Pembinaan Instrumen Saringan (Screening) bagi Kanak ...
91
1 Pembinaan Instrumen Saringan (Screening) bagi Kanak-kanak Sindrom Asperger dan Manual Kod Penyelidikan / Research Code : 2015-0082-107-04 Tajuk Penyelidikan / Research Title : Pembinaan Instrumen Saringan (Screening) dan Manual bagi Kanak-kanak Sindrom Asperger Ketua Penyelidik / Principal Researcher : Assoc. Prof. Dr. Siti Rafiah Abd Hamid Penyelidik Bersama/Co-researchers : 1) Prof. Dr Nik Ahmad Hisham Ismail 2) Assoc.Prof.Dr.Haniz Ibrahim 3) Assoc.Prof.Dr.Nik Suryani Nik Abd Rahman 2) Asst.Prof.Dr.Supiah Saad 3) Asst.Prof.Dr.Khamsiah Ismail
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Pembinaan Instrumen Saringan (Screening) bagi Kanak ...

1
Pembinaan Instrumen Saringan (Screening) bagi
Kanak-kanak Sindrom Asperger dan Manual
Kod Penyelidikan / Research Code : 2015-0082-107-04
Tajuk Penyelidikan / Research Title : Pembinaan Instrumen Saringan (Screening) dan Manual bagi Kanak-kanak Sindrom Asperger
Ketua Penyelidik / Principal Researcher : Assoc. Prof. Dr. Siti Rafiah Abd Hamid
Penyelidik Bersama/Co-researchers :
1) Prof. Dr Nik Ahmad Hisham Ismail
2) Assoc.Prof.Dr.Haniz Ibrahim
3) Assoc.Prof.Dr.Nik Suryani Nik Abd Rahman
2) Asst.Prof.Dr.Supiah Saad
3) Asst.Prof.Dr.Khamsiah Ismail

2
Development of Screening Instrument and Manual for
Children with Asperger Syndrome (ISSAKKM / SIMCAS)
Final Inception Report
Prepared by
SIMCAS Team
International Islamic University Malaysia (IIUM) & Sultan Idris Education University
(UPSI)
Table of content Page
Chapter 1:
1.0 Introduction 5
1.1 Executive summary 6
Chapter 2:
Overview of Literature Review 8
2.0 Background 9
2.1 Parental Awareness 9
2.2 Characteristics of Autism 10
2.3 Asperger Syndrome 11
2.4 Importance of Early Intervention 15
2.4.1 Benefits of Early Intervention 15
2.4.2 Early Childhood 15
2.5 Special Education 17
2.6 Effectiveness of Early Intervention 20
2.7 Diagnosis & Proposed Intervention of Asperger
Syndrome 24
2.8 The Problem Statement 29
2.9 The Proposed DSIMCAS 30
2.10 Objectives of DSIMCAS 32
2.11 Scope of Study 33
2.12 Research Objectives 33
2.13 Study Framework 34
Chapter 3:
3.0 Introduction 35

3
3.1Research Methodology 35
3.2 Sampling Procedures & Data Collection 36
3.3 Data Analysis – Framework 36
3.4 Scope of Final Report 37
3.5 DSIMCAS Team 38
3.6 Research Team 38
3.7 Project Steering Committee 38
3.8 Pilot Study for SIMCAS 38
3.8.0 Introduction 38
3.8.1 Domains & Constructs 38
3.8.2 Pilot Study 40
3.8.3 Reliability Estimates of the ISSAKKM / SIMCAS 41
3.8.4 Means & Standard Deviation of Measures 42
3.8.5 Validity of ISSAKKM / SIMCAS items 43
3.8.6 Face Validity 43
3.8.7 Content Validity 43
3.8.8 Construct Validity 44
3.8.9 Summary of Analysis 45
Chapter 4:
4.0 Findings from Focus Group Discussion (FGD) 46
4.1 Difficulties in Identifying Asperger Syndrome & Other
Disorders 48
4.1.0 Students’ Attitude 48
4.1.1 Teacher’s Knowledge of AS & Type of Disorders 49
4.1.2 Useful Information from other sources 51
4.1.2.0 Parents as the source of information 52
4.1.2.1 Subjects learnt – source of information 52
4.1.2.2 Cultural Belief & Practices –
source of information 53
4.2 Least Exposure to Instruments 54
4.2.0 Unfamiliar to any related instruments 54
4.2.1 The Need for ISSAKKM / SIMCAS 55
4.3 RQ2 - Findings from Confirmatory Factor Analysis – CFA 56
4.3.0 Validating Social Interaction & Language
Difficulties Constructs 58

4
4.3.1 Validating Cognitive Difficulties 61
4.3.2 Validating Senses Sensitiveness 63
4.3.3 Validating Limited Interests & Rigidity in
Daily Routines 65
4.3.4 Validating Motor Skills Difficulties 69
4.4 RQ3 – Estimating the Prevalence Rate of Asperger syndrome
among Malaysian mainstream children 71
4.4.0 Setting the ISSAKKM / SIMCAS Benchmark 72
4.4.1 Reliability & Validity of ISSAKKM / SIMCAS 74
4.4.2 Benchmark for ISSAKKM / SIMCAS 74
4.5 Summary of Findings for RQ1, RQ2 & RQ3 75
Chapter 5: Discussion & Recommendations 77
5.0 Introduction 77
5.1 Limitations & Delimitations 79
5.2 Future Research 80
List of Figures:
Figure 1: Overview of DSIMCAS 31
Figure 2: The Framework of the Study 35
Figure 3: Limited Interests & Rigidity in Daily Routines 69
List of Tables
Table 1.0: Social Interaction & Communication. 14
Table 2.0: DSIMCAS Components 31
Table 2.1: ISSAKKM / SIMCAS Benefits to ECE Field. 32
Table 2.2: Examples of ISSAKKM / SIMCAS Reporting 32
Table 3.0: Sampling Procedure & Data Collection 36
Table 3.1: Domains, Constructs & Items in ISSAKKM / SIMCAS 39
Table 3.2: Internal Consistency Validity – ISSAKKM / SIMCAS
Domains for pilot study 1 & 2 42
Table 3.3: Means & Standard Deviation for the Six (6)
Domains 42
Table 3.4: IDEAS Autism Centres & Tadika Bitara –
Pilot Study 1 44

5
Table 3.5: NASOM Centres – Pilot Study 2 45
Table 4.0: Findings for Thematic Analysis for
Research Question 1 – RQ1 47
Table 4.1: General Findings for RQ1 47
Table 4.2: Difficulties in Identifying Asperger Syndrome 48
Table 4.3: Useful Information from other resources 52
Table 4.4: Effects of Exposure to Experiments 54
Table 4.5: Domains & Constructs Undertaken by the study 57
Table 4.6: Factor Loadings 59
Table 4.7: Correlations Across Factors/Constructs 60
Table 4.8: Confirmatory Factor Analysis -CFA (Group 1 & 2) 61
Table 4.9: CFA – Analysis for Cognitive Issues 62
Table 4.10: CFA - Cognitive Issues - Goodness of fit measures
Across two groups 63
Table 4.11: CFA – Senses Sensitiveness 64
Table 4.12: Correlations Across Constructs – Senses
Sensitiveness 64
Table 4.13: Goodness of fit – Senses Sensitiveness 65
Table 4.14: Limited interests & Rigidity in Daily Routines 66
Table 4.15: Correlation Across Limited interests & Rigidity
in Daily Routines 67
Table 4.16: Correlations Across Motor Clumsiness Construct 70
Table 4.17: Goodness of Fit – Motor Clumsiness 70
Table 4.18: ISSAKKM / SIMCAS Internal Consistency 75
Table 4.19: Determining Criteria & Potential AS via ISSAKKM /
SIMCAS 75
References: 81
Appendixes:
Sample of ISSAK / SIMCAS 87
Note:
ISSAKIM stands for the name of screening instrument in Bahasa Malaysia and
SIMCAS is the English version
6
Chapter 1
1. Introduction
Development of the screening instrument and manual for Children with Asperger
Syndrome (DSIMCAS) is an EPU funded project to produce user-friendly documents for
the screening of Asperger’s Syndrome for children at an early age (5 years old and
below). The purpose of this inception report is to simplify the objectives, methodology,
and scope of the final report and research team of this study. A group of experts, relevant
stakeholders and assistant researcher for preliminary conceptualization of DSIMCAS is
set out for implementation of the study.
1.1 Executive summary
Children with Asperger syndrome (high-functioning autism spectrum disorder) develop
into adulthood along diverse paths, and some often experience problems in school or
occupational settings despite their high intellectual or language abilities. Better quality
of life was associated with factors such as suitable medication, mother’s support and
early diagnosis, while poorer quality of life was associated with the presence of
aggressive behaviors. In line with the development of special education programmes for
children with special needs, early detection of asperger syndrome cases could help the
ECCE program provider to cater for early intervention program for children with
asperger syndrome. Early intervention serves as a meaningful starting point in providing
an appropriate program for children with asperger syndrome.
This study will utilize the mixed method approach. In the initial stage instrument
development (items/variables development) the qualitative approach (interviews) was
employed with clinical experts in this area in order to gauge variables affecting asperger
syndrome and as well as the asperger syndrome attributes. Series of observation were
conducted on children at the age of five (5) and below at Permata Childcare Centres and
other centers established by goverment agensies as well as private schools. The end
product or contribution of this research is the validated instrument for screening asperger

7
syndrome based on the Malaysian experience and subjects and as well as the
development of Malaysian asperger syndrome manual which can be referred to by special
needs practitioners in the Malaysian context.
The establishment of this instrument/questionnaire and interview protocol (focus group
purposes), special needs educators and child caretakers will create awareness of this
problem among children at the preschool level. Such awareness will enable teachers and
childcare takers to select suitable teaching-learning strategies and resources. Teachers
will also be capable of catering the emotional and social needs of these children. As for
serious Asperger cases, these potential cases will be referred to the medical practitioners.
Standardized screening instrument for AS have been developed in other countries and
they are not exactly suitable because of cultural differences. So far not many (if any),
screening instrument for early detection of Asperger syndrome based on the Malaysian
norms can be found in Malaysia. As such this study is important and pertinent to child
caretakers and teachers so that they will be able to ascertain that these children’s
emotional and social needs are met.
This study was lead by Dr Supiah Saad initially and later taken over by Dr Siti Rafiah
Abd Hamid later on due to inevitable circumstances. This team is supported by a host of
experts which include psychologists, early childhood professional, clinical psychologists
and special education profesional from IIUM and UPSI. The objectives of this study are
to develop items for the instruments and validate the instrument for screening children
with Asperger syndrome (SIMCAS) below 5 years old. The other objective is to generate
comprehensive and integrated report for policy makers and intervention / programme
providers as well as to provide insights of the degree of AS related behaviors in children
at five years old and below based on statistical data and qualitative data.
The objectives of having SIMCAS which is reflective of DSIMCAS study:
1. To explore preschool educators’ knowledge, skills and awareness related to children
with Asperger Syndrome.
2. Identify the capability of SIMCAS in assisting educators and childcare takers in
screening children with Asperger Syndrome develop and validate SIMCAS
(develop and validate SIMCAS)

8
3. discover the prevalence rate of potential Asperger syndrome in Malaysian children
aged 5 and below.
4. Outreach information related to Asperger syndrome to educators/caregivers
An instrument will be developed and is known as the Screening Instrument and Manual
for Asperger Syndrome (SIMCAS). It will be validated before the real data collection.
This instrument may be regarded as one of the significant contribution of this study.
Since this study is based on broad field work procedures, the methodology used may
contribute some background for further inquiry by researchers who are interested in
special needs education.

9
Chapter 2
Literature Review
2.0 Background
Asperger syndrome is part and parcel of the pervasive developmental disorder. It
resembles the classic autistic pattern of behavior. However, children with Asperger
syndrome exhibit high cognitive ability and verbal communication ability together with
the selected area of communication (based on their interest). According to Teitelbaum,
Benton, Shah, Prince and Kelly (2004); Russel and Sofronoff (2005); and Moyes (2002)
children with Asperger syndrome typically have normal or high IQ but they lacked
emotional intelligence and social skills. Most of these children were found as high
functioning children however the Asperger symptoms deter them from achieving
optimum level of performance in school. As a result, these symptoms sometimes overlap
with the expected developmental milestone of any typical child. As reported in many
literatures, late detection results in the children deprived the rights to get special
education provision in mainstream classroom. As such the screening tool based on
Malaysian norms necessary to identify the attributes and subject to diagnosis by the
qualified personnel. Once diagnosed, these children can be referred to MOE for
educational provisional suitable for their needs. In April 2012, a proposal was submitted
to seek funding allocation to carry out this study. However due to inevitable
circumstances, the real study was embarked in July 2015.
2.1 Parental Awareness
Parents are experts on their own children and nobody else would. If parents suspect that
there is something wrong about the child, they are on the right track in seeking
professional help. On the contrary, figuring what the real underlying problem is may be
a problem for many parents and as well as where to get professional help. The difficulty
is often in working out what the problem might be, how serious it is and with whom to
check out your worries. Most parents would discuss these anxieties with their family and
friends instantly and later consult a health professional (such as a health visitor or doctor)
if their concerns still remained. Often parents are reassured and, either quickly or
gradually, the behaviours that were of concern to us disappear. If the child’s behaviour

10
display a recurring pattern, parental worries may remain. In most cases, most parents may
need to consult a health professional again.
2.2 Characteristics of Autism
Autism Spectrum Disorder (ASD) is a developmental disorder that normally becomes
evident in the first three years of a child’s life (Williams & Wrights, 2004). Current
estimates are that ASD including all the spectrum diagnoses occurs in approximately two
to seven per 1000 person. It is about one-tenth of this for the severe end of the autism
spectrum. This varies depending on which research you read and also in which countries
the research was carried out; it is also probably to do with the way diagnosis is made and
the criteria used. It is about three to four times more common in boys than in girls. ASD
affects communication, social interaction, imagination and behaviour. It is not something
a child can catch. Parents do not cause it. It is a condition that carries on into adolescence
and adulthood. However, all children with ASD will continue to continue to make
developmental progress and there is a great deal that can be done to help.
The children with autistic personality disorder and remarkably perceptive description of
the children’s difficulties and abilities; delayed and some aspects of their social abilities
were quite unusual at any stage of development; had difficulty making friends and they
were often teased by other children; impairment in verbal and non-verbal
communication, especially the conversation aspects of language (Attwood, 2007). The
children’s use of language was pedantic, and some children had an unusual prosody that
affected the tone, pitch and rhythm of speech.
Autism Spectrum Disorder is the term that is currently used to describe the broad range
of pervasive developmental disorders. These disorders include Autistic Disorder,
Aspergers Disorder (also referred to as Asperger's syndrome), Rett's Disorder, Childhood
Dis-integrative Disorder, and Pervasive Developmental Disorder Not Otherwise
Specified (PDD-NOS (Dawson & Toth, 2006). According to the researchers, Autism
spectrum disorders involve impairments in reciprocal social interaction and
communication and the restricted, stereotyped, and repetitive interests and behaviors. Of
these three symptom domains, impairments in social interaction are considered a primary
feature of these disorders. These impairments include a lack of social and emotional

11
reciprocity; atypical nonverbal behaviors such as atypical eye-to-eye gaze, facial
expressions, body postures, and gestures to regulate social interaction; lack of interest
and/or difficulty relating to others, particularly peers; and a failure to share enjoyment
and interests with others. A great deal of heterogeneity exists among the Autism spectrum
disorders in terms of the number and severity of symptoms across the three domains
(social, communication, and stereotyped/restricted interests and behaviors) and in
cognitive and adaptive functioning. Further, within each diagnostic category,
impairments differ across individuals and, for any given individual, symptoms may
change across the life span.
Autism is a severe, chronic development disorder, involving marked retardation of
aptitudes for social interaction, communication and play. The detection of autism and
other general developmental disorders in very young children is quite difficult since
delayed development may not be identified until the child is given the opportunity to
interact in social environments other than the family setting. In addition, at the most
severe levels, the differential diagnosis between autism and mental retardation is more
difficult, especially among children of preschool age (de Bildt, Sytema, Ketelaars,
Kraijer, Mulder, Volkmar, & Minderaa. (2004). As in autism, Asperger syndrome shows
impaired reciprocal social interaction and restricted, repetitive or stereotyped patterns of
behavior, interests and activities. Unlike autism, intellectual ability and syntactical
speech are normal (Berney, 2004).
2.3 Asperger’s Syndrome
Parent of a young child with Asperger’s Syndrome often question if their child’s
behaviour and is within the “normal” range. The world of the young child is a rich and
complicated place with so many things happening developmentally. Given the
complexities of the world of the young child, we feel that it is important to develop a
shared understanding of the developmental tasks salient at this age. What can make this
time period both rewarding and challenging for parents, teachers and children in that the
children are undergoing major charges at varying rates in differing areas of development
(Leventhal-Belfer & Coe, 2004). With this in mind we will examine the developmental
task which are characteristic of the Asperger’s such as sensory-motor development,
communication, cognition, play, emotional and social functioning, relationships with

12
caregivers and peers and the child’s capacity to cope with stressful events.
The characteristics that define Asperger's Disorder include intact formal language skills
(e.g., vocabulary, grammar), with impairments in the social use of language and in
nonverbal expression, social awkwardness, and idiosyncratic and consuming interests
(Volkmar & Klin, 2001). Although motor clumsiness is not a defining feature of
Asperger's Disorder, it is often observed (Volkmar & Klin, 2001). The DSM-IV
diagnostic criteria for Asperger's Disorder include at least two symptoms in the domain
of social interaction and one symptom in the domain of restricted interests and behaviors.
Further, individuals with Asperger's Disorder do not demonstrate clinically significant
delays in general cognitive ability, self-help skills, and adaptive development (Dawson
& Toth, 2006). Differentiating Asperger's Disorder and high-functioning Autism is often
difficult to do clinically, and the empirical validity of such a distinction has not yet been
unequivocally established (Ozonoff & Griffith, 2000; Volkmar & Klin, 2001). Asperger's
Disorder was included as a separate diagnostic category only in the more recent revisions
of the DSM IV and ICD-10 classification systems, and epidemiologic data on this subtype
of Autism Spectrum Disorder are scarce. The first systematic epidemiologic study of
Asperger's Disorder was conducted in Sweden and yielded a prevalence rate of 28.5 per
10,000 (Ehlers & Gillberg, 1993).
In a review of epidemiology surveys, Fombonne and Tidmarsh (2003) concluded that the
number of children with Autism was five times that of children with Asperger's Disorder,
on average, suggesting that the prevalence of Asperger's is approximately two per 10,000.
The authors note that future studies should focus on slightly older children (ages 8 to 12
years) as Asperger's Disorder is often diagnosed much later than Autism. According to
Fombonne and Tidmarsh (2003), Asperger syndrome (AS) is a developmental disorder
that is marked by:
i.limited interests or an unusual preoccupation with a particular subject to the
exclusion of other activities
ii.repetitive routines or rituals
iii. peculiarities in speech and language, such as speaking in an overly formal manner
or in a monotone, or taking figures of speech literally
iv.socially and emotionally inappropriate behavior and the inability to interact
successfully with peers

