
Functional and Anatomic Alterations in the Gentamicin-Damaged Vestibular System in the Guinea Pig
Upload
independentCategory
view
5download
0
The Journal of Arthroplasty Vol. 24 No. 1 2009
Long-Term Remodeling in Proximal Femur Around aHydroxyapatite-Coated Anatomic Stem
Ten Years Densitometric Follow-Up
Juan J. Panisello, PhD, Luis Herrero, PhD, Vicente Canales, PhD, Antonio Herrera, PhD,Angel A. Martínez, PhD, and Jesús Mateo, MD
Abstract: Bone remodeling after a hip arthroplasty has been quantified with dualenergy x-ray absorptiometry, usually for short-term follow-up. We used thistechnique to determine the long-term remodeling produced by a hydroxyapatite-coated, anatomic stem. Eighty patients with unilateral hip osteoarthritis wereincluded in the study. The contralateral, healthy hip was taken as control. Bilateraldual energy x-ray absorptiometry scans were done before the surgery, at 15 days, and1 and 10 years postoperatively. There was a decrease of bone mineral density inzones 1 and 7, which ranged from 12.2% to 27.3% at the end of the first year. Therewere no changes in zones 1 to 6 from the 1st to the 10th year, but there was a latedecrease, up to 42.9%, in zone 7. The changes of bone mineral density promoted bythis stem occurred in the first postoperative year. Late loss was seen only in area 7.Key words: cementless hip prostheses, densitometry, anatomic stem, boneremodeling, stress shielding.© 2009 Elsevier Inc. All rights reserved.
Bone remodeling after a hip arthroplasty is acommon event observed in all designs of hipprostheses. Nevertheless, the amount of this remo-deling can vary depending on factors related to thepatients (mainly preoperative bone quality) andfactors related to the stem (alloy, size, shape, design,and surface texture) [1-4]. It is generally acceptedthat most of the changes of bone mass around thefemoral stem occur in the first 3 years after theprocedure [5-7]; however, little is known about
From the Department of Orthopaedic Surgery. Miguel ServetUniversity Hospital, Zaragoza, Spain.
Submitted February 4, 2007; accepted December 11, 2007.No benefits or funds were received in support of this study.Reprint requests: Juan José Panisello, PhD, Sebastiá. 3 Maria
Espinosa, Street, First floor, Door O. 50018 Zaragoza, Spain.© 2009 Elsevier Inc. All rights reserved.0883-5403/08/2401-0010$36.00/0doi:10.1016/j.arth.2007.12.017
56
the effect of long-term remodeling and age-relatedchanges on stem fixation.
Dual x-ray absorptiometry (DEXA) has beenwidely used to quantify the extent of periprostheticbone loss around joint implants [8-11]. This methodhas been proven to be accurate and reliable, and it isconsidered ideal for repeated examinations on thesame patient.
To know the pattern of long-term remodelingproduced by a hydroxyapatite (HA)-coated ana-tomic stem, we designed a prospective, controlledstudy with 80 patients who have unilateral osteoar-thritis. Each patient was treated with this type ofstem and evaluated with DEXA throughout the first10 postoperative years. The aims of this study wereto determine the pattern of remodeling produced bythis stem, to quantify the changes of bone density inthe 7 zones of Gruen throughout the follow-up, toprove or reject the presence of positive long termremodeling, and to quantify the effect of aging onperiprosthetic bone density.

Fig. 1. ABG-I stem. An anatomical design with scale-shaped recesses underneath the HA coating in themetaphyseal portion of the implant.
