Long-term results of the AIEOP LNH-97 protocol for childhood lymphoblastic lymphoma
7
Pediatr Blood Cancer Long-Term Results of the AIEOP LNH-97 Protocol for Childhood Lymphoblastic Lymphoma Marta Pillon, MD, 1 * Maurizio Arico `, MD, 2 Lara Mussolin, PhD, 3 Elisa Carraro, BS, 1 Valentino Conter, MD, 4 Alessandra Sala, MD, 4 Salvatore Buffardi, MD, 5 Alberto Garaventa, MD, 6 Paolo D’Angelo, MD, 7 Luca Lo Nigro, MD, 8 Nicola Santoro, MD, 9 Matilde Piglione, MD, 10 Alessandra Lombardi, MD, 11 Fulvio Porta, MD, 12 Simone Cesaro, MD, 13 Maria L. Moleti, MD, 14 Fiorina Casale, MD, 15 Rossella Mura, MD, 16 Emanuele S. G. d’Amore, MD, 17 Giuseppe Basso, MD, 1 and Angelo Rosolen, MD 1,† INTRODUCTION Non-Hodgkin lymphomas (NHL) represent approximately 10– 15% of childhood and adolescence high-grade tumors according to the National Cancer Institute (NCI) Working Formulation [1–2]. They comprise the B-cell types Burkitt lymphoma and large cell lymphoma, T-cell anaplastic large cell lymphoma, and lymphoblastic lymphoma (LBL). In Europe and the United States, about 30% of all pediatric NHL are LBL, most of them have a precursor T-cell immunophenotype and present at an advanced stage. During the last 30 years, NHL are among pediatric malignancies that have benefited the most from advances in treatment, largely due to the use of sequential protocols with increasingly intensive chemotherapy regimens, tailored according to clinical stage and immunohistochemistry [3–5]. Contemporary regimens offer to at least 75% of children with advanced-stage LBL the opportunity to be cured. This has been achieved largely thanks to the great amount of research and subsequent advances made in the field of acute lymphoblastic leukemia (ALL) [6]. In a prospective Children’s Cancer Group trial, a comparison of two pioneer regimens, COMP based on use of cyclophosphamide and the 10-drug LSA 2 L 2 (used for ALL) showed the superiority of the LSA 2 L 2 regimen [7]. Taking into account these results, subsequent LBL chemotherapy treat- ments were designed including new drugs, optimization of central nervous system (CNS) prophylaxis, and intensification of treat- ment [8–10]. Between 1992 and 1997 the Italian cooperative study group “Associazione Italiana Ematologia Oncologia Pediatrica” (AIEOP) conducted its first trial for treatment of childhood LBL, named “AIEOP LNH-92,” based on the LSA2-L2 backbone. The outcome of this study was comparable to that of contemporary studies, with a 5-year event free survival (EFS) of 69% and, in particular, of 65% for patients with stages III and IV [11]. The main cause for treatment failure in that study was disease relapse, Background. Treatment intensification was considered a suitable strategy to increase the cure rate of lymphoblastic lymphoma (LBL) in children. Procedure. The AIEOP LNH-97 trial was run between 1997 and 2007 for newly diagnosed LBL in patients aged less than 18 years. Treatment schedule was based on the previous, LSA2-L2 derived, AIEOP LNH-92 protocol. Modifications included: increased dose of upfront cyclophosphamide and methotrexate, use of L-Asparaginase during induction therapy, intensive block therapy for slow respond- ers, and late intensification (“Reinduction”) for patients with advanced stage disease. Total therapy duration was 12 months for stage I and II, and 24 months for stage III and IV. Central nervous system prophylaxis did not include cranial irradiation. Results. 114 eligible patients were enrolled, 84 males and 30 females; median age was 9 years. Complete remission was obtained in 98% of patients. After a median follow-up time of seven years, 29 patients failed due to progression of disease (n ¼ 2), relapse (n ¼ 25), or second malignancy (n ¼ 2). The 7-year overall survival was 82% (standard error [SE] 4%) and the 7-year event-free survival was 74% (SE 4%). No subgroup showed significantly different event free survival. None of the patients died of front line chemotherapy-related toxicity. Conclusions. Treatment intensification was associated with good outcome in children and adolescents with LBL, with limited toxicity. Prognosis after relapse was better for patients who underwent allogeneic hematopoietic stem cell transplantation. Measurements of biological markers and treatment response are necessary for achieving further improvement through more accurate identification and stratification of patients at risk of disease relapse. Pediatr Blood Cancer # 2015 Wiley Periodicals, Inc. Key words: childhood; long-term outcome; lymphoblastic lymphoma; non-Hodgkin lymphoma; treatment 1 Clinic of Pediatric Hemato-Oncology, Department of Women’s and Children’s Health, University of Padova, Padova, Italy; 2 Azienda Sanitaria Provinciale, Ragusa, Italy; 3 Istituto di Ricerca Pediatrica, Fondazione Citta `, della Speranza, Padova, Italy; 4 Clinica Pediatrica, Universita ` degli Studi di Milano-Bicocca, Azienda Ospedaliera San Gerardo, Monza, Italy; 5 Pediatric Oncology Department, Santobono- Pausilipon Hospital of Napoli, Napoli, Italy; 6 Department of Hematology-Oncology, Istituto Giannina Gaslini, Genova, Italy; 7 Department of Oncology, Pediatric Hematology and Oncology Unit, A.R.N.A.S. Ospedali Civico Di Cristina e Benfratelli, Palermo, Italy; 8 Pediatric Hematology-Oncology, Policlinico di Catania, Catania, Italy; 9 Division of Paediatric Haematology-Oncology, Department of Pediatrics, Bari, Italy; 10 Division of Pediatric Onco-Hematology, Regina Margherita Children’s Hospital, Torino, Italy; 11 Dipartimento di Onco-Ematologia Pediatrica, Ospedale Bambino Gesu `, Roma, Italy; 12 Oncology-Haematology and BMT Unit, Ospedale dei Bambini, Spedali Civili, Brescia, Italy; 13 Pediatric Hematology-Oncology, Azienda Ospedaliera Universitaria Integrata Verona, Verona, Italy; 14 Hematology, Department of Cellular Biotechnologies and Hematol- ogy, Roma, Italy; 15 Pediatric Oncology Service,, Pediatric Department, Second University of Napoli, Napoli, Italy; 16 Pediatric Hematology- Oncology, Ospedale Pediatrico Microcitemico, Cagliari, Italy; 17 De- partment of Pathology, San Bortolo Hospital, Vicenza, Italy † Deceased in December 2013. Conflict of interest: Nothing to declare. Correspondence to: Marta Pillon, Clinic of Pediatric Hemato- Oncology, Department of Women’s andChildren’s Health, University of Padova, Via Giustinani 3, 35128 Padova, Italy. E-mail: [email protected] Received 16 September 2014; Accepted 2 October 2014 C 2015 Wiley Periodicals, Inc. DOI 10.1002/pbc.25469 Published online in Wiley Online Library (wileyonlinelibrary.com).
