Needs - Journal - World Neurosurgery.pdf
12
Evolving Societal Risks and Necessary Precautions in the Age of Nuclear Power and Therapeutic Radiation: An American Perspective Martin H. Pham 1 , Cheng Yu 1,3 , Mairead Rusch 4 , Charles Holloway 5 , Eric Chang 2 , Michael L. J. Apuzzo 1 INTRODUCTION The terrorist attacks on September 11, 2001, in the United States have generated a national climate of heightened awareness to the ever-present risk of violence against large civilian populations. Deliberate at- tacks by terrorist organizations using chemical, biologic, radiologic, or nuclear agents can terrify and disrupt large por- tions of society, which renders these agents tremendously more dangerous than conventional weaponry. In our age of nu- clear therapeutics, the acquisition of radioactive materials with the intention to perpetrate radiologic or nuclear terrorism is a constant possibility. This fact is underscored in light of the death of a Russian spy in London from polonium-210 as well as 2 radiation exposure devices left in Moscow in the mid-1990s (14). Many iterations of radiologic and nuclear terrorism exist with the possession of radioactive material, and awareness of the potential use of these radioactive sources is an essential first step toward protection and prevention. A successfully executed attack in the United States would have far-ranging consequences across the social, political, economic, and medical landscapes. As yet, there have been no major radiologic attacks in the United States. However, the threat of hazard remains. This article discusses terrorism involving nuclear and radiologic weapons in the context of our current ubiquitous use and access to nuclear therapeutics. Special focus is placed on cobalt-60 and the Lek- sell Gamma Knife (Elekta AB, Stockholm, Sweden) because of its high potential for use in a weaponized radiologic device. Although many of the rules and regula- tions discussed are requirements regarding radiation safety, security, and protection in the United States, the po- tential dangers inherent with using high-energy radioisotopes are present worldwide. RADIATION Much of the terror from a radiologic or nuclear device detonation comes from the harmful radiation exposure and area contamination from radioactive fallout. Harmful radiation injures cells through both somatic and genetic effects. Imme- diate somatic effects involve damage and destruction to enzymes, structural pro- teins, and other organelles and molecules required for cellular function. This is typically a consequence of high-radiation exposure and results in cell damage, tissue injury, and organ failure. Genetic effects are typically delayed and can result from both low-radiation and high-radiation doses. These effects are largely due to ra- diation injury on cellular DNA, which render it susceptible to mutation and carcinogenesis (34). Harmful radiation can be in the form of particles (alpha particles, beta particles, neutrons) or energy in the form of electromagnetic radiation (ultra- violet, x-ray, and gamma rays). Table 1 summarizes the different types of radia- tion that are commonly encountered in everyday life and in the medical and commercial industries. NUCLEAR MEDICINE AND MEDICAL RADIATION THERAPEUTICS With regard to nuclear therapeutics, a difference exists between radioactivity Terrorism involving nuclear or radiologic weapons can devastate populations, city infrastructures, and entire sociopolitical systems. In our age of nuclear medicine and therapeutic radiation delivery, the unauthorized and illegal acquisition of radioactive materials needed for such an attack is always a possibility and risk. Physicians handling high-energy isotopes for medical radiotherapy must be aware of the basic security requirements as outlined by the Nuclear Regulation Commission, which include background checks and authorized access, physical protection during radionuclide use, and physical protection during its transit. The Leksell Gamma Knife and its Category 1 cobalt- 60 radioactive source are discussed because of their significant potential for deployment in a weaponized device. Although this article presents a perspective relating to American rules and regulations, these precautions are applicable anywhere that similar situations exist. Understanding these materials and the security they require is essential to preventing the disastrous outcomes should these isotopes fall into terrorists’ hands. Key words - Dirty bomb - Gamma Knife - Nuclear weapon - Radiation dispersion device - Radiosurgery - Terrorism Abbreviations and Acronyms BWR: Boiling water reactor CFR: Code of Federal Regulations NRC: Nuclear Regulatory Commission RDD: Radiation dispersion device From the Departments of 1 Neurosurgery and 2 Radiation Oncology, Keck School of Medicine, Los Angeles; and 3 Department of Radiation Physics, 4 Gamma Unit, and 5 Security Operations, Keck Hospital of USC, Los Angeles, California, USA To whom correspondence should be addressed: Martin H. Pham, M.D. [E-mail: [email protected]] Citation: World Neurosurg. (2014) 82, 6:1060-1070. http://dx.doi.org/10.1016/j.wneu.2014.09.007 Supplementary digital content available online. Journal homepage: www.WORLDNEUROSURGERY.org Available online: www.sciencedirect.com 1878-8750/$ - see front matter Published by Elsevier Inc. 1060 www.SCIENCEDIRECT.com WORLD NEUROSURGERY, http://dx.doi.org/10.1016/j.wneu.2014.09.007 SPECIAL ARTICLE Peer-Review Reports
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Needs - Journal - World Neurosurgery.pdf

SPECIA
LARTIC
LE
Peer-Review Reports
Evolving Societal Risks and Necessary Precautions in the Age of Nuclear Power and
Therapeutic Radiation: An American Perspective
Martin H. Pham1, Cheng Yu1,3, Mairead Rusch4, Charles Holloway5, Eric Chang2, Michael L. J. Apuzzo1
Terrorism involving nuclear or radiologic weapons can devastate populations,city infrastructures, and entire sociopolitical systems. In our age of nuclearmedicine and therapeutic radiation delivery, the unauthorized and illegalacquisition of radioactive materials needed for such an attack is always apossibility and risk. Physicians handling high-energy isotopes for medicalradiotherapy must be aware of the basic security requirements as outlined bythe Nuclear Regulation Commission, which include background checks andauthorized access, physical protection during radionuclide use, and physicalprotection during its transit. The Leksell Gamma Knife and its Category 1 cobalt-60 radioactive source are discussed because of their significant potential fordeployment in a weaponized device. Although this article presents a perspectiverelating to American rules and regulations, these precautions are applicableanywhere that similar situations exist. Understanding these materials and thesecurity they require is essential to preventing the disastrous outcomes shouldthese isotopes fall into terrorists’ hands.
Key words- Dirty bomb- Gamma Knife- Nuclear weapon- Radiation dispersion device- Radiosurgery- Terrorism
Abbreviations and AcronymsBWR: Boiling water reactorCFR: Code of Federal RegulationsNRC: Nuclear Regulatory CommissionRDD: Radiation dispersion device
From the Departments of 1Neurosurgery and2Radiation Oncology, Keck School of Medicine,
Los Angeles; and 3Department of Radiation Physics, 4GammaUnit, and 5Security Operations, Keck Hospital of USC, LosAngeles, California, USA
To whom correspondence should be addressed:Martin H. Pham, M.D.[E-mail: [email protected]]
Citation: World Neurosurg. (2014) 82, 6:1060-1070.http://dx.doi.org/10.1016/j.wneu.2014.09.007
Supplementary digital content available online.
Journal homepage: www.WORLDNEUROSURGERY.org
Available online: www.sciencedirect.com
INTRODUCTION
The terrorist attacks on September 11,2001, in the United States have generated anational climate of heightened awarenessto the ever-present risk of violence againstlarge civilian populations. Deliberate at-tacks by terrorist organizations usingchemical, biologic, radiologic, or nuclearagents can terrify and disrupt large por-tions of society, which renders theseagents tremendously more dangerous thanconventional weaponry. In our age of nu-clear therapeutics, the acquisition ofradioactive materials with the intention toperpetrate radiologic or nuclear terrorismis a constant possibility. This fact isunderscored in light of the death of aRussian spy in London from polonium-210as well as 2 radiation exposure devices leftin Moscow in the mid-1990s (14). Manyiterations of radiologic and nuclearterrorism exist with the possession of
1878-8750/$ - see front matter Published by Elsevier Inc.
