
The costs of planned cesarean versus planned vaginal birth in the term breech trial
Upload
independentCategory
view
0download
0
Accepted Manuscript
Autologous in vitro cultured vaginal tissue for vaginoplasty in women with Mayer–Von-Rokitansky–Küster–Hauser syndrome: anatomical and functional results
Pierluigi Benedetti Panici, M.D. Diana Maffucci, M.D. Simona Ceccarelli, PhD EnricaVescarelli, Giorgia Perniola, M.D. Ludovico Muzii, M.D. Cinzia Marchese, PhD
PII: S1553-4650(14)01421-6
DOI: 10.1016/j.jmig.2014.09.012
Reference: JMIG 2393
To appear in: The Journal of Minimally Invasive Gynecology
Received Date: 9 June 2014
Revised Date: 25 September 2014
Accepted Date: 28 September 2014
Please cite this article as: Benedetti Panici P, Maffucci D, Ceccarelli S, Vescarelli E, Perniola G, MuziiL, Marchese C, Autologous in vitro cultured vaginal tissue for vaginoplasty in women with Mayer–Von-Rokitansky–Küster–Hauser syndrome: anatomical and functional results, The Journal of MinimallyInvasive Gynecology (2014), doi: 10.1016/j.jmig.2014.09.012.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT1
1
TITLE
Autologous in vitro cultured vaginal tissue for vaginoplasty in women with Mayer–Von-
Rokitansky–Küster–Hauser syndrome: anatomical and functional results.
Pierluigi BENEDETTI PANICI M.D.1, Diana MAFFUCCI M.D.1*, Simona CECCARELLI PhD2,
Enrica VESCARELLI2, Giorgia PERNIOLA M.D.1, Ludovico MUZII M.D.1, Cinzia MARCHESE
PhD2.
1 Department of Gynecologic-Obstetrical and Urologic Sciences .“Sapienza” University of Rome.
Viale del Policlinico, 155 – 00161, Rome. Italy
2 Department of Experimental Medicine - Unit of Regenerative Medicine. “Sapienza” University of
Rome. Viale Regina Elena, 324 – 00161, Rome. Italy
The Authors report no conflict of interest
The authors have no disclosure to report
*Corresponding author: Diana Maffucci, M.D.
E-mail: [email protected]
Business telephone number: + 393395018918
Fax: + 39064454820

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT2
2
PRÉCIS
This study presents the procedure and the results of a technique in which in vitro autologous cell
cultures were used for the canal lining in patients with Mayer–von-Rokitansky–Küster–Hauser
syndrome (MRKHS)

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT3
3
STRUCTURED ABSTRACT
STUDY OBJECTIVE: To present the procedure and the results of a technique in which in vitro
autologous cell cultures were used for the canal lining in patients with Mayer–von-Rokitansky–
Küster–Hauser syndrome (MRKHS) subjected to vaginoplasty with a modified Abbè–McIndoe
technique. MRKHS is a rare anomaly characterized by vaginal agenesis with variable Müllerian
duct abnormalities. The Abbè-McIndoe procedure is one of the most frequent surgical treatments
adopted in these women. In the last decades several modifications have been introduced by different
authors, mostly changing the lining material, but no consensus has been reached on what material
should be used for the neovagina canal wall lining.
DESIGN: Pilot study.
DESIGN CLASSIFICATION: II-1 according to the Canadian Task Force Classification of Study
Designs.
SETTING: Policlinico Umberto I, “Sapienza” University of Rome.
PATIENTS: A consecutive series of 23 women with MRKHS underwent neovaginoplasty with
autologous vaginal tissue as graft material, between 2006 and 2013.
INTERVENTIONS: Each patient with MRKHS was subjected to a full-thickness mucosal biopsy
from the vaginal vestibule. Following enzymatic dissociation, cells were inoculated onto collagen
IV-coated plates and cultured for 2-3 weeks. The patients were subjected to a vaginoplasty with a
modified Abbè–McIndoe technique with autologous in vitro cultured vaginal tissue. Patients
underwent clinical follow-up visits at 1, 3, 6 and 12 months after surgery and every year thereafter.
Anatomical, functional and sexual results were assessed.
MEASUREMENTS AND MAIN RESULTS: In all cases the vagina appeared normal in length
and depth. A vaginal cytology and a vaginal biopsy obtained at 3 month follow-up visit revealed
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT4
4
physiological vaginal tissue. All 23 patients completed the Female Sexual Function Index (FSFI)
questionnaire at 12 months after surgery. The results showed a total score of 27.2.
