
Outcomes of anterior cruciate ligament reconstruction from 2 ...
Upload
bergmankliniekCategory
view
4download
0
Systematic Review
USti(MDU
fu
1
Preoperative Patient and Injury Factors of SuccessfulRehabilitation After Anterior Cruciate LigamentReconstruction With Single-Bundle Techniques
Eduard J. de Valk, M.Sc., Maarten H. Moen, M.D., Ph.D., Marinus Winters, M.Sc.,Eric W. P. Bakker, Ph.D., Rob Tamminga, and Henk van der Hoeven, M.Sc.
Purpose: The aim of this systematic review was to determine which patient determinants and injury factors, beforeanterior cruciate ligament reconstruction by arthroscopic single-bundle techniques, affect postoperative rehabilitation.Methods: A search of PubMed, Embase, and the Cochrane Database of Clinical Trials was performed up to February2013. After application of our inclusion criteria, a final selection was made based on studies’ methodologic score assessedwith the Newcastle-Ottawa Scale. Meta-analysis was planned for each prognostic factor when data were consideredclinically and statistically homogeneous. Results: Meta-analysis showed that male patients have better functionaloutcomes. Qualitative synthesis from 18 high-quality studies showed that patients operated on before 30 years of agereach higher activity levels. Patients with high baseline body mass index have lower activity levels after surgery. Smokingresults in more symptoms and lower activity levels and subjective scores. Reconstruction before 3 months results in higheractivity levels. Preoperatively, a less than 20% quadriceps strength difference, 50� of tibial external rotation or less,absence of flexion deficits, low knee influence on the patient’s activity level, and less anterior knee pain result in higherfunctional scores. Preoperative anterior laxity difference does not predict functional scores. The prognostic value ofpreoperative activity and competition level for postoperative functional outcome is controversial. Patients withconcomitant meniscal injuries have worse functional outcomes. The prognostic value of concomitant chondral pathologyfor postoperative functional outcome is controversial. Collateral ligament injury could predict functional scores or activitylevel. Conclusions: Male gender, patient age younger than 30 years, reconstruction before 3 months, and high baselineactivity level contribute to better functional outcomes. Smoking, high body mass index, quadriceps strength, and range-of-motion deficits affect rehabilitation negatively. Preoperative anterior laxity does not influence rehabilitation. The role ofpreoperative prognostic injury factors remains unclear because of limited evidence. Level of Evidence: Level III,systematic review of Level II and III studies.
nterior cruciate ligament (ACL) deficiency of the
Aknee can lead to loss of stability, resulting in limi-tation or discontinuation of preinjury sporting activi-ties. Nonoperative management is often indicated forFrom the Faculty of Medicine, Health and Life Sciences, Maastrichtniversity (E.J.d.V.), Maastricht; Department of Orthopedic Surgery andports Medicine, Bergman Clinics (M.H.M., H.v.d.H.), Naarden; Rehabilita-on, Nursing Science & Sports Department, University Medical Centre Utrecht.W.), and Medicort, Sports & Orthopedic Care (R.T.), Utrecht; and theivision of Clinical Methods and Public Health, Academic Medical Centre,niversity of Amsterdam (E.W.P.B.), Amsterdam, The Netherlands.The authors report the following potential conflict of interest or source ofnding: H.v.d.H. receives support from Arthrex.Received June 8, 2013; accepted July 24, 2013.Address correspondence to Eduard J. de Valk, M.Sc., Hasebroekstraat 87-3,
053 CR, Amsterdam, The Netherlands. E-mail: [email protected]� 2013 by the Arthroscopy Association of North America0749-8063/13382/$36.00http://dx.doi.org/10.1016/j.arthro.2013.07.273
Arthroscopy: The Journal of Arthroscopic and Related Surg
patients who are less active, have minimal instability, orare unable to undergo an operation and/or rehabilita-tion protocol. Surgical ACL reconstruction continues tobe the standard of care for ACL-deficient patients withthe desire to return to sporting activities.1,2
Postoperative rehabilitation plays a critical role inreturning patients to their preinjury level of sport. OfACL-reconstructed patients, 82% return to some kind ofsports participation. Only 63% return to their preinjurylevel of sport, and 44% return to competitive sports. Inview of this moderate success rate, it is remarkable that85% to 90% of ACL-reconstructed patients reportednormal or nearly normal knee function.3 Apparently,factors other than only recovering knee function areassociated with return to preinjury level of sport. In theliterature several patient- and injury-related prognosticfactors before ACL reconstruction have been suggestedthat could be associated with recovery.4-6 A better
ery, Vol 29, No 11 (November), 2013: pp 1879-1895 1879

1880 E. J. DE VALK ET AL.
understanding of the relation between preoperativefactors and rehabilitation could be helpful in preopera-tive training strategies (better in, better out principle)and/or adjustment of expected postoperative results.The aim of this systematic review was to determinewhich patient and injury factors before ACL recon-struction by arthroscopic single-bundle techniques areassociated with successful or prolonged rehabilitation.
Methods
Research QuestionWe sought to determine which prognostic patient and
injury factors before ACL reconstruction by arthros-copic single-bundle techniques are associated withsuccessful or prolonged rehabilitation.
Inclusion and Exclusion Criteria
Type of StudiesFull-text reports of published and non-published,
randomized and nonrandomized controlled trials, pro-spective and retrospective cohort studies, and case-control studies were eligible for inclusion.
Type of ParticipantsPatients (aged 13 to 62 years) with an ACL rupture
identified by magnetic resonance imaging or arthros-copy and treated with an ACL repair were eligible forinclusion.
Type of Prognostic VariablesDemographic variables, time to surgery, preoperative
function (patient factors), and concomitant injuries(injury factors) were investigated.
Type of InterventionArthroscopic single-bundle techniques, both 1- and
2-incision techniques, were eligible for inclusion, irre-spective of the type of graft. Studies reporting on openor double-bundle techniques were excluded. If thedescription of the surgical technique used was unclear,the corresponding author was contacted.
Type of OutcomeThe following outcome measures, either objective or
subjective, were included: muscle strength, knee func-tion, and activity level (including return to sport).Studies were excluded if outcome measures concerningknee function were measured postoperatively withoutpreoperative reference measurements.
Length of Follow-UpTotal rehabilitation must be fulfilled. Assuming that
a regular rehabilitation program takes about 9 monthsto complete, a minimal follow-up length of 1 year waschosen, taking possible delay in recovery into account.
Search StrategyMedline (PubMed), Embase, the Cochrane Library of
Clinical Trials, and the Trip Database were searchedfrom their inception until February 18, 2013, to identifyall relevant reports. Our search strategy was based oncontrolled vocabulary (MeSH terms) and free textterms. No language restrictions were imposed.We searched national (www.trialregister.nl) and inter-
national (www.controlled-trials.com, ClinicalTrials.gov,http://apps.who.int/trialsearch/) trial registries to identifyongoing studies. When an ongoing study was found,attemptsweremade to contact its primary investigator tocollect further information.After the initial search and removal of duplicates, 2
reviewers (E.J.d.V. and M.H.M.) independently appliedthe selection criteria to identified titles and abstracts toselect potentially relevant studies. Full text of all therelevant reports was obtained. The 2 reviewers inde-pendently applied the selection criteria to the full-textarticles. Disagreements were resolved by consensusmeetings or, if disagreement persisted, by a thirdreviewer (H.v.d.H.). Reference lists of all included articleswere searched to retrieve additional published studiesnot identified by the computerized database search.
Quality AssessmentThe Newcastle-Ottawa Scale (NOS) was used to assess
methodologic quality of the included studies.7 Everystudy was appraised on 3 domains: the selection of thestudy groups, the comparability of the groups, and theascertainment of the exposure and outcome of interest.High-quality choices are identified with a star. Theassessed study canbe awarded amaximumof one star foreach numbered itemwithin the “selection” (4 numbereditems) and “outcome” (3 numbered items) categories.For “comparability” (one numbered item), a maximumof 2 stars can be given. The sum of all items rated witha star was calculated, resulting in a total quality score,with amaximumscore of 9 stars.We somewhatmodifiedthe NOS for the purpose of this review (Table 1).
Levels of EvidenceThe Oxford Levels of Evidence as produced by the
Oxford Centre for Evidence-Based Medicine8 were usedto further assessmethodologic quality. This tool classifiessystematic randomized clinical trials and inceptioncohort studies as Level II evidence, cohort studies orcontrol arm of randomized trials as Level III evidence,and case series or case-control studies or poor-qualityprognostic cohort studies as Level IV evidence.
Data ExtractionData were extracted by the 2 reviewers indepen-
dently, using a priori standardized forms. Data consistedof inclusion criteria; population; baseline characteristics;prognostic factors; outcomes and results (i.e., risk

Table 1. Newcastle-Ottawa Scale
Stars
Selection (maximum of 4 stars)1. Representativeness of exposed cohortA. Truly representative of the average. [describe] in the
community+
B. Somewhat representative of the average . [describe]in the community
+
C. Selected group of usersD. No description of the derivation of the cohort
2. Selection of non-exposed cohortA. Drawn from the same community as the exposed
cohort+
B. Drawn from a different sourceC. No description of the derivation of the non exposed
cohort3. Ascertainment of exposureA. Secure record +B. Structured interview +
C. Written self-reportD. No description
4. Demonstration that outcome of interest was not presentat start of study
A. Yes +
B. NoComparability (maximum of 2 stars)
1. Comparability of cohorts on the basis of the design oranalysisA. Study controls for. [select the most important factor]
(or determination of baseline predictors*)+
B. Study controls for any additional factor (or performmultivariate analysis of selected predictors*)
+
Outcome (maximum of 3 stars)1. Assessment of outcomeA. Independent blind assessment +
B. Record linkage +C. Self-reportD. No description
2. Was follow-up long enough for outcomes to occurA. Yes (select an adequate follow-up period for outcome
of interest)+
B. No3. Adequacy of follow-up of cohortsA. Complete follow-updall subjects accounted for +B. Subjects lost to follow-up unlikely to introduce
biasdsmall number lost . [select an adequatepercent] follow-up or description provided of thoselost to follow-up
+
C. Follow-up rate <.% (select an adequate %) and nodescription of those lost
D. No statement
*Modified item.
