
Functional and Anatomic Alterations in the Gentamicin-Damaged Vestibular System in the Guinea Pig
International Journal of
Radiation Oncologybiology physics
www.redjournal.org
Clinical Investigation: Late Effect
Incidence, Causative Mechanisms, and AnatomicLocalization of Stroke in Pituitary Adenoma PatientsTreated With Postoperative Radiation Therapy VersusSurgery AloneMargriet G.A. Sattler, MD,*,x Patrick C. Vroomen, MD, PhD,y Wim J. Sluiter, PhD,z
Henk J. Schers, MD, PhD,k Gerrit van den Berg, MD, PhD,z
Johannes A. Langendijk, MD, PhD,* Bruce H.R. Wolffenbuttel, MD, PhD,z
Alphons C.M. van den Bergh, MD, PhD,* and Andre P. van Beek, MD, PhDz
Departments of *Radiation Oncology, yNeurology, and zEndocrinology and Metabolic Diseases, University of Groningen,University Medical Center Groningen, Groningen, The Netherlands; xDepartment of Radiation Oncology, SunnybrookHealth Sciences Centre, University of Toronto, Toronto, ON, Canada; and kDepartment of Primary and Community Care,Radboud University Nijmegen Medical Centre, The Netherlands
Received Jan 23, 2013, and in revised form Apr 28, 2013. Accepted for publication May 1, 2013
Summary
The incidence of stroke inirradiated pituitary adenomapatients was compared withthat in surgery-alone patientsand in a normal referencepopulation. In both treatmentgroups (1) several other well-established stroke riskfactors were assessed; (2)additional CT imaging wasused to confirm stroke diag-nosis and stroke type; and (3)causative mechanism andanatomic localization ofischemic stroke were
Reprint requests to: Margriet G. A. Sattler, M
tion Oncology, University Medical Center Gron
Box 30.001, 9700 RB, Groningen, The Net
3611190; E-mail: [email protected]
Int J Radiation Oncol Biol Phys, Vol. 87, No. 1
0360-3016/$ - see front matter � 2013 Elsevie
http://dx.doi.org/10.1016/j.ijrobp.2013.05.006
Purpose: To assess and compare the incidence of stroke and stroke subtype in pituitary adenomapatients treated with postoperative radiation therapy (RT) and surgery alone.Methods and Materials: A cohort of 462 pituitary adenoma patients treated between 1959 and2008 at theUniversityMedicalCenterGroningen inTheNetherlandswas studied.Radiation therapywas administered in 236 patients. The TOAST (Trial of ORG 10172 inAcute Stroke Treatment) andthe Oxfordshire Community Stroke Project classificationmethods were used to determine causativemechanism and anatomic localization of stroke. Stroke incidences in patients treated with RTwerecompared with that observed after surgery alone. Risk factors for stroke incidence were studied bylogerank test, without andwith stratification for other significant risk factors. In addition, the strokeincidence was compared with the incidence rate in the general Dutch population.Results: Thirteen RT patients were diagnosed with stroke, compared with 12 surgery-alonepatients. The relative risk (RR) for stroke in patients treated with postoperative RTwas not signif-icantly different comparedwith surgery-alone patients (univariate RR0.62, 95% confidence interval[CI] 0.28-1.35, PZ.23). Stroke risk factors were coronary or peripheral artery disease (univariateand multivariate RR 10.4, 95% CI 4.7-22.8, P<.001) and hypertension (univariate RR 3.9, 95%CI 1.6-9.8, PZ.002). There was no difference in TOAST and Oxfordshire classification of stroke.In this pituitary adenoma cohort 25 strokes were observed, compared with 16.91 expected (standardincidence ratio 1.48, 95% CI 1.00-1.96, PZ.049).
D, Department of Radia-
ingen, Hanzeplein 1, P.O.
herlands. Tel: (þ31) 50-
This study was presented in part at the 53rd Annual Meeting of the
American Society for Radiation Oncology (ASTRO), Miami Beach, FL,
October 2-6, 2011.
Conflict of interest: none.
AcknowledgmentsdThe authors thank Mrs. M. A. Groeneveld for her help
in the data collection.
, pp. 53e59, 2013
r Inc. All rights reserved.

Sattler et al. International Journal of Radiation Oncology � Biology � Physics54
assessed. Postoperative
radiation therapy was notassociated with an increasedrisk of stroke compared withsurgery alone.Conclusions: In pituitary adenoma patients, an increased incidence of stroke was observedcompared with the general population. However, postoperative RT was not associated with anincreased incidence of stroke or differences in causative mechanism or anatomic localization ofstroke compared with surgery alone. The primary stroke risk factor was pre-existent coronary orperipheral artery disease. � 2013 Elsevier Inc.
