
Anatomic Single and Double-Bundle Anterior Cruciate Ligament Reconstruction, Part 2: Clinical...
11
Anatomic Single- and Double-Bundle Anterior Cruciate Ligament Reconstruction, Part 2 Clinical Application of Surgical Technique Jon Karlsson, * MD, PhD, James J. Irrgang, y PT, PhD, ATC, FAPTA, Carola F. van Eck, y MD, PhD, Kristian Samuelsson, * MD, Hector A. Mejia, y MD, and Freddie H. Fu, yz MD, DSc The anterior cruciate ligament has been and is of great interest to scientists and orthopaedic surgeons worldwide. Anterior cru- ciate ligament reconstruction was initially performed using an open approach. When the approach changed from open to arthro- scopic reconstruction, a 2- and, later, 1-incision technique was applied. With time, researchers found that traditional arthroscopic single-bundle reconstruction did not fully restore rotational stability of the knee joint and a more anatomic approach to reconstruct the anterior cruciate ligament has been proposed. Anatomic anterior cruciate ligament reconstruction intends to replicate normal anatomy, restore normal kinematics, and protect long-term knee health. Although double-bundle anterior cruciate ligament reconstruction has been shown to result in better rotational stability in both biomechanical and clinical studies, it is vital to differ- entiate between anatomic and double-bundle anterior cruciate ligament reconstruction. The latter is merely a step closer to reproducing the native anatomy of the anterior cruciate ligament; however, it can still be done nonanatomically. To evaluate the potential benefits of reconstructing the anterior cruciate ligament in an anatomic fashion, accurate, precise, and reliable out- come measures are needed. These include, for example, T2 magnetic resonance imaging mapping of cartilage and quantification of graft healing on magnetic resonance imaging. Furthermore, there is a need for a consensus on which patient-reported outcome measures should be used to facilitate homogeneous reporting of outcomes. Keywords: anterior cruciate ligament; anatomic; single-bundle; double-bundle; graft; imaging; outcome The anterior cruciate ligament (ACL) has been and contin- ues to be of great interest to scientists and orthopaedic sur- geons worldwide. This interest is easily demonstrated by the vast number of publications on this subject. Reasons for this interest are the high incidence of ACL ruptures, 30 especially in young athletes; difficulties restoring normal anatomy of the ACL; and orthopaedic surgeons’ concern to provide the best care for their patients. The extensive research in the area has yielded several breakthroughs and changes in the treatment of ACL injuries. Treatment options are numerous and range from nonoperative treatment to different methods to surgically reconstruct the ACL that vary in graft type, number of tunnels and bundles, method of fixation, and more. The surgical methods to reconstruct the ACL have taken several sharp turns since the development of the arthro- scopically assisted reconstruction that was initially per- formed by Dandy in 1980. 22 The major reason for changing from open to arthroscopically assisted techniques was to reduce surgical morbidity. The transtibial single- bundle technique was—and probably still is—the most com- mon technique. Initially there was great focus on graft selection and attempts were made with different artificial grafts, allografts, and autografts. 35 We are in the midst of yet another important change in the surgical technique of ACL reconstruction. Focus is now changing toward ana- tomic reconstruction with greater emphasis on tunnel posi- tion in the native ACL footprint. The traditional transtibial technique has come under scrutiny as it has been shown that a transtibial technique results in nonanatomic recon- struction with regard to the native ACL footprints. 43 Recently, the medial portal femoral drilling technique, using the accessory medial portal, together with better understanding of bone tunnel positioning has allowed for anatomic single- or double-bundle ACL reconstruc- tion. 11,20,33 Furthermore, double-bundle ACL reconstruction M z Address correspondence to Freddie H. Fu, MD, DSc, Kaufman Building Suite 1011, 3471 Fifth Avenue, Pittsburgh, PA 15213 (e-mail: [email protected]). *Department of Orthopaedics, Sahlgrenska University Hospital, Mo ¨ ln- dal, Sweden. y Department of Orthopaedic Surgery, University of Pittsburgh, Pitts- burgh, Pennsylvania. One or more of the authors has declared the following potential con- flict of interest or source of funding: The Department of Orthopaedic Sur- gery of the University of Pittsburgh receives funding from Smith & Nephew to support research related to reconstruction of the ACL. The American Journal of Sports Medicine, Vol. 39, No. 9 DOI: 10.1177/0363546511402660 Ó 2011 The Author(s) 2016 Spotlight on Surgical Techniques by KAREN MOHR on October 5, 2011 ajs.sagepub.com Downloaded from
Transcript of Anatomic Single and Double-Bundle Anterior Cruciate Ligament Reconstruction, Part 2: Clinical...

Anatomic Single- and Double-BundleAnterior Cruciate LigamentReconstruction, Part 2
Clinical Application of Surgical Technique
Jon Karlsson,* MD, PhD, James J. Irrgang,y PT, PhD, ATC, FAPTA, Carola F. van Eck,y MD, PhD,Kristian Samuelsson,* MD, Hector A. Mejia,y MD, and Freddie H. Fu,yz MD, DSc
The anterior cruciate ligament has been and is of great interest to scientists and orthopaedic surgeons worldwide. Anterior cru-ciate ligament reconstruction was initially performed using an open approach. When the approach changed from open to arthro-scopic reconstruction, a 2- and, later, 1-incision technique was applied. With time, researchers found that traditional arthroscopicsingle-bundle reconstruction did not fully restore rotational stability of the knee joint and a more anatomic approach to reconstructthe anterior cruciate ligament has been proposed. Anatomic anterior cruciate ligament reconstruction intends to replicate normalanatomy, restore normal kinematics, and protect long-term knee health. Although double-bundle anterior cruciate ligamentreconstruction has been shown to result in better rotational stability in both biomechanical and clinical studies, it is vital to differ-entiate between anatomic and double-bundle anterior cruciate ligament reconstruction. The latter is merely a step closer toreproducing the native anatomy of the anterior cruciate ligament; however, it can still be done nonanatomically. To evaluatethe potential benefits of reconstructing the anterior cruciate ligament in an anatomic fashion, accurate, precise, and reliable out-come measures are needed. These include, for example, T2 magnetic resonance imaging mapping of cartilage and quantificationof graft healing on magnetic resonance imaging. Furthermore, there is a need for a consensus on which patient-reported outcomemeasures should be used to facilitate homogeneous reporting of outcomes.
Keywords: anterior cruciate ligament; anatomic; single-bundle; double-bundle; graft; imaging; outcome
The anterior cruciate ligament (ACL) has been and contin-ues to be of great interest to scientists and orthopaedic sur-geons worldwide. This interest is easily demonstrated bythe vast number of publications on this subject. Reasonsfor this interest are the high incidence of ACL ruptures,30
especially in young athletes; difficulties restoring normalanatomy of the ACL; and orthopaedic surgeons’ concernto provide the best care for their patients. The extensiveresearch in the area has yielded several breakthroughsand changes in the treatment of ACL injuries. Treatmentoptions are numerous and range from nonoperative
treatment to different methods to surgically reconstructthe ACL that vary in graft type, number of tunnels andbundles, method of fixation, and more.
The surgical methods to reconstruct the ACL have takenseveral sharp turns since the development of the arthro-scopically assisted reconstruction that was initially per-formed by Dandy in 1980.22 The major reason forchanging from open to arthroscopically assisted techniqueswas to reduce surgical morbidity. The transtibial single-bundle technique was—and probably still is—the most com-mon technique. Initially there was great focus on graftselection and attempts were made with different artificialgrafts, allografts, and autografts.35 We are in the midst ofyet another important change in the surgical technique ofACL reconstruction. Focus is now changing toward ana-tomic reconstruction with greater emphasis on tunnel posi-tion in the native ACL footprint. The traditional transtibialtechnique has come under scrutiny as it has been shownthat a transtibial technique results in nonanatomic recon-struction with regard to the native ACL footprints.43
Recently, the medial portal femoral drilling technique,using the accessory medial portal, together with betterunderstanding of bone tunnel positioning has allowed foranatomic single- or double-bundle ACL reconstruc-tion.11,20,33 Furthermore, double-bundle ACL reconstruction
M
zAddress correspondence to Freddie H. Fu, MD, DSc, KaufmanBuilding Suite 1011, 3471 Fifth Avenue, Pittsburgh, PA 15213 (e-mail:[email protected]).