PROGNOSTIC FACTORS OF SUCCESSFUL REHABILITATION 1881
estimate [e.g., odds ratio (OR)] adjusted for relevantconfounders); information on statistical significance;and, where possible, a measure of precision (e.g.,confidence interval [CI]). Disagreements were resolvedby consensus meeting or, if disagreement persisted, bya third author (H.v.d.H.).
Data SynthesisStudies that were awarded 7 or more stars on the
NOS and, in addition, were awarded 2 stars for the
comparability domain were eligible for data synthesis. Aquantitative synthesis was planned, taking the expectedhomogeneity between studies into account. For dataanalysis, we used univariate and multivariate outcomedata. A pooled OR was calculated based on availabledata. Data on meta-analysis were expressed as ORs forthe retrospective design of included primary studies.Meta-analysis was conducted to increase power and tocalculate a pooled effect estimate. The standard error ofthe pooled effect estimate was used for the precision ofthe summary estimate of individual studies by a CI.When the preferred outcome was measured in differentways, standardized mean differences were used. Todetermine possible variation across studies, heteroge-neity had to be considered. Heterogeneity was assessedby P values from c2 statistics and I2 using random effectsmodels. I2 describes the percentage of variability in effectestimates due to heterogeneity. Heterogeneity wasregarded possibly unimportant when the I2 value wasless than 40% and considerable when more than 75%.9
If necessary, ORs were calculated from 2 � 2 tables foreach individual study. A pooled effect estimate wascalculated as a weighted average of the effects estimatedin the individual studies. The weights represent theamount of information from each study. Studies withlarger sample sizes were weighted more heavily onmeta-analysis than studies with smaller sample sizes.Meta-analysis was conducted with Review Manager5.2.3.9 When considerable heterogeneity betweenstudies occurred or data did not provide sufficientinformation to perform meta-analysis, a qualitativesynthesis was conducted.
Results
Study SelectionThe initial search strategy resulted in 1,570 hits. After
the first selection, 65 articles were screened based onfull text. Thirty-six studies were scored for their meth-odologic quality. On the basis of quality assessment, 18studies were further analyzed. The article selection withapplication of the inclusion and exclusion and NOScriteria is summarized in Fig 1.
Quality AssessmentOn the basis of the final NOS score, an arbitrary
threshold score of 7 stars or greater, of which 2 starswere earned for “comparability,” was chosen to distin-guish between “good”- and “poor”-quality studies.10
Studies that scored below this cutoff were excludedfrom further analysis.Many studies were rewarded one star automatically
for items 2 and 4 of the “selection” subcategory forbeing a cohort study and for the logical conclusion thatthe outcome of interest, a successful or prolongedrehabilitation, was not present at the start of the study.

Original search: 1570 hits
Title selection: 151
Abstract selection: 65
Full text selection: 36
Animal studies: 104Pediatric patients only: 35Revision surgery: 29Posterior cruciate ligament: 38Irrelevant: 1217
Follow -up measurements: 14Psychological factors: 3Review: 21No group comparison: 8Graft selection: 19Costs: 1Editorial piece: 2Conservative only: 3No prognostic factor: 9Double-bundle technique: 2Ongoing studies: 4
Final selection: 18
Open technique: 8Double-bundle technique: 5No surgical information: 3Conservative included: 1Meniscus surgery: 1No prognostic factor: 4No comparison to ACL rupture alone: 5Insufficient follow -up: 2
Poor quality based on NOS: 18
Ongoing studies: 4
Fig 1. Article selection.
1882 E. J. DE VALK ET AL.
Table 2 provides an overview of the 36 studies with thecorresponding methodologic NOS scores. Less than10% loss to follow-up was chosen as acceptable andunlikely to introduce bias. Seven included studies (�7stars) reported more than 10% loss to follow-up ormade no statement at all.
Description of Included StudiesOne randomized controlled trial and 8 prospective and
9 retrospective cohort studies were included. They werepublished between 1997 and 2012. In total, 3,073patients were reviewed, of whom 1,793 were malepatients and 1,280 were female patients. The largestpopulation consisted of 402 patients11; the smallestcomprised 40 patients.12 Different graft types were used:boneepatellar tendonebone (11 studies), hamstring(11 studies), and alternative grafts (iliotibial band,quadriceps tendon, Achilles tendon) (2 studies). Themean follow-up duration varied between 1 year13,14 and7 years15 postoperatively. An overview of the extracteddata of the 18 included studies is given in Table 3.
Effect of Preoperative Prognostic Patient Factors
DemographicsGender. Return to sport is the end stage of rehabilita-tion after ACL reconstruction. Therefore activity level
was chosen as an outcome measure in the meta-analysis. From 3 studies, sufficient data could becollected for statistical pooling.15-17 Standardizedmean differences were used to correct for differentoutcome measures. On the basis of this meta-analysis,male patients have a higher level of activity thanfemale patients (effect size, 0.28; 95% CI, 0.05 to0.51; P ¼ .02) at a minimum of 1 year of follow-up(Fig 2).Three other studies not included in the meta-analysis
reported gender differences. The finding of one study isin line with the meta-analysis outcome. Spindleret al.18 concluded that female gender (P < .001) isa predictor of lower activity level at 6 years. The 2 otherstudies did not find a significant gender difference infunctional outcome after 1 year13 and 26 months19
postoperatively.In summary, meta-analysis concluded that male
patients have better functional outcomes after ACLreconstruction (Level III evidence).
Age. Three studies examined age as a factor for recovery.The first study concluded that young patients (aged 20 to24 years) had a higher Tegner activity level (P ¼ .032)at a minimal follow-up of 22 months comparedwith patients aged older than 40 years.20 InternationalKnee Documentation Committee Subjective Knee Form

Table 2. Quality Assessment of Included Studies (36 Studies)
Study
Selection Comparability Outcome
Total Score1 2 3 4 1 1 2 3
Ahldén et al.,16 2012* + + + + + + + + + 9Ahlén and Lidén,22 2011* + + + + + + + + + 9Brandsson et al.,20 2000* + + + + + + + + + 9Hamada et al.,27 2000* + + + + + + + + + 9Heijne et al.,13 2009* + + + + + + + + + 9Karim et al.,21 2006* + + + + + + + + + 9Kim et al.,28 2011* + + + + + + + + + 9Kowalchuk et al.,11 2009* + + + + + + + + + 9Raviraj et al.,24 2010* + + + + + + + + + 9Barber-Westin et al.,19 1997* + + + + + + + + d 8Dunn et al.,17 2010* + + + + + + + + d 8Eitzen et al.,26 2009* + + + + + + + + d 8Karlsson et al.,23 1999* d + + + + + + + + 8Melikoglu et al.,14 2008* + + + + + + + + d 8Salmon et al.,15 2006* + + + + + + + + d 8Spindler et al.,18 2011* + + + + + + + + d 8Harner et al.,35 1992 + + + + d d + + + 7Jerre et al.,36 2001 + + + + d d + + + 7Kim et al.,37 2010 + + + + d d + + + 7Laxdal et al.,38 2005 + + + + d d + + + 7Osti et al.,12 2011* d d + + + + + + + 7Sakai et al.,39 2011 + + + + d d + + + 7Sgaglione et al.,40 1993 + + + + d d + + + 7Sterett et al.,25 2003* d + + + + + + + d 7Tambe et al.,41 2006 + + + + d d + + + 7Wiger et al.,42 1999 d + + + d + + + + 7Ferrari et al.,43 2001 + + + + d d + + d 6Marcacci et al.,44 1995 + + + + d d + + d 6McHugh et al.,45 2002 d + + + + + + d d 6Ott et al.,46 2003 d + + + d d + + + 6Wu et al.,47 2002 + + + + d d + + d 6Asano et al.,48 2002 + + + + d d d + d 5de Jong et al.,49 2007 d + + + d d + + d 5Mauro et al.,50 2008 + + + + d d + d d 5Yüksel et al.,51 2011 d + + + + d + d d 5McHugh et al.,52 1998 d + + + d d + d d 4
*Selected for data extraction (�7 stars, with 2 stars earned for “comparability”).
PROGNOSTIC FACTORS OF SUCCESSFUL REHABILITATION 1883
(IKDC) scores, Lysholm scores, anterior laxity, and one-leg hop test results were not significantly differentbetween the groups. In the second study, patients agedyounger than 30 years had significantly higher IKDCsports activity level rates compared with patients agedolder than 50 years (P < .05), but a nonsignificantintergroup difference was found for Lysholm scores.12
The final study concluded that age was a significantpredictor (P ¼ .031) of IKDC score at 6 years.18
In summary, patients aged younger than 30 yearsreach higher activity levels than older patients afterACL reconstruction (Level III evidence).