Introduction
In patients with nonfunctioning adenomas, growth hormone-secreting adenomas, and adrenocorticotropic hormone-secretingadenomas, surgery is considered the treatment of first choice. Post-operative radiation therapy (RT) is usually applied as an adjuvanttreatment modality to prevent tumor progression after incompleteresection, in case of secreting adenomas for which hormonal controlcannot be achieved with surgery alone and medical treatment, or assalvage treatment for a local recurrence after surgery. Radiationtherapy results in excellent long-term local tumor control, withreported rates of 90%-97% at 10 years (1-4). Furthermore, animprovement of excessive hormonal secretion has been reported in80%-85% of Cushing’s disease patients and in 60%-76% ofacromegaly patients at 10 years (5-8).
Nevertheless, the role of postoperative RT has been debatedbecause of concerns related to possible long-term side effects,such as stroke. A number of case reports describe stroke devel-oping after RT for pituitary adenoma (9, 10). Pituitary adenomacohort studies regarding RT and stroke have shown conflictingresults. An increased stroke risk has been reported (11), whereasothers reported no increased stroke incidence (12). These previousstudies compared the stroke incidence in irradiated pituitaryadenoma patients with the incidence observed in a normal refer-ence population. Such comparisons could be biased by imbalancesin the presence of other stroke risk factors that are related to thepituitary adenoma disease and/or other treatments.
To evaluate the concerns related to RT and stroke a directcomparison should be made with similar patients treated withsurgery alone. In this study, the incidence, the stroke subtype, andin ischemic stroke, the causative mechanism and anatomic local-ization, were assessed and compared between pituitary adenomapatients treated with postoperative RT and surgery alone. Thestroke incidence in this cohort was also compared with generalpopulation rates by using a large Dutch population-basedmorbidity registry (13).
Methods and Materials
Patients and follow-up
A total of 462 pituitary adenoma patients underwent treatmentbetween January 1959 and March 2008 in the University MedicalCenter Groningen. The pituitary adenoma patient characteristicsare shown in Table 1. All patients were treated with surgery asprimary treatment with or without postoperative RT. The pituitaryadenoma diagnosis was based on the patient’s clinical history andpresentation, endocrine evaluation, and pituitary imaging and wasconfirmed by postoperative histopathologic findings.
All patients were followed from the onset of pituitary adenomadiagnosis until January 2009 or date of death. For patients whowere not seen in our center for follow-up appointments after
January 2008, information requests were sent to the referringhospital or general practitioner.
Stroke diagnosis was retrieved retrospectively by reviewing thehospital records. The date of stroke was that of the first recordedstroke after pituitary adenoma diagnosis. Besides RT as potentialrisk factor, several other established stroke risk factors wereassessed (Table 1).
In patients diagnosed with stroke, information about theirprevious medical history, including well-established (cardiovas-cular) risk factors, the clinical course of stroke, and results ofgeneral physical and neurological examination and of studiesinvestigating a possible peripheral source of emboli, if indicated,were obtained. Furthermore, neuroimaging studies of the brain(CT/MRI) were retrieved to further define stroke subtype and sothat a classification into hemorrhagic and ischemic stroke couldbe assessed for all stroke patients. The most widely usedmethods for stroke subtype classification are the TOAST (Trialof ORG 10172 in Acute Stroke Treatment) and the OxfordshireCommunity Stroke Project method (14, 15). To determine thecausative mechanism of ischemic stroke the TOAST classifica-tion method was used (14). This diagnostic classificationdistinguishes 5 different clinical stroke subtypes based mainly onthe pathophysiologic mechanisms of infarction that are recog-nized as the cause of most strokes. The TOAST subtypes are (1)large artery atherosclerosis; (2) cardioembolism; (3) small vesselocclusion; (4) stroke of other determined etiology; and (5) strokeof undetermined etiology. In the last subtype the stroke causecannot be determined with any degree of confidence or includesthose with 2 or more potential causes identified, or those witha negative or incomplete evaluation. In addition, the OxfordshireCommunity Stroke Project classification method was used todetermine the anatomic localization of ischemic stroke (15).This method subdivides stroke according to the anatomicdistribution into 4 groups: (1) total anterior circulation; (2)partial anterior circulation; (3) posterior circulation; and (4)lacunar stroke.
The median follow-up time after pituitary adenoma diagnosisfor the entire cohort was 9 years (range, 1-49 years). The totalcumulative follow-up time in patients treated with RT was 3575patient-years, compared with 1586 patient-years in patients treatedwith surgery alone. In the time-to-event analyses, differences infollow-up time between the 2 treatment groups were taken intoaccount (see below, “Statistical methods”).
Postoperative RT
Indications for RT were (1) postoperative for local control oftumor growth and/or control of hormone excess in case ofresidual disease after incomplete resection and medical therapy,or (2) salvage treatment in patients with recurrent disease aftersurgery.