Hydroxyapatite-Coated Anatomic Stem � Panisello et al 57
Materials and Methods
A prospective, controlled study was designed toinvestigate the periprosthetic remodeling broughtabout by the ABG-I stem. The size of the sample wascalculated considering the average loss of bonemineral density (BMD) reported in previous studiesin the 7 zones of Gruen [1,4,7,9,12-15], which was130 mg of HA per cm2, and the variation of bonedensity in the preoperative scans. It was considerednecessary to include a minimum of 60 patients inthe study group. To keep a sufficient number ofpatients throughout the follow-up, we included20 additional patients. The inclusion criteria werethe following: firstly, the type of implant beingstudied should be indicated by the patients' condi-tion according to the shape of the femur and theirbone quality; secondly, involvement should beunilateral because the healthy opposite hip wasused as a control; and finally, patients had to sign adocument granting their informed consent toparticipate in the study. The local Research EthicsCommittee authorized the study. Osteoarthritis wasdiagnosed in all the cases. Patients were included inthe study between February and October 1994.Eighty patients met the inclusion criteria and wereincluded in the study; however, only 61 of themcompleted the 10-year follow-up period (32 menand 29women), with a mean age of 59 years (range,38-76 years) and a mean body weight of 79.3 kg(range, 49-110 kg) at the time of the surgery. Thedata related to those 19 patients who did notcomplete the 10-year follow-up were not includedin the study. The following were the reasons for theexclusion: 2 of the 19 patients developed severediseases not related to their hip arthroplasty thatprevented them from walking; 3 had severeosteolysis around the stem that required revision;6 moved to different cities and were removed fromthe follow-up; and finally, 8 needed a latercontralateral arthroplasty.The implant used was the ABG-I stem (Stryker,
Howmedica), with a cementless, modular, press-fitcup belonging to the ABG-I system (the cup was notpart of the study). The ABG-I is a cementlessanatomic stem with press-fit metaphyseal fixationmade of an alloy of titanium (Ti6Al4V) (Fig. 1). Atthe metaphyseal level, the implant is covered by a70-μm-deep HA layer of 97% of crystallinity andfeatures a scale-shaped anterior and posterior designthat increases its stability. The distal portion of theimplant is short and thin to avoid endomedullarycontact with the diaphysis.All the patients were operated on using a standard
posterolateral approach by the same group of 4
surgeons. The femoral canal was prepared withdiaphyseal reaming (1 mm more than the tipdiameter calculated preoperatively) and progressivebroaching leaving 2 to 3 mm of metaphysealcancellous bone around the stem. The bearingsurface was metal on polyethylene in all the cases.Postoperatively, all the patients received low-mole-cular-weight heparin for prophylaxis against deepvenous thrombosis and antibiotic prophylaxis forthe first 48 hours. Partial weight bearing with 2crutches was allowed during the first 6 weeks; andwalking with a walking stick was recommended foranother 6 weeks.
Clinical assessment was done using the MerleD'Aubigné score preoperatively and every year afterthe surgery. Radiographs were obtained annually todetermine changes in cup or stem position andany other radiographic findings according to Engh'scriteria [16].
The evolution criterion used were the BMDvariations in a series of small 30 × 30 pixel framesfor each 1 of the 7 Gruen zones, both in the operatedand in the healthy hip (Fig. 2). To ensure the preciseplacement of the bones throughout the study, weused the scan comparison software provided byHologic for the densitometer used in the study. Bonedensity measurements were made with a HOLOGICQDR 1000 densitometer (Hologic Inc, Waltham,MA), using the Hologic metal exclusion software, onboth hips during the preoperative, 15th postopera-tive day, and 1 and 10 years after surgery. In
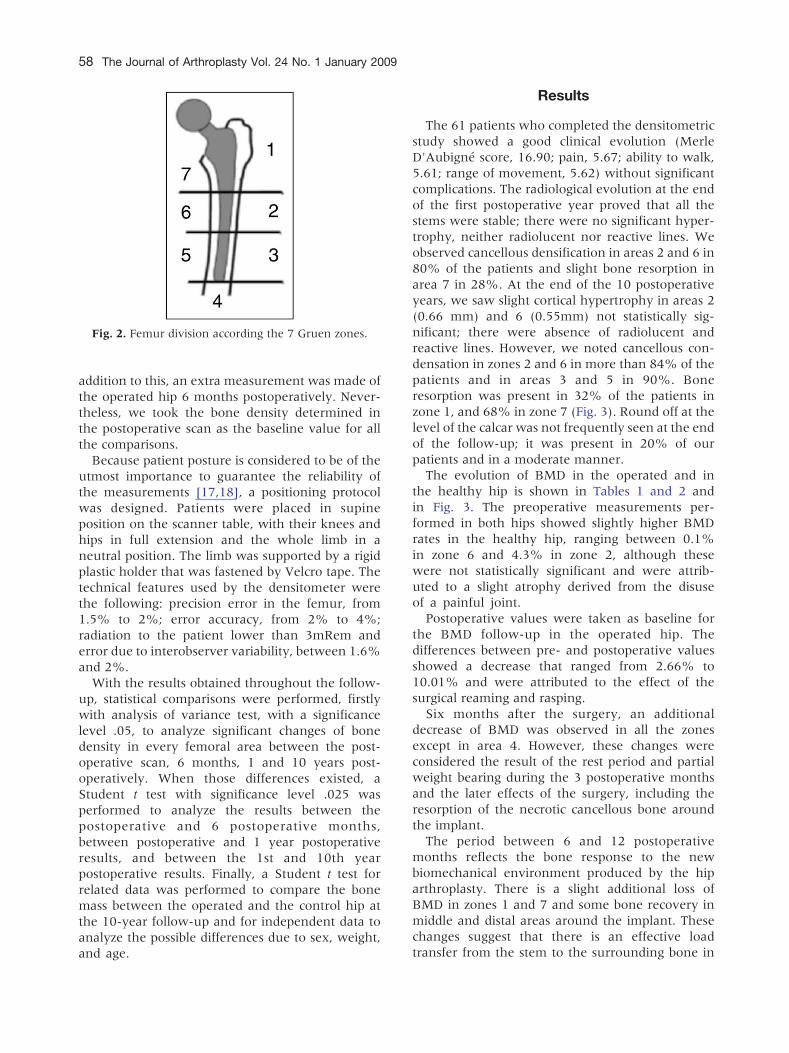
Fig. 2. Femur division according the 7 Gruen zones.