Body Mass Index. Four studies investigated body massindex (BMI) as a prognostic factor. Patients witha lower baseline BMI had a higher activity level at2 years’ follow-up (OR, 1.37; 95% CI, 1.04 to 1.82;P ¼ .027).17 Low BMI was found to be a significantpredictor (R2 ¼ 0.08) of a higher Knee Injury andOsteoarthritis Outcome Score (KOOS) for the quality-
of-life domain (KOOSQOL) at 1 year as well.13
Another study highlighted that obese patients (BMI>30) had 0.35 the odds of success when comparedwith patients with a normal BMI (P < .01) at a meanof 6.3 years’ follow-up.11 This is in line with thefinding that lower BMI was a significant predictor ofhigher IKDC scores (P ¼ .022) and KOOS sports andrecreation subscale (KOOSsport/rec) scores (P ¼ .0497)at 6 years.18
In summary, patients with a high baseline BMI havelower activity levels after ACL reconstruction comparedwith patients with a normal BMI (Level III evidence).
Smoking. Four studies investigated smoking in relationto rehabilitation. Smoking within 6 months beforesurgery (OR, 0.55; 95% CI, 0.33 to 0.92; P ¼ .023) wasassociated with lower activity 2 years after ACLreconstruction, and smokers had 0.36 times the odds ofsuccess as nonsmokers.11,17 Smoking resulted in worsemean IKDC scores (P < .001), a higher frequency

Table 3. Study Characteristics (18 Studies)
Authors Inclusion Criteria Population Baseline CharacteristicsPrognosticsFactors Measures Results LOE
Ahldén et al.,16
2012Primary ACL
reconstruction; revisions,PCL reconstructions,
MCL/LCL injuries morethan grade 1,
radiographically visibleosteoarthritis or visiblesubchondral bone at
index operation, fracture/suture/previous majorknee surgery, BPTB
grafts, contralateral ACLinjury, reconstructions<2 mo, unavailablepreoperative or
postoperative data wereexcluded.
NU HospitalOrganisation: 244
patientsGroup 1: 141Group 2: 103
Follow-up, 25 mo
Group 1: age, 29 yr(15-61 yr); only M; TTS,
13 mo (2-360 mo)Group 2: age, 26 yr
(13-53 yr); only F; TTS,15 mo (2-276 mo)
Graft type: 4-strand ST/G
Gender KT-1000, Lachman,ROM, one-leg hop test,
Lysholm, Tegner
One-leg hop test at 2-yr follow-up: 91 (0-162) in group 1 and
84 (0-113) in group 2,P < .001
No significant differences atfollow-up between men andwomen in terms of Tegner
activity level (P ¼ .07), Lysholmscore (P ¼ .19), extension
(P ¼ .20) or flexion (P ¼ .95)deficits, KT-1000 (P ¼ .07), or
Lachman (P ¼ .31)
III
Ahlén andLidén,22 2011
Unilateral ACL ruptureand primary
reconstruction withST or ST/G autograft
No description: 61patients
Group 1:30Group 2: 31
Follow-up, 2 yr
Group 1: age, 26 � 9 yr;M/F, 15/15; TTS, 3 mo
(2-5 mo)Group 2: age, 27 � 6 yr;M/F, 19/12; TTS, 30 mo
(24-48 mo)Graft type: ST, ST/G
Time to surgery Lysholm, Tegner,manual Lachman, KT-
1000, ROM, one-leg hoptest, kneeling ability
Lysholm at follow-up: 90(58-100) in group 1 and 81(38-100) in group 2, P ¼ .01Tegner at follow-up: 6 (2-9) ingroup 1 and 5 (0-9) in group
2, P ¼ .01No significant difference
between groups in terms of KT-1000, Lachman, ROM, kneelingability, and one-leg hop test at
2-yr follow-up
III
Barber-Westinet al.,19 1997
No other ligamentruptures, minimum of2-yr follow-up, intactcontralateral knee
Participants ina prospective study onthe efficacy of patellartendon ACL autograftreconstruction: 94
patientsGroup 1a: 27Group 1b: 27Group 2a: 20Group 2b: 20
Follow-up: 26 mo
Group 1a, chronic repair:age, 29 yr (15-45 yr);only M; TTS, 71 mo
(7-348 mo)Group 1b, chronic repair:age, 29 yr (16-54 yr);only F; TTS, 73 mo
(5-278 mo)Group 2a, acute repair:age, 24 yr (15-41 yr);only M; TTS, 7.1 wk
(2-12 wk)Group 2b, acute repair:age, 26 yr (14-51 yr);only F; TTS, 5.2 wk
Gender KT-2000 (MEDmetric),isokinetic quadriceps and
hamstring testing,comprehensive knee
examination, subjectivequestionnaire, interview
No statistically significantdifference between men andwomen in either subgroup forKT-2000, pivot shift, kneemotion, patellofemoral
complications, muscle strength,subjective symptoms, functionalevaluation, or overall rating
III
(continued)
1884
E.J.
DEVALKETAL.

Table 3. Continued
Authors Inclusion Criteria Population Baseline CharacteristicsPrognosticsFactors Measures Results LOE
(1-12 wk)Graft type: BPTB
Brandssonet al.,20
2000
Uninjured contralateralknee
Database: 67 patientsGroup 1: 30Group 2: 37
Follow-up: 31 mo
Group 1: age, 43 yr(40-51 yr); M/F, 21/9;TTS, 36 mo (6-360 mo)Group 2: age, 23 yr
(21-24 yr); M/F, 24/13;TTS, 23 mo (9-108 mo)Graft type: not specified
Age Lysholm, Tegner, IKDC,patellofemoral pain,knee-walking ability,KT-1000, one-leg hop
test, ROM
Tegner at follow-up: 5 (3-9) ingroup 1 and 6 (1-9) in group 2,
P ¼ .032“Excellent” overall results atfollow-up: n ¼ 16 in group 1
and n ¼ 10 in group 2, P < .05No significant difference
between groups in terms ofLysholm, IKDC, KT-1000, 1-leghop test, knee-walking ability,
or ROM
III
Dunn et al.,17
2010Unilateral ACLreconstruction;
participants undergoingbilateral ACL
reconstruction wereexcluded
Multicenter OrthopaedicOutcomes Network: 393
patientsFollow-up: 2 yr
Age, 23 yr (17-35) yr; M/F, 222/171; TTS, not
specifiedGraft type: BPTB, ST/G,
iliotibial band,quadriceps tendon,Achilles tendon
Preinjury Marx level,gender, BMI, smoking
status
Marx activity level,KOOS, IKDC
Higher baseline activity (IQROR, 3.84; 95% CI, 1.98-7.43;
P < .0001); lower baseline BMI(IQR OR, 1.37; 95% CI, 1.04-
1.82; P ¼ .027); highercompetition level (P ¼ .027)compared with recreational
level, competing at high schoollevel (OR, 2.52; 95% CI, 1.27-5.01) or college level (OR, 4.23;95% CI, 1.85-9.66); and type ofactivity at injury (P ¼ .023)were associated with higher
activity levels at 2 yr.Female gender (OR, 0.60; 95%CI, 0.39-0.91, P ¼ .015) andsmoking within 6 mo beforesurgery (OR, 0.55; 95% CI,0.33-0.92; P ¼ .023) were
associated with lower activitylevel.
III
Eitzen et al.,26
2009Unilateral complete
rupture of ACL; date ofinjury maximum of 3 yr
before scheduledsurgery; potentialcandidates were
excluded if they had anyhistory of injury and/orsurgical intervention ineither the ACL-deficientor contralateral knee,meniscus injury that
Orthopaedic Centre,Ullevål University
Hospital Oslo: 73 patientsFollow-up: 2 yr
Age, 29.5 yr (16.7-40.3yr) in M and 26.8 yr
(19.8-38.0 yr) in F; M/F,47/26; TTS, not specified
Graft type: BPTB
Meniscus injury, SF-36BP subscore, VAS globalfunction, triple-hop test,quadriceps strength,
stair-hop test
Cincinnati Knee Score Preoperative quadricepsstrength, meniscus injury, and
SF-36 BP subscore weresignificant predictors for the
Cincinnati Knee Score.Preoperative quadriceps
strength alone explained 15.6%of the regression, preoperatievequadriceps and meniscus injury
explained 24% of theregression, and the SF-36 BP
subscore increased the
III
(continued)
PROGNOST
ICFACTORSOFSU
CCESSF
ULREHABILITATION
1885

Table 3. Continued
Authors Inclusion Criteria Population Baseline CharacteristicsPrognosticsFactors Measures Results LOE
required repair, orfull-depth cartilagedefects affectingsubchondral bone
explained variation to 30.7%.Patients with a quadricepsstrength deficit >20% at
baseline had lower CincinnatiKnee Scores (P ¼ .008) and
quadriceps strength (P ¼ .001).Patients with meniscus injury atbaseline had lower CincinnatiKnee Scores (P ¼ .036) and SF-36 BP subscores (P ¼ .028).