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Long-term results of the AIEOP LNH-97 protocol for childhood lymphoblastic lymphoma

Pediatr Blood Cancer
Long-Term Results of the AIEOP LNH-97 Protocol for Childhood
Lymphoblastic Lymphoma
Marta Pillon, MD,1* Maurizio Arico, MD,2 Lara Mussolin, PhD,3 Elisa Carraro, BS,1 Valentino Conter, MD,4
Alessandra Sala, MD,4 Salvatore Buffardi, MD,5 Alberto Garaventa, MD,6 Paolo D’Angelo, MD,7 Luca Lo Nigro, MD,8
Nicola Santoro, MD,9 Matilde Piglione, MD,10 Alessandra Lombardi, MD,11 Fulvio Porta, MD,12 Simone Cesaro, MD,13
Maria L. Moleti, MD,14 Fiorina Casale, MD,15 Rossella Mura, MD,16 Emanuele S. G. d’Amore, MD,17
Giuseppe Basso, MD,1 and Angelo Rosolen, MD1,†
INTRODUCTION
Non-Hodgkin lymphomas (NHL) represent approximately 10–
15% of childhood and adolescence high-grade tumors according
to the National Cancer Institute (NCI) Working Formulation
[1–2]. They comprise the B-cell types Burkitt lymphoma and
large cell lymphoma, T-cell anaplastic large cell lymphoma, and
lymphoblastic lymphoma (LBL). In Europe and the United States,
about 30% of all pediatric NHL are LBL, most of them have a
precursor T-cell immunophenotype and present at an advanced
stage.
During the last 30 years, NHL are among pediatric malignancies
that have benefited the most from advances in treatment, largely due
to the use of sequential protocols with increasingly intensive
chemotherapy regimens, tailored according to clinical stage and
immunohistochemistry [3–5]. Contemporary regimens offer to at
least 75% of children with advanced-stage LBL the opportunity to
be cured. This has been achieved largely thanks to the great amount
of research and subsequent advances made in the field of acute
lymphoblastic leukemia (ALL) [6]. In a prospective Children’s
Cancer Group trial, a comparison of two pioneer regimens, COMP
based on use of cyclophosphamide and the 10-drug LSA2L2 (used
for ALL) showed the superiority of the LSA2L2 regimen [7]. Taking
into account these results, subsequent LBL chemotherapy treat-
ments were designed including new drugs, optimization of central
nervous system (CNS) prophylaxis, and intensification of treat-
ment [8–10].
Between 1992 and 1997 the Italian cooperative study group
“Associazione Italiana Ematologia Oncologia Pediatrica”
(AIEOP) conducted its first trial for treatment of childhood LBL,
named “AIEOP LNH-92,” based on the LSA2-L2 backbone.
The outcome of this study was comparable to that of contemporary
studies, with a 5-year event free survival (EFS) of 69% and, in
particular, of 65% for patients with stages III and IV [11]. The main
cause for treatment failure in that study was disease relapse,
Background. Treatment intensification was considered a suitable
strategy to increase the cure rate of lymphoblastic lymphoma (LBL) in
children. Procedure. The AIEOP LNH-97 trial was run between 1997and 2007 for newly diagnosed LBL in patients aged less than 18 years.
Treatment schedule was based on the previous, LSA2-L2 derived,
AIEOP LNH-92 protocol. Modifications included: increased dose of
upfront cyclophosphamide and methotrexate, use of L-Asparaginaseduring induction therapy, intensive block therapy for slow respond-
ers, and late intensification (“Reinduction”) for patients with
advanced stage disease. Total therapy duration was 12 months for
stage I and II, and 24 months for stage III and IV. Central nervoussystem prophylaxis did not include cranial irradiation. Results. 114
eligible patients were enrolled, 84 males and 30 females; median age
was 9 years. Complete remission was obtained in 98% of patients.
After a median follow-up time of seven years, 29 patients failed due
to progression of disease (n¼2), relapse (n¼25), or second
malignancy (n¼2). The 7-year overall survival was 82% (standarderror [SE] 4%) and the 7-year event-free survival was 74% (SE 4%).
