
TO GRAFT OR NOT TO GRAFT? AN UPDATE ON GINGIVAL ...
76
TO GRAFT OR NOT TO GRAFT? AN UPDATE ON GINGIVAL GRAFTING DIAGNOSIS AND TREATMENT MODALITIES Richard J. Nagy, DDS Journa CALIFORNIA DENTAL ASSOCIATION Gingival Recession Autogenous Soft Tissue Grafting Tissue Engineering October 2018
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of TO GRAFT OR NOT TO GRAFT? AN UPDATE ON GINGIVAL ...

TO GRAFT OR NOT TO GRAFT?
AN UPDATE ON GINGIVAL GRAFTING DIAGNOSIS AND
TREATMENT MODALITIESRichard J. Nagy, DDS
JournaC A L I F O R N I A D E N T A L A S S O C I A T I O N
Gingival Recession
Autogenous Soft Tissue Grafting
Tissue Engineering
October 2018

Let’s go!Discover The Dentists Supply Company’s
online shopping experience that delivers
CDA members the supplies they need at
discounts that make a difference.
Price compare and save at tdsc.com.
Ready to save
Price comparisons are made to the manufacturer’s list price. Actual savings on tdsc.com will vary on a product-by-product basis.
20%?
C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 603
To Graft or Not To Graft? An Update on Gingival Grafting Diagnosis and Treatment Modalities
An introduction to the issue.Richard J. Nagy, DDS
Gingival Recession: What Is It All About?
This article reviews factors that enhance the risk for gingival recession, describes at what stage interceptive treatment should be recommended and expected outcomes.Debra S. Finney, DDS, MS, and Richard T. Kao, DDS, PhD
Autogenous Soft Tissue Grafting for the Treatment of Gingival Recession
This article reviews the use of autogenous soft tissue grafting for root coverage. Advantages and disadvantages of techniques are discussed. Case types provide indications for selection and treatment.Elissa Green, DMD; Soma Esmailian Lari, DMD; and Perry R. Klokkevold, DDS, MS
Acellular Dermal Matrix Allografts in Periodontal Therapy
This article reviews the material, techniques and rationale for ACD when there is inadequate autogenous donor tissue for the treatment site or the patient prefers a single surgical site.Joan Otomo-Corgel, DDS, MPH; Chanook David Ahn, DMD; and Allen Gunn, DDS
The Pinhole Surgical Technique: A Clinical Perspective and Treatment Considerations From a Periodontist
This commentary is intended to help guide clinicians in the decision-making process when considering root-coverage strategies.Tina M. Beck, DDS, MS
Tissue Engineering for Improving Periodontal Phenotype
This article provides clinicians with an understanding of how certain biotechnologies associated with tissue engineering may be incorporated into mucogingival surgery.Cherissa Chong, DMD, MS; Yung-Ting Hsu, DDS, MDSc; Paul Y. Lee, DDS; and Richard T. Kao, DDS, PhD
615
617
625
639
647
653
Oct. 2018
D E PA R TM E N T S
F E AT U R E S
609
The Editor/Nothing but the Tooth
Letter to the Editor
Impressions
RM Matters/Are Your Patients Who They Say They Are? Preventing Medical Identity Theft
Regulatory Compliance/OSHA Regulations: Fire Extinguishers, Eyewash, Exit Signs
Tech Trends
605
607
609
663
667
674

C DA J O U R N A L , V O L 4 6 , Nº 1 0
604 O C TO B E R 2 01 8
Volume 46, Number 10 October 2018
JournaC A L I F O R N I A D E N T A L A S S O C I A T I O N
CDA classifieds work harder to
bring you results. Selling a practice
or a piece of equipment? Now you
can include photos to help buyers
see the potential.
And if you’re hiring, candidates
anywhere can apply right from
the site. Looking for a job? You can
post that, too. And the best part—
it’s free to all CDA members.
All of these features are designed to
help you get the results you need,
faster than ever. Check it out for
yourself at cda.org/classifieds.
CDA Classifieds. Free postings.Priceless results.
CDA classifieds work harder to
bring you results. Selling a practice
or a piece of equipment? Now you
CDA Offi cersNatasha A. Lee, DDSPRESIDENT
R. Del Brunner, DDSPRESIDENT-ELECT
Richard J. Nagy, DDS VICE PRESIDENT
Judee Tippett-Whyte, DDS SECRETARY
Steven J. Kend, DDSTREASURER
Craig S. Yarborough, DDS, MBASPEAKER OF THE HOUSE
Clelan G. Ehrler, DDSIMMEDIATE PAST PRESIDENT
ManagementPeter A. DuBoisEXECUTIVE DIRECTOR
Carrie E. GordonCHIEF STRATEGY OFFICER
Kristine AllingtonVICE PRESIDENT, MARKETING
AND MEMBERSHIP
Alicia MalabyCOMMUNICATIONS
DIRECTOR
EditorialKerry K. Carney, DDS, CDEEDITOR-IN-CHIEF
Ruchi K. Sahota, DDS, CDEASSOCIATE EDITOR
Brian K. Shue, DDS, CDEASSOCIATE EDITOR
Gayle Mathe, RDHSENIOR EDITOR
Richard J. Nagy, DDSGUEST EDITOR
Andrea LaMattina, CDEPUBLICATIONS MANAGER
Kristi Parker JohnsonEDITORIAL SPECIALIST
Blake EllingtonTECH TRENDS EDITOR
Jack F. Conley, DDSEDITOR EMERITUS
Robert E. Horseman, DDSHUMORIST EMERITUS
ProductionVal B. MinaSENIOR GRAPHIC DESIGNER
Randi TaylorSENIOR GRAPHIC DESIGNER
Upcoming Topics November/General TopicsDecember/BiomaterialsJanuary/CAMBRA/PBRN
AdvertisingSue Gardner ADVERTISING SALES
Permission and ReprintsAndrea LaMattina, CDEPUBLICATIONS MANAGER
Manuscript Submissionswww.editorialmanager.com/jcaldentassoc
Letters to the Editorwww.editorialmanager.com/jcaldentassoc
SubscriptionsSubscriptions are available only to active members of the Association. The subscription rate is $18 and is included in membership dues. Nonmembers can view the publication online at cda.org/journal.
Manage your subscription online: go to cda.org, log in and update any changes to your mailing information.Email questions or other changes to [email protected].
published by the California Dental Association 1201 K St., 14th Floor Sacramento, CA 95814 800.232.7645 cda.org
Journal of the California Dental Association (ISSN 1043–2256) is published monthly by the California Dental Association, 1201 K St., 14th Floor, Sacramento, CA 95814, 916.554.5950. Periodicals postage paid at Sacramento, Calif. Postmaster: Send address changes to Journal of the California Dental Association, P.O. Box 13749, Sacramento, CA 95853.
The California Dental Association holds the copyright for all articles and artwork published herein. The Journal of the California Dental Association is published under the supervision of CDA’s editorial staff . Neither the editorial staff , the editor, nor the association are responsible for any expression of opinion or statement of fact, all of which are published solely on the authority of the author whose name is indicated. The association reserves the right to illustrate, reduce, revise or reject any manuscript submitted. Articles are considered for publication on condition that they are contributed solely to the Journal.
Copyright 2018 by the California Dental Association. All rights reserved.
Stay Connected cda.org/journal

C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 605
Editor
A picture is worth a thousand words.” Some might say that is an understatement. There was a graduate student in anthropology who wrote
her entire master’s thesis based on one photograph. Her advisor had given her an old photo of the studio of a well-known artist from a northwest coast Native American culture. She meticulously cataloged every identifi able item in the photo of the cluttered studio. She devised a relative ruler and gave the dimensions of the visible artworks. She researched the motifs used in the sculptures and their cultural relevance. She was able to track down some of the pieces and place them in the three-dimensional world of today. That picture was worth much more than a thousand words.
In the same way that a tattered photograph was a repository of volumes of data, which needed only to be recognized and interpreted, so too can a single tooth be worth more than a thousand words.
The tooth is the basic unit of our science. In the profession of dentistry we are usually interested in a more “macro” view. Our attention is focused not so much on the single tooth but on how each tooth functions together with the other teeth, the supporting periodontal structures and how they fulfi ll the functional requirements of oral health. In an expanded view, all the teeth perform their part in the psychosocial health of the individual through a healthy smile. In an even more universal view, teeth serve as bits of evidential data we rely on in formulating policy decisions aimed at promoting oral health on a global scale.
Why is the tooth such a treasure trove of information? What if we zoom in on that tooth and consider nothing but the tooth. What is it about that small organ, the tooth, that makes it so special?
“
The tooth endures. It can last millions of years. The enamel of teeth in fossilized remains is the original enamel that was laid down during the developmental period of the individual’s lifetime. Enamel demarcation lines can be delineated and counted. The enamel lines are somewhat similar to tree rings. They seem to demarcate a short daily pattern and a longer eight-day period. If the individual died before the tooth was completely developed, it is possible to count the lines from the birth demarcation line and estimate the individual’s age at death and compare rates of maturation with modern Homo sapiens. That rate can be contrasted with nonhuman primate maturation. The tooth supplies evidence that our prehistoric ancestors manifested a change in the rate of maturation. The prolongation of childhood that we observe today can be seen in the fossil record and documented through enamel lines.
The tooth is a biochemical archive. The proportions of carbon isotopes C-13 and C-12 are different in tropical grasses and sedges compared to fruits and nuts. During maturation, a record of the categories of plants that were being ingested is incorporated into the enamel. There are also biochemical markers that help estimate the proportion of meat-to-plant intake.
Tooth enamel samples divulge that more than 3 million years ago our ancestors had diversifi ed their diet beyond that of chimpanzees.
The tooth is a tool. It is a tool for mastication as well as a cultural tool. It can tell us what kind of food it can best process: meat, grains, grasses. It can tell us how it was used and abused. We can tell if it was worn down by the incorporation of abrasives like sand into the daily diet. This can tell us something about how and where food was gathered and processed.
We can tell from the wear marks on a tooth if it was used in the preparation of materials for clothing or in the adapting of materials for building or food gathering or cultivating. Wear patterns may indicate if sinew or plant fi bers were chewed or scraped to prepare them for use in the making of clothing, baskets or weapons.
The tooth is a thing of beauty. We can tell if it was adapted or adorned for cultural reasons. Was it fi led into a point to refl ect a cultural preference for or admiration of a dagger smile? Was there an inlay of stone or jade? Was it abraded by contact with a lip ornament like a labret? Was it otherwise modifi ed for aesthetic reasons?
Morphological characteristics like the shovel shape of an incisor or an extra talon or cusp can indicate the probability of a genetic commonality with a population from a specifi c geographic area.
Nothing but the ToothKerry K. Carney, DDS, CDE
What if we zoom in on that tooth and consider nothing but the tooth. What is it about that small organ, the tooth, that makes it so special?

C DA J O U R N A L , V O L 4 6 , Nº 1 0
606 O C TO B E R 2 01 8
Tonya Lanthier became a Registered Dental Hygienist (RDH) in the Atlanta area in 1995. She quickly recognized the need for a place where dental professionals could connect and create teams that excel. By design, three babies were born - twin girls and DentalPost!
DentalPost has grown into the leading dental industry job board and community serving more than 700,000 dental professionals. We believe in using data for a
nya Lanthier becaaameameme a aaa a RegRegRRRegRegRegistisististstereereereereddd Dd Dental Hyygygygygygygygygygygygygygygyggygygyygygyyyggienieieenenenienenenenniennnenenenenennneeeneeeeeeienistii ti tistttiststtistttttistttttiissisistststttsissistttistiiisisisttististististsistsistisstststst (R(R(R((R(R(R(R((R((R(R(RR((R((RRR(R(RRR((RRRRRRRR(R(R(R(RRRRR(RR(RR(R(R(R(R(R(R(R(( DHDH)DHH)DH)DH)DH)DH))))H)H))))HHDHDH))DH))HHHHHDH))DDDHDHHHDHDHDH)H)DDDDHHHDH))DDH))DH))HHHH)DH)DH)DDDDHDHDHHDH)DH)DH)DDH)H)D ))) iiiiiiiininiinnininniinnnnininnniiiinnnn ththththhhhhhththhhhhthhththhthththhhththhththththththhhhthththhhhthhh AAe AAAAe Ae Ae Ae AAAe Ae Ae Ae Aee Ae Ae Atlattlatlatllalalatlalaltlatlalalaaaaaantantantantatataaatntatatantattaantantantantantantantataantantaantaaaantaantantaanta araararrarrarrraaaaraaraarrraraaaaara eaeeaeeaeaeaaaaaeeeeaeeeaaeaeeaeeeaeaaea ea eeaeaeaeaaa1995. She quickly recrecrececececcecognognognogognognognognognognog izeizeizezeizeizizizi d tdd he need for aa pa pa ppa pa ppppllllalalacacacaclaclaaccl ce we wwe wwe we we we we wwe we wwe wwwe e wherherherhereee de dental a proofesfe sionalss
O C T . 2 0 1 8 E D I T O R
The presence of naturally occurring fl uorosis in the tooth can help narrow the probable locations where the individual grew up. Certain genetic disorders are expressed in the development of the tooth and can tell us about the distribution of that trait within a population.
In the fossil record, the enamel is a treasure trove of information. In the living tooth, there are soft tissue resources to investigate. Research has shown that stem cells can be harvested from primary teeth and banked for later use. Postmortem identifi cation need not rely solely on forensic analysis of
radiographic matches of hard tooth structure morphology or restorations to confi rm an individual’s identity. Now pulpal tissue may supply the DNA sample necessary to aid in identifi cation.
Sometimes in catastrophic plane crashes or battlefi eld disasters, the only surviving body part is a tooth. It may be a single tooth that establishes identity. The identifi cation provided by a single tooth may allow a military honor guard to demonstrate respect for those who have made the ultimate sacrifi ce for our constitution. A military dentist told me that the coffi n they
salute at interment might hold only a single tooth. It may be the information from a single tooth that helps provide closure for a family in mourning.
The single tooth is not the only thing that concerns us in the practice of dentistry. But it is an amazing, long-lasting, informative little organ. The tooth can be worth more than a thousand words. That is the tooth, the whole tooth and nothing but the tooth. ■
C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 607
Letter
Et tu, CDA?
Daniel N. Jenkins, DDS, CDE
CRANIOFACIAL PHYSIOLOGY:
el N JenkinsDaniee DDS C
PHYSIOLOGY:YWHAT MAKES US TICK?
JournaC A L I F O R N I A D E N T A L A S S O C I A T I O N
Tooth Eruption
Pathophysiology of Oral Cancer
Sleep Physiology
August 2018
I have been a member of CDA since joining as a University of California, San Francisco, student in the 1960s. CDA has done a lot for organized dentistry and in protecting dentists from OSHA witch hunts, fi ghting penalties assessed for noncompliance of ill-defi ned nonestablished rules. But now with CDA’s support of a tax on sweetened drinks, CDA and I part company.
Ever notice when an activist dislikes something it gets the label “Big?” Big Tobacco. Big Oil. Big Government. Now it’s Big Soda. There is a tremendous difference between the harmful ingredients from smoking cigarettes to drinking soft drinks. Smoking cigarettes exposes one to acetone, lead, benzene, formaldehyde, nicotine, tar, carbon dioxide and a host of other toxic substances. Coca-Cola exposes us to carbonated water, sugar, caffeine and some fl avoring. None of these are toxic!
The CDC’s report shows only 49 percent of adults and 63 percent of youths drank sugar drinks per day.1 This amounts to only 145 and 143 calories respectively per day! Visit Starbucks and eat a butter croissant (260 calories), a chocolate chip cookie (570), coffee cake (390) or a plain bagel (280)2 and you far exceed the average calories from a sugar-sweetened soda plus any sugar you may need to sweeten your coffee. Eating these foods exposes you to 29 grams of fat that you won’t fi nd in soft drinks. You also get up to 320 mg sodium versus 45 mg in a can of Coke.3 Sodium causes water retention that strains the kidneys, heart, arteries and brain, leading to arterial damage, heart damage, heart attacks and strokes. If these activists leading the attack on sugary drinks were serious, they would be banning Starbucks from selling anything except coffee and tea. Or is Big Activism’s next goal banning your morning croissant and your child’s chocolate chip cookie?
It is time we look at this rationally.
Activists merely want tax money for their pet projects. Otherwise they would call for a ban on sugary drinks completely. A 1-cent tax on an ounce amounts to 12 cents per can or 72 cents per six-pack. This tax is falling mostly on the poor laborer who can ill afford it and just wants some sugar to replace the energy he expended working each day. These greedy activists today attack soft drinks. Will your croissant or bagel be next? The CDA-CMA ballot initiative will amount to $1.7 BILLIONa year! That is billion with a “B!”
Our personal freedoms have decreased in the name of helping us. Those useful plastic bags that grocery stores once used are gone. Plastic straws are next. Taxes may shift consumer choices, but why should government taxation restrict our freedom of choice. Don’t let the CDA take away or tax our choice of drinks.
REFERENCES
1. Centers for Disease Control and Prevention. Get the Facts: Sugar-Sweetened Beverages and Consumption. cdc.gov/nutrition/data-statistics/sugar-sweetened-beverages-intake.html.2. Starbucks. Explore Our Menu. starbucks.com/menu/catalog/nutrition?food=all#view_control=nutrition.3. Coca-Cola Company. Nutritional facts from a can of sugared Coke.
M U R R AY S . L E V I N E , D D S
Encino, Calif.
The Editor-in-Chief RespondsWith $195 billion in U.S. sales,
dubious political tactics and proven adverse health effects, the soda industry has earned the moniker “Big Soda.” Overwhelming evidence links consumption of sugar-sweetened beverages to obesity, diabetes, tooth decay and heart disease.
CDA adopted policy in 2008 that directs the organization to pursue the enactment of a manufacturer’s fee on the syrup used to produce soda, sport and energy drinks to fund disease prevention and treatment programs. The soda
industry’s recent strong-arming of the legislature to ban local soda taxes for 12 years to protect profi ts prompted CDA and the California Medical Association to fi ght back with a 2020 ballot measure that taxes sugar-sweetened beverages.
An average bottle of soda is 20 ounces, which contains more than 15 teaspoons of sugar,1 far more than the added sugar per day recommended by the American Heart Association.2 These liquid calories do not suppress “the hunger hormone” in the same way that sugar does in complex solid foods, leading to an increase in total caloric intake.3
As dentists, we see fi rsthand the damage caused from soda drinking, but the ill health effects go far beyond tooth enamel. People who consume one or more sugary drinks per day have a 26 percent higher risk of diabetes.4
Among adults, even after adjusting for race and household income, people who drink one or more sodas each day are 27 percent more likely to be overweight or obese than adults who do not drink soda.5 California adolescents drink 1.2 sodas per day on average, which equates, conservatively, to 39 pounds of sugar each year.5
The economic burden of diseases related to sugar-sweetened beverages is staggering. More than 2.5 million
C DA J O U R N A L , V O L 4 6 , Nº 1 0
608 O C TO B E R 2 01 8
adult Californians have diabetes with health care costs of $12.98 billion.6
The estimated $2 billion to $3 billion raised from a statewide soda tax would reduce consumption by 15 to 35 percent.7 Consumers will still have a wide choice of beverages, including sweetened ones with nutritional value that would not include a public health tax. Additionally, voters will have the choice to approve or defeat the statewide soda tax at the 2020 ballot box — a right that Big Soda circumvented.
REFERENCES
1. Coca-Cola Co. Product Facts. coca-colaproductfacts.com/en/products/coca-cola/original/20-oz.2. American Heart Association. Added Sugars. heart.org/en/healthy-living/healthy-eating/eat-smart/sugar/added-sugars.3. Mourao DM, et al. Eff ects of food form on appetite and energy intake in lean and obese young adults. Int J Obes (Lond) 2007 Nov;31(11):1688–1695. Epub 2007 Jun 19.4. Soft Drinks and Disease. Harvard School of Public Health.5. Bubbling Over: Soda Consumption and Its Link to Obesity in California. UCLA Health Policy Research Brief, 2009.6. Economic Burden of Chronic Disease in California, 2015. California Department of Public Health7. lao.ca.gov/ballot/2018/180384.pdf.
The Journal welcomes lettersWe reserve the right to edit all
communications. Letters should discuss an item published in the Journal within the last two months or matters of general interest to our readership. Letters must be no more than 500 words and cite no more than fi ve references. No illustrations will be accepted. Letters should be submitted at editorialmanager.com/jcaldentassoc. By sending the letter, the author certifi es that neither the letter nor one with substantially similar content under the writer’s authorship has been published or is being considered for publication elsewhere, and the author acknowledges and agrees that the letter and all rights with regard to the letter become the property of CDA.
O C T . 2 0 1 8 L E T T E R
House 1/2 island
cda.org
®
TOGETHERWE ARE
LIMITLESS

C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 609
Impressions
The nub:
1. The reputation of the profession matters just as the reputation of its members does.
2. It is a double ethical challenge to act based on what we know unless we have permission to know that sort of thing.
3. Ethical principles are sometimes used as an excuse to cover systemic ethical weakness.
David W. Chambers, EdM, MBA, PhD, is a professor of dental education at the University of the Pacifi c, Arthur A. Dugoni School of Dentistry, San Francisco, and the editor of the American College of Dentists.
Disclosing Ethical SecretsDavid W. Chambers, EdM, MBA, PhD
The marketing folks tell us that “leaked secrets” is an inviting phrase and much more likely to prompt interest than the word “ethics.” My point will be that there is even greater power in being able to suppress ethical secrets. It is one of the new ethical norms: “I know something that could help others, but I can’t tell because I am so ethical.”
A colleague sent me a CV to review as he was considering nominating this individual for fellowship in the American College of Dentists. On paper, this was a clear shot. But I happened to know a little background about the case because of a “need to know” relationship with the university. The possible candidate was under administrative sanction for violation of ethical standards. The university had screened my colleague and others from getting this information. What should I say?
The rationale for the secrecy was to protect the faculty member’s reputation. Quite possibly the university was protecting itself as well from bad publicity and possible legal action. But a penalty that no one knows about has to be considered a strange one.
Ethicists debate these things: If you have been damaged (say, by praising someone who should not be praised) but are not aware that you have misled others, is it wrong? Yes, and the fault lies with the third party that has unnecessarily covered an ethical secret for its own advantage.
Disciplined licenses for dentists are public records and a quick check will show that the proportion of disciplinary actions in some states, such as California, is two or three times the rate in other states. It is not because California dentists are unethical. Phone conversations with responsible agents indicate that many states simply lack suffi cient enforcement resources and others try to suppress information about inconvenient facts.
Several billboards appeared in 2016 in another state asking motorists to consider whether their dentist was honest. The phone number of the state association was displayed at the bottom of the message inviting drivers to phone and fi nd out. This is a frightening use of innuendo. I know exactly what happened, but no one I talked with in the state or nationally seems to have any knowledge of this ethical secret.
There are two levels of ethical knowledge: What one knows and what one is allowed to know.
These are tough cases, but generally it works well to keep the secret when there is a potential for harm to others. If there is potential harm in keeping the secret, think about speaking up. If it is really a tight situation, confront the person or organization that is responsible for the gag order and challenge them to be ethical. ■

C DA J O U R N A L , V O L 4 6 , Nº 1 0
610 O C TO B E R 2 01 8
Dental Care Could Benefi t Patients Scheduled for Cancer Surgery
Preoperative oral care by a dentist may help reduce postoperative complications, such as pneumonia that may be caused by aspiration of oral and pharyngeal secretions, in patients who undergo cancer surgery, according to a new British Journal of Surgery study conducted by Miho Ishimaru, PhD, of the department of clinical epidemiology and health economics, School of Public Health at the University of Tokyo in Japan.
The retrospective cohort study was undertaken to assess the association between preoperative oral care and postoperative complications among patients who underwent major surgery for head and neck, oesophageal, gastric, colorectal, lung or liver cancer between May 2012 and December 2015. The nationwide administrative claims database in Japan was analyzed.
Of 509,179 patients studied, 16 percent received preoperative oral care from a dentist. When a surgeon requested that a dentist provide preoperative oral care to a patient with cancer, the dentist checked the patient’s oral condition, provided professional tooth cleaning, taught the patient self-cleaning methods for the teeth and provided any treatment needed, according to the study.
The researchers found that 15,724 patients (3.09 percent) developed postoperative pneumonia and 1,734 (0.34 percent) died within 30 days of surgery. After adjustments, preoperative oral care by a dentist was linked with a decrease in postoperative pneumonia (3.28 percent versus 3.76 percent) and death within 30 days (0.30 percent versus 0.42 percent).
“The findings could help improve strategies for the prevention of postoperative complications,” Dr. Ishimaru said.
Read more of this study in the British Journal of Surgery (2018); doi.org/10.1002/bjs.10915.
O C T . 2 0 1 8 I M P R E S S I O N S
Scanning electron microscope image of silver nanoparticles. (Credit: Dr. T. Theivasanth/Wikimedia Commons)
Catalytic Nanoparticles Prevent Tooth Decay
In a study published in Nature Communications, researchers led by Hyun (Michel) Koo, DDS, MS, PhD, of the University of Pennsylvania School of Dental Medicine, used FDA-approved nanoparticles to effectively disrupt biofi lms and prevent tooth decay in both an experimental human plaque-like biofi lm and in an animal model that mimicked early childhood caries.
The nanoparticles break apart dental plaque through a unique pH-activated antibiofi lm mechanism. Because caries-causing plaque is highly acidic, the new therapy is able to precisely target areas of the teeth harboring pathogenic biofi lms, without harming the surrounding oral tissues or microbiota, according to the study.
The iron-containing nanoparticle used in the experiments, ferumoxytol, is already FDA-approved to treat iron defi ciency, which indicates that a topical application of the same nanoparticle would also be safe for human use, according to the study. Though some scientists have questioned whether coatings used on ferumoxytol and other nanoparticles used for medical applications would render them catalytically inert, the researchers demonstrated that they maintained peroxidase-like activity, activating hydrogen peroxide.
After testing the ferumoxytol-hydrogen peroxide combination on a
tooth-enamel-like material, the team moved on to an experimental set-up that more closely replicated the conditions of the human mouth.
“We used plaque samples from caries-active subjects to reconstruct these highly pathogenic biofi lms on real human tooth enamel,” Dr. Koo said. “This simulation showed that our treatment not only disrupts the biofi lm but also prevents mineral destruction of the tooth’s surface.”
Further studies in a rodent model that closely mirrored the stages of caries development in humans showed that twice-a-day rinses of ferumoxytol and hydrogen peroxide greatly reduced the severity of caries on all of the surfaces of the teeth and completely blocked the formation of cavities in the enamel.
Learn more about this study at Nature Communications (2018); doi.org/10.1038/s41467-018-05342-x.
C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 611
Nearly a third of older adults have received a prescription for an opioid pain medicine in the past two years, but the associated dangers often go unaddressed, according to fi ndings from the National Poll on Healthy Aging published in an article on the University of Michigan Health Lab website.
The poll of 2,013 adults aged
50–80, conducted by the University of Michigan Institute for Healthcare Policy and Innovation and sponsored by AARP and Michigan Medicine, U-M’s academic medical center, found that many patients didn’t get enough counseling about the risks that come with the potent painkillers, how to reduce their use, when to switch to a non-opioid
option or what to do with leftover pills.Additionally, nearly three-quarters
of surveyed older adults would support limits on how many opioid pills a doctor could prescribe at once. And even more supported other efforts to limit exposure to these medications and potentially combat the national epidemic of opioid misuse due to medication diversion, according to the poll.
The poll results suggest that health care providers who prescribe or dispense opioids should do more to help patients understand how to safely use and dispose of them, in language that patients understand, the article states. This should include a disposal plan that helps patients understand why and how they should dispose of extra medications.
Jennifer Waljee, MD, MPH, MS, the co-director of the Michigan Opioid Prescribing Engagement Network (Michigan OPEN) and an associate professor of surgery at Michigan Medicine, said when patients are prescribed an opioid, many other aspects of care are often at the forefront of their minds, such as their diagnosis, social stressors, work-related concerns and caring for loved ones, which can result in education fatigue.
“But we spend a lot of time educating our patients on when they can drive, return to work and take care of their painful condition or surgical incision sites. Similarly, we need to educate our patients on what to expect following pain, the role and risks of opioids and important alternatives such as over-the-counter analgesics, breathing, exercise and sleep,” Dr. Waljee said.
Learn more about the poll at labblog.uofmhealth.org.
Physicians Don’t Educate Older Patients About Opioids
Researchers Sequence Rare Bacteria That Causes Tooth Decay
A team of bioengineering researchers led by Paul Jensen, PhD, assistant professor at the University of Virginia, has successfully sequenced the complete genomes of three strains of S. sobrinus, a harmful bacteria that accelerates tooth decay. While scientists know much about the bacteria Streptococcus mutans, which also causes cavities, little has been known about S. sobrinus until now. The research was published in the journal Microbiology Resource Announcements in June 2018.
According to Dr. Jensen, S. sobrinus is difficult to work with in the lab and is not present in all people, so researchers have instead focused their efforts over the years on understanding the more stable and prevalent S. mutans, which was sequenced in 2002.
“Although it is rare, S. sobrinus produces acid more quickly and is associated with the poorest clinical outcomes, especially among children,” Jensen said. “If S. sobrinus is present along with S. mutans, you’re at risk for rampant tooth decay, which means there’s some level of communication or synergy between the two that we don’t understand yet.”
Now that the S. sobrinus sequencing is complete, Dr. Jensen and his students are building computational models to better understand how the two bacteria interact and why S. sobrinus can cause such potent tooth decay when combined with S. mutans.
Already they have confirmed, for example, that S. sobrinus lacks complete pathways for quorum sensing, which is the ability bacteria have to sense and react to nearby bacteria and ultimately proliferate.
Read more of this study in Microbiology Resource Announcements (2018); doi:10.1128/MRA.00804-18.
Viridans streptococci. (Credit: Wikimedia Commons)

C DA J O U R N A L , V O L 4 6 , Nº 1 0
612 O C TO B E R 2 01 8
demonstrated elevated nicotine and TSNA concentrations relative to non-users. TSNA exposures were highest among smokeless tobacco users, whether used alone or together with other product types. Exclusive e-cigarette users were exposed to lower NNN and NNAL levels than other product users, despite comparable nicotine exposure. However, most e-cigarette users concurrently used combustible tobacco resulting in TSNA exposure similar to exclusive cigarette smokers.
metabolite of lung carcinogen (NNK) and total nicotine equivalents.
Participants were categorized according to use of combustible, which includes cigarettes, cigars, water pipes, pipes, blunts (marijuana-containing cigars), smokeless, which includes moist snuff, chewing tobacco and snus, e-cigarettes and nicotine replacement products. For each product, recent use was defi ned as within the prior three days and non-use defi ned as none within 30 days.
All tobacco use categories
E-cigarettes, Tobacco-Product Use Linked to Increased Oral Cancer Risk
A vast majority of noncigarette tobacco users are exposed to carcinogen levels comparable to or exceeding exposure among exclusive cigarette smokers — levels that are likely to place users at substantial risk, according to a poster entitled “Nicotine and Carcinogen Exposure by Tobacco Product Type and Dual-Use” presented at the 96th General Session of the International Association for Dental Research (IADR) held in conjunction with the IADR Pan European Regional (PER) Congress in England in July 2018.
Tobacco use remains a leading cause of oral cancer but the tobacco landscape is evolving with increasing use of noncigarette tobacco products and dual-use of multiple product types. Co-authors Benjamin Chaffee, DDS, MPH, PhD, and Neal Benowitz, MD, of the University of California, San Francisco, evaluated exposure to known carcinogens according to recent use of different tobacco product types, alone or in combination.
Data was analyzed from the Population Assessment of Tobacco and Health, which included a sample of U.S. adults who provided urine specimens for analysis of tobacco-specifi c nitrosamines (TSNAs) N’-nitrosonornicotine (NNN), a known oral and esophageal carcinogen, 4-(methylnitrosamino)-1-(3)-pyridyle-1-butanol (NNAL), a
Opioids Unwise for Teens Who Have Wisdom Teeth Removed
Young people aged 13 to 30 who filled an opioid prescription immediately before or after they had their wisdom teeth out were nearly 2.7 times as likely as their peers to still be filling opioid prescriptions weeks or months later, according to new research from a University of Michigan team.
Those in their late teens and 20s had the highest odds of persistent opioid use, compared with those of middle-school and high-school age, the researchers report in a research letter published in the August 2018 issue of the Journal of the American Medical Association.
Led by Calista Harbaugh, MD, a U-M research fellow and surgical resident, the researchers used insurance data to focus on young people who were “opioid naïve” — who hadn’t had an opioid prescription in the six months before their wisdom teeth came out and who didn’t have any other procedures requiring anesthesia in the following year.
“Wisdom tooth extraction is performed 3.5 million times a year in the United States, and many dentists routinely prescribe opioids in case patients need it for postprocedure pain,” said Dr. Harbaugh. “Until now, we haven’t had data on the long-term risks of opioid use after wisdom tooth extraction. We now see that a sizable number go on to fill opioid prescriptions long after we would expect they would need for recovery, and the main predictor of persistent use is whether or not they fill that initial prescription.”
Learn more about this study in the Journal of the American Medical Association (2018); doi:10.1001/jama.2018.9023.
O C T . 2 0 1 8 I M P R E S S I O N S
By Steven Fruitsmaak (Credit: Wikimedia Commons)
(Credit: Wikimedia Commons)

C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 613
An examination of research on oral health commissioned by the World Health Organization (WHO) has indicated that sticking to whole grain carbohydrates and avoiding processed ones, especially if sweet, is best for oral health. The fi ndings, published in August 2018 in the Journal of Dental Research, came from a review of 33 academic papers on starch and oral health.
Although researchers found no association between the total amount of starch eaten and tooth decay, they did fi nd that more processed forms of starch increased the risk of cavities. This is because they can be broken down into sugars in the mouth by amylase found in saliva, according to the research.
Further fi ndings, although based on
very few available studies and weaker data, suggested a lower risk of oral cancer from consuming whole grain starches and that whole grains may also offer protection against gum disease.
Paula Moynihan, PhD, professor of nutrition and oral health at Newcastle University, U.K., who led the research, said the evidence suggests that a diet rich in whole grain carbohydrates is less likely to damage your oral health than one containing processed starches.
In the review, 33 papers were included of studies on foods containing what were characterized as rapidly digestible starches (e.g., white bread, crackers, biscuits, cakes, pretzels) and slowly digestible starches (e.g., whole grains, legumes) and their relationships with dental caries, oral cancer and gum disease.
The WHO, which is currently updating its guidance on carbohydrate intake, recommends reducing free-sugar intake to less than 10 percent of total energy (calorie) intake and suggests further reduction to less than 5 percent for additional health benefi ts, according to the published study. Free sugars are sugars that are added to foods by the manufacturer, cook or consumer, plus those naturally present in honey, syrups, fruit juices and fruit juice concentrates.
Additional research commissioned by the WHO into the effects of carbohydrate quality on other health outcomes, including cardiovascular diseases, cancer and Type 2 diabetes, will be used to inform the forthcoming guideline.
Read more of this study in the Journal of Dental Research (2018); doi.org/10.1177/0022034518788283.
Avoid Processed Starch for Better Oral Health
Doctors Prescribed Fewer Opioids After Learning of Patient Overdose
A study published in the journal Science in August 2018 found that when a clinician learned one of their patients had suffered a fatal overdose, they reduced the amount of opioids prescribed by almost 10 percent in the following three months. The study leveraged behavioral insights and psychology to give prescribers personal experience with the risk associated with opioids.
“Clinicians may never know a patient they prescribed opioids to suffered a fatal overdose,” said lead author Jason Doctor, PhD, the director of health informatics at the USC Schaeffer Center for Health Policy and Economics and associate professor at the Price School of Public Policy. “What we wanted to evaluate is whether closing that information gap will make them more judicious prescribers.”
Dr. Doctor and his colleagues conducted a randomized trial between July 2015 and June 2016 of 861 clinicians who had prescribed to 170 patients who subsequently suffered a fatal overdose involving prescription opioids. Half the clinicians were randomly selected to receive a letter from the San Diego County medical examiner notifying them that a patient they had prescribed opioids to in the past 12 months had a fatal overdose. The letter, which was supportive in tone, also provided information on safe prescribing guidelines from the Centers for Disease Control and Prevention, nudging clinicians toward better prescribing habits.
In the three months after receiving the letter, prescribing decreased by 9.7 percent compared to the control group that didn’t receive a letter. Furthermore, clinicians who received the letter were 7 percent less likely to start a new patient on opioids and less likely to prescribe higher doses.
“Interventions that use behavioral insights to nudge clinicians to correct course are powerful, low-cost tools because they maintain the autonomy of the physician to ultimately decide the best course of care for their patient,” Dr. Doctor said.
Read more of this study in Science (2018); doi:10.1126/science.aat4595.