Hamada et al.,27
2000No prior intra- or extra-
articular ligamentreconstruction; absenceof posterior drawer sign,varus/valgus instability,excessive external tibialrotation, recurvatum, or
reversed pivot shift;healthy contralateral
knee; no severeosteoarthritic changes byradiography; no loss ofmotion >5� of extensionor flexion; no acute cases
of injury sustainedwithin 3 wk
Consecutive series ofpatients operated on atOsaka Rosai Hospital: 86
patientsGroup 1: 27Group 2: 48Group 3: 11
Follow-up: 2 yr
Group 1: age, 24.3 � 10yr; M/F, 11/16; TTS,
13.8 � 32.4 moGroup 2: age, 25.2 � 7.5
yr; M/F, 26/22; TTS,26.3 � 36.5 mo
Group 3: age, 21.8 � 4.4yr; M/F, 6/5; TTS, 19.4 �
29.9Graft type: HT
Preoperative knee jointlaxity
IKDC, Knee LaxityTester, flexion and
extension peak torques
Preoperative AL-D did notinfluence postoperative
stability.AL-D postoperatively: 0.8 � 1.7mm in group 1, 1.1 � 1.6 mmin group 2, and 1.5 � 1.4 mm in
group 3; P ¼ .40No positive correlation betweenpreoperative and postoperativeCorrelation coefficient for AL-D:
0.15
III
Heijne et al.,13
2009Asymptomatic
contralateral knee, noknown knee injury
Patients withconcomitant medial orlateral meniscus tearand/or MCL injury,grade I, for which
surgical repair was notindicated, were also
eligible.Exclusion criteria weremore grade II and III
meniscus injuries, gradeII or III MCL injuries,
meniscus lesions suitablefor fixation, and grafts
harvested fromcontralateral knee.
Patients involved ina preoperative
physiotherapy regimenat a sport rehabilitationclinic or invited throughinformation from thehospital: total of 64
patientsFollow-up: 1 yr
Age: 30.1 � 7.8 yr; M/F,35/29; TTS <6 mo/7-12mo/>13 mo, 26/20/18Graft type: BPTB (n ¼32), ST (n ¼ 22), and
ST/G (n ¼ 10)
AKP, knee flexiondeficits, influence on
activity (IKDC), gender,cartilage damage, BMI,anterior knee laxity,eccentric/concentric
quadriceps torque, graft,time to surgery
KOOSsport/rec, KOOSQOL,1-leg hop test, Tegner
AKP, knee function, kneeflexion deficits, influence onactivity level, gender, andcartilage damage together
explained 37% of the outcomevariance in KOOSsport/rec
(P ¼ .002).Less AKP is a significant
predictor of a high KOOSsport/recscore (P ¼ .05).
Knee flexion deficits, AKP, kneefunction, BMI, anterior knee
laxity, and eccentric quadricepstorques explained 44% of the
outcome in KOOSQOL(P ¼ .001).
Less AKP, no loss of flexion, lowBMI, and eccentric quadriceps
torque were significant
III
(continued)
1886
E.J.
DEVALKETAL.
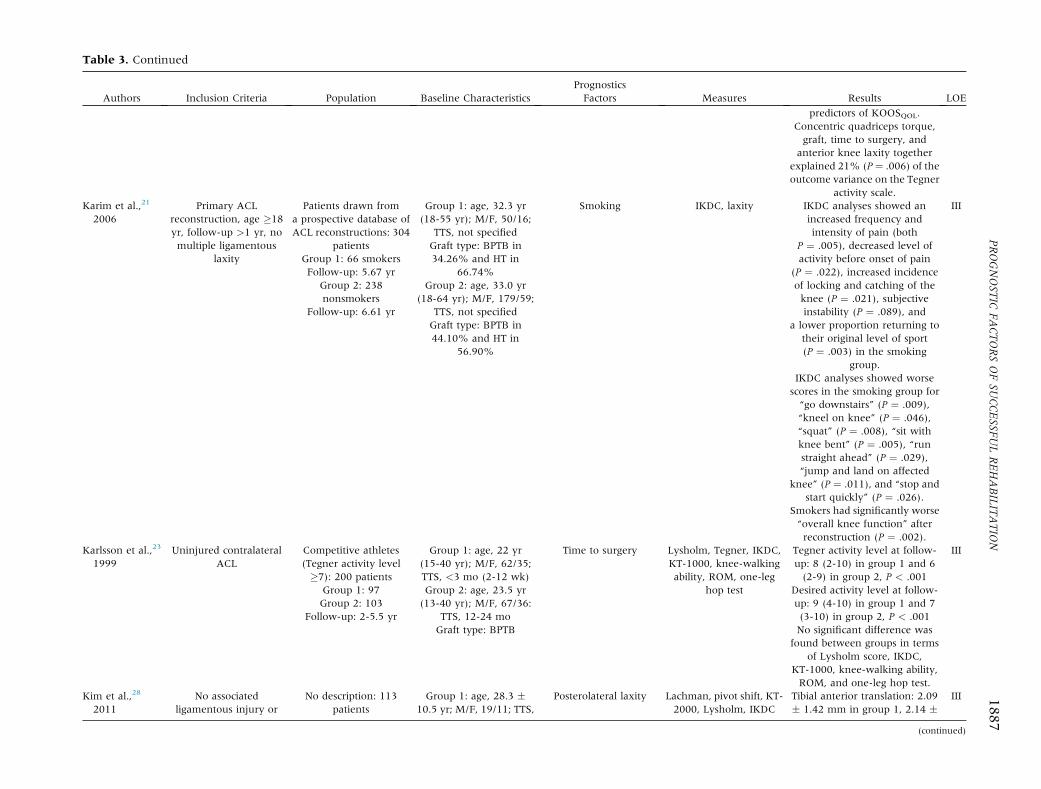
Table 3. Continued
Authors Inclusion Criteria Population Baseline CharacteristicsPrognosticsFactors Measures Results LOE
predictors of KOOSQOL.Concentric quadriceps torque,graft, time to surgery, and
anterior knee laxity togetherexplained 21% (P ¼ .006) of theoutcome variance on the Tegner
activity scale.Karim et al.,21
2006Primary ACL
reconstruction, age �18yr, follow-up >1 yr, nomultiple ligamentous
laxity
Patients drawn froma prospective database ofACL reconstructions: 304
patientsGroup 1: 66 smokersFollow-up: 5.67 yr
Group 2: 238nonsmokers
Follow-up: 6.61 yr
Group 1: age, 32.3 yr(18-55 yr); M/F, 50/16;
TTS, not specifiedGraft type: BPTB in34.26% and HT in
66.74%Group 2: age, 33.0 yr
(18-64 yr); M/F, 179/59;TTS, not specifiedGraft type: BPTB in44.10% and HT in
56.90%
Smoking IKDC, laxity IKDC analyses showed anincreased frequency andintensity of pain (both
P ¼ .005), decreased level ofactivity before onset of pain
(P ¼ .022), increased incidenceof locking and catching of theknee (P ¼ .021), subjectiveinstability (P ¼ .089), and
a lower proportion returning totheir original level of sport(P ¼ .003) in the smoking
group.IKDC analyses showed worse
scores in the smoking group for“go downstairs” (P ¼ .009),“kneel on knee” (P ¼ .046),“squat” (P ¼ .008), “sit withknee bent” (P ¼ .005), “runstraight ahead” (P ¼ .029),“jump and land on affected
knee” (P ¼ .011), and “stop andstart quickly” (P ¼ .026).
Smokers had significantly worse“overall knee function” afterreconstruction (P ¼ .002).
III
Karlsson et al.,23
1999Uninjured contralateral
ACLCompetitive athletes(Tegner activity level�7): 200 patients
Group 1: 97Group 2: 103
Follow-up: 2-5.5 yr
Group 1: age, 22 yr(15-40 yr); M/F, 62/35;TTS, <3 mo (2-12 wk)Group 2: age, 23.5 yr(13-40 yr); M/F, 67/36:
TTS, 12-24 moGraft type: BPTB
Time to surgery Lysholm, Tegner, IKDC,KT-1000, knee-walkingability, ROM, one-leg
hop test
Tegner activity level at follow-up: 8 (2-10) in group 1 and 6(2-9) in group 2, P < .001
Desired activity level at follow-up: 9 (4-10) in group 1 and 7(3-10) in group 2, P < .001No significant difference was
found between groups in termsof Lysholm score, IKDC,
KT-1000, knee-walking ability,ROM, and one-leg hop test.
III
Kim et al.,28
2011No associated
ligamentous injury orNo description: 113
patientsGroup 1: age, 28.3 �
10.5 yr; M/F, 19/11; TTS,Posterolateral laxity Lachman, pivot shift, KT-
2000, Lysholm, IKDCTibial anterior translation: 2.09� 1.42 mm in group 1, 2.14 �
III
(continued)
PROGNOST
ICFACTORSOFSU
CCESSF
ULREHABILITATION
1887

Table 3. Continued
Authors Inclusion Criteria Population Baseline CharacteristicsPrognosticsFactors Measures Results LOE
contralateral knee injury;negative dial test; single-
bundle ACLreconstruction withBPTB autograft; nohistory of additional
surgery involving lowerextremities; no axial orrotational malalignmentof lower extremities; nochondral lesion greater
than grade II(Outerbridge); intact or
partially resectedmeniscus with remaininghoop tension; minimum
follow-up of 24 mo
Group 1: 30Group 2: 41Group 3: 42;
Follow-up: 2 yr
14.5 � 8.3 moGroup 2: age, 27.9 � 9.3yr; M/F, 25/16; TTS, 12.6
� 7.9 moGroup 3: age, 29.0 � 8.9yr; M/F, 27/15; TTS, 15.4
� 9.3 moGraft type: BPTB
1.53 mm in group 2, and 3.38 �1.65 mm in group 3; P < .001IKDC score (normal or nearlynormal): 26 (86.7%) in group 1,36 (87.8%) in group 2, and 32(76.2%) in group 3; P < .001Lysholm score: 93.7 � 5.6
points in group 1, 92.3 � 6.2points in group 2, and 86.4 �8.1 points in group 3; P < .001
Kowalchuket al.,11
2009
Minimum of 2-yr follow-up with completed IKDCSubjective Knee Form
Patients with incompletesurvey data were
excluded.