External beam RT was applied in 236 of the 462 pituitaryadenoma patients. All individual RT data were retrieved from the

Table 1 Characteristics of pituitary adenoma patients treated with postoperative radiation therapy (RT) or surgery alone
Characteristic RTþ RT� P*
N 236 226Sex (male/female) 110/126 107/119 .948Age at diagnosis (y) 46 (10-83) 51 (19-81) .001Age at end of follow-up (y) 62 (21-89) 57 (23-89) .005Duration of follow-up (y) 14 (1-49) 6 (1-34) <.001Type of adenoma .013
Nonfunctioning adenoma 143 (61) 113 (50)GH-secreting adenoma 69 (29) 70 (31)ACTH-secreting adenoma 24 (10) 43 (19)
Primary treatment <.001Transsphenoidal surgery 172 (73) 218 (96)Craniotomy 64 (27) 8 (4)Second surgical treatment 40 (17) 22 (10)
Control of hormone excess <.001(GH- and ACTH-secreting adenoma) 50 (54) 90 (80)
Hormonal substitutionNo. of hormone replacements (0/1/2/3/4/5) (40/41/60/61/32/0) (81/64/36/30/11/4) <.001Glucocorticoids 158 (67) 105 (46) <.001Thyroid hormone 156 (66) 74 (33) <.001Growth hormone 37 (16) 23 (10) .106Sex hormones 104 (44) 62 (27) <.001Desmopressin 21 (9) 22 (10) .843
Postoperative RTAge at RT (y) 49 (19-84) dTime between first surgery and RT (y) 1 (1-32) dRadiation therapy dose (Gy)�44 4 d45-49 173 d� 50 55 dUnknown 4 d
Stroke risk factorsHypertension 108 (46) 107 (47) .805Atrial fibrillation 14 (6) 6 (3) .137Hypercholesterolemia 66 (28) 52 (23) .266Diabetes mellitus 41 (17) 41 (18) .902Coronary or peripheral artery disease 39 (17) 37 (16) .907Open foramen ovale 0 0Prior stroke 0 5 (2) .070Prior transient ischemic attack 1 (0) 2 (1) .595
Abbreviations: ACTHZ adrenocorticotropic hormone; GHZ growth hormone; RTþZ patients with postoperative radiation therapy; RT�Z patients
with surgery alone.
Data are given as absolute numbers, median (range), or number (percentage).
* RTþ versus RT� by c2 test or Mann-Whitney U test.
Volume 87 � Number 1 � 2013 Stroke in pituitary adenoma patients 55
patient charts. The median total RT dose was 45 Gy (range, 30-55Gy). Most patients received an RT fractionation scheme of 25daily fractions of 1.8 Gy in 5 weeks.
Patients were treated with RT from 1962 to 2008, and differentRT techniques were used: rotational (nZ8), 2 fields (nZ19), 2fields and 3 fields (nZ16), 2 fields and 5 fields (nZ29), 3 fields(nZ68), 3 fields and 5 fields (nZ2), 4 fields (nZ3), tetraedertechnique (nZ47), 5-fields technique (nZ41), and unknown(nZ3). One patient was treated with 200-kV x-rays and 2 patientswith 60Co. All other patients were treated with external beam RTwith 4- to 18-MeV photons. In the 1990s 3-dimensional radiationtreatment planning techniques were used. The planning targetvolume was defined as the gross tumor volume plus a 1-cm margin.
The RT dose to the tumor was prescribed at the tumor-encompassing isodose in the time period 1962-1990. From 1991to 2008 the dose was prescribed at a central point in the tumoraccording to the recommendations of the International Commis-sion on Radiation Units and Measurements (www.icru.org).
General population stroke rate
Reference data were derived from the Continuous MorbidityRegistration Nijmegen (CMRN), a practice-based registrationnetwork of the Department of Primary and Community care at theRadboud University Nijmegen (13).
