WMT-pre-course-reading-bundle-2020.pdf - Wilderness ...
128
WMT Pre-course Reading Bundle (revised January 2020) Pre-course reading is not required but these papers will prime medics attending WMT course. Laypeople (on Explorer courses) may also find this information useful and accessible. This reading may count towards CPD and be a useful future point of reference. Introduction Faculty of Prehospital Care, Royal College of Surgeons Edinburgh guidance for medical provision for wilderness medicine Mountain Medicine Wilderness Medical Society Practice Guidelines for the Prevention and Treatment of Acute Altitude Illness: 2019 Update The 2018 Lake Louise Acute Mountain Sickness Score Wilderness Medical Society Practice Guidelines for the Prevention and Treatment of Frostbite: 2019 update Retrospective study of 70 cases of severe frostbite lesions: a proposed new classification scheme. Wild Envir Med 12: 248-255 Wilderness Medical Society Clinical Practice Guidelines for the Out-of-Hospital Evaluation and Treatment of Accidental Hypothermia: 2019 Update Heat Illness Wilderness Medical Society Practice Guidelines for the Prevention and Treatment of Heat Illness: 2019 Update Drowning Wilderness Medical Society Clinical Practice Guidelines for the Treatment and Prevention of Drowning: 2019 Update Water Purification Wilderness Medical Society Clinical Practice Guidelines for Water Disinfection for Wilderness, International Travel, and Austere Situations
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of WMT-pre-course-reading-bundle-2020.pdf - Wilderness ...

WMT Pre-course Reading Bundle (revised January 2020)
Pre-course reading is not required but these papers will prime medics attending WMT course. Laypeople (on Explorer courses) may also find this information useful and accessible. This reading may count towards CPD and be a useful future point of reference. Introduction Faculty of Prehospital Care, Royal College of Surgeons Edinburgh guidance for medical provision for wilderness medicine Mountain Medicine Wilderness Medical Society Practice Guidelines for the Prevention and Treatment of Acute Altitude Illness: 2019 Update The 2018 Lake Louise Acute Mountain Sickness Score Wilderness Medical Society Practice Guidelines for the Prevention and Treatment of Frostbite: 2019 update Retrospective study of 70 cases of severe frostbite lesions: a proposed new classification scheme. Wild Envir Med 12: 248-255 Wilderness Medical Society Clinical Practice Guidelines for the Out-of-Hospital Evaluation and Treatment of Accidental Hypothermia: 2019 Update Heat Illness Wilderness Medical Society Practice Guidelines for the Prevention and Treatment of Heat Illness: 2019 Update Drowning Wilderness Medical Society Clinical Practice Guidelines for the Treatment and Prevention of Drowning: 2019 Update Water Purification Wilderness Medical Society Clinical Practice Guidelines for Water Disinfection for Wilderness, International Travel, and Austere Situations

Mellor et al. Extrem Physiol Med (2015) 4:22 DOI 10.1186/s13728-015-0041-x
COMMENTARY
Faculty of Prehospital Care, Royal College of Surgeons Edinburgh guidance for medical provision for wilderness medicineAdrian Mellor1,2,3*, Naomi Dodds4, Raj Joshi5,6, John Hall7,8, Sundeep Dhillon9,10, Sarah Hollis11,12, Pete Davis13,14, David Hillebrandt15,16, Eva Howard17, Matthew Wilkes18,19, Burjor Langdana20,21, David Lee22, Nigel Hinson22, Thomas Harcourt Williams22, Joe Rowles22 and Harvey Pynn13,23,24,25
Abstract
To support leaders and those involved in providing medical care on expeditions in wilderness environments, the Faculty of Pre-Hospital Care (FPHC) of The Royal College of Surgeons of Edinburgh convened an expert panel of lead-ing healthcare professionals and expedition providers. The aims of this panel were to: (1) provide guidance to ensure the best possible medical care for patients within the geographical, logistical and human factor constraints of an expedition environment. (2) Give aspiring and established expedition medics a ‘benchmark’ of skills they should meet. (3) Facilitate expedition organisers in selecting the most appropriate medical cover and provider for their planned activity. A system of medical planning is suggested to enable expedition leaders to identify the potential medical risks and their mitigation. It was recognised that the scope of practice for wilderness medicine covers elements of primary healthcare, pre-hospital emergency medicine and preventative medicine. Some unique competencies were also identified. Further to this, the panel recommends the use of a matrix and advisory expedition medic competencies relating to the remoteness and medical threat of the expedition. This advice is aimed at all levels of expedition medic, leader and organiser who may be responsible for delivering or managing the delivery of remote medical care for par-ticipants. The expedition medic should be someone equipped with the appropriate medical competencies, scope of practice and capabilities in the expedition environment and need not necessarily be a qualified doctor. In addition to providing guidance regarding the clinical competencies required of the expedition medic, the document provides generic guidance and signposting to the more pertinent aspects of the role of expedition medic.
Keywords: Expedition, Risk assessment, Medical planning, Wilderness medicine, Austere environment
© 2015 Mellor et al. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
BackgroundThe Oxford English dictionary defines an expedition as “a journey undertaken by a group of people with a particu-lar purpose”. This definition highlights the broad scope of expeditions and de facto, expedition medical plan-ning. Medical care provided in an austere environment is often referred to as “wilderness medicine”. This was described by Backer and was defined by its remoteness, physiology, need for improvisation and dependence upon
clinical examination and judgement [1]. The scope of this guidance is intended to cover the planning and compe-tencies that facilitate the understanding of the challenges described by Backer and therefore the delivery of good quality clinical care.
The practice of wilderness medicine occurs in many environments and this document is not intended to pro-vide specific advice to specialist expeditions (e.g. deep cave exploration or pioneering extreme new routes in the mountains). The concept of competencies in pre-hospital care has previously been described [2] and competent individuals are those deemed to have the “ability to apply knowledge, understanding and skills” to perform to an accepted standard. The competencies discussed consider
Open Access
*Correspondence: [email protected] 2 Cardiothoracic Anaesthesia, James Cook University Hospital, Middlesbrough TS4 3BW, UKFull list of author information is available at the end of the article

Page 2 of 10Mellor et al. Extrem Physiol Med (2015) 4:22
pre-hospital and primary care skills relevant to medical providers on expeditions in remote areas with some con-sideration of more specialist environments.
Death and serious injury or illness on expeditions is thankfully rare. Aside from extreme sports in the wilder-ness, the risks faced by participants on a well-planned expedition are equivalent to those faced by an active person living in the UK. For example, road traffic acci-dents cause approximately 50 % of unexpected deaths on expeditions per annum [3]. Anderson and Johnson [4] reviewed the data from 246 expeditions with 1263 medical problems (gastrointestinal disease 30 %, medi-cal problems 21 %, orthopaedic problems 19 %, environ-mental problems 14 %) and a 10 % evacuation rate. More recent published data reviewed charity expeditions over a 5-year period provided by one company. Overall 1564 incidents were reported during 42,482 expedition days. 94 % of the incidents reported were minor and 1 % severe giving a risk of a severe injury or condition of 0.47 per 1000 participant days [5]. Even on potentially high threat expeditions to Denali in Alaska, medical incidents were rare with only 3.5 % of 24,079 climbers request-ing medical assistance and only 15 % of these requiring evacuation by the National Park Service [6]. It is worth bearing such figures in mind when planning an expedi-tion, and considering the relatively low prevalence of problems, whilst being mindful of the potentially higher impact should they occur. In addition to medical pro-vision the expedition medic will be responsible for the dental health of participants as well as environmental health. Dental problems, in particular, present a poten-tial burden to the expedition with one expedition report-ing 50/309 (16.5 %) of expedition members suffering dental symptoms potentially treatable with a simple den-tal first aid kit [7].
This document not only provides guidance on the clini-cal competencies required of the expedition medic but also on other pertinent aspects of the role such as medi-cal planning, risk management, human factors, clinical governance and medical kits.
MethodsAn initial meeting was convened by the FPHC. Members were invited based on their contribution to wilderness medicine in terms of research, teaching, military expe-rience or were selected as representatives of UK-based expedition providers. It was identified that the compe-tencies required for wilderness medicine were wide rang-ing and evidence for what skills and interventions are required was lacking. For this reason, the panel elected to use the existing FPHC competency framework and adapted it (based on expert opinion) for wilderness medi-cine use. Members of the panel were then selected to
undertake literature reviews and to author specific parts of this consensus document.
The key drivers to any medical plan are:
1. The degree of remoteness of the potential incident.2. The medical threat—the likelihood of a medical inci-
dent occurring.
Remoteness was considered as the time taken to access advanced medical care defined in varying ways depend-ing on the injury or illness. For the purposes of this document, it is a facility where a doctor, basic diagnos-tics, pharmacy, etc., are available and the injury or illness can be managed in a timely and definitive manner. It is accepted that this definition is flexible, as definitive care could potentially be delivered within a well-equipped and appropriately staffed expedition setup and is dependent on the presenting condition.
For the purposes of discussing the required medi-cal competencies, three measures of remoteness from advanced medical care were considered:
1. Time 1: less than 4 h away.2. Time 2: 4–12 h away.3. Time 3: more than 12 h away.
These timelines were considered alongside the levels of medical threat that take into account the demographics of the group, the location and the planned activity.
1. Low—such as young, fit group trekking in foothills of Atlas Mountains, Morocco.
2. Medium—such as vehicle borne overland expedi-tion across Eastern Africa with diverse middle aged group.
3. High—such as a ski mountaineering in remote area of Greenland or a medically unscreened group doing charity trek up Mt Kilimanjaro.
Using this model, two main assumptions were made, firsty that time is based on typical estimated travelling time, e.g. summer rather than winter and not worse case. However, planning should take into account a range of travel time most likely to be encountered. Secondly, specific competen-cies will be dictated by environment (cold, high, hot or any unusual endemic diseases identified by the medical plan).
Priorities for care and evacuation, and therefore com-petencies for each, could then be agreed upon and are summarised as;
• Less than 4 h: emergency field care. • 4–12 h: commence definitive treatment in the field. • 12 h plus: prolonged field care.
Page 3 of 10Mellor et al. Extrem Physiol Med (2015) 4:22
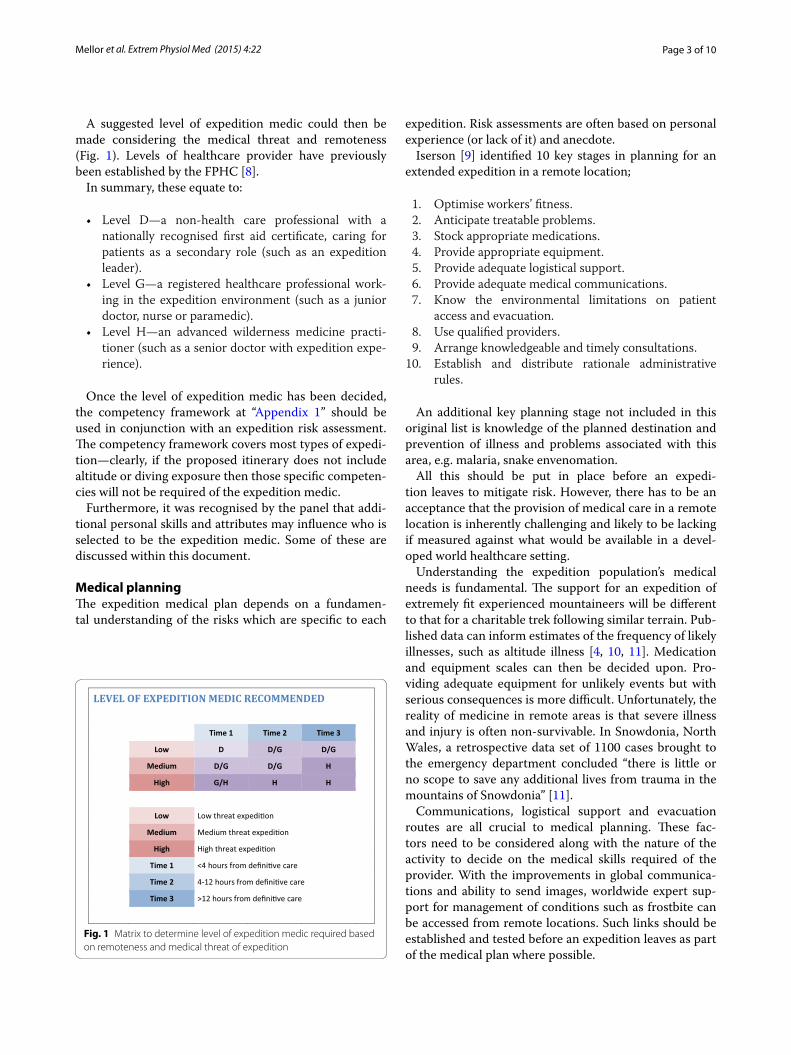
A suggested level of expedition medic could then be made considering the medical threat and remoteness (Fig. 1). Levels of healthcare provider have previously been established by the FPHC [8].
In summary, these equate to:
• Level D—a non-health care professional with a nationally recognised first aid certificate, caring for patients as a secondary role (such as an expedition leader).
• Level G—a registered healthcare professional work-ing in the expedition environment (such as a junior doctor, nurse or paramedic).
• Level H—an advanced wilderness medicine practi-tioner (such as a senior doctor with expedition expe-rience).
Once the level of expedition medic has been decided, the competency framework at “Appendix 1” should be used in conjunction with an expedition risk assessment. The competency framework covers most types of expedi-tion—clearly, if the proposed itinerary does not include altitude or diving exposure then those specific competen-cies will not be required of the expedition medic.
Furthermore, it was recognised by the panel that addi-tional personal skills and attributes may influence who is selected to be the expedition medic. Some of these are discussed within this document.
Medical planningThe expedition medical plan depends on a fundamen-tal understanding of the risks which are specific to each
expedition. Risk assessments are often based on personal experience (or lack of it) and anecdote.
Iserson [9] identified 10 key stages in planning for an extended expedition in a remote location;
1. Optimise workers’ fitness. 2. Anticipate treatable problems. 3. Stock appropriate medications. 4. Provide appropriate equipment. 5. Provide adequate logistical support. 6. Provide adequate medical communications. 7. Know the environmental limitations on patient
access and evacuation. 8. Use qualified providers. 9. Arrange knowledgeable and timely consultations. 10. Establish and distribute rationale administrative
rules.
An additional key planning stage not included in this original list is knowledge of the planned destination and prevention of illness and problems associated with this area, e.g. malaria, snake envenomation.
All this should be put in place before an expedi-tion leaves to mitigate risk. However, there has to be an acceptance that the provision of medical care in a remote location is inherently challenging and likely to be lacking if measured against what would be available in a devel-oped world healthcare setting.
Understanding the expedition population’s medical needs is fundamental. The support for an expedition of extremely fit experienced mountaineers will be different to that for a charitable trek following similar terrain. Pub-lished data can inform estimates of the frequency of likely illnesses, such as altitude illness [4, 10, 11]. Medication and equipment scales can then be decided upon. Pro-viding adequate equipment for unlikely events but with serious consequences is more difficult. Unfortunately, the reality of medicine in remote areas is that severe illness and injury is often non-survivable. In Snowdonia, North Wales, a retrospective data set of 1100 cases brought to the emergency department concluded “there is little or no scope to save any additional lives from trauma in the mountains of Snowdonia” [11].
Communications, logistical support and evacuation routes are all crucial to medical planning. These fac-tors need to be considered along with the nature of the activity to decide on the medical skills required of the provider. With the improvements in global communica-tions and ability to send images, worldwide expert sup-port for management of conditions such as frostbite can be accessed from remote locations. Such links should be established and tested before an expedition leaves as part of the medical plan where possible.
LEVEL OF EXPEDITION MEDIC RECOMMENDED
Time 1 Time 2 Time 3
Low D D/G D/G
Medium D/G D/G H
High G/H H H
Low Low threat expedi�on
Medium Medium threat expedi�on
High High threat expedi�on
Time 1 <4 hours from defini�ve care
Time 2 4-12 hours from defini�ve care
Time 3 >12 hours from defini�ve care
Fig. 1 Matrix to determine level of expedition medic required based on remoteness and medical threat of expedition

Page 4 of 10Mellor et al. Extrem Physiol Med (2015) 4:22
Consideration should be given to medical plans in the absence of the lead expedition medic, i.e. small groups operating from one base location or climbers split across different camps. Diagnostic algorithms for likely con-ditions such as heat illness or altitude sickness can be placed with medical kits as well as protocols for admin-istration of emergency medication. The lead expedition medic will often be able to communicate emergency medical advice over radio or satellite phone to remote teams, however, algorithms should be robust enough for independent use in emergent situations. The role of expe-dition medic will include briefing these teams in usage of emergency medical treatments. There is no suggested guidance on the ratio of medics to participants required on an expedition but should be considered on a case-by-case basis in the planning phase.
Medical planning relies on the ability to assess the like-lihood of adverse medical events. This is dependent on published data to detect the underlying rate of injury such as discussed above. It is therefore important that, wherever practicable, the incidence of medical problems during expeditions are well recorded and accessible. This is now facilitated by a range of open access journals or online resources.
The purpose of this guideline is to inform best practice and inform expedition planning. It does not seek to pro-vide a mandated framework beyond which none should go. It is accepted that the degree to which the guidelines are implemented may legitimately vary with the nature of the expedition.
Clinical governance in wilderness medicineClinical governance is the framework used to maintain and improve standards of medical care, in which ‘organi-sations are accountable for continuously improving the quality of their services and safeguarding high standards of care…’ [12].
There are several domains to clinical governance that all have a part to play in an expedition setting:
• Risk management. • Continuing professional development. • Evidence based and effective clinical care. • Audit. • Patient satisfaction.
These features remain applicable during the pre-expedition, expedition, and post-expedition phases and should not be viewed as optional simply because a prac-titioner is working outside the health system of the UK. Participants in an expedition should have care provided by someone working within an appropriate scope of practice.
Responsibility for clinical governance rests with both the expedition medic and the expedition organisers. For instance, the organisation must ensure that it carefully selects the expedition medic, that it provides them with timely and accurate information about the participants and the nature of the expedition and that it encourages a culture of openness through the sharing of [medical] risk assessments and post-expedition [medical] reports. The expedition medic is responsible for maintaining their own personal and medical competencies, for precise and robust documentation and for the safe usage and main-tenance of medical kit and equipment. Both are respon-sible for reporting identified problems of any nature and recording these in such a way that incidents can be learned from and mitigated against in the future. Clinical audit should be encouraged.
It is good practice to have a contract between the expe-dition medic and organisation. An example of such is the UIAA’s Model Contract for Health Care on Trekking and Expeditions [13].
Other factors that the expedition medic and expedition organisers should agree on are listed:
• Provision of medical kit and supply/resupply. • Work place and distant supervision of expedition
medics. • Responsibility for arranging the provision of special-
ist medical advice. • Security and ownership of confidential medical infor-
mation. • Responsibility for development and use of Medical
Standard Operating Procedures. • Standardised medical record keeping.
The liability for providing adequate medical care for all expedition members ultimately lies with the expedition organisers. In addition, all Level G and H practitioners should discuss any proposed expedition with their pro-fessional indemnifiers.
Risk managementPre-emptive risk management is essential for manag-ing safety while on expeditions. An understanding of the terms used in risk management is needed to manage risk appropriately.
A threat is something that can cause harm. This may be harm to an individual, to property or to the expedition itself. For example malaria may constitute a threat to an individual, theft is a risk to property and a hurricane may represent a threat to all three. The result of the threat is the consequence of that occurrence.
Likelihood: This is the chance of a threat occurring. For example, acute mountain sickness (AMS) is a threat to

Page 5 of 10Mellor et al. Extrem Physiol Med (2015) 4:22
which climbers in Scotland will not be exposed. However, for the Himalayan mountaineer, AMS is a threat to which he or she is vulnerable.
The likelihood multiplied by the consequences gives an index of the threat [14]. The assessment of the threat must take place within the context of the expedition. With this context comes the important concept of resid-ual risk. Residual risk describes the risks that remain despite mitigation attempts. For example, while driving a car, a driver may mitigate the risks of crashing by ensur-ing the car is roadworthy, not driving at night and not exceeding the speed limit. However, the threat of error by another driver causing an accident is difficult to mitigate. This is known as a residual risk.
Once a threat has been assessed and is deemed to be above the threshold of risk for an expedition steps may be taken to reduce the impact of the threat. There are three main ways to mitigate risk:
1. Remove or diminish the threat.2. Reduce the exposure to the threat.3. Take measures to reduce the impact of the threat.
For example, an expedition to the Honduran jungle may consider the threat of envenomation by snake-bite. The threat may be diminished by ensuring eve-ryone on the expedition wears boots. The exposure to the threat can be reduced by running a teaching ses-sion about the snake habitat and how to avoid coming into contact with snakes. The impact could be reduced by ensuring timely evacuation is available to a facility where appropriate care is available. These measures may change an unacceptable risk into a risk accepted by the expedition.
Risk assessment should be carried out at three levels; generic risk assessment for the activity, a daily risk assess-ment documented for the activity and local conditions and then dynamic risk assessment during the course of the activity.
Incidents that cause harm should be documented, as should ‘near misses’. This will aid future expeditions in building an evidence base of hazards and mitigation strategies. Expedition providers have a legal responsibil-ity for the safety of both paying clients (under Package Travel Regulations 1992) and staff, including any locally employed staff (Employer’s Liability). Thorough risk assessment is key to providing both physical and legal protection for both staff and clients.
Medical threats and mitigationExpeditions to remote areas are, by their very nature, complex and normal medical risk assumptions and miti-gation may not apply.
The experiential evidence backed up by limited pub-lished evidence suggest serious incidents on expeditions are unusual [3–6]. Most medical conditions or injuries seen during expeditions can be managed by a competent expedition medic with basic skills. However, incidents in the wilderness environment are compounded by a num-ber of factors;
• The incident occurs in a different location to the expedition medic.
• The casualty may be travelling alone (e.g. between camps in a jungle or on a mountain).
• The casualty may not have the means, capacity or capability to identify their location.
• The casualty may not have the means, capacity or capability to communicate and request help.
• Bad weather/night/visibility/poor communications may hinder the realisation that someone is missing, that a medical incident has occurred and therefore delay any response.
Good medical screening can reduce, but not elimi-nate, the medical risks to an expedition and should be an essential part of any medical planning. Consideration should be given to who has access to this medically con-fidential information and whether a certificate and dis-closure from the participants’ medical practitioner may be required. In addition to screening, education as to the likely hazards is a key part of reducing the medical risks on an expedition. It should be borne in mind that partici-pants often fail to disclose key medical information and this only comes to light once the expedition starts. Par-ticipants should be medically risk assessed again if new information becomes available.
On many expeditions it may be impossible, impractical or unreasonable (as it would fundamentally change the character of the expedition) to provide the highest level of medical care and participants should be sufficiently well informed to accept this risk. Suitable planning and development of guidelines and protocols for manage-ment of likely hazards is an important part of medical planning and may remove the need for a medical profes-sional on an expedition.
Human factorsHuman factors refer to the non-clinical aspects of wilder-ness medicine. It is important to recognise that the role of the expedition medic goes beyond the simple provi-sion of medical care. They often form part of the leader-ship team, with all the associated responsibilities that this entails.
In the best case, the expedition medic is an independ-ent experienced professional who puts the health and

Page 6 of 10Mellor et al. Extrem Physiol Med (2015) 4:22
safety of the participants above the objectives of the expe-dition. For every trip, the expectations and requirements of the expedition medic, from the participants, expedi-tion leaders and the organisers will be subtly different. On occasions, they may even be a source of conflict.
Therefore, the expedition medic does not merely require appropriate clinical skills to deliver care in a wilderness setting but should have the personal skills to work within a team and the technical skills to be able to live comfortably in that environment. A deficiency in any part of the clinical–personal–technical triad will render the expedition medic less effective.
Personal skillsPersonal/interpersonal skills do not always come natu-rally yet are a vital part of being a functioning, respected team member. The manner in which one employs these ‘soft’ skills will vary depending on the expedition. For example, interaction with a group of ultra-marathon athletes will differ considerably from an inexperienced charity clientele group. The following areas should be considered:
• Communication skills and self-awareness. • Teamwork. • Leadership. • Decision making. • Coping with fatigue and stress.
The ability to communicate and interact successfully with a team whilst living alongside them is incredibly important, particularly when fostering therapeutic rela-tionships. The expedition medic must be aware of subtle differences in ‘sense of humour’, the need for compassion even with the trivial and regularly reflect on the need to adapt. Instructions or advice should be clear and unam-biguous for those to whom they are directed. The expe-dition medic will often spend the majority of their time as an equal team colleague and friend. It is important to ensure boundaries are well defined and it is clear to par-ticipants when there is a swap to the “medic role”.
Leadership styles vary greatly. The expedition medic should be capable of adapting their leadership skills to the needs and requirements of the group. Clear demar-cation of roles, responsibilities and decision-making frameworks should be clarified before departure thus minimising the potential for conflict during times of increased stress. Both expedition leader and medic require clarity of jurisdiction, not only during a medical incident/s, but also in a situation where failure to inter-vene pre-emptively may result in harm.
Decision making on expedition carries with it far more responsibility than purely arriving at a treatable
diagnosis. The decisions made will have consequences varying from temporary cessation of activities to perma-nent casualty evacuation, with all the associated logisti-cal, financial and emotional implications.
The demands placed on the expedition medic have the potential to exceed any other expedition participant. Expedition medics should be prepared to carry out a full day’s expedition activities and then face the possibility of providing the full range of expedition healthcare, irre-spective of the time of day or night, including a complex casualty evacuation. Mental resilience and physical fit-ness are important, as stressors on expedition are many and varied. They include clinical pressures associated with independent/autonomous decision making, stress-ors of living in a close-knit community or the difficulties of just living and surviving in uncomfortable surround-ings with reduced communication with home.
Expedition skillsThe expedition medic will need a range of skills specific to the expedition objectives. These skills are beyond the scope of this document.
Real-life examples of the impact of personal or expedi-tion skill deficiencies can be found at “Appendix 2”.
Medical kitDesigning and gathering a fit-for-purpose medical kit is frequently overlooked by expedition planners but it is a multifaceted and time-consuming job. It must be clear whose responsibility it will be to provide and pay for medical kit and it must be checked regularly for accept-able quality, including for damage, stock level and out-of-date contents. Meticulous labelling, organisation of the kit and a contents spreadsheet are of paramount importance.
The expedition medic must have knowledge of the indi-cations and side effects of each medication carried, this will depend on the level of medical provider, but any pro-vider must be competent dispensing or administering those medications and be familiar with the identification and timely treatment of any complications occurring. All expedition medics should have access to reference mate-rial in this regard. For example, the British National For-mulary (BNF) is available electronically as an App.
Medical kits should be bespoke to the expedition in question. Their composition will vary based on team composition, demographics and number of participants as well as destination and the duration of the trip. Kits should reflect the likely illness and injury patterns of the planned activities and to some extent, the level and skills of the expedition medic. Published surveys suggest that first responder medical kits tend to be well equipped to support trauma but less well equipped for medical

Page 7 of 10Mellor et al. Extrem Physiol Med (2015) 4:22
emergencies [15]. It should also be remembered that the majority of medical presentations on expeditions are not high-level trauma or medical emergencies and medi-cal kits should reflect this by including medications and equipment for treating simple illness and injuries.
Comprehensive advice on provision of medical kits is beyond the scope of this publication. Broad areas for consideration are listed below.
1. A medical kit should be dictated by the medical plan and wilderness environment.
2. Medications (unlike dressings) cannot be improvised and expeditions need to have adequate supplies of trustworthy medications.
3. Import and export restrictions for medications vary between countries.
4. Medications that have a variety of uses should be taken.
5. Practitioners should be aware of expedition members with drug allergies or on regular medications and be aware of any interactions these may have.
6. Group medical kits should be appropriately and securely stored.
7. Ensure adequate means of diluting and administering drugs are available.
8. Individuals should have a personal first aid kit on their person at all times.
9. If travelling in areas with high incidence of HIV or hepatitis consider carrying sterile needles, etc.
These points are expanded in “Appendix 3”.
Cardiopulmonary resuscitation in the wilderness environmentThe decision whether to attempt resuscitation or not in the event of cardio-respiratory arrest in the wilderness is a complex one and requires a pragmatic and realistic decision-making process. Resuscitation efforts and extri-cation may take place in hazardous terrain and in extreme meteorological conditions. Additionally, resources may be very limited, and there may be multiple casualties amongst who these resources must be shared. Multiple casualty emergencies may fit the definition criteria for a major incident and appropriate Major Incident Medical Management systems may need to be applied in a wilder-ness setting to effectively utilise available resources.
In 2012, Paal et al. [16] published a position paper to establish scientifically supported guidelines under which cardiopulmonary resuscitation (CPR) could be termi-nated during mountain rescue. This guidance was sub-sequently adopted as a formal recommendation by the
International Commission for Alpine Rescue (ICAR/CISA) and it is applicable both to medical and non-med-ical personnel.
As the same principles apply both to organised res-cue in the mountains and to wilderness expeditions in terms of decision-making algorithms. The aim of these guidelines is to reduce unnecessary CPR, diminish risk to expedition members or rescuers, apportion limited human and material resources effectively and to iden-tify special circumstances where extended CPR may be indicated.
These circumstances permit the termination of CPR in a patient with unwitnessed loss of vital signs in the wilderness:
1. No return of spontaneous circulation during 20 min of CPR.
AND
2. No special circumstance (see below) warranting extended CPR.
AND
3. When professional medical support is available, either that no shock is advised by an Automated External Defibrillator (AED) at any time, or that only asystole is observed by electrocardiogram (ECG) monitoring.
Special circumstances are hypothermia, lightning strike and submersion (drowning). With these, prolonged CPR may be associated with a good neurological outcome and functional recovery.
ConclusionThe role of an expedition medic can fall to either medi-cally qualified professionals or to others providing medi-cal care in addition to their primary duty. It is important to recognise that the role of expedition medic is multi-faceted and requires an extensive skill set in addition to suitable underpinning medical knowledge and skills. Expedition medical planning should enable all these aspects to be considered so that appropriate personnel are selected and medical threats recognised and miti-gated against.
Additional file
Additional file 1. Expedition medic competencies.

Page 8 of 10Mellor et al. Extrem Physiol Med (2015) 4:22
AbbreviationsAED: automated external defibrillator; AMS: acute mountain sickness; BNF: British National Formulary; CPR: cardiopulmonary resuscitation; ECG: electro-cardiogram; FPHC: Faculty of prehospital care of the Royal College of Surgeons of Edinburgh; ICAR: International Commission for Alpine Rescue; UIAA: International Climbing and Mountaineering Federation (Union International des Associations d’Alpinisme).
Authors’ contributionsAll authors contributed to the FPHC working group in expedition medical capability and contributed to the manuscript. JH chaired the working group, ND collated authors’ initial drafts, AM and HP drafted the final manuscript and AM, HP, JH, ND edited the final version of the manuscript. RJ, MW, TH-W, JR drafted the human factors, threats and medical planning sections, NH and DL drafted the personal skills section, BL contributed to the dental and medical kit sections, ND, JH, SD, DH, EH, SH, DL and NH drafted the competency matrix, PD drafted the section on CPR. All listed authors reviewed and revised the final version of the manuscript. All authors read and approved the final manuscript.
Author details1 Academic Department of Military Anaesthesia and Critical Care, RCDM, Birmingham, UK. 2 Cardiothoracic Anaesthesia, James Cook University Hos-pital, Middlesbrough TS4 3BW, UK. 3 Carnegie Institute for Sport and Human Performance, Leeds Beckett University, Leeds, UK. 4 Academic Critical Care Foundation Doctor, Aberdeen Royal Infirmary, Aberdeen, UK. 5 Centre for Health and Human Performance, London, UK. 6 Summerfield Urgent Care Centre, Birmingham, UK. 7 Department of Emergency Care, University of Birmingham, Birmingham, UK. 8 Faculty of Pre Hospital Care, Royal College of Surgeons of Edinburgh, Edinburgh, UK. 9 The Centre for Altitude Space and Extreme Environment Medicine (CASE Medicine), Institute for Sport, Exercise and Health (ISEH), London, UK. 10 Medical Cell, The Royal Geographi-cal Society, 1 Kensington Gore, London, UK. 11 Primary Care and Occupational Medicine, Ministry of Defence, London, UK. 12 Ultimate Travel Company, Lon-don, UK. 13 Department of Emergency Medicine, Defence Medical Services, Whittington, UK. 14 Department of Emergency Medicine, Queen Elizabeth University Hospital and Emergency Medical Retrieval Service, Glasgow, UK. 15 UIAA Medcom, Manchester, UK. 16 British Mountaineering Council, Manchester, UK. 17 Queen Elizabeth Hospital, Birmingham, UK. 18 Adventure Medic Ltd, Edinburgh, UK. 19 Royal Infirmary of Edinburgh, Edinburgh, UK. 20 Adventure Medic, Edinburgh, UK. 21 Expedition and Wilderness Medicine, Devon, UK. 22 Gloucestershire, UK. 23 Department of Emergency Medicine, University Hospitals Bristol, Bristol, UK. 24 Great Western Air Ambulance, Bristol, UK. 25 Wilderness Medical Training, Kendal, UK.
AcknowledgementsThe authors would like to acknowledge the very extensive contribution to the content of this manuscript from the following additional members of the FPHC working group; Mr. James Moore, Dr. Alex Rowe, Dr. Caroline O’Keeffe, Mr. Mark Hannaford, Mr. James Yates, Mr. Mark Brazier, Mr. Mark Turner, Dr. Sean Hudson, Dr. Paul Richards, Dr. J. Dallimore.
Competing interestsA number of the authors have affiliations to commercial medical training providers but none view this as a conflict of interest in contributing to these guidelines.
Appendix 1The FPHC competencies are available as an additional file please see Additional file 1.
Appendix 2This appendix includes examples of where the expedition medic without the appropriate personal or expedition skills could potentially put themselves and others at risk. These examples are based on the real-life experiences of those on the panel.
1. The expedition medic has never been to altitude and therefore has a lack of environmental experience. As a result is unable to cope with working at altitude and is less effective in providing medical care. Eventually falls prey to altitude illness and has to be evacuated to definitive medical care. The group is left without the originally intended medical care.
2. Expedition medic is required to independently arrive at a casualty in a remote environment. The expedi-tion medic is not competent in navigating and fails to arrive at the casualty. The expedition medic poten-tially becomes a lost person and requires additional resources to mount a search and rescue effort.
3. Expedition medic lacks situational awareness and as a result becomes targeted by assailants at a mar-ket place in a foreign country. They are attacked and robbed of possessions. The expedition medic is psy-chologically affected for the duration of the expedi-tion and is less effective in providing care with poten-tial long-term health implications.
4. Expedition medic does not have experience in camp craft and lacks necessary personal admin skills. The expedition medic is late each morning in properly organising own equipment. As a result is not ready when the rest of group is ready and either the expe-dition is delayed or the group is left without the intended medical care until later.
5. A commercial television production taking expedition naive individuals to a hostile environment and filming the outcome. Production aims are to stress individuals physically, socially and mentally whilst filming results. Production company staff have limited understanding of both risk and consequence of harm in the expedi-tion environment and as such encourage risky activi-ties. Intervention by the expedition medic to mitigate risk is frowned upon as this reduces ‘story potential’. These issues will be predicted by experienced expedi-tion medics and mitigated for.
6. Expedition medic is required to treat a casualty on more technical terrain. Expedition medic does not have sufficient technical skills such as appropriate rope work to move competently over technical ter-rain. They become stranded as a result and require rescuing.
7. A production company wish to film a sequence where a presenter is attempting to recover a vehicle trapped in soft sand. Expedition porters are placing rocks and sand ladders in front of spinning wheels whilst the presenter is positioned behind the vehicle at great risk of being hit by flying debris. An astute and experienced medic with identify a significant risk of injury to the presenter and intervene promptly.

Page 9 of 10Mellor et al. Extrem Physiol Med (2015) 4:22
The above examples can happen to anyone even with sound non-medical skills and experience in the wilder-ness environment. However, expedition medics that have the required operational capability reduce any risk.
Appendix 3This annex composes some of the lessons identified from the experience of the panel with regard to preparing an expedition medical kit.
1. Know your environment and adapt the team medi-cal kit accordingly. For example, for tropical envi-ronments where the risk of infection is high, take broad spectrum antibiotics, a malarial detection kit (with high sensitivity) and stand-by treatment. For high altitude environments, include medications fol-lowing the most recent guidance in the treatment of acute mountain sickness, high altitude pulmonary and cerebral oedema.
2. You cannot improvise medications. Dressings and splints can be improvised whereas medications can-not be. You cannot guarantee the quality of medica-tions bought in many countries so whilst they may be easily available, they may not be as efficacious.
3. Know the import and export restrictions for coun-tries. Know the Medicines Health and Regulatory Agency (MHRA) scheduling of different drugs and the restrictions that this imposes. Be aware of the restrictions imposed by other countries; for example, drugs such as codeine are robustly regulated in the Middle Eastern countries. The FCO website is a use-ful resource for more details of restrictions for indi-vidual countries.
4. Take medications with more than one use. For exam-ple, codeine has analgesic, antitussive and anti diar-rhoeal properties so is extremely versatile. Antibi-otics such as co-amoxiclav and azithromycin have broad spectrums of cover so can be used to treat a wide range of infection.
5. Beware of interactions between medicines in the medical kit. For example, ciprofloxacin and ibupro-fen in combination can reduce the seizure threshold so make epileptics more prone to seize. Be aware what regular medications are being taken by group members and compile the group medical kit accord-ingly.
6. Choose the most appropriate container for the medi-cal kit. Be aware that in a tropical environment, the medical kit will need to be stored in a damp proof, sealable container.
7. Ensure that all participants have their own personal medical kits containing basic medical supplies such as blister prevention and treatment, simple analgesia,
dressings and a plentiful supply of their own regular medication.
8. Be aware that certain medications used for intra-muscular injection have specific diluents. For exam-ple, ceftriaxone for intramuscular injection uses 1 % lignocaine for reconstitution and injection. This is particularly important for groups where the medic is not confident or unable to achieve intravenous can-nulation.
9. If travelling to regions of the world with a high inci-dence of HIV, consider taking a set of sterile needles and cannulae in the event that a participant requires local hospital admission.
10. Remember that other issues not normally associated with developed world medicine will fall to the expe-dition medic. For example, issues with contact lenses and hearing aids. Contact lenses can be problematic on expedition. The risk of keratitis is greater in con-tact lens wearers. Ensure all participants that plan to wear contact lenses take their glasses in addition. Ensure that anyone with a hearing aid takes spare batteries and that you and they know how to change them. If participants travel with specific pieces of equipment to manage their condition, consider ask-ing for a demonstration on usage before the trip, for example, an insulin pump. A plan for dealing with failure of equipment (e.g. insulin pump) should be in place.
Received: 3 October 2015 Accepted: 4 November 2015
References 1. Backer H. What is wilderness medicine? Wilderness Env Med. 1995;6:3–10. 2. Clements R, Mackenzie R. Competence in prehospital care: evolving
concepts. Emerg Med J. 2005;22:516–9. 3. Johnson C, Anderson S, Dallimore J, Winser S, Warrell D. Oxford handbook
of expedition and wilderness medicine. 2nd ed. Oxford: Oxford Univeristy Press; 2008.
4. Anderson SR, Johnson CJ. Expedition health and safety: a risk assessment. J R Soc Med. 2000;93(11):557–62.
5. Lyon R, Wiggins C. Expedition medicine—risk of illness and injury. Wilder-ness Env Med. 2010;21:318–24.
6. McIntosh SE, Campbell A, Weber D, Dow J, Joy E, Grissom CK. Mountain-eering medical events and trauma on Denali, 1992–2011. High Alt Med Biol. 2012;13(4):275–80.
7. Kupper T, Hettlich M, Horz HP, Lechner K, Scharfenberg C, Conrads G, et al. Dental problems and emergencies of trekkers—epidemiology and prevention. Results of the ADEMED Expedition 2008. High Alt Med Biol. 2014;15(1):39–45.
8. Faculty of Pre-Hospital Care, The Royal College of Surgeons Edinburgh, PHEM Skills Framework. http://www.fphc.co.uk/content/LatestNews/PHEMSkillsFramework.aspx. Accessed 7 Sept 2015.
9. Iserson KV. Medical planning for extended remote expeditions. Wilder-ness Environ Med. 2013;24(4):366–77.
10. Barry PW, Pollard AJ. Altitude illness. BMJ. 2003;326(7395):915–9.