Retrospective database ofpatients who underwent
primary ACLreconstruction between1986-2002: 402 patients
Follow-up: 6.3 yr
Age, 28.4 � 11.59 yr; M/F, 209/193; TTS, 22 mo
(1 d-328 mo)Graft type: BPTB, HT,
Achilles tendon
BMI, occupation,smoking, educationlevel, marital status,activity level before
surgery, mechanism ofinjury, No. of episodes of
giving way beforesurgery, previous
meniscectomy, surgicalvariables
IKDC Univariate logistic regressionOverweight: OR, 0.92; SE, 0.31;P ¼ .82; 95% CI, 0.47-1.80Obese: OR, 0.35; SE, 0.13;P < .01; 95% CI, 0.17-0.71
Current smoker: OR, 0.34; SE,0.14; P ¼ .01; 95% CI,
0.15-0.76Medial meniscal surgery: OR,
0.42; SE, 0.18; P ¼ .05; 95% CI,0.17-0.99
Severe medial compartmentchondrosis: OR, 0.38; SE, 0.16;P ¼ .02; 95% CI, 0.18-0.87
Multivariate regressionmodeling
Overweight: OR, 0.93; SE, 0.32;P ¼ .84; 95% CI, 0.47-1.84Obese: OR, 0.34; SE, 0.13;P < .01; 95% CI, 0.14-0.81
Current smoker: OR, 0.34; SE,0.15; P ¼ .01; 95% CI,
0.14-0.81Medial compartment
chondrosis: OR, 0.38; SE, 0.17;P ¼ .03; 95% CI, 0.15-0.93
III
Melikogluet al.,14 2008
Unilateral ACL ruptureassessed by a positive
No description: 98patients
Group 1: age, 32.4 � 6.6yr; M/F, 32/5; TTS, 5.0 �
Time to surgery After 2 mo from surgery,P < .05
III
(continued)
1888
E.J.
DEVALKETAL.

Table 3. Continued
Authors Inclusion Criteria Population Baseline CharacteristicsPrognosticsFactors Measures Results LOE
Lachman test and/ormagnetic resonance
imagingExclusion criteria wereage >50 yr, bilateral
injuries, other ligamentinstability, previous ACLreconstruction, or signsof osteoarthritis on
radiography.
Group 1: 37Group 2a: 32Group 2b: 29
Follow-up: 1 yr
3.8 moGroup 2a: age, 25.4 �5.6 yr; M/F, 29/3; TTS,
25.4 � 5.6 moGroup 2b: age, 34.6 �16.0 yr; M/F, 24/5; TTS,
62.4 � 16.0 moGraft type: BPTB
Quadriceps strength,hamstring strength,
isokinetic data, KT-1000
Extension PT in 60�/sGroup 1: 28.3 � 35.0Group 2: 45.12 � 24.2Extension PT in 240�/sGroup 1: 13.5 � 8.8Group 2: 21.8 � 19.6Extension enduranceGroup 1: 4.0 � 21.2)Group 2: 19.0 � 38.5
After 6 months from surgery,P < .05
Extension endurance:Group 1: 2.8 � 23.4Group 2: 6.1 � 17.2
Osti et al.,12
2011Physically active;diagnosed with
symptomatic ACLdeficiency unresponsive
to conservativemanagement detected on
clinical grounds andmagnetic resonanceimaging; history of
activity-related pain andrestricted range of
motionExclusion criteriaincluded history of
previous knee surgery,severe osteoarthritic
changes, multiligamentinvolvement,
concomitant lowerextremity fracture,
cardiovascular disease,Workers’ Compensationclaims, or psychiatric
illness.
No description: 40patients
Group 1: 20Group 2: 20
Follow-up: 2 yr
Group 1: age, 56 (50-62);M/F, 12/8; TTS, 86 (72-
100)Group 2: age, 27 (17-30);M/F, 12/8; TTS, 84 (74-
94)Graft type: 4-strand ST/G
Age Lachman, pivot shift, KT-1000, IKDC, Lysholm
IKDC improvement:preoperatively and last
follow-upGroup 1: 46 (30-60) and 91
(80-100); P < .001Group 2: 50 (39-67) and 92 (80-
100); P < .001IKDC sports activity level at lastfollow-up/return to preinjuryactivity level: 12 (60%) in group1 and 18 (90%) in group 2,
P < .05There were no intergroup
significant differences in termsof postoperative Lysholm
scores, Lachman, pivot shift,and KT-1000 at 24-mo
follow-up.
III
Raviraj et al.,24
2010Diagnosed with a torn
ACL as seen ona magnetic resonance
scanPatients with
concomitant ligamentousinjuries, ipsilateral long-
Patients who presentedto the emergency
department: 99 patientsGroup 1: 51Group 2: 48
Follow-up: 32 mo
Group 1: age, 31.6 � 5.3yr; M/F, 25/26; TTS, 7
d (2-14 d)Group 2: age, 31.2 � 5.3yr; M/F, 26/22; TTS, 32
d (29-42 d)Graft type: ST/G
Time to surgery Lysholm, Tegner, ROM,clinical examination, KT-
1000
The recovery of the range ofmovement at various intervalsshowed no statistical difference
between the 2 groups.No statistically significant
difference was found for theLysholm score (P ¼ .86) and
II
(continued)
PROGNOST
ICFACTORSOFSU
CCESSF
ULREHABILITATION
1889
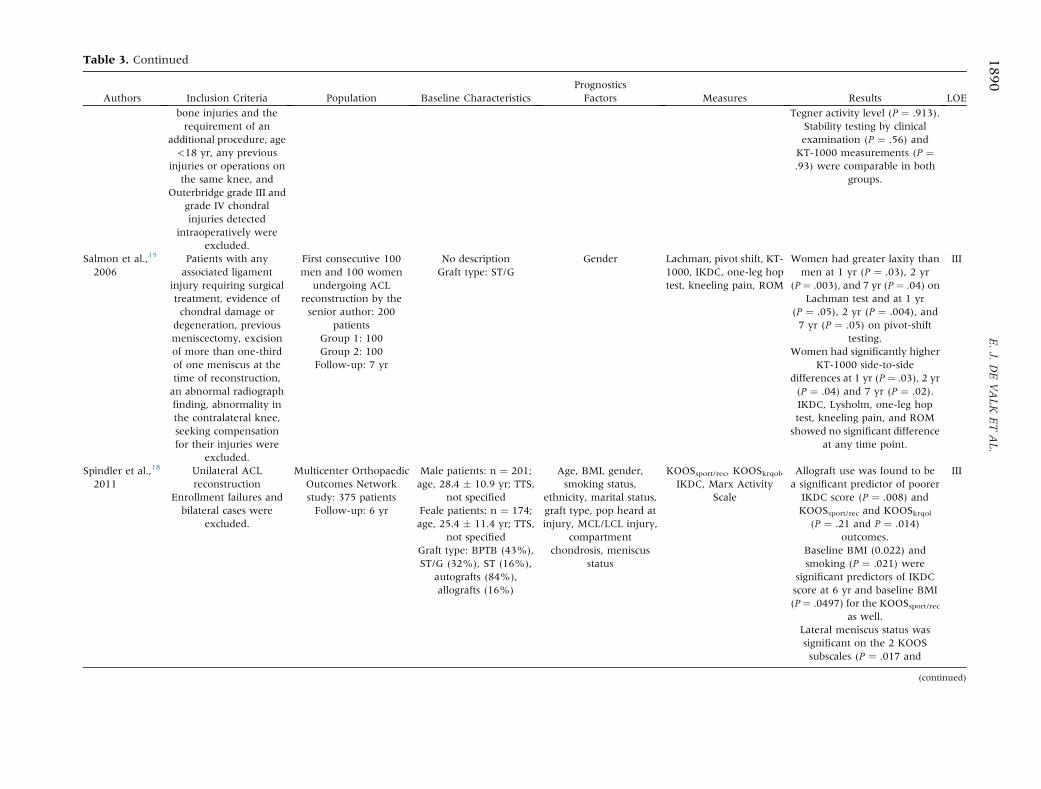
Table 3. Continued
Authors Inclusion Criteria Population Baseline CharacteristicsPrognosticsFactors M es Results LOE
bone injuries and therequirement of an
additional procedure, age<18 yr, any previous
injuries or operations onthe same knee, and
Outerbridge grade III andgrade IV chondralinjuries detected
intraoperatively wereexcluded.
Tegner activity level (P ¼ .913).Stability testing by clinicalexamination (P ¼ .56) and
KT-1000 measurements (P ¼.93) were comparable in both
groups.
Salmon et al.,15
2006Patients with anyassociated ligament
injury requiring surgicaltreatment, evidence ofchondral damage or
degeneration, previousmeniscectomy, excisionof more than one-thirdof one meniscus at thetime of reconstruction,an abnormal radiographfinding, abnormality inthe contralateral knee,seeking compensationfor their injuries were
excluded.