This results demonstrate a satisfactory quality of sexual life.
CONCLUSION: The modified Abbè–McIndoe technique with autologous vaginal tissue appears
safe and feasible. This technique allows normal and satisfying sexual intercourse. Larger series with
longer follow-up will be necessary to confirm if this technique represents the ideal procedure for
vaginal agenesis.
Key Words: Abbè-McIndoe, Autologous Tissue, Mayer-Rokitansky-Küster-Hauser syndrome,
vaginal agenesis, vaginoplasty.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT5
5
TEXT
Introduction
The estimated incidence of Mayer–von-Rokitansky–Küster–Hauser syndrome (MRKHS) is 1:
5.000 live-born females (1-2). The aetiology of MRKHS is considered multifactorial (3).
Women affected by MRKHS have normal female phenotype and karyotype (46, XX).
Ovarian function is usually preserved. Most women have a complete uterine agenesis or a non-
functional rudimental uterus. Patients suffering from MRKHS usually maintain a normal vaginal
vestibule and sometimes a vaginal dimple.
The symptom that usually leads to diagnosis is primary amenorrhea. In patients with MRKHS,
vaginal aplasia/hypoplasia is frequently associated with other congenital abnormalities.
Approximately a third of these women have renal system abnormalities and skeletal malformations
and a minority of the cases may have cardiovascular anomaly. Müllerian remnants can be
frequently observed in these patients (4).
The objective of the treatment of vaginal agenesis is to allow women to have a satisfactory sexual
life. The ideal treatment should aim to achieve an anatomically and functionally normal vagina.
Ideally, the procedure should be able to be permanent, require minimal use of dilators and be non or
minimally invasive without leaving visible scars.
Several methods have been suggested for the treatment of vaginal agenesis. Currently, the
American College of Obstetrics and Gynecology (ACOG) suggests a conservative approach (5-6) as
first line treatment and reserve surgery as a second line treatment in patients who failed progressive
dilation or who are not compliant (2).
Several surgical techniques have been developed for the treatment of vaginal agenesis.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT6
6
Recently, the interest of most gynaecologists has been directed towards minimally invasive
techniques (7). The most widely adopted minimally invasive methods are the laparoscopic
Vecchietti’s technique and the Abbé-McIndoe procedure.
The Vecchietti’s technique (8) traditional or laparoscopically-modified (9-10), commonly used in
European countries, is carried out using an acrylic olive placed in the vaginal dimple with two
threads that are passed through the abdominal cavity which are attached to a traction device placed
on the sovrapubic region. The threads are subjected to a progressive traction until the vaginal
dimple is elongated to the desired length; so the patients have to adjust the tension every 48 hours.
The critical point of this procedure is the prolonged time required, usually between 6 and 9 days,
necessary to obtain an adequate vaginal length. The postoperative period is uncomfortable and
furthermore an excessive traction may cause necrosis of epithelium, whereas limited traction would
not allow lengthening of the neovagina.
The Abbè-McIndoe technique (11) is a minimally invasive procedure that is widely adopted for the
treatment of vaginal agenesis. This technique consists in the creation of a canal in between the
bladder and the rectum, which is covered with a skin graft. Several modifications of this original
technique have been attempted, mostly changing the different tissue adopted for the canal lining.
Here we present our continued experience with this novel treatment initially described by our group
in a case report (12) in which in vitro autologous vaginal cell cultures obtained from biopsies from
the vaginal vestibule were used for the epithelialization of the neovaginal walls.
This prospective pilot study was carried out on 23 women with MRKH syndrome who were treated
in our Department between 2006 and 2013.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT7
7
Methods
IRB approval was obtained.
Preoperative workup
Between 2006 and 2013, 23 caucasian women with MRKH syndrome were addressed to our
institution. All patients exhibited primary amenorrhoea, normal secondary sex characteristics, and a
vaginal dimple without vaginal orifice.
All women underwent a pre-operative work-up, which included chromosome analysis, abdomino-
pelvic MRI, echocardiogram, ECG and chest X-ray.
Patients were counseled, before surgery, regarding the non-surgical technique (Frank’s method) and
alternative surgical techniques, as well as the possible complications of the modified Abbè–
McIndoe technique with autologous in vitro cultured vaginal tissue.
The technique has been described by our groups previously (12).
Surgical technique
The technique consists in a two-step procedure. The patient is subjected to a preliminary full
thickness biopsy from the vaginal vestibule of approximately 1cm2 (Figure 1).