C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 615
i n t r o d u c t i o n
GUEST EDITOR
Richard J. Nagy, DDS, is a board-certifi ed periodontist and has actively integrated academic pursuits with a private practice limited to periodontics, sedation and implant therapy in Santa Barbara, Calif. Dr. Nagy is the former director of postgraduate periodontics and department chairman at the Greater Los Angeles VA Healthcare System and has published numerous scientifi c papers and abstracts in peer-reviewed journals and textbook chapters. He is the former editor of Periodontal Abstracts and past president of the California Society of Periodontists and the Western Society of Periodontology. Dr. Nagy, a diplomate of the American Board of Periodontology, is currently the vice president of the California Dental Association.Confl ict of Interest Disclosure: None reported.
Patients present to our practices with either localized or generalized gingival recessions that they may or may not be aware of. Some patients may ask about the recessions and
what may need to be done. These patients usually are most concerned about the effect the recessions have on aesthetics and/or they are dealing with sensitivity issues on these teeth. Then there is you, the dental practitioner, who feels teeth with recessions as well as teeth with thin unattached tissues regardless of recession need to be addressed due to concerns for either tooth loss or restorative issues. These patients are typically not aware of their recessions or mucogingival problem. As a periodontist, I often get questions from general dentists and dental hygienists on when to perform gingival grafting: Who are the acceptable candidates, what are the treatable defects and what are the available and most predictable techniques? It is important that not just the periodontist but all members of the dental team understand the thought process of how to address recessions and other mucogingival defects so that all dental practitioners can help explain to patients the diagnosis and treatment options for the best and most predictable outcomes, whether the clinician will be doing the corrective procedure or referring the case to a specialist.
This issue of the Journal was designed to help the reader answer these questions. In their manuscript “Gingival Recession: What Is It All About?” Debra S. Finney, DDS, MS, and Richard T. Kao, DDS, PhD, discuss diagnosis, terminology, classifi cation systems and case selection that will
To Graft or Not To Graft? An Update on Gingival Grafting Diagnosis and Treatment ModalitiesRichard J. Nagy, DDS
guide which patients may or may not be acceptable candidates as well as defects for grafting. Perry Klokkevold, DDS, MS, Elissa Green, DMD, and Soma Esmailian Lari, DMD, discuss autogenous gingival grafting, looking at the connective tissue graft as the current standard of care, and the free gingival graft and other autogenous grafting techniques in their manuscript “Autogenous Soft Tissue Grafting for the Treatment of Gingival Recession.” Joan Otomo-Corgel, DDS, MPH, Chanook David Ahn, DMD, and Allen Gunn, DDS, discuss the use of acellular dermal matrix allografting as an alternative to autogenous grafting. Tina M. Beck, DDS, MS, explains her experience with the Pinhole Surgical Technique, which has received much press these days. These treatment modality papers attempt to discuss surgical technique and posttreatment outcomes. Cases are used to emphasize the appropriate use of surgical approaches and to provide readers with examples of the aesthetic improvements. These papers also discuss the literature and the authors’ personal experiences of the advantages, disadvantages and case selection specifi cs for that procedure. Finally, Cherissa Chong, DMD, MS, Yung-Ting Hsu, DDS, MDSc, Paul Y. Lee, DDS, and Richard T. Kao, DDS, PhD, discuss the future of grafting with the current and future use of biologics on teeth with recessions and mucogingival defects as well as in conjunction with surgically facilitated orthodontic treatment. It is hoped this issue will provide readers with a greater understanding of the diagnosis, treatment planning and treatment modalities associated with recessions, mucogingival defects without recession and gingival grafting. ■

(855) 886-4824 | rstrepublic.com | New York Stock Exchange symbol: FRCMEMBER FDIC AND EQUAL HOUSING LENDER
“We treat our patients with respect and great service. Th at’s exactly how First Republic treats us.”
L E E & YO U N G O RT H O D O N T I C S
Rodney Lee, D.D.S., Owner (left ); Glen Young, D.D.S., Owner (right)
CDAJour Oct_18 LeeYoung ND2017.indd 1 8/21/18 12:09 PM
C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 617
g i n g i v a l r e c e s s i o n
AUTHORS
Debra S. Finney, DDS, MS, a board-certifi ed periodontist, practices in Folsom, Calif. She was president of the California Dental Association in 2004 and has held numerous positions with the CDA and the ADA.Confl ict of Interest Disclosure: None reported.
Richard T. Kao, DDS, PhD, is a clinical professor at the University of California, San Francisco, School of Dentistry and is in private practice in Cupertino, Calif.Confl ict of Interest Disclosure: None reported.
Gingival Recession: What Is It All About?Debra S. Finney, DDS, MS, and Richard T. Kao, DDS, PhD
A B S T R AC T Gingival recession is a common dental problem that escalates with increasing age. From the patient’s perspective, this may be associated with intensifi ed symptoms of dentinal hypersensitivity, impaired aesthetics, plaque retention with increased localized infl ammation and greater susceptibility to root caries. This article reviews factors that enhance the risk for gingival recession, describes at what stage interceptive treatment should be recommended and expected outcomes.
Gingival recession is one of the most common forms of mucogingival deformities. It is a prevalent but often overlooked problem. The
2012 National Health and Nutrition Examination Survey study reported a prevalence of gingival recession in 50 percent of those aged 18 to 64 and that 88 percent of those 65 and older have at least one site. It increases with age and males have more recession defects than females.1
Once recession is present, a 3-mm recession will worsen 67 percent of the time and a 4-mm recession will worsen 98 percent of the time.2 In the clinical evaluation and monitoring process, determining the causes of gingival recession is important in defi ning if the mucogingival defects need to be addressed. Etiologic causes for gingival recession include traumatic oral hygiene habits, chronic periodontal infl ammation, malposition of the tooth, orthodontic movement, regional frenum pull, biological width invasion and underlying bony dehiscence. Experience, careful observation of the dental environment and good history intake will help the clinician discern the true etiology.
Mucogingival Assessment and Phenotype
Gingival recession results when the marginal tissue migrates apical to the cementoenamel junction (CEJ), exposing the root surface. Recession is measured from the CEJ to the coronal tissue margin. In addition, it is important to measure and monitor the width of attached gingiva, which can be determined by measuring the distance from the coronal margin of the gingiva to the mucogingival junction (MGJ) and subtracting the sulcular probing depth. At times, especially if the gingiva is thin, it can be challenging to identify the MGJ. Gently rolling the mucosa with an instrument such as a periodontal probe (FIGURE 1) can be helpful in locating the apical extent of the attached gingiva. The position of frenum attachments should also be noted as part of the mucogingival evaluation. A frenum attachment at or near the gingival margin may contribute to recession (FIGURE 2).
Another signifi cant parameter in assessing mucogingival health and treatment planning for restorative procedures is the tissue type. Ochsenbein and Ross fi rst described the concept
C DA J O U R N A L , V O L 4 6 , Nº 1 0
618 O C TO B E R 2 01 8
of thick and thin gingival biotypes.3 More recently, the 2017 American Academy of Periodontology World Workshop on Disease Classifi cation has described this not as biotypes but as gingival phenotypes.4 Appreciating the gingival phenotype will help the clinician predict how fast recession or attachment loss may occur. Employing gingival phenotype as a prognostic indicator for further gingival recession/attachment loss is a skill that clinicians learn over time with clinical experience. In defi ning and identifying the gingival phenotype, the components of the mucogingival complex that should be considered include the gingival thickness (GT), keratinized tissue width (KTW), gingival morphotype (GM), bone morphotype (BM) and tooth dimension. Utilizing these parameters, one recent classifi cation system categorized gingival phenotypes into three categories:5
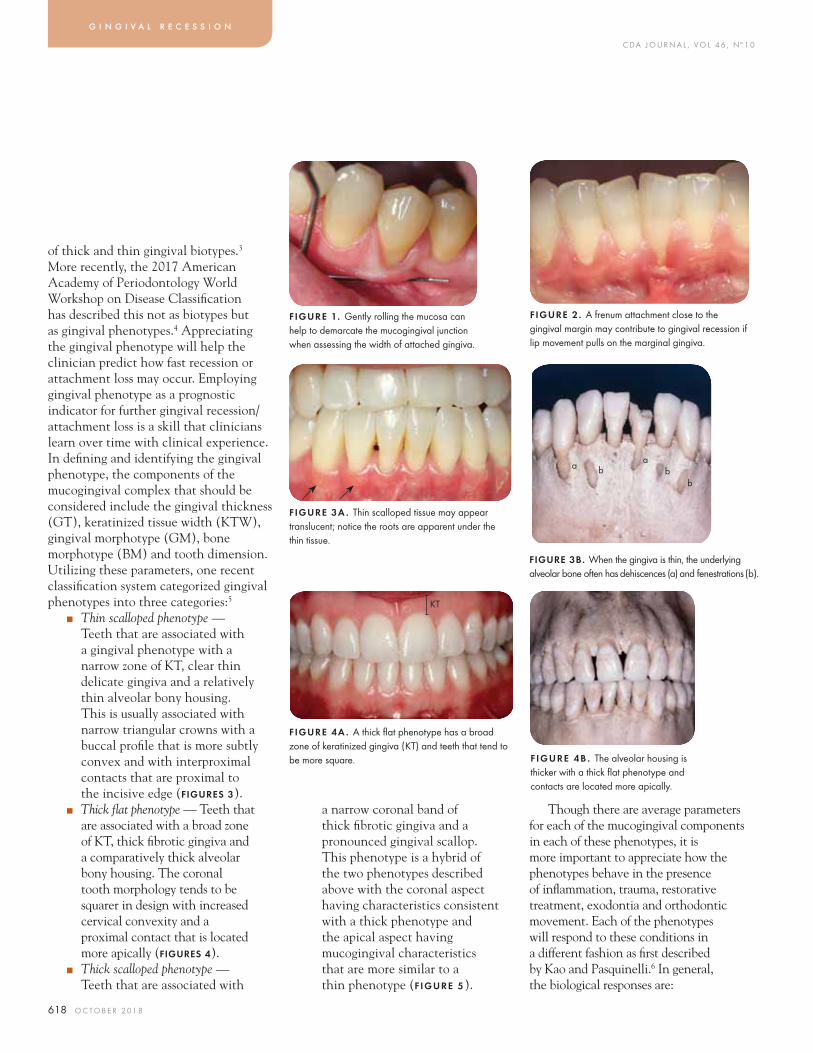
■ Thin scalloped phenotype — Teeth that are associated with a gingival phenotype with a narrow zone of KT, clear thin delicate gingiva and a relatively thin alveolar bony housing. This is usually associated with narrow triangular crowns with a buccal profi le that is more subtly convex and with interproximal contacts that are proximal to the incisive edge (FIGURES 3).
■ Thick fl at phenotype — Teeth that are associated with a broad zone of KT, thick fi brotic gingiva and a comparatively thick alveolar bony housing. The coronal tooth morphology tends to be squarer in design with increased cervical convexity and a proximal contact that is located more apically (FIGURES 4).
■ Thick scalloped phenotype — Teeth that are associated with
g i n g i v a l r e c e s s i o n
a narrow coronal band of thick fi brotic gingiva and a pronounced gingival scallop. This phenotype is a hybrid of the two phenotypes described above with the coronal aspect having characteristics consistent with a thick phenotype and the apical aspect having mucogingival characteristics that are more similar to a thin phenotype (F IGURE 5).
Though there are average parameters for each of the mucogingival components in each of these phenotypes, it is more important to appreciate how the phenotypes behave in the presence of infl ammation, trauma, restorative treatment, exodontia and orthodontic movement. Each of the phenotypes will respond to these conditions in a different fashion as fi rst described by Kao and Pasquinelli.6 In general, the biological responses are:
FIGURE 1. Gently rolling the mucosa can help to demarcate the mucogingival junction when assessing the width of attached gingiva.
FIGURE 2. A frenum attachment close to the gingival margin may contribute to gingival recession if lip movement pulls on the marginal gingiva.
FIGURE 3B. When the gingiva is thin, the underlying alveolar bone often has dehiscences (a) and fenestrations (b).
F IGURE 4B . The alveolar housing is thicker with a thick fl at phenotype and contacts are located more apically.
FIGURE 3A . Thin scalloped tissue may appear translucent; notice the roots are apparent under the thin tissue.
FIGURE 4A . A thick fl at phenotype has a broad zone of keratinized gingiva (KT) and teeth that tend to be more square.
a ab b
b
KT
C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 619
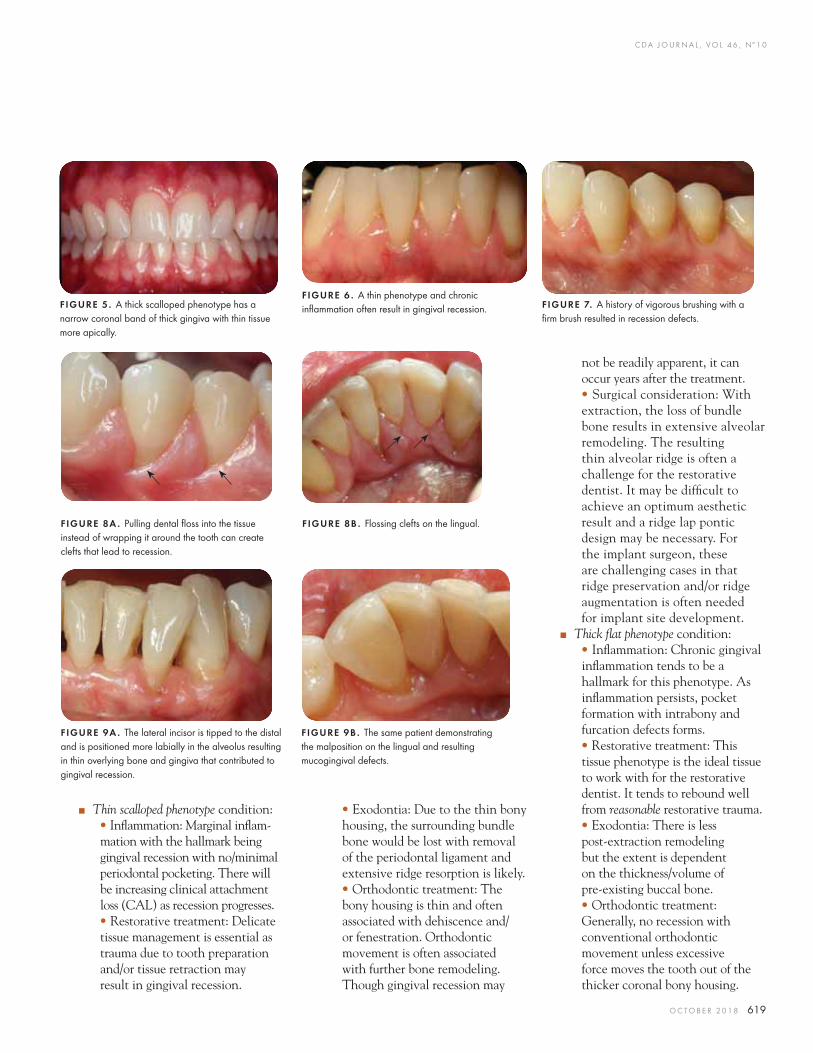
• Exodontia: Due to the thin bony housing, the surrounding bundle bone would be lost with removal of the periodontal ligament and extensive ridge resorption is likely.• Orthodontic treatment: The bony housing is thin and often associated with dehiscence and/or fenestration. Orthodontic movement is often associated with further bone remodeling. Though gingival recession may
■ Thin scalloped phenotype condition:• Infl ammation: Marginal infl am-mation with the hallmark being gingival recession with no/minimal periodontal pocketing. There will be increasing clinical attachment loss (CAL) as recession progresses. • Restorative treatment: Delicate tissue management is essential as trauma due to tooth preparation and/or tissue retraction may result in gingival recession.
not be readily apparent, it can occur years after the treatment.• Surgical consideration: With extraction, the loss of bundle bone results in extensive alveolar remodeling. The resulting thin alveolar ridge is often a challenge for the restorative dentist. It may be diffi cult to achieve an optimum aesthetic result and a ridge lap pontic design may be necessary. For the implant surgeon, these are challenging cases in that ridge preservation and/or ridge augmentation is often needed for implant site development.
■ Thick fl at phenotype condition:• Infl ammation: Chronic gingival infl ammation tends to be a hallmark for this phenotype. As infl ammation persists, pocket formation with intrabony and furcation defects forms.• Restorative treatment: This tissue phenotype is the ideal tissue to work with for the restorative dentist. It tends to rebound well from reasonable restorative trauma.• Exodontia: There is less post-extraction remodeling but the extent is dependent on the thickness/volume of pre-existing buccal bone.• Orthodontic treatment: Generally, no recession with conventional orthodontic movement unless excessive force moves the tooth out of the thicker coronal bony housing.
FIGURE 5. A thick scalloped phenotype has a narrow coronal band of thick gingiva with thin tissue more apically.
FIGURE 7. A history of vigorous brushing with a fi rm brush resulted in recession defects.
FIGURE 6 . A thin phenotype and chronic infl ammation often result in gingival recession.
FIGURE 8A . Pulling dental fl oss into the tissue instead of wrapping it around the tooth can create clefts that lead to recession.
FIGURE 8B . Flossing clefts on the lingual.
FIGURE 9A . The lateral incisor is tipped to the distal and is positioned more labially in the alveolus resulting in thin overlying bone and gingiva that contributed to gingival recession.
FIGURE 9B . The same patient demonstrating the malposition on the lingual and resulting mucogingival defects.

C DA J O U R N A L , V O L 4 6 , Nº 1 0
620 O C TO B E R 2 01 8
These mucogingival parameters are an important component of a comprehensive periodontal evaluation and should be obtained as a baseline on adult patients and anyone who presents with a mucogingival defect.8 Mucogingival abnormalities should be evaluated at each exam to determine if there has been progression.
Etiology and Contributing FactorsEtiologic factors must also be identifi ed
to allow them to be addressed as part of the corrective treatment if indicated. The most common causes of gingival recession are plaque-induced infl ammation and mechanical trauma.2,9 Chronic periodontal infl ammation can result in gingival recession and attachment loss, especially with thin anatomy (FIGURE 6). Mechanical trauma may occur as a result of brushing with a hard toothbrush10 especially with a vigorous brushing technique and/or using an abrasive dentifrice (FIGURE 7). Buccal gingival recession is noted more frequently on the left side of the jaw, most likely related to the fact that most people are right-handed and brush more thoroughly on the left sides of their mouths. In patients with dentin hypersensitivity, more gingival recession and sensitivity are found on the left side of the mouth and the lowest amount of plaque is seen on teeth with recession and sensitivity.11 Improper fl ossing technique can lead to fl ossing clefts in the gingiva (FIGURES 8), which may contribute to gingival recession. Improper and aggressive use of other interproximal aids may also lead to mucogingival defects.
Anatomical abnormalities often result in teeth with a thin phenotype because
• Surgical consideration: Though this is the ideal gingival phenotype to work with both from a restorative and surgical perspective, ridge preservation strategy should be taken when there is concern for extensive ridge remodeling post-extraction. This is so the ideal ridge for an ovate pontic or implant placement can be developed.
■ Thick scalloped phenotype condition: The behavior of this phenotype is dependent on whether the problem area is limited to the thicker coronal band. If this is the case, the tissue behaves similar to the thick fl at phenotype. If recession is present or the trauma spreads to the more apical thinner phenotype, recession and mucogingival remodeling may occur at a much more rapid rate. With implant placement, the surgeon must take caution in that the apical portion is quite thin and care must be taken to avoid buccal plate perforation. This is easy to do because the coronal aspect gives the false image that there is a thick bony housing.
While it is not the purview of this paper, it should be mentioned that these characteristics also apply to the mucogingival complex around implants. The conclusion of a systematic review indicated that based on current evidence, a lack of adequate keratinized gingiva around implants is associated with more plaque accumulation, tissue infl ammation, gingival recession and attachment loss.7
they are positioned more buccal or lingual in the alveolar bone (FIGURES 9). Such teeth may incur greater forces during oral hygiene because they are more prominent (FIGURE 10). Canines and the mesial buccal root of fi rst molars are often prominent in the arch and may be subject to heavier brushing forces contributing to recession defects (FIGURES 11). Patients should be made aware of these conditions and educated in proper oral hygiene to reduce the possibility of gingival recession.
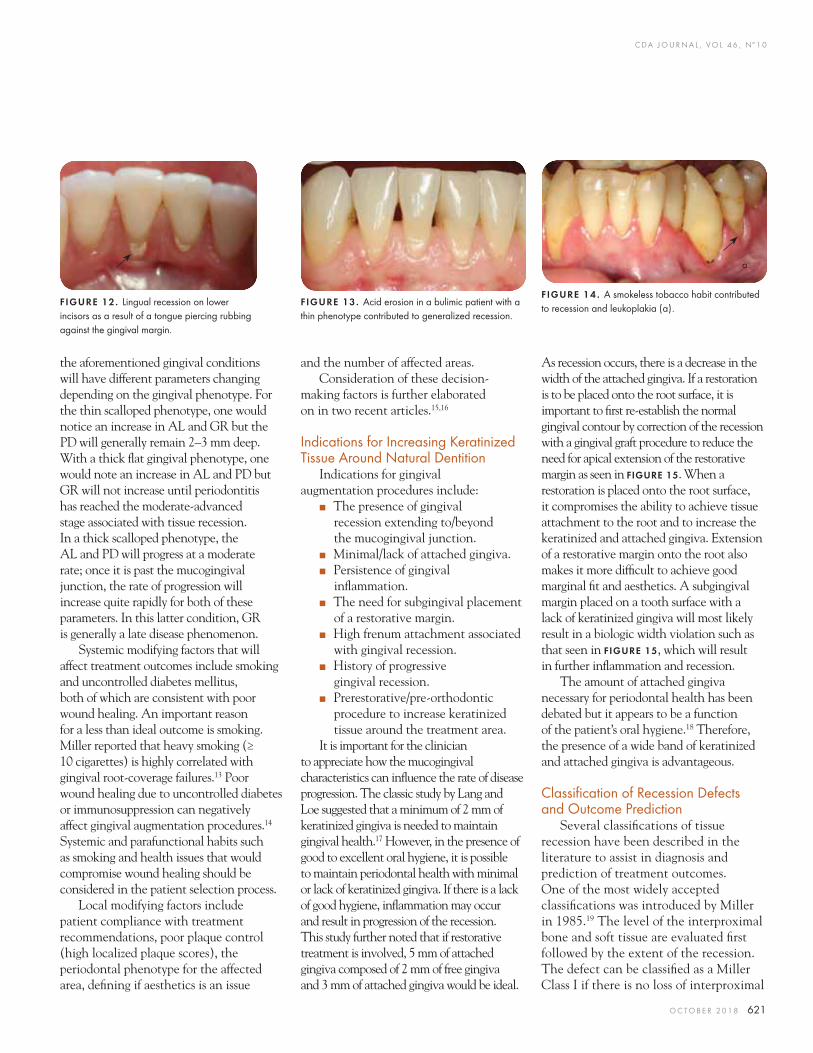
Mechanical trauma leading to gingival recession may also be the result of oral piercings. A tongue piercing can rub on the lingual aspect of the lower incisors (FIGURE 12) and lip piercings may affect the buccal aspect. Other contributing factors include chemical erosion from acid refl ux or bulimia (FIGURE 13) or the combined chemical and mechanical action of smokeless tobacco (FIGURE 14).
Gingival recession is typically the result of several factors but not necessarily simultaneously or equally.
Disease Progression and Modifying Factors
Once the putative etiologic contributing factor(s) and the gingival phenotype have been identifi ed, the greatest challenge to the clinician is to defi ne the rate of disease progression. To defi ne how fast the disease is progressing, clinical records must provide a history of the progress of gingival recession. This may at times prove challenging in that it would require diligent monitoring of attachment loss (AL), pocket depth (PD) and gingival recession (GR). This challenge has been previously described.12 Each of
g i n g i v a l r e c e s s i o n
FIGURE 10 . The fi rst premolar is displaced toward the buccal making it more prominent and more likely to incur toothbrush trauma resulting in gingival recession.
FIGURE 11A . Premolar and fi rst molar roots are prominent and have more recession defect.
FIGURE 11B . Canines commonly have prominent roots that exhibit recession.
C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 621
the aforementioned gingival conditions will have different parameters changing depending on the gingival phenotype. For the thin scalloped phenotype, one would notice an increase in AL and GR but the PD will generally remain 2–3 mm deep. With a thick fl at gingival phenotype, one would note an increase in AL and PD but GR will not increase until periodontitis has reached the moderate-advanced stage associated with tissue recession. In a thick scalloped phenotype, the AL and PD will progress at a moderate rate; once it is past the mucogingival junction, the rate of progression will increase quite rapidly for both of these parameters. In this latter condition, GR is generally a late disease phenomenon.
Systemic modifying factors that will affect treatment outcomes include smoking and uncontrolled diabetes mellitus, both of which are consistent with poor wound healing. An important reason for a less than ideal outcome is smoking. Miller reported that heavy smoking (≥ 10 cigarettes) is highly correlated with gingival root-coverage failures.13 Poor wound healing due to uncontrolled diabetes or immunosuppression can negatively affect gingival augmentation procedures.14 Systemic and parafunctional habits such as smoking and health issues that would compromise wound healing should be considered in the patient selection process.
Local modifying factors include patient compliance with treatment recommendations, poor plaque control (high localized plaque scores), the periodontal phenotype for the affected area, defi ning if aesthetics is an issue
and the number of affected areas.Consideration of these decision-
making factors is further elaborated on in two recent articles.15,16
Indications for Increasing Keratinized Tissue Around Natural Dentition
Indications for gingival augmentation procedures include:
■ The presence of gingival recession extending to/beyond the mucogingival junction.
■ Minimal/lack of attached gingiva. ■ Persistence of gingival
infl ammation. ■ The need for subgingival placement
of a restorative margin. ■ High frenum attachment associated
with gingival recession. ■ History of progressive
gingival recession. ■ Prerestorative/pre-orthodontic
procedure to increase keratinized tissue around the treatment area.
It is important for the clinician to appreciate how the mucogingival characteristics can infl uence the rate of disease progression. The classic study by Lang and Loe suggested that a minimum of 2 mm of keratinized gingiva is needed to maintain gingival health.17 However, in the presence of good to excellent oral hygiene, it is possible to maintain periodontal health with minimal or lack of keratinized gingiva. If there is a lack of good hygiene, infl ammation may occur and result in progression of the recession. This study further noted that if restorative treatment is involved, 5 mm of attached gingiva composed of 2 mm of free gingiva and 3 mm of attached gingiva would be ideal.
As recession occurs, there is a decrease in the width of the attached gingiva. If a restoration is to be placed onto the root surface, it is important to fi rst re-establish the normal gingival contour by correction of the recession with a gingival graft procedure to reduce the need for apical extension of the restorative margin as seen in FIGURE 15. When a restoration is placed onto the root surface, it compromises the ability to achieve tissue attachment to the root and to increase the keratinized and attached gingiva. Extension of a restorative margin onto the root also makes it more diffi cult to achieve good marginal fi t and aesthetics. A subgingival margin placed on a tooth surface with a lack of keratinized gingiva will most likely result in a biologic width violation such as that seen in FIGURE 15, which will result in further infl ammation and recession.
The amount of attached gingiva necessary for periodontal health has been debated but it appears to be a function of the patient’s oral hygiene.18 Therefore, the presence of a wide band of keratinized and attached gingiva is advantageous.
Classifi cation of Recession Defects and Outcome Prediction
Several classifi cations of tissue recession have been described in the literature to assist in diagnosis and prediction of treatment outcomes. One of the most widely accepted classifi cations was introduced by Miller in 1985.19 The level of the interproximal bone and soft tissue are evaluated fi rst followed by the extent of the recession. The defect can be classifi ed as a Miller Class I if there is no loss of interproximal
FIGURE 12. Lingual recession on lower incisors as a result of a tongue piercing rubbing against the gingival margin.
FIGURE 13. Acid erosion in a bulimic patient with a thin phenotype contributed to generalized recession.
FIGURE 14 . A smokeless tobacco habit contributed to recession and leukoplakia (a).
a
C DA J O U R N A L , V O L 4 6 , Nº 1 0
622 O C TO B E R 2 01 8
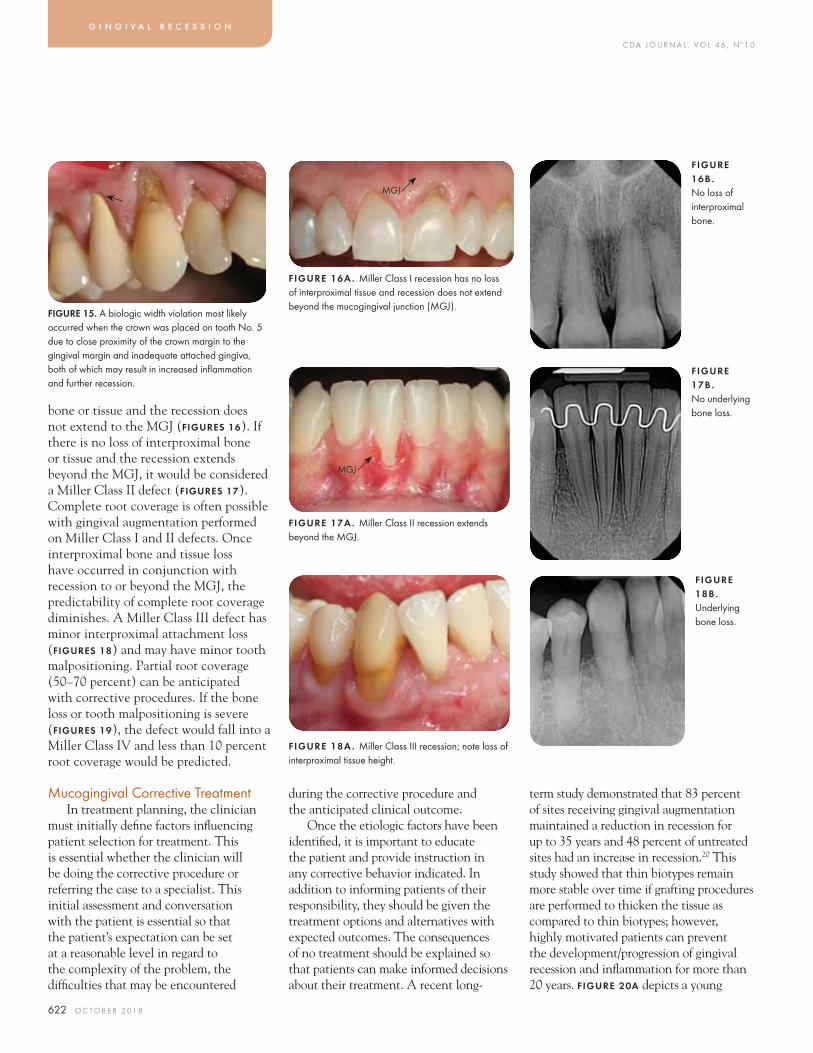
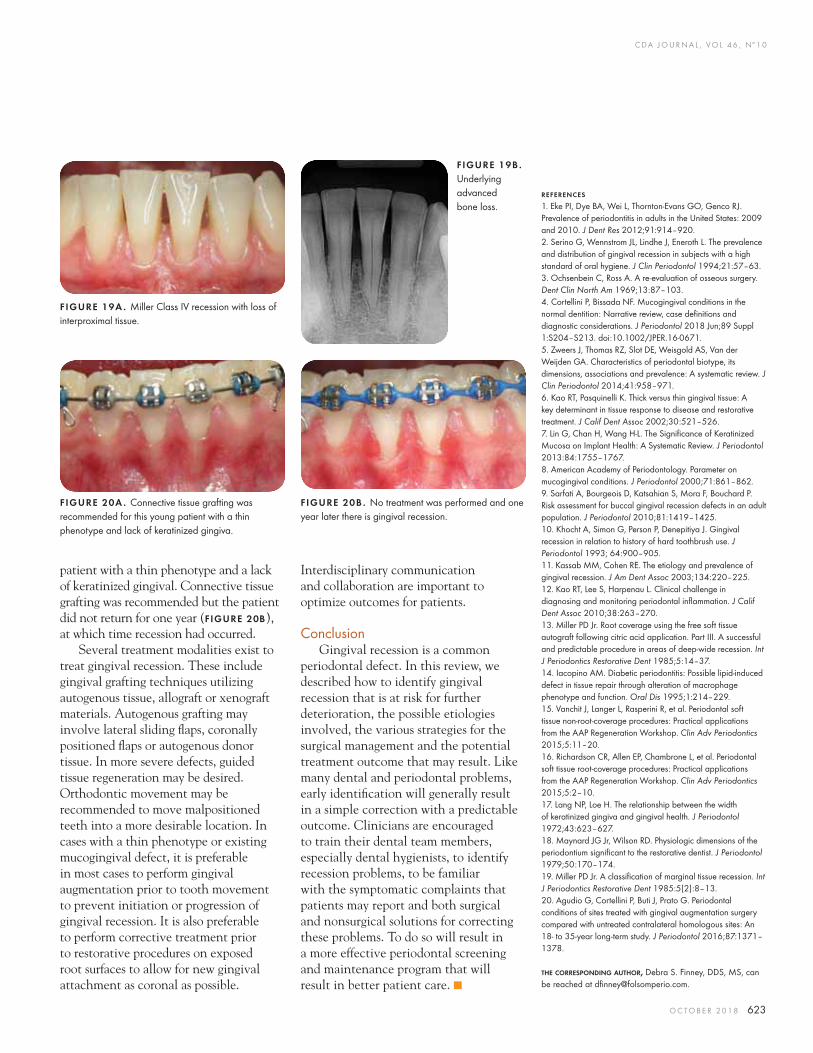
bone or tissue and the recession does not extend to the MGJ (FIGURES 16). If there is no loss of interproximal bone or tissue and the recession extends beyond the MGJ, it would be considered a Miller Class II defect (FIGURES 17). Complete root coverage is often possible with gingival augmentation performed on Miller Class I and II defects. Once interproximal bone and tissue loss have occurred in conjunction with recession to or beyond the MGJ, the predictability of complete root coverage diminishes. A Miller Class III defect has minor interproximal attachment loss (FIGURES 18) and may have minor tooth malpositioning. Partial root coverage (50–70 percent) can be anticipated with corrective procedures. If the bone loss or tooth malpositioning is severe (FIGURES 19), the defect would fall into a Miller Class IV and less than 10 percent root coverage would be predicted.
Mucogingival Corrective TreatmentIn treatment planning, the clinician
must initially defi ne factors infl uencing patient selection for treatment. This is essential whether the clinician will be doing the corrective procedure or referring the case to a specialist. This initial assessment and conversation with the patient is essential so that the patient’s expectation can be set at a reasonable level in regard to the complexity of the problem, the diffi culties that may be encountered
during the corrective procedure and the anticipated clinical outcome.
Once the etiologic factors have been identifi ed, it is important to educate the patient and provide instruction in any corrective behavior indicated. In addition to informing patients of their responsibility, they should be given the treatment options and alternatives with expected outcomes. The consequences of no treatment should be explained so that patients can make informed decisions about their treatment. A recent long-
term study demonstrated that 83 percent of sites receiving gingival augmentation maintained a reduction in recession for up to 35 years and 48 percent of untreated sites had an increase in recession.20 This study showed that thin biotypes remain more stable over time if grafting procedures are performed to thicken the tissue as compared to thin biotypes; however, highly motivated patients can prevent the development/progression of gingival recession and infl ammation for more than 20 years. FIGURE 20A depicts a young
g i n g i v a l r e c e s s i o n
FIGURE 15. A biologic width violation most likely occurred when the crown was placed on tooth No. 5 due to close proximity of the crown margin to the gingival margin and inadequate attached gingiva, both of which may result in increased infl ammation and further recession.
FIGURE 16A . Miller Class I recession has no loss of interproximal tissue and recession does not extend beyond the mucogingival junction (MGJ).
FIGURE 16B . No loss of interproximal bone.
FIGURE 17A . Miller Class II recession extends beyond the MGJ.
FIGURE 17B . No underlying bone loss.
FIGURE 18A . Miller Class III recession; note loss of interproximal tissue height.
FIGURE 18B . Underlying bone loss.
MGJ
MGJ
C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 623
patient with a thin phenotype and a lack of keratinized gingival. Connective tissue grafting was recommended but the patient did not return for one year (FIGURE 20B), at which time recession had occurred.
Several treatment modalities exist to treat gingival recession. These include gingival grafting techniques utilizing autogenous tissue, allograft or xenograft materials. Autogenous grafting may involve lateral sliding fl aps, coronally positioned fl aps or autogenous donor tissue. In more severe defects, guided tissue regeneration may be desired. Orthodontic movement may be recommended to move malpositioned teeth into a more desirable location. In cases with a thin phenotype or existing mucogingival defect, it is preferable in most cases to perform gingival augmentation prior to tooth movement to prevent initiation or progression of gingival recession. It is also preferable to perform corrective treatment prior to restorative procedures on exposed root surfaces to allow for new gingival attachment as coronal as possible.
Interdisciplinary communication and collaboration are important to optimize outcomes for patients.
ConclusionGingival recession is a common
periodontal defect. In this review, we described how to identify gingival recession that is at risk for further deterioration, the possible etiologies involved, the various strategies for the surgical management and the potential treatment outcome that may result. Like many dental and periodontal problems, early identifi cation will generally result in a simple correction with a predictable outcome. Clinicians are encouraged to train their dental team members, especially dental hygienists, to identify recession problems, to be familiar with the symptomatic complaints that patients may report and both surgical and nonsurgical solutions for correcting these problems. To do so will result in a more effective periodontal screening and maintenance program that will result in better patient care. ■
REFERENCES
1. Eke PI, Dye BA, Wei L, Thornton-Evans GO, Genco RJ. Prevalence of periodontitis in adults in the United States: 2009 and 2010. J Dent Res 2012;91:914–920.2. Serino G, Wennstrom JL, Lindhe J, Eneroth L. The prevalence and distribution of gingival recession in subjects with a high standard of oral hygiene. J Clin Periodontol 1994;21:57–63.3. Ochsenbein C, Ross A. A re-evaluation of osseous surgery. Dent Clin North Am 1969;13:87–103.4. Cortellini P, Bissada NF. Mucogingival conditions in the normal dentition: Narrative review, case defi nitions and diagnostic considerations. J Periodontol 2018 Jun;89 Suppl 1:S204–S213. doi:10.1002/JPER.16-0671.5. Zweers J, Thomas RZ, Slot DE, Weisgold AS, Van der Weijden GA. Characteristics of periodontal biotype, its dimensions, associations and prevalence: A systematic review. J Clin Periodontol 2014;41:958–971.6. Kao RT, Pasquinelli K. Thick versus thin gingival tissue: A key determinant in tissue response to disease and restorative treatment. J Calif Dent Assoc 2002;30:521–526.7. Lin G, Chan H, Wang H-L. The Signifi cance of Keratinized Mucosa on Implant Health: A Systematic Review. J Periodontol 2013:84:1755–1767.8. American Academy of Periodontology. Parameter on mucogingival conditions. J Periodontol 2000;71:861–862.9. Sarfati A, Bourgeois D, Katsahian S, Mora F, Bouchard P. Risk assessment for buccal gingival recession defects in an adult population. J Periodontol 2010;81:1419–1425.10. Khocht A, Simon G, Person P, Denepitiya J. Gingival recession in relation to history of hard toothbrush use. J Periodontol 1993; 64:900–905.11. Kassab MM, Cohen RE. The etiology and prevalence of gingival recession. J Am Dent Assoc 2003;134:220–225.12. Kao RT, Lee S, Harpenau L. Clinical challenge in diagnosing and monitoring periodontal infl ammation. J Calif Dent Assoc 2010;38:263–270.13. Miller PD Jr. Root coverage using the free soft tissue autograft following citric acid application. Part III. A successful and predictable procedure in areas of deep-wide recession. Int J Periodontics Restorative Dent 1985;5:14–37.14. Iacopino AM. Diabetic periodontitis: Possible lipid-induced defect in tissue repair through alteration of macrophage phenotype and function. Oral Dis 1995;1:214–229.15. Vanchit J, Langer L, Rasperini R, et al. Periodontal soft tissue non-root-coverage procedures: Practical applications from the AAP Regeneration Workshop. Clin Adv Periodontics 2015;5:11–20.16. Richardson CR, Allen EP, Chambrone L, et al. Periodontal soft tissue root-coverage procedures: Practical applications from the AAP Regeneration Workshop. Clin Adv Periodontics 2015;5:2–10.17. Lang NP, Loe H. The relationship between the width of keratinized gingiva and gingival health. J Periodontol 1972;43:623–627.18. Maynard JG Jr, Wilson RD. Physiologic dimensions of the periodontium signifi cant to the restorative dentist. J Periodontol 1979;50:170–174.19. Miller PD Jr. A classifi cation of marginal tissue recession. Int J Periodontics Restorative Dent 1985:5(2):8–13.20. Agudio G, Cortellini P, Buti J, Prato G. Periodontal conditions of sites treated with gingival augmentation surgery compared with untreated contralateral homologous sites: An 18- to 35-year long-term study. J Periodontol 2016;87:1371–1378.
THE CORRESPONDING AUTHOR, Debra S. Finney, DDS, MS, can be reached at dfi [email protected].
FIGURE 19A . Miller Class IV recession with loss of interproximal tissue.
FIGURE 19B . Underlying advanced bone loss.
FIGURE 20A . Connective tissue grafting was recommended for this young patient with a thin phenotype and lack of keratinized gingiva.
FIGURE 20B . No treatment was performed and one year later there is gingival recession.