0
0,1
0,2
0,3
0,4
0,5
-70 -60 -50 -40 -30 -20 -10 0 10
Minus Median Life Expectancy
Cu
mu
la
tiv
e P
ro
po
rtio
n
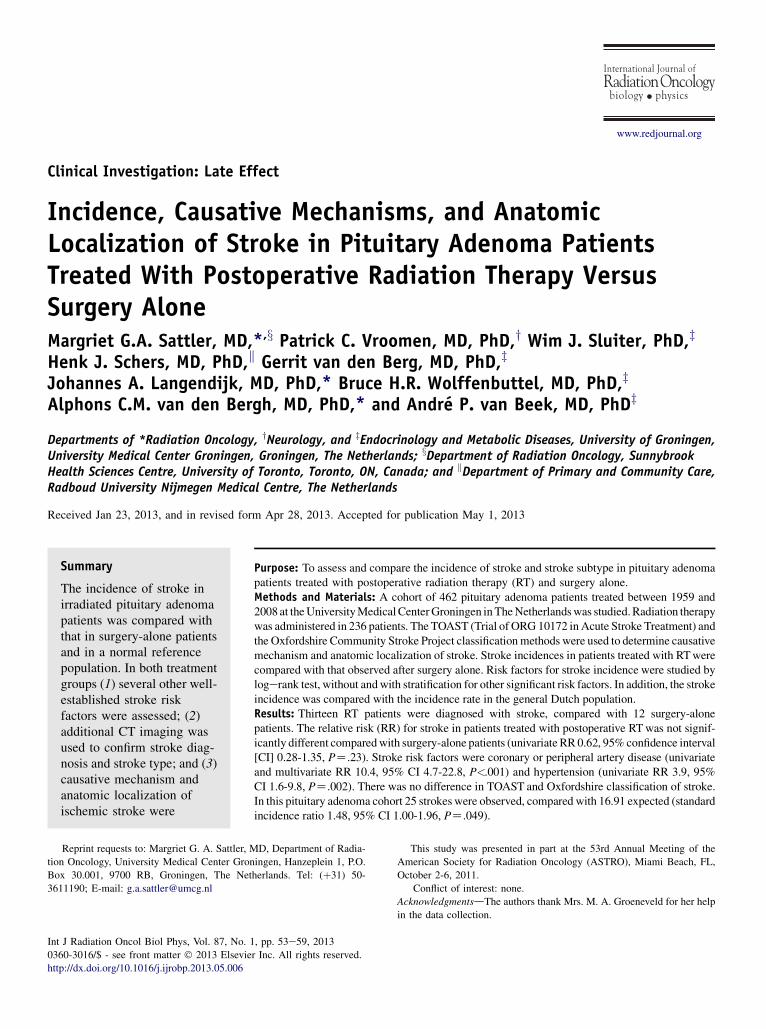
Fig. 2. Incidence of stroke in pituitary adenoma patientscompared with the expected incidence of stroke in the Dutchreference population. Solid line: Observed median life expectancyat stroke diagnosis in pituitary adenoma patients. Dashed line:Expected median life expectancy at stroke diagnosis in Dutchreference population.
Sattler et al. International Journal of Radiation Oncology � Biology � Physics56
For more than 40 years the CMRN has recorded all morbidityin the Dutch general population in relation to the sociodemo-graphic characteristics of this population. The patient populationin the CMRN is representative for the Dutch general population.The diagnosis stroke is registered in a primarily disease-orientedclassification system based on the International Classification ofHealth Problems in Primary Care. A limitation of this databasewas that stroke diagnosis was not classified into hemorrhagic orischemic stroke.
Statistical methods
The registration of strokes started from the date of pituitaryadenoma diagnosis, allowing a direct comparison of both treat-ment groups (postoperative RT and surgery alone) from a fixedpoint in time.
Age at pituitary adenoma diagnosis was transformed to medianlife expectancy (MLE) using the annual life tables of the CentralOffice of Statistics (CBS) according to sex and year of birth (www.cbs.nl). We used MLE (projected negative on the x-axis in Figs. 1and 2) instead of age, to account for differences in life expec-tancy due to differences in follow-up time, sex, and birth cohorteffects. For example, an MLE of�30 means an MLE of 30 years atthe moment of pituitary adenoma diagnosis. After 10 years offollow-up the MLE is decreased to 20 years and projected negativeon the x-axis as�20 in Figures 1 and 2. In this way, patients with thesame MLE are compared. The MLE at the event (stroke) instead ofsurviving time is the outcome parameter (16). The MLEs at pitui-tary adenoma diagnosis in patients treated with RTwere comparedwith those in surgery-alone patients and with the expected MLE ofstroke in the Dutch reference population. Left and right censoringwere used, and logerank test and Kaplan-Meier curves can beperformed without objection this way.
