110845.htm 36 http://www.cdc.gov/parasites/scabies/health_professionals/meds.html 37 United Kingdom national guideline on the management of scabies infestation http://www.guideline.gov/content.aspx?id=12287&search=scabies 38 Heukelbach, J. and Feldmeier. 2006. Scabies. The Lancet 367:1767-1774

UNEP/POPS/COP.5/INF/13/Rev.1
18
(f) Comparison of three treatment modalities in scabies for safety, efficacy, and economy in a local population of Nagpur, India, Conclusion: Benzyl benzoate as first line intervention and ivermectin in the remaining gave best cost-effective results in the study patients of scabies40.
(g) Comparison the effectiveness of oral ivermectin (IV) and two different modalities of topical benzyl benzoate (BB) for treating scabies in a community setting. Conclusion: Topical BB was clearly more effective than oral IV for treating scabies in a Senegalese community41.
(h) Search of the Cochrane Infectious Diseases Group Specialized Register, CENTRAL (The Cochrane Library 2010, Issue 2), MEDLINE, EMBASE, LILACS, and INDMED, in June 2010 and search of the grey literature and sources for registered trials, in August 2010, as well as checking the reference lists of retrieved studies, led to the conclusions that: Topical permethrin appears to be the most effective treatment for scabies. Ivermectin appears to be an effective oral treatment. More research is needed on the effectiveness of malathion, particularly when compared to permethrin, and on the management of scabies in an institutional setting and at a community level.42 It is important to note that this research is confirming that lindane is not needed. In this research twenty-two small trials involving 2676 people were included and also lindane has been included. Following statements were made: Topical permethrin appeared more effective than oral ivermectin (140 participants, 2 trials), topical crotamiton (194 participants, 2 trials), and topical lindane (753 participants, 5 trials). Permethrin also appeared more effective in reducing itch persistence than either crotamiton (94 participants, 1 trial) or lindane (490 participants, 2 trials). No significant difference was detected in the number of treatment failures between crotamiton and lindane (100 participants, 1 trial), lindane and sulfur (68 participants, 1 trial), benzyl benzoate and sulfur (158 participants, 1 trial), and benzyl benzoate and natural synergized pyrethrins (240 participants, 1 trial); all were topical treatments.
(i) Scabies is a common dermatological problem that can be managed effectively if physicians possess an appropriate knowledge of the available drugs and instructs patients appropriately. It requires a willing physician and a cooperative patient to successfully treat this disease43.
(j) Comparison the effectiveness of oral ivermectin (200 microg/kg) with topical 25% benzyl benzoate and monosulfiram soap in 210 subjects of age 5 to 65 years with scabies. Compared with topical benzyl benzoate and monosulfiram in the treatment of scabies ivermectin was at least as effective and led to more rapid improvement44.
(k) A total of 240 convicted patients, enrolled in eight National Jail Institutions, with a clinical diagnosis of scabies, were treated with PF (n = 120) for three consecutive days or BB (n = 120) for five consecutive days. Conclusion: results show that a 3-day treatment with pyrethrins thermofobic foam is at least as effective as a 5-day treatment with benzyl benzoate lotion in convicted subjects with scabies. The foam formulation is better tolerated than the benzyl benzoate lotion45.
39 Apgar, B. 2000. American Family Physician 61(2): January 15, 2000 40 Bachewar NP, Thawani VR, Mali SN, Gharpure KJ, Shingade VP, Dakhale GN, Comparison of safety, efficacy, and cost effectiveness of benzyl benzoate, permethrin, and ivermectin in patients of scabies, JMF's ACPM Med. College, Dhule, India. Indian J Pharmacol 2009 Feb; 41(1):9-14bb 41 Ly F, Caumes E, Ndaw CA, Ndiaye B, Mahé A, Ivermectin versus benzyl benzoate applied once or twice to treat human scabies in Dakar, Senegal: a randomized controlled trial. Bull. World Health Organ. 2009 Jun; 87(6):424-30 42 Mark Strong1, Paul Johnstone2, Interventions for treating scabies, 1School of Health and Related Research, University of Sheffield, Sheffield, UK. 2NHS Yorkshire and the Humber, Blenheim House, Leeds, UK, Contact address: Mark Strong, School of Health and Related Research, University of Sheffield, Regent Court, 30 Regent Street, Sheffield, S1 4DA, UK. [email protected]. Editorial group: Cochrane Infectious Diseases Group., Publication status and date: New search for studies and content updated (no change to conclusions), published in Issue 10, 2010. Review content assessed as up-to-date: 10 August 2010. Citation: Strong M, Johnstone P. Interventions for treating scabies. Cochrane Database of Systematic Reviews 2007, Issue 3. Art. No.: CD000320. DOI: 10.1002/14651858.CD000320.pub2. Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd. 43 K Karthikeyan, Treatment of scabies: newer perspectives, Postgrad Med J 2005;81:7–11. doi: 10.1136/pgmj.2003.018390 44 Sule HM, Thacher TD, Department of Family Medicine, Jos University Teaching Hospital, Jos, Nigeria. Comparison of ivermectin and benzyl benzoate lotion for scabies in Nigerian patients. Am. J. Trop. Med. Hyg. 2007 Feb; 76(2):392-5 45 Biele M, Campori G, Colombo R, De Giorgio G, Frascione P, Sali R, Starnini G, Milani M, ISaC Investigator Group Dermatology Service, Casa Circondariale Civitavecchia, Rome, Italy. Efficacy and tolerability of a new synergized pyrethrins thermofobic foam in comparison with benzyl benzoate in the treatment of scabies in convicts: the ISAC study (Studio Della scabbia in ambiente carcerario). J Eur Acad Dermatol Venereol 2006 Jul; 20(6):717-20
UNEP/POPS/COP.5/INF/13/Rev.1
19
Appendix 5: Outreach by the North American Regional Action Plan (NARAP) on Lindane and other Hexachlorocyclohexane (HCH) Isomers The information below is provided by personal correspondence with Ms. Kristen J. Hendricks, Office of Pesticide Programs (OPP), Field and External Affairs Division (FEAD), US EPA, 10 January 2011.
North American Regional Action Plan (NARAP) on lindane and other Hexachlorocyclohexane (HCH) Isomers The “North American Regional Action Plan (NARAP) on lindane and other Hexachlorocyclohexane (HCH) Isomers” is a regional undertaking stemming from the North American Agreement on Environmental Cooperation (NAAEC) between the governments of Canada, Mexico and the United States of America.
NARAPs reflect regional commitments by the Parties to work cooperatively on chemicals of mutual concern and build upon international environmental agreements and on existing policies and laws by:
(a) bringing regional perspectives to international initiatives that are in place or being negotiated with respect to persistent toxic substances;
(b) promoting cooperation among Latin American and Caribbean nations and countries that have territories in the high Arctic;
(c) encouraging harmoniy in trade and environment policies so that they are conducive to the conservation, protection and enhancement of the environment in their territories;
(d) and sharing information, risk assessments, and other expertise and experience.