C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 625
AUTHORS
Elissa Green, DMD, earned a bachelor’s degree in molecular cell biology at the University of California, Berkeley in 2009. She earned her doctor of dental medicine degree at Tufts University in 2015 and recently completed the periodontics residency and a master’s degree in periodontics and oral biology at the University of California, Los Angeles.Confl ict of Interest Disclosure: None reported.
Soma Esmailian Lari, DMD, earned a bachelor’s degree in biomedical engineering at the University of California, Los Angeles, in 2011 and her doctor of dental medicine degree at the Western University of Health Sciences, School of Dentistry in 2015. She recently completed the periodontics residency at UCLA.Confl ict of Interest Disclosure: None reported.
Perry R. Klokkevold, DDS, MS, earned a doctor of dental science degree at the University of California, San Francisco, in 1986. His postdoctoral training at UCLA includes the hospital-based general practice residency, the periodontics residency and the surgical implant fellowship at UCLA. He earned a master’s degree in oral biology concurrently with his specialty training. He is a diplomate of the American Board of Periodontology and a fellow of the American College of Dentists. He is professor of clinical dentistry and currently serves as the periodontics residency program director at UCLA.Confl ict of Interest Disclosure: None reported.
Autogenous Soft Tissue Grafting for the Treatment of Gingival RecessionElissa Green, DMD; Soma Esmailian Lari, DMD; and Perry R. Klokkevold, DDS, MS
A B S T R AC T Gingival recession is prevalent. It can adversely affect the health, stability and appearance of the involved teeth. Exposed root surfaces may be susceptible to caries, root sensitivity or result in aesthetic concerns. A variety of procedures are described in the literature for the treatment of gingival recession. This article reviews the use of autogenous soft tissue grafting for root coverage. Advantages and disadvantages of techniques are discussed. Case types provide indications for selection and treatment.
Gingival recession is a prevalent condition that can adversely affect the health, stability and appearance of the involved teeth. Exposed
root surfaces may increase susceptibility to caries and root sensitivity and/or result in aesthetic concerns for the patient. There are a variety of periodontal plastic surgery procedures that have been developed and described in the literature for the treatment of gingival recession. This article reviews the use of autogenous soft tissue grafting as a predictable and effective treatment when indicated for gingival recession, focusing on the goal of root coverage. Various procedures are presented in a historical context. Advantages and disadvantages of each technique are discussed and gingival recession case types are defi ned to provide indications and guidelines for case selection. A completed case with long-term follow-up is presented to demonstrate the use of the subepithelial connective tissue graft with a tunnel approach and coronally advanced fl ap as a predicable technique for aesthetic root coverage.
IntroductionGingival recession is a prevalent
condition, reported to affect about 50 percent of the adult population aged 18–64 and 88 percent of those over 65 years old.1 It is described as the apical displacement of the gingival margin away from the cementoenamel junction (CEJ) resulting in exposed root structure. Depending on the extent of periodontal attachment and bone loss, gingival recession can adversely affect the health, stability and appearance of involved teeth. It may increase susceptibility to caries, root sensitivity and, based on the location, gingival recession may cause signifi cant aesthetic concerns for the patient.
Topical agents are available to reduce root sensitivity and aid in the prevention of caries. However, these medicaments tend to be palliative and do not correct the anatomical defects. Class V composite restorations have also been advocated as a treatment to mask root sensitivity, correct cervical abrasion, cover dark, unsightly roots and repair tooth structure lost to caries or abrasion/abfraction.
S O F T T I S S U E G R A F T I N G
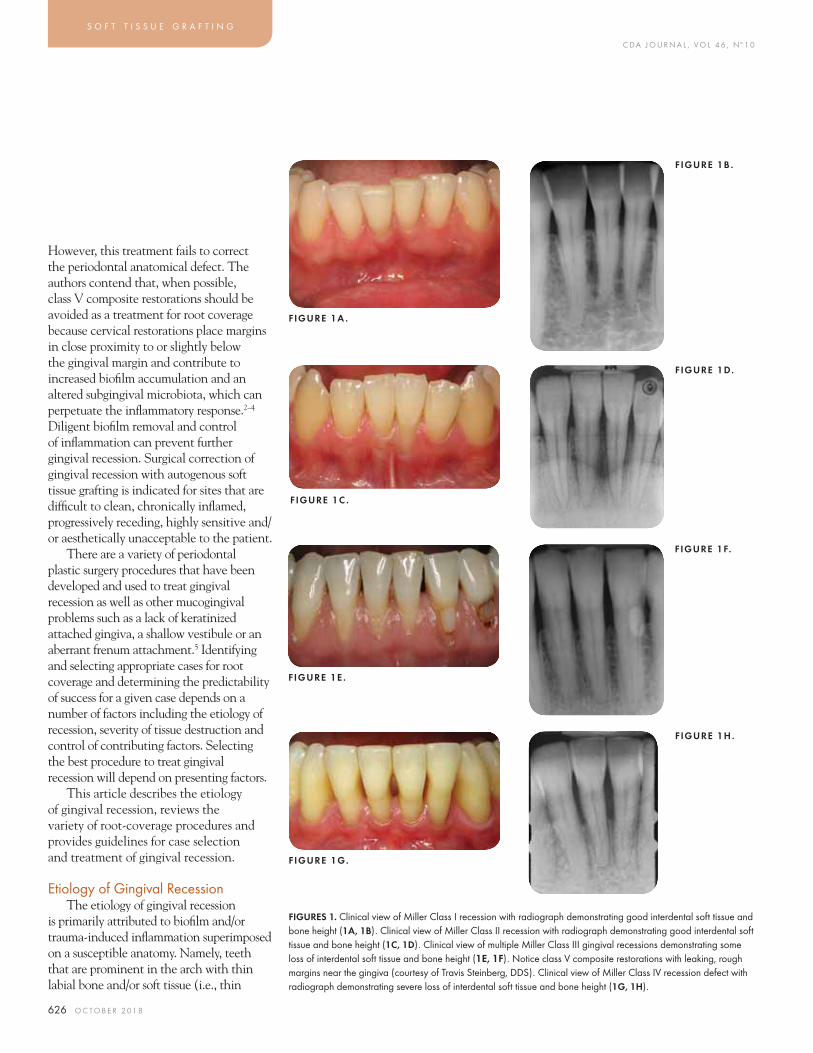
C DA J O U R N A L , V O L 4 6 , Nº 1 0
626 O C TO B E R 2 01 8
S O F T T I S S U E G R A F T I N G
However, this treatment fails to correct the periodontal anatomical defect. The authors contend that, when possible, class V composite restorations should be avoided as a treatment for root coverage because cervical restorations place margins in close proximity to or slightly below the gingival margin and contribute to increased biofi lm accumulation and an altered subgingival microbiota, which can perpetuate the infl ammatory response.2–4 Diligent biofi lm removal and control of infl ammation can prevent further gingival recession. Surgical correction of gingival recession with autogenous soft tissue grafting is indicated for sites that are diffi cult to clean, chronically infl amed, progressively receding, highly sensitive and/or aesthetically unacceptable to the patient.
There are a variety of periodontal plastic surgery procedures that have been developed and used to treat gingival recession as well as other mucogingival problems such as a lack of keratinized attached gingiva, a shallow vestibule or an aberrant frenum attachment.5 Identifying and selecting appropriate cases for root coverage and determining the predictability of success for a given case depends on a number of factors including the etiology of recession, severity of tissue destruction and control of contributing factors. Selecting the best procedure to treat gingival recession will depend on presenting factors.
This article describes the etiology of gingival recession, reviews the variety of root-coverage procedures and provides guidelines for case selection and treatment of gingival recession.
Etiology of Gingival RecessionThe etiology of gingival recession
is primarily attributed to biofi lm and/or trauma-induced infl ammation superimposed on a susceptible anatomy. Namely, teeth that are prominent in the arch with thin labial bone and/or soft tissue (i.e., thin
FIGURES 1. Clinical view of Miller Class I recession with radiograph demonstrating good interdental soft tissue and bone height (1A, 1B). Clinical view of Miller Class II recession with radiograph demonstrating good interdental soft tissue and bone height (1C, 1D). Clinical view of multiple Miller Class III gingival recessions demonstrating some loss of interdental soft tissue and bone height (1E, 1F). Notice class V composite restorations with leaking, rough margins near the gingiva (courtesy of Travis Steinberg, DDS). Clinical view of Miller Class IV recession defect with radiograph demonstrating severe loss of interdental soft tissue and bone height (1G, 1H).
FIGURE 1A .
FIGURE 1B .
FIGURE 1D.
FIGURE 1C .
FIGURE 1F.
FIGURE 1E .
FIGURE 1H.
FIGURE 1G.

C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 627
periodontal biotype) are more susceptible to gingival recession than teeth in a normal or lingual/palatal position with a thick biotype. Factors that increase the risk of gingival recession include aggressive toothbrushing, tooth malposition, alveolar bone dehiscence, high muscle/frenum attachment, plaque-induced infl ammatory lesions, iatrogenic habits and factors related to restorative and periodontal treatments.5,6
Classifi cation of Gingival RecessionIn 1985, P.D. Miller published a
classifi cation scheme for gingival recession and associated the prognosis for root coverage with each type.7 He correlated the predictability of therapeutic success (i.e., root coverage) with the extent of the recession defect and the height of adjacent interdental soft and hard tissues. Miller Class I defects are defi ned as gingival margin recession that does not extend beyond the mucogingival junction with no loss of interdental tissues. Miller Class II defects are defi ned as gingival margin recession that extends to or beyond the mucogingival junction with no loss of interdental tissues. Miller Class III defects are defi ned as gingival margin recession that extends to or beyond the mucogingival junction with some loss of interdental bone or soft tissues and/or malpositioning of teeth. Miller Class IV defects are defi ned as gingival margin recession that extends to or beyond the mucogingival junction with severe loss of interdental bone or soft tissues and/or malpositioning of teeth (FIGURES 1).
According to Miller, complete root coverage can be anticipated in Miller Class I and Miller Class II recession defects where there is no interproximal attachment loss, partial root coverage can be expected in Miller Class III defects where there is some loss of interproximal bone and soft tissue height and no root coverage is expected in Miller Class IV defects where there is severe interproximal attachment loss.
Root-Coverage ProceduresThe methods used to treat gingival
recession have progressively advanced over time from early basic attempts to transplant gingival soft tissue from one site to another to more sophisticated techniques of creating recipient sites with an envelope, pouch or tunnel approach and the use of subepithelial connective tissue grafts with or without biologic mediators and biomaterials. Regardless of surgical techniques or materials used for root coverage, all procedures share the common endpoint
objective to cover exposed roots with tissues that are stable, healthy and aesthetic. In a patient with high aesthetic demands, obtaining complete root coverage is the primary objective.8 Secondary objectives, depending on specifi c case fi ndings, may be to increase the amount of keratinized tissue and/or to decrease dentin hypersensitivity.
Root-coverage procedures must also result in tissue coverage that is well adapted and adherent to the previously exposed root surface. It would be problematic, and considered a failure, if the soft tissue grafting resulted in periodontal pocket formation. The ideal outcome of soft tissue grafting for root coverage would be a true regeneration of the periodontal attachment with new cementum, periodontal ligament,
inserting connective tissue fi bers and new bone; this can only be determined with histology. Although true periodontal regeneration seems to be an elusive goal, there is limited human histologic evidence that it has been achieved with autogenous soft tissue grafting over exposed root surfaces.9–12 The periodontal regeneration achieved in these cases always formed at the apical extent of the grafted site from the existing periodontium with the more coronal aspect consisting of closely adapted connective tissue fi bers running parallel to the root surface (i.e., not inserting perpendicular) and a long junctional epithelial attachment above it. The most likely and predominant form of attachment following autogenous soft tissue grafting for root coverage will be an apical zone of connective tissue adherence with fi bers running parallel to the root surface, little or no new cementum or bone and a coronal zone of long junctional epithelial attachment.13 This attachment will be predictable and stable long term.14,15
Autogenous soft tissue grafting techniques are reviewed here in the order that they were fi rst described in the literature. Procedures include the laterally positioned fl ap16 (Grupe and Warren, 1956), free gingival grafts17 (Sullivan and Atkins, 1968), free connective tissue grafts18 (Edel, 1974), coronally advanced fl aps19 (Bernimoulin et al., 1975), subepithelial connective tissue grafts in combination with coronally advanced fl aps20 (Langer and Langer, 1985) and variations of these techniques. While all soft tissue grafting techniques provide reduction in gingival recession, some are more effective than others. See other articles in this issue regarding the use of biomaterials, allografts and biologic mediators as adjuncts to root-coverage procedures.
While all soft tissue grafting techniques provide reduction in gingival recession, some are more eff ective than others.

C DA J O U R N A L , V O L 4 6 , Nº 1 0
628 O C TO B E R 2 01 8
Laterally Positioned Pedicle GraftThe laterally positioned pedicle
graft technique was introduced by Grupe and Warren in 1956.6 It utilizes a split-thickness fl ap design with vertical incisions directed apically toward the recipient site thereby allowing keratinized tissue from an adjacent location to be repositioned over an exposed root surface while remaining attached at the base. Tissues adjacent to the area of recession are de-epithelialized with a split-thickness fl ap to expose a connective tissue bed for attachment and nutrients (blood supply) of the laterally positioned fl ap. Tissue survival and root coverage depends on a fl ap design with a wide base that allows good blood supply, adequate fl ap (periosteum) release, connective tissue exposure for blood supply at the recipient site, intimate adaptation and fl ap stabilization with sutures. Advantages of the laterally positioned pedicle graft are relative ease of procedure, time effi ciency, excellent aesthetic results and avoidance of a second surgical site. Disadvantages are the limited applicability to isolated recession defects and the possible risk of creating gingival recession, dehiscence or fenestration at the adjacent donor site. There is also a requirement for adequate keratinized tissue at a neighboring donor site along with a deep vestibule.
The success rate of the laterally positioned pedicle graft for root coverage is limited, ranging from 61 percent to 77 percent.21,22 The
predictability of this technique has not been evaluated in a systematic review or meta-analysis.
Variations of the laterally positioned fl ap procedure include the double papilla graft (Cohen and Ross, 1968)23 and the obliquely rotated graft (Pennel et al., 1965).24 It is important to recognize that all of these rotational pedicle grafts work best when the adjacent donor papilla and zone of keratinized tissue is wide.
Free Gingival GraftThe free gingival graft (FGG)
technique was introduced by Sullivan and Atkins in 1968.17 The FGG is harvested from the surface of a keratinized area on the palate and placed on a de-epithelialized recipient bed at the defect site (FIGURES 2). Survival of the graft depends on the intimate contact of the graft with an adequate area of exposed connective tissue/vascular bed and stabilization of the
S O F T T I S S U E G R A F T I N G
FIGURE 2A . FIGURE 2B . FIGURE 2C .
FIGURES 2. Miller Class III recession of mandibular central incisor (2A). There is slight loss of interdental papilla height. Notice the lack of keratinized tissue and high frenum attachment at the gingival margin. There is also evidence of calculus on the root surface. Recipient site was prepared by de-epithelializing the adjacent tissues and resecting the mucosa/frenum (2B). Healed site more than fi ve years later (2C). Notice the incomplete root coverage with increased zone of keratinized, attached tissue. There is also a clear color demarcation outlining the free gingival graft.
FIGURE 3A .
FIGURE 3C .
FIGURE 3B .
FIGURE 3D.
FIGURES 3 . Miller Class I recession aff ecting several maxillary incisors (3A). Split-thickness fl ap preparation of recipient site with vertical releasing incisions on the distal aspect of the papilla adjacent to recession defects (3B). Periosteum is released at the base of the fl ap. Coronally advanced fl ap to cover recession defects (3C). Flap is secured coronally with interrupted and mattress sutures. Healed site about six months after surgery. Root coverage of the treated sites is nearly complete (3D).
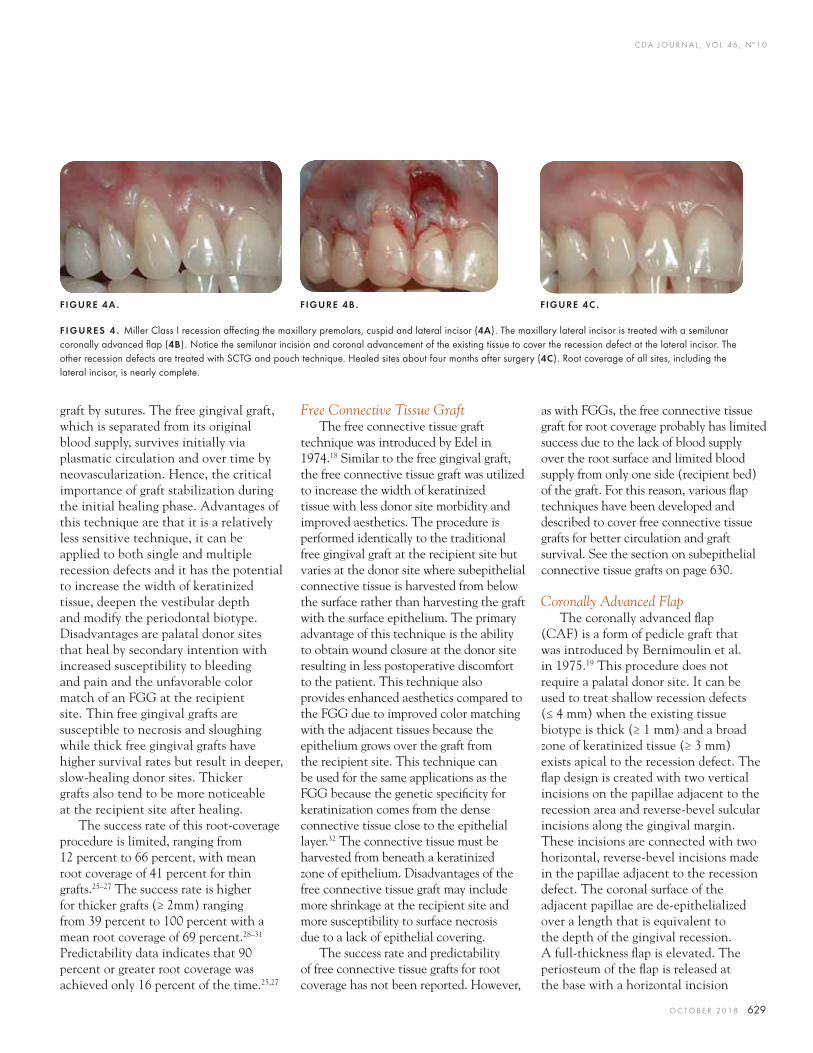
C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 629
graft by sutures. The free gingival graft, which is separated from its original blood supply, survives initially via plasmatic circulation and over time by neovascularization. Hence, the critical importance of graft stabilization during the initial healing phase. Advantages of this technique are that it is a relatively less sensitive technique, it can be applied to both single and multiple recession defects and it has the potential to increase the width of keratinized tissue, deepen the vestibular depth and modify the periodontal biotype. Disadvantages are palatal donor sites that heal by secondary intention with increased susceptibility to bleeding and pain and the unfavorable color match of an FGG at the recipient site. Thin free gingival grafts are susceptible to necrosis and sloughing while thick free gingival grafts have higher survival rates but result in deeper, slow-healing donor sites. Thicker grafts also tend to be more noticeable at the recipient site after healing.
The success rate of this root-coverage procedure is limited, ranging from 12 percent to 66 percent, with mean root coverage of 41 percent for thin grafts.25–27 The success rate is higher for thicker grafts (≥ 2mm) ranging from 39 percent to 100 percent with a mean root coverage of 69 percent.28–31 Predictability data indicates that 90 percent or greater root coverage was achieved only 16 percent of the time.25,27
Free Connective Tissue GraftThe free connective tissue graft
technique was introduced by Edel in 1974.18 Similar to the free gingival graft, the free connective tissue graft was utilized to increase the width of keratinized tissue with less donor site morbidity and improved aesthetics. The procedure is performed identically to the traditional free gingival graft at the recipient site but varies at the donor site where subepithelial connective tissue is harvested from below the surface rather than harvesting the graft with the surface epithelium. The primary advantage of this technique is the ability to obtain wound closure at the donor site resulting in less postoperative discomfort to the patient. This technique also provides enhanced aesthetics compared to the FGG due to improved color matching with the adjacent tissues because the epithelium grows over the graft from the recipient site. This technique can be used for the same applications as the FGG because the genetic specifi city for keratinization comes from the dense connective tissue close to the epithelial layer.32 The connective tissue must be harvested from beneath a keratinized zone of epithelium. Disadvantages of the free connective tissue graft may include more shrinkage at the recipient site and more susceptibility to surface necrosis due to a lack of epithelial covering.
The success rate and predictability of free connective tissue grafts for root coverage has not been reported. However,
as with FGGs, the free connective tissue graft for root coverage probably has limited success due to the lack of blood supply over the root surface and limited blood supply from only one side (recipient bed) of the graft. For this reason, various fl ap techniques have been developed and described to cover free connective tissue grafts for better circulation and graft survival. See the section on subepithelial connective tissue grafts on page 630.
Coronally Advanced FlapThe coronally advanced fl ap
(CAF) is a form of pedicle graft that was introduced by Bernimoulin et al. in 1975.19 This procedure does not require a palatal donor site. It can be used to treat shallow recession defects (≤ 4 mm) when the existing tissue biotype is thick (≥ 1 mm) and a broad zone of keratinized tissue (≥ 3 mm) exists apical to the recession defect. The fl ap design is created with two vertical incisions on the papillae adjacent to the recession area and reverse-bevel sulcular incisions along the gingival margin. These incisions are connected with two horizontal, reverse-bevel incisions made in the papillae adjacent to the recession defect. The coronal surface of the adjacent papillae are de-epithelialized over a length that is equivalent to the depth of the gingival recession. A full-thickness fl ap is elevated. The periosteum of the fl ap is released at the base with a horizontal incision
FIGURE 4A . FIGURE 4B . FIGURE 4C .
F IGURES 4 . Miller Class I recession aff ecting the maxillary premolars, cuspid and lateral incisor (4A). The maxillary lateral incisor is treated with a semilunar coronally advanced fl ap (4B). Notice the semilunar incision and coronal advancement of the existing tissue to cover the recession defect at the lateral incisor. The other recession defects are treated with SCTG and pouch technique. Healed sites about four months after surgery (4C). Root coverage of all sites, including the lateral incisor, is nearly complete.

C DA J O U R N A L , V O L 4 6 , Nº 1 0
630 O C TO B E R 2 01 8
and the fl ap is coronally positioned to cover the recession. Alternatively, a partial-thickness fl ap can be used. Tissue adjacent to the area of recession is de-epithelialized with a split-thickness fl ap to expose connective tissue and provide a blood supply for the advanced fl ap. The coronally advanced fl ap is sutured at a level to cover exposed root surfaces (FIGURES 3). This procedure can be applied at single or multiple recession sites with adequate keratinized tissue apical to the root exposure. With this approach, the soft tissue used to cover the root exposure is similar in color, texture and thickness to that originally present at the labial aspect of the tooth with the recession defect, providing a satisfactory aesthetic result. Advantages of the coronally advanced fl ap procedure include relative ease, good aesthetics and no secondary donor site required. Disadvantages are that this procedure does not increase the zone of keratinized tissue and may be susceptible to fl ap retraction and relapse of the recession if the fl ap is not adequately released and sutured. The CAF procedure cannot be used if there is a lack of keratinized tissue, a cleft through the gingival margin, a high frenum attachment at the gingival margin or a shallow vestibule.
The coronally advanced fl ap procedure for root coverage was shown to be successful with mean root coverage of 79 percent.33 Predictability data showed that complete root coverage was achieved 40 percent of the time.34,35
Semilunar Coronally Advanced FlapSeveral variations of the coronally
advanced flap have been proposed. Tarnow described the semilunar coronally repositioned flap in 1986.36 This technique uses a semilunar incision that is parallel to the gingival margin above the recession defect. A split-thickness incision is made through the sulcus to elevate and coronally advance the tissue over the denuded root (FIGURES 4). Advantages include no tension, no shortening of the vestibule and no manipulation of interdental papilla. Disadvantages are similar to the CAF procedure. Namely, it does not increase the zone of keratinized tissue, may be susceptible to retraction and cannot be used in cases with a gingival cleft, high frenum attachment or shallow vestibule.
Modifi ed Coronally Advanced FlapDe Sanctis and Zucchelli (2007)
proposed a modifi ed surgical approach of split-full-split-thickness fl ap compared to the conventional CAF procedure with vertical releasing incisions for the treatment of localized gingival recessions.37 For multiple recession types, Zucchelli and de Sanctis (2000, 2007) presented further changes to the CAF procedure to improve the predictability of multiple recession-type defects.38,39 The authors proposed the use of a horizontal incision and a split-full-split approach to create an “envelope fl ap” with no vertical releasing incisions in
order to preserve the maximum soft tissue thickness above the root exposure. This incision should be extended laterally to include at least one adjacent tooth on each side of the gingival recession.
Subepithelial Connective Tissue Graft With Flap Coverage
The use of a “submerged” subepithelial connective tissue graft (SCTG) for root coverage was originally introduced by Langer and Langer in 1985.20 The technique utilized an SCTG and split-thickness CAF with releasing vertical incisions that is repositioned over the connective tissue graft to partially cover it. Advantages of this technique are the dual blood supply contributing to the high predictability and improved aesthetics compared to the free gingival graft or the free connective tissue graft. The SCTG with CAF provides more tissue thickness than the CAF alone. Furthermore, harvesting SCTG from the donor site involves less postoperative morbidity as compared to the donor site for free gingival grafts. In situations where the overlying fl ap does not completely cover the connective tissue, the exposed tissue becomes keratinized thereby potentially increasing the zone of keratinized tissue. The disadvantage of this technique is the use of vertical releasing incisions, which may compromise vascularization in wound healing and result in fi brotic scars.
Following the introduction of the original Langer and Langer technique, several modifi cations of the recipient site preparation have been proposed.
S O F T T I S S U E G R A F T I N G
FIGURE 5A . FIGURE 5B . FIGURE 5C .
FIGURES 5. Free gingival graft donor site (5A). Free gingival graft harvested (5B). Donor site healing at one week (5C).

C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 631
Envelope fl aps were introduced to avoid the use of vertical incisions with the SCTG either completely covered or left partially exposed.40 Further modifi cations include combining the free connective tissue graft with partial- or full-thickness fl aps, single-tooth tunnel or pouch technique, subpedicle fl aps and double papilla pedicle fl aps.41 All of these techniques offer a bilaminar blood supply increasing the chance for revascularization of the graft and complete root coverage. In 2005, Harris compared various recipient site fl ap designs used to cover SCTG and found them all to be equally effective in obtaining root coverage and improving clinical parameters.42
Another bilaminar technique using a dual blood supply was introduced by Zadeh in 2011.43 He proposed a variation of the SCTG that used a midline vestibular incision and subperiosteal tunnel approach (VISTA) to prepare the recipient site. The VISTA technique utilizes a vertical incision in the vestibule, away from the recession area, to provide access for full-thickness, tension-free soft tissue elevation and insertion of graft materials (i.e., subepithelial connective tissue or acellular dermal matrix). The outer “fl ap” tissue is coronally advanced along with the graft and stabilized with suspensory sutures that are tacked to the crowns with composite.
Subepithelial connective tissue grafts with fl ap coverage have clearly been established as a highly effective means of covering recession defects providing the most signifi cant gains in root coverage and the greatest long-term stability.44 It is
reported to be a highly successful method with mean root-coverage outcomes of 91.1 percent and 95.8 percent for molar and non-molar sites, respectively.45,46 Predictability data indicates that complete root coverage and long-term success of the SCTG with fl ap coverage for Miller I and II recession defects is 98.4 percent.47 This is the gold standard for root coverage in terms of predictability, percentage of coverage and long-term stability. See the following case presentation.
Recipient Site Considerations
Recipient Site PreparationRecipient site preparation includes
soft tissue fl ap design and root surface treatment. The primary purpose of the recipient site soft tissue fl ap preparation is to expose stable connective tissue that serves to provide nutrients (blood supply) and an area for attachment (suturing and healing) of the graft. In the case of free gingival grafts or free connective tissue grafts, the recipient site is prepared by dissecting the epithelium, connective tissue and muscle fi bers, leaving the periosteum as the base. The recipient bed should be nonmobile. It should be even and the donor tissue should be well adapted to prevent blood pooling, which can lead to a hematoma and subsequent necrosis.17 In the case of subepithelial connective tissue graft with fl ap coverage, the recipient site is prepared by elevating a full- or partial-thickness fl ap with or without vertical incisions and repositioning the fl ap over
the graft either completely or partially. In the case of a tunnel or pouch technique, incisions are made through the sulcus and horizontal incisions across interdental papilla are avoided; the fl ap is extended beyond the mucogingival junction and under each papilla to allow passive, tension-free coronal mobilization of the overlying fl ap. The tissues are less likely to retract when using this fl ap design because the interdental tissues are not severed. Incisions and fl ap refl ection are accomplished entirely through the gingival sulcus.
The etiology of the lesion must be identifi ed and addressed prior to surgical therapy. This may include the removal and control of biofi lm, modifi cation of oral hygiene techniques, orthodontic tooth movement, surgical reduction of prominent root surfaces and complete removal of class V restorations.
Root surfaces must be thoroughly cleaned prior to surgical preparation of the recipient site. Typically, roots are scaled and root planed. Root surface biomodifi cation may be performed, although the clinical benefi t is unclear.48 The purpose, in conjunction with scaling and root planing, is to remove the smear layer, expose collagen fi bers within the dentin and eliminate any toxic substances on the root surface. Citric acid, tetracycline, sodium hypochlorite and ethylenediaminetetraacetic acid (EDTA) are chemical agents commonly used to remove the smear layer and prepare the root surface. The use of lasers to clean and prepare root surfaces has also been
FIGURE 6A .
FIGURE 6B . FIGURE 6C .
FIGURES 6 . Strip gingival autograft donor site (6A). Strip gingival grafts (6B). Donor site healing at one week (6C). Notice the shallow depth and rapid re-epithelialization as compared to the typical FGG donor site.

