Hippocampal spatial representations require vestibular input
Upload
independentCategory
view
1download
0
Natural History of Hearing Deterioration inIntracanalicular Vestibular Schwannoma
BACKGROUND: Intracanalicular vestibular schwannomas have a range of treatmentoptions that can preserve hearing: microsurgery, stereotactic radiotherapy, and con-servative observation.
OBJECTIVE: To evaluate the natural course of hearing deterioration during a period ofconservative observation.
METHODS: A retrospective case review was performed on 47 patients with a unilateralintracanalicular vestibular schwannoma. Evaluation of growth was monitored by repeatMRI scanning. Repeated pure-tone and speech audiometry results were evaluated forsubgroups of patients showing growth or no growth and by subsite location of tumor inthe internal auditory canal.
RESULTS: Patients had a mean follow-up of 3.6 years. Over the entire population, thepure-tone average thresholds at 0.5, 1, 2, and 3 kHz and the word recognition scoresboth significantly deteriorated from 38 to 51 dB HL, and from 66% to 55%, respectively.Overall, 74% of subjects with good hearing, according to the 50/50 rule, maintainedhearing above this rule. There were no significant differences in hearing loss by subsite inthe internal auditory canal (porus, fundus, central) or by growth status (stable, growing,shrinking). Only 6 patients showed a large hearing change. This happened early duringfollow-up, with relatively stable hearing after this.
CONCLUSION: Hearing will deteriorate in some intracanalicular vestibular schwanno-mas, regardless of tumor growth. Hearing deterioration, if on a large scale, most likelyoccurs early in follow-up. The present results using conservative management in thesetumors appear similar to those reported for stereotactic radiotherapy or microsurgery.
KEY WORDS: Acoustic neuroma, Hearing, Hearing preservation, Intracanalicular, Microsurgery, Stereotactic
radiotherapy, Vestibular schwannoma
Neurosurgery 68:68–77, 2011 DOI: 10.1227/NEU.0b013e3181fc60cb www.neurosurgery-online.com
Avestibular schwannoma (often used syn-onymously with the term acoustic neu-roma) is a benign tumor arising from the
Schwann cell covering of the eighth cranialnerve. These tumors often first present withasymmetric hearing loss. Other symptoms may betinnitus, aural fullness, poor speech discrimination,imbalance, or, rarely, vertigo. Varied explanationsfor the etiology of hearing deterioration in patientswith vestibular schwannomas, including tumor-
induced expansion with subsequent increase ofpressure in the internal auditory canal, cochlearhair cell loss, vascular compromise, and a change ininner ear fluid composition, have been reported.1,2
As accessibility to MRI scanning has im-proved, the number of patients with a diagnosisof vestibular schwannoma has increased, and thesize of tumor at diagnosis appears to be smaller.In recent years, the management of vestibularschwannomas has become controversial, becauseseveral different treatment strategies have beenproposed.Intracanalicular tumors present several valid
management choices. Their small size allows forthe possibility of hearing preservation after sur-gery, but also for policies of conservative
Ronald J. E. Pennings, MD, PhD*
David P. Morris, MBBS, FRCS(ORL-HNS)*
Linda Clarke, RN†
Stefan Allen†
SimonWalling, MBChB, FRCSC*
Manohar L. Bance, MB, MSc,FRCSC*
*Division of Otolaryngology – Head &
Neck Surgery; and †Division of Neuro-
surgery, Department of Surgery, Dalhou-
sie University, Halifax, Nova Scotia,
Canada
Correspondence:
Ronald Pennings, MD, PhD,
Dalhousie University,
Department of Surgery,
Division of Otolaryngology – Head &
Neck Surgery,
1278 Tower Road,
3184 Dickson Building,
VGH Site, QEII HSC, Capital Health,
B3H 2Y9, Halifax, Nova Scotia, Canada.
E-mail: [email protected]
Received, September 9, 2009.
Accepted, April 30, 2010.
Copyright ª 2010 by the
Congress of Neurological Surgeons
ABBREVIATIONS: ANOVA, analysis of variance; HL,
hearing level; IAC, internal auditory canal; PTA,
pure-tone average; SRT, stereotactic radiotherapy;
WRS, word recognition score
68 | VOLUME 68 | NUMBER 1 | JANUARY 2011 www.neurosurgery-online.com
RESEARCH—HUMAN—CLINICAL STUDIESTOPIC Research—Human—Clinical Studies
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.
observation (‘‘wait-and-scan’’) and of stereotactic radiotherapy.Larger tumors offer more circumscribed options, because hearingpreservation following surgery is much less likely with largertumors, and size alone may dictate surgical intervention to pre-vent immediate risk to the patient. In intracanalicular tumors, themanagement decisions are more complex, and the impact of theavailable treatment options on hearing outcomes becomes ofmuch greater importance.
This report documents the auditory consequences of conser-vative management in a cohort of patients with intracanaliculartumors to aid this decision-making and management strategycomparison process.
To date, very few studies3-5 have examined the natural courseof auditory function in purely intracanalicular vestibularschwannomas. Only one study3 reported the results on more than20 patients. We discuss comparisons with the hearing resultsobtained after intervention with surgical and stereotactic radio-therapeutic options.
PATIENTS AND METHODS
Informed consent is taken at first presentation to enter all patientdetails into a database for follow-up and research purposes. Ethics ap-proval for this study was obtained from the Capital Health ResearchEthics Board #CDHA-RS/2009-270.
Conservative Management Protocol
Our policy is that purely intracanalicular vestibular schwannomas arefollowed by a conservative observational ‘‘wait-and-scan’’ protocol,which is systematically followed. After the first MRI scan, the secondMRI scan is performed at 6 months. If no growth is seen, annual MRIscans are performed up to 5 years. Between 5 and 10 years, scanning isperformed every 2 years, and after this period every 5 years.