58 The Journal of Arthroplasty Vol. 24 No. 1 January 2009
addition to this, an extra measurement was made ofthe operated hip 6 months postoperatively. Never-theless, we took the bone density determined inthe postoperative scan as the baseline value for allthe comparisons.Because patient posture is considered to be of the
utmost importance to guarantee the reliability ofthe measurements [17,18], a positioning protocolwas designed. Patients were placed in supineposition on the scanner table, with their knees andhips in full extension and the whole limb in aneutral position. The limb was supported by a rigidplastic holder that was fastened by Velcro tape. Thetechnical features used by the densitometer werethe following: precision error in the femur, from1.5% to 2%; error accuracy, from 2% to 4%;radiation to the patient lower than 3mRem anderror due to interobserver variability, between 1.6%and 2%.With the results obtained throughout the follow-
up, statistical comparisons were performed, firstlywith analysis of variance test, with a significancelevel .05, to analyze significant changes of bonedensity in every femoral area between the post-operative scan, 6 months, 1 and 10 years post-operatively. When those differences existed, aStudent t test with significance level .025 wasperformed to analyze the results between thepostoperative and 6 postoperative months,between postoperative and 1 year postoperativeresults, and between the 1st and 10th yearpostoperative results. Finally, a Student t test forrelated data was performed to compare the bonemass between the operated and the control hip atthe 10-year follow-up and for independent data toanalyze the possible differences due to sex, weight,and age.
Results
The 61 patients who completed the densitometricstudy showed a good clinical evolution (MerleD'Aubigné score, 16.90; pain, 5.67; ability to walk,5.61; range of movement, 5.62) without significantcomplications. The radiological evolution at the endof the first postoperative year proved that all thestems were stable; there were no significant hyper-trophy, neither radiolucent nor reactive lines. Weobserved cancellous densification in areas 2 and 6 in80% of the patients and slight bone resorption inarea 7 in 28%. At the end of the 10 postoperativeyears, we saw slight cortical hypertrophy in areas 2(0.66 mm) and 6 (0.55mm) not statistically sig-nificant; there were absence of radiolucent andreactive lines. However, we noted cancellous con-densation in zones 2 and 6 in more than 84% of thepatients and in areas 3 and 5 in 90%. Boneresorption was present in 32% of the patients inzone 1, and 68% in zone 7 (Fig. 3). Round off at thelevel of the calcar was not frequently seen at the endof the follow-up; it was present in 20% of ourpatients and in a moderate manner.
The evolution of BMD in the operated and inthe healthy hip is shown in Tables 1 and 2 andin Fig. 3. The preoperative measurements per-formed in both hips showed slightly higher BMDrates in the healthy hip, ranging between 0.1%in zone 6 and 4.3% in zone 2, although thesewere not statistically significant and were attrib-uted to a slight atrophy derived from the disuseof a painful joint.
Postoperative values were taken as baseline forthe BMD follow-up in the operated hip. Thedifferences between pre- and postoperative valuesshowed a decrease that ranged from 2.66% to10.01% and were attributed to the effect of thesurgical reaming and rasping.
Six months after the surgery, an additionaldecrease of BMD was observed in all the zonesexcept in area 4. However, these changes wereconsidered the result of the rest period and partialweight bearing during the 3 postoperative monthsand the later effects of the surgery, including theresorption of the necrotic cancellous bone aroundthe implant.
The period between 6 and 12 postoperativemonths reflects the bone response to the newbiomechanical environment produced by the hiparthroplasty. There is a slight additional loss ofBMD in zones 1 and 7 and some bone recovery inmiddle and distal areas around the implant. Thesechanges suggest that there is an effective loadtransfer from the stem to the surrounding bone in

Fig. 3. (A) Preoperative x-ray showing unilateral osteoarthritis (required to be included in the study). (B) Six monthspostoperative x-ray showing theABG-1 stemwith appropriate fit in themetaphyseal area. (C) Ten-year postoperative x-ray.The stem was stable, no subsidence was noted. The picture shows the usual radiographic evolution of this stem at 10-yearfollow-up: slight cortical hypertrophy in areas 2 to 6 and some osteopenia in areas 1 and 7. Cancellous condensation isobserved in zones 2, 3, 5, and 6. The shape of the proximal femur is usually preserved because round offwas not often seen inthe calcar with this stem. (D) DEXA of the same hip at 10-year follow-up, showing the average changes of BMD at the end ofthe follow-up. There is a decrease of bone density in areas 1 and 7, whereas in areas 2, 3, 5, and 6, there are almost nochanges of bone density, suggesting an adequate load transfer that promotes bone mass preservation.