C DA J O U R N A L , V O L 4 6 , Nº 1 0
632 O C TO B E R 2 01 8
reported but without advantages.49,50 In fact, root surface biomodifi cation with the Nd:YAG laser was found to be detrimental to the success of root-coverage procedures.49 No particular root surface biomodifi cation technique has been shown to produce any advantage over another, including no treatment.51
Donor Site Considerations
Donor Site: Harvesting Free Gingival Graft
The free gingival graft must be harvested from an area of keratinized epithelium with a dense lamina propria. This can include edentulous ridge tissue, attached gingiva and palatal mucosa.17 A minimum palatal thickness of 3 mm is recommended for this technique. Graft thickness relates to graft survival, shrinkage and appearance. Thinner grafts blend better than thicker grafts but may not survive as well over root surfaces. An FGG for root coverage requires a thicker graft than for gaining attached gingiva.52 Overall, a graft thickness of 1–1.5 mm has been reported to be functionally optimal5 (FIGURES 5).
The strip gingival autograft technique has been described as a technique to address the disadvantage of large, slow healing palatal donor sites with the traditional FGG.53,54 Donor tissue is harvested in thin and narrow (2 mm wide) strips from multiple separate sites to create small, shallow donor site wounds with more wound edges and less exposed connective tissue area for rapid epithelialization and decreased discomfort for the patient (FIGURES 6). This technique cannot be used for root coverage because the donor tissue is too thin to survive over root surfaces; it may be used in combination with a subsequent coronally advanced fl ap procedure to cover exposed roots.
Donor Site: Harvesting Subepithelial Connective Tissue Graft
There are important anatomical structures that must be considered when electing to harvest SCTGs from the palate. The depth of the palatal vault must be evaluated prior to surgery. The primary concern is violation of the neurovascular bundle that extends from the greater palatine foramen anteriorly in the palatal vault. It has been reported that the greater palatine vascular bundle is located 7 mm apical to the free gingival margin in shallow palates, 12 mm apical to the free gingival margin in average palates and 17 mm apical to the free gingival margin in steep palates.55 In shallow palates, the harvest site must be restricted to a position closer to the teeth and limited in depth. The optimal location for harvesting SCTGs is palatal to the maxillary premolars and fi rst molar sites. Harvesting of SCTGs must be limited to the depth that avoids injury to the major vessels. Based on the estimated position
of the greater palatine artery in 198 periodontally healthy individuals, it was determined that it is possible to harvest a connective tissue graft measuring 5 mm in height for all cases and approximately 8 mm in height for 93 percent of cases in the premolar region.56 Direct evaluation of the greater palatine artery in 41 human cadavers confi rmed that it is possible to harvest a connective tissue graft measuring at least 5 mm in height.57 Palatal tissue thickness is thinner in younger individuals and females as compared to older individuals and males, respectively. The amount of tissue that can be harvested varies depending on the height of the palatal vault and thickness of tissue.56,58
There are multiple methods for the harvesting of subepithelial connective tissue grafts. The overall goals are to achieve a graft of desired dimensions while respecting anatomical landmarks and minimizing tissue sloughing during healing. The overlying fl ap tissue must remain thick enough to survive and to be sutured adequately for
S O F T T I S S U E G R A F T I N G
FIGURE 7C . FIGURE 7D.
FIGURE 7A . FIGURE 7B .
FIGURES 7. Trap door technique donor site with vertical incisions at both ends (7A). Harvesting SCTG from trap door (7B). SCTG harvested from trap door (7C). Trap door donor site sutured with mattress and interrupted sutures (7D).
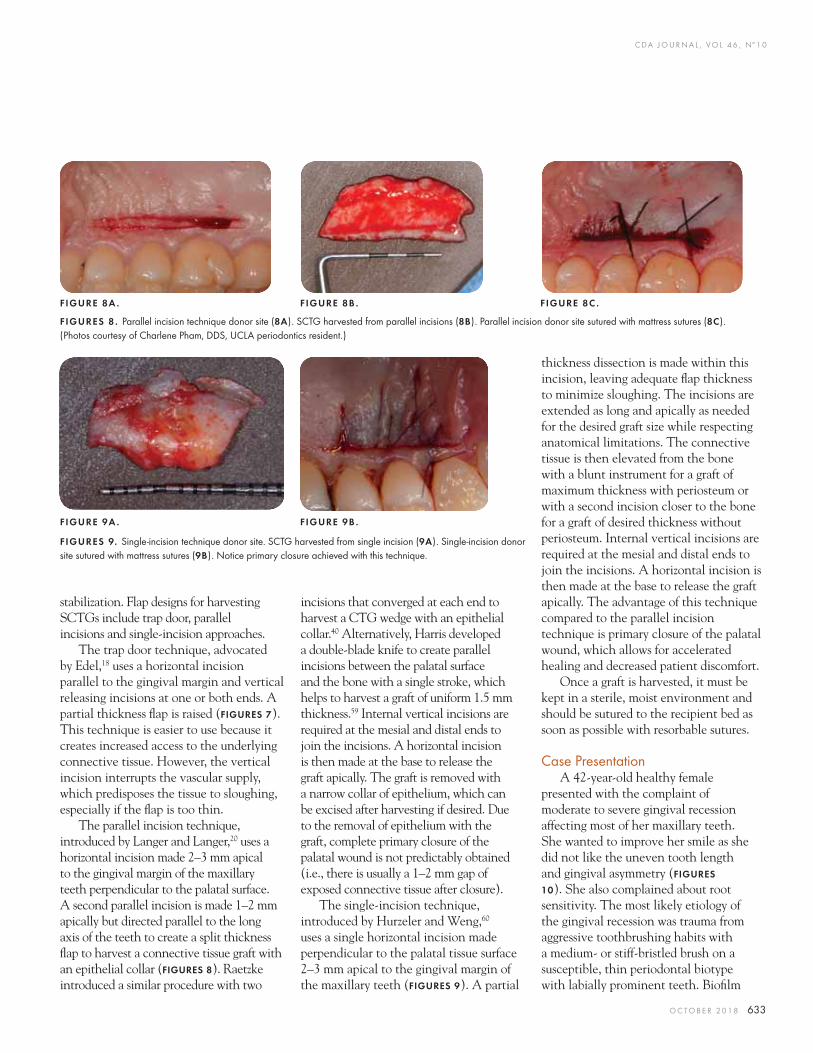
C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 633
stabilization. Flap designs for harvesting SCTGs include trap door, parallel incisions and single-incision approaches.
The trap door technique, advocated by Edel,18 uses a horizontal incision parallel to the gingival margin and vertical releasing incisions at one or both ends. A partial thickness fl ap is raised (FIGURES 7). This technique is easier to use because it creates increased access to the underlying connective tissue. However, the vertical incision interrupts the vascular supply, which predisposes the tissue to sloughing, especially if the fl ap is too thin.
The parallel incision technique, introduced by Langer and Langer,20 uses a horizontal incision made 2–3 mm apical to the gingival margin of the maxillary teeth perpendicular to the palatal surface. A second parallel incision is made 1–2 mm apically but directed parallel to the long axis of the teeth to create a split thickness fl ap to harvest a connective tissue graft with an epithelial collar (FIGURES 8). Raetzke introduced a similar procedure with two
incisions that converged at each end to harvest a CTG wedge with an epithelial collar.40 Alternatively, Harris developed a double-blade knife to create parallel incisions between the palatal surface and the bone with a single stroke, which helps to harvest a graft of uniform 1.5 mm thickness.59 Internal vertical incisions are required at the mesial and distal ends to join the incisions. A horizontal incision is then made at the base to release the graft apically. The graft is removed with a narrow collar of epithelium, which can be excised after harvesting if desired. Due to the removal of epithelium with the graft, complete primary closure of the palatal wound is not predictably obtained (i.e., there is usually a 1–2 mm gap of exposed connective tissue after closure).
The single-incision technique, introduced by Hurzeler and Weng,60 uses a single horizontal incision made perpendicular to the palatal tissue surface 2–3 mm apical to the gingival margin of the maxillary teeth (FIGURES 9). A partial
thickness dissection is made within this incision, leaving adequate fl ap thickness to minimize sloughing. The incisions are extended as long and apically as needed for the desired graft size while respecting anatomical limitations. The connective tissue is then elevated from the bone with a blunt instrument for a graft of maximum thickness with periosteum or with a second incision closer to the bone for a graft of desired thickness without periosteum. Internal vertical incisions are required at the mesial and distal ends to join the incisions. A horizontal incision is then made at the base to release the graft apically. The advantage of this technique compared to the parallel incision technique is primary closure of the palatal wound, which allows for accelerated healing and decreased patient discomfort.
Once a graft is harvested, it must be kept in a sterile, moist environment and should be sutured to the recipient bed as soon as possible with resorbable sutures.
Case PresentationA 42-year-old healthy female
presented with the complaint of moderate to severe gingival recession affecting most of her maxillary teeth. She wanted to improve her smile as she did not like the uneven tooth length and gingival asymmetry (FIGURES
10). She also complained about root sensitivity. The most likely etiology of the gingival recession was trauma from aggressive toothbrushing habits with a medium- or stiff-bristled brush on a susceptible, thin periodontal biotype with labially prominent teeth. Biofi lm
FIGURES 9. Single-incision technique donor site. SCTG harvested from single incision (9A). Single-incision donor site sutured with mattress sutures (9B). Notice primary closure achieved with this technique.
FIGURE 8A .
FIGURE 9A .
FIGURE 8B .
FIGURE 9B .
FIGURE 8C .
FIGURES 8 . Parallel incision technique donor site (8A). SCTG harvested from parallel incisions (8B). Parallel incision donor site sutured with mattress sutures (8C). (Photos courtesy of Charlene Pham, DDS, UCLA periodontics resident.)

C DA J O U R N A L , V O L 4 6 , Nº 1 0
634 O C TO B E R 2 01 8
S O F T T I S S U E G R A F T I N G
FIGURES 10 . Patient presents with several Miller Class II recession defects aff ecting most maxillary teeth (10A). Gingival margins are uneven and asymmetrical. Preoperative clinical view of many recession defects (10B–10D). Recession defects treated with SCTGs using a pouch technique to mobilize and advanced tissues through the sulcular incisions (10E–10G). Palatal stent fabricated for patient comfort to cover donor site wounds during initial healing phase (10H). Healed sites about four months after surgery prior to restorations. (10 I–10K). Smile view about six years after surgery and restorations (10L). Healed sites about six years after surgery (10M–10O). The combined treatment of SCTGs and restorative treatment provided an excellent aesthetic result that is stable.
FIGURE 10D. FIGURE 10E .
FIGURE 10A . FIGURE 10B .
FIGURE 10C .
FIGURE 10G.
FIGURE 10H.
FIGURE 10 I .
FIGURE 10J .FIGURE 10K.
FIGURE 10 L .
FIGURE 10M .FIGURE 10 N.
FIGURE 10 O.
FIGURE 10F.FIGURE 10D. FIGURE 10E .

C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 635
control was fair and there was slight marginal gingival infl ammation. The maxillary central incisor No. 9 had a PFM crown with a gingival margin that was 2–3 mm more apical than the contralateral unrestored central incisor No. 8. Exposed root surfaces were clean and smooth with a glassy, polished appearance. Slight surface wear was noted on roots, especially the patient’s left side, which also presented with greater recession depth. Although there was some incipient loss of interdental papilla, the interproximal spaces were nearly full with peaked papillary tissues and interproximal bone levels were normal.
The patient was advised to use a soft-bristled toothbrush and her brushing habits were modifi ed. The treatment, which was planned in coordination with her restorative dentist, was to improve gingival margin
levels with autogenous soft tissue grafts to provide root coverage for teeth Nos. 5, 6, 7, 10, 11 and 12 and to crown lengthen tooth No. 8. The crown No. 9 would be replaced and veneers were planned for adjacent teeth to level incisal edges and balance tooth dimensions and contours.
The procedure was performed under local anesthesia with 2% lidocaine with 1:100,000 epinephrine. All exposed root surfaces were scaled and root planed. The recipient sites were prepared with a pouch technique. Sulcular incisions were made with a microblade. A split-thickness pouch was prepared with sharp dissection beyond the mucogingival junction until the entire area was separated and mobilized. Continuity of the pouch space from end to end was confi rmed by passing an instrument through the tunnel. Two SCTGs were harvested from the right and left palate using the parallel incision technique. Donor sites were well adapted and closed with mattress sutures (5-0 chromic gut). The connective tissue grafts were inserted through the sulcus at one end, pulled through the tunnel with a suture passed in from the other end, positioned and secured in place over exposed root surfaces with sutures (5-0 chromic gut). The fl ap was secured with mattress sutures (5-0 chromic and 6-0 prolene). Stability of grafts and fl aps was verifi ed with careful examination. Tooth No. 8 was crown lengthened with a gingival excision of approximately 2–3 mm. The labial bone level was assessed and reduced through the sulcular incision using hand instruments.
A palatal stent was provided to protect the donor site wounds — mostly as an aid for patient comfort during the initial healing. Postoperative instructions were provided and the patient was scheduled to return for postoperative care and suture removal.
The patient healed uneventfully. Tissues were allowed to heal and mature four months prior to initiating restorative
dentistry. Examination about six years after the surgical procedure reveals good healing, nearly complete root coverage and good gingival contours. The patient reports no root sensitivity. The combined treatment of SCTGs and restorative dentistry provided an excellent aesthetic result that is stable.
Postoperative Complications Complications following autogenous
soft tissue grafts can include pain, bleeding, infection and necrosis. These can be minimized through patient selection, careful surgical technique and adherence to postoperative instructions.
Postoperative InstructionsTreatment of gingival recession
with autogenous soft tissue grafting typically involves two surgical sites that need to be carefully managed after surgery. Prior to patient discharge, both donor and recipient sites should be carefully inspected to assess hemostasis and wound stability. Postoperative instructions should advise patient to avoid manipulation of the surgical sites.
Specifi c instructions may include: ■ Avoid manipulation of
the surgical area. ■ Avoid attempting to look at
or inspect the surgical sites. ■ Brush all teeth normally except
those in surgical sites. ■ Biofi lm should be gently removed
from treated teeth with an extra soft brush and/or a cotton swab.
■ Gently rinse two to four times a day with salt water (or prescribed antimicrobial mouthwash) during the fi rst two weeks.
■ Use ice pack and cold water to keep surgical sites cool during fi rst two days.
■ Limit diet to mild, soft foods. ■ Avoid hot, spicy, hard
or crunchy foods.
TABLE
Factors That Can Adversely Influence the Expected Outcomes of Root-Coverage Procedures
Patient-related factors
■ Smoking
■ Systemic conditions that adversely aff ect healing
■ Inadequate biofi lm control
■ Poor compliance or inability to follow instructions
■ Psychological impairment
■ Unrealistic expectations
Defect-related factors
■ Recession type
■ Single or multiple recession defects
■ Mucogingival defects
■ Amount of keratinized tissue
■ Periodontal biotype
■ Vestibule depth
■ Subgingival restorations
■ Caries or noncarious cervical lesions
Technique-related factors
■ Stability of graft and fl ap
■ Position of the gingival margin
■ Adequate vascular supply
■ Adequate release of fl ap tension
■ Appropriate technique

C DA J O U R N A L , V O L 4 6 , Nº 1 0
636 O C TO B E R 2 01 8
■ Take anti-infl ammatory/analgesic medications as directed or needed for pain.
■ Use palatal stent to protect donor site wound as needed for fi rst two weeks (optional).
Therapeutic Endpoint of SuccessThe therapeutic endpoints of success
for the treatment of gingival recession are to achieve complete root coverage and improve aesthetics. Secondary benefi ts may include reducing sensitivity and increasing gingival width and thickness. As with most surgical procedures, there are risk factors that may diminish the success of root coverage. There are patient-related, site-related and technique-related factors that can adversely infl uence the expected outcomes of root-coverage procedures (TABLE). Hence, it is important to select the most predictable and easy-to-perform surgical technique with careful evaluation and consideration of these risk factors.
Patient-Related FactorsSome of the patient-related factors
that may adversely affect the outcome of root-coverage procedures include smoking, systemic conditions, biofi lm and poor patient compliance. Smokers had 17.5 percent less root coverage and about 36 percent fewer sites with complete root coverage when treated with SCTG.61 Systemic conditions such as poorly controlled diabetes and immune-compromised conditions can adversely affect healing and may impair the results of root-coverage procedures. Inadequate or poor biofi lm control following surgery may adversely affect the results of root-coverage procedures. Poor compliance with or an inability to follow instructions may adversely affect healing and results. Psychological impairment as well as unrealistic expectations can have an adverse effect on the result of root-coverage procedures.62
Defect-Related FactorsThe severity of the recession defect
(Miller’s classifi cation) and surrounding tissues can adversely affect the outcome of root-coverage procedures. Teeth that are labially prominent in the arch, malaligned or crowded with a thin biotype pose a greater challenge for root-coverage procedures. Likewise, recession defects associated with little or no keratinized tissue, a lack of vestibular depth, subgingival restorations, caries or noncarious cervical lesions pose a greater challenge for root coverage. Covering multiple recession defects can be less predictable than single recession defects. Initial tissue thickness directly correlates with the predictability of complete root coverage. Increasing tissue thickness results in complete root coverage irrespective of width of keratinized tissue or recession depth. Complete coverage with a coronally positioned fl ap requires soft tissue thickness ≥ 1 mm (less results in incomplete coverage).
Technique-Related FactorsPrecise, careful surgical management of
soft tissues at the recipient and donor sites is essential to the success of root-coverage procedures. Blood supply, blood supply, blood supply. Adequate vascular supply obtained from the bone, periosteum, PDL or overlying fl ap at the recipient site is essential for complete root coverage regardless of procedure or technique used. Recipient sites must be designed and managed to optimize the blood supply to the graft. Bilaminar vascular supply with an overlying fl ap is preferred as it contributes to increased predictability of root coverage by subepithelial connective tissue grafts as compared to free gingival and free connective tissue grafts. Surgical positioning of the tissue margin coronal to the cementoenamel junction is an important factor that improves root coverage outcomes.63 Releasing the periosteum and
using tension-free fl aps and suturing techniques are essential to minimize retraction during healing because increased fl ap tension causes tissues to retract. The utilization of pouch, envelope and tunnel procedures, which avoid making incisions across or through interdental papilla, also helps to reduce the likelihood of fl ap retraction.
ConclusionGingival recession is a common
condition. Consequences of gingival recession include loss of clinical attachment, root sensitivity, susceptibility to root caries and abrasion, challenges to effective biofi lm control and poor aesthetics. The ultimate goal of treatment for gingival recession is achieving complete root coverage with a healthy, thick and suffi ciently broad zone of keratinized gingiva. It is also important for the newly formed tissue to blend in with the surrounding tissues in terms of color, surface texture and harmony.64 The coronally advanced fl ap with subepithelial connective tissue graft has been consistently reported as the most effective and predictable procedure for root coverage, often referred to as the gold standard. This article reviews the etiology and classifi cation of gingival recession, the evolution of autogenous soft tissue grafting and describes techniques used for root coverage. ■
REFERENCES
1. Kassab MM, Cohen RE. The etiology and prevalence of gingival recession. J Am Dent Assoc 2003;134:220–225.2. Broadbent JM, Williams KB, Thomson WM, Williams SM. Dental restorations: A risk factor for periodontal attachment loss? J Clin Periodontol 2006;33(11):803–10.3. Kois JC. The restorative-periodontal interface: Biological parameters. Periodontol 2000 1996;11:29–38.4. Paolantonio M, D’ercole S, Perinetti G, Tripodi D, Catamo G, Serra E, Bruè C, Piccolomini R. Clinical and microbiological eff ects of diff erent restorative materials on the periodontal tissues adjacent to subgingival class V restorations. J Clin Periodontol 2004;31(3):200–7.5. Takei HH, Scheyer ET, Azzi RR, et al. Periodontal Plastic and Esthetic Surgery. In: Newman MG, Takei HH, Klokkevold PR, Carranza FA eds. Carranza’s Clinical Periodontology, 12th ed. St. Louis: Elsevier; 2015.6. Checchi L, Daprile G, Gatto MR, et al. Gingival recession and
S O F T T I S S U E G R A F T I N G

C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 637
toothbrushing in an Italian school of dentistry: A pilot study. J Clin Periodontol 1999;26:276–280.7. Miller PD Jr. A classifi cation of marginal tissue recession. Int J Periodontics Restorative Dent 1985;5:8–13.8. Stefanini M, Marzadori M, Aroca S, et al. Decision making in root-coverage procedures for the esthetic outcome. Periodontol 2000 2018;77:54–64.9. Goldstein M, Boyan BD, Cochran DL, Schwartz Z. Human histology of new attachment after root coverage using subepithelial connective tissue graft. J Clin Periodontol 2001 Jul;28(7):657–62.10. E. Rasperini G, Silvestri M, Schenk RK, Nevins ML. Clinical and histologic evaluation of human gingival recession treated with a subepithelial connective tissue graft and enamel matrix derivative (Emdogain): A case report. Int J Periodontics Restorative Dent 2000 Jun;20(3):269–75.11. Harris RJ. Successful root coverage: A human histologic evaluation of a case. Int J Periodontics Restorative Dent 1999 Oct;19(5):439–47.12. Pasquinelli KL. The histology of new attachment utilizing a thick autogenous soft tissue graft in an area of deep recession: A case report. Int J Periodontics Restorative Dent 1995 Jun;15(3):248–57.13. Majzoub Z, Landi L, Grusovin MG, Cordioli G. Histology of connective tissue graft. A case report. J Periodontol 2001 Nov;72(11):1607–15.14. Harris RJ. The connective tissue with partial thickness double pedicle graft: The results of 100 consecutively treated defects. J Periodontol 1994 May;65(5):448–61.15. Pini Prato GP, Franceschi D, Cortellini P, Chambrone L. Long-term evaluation (20 years) of the outcomes of subepithelial connective tissue graft plus coronally advanced fl ap in the treatment of maxillary single recession-type defects. J Periodontol 2018 Jun 6. doi: 10.1002/JPER.17-0619. [Epub ahead of print] PubMed PMID: 29873085.16. Grupe H, Warren R. Repair of gingival defects by a sliding fl ap operation. J Periodontol 1956;27:92–95.17. Sullivan HC, Atkins JH. Free autogenous gingival grafts. 3. Utilization of grafts in the treatment of gingival recession. Periodontics 1968;6:152–160.18. Edel A. Clinical evaluation of free connective tissue grafts used to increase the width of keratinised gingiva. J Clin Periodontol 1974;1:185–196.19. Bernimoulin JP, Luscher B, Muhlemann HR. Coronally repositioned periodontal fl ap. Clinical evaluation after one year. J Clin Periodontol 1975;2:1–13.20. Langer B, Langer L. Subepithelial connective tissue graft technique for root coverage. J Periodontol 1985;56:715–720.21. Smukler H. Laterally positioned mucoperiosteal pedicle grafts in the treatment of denuded roots. A clinical and statistical study. J Periodontol 1976;47:590–595.22. Caff esse RG, Espinel MC. Lateral sliding fl ap with a free gingival graft technique in the treatment of localized gingival recessions. Int J Periodontics Restorative Dent 1981;1:22–29.23. Cohen DW, Ross SE. The double papillae repositioned fl ap in periodontal therapy. J Periodontol 1968;39:65–70.14. Pennel BM, Higgason JD, Towner JD, et al. Oblique Rotated Flap. J Periodontol 1965;36:305–309.25. Mlinek A, Smukler H, Buchner A. The use of free gingival grafts for the coverage of denuded roots. J Periodontol 1973;44:248–254.26. Livingston HL. Total coverage of multiple and adjacent denuded root surfaces with a free gingival autograft. A case report. J Periodontol 1975;46:209–216.27. Matter J. Creeping attachment of free gingival grafts. A fi ve-year follow-up study. J Periodontol 1980;51:681–685.
28. Miller PD Jr. Root coverage using the free soft tissue autograft following citric acid application. III. A successful and predictable procedure in areas of deep-wide recession. Int J Periodontics Restorative Dent 1985;5:14–37.29. Borghetti A, Gardella JP. Thick gingival autograft for the coverage of gingival recession: A clinical evaluation. Int J Periodontics Restorative Dent 1990;10:216–229.30. Jahnke PV, Sandifer JB, Gher ME, et al. Thick free gingival and connective tissue autografts for root coverage. J Periodontol 1993;64:315–322.31. Paolantonio M, di Murro C, Cattabriga A, et al. Subpedicle connective tissue graft versus free gingival graft in the coverage of exposed root surfaces. A fi ve-year clinical study. J Clin Periodontol 1997;24:51–56.32. Karring T, Lang NP, Loe H. The role of gingival connective tissue in determining epithelial diff erentiation. J Periodontal Res 1975;10:1–11.33. Wennstrom JL, Zucchelli G. Increased gingival dimensions. A signifi cant factor for successful outcome of root coverage procedures? A two-year prospective clinical study. J Clin Periodontol 1996;23:770–777.34. Pini-Prato G, Baldi C, Pagliaro U, et al. Coronally advanced fl ap procedure for root coverage. Treatment of root surface: Root planing versus polishing. J Periodontol 1999;70:1064–1076.35. Saletta D, Pini Prato G, Pagliaro U, et al. Coronally advanced fl ap procedure: Is the interdental papilla a prognostic factor for root coverage? J Periodontol 2001;72:760–766.36. Tarnow DP. Semilunar coronally repositioned fl ap. J Clin Periodontol 1986;13:182–185.37. de Sanctis M, Zucchelli G. Coronally advanced fl ap: A modifi ed surgical approach for isolated recession-type defects: three-year results. J Clin Periodontol. 2007;34:262–268.38. Zucchelli G, De Sanctis M. The coronally advanced fl ap for the treatment of multiple recession defects: A modifi ed surgical approach for the upper anterior teeth. J Int Acad Periodontol 2007;9:96–103.39. Zucchelli G, De Sanctis M. Treatment of multiple recession-type defects in patients with esthetic demands. J Periodontol 2000;71:1506–1514.40. Raetzke PB. Covering localized areas of root exposure employing the “envelope” technique. J Periodontol 1985;56:397–402.41. Nelson SW. The subpedicle connective tissue graft. A bilaminar reconstructive procedure for the coverage of denuded root surfaces. J Periodontol 1987;58:95–102.42. Harris RJ, Miller LH, Harris CR, et al. A comparison of three techniques to obtain root coverage on mandibular incisors. J Periodontol 2005;76:1758–1767.43. Zadeh HH. Minimally invasive treatment of maxillary anterior gingival recession defects by vestibular incision subperiosteal tunnel access and platelet-derived growth factor BB. Int J Periodontics Restorative Dent 2011;31:653–660.44. Chambrone L, Pannuti CM, Tu YK, et al. Evidence-based periodontal plastic surgery. II. An individual data meta-analysis for evaluating factors in achieving complete root coverage. J Periodontol 2012;83:477–490.45. Harris RJ. A comparative study of root coverage obtained with an acellular dermal matrix versus a connective tissue graft: Results of 107 recession defects in 50 consecutively treated patients. Int J Periodontics Restorative Dent 2000;20:51–59.46. Harris RJ. Root coverage in molar recession: Report of 50 consecutive cases treated with subepithelial connective tissue grafts. J Periodontol 2003;74:703–708.
47. Harris RJ. Root coverage with connective tissue grafts: An evaluation of short- and long-term results. J Periodontol 2002;73:1054–1059.48. Oliveira GH, Muncinelli EA. Effi cacy of root surface biomodifi cation in root coverage: A systematic review. J Can Dent Assoc 2012;78:c122.49. Dilsiz A, Aydin T, Canakci V, et al. Root surface biomodifi cation with Nd:YAG laser for the treatment of gingival recession with subepithelial connective tissue grafts. Photomed Laser Surg 2010;28:337–343.PMC2966850.50. Dilsiz A, Aydin T, Yavuz MS. Root surface biomodifi cation with an Er:YAG laser for the treatment of gingival recession with subepithelial connective tissue grafts. Photomed Laser Surg 2010;28:511–517.PMC2966853.51. Karam PS, Sant’Ana AC, de Rezende ML, et al. Root surface modifi ers and subepithelial connective tissue graft for treatment of gingival recessions: A systematic review. J Periodontal Res 2016;51:175–185.52. Miller PD Jr. Root coverage with the free gingival graft. Factors associated with incomplete coverage. J Periodontol 1987;58:674–681.53. Han TJ, Takei HH, Carranza FA. The strip gingival autograft technique. Int J Periodontics Restorative Dent 1993;13:180–187.54. Han TJ, Klokkevold PR, Takei HH. Strip gingival autograft used to correct mucogingival problems around implants. Int J Periodontics Restorative Dent 1995;15:404–411.55. Ricci G, Aimetti M. Gingival surgery, mucogingival therapy and periodontal plastic surgery. In: Ricci G ed. Periodontal Diagnosis and Therapy. Milan: Quintessenza Edizioni; 2014.56. Monnet-Corti V, Santini A, Glise JM, et al. Connective tissue graft for gingival recession treatment: Assessment of the maximum graft dimensions at the palatal vault as a donor site. J Periodontol 2006;77:899–902.57. Klosek SK, Rungruang T. Anatomical study of the greater palatine artery and related structures of the palatal vault: Considerations for palate as the subepithelial connective tissue graft donor site. Surg Radiol Anat 2009;31:245–250.58. Ksv R, P S, V K, et al. Assessment of thickness of palatal masticatory mucosa and maximum graft dimensions at palatal vault associated with age and gender — a clinical study. J Clin Diagn Res 2014;8:ZC09–13.PMC4080056.59. Harris RJ. The connective tissue with partial thickness double pedicle graft: The results of 100 consecutively treated defects. J Periodontol 1994;65:448–461.60. Hurzeler MB, Weng D. A single-incision technique to harvest subepithelial connective tissue grafts from the palate. Int J Periodontics Restorative Dent. 1999;19:279–287.61. Chambrone L, Tatakis DN. Periodontal soft tissue root-coverage procedures: A systematic review from the AAP Regeneration Workshop. J Periodontol 2015;86:S8–51.62. Bouchard P, Malet J, Borghetti A. Decision-making in aesthetics: Root coverage revisited. Periodontol 2000 2001;27:97–120.63. Pini Prato GP, Baldi C, Nieri M, et al. Coronally advanced fl ap: The post-surgical position of the gingival margin is an important factor for achieving complete root coverage. J Periodontol 2005;76:713–722.64. Cortellini P, Pini Prato G. Coronally advanced fl ap and combination therapy for root coverage. Clinical strategies based on scientifi c evidence and clinical experience. Periodontol 2000 2012;59:158–184.
THE CORRESPONDING AUTHOR, Perry R. Klokkevold, DDS, MS, can be reached at [email protected].
New cyber protection.Better tools to respond.
Add Cyber Suite Liability coverage to your TDIC Business Owner’s policy.Our comprehensive Cyber Suite Liability protection is more than just data compromise coverage. We help business owners respond to a full range of cyber incidents, including:
• Data compromise response expense
• Computer attack and cyber extortion
• Liability coverage for data compromise, including regulatory proceedings, network security and electronic media
TDIC Commercial Property policyholders with Business Owner’s coverage can add Cyber Suite Liability insurance at any time.
To apply for coverage or learn more, visit tdicinsurance/cyber.
Protecting dentists. It’s all we do.®
800.733.0633 | tdicinsurance.com | CA Insurance Lic. #0652783
Coverage specifically underwritten by The Dentists Insurance Company includes Professional Liability, Commercial Property and Employment Practices Liability. TDIC also underwrites Workers’ Compensation in California. TDIC Insurance Solutions offers other coverages as an agent or broker by agreements with our partner insurance carriers. Available coverage limits and discounts vary by carrier and are subject to carrier underwriting. Special Features and Optional Riders offered in policies may vary by carrier. The information provided here is an overview of the referenced product and is not intended to be a complete description of all terms, conditions and exclusions.

C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 639
Gingival augmentation is a periodontal procedure performed to enhance keratinized tissues around teeth and dental implants.
Patients today are interested in the long-term health, aesthetics and function of their periodontium. Periodontics involves advanced training to evaluate the individual patient and site for indications, as well as contraindications, for the myriad options for gingival augmentation. These procedures have been extensively studied for long-term stability, histology, comparability and outcomes based on the severity of the gingival recession (Miller’s Classifi cation) or tissue thickness. It is known that thicker biotypes with adequate zones of keratinized tissue around teeth and implants have improved long-term gingival stability. The purpose of this section is to provide the current status of one option to achieve enhanced gingival tissue thickness and
Acellular Dermal Matrix Allografts in Periodontal TherapyJoan Otomo-Corgel, DDS, MPH; Chanook David Ahn, DMD; and Allen Gunn, DDS
A B S TAC T Adequate keratinized tissue thickness and height enhance periodontal and implant stability. In order to correct gingival recession or augment keratinized gingival tissue, acellular dermal matrix (ACD) grafts from human donors provide an option for the clinician. This article reviews the material, techniques and rationale for ACD when there is inadequate autogenous donor tissue for the treatment site or the patient prefers a single surgical site.
AUTHORS
Joan Otomo-Corgel DDS, MPH, is a clinical associate professor at the University of California, Los Angeles, School of Dentistry, department of periodontics and faculty at the Greater Los Angeles VA Healthcare Center Dental Service. She is the past president of the American Academy of Periodontology, California Society of Periodontists and Western Society of Periodontology. She has a private practice limited to periodontics, oral medicine and implantology in Los Angeles.Confl ict of Interest Disclosure: None reported.
g i n g i v a l a u g m e n t a t i o n
root coverage, acellular dermal matrix (ADM) from human donor tissue. Note that ADM is also available from bovine, equine, porcine and plant sources.
Acellular dermal matrices were initially used for the resurfacing of burn injuries,1–3 replacement of tympanic membranes,4–8 dural repairs,9
abdominal wall repairs,10–12 tendon/joint repairs13–16 that are “hard to heal”17,18 and reconstructive breast surgery.19–22 Studies for use in urethral reconstruction23 are also under review. ADM are created by a process that decellularizes human donor soft tissue leaving the extracellular matrix intact. This matrix provides repopulation by the patient’s own cells as well as revascularization of the implanted ADM tissue. The donor tissue epidermal layer is removed with all the dermal cellular structures, thus removing the factors responsible for graft rejection and infection.24 It is a freeze-dried, cell-free dermal matrix with a structurally
Chanook David Ahn, DMD, is a periodontist who completed his periodontics residency at the VA Greater Los Angeles Healthcare System. Dr. Ahn graduated from Tufts School of Dental Medicine and then completed a general practice residency at Yale New Haven Hospital.Confl ict of Interest Disclosure: None reported.
Allen Gunn, DDS, is a 2018 graduate of the VA Greater Los Angeles Healthcare System residency in periodontics. Dr. Gunn graduated from the Columbia University College of Dental Medicine and fi nished a one-year AEGD with the U.S. Air Force, followed by four years of active duty service.Confl ict of Interest Disclosure: None reported.