1060 www.SCIENCEDIRECT.com
radioactive material, and awareness of thepotential use of these radioactive sourcesis an essential first step toward protectionand prevention. A successfully executedattack in the United States would havefar-ranging consequences across thesocial, political, economic, and medicallandscapes.As yet, there have been no major
radiologic attacks in the United States.However, the threat of hazard remains.This article discusses terrorism involvingnuclear and radiologic weapons in thecontext of our current ubiquitous use andaccess to nuclear therapeutics. Specialfocus is placed on cobalt-60 and the Lek-sell Gamma Knife (Elekta AB, Stockholm,Sweden) because of its high potential foruse in a weaponized radiologic device.Although many of the rules and regula-tions discussed are requirementsregarding radiation safety, security, andprotection in the United States, the po-tential dangers inherent with usinghigh-energy radioisotopes are presentworldwide.
RADIATION
Much of the terror from a radiologic ornuclear device detonation comes from the
WORLD NEUROSURGERY, http://
harmful radiation exposure and areacontamination from radioactive fallout.Harmful radiation injures cells throughboth somatic and genetic effects. Imme-diate somatic effects involve damage anddestruction to enzymes, structural pro-teins, and other organelles and moleculesrequired for cellular function. This istypically a consequence of high-radiationexposure and results in cell damage, tissueinjury, and organ failure. Genetic effectsare typically delayed and can result fromboth low-radiation and high-radiationdoses. These effects are largely due to ra-diation injury on cellular DNA, whichrender it susceptible to mutation andcarcinogenesis (34). Harmful radiation canbe in the form of particles (alpha particles,beta particles, neutrons) or energy in theform of electromagnetic radiation (ultra-violet, x-ray, and gamma rays). Table 1summarizes the different types of radia-tion that are commonly encountered ineveryday life and in the medical andcommercial industries.
NUCLEAR MEDICINE AND MEDICALRADIATION THERAPEUTICS
With regard to nuclear therapeutics, adifference exists between radioactivity
dx.doi.org/10.1016/j.wneu.2014.09.007

Table 1. Types of Radiation
UV Rays X-Rays Gamma Rays Neutrons Beta Particles Alpha Particles
Ionizing energy Low High High Very high Very high Very high
Body penetration Superficial Deep Deep Deep Moderate Superficial
Potential for harm Moderate Moderate Moderate High High Moderate
Common source Sun, welding Medical imaging Cosmic radiation,radioactive decay
Cosmic radiation,radioactive decay
Cosmic radiation,radioactive decay
Cosmic radiation,radioactive decay
Materials that block Sunscreen, UV eyeprotection, anythingblocking visible light
Lead and othermetals
Thick metal suchas lead, tungsten,steel
Paraffin, water Thick aluminum,plastic glass
Paper, clothes,water, skin
The types of electromagnetic and particle radiation commonly encountered either in daily life or in the medical and commercial sectors are compared. Different radiation types have differentenergies, abilities to penetrate the body, and potential for harm. Common sources of these types of radiation and routine blocking materials are compared as well.
UV, ultraviolet.From Yamamoto LG: Risks and management of radiation exposure. Pediatr Emerg Care 29:1016-1026 [quiz 1027-1029], 2013 (34).
Table 2. Characteristics of Various Diagnostic and Therapeutic Medical Isotopes
RadioactiveSubstance Half-Life Medical Use
DisintegrationRadiationRelease
Cesium-137 30 years Medical radiotherapy Beta, gamma
Cobalt-57 272 days Schilling test for vitaminB12 excretion
Beta, gamma
Cobalt-60 5.3 years Stereotactic radiotherapy,sterilization of equipment
Beta, gamma
Gallium-67 3 days Nuclear medicine imaging Gamma
Technetium-99m 6 hours Nuclear medicine imaging Beta, gamma
Indium-11 3 days Nuclear medicine imagingfor white blood cell scans
Gamma
Iodine-123 13 hours Nuclear medicine imagingfor thyroid scans
Gamma
Iodine-131 8 days Thyroid radiation ablationtreatment
Beta, gamma
Iridium-192 74 days Brachytherapy Beta, gamma
Radium-223 11 days Bone metastasis treatment Alpha, beta, gamma
Strontium-89 51 days Bone metastasis treatment Beta, gamma
Strontium-90 29 years Bone metastasis treatment Beta
Xenon-133 5 days Ventilation/perfusion lungscan
Beta, gamma
Thallium-201 3 days Cardiac stress test Gamma
Radionuclides used in medical radiotherapy and radiosurgery are listed with half-lives, typical medical uses, and type ofradiation decay.
From Yamamoto LG: Risks and management of radiation exposure. Pediatr Emerg Care 29:1016-1026 [quiz 1027-1029],2013 (34).
SPECIA
LARTIC
LE
PEER-REVIEW REPORTS
MARTIN H. PHAM ET AL. NUCLEAR POWER AND THERAPEUTIC RADIATION
and radiation. A radioactive substancecontinuously decays and emits ionizingradiation secondary to an inherentinstability of its atomic structure. Cobalt-60, iridium-192, and cesium-137 are ex-amples of radioactive isotopes used fortherapeutic radiotherapy. Conversely, aradiation device such as an x-ray ma-chine or linear accelerator are sources ofradiation when turned on, but becausethey are not radioactive substances, theydo not emit ionizing radiation when theyare off (34). Table 2 lists several radio-active isotopes that are commonly usedin nuclear imaging and medicalradiotherapy.Radioactive sources typically used by
the military and nuclear power plant in-dustry are known as the “military 4”(tritium, uranium-235, plutonium-239, andamericium-241) and are well guarded withsophisticated security systems (24, 34).University research hospitals as well ascommercial industry are typically associ-ated with a different set of radioactivesources termed the “university 7” (tritium,carbon-14, phosphorus-32, cobalt-60,iodine-125, iodine-131, and californium-252) and the “industrial 3” (iridium-192,cesium-137, and cobalt-60) (24, 34). All 3industry-associated radionuclides are alsoused in therapeutic radiation delivery andare often found in the hospital or univer-sity setting as well. This grouping lies inthe relatively lower security protocolsassociated with these latter isotopes,which means there is an increased risk oftheir acquisition by terrorist organizationsfor destructive purposes.
WORLD NEUROSURGERY 82 [6]: 1060-10
NUCLEAR WEAPONS AND RADIATIONDEVICES
The method of a terrorist attack usingradioactive material can take the form of
70, DECEMBER 2014 www
both nuclear and radiologic weapons.Nuclear fission bombs (also known asatomic bombs) use either uranium orplutonium to create a chain reaction
.WORLDNEUROSURGERY.org 1061

SPECIA
LARTIC
LE
PEER-REVIEW REPORTS
MARTIN H. PHAM ET AL. NUCLEAR POWER AND THERAPEUTIC RADIATION
through the impact of a sudden criticalmass. The subsequent explosion istremendous and would be similar to whatoccurred at Hiroshima and Nagasaki.Nuclear fusion bombs (also known ashydrogen or thermonuclear bombs) usethe fusion of deuterium and tritium intohelium first through an internal fissiondetonation; the resulting fusion releases amassive explosion several orders ofmagnitude greater than their fission bombcounterparts (34). In addition to thedestructive blast wave and firestorms, bothtypes of nuclear devices would cause sig-nificant radioactive fallout from theincomplete fissile material. A fusion bombwould release its radioactive substanceswith a greater dispersive energy secondaryto its greater blast effect.The detonation of a true nuclear
weapon by a terrorist organization wouldhave to occur through the illegal acquisi-tion and subsequent importation of astolen nuclear weapon for use against theUnited States. The devastation to thepopulation, the environment, and thelong-term economic and political climatewould be tremendous. The likelihood ofthis event occurring is not very high (32).Similarly, the likelihood of a terroristgroup creating its own nuclear weaponthrough the use of an improvised nucleardevice is a low-probability event (5). Thetechnical challenges of assembling animprovised nuclear device along with thedifficulty of obtaining large enoughamounts of weapons-grade uranium orplutonium are regarded as barriers toogreat to make this a probable method of anuclear attack (2, 32).Any discussion of nuclear or radiologic
terrorism must include the considerationof an attack on a nuclear power plant fa-cility as a means of contaminating theenvironment and atmosphere with highlyradioactive material. The effect of violentsabotage of a nuclear power plant wouldlikely resemble the outcomes of the 3 mostwell-known plant accidents involving the1979 Three Mile Island (Pennsylvania,USA), 1986 Chernobyl (Ukraine in theformer Soviet Union), and 2011 Fukushima(Japan) nuclear reactor accidents (3, 4, 34).Although destructive, a terrorist attack ona nuclear power plant is also a low-prob-ability event because of their multiplecontainment protocols and high-securitysafeguards (32).