The fresh biopsy is transferred to the Department of Experimental Medicine for cell extraction and
tissue culture. Following enzymatic dissociation, the keratinocyte suspension is inoculated onto five
collagen IV (10 mg/ml)-coated culture plates, as previously reported (12). Cells are seeded at cell
density of 2.5 X 105 cells/plate and maintained in Keratinocyte Basal Medium (KBM, Lonza
Milano S.r.l., Milano, Italy) supplemented with Keratinocyte Growth Medium (KGM) single quotes
(Lonza), with medium change twice a week. The size of the tissue culture is determined by the
number and size of the plates adopted.
After 1-2 weeks of culture, cells reach 70–80% of confluence, being cultured for additional 8 days
in order to obtain a fully differentiated mucosal tissue. Autologous reconstructed vaginal tissues are
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT8
8
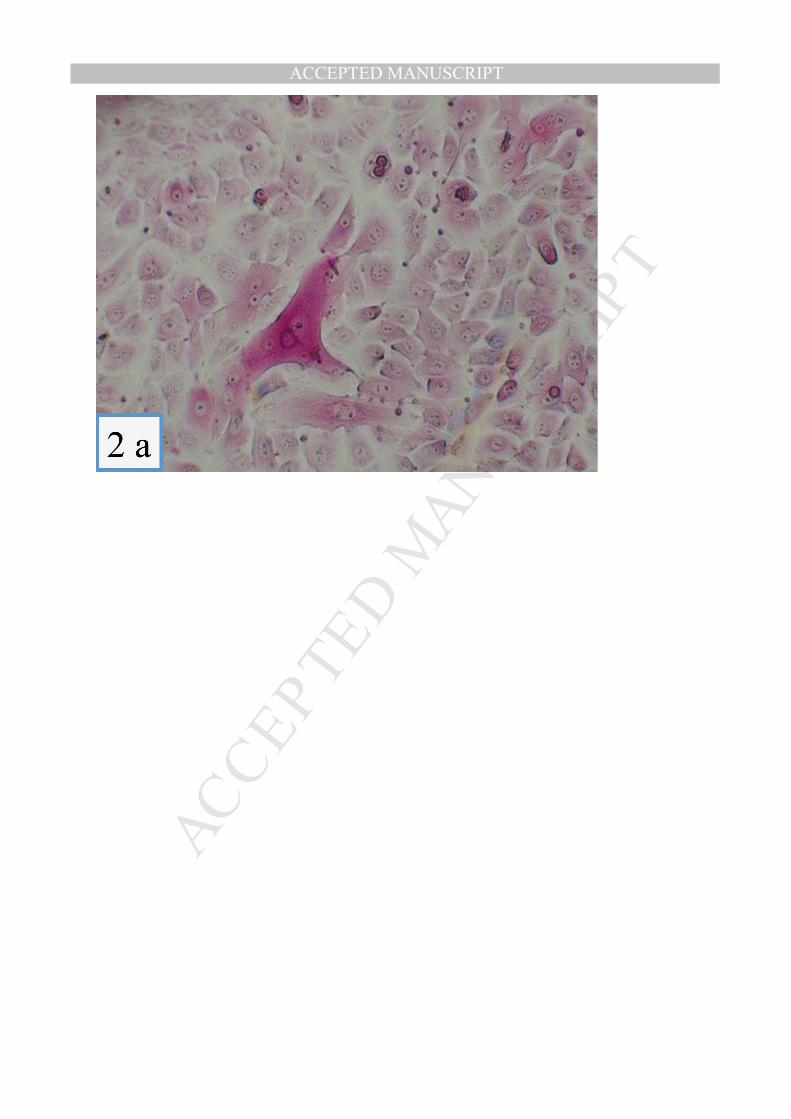
then harvested from the culture plates by incubation with dispase II (2.5 mg/ml), washed in PBS,
mounted onto 2 mg/10 cm² hyaluronic acid embedded gauze to maintain the orientation of the
mucosal tissue and transferred to the operative theatre, taking care that the basal epithelial cell layer
faced away from the gauze (Figure 2: 2a-2b-2c).
The time interval between the biopsy and the development of a fully differentiated mucosal tissue is
approximately 2-3 weeks.
Before the second-step surgery, the patients are treated with antibiotics prophylaxis and a bowel
enema. In the operative room, the patients are placed in a lithotomic position with a Foley catheter.
The vaginal canal is developed as described in the Abbè-McIndoe technique: a midline incision at
the vaginal introitus is made, and a 10 cm canal is made between the bladder and the rectum using a
blunt digital and scissor dissection reaching the pouch of Douglas.