No subgroup showed significantly different event free survival. None
of the patients died of front line chemotherapy-related toxicity.
Conclusions. Treatment intensification was associated with goodoutcome in children and adolescents with LBL, with limited toxicity.
Prognosis after relapse was better for patients who underwent
allogeneic hematopoietic stem cell transplantation. Measurements of
biological markers and treatment response are necessary forachieving further improvement through more accurate identification
and stratification of patients at risk of disease relapse. Pediatr Blood
Cancer # 2015 Wiley Periodicals, Inc.
Key words: childhood; long-term outcome; lymphoblastic lymphoma; non-Hodgkin lymphoma; treatment
1Clinic of Pediatric Hemato-Oncology, Department of Women’s and
Children’s Health, University of Padova, Padova, Italy; 2Azienda
Sanitaria Provinciale, Ragusa, Italy; 3Istituto di Ricerca Pediatrica,
Fondazione Citta, della Speranza, Padova, Italy; 4Clinica Pediatrica,
Universita degli Studi di Milano-Bicocca, Azienda Ospedaliera San
Gerardo, Monza, Italy; 5Pediatric Oncology Department, Santobono-
Pausilipon Hospital of Napoli, Napoli, Italy; 6Department of
Hematology-Oncology, Istituto Giannina Gaslini, Genova, Italy;7Department of Oncology, Pediatric Hematology and Oncology Unit,
A.R.N.A.S. Ospedali Civico Di Cristina e Benfratelli, Palermo, Italy;8Pediatric Hematology-Oncology, Policlinico di Catania, Catania,
Italy; 9Division of Paediatric Haematology-Oncology, Department of
Pediatrics, Bari, Italy; 10Division of Pediatric Onco-Hematology,
Regina Margherita Children’s Hospital, Torino, Italy; 11Dipartimento di
Onco-Ematologia Pediatrica, Ospedale Bambino Gesu, Roma, Italy;12Oncology-Haematology and BMT Unit, Ospedale dei Bambini,
Spedali Civili, Brescia, Italy; 13Pediatric Hematology-Oncology,
Azienda Ospedaliera Universitaria Integrata Verona, Verona, Italy;14Hematology, Department of Cellular Biotechnologies and Hematol-
ogy, Roma, Italy; 15Pediatric Oncology Service,, Pediatric Department,
Second University of Napoli, Napoli, Italy; 16Pediatric Hematology-
Oncology, Ospedale Pediatrico Microcitemico, Cagliari, Italy; 17De-
partment of Pathology, San Bortolo Hospital, Vicenza, Italy
† Deceased in December 2013.
Conflict of interest: Nothing to declare.
�Correspondence to: Marta Pillon, Clinic of Pediatric Hemato-
Oncology, Department of Women’s and Children’s Health, University
of Padova, Via Giustinani 3, 35128 Padova, Italy.
E-mail: [email protected]
Received 16 September 2014; Accepted 2 October 2014
C 2015 Wiley Periodicals, Inc.DOI 10.1002/pbc.25469Published online in Wiley Online Library(wileyonlinelibrary.com).

occurring in 24% of patients, often during the first phase of
maintenance therapy. By the time these data became available,
preliminary results of some ongoing studies suggested that
treatment intensification might contribute to reduce the risk of
treatment failure, as in the Berlin–Frankfurt–Muenster (BFM)
experience [12].
Based on this background, in the following AIEOP LNH-97
study, treatment was intensified by the following changes: earlier
exposure to native L-asparaginase (the Escherichia coli product
was used in most patients), increased dose of cyclophosphamide,
and use of high dose of methotrexate (MTX) during induction
therapy. Patients with slow response at the end of induction were
treated with six courses of high-risk ALL type blocks [8].
Moreover, a late intensification (Reinduction) with a BFM-type
protocol II [12] was introduced for patients with more advanced
(stage III and IV) disease. A simplified continuation therapy was
applied for a total duration of treatment of 12 months in stages I
and II, or 24 months in stages III and IV. We report the long-term
treatment outcome of patients with LBL treated in this trial.
PATIENTS AND METHODS
Patients
From October 1997 to August 2007, children and adolescents
aged less than 18 years with newly diagnosed LBL, were
eligible for the AIEOP LNH-97 trial. Exclusion criteria were:
bone marrow (BM) massive involvement (�25% of blasts),
pre-existing severe congenital or acquired immunodeficiency,
previous cytostatic treatment, NHL as a second malignancy, post-
transplantation lymphoma, and any other condition prohibiting
chemotherapy. The study was approved by local institutional
review boards and written informed consent was obtained for
every patient enrolled.
Diagnosis and Staging
The diagnosis was established by analysis of lesional tissue,
obtained by lymph node or tumor biopsy, or malignant effusion.
All cases with available tissue underwent central pathology
review by two independent pathologists to confirm the diagnosis
and the cell lineage (precursor T or precursor B). Formalin-fixed
paraffin-embedded tumor biopsies were analyzed by immuno-
histochemistry using a wide panel of antibodies including T- and
B-lineage markers (TdT, CD1a, CD2, CD3, CD4, CD5, CD7,
CD8, CD10, CD19, CD20, CD43, CD79a, m heavy chain, and k
and l light chains). In selected cases, additional immunostains
were used (myeloperoxidase, CD33, CD123, CD68, CD163,
and CD11c). Cases were classified according to the WHO
classification [13].