C DA J O U R N A L , V O L 4 6 , Nº 1 0
640 O C TO B E R 2 01 8
integrated basement membrane and extracellular matrix in which collagen bundles and elastic fi bers are the main components. This bioactive scaffold provides for fi broblast, epithelial cell and endothelial cell migration, providing integration into host tissues.25,26
There are currently various acellular dermal graft products applicable to periodontics according to Silc and Petrunagro.27 Their article provided information comparing the available materials. They reviewed the differences among fi ve main products (TABLE 1). Acellular dermal matrix has two sizes: the 0.25 mm to 1.25 mm thin-size grafts are recommended for root coverage and soft-tissue ridge augmentation. Thicker sized grafts (0.8 mm to 1.8 mm) are recommended for guided bone regeneration and barrier membrane function. The thickness of the ADM used is predicated, however, on the needs of the individual site to be treated.
The following is a review of the preparation and differentiation of allograft ADM materials from Silc and Petrugaro’s article:26
AlloDerm Regenerative Tissue Matrix (BioHorizons IPH Inc., Birmingham, Ala.) is an acellular dermal matrix derived from donated human skin. It has an excellent safety history, having been used in more than 1 million procedures ranging from general/urogenital, orthopedic and dental. In the procurement and safety process of AlloDerm, tissue is accepted from tissue banks in compliance with the American Association of Tissue Banks (AATB) guidelines. AlloDerm processing from donor tissue involves a multistep proprietary process that removes the epidermis and cells in the dermis that can lead to graft rejection and/or failure of recipient responses. The extracellular matrix that remains is then put through a proprietary freeze-drying step that preserves
the tissue without damage from ice crystal formation. Histologic testing is then done on each fi nal lot to verify cell removal.
Puros Dermis Allograft Tissue Matrix (Zimmer Biomet Dental, Palm Beach Gardens, Fla.) is recovered following the rigorous standards of both the Food and Drug Administration and the AATB with either a scalpel or dermatome from the back of the thighs of the cadaver donor. The tissue is recovered by a recovery team within 24 hours of death using an aseptic process that meets the standards set by the AATB. The tissue enters the Tutoplast tissue sterilization process (Tutogen Medical/RTI Biologics Inc., Alachua, Fla.) only after it passes serological tests, such as those for human immunodefi ciency virus, hepatitis, human T-lymphotropic virus and syphilis. The multistep Tutoplast process removes all antigenicity, inactivates all kinds of pathogens, preserves tissue structure and collagen, preserves biomechanics, guarantees sterility and results in graft healing comparable to autografts. The process itself consists of donor selection, osmotic treatment, oxidative treatment, alkaline treatment (different from bone) and solvent dehydration. Tutoplast processing of Puros Dermis involves a limited-dose gamma irradiation, which provides a sterility level that preserves graft integrity. The Puros Dermis tissue allograft has a strength-to-failure measurement of 5 pounds ± 0.8 pounds, can be stored at room temperature, has a fi ve-year shelf life and, because of the Tutoplast process, has no residual chemicals when it is packed and delivered to the clinician.
PerioDerm Acellular Dermis (Dentsply Sirona, York, Pa.) undergoes a three-phase process that gently cleans, decellularizes and disinfects without crosslinking or compromising the integrity of the dermal matrix. Each piece is quality controlled for 90%+ uniformity in thickness. Biologic integrity is maximized via a proprietary process that avoids high-dose gamma irradiation. PerioDerm is aseptically processed by the Musculoskeletal Transplant Foundation and is rendered sterile per United States Pharmacopeia Standard 71 (USP 71). PerioDerm has a shorter hydration period, no need for refrigeration, no added antibiotics and a three-year shelf life.
Oracell (LifeNet Health, Virginia Beach, Va.) is decellularized with LifeNet Health’s patented technology called Matracell, which renders the product acellular without compromising biomechanical or biologic properties. More than 97 percent of the DNA is removed from the dermis, so immunogenic potential is low. Oracell is infused with glycerin-based solution to replace rehydration at chairside.
SureDerm (Hans Biomed, Daejeon, Korea) is transported in ambient temperature but requires refrigeration to preserve better shelf life. It is packaged in antibiotics and requires a separate rehydration rinse similar to AlloDerm.
Although the “gold standard” is the autograft, acellular dermal matrix provides the potential to enhance soft-tissue root coverage and increase the gingival width/thickness without the morbidity of a donor site. Often, there is an inadequate amount
g i n g i v a l a u g m e n t a t i o n
TABLE 1
Acellular Dermal Matrix Graft Products
Tissue Distribution agent Processor
AlloDerm BioHorizons IPH Inc. LifeCell
Puros Dermis Zimmer Biomet Tutogen via RTI Biologics
PerioDerm Dentsply Implants Musculoskeletal Transplant Foundation (MTF)
Oracell Puragraft/LifeNet Health Oracell
SureDerm Hiossen Hans Biomed
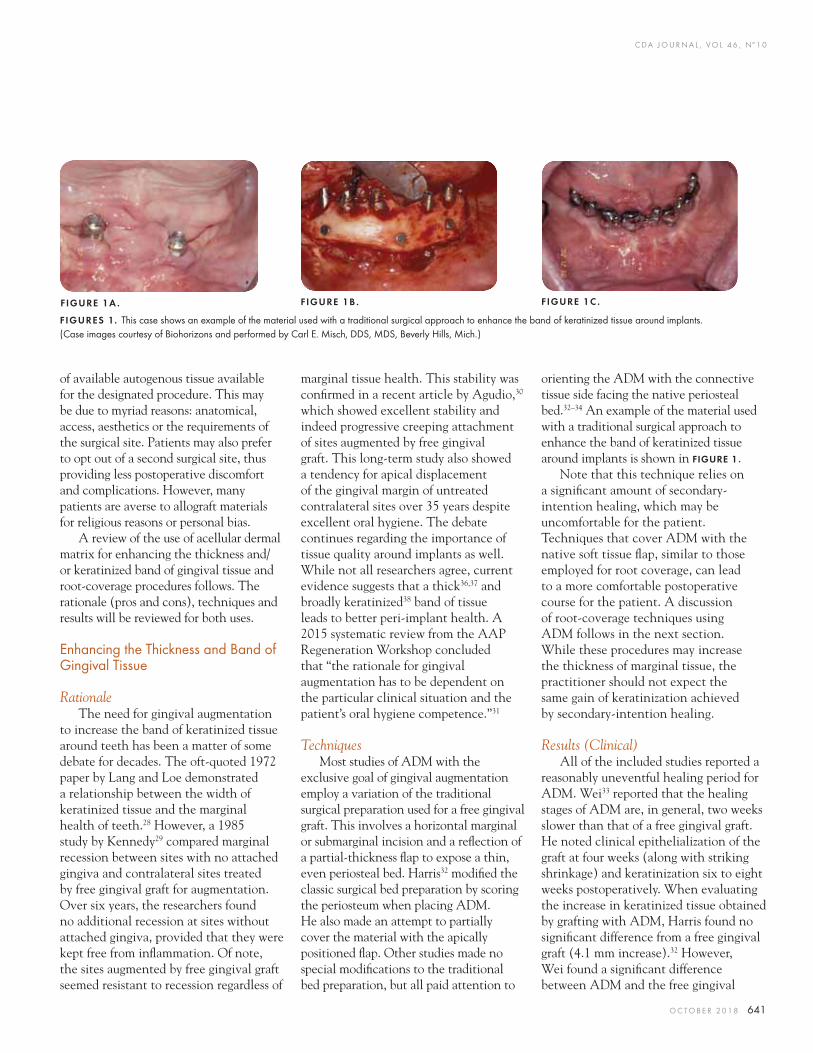
C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 641
of available autogenous tissue available for the designated procedure. This may be due to myriad reasons: anatomical, access, aesthetics or the requirements of the surgical site. Patients may also prefer to opt out of a second surgical site, thus providing less postoperative discomfort and complications. However, many patients are averse to allograft materials for religious reasons or personal bias.
A review of the use of acellular dermal matrix for enhancing the thickness and/or keratinized band of gingival tissue and root-coverage procedures follows. The rationale (pros and cons), techniques and results will be reviewed for both uses.
Enhancing the Thickness and Band of Gingival Tissue
RationaleThe need for gingival augmentation
to increase the band of keratinized tissue around teeth has been a matter of some debate for decades. The oft-quoted 1972 paper by Lang and Loe demonstrated a relationship between the width of keratinized tissue and the marginal health of teeth.28 However, a 1985 study by Kennedy29 compared marginal recession between sites with no attached gingiva and contralateral sites treated by free gingival graft for augmentation. Over six years, the researchers found no additional recession at sites without attached gingiva, provided that they were kept free from infl ammation. Of note, the sites augmented by free gingival graft seemed resistant to recession regardless of
marginal tissue health. This stability was confi rmed in a recent article by Agudio,30 which showed excellent stability and indeed progressive creeping attachment of sites augmented by free gingival graft. This long-term study also showed a tendency for apical displacement of the gingival margin of untreated contralateral sites over 35 years despite excellent oral hygiene. The debate continues regarding the importance of tissue quality around implants as well. While not all researchers agree, current evidence suggests that a thick36,37 and broadly keratinized38 band of tissue leads to better peri-implant health. A 2015 systematic review from the AAP Regeneration Workshop concluded that “the rationale for gingival augmentation has to be dependent on the particular clinical situation and the patient’s oral hygiene competence.”31
TechniquesMost studies of ADM with the
exclusive goal of gingival augmentation employ a variation of the traditional surgical preparation used for a free gingival graft. This involves a horizontal marginal or submarginal incision and a refl ection of a partial-thickness fl ap to expose a thin, even periosteal bed. Harris32 modifi ed the classic surgical bed preparation by scoring the periosteum when placing ADM. He also made an attempt to partially cover the material with the apically positioned fl ap. Other studies made no special modifi cations to the traditional bed preparation, but all paid attention to
orienting the ADM with the connective tissue side facing the native periosteal bed.32–34 An example of the material used with a traditional surgical approach to enhance the band of keratinized tissue around implants is shown in FIGURE 1.
Note that this technique relies on a signifi cant amount of secondary-intention healing, which may be uncomfortable for the patient. Techniques that cover ADM with the native soft tissue fl ap, similar to those employed for root coverage, can lead to a more comfortable postoperative course for the patient. A discussion of root-coverage techniques using ADM follows in the next section. While these procedures may increase the thickness of marginal tissue, the practitioner should not expect the same gain of keratinization achieved by secondary-intention healing.
Results (Clinical)All of the included studies reported a
reasonably uneventful healing period for ADM. Wei33 reported that the healing stages of ADM are, in general, two weeks slower than that of a free gingival graft. He noted clinical epithelialization of the graft at four weeks (along with striking shrinkage) and keratinization six to eight weeks postoperatively. When evaluating the increase in keratinized tissue obtained by grafting with ADM, Harris found no signifi cant difference from a free gingival graft (4.1 mm increase).32 However, Wei found a signifi cant difference between ADM and the free gingival
FIGURE 1A . FIGURE 1B . FIGURE 1C .
FIGURES 1. This case shows an example of the material used with a traditional surgical approach to enhance the band of keratinized tissue around implants. (Case images courtesy of Biohorizons and performed by Carl E. Misch, DDS, MDS, Beverly Hills, Mich.)
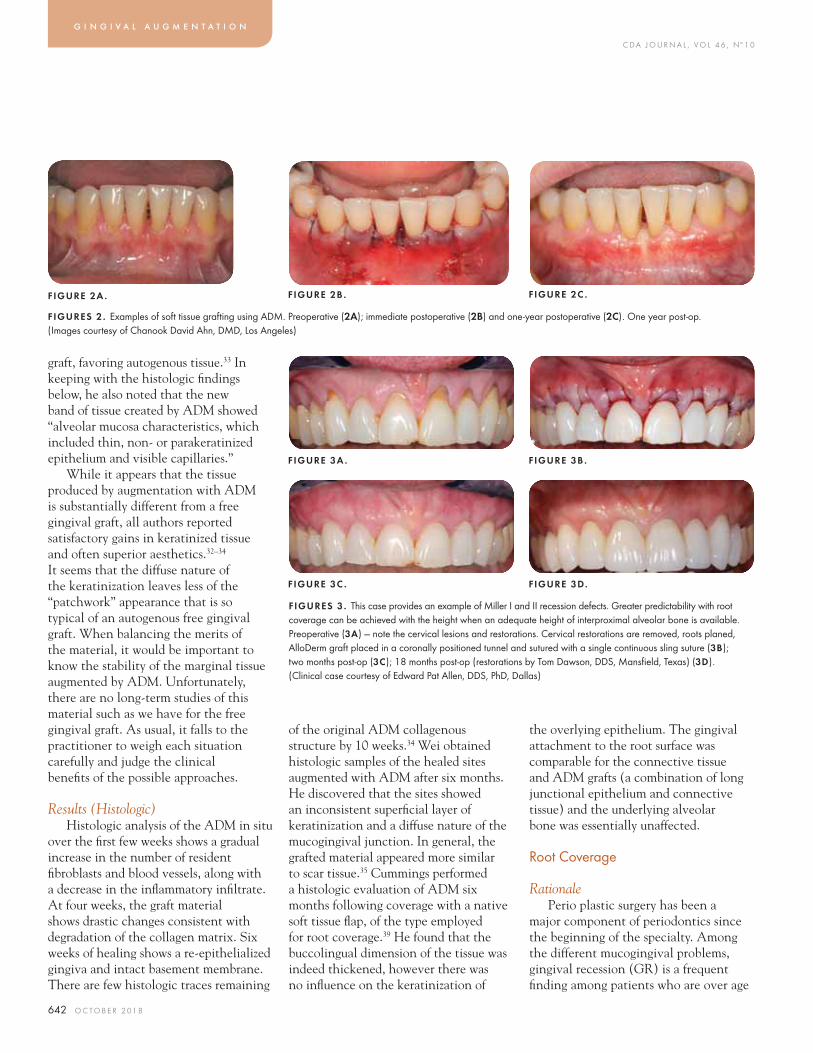
C DA J O U R N A L , V O L 4 6 , Nº 1 0
642 O C TO B E R 2 01 8
graft, favoring autogenous tissue.33 In keeping with the histologic fi ndings below, he also noted that the new band of tissue created by ADM showed “alveolar mucosa characteristics, which included thin, non- or parakeratinized epithelium and visible capillaries.”
While it appears that the tissue produced by augmentation with ADM is substantially different from a free gingival graft, all authors reported satisfactory gains in keratinized tissue and often superior aesthetics.32–34 It seems that the diffuse nature of the keratinization leaves less of the “patchwork” appearance that is so typical of an autogenous free gingival graft. When balancing the merits of the material, it would be important to know the stability of the marginal tissue augmented by ADM. Unfortunately, there are no long-term studies of this material such as we have for the free gingival graft. As usual, it falls to the practitioner to weigh each situation carefully and judge the clinical benefi ts of the possible approaches.
Results (Histologic)Histologic analysis of the ADM in situ
over the fi rst few weeks shows a gradual increase in the number of resident fi broblasts and blood vessels, along with a decrease in the infl ammatory infi ltrate. At four weeks, the graft material shows drastic changes consistent with degradation of the collagen matrix. Six weeks of healing shows a re-epithelialized gingiva and intact basement membrane. There are few histologic traces remaining
of the original ADM collagenous structure by 10 weeks.34 Wei obtained histologic samples of the healed sites augmented with ADM after six months. He discovered that the sites showed an inconsistent superfi cial layer of keratinization and a diffuse nature of the mucogingival junction. In general, the grafted material appeared more similar to scar tissue.35 Cummings performed a histologic evaluation of ADM six months following coverage with a native soft tissue fl ap, of the type employed for root coverage.39 He found that the buccolingual dimension of the tissue was indeed thickened, however there was no infl uence on the keratinization of
the overlying epithelium. The gingival attachment to the root surface was comparable for the connective tissue and ADM grafts (a combination of long junctional epithelium and connective tissue) and the underlying alveolar bone was essentially unaffected.
Root Coverage
RationalePerio plastic surgery has been a
major component of periodontics since the beginning of the specialty. Among the different mucogingival problems, gingival recession (GR) is a frequent fi nding among patients who are over age
g i n g i v a l a u g m e n t a t i o n
FIGURES 3 . This case provides an example of Miller I and II recession defects. Greater predictability with root coverage can be achieved with the height when an adequate height of interproximal alveolar bone is available. Preoperative (3A) — note the cervical lesions and restorations. Cervical restorations are removed, roots planed, AlloDerm graft placed in a coronally positioned tunnel and sutured with a single continuous sling suture (3B); two months post-op (3C); 18 months post-op (restorations by Tom Dawson, DDS, Mansfi eld, Texas) (3D). (Clinical case courtesy of Edward Pat Allen, DDS, PhD, Dallas)
FIGURE 2A . FIGURE 2B . FIGURE 2C .
FIGURES 2. Examples of soft tissue grafting using ADM. Preoperative (2A); immediate postoperative (2B) and one-year postoperative (2C). One year post-op. (Images courtesy of Chanook David Ahn, DMD, Los Angeles)
FIGURE 3A .
FIGURE 3C .
FIGURE 3B .
FIGURE 3D.
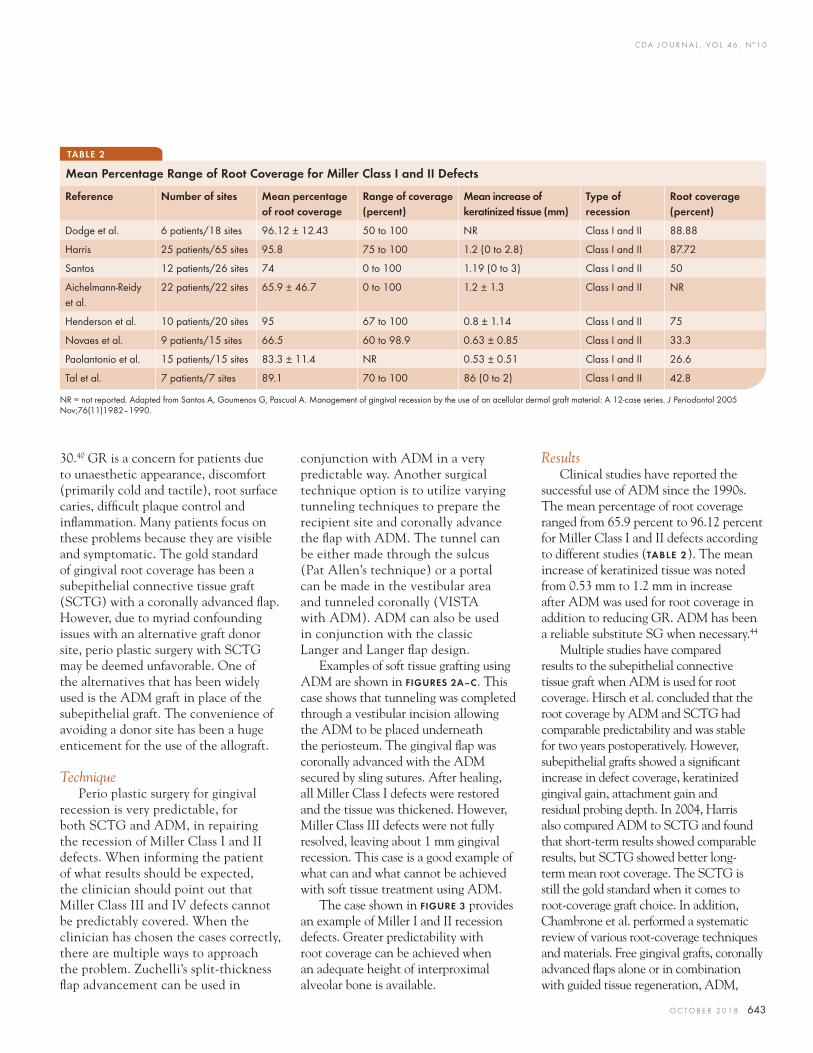
C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 643
TABLE 2
Mean Percentage Range of Root Coverage for Miller Class I and II Defects
30.40 GR is a concern for patients due to unaesthetic appearance, discomfort (primarily cold and tactile), root surface caries, diffi cult plaque control and infl ammation. Many patients focus on these problems because they are visible and symptomatic. The gold standard of gingival root coverage has been a subepithelial connective tissue graft (SCTG) with a coronally advanced fl ap. However, due to myriad confounding issues with an alternative graft donor site, perio plastic surgery with SCTG may be deemed unfavorable. One of the alternatives that has been widely used is the ADM graft in place of the subepithelial graft. The convenience of avoiding a donor site has been a huge enticement for the use of the allograft.
TechniquePerio plastic surgery for gingival
recession is very predictable, for both SCTG and ADM, in repairing the recession of Miller Class I and II defects. When informing the patient of what results should be expected, the clinician should point out that Miller Class III and IV defects cannot be predictably covered. When the clinician has chosen the cases correctly, there are multiple ways to approach the problem. Zuchelli’s split-thickness fl ap advancement can be used in
conjunction with ADM in a very predictable way. Another surgical technique option is to utilize varying tunneling techniques to prepare the recipient site and coronally advance the fl ap with ADM. The tunnel can be either made through the sulcus (Pat Allen’s technique) or a portal can be made in the vestibular area and tunneled coronally (VISTA with ADM). ADM can also be used in conjunction with the classic Langer and Langer fl ap design.
Examples of soft tissue grafting using ADM are shown in FIGURES 2A–C. This case shows that tunneling was completed through a vestibular incision allowing the ADM to be placed underneath the periosteum. The gingival fl ap was coronally advanced with the ADM secured by sling sutures. After healing, all Miller Class I defects were restored and the tissue was thickened. However, Miller Class III defects were not fully resolved, leaving about 1 mm gingival recession. This case is a good example of what can and what cannot be achieved with soft tissue treatment using ADM.
The case shown in FIGURE 3 provides an example of Miller I and II recession defects. Greater predictability with root coverage can be achieved when an adequate height of interproximal alveolar bone is available.
ResultsClinical studies have reported the
successful use of ADM since the 1990s. The mean percentage of root coverage ranged from 65.9 percent to 96.12 percent for Miller Class I and II defects according to different studies (TABLE 2). The mean increase of keratinized tissue was noted from 0.53 mm to 1.2 mm in increase after ADM was used for root coverage in addition to reducing GR. ADM has been a reliable substitute SG when necessary.44
Multiple studies have compared results to the subepithelial connective tissue graft when ADM is used for root coverage. Hirsch et al. concluded that the root coverage by ADM and SCTG had comparable predictability and was stable for two years postoperatively. However, subepithelial grafts showed a signifi cant increase in defect coverage, keratinized gingival gain, attachment gain and residual probing depth. In 2004, Harris also compared ADM to SCTG and found that short-term results showed comparable results, but SCTG showed better long-term mean root coverage. The SCTG is still the gold standard when it comes to root-coverage graft choice. In addition, Chambrone et al. performed a systematic review of various root-coverage techniques and materials. Free gingival grafts, coronally advanced fl aps alone or in combination with guided tissue regeneration, ADM,
NR = not reported. Adapted from Santos A, Goumenos G, Pascual A. Management of gingival recession by the use of an acellular dermal graft material: A 12-case series. J Periodontol 2005 Nov;76(11)1982–1990.
Reference Number of sites Mean percentage of root coverage
Range of coverage (percent)
Mean increase of keratinized tissue (mm)
Type of recession
Root coverage (percent)
Dodge et al. 6 patients/18 sites 96.12 ± 12.43 50 to 100 NR Class I and II 88.88
Harris 25 patients/65 sites 95.8 75 to 100 1.2 (0 to 2.8) Class I and II 87.72
Santos 12 patients/26 sites 74 0 to 100 1.19 (0 to 3) Class I and II 50
Aichelmann-Reidy et al.
22 patients/22 sites 65.9 ± 46.7 0 to 100 1.2 ± 1.3 Class I and II NR
Henderson et al. 10 patients/20 sites 95 67 to 100 0.8 ± 1.14 Class I and II 75
Novaes et al. 9 patients/15 sites 66.5 60 to 98.9 0.63 ± 0.85 Class I and II 33.3
Paolantonio et al. 15 patients/15 sites 83.3 ± 11.4 NR 0.53 ± 0.51 Class I and II 26.6
Tal et al. 7 patients/7 sites 89.1 70 to 100 86 (0 to 2) Class I and II 42.8

C DA J O U R N A L , V O L 4 6 , Nº 1 0
644 O C TO B E R 2 01 8
enamel matrix derivative protein, xenogenic collagen matrix grafts or other biomaterials were reviewed in the study. All techniques that were reviewed showed predictable root coverage in Miller I and II defects. Superiority was noticed in SCTG in their percentage of mean and complete root coverage and increase in keratinized tissue. However, ADM is a suitable alternative when it is not plausible to obtain SG.
Barker et al. (2010) compared the treatment of localized tissue recession when using AlloDerm and Puros on the results of this study and found there was no statistical or clinical difference in root coverage, probing depth or keratinized tissue in coronally advanced fl aps for root coverage among the two acellular dermal matrix materials. They determined that both materials were successful in achieving root coverage.
ConclusionThe focus of periodontics is to save
teeth, regenerate lost gingival and osseous tissues and reduce infl ammation, thus improving the periodontal condition and possibly decreasing the risk for systemic diseases. This section emphasized one aspect of periodontal training — the regeneration of lost or inadequate gingival tissues via acellular dermal matrix allografts. ADM has been shown to be easy to handle, capable of integrating into human host sites without adverse effect, capable of epithelialization and possessing satisfactory clinical results. These procedures, however, require an in-depth knowledge of wound healing, indications/contraindications, site selection, site preparation, material selection, surgical fl ap management and postoperative management. When all of these factors align, acellular dermal matrix allograft material is a viable option for gingival augmentation. ■
REFERENCES
1. Wainright D. The use of an allograft dermal matrix in the management of full thickness burns. Burns 1995;21:243–8.2. Walter RJ, Matsuda T, Reyes HM, et al. Characterization of acellular dermal matrices (ADMs) prepared by two different methods. Burns 1998 Mar;24(2):104–113.3. Askari M, Cohen MJ, Grossman PH, et al. The use of acellular dermal matrix in release of burn contracture scars in the hand. Plast Reconstr Surg 2011 Apr;127(4):1593–1599. doi:10.1097/PRS.0b013e31820a6511.4. Downey TJ, Champeaux AL, Silva AB. AlloDerm tympanoplasty of tympanic membrane perforations. Am J Otolaryngol 2003 Jan–Feb;24(1):6–13.5. Haynes DS, Vos JD, Labadie RF. Acellular allograft dermal matrix for tympanoplasty. Curr Opin Otolarynol Head Neck Surg 2005 Oct;13(5):283–6.6. Qin J, Sun J, Li X, et al. An experimental study on tympanic membrane reconstruction with acellular dermal matrix. Acta Otolaryngol 2012 Dec;132(12)1266–70. doi:10.3109/00016489.2012.701327. Epub 2012 Jul 25.7. Vos JD, Latev MD, Labadie RF, et al. Use of AlloDerm in type I tympanoplasty: A comparison with native tissue grafts. Laryngoscope 2005 Sep;115(9):1599–602.8. Farahani F, Yazdi AK, Ghasemi MA, et al. Results of acellular dermis matrix graft used for tympanoplasty in guinea pig model. Iran J Otorhinolaryngol 2015 Mar;27(79):95–100.9. Chaplin JM, Costantino MD, Wolpoe BA, et al. Use of an acellular dermal allograft for dural replacement: An experimental study. Neurosurg 1999 Aug;45(2):320–326.10. Zhong T, Janis JE, Ahmad J, et al. Outcomes after abdominal wall reconstruction using acellular dermal matrix: A systematic review. J Plast Reconstr Aesthet Surg 2011 Dec;64(12):1562–71. doi:10.1016/j.bjps.2011.04.035. Epub 2011 May 31.11. Holton LH, Kim D, Silvermn RP, et al. Human acellular dermal matrix for repair of abdominal wall defects: Review of clinical experience and experimental data. J Long Term Eff Med Implants 2005;15(5):547–58.12. Janis JE, O’Neill AC, Ahmad J, et al. Acellular dermal matrices in abdominal wall reconstruction: A systematic review of the current evidence. Plast Reconstr Surg 2012 Nov;130(5 Supple 2):183S–93S. doi:10.1097/PRS.0b013e3182605cfc.13. Barber FA, McGarry JE, Herbert MA, Anderson RB. A biomechanical study of Achilles tendon repair augmentation using GraftJacket Matrix. Foot Ankle Int 2008 Mar;29(3)329–33. doi:10.3113/FAI.2008.0329.14. Snyder SJ, Arnoczky SP, Bond JL, Dopirak R. Histologic evaluation of a biopsy specimen obtained three months after rotator cuff augmentation with GraftJacke matrix. Arthroscopy 2009: Mar;25(3):329–333. doi:10.1016/j.arthro.2008.05.023. Epub 2008 Jul 24.15. Lavenda AC, Sanders NR. A Simplified approach for arthroscopic repair of rotator cuff tear with dermal patch augmentation. Adv Orthoped Surg 2015;Article ID 423949;1–7.16. Wong I, Burns J, Snyder S. Arthroscopic GraftJacket repair of rotator cuff tears. J Shoulder Elbow Surg 2010 Mar;19(2 Suppl):104–109. doi:10.1016/j.jse.2009.12.017.17. Yonehiro L, Burleson G, Sauer V. Use of a new acellular dermal matrix for treatment of nonhealing wounds in the
lower extremities of patients with diabetes. Wounds 2013 Dec;25(12):340–4.18. Harding K, Kirsner R, Lee D, et al. International Consensus — Acellular matrices for the treatment of wounds. An expert working group review. Wounds International 2010. www.woundsinternational.com/media/issues/380/files/content_9732.pdf.19. Macadam, SA, Lennox PA. Acellular dermal matrices: Use in reconstructive and aesthetic breast surgery. Can J Plast Surg 2012 Summer;20(2):75–89.20. Lanier ST, Wang EF, Chen JJ, et al. The effect of acellular dermal matrix use on complication rates in tissue expander/implant breast reconstruction. Ann Plast Surg 2010 May;64(5):674–8. doi:10.1097/SAP.0b013e3181dba892.21. Spear SL, Parikh PM, Reisin E, et al. Acellular dermis-assisted breast reconstruction. Aesthetic Plast Surg 2008 May;32(3):418–25. doi:10.1007/s00266-008-9128-8.22. Kim JYS, Long JN, Davila A, et al. Breast reconstruction with acellular dermis. emedicine.medscape.com. July 16, 2017.23. Cheng L, Lin J, Wang Z. MP26-02 cell-seeded acellular dermal matrix graft for reconstruction of long urethral defects in a canine model. J Urol 2017;2017:197:e466.24. Jhaveri HM, Chavan MS, Tomar GB, Deshmukh VL, Wani MR, Miller PD Jr. Acellular dermal matrix seeded with autologous gingival fibroblasts for the treatment of gingival recession: A proof-of-concept study. J Periodontol 2010 Apr;81(4):616–25. doi:10.1902/jop.2009.090530.25. Barker TS, Cueva MA, Rivera-Hidalgo F, et al. A comparative study of root coverage using two different acellular dermal matrix products. J Peridontol 2010;68:1596-1603.26. Jhaveri HM, Chavan MS, Tomar GB, Deshmukh VL, Wani MR, Miller PD Jr. Acellular dermal matrix seeded with autologous gingival fibroblasts for the treatment of gingival recession: A proof-of-concept study. J Periodontol 2010 Apr;81(4):616–25. doi:10.1902/jop.2009.090530.27. Silc JT, Petrungaro PS. Acellular dermal matrix grafts for root-coverage procedures: Review of products and introduction of a new technique. Compend Contin Educ Dent 2012 Jun;34(6):408–414.28. Lang NP, Loe H. The relationship between the width of keratinized gingiva and gingival health. J Periodontol 1972 Oct;43(10):623–627.29. Kennedy JE, Bird WC, Palcanis KG, Dorfman HS. A longitudinal evaluation of varying widths of attached gingiva. J Clin Periodontol 1985 Sep;12(8):667–675.30. Agudio G, Cortellini P, Buti J, Pini Prato G. Periodontal conditions of sites treated with gingival augmentation surgery compared with untreated contralateral homologous sites: an 18- to 35-year long-term study. J Periodontol 2016 Dec;87(12):1371–1378. Epub 2016 Aug 13.31. Kim DM, Neiva R. Periodontal soft tissue nonroot- coverage procedures: A systematic review from the AAP regeneration workshop. J Periodontol 2015 Feb;8 (2 Suppl):S56–72. doi:10.1902/jop.2015.130684.32. Harris RJ. Clinical evaluation of three techniques to augment keratinized tissue without root coverage J Periodontol 2001;72:932–938.33. Wei PC, Laurell L, Geivelis M, et al. Acellular dermal matrix allografts to achieve increased attached gingiva. Part 1. A clinical study. J Periodontol 2000 Aug;71(8):1297–1305.
g i n g i v a l a u g m e n t a t i o n

C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 645
34. Scarano A, Barros RM, Lezzi G, et al. Acellular dermal matrix graft for gingival augmentation: A preliminary clinical, histologic and ultrastructural evaluation. J Periodontol 2009;80:253–259.35. Wei PC, Laurell L, Lingen MW, Geivelis M. Acellular dermal matrix allografts to achieve increased attached gingiva. Part 2. A histological comparative study. J Periodontol 2002 Mar;73(3):257–265.36. Linkevicius T, Puisys A, Steigmann M, Vindasiute E, Linkeviciene L. Influence of vertical soft tissue thickness on crestal bone changes around implants with platform switching: A comparative clinical study. Clin Implant Dent Relat Res 2015 Dec;17(6):1228–1236. doi:10.1111/cid.12222. Epub 2014 Mar 28.37. Suarez-Lopez del Amo F, Lin G, Monje A, Galindo-Moreno P, Wang HL. Influence of soft tissue thickness on peri-implant marginal bone loss: a systematic review and meta-analysis. J Periodontol 2016; 87 (6)690–699.38. Lin G, Chang HL, Wang HL. The significance of keratinized mucosa on implant health: A systematic review. J Periodontol 2013 Dec;84(12):1755–1767. doi:10.1902/jop.2013.120688. Epub 2013 Mar 1.39. Cummings LC, Kaldahl, WB, Allen EP. Histologic evaluation of autogenous connective tissue and acellular dermal matrix grafts in humans. J Periodontol 2005 Feb;76(2):178–186.40. Barker TS, Cueva MA, Rivera-Hidalgo F, et al. A comparative study of root coverage using two different cellular dermal matrix products. J Periodontol 2010 Nov;81(11):1596–1603. doi:10.1902/jop.2010.090291. Epub 2010 Jul 14.41. Richardson CR, Allen EP, Chambrone L, et al. Periodontal soft tissue root-coverage procedures: Practical applications from the AAP regeneration workshop. Clin Adv Periodontics 2015;5:2–10.42. Harris RJ. A short-term and long-term comparison of root coverage with an acellular dermal matrix and a subepithelial graft. J Periodontol 2004 May;75(5):734–743.43. Hirsch A, Goldstein M, Goultschin J, et al. A two-year follow-up of root coverage using subpedicle acellular dermal matrix allografts and subepithelial connective tissue autografts. J Periodontol 2005 Aug;76(8):1323–1328.44. Santos A, Goumenos G, Pascual A. Management of gingival recession by the use of an acellular dermal graft material: A 12-case series. J Periodontol 2005 Nov;76(11)1982–1990.45. Chambrone L, Tatakis DN. Periodontal soft tissue root-coverage procedures: A systematic review from the AAP regeneration workshop. J Periodontol 2015 Feb;86,(2 Suppl):S8–51. doi:10.1902/jop.2015.130674.
THE CORRESPONDING AUTHOR, Joan Otomo-Corgel, DDS, MPH, can be reached at [email protected].
Give health, hope and happiness. By contributing your time and talent, you relieve pain,
restore dignity and create smiles for thousands of people
who face barriers to care. Volunteer at CDA Cares Modesto
to help provide essential dental care to those in need.
CDA Cares Modesto
October 26–27, 2018
Modesto Centre Plaza
Join us. cdafoundation.org/cdacares
®
ENDORSEDPROGRAMS
CDA has leveraged the strength of our large membership
to deliver even more value, including resources to support
you in the business side of practice. Endorsed Programs provide money-saving solutions from vendors that have
been vetted by a team of CDA dentists.
cda.org/endorsedprograms
STRENGTH.SAVINGS.CONFIDENCE.
Increase case acceptance by offering friendly financing options and connect to new patients who are looking for more flexibility to budget their treatment. As a CDA member, you have a special rate to start offering healthcare credit cards from CareCredit.
CareCredit is accepted by more than 100,000 dental teams, making it easier for patients to manage out-of-pocket investments and say yes to treatment. Explore free resources to address financial conversations with patients and see how you can get started for only $30.
F E AT U R E D E N D O R S E D P R O G R A M

C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 647
AUTHOR
Tina M. Beck, DDS, MS, is a diplomat of the American Board of Periodontology and a solo practitioner in San Diego. Her professional career has been dedicated to leadership in organized dentistry and patient care. She is published in the Journal of the American Academy of Periodontology.Confl ict of Interest Disclosure: None reported.
The Pinhole Surgical Technique: A Clinical Perspective and Treatment Considerations From a PeriodontistTina M. Beck, DDS, MS
A B S T R AC T Multiple treatment options exist when considering therapeutic approaches for the management of gingival recession. The patented Pinhole Surgical Technique is one of the most recent of such procedures and one of the most poorly understood. The following commentary is intended to help guide clinicians in the decision-making process when considering root-coverage strategies.
Numerous therapeutic solutions have been proposed for the treatment of gingival recession.1
One of the most recent root-coverage techniques, the Pinhole Surgical Technique (PST), has rapidly gained popularity over the last few years but is poorly understood by many clinicians. Even more confusing is the fact that there are numerous options available for gingival recession treatment, each with its own benefi ts and limitations. As a periodontist well trained in a vast array of techniques, incorporating PST into my practice four years ago was a bit of a treatment-planning challenge. Like many periodontists, my preferred technique had been subepithelial connective tissue grafting because of its ability to predictably cover exposed root surfaces,
c o m m e n t a r y
change the gingival phenotype and increase the band of attached keratinized gingiva.2–5 I was initially hesitant to offer PST as a viable treatment option because of the lack of long-term studies, specifi cally on its effi cacy and stability. However, through trial and error and more than 100 cases completed with a minimum of one-year follow-up, I have established some guidelines that I use in my decision-making process when considering treatment options for recession defects. The purpose of this discussion is to elucidate how PST is performed, review its benefi ts and limitations and share my personal decision-making process in order to assist other clinicians in determining when this procedure would be a viable treatment option as well as answer some of the most commonly asked questions regarding this novel technique.

C DA J O U R N A L , V O L 4 6 , Nº 1 0
648 O C TO B E R 2 01 8
The most alluring aspect of this procedure for the general public, and some clinicians, is that PST does not require the use of autogenous or allogenic graft material (tissue harvested from a different site from the same patient or from a cadaver, respectively). Instead, the patient’s existing gingiva is simply moved coronally to cover the exposed root surface. This is achieved using a 16-gauge sterile hypodermic needle to penetrate the alveolar mucosa and pierce the periosteum apical to the recessed area creating a “pinhole” through which instruments can be inserted. In cases with multiple adjacent sites, multiple pinholes may be required. Specifi cally designed instruments are inserted through the pinhole to elevate a full-thickness fl ap without severing the interproximal papillae to move the tissue to the desired coronal position. In my mind, I thought of the PST elevation technique to be an alternative method for achieving a full-thickness fl ap while keeping the papillae intact, similar to popular tunneling and modifi ed tunneling procedures6,7 or the vestibular incision subperiosteal tunnel access (VISTA) technique,8 which many surgeons utilize to prepare a site for graft placement.
A critical factor for the success of most root-coverage procedures is the elimination of tension on the gingival margin of the newly positioned tissue.9 With PST, wound stabilization is achieved with the use of a malleable, noncross-linked bioresorbable porcine collagen membrane (Bio-Gide, Geistlich, Princeton, N.J.) that is carefully inserted through the pinhole and tucked under the gingival tissues, over the root surfaces, supporting the fl ap in the desired coronal position, without the need for suturing, dressings or tissue adhesive. Wound stabilization is thus achieved by distending the fl ap with the collagen membrane, resulting in adequate
tissue support to secure the marginal gingiva in the new position. The use of such a membrane is not new in the periodontal literature and has a long history of being safe and effective both in the treatment of gingival recession10 as well as periodontal regeneration.11
The elimination of the need for sutures is another unique aspect of this procedure. In order to allow tension-free coronal repositioning of the gingival margin without using sutures, it is necessary to also elevate and coronally advance the gingival tissues of several adjacent teeth, both mesially and distally to the treatment area. This requirement is of clinical signifi cance for some patients who want to minimize the area of treatment for faster recovery. For example, it would not be uncommon to require release from fi rst molar to fi rst molar to treat a single, deep recession defect of a mandibular incisor. The more severe the recession defect, the
more lateral extension and fl ap release will be required to allow tension-free coronal advancement of the gingival margin at the site of recession. For this reason, many of my patients prefer a technique that allows for a smaller surgical area, like a subepithelial connective tissue graft with a double papilla fl ap technique.12
Postsurgically, the pinhole is left to heal by primary intention without suturing and is often healed within 48 hours. Patients are instructed to bathe the surgical area with 0.12% chlorhexidine gluconate oral rinse and avoid brushing or fl ossing the area for six to 12 weeks. Although patients experience very little pain following the procedure, there can be a considerable amount of swelling that subsides after about seven days. The collagen membrane is slowly resorbed over the next three to four months, as the newly coronally advanced gingiva settles and re-establishes periodontal
c o m m e n t a r y
FIGURE 1A . FIGURE 1B .
FIGURES 1. Maxillary central incisors with Class I Miller recession (1A). One year after PST (1B).
FIGURE 2A .
FIGURE 2B .
FIGURE 2C .FIGURE 2D.
FIGURES 2. 2A and 2B show pretreatment of Class II Miller recession defects with thin biotype and no attached gingiva on teeth Nos. 21, 23, 28. 2C and 2D are one year after PST and demonstrate complete root coverage.