13
v.problems with non-verbal communication, including the restricted use of gestures,
limited or inappropriate facial expressions, or a peculiar, stiff gaze clumsy and
uncoordinated motor movements
Asperger syndrome is an autism spectrum disorder (ASD), one of a distinct group of
neurological conditions characterized by a greater or lesser degree of impairment in
language and communication skills, as well as repetitive or restrictive patterns of thought
and behavior. Other ASDs include: classic autism, Rett syndrome, childhood dis-
integrative disorder, and pervasive developmental disorder not otherwise specified
(usually referred to as PDD-NOS).
Parents usually sense there is something unusual about a child with AS by the time of his
or her third birthday, and some children may exhibit symptoms as early as infancy.
Unlike children with autism, children with AS retain their early language skills. Motor
development delays – crawling or walking late, clumsiness – are sometimes the first
indicator of the disorder. The incidence of AS is not well established, but experts in
population studies conservatively estimate that two out of every 10,000 children have the
disorder. Boys are three to four times more likely than girls to have AS.
Studies of children with AS suggest that their problems with socialization and
communication continue into adulthood. Some of these children develop additional
psychiatric symptoms and disorders in adolescence and adulthood. Although diagnosed
mainly in children, AS is being increasingly diagnosed in adults who seek medical help
for mental health conditions such as depression, obsessive-compulsive disorder (OCD),
and attention deficit hyperactivity disorder (ADHD). No studies have yet been conducted
to determine the incidence of AS in adult populations. (Available at:
http://childdevelopmentinfo.com/child-psychology/autism-aspergers/asperger/).
Asperger syndrome comes not only with its own characteristics, but also with a wide
variety of comorbid conditions such as depression, anxiety, obsessive–compulsive
disorder, attention-deficit hyperactivity disorder (ADHD) and alcoholism, and
relationship difficulties (including family/marital problems). It may predispose
individuals to commit offences and can affect their mental capacity and level of

14
responsibility as well as their ability to bear witness or to be tried (Tantam, 2003). The
syndrome can color psychiatric disorder, affecting both presentation and management,
for children and adults across a wide range of functional ability. Families have taken an
active legalistic approach, alleging misdiagnosis and mistreatment and demanding clarity
as to the relationship between Asperger syndrome and other diagnostic concepts. The
characteristics of Asperger syndrome in adulthood (Gillberg, et al. 2001) which includes
at the childhood onset are listed in Table 1.0 below:
Table 1.0: Limited Social Relationship
No. Social Relationship
i. Few/no sustained relationships; relationships that vary from too distant to too
intense
ii. Awkward interaction with peers
iii. Unusual egocentricity, with little concern for others or awareness of their
viewpoint; little empathy or sensitivity
iv. Lack of awareness of social rules; social blunders Problems in communication
v. An odd voice, monotonous, perhaps at an unusual volume
vi. Talking ‘at’ (rather than ‘to’) others, with little concern about their response
vii. Superficially good language but too formal/stilted/pedantic; difficulty in
catching any meaning other than the literal
viii. Lack of non-verbal communicative behavior: a wooden, impassive appearance
with few gestures; a poorly coordinated gaze that may avoid the other’s eyes or
look through them
ix. An awkward or odd posture and body language Absorbing and narrow interests
x. Obsessively pursued interests
xi. Very circumscribed interests that contribute little to a wider life, e.g. collecting
facts and figures of little practical or social value
xii. Unusual routines or rituals; change is often upsetting
Asperger syndrome, a form of autism with normal ability and normal syntactical speech,
is associated with a variety of comorbid psychiatric disorders. The disorder is well known
to child psychiatry, and we are beginning to recognize the extent of its impact in
adulthood. The article reviews the diagnosis and assessment of Asperger syndrome and
its links with a wide range of psychiatric issues, including mental disorder, offending and
mental capacity. It also describes the broader, non-psychiatric management of Asperger
syndrome itself, which includes social and occupational support and education, before
touching on the implications the disorder has for our services (Berney, 2004).
15
2.4 Importance of early intervention
2.4.1 Definition of early intervention
Early intervention is defined as the experience and opportunities afforded infants and
toddlers with disabilities by the children’s parents and other primary caregivers that are
intended to promote the children’s acquisition and use of behavioural competencies to
shape and influence their pro-social interactions with people and objects (Dunst, 2007).
There three principles that guide the ways in which early intervention is operationalized
and practiced such as principle 1: The experiences and opportunities afforded infants and
toddlers with disabilities should strengthen children’s self-initiated and self-directed
learning and development to promote acquisition of functional behavioural competencies
and children’s recognition of their abilities to produce desired and expected effects and
consequences; principle 2. Parent-mediated child learning is effective to the extent that
it strengthens parents’ confidence and competence in providing their children with
development-investigating and development-enhancing learning experiences and
opportunities; and principle 3. The role of early-intervention practitioners in parent-
mediated child learning is to support and strengthen parent capacity to provide their
children with experiences and opportunities of known qualities and characteristics (i.e.,
evidence based) that are most likely to support and strengthen both parent and child
capacity.
2.4.2 Early childhood and the Malaysian Experience
Malaysia has always place great effort in ensuring education and care for all children.
These efforts are manifested through the many sectors involving in ECCE and the amount
of allocation given to ECCE each year. ECCE in Malaysia is broadly divided into two
main groups, which is the 0-4 years old and the 4-6 years old. In Malaysia, early
childhood care and family development is the jurisdiction of the Ministry of Women,
Family and Community Development (MWFCD). MWFCD is the coordinator for
national programs on the growth and development of children. Through its Department
of Social Welfare, MWFCD registers all Childcare centers (TASKA, an acronym in the
local language). TASKA offers care and education for children in the age group of 0-4
years old (Ministry of Education Malaysia (2007).

16
Early childhood education for the 4-6 years old group falls under the responsibilities of
three Ministries, i.e. Ministry of Education, Ministry of Rural and Regional
Development, as well as Department of National Unity and Integration under the Prime
Minister Department. Ministry of Rural Development is the pioneer in setting up
preschools in Malaysia (beginning early 1970‟s), currently there are 8307 preschools set
up by this Ministry which are commonly known as the KEMAS preschool. KEMAS
preschools are located in rural or suburban and are set up based on request by the local
authority. In the late 1970‟s Department of National Unity and Integration set up
preschools in the urban areas where there are, Rukun Tetangga’, a friendly neighborhood
scheme, these preschools are generally known as the PERPADUAN preschools,
PERPADUAN preschools must accept students from the different races, currently, there
are 1496 PERPADUAN preschools.
Ministry of Education (MOE) is the latest in setting up preschools. In the year 1992,
preschool was set up by MOE in the form of pilot project as an annex to the existing
primary school, in the year 2003, MOE preschool project was rolled out to whole nation;
currently there are 5,905 of these preschools which are situated all over the country. Other
than MOE, KEMAS and PERPADUAN, other providers of preschool education include
also the State Religious Department (JAIN) and the Islamic (ABIM). There are various
kinds of childcare centers in Malaysia, these centers are generally named as TASKA.
Categories of childcare centers found in Malaysia are as Government own childcare
center (TASKA dalam komuniti) (since 2006); Workplace childcare center; Institutional
childcare center; Plantation childcare center; and Home based childcare center
(Gallagher, Clifford, & Maxwell, 2004).
The development, care, and education of children from birth to age 5 has been the focus
of rapidly increasing public interest, and numerous early childhood public policy
initiatives have focused attention on a major problem of coordination and collaboration
of services for young children. Four segments of services for young children—(1) child
care, (2) Head Start, (3) services for children with disabilities, and (4) preschool
programs—have all been major players in providing services for differing, and
sometimes overlapping, populations of young children.

17
Each group has a similar mission: to help children (most often with special needs or
limited opportunities) master the skills and knowledge needed to adapt effectively to
kindergarten at age 5. Each group has its own history and has developed more or less
independently of the others. Because the groups developed independently, they have
overlapping personnel preparation programs, evaluation efforts, and data systems. This
paper explores some strategies for moving from independent and overlapping services
toward a seamless system of early child care and nurturance provided by these four
diverse players (Gallagher, Clifford & Maxwell, 2004). Voluntary collaborations between
these players seem unlikely because of self-interest and bureaucratic challenges. Barriers
to reform exist in institutional, psychological, sociological, economic, political, and
geographic domains. This paper proposes that four engines of change namely legislation,
court decisions, administrative rule making, and professional initiatives - be energized to
move toward a seamless system. Such collaboration can begin by merging support
systems such as personnel preparation, technical assistance, and evaluation. The paper
concludes with specific recommendations for achieving an integrated early childhood
system.
2.5 Special Education in Malaysia
Cabinet Committee Report 1979 stated that special children education is the responsibility
of the government and NGOs are to be involved in this endeavour (Ministry of Education
Malaysia, 2007). Education for the special children are taken care of by both the Ministry
of Woman, Family and Community Development as well as the Ministry of Education.
Ministry of Education is in charge of program in the special schools and also in the special
integrated primary schools for children. Ministry of Woman, Family and Community
Development will be in charge of the other special programs. Since 2000, the existing special
schools then have started early intervention program for the 4-6 age group on their own
initiative (Ministry of Education Malaysia, 2007). These programs run without any
allocation or training for the teachers specifically to teach preschool. In the year 2003, MOE
has approved the conversion of these early intervention programs in the 28 special schools
to preschool programs for special need children.

18
These 28 programs made up of 22 for the hearing impaired, 5 for visually impaired and 1 for
learning disability The program run by the Department of Social Welfare, Ministry of
Woman, Family and Community Development are specially for the severely disabled
children. The purpose is to enhance the quality of life of these people. The National Welfare
Policy and National Social Policy has been introduced to serve this purpose. There are also
special grant given to the NGO‟s to help run these special programs for special children
below four (4) years old.
We now know that professionals can diagnose children with autism when they are as
young as 2 years of age (Lord, 1995). Screening and the role of the pediatrician have
become even more critical as we have recognized the stability of early diagnosis over
time and the importance of early intervention. At this point, experts working with
children with autism agree that early intervention is critical (Corsello, 2005). There is
professional consensus about certain crucial aspects of treatment (intensity, family
involvement, focus on generalization) and empirical evidence for certain intervention
strategies.
However, there are many programs developed for children with autism that differ in
philosophy and a lack of research comparing the various intervention programs
(Corsello, 2005). Most of the programs for children with autism that exist are designed
for children of preschool age, and not all are widely known or available. While outcome
data are published for some of these programs, empirical studies comparing intervention
programs are lacking. In this review, existing intervention programs and empirical studies
on these programs will be reviewed, with a particular emphasis on the birth to 3 age
group.
There has been a dramatic rise in the number of children being diagnosed with autism
spectrum disorders (ASD), which has led to increased attention paid to assessment and
intervention issues (Koegel , Koegel , Ashbaugh & Bradshaw, 2014). This manuscript
agrees with Camarata (2014) that the evidence base for early assessment and intervention
should be expanded. However, it disagrees with Warren et al. (2011) assumption that
there are not empirically validated early interventions. Reliable diagnosis has been
documented during infancy and toddler hood, and evidence suggests that the earlier the
onset of intervention, the greater likelihood of an improved developmental trajectory.
19
It is argued that early intervention is more costly and time efficient than a “wait and see”
approach. With regard to published studies, the large amount of heterogeneity in the ASD
population supports the use of rigorous single case experimental design research. It is an
error to limit empirical evidence for treatments to only randomized clinical trials, which
have the weakness of masking individual differences.
Single case experimental designs examine the effects of intervention beyond typical
maturation by allowing for clear estimations of developmental trajectories prior to the
onset of intervention, followed by evaluation of the impact of the intervention. This
commentary discusses the short- and long-term benefit ts of early diagnosis and
intervention.
According to Dawson and Toth (2006) some parents of children whose children are
disgnosed with Autism Syndrome were concerned about their child's development since
birth, and, by 18 months, most parents raise concerns with their primary health care
provider (Howlin & Asgharian, 1999; Rogers, 2001; Siegel, Pilner, Eschler, & Elliot,
1988). However, the age at which a diagnosis is confirmed tends to be much older. In a
survey of 770 parents of children with Autism and Asperger's Disorder, the average age
at which a formal diagnosis was confirmed was 5.5 years for Autism and 11years for
Asperger's Disorder (Howlin & Asgharian,1999). Refining methods of early
identification and diagnosis allows for early intervention and better outcomes for young
children with these disorders
Early social and language input is critical for normal brain development (Dawson & Toth,
2006). If Autism can be identified early and intervention can begin during the first few
sensitive years of life, there is the greatest potential for having a significant impact on
the developing nervous system and improved social and behavioral outcomes for children
with Autism (G. Dawson Ashman, et al., 2000; Rogers, 1998).As summarized by G.
Dawson and Osterling, Green, Brennan, and Fein (2002), Rogers, and the National
Research Council (2001), although intervention approaches have varied across different
outcome studies, most have several features in common:

20
i. A focus on the curriculum domains of attention, imitation, language, toy play,
and social interaction;
ii. Programs that incorporate developmental sequence;
iii. Teaching strategies that offer a high level of support for the child, many of which
rely on principles of applied behavioral analysis (see later discussion);
iv. Specific strategies focused on reducing interfering /problem behaviors;
v. A high level of involvement of parents;
vi. Careful transitioning from one-to-one teaching to small groups;
vii. Highly trained staff;
viii. High levels of supervision of therapists;
ix. Intensive intervention consisting of about 25 hours a week of structured
intervention lasting for at least 2 years; and
x. Onset of intervention by 2 to 4 years.
2.6 Effectiveness of early intervention
There has been a heated debate over the last several decades about when the education
of young children should begin, with many researchers claiming the growth and
development starts at birth or even during the prenatal period. Regardless of the earliest
starting point, scientists who carry out brain development research have at least
concurred with one key finding: learning during the early years is critical (Lee & Hayden,
2009). The consensus seems to be that early exposure to learning experiences in a
stimulating environment will lead children to perform better in primary schools. In time
these individuals become more productive, healthier citizens in democratic society (Lee
& Hayden, 2009). Researchers have determined that the long-term effect of early learning
and education can be observed in all children with varying abilities, including those with
or at risk of developmental delay.
This movement in education has been almost universal. Many developed countries have
begun to turn their attention to “very early” education of children from birth to pre-
primary ages. By drawing on a variety of funding resources, effort have focused on
generating and choreographing various early childhood education programs. The
introduction of universal preschool programs in North American and West European
countries is one example. In addition, more early childhood professionals have involved

21
families and communities in order to improve quality care and development of young
children especially from birth through age three. Due to the proliferation of the variety
of such programs it has become critical to ensure program quality and administration.
In accordance with the recent change in the climate of early childhood education, this
trend seems to be spreading to developing countries as well. According to UNESCO the
global pre-primary gross enrolment ratio grew from 33% to 40% between 1999 and 2005
(United Nations Educational Scientific and Cultural Organization (UNESCO), 2008).
The data confirms that more countries are advocating the compulsory pre-primary
education programs of 5-year-old children, specifically before their entrance into formal
primary education. In addition, these developing countries have further expanded their
public childcare, family and social and welfare services. These services target lower-
income families and working parents as well as private early childhood programs in
urban cities for families with more resources.
The primary goals of early intervention for children with developmental disabilities or
delays are to enhance the quality of life for individual children and their families and to
increase opportunities for developmental progress (Lee & Miller, 2009). In Washington,
the Infant Toddler Early Intervention Program (ITEIP) provides a framework for services
for children with developmentally disabilities and developmental delays, aged birth to
three. ITEIP is governed under the federal Individuals with Disabilities Education Act
(IDEA), Part C, which enables states to receive federal funding to “maintain and
implement a statewide, comprehensive, coordinated, multidisciplinary, inter-agency
system to provide early intervention services for infants and toddlers with disabilities and
their families”. Through the ITEIP program, children and their families may receive a
variety of individualized services, depending on a child’s needs. These services can
include:
i. Assistive technology devices and services
ii. Audiology (hearing)
iii. Occupational therapy
iv. Family resources coordination
v. Family training, counseling, and home visits
vi. Medical services only for diagnostic or evaluation purposes

22
vii. Nursing services
viii. Early identification, screening, and assessment
ix. Physical therapy
x. Psychological services
xi. Social work services
xii. Special instruction
xiii. Speech-language pathology
xiv. Transportation and related costs necessary to enable receipt of early
intervention services
xv. Vision services
Services for infants and toddlers are funded through public education, county human
service agencies, and the Department of Health. In addition, Medicaid funds and military
and private health care coverage are often utilized for these services (Lee & Miller, 2009).
ITEIP is the payer of last resort. The aim of ITEIP is to reduce the need for special
education services when the child becomes three years old.
According to ITEIP records, 27 percent of the children who transitioned out of early
intervention services from October 2007 through September 2008 did not need special
education at age three.
Research on interventions for infants and toddlers with developmental disabilities is
limited. Most studies on early intervention focus on “at-risk” populations, such as infants
in impoverished families, or those biologically at-risk (e.g., born pre-term or at a very
low birth weight). Well-controlled comparison group studies have shown long-term
educational, economic, and other societal benefits of some early intervention programs
for these at-risk populations Ethical and legal considerations may pose obstacles to the
study of treatments for infants and toddlers with developmental disabilities.
In some instances, these obstacles can be overcome when opportunities for comparison
group research naturally arise. For example, there may be insufficient resources to treat
all children with a particular intervention. A researcher could randomly assign clients to
a “treatment” group or to a “service as usual” group, measure the clients at intake, then

23
track the outcomes of both groups over time. Alternatively, clients could be randomly
assigned to a waiting list to receive the treatment at a later time. Research as devised
above would enable researchers to draw conclusions about the relative efficacy of
different interventions
Focused development of early childhood education programs is now in demand. The
general disposition is that the age-scope of early childhood education should extended
from preschool and pre-primary ages to all young children from birth. Due to the wide
gap among these young children development and learning, a variety of childcare and
educational models has been proposed in all countries (Gallagher, Clifford, & Maxwell,
2004). Bearing in mind the importance of family involvement in this age group, there is
an ongoing reification of programs that are family-based, community-based, or parenting
education programs versus traditional center-based preschool programs.
Furthermore, instead of replicating the program models from developed countries, these
developing countries’ programs tend to consider the individual families’ culture and
background (Gallagher, Clifford, & Maxwell, 2004). For example, it is acknowledged
that families in many Middle Eastern and Asian countries particularly favor home-based
childcare services rather than center-based services until children are provided with
compulsory primary education (UNESCO, 2008). Thus, the great need of early childhood
care and education programs should not overshadow the method used. Actual
implementation should be carefully planned based upon each country’s culture, rather
than counting on the idea and belief projected by developed countries’ research.
This study investigated the unique contributions of joint attention, imitation, and toy play
to language ability and rate of development of communication skills in young children
with autism spectrum disorder (ASD). Sixty preschool-aged children with ASD were
assessed using measures of joint attention, imitation, toy play, language, and
communication ability (Toth , Munson, Meltzoff & Dawson, 2006). Two skills, initiating
proto declarative joint attention and immediate imitation, were most strongly associated
with language ability at age 3–4 years, whereas toy play and deferred imitation were the
best predictors of rate of communication development from age 4 to 6.5 years.