1062 www.SCIENCEDIRECT.com
The creation of a radioactive dirtybomb, also known as a radiation disper-sion device (RDD), is an event of muchhigher probability. By combining a con-ventional explosive with a radioactivesubstance that is relatively easier to obtain,the subsequent detonation would use thebomb blast as the delivery method forradioactive contamination over theaffected area (1, 34). This radiologicterrorism scenario has the highest proba-bility of successful execution because ofthe relatively simple assembly required ofthe device. The most difficult step wouldbe obtaining and handling the radioactivematerial for placement within the con-ventional explosive (32). Another scenarioas an extension of this principle would bethe use of a concealed radiation exposuredevice. The goal of a radiation exposuredevice would be to expose people toionizing radiation without their knowl-edge (1). This possibility is highlighted inthe 1993 placement of a gamma ray sourcein a Moscow businessman’s office and the1995 irradiation of a Moscow park withcesium-137 by Chechen rebels (14).A successful radiologic attack within the
United States would have significant social,political, economic, and long-lasting med-ical repercussions. Kelly (13) described 3scenarios modeling the use of RDDs beforethe Senate Foreign Relations committee in2002; 2 scenarios used high-energy gammaemitters, and the third used an alpha par-ticle emitter. The first scenario was a pea-sized source of cesium-137 within an RDDdetonated at Union Station in Washington,D.C. The second scenario used a cobalt-60explosion at the southern end of Manhat-tan. The third scenario employed a smallsource of americium-241 with 1 lb of 2,4,6-trinitrotoluene at Times Square in NewYork (13, 32).In all 3 scenarios, the acute effects would
mostly be from the blast injury radius of theexplosion itself. The long-term effectswould come from the resulting panic,decontamination process, impact on thelocal and national economy, and potentialincrease in cancer risk from latent radia-tion. Following stringent EnvironmentalProtection Agency guidelines concerningpermissible levels of residual radioactivity,the potential cleanup of americium-241around Times Square would cost >$50billion, whereas cleanup of the more highlycontaminated cobalt-60-irradiated areas of
WORLD NEUROSURGERY, http://
Manhattan could cost almost $2 trillion (13,32). The level and area of contaminationwould be the greatest in the cobalt-60 sce-nario because it has the largest specific ac-tivity of the 3 radioactive agents.
COBALT-60 AND LEKSELL GAMMA KNIFE
The development of a RDD has the high-est possibility of being used as a terroristradiologic attack because of the social,economic, and political disruption causedspecifically by the radiation fallout.Although uranium and plutonium havereceived significant attention because oftheir use in nuclear weapons, the specificactivity of these radionuclides is muchlower than many commonly used radio-isotopes in medicine. For example, thespecific activity of uranium-235 is 2.1 mCiper gram, whereas that of cobalt-60 is 1100Ci per gram; this means it would take>1000 lb of enriched uranium-235 to equalthe radioactivity of 1 mg of cobalt-60.The highly radioactive and portable na-
ture of these therapeutic radioisotopesputs the risks of successfully developing a“dirty bomb” not at nuclear reactors andweapons facilities but at relatively moreaccessible medical and industrial unitsusing these sources. The potential risk ofuse of cobalt-60 in a RDD is particularlyhigh because of its high specific activityand long half-life. This section discussesthe synthetic creation of cobalt-60 andsubsequent incorporation into the LeksellGamma Knife for therapeutic radio-surgery. Because the Leksell Gamma Knifedevice houses these cobalt-60 sources,special attention is given to its design andthe rules and regulations that govern itsuse. Although the Leksell Gamma Knife iselegantly sophisticated in its role as atherapeutic radiosurgical instrument, it isa potential source of danger that must beprotected and safeguarded.
Cobalt-60 RadioisotopeThe cobalt-60 radioisotope is createdthrough neutron activation of the naturallyoccurring stable element cobalt-59. Thisneutron activation process occurs throughthe substitution of the steel control rodswith cobalt-59 rods in a CANada Deute-rium Uranium nuclear reactor or includingcobalt-59 pellets within the fuel assem-blies in the reactor core of a boiling waterreactor (BWR) nuclear power plant. In
dx.doi.org/10.1016/j.wneu.2014.09.007

Figure 1. Photograph and schematic diagram of the cobalt-60 bushing andcap. (A) Photograph shows the aluminum bushing holder and its steel cap.(B) Schematic demonstrates how the 8-mm double stainless steel weldedcapsule containing the cobalt-60 pellets is held within the bushing.
SPECIA
LARTIC
LE
PEER-REVIEW REPORTS
MARTIN H. PHAM ET AL. NUCLEAR POWER AND THERAPEUTIC RADIATION
each circumstance, cobalt-59 is exposed tothe significant neutron flux within thenuclear plant and becomes the syntheticradionuclide cobalt-60. This activationprocess alone takes 18e24 months (9, 17,18). Once created, cobalt-60 has a half-lifeof 5.27 years and undergoes beta decayinto nickel-60, releasing high-energygamma rays in the process.The production of cobalt-60 has mostly
come from international CANada Deute-rium Uranium power reactors, whichinclude Bruce B, Pickering, Gentilly, andChalk River stations in Canada; Embalseand Atucha 1 in Argentina; Qinshan PhaseIII units 1 and 2 in China; and Wolsong 1and 2 in South Korea. Canada’s nuclearresearch reactor at Chalk River producesroughly 75% of the global supply of cobalt-60 (21). In 2010, the Clinton NuclearGenerating Station near Clinton, Illinois,USA, began production of cobalt-60 usingits single BWR (27); it was subsequentlyjoined by the Hope Creek GeneratingStation in Lower Alloways Creek Town-ship, New Jersey, USA, later that year us-ing its single BWR as well (29). Both ofthese nuclear reactors use technologyprovided by GE Hitachi Nuclear Energy(Wilmington, North Carolina, USA), andthe raw cobalt-60 from each BWR is pro-cessed at GE Hitachi Nuclear Energy. Thecobalt-60 from Canada’s Chalk River nu-clear research reactor is processed andmanufactured by Nordion, Inc. (Ottawa,Ontario, Canada).In 2006, the U.S. Nuclear Regulatory
Commission (NRC) implemented regula-tions for the National Source TrackingSystem to provide a centralized registry forcertain high-risk radioactive materials,including cobalt-60 (28). This registry wascreated as a mandate by Congress in theEnergy Policy Act of 2005 and developedfollowing recommendations by the jointNRCeDepartment of Energy report in 2003on the potential use of RDDs or “dirtybombs” employing radioactive sources (23,31). The tracking system was subsequentlydeployed in January 2009 to account forhigh-risk radioactive sources used in in-dustry, medicine, and research (30). Whencobalt-60 is created and processed forcommercial or industrial use, it is assigneda permanent NRC tracking number tomonitor its location, use, and subsequentdisposal in the interests of public safety andsecurity.
WORLD NEUROSURGERY 82 [6]: 1060-10
In preparation for implementation forGamma Knife radiosurgery, the cobalt-60sources themselves aremanufactured in theform of a double stainless steel weldedcapsule. This capsule has an outer diameterof 8mmand aheight of 27mmand contains20 cobalt-60 pellets that are nominally 1mm in diameter with a length of 1 mm (6).The sealed cobalt-60 may also be in theform of a powder or a solid rod. Thesesource capsules are placed in aluminumbushings with stainless steel threaded lidsthat are 28 mm in diameter and 31.4 mm inlength (Figure 1). Each source capsule andits matching bushing are engraved with aunique NRC serial tracking number. Thesesource bushings are placed within theGamma Knife housing for subsequentradiosurgical delivery.