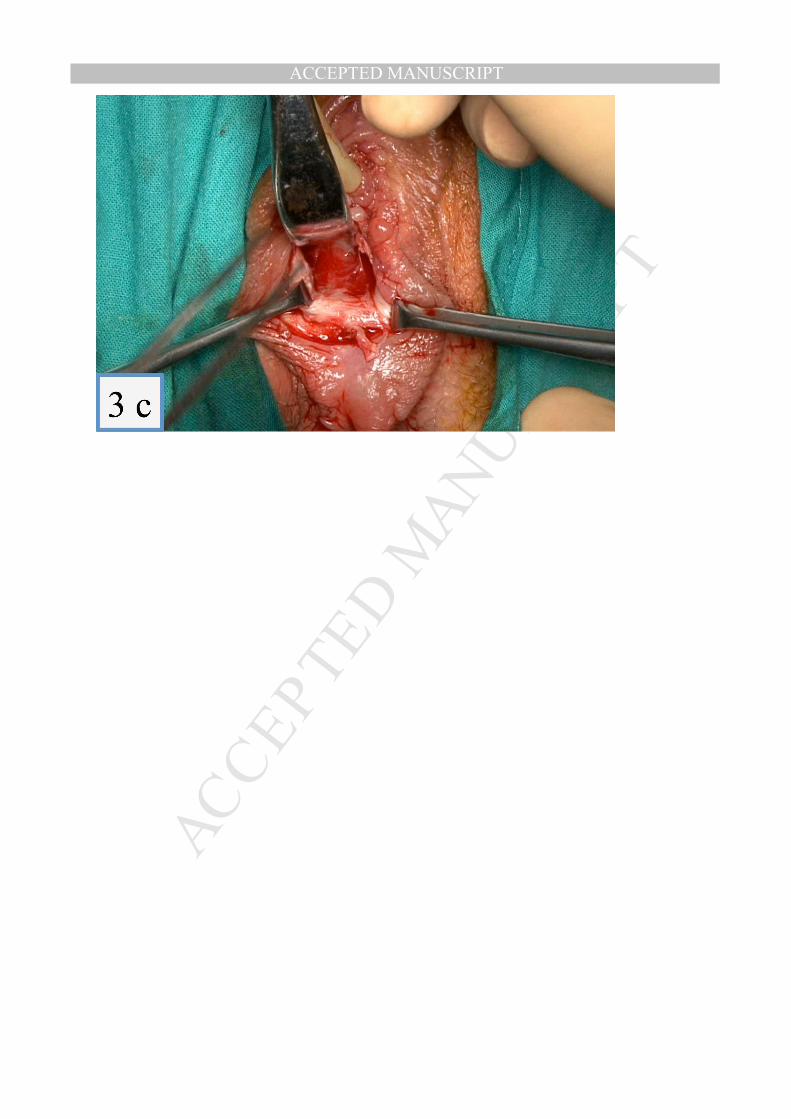
Complete haemostasis is obtained with electrocautery (Figure 3: 3a-3b-3c-3d). The tunnel is
covered with the gauze with the cell stratum facing the canal walls. The gauzes are kept in place by
a 2 cm in diameter and 12 cm in length vaginal mould (Figure 4: 4a-4b-4c). The mould is fixed to
the perineum. No stitches are used to keep the gauze in place.
The gauzes, the Foley catheter and the mould are kept in place for 5 post-operative days. At this
point, the mould is removed, the vagina is rinsed and the percentage of take is evaluated. The Foley
catheter was kept in place until the patients started using the dilators autonomously.
The patients are advised to wear the vaginal mould day and night during the initial 6 weeks post-
operative period, after which the mould is kept at night until regular sexual intercourse is
commenced.
Patients underwent clinical follow-up visits at 1, 3, 6 and 12 months after surgery and every year
thereafter. Clinical follow-up included vaginal examination and vaginoscopy.
Both vaginal cytology and vaginal biopsy were obtained at the 3 months follow-up visit.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT9
9
Functional results were assessed by using Female Sexual Function Index (FSFI) questionnaire , at
12 months after surgery.
The highest total FSFI score that may be obtained is 36. On the basis of literature data, 30 is the
mean score in the normal population, so a functional result can be considered as good when the total
score is between 30 and 36, satisfactory when between 23 and 29, poor when is 23 or less (13).