0
0,1
0,2
0,3
0,4
0,5
-70 -60 -50 -40 -30 -20 -10 0 10
Minus Median Life Expectancy
Cu
mu
lative P
ro
po
rtio
n
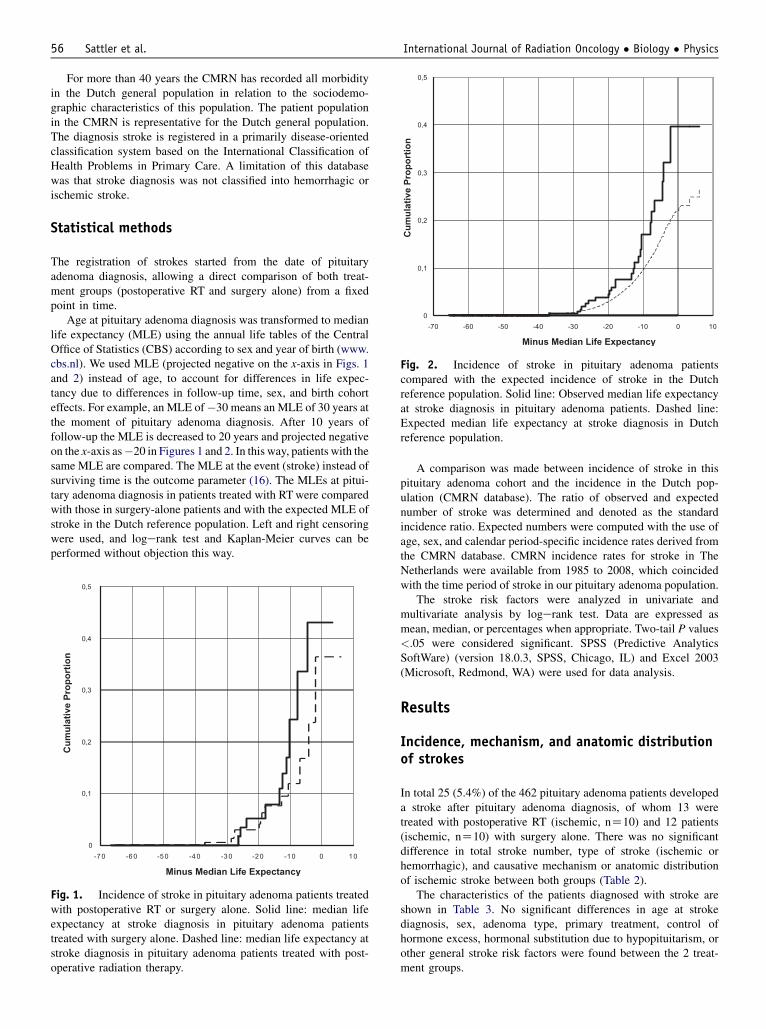
Fig. 1. Incidence of stroke in pituitary adenoma patients treatedwith postoperative RT or surgery alone. Solid line: median lifeexpectancy at stroke diagnosis in pituitary adenoma patientstreated with surgery alone. Dashed line: median life expectancy atstroke diagnosis in pituitary adenoma patients treated with post-operative radiation therapy.
A comparison was made between incidence of stroke in thispituitary adenoma cohort and the incidence in the Dutch pop-ulation (CMRN database). The ratio of observed and expectednumber of stroke was determined and denoted as the standardincidence ratio. Expected numbers were computed with the use ofage, sex, and calendar period-specific incidence rates derived fromthe CMRN database. CMRN incidence rates for stroke in TheNetherlands were available from 1985 to 2008, which coincidedwith the time period of stroke in our pituitary adenoma population.
The stroke risk factors were analyzed in univariate andmultivariate analysis by logerank test. Data are expressed asmean, median, or percentages when appropriate. Two-tail P values<.05 were considered significant. SPSS (Predictive AnalyticsSoftWare) (version 18.0.3, SPSS, Chicago, IL) and Excel 2003(Microsoft, Redmond, WA) were used for data analysis.
Results
Incidence, mechanism, and anatomic distributionof strokes
In total 25 (5.4%) of the 462 pituitary adenoma patients developeda stroke after pituitary adenoma diagnosis, of whom 13 weretreated with postoperative RT (ischemic, nZ10) and 12 patients(ischemic, nZ10) with surgery alone. There was no significantdifference in total stroke number, type of stroke (ischemic orhemorrhagic), and causative mechanism or anatomic distributionof ischemic stroke between both groups (Table 2).
The characteristics of the patients diagnosed with stroke areshown in Table 3. No significant differences in age at strokediagnosis, sex, adenoma type, primary treatment, control ofhormone excess, hormonal substitution due to hypopituitarism, orother general stroke risk factors were found between the 2 treat-ment groups.