First consecutive 100men and 100 women
undergoing ACLreconstruction by thesenior author: 200
patientsGroup 1: 100Group 2: 100Follow-up: 7 yr
No descriptionGraft type: ST/G
Gender Lachman t shift, KT-1000, IK e-leg hoptest, kne ain, ROM
Women had greater laxity thanmen at 1 yr (P ¼ .03), 2 yr
(P¼ .003), and 7 yr (P ¼ .04) onLachman test and at 1 yr
(P ¼ .05), 2 yr (P ¼ .004), and7 yr (P ¼ .05) on pivot-shift
testing.Women had significantly higher
KT-1000 side-to-sidedifferences at 1 yr (P¼ .03), 2 yr(P ¼ .04) and 7 yr (P ¼ .02).IKDC, Lysholm, one-leg hoptest, kneeling pain, and ROMshowed no significant difference
at any time point.
III
Spindler et al.,18
2011Unilateral ACLreconstruction
Enrollment failures andbilateral cases were
excluded.
Multicenter OrthopaedicOutcomes Networkstudy: 375 patientsFollow-up: 6 yr
Male patients: n ¼ 201;age, 28.4 � 10.9 yr; TTS,
not specifiedFeale patients: n ¼ 174;age, 25.4 � 11.4 yr; TTS,
not specifiedGraft type: BPTB (43%),ST/G (32%), ST (16%),
autografts (84%),allografts (16%)
Age, BMI, gender,smoking status,
ethnicity, marital status,graft type, pop heard atinjury, MCL/LCL injury,
compartmentchondrosis, meniscus
status
KOOSspo OOSkrqol,IKDC, Activity
Allograft use was found to bea significant predictor of poorer
IKDC score (P ¼ .008) andKOOSsport/rec and KOOSkrqol
(P ¼ .21 and P ¼ .014)outcomes.
Baseline BMI (0.022) andsmoking (P ¼ .021) were
significant predictors of IKDCscore at 6 yr and baseline BMI(P¼ .0497) for the KOOSsport/rec
as well.Lateral meniscus status wassignificant on the 2 KOOSsubscales (P ¼ .017 and
III
(continued)
1890
E.J.
DEVALKETAL.
easur
, pivoDC, oneling p
rt/rec, KMarxScale

Tab
le3.
Continued
Authors
InclusionCriteria
Population
BaselineCharacteristics
Progn
ostics
Factors
Mea
sures
Results
LOE
P¼
.027).
Marxactivity
scoreswerelower
forfemalepatients
(P<
.001).
Sterettet
al.,25
2003
Nodescription
Nodescription:160
patients
Group1:80
Group2:80
Follow-up:1yr
Group1:ag
e,28.5
(15-50);M/F,43/37;
TTS,7.3
d(1-21d)
Group2:ag
e,30.6
yr(14-49yr);M/F,41/39;
TTS
,1,243d(22-10,920
d)Grafttype
:BPT
B
Tim
eto
surgery
ROM
Therewerenostatistical
differencesin
rate
ofdecreased
range
ofmotionbe
tweenthe
acute
andch
ronic
groups
(P¼
.316)at
3moan
dfinal
follow-up.
III
NOTE.Grade1,incomplete
rupture
withminim
alsymptoms.Grade2,incomplete
tearswithinstab
ility
complaints
andsw
elling.
Grade3,complete
tear.
AL-D
,an
teriorlaxitydifference;AKP,an
teriorknee
pain;BP,bo
dily
pain;BPTB,bo
nee
patellartendonebo
ne;
F,female;
G,gracilis;HT,ham
stringtendon;IQ
R,interquartile
range
;KOOSkrqol,Knee
injury
andOsteo
arthritisOutcomeScore
(KOOS)knee
relatedqualityoflife;LCL,lateralcollateral
liga
men
t;LOE,leve
lofev
iden
ce;M,male;
MCL,med
ialcollateral
liga
men
t;PCL,posteriorcruciateliga
men
t;PT,peaktorque;
ROM,range
ofmotion;SF-36,Short
Form
36Hea
lthSurvey
;ST,semiten
dinosus;TTS,timeto
surgery;
VAS,visual
analogscale
score.
PROGNOSTIC FACTORS OF SUCCESSFUL REHABILITATION 1891
(P ¼ .005) and intensity (P ¼ .005) of pain, a decreasedlevel of activity before the onset of pain (P ¼ .022), anincreased incidence of locking and catching of the knee(P ¼ .021), and a higher side-to-side difference in kneelaxity (P ¼ .001). Smokers were also less likely to returnto their original preinjury level of sport (P ¼ .003) andhad an overall worse final IKDC score (P ¼ .002).21
Moreover, at 6 years’ follow-up, not smoking atbaseline was a predictor (P ¼ .021) for higher IKDCscores.18
In summary, smoking results in more symptoms,lower activity levels, and lower subjective IKDC andKOOS scores after ACL reconstruction (Level IIIevidence).
Time to SurgeryFive studies investigated the relation between the
time between ACL tear and repair and functionaloutcomes. The first study found that patients operatedon within 3 months after injury showed betteroutcomes in terms of Lysholm score (P ¼ .01) andTegner activity level (P ¼ .01) at 2 years’ follow-upcompared with patients operated on more than 24months after injury.22 The second study, in whichcompetitive athletes were included (Tegner activitylevel �7), showed that patients operated on early (2 to12 weeks) reached a higher Tegner activity level(P < .001), reached a higher desired Tegner activitylevel (P < .001), and had fewer meniscal injuries(P < .01) compared with the control group (12 to 24months).23 Lysholm scores, KT-1000 total side-to-sidedifferences (MEDmetric, San Diego, CA), and one-leghop test results were not statistically different betweenthe groups at 2 years’ follow-up. Another studyconfirmed that time between injury and surgery wasassociated with Tegner activity level (P ¼ .02) at 1 yearaccording to stepwise regression, but a shorter timebetween injury and surgery and a higher activity levelwere not independently associated.13 A fourth studyshowed that surgery within 2 weeks compared withsurgery 4 to 6 weeks after injury was not statisticallysignificantly different regarding Lysholm (P ¼ .860) orTegner (P ¼ .913) score at a mean follow-up of 32months.24 The final study showed no statisticallysignificant difference in the rate of decreased range ofmotion between patients operated on within 3 weeksand those operated on after 3 weeks (P ¼ .316).25
In summary, early reconstruction, between 2 weeksand 3 months, results in higher activity levels after ACLreconstruction (Level II and III evidence).
Preoperative Knee FunctionStrength. Two studies investigated the relation betweenpreoperative knee strength and functional outcomeafter ACL repair. The first study showed that patientswith a quadriceps strength deficit greater than 20%

Fig 2. Forest plot for gender and activity level.
1892 E. J. DE VALK ET AL.
compared with the uninvolved leg at baseline had lowerCincinnati Knee Scores (P ¼ .008) and quadricepsstrength (P ¼ .001) 2 years after surgery.26 Moreover,quadriceps strength was still significantly lower (P ¼.001) 2 years after surgery among patients who haddeficits greater than 20% at baseline. Preoperativequadriceps strength was a significant predictor for theCincinnati Knee Score and explained 15.6% of theregression. This is in agreement with another studythat found that low preoperative eccentric quadricepstorque, as compared with the uninvolved knee, wasa significant predictor of a lower KOOSQOL score at 12months’ follow-up.13 Together with 5 other variables,low eccentric quadriceps torque explained 44% of theoutcome on the KOOSQOL.In summary, preoperative quadriceps strength deficits
greater than 20% and low preoperative eccentricquadriceps torques, as compared with the uninvolvedknee, lead to a lower Cincinnati Knee Score andKOOSQOL score, respectively (Level III evidence).
Range of Motion. One study reported that preoperativeabsence of knee flexion deficit was a significantpredictor (adjusted R2 ¼ 0.26) of high KOOSQOL
outcome scores.13
Subjective Experience of Knee Function and Anterior KneePain. When the influence of the injured knee on thepatient’s activity level is low, as measured by the IKDCform, KOOSsport/rec scores are higher. Less anterior kneepain was found to be a significant (P < .05) preopera-tive predictor of a high score on the KOOSsport/rec aswell. These 2 independent variables together explained31% of the outcome variance.13
Knee Joint Laxity. Two studies examined anterior kneelaxity as a predictive factor. The first study divided 86patients into 3 groups (<5 mm, 5 to 9 mm, and >10mm) according to the preoperative anterior laxity side-to-side difference measured with the Knee Laxity Tester(Orthopedic Systems, Union City, CA).27 The authorsfound no significant statistical differences betweengroups in postoperative anterior laxity difference. Inaddition, there was no positive correlation (g ¼ 0.15)between the preoperative and postoperative anteriorlaxity difference. The second study did not find
a significant relation between anterior laxity andKOOSQOL.
13
One study investigated the influence of posterolaterallaxity in patients scheduled for ACL reconstruction onclinical outcomes measured by the Lysholm and IKDCscales at 2 years’ follow-up.28 There was an inversecorrelation between the degree of tibial external rota-tion at 90� and the Lysholm score (P ¼ .015,r ¼ �0.146) and IKDC score (P ¼ .003, r ¼ �0.205) at24 months’ follow-up. After ACL reconstruction,patients with 50� of tibial external rotation or greater at90� had increased anterior translation and worsefunctional outcomes in comparison with those who hadless than 50� of tibial external rotation.In summary, preoperative anterior laxity difference is
not a predictive factor of postoperative anterior laxitydifference and KOOSQOL. Patients with 50� of tibialexternal rotation or greater have worse functionaloutcomes and increased postoperative anterior trans-lation (Level III evidence).