C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 649
attachment to the previously exposed root surface. Histological studies are currently lacking to determine the exact biology of the healing process, either connective tissue attachment, long junctional epithelium or perhaps even some bone regeneration. Clinically, probing depths usually range from 1–3 mm when measured six months after surgery.
Like all surgical techniques, there are limitations to the success of PST that must be considered when determining treatment options. Most important, the patient must be healthy enough to be considered a surgical candidate, similar to all the other treatment modalities. Heavy smoking, uncontrolled or poorly controlled diabetes and certain medications are just some of the factors that can compromise the healing process and increase the risk of complications,1 which may outweigh the benefi t of treating the condition at all. As with other root-coverage therapies, patients should be free of active periodontal disease or severe gingival infl ammation prior to performing PST and should demonstrate compliance with periodontal recall appointments and home care instructions. Also similar to other surgical therapies, occlusal discrepancies and nocturnal bruxism or clenching should be appropriately identifi ed and managed.
There are many anatomical factors to account for when considering treatment options, including but not limited to location of defect, severity of defect, presence or absence of bone loss, number of teeth involved, amount of attached keratinized gingiva and gingival phenotype. Miller’s classifi cation of gingival recession13 is the most widely used method for categorization of the different types and severities of recession defects and is useful to establish general guidelines for clinicians when predicting the success of various gingival recession
treatments. Miller explained that class I and II recession defects can expect 100 percent root coverage, class III defects can expect only partial root coverage and class IV defects are highly unpredictable and little to no root coverage can be expected due to the presence of horizontal bone loss and loss of interdental papillae. These same guidelines should apply to PST as well. Additional limitations include the inability to treat recession defects located on palatal surfaces, diffi culty in physically accessing mandibular lingual areas using the PST
protocol and instruments and anatomical considerations involving the sublingual spaces and related structures that may present signifi cant risk in an apical-style approach for mandibular lingual surfaces.
When considering soft tissue biotype and attached keratinized gingiva, autogenous grafting is the most documented procedure demonstrating predictable and stable increases in tissue volume, i.e., altering the soft tissue biotype and amount of attached keratinized gingiva.2–5 However, analogous to alternative treatment modalities including allogenic soft tissue grafting and guided tissue regeneration, anecdotal evidence suggests that PST is capable of increasing tissue volume and attached keratinized gingiva,14 but currently there is limited evidence to
support these claims. When discussing treatment options with my patients, they are fully informed of this fact and it is left to them to make an educated decision. They usually choose subepithelial grafting in cases where there is only a single tooth with little to no attached keratinized gingiva. Initially, I only offered PST to patients who have ample attached gingiva and thick phenotypes (FIGURE 1). However, after my experience with the procedure and witnessing fi rst-hand some of the dramatic results it can produce, I began to offer it for more complex cases (FIGURE
2). In cases where there are several teeth in a single arch with recession and minimal attached gingiva, patients often want to try PST over the multiple rounds of surgery required for connective tissue grafting of an entire arch. FIGURE 2 demonstrates that good root coverage and some gain in attached gingiva is possible with PST and I consider it an acceptable treatment option despite the lack of documented stability, as long as patients are made aware of this fact. Additionally, I evaluate the gingival phenotype of the recession site and explain that PST might not alter it signifi cantly, increasing the risk of recurrence. Due to the lack of evidence regarding the long-term stability of PST in cases with very thin biotypes and minimal or no attached gingiva, I ensure that these patients understand that additional procedures may be required if the desired results are not achieved, although I have yet to see such recurrence. This word of caution is based on existing studies involving coronally positioned fl aps that suggest a minimum tissue thickness of 0.8–1mm for predictable and stable root coverage.15–17 Notwithstanding these limitations, there are some unique and signifi cant advantages to PST for both the patient and clinician.
Patients should be free of active periodontal disease or severe gingival infl ammation prior to performing PST.
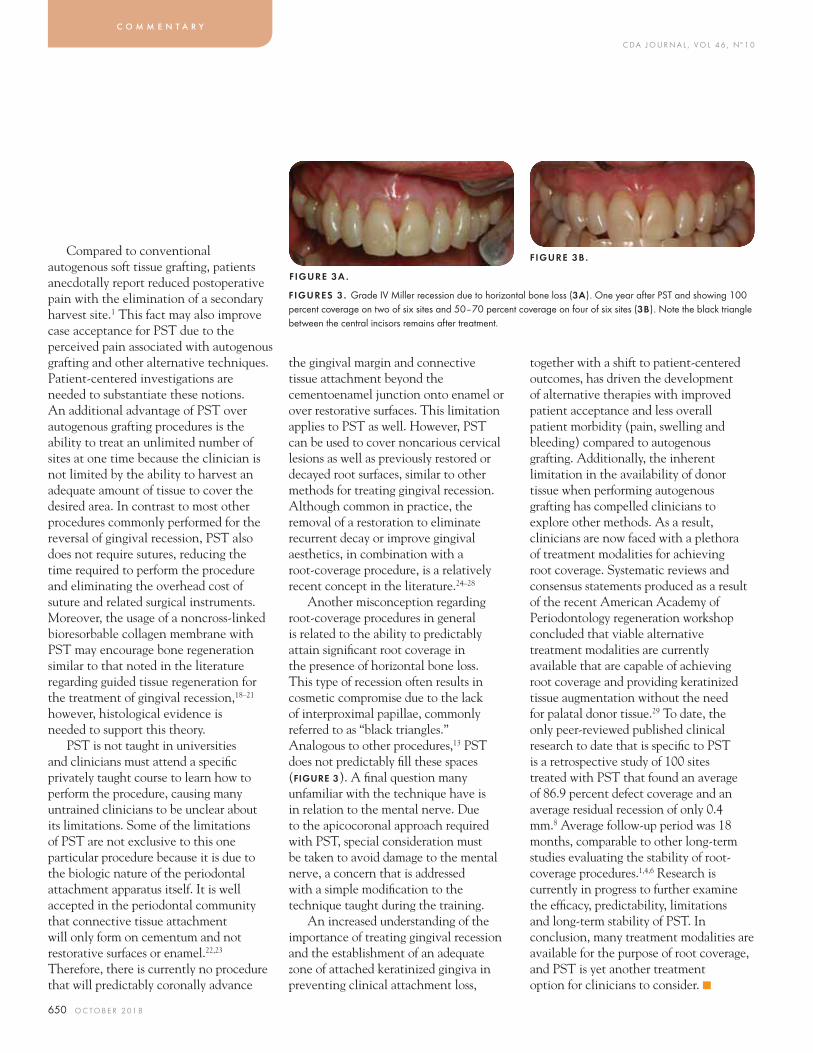
C DA J O U R N A L , V O L 4 6 , Nº 1 0
650 O C TO B E R 2 01 8
Compared to conventional autogenous soft tissue grafting, patients anecdotally report reduced postoperative pain with the elimination of a secondary harvest site.1 This fact may also improve case acceptance for PST due to the perceived pain associated with autogenous grafting and other alternative techniques. Patient-centered investigations are needed to substantiate these notions. An additional advantage of PST over autogenous grafting procedures is the ability to treat an unlimited number of sites at one time because the clinician is not limited by the ability to harvest an adequate amount of tissue to cover the desired area. In contrast to most other procedures commonly performed for the reversal of gingival recession, PST also does not require sutures, reducing the time required to perform the procedure and eliminating the overhead cost of suture and related surgical instruments. Moreover, the usage of a noncross-linked bioresorbable collagen membrane with PST may encourage bone regeneration similar to that noted in the literature regarding guided tissue regeneration for the treatment of gingival recession,18–21 however, histological evidence is needed to support this theory.
PST is not taught in universities and clinicians must attend a specifi c privately taught course to learn how to perform the procedure, causing many untrained clinicians to be unclear about its limitations. Some of the limitations of PST are not exclusive to this one particular procedure because it is due to the biologic nature of the periodontal attachment apparatus itself. It is well accepted in the periodontal community that connective tissue attachment will only form on cementum and not restorative surfaces or enamel.22,23 Therefore, there is currently no procedure that will predictably coronally advance
the gingival margin and connective tissue attachment beyond the cementoenamel junction onto enamel or over restorative surfaces. This limitation applies to PST as well. However, PST can be used to cover noncarious cervical lesions as well as previously restored or decayed root surfaces, similar to other methods for treating gingival recession. Although common in practice, the removal of a restoration to eliminate recurrent decay or improve gingival aesthetics, in combination with a root-coverage procedure, is a relatively recent concept in the literature.24–28
Another misconception regarding root-coverage procedures in general is related to the ability to predictably attain signifi cant root coverage in the presence of horizontal bone loss. This type of recession often results in cosmetic compromise due to the lack of interproximal papillae, commonly referred to as “black triangles.” Analogous to other procedures,13 PST does not predictably fi ll these spaces (FIGURE 3). A fi nal question many unfamiliar with the technique have is in relation to the mental nerve. Due to the apicocoronal approach required with PST, special consideration must be taken to avoid damage to the mental nerve, a concern that is addressed with a simple modifi cation to the technique taught during the training.
An increased understanding of the importance of treating gingival recession and the establishment of an adequate zone of attached keratinized gingiva in preventing clinical attachment loss,
together with a shift to patient-centered outcomes, has driven the development of alternative therapies with improved patient acceptance and less overall patient morbidity (pain, swelling and bleeding) compared to autogenous grafting. Additionally, the inherent limitation in the availability of donor tissue when performing autogenous grafting has compelled clinicians to explore other methods. As a result, clinicians are now faced with a plethora of treatment modalities for achieving root coverage. Systematic reviews and consensus statements produced as a result of the recent American Academy of Periodontology regeneration workshop concluded that viable alternative treatment modalities are currently available that are capable of achieving root coverage and providing keratinized tissue augmentation without the need for palatal donor tissue.29 To date, the only peer-reviewed published clinical research to date that is specifi c to PST is a retrospective study of 100 sites treated with PST that found an average of 86.9 percent defect coverage and an average residual recession of only 0.4 mm.8 Average follow-up period was 18 months, comparable to other long-term studies evaluating the stability of root-coverage procedures.1,4,6 Research is currently in progress to further examine the effi cacy, predictability, limitations and long-term stability of PST. In conclusion, many treatment modalities are available for the purpose of root coverage, and PST is yet another treatment option for clinicians to consider. ■
c o m m e n t a r y
FIGURE 3A .
FIGURE 3B .
FIGURES 3 . Grade IV Miller recession due to horizontal bone loss (3A). One year after PST and showing 100 percent coverage on two of six sites and 50–70 percent coverage on four of six sites (3B). Note the black triangle between the central incisors remains after treatment.

C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 651
DISCLOSURE
John Chao, DDS, holds patents for PST instruments and trademarks for the Pinhole Surgical Technique.
ACKNOWLEDGMENT
The author thanks Richard Nagy, DDS, for inviting her to write an article for this issue of the Journal.
REFERENCES
1. Chambrone L, Tatakis D. Long Term Outcomes of Untreated Buccal Gingival Recessions: A Systematic Review and Meta-Analysis. J Periodontol 2016;87:796–808.2. Oates T, Robinson M, Gunsolley J. Surgical Therapies for the Treatment of Gingival Recession: A Systematic Review. Ann Periodontol 2003;8:303–320.3. Roccuzzo M, Bunino M, Needleman I, Sanz M. Periodontal Plastic Surgery for the Treatment of Localized Gingival Recessions: A Systematic Review. J Clin Periodontol 2003;29:178–194.4. Cairo F, Pagliaro U, Nieri M. Treatment of Gingival Recession with Coronally Advanced Flap Procedures: A Systematic Review. J Clin Periodontol 2008;35:136–162.5. Chambrone L, Sukekava F, Arujo M, Pustiglioni F, Chambhone L, Lima L. Root-Coverage Procedures for the Treatment of Localized Recession-Type Defects: A Cochrane Systematic Review. J Periodontol 2010;81:452–478.6. Allen AL. Use of the Supraperiosteal Envelope in Soft Tissue Grafting for Root coverage I. Rationale and Technique. Int J Periodontics Restorative Dent 1994;14:216–27.7. Tözüm TF, Dini FM. Treatment of Adjacent Gingival Recessions with Subepithelial Connective Tissue Grafts and the Modified Tunnel Technique. Quintessence Int 2003;34:7–13.8. Zadeh H. Minimally Invasive Treatment of Maxillary Anterior Gingival Recession Defects by Vestibular Incision Subperiosteal Tunnel Access and Platelet-Derived Growth Factor BB. Int J Periodontics Restorative Dent 2011;31(6):653–660.9. Pini Prato G, Pagliaro U, Baldi C, et al. Coronally Advanced Flap Procedure For Root coverage. Flap Tension versus Flap Without Tension: A Randomized Controlled Clinical Study. J Periodontol 2000; 71:188–201.10. Al-Hamdan K, Eber R, Sarment D, Kowalski C, Wang HL. Guided Tissue Regeneration-Based Root coverage: Meta-Analysis. J Periodontol 2003;74:1520–1533.11. Murphy K, Gunsolley J. Guided Tissue Regeneration for the Treatment of Periodontal Intraboney and Furcation Defects. A Systematic Review. Ann Periodontol 2003;8:266–302.12. Cohen W, Ross S. The Double Papillae Repositioned Flap in Periodontal Therapy. J Periodontol 1968;39:65–70.13. Miller PD Jr. A Classification of Marginal Tissue Recession. Int J Periodontics Restorative Dent 1985;5(2):8–13.14. Chao J. A Novel Approach to Root coverage: The Pinhole Surgical Technique. Int J Periodontics Restorative Dent 2012;32:521–531.15. Baldi C, Pini-Prato G, Pagliaro U, et al. Coronally Advanced Flap Procedure for Root coverage: Is Flap
Thickness a Relevant Predictor to Achieve Root coverage? A 19-Case Series. J Periodontol 1999;70:1077–1084.16. Berlucchi I, Francetti L, Del Fabbro M, Basso M, Weinstein RL. The Influence of Anatomical Features on the Outcome of Gingival Recessions Treated With Coronally Advanced Flap and Enamel Matrix Derivative: A One-Year Prospective Study. J Periodontol 2005;76:899–907.17. Huang LH, Neiva RE, Wang HL. Factors Affecting the Outcomes of Coronally Advanced Flap Root-coverage Procedure. J Periodontol 2005;76:1729–1734.18. Vincenzi G, De Chiesa A, Trisi P. Guided Tissue Regeneration Using a Resorbable Membrane in Gingival Recession-Type Defects: A Histological CAs Report in Humans. Int J Periodontics Restorative Dent 1998;18:24–33.19. Cortellini P, Clauser C, Prato GP. Histological Assessment of New Attachment Following the Treatment of Human Buccal Recession By Means of a Guided Tissue Regeneration Procedure. J Periodontol 1993;64:387–391.20. Parma-Benefanti S, Tinti C. Histologic Evaluation of New Attachment Utilizing a Titanium-Reinforced Barrier Membrane in a Mucogingival Recession Defect. A Case Report. J Periodontol 1998;69:834–839.21. McGuire MK, Cochran DL. Evaluation of Human Recession Defects Treated with Coronally Advanced Flap and Either Enamel Matrix Derivative or Connective Tissue. J Periodontol 2003;74:1126–1135.22. Martins T, Bosco A, Nobrega F, Nagata M, Garcia V, Fucini S. Periodontal Tissue Response to Coverage of Root Cavities Restored With Resin Materials: A Histomorphometric Study in Dogs. J Periodontol 2007;78:1075–1082.23. McGuire MK. Soft Tissue Augmentation on Previously Restored Root Surfaces. Int J Periodontics Restorative Dent 1996;16(6):570–581.24. Golstein M, Nasatzky E, Goultschin J, Boyan B, Schwartz Z. Coverage of Previously Carious Roots Is Predictable a Procedure as Coverage as Intact Roots. J Periodontol 2002;73:1419–1426.25. Anson D. Periodontal Esthetics and Soft-Tissue Root coverage for the Treatment of Cervical Root Caries. Compend Contin Educ Dent 1999;20(11):1043–1046.26. Corsair A. Root coverage of a Previously Restored Tooth. A Case Report With a Seven-Year Follow-up. Clin Cosmet Investig Dent 2009;1:35–38.27. Fourel J. Gingival Reattachment on Carious Tooth Surfaces. A Four-Year Follow-Up. J Clin Periodontol 1982;9:285-289.28. Prato GP, Tinti C, Tortellini P, Magnani C, Clauser C. Periodontal Regenerative Therapy with the Coverage of Previously Restored Root Surfaces: Case Reports. Int J Periodontics Restorative Dent 1992;12:450–461.29. Richardson C, Allen E, Chambrone L, Langer B, McGuire M, Zabalegui I, Zadeh H, Tatakis D. Periodtonal Soft Tissue Root-Coverage Procedures: Practical Applications From the AAP Regeneration Workshop. Clin Adv Periodontics 2015;5:2–10.
THE AUTHOR, Tina M. Beck, DDS, MS, can be reached at [email protected].

WE HAVE ANSWERS.In the dynamic world of dental benefit plans, our
smart analysts can help you decode provider
agreement requirements, manage claims efficiently
and better understand your appeal rights. Get
support challenging a decision or filing a claim
from our experts, and use our Dental Benefit Plan
Handbook to navigate the dispute resolution process.
QUESTIONS ABOUTNAVIGATING DENTAL
BENEFIT PLANS?
800.232.7645cda.org/practicesupport
®
Practice ManagementEmployment PracticesDental Benefit PlansRegulatory Compliance
PRACTICE SUPPORT
C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 653
Paul Y. Lee, DDS, is in private practice in Cupertino, Calif.Confl ict of Interest Disclosure: None reported.
Richard T. Kao, DDS, PhD, is a clinical professor at the University of California, San Francisco, School of Dentistry and is in private practice in Cupertino, Calif.Confl ict of Interest Disclosure: None reported.
AUTHORS
Cherissa Chong, DMD, MS, is a diplomate of the American Board of Orthodontics and the American Board of Periodontology. She is in private practice in Saratoga, Calif.Confl ict of Interest Disclosure: None reported.
Yung-Ting Hsu, DDS, MDSc, MS, is a diplomate of the American Board of Periodontology and is a clinical assistant professor, department of graduate periodontology at the University of Detroit Mercy School of Dentistry, and an adjunct clinical assistant professor, department of periodontics and oral medicine at the University of Michigan.Confl ict of Interest Disclosure: None reported.
Tissue Engineering for Improving Periodontal PhenotypeCherissa Chong, DMD, MS; Yung-Ting Hsu, DDS, MDSc; Paul Y. Lee, DDS; and Richard T. Kao, DDS, PhD
A B S T R AC T Tissue engineering is a new fi eld whereby healing and regeneration is manipulated for an improved result. There are two main approaches. The fi rst is to use tissue engineering as an approach to repair the recession defect. The second is to augment the soft and hard tissue in preparation of teeth for orthodontic movements. From this review, clinicians will be able to appreciate some new strategies for the correction of recession defects.
In this issue, the importance of correcting gingival recession and mucogingival defects for periodontal health has been advocated. Though this is an ideal goal, our patients often have
hesitation due to surgical concerns. These concerns center on the lack of adequate autogenous donor tissue, multiple surgeries to gain adequate bone/soft tissue volume, pain associated with donor site, increased risk for bleeding, necrosis of the donor site and delayed healing. Tissue engineering is a highly promising fi eld whereby biotechnologies are used to facilitate regeneration of a particular tissue (FIGURE 1). A tissue engineering approach consists of applying biologic signaling molecules (e.g., growth/differentiation factors and plasma preparations), cells (stem cells) and/or scaffolding matrices to promote regeneration whereby the new tissue is characteristically and functionally indistinguishable from the original tissue.1 This article provides
t i s s u e e n g i n e e r i n g
clinicians with an understanding of how certain biotechnologies associated with tissue engineering may be incorporated into mucogingival surgery. It focuses on clinically available biotechnologies, their scientifi c merit or potential to improve clinical outcomes and considerations for incorporation into clinical practice. More important, it addresses some of our patients’ concerns regarding mucogingival augmentation.
There are two basic strategies for applying a tissue engineering approach for correcting recession defects. The fi rst is to repair and change a thin phenotype into a thick phenotype. This is applicable in gingival recession cases where there is a need to repair the recession and obtain root coverage with a secondary goal of thickening the mucogingival tissue to prevent future recession. It should be appreciated that, in these situations, the repair process is the “masking” of the loss of bony plate
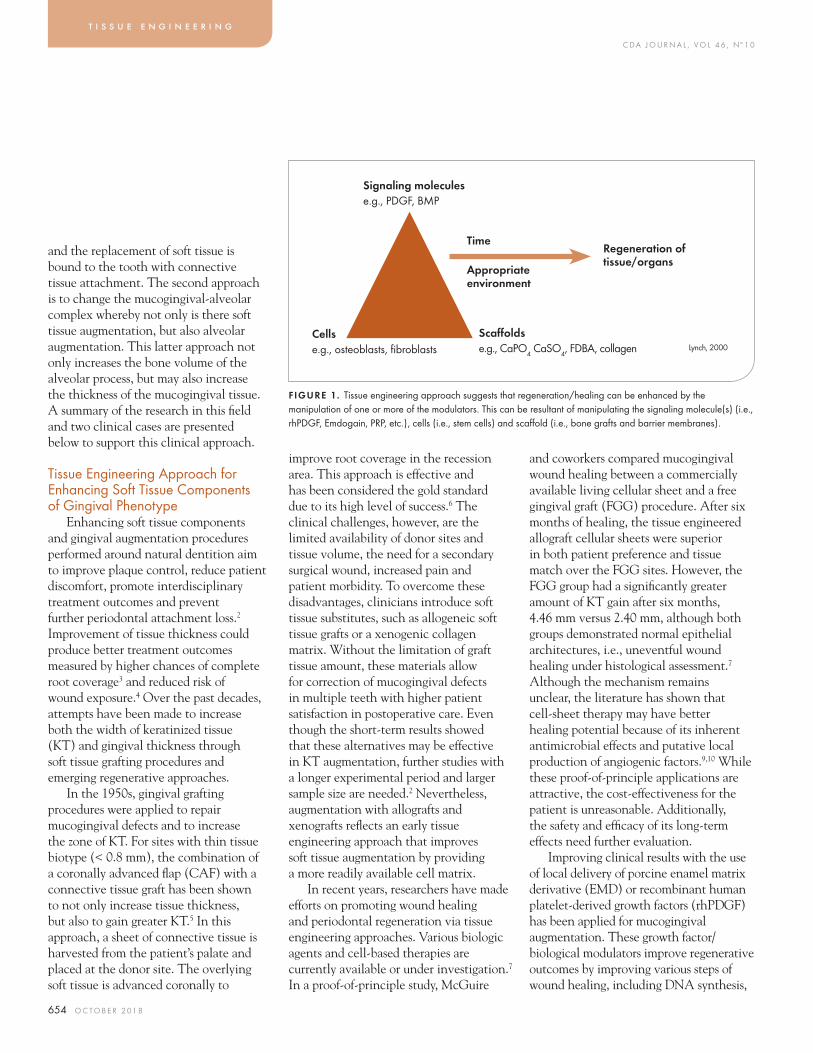
C DA J O U R N A L , V O L 4 6 , Nº 1 0
654 O C TO B E R 2 01 8
and the replacement of soft tissue is bound to the tooth with connective tissue attachment. The second approach is to change the mucogingival-alveolar complex whereby not only is there soft tissue augmentation, but also alveolar augmentation. This latter approach not only increases the bone volume of the alveolar process, but may also increase the thickness of the mucogingival tissue. A summary of the research in this fi eld and two clinical cases are presented below to support this clinical approach.
Tissue Engineering Approach for Enhancing Soft Tissue Components of Gingival Phenotype
Enhancing soft tissue components and gingival augmentation procedures performed around natural dentition aim to improve plaque control, reduce patient discomfort, promote interdisciplinary treatment outcomes and prevent further periodontal attachment loss.2 Improvement of tissue thickness could produce better treatment outcomes measured by higher chances of complete root coverage3 and reduced risk of wound exposure.4 Over the past decades, attempts have been made to increase both the width of keratinized tissue (KT) and gingival thickness through soft tissue grafting procedures and emerging regenerative approaches.
In the 1950s, gingival grafting procedures were applied to repair mucogingival defects and to increase the zone of KT. For sites with thin tissue biotype (< 0.8 mm), the combination of a coronally advanced fl ap (CAF) with a connective tissue graft has been shown to not only increase tissue thickness, but also to gain greater KT.5 In this approach, a sheet of connective tissue is harvested from the patient’s palate and placed at the donor site. The overlying soft tissue is advanced coronally to
improve root coverage in the recession area. This approach is effective and has been considered the gold standard due to its high level of success.6 The clinical challenges, however, are the limited availability of donor sites and tissue volume, the need for a secondary surgical wound, increased pain and patient morbidity. To overcome these disadvantages, clinicians introduce soft tissue substitutes, such as allogeneic soft tissue grafts or a xenogenic collagen matrix. Without the limitation of graft tissue amount, these materials allow for correction of mucogingival defects in multiple teeth with higher patient satisfaction in postoperative care. Even though the short-term results showed that these alternatives may be effective in KT augmentation, further studies with a longer experimental period and larger sample size are needed.2 Nevertheless, augmentation with allografts and xenografts refl ects an early tissue engineering approach that improves soft tissue augmentation by providing a more readily available cell matrix.
In recent years, researchers have made efforts on promoting wound healing and periodontal regeneration via tissue engineering approaches. Various biologic agents and cell-based therapies are currently available or under investigation.7 In a proof-of-principle study, McGuire
and coworkers compared mucogingival wound healing between a commercially available living cellular sheet and a free gingival graft (FGG) procedure. After six months of healing, the tissue engineered allograft cellular sheets were superior in both patient preference and tissue match over the FGG sites. However, the FGG group had a signifi cantly greater amount of KT gain after six months, 4.46 mm versus 2.40 mm, although both groups demonstrated normal epithelial architectures, i.e., uneventful wound healing under histological assessment.7 Although the mechanism remains unclear, the literature has shown that cell-sheet therapy may have better healing potential because of its inherent antimicrobial effects and putative local production of angiogenic factors.9,10 While these proof-of-principle applications are attractive, the cost-effectiveness for the patient is unreasonable. Additionally, the safety and effi cacy of its long-term effects need further evaluation.
Improving clinical results with the use of local delivery of porcine enamel matrix derivative (EMD) or recombinant human platelet-derived growth factors (rhPDGF) has been applied for mucogingival augmentation. These growth factor/biological modulators improve regenerative outcomes by improving various steps of wound healing, including DNA synthesis,
t i s s u e e n g i n e e r i n g
FIGURE 1. Tissue engineering approach suggests that regeneration/healing can be enhanced by the manipulation of one or more of the modulators. This can be resultant of manipulating the signaling molecule(s) (i.e., rhPDGF, Emdogain, PRP, etc.), cells (i.e., stem cells) and scaff old (i.e., bone grafts and barrier membranes).
Time
Appropriate environment
Signaling moleculese.g., PDGF, BMP
Cellse.g., osteoblasts, fi broblasts
Scaff oldse.g., CaPO4 CaSO4, FDBA, collagen
Regeneration of tissue/organs
Lynch, 2000

C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 655
chemotaxis, cell differentiation and matrix synthesis.11 Clinically, EMD application in conjunction with CAF graft procedures have been advantageous for correction of Miller Class I or II defects.12 Despite this, increase in KT gain with EMD is not as effective as using either a subepithelial connective tissue graft or xenogenous collagen matrix.13,14 In precursor studies to the use of rhPDGF, platelet concentrate was shown to improve root-coverage procedures but failed to show superiority on KT gain.15,16 When rhPDGF concentrate was used, a similar trend was noted in the treatment of gingival defects.17,18 A recent study utilizing the combination therapy of rhPDGF and acellular dermal matrix showed improved healing (35 percent) compared to the sites with acellular dermal matrix (15 percent) only one week postoperatively.19 These studies suggest that EMD, rhPDGF and platelet concentrate may aid and enhance healing, but if the outcome criteria are to gain an increased band of attached tissue, an autologous grafting approach may be superior.
From a histological perspective of healing, tissue engineering approaches not only accelerate wound healing but also improve the healing outcomes from new attachment to regeneration. Conventionally, soft tissue grafts or their substitutes adhere to the root surface primarily by epithelial and connective tissue attachment.20,21 Additional improvement in root coverage and increased KT can potentially be gained over time by creeping attachment, a
postoperative coronal migration of gingival margin.22,23 Though epithelial and connective tissue attachment can be stable, a histologically more appealing type of graft attachment to teeth has been demonstrated when EMD or PDGF has been used. In a case report, the EMD-treated site exhibited signs of new cementum, periodontal ligament fi ber and islands of bone after six months of healing.21
Similar fi ndings of periodontal regeneration have also been reported with the use of PDGF.24 In KT augmentation, tissue-engineered cell therapy was capable of gaining KT that was integrated within the host connective tissue.8 It can be argued that these histological tooth forms of regeneration and healing may be more stable than epithelial and connective tissue attachment, but further evidence and longitudinal studies are needed.25
Case 1: The use of a tissue engineering approach for altering gingival phenotype may be benefi cial in complex cases where one is concerned whether the conventional approach may not provide adequate correction of the recession defect. In the clinical case shown in FIGURE 2A, the patient presented with multiple recession issues particularly in the area of teeth Nos. 5-6 and 11-12. Additionally, aesthetic concerns included the need to increase clinical length for tooth No. 7 and decrease the crown length on tooth No. 10. It was decided to accept the clinical crown length of Nos. 8-9. In attempting to resolve these issues, the restorations were removed
revealing a large class V composite on the area to be grafted (FIGURE 2B). The composite was removed and the area was root planed. The area remained stained and there were concerns whether root coverage was possible. To enhance root coverage for this area, EMD was used in conjunction with the placement of the connective tissue graft. The buccal fl ap was advanced coronally to ensure blood supply for the area. Though it may be debatable whether EMD was necessary, it provided regional enrichment of growth factors that may have enhanced the success of the graft. Soon after the fi nal delivery of the veneers and crowns, one can see a more balanced smile where aesthetic root coverage was achieved for teeth Nos. 5-6, 10 and 11-12 (FIGURE 2C). Due to the increased cost for the use of biologics, the clinician must be prudent and have justifi cation for its use only in situations whereby conventional approach will not or cannot reliably achieve satisfactory results.
Tissue Engineering Approach for Altering Gingival Phenotype for Orthodontic Treatment
Poor dental alignment and malocclusion are the most common reasons people seek orthodontic treatment. As teeth are repositioned for more ideal occlusal scheme, one needs to consider if there is an adequate volume of bone and soft tissue that will heal with no long-term negative results such as gingival recession. These deleterious consequences may be immediately evident, but at times
FIGURE 2A . FIGURE 2B . FIGURE 2C .
FIGURES 2. This elderly female patient presented with a chief complaint of wanting to improve her appearance (2A). Tooth No. 7 was aesthetically crown lengthened. Gingival recession was present on teeth Nos. 5–6 and 11–12 that were treated with CTG with coronal advancement of the buccal fl ap. Tooth No. 10 had a composite in the Cl V area that was removed and the graft bed had odontoplasty and was treated with EMD to enhance healing and root coverage (2B). Clinical presentation immediately after the delivery of restorations (2C). Note that gingival infl ammation was still present from the mandibular veneers.

C DA J O U R N A L , V O L 4 6 , Nº 1 0
656 O C TO B E R 2 01 8
it may take several years or more before they appear. Therefore, as the orthodontist is planning for orthodontic tooth movement, the gingival biotype needs to be considered. Orthodontic movement in a thick phenotype environment is both predictable and without any deleterious results. This is because there is adequate volume of bone and soft tissue that will permit remodeling and healing. However, moving teeth in a thin phenotype environment can be challenging. This is because teeth that are moved in a thin bony plate often are compromised with increased incidence of fenestrations and dehiscence. As these thin bony plates remodel, there may be compromised healing or bone deposition that may result in gingival recession during treatment many years afterward. Additionally, the overlying gingiva is often so thin that orthodontic movement may result in gingival recession. Recently, utilizing a combination of gingival augmentation, alveolar bone grafting and periodontally accelerated osteogenic orthodontics (PAOO — also called Wilckodontics or surgically facilitated orthodontic therapy, SFOT), it is now possible to create an environment whereby teeth can be moved to an ideal position, reinforced with increased osseous volume and augmented with soft tissue such that there is an adequate zone of attached gingiva.
While there are several reviews on gingival augmentation and bone grafting, PAOO is a relatively new surgical technique that, when performed in conjunction with traditional orthodontics, can accelerate tooth movement and expand the scope of conventional orthodontic treatment by two- to threefold in most spatial dimensions26 and accelerate tooth movement 1 ½ times to four times26–28 the normal rate of traditional orthodontic tooth movement.
Decortication of the alveolar housing creates transient demineralization and the resulting soft tissue matrix of the bone can be carried out with the root during orthodontic tooth movement. Remineralization of the bone occurs after orthodontic treatment is completed. During this time, there is an accelerated rate of tooth movement due to the altered physiologic response known as the regional acceleratory phenomenon (RAP) effect. The regional acceleratory phenomenon was fi rst described by
Frost,29–31 where injury to bone results in acceleration of all processes involved in healing, including remodeling, cell turnover, metabolism and repair. The biologic limits of tooth movement are determined by the alveolar bone and surrounding soft tissues. Movement of teeth outside the alveolar housing can result in fenestrations and dehiscence in the alveolar bone. In individuals with thin gingival biotype, movement of the teeth outside of the thin bony housing may present clinically as root recession. This may present itself immediately after orthodontic treatment or in years following treatment. By combining soft tissue augmentation and bone grafting techniques, it is now possible to convert the thin phenotype environment into a thick phenotype.
PAOO has been shown to be effi cacious in the treatment of malocclusions, as well as presurgical decompensation for orthognathic surgeries.26 The benefi ts of PAOO include accelerated treatment time,32 greater stability of clinical outcomes and less relapse,29 enhanced scope of the treatment of malocclusion and increased alveolar volume and enhanced periodontium.26 Clinical studies have shown the application of PAOO to resolve crowding of the dentition,33 accelerate canine retraction in closing extraction spaces,33 facilitate the eruption of impacted teeth34 and facilitate orthodontic expansion in borderline orthognathic cases,35 dental intrusion and open bite correction.26,36 PAOO has been proposed as an alternative treatment plan for borderline orthognathic/orthodontic surgical cases. Combining proper diagnosis and patient desires, PAOO may be a feasible treatment for tooth movement necessary beyond orthodontic “camoufl age” but not severe enough to warrant orthognathic surgery.37 Wilcko et al. demonstrated that orthodontic therapy combined with alveolar decortication results in a signifi cant increase in keratinized tissue height. The authors found that 1½ years after completion of active orthodontic treatment, keratinized gingival tissue height increased signifi cantly, by 0.78 mm (P < 0.001) in the corticotomy group, and decreased by 0.38 mm (P = 0.002) in the conventional group treated without corticotomy.38 Stability post-orthodontic treatment is also a key benefi t of PAOO. It is believed that PAOO patients have fewer tendencies for relapse post-orthodontic treatment because scarring of the alveolar cortex initiates an infl ammatory healing, i.e., RAP, which increases tissue turnover.39 This tissue turnover may be partly responsible for the loss in tissue memory,
t i s s u e e n g i n e e r i n g
PAOO is a relatively new surgical technique that, when performed in conjunction with traditional orthodontics, can accelerate tooth movement.

C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 657
which allows for bone augmentation that increases cortical thickness of the alveolar bone surrounding the dentition. The increased thickness of the alveolar bone is believed to enhance post-orthodontic stability of the dentition.40 In a 2016 systematic review,32 corticotomy did not appear to have any important sequelae on periodontal health, including periodontal probing depths, plaque indices, gingival recession, clinical attachment levels and alveolar crestal bone heights. While many studies have shown that PAOO is safe for the oral tissues and accompanied by a phase of accelerated tooth movement, further well-designed prospective studies are needed to draw valid conclusions on this technique.41,42
Case 2: To demonstrate the principle of utilizing tissue engineering with orthodontic mechanical strategy, this 42-year-old Asian female presented with a chief complaint of crowding but refused further extractions (FIGURE 3A). Patient presented with thin gingival biotype with areas of existing gingival recession and generalized dental wear on her teeth. A cone beam computed tomography (CBCT) was taken prior to PAOO, which showed the prevalence of a thin cortical plate, if any, in several areas from canine to canine. A sample pre-op CBCT is presented in FIGURE 3G. The goal of tooth movement was to enhance the thickness of the alveolus to allow for protraction of the upper and lower anterior teeth and alleviate crowding. To achieve this, a PAOO-RAP approach was utilized with the addition of a tissue engineering modifi cation (i.e., bone grafting).
Bracket placement was performed one week before surgery, however it has been suggested that bracketing can occur up to one week after surgery.43 Initiation of orthodontic force should not be delayed more than two weeks after surgery in order to take full advantage of the four- to six-month RAP phenomenon or “window”
FIGURES 3 . Conventional PAOO treatment. 3A is the clinical presentation at pretreatment; 3B–D is the surgical view and with corticotomy; 3E is the surgical area bone grafted; 3F is the clinical presentation after treatment; and 3G are the representative pre- and post-op CBCT.
of accelerated tooth movement.43 A full-thickness mucoperiosteal fl ap was raised in the coronal portion and a split-thickness dissection was made in the apical portion. The purpose of the split-thickness dissection is to provide mobility of the fl ap and reduce tension in the fl ap. Upon fl ap refl ection, it is evident that prior to any orthodontic treatment, this patient already had several existing dehiscence and fenestrations. If orthodontic treatment was performed under such conditions and teeth were moved further buccally, this patient would be predisposed to developing
gingival recession. Decortication was performed at each inter-radicular area, as well as apical to each root apex. Vertical grooves were made extending just below the interproximal alveolar bone margin to beyond the apex of each tooth. Horizontal grooves were made to join the apical extensions of the vertical grooves39 (FIGURES 3B–D). The purpose of decortication is to initiate the RAP phenomenon and bone turnover. It is recommended that the corticotomy cut minimally breaks through the cortical plate into the medullary bone on the
FIGURE 3A .
FIGURE 3C .
FIGURE 3E .
FIGURE 3G.
FIGURE 3B .
FIGURE 3D.
FIGURE 3F.

