
New-onset graft dysfunction after heart transplantation—incidence and mechanism-related outcomes
10
New-onset graft dysfunction after heart transplantation—incidence and mechanism-related outcomes Khurram Shahzad, MD, a Quratul Ain Aziz, MD, a Jean-Paul Leva, BS, a Martin Cadeiras, MD, a Eric K. Ho, MD, b George Vlad, MD, b E. Rodica Vasilescu, MD, b Farhana Latif, MD, a Anshu Sinha, PhD, c Elizabeth Burke, a Linda J. Addonizio, MD, d Susan W. Restaino, MD, a Charles C. Marboe, MD, b Nicole Suciu-Foca, MD, b Yoshifumi Naka, MD, PhD, e Donna Mancini, MD, a and Mario C. Deng, MD a From the a Department of Medicine, Division of Cardiology; b Department of Pathology; c Department of Biomedical Informatics; d Department of Pediatrics, Division of Pediatric Cardiology; and e Department of Surgery, Columbia University, New York, New York. BACKGROUND: Graft dysfunction (GD) after heart transplantation (HTx) is a major cause of mor- bidity and mortality. The impact of different pathophysiologic mechanisms on outcome is unknown. In this large, single-center study we aimed to assess the incidence of GD and compare the outcomes with different histopathologic mechanisms of rejection. METHODS: We analyzed a data set of 1,099 consecutive patients after their HTx at Columbia University Medical Center between January 1994 and March 2008, and identified all patients hospi- talized with new-onset GD. Based on the histopathologic data, patients were divided into GD- unexplained (Group-GD-U), GD-antibody-mediated rejection (Group-GD-AMR), GD-cardiac allograft vasculopathy (Group-GD-CAV) and GD-acute cellular rejection (Group-GD-ACR) groups. We com- pared the in-hospital and 3-, 6- and 12-month mortality across these groups using the chi-square test. We also compared the 3-, 6- and 12-month survival curves across groups using the log-rank test. RESULTS: Of 126 patients (12%) identified with GD, complete histology data were available for 100 patients. There were 21, 20, 27 and 32 patients identified in Group-GD-U, Group-GD-AMR, Group- GD-CAV and Group-GD-ACR, respectively. The in-hospital mortality rates were 52%, 20%, 15% and 6%, respectively. The in-hospital mortality rate was significantly higher in Group-GD-U compared with all other groups (p 0.0006). The 3-, 6- and 12-month survival rate was also significantly lower in Group-GD-U compared with all other groups. CONCLUSION: A significant proportion of patients presenting with new-onset GD have unexplained histopathology. Unexplained GD is associated with a significantly higher mortality rate. New diagnostic tools are necessary to better understand and detect/predict this malignant phenotype. J Heart Lung Transplant 2011;30:194 –203 Crown Copyright © 2011 Published by Elsevier Inc. All rights reserved. KEYWORDS: heart transplant; graft dysfunction; acute cellular rejection; antibody-mediated rejection; cardiac allograft vasculopathy; unexplained graft dysfunction Allograft rejection has been the central focus and chal- lenge in the clinical practice of transplantation medicine. In heart transplant patients, this challenge emerges from the development of acute cellular rejection (ACR), antibody- mediated rejection (AMR) and cardiac allograft vasculopa- thy (CAV). Acute cellular rejection is diagnosed by endo- myocardial biopsy (EMB) and graded depending on the degree of lymphocyte infiltration into myocardial tissue, 1,2 AMR is diagnosed by positive C4d staining of endothelial tissue, and CAV is diagnosed by annual coronary angiog- raphy or intracoronary/vascular ultrasound (IVUS). With the recent development in molecular biologic techniques and availability of novel tools to better understand the immune mechanisms of cardiac allograft rejection, different non-invasive biomarkers, including leukocyte gene expres- sion and N-terminal B-type natriuretic peptide (BNP) as important non-invasive markers of hemodynamic changes Reprint requests: Mario C. Deng, MD, Department of Medicine, Di- vision of Cardiology, Columbia University, 622 West 168th Street, PH12 STEM, Room 134, New York, NY 10032. Telephone: 212-305-0200. Fax: 212-305-7439. E-mail address: [email protected] http://www.jhltonline.org 1053-2498/$ -see front matter Crown Copyright © 2011 Published by Elsevier Inc. All rights reserved. doi:10.1016/j.healun.2010.08.026
Transcript of New-onset graft dysfunction after heart transplantation—incidence and mechanism-related outcomes
NtKMFSYFo
lhdmt
vS2
http://www.jhltonline.org
1d
ew-onset graft dysfunction after heartransplantation—incidence and mechanism-related outcomeshurram Shahzad, MD,a Quratul Ain Aziz, MD,a Jean-Paul Leva, BS,a
artin Cadeiras, MD,a Eric K. Ho, MD,b George Vlad, MD,b E. Rodica Vasilescu, MD,b
arhana Latif, MD,a Anshu Sinha, PhD,c Elizabeth Burke, a Linda J. Addonizio, MD,d
usan W. Restaino, MD,a Charles C. Marboe, MD,b Nicole Suciu-Foca, MD,b
oshifumi Naka, MD, PhD,e Donna Mancini, MD,a and Mario C. Deng, MDa
rom the aDepartment of Medicine, Division of Cardiology; bDepartment of Pathology; cDepartment of Biomedical Informatics; dDepartment
f Pediatrics, Division of Pediatric Cardiology; and eDepartment of Surgery, Columbia University, New York, New York.BACKGROUND: Graft dysfunction (GD) after heart transplantation (HTx) is a major cause of mor-bidity and mortality. The impact of different pathophysiologic mechanisms on outcome is unknown. Inthis large, single-center study we aimed to assess the incidence of GD and compare the outcomes withdifferent histopathologic mechanisms of rejection.METHODS: We analyzed a data set of 1,099 consecutive patients after their HTx at ColumbiaUniversity Medical Center between January 1994 and March 2008, and identified all patients hospi-talized with new-onset GD. Based on the histopathologic data, patients were divided into GD-unexplained (Group-GD-U), GD-antibody-mediated rejection (Group-GD-AMR), GD-cardiac allograftvasculopathy (Group-GD-CAV) and GD-acute cellular rejection (Group-GD-ACR) groups. We com-pared the in-hospital and 3-, 6- and 12-month mortality across these groups using the chi-square test.We also compared the 3-, 6- and 12-month survival curves across groups using the log-rank test.RESULTS: Of 126 patients (12%) identified with GD, complete histology data were available for 100patients. There were 21, 20, 27 and 32 patients identified in Group-GD-U, Group-GD-AMR, Group-GD-CAV and Group-GD-ACR, respectively. The in-hospital mortality rates were 52%, 20%, 15% and6%, respectively. The in-hospital mortality rate was significantly higher in Group-GD-U compared withall other groups (p � 0.0006). The 3-, 6- and 12-month survival rate was also significantly lower inGroup-GD-U compared with all other groups.CONCLUSION: A significant proportion of patients presenting with new-onset GD have unexplainedhistopathology. Unexplained GD is associated with a significantly higher mortality rate. New diagnostictools are necessary to better understand and detect/predict this malignant phenotype.J Heart Lung Transplant 2011;30:194–203 Crown Copyright © 2011 Published by Elsevier Inc. Allrights reserved.
KEYWORDS:heart transplant;graft dysfunction;acute cellularrejection;antibody-mediatedrejection;cardiac allograftvasculopathy;unexplained graftdysfunction
mdAtrtains
Allograft rejection has been the central focus and chal-enge in the clinical practice of transplantation medicine. Ineart transplant patients, this challenge emerges from theevelopment of acute cellular rejection (ACR), antibody-ediated rejection (AMR) and cardiac allograft vasculopa-
hy (CAV). Acute cellular rejection is diagnosed by endo-
Reprint requests: Mario C. Deng, MD, Department of Medicine, Di-ision of Cardiology, Columbia University, 622 West 168th Street, PH12TEM, Room 134, New York, NY 10032. Telephone: 212-305-0200. Fax:12-305-7439.
iE-mail address: [email protected]
053-2498/$ -see front matter Crown Copyright © 2011 Published by Elsevier Inoi:10.1016/j.healun.2010.08.026
yocardial biopsy (EMB) and graded depending on theegree of lymphocyte infiltration into myocardial tissue,1,2
MR is diagnosed by positive C4d staining of endothelialissue, and CAV is diagnosed by annual coronary angiog-aphy or intracoronary/vascular ultrasound (IVUS). Withhe recent development in molecular biologic techniquesnd availability of novel tools to better understand themmune mechanisms of cardiac allograft rejection, differenton-invasive biomarkers, including leukocyte gene expres-ion and N-terminal B-type natriuretic peptide (BNP) as
mportant non-invasive markers of hemodynamic changesc. All rights reserved.