Preoperative Activity Level. Two studies investigatedpreoperative activity level as a preoperative prognosticfactor. A higher baseline Marx activity level (OR, 3.84;95% CI, 1.98 to 7.42; P < .0001) is associated withhigher activity levels at 2 years after ACL reconstruc-tion.17 A higher level of competition (P ¼ .027), ascompared with patients at a recreational level,competing at high school level (OR, 2.52; 95% CI, 1.27to 5.01) or college level (OR, 4.23; 95% CI, 1.85 to9.66), is associated with higher activity levels at 2 yearsas well. This is in contrast to another study in whichactivity level before surgery was not found to bea predictor independently associated with IKDC score(P ¼ .05).11
In summary, the prognostic value of preoperativeactivity and competition level for postoperative func-tional outcome is controversial (Level III evidence).
Effect of Preoperative Prognostic Injury Factors
Meniscal StatusThe first of 4 studies found that meniscal injury was
a significant predictor of the Cincinnati Knee Score 2years after ACL reconstruction and explained 8.4% ofthe regression.26 Patients with meniscal injuries at

PROGNOSTIC FACTORS OF SUCCESSFUL REHABILITATION 1893
baseline had a significantly lower Cincinnati Knee Score(P ¼ .036) and Short Form 36 bodily pain subscore (P ¼.028). Lateral meniscus status was also a significantpredictor of the KOOSsport/rec and KOOSQOL at 6 years’follow-up.18 The possible indirect effect of prior menis-cectomy through chondrosis on IKDC scores was inves-tigated as well but was not significant.11 The fourth studydid not find a significant correlation between meniscalinjury and KOOSsport/rec, KOOSQOL, one-leg hop testresult, or Tegner activity scale at 1 year of follow-up.13
In summary, patients with concomitant meniscalinjuries have worse functional outcomes 2 to 6 yearsafter surgery (Level III evidence).
Chondral PathologyOne study showed that cartilage damage was not
significantly (P ¼ .07) associated with KOOSsport/rec at 1year of follow-up.13 Neither medial nor lateral chond-rosis was a significant predictor of IKDC score, KOOS,or Marx score at long-term follow-up (6 years).18 Thesefindings are in contrast with another study that showedthat severe medial chondrosis was a significantpredictor of the IKDC score (OR, 0.38; 95% CI, 0.15 to0.93; P ¼ .03).11
In summary, the prognostic value of concomitantchondral pathology for postoperative functional outcomeis controversial (Level III evidence).
Collateral Ligament InjuryOne study investigated concomitant collateral injuries
and concluded that neither medial nor lateral collateralligament injury could predict IKDC score, KOOS, orMarx score at 6 years’ follow-up.18
DiscussionThis is the first systematic review with meta-analysis
investigating preoperative patient and injury factors inrelation to rehabilitation after ACL reconstruction withsingle-bundle techniques. Concerning preoperativepatient factors, the following can be concluded: malepatients and patients aged younger than 30 years ach-ieve higher activity levels after rehabilitation. Earlyreconstruction before 3 months after injury is superiorto late reconstruction. Quadriceps strength and range-of-motion deficits are associated with lower kneefunction after rehabilitation; high BMI and smokingaffect rehabilitation negatively as well. The amount ofanterior laxity does not affect rehabilitation.Only a few included studies investigated preoperative
injury factors, although firm conclusions cannot bedrawn. Patients with concomitant meniscal injurieshave worse functional outcomes 2 to 6 years aftersurgery. The prognostic value of concomitant chondralpathology and baseline activity level for postoperativefunctional outcome is controversial. Collateral ligament
injury did not predict functional scores or activity levelat 6 years’ follow-up.Of the factors that influence outcome, quadriceps
strength, range of motion, BMI, and smoking arefactors that can be modified preoperatively. Quadri-ceps strength and range of motion could be improvedby preoperative training. Although evidence forpreoperative thresholds is still lacking, the optimalpreoperative knee status consists of decreasedswelling and full range of motion, and the quadricepsstrength deficit should be less than 20% comparedwith the uninvolved leg.26,29
BMI should be reduced to normal or minimal ranges,and smoking should be stopped. An exact timeframe forreconstruction is hard to provide based on the foundliterature, but the timeframe should preferably bebetween 2 and 12 weeks after injury.Future research should focus on preoperative injury
characteristics in relation to rehabilitation. The effect ofchondral pathology and collateral ligament injury is stillunclear. Further clarification and modification ofknown and indistinct preoperative factors will help tofurther improve outcome after ACL reconstruction.
LimitationsThis systematic review has a few limitations. We
limited this review to the most commonly used, single-bundle techniques. Double-bundle ACL reconstructioncould have slightly better outcomes with regard torotational laxity, stability, IKDC knee examination, andreturn to preinjury level of sports.30,31 However,single- and double-bundle techniques have not beenshown to be significantly different in terms of subjec-tive functional knee scores, complications, or graftfailure.31,32 Another limitation could be the use ofdifferent graft types. Rehabilitation might be influ-enced by the use of different graft types, althoughboneepatellar tendonebone and hamstring graftsshowed similar outcomes in terms of functionalassessment, return to activity, and subjective measuresof outcome.33 A final limitation may be the tool used toassess methodologic quality. No widely accepted toolexists for the quality assessment of cohort studies.However, the NOS tool is one of the recommendedtools in the report of Deeks et al.34 and is commonlyused to assess cohort studies’ methodologic quality.Data synthesis was hampered by heterogeneity across
studies and missing data. Only data for gender could besynthesized quantitatively. Possible determinants ofheterogeneity were different definitions of early andlate reconstruction, as well as young and old patients,and different outcome measures used. Correction forpossible confounders between groups and correct use ofstatistical methods with mentioning of all relevantstatistical values would have led to more possibilities formeta-analysis.

1894 E. J. DE VALK ET AL.
ConclusionsRehabilitation and return to sport after ACL recon-
struction are influenced by preoperative patient andinjury factors as shown by this systematic review withmeta-analysis. Male patients, patients aged youngerthan 30 years, and patients who undergo early recon-struction have better functional outcomes. Smoking,high BMI, quadriceps strength deficits, and range-of-motion deficits affect rehabilitation negatively. Preop-erative anterior laxity does not affect rehabilitationsuccess. There is limited evidence for any prognosticinjury factor. ACL reconstruction is the standard ofcare in ACL-deficient patients, but results may beoptimized when modifiable factors such as strengthdeficits, range-of-motion deficits, BMI, and smoking arereduced.
References1. Hewett TE, Di Stasi SL, Myer GD. Current concepts for
injury prevention in athletes after anterior cruciate liga-ment reconstruction. Am J Sports Med 2013;41:216-224.
2. Kvist J. Rehabilitation following anterior cruciate liga-ment injury: Current recommendations for sports partic-ipation. Sports Med 2004;34:269-280.
3. Ardern CL, Webster KE, Taylor NF, Feller JA. Return tosport following anterior cruciate ligament reconstructionsurgery: A systematic review and meta-analysis of thestate of play. Br J Sports Med 2011;45:596-606.
4. Thomeé R, Kaplan Y, Kvist J, et al. Muscle strength andhop performance criteria prior to return to sports afterACL reconstruction. Knee Surg Sports Traumatol Arthrosc2011;19:1798-1805.
5. Te Wierike SC, van der Sluis A, van den Akker-Scheek I,Elferink-Gemser MT, Visscher C. Psychosocial factorsinfluencing the recovery of athletes with anterior cruciateligament injury: A systematic review. Scand J Med SciSports. 4 November, 2012. [Epub ahead of print.]
6. Thomeé P, Währborg P, Börjesson M, Thomeé R,Eriksson BI, Karlsson J. Self-efficacy of knee function asa pre-operative predictor of outcome 1 year after anteriorcruciate ligament reconstruction. Knee Surg Sports Trau-matol Arthrosc 2008;16:118-127.
7. WellsGA, SheaB,O'Connell D, et al. TheNewcastle-OttawaScale (NOS) for assessing the quality of nonrandomisedstudies in meta-analyses. Available from: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. AccessedDecember 13, 2012.
8. Oxford Centre for Evidence-Based Medicine. OCEBMlevels of evidence system. Available from: http://www.cebm.net/index.aspx?o=5653. Accessed December 13,2012.
9. Higgins JPT, Green S, editors. Cochrane handbook forsystematic reviews of interventions. Version 5.1.0 [updatedMarch 2011]. The Cochrane Collaboration, 2011. Avail-able from: http://www.cochrane-handbook.org. AccessedFebruary 12, 2013.
10. McPheeters ML, Kripalani S, Peterson NB. Quality improve-ment interventions to address health disparities. Closing thequality gap: Revisiting the state of the science. Evidence
Report No. 208. AHRQ Publication No. 12-E009-EF. Rock-ville, MD: Agency for Healthcare Research and Quality,2012. Available from: http://www.effectivehealthcare.ahrq.gov/reports/final.cfm. Accessed December 13, 2012.
11. Kowalchuk DA, Harner CD, Fu FH, Irrgang JJ. Predictionof patient-reported outcome after single-bundle anteriorcruciate ligament reconstruction. Arthroscopy 2009;25:457-463.