C DA J O U R N A L , V O L 4 6 , Nº 1 0
658 O C TO B E R 2 01 8
buccal and lingual aspect in order to enhance suffi cient vascularization of the overlying graft to occur. A combination of demineralized freeze-dried bone allograft-mineralized freeze-dried allograft (DFDBA-FDBA) mixture was used to augment the bone (FIGURE 3E). Gingival fl aps were repositioned and sutured in place. Healing was uneventful. Ten days following the periodontal bone grafting procedure, traditional nitinol wires were placed to begin leveling and aligning. The patient was seen every two weeks to assess alignment and maintain effi cient tooth movement during the “window” of accelerated tooth movement. Finishing and detailing was completed in a comparable time frame as a traditional orthodontic case. The overall goal of alleviating crowding and enhancing alveolar housing had been achieved. A follow-up CBCT scan taken six months postsurgery showed the presence of a robust thickness of alveolar bone. Simultaneous coronal repositioning for the mucoperiosteal fl ap in conjunction with bone grafting corrected recession defects shown on several teeth in the initial scan (FIGURE 3F). Pre- and postoperative CBCT scans demonstrated radiographic suggestion of thickened labial plate (FIGURE 3G). Many cases are now being treated with a combination of soft tissue grafting or with the addition of stem cells in order to enhance the soft tissue quality.
This case demonstrates the potential benefi ts as well as some of the complications that may result from the PAOO procedure. Without doing the PAOO procedure, the preoperative CBCT and surgical observations suggest that it would not have been possible to have treated this case orthodontically. The negative consequences of pursuing treatment without PAOO would be to orthodontically move teeth out of the bony housing. This would have resulted
t i s s u e e n g i n e e r i n g
in increased mobility as well as extensive gingival recession. In this particular case, slight recession did occur at the completion of treatment. The corrective procedure would have been a root-coverage procedure. Because there was adequate zone of attached gingiva and lack of dentinal hypersensitivity, the patient elected not to have further surgical treatment and the additional expense. She was happy with the aesthetic results and the improved stability of her dentition. This case demonstrates that PAOO can provide increased opportunities for achieving better occlusion
and improving oral hygiene access. One possible negative consequence, however, is this may result in minor gingival recession that may require an additional gingival root-coverage procedure.
Case 3: In this case, a 30-year-old female with a severe Class III malocclusion and extremely thin phenotype was presented for treatment (FIGURES 4A–C). The basic strategy was to convert the thin biotype characteristics in the mandibular anterior segment into thick phenotype. This would be done prior to initial orthodontic and subsequent orthognathic treatment. Given the thin gingival tissue, there were surgical concerns that simply refl ecting the mucogingival fl ap would result in tissue necrosis. Therefore, the case was planned in two phases. The fi rst phase centered on thickening the gingiva and
the second phase focused on PAOO with a commercially available stem cell preparation. The fi rst surgery was performed as an autogenous connective tissue graft from teeth Nos. 20–29. In order to assure the survival of the graft and the overlying gingiva, rhPDGF was used with the objective of improving healing. After the fi rst phase, the area was allowed to heal. It should be noted that during this healing phase, there were small areas of epithelial sloughing. This suggests that in extremely thin cases, the simple act of lifting the mucoperiosteal fl ap may compromise the blood supply such that some superfi cial tissue necrosis may occur. It is these authors’ contention that the rhPDGF improved wound healing, but this is an observation that requires further confi rmation. Furthermore, this preliminary CTG grafting provided a thicker gingiva and increased the zone of attached gingiva. On re-entry, one can see numerous areas of fenestrations and dehiscence that were previously present but may have been accentuated due to fl ap refl ection for the previous connective tissue grafting procedure (FIGURE 4D). The area was decorticated on both the buccal as well as the lingual aspect as previously described in Case 1 and augmented with stem cell allograft preparation that consisted of stem cells seeded onto DFDBA (Osteocel). In order to prevent dispersal of the graft material, a resorbable collagen membrane was used to contain the graft in the area of interest. The collagen membrane helped by keeping the graft materials in the proper place; without the use of membrane, there is a tendency for the graft material to pool apically. The area was sutured and allowed to heal (FIGURE 4E). Note that three months after healing, the tissue on the buccal of tooth No. 22 was still remodeling. When very thin soft tissue is grafted with connective tissue, remodeling may occur up to six months after the grafting procedure. Additionally, it should be noted that the
Many cases are now being treated with a combination of soft tissue grafting or with the addition of stem cells in order to enhance the soft tissue quality.
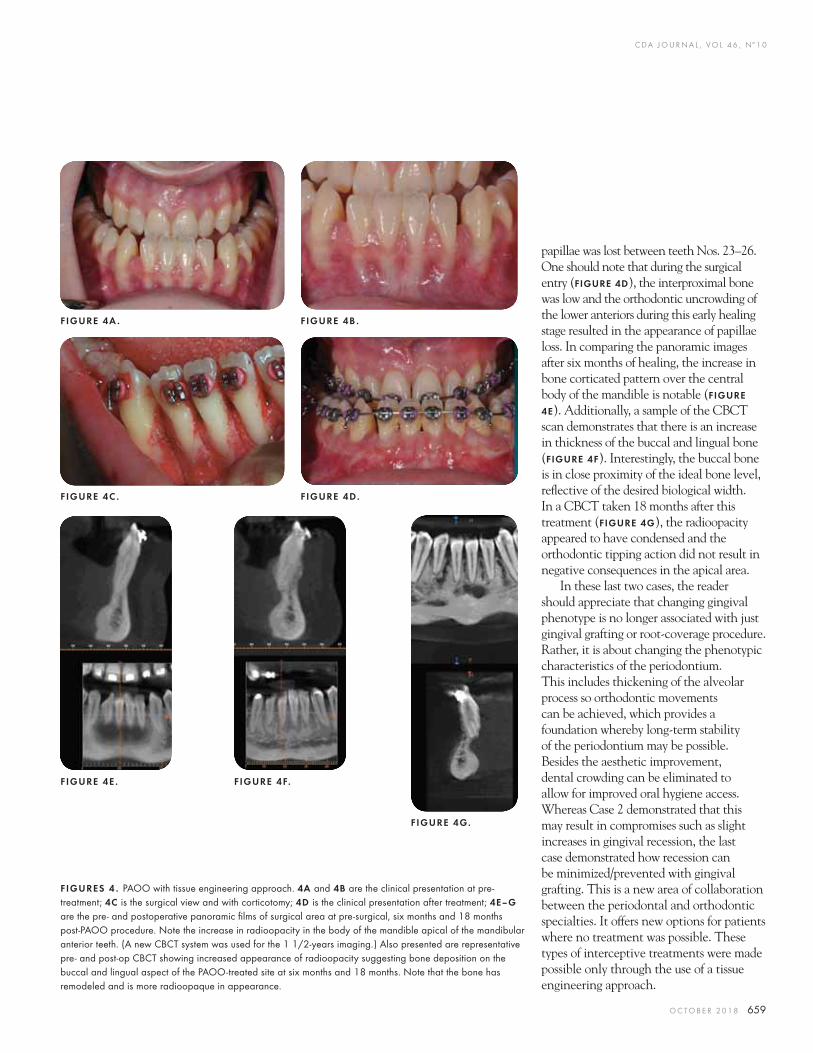
C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 659
papillae was lost between teeth Nos. 23–26. One should note that during the surgical entry (FIGURE 4D), the interproximal bone was low and the orthodontic uncrowding of the lower anteriors during this early healing stage resulted in the appearance of papillae loss. In comparing the panoramic images after six months of healing, the increase in bone corticated pattern over the central body of the mandible is notable (FIGURE
4E). Additionally, a sample of the CBCT scan demonstrates that there is an increase in thickness of the buccal and lingual bone (FIGURE 4F). Interestingly, the buccal bone is in close proximity of the ideal bone level, refl ective of the desired biological width. In a CBCT taken 18 months after this treatment (FIGURE 4G), the radioopacity appeared to have condensed and the orthodontic tipping action did not result in negative consequences in the apical area.
In these last two cases, the reader should appreciate that changing gingival phenotype is no longer associated with just gingival grafting or root-coverage procedure. Rather, it is about changing the phenotypic characteristics of the periodontium. This includes thickening of the alveolar process so orthodontic movements can be achieved, which provides a foundation whereby long-term stability of the periodontium may be possible. Besides the aesthetic improvement, dental crowding can be eliminated to allow for improved oral hygiene access. Whereas Case 2 demonstrated that this may result in compromises such as slight increases in gingival recession, the last case demonstrated how recession can be minimized/prevented with gingival grafting. This is a new area of collaboration between the periodontal and orthodontic specialties. It offers new options for patients where no treatment was possible. These types of interceptive treatments were made possible only through the use of a tissue engineering approach.
FIGURES 4 . PAOO with tissue engineering approach. 4A and 4B are the clinical presentation at pre-treatment; 4C is the surgical view and with corticotomy; 4D is the clinical presentation after treatment; 4E–G are the pre- and postoperative panoramic fi lms of surgical area at pre-surgical, six months and 18 months post-PAOO procedure. Note the increase in radioopacity in the body of the mandible apical of the mandibular anterior teeth. (A new CBCT system was used for the 1 1/2-years imaging.) Also presented are representative pre- and post-op CBCT showing increased appearance of radioopacity suggesting bone deposition on the buccal and lingual aspect of the PAOO-treated site at six months and 18 months. Note that the bone has remodeled and is more radioopaque in appearance.
FIGURE 4A .
FIGURE 4C .
FIGURE 4E . FIGURE 4F.
FIGURE 4G.
FIGURE 4B .
FIGURE 4D.

C DA J O U R N A L , V O L 4 6 , Nº 1 0
660 O C TO B E R 2 01 8
ConclusionTissue engineering has the potential to
alter gingival phenotype. This approach can thicken gingival thickness and provide root coverage in situations where there is recession or increase the gingival resistance to infl ammatory or restorative trauma. Additionally, when used in conjunction with a PAOO approach, augmentation with both soft tissue and stem cells can increase the bone volume and permit nontraditional orthodontic movement. These new exciting clinical translational applications may be applied in areas with compromised periodontal phenotypes where no treatment would have been considered in the recent past. ■
REFERENCES
1. Lynch SE (1999) Introduction to tissue engineering. In: Lynch SE, Genco RJ, Marx RE eds. Tissue Engineering: Applications in Maxillofacial and Periodontics. Chicago: Quintessence; 1999:xi–xviii.2. Kim DM, Neiva R. Periodontal soft tissue non-root-coverage procedures: A systematic review from the AAP Regeneration Workshop. J Periodontol 2015;86(2 Suppl):S56–72.3. Richardson CR, Allen EP, Chambrone L, et al. Periodontal soft tissue root-coverage procedures: Practical applications from the AAP Regeneration Workshop. Clinical Adv Periodontics 2015;5(1):2–10.4. Chao YC, Chang P, Fu J, Wang H, Chan H. Surgical site assessment for soft tissue management in ridge augmentation procedures. Int J Periodontics Restorative Dent 2015;35(5):e75–83.5. Cairo F, Cortellini P, Pilloni A, et al. Clinical effi cacy of coronally advanced fl ap with or without connective tissue graft for the treatment of multiple adjacent gingival recessions in the aesthetic area: A randomized controlled clinical trial. J Clin Periodontol 2016;43(10):849–56.6. Scheyer ET, Sanz M, Dibart S, et al. Periodontal soft tissue non-root-coverage procedures: A consensus report from the AAP Regeneration Workshop. J Periodontol 2015;86(2 Suppl):S73–6.7. Ishikawa I, Iwata T, Washio K, et al. Cell sheet engineering and other novel cell-based approaches to periodontal regeneration. Periodontol 2000 2009;51:220–38.8. McGuire MK, Scheyer ET, Nunn ME, Lavin PT. A pilot study to evaluate a tissue-engineered bilayered cell therapy as an alternative to tissue from the palate. J Periodontol 2008;79(10):1847–56.9. Falanga V, Isaacs C, Paquette D, et al. Wounding of bioengineered skin: Cellular and molecular aspects after injury. J Invest Dermatol 2002;119(3):653–60.10. Villar CC, Zhao XR, Livi CB, Cochran DL. Eff ect of living cellular sheets on the angiogenic potential of human microvascular endothelial cells. J Periodontol 2015;86(5):703–12.
11. Anusaksathien O, Giannobile WV. Growth factor delivery to re-engineer periodontal tissues. Curr Pharm Biotechnol 2002;3(2):129–39.12. Alkan EA, Parlar A. EMD or subepithelial connective tissue graft for the treatment of single gingival recessions: A pilot study. J Periodontal Res 2011;46(6):637–42.13. Alexiou A, Vouros I, Menexes G, Konstantinidis A. Comparison of enamel matrix derivative (Emdogain) and subepithelial connective tissue graft for root coverage in patients with multiple gingival recession defects: A randomized controlled clinical study. Quintessence Int 2017;48(5):381–89.14. Sangiorgio JPM, Neves F, Rocha Dos Santos M, et al. Xenogenous Collagen Matrix and/or Enamel Matrix Derivative for Treatment of Localized Gingival Recessions: A Randomized Clinical Trial. Part I: Clinical Outcomes. J Periodontol 2017;88(12):1309–18.15. Oncu E. The Use of Platelet-Rich Fibrin Versus Subepithelial Connective Tissue Graft in Treatment of Multiple Gingival Recessions: A Randomized Clinical Trial. Int J Periodontics Restorative Dent 2017;37(2):265–71.16. Lafzi A, Faramarzi M, Shirmohammadi A, et al. Subepithelial connective tissue graft with and without the use of plasma rich in growth factors for treating root exposure. J Periodontal Implant Sci 2012;42(6):196–203.17. McGuire MK, Scheyer ET, Snyder MB. Evaluation of recession defects treated with coronally advanced fl aps and either recombinant human platelet-derived growth factor-BB plus beta-tricalcium phosphate or connective tissue: Comparison of clinical parameters at fi ve years. J Periodontol 2014;85(10):1361–70.18. Rubins RP, Tolmie PN, Corsig KT, Kerr EN, Kim DM. Subepithelial connective tissue graft with growth factor for the treatment of maxillary gingival recession defects. Int J Periodontics Restorative Dent 2013;33(1):43–50.19. Carney CM, Rossmann JA, Kerns DG, et al. A comparative study of root defect coverage using an acellular dermal matrix with and without a recombinant human platelet-derived growth factor. J Periodontol 2012;83(7):893–901.20. Goldstein M, Boyan BD, Cochran DL, Schwartz Z. Human histology of new attachment after root coverage using subepithelial connective tissue graft. J Clin Periodontol 2001;28(7):657–62.21. McGuire MK, Cochran DL. Evaluation of human recession defects treated with coronally advanced fl aps and either enamel matrix derivative or connective tissue. Part 2: Histological evaluation. J Periodontol 2003;74(8):1126–35.22. Harris RJ. A short-term and long-term comparison of root coverage with an acellular dermal matrix and a subepithelial graft. J Periodontol 2004;75(5):734–43.23. Zucchelli G, Mounssif I, Mazzotti C, et al. Coronally advanced fl ap with and without connective tissue graft for the treatment of multiple gingival recessions: A comparative short- and long-term controlled randomized clinical trial. J Clin Periodontol 2014;41(4):396–403.24. Kaigler D, Avila G, Wisner-Lynch L, et al. Platelet-derived growth factor applications in periodontal and peri-implant bone regeneration. Expert Opin Biol Ther 2011;11(3):375–85.25. Vignoletti F, Nunez J, Sanz M. Soft tissue wound healing at teeth, dental implants and the edentulous ridge when using barrier membranes, growth and diff erentiation factors and soft tissue substitutes. J Clin Periodontol 2014;41 Suppl 15:S23–35.26. Ferguson DJ, Wilcko MT, Wilcko WM, Makki L. Scope of treatment with periodontally accelerated osteogenic orthodontic
therapy. Sem Orthod 2015;21:176–186.27. Bockow R. Treatment Planning with Corticotomy Facilitated Orthodontics. Sem Orthod 2014;20:228–238.28. Wilcko MT, Ferguson DJ, Makki L, Wilcko W. Keratinized gingiva height increases after alveolar corticotomy and augmentation bone grafting. J Periodontol 2015 Oct;86(10):1107–1115. doi: 10.1902/jop.2015.150074. Epub 2015 Jul 3.29. Makki L, Ferguson DJ. Stability of Mandibular Irregularity Index With and Without PAOO: A Review. Adv Dent & Oral Health 2017;4:1–3.30. Ferguson DJ, Machado I, Wilcko MT, Wilcko W. Root resorption following periodontally accelerated osteogenic orthodontics. APOS Trends in Orthodontics 2016;6:78–84.31. Murphy KG, Wilcko MT, Wilcko WM, Ferguson DJ. Periodontal Accelerated Osteogenic Orthodontics: A Description of the Surgical Technique. J Oral Maxillofac Surg 2009 Oct;67(10):2160–2166. doi: 10.1016/j.joms.2009.04.124.32. Wilcko MT, Wilcko WM, Bissada NF. An evidence-based analysis of periodontally accelerated orthodontic and osteogenic techniques: A synthesis of scientifi c perspectives. Sem Orthod 2008;14:305–16.33. Aboul-Ela SM, El-Beialy AR, El-Sayed KM, Selim EM, El Mangoury NH, Mostafa YA. Miniscrew implant-supported maxillary canine retraction with and without corticotomy-facilitated orthodontics. Am J Orthod Dentofacial Orthop 2011;139:252–9.34. Fischer TJ. Orthodontic treatment acceleration with corticotomy-assisted exposure of palatally impacted canines. Angle Orthod 2007; 77:417–20.35. Vercellotti T, Podesta A. Orthodontic microsurgery: A new surgically guided technique for dental movement. Int J Periodontics Restorative Dent 2007;27:325–31.36. Akay MC, Aras A, Gunbay T, Akyalcin S, Koyuncue BO. Enhanced eff ect of combined treatment with corticotomy and skeletal anchorage in open bite correction. J Oral Maxillofac Surg 2009; 67:563–9.37. Gantes B, Rathbun E, Anholm M. Eff ects on the Periodontium Following Corticotomy-Facilitated Orthodontics. Case Reports. J Periodontol 1990; 61:234–238.38. Frost HM. The regional acceleratory phenomenon: A review. Henry Ford Hosp Med J 1983;31(1):3–9.39. Frost HM. The biology of fracture healing. An overview for clinicians Part II. Clin Orthop Relat Res 1989 Nov (248): 294–309.40. Frost HM. The biology of fracture healing. An overview for clinicians. Part I. Clin Orthop Relat Res 1989;248:283–293.41. Patterson BM, Dalci O, Darendeliler MA, Papadopoulou AK. Corticotomies and Orthodontic Tooth Movement: A Systematic Review. J Oral Maxillofac Surg 2016 Mar;74(3):453–473. doi: 10.1016/j.joms.2015.10.011. Epub 2015 Oct 24.42. Hoogeveen EJ, Jansma J, Ren, Y. Surgically facilitated orthodontic treatment: A Systematic Review. Am J Orthod Dentofacial Orthop 2014; 145: S51–64.43. Al-Naoum F, Hajeer MY, Al-Jundi A. Does alveolar corticotomy accelerate orthodontic tooth movement when retracting upper canines? A split-mouth design randomized controlled trial. J Oral Maxillofac Surg 2014;72:1880.
THE CORRESPONDING AUTHOR, Richard T. Kao, DDS, PhD, can be reached at [email protected].
t i s s u e e n g i n e e r i n g
®
TOTOTTOTOTOOOOTOOOTOOGEGEGEGEGEGEGEGEGEGEGEGEGEGGGETHTHTHTHTHTHTHTHTHTHTHTHTHTTHERERERERRERERERERERERWEWEWEWEWEWEWEWEWEWEWEWEWEWWWWW AAAAAAAAAAAAAARERERERERERERERERERRERRR
LILILILILILILILILILILLILL MIMIMIMIMIMIMIMIMIMIMMIMIMMMM TLTLTLTLTLTLTLTLTLTLLLTLTLESESESESESESESESESSSESESSSSSSSSSSSSSSS
CDA. THIS IS WHERE WE
MEET YOU.
Dedicated legislative advocacy
means that California dentists have
more protection today and tomorrow.
Just one of the limitless member
benefits at cda.org.
A louder voice.
Specializing in selling and appraising dental practices for over 40 years!
CONTACT US FOR A FREE CONSULTATION Phone: (800) 697-5656
WWW.CALPRACTICESALES.COM CA BRE #00283209
youtube.com/mycpsteam faceboook.com/mycpsteam
Visit our Website and Social Media pages for Prac ce Photos and Videos
LOS ANGELES COUNTY
CARSON— Price Reduced!! Long established GP in a small shopping center. Grossed $277K in 2017. Net $132K. Has 3 eq ops & 2 plmbd not eq. Re ring seller work 3 days/wk. Great street visibility. Prop-erty ID #5181.
ENCINO - GP w/ 4 eq ops in a prof. bldg. w/ widow views to the mountain. Fee for service. Net $144K. Gross. $488K in 2017. Property ID #5210.0
GLENDALE—Beau ful office w/ 3 eq ops in a 850 sq . LH & Equip Only! Great starter office. Near resi-
den al & commercial area. Property ID #5208.
GLENDALE - GP located in a med bldg w/3 eq ops in a 1,123 sq ste. Ins & Cash Only! Est. in 1994. Grossed $473K in 2017. Prop. #5216.
LANCASTER (GP + Bldg) Long established prac ce w / 4 eq ops in a 1,600 sq office. Grossed $693K in 2017. NET $220K. Property ID #5222.
MOTEBELLO—Grossed approx. $1M in 2017, locat-ed in a free standing bldg w/ 5 eq ops. Established in 2002. Property ID #5168
SANTA CLARITA—GP w/ 36 yrs of goodwill in prof. bldg. w/ 5 eq ops. Grossed $449K in 2017. Property ID #5207.
TARZANA - Established in 1929 w/ 5 eq ops in a 1,552 sq suite. Delta Premier and Cash Only! Grossed $681K in 2017. Buyer’s Net $225K. Proper-ty #5226.
WOODLAND HILLS - Well established GP in a 5 story med/dent bldg with 4 eq ops and 1 plmbd not eq. Projec ng $1M for 2018. Property ID #5246.
KERN, VENTURA, & SAN LUIS OBISPO COUNTIES
FRESNO— GP 4 eq ops in a retail shopping center. Grossed $448K in 2017. NET $202K. Prop. #5214.
GOLETA—GP w/ 27 yrs of gdwll in a 2 story mix bldg. 4 eq ops. Grossed $572K. Prop. #5205.
OXNARD—Est, in 1973 w/ 4 eq ops in a 1,100 sq suite. Grossed $585K Net $186K. Prop. #5206.
SIMI VALLEY— GP + Real Estate. Prac ce has 4 eq ops & 2 plmbd not eq ops. Net of $92K. ID #5185.
ORANGE COUNTY
GARDEN GROVE - LH & Equip Only! Has 3 eq ops, 1 plmbd not equip in a 2 story professional bldg. Great for a Perio or GP. Property ID #5239.
IRVINE - Well established Cash Only GP w/ 5 eq ops in a1,915 sq office . Grossed approx. $482K in 2017. Property ID #5193.
LA PALMA— With 60 years of goodwill this GP prac ce is located in 2 story dental bldg w/ 4 eq ops. Grossed $443K in 2017. Property ID # 5234.
ORANGE— Est. in 1978 GP in one story free stand-ing duplex w/ 3 eq ops. Grossed approx. $386K in 2017. Property ID #5213.
ORANGE— LH & Equip Only! Beau ful office w/ 4 eq ops in a 1,300 sq office in single free standing bldg. Property ID #5229.
SANTA ANA— Well established prac ce. PPO & Cash only. Gross. approx. $500K. Prop. ID #5113.
TUSTIN—Well established GP in a 2 story busy shopping center. Projec ng $1.8M in 2018. Has 3 eq ops in 1,222 sq suite. Property # 5236.
TUSTIN— LH & EQUIP ONLY! Beau ful remodeled office with 3 eq op and 1 plmbd not eq. Located in a single story professional building. Has two price points. Property ID #5244.
RIVERSIDE & SAN BERNARDINO COUNTIES
CHINO HILLS— GP in busy shopping center. Grossed $352K . NET $141K. PPO & Cash Only! Has 3 eq ops and 1 plmbed op. Established in 1992. Property ID #5219.
CORONA— Beau ful GP w/ 6 eq ops / 4 plmbd not eq for expansion in a 3,700 sq office. Located on a one story free standing building next to a busy shop-ping center. Grossed $346K in 2017. Great poten al for a full me den st. Property ID #5224.
DESERT HOT SPRINGS— GP + Real Estate! Two partners one office. Consists of 4 eq ops / 1 plmbd not eq. Est. in 1986. Proj. approx. $802K for 2017. Property ID #5198.
FONTANA— GP + Real Estate!! Premier office with 50 years of goodwill. In a 3,000 sq bldg with 8 eq ops. Has the latest technology. Grossed approx. $2.3M in 2016. Net of $968K. Property ID #5140.
PALM DESERT— Beau ful GP located in a single story corner building. Heavy traffic flow. Consists of 4 eq ops in a 1,800 sq office. Reasonable rent. Monthly revenues of $132K. Grossed $1.4M in 2017. NET $383K. Property ID #5217.
PALM SPRINGS – General prac ce with 3 equipped ops located in a free standing bldg. Established in 2005. Suite is approx. 1,200. Seller work 5 days/wk. BUYER’S NET OF $311K. Property ID #4487.
RANCHO CUCAMONGA— GP established in 2004 in busy shopping center. Consists of 3 eq ops in a 1,200 sq suite. Grossed $422K in 2017. Net $149K. Prop-erty ID #5169.
UPLAND—Pediatric dental prac ce located in a medical bldg with 40 years of goodwill. Consists of 4 chairs in open with Alpha-Dent so ware. Grossed $271K in 2016. Property ID #5188.
COMING SOON IN LEMOORE, RANCHO BERNARDO, SAN DIEGO AND TEMECULA
SAN DIEGO COUNTY
LA JOLLA— 4 eq ops in 2 story med building. PPO & Cash Only! Grossed approx. $1.1M in 2017. Property ID #5220.
LA MESA— Beau ful GP office in shopping center w/ 5 eq ops & 1 plumbd not eq. Sees 80-100 new pa ents/mo. Grossed $1.5M in 2017. Net $368K. Prop.#5228.
OCEANSIDE— Orthodon c prac ce w/4 chairs in open bay in a 1,550 sq office. Grossed $263K in 2017. Property ID #5225.
SAN DIEGO— Price Reduced!! GP in med/dent bldg. w/ 3 eq ops. Fee for service. Estab. circa 1950. Grossed $301K in 2017. Net $117K. Prop-erty ID # 5212.
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 663
RM Matters
A dental professional can treat dozens of patients each day. Patients present, provide their information, get checked in and proceed with treatment.
Do you ever stop to wonder whether your patients are who they say they are?
In a case reported to The Dentist Insurance Company’s Risk Management Advice Line, a patient presented for a root canal treatment. The patient provided a name, date of birth, phone number, insurance information and Social Security number. The dentist completed the treatment without incident and the offi ce submitted a claim to the insurance company to receive payment for services rendered.
The offi ce staff realized they had been given false information when they received a call from the individual whose Social Security number and insurance information were used to obtain treatment. The caller questioned why his insurance was billed when he was not even a patient at that practice. The offi ce tried calling the individual who was treated, but the woman who answered stated that there was no one there by that name.
Once the offi ce realized that they did not know the true identity of the individual they treated, they contacted the Advice Line for guidance. The Risk Management analyst advised the dentist not to release any information about the mystery patient to the individual whose identity was stolen. The analyst also recommended that the dentist fi le a police report and report the incident to the dental benefi ts plan provider.
This case illustrates the unfortunate reality that medical identity theft has made its way into the dental offi ce. And just as dental offi ces have an obligation to prevent fi nancial identity theft by protecting patients’ personal data, so too do they have an obligation to prevent medical identity theft.
Are Your Patients Who They Say They Are? Preventing Medical Identity Theft
TDIC Risk Management Staff
According to the Ponemon Institute, a private cybersecurity research fi rm, more than 2.3 million people became victims of medical identity theft between 2014 and 2015, representing uninsured individuals seeking care under a stolen identity or, more commonly, obtaining prescription medications fraudulently. On average, patients spent $13,500 to resolve a case of stolen medical identity. But the nonmonetary costs are even greater. Patients report a lack of trust in their medical providers for failing to protect their private data.
According to the Federal Trade Commission, medical identity theft stems from several scenarios. The most common are data breaches within medical care providers, where thieves gain access to medical data systems, and “friendly fraud,” where someone known to the victim assumes his or her identity. Another type of scenario is one wherein thieves target unsuspecting individuals by posing as an employee of an insurance company, pharmacy or medical or dental offi ce and asking for personal information, including plan numbers or Social Security numbers.
You are not a sales goal.
You are a dentist deserving of an insurance company relentless
in its pursuit to keep you protected. At least that’s how we see
it at The Dentists Insurance Company, TDIC. Take our Risk
Management program. Be it seminars, online resources or our
Advice Line, we’re in your corner every day. With TDIC,
you are not a sales goal or a statistic. You are a dentist.
Protecting dentists. It’s all we do.®
800.733.0633 | tdicinsurance.com | CA Insurance Lic. #0652783
C DA J O U R N A L , V O L 4 6 , Nº 1 0
664 O C TO B E R 2 01 8
O C T . 2 0 1 8 R M M A T T E R S
Commonly, these thieves will make false offers of free or discounted care.
Another common source of medical identity theft is a dishonest employee who either steals patients’ private data to sell on the black market or allows uninsured friends or family members to use stolen identity to obtain free dental care.
It’s crucial that dentists know and trust their staff, says Taiba Solaiman, senior risk management analyst at The Dentists Insurance Company. Conducting comprehensive background screenings and random audits of charts and billing activity for any friends or family members who have been seen in the offi ce can go a long way in catching and thwarting illegal activity.
Preventing fraud begins at the front desk. Therefore, it is imperative to instruct employees to ask for photo identifi cation as patients present. It is not a violation of HIPAA and, while it is not required, it is highly recommended. Most dental patients are already familiar and comfortable with providing photo identifi cation when visiting their medical care providers.
Some offi ces take photos of their patients, making it easier to identify patients when they arrive. Many dental software programs have built-in features
to capture photos. If patients are hesitant to have their pictures taken, reassure them that it is only for internal use and will not be posted on social media or used for any marketing purposes. Let them know of your commitment to protect their personal information and prevent fraud.
When training your staff on spotting possible fraudulent patient activities, some red fl ags to look for are:
■ Questionable or altered documents or signatures.
■ Information not matching with information previously collected.
■ Suspicious behavior, such as an inability to quickly answer basic questions.
■ Refusing to present identifi cation or provide identifying information when requested.
■ Forms of identifi cation that don’t match the description of the patient producing them.
■ An accompanying individual addressing the presenting individual with a different name.
Should your practice team spot a red fl ag, it’s advisable to alert the authorities. It is not advisable to refuse treatment; instead, inform the patient that there are discrepancies that need to be looked into
further and then make other arrangements for payment until the issue is resolved.
In addition, ensure that your staff is trained to educate patients on best practices for keeping their private data private. For example, patients should be informed that your staff will never ask for Social Security numbers or dental benefi t plan numbers over the phone, so if they receive unsolicited calls from people requesting this information, they should hang up immediately. Remind patients to carefully review statements from insurance companies to look for suspicious or unauthorized treatments or payments.
Medical identity theft is a multifaceted, complex crime and it takes the diligence of all players — medical and dental professionals, patients, insurance providers and law enforcement — to halt its progress. And while dentists certainly aren’t expected to take on the role of crime fi ghter, there are simple steps they can take to ensure their patients and their practice remain free from fraud. ■
To schedule a confi dential consultation with an experienced risk management analyst, visit tdicinsurance.com/RM consult or call 800.733.0633. TDIC’s Risk Management Advice Line is a benefi t of CDA membership.
usbank.com/practicefinance
Financial options tailored to your practice.Whether you are establishing your career or have an existing
practice, U.S. Bank Practice Finance is your provider for
customized practice financing that may help your business grow.
Advantages of U.S. Bank Practice Finance
• Competitive fixed rates
• Term up to 10 years
• 100% financing options on acquisitions
• No prepayment penalty options
Contact a practice finance specialist today.
Jeramie Eimers | 605.681.7371 | [email protected]
Financing maximums and terms are determined by borrower qualification and use of funds. Credit products offered by U.S. Bank National Association and are subject to normal credit approval and program guidelines. See a banker for details. Deposit products offered by U.S. Bank National Association. Member FDIC. ©2018 U.S. Bank. 36901 6/18

4248 MENLO PARK FACILITY Remodeled, 930 sq. ft. dental facility with2 fully equipped ops. and plumbed for 2 additional ops, reception area,doctor's office, sterilization, lab, storage and restroom. Medical/Dentalbuilding in highly desirable location. Asking $135K.
4246 SUNNYVALE GP Retiring seller offering a well est. general practicewith loyal staff in organized office with 3 fully-euipped ops. Located in highlydesirable neighborhood. 2017 Gross Receipts $540K+. Asking $390K.
4269 SAN JOSE GP Well established practice offering 46 yrs of goodwill.Excellent West San Jose location. 7ops, 5 fully equipped in 2,000 sq. ftfacility. Approx 3,000 active patients, all fee-for-service. 9 days of hygiene/week. Outstanding staff. Average annual GR $1.3M with an adjusted net of$473K. Asking price $1,015,000. Potential to purchase bldg interest, priceto be determined. Owner willing to help in the transition.
4261 CAPITOLA GP Retiring doctor offering an established practice inprofessional office complex built around a garden setting. Beautiful andmodern 1,465 square foot facility with 4 fully-equipped operatories. Averagegross $743K+ with 3 doctor days and 6 hygiene days per week.Approximately 1,800 active patients. Asking $562K.
4267 SAN JOSE GP 36-year established 4 op practice near Willow Glenarea grossing $650K average. 950+ active patients. Beautifully maintainedand updated 1,450 sq. ft. facility. 3-day doctor week, 3 hygiene days.Asking $450K.
4233 SF GP Seller offering 26+ year general practice in SF Financial district.Ground floor office with high volume foot traffic. Approx. 1,200 sq. ft. facilitywith 4 fully-equipped ops. $930K+ avg. annual GR. Seller willing to help for asmooth transition. Asking $640K.
4271 SOUTH SF DENTAL FACILITY Turnkey facility in well knownbeautiful, professional building with dedicated parking lot. Incredible locationwith EZ freeway access to Hwys 280, 380 and 101. Asking only $30K.
4198 PETALUMA DENTAL BUILDING Condominiumized dental officeconveniently located close to Petaluma Valley Hospital and nearby shops,with easy access to Highway 101 and with ample, dedicated parking.Approximately 1,600+ square feet with five (5) fully-equipped operatories setup for right hand delivery. There is a reception area, business office, consultroom, staff lounge, lab, sterilization area, private office and separate storagearea. Asking $495K.
4178 SONOMA COUNTY PERIO Seller retiring from 21 year practice withtrained, seasoned staff and great location. Exceptional 2,100 sq. ft. ampleoffice with 6 fully equipped ops. Majority of equipment purchased in 2002. 4doctor-days & 3 hygiene days per week. Average gross receipts $1M+.Asking $677K.
4225 EUREKA GP & BUILDING Established since 1981 in charmingNorthern California port city. Retiring doctor is offering practice and building.Practice has approximately 1,200 active patients with new patients acceptedon a selective basis. Average Gross Receipts of $765K+ with 61% averageoverhead. Beautiful 1,400 square foot office with four (4) fully-equippedoperatories. Asking price for practice $468K.
4321 SAN JOSE GP Incredible location on the corner of two majorthoroughfares. Seller retiring after 20+ years. Solid, loyal staff and patientbase. 1,200 active patients (Seller is contracted with Delta PPO & Premier) 4ops in 1,400 sq. ft. Seller works 4 days/wk with 4+ hygiene days. AverageGR $739K with average adj net of $282K. Asking price $561K.
4216 SIERRA NEVADA FOOTHILLS 23 year practice located in the heartof the Sierra Nevada foothills in modern building close to downtown area.1,024 square foot office with 4 fully- equipped ops., upgraded majorequipment and digital radiography. Average Gross Receipts $890K+ with56% average overhead. Asking price for practice $604K. Seller is offeringreal estate for sale to the buyer of his practice.
4172 NAPA GP Amazing opportunity to own the practice of your dreams inone of the world’s premier wine destinations! Situated in a primeneighborhood close to many amenities. 1,200 square foot office with 4 fully-equipped and updated operatories. Over 1,000 active patients. Averageannual gross receipts over $700K. Asking price for practice $484K. Buildingavailable for purchase.
4322 MENLO PARK GP Practice in seller owned facility in desireablecorner location in the heart of Menlo Park, 1 block fron Santa Cruz Ave. 60%of patients are private pay. Great upside potential from retiring seller. Asking$25K.
4326 SANTA CLARA GP Practice with an emphasis on Restorativedentistry with over 1,000 active patients located in sought-afterneighborhood close to major routes, shopping centers and hospitals.Approximately 850 sq. ft. facility with 3 fully-equipped ops. pljus a seasonedand loyal staff. Avg. Gross Receipts $617K.
4324 SF GP Seller offering 33 years of goodwill in busy financial districtbldg. Gorgeous 890 sq. ft. office with 3 fully equipped ops (plumbed for 4).Incredible panoramic views with amazing natural light pouring into eachwindow. 500+ active patients. 2 days of hygiene/wk. Current average GRapprox. $410K with adj net of $115K. Asking $282K.
4210 UNION CITY GP Retiring GP offering 40+ years of goodwill. 5 ops in1,100 sq. ft. 350 active patients, all fee-for-service. 2 yr average GR$177K. Asking $85K.
4262 MOUNTAIN VIEW GP Desirable 1,700 square foot Mountain Viewlocation. 5 fully equipped operatories. Average Gross Receipts $886K+ with4 doctor days and 6 hygiene days. Practice with an emphasis on Restorativeand Preventative care. Seller retiring. Great opportunity for a skilled dentist totake over a 35 year practice with seasoned staff and loyal patient base.Asking $619K.
carroll.company [email protected] (650) 362-7004 (650) 362-7007
CARROLL& C O M P A N YV “Matching the Right Dentist to the Right Practice”
SOLD
Mike Carroll Pamela Carroll-Gardiner Mary McEvoy Carroll
Carroll & Company2055 Woodside Road, Suite 160Redwood City, CA 94061BRE #00777682
PENDING
PENDING
SOLD

Making your transition a reality.
www.henryscheinppt.com 1.888.685.81001.800.519.3458
Dr. Lee Maddox
LIC #01801165(949) 675-5578
Dr. Thomas Wagner
Dr. Russell Okihara
Jim Engel
Kerri McCullough
Gina Miller
Steve Caudill
Thinh Tran
Jaci Hardison
• • • ••
C DA J O U R N A L , V O L 4 6 , Nº 1 0
O C TO B E R 2 0 1 8 667
Dental professionals hear much about Cal/OSHA’s blood-borne pathogens, hazard communication and injury and illness prevention regulations
because they require employers to develop written plans and train employees on specifi c elements. These are not the only Cal/OSHA regulations, however. Employers should be aware of other occupational safety regulations applicable to dental facilities. These are found in the California Code of Regulations Title 8 Chapter 4 Subchapter 1 Unfi red Pressure Vessel Safety Orders, Subchapter 3 Compressed Air Safety Orders, Subchapter 5 Electrical Safety Orders and Subchapter 7 General Industry Safety Orders and can be viewed on the Department of Industrial Relations website, dir.ca.gov. This article reviews Cal/OSHA regulations on:
■ Portable fi re extinguishers. ■ Eyewash stations. ■ Exit signs. ■ Maintenance and access to exits.
§6151 Portable Fire ExtinguishersThe regulation applies to the
placement, use, maintenance and testing of portable fi re extinguishers provided for the use of employees. In offi ces where extinguishers are provided but are not intended for employee use and the employer has an emergency action plan and a fi re prevention plan that meet Cal/OSHA requirements, then the employer need only meet the following inspection, maintenance and testing requirements:
■ Monthly visual inspection. ■ Annual maintenance check.
Record date of maintenance check and retain record for one year after last entry.
Other Cal/OSHA Regulations: Fire Extinguishers, Eyewash, Exit SignsCDA Practice Support
Regulatory Compliance
■ Alternate protection must be provided when portable extinguisher is removed from service for maintenance and recharging.
■ Empty and recharge every six years a stored pressure dry chemical extinguisher that requires a 12-year hydrostatic test except if it has a nonrefi llable disposable container.
■ Hydrostatic testing performed by a trained individual with suitable testing equipment and facilities.
Employers should be aware of other occupational safety regulations applicable to dental facilities. These are found in the California Code of Regulations Title 8 Chapter 4.