ip
mprak(cm
M
S
WtUMrcctmbtcwtp
S
Tpvtwmrw
D
AplFflwdat(BGCm
(tatppa
A
Pdc(Tsdpw
G
Aeo2pmafdPhccn
D
DNagtFC
S
D(bfiimtmt1l
195Shahzad et al. New-onset Graft Dysfunction Post-HTx
n heart transplant patients, have been identified to detect/redict cardiac allograft rejection.3,4
Graft dysfunction (GD) is a major cause of morbidity andortality in heart transplant patients.5 The impact of different
athophysiologic mechanisms of rejection on outcome is cur-ently unknown. In this large, single-center study we aimed tossess the incidence of GD and hypothesized that currentlynown histopathologic mechanisms of allograft rejectionACR, AMR and CAV) fail to explain all clinical cases ofardiac allograft dysfunction, and that GD with unexplainedechanisms is associated with worse clinical outcomes.
ethods
tudy population
e retrospectively analyzed a data set of 1,099 consecutive pa-ients, who underwent heart transplantation (HTx) at the Columbianiversity Medical Center (CUMC) between January 1994 andarch 2008. The study protocol was approved by the institutional
eview board (IRB) of the CUMC. All transplant recipients re-eived double- or triple-drug immunosuppressive therapy withombinations of the following drugs: prednisone, cyclosporine,acrolimus or sirolimus and azathioprine or mycophenolateofetil. Standards of treatment for AMR at our institution have
een described elsewhere.6 All patients were managed according tohe CUMC’s standard of care.7 Clinical data were retrospectivelyollected from the charts and electronic medical records. Patientsere selected for analysis if they underwent echocardiogram at the
ime of hospitalization with new-onset (as defined by �3 monthsost-HTx) heart failure.
urveillance of transplant rejection
o rule out ACR and AMR, EMBs were performed routinely atre-specified time intervals based on the CUMC’s rejection sur-eillance protocol for HTx recipients; that is, every week duringhe first month, every 2 weeks during the next 2 months, every 4eeks until month 6, every 8 weeks up to the first year, every 3 to 6onths during the second year, and every 3 to 12 months during the
est of follow-up. For CAV, patients were followed on an annual basisith coronary angiography and/or dobutamine echocardiography.
iagnosis of rejection
t the time of hospitalization with suspected rejection, the EMBrocedure was performed using a standard technique.8,9 Acute cellu-ar cardiac allograft rejection was defined as ISHLT Grade �1R/1B.or AMR, immunoglobulin (Ig) deposition was tested by immuno-uorescence and endothelial swelling, capillary leak and hemorrhageere also assessed. Since 2005, staining for C4d was added foriagnosis of AMR. Cardiac allograft vasculopathy was defined asngiographic evidence of coronary artery blockage of �25% in any ofhe 3 main coronary arteries, including the left anterior descendingLAD), left circumflex (LCX) and right coronary (RCA) arteries.ased on these criteria patients were divided into a GD-ACR (Group-D-ACR), GD-AMR (Group-GD-AMR) or GD-CAV (Group-GD-AV) group, respectively. All patients with no evidence of the afore-
entioned histopathologic mechanisms were labeled as unexplained GGroup-GD-U). Positive autopsy findings, if available, were utilizedo make the decision in case of negative findings on histopathologynd coronary angiography. Clinical consensus was developed amonghe CUMC transplant cardiologists, transplant pathologists and trans-lant immunologists who were involved in the clinical care of theseatients in order to accurately allocate the patients among the 4 groupss defined by the pathophysiologic mechanisms.
nti-HLA antibodies
atients’ sera were obtained at the time of each EMB and tested foronor-specific antibodies (DSA) by direct cross-matching withryopreserved donor lymphocytes. Panel-reactive antibodiesPRA) were analyzed on an HLA-A, -B, -DR, -DQ reference set of
and B cells from 70 donors and the frequency and anti-HLApecificity of complement-fixing lymphocytotoxic antibodies wasetermined. Sera with PRA �10% and/or antibodies against arivate or public epitope of donor HLA Class I or II antigen(s)ere considered positive.10
raft dysfunction
t the time of hospitalization, patients underwent transthoracicchocardiography (TTE) to evaluate allograft function along withther laboratory testing. Echocardiography was performed with-dimensional sector scanning, Doppler color flow mapping andulsed- and continuous-wave Doppler interrogation. Most com-on echocardiographic parameters of allograft function were an-
lyzed, including ventricular wall motion, left ventricular ejectionraction (LVEF), valvular assessment and assessment for pericar-ial disease. Graft dysfunction was defined as LVEF �30%.11,12
atients were followed from �3 months post-HTx onward for aospitalization with a new-onset graft failure as defined by LVEFriteria. In the case of multiple episodes, the first episode withomplete (100%) data available on all pathophysiologic mecha-isms (i.e., AMR, CAV and ACR) was selected for the analysis.
onor clinical characteristics
onor-related clinical data were collected as reported to the Unitedetwork of Organ Sharing (UNOS) from the database maintained
t Center for Advanced Cardiac Care (CACC) and included age,ender, cytomegalovirus (CMV) status, toxoplasmosis (Toxo) sta-us, blood group, body surface area (BSA) and cold ischemia time.rom these data, known parameters of mismatch, such as gender,MV and Toxo mismatches, were constructed.
tatistical analysis
ata were analyzed using SPSS (version 15.0) statistical softwareSPSS, Inc., Chicago, IL). All variables were assessed for distri-ution characteristics. Outliers, defined as �2 standard deviationsrom the mean, were not considered in the analysis. Mortalitynformation was collected using clinical charts and electronic med-cal records. Time-to-event analysis was performed and in-hospitalortality rates as an outcome were compared across groups using
he chi-square test. In addition, mortality rates at 3, 6 and 12onths were also compared across groups using the chi-square
est. Kaplan–Meier survival analysis was performed and 3-, 6- and2-month survival curves were compared across groups using theog-rank test. To understand the causes of adverse outcomes for
D-U patients, augmented immunosuppression therapy received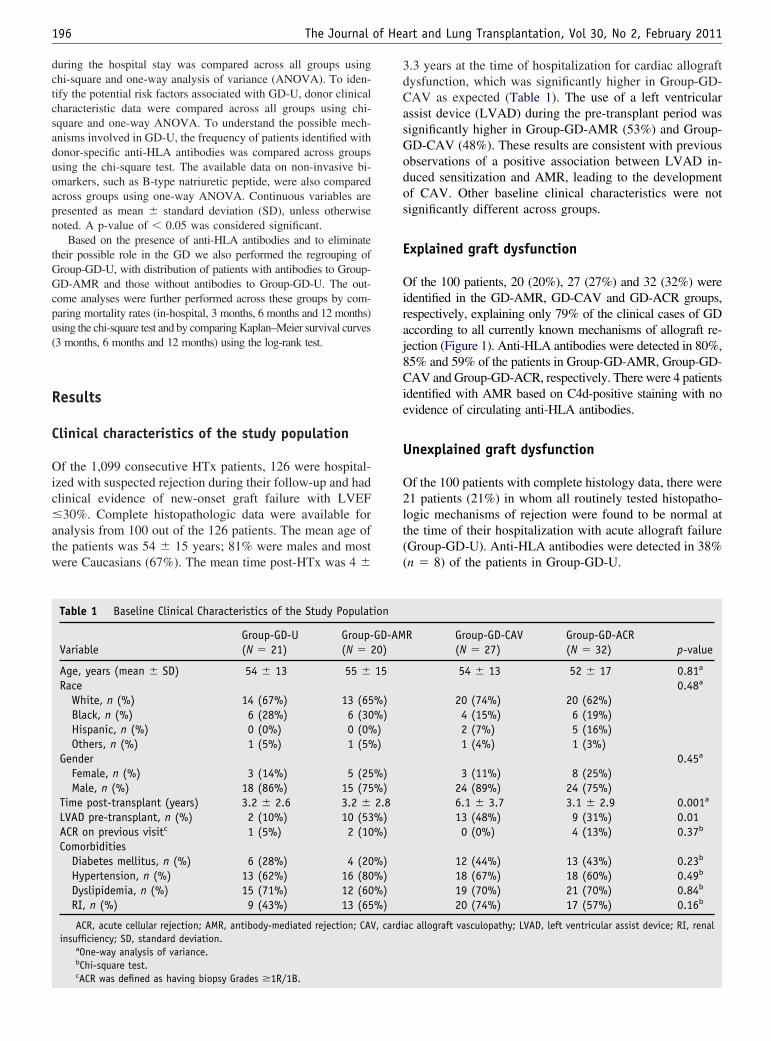
dctcsaduoapn
tGGcpu(
R
C
Oic�atw
3dCasGodos
E
Oiraj8Cie
U
O2lt((
196 The Journal of Heart and Lung Transplantation, Vol 30, No 2, February 2011
uring the hospital stay was compared across all groups usinghi-square and one-way analysis of variance (ANOVA). To iden-ify the potential risk factors associated with GD-U, donor clinicalharacteristic data were compared across all groups using chi-quare and one-way ANOVA. To understand the possible mech-nisms involved in GD-U, the frequency of patients identified withonor-specific anti-HLA antibodies was compared across groupssing the chi-square test. The available data on non-invasive bi-markers, such as B-type natriuretic peptide, were also comparedcross groups using one-way ANOVA. Continuous variables areresented as mean � standard deviation (SD), unless otherwiseoted. A p-value of � 0.05 was considered significant.