Sample characteristics
The present cohort consists of patients with an intracanalicular ves-tibular schwannoma identified on MRI scanning who presented to ourSkull Base Clinic between 1998 and 2007. Exclusion criteria includedintralabyrinthine lesions (n = 2), neurofibromatosis type 2 (n = 1), andcases (n = 17) with fewer than 3 consecutive MRI scans. In addition, onemore patient was excluded because of insufficient data. After a 2-yearfollow-up, significant growth of tumor was seen and he was referred forstereotactic radiotherapy (SRT). However, only one pre-SRT audiogramwas made; therefore, it was decided to exclude this patient. In total, 47(28 female and 19 male) patients with purely intracanalicular vestibularschwannomas were included in the study. The median age at the firstaudiogram was 55.7 years with a range of 26.3 to 80.0 years. The meanfollow-up time (difference in time between the first and last audiogram)was 3.6 years with a range of 0.7 to 7.0 years.
Tumor Designations and Nomenclature
Significant growth of tumor was defined as an increase in size of morethan 2 mm in diameter between the first and last MRI scan.6 Using thiscriterion, tumors were labeled as ‘‘growing’’ (40% or 19/47), ‘‘stable’’(51% or 24/47), or, if they shrank by more than 2 mm, as ‘‘shrinking’’
(9% or 4/47). In 18 patients growth of tumor was seen into the cer-ebellopontine angle. Details of growth will be published separately.Tumors were also characterized by location in the internal auditory canal(IAC). Lateral ones were designated as ‘‘fundus’’ (n = 16), midportion as‘‘central’’ (n = 24), and medial as ‘‘porus’’ (n = 7). In fundus tumors therewas no cerebrospinal fluid (CSF) between tumor and cochlea, in centraltumors there was CSF on both sides of the tumor, or the tumors filledthe entire IAC, and in porus tumors there was CSF between tumor andcochlea.1 There was no significant difference in size at the time ofdiagnosis in these 3 subsite locations of tumors. The average follow-uptimes for the subtypes of tumors (years in parentheses) were growing(3.2), stable (3.7), shrinking (5.1), fundus (4.0), central (3.7), and porus(2.5). These were not significantly different on analysis of variance(ANOVA) testing.
Hearing Assessment
All patients monitored in our clinic undergo audiometric testing at thesame time that their MRI scans are repeated. Pure-tone audiogram andspeech recognition scores are tested in standard sound-attenuating au-diology booths, following standard American National Standards In-stitute calibration and sound-level protocols. The pure-tone average(PTA) of the hearing thresholds at index frequencies of 0.5, 1, 2, and 3kHz (PTA0.5,1,2,3 kHz) was used according to the recommendations ofthe Committee on Hearing and Equilibrium of the American Academyof Otolaryngology-Head and Neck Surgery.7 If patients underwenttreatment, pre- and posttreatment hearing was also categorized accordingto the American Academy of Otolaryngology and Head and NeckSurgery (AAOHNS) classification. The first audiogram at diagnosis andthe last audiogram (before treatment) were used to evaluate deteriorationof hearing caused by the policy of conservative management. Hearingresults were analyzed for the whole group (n = 47), and separately for thesubgroups of growing, stable, and shrinking tumors, and for subsitelocation in the IAC.In those cases where MRI scanning showed tumor growth, an in-
dividualized decision was made about rescanning or referral for SRTbased on size of tumor, degree of growth, and patient factors such as ageand medical condition. The decrease in hearing after treatment wasevaluated separately and is not reported as part of the conservativemanagement strategy.
Statistical Analyses
For comparisons between the groups, paired t tests, Pearson corre-lation tests, and one-way ANOVA followed by the Tukey multiplecomparison test were performed after testing for a Gaussian distributionwith the normality test. Criteria for significant differences was P , .05.Because the distribution is often not Gaussian, nonparametric tests werealso used. Actuarial survival curves were also generated for hearing re-tention. The computer software program Prism version 3.03 (GraphPadSoftware Inc., San Diego, California) was used for statistical analysis.
RESULTS
Overall Results
Table 1 shows the deterioration in hearing for all 47 patientswith an intracanalicular vestibular schwannoma. The meanPTA0.5,1,2,3 kHz threshold at the initial audiogram was 37.5 decibelhearing level (dB HL). After follow-up, the mean threshold
HEARING IN INTRACANALICULAR VESTIBULAR SCHWANNOMA
NEUROSURGERY VOLUME 68 | NUMBER 1 | JANUARY 2011 | 69
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.