Page 10 of 10Mellor et al. Extrem Physiol Med (2015) 4:22
11. Bangor Mountain Medicine Project, Ysbyty Gwynedd Mountain Medicine database. http://www.mountainmedicine.co.uk/Mountain_Medicine_Bangor/Mountain_Medicine.html. Accessed 29 August 2015.
12. Scally G, Donaldson LJ. The NHS’s 50 anniversary. Clinical governance and the drive for quality improvement in the new NHS in England. BMJ. 1998;317(7150):61–5.
13. Küpper T, Nies I, Hillebrandt D, Milledge J, Basnayt B. Model contract for health care on trekking and expeditions for doctors. Intended for doctors, interested non-medical persons and trekking or expedition operators. UIAA. 2008. http://theuiaa.org/medical_advice.html. Accessed 29 August 2015.
14. Woodruff JM. Consequence and likelihood in risk estimation: a matter of balance in UK health and safety risk assessment practice. Saf Sci. 2005;43:345–53.
15. Elsensohn F, Soteras I, Resiten O, Ellerton J, Brugger H, Paal P. Equip-ment of medical backpacks in mountain rescue. High Alt Med Biol. 2011;12(4):343–7.
16. Paal P, Milani M, Brown D, Boyd J, Ellerton J. Termination of car-diopulmonary resuscitation in mountain rescue. High Alt Med Biol. 2012;13(3):200–8.
Submit your next manuscript to BioMed Centraland take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
• Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution
Submit your manuscript at www.biomedcentral.com/submit

WILDERNESS MEDICAL SOCIETY PRACTICE GUIDELINES
Wilderness Medical Society Practice Guidelines for thePrevention and Treatment of Acute Altitude Illness:2019 Update
Andrew M. Luks, MD1; Paul S. Auerbach, MD, MS2; Luanne Freer, MD3,4,5; Colin K. Grissom, MD6,7;
Linda E. Keyes, MD8,9; Scott E. McIntosh, MD, MPH10; George W. Rodway, PhD, APRN11;
Robert B. Schoene, MD12; Ken Zafren, MD2,13; Peter H. Hackett, MD14
1Division of Pulmonary, Critical Care and Sleep Medicine, University of Washington, Seattle, WA; 2Department of Emergency Medicine, Stanford
University School of Medicine, Stanford, CA; 3Yellowstone National Park, WY; 4Midway Atoll National Wildlife Refuge, Honolulu, HI; 5Everest ER,
Himalayan Rescue Association, Kathmandu, Nepal; 6Division of Pulmonary and Critical Care Medicine, Intermountain Medical Center, Salt Lake
City, UT; 7Division of Pulmonary and Critical Care Medicine, University of Utah, Salt Lake City, UT; 8Department of Emergency Medicine,
University of Colorado, Denver, CO; 9Boulder Community Health, Boulder, CO; 10Division of Emergency Medicine, University of Utah, Salt Lake
City, UT; 11University of California, Davis School of Nursing, Sacramento, CA; 12Division of Pulmonary and Critical Care Medicine, Sound
Physicians, St. Mary’s Medical Center, San Francisco, CA; 13Himalayan Rescue Association, Kathmandu, Nepal; 14Altitude Research Center,
Division of Pulmonary Sciences and Critical Care Medicine, Department of Medicine, University of Colorado Anschutz Medical Campus, Aurora, CO
To provide guidance to clinicians about best preventive and therapeutic practices, the Wilderness Medi-
cal Society (WMS) convened an expert panel to develop evidence-based guidelines for prevention and
treatment of acute mountain sickness, high altitude cerebral edema, and high altitude pulmonary edema.
Recommendations are graded based on the quality of supporting evidence and the balance between the
benefits and risks/burdens according to criteria put forth by the American College of Chest Physicians.
The guidelines also provide suggested approaches to prevention and management of each form of acute
altitude illness that incorporate these recommendations. This is an updated version of the original
WMS Consensus Guidelines for the Prevention and Treatment of Acute Altitude Illness published in
2010 and subsequently updated as the WMS Practice Guidelines for the Prevention and Treatment of
Acute Altitude Illness in 2014.
Keywords: high altitude, acute mountain sickness, high altitude pulmonary edema, high altitude cere-
bral edema, acetazolamide, dexamethasone, nifedipine
Introduction
Travel to elevations above 2500 m is associated with risk
of developing 1 or more forms of acute altitude illness:
acute mountain sickness (AMS), high altitude cerebral
edema (HACE), and high altitude pulmonary edema
(HAPE). Because large numbers of people travel to such
elevations, many clinicians are faced with questions
from patients about the best means to prevent these dis-
orders. In addition, clinicians working at facilities in
high altitude regions or as members of expeditions
traveling to such areas can expect to see persons who are
experiencing these illnesses and must be familiar with
prophylactic regimens and proper treatment protocols.
To provide guidance to clinicians and disseminate knowl-
edge about best practices, the Wilderness Medical Society
(WMS) convened an expert panel to develop evidence-based
guidelines for prevention and treatment of acute altitude ill-
ness. Preventive and therapeutic modalities are presented
and recommendations made for each form of acute altitude
illness. Recommendations are graded based on the quality of
supporting evidence and consideration of benefits and risks/
burdens associated with each modality. These recommenda-
tions are intended to apply to all travelers to high altitude,
whether they are traveling to high altitude for work, recrea-
tion, or various activities including hiking, skiing, trekking,
and mountaineering.
Corresponding author: Andrew Luks, MD, Pulmonary, Critical Care
and Sleep Medicine, Harborview Medical Center, 325 Ninth Avenue,
Box 359762, Seattle, WA 98104; e-mail: [email protected].
Submitted for publication November 2018.
Accepted for publication April 2019.
ARTICLE IN PRESS
Wilderness & EnvironmentalMedicine 2019; 00(00): 1�16

Methods
The original expert panel was convened at the 2009
annual meeting of the WMS in Snowmass, Colorado.
Members were selected by the WMS based on their clini-
cal and/or research experience. Relevant articles were
identified through the MEDLINE database by keyword
search using the terms acute mountain sickness, high
altitude pulmonary edema, high altitude cerebral edema,
treatment, prevention, acetazolamide, dexamethasone,
ibuprofen, nifedipine, tadalafil, sildenafil, and salme-
terol. English-language, peer-reviewed studies including
adults and/or children that were related to prevention
and treatment of acute altitude illnesses, including ran-
domized controlled trials, observational studies, and case
series, were reviewed, and the level of evidence support-
ing various preventive and treatment modalities was
assessed. Animal studies and abstract-only studies were
not included. Conclusions from review articles were not
considered in the formulation of recommendations but
are cited to provide background information on the acute
altitude illnesses and their management. The panel used a
consensus approach to develop recommendations and
graded each recommendation according to criteria stipulated
in the American College of Chest Physicians statement on
grading recommendations and strength of evidence in clini-
cal guidelines (online Supplementary Table 1).1
This set of guidelines is an updated version of the orig-
inal Wilderness Medical Society Consensus Guidelines
for the Prevention and Treatment of Acute Altitude Ill-
ness published in 20102 and the update as the Wilderness
Medical Society Practice Guidelines for the Prevention
and Treatment of Acute Altitude Illness published in
2014.3 As for the 2014 update, the panel used the
approach described to identify relevant studies, adding
additional search terms to reflect updates in the litera-
ture. The new search terms for the current version
included budesonide, acetaminophen, continuous posi-
tive airway pressure (CPAP), and hypoxic tents.
Defining the threshold for “high altitude” and when
to apply these guidelines
Unacclimatized individuals are at risk of high altitude ill-
ness when ascending to altitudes above 2500 m. Prior
studies and extensive clinical experience, however, sug-
gest that susceptible individuals can develop AMS, and
potentially HAPE, at elevations as low as 2000 m.4�6
HACE is typically encountered at higher elevations but
has also been reported at around 2500 m in patients with
concurrent HAPE.7 Part of the difficulty in defining a
specific threshold at which altitude illness can develop is
the fact that the symptoms and signs of AMS, the most
common form of altitude illness, are nonspecific, as
demonstrated in several studies in which participants
met criteria for the diagnosis of AMS despite no gain in
altitude.8�10 As a result, studies assessing AMS inci-
dence at modest elevations may label individuals as hav-
ing altitude illness when, in fact, symptoms are related to
some other process, thereby falsely elevating the
reported incidence of AMS at that elevation.
Recognizing the difficulty in defining a clear thresh-
old, the expert panel recommends an approach to pre-
venting and treating acute altitude illness that does not
depend strictly on the altitude to which an individual is
traveling. Preventive measures should be considered
based on the altitude to which the individual is traveling
and also account for factors such as history of perfor-
mance at high altitude, rate of ascent, and availability of
acclimatization days (described in greater detail later).
Diagnoses of AMS, HAPE, or HACE should not be
excluded based on the fact that an ill individual is below
2500 m. These diagnoses should be strongly considered
in the presence of compatible clinical features, with care-
ful attempts to exclude other entities such as severe
dehydration, hyponatremia, pneumonia, carbon monox-
ide poisoning, and hypoglycemia.
Acute mountain sickness and high altitude cerebral
edema
Information on the epidemiology, clinical presentation,
and pathophysiology of AMS and HACE is provided in
several extensive reviews.11�14 From a clinical stand-
point, HACE represents an extremely severe form of
AMS; therefore, preventive and treatment measures for
the 2 disorders can be addressed simultaneously.
PREVENTION
Measures considered for prevention of AMS and HACE
include the following.
Gradual ascent
Controlling the rate of ascent, in terms of the number of
meters gained per day, is a highly effective means of pre-
venting acute altitude illness; however, aside from 2
recent prospective studies,15,16 this strategy has largely
been evaluated retrospectively.17 In planning the rate of
ascent, the altitude at which someone sleeps is consid-
ered more important than the altitude reached during
waking hours.
Recommendation. Gradual ascent, defined as a slow
increase in sleeping elevation, is recommended for AMS
and HACE prevention. A specific approach is described
further later in the text. Recommendation Grade: 1B
ARTICLE IN PRESS
2 Luks et al

Acetazolamide
Multiple trials have established a role for acetazolamide
in prevention of AMS.18�21
Acetazolamide contains a sulfa moiety but carries an
extremely low risk of inciting an allergic reaction in per-
sons with sulfonamide allergy. As a result, persons with
known allergy to sulfonamide medications can consider a
supervised trial of acetazolamide before the trip, particu-
larly if planning travel to a location remote from medical
resources.22 Prior anaphylaxis to a sulfonamide medication
or a history of Stevens-Johnson syndrome should be con-
sidered a contraindication to acetazolamide.
Some studies suggest that acetazolamide may have an
adverse effect on maximum exercise capacity,23 perceived
dyspnea during maximal exercise tests,24 and respiratory
muscle function at high levels of work.25 The small
observed changes, however, are unlikely to affect overall
exercise performance for the majority of activities in which
high altitude travelers engage (hiking, skiing) or the chance
of summit success for climbers at moderate and even
extreme elevations. These changes should not be viewed as
a reason to avoid acetazolamide.
The recommended adult dose for prophylaxis is 125 mg
every 12 h (Table 1). Although doses up to 750 mg daily
are effective at preventing AMS compared to placebo, they
are associated with more frequent and/or pronounced side
effects, do not convey greater efficacy, and are not recom-
mended for prevention. A recent, small study suggested
that 62.5 mg every 12 h was noninferior to 125 mg every
12 h,26 but further research with greater numbers of partici-
pants in different high altitude settings should be completed
before a change in dose can be recommended. The pediat-
ric dose of acetazolamide is 2.5 mg¢kg¡1¢dose¡1 (maximum
125 mg¢dose¡1) every 12 h.27
Recommendation. Acetazolamide should be strongly
considered in travelers at moderate or high risk of AMS
with ascent to high altitude. Recommendation Grade: 1A.
Recommendation. Acetazolamide can be used in chil-
dren for prevention of AMS. Recommendation Grade: 1C.
Dexamethasone
Although dexamethasone does not facilitate acclimatization
like acetazolamide, prospective trials have established a
benefit for dexamethasone in AMS prevention.28,29 The
recommended adult doses are 2 mg every 6 h or 4 mg every
12 h. Very high doses (4 mg every 6 h) may be considered
in very high-risk situations, such as military or search and
rescue personnel being airlifted to altitudes >3500 m with
Table 1. Recommended dosages for medications used in the prevention and treatment of altitude illness
Medication Indication Route Dosage
Acetazolamide AMS, HACE prevention Oral 125 mg every 12 ha
Pediatrics: 2.5 mg¢kg¡1 every 12 h
AMS treatmentb Oral 250 mg every 12 h
Pediatrics: 2.5 mg¢kg¡1 every
12 h (maximum: 125 mg per dose)
Dexamethasone AMS, HACE prevention Oral 2 mg every 6 h or 4 mg every 12 ha
Pediatrics: Should not be used for prophylaxis
AMS, HACE treatment Oral, IV, IM AMS: 4 mg every 6 h
HACE: 8 mg once, then 4 mg every 6 h
Pediatrics: 0.15 mg¢kg¡1¢dose¡1 every
6 h (Maximum: 4 mg per dose)
Ibuprofen AMS prevention Oral 600 mg every 8 h
Nifedipine HAPE prevention Oral 30 mg ER version, every 12 h or 20 mg ER version every 8 hc
HAPE treatment Oral 30 mg ER version, every 12 h or 20 mg ER version every 8 h
Tadalafil HAPE prevention Oral 10 mg every 12 hc
Sildenafil HAPE prevention Oral 50 mg every 8 hc
AMS, acute mountain sickness; HACE, high altitude cerebral edema; IM, intramuscularly; ER, extended release; HAPE, high altitude pulmo-
nary edema.a For individuals ascending to and remaining at a given elevation, after arrival at the target elevation, the medication should be continued for 2 d
in individuals adhering to the recommended ascent rate and 2 to 4 d in individuals ascending faster than recommended rates. Individuals who
ascend to a target elevation and immediately descend can stop the medication once descent is initiated.bAcetazolamide can also be used at this dose as an adjunct to dexamethasone in HACE treatment, but dexamethasone remains the primary treat-
ment for HACE.cFor individuals ascending to and remaining at a given elevation, after arrival at the target elevation, the medication should be continued for 4 d
in individuals adhering to the recommended ascent rate and 4 to 7 d in individuals ascending faster than recommended rates. Individuals who
ascend to a target elevation and immediately descend can stop the medication once descent is initiated.
ARTICLE IN PRESS
Altitude Illness Practice Guidelines 3

immediate performance of physical activity, but should not
be used except in these limited circumstances. Prolonged
use carries a risk of adrenal suppression. Although some
resources state that use of less than 2-wk duration does not
require a taper,30 in remote mountain environments a more
conservative approach is warranted. If used for longer than
10 d, the medication should be tapered over a 1-wk period
rather than stopped abruptly. Given the absence of data on
the use of dexamethasone for AMS prevention in children
and the availability of other safe alternatives—specifically,
graded ascent and acetazolamide—dexamethasone is not
recommended for AMS prevention in children.
Recommendation. Dexamethasone can be used as an
alternative to acetazolamide for adult travelers at moder-
ate or high risk of AMS. Recommendation Grade: 1A.
Inhaled budesonide
Two studies indicated that inhaled budesonide 200
micrograms twice daily was effective at preventing
AMS when compared to placebo.31,32 These studies
were limited by methodological issues such as timing of
the assessment for AMS31 and number of participants in
each study arm.32 A clear mechanism of action was not
apparent in these studies, but small improvements in spi-
rometry and oxygen saturation—both of little clinical
significance—were suggested as evidence that the bene-
fit might derive from a direct lung effect. More recent,
well-designed randomized controlled trials failed to rep-
licate these results.33,34
Recommendation. Inhaled budesonide should not be
used for altitude illness prophylaxis. Recommendation
Grade: 1C
Ginkgo biloba
Although 2 trials demonstrated a benefit of Ginkgo in AMS
prevention,35,36 2 other negative trials have also been pub-
lished.37,38 This discrepancy may result from differences in
the source and composition of the Ginkgo products.39
Ginkgo should be avoided in pregnant women40 and used
with caution in people taking anticoagulants.41 Acetazol-
amide is considered far superior for AMS prevention.
Recommendation. Ginkgo biloba should not be used
for AMS prevention. Recommendation Grade: 1C
Ibuprofen
Two trials demonstrated that ibuprofen (600 mg 3 times
daily) is more effective than placebo at preventing
AMS,42,43 while a third, smaller study showed no benefit.44
Another study claimed to show benefit, but the trial did not
include a placebo arm and instead compared the incidence
of AMS with ibuprofen with historically reported rates
from the region in which the study was conducted.45
Although no studies have compared ibuprofen with dexa-
methasone, 2 studies have compared ibuprofen with acet-
azolamide. The first found an equal incidence of high
altitude headache and AMS in the acetazolamide and ibu-
profen groups, with both showing significant protection
compared to placebo.46 A more recent trial failed to show
that ibuprofen was noninferior to acetazolamide (ie, ibupro-
fen is inferior to acetazolamide for AMS prophylaxis).47
The aforementioned trials all used the medication for a
short duration (»24�48 h). As a result, efficacy and safety
(eg, the risk of gastrointestinal bleeding or renal dysfunc-
tion) over longer periods of use at high altitude remain
unclear. For these reasons, as well as more extensive clini-
cal experience with acetazolamide and dexamethasone,
ibuprofen cannot be recommended over these medications
for AMS prevention for rapid ascent.
Recommendation. Ibuprofen can be used for AMS
prevention in persons who do not wish to take acetazol-
amide or dexamethasone or have allergies or intolerance
to these medications. Recommendation Grade: 2B.
Acetaminophen
A single study demonstrated that acetaminophen
1000 mg 3 times daily was as effective as ibuprofen at
preventing AMS in trekkers travelling between 4370 and
4940 m in elevation.45 Rather than including a placebo
arm, the study attempted to establish the benefit of acet-
aminophen by comparing the incidence rates in the study
with those of untreated trekkers from prior studies that
used the same ascent profile. Based on these data, acet-
aminophen is not recommended for use as a preventive
agent over acetazolamide or dexamethasone.
Recommendation. Acetaminophen should not be used
for AMS prevention. Recommendation Grade: 1C
Staged ascent and preacclimatization
Two studies showed that spending 6 to 7 d at moderate
altitude (»2200�3000 m) before proceeding to higher
altitude (referred to as “staged ascent”) decreases the
risk of AMS, improves ventilation and oxygenation, and
blunts the pulmonary artery pressure response after sub-
sequent ascent to 4300 m.16,48 Many travelers to high
altitude visit mountain resorts at more moderate eleva-
tions between 2500 and 3000 m. The value of short stays
at intermediate elevations of »1500 m for decreasing the
risk of AMS during such ascents makes sense from a
physiologic standpoint. However, this approach has not
been studied in a randomized fashion, aside from 1
cross-sectional study finding a decreased risk of AMS in
travelers who spent 1 night at 1600 m before ascent to
resort communities between 1920 and 2950 m.5
ARTICLE IN PRESS
4 Luks et al

A larger number of studies examining the effects of
repeated exposures to hypobaric or normobaric hypoxia in
the days and week preceding high altitude travel (referred to
as “preacclimatization”) showed mixed results, with some
studies finding benefit in terms of decreased AMS incidence
or severity49�51 and others showing no effect.52�55 A signifi-
cant challenge in interpreting the literature on preacclimati-
zation is the variability among the hypoxic exposure
protocols used, as well as the fact that not all studies include
evidence that their protocols induced physiologic responses
consistent with acclimatization.
Implementation of either staged ascent or preacclima-
tization may be logistically difficult for many high alti-
tude travelers. In general, short-term exposures (eg,
15�60 min of exposure to hypoxia, or a few hours of
hypoxia a few times before ascent) are unlikely to aid
acclimatization, whereas longer exposures (eg, >8 h
daily for >7 d) are more likely to yield benefit. Hypo-
baric hypoxia is more effective than normobaric hypoxia
in facilitating preacclimatization and preventing AMS.56
Because the optimal methods for preacclimatization and
staged ascent have not been fully determined, the panel
recommends consideration of these approaches but does
not endorse a particular protocol.
Recommendation. When feasible, staged ascent and
preacclimatization can be considered as a means for
AMS prevention. Recommendation Grade: 1C
Hypoxic tents
Commercial products are available that allow individuals to
sleep or exercise in hypoxic conditions for the purpose of
facilitating acclimatization before a trip to high altitude.
Only 1 placebo-controlled study has examined their utility.57
Although this study demonstrated a lower incidence of AMS
in persons who slept in simulated high altitude conditions
compared to normoxia, technical difficulties with the system
resulted in a substantial number of study participants not
receiving the intended hypoxic dose. Although the systems
are marketed to be of benefit and anecdotal reports suggest
they are widely used by climbers and other athletes compet-
ing at high altitude, there are no data indicating increased
likelihood of summit success or improved physical perfor-
mance. As with the preacclimatization approaches previ-
ously described, any benefit that may accrue from these
systems is more likely with long hypoxic exposures (>8 h
per day) for at least several weeks before planned high alti-
tude travel. Short and/or infrequent exposures, including
exercise training, are likely of no benefit. In addition to the
cost of the systems and power needed to run them, individu-
als face the risk of poor sleep, which over a long period of
time could have deleterious effects on performance during
an expedition.
Recommendation. Hypoxic tents can be used for
facilitating acclimatization and preventing AMS, pro-
vided sufficiently long exposures can be undertaken reg-
ularly over an appropriate number of weeks and other
factors, such as sleep quality, are not compromised. Rec-
ommendation Grade: 2B
Other options
Chewed coca leaves, coca tea, and other coca-derived prod-
ucts are commonly recommended for travelers in the Andes
mountains for AMS prevention. Their utility in prevention
of altitude illness has not been properly studied, so they
should not be substituted for other established preventive
measures described in these guidelines. Multiple studies
have sought to determine whether other agents, including
antioxidants,58 iron,59 dietary nitrates,60 leukotriene receptor
blockers,61,62 phosphodiesterase inhibitors,63 salicylic acid,64
spironolactone,65 and sumatriptan66 can prevent AMS, but
the current state of evidence does not support their use.
“Forced” or “over” hydration has never been found to pre-
vent altitude illness and might increase the risk of hyponatre-
mia; however, maintenance of adequate hydration is
important because symptoms of dehydration can mimic
those of AMS. Nocturnal expiratory positive airway pressure
(EPAP) administered via a single-use nasal strip during sleep
is not effective for AMS prophylaxis,67 nor is a regimen of
remote ischemic preconditioning.68
No studies have examined short-term oxygen use in
the form of either visits to oxygen bars or over-the-
counter oxygen delivery systems by which individuals
inhale oxygen-enriched gas from a small prefilled canis-
ter. Due to the small volume of gas (2�10 L/canister)
and short duration of administration, these interventions
are unlikely to be of benefit and, as a result, have no role
in AMS/HACE prevention. Other over-the-counter prod-
ucts, such as powdered drink mixes, also lack any evi-
dence of benefit.
SUGGESTED APPROACH TO AMS/HACE
PREVENTION
Because the rates of acclimatization and physiologic
responses to high altitude vary considerably between indi-
viduals, clinicians must recognize that the recommendations
that follow, although generally effective, do not guarantee
successful prevention in all high altitude travelers.
The approach to prevention of AMS and HACE
should be a function of the risk profile of the individual
traveling to high altitude (Table 2). The first priority
should be ensuring gradual ascent to the target elevation.
Travelers can lower their risk by sleeping 1 night at an
intermediate altitude. For example, sea-level residents
traveling to Colorado resort areas over 2800 m can spend
ARTICLE IN PRESS
Altitude Illness Practice Guidelines 5

1 night in Denver (1600 m). It should be recognized that
a large number of people will travel directly by car or
plane to commonly visited mountain high altitude loca-
tions, often located between 2500 and 3000 m, and may
be unable to ascend gradually because of various logisti-
cal factors. In such situations, pharmacologic prophy-
laxis can be considered. Such individuals should also
take care to slow the rate of further ascent beyond the
altitude achieved at the start of their visit.
With travel above 3000 m, individuals should not
increase their sleeping elevation by more than 500 m¢d¡1
and should include a rest day (ie, no ascent to higher
sleeping elevation) every 3 to 4 d. The increase in sleep-
ing elevation should be less than 500 m for any given
day of a trip. In many areas, terrain and other logistical
factors prevent strict adherence to this approach and
mandate larger gains in sleeping elevation over a single
day. In such cases, acclimatization days should be
strongly considered before and/or after these large gains
in elevation and elsewhere in the itinerary to ensure—at
the very least and as an approximation of properly con-
trolled ascent—that the overall ascent rate averaged over
the entire trip (ie, total elevation gain divided by the
number of days of ascent during the trip) is below the
500 m¢d¡1threshold.
Prophylactic medications are not necessary in low-risk
situations but should be considered in addition to gradual
ascent for use in moderate- to high-risk situations (Table 2).
Acetazolamide is the preferred medication; dexamethasone
may be used as an alternative in individuals with a history
of intolerance of or allergic reaction to acetazolamide. In
rare circumstances (eg, military or rescue teams that must
ascend rapidly to and perform physical work at >3500 m),
consideration can be given to concurrent use of acetazol-
amide and dexamethasone. This strategy should be avoided
except in these particular or other emergency circumstances
that mandate very rapid ascent.
Acetazolamide and dexamethasone should be started
the day before ascent but still have beneficial effects if
started on the day of ascent. For individuals ascending to
and staying at the same elevation for more than several
days, prophylaxis may be stopped after 2 d at the highest
altitude. Individuals ascending faster than the recom-
mended ascent rates may consider continuing preventive
medication for 2 to 4 d after arrival at the target altitude,
but there are no data to support this approach. For indi-
viduals ascending to a high point and then descending
toward the trailhead (eg, descending from the summit of
Mt. Kilimanjaro), in the absence of AMS/HACE symp-
toms, preventive medications should be stopped when
descent is initiated.
TREATMENT
Potential therapeutic options for AMS and HACE include
the following.
Descent
Descent remains the single best treatment for AMS and
HACE, but it is not necessary in all circumstances (dis-
cussed further later in the text). Individuals should
descend until symptoms resolve unless terrain, weather,
or injuries make descent impossible. Symptoms typically
resolve after descent of 300 to 1000 m, but the required
decrease in altitude varies among individuals. Individu-
als should not descend alone, particularly if they are
experiencing HACE.
Recommendation. Descent is effective for any degree
of AMS/HACE and is indicated for individuals with
severe AMS, AMS that fails to resolve with other meas-
ures, or HACE. Recommendation Grade: 1A
Table 2. Risk categories for acute mountain sickness
Risk category Description
Low � Individuals with no history of altitude illnessand ascending to �2800 m
� Individuals taking �2 d to arrive at
2500�3000 m with subsequent increases in
sleeping elevation <500 m¢d¡1and an extra
day for acclimatization every 1000 m
Moderate � Individuals with history of AMS and
ascending to 2500�2800 m in 1 d� No history of AMS and ascending to
>2800 m in 1 d� All individuals ascending >500 m¢d¡1
(increase in sleeping elevation) at altitudes
above 3000 m but with an extra day for
acclimatization every 1000 m
High � Individuals with a history of AMS and
ascending to >2800 m in 1 d� All individuals with a history of HACE or
HAPE� All individuals ascending to >3500 m in 1 d� All individuals ascending >500 m¢d¡1
(increase in sleeping elevation) above
>3000 m without extra days for
acclimatization� Very rapid ascents (eg, <7 d ascents of Mt.
Kilimanjaro)
AMS, acute mountain sickness; HACE, high altitude cerebral edema;
HAPE, high altitude pulmonary edema.
Altitudes listed in the table refer to the altitude at which the person
sleeps.
Ascent is assumed to start from elevations <1200 m.
The risk categories described pertain to unacclimatized individuals.
ARTICLE IN PRESS
6 Luks et al

Supplemental oxygen
Oxygen delivered by nasal cannula or mask at flow rates
sufficient to relieve symptoms provides a suitable alterna-
tive to descent. A peripheral capillary oxygen saturation
(SpO2) >90% is usually adequate. Use of oxygen is not
required in all circumstances and is generally reserved for
mountain clinics and hospitals where supply is abundant. It
should also be used when descent is recommended but not
feasible or during descent in severely ill individuals. The
inspired oxygen fraction will vary significantly between
oxygen delivery systems, including nasal cannula, simple
facemasks, Venturi masks, or non-rebreather masks. In
addition, because of interindividual variability in inspiratory
flow rates and minute ventilation, the inspired fractional
concentration of oxygen (FIO2) can vary significantly
between patients for any given common oxygen delivery
system, with the exception of high flow systems. For this
reason, supplemental oxygen should be administered to tar-
get an SpO2 of >90% rather than a specific FIO2. Oxygen
supply may be limited at remote high altitude clinics or on
expeditions, necessitating judicious use. Short-term oxygen
use in the form of visits to oxygen bars or use of over-the-
counter oxygen canisters has not been studied for AMS
treatment and should not be relied on for this purpose.
Recommendation. When available, ongoing supple-
mental oxygen sufficient to raise SpO2 to >90% or to
relieve symptoms can be used while waiting to initiate
descent or when descent is not practical. Recommenda-
tion Grade: 1A
Portable hyperbaric chambers
Portable hyperbaric chambers are effective for treating
severe altitude illness69,70 but require constant tending by
care providers and are difficult to use with claustrophobic or
vomiting patients. Symptoms may recur when individuals
are removed from the chamber,71 but this should not pre-
clude use of the chamber when indicated. In many cases, ill
individuals may improve sufficiently to enable them to assist
in their evacuation and descend once symptoms improve.
Use of a portable hyperbaric chamber should not delay
descent in situations where descent is required.
Recommendation. When available, portable hyper-
baric chambers should be used for patients with severe
AMS or HACE when descent is infeasible or delayed
and supplemental oxygen is not available. Recommenda-
tion Grade: 1B
Acetazolamide
Only 1 study has examined acetazolamide for AMS treat-
ment. The dose studied was 250 mg every 12 h; whether a
lower dose might suffice is unknown.72 No studies have
assessed AMS treatment with acetazolamide in pediatric
patients, but anecdotal reports suggest it has utility. The
pediatric treatment dose is 2.5 mg¢kg¡1¢dose¡1 every 12 h
up to a maximum of 250 mg¢dose¡1.
Recommendation. Acetazolamide should be consid-
ered for treatment of AMS. Recommendation Grade: 1C
Dexamethasone
Dexamethasone is very effective for treating AMS.73�75
The medication does not facilitate acclimatization, so
further ascent should be delayed until the patient is
asymptomatic while off the medication. Although sys-
tematic studies have not been conducted, extensive clini-
cal experience supports using dexamethasone in patients
with HACE. It is administered as an 8 mg dose (intra-
muscularly, IV, or orally) followed by 4 mg every 6 h
until symptoms resolve. The pediatric dose is 0.15
mg¢kg¡1¢dose¡1 every 6 h.27
Recommendation. Dexamethasone should be consid-
ered for treatment of AMS. Recommendation Grade 1B.
Recommendation. Dexamethasone should be adminis-
tered to patients with HACE. Recommendation Grade: 1B
Acetaminophen
Acetaminophen has been found to relieve headache at
high altitude76 but has not been found to improve the full
spectrum of AMS symptoms or effectively treat HACE.
Recommendation. Acetaminophen can be used to
treat headache at high altitude. Recommendation Grade:
1C.
Ibuprofen
Ibuprofen has been found to relieve headache at high
altitude76 but has not been shown to improve the full
spectrum of AMS symptoms or effectively treat HACE.
Recommendation. Ibuprofen can be used to treat
headache at high altitude. Recommendation Grade: 1C.
Continuous positive airway pressure
Rather than affecting barometric pressure, CPAP works
by increasing transmural pressure across alveolar walls,
thereby increasing alveolar volume and improving venti-
lation-perfusion matching and gas exchange. Two
reports have demonstrated the feasibility of administer-
ing CPAP to treat AMS,77,78 but this has not been studied
in a systematic manner. Logistical challenges to use in
field settings include access to power and the weight and
bulk of these systems.
Recommendation. Because of lack of data, no recom-
mendation can be made regarding use of CPAP for AMS
treatment.
ARTICLE IN PRESS
Altitude Illness Practice Guidelines 7

SUGGESTED APPROACH TO AMS/HACE
TREATMENT
Care should be taken to exclude disorders whose symp-
toms and signs resemble those seen with AMS and
HACE, such as carbon monoxide poisoning, dehydra-
tion, exhaustion, hypoglycemia, hypothermia, and hypo-
natremia. Persons with AMS of any severity or HACE
should cease ascending and may need to consider
descent, depending on the severity of illness and the cir-
cumstances (Table 3).11 Patients with AMS can remain
at their current altitude and use nonopioid analgesics for
headache and antiemetics for nausea and vomiting.
These individuals should be closely observed for signs
of progression of altitude illness. Descent should be initi-
ated for AMS if symptoms worsen or fail to improve
after 1 to 2 d of appropriate interventions.
Although acetazolamide facilitates acclimatization
and is somewhat effective for treating mild illness, it is
likely better for prevention than for treatment. Dexa-
methasone is considered to be a more reliable treatment
for moderate to severe AMS, which often also requires
descent. Individuals with AMS may resume ascending
once symptoms resolve. Further ascent or reascent to a
previously attained altitude should never be undertaken
if there are ongoing symptoms. After resolution of AMS,
taking acetazolamide at preventive doses during reascent
is prudent.
HACE is differentiated from severe AMS by neu-
rological signs such as ataxia, confusion, or altered
mental status in the setting of acute ascent to high
altitude and may follow AMS or occur concurrently
with HAPE. Individuals developing HACE in loca-
tions with access to hospitals or specialized clinics
should be started on dexamethasone and supplemen-
tal oxygen sufficient to achieve an SpO2 >90%. In
remote areas away from medical resources, descent
should be initiated in any suspected cases of HACE
or if symptoms of AMS are worsening despite treat-
ment with acetazolamide or dexamethasone. If
descent is not feasible, supplemental oxygen or a por-
table hyperbaric chamber should be used. Persons
with HACE should also be started on dexamethasone.
There are no systematic data or case reports about
reascent during the same trip or expedition after reso-
lution of HACE. The prudent course is to avoid reas-
cent in this situation, but if it is to be attempted, at a
minimum the individual should be asymptomatic and
no longer taking dexamethasone for at least 2 to 3 d
before reascent.
High altitude pulmonary edema
Information on the epidemiology, clinical presentation,
and pathophysiology of HAPE, the majority of which
comes from studies in adults, is provided in extensive
reviews.13,14,79,80 Although some of the prophylactic and
therapeutic modalities are the same for HAPE as for
AMS and HACE, important differences in the underly-
ing pathophysiology mandate certain alternative preven-
tion and treatment approaches.
PREVENTION
Potential preventive measures for HAPE include the fol-
lowing.
Gradual ascent
No studies have prospectively assessed whether limiting
the rate of increase in sleeping elevation prevents
HAPE; however, there is a clear relationship between
rate of ascent and disease incidence.17,81,82
Recommendation. Gradual ascent is recommended to
prevent HAPE. Recommendation Grade: 1B
Table 3. Acute mountain sickness classification
Category Mild AMS Moderate�Severe AMS High altitude cerebral
edema (HACE)
Symptoms Headache plus 1 or more other
symptoms (nausea/vomiting,
fatigue, lassitude, dizziness)
Headache plus 1 or more other symptoms
(nausea/vomiting, fatigue, lassitude, dizziness)
Worsening of symptoms seen
in moderate to severe AMS
All symptoms of mild intensity All symptoms of moderate�severe intensity
Signs None None Ataxia, severe lassitude, altered
mental status, encephalopathy
Lake Louise
AMS Scorea3�5 6�12 Not applicable
AMS, acute mountain sickness.a Self-report AMS score. Roach et al.103
ARTICLE IN PRESS
8 Luks et al

Nifedipine
A single, randomized, placebo-controlled study83 and
extensive clinical experience have established a role
for nifedipine in HAPE prevention in susceptible
individuals. The recommended dose is 30 mg of
the extended-release preparation administered every
12 h. Hypotension was not noted in the study83 and is
generally not a concern with the extended-release
version of the medication but may occur in a limited
number of individuals.
Recommendation. Nifedipine is recommended for
HAPE prevention in HAPE-susceptible people. Recom-
mendation Grade: 1B
Salmeterol
In a single randomized, placebo-controlled study, the long-
acting inhaled beta-agonist salmeterol decreased the inci-
dence of HAPE by 50% in susceptible individuals.84 Very
high doses (125 micrograms twice daily) that are often
associated with side effects, including tremor and tachycar-
dia, were used in the study. Clinical experience with salme-
terol at high altitude is limited.
Recommendation. Salmeterol is not recommended for
HAPE prevention. Recommendation Grade: 2B.
Tadalafil
In a single, randomized placebo-controlled trial,
10 mg of tadalafil every 12 h was effective in prevent-
ing HAPE in susceptible individuals.85 The number
of individuals in the study was small, and 2 developed
incapacitating AMS. Clinical experience with tadalafil
is lacking compared to nifedipine. As a result, further
data are necessary before tadalafil can be recom-
mended over nifedipine.
Recommendation. Tadalafil can be used for HAPE
prevention in known susceptible individuals who are not
candidates for nifedipine. Recommendation Grade: 1C
Dexamethasone
In the same study that assessed the role of tadalafil in
HAPE prevention, dexamethasone (8 mg every 12 h)
was also found to prevent HAPE in susceptible individu-
als.85 The mechanism for this effect is not clear, and
there is very little clinical experience in using dexameth-
asone for this purpose. Further data are necessary before
it can be recommended for HAPE prevention.
Recommendation. Dexamethasone can be used for
HAPE prevention in known susceptible individuals who
are not candidates for nifedipine and tadalafil. Recom-
mendation Grade: 1C
Acetazolamide
Because acetazolamide hastens acclimatization, it should
be effective at preventing all forms of acute altitude ill-
ness. It has also been shown to blunt hypoxic pulmonary
vasoconstriction, a key factor in HAPE pathophysiology,
in animal models86�88 and in a single study in humans,89
but there are no data specifically supporting a role in
HAPE prevention. Clinical observations suggest acet-
azolamide may prevent reentry HAPE,90 a disorder seen
in individuals who reside at high altitude, travel to lower
elevation, and then develop HAPE upon rapid return to
their residence.
Recommendation. Because of lack of data, no recom-
mendation can be made regarding use of acetazolamide
for HAPE prevention.
Recommendation. Acetazolamide can be considered
for prevention of reentry HAPE in people with a history
of the disorder. Recommendation Grade: 1C
Preacclimatization and staged ascent
No study has examined whether preacclimatization strate-
gies are useful for HAPE prevention. Staged ascent, with
7 d of residence at moderate altitude (»2200 m), has been
found to blunt the hypoxia-induced increase in pulmonary
artery pressure.48 However, uncertainty remains as to the
magnitude and duration of moderate altitude exposure
necessary to yield benefit, and no study has specifically
investigated whether the strategy is of benefit in HAPE-
susceptible individuals. Although the risks of preacclimati-
zation and staged ascent are likely low, feasibility is a
concern for many high altitude travelers. Because the opti-
mal methods for preacclimatization and staged ascent have
not been fully determined, the panel recommends consider-
ation of these approaches but cannot endorse a particular
protocol for implementation.
Recommendation. When feasible, staged ascent and
preacclimatization can be considered as a means for
HAPE prevention. Recommendation Grade: 1C
SUGGESTED APPROACH TO HAPE PREVENTION
As noted earlier, because the rates of acclimatization and
physiologic responses to high altitude vary considerably
among individuals, the recommendations that follow,
although generally effective, do not guarantee prevention
in all high altitude travelers. A gradual ascent profile is the
primary method for preventing HAPE; the recommenda-
tions provided for AMS and HACE prevention also apply
to HAPE prevention. Pharmacologic prophylaxis should
only be considered for individuals with a history of HAPE,
especially multiple episodes. Nifedipine is the preferred
drug in such situations; it should be started the day before
ARTICLE IN PRESS
Altitude Illness Practice Guidelines 9

ascent and continued either until descent is initiated or the
individual has spent 4 d at the highest elevation, perhaps up
to 7 d if the individual’s rate of ascent was faster than rec-
ommended. Note that these durations are longer than use of
acetazolamide for AMS prevention. For individuals ascend-
ing to a high point and then descending toward the trailhead
(eg, descending from the summit of Kilimanjaro), prophy-
lactic medications should be stopped when descent is initi-
ated. Further research is needed before tadalafil or
dexamethasone can be recommended over nifedipine for
prevention. Acetazolamide facilitates acclimatization in
general but should not be relied upon as the sole preventive
agent in known HAPE-susceptible individuals.
TREATMENT
Therapeutic options for HAPE include the following.
Descent
As with AMS and HACE, descent remains the single best
treatment for HAPE. Individuals should try to descend
at least 1000 m or until symptoms resolve. They should
exert themselves as little as possible while descending (eg,
travel without a pack or via motor vehicle, helicopter, or ani-
mal transportation) because exertion can further increase
pulmonary artery pressure and exacerbate edema formation.
Recommendation. Descent is indicated for individualswith HAPE. Recommendation Grade: 1A
Supplemental oxygen
Oxygen delivered by nasal cannula or mask at flow rates
sufficient to achieve an SpO2 >90% provides a suitable
alternative to descent, particularly when patients can access
healthcare facilities and be closely monitored.91�93 As
noted earlier in the section on AMS/HACE treatment, pro-
viders should target an SpO2 of>90% rather than a particu-
lar FIO2. Short-term use in the form of visits to oxygen bars
or use of over-the-counter oxygen canisters has no role in
HAPE treatment.
Recommendation.When available, supplemental oxy-
gen sufficient achieve an SpO2 of >90% or to relieve
symptoms should be used while waiting to initiate
descent when descent is infeasible and during descent in
severely ill patients. Recommendation Grade: 1A
Portable hyperbaric chambers
As for AMS and HACE, portable hyperbaric chambers
can be used for HAPE treatment. They have not been
systematically studied for this purpose, but their use for
HAPE has been reported in the literature.94 Use of a por-
table hyperbaric chamber should not delay descent in sit-
uations where descent is feasible.
Recommendation. When descent is infeasible or delayed
or supplemental oxygen is unavailable, a portable hyperbaric
chamber may be used to treat HAPE. Recommendation
Grade: 1C
Nifedipine
A single, nonrandomized, unblinded study demonstrated
utility of nifedipine (10 mg of the short-acting version fol-
lowed by 20 mg slow-release every 6 h) for HAPE treatment
when oxygen or descent was not available.95 Although par-
ticipants in this study received a loading dose of the short-
acting version of the medication, this initial dose is no longer
employed because of concerns about provoking systemic
hypotension. Although hypotension is less common with the
extended-release preparation, it may develop when nifedi-
pine is given to patients with intravascular volume depletion.
A prospective, cross-sectional study of individuals with
HAPE demonstrated that addition of nifedipine (30 mg sus-
tained release every 12 h) to descent, oxygen, and rest
offered no additional benefit in terms of time to resolution of
hypoxemia and radiographic opacities or hospital length
of stay.96
Recommendation. Nifedipine should be used for HAPE
treatment when descent is impossible or delayed and reliable
access to supplemental oxygen or portable hyperbaric ther-
apy is unavailable. Recommendation Grade: 1C
Beta-agonists
Although there are reports of beta-agonist use in HAPE
treatment97 and the risks of use are likely low, no data
support a benefit from salmeterol or albuterol in patients
experiencing HAPE.
Recommendation. No recommendation can be made
regarding beta-agonists for HAPE treatment due to lack
of data.
Phosphodiesterase inhibitors
By virtue of their ability to cause pulmonary vasodilation
and decrease pulmonary artery pressure, there is a strong
physiologic rationale for using phosphodiesterase inhibi-
tors in HAPE treatment. Although reports document
their use for this purpose,97,98 no systematic study has
examined the role of tadalafil or sildenafil in HAPE treat-
ment as either mono- or adjunctive therapy. Combined
use of nifedipine and sildenafil or tadalafil should be
avoided because of risk of hypotension.
Recommendation. Tadalafil or sildenafil can be used forHAPE treatment when descent is impossible or delayed,
access to supplemental oxygen or portable hyperbaric ther-
apy is impossible, and nifedipine is unavailable. Recom-
mendation Grade: 2C
ARTICLE IN PRESS
10 Luks et al

Continuous positive airway pressure
As noted earlier, positive airway pressure works by increasing
transmural pressure across alveolar walls, thereby increasing
alveolar volume and improving ventilation-perfusion match-
ing and, as a result, gas exchange. A small study demon-
strated that EPAP, in which a mask system is used to increase
airway pressure during exhalation only, improved gas
exchange in patients with HAPE.99 However, although sev-
eral reports document use of CPAP for management of
HAPE in hospital and field settings,6,78 there is no systematic
evidence that CPAP or EPAP improves patient outcomes
compared to oxygen alone or in conjunction with medica-
tions. Given the low risks associated with the therapy, CPAP
can be considered an adjunct to oxygen administration in a
medical facility, provided the patient has normal mental status
and can tolerate the mask. Although lithium battery�powered
devices and decreased size and weight of CPAP machines
have increased feasibility of field use, logistical challenges
remain and currently limit overall utility in this setting.
Recommendation. CPAP or EPAP may be considered
for treatment of HAPE when supplemental oxygen or
pulmonary vasodilators are not available or as adjunctive
therapy in patients not responding to supplemental oxy-
gen alone. Recommendation Grade: 2C
Diuretics
Although their use is documented in older reports,100
diuretics have no role in HAPE treatment, particularly
because many patients with HAPE have intravascular
volume depletion.
Recommendation. Diuretics should not be used for
treatment of HAPE. Recommendation Grade: 1C.
Acetazolamide
Although clinical reports document use of acetazolamide
for treatment of HAPE,97,98 there are no systematic stud-
ies examining its role in HAPE treatment. The diuretic
effect might provoke hypotension in the intravascularly
depleted patient, and the added stimulus to ventilation
might worsen dyspnea.
Recommendation. Acetazolamide should not be used
for treatment of HAPE. Recommendation Grade: 1C
Dexamethasone
Considering its potential role in HAPE prevention noted
earlier and studies demonstrating effects on maximum
exercise capacity,101 pulmonary inflammation, and ion
transporter function in hypoxia,102 dexamethasone may
have a role in HAPE treatment. Although reports docu-
ment clinical use in this regard,98 no study has estab-
lished whether it is effective for this purpose.
Recommendation. Because of insufficient evidence,
no recommendation can be made regarding dexametha-
sone for HAPE treatment.
SUGGESTED APPROACH TO HAPE TREATMENT
Before initiating treatment, consideration should be given to
other causes of respiratory symptoms at high altitude, such
as asthma, bronchospasm, mucous plugging, pneumonia,
pneumothorax, pulmonary embolism, viral upper respira-
tory tract infection, or myocardial infarction. If HAPE is
suspected or diagnosed, oxygen should be started if avail-
able, and descent to lower elevation should be initiated. If
descent is infeasible or delayed, supplemental oxygen
should be continued or the individual should be placed in a
portable hyperbaric chamber. Patients who have access to
supplemental oxygen and can be adequately monitored in a
medical setting (eg, urgent care clinic or emergency depart-
ment) may not need to descend to lower elevation and can
be treated with oxygen alone at the current elevation.
Descent should be initiated, however, if oxygenation fails to
improve with supplemental oxygen and/or CPAP, if the
patient’s condition deteriorates despite achieving an oxygen
saturation >90%, or if the patient fails to show signs of
improvement with appropriate interventions for HAPE. In
more remote settings, early descent should be considered.
Addition of nifedipine may not yield additional benefit
in well-monitored settings.93,96 In the field setting, where
resources are limited, nifedipine can be used as an
adjunct to descent, supplemental oxygen, or portable
hyperbaric therapy. It should only be used as primary
therapy if none of these other measures is available. A
phosphodiesterase inhibitor may be used if nifedipine is
not available, but concurrent use of multiple pulmonary
vasodilators is not recommended. In the hospital setting,
CPAP can be considered as an adjunct to supplemental
oxygen and nifedipine can be added if the patient fails to
respond to oxygen therapy alone. There is no established
role for beta-agonists, diuretics, acetazolamide, or dexa-
methasone in the treatment of HAPE, although, as noted
below, dexamethasone should be considered when con-
cern is raised for concurrent HACE.
Selected patients (able to achieve an oxygen saturation
>90%, with adequate support from family or friends,
with adequate housing or lodging arrangements) may be
discharged from direct medical care if they can continue
using supplemental oxygen rather than being admitted to
a healthcare facility. Individuals treated in this manner
should be admitted to the hospital if they develop wors-
ening symptoms and/or oxygen saturation while on sup-
plemental oxygen. Descent to lower elevation should be
pursued if oxygenation or other aspects of their condition
worsen despite appropriate interventions for HAPE, as
ARTICLE IN PRESS
Altitude Illness Practice Guidelines 11

this suggests they may have alternative pathology that
requires further evaluation and management.
Individuals who develop HAPE may consider further
ascent to higher altitude or reascent only when symp-
toms of HAPE have completely resolved and they main-
tain stable oxygenation at rest and with mild exercise
while off supplemental oxygen and/or vasodilator ther-
apy. Consideration may be given to using nifedipine or
another pulmonary vasodilator upon resuming ascent.
SUGGESTED APPROACH FOR PATIENTS WITH
CONCURRENT HAPE AND HACE
Dexamethasone should be added to the treatment regimen
of patients with concurrent HAPE and HACE at the doses
described earlier for patients with HACE. Some patients
with HAPE may have neurologic dysfunction caused by
hypoxic encephalopathy rather than caused by HACE, but
making the distinction between hypoxic encephalopathy
and HACE in the field can be difficult. Therefore, dexa-
methasone should be added to the treatment regimen for
patients with HAPE with neurologic dysfunction that does
not resolve rapidly with administration of supplemental
oxygen and improvement in oxygen saturation. If supple-
mental oxygen is not available, dexamethasone should be
started in addition to the medications for HAPE in patients
with altered mental status and/or suspected concurrent
HACE. Nifedipine or other pulmonary vasodilators may
be used in patients with concurrent HAPE and HACE,
with care to avoid lowering mean arterial pressure, as this
may decrease cerebral perfusion pressure and thus
increase the risk for cerebral ischemia.
Conclusions
We have provided evidence-based guidelines for preven-
tion and treatment of acute altitude illnesses, including
the main prophylactic and therapeutic modalities for
AMS, HACE, and HAPE, and recommendations regard-
ing their role in disease management. Although these
guidelines cover many of the important issues related to
prevention and treatment of altitude illness, several
important questions remain to be addressed and should
serve as a focus for future research. Such research
includes determining the optimal rate of ascent to pre-
vent altitude illness, the role of acetazolamide in HAPE
prevention and treatment, proper dosing regimens for
prevention and treatment of altitude illness in the pediat-
ric population, and the role of staged ascent, preacclima-
tization, and hypoxic tents in altitude illness prevention.
Author Contributions: All authors participated in a review of the lit-
erature and analysis of studies. AML drafted the original manuscript.
All authors participated in critical revision of the manuscript and
approved the final manuscript.
Financial/Material Support: None.
Disclosures: None.
Supplementary materials
Supplementary material associated with this article
can be found in the online version at doi:10.1016/j.
wem.2019.04.006.
References
1. Guyatt G, Gutterman D, Baumann MH, Addrizzo-Harris D,
Hylek EM, Phillips B, et al. Grading strength of recommen-
dations and quality of evidence in clinical guidelines: report
from an American College of Chest Physicians task force.
Chest. 2006;129(1):174–81.
2. Luks AM,McIntosh SE, Grissom CK, Auerbach PS, Rodway
GW, Schoene RB, et al. Wilderness Medical Society consen-
sus guidelines for the prevention and treatment of acute alti-
tude illness.Wilderness Environ Med. 2010;21(2):146–55.
3. Luks AM, McIntosh SE, Grissom CK, Auerbach PS, Rod-
way GW, Schoene RB, et al. Wilderness Medical Society
Practice Guidelines for the prevention and treatment of
acute altitude illness: 2014 update. Wilderness Environ
Med. 2014;25(4S):S4–14.
4. Montgomery AB, Mills J, Luce JM. Incidence of acute
mountain sickness at intermediate altitude. JAMA. 1989;
261(5):732–4.
5. Honigman B, Theis MK, Koziol-McLain J, Roach R, Yip
R, Houston C, et al. Acute mountain sickness in a general
tourist population at moderate altitudes. Ann Intern Med.
1993;118(8):587–92.
6. Gabry AL, Ledoux X, Mozziconacci M, Martin C. High-alti-
tude pulmonary edema at moderate altitude (< 2,400 m;
7,870 feet): a series of 52 patients. Chest. 2003;123(1):49–53.
7. Hackett PH, Yarnell PR, Weiland DA, Reynard KB.
Acute and evolving MRI of high-altitude cerebral edema:
microbleeds, edema, and pathophysiology. AJNR Am J
Neuroradiol. 2019;40(3):464–9.
8. Southard A, Niermeyer S, Yaron M. Language used in
Lake Louise Scoring System underestimates symptoms of
acute mountain sickness in 4- to 11-year-old children.
High Alt Med Biol. 2007;8(2):124–30.
9. Muhm JM, Rock PB, McMullin DL, Jones SP, Lu IL,
Eilers KD, et al. Effect of aircraft-cabin altitude on pas-
senger discomfort. N Engl J Med. 2007;357(1):18–27.
10. Theis MK, Honigman B, Yip R, McBride D, Houston CS,
Moore LG. Acute mountain sickness in children at 2835
meters. Am J Dis Child. 1993;147(2):143–5.
11. Hackett PH, Roach RC. High-altitude illness. N Engl J
Med. 2001;345(2):107–14.
12. Hackett PH, Roach RC. High altitude cerebral edema.
High Alt Med Biol. 2004;5(2):136–46.
13. Bartsch P, Swenson ER. Clinical practice: acute high-alti-
tude illnesses. N Engl J Med. 2013;368(24):2294–302.
ARTICLE IN PRESS
12 Luks et al