Based on the presence of anti-HLA antibodies and to eliminateheir possible role in the GD we also performed the regrouping ofroup-GD-U, with distribution of patients with antibodies to Group-D-AMR and those without antibodies to Group-GD-U. The out-
ome analyses were further performed across these groups by com-aring mortality rates (in-hospital, 3 months, 6 months and 12 months)sing the chi-square test and by comparing Kaplan–Meier survival curves3 months, 6 months and 12 months) using the log-rank test.
esults
linical characteristics of the study population
f the 1,099 consecutive HTx patients, 126 were hospital-zed with suspected rejection during their follow-up and hadlinical evidence of new-onset graft failure with LVEF30%. Complete histopathologic data were available for
nalysis from 100 out of the 126 patients. The mean age ofhe patients was 54 � 15 years; 81% were males and mostere Caucasians (67%). The mean time post-HTx was 4 �
Table 1 Baseline Clinical Characteristics of the Study Populat
VariableGroup-GD-U(N � 21)
Group-(N � 2
Age, years (mean � SD) 54 � 13 55 �Race
White, n (%) 14 (67%) 13 (65Black, n (%) 6 (28%) 6 (30Hispanic, n (%) 0 (0%) 0 (0%Others, n (%) 1 (5%) 1 (5%
GenderFemale, n (%) 3 (14%) 5 (25Male, n (%) 18 (86%) 15 (75
Time post-transplant (years) 3.2 � 2.6 3.2 �LVAD pre-transplant, n (%) 2 (10%) 10 (53ACR on previous visitc 1 (5%) 2 (10Comorbidities
Diabetes mellitus, n (%) 6 (28%) 4 (20Hypertension, n (%) 13 (62%) 16 (80Dyslipidemia, n (%) 15 (71%) 12 (60RI, n (%) 9 (43%) 13 (65
ACR, acute cellular rejection; AMR, antibody-mediated rejection; CAVinsufficiency; SD, standard deviation.
aOne-way analysis of variance.bChi-square test.c
ACR was defined as having biopsy Grades �1R/1B..3 years at the time of hospitalization for cardiac allograftysfunction, which was significantly higher in Group-GD-AV as expected (Table 1). The use of a left ventricularssist device (LVAD) during the pre-transplant period wasignificantly higher in Group-GD-AMR (53%) and Group-D-CAV (48%). These results are consistent with previousbservations of a positive association between LVAD in-uced sensitization and AMR, leading to the developmentf CAV. Other baseline clinical characteristics were notignificantly different across groups.
xplained graft dysfunction
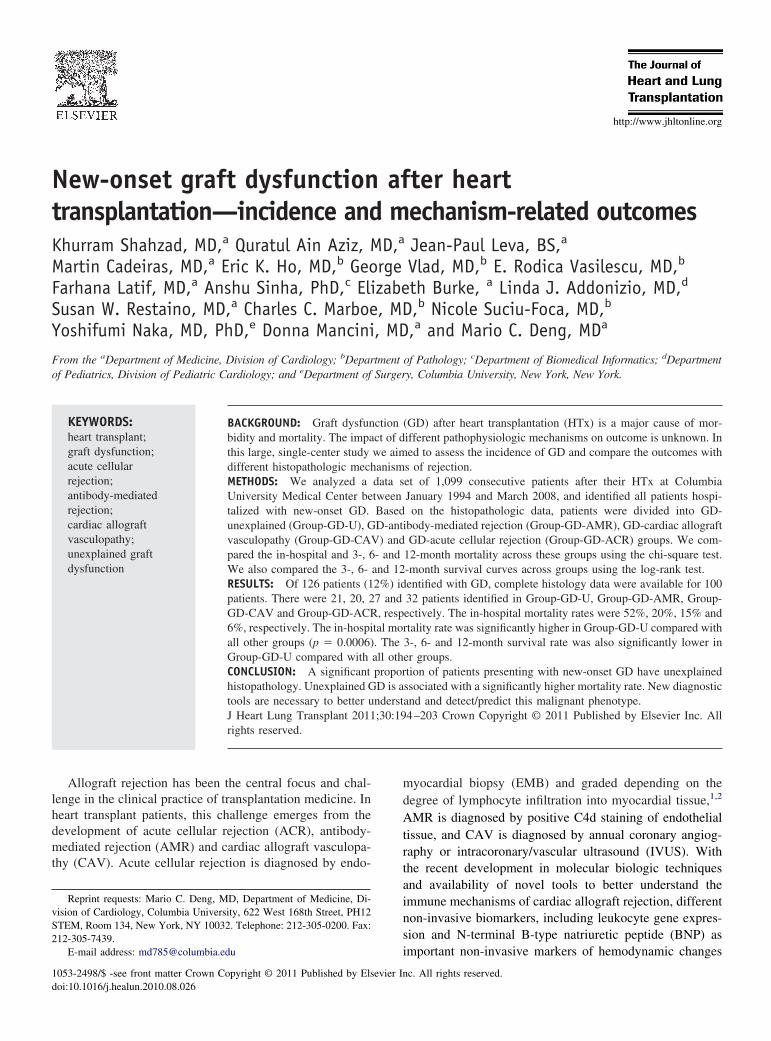
f the 100 patients, 20 (20%), 27 (27%) and 32 (32%) weredentified in the GD-AMR, GD-CAV and GD-ACR groups,espectively, explaining only 79% of the clinical cases of GDccording to all currently known mechanisms of allograft re-ection (Figure 1). Anti-HLA antibodies were detected in 80%,5% and 59% of the patients in Group-GD-AMR, Group-GD-AV and Group-GD-ACR, respectively. There were 4 patients
dentified with AMR based on C4d-positive staining with novidence of circulating anti-HLA antibodies.
nexplained graft dysfunction
f the 100 patients with complete histology data, there were1 patients (21%) in whom all routinely tested histopatho-ogic mechanisms of rejection were found to be normal athe time of their hospitalization with acute allograft failureGroup-GD-U). Anti-HLA antibodies were detected in 38%n � 8) of the patients in Group-GD-U.