*Department of Orthopaedics, Sahlgrenska University Hospital, Moln-dal, Sweden.
yDepartment of Orthopaedic Surgery, University of Pittsburgh, Pitts-burgh, Pennsylvania.
One or more of the authors has declared the following potential con-flict of interest or source of funding: The Department of Orthopaedic Sur-gery of the University of Pittsburgh receives funding from Smith &Nephew to support research related to reconstruction of the ACL.
The American Journal of Sports Medicine, Vol. 39, No. 9DOI: 10.1177/0363546511402660� 2011 The Author(s)
2016
Spotlight on Surgical Techniques
by KAREN MOHR on October 5, 2011ajs.sagepub.comDownloaded from

is gaining interest because of its potential to more closelymimic the native ACL anatomy.53 The biomechanicaladvantages in terms of double-bundle reconstruction havebeen demonstrated in several studies.65,74-76 Currently, sev-eral clinical trials are being conducted to evaluate the ben-efit of the double-bundle technique. This is all in light oftrying to improve patient outcomes, especially reducingthe risk of osteoarthritis in the medium and long term. Toevaluate this aim, new and better outcome measures aresought including better patient-reported and clinician-mea-sured outcomes measures. In addition, the option of ana-tomic single-bundle reconstruction is being explored,which has the potential benefits of anatomic placementwithout the increased procedural difficulty of double-bundlereconstruction.64
This article will report the current concepts in anatomicACL reconstruction, including the principles, surgical tech-nique descriptions for anatomic single-bundle as well as ana-tomic double-bundle reconstruction, the pearls and pitfalls,postoperative evaluation, rehabilitation, and clinical outcome.Finally, current trends in the literature will be discussed.
PRINCIPLES OF ANATOMIC ACL RECONSTRUCTION
When considering anatomic ACL reconstruction, there are4 major principles. In our opinion, it is the application ofthese principles that makes the concept of anatomic ACLreconstruction suitable for primary and revision surgery,as well as for augmentation surgery, and single- anddouble-bundle reconstruction.59 The first principleinvolves restoring the native insertion site anatomy. TheACL footprint remnants, on both the femoral and tibialside, should be used to indicate the tunnel positions.Also, the native ACL insertion site size and shape shouldbe replicated when doing so. The second principle logicallyfollows the first and is to restore the 2 functional bundles ofthe ACL. The anteromedial (AM) and posterolateral (PL)bundles may be restored as 1 single graft (anatomic single-bundle reconstruction) if certain factors are present.However, the graft(s) should try to restore the functionalanatomy of the native ACL. The third principle is to addressthe tension behavior of the native ACL. The AM componentis taut throughout the entire range of motion of the knee,with a peak between 45� and 60�.19,26,28,67 The PL compo-nent is primarily taut in extension. The reconstructed single-or double-bundle graft should mimic this native tensioningbehavior. Lastly, the fourth principle is to individualize thesurgical procedure for each patient. Either an anatomic sin-gle-bundle or anatomic double-bundle procedure, graft type,tunnel size, and graft diameter should be dictated by mor-phologic characteristics of the knee and native ACL anatomyof each patient. A small native insertion site may be unableto accommodate a double-bundle procedure and, inversely,a large native insertion site may be insufficiently restoredwith a single-bundle graft. The goal of anatomic ACL recon-struction is to tailor each procedure with each patient’s ana-tomic, biomechanical, and functional demands, in order toensure favorable long-term outcome.
PREOPERATIVE ASSESSMENT
A thorough history, physical examination, and imagingare vital in the diagnosis of an ACL injury, and can alsoprovide useful information regarding what treatmentoptions are available and appropriate.67 The history givesthe clinician an idea of the patient’s activity level andmechanism of injury, which can help determine the rup-ture pattern of the ACL bundles.79 The preoperative phys-ical examination for diagnostic purposes is essential, as ithas been shown to be as sensitive and specific as imagingmodalities.13 The Lachman and pivot-shift tests are diag-nostic for an ACL tear, and discrepancies between thetests can indicate 1-bundle tears.68 A positive Lachmantest in the absence of a positive pivot shift may indicatean AM bundle tear. Magnetic resonance imaging can con-firm the diagnosis of an ACL injury,62 but more impor-tantly it also allows the surgeon to examine the rupturepattern,60,63 measure the native ACL insertion sitedimensions and inclination angles, evaluate for other lig-amentous or bony injuries, and evaluate meniscus andcartilage status2 (Figure 1).
INTRAOPERATIVE EVALUATION
Before the start of the arthroscopic reconstruction, an exam-ination of the knee under anesthesia should be performed tobetter evaluate the degree of instability. It has been shownthat the examination under anesthesia is often quite differ-ent than that performed in the clinic, specifically with regardto the pivot-shift test.13 Intraoperative evaluation viaarthroscopy can confirm the rupture pattern as assessed byphysical examination and MRI. The rupture pattern of theACL can be used to individualize surgical treatment. Forexample, a 1-bundle tear could be amendable to a single-bundle augmentation of the injured bundle as opposed tosingle-bundle or double-bundle ACL reconstruction. In addi-tion, the remnants of the native ACL can be followed to iden-tify the native femoral and tibial insertion sites.
THREE-PORTAL APPROACH
The femoral and tibial insertion sites can best be visualizedusing a 3-portal approach20 (Figure 2). This approachmakes use of the standard anterolateral and centralmedial portals and in addition an accessory AM portal.The central portal is created under arthroscopic visualiza-tion through the lateral portal with a spinal needle. Thespinal needle should be in the center portion of the notchin the coronal plane and in the lower third of the notchin the proximal to distal direction. The accessory AM portalis ideally located superior to the medial joint line approxi-mately 2 cm medial to the medial border of the patellartendon. Using all 3 portals as viewing and instrumentationportals allows for complete visualization of the entire ACLand its femoral and tibial insertion sites. The femoral tun-nels can be drilled through the accessory medial portal,
Vol. 39, No. 9, 2011 Anatomic Single- and Double-Bundle ACL Reconstruction 2017
by KAREN MOHR on October 5, 2011ajs.sagepub.comDownloaded from

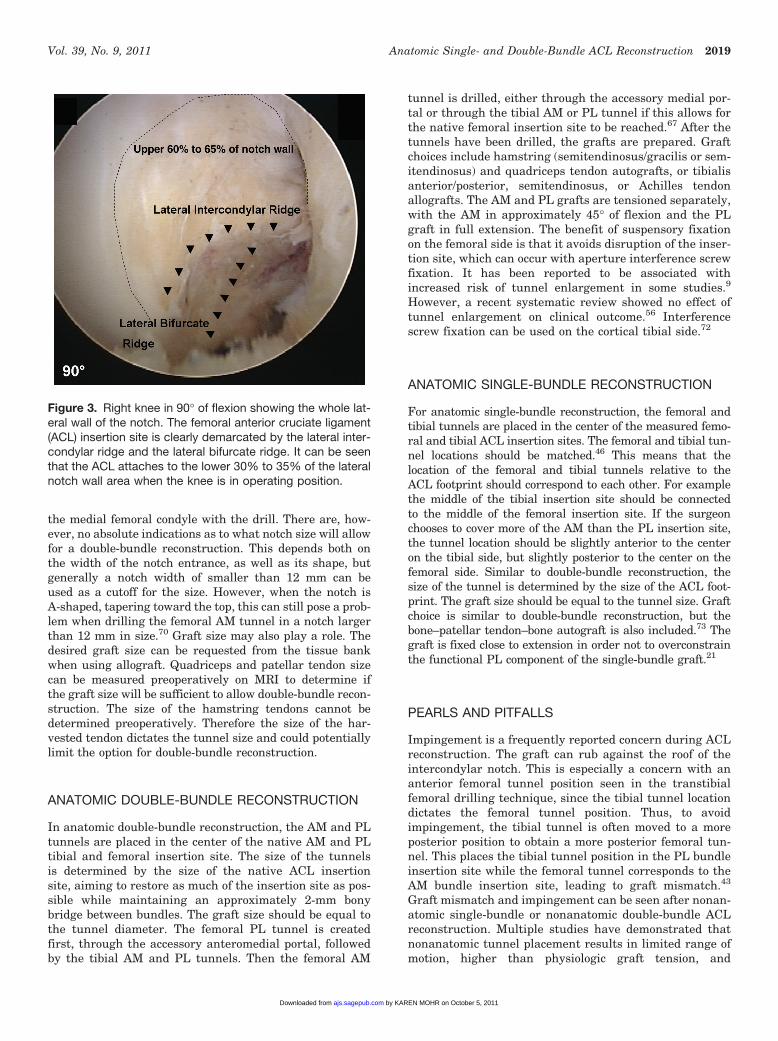
under direct visualization through the central medial por-tal. In addition to the ACL remnants, other anatomicstructures can be used to locate the ACL insertion sitesfor anatomic tunnel placement. On the femoral side, thebony landmarks—the lateral intercondylar ridge and lat-eral bifurcate ridge25—may be used, as well as the poste-rior cartilage border. These landmarks are especiallyuseful for chronic ACL injuries.71 If the femoral insertionsite cannot be determined using these anatomic land-marks, then it is important to obtain visualization of thewhole medial wall of the lateral femoral condyle as thefemoral insertion site encompasses the lower 30% to 35%of the notch wall with the knee in 90� of flexion (Figure3). On the tibial side, the close relationship of the ACLinsertion site with the tibial spines, anterior and posteriorhorns of the lateral meniscus and posterior cruciate liga-ment insertion site can be used as surgical landmarks.