24
The implications of these results for understanding the nature and course of language
development in autism and for the development of targeted early interventions are
discussed. the results of the present study shed light on the relationship between early
skill domains and the development of language and communication in young children
with autism, and suggest specific targets for early intervention (Toth , Munson, Meltzoff
& Dawson, 2006). Early abilities involved in social exchange and communication,
namely, joint attention and immediate imitation, appear to be important for setting the
stage for early language learning in autism, while representational skills, demonstrated
through toy play and deferred imitation, contribute to the continued expansion of
language and communication skills over the preschool and early school age years. Each
of these skill areas represents an important target for early intervention programs that
promote communicative competence and improved outcomes for young children with
autism.
2.7 Diagnosis and Proposed Interventions of Asperger syndrome
Clinical and practical knowledge about Asperger syndrome is accumulating, but we do
not yet know how frequent Asperger syndrome is (Uta, 2004). Of course, we can only
know how many cases there are if we know what a case is! There is reason to believe
that in current clinical practice the label Asperger syndrome is used rather
indiscriminately. Asperger syndrome has a special cachet that hints at superior
intelligence and perhaps even genius. The label high- functioning autism, because it is
sometimes applied to individuals who are only relatively high functioning, possibly
carries less of such an implication. In reality, the label is given to many children and
adults on the autism spectrum who are simply atypical in their presentation, talkative
rather than withdrawn, but not necessarily of high ability. Asperger syndrome, or high-
functioning autism as identified in many clinics today, comprises a far too heterogeneous
group, including cases of well below average ability and poor social adaptation, as well
as those of superior intelligence and good social adaptation.
According to Dawson and Toth (2006), the Diagnostic and Statistical Manual of Mental
Disorders, fourth edition (DSM-IV; American Psychiatric Association, 1994) and the
International Classification of Diseases, 10th edition (ICD-10; World Health
Organization, 1992) suggests two widely used systems for diagnosing Autism spectrum
disorders.

25
Although much research has been done, concerns and issues in early childhood education
exist throughout the world. Most importantly, the quality of these early childhood
education programs needs to be examined (Lee & Hayden, 2009). Although the
development and expansion of early childhood programs has greatly increased (Barnett,
1995), there have been only limited number of instruments to monitor their
implementation and measure their overall quality (NICHD Early Child Care Research
Network, 2000).
It remains unknown how these early childhood programs are operated and if they are
truly offering learning experiences and environments for young children growth and
development. Improve and systematic program evaluation and monitoring are needed.
As a result, professional teacher training and development programs have been targeted
for analysis. Secondly, more support and advocacy in the field of early childhood
education and development is needed in today’s political climate. In order to promote
early childhood programs and their quality, it is necessary to provide a policy framework
of standards and norms that serve as the foundation of those programs. Based on this
framework, then, increased government budgets or other alternative financial resources
may in due course become available. Lastly, within the international context of early
childhood education, a greater attention to diverse, particular populations should be
given. These groups include indigenous populations, low income families, rural
communities, and groups from non-mainstreamed cultures, among others.
This study investigated child-assessment practices in the context of Korean early
childhood education and care settings (Nah & Kwak, 2011). Interviews with educators
and documents obtained from educational and care settings were analyzed. In general,
the results support the rigorous implementation of child-assessment procedures since the
recent implementation of kindergarten evaluation and childcare accreditation by the
government.
However, some settings have not implemented these procedures systematically, resulting
in wide variation in the types of assessment conducted and the forms used across
environments, as well as superficial goals and limited information regarding children
(Nah & Kwak, 2011). To enable efficient child assessment and the transfer and sharing
of information about each child among providers and schools, a common framework

26
should be provided, with common tools and recording forms, together with guidelines
for child assessment and training services for educators and staff.
The most effective evaluation of young children utilized both formal and informal
assessments, including information from standardized tests, such as medical check-ups
that assess physical development, personal reports, tests created by teachers, work
samples, and/or observations of children during activities, which represents the most
informal approach to assessment (Nah & Kwak, 2011). The use of informal assessment
to obtain information to inform teaching and decision making about young children has
been widely accepted (Morrison, 2009), and observation has emerged as one of the most
widely used methods of informal assessment (Beaty, 2006; Mindes, 2003). The context
of assessment can affect the performances of young children, who can perform best when
they work in familiar, comfortable, natural, and informal settings (Cazden, 2001).
Thus, information used to assess young children must be gathered not only during adult-
led activities, but also during free play, everyday routines, and child-initiated activities.
Observation of daily activities, play, and work is more appropriate than formal tests using
structured tasks in assessments of young children (Schweinhart, 1993; Hills, 1993;
Pellegrini, 2001).
This study aimed to identify what and how often quality control practices are
implemented in Early Intervention (EI) centers (Jeanette, 2010). Focus group discussions
(FGDs) among 22 participants yielded several aspects of early intervention in four
domains: the child and the EI program; parent-professional collaboration; government,
non-government, and community linkages; and legislation and societal values. Results
were used in constructing a 50-item survey questionnaire, administered to 30 respondents
working in 17 EI centers for different age groups. Results showed that almost all the EI
centers had these daily activities: development of self-help skills, use of sensorial
materials, parent-teacher consultations, and beginning reading, writing, and numeracy
lessons. In general, the EI centers concentrate on direct instruction of the child but do not
prioritize macro components such as implementation of accessibility laws.
Recommendations include standardization of quality control in EI centers, especially the
requirement of a transition plan upon exit from the EI program.

27
The high-functioning Autism Spectrum Screening Questionnaire (ASSQ) is a 27-item
checklist for completion by lay informants when assessing symptoms characteristic of
Asperger syndrome and other high-functioning autism spectrum disorders in children
and adolescents with normal intelligence or mild mental retardation (Ehlers, Gillberg,
& Wing (1999) . Data for parent and teacher ratings in a clinical sample are presented
along with various measures of reliability and validity. Optimal cutoff scores were
estimated, using Receiver Operating Characteristic analysis. Findings indicate that the
ASSQ is a useful brief screening device for the identification of autism spectrum
disorders in clinical settings.
To examine the concurrent and criterion validity of the Autism Behavior Checklist
(ABC). Methods: Three groups, comprising 38 mothers of children previously diagnosed
with autism (DSM IV-TR, 2002), 43 mothers of children with language disorders other
than autism, and 52 mothers of children who had no linguistic or behavioral complaints,
were interviewed (Marteleto & Pedromonico, 2005). In order to minimize the effect of
maternal level of education, the questionnaire was completed by the researcher.
To determine the concurrent validation, ANOVA and discriminant analysis were used.
The ROC curve was used to establish the cutoff score of the sample and to examine the
criterion validity. Results: The mean total score was significantly higher in the group of
mothers of autistic children than in the other groups. The ABC correctly identified 81.6%
of the autistic children. The ROC curve cutoff score was 49, and the sensitivity was
92.1%, higher than the 57.89% found when a cutoff score of 68 was used. The specificity
was 92.6%, similar to the 94.73% obtained with a cutoff score of 68. Conclusions: The
ABC shows promise as an instrument for identifying children with autistic disorders,
both in clinical and educational contexts, especially when a cutoff score of 49 is used
(Marteleto & Pedromonico, 2005).
Diagnostic Observation Schedule-Generic (ADOS-G) and clinical classification was
studied in 184 children and adolescents with Mental Retardation (MR). The agreement
between the ADI-R and ADOS-G was fair, with a substantial difference between younger
and older children (5–8 vs. 8+ years) (Bildt, Sytema, Ketelaars, Kraijer, Mulder, Volkmar,
& Minderaa. (2004). Compared with the Diagnostic and Statistical Manual of Mental
Disorders-IV-TR (DSM-IV-TR) classification of Autistic Disorder (AD) and Pervasive

28
Developmental Disorder (PDD), both instruments measure AD or PDD validly and
reliably. Even in low-functioning children the interrelationship between the instruments
and the clinical classification was satisfactory (Bildt, Sytema, Ketelaars, Kraijer, Mulder,
Volkmar, & Minderaa. (2004). . The combination of ADI-R and ADOS-G identifies AD
or PDD, as described in the DSM-IV-TR, most appropriately. Both instruments seem to
be of great value in the diagnostic process of PDD in children and adolescents with MR.
Early diagnosis is very important since the sooner the recommended orientation of
procedures is carried out, the more likely it is that such children will develop social and
communicative skills, and the less stereotyped their behavior will be (Bildt, Sytema,
Ketelaars, Kraijer, Mulder, Volkmar, & Minderaa. (2004). .
Several psychiatric conditions, both internalizing and externalizing, have been
documented in comorbidity with Asperger Syndrome (AS) and High Functioning Autism
(HFA) (Mazzone, Ruta & Reale, 2012). In this review we examine the interplay between
psychiatric comorbidities and AS/HFA. In particular, we will focus our attention on three
main issues. First, we examine which psychiatric disorders are more frequently
associated with AS/HFA. Second, we review which diagnostic tools are currently
available for clinicians to investigate and diagnose the associated psychiatric disorders
in individuals with AS/HFA. Third, we discuss the challenges that clinicians and
researchers face in trying to determine whether the psychiatric symptoms are phenotypic
manifestations of AS/HFA or rather they are the expression of a distinct, though
comorbid, disorder. We will also consider the role played by the environment in the
manifestation and interpretation of these symptoms. Finally, we will propose some
strategies to try to address these issues, and we will discuss therapeutic implications
(Mazzone, Ruta & Reale, 2012) .
Although Head Start has a mandate to serve children with disabilities as at least 10% of
its population, few systematic data are available on identification of children in various
disability categories in the years immediately following their preschool experience
(Forness, Ramey, Ramey, Hsu, Brezausek, MacMillan, Kavale & Zima, 1998). In an
extensive study, a team of researchers (Forness, Ramey, Ramey, Hsu, Brezausek,
MacMillan, Kavale & Zima, 1998) identified children in various disability categories in
the years immediately following their preschool experience.

29
Two cohorts of 4,161 children across 30 sites were followed through first grade as part
of a larger study on transition assistance in which at-risk status was assessed at the
beginning of kindergarten by developing research diagnostic criteria (RDC) for four
major special education categories using clinical cut-off points on language, achievement,
and social skills measures and indicators of speech or mental health problems on parent
interviews. The school identification of study participants in each RDC was determined
by a search of school archival records in the spring of first grade. It was found that only
26% of the children meeting RDC in the four major categories were identified by the
schools, and little concordance was observed among categories. Findings assume that
there was an under identification of children with emotional or behavioral disorders.
However, the identification of children with disabilities in the schools has changed
substantially, however, since the original studies evaluating Head Start, especially in the
largest and most controversial special education categories such as mental retardation
(MR), learning disabilities (LD), speech or language impairments (SL), and emotional
disturbance (ED) (U.S. Department of Education, 1995).
Scott at.el (2002) conducted a pilot and follow-up study of the preliminary development
of a new tool to screen for Asperger syndrome (AS) and related social and communication
conditions (the Childhood Asperger Syndrome Test, CAST) in children aged 4–11 years,
in a non-clinical setting. In the pilot study, parents of 13 children with AS and of 37
typically developing children completed the CAST. There were significant differences
between the AS and typical sample means. The pilot was used to establish preliminary
cut-off scores for the CAST. In the main study, parents of 1150 primary-school-age
children were sent the CAST, and 174 took part in the full data analysis. Results suggest
that compared with other tools currently available, the CAST may be useful for
identifying children at risk for AS and related conditions, in a mainstream non-clinical
sample.
2.8 The problem statement
Characteristic features of Asperger syndrome that predispose to criminal offending
(Berney, 2004):
i. An innate lack of concern for the outcome can result in, for example, an assault
that is disproportionately intense and damaging. Individuals often lack insight

30
and deny responsibility, blaming someone else; this may be part of an inability
to see their inappropriate behavior as others see it.
ii. An innate lack of awareness of the outcome that allows individuals to embark on
actions with unforeseen consequences; for example, fire-setting may result in a
building’s destruction, and assault in death.
iii. Impulsivity, sometimes violent, can be a component of comorbid ADHD or of
anxiety turning into panic.
iv. Social naïvety and the misinterpretation of relationships can leave the individual
open to exploitation as a stooge. Their limited emotional knowledge can lead to
a childish approach to adult situations and relationships, resulting, for example,
in the mistaking of social attraction or friendship for love.
v. Misinterpreting rules, particularly social ones, individuals find themselves
unwittingly embroiled in offences such as date rape.
vi. Difficulty in judging the age of others can lead the person into illegal
relationships and acts such as sexual advances to somebody under age.
vii. Overriding obsessions can lead to offences such as stalking or compulsive theft.
Admonition can increase anxiety and consequently a ruminative thinking of the
unthinkable that increases the likelihood of action.
viii. In formal interviews, misjudging relationships and consequences can permit an
incautious frankness and the disclosure of private fantasies which, although no
more lurid than any adolescent’s, are best not revealed.
ix. Lacking motivation to change, individuals may remain stuck in a risky pattern of
behaviour.
2.9 The Proposed DSIMCAS
The idea of DSIMCAS is the development of a screening instrument for children with
Asperger syndrome and its manual. The development of this instrument is proposed with
consideration that it is high time for early detection of Asperger syndrome children in
supporting the implementation of effective early intervention programs for children with
special needs. Appropriate intervention with support at early age could lead the child to
engage in learning process successfully. The right and effective instrument is needed for
early detection process. DSIMCAS is expected to produce the user-friendly instrument.
The data from this study are expected to be the initial figure of the young children with
Asperger syndrome in Malaysia.

31
The suitability and practicality of SIMCAS, is critically important if it is to be promoted
as a standardized instrument (after further research) and it can be used in child care
centers for early detection purposes. Overview of DSIMCAS is as in Figure 2.1.
Figure 1: Overview of DSIMCAS
The component of the DSIMCAS comprising mainly the information related to the
child’s behaviors. Particulars about parents, teachers/caregivers, childcare centers, and
institution related to ECCE are also relevant. Table 2.0 is describing about the
DSIMCAS.
Table 2.0: DSIMCAS components
Components Detail contents
ECCE target group Children 5 years old and below
Workshop Confirmatory Factor Analysis (CFA) & Rasch Model
Development Items of SIMCAS
Pilot testing Two tiers of pilot testing of SIMCAS items pilot
testing.
Tier 1 with trained & qualified educators in Autism at
IDEAS & NCDRC (for expert views via interview
with teachers for level of difficulties and constructs) –
UPSI.
Tier 2 with NASOM centers in Lembah Klang &
Ipoh.
Real data collection:
quantitative via
1,100 children in mainstream preschool were
identified via multistage random sampling procedure
and were observed by their classroom teachers and
PERMATA
ECCE
E
I
Early Detection Through Screening
OTHER AGENCIES
INTERVENTION

32
questionnaires –
SIMCAS
assessed. 1,041 questionnaires were returned (return
rate is 95% - 95% confidence interval with +/ - 3)
Analyses of data SPSS package
Qualitative data analyses – Verbatim & Major & sub
themes
Identification ECCE children with potential AS
The data derived from SIMCAS will benefit several stakeholders of ECCE field. Table
2.1 shows how SIMCAS will assist the stakeholders.
Table 2.1: SIMCAS Benefits’ to ECCE Field
Stakeholders Benefits
Government
(MOE)
i. Early childhood education planning
ii. special education policies
Teachers/childcare
takers
Early intervention planning
Parents Early detection
Institutions Teachers/caretakers qualifications and
competencies
DSIMCAS also able to generate reports related to insights in special educational needs
in ECCE. Table 2.2 shows some of the examples.
Table 2.2: Example of DSIMCAS Reporting.
Reports Type of reports
Instrument (SIMCAS) Training in implementation of SIMCAS;
Psychometric property;
Teachers/child caretakers Asperger
syndrome awareness level
Inclusive education and teachers’ training
Prevalent rate of potential Asperger
syndrome
Special education programme for children with
autism in Malaysia
Research in special education SIMCAS in assisting educators and childcare
takers in screening children with Asperger
syndrome?
2.10 Objectives of DSIMCAS
The establishment of DSIMCAS aims to fulfill two main objectives, namely:
i. develop and validate the instrument for screening children with Asperger
syndrome (SIMCAS) below 5 years old.

33
ii. generate comprehensive and integrated report for policy makers and intervention /
programme providers
iii. provide insights of the degree of AS related behaviors in children at five years old
and below based on statistical data and qualitative data
2.11 Scope of Study
The scope of this study explain in this section covers the objectives, methodology,
sampling and data collection as well as the framework of the quantitative and qualitative
data analyses.
2.12 Research Objectives
This study intent to develop and validate the instrument for screening Malaysian children
with Asperger syndrome for five (5) years old and below. The study aims to develop an
instrument and manual for screening of Malaysian children with Asperger’s syndrome at
the age of five years old and below. As this instrument intended to be utilized by the
Malaysia educators and childcare takers, this study will verify the extend the developed
instrument capable of assisting educators and childcare takers in screening children with
Asperger syndrome. Basic empirical statistics of Malaysian children with reference to
Asperger characteristics.
The collected data is expected to give insight of the tendency of children AS in age group
below 5 years old. The construction of the instrument will be based on a review that
provides an indication of the symptoms of Asperger’s. This will be incorporated within
the qualitative data (observation and interview) in order to seek new insights of the degree
of AS related behaviors in children at Tabika.
i. To review the standardized instrument for screening AS used at the international
level and discovering relevant facts from the experts and selected stakeholders
regarding evaluation of AS cases in Malaysia via:
a. Round-table discussion
b. Library search
c. Small scale seminar
ii. Field work:
The number and scoring of items chosen should be easier to manage.

34
2.13 Study Framework
Initially, the duration of this study is set for 12 months from 1st April 2015 to 31st
March 2016. However, the real study was approved and embarked in July 2015 and
extended to 21st November 2016 due to inevitable circumstances.