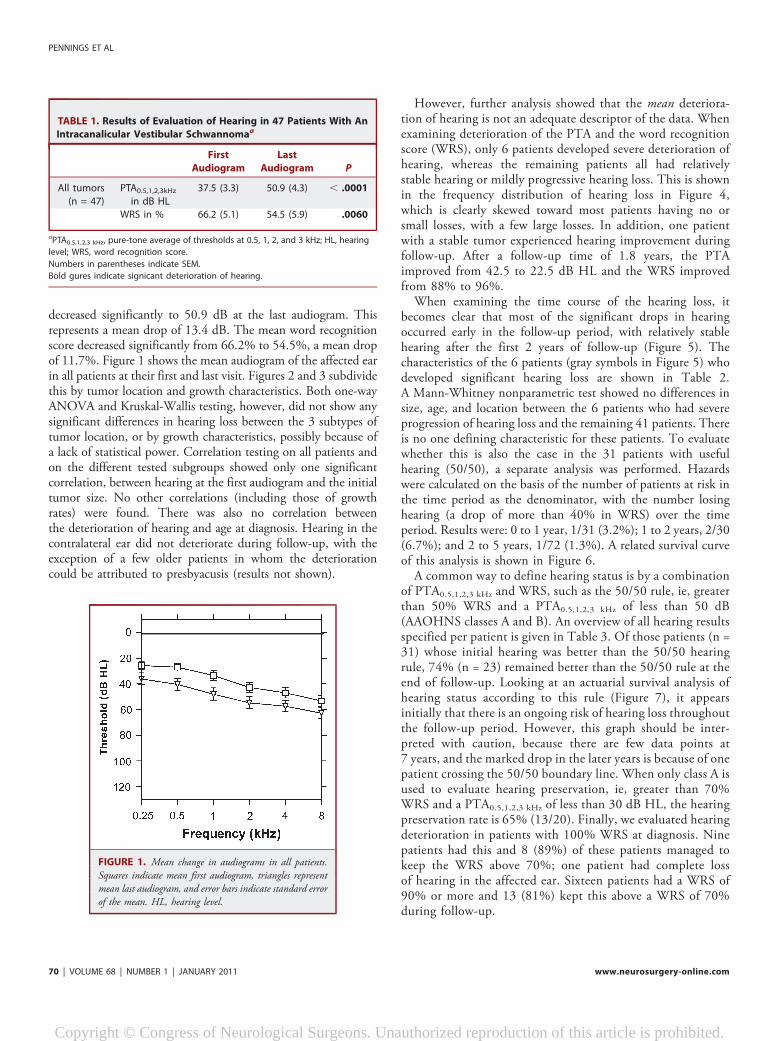
decreased significantly to 50.9 dB at the last audiogram. Thisrepresents a mean drop of 13.4 dB. The mean word recognitionscore decreased significantly from 66.2% to 54.5%, a mean dropof 11.7%. Figure 1 shows the mean audiogram of the affected earin all patients at their first and last visit. Figures 2 and 3 subdividethis by tumor location and growth characteristics. Both one-wayANOVA and Kruskal-Wallis testing, however, did not show anysignificant differences in hearing loss between the 3 subtypes oftumor location, or by growth characteristics, possibly because ofa lack of statistical power. Correlation testing on all patients andon the different tested subgroups showed only one significantcorrelation, between hearing at the first audiogram and the initialtumor size. No other correlations (including those of growthrates) were found. There was also no correlation betweenthe deterioration of hearing and age at diagnosis. Hearing in thecontralateral ear did not deteriorate during follow-up, with theexception of a few older patients in whom the deteriorationcould be attributed to presbyacusis (results not shown).
However, further analysis showed that the mean deteriora-tion of hearing is not an adequate descriptor of the data. Whenexamining deterioration of the PTA and the word recognitionscore (WRS), only 6 patients developed severe deterioration ofhearing, whereas the remaining patients all had relativelystable hearing or mildly progressive hearing loss. This is shownin the frequency distribution of hearing loss in Figure 4,which is clearly skewed toward most patients having no orsmall losses, with a few large losses. In addition, one patientwith a stable tumor experienced hearing improvement duringfollow-up. After a follow-up time of 1.8 years, the PTAimproved from 42.5 to 22.5 dB HL and the WRS improvedfrom 88% to 96%.When examining the time course of the hearing loss, it
becomes clear that most of the significant drops in hearingoccurred early in the follow-up period, with relatively stablehearing after the first 2 years of follow-up (Figure 5). Thecharacteristics of the 6 patients (gray symbols in Figure 5) whodeveloped significant hearing loss are shown in Table 2.A Mann-Whitney nonparametric test showed no differences insize, age, and location between the 6 patients who had severeprogression of hearing loss and the remaining 41 patients. Thereis no one defining characteristic for these patients. To evaluatewhether this is also the case in the 31 patients with usefulhearing (50/50), a separate analysis was performed. Hazardswere calculated on the basis of the number of patients at risk inthe time period as the denominator, with the number losinghearing (a drop of more than 40% in WRS) over the timeperiod. Results were: 0 to 1 year, 1/31 (3.2%); 1 to 2 years, 2/30(6.7%); and 2 to 5 years, 1/72 (1.3%). A related survival curveof this analysis is shown in Figure 6.A common way to define hearing status is by a combination
of PTA0.5,1,2,3 kHz and WRS, such as the 50/50 rule, ie, greaterthan 50% WRS and a PTA0.5,1,2,3 kHz of less than 50 dB(AAOHNS classes A and B). An overview of all hearing resultsspecified per patient is given in Table 3. Of those patients (n =31) whose initial hearing was better than the 50/50 hearingrule, 74% (n = 23) remained better than the 50/50 rule at theend of follow-up. Looking at an actuarial survival analysis ofhearing status according to this rule (Figure 7), it appearsinitially that there is an ongoing risk of hearing loss throughoutthe follow-up period. However, this graph should be inter-preted with caution, because there are few data points at7 years, and the marked drop in the later years is because of onepatient crossing the 50/50 boundary line. When only class A isused to evaluate hearing preservation, ie, greater than 70%WRS and a PTA0.5,1,2,3 kHz of less than 30 dB HL, the hearingpreservation rate is 65% (13/20). Finally, we evaluated hearingdeterioration in patients with 100% WRS at diagnosis. Ninepatients had this and 8 (89%) of these patients managed tokeep the WRS above 70%; one patient had complete lossof hearing in the affected ear. Sixteen patients had a WRS of90% or more and 13 (81%) kept this above a WRS of 70%during follow-up.