CONTRAINDICATIONS FOR DOUBLE-BUNDLERECONSTRUCTION
The tibial and femoral insertion sites of the ACL should bemarked and measured to determine tunnel location andsize. When a patient has an insertion site less than14 mm in diameter, a double-bundle reconstruction canpresent a challenge. Other indications for single-bundlereconstruction are open physes, severe bone bruising,a narrow notch and arthritis changes, and multiple liga-mentous injuries.59 A narrow notch can make it difficultto place the guide pins, especially the AM guide pin, inthe native femoral insertion site. With such a narrow notch,it is difficult to drill the femoral tunnels without damaging
Figure 2. Right knee in 90� of flexion showing the 3-portaltechnique. There is a central medial portal (CMP) and a stan-dard lateral portal (LP). In addition, an accessory medial por-tal (AMP) is applied.
Figure 1. Special MRI cuts of the anterior cruciate ligament: A, oblique sagittal cut showing the anteromedial (AM) and postero-lateral (PL) bundles; B, oblique coronal cut showing the AM bundle; and C, oblique coronal cut showing the PL bundle.
2018 Karlsson et al The American Journal of Sports Medicine
by KAREN MOHR on October 5, 2011ajs.sagepub.comDownloaded from
the medial femoral condyle with the drill. There are, how-ever, no absolute indications as to what notch size will allowfor a double-bundle reconstruction. This depends both onthe width of the notch entrance, as well as its shape, butgenerally a notch width of smaller than 12 mm can beused as a cutoff for the size. However, when the notch isA-shaped, tapering toward the top, this can still pose a prob-lem when drilling the femoral AM tunnel in a notch largerthan 12 mm in size.70 Graft size may also play a role. Thedesired graft size can be requested from the tissue bankwhen using allograft. Quadriceps and patellar tendon sizecan be measured preoperatively on MRI to determine ifthe graft size will be sufficient to allow double-bundle recon-struction. The size of the hamstring tendons cannot bedetermined preoperatively. Therefore the size of the har-vested tendon dictates the tunnel size and could potentiallylimit the option for double-bundle reconstruction.
ANATOMIC DOUBLE-BUNDLE RECONSTRUCTION
In anatomic double-bundle reconstruction, the AM and PLtunnels are placed in the center of the native AM and PLtibial and femoral insertion site. The size of the tunnelsis determined by the size of the native ACL insertionsite, aiming to restore as much of the insertion site as pos-sible while maintaining an approximately 2-mm bonybridge between bundles. The graft size should be equal tothe tunnel diameter. The femoral PL tunnel is createdfirst, through the accessory anteromedial portal, followedby the tibial AM and PL tunnels. Then the femoral AM
tunnel is drilled, either through the accessory medial por-tal or through the tibial AM or PL tunnel if this allows forthe native femoral insertion site to be reached.67 After thetunnels have been drilled, the grafts are prepared. Graftchoices include hamstring (semitendinosus/gracilis or sem-itendinosus) and quadriceps tendon autografts, or tibialisanterior/posterior, semitendinosus, or Achilles tendonallografts. The AM and PL grafts are tensioned separately,with the AM in approximately 45� of flexion and the PLgraft in full extension. The benefit of suspensory fixationon the femoral side is that it avoids disruption of the inser-tion site, which can occur with aperture interference screwfixation. It has been reported to be associated withincreased risk of tunnel enlargement in some studies.9
However, a recent systematic review showed no effect oftunnel enlargement on clinical outcome.56 Interferencescrew fixation can be used on the cortical tibial side.72
ANATOMIC SINGLE-BUNDLE RECONSTRUCTION
For anatomic single-bundle reconstruction, the femoral andtibial tunnels are placed in the center of the measured femo-ral and tibial ACL insertion sites. The femoral and tibial tun-nel locations should be matched.46 This means that thelocation of the femoral and tibial tunnels relative to theACL footprint should correspond to each other. For examplethe middle of the tibial insertion site should be connectedto the middle of the femoral insertion site. If the surgeonchooses to cover more of the AM than the PL insertion site,the tunnel location should be slightly anterior to the centeron the tibial side, but slightly posterior to the center on thefemoral side. Similar to double-bundle reconstruction, thesize of the tunnel is determined by the size of the ACL foot-print. The graft size should be equal to the tunnel size. Graftchoice is similar to double-bundle reconstruction, but thebone–patellar tendon–bone autograft is also included.73 Thegraft is fixed close to extension in order not to overconstrainthe functional PL component of the single-bundle graft.21
PEARLS AND PITFALLS
Impingement is a frequently reported concern during ACLreconstruction. The graft can rub against the roof of theintercondylar notch. This is especially a concern with ananterior femoral tunnel position seen in the transtibialfemoral drilling technique, since the tibial tunnel locationdictates the femoral tunnel position. Thus, to avoidimpingement, the tibial tunnel is often moved to a moreposterior position to obtain a more posterior femoral tun-nel. This places the tibial tunnel position in the PL bundleinsertion site while the femoral tunnel corresponds to theAM bundle insertion site, leading to graft mismatch.43
Graft mismatch and impingement can be seen after nonan-atomic single-bundle or nonanatomic double-bundle ACLreconstruction. Multiple studies have demonstrated thatnonanatomic tunnel placement results in limited range ofmotion, higher than physiologic graft tension, and
Figure 3. Right knee in 90� of flexion showing the whole lat-eral wall of the notch. The femoral anterior cruciate ligament(ACL) insertion site is clearly demarcated by the lateral inter-condylar ridge and the lateral bifurcate ridge. It can be seenthat the ACL attaches to the lower 30% to 35% of the lateralnotch wall area when the knee is in operating position.
Vol. 39, No. 9, 2011 Anatomic Single- and Double-Bundle ACL Reconstruction 2019
by KAREN MOHR on October 5, 2011ajs.sagepub.comDownloaded from

ultimately graft failure.3,41 Mismatched grafts are more ver-tical in orientation and can lead to rotational instabilitywhen compared with the intact ACL or anatomic ACLreconstruction as shown in biomechanical studies.80 Medialportal drilling can establish a femoral tunnel independent ofthe tibial tunnel location, and allows for anatomic ACLreconstruction with regard to its respective insertion siteand matching of bundles.59 However, compared with trans-tibial drilling, medial portal drilling holds a higher risk ofshort femoral tunnel and posterior wall blow-out.12 Thisrisk can be decreased by hyperflexing the knee during fem-oral tunnel drilling. In case of double-bundle reconstruction,the tunnels should be drilled in a divergent manner. If pos-terior wall blowout does occur, a potential solution is toplace the graft using the over-the-top technique. The medialwall of the lateral femoral condyle is rasped first to increasegraft-to-bone healing. Then, the passing wire is routedaround the lateral condyle and out through the lateral thighincision. The graft is routed using this passing wire andfixed with a post and suture construct on the femoral side,using an AO screw and washer.