Table 3 Characteristics of stroke patients treated withpostoperative RT or surgery alone
Characteristic RTþ RT� P*
N 13 12Age at stroke diagnosis (y) .602�49 1 150-59 3 1�60 9 10
Sex .509Male 6 3Female 7 9
Type of adenoma .090Nonfunctioning adenoma 9 8GH-secreting adenoma 3 0ACTH-secreting adenoma 1 4
Primary treatment .154Transsphenoidal surgery 6 10Craniotomy 7 2Second surgical treatment 2 2
Time since surgery (y) .007�9 4 1110-19 4 1�20 5 0
Time since postoperativeRT (y)
d
� 9 4 d10-19 7 d�20 2 d
Total RT dose (Gy) d�44 2 d45-49 7 d�50 4 d
Control of hormone excess(GH- and ACTH-secretingadenoma)
4 of 4 3 of 4 .559
Hormonal substitution .704No. of hormonereplacements(0/1/2/3/4/5)
(2/0/3/7/1/0) (2/5/2/3/0/0)
Glucocorticoids 11 9Thyroid hormone 11 4Growth hormone 1 1Sex hormones 6 2Desmopressin 2 2
Stroke risk factors .858Hypertension 10 10Atrial fibrillation 3 1Hypercholesterolemia 4 5Diabetes mellitus 6 4Coronary or peripheralartery disease
11 9
Prior stroke 0 0Prior transient ischemicattack
0 0
Table 2 Number and type of stroke in pituitary adenomapatients treated with postoperative RT or surgery alone
Parameter RTþ RT� P*
Total stroke 13 12 .764Total ischemic stroke 10 10Total hemorrhagic stroke 3 2
TOAST classification (ischemic stroke only)Large artery atherosclerosis 0 0 dCardioembolism 0 0 dSmall vessel occlusion 6 3 .389Stroke of other determined etiology 0 0 dStroke of undetermined etiology 3 7 .197Unknown 1 0 d
Oxfordshire classification (ischemic stroke only)Total anterior circulation stroke 0 3 .241Lacunar stroke 6 3 .389Partial anterior circulation stroke 3 2 .808Posterior circulation stroke 0 2 .428Unknown 1 0 d
Abbreviation: TOAST Z Trial of ORG 10172 in Acute Stroke
Treatment. Other abbreviations as in Table 1.
* RTþ versus RT� by c2 test.
Volume 87 � Number 1 � 2013 Stroke in pituitary adenoma patients 57
Stroke risk factors
Incidence and relative risk of risk factors for stroke in pituitaryadenoma patients are shown in Table 4.
In univariate analyses the incidence of stroke in patients treatedwith RT was not significantly different compared with surgeryalone (RR 0.62, 95% confidence interval [CI] 0.28-1.35, PZ.23).Only coronary or peripheral artery disease (RR 10.4, 95% CI 4.7-22.8, P<.001) and hypertension (RR 3.9, 95% CI 1.6-9.8,PZ.002) were identified as risk factors for stroke (Table 4).
In multivariate analyses coronary or peripheral artery diseasewas the only independent risk factor for stroke. Postoperative RTwas not an independent risk factor for stroke (data not shown).
All stroke patients were stratified for coronary or peripheralartery disease to further investigate the role of RT as a stroke riskfactor. In stroke patients diagnosed with or without coronary orperipheral artery disease, postoperative RT was not associatedwith an increased incidence of stroke compared with the surgery-alone patients (data not shown).
Incidence of stroke compared with the generalDutch population
In 462 pituitary adenoma patients 25 strokes were observed,compared with 16.91 expected (standard incidence ratio 1.48,95% CI 1.00-1.96, PZ.049). There was an increased incidence ofstroke in the pituitary adenoma population compared with an age-and sex-matched Dutch reference population (Fig. 2).
Abbreviations as in Table 1.
* RTþ versus RT� by c2 test.
DiscussionIn this study postoperative RT was not associated with anincreased risk of stroke compared with patients treated withsurgery alone.
To our knowledge this is the first study that compared theincidence of stroke in irradiated pituitary adenoma patients withthat in nonirradiated patients as a reference group instead of

Table 4 Incidence and relative risk of stroke risk factors inpituitary adenoma patients diagnosed with stroke
Riskfactor Observed Expected
Relativerisk 95% CI
P(univariate)
RTNo 12 9.11Yes 13 15.88 0.62 (1.35-0.28) .230
HypertensionNo 5 12.45Yes 20 12.54 3.96 (1.60-9.82) .002
Atrial fibrillationNo 21 20.59Yes 4 4.40 0.89 (2.59-0.30) .831
HypercholesterolemiaNo 16 17.01Yes 9 7.98 1.19 (0.53-2.70) .664
Diabetes mellitusNo 15 18.56Yes 10 6.43 1.92 (0.87-4.21) .103
Coronary or peripheral artery diseaseNo 5 18.06Yes 20 6.93 10.4 (4.74-22.89) <.001
Hormonal substitutionNo 4 3.94Yes 21 21.05 0.98 (2.86-0.33) .974
Abbreviations: CI Z confidence interval; RT Z patients with
postoperative radiation therapy.
Sattler et al. International Journal of Radiation Oncology � Biology � Physics58
a normal reference population, assessed several other well-established stroke risk factors, used additional CT imaging toconfirm stroke diagnosis and assess stroke subtype, and assessedcausative mechanism and anatomic localization of ischemicstroke. In a previously published article we showed that in thissame pituitary adenoma cohort no difference was seen in deathevents in patients treated with postoperative RT compared withpatients treated with surgery alone and that there was an increasedincidence of death events in the entire study population comparedwith an age- and sex-related Dutch reference population (17).