TABLE 1. Results of Evaluation of Hearing in 47 Patients With An
Intracanalicular Vestibular Schwannomaa
First
Audiogram
Last
Audiogram P
All tumors
(n = 47)
PTA0.5,1,2,3kHz
in dB HL
37.5 (3.3) 50.9 (4.3) , .0001
WRS in % 66.2 (5.1) 54.5 (5.9) .0060
aPTA0.5,1,2,3 kHz, pure-tone average of thresholds at 0.5, 1, 2, and 3 kHz; HL, hearing
level; WRS, word recognition score.
Numbers in parentheses indicate SEM.
Bold gures indicate signicant deterioration of hearing.
FIGURE 1. Mean change in audiograms in all patients.Squares indicate mean first audiogram, triangles representmean last audiogram, and error bars indicate standard errorof the mean. HL, hearing level.
PENNINGS ET AL
70 | VOLUME 68 | NUMBER 1 | JANUARY 2011 www.neurosurgery-online.com
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.

Treatment and Subsequent Hearing Change inGrowing Tumors
Based on individual evaluation it was decided that 8 of the 19patients with a growing intracanalicular vestibular schwannomaneeded treatment (17% of all patients). Most of those patientsthat showed growth of tumor have not (as of yet) been referredfor radiation, because they have relatively small tumors andthe decision was made to continue to closely follow them. Onepatient opted for surgery using a translabyrinthine approach. Shehad no useful hearing in that ear before surgery. The 7 remainingpatients underwent SRT. Three of them did not have any usefulhearing before treatment. One patient, who moved out-of-province after SRT, had no follow-up audiometry. The remaining3 patients experienced deterioration of hearing from a mean pre-SRT PTA0.5,1,2,3 kHz value of 36.7 dB to a post-SRT value of 52.9dB. The mean word recognition score decreased from 83.3% to68.0% over a mean follow-up time of 2.5 years post-SRT.
DISCUSSION
The present study reports on the natural course of auditoryfunction in 47 patients with a purely intracanalicular vestibular
schwannoma, with the use of conservative management (‘‘wait-and-scan’’ policy). Taken as a whole group, hearing deterioratedsignificantly in this group of patients from a mean PTA0.5,1,2,3 kHz
of 37.5 dB HL at the first audiogram to 50.9 dB HL at the last-visit audiogram. The word recognition score deteriorated sig-nificantly from 66.2% to 54.5%. ANOVA testing showed therewas no significant difference in hearing deterioration betweengrowing, stable, or shrinking tumors nor between central, fundus,and porus tumors (acknowledging that there is a decrease inpower with smaller numbers in each subgroup). Eight patients(17% of all patients) eventually required intervention (surgery orSRT) because of tumor growth.Conservative management in even this small tumor population
has some risks to hearing. Analysis of the deterioration of hearing,however, showed that only a few patients experienced severedeterioration of hearing and this appears to occur relatively early,with relatively stable hearing following this. This is an importantmessage, and one that has not been previously emphasized inthe literature. This early-loss effect can also be seen in the data ofCaye-Thomasen et al3 whose data show that hearing is mainlylost during the very first years after diagnosis. Early hearing lossis also seen in the data sample of Warrick et al,8 although not
FIGURE 2. Mean change in audiogram subdivided by tumor growth subtype. Squares indicate first audiogram, trianglesrepresent last audiogram, and error bars indicate standard error of the mean. HL, hearing level; VS, vestibular schwannoma.
FIGURE 3. Mean change in audiogram subdivided by tumor subsite. Squares indicate first audiogram, triangles represent lastaudiogram, and error bars indicate standard error of the mean. HL, hearing level; VS, vestibular schwannoma.
HEARING IN INTRACANALICULAR VESTIBULAR SCHWANNOMA
NEUROSURGERY VOLUME 68 | NUMBER 1 | JANUARY 2011 | 71
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.

explicitly acknowledged. The hearing loss data shown in Figure 6imply a continual deterioration, but this is because an arbitraryline (the 50/50 rule) is chosen as a ‘‘pass/fail’’ criterion. Hence,ongoing small deteriorations in hearing in the order of 10 to20 dB push some patients past this 50/50 rule if they were closeto it to begin with. The lack of data points at longer follow-upintervals also magnifies the effect of change in even one patient,because the percentage of change is calculated in actuarial analysisas a percentage of remaining data points. Appreciating that mostlarge changes in hearing occur early during the follow-up periodhas important clinical implications. If a patient has been moni-tored for more than 3 years and has good hearing, the riskof catastrophic hearing loss is probably small at that time. Thisshould be factored into the equation if choosing differingmanagement options in patients who have been monitored forsome time, such as when taking over care from other centers.
Definition of Useful Hearing and Hearing Preservation
In the past decade, there has been much discussion aboutwhether hearing preservation surgery in small intracanalicularvestibular schwannomas with useful hearing should be the fa-vored strategy for preserving this hearing, compared with a wait-and-scan policy or SRT. The reported hearing results for thesetreatments are variable, and this is muddied by the differentcriteria applied for defining useful hearing and by the variousdefinitions of what hearing preservation means after surgery.Most studies describe useful hearing as a PTA0.5,1,2,3 kHz of lessthan 50 dB HL with a word recognition score higher than 50%(50/50 rule). This equates to classes A and B by the AAOHNS,7
based on the classes I and II as defined by Gardner and
FIGURE 4. Frequency distribution of the deterioration of PTA0.5,1,2,3 kHz (A)and WRS (B). The deterioration in hearing is plotted against the number ofpatients that have a specific amount of deterioration. HL, hearing level; PTA,pure-tone average; WRS, word recognition score.