14. Hackett PH, Luks AM, Lawley JS, Roach RC. High altitude
medicine and pathophysiology. In: Auerbach PS, ed.
Auerbach’s Wilderness Medicine. Philadelphia: Elsevier;
2017.
15. Bloch KE, Turk AJ, Maggiorini M, Hess T, Merz T,
Bosch MM, et al. Effect of ascent protocol on acute
mountain sickness and success at Muztagh Ata, 7546 m.
High Alt Med Biol. 2009;10(1):25–32.
16. Beidleman BA, Fulco CS, Muza SR, Rock PB, Staab JE,
Forte VA, et al. Effect of six days of staging on physiologic
adjustments and acute mountain sickness during ascent to
4300 meters. High Alt Med Biol. 2009;10(3):253–60.
17. Hackett PH, Rennie D, Levine HD. The incidence, impor-
tance, and prophylaxis of acute mountain sickness. Lan-
cet. 1976;2(7996):1149–55.
18. Forwand SA, Landowne M, Follansbee JN, Hansen JE.
Effect of acetazolamide on acute mountain sickness. N
Engl J Med. 1968;279(16):839–45.
19. Basnyat B, Gertsch JH, Holck PS, Johnson EW, Luks AM,
Donham BP, et al. Acetazolamide 125 mg BD is not signifi-
cantly different from 375 mg BD in the prevention of acute
mountain sickness: the prophylactic acetazolamide dosage
comparison for efficacy (PACE) trial. High Alt Med Biol.
2006;7(1):17–27.
20. van Patot MC, Leadbetter 3rd G, Keyes LE, Maakestad
KM, Olson S, Hackett PH. Prophylactic low-dose acet-
azolamide reduces the incidence and severity of acute
mountain sickness. High Alt Med Biol. 2008;9(4):
289–93.
21. Low EV, Avery AJ, Gupta V, Schedlbauer A, Grocott MP.
Identifying the lowest effective dose of acetazolamide for
the prophylaxis of acute mountain sickness: systematic
review and meta-analysis. BMJ. 2012;345:e6779.
22. Luks AM, Swenson ER. Medication and dosage consider-
ations in the prophylaxis and treatment of high-altitude
illness. Chest. 2008;133(3):744–55.
23. Elisabeth E, Hannes G, Johannes B, Martin F, Elena P,
Martin B. Effects of low-dose acetazolamide on exercise
performance in simulated altitude. Int J Physiol Patho-
physiol Pharmacol. 2017;9(2):28–34.
24. Bradwell AR, Myers SD, Beazley M, Ashdown K, Harris
NG, Bradwell SB, et al. Exercise limitation of acetazol-
amide at altitude (3459 m). Wilderness Environ Med.
2014;25(3):272–7.
25. Gonzales JU, Scheuermann BW. Effect of acetazolamide
on respiratory muscle fatigue in humans. Respir Physiol
Neurobiol. 2013;185(2):386–92.
26. McIntosh SE, Hemphill M, McDevitt MC, Gurung TY,
Ghale M, Knott JR, et al. Reduced acetazolamide dosing
in countering altitude illness: a comparison of 62.5 vs
125 mg (the RADICAL Trial). Wilderness Environ Med.
2019;30(1):12–21.
27. Pollard AJ, Niermeyer S, Barry P, Bartsch P, Berghold F,
Bishop RA, et al. Children at high altitude: an interna-
tional consensus statement by an ad hoc committee of the
International Society for Mountain Medicine, March 12,
2001. High Alt Med Biol. 2001;2(3):389–403.
28. Ellsworth AJ, Larson EB, Strickland D. A randomized trial
of dexamethasone and acetazolamide for acute mountain
sickness prophylaxis. Am J Med. 1987;83(6):1024–30.
29. Ellsworth AJ, Meyer EF, Larson EB. Acetazolamide or
dexamethasone use versus placebo to prevent acute
mountain sickness on Mount Rainier. West J Med. 1991;
154(3):289–93.
30. Chrousos G, Pavlaki AN, Magiakou MA, et al. Glucocor-
ticoid therapy and adrenal suppression. In: De Groot LJ,
Chrousos G, Dungan K, eds. Endotext. South Dartmouth,
MA: MDText.com; 2011.
31. Zheng CR, Chen GZ, Yu J, Qin J, Song P, Bian SZ, et al.
Inhaled budesonide and oral dexamethasone prevent acute
mountain sickness. Am J Med. 2014;127(10):1001–9. e2.
32. Chen GZ, Zheng CR, Qin J, Yu J, Wang H, Zhang JH,
et al. Inhaled budesonide prevents acute mountain sick-
ness in young Chinese men. J Emerg Med. 2015;48
(2):197–206.
33. Berger MM, Macholz F, Sareban M, Schmidt P, Fried S,
Dankl D, et al. Inhaled budesonide does not prevent acute
mountain sickness after rapid ascent to 4559 m. Eur
Respir J. 2017;50(3).
34. Lipman GS, Pomeranz D, Burns P, Phillips C, Cheffers
M, Evans K, et al. Budesonide versus acetazolamide for
prevention of acute mountain sickness. Am J Med.
2018;131(2):e9–16.
35. Roncin JP, Schwartz F, D’Arbigny P. EGb 761 in control
of acute mountain sickness and vascular reactivity to cold
exposure. Aviat Space Environ Med. 1996;67(5):445–52.
36. Moraga FA, Flores A, Serra J, Esnaola C, Barriento C.
Ginkgo biloba decreases acute mountain sickness in people
ascending to high altitude at Ollague (3696 m) in northern
Chile.Wilderness Environ Med. 2007;18(4):251–7.
37. Gertsch JH, Basnyat B, Johnson EW, Onopa J, Holck PS.
Randomised, double blind, placebo controlled compari-
son of Ginkgo biloba and acetazolamide for prevention of
acute mountain sickness among Himalayan trekkers: the
prevention of high altitude illness trial (PHAIT). BMJ.
2004;328(7443):797.
38. Chow T, Browne V, Heileson HL, Wallace D, Anholm J,
Green SM. Ginkgo biloba and acetazolamide prophylaxis
for acute mountain sickness: a randomized, placebo-
controlled trial. Arch Intern Med. 2005;165(3):296–301.
39. Leadbetter G, Keyes LE, Maakestad KM, Olson S, Tissot
van Patot MC, Hackett PH. Ginkgo biloba does—and
does not—prevent acute mountain sickness. Wilderness
Environ Med. 2009;20(1):66–71.
40. Dugoua JJ, Mills E, Perri D, Koren G. Safety and efficacy
of ginkgo (Ginkgo biloba) during pregnancy and lacta-
tion. Can J Clin Pharmacol. 2006;13(3):e277–84.
41. Stoddard GJ, Archer M, Shane-McWhorter L, Bray BE,
Redd DF, Proulx J, et al. Ginkgo and warfarin interaction
in a large veterans administration population. AMIA Annu
Symp Proc. 2015;2015:1174–83.
42. Gertsch JH, Corbett B, Holck PS, Mulcahy A, Watts M,
Stillwagon NT, et al. Altitude Sickness in Climbers and Effi-
cacy of NSAIDs Trial (ASCENT): randomized, controlled
ARTICLE IN PRESS
Altitude Illness Practice Guidelines 13

trial of ibuprofen versus placebo for prevention of altitude
illness.Wilderness Environ Med. 2012;23(4):307–15.
43. Lipman GS, Kanaan NC, Holck PS, Constance BB,
Gertsch JH. Ibuprofen prevents altitude illness: a random-
ized controlled trial for prevention of altitude illness with
nonsteroidal anti-inflammatories. Ann Emerg Med. 2012;
59(6):484–90.
44. Lundeberg J, Feiner JR, Schober A, Sall JW, Eilers H,
Bickler PE. Increased cytokines at high altitude: lack of
effect of ibuprofen on acute mountain sickness, physio-
logical variables, or cytokine levels. High Alt Med Biol.
2018;19(3):249–58.
45. Kanaan NC, Peterson AL, Pun M, Holck PS, Starling J,
Basyal B, et al. Prophylactic acetaminophen or ibuprofen
results in equivalent acute mountain sickness incidence at
high altitude: a prospective randomized trial. Wilderness
Environ Med. 2017;28(2):72–8.
46. Gertsch JH, Lipman GS, Holck PS, Merritt A, Mulcahy A,
Fisher RS, et al. Prospective, double-blind, randomized,
placebo-controlled comparison of acetazolamide versus ibu-
profen for prophylaxis against high altitude headache: the
Headache Evaluation at Altitude Trial (HEAT). Wilderness
Environ Med. 2010;21(3):236–43.
47. Burns P, Lipman GS, Warner K, Jurkiewicz C, Phillips C,
Sanders L, et al. Altitude sickness prevention with ibupro-
fen relative to acetazolamide. Am J Med. 2019;132
(2):247–51.
48. Baggish AL, Fulco CS, Muza S, Rock PB, Beidleman B,
Cymerman A, et al. The impact of moderate-altitude stag-
ing on pulmonary arterial hemodynamics after ascent to
high altitude. High Alt Med Biol. 2010;11(2):139–45.
49. Lyons TP, Muza SR, Rock PB, Cymerman A. The effect
of altitude pre-acclimatization on acute mountain sickness
during reexposure. Aviat Space Environ Med. 1995;66
(10):957–62.
50. Beidleman BA, Muza SR, Fulco CS, Cymerman A, Dit-
zler D, Stulz D, et al. Intermittent altitude exposures
reduce acute mountain sickness at 4300 m. Clin Sci
(Lond). 2004;106(3):321–8.
51. Wille M, Gatterer H, Mairer K, Philippe M, Schwarzen-
bacher H, Faulhaber M, et al. Short-term intermittent hyp-
oxia reduces the severity of acute mountain sickness.
Scand J Med Sci Sports. 2012;22(5):e79–85.
52. Burse RL, Forte Jr VA. Acute mountain sickness at
4500 m is not altered by repeated eight-hour exposures to
3200�3550 m normobaric hypoxic equivalent. Aviat
Space Environ Med. 1988;59(10):942–9.
53. Schommer K, Wiesegart N, Menold E, Haas U, Lahr K,
Buhl H, et al. Training in normobaric hypoxia and its
effects on acute mountain sickness after rapid ascent to
4559 m. High Alt Med Biol. 2010;11(1):19–25.
54. Fulco CS, Muza SR, Beidleman BA, Demes R, Staab JE,
Jones JE, et al. Effect of repeated normobaric hypoxia
exposures during sleep on acute mountain sickness, exer-
cise performance, and sleep during exposure to terrestrial
altitude. Am J Physiol Regul Integr Comp Physiol. 2011;
300(2):R428–36.
55. Faulhaber M, Pocecco E, Gatterer H, Niedermeier M,
Huth M, Dunnwald T, et al. Seven passive 1-h hypoxia
exposures do not prevent AMS in susceptible individuals.
Med Sci Sports Exerc. 2016;48(12):2563–70.
56. Fulco CS, Beidleman BA, Muza SR. Effectiveness of pre-
acclimatization strategies for high-altitude exposure.
Exerc Sport Sci Rev. 2013;41(1):55–63.
57. Dehnert C, Bohm A, Grigoriev I, Menold E, Bartsch P.
Sleeping in moderate hypoxia at home for prevention of
acute mountain sickness (AMS): a placebo-controlled,
randomized double-blind study. Wilderness Environ Med.
2014;25(3):263–71.
58. Baillie JK, Thompson AA, Irving JB, Bates MG, Sutherland
AI, Macnee W, et al. Oral antioxidant supplementation does
not prevent acute mountain sickness: double blind, random-
ized placebo-controlled trial.QJM. 2009;102(5):341–8.
59. Talbot NP, Smith TG, Privat C, Nickol AH, Rivera-Ch M,
Leon-Velarde F, et al. Intravenous iron supplementation
may protect against acute mountain sickness: a random-
ized, double-blinded, placebo-controlled trial. High Alt
Med Biol. 2011;12(3):265–9.
60. Rossetti GMK, Macdonald JH, Wylie LJ, Little SJ, New-
ton V, Wood B, et al. Dietary nitrate supplementation
increases acute mountain sickness severity and sense of
effort during hypoxic exercise. J Appl Physiol (1985).
2017;123(4):983–92.
61. Grissom CK, Richer LD, Elstad MR. The effects of a
5-lipoxygenase inhibitor on acute mountain sickness and
urinary leukotriene e4 after ascent to high altitude. Chest.
2005;127(2):565–70.
62. Luks AM, Henderson WR, Swenson ER. Leukotriene
receptor blockade does not prevent acute mountain sick-
ness induced by normobaric hypoxia. High Alt Med Biol.
2007;8(2):131–8.
63. Bates MG, Thompson AA, Baillie JK, Sutherland AI, Irv-
ing JB, Hirani N, et al. Sildenafil citrate for the prevention
of high altitude hypoxic pulmonary hypertension: double
blind, randomized, placebo-controlled trial. High Alt Med
Biol. 2011;12(3):207–14.
64. Kayser B, Hulsebosch R, Bosch F. Low-dose acetylsali-
cylic acid analog and acetazolamide for prevention of
acute mountain sickness. High Alt Med Biol. 2008;9
(1):15–23.
65. Basnyat B, Holck PS, Pun M, Halverson S, Szawarski P,
Gertsch J, et al. Spironolactone does not prevent acute
mountain sickness: a prospective, double-blind, random-
ized, placebo-controlled trial by SPACE Trial Group (spi-
ronolactone and acetazolamide trial in the prevention of
acute mountain sickness group). Wilderness Environ
Med. 2011;22(1):15–22.
66. Jafarian S, Gorouhi F, Salimi S, Lotfi J. Sumatriptan for
prevention of acute mountain sickness: randomized clini-
cal trial. Ann Neurol. 2007;62(3):273–7.
67. Lipman GS, Kanaan NC, Phillips C, Pomeranz D, Cain P,
Fontes K, et al. Study Looking at End Expiratory Pressure
for Altitude Illness Decrease (SLEEP-AID). High Alt
Med Biol. 2015;16(2):154–61.
ARTICLE IN PRESS
14 Luks et al

68. Berger MM, Macholz F, Lehmann L, Dankl D, Hochreiter
M, Bacher B, et al. Remote ischemic preconditioning
does not prevent acute mountain sickness after rapid
ascent to 3,450 m. J Appl Physiol (1985). 2017;123
(5):1228–34.
69. Bartsch P, Merki B, Hofstetter D, Maggiorini M, Kayser B,
Oelz O. Treatment of acute mountain sickness by simulated
descent: a randomised controlled trial. BMJ. 1993;306
(6885):1098–101.
70. Keller HR, Maggiorini M, Bartsch P, Oelz O. Simulated
descent v dexamethasone in treatment of acute mountain
sickness: a randomised trial. BMJ. 1995;310(6989):
1232–5.
71. Taber RL. Protocols for the use of portable hyperbaric
chambers for the treatment of high altitude disorders.
J Wild Med. 1990;1:181–92.
72. Grissom CK, Roach RC, Sarnquist FH, Hackett PH. Acet-
azolamide in the treatment of acute mountain sickness:
clinical efficacy and effect on gas exchange. Ann Intern
Med. 1992;116(6):461–5.
73. Ferrazzini G, Maggiorini M, Kriemler S, Bartsch P, Oelz
O. Successful treatment of acute mountain sickness with
dexamethasone. Br Med J (Clin Res Ed). 1987;294
(6584):1380–2.
74. Hackett PH, Roach RC, Wood RA, Foutch RG, Meehan
RT, Rennie D, et al. Dexamethasone for prevention and
treatment of acute mountain sickness. Aviat Space Envi-
ron Med. 1988;59(10):950–4.
75. Levine BD, Yoshimura K, Kobayashi T, Fukushima M,
Shibamoto T, Ueda G. Dexamethasone in the treatment
of acute mountain sickness. N Engl J Med. 1989;321
(25):1707–13.
76. Harris NS, Wenzel RP, Thomas SH. High altitude headache:
efficacy of acetaminophen vs. ibuprofen in a randomized,
controlled trial. J Emerg Med. 2003;24(4):383–7.
77. Johnson PL, Johnson CC, Poudyal P, Regmi N,
Walmsley MA, Basnyat B. Continuous positive airway
pressure treatment for acute mountain sickness at
4240 m in the Nepal Himalaya. High Alt Med Biol.
2013;14(3):230–3.
78. Walmsley M. Continuous positive airway pressure as
adjunct treatment of acute altitude illness. High Alt Med
Biol. 2013;14(4):405–7.
79. Stream JO, Grissom CK. Update on high-altitude pulmo-
nary edema: pathogenesis, prevention, and treatment.Wil-
derness Environ Med. 2008;19(4):293–303.
80. Bartsch P, Mairbaurl H, Maggiorini M, Swenson ER.
Physiological aspects of high-altitude pulmonary edema.
J Appl Physiol. 2005;98(3):1101–10.
81. Bartsch P, Maggiorini M, Mairbaurl H, Vock P, Swenson
ER. Pulmonary extravascular fluid accumulation in
climbers. Lancet. 2002;360(9332):571; author reply �2.
82. Singh I, Kapila CC, Khanna PK, Nanda RB, Rao BD. High-
altitude pulmonary oedema. Lancet. 1965;191:229–34.
83. Bartsch P, Maggiorini M, Ritter M, Noti C, Vock P, Oelz
O. Prevention of high-altitude pulmonary edema by nifed-
ipine. N Engl J Med. 1991;325(18):1284–9.
84. Sartori C, Allemann Y, Duplain H, Lepori M, Egli M, Lipp
E, et al. Salmeterol for the prevention of high-altitude pul-
monary edema. N Engl J Med. 2002;346(21):1631–6.
85. Maggiorini M, Brunner-La Rocca HP, Peth S, Fischler M,
Bohm T, Bernheim A, et al. Both tadalafil and dexameth-
asone may reduce the incidence of high-altitude pulmo-
nary edema: a randomized trial. Ann Intern Med. 2006;
145(7):497–506.
86. Hohne C, Krebs MO, Seiferheld M, Boemke W, Kacz-
marczyk G, Swenson ER. Acetazolamide prevents hyp-
oxic pulmonary vasoconstriction in conscious dogs. J
Appl Physiol. 2004;97(2):515–21.
87. Shimoda LA, Luke T, Sylvester JT, Shih HW, Jain A,
Swenson ER. Inhibition of hypoxia-induced calcium
responses in pulmonary arterial smooth muscle by acet-
azolamide is independent of carbonic anhydrase inhibi-
tion. Am J Physiol Lung Cell Mol Physiol. 2007;292(4):
L1002–12.
88. Pickerodt PA, Francis RC, Hohne C, Neubert F, Telalba-
sic S, Boemke W, et al. Pulmonary vasodilation by acet-
azolamide during hypoxia: impact of methyl-group
substitutions and administration route in conscious, spon-
taneously breathing dogs. J Appl Physiol (1985). 2014;
116(7):715–23.
89. Teppema LJ, Balanos GM, Steinback CD, Brown AD,
Foster GE, Duff HJ, et al. Effects of acetazolamide on
ventilatory, cerebrovascular, and pulmonary vascular
responses to hypoxia. Am J Respir Crit Care Med. 2007;
175(3):277–81.
90. Liptzin DR, Abman SH, Giesenhagen A, Ivy DD. An
approach to children with pulmonary edema at high alti-
tude. High Alt Med Biol. 2018;19(1):91–8.
91. Marticorena E, Hultgren HN. Evaluation of therapeutic
methods in high altitude pulmonary edema. Am J Cardiol.
1979;43(2):307–12.
92. Zafren K, Reeves JT, Schoene R. Treatment of high-alti-
tude pulmonary edema by bed rest and supplemental oxy-
gen.Wilderness Environ Med. 1996;7(2):127–32.
93. Yanamandra U, Nair V, Singh S, Gupta A, Mulajkar D,
Yanamandra S, et al. Managing high-altitude pulmonary
edema with oxygen alone: results of a randomized con-
trolled trial. High Alt Med Biol. 2016;17(4):294–9.
94. Freeman K, Shalit M, Stroh G. Use of the Gamow Bag by
EMT-basic park rangers for treatment of high-altitude
pulmonary edema and high-altitude cerebral edema. Wil-
derness Environ Med. 2004;15(3):198–201.
95. Oelz O, Maggiorini M, Ritter M, Waber U, Jenni R, Vock P,
et al. Nifedipine for high altitude pulmonary oedema. Lan-
cet. 1989;2(8674):1241–4.
96. Deshwal R, Iqbal M, Basnet S. Nifedipine for the treat-
ment of high altitude pulmonary edema. Wilderness Envi-
ron Med. 2012;23(1):7–10.
97. Fagenholz PJ, Gutman JA, Murray AF, Harris NS. Treat-
ment of high altitude pulmonary edema at 4240 m in
Nepal. High Alt Med Biol. 2007;8(2):139–46.
98. Jones BE, Stokes S, McKenzie S, Nilles E, Stoddard GJ.
Management of high altitude pulmonary edema in the
ARTICLE IN PRESS
Altitude Illness Practice Guidelines 15
Himalaya: a review of 56 cases presenting at Pheriche
medical aid post (4240 m). Wilderness Environ Med.
2013;24(1):32–6.
99. Schoene RB, Roach RC, Hackett PH, Harrison G, Mills Jr
WJ. High altitude pulmonary edema and exercise at 4,400
meters on Mount McKinley. Effect of expiratory positive
airway pressure. Chest. 1985;87(3):330–3.
100. Singh I, Lal M, Khanna PK, Mathew NT. Augmentation
of frusemide diuresis by morphine in high altitude pulmo-
nary oedema. Br Heart J. 1967;29(5):709–13.
101. Siebenmann C, Bloch KE, Lundby C, Nussbamer-Ochsner Y,
Schoeb M, Maggiorini M. Dexamethasone improves maxi-
mal exercise capacity of individuals susceptible to high alti-
tude pulmonary edema at 4559 m. High Alt Med Biol.
2011;12(2):169–77.
102. Urner M, Herrmann IK, Booy C, Z’Graggen BR, Mag-
giorini M, Beck-Schimmer B. Effect of hypoxia and
dexamethasone on inflammation and ion transporter
function in pulmonary cells. Clin Exp Immunol. 2012;
169(2):119–28.
103. Roach RC, Hackett PH, Oelz O, Bartsch P, Luks AM,
MacInnis MJ, et al. The 2018 Lake Louise Acute Moun-
tain Sickness Score. High Alt Med Biol. 2018;19(1):
4–6.
ARTICLE IN PRESS
16 Luks et al

Special Reports
The 2018 Lake Louise Acute Mountain Sickness Score
Robert C. Roach,1 Peter H. Hackett,1 Oswald Oelz,2 Peter Bartsch,3 Andrew M. Luks,4 Martin J. MacInnis,5
J. Kenneth Baillie,6,7 and The Lake Louise AMS Score Consensus Committee
Abstract
Roach, Robert C., Peter H. Hackett, Oswald Oelz, Peter Bartsch, Andrew M. Luks, Martin J. MacInnis,J. Kenneth Baillie, and The Lake Louise AMS Score Consensus Committee. The 2018 Lake Louise AcuteMountain Sickness Score. High Alt Med Biol. 19:4–6, 2018.— The Lake Louise Acute Mountain Sickness (AMS)scoring system has been a useful research tool since first published in 1991. Recent studies have shown that disturbedsleep at altitude, one of the five symptoms scored for AMS, is more likely due to altitude hypoxia per se, and is notclosely related to AMS. To address this issue, and also to evaluate the Lake Louise AMS score in light of decades ofexperience, experts in high altitude research undertook to revise the score. We here present an international consensusstatement resulting from online discussions and meetings at the International Society of Mountain Medicine WorldCongress in Bolzano, Italy, in May 2014 and at the International Hypoxia Symposium in Lake Louise, Canada, inFebruary 2015. The consensus group has revised the score to eliminate disturbed sleep as a questionnaire item, and hasupdated instructions for use of the score.
Keywords: AMS; high altitude illness; history; Lake Louise; symptom scores
Committee members: Eric Achatz, United States; Edi Albert, Australia; Jon S. Andrews, United States; James D.Anholm, United States; Mohammad Zahid Ashraf, India; Paul Auerbach, United States; Buddha Basnyat, Nepal; Beth A.Beidleman, United States; R.R. Berendsen, The Netherlands; Marc Moritz Berger, Austria; Konrad E. Bloch, Switzerland;Hermann Brugger, Italy; Annalisa Cogo, Italy; Ricardo Gonzalez Costa, Argentina; Andrew Cumpstey, United Kingdom;Allen Cymerman, United States; Tadej Debevec, Slovenia; Catriona Duncan, United Kingdom; David Dubowitz, UnitedStates; Angela Fago, Denmark; Michael Furian, Switzerland; Matt Gaidica, United States; Prosenjit Ganguli, India;Michael P.W. Grocott, United Kingdom; Debra Hammer, Canada; David Hall, United Kingdom; David Hillebrandt,United Kingdom; Matthias Peter Hilty, Switzerland; Gigugu Himashree, India; Benjamin Honigman, United States; NedGilbert-Kawai, United Kingdom; Bengt Kayser, Switzerland; Linda Keyes, United States; Michael Koehle, Canada;Samantha Kohli, India; Arlena Kuenzel, United Kingdom; Benjamin D. Levine, United States; Mona Lichtblau, Swit-zerland; Jamie Macdonald, United Kingdom; Monika Brodmann Maeder, Italy; Marco Maggiorini, Switzerland; DanielMartin, United Kingdom; Shigeru Masuyama, Japan; John McCall, Canada; Scott McIntosh, United States; GregoireMillet, Switzerland; Fernando Moraga, Chile; Craig Mounsey, United Kingdom; Stephen R. Muza, United States; SamuelOliver, United Kingdom; Qadar Pasha, India; Ryan Paterson, United States; Lara Phillips, United States; Aurelien Pichon,France; Philipp A. Pickerodt, Germany; Matiram Pun, Canada; Manjari Rain, India; Drummond Rennie, United States; GeRi-Li, P.R. China; Steven Roy, Canada; Samuel Verges, France; Tatiana Batalha Cunha dos Santos, Brazil; Robert B.Schoene, United States; Otto D. Schoch, Switzerland; Surinderpal Singh, India; Talant Sooronbaev, Kyrgyz Republic;Craig D. Steinback, Canada; Mike Stembridge, United Kingdom; Glenn Stewart, United States; Tsering Stobdan, UnitedStates; Giacomo Strapazzon, Italy; Andrew W. Subudhi, United States; Erik Swenson, United States; A. A. RogerThompson, United Kingdom; Martha Tissot van Patot, United States; Rosie Twomey, Canada; Silvia Ulrich, Switzerland;Nicolas Voituron, France; Dale R. Wagner, United States; Shih-hao Wang, Taiwan; John B. West, United States; MattWilkes, United Kingdom; Gabriel Willmann, Germany; Michael Yaron, United States; Ken Zafren, United States.
1Altitude Research Center, Division of Pulmonary Sciences and Critical Care Medicine, Department of Medicine, University ofColorado School of Medicine, Anschutz Medical Campus, Aurora, Colorado.
2Department of Internal Medicine, University of Zurich, Switzerland.3Department of Internal Medicine, University Hospital, Heidelberg, Germany.4Division of Pulmonary, Critical Care and Sleep Medicine, Department of Medicine, University of Washington, Seattle, WA.5Department of Kinesiology, McMaster University, Hamilton, Canada.6Roslin Institute, University of Edinburgh, Easter Bush, Midlothian, United Kingdom.7Intensive Care Unit, Royal Infirmary Edinburgh, Edinburgh, United Kingdom.
HIGH ALTITUDE MEDICINE & BIOLOGYVolume 19, Number 1, 2018ª Mary Ann Liebert, Inc.DOI: 10.1089/ham.2017.0164
4

Introduction
Acute mountain sickness (AMS) is the most commonform of acute altitude illness and typically occurs in
unacclimatized persons ascending to altitudes >2500 m, al-though it can develop at lower altitudes in highly susceptibleindividuals. Established risk factors include rate of ascent,altitude reached, and individual predisposition. With 25 yearsof use in hundreds of publications, the Lake Louise AMS scorehas provided a robust and practical tool for researchers todiagnose and to score the severity of AMS. Recent opinion(Milledge, 2014) and research (MacInnis et al., 2013; Hallet al., 2014) have suggested that updating the Lake LouiseAMS score is in order. This article outlines the brief historicalbackground, reviews diagnostic criteria, describes modifica-tions to the score, and offers suggested experimental proce-dures that may improve the use of the score in future studies.
Background
At the 1991 International Hypoxia Symposium, the partici-pants executed a consensus process chaired by Peter Hackett andOswald Oelz (Hackett et al., 1992; supplementary reprint oforiginal article is available online at www.liebertpub.com/ham)to define and quantify the various altitude illnesses. Subsequentlyat the 1993 conference, all delegates were given the opportunityto have input into the preparation of the document. The score forAMS consisted of the five symptoms (headache, gastrointestinalupset, fatigue/weakness, dizziness/light-headedness, and sleepdisturbance), rated on a scale of severity from 0 to 3. The double-worded terms were to facilitate understanding as well as trans-lation into many languages (Roach et al., 1993; supplementaryreprint of original article is available online at www.liebertpub.com/ham). A total score ‡3, in the presence of a headache, wasconsidered diagnostic for AMS.
Methods
This effort is the result of online discussions and meetingsat the International Society of Mountain Medicine WorldCongress in Bolzano, Italy, in May 2014 and at the Interna-tional Hypoxia Symposium in Lake Louise, Canada, inFebruary 2015. Members of the consensus committee arethose who have participated in the online or in-person dis-cussions and are listed in alphabetical order in the box.
Rationale for Revising the Lake Louise AMS Score
Although use of the scoring system has helped standardizethe diagnosis and severity of AMS across research studies,debate has persisted since its inception regarding whether sleepshould be included in the diagnostic criteria. Recently thisdiscussion has intensified. Two independent reports in 2013provided empirical evidence that sleep disturbance is discordantfrom other symptoms of AMS (MacInnis et al., 2013; Hallet al., 2014). Hall et al. (2014) used network analysis of datafrom 292 research volunteers exposed to altitudes from 3650 to5200 m to demonstrate that sleep disturbance correlated poorlywith other symptoms of AMS. Importantly, sleep disturbancewas absent in 40% of cases with severe headache, long con-sidered a hallmark of AMS. MacInnis et al. (2013) appliedfactor analysis to Lake Louise AMS scores of 491 Nepalesepilgrims at 4390 m and revealed that sleep had only a weakrelationship with the other four symptoms in the score. Milledge
also expressed doubt as to whether sleep disturbance was asymptom of AMS, or rather an effect of hypoxia per se, basedon his own experience with AMS studies (Milledge, 2014).Another problem recognized over time is that many studies ofAMS have used only daytime exposures, making the sleepcomponent irrelevant. Without a score for sleep in these studies,comparison with overnight studies is difficult. Based on theseconcerns, the consensus committee recommends that the sleepcomponent be removed from the Lake Louise AMS score.
Diagnostic Criteria and Assessment of AMS
AMS is defined as a Lake Louise AMS score total of threeor more points from the four rated symptoms, including atleast one point from headache in the setting of a recent ascentor gain in altitude (Roach et al., 2011; West, 2011) (Table 1).Some authors have suggested a higher cutoff for diagnosingAMS (Maggiorini et al., 1998; Bartsch et al., 2004), but theconsensus committee believes that by eliminating the sleepquestion, more people with true AMS will be identified at thethreshold of three points, including headache. Sufficient re-search is lacking to divide the score into severity rankings.For those who wish to do so, we suggest mild AMS as 3–5points, moderate AMS as 6–9 points, and severe AMS as 10–12 points. Although symptoms can develop within 6 hours ofgain in altitude, we recommend assessing AMS score onlyafter 6 hours, to avoid confusing AMS with confoundingsymptoms from travel or responses to acute hypoxia (e.g.,vagal responses). If investigators wish to assess the impact ofAMS symptoms on overall function at high altitude, the‘‘AMS Clinical Functional Score’’ is available (Table 1).
Table 1. 2018 Lake Louise Acute Mountain
Sickness Score
Headache0—None at all1—A mild headache2—Moderate headache3—Severe headache, incapacitating
Gastrointestinal symptoms0—Good appetite1—Poor appetite or nausea2—Moderate nausea or vomiting3—Severe nausea and vomiting, incapacitating
Fatigue and/or weakness0—Not tired or weak1—Mild fatigue/weakness2—Moderate fatigue/weakness3—Severe fatigue/weakness, incapacitating
Dizziness/light-headedness0—No dizziness/light-headedness1—Mild dizziness/light-headedness2—Moderate dizziness/light-headedness3—Severe dizziness/light-headedness, incapacitating
AMS Clinical Functional ScoreOverall, if you had AMS symptoms, how did they affect
your activities?0—Not at all1—Symptoms present, but did not force any change in
activity or itinerary2—My symptoms forced me to stop the ascent or to go
down on my own power3—Had to be evacuated to a lower altitude
2018 LAKE LOUISE AMS SCORE 5

AMS must not be confused with high-altitude cerebral edema(HACE). AMS alone exhibits no neurological findings, and isself-limited. In contrast, HACE, which usually comes on be-tween 24 and 72 hours after a gain in altitude, is characterized bychange in mental status and/or ataxia, occurs usually in a personwith AMS or high-altitude pulmonary edema, and is a medicalemergency (Hackett and Roach, 2004; Willmann et al., 2014).
Directions for Using the Lake Louise AMS Score
This Lake Louise AMS score is for use by investigatorsstudying AMS. It is not intended for use by clinicians, pro-fessional outdoor guides, and laypersons to diagnose ormanage AMS. After a recent gain in altitude or induction ofhypoxia, and an exposure of at least 6 hours duration, theAMS score is used as follows:
1. The Lake Louise AMS score is designed as a self-report questionnaire that research volunteers completeon their own. However, some investigators prefer toread the question to the volunteer and record the an-swers, whereas others use a two-step method whereinthe volunteer first completes the score, then the in-vestigator verbally verifies the answers. These optionsare acceptable as long as a uniform approach is usedwith all subjects in a study and the method of col-lecting data is clearly described in subsequent reports.
2. The Lake Louise AMS score for an individual is the sumof the score for the four symptoms (headache, nausea/vomiting, fatigue, and dizziness/light-headedness). For apositive AMS definition, it is mandatory to have a head-ache score of at least one point, and a total score of at leastthree points.
Example 1: A total score greater than two points butwith no headache is defined as NO AMS for researchpurposes, although absence of a headache does notexclude a diagnosis for clinical purposes.Example 2: A score of three points for a severe head-ache, with no other AMS symptoms, is defined as AMS.
3. We suggest using the AMS clinical functional scoreand reporting it when suitable to the study design(Roach et al., 1993; supplementary reprint of originalarticle is available online at www.liebertpub.com/ham;Meier et al., 2017).
Avenues for Future Research
Further research should focus on the following areas: (1) bestmethods for Lake Louise AMS score administration; that is,is investigator-led scoring different/better than volunteer-completed scores? (2) the impact of experimental design, thetesting environment, and expectations of research volunteers(i.e., nocebo) (Benedetti et al., 2014) on reliability of LakeLouise AMS score; (3) the clinical and functional impact(s) ofAMS score severity; (4) best practices for use of the Lake LouiseAMS score and clinical functional score by nonexpert clinicians,mountain guides, and laypersons (Roach et al., 1993; supple-mentary reprint of original article is available online at www.liebertpub.com/ham; Meier et al., 2017); (5) the impact of dis-turbed sleep on overall well-being at high altitude, independentof AMS; and (6) the pathophysiology of typical AMS vs. pre-sentation without headache (Roach et al., 2011; West, 2011). Inaddition, we strongly encourage researchers to publish all in-
dividual scores for all volunteers and all symptoms. This willallow other researchers to directly compare patterns of illness,to compile meta-analyses, and to examine the raw data for ideasand observations that will further refine the consensus defini-tion and scoring of AMS.
Author Disclosure Statement
No competing financial interests exist.
References
Bartsch P, Bailey DM, Berger MM, Knauth M, and Baum-gartner RW. (2004). Acute mountain sickness: Controversiesand advances. High Alt Med Biol 5:110–124.
Benedetti F, Durando J, and Vighetti S. (2014). Nocebo and pla-cebo modulation of hypobaric hypoxia headache involves thecyclooxygenase-prostaglandins pathway. Pain 155:921–928.
Hackett PH, and Oelz O. (1992). The Lake Louise Consensuson the definition and quantification of altitude illness. In:Hypoxia and Mountain Medicine. JR Sutton, CS Houston, GCoates, eds. Queen City Press, Burlington, VT. pp 327–330.
Hackett PH, and Roach RC. (2004). High altitude cerebraledema. High Alt Med Biol 5:136–146.
Hall DP, MacCormick IJ, Phythian-Adams AT, RzechorzekNM, Hope-Jones D, Cosens S, Jackson S, Bates MG, CollierDJ, Hume DA, et al. (2014). Network analysis reveals distinctclinical syndromes underlying acute mountain sickness. PLoSOne 9:e81229.
MacInnis MJ, Lanting SC, Rupert JL, and Koehle MS. (2013). Ispoor sleep quality at high altitude separate from acute mountainsickness? Factor structure and internal consistency of the LakeLouise Score Questionnaire. High Alt Med Biol 14:334–337.
Maggiorini M, Muller A, Hofstetter D, Bartsch P, and Oelz O. (1998).Assessment of acute mountain sickness by different score proto-cols in the Swiss Alps. Aviat Space Environ Med 69:1186–1192.
Meier D, Collet TH, Locatelli I, Cornuz J, Kayser B, Simel DL,and Sartori C. (2017). Does this patient have acute mountainsickness?: The rational clinical examination systematic re-view. JAMA 318:1810–1819.
Milledge JS. (2014). Should sleep quality be part of the Lake LouiseAcute Mountain Sickness Score? High Alt Med Biol 15:208.
Roach RC, Bartsch P, Hackett PH, and Oelz O. (1993). TheLake Louise Acute Mountain Sickness Scoring System. In:Hypoxia and Molecular Medicine. JR Sutton, CS Houston, GCoates, eds. Queen City Press, Burlington, VT. pp 272–274.
Roach RC, Kayser B, and Hackett PH. (2011). Pro: Headacheshould be a required symptom for the diagnosis of acutemountain sickness. High Alt Med Biol 12:21–22.
West JB. (2011). Con: Headache should not be a requiredsymptom for the diagnosis of acute mountain sickness. HighAlt Med Biol 12:23–25.
Willmann G, Gekeler F, Schommer K, and Bartsch P. (2014).Update on high altitude cerebral edema including recent workon the eye. High Alt Med Biol 15:112–122.
Address correspondence to:Robert C. Roach, PhD
Altitude Research CenterDivision of Pulmonary Sciences and Critical Care Medicine
Department of MedicineAnschutz Medical Campus
University of Colorado School of MedicineAurora CO 80045
E-mail: [email protected]
6 ROACH ET AL.