35
Chapter 3
Methodology and Instrumentation
3.0 Introduction
This study employed both qualitative and quantitative approach. At the initial stage of
the items development, focus group discussion (FGD) with early childhood practitioners
and caretakers was conducted to gauge in-depth understanding of what special needs
concepts is all about and knowledge and awareness related to Asperger Syndrome. In the
second stage of this study interview was conducted with NASOM educators to tap
insights related to autism and Asperger syndrome as experienced by these educators. The
final stage of this study is developing the items based on six (6) domains and
administering two pilot tests at special needs centers in Wilayah Persekutuan Kula
Lumpur and Perak. Finally, it involved real data collection at identified preschools via
stratified sampling procedure (at government-run preschools and private child-care
centers) throughout Peninsular Malaysia. This chapter discusses the methodology
employed by this study in detail.
3.1 Research Methodology
Mixed method study was utilized by this study. The framework is as displayed in the
Figure 2 below.
Figure 2: The Framework of The Study
DSIMCAS Quantitative data Qualitative data – Focus
Group Discussion (FGD) -
accomplished
1100 children (SIMCAS ) - Observed by 200 teachers /caregivers
Select 20 potential AS –
next study using
different research grant
Non potential AS Potential AS – 9
children identified
50 parents of children with potential AS
(to be conducted in the next study) Observations (20
selected children) - NIL
Interviews protocol
(respective parents and
teachers) -NIL

36
As illustrated in Figure 2 there are four instruments that is needed in the study. The
screening instrument (SIMCAS) will be used to collect quantitative data from
teachers/childcare givers and parents. The qualitative data will be collected through
individual and focus group interviews (FGD – using interview protocol) with selected
respondents (early childhood practitioners namely caregivers, teachers and parents) and
observation of children’s behavior. The items in the instruments intent to gain
quantitative data include demographic background, Asperger syndrome symptoms
exhibited by the child (as rated by their teachers/childcare givers).
Pilot studies will be carried out to determine the scoring profile of the instrument and
procedures developed for data collection. Eight (8) teachers/care givers from selected
programs will be involved in the pilot study. In pilot study 1, five teachers were involved
in the observation of children who have diagnosed from mild to severe autism at IDEAS’
Autism center, Rawang, Selangor and Tadika Bitara, NCDRC – UPSI childcare center.
Pilot study two (2) covered quite a number of NASOM childcare centers in the Klang
Valley and Ipoh, Perak. The teachers and childcare practitioners were required to observe
and rate the children whom they have known for at least six months. Test re-test
reliability study with two weeks’ interval was utilized by this study.
3.2 Sampling Procedure and Data Collection
Respondents for quantitative data collection are amongst teachers and caregivers. A
number of 200 teachers/caregivers are expected to do the rating for minimum of 10
children under their care. The collected data will be analyzed and the children (with
positive cut-off point) will be shortlisted for random sampling for participants of second
phase of the study, structured observations and interviews. A total of 22 children were
involved for observations and their teachers / caregivers will be interviewed (done during
the tier 1 pilot study). Table 3.0 show the sampling and data collection in this study.
Table 3.0: Sampling and Data Collection
Data Preschool/play
school Children
Teachers /childcare
givers
Parents
SIMCAS rating 1100 children (5 yrs and
below)
200 teachers/childcare givers
from permata negara centers
and other agencies
50 parents of children
rated by teacher as
potential AS – to be
conducted in the
follow-up study
Observation 20 children rated as
potential Asperger

37
syndrome (AS) – will be
conducted in the next
study using different
research grant
Interviews – next study 20 teachers/childcare givers
with potential AS children
20 parents with
potential AS children
3.3 Data Analyses Framework
Quantitative approach in the main data collection using Asperger syndrome screening
instrument will be analyzed using SPSS package. The distribution of the scores of each
item in the instrument is expected to give the pattern for subscale of behaviors related to
AS symptoms (derived using factor analysis). Statistical analyses are used to draw the
psychometric properties of the instruments.
Children rated with high score will be short listed for qualitative data collection and 20
children will be selected at random for observation. The data collected will be analyzed
using standard qualitative data analysis procedures.
3.4 Scope of Final Report
The final report will consist of;
i. The current scenario of special needs children in Malaysia – FGD findings –
RQ1
ii. Asperger syndrome in young children and the new diagnostic criteria via CFA
analysis (DSM- IV and DSM-V) – RQ2
iii. Terms of reference and objectives of study – items selected representing
Asperger attributes – Asperger Syndrome Screening Instrument and Manual
iv. Data analysis and findings
v. Implication of study – liability versus asset to the nation
vi. Recommendation and conclusion – this is preliminary findings, thus further
refinement of the DSIMCAS and testing on random and bigger sample are
necessary

38
3.5 DSIMCAS Team
The study team consist of research adviser, research leader, consultants (child
psychologist, language experts, special needs education, autism - Asperger Syndrome
experts), technical assistant, research assistants.
3.6 Research Team
Asst. Prof. Dr. Supiah Saad (Special Education-IIUM)
Asst. Prof. Dr. Khamsiah Ismail (Clinical Psychology – IIUM)
Assoc. Prof. Dr. Siti Rafiah Abd Hamid (Educational Psychology - UM)
Prof. Dr. Nik Ahmad Hisham Ismail (Social Psychology -IIUM)
Assoc. Prof. Dr Haniz Ibrahim (Special Education- UPSI)
Assoc. Prof. Dr.Nik Suryani Nik Abd Rahman (Maths Education - UM)
3.7 Project Steering Committee
The steering committee comprises of representatives from Ministry of Education and
UPSI. The study team reports directly to the committee chair person about the progress
of the study.
3.8 Pilot Study Report for Asperger Syndrome Screening Instrument
3.8.0 Introduction:
In developing this screening instrument, literature review (Scott, Cohen, Bolton, Brayne,
2002; Williams, Scott, Stott, et al., 2004; Mayes, Calhoun, Murray, Morrow, Yurich,
Mahr, Fauzia, Cothren, Purichia, Bouder, & Petersen, 2009; Robins, Fein, & Barton,
2009; Squires & Bricker, 2009; Helland, 2014) was undertaken to identify empirical
domains and constructs (reliable and valid) which represent Asperger Syndrome. In this
search six domains were identified and were later six constructs as explained in the
following section.
3.8.1 Domains and Construct in Asperger Syndrome Screening
Instrument
The items in Asperger Syndrome Screening Instrument were categorized into six
domains. They are:

39
i. Social - measures difficulties in reciprocal social interactions particularly the
ability and the desire to interact with same-age peers.
ii. Language - measures impairment in language skills. This domain is refers to three
areas which are difficulties in interacting with people and language processing;
iii. Interest and routine - measures limitation in interest and rigidity in routines, which
include rigidity in worldview, obsession and abilities in following routines and
order.
iv. Motor clumsiness - difficulties with motor functioning and planning that focus on
difficulties gross and fine motor skills respectively.
v. Cognitive issues - measures children ability to make inferences about what another
person is thinking; cognitive flexibility; impairment of imaginative play; visual
learning strength and specific strengths in cognitive areas.
vi. Senses sensitives - measures abnormalities of the senses an individual may have
which are visual, auditory, olfactory, tactile and gustatory areas respectively.
The following Table 3.1 provides details of the constructs found in each domain in
SIMCAS.
Table 3.1: Domain, Constructs & Items in SIMCAS
Domain Constructs No. of Constructs Items
1. Social Interaction i. Inability and/or a lack of desire to
interact with peers (1-i)
3 1 – 73 = 73
ii. Socially and emotionally
inappropriate behaviors (1-ii)
iii. Limited or abnormal use of nonverbal
communication (1-iii)
2. Language Skills i. Inability use to in interact
/communicate with other people, and
difficulties in semantic and poetic
language (2-i)
2 74 – 113 =
39
ii. Difficulties in language processing (2-
ii)
3. Interest & Routine i. limitation in interest and rigidity in
routines (3-i)
1 114 – 143 =
29
4. Motor Skills i. Difficulties with motor functioning
and planning that focus on difficulties
gross and fine motor skills (4-i)
1 144 – 156 =
12

40
3.8.2 Pilot Study
Prior to the actual study, pilot study were conducted at two special needs centers in
Selangor and Perak respectively. This procedure was conducted to establish the internal
consistency of the 213 items pilot-tested on a sample of n = 22 children aged between three
to nine years old from IDEAS Autistic Center, Rawang, Selangor and Tadika Bitara –
NCDRC – UPSI. The main intention of this study was to gauge experts’ views on what autism
is all about and also to tap information on high functioning autism among the children
observed. Most of the educators at IDEAS Autism Centre, Rawang are trained, experienced,
qualified and specialized in Autism. The items in the Asperger Syndrome screening
instrument were developed from Autism items and were adopted and adapted for the
Asperger Syndrome Screening Instrument. The internal consistency reliability / Cronbach’s
alpha obtained for pilot 1 was α = .77 and an alpha based on standardizing the items was α
=.77 classified under six domains (6).
Pilot study two (2) was conducted at the National Autism Society of Malaysia or NASOM
(basically in Klang Valley and Ipoh). Approximately 114 children in the centers were
observed by their class teachers who have known them for a minimum duration of 6 months.
The NASOM centers were selected because they are mainly managed by practitioners and
5. Cognitive Issues i. Ability to make inferences about what
another person is thinking - inability
to distinguish the relationship between
internal and external situations (5-i)
5 157 – 210 =
53
ii. Lack of cognitive flexibility – ability
to solve problems; engage in and
maintain mental planning; to exert
impulse control; to be flexible in
thoughts and actions, and to stay
focused on a goal until its completion
(5-ii)
iii. Impaired imaginative play - ability to
create and act out novel play
scenarios (5-iii)
iv. Visual learning strength (5-iv)
v. Specific strengths in cognitive areas
(5-v)
6. Senses Sensitiveness i. Visual areas (6-i)
ii. Auditory areas (6-ii)
iii. Olfactory areas (6-iii)
iv. Tactile areas (6-iv)
v. Gustatory areas (6-v)
41
volunteers who have vast experience in handling children with autism. As for the Asperger
Syndrome screening instrument, the items were adopted and adapted from Autism items
and were refined and validated for the Asperger Syndrome Screening Instrument. The next
step was to identify double-barrel items which were further breakdown, simplified and
translated from English language to Malay Language (Bahasa Malaysia) and back to
English (back translation) and became a bilingual survey. The idea of conducting “back
translation” is to keep the original meaning intact. Warwick and Osherson (1973) advised
researchers not only to get respondents’ answers but also to get the interpretation of the
meaning of the items, which are unclear to them. In addition to that, the pilot study was
intended to examine the relevancy of the items and terminologies found in the instruments .
The teachers at NASOM centers were also interviewed and consulted for the simplicity
and level of difficulties of the items found in the improved and refined instrument. In pilot
study 2, n = 114 and the six (6) domains remained intact. The internal consistency reliability
/ Cronbach’s alpha obtained for pilot 2 was α = .913 and an alpha based on standardizing the
items was α = .916.
3.8.3 Reliability Estimates of SIMCAS
The reliability of a measurement is indicated by its consistency (Shaughnessy & Zechmeister,
1997). In other words, reliability refers to the attribute of consistency in measurement
(Swerdlik, Sturman & Cohen, 2012). It indicates the degree to which a test consistently
measures whatever it is measuring (Gay, Mills & Airasian, 2012). Two types of reliability tests
to estimate the internal consistency of the scales. Cronbach alpha reliability coefficients were
used on the Asperger Syndrome Screening Instrument as this screening tool used Likert scales.
Items were deleted as the deletion increases the Cronbach alpha value of the scales, and
subsequently dropped from further analyses. Comparatively, data obtained from the two pilot
studies showed tremendous improvement in terms of its internal consistency reliability
estimates. Overall for the two pilot studies the instrument has a high internal consistency
reliability estimate value of α = .84. This suggests that all items are valid and reliable to
be utilized in the actual study. Reliability analysis was also conducted on the instrument
based on the six domains mentioned above. The results demonstrate high reliability indices
for all components that ranged from a low α = .65 to a high α = .77 (in pilot study 1).
Comparatively, in pilot study 2 the range of alpha is from a low α = .88 to a high α = .91
Refer Appendix 1 for details of the reliability indices of all items Table 3.2 below provides
summary of the alpha values of the instrument.

42
Table 3.2: Reliability Estimates of the Domains in SIMCAS for Pilot Study 1 & Pilot
Study 2
Domains Reliability
(α) for
Pilot Study
1
No.
of
Items
Reliability (α)
for Pilot
Study 2
No.
of
Items
1. Difficulty in Social
Interaction &
Communication
.753 43 .898 73
2. Impairment in Language
Skills
.734 34 .909 39
3. Narrow Range of Interest
& Insistence
.726 28 .900 29
4. Motor Clumsiness .725 12 .894 12
5. Cognitive Issues .766 51 .882 53
6. Sensory Sensitivities .652 39 .903 34
Overall (all items) .770 207 .913 240
3.8.4 Means and Standard Deviations
Descriptive analyses were employed to obtain means and standard deviation the
measures used in this study. Sum of the scores of each measure were computed and the mean
scores of each scale was obtained by dividing the sum of the total score with the number of
items in each of the respective scale. Table 3.3 summarizes the means and standard deviation
of the measures.
Table 3.3: Means and Standard Deviations for the Six Domains - Pilot Study 1
& Study 2
No. Domains Range of Means Range of Standard
Deviation
Pilot 1 Pilot 2 Pilot 1 Pilot 2
1. Difficulty in Social
Interaction
3.95 4.32 .976 1.57
2. Impairment in Language
Skills & Communication
4.28 5.00 1.71 1.94

43
3. Narrow Range of Interest
& Insistence
3.33 4.40 1.14 2.05
4. Motor Clumsiness 3.70 3.93 .965 1.82
5. Cognitive Issues 3.62 4.83 .765 1.81
6. Sensory Sensitivities 3.21 3.99 .921 1.87
Overall (all items)
3.8.5 Validity of SIMCAS Items
Validity concerns with the appropriateness of the interpretations made from the test (Gay, Mills
& Airasian, 2012). “Traditionally, validity has been defined as the extent to which a test
measures what is designed to measure” (Aiken, 2003, p. 94). In view of that, the concept of
validity refers to the appropriateness, meaningfulness, and usefulness of the specific inferences
from the test scores (American Psychological Association, 1985).
Four types of validity were determined for the measures utilized in for the purpose of
the this study: (1) face validity (2) content validity, (3) criterion-related validity, and (4)
construct validity.
3.8.6 Face Validity
Face validity “pertains to whether the test ‘look valid’ to the examinees, the administrative
personnel who decide on its use and other technically untrained observers” (Anastasi & Urbina,
1997). It refers to the degree to which a test appears to measure what it claims to measure (Gay
& Airasian, 2003).
Briefly, for face validity, the instrument used in this study was purposely developed for
measuring the traits of Asperger Syndrome among children and adolescents. Literature review
(Scott, Cohen, Bolton, Brayne, 2002; Williams, Scott, Stott, Allison, Bolton, Cohen, & Brayne,
, 2004; Mayes, Calhoun, Murray, Morrow, Yurich, Mahr, Fauzia, Cothren, Purichia, Bouder,
& Petersen, 2009; Robins, Fein, & Barton, 2009; Squires & Bricker, 2009; Helland, 2014)
have provided empirical evidences of the items. Determining face validity though is not a
psychometrically sound way of estimating validity. Hence, face validity of the instrument is
established.

44
3.8.7 Content Validity
Content validity concerns with whether the content of a test elicits a range of responses that are
representative of the entire domain, or universe skills, understandings, and other behaviours,
the test is supposed to measure (Aiken, 2003). Conceptually, this type of validity describes “the
degree to which a test measures the intended content area” (Gay & Airasian, 2003, p. 136).
Nonetheless, responses to the sample of items on a well-designed test are presumably indicative
of what the responses would be to the entire universe of behaviours of interest (Aiken, 2003).
As mentioned above, numerous literature reviews supports content validity established in the
instrument. This questionnaire including the translated version has been validated by two
experts (Dr. Haniz Ibrahim – UPSI and Dr. Supiah Saat - IIUM) who are senior lectures and
have doctorate degree in special educational need and have a lot of experience working in
numerous special education settings.
3.8.8 Construct Validity
Construct validity is the extent to which an instrument measures the construct that it is
intended to measure. This type of validity requires a definition with clearly specified
conceptual limits (Newman, 2002) and concerned with the primary attributes rather than with
the scores the instrument produces (Salkind, 2000). Analysis of validity using Pearson’s
bivariate correlations was performed on the data of pilot study to provide preliminary
evidence of convergent and discriminant validity of the instrument.

45
Table 3.4: IDEAS Autism Centre & Tadika Bitara (Pilot Study 1; n = 22)
**Correlation is significant at p = 0.01 level (2-tailed)
Table 3.4 and Table 3.5 demonstrate details of bivariate correlations of the constructs in
Asperger Screening Instrument from IDEAS and NASOM data respectively.
Result of the analyses shows that the correlations between the constructs range between r =
.526 p < .001 and r = .813 p = <.001 for Pilot Study 1. Consistently the results for Pilot Study
2 also demonstrates correlations of between r = .635 p < .001 and r = .821 p = <.001. In sum,
the result of bivariate correlation analysis indicates that the constructs in the instrument are
measuring different aspects in the spectrum of Asperger Syndrome.
Table 3.5: National Autism Society of Malaysia or NASOM (Pilot Study 2; n = 114)
1 - Social Interation and
Communication difficulties
2 - Language difficulties
3 - Limited interests and
rigidity in daily routines
4 - Motor Clumsiness
5 - Cognitive Issues
6 - Senses Sensitiveness
1 - Social Interaction & Communication difficulties
1.00 .78 .58 .64 .74 .53
2 - Language difficulties
.78 1.00 .56 .48 .75 .39
3 - Limited interests & rigidity in daily routines
.58 .56 1.00 .66 .68 .69
4 - Motor Clumsiness
.64 .48 .66 1.00 .76 .78
5 - Cognitive Issues .74 .75 .68 .76 1.00 .67
6 - Senses Sensitiveness
.53 .39 .69 .78 .67 1.00
** Correlation is significant at p = 0.01 level (2-tailed)
Domain Social
Interaction
Language &
Communication
Cognitive
Issues
Motor skills
(gross & fine)
Limited
interests
& Rigidity in
Daily Routines
Senses
Sensitiveness
Social Interaction
1.00 .63 .16 .65 .09 -.24
Language &
Communication
.63 1.00 .59 .61 .50 .23
Cognitive Issues .16 .59 1.00 .18 .45 .62
Motor skills
(gross & fine)
.65 .61 .18 1.00 .14 .20
Limited interests
& Rigidity in
Daily Routines
.09 .50 .45 .14 1.00 .58
Senses
Sensitiveness
-.24 .23 .62 .20 .58 1.00

46
4.3.10 Summary of Analysis
Results of the preliminary analysis of the instrument or rather pilot study involving 213 items,
categorized into six domains on 22 children in pilot study one (1) from two autism centres
indicated sound psychometric properties. The reliability indices of the domains are high enough
to suggest that all items can be utilized in the actual study. Similarly, in pilot study two (2)
which observed 214 children from NASOM centres in the KLang Valley and Ipoh, Perak and
engaging 240 items. As for construct validity, no correlation between the domains exceeds the
correlation value of .90 that could indicate pattern of multi-collinearity (Hair et al, 1998) among
the domain measured. This demonstrates that the domains are measuring different factors in
traits of Asperger.

47
Chapter 4 – Findings
4.0 RQ1 (FGD) Degree of AS related behaviours in Students as Perceived by Preschool
Practitioners
In addressing research question 1, a focus group discussion (FGD) was held with six educators
who were involved directly or indirectly with AS students. From the data analysis, seven
categories have emerged and they were further categorized into three general themes.
Table 4.0: Thematic analysis of Research Findings
Research
Question
Themes Categories
How do you
identify AS and
other disorders?
Difficulties in
identifying Asperger
Syndrome and other
disorders
Students’ attitude
Teachers’
knowledge on AS
and other
disorder
Useful information
from other sources
Parent as a source
of information
Subject learnt as
a source of
information
Cultural belief as
a source of
information
What do you know
about any
instrument for AS
and other
disorders?
Exposure to
instruments No specific
instrument
The need of
instrument
Some of the respondents had similar experiences in handling students with AS and
other disorders as well as the instruments, while others did not. It can be seen from
table below.