Gamma Knife Housing DesignAn understanding of the Gamma Knifehousing is needed to appreciate how thecobalt-60 sources are contained and usedwithin the unit. The threat of a terroristattempt to remove these cobalt-60 sourcesforcibly from the Gamma Knife housingexists; the security and safeguards of thesesources are discussed later in this article.Although removal of the cobalt-60 sourceswould expose the unshielded individualattempting the theft to an enormousamount of gamma radiation, this may notbe a concern to terrorist organizations inan era of suicide bombings andmartyrdom.The first Gamma Knife prototype unit
was originally introduced by Swedishneurosurgeon Lars Leksell in 1967. Since
70, DECEMBER 2014 www
then, the Gamma Knife radiosurgical de-vice has been used to treat variousneoplastic, vascular, and intractable painsyndromes. The initial Gamma Knife ra-diation housing designs were, in chrono-logic order, Models S, U, B, C/4C, andPerfexion. The current Perfexion unit iscompletely redesigned and differs signifi-cantly from prior designs.The initial designs of the Gamma Knife
housing units incorporated 201 cobalt-60sources housed in the central body of theunit. These sources produced 201 colli-mated beams to a single focal point at themachine’s isocenter. The radiation unitsthemselves had a hemispherical orienta-tion at different gantry angles dependingon the specific model design. The newerPerfexion unit instead uses 192 cobalt-60sources housed along movable sectors in acone-section configuration. This designreduces the amount of radiation goingthrough the long axis of the patient’s body(Figure 2) (15).Earlier Gamma Knife models had 1 pri-
mary collimator within the housing unitand 4 interchangeable secondary collimatorhelmets that were mounted manually.These collimator helmets were attached tothe bed, and the patient’s head wasattached to the helmet via the stereotacticframe. The stereotactic frame was movedsmall distances to center the radiation de-livery at the intended targets throughmanual trunnion adjustments or with arobotic automatic positioning system in theModel C. Choices of collimator helmetsincluded apertures of 4 mm, 8 mm, 14 mm,and 18 mm (Figure 3). For the Perfexion
.WORLDNEUROSURGERY.org 1063
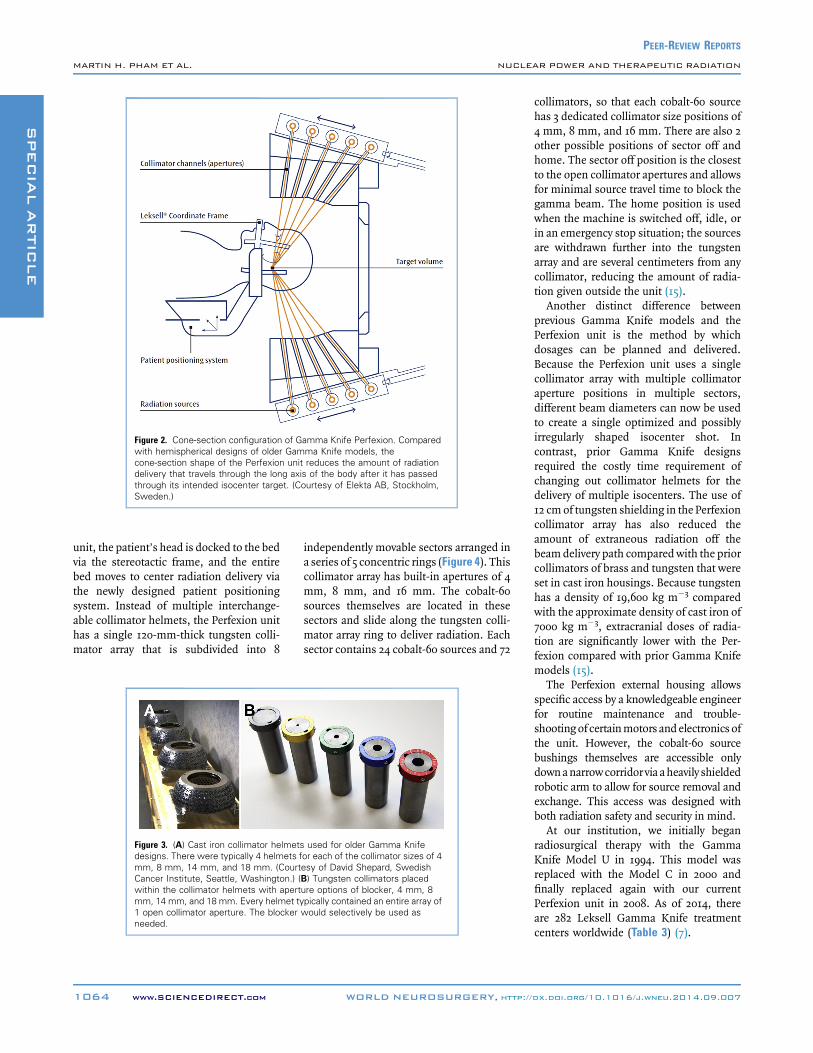
Figure 2. Cone-section configuration of Gamma Knife Perfexion. Comparedwith hemispherical designs of older Gamma Knife models, thecone-section shape of the Perfexion unit reduces the amount of radiationdelivery that travels through the long axis of the body after it has passedthrough its intended isocenter target. (Courtesy of Elekta AB, Stockholm,Sweden.)
SPECIA
LARTIC
LE
PEER-REVIEW REPORTS
MARTIN H. PHAM ET AL. NUCLEAR POWER AND THERAPEUTIC RADIATION
unit, the patient’s head is docked to the bedvia the stereotactic frame, and the entirebed moves to center radiation delivery viathe newly designed patient positioningsystem. Instead of multiple interchange-able collimator helmets, the Perfexion unithas a single 120-mm-thick tungsten colli-mator array that is subdivided into 8
Figure 3. (A) Cast iron collimator helmetdesigns. There were typically 4 helmets fmm, 8 mm, 14 mm, and 18 mm. (CourtCancer Institute, Seattle, Washington.) (within the collimator helmets with apertmm, 14 mm, and 18 mm. Every helmet t1 open collimator aperture. The blockerneeded.
1064 www.SCIENCEDIRECT.com
independently movable sectors arranged ina series of 5 concentric rings (Figure 4). Thiscollimator array has built-in apertures of 4mm, 8 mm, and 16 mm. The cobalt-60sources themselves are located in thesesectors and slide along the tungsten colli-mator array ring to deliver radiation. Eachsector contains 24 cobalt-60 sources and 72
s used for older Gamma Knifeor each of the collimator sizes of 4esy of David Shepard, SwedishB) Tungsten collimators placedure options of blocker, 4 mm, 8ypically contained an entire array ofwould selectively be used as
WORLD NEUROSURGERY, http://
collimators, so that each cobalt-60 sourcehas 3 dedicated collimator size positions of4 mm, 8 mm, and 16 mm. There are also 2other possible positions of sector off andhome. The sector off position is the closestto the open collimator apertures and allowsfor minimal source travel time to block thegamma beam. The home position is usedwhen the machine is switched off, idle, orin an emergency stop situation; the sourcesare withdrawn further into the tungstenarray and are several centimeters from anycollimator, reducing the amount of radia-tion given outside the unit (15).Another distinct difference between
previous Gamma Knife models and thePerfexion unit is the method by whichdosages can be planned and delivered.Because the Perfexion unit uses a singlecollimator array with multiple collimatoraperture positions in multiple sectors,different beam diameters can now be usedto create a single optimized and possiblyirregularly shaped isocenter shot. Incontrast, prior Gamma Knife designsrequired the costly time requirement ofchanging out collimator helmets for thedelivery of multiple isocenters. The use of12 cmof tungsten shielding in the Perfexioncollimator array has also reduced theamount of extraneous radiation off thebeamdelivery path comparedwith the priorcollimators of brass and tungsten that wereset in cast iron housings. Because tungstenhas a density of 19,600 kg m�3 comparedwith the approximate density of cast iron of7000 kg m�3, extracranial doses of radia-tion are significantly lower with the Per-fexion compared with prior Gamma Knifemodels (15).The Perfexion external housing allows
specific access by a knowledgeable engineerfor routine maintenance and trouble-shootingof certainmotors and electronics ofthe unit. However, the cobalt-60 sourcebushings themselves are accessible onlydownanarrowcorridor via aheavily shieldedrobotic arm to allow for source removal andexchange. This access was designed withboth radiation safety and security in mind.At our institution, we initially began
radiosurgical therapy with the GammaKnife Model U in 1994. This model wasreplaced with the Model C in 2000 andfinally replaced again with our currentPerfexion unit in 2008. As of 2014, thereare 282 Leksell Gamma Knife treatmentcenters worldwide (Table 3) (7).