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT10
10
Results
The operation was performed successfully in all 23 patients. Patients characteristics and primary
results are presented in Table I. The mean age of patients at surgery was 21.7 years-old (range 17-
49 years-old). The measure of the vaginal biopsy ranged from 0.5 to 2 cm² (mean 1.4 cm²).
The mean operative time was 21.5 minutes (range 18- 25 min) and mean blood loss was 94 ml
(range 80 -110 ml). The time interval between the biopsy and the development of the fully
differentiated mucosal tissue ranged from 15 to 27 days (mean time 20.4 days).
The vaginal tissue percentage of take was between 70 and 100% (mean percentage 83%).
The evaluation of neovagina with gynecologic examination, carried out after 5 days from surgery,
demonstrated that the vaginal tissue covered the 70-100 % of the vaginal wall, whereas the
remainder of neovagina appeared covered by granulation tissue, which was successively replaced
by vaginal tissue up to 2 weeks after.
Post-operatively, all the patients were placed on a liquid diet until day 5. The Foley catheter was
kept in place until the patients started using the dilators autonomously.
All patients urinated smoothly after bladder training. The hospitalization stay ranged from 2 to 16
days. Patients started using the dilators autonomously after a mean post-operative time of 12 days
(range 9-16 days).
At time of discharge patients were suggested to use liquid lubricants in order to improve the
compliance to the use of dilators.
One patient suffered from postoperative bleeding that was treated with vaginal packing and medical
therapy administering intravenously tranexamic acid.
One patient suffered from vaginal spotting at three month from surgery for granulomatous tissue.
Anatomic and functional success was achieved in all patients. Sexual activity was commenced from

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT11
11
1 to 4 month after surgery. Patients started a regular sexual activity after a mean post-operative time
of 7 weeks (range 4-16 weeks).
Mean vaginal length was 8 cm ranging from 6 cm to 10 cm, and the width was about two fingers in
all patients. The vaginal length and depth at 12 months of follow-up did not differ, compared with
that at 6 post-operative months.
There was no exudate, and the vaginal tunnel was covered with a pink smooth lining.
The vaginal cytology and the vaginal biopsy of the neovagina obtained at 3 month follow-up visit
did not reveal atrophy and showed a normal epithelium (Figure 5).
All 23 patients completed the FSFI questionnaire at 12 months after surgery. The results showed a
total score of 27.2. This results demonstrate a satisfactory quality of sexual life. This finding
demonstrates that vaginoplasty with autologous in vitro cultured vaginal tissue permits normal and
satisfying sexual intercourse.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT12
12
Discussion
Various treatments have been proposed in the last century for vaginal agenesis.
Every technique shows advantages and disadvantages, so the ideal treatment of MRKHS remains a
matter of debate. Invasive reconstruction of the vaginal canal can be carried out using bowel
segments (14-15) or skin flaps (16).
In recent years, several Authors have advocated the use of non-invasive methods or minimally
invasive procedures as the ideal strategies to create a functional vagina.
Currently, the conservative approach such as the Frank or the Ingram method (5-6) represents the
standard first line treatments in motivated patients with favourable anatomic conditions (2), but the
long duration of treatment often leads to prefer surgery.
The most widely adopted minimally invasive methods are the laparoscopic Vecchietti’s technique
(8) and the Abbé-McIndoe procedure (11).
Since the first description of Abbè, several modifications of the original procedure have been
proposed, the most relevant ones regarding the tissue for the canal lining.
The original technique has demonstrated to be highly feasible and yield high success rates but carry
the inherited disadvantage of leaving a scar in the donor site.
Modified techniques can obviate several of these inconveniences and various modifications have
been proposed. These include the use of the peritoneum (17-18), the amnion (19-20), allogeneic
epidermal sheets (21-22), Interceed (23) and autologous buccal mucosa (24).
The use of peritoneum has the disadvantage of being complex, requires the opening of the
peritoneal cavity and the retraction of the labia minor in the vagina has been reported (25).
Vaginoplasty with amniotic membranes is a rapid procedure and does not leave any scar.
Furthermore, membranes can be stored for several days, and this allows physicians to have time to
organize the transplant. Epithelialization has constantly been shown to be rapid.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT13
13
The use of allogeneic tissues such as amnion sheets carries the inherited disadvantage of allograft
rejection and risk of human-to-human transmission of infective disease. Lastly, amniotic
membranes have been shown to be easily contaminated before or after being transplanted.