Disease stage was defined according to the Murphy modified
system, [14] including physical examination, computed tomogra-
phy or magnetic resonance imaging, bone scan, complete blood
count, BM examination, cerebrospinal fluid (CSF) cell count, and
lactate dehydrogenase (LDH) level. CNS involvement was defined
as >5 cells/ml with lymphoblasts in the CSF, and/or CNS mass
lesion. BM involvement was considered as the presence of blasts
between 5% and <25%.
Treatment and Response Criteria
All patients received the same induction therapy, based on the
LSA2-L2 strategy, largely derived from the previous AIEOP LNH-
92 study [11]. The outline of the protocol and the treatment
elements are summarized in Figure 1 and Table I. While patients in
stage I or II received Induction followed by Consolidation and
Maintenance part I and II, patients in stages III or IValso received a
Reinduction after Consolidation. Patients with CNS involvement
received intensified therapy with high-dose cytarabine during
Consolidation, additional intrathecal therapy and cranial radiother-
apy (CRT) at the end of reinduction therapy in children�1 year old
(18 Gy in children <2 year old, 24 Gy in those aged�2 years). The
total therapy duration was 12 months for stages I and II, and
24 months for stages III and IV.
Early response to treatment was evaluated on day 15. The time
points for complete remission (CR) assessment were the end of
Induction and the end of Consolidation. CR was defined as the
absence of any residual mass and no blasts in the BM and in the
CSF. Patients in partial remission (PR), defined as a residual mass
<30% of the initial volume at the end of Induction, remained in the
same treatment group. Patients with residual tumor mass >30% at
the end of Induction received intensified chemotherapy with six
Figure 1. Treatment schema of AIEOP LNH-97 protocol.
Pediatr Blood Cancer DOI 10.1002/pbc
2 Pillon et al.

courses of high-risk ALL blocks, instead of Consolidation; if CR
was achieved, they completed the treatment program with
Reinduction and Maintenance; on the contrary, in case of
incomplete response, a second line treatment including allogeneic
hematopoietic stem cell transplantation (HSCT) was indicated.
Statistical Analysis
Analyses of overall survival (OS) and EFS were performed
using the Kaplan–Meier method, with differences compared by the
log-rank test [15,16]. OS was calculated from the date of diagnosis
to death from any cause or to the date of last follow-up. EFS was
calculated from the date of diagnosis to the first event (induction
failure, relapse, second malignancy, or death from any cause) or to
the date of last follow-up. Disease free survival (DFS) was defined
as the time from CR until tumor relapse or death from any cause or
to the last follow up. Patients lost to follow-up were censored at the
time of their withdrawal. Statistical analysis was carried out by
using the SAS statistical program (SAS-PC, version 9.3, SAS
Institute, Inc., Cary, NC).
TABLE I. Treatment Schedule
Phase Dose Administration route Days
Induction
Cyclophosphamide 1,000 mg/m2/day in 1 hr i.v. 1
Cyclophosphamide 600 mg/m2/day in 1 hr i.v. 8
Asparaginasea 5,000 U/m2/day i.m. 15, 18, 21, 24, 27, 30, 33, 36
Prednisone 60 mg/m2/day Orally 1–36
Vincristine 1.5 mg/m2/day i.v. 8, 15, 22, 29, 36
Daunorubicin 30 mg/m2/day in 4 hr i.v. 15, 22, 29, 36
HD-MTX 5 g/m2/day in 24 hr i.v. 36b
MTXþAra-CþPdn 12 mgþ30 mgþ10 mgc IT 1, 3d, 8, 15d, 22, 29d, 36
Consolidation
Mercaptopurine 25 mg/m2/day Orally 1–42
Ara-C 100 mg/m2/day i.v. 1–4, 8–11
HD-Ara-Ce 3 g/m2/every 12 hr in 3 hr i.v. 4, 5
Etoposide 100 mg/m2/day in 1 hr i.v. 1–4
HD-MTX 3 g/m2/day in 24 hr i.v. 1f, 22f, 36f
MTXþAra-CþPdn 12 mgþ 30 mgþ 10 mgc IT 1, 22, 36
Cranial RTg 2,400 cGyh At the end of Consolidation
Reinductioni
Cyclophosphamide 600 mg/m2/day in 1 hr i.v. 1
Doxorubicin 30 mg/m2/day in 4 hr i.v. 1, 8, 15
Dexamethasone 6 mg/m2/day Orally/i.v. 1–15
Asparaginasea 5,000 U/m2/day i.m. 8, 11, 14, 17
Vincristine 1.5 mg/m2/day i.v. 1, 8, 15, 22
Ara-C 100 mg/m2/day i.v. 29–32, 36–39
HD-MTX 3 g/m2/day in 24 hr i.v. 29f, 43f
Thioguanine 75 mg/m2/day Orally 29–43
MTXþAra-CþPdnj 12 mgþ 30 mgþ10 mgc IT 1, 15, 29, 43
Maintenance part I 2 cycles of 22 days each
Cyclophosphamide 600 mg/m2/day in 1 hr i.v. 1
Thioguanine 60 mg/m2/day Orally 1–7
MTX 40 mg/m2/day Orally 10
Vincristine 1.5 mg/m2/day i.v. 10
Prednisone 60 mg/ m2/day Orally 10–14
Ara-C 100 mg/m2/day i.v. 18–21
Etoposide 100 mg/m2/day in 1 hr i.v. 18–21
MTXþAra-CþPdnj 12 mgþ 30 mgþ 10 mgc IT 10
Maintenance part II k Time
MTX 20 mg/m2/week i.m. Weekly
MTXþAra-CþPdnl 12 mgþ 30 mgþ 10 mgc IT Every 8 week
Mercaptopurine 50 mg/m2/day Orally Daily
i.v., intravenously; HD, high-dose; MTX, methotrexate; Ara-C, cytosine arabinoside; Pdn, prednisolone; IT, intrathecal therapy; i.m.,
intramuscularly; RT, radiotherapy. aNative Escherichia coli Asparaginasi. bL-leucovorin rescue was administered at 42 hr (15 mg/m2 i.v.), at 48 and
54 hr (7.5 mg/m2 i.v.) from the beginning of HD-MTX infusion and subsequently every 6 hr till serum MTX values <0.25 mmol/L. cDose of IT
therapy was adjusted for children <3 years. dOnly if CNS positive. eHD-Ara-C only in CNS positive patients instead of low-dose Ara-C. fL-
leucovorin rescue, 7.5 mg/m2 i.v., was administered at 42, 48, and 54 hr from the beginning of HD-MTX infusion and subsequently every 6 hr till
serum MTX values<0.25 mmol/L. gCranial RTonly for CNS involvement. hCranial RT dose was adjusted for children>1 year and<2 years (1,800
cGy), but not administered in children<1 year. iOnly for stages III and IV. jIT not administered in children treated with cranial RT. kFor stages I and
II, up to 12 months of therapy; for stages III and IV, up to 24 months of therapy. lOnly for patients with CNS involvement but not irradiated.