R Group-GD-CAV(N � 27)
Group-GD-ACR(N � 32) p-value
54 � 13 52 � 17 0.81a
0.48a
20 (74%) 20 (62%)4 (15%) 6 (19%)2 (7%) 5 (16%)1 (4%) 1 (3%)
0.45a
3 (11%) 8 (25%)24 (89%) 24 (75%)6.1 � 3.7 3.1 � 2.9 0.001a
13 (48%) 9 (31%) 0.010 (0%) 4 (13%) 0.37b
12 (44%) 13 (43%) 0.23b
18 (67%) 18 (60%) 0.49b
19 (70%) 21 (70%) 0.84b
20 (74%) 17 (57%) 0.16b
ac allograft vasculopathy; LVAD, left ventricular assist device; RI, renal
ion
GD-AM0)
15
%)%)))
%)%)2.8%)%)
%)%)%)%)
, cardi
I
OhG(2daiGAaw
M
IdTG5rG
Gw(GG(rGg
K1
OAtsGsw
FpgGwca
Fw
197Shahzad et al. New-onset Graft Dysfunction Post-HTx
n-hospital mortality and time-to-event analysis
verall, there were 21 patients (21%) who died during theirospital stay. Group-GD-AMR, Group-GD-CAV androup-GD-ACR had in-hospital mortality rates of 20%
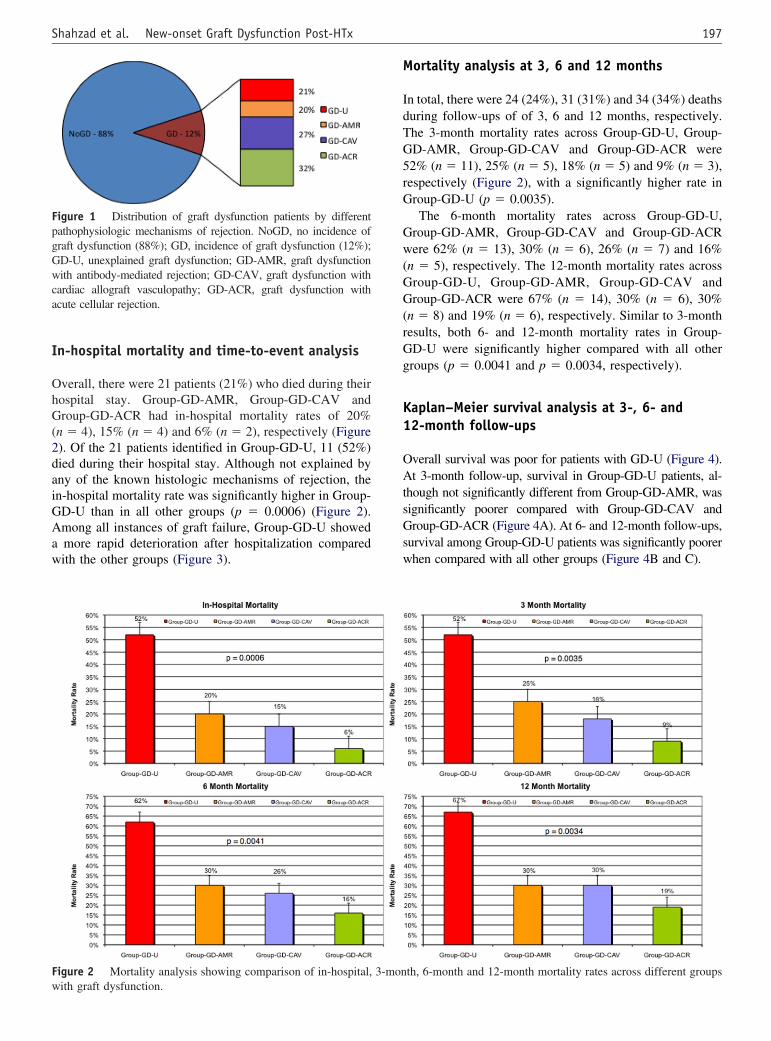
n � 4), 15% (n � 4) and 6% (n � 2), respectively (Figure). Of the 21 patients identified in Group-GD-U, 11 (52%)ied during their hospital stay. Although not explained byny of the known histologic mechanisms of rejection, then-hospital mortality rate was significantly higher in Group-D-U than in all other groups (p � 0.0006) (Figure 2).mong all instances of graft failure, Group-GD-U showedmore rapid deterioration after hospitalization comparedith the other groups (Figure 3).
igure 1 Distribution of graft dysfunction patients by differentathophysiologic mechanisms of rejection. NoGD, no incidence ofraft dysfunction (88%); GD, incidence of graft dysfunction (12%);D-U, unexplained graft dysfunction; GD-AMR, graft dysfunctionith antibody-mediated rejection; GD-CAV, graft dysfunction with
ardiac allograft vasculopathy; GD-ACR, graft dysfunction withcute cellular rejection.
igure 2 Mortality analysis showing comparison of in-hospital,
ith graft dysfunction.ortality analysis at 3, 6 and 12 months
n total, there were 24 (24%), 31 (31%) and 34 (34%) deathsuring follow-ups of of 3, 6 and 12 months, respectively.he 3-month mortality rates across Group-GD-U, Group-D-AMR, Group-GD-CAV and Group-GD-ACR were2% (n � 11), 25% (n � 5), 18% (n � 5) and 9% (n � 3),espectively (Figure 2), with a significantly higher rate inroup-GD-U (p � 0.0035).The 6-month mortality rates across Group-GD-U,
roup-GD-AMR, Group-GD-CAV and Group-GD-ACRere 62% (n � 13), 30% (n � 6), 26% (n � 7) and 16%
n � 5), respectively. The 12-month mortality rates acrossroup-GD-U, Group-GD-AMR, Group-GD-CAV androup-GD-ACR were 67% (n � 14), 30% (n � 6), 30%
n � 8) and 19% (n � 6), respectively. Similar to 3-monthesults, both 6- and 12-month mortality rates in Group-D-U were significantly higher compared with all otherroups (p � 0.0041 and p � 0.0034, respectively).
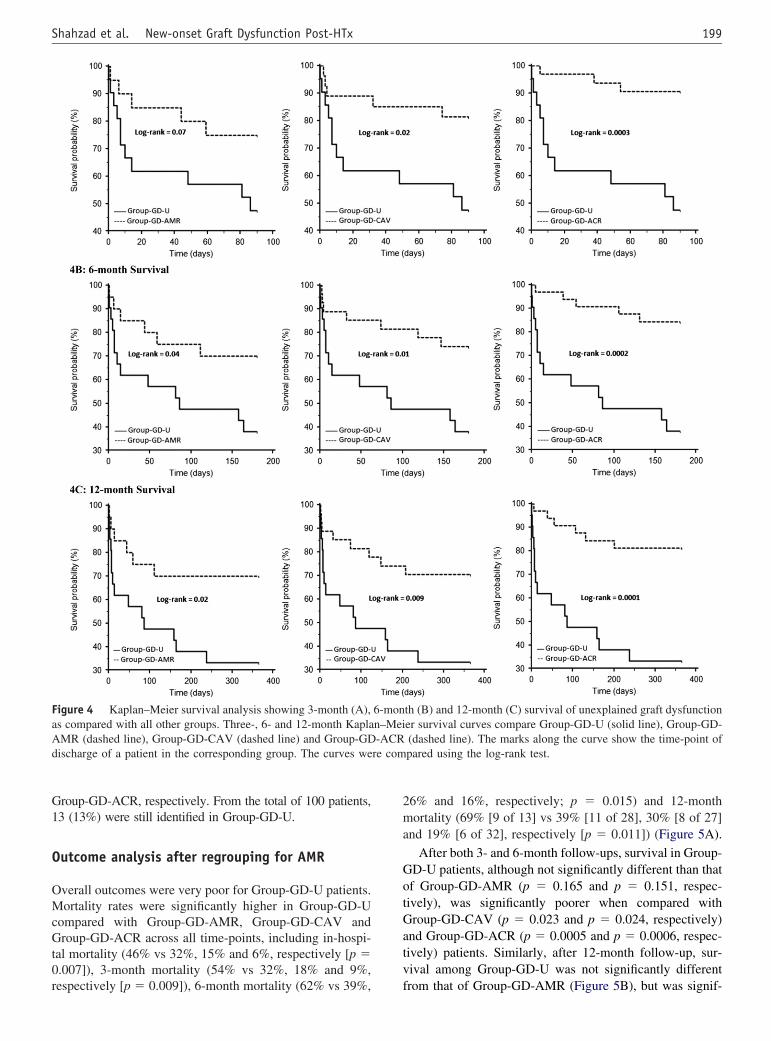
aplan–Meier survival analysis at 3-, 6- and2-month follow-ups
verall survival was poor for patients with GD-U (Figure 4).t 3-month follow-up, survival in Group-GD-U patients, al-
hough not significantly different from Group-GD-AMR, wasignificantly poorer compared with Group-GD-CAV androup-GD-ACR (Figure 4A). At 6- and 12-month follow-ups,
urvival among Group-GD-U patients was significantly poorerhen compared with all other groups (Figure 4B and C).