Inert materials are inexpensive, readily available, sterile, and allow fast operative times with no
cutaneous scars. With these materials, epithelialization occurs either from metaplasia or from
keratinocyte colonization from the vaginal vestibule and therefore the interval between surgery and
the beginning of intercourse is relatively long.
Buccal mucosa appears as a promising lining material for the neovagina . Regarding vaginoplasty
performed with autologous buccal micromucosa, Li et al (26) recently reported the long-term
outcome of 38 patients subjected to this type of technique. They demonstrated that this technique is
an effective and feasible approach, but needs a long operative times and two operative teams: one
for oral mucosa graft harvesting and the other for reconstruction of the neovaginal cavity. Other
possible problems related to this method are morbidity connected with the removal of the mucosa
from the donor site and the relatively long time necessary to achieve a functional vagina.
Comparing to our technique, vaginoplasty with oral micromucosa showed a longer operative time
(86.4 minutes vs 21.5 minutes) but similar FSFI score (28.8 vs 27.2).
The idea of regenerate tissue through a process of cultured cells is an attractive paradigm to be
explored. A pilot cohort study assessing the use of engineered vaginal organs in four patients with
MRKHS was recently published (27).
The use of in vitro cultured vaginal mucosa is in its early infancy and more experience needs to be
acquired before drawing definite conclusions.
In our patients no use of resorbable scaffolds, growth factors and peptides has been exploited for
controller delivery and release of the new mucosal tissue. Since these reconstructed mucosal
equivalents are fragile and difficult to handle in the clinical setting, only epithelial/mucosal sheets

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT14
14
covered by a gauze of degradable hyaluronic acid, that confers both mechanical stability and high
biocompatibility and allowed the orientation of the epithelial layer has been used.
The technique appears to carry several advantages. The graft is autologous and orthotopic with no
risk of rejection or donor-derived infections.
The procedure is fast and leaves no visible scars. Epithelialization is rapid since there is no need to
“mesh” the material, but there is the possibility of having enough tissue to cover the entire canal
surface.
Furthermore, after removing the gauze and the mould, adopted in order to maintain in place and to
increase the pressure on the gauzes with vaginal tissue, the epithelialization could be seen through
the entire neovaginal wall and this suggest that epithelialization occurred from the transplanted
tissue and not as with other techniques from the vaginal vestibule.
As expected, the initial percentage of epithelialization of neovagina was variable between
individual patients. We didn’t investigate the possible reasons of this variability. Future
investigation will clarify the role of age, cell characteristics, medications and/or environmental
factors in determining the lining of neovagina.
In addition, women’s perception to have the vagina lined by physiological vaginal tissue is likely to
play an important psychological role in the achievement of a normal sexual life.
Moreover, we recently published a detailed characterization of cultured vaginal mucosa cells,
demonstrating their epithelial features and the presence of mucified cells interspersed among cell
cultures, which might contribute to maintain a normal glandular function of the neovagina (28).
Disadvantages include that the cell-based therapies can only be carried out in culture conditions
compliant with Good Manufacturing Practice (GMP) which require centres who have dedicated
tissue culture laboratories (such as referral centres or hospitals with burn units). Moreover, the fact
that the procedure is carried out in two steps means that the operative theatre organization need to

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT15
15
be coordinated with the laboratories in order to program the surgical procedure when the tissue is
ready.
The quality of sexual life is the main objective of the treatment. The FSFI is the questionnaire used
to evaluate the satisfactory or unsatisfactory sexual intercourse after the surgery. The results
demonstrate a satisfactory quality of sexual life.
Future studies should also consider to extend the use of autologous vaginal tissue for the
reconstruction of acquired defects of the vagina resulting from extirpative oncologic surgery of
cervical, vaginal or urinary tract malignancies, or from traumas or infections with soft tissue
necrosis and subsequent extensive debridement. Such defects are generally repaired or
reconstructed with fasciocutaneous and myocutaneous flaps, but in oncologic patients previously
treated with radiotherapy the surrounding tissues are often subjected to an increased risk of wound
healing complications. The use of autologous cultured vaginal tissue could prevent this problem
since vaginal biopsy could be obtained before the beginning of radiotherapy.
In conclusion, we demonstrated that autologous in vitro cultured vaginal tissue combines the best
material characteristics with important psychological implications. Larger series with longer follow
up will be required to confirm if this technique represents the ideal procedure for vaginal agenesis
and if it can be applied also for reconstruction of acquired vaginal defects.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT16
16
REFERENCES
1. Rock JA, Azziz R. Genital anomalies in childhood. Clin Obstet Gynecol. 1987; 30: 682-696.
2. American College of Obstetrics and Gynecology. ACOG committee opinion. Nonsurgical
diagnosis and management of vaginal agenesis. Number 274, July 2002. Committee on
Adolescent Health Care. American College of Obstetrics and Gynecology. Int J Gynaecol
Obstet. 2002; 79: 167-170.