An important dimension of NARAPs is the formation of close working relationships among the national governmental bodies that address persistent and toxic substances in each of the three countries. NARAPs are also intended to facilitate meaningful participation of the public, including: non-governmental organizations, business and industry, indigenous peoples, provincial, state and municipal governments, academia and technical and policy experts. At the same time, each NARAP is unique and recognizes the different responsibilities in each of the three partner countries. Council Resolution 95-05 and the Regional Action Plans developed pursuant to it, also take into account each country’s respective natural endowments, climate and geographical conditions, and economic, technological and infrastructural capabilities. NARAPs have been developed for polychlorinated biphenyls (PCBs), dichlorodiphenyltrichloroethane (DDT), chlordane and mercury. Canada, Mexico, and the United States of America, under the auspices of the North American Commission for Environmental Cooperation (CEC), have recognized that the organochlorine pesticide lindane and other isomers of HCH may constitute a risk to human health and the environment.
The three Parties to the CEC also recognize that lindane and other isomers of HCH meet several internationally accepted criteria for persistence, bioaccumulation factors and toxicity. While lindane is no longer produced in North America, it continues to be used for various applications in different quantities in the three countries. Consequently, the Parties, through the development of this trilateral action plan, will reduce the risks that arise from exposure to the various isomers of HCH, and where warranted, eliminate or ban uses of lindane in particular. This will be accomplished through regulatory and managemental actions, outreach and education efforts, science and research, capacity building, and collaborative cross-border activities.
On a regional basis, the three Parties will work together to implement the actions described in this plan. A key recommendation is to establish a tri-lateral implementation task force consisting of national representatives with expertise in the fields of health and environmental aspects of lindane and other HCH isomers, to oversee these activities. In addition, based on information gained through the development of this regional action plan, the Parties will participate in other international initiatives to promote emissions reductions from other global sources of lindane.
On a national basis, each Party will address lindane and other isomers of HCH as indicated in the action plan. As of January 1, 2005, there are no registered agricultural or veterinary uses of lindane in Canada. Canada has agreed to assess and manage risks from its sole remaining use of lindane as a pharmaceutical drug. Canada will address waste management issues, promote science and research, and strengthen outreach and education.
Mexico has agreed to eliminate all agricultural, veterinary, and pharmaceutical uses of lindane through a prioritized, phase-out approach. Reasonable timeframes for a voluntary phase out are currently being negotiated between the Federal Commission for Sanitary Risks Protection, Ministry of Health (COFEPRIS) and industry. Lindane is currently authorized for use in Mexico on livestock, as a seed treatment on six crops, as a flea treatment on domestic animals, and for public health campaigns. Lindane is also authorized for pharmaceutical use to control scabies and lice.

UNEP/POPS/COP.5/INF/13/Rev.1
20
The United States has received requests for voluntary cancellation from all lindane. The United States registrants for all remaining the United States registrations of lindane pesticide products and plans to accept the producers' voluntary cancellation requests. The United States has reviewed the six remaining lindane seed treatment uses and determined that the remaining uses are not eligible for re-registration. The United States will facilitate development of alternatives to lindane to treat lice and scabies, and to strengthen awareness raising initiatives regarding the remaining use of lindane as a pharmaceutical drug for lindane NARAP five applications involving children. There are no registered uses of lindane for veterinary purposes in the United States.
The Parties enlisted and received input through a regional task force, from various experts and representatives of indigenous peoples, children's health interests, environmental organizations, and industry in preparing this "North American Regional Action Plan on lindane and other HCH Isomers." Public meetings were held to solicit additional input and to enlist the aid of experts in toxicology, atmospheric transport, epidemiology, wildlife concerns and indigenous/tribal issues.
Prior to its approval, this plan will have undergone extensive national public and private stakeholder review. This document represents the consensus opinion of the three national governments. It is anticipated that the implementation of this action plan will be conducted in stages, with short term, medium term, and long term goals over the next 10 years. Lindane NARAP's Implementation Task Force
After the finalization of the lindane NARAP in November 2006, the lindane NARAP's Implementation Task Force was established to ensure that all the commitments agreed to in the lindane NARAP were implemented. Furthermore, it was anticipated that the implementation of the NARAP action plan would be conducted in stages, with short term, medium term, and long term goals over the next 10 years. The Lindane Implementation Task Force is made up of representatives from the United States, Canada, and Mexico and is chaired by the CEC Secretariat. The Lindane Implementation Task Force meets regularly, several times per year, mostly via teleconference. However, the most recent meeting was a two-day face-to-face meeting in the Washington DC area. At that meeting, representatives from Mexico, Canada, the Unite States, and the CEC attended in person to discuss progress on the actions/commitments made by their country in order to implement the actions contained in Section 4 of the the lindane NARAP. Further, the possibility of initiating the lindane NARAP's close-out process in 2011 was discussed. Information on lindane NARAP and the Lindane Implementation Task Force's activities are available on CEC's website at:
http://www.cec.org/Page.asp?PageID=924&SiteNodeID=430 .
Examples of outreach and awareness programs in the US, Canada, and Mexico Mexico's lindane in Milk Project: For the last several years, Mexico has been working on lindane in milk project to determine if lindane or its alpha and beta-HCH isomers are found in cow's milk. At this time, there is no publically available information on the study yet.
The lindane NARAP Implementation Matrix of outreach and awareness programs is in all 3 countries: All 3 governments; the United States, Canada, and Mexico, have been doing various activities to implement the actions/commitments agreed to in Section 4 of the lindane NARAP. Through the Lindane Implementation Task Force, one has been keeping track of our efforts in an informal and internal working document called "the matrix". The Lindane Implementation Task Force thoroughly updated the matrix document at the face-to-face meeting held in November 2010.
NARAP results and real achievements: Regarding the real achievements, the NARAP process was a force behind all 3 countries canceling the agricultural uses of lindane in the North American region, as well as almost all of the pharmaceutical uses of lindane. Further, Mexico was able to use information from the lindane NARAP process to initiate the nomination process for lindane and the Alpha and Beta-HCH isomers to the Stockholm Convention. There is common agreement that these are significant results and substantive achievements of the NARAP process.

UNEP/POPS/COP.5/INF/13/Rev.1
21
Appendix 6: Articles related to scabies This appendix contains English translation of two articles (“Scabies in children” and “The modern view on the treatment of scabies”) published in Russian. 1. “Scabies in children”
Source: http://www.epidemiolog.ru/publications/detail.php?ID=4280 Information collected in December 2010 Trade House Allergen 27.08.2009 KN Suvorova, RB Oparin, T. A. Sysoev, OB Tamrazova, TN Grishko Russian Medical Academy of Postgraduate Education, Moscow; City clinical dermatological and venereal hospital number 14 named. Korolenko, Moscow Scabies has been known in human society since ancient times and remains as the most common parasitic disease for the skin. The lecture is based on an analysis of literature and observations, and the authors outline the history of the disease, clinical picture and its peculiarities in children and adults, as well as provide a detailed description of the major acaricide drugs.