Pediatr Blood Cancer DOI 10.1002/pbc
AIEOP LNH-97 Protocol Results 3

RESULTS
Diagnosis and Clinical Features
Of the 131 patients registered in the study, 17 were not eligible
because of age>18 years (n¼ 1), pre-treatment (n¼ 5), blasts in the
BM �25% (n¼ 6), other diagnosis at central review (n¼ 2),
treatment with another protocol (n¼ 2), and NHL as second
malignancy (n¼ 1). Thus a total of 114 patients were eligible. Their
median age at diagnosis was 9 years (range, 1.3–16.6). Central review
of the histological diagnosis was obtained in 90% of the cases;
immunophenotype analysis showed T-cell lineage in 88 cases (77%),
B-lineage in 26 cases. One patient was in stage I, 10 in stage II, 71 in
stage III, and 32 in stage IV (one due to isolated CNS involvement).
Median serum LDH value was 635 IU/L (range, 146–4,441). The
tumor involved a single site in 63 patients: mediastinum (n¼ 47),
lymph node (n¼ 7), parotid gland (n¼ 3), tonsil (n¼ 2), bowel
(n¼ 2), or skin (n¼ 2). In the remaining 51 patients (43%), multiple
sites were involved: in 29 cases mediastinal mass was combined with
other localization (BM, n¼ 16; lymph nodes, n¼ 10; tonsil, n¼ 2;
kidney, n¼ 1); in 15 cases BM involvement was combined with
lymph node (n¼ 9), skin (n¼ 2), bone (n¼ 2), kidney (n¼ 1), or
nasopharynx (n¼ 1); in 7 cases the disease involved lymph node and
testis (n¼ 1), or orbit (n¼ 2), or kidney (n¼ 3), or CNS (n¼ 1).
Response to Treatment and Outcome
Overall, CR was achieved in 112 patients (98%), in 19 already
on day þ15, in 46 at the end of Induction, in the remaining 46 only
at the end of Consolidation; one patient, with a residual mass>30%
at the end of Induction, received six courses of high-risk ALL
blocks (instead of Consolidation), achieving the first CR after the
third block therapy, and completed the scheduled chemotherapy.
Due to the late CR, this patient received an unrelated donor HSCTas
intensification therapy, by local treating physician decision, and
remains alive and disease free at last follow up. No statistically
significant difference in DFS was observed between patients who
obtained early CR (at dayþ15) or late CR (P¼ 0.36). Two patients
failed to achieve CR because of refractory disease and died of
progressive disease (PD), in one case after autologous HSCT.
Twenty-five patients (22%) developed a single site (n¼ 12) or
combined (n¼ 13) relapse at a median time of 14 months (range,
1.7–78 months) from CR, including nine patients who relapsed after
a median time of 14 months (range, 11–61 months) from completion
of therapy. Of the 25 patients who relapsed, 21 (84%) had a T-lineage
LBL (2 stage II, 12 stage III, 7 stage IV CNS negative) while four
patients (16%) had a B-lineage LBL (three stage III, one stage IV
CNS negative). Median time from diagnosis to relapse for T-LBL
patients was 1.3 years (range, 0.3–6.4 years) while median time for
B-lineage LBL was 3.1 years (range, 1.7–7.0). Twelve patients had an
isolated relapse in BM (n¼ 6), mediastinum (n¼ 2), skin (n¼ 2), and
CNS (n¼ 2, both in stage III at diagnosis), whereas 13 experienced a
combined relapse in mediastinum and lymph node (n¼ 2),
mediastinum and BM (n¼ 4), mediastinum plus BM and lymph
node (n¼ 4), BM and lymph node (n¼ 2), BM and testis, BM and
lymph node, thyroid and lymph node (n¼ 1), respectively.