Another benefit of medial portal drilling is that the AMand PL tunnels can be drilled in a divergent manner. Analternative way to create diverging tunnels is to drill thePL tunnel through the medial portal and to drill the femoralAM tunnel through the tibial PL tunnel in a transtibialfashion. This will change the tunnel direction between theAM and PL. If there is no bony bridge between the femoralAM and PL tunnels, drilling the tunnels in a divergent man-ner ensures that the tunnels will not merge.
Another way to avoid graft impingement is to performa notchplasty. However, notchplasty is mostly unnecessary
when an anatomic ACL reconstruction is performed. The the-ory is that if the native ACL does not impinge, then the ana-tomically reconstructed ACL should not impinge either. Anotchplasty can also be performed to obtain better visualiza-tion of the PL margin of the intercondylar area,7 but thismakes anatomic reconstruction more difficult as all osseouslandmarks of the femoral ACL insertion are removed. Also,the removal of the bony ridges can complicate anatomic tun-nel placement and regrowth or overgrowth after previousnotchplasty has been linked to graft rupture.47 The recentlypreferred technique is the use of a 3-portal technique, whichuses an accessory AM portal that allows the surgeon clearvisualization of the intercondylar space.20
EVALUATION OF GRAFT AND TUNNEL POSITION
There are many ways to evaluate the tunnel position, bothintra- and postoperatively. Intraoperative fluoroscopy canbe used to assess guidewire placement and to evaluate tun-nel position before drilling of the tunnels. Postoperatively,AP and lateral radiographs can be used. These allow visu-alization of the bone tunnel angle and hardware.42 MRIcan be used to determine if the graft is intact and to eval-uate postoperative insertion site size and inclination angle.These findings can be compared with the preoperativeMRI2 (Figure 4). This is most useful in the setting of rein-jury or the concern for intactness of the graft. However, 3-dimensionally reconstructed CT is the best imaging tech-nique to critically evaluate tunnel position27,43
(Figure 5). This can prove to be especially useful when it
Figure 4. Bilateral MRI scans of a patient after right knee anterior cruciate ligament (ACL) reconstruction. A, left knee sagittalimage showing a native tibial ACL insertion site size of 18.4 mm and an inclination angle of 48�. B, right knee sagittal MRIscan after anatomic double-bundle ACL reconstruction showing a tibial insertion site size of 18.0 mm and a graft inclination angleof 49�, indicating that the native ACL is closely restored.
2020 Karlsson et al The American Journal of Sports Medicine
by KAREN MOHR on October 5, 2011ajs.sagepub.comDownloaded from

comes to revision surgery. This can help determine if theold tunnels can be reused, or if new tunnels are warranted.It can also help quantify bone loss or tunnel expansion forpreoperative determination of a single versus staged proce-dure.59 Tunnel enlargement can be quantified and if thetunnel size is larger than the expected size of the graftthat is going to be used in the revision, or if the bone qual-ity surrounding the tunnels is deemed to be poor, a 2-stageprocedure can be planned.
CLINICAL OUTCOMES
There are several outcome measures available to evaluatethe results of ACL reconstruction. Patient-reported out-comes, such as the International Knee DocumentationCommittee (IKDC) subjective knee form, Knee injury andOsteoarthritis Outcome Score (KOOS), Tegner activity score,and Marx activity score, can be used to evaluate symptoms,functioning, and sports activity. Restoration of range ofmotion symmetrical to the noninvolved knee is an importantoutcome. A side-to-side difference of greater than 3� forextension has been associated with persistent pain and thedevelopment of osteoarthritis.50 Manual laxity tests,including the Lachman, anterior drawer, and pivot-shifttests can be used to grade the degree of anterior-posteriorand rotational laxity of the knee. Instrumented measure-ment of knee laxity with an arthrometer, such as
KT-1000 arthrometer (MEDmetric, San Diego, California)testing, can provide a numeric value of anterior transla-tion compared with the uninjured side. Because of individ-ual differences in laxity, laxity of the surgicallyreconstructed knee must be compared with the nonin-volved knee and should be graded according to guidelinesestablished by the IKDC.36 For the office examination, itshould be remembered that any degree of laxity in com-parison with the contralateral knee cannot be considereda normal finding of knee laxity. In addition, normal kneelaxity during the office examination does not necessarilyimply that normal kinematics of the knee have beenrestored. Other outcome measures that should be consid-ered are graft failure and the need for revision ACLreconstruction.
To optimally evaluate the outcome of ACL surgery, theoutcome measures need to be both reliable and valid. Clin-ical studies have been conducted to compare differentmethods of reconstruction, graft types, and tunnel posi-tions. Systematic reviews and meta-analyses of these stud-ies overwhelmingly show only minor differences in most ofthe reported outcomes.31,35,48,56 However, this may beattributable to the ability of the available outcome meas-ures to detect differences, or the way these outcome meas-ures are applied. The IKDC Knee Ligament Guidelinessuggest that joint laxity, such as for the pivot-shift, Lach-man, and KT-1000 arthrometer tests be reported as normal,nearly normal, abnormal, or severely abnormal in compari-son with the contralateral normal knee.38 However, whenresults are reported in the literature, normal and nearlynormal outcomes are often combined into a single group,implying that ‘‘nearly normal is good enough.’’39 Osteoar-thritic changes after ACL reconstruction are not uncom-mon,45 leaving room for improvement in treatmentstrategies, but also in outcome measures. More preciseinstruments, such as T2 and T1rho MRI mapping10 thatmay detect early cartilage changes and dynamic stereoradiographs to precisely quantify in vivo knee kinematics,66
may be needed. Detailed evaluation is needed to demon-strate the potential benefits of anatomic ACL reconstruc-tion. Moreover, large randomized clinical trials withsimilar groups are needed. For example, to know ifdouble-bundle reconstruction is superior to single-bundlereconstruction, prospective randomized trials are neededto compare anatomic single-bundle to anatomic double-bundle reconstruction with similar grafts and fixation.
TRENDS IN THE LITERATURE
Treatment Perspectives
Open Versus Arthroscopic Techniques. The techniquefor ACL reconstruction has taken several, and sometimessharp, turns since the dramatic start of the arthroscopi-cally assisted reconstruction, which was initially per-formed by Dandy in 1980.22 Before the arthroscopicrevolution, ACL reconstruction was performed as arthrot-omy, with the goal to restore the normal anatomy of theACL. Arthrotomy is a more traumatic operation and has
Figure 5. Three-dimensional CT scans after anatomicsingle-bundle reconstruction (A) and anatomic double-bundle reconstruction (B) of the anterior cruciate ligament.
Vol. 39, No. 9, 2011 Anatomic Single- and Double-Bundle ACL Reconstruction 2021
by KAREN MOHR on October 5, 2011ajs.sagepub.comDownloaded from

less theoretical advantages than arthroscopic ACL recon-struction, although studies found only minor differencesin postoperative morbidity.16,17,55,58 The general changetoward minimally invasive surgical techniques and theincreasing knowledge of the function of the ACL led to anincrease of arthroscopically assisted ACL reconstructions.