Historical background The appearance of scabies refers to the ancient times, with domesticated animals to man have become crawl zudnevye mites, one of their smaller varieties adapted to the intradermal parasitism in humans and has lost the ability to cause disease in animals L-LI. Scabies is mentioned in Egyptian papyri, was known in Assyria, Babylon and China. In ancient Greek, medicine did exist. The term "psora" means –“Itch, mange or scab” in Greek. Hippocrates, included a description of a chronic and severe itch in his essay “epidemic”. In ancient Rome (Aulus Cornelius Celsus), scabies was called "scab" (The Latin word scabo means “itch”). Abu Ali ibn Sina (tenth-eleventh centuries, BC) argued that scabies is contagious like lice and leprosy. Since ancient times, isolation was the way to prevent the spread of infectious diseases. For example, in the 13 century, in the cities of medieval Europe, patients with scabies were considered to be as contagious as the patients with leprosy, erysipelas, smallpox, or any feverwith a rash, and were exiled outside the city boundaries.
Despite the small size of scabies treatment (about 0.33 mm), it failed to consider: the tick seen in patients with scabies and believed the cause of the disease by Arabic scholar Avenzoar (twenty-first century AD), French doctors and Guy de Sholiak (fourteenth century) and Ambroise Paré (sixteenth century). In the second half of the seventeenth century, microscopic structural details of mite have observed by doctors Mouffe, Hauptmann, Entmyuller and Cheston, especially to describe and depict in detail, also to indicate the routes of transmission. Leghorn doctor Bonomo in 1687. In 1796, a doctor called Wichmann transferd the mites from his patient to himself. In 1834, Renuchchi publicly demonstrated the causative agent of scabies in a skin clinic in Paris, Jean Louis Aliber. In 1844, F. Algebra scientifically identified parasitic mange as a separate nosological unit. His research laid the basis for nosologic differentiation of the largest and the most complex etiologically heterogeneous group of itching dermatoses. The high authority of the Viennese dermatological school Algebra F., ended in the III decade of the nineteenth century. Holding a leading position in Europe, it was instrumental in introducing new perspectives on parasitic mange and differentiating the forms of prurigo and eczema in the practice of dermatology and in clinical thinking in many countries. Ernest Besnier, who wasa head of the Paris School of dermatology for over 30 years, separated an independent nosologic unit of disease in 1892, now known as atopic dermatitis, and called it "ekzemato-lichenoid form diatezicheskogo prurigo algebra”. Pierre Antoine Ernest Bazin, developed versions of the constitutional diathesis, making France one of the first countries to recognize the etiological role of the mite. Alfred Hardy (Chairman of the First International Dermatological Congress in Paris in 1889) described the typical symptom of scabies as the form of clusters on the elbows vezikulezno-impetiginoznyh cortical elements, translated into Russian by F. Algebra and his disciple M. Kaposi and was published in Russia (in 1876, 1881 and 1883). N. Mansurov, the ancestor of the Moscow School of Dermatology and the author of the first Russian leadership "Skin diseases(1863, 1873)”, developed in 1884, the diagnostic method of taking the material for microscopic mite by sections tires vesicles. Further investigation of scabies was conducted in Russia, and improved diagnosis and therapy were reflected in the theses, manuals, monographs and methodical recommendations LII-LVII. Universal recognition was given throughout the world to the prominent biologist and parasitologist E. N. Pavlovsky, whose teaching of evolutionary formation antroponoznyh parasitosis became the basis for understanding the epidemiology of scabies in humans and of tick dermatitis.
UNEP/POPS/COP.5/INF/13/Rev.1
22
Epidemiology Scabies is very contagious; Ricinus replenished very rapidly (upto 150 million mites on a three-months-old female baby) LVIII.
By the twentieth century, as it is well known that scabies are a contagious parasitosis, and are observed in all population strata and age groups, most often when met with prostitutes or in crowded and populated living areas LIX. In some villages in pre-revolutionary Russia, most of the population was infected with scabby LX. In 1913 Russia, there were 5.5 million patients with scabies, and in 1914, patients with scrabies accounted for 3.7% of the total Russian population. In the early 1920s, in USSR, the share of scabies accounted for more than 30% of all skin diseases LX. Large rise in the incidence was observed during the First and Second World Wars. In 1944-46, in Europe, 10-15% of patients suffered from skin itch. In the 1950's, the prevalence of scabies went down to 1-2% of all skin diseases in the USSR, and by 1960, there were only sporadic cases of scabies LII-LIII. But soon in different parts of the world began the cyclic fluctuations of incidence. In 1960-70, despite improvements in living standards, the frequency of regional outbreaks of scabies increased in Europe and North America, reaching almost pandemic levels in some places by 1980, with subsequent reduction in the form prevailed loop routine cases. The reasons for these fluctuations were not always clear, a high incidence of children explains intra direct infection (mother), young adults demonstrates the importance of especially frequent venereal route of infection and the role of promiscuity in cases of regional outbreaks observed value heaped cohabitation.
The HIV epidemic in some areas is combined with a pandemic of scabies LXI-LXIII. In Russia, according to statistics, the incidence of scabies has been reduced: in 1997, 217.6 per 100 000 inhabitants got infected. The number was reduced to 157 in 2001, and 131.4 in 2005; For children, the figure was 324, 3 per 100 000 child population in 2005. Many authors believe that the true incidence of scrabies is much higher due to unsatisfactory level of hypo diagnosis by general practitioners, private dermatologists, as well as laboratories LV-LXIV. In St. Petersburg in 2005, the incidence of scabies has declined by 9.8%, but at the same time, the authors note that incomplete registration of contagious disease distorts the statistics LXV.
Our clinical observations suggest that scabies is now much more frequent than in the 1970-80s. Among children with skin diseases between several months to 16 years of age surveyed in Tooshino City Children's hospital in Moscow for 3.5 years, acarian dermatoses were established in 238 patients, which accounted for 13.58% of the 1,752 surveyed children with skin diseases LXVI. Among the 238 child patients, 226 were diagnosed as scabies (12.9%) and the other 12 contracted mite dermatitis during contact with animals (0.68%). 63 (26,5%) children came from orphanages or shelters, 132 (55,5%) were stray children or children from dysfunctional families, and 43 came from socially disadvantaged families(18%). Between the following two groups, there were differences in the course of the disease: children from orphanages and boarding schools had more common and uncomplicated fresh forms (sometimes without scabies mite moves); but stray children in most cases had scabies complicated by pyoderma, and children from socially advantaged families had common scabies with the duration longer than 3 months.
In the children's skin department of Venereal Diseases Hospital, Korolenko, Moscow often received children with long-flowing and uncomplicated scabies (a tick-borne nail infections, or in rare cases, with a picture of the cortical "Norwegian" scabies).
Consultations were given to the parents who came with kids (with a previously undiagnosed scabies) for further diagnosis and therapy, the prevalence of chronic itchy skin lesions, do not succumb to traditional treatment of corticosteroid and antihistamines, the most frequent erroneous diagnoses were atopic dermatitis (which in some patients accompanied itching), food allergies, dysbiosis, pyoderma, diathesis, etc.