dx.doi.org/10.1016/j.wneu.2014.09.007

Figure 4. Gamma Knife Perfexion tungsten collimator array and a schematicwithin its housing unit. (A) The single tungsten collimator array is dividedinto 8 sectors arranged in a series of 5 concentric rings. The sectorsthemselves can move independently of each other to acquire 4-mm, 8-mm,or 16-mm beams. (B) Schematic with the collimator array within thePerfexion outer housing unit. (Courtesy of Paula Petti, Taylor McAdam BellNeuroscience Institute, Fremont, California.)
Table 4. Nuclear RegulatoryCommission Title 10 Code of FederalRegulations Part 20 Radiation Limits
Occupational Radiation Dose Limits(annual, in mSv)
Total dose 50
Sum deep-dose to anyindividual organ (except lens)
500
Lens of eye 150
Skin 500
Public Radiation Dose Limits (annual, inmSv)
Total dose 1
Total dose (for visitors) 5
Dose from any unrestrictedarea
0.02 in anygiven hour
The Nuclear Regulatory Commission developed guide-lines to provide standards for protection againstionizing radiation. These guidelines were created toensure that the receipt, possession, use, transfer,and disposal of radioactive material do not exceedthese safety levels.
SPECIA
LARTIC
LE
PEER-REVIEW REPORTS
MARTIN H. PHAM ET AL. NUCLEAR POWER AND THERAPEUTIC RADIATION
Radiation Vault Design and ShieldingThe terrorist use of a RDD would haveconsiderable repercussions because of thewidespread radiation exposure from deto-nation of such a device. The importance ofradiation protection is highlighted in theNRC Title 10 Code of Federal Regulations
Table 3. Leksell Gamma KnifeTreatment Centers Worldwide
Region Number of Centers
Africa 3
Asia/Pacific 35
China 18
Europe/Middle East 44
Japan 48
Latin America 8
North America 126
As of September 2, 2014, these are the number ofGamma Knife treatment centers worldwide as pro-vided by Elekta AB, Stockholm, Sweden.
WORLD NEUROSURGERY 82 [6]: 1060-10
(CFR) Part 20, which discusses several re-quirements regarding safe radiation expo-sure levels to medical personnel and thepublic when using high-energy therapeuticradiation devices (Table 4) (25). The sig-nificant protective shielding requirementsdiscussedhere demonstrate the devastatingand dangerous nature of the unshieldedrelease of these radioactive substancesinto the general public by terroristorganizations.Per NRC Title 10 CFR Part 20, total
annual occupational radiation levels mustnot exceed 50 mSv or a sum of deep-doseradiation to any individual organsexcluding skin and eyes of 500 mSv. Thelens of the eyemust not exceed an exposureof 150 mSv, and the skin has a limit of 500mSv. Annual radiation limits to the publicmust not exceed 1mSv or 5mSv for visitors.Radiation doses in any unrestricted areaaccessible to the public cannot exceed 0.02mSv in any given hour. Annual backgroundradiation doses fromnatural sources withinthe United States are roughly 3.1 mSv peryear (20).
70, DECEMBER 2014 www
Specifically for the Gamma Knife, Na-tional Council on Radiation ProtectionReport 151 was released in 2005 to guidestructural shielding designs specifically formegavoltage x-ray and gamma-ray radio-therapy devices. These guidelines statethat shielding designs should have goalssuch that uncontrolled areas receive radi-ation exposure levels of 1 mSv per year,whereas controlled areas receive levels of 5mSv per year (19, 33).The design of the radiation vault is a
complicated endeavor that is typicallydone with the aid of contracted radiationphysicists. In designing the bunker, loca-tions are identified that require shieldingcalculations based on estimated shieldeddose rates from the radiation source.These shielding calculations include ma-terial barrier thickness, the material’stenth-value layer, workload, occupancyfactor, and distance to the radiation source(16). When these calculations are com-plete, they are communicated to both thearchitect and the contractor for subse-quent adaptation to the construction ofthe vault. Typical materials used for radi-ation vault construction include steel,lead, concrete, and high-density concrete.
.WORLDNEUROSURGERY.org 1065

Table 5. Densities of CommonMaterials Used in Radiation VaultDesign and Shielding
Material Density (lb/ft3)
Asphalt 125
Concrete 147
Concrete (high-density) 288
Earth 94
Lead 708
Steel 484e503
Gamma rays are better absorbed by materials with highatomic numbers and high density, although the mostimportant factor is the total mass per area in thepath of the gamma ray.
SPECIA
LARTIC
LE
PEER-REVIEW REPORTS
MARTIN H. PHAM ET AL. NUCLEAR POWER AND THERAPEUTIC RADIATION
Asphalt can be used as ceiling shielding ifthere is a parking lot placed over the ra-diation vault. Table 5 lists the densities ofthese materials used in calculations forradiation bunker designs (19).
At our institution, the radiation vaultwas initially designed and constructed in1994 in preparation for the Gamma KnifeModel U (Figure 5). Because the gammaunit is 1 level underground, architecturaldesigns included a ceiling hatch thatallowed for lowering of the Gamma Knifehousing down into the treatment area.Our ceiling hatch design incorporated aclosed ceiling cover owing to a parkinglot right above our underground gammaunit; other institutions with above-groundgamma units have shielded their ceilinghatches to function as skylights as well(10, 12). Radiation calculations provided arequirement of at least 12e14 inches ofhigh-density concrete around our gammaroom and treatment area during thera-peutic Gamma Knife use (Figure 6).However, the initial unshielded loadingof the cobalt-60 sources into the GammaKnife Model U unit housing released asignificant amount of radiation. To ac-count for this release of radiation, thefoot section of the gamma unit room wasconstructed with 3e4 feet of concrete and
Figure 5. Early architectural design of the gamma uniSouthern California. The gamma room was designedtable and hoists required of early Gamma Knife designcameras were installed for both patient monitoring and
1066 www.SCIENCEDIRECT.com
built with a temporary concrete wall toshield the significant radiation exposureduring this step. Once the cobalt-60sources were loaded into the GammaKnife with its supplementary built-inshielding, the temporary wall wasremoved, and the Gamma Knife wasmoved into its permanent therapeuticlocation. Total time from design tofinished construction was roughly 3e6months. A radiation survey of our gamma
t at the University ofto include the helmets. Multiple televisionsecurity. The ceiling
hatch within the vestibule tGamma Knife units from abincorporated in this plan for
WORLD NEUROSURGERY, http://
unit conducted after installation of theGamma Knife Model U demonstratedradiation exposures of 0.009e0.01 mSv inany given hour, well below the re-quirements of NRC Title 10 CFR Part 20.When we acquired the Model C in
2000, a small temporary concrete bunkerwas constructed above ground to facili-tate shielded loading of the cobalt-60sources within the new unit. This tem-porary bunker was much more cost-effective than recreating the temporarywall below ground as we had done withthe Model U. It also significantlyreduced the clinical downtime of thegamma unit and allowed us to continueradiosurgical treatment of patients withthe Model U until the Model C wasloaded with its radiation sources. TheModel C was exchanged with the ModelU and placed into the undergroundgamma room via the ceiling hatch. In2008, the newly redesigned GammaKnife Perfexion unit (Figure 7) wasinstalled. Because of its superior internaltungsten collimator array shielding, aseparate concrete cell was not needed forcobalt-60 source loading. Our currentradiation vault design exceeded its radi-ation shielding requirements, and wewere able to exchange Gamma Knife
hat allowed for both delivery and exchange ofove ground is shown. An examination room isframe placement.
dx.doi.org/10.1016/j.wneu.2014.09.007

Figure 6. Gamma treatment area layout including required thickness ofhigh-density concrete to meet radiation shielding standards. (A) Overall floorlayout of thegammaunit demonstrating thesignificantshielding requirementsspecifically around both the gamma room and the unit. Clinician workroomsare seen just outside the gamma unit to be used for daily work and planning.