In this study the median follow-up time for patients treated withRTwas 14 (range, 1-49) years, compared with 6 (range, 1-34) yearsin patients treated with surgery alone. The patients were diagnosedand treated from 1959 to 2008, a period of almost 50 years. Becauseof improvements over time in neurosurgery and pituitary imagingtechniques (CT/MRI), the indication for RT decreased. Thisexplains the differences in follow-up time between patients treatedwith postoperative RT and surgery alone. Despite a longer follow-up time for patients treated with RT, no difference was seen instroke incidence between the 2 treatment groups.
In this large, retrospective study, collecting stroke data mayhave resulted in underreporting of stroke diagnoses. In addition,the small numbers of stroke found limit the power of the study torelate particular stroke characteristics to RT. However, despitea perhaps relatively low absolute number of strokes, the strokeincidence in this pituitary adenoma cohort was significantlyincreased compared with an age- and sex-related Dutch referencepopulation.
Our results on stroke are in agreement with investigators whoreported on increased stroke incidence in pituitary adenomapatients treated with RT compared with a normal reference
population (4, 11). Brada et al (11) reported an RR of stroke of 4.1compared with a normal reference population. Sixty-four (19%) ofthese 331 patients treated between 1962 and 1986 in the UnitedKingdom were diagnosed with stroke. The stroke frequency wasassessed from hospital records and clinicians, by postal ques-tionnaire of referring hospitals and general practitioners, and byexamination of all death certificates. The precise clinicopathologicclassification of stroke could not be determined, with the excep-tion of 5 recorded aneurysms presenting with subarachnoidhemorrhage. Furthermore, the expected stroke incidence wascalculated from a different calendar-year period. The medianfollow-up time of this pituitary adenoma cohort was 15 (range,0.5-33) years. In a more recent study by Erridge et al (4), an RR of1.45 (CI 1.05-1.18, PZ.03) in men and 2.22 (1.56-3.08, P<.01) inwomen matched with a Scottish reference population was re-ported. Seventy-eight (20%) of 385 pituitary adenoma patientstreated with RT between 1974 and 2003 in Edinburgh werediagnosed with stroke, of which 40% were fatal, and identified byeither review of case notes or data linkage with hospital dischargedata. The median follow-up time was 9.1 (range, 0.1-30.4) years.
However, a study by Flickinger et al (12) demonstrated noincreased incidence of ischemic stroke in irradiated pituitaryadenoma patients compared with a normal reference population.Seven (4.5%) of the 156 patients treated from 1964 to 1987 inPittsburgh experienced stroke. The ratio of observed to expectednumber of strokes was 1.98 and was not significantly elevated(PZ.078). The expected stroke incidence was calculated froma different calendar-year period. Arteriographic studies wereperformed in only 1 patient after stroke. Three stroke patients hadevidence of vascular disease outside the treatment field. Sixstrokes occurred in patients treated with a radiation dose of 41.80Gy in 22 fractions or more. The observed to expected ratio in thehigh-dose RT group was 3.87 and significantly elevated (P<.001).Univariate logerank analyses showed a significantly higher risk ofstroke (PZ.010) in patients treated with a total dose of 41.80 Gyor more compared with the lower-dose group. However, multi-variate analyses demonstrated that an increased risk of stroke wasassociated only with increasing age (P<.0001).
In the present study the strokes diagnosed in patients treatedwith postoperative RT may still represent a late side effect of RT.Vascular damage and atherosclerosis due the effects of RT on thecerebral vasculature can be considered as a possible underlyingmechanism in irradiated pituitary adenoma patients diagnosedwith stroke (18). However, the TOAST and Oxfordshire classifi-cation methods showed no significant differences in causativemechanism or anatomic localization of ischemic stroke betweenpatients treated with RT or surgery alone.
These results suggest that risk factors other than RT may havecontributed to the development of stroke. Indeed, in our studymultivariate analysis showed that the primary risk factor for strokewas pre-existent coronary or peripheral artery disease. However,some argue that surgical trauma to the vasculature or extent ofsurgery (11, 18) may play a role in the risk of stroke. In addition,hormone excess (Cushing’s disease or acromegaly) or hormonedeficiency (hypopituitarism due to pituitary adenoma disease,surgery, and/or RT) may act as risk factors for stroke (18) indi-rectly by inducing secondary hypertension, insulin resistance, ordyslipidemia, and directly by interactions with cellular pathwaysthat are important in the process of atherosclerotic plaqueformation, plaque instability, and thrombosis (19). Finally,well-established stroke risk factors, such as advanced age,hypertension, previous stroke or transient ischemic attack,

Volume 87 � Number 1 � 2013 Stroke in pituitary adenoma patients 59
asymptomatic carotid stenosis, diabetes mellitus, hyperlipidemia,cigarette smoking, and atrial fibrillation and other cardiac disease(20), may also predispose to stroke in pituitary adenoma patients.
In pituitary adenoma patients, early detection of patients at riskfor stroke (ie, patients with evidence of pre-existent coronary orperipheral artery disease), adequate treatment of hormone excessand hormone deficiencies, and preventive management of modi-fiable cardiovascular risk factors may help in reduce stroke risk.