FIGURE 5. Deterioration of PTA0.5,1,2,3 kHz and WRS plotted against follow-uptime. Black and white symbols indicate the difference (deterioration) between thefirst and last audiogram for all individuals during follow-up. White symbolsindicate patients with more than 70 dB HL on the first audiogram. Blacksymbols present the deterioration of hearing in all remaining patients. Graysymbols represent longitudinal hearing results in 6 patients with severe (.45 dBHL PTA or .35% WRS) deterioration of hearing (the characteristics aredescribed in more detail in Table 2). HL, hearing level; PTA, pure-tone average;WRS, word recognition score.
PENNINGS ET AL
72 | VOLUME 68 | NUMBER 1 | JANUARY 2011 www.neurosurgery-online.com
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.

Robertson.9 Sanna et al10 describe useful hearing as a PTA0.5,1,2,3 kHz
better than 30 dB and a word recognition score of more than70% (70/30 rule). In 2006, Meyer et al11 suggested use of onlythe word recognition scores to evaluate hearing in vestibularschwannoma.
A previous study by our group demonstrated that there wasno ‘‘magic change’’ in ability to hear in background noise at the50/50 or 70/30 rule when measured objectively, but rather acontinuous decrease in speech comprehension as the PTA0.5,1,2,3 kHz
decreased.12 This is particularly relevant to Figure 6, because thiskind of ‘‘pass/fail’’ plot is based on the assumption that there issome nonlinear change in hearing ability when the 50/50 rule lineis crossed. Our previous study showed no such nonlinearity, butrather a gradual decline as WRS and PTA in the tumor ear fell. Inaddition, the 50/50 rule may not be ideal in all cases. Somepatients with more than 50 dB HL loss and near to normal speechperception may still benefit from amplification. Finally, locali-zation of sound can still benefit from hearing levels below the50/50 rule.
Comparison of Present Results With the Literature
Only a few studies reported both PTA0.5,1,2,3 kHz and WRSresults after management of purely intracanalicular vestibularschwannomas. Table 4 shows the hearing results from the presentstudy compared with results reported by other studies. Because ofthe variations in criteria used to define hearing preservation, somestudies with large samples such as those reported by Samiiand Matthies,13 and more recently, Iwai et al,14 could not beincluded.
The hearing results in our study are different from those re-ported by Caye-Thomasen et al3 (Table 4), who reported pres-ervation rates (using the 50/50 rule) of 47% (21/45) and (usingthe 70/30 rule) of 47% (9/19), compared with our preservationrate of 74% (23/31) and 65% (13/20), respectively. Their studyhas so far reported on the largest group of patients with thelongest follow-up of intracanalicular vestibular schwannomasmanaged with a wait-and-scan policy. In general, their patientshad worse hearing on initial testing than the patients reported inthe present study. This might be related to the fact that theirstudy started much earlier than ours (since 1975; present study,
since 1998) and therefore included more patients that wereidentified in a timeframe when MRI scanning was less available,and hence tumor size or location less exact. In addition, theirmean follow-up time is longer (4.6 years) than reported in ourstudy (3.6 years). A pass-fail rule like the 50/50 rule is verysensitive to how many patients start off close to the 50/50 border;two studies with equal median deterioration can report verydifferent preservation rates if in one study most patients were wellabove or below the 50/50 rule, and in another they were closeto it. Because our study appears to have started out with morebetter-hearing subjects, not many will cross the 50/50 line withsmall changes. Both studies have shown that hearing deteriorateswhen comparing the first and last audiogram. However, in thepresent study this effect seems to be related mainly to the fewpatients who had severe deterioration of hearing early in thefollow-up period.In another article from the same Danish group, evaluation of
their large series of patients with vestibular schwannomas dem-onstrated that the main predictive factor is the initial speechdiscrimination.15 A more recent article demonstrated that, ofthose patients with 100% speech discrimination at diagnosis,
TABLE 2. Patient Characteristics of 6 Patients Who Had More Than 40 dB Deterioration of the PTA0.5,1, 2, 3 kHz or More Than 35% Loss of WRSa
Patient
No.
Age,
y
First PTA,
dB HL
Last PTA,
dB HL
Deterioration,
dB HL
First
WRS, %
Last
WRS, %
Deterioration,
%
Subsite
Location
Growth
Status
Size at First
Diagnosis, mm
Size at Last
Diagnosis, mm
32 37 23 64 41 100 0 100 Central Growth 13.8 19.7
35 69 52 110 58 80 0 80 Central Growth 8.9 13.7
38 51 34 60 26 88 4 84 Central Growth 9.7 14.7
42 56 31 55 24 92 48 44 Central Stable 8.8 10.4
45 37 62 111 49 38 0 38 Central Stable 3.1 3.5
58 50 21 110 81 80 0 80 Fundus Stable 0.9 1.2
aPTA0.5,1,2,3 kHz, pure-tone average of thresholds at 0.5, 1, 2, and 3 kHz; HL, hearing level; WRS, word recognition score.
FIGURE 6. Cumulative risk of losing less than 40% inWRS during follow-up in all patients with initial usefulhearing according to the 50/50 rule. WRS, word recognitionscore; FU, follow-up.
HEARING IN INTRACANALICULAR VESTIBULAR SCHWANNOMA
NEUROSURGERY VOLUME 68 | NUMBER 1 | JANUARY 2011 | 73
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.

TABLE 3. Hearing Results for Patients With Growing, Stable, and Shrinking Tumorsa
Patient No.
Diagnostic Evaluation Follow-up Evaluation
PTA0.5,1,2,3 WRS AAOHNS PTA0.5,1,2,3 WRS AAOHNS F.U.