About 83.3% of patients with scabies were represented by the children; small children were infected in the family, and teens from his peers. Test was conducted to people who have not received any treatment for scrabies.13,9% patients took acaricidal treatment (short-term improvements), but those treatments were conducted at home without a proper survey, without consulting a pediatric dermatology and without follow-up preventive measures. As a result, complete recovery did not occur and treatment had to be repeated with corticosteroid ointments.
We carried out a course of pediatric dermato-venerology which showed the following results;
- experienced pediatric dermatologists have more success to detect the scabies;
- 42% of pediatric dermatologists are not satisfied with the laboratory diagnosis of this disease. Therefore, once the scabies are identified, the illness is diagnosed differently and the treatment is carried out with acaricide means (Spregal, benzyl).
The clinical description Scabious eruption characterized by a true polymorphism and includes elements caused by the direct action of the mite, and the secondary rash.
UNEP/POPS/COP.5/INF/13/Rev.1
23
Pathognomonic itch elements: * Motherboard itch moves. Their fertilized females burrow into the horny layer of the skin, laying eggs and making the cover of the pinhole to yield larvae that hatch from eggs in 3-4 days. The moves are kind of thin grayish-whitish lines, 5-7 mm in length (rarely up to 1.5 cm or more), curved or straight, they can be seen with the naked eye and to determine by palpation (symptom Sézary). At the head end of the blind, we can consider the transmission through the stratum corneum mite (itch elevation "Bazin”), sometimes alongside “pearl” bubble. In addition to the initial stroke, distinguish jet options to form a course of small vesicles (rare bladder), shrinking in point or linear crust;
* Lenticular papules or benign scabious nodule on the skin (red-brown, persistent, indurative edema, or nodules, up to 10-13 mm in diameter). This perivascular infiltration of the dermis with hyperplasia of lymphoid tissue by passages in the epidermis filled with egg shells, dead embryos and larvae, to treat them can use live mites. The appearance of these elements is associated with elevated skin reactions to antigens of mites and their feces LXVII;
* Metamorphic scabious eruptions (scattered, small, 2 mm, follicular papules, some with microvesicles, as well as isolated large noninflammatory vesicles) occur both in typical scabies with strokes, and in short-term phase of scabies without stroke (when infected larvae) and connected with the life cycle of ticks: larvae introduced under flakes in the hair follicles, where over 2 weeks metamorphosis occurs through two stages of the nymphs to mature individuals.
Secondary elements of rash caused by complications: * Pyoderma (staphylococcal impetigo, folliculitis, furuncles, ecthyma);
* Sensitization to tick and microbial antigens (eczematization, urticaria papules);
* Reaction to external agents (allergic or irritant dermatitis);
* Excoriation and scratching (scattered small hemorrhagic crust on the top of the follicles, linear scratches).
Localization scabious eruption eruptive elements determined not place the initial contact with ticks on the skin, and their biology, disease duration, the influence of age and sex of patients, the level of hygiene. In the reproductive stage, females settle and pave the moves in the field with a sufficiently thin skin, a minimum of lardaceous hair follicle structures, with a relative predominance of the thickness of the stratum corneum over malpighian and low rate of desquamation, to have time to mature and the larvae to hatch (distal parts of limbs, especially hands), hence then there is the resettlement of larvae and adult ticks by remedies of migration or transfer hands of the host (Table 1). A characteristic feature of the itch is a rash with respect to symmetric, trace elements may spread throughout the skin, sometimes with involvement of nails.
Table 1. Localization rash classic form of scabies Elements of the rash
Typical itch moves Initial moves; on the hands, wrists, fingers and toes. Typical areas where itch occurs are; the lateral surfaces of the fingers, interdigital folds, ulnar edge of the palms, palmar surface of the wrist, foot (arch area), Achilles tendon, ankle, interdigital folds. Areas where long-term illness occurs are; the skin of genitals (in men), the areola of the mammary glands (females), the elbows, around the navel and below the abdomen, buttocks, thighs, legs and sometimes on the palms and palmar surfaces of fingers.
Lenticular papules Occur only in closed areas: in the inguinal folds, on the scrotum, penis, breasts, on the front of the armpits, elbows and stomach.
Follicular papules Occur mainly on the front and sides of the torso, buttocks and anterior-inner thighs. Noninflammatory vesicles
Predominantly occur on the hands, wrists and feet where the itch moves. The “itch without stroke” occurs in interdigital folds on the sides of the fingers.
In children and infants, localization itch rash has some differences: the rash quickly spreads through the body, involving the scalp, face, neck, back, namely sites that are rarely marveling at older children and adults LXVIII-LXX. The scars are quickly destroyed or masked by eczema and pyoderma when the young children have a daily bath. In case of difficulties in identifying the scabby moves in clinical diagnosis it can be used the full range of clinical presentations and during the medical examination of a young child, all the children and adults contacts are carefully examined. If the scabies are identified, there are possibilities of an identical disease in children. Therefore, the pediatrician should know about clinical symptoms of scabies in infants and young children:
(a) Pronounced exudative nature of eruptive elements: blisters, urticaria papules, vesicles, blisters, pustules, erythematous patches and moisture;
(b) A tendency to the appearance of elements of "nodular scabies" (scabious limfoplazii skin);
(c) Fast generalization lesions;
(d) Involvement of the face, head, neck and back;
UNEP/POPS/COP.5/INF/13/Rev.1
24
(e) Very often defeat the soles and palms (moves, vesicles, pustules);
(f) Rapid destruction of the itch moves;
(g) Frequent complications (eczema and impetigo) masking scabious eruptions;
(h) More often than adults, meets defeat nails, paronychia;
(i) Itching can be very strong, but some of the children is weak;
(j) General effects and complications: increased irritability, urinary tract infection, albuminuria, lymphangitis, lymphadenitis, eosinophilia, and leukocytosis in the peripheral blood.
Diagnosis Epidemiological history: Take into account all possible indications of contact with sick itch; particularly important diagnostic confrontation with a tour of family members and carers of the child entities. For the older children we also look into the possibility of infection to other teams, during tourist trips and sporting activities.
Inspection: Scabious specific elements in children is not always easy to determine, since the moves are rapidly destroyed (the longer they remain on the soles) and can be found in unusual places (on the face, scalp, neck and back). Additional lesions in children, masking specific rash, often the cause of diagnostic errors. In older children and adolescents, it affected wrist, elbow (symptom Hardy: the presence of pustules with impetiginoznymi crusts on the elbows; symptom Gorchakov: points scattered hemorrhagic crusts on the elbows and around them), feet, buttocks, perimamillyarnye area, genitals, mezhyagodichnye folds (symptom Michaelis: hemorrhagic crusts and impetiginoznye elements mezhyagodichnoy fold, extending to the sacrum and the rhombus of Michaelis).
Laboratory diagnosis: In order to identify strokes blur skin using aniline dye, 2% iodine solution, 0.1% solution of fluorescein sodium. While living mite is sometimes possible to consider even the naked eye, microscopy scrapes or cuts needed gatherings while found adults, larvae, nymphs, egg shells, linechnye skins. Positive laboratory tests for tick is mandatory for emergency notification.