48
Table 4.1: General findings from Focus Group Discussion – FGD (Qualitative
Approach)
Themes Categories S
R
A
D
F
A
I
Z
P
U
S
D
Difficulties
in
identifying
AS and
other
disorders
Students’
attitude
Teachers’
knowledge
on AS and
other
disorder
X
X
X
X
X
X
X
Useful
information
from other
sources
Exposure to
instruments
Parent as a
source of
inforation
Subject
learnt as a
source of
inforation
Cultural
belief as a
source of
information
No specific
instrument
The need
of
instrument
X
X
X
X
X
X
X
X
X
X
X
X
X
X
4.1 DIFFICULTIES IN IDENTIFYING AS AND OTHER DISORDERS
There are two difficulties found by the educators in identifying Asperger Syndrome
(AS) and other disorders as summarized in Table 4.2 below.
Table 4.2: Difficulties in identifying AS and other disorders
Theme Categories
Difficulties in identifying
Asperger Syndrome and
other disorders
Students’ attitude
Teachers’ knowledge on AS and
other disorder

49
4.1.0 Students’ Attitude
One of the factors that the educators face difficulties in identifying the Asperger
Syndrome (AS) as well as its symptoms among their students is regarding the students’
attitude towards them. From the interview, it is believed that some of the students behave
differently in school as compared to the way they interact with their parents at home. It
can be illustrated through some of the respondents’ statement below. (Refer to the
Discourse Unit as attached in Appendix).
“Ha, dia jadi macam passive, orang kata behaviour yang kedua. Dia ada
dua, dua personality la. Lepas itu bila mak dia, kan haritu ada Report
Day kan, mak dia cerita kata kat rumah dia banyak sangat cakap sampai
ke malam. Tapi dia dekat sekolah dia diam…” (IZ/ DU 39)
From the above statement, it can be seen that the students show different acts in front of
the teacher at the school. It is undeniable that this kind of barrier would be faced by most
of the early childhood teachers as these students may perceive them as strangers in the
beginning of meeting. Hence, the teachers would also face difficulties when reporting to
the parents regarding their children’s progress at school. This is due to some of the
students are very responsive in doing their homeworks at home but they are not
responding to the teachers at the school during the lesson. It can be illustrated through
the statement below.
“Mungkin dia (ibu bapa) akan cakap, oh kenapa dekat sekolah jadi
macam ini. So macam bila ada, kita akan tahu selama ini yang kita ajar
budak itu dapat ke tak. Sebab tak semua budak yang akan jawab bila kita
tanya.” (FA/ DU 34)
This statement indicates that the teachers face difficulties in detecting any symptoms
from the students due to this incompatible information.
4.1.1 Teachers’ Knowledge on AS and Other Disorders
Throughout the focus group discussion, questions regarding teachers’ knowledge on the
AS and other disorders are also being asked by the researchers. Majority of the
respondents agree that they only know some of the symptoms of AS and other disorders
such as Autism Spectrum Disorder, and Dyslexia.
As for Autism Spectrum Disorder (ASD), the teachers’ knowledge about this can
be illustrated through the following statements.
“and personality budak tu pun kita dah tahu dia adalah Autism. Dia
dengan dunia dia sendiri, ha ikut dia lah…” (IZ/ DU 83)

50
Similarly, another respondent also noted the symptoms of ASD as described in the
following statement.
“Sampai lah sekarang still, masa dia 7 years old, dia still tak boleh jalan,
duduk atas wheel chair, itu memang yang very low functioning, memang
eye contact apa semua tak ada.” (PU/ DU 194)
Both of these statements show that the early childhood teachers do have some knowledge
about the ASD, but perhaps it is incomprehensive.
Other than that, some of the teachers also noted the symptom of Dyslexia however it is
interconnected with slow learner students. It can be described through the statement
below.
“Kadang-kadang macam tengok bila macam reading tu kan susah nak
dapat. Satu satu tu, macam, a i u, kadang-kadang kita ulang banyak kali
pun dia macam susah nak tangkap. Kadang-kadang macam dia tulis pun
macam terbalik, macam A terbalik,” (IZ/ DU 110)
Similarly, the teachers do have some knowledge regarding psychological disorder
particularly Dyslexia among children, yet it is confused with other learning disability.
Above all, majority of the respondents indicate that they have similar knowledge in
identifying the symptom of Asperger Syndrome (AS). It can be best illustrated through
the following statement.
“Yang saya faham it is one kind of Autism Spectrum disorder lah.
Because they have high functioning mild functioning. But this one
categorized under high functioning, not mild functioning, tak tahulah
kalau saya silap. Ada special interest, their problem is the communication
skill, no social interaction, no eye contact with people, lepastu dia tak
boleh pergi tempat yang ramai-ramai orang, semua ini. Basically that is
what I know lah. They are very very good in certain thing. And mostly tak
tahu kenapa they are very good in English, mostly kalau dia speak
English dia akan guna American slang.” (PU/ DU 170)
Based on this statement, some of the respondents indicate that AS is a type of Autism
Spectrum Disorder and some of them do not mention that AS is categorized under high
functioning. The teachers also notice that students with AS have very low eye-contact
with other people. Interestingly, majority of them noted similar concern on one of the
symptoms of AS which students with AS are believed to have high interest in one thing.

51
Regarding this matter, another example of students with AS who have special interest in
certain subject can be described as the following statement.
“Tapi dia akan ada satu benda yang akan show dia punya attention lain,
contohnya ada anak itu dia lebih kepada Math. So dia akan sangat expert
dalam Math.” (SD/ DU 93)
Other than Mathematics, students with AS are also being reported to be expert in other
subjects such as English, Music as well as Drawing.
Teachers’ knowledge on psychological disorder among children is quite important as it
may affect the education of these students. One of the respondents indicates about this
matter as stated in the statement below.
“Tapi masa dia tadika memang cikgu-cikgu tak tahu kan, so memang
selalu lah sampai report kata memang tak pay attention tak belajar tak
buat kerja, so all the negative remarks daripada cikgu-cikgu. Cikgu tak
tengok apa yang positif daripada dia. So memang focus on negative
negative remarks kan. Sampai dia jadi memberontak lah tak nak pergi
sekolah semua. So bila masuk Darjah 1, cikgu dekat situ dia ada PPKI
kan, so cikgu ni is quite aware pasal Dyslexia apa semua ini, so cikgu ni
observe lepastu cikgu ni inform kita punya kawan tu dia kata most
probably macam mana symptoms Dyslexia.” (PU/ DU 246)
Other than above information, majority of the respondents also mention that they are not
provided with training to cater these students. Therefore, there is a need for knowledge
regarding this matter especially among early childhood teachers so that the future of these
students will be guaranteed. Plus, early interventions could be carried out to these
students if the teachers become more aware of the symptoms.
4.3 USEFUL INFORMATION FROM OTHER SOURCES
Other than the teachers’ existing knowledge in identifying the symptoms of AS and other
disorders, they also reported to have some sources of information on the psychological
disorders. There are three sources of information about this matter as summarized in the
table below.

52
Table 4.3: Useful information from other sources
Theme Categories
Useful information from
other sources
Parent as a source of
information
Subject learnt as a source of
information
Cultural belief as a source of
information
4.1.2.0 Parent as a Source of Information
Based on the information given, some of the respondents indicate that they get the
information regarding the students’ background from parents. It means that parents bring
some documents regarding their children’s problem to these early childhood teachers so
that it would be easier for the teachers to cater these students in the classroom. It can be
illustrated through the following statement where one of the respondents claims to have
received the medical record from the parents.
“Parents tu sendiri, ha dia bawa lah dari segi medical record, and
personality budak tu pun kita dah tahu dia adalah Autism. Dia dengan
dunia dia sendiri, ha ikut dia lah…” (IZ/ DU 83)
“Saya kena isi, saya kena isi very detail, semua the symptoms of physical Other than
that, parents also need to fill up a form regarding their children in the enrolment day.
Statement below described about some of the details of the children.
development, social development, semua kan.” (PU/ DU 42)
It shows that the teachers are receiving some particular details about the students during
the beginning of the school. They also reported to have information regarding students’
interest from parents which may help them a lot in the learning session.
4.1.2.1 Subject Learnt as a Source of Information
Second source of information about any symptoms of AS or other disorders is through
revising the subject that these teachers have learnt during their Diploma. However, there
is only one subject that they have learnt regarding psychological disorders among
children. For example, one of the respondents describes about the subject in the following
statement.

53
“Apa yang penekanannya dalam subjek itu sendiri adalah kita identify ja
semua jenis disorder. Sebab kita ada disability dan disorder kan.
Disability kita senang sebab kita tengok dari segi physical, tapi kalau
disorder ini complicated lah sebab dia termasuk semua tu. Semua jenis
difficulty macam Dyslexia, Autism, ADHD and then dia complicated bila
dia bergabung, ADHD contoh nya macam Autism ataupun ADHD
campur Dyslexia.” (SD/ DU 153)
Other than this, they also reported to have learnt about early childhood education and
children development. Hence, some of the symptoms among the children are noticed by
these teachers in the school based on theories of various types of disorder.
4.1.2.2 Cultural Belief as a Source of Information
The last source of information regarding AS or any other disorders known by the teachers
is through the cultural belief. This is refers to Malay culture in explaining the causes of
any illness. According to one of the respondents, a pregnant mother must be careful in
speaking because it may affect the child after birth according to Malay culture. It can be
described through the statement below.
“Orang cakap, jangan cakap benda tak baik, so nanti effect pada anak.
Tu Malaysian punya, ye lah tu. Masa pregnant memang kena jaga kata-
kata perbuatan semua.” (SD/ DU 213)
Likewise, another respondent also indicates that there is a cultural belief among
Malaysian regarding the causes of an illness. The following statement described on how
marriage can be one of the reasons of any illness among children after birth.
“Kalau macam apa ni, what happen to my nephew ada orang tua-tua
cakap sebab ‘panas’. Sebab Puteri ni kahwin dengan Megat. Dia kata
‘panas’ tu. Tu anak jadi macam tu.” (PU/ DU 222)
Therefore, cultural belief also becomes an indicator of any disorder including AS among
children as stated by the teachers.

54
4.2 LEAST EXPOSURE TO INSTRUMENTS
The last theme that has derived from the focus group discussion is exposure to
instruments. This is refers to whether the teachers know any instrument especially
regarding the screening the symptoms of Asperger Syndrome (AS) and other disorders.
There are two categories under this general theme as summarized in the table below.
Table 4.4: Exposure to instruments
Theme Categories
Exposure to
instruments No specific instrument
The need of instrument
4.2.0 Unfamiliar to any related Instrument
Based on the information given by the teachers, they are reporting that there is only one
instrument that they had used in collecting the data about students’ background during
the Enrolment Day. For example, the early childhood teachers claim to have an
instrument as stated in the statement below.
“Dekat enrolment ini lah, memang ada. Kira tu first thing lah.”
(IZ/ DU 48)
The respondents claim that this instrument is used to identify the students’ health problem
during the Enrolment Day. They further say that the instrument contains the details on
students’ regular behaviour and special interest. This instrument is believed to be filled
up by the parents during that day.
However, some of them also indicate that there is no specific instrument for
screening the symptoms of AS and other disorders among these students. The teachers
are reporting about their observations on the children’s behaviour in the classroom which
can be illustrated in the following statement.
“Sebab kita tak dedahkan diaorang kepada instrument. Maybe setiap
centre itu instrument dia berbeza-beza kan. Jadi itulah yang kita boleh
beri dengan student kita. Jadi bila student ini ternampak oh ini early
symptoms of Dyslexia jadi bila dia berdepan dengan real experience, dia
syak… So apa dia perlu buat dia kena kumpul bukti. Evidences. Masa
Report Day dia kena tunjuk. Parents dia bukan based on dia punya
personal judgement tapi dia based on dia punya pemerhatian.” (SD/ DU
153)

55
This statement summarized that the early childhood teachers are not exposed to any kind
of instrument especially in screening the AS and other disorders. It also stated that these
teachers only do some observations on the students in the classroom and they will report
their observations to the parents later on.
4.2.1 The Need of Asperger Syndrome Screening Instrument
Based on the above information, it is believed that the early childhood teachers need to
be exposed to the instrument especially in doing screening the symptoms of AS and other
disorders among their students. Majority of the respondents agree that it would be a great
help if they are exposed to the instrument. The following statement indicates about the
need of instrument.
“Misalnya dapat membantu dari segi pendidikan budak-budak juga tapi
improve dia punya behaviour, emotional, semua. Dan dia akan memberi
membantu ibu bapa lebih faham lah. Tapi bagi saya okay lah bagus lah
dia punya semua tu.” (AD/ DU 199)
Above statement indicates that the instrument could help the development of the children
especially in terms of their behaviour and emotional as well as provide an insight for the
parents regarding the development of their children.
Some of the respondents agree that the instrument would provide an insight for the
parents as well, however some of them only stress on improving teachers’ knowledge
regarding AS and other disorders. It can be illustrated in the statement below.
“It is good untuk cikgu punya knowledge. Tapi bukan untuk cikgu share
dengan parents sebab dia macam taboo ya untuk cikgu nak sampaikan
kepada parents. Tapi bila dengar kata daripada expert daripada HKL tu
balik, it takes time for him to accept. Sampaikan *marah marah doctor
tak boleh terima, so apatah lagi kalau daripada cikgu.” (PU/ DU 207)
Therefore, the usage of the instrument should be only among the teachers as to gain some
insight regarding the AS and other disorders as well as to improve their skills in dealing
with these students.

56
4.3 RQ2: Quantitative – Confirmatory Factor Analysis (CFA) – Validating the
Factors
Research question 2 was meant to develop and validate the instrument for screening
children with Asperger syndrome below 5 years old. The following is the structure of
Research Question 2:
“To what extent is the screening instrument developed capable of assisting educators
and childcare takers in screening children with Asperger syndrome?”
To address Research Question 2, a series of Confirmatory Factor Analyses (CFA) have
been carried out to validate all the constructs. The constructs are as follow and
accompanied by formulated hypotheses:
(i). Social and Language were combined as a four-factor construct. Thus, the alternative
hypotheses were formulated as the following and further tested.
HA: Social and Language interactions is a four-factor measurement model.
HB: The four-factor measurement model of Social and Language interactions fits
across two sets of data
(ii). Cognitive difficulties are a three-factor model. Thus, the alternative hypotheses
were formulated as the following and further tested.
H2A: Cognitive difficulties is a three-factor measurement model
H2B: The three-factor measurement model of Cognitive difficulties fits across two
sets of data.
(iii). Senses Sensitiveness is a five-factor model. Thus, the alternative hypotheses were
formulated as the following and further tested.
H3A: The Senses Sensitiveness construct is a five-factor measurement model
H3B: The Senses Sensitiveness measurement model fits across two sets of data.
(iv) Limited Interest and Rigidity in Daily Routine, thus the hypotheses were formulated
as the following and further tested.
H4A: Limited Interest and Rigidity in Daily Routine is a two-factor model
(v) Motor Clumsiness or difficulties is a two-factor model.
H5A: Motor clumsiness is a two-factor model

57
H5B: The motor clumsiness two factor model fits in both data sets
The following Table 4.5 tabulates the 6 domains and constructs:
Table 4.5: Domains and Constructs of this study
Constructs Section Domains No.
of
Items
Social IA Difficulties in Social
Interaction
13
IB Socially and
Emotionally
Inappropriate Behavior
4
IC Limited or Abnormal
Use of Non-Verbal
Communication
9
Language
Limited
Interests &
Rigid
Routines
IIA Difficulties in Oral
Communication
5
IIB Difficulties in Semantic
and Poetic Language
5
IIC
Difficulties in Language
Processing
6
IIIABC Worldview, Interests,
Regulations & Routines
10
Psychomotor IVAB Retardation in Motor
Development - Gross
and Fine Motor Skills
10
Cognitive VA "Buta Minda" Inability
to relate to internal and
external situations
5
VB Lacked of Cognitive
Flexibility - lacked
focus - Rigid - one way
of problem solving
14
VC Cognitive Issues - Weak
Imaginative Play
4
VD Strength in Visual
Learning
5
VE Specific Cognitive
Strengths
5
Senses VIA Difficulties in Sight 4
VIB Difficulties in
Managing Sound
5
VIC Difficulties in Olfactory
Aspects
5

58
VID Difficulties in Touch 10
VIE Difficulties in
Managing Sense of
Taste
11
4.3.0 Validating the instrument of Asperger Syndrome in Social and Language
Difficulties
HA: Social and Language interactions is a four factors measurement model has been
accepted
The instrument measuring Asperger Syndrome (AS) specifically detecting social and
language difficulties has been postulated to be in four constructs namely lack of interest
to interact with peers, showing inappropriate behaviors socially and emotionally, having
abnormality in non-verbal communication and difficulties to communicate from the
aspects of semantic and poetic language.
Based on the inability to interact, three items were detected to explain the
construct of lack of interaction with IA2a (unable to interact orally – inefficient in using
language in social communication); IA2b (lacked of skills in initiating communication);
and IA2c (unable to understand the flow of discussion). IA2b (lacked of skills in initiating
communication) determines the highest squared multiple correlations which indicates the
highest contribution of 82.4% to the construct. IBa (display of strange behaviors), IBc
(passing inappropriate remarks) and IBd (display anger when someone disobey the rules
and regulations) explain inappropriate behavior. IBc contributes to the next highest
explanation of inappropriate display of social behavior marked by 68.8%. IC1b (unable
to understand body language), IC1c (facial expression doesn’t correlate well with
emotional display), IC1d (lacked of facial expression when communicating with others)
and IC1e (unable to understand others’ facial expressions) determine difficulties in
abnormal non -verbal communication. ICId (lacked of facial expression when

59
communicating with others) contributes to the highest explanation of the construct with
72.5%.
The last construct (weak in communicational skills) is determined by four items namely
IIDa (unable to distinguish relevant from irrelevant information during information
processing), IIDc (easily irritated by surrounding stimulants), IIDd (late in responding to
questions asked) and IIDe (difficult to stay focused). IIDd (late in responding to questions
asked) indicates the highest explanation with 74.1% to its construct. The correlations
show distinct factors where they fall below .85 as suggested by Hair,et.al. (2005). Thus,
the factors in the hypothesized model have accomplished discriminant validity. However,
it is imperative for the researchers to address the factors seriously as “difficulties in
language processing” and “abnormality in non-verbal” as they are considered weak with
a high association of .806. This indicate that some closely related factors may tend to
measure similar construct. Thus, future research needs to address the matter and more
empirical evidence is needed to further validate the findings.
Table 4.6: Factor Loading
Items Factor/construct Loadings
IA2a lack to interact .853
IA2b lack to interact .908
IA2c lack to interact .815
Iba inappropriate behaviour .519
IBc inappropriate behaviour .830
IBd inappropriate behaviour .705
IC1b abnormal nonverbal .831
IC1c abnormal nonverbal .766
IC1d abnormal nonverbal .851
IC1e abnormal nonverbal .833
IIDa difficult in language_ processing .716
IIDc difficult in language_ processing .726
IIDd difficult in language_ processing .861
IIDe difficult in language_ processing .840