Growing Tumors
1 30.00 84 A 42.50 72 B 6.96
2 27.50 96 A 41.25 64 B 5.63
4 45.00 80 B 45.00 96 B 4.04
6 98.75 0 D 110.00 0 D 5.16
11 43.75 92 B 53.75 100 C 6.54
14 45.00 0 D 52.50 0 D 4.93
21 96.25 0 D 110.00 0 D 1.50
25 43.75 52 B 53.75 36 D 4.03
32 22.50 100 A 63.75 0 D 2.87
33 12.50 100 A 23.75 90 A 1.63
34 12.50 96 A 13.75 100 A 4.28
35 52.50 80 C 110.00 0 D 1.55
38 33.75 88 B 60.00 4 D 3.09
39 20.00 84 A 47.50 56.00 B 1.18
50 16.25 92 A 15.00 96 A 1.32
51 17.50 100 A 18.75 96 A 2.37
57 21.25 100 A 23.75 100 A 0.96
60 47.50 22 D 56.25 41 D 1.61
65 20.00 90 A 37.50 100 B 1.93
Stable Size Tumors
8 46.25 60 B 58.75 28 D 5.09
9 55.00 12 D 63.75 0 D 6.11
10 32.50 40 D 58.75 48 D 6.29
13 10.00 100 A 28.75 100 A 5.61
19 67.50 68 C 66.25 72 C 4.97
20 30.00 70 A 58.75 64 C 5.57
23 47.50 16 D 61.25 16 D 4.59
24 63.75 4 D 98.75 0 D 6.02
26 66.25 20 D 76.25 0 D 3.06
28 25.00 76 A 26.25 68 B 3.00
29 7.50 100 A 13.75 100 A 5.65
30 61.25 44 D 63.75 56 C 2.35
36 15.00 100 A 18.75 100 A 3.49
40 37.50 96 B 47.50 100 B 2.65
41 38.75 76 B 43.75 56 B 1.78
42 31.25 92 B 55.00 48 D 3.02
43 52.50 56 C 58.75 44 D 2.92
45 62.50 38 D 111.25 0 D 2.15
48 7.50 100 A 10.00 100 A 1.92
49 25.00 68 B 22.50 76 A 0.73
54 10.00 100 A 13.75 92 A 0.65
58 21.25 80 A 110.00 0 D 4.41
62 30.00 88 A 33.75 92 B 4.21
63 42.50 88 B 22.50 96 A 1.84
Shrinking Tumors
5 80.00 0 D 76.25 0 D 5.82
12 30.00 68 B 33.75 80 B 4.39
15 7.50 96 A 8.75 100 A 4.59
74 53.75 0 D 72.50 20 D 5.75
aPTA0.5,1,2,3 kHz, pure-tone average of thresholds at 0.5, 1, 2 and 3 kHz in dB HL; HL, hearing level; WRS, word recognition score in percent; AAOHNS, the classification according
to the American Academy of Otolaryngology and Head and Neck Surgery; F.U., follow-up in years.
PENNINGS ET AL
74 | VOLUME 68 | NUMBER 1 | JANUARY 2011 www.neurosurgery-online.com
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.

after more than 10 years observation, 69% maintain goodhearing, compared with 38% of the patients with even a smalldiscrimination loss at diagnosis.16 These two studies on the samepatient groups deal with all types of vestibular schwannomas,whereas we only present data on intracanalicular vestibularschwannomas. The present study shows similar results witha 88% preservation rate for patients with 100% speech dis-crimination at diagnosis, although our follow-up needs to beextended for many more years to confirm these data.
Comparison With Other Treatments for IntracanalicularVestibular Schwannomas
On the balance of reported results (Table 4), hearing preser-vation surgery and SRT appear to be equally capable of preservinghearing in small tumors (approximately 60%). Recently, anoverview of the hearing preservation results of microsurgery werepublished by Noudel et al.17 They reported a hearing preservationrate of 58% for the retrosigmoid approach and 62% for themiddle fossa approach (not significantly different). Most hearingpreservation microsurgical studies state that hearing preservationsurgery is especially important in young patients, because theyhave more to lose and can handle extensive surgery better. Ourstudy shows there is no correlation between hearing deteriorationand age at diagnosis. Because the present result of 74% hearingpreservation with wait-and-scan appears better than the ap-proximately 60% reported for microsurgery, we feel that youngerpatients also deserve the option of a wait-and-scan policy, as analternative to microsurgery. A disadvantage in most studies of themicrosurgical treatment of intracanalicular vestibular schwan-nomas is that the follow-up time is relatively short. Only a fewstudies have reported long-term hearing results after hearingpreservation surgery. A study by Shelton et al18 demonstratedthat 56% of the patients who had had operations experienceda decline in hearing quality during a follow-up time of 8 to 20years. In another study by Chee et al19 the direct postoperativeserviceable hearing rate was 77%; however, this dropped to 57%at a late evaluation with a mean follow-up of 9.4 years. TranBa Huy reported on the results of a questionnaire he sent outto French nonotologist ears, nose, and throat doctors and
FIGURE 7. Cumulative risk of maintaining hearing above 50 dB forPTA0.5,1,2,3 kHz and 50% for WRS (the 50/50 rule) and maintaining hearingabove 70% WRS. n, the number of patients; WRS, word recognition score; FU,follow-up.
TABLE 4. Overview of Some of the Reported Results in Literature on the Evaluation of Useful Hearing and Preservation of Hearing for
Different Types of Treatment for Intracanalicular Vestibular Schwannomasa
Study Year No. of Patients Approach
% Hearing Preservation
Using 50/50
Mean/Median Follow-Up
Time (in Years)
Noudel et al17 2009 Review RSA/MCFA 58-62 Variable, usually
not long-term
Niranjan et al22 2008 96 Radiotherapy 61 3.5/2.3
Caye-Thomasen et al3 2007 156 Wait-and-scan 47 4.6/NA
Present study 47 Wait-and-scan 74 3.6/3.6
aPTA, pure-tone average; WRS, word recognition score; 70/30, PTA #30 dB and WRS $70%; 50/50, PTA #50 dB and WRS $50%; NA, not available; RSA, retrosigmoid approach;
MCFA, middle cranial fossa approach.