Initially, arthroscopically assisted ACL reconstructionwas performed using a 2-incision technique, also calledthe ‘‘rear-entry’’ technique, in which the femoral bonetunnels were drilled from outside in. However, in the early1990s there was a trend toward 1-incision technique, alsoknown as an ‘‘endoscopic,’’ ‘‘all-inside,’’ or ‘‘transtibial’’technique, in which the femoral bone tunnels were drilledfrom inside out. The potential benefits for the new1-incision technique included shorter operating time, lowercosts, improved cosmesis, less postoperative pain, andpotentially faster rehabilitation. Several orthopaedic sur-geons were concerned that the new technique would yieldless optimal femoral tunnel placement and greater riskfor posterior wall break-out.12 This was contested by advo-cates of the 1-incision ACL reconstruction who proposednotchplasty or use of the AM portal for better visualizationof the posterior femur. Clinical studies comparing the 1-and 2-incision techniques found only minimal differencesbetween the 2 techniques,34,37 except for the study byPanni et al,54 which found more vertical femoral tunnelplacement in the 1-incision group. However, it is likelythat both techniques failed to consistently place the femo-ral tunnel in the center of the ACL footprint. For almosta decade, 1-incision ACL reconstruction with transtibialfemoral tunnel drilling was the standard ACL reconstruc-tion and it is still widespread. During this time, severalsurgical principles were further developed and widely uti-lized, including the concepts of isometry, notchplasty, andclockface position. Unfortunately, although fast and effi-cient, these principles, together with transtibial femoraltunnel drilling, promoted reconstruction of the ACL ina nonanatomic position.
Isometry. Isometric graft placement means that the dis-tance between the femoral and tibial attachments remainsconstant during motion in the knee joint.4 Isometric place-ment evolved from several well-grounded theories in whichthe major theory was that a tendon that is elongated morethan 4% under repetitive motion will be irreversiblystretched.81 Also, isometric graft placement was thoughtto produce better functional knee joint movement, and clin-ical studies revealed positive effects of isometric place-ment.61 However, the native ACL is not isometric, buthas a complex, nonuniform, double-bundle fiber anatomy.Furthermore, the best isometry for the femoral tunnel ishigh in the femoral notch49 and points close to the proximalend of the Blumensaat line.81 This location is very differentfrom the location of the native ACL footprint, which is lowon the wall of the lateral femoral condyle. Finally, an invitro study by Musahl et al49 found that placement of thefemoral graft in the femoral footprint of the native ACLresulted in closer knee joint kinematics than the isometricfemoral position. Therefore isometric placement of the ACL
graft is a poor substitute for restoration of the native anat-omy of the ACL and is no longer an accepted goal of ACLreconstruction.
Clockface Reference. Reference to the clockface positionfor placement of the femoral tunnel was developed in thecradle of the arthroscopic knee surgery. It is now familiarto orthopaedic surgeons worldwide and is commonly used.Even though it is easy to use the clockface position asa reference, there are several limitations: it refers toa 2-dimensional structure and therefore neglects thedepth of the notch, its position varies with knee flexion,and it is not universally employed because of the asym-metric anatomy of the notch and therefore actuallydenotes different points on the femur to different ortho-paedic surgeons.59,68 Because of the aforementioned limi-tations, the clockface method is not an accurate way todocument the tunnel placement. Instead, arthroscopicimages with the angle of knee flexion defined or radio-graphic images should be used, depicting the tunnel inrelation to constant anatomic landmarks.71 Reportingthe knee flexion angle with images allows for easy inter-pretation, especially since both the anatomic nomencla-ture (anterior, posterior) and arthroscopic nomenclature(shallow versus deep, high versus low) are used inter-changeably in the literature24 (Figure 6).
Anatomic ACL Reconstruction. One-incision arthroscopi-cally assisted ACL reconstruction introduced drilling ofthe femoral tunnel through a tibial tunnel, the so-calledtranstibial technique. The positive aspects of the transtibialtechnique are that it is simple, quick, and it does not requirethe knee to be flexed beyond 90� when the femoral tunnel isdrilled. However, in the beginning of the 21st century, ourunderstanding of the native ACL and its kinematics quicklyexpanded and new recommendations were developed withregard to placement of bone tunnels. Emphasis shifted toanatomic graft placements to recreate normal physiologicgraft tensions and studies confirmed nearly normal kneejoint kinematics when the bone tunnels were in the centerof the native ACL footprint.44,57,75-77 Orthopaedic surgeonsand researchers started to criticize the transtibial techniqueand suggested that this technique failed to place the bonetunnels in the center of the native ACL footprint, especiallyin the femur. Several disadvantages were identified; themost serious of which is the dependence of the 2 tunnelson each other since the femoral tunnel is drilled throughthe tibial tunnel. This restriction in femoral tunnel locationoften leads to a nonanatomic femoral tunnel position that istoo high and deep in the intercondylar notch.23,43 This,together with a more posteriorly placed tibial tunnel, willproduce a nonanatomic vertical ACL graft that reducesanterior-posterior laxity but fails to decrease the rotationalinstability.74,75 The deficiencies of the transtibial techniqueto restore normal kinematics of the knee led to the develop-ment of an accessory medial portal technique to create thefemoral tunnel.6,32 When using the medial portal technique,the femoral tunnel is drilled independent of the tibial tunnelthrough the AM or the accessory medial portal. This facili-tates anatomic placement of the ACL graft and allows
2022 Karlsson et al The American Journal of Sports Medicine
by KAREN MOHR on October 5, 2011ajs.sagepub.comDownloaded from

preservation of the remaining intact ACL fibers, which inturn facilitates isolated reconstruction of the AM or PL bun-dle. Also, there are few restrictions concerning graft type,graft fixation, or instrumentation.18
Single- or Double-Bundle Reconstruction. The nativeACL consists of 2 functional bundles that work together tocontrol anterior-posterior and rotational stability, respec-tively. Reconstruction of the ACL has traditionally concen-trated on replacing the ACL as a single bundle thatapproximates the AM bundle. Although this will restoreanterior-posterior laxity, biomechanical studies have shownthat it fails to fully restore rotational laxity.74,75 Further-more, the nonanatomic single-bundle ACL reconstructionhas not been shown to prevent the development of earlyosteoarthritis after ACL injury.56 This has led to thehypothesis that double-bundle reconstruction could moreclosely restore the normal function of the native ACL andtherefore yield better functional results and hopefully min-imize the risk of osteoarthritis. However, it is vital to under-stand that double-bundle reconstruction is not the same asanatomic ACL reconstruction. It is merely a step closer toreproducing native ACL anatomy. We define anatomicreconstruction as the functional restoration of the ACL toits native dimensions, collagen orientation, and insertionsites.88 Anatomic ACL reconstruction can be performed asa single- or double-bundle procedure. Biomechanical studieshave shown that double-bundle reconstruction is more suc-cessful in restoring rotational stability and normal kneekinematics.75 A systematic review by Samuelsson et al56
assessed all randomized controlled trials comparing single-and double-bundle reconstruction and found that all but 1of them reported significantly less rotational laxity usingdouble-bundle techniques compared with the single-bundletechniques; however, there were no differences in clinicaloutcome.56 It should be noted that there are no availablestudies with long-term follow-up comparing the 2 surgical
techniques, and therefore the answer to whether double-bundle ACL reconstructions reduces osteoarthritis lies inthe future. In addition, some clinical studies comparenonanatomic single-bundle reconstruction to anatomic dou-ble-bundle reconstruction, which does not pose a fair com-parison.1,78 Double-bundle reconstruction also has severallimitations. It is much more technically demanding andtherefore requires more surgical time and expertise. Thequadrupled tunnels increase the risk of tunnel malplace-ment, posterior blowout, fracture, and confluence of the tun-nels, which can lead to fixation failure. It is also moreexpensive than single-bundle ACL reconstruction becauseof longer surgical time and more fixation material. Finally,it is only suited for a selective group of patients because ofminimal requirements in knee size.
Graft Options
Allografts. The major theoretical advantage of allograftcompared with autograft is the decreased harvest sitemorbidity with intact flexor and extensor mechanism inthe knee joint. However, allografts were initially seldomused especially because of possible risk of disease trans-mission, inferior tensile properties, and limited availabil-ity. These issues have largely been resolved with bettersterilization techniques and increased availability withgreater demand. It has been shown that the allograftdoes revascularize after implantation5 and clinical stud-ies show similar results to autografts.8,51 However, grafthealing is slower for the allograft than autograft40 andthe use of allograft tissue in young active individualshas been associated with a higher incidence of graft fail-ure.15 The strongest indications for allograft have been,and still are, athletes who may be negatively affected byharvest site symptoms or functional deficits, and people
Figure 6. This figure illustrates the anatomic nomenclature versus the arthroscopic nomenclature as demonstrated in a right kneecadaveric specimen. A, the knee is in full extension and the anatomic nomenclature is easy to interpret. B, the knee is in 90� offlexion and both the anatomic and the corresponding arthroscopic nomenclature are shown.