Hydroxyapatite-Coated Anatomic Stem � Panisello et al 59
zones 2 and 6 helping to promote bone preservationand some bone restoration from these points todistal areas. Nevertheless, the load transfer toproximal zones, 1 and 7, seemed to be insufficientto preserve the bone density.There were no significant changes of BMD in the
period between the end of the 1st year and the 10thpostoperative year in zones 1 to 6, which seemed tohave reached a plateau, with some small bonerecovery in zones 2 to 6.However, there was a decrease of BMD in zone 7
in the period between the 1st and the 10thpostoperative year, which reached up to 42.9%.
To determine the cause of these late changes in zone7, we reviewed all the radiographs corresponding tothat period. In all the cases, the radiographs showedstable stems but with some bone resorption in twothirds of the patients, which was not found in thefirst postoperative treatment.
The BMD in the contralateral, healthy hip,showed slight differences in this period. At the endof the study, the decreases ranged from 0.9% to7.2% and were more evident in the proximal part ofthe femur, richer in cancellous bone, and reflectedthe regressive changes of aging. When comparedwith the operated hip, the BMD in middle and distal

Table 1. Bone Density Changes in the Operated Hip Throughout the Follow-Up
Femur Preoperative Postoperative (baseline) 6 mo 1 y 10 y
Zone 1 746 680 622 596 594SD 169.5 145.4 228.5 182.3 188.1Min-Max 385-1167 389-986 322-1268 349-1195 376-77695% CI −174.3 to −1.3 −159.6 to −75.2 −290.4 to −50.3% change −8.52 −12.35 −12.64P .026 .002* .020*Zone 2 1166 1125 1072 1095 1138SD 265.2 209.0 291.5 276.7 344.8Min-Max 773-1772 607-1655 680-1769 667-1948 568-166995% CI −153.8 to 15.5 −125.2 to 32.7 −291.4 to 243.2% change −4.71 −2.66 +1.01P .393 .239 .668Zone 3 1488 1411 1299 1374 1354SD 282.4 181.6 263.8 260.3 293.5Min-Max 968-2079 1072-1809 941-1913 853-2103 877-183595% CI −194.2 to −38.4 −141.5 to 5.5 −461.5 to 274.6% change −7.93 −2.62 −4.03P .053 .169 .478Zone 4 1582 1482 1485 1497 1433SD 273.5 211.9 263.4 231.4 315.1Min-Max 1119-2122 1039-1916 1025-2076 1094-2008 1065-201695% CI −46.2 to 68.9 −54.3 to 71.8 −371.5 to 227.6% change +0.20 +1.01 −3.30P .881 .776 .907Zone 5 1545 1462 1440 1446 1442SD 360.0 301.6 284.3 273.5 321.5Min-Max 934-2589 870-2250 868-2106 805-2174 906-214295% CI −149.7 to −3.2 −150.1 to 7.5 −344.5 to 299.7% change −1.50 −1.09 −1.37P .206 .274 .288Zone 6 1353 1317 1188 1197 1327SD 383.7 315.1 309.4 310.8 350.9Min-Max 695-2386 750-2045 594-1968 657-1927 643-220995% CI −331.7 to −84.2 −316.8 to −62.9 −445.3 to 302.8% change −9.79 −9.11 +0.7P .048 .055 .456Zone 7 1285 1172 896 852 669SD 304.2 305.6 321.9 310.3 274.6Min-Max 634-1997 643-2056 474-1671 409-1848 398-102595% CI −423.1 to −247.8 −436.9 to −252.1 −719.1 to −139.% change −24.06 −27.3 −42.91P .022* .018* .001*
The bone density is expressed in mg of HA per cm2.The percentage of variation is related to the postoperative scan, considered as the baseline values.CI indicates confidence interval.*Statistically significant change.
60 The Journal of Arthroplasty Vol. 24 No. 1 January 2009
areas were similar in both hips. Only in zones 1 and7 were there significantly reduced values on theoperated hip.To analyze the influence of factors such as
patients' age, weight, and sex, we carried out newanalyses. Firstly, the influence of age was analyzedby classifying patients into 2 age groups: patientsyounger or older than 65 years. This factor was notfound to have a statistically significant influence onthe periprosthetic remodeling of any of the zonesstudied. Similar results were obtained when com-paring bone stock rates and remodeling evolutionbetween patients with weight less than 75 kg andthose with weight greater than 75 kg. Similar
findings related to the patients' sex were obtained,that showed no significant differences.