HEARING IN INTRACANALICULAR VESTIBULAR SCHWANNOMA
NEUROSURGERY VOLUME 68 | NUMBER 1 | JANUARY 2011 | 75
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.

questioned them whether they would choose surgery or a wait-and-scan policy. There was a very clear answer: 87% favoredfollow-up over surgery.20
With regard to the third option, SRT, in the past few yearsmany reports had emerged on hearing preservation by Gammaknife radiotherapy or fractionated radiation therapy. So far, onlyone group has published results specifically on intracanalicularvestibular schwannomas.21,22 Niranjan et al21 first publishedtheir results on 15 patients with purely intracanalicular vestibularschwannomas and found improved results for hearing preserva-tion when the tumor was smaller (4 mm vs 5-7 mm) and whensmall beam parameters were used (4 mm isocenters vs 4 and 8mm isocenters). A second, more recent study by the same groupdescribed the auditory performance after Gamma knife radio-therapy in a larger group of patients (n = 96) with purely in-tracanalicular vestibular schwannomas.22 This study showed that,after a mean follow-up of 3.5 years, the hearing preservation ratewas 61% (using the 50/50 rule) and therefore lower than thatreported in our study (74%), which has a similar follow-up time.In our study, 2 of the 3 patients who had residual hearing beforefractionated linear accelerator (LINAC)-based SRT showed de-terioration of hearing after treatment.
Massager et al23 evaluated the hearing outcome of patients withvestibular schwannomas after Gamma knife radiotherapy. Theynoted that the volume of the intracanalicular part of the vestibularschwannoma is significantly associated with the hearing outcomesafter radiotherapy. A higher volume of the tumor in the IAC sig-nificantly increases the risk of deterioration of hearing after radio-therapy. Vermeulen et al24 noticed that patients with intracanalicularvestibular schwannomas are more prone to develop complicationsafter Gamma knife radiotherapy, especially vestibulocochlear nerveinjury. However, their high complication rate might also be causedby the higher dose of radiation they used in their patients (18 Gy vs,14 Gy in more recent series). The Pittsburgh group also reportedtheir results on Gamma knife radiotherapy of vestibular schwan-nomas and reported a hearing preservation rate of almost 80%(classes A and B according to AAOHNS).25 Recently, however, theyreported long-term hearing preservation results and noticed anongoing deterioration in serviceable hearing after treatment. Theactuarial rate of keeping the same Gardner and Robertson leveldeclined to 44% after 10 years, with very few tumors exhibitinggrowth, indicating that the deterioration was not due to continuedtumor growth.26 It is possible that the wait-and-scan results in ourcohort will show similar deterioration with time, but there does notappear to be evidence that SRT ‘‘protects’’ against hearing losswith time.
Because the current results with a wait-and-scan policy anda similar follow-up time appear as good as or better than thosereported for SRT, there is no evidence that SRT stabilizes hearingin these tumors, and a wait-and-scan policy may offer equivalenthearing results with less risk of complications. We acknowledge thatcomplications of expertly performed SRT are quite low, in partic-ular, for intracanalicular tumors, but these complications do includethe risks of facial nerve paresis and vestibular loss, and the rare risk of
development of malignancy with time. Any definitive treatmentrecommendation would have to await truly long-term comparisons(.10 years) between SRT and conservative management.
CONCLUSION
In our cohort of patients with purely intracanalicular vestibularschwannomas, most major hearing losses occurred early in thefollow-up period. Hearing was relatively stable after this period,although smaller hearing losses did occur. In comparing ourresults with other treatment modalities available to this patientgroup, the wait-and-scan policy seems to offer hearing results thatare as good as, and possibly better than, surgery or SRT. Hence,we continue to recommend a conservative management approachin intracanalicular vestibular schwannomas.We acknowledge our relatively short follow-up time. However,
compared with the published literature, our follow-up is similar to orlonger than many other studies describing different modalities oftreatment. Hearing will continue to decrease with time, and finalcomparisons at 10 years will be much more important. However,because both SRT and surgery have been described to have long-term deterioration in hearing, it is unlikely that the wait-and-watchresults will decline in isolation compared with the other twomodalities in the long term. We offer a comparison with othermodalities of treatment at a relatively early window of observation.
Disclosure
This research was funded in part by a Niels Stensen stipendium (to R.P.).The other authors have no personal financial or institutional interest in any of thedrugs, materials, or devices described in this article.
REFERENCES
1. Kobayashi T, Aslan A, Chiba T, Takaska T, Sanna M. Measurement of endo-cochlear DC potentials in ears with acoustic neuromas: a preliminary report. ActaOtolaryngol. 1996;116(6):791-795.
2. Prasher D, Tun T, Brookes G, Luxon L. Mechanisms of hearing loss in acousticneuroma: an otoacoustic emission study. Acta Otolaryngol. 1995;115(3):375-381.
3. Caye-Thomasen P, Dethloff T, Hansen S, Stangerup SE, Thomsen J. Hearing inpatients with intracanalicular vestibular schwannomas. Audiol Neurootol. 2007;12(1):1-12.
4. Graamans K, van Dijk JF, Janssen LW. Hearing deterioration in patients witha non-growing vestibular schwannoma. Acta Otolaryngol. 2003;123(1):51-54.
5. Massick DD, Welling DB, Dodson EE, et al. Tumor growth and audiometric changein vestibular schwannomas managed conservatively. Laryngoscope. 2005;115:292-296.