WILDERNESS MEDICAL SOCIETY PRACTICE GUIDELINES
Wilderness Medical Society Practice Guidelines for thePrevention and Treatment of Frostbite: 2019 Update
Scott E. McIntosh, MD, MPH1; Luanne Freer, MD2,3; Colin K. Grissom, MD4; Paul S. Auerbach, MD, MS5;
George W. Rodway, PhD, APRN6; Amalia Cochran, MD7; Gordon G. Giesbrecht, MD8;
Marion McDevitt, DO, MPH9; Christopher H. Imray, MD10; Eric L. Johnson, MD11; Prativa Pandey, MD12;
Jennifer Dow, MD13; Peter H. Hackett, MD14,15
1Division of Emergency Medicine, University of Utah, Salt Lake City, UT; 2Everest Base Camp Medical Clinic, Nepal; 3Yellowstone National
Park, WY; 4Division of Critical Care Medicine, Intermountain Medical Center, Salt Lake City, UT; 5Department of Emergency Medicine, Stanford
University, School of Medicine, Palo Alto, CA; 6College of Nursing and School of Medicine, UC Davis, Davis, CA; 7Department of Surgery, The
Ohio State University, Columbus, OH; 8Faculty of Kinesiology and Recreation Management, Departments of Anesthesia and Emergency Medicine,
University of Manitoba, Winnipeg, Canada; 9Emergency Medicine, Peace Health Ketchikan Medical Center, Ketchikan, AK; 10Warwick Medical
School, University Hospital Coventry and Warwickshire NHS Trust, Coventry, UK; 11Wound & Hyperbaric Medicine, Bozeman Health, Bozeman,
MT; 12CIWEC Hospital, Kathmandu, Nepal; 13Denali National Park and Preserve, AK; 14Division of Emergency Medicine, Altitude Research
Center, University of Colorado Denver School of Medicine, Denver, CO; 15Institute for Altitude Medicine, Telluride, CO
The Wilderness Medical Society convened an expert panel to develop a set of evidence-based guide-
lines for prevention and treatment of frostbite. We present a review of pertinent pathophysiology. We
then discuss primary and secondary prevention measures and therapeutic management. Recommenda-
tions are made regarding each treatment and its role in management. These recommendations are
graded on the basis of the quality of supporting evidence and balance between the benefits and risks or
burdens for each modality according to methodology stipulated by the American College of Chest
Physicians. This is an updated version of the guidelines published in 2014.
Keywords: hypothermia, rewarming, aloe vera, thrombolysis, tPA, iloprost
Introduction
The Wilderness Medical Society (WMS) convened an
expert panel to develop a set of evidence-based guide-
lines for prevention and treatment of frostbite to guide
clinicians and first responders and disseminate knowl-
edge about best practices in this area of clinical care. We
present the main prophylactic and therapeutic modalities
and make recommendations about their role in injury
management. Recommendations are graded on the basis
of the quality of supporting evidence and balance
between the benefits and risks or burdens for each
modality. We then provide suggested approaches for pre-
vention and management that incorporate these recom-
mendations.
The original expert panel was convened at the 2010
Annual Winter Meeting of the WMS in Park City, UT.
Members were selected on the basis of their clinical or
research experience. Relevant articles were identified
through the MEDLINE database using the search terms
frostbite, frostbite management, prehospital frostbite treat-
ment, prehospital frostbite management, frostbite preven-
tion, first aid frostbite treatment, and first aid frostbite and
were restricted to the English language. Studies in these cat-
egories were reviewed, and level of evidence was assessed.
The panel used a consensus approach to develop recom-
mendations regarding each modality and graded each rec-
ommendation according to criteria stipulated by the
American College of Chest Physicians statement on grading
recommendations and strength of evidence in clinical
guidelines (online Supplementary Table 1).1 This is an
updated version of the guidelines published in 2014.2
Pathophysiology of frostbite
Frostbite is a freezing injury that may be divided into 4
overlapping pathologic phases: prefreeze, freeze�thaw,
Corresponding author: Scott E. McIntosh, MD, MPH, University of
Utah, Division of Emergency Medicine, 50 North Medical Drive, Salt
Lake City, UT 84132; e-mail: [email protected].
Submitted for publication December 2018.
Accepted for publication May 2019.
ARTICLE IN PRESS
Wilderness & EnvironmentalMedicine 2019; 00(00): 1�14

vascular stasis, and late ischemic. The prefreeze phase
consists of tissue cooling with accompanying vasocon-
striction and ischemia and without actual ice crystal for-
mation. Neuronal cooling and ischemia produce
hyperesthesia or paresthesia. In the freeze�thaw phase,
ice crystals form intracellularly (during a more rapid-onset
freezing injury) or extracellularly (during a slower freeze),
causing protein and lipid derangement, cellular electrolyte
shifts, cellular dehydration, cell membrane lysis, and cell
death.3 The thawing process may initiate ischemia, reper-
fusion injury, and an inflammatory response. In the vascu-
lar stasis phase, vessels fluctuate between constriction and
dilation; blood may leak from vessels or coagulate within
them.4�6 The late ischemic phase results from progressive
tissue ischemia and infarction from a cascade of events,
including inflammation mediated by thromboxane A2,
prostaglandin F2alpha, bradykinin, and histamine; inter-
mittent vasoconstriction of arterioles and venules; contin-
ued reperfusion injury; showers of emboli coursing
through the microvessels7,8; and thrombus formation in
larger vessels.9 Destruction of the microcirculation is the
main factor leading to cell death.10 The initial cellular
damage caused by ice crystals and the subsequent post-
thawing processes are made worse if refreezing follows
thawing of injured tissues.11,12
Classification of frostbite
Frostnip is superficial nonfreezing cold injury associated
with intense vasoconstriction on exposed skin, usually
cheeks, ears, or nose. Ice crystals, appearing as frost,
form on the skin surface. Frostnip is distinct from and
may precede frostbite. With frostnip, ice crystals do not
form within the tissue and tissue loss does not occur.
Numbness and pallor resolve quickly after warming the
skin with appropriate clothing, direct contact, breathing
with cupped hands over the nose, or gaining shelter. No
long-term damage occurs. Frostnip signals conditions
favorable for frostbite; appropriate action should be
undertaken immediately to prevent injury.
Frostbite has historically been divided into 4 tiers or
“degrees” of injury following the classification scheme
for thermal burn injury. These classifications are based
on acute physical findings and advanced imaging after
rewarming.13 The classifications can be difficult to assess
in the field before rewarming because the still-frozen tis-
sue is hard, pale, and anesthetic. An alternate 2-tiered
classification more appropriate for field use (after
rewarming but before imaging) is suggested with the fol-
lowing the 4-tier classification:
� First-degree frostbite causes numbness and erythema.
A white or yellow, firm, and slightly raised plaque
develops in the area of injury. No gross tissue
infarction occurs; there may be slight epidermal
sloughing. Mild edema is common.� Second-degree frostbite injury causes superficial skin
vesiculation; a clear or milky fluid is present in the
blisters, surrounded by erythema and edema.� Third-degree frostbite causes deeper hemorrhagic blis-
ters, indicating that the injury has extended into the retic-
ular dermis and beneath the dermal vascular plexus.� Fourth-degree frostbite extends completely through
the dermis and involves the comparatively avascular
subcutaneous tissues, with necrosis extending into
muscle and bone.
For field classification, after spontaneous or formal
rewarming but before imaging, we favor the following 2
tier classification scheme:
� Superficial—no or minimal anticipated tissue loss,
corresponding to first- and second-degree injury.� Deep—anticipated tissue loss, corresponding to third-
and fourth-degree injury.
Severity of frostbite may vary within a single extrem-
ity.
Once thawing occurs and a patient reaches a field
clinic or hospital, one can further classify or characterize
the frostbite injury via 2 additional methods. The Henne-
pin score14 uses a system similar to that for measuring
burns by total body surface area. The effect of treatment
can then be quantified retrospectively. The Cauchy clas-
sification method13 measures extent of frostbite anatomi-
cally using the following grades: 0—no lesion; 1—
lesion on the distal phalanx; 2—lesion on the middle
phalanx or proximal phalanx for the thumb/big toe; 3—
lesion on the proximal phalanx except for the thumb/big
toe; 4—lesion on the metacarpal/metatarsal; 5—lesion
on the carpal/tarsal. Although not validated, grades cor-
relate well with bone scans and clinical outcomes and
may assist caregivers in predicting tissue loss. The
Cauchy classification method may assist caregivers in
predicting amputation risk, which helps to inform evacu-
ation decisions. For example, a necrotic fingertip
(labeled grade 4 by the 4-tiered system but unlikely to
involve significant amputation) would be designated a
grade 1 on the Cauchy classification method, designating
lower severity. Higher grades in the Cauchy classifica-
tion method designate more proximal injuries with
greater risk for functionally important amputation.
Prevention
The adage that “prevention is better than treatment” is
especially true for frostbite, which is typically prevent-
able and often not improved by treatment. Underlying
ARTICLE IN PRESS
2 McIntosh et al

medical problems may increase risk of frostbite, so pre-
vention must address both environmental and health-
related aspects. Frostbite injury occurs when tissue heat
loss exceeds the ability of local tissue perfusion to pre-
vent freezing of soft tissues (blood flow delivers heat).
One must both ensure adequate perfusion and minimize
heat loss to prevent frostbite. The adventurer should rec-
ognize cold-induced “numbness” as a warning that frost-
bite injury may be imminent if protective or avoidance
measures are not taken to decrease tissue cooling. Subse-
quent loss of sensation does not mean the situation has
improved; rather, receptors and nerves are not conduct-
ing pain/cold signals because they are nearing the freez-
ing point.
MAINTAINING PERIPHERAL PERFUSION
Preventive measures to ensure local tissue perfusion
include: 1) maintaining adequate core temperature and
body hydration; 2) minimizing the effects of known dis-
eases, medications, and substances (including awareness
and symptoms of alcohol and drug use) that might
decrease perfusion; 3) covering all skin and the scalp to
insulate from the cold; 4) minimizing blood flow restric-
tion, such as occurs with constrictive clothing, footwear,
or immobility; 5) ensuring adequate nutrition; and 6)
using supplemental oxygen in severely hypoxic condi-
tions (eg, >7500 m). Recommendation Grade: 1C.
EXERCISE
Exercise is a specific method to maintain peripheral per-
fusion. Exercise enhances the level and frequency of
cold-induced peripheral vasodilation. In one study, exer-
cise resulted in cold-induced peripheral vasodilation in
the toes of 58% of exercising subjects vs 28% in non-
exercising subjects.15 Another study found increased
skin temperature in the hands during exercise.16 How-
ever, using exercise to increase warmth can lead to
exhaustion, with subsequent profound systemic heat loss
should exhaustion occur. Recognizing this caveat, exer-
cise and its associated elevation in core and peripheral
temperatures can be protective in preventing frostbite.
Recommendation Grade: 1B.
PROTECTION FROM COLD
Measures should be taken to minimize exposure of tissue
to cold. These measures include the following: 1) avoid-
ing environmental conditions that predispose to frostbite,
specifically below ¡15˚C, even with low wind speeds17;
2) protecting skin from moisture, wind, and cold; 3)
avoiding perspiration or wet extremities; 4) increasing
insulation and skin protection (eg, by adding clothing
layers, changing from gloves to mitts); 5) ensuring bene-
ficial behavioral responses to changing environmental
conditions (eg, not being under the influence of illicit
drugs, alcohol, or extreme hypoxemia)18; 6) using chem-
ical hand and foot warmers and electric foot warmers to
maintain peripheral warmth (note: warmers should be
close to body temperature before being activated and
must not be placed directly against skin or constrict flow
if used within a boot); 7) regularly checking oneself and
the group for extremity numbness or pain and warming
the digits and/or extremities as soon as possible if there
is concern that frostbite may be developing; 8) recogniz-
ing frostnip or superficial frostbite before it becomes
more serious; and 9) minimizing duration of cold expo-
sure. Emollients do not protect against—and might even
increase—risk of frostbite.19 The time that a digit or
extremity can remain numb before developing frostbite
is unknown; thus, digits or extremities with paresthesia
should be warmed as soon as possible. An extremity at
risk for frostbite (eg, numbness, poor dexterity, pale
color) should be warmed with adjacent body heat from
the patient or a companion, using the axilla or abdomen.
Recommendation Grade: 1C.
Field treatment and secondary prevention
If a body part is frozen in the field, the frozen tissue
should be protected from further damage. Remove jew-
elry or other constrictive extraneous material from the
body part. Do not rub or apply ice or snow to the affected
area.20
REFREEZING INJURY
A decision must be made whether to thaw the tissue. If
environmental conditions are such that thawed tissue could
refreeze, it is safer to keep the affected part frozen until a
thawed state can be maintained. Prostaglandin and throm-
boxane release associated with the freeze�thaw cycle20�22
causes vasoconstriction, platelet aggregation, thrombosis,
and, ultimately, cellular injury. Refreezing thawed tissue
further increases release of these mediators, and significant
morbidity may result. One must absolutely avoid refreez-
ing if field thawing occurs. Recommendation Grade: 1B.
SPONTANEOUS OR PASSIVE THAWING
Most frostbite thaws spontaneously and should be
allowed to do so if rapid rewarming (described in the fol-
lowing) cannot be readily achieved. Do not purposefully
keep tissue below freezing temperatures because this
will increase the duration that the tissue is frozen and
might result in more proximal freezing and greater mor-
bidity. If environmental and situational conditions allow
ARTICLE IN PRESS
WMS Practice Guidelines for Frostbite 3

for spontaneous or slow thawing, tissue should be
allowed to thaw. Recommendation Grade: 1C.
Strategies for 2 scenarios are presented:
Scenario 1: The frozen part has the potential for
refreezing and is not actively thawed.
Scenario 2: The frozen part is thawed and kept warm
without refreezing until evacuation is completed.
THERAPEUTIC OPTIONS FOR BOTH SCENARIOS
Many of these guidelines parallel the State of Alaska
cold injuries guidelines.23 Therapeutic options include
the following:
Treatment of hypothermia
No studies examine concurrent hypothermia and frost-
bite. Hypothermia frequently accompanies frostbite and
causes peripheral vasoconstriction that impairs blood
flow to the extremities. Mild hypothermia may be treated
concurrently with frostbite injury. Moderate and severe
hypothermia should be treated effectively before treating
frostbite injury. Recommendation Grade: 1C.
Hydration
Vascular stasis can result from frostbite injury. No stud-
ies have specifically examined the effect of hydration
status on frostbite outcomes, but it is believed that appro-
priate hydration and avoidance of hypovolemia are
important for frostbite recovery. Oral fluids may be
given if the patient is alert, capable of purposeful swal-
lowing, and not vomiting. If the patient is nauseated or
vomiting or has an altered mental status, IV normal
saline should be given to maintain normal urine output.
Intravenous fluids should optimally be warmed (mini-
mally to 37˚C but preferably to 40 to 42˚C with a method
that has been proven to be effective in the present envi-
ronmental conditions) before infusion and be infused in
small (eg, 250 mL), rapid boluses because slow infusion
will result in fluid cooling and even freezing as it passes
through the tubing. Fluid administration should be opti-
mized to prevent clinical dehydration. RecommendationGrade: 1C.
Low molecular weight dextran
Intravenous low molecular weight dextran (LMWD)
decreases blood viscosity by preventing red blood cell
aggregation and formation of microthrombi and can be
given in the field once it has been warmed. In some ani-
mal studies, the extent of tissue necrosis was found to be
significantly less than in control subjects when LMWD
was used24�27 and was more beneficial if given early.28
In one animal trial,28 tissue in the LMWD group thawed
slightly more rapidly, but overall tissue loss was no dif-
ferent from that of control animals. Give a test dose
before administration because of the low risk of anaphy-
laxis. This low risk of anaphylaxis should not deter
administration. The slight risk of bleeding is minimal,
and benefits seem to outweigh this risk; however, avail-
ability is limited in the United States. The use of LMWD
has not been evaluated in combination with other treat-
ments such as thrombolytics. LMWD should be given if
the patient is not being considered for other systemic
treatments, such as thrombolytic therapy. Recommenda-tion Grade: 2C.
Ibuprofen
Nonsteroidal anti-inflammatory drugs (NSAIDs) block the
arachidonic acid pathway and decrease production of
prostaglandins and thromboxanes.29 These mediators can
lead to vasoconstriction, dermal ischemia, and further tis-
sue damage. No studies have demonstrated that any par-
ticular anti-inflammatory agent or dosing is clearly related
to outcome. Aspirin has been proposed as an option and is
used in many parts of the world for anti-inflammatory and
platelet inhibition effects. One rabbit ear model study
showed 23% tissue survival with aspirin vs 0% in the con-
trol group.30 However, aspirin theoretically blocks pro-
duction of certain prostaglandins that are beneficial to
wound healing,31 and the authors of the rabbit ear model
study recommend ibuprofen in their treatment algorithm.
No studies specifically compare aspirin with ibuprofen
in frostbite. Ibuprofen should be started in the field at a
dose of 12 mg¢kg¡1 per day divided twice daily (minimum
to inhibit harmful prostaglandins29) to a maximum of
2400 mg¢d¡1 divided 4 times daily. RecommendationGrade: 2C.
SPECIFIC RECOMMENDATIONS—SCENARIO 1
Therapeutic options for frostbite in Scenario 1 (no active
thawing) include the following:
Dressings
No evidence supports applying a dressing to a frostbitten
part intended to remain frozen until rewarming can
safely be achieved. If this is considered, it should only
be done if practical and will not interfere with mobility.
Bulky, clean, and dry gauze or sterile cotton dressings
should be applied to the frozen part and between the toes
and fingers. Recommendation Grade: 2C.
ARTICLE IN PRESS
4 McIntosh et al

Ambulation and protection
If at all possible, a frozen extremity should not be used
for walking, climbing, or other maneuvers until defini-
tive care is reached. If use of the frozen extremity for
mobility is considered, a risk�benefit analysis must con-
sider the potential for further trauma and possible poorer
outcome. Although it is reasonable to walk on a foot
with frostbitten toes for evacuation purposes, it is inad-
visable to walk on an entirely frostbitten foot because of
the potential for resulting morbidity. This risk is theoreti-
cal and based on the panel’s opinion. Mills described
frostbite patients who ambulated on frozen extremities
for days and sustained no or limited amputation.32 If
using a frozen extremity for locomotion or evacuation is
unavoidable, the extremity should be padded, splinted,
and kept as immobile as possible to minimize additional
trauma. Recommendation Grade: 2C.
SPECIFIC RECOMMENDATIONS—SCENARIO 2
Therapeutic options for frostbite in Scenario 2 (thawing
and continued warming) include the following:
Rapid field rewarming of frostbite
Field rewarming by warm water bath immersion can and
should be performed if the proper resources are available
and definitive care is more than 2 h distant. Other heat
sources (eg, fire, space heater, oven, heated rocks) should
be avoided because of the risk of thermal burn injury.
Rapid rewarming by water bath has been found to result
in better outcomes than slow rewarming.20,27,32 Field
rewarming should only be undertaken if the frozen part
can be kept thawed and warm until the victim arrives at
definitive care. Water should be heated to 37 to 39˚C
(98.6 to 102.2˚F), using a thermometer to maintain this
range.33 If a thermometer is not available, a safe water
temperature can be determined by placing a caregiver’s
uninjured hand in the water for at least 30 s to confirm
that the water temperature is tolerable and will not cause
burn injury. Circulation of water around the frozen tissue
will help maintain correct temperature.34,35 Because the
water may cool quickly after the rewarming process is
started, the water should be continuously and carefully
warmed to the target temperature. If the frozen part is
being rewarmed in a pot, skin should not press against the
bottom or sides. Rewarming is complete when the
involved part takes on a red or purple appearance and
becomes soft and pliable to the touch. This is usually
accomplished in approximately 30 min, but the time is
variable depending on the extent and depth of injury. The
affected tissues should be allowed to air dry or be gently
dried with a blotting technique (not rubbing) to minimize
further damage. Under appropriate circumstances, this
method of field rewarming is the first definitive step in
frostbite treatment. Recommendation Grade: 1B.
Antiseptic solution
Most injuries do not become infected, but adding an anti-
septic solution (eg, povidone-iodine, chlorhexidine) to
the rewarming water has theoretical benefits of reducing
skin bacteria. Evidence for this practice does not exist
for frostbite care, however. Adding an antiseptic solution
to the water while rewarming is unlikely to be harmful
and might reduce the risk for cellulitis if severe edema is
present in the affected extremity. RecommendationGrade: 2C.
Pain control
During rewarming, pain medication (eg, NSAIDs or an
opiate analgesic) should be given to control symptoms
as dictated by individual patient situation. Recommenda-tion Grade: 1C.
Spontaneous or passive thawing
According to the foregoing guidelines, rapid rewarming
is strongly recommended. If field rewarming is not possi-
ble, spontaneous or slow thawing should be allowed.
Slow rewarming is accomplished by moving to a warmer
location (eg, tent or hut) and warming with adjacent
body heat from the patient or a caregiver, as previously
described. The expert panel agrees that slow thawing is a
reasonable course of action to initiate the rewarming pro-
cess if it is the only means available. RecommendationGrade: 1C.
Debridement of blisters
Debridement of blisters should not be routinely per-
formed in the field. If a clear, fluid-filled blister is tense
and at high risk for rupture during evacuation, blister
aspiration and application of a dry gauze dressing should
be performed in the field to minimize infection risk.
Hemorrhagic bullae should not be aspirated or debrided
in the field. These recommendations are common prac-
tice but lack evidence beyond case series.29 Recommen-dation Grade: 2C.
Topical aloe vera
Aloe vera ointment has been shown in an observational
study36 and an animal model30 to improve frostbite out-
come by reducing prostaglandin and thromboxane for-
mation. Topical agents do not penetrate far into tissues,
however, so aloe vera is theoretically only beneficial for
ARTICLE IN PRESS
WMS Practice Guidelines for Frostbite 5

superficially injured areas. The study supporting the
benefit of aloe vera examined its application on unroofed
blebs where it would be able to penetrate underlying
tissue. Topical aloe vera should be applied to thawed
tissue before application of dressings. RecommendationGrade: 2C.
Dressings
Bulky, dry gauze dressings should be applied to the
thawed parts for protection and wound care. Substantial
edema should be anticipated, so circumferential dress-
ings should be wrapped loosely to allow for swelling
without placing pressure on the underlying tissue. Rec-ommendation Grade: 1C.
Ambulation and protection
A risk�benefit analysis must consider the potential for
further trauma and, ultimately, potentially higher mor-
bidity if a thawed part is used for ambulation. For exam-
ple, it might be reasonable to walk on a foot with thawed
toes for evacuation purposes, but it is inadvisable to
walk on a recently thawed frostbitten foot because of the
potential resulting morbidity. Very little evidence is
available to guide recommendations. In one study, mobi-
lization within 72 h after thawing did not affect tissue
loss, complications, or hospital length of stay.37 After
the rewarming process, swelling should be anticipated. If
passive thawing has occurred, boots (or inner boots) may
need to be worn continuously to compress swelling.
Boots that were removed for active rewarming may not
be able to be re-donned if tissue swelling has occurred
during the warming process. The panel’s clinical experi-
ence supports the concept that a recently thawed extrem-
ity should ideally not be used for walking, climbing, or
other maneuvers and should be protected to prevent fur-
ther trauma.36,38 Recommendation Grade: 2C.
Elevation of extremity
If possible, the thawed extremity should be elevated above
the level of the heart, which might decrease formation of
dependent edema. Recommendation Grade: 1C.
Oxygen
Recovery of thawed tissue partly depends on the level
of tissue oxygenation in the postfreezing period. One
small study that measured hand temperature at normo-
baric hypoxia found decreased skin temperatures with
decreasing FIO2.39 However, hyperoxia has been
found to cause vasoconstriction in the extremities40;
therefore, oxygen should not be applied routinely to
patients who are not hypoxic. Although evidence is
lacking to support use of supplemental oxygen for
frostbite, oxygen may be delivered by face mask or
nasal cannula if the patient is hypoxic (oxygen satura-
tion <88%) or at high altitude above 4000 m. Recom-mendation Grade: 2C.
For a summary of the suggested approach to the field
treatment of frostbite, see Table 1.
Immediate medical therapy—hospital (or high-level
field clinic)
Once the patient reaches the hospital or field clinic, a
number of treatments should be initiated. After reaching
the hospital or field clinic, potential therapeutic options
for frostbite include the following:
TREATMENT OF HYPOTHERMIA
Similar recommendations apply to hospital or field clinic
treatment of hypothermia before frostbite treatment (see
previous). Recommendation Grade: 1C.
HYDRATION
Similar recommendations apply in the hospital or field
clinic regarding hydration (see previous). Recommenda-tion Grade: 1C.
LOWMOLECULARWEIGHT DEXTRAN
Similar recommendations apply in the hospital or field
clinic regarding LMWD (see previous). Recommenda-tion Grade: 2C.
Table 1. Summary of field treatment of frostbite (>2 h from
definitive care)
Treat hypothermia or serious trauma
1. Remove jewelry or other extraneous material from the body
part.
2. Rapidly rewarm in water heated and maintained between 37
and 39˚C (98.6 to 102.2˚F) until area becomes soft and pliable
to the touch (approximately 30 min); allow spontaneous or
passive thawing if rapid rewarming is not possible.
3. Ibuprofen (12 mg¢kg¡1 per day divided twice daily) if
available.
4. Pain medication (eg, opiate) as needed.
5. Air dry (ie, do not rub at any point).
6. Protect from refreezing and direct trauma.
7. Apply topical aloe vera cream or gel if available.
8. Dry, bulky dressings.
9. Elevate the affected body part if possible.
10. Systemic hydration.
11. Avoid ambulation on thawed lower extremity (unless only
distal toes are affected).
ARTICLE IN PRESS
6 McIntosh et al

RAPID REWARMING OF FROZEN TISSUES
Frozen tissue should be assessed to determine whether
spontaneous thawing has occurred. If tissue is
completely thawed, further rewarming will not be benefi-
cial. Rapid rewarming should be undertaken according to
the field protocol described previously if the tissue
remains partially or completely frozen. Recommenda-tion Grade: 1B.
MANAGEMENT OF BLISTERS
Clear or cloudy blisters contain prostaglandins and throm-
boxanes that may damage underlying tissue. Hemorrhagic
blisters are thought to signify deeper tissue damage
extending into the dermal vascular plexus. Common prac-
tice is to drain clear blisters (eg, by needle aspiration)
while leaving hemorrhagic blisters intact.34,36,38,41,42
Although this approach to frostbite blister management is
recommended by many authorities, comparative studies
have not been performed and data are insufficient to make
absolute recommendations. Some authors argue that
unroofing blisters might lead to the desiccation of exposed
tissue and that blisters should only be removed if they are
tense, likely to break or be infected, or interfere with the
patient’s range of motion.43 In a remote field situation,
draining or unroofing blisters may not be under control
of the provider. Blisters most often will have been broken
by the patient’s boots. In this case, the most important
treatment is applying aloe vera and a sterile dressing
to the unroofed blister. Debridement or aspiration of
clear, cloudy, or tense blisters is at the provider’s discre-
tion, with consideration of patient circumstances, until
better evidence becomes available. RecommendationGrade: 2C.
TOPICAL ALOE VERA
Topical aloe vera cream or gel should be applied to the
thawed tissue before application of dressings. Aloe vera
is reapplied at each dressing change or every 6 h.36 Rec-ommendation Grade: 2C.
SYSTEMIC ANTIBIOTICS
Frostbite is not an inherently infection-prone injury.
Therefore, antibiotic administration specifically for pre-
venting infection during or after frostbite injury is not
supported by evidence. Some authorities reserve antibi-
otics for situations when edema occurs after thawing
because of the notion that edema increases skin suscepti-
bility to infection by gram-positive bacteria.38 However,
this practice is not based on evidence. Systemic antibiot-
ics, either oral or parenteral, should be administered
to patients with significant trauma, other potential
infectious sources, or signs and symptoms of cellulitis or
sepsis. Recommendation Grade: 1C.
TETANUS PROPHYLAXIS
Tetanus prophylaxis should be administered according to
standard guidelines. Recommendation Grade: 1C.
IBUPROFEN
If NSAIDs have not been initiated in the field, ibuprofen
should be administered at a dose of 12 mg¢kg¡1 divided
twice daily (to inhibit harmful prostaglandins but remain
less injurious to the gastrointestinal system29) until the
frostbite wound is healed or surgical management occurs
(typically for 4�6 wk). Recommendation Grade: 2C.
THROMBOLYTIC THERAPY
The goal of thrombolytic therapy in frostbite injury is to
lyse and clear microvascular thromboses. For deep frost-
bite injury with potential significant morbidity, angiogra-
phy and use of either IV or intra-arterial tissue
plasminogen activator (tPA) within 24 h of thawing may
salvage some or all tissue at risk. A retrospective, single-
center review by Bruen et al44 demonstrated reduction in
digital amputation rates from 41% in those patients who
did not receive tPA to 10% in patients receiving tPA
within 24 h of injury. The 20-y series presented by the
Regions Hospital group found that two-thirds of patients
who received intra-arterial tPA responded well and that
amputation rate correlated closely with angiographic
findings.45 The Massachusetts General Hospital group
has proposed a screening and treatment tool for thrombo-
lytic management of frostbite based on a case report and
their evaluation of the Utah and Minneapolis experien-
ces.46 Twomey et al47 from Hennepin County Medical
Center have developed a specific protocol based on a
small group of good outcomes with intravenous tPA.
Further study is needed to compare intra-arterial vs IV
tPA on tissue salvage and functional outcome. Animal
studies demonstrate benefit from thrombolytics.48
When considering using a thrombolytic, a risk�benefit
analysis should be performed. Only deep injuries with
potential for significant morbidity (eg, extending into the
proximal interphalangeal joints of digits) should be consid-
ered for thrombolytic therapy. Potential risks of tPA include
systemic and catheter site bleeding, compartment syndrome,
and failure to salvage tissue. The long-term, functional con-
sequences of digit salvage using tPA have not been fully
evaluated.
Thrombolytic treatment should be undertaken in a facil-
ity familiar with the technique and with intensive care
monitoring capabilities. If a frostbite patient is being cared
ARTICLE IN PRESS
WMS Practice Guidelines for Frostbite 7

for in a remote area, transfer to a facility with tPA admin-
istration and monitoring capabilities should be considered
if tPA can be started within 24 h of tissue thawing. Time
to thrombolysis appears to be very important, with best
outcomes within 12 h and ideally as soon as possible.
Recent work from Hennepin County has found that each
hour of delay of thrombolytic therapy results in a 28%
decrease in salvage.49 Rare use of tPA in the field has
shown variable success50 and should only be undertaken
with extreme caution because bleeding complications
may be impossible to detect and treat. If other treatment
options are limited or unavailable, tPA should be consid-
ered for field treatment only of severe frostbite extending
to the proximal interphalangeal joint or more proximally
(eg, Cauchy classification grade 3�5).
Method of administration
Dosing is typically a 3 mg bolus (30 mL of 0.1 mg¢mL¡1
solution) followed by infusion of 1 mg¢mL¡1 (10 mL¢h¡1)
until specialists (eg, vascular, burn, radiology) recom-
mend discontinuation. Heparin is administered concur-
rently: 500 units¢h¡1.51
Intra-arterial angiography or IV pyrophosphate scan-
ning should be used to evaluate the initial injury and
monitor progress after tPA administration as directed by
local protocol and resources. As of the end of 2018,52 the
following have been published on tPA use in frostbite: 1
randomized controlled prospective trial (tPA plus ilo-
prost, 16 patients),53 3 retrospective cohort studies (59
patients),44,49,54 8 retrospective case series (130
patients),47,55�61 and 3 case reports.46,62,63 Although fur-
ther studies are needed to determine the absolute efficacy
of tPA for frostbite injury and to compare intra-arterial
tPA to IV prostacyclin, we recommend IV or intra-arte-
rial tPA within 24 h of injury as a reasonable choice in
an environment with appropriate monitoring capabilities.
Recommendation Grade: 1C.
IMAGING
In patients with delayed presentation (4�24 h from the
time of the frostbite thawing), noninvasive imaging with
technetium pyrophosphate13 or magnetic resonance angi-
ography64 can be used at an early stage to predict the
likely levels of tissue viability for amputation. Cauchy et
al13 described the combination of a clinical scoring sys-
tem and technetium scanning to successfully predict sub-
sequent level of amputation on day 2 after frostbite
rewarming. Single photon emission computed tomogra-
phy (CT)/CT combines the anatomic precision of CT
with the functional vascular information obtained from
multiphase bone scintigraphy. Kraft et al used single
photon emission CT/CT for 7 patients with frostbite and
found it improved surgical planning for deep frostbite
injuries by enabling early and precise anatomic localiza-
tion of nonviable tissues.65,66
If available, appropriate imaging should be used to
assess tissue viability and guide timing and extent of
amputation. Recommendation Grade: 1C.Other potential useful imaging techniques include
Doppler ultrasound55; triple phase technitium58,67;
indocyanine green microangiography68; and thermal
imaging.39 Although some of these techniques show
potential, further studies are required to determine their
exact role.
ILOPROST
Iloprost, a prostacyclin (PGI2) analogue, is a potent
vasodilator that also inhibits platelet aggregation, down-
regulates lymphocyte adhesion to endothelial cells,69
and may have fibrinolytic activity.70 Intravenous iloprost
was first used for treatment of frostbite by Groechenig in
1994, in 5 patients with second- and third-degree frost-
bite. He infused iloprost daily, starting at 0.5 ng¢kg¡1 and
increasing to 2.0 ng¢kg¡1 total dose over 3 d, and then
continued for between 14 and 42 d.71 Recovery without
amputation was achieved in all patients.
A randomized trial by Cauchy et al assessed the effi-
cacy of aspirin plus: 1) buflomedil, an alpha-blocker
vasodilator; 2) iloprost; or 3) intravenous tPA plus ilo-
prost.53 Forty-seven patients with severe frostbite, with
407 digits at risk, were randomly assigned to 8 d of treat-
ment with the 3 different regimens. Iloprost alone (0%
amputation rate) was found superior to tPA plus iloprost
(19%) and buflomedil (60%) groups. A limitation of this
study was that ischemia was not documented with angi-
ography or technetium scanning before treatment;
groups were randomized according to clinical severity.
A Canadian study documented full recovery of grade 3
frostbite when iloprost was started within 48 h of injury
in 2 long distance runners.72 In a Finnish study, iloprost
was partially beneficial with digit salvage rate of 78% in
4 persons: 2 with contraindication for tPA, 1 with failed
tPA therapy, and 1 with vasospasm without thrombosis
on angiography.55 One patient with minimal response to
tPA had complete reperfusion with iloprost.
Despite the limitations of these initial studies, iloprost
has shown consistently favorable effects.73 Extending
the treatment window, Pandey et al74 reported good
results with iloprost therapy up to 72 h after injury. In 5
Himalayan climbers with 34 digits at risk, 5 d of daily
iloprost infusion produced excellent outcomes in 4 of 5
patients. Treatment delayed beyond 72 h has not been
beneficial except in 1 patient.74,75 No serious side effects
have been noted in these studies.
ARTICLE IN PRESS
8 McIntosh et al

Intravenous iloprost should be considered first-line
therapy for grade 3 and 4 frostbite <72 h after injury,
when tPA is contraindicated, and in austere environ-
ments where tPA infusion is considered risky or evacua-
tion to a treatment facility will be delayed. Field use of
both iloprost and IV tPA has been advocated to reduce
delay in treatment for mountaineers who will invariably
take >48 h for evacuation to a hospital.50 In these
situations, iloprost may be the safer alternative. The IV
form of iloprost is not approved by the US Food and
Drug Administration, however. Consider iloprost for
deep frostbite to or proximal to the proximal interphalan-
geal joint; within 48 h after injury, especially if angiogra-
phy is not available; or with contraindications to
thrombolysis. Expedition physicians should consider
adding iloprost to their medical armamentarium, espe-
cially if it can be safely sourced and when treatment is
occurring outside of the United States. RecommendationGrade: 1B.
Method of administration
Iloprost dosage is given IV via controlled infusion or
syringe pump. Iloprost is mixed with normal saline or
dextrose in water. On days 1 through 3, start at an initial
rate of 0.5 ng¢kg¡1¢min¡1, then gradually increase by 0.5
ng¢kg¡1¢min¡1 at 30-min intervals to a maximum dose of
2.0 ng¢kg¡1¢min¡1. If intolerable side effects (nausea, head-
ache, flushing) emerge or blood pressure or heart rate are
outside normal limits, reduce the rate by 0.5 ng¢kg¡1¢min¡1
until side effects are tolerable or vital signs normalize.
Mild and tolerable side effects can be treated symptomati-
cally, whereas hypotension or severe symptoms require
dose reduction. Continue the highest dose achieved or a
maximum of 2.0 ng¢kg¡1¢min¡1 for 6 h total. For days 4
through 5, start directly at the highest/optimum rate or a
maximum of 2.0 ng¢kg¡1¢min¡1 for 6 h daily.51 Some pro-
tocols recommend up to 8 d of treatment; the first dose is
considered the most important.
HEPARIN
No evidence supports use of low molecular weight hepa-
rin or unfractionated heparin for initial management of
frostbite in the field or hospital, although climbers and
practitioners in many regions use these medications. Evi-
dence supports use of heparin as adjunctive therapy in
tPA protocols, as described previously. Heparin has been
used in conjunction with iloprost as well; the 5 patients
in the 1994 Groechenig iloprost study,71 the 1 Israeli
traveler with excellent outcome in the Kathmandu
study,74 and 4 patients in the Finnish study55 were
treated with low molecular weight heparin (enoxaparin)
in addition to iloprost. Whether low molecular weight
heparin offers additional benefit when combined with
iloprost requires further investigation; currently data are
insufficient for a recommendation on this combination.
Recommendation Grade: Not recommended as mono-
therapy owing to insufficient data.
OTHER VASODILATOR THERAPY
Vasodilators, such as prostaglandin E1,76 nitroglycerin,46
pentoxifylline,77,78 phenoxybenzamine, nifedipine, reser-
pine,79,80 and buflomedil,53,81,82 have been used as primary
and adjunctive therapies for treatment of frostbite. In addi-
tion to vasodilation, some of these agents might also prevent
platelet aggregation and microvascular occlusion. Sheridan
et al46 recommend intra-arterial infusion of nitroglycerin
during angiography before tPA infusion. A study in rabbits
that did not undergo rapid rewarming found benefit from
intra-arterial administration of prostaglandin E1.76 Buflome-
dil is an alpha-adrenolytic agent that is used widely in
Europe with preliminary and anecdotal evidence of good
results53,82; however, animal models have not replicated
these findings.81 This medication is not approved by the US
Food and Drug Administration. Intra-arterial reserpine stud-
ied in a controlled trial was found not to be effective.79
Pentoxifylline, a methylxanthine-derived phosphodi-
esterase inhibitor, has been widely used for treatment of
peripheral vascular disease and yielded promising results
in animal78,83,84 and human frostbite.77 Hayes et al77 rec-
ommend pentoxifylline in the controlled-release form of
one 400 mg tablet 3 times a day with meals, continued
for 2 to 6 wk. Controlled studies of pentoxifylline in
management of frostbite have not been performed.
Certain vasodilators have the potential to improve out-
comes and can be used with minimal risk. However, as
discussed earlier, data demonstrating benefit are limited.
Iloprost is the only vasodilator with reasonable scientific
evidence supporting its use.
For a summary of the suggested approach to hospital
or advanced field clinic treatment of frostbite, see
Table 2.
Other post-thaw medical therapy
Once the patient has received initial frostbite therapy,
long-term management is initiated to reduce long-term
sequelae. Therapeutic options for frostbite after thawing
include the following:
HYDROTHERAPY
Daily or twice-daily hydrotherapy at 37 to 39˚C (98.6 to
102.2˚F) has been recommended in the post-thaw peri-
od.32,34�36,85 Hydrotherapy theoretically increases cir-
culation, removes superficial bacteria, and debrides
ARTICLE IN PRESS
WMS Practice Guidelines for Frostbite 9

devitalized tissue.38 No trials support improved out-
comes, but the practice has few negative consequences
and has the potential to benefit recovery. Data are insuf-
ficient to recommend specific temperature, timing, or
duration of therapy. Recommendation Grade: 1C.
HYPERBARIC OXYGEN THERAPY
Many types of nonfrostbite wounds show accelerated
or more complete healing as a result of increased
tissue oxygenation from hyperbaric oxygen therapy
(HBOT).86 Because oxygen under pressure increases
oxygen tension in the blood, HBOT is typically effec-
tive only if blood supply to distal tissues is competent
and, therefore, may not be successful in frostbite. How-
ever, HBOT may have other effects such as making
erythrocytes more malleable and decreasing bacterial
load. Despite anecdotal success in extremely limited
case series,87�90 controlled studies have not been
conducted. The time, expense, and availability of
HBOT also limit its use. At this time, data are insuffi-
cient to recommend HBOT for frostbite treatment. Rec-ommendation Grade: Not recommended owing to
insufficient data.
SYMPATHECTOMY
Because blood flow is partly determined by sympathetic
tone, chemical or surgical sympathectomy has been pro-
posed in the immediate postexposure phase to reduce tis-
sue loss. In a rat lower limb model, early surgical
denervation (within 24 h of exposure) reduced tissue loss
but had no effect if performed after 24 h.91 In a rabbit
ear model, procaine-induced sympathectomy had no
demonstrable beneficial effect.92 Frostbite patients often
experience long-term delayed symptoms, such as pain,
paresthesia, and numbness. Chemical or surgical sympa-
thectomy to treat these symptoms has been performed
with variable results. In some studies, surgical sympa-
thectomy has been found to reduce duration of pain and
expedite demarcation of tissue necrosis. However, it has
not been found to reduce the ultimate extent of tissue
loss.41,93 Acute treatment success with IV guanethidine
has been reported94 but was not beneficial in another
case report.95 Sympathectomy may have a role in pre-
venting certain long-term sequelae of frostbite such as
pain (putatively caused by vasospasm), paresthesia, and
hyperhidrosis.96,97 Despite many years of study, the data
on surgical sympathectomy are limited and conflicting;
therefore, a recommendation for their use cannot be
made. Recommendation Grade: Not recommended
owing to insufficient data.
HOSPITALIZATION
Hospital admission and discharge are determined on an
individual basis. Factors should include severity of the
injury, coexisting injuries, comorbidities, and need for
hospital-based interventions (tPA, vasodilators, surgery)
or supportive therapy, as well as ease of access to appro-
priate community medical and nursing support. Signifi-
cant swelling should prompt evaluation for compartment
syndrome and admission for observation. Patients with
superficial frostbite can usually be managed as outpatients
or with brief inpatient stays followed by wound care
instructions. Initially, deep frostbite should be managed in
an inpatient setting. Recommendation Grade: 1C.
FASCIOTOMY
Thawing results in reperfusion of ischemic tissue and, in
turn, sometimes results in elevated pressures within
closed soft-tissue compartments. Compartment syn-
drome clinically manifests as tense, painful distention
with reduced movement and sensation. Urgent attention
is necessary to evaluate compartment pressures. If ele-
vated compartment pressures are present, prompt surgi-
cal decompression is indicated for limb salvage.20
Recommendation Grade: 1C.
Table 2. Summary of initial hospital management of frostbite
1. Treat hypothermia or serious trauma.
2. Rapidly rewarm in water heated and maintained between
37 and 39˚C (98.6 to 102.2˚F) until area becomes soft and
pliable to the touch (approximately 30 min).
3. Ibuprofen (12 mg¢kg¡1 per day divided twice daily).
4. Pain medication (eg, opiate) as needed.
5. Tetanus prophylaxis.
6. Air dry (ie, do not rub at any point).
7. Debridement: selectively drain (eg, by needle aspiration)
clear blisters and leave hemorrhagic blisters intact.
8. Topical aloe vera every 6 h with dressing changes.
9. Dry, bulky dressings.
10. Elevate the affected body part if possible.
11. Systemic hydration.
12. Thrombolytic therapy: consider for deep frostbite at the
distal interphalangeal joint or proximal if less than 24 h
after thawing; use angiography for prethrombolytic
intervention and monitoring of progress. Consider
intravenous thrombolysis if angiography is not available.
13. Iloprost therapy: consider for deep frostbite to or proximal
to the proximal interphalangeal joint, within 48 h after
injury, especially if angiography is not available or with
contraindications to thrombolysis.
14. Clinical examination (plus angiography or technetium-99
bone scan if necessary) to assist determination of surgical
margins. Evaluation by an experienced surgeon for
possible intervention.
ARTICLE IN PRESS
10 McIntosh et al