th, 6-month and 12-month mortality rates across different groups
3-mon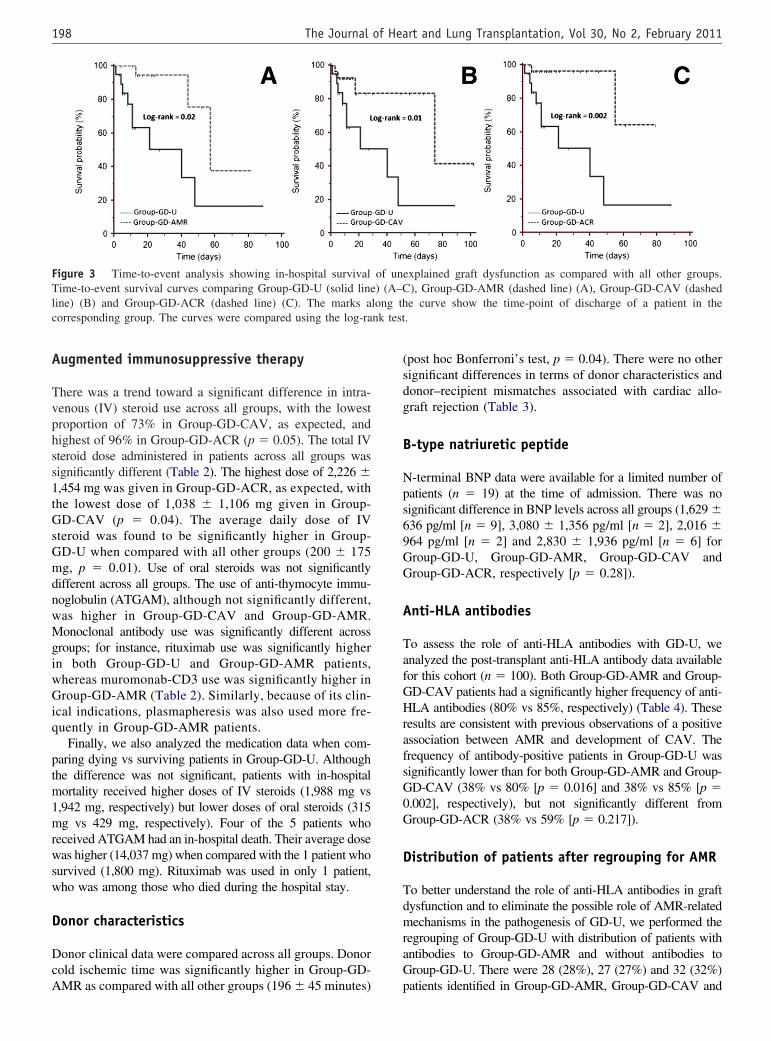
A
Tvphss1tGsGmdnwMgiwGiq
ptm1mrwsw
D
DcA
(sdg
B
Nps69GG
A
TafGHrafsG0G
D
TdmraG
FTlc nk test
198 The Journal of Heart and Lung Transplantation, Vol 30, No 2, February 2011
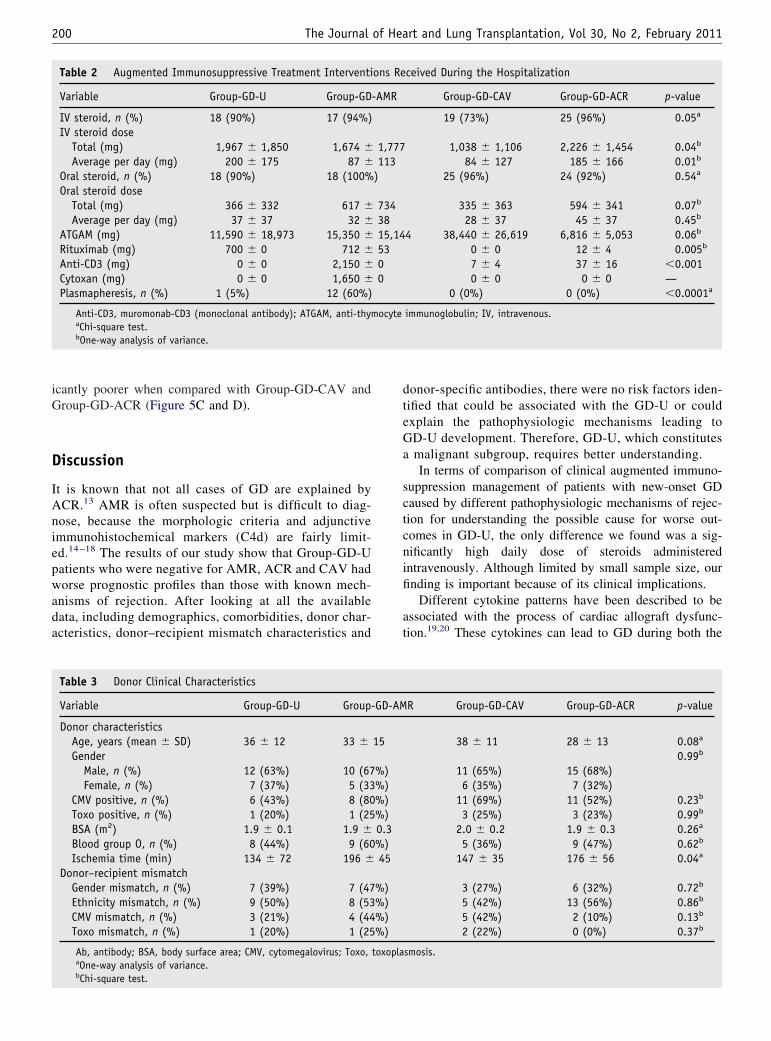
ugmented immunosuppressive therapy
here was a trend toward a significant difference in intra-enous (IV) steroid use across all groups, with the lowestroportion of 73% in Group-GD-CAV, as expected, andighest of 96% in Group-GD-ACR (p � 0.05). The total IVteroid dose administered in patients across all groups wasignificantly different (Table 2). The highest dose of 2,226 �,454 mg was given in Group-GD-ACR, as expected, withhe lowest dose of 1,038 � 1,106 mg given in Group-D-CAV (p � 0.04). The average daily dose of IV
teroid was found to be significantly higher in Group-D-U when compared with all other groups (200 � 175g, p � 0.01). Use of oral steroids was not significantly
ifferent across all groups. The use of anti-thymocyte immu-oglobulin (ATGAM), although not significantly different,as higher in Group-GD-CAV and Group-GD-AMR.onoclonal antibody use was significantly different across
roups; for instance, rituximab use was significantly highern both Group-GD-U and Group-GD-AMR patients,hereas muromonab-CD3 use was significantly higher inroup-GD-AMR (Table 2). Similarly, because of its clin-
cal indications, plasmapheresis was also used more fre-uently in Group-GD-AMR patients.
Finally, we also analyzed the medication data when com-aring dying vs surviving patients in Group-GD-U. Althoughhe difference was not significant, patients with in-hospitalortality received higher doses of IV steroids (1,988 mg vs
,942 mg, respectively) but lower doses of oral steroids (315g vs 429 mg, respectively). Four of the 5 patients who
eceived ATGAM had an in-hospital death. Their average doseas higher (14,037 mg) when compared with the 1 patient who
urvived (1,800 mg). Rituximab was used in only 1 patient,ho was among those who died during the hospital stay.
onor characteristics
onor clinical data were compared across all groups. Donorold ischemic time was significantly higher in Group-GD-
igure 3 Time-to-event analysis showing in-hospital survivalime-to-event survival curves comparing Group-GD-U (solid line
ine) (B) and Group-GD-ACR (dashed line) (C). The marks aorresponding group. The curves were compared using the log-ra
MR as compared with all other groups (196 � 45 minutes) p
post hoc Bonferroni’s test, p � 0.04). There were no otherignificant differences in terms of donor characteristics andonor–recipient mismatches associated with cardiac allo-raft rejection (Table 3).