(B and C) Cross sections through the gamma room demonstrating extra-thickconcrete to account for initial unshielded source loading of the Gamma KnifeModel U. The requirement of 2e4 feet of high-density concrete around thetemporary room and wall established within the gamma room itself to blockthe radiation from the source loading is noted.
SPECIA
LARTIC
LE
PEER-REVIEW REPORTS
MARTIN H. PHAM ET AL. NUCLEAR POWER AND THERAPEUTIC RADIATION
units and load the Perfexion unit cobalt-60 sources in our existing gammaroom without further construction. The
Figure 7. Gamma Knife Perfexion unit inunit was installed into our gamma roomfinal location. Its position is the same as
WORLD NEUROSURGERY 82 [6]: 1060-10
design and construction of a typical ra-diation vault costs approximately $1e2million (6).
its radiation vault. The Perfexionin 2008 and is shown here in itsthe prior Model U and Model C.
70, DECEMBER 2014 www
Security Regulations and VulnerabilitiesMost significant with regard to the securityand protection of the Gamma Knife arethe standardized national requirements setforth by the NRC to protect cobalt-60 as aCategory 1 radioactive source. Describedin their NRC Title 10 CFR Part 37 guide-lines, they are broken down into back-ground checks and authorized access,physical protection during radionuclideuse, and physical protection during itstransit (26). They are structured to providea basis for institutions to develop a secu-rity program that prevents theft or sabo-tage of the high-energy radioisotope.Table 6 summarizes these requirements.With regard to background check and
access to the radioactive source, the NRCrequires a system in place to review the“trustworthiness and reliability” ofpersonnel with unescorted access autho-rizations as well as the individuals whogrant such determinations. This system
.WORLDNEUROSURGERY.org 1067

Table 6. Outline of Nuclear Regulatory Commission Title 10 Code of Federal Regulations Part 37 Materials Security Programs
� Background Investigations and Access Authorization Program
B Procedures to appoint and certify “reviewing officials” who will then be making “trustworthiness and reliability determinations” for unescorted access in additionto background investigations and fingerprinting; certification of reviewing officials requires personal history disclosure, fingerprint check, background in-vestigations, and an FBI criminal history records check
B Background investigations include fingerprinting, FBI identification and criminal history records check, verification of true identity, verification of employmenthistory, verification of education, determination of character and reputation, and any other information
� Physical Protection Requirements During Use
B Requires implementation of a security program designed to monitor, detect, assess, and respond to an actual or attempted unauthorized access, to includenonbusiness hours as well
B Should have a training program to include instruction on the purpose of function of the security measures themselves, the appropriate response time to securityalarms, and the responsibility to report to LLEA about an actual or attempted theft, sabotage, or diversion
B Verification of coordination with LLEA to include a description of the facility, security measures, and the requirement of an armed response in a timely fashion
B Use and storage of radioactive material within designated security zones to provide isolation of material and a physical barrier that allows access through accesscontrol points
B Capability to monitor continuously and detect all unauthorized entries into security zones and provide an alarm and response even in the event of loss of primarypower
B Monitoring and detection must be by monitored intrusion system linked to onsite/offsite central station, an electronic device for alarm detection that will alertnearby personnel, a monitored video surveillance system, or direct visual surveillance by approved individuals in or outside the security zones
B Verification of means to detect unauthorized removal of radioactive material from the security zone
� Physical Protection in Transit
B Location for requested delivery of radioactive material must be authorized and verified
B A safe haven for shipments include these criteria: located near the transportation route and readily available for the transport vehicle, law enforcement is presentor accessible for a timely response, site is readily identified and well-lit with parking and emergency access on a 24-hour basis, and additional communicationssystems are available if the transport vehicle system fails
B Advanced notification required to the NRC and governor of the state
B Physical protection of shipments by road require a movement control center, redundant communications, continuous and active telemetric position monitoringsystem, individual accompanying driver, and contingency procedures
B Movement control center should be a remote location providing 24-hour monitoring, communication, and emergency service with appropriate law enforcementagencies; redundant communications include cellular phones, satellite phones, or 2-way radios; telemetric position monitoring through radiofrequency identi-fication or satellite-based GPS system
The NRC developed requirements for the physical protection of any facility that houses or uses a Category 1 or 2 radioactive source, which includes cobalt-60. The requirements are structuredto provide a basis for institutions to prevent theft, sabotage, or interference of their radioisotope. The requirements themselves are subdivided into 3 major sections: Background In-vestigations and Access Authorization Program, Physical Protection Requirements During Use, and Physical Protection in Transit.
FBI, Federal Bureau of Investigation; LLEA, local law enforcement agencies; NRC, Nuclear Regulatory Commission; GPS, Global Positioning System.
SPECIA
LARTIC
LE
PEER-REVIEW REPORTS
MARTIN H. PHAM ET AL. NUCLEAR POWER AND THERAPEUTIC RADIATION
must include background investigationsvia fingerprinting, Federal Bureau ofInvestigation identification and criminalhistory records checks, verification ofidentity, verification of both education andemployment history, and a determinationof character and reputation.The requirement of physical protection
of the radioactive source during use re-volves around the implementation of asecurity program that allows for contin-uous monitoring, detection, assessment,and response to unauthorized access evenin the loss of primary power. There is anexpectation that this security program is incoordination with local law enforcement
1068 www.SCIENCEDIRECT.com
agencies that would provide an armedresponse in a timely fashion as well. Theradioactive source must be in a designatedsecurity zone that would provide bothisolation and a physical barrier throughwhich access is obtained only through anaccess control point. There must also be ameans to monitor, detect, and respond tounauthorized removal of the radioactivematerial from the security zone itself.Lastly, the NRC has delineated pre-
requisites for the transportation and de-livery of a Category 1 radioactive sourcesuch as cobalt-60. The location for requestdelivery must be authorized and verified,and advanced notification must be sent to
WORLD NEUROSURGERY, http://
both the NRC and the governor of thestate. This safe haven location must bereadily accessible to the transport vehicle,must be well lit with parking and emer-gency access on a 24-hour basis, and musthave communications capability shouldthe transport vehicle system fail. In addi-tion, law enforcement must be present oraccessible for a timely response. Thephysical protection of the transport vehiclemust include a remote movement controlcenter for 24-hour monitoring, communi-cation, and emergency services with lawenforcement agencies. The vehicle mustalso have redundant communicationsabilities via cellular phone, satellite phone,
dx.doi.org/10.1016/j.wneu.2014.09.007

Table 7. Basic Security Measures toBe Considered with High-EnergyRadioactive Isotopes
� Security Department
B Open communication
SPECIA
LARTIC
LE
PEER-REVIEW REPORTS
MARTIN H. PHAM ET AL. NUCLEAR POWER AND THERAPEUTIC RADIATION
or 2-way radios and must be equippedwith a continuously active telemetricposition monitoring system via radio-frequency identification or a satellite-based Global Positioning System.The time period during which an old
cobalt-60 source needs to be exchangedwith a fresh source is generally consideredto be the most vulnerable to terroristacquisition of the radioisotope. At thatparticular time, there are 2 sources in 1location that could be targeted. In addi-tion, the cobalt-60 sources have now beenremoved from the unwieldy Gamma Knifehousing unit and are transported insteadin a smaller heavily shielded safe. Becauseof the significant dangers associated withthe loss of either the old or the new cobalt-60 radionuclides, the security team at ourfacility works closely with local lawenforcement and SWAT team units toensure that this exchange occurs safely.The overall time required for a
completed changing over of devices isroughly 1 week. Exchange of the cobalt-60sources themselves typically takes 10e20hours with the assistance of a shieldedrobotic arm “source reloader,” with therest of the week dedicated to setup, cali-bration, and testing for appropriatestrength, position, and radiation distribu-tion of the new cobalt-60 sources. At ourfacility, security personnel and heavilyarmed law enforcement are present at alltimes during this process.