Diagnosis ex juvantibus: It is also possible formulation of a presumptive diagnosis on the positive effect of a particular acaricidal therapy should take into account the lack of improvement in the treatment of corticosteroid and antihistamines, as well as a sufficient effect on the traditional protivoekzematoznoy and antimicrobial therapy.
Differential diagnosis is carried out with dermatitis (contact, tick-borne, infantile seborrheic and atopic) eczema disgidroziformnoy, strofulyusom, papular urticaria, lice, insect bites and other itchy skin lesions in children. Treatment There are modern acaricidal remedies that destroy quickly and completely the mites, all their metamorphic stage and eggs without causing any complications. Such a vast arsenal of scabicide that lets you choose the products suitable for the patient's age, case and severity of scabies, did not appear immediately. In the XIXs, the treatment of scabies was dominated by preparations of sulfur. In the sulfur ointment, tar (antiscabious sernodegtyarnaya ointment Wilkinson), balms, naphthol, green soap, also some insecticide like pyrethrum (powder Dalmatian daisy), Lysol and other phenolic remedies were added. In popular methods of treatment of the scabies, ash lye, kerosene, gasoline, avtolom, fuel oil, fresh tar and crude oil were used. All of the above remedies, that are able to kill the mites, have the side effects (skin irritation), toxic effects (which is especially dangerous for small children) and great inconvenience in use. In the 1930s, XX century the method of Hyposulphite is widely used for fighting the scabies (MP Dem'yanovich): sodium thiosulfate in the presence of hydrochloric acid decomposes into sulfur dioxide and sulfur to oxides form and pentationov acid producing paralytic effect on the mite.
Modern scabicides (and insecticides) act on the tick as neurotoxic poisons. These include:
* Organophosphates (Malathion - acts as an inhibitor of acetyl cholinesterase by phosphorylating its parts of esterase which causes an excessive accumulation of acetylcholine and the paralysis of the tick);
* Aromatic hydrocarbons (N-ethyl-0-krotonotoluidid - Crotamiton, benzyl);
* Halogenated hydrocarbons (hexachlorocyclohexane - lindane exerts neurotoxic effects by inactivating the sodium pump in the excited membranes, by inhibiting the transport of calcium ions and repolarisation, and by increasing the excitability of neurons that causes the tetanic paralysis);
* Improved pyrethrins and synthetic pyrethroids (permethrin, Spregal, A Pairs which the mechanism of action is similar to that of halogenated hydrocarbons).
The form of drugs has also changed. It is now mostly liquid, sprays, creams, which are suitable for use in any situation. Their high efficiency at all stages of the extermination of ticks allowed shortening the treatment course: 1-2 (lindane, Spregal, permethrin) or 3-5 days (benzyl benzoate, Crotamiton).
The choice of drugs depends on their potential toxicity, allergenicity and irritating properties. Toxicity depends on the resorption of acaricide from the skin into the systemic circulation, the rate of metabolism and excretion of drugs.
UNEP/POPS/COP.5/INF/13/Rev.1
25
Suction ability is more represented for lipophilic drugs: lindane is absorbed at 10% of the dose applied to the skin and slowly metabolized, excreted in the urine over 5 days and can be accumulated in lipid-rich tissues: the brain. When using Malathion, it is absorbed 8% of applied drug on the skin. Permethrin slightly penetrates into the skin: less than 2% of the dose is rapidly metabolized and removed. The sulfur, benzyl benzoate and Crotamiton are not absorbed.
However, in certain manuals there are age restrictions in the treatment of benzyl benzoate: absolute contra-indications in infancy, and the relative: for small children or the complete abandonment of the use on the children under 3 years. Such restrictions are associated with the possibility of gasping syndrome (severe state of metabolic acidosis, encephalopathy, puerperal, respiratory depression) observed in preterm children; it was assumed to do the benzyl alcohol intoxication, which was used as a preservative or bacteriostatic for injection. Although benzyl benzoate has been used over 50 years for the treatment of scabies, not one case of gasping syndrome has been discovered. German pediatric dermatologists do not recommend the use of benzyl benzoate for infants, as it is known that when using the hydrolysis of benzyl benzoate, other chemical remedies were formed (benzoic acid and benzyl alcohol).
Restrictions on administration of these drugs with potential toxicity and the rapid absorption concern for: the newborns and infants, pregnant women, nursing mothers and patients with convulsive syndrome. By reducing the contact time of the drug with the patient the risk of skin toxicity is reduced. Therefore, the prescribed treatment regimen should be respected and the drug should not be left on the skin longer than it is recommended. Lindane should be on the skin of the patient for 6-8 hours, permethrin for 8-14 hours, and Spregal for 12 hours. However, many use the drugs for a few days (2-7), repeating the application on a daily basis (Crotamiton for 2-5 days, and sulfur ointment for 3-7 days) or with a break (benzyl benzoate applied in the first and fourth day of treatment). Procedure is carried out at night, when female mite is most active. Before applying scabicide, patients should wash with soap and a washcloth (in this case partly destroyed tunnels) at the end of the treatment, until the drug is thoroughly washed off from the skin. However, while using lindane (rapidly absorbed into the bloodstream), a pre-washing is not recommended. Prescription of lindane foryoung children with thin skin and disturbed epidermal barrier (scratching, erosion, and moisture) is not recommended. Treatment of children must be conducted under daily supervision of a physician, and infants should always be treated in a hospital.
To prevent toxic effects of scabicides on human, its concentration in the product is reduced, but the effectiveness remains the same. In order to get this effect, the combined remedies are produced with the substance that blocks the protective enzymes of the mite: piperonyl butoxide (in preparations of Spregal and A-pairs, which complement the treatment of scabies and are used for disinfection of clothing, bedding, shoes and other things), pyrethrum (insecticide spray-Pax ), permethrin (treated with insecticides Pair Plus, in this product is additionally included organophosphates Malathion, acting at the level of motor nerves, by forming a covalent bond with cholinesterase). The effectiveness of antiparasitic action of such combination of therapies is significantly increased, although the concentration of the inclusion of remedies is not much and is not toxic to humans.
Non-compliance with the drug-taking practices (for example, the recommended time frame, especially, prolonged use of the medicine by parents or patients) is often the cause to skin irritation (irritant dermatitis) and sensory irritation (burning, tingling, numbness, short-term enhancement of itch). Irritant dermatitis often cause hiposulphite therapy, benzyl benzoate and even Crotamiton giving rise to antipruritic effect. After the treatment, the patients with scabies are not recognized by hormonal ointments, the development of irritant dermatitis on the use of scabicide is observed more frequently; antiscabious treatment in patients with atopic dermatitis often leads to the same side effects.
Application of the Hyposulphite method for more than 3 days is often complicated by irritant contact dermatitis in children. That’s why the dermatologists believe that for young children, this method of treatment is not suitable.
Modern pyrethroids (esters of chrisantem acids and various cyclic alcohols) with minimal toxic and irritant effect in rare cases cause allergic dermatitis (with cross-hypersensitivity to the genus Chrysanthemum) and are widely used in pediatric practices. In the United States, among scabicides, permethrin is the most effective and the safest, and lindane is the most expensive. In Germany, dermatologists prefer a combination of pyrethroids andh piperonyl butoxide (Allethrin, Spregal) for treatment of children.