-type natriuretic peptide
-terminal BNP data were available for a limited number ofatients (n � 19) at the time of admission. There was noignificant difference in BNP levels across all groups (1,629 �36 pg/ml [n � 9], 3,080 � 1,356 pg/ml [n � 2], 2,016 �64 pg/ml [n � 2] and 2,830 � 1,936 pg/ml [n � 6] forroup-GD-U, Group-GD-AMR, Group-GD-CAV androup-GD-ACR, respectively [p � 0.28]).
nti-HLA antibodies
o assess the role of anti-HLA antibodies with GD-U, wenalyzed the post-transplant anti-HLA antibody data availableor this cohort (n � 100). Both Group-GD-AMR and Group-D-CAV patients had a significantly higher frequency of anti-LA antibodies (80% vs 85%, respectively) (Table 4). These
esults are consistent with previous observations of a positivessociation between AMR and development of CAV. Therequency of antibody-positive patients in Group-GD-U wasignificantly lower than for both Group-GD-AMR and Group-D-CAV (38% vs 80% [p � 0.016] and 38% vs 85% [p �.002], respectively), but not significantly different fromroup-GD-ACR (38% vs 59% [p � 0.217]).
istribution of patients after regrouping for AMR
o better understand the role of anti-HLA antibodies in graftysfunction and to eliminate the possible role of AMR-relatedechanisms in the pathogenesis of GD-U, we performed the
egrouping of Group-GD-U with distribution of patients withntibodies to Group-GD-AMR and without antibodies toroup-GD-U. There were 28 (28%), 27 (27%) and 32 (32%)
explained graft dysfunction as compared with all other groups.), Group-GD-AMR (dashed line) (A), Group-GD-CAV (dashede curve show the time-point of discharge of a patient in the
.
of un) (A–C
long th
atients identified in Group-GD-AMR, Group-GD-CAV and
G1
O
OMcGt0r
2ma
GotGatv
FaAd re com
199Shahzad et al. New-onset Graft Dysfunction Post-HTx
roup-GD-ACR, respectively. From the total of 100 patients,3 (13%) were still identified in Group-GD-U.
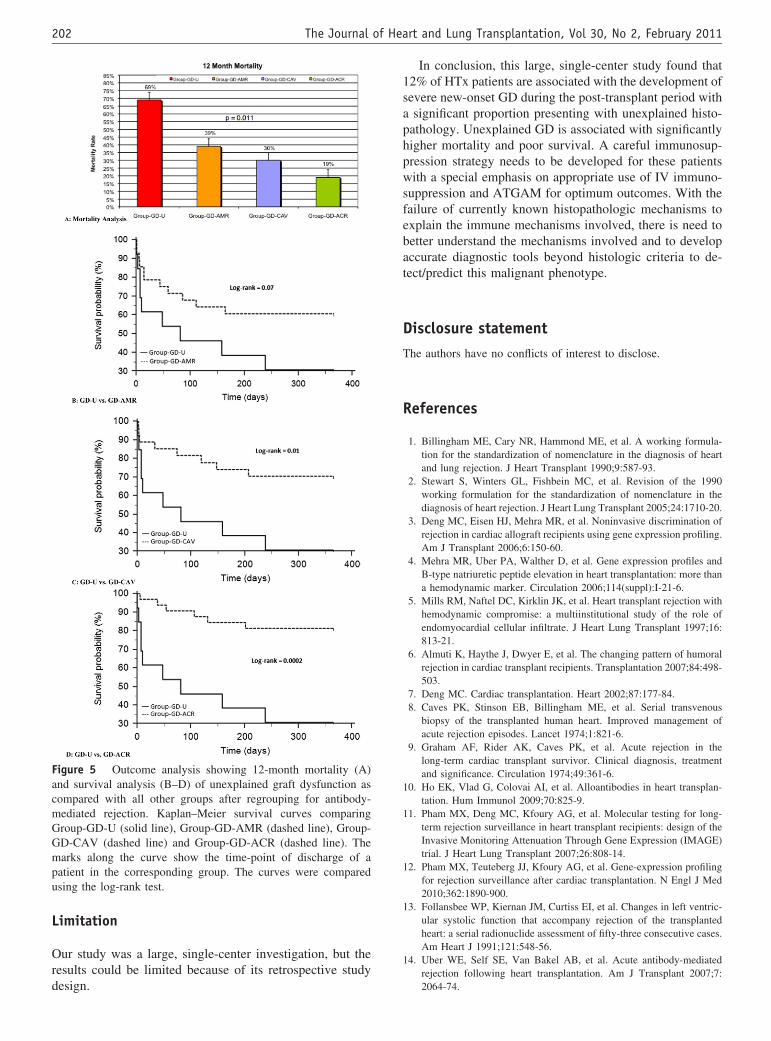
utcome analysis after regrouping for AMR
verall outcomes were very poor for Group-GD-U patients.ortality rates were significantly higher in Group-GD-U
ompared with Group-GD-AMR, Group-GD-CAV androup-GD-ACR across all time-points, including in-hospi-
al mortality (46% vs 32%, 15% and 6%, respectively [p �.007]), 3-month mortality (54% vs 32%, 18% and 9%,
igure 4 Kaplan–Meier survival analysis showing 3-month (A),s compared with all other groups. Three-, 6- and 12-month KaplaMR (dashed line), Group-GD-CAV (dashed line) and Group-GDischarge of a patient in the corresponding group. The curves we
espectively [p � 0.009]), 6-month mortality (62% vs 39%, f
6% and 16%, respectively; p � 0.015) and 12-monthortality (69% [9 of 13] vs 39% [11 of 28], 30% [8 of 27]
nd 19% [6 of 32], respectively [p � 0.011]) (Figure 5A).
After both 3- and 6-month follow-ups, survival in Group-D-U patients, although not significantly different than thatf Group-GD-AMR (p � 0.165 and p � 0.151, respec-ively), was significantly poorer when compared withroup-GD-CAV (p � 0.023 and p � 0.024, respectively)
nd Group-GD-ACR (p � 0.0005 and p � 0.0006, respec-ively) patients. Similarly, after 12-month follow-up, sur-ival among Group-GD-U was not significantly different
th (B) and 12-month (C) survival of unexplained graft dysfunctioner survival curves compare Group-GD-U (solid line), Group-GD-(dashed line). The marks along the curve show the time-point ofpared using the log-rank test.
6-monn–Mei-ACR
rom that of Group-GD-AMR (Figure 5B), but was signif-
iG
D
IAniepwada
dteGa
sctcnifi
at
200 The Journal of Heart and Lung Transplantation, Vol 30, No 2, February 2011
cantly poorer when compared with Group-GD-CAV androup-GD-ACR (Figure 5C and D).
iscussion
t is known that not all cases of GD are explained byCR.13 AMR is often suspected but is difficult to diag-ose, because the morphologic criteria and adjunctivemmunohistochemical markers (C4d) are fairly limit-d.14 –18 The results of our study show that Group-GD-Uatients who were negative for AMR, ACR and CAV hadorse prognostic profiles than those with known mech-
nisms of rejection. After looking at all the availableata, including demographics, comorbidities, donor char-cteristics, donor–recipient mismatch characteristics and
Table 2 Augmented Immunosuppressive Treatment Interventi
Variable Group-GD-U Group-GD
IV steroid, n (%) 18 (90%) 17 (94%)IV steroid dose
Total (mg) 1,967 � 1,850 1,674 �Average per day (mg) 200 � 175 87 �
Oral steroid, n (%) 18 (90%) 18 (100%Oral steroid dose
Total (mg) 366 � 332 617 �Average per day (mg) 37 � 37 32 �
ATGAM (mg) 11,590 � 18,973 15,350 �Rituximab (mg) 700 � 0 712 �Anti-CD3 (mg) 0 � 0 2,150 �Cytoxan (mg) 0 � 0 1,650 �Plasmapheresis, n (%) 1 (5%) 12 (60%)
Anti-CD3, muromonab-CD3 (monoclonal antibody); ATGAM, anti-thymaChi-square test.bOne-way analysis of variance.