Only seven patients with relapse (28%) survived after second line
chemotherapy and HSCT, either autologous (n¼ 1) or allogeneic
(n¼ 6). The remaining 18 patients died, eight of PD after second line
chemotherapy, and 10 after HSCT, due to: PD (n¼ 4), multiple
organ failure (MOF) (n¼ 2), cytomegalovirus pneumonia (n¼ 1),
adenovirus pneumonia (n¼ 1), sepsis of unknown etiology (n¼ 1),
and gram negative septicemia in second relapse (n¼ 1). Two
patients developed a second malignant neoplasm as their first
adverse event: one patient developed thyroid carcinoma 24 months
after the end of treatment and is still alive after surgical resection; the
second patient had M5 acute myeloid leukemia seven months after
completion of therapy and is in CR after allogeneic HSCT (Table II).
At a median follow-up of seven years (range, 0.7–12.4 years), OS
(standard error [SE]) and EFS (SE) were 82% (4%) and 74% (4%),
respectively (Fig. 2A). The 7 year EFS was 82% (12%) for stage I–II,
74% (5%) for stage III, and 72% (8%) for stage IV, P¼ 0.76
(Fig. 2B). Of note, the late events were three relapses: one in stage II
and two in stage III, at 6.4, 5.5, and 7 years, respectively. The 5-year
OS for the 27 patients who suffered relapse or PD was 24% (9%).
Univariate analysis of age, gender, tumor lineage, LDH value, BM
involvement, mediastinal mass, and stage, early response did not
show any subgroup at significantly different EFS (Table III).
Toxicity
Grade III/IV cytopenia was observed in all treatment phases: in
40% of patients during induction, in 57% during consolidation, in
TABLE II. Treatment Results and Outcome of 114 Children and Adolescents With Lbl, According to Immunophenotype and Disease Stage
Immunophenotype
TotalPre-B T
114 26 88
I II III IV I II III IV
Stage 114 1 6 8 11* 0 4 63 21
Early toxic death 0 0 0 0 0 0 0 0 0
Remission failure 2 0 0 0 0 0 0 2 0
CR 112 1 6 8 11 0 4 61 21
Alive in first CR 85 1 6 5 10a 0 2 48 13
Death in first CR 0 0 0 0 0 0 0 0 0
Second malignancy 2 0 0 0 0 0 0 1 1
Relapses 25 0 0 3 1 0 2 12 7
Alive after relapse 7 2 1 0 2 1 1
CR, complete remission. aIncluding one patient with CNS involvement.
Pediatr Blood Cancer DOI 10.1002/pbc
4 Pillon et al.

52% during reinduction and in 58% during maintenance therapy.
Liver toxicity episodes, mainly transaminase elevation, were
reported in 39% of patients; gastrointestinal toxicity episodes,
mainly due to stomatitis, occurred in 41% of patients; 21% of patients
developed clotting abnormalities, including two cases of thrombosis.
No toxic deaths were reported during first line treatment; six
study patients (5%) died after relapse, during salvage therapy, soon
after HSCT performed as consolidation of second remission, due to
multiorgan failure (n¼ 2) or septicemia (n¼ 4).
DISCUSSION
The main aim of this study was to increase the cure rate in
children with LBL, and particularly in those with advanced disease,
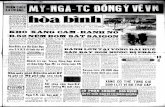
Figure 2. A: 7-year overall survival (OS; OS� standard error [SE], 82� 4%) and 7-year event-free survival (EFS; EFS�SE, 74� 4%) for the
entire study cohort. B: Seven-year EFS according to disease stage (EFS� SE), stage I–II, 82� 12%; stage III, 74� 5%; stage IV, 72� 8%; P: 0.76.
Pediatr Blood Cancer DOI 10.1002/pbc
AIEOP LNH-97 Protocol Results 5

who in the previous study had an EFS of 62% in stage III, and 75%
in stage IV [11]. To achieve this goal, late intensification
(“Reinduction”) was introduced for stage III and IV patients,
based on the favorable impact of this modification made by the
BFM group in their BFM-ALL-86 trial [10]. Also, initial
chemotherapy was intensified for all patients by increasing the
doses of cyclophosphamide (1,000 mg/m2 in 1 hr infusion on day
one, and 600 mg/m2 in 1 hr infusion on day 8 vs. 600 mg/m2/every
12 hr) and of MTX (5 g/m2 over 24 hr, vs. 3 g/m2 over 3 hours). L-
Asparaginase was administered in the induction phase, instead of
consolidation phase, to allow an earlier exposure. Comparative
analyses of AIEOP LNH-92 and AIEOP LNH-97 studies show that
treatment intensification was associated with a higher proportion of
cases achieving survival and EFS at 5 years (from 74% to 83%, and
from 69% to 77%, respectively) although this difference did not
reach statistical significance (P¼ 0.11 and P¼ 0.33, respectively).
These results are comparable with those achieved by major
cooperative groups in contemporary international studies in Europe
and North America [3–7,17–20]. The treatment intensification
applied was not associated with an increase of toxicity, in particular
we did not observe any toxic or infectious deaths.
The main cause for treatment failure was LBL relapse, observed
in 22% of patients. Unfortunately, the majority of them could not be
rescued by second line therapies; remarkably, all the patients still
alive received an allogeneic HSCT as part of their retreatment. This
is in keeping with the report of significantly lower progression rate,
and improved EFS, in patients with LBL after allogeneic HSCT
compared to autologous [21]. An older study had failed to
demonstrate the superiority of allogeneic versus autologous HSCT
for LBL [22]. However, in that study fewer than 20% of the study
population was aged �18 years. The outcome of patients who
failed, due to PD (rarely) or relapse was very poor, with a survival of
only 24%. As in our previous study, AIEOP LNH-92, and despite
the good results, the current analysis of presenting features was not
able to identify any prognostic factors associated with a higher risk
of treatment failure, that is, of lymphoma relapse. Thus, additional
tools for better stratification of patients with LBL still represent an
unmet need. Recent availability of molecular or flow-cytometry
markers could represent a critical tool to detect minimal residual
disease (MRD) with potential to predict clinical relapse, suitable for
therapeutic intervention. To this issue, Coustan-Smith et al.[23]
reported that flow cytometry and real-time quantitative PCR for T-
cell receptor rearrangements could identify submicroscopic BM
involvement associated with inferior outcome. The BFM Study
Group found a clear association between LOH at chromosome 6q,
seen in 19% of T-lineage LBL, and an increased risk of relapse [24].