3. Schätz T, Huber J, Wenzl R. Creation of a neovagina according to Wharton-Sheares-George in
patients with Mayer-Rokitansky-Küster-Hauser syndrome. Fertil Steril. 2005; 83: 437-441.
4. Griffin JE, Edwards C, Madden JD et al. Congenital absence of the vagina. The Mayer-
Rokitansky-Kuster-Hauser syndrome. Ann Intern Med. 1976; 85: 224-236.
5. Frank RT. The formation of an artificial vagina without operation. Am J Obstet Gynecol. 1938;
135: 1053–1055.
6. Ingram JM. The bicycle seat stool in the treatment of vaginal agenesis and stenosis: a
preliminary report. Am J Obstet Gynecol. 1981; 140: 867-873.
7. Benedetti Panici P, Ruscito I, Gasparri ML et al. Vaginal reconstruction with the Abbè-McIndoe
technique: from dermal grafts to autologous in vitro cultured vaginal tissue transplant. Semin
Reprod Med. 2011; 29(1): 4
8. Vecchietti G. Creation of an artificial vagina in Rokitansky-Küster-Hauser syndrome. Attual
Ostet Ginecol. 1965; 11: 131-147.
9. Borruto F, Chasen ST, Chervenak FA et al. The Vecchietti procedure for surgical treatment of
vaginal agenesis: comparison of laparoscopy and laparotomy. Int J Gynaecol Obstet. 1999; 64:
153-158.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT17
17
10. Fedele L, Bianchi S, Frontino G et al. The laparoscopic Vecchietti's modified technique in
Rokitansky syndrome: anatomic, functional, and sexual long-term results. Am J Obstet Gynecol.
2008; 198(4):377.e 1-6
11. McIndoe AH, Banniser JB. An operation for the cure of congenital absence of the vagina. J
Obstet Gynaecol Br Emp. 1938; 45: 490–494.
12. Benedetti Panici P, Bellati F, Boni T et al. Vaginoplasty using autologous in vitro cultured
vaginal tissue in a patient with Mayer-von-Rokitansky-Kuster-Hauser syndrome. Hum Reprod.
2007; 22(7): 2025-8
13. Rosen R, Brown C, Heiman J, et al. The Female Sexual Function Index (FSFI): A
multidimensional self-report instrument for the assessment of female sexual function. J Sex
Marital Ther 2000;26:191-208.
14. Khen-Dunlop N, Lortat-Jacob S, Thibaud E et al. Rokitansky syndrome: clinical experience and
results of sigmoid vaginoplasty in 23 young girls. J Urol. 2007; 177: 1107-1111.
15. Imparato E, Alfei A, Aspesi G et al. Long-term results of sigmoid vaginoplasty in a consecutive
series of 62 patients. Int Urogynecol J Pelvic Floor Dysfunct. 2007; 18: 1465-1469.
16. Purushothaman V. Horse shoe flap vaginoplasty--a new technique of vaginal reconstruction
with labia minora flaps for primary vaginal agenesis. Br J Plast Surg. 2005; 58: 934-939.
17. Rothman D. The use of peritoneum in the construction of a vagina. Obstet Gynecol . 1972; 40:
835–838.
18. Davydov SN, Zhvitiashvili OD. Formation of vagina (colpopoiesis) from peritoneum of
Douglas pouch. Acta Chir Plast. 1974; 16: 35-41.
19. Dhall K. Amnion graft for the treatment of congenital absence of the vagina. Br J Obstet

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT18
18
Gynaecol. 1984; 91: 279–282.
20. Ashworth MF, Morton KE, Dewhurst J et al. Vaginoplasty using amnion. Obstet Gynecol.
1986; 67: 443-446.
21. Carranza-Lira S, Sauer-Ramirez R, Bolivar-Flores YJ. Neovagina with cultured allogenic
epidermal sheets. Eur J Obstet Gynecol Reprod Biol. 1999; 82: 77–79.
22. Noguchi S, Nakatsuka M, Sugiyama Y et al. Use of artificial dermis and recombinant basic
fibroblast growth factor for creating a neovagina in a patient with Mayer-Rokitansky-Kuster-
Hauser syndrome. Hum Reprod. 2004; 19: 1629-1632.