B Drills and notification protocols
B Existing relationship with localauthorities
B Consultation with independentsecurity firm to tailor protection
� Physical Treatment Area
B Layered rooms
B Closed-circuit monitoring video
B Biometric identifier access
B Automated alarm and notifica-tion of unauthorized access
� Unescorted Access Control
B Background and criminal checks
B Security access badges
Suggested implementations of the Nuclear RegulatoryCommission Title 10, Code of Federal Regulations,Part 37, Materials Security Programs requirementswith regard to security of the facility and its radi-ation vault are summarized.
DETERRENCE, SECURITY, ANDPROTECTIVE MEASURES
The protective capabilities and goals ofsafeguarding radioactive material differbetween the military and university sec-tors. Because of the very real, albeit lowpossibility of an attack on a nuclear powerplant facility, many protective measuresare in place both to secure the safety of theradioactive material and to prevent itsrelease into the environment. Nuclearpower plants operationally are protectedvia complex design safeguards and safetysystems redundancies, and their extensivesecurity measures and training exercisesare often likened to military fortresses (2,32). Power plant containment vessels aredesigned and placed such that even anattack from the air similar to the assaulton the World Trade Center and thePentagon would not pose a threat
WORLD NEUROSURGERY 82 [6]: 1060-10
to containment vessel integrity from any-thing smaller than a large jetliner (2).Given that their security is so rigorous,
the probability of radiologic terrorismaimed at nuclear power plants is quite low(8, 32). Because other, less standardizedcivilian targets would then be considered,some deliberation and thought must begiven with regard to the basic protectivemeasures of radioactive sources that hos-pitals use. In adherence to NRC Title 10CFR Part 37, some suggestions are madehere for the practical application of thoseguidelines (Table 7).First, open communication with the
facility’s security team and department isparamount. Personnel must appreciatethe significance of having radioactivesources on site and be aware of therequisite security measures and protocolsassociated with protection, including,but not limited to, urgent notificationdrills, emergency lockdown situations,and appropriate response times. Thefacility’s security team should also haveprotocols in place for the notification oflocal authorities, including, but not
70, DECEMBER 2014 www
limited to, police, fire, special teams,and Hazmat. Further consultation with asecurity firm may be required to tailorthe protective layers around the capabil-ities of each individual facility.The physical design of the radiation
vault and unit can include the use oflayered rooms so that the innermost roomhousing the radioactive source could beused as a safe room in the event of anattempted forcible capture. Closed-circuitmonitoring would allow individuals insidethe unit to review the identities and needof entry for unauthorized personnel. Ac-cess badges can be used for basic entrycontrol into the unit, of which appropriateapproval should be stringently reviewed bythe facility’s security department. Anautomated notification system should alsobe put in place such that unauthorizedaccess or removal of a radioactive sourcetriggers an alarm to facility security orlocal authorities depending on theperceived severity of the trigger.For access of the radioactive source itself
during therapeutic treatment, supplemen-tary security measures can also be used torestrict entry to only a handful of personnel.Installation of a biometric identificationsystem is 1 option for final source accessthat would make unauthorized entry muchmore difficult and eliminate the possibilityof entry simply from a stolen access card.Examples of biometric identifiers include,but are not limited to, fingerprint, palmprint, face, iris, retina, and voice recogni-tion (11, 22).Lastly, background checks must be
conducted for all personnel with access tothe unit per NRC Title 10 CFR Part 37 re-quirements. Although this security mea-sure may be obvious for clinical staffinvolved with daily radiosurgery, otherhospital workers must also be scrutinized.The most unassuming of personnel withsome token access to or near the radio-logic unit sometimes may be the mostvaluable to terrorist groups who wish togather information. Waste management,food service, and systems maintenancestaff are examples of employees whotypically do not garner much attention ona daily basis.
CONCLUSIONS
In our age of common use of nucleartherapeutics, radiologic terrorism is a
.WORLDNEUROSURGERY.org 1069

SPECIA
LARTIC
LE
PEER-REVIEW REPORTS
MARTIN H. PHAM ET AL. NUCLEAR POWER AND THERAPEUTIC RADIATION
significant risk and possibility. One of themost important things that physiciansneed in this potentially devastating sce-nario is the invested awareness of theharmful potential that these radiologicsources carry. The NRC has developedguidelines for practical application of se-curity measures for the protection ofCategory 1 radionuclides, which includesthe cobalt-60 sources in the LeksellGamma Knife. Although these regulationsare specific to the United States, physi-cians worldwide who use radioactivesources for therapeutic use should beaware, appreciate, and endorse the requi-site protective measures needed to preventthese materials from falling into the wronghands. Certain terrorist organizationsdepend on complacency and unfamiliarity,which could subsequently lead to thecatastrophic loss of a radioactive source.
REFERENCES
1. Anderson PD, Bokor G: Nuclear and radiologicalterrorism: continuing education article. J PharmPract 26:171-182, 2013.
2. Anet B: Assessing the risk of radiologicalterrorism: how real is the threat? Presented at:Fourth International Chemical and BiologicalMedical Treatment Symposium; Spiez,Switzerland, April 28 to May 3, 2002.
3. Balk S, Miller R: Radiation disasters and children.Pediatrics 111:1455-1466, 2003.
4. Biddle W: A Field Guide to Radiation. New York:Penguin Books; 2012.
5. Burchfield L: Radiation Safety: Protection andManagement for Homeland Security and Emer-gency Response. Hoboken, NJ: Wiley; 2009.
6. Committee on Radiation Source Use andReplacement Nuclear and Radiation StudiesBoard Division on Earth and Life Studies NationalResearch Council: Radiation Source Use andReplacement: Abbreviated Version. Washington,DC: National Academies Press; 2008.
7. Elekta AB: Treatment Centers. Available at: http://www.elekta.com/patients/treatment-information/treatment-centers.html. Accessed September 5,2014.
8. Gottemoeller R: House Subcommittee on NationalSecurity, Veterans Affairs and International Re-lations; Washington, DC, 2002. Available at: http://www.iraqwatch.org/government/US/HearingsPreparedstatements/hgrc-gottemoeller-092402.htm. Ac-cessed August 26, 2014.
9. Gugiu D, Dumitrache I: Monte Carlo estimationof the dose and heating of cobalt adjuster rodsirradiated in the CANDU 6 reactor core. RadiatProt Dosimetry 116:69-72, 2005.
1070 www.SCIENCEDIRECT.com
10. Hines J: Planning the Gamma Knife Unit: TheGamma Knife Center of the Carolinas. TheAcademy Journal 2, 1999.
11. Jain AK: Technology: biometric recognition. Na-ture 449:38-40, 2007.
12. Kalend A, Bhatnagar J, Coletti J: An open ceilingradiosurgery vault for the practical source reload-ing of the Leksell Gamma Knife Unit. Presentedat: American Association of Physicists in Medicine46th Annual Meeting; Pittsburgh, July 25-29, 2004.
13. Kelly H: Dirty bombs: response to a threat.Washington, DC: Senate Foreign Relations Com-mittee; 2002. Available at: http://fas.org/ssp/docs/030602-kellytestimony.htm. Accessed August 26,2014.