6. Solares CA, Panizza B. Vestibular schwannoma: an understanding of growthshould influence management decisions. Otol Neurotol. 2008;29(6):829-834.
7. Committee on Hearing and Equilibrium. Committee on Hearing and Equilib-rium guidelines for the evaluation of hearing preservation in acoustic neuroma(vestibular schwannoma). Otolaryngol Head Neck Surg. 1995;113(3):179-180.
8. Warrick P, Bance M, Rutka J. The risk of hearing loss in nongrowing, conser-vatively managed acoustic neuromas. Am J Otol. 1999;20(6):758-62.
9. Gardner G, Robertson J. Hearing preservation in bilateral acoustic neuromasurgery. Am J Otol. 1993;14(6):562-565.
10. Sanna M, Khrais T, Russo A, Piccirillo E, Augurio A. Hearing preservation surgeryin vestibular schwannoma: the hidden truth. Ann Otol Rhinol Laryngol.2004;113(2):156-163.
11. Meyer TA, Canty PA, Wilkinson EP, Hansen MR, Rubinstein JT, Gantz BJ.Small acoustic neuromas: surgical outcomes versus observation or radiation. OtolNeurotol. 2006;27(3):380-392.
PENNINGS ET AL
76 | VOLUME 68 | NUMBER 1 | JANUARY 2011 www.neurosurgery-online.com
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.

12. Lee A, Clarke L, Bance M. Vestibular schwannoma: how much residual hearing isuseful? J Otolaryngol Head Neck Surg. 2008;37(3):399-410.
13. Samii M, Matthies C. Management of 1000 vestibular schwannomas (acousticneuromas): hearing function in 1000 tumor resections. Neurosurgery.1997;40(2):248-262.
14. Iwai Y, Yamanaka K, Kubo T, Aiba T. Gamma knife radiosurgery for intra-canalicular acoustic neuromas. J Clin Neurosci. 2008;15(9):993-997.
15. Stangerup SE, Caye-Thomasen P, Tos M, Thomsen J. Change in hearing during�wait and scan� management of patients with vestibular schwannoma. JLO.2008;122(7):673-681.
16. Stangerup S-E, Thomsen J, Tos M, Caye-Thomasen P. Long-term hearingpreservation in vestibular schwannoma. Otol Neurotol. 2010;31(2):271-275.
17. Noudel R, Gomis P, Duntze J, Marnet D, Bazin A, Roche PH. Hearing pres-ervation and facial nerve function after microsurgery for intracanalicular vestibularschwannomas: comparison of middle fossa and retrosigmoid approaches. ActaNeurochir. 2009;151(8):935-944.
18. Shelton C, Hitselberger WE, House WF, Brackmann DE. Hearing preservation afteracoustic tumor removal: long-term results. Laryngoscope. 1990;100(2 pt 1):115-119.
19. Chee GH, Nedzelski JM, Rowed D. Acoustic neuroma surgery: the results of long-term hearing preservation. Otol Neurotol. 2003;24(4):672-676.
20. Tran Ba Huy P. Operating on intracanalicular vestibular schwannoma – whatwould ENT doctors chose for themselves? Lancet. 1998;351(9113):1406.
21. Niranjan A, Lunsford LD, Flickinger J, Maitz A, Kondziolka D. Dose reductionimproves hearing preservation rates after intracanalicular acoustic tumor radio-surgery. Neurosurgery. 1999;45(4):753-762.
22. Niranjan A, Mathieu D, Flickinger JC, Kondziolka D, Lunsford LD. Hearingpreservation after intracanalicular vestibular schwannoma radiosurgery. Neuro-surgery. 2008;63(6):1054-1063.
23. Massager N, Nissim O, Delbrouck C, et al. Role of intracanalicular volumetric anddosimetric parameters on hearing preservation after vestibular schwannomaradiosurgery. Int J Radiat Oncol Biol Phys. 2006;64(5):1331-1340.
24. Vermeulen S, Young R, Posewitz A, et al. Stereotactic radiosurgery toxicity inthe treatment of intracanalicular acoustic neuromas: the Seattle Northwest GammaKnife experience. Stereotact Funct Neurosurg 1998;70(Suppl 1):80–87.
25. Lunsford LD, Niranjan A, Flickinger JC, Maitz A, Kondziolka D. Radiosurgeryof vestibular schwannomas: summary of experience in 829 cases. J Neurosurg.2005;102(Suppl):195-199.
26. Chopra R, Kondziolka D, Niranjan A, Lunsford LD, Flickinger JC. Long-termfollow-up of acoustic schwannoma radiosurgery with marginal tumor doses of 12to 13 Gy. Int J Radiat Oncol Biol Phys. 2007;68(3):845-851.
The Cyrus Cylinder is an ancient clay cylinder, now broken into several fragments, on which is written a declaration in Akkadian cuneiform script inthe name of the Achaemenid Persian king Cyrus the Great. The UN classifies and promotes the Cyrus Cylinder as ‘‘an ancient declaration of human rights.’’The Universal Declaration of Human Rights is a declaration adopted by the United Nations General Assembly on Dec. 10, 1948 at the Palais de Chaillot inParis. The Declaration arose directly from the experience of the Second World War and represents the first global expression of rights to which all humanbeings are entitled. It consists of 30 articles that have been elaborated in subsequent international treaties, regional human rights instruments, nationalconstitutions and laws.
HEARING IN INTRACANALICULAR VESTIBULAR SCHWANNOMA
NEUROSURGERY VOLUME 68 | NUMBER 1 | JANUARY 2011 | 77
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.
Copyright © 2022 FDOKUMEN