Vol. 39, No. 9, 2011 Anatomic Single- and Double-Bundle ACL Reconstruction 2023
by KAREN MOHR on October 5, 2011ajs.sagepub.comDownloaded from

undergoing revision ACL reconstruction and multiple lig-ament reconstructions.15
Autografts. Bone–patellar tendon–bone (BPTB) grafthas traditionally been the ‘‘gold standard’’ for ACL recon-struction for almost 3 decades. Its major advantage isthat it has bone plugs on both ends of the graft, which facil-itates graft fixation and incorporation. This probablyaccounts for the success of BPTB ACL reconstruction inlong-term follow-up. It also allows early return to sportsactivities. Advocates of the BPTB graft have also indicatedthat the BPTB graft yields less knee joint laxity than thehamstrings tendon (HT) graft, but this is not strongly sup-ported by literature.14 Also, it is easy to preoperativelyassess the thickness of the graft with MRI, which thereforeprovides the opportunity for better preoperative planning.This is in contrast to the HT, in which the size can only bedetermined after harvesting the tendon. The BPTB grafthas lost some favor in the past decade and is now less fre-quently used than HT grafts. The reasons are mostly basedon the harvest site morbidity in form of anterior knee pain,kneeling pain, quadriceps weakness, possible patellar frac-ture, and risk of rupture of the patellar tendon. A system-atic review by Samuelsson et al56 confirmed that the BPTBgraft produced more anterior knee pain and kneeling painthan the HT graft; however, the difference might disappearwith time. In addition, BPTB harvesting affected quadri-ceps muscle strength initially; however this resolved overtime.56 There were no clear differences in the restorationof knee laxity and osteoarthritis risk between the 2groups.53 The quadrupled HT has also been shown to bestronger and stiffer than BPTP.52 However, there are sev-eral concerns with the HT grafts and the majority reflectson the fact that the graft has soft tissue–to-bone fixationand the negative effect on hamstring strength in deep flex-ion and internal rotation. Studies have confirmed that softtissue–to-bone healing time is longer than the time forbone-to-bone healing; however, it does not affect the resto-ration of joint laxity.56
The quadriceps tendon is an excellent graft option forACL reconstruction with several advantages. It can easilybe harvested with or without a patellar bone block, it ismore often sufficient for both single- and double-bundlereconstruction than a BPTB graft, and it produces lessanterior knee pain and numbness than the BPTB graft.29
Furthermore, the quadriceps tendon graft has excellentbiomechanical properties52 that are probably attributableto its larger cross-sectional area than the BPTB graft.
CONCLUSION
Anatomic ACL reconstruction intends to replicate normalanatomy, restore normal kinematics, and protect long-term knee health. The road to anatomic ACL reconstruc-tion has been long and winding. It is a detailed surgicalprocedure with a steep learning curve and many pitfalls.In the future, more reliable, accurate, precise, and vali-dated outcome measures are needed to evaluate itsresults.
An online CME course associated with this article isavailable for 1 AMA PRA Category 1 CreditTM at http://ajsm-cme.sagepub.com. In accordance with the standardsof the Accreditation Council for Continuing Medical Edu-cation (ACCME), it is the policy of The American Ortho-paedic Society for Sports Medicine that authors, editors,and planners disclose to the learners all financial rela-tionships during the past 12 months with any commercialinterest (A ‘commercial interest’ is any entity producing,marketing, re-selling, or distributing health care goodsor services consumed by, or used on, patients). Any andall disclosures are provided in the online journal CMEarea which is provided to all participants before theyactually take the CME activity. In accordance withAOSSM policy, authors, editors, and planners’ participa-tion in this educational activity will be predicated upontimely submission and review of AOSSM disclosure. Non-compliance will result in an author/editor or planner to bestricken from participating in this CME activity.
REFERENCES
1. Aglietti P, Giron F, Cuomo P, Losco M, Mondanelli N. Single-and
double-incision double-bundle ACL reconstruction. Clin Orthop Relat
Res. 2007;454:108-113.
2. Ahn JH, Lee SH, Yoo JC, Ha HC. Measurement of the graft angles for
the anterior cruciate ligament reconstruction with transtibial technique
using postoperative magnetic resonance imaging in comparative
study. Knee Surg Sports Traumatol Arthrosc. 2007;15(11):1293-1300.
3. Allen CR, Giffin JR, Harner CD. Revision anterior cruciate ligament
reconstruction. Orthop Clin North Am. 2003;34(1):79-98.
4. Amis AA, Zavras TD. Isometricity and graft placement during anterior
cruciate ligament reconstruction. Knee. 1995;2(1):5-17.
5. Arnoczky SP, Warren RF, Ashlock MA. Replacement of the anterior
cruciate ligament using a patellar tendon allograft: an experimental
study. J Bone Joint Surg Am. 1986;68(3):376-385.
6. Arnold MP, Kooloos J, van Kampen A. Single-incision technique
misses the anatomical femoral anterior cruciate ligament insertion:
a cadaver study. Knee Surg Sports Traumatol Arthrosc. 2001;9(4):
194-199.
7. Asahina S, Muneta T, Ezura Y. Notchplasty in anterior cruciate liga-
ment reconstruction: an experimental animal study. Arthroscopy.
2000;16(2):165-172.
8. Baer GS, Harner CD. Clinical outcomes of allograft versus autograft
in anterior cruciate ligament reconstruction. Clin Sports Med.
2007;26(4):661-681.
9. Baumfeld JA, Diduch DR, Rubino LJ, et al. Tunnel widening following
anterior cruciate ligament reconstruction using hamstring autograft:
a comparison between double cross-pin and suspensory graft fixa-
tion. Knee Surg Sports Traumatol Arthrosc. 2008;16(12):1108-1113.
10. Bear DM, Williams A, Chu CT, Coyle CH, Chu CR. Optical coherence
tomography grading correlates with MRI T2 mapping and extracellu-
lar matrix content. J Orthop Res. 2010;28(4):546-552.
11. Bedi A, Altchek DW. The ‘‘footprint’’ anterior cruciate ligament tech-
nique: an anatomic approach to anterior cruciate ligament recon-
struction. Arthroscopy. 2009;25(10):1128-1138.
12. Bedi A, Raphael B, Maderazo A, Pavlov H, Williams RJ 3rd. Transti-
bial versus anteromedial portal drilling for anterior cruciate ligament
reconstruction: a cadaveric study of femoral tunnel length and obliq-
uity. Arthroscopy. 2010;26(3):342-350.
13. Benjaminse A, Gokeler A, van der Schans CP. Clinical diagnosis of an
anterior cruciate ligament rupture: a meta-analysis. J Orthop Sports
Phys Ther. 2006;36(5):267-288.
2024 Karlsson et al The American Journal of Sports Medicine
by KAREN MOHR on October 5, 2011ajs.sagepub.comDownloaded from

14. Biau DJ, Tournoux C, Katsahian S, Schranz PJ, Nizard RS. Bone-
patellar tendon-bone autografts versus hamstring autografts for
reconstruction of anterior cruciate ligament: meta-analysis. BMJ.
2006;332(7548):995-1001.
15. Borchers JR, Pedroza A, Kaeding C. Activity level and graft type as
risk factors for anterior cruciate ligament graft failure: a case-control
study. Am J Sports Med. 2009;37(12):2362-2367.
16. Buss DD, Warren RF, Wickiewicz TL, Galinat BJ, Panariello R. Arthro-
scopically assisted reconstruction of the anterior cruciate ligament
with use of autogenous patellar-ligament grafts: results after
twenty-four to forty-two months. J Bone Joint Surg Am. 1993;75(9):
1346-1355.