Table 3 Donor Clinical Characteristics
Variable Group-GD-U Group
Donor characteristicsAge, years (mean � SD) 36 � 12 33 �Gender
Male, n (%) 12 (63%) 10 (67Female, n (%) 7 (37%) 5 (33
CMV positive, n (%) 6 (43%) 8 (80Toxo positive, n (%) 1 (20%) 1 (25BSA (m2) 1.9 � 0.1 1.9 �Blood group O, n (%) 8 (44%) 9 (60Ischemia time (min) 134 � 72 196 �
Donor–recipient mismatchGender mismatch, n (%) 7 (39%) 7 (47Ethnicity mismatch, n (%) 9 (50%) 8 (53CMV mismatch, n (%) 3 (21%) 4 (44Toxo mismatch, n (%) 1 (20%) 1 (25
Ab, antibody; BSA, body surface area; CMV, cytomegalovirus; Toxo,aOne-way analysis of variance.b
Chi-square test.onor-specific antibodies, there were no risk factors iden-ified that could be associated with the GD-U or couldxplain the pathophysiologic mechanisms leading toD-U development. Therefore, GD-U, which constitutesmalignant subgroup, requires better understanding.In terms of comparison of clinical augmented immuno-
uppression management of patients with new-onset GDaused by different pathophysiologic mechanisms of rejec-ion for understanding the possible cause for worse out-omes in GD-U, the only difference we found was a sig-ificantly high daily dose of steroids administeredntravenously. Although limited by small sample size, ournding is important because of its clinical implications.
Different cytokine patterns have been described to bessociated with the process of cardiac allograft dysfunc-ion.19,20 These cytokines can lead to GD during both the
ceived During the Hospitalization
Group-GD-CAV Group-GD-ACR p-value
19 (73%) 25 (96%) 0.05a
1,038 � 1,106 2,226 � 1,454 0.04b
84 � 127 185 � 166 0.01b
25 (96%) 24 (92%) 0.54a
335 � 363 594 � 341 0.07b
28 � 37 45 � 37 0.45b
4 38,440 � 26,619 6,816 � 5,053 0.06b
0 � 0 12 � 4 0.005b
7 � 4 37 � 16 �0.0010 � 0 0 � 0 —
0 (0%) 0 (0%) �0.0001a
immunoglobulin; IV, intravenous.
R Group-GD-CAV Group-GD-ACR p-value
38 � 11 28 � 13 0.08a
0.99b
11 (65%) 15 (68%)6 (35%) 7 (32%)
11 (69%) 11 (52%) 0.23b
3 (25%) 3 (23%) 0.99b
2.0 � 0.2 1.9 � 0.3 0.26a
5 (36%) 9 (47%) 0.62b
147 � 35 176 � 56 0.04a
3 (27%) 6 (32%) 0.72b
5 (42%) 13 (56%) 0.86b
5 (42%) 2 (10%) 0.13b
2 (22%) 0 (0%) 0.37b
smosis.
ons Re
-AMR
1,777113
)
7343815,145300
ocyte
-GD-AM
15
%)%)%)%)0.3%)45
%)%)%)%)
toxopla

ptiospttwpktamnmct
ahttsAsAalwAGm
AobtlatgA
cwv
LIGwtaktat
nnphop
uPpiaeoC(scjcgtelprtavbprps
201Shahzad et al. New-onset Graft Dysfunction Post-HTx
rocess of rejection and sepsis. The balance between rejec-ion and sepsis that is critically affected by augmentedmmunosuppression needs to be maintained in order toptimally treat GD. These cytokine patterns could be re-ponsible for the GD-U. From the clinical managementoint of view, many transplant centers advocate augmenta-ion of immunosuppression, assuming that EMB is insensi-ive in diagnosis of rejection.21 These patients are treatedith clinically indicated over-immunosuppression. Thisractice, in the absence of an objective criteria and withoutnowing the appropriate diagnosis, leads to imbalance inhe cytokine patterns, which complicates the clinical coursend leads to death in some cases.22 The reports of improve-ent in some patients by treatment with enhanced immu-
osuppression21 also suggest the role of possible immune-ediated mechanisms along with the immunoregulatory
ytokines. Further studies are required to better understandhe immune mechanisms involved in this phenotype.
In many cases, AMR is the default diagnosis in thebsence of supporting evidence for ACR. AMR has beenistorically diagnosed by immunoglobulin deposition asested by immunofluorescence with the presence of endo-helial swelling, capillary leak and hemorrhage. Since 2005,taining for C4d complement was added for diagnosis ofMR. Recently, it was suggested that inclusion of C3d
taining to C4d staining is more helpful for the diagnosis ofMR.23 Because there are no consensus guidelines avail-
ble as yet, AMR diagnosis still remains a clinical chal-enge. Further analysis in our study by including patientsith only DSA in the absence of histology into Group-GD-MR, which showed still worse outcomes for Group-D-U, rules out the possibility of any role of AMR-relatedechanisms involved in the pathogenesis of GD-U.The observation in our study of 3 patients identified with
MR based on positive C4d staining but having no evidencef circulating anti-HLA antibodies may be explained by C4dinding to anti-endothelial non-HLA antibodies. It is of interesthat patients with GD-U have the lowest frequencies of circu-ating antibodies. The frequency of patients with anti-HLAntibodies positive was higher in CAV and AMR groups, andhis frequency was significantly higher than in the unexplainedroup, suggesting the role of an immune mechanism beyondMR in patients with GD-U.Graft dysfunction can be defined using different LVEF
riteria—for example, LVEF �45% was used by the ISHLTorking formulation for the standardized nomenclature de-
Table 4 Donor-specific Antibodies inExplained Groups
Comparison groups An
Group-GD-U vs Group-GD-AMR 38Group-GD-U vs Group-GD-CAV 38Group-GD-U vs Group-GD-ACR 38
Ab, antibody; HLA, human leukocyte antiaChi-square test.
elopment for CAV.24 In our study, GD was defined as b
VEF �30% being representative of a severe form of GD.n our clinical observations there have been clinical cases ofD-U with a less severe decrease in LVEF. Perhaps theorse outcomes, as observed in this study, are the charac-
eristic of severe GD cases when they are treated withggressive IV immunosuppression in the absence of allnown pathophysiologic mechanisms of rejection. Al-hough less severe cases were not included in the currentnalysis, it would be of interest to see how such cases arereated in clinical practice and their related outcomes.
With the early and non-invasive detection of clinical phe-otype as the key concept in the management of HTx patients,on-invasive markers, such as BNP, represent potentially im-ortant markers of ventricular wall stress and are predictive ofemodynamic abnormalities in heart transplantation.25,26 Inur study, BNP data were available in a limited number ofatients, so it is difficult to make any significant conclusion.
We will need to use novel tools to reach the goal ofnderstanding the immune mechanisms involved in GD-U.eripheral blood mononuclear cells (PBMC), being an im-ortant part of the immune system, play a pivotal role innflammation, sepsis and transplant immunobiology. Forcute cellular rejection, based on the rationale that genexpression profiling (GEP) of PBMC reflects the activationf host responses by the cardiac allograft, the multicenterardiac Allograft Rejection Gene expression Observational
CARGO) study developed and validated a molecular clas-ifier to distinguish ISHLT Grade 0 rejection (i.e., quies-ence) from moderate/severe (ISHLT Grade �3A/2R) re-ection.3 The concept that early immune activation byontinuous interaction between recipient leukocytes and allo-raft endothelial cells leads to complementary changes in theransplanted myocardium (according to electrocardiogram/chocardiogram) is intriguing.4 We have shown that such aink exists between the cardiac allograft and the recipienteripheral leukocytes.27–29 In addition, we have shown theelationship of leukocyte GEP in patients with AMR.30 Usinghe whole transcriptome-wide leukocyte GEP approach asdopted in acute cellular allograft rejection, specifically di-ided into subtypes including B cells and T cells, may help usetter understand the immune mechanisms of GD. This ap-roach can also help us delineate inflammation- and sepsis-elated mechanisms, such as cytokine patters involved in theathogenesis of GD. If identified in prospectively designedtudies, the results can be used to develop novel biomarkers,
ained Group as Compared With the
-Ab positive p-value
f 21) vs 80% (16 of 20) 0.016a
f 21) vs 85% (23 of 27) 0.002a
f 21) vs 59% (19 of 32) 0.217a
Unexpl
ti-HLA
% (8 o% (8 o% (8 o
gen.
eyond histology, for the early diagnosis of GD-U patients.