14. Levett J: Radiological terrorism scenarios. PrehospDisaster Med 22:346, 2007.
15. Lindquist C, Paddick I: The Leksell Gamma KnifePerfexion and comparisons with its predecessors.Neurosurgery 61:130-140, 2007; discussion 140-141.
16. Martin M: Shielding design methods for radiationoncology departments. Presented at AmericanCollege of Medical Physics 25th Annual Meeting;Seattle, May 3-5, 2008.
17. Mushtaq A: Producing radioisotopes in powerreactors. Journal of Radioanalytical and NuclearChemistry 292:793-802, 2011.
18. Mylvaganam C, Ronchka R: New avenues in co-balt-60 production at Ontario hydro. InternationalJournal of Radiation Applications and Instru-mentation. Part C. Radiation Physics and Chem-istry 35:602-605, 1990.
19. National Council on Radiation Protection: NCRPReport No. 151, Structural Shielding Design andEvaluation for Megavoltage X- and Gamma-RayRadiotherapy Facilities. Bethesda, MD: NRCP;2005.
20. Schauer DA, Linton OW: NCRP Report No. 160,Ionizing Radiation Exposure of the Population ofthe United States, medical exposure—are we do-ing less with more, and is there a role for healthphysicists? Health Phys 97:1-5, 2009.
21. Slack J, Norton J, Malkoske G: Cobalt-60 produc-tion in CANDU power reactors. Presented at: In-ternational Symposium on Nuclear Energy;Bucharest, Romania, October 22-25, 2003.
22. Snelick R, Uludag U, Mink A, Indovina M, Jain A:Large-scale evaluation of multimodal biometricauthentication using state-of-the-art systems.IEEE Trans Pattern Anal Mach Intell 27:450-455,2005.
23. U.S. Department of Energy and Nuclear Regula-tory Commission Working Group: RadiologicalDispersal Devices: An Initial Study to IdentifyRadioactive Materials of Greatest Concern andApproaches to their Tracking, Tagging, andDisposition. Report to the Nuclear RegulatoryCommssion and the Secretary of Energy; 2003.Available at: http://www.energy.gov/sites/prod/
WORLD NEUROSURGERY, http://
files/edg/media/RDDRPTF14MAYa.pdf. AccessedAugust 27, 2014.
24. U.S. Military AFRRIA: Medical Management ofRadiological Casualties—Third Edition 2010—Ionizing Radiation and Radionuclide EmergencyTreatment, Acute Radiation Syndrome, Skin In-juries, Decontamination, Delayed Effects.Bethesda, MD: Armed Forces RadiobiologyResearch Institute; 2011.
25. U.S. Nuclear Regulatory Commission: NRC 10CFR Part 20—Standards for Protection AgainstRadiation. Washington, DC: NRC; 2014.
26. U.S. Nuclear Regulatory Commission: NRC 10CFR Part 37—Physical Protection of Category 1and Category 2 Quantities of Radioactive Material.Washington, DC: NRC; 2014, 2014.
27. U.S. Nuclear Regulatory Commission: NRC Ap-proves Co-60 Pilot Program at Clinton. Washing-ton, DC: NRC; 2010.
28. U.S. Nuclear Regulatory Commission: NRC Ap-proves Final Rule on National Source TrackingSystem for Radioactive Materials of Concern.Washington, DC: NRC; 2006.
29. U.S. Nuclear Regulatory Commission: NRC Ap-proves Pilot Program for Co-60 Production atHope Creek Nuclear Power Plant. Washington,DC: NRC; 2010.
30. U.S. Nuclear Regulatory Commission: NRC De-ploys National Source Tracking System: Milestonein Security of Radioactive Materials. Washington,DC: NRC; 2009.
31. U.S. Congress: Energy Policy Act of 2005; Wash-ington, DC, 2005.
32. Van Moore A Jr: Radiological and nuclearterrorism: are you prepared? J Am Coll Radiol 1:54-58, 2004.
33. Wu R: Overview and Basis of Design for NCRPReport 151. In: Shielding Methods for MedicalFacilities: Diagnostic Imaging, PET and RadiationTherapy; Collegeville, MN, 2007. Available at:http://www.aapm.org/meetings/07ss/documents/revNCRP151AAPM.pdf. Accessed August 27, 2014.
34. Yamamoto LG: Risks and management of radia-tion exposure. Pediatr Emerg Care 29:1016-1026[quiz 1027-1029], 2013.
Conflict of interest statement: The authors declare that thearticle content was composed in the absence of anycommercial or financial relationships that could be construedas a potential conflict of interest.
Received 6 September 2014; accepted 7 September 2014;published online 11 September 2014
Citation: World Neurosurg. (2014) 82, 6:1060-1070.http://dx.doi.org/10.1016/j.wneu.2014.09.007
Journal homepage: www.WORLDNEUROSURGERY.org
Available online: www.sciencedirect.com
1878-8750/$ - see front matter Published by Elsevier Inc.
dx.doi.org/10.1016/j.wneu.2014.09.007

SPECIA
LARTIC
LE
PEER-REVIEW REPORTS
MARTIN H. PHAM ET AL. NUCLEAR POWER AND THERAPEUTIC RADIATION
APPENDIX: GLOSSARY
Alpha decay: Radioactive decay inwhich the atomic nucleus emits an alphaparticle, which is an He2þ ionBeta decay: Radioactive decay in which
a free neutron decays into a proton andreleases an electron or positronBoiling water reactor (BWR): A light
water nuclear reactorCANDU (CANada Deuterium Uranium)
nuclear reactor: A Canadian-inventedpressurized heavy water nuclear reactorusing deuterium oxide and uranium fuelGamma ray: Ionizing radiation of
extremely high frequency and high energyper photonImprovised nuclear device (IND): A
device built by a terrorist group usingnuclear material (uranium or plutonium)that would produce a nuclear explosionIonizing radiation: Radiation that
carries enough energy to liberate electronsfrom atoms or molecules, ionizing themand giving them a positive charge (ornegative charge if they acquire an electron)Isotope: A variant of a particular
chemical element, having the same
WORLD NEUROSURGERY 82 [6]: 1060-10
number of protons but differing innumber of neutronsNeutron activation: The process by
which neutron radiation induces radioac-tivity; when an atomic nucleus capturesthe free neutrons and becomes unstableNRC Title 10 CFR Part 20: Nuclear Reg-
ulatory Commission Title 10 Code of Fed-eral Regulations Part 20, providingrequirements on acceptable radiationexposure levels to occupational employeesand the general publicNRC Title 10 CFR Part 37: Nuclear Reg-
ulatory Commission Title 10 Code of Fed-eral Regulations Part 37, providingrequirements for the physical protection ofCategory 1 radioactive sourcesNuclearRegulatory Commission (NRC):
U.S. government agency responsible forprotecting public health and safety withissues relating to nuclear energyOccupancy factor: The level of human
occupancy of an area adjacent to a radiationsource, used as a modifier for shieldingrequirements of a particular barrier. Thisfactor ranges from a factor of 1 (full-occu-pancy areas occupied full-time) to 1/40
70, DECEMBER 2014 www.WO
(transient pedestrian traffic such as unat-tended parking lots or stairways)Radiation dispersion device (RDD): A
weapon designed with the purpose ofspreading radioactive material; also knownas a “dirty bomb,” where a conventionalexplosive is used to spread radioactivematerialRadiation exposure device (RED): A
hidden or concealed device containingradioactive material that is meant toexpose people to ionizing radiationwithout their knowledgeSievert (Sv): The equivalent biologic
effect of the deposition of 1 J of radiationenergy in 1 kg of human tissueSpecific activity: Radioactivity per unit
mass, usually expressed in curie (Ci) pergram (g)Tenth-value layer (TVL): The thickness
of a material at which it has absorbed 90%of the radiation and reduced it to onetenth of its original intensityWorkload: The average absorbed dose
of radiation produced by a source over aspecific time at a specific location for thebarrier in question
RLDNEUROSURGERY.org 1070.E1