17. Cameron SE, Wilson W, St Pierre P. A prospective, randomized com-
parison of open vs arthroscopically assisted ACL reconstruction.
Orthopedics. 1995;18(3):249-252.
18. Cha PS, Chhabra A, Harner CD. Single-bundle anterior cruciate liga-
ment reconstruction using the medial portal technique. Oper Tech
Orthop. 2005;15(2):89-95.
19. Chhabra A, Starman JS, Ferretti M, Vidal AF, Zantop T, Fu FH. Ana-
tomic, radiographic, biomechanical, and kinematic evaluation of the
anterior cruciate ligament and its two functional bundles. J Bone
Joint Surg Am. 2006;88 Suppl 4:2-10.
20. Cohen SB, Fu FH. Three-portal technique for anterior cruciate liga-
ment reconstruction: use of a central medial portal. Arthroscopy.
2007;23(3):325 e321-e325.
21. Cuomo P, Rama KR, Bull AM, Amis AA. The effects of different ten-
sioning strategies on knee laxity and graft tension after double-
bundle anterior cruciate ligament reconstruction. Am J Sports Med.
2007;35(12):2083-2090.
22. Dandy DJ. Arthroscopic surgery of the knee. Br J Hosp Med.
1982;27(4):360, 362, 365.
23. Dargel J, Schmidt-Wiethoff R, Fischer S, Mader K, Koebke J,
Schneider T. Femoral bone tunnel placement using the transtibial tun-
nel or the anteromedial portal in ACL reconstruction: a radiographic
evaluation. Knee Surg Sports Traumatol Arthrosc. 2009;17(3):220-227.
24. Edwards A, Bull AM, Amis AA. The attachments of the anteromedial
and posterolateral fibre bundles of the anterior cruciate ligament: part
2, femoral attachment. Knee Surg Sports Traumatol Arthrosc.
2008;16(1):29-36.
25. Ferretti M, Ekdahl M, Shen W, Fu FH. Osseous landmarks of the fem-
oral attachment of the anterior cruciate ligament: an anatomic study.
Arthroscopy. 2007;23(11):1218-1225.
26. Ferretti M, Levicoff EA, Macpherson TA, Moreland MS, Cohen M, Fu
FH. The fetal anterior cruciate ligament: an anatomic and histologic
study. Arthroscopy. 2007;23(3):278-283.
27. Forsythe B, Kopf S, Wong AK, et al. The location of femoral and tibial
tunnels in anatomic double-bundle anterior cruciate ligament recon-
struction analyzed by three-dimensional computed tomography
models. J Bone Joint Surg Am. 2010;92(6):1418-1426.
28. Gabriel MT, Wong EK, Woo SL, Yagi M, Debski RE. Distribution of in
situ forces in the anterior cruciate ligament in response to rotatory
loads. J Orthop Res. 2004;22(1):85-89.
29. Geib TM, Shelton WR, Phelps RA, Clark L. Anterior cruciate ligament
reconstruction using quadriceps tendon autograft: intermediate-term
outcome. Arthroscopy. 2009;25(12):1408-1414.
30. Gianotti SM, Marshall SW, Hume PA, Bunt L. Incidence of anterior
cruciate ligament injury and other knee ligament injuries: a national
population-based study. J Sci Med Sport. 2009;12:622-627.
31. Goldblatt JP, Fitzsimmons SE, Balk E, Richmond JC. Reconstruction
of the anterior cruciate ligament: meta-analysis of patellar tendon
versus hamstring tendon autograft. Arthroscopy. 2005;21(7):791-803.
32. Hantes ME, Zachos VC, Liantsis A, Venouziou A, Karantanas AH,
Malizos KN. Differences in graft orientation using the transtibial and
anteromedial portal technique in anterior cruciate ligament recon-
struction: a magnetic resonance imaging study. Knee Surg Sports
Traumatol Arthrosc. 2009;17(8):880-886.
33. Harner CD, Honkamp NJ, Ranawat AS. Anteromedial portal tech-
nique for creating the anterior cruciate ligament femoral tunnel.
Arthroscopy. 2008;24(1):113-115.
34. Harner CD, Marks PH, Fu FH, Irrgang JJ, Silby MB, Mengato R. Ante-
rior cruciate ligament reconstruction: endoscopic versus two-incision
technique. Arthroscopy. 1994;10(5):502-512.
35. Harner CD, Olson E, Irrgang JJ, Silverstein S, Fu FH, Silbey M. Allo-
graft versus autograft anterior cruciate ligament reconstruction: 3- to
5-year outcome. Clin Orthop Relat Res. 1996;324:134-144.
36. Hefti F, Muller W, Jakob RP, Staubli HU. Evaluation of knee ligament
injuries with the IKDC form. Knee Surg Sports Traumatol Arthrosc.
1993;1(3-4):226-234.
37. Hess T, Duchow J, Roland S, Kohn D. Single- versus two-incision
technique in anterior cruciate ligament replacement: influence on
postoperative muscle function. Am J Sports Med. 2002;30(1):27-31.
38. Irrgang JJ, Anderson AF, Boland AL, et al. Development and valida-
tion of the International Knee Documentation Committee subjective
knee form. Am J Sports Med. 2001;29(5):600-613.
39. Irrgang JJ, Bost JE, Fu FH. Re: Outcome of single-bundle versus dou-
ble-bundle reconstruction of the anterior cruciate ligament: a meta-
analysis. Am J Sports Med. 2009;37(2):421-422; author reply 422.
40. Jackson DW, Grood ES, Goldstein JD, et al. A comparison of patellar
tendon autograft and allograft used for anterior cruciate ligament
reconstruction in the goat model. Am J Sports Med.
1993;21(2):176-185.
41. Johnson DL, Swenson TM, Irrgang JJ, Fu FH, Harner CD. Revision
anterior cruciate ligament surgery: experience from Pittsburgh. Clin
Orthop Relat Res. 1996;325:100-109.
42. Kondo E, Yasuda K, Ichiyama H, Azuma C, Tohyama H. Radiologic
evaluation of femoral and tibial tunnels created with the transtibial
tunnel technique for anatomic double-bundle anterior cruciate liga-
ment reconstruction. Arthroscopy. 2007;23(8):869-876.
43. Kopf S, Forsythe B, Wong AK, et al. Nonanatomic tunnel position in
traditional transtibial single-bundle anterior cruciate ligament recon-
struction evaluated by three-dimensional computed tomography. J
Bone Joint Surg Am. 2010;92(6):1427-1431.
44. Loh JC, Fukuda Y, Tsuda E, Steadman RJ, Fu FH, Woo SL. Knee sta-
bility and graft function following anterior cruciate ligament recon-
struction: comparison between 11 o’clock and 10 o’clock femoral
tunnel placement, 2002 Richard O’Connor Award paper. Arthros-
copy. 2003;19(3):297-304.
45. Lohmander LS, Ostenberg A, Englund M, Roos H. High prevalence of
knee osteoarthritis, pain, and functional limitations in female soccer
players twelve years after anterior cruciate ligament injury. Arthritis
Rheum. 2004;50(10):3145-3152.
46. Martins CAQ, Kropf EJ, Shen W, van Eck CF, Fu FH. The concept of
anatomic anterior cruciate ligament reconstruction. Oper Tech
Sports Med. 2008;16:104-115.
47. May DA, Snearly WN, Bents R, Jones R. MR imaging findings in ante-
rior cruciate ligament reconstruction: evaluation of notchplasty. AJR
Am J Roentgenol. 1997;169(1):217-222.
48. Meredick RB, Vance KJ, Appleby D, Lubowitz JH. Outcome of
single-bundle versus double-bundle reconstruction of the anterior
cruciate ligament: a meta-analysis. Am J Sports Med. 2008;36(7):
1414-1421.
49. Musahl V, Plakseychuk A, VanScyoc A, et al. Varying femoral tunnels
between the anatomical footprint and isometric positions: effect on
kinematics of the anterior cruciate ligament-reconstructed knee.
Am J Sports Med. 2005;33(5):712-718.