In many countries of the world, for infants and for pregnant or nursing mothers, though it is inconvenient to use because of it has strong odor, creates stains in skin and clothes, and requires longer course of treatment than other medicies, the safest medicine has traditionally been the sulfuric ointment

UNEP/POPS/COP.5/INF/13/Rev.1
26
Table 1 shows the age restrictions for use of scabicides in pediatric practice.
Table 1. Acaricidal drugs used in pediatric dermatology Age Safe and effective may be allowed with
caution contra-indicated and/or not
advisable Newborn babies
under the age of 2 months
Ointment or suspension with the sedimentary sulfur 3-5%
Spregal, benzyl, soap water emulsion
10%
Lindane, Malathion, Permethrin,
Crotamiton, Wilkinson ointment,
YAM* ointment Hyposulphite therapy
Up to 1 year 5-6% Sulfur ointment, Spregal, Benzyl benzoate 10%, soap
water emulsion
Hyposulphite therapy Permethrin (after 2
months),
Lindane, Wilkinson ointment, YAM* ointment, Malathion
From 1 year to 5 years
Sulphuric ointment 10%, Spregal, benzyl benzoate 10%,
soap water emulsion, permethrin
Hyposulphite therapy Malathion (after 2.5
years)
Lindane
* Composition: Ac. salicylici 5,0; Sulfuris praecipitati 10,0; Ol.Terebuithinae rectificati 2,0; Picta liquidae Betulae 5,0; Lisoli 5,0; Novocaini 1,0; Zinci oxydi 10,0; Lanolini 25,0; Ol. olivarum 2,0.
Ambulatory, for adults and older children, an inexpensive drug with 10% or 20% emulsion of benzyl benzoate or Spregal are assigned and for kids.
Benzyl benzoate is rubbed (at night) into the skin in a certain sequence (upper limbs, fingers, torso, feet, soles and toes), and after 10 minutes the procedure is repeated. And then, the clean clothes are worn and bed linens are changed. The hands should not be washed for 3 hours (or after each hand washing, the emulsion should be rubbed again). After 4 days, the procedure of applying the medicine to the skin is repeated. At the fifth day, the patient is washed with soap and again the clothes and linens are changed. At the same time, the disinfection of the house and treatment of the contact persons are carried out. In leather treatment by emulsion, a burning or itchy sensation on skin may appear, but it goes away quickly.
Spregal is particularly convenient for use in young children with soft and thin skin: it is sprayed on the skin of the body while covering the mouth, nose and eyes of a child with a tissue. Only the scalp and face are wiped with a swab dipped in Spregal. After the treatment, the sleeves need to be sewed in order to ensure that the child does not put in his mouth the drug from the skin. The treatment is done only once in the evening, and after each treatment, the room is thoroughly ventilated. Particularly, it is appropriate to use the spray for children with bullous dermatoses (bullous Epidermolysis), bullous form of scabies, erosions and weeping when unction is not recommended. After 12 hours, the ointment is thoroughly washed with soap and water. Clothes, toys and other things can be treated with A-Par.
In the children's department of Venereal Diseases of the Hospital number 14, Moscow, the common forms of treatment of scabies is carried out mainly by benzyl benzoate, in a mode referred to above. In a case of cortical forms it is recommended to prolong the treatment. In Tooshino City Children's hospital in Moscow, the Spregal is applied for all the children with scabies. With the proper technology of application of the above remedies, we did not observe any complication or incomplete healing.
Proper use of modern acaricide drugs (including characteristics of the patient, his age and the severity of the disease) provides 100% cure for scabies. Autumn and winter are the seasons with the highest incidence of scabies among the children and adolescents, especially, when they return from summer trips and contact with each other in kindergarten and schools. Pediatricians should be prepared for these seasons by raising their suspicion for scabies. The most safe and effective in pediatric practice (as in inpatient and outpatient care) is the Spregal medicine.
UNEP/POPS/COP.5/INF/13/Rev.1
27
2. “The modern view on the treatment of scabies”
Source: http://www.mymed.su/?articles/read/165 December 2010, Printable version From parasitic dermatoses itch is the most common skin disease. High numbers of official statistics on the incidence of scabies, the Russian population does not reflect the real state of the problem. Sometimes doctors, unwilling to engage in anti-epidemic measures in the foci of the disease, conducting patient antiscabious treatment, have resorted to "tricks", diagnosing scabies as "hives", "insect bites" or "atopic dermatitis". Self-medication of patients and treatment by private practice doctors, also bring about the problem of undercounting the cases of patients suffering from this disease.
The usual social phenomena of our days such as migration, non-personal hygiene, early sexual activity and the deterioration of material living standards are also the causes of high incidence of scabies. Currently, the most urgent problem with scabies in Russia is the high morbidity rate in the Armed Forces of the Russian Federation, which exceeds the incidence rate among the civilian population by six times.
ETIOLOGY Scabies, or proceeding from the specific name of agent, Scabies, are caused by itch mite Sarcoptes scabiei. Similar diseases in veterinary medicine are called sarcoptic mange; the generic name for the pathogen. Pathological process that occurs in humans who had contact with scabies mites from animals by analogy are called psevdosarkoptozom.
Itch mite belongs to the permanent (obligate) parasites, whose feature is to transfer only from person to person, but its type determines the characteristics of parasitism of etiology, epidemiology and clinical disease, diagnosis and treatment tactics. Ticks spend most of their lives in the skin of the host and only during a short period of resettlement are ektoparazitichesky lives on the skin surface. Sarcoptes scabiei parasite lives in the surface layers of the skin, but in complicated forms and can affect deeper layers of skin.
The life cycle of itch zudnya presented in two stages: the reproductive and metamorphic. Reproductive stage of the tick is as follows: eggs are laid by the female itch during which the larvae then appear. Unlike other insect larvae, scabies treatment is targeted in the egg which are already beginning to move, then gradually dropping off the egg shell. If on skin, they penetrate into the hair follicles, forming a follicular papules. Metamorphic stage is determined by the appearance of the larvae, which penetrate through the course of the skin and after molting become protonymph, then - in teleonimfy, which then in turn, turning into adults, located on the skin of the patient in papules and vesicles. The next two weeks developing atypical scabies (scabies without stroke), while the development of the larvae to mature females capable of laying the moves, takes two weeks. Himself itch progress can be stored up to six months and serve as a source of infection.
EPIDEMIOLOGY Longevity of itch zudnya at room temperature 22 ° C and 35% humidity is about 4 days. At a temperature of -60, mites die within hours, and at a temperature below 0 ° C, almost immediately. Only young females and larvae are invasive stages of scabies treatment. The average duration of survival of female scabies mite is about three days, and Larvae - two days.
It is in these stages that a tick can jump from a host to another human and exist sometime in an external environment. And the house-dust, wood surfaces, as well as natural fabrics are the most favorable habitats for sarcoptes scabiei outside the host. It should be noted that a pair of sulfur dioxide can kill scabies for 2-3 minutes. Mites and eggs are more resistant to various acaricidal drugs.