60
Table 4.7: Correlations between factors/constructs
Factors correlations
abnormal
nonverbal <-->
difficult in language_
processing .806
inappropriate
behaviour <--> abnormal nonverbal .555
lack to interact <--> inappropriate behaviour .392
inappropriate
behaviour <-->
difficult in language_
processing .564
lack to interact <--> difficult in language_
processing .626
lack to interact <--> abnormal nonverbal .655
HB: The four-factor measurement model of Social and Language interactions fits in
both sets of data has been accepted.
The comparison of results reveals a slight change in normed relative chi-square with
group 2 (500 sample size) is higher than group 1 (537 samples). The results have
proven that by cross validating with another set of data yield almost similar results that
satisfy the model fit for a four-factor model of Asperger Syndrome in social and
language difficulties.
Table 4.8: RMSEA, CFI, TLI & CMIN/df
Group 1 Group
2
RMSEA .77 .68
CFI .951 .950
TLI .937 .936
CMIN/df 4.14 4.89

61
Table 4.8: Confirmatory Factor Analysis (CFA) for Group 1 & Group 2
CFA in group 1 CFA in group 2
4.3.1 Validating the instrument of Asperger Syndrome in Cognitive Difficulties
H2A:cognitive difficulties is a three factor measurement model has been accepted.
The construct of Mind Blindness is denoted by perceiving the world in black and white;
demonstrated lack of empathy towards others; don’t realize words can hurt other
people; not realizing the word forgiveness means a lot to people.
The construct of lack of cognitive flexibility is determined through the items related to
having difficulties in organizing skills and how to do it; difficulties in arrangement and
sequences; and difficult to take instructions.
The construct of imagination in playing games is determined through the items include
attempt by others to change the game is opposed strongly; involve in imagination of
lack to interact
inappropriate behav
abnormal nonverbal
.73
IA2a e1.85
.82
IA2b e2.91
.66
IA2c e4
.81
.27
IBa e5.52
.69
IBc e7.83
.50
IBd e8
.71
.69
IC1b e10.83 .59
IC1c e11.77
.73
IC1d e12
.85
.69
IC1e e13
.83
difficult in language
processing
.51
IIDa e19.72
.53
IIDc e21.73
.74
IIDd e22
.86
.71
IIDe e23
.84
p=.000
rmsea=.077
cfi=.951
tli=.937
.81
.56
.39
.56
.63
.66
lack to interact
inappropriate behav
abnormal nonverbal
.77
IA2a e1.88
.76
IA2b e2.87
.80
IA2c e4
.89
.47
IBa e5.68
.78
IBc e7.88
.47
IBd e8
.68
.75
IC1b e10.87 .72
IC1c e11.85
.80
IC1d e12
.90
.72
IC1e e13
.85
difficult in language
processing
.57
IIDa e19.76
.74
IIDc e21.86
.75
IIDd e22
.86
.79
IIDe e23
.89
p=.000
rmsea=.088
cfi=.950
tli=.936
.78
.64
.61
.52
.67
.71
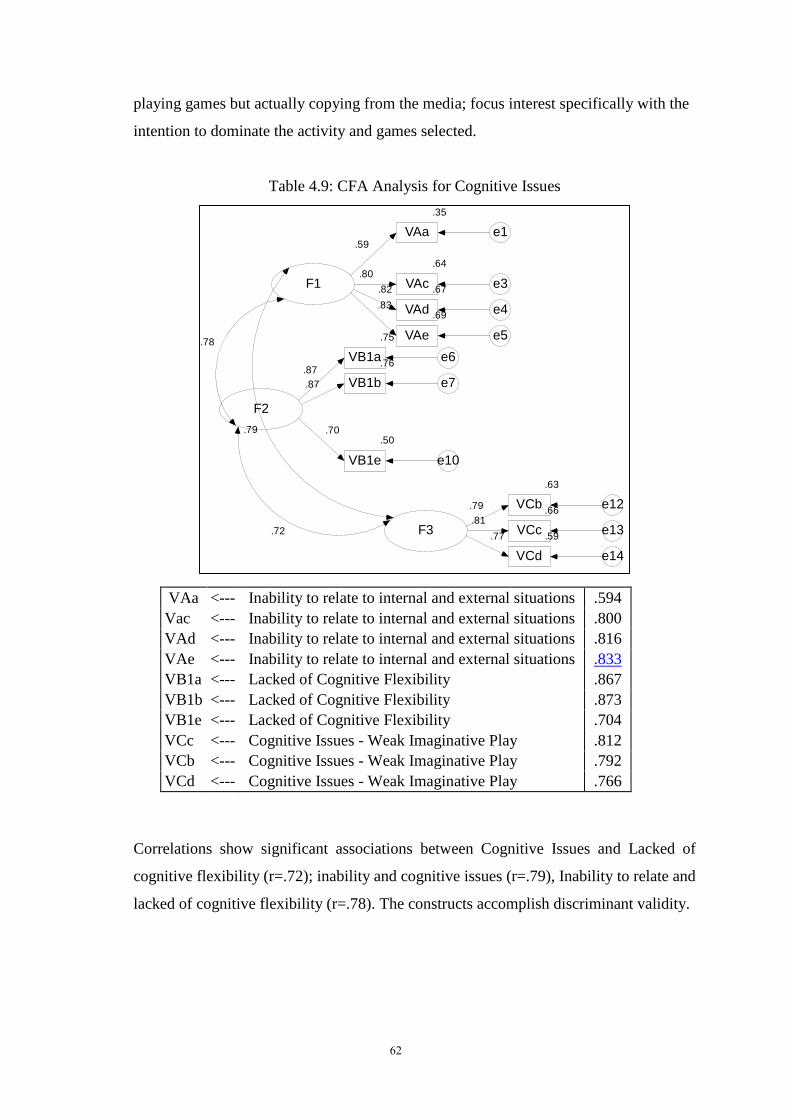
62
playing games but actually copying from the media; focus interest specifically with the
intention to dominate the activity and games selected.
Table 4.9: CFA Analysis for Cognitive Issues
Correlations show significant associations between Cognitive Issues and Lacked of
cognitive flexibility (r=.72); inability and cognitive issues (r=.79), Inability to relate and
lacked of cognitive flexibility (r=.78). The constructs accomplish discriminant validity.
F1
.35
VAa e1.59
.64
VAc e3.80
.67
VAd e4
.82
.69
VAe e5
.83
F2
.75
VB1a e6.76
VB1b e7
.50
VB1e e10
.87
.87
.70
F3
.63
VCb e12.66
VCc e13.59
VCd e14
.79
.81
.77.72
.78
.79
VAa <--- Inability to relate to internal and external situations .594
Vac <--- Inability to relate to internal and external situations .800
VAd <--- Inability to relate to internal and external situations .816
VAe <--- Inability to relate to internal and external situations .833
VB1a <--- Lacked of Cognitive Flexibility .867
VB1b <--- Lacked of Cognitive Flexibility .873
VB1e <--- Lacked of Cognitive Flexibility .704
VCc <--- Cognitive Issues - Weak Imaginative Play .812
VCb <--- Cognitive Issues - Weak Imaginative Play .792
VCd <--- Cognitive Issues - Weak Imaginative Play .766

63
H2B: The three-factor measurement model of Cognitive difficulties fits across two sets
of data.
The hypothesis has been accepted since both data accommodates the model with only a
slight difference for all the indices tested.
Table 4.10: Goodness of Fit for Cognitive Issues Across 2 Groups of Data.
Group IFI TLI RMSEA CMIN/DF
1 .962 .946 .084 4.741
2 .986 .981 .058 2.666
CFA in
CFA in group 1 CFA in group 2
4.3.2 Validating Senses Sensitiveness – It is initially a five-factor model. Thus,
the alternative hypotheses were tested.
H3A: The Senses Sensitiveness construct is a five-factor measurement model
The factors or constructs involve “difficulties in vision, hearing, smell (olfactory),
touch, and taste”.
The construct of difficulties in vision include “not having sharp vision, avoid confronting
eyes to eyes and difficulties to stand too close with others”.

64
The construct of hearing is determined by “closing eyes when hearing something, show
extreme fright when hearing unexpected sound, not able to focus when hearing
unexpected sounds; not able to focus when a few sounds are at similar time, purposely
run away from sounds and lastly scared of specific sounds”.
The construct of difficulties in smell is indicated by the items of can detect certain smell
when it is strong and unpleasant, can sense the smell faster than others; must smell certain
thing before using it. The construct of difficulties in touch shows the items difficult to be
touched and pinched; show anxiety when touch something at sudden; and difficult with
plated short or with tagging.
The construct of difficulties in taste is determined by making limited choice of food, only
accept food with certain texture and colour and must touch the food before eating.
Table 4.11: Senses Sensitiveness
Table 4.12: Correlations Across constructs of
Senses Sensitiveness
Codes Items Loadings
VIAa <--- Difficulties in vision .717
VIAb <--- Difficulties in vision .803
VIAc <--- Difficulties in vision .686
VIBa <--- Sensitive to noise .756
VIBb <--- Sensitive to noise .853
VIBc <--- Sensitive to noise .852
VIBd <--- Sensitive to noise .876
VIBe <--- Sensitive to noise .855
VICa <--- Sense of smell .706
VICc <--- Sense of smell .757
VICe <--- Sense of smell .857
VIDa <--- Sense of touch .863
VIDb <--- Sense of touch .832
VIDe <--- Sense of touch .725
VIEa <--- Sense of taste .725
VIEb <--- Sense of taste .877
VIEc <--- Sense of taste .724
F1 <--> F2 .629
F2 <--> F3 .547
F3 <--> F4 .560
F4 <--> F5 .644
F3 <--> F5 .512

65
No correlation is found to be more than .08. Thus, all the constructs are discriminant.
H3B: The Senses Sensitiveness measurement model fits across two sets of data
Table 4.13: Goodness of Fit for Senses Sensitiveness
Group IFI TLI RMSEA CMIN/DF
1 .930 .912 .085 4.582
2 .944 .929 .078 4.566
Both models have shown goodness of fit where only a slight change in fit indices. The
items were detected to show similarities in both models.
CFA in group 1 CFA in group 2
F2 <--> F5 .493
F1 <--> F5 .571
F1 <--> F3 .488
F2 <--> F4 .641
F1 <--> F4 .730

66
4.3.3 Validating – Rigidity, Limited Interest & Daily Routine
H4A: Rigidity, Narrow Range of Interest and Daily Routine - A three-factor
measurement Model has been accepted.
The rigidity, limited interest and daily routine construct are explained by three measurement
factors which are: a) rigidity in the thinking process, b) limited interests, and c) inability to
adhere to rules and daily routines.
In general, behavioral rigidity refers to a child’s difficulty in maintaining appropriate
behavior in new and unfamiliar situations. The opposite of rigidity would be flexibility,
which enables children to shift effortlessly from task to task in the classroom, from topic to
topic in conversation, from one role to another in games, etc.
Rigidity can also affect thinking. Cognitive rigidity occurs when the child is unable to
consider alternatives to the current situation, alternative viewpoints, or innovative solutions to
a problem. The child with rigid thinking tends to view things in “either-or” terms (e.g., things
are either right or wrong, good or bad). He or she wants concrete, black and white answers.
The “gray areas” of life are very uncomfortable (e.g., often has an exact way of doing things
with no variations).
Children with Asperger’s (AS) and High-Functioning Autism (HFA) often demonstrate
extreme forms of rigidity or inflexibility. This may manifest itself as (a) difficulty
ending an intense emotional feeling, (b) making transitions during the school day (e.g.,
from lunch back to the classroom), and (c) tolerating changes in schedules or everyday
routines.
Children with Asperger Syndrome display narrow range of interests and insistence on
Set Routines – These set of attributes address the Aspergers child’s rigidity, obsessions,
perseverations, and need for structure/routine/order. Rules are very important as the
world is seen as black or white:
i. Takes perfectionism to an extreme — one wrong answer is not tolerable, and
the child must do things perfectly
ii. Has difficulty with any changes in the established routine
iii. Has a set routine for how activities are to be done
iv. Has rules for most activities, which must be followed (this can be extended to
all involved)
Children with Asperger syndrome too have few interests, but those present are unusual
and treated as obsessions:
i. Patterns, routines, and rituals are evident and interfere with daily functioning
(note: this is driven by the child’s anxiety; the world is confusing for her; she is
unsure what to do and how to do it; if she can impose structure, she begins to
have a feeling of control)

67
ii. Has developed narrow and specific interests; the interests tend to be atypical
(note: this gives a feeling of competence and order; involvement with the area
of special interest becomes all-consuming)
iii. Displays rigid behaviour
Findings for goodness fit of model for group 1 and group 2 via CFA analysis is
tabulated as the following Table 4.14.
Table 4.14: Goodness of Fit for the three factors measurement model of
Rigidity, Limited Interests & Daily Routines
Group IFI TLI RMSEA CMIN/DF
1 .930 .931 .090 5.33
2 .980 .966 .080 4.22
The correlation of items across three constructs are tabulated in Table 4.15 below.
Table 4.15: Correlations Across Constructs of Rigidity (F1),
Limited Interest (F2) & Daily Routines (F3)
Codes Items Estimate
IIIAa <--- F1 .73
IIIAb <--- F1 .86
IIIBa <--- F2 .69
IIIBb <--- F2 .71
IIIBc <--- F2 .75
IIIBd <--- F2 .77
IIIBe <--- F2 .76
IIICa <--- F3 .75
IIICb <--- F3 .77
IIICc <--- F3 .82

68
Group 1
RIGIDITYIIIAa e1
.73
IIIAb e2.88
INTEREST
IIIBa e3.69
IIIBb e4.71
IIIBc e5.75
IIIBd e6
.77
IIIBe e7
.76
ROUTINES
IIICa e8.75
IIICb e9.77
IIICc e10.82
.84
.81
.77

69
Group 2
Figure 3: Three Factors Model for Limited Interests & Rigidity in Daily Routines for
Group 1 and Group 2
H4B: The Limited Interests, Rigidity and Daily Routines constructs as a three factor
model fits in both data sets has been accepted based on overall results. However, the
results are weak due to relative chi-squared (CMIN/DF) for group 1 is greater than
accepted threshold value of less than 5.00. Further RMSEA values for both groups are
within the acceptable low and high range. The correlation remains high at .084 for group
2. Thus, the three-factors model is relevant to be explained by the items and factors
involved.

70
4.3.4 Validating - Motor Clumsiness or difficulties is a two-factor model.
H5A: Motor clumsiness is a two-factor model has been accepted.
Motor clumsiness is explained by two factors namely “difficulties in rough motor
skills” and “soft and delicate motor skills”. The items of “awkward body movement
when moving, difficulties in catching and throwing ball, difficulties in body
coordination explain the rough motor skills”. The soft motor skills are explained
through the “difficulties in writing, holding pen or pencil, and too fast in completing a
task”.
Table 4.16: Correlations Across Constructs of Motor Clumsiness
Codes Items Estimate
IVAa <--- F1 .688
IVAc <--- F1 .886
IVAd <--- F1 .904
IVBa <--- F2 .814
IVBb <--- F2 .891
IVBc <--- F2 .660
Correlation between both constructs is .85 (highly correlated). The constructs are not
discriminant and the hypothesis of two factor model can be rejected.
H5B: The motor clumsiness as a two factor model fits in both data sets has been accepted
based on overall results. However, the results are weak due to relative chi-squared for
group 2 is greater than accepted value of less than 5.00. Further RMSEA also shows
greater than expected value of less than .08 in group 2. The correlation remains high at
.084 for group 2. Thus, the two-factor model is not relevant to be explained by the items
and factors involved.
Table 4.17: Goodness of Fit – Motor Clumsiness
Group IFI TLI RMSEA CMIN/DF
1 .985 .971 .084 4.811
2 .967 .982 .098 5.815

71
CFA in group 1 CFA in group 2
4.4 RQ3 : Estimating the Prevalence Rate of Asperger Syndrome Among Malaysian
Mainstream Children
In addressing research question three, ie. to estimate the prevalence rate of children with
potential Asperger Syndrome, new criteria have been set to ascertain the Single Spectrum but
Significant Individual Variability which is based on DSM 5. The criteria include:
i. Severity of ASD Symptoms
ii. Pattern of Onset and Clinical Course
iii. Etiologic factors
iv. Cognitive abilities (IQ)
v. Associated conditions

72
Under the current DSM-5, the diagnosis of autism requires that at least six developmental and
behavioral characteristics are observed, that problems are present before the age of three and
that there is no evidence of certain other conditions that are similar.
There are two domains where people with ASD must display persistent deficits namely:
i. challenges with social communication and social interaction
ii. restricted and repetitive patterns of behavior
Specifically, people with ASD must demonstrate (either in the past or in the present) deficits in
social-emotional reciprocity, deficits in nonverbal communicative behaviors used for social
interaction and deficits in developing, maintaining and understanding relationships. In
addition, they must show at least two types of repetitive patterns of behavior, including
stereotyped or repetitive motor movements, insistence on sameness or inflexible adherence to
routines, highly restricted, fixated interests, hyper or hypo reactivity to sensory input or unusual
interest in sensory aspects of the environment. Symptoms can be currently present or reported
in past history.
4.4.0 Setting the SIMCAS Benchmark
Before embarking on this study, the rule thumb was set in that the preschool teachers need to
know the children under observation not less than six (6) months. Further, based on the 6 points
Likert Scale in SIMCAS, any child with a score on the SIMCAS’s item between the Likert
Scale of 5 and 6 were taken into consideration as having the AS criteria whereas the score of 1
through 4 are considered as free from the established norms of Asperger Syndrome. The cut-
offs points were chosen from each item to be calculated to approximately 0 .7% of the children
undertaken by the study. In one epidemiological study estimating a population prevalence rate
of 0.7% (Ehlers, Gillberg, 1993) in a clinical work-up - a minimum prevalence of 3.6 per 1.000
children (7-16 years of age) was adopted using Gillberg and Gillberg's criteria and a male to
female ratio of 4:1. This also includes suspected and possible Asperger syndrome cases, the
prevalence rose to 7.1 per 1.000 children and the male:female ratio dropped to 2.3:1. These
findings are discussed as they relate to previously published results in the field and to findings
obtained using Szatmari et al.’s and ICD -10 draft criteria for the disorder (Ehlers S, Gillberg
C. (1993).