More recently, Callens et al.[25] showed that NOTCH1/FBXW7
mutations, found in 55% of T-lineage LBL, were associated
with improved EFS and OS. Thus, molecular screening at the
diagnosis and timely evaluation of MRD during the early phase of
treatment should be major components of any future study design in
childhood LBL.
In summary, the long-term results of the AIEOP LNH-97
protocol show that treatment intensification was associated with a
good outcome in children and adolescents with LBL, stratified
according to Murphy system, and that allogeneic HSCT is strongly
indicated for relapsed patients. A combination of clinical and
biological parameters is in the pipeline of current international
collaboration to achieve refined stratification and further improve-
ment in treatment results.
REFERENCES
1. National Cancer Institute sponsored study of classifications of non-Hodgkin’s lymphomas: Summary and
description of a working formulation for clinical usage. The non-hodgkin’s lymphoma pathologic
classification project. Cancer. 1982;49:2112–2135.
2. Jaffe ES, Harris NL, Stein H, Vardiman JW. Pathology and Genetics of Tumours of Haematopoietic and
Lymphoid Tissues. Lyon: IARC Press 2001.
3. Sandlund JT, Pui CH, Zhou Y, Onciu M, Campana D, Hudson MM, Inaba H, Metzger ML, Bhojwani D,
Ribeiro RC. Results of treatment of advanced-stage lymphoblastic lymphoma at St Jude Children’s
Research Hospital from 1962 to 2002. Ann Oncol 2013;24:2425–2429.
4. Mora J, Filippa DA, Qin J, Wollner N. Lymphoblastic lymphoma of childhood and the LSA2-L2
protocol: The 30-year experience at Memorial-Sloan-Kettering Cancer Center. Cancer 2003;98:1283–
1291.
5. Patte C, Kalifa C, Flamant F, Hartmann O, Brugieres L, Valteau-Couanet D, Bayle C, Caillaud JM,
Lemerle J. Results of the LMT81 protocol, a modified LSA2L2 protocol with high dose methotrexate,
on 84 children with non-B-cell (lymphoblastic) lymphoma. Med Pediatr Oncol 1992;20:105–113.
6. Uyttebroeck A, Suciu S, Laureys G, Robert A, Pacquement H, Ferster A, Marguerite G, Mazingue F,
Renard M, Lutz P, Rialland X, Mechinaud F, Cave H, Baila L, Bertrand Y. Treatment of childhood
T-cell lymphoblastic lymphoma according to the strategy for acute lymphoblastic leukaemia,
without radiotherapy: Long term results of the EORTC CLG 58881 trial. Eur J Cancer 2008;44:
840–846.
7. Anderson JR, Jenkin RD, Wilson JF, Kjeldsberg CR, Sposto R, Chilcote RR, Coccia PF, Exelby PR, Siegel
S, Meadows AT. Long-term follow-up of patients treated with COMP or LSA2L2 therapy for childhood
non-Hodgkin’s lymphoma: A report of CCG-551 from the Childrens Cancer Group. J Clin Oncol
1993;11:1024–1032.
8. Reiter A, Schrappe M, Parwaresch R, Henze G, Muller-Weihrich S, Sauter S, Sykora KW, Ludwig WD,
Gadner H, Riehm H. Non-Hodgkin’s lymphomas of childhood and adolescence: results of a treatment
stratified for biologic subtypes and stage—A report of the Berlin-Frankfurt-Munster Group. J Clin Oncol
1995;13:359–372.
9. Tubergen DG, Krailo MD, Meadows AT, Rosenstock J, Kadin M, Morse M, King D, Steinherz PG, Kersey
JH. Comparison of treatment regimens for pediatric lymphoblastic non-Hodgkin’s lymphoma: A
Childrens Cancer Group study. J Clin Oncol 1995;13:1368–1376.
10. Reiter A, Schrappe M, Ludwig WD, Hiddemann W, Sauter S, Henze G, Zimmermann M, Lampert F,
Havers W, Niethammer D, Odenwald E, Ritter J, Mann G, Welte K, Gadner H, Rihem H. Chemotherapy in
998 unselected childhood acute lymphoblastic leukemia patients results and AT of the multicenter trial
ALL-BFM 86. Blood 1994;84:3122–3133.
11. Pillon M, Piglione M, Garaventa A, Conter V, Giuliano M, Arcamone G, Mura R, Cellini M, D’Amore ES,
Varotto S, Mussolin L, Rosolen A. Long-term results of AIEO P LNH–92 protocol for the treatment of
pediatric lymphoblastic lymphoma: A report of the Italian association of pediatric hematology and
oncology. Pediatr Blood Cancer 2009;53:953–959.
12. Reiter A, Schrappe M, Ludwig WD, Tiemann M, Parwaresch R, Zimmermann M, Schirg E, Henze G,
Schellong G, Gadner H, Riehm H. Intensive ALL-type therapy without local radiotherapy provides a 90%
TABLE III. Univariate Analysis of Risk Factors
Patients
No.