The incidence of scabies increases in autumn and winter period, due primarily to a sharp increase in fertility tick. This is confirmed by the fact that the specific abundance of young do not put in the itch moves eggs, the females in autumn drops to zero. Infection occurs in 95% for live transmission of the mite from a sick man (and half the time during sexual contact) or indirectly (through the objects used by the patient). The low incidence of the indirect route of infection due to poor viability mite in the environment because the agent often is transmitted by common use of bedding: washcloths, toys and stationery. Infection can also occur in the showers, bathhouses, hotels, trains and other public places subject to violations of sanitary regime.
CLINIC Scabies infection in the case of females during the incubation period is virtually absent. The female immediately begins to gnaw through the passage and lay eggs. Upon infection, the larvae incubation period is about 2 weeks, which corresponds to the time of metamorphosis of mites.
Ground and the first subjective symptoms are itching, which worsens at night. Its intensity often increases with increasing duration of illness, which in turn depends on the size of the parasite and the individual characteristics of the organism. The latter include the sensitization to mite and products of its activity (faeces, oral secret, which is shed for gnawing course, the secret glands of the oviduct) and the condition of the nervous system of the patient (degree of

UNEP/POPS/COP.5/INF/13/Rev.1
28
irritation of the nerve endings of the parasite in the motion). Number and distribution in skin itch moves not by chance and by the rate of regeneration of the epidermis, the structure and the thermal regime of skin. In most cases, itch moves are on the skin areas with lower temperature, minimal or absent hair, and the maximum thickness of the stratum corneum of the epidermis (hands, wrists and feet). The latter factor allows the larvae hatch out of eggs, and not cut off with horny scales.
Rashes in infants often capture skin in areas such as the face and head, soles and palms areas which for adults are only rarely affected. And sometimes the phenomenon of scabies on the face and head "masked" the clinical picture of acute weeping eczema resistant to conventional therapy. In children, the first months of itch can often give the first impression of child urticaria, since it causes on the face, back and buttocks a large number of scratching and bloody crusts and blisters. In children, scabies may be complicated by severe sepsis, pyoderma and maybe even the death of the patient. It should be noted that students with complication of scabies in the form of secondary pyoderma often mask parasitic process under the clinical picture of acute eczema, pyoderma and pruritus. Elderly clinical pictures showed bloody crusts and scratching in the absence of vesicles and in the presence of single itch moves.
When the complications of the disease set in, there are phenomena of repeated Pyoderma in form of impetiginous elements. Complication of the disease is the formation of post scabious nodules as reactive hyperplasia of lymphoid tissue.
Distinguish individual forms of scabies: nodular (postskabioznaya limfoplaziya skin), scabies in children, Norwegian, psevdochesotku.
DIAGNOSIS Clinical criteria for diagnosis of scabies is the presence of scabies moves, papules, vesicles, serous crusts, which appear in typical places in the interdigital folds of hands, wrists, abdomen, genitals, breasts, buttocks and thighs (Table 1).
Table 1. Criteria for the diagnosis of scabies Clinical criteria for diagnosis of scabies Epidemiological criteria for the diagnosis of scabies Itching, worse at night time Itching dermatosis presence of one or more family
members The presence of typical scabies moves, isolated vesicles and itching follicular papules lenticular
The presence of itching dermatosis among members of the invasive-contact group (dormitory, kindergarten, boarding school, barracks, etc.)
The presence of typical symptoms of scabies: Ardi, Gorchakov, Bazin, Michaelis, Cesar
Sequential emergence of new patients in the outbreak
The predominance of staphylococcal impetigo on the hands, wrists, feet, ecthyma - in the legs and buttocks; folliculitis and boils on the trunk and buttocks. Lack of effect of treatment of antihistamines, antisensitizer inside, anti-inflammatory, including corticosteroid ointments implementation
Indirect route of infection only in the presence of several patients in the outbreak or high parasite index in one patient
Laboratory criteria: detection of the causative agent of scabies with one of the available methods
Therapeutic diagnostic criteria: the disappearance of itching after the first treatment and resolution of lesions by the end of the week with ex juvantibus therapy
The clinical description of scabies may also be presented erosion, hemorrhagic crusts, excoriations, erythematous-infiltrative foci of nature. Often found worn form of scabies, which lead to an erroneous diagnosis, often regarded as allergic.
The diagnosis of scabies is established on the basis of clinical symptoms, epidemiological data and laboratory results. Known methods of treatment mite needle, thin slices, layer scraping, preparation of alkaline skin. Rapid diagnosis of scabies is carried out using 40% aqueous solution of lactic acid. Rarely diagnosed on the basis of a positive effect in the treatment of ex juvantibus one of acaricidal preparations.
TREATMENT (a) Treatment of patients identified in one nidus, should be carried out simultaneously in order to avoid the re-
invasion
(b) Children under 3 years should be rubbed with antiscabious drugs in the whole skin, for the other patients the drug should not be rubbed on the face and scalp
(c) Rubbing of the preparations is done only by hand for a better penetration of the scabicide
(d) Treatment is carried out in the evening, which is associated with circadian rhythm activity of the pathogen

UNEP/POPS/COP.5/INF/13/Rev.1
29
(e) Treatment of complications of scabies is performed simultaneously with the main treatment
(f) Those who were in contact with the patient with scabies, are treated by avoiding "ping-pong" infection. It consists of a single treatment of any drug antiscabious
(g) It is recommended to wash the patient before and after treatment. If necessary, the drug can be washed off each morning, since its exposure on the skin should be not less than 12 hours, including night-time
(h) Change of underwear and bed linen is carried out at the end of therapy
(i) Post-scabious itch, after a full treatment, is not an indication for an additional year of specific therapy
(j) Persistent scabious lymphoplasia of the skin does not require any specific therapy
For the treatment of the scabies,quite a lot of drugs and therapeutic schemes are being used.
The most commonly used drugs are presented in Table 2.
Table 2. Effectiveness of the main remedies of acaricidal preparations Preparations Efficiency,% Sulphur 95 - Esdepalletrin 80-91 Krotamion 72-91 Tiobendazol 72-90 Benzyl benzoate 73-87 Lindane 60-80 *
* Depending on the percentage of active substance
Nevertheless, before starting the treatment, taking a hot shower with sponge and soap is advisable in order to remove the ticks from the skin, secretions of the sebaceous glands, and for loosening the horny layer of the epidermis which improves the adhesion of anti scabious remedies. However, in a case of the phenomenon of secondary pyoderma, the water treatments are contraindicated.
The treatment with the method of Dem'yanovich is carried out by two solutions: number 1 (60% solution of sodium thiosulfate) and number 2 (6% solution of hydrochloric acid). In previous years, it was the most common treatment for scabies. The method is recommended for the local form of scabies. In a case of common forms, it is advisable to combine with a subsequent three-day rubbing sulfur ointment. This methodology is based on the acaricidal effect of sulfur and sulfur dioxide that are emitted during the interaction of hydrochloric acid and sodium hyposulfite. This method has its drawbacks. Among them are; labor-intensive, frequent medication Dermatitis and low efficiency when used in outpatient treatment.