Discussion
Bone remodeling after a hip arthroplasty has amultifactorial origin [4,5,19]. In the early stages, arapid bone loss can be detected during the first 3 to6 months and vary between 20% and 50%depending on the type of implant and the studymethodology. This loss is caused by different factors,including postoperative rest, partial weight bearing,and surgical technique. The bone mass is affected
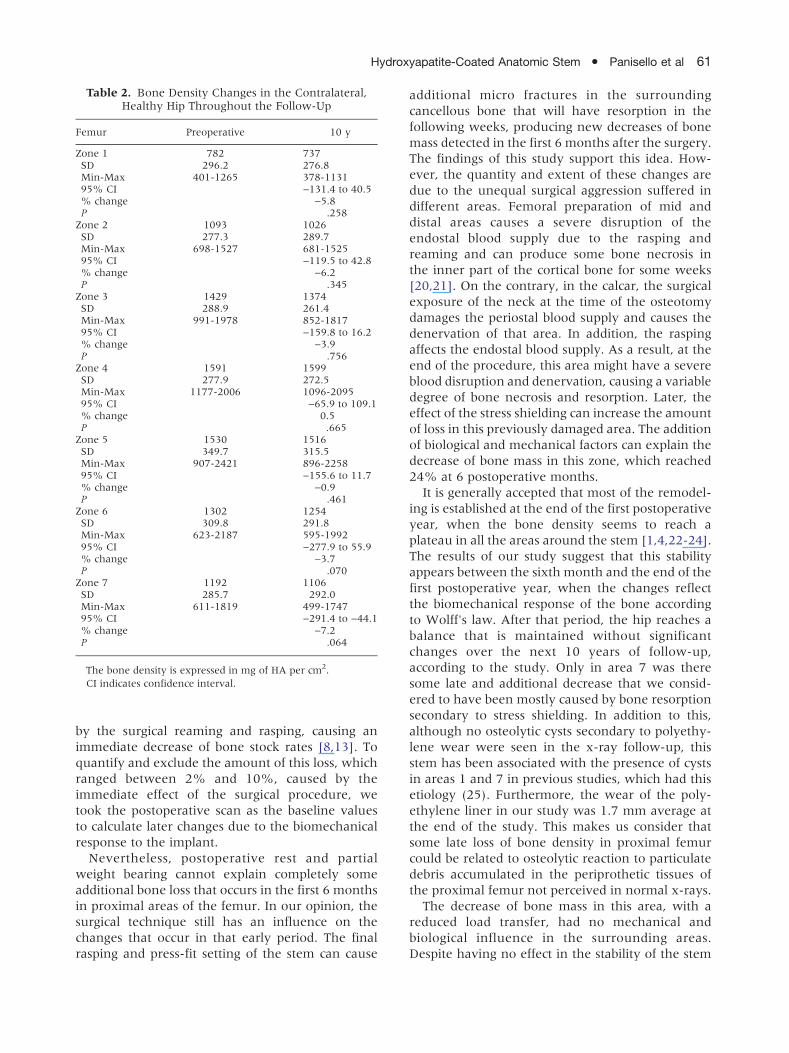
Table 2. Bone Density Changes in the Contralateral,Healthy Hip Throughout the Follow-Up
Femur Preoperative 10 y
Zone 1 782 737SD 296.2 276.8Min-Max 401-1265 378-113195% CI −131.4 to 40.5% change −5.8P .258Zone 2 1093 1026SD 277.3 289.7Min-Max 698-1527 681-152595% CI −119.5 to 42.8% change −6.2P .345Zone 3 1429 1374SD 288.9 261.4Min-Max 991-1978 852-181795% CI −159.8 to 16.2% change −3.9P .756Zone 4 1591 1599SD 277.9 272.5Min-Max 1177-2006 1096-209595% CI −65.9 to 109.1% change 0.5P .665Zone 5 1530 1516SD 349.7 315.5Min-Max 907-2421 896-225895% CI −155.6 to 11.7% change −0.9P .461Zone 6 1302 1254SD 309.8 291.8Min-Max 623-2187 595-199295% CI −277.9 to 55.9% change −3.7P .070Zone 7 1192 1106SD 285.7 292.0Min-Max 611-1819 499-174795% CI −291.4 to −44.1% change −7.2P .064
The bone density is expressed in mg of HA per cm2.CI indicates confidence interval.