C DA J O U R N A L , V O L 4 6 , Nº 1 0
668 O C TO B E R 2 01 8
If it is intended for employees to use the fi re extinguishers, an employer must provide training to employees to familiarize them with the general principles of fi re extinguisher use and hazards of their use. Training must be done upon employment and at least annually thereafter. Mount extinguishers on the wall and identify and maintain them in a fully charged and operable condition. They should be kept in their designated locations at all times except during use.
Selection and distribution of fi re extinguishers within the dental facility must be based on type of fi res anticipated in the work place.
OC T. 2018 REGUL ATORY COMPL IANCE
Fire Classifi cation ■ Class A fires include wood,
paper and textiles — place extinguisher every 75 feet or less.
■ Class B fires include flammable liquids — place extinguisher every 50 feet or less.
■ Class C fires include electrical equipment — extinguisher placement dependent on placement of other extinguishers.
■ Class D fires include metal powders and shavings — place extinguisher every 75 feet or less.
Extinguisher Type ■ Water and foam – for
Class A fi res only. ■ Carbon dioxide – for Class
B and C fi res; ineffective on Class A fi res.
■ Dry chemical, multipurpose – for Class A, B and C fi res.
■ Dry chemical, ordinary – for Class B and C fi res.
■ Wet chemical – for kitchen fi res (deep-fat fryers).
■ Clean agent – Class A, B and C fi res.
■ Dry powder – Class D fi res only; ineffective on all other fi res.
■ Water mist – Class A and C fi res. ■ Cartridge-operated dry chemical.1
§5162 Emergency Eyewash and Shower Equipment
A dental facility must have a plumbed or self-contained eyewash or eye/facewash equipment that meets at a minimum the standards set in section 5, 7 or 9 of ANSI Z358.1–1981, “Emergency Eyewash and Equipment.” Personal eyewash units or drench hoses may be used in support of the required equipment but not in lieu of them. The equipment must be in an accessible location that requires no more than 10 seconds for an injured person to reach. Keep the area around the equipment free of obstructions.
The required equipment must be able to supply potable water at 1.5 liters per minute for 15 minutes, which is the fl ow rate and time duration specifi ed in the ANZI standard. The control valve must allow the water fl ow to remain on without requiring the use of an operator’s hands, and the valve must remain activated until intentionally shut off.
CONTINUES ON 670

Lee Skarin & Associates have been successfully assisting Sellers and Buyers of Dental Practices for nearly 30 years in providing the answers to these and other questions that have been of concern to Dentists.
Call at anytime for a no obligation response to any or all of your questionsVisit our website for current listings: www.LeeSkarinandAssociates.com
QUESTIONS MOST OFTEN ASKED BY SELLERS:1. Can I get all cash for the sale of my practice?
2. If I decide to assist the Buyer with financing, how can I be guaranteed payment of the balance of the sales price?
3. Can I sell my practice and continue to work on a part time basis?
4. How can I most successfully transfer my patients to the new dentist?
5. What if I have some reservation about a prospective Buyer of my practice?
6. How can I be certain my Broker will demonstrate absolute discretion in handling the transaction in all aspects, including dealing with personnel and patients?
7. What are the tax and legal ramifications when a dental practice is sold?
QUESTIONS MOST OFTEN ASKED BY BUYERS:1. Can I afford to buy a dental practice?
2. Can I afford not to buy a dental practice?
3. What are ALL of the benefits of owning a practice?
4. What kinds of assets will help me qualify for financing the purchase of a practice?
5. Is it possible to purchase a practice without a personal cash investment?
6. What kinds of things should a Buyer consider when evaluating a practice?
7. What are the tax consequences for the Buyer when purchasing a practice?
805.777.7707 818.991.6552 800.752.7461
CA DRE #00863149
LEE S
KARI
N&
ASSO
CIAT
ES IN
C.
C DA J O U R N A L , V O L 4 6 , Nº 1 0
670 O C TO B E R 2 01 8
Activate plumbed eyewash equipment monthly to fl ush the line and verify proper operation. Logging this activity is highly recommended. Maintain a self-contained unit in accordance with manufacturer’s instructions. Improperly maintained eyewash stations may cause damage to employees’ eyes.2
§3216 Exit SignsExit signs are required for any room
or building that has an occupant load of more than 50. The words on the exit sign must be in block letters at least 6 inches in height with a stroke of not less than 3/4 of an inch. The color or design of the letters must be in strong contrast to the sign background. The luminance on the
face of the sign may not be less than 50 lux. An exit sign must be at every exit door, at the intersection of corridors, at exit stairways or ramps and at other locations and intervals deemed necessary to inform individuals. Exit signs that are required to be electrically illuminated should be lighted with two bulbs, either one of which shall be suffi cient to provide the required luminance on the face of the sign.
§3225 Maintenance and Access to Exits
Every required exit must be kept free of obstructions or impediments at all times. Do not hang draperies, mirrors or other hangings that can conceal or obscure an exit door. No mirror may be placed
adjacent to an exit door. The path to an exit should be kept clear and should not require an individual to pass through a restroom, closet or high-hazard area. ■
REFERENCES
1. Fire Equipment Manufacturers Association. www.femalifesafety.org/types-of-extinguishers.html. Accessed July 27, 2018.2. OSHA InfoSheet. Health Eff ects from Contaminated Water in Eyewash Stations, undated. www.osha.gov/Publications/OSHA3818.pdf. Accessed Aug. 7, 2018.
Regulatory Compliance appears monthly and features resources about laws that impact dental practices. Visit cda.org/practicesupport for more than 600 practice support resources, including practice management, employment practices, dental benefi ts plans and regulatory compliance.
OC T. 2018 REGUL ATORY COMPL IANCE
CONTINUED FROM 668
GET REWARDED THREE WAYS.
SHAREMEMBER BENEFITS.
Offer subject to change. See official guidelines at cda.org/mgm. 1 Rewards issued to referring member once referral joins and pays required dues. Total rewards possible per calendar year are limited to $500 in gift cards from ADA and $500 in value from CDA. 2 Rewards issued to referring member once referral joins, pays required dues and spends $250+ at tdsc.com by December 31, 2018.
THE MORE NEW MEMBERS YOU REFER, THE MORE REWARDS!
Get started at cda.org/mgm.
THERE’S NO BETTER TIME for a member to get a new member. Our newest benefit? Big savings on dental supplies you love from brands you trust through tdsc.com.
1. RECEIVE A $100 AMERICAN EXPRESS® GIFT CARD from ADA.1
2. RECEIVE $100 TO SHOP TDSC.COM from CDA.1
3. RECEIVE $50 MORE to shop tdsc.com if the new member places orders totaling $250.2
Refer your colleagues and be rewarded.
®
6150 HAYWARD Strong Dental DNA. Well-designed 5-op office. Digital radiography computers. 2018 trending $850,000+. 5-days of hygiene. Full Price $200,000. 6149 NOVATO Stand-alone building at busy stop light intersection off Highway 101. All new 2-years ago. 4-ops, digital, paperless, Pano with Ceph at cost of $280,000. At doorway into Hamilton neighborhood with hundreds of homes. No competition. Perfect for nearby DDS to
or Growing Group ing perfect location. Building turn-key office available for purchase. 6148 SAN LEANDRO Great location on Hesperian Boulevard. Absentee owned. Shall collect $400,000 in 2018. Has done $670,000 in recent past with owner here. Associate relocating. Seller’s daughter shall provide transition assistance. 6147 SAN FRANCISCO BAY AREA – “OUT-OF-NETWORK” 2017 collected $2 Million. 2018 tracking $2.15 Million. Hygiene produces $1+ Million. Seller available for long transition. 6146 LOWER SACRAMENTO FOOTHILLS Highly regarded family community. 6-days of hygiene evidences strong foundation. 2017 collected $880,000. 2018 projecting $950,000. 6145 MARIN COUNTY - NOVATO Excellent foundation. Best location, beautiful office, Adec equipped with everything new since 2014. 500-active files. 2018 tracking $250,000. Full Price $125,000.6144 SACRAMENTO AREA 14-days of Hygiene. 2017 collected $1.85 Million. Strong staff. 7-ops. Great location. Condo optional purchase.6143 BERKELEY’S ALTA BATES VILLAGE Perfect for nearby Premier Dentist to relocate their practice into stand-alone building on Webster Street. 3-day week collected $550,000 in 2017. 4-days of Hygiene.6142 OAKLAND’S PIEDMONT - “OUT-OF-NETWORK” 3-ops, paperless and Planmeca ProMax. 2017 collected $667,000. Profits $300,000+. Successor should be proficient in Ortho or willing to learn.Seller available for transition.6141 NAPA VALLEY’S ST. HELENA 3-day per week PPO practice.3-days Hygiene. 2017 Collected $359,000. Attractive 3-op office.15- m th. Full Price $100,000.6140 SAN RAFAEL entist retir . Delta PPO provider. Has averaged $390,000 in collections on 26.5-hour week. $223,000+ in Profits in 2017. Full Price $125,000.6139 S BAY AREA PROS PRACTICE - “OUT-OF-NETWORK” 2017 billed $1.2 Million, collected $1.19 Million. 4-days of Hygiene. Owner available for transition. 6138 SILICON VALLEY Best technology and well-designed suite.2017 collected $900,000+ with Profits of $420,000. Perfect for Dentist wishing to create high-end brand.6129 FOSTER CITY – “OUT-OF-NETWORK” Wish to infuse your nearby practice with quality patients? $5 0,000 in
part-time schedule. Seller and Hygienist shall relocate into Buyer’s practice to transition patients. Full Price $100,000.6122 SANTA CLARA Best exposure in beautiful strip center on El Camino Real. 5-Ops. Delta PPO practice currently trending $1 Million in Collections on 4-days. Perfect platform to operate 6-days a week.Wants to do $1.5+ Million.
YWARDW Strong Dental DNA Well-designed 5-op off
NORTHERN CALIFORNIA(415) 899-8580 – (800) 422-2818
Raymond and Edna [email protected]
California DRE License 1422122
SOUTHERN CALIFORNIA(714) 832-0230 – (800) 695-2732Thomas Fitterer and Dean George
California DRE License 324962
ALTA LOMA Hi dentity Grossing $700 . 5 ops 3-equipped.
BAKERSFIELD Will do $1 Million. $650 includes RE. BAKERSFIELD Grossing $1 . Owne works 16-
Nets $300 . BAKERSFIELD AREA Grossing $40K/mth on 2-days. 5-ops. BELLFLOWER Part-time doing $100 . FP $65
Latino. Absentee. Grosses $350 . 5-ops. CORONA Near Capistrano Beach exit. Part-time grossing $200 DEL MAR -- ENCINITAS grossing near $400K. 4-ops. DIAMOND BAR Million Dollar location-to-be. 4-ops digital pan. DIAMOND BAR Hi dentity Asian center. 5-ops. ill do $1 Million.GARDENA Did $2 Million when Owner here. Doing $1.5 GLENDALE / BURBANK Grosses $840 . Includes apt. INLAND EMPIRE Adec, cone beam. Gross $1.3. Incl RE. INLAND EMPIRE DentiCal gross near $300K. FP $150 . INLAND EMPIRE Union Practice can do $1+ Million. INLAND EMPIRE 2 practices grossing $1.8 Right
does $3 GorgeousIRVINE rossing $1.2 Million. 5-ops. LA MIRADA Like new 5-ops, 3-equipped. Grossing $450 . LANCASTER Successor will do $1 2 Area booming. NORTH LONG BEACH Hi Identity. 50% Latino. Only $75K.
Million practice. 5-op across from Starbucks.
OC BEACH 6-ops, Dentrix, digital, computerized. FP $150 OC BEACH Absentee owned, grossing $550 . 4-ops. OC BEACH Grossed $100K last month. F $900,000.OC BEACH Grossing $1 Million. 4-ops cone beam. OC’S FASHION ISLAND Grossing $650K. Rare opportunity.
Doing $1.5 but can do $2 Million. PEDO Chinese & Latino. Grosses $450 . F $285,000. REDLANDS Once did $1 Million. Grossing over $400 .
Empty 9-op office in 10,000 sq.ft. building near 210. Did $1+ Million.RIVERSIDE Grossing $250 . 30-new pts/mth. FP $165 .SANTA CLARITA 70,000 cars pass daily. 8-ops. FP $250K.THOUSAND OAKS / AGOURA HILLS 5-ops, part-time
rossing $500 TORRANCE Entrance to P Verdes. Grossing $300
. F $290 .Grossing $135 part-time. 3-ops.
WEST COVINA Grossing $650 . 2 days hygiene.
PracticesWanted
NORT
Specialists in the Sale and Appraisal of Dental PracticesServing California Dentists since 1966
How much is your practice worth??Selling or Buying, Call PPS today!

Largest Broker in Northern California
Over $34.5M in 2017 sales
Extensive Buyer Database &
Unsurpassed Exposure allows us to offer you
Better Candidate
Better Fit
Better Price
BAY AREA CONTINUED CC-846 SAN RAFAEL: Prof/Retail Building Complex. 3 ops 640 sf Collections $433k in 2017 $$295k CG-616 NAPA: State-of-the-Art practice and on track to do $100k more in 2018. SSeller is ready for retirement! $425k CG-859 SONOMA: On track to collect over $700k in 2018! 2000sf w/ 4 ops highly esteemed FFS Prac-tice $$395k CN-878 VALLEJO: Highly desirable thriving communi-ty! 2 story prof bldg. 2000 sf w/4 ops $$315k DC-812 REDWOOD CITY Facility: Reasonable rent and great landlord! 740 sf w/ 3 fully equipped ops $65k DG-844 SAN JOSE: Beloved prac ce delivers quality care and warm rela onships which pa ents have come to expect. 1500sf 3 ops + 1 add’l. $$195k/ Real Estate Available! DG-854 SUNNYVALE: Do your best den stry here to an educated, diverse, family-oriented, business-friendly popula on! 782sf w/ 3 ops $$875k DG-862 MID-PENINSULA: Prac ce is a rare gem with up to 7 operatories in the Bay Area!! 1800sf w/ 6ops + 1 add’l. $475k DG-865 SANTA MARIA: Live and prac ce in this de-sirable collegiate coastal community! 930sf w/ 3 ops $$395k DG-868 SUNNYVALE: Hesitate and you might lose out on the prac ce of your dreams! 1350sf w/ 5 ops. $$725k DN-771 SOQUEL Facility: The perfect place to sink down roots, raise a family & build an empire! 1100sf w/2 ops + 1 add’l. $$38,500 DG-785 SANTA CRUZ: Great price and cash flow for only 3 days a week!! 1000sf w/ 4 ops. Seller Mo -vated: $165k DG-842 FREMONT: Imagine being able to live, prac ce and play here! 3200 sf w/ 10 ops $$395k DG-857 SAN JOSE: Do the math - this associate-driven prac ce with profitability consistently! 1709 sf w/5 ops $$595k DG-892 SAN JOSE: Excellent loca on and stellar reputa on in a one-of-a-kind se ng! 1500 sf w/ 3 ops + 2 add’l. $$295k DN-806 WATSONVILLE: This quality, family-oriented prac ce thrives $ focuses on delivering quality care. 1,182 SF W/ 4 OPS. $$495K/ Real Estate TBD DN-845 FREMONT Facility: Build your dream Prac ce! Primed for success in this proven loca-
on! 1800sf w/3 ops + 2 add’l. $$90k
BAY AREA AC-782 SAN FRANCISCO: Well maintained, mul -level Professional Medical Complex. 1450 sf w/ 5 ops $$195k AC-886 SAN FRANCISCO (Facility): Unsurpassed visibility & loca on! Poten al here is limitless! 850 sf w/ 3 ops $85k AC-893 SAN FRANCISCO (Facility): Amazing Move In Ready Facility in Union Square. 1000 sf w/ 3 ops $75k AG-852 SAN FRANCISCO: PRIME LOCATION! 600 sf w/ 2 fully equipped, computerized ops. RReduced Price: $365k AG-871 SAN FRANCISCO: The LOCATION of this office is the envy of all! 600 sf w/ 2 ops $$88k AG-880 SAN FRANCISCO: Seller re ring a er 39 years! Remodeled in 2010. ~ 700 sf w/ 2 ops $$350k AG-895 SAN FRANCISCO: This prac ce has a stellar reputa on and delivers the highest quality of den s-try! 1500 sf w/ 4 ops $675k AG-896 SAN FRANCISCO: Don’t less this opportunity pass you by! ~ 1300 sf w/ 2 ops $$600k AG-900 SAN FRANCISCO: State-of-the-art equip-ment in this prac ce, already primed for proven success at this loca on. 2000sf w/ 5 ops $$695k BC-710 WALNUT CREEK: Desirable location. Stand-alone, single-story bldg. 1313sf w/ 3 ops $$150k BC-741 DANVILLE (FACILITY): Move in Ready facility to build the practice of your dreams! ~ 1600sf w/ 3 fully equipped ops $$150k BC-789 OAKLAND (Facility): Perfect layout for Pedo or Ortho. 2800 sf w/ 6 fully equipped ops. Plumb-er for 2 add’l $$135k BC-894 BRENTWOOD: Perfect loca on – Will be your best purchase ever! 1230 sf w/ 2 ops. Plumbed for 2 add’l $$225k BG-734 ANTIOCH: The perfect place to work, live and play! Located in desirable professional neigh-borhood. 1,323 sf w/ 4 ops. $$315k BG-839 PINOLE: Sink your roots into this community which retains many “turn-of-the-century” buildings! 1212sf w/ 3 ops + 1 add’l. $$350k BN-891 PINOLE: This one won’t last! Build your dental empire in this bedroom community! 1300sf w/3 ops. $$425k CC-798 PETALUMA: Partially equipped dental office for lease. Only $2500/mo for 1400 sf! Call for De-tails! CC-802 SANTA ROSA: Retail shopping center w/ 1200 sf and 4 fully equipped ops $$220k or $260k w/CT Scanner
NORTHERN CALIFORNIA EC-729 GREATER SACRAMENTO AREA:
Call for details!EN-664 SACRAMENTO Facility:
Now Only: $30k EN-755 FOLSOM:
Now Only: $100k EN-791 SO. SACRAMENTO CO:
$495k EG-788 ROSEVILLE:
. Reduce Price $275k/ Real Estate Available EG-849 AUBURN:
$350k EG-887 FOLSOM Facility:
Priced for quick Sale! $50k EN-797 WOODLAND:
Prac ce $575k/ Real Estate TBD EN-831 SACRAMENTO“a cut above” Now Only: $650k EN-836 CITRUS HEIGHTS:
$188k EN-858 ORANGEVALE:
Priced to Sell Only $70k! EN-885 ROSEVILLE Facility:
$95k EN-899 DIXON:
$195k FC-650 FORT BRAGG:
$350k for the Prac ce & $400k for the Real Estate FG-841 ARCATA:
$275k/Real Estate TBD FN-754 SO. HUMBOLDT:
Now $150k! FN-855 NO. HUMBOLDT:
$275kGG-769 REDDING AREA:
Prac ce $390k/ Real Estate $540k GN-799 PARADISE:
Prac ce $375k, Real Estate $325k GN-853 REDDING:
$595k GN-884 YUBA CITY Real Estate w/ Equip:
$400kHG-815 SIERRA CO: Reduced Price: $165k/ Real Estate $437k HG-827 SO. LAKE TAHOE:
$310k HG-851 SO LAKE TAHOE:
$425k
NORTHERN CALIFORNIA CONTINUED HN-618 SIERRA FOOTHILLS:
$65k HN-740 SHASTA CO:
$475k/ Real Estate $350k HN-773 SUTTER CREEK: Seller Mo vated!
! $175k HN-816 CHESTER/ALMANOR AREA:
Prac ce $140k/ Real Estate TBD HN-879 SONORA:
$275k
CENTRAL VALLEY & SOUTHERN CALIFORNIA IG-832 OAKHURST: $235k/ Real Estate 375kIG-881 TURLOCK:
$360K IN-764 STOCKTON:
$267.5k JC-811 FRESNO COUNTY:
$350kJC-823 LOS BANOS:
$80kJG-778 FRESNO:
$275k JG-807 FRESNO:
Seller Mo vated $99kKG-779 SAN CLEMENTE Ortho:
$325k/ Real Estate Available!
SPECIALTY PRACTICES AC-748 SAN FRANCISCO Perio:
$750kBC-784 CENTRAL CONTRA COSTA CO Perio:
$395k BG-843 WALNUT CREEK Perio
Reduced Price: $595kEG-903 CARMICHAEL Oral Surgery:
Amazingly Priced: $450k EN-821 DAVIS Perio:
$385k EN-822 SACRAMENTO Perio:
$790k JG-757 VISALIA Perio:
Reduced Price: $350k
800.641.4179 [email protected] “ASK THE BROKER” WWW.WESTERNPRACTICESALES.COM

Largest Broker in Northern California
Over $34.5M in 2017 sales
Extensive Buyer Database &
Unsurpassed Exposure allows us to offer you
Better Candidate
Better Fit
Better Price
BAY AREA CONTINUED CC-846 SAN RAFAEL:
$295kCG-616 NAPA:
Seller is ready for retirement! $425k CG-859 SONOMA:
$395kCN-878 VALLEJO:
$315kDC-812 REDWOOD CITY Facility:
$65k DG-844 SAN JOSE:
$195k/ Real Estate Available!DG-854 SUNNYVALE
$875kDG-862 MID-PENINSULA:
$475k DG-865 SANTA MARIA:
$395k DG-868 SUNNYVALE:
$725kDN-771 SOQUEL Facility:
$38,500 DG-785 SANTA CRUZ:
Seller Mo -vated: $165k DG-842 FREMONT:
$395kDG-857 SAN JOSE:
$595k DG-892 SAN JOSE:
$295k DN-806 WATSONVILLE:
$495K/ Real Estate TBD DN-845 FREMONT Facility:
$90k
BAY AREA AC-782 SAN FRANCISCO:
$195kAC-886 SAN FRANCISCO (Facility):
$85k AC-893 SAN FRANCISCO (Facility):
$75kAG-852 SAN FRANCISCO:
Reduced Price: $365k AG-871 SAN FRANCISCO:
$88k AG-880 SAN FRANCISCO:
$350k AG-895 SAN FRANCISCO:
$675k AG-896 SAN FRANCISCO:
$600kAG-900 SAN FRANCISCO:
$695k BC-710 WALNUT CREEK:
$150kBC-741 DANVILLE (FACILITY):
$150kBC-789 OAKLAND (Facility):
$135kBC-894 BRENTWOOD:
$225kBG-734 ANTIOCH:
$315k BG-839 PINOLE:
$350k BN-891 PINOLE: This one won’t last!
$425k CC-798 PETALUMA:
CC-802 SANTA ROSA:$220k or $260k w/CT
Scanner
Jon B. Noble, MBA Mona Chang, DDS John M. Cahill, MBA
NORTHERN CALIFORNIA EC-729 GREATER SACRAMENTO AREA: Seller re ring! FFS Prac ce and Real Estate Available! CCall for details! EN-664 SACRAMENTO Facility: Great corner loca on, excellent visibility & easy access! 2300sf w/ 4 ops. NNow Only: $30k EN-755 FOLSOM: A perfect loca on, envied by all! Enjoy an amazing qual-ity lifestyle in this thriving city. 1200sf w/ 4 ops. NNow Only: $$100k EN-791 SO. SACRAMENTO CO: Highly esteemed prac ce to an adoring & apprecia ve pa ent base! 1950sfw/ 5 ops. $$495k EG-788 ROSEVILLE: Do not pass up on this remarkable opportunity! 2700sf w/ 6 ops.. Reduce Price $275k/ Real Estate Available EG-849 AUBURN: Imagine living in a peaceful, rural town that has an ideal climate and “big city” ameni es less than an hour away. 1400 sf w/ 4 ops $350k EG-887 FOLSOM Facility: Build the prac ce of your dreams here! 1200 sf w/ 2 ops Priced for quick Sale! $50k EN-797 WOODLAND: Do not hesitate or this enviable opportunity will fulfill someone else’s dream! 2316sf w/ 6 ops. PPrac ce $575k/ Real Estate TBD EN-831 SACRAMENTO: Loca on & prac ce philosophy make this opportunity “a cut above” others! ~1600sf w/4 ops. NNow Only: $$650k EN-836 CITRUS HEIGHTS: well-established, quality prac ce comes loaded W/ 30+ years of goodwill. 1300sf w/3 ops + 2 add’l. $$188k EN-858 ORANGEVALE: Perfect for a second loca on or satellite situa on! 850 sf w/ 3 ops. PPriced to Sell Only $70k! EN-885 ROSEVILLE Facility: Looking for the ideal loca on, great visibility, and close to just about anything? Here it is! 1000sf w/3 ops. $$95k EN-899 DIXON: State-of–the-art office, with all the “bells and whis-tles”! This fantas c prac ce has 3 ops. $$195k FC-650 FORT BRAGG: Family-oriented prac ce. 5 ops in 2000sf, 6 npts/mo $$350k for the Prac ce & $400k for the Real Estate FG-841 ARCATA: Live and own a little slice of heaven, when you practice here! 1114sf w/3 ops $$275k/Real Estate TBD FN-754 SO. HUMBOLDT: If you love the lure of sea air, a relaxed lifestyle & charm of coastal living, then look no further! 1500sf w/ 3 ops + 1 add’l. Now $$150k! FN-855 NO. HUMBOLDT: Seller reloca ng! Long-established, quality 100% fee-for-service prac ce could be yours! 1600sf w/ 3ops + 1 add’l. $$275k GG-769 REDDING AREA: Offering a full spectrum of general den stry and total care! 2700sf w/ 6ops. PPrac ce $390k/ RReal Estate $540k GN-799 PARADISE: This remarkable opportunity is undeniably too good to be true! 1800sf w/ 4 ops. PPrac ce $375k, Real Estate $325k GN-853 REDDING: A great place to visit…and an even be er place to live, work and play! 1450sf w/ 5 ops $$595k GN-884 YUBA CITY Real Estate w/ Equip: Designed specifically w/ pa ent flow &efficiency in mind. 1750sf w/ 5 ops. $$400k HG-815 SIERRA CO: Perfect location for outdoor enthusiast! 1000 sf w/ 3 ops Reduced Price: $165k/ Real Estate $437k HG-827 SO. LAKE TAHOE: Ski, live, play and prac ce here where your lifestyle can’t be beat! 1200sf w/4 ops. $310k HG-851 SO LAKE TAHOE: Don’t wait another day to start living your dream of a serene lifestyle! 2100 sf w/ 5 ops $$425k
NORTHERN CALIFORNIA CONTINUED HN-618 SIERRA FOOTHILLS: Seller Retiring! Huge opportunity for growth by increasing office hours! 750sf w/ 2 ops $$65k HN-740 SHASTA CO: Beau ful mountain community, well-established prac ce, excep onal long-term staff. 2400+sf w/5 ops + 1 add’l. $$475k/ Real Estate $350k HN-773 SUTTER CREEK: Seller Mo vated! Loca on known for beau ful scen-ery, excellent wine & rich history! 1536sf w/4 ops + 1 add’l!! $175k HN-816 CHESTER/ALMANOR AREA: The perfect place to work, live and play! Do not hesitate, or this prac ce will be gone! 1250 sf w/ 4ops. Prac ce $140k/ Real Estate TBD HN-879 SONORA: Live and prac ce in the cap va ng beauty of this family-oriented, scenic town in Tuolumne County! 2950 sf w/ 3 ops $275k
CENTRAL VALLEY & SOUTHERN CALIFORNIA IG-832 OAKHURST: 2048sf w/3 ops + 1 add’l. $$235k/ Real Estate 375k IG-881 TURLOCK: Offering a philosophy to provide “Nothing but the Very Best” in dental care! 10 ops $$360K IN-764 STOCKTON: Well-established, fully computerized, paperless, digital-ized prac ce just wai ng for your talent & skill! 5,000sf w/10 ops $$267.5k JC-811 FRESNO COUNTY: Amazing Opportunity! Considerable Goodwill in Community! 3,000 sf w/ 6 ops $$350k JC-823 LOS BANOS: Unique opportunity. Heavy emphasis on hygiene. Growth poten al by increasing DDS days. 1000 sf w/ 3 ops $$80k JG-778 FRESNO: What a steal. Consistent collec ons over $600k with cash flow over $300k!! 1452 sf w/ 4 ops $$275k JG-807 FRESNO: Reasonable Overhead, Stellar Reputa on, Excellent Loca-
on! 1000 sf w/3 ops SSeller Mo vated $$99k KG-779 SAN CLEMENTE Ortho: Huge growth potential by expanding work week! 2896 sf w/ 6 open bay chairs $$325k/ Real Estate Available!
SPECIALTY PRACTICES AC-748 SAN FRANCISCO Perio: Reputable PERIO practice with million dollar Bay views! 980 sf w/ 3 ops $$750k BC-784 CENTRAL CONTRA COSTA CO Perio: Seasoned Staff. Office runs like well-oiled machine! 3 ops $$395k BG-843 WALNUT CREEK Perio: Collec ons over $1M! Great gross and profit for only 2 ½ days per week! 1085sf w/ 4 ops RReduced Price: $595k EG-903 CARMICHAEL Oral Surgery: Gross receipts were over $1.1 million in 2017! Stable pa ent base won’t be affected by transi on! 2282sf w/ 5 ops Amazingly Priced: $450k EN-821 DAVIS Perio: Live, prac ce & play here! It’ll be the BEST decision you’ll ever make! 1700sf w/4 ops + 1 add’l. $$385k EN-822 SACRAMENTO Perio: This prac ce is known throughout Sacramento for its stellar reputa on! 2200sf w/ 5 ops + 1add’l. $$790k JG-757 VISALIA Perio: Keep implants in house and imagine the growth possibilities! 9 hygiene days per week! Rare Gem! 2,000 sf w/ 5 ops Reduced Price: $350k
Edmond P. Cahill, JD Timothy Giroux, DDS
800.641.4179 [email protected] “ASK THE BROKER” can now be found at WWW.WESTERNPRACTICESALES.COM
C DA J O U R N A L , V O L 4 6 , Nº 1 0
674 O C TO B E R 2 01 8
A look into the latest dental and general technology on the market
Tech Trends
Dental Patient Education ($49.99, 3D4Medical)
The ability to take three-dimensional, layered models of the human anatomy to demonstrate dental conditions and procedures for patients has long been a goal of every provider looking to educate their patients using technology. Physical models and expensive professional videos have tried to meet this goal with limited success. 3D4Medical, an award-winning creator of medical and fi tness software, developed the Dental Patient Education app, available on macOS and iPad, to integrate valuable patient education content with the latest in 3D technology.
The Dental Patient Education app (iPad version) centers on a beautifully detailed 3D model of the human head. Users can swipe to rotate and use single- and multiple-fi nger double-tap gestures to zoom in and out of the model. Layers of anatomy can be explored by adding and removing them at a tap of a button. Certain anatomical objects in specifi c layers, such as teeth, can be further isolated by a double tap on superimposed blue zoom icons located throughout various layers in the 3D model. Users can subsequently take these isolated objects and apply drag gestures to cut and view them cross-sectionally. Every part of the anatomy is labeled in a searchable index that points users to a specifi c layer and area on the 3D model. No matter which layer is being viewed on the 3D model, users can easily navigate back to the top layer through a home icon on the upper left. Custom pins and annotations can be placed anywhere for quick reference. In addition to anatomy, the app contains a searchable index of more than 200 animation videos with audio narration categorized by conditions, treatment, prevention and diagnostics to off er patients a unique chairside educational experience. Providers can take any image of the 3D model viewed and send it to patients through text messaging or email attachment using the share button.
The user interface is rich with features, but discovering them is not intuitive. Navigation tips are prominently displayed throughout the app to help users learn the interface.
— Hubert Chan, DDS
CephNinja (Free to $49 per year)
Reliable handheld devices with responsive touch interfaces, minimal maintenance costs and information synchronization can streamline many practice workfl ows, from patient chart management to laboratory case tracking. However, the reality of mobile clinical technology contrasts with this envisioned ideal, replete with pitfalls like HIPAA security concerns, information barriers between diff erent applications and general user-unfriendliness. CephNinja, a subscription-based Android and iOS cephalometric analysis application, highlights both the great potential and frustrating obstacles of mobile technology for clinical dentistry. This review utilized an iPhone X and focuses on the free version of the application, which has limited access to the gamut of orthodontic analyses and contains commercial ads.
Described by the CephNinja creators as a “powerful cephalometric analysis and patient management tool,” it presents itself as a comprehensive solution for those interested in performing orthodontic treatment. Its main screen is dedicated to information entry as it has options to upload radiographs, add photographs, input progress notes and even manage 3D models. Patient information can be transferred into CephNinja via email, the mobile device’s camera roll or Microsoft’s OneDrive. Once a ceph has been uploaded, the analysis workfl ow is identical to other cephalometric analysis software: crop the image, calibrate the ruler, pick the analysis, then plot the points. According to Cyncronus, there have been two studies that compared CephNinja’s results favorably versus hand tracing. The basic Wit’s analysis, which was available in the free version, appeared to be accurate and repeatable across multiple uses. The resulting analysis can be saved then shared as a PDF through email, text message or any cloud storage system.
Despite the promising ease of use and seeming accuracy in its analyses, CephNinja has no discernible security measures — anyone with access to the phone will have access to CephNinja’s patient records. Transferring patients both to and from CephNinja relies on potentially HIPAA noncompliant methods like email and cloud storage. Finally, CephNinja does not appear to have any integrations with any other EHRs, making the information diffi cult to use as it has no other patient management functionality (patient billing comes to mind as a potential hurdle if CephNinja is used). CephNinja is undoubtedly promising and, for instruction in an educational setting, imminently useful as only de-identifi ed patient information is being used. For an active clinical practice, CephNinja does not address the security concerns.
— Alexander Lee, DMD

The Artand Scienceof Dentistry
See what brings the best and brightest in dentistry together.
FIND YOUR WONDER
ENGAGE with speakers, experts and your team
EXPAND your education with new C.E. courses
EXPLORE innovations and deals from exhibitors
EXHALE at local attractions and events after hours
Discover all the nation’s premier dental convention
has to offer during three days of memorable
learning, skill-building and networking. Learn more
at cdapresents.com.
Anaheim, CA May 16–18, 2019*May 14–16, 2020
at CDA Presents
*Registration opens Jan. 2, 2019
San Francisco2019 – ADA meetingSept. 10–12, 2020

THE NEXT GENERATION of the Ultrapro Tx Prophylaxis Equipment Family
Our next generation Ultrapro Tx prophylaxis equipment family features an
ergonomic handpiece, innovative prophy angle cup designs, and splatter-
free prophy pastes. Together they offer a powerful, comfortable, and
effective solution to all your polishing needs.
ULTRADENT. COM800.552.5512
Learn more at ultradent.com/ultraprotx




