12. Osti L, Papalia R, Del Buono A, Leonardi F, Denaro V,Maffulli N. Surgery for ACL deficiency in patients over 50.Knee Surg Sports Traumatol Arthrosc 2011;19:412-417.
13. Heijne A, Ang BO, Werner S. Predictive factors for 12-month outcome after anterior cruciate ligament recon-struction. Scand J Med Sci Sports 2009;19:842-849.
14. Melikoglu MA, Balci N, Samanci N, et al. Timing ofsurgery and isokinetic muscle performance in patientswith anterior cruciate ligament injury. J Back MusculoskeletRehabil 2008;21:23-28.
15. Salmon LJ, Refshauge KM, Russell VJ, Roe JP, Linklater J,Pinczewski LA. Gender differences in outcome afteranterior cruciate ligament reconstruction with hamstringtendon autograft. Am J Sports Med 2006;34:621-629.
16. Ahldén M, Sernert N, Karlsson J, Kartus J. Outcome ofanterior cruciate ligament reconstruction with emphasison sex-related differences. Scand J Med Sci Sports 2012;22:618-626.
17. Dunn WR, Spindler KP, MOON Consortium. Predictors ofactivity level 2 years after anterior cruciate ligamentreconstruction (ACLR): A Multicenter OrthopaedicOutcomes Network (MOON) ACLR cohort study. Am JSports Med 2010;38:2040-2050.
18. Spindler KP, Huston LJ, Wright RW, et al. The prognosisand predictors of sports function and activity atminimum6years after anterior cruciate ligament reconstruction: Apopulation cohort study.Am J Sports Med 2011;39:348-359.
19. Barber-Westin SD, Noyes FR, Andrews M. A rigorouscomparison between the sexes of results and complica-tions after anterior cruciate ligament reconstruction. Am JSports Med 1997;25:514-525.
20. Brandsson S, Kartus J, Larsson J, Eriksson BI, Karlsson J.A comparison of results in middle-aged and youngpatients after anterior cruciate ligament reconstruction.Arthroscopy 2000;16:178-182.
21. Karim A, Pandit H, Murray J, Wandless F, Thomas NP.Smoking and reconstruction of the anterior cruciateligament. J Bone Joint Surg Br 2006;88:1027-1031.
22. Ahlén M, Lidén M. A comparison of the clinical outcomeafter anterior cruciate ligament reconstruction usinga hamstring tendon autograft with special emphasis onthe timing of the reconstruction. Knee Surg Sports Trau-matol Arthrosc 2011;19:488-494.
23. Karlsson J, Kartus J, Magnusson L, Larsson J, Brandsson S,Eriksson BI. Subacute versus delayed reconstruction of theanterior cruciate ligament in the competitive athlete. KneeSurg Sports Traumatol Arthrosc 1999;7:146-151.
24. Raviraj A, Anand A, Kodikal G, Chandrashekar M, Pai S.A comparison of early and delayed arthroscopically-assistedreconstruction of the anterior cruciate ligament usinghamstring autograft. J Bone Joint Surg Br 2010;92:521-526.
25. SterettWI, Hutton KS, Briggs KK, Steadman JR. Decreasedrange of motion following acute versus chronic anterior

PROGNOSTIC FACTORS OF SUCCESSFUL REHABILITATION 1895
cruciate ligament reconstruction. Orthopedics 2003;26:151-154.
26. Eitzen I, Holm I, Risberg MA. Preoperative quadricepsstrength is a significant predictor of knee function twoyears after anterior cruciate ligament reconstruction. Br JSports Med 2009;43:371-376.
27. Hamada M, Shino K, Horibe S, Mitsuoka T, Miyama T,Toritsuka Y. Preoperative anterior knee laxity did not in-fluence postoperative stability restored by anterior cruciateligament reconstruction. Arthroscopy 2000;16:477-482.
28. Kim SJ, Choi DH, Mei Y, Hwang BY. Does physiologicposterolateral laxity influence clinical outcomes of ante-rior cruciate ligament reconstruction? J Bone Joint Surg Am2011;93:2010-2014.
29. Shelbourne KD, Foulk DA. Timing of surgery in acuteanterior cruciate ligament tears on the return of quadricepsmuscle strength after reconstruction using an autogenouspatellar tendon graft. Am J Sports Med 1995;23:686-689.
30. Howell SM, Deutsch ML. Comparison of endoscopic andtwo-incision techniques for reconstructing a torn anteriorcruciate ligament using hamstring tendons. Arthroscopy1999;15:594-606.
31. Kongtharvonskul J, Attia J, Thamakaison S,Kijkunasathian C, Woratanarat P, Thakkinstian A. Clinicaloutcomes of double- vs single-bundle anterior cruciateligament reconstruction: A systematic review of random-ized control trials. Scand J Med Sci Sports 2013;23:1-14.
32. Tiamklang T, Sumanont S, Foocharoen T, Laopaiboon M.Double-bundle versus single-bundle reconstruction foranterior cruciate ligament rupture in adults. CochraneDatabase Syst Rev 2012;11:CD008413.
33. Mohtadi NGH, Chan DS, Dainty KN, Whelan DB. Patellartendon versus hamstring tendon autograft for anteriorcruciate ligament rupture in adults. Cochrane Database SystRev 2011;(9):CD005960.
34. Deeks JJ, Dinnes J, D’Amico R, et al. Evaluating non-randomised intervention studies. Health Technol Assess2003;7: iii-x, 1-173.
35. Harner CD, Irrgang JJ, Paul J, Dearwater S, Fu FH. Loss ofmotion after anterior cruciate ligament reconstruction.Am J Sports Med 1992;20:499-506.
36. Jerre R, Ejerhed L, Wallmon A, Kartus J, Brandsson S,Karlsson J. Functional outcome of anterior cruciate liga-ment reconstruction in recreational and competitiveathletes. Scand J Med Sci Sports 2001;11:340-342.
37. Kim SJ, Moon HK, Kim SG, Chun YM, Oh KS. Doesseverity or specific joint laxity influence clinical outcomesof anterior cruciate ligament reconstruction? Clin OrthopRelat Res 2010;468:1136-1141.
38. Laxdal G, Kartus J, Ejerhed L, et al. Outcome and riskfactors after anterior cruciate ligament reconstruction:a follow-up study of 948 patients. Arthroscopy 2005;21:958-964.
39. Sakai H, Hisatada H, Yashiki M. Gravity-assisted pivot-shift test can predict the function of the reconstructedanterior ligament. Knee Surg Sports Traumatol Arthrosc2011;19:572-578.
40. Sgaglione NA, Del Pizzo W, Fox JM, Friedman MJ.Arthroscopically assisted anterior cruciate ligamentreconstruction with the pes anserine tendons. Am J SportsMed 1993;21:249-256.
41. Tambe AD, Godsiff S, Mulay S, Joshi M. Anterior cruciateligament insufficiency: does delay in index surgery affectoutcome in recreational athletes. Int Orthop 2006;30:104-109.
42. Wiger P, Brandsson S, Kartus J, Eriksson BI, Karlsson J. Acomparison of results after arthroscopic anterior cruciateligament reconstruction in female and male competitiveathletes. Scand J Med Sci Sports 1999;9:290-295.
43. Ferrari JD, Bach BR, Bush-Joseph CA, Wang T,Bojchuk J. Anterior cruciate ligament reconstruction inmen and women: an outcome analysis comparing gender.Arthroscopy 2001;17:588-596.
44. Marcacci M, Zaffagnini S, Iacono F, Neri MP, Petitto A.Early versus late reconstruction for anterior cruciateligament rupture. Am J Sports Med 1995;23:690-693.
45. McHugh MP, Tyler TF, Browne MG, Gleim GW,Nicholas SJ. Electromyography predictors of residualquadriceps muscle weakness after anterior cruciate liga-ment reconstruction. Am J Sports Med 2002;30:334-339.
46. Ott SM, Ireland ML, Ballantyne BT, Willson JD, McClayDavis IS. Comparison of outcome between males andfemales after anterior cruciate ligament reconstruction.Knee Surg Sports Traumatol Arthrosc 2003;11:75-80.
47. Wu WH, Hackett T, Richmond JC. Effects of meniscal andarticular surface status on knee stability, function, andsymptoms after anterior cruciate ligament reconstruction.Am J Sports Med 2002;30:845-850.
48. Asano H, Muneta T, Shinomiya K. Evaluation of clinicalfactors affecting knee pain after anterior cruciate ligamentreconstruction. J Knee Surg 2002;15:23-28.
49. de Jong SN, van Caspel DR, van Haeff MJ, Saris DBF.Functional assessment and muscle strength before andafter reconstruction of chronic anterior cruciate ligamentlesions. Arthroscopy 2007;23:21-28.
50. Mauro CS, Irrgang JJ, Williams BA, Harner CD. Loss ofextension following anterior cruciate ligament recon-struction: analysis of incidence and etiology using IKDCcriteria. Arthroscopy 2008;24:146-153.
51. Yüksel HY, Erkan S, Uzun M. Factors affecting isokineticmuscle strength before and after anterior cruciate liga-ment reconstruction. Acta Orthop Belg 2011;77:339-348.
52. McHugh MP, Tyler TF, Gleim GW, Nicholas SJ. Preoper-ative indicators of motion loss and weakness followinganterior cruciate ligament reconstruction. J Orthop SportsPhys Ther 1998;27:407-411.
Copyright © 2022 FDOKUMEN




