Hydroxyapatite-Coated Anatomic Stem � Panisello et al 61
by the surgical reaming and rasping, causing animmediate decrease of bone stock rates [8,13]. Toquantify and exclude the amount of this loss, whichranged between 2% and 10%, caused by theimmediate effect of the surgical procedure, wetook the postoperative scan as the baseline valuesto calculate later changes due to the biomechanicalresponse to the implant.Nevertheless, postoperative rest and partial
weight bearing cannot explain completely someadditional bone loss that occurs in the first 6 monthsin proximal areas of the femur. In our opinion, thesurgical technique still has an influence on thechanges that occur in that early period. The finalrasping and press-fit setting of the stem can cause
additional micro fractures in the surroundingcancellous bone that will have resorption in thefollowing weeks, producing new decreases of bonemass detected in the first 6 months after the surgery.The findings of this study support this idea. How-ever, the quantity and extent of these changes aredue to the unequal surgical aggression suffered indifferent areas. Femoral preparation of mid anddistal areas causes a severe disruption of theendostal blood supply due to the rasping andreaming and can produce some bone necrosis inthe inner part of the cortical bone for some weeks[20,21]. On the contrary, in the calcar, the surgicalexposure of the neck at the time of the osteotomydamages the periostal blood supply and causes thedenervation of that area. In addition, the raspingaffects the endostal blood supply. As a result, at theend of the procedure, this area might have a severeblood disruption and denervation, causing a variabledegree of bone necrosis and resorption. Later, theeffect of the stress shielding can increase the amountof loss in this previously damaged area. The additionof biological and mechanical factors can explain thedecrease of bone mass in this zone, which reached24% at 6 postoperative months.
It is generally accepted that most of the remodel-ing is established at the end of the first postoperativeyear, when the bone density seems to reach aplateau in all the areas around the stem [1,4,22-24].The results of our study suggest that this stabilityappears between the sixth month and the end of thefirst postoperative year, when the changes reflectthe biomechanical response of the bone accordingto Wolff's law. After that period, the hip reaches abalance that is maintained without significantchanges over the next 10 years of follow-up,according to the study. Only in area 7 was theresome late and additional decrease that we consid-ered to have been mostly caused by bone resorptionsecondary to stress shielding. In addition to this,although no osteolytic cysts secondary to polyethy-lene wear were seen in the x-ray follow-up, thisstem has been associated with the presence of cystsin areas 1 and 7 in previous studies, which had thisetiology (25). Furthermore, the wear of the poly-ethylene liner in our study was 1.7 mm average atthe end of the study. This makes us consider thatsome late loss of bone density in proximal femurcould be related to osteolytic reaction to particulatedebris accumulated in the periprothetic tissues ofthe proximal femur not perceived in normal x-rays.
The decrease of bone mass in this area, with areduced load transfer, had no mechanical andbiological influence in the surrounding areas.Despite having no effect in the stability of the stem

62 The Journal of Arthroplasty Vol. 24 No. 1 January 2009
after 10 years of follow-up, the possible increase inbone resorption can compromise the long-termstability of the stem.The pattern of remodeling produced by this
anatomic, cementless stem was quite similar tothose shown by other second-generation cementlessstems. Several densitometric studies [1,7,22,23,25]have observed a decrease of bone mass thatranged between 20% and 25% in proximal areas,between 5% to 15% in intermediate parts, andwith no significant loss in distal areas. Thesechanges were stable after 1 to 2 years of post-operative evolution.However, long term remodeling can be influenced
by different factors such as age-related changes.There are several studies proving that aging affectsboth trabecular and cortical bone [4,6,19,26]. None-theless, the amount of these changes in our studyat the 10-year follow-up was reduced, rangingfrom 0.9% to 7.2%, mostly trabecular and withminimal effect in cortical bone. These changescoincided with the changes of bone density observedin the Spanish population, which had an averagedecrease of 3.7% between groups 50-59 and 60-69 years old [27]. Thus, the differences of BMDobserved between the operated and healthy hipwere significant only in proximal zones. These factsallow us to propose that the age-related effects inpeople who are 60 years old at the time of thesurgery have a minimal influence in their BMD10 years after a hip arthroplasty. Secondly, thisanatomic cementless stem provides a model of loadtransfer that helps to preserve similar rates of bonedensity in the mid and distal zones of the femurwhen compared with the contralateral, healthy hip.Changes of BMD related to stress shielding are
usually detected at the end of the first postoperativeyear. In a normal proximal femur, load transfer istransmitted from the femoral head to the lessertrochanter that withstands greater compressiveforces than the more diaphyseal parts of the femur[12]. After a hip arthroplasty, this pattern of loadtransfer is reversed. Most of the compressive loadsare transmitted to diaphyseal areas by the stem,which causes a proximal unloading and, as a result,bone resorption. In densitometric studies, first-generation cementless stems were associated withhigh proximal losses attributable to adaptive boneremodeling that reached up to 45% of bone mass.These changes were stable after the first or secondyear [3,4,19]. Second-generation cementless stems,made of titanium and with anatomic design toimprove the stem-canal fill, still showed a decreaseof BMD at the end of the second year that rangedfrom 20% to 25% [7,23,25]. Tapered femoral
components, often used in Europe, had a proximalloss between 10% and 30% [1,10,28]. Custom-made implants had the best results with regardproximal loss of BMD, but they still had a fallbetween 10% and 15% at the end of the third year[29-31]. More recently, femoral stems with reducedstiffness showed a 15% reduction of BMD in calcarat the end of the second year and even 10 to 15 yearsafter the surgery [2,22,32].