73
Criteria for Screening Asperger Syndrome follows the “Golden Standard” namely:
i) Difficulties in social interaction and communication.
ii) Limited interests and rigidity in daily routines.
iii) Display normal cognitive and language development
iv) Difficulties in gross and fine motor skills
v) Senses sensitiveness
(cited in the American Psychiatric Association, 2000; Szatmari, Bremner, Nagy,1989;
Gillberg & Gillberg, 1989).
In this study, the SIMCAS is a 44-item rating scale that requires the respondent to indicate the
presence or absence of behaviors indicative of Asperger syndrome. The SIMCAS contains five
subscales:
i. Social Interaction and Communication,
ii. Difficulties in Language development (excluded in the final calculation of AS),
iii. Limited Interests and Rigid Daily Routines (were included back again)
iv. Gross and Fine Motor Difficulties
v. Cognitive Issues (excluded in the final calculation AS),
vi. Sensory Sensitiveness
All raw scores were added (by excluding scores for Cognitive issues and Language
Development domains which must yield zero “0” score) within the six (4) domains. The items
were added (using SPSS -summation notation analysis) for the entire scale to yield an Asperger
Syndrome scores.
Findings from this analysis indicated that of the 1041 respondents examined by this study, 9
children (8 Males:1 Female) were identified as having the potentials of Asperger Syndrome
criteria. The prevalence rate is 0.86% which is slightly higher that rate found by other studies.
Hence, another follow-up study employing bigger sample size which includes Sabah and
Sarawak has to be undertaken. This must also include interview with the children identified as
having Asperger Syndrome potentials.

74
4.4.1 Reliability & Validity of the SIMCAS
Table 4.17 tabulates the SIMCAS’s internal consistency rate for each construct.
Table 4.18: The SIMCAS Internal Consistency
4.4.2 Benchmark for ISSAK / SIMCAS
DSM-IV criteria for Asperger Syndrome (AS) was used as the yardstick against which the
SIMCAS was evaluated. The development of screening questionnaires is important because all
diagnostic interviews involve a lengthy assessment those who are highly likely to have an AS
go through this diagnostic process. SIMCAS was developed for possible cases of Asperger
Syndrome in Malaysia. But this screening questionnaire is a non-clinical instrument designed
for use with young children (3-5 years) and is a user-friendly for preschool educators and
parents alike.
i. Educational services to assess for the possibility of Asperger Syndrome screening at
an early stage
ii. able to identify those children who are most likely to have potential AS
iii. results should support the SIMCAS as a useful screening instrument in school settings
for early identification.
iv. SIMCAS has acceptable properties to allow it to be used as a screening instrument in
educational settings
TOTAL
SIMCAS
Social
interaction
Language Interest Motor
development
Cognitive Sensory
No of cases 1041 1041 1041 1041 1041 1041 1041
No of items
(clean set)
44 9 3 0 6 9 17
Alpha .94 .84 .82 .80 .86 .89
No of item
(Original set)
130
items
26 items 16 items 10 items 10 items 33 items 35 items
.99 .96 .95 .92 .95 .95 .97

75
Table 4.18: Determining Criteria & AS Potential - Identified via SIMCAS (30 items sample –
Malaysian Study)
Criteria (N=1041) N % _ve Notes
1. No of cases without language symptoms
(without score 5 or 6) 26 items
628 60.3 413 0
1-16
2. No of cases without cognitive symptoms
(without score 5 or 6) 33 items
420 40.3 621 0
1-32
3. No of cases with at least 2 symptoms in Social
interaction (with score 5 or 6) 10 items
373 35.8 668 0-1
2- 10
4. No of cases with at least 1 symptoms restricted
interest, obsessive, etc.
(with score 5 or 6) 45 items
317 30.5 724
No of students with all in criteria 1- 4 9 0.86 1032
4.5 Summary of Findings for RQ1, RQ2 & RQ3
In summary, several conclusions can be derived from the data analysis in chapter 4 and it
is simplified in Table 4.19. Similarly, the recommendations are suggested side by side for
the ease of reading:
Table 4.19: Summary of Findings for RQ1, RQ2 & RQ3
Research
Questions
Findings
RQ1:
Focus
Group
Discussion
(FGD)
Major Themes:
4.5.1 Difficulties in identifying
Asperger Syndrome and other
disorders
4.5.2 Useful information from other
sources
4.5.3 Exposure to instruments
Sub Themes:
a) Students’ attitude
b) Teachers’ knowledge
on AS and other
disorder
a) Parent as a source of
information
b) Subject learnt as a
source of information
c) Cultural belief as a
source of information
a) No specific instrument
b) The need of screening
instrument user-

76
friendly for parents
and teachers alike
RQ2:
Development
of DSIMCAS
Validating
The domain &
items
i. High internal consistency rate for the
two studies:
ii. Confirmatory Factor Analysis (CFA)
indicted that:
iii. Items clustered under the six
domains – analyzed & reduced via
CFA & identified using Malaysian
norms are:
a) Pilot study 1 at IDEAS
Rawang & Tadika
Bitara (n = 22; α =
.77)
b) Pilot study 2 –
NASOM Centers (n =
114; α = .93).
a) Motor Clumsiness is a
2 Factor(s)
measurement model &
constructs include:
difficulties in gross &
fine motor skills.
b) Limited in Interests &
Rigidity in daily
routines is 2 Factor(s)
model -
c) Cognitive Issues is 3
Factor(s) Measurement
Model & Constructs
include; Mind
Blindness (,); Lacked
of Cognitive
Flexibility (,) &
Imaginative Play (,)
d) Difficulties in Social
Interaction &
Language processing
(combined) is a 4
factor(s) model.
e) Senses Sensitiveness
is a 5 Factor(s) model.
RQ3:
Crosstabulation
& Percentages
i. Prevalence rate for potential
Malaysian children with Asperger
Syndrome.
iii. Breakdown / Ratio of male: female.
- The prevalence rate is
0.86% which is
slightly higher that rate
found by other studies.
- Findings from this
analysis indicated that
of the 1041
respondents examined
by this study, 9
children (8 Males :1
Female) were found
having the potentials
of Asperger Syndrome
criteria.

77
Chapter 5
Discussion & Recommendation
5.0 Introduction:
This study was undertaken when the existence of Asperger Syndrome instrument based
on Malaysian norms is almost non existence. Prior to this, a meta analysis of studies
related to Asperger Syndrome and children was conducted. The findings indicated that
there is a gap in the development of Asperger Syndrome screening instrumentbased on
the Malaysian children and Malaysian norms. Hence, it is imperative for this study to
examine the special needs education practitioners as regard to their needs which include;
1) their awareness of what is classified in DSM IV as Asperger Syndrome, 2) their
knowledge and experience related to Asperger Sydrome, 3) their experiences in handling
special needs children of any kind, 4) their source of references and information, and
finally, 5) availability of any support system for children identified as having Asperger
Syndrome in this country.
This study employed the mixed method in which the qualitative data was obtained via
focus group discussion and the quantitative data was collected through the survey
method. The focus group discussion, probive insights from the special needs education
practitioners. The sharing session highlighted; i) the practitioners’ difficulties in
identifying Asperger Syndrome and other disorders as children do not display the traits
until they are diagnosed clinically by certified psychitrists, or professionals in the related
field, ii) inadequate information from other sources such as parents, subjects learnt and
cutural beliefs, iii) lacked of exposure to screening instruments for Asperger Syndrome
among Malaysian children.
As RQ2, quantatively the findings demonstrated that there was a high internal
consistency rate for the instrumentas examined in two pilot studies. Confirmatory Factor
Analysis on the other hand, suggested the following:
i) Two-factor measurement model for motor clumsiness – difficulties in gross &
fine motor skills
ii) Two-factor model in rigidity in daily routine and limited interests

78
iii) Three factor model in cognitive issues – mind-blindness, lacked of cognitive
flexibility & imaginative play
iv) Four-factor model for difficulties in social interaction & language processing
v) Five factor model for senses sensitivity
In addressing RQ3, quantitative analysis was again utilised. The result indicated that the
prevalence rate for potential Malaysian with Aspeger Syndrome is 0.86%. This means
that approximately 9 children (8:1) 8 males and 1 female of 1041 respondents examined
were found having asperger syndrome potentials.
According to de Bildt, Sytema, Ketelaars, Kraijer, Mulder, Volkmar, and Minderaa.
(2004), the characteristics that define Asperger’s Disorder include intact formal language
skills (e.g., vocabulary, grammar), with impairments in the social use of language and in
non-verbal expression, social awkwardness, and idiosyncratic and consuming interests
(Volkmar & Klin, 2001). Although motor clumsiness is not a defining feature of
Asperger's Disorder, it is often observed (Volkmar & Klin, 2001). Further as reported in
many special needs journals, parents usually sense there is something unusual about a
child with AS by the time of his or her third birthday, and some children may exhibit
symptoms as early as infancy. Unlike children with autism, children with AS retain their
early language skills. Motor development delays – crawling or walking late, clumsiness
– are sometimes the first indicator of the disorder.
The DSM-IV diagnostic criteria for Asperger's Disorder include at least two symptoms
in the domain of social interaction and one symptom in the domain of restricted interests
and behaviors.
The practitioners’ inability to identify and screen may dampen or impede the child’s
rights to early intervention and tutelage under trained professionals in Asperger
Syndrome. Early intervention is defined as the experience and opportunities afforded
infants and toddlers with disabilities by the children’s parents and other primary
caregivers that are intended to promote the children’s acquisition and use of behavioural
competencies to shape and influence their pro-social interactions with people and objects
(Dunst, 2007).

79
The lack of exposure and knowledge as regard to what is known as children with
Asperger Syndrome is a big concern especially for parents and special needs educators
in Malaysia. Workshops on Asperger Syndrome and related skills in handling children
with Asperger Syndrome is crucial and critical especially to special needs educators,
childcare-minders, practitioners and parents.
Exposure and knowledge related to Asperger Syndrome is pertinent to parents and
teachers alike. According to Dawson and Toth (2006) some parents of children whose
children are disgnosed with Autism Syndrome were concerned about their child's
development since birth, and, by 18 months, most parents raise concerns with their
primary health care provider (Howlin & Asgharian, 1999; Rogers, 2001; Siegel, Pilner,
Eschler, & Elliot, 1988).
However, the age at which a diagnosis is confirmed tends to be much older. In a survey
of 770 parents of children with Autism and Asperger's Disorder for instance, the average
age at which a formal diagnosis was confirmed was 5.5 years for Autism and 11 years
for Asperger's Disorder (Howlin & Asgharian, 1999). Empirically it is quite impossible
to ascertain that a child is having Asperger Syndrome when the ripe age for detecting it
is only at 11 years old as reported by many medical research journals. As such screening
children for Asperger Syndrome at the age of 6 years old and below may not yield
positive outcomes.
As for SIMCAS, the screening instrument for Asperger Syndrome based on Malaysian
norms, it is still premature to conclude that the items developed may correctly screen the
Asperger Syndrome traits or attributes as the AS traits may only be visible when the child
turns 11 years old. The Confirmatory Factor Analysis for example, employed by this
study to screen “limited interests and rigidity in daily routines” among mainstream
Malaysian children didn’t indicate the presence of such traits. Hence, this finding is
consistence with findings from other studies that such AS traits may only reveal itself at
the onset of adolescence (Howlin & Asgharian, 1999).

80
5.1 Limitation
Limitation of the study includes:
i) pool of items were too large in that it was too taxing for the class teachers;
ii) many teachers and parents were reluctant to participate in the survey as they associate
the information collected with “stigma and labelling” – issue of confidentiality;
iii) double-barrel items and lengthy statements – items were adoptedand adapted from
existing instruments used for children in the western culture, hence simplification of
the items and adapting them according to the local culture and understanding took
longer time.
5.2 Future Research
Further duplicate study is imperative to cross-validate the findings but it has to be with
larger sample size that comprehend all children in West and East Malaysia randomly

81
References
Adolphs R, Sears L, Piven J. (2001). Abnormal processing of social information from faces
in autism. J Cognitive Neurosci. v13: p232–240.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th
edition, text revision. Washington, DC; 2000
Annelies de Bildt, Sjoerd Sytema, Cees Ketelaars, Dirk Kraijer, Erik Mulder, Fred Volkmar,
and Ruud Minderaa. (2004). Interrelationship between Autism Diagnostic Observation
Schedule-Generic (ADOS-G), Autism Diagnostic Interview- Revised (ADI-R), and the
Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-RQTR) Classification
in Children and Adolescents with Mental Retardation. Journal of Autism and
Developmental Disorders, Vol. 34, No. 2, April 2004 . Plenum Publishing Corporation.
Asperger Disorder, (2016). Raising Children Network Australia. Available at:
raisingchildren,net.au
Aston MC. (2001). The other half of Asperger's syndrome: a guide to living in an intimate
relationship with a partner who has Asperger syndrome. London: The National Autistic
Society.
Attwood T. (2007). The Complete Guide to Asperger’s Syndrome. Jessica Kingsley Publishers.
https://books.google.com.my/books?id=ZwQGsuCNMPYC&pg=PA14&dq=developme
ntal++in+autism+and+Asperger+syndrome:+from+early+childhood&hl=en&sa=X&ve
d=0ahUKEwj01qmQr7zKAhVHSY4KHXECCAMQ6AEIHTAA#v=onepage&q=devel
opmental%20%20in%20autism%20and%20Asperger%20syndrome%3A%20from%20
early%20childhood&f=false
Attwood T. (1998). Asperger's syndrome: a guide for parents and professionals. London:
Jessica Kingsley Publishers.
Baron-Cohen S, Ring HA, Wheelwright S, Bullmore ET, Brammer MJ, Simmons A, et al.
(1999). Social intelligence in the normal autistic brain: an FMRI Study. Eur J Neurosci.
v11: p1891–1898.
Bauminger N, Kasari C. (2000). Loneliness and friendship in high functioning children with
autism. Child Dev.v (71): p 447–456.
Baron-Cohen S, Jolliffe T. (1997). Another advanced test of theory of mind: evidence from
very high functioning adults with autism or Asperger disorder. J Child Psychol
Psychiatry. v38: p813–822.
Baron-Cohen S, O'Riordan M, Stone V, Jones R, Plaisted K. (1999).Recognition of faux pas
by normally developing children and children with Asperger disorder or high
functioning autism. J Autism Devel Disord.v29: p407–418.
Blackshaw AJ, Kinderman P, Hare DJ, Hatton C. (2001). Theory of mind, causal attribution
and paranoia in Asperger disorder. Autism.;5(2):147–163.
Bolton P, Pickles A, Murphy M, Rutter M. (1988). Autism affective and other psychiatric
disorders: patterns of familial aggregation. Psych Med.; v28: p385–395.

82
Brenda, C. (2013). Special care needed for children afflicted with Asperger's Syndrome,
Community, The STAR Online.
Carrington S, Graham L. (2000). Perceptions of school by two teenage boys with Asperger
syndrome and their mothers: a qualitative study. Autism. v5:37–48.
Carl J. Dunst (2007). Early intervention for infants and toddlers with developmental disabilities.
Handbook of Developmental Disabilities. Edited by Samuel L. Odom, Robert H.
Horner, Martha E. Snell, and Jan B. Blacher (2007). The Guilford Press, London.
Chris Williams and Barry Wright (2004). How to Live with Autism and Asperger Syndrome.
Practical Strategies for Parents and Professionals. Jessica Kingsley Publishers London
and Philadelphia.
Christina M. Corsello. (2015). Early Intervention in Autism. Infants & Young Children. Vol.
18, No. 2, pp. 74–85 Lippincott Williams & Wilkins, Inc.
Church C, Alisanski S, Amanullah S. (2000). The social, behavioural and academic
experiences of children with Asperger disorder. Focus on Autism and Other
Developmental Disabilities. v15(1): p12–20.
Critchley HD, Daly EM, Bullmore ET, Williams SCR, Van Amelsvoort T, Robertson DM, et
al. (2000). The functional neuroanatomy of social behaviour. Brain. v123: p2203–2212.
Dawson, G., & Toth, K. (2006). Autism spectrum disorders. In D. Cicchetti & D. J.
Cohen (Eds.), Developmental psychopathology, second edition, volume three: Risk,
disorder, and adaptation (pp. 317-357). Hoboken, NJ: Wiley.
De Long G.R, Dwyer J.T. (n.d). Correlation of family history with specific autistic
subgroups: Asperger's disorder and bipolar affective disease. J Autism Dev Disord.v18:
p593–600.
de Villiers, J. G. & de Villiers, P. A. (2014). The role of language in theory of mind
development. Topics in Language Disorders, v34(4), p313-328.
Dougal Julian Hare, Jonathan Paul Robin Jones, Claire Paine, (2016). Approaching Reality:
The Use of Personal Construct Assessment in Working with People with Asperger
Syndrome, Autism, Manchester Joint Service for Learning Disabilities, UK. University
of Plymouth, UK
Eisenmajer R, Prior M, Leekman S, Wing L, Gould J, Welham M, et al. (1996). Comparison
of clinical symptoms in autism and Asperger's disorder. J Am Acad Child Adolescent
Psychiatry.v35: p1523–1531.
Fine C, Lumsden J, Blair RJR. (2001). Dissociation between theory of mind and executive
functions in a patient with early left amygdala damage. Brain J Neurol. v124: p287–
298.
Frith, Uta. (2004). Emanuel Miller lecture: Confusions and controversies about Asperger
syndrome. Journal of Child Psychology and Psychiatry and Allied Disciplines. 45:4
(2004), pp 672–686.

83
Gallagher, J., Clifford, R., & Maxwell, K. (2004). Getting from here to there: To an ideal early
preschool system. Early Childhood Research and Practice, 6(1), 1-28. Retrieved
Oktober 12, 2015, from http://ecrp.uiuc.edu/v6n1/clifford.html.
Gillberg, C., Gillberg, C., Rastam, M., et al. (2001). The Asperger Syndrome (and
high-functioning autism) Diagnostic Interview (ASDI). A preliminary study of a new
structured clinical interview. Autism, 5, 57–66.
Ghazuddin M, Wieder-Mikhail W, Ghaziuddin N. (1998). Comorbidity of Asperger
syndrome: a preliminary report. J Intellect Disabil Res. v42: p279–283.
Ghaziuddin M, Greden J. (1998). Depression in children with autism/pervasive
developmental disorders: a case-control family history study. J Autism Devel Disord.
v28: p111–115.
Gillot A, Furniss F, Walter A. (2001). Anxiety in high-functioning children with autism.
Autism. v5(3): p277–286.
Goldman, A. I. (2012). Theory of Mind, in: Oxford Handbook of Philosophy and Cognitive
Science, Edited by Eric Margolis, Richard Samuels, and Stephen Stich.
Green J, Gilchrist A, Burton D, Cox A. (2000). Social and psychiatric functioning in
adolescents with Asperger disorder compared with conduct disorder. J Autism Dev
Disord. v30(4):279–293.
Heavey L, Phillips W, Baron-Cohen S, Rutter M. (2000). The awkward moments test: a
naturalistic measure of social understanding in autism. J Autism Dev Disord. v30:
p225–236.
Howlin P, Baron-Cohen S, Hadwin J. (1999). Teaching children with autism to mind-read: a
practical guide. Chichester: Wiley.
Holliday-Willey L.(1999). Pretending to be normal. London: Jessica Kingsley Publishers.
Kim JA, Szatmari P, Bryson SE, Streiner DL, Wilson F. (2000). The prevalence of anxiety
and mood problems among children with autism and Asperger disorder. Autism. v4:
p117–132.
Karen Toth, Jeffrey Munson, Andrew N. Meltzoff, Geraldine Dawson. (2006). Early
Predictors of Communication Development in Young Children with Autism
Spectrum Disorder: Joint Attention, Imitation, and Toy Play. J Autism Dev Disord
(2006) 36:993–1005. Springer Science+Business Media, Inc.
Koegel, L. K., Koegel,R.L., Ashbough, , K., Bradshaw, J. (2014). The Importance of early detection
and intervention for children with or at-risk for autism spectrum disorders, International Journal
od Speech-Language Pathology, v16(1), p 50-56K.
Kleinman J, Marciano P, Ault R. (2001). Advanced theory of mind in high-functioning adults
with autism. J Autism Dev Disord. v31: p29–36.