L
Ord
1saphpwsfebat
DT
R
1
1
1
1
1
FacmGGmpu
202 The Journal of Heart and Lung Transplantation, Vol 30, No 2, February 2011
imitation
ur study was a large, single-center investigation, but theesults could be limited because of its retrospective study
igure 5 Outcome analysis showing 12-month mortality (A)nd survival analysis (B–D) of unexplained graft dysfunction asompared with all other groups after regrouping for antibody-ediated rejection. Kaplan–Meier survival curves comparingroup-GD-U (solid line), Group-GD-AMR (dashed line), Group-D-CAV (dashed line) and Group-GD-ACR (dashed line). Thearks along the curve show the time-point of discharge of a
atient in the corresponding group. The curves were comparedsing the log-rank test.
esign.
In conclusion, this large, single-center study found that2% of HTx patients are associated with the development ofevere new-onset GD during the post-transplant period withsignificant proportion presenting with unexplained histo-
athology. Unexplained GD is associated with significantlyigher mortality and poor survival. A careful immunosup-ression strategy needs to be developed for these patientsith a special emphasis on appropriate use of IV immuno-
uppression and ATGAM for optimum outcomes. With theailure of currently known histopathologic mechanisms toxplain the immune mechanisms involved, there is need toetter understand the mechanisms involved and to developccurate diagnostic tools beyond histologic criteria to de-ect/predict this malignant phenotype.
isclosure statementhe authors have no conflicts of interest to disclose.
eferences
1. Billingham ME, Cary NR, Hammond ME, et al. A working formula-tion for the standardization of nomenclature in the diagnosis of heartand lung rejection. J Heart Transplant 1990;9:587-93.
2. Stewart S, Winters GL, Fishbein MC, et al. Revision of the 1990working formulation for the standardization of nomenclature in thediagnosis of heart rejection. J Heart Lung Transplant 2005;24:1710-20.
3. Deng MC, Eisen HJ, Mehra MR, et al. Noninvasive discrimination ofrejection in cardiac allograft recipients using gene expression profiling.Am J Transplant 2006;6:150-60.
4. Mehra MR, Uber PA, Walther D, et al. Gene expression profiles andB-type natriuretic peptide elevation in heart transplantation: more thana hemodynamic marker. Circulation 2006;114(suppl):I-21-6.
5. Mills RM, Naftel DC, Kirklin JK, et al. Heart transplant rejection withhemodynamic compromise: a multiinstitutional study of the role ofendomyocardial cellular infiltrate. J Heart Lung Transplant 1997;16:813-21.
6. Almuti K, Haythe J, Dwyer E, et al. The changing pattern of humoralrejection in cardiac transplant recipients. Transplantation 2007;84:498-503.
7. Deng MC. Cardiac transplantation. Heart 2002;87:177-84.8. Caves PK, Stinson EB, Billingham ME, et al. Serial transvenous
biopsy of the transplanted human heart. Improved management ofacute rejection episodes. Lancet 1974;1:821-6.
9. Graham AF, Rider AK, Caves PK, et al. Acute rejection in thelong-term cardiac transplant survivor. Clinical diagnosis, treatmentand significance. Circulation 1974;49:361-6.
0. Ho EK, Vlad G, Colovai AI, et al. Alloantibodies in heart transplan-tation. Hum Immunol 2009;70:825-9.
1. Pham MX, Deng MC, Kfoury AG, et al. Molecular testing for long-term rejection surveillance in heart transplant recipients: design of theInvasive Monitoring Attenuation Through Gene Expression (IMAGE)trial. J Heart Lung Transplant 2007;26:808-14.
2. Pham MX, Teuteberg JJ, Kfoury AG, et al. Gene-expression profilingfor rejection surveillance after cardiac transplantation. N Engl J Med2010;362:1890-900.
3. Follansbee WP, Kiernan JM, Curtiss EI, et al. Changes in left ventric-ular systolic function that accompany rejection of the transplantedheart: a serial radionuclide assessment of fifty-three consecutive cases.Am Heart J 1991;121:548-56.
4. Uber WE, Self SE, Van Bakel AB, et al. Acute antibody-mediatedrejection following heart transplantation. Am J Transplant 2007;7:
2064-74.
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
203Shahzad et al. New-onset Graft Dysfunction Post-HTx
5. Reed EF, Demetris AJ, Hammond E, et al. Acute antibody-mediatedrejection of cardiac transplants. J Heart Lung Transplant 2006;25:153-9.
6. Reed E, Cohen DJ, Barr ML, et al. Effect of anti-HLA and anti-idiotypic antibodies on the long-term survival of heart and kidneyallografts. Transplant Proc 1992;24:2494-5.
7. Cherry R, Nielsen H, Reed E, et al. Vascular (humoral) rejection inhuman cardiac allograft biopsies: relation to circulating anti-HLAantibodies. J Heart Lung Transplant 1992;11:24-9.
8. Suciu-Foca N, Reed E, Marboe C, et al. The role of anti-HLA anti-bodies in heart transplantation. Transplantation 1991;51:716-24.
9. Deng MC, Erren M, Roeder N, et al. T-cell and monocyte subsets,inflammatory molecules, rejection, and hemodynamics early after car-diac transplantation. Transplantation 1998;65:1255-61.
0. Deng MC, Erren M, Kammerling L, et al. The relation of interleukin-6,tumor necrosis factor-alpha, IL-2, and IL-2 receptor levels to cellularrejection, allograft dysfunction, and clinical events early after cardiactransplantation. Transplantation 1995;60:1118-24.
1. McNamara D, Di Salvo T, Mathier M, et al. Left ventricular dysfunc-tion after heart transplantation: incidence and role of enhanced immu-nosuppression. J Heart Lung Transplant 1996;15:506-15.
2. Boilson BA, Miller DV, Pereira NL. Late allograft failure after hearttransplantation: 2 unusual cases. J Heart Lung Transplant 2008;27:1050-4.
3. Tan CD, Sokos GG, Pidwell DJ, et al. Correlation of donor-specificantibodies, complement and its regulators with graft dysfunction in car-
diac antibody-mediated rejection. Am J Transplant 2009;9:2075-84.4. Mehra MR, Crespo-Leiro MG, Dipchand A, et al. International Societyfor Heart and Lung Transplantation working formulation of a stan-dardized nomenclature for cardiac allograft vasculopathy—2010.J Heart Lung Transplant 2010;29:717-27.
5. Park MH, Uber PA, Scott RL, et al. B-type natriuretic peptide in hearttransplantation: an important marker of allograft performance. HeartFail Rev 2003;8:359-63.
6. Mehra MR, Uber PA, Potluri S, et al. Usefulness of an elevated B-typenatriuretic peptide to predict allograft failure, cardiac allograft vascu-lopathy, and survival after heart transplantation. Am J Cardiol 2004;94:454-8.
7. Cadeiras M, Shahzad K, John MM, et al. Relationship between avalidated molecular cardiac transplant rejection classifier and routineorgan function parameters. Clin Transplant 2009;24:321-7.
8. Shahzad K, He J, Li Q, et al. Relationship between prolonged QTc-interval, cardiac allograft dysfunction and elevated molecular geneexpression profiling test score after heart transplantation. J Heart LungTransplant 2010;29:711-3.
9. Shahzad K, Cadeiras M, Arai K, et al. Unexplained graft dysfunction afterheart transplantation—role of novel molecular expression test score andQTc-interval: a case report. Cardiol Res Pract 2010;230810.
0. Cadeiras M, Burke E, Dedrick R, et al. Gene expression profiles ofpatients with antibody-mediated rejection after cardiac transplantation.
J Heart Lung Transplant 2008;27:932-4.



