23. Jackson ND, Rosenblatt PL. Use of Interceed Absorbable Adhesion Barrier for vaginoplasty.
Obstet Gynecol. 1994; 84: 1048-1050.
24. Lin WC, Chang CY, Shen YY et al. Use of autologous buccal mucosa for vaginoplasty: a study
of eight cases. Hum Reprod. 2003; 18: 604-607.
25. Rangaswamy M, Machado NO, Kaur S et al. Laparoscopic vaginoplasty: using a sliding
peritoneal flap for correction of complete vaginal agenesis. European Journal of Obstetrics,
Gynecology, and Reproductive Biology 2001; 98: 244-248.
26. Li FY, Xu YS, Zhou CD, Zhou Y, Li SK, Li Q. Long-term outcomes of vaginoplasty with
autologous buccal micromucosa. Obstet Gynecol. 2014 May;123(5):951-6.
27. Raya-Rivera A, Esquiliano D, Fierro-Pastrana R et al. Tissue-engineered autologous vaginal
organs in patients: a pilot cohort study. Lancet 2014; S0140-6736(14) 60542-0
28. Nodale C, Vescarelli E, D'Amici S et al. Characterization of human vaginal mucosa cells for
autologous in vitro cultured vaginal tissue transplantation in patients with MRKH syndrome.
BioMed Res Int. 2014;2014:201518.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT19
19
TABLE
Table 1: Patients characteristics and primary results.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT20
20
FIGURE LEGENDS
Figure 1: Full-thickness mucosal biopsy obtained from the vaginal vestibule.
Figure 2 (2a-2b-2c): In vitro culture of vaginal mucosa cells (PAS staining, identifying mucinous
cells and phase contrast) and detached tissues with application of hyaluronic acid embedded gauzes.
Figure 3 (3a-3b-3c-3d): Modified Abbè–McIndoe vaginoplasty: a canal reaching the pouch of
Douglas was made between the bladder and the rectum using blunt digital and scissor dissection.
Figure 4 (4a-4b-4c): Modified Abbè–McIndoe vaginoplasty: the tunnel was covered with the
gauzes with the mounted cell stratum facing the canal walls.
Figure 5: Vaginoscopy carried out during a 3- months interval patient’s follow-up visit.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
CASE AGE Biopsy
specimen
size
(cm²)
Blood
loss
(ml)
Operative
time
(min.)
Tissue
take
(%)
Time
of in
vitro
culture
(days)
Starting
autonomous
use of
dilators
(days)
Sexual
activity
initiation
(weeks)
FSFI score
(min. 2.0-
max 36)
CASE 1 28 1 80 18 90 15 16 12 24.5
CASE 2 17 0.5 85 19 90 20 15 8 24
CASE 3 17 1.5 90 20 100 18 14 6 25.7
CASE 4 24 1 95 21 70 23 14 8 26.9
CASE 5 20 1 100 22 100 19 13 6 28.1
CASE 6 25 1.5 105 23 80 15 11 4 29.3
CASE 7 49 1 110 24 90 20 12 16 23.3
CASE 8 18 0.5 110 25 80 27 13 8 30.5
CASE 9 22 2 100 23 80 22 12 10 29.3
CASE 10 18 1.5 95 22 80 21 10 10 24.5
CASE 11 18 1.5 90 20 70 23 9 10 25.7
CASE 12 29 2 85 19 70 22 9 8 28.1
CASE 13 17 1.5 80 18 90 20 11 6 30.5
CASE 14 19 2 90 18 80 19 12 6 25.7
CASE 15 20 2 105 25 80 16 11 4 23.3
CASE 16 20 1.5 110 23 100 23 10 4 29.3
CASE 17 17 1.5 80 21 70 18 13 4 30.5
CASE 18 18 2 85 24 80 28 12 4 28.1
CASE 19 23 1 95 25 70 20 11 6 25.7
CASE 20 21 1,5 100 20 80 21 10 5 29.3
CASE 21 19 0,5 80 25 100 22 12 4 28.1
CASE 22 20 2 85 20 90 18 13 6 30.5
CASE 23 22 1,5 110 20 70 19 15 6 24.5
MEAN 21.7 1.4 94 21.5 83 20.4 12 7 27.2

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
http://www.AAGL.org/jmig-22-2-JMIG-D-14-00294

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
http://www.AAGL.org/jmig-22-2-JMIG-D-14-00294
Copyright © 2022 FDOKUMEN




