SURGICAL TREATMENT OR AMPUTATION
After frostbite occurs, complete demarcation of tissue
necrosis may take 1 to 3 mo. Angiography, technetium-
99 bone scan, or magnetic resonance imaging may be
used to assist determination of surgical margins42,64,98 in
conjunction with clinical findings. If the patient exhibits
signs and symptoms of sepsis attributed to infected frost-
bitten tissue, amputation should be performed expedi-
tiously.85 Otherwise, amputation should be delayed until
definitive demarcation occurs. The affected limb is often
insensate. Therefore, an approach that addresses foot-
wear and orthotics is essential to provide optimal func-
tion. Our experience has found that early involvement of
a multidisciplinary rehabilitation team produces better
long-term functional results. Telemedicine or electronic
consultation with a surgical frostbite expert to guide
local surgeons should be considered when no local
expert is available. Because significant morbidity may
result from unnecessary or premature surgical interven-
tion, a surgeon with experience evaluating and treating
frostbite should assess the need for and the timing of any
amputation. Recommendation Grade: 1C.
Conclusions
This summary provides evidence-based guidelines for
prevention and treatment of frostbite. Many important
questions remain and should serve as a focus for future
research. This includes elucidation of pathophysiology,
medications to assist in the prevention of frostbite, peri-
thawing procedures to reduce injury and decrease mor-
bidity, and post-thaw therapies that might improve long-
term outcomes.
Author Contributions: Drafting of the manuscript (SEM, LF, CKG,
PSA, GWR, AC, GGG, MM, CHI, ELJ, PP, JD, PHH); critical revision
of the manuscript (SEM, LF, CKG, PSA, GWR, AC, GGG, MM, CHI,
ELJ, PP, JD, PHH); and approval of final manuscript (SEM, LF, CKG,
PSA, GWR, AC, GGG, MM, CHI, ELJ, PP, JD, PHH).
Financial/Material Support: None.
Disclosures: None.
Supplementary materials
Supplementary material associated with this article can
be found in the online version at doi:10.1016/j.
wem.2019.05.002.
References
1. Guyatt G, Gutterman D, Baumann MH, Addrizzo-Harris
D, Hylek EM, Phillips B, et al. Grading strength of recom-
mendations and quality of evidence in clinical guidelines:
report from an American College of Chest Physicians Task
Force. Chest. 2006;129(1):174–81.
2. McIntosh SE, Opacic M, Freer L, Grissom CK, Auerbach
PS, Rodway GW, et al. Wilderness Medical Society
practice guidelines for the prevention and treatment of
frostbite: 2014 update. Wilderness Environ Med. 2014;
25(4 suppl):S43–54.
3. Mazur P. Causes of injury in frozen and thawed cells. Fed
Proc. 1965;24:S175–82.
4. Lange K, Boyd LJ, Loewe L. The functional pathology of
frostbite and the prevention of gangrene in experimental
animals and humans. Science. 1945;102(2641):151–2.
5. Meryman HT. Tissue freezing and local cold injury. Phys-
iol Rev. 1957;37(2):233–51.
6. Quintanilla R, Krusen FH, Essex HE. Studies on frost-bite
with special reference to treatment and the effect on minute
blood vessels. Am J Physiol. 1947;149(1):149–61.
7. Robson MC, Heggers JP. Evaluation of hand frostbite blis-
ter fluid as a clue to pathogenesis. J Hand Surg Am. 1981;6
(1):43–7.
8. Zacarian S. Cryogenics: The cryolesion and the pathogene-
sis of cryonecrosis. In: Zacarian S, ed. Cryosurgery for
Skin Cancer and Cutaneous Disorders. St. Louis: Mosby;
1985.
9. Kulka JP. Microcirculatory impairment as a factor in
inflammatory tissue damage. Ann N Y Acad Sci.
1964;116:1018–44.
10. Daum PS, Bowers WD Jr, Tejada J, Hamlet MP. Vascular
casts demonstrate microcirculatory insufficiency in acute
frostbite. Cryobiology. 1987;24(1):65–73.
11. Bhatnagar A, Sarker BB, Sawroop K, Chopra MK, Sinha
N, Kashyap R. Diagnosis, characterisation and evaluation
of treatment response of frostbite using pertechnetate scin-
tigraphy: a prospective study. Eur J Nucl Med Mol Imag-
ing. 2002;29(2):170–5.
12. Petrone P, Kuncir EJ, Asensio JA. Surgical management
and strategies in the treatment of hypothermia and cold
injury. Emerg Med Clin North Am. 2003;21(4):1165–78.
13. Cauchy E, Chetaille E, Marchand V, Marsigny B. Retro-
spective study of 70 cases of severe frostbite lesions: a pro-
posed new classification scheme. Wilderness Environ Med.
2001;12(4):248–55.
14. Nygaard RM, Whitley AB, Fey RM, Wagner AL. The
Hennepin score: quantification of frostbite management
efficacy. J Burn Care Res. 2016;37(4):e317–22.
15. Dobnikar U, Kounalakis SN, Mekjavic IB. The effect of
exercise-induced elevation in core temperature on cold-
induced vasodilatation response in toes. Eur J Appl Phys-
iol. 2009;106(3):457–64.
16. Geurts CL, Sleivert GG, Cheung SS. Local cold acclima-
tion during exercise and its effect on neuromuscular func-
tion of the hand. Appl Physiol Nutr Metab. 2006;31
(6):717–25.
17. Danielsson U. Windchill and the risk of tissue freezing.
J Appl Physiol. 1996;81(6):2666–73.
18. Urschel JD, Urschel JW, Mackenzie WC. The role of alco-
hol in frostbite injury. Scand J Soc Med. 1990;18(4):273.
19. Lehmuskallio E. Emollients in the prevention of frostbite.
Int J Circumpolar Health. 2000;59(2):122–30.
ARTICLE IN PRESS
WMS Practice Guidelines for Frostbite 11

20. Mills WJ Jr. Frostbite. A discussion of the problem and a
review of the Alaskan experience. 1973. Alaska Med.
1993;35(1):29–40.
21. Mills WJ Jr. Summary of treatment of the cold injured
patient: frostbite. 1983. Alaska Med. 1993;35(1):61–6.
22. Mills WJ Jr. Summary of treatment of the cold injured
patient. 1980. Alaska Med. 1993;35(1):50–3.
23. McLeron K. State of Alaska Cold Injury Guidelines. 7th ed.
Juneau, AK: Department of Health and Social Services
Division of Public Health Section of Community Health
and EMS; 2003.
24. Martinez Villen G, Garcia Bescos G, Rodriguez Sosa V,
Morandeira Garcia JR. Effects of haemodilution and
rewarming with regard to digital amputation in frostbite
injury: an experimental study in the rabbit. J Hand Surg
Br. 2002;27(3):224–8.
25. Talwar JR, Gulati SM, Kapur BM. Comparative effects of
rapid thawing, low molecular dextran and sympathectomy
in cold injury in the monkeys. Indian J Med Res. 1971;59
(2):242–50.
26. Weatherley-White RC, Sjostrom B, Paton BC. Experimen-
tal studies in cold injury. II. the pathogenesis of frostbite. J
Surg Res. 1964;4:17–22.
27. Webster DR, Bonn G. Low-molecular-weight dextran in
the treatment of experimental frostbite. Can J Surg. 1965;8
(4):423–7.
28. Kapur BM, Gulati SM, Talwar JR. Low molecular dextran
in the management of frostbite in monkeys. Indian J Med
Res. 1968;56(11):1675–81.
29. Rainsford KD. Ibuprofen: pharmacology, efficacy and
safety. Inflammopharmacology. 2009;17(6):275–342.
30. Heggers JP, Robson MC, Manavalen K, Weingarten MD,
Carethers JM, Boertman JA, et al. Experimental and clini-
cal observations on frostbite. Ann Emerg Med. 1987;16
(9):1056–62.
31. Robson MC, DelBeccaro EJ, Heggers JP, Loy GL. Increas-
ing dermal perfusion after burning by decreasing throm-
boxane production. J Trauma. 1980;20(9):722–5.
32. Mills WJ Jr. Frostbite. A method of management including
rapid thawing. Northwest Med. 1966;65(2):119–25.
33. Malhotra MS, Mathew L. Effect of rewarming at various
water bath temperatures in experimental frostbite. Aviat
Space Environ Med. 1978;49(7):874–6.
34. Imray C, Grieve A, Dhillon S. Cold damage to the extremi-
ties: frostbite and non-freezing cold injuries. Postgrad Med
J. 2009;85(1007):481–8.
35. Mills WJ, Whaley R. Frostbite: experience with rapid
rewarming and ultrasonic therapy. 1960-1. Wilderness
Environ Med. 1998;9(4):226–47.
36. McCauley RL, Hing DN, Robson MC, Heggers JP. Frost-
bite injuries: a rational approach based on the pathophysi-
ology. J Trauma. 1983;23(2):143–7.
37. Dole M, Endorf FW, Gayken J, Fey R, Nygaard RM. Early
mobilization in lower extremity frostbite injury: prelimi-
nary experience at a single burn center. J Burn Care Res.
2018;39(3):339–44.
38. Reamy BV. Frostbite: review and current concepts. J Am
Board Fam Pract. 1998;11(1):34–40.
39. Jones D, Covins SF, Miller GE, Morrison KI, Clark AG,
Calcott SD, et al. Infrared thermographic analysis of sur-
face temperature of the hands during exposure to normo-
baric hypoxia. High Alt Med Biol. 2018;19(4):388–93.
40. Rousseau A, Steinwall I, Woodson RD, Sjoberg F. Hyper-
oxia decreases cutaneous blood flow in high-perfusion
areas.Microvasc Res. 2007;74(1):15–22.
41. Golant A, Nord RM, Paksima N, Posner MA. Cold expo-
sure injuries to the extremities. J Am Acad Orthop Surg.
2008;16(12):704–15.
42. Murphy JV, Banwell PE, Roberts AH, McGrouther DA.
Frostbite: pathogenesis and treatment. J Trauma. 2000;48
(1):171–8.
43. Biem J, Koehncke N, Classen D, Dosman J. Out of the
cold: management of hypothermia and frostbite. CMAJ.
2003;168(3):305–11.
44. Bruen KJ, Ballard JR, Morris SE, Cochran A, Edelman LS,
Saffle JR. Reduction of the incidence of amputation in
frostbite injury with thrombolytic therapy. Arch Surg.
2007;142(6):546–51; discussion 551�3.
45. Jenabzadeh K, Mohr W, Ahrenholz D. Frostbite: a single
institution’s twenty year experience with intraarterial
thrombolytic therapy. J Burn Care Research. 2006;30(2):
S103.
46. Sheridan RL, Goldstein MA, Stoddard FJ Jr, Walker TG
Case records of the Massachusetts General Hospital. Case
41-2009. A 16-year-old boy with hypothermia and frost-
bite. N Engl J Med. 2009;361(27):2654–62.
47. Twomey JA, Peltier GL, Zera RT. An open-label study to
evaluate the safety and efficacy of tissue plasminogen acti-
vator in treatment of severe frostbite. J Trauma. 2005;59
(6):1350–4. discussion 1354�5.
48. Zdeblick TA, Field GA, Shaffer JW. Treatment of experi-
mental frostbite with urokinase. J Hand Surg Am. 1988;13
(6):948–53.
49. Nygaard RM, Lacey AM, Lemere A, Dole M, Gayken JR,
Lambert Wagner AL, et al. Time matters in severe frost-
bite: assessment of limb/digit salvage on the individual
patient level. J Burn Care Res. 2017;38(1):53–9.
50. Cauchy E, Davis CB, Pasquier M, Meyer EF, Hackett PH. A
new proposal for management of severe frostbite in the aus-
tere environment.Wilderness Environ Med. 2016;27(1):92–9.
51. Handford C, Buxton P, Russell K, Imray CE, McIntosh SE,
Freer L, et al. Frostbite: a practical approach to hospital
management. Extrem Physiol Med. 2014;3:7.
52. Hutchison RL, Miller HM, Michalke SK. The use of tPA in
the treatment of frostbite: a systematic review. Hand (N Y).
2019;14(1):13–8.
53. Cauchy E, Cheguillaume B, Chetaille E. A controlled trial
of a prostacyclin and rt-PA in the treatment of severe frost-
bite. N Engl J Med. 2011;364(2):189–90.
54. Patel N, Srinivasa DR, Srinivasa RN, Gemmete JJ, Krish-
namurthy V, Dasika N, et al. Intra-arterial thrombolysis for
extremity frostbite decreases digital amputation rates and
ARTICLE IN PRESS
12 McIntosh et al

hospital length of stay. Cardiovasc Intervent Radiol.
2017;40(12):1824–31.
55. Lindford A, Valtonen J, Hult M, Kavola H, Lappalai-
nen K, Lassila R, et al. The evolution of the Helsinki
frostbite management protocol. Burns. 2017;43(7):
1455–63.
56. Wexler A, Zavala S. The use of thrombolytic therapy in the
treatment of frostbite injury. J Burn Care Res. 2017;38(5):
e877–e81.
57. Johnson AR, Jensen HL, Peltier G, DelaCruz E. Efficacy of
intravenous tissue plasminogen activator in frostbite
patients and presentation of a treatment protocol for frost-
bite patients. Foot Ankle Spec. 2011;4(6):344–8.
58. Jones LM, Coffey RA, Natwa MP, Bailey JK. The use of
intravenous tPA for the treatment of severe frostbite.
Burns. 2017;43(5):1088–96.
59. Ibrahim AE, Goverman J, Sarhane KA, Donofrio J, Walker
TG, Fagan SP. The emerging role of tissue plasminogen
activator in the management of severe frostbite. J Burn
Care Res. 2015;36(2):e62–6.
60. Tavri S, Ganguli S, Bryan RG Jr, Goverman J, Liu R, Irani
Z, et al Catheter-directed intraarterial thrombolysis as part
of a multidisciplinary management protocol of frostbite
injury. J Vasc Interv Radiol. 2016;27(8):1228–35.
61. Gonzaga T, Jenabzadeh K, Anderson CP, Mohr WJ,
Endorf FW, Ahrenholz DH. Use of intra-arterial thrombo-
lytic therapy for acute treatment of frostbite in 62 patients
with review of thrombolytic therapy in frostbite. J Burn
Care Res. 2016;37(4):e323–34.
62. Saemi AM, Johnson JM, Morris CS. Treatment of bilateral
hand frostbite using transcatheter arterial thrombolysis
after papaverine infusion. Cardiovasc Intervent Radiol.
2009;32(6):1280–3.
63. Wagner C, Pannucci CJ. Thrombolytic therapy in the acute
management of frostbite injuries. Air Med J. 2011;30
(1):39–44.
64. Barker JR, Haws MJ, Brown RE, Kucan JO, Moore WD.
Magnetic resonance imaging of severe frostbite injuries.
Ann Plast Surg. 1997;38(3):275–9.
65. Millet JD, Brown RK, Levi B, Kraft CT, Jacobson JA,
Gross MD, et al. Frostbite: spectrum of imaging findings
and guidelines for management. Radiographics. 2016;36
(7):2154–69.
66. Kraft C, Millet JD, Agarwal S, Wang SC, Chung KC,
Brown RK, et al. SPECT/CT in the evaluation of frostbite.
J Burn Care Res. 2017;38(1):e227–34.
67. Handford C, Thomas O, Imray CHE. Frostbite. Emerg Med
Clin North Am. 2017;35(2):281–99.
68. Masters T, Omodt S, Gayken J, Logue C, Westgard B,
Hendriksen S, et al. Microangiography to monitor treat-
ment outcomes following severe frostbite injury to the
hands. J Burn Care Res. 2018;39(1):162–7.
69. Della Bella S, Molteni M, Mocellin C, Fumagalli S, Bonara
P, Scorza R. Novel mode of action of iloprost: in vitro
down-regulation of endothelial cell adhesion molecules.
Prostaglandins Other Lipid Mediat. 2001;65(2-3):73–83.
70. Candela M, Pansoni A, Jannino L, Menditto VG, Natalini
M, Ravaglia F, et al. Coagulative modifications in patients
with systemic sclerosis treated with iloprost or nifedipine.
Ann Ital Med Int. 2001;16(3):170–4.
71. Groechenig E. Treatment of frostbite with iloprost. Lancet.
1994;344(8930):1152–3.
72. Poole A, Gauthier J. Treatment of severe frostbite with ilo-
prost in northern Canada. CMAJ. 2016;188(17-18):1255–8.
73. Kaller M. BET 2: treatment of frostbite with iloprost.
Emerg Med J. 2017;34(10):689–90.
74. Pandey P, Vadlamudi R, Pradhan R, Pandey KR, Kumar A,
Hackett P. Case report: severe frostbite in extreme altitude
climbers—the Kathmandu iloprost experience. Wilderness
Environ Med. 2018;29(3):366–74.
75. Irarrazaval S, Besa P, Cauchy E, Pandey P, Vergara J. Case
report of frostbite with delay in evacuation: field use of ilo-
prost might have improved the outcome. High Alt Med
Biol. 2018;19(4):382–7.
76. Yeager RA, Campion TW, Kerr JC, Hobson RW 2nd,
Lynch TG Treatment of frostbite with intra-arterial prosta-
glandin E1. Am Surg. 1983;49(12):665–7.
77. Hayes DW Jr, Mandracchia VJ, Considine C, Webb GE
Pentoxifylline. Adjunctive therapy in the treatment of pedal
frostbite. Clin Podiatr Med Surg. 2000;17(4):715–22.
78. Miller MB, Koltai PJ. Treatment of experimental frostbite
with pentoxifylline and aloe vera cream. Arch Otolaryngol
Head Neck Surg. 1995;121(6):678–80.
79. Bouwman DL, Morrison S, Lucas CE, Ledgerwood AM.
Early sympathetic blockade for frostbite—is it of value? J
Trauma. 1980;20(9):744–9.
80. Espinosa GA. Management of frostbite injuries. J Natl Med
Assoc. 1981;73(12):1125–31.
81. Daum PS, Bowers WD Jr, Tejada J, Morehouse D, Hamlet
MP An evaluation of the ability of the peripheral vasodila-
tor buflomedil to improve vascular patency after acute
frostbite. Cryobiology. 1989;26(1):85–92.
82. Foray J, Baisse PE, Mont JP, Cahen C. Treatment of frost-
bites. Analysis of results in twenty patients with buflomedil
chlorhydrate (author’s transl) [in French]. Sem Hop.
1980;56(9-10):490–7.
83. Purkayastha SS, Roy A, Chauhan SK, Verma SS, Selva-
murthy W. Efficacy of pentoxifylline with aspirin in the
treatment of frostbite in rats. Indian J Med Res.
1998;107:239–45.
84. Purkayastha SS, Bhaumik G, Chauhan SK, Banerjee PK,
Selvamurthy W. Immediate treatment of frostbite using
rapid rewarming in tea decoction followed by combined
therapy of pentoxifylline, aspirin & vitamin C. Indian J
Med Res. 2002;116:29–34.
85. Jurkovich GJ. Environmental cold-induced injury. Surg
Clin North Am. 2007;87(1):247–67. viii.
86. Thom SR. Hyperbaric oxygen: its mechanisms and effi-
cacy. Plast Reconstr Surg. 2011;127(suppl 1):131S–41S.
87. Finderle Z, Cankar K. Delayed treatment of frostbite injury
with hyperbaric oxygen therapy: a case report. Aviat Space
Environ Med. 2002;73(4):392–4.
ARTICLE IN PRESS
WMS Practice Guidelines for Frostbite 13
88. Folio LR, Arkin K, Butler WP. Frostbite in a mountain
climber treated with hyperbaric oxygen: case report. Mil
Med. 2007;172(5):560–3.
89. von Heimburg D, Noah EM, Sieckmann UP, Pallua N.
Hyperbaric oxygen treatment in deep frostbite of both
hands in a boy. Burns. 2001;27(4):404–8.
90. Lansdorp CA, Roukema GR, Boonstra O, Dokter J. Delayed
treatment of frostbite with hyperbaric oxygen: a report of
two cases. Undersea Hyperb Med. 2017;44(4):365–9.
91. Gildenberg PL, Hardenbergh E. The effect of immediate
sympathectomy on tissue survival following experimental
frostbite. Ann Surg. 1964;160:160–8.
92. Fuhrman FA, Crismon JM. Studies on gangrene following
cold injury; the effect of rutin and other chemical agents
on the course of experimental frostbite in rabbits. J Clin
Invest. 1948;27(3 Pt 1):364–71.
93. Christenson C, Stewart C. Frostbite. Am Fam Physician.
1984;30(6):111–22.
94. Kaplan R, Thomas P, Tepper H, Strauch B. Treatment
of frostbite with guanethidine. Lancet. 1981;2
(8252):940–1.
95. Engkvist O. The effect of regional intravenous guanethi-
dine block in acute frostbite. Case report. Scand J Plast
Reconstr Surg. 1986;20(2):243–5.
96. Khan MI, Tariq M, Rehman A, Zafar A, Sheen SN. Effi-
cacy of cervicothoracic sympathectomy versus conserva-
tive management in patients suffering from incapacitating
Raynaud’s syndrome after frost bite. J Ayub Med Coll
Abbottabad. 2008;20(2):21–4.
97. Taylor MS. Lumbar epidural sympathectomy for frostbite
injuries of the feet.Mil Med. 1999;164(8):566–7.
98. Cauchy E, Marsigny B, Allamel G, Verhellen R, Chetaille
E. The value of technetium 99 scintigraphy in the progno-
sis of amputation in severe frostbite injuries of the extremi-
ties: A retrospective study of 92 severe frostbite injuries.
J Hand Surg Am. 2000;25(5):969–78.
ARTICLE IN PRESS
14 McIntosh et al

Seediscussions,stats,andauthorprofilesforthispublicationat:https://www.researchgate.net/publication/11587763
Retrospectivestudyof70casesofsevere
frostbitelesions:aproposednew
classificationscheme.WildEnvirMed12:
248-255
ArticleinWildernessandEnvironmentalMedicine·February2001
ImpactFactor:1.2·DOI:10.1580/1080-6032(2001)012[0248:RSOCOS]2.0.CO;2·Source:PubMed
CITATIONS
34
READS
57
4authors,including:
EmmanuelCauchy
InstitutdeFormationetdeRechercheen…
39PUBLICATIONS368CITATIONS
SEEPROFILE
Availablefrom:EmmanuelCauchy
Retrievedon:01June2016




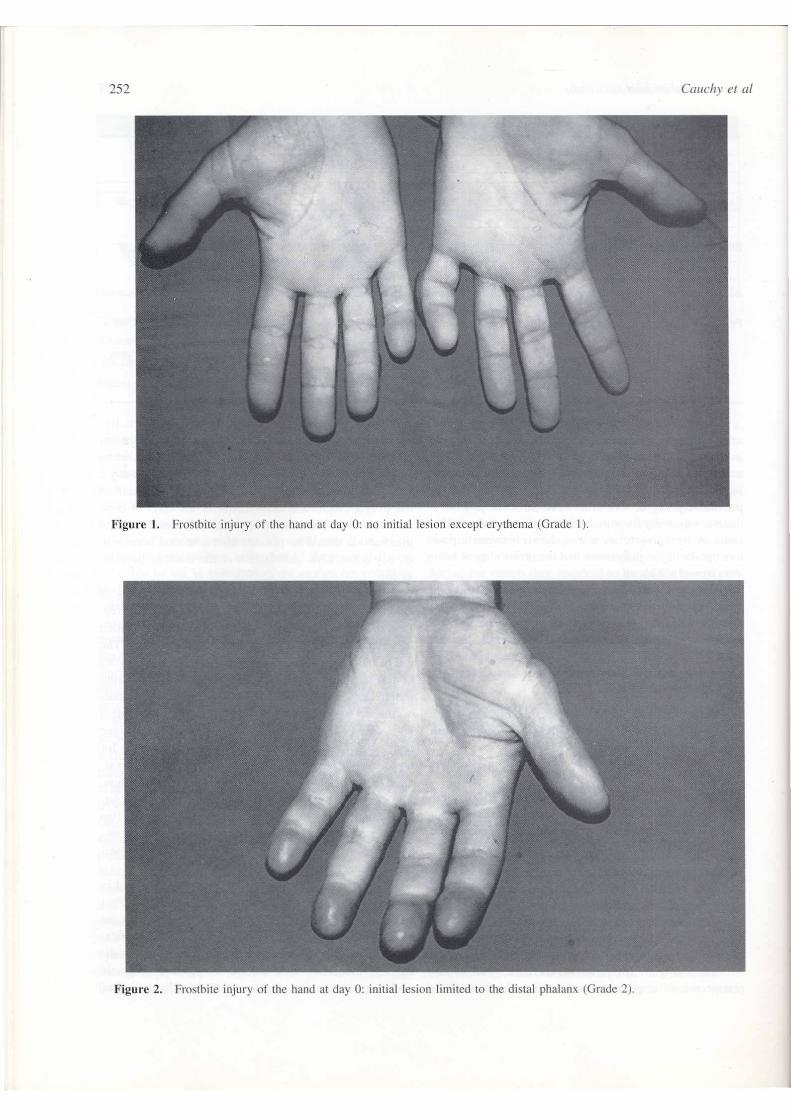



WILDERNESS MEDICAL SOCIETY CLINICAL PRACTICE GUIDELINES
Wilderness Medical Society Clinical Practice Guidelinesfor the Out-of-Hospital Evaluation and Treatment ofAccidental Hypothermia: 2019 UpdateJennifer Dow, MD, MHA 1; Gordon G. Giesbrecht, PhD 2; Daniel F. Danzl, MD 3; Hermann Brugger, MD 4,5;Emily B. Sagalyn, MD, MPH 6; Beat Walpoth, MD 7; Paul S. Auerbach, MD 8; Scott E. McIntosh, MD, MPH 9;M!aria N!emethy, MD 10;MarionMcDevitt, DO,MPH 10; Robert B. Schoene, MD 11; GeorgeW. Rodway, PhD, APRN 12;Peter H. Hackett, MD 13,14; Ken Zafren, MD 4,8; Brad L. Bennett, PhD 15; Colin K. Grissom, MD 16
1Alaska Regional Hospital Anchorage, Anchorage, AK; National Park Service: Alaska Region, Anchorage, AK; 2Faculty of Kinesiology and RecreationManagement, Departments of Anesthesia and Emergency Medicine, University of Manitoba, Winnipeg, Canada; 3Department of Emergency Medicine,University of Louisville, School of Medicine, Louisville, KY; 4International Commission for Mountain Emergency Medicine (ICARMEDCOM), Bolzano,Italy; 5Institute of Mountain Emergency Medicine, EURAC Research, Bolzano, Italy; 6University of Nevada School of Medicine, Reno, NV; 7Service ofCardiovascular Surgery, University Hospital of Geneva, Geneva, Switzerland; 8Departments of Emergency Medicine and Surgery, Stanford UniversitySchool of Medicine, Stanford, CA; 9Division of Emergency Medicine, University of Utah, Salt Lake City, UT; 10PeaceHealth Ketchikan Medical Center,Ketchikan, AK; 11University of Washington, Seattle, WA; 12School of Nursing, University of California, Davis, Sacramento, CA; 13Division of EmergencyMedicine, Altitude Research Center, University of Colorado School of Medicine, Denver, CO; 14Institute for Altitude Medicine, Telluride, CO; 15Military& EmergencyMedicine Department, F. EdwardH!ebert School of Medicine, Uniformed Services University of the Health Sciences, Bethesda, MD; 16Divi-sion of Pulmonary and Critical Care Medicine, Intermountain Medical Center and the University of Utah, Salt Lake City, UT
To provide guidance to clinicians, the Wilderness Medical Society convened an expert panel to develop evi-dence-based guidelines for the out-of-hospital evaluation and treatment of victims of accidental hypother-mia. The guidelines present the main diagnostic and therapeutic modalities and provide recommendationsfor the management of hypothermic patients. The panel graded the recommendations based on the qualityof supporting evidence and a balance between benefits and risks/burdens according to the criteria publishedby the American College of Chest Physicians. The guidelines also provide suggested general approaches tothe evaluation and treatment of accidental hypothermia that incorporate specific recommendations. This isthe 2019 update of the Wilderness Medical Society Practice Guidelines for the Out-of-Hospital Evaluationand Treatment of Accidental Hypothermia: 2014 Update.
Keywords: rewarming, resuscitation, wilderness medicine, cold, shivering
Introduction
Accidental hypothermia is defined as an unintentional dropin core temperature to 35!C or lower. Accidental hypother-mia due to environmental exposure can occur during anyseason and in most climates, with cold and wet environ-ments posing the greatest risk. Throughout history, it hasbeen a disease of war and disasters, but those who work
and recreate outside, especially in the wilderness, placethemselves at risk for hypothermia.
In addition to occurring in wilderness environments,hypothermia is associated with urban homelessness, parti-cularly with the use of alcohol and other intoxicating sub-stances. Hypothermia can occur during resuscitation inemergency settings (iatrogenic hypothermia); is notablyassociated with trauma; and may be a feature of sepsis, dis-eases that decrease metabolic rate (including hypoendo-crine states), and diseases that affect thermoregulation.Therapeutic hypothermia is beyond the scope of thisreview.
Hypothermia is the result of net heat loss from the body.Heat can be lost or gained by conduction, convection, and
WILDERNESS & ENVIRONMENTAL MEDICINE XXXX; XXX(XXX): 1e23
Corresponding author: Jennifer Dow,MD, National Park Service AlaskaRegion, POBox 1229,Girdwood, AK99587.; e-mail: [email protected].
Submitted for publication March 2019.Accepted for publication October 2019.

radiation and lost through evaporation. Conduction is directtransfer of heat from warmer to cooler objects that are incontact. Convection is transfer of heat to or from a gas ora liquid that is in motion. Radiation is transfer of heat inthe form of electromagnetic energy between 2 objects thatare visible to each other. Evaporation is loss of heat byvaporizing liquid (usually water from sweat or externalsources) from the skin, clothing that is in contact with theskin, or respiration.
The human body attempts to maintain a core tempera-ture at or near 37!C. The thermoregulatory control centerin the hypothalamus receives input from central and periph-eral thermal receptors. The integrated thermal signal trig-gers autonomic reflexes that control the initiation ofcooling responses such as vasodilation or sweating (heatloss) or warming responses such as vasoconstriction (heatretention) or shivering (heat production).1 Peripheralblood flow is also partly regulated by local skintemperature.
Humans originated in the tropics and have limited phy-siologic means to avoid developing hypothermia. Exerciseand shivering can raise the metabolic rate to preventhypothermia if nutritional reserves and insulation are ade-quate, but the benefit may be limited by environmental con-ditions. Prevention of hypothermia in humans mostlydepends on behavior, chiefly wearing insulating clothingand using shelter.
Methods
TheWildernessMedical Society (WMS) convened an expertpanel to develop evidence-based clinical guidelines for pre-vention and out-of-hospital diagnosis and treatment of vic-tims of accidental hypothermia to update the previousWMSPracticeGuidelines for theOut-of-Hospital Evaluationand Treatment of Accidental Hypothermia: 2014 Update.2
Panelists were selected by the WMS based on clinical and/or research experience and generated a set of questions(Figure 1) to define the most significant areas of interest. Aspart of the update process, the current panel identified addi-tional questions not previously considered. A literaturesearch identified relevant articles with a key word search oftheMEDLINE database. Keywords were hypothermia, acci-dental hypothermia, wilderness hypothermia, shivering,rewarming, core temperature, and resuscitation. The panelconsidered only peer-reviewed randomized controlled trials,observational studies, case series, and case reports related toevaluation and treatment of accidental hypothermia.Although all articles were considered, those publishedbetween 2013 andMarch 2019 were the focus of this review.
The panel assessed the level of evidence supporting eachdiagnostic and therapeutic modality. Conclusions fromreview articles were not used in the formulation of recom-mendations, but the guidelines cite review articles whennecessary to provide background information.
Questions considered by the panel
FIELD ASSESSMENT• How should the level of hypothermia be classified?• What is the best way to measure core temperature?
PREHOSPITAL TREATMENT• What is the best treatment for a cold patient who is not hypothermic or for a patient with mild hypothermia in
the field?• What is the safest way to handle a patient with moderate to severe hypothermia in the field?• What is the best treatment for moderate to severe hypothermia?• When should a hypothermic patient without signs of life be resuscitated?• Are there specific considerations regarding hypothermia in a trauma patient?• Are there specific considerations regarding burn prevention in an actively warmed patient?• When should rescuers start cardiopulmonary resuscitation (CPR) on a hypothermic patient?• When and how should a hypothermic patient be defibrillated?• What is the best method for giving CPR to a hypothermic patient?• What are recommendations for delayed, intermittent, and prolonged CPR?• What is the best way to manage the airway in a severely hypothermic patient?• What is the best way to obtain vascular access in a hypothermic patient?• What is the best way to manage fluids in a hypothermic patient?• What is the role of Advanced Life Support (ALS) drugs in a hypothermic patient?• Is there a role for transcutaneous cardiac pacing in a hypothermic patient?• How should atrial dysrhythmias be managed during rewarming for a hypothermic patient?• Is there a simple decision aid that can be used by any responders in the field?
TRANSPORT/TRIAGE• How should the destination hospital be determined for a hypothermic patient?• What is the tole of ECLS in the hypothermic patient?• How can serum potassium be used to determine if CPR should be continued on a hypothermic patient?
Figure 1. Questions considered by the authors for the development of these practice guidelines.
Dow et al2

The panel used a consensus approach to develop recom-mendations regarding each evaluation technique and inter-vention and its role in management. The panel gradedeach recommendation based on the quality of supportingevidence and balance between the benefits and risks/bur-dens, according to the criteria of the American College ofChest Physicians (see online Supplementary Table).3
PATHOPHYSIOLOGY OF HYPOTHERMIA
The primary physiologic effects of tissue cooling aredecreased resting metabolism and inhibition of central andperipheral neurologic function. During the initial stages ofcooling of a neurologically intact victim, secondaryresponses to skin cooling predominate.1 Shivering thermo-genesis, triggered by skin cooling, results in increasedmetabolism due to the work of shivering and increased ven-tilation, cardiac output, and mean arterial pressure.4 Thesephysiologic parameters initially increase as core tempera-ture decreases to approximately 32!C. The parametersthen decrease with a further drop in core temperature.1 Shi-vering ceases at and below a core temperature of approxi-mately 30!C.5 Once this occurs, metabolism decreaseswith further decreases in core temperature.
Clinical manifestations of accidental hypothermia relatepredominantly to cerebral and cardiorespiratory effects.Brain activity begins to decline at a core temperature ofapproximately 33 to 34!C and continues to decline withfurther cooling.6,7 Cooling of the brain leads to irritability,confusion, apathy, poor decision making, lethargy, somno-lence, and eventually coma. Brain cooling decreases cere-bral oxygen requirements.8 This provides temporaryprotection during anoxic conditions such as cold-inducedcardiac standstill and cold-water drowning. Cold stressreduces circulating blood volume due a combination ofcold-induced diuresis, extravascular plasma shift, andinadequate fluid intake.9 As the heart cools below 30!C,cardiac output decreases markedly, and bradycardia usuallyoccurs. Abnormalities in electrical conduction lead to dys-rhythmias such as premature atrial and ventricular contrac-tions, atrial fibrillation, and ventricular fibrillation (VF).10
Below 28!C, the heart is susceptible to VF, which can betriggered by acidosis, hypocarbia, hypoxia, or movement.1
Decreased ventilatory response to carbon dioxide leads tohypoventilation and respiratory acidosis.11
FIELD ASSESSMENT
Classification of hypothermia
Most guidelines use a standard classification of hypother-mia based on core temperature. Hypothermia is classifiedas mild at 35 to 32!C; moderate at 32 to 28!C; or severeat <28!C.12e14 Some experts advocate a further category,
profound hypothermia, at <24!C12 or <20!C.1 The chanceof survival appears to bemuch lower in this range, probablybecause of a high likelihood of cardiac arrest. In cases ofhypothermia secondary to cold water immersion, loss ofairway protection and drowning may also contribute tocauses of death. Although core temperature is used to clas-sify hypothermia, individual variation to core temperatureis wide, as is true of other physiologic parameters. Measur-ing core temperature is not always feasible in the out-of-hospital environment.15
Factors to guide treatment
The standard classification of hypothermia by core tem-perature correlates with the status of the thermoregulatorysystem. From 35 to 32!C (mild hypothermia) thermoregu-latory shivering control is functional and increases as coretemperature decreases.16 With further cooling, shiveringgenerally becomes less effective, although it can still bestrong at 31!C.5 Below 32!C (moderate hypothermia),thermoregulation becomes less effective and rewarming ispossible only with addition of exogenous heat. As thecore temperature decreases below 32!C, level of conscious-ness decreases. Below 28!C (profound/severe hypother-mia), most patients are unconscious and not shivering,and the risk of VF or asystole is high.17
Recommendation. The key factors guiding hypothermiatreatment are level of consciousness, alertness, shiveringintensity, physical performance, and cardiovascular stabi-lity, which is based on blood pressure and cardiac rhythm(Figure 2). Core temperature can provide additional helpfulinformation, but it is difficult to accurately obtain in thefield, and the panel recommends that this should not bethe sole basis for treatment (Evidence grade: 1C).
Simplified decision aid for field use
We have developed a simplified “Cold Card”18 (Figure 3)corresponding to the more technical flowchart in Figure 2.
Recommendation. It is the recommendation of the workinggroup that this decision aid be considered to facilitate eva-luation and treatment of accidental hypothermia in theout-of-hospital setting for responders with varying levelsof medical training.
Some patients are cold, but not hypothermic
Patients can be cold and shivering, but not hypothermic.Shivering is triggered by skin cooling as a mechanism forpreventing hypothermia. A shivering patient with a coretemperature >35!C is cold-stressed, but not hypothermic.If temperature measurement is not possible, clinical judg-ment may be helpful to distinguish whether a patient is
Hypothermia Clinical Practice Guidelines 3
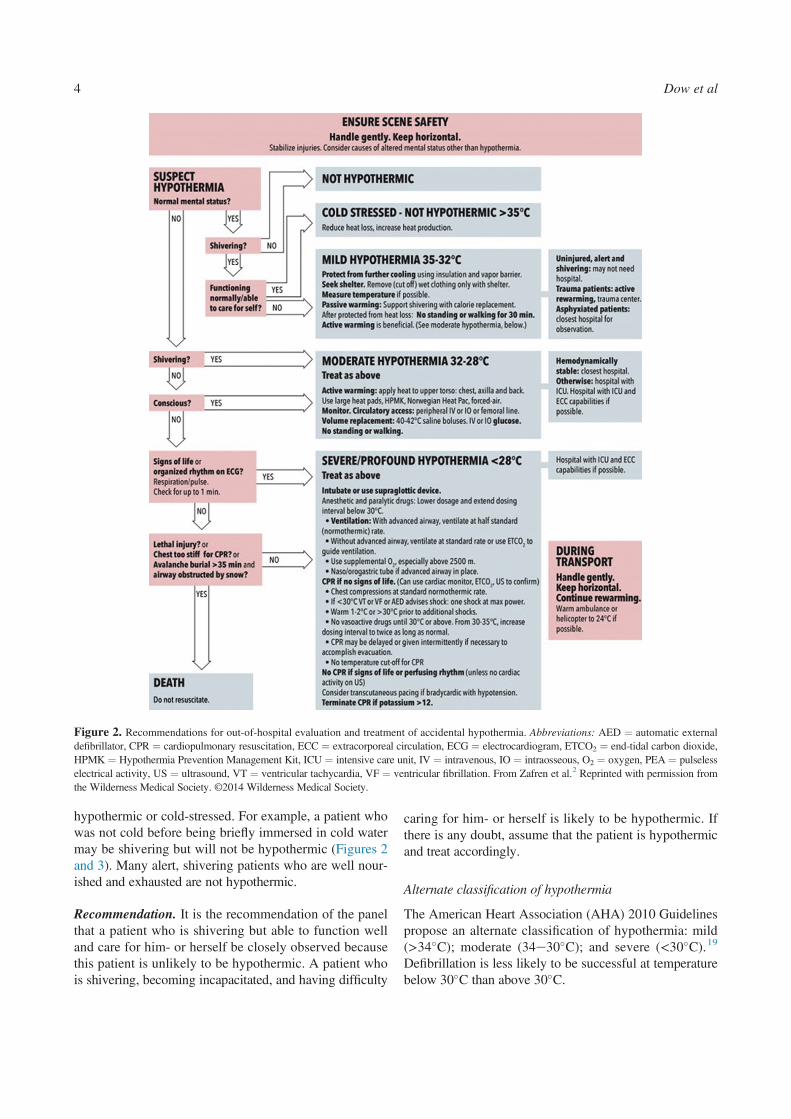
hypothermic or cold-stressed. For example, a patient whowas not cold before being briefly immersed in cold watermay be shivering but will not be hypothermic (Figures 2and 3). Many alert, shivering patients who are well nour-ished and exhausted are not hypothermic.
Recommendation. It is the recommendation of the panelthat a patient who is shivering but able to function welland care for him- or herself be closely observed becausethis patient is unlikely to be hypothermic. A patient whois shivering, becoming incapacitated, and having difficulty
caring for him- or herself is likely to be hypothermic. Ifthere is any doubt, assume that the patient is hypothermicand treat accordingly.
Alternate classification of hypothermia
The American Heart Association (AHA) 2010 Guidelinespropose an alternate classification of hypothermia: mild(>34!C); moderate (34e30!C); and severe (<30!C).19
Defibrillation is less likely to be successful at temperaturebelow 30!C than above 30!C.
Figure 2. Recommendations for out-of-hospital evaluation and treatment of accidental hypothermia. Abbreviations: AED ¼ automatic externaldefibrillator, CPR ¼ cardiopulmonary resuscitation, ECC ¼ extracorporeal circulation, ECG ¼ electrocardiogram, ETCO2 ¼ end-tidal carbon dioxide,HPMK ¼ Hypothermia Prevention Management Kit, ICU ¼ intensive care unit, IV ¼ intravenous, IO ¼ intraosseous, O2 ¼ oxygen, PEA ¼ pulselesselectrical activity, US ¼ ultrasound, VT ¼ ventricular tachycardia, VF ¼ ventricular fibrillation. From Zafren et al.2 Reprinted with permission fromthe Wilderness Medical Society. ©2014 Wilderness Medical Society.
Dow et al4

Recommendation. The panel recommends that the AHAscheme should not be used as the standard classificationfor out-of-hospital treatment of hypothermia because itchanges the widely accepted definition of hypothermiaand emphasizes response to defibrillation rather than phy-siologic changes.
Field classification of hypothermia: the “Swiss” system
The “Swiss” hypothermia classification was developed tohelp rescuers estimate core temperature by observing clini-cal signs.12 Because individuals have variability inresponse to cold, estimating core temperature on the basis
Figure 3. (A) Front of cold cardd “assess cold patient”. (B) Back of cold cardd “care for cold patient.” FromGiesbrecht.18 Reprinted with permissionfrom the Wilderness Medical Society. ©2018 Wilderness Medical Society
Hypothermia Clinical Practice Guidelines 5

of clinical signs is only an approximation. The stages of the“Swiss” hypothermia (abbreviated “HT”) grading systemwith descriptions and estimated core temperature are asfollows:
#HT Idclear consciousness with shivering: 35 to 32!C#HT IIdimpaired consciousness without shivering: 32 to28!C
#HT IIIdunconscious: 28 to 24!C#HT IVdapparent death: 24 to 13.7!C#HT Vddeath due to irreversible hypothermia: <13.7!C?(<9!C?)12
A limitation of this system is that individuals vary inphysiologic response to hypothermia. Shivering may be
Figure 3 (continued).
Dow et al6

maximal at 32 to 33!C but may continue at 31!C and maynot cease until core temperature drops to approximately30!C. A shivering patient with impaired consciousnessshould be treated for moderate, not mild, hypothermia.Temperature ranges for hypothermia stages should not beconsidered absolute but rather correlated with clinicalobservations. An analysis of reported cases of hypothermiarevealed clinically significant temperature overlap withrespect to hypothermia staging. The lowest recorded tem-perature was 28.1!C for HT I, 22!C for HT II, and19.3!C for HT III.20 It is advised that rescuers focus onthe entire clinical picture rather than just shivering. Manycase reports describe hypothermic patients with vital signswho had core temperatures below 24!C.21e25 Individualswith core temperatures below 24!C are very susceptible toVF. Although the Swiss HT system can help guide rescuersin certain situations, we prefer to use the terms mild, mod-erate, severe, and profound hypothermia.
Recommendation. Rescuers should classify hypothermiaas mild, moderate, severe, and profound on the basis ofclinical observations, remembering that shivering canoccur below 32!C, usually with altered mental status, andthat patients can have detectable vital signs with core tem-peratures below 24!C. Furthermore, rescuers should beaware of core temperature overlap between classificationcategories20,25 (Evidence grade: 1C).
Associated conditions complicating the field classificationof hypothermia
In addition to hypothermia, many conditions can causealtered mental status and decreased level of consciousness.Conditions such as sepsis and severe trauma can decreasephysiologic reserves and may decrease or abolishshivering.26 Many drugs and medications27 suppressshivering.28
Recommendation. Clinicians should consider causes otherthan hypothermia to explain altered mental status or lack ofshivering that do not correlate with the measured core tem-perature or are associated with a history of minimal coldexposure (Evidence grade: 1B).
MEASUREMENT OF CORE TEMPERATURE
Esophageal temperature
The most accurate minimally invasive method of measur-ing core temperature is esophageal temperature, with theprobe inserted into the lower third of the esophagus.29
The degree of accuracy afforded by esophageal temperaturemonitoring is helpful to guide treatment of patients withmoderate or severe hypothermia. Placement of an
esophageal probe via the pharynx may cause vomitingand aspiration. The airway must be protected with an endo-tracheal tube or supraglottic device that allows passage of agastric tube before placement of an esophageal probe.Heated humidified oxygen does not significantly raise thetemperature measured by a properly inserted esophagealprobe.30e32 If the esophageal probe is not inserted intothe lower third of the esophagus, an average of 24 cmbelow the larynx in adults,1 use of heated humidified oxy-genmay result in a falsely elevated esophageal temperature.Esophageal probes that do not have markings can be mea-sured visually against the patient and marked to ensurethe correct depth of insertion. Field conditions will rarelyallow for placement of an esophageal probe; however,transporting air or ground medical services that have thiscapacity should place a probe as soon as possible.
Recommendation. If available, an esophageal temperatureprobe should be placed in a patient whose airway hasbeen protected and secured. Esophageal temperature is thepreferred method of core temperature measurement (Evi-dence grade: 1C).
Epitympanic temperature
Epitympanic (ear canal) temperature, measured using a softprobe with a thermistor in proximity to the tympanic mem-brane, reflects carotid artery temperature.33 Epitympanicthermometers should not be confused with the more com-mon and much less accurate infrared “tympanic” thermo-meters. In patients with adequate cardiac output,epitympanic temperature reflects core temperature. Epitym-panic temperature can be lower than esophageal tempera-ture during low flow (decreased cardiac output) or no-flow (cardiac arrest) states.28 In out-of-hospital settingscare must be taken to insulate the ear canal from the envir-onment. With cold ambient temperature, epitympanic tem-perature may be falsely low, especially if the externalauditory canal is blocked by cerumen, filled with snow, ornot adequately sealed and properly covered with an isolat-ing “cap.”33 Epitympanic temperature is much lower thanesophageal temperature during initial cooling of the headin normothermic subjects. After 10 min of isolated headcooling, the mean difference between epitympanic and eso-phageal temperatures is about 1 to 2!C.34 Epitympanicthermometers for use in the operating room are not suitablefor field use; they are not designed for use in coldenvironments.
Recommendation. Use an epitympanic thermometerdesigned for field conditions with an isolating ear cap in apatient whose airway has not been secured by endotrachealintubation or a supraglottic airway, or in a patient with asecured airway if an esophageal probe is not available
Hypothermia Clinical Practice Guidelines 7