The pattern of remodeling observed with the ABGstem was similar to those reported by otheranatomic stems, with proximal loss of bone massdue to the new biomechanical environment causedby the hip arthroplasty. Adaptive changes mayappear in response to the design, size, and alloyonce the stem reaches the biological fixation. Atthe end of the first postoperative year, these changesseem to reach a balance and, providing both bio-logical and mechanical disturbances do not exist,no significant changes of BMD should be detected.In that way, this study has not observed any signof positive bone remodeling reported in otherarticles [12]. Once an arthroplasty changes thebiomechanics of the hip, the BMD varies accordingto the “adaptive bone remodeling” produced byeach different design, and their mechanical effectsare permanent.
We acknowledge several limitations of this study.First, the bone remodeling is considered to be aresponse to the new biomechanical environmentdetermined by the implant, according to its design,size, and alloy; however, little is known about theeffect of the HA layer in the early stages of thisremodeling. It is said that HA promotes bonefixation on the implant, and this event can providean increased area of contact between bone andimplant and a slightly different pattern of loadtransfer. Second, the size of the implant was decidedto obtain a solid metaphyseal fixation and aminimum of 2 or 3 mm of cancellous bone aroundthe implant. However, some patients with moredense cancellous bone allowed us to use smallerimplants and leave more metaphyseal bone thanothers, which can possibly cause some changes inthe pattern of load transfer. Finally, the follow-up ofthis study may be insufficient, above all because it isin more elderly patients that the changes due tolong-term remodeling can have a more intenseeffect and produce more consequences on theimplant fixation.
To sum up, we consider that the pattern ofremodeling produced by the ABG stem was estab-lished in the period between 6 and 12 postoperativemonths and then remained stable throughout theentire follow-up. Additional loss was observed in
Hydroxyapatite-Coated Anatomic Stem � Panisello et al 63
response to stress shielding but confined to thecalcar and without clinical effect. In relatively youngpatients, the changes related to age had nosignificant consequences on BMD; longer follow-up is required to determine the influence of endostalbone resorption on stem stability. The biomechani-cal response of the bone after the hip arthroplastyproduces an adaptive remodeling that remains,provided that no metabolic, mechanical, or biologi-cal events affect the hip.
References
1. Gibbons C, Davis A, Olearnik H, et al. Periprostheticbone mineral density changes with femoral compo-nents of different design philosophy. Int Orthop2001;25:89.
2. Glassman AH, Crowninshield RD, Schenck R, et al. Alow stiffness composite biologically fixed prostheses.Clin Orthop Relat Res 2001;393:128.
3. McAuley J, Sychterz CH, Ench CA. Influence ofporous coating level on proximal femoral remodeling.Clin Orthop Relat Res 2000;371:146.
4. Sychter CJ, Engh CA. The influence of clinical factoron periprosthetic bone remodeling. Clin Orthop RelatRes 1996;322:285.
5. Braun A, Papp J, Reiter A. The periprosthetic boneremodeling process signs of vital bone reaction. IntOrthop 2003;27(S1):7.
6. Bugbee W, Culpepper W, Engh A, et al. Long termclinical consequences of stress-shielding after total hiparthroplasty without cement. J Bone Joint Surg Am1997;79:1007.
7. Tanzer M, Kantor S, Rosenthall L, et al. Femoralremodelling after porous-coated hip arthroplasty withand without hydroxyapatite-tricalcium phosphatecoating. A prospective randomized trial. J Arthro-plasty 2001;16:552.
8. Kroger H, Miettinen H, Arnala I, et al. Evaluation ofperiprosthetic bone using dual energy x-ray absorp-tiometry: precision of the method and effect ofoperation on bone mineral density. J Bone MinerRes 1996;11:1526.
9. Rosenthall L, Bobyn JD, Tanzer M. Bone densitome-try: influence of prosthetic design and hydroxyapatitecoating on regional adaptative bone remodeling. IntOrthop 1999;23:325.
10. Schmidt R, Nowak T, Mueller L, et al. Osteodensito-metry after total hip replacement with uncementedtaper-design stem. Int Orthop 2004;28:74.