84
Klin A. (2000). Attributing social meaning to ambiguous visual stimuli in higher-functioning
autism and Asperger syndrome: the social attribution task. J Child Psychiatry. 41:831–
846.
Koning C, Magill-Evans J. (2001). Social and language skills in adolescent boys with
Asperger's disorder. Autism. v5(1): p23–36.
Kurita H. (1999). Delusional disorder in a male adolescent with high-functioning PDD-NOS
[brief report]. J Autism Dev Disord. v29(5): p419–423.
Kimbi, Y. (2014). Theory of mind abilities and deficits in autism spectrum disorders. Topics
in Language Disorders, 34(4), 329-343.
Kwi-Ok Nah & Jung-In Kwak. (2011). Child Assessment in Early Childhood Education and
Care Settings in South Korea. Asian Social Scienc. Vol. 7, No. 6; June 2011. ISSN 1911-2017 E-
ISSN 1911-2025. Canadian Center of Science and Education.
Laurie Leventhal-Belfer, Cassandra Coe (2004). Asperger’s Syndrome in Young Children. A
Developmental Guide for Parents and Professionals. Athenaeum Press, Gateshead, Tyne
and Wear.
Luigi Mazzone, Liliana Ruta and Laura Reale (2012). Psychiatric comorbidities in asperger
syndrome and high functioning autism: diagnostic challenges. Annals of General
Psychiatry 2012 11:16. Mazzone et al.; licensee BioMed Central Ltd
Lynn Kern Koegel , Robert l. Koegel , Kristen Ashbaugh & Jessica Bradshaw. (2014). The
importance of early identification and intervention for children with or at risk for autism
spectrum disorders. Importance of early identification and intervention for ASD.
International Journal of Speech-Language Pathology, 2014; 16(1): 50–56
Marcia Regina Fumagalli Marteleto & Marcia Regina Marcondes Pedromonico (2005).
Validity of Autism Behavior Checklist (ABC): preliminary study. Financing:
Coordenação de Aperfeiçoamento de Pessoal de. Rev Bras Psiquiatr.
2005;27(4):295-301
McAfee J. (2001). Navigating the social world. A curriculum for individuals with Asperger's
syndrome, high-functioning autism and related disorders. London: Jessica Kingsley
Publishers.
Miller, S. A. (2012). Theory of mind: Beyond the preschool years. New York, NY: Psychology
Press.
Ministry of Education Malaysia. (2007). Early Childhood Care and Education Policy
Implementation Review. ppk/ups/nsb/ECCE Policy Review 24 Jan 2008.
http://www.scielo.br/pdf/rbp/v27n4/a08v27n4.pdf
Muris, P, Steerneman P, Meesters C, Merckelbach H, Horselenberg R, Van Den Hogan T, et
al. (2001). The TOM test: a new instrument for assessing theory of mind in normal
children and children with pervasive developmental disorders. J Autism Dev Disord.
v29: p67–80.

85
Nyden A, Gillberg C, Hjelmquist E, Heiman M. (1999). Executive function/attention deficits
in boys with Asperger disorder, attention disorder and reading/writing disorder. Autism.
v3: p213–228.
Ozonoff S, South M, Miller J. (2000). DSM-IV defined Asperger disorder: cognitive,
behavioural and early history differentiation from high-functioning autism. Autism. v4:
p29–46.
Piven J, Palmar R. (1999). Psychological disorder and the broad autism phenotype: evidence
from a family study of multiple-incidence autism families. Am J Psychiatry; v156:
p557–563.
Peterson, C. C., Wellman, H. M. & Slaughter, V. (2012). The mind behind the message:
Advancing theory-of-mind scales for typically developing children, and those with
deafness, autism, or asperger syndrome. Child Development, v83(2), p469-485.
Pennington BF, Ozonoff S. (1996). Executive functions and developmental psychopathology.
J Child Psychol Psychiatry Ann Res Rev. v37: p51–87.
Rebecca S. New and Moncrieff Cochran. (2007). Early childhood education (four volumes).
An international encyclopedia. Greenwood Publishing Group, Inc.
Rosen, P. (2016). The importance of Early Detection, Parents.
Ruffman, T., Slade, L., & Crowe, E. (2003). The relation between children’s and mothers’
mental state language and theory-of-mind understanding. Child Development, 73(3), 734-
751.
Scott F., Cohen S. Bolton P & Brayne C. (2002). The CAST (Childhood Asperger Syndrome
Test) Preliminary development of a UK screen for mainstream primary-school-age
children. Aut.sagepub.com. SAGE Publications and The National Autistic Society. Vol
6(1) 9–31; 021321. 1362-3613(200203)6:1.
Stephan Ehlers,Christopher Gillberg, & Lorna Wing (1999).A Screening Questionnaire for
Asperger Syndrome and Other High-Functioning Autism Spectrum Disorders in School
Age Children. Journal of Autism and Developmental Disorders, Vol. 29, No. 2, 1999.
Plenum Publishing Corporation
Stephanie Lee & Marna Miller. (2009). Children and adults with developmental
disabilities: Services in Washington, research evidence. Olympia: Washington State
Institute for Public Policy, Document No. 09-10-3901.
Steven R. Forness, Sharon L. Ramey, Craig T. Ramey, Chuanchieh Hsu, Carl M. Brezausek,
Donald L. MacMillan, Kenneth A. Kavale and Bonnie T. Zima. (1998). Head Start
Children Finishing First Grade: Preliminary Data on School Identification of Children
at Risk for Special Education. Behavioral Disorders, 23(2), 111-124.
Slaughter, V., Peterson, C., & Mackintosh, E. (2007). Mind what mother says: Narrative input
and theory of mind in typical children and those on the autism spectrum. Child
Development, 78, 839-858.

86
Susan Jeanette G. Ealdama. (2010). Quality Control in Early Intervention Centers for
Young Children with Special Needs. EDUCATION QUARTERLY, December 2010,
Vol. 68 (1), 36-54 U.P. College of Education.
Schopler E, Mesibov GB, Kunce LJ. (1998). In: Asperger syndrome and high-functioning
autism?. New York: Plenum Press; p. 167–198.
Tantam D. (2000). Psychological disorder in adolescents and adults with Asperger disorder.
Autism.; v4: p47–62.
Tantam, D. (2003) The challenge of adolescents and adults with Asperger syndrome.
Child and Adolescent Psychiatric Clinics of North America, 12, 143–163, vii–viii.
Tom Berney. (2004). Asperger syndrome from childhood into adulthood. Advances in
Psychiatric Treatment (2004), vol. 10, 341–351
Tantam D. (2000). Psychological disorder in adolescents and adults with Asperger disorder.
Autism. v4:p47–62.
Tonge B, Brereton A, Gray K, Einfeld S. (1999). Behavioural and emotional disturbance in
high-functioning autism and Asperger disorder. Autism. v3: p117–130.
Sussman, F. (2006). TalkAbility – People skills for verbal children on the autism spectrum: A
guide for parents. Toronto, ON: Hanen Early Language Program.
United Nations Educational Scientific and Cultural Organization. (2008). What approaches to
linking ECCE and Primary Education? United Nations Policy Brief on Early Childhood.
U.S. Department of Education. (1995). Seventeenth annual report to Congress on
implementation of the Individuals with Disabilities Education Act. Washington, DC: U.S.
Office of Special Education.
Walter, R. (2016). Asperger Syndrome, KidsHealth, Nemours Foundation.
Wellman, H. M. & Liu, D. (2004). Scaling theory of mind tasks. Child Development, 75, 759-
763.
Westby, C. & Robinson, L. (2014). A developmental perspective for promoting theory of mind.
Topics in Language Disorders, v34(4), p362-383.
Yoon Lee & Matthew Hayden. (2009). Early childhood care and education: Worldwide
challenges and progresses. Current issues in comparative education. Volume 11/ 2009.
ISSN 1523-1615.

87
Tanda tangan penilai Tarikh:
___________
_________________________________
KOD
A. MAKLUMAT DEMOGRAFI:
(Bahagian ini perlu diisi oleh guru: Sila baca setiap pernyataan dengan teliti dan
tandakan jawapan anda).
1. Nama Murid: _______________________________________
2. Jantina: 1. Lelaki
2. Perempuan
3. Nama sekolah: ___________________________________________
4. Tarikh penilaian: ____________________
5. Umur pada tarikh penilaian: tahun ______bulan ________
6. Nama guru
penilai:_______________ _________________________
7. Tempoh penilai mengenali pelajar: ______________________________________
8. Kategori ketidakupayaan /
kecacatan (jika ada) : 1. Pendengaran
2. Penglihatan
3. Pertuturan
4. Fizikal
5. Masalah pembelajaran
6. Mental
7. Pelbagai ketidakupayaan
8. Lain-lain. Sila jelaskan: __________
9. Masalah Pembelajaran : 1. Lewat perkembangan global
2. Sindrom down
3. ADHD
4. Austisma
5. Kurang upaya intelektual
6. Masalah pembelajaran spesifik

88
BAHAGIAN B: PEMARKAHAN
(diisi oleh penilai)
Jumlah Ya Tidak
(5 & 6)
1.Interaksi Sosial : Skor bagi konstruk 5 & 6
(item 1 – 10)
2.Kemahiran Bahasa : Skor bagi konstruk 5 & 6
(item 11 – 13)
3.Rutin Harian & Minat : Skor bagi konstruk 5 & 6
(item 14 - 22)
4.Kemahiran Motor : Skor bagi konstruk 5 & 6
(item 23 - 28)
5.Sensorideria : Skor bagi konstruk 5 & 6
(item 29 - 43)
6.Kognitif : Skor bagi konstruk 5 & 6
(item 44-52)
BAHAGIAN C: PELAJAR YANG BERPOTENSI DIKELASIFIKASIKAN SEBAGAI
SINDROM ASPERGER (SA)
(disaring oleh penilai)
1. Interaksi Sosial – jumlah skor 5 & 6 – minima 2 item ke atas.
2. Kemahiran Bahasa – jumlah skor 5 & 6 – MESTI sifar (0).
3. Rutin & Minat, Kemahiran motor & sensori - jumlah skor 5 & 6 – minimum 1 item
4. Kemahiran kognitif - jumlah skor 5 & 6 - MESTI sifar (0).
BAHAGIAN D:
(diisi oleh penilai berkaitan)
Rumusan
Murid berkemungkinan mempunyai sindrom Asperger
Murid berkemungkinan tidak menpunyai sindrom Asperger
Tandatangan : _________________________
Nama : __________________________________________
Disahkan
Tandatangan Guru Besar: _________________________ Cop Sekolah
Nama : ________________________________________________

89
I. INTERAKSI SOSIAL DUA HALA
A. Ketidakupayaan dan/atau kurang keinginan untuk berinteraksi dengan rakan sebaya.
1.Kurang mahir menggunakan bahasa dalam hubungan sosial. 1 2 3 4 5 6
2.Kurang berkemampuan untuk memulakan perbualan. 1 2 3 4 5 6
3.Kurang keupayaan memahami aliran perbualan (Contoh: ini menyebabkan salah
faham dalam berinteraksi)
1 2 3 4 5 6
B. Tingkah laku yang tidak sesuai secara emosi atau sosial.
4.Tingkah laku pelik (Contoh: Ketawa terhadap sesuatu yang menyedihkan,
bertanya soalan yang terlalu peribadi).
1 2 3 4 5 6
5.Tidak menyedari akan peraturan yang tersirat (Contoh: 'melaporkan' perbuatan
rakan sebaya, melanggar 'kod rahsia' yang ada menyebabkan orang lain marah
kepadanya).
1 2 3 4 5 6
6.Bertindak balas dengan marah apabila orang lain tidak mengikut peraturan
(Contoh: Mendisiplinkan orang lain mengikuti gaya guru atau ibu bapa).
1 2 3 4 5 6
C. Penggunaan komunikasi bukan lisan yang terhad atau tidak normal.
7.Tidak memahami isyarat bahasa badan orang lain. 1 2 3 4 5 6
8. Ekspresi muka tidak sama dengan emosi yang ditonjolkan. 1 2 3 4 5 6
9. Kurang ekspresi muka ketika berkomunikasi. 1 2 3 4 5 6
10.Tidak berupaya memahami ekspresi muka orang lain 1 2 3 4 5 6
II. KEMAHIRAN BERTUTUR
A. Kurang upaya dalam pemprosesan bahasa.
11.Sukar membezakan antara maklumat yang relevan dan tidak relevan semasa
pemprosesan bahasa.
1 2 3 4 5 6
12.mudah terganggu oleh rangsangan persekitaran 1 2 3 4 5 6
13.Sukar mengekalkan tumpuan ( mudah terganggu). 1 2 3 4 5 6
III.PILIHAN KEGEMARAN/MINAT
A. Peraturan amat penting apabila dunia dilihat dalam bentuk hitam (buruk) dan putih (baik).
14.mengamalkan kesempurnaan yang melampau. 1 2 3 4 5 6
15.Menghadapi kesukaran untuk merubah rutin sedia ada. 1 2 3 4 5 6
B. Individu mempunyai minat yang terhad.
16.Telah membentuk minat yang atipikal (Contoh: khusus, sempit, dan perasaan
cekap dan terkawal).
1 2 3 4 5 6
17.Bermain dengan alat permainan secara berulang-ulang. 1 2 3 4 5 6
18.Menyusun objek dalam cara yang khusus. 1 2 3 4 5 6

90
19.Tidak boleh menukar cara yang telah dipelajari bagi menyelesaikan
sesuatu tugas.
1 2 3 4 5 6
C. Kegagalan mengikuti peraturan dan rutin menyebabkan masalah sikap.
Ini mungkin termasuk:
20.Keresahan. 1 2 3 4 5 6
21.Bersikap tentarum (contoh: menangis, kekasaran, memusnahkan barang, 1 2 3 4 5 6
menjerit, perbalahan lisan) 1 2 3 4 5 6
22.Tidak mampu mengelak sikap reaksi melampau(contoh: tidak mampu
menggunakan teknik menenang atau menyesuaikan diri.
1 2 3 4 5 6
IV. KERENCATAN PERKEMBANGAN MOTOR.
A. Kesukaran dengan kemahiran motor kasar
23.Ayunan badan yang pelik ketika bergerak. 1 2 3 4 5 6
24.Kesukaran ketika membaling atau menangkap bola (kelihatan takut kepada
bola tersebut).
1 2 3 4 5 6
25.Kesukaran dalam mengkoordinasi anggota badan yang berlainan (mengikat
tali kasut, mengayuh basikal).
1 2 3 4 5 6
B. Kesukaran dengan kemahiran motor halus.
26.Kesukaran dalam kemahiran menulis. 1 2 3 4 5 6
27.Cara memegang pensel/pen yang pelik. 1 2 3 4 5 6
28.Tergesa-gesa dalam menyiapkan tugas yang membabitkan motor halus. 1 2 3 4 5 6
V. SENTITIVITI DERIA.
A. Mempunyai kesukaran dalam aspek penglihatan
29.Membuat renungan yang tajam. 1 2 3 4 5 6
30.Mengelak daripada bertentangan mata. 1 2 3 4 5 6
31.Berdiri terlalu dekat pada objek atau orang. 1 2 3 4 5 6
B. Mengalami kesukaran dalam aspek bunyi.
32.Menutup telinga apabila bunyi tertentu dihasilkan. 1 2 3 4 5 6
33.Tidak mampu memberi tumpuan kepada beberapa jenis bunyi yang berlaku pada
masa yang sama
1 2 3 4 5 6
34.Takut kepada bunyi-bunyi khususnya yang dihasilkan objek tertentu (mesin
hampagas, pengisar, pencuci debu)
1 2 3 4 5 6
C. Mengalami kesukaran dalam aspek olfaktori (penghiduan).
35.Merasakan sesetengah bau terlalu kuat atau tidak enak sehingga berasa mual. 1 2 3 4 5 6
36.Boleh mengenalpasti bau lebih cepat daripada orang lain. 1 2 3 4 5 6
37.Perlu mencium bau bahan tertentu sebelum menggunakannya. 1 2 3 4 5 6

91
D. Mengalami kesukaran dalam aspek sentuhan.
38.mengalami kesukaran apabila disentuh orang lain, walaupun cuma dicuit sedikit
(khususnya di bahu dan kepala).
1 2 3 4 5 6
39.Menunjukkan keresahan apabila disentuh secara tiba-tiba. 1 2 3 4 5 6
40.Mengalami kesukaran dengan baju yang berkelim atau mempunyai tag. 1 2 3 4 5 6
E. Mengalami kesukaran dalam aspek deria rasa
41.Membuat pilihan makanan yang terhad (tertentu). 1 2 3 4 5 6
42.Hanya menerima makanan dengan tekstur atau warna tertentu. 1 2 3 4 5 6
43.Perlu menyentuh makanan sebelum makan. 1 2 3 4 5 6
VI. ISU_ISU KOGNITIF
A. Buta minda (Teori Akal).
44.Melihat dunia dalam hitam dan putih (Contoh: mengakui melanggar satu
peraturan walaupun mengetahui ada risiko untuk ditangkap).
1 2 3 4 5 6
45.Tidak menyedari bahawa orang lain mempunyai sudut pandangan berbeza
daripada dirinya
1 2 3 4 5 6
46.Tidak menyedari dia boleh mengatakan sesuatu yang mengguris perasaan orang
lain.
1 2 3 4 5 6
B. Kurang fleksibiliti kognitif.
47.Menghadapi kesukaran dalam kemahiran mengorganisasikan (Contoh: apa
yang perlu saya lakukan, dan bagaimana saya boleh melakukannya?).
1 2 3 4 5 6
48.Mempunyai kesukaran dengan urutan susun atur (Contoh: apakah urutan /
susunan yang digunakan untuk menyelesaikan sesuatu tugas?).
1 2 3 4 5 6
49.Mempunyai kesukaran mengikut arahan. 1 2 3 4 5 6
C. Permainan Imaginasi :
50.Cuba mengawal semua aspek aktiviti permainan; (Contoh: Sebarang cubaan pihak
lain untuk mengubah permainan itu akan ditentang dengann keras).
1 2 3 4 5 6
51.Terlibat dalam permainan yang kelihatan berimaginasi tetapi sebenarnya ditiru
daripada media (Contoh: Filem / rancangan TV / buku yang diminatinya).
1 2 3 4 5 6
52.Fokus kepada minat khusus sehingga mereka mendominasi permainan dan pilihan
aktiviti.
1 2 3 4 5 6