(Evidence grade: 1C). Infrared tympanic thermometersshould never be used to measure core temperature in ahypothermic patient15 (Evidence grade: 1A).
Rectal temperature in the field
The use of rectal thermometers is not advisable before thepatient has been removed from the cold environmentbecause the patient must be further exposed, increasingheat loss and potentially worsening hypothermia.
Recommendation.Rectal temperature measurement shouldnot be used unless the patient is in a warm environment(Evidence grade: 1C).
Rectal and bladder temperatures during rewarming
Rectal and bladder temperatures lag behind core tempera-ture changes by as much as an hour and can give the falseimpression that the patient is still cooling.4,9,35 Rectal andbladder temperature overestimate heart temperature duringcooling and underestimate heart temperature duringrewarming.
Recommendation. Monitor rectal or bladder temperatureduring rewarming of an unconscious patient only if an eso-phageal or epitympanic probe is not available. If rectal orbladder temperature is used for monitoring during rewarm-ing, allow for inaccuracy due to the time lag behind coretemperature changes (Evidence grade: 1A).
Oral temperature
Oral temperatures are useful only to rule out hypothermia.Nonelectronic thermometers are typically unable to mea-sure temperatures below 35.6!C. If mercury or alcohol ther-mometers are used to diagnose hypothermia, they must bespecial “low reading” thermometers.1
Recommendation. Oral temperature measurement with athermometer that cannot read below 35!C should not beused to diagnose hypothermia (Evidence grade: 1A).
“Temporal artery” thermometer
“Temporal artery” thermometers, used on the skin surface,do not provide accurate temperature measurements inhypothermia.36
Recommendation. Do not use a temporal artery thermo-meter in a possibly hypothermic patient (Evidence grade:1C).
Zero-heat flux thermometer
A noninvasive heat flux or “double sensor” thermometer iscurrently under development.37 This technology, whichcombines a skin temperature sensor with a heat flux sensor,
correlates well with esophageal temperature in operativeand intensive care unit settings.38,39
Recommendation. Because this technology has not beenvalidated in field settings, no recommendation can bemade at this time.
OUT-OF-HOSPITALTREATMENT
Safety of the rescuers
Rescuer safety is the first priority during rescue. The scenemay be unsafe to enter, or the safety officer in a rescue mayallow only brief entry. Unless there are obvious fatal inju-ries, rescuers might need to move the patient to a safeplace before deciding to resuscitate.
Recommendation. The decision to rescue or resuscitate apatient can only be made after the scene is secure and safefor the rescuers to enter and make an evaluation (Evidencegrade: 1A). After rescuer safety has been assured, the prio-rities for out-of-hospital treatment of a hypothermic patientwho is not in cardiac arrest are to avoid causing cardiovas-cular collapse during rescue, prevent further decrease incore temperature (afterdrop), and rewarm the patient in asafe manner. If a hypothermic patient is in cardiac arrest,rescuers should, if indicated, initiate resuscitation.
Core temperature afterdrop
Core temperature afterdrop refers to continued core coolingafter removal from a cold environment. Afterdrop is causedby a combination of conductive heat loss from the warmercore to cooler peripheral tissue and convective heat lossfrom blood due to increased flow to cooler tissue and subse-quent return to the central circulation and heart.40e42 Theconvective component transfers more heat, and, unlike theconductive component, is affected by the method ofrewarming. In a hypothermia victim, peripheral tissue iscolder than the heart. Therefore, any action that increasesblood flow to cold peripheral tissue (eg, hoisting or holdingvictim in a vertical position, allowing the victim to stand orwalk, active or passive limbmovement, immersion in warmwater) will increase the volume of cold blood returning tothe heart. This increases cardiac work and further decreasescore temperature.
Afterdrop may be clinically important in victims whoare at the threshold of moderate to severe hypothermiabecause they are susceptible to cardiovascular instabilitywith a small further drop in core (heart) temperature. After-drop of as much as 5 to 6!C has been reported in hypother-mic patients.21,42e44 Therefore, care should be taken toprevent increased blood flow to the limbs during and afterrescue.
Dow et al8

Circumrescue collapse
Circumrescue collapse refers to light-headedness, collapse,syncope, or sudden death occurring in victims of cold-waterimmersion just before, during, or after rescue and removalfrom water.45 Circumrescue collapse can be caused bymental relaxation and decreased catecholamine outputcausing life-threatening hypotension or by sudden onsetof cardiac dysrhythmia, likely VF.4
The act of removing a victim from water decreaseshydrostatic pressure,4 which is normally greatest aroundthe legs. Removing hydrostatic pressure allows blood topool in dependent areas, causing decreased blood returnwith resultant hypotension or cardiovascular collapse. Acold heart may not be able to compensate for decreasingblood pressure by increasing cardiac output. Blood thatdoes return from dependent areas will be cooled and willcontribute to core temperature afterdrop. Afterdrop isincreased if the victim has to perform work to assist in res-cue (eg, having to climb a ladder onto a boat).45,46Mechan-ical stimulation of the heart during rescue andextricationdcombined with hypotension, afterdrop, andacidosisdmay precipitate fatal dysrhythmias.47
When rescue is imminent, mental relaxation in con-scious patients may be associated with decreased catechola-mine release, causing decreased blood pressure with loss ofconsciousness and subsequent drowning.47 Circumrescuecollapse has also been described in terrestrial rescuesituations.23,48
Handling of a hypothermic patient during rescue
Keeping the patient in a horizontal position mitigates theeffects of decreased hydrostatic pressure during rescue.45
Avoiding physical effort protects against afterdrop.46 Con-tinued mental stimulus may help maintain catecholaminestimulus.
Recommendation. Rescuers should keep a hypothermicpatient horizontal, especially during rescue from water ora crevasse (Evidence grade: 1B) and should limit physicaleffort by the patient during rescue (Evidence grade: 1B). Aconscious patient should be encouraged to be attentive andfocus on survival (Evidence grade: 1C).
Gentle handling to prevent ventricular fibrillation
Hypothermia lowers the threshold for VF, especially at coretemperatures below 28!C.1 Movement or significant warm-ing of the extremities, as with warm water immersion,increases blood flow to colder tissues. Blood flows to theperiphery, is cooled, and has the potential to cool the heartupon return to the core, increasing the risk of VF.17,49,50
Additional blood return may also cause increased load ona heart that is already pumping ineffectively.
Recommendation. Handle a hypothermic patient gentlyand continue to keep the patient horizontal (Evidencegrade: 1B). Avoid any disturbance, especially movementof the extremities that might precipitate VF (Evidencegrade: 1B). In an effort to minimize movement, clothesshould be cut off of a patient once in a warm environment(Evidence grade: 1B).
Protection from further heat loss
After rescue, the next priority for care of a hypothermicpatient in the out-of-hospital setting is to maintain core tem-perature by preventing further heat loss.
Insulation protects from heat loss. Insulating materialsinclude extra clothing, blankets, quilts, sleeping bags, insu-lated pads, and bubble wrap.51,52 A sleeping bag should notbe used like a blanket; rather the patient should be placedinside, and the enclosure should be completely zipped up.Multiple sleeping bags, if available, can be placed withineach other to create a multilayered enclosure. Any availableinsulation (eg, spare parkas) should be incorporated withinor outside the enclosure in such a way as to not compromiseloft. Bubble wrap is an effective vapor barrier, but it pro-vides less insulation than the other materials.51,52 A largeamount of heat can be lost to the ground by conduction.53
Significant heat can also be lost from the head and neckdue to necessary exposure of the face to allowbreathing.53,54
Vapor barriers protect against convective and evapora-tive cooling (substantially reducing heat loss) and impor-tantly also keep the insulation dry and more effective.Barriers can be made from bubble wrap, tarps, sheets ofplastic, reflective blankets, or garbage bags with a hole cutout for the face. The vapor barrier(s) may be placed insidethe insulation (to keep the insulation dry if the patient ispackaged wet) and/or outside the insulation to protect theinsulation from a wet environment.52,55
Extra insulation can compensate for the absence of awindproof layer or vapor barrier.55 A combined methodusing 2 vapor barriers (1 against the patient and 1 outsidethe insulating layers) will protect the insulation frombecoming wet from all sources.52
Recommendations. Protect from further cooling by usinginsulation and vapor barriers until the patient has reacheda warm environment, such as the warmed interior of anambulance. Remove wet clothes, preferably by cuttingthem off, only when the patient has been protected fromthe cold (Evidence grade: 1C). Insulate the patient fromthe ground (eg, with sleeping pads) to protect from conduc-tive heat loss. Minimize heat loss from the head and neckby covering these areas as effectively as possible (eg,toque, watch cap, hood, jacket) (Evidence grade: 1C).
Hypothermia Clinical Practice Guidelines 9

Protection from windy conditions
In windy conditions, a windproof layer, ideally a vapor bar-rier, provides substantial protection from convective heatloss.51
Recommendation. An outer windproof layer should beused to protect the patient from wind and especially fromrotor wash when loading or unloading from a helicopter.If possible, add a second vapor barrier against the victimto protect the insulating layers (Evidence grade: 1C).
FIELD REWARMINGOnce a hypothermic patient has been protected from furtherheat loss, the next priority is to rewarm the patient. Therewarming methods described in this section achieve thesafe rewarming rate of 1 to 2!C$h-1 and minimize the riskof afterdrop. Afterdrop can lead to hemodynamic instabilityand VF. The risk of afterdrop is reduced by limiting limbmovement and by keeping the patient horizontal. Mostpatients with altered consciousness will require activerewarming.
It is important to recognize that the optimal rate ofrewarming may not be the fastest rate. Even profoundhypothermia may require slow, controlled rewarming.Only patients with hemodynamic instability should be con-sidered for rapid rewarming via extracorporeal life support(ECLS).
Shivering
Vigorous shivering can increase heat production by 5 to 6times the resting metabolic rate and up to 50% of maximal
metabolic rate (V:O2max).
5,56 Shivering can raise core tem-perature by 3 to 4!C$h-1,16,28,57 but it uses a large amountof energy, stresses the cardiovascular system, and causespatient discomfort.17
Recommendation. Shivering is an effective method ofrewarming in a patient who is cold-stressed or mildlyhypothermic. The patient must be adequately insulatedfrom the environment to retain the generated heat (Evi-dence grade: 1A). An alert patient who is shivering, andwho is not at risk for aspiration, should receive high-carbo-hydrate liquids and/or food. Liquids and food may bewarmed but should not be hot enough to burn the esopha-gus (Evidence grade: 1C).
Delay exercise to protect against afterdrop
Once a patient is protected from further heat loss and hasadequate energy reserves, the most effective means of res-cue may be for the patient to walk. Allowing the patientto shiver and rewarm, while insulated and before exercise,should help minimize afterdrop.46 This time period should
last 30 min but will depend upon the situation. Standingupright increases blood flow to and from the legs, worsen-ing afterdrop and potentially decreasing blood pressure.29
Walking or other exercise generates additional heat, but ifinitiated immediately after rescue, may cause a greaterafterdrop in core temperature than if the patient remains atrest.46 There may be situations when immediate movementis necessary to relocate a patient to a safer environment.When this is necessary, close monitoring is prudent.
Recommendation. A shivering patient who may behypothermic should be kept as warm as possible, given cal-orie replacement, and observed before exercising. After thisperiod of observation, the alert patient may be allowed tostand. If the patient can stand without difficulty, exerciseintensity should start low and increase gradually as toler-ated. The patient should be closely monitored; if the condi-tion worsens, the patient should stop exercising and betreated accordingly (Evidence grade: 1C).
Active external rewarming
Field methods of external rewarming are useful in both shi-vering and nonshivering patients. Active (exogenous)rewarming methods, such as large electric heat pads orblankets,58 large chemical heat pads,59,60 warmwater bottles,61 and the Norwegian charcoal-burning HeatPac,17,58,62 all provide significant external heat. In a shiver-ing patient, the added heat attenuates shivering heat produc-tion. This results in a rate of core rewarming similar to thatproduced by shivering but has the advantages of increasedcomfort and decreased energy use with lower cardiac work-load. In a nonshivering patient, added heat will warm thecore, even if slowly, in a patient lacking capacity for endo-genous heat production. The Heat Pac should be used withcaution because it can generate potentially toxic levels ofcarbon monoxide (CO).32
Tomaximize total body net heat gain, active heating willbe more effective in conjunction with insulation and vaporbarrier(s) to create an effective hypothermia enclosure sys-tem. Five such systems were compared on normothermicsubjects inL20!C conditions.63 The systems (all includingactive heating and vapor barrier) included 3 commercialsystems using heavy insulation enclosures, a user-assembled system using a 3-season sleeping bag, and theHypothermia Prevention Management Kit (HPMK).63
Initially evaluated for effectiveness between other rewarm-ing systems,64 the HPMKwas commercially developed forthe Department of Defense-Joint Trauma System (JTS) as alightweight, compact kit designed for field use that com-bines an oxygen-activated self-heating liner with a vaporbarrier. The HPMK was part of the JTS theater-wide strat-egy for battlefield casualties and has been used extensively
Dow et al10

in military operations to decrease mortality from trauma-induced hypothermia.65e67 System effectiveness (netbody heat gain) generally depended on the mass of the insu-lation enclosure.63 The 3 commercial systems were heavyand bulky and therefore only applicable at a point of careor if they could be delivered by sled or vehicle. The user-assembled and HPMK systems could both be transportedby backpack; however, the HPMK was smaller and lighterand therefore more portable, but at the expense of providingless net body heat gain. Therefore, factors such as mass,volume, effectiveness, and cost will affect the type of sys-tem used in the field. Search and rescue teams, whichusually consist of 2 to 4 persons, could realistically carrya more-effective user-assembled system because the itemscan be separated and dispersed to multiple backpacks(Figure 3). Alternatively, the HPMK should be comple-mented by incorporating a sleeping bag (or blankets) overthe heated liner and inside the vapor barrier.
Recommendations. Active sources of heat should be used(Evidence grade: 1B). Rewarming devices should beused in conjunction with vapor barriers and insulation (Evi-dence grade: 1B). The Heat Pac should only be used out-doors or with proper ventilation that is carefullymonitored to prevent CO accumulation (Evidence grade:1B). The single-package, small, and light HPMK is a prac-tical system for transport in a single backpack and useful formilitary operations and should be used with an added layerof insulation if possible (Evidence grade: 1C).
Body-to-body rewarming
Body-to-body rewarming of a shivering patient with awarm person in a sleeping bag blunts the increase in shiver-ing thermogenesis, resulting in rewarming rates no greaterthan shivering alone.57,58 Body-to-body rewarming maymake the cold patient more comfortable due to decreasedshivering, but at the cost of delaying evacuation.
Recommendation. Body-to-body rewarming can be usedin mild hypothermia to increase patient thermal comfort ifenough personnel are available and it does not delay eva-cuation to definitive care (Evidence grade: 1B).
Applying heat to the axillae, chest, and back
External heat is most effective if concentrated on the axil-lae, chest, and back (in that order), which are the areaswith the highest potential for conductive heat transfer.53
Upper torso rewarming is more effective than extremityrewarming.68 Some scenarios may. however, precludeapplying heat to the chest (eg, cardiopulmonary resuscita-tion [CPR] in progress or treatment of chest injury). Apply-ing heat to the head, although requiring more technique to
insulate and apply the heat, has been shown to be equallyeffective in shivering and nonshivering subjects, thus pro-viding an alternative warming approach in extenuatingcircumstances.69
Recommendations. Apply heat sources to the axillae,chest, and back. A large heat pad or blanket should beplaced over the chest and, if large enough, extend into theaxillae and under the back (Evidence grade: 1B). Addi-tional heat can be applied to the neck if precautions aretaken to prevent heat loss through any neck opening (Evi-dence grade: 1C). Avoid applying external heat to theextremities, although it is not necessary to insulate thearms from heat applied to the torso (Evidence grade:1B). If application of heat to the chest is contraindicated(eg, CPR or some chest injuries), heat sources may be stillbe applied under the patient’s upper back or to the head(Evidence grade: 1B). If applying heat sources to theback, rescuers must be able to observe for the developmentof burns on a regular basis (Evidence grade: 1C).
Protection of cold skin
Cold skin is very susceptible to injury from pressure orheat.70 There have been reports of burns associated withuse of a hot water bottle with lukewarm water applieddirectly to hypothermic skin,71 the HPMK,64 water-per-fused warming blankets, a Heat Pac, and hot pads.72
Burns have been reported both in controlled settings whileresearching rewarming methods and during rescue ofhypothermic patients. It is important to visually inspectthe heated skin at regular intervals (eg, 20 to 30 min) toobserve for excess reddening or other signs of pendingburns; in these cases, active heating should be stopped inthe affected areas. This must be done segmentally and care-fully to minimize heat loss. Heated pads should be appliedwith great caution to areas such as the back that are difficultto visualize or under constant pressure from body weight orimmobilization systems.
Recommendation. Avoid localized pressure to cold skin.Apply heat sources according to manufacturer instructions;this often precludes direct contact with the skin by placingsome thin insulating material between the skin and heatsource to prevent burning the skin (Evidence grade: 1C).Skin should be assessed every 20 to 30 min for excess red-dening or other signs of impending thermal burns whenactive heat sources are being applied (Evidence grade:1C).
Do not use small chemical heat packs for rewarming
Small chemical heat packs (eg, those used for hand and footwarming) do not provide sufficient heat to affect core
Hypothermia Clinical Practice Guidelines 11

temperature. In addition, the high surface temperature ofsmall chemical heat packs creates a risk of thermal burns.
Recommendation. Do not use small chemical heat packsfor core rewarming of a hypothermic patient (Evidencegrade: 1B). However, these small chemical heat packscan be used to prevent local cold injury to the hands andfeet during treatment and transport (Evidence grade: 1C).
Heated humidified oxygen
Although heated humidified oxygen prevents respiratoryheat loss, the respiratory tract allows limited heat exchange.Heated humidified oxygen is not effective as a solitaryrewarming method,30e32 but it can be used as an adjunctto other methods.26 Heated humidified oxygen has thepotential to cause facial burns.32
Recommendations.Heated humidified oxygen can be usedin combination with other rewarming methods (Evidencegrade: 2C), but it should not be relied on as the onlyrewarming method (Evidence grade: 1B).
Do not use warm showers or baths for rewarming
A warm shower or bath markedly increases peripheralblood flow, increasing afterdrop and potentially causinghypotension.29,42 Using a warm shower or bath, even in apatient who is mildly hypothermic, may cause cardiovascu-lar collapse. This method of warming may be consideredfor patients who are cold-stressed or after an initial periodof rewarming for those with mild hypothermia.
Recommendation. A warm shower or bath should not beused for initial rewarming, even if a patient appears to beonly mildly hypothermic (Evidence grade: 1C).
Distal limb warming
Distal limb warming in 42 to 45!C water to the elbows andknees is effective for warming alert, mildly hypothermicpatients.9 This method works by opening arteriovenousanastomoses in the hands and feet, causing increased returnflow of warmed blood directly from the arms and legs to thecore. This is an exception to the general rule that peripheralrewarming is contraindicated in hypothermic patients.Because the warmed superficial venous blood bypassesthe cold arteries in the extremities, there is little countercur-rent heat exchange. In the 1 laboratory study that used thismethod, the afterdrop was less than the afterdrop forshivering.9 Distal limb rewarming in water was designedfor use on watercraft and is difficult to apply for otherout-of-hospital transport.
Recommendation. Distal limb warming to the elbows andknees in 42 to 45!C water can be used for rewarming apatient with mild hypothermia if the clinical setting isappropriate (Evidence grade: 1C).
Rewarming during transport
Continued rewarming is challenging during transport. Arandomized, controlled study of care in helicopter andground advanced life support units showed a small increasein core temperature with using large chemical heat pads butdecreased core temperature with passive rewarming, reflec-tive blankets, warm IV fluids, and warm IV fluids plusreflective blankets.60
Forced air warming, usually with an air-filled plasticbaffled blanket with continuous heated airflow through per-forations in the bottom of the blanket, is an effective way torewarm a hypothermic patient.30,73,74 In 1 study, afterdropwith forced air warming was less than with shivering.75
Forced air warming is more effective and more practicalthan a liquid-filled heating blanket.
Recommendations. Forced air warming should be usedduring air or ground transport, if available (Evidencegrade: 1A). If forced air warming is not available, use ofother heat sources can be continued. Care must be takento prevent CO buildup with the charcoal Heat Pac in aground ambulance; this can be done by igniting the deviceoutside the vehicle, bringing it inside only after initialsmoke production subsides, ventilating the vehicle com-partment, and monitoring CO (Evidence grade: 1C). Acharcoal Heat Pac should not be used in an aircraft (Evi-dence grade: 1C).
Temperature in air or ground ambulances
The temperature in patient compartments should ideally be28!C, which is the temperature at which unclothed restingnormothermic humans will neither gain nor lose heat.1
Warming the patient compartment will protect patientsfrom further heat loss when exposed for monitoring orother procedures. However, an air temperature of 28!C isusually uncomfortably hot for pilots, drivers, and medicalproviders. A slightly cooler temperature of 24!C will limitheat loss and is better tolerated by ambulance personnel.
Recommendation. Patient compartments in ground and airambulances should be heated to at least 24!C, if possible, todecrease further heat loss (Evidence grade: 1C).
Treatment of cold stressed patients who are nothypothermic
A cold patient who is alert and shivering but who has ade-quate energy reserves and is not hypothermic is at low riskfor afterdrop or circumrescue collapse.
Dow et al12

Recommendation. It is the consensus of the panel that acold-stressed patient who is not hypothermic need not bekept horizontal. The patient may be allowed to remove hisor her own wet clothing and to put on dry clothing withoutshelter, if necessary. The patient may be allowed to rest in asitting position, to eat and drink to maintain energy reservesand hydration, and to move or keep moving, if necessary.These patients will need close monitoring to ensure theydo not become hypothermic.
RESUSCITATION OF HYPOTHERMIC PATIENTS
Decision to resuscitate hypothermic patients without signsof life
Hypothermic patients have survived with normal neurolo-gic function even after cardiac arrest.23,76e78 Many of theusual indicators of death, such as fixed, dilated pupils andapparent rigor mortis, are unreliable in hypothermicpatients.76,77 Dependent lividity is an unpredictable indica-tor of death in hypothermia.
Recommendations. Fixed, dilated pupils, apparent rigormortis, and dependent lividity are not considered contrain-dications to resuscitation of a severely hypothermic patient(Evidence grade: 1A for fixed, dilated pupils and apparentrigor mortis). Rescuers should attempt CPR and resuscita-tion unless contraindications exist (Evidence grade: 1A).
Contraindications to resuscitation of hypothermic patients
The dictum that “no one is dead until they are warm anddead” is based on the difficulty of diagnosing death in ahypothermic patient in the field. However, some patientsreally are cold and dead. General contraindications toattempted resuscitation in the field include obvious fatalinjuries, such as decapitation, open head injury withloss of brain matter, truncal transection, incineration, ora chest wall that is so stiff that compressions are notpossible.79
Recommendation. Do not attempt to resuscitate a patientwith obvious fatal injuries or whose chest wall is too stifffor compressions (Evidence grade: 1A).
Indication for cardiopulmonary resuscitation
CPR is only indicated in cardiac arrest and is contraindi-cated if there are signs of life. In a hypothermic patient inthe out-of-hospital setting, signs of life may be very dif-ficult to detect. The heart rate can be very slow and pulsesdifficult to palpate. The traditional method of checking apulse by trying to feel the pulse with a finger placed overthe presumed location of an artery is limited by cold.Cold fingers have decreased sensitivity to tactile stimuli.
Breathing can be very slow and shallow but may bedetectible in the absence of palpable pulses.22 If cardiacmonitoring is not available, the diagnosis of cardiacarrest can be difficult.
Recommendation. Rescuers should make every effort tomove the patient to a warm setting, such as a ground orair ambulance or a medical facility where cardiac moni-toring is available to guide resuscitation and to startrewarming (Evidence grade: 1C). Prior to startingCPR, feel for a carotid pulse for 1 min. If a pulse is notpalpated after 1 min, start CPR, including rescue breath-ing (Evidence grade: 1C).
No cut-off temperature for resuscitation
The lowest known core temperature from which a patientwith accidental hypothermia has been successfully resusci-tated is 13.7!C.80 The lowest core temperature ever inducedtherapeutically is 9!C.81 Both patients survived neurologi-cally intact. Induced hypothermia for cardiac or vascularsurgery is usually to 18!C anddunlike accidentalhypothermiada very controlled situation. The lowest tem-perature from which humans with accidental hypothermiacan be successfully resuscitated is not known, and reportsof recovery from extremely low core temperatures makeestablishing a temperature cut-off for resuscitationchallenging.
Recommendation. Resuscitation attempts should be con-tinued regardless of the measured core temperature (Evi-dence grade: 2C).
Electrocardiographic monitoring
Electrocardiographic monitoring is the best way to diag-nose cardiac arrest in the field. An organized rhythm with-out detectible pulses may be pulseless electrical activity ormay be a perfusing rhythm with very weak pulses. Inhypothermic patients, the amplitude of the QRS complexesmay be decreased.10
Starting CPR in a hypothermic patient with an organizedcardiac rhythm carries a risk of causing VF that wouldconvert a perfusing rhythm to a nonperfusing rhythm. Ifend-tidal CO2 (ETCO2) monitoring is available, lack ofwaveform indicates lack of circulation or absence ofmetabolism.13 If ultrasound is available, echocardiographycan be used to determine if cardiac contractions correspondto electrical activity.13
Recommendation. CPR should be started if a nonperfusingrhythm, including ventricular tachycardia, VF, or asystole,is detected. If there is a cardiac rhythm with organizedQRS complexes, CPR should not be performed (Evidence
Hypothermia Clinical Practice Guidelines 13

grade: 1C) unless ETCO2 monitoring confirms lack of per-fusion or echocardiography shows that there are no cardiaccontractions corresponding to electrical activity (Evidencegrade: 1B). Use maximal amplification on the monitor tosearch for QRS complexes (Evidence grade: 1C).
Delaying CPR, intermittent CPR, and prolonged CPR
Cooling reduces resting oxygen consumption of mosthuman tissue by about 6% per 1!C decrease, with a greaterdecrease in brain tissue. Hypothermia preferentially pro-tects the brain from hypoxia. At a core temperature of28!C, whole body oxygen consumption is about 50% ofnormal,1 while brain oxygen consumption may be reducedto about 35% of normal.8 Surgical procedures employingdeep hypothermic circulatory arrest (DHCA) have demon-strated a 7% decrease in cerebral oxygen consumption forevery 1!C decrease in core temperature. Sixty percent ofpatients with a core temperature less than 18!C demonstratean isoelectric electroencephalogram. DHCA is a controlled,rapid, decrease of core temperature from 18 to 20!C.Patients over the age of 60 y undergoing DHCA only toler-ated an estimated 25 min of cardiac arrest, based upon inci-dence of postprocedural cognitive injury. Children toleratelonger periods of time, but there is a dearth of informationfor young and middle-aged adults.82,83 There are manydocumented cases of full neurologic recovery, even afterextended periods of cardiac arrest as long as 9 h84,85 in per-sons who did not have asphyxia before they becamehypothermic. Severely hypothermic patients have beenresuscitated with good neurologic status after as long as 6h 30 min of CPR.23,86e88 Prolonged cardiac arrest inseverely hypothermic patients does not necessarily causebrain injury as it does in normothermic patients.
In cardiac arrest, the classic teaching is that CPRmust bestarted promptly and continued without interruption untilreturn of spontaneous circulation (ROSC) can be estab-lished or death is confirmed. This CPR strategy may notbe possible or warranted in patients with severe hypother-mia.Multiple case reports describe survival with neurologicrecovery when initiation of CPR was delayed and per-formed intermittently.85,89 In 1 case report, a hypothermicavalanche victim was successfully resuscitated with com-plete neurologic recovery, although CPR was not startedfor 15 min after a monitored cardiac arrest.23 In anothercase report, an avalanche victim was extricated apneic andpulseless after a 5 h burial in a crevasse. No attempt wasmade to resuscitate the patient, but the patient was flownto a nearby hospital where ECG showed asystole. CPRwas started 70min after rescue. The patient made a full neu-rologic recovery.48 A third case report described successfulresuscitation with good neurologic recovery of a hypother-mic patient in cardiac arrest who was treated during
evacuation with CPR in a stationary litter for 1-min periodsalternating with 1-min periods of being carried withoutCPR.86
Continuous compressions are ideal, but intermittentcompressions may be necessary to successfully and safelyevacuate the patient. With properly performed compres-sions, it takes an estimated 5 min of cerebral oxygenationto overcome the ischemic threshold.90
Recommendation. Immediate, high-quality CPR should beperformed for a hypothermic patient in cardiac arrest. If it isimpossible or unsafe to perform immediate and continuousCPR, rescuers should perform delayed or intermittent CPR.Ideally, compressions will not be delayed for longer than 10min, a conservative interval based on the uncontrolled nat-ure of out-of-hospital hypothermic cardiac arrest (Evidencegrade: 1C). If CPR cannot be performed continuously,compressions should be performed for a minimum of 5min, with interruptions between periods of compressionsthat should not exceed 5 min (Evidence grade: 1C).
CPR technique in hypothermia
A hypothermic patient will have a stiff chest wall that limitsthe effectiveness of chest compressions and bag-valve-mask ventilation. Myocardial and pulmonary complianceare also markedly reduced in severe hypothermia. Duringhypothermic cardiac arrest with CPR91 in a swine model,cardiac output, cerebral blood flow, and myocardial bloodflow averaged 50, 55, and 31%, respectively, of thoseachieved during normothermic closed-chest compressions.However, metabolic demands are also decreased. Althoughthere are no data to support increased survival when amechanical compression device is used,92 mechanicaldevices reduce the incidence of rescuer fatigue and maypermit longer periods of uninterrupted compressions, espe-cially when bridging to ECLS.86,93
Recommendation. Patients in cardiac arrest should havechest compressions delivered at the same rate as for nor-mothermic patients (Evidence grade: 1C). Using amechanical compression device may decrease interruptionsand reduce rescuer fatigue (Evidence grade: 1C).
Automated external defibrillator
If an automated external defibrillator (AED) with a cardiacmonitor is available, it can be used for cardiac monitoring.An AED without a cardiac monitor can also be used fordiagnosis. The cardiac rhythms that may benefit from cardi-oversion or defibrillation (shockable rhythms) are VT andVF. VT is rare during moderate or severe hypothermia.The instruction “shock is advised” means that the rhythmis VT or VF. The instruction “no shock advised” on an
Dow et al14

AED without monitoring capability can mean that therhythm is asystole or an organized rhythm, which may bepulseless electrical activity. Current AHA guidelinesrecommend a single shock.19
Recommendation. If shock is advised by the AED, rescuersshould attempt defibrillation and start CPR. If no shock isadvised on an AED, no carotid pulse is found after palpat-ing for at least 1 min, normal breathing or other signs oflife are not observed, and ultrasound is not available to ver-ify cardiac activity or pulse, start CPR (Evidence grade:1C).
Initial defibrillation in hypothermia
Defibrillation is only indicated for a shockable rhythm (pul-seless VT or VF). An AED will only advise a shock if therhythm is VT or VF. Current resuscitation guidelinesrecommend a single shock at maximum power for a patientwhose core temperature is below 30!C.13,17,94
Recommendation. If a monitor/defibrillator shows VT orVF in a patient whose core temperature is thought to bebelow 30!C, a single shock should be given at maximumpower (Evidence grade: 1C).
Repeat defibrillation attempts in hypothermia
Patients have been successfully defibrillated at core tem-peratures below 26!C.95e98 If defibrillation below 30!C isunsuccessful, delay further shocks until the temperature isgreater than 30!C; below 30!C, defibrillation is less likelyto be successful. Defibrillation in a patient whose core tem-perature has reached 30!C should follow guidelines for nor-mothermic patients.13
Recommendations.Wait until a patient has been rewarmedto 30!C before attempting further shocks (Evidence grade:2C). Once the core temperature reaches 30!C, follow defi-brillation guidelines for normothermic patients (Evidencegrade: 1C).
Airway management in hypothermia
The principles of airway management are the same in ahypothermic patient as in a normothermic patient. In apatient who is not breathing spontaneously orwho is breath-ing spontaneously but not protecting their airway owing to adecreased level of consciousness, advanced airwaymanage-ment with endotracheal intubation or a supraglottic airwaydevice is indicated to provide adequate ventilation and toprotect against aspiration.13,99 Although there are casereports of VF occurring during endotracheal intubation ofa hypothermic patient,21,50,100,101 this is an uncommoncomplication. In a multicenter study, 117 hypothermic
patients were intubated endotracheally after preoxygenationwith 100% oxygen with no induced dysrhythmias.102
Recommendations. The advantages of advanced airwaymanagement outweigh the risk of causing VF (Evidencegrade: 1C). A nasogastric or orogastric tube should beplaced after the airway is secured to decompress the sto-mach (Evidence grade: 1C).
Practical considerations. Rapid-sequence intubation withparalysis may not be effective if the paralytic agent is unableto overcome the trismus produced by profound hypother-mia. Fiber optic intubation or cricothyroidotomy may berequired to place an endotracheal tube if cold-induced tris-mus prevents laryngoscopy. A supraglottic device may bepreferable to endotracheal intubation in these conditions.Overinflation of an endotracheal tube or supraglottic devicecuff with cold air should be avoided because the air insidethe cuff will expand as the victim rewarms, potentially kink-ing the tube or rupturing the cuff.
Ventilation in hypothermia without an advanced airway
Hyperventilation has many potentially adverse effects inhypothermia, including decreased cerebral blood flow. Asshown in the swine model, ventilation without an advancedairway is limited by decreased thoracic compliance.91,103 Ifavailable, ETCO2 monitoring can be used to preventhyperventilation.
Recommendation. In the absence of ETCO2 monitoring,ventilation should be delivered at the same rate recom-mended for a normothermic patient,13,19 unless an advancedairway is in place (see below) (Evidence grade: 2C).
Ventilation in hypothermia with advanced airway
If the patient is intubated or has a supraglottic device, ven-tilation is more effective than in a patient without advancedairway management.
Recommendation. In a patient with an advanced airway,if ETCO2 monitoring is not available, ventilationshould be delivered at half the rate recommended for a nor-mothermic patient to avoid hyperventilation (Evidencegrade: 1C).
Management of ETCO2
ETCO2 monitoring can be used to keep ETCO2 in the nor-mal range. This range depends on altitude.
Recommendation. If ETCO2 monitoring is available,ETCO2 should be kept within the normal range. In rescuesat altitudes above 1200 m, advanced life support personnelshould be aware of the normal range of ETCO2 at a givenaltitude (Evidence grade: 1C).
Hypothermia Clinical Practice Guidelines 15

Anesthetic and neuromuscular blocking agents inhypothermia
At low core temperatures, drug metabolism is decreased;anesthesia and neuromuscular blockade areprolonged.104e106
Recommendation. In patients with core temperatures lowerthan 30!C, dosages of anesthetic and neuromuscular block-ing agents should be decreased, and intervals should beextended according to the degree of hypothermia. Currentdata are insufficient to recommend specific protocols (Evi-dence grade: 1C).
Supplemental oxygen
Oxygen extraction is not a limiting factor in survival inhypothermia at sea level.107
Recommendation. A hypothermic patient should receivesupplemental oxygen, especially at altitudes over 2500 m,because of potential benefits and no known harm (Evi-dence grade: 1C).
Circulatory access in hypothermia
Obtaining intravenous (IV) access is often difficult inhypothermic patients. Intraosseous (IO) access is fast andreliable. Because the myocardium is irritable in hypother-mia, catheters that contact the heart may cause dysrhyth-mias. Internal jugular or subclavian central lines thatextend into the right atrium are contraindicated unless ashort catheter is inserted. There is a risk of causing VF ifthe wire used during placement of a central venous catheterusing the Seldinger technique is advanced into the heart.The femoral vein approach allows central venous accesswithout the danger of inducing dysrhythmias, but it maybe difficult in the field. Unsuccessful attempts often causehematomas.
Recommendations. If circulatory access cannot immedi-ately be obtained with a peripheral IV catheter, accessshould be obtained by the IO method (Evidence grade:1C). Central venous access can be obtained using a femoralline if no other option is available (Evidence grade: 1C).
Volume replacement in hypothermia
Circulating blood volume in moderate and severe hypother-mia is reduced.9,107 During rewarming, vasoconstrictionthat previously limited the vascular space is abolished.Volume should be replaced to avoid severe volume deple-tion with resultant shock, while avoiding administration offluid sufficient to cause volume overload. To preventfurther core temperature cooling, IV/IO fluid should be
warmed to at least 40!C and preferably to 42!C. In thefield, IV/IO bags and tubing should be insulated. Fluid war-mers, preferably commercial products that have been pro-ven effective, should be used. Because the effectiveperfused mass (thermal core) is decreased in hypothermiaas a result of intense peripheral vasoconstriction,9 adminis-tration of fluid warmed to 40 to 42!C may help increasecore temperature. Because metabolism is depressed, glu-cose-containing fluid is not essential. The fluid of choicefor volume replacement is normal saline. Lactated Ringer’ssolution should not be used in a hypothermic patientbecause the cold liver cannot metabolize lactate.1 Someclinicians use a mixture of crystalloid and colloid.1
Recommendation. Resuscitate a hypothermic patient withnormal saline warmed to 40 to 42!C given IV or IO. Usecaution to prevent volume overload (Evidence grade: 1B).
Fluid management in hypothermia
Giving fluids in boluses, as rapidly as possible, rather thanby continuous infusion will alleviate problems with coolingof fluid or freezing of lines, which can occur even if linesare insulated. The ideal method is to saline lock the linewhen there will be a long pause after a bolus. Boluses of500 mL can be titrated to maintain adequate systolicblood pressure, depending on the degree of hypothermia.There is no available evidence to quantify a target systolicblood pressure.
Recommendations.When practical, fluids should be givenas boluses rather than by continuous infusion (Evidencegrade: 1C). The goal of fluid administration should be tomaintain systolic blood pressure at a level that providesadequate perfusion, depending on the degree of hypother-mia (Evidence grade: 1C).
Use of exogenous glucose and insulin in hypothermia
Hypo- and hyperglycemia have been reported inhypothermia.96,108 Point-of-care glucose testing is routinein patients with an altered level of consciousness but maynot be available in an out-of-hospital setting. Hyperglyce-mia has not been shown to be deleterious in hypothermicpatients.96
Recommendation. Glucose should be administered to thehypothermic patient who is hypoglycemic (Evidencegrade: 1A). Insulin is not initially indicated for hyperglyce-mia (Evidence grade: 1B). If glucose testing is not avail-able, IV glucose can be administered empirically to thehypothermic patient with altered mental status (Evidencegrade: 1C).
Dow et al16

Effects of vasoactive and antidysrhythmic drugs inhypothermia
There is limited evidence regarding drug effects inhypothermic cardiac arrest in humans. Most of the evi-dence comes from animal studies.109 The cold heart haslong been considered to be unresponsive to vasopressoror antiarrhythmic medications, although some animal stu-dies have suggested otherwise. In a study of hypothermicdogs, epinephrine increased coronary perfusion pressureand ROSC after defibrillation.110 In a hypothermic pigstudy, vasopressin increased coronary perfusion pressurewith active compression-decompression CPR using animpedance threshold valve, but not with standardCPR.111 Vasopressin improved ROSC and 1-h survivalafter defibrillation in a study of hypothermic pigs.112
There is a case report of ROSC with vasopressin follow-ing unsuccessful use of epinephrine (2 mg) in a hypother-mic patient, but the patient subsequently died OFmultisystem failure.113
The ideal pharmacologic approach to ventricular dys-rhythmias remains unresolved. Class III agents, such as bre-tylium and amiodarone, are theoretically ideal because theyact directly against fibrillation. Amiodarone is less effectivein hypothermia than in normothermia and carries a risk ofinducing torsades des pointes.114 The safety of amiodaronein hypothermia is not known. In a study of hypothermicdogs, the combination of epinephrine and amiodaroneincreased ROSC after defibrillation following administra-tion of epinephrine alone.110 Bretylium failed to increasethe incidence of ROSC in a study of hypothermicdogs.115 In another dog study, neither amiodarone nor bre-tylium improved ROSC.116 There are 2 clinical reports ofresolution of VF following infusion of bretylium.117,118
Recommendation. The panel concurs that no recommenda-tion can be made at this time owing to the limited evidenceavailable.
Dosing of drugs in hypothermia
In hypothermia, drug metabolism is decreased and proteinbinding is increased.11 Drugs given have little activitywhile the patient is hypothermic but may reach toxic levelswith rewarming.
Recommendations. Do not administer vasoactive drugsuntil the patient has been rewarmed to 30!C (Evidencegrade: 1C). To minimize the potential for toxic accumula-tion of medications, the usual dose can be given, but dosingintervals should be twice as long as usual when the coretemperature is 30 to 35!C (Evidence grade: 2C).
Transcutaneous cardiac pacing in hypothermia
Two case reports suggest that transcutaneous pacing maybe beneficial in the hypothermic patient.119 In both cases,transcutaneous pacing was instituted to increase blood pres-sure to facilitate arteriovenous rewarming rather than tocontrol heart rate.
Recommendation. It is the consensus of the panel thattranscutaneous pacing may be beneficial in hypothermiain the setting of bradycardia with hypotension dispropor-tionate to the core temperature (Evidence grade: 2C).
Management of atrial dysrhythmias during rewarming of ahypothermic patient
Atrial dysrhythmias in hypothermic patients duringrewarming are common and resolve spontaneously oncethe patient has been sufficiently rewarmed.120
Recommendation. No treatment is indicated for atrial dys-rhythmias in a hemodynamically stable patient duringrewarming (Evidence grade: IB).
TRANSPORT/TRIAGE
Severe trauma
Core temperatures <35!C are associated with decreasedsurvival in patients with severe trauma.121,122 Severetrauma can cause acidosis and coagulopathy. In traumapatients with hemorrhagic shock, the “lethal triad” of acido-sis, coagulopathy, and hypothermia is associated withmultiorgan system dysfunction123 and extremely highmortality.124
Recommendation. To prevent hypothermia, the severelyinjured patient should be treated early and aggressivelywith active rewarming during all phases of out-of-hospitalcare (Evidence grade: 1B).
Stabilizing injuries for transport
Stabilization of injuries for transport is the same in ahypothermic patient as in a normothermic patient.
Recommendations.When preparing a patient for transport,potential spinal injuries should be stabilized125 (Evidencegrade: 1C). Fractures and dislocations should be reducedas much as possible to normal anatomic configuration (Evi-dence grade: 1C). Open wounds should be covered (Evi-dence grade: 1C).
Patients with mild hypothermia who are alert
Alert patients with mild hypothermia can be treated in thefield.
Hypothermia Clinical Practice Guidelines 17