7-year EFS
% (SE) Events P value
Gender
Male 84 73 (5) 22 0.69
Female 30 76 (8) 7
Median age at diagnosis
< 9 years 57 71 (6) 16 0.49
� 9 years 57 77 (6) 13
Immunophenotype
T 88 71 (5) 25 0.17
Pre-B 26 83 (8) 4
LDH
<500 IU/L 43 69 (7) 13 0.56
�500 IU/L 71 77 (5) 16
Bone marrow involvement
Yes 31 71 (8) 9 0.61
No 83 75 (5) 20
Mediastinal mass
Yes 76 75 (5) 19 0.91
No 38 72 (8) 10
Stage
Iþ II 11 82 (12) 2 0.48
IIIþ IV 103 73 (4) 27
Early response
CR on day þ15 19 83 (9) 3 0.36
CR after day þ15 93 74 (5) 24
EFS, event free survival; SE, standard error; LDH, lactate dehydroge-
nase; CR, complete remission.
Pediatr Blood Cancer DOI 10.1002/pbc
6 Pillon et al.

event-free survival for children with T-cell lymphoblastic lymphoma: A BFM group report. Blood
2000;95:416–421.
13. Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J, Vardiman JW.
WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. 4th Edition. Lyon: IARC
2009.
14. Murphy SB. Classification, staging and end results of treatment in childhood non Hodgkin’s lymphoma:
Dissimilarities from lymphomas in adults. Sem Oncol 1980;7:332–339.
15. Peto R, Peto J. Asymptotically efficent rank invariant test procedures. J R Stat Soc Ser A 1972;135:
185–198.
16. Kaplan EL, Meier P. Nonparametric estimation from incomplete observation. J Am Stat Assoc
1958;53:457–481.
17. Gao YJ, Pan C, Tang JY, Lu FJ, Chen J, Xue HL, Zhai XW, Li J, Ye QD, Zhou M, Wang HS, Miao H, Qian
XW, Xu Z, Meng JH. Clinical outcome of childhood lymphoblastic lymphoma in Shanghai China 2001–
2010. Pediatr Blood Cancer 2014;61:659–663.
18. Burkhardt B, Woessmann W, Zimmermann M, Kontny U, Vormoor J, Doerffel W, Mann G, Henze G,
Niggli F, Ludwig WD, Janssen D, Riehm H, Schrappe M, Reiter A. Impact of cranial radiotherapy on
central nervous system prophylaxis in children and adolescents with central nervous system-negative stage
III or IV lymphoblastic lymphoma. J Clin Oncol 2006;24:491–499.
19. Abromowitch M, Sposto R, Perkins S, Zwick D, Siegel S, Finlay J, Cairo MS. Shortened intensified multi-
agent chemotherapy and non-cross resistant maintenance therapy for advanced lymphoblastic lymphoma
in children and adolescents: Report from the Children’s Oncology Group. Br J Haematol 2008;143:
261–267.
20. Termuhlen AM, Smith LM, Perkins SL, Lones M, Finlay JL, Weinstein H, Gross TG, Abromowitch M.
Disseminated lymphoblastic lymphoma in children and adolescents: Results of the COG A5971 trial: A
report from the Children’s Oncology Group. Br J Haematol 2013;162:792–801.
21. Gross TG, Hale GA, He W, Camitta BM, Sanders JE, Cairo MS, Hayashi RJ, Termuhlen AM, Zhang MJ,
Davies SM, Eapen M. Hematopoietic stem cell transplantation for refractory or recurrent non-hodgkin
lymphoma in children and adolescents. Biol Blood Marrow Transplant 2010;16:223–230.
22. Levine JE, Harris RE, Loberiza FR Jr, Armitage JO, Vose JM, Van Besien K, Lazarus HM, Horowitz MM,
Bashey A, Bolwell BJ, Burns LJ, Cairo MS, Champlin RE, Freytes CO, Gibson J, Goldstein SC, Laughlin
MJ, Lister J, Marks DI, Maziarz RT, Miller AM, Milone GA, Pavlovsky S, Pecora AL, Rizzo JD, Schiller
G, Schouten HC, Zhang MJ. A comparison of allogeneic and autologous bone marrow transplantation for
lymphoblastic lymphoma. Blood 2003;101:2476–2482.
23. Coustan-Smith E, Sandlund JT, Perkins SL, Chen H, Chang M, Abromowitch M, Campana D. Minimal
disseminated disease in childhood T-cell lymphoblastic lymphoma: A report from the children’s oncology
group. J Clin Oncol 2009;27:3533–3539.
24. Burkhardt B, Moericke A, Klapper W, Greene F, Salzburg F, Damm-Welk J, Zimmermann C, Strauch M,
Ludwig K, Schrappe WD, Reiter M. Pediatric precursor T lymphoblastic leukemia and lymphoblastic
lymphoma: Differences in the common regions with loss of heterozygosity at chromosome 6q and their
prognostic impact. Leuk Lymphoma 2008;49:451–461.
25. Callens C, Baleydier F, Lengline E, Ben A, Petit R, Villarese A, Cieslak P, Minard-Colin A, Rullier V,
Moreau A, Baruchel A, Schmitt A, Asnafi C, Bertrand V, Macintyre Y. Clinical impact of NOTCH1 and/or
FBXW7 mutations, FLASH deletion, and TCR status in pediatric T-cell lymphoblastic lymphoma. J Clin
Oncol 2012;30:1966–1973.
Pediatr Blood Cancer DOI 10.1002/pbc
AIEOP LNH-97 Protocol Results 7