11. Smart RC, Barbagallo S, Slater G, et al. Measurementof periprosthetic bone density in hip arthroplastyusing a dual energy x-ray absorptiometry. J Arthro-plasty 1996;11:445.
12. Karachalios T, Tsatsaronis CH, Efraimis G, et al.The long-term clinical relevance of calcar atrophycaused by stress shielding in total hip arthroplasty.J Arthroplasty 2004;19:469.
13. Kobayashi O, Saito N, Nawata M, et al. Sequentialchanges in periprosthetic bone mineral densityfollowing total hip arthroplasty: a 3-year follow-up.J Bone Miner Metab 2003;21:229.
14. Nishii T, Sugano N, Masuhara K, et al. Longitudinalevaluation of time related bone remodeling aftercementless total hip arthroplasty. Clin Orthop RelatRes 1997;339:121.
15. Rahmy AI, Gosens T, Blake GM, et al. Periprostheticbone remodeling of two types of uncementedfemoral implant with proximal hydroxyapatite coat-ing: a 3-year follow up study addressing theinfluence of prosthetic design and preoperativebone density on periprosthetic bone loss. OsteoporosInt 2004;15:281.
16. Engh CA, Massin P, Suthers KE. Roentgenographicassessment of the biologic fixation of porous-surfacedfemoral component. Clin Orthop Relat Res 1990;257:107.
17. Cohen B, Rushton N. Accuracy of DEXA measure-ment of bone mineral density after total hip arthro-plasty. J Bone Joint Surg Br 1995;77:479.
18. Mortimer ES, Rosenthall L, Paterson I, et al. Effect ofrotation on periprosthetic bone mineral measure-ments in a hip phantom. Clin Orthop Relat Res1996;324:269.
19. Sychterz CJ, Claus AM, Engh CA. What we havelearned about long-term cementless fixation fromautopsy retrieval. Clin Orthop Relat Res 2002;405:79.
20. elMaraghy AW, Schemitsch EH, Waddell JP. Greatertrochanter blood flow during total hip arthroplastyusing a posterior approach. Clin Orthop Relat Res1999;363:151.
21. Hupel TM, Schemitsch EH, Aksenov SA, et al. Bloodflow changes to the proximal femur during total hiparthroplasty. Can J Surg 2000;43:359.
22. Kärrholm J, Anderberg CH, Snorrason F, et al.Evaluation of a femoral stem with reduced stiffness.J Bone Joint Surg Am 2002;84:1651.
23. Niinimäki T, Junila J, Jalovaara P. A proximal fixedanatomic femoral stem reduces stress shielding. IntOrthop 2001;25:85.
24. Theis JC, Beabel G. Changes in proximal femoral bonemineral density around a hydroxyapatite coated hipjoint arthroplasty. J Orthop Surg 2003;11:48.
25. Tonino A, Rahmy A, et al. The hydroxyapatite ABGhip system. J Arthroplasty 2000;15:274.
26. Ahlborg H, Johnell O, Karlsson M. An age-relatedmedullary expansion can have implications for thelong-term fixation of hip prostheses. Acta OrthopScand 2004;75:154.
27. Carrasco JL, Díaz M, Honorato J, et al. DensidadMineral Ósea en Cuello Femoral. En: ProyectoMulticéntrico de Investigación en Osteoporosis. Estu-dio de la Densidad Osea de la Población Española. Ed:Pharma Consult. 1992 Madrid.
28. Brodner W, Bitzan P, Lomoschitz F, et al. Changes inbone mineral density in the proximal femur after thecementless total hip arthroplasty. A five year long-itudinal study. J Bone Joint Surg 2004;86:20.

64 The Journal of Arthroplasty Vol. 24 No. 1 January 2009
29. Leichtle UG, Leichtle CI, Schmidt B, et al. Peripros-thetic bone density after implantation of a custommade femoral component. J Bone Joint Surg (Br)2006;88-B:467.
30. Martini F, Sell S, Kremling E, et al. Determination ofperiprosthetic bone density with the DEXA methodafter implantation of custom-made uncementedfemoral stems. Int Orthop 1996;20:218.
31. Zerahn B, Storgaard M, Johansen T, et al. Changes inbonemineral density adjacent to two biomechanicallydifferent types of cementless femoral stems in totalhip arthroplasty. Int Orthop 1998;22:225.
32. Nagi ON, Kumar S, Aggarwal S. The uncementedisoelastic/isotitan total hip arthroplasty. A 10-15 yearsfollow-up with bone mineral density evaluation. ActaOrthop Belg 2006;72:55.
Copyright © 2022 FDOKUMEN




