Recommendation. An uninjured patient who is completelyalert and shivering may be treated without being trans-ported to a hospital (Evidence grade: 1B).
Choice of destination hospital for hypothermic patients
Profoundly hypothermic patients (<28!C) and those withhemodynamic instability and witnessed out-of-hospital car-diac arrest may benefit from transport to centers capable ofECLS. ECLS includes the techniques of extracorporeal cir-culation, extracorporeal membrane oxygenation (ECMO),and coronary bypass. ECLS provides both oxygenationand hemodynamic support for unstable patients whileallowing for controlled rewarming.
Patients who are not profoundly hypothermic or hemo-dynamically unstable should be transported to the nearestfacility.87,126e131
Hypothermic patients with hemodynamic instability
Hemodynamically unstable patients require critical careand may benefit from ECLS with ECMO or CPB. ECMOis preferred overCPB,127 but both have been used success-fully to rewarm severely hypothermic patients. Profoundlyhypothermic patients with witnessed cardiac arrest, regard-less of return to spontaneous circulation in the field, have agreater chance of survival if transferred to a center whereECLS can be initiated.87,126e131
Many geographic areas do not have a hospital capable ofECLS. Bad weather or other factors may prevent transfer ofa patient to a hospital with ECLS. Hemodynamicallyunstable hypothermic patients, including hypothermicpatients in cardiac arrest, have been successfully resusci-tated with complete neurologic recovery without usingECLS.88,132e134
Recommendations. A patient with moderate to severehypothermia who is hemodynamically stable can be trans-ferred to the closest hospital or other appropriate medicalfacility, such as a rural clinic (Evidence grade: 1C). Apatient who is hemodynamically unstable or with a coretemperature <28!C should be transferred to a hospital cap-able of providing critical care and ECLS. If this will requiresignificant additional timedgenerally more than an addi-tional hourdof noncritical care transport, the patient shouldfirst be stabilized at a closer facility (Evidence grade: 1C).A patient in cardiac arrest should be transferred to a hospitalcapable of providing ECLS if possible. If all other factorsare equal, ECMO is preferable over CPB (Evidencegrade: 1B).
In geographic regions where there is no hospital capableof providing ECLS or when a hospital capable of providingECLS is not accessible, transport a patient in cardiac arrestto the closest hospital where serum potassium can be
measured and resuscitation methods not involving ECLScan be attempted for a patient whose serum potassium is<12 mmol$L-1 (Evidence grade: 1C). (Please see sectionfor use of biochemical markers.)
Hypothermic patients who are alert but have comorbidities,including trauma or asphyxia
Hypothermic patients with injuries or other medical comor-bidities should be transferred to a facility able to appropri-ately manage the patient. Comorbidities can alter theclinical presentation of hypothermia and could potentiallydelay recognition of severe hypothermia.135 Asphyxiatedpatients (from avalanche or drowning) may appear stablebut are at risk for delayed complications and are likely torequire a higher level of care.127
Recommendations. A patient with injuries meeting traumacriteria should be transported to a trauma center (Evidencegrade: 1B). The asphyxiated patient should be transportedto a hospital for observation (Evidence grade: 1B).
Use of biochemical markers to determine if resuscitationshould be continued in a hypothermic patient without vitalsigns. Increased serum potassium in a hypothermicpatient usually indicates that hypothermia was precededby hypoxia. As such, it is a marker of cell lysis anddeath. The highest potassium in a patient resuscitatedfrom hypothermia was 11.8 mmol$L-1 in a 31-mo-oldchild. This level is questionable because the repeat potas-sium 25 min later was 4.8 mmol$L-1 without mention oftherapeutic intervention.136 The highest levels recordedin patients who were resuscitated were 9.5 mmol$L-1 ina 13-y-old137 and 7.9 mmol$L-1 in a 34-y-old.138
Recommendation. If an adult hypothermic patient has apotassium >12 mmol$L-1, CPR should be terminated (Evi-dence grade: 1B).
Conclusions
To assist medical providers caring for patients with acci-dental hypothermia in the out-of-hospital setting, we haveprovided evidence-based recommendations for evaluationand treatment. There are several important areas of uncer-tainty that warrant future research. These areas include opti-mal methods for evaluating patients with accidentalhypothermia, best treatments for patients with mild to mod-erate hypothermia, and optimal methods of resuscitatinghypothermic patients in cardiac arrest.
Dow et al18

Author Contributions: All authors contributed to manuscript conceptua-lization, data collection and review, and manuscript preparation.
Financial/Material Support: None.Disclosures: None.
Supplementary materials
Supplementary material associated with this article can befound in the online version at https://doi.org/10.1016/j.wem.2019.10.002.
References
1. Danzl DF. Accidental hypothermia. In: Auerbach PS,Cushing TA, Harris NS, eds. Auerbach's Wilderness Medi-cine. 7th ed. Philadelphia, PA: Elsevier; 2017:135e62.
2. Zafren K, Giesbrecht GG, Danzl DF, Brugger H,Sagalyn EB, Walpoth B, et al. Wilderness Medical Societypractice guidelines for the out-of-hospital evaluation andtreatment of accidental hypothermia: 2014 update. Wilder-ness Environ Med. 2014;25(4 Suppl):S66e85.
3. Guyatt G, Gutterman D, Baumann MH, Addrizzo-Harris D,Hylek EM, Phillips B, et al. Grading strength of recommen-dations and quality of evidence in clinical guidelines: reportfrom an american college of chest physicians task force.Chest. 2006;129(1):174e81.
4. Giesbrecht GG. Cold stress, near drowning and accidentalhypothermia: a review. Aviat Space Environ Med.2000;71(7):733e52.
5. Bristow GK, Giesbrecht GG. Contribution of exercise andshivering to recovery from induced hypothermia (31.2degrees C) in one subject. Aviat Space Environ Med.1988;59(6):549e52.
6. FitzGibbon T, Hayward JS, Walker D. EEG and visualevoked potentials of conscious man during moderatehypothermia. Electroencephalogr Clin Neurophysiol.1984;58(1):48e54.
7. Giesbrecht GG, Arnett JL, Vela E, Bristow GK. Effect oftask complexity on mental performance during immersionhypothermia. Aviat Space Environ Med. 1993;64(3 Pt 1):206e11.
8. Michenfelder JD, Milde JH. The relationship among caninebrain temperature, metabolism, and function duringhypothermia. Anesthesiology. 1991;75(1):130e6.
9. Vanggaard L, Eyolfson D, Xu X,Weseen G,Giesbrecht GG.Immersion of distal arms and legs in warm water (AVArewarming) effectively rewarms mildly hypothermichumans. Aviat Space Environ Med. 1999;70(11):1081e8.
10. Duguid H, Simpson RG, Stowers JM. Accidental hypother-mia. Lancet. 1961;2(7214):1213e9.
11. Giesbrecht GG. The respiratory system in a cold environ-ment. Aviat Space Environ Med. 1995;66(9):890e902.
12. Durrer B, Brugger H, SymeD, International Commission forMountain Emergency Medicine. The medical on-site treat-ment of hypothermia: ICAR-MEDCOM recommendation.High Alt Med Biol. 2003;4(1):99e103.
13. Soar J, Perkins GD, Abbas G, Alfonzo A, Barelli A,Bierens JJ, et al. European Resuscitation Council Guidelinesfor Resuscitation 2010 Section 8. Cardiac arrest in specialcircumstances: Electrolyte abnormalities, poisoning, drown-ing, accidental hypothermia, hyperthermia, asthma, anaphy-laxis, cardiac surgery, trauma, pregnancy, electrocution.Resuscitation. 2010;81(10):1400e33.
14. ZafrenK,Giesbrecht GG. State of Alaska Cold InjuryGuide-lines. Juneau: State of Alaska; 2014.
15. Strapazzon G, Procter E, Paal P, Brugger H. Pre-hospitalcore temperature measurement in accidental and therapeutichypothermia. High Alt Med Biol. 2014;15(2):104e11.
16. Tikuisis P, Giesbrecht GG. Prediction of shivering heat pro-duction from core and mean skin temperatures. Eur J ApplPhysiol Occup Physiol. 1999;79(3):221e9.
17. Giesbrecht GG. Emergency treatment of hypothermia.Emerg Med (Fremantle). 2001;13(1):9e16.
18. Giesbrecht GG. “Cold Card” to guide responders in theassessment and care of cold-exposed patients. WildernessEnviron Med. 2018;29(4):499e503.
19. Vanden Hoek TL, Morrison LJ, Shuster M, Donnino M,Sinz E, Lavonas EJ, et al. Part 12: cardiac arrest in specialsituations: 2010 American Heart Association Guidelinesfor Cardiopulmonary Resuscitation and Emergency Cardio-vascular Care.Circulation. 2010;122(18 Suppl 3):S829e61.
20. Deslarzes T, Rousson V, Yersin B, Durrer B, Pasquier M.An evaluation of the Swiss staging model for hypothermiausing case reports from the literature. Scand J TraumaResusc Emerg Med. 2016;24:16.
21. Baumgartner FJ, Janusz MT, Jamieson WR, Winkler T,Burr LH, Vestrup JA. Cardiopulmonary bypass for resusci-tation of patients with accidental hypothermia and cardiacarrest. Can J Surg. 1992;35(2):184e7.
22. Feiss P, Mora C, Devalois B, Gobeaux R, Christides C.[Accidental deep hypothermia and circulatory arrest. Treat-ment with extracorporeal circulation]. Ann Fr Anesth Rea-nim. 1987;6(3):217e8.
23. Oberhammer R, Beikircher W, Hormann C, Lorenz I,Pycha R, Adler-Kastner L, et al. Full recovery of an ava-lanche victim with profound hypothermia and prolongedcardiac arrest treated by extracorporeal re-warming. Resusci-tation. 2008;76(3):474e80.
24. Papenhausen M, Burke L, Antony A, Phillips JD. Severehypothermia with cardiac arrest: complete neurologic recov-ery in a 4-year-old child. J Pediatr Surg. 2001;36(10):1590e2.
25. Pasquier M, Zurron N, Weith B, Turini P, Dami F,Carron PN, et al. Deep accidental hypothermia with coretemperature below 24!C presenting with vital signs. HighAlt Med Biol. 2014;15(1):58e63.
26. Stoner HB. Thermoregulation after injury. Adv Exp MedBiol. 1972;33(0):495e9.
27. Jain A, Gray M, Slisz S, Haymore J, Badjatia N, Kulstad E.Shivering treatments for targeted temperature management:a review. J Neurosci Nurs. 2018;50(2):63e7.
28. Giesbrecht GG, Goheen MS, Johnston CE, Kenny GP,Bristow GK, Hayward JS. Inhibition of shivering increases
Hypothermia Clinical Practice Guidelines 19

core temperature afterdrop and attenuates rewarming inhypothermic humans. J Appl Physiol (1985). 1997;83(5):1630e4.
29. Hayward JS, Eckerson JD, Kemna D. Thermal and cardio-vascular changes during three methods of resuscitationfrom mild hypothermia. Resuscitation. 1984;11(1e2):21e33.
30. Goheen MS, Ducharme MB, Kenny GP, Johnston CE,Frim J, Bristow GK, et al. Efficacy of forced-air and inhala-tion rewarming by using a human model for severehypothermia. J Appl Physiol (1985). 1997;83(5):1635e40.
31. Mekjavic IB, Eiken O. Inhalation rewarming from hypother-mia: an evaluation in -20 degrees C simulated field condi-tions. Aviat Space Environ Med. 1995;66(5):424e9.
32. Sterba JA. Efficacy and safety of prehospital rewarmingtechniques to treat accidental hypothermia. Ann EmergMed. 1991;20(8):896e901.
33. Walpoth BH, Galdikas J, Leupi F, Muehlemann W,Schlaepfer P, Althaus U. Assessment of hypothermia witha new “tympanic” thermometer. J Clin Monit. 1994;10(2):91e6.
34. Skaiaa SC, Brattebø G, Aßmus J, Thomassen Ø. Theimpact of environmental factors in pre-hospital thermistor-based tympanic temperature measurement: a pilot fieldstudy. Scand J Trauma Resusc Emerg Med. 2015;23:72.
35. Grissom CK, Harmston CH, McAlpine JC, Radwin MI,Ellington B, Hirshberg EL, et al. Spontaneous endogenouscore temperature rewarming after cooling due to snow bur-ial. Wilderness Environ Med. 2010;21(3):229e35.
36. Kimberger O, Cohen D, Illievich U, Lenhardt R. Temporalartery versus bladder thermometry during perioperative andintensive care unit monitoring. Anesth Analg. 2007;105(4):1042e7.
37. Gunga HC, Werner A, Stahn A, Steinach M, Schlabs T,Koralewski E, et al. The double sensor-a non-invasivedevice to continuously monitor core temperature in humanson earth and in space. Respir Physiol Neurobiol.2009;169(Suppl 1):S63e8.
38. Kimberger O, Thell R, Schuh M, Koch J, Sessler DI,Kurz A. Accuracy and precision of a novel non-invasivecore thermometer. Br J Anaesth. 2009;103(2):226e31.
39. Dahyot-Fizelier C, Lamarche S, Kerforne T, Benard T,Giraud B, Bellier R, et al. Accuracy of zero-heat-flux cuta-neous temperature in intensive care adults. Crit Care Med.2017;45(7):e715e7.
40. Giesbrecht GG, Bristow GK. A second postcooling after-drop: more evidence for a convective mechanism. J ApplPhysiol (1985). 1992;73(4):1253e8.
41. Golden FS, Hervey GR. The mechanism of the after-dropfollowing immersion hypothermia in pigs [proceedings].J Physiol. 1977;272(1):26Pe7P.
42. Romet TT. Mechanism of afterdrop after cold water immer-sion. J Appl Physiol (1985). 1988;65(4):1535e8.
43. Fox JB, Thomas F, Clemmer TP, Grossman M.A retrospective analysis of air-evacuated hypothermiapatients. Aviat Space Environ Med. 1988;59(11 Pt 1):1070e5.
44. Stoneham MD, Squires SJ. Prolonged resuscitation in acutedeep hypothermia. Anaesthesia. 1992;47(9):784e8.
45. Golden FS, Hervey GR, Tipton MJ. Circum-rescuecollapse: collapse, sometimes fatal, associated with rescueof immersion victims. J R Nav Med Serv. 1991;77(3):139e49.
46. Giesbrecht GG, Bristow GK. The convective afterdrop com-ponent during hypothermic exercise decreases with delayedexercise onset. Aviat Space Environ Med. 1998;69(1):17e22.
47. Giesbrecht GG, Hayward JS. Problems and complicationswith cold-water rescue. Wilderness Environ Med.2006;17(1):26e30.
48. Althaus U, Aeberhard P, Schupbach P, Nachbur BH,Muhlemann W. Management of profound accidentalhypothermia with cardiorespiratory arrest. Ann Surg.1982;195(4):492e5.
49. Lee CH, Van Gelder C, Burns K, Cone DC. Advancedcardiac life support and defibrillation in severehypothermic cardiac arrest. Prehosp Emerg Care.2009;13(1):85e9.
50. Osborne L, Kamal El-Din AS, Smith JE. Survival after pro-longed cardiac arrest and accidental hypothermia. Br Med J(Clin Res Ed). 1984;289(6449):881e2.
51. Henriksson O, Lundgren JP, Kuklane K, Holmer I,Bjornstig U. Protection against cold in prehospital care-thermal insulation properties of blankets and rescue bagsin different wind conditions. Prehosp Disaster Med.2009;24(5):408e15.
52. Thomassen Ø, Faerevik H, Osteras Ø, Sunde GA,Zakariassen E, Sandsund M, et al. Comparison of three dif-ferent prehospital wrapping methods for preventinghypothermia–a crossover study in humans. Scand J TraumaResusc Emerg Med. 2011;19:41.
53. Hayward JS, Collis M, Eckerson JD. Thermographic evalua-tion of relative heat loss areas of man during cold waterimmersion. Aerosp Med. 1973;44(7):708e11.
54. Pretorius T, Bristow GK, Steinman AM, Giesbrecht GG.Thermal effects of whole head submersion in cold wateron nonshivering humans. J Appl Physiol (1985).2006;101(2):669e75.
55. Henriksson O, Lundgren P, Kuklane K, Holmer I, Naredi P,Bjornstig U. Protection against cold in prehospital care: eva-porative heat loss reduction by wet clothing removal or theaddition of a vapor barrier–a thermal manikin study.PrehospDisaster Med. 2012;27(1):53e8.
56. Iampietro PF, Vaughan JA, Goldman RF, Kreider MB,Masucci F, Bass DE. Heat production from shivering.J Appl Physiol. 1960;15:632e4.
57. Giesbrecht GG, Sessler DI, Mekjavic IB, Schroeder M,Bristow GK. Treatment of mild immersion hypothermia bydirect body-to-body contact. J Appl Physiol (1985).1994;76(6):2373e9.
58. Hultzer MV, Xu X, Marrao C, Bristow G, Chochinov A,Giesbrecht GG. Pre-hospital torso-warming modalities forsevere hypothermia: a comparative study using a humanmodel. CJEM. 2005;7(6):378e86.
Dow et al20

59. Watts DD, Roche M, Tricarico R, Poole F, Brown JJ Jr,Colson GB, et al. The utility of traditional prehospital inter-ventions in maintaining thermostasis. Prehosp Emerg Care.1999;3(2):115e22.
60. Lundgren P, Henriksson O,Naredi P, Bjornstig U. The effectof active warming in prehospital trauma care during road andair ambulance transportation - a clinical randomized trial.Scand J Trauma Resusc Emerg Med. 2011;19:59.
61. Lundgren JP, Henriksson O, Pretorius T, Cahill F,Bristow G, Chochinov A, et al. Field torso-warming modal-ities: a comparative study using a human model. PrehospEmerg Care. 2009;13(3):371e8.
62. Giesbrecht GG, Bristow GK, Uin A, Ready AE, Jones RA.Effectiveness of three field treatments for induced mild(33.0 degrees C) hypothermia. J Appl Physiol (1985).1987;63(6):2375e9.
63. Dutta R, Kulkarni K, Gardiner P, Steinman A, Giesbrecht G.PW 2321 Human responses to five heated hypothermiaenclosure systems in a cold environment. Injury Prevention.2018;24:A216.1eA.
64. Allen PB, Salyer SW, Dubick MA, Holcomb JB,Blackbourne LH. Preventing hypothermia: comparison ofcurrent devices used by the US Army in an in vitro warmedfluid model. J Trauma. 2010;69(Suppl 1):S154e61.
65. Arthurs Z, Cuadrado D, Beekley A, Grathwohl K, Perkins J,Rush R, et al. The impact of hypothermia on trauma care atthe 31st combat support hospital. Am J Surg. 2006;191(5):610e4.
66. Palm K, Apodaca A, Spencer D, Costanzo G, Bailey J,Blackbourne LH, et al. Evaluation of military trauma systempractices related to damage-control resuscitation. J TraumaAcute Care Surg. 2012;73(6 Suppl 5):S459e64.
67. Bennett BL, Holcomb JB. Battlefield trauma-inducedhypothermia: transitioning the preferred method of casualtyrewarming. Wilderness Environ Med. 2017;28(2S):S82e9.
68. Ducharme MB, Tikuisis P. Role of blood as heat source orsink in human limbs during local cooling and heating.J Appl Physiol (1985). 1994;76(5):2084e94.
69. Kulkarni K, Hildahl E, Dutta R, Webber SC, Passmore S,McDonald GK, et al. Efficacy of head and torso rewarmingusing a human model for severe hypothermia. WildernessEnviron Med. 2019;30(1):35e43.
70. SteinmanAM. Cardiopulmonary resuscitation and hypother-mia. Circulation. 1986;74(6 Pt 2):IV29e32.
71. Giesbrecht GG. Immersion into cold water. In: Auerbach PS,Cushing TA, Harris NS, eds. Auerbach's Wilderness Medi-cine. 7th ed. Vol 1. Philadelphia, PA: Elsevier; 2017:162.
72. Giesbrecht GG, Walpoth B. Risk of burns during activeexternal rewarming for accidental hypothermia. WildernessEnviron Med. 2019 [Epub ahead of print].
73. Ducharme MB, Giesbrecht GG, Frim J, Kenny GP,Johnston CE, Goheen MS, et al. Forced-air rewarming in-20 degrees C simulated field conditions. Ann N Y AcadSci. 1997;813:676e81.
74. Steele MT, Nelson MJ, Sessler DI, Fraker L, Bunney B,Watson WA, et al. Forced air speeds rewarming in acciden-tal hypothermia. Ann Emerg Med. 1996;27(4):479e84.
75. Giesbrecht GG, Schroeder M, Bristow GK. Treatment ofmild immersion hypothermia by forced-air warming. AviatSpace Environ Med. 1994;65(9):803e8.
76. Ko CS, Alex J, Jeffries S, Parmar JM. Dead? Or just cold:profoundly hypothermic patient with no signs of life.Emerg Med J. 2002;19(5):478e9.
77. Leitz KH, Tsilimingas N, Guse HG, Meier P, Bachmann HJ.[Accidental drowning with extreme hypothermia–rewarm-ing with extracorporeal circulation]. Chirurg. 1989;60(5):352e5.
78. Walpoth BH, Walpoth-Aslan BN, Mattle HP, Radanov BP,Schroth G, Schaeffler L, et al. Outcome of survivors of acci-dental deep hypothermia and circulatory arrest treated withextracorporeal blood warming. N Engl J Med.1997;337(21):1500e5.
79. Paal P, Milani M, Brown D, Boyd J, Ellerton J. Terminationof cardiopulmonary resuscitation in mountain rescue. HighAlt Med Biol. 2012;13(3):200e8.
80. Gilbert M, Busund R, Skagseth A, Nilsen PA,Solbo JP. Resuscitation from accidental hypothermiaof 13.7 degrees C with circulatory arrest. Lancet.2000;355(9201):375e6.
81. Niazi SA, Lewis FJ. Profound hypothermia in man; report ofa case. Ann Surg. 1958;147(2):264e6.
82. Englum BR, Andersen ND, Husain AM, Mathew JP,Hughes GC. Degree of hypothermia in aortic arch surgery- optimal temperature for cerebral and spinal protection:deep hypothermia remains the gold standard in the absenceof randomized data. Ann Cardiothorac Surg. 2013;2(2):184e93.
83. Svensson LG, Crawford ES, Hess KR, Coselli JS, Raskin S,Shenaq SA, et al. Deep hypothermia with circulatory arrest.Determinants of stroke and early mortality in 656 patients.J Thorac Cardiovasc Surg. 1993;106(1):19e28.
84. Meyer M, Pelurson N, Khabiri E, Siegenthaler N,Walpoth BH. Sequela-free long-term survival of a 65-year-old woman after 8 hours and 40 minutes of cardiac arrestfrom deep accidental hypothermia. J Thorac CardiovascSurg. 2014;147(1):e1e2.
85. Forti A, Brugnaro P, Rauch S, Crucitti M, Brugger H,Cipollotti G, et al. Hypothermic cardiac arrest withfull neurologic recovery after approximately ninehours of cardiopulmonary resuscitation: managementand possible complications. Ann Emerg Med.2019;73(1):52e7.
86. Boue Y, Lavolaine J, Bouzat P, Matraxia S, Chavanon O,Payen JF. Neurologic recovery from profound accidentalhypothermia after 5 hours of cardiopulmonary resuscitation.Crit Care Med. 2014;42(2):e167e70.
87. Hilmo J, Naesheim T, Gilbert M. “Nobody is dead untilwarm and dead”: prolonged resuscitation is warranted inarrested hypothermic victims also in remote areas–a retro-spective study from northern Norway. Resuscitation.2014;85(9):1204e11.
88. Lexow K. Severe accidental hypothermia: survival after 6hours 30 minutes of cardiopulmonary resuscitation. ArcticMed Res. 1991;50(Suppl 6):112e4.
Hypothermia Clinical Practice Guidelines 21

89. Gordon L, Paal P, Ellerton JA, Brugger H, Peek GJ,Zafren K. Delayed and intermittent CPR for severe acciden-tal hypothermia. Resuscitation. 2015;90:46e9.
90. Imberti R, Bellinzona G, Riccardi F, Pagani M, Langer M.Cerebral perfusion pressure and cerebral tissue oxygen ten-sion in a patient during cardiopulmonary resuscitation. Inten-sive Care Med. 2003;29(6):1016e9.
91. Maningas PA, DeGuzman LR, Hollenbach SJ, Volk KA,Bellamy RF. Regional blood flow during hypothermicarrest. Ann Emerg Med. 1986;15(4):390e6.
92. Pietsch U, Lischke V, Pietsch C, Kopp KH. Mechanicalchest compressions in an avalanche victim with cardiacarrest: an option for extreme mountain rescue operations.Wilderness Environ Med. 2014;25(2):190e3.
93. Wik L, Kiil S. Use of an automatic mechanical chest com-pression device (LUCAS) as a bridge to establishing cardio-pulmonary bypass for a patient with hypothermic cardiacarrest. Resuscitation. 2005;66(3):391e4.
94. Ujhelyi MR, Sims JJ, Dubin SA, Vender J,Miller AW. Defi-brillation energy requirements and electrical heterogeneityduring total body hypothermia. Crit Care Med. 2001;29(5):1006e11.
95. DaVee TS, Reineberg EJ. Extreme hypothermia and ventri-cular fibrillation. Ann Emerg Med. 1980;9(2):100e2.
96. Koller R, Schnider TW, Neidhart P. Deep accidentalhypothermia and cardiac arrest–rewarming with forced air.Acta Anaesthesiol Scand. 1997;41(10):1359e64.
97. Thomas R, Cahill CJ. Successful defibrillation in profoundhypothermia (core body temperature 25.6 degrees C). Resus-citation. 2000;47(3):317e20.
98. Mair P, Gasteiger L, Mair B, Stroehle M, Walpoth B. Suc-cessful defibrillation of four hypothermic patients withwitnessed cardiac arrest. High Alt Med Biol. 2019;20(1):71e7.
99. Morrison LJ, Deakin CD, Morley PT, Callaway CW,Kerber RE, Kronick SL, et al. Part 8: Advanced life support:2010 International Consensus on Cardiopulmonary Resusci-tation and Emergency Cardiovascular Care Science WithTreatment Recommendations. Circulation. 2010;122(16Suppl 2):S345e421.
100. Binnema R, van der Wal A, Visser C, Schepp R, Jekel L,Schroder P. Treatment of accidental hypothermia with cardi-opulmonary bypass: a case report. Perfusion. 2008;23(3):193e6.
101. Hauty MG, Esrig BC, Hill JG, LongWB. Prognostic factorsin severe accidental hypothermia: experience from the Mt.Hood tragedy. J Trauma. 1987;27(10):1107e12.
102. Danzl DF, Pozos RS, Auerbach PS, Glazer S, Goetz W,Johnson E, et al. Multicenter hypothermia survey. AnnEmerg Med. 1987;16(9):1042e55.
103. Deal CW, Warden JC, Monk I. Effect of hypothermia onlung compliance. Thorax. 1970;25(1):105e9.
104. Caldwell JE, Heier T, Wright PM, Lin S, McCarthy G,Szenohradszky J, et al. Temperature-dependent pharmacoki-netics and pharmacodynamics of vecuronium. Anesthesiol-ogy. 2000;92(1):84e93.
105. Heier T, Caldwell JE. Impact of hypothermia on theresponse to neuromuscular blocking drugs. Anesthesiology.2006;104(5):1070e80.
106. Leslie K, Sessler DI, Bjorksten AR, Moayeri A. Mildhypothermia alters propofol pharmacokinetics and increasesthe duration of action of atracurium. Anesth Analg.1995;80(5):1007e14.
107. Kondratiev TV, Flemming K, Myhre ES, Sovershaev MA,Tveita T. Is oxygen supply a limiting factor for survival dur-ing rewarming from profound hypothermia? Am J PhysiolHeart Circ Physiol. 2006;291(1):H441e50.
108. Strapazzon G, Nardin M, Zanon P, Kaufmann M,Kritzinger M, Brugger H. Respiratory failure and sponta-neous hypoglycemia during noninvasive rewarming from24.7 degrees C (76.5 degrees F) core body temperatureafter prolonged avalanche burial. Ann Emerg Med.2012;60(2):193e6.
109. Wira CR, Becker JU,Martin G, DonninoMW.Anti-arrhyth-mic and vasopressor medications for the treatment of ventri-cular fibrillation in severe hypothermia: a systematic reviewof the literature. Resuscitation. 2008;78(1):21e9.
110. Wira C, Martin G, Stoner J, Margolis K, Donnino M. Appli-cation of normothermic cardiac arrest algorithms tohypothermic cardiac arrest in a canine model. Resuscitation.2006;69(3):509e16.
111. Raedler C, Voelckel WG, Wenzel V, Bahlmann L,Baumeier W, Schmittinger CA, et al. Vasopressor responsein a porcine model of hypothermic cardiac arrest is improvedwith active compression-decompression cardiopulmonaryresuscitation using the inspiratory impedance thresholdvalve. Anesth Analg. 2002;95(6):1496e502.
112. Schwarz B, Mair P, Raedler C, Deckert D, Wenzel V,Lindner KH. Vasopressin improves survival in a pig modelof hypothermic cardiopulmonary resuscitation. Crit CareMed. 2002;30(6):1311e4.
113. Sumann G, Krismer AC, Wenzel V, Adelsmayr E,Schwarz B, Lindner KH, et al. Cardiopulmonary resuscita-tion after near drowning and hypothermia: restoration ofspontaneous circulation after vasopressin. Acta AnaesthesiolScand. 2003;47(3):363e5.
114. Khan JN, PrasadN, Glancy J. Amiodarone use in therapeutichypothermia following cardiac arrest due to ventriculartachycardia and ventricular fibrillation. Europace.2009;11(11):1566e7.
115. Elenbaas RM, Mattson K, Cole H, Steele M, Ryan J,Robinson W. Bretylium in hypothermia-induced ventricularfibrillation in dogs. Ann Emerg Med. 1984;13(11):994e9.
116. Stoner J, Martin G, O'Mara K, Ehlers J, Tomlanovich M.Amiodarone and bretylium in the treatment of hypothermicventricular fibrillation in a canine model. Acad EmergMed. 2003;10(3):187e91.
117. Danzl DF, Sowers MB, Vicario SJ, Thomas DM,Miller JW.Chemical ventricular defibrillation in severe accidentalhypothermia. Ann Emerg Med. 1982;11(12):698e9.
118. Lloyd EL. Accidental hypothermia. Resuscitation.1996;32(2):111e24.
Dow et al22

119. Ho JD, Heegaard WG, Brunette DD. Successful transcuta-neous pacing in 2 severely hypothermic patients. AnnEmerg Med. 2007;49(5):678e81.
120. Rankin AC, Rae AP. Cardiac arrhythmias during rewarmingof patients with accidental hypothermia. Br Med J (Clin ResEd). 1984;289(6449):874e7.
121. Jurkovich GJ, Greiser WB, Luterman A, Curreri PW.Hypothermia in trauma victims: an ominous predictor of sur-vival. J Trauma. 1987;27(9):1019e24.
122. Martin RS, Kilgo PD, Miller PR, Hoth JJ, Meredith JW,Chang MC. Injury-associated hypothermia: an analysis ofthe 2004 National Trauma Data Bank. Shock. 2005;24(2):114e8.
123. Beilman GJ, Blondet JJ, Nelson TR, Nathens AB,Moore FA, Rhee P, et al. Early hypothermia in severelyinjured trauma patients is a significant risk factor for multipleorgan dysfunction syndrome but not mortality. Ann Surg.2009;249(5):845e50.
124. Mitra B, Tullio F, Cameron PA, Fitzgerald M. Traumapatients with the 'triad of death'. Emerg Med J. 2012;29(8):622e5.
125. Quinn R, Williams J, Bennett B, Stiller G, Islas A,McCord S, et al. Wilderness Medical Society practice guide-lines for spine immobilization in the austere environment.Wilderness Environ Med. 2013;24(3):241e52.
126. Debaty G, Moustapha I, Bouzat P, MaignanM, Blancher M,Rallo A, et al. Outcome after severe accidental hypothermiain the French Alps: A 10-year review. Resuscitation.2015;93:118e23.
127. Ruttmann E,Weissenbacher A, Ulmer H,Muller L, Hofer D,Kilo J, et al. Prolonged extracorporeal membrane oxygena-tion-assisted support provides improved survival inhypothermic patients with cardiocirculatory arrest.J Thorac Cardiovasc Surg. 2007;134(3):594e600.
128. Ruttmann E, Dietl M, Kastenberger T, El Attal R, StrohleM,Ulmer H, et al. Characteristics and outcome of patients withhypothermic out-of-hospital cardiac arrest: experience froma European trauma center. Resuscitation. 2017;120:57e62.
129. Khorsandi M, Dougherty S, Young N, Kerslake D,Giordano V, Lendrum R, et al. Extracorporeal life supportfor refractory cardiac arrest from accidental hypothermia: a
10-year experience in Edinburgh. J Emerg Med.2017;52(2):160e8.
130. Darocha T, Kosinski S, Jarosz A, Sobczyk D,Galazkowski R, Piatek J, et al. The chain of survival inhypothermic circulatory arrest: encouraging preliminaryresults when using early identification, risk stratificationand extracorporeal rewarming. Scand J Trauma ResuscEmerg Med. 2016;24:85.
131. Jarosz A, Darocha T, Kosinski S, Galazkowski R, Mazur P,Piatek J, et al. Profound accidental hypothermia: systematicapproach to active recognition and treatment. ASAIO J.2017;63(3):e26e30.
132. Gruber E, Beikircher W, Pizzinini R, Marsoner H,Pornbacher M, Brugger H, et al. Non-extracorporealrewarming at a rate of 6.8!C per hour in a deeplyhypothermic arrested patient. Resuscitation. 2014;85(8):e119e20.
133. Roggero E, Stricker H, Biegger P. [Severe accidentalhypothermia with cardiopulmonary arrest: prolonged resus-citation without extracorporeal circulation]. Schweiz MedWochenschr. 1992;122(5):161e4.
134. Turtiainen J, Halonen J, Syvaoja S, Hakala T. Rewarminga patient with accidental hypothermia and cardiac arrestusing thoracic lavage. Ann Thorac Surg. 2014;97(6):2165e6.
135. Woehrle T, Lichtenauer U, Bayer A, Brunner S,Angstwurm M, Schafer ST, et al. Misleading symptomsand successful noninvasive rewarming of a patient withsevere hypothermia (23.1!C). Anaesthesist. 2018;67(12):931e5.
136. Dobson JA, Burgess JJ. Resuscitation of severe hypothermiaby extracorporeal rewarming in a child. J Trauma.1996;40(3):483e5.
137. von Segesser LK, Garcia E, Turina M. Perfusionwithout systemic heparinization for rewarming in acci-dental hypothermia. Ann Thorac Surg. 1991;52(3):560e1.
138. Farstad M, Andersen KS, Koller ME, Grong K, Segadal L,Husby P. Rewarming from accidental hypothermia by extra-corporeal circulation. A retrospective study. Eur J Cardi-othorac Surg. 2001;20(1):58e64.
Hypothermia Clinical Practice Guidelines 23

WILDERNESS MEDICAL SOCIETY PRACTICE GUIDELINES
Wilderness Medical Society Practice Guidelines for thePrevention and Treatment of Heat Illness: 2019 Update
Grant S. Lipman, MD1; Flavio G. Gaudio, MD2; Kurt P. Eifling, MD3; Mark A. Ellis, MD4; Edward M. Otten, MD5;
Colin K. Grissom, MD6
1Department of Emergency Medicine, Stanford University School of Medicine, Stanford, CA; 2Department of Emergency Medicine, New York-
Presbyterian Hospital/Weill Cornell Medical College, New York, NY; 3Division of Emergency Medicine, Larner College of Medicine at the
University of Vermont, Burlington, VT; 4Department of Emergency Medicine, Spartanburg Regional Healthcare System, Spartanburg, SC;5Department of Emergency Medicine, University of Cincinnati, Cincinnati, OH; 6Pulmonary and Critical Care Division, Intermountain Medical
Center and the University of Utah, Salt Lake City, UT
The Wilderness Medical Society convened an expert panel in 2011 to develop a set of evidence-based
guidelines for the recognition, prevention, and treatment of heat illness. We present a review of the clas-
sifications, pathophysiology, and evidence-based guidelines for planning and preventive measures, as
well as best practice recommendations for both field- and hospital-based therapeutic management of
heat illness. These recommendations are graded based on the quality of supporting evidence and
balance the benefits and risks or burdens for each modality. This is an updated version of the original
Wilderness Medical Society Practice Guidelines for the Treatment and Prevention of Heat-Related
Illness published in 2013.
Keywords: heat stroke, hyperthermia, prevention, recognition, treatment
Introduction
Heat illness is a common occurrence worldwide. The
European heat wave of 2003 resulted in at least 70,000
fatalities,1 and in the last decade the United States aver-
aged over 600 deaths annually associated with excessive
heat exposure.2 Currently, heat illness is the leading
cause of morbidity and mortality among US high school
athletes.3 Heat stroke mortality approaches 10%4 and
when presenting with hypotension increases to 33%.5
Outcome is directly attributed to both the magnitude and
duration of hyperthermia,6�8 making early recognition
and treatment a priority. The Wilderness Medical Soci-
ety convened an expert panel to develop a set of practice
guidelines for the recognition, prevention, and treatment
of heat illness. We present a review of the classifications,
pathophysiology, and evidence-based guidelines for
planning and preventive measures, as well as best prac-
tice recommendations for both field- and hospital-based
therapeutic management of heat illness. Although the
spectrum of heat illness is discussed, this practice
group’s focus was on the exploration of exertional heat
stroke (EHS), which is synonymous with the term “heat
stroke” in this article unless otherwise specified.
Methods
Specialists in emergency medicine, primary care, and
critical care from both civilian and military backgrounds
were chosen based on their clinical or research experi-
ence. In 2011,9 and for subsequent practice guideline
updates,10 relevant articles were identified through the
PubMed database using the following key words: hyper-
thermia, heat stroke, heat illness, heat syncope, and heat
exhaustion. This was supplemented by a hand search of
articles from references in the initial PubMed search.
Studies in these categories, including randomized con-
trolled trials, observational studies, and case series, were
reviewed. Abstract-only reports were not included. Con-
clusions from review articles were cited to provide back-
ground information but were not considered in the
formulation of recommendation grades. The panel used
a consensus approach to develop recommendations for
Corresponding author: Grant S. Lipman, MD, Department of Emer-
gency Medicine, Stanford University School of Medicine, Suite #350,
900 Welch Rd, Palo Alto, CA 94304; e-mail: [email protected].
Submitted for publication June 2018.
Accepted for publication October 2018.
ARTICLE IN PRESS
Wilderness & EnvironmentalMedicine 2018; 00(00): 1�14

the recognition and management of heat illness, with
level of evidence assigned according to methodology
stipulated by the American College of Chest Physicians
for grading of evidence and recommendations (Supple-
mentary Table 1). These recommendations are graded
based on the quality of supporting evidence and balance
between the benefits and risks or burdens for each
modality or intervention.
Definition of heat illness
Heat illness can be manifested as a spectrum of disease
from minor to severe, such as heat cramps, heat syncope,
heat exhaustion, and life-threatening heat stroke. Hyper-
thermia is a deviation above the body’s normal physio-
logic setpoint and should be considered separately from
the concept of heat illness. It is an expected physiologic
response when core body temperature rises as a result of
exposure to elevated ambient temperatures or when
internally generated heat from muscular activity accu-
mulates faster than it can be dissipated. Hyperthermia is
a natural outcome of exertion, and increased metabolic
rate has been shown to be the most important factor in
elevation of body temperature.11 Studies of asymptom-
atic runners have found 15 to 56% with core tempera-
tures �40˚C and 11% �42˚C.12,13 As such, absolute
temperature thresholds alone should not be routinely
applied to asymptomatic individuals as a pathologic indi-
cator of heat illness.
As with any syndrome, the terms used to define heat ill-
ness do not necessarily confer direct cause and effect but
rather a strong contextual association that may have descrip-
tive, prognostic, and epidemiological merit, if not patho-
physiologic precision.14,15 Heat cramps were initially
defined in the 1930s to describe the clinical phenomenon of
involuntary diffuse large-muscle contractions associated
with exertion in hot environments.16 These heat cramps
are likely distinct from the focal muscle cramping in an ath-
lete during repetitive exercises.17 Dehydration and electro-
lyte disturbances have been associated with heat cramps,18
and isotonic rehydration has been found to be restorative.16
Heat edema is a benign self-limiting condition. Interstitial
fluid accumulates in dependent extremities as a result of
hydrostatic pressure, vascular leak, and cutaneous vasodila-
tion. Heat syncope refers to a multifactorial syndrome
involving transient loss of consciousness in the context of
heat exposure with a relatively rapid return to normal func-
tion and baseline. Contributing factors may include periph-
eral vasodilation, orthostatic pooling of blood, prolonged
standing, advanced age, dehydration, and coexisting medical
conditions such as ischemic heart disease that reduces car-
diac output. Although syncope can occur in both milder and
more severe forms of heat illness, heat syncope generally
refers to a more benign clinical condition that should resolve
with rest and possibly rehydration at comfortable ambient
temperatures.19,21 Syncope may also occur during exertion
from impaired baroreceptor reflex and lower extremity
venous pooling in the absence of hyperthermia or dehydra-
tion, a syndrome known as exercise-associated collapse.19
Heat exhaustion results from exposure to high ambient
temperature or strenuous exertion. It manifests as a con-
stellation of symptoms that range from uncomfortable to
debilitating6,21 and may limit continuation of exercise in
the heat.6 Symptoms are variable and may include weak-
ness, fatigue, thirst, headache, nausea, dizziness, and
muscle aches.21 This mild to moderate heat illness may
progress to heat stroke if left untreated or unrecognized
in a hot environment, although heat stoke does occur as
a fulminant illness without preceding heat exhaustion.
Heat stroke is traditionally defined as a core temperature
above 40˚C (104˚F) with central nervous system involve-
ment (eg, encephalopathy, seizures, or coma). Heat
stroke is generally divided into 2 categories: classic heat
stroke resulting from passive exposure to high environ-
mental temperatures and EHS resulting from pathologic
Table 1. Categories of heat illness
Condition Definition
Hyperthermia A rise in body temperature above the hypo-
thalamic set point when heat-dissipating
mechanisms are impaired (by clothing or
insulation, drugs, or disease) or over-
whelmed by external (environmental) or
internal (metabolic) heat production.
Heat edema Dependent extremity swelling due to intersti-
tial fluid pooling.
Heat cramps Exercise-associated painful involuntary
muscle contractions during or immediately
after exercise.
Heat syncope Transient loss of consciousness with sponta-
neous return to normal mentation.
Heat exhaustion Mild to moderate heat illness due to exposure
to high environmental heat or strenuous
physical exercise; signs and symptoms
include intense thirst, weakness, discom-
fort, anxiety, dizziness, syncope; core tem-
perature may be normal or slightly elevated
>37˚C (98.6˚F) but <40˚C (104˚F).
Heat stroke Severe heat illness characterized by a core
temperature >40˚C (104˚F) and central
nervous system abnormalities such as
altered mental status (encephalopathy),
seizure, or coma resulting from passive
exposure to environmental heat (classic
heat stroke) or strenuous exercise (exer-
tional heat stroke).
ARTICLE IN PRESS
2 Lipman et al