Conclusions
An increased incidence of stroke in the entire pituitary adenomastudy population was observed compared with an age- and sex-matched reference population. However, postoperative RT forpituitary adenoma patients was not associated with an increasedincidence of stroke compared with patients who were treated withsurgery alone, and stroke type (ischemic or hemorrhagic) was notdifferent between the 2 treatment groups. Furthermore, in ischemicstroke patients, RT did not show a difference in causative mecha-nism or anatomic localization compared with patients treated withsurgery alone. Finally, the primary risk factor for stroke waspre-existent coronary or peripheral artery disease.
References
1. Gittoes NJ, Bates AS, Tse W, et al. Radiotherapy for non-function
pituitary tumours. Clin Endocrinol (Oxf) 1998;48:331-337.
2. Park P, Chandler WF, Barkan AL, et al. The role of radiation therapy
after surgical resection of nonfunctional pituitary macroadenomas.
Neurosurgery 2004;55:100-106.
3. van den Bergh AC, van den Berg G, Schoorl MA, et al. Immediate
postoperative radiotherapy in residual nonfunctioning pituitary
adenoma: Beneficial effect on local control without additional nega-
tive impact on pituitary function and life expectancy. Int J Radiat
Oncol Biol Phys 2007;67:863-869.
4. Erridge SC, Conkey DS, Stockton D, et al. Radiotherapy for pituitary
adenomas: Long-term efficacy and toxicity. Radiother Oncol 2009;93:
597-601.
5. Estrada J, Boronat M, Mielgo M, et al. The long-term outcome of
pituitary irradiation after unsuccessful transsphenoidal surgery in
Cushing’s disease. N Engl J Med 1997;336:172-177.
6. Minniti G, Osti M, Jaffrain-Rea ML, et al. Long-term follow-up
results of postoperative radiation therapy for Cushing’s disease. J
Neurooncol 2007;84:79-84.
7. Jenkins PJ, Bates P, Carson MN, et al. Conventional pituitary irradi-
ation is effective in lowering serum growth hormone and insulin-like
growth factor-I in patients with acromegaly. J Clin Endocrinol
Metab 2006;91:1239-1245.
8. Biermasz NR, Dulken HV, Roelfsema F. Postoperative radiotherapy in
acromegaly is effective in reducing GH concentration to safe levels.
Clin Endocrinol (Oxf) 2000;53:321-327.
9. Bowen J, Paulsen CA. Stroke after pituitary irradiation. Stroke 1992;
23:908-911.
10. Ogaki S, Suzuki S, Suzuki H, et al. Cerebral hemorrhagic infarc-
tion after radiation for pituitary adenoma. Intern Med 2002;41:
834-838.
11. Brada M, Burchell L, Ashley S, et al. The incidence of cerebrovascular
accidents in patients with pituitary adenoma. Int J Radiat Oncol Biol
Phys 1999;45:693-698.
12. Flickinger JC, Nelson PB, Taylor FH, et al. Incidence of cerebral
infarction after radiotherapy for pituitary adenoma. Cancer 1989;63:
2404-2408.
13. Van Weel C. The continuous morbidity registration Nijmegen: Back-
ground and history of a Dutch general practice database. Eur J Gen
Pract 2008;14(Suppl. 1):5-12.
14. Adams HP Jr., Bendixen BH, Kappelle LJ, et al. Classification of
subtype of acute ischemic stroke. Definitions for use in a multicenter
clinical trial. TOAST. Trial of ORG 10172 in Acute Stroke Treatment.
Stroke 1993;24:35-41.
15. Bamford J, Sandercock P, Dennis M, et al. Classification and natural
history of clinically identifiable subtypes of cerebral infarction. Lancet
1991;337:1521-1526.
16. Korn EL, Graubard BI, Midthune D. Time-to-event analysis of
longitudinal follow-up of a survey: Choice of the time-scale. Am J
Epidemiol 1997;145:72-80.
17. Sattler MG, van Beek AP, Wolffenbuttel BH, et al. The incidence of
second tumours and mortality in pituitary adenoma patients treated
with postoperative radiotherapy versus surgery alone. Radiother Oncol
2012;104:125-130.
18. Erfurth EM, Hagmar L. Cerebrovascular disease in patients with
pituitary tumors. Trends Endocrinol Metab 2005;16:334-342.
19. van Zaane B, Reuwer AQ, Buller HR, et al. Hormones and cardio-
vascular disease: A shift in paradigm with clinical consequences?
Semin Thromb Hemost 2009;35:478-487.
20. Elkind MS, Sacco RL. Stroke risk factors and stroke prevention. Semin
Neurol 1998;18:429-440.
Copyright © 2022 FDOKUMEN




