To prepare the benzyl benzoate emulsion (10% - for children, 20% - for adults), dissolvle in 780-800 ml of warm boiled water 20 grams of green soap, laundry soap or shampoo and add 200 mg of benzyl benzoate. The suspension is stored in a dark place at room temperature for more than a week. A person that is going to carry out the rubbing, before the treatment, has to wash his/her hands with soap and water. Emulsion is shook and rubbed with hands on the skin, except the scalp, face and neck. First, the drug is rubbed into the skin of both hands, and then in the right and left upper limb, and after in the skin of the trunk (chest - abdomen - back - the buttocks - the genitals) and then the lower extremities, including the soles and toes. For two days, it should be conducted for two successive times, each rubbing for 10 minutes with the same break to let the skin dry. After completion of treatment, the bed and underwear should be changed. Hands should be washed after each treatment. On the third day, the patient should be cleaned and the linen should be changed once again.
In order to treat the children less than 3 years old,10% solution is used, which is prepared by diluting a 20% suspension with the same amount of water. The drug is slightly rubbed into the scalp and face with care, avoiding contact with the eye.
When there are complications or common form of scabies, when during the treatment there the new elements appear on the skin and the patient complains of continued itching of the evening and night time, it is advisable to extend therapy to three days or reappointed two-day course of therapy, three days after the completion of the first.
Benzyl benzoate, which is a part of soapy water and a suspension has both anti-scabious and anesthetic effect. Its use is most advisable under unfavorable epidemic situation. The disadvantages include the local irritant effect of the drug, which can cause subjective sensations and pain during application of the skin.
Currently, the ointments containing sulfur or tar (Wilkinson ointment, 20-30% sulfuric acid ointment), is rubbed on the skin for 10 minutes, except on face and scalp. Rubbing is carried out five consecutive days. The use is better at night, especially vigorously applying the ointment in the mite’s favorite locations such as hands, wrists, elbows and stomach. After a day, at the end of therapy, the patient is washed with soap and water and changes the underwear and
UNEP/POPS/COP.5/INF/13/Rev.1
30
bed linen. In the areas with sensitive skin such as genital organs, peripapillary region, groin, thigh and other folds, the ointment is rubbed carefully in order to prevent the dermatitis. Sulfur, in addition to antiscabious effect, also has keratolytic effect, which provides better access of the drug to the activator. In the presence of secondary pyoderma, it is necessary to first arrest these phenomena with antibiotics or antibacterial ointments. When there is an expressed eczematization, accompanied by parasitic process, it is prescribed an antihistamines and corticosteroids remedies. Following shortcomingsof this treatment method should be taken into account: the duration of therapy, odor, and frequent development of complications. These ointments are not assigned to persons suffering from eczema or to children.
Lindane lotion (1%) has high efficiency but low cost, which is applied once to the entire surface of the skin, left for six hours, and then is washed off. In hot climates, the drug in powder form (15,0-20,0g powder rubbed into the skin 2-3 times a day and take a shower and change clothes after a day) is especially useful. The drug is also used as a 1% cream, shampoo, or 1.2% ointment. 12-24 hours of exposure is enough for one treatment for a complete cure. Because of some toxicity, its use is strictly prohibited in children up to 2 years, pregnant women, patients with multiple scratching, eczema or atopic dermatitis, as it may aggravate the disease. Recently, in connection with its application, some cases of lindane-resistant scabies are described, for which even repeated treatment of this drug does not lead to recovery of the patient.
Krotamion is used as a 10% cream, lotion or ointment. It is rubbed twice a day after washing with a daily interval, or four times every twelve hours during the day. Daily treatment is required for five days because the drug is characterized by low scabicidious activity and, consequently, the emergence of cases of resistance of the mites to the krotamion.
Solutions of esdepallethrine and piperonyl butoxide are applied, in the evening, to the skin from the neck area to the soles (first on the skin of the trunk, then on the lower extremities). The Aerosol can be applied to the entire surface of the skin and provides the penetration of active substances in the itch moves. After 12 hours the drug is carefully washed off. When it is necessary, the anti-scabious remedies could be used again 10-12 days after the first treatment. The effectiveness of this preparation is 80-91%, even in the case of treating the itching and other symptoms may persist for eight to ten days. The drug is used in all age groups and has no contraindications. Before use, it is necessary to cure the effects of secondary infection (impetigo) or eczematization.
Malathion as a liquid is applied to the areas of skin where the patient suffers from scabies. Malathion is used in a 0.5% lotion (1% shampoo is used for lice). The skin treatment is carried out in the evening. All family members are involved in the therapeutic process. The drug is applied to the entire skin surface except the face and scalp. The remedy is washed off twelve hours after its application on the skin. Retreatment is available in 8-10-days. Be sure to change the bedding and underwear. Careful when using the drug to patients suffering from bronchial asthma and children to prevent the inhalation of fumes on alcohol base. Therefore the use of aqueous lotion is more appropriate.
Permethrin is an effective and safe treatment for scabies. After only one treatment at the night, 89-98% of the patients are effectively cured. The drug is applied for 8-12 hours (overnight), and clean clothes are put on after washing off the drug. The treatment could be repeated at the seventh or tenth day of the therapy. The drug has several advantages: good tolerability when used in high temperature and humid environment, can be used for complications of scabies (atopic dermatitis, pyoderma, microbial eczema), permissible use for the disinfection of underwear and bed linen in the treatment of other parasitic diseases (pediculosis and ftiriaz).
Prevention of scabies consists of identifying the source of infection, and persons exposed to the patients with a view to involve them in the preventive treatment. It is necessary to establish the degree of contact (direct / indirect), to identify and eliminate pockets of scabies, make dispensary observation of patients, carry out the disinfection at the source of infection.
The sanitization of the things, clothes and rooms enhances the efficacy of therapy by acaricidal remedies because it warns the possible recurrence of the disease.
To treat the things that cannot be boiled, the highly effective remedies such as permethrin, piperonyl butoxide and esdepalletrin in aerosol packaging are used. These remedies are highly effective also in treating various types of head lice, scabies, during infection from random parasites species (fleas, bedbugs).
The lingerie of the patients has to be boiled, washed, thoroughly ironed or aerated for five days or for one day during the cold days.

UNEP/POPS/COP.5/INF/13/Rev.1
31
The control of cure is carried out in three days after the treatment and then every ten days for six weeks. Treatment success is defined by the drug itself and its concentration, the choice of which depends on the patient's age, presence of pregnancy, the degree of development process, the presence of complications and their severity. An important role has the proper use of the drugs. Rubbing of any remedies have to be done by the hands only and it is better to do it in the evening. This is because of the nocturnal activity of the pathogen and the fact that 6-8 hours of sleep are enough for the death of the active stages of the scabies.
Of course, the scabies are an important problem of modern dermatology, but due to successful etiopathogenetic and epidemiological developments in recent years and to accumulated clinical, diagnostic and therapeutic experience, the solution to this problem does not seem an impossible task for the doctors of any profile.
________________