50. Neuman P, Kostogiannis I, Friden T, Roos H, Dahlberg LE, Englund
M. Patellofemoral osteoarthritis 15 years after anterior cruciate liga-
ment injury–a prospective cohort study. Osteoarthritis Cartilage.
2009;17(3):284-290.
51. Noyes FR, Barber-Westin SD. Reconstruction of the anterior cruciate
ligament with human allograft: comparison of early and later results. J
Bone Joint Surg Am. 1996;78(4):524-537.
52. Noyes FR, Butler DL, Grood ES, Zernicke RF, Hefzy MS. Biomechan-
ical analysis of human ligament grafts used in knee-ligament repairs
and reconstructions. J Bone Joint Surg Am. 1984;66(3):344-352.
53. Odensten M, Gillquist J. Functional anatomy of the anterior cruciate
ligament and a rationale for reconstruction. J Bone Joint Surg Am.
1985;67(2):257-262.
Vol. 39, No. 9, 2011 Anatomic Single- and Double-Bundle ACL Reconstruction 2025
by KAREN MOHR on October 5, 2011ajs.sagepub.comDownloaded from

54. Panni AS, Milano G, Tartarone M, Demontis A, Fabbriciani C. Clinical
and radiographic results of ACL reconstruction: a 5- to 7-year follow-
up study of outside-in versus inside-out reconstruction techniques.
Knee Surg Sports Traumatol Arthrosc. 2001;9(2):77-85.
55. Raab DJ, Fischer DA, Smith JP, Markman AW, Steubs JA. Compar-
ison of arthroscopic and open reconstruction of the anterior cruciate
ligament: early results. Am J Sports Med. 1993;21(5):680-684.
56. Samuelsson K, Andersson D, Karlsson J. Treatment of anterior cruci-
ate ligament injuries with special reference to graft type and surgical
technique: an assessment of randomized controlled trials. Arthros-
copy. 2009;25(10):1139-1174.
57. Scopp JM, Jasper LE, Belkoff SM, Moorman CT 3rd. The effect of
oblique femoral tunnel placement on rotational constraint of the
knee reconstructed using patellar tendon autografts. Arthroscopy.
2004;20(3):294-299.
58. Shelbourne KD, Wilckens JH. Intraarticular anterior cruciate ligament
reconstruction in the symptomatic arthritic knee. Am J Sports Med.
1993;21(5):685-689.
59. Shen W, Forsythe B, Ingham SM, Honkamp NJ, Fu FH. Application of
the anatomic double-bundle reconstruction concept to revision and
augmentation anterior cruciate ligament surgeries. J Bone Joint
Surg Am. 2008;90 Suppl 4:20-34.
60. Siebold R, Fu FH. Assessment and augmentation of symptomatic
anteromedial or posterolateral bundle tears of the anterior cruciate
ligament. Arthroscopy. 2008;24(11):1289-1298.
61. Sommer C, Friederich NF, Muller W. Improperly placed anterior cru-
ciate ligament grafts: correlation between radiological parameters
and clinical results. Knee Surg Sports Traumatol Arthrosc.
2000;8(4):207-213.
62. Steckel H, Vadala G, Davis D, Fu FH. 2D and 3D 3-tesla magnetic
resonance imaging of the double bundle structure in anterior cruciate
ligament anatomy. Knee Surg Sports Traumatol Arthrosc.
2006;14(11):1151-1158.
63. Steckel H, Vadala G, Davis D, Musahl V, Fu FH. 3-T MR imaging of
partial ACL tears: a cadaver study. Knee Surg Sports Traumatol
Arthrosc. 2007;15(9):1066-1071.
64. Steiner M. Anatomic single-bundle ACL reconstruction. Sports Med
Arthrosc. 2009;17(4):247-251.
65. Tashman S, Collon D, Anderson K, Kolowich P, Anderst W. Abnormal
rotational knee motion during running after anterior cruciate ligament
reconstruction. Am J Sports Med. 2004;32(4):975-983.
66. Tashman S, Kolowich P, Collon D, Anderson K, Anderst W. Dynamic
function of the ACL-reconstructed knee during running. Clin Orthop
Relat Res. 2007;454:66-73.
67. Tischer T, Ronga M, Tsai A, et al. Biomechanics of the goat three
bundle anterior cruciate ligament. Knee Surg Sports Traumatol
Arthrosc. 2009;17(8):935-940.
68. van Eck CF, Lesniak BP, Schreiber VM, Fu FH. Anatomic single- and
double-bundle anterior cruciate ligament reconstruction flowchart.
Arthroscopy. 2010;26(2):258-268.
69. van Eck CF, Martins CA, Lorenz SG, Fu FH, Smolinski P. Assessment
of correlation between knee notch width index and the three-dimen-
sional notch volume. Knee Surg Sports Traumatol Arthrosc.
2010;18(9):1239-1244.
70. van Eck CF, Martins CA, Vyas SM, Celentano U, van Dijk CN, Fu FH.
Femoral intercondylar notch shape and dimensions in ACL-injured
patients. Knee Surg Sports Traumatol Arthrosc. 2010;18(9):1257-1262.
71. van Eck CF, Morse KR, Lesniak BP, et al. Does the lateral intercon-
dylar ridge disappear in ACL deficient patients? Knee Surg Sports
Traumatol Arthrosc. 2010;18(9):1184-1188.
72. van Eck CF, Schreiber VM, Liu TT, Fu FH. The anatomic approach to
primary, revision and augmentation anterior cruciate ligament recon-
struction. Knee Surg Sports Traumatol Arthrosc. 2010;18(9):1154-1163.
73. West RV, Harner CD. Graft selection in anterior cruciate ligament
reconstruction. J Am Acad Orthop Surg. 2005;13(3):197-207.
74. Woo SL, Kanamori A, Zeminski J, Yagi M, Papageorgiou C, Fu FH.
The effectiveness of reconstruction of the anterior cruciate ligament
with hamstrings and patellar tendon: a cadaveric study comparing
anterior tibial and rotational loads. J Bone Joint Surg Am.
2002;84(6):907-914.
75. Yagi M, Wong EK, Kanamori A, Debski RE, Fu FH, Woo SL. Biome-
chanical analysis of an anatomic anterior cruciate ligament recon-
struction. Am J Sports Med. 2002;30(5):660-666.
76. Yamamoto Y, Hsu WH, Woo SL, Van Scyoc AH, Takakura Y, Debski
RE. Knee stability and graft function after anterior cruciate ligament
reconstruction: a comparison of a lateral and an anatomical femoral
tunnel placement. Am J Sports Med. 2004;32(8):1825-1832.
77. Yasuda K, Kondo E, Ichiyama H, et al. Anatomic reconstruction of the
anteromedial and posterolateral bundles of the anterior cruciate
ligament using hamstring tendon grafts. Arthroscopy. 2004;20(10):
1015-1025.
78. Yasuda K, Kondo E, Ichiyama H, Tanabe Y, Tohyama H. Clinical eval-
uation of anatomic double-bundle anterior cruciate ligament recon-
struction procedure using hamstring tendon grafts: comparisons
among 3 different procedures. Arthroscopy. 2006;22(3):240-251.
79. Zantop T, Brucker PU, Vidal A, Zelle BA, Fu FH. Intraarticular rupture
pattern of the ACL. Clin Orthop Relat Res. 2007;454:48-53.
80. Zantop T, Diermann N, Schumacher T, Schanz S, Fu FH, Petersen W.
Anatomical and nonanatomical double-bundle anterior cruciate liga-
ment reconstruction: importance of femoral tunnel location on knee
kinematics. Am J Sports Med. 2008;36:678-685.
81. Zavras TD, Race A, Bull AM, Amis AA. A comparative study of ‘iso-
metric’ points for anterior cruciate ligament graft attachment. Knee
Surg Sports Traumatol Arthrosc. 2001;9(1):28-33.
For reprints and permission queries, please visit SAGE’s Web site at http://www.sagepub.com/journalsPermissions.nav
2026 Karlsson et al The American Journal of Sports Medicine
by KAREN MOHR on October 5, 2011ajs.sagepub.comDownloaded from




