(nonphysiologic) hyperthermia during strenuous exercise
(Table 1).22
Heat dissipation and pathophysiology
Heat loss is controlled by peripheral centers in the skin
and organs and the central nervous system via the hypo-
thalamus, with a greater cooling response to temperature
elevation via central sensors.23 A temperature gradient
exists between the body core and skin that promotes heat
dissipation when core temperature is higher than surface
temperature. A rise in blood temperature by less than 1˚C
triggers hypothalamic thermoregulation to increase blood
flow to the skin by up to 8 L¢min¡1 via sympathetic cuta-
neous vasodilation, with sixfold blood flow increases to
the forearms and the arteriovenous anastomotic microvas-
cular structures deep to the glabrous skin areas, with their
unique intrinsic heat transfer capabilities.24,25 As blood is
shunted to the periphery to facilitate heat loss, renal and
splanchnic perfusion is reduced by 30%.24
However, when the core temperature increases dur-
ing exercise and skin temperature also rises as a result
of the environment or internal heat production, heat dis-
sipation is reduced. Similarly, when the body’s meta-
bolic heat production outpaces heat transfer, core
temperature rises, and heat illness can occur.26 Heat
stroke occurs when internal core temperatures rise
above a critical level, leading to a cascade of cellular
and systemic responses. These responses include ther-
moregulatory dysfunction, an acute phase response, and
a heat shock protein response. The acute phase response
to heat stress involves an inflammatory reaction of
interleukins, cytokines, and proteins that progresses in
a sequence similar to that seen in sepsis. It is theorized
that an exaggerated acute phase and inflammatory
response mark the progression from heat stress to heat
stroke, possibly incited by the hypoperfused gastroin-
testinal tract.22 Increased mucosal permeability from
inflammatory mediators allows endotoxins from the gut
to enter the systemic circulation. This combination of
endotoxemia and cascade of inflammatory cytokines
leads to alterations in the microcirculation, further
endothelial and tissue injury, and impaired thermoregu-
lation, thus precipitating heat stroke and hypotension.
An overlapping hypothesis presupposes that at a similar
threshold temperature, the expression of protective
heat-shock proteins is altered, decreasing their ability
to prevent thermal denaturation of structural proteins
and enzymes that start to fail at a cellular level, with
ensuing end organ dysfunction.22,27 At critical levels of
hyperthermia, heat causes direct tissue injury and death
via apoptosis or necrosis, with the severity of injury
dictated by both the level and duration of thermal
stress.28,29 This complex constellation of overlapping
events leads to thermoregulatory failure, heat stroke,
and circulatory shock.
Prevention and planning
The proverb that “an ounce of prevention is worth a
pound of cure” is especially apt in light of the potentially
fatal nature of heat illness. Deliberate strategies for pre-
vention should be included when planning for activities
with a credible risk. Structured risk assessments can be
built and validated for population-level use,30,31 or the
practitioner considering a particular scenario should con-
sider the risk incurred by the individual participant’s fac-
tors including physiology, the environment, and the
planned athletic activity.32
INDIVIDUAL FACTORS
Any condition that limits heat loss through the skin may
lead to heat retention, including hypohydrosis, extensive
scars, and diminished cardiopulmonary reserve at the
extremes of age. Small studies have linked acute sunburn
with impaired sweating, which persisted for 7 d, consid-
erably longer than the associated pain and erythema.33,34
Impaired sweating is a risk factor for heat accumulation,
but otherwise the risks of sunburn are of indeterminate
clinical significance.
Certain drugs can predispose individuals to heat
injury by 2 primary pathways, increased heat produc-
tion resulting from drug actions and compromised func-
tion of thermoregulatory centers (Table 2).35,36
Moderate caffeine intake appears to have no detrimen-
tal effect.18 A large prospective study of military
Table 2. Medications and drugs that may contribute to heat
illness
Alcohol
Alpha adrenergics
Amphetamines
Anticholinergics
Antihistamines
Antipsychotics
Benzodiazepines
Beta blockers
Calcium channel blockers
Clopidogrel
Cocaine
Diuretics
Laxatives
Neuroleptics
Phenothiazines
Thyroid agonists
Tricyclic antidepressants
ARTICLE IN PRESS
WMS Practice Guidelines for Heat-Related Illness 3

recruits found a significantly increased risk of heat
illness among those who were obese or overweight
compared with fitter individuals.37
Heat acclimatization, as induced by 1 to 2 h of heat-
exposed exertion per day over 10 to 14 d, results in
reproducible adaptations that increase the body’s ability
to tolerate and divest heat.38�40 These adaptations may
persist for up to a month.41,42 Evidence suggests that a
bout of heat stroke may acutely reset these thermoregula-
tory adaptations and cause elevated risk for subsequent
heat injury for months after the initial event,43 although
case reports indicate that heat tolerance can be recovered
fully.44,45 Individuals with high levels of cardiopulmo-
nary fitness tolerate more activity in heat-strained condi-
tions and acclimatize to heat more rapidly because they
have increased sweat volumes and higher subjective tol-
erance for activity when hyperthermic.
The most readily modifiable physiologic risk factor is
hydration status. Although endurance athletes may com-
fortably tolerate weight losses of 3 to 4% during
events,46,47 fluid losses that result in a 2 to 3% decrease
in body weight correlate with greater core temperatures
at a given work load in the heat.39,48,49 Dehydration has
been found to increase physiologic strain, decrease sweat
rates, increase perceived exertion, and increased core
temperatures.23,50,51
Hyperhydration before activity has not been shown to
have a significant effect on heat tolerance, nor has active
body cooling before activity.52 One investigation on the
effect of sex as a risk factor on thermal recovery was
confounded by body mass index differences, such that
no conclusion could be reached.53 The luteal phase of
the menstrual cycle, which is associated with increased
core temperatures, does not appear to induce heat intoler-
ance in women on oral contraceptive pills.54 The physi-
ology of pediatric and elderly populations differs enough
from healthy adults to warrant special considerations
that are outside this panel’s scope but are discussed at
length elsewhere.55�57
Recommendations. Screen for significant pre-existing
medical conditions (1B). Minimize use of medications
that could limit the thermoregulatory response (1C).
Recognize that an overweight body habitus is associated
with greater risk of heat illness (1B). Promote regular
aerobic activity before heat exposure (1C). Allow for
acclimatization with 1 to 2 h per d of heat-exposed exer-
tion for at least 8 days (1C). Ensure euhydration before
activity (1B). Ensure ongoing rehydration with a “drink
to thirst” approach sufficient to prevent >2% loss of
body weight (1B). Consider history of heat injury as a
reversible risk factor for recurrence (1C).
ENVIRONMENTAL CONSIDERATIONS
The body and the environment exchange heat through sev-
eral mechanisms: conduction (heat transfer from the body
to the surrounding environment along a temperature gradi-
ent by direct contact), evaporation (heat transfer from the
body to sweat, resulting in transition of water from the liq-
uid to vapor phase), thermal radiation (infrared rays given
off by any mass as a function of the temperature of that
mass), or convection (transfer of heat from the body to
free fluids or gas moving across the skin surface).
As the environmental temperature increases, the body
will eventually incur a net heat gain through conductive,
convective, and radiative processes, leaving evaporation as
the only cooling mechanism. The vaporization of 1.7 mL of
sweat consumes 1 kcal of heat58; however, evaporative
cooling is less effective in highly humid environments,
which have a lower water vapor pressure difference
between the sweat on the skin and the water in the surround-
ing air. The wet-bulb globe temperature index (WBGT) is a
composite index of temperature, humidity, and solar radia-
tion that expresses the total thermal strain that an individual
experiences. A series of WBGT values can be designated as
cautionary warnings and triggers to activate guidelines for
rehydration, active cooling, and limitations (or even cancel-
lation) of physical activity.34 An alternative to the WBGT
that is more readily available is the heat index, which is a
measure of the contribution that high temperature and high
humidity (expressed as either relative humidity or dew point
temperature) make in reducing the body’s ability to cool
itself. Although the wet bulb globe temperature is a metric
likely not readily available to individual medical practi-
tioners, its current use by military,59 occupational,60 and
civilian groups26,55 makes it the standard when discussing
environmental thermal strain and choosing activity levels
for ambient conditions. Guidelines that correlate the heat
index with the risk of heat injury and outline parameters for
limiting physical activity are readily available.61
Recommendation. WBGT should be used for the
assessment of heat risk (1A).
ACTIVITY CONSIDERATIONS
The metabolic thermal output of an activity is the product
of its intensity and duration. The accumulation of heat by
the body is tempered in some circumstances by an activity
that can enhance heat transfer with the environment (eg,
water convection on a swimmer or wind past a cyclist).
Occupational,60,62 military,59 and medical24 guidelines rec-
ommend breaks in proportion to metabolic demand and
ambient conditions, but there are few studies examining
how to optimize the dosing of breaks.
ARTICLE IN PRESS
4 Lipman et al

Recommendation. Consider which mechanisms of heat
accumulation or dissipation are dominant during an activity,
and consider heat loss as a key feature of breaks (1C).
CLOTHING AND EQUIPMENT
Clothing or other equipment worn during an activity may
limit or enhance the body’s thermoregulatory efficiency.
Of particular importance is equipment that occludes
regions of skin, resulting in compromise of evaporative,
convective, radiative, or conductive heat transfer. For
example, the American football uniform prevents full
heat exchange across much of the torso and head and can
therefore contribute to heat accumulation,63 similar to
military helmets and body armor.64 Preventing heat
exchange may be protective, as in the case of firefighting
gear that prevents heat in a superheated environment
from entering the body by conduction or radiation.
Sports medicine guidelines and military occupational
guidelines have set examples of systematic reductions in
clothing and equipment based on WBGT thresholds.26,65
Recommendation. Clothing and equipment for a
given activity should be evaluated and modified as
needed to optimize evaporative, convective, conductive,
and radiative heat exchange or isolation (1C).
Field treatment
Optimal field management of heat illness may be challeng-
ing because of resource limitations or extreme settings. The
ideal treatment, as emphasized in the previous section, is
prevention via avoiding high-exertion activities in exposed
or hot areas. The method and aggressiveness of cooling in
the field depend on the type of heat illness encountered
(Table 3). Regardless of the underlying cause, removal
from the heat and rapid cooling is critical because the extent
of morbidity is directly related to both to the degree and
duration of hyperthermia.8,37,66�69 All treatment in the field
is first directed to stabilization of the patient’s airway,
breathing, and circulation before proceeding to more spe-
cific cooling therapy. If no life-threatening complications
exist, the implementation of on-site cooling before evacua-
tion should be implemented (Figure 1).26 In transitioning
patient care to emergency medical service providers, it is
important to communicate any cooling techniques begun in
the field and to emphasize continued cooling of the patient
by best available means en route to the destination.
MINOR HEAT ILLNESS TREATMENT
There is scant evidence supporting treatments of minor
and moderate heat illness. Most treatments are anecdotal
but effective and generalizable from the evidence-based
treatment for more severe forms of heat illness (Table 3).
Heat cramps, which are historically described as general-
ized,16 differ from the focal exercise-associated muscle
cramps seen in endurance athletes. Heat cramps are
relieved with oral salt solutions or electrolyte replacement
that may be isotonic or hypertonic,16 compared with
exercise-associated muscle cramps that occur with neuro-
muscular fatigue and are relieved with passive stretch-
ing.70 Heat edema is reversed by extremity elevation or
wearing of compression stockings. Diuretics are ineffec-
tive and may worsen volume depletion.71
Heat syncope by definition is self-limiting. After con-
sideration of other medical causes of syncope or resul-
tant trauma from a fall, treatment consists of ensuring
replacement of vascular volume with isotonic oral fluids
and rest in a cool environment.19 Individuals at risk for
heat syncope should move often and flex their larger leg
muscles to prevent peripheral pooling of blood from
cutaneous vasodilation. An individual with heat syncope
is likely underacclimatized to the heat, and caution is
warranted before immediate return to regular activity.
Table 3. Heat illness treatments
Severity of heat-
related illness
Diagnosis Treatment
Mild Heat cramps Oral isotonic or hyper-
tonic fluid replacement
Heat edema Extremity elevation
Compression stockings
Moderate Heat syncope Remove from heat source
Passive cooling
Oral isotonic or hyper-
tonic fluid hydration
Heat exhaustion Remove from heat source
Evaporative, convective,
or conductive cooling
Oral or intravenous iso-
tonic or hypertonic fluid
hydration
Severe Heat stroke Remove from heat source
Supportive care of airway,
breathing, and circulation
Cold water immersion
Whole-body conductive
cooling
Intravenous hydrationa
Evacuationb
a Intravenous hydration with isotonic (0.9% sodium chloride) or
hypertonic (D5NS) fluids, with 3% sodium chloride indicated if con-
cern for exercise-associated hyponatremia as cause of encephalopathy.b Initiate emergency medical services if unable to rapidly cool
patient, prolonged encephalopathy, or concern of multiorgan
dysfunction.
ARTICLE IN PRESS
WMS Practice Guidelines for Heat-Related Illness 5

Signs or symptoms of heat illness?
Signs or symptoms of central nervous system alterations?
Confirmed or suspected temperature > 40°C (104°F)?
Yes No
No Yes
Treat for heat stroke: - Address airway, breathing and
circulation- Initiate rapid cooling (immersion /
conductive cooling is most effective)- Initiate intravenous fluids (if possible)- Arrange for transport to emergency
care
Mild heat illness: Heat exhaustion, heat
syncope, or heat cramps
Consider alternatives:
--
Treat for mild heat illness: - Orally hydrate- Cool with convection, conduction, or
evaporation- Consider giving salty food or oral
electrolyte fluids in addition to water- Observe for symptom resolution
Symptoms persist or have worsened?
Yes No
- Relative rest- Remain in cool place- Education on symptoms
and signs of heat illness- Consider not returning
to activity
- Consider more aggressive cooling- Consider an alternative diagnosis- Arrange transport for evacuation
- Hypoglycemia- Seizure- Severe exercise-associated hyponatremia- Hypernatremia
Central nervous system diseaseHigh altitude cerebral edema
- Infection- Endocrine issue- Toxic ingestion / drugs
Figure 1. Heat illness treatment algorithm.
ARTICLE
INPRESS
6Lipmanetal

Heat exhaustion, like heat stroke, results from a combi-
nation of both cardiovascular and thermal strain, and vari-
ous forms of rest and whole-body cooling are dictated by
severity of symptoms. Mild cases generally resolve with
removing the patient from the hot environment, cessation
of physical activity, and rehydration with oral isotonic flu-
ids. Severe heat exhaustion typically has more pro-
nounced volume depletion and may require intravenous
replacement of fluids as well as conductive and convec-
tive cooling. Because heat exhaustion can lead to cessa-
tion of physical activity and collapse,6 it is important to
actively reverse the process of heat exhaustion, which can
progress to heat stroke without proper cooling techniques.
Case reports have linked heat exhaustion or acute heat
stress to precipitating electrocardiogram changes, symp-
tomatic arrhythmias, and cardiac arrest with features of
underlying Brugada syndrome.72,73
Recommendation. Heat syncope patients whose eventis recurrent and inconsistent with exercise-associated
collapse or other clear explanation should be referred for
further cardiology diagnostics (2C).
TEMPERATURE MEASUREMENT
When possible, obtaining an accurate body temperature
is an important diagnostic step in differentiating heat
stroke from less severe heat illness. Rectal temperature
is widely considered the standard field measurement,25,67
because it is a reliable and practical measure of core tem-
perature that is more accurate than temporal, axillary,
oral, or aural thermometry.74,75 Esophageal and ingest-
ible thermistors have been validated and provide a
more accurate measurement of core temperature but are
impractical in the wilderness setting. Rectal temperature
measurement carries implicit challenges in maintaining
patient privacy and hygiene, so initial assessment and
aggressive cooling should be implemented based on the
clinical suspicion, regardless of the degree of hyperther-
mia or mode of measurement.
Recommendations. When available, rectal temperature
should be considered the most accurate measurement of
core hyperthermia compared to axillary, oral, or aural
thermometry (1B). In a hyperthermic individual with an
altered sensorium, the initiation of empiric cooling for
heat stroke should not be delayed by a measurement value
that may be below the diagnostic threshold of 40˚C (1B).
PASSIVE COOLING
Simple measures can be easily taken to reduce the patient’s
exposure to heat. Moving the victim into the shade can exter-
nally decrease the ambient temperature; however, this is
most effective when temperatures are <20˚C (68˚F).67
Conduction of heat from the ground can be decreased by
placing the victim on cool ground, if available, or on an insu-
lating barrier such as sleeping pad or sleeping bag. Loosen-
ing or removing any tight-fitting clothing to optimize air
circulation aids in convective heat exchange.76
Recommendation. Passive cooling measures should
be used to minimize thermal strain and maximize heat
loss (1C).
HYDRATION
Euhydration is an important factor in reducing hyper-
thermia.76,77 Body water losses through increased sweat
rates, vomiting, diarrhea, or insufficient oral intake
increase the risk of potential heat injury resulting from
poor hydration status. Dehydration predisposes patients
to hyperthermia by decreasing sweat rates and increases
thermal strain at a given temperature.50,77�79 Oral and
intravenous hydration have been shown to be equally
effective in replenishing water deficiencies related to
heat stress.77,80
Recommendation. Dehydration should be minimized
in heat illness (1C).
Optimizing hydration in heat stroke decreases both the
cardiovascular and thermal strain. In a heat stroke victim
with altered mental status and risk of seizure, the intrave-
nous route minimizes aspiration risk and subsequent air-
way compromise. Few data exist on the optimal
intravenous fluid type and amount relating specifically to
heat illness. Because those with EHS may be volume
depleted from insensible fluid losses, the reasonable
choices of replenishment are 1 to 2 L of isotonic (0.9%
normal saline or normal saline with 5% dextrose) fluids.
Because heat stroke can occur in both euhydrated and
dehydrated individuals, care should be taken to not over-
hydrate patients (especially those with coronary comor-
bidity) because this may increase the risk of pulmonary
edema.79 Any effort to provide hydration in suspected
heat stroke should not delay rapid whole-body cooling.82
If intravenous hydration is provided, field monitoring of
blood pressure, heart rate, lightening of urine color, and
increase in urine output can help guide patient response
and fluid status.
Recommendation. Intravenous fluids should be used
for rehydration in EHS (1B).
Symptomatic exercise-associated hyponatremia
may present similarly to heat exhaustion,21 and the
presence of altered mental status (eg, obtundation,
coma, or seizures) without other explanation, such as
hypoglycemia or trauma, in the absence of hyperther-
mia may indicate severe exercise-associated hypona-
tremia. This is a critical illness that ideally should be
confirmed with serum sodium measurement, but in
the absence of point-of-care testing the patient should
ARTICLE IN PRESS
WMS Practice Guidelines for Heat-Related Illness 7

empirically be resuscitated with up to 3, 100 mL 3%
sodium chloride boluses given every 10 min, or until
resolution of altered mental status, with rapid transfer
to a medical facility.83
COLD WATER IMMERSION THERAPY
Cold water immersion therapy is the optimal field treat-
ment to achieve rapid temperature reduction below criti-
cal levels in heat stroke. Immersion is a conductive
method of cooling that takes advantage of water’s high
thermal conductivity, which is 24 times greater than that
of air,84 and the high thermal gradient that exists
between cold water and skin,85 which translates into a
greater capacity for heat transfer. The colder the water,
the faster the rate of cooling.86 The theoretical concern
that cold-water immersion causes peripheral vasocon-
striction and shivering that slow cooling, or may even
increase the core temperature, is a prevalent misconcep-
tion, possibly stemming from a misinterpretation of the
“Currie response.”87 This 18th century observation
found an increase in the core temperature of shivering
normothermic individuals by 0.1 to 0.2˚C. Although
shivering has been observed in immersions lasting longer
than 10 min in healthy volunteers,88,89 such shivering
may be less problematic in actual heat stroke patients
with failing thermoregulation.90 In addition, the hin-
drance of cooling EHS by heat-generating shivering has
been physiologically refuted.86,91 Cold-water immersion
is achieved by removing insulating clothes and equip-
ment and submersing the patient’s trunk and extremities
in a bath of cold water or tub of ice water. Alternatively,
water may be applied onto a patient covered in crushed
ice and lying on a plastic sheet or tarp with its sides
folded upright to keep the slurry in place (“tarp taco”).92
Ice water cooling has been shown to be twice as rapid in
reducing core temperature as covering the body in
soaked towels to enhance evaporative cooling (0.20˚
C¢min¡1 vs 0.11˚C¢min
¡1).66
In the field, using a natural body of water such as a
stream, pond, river, or lake may be another treatment
option. Special care should be taken to protect against
currents and to ensure the head does not go underwater
and the airway is protected; the patient should never be
left alone owing to risk of aspiration and drowning. In
lieu of a cold-water source, repeated dousing with cold
water or snow, if available, is encouraged. Multiple mili-
tary studies on immersion cooling of comparatively
young and healthy EHS patients boast a 0% fatality
rate,93 strongly supporting that rapid treatment with this
cooling modality has the best outcomes.
Recommendation. Cold water immersion is the opti-
mal cooling method for heat stroke (1A).
EVAPORATIVE COOLING
If immersion or conductive cooling is unavailable, evap-
orative cooling measures should be initiated by loosen-
ing or removing clothing and dousing the patient with
cold water to maximize the water�vapor skin inter-
face.94 Convection is then facilitated with air movement
by fanning. Cooling by evaporation plus convection has
been studied predominantly in patients with non-EHS,95
with mean cooling times of 40 to 68 min.91,96 Limited
studies on traditional evaporative cooling have been
done with EHS or heat exhaustion, with reported cooling
rates half as fast as immersion cooling.97
Recommendation. Evaporative or convective cooling
can be considered as adjunct cooling methods if cold
water immersion is unavailable (1C).
CHEMICAL COLD PACKS/ICE PACKS
There is a traditional advocacy for the use of ice packs or
chemical cold packs strategically applied to the skin cover-
ing the neck, axillae, and groin to cool blood flow passing
in the major vessels as an adjunctive cooling measure.98
Limited studies show no benefit in heat reduction with ice
packs or chemical cold packs applied to these areas.99,100
Ice packs have been found to have greater cooling capacity
than chemical cold packs,101 and if used, are most effica-
cious when wet and covering the entire body (to optimize
conductive cooling).99 A small translational study applied
chemical cold packs to the glabrous skin of the palms, soles,
and cheeks and found twice the cooling rate over traditional
major vascular locations,102 using the high-capacity blood
flow of the subcutaneous arteriovenous anastomoses.
Recommendations. Ice packs should be applied to
cover the entire body (1C). If chemical cold packs are
used, they should be applied to the cheeks, palms, and
soles rather than the skin covering the major vessels (1C).
ANTIPYRETICS
As clinicians, we generally treat elevated temperatures
with antipyretics. This class of medications, such as ibu-
profen and aspirin, works by inhibiting prostaglandin
formation, and acetaminophen lowers the thermoregula-
tory setpoint.103 Although this may be elevated in infec-
tious causes of hyperthermia, this is not the case in
exercise-induced hyperthermia. Antipyretic drugs are
ineffectual and should be avoided.104,105
Recommendation. Antipyretics should be avoided in
heat illness (2B).
Hospital treatment
Generally, patients with heat stroke should be transported to
a medical facility capable of critical care management of
ARTICLE IN PRESS
8 Lipman et al

patients with multiple organ failure. Exceptions to this
guideline have included soldiers or athletes treated in the
field with ice-water immersion immediately at the onset of
EHS with complete resolution of symptoms and subsequent
observation in a medical station or infirmary.106,107 In a hos-
pital setting, the primary goals of treatment for heat stroke
are rapidly lowering core body temperature and supporting
organ system function22 because patients may develop mul-
tiple organ failure with shock, acute respiratory failure,
acute kidney injury, disseminated intravascular coagulop-
athy, and intestinal ischemia. Depending on the patient’s
clinical status, supportive treatment may include adminis-
tering supplemental oxygen, performing intubation and
mechanical ventilation, establishing adequate intravascular
access, restoring intravascular volume with intravenous iso-
tonic crystalloid solution, placing a bladder catheter to mon-
itor urine output, and initiating vasopressors to support
blood pressure (after adequate volume resuscitation).
The evidence on different cooling methods has
involved a heterogeneous range of subjects experiencing
EHS or classic heat stroke. Of the studies comparing dif-
ferent cooling methods, those involving randomized tri-
als generally have been performed on healthy volunteers
with exercise-induced hyperthermia and have enrolled
relatively few subjects. The remaining studies on treating
heat stroke patients have for the most part been case
series reports or nonrandomized comparisons of treat-
ment methods, with considerable variations in the base-
line characteristics of subjects from one study to the
next. Such heterogeneity and variation have reduced
the comparative conclusions that can be drawn. Despite
this limitation, the historical record has promoted 2
methods of cooling in a hospital setting: 1) conductive
cooling via cold water immersion of the patient; and 2)
evaporative and convective cooling via the application
of sprayed water and forced air currents over the body.
CONDUCTIVE COOLING
Cold water immersion is safe and effective for young,
athletic patients with EHS. A cooling protocol used for
over 15 y involving an ice-water slurry has been applied
effectively with no fatalities or adverse effects in hun-
dreds of civilian and military individuals.18,106,108 Agita-
tion, intolerance, or combativeness may occur in
encephalopathic heat stroke patients, and benefits of
immersive cooling should be balanced with the theoreti-
cal concerns of impaired access to an immersed patient
who may require advanced cardiac monitoring or resus-
citation, especially among older patients.90,94,109 Cold-
water immersion may be considered in non-EHS,
although this may not be practical for the typically older
patients with multiple comorbidities in the critical care
environment.90,110 In the absence of cold-water immer-
sion, wetted ice packs covering the entire body can cool
through conduction.99
Recommendations. Cold water immersion should be
considered for EHS in the hospital setting (1A). Cold
water immersion can be considered for treatment of clas-
sic heat stroke patients (1C).
EVAPORATIVE AND CONVECTIVE COOLING
Evaporative cooling in elderly patients may offer sev-
eral theoretical advantages, such as greater patient
comfort and less agitation as well as easier access to
patients who may need advanced monitoring or resus-
citative procedures. In general, studies on evaporative
and convective cooling have involved classic heat
stroke patients and experimental volunteers with exer-
cise-induced hyperthermia but not patients with actual
EHS. The larger studies using a specially constructed
device, termed a body cooling unit, have produced
cooling rates ranging from 0.04 to 0.11˚C¢min¡1, with
an average cooling of time of 68 to 78 min and 10%
mortality.94,95 No direct comparisons between the
body cooling unit with cold water immersion are avail-
able, but extrapolation of cooling rates suggests evap-
orative and convective cooling is an order of
magnitude less efficacious. Because classic heat stroke
patients are more likely to be older, obese, and with
medical conditions such as diabetes, high blood pres-
sure, and heart disease, the evidence suggests that the
evaporative plus convective cooling technique by wet-
ting and fanning the skin has a passable hospital-based
role in the treatment of classic heat stroke but cools
more slowly than conductive cooling and is not indi-
cated in EHS.
Recommendation. Evaporative and convective cool-
ing may be considered in classic heat stroke in the hospi-
tal setting, but cooling rates with this method are inferior
to those with conductive cooling. Evaporative and con-
vective cooling is not indicated in EHS, unless effective
conductive cooling is not available (1C).
TARGET COOLING TEMPERATURES
The target cooling temperatures of EHS and exercise-
induced hyperthermia to less than 39˚C by ice water
immersion have been well tolerated, with no fatalities,
adverse outcomes, or core temperature “afterdrop”
resulting in hypothermia.18,106,108,111 Practitioners
should also be cautious of falsely elevated rectal temper-
ature measurements in the recovery phase resulting from
the insulating effect of body mass.112
ARTICLE IN PRESS
WMS Practice Guidelines for Heat-Related Illness 9

Recommendation. Heat stroke patients should be
cooled to a target temperature of no less than 39˚C
(1B).
ADJUNCTIVE COOLING TREATMENTS
If intravenous fluids are available, it is beneficial to use
cold fluids (4˚C) whenever possible. These can decrease
core temperature at a twofold rate compared with room
temperature fluids but provide insufficient cooling as a
primary treatment for heat stroke. More invasive techni-
ques of body cavity lavage with cold isotonic fluid have
been reported but have not been adequately stud-
ied.113,114 Intravascular cooling catheters are suggested
to decrease morbidity when added to evaporative and
convective cooling.115
Recommendations. Cold intravenous fluids should be
given for adjunctive cooling in heat stroke (1C). Intra-
vascular cooling catheters or cold water lavage are not
recommended primary treatments for heat stroke (2C).
PHARMACOLOGIC TREATMENT
No pharmacologic agent has been shown to be helpful as
a treatment for heat stroke. Dantrolene has been used for
treatment of malignant hyperthermia. It acts by impair-
ing calcium release from the sarcoplasmic reticulum,
thereby reducing the muscular rigidity and hypertonicity
typical of this condition. A well-designed randomized
clinical trial of dantrolene vs placebo in classic heat
stroke found no difference in cooling rates or outcome,
concluding that this pharmacologic treatment should not
be used in heat stroke patients.116
Recommendation. Dantrolene should be avoided for
treatment of heat stroke patients (2B).
Conclusion
This article provides evidence-based guidelines for the
prevention, recognition, and treatment of heat illness.
Most of the available data are based on case series or
extrapolation of results stemming from exercise-associ-
ated hyperthermia, which is an accepted research model,
because randomized controlled trials for treatments of
EHS are ethically challenging to justify. These guide-
lines apply the strength of the evidence to 2 distinct pop-
ulations of heat stroke patients, and although the patient
with EHS is more likely to be found in the wilderness
environment, the medical provider should be aware of
all therapeutic modalities and their inherent risks and
benefits. We recommend that patients with heat stroke
be cooled by conductive means by whole-body ice water
or cold-water immersion (the preferential method in
EHS). Evaporative and convective cooling of classic
heat stroke may be augmented with the addition of ice
packs over the entire body to promote conductive cool-
ing. Future areas of research should include direct com-
parisons of available cooling modalities in controlled
models, as well as further evaluation of endovascular
catheters and hospital-based systems for optimum cool-
ing of critical patients.
Author Contributions: All authors contributed to manuscript concep-
tualization, data collection and review, and manuscript preparation.
Financial/Material Support: None.
Disclosures: None.
Supplementary materials
Supplementary material associated with this article can
be found in the online version at doi:10.1016/j.
wem.2018.10.004.
References
1. Robine JM, Cheung SL, Le Roy S, Van Oyen H, Griffiths
C, Michel JP, et al. Death toll exceeded 70,000 in Europe
during the summer of 2003. C R Biol. 2008;331(2):171–8.
2. Xu J. QuickStats: Number of heat-related deaths, by
sex�national vital statistics system, United States,
1999�2010. MMWR Morb Mortal Wkly Rep. 2012;61
(36):729.
3. Gilchrist J, Haileyesus T, Murphy M, Comstock RD,
Collins C, Yard E. Heat illness among high school athle-
tes�United States, 2005�2009. MMWR Morb Mortal
Wkly Rep. 2010;59(32):1009–13.
4. Centers of Disease Control and Prevention. Heat-related
illnesses and deaths�United States, 1994�1995. MMWR
Morb Mortal Wkly Rep. 1995;44(25):465–8.
5. Austin MG, Berry JW. Observations on one hundred
cases of heatstroke. J Am Med Assoc. 1956;161(16):
1525–9.
6. Adolph EF. Tolerance to heat and dehydration in several
species of mammals. Am J Physiol. 1947;151(2):564–75.
7. Overgaard J, Suit HD. Time-temperature relationship in
hyperthermic treatment of malignant and normal tissue in
vivo. Cancer Res. 1979;39(8):3248–53.
8. Vicario SJ, Okabajue R, Haltom T. Rapid cooling in clas-
sic heatstroke: effect on mortality rates. Am J Emerg
Med. 1986;4(5):394–8.
9. Lipman GS, Eifling KP, Ellis MA, Gaudio FG, Otten EM,
Grissom CK. Wilderness Medical Society practice guide-
lines for the prevention and treatment of heat-related ill-
ness.Wilderness Environ Med. 2013;24(4):351–61.
10. Lipman GS, Eifling KP, Ellis MA, Gaudio FG, Otten EM,
Grissom CK. Wilderness Medical Society practice guide-
lines for the prevention and treatment of heat-related
illness: 2014 update. Wilderness Environ Med. 2014;25
(4 Suppl):S55–65.
ARTICLE IN PRESS
10 Lipman et al
11. Noakes TD, Myburgh KH, du Plessis J, Lang L, Lambert M,
van der Riet C, et al. Metabolic rate, not percent dehydra-
tion, predicts rectal temperature in marathon runners. Med
Sci Sports Exerc. 1991;23(4):443–9.
12. Byrne C, Lee JK, Chew SA, Lim CL, Tan EY. Continu-
ous thermoregulatory responses to mass-participation dis-
tance running in heat. Med Sci Sports Exerc. 2006;38
(5):803–10.
13. Veltmeijer MT, Eijsvogels TM, Thijssen DH, Hopman
MT. Incidence and predictors of exertional hyperthermia
after a 15-km road race in cool environmental conditions.
J Sci Med Sport. 2015;18(3):333–7.
14. Lipman GS, Eifling KP, Ellis MA, Gaudio FG, Otten EM,
Grissom CK. Keeping a broad perspective: reply regard-
ing the Wilderness Medical Society practice guidelines
for the prevention and treatment of heat-related illness.
Wilderness Environ Med. 2014;25(2):251–2.
15. Nelson DA, Deuster PA, O’Connor FG, Kurina LM. Timing
and predictors of mild and severe heat illness among newmil-
itary enlistees.Med Sci Sports Exerc. 2018;50(8):1603–12.
16. Talbott JH, Michelsen J. Heat cramps. A clinical and
chemical study. J Clin Invest. 1933;12(3):533–49.
17. Schwellnus MP. Cause of exercise associated muscle cramps
(EAMC)�altered neuromuscular control, dehydration or
electrolyte depletion? Br J Sports Med. 2009;43(6):401–8.
18. Costrini AM, Pitt HA, Gustafson AB, Uddin DE. Cardio-
vascular and metabolic manifestations of heat stroke and
severe heat exhaustion. Am J Med. 1979;66(2):296–302.
19. Asplund CA, O’Connor FG, Noakes TD. Exercise-associ-
ated collapse: an evidence-based review and primer for
clinicians. Br J Sports Med. 2011;45(14):1157–62.
20. Casa DJ, DeMartini JK, Bergeron MF, Csillan D, Eichner
ER, Lopez RM, et al. National Athletic Trainers’ Associa-
tion Position Statement: exertional heat illnesses. J Athl
Train. 2015;50(9):986–1000.
21. Backer HD, Shopes E, Collins SL, Barkan H. Exertional
heat illness and hyponatremia in hikers. Am J Emerg
Med. 1999;17(6):532–9.
22. Bouchama A, Knochel JP. Heat stroke. N Engl J Med.
2002;346(25):1978–88.
23. Sawka MN, Wenger CB. Physiological Responses to
Acute Exercise-Heat Stress. Indianapolis, IN: Benchmark
Press; 1988.
24. Rowell LB. Cardiovascular aspects of human thermoreg-
ulation. Circ Res. 1983;52(4):367–79.
25. Heller HC, Grahn DA. Enhancing thermal exchange in
humans and practical applications. Disrupt Sci Technol.
2012;1(1):11–9.
26. Armstrong LE, Casa DJ, Millard-Stafford M, Moran DS,
Pyne SW, Roberts WO. American College of Sports Medi-
cine position stand. Exertional heat illness during training
and competition.Med Sci Sports Exerc. 2007;39(3):556–72.
27. Leon LR, Helwig BG. Heat stroke: role of the systemic
inflammatory response. J Appl Physiol (1985). 2010;109
(6):1980–8.
28. Sakaguchi Y, Stephens LC, Makino M, Kaneko T, Strebel
FR, Danhauser LL, et al. Apoptosis in tumors and normal
tissues induced by whole body hyperthermia in rats. Can-
cer Res. 1995;55(22):5459–64.
29. Buckley IK. A light and electron microscopic study of
thermally injured cultured cells. Lab Invest. 1972;26
(2):201–9.
30. Eberman LE, Cleary MA. Development of a heat-illness
screening instrument using the Delphi panel technique.
J Athl Train. 2011;46(2):176–84.
31. Toloo GS, Fitzgerald G, Aitken P, Verrall K, Tong S. Are
heat warning systems effective? Environ Health. 2013;12:27.
32. Pryor RR, Bennett BL, O’Connor FG, Young JM,
Asplund CA. Medical evaluation for exposure extremes:
heat.Wilderness Environ Med. 2015;26(4 suppl):S69–75.
33. Pandolf KB, Gange RW, Latzka WA, Blank IH, Kraning
II KK, Gonzalez RR. Human thermoregulatory responses
during heat exposure after artificially induced sunburn.
Am J Physiol. 1992;262(4 Pt 2):R610–6.
34. Pandolf KB, Gange RW, Latzka WA, Blank IH, Young
AJ, Sawka MN. Human thermoregulatory responses dur-
ing cold water immersion after artificially induced sun-
burn. Am J Physiol. 1992;262(4 Pt 2):R617–23.
35. Glazer JL. Management of heatstroke and heat exhaus-
tion. Am Fam Physician. 2005;71(11):2133–40.
36. Bruning RS, Dahmus JD, Kenney WL, Alexander LM.
Aspirin and clopidogrel alter core temperature and skin
blood flow during heat stress. Med Sci Sports Exerc.
2013;45(4):674–82.
37. Bedno SA, Li Y, Han W, Cowan DN, Scott CT, Cavicchia
MA, et al. Exertional heat illness among overweight US
army recruits in basic training. Aviat Space Environ Med.
2010;81(2):107–11.
38. Brazaitis M, Skurvydas A. Heat acclimation does not
reduce the impact of hyperthermia on central fatigue. Eur
J Appl Physiol. 2010;109(4):771–8.
39. Cheung SS, McLellan TM. Heat acclimation, aerobic fit-
ness, and hydration effects on tolerance during uncom-
pensable heat stress. J Appl Physiol (1985). 1998;84
(5):1731–9.
40. Garrett AT, Goosens NG, Rehrer NJ, Patterson MJ, Cotter
JD. Induction and decay of short-term heat acclimation.
Eur J Appl Physiol. 2009;107(6):659–70.
41. Weller AS, Linnane DM, Jonkman AG, Daanen HA.
Quantification of the decay and re-induction of heat accli-
mation in dry-heat following 12 and 26 days without
exposure to heat stress. Eur J Appl Physiol. 2007;102
(1):57–66.
42. Daanen HA, Jonkman AG, Layden JD, Linnane DM,
Weller AS. Optimising the acquisition and retention of
heat acclimation. Intl J Sports Med. 2011;32(11):822–8.
43. Armstrong LE, De Luca JP, Hubbard RW. Time course of
recovery and heat acclimation ability of prior exertional heat-
stroke patients.Med Sci Sports Exerc. 1990;22(1):36–48.
44. Kazman JB, Heled Y, Lisman PJ, Druyan A, Deuster PA,
O’Connor FG. Exertional heat illness: the role of heat tol-
erance testing. Curr Sports Med Rep. 2013;12(2):101–5.
45. Johnson EC, Kolkhorst FW, Richburg A, Schmitz A,
Martinez J, Armstrong LE. Specific exercise heat stress
ARTICLE IN PRESS
WMS Practice Guidelines for Heat-Related Illness 11

protocol for a triathlete’s return from exertional heat
stroke. Curr Sports Med Rep. 2013;12(2):106–9.
46. Sharwood KA, Collins M, Goedecke JH, Wilson G,
Noakes TD. Weight changes, medical complications, and
performance during an Ironman triathlon. Br J Sports
Med. 2004;38(6):718–24.
47. Wharam PC, Speedy DB, Noakes TD, Thompson JM,
Reid SA, Holtzhausen LM. NSAID use increases the risk
of developing hyponatremia during an Ironman triathlon.
Med Sci Sports Exerc. 2006;38(4):618–22.
48. Maughan RJ, Watson P, Shirreffs SM. Heat and cold:
what does the environment do to the marathon runner?
Sports Med. 2007;37(4-5):396–9.
49. Wall BA, Watson G, Peiffer JJ, Abbiss CR, Siegel R,
Laursen PB. Current hydration guidelines are erroneous:
dehydration does not impair exercise performance in the
heat. Br J Sports Med. 2015;49(16):1077–83.
50. Sawka MN, Latzka WA, Matott RP, Montain SJ. Hydra-
tion effects on temperature regulation. Int J Sports Med.
1998;19(Suppl 2):S108–10.
51. Sawka MN, Young AJ, Latzka WA, Neufer PD, Quigley
MD, Pandolf KB. Human tolerance to heat strain during
exercise: influence of hydration. J Appl Physiol (1985).
1992;73(1):368–75.
52. Duffield R, Steinbacher G, Fairchild TJ. The use of
mixed-method, part-body pre-cooling procedures for
team-sport athletes training in the heat. J Strength Cond
Res. 2009;23(9):2524–32.
53. Lemire B, Gagnon D, Jay O, Dorman L, DuCharme MB,
Kenny GP. Influence of adiposity on cooling efficiency in
hyperthermic individuals. Eur J Appl Physiol. 2008;104
(1):67–74.
54. Tenaglia SA, McLellan TM, Klentrou PP. Influence of
menstrual cycle and oral contraceptives on tolerance to
uncompensable heat stress. Eur J Appl Physiol Occup
Physiol. 1999;80(2):76–83.
55. Bergeron MF, Devore C, Rice SG. Policy statement—
Climatic heat stress and exercising children and ado-
lescents. Pediatrics. 2011;128(3):e741–e7.
56. Basu R, Samet JM. Relation between elevated ambient
temperature and mortality: a review of the epidemiologic
evidence. Epidemiol Rev. 2002;24(2):190–202.
57. Bouchama A, Dehbi M, Mohamed G, Matthies F, Shoukri
M, Menne B. Prognostic factors in heat wave related deaths:
a meta-analysis. Arch Intern Med. 2007;167(20):2170–6.
58. Nelson N, Eichna LW, Horvath SM, Shelley WB, Hatch
TF. Thermal exchanges of man at high temperatures. Am
J Physiol. 1947;151(2):626–52.
59. United States Department of the Navy, Bureau of Medi-
cine and Surgery. Manual of Naval Preventive Medicine
(NAVMED P-5010-3). Washington, DC: Department of
the Navy, US Department of Defense; 2009.
60. Occupational Health and Safety Administration. OSHA
Technical Manual (TED1-00-015). Washington, DC:
Occupational Health and Safety Administration, US
Department of Labor; 1999.
61. National Climactic Data Center. Heat Index Charts.
Asheville, NC: National Oceanic and Atmospheric
Administration, National Climactic Data Center; 2000.
62. Jackson LL, Rosenberg HR. Preventing heat-related illness
among agricultural workers. J Agromedicine. 2010;15
(3):200–15.
63. Armstrong LE, Johnson EC, Casa DJ, Ganio MS, McDer-
mott BP, Yamamoto LM, et al. The American football
uniform: uncompensable heat stress and hyperthermic
exhaustion. J Athl Train. 2010;45(2):117–27.
64. Porter AM. Heat illness and soldiers. Mil Med. 1993;158
(9):606–9.
65. Biery Jr JC, Blivin SJ, Pyne SW. Training in ACSM black
flag heat stress conditions: how US marines do it. Curr
Sports Med Rep. 2010;9(3):148–54.
66. Armstrong LE, Crago AE, Adams R, Roberts WO, Mar-
esh CM. Whole-body cooling of hyperthermic runners:
comparison of two field therapies. Am J Emerg Med.
1996;14(4):355–8.
67. Hadad E, Moran DS, Epstein Y. Cooling heat stroke
patients by available field measures. Intensive Care Med.
2004;30(2):338.
68. Hadad E, Rav-Acha M, Heled Y, Epstein Y, Moran DS.
Heat stroke: a review of cooling methods. Sports Med.
2004;34(8):501–11.
69. Shapiro Y, Seidman DS. Field and clinical observations
of exertional heat stroke patients. Med Sci Sports Exerc.
1990;22(1):6–14.
70. Schwellnus MP, Derman EW, Noakes TD. Aetiology of
skeletal muscle ‘cramps’ during exercise: a novel hypoth-
esis. J Sports Sci. 1997;15(3):277–85.
71. Lugo-Amador NM, Rothenhaus T, Moyer P. Heat-related
illness. Emerg Med Clin North Am. 2004;22(2):315–27. viii.
72. Canpolat U, Bayazit Y, Aytemir K. Brugada syndrome
unmasked by heat exhaustion. Ann Noninvasive Electro-
cardiol. 2017;22(1).
73. Molina Borao I, Calvo Galiano N, Urmeneta Ulloa J, Rivero
Fernandez E, Oloriz Sanjuan T, Asso Abadia A. Heat wave:
a trigger of electrical storm in a patient with Brugada
syndrome. Rev Esp Cardiol (Engl Ed.). 2016;69(12):
1228–30.
74. Binkley HM, Beckett J, Casa DJ, Kleiner DM, Plummer PE.
National Athletic Trainers’ Association position statement:
exertional heat illnesses. J Athl Train. 2002;37(3):329–43.
75. Casa DJ, Becker SM, Ganio MS, Brown CM, Yeargin
SW, Roti MW, et al. Validity of devices that assess body
temperature during outdoor exercise in the heat. J Athl
Train. 2007;42(3):333–42.
76. Gonzalez-Alonso J, Calbet JA, Nielsen B. Metabolic and
thermodynamic responses to dehydration-induced reduc-
tions in muscle blood flow in exercising humans. J Phys-
iol. 1999;520(Pt 2):577–89.
77. Casa DJ, Armstrong LE, Hillman SK, Montain SJ, Reiff
RV, Rich BS, et al. National Athletic Trainers’ Association
position statement: fluid replacement for athletes. J Athl
Train. 2000;35(2):212–24.
ARTICLE IN PRESS
12 Lipman et al

78. Lopez RM, Casa DJ, Jensen KA, DeMartini JK, Pagnotta
KD, Ruiz RC, et al. Examining the influence of hydration
status on physiological responses and running speed dur-
ing trail running in the heat with controlled exercise inten-
sity. J Strength Cond Res. 2011;25(11):2944–54.
79. Sawka MN. Physiological consequences of hypohydra-
tion: exercise performance and thermoregulation. Med
Sci Sports Exerc. 1992;24(6):657–70.
80. Castellani JW, Maresh CM, Armstrong LE, Kenefick
RW, Riebe D, Echegaray M, et al. Intravenous vs. oral
rehydration: effects on subsequent exercise-heat stress. J
Appl Physiol (1985). 1997;82(3):799–806.
81. Epstein Y, Shani Y, Moran DS, Shapiro Y. Exertional
heat stroke�the prevention of a medical emergency.
J Basic Clin Physiol Pharmacol. 2000;11(4):395–401.
82. Hostler D, Reis SE, Bednez JC, Kerin S, Suyama J. Com-
parison of active cooling devices with passive cooling for
rehabilitation of firefighters performing exercise in ther-
mal protective clothing: a report from the Fireground
Rehab Evaluation (FIRE) trial. Prehosp Emerg Care.
2010;14(3):300–9.
83. Hew-Butler T, Rosner MH, Fowkes-Godek S, Dugas JP,
Hoffman MD, Lewis DP, et al. Statement of the Third
International Exercise-Associated Hyponatremia Consen-
sus Development Conference, Carlsbad, California, 2015.
Clin J Sport Med. 2015;25(4):303–20.
84. McArdle WD, Magel JR, Lesmes GR, Pechar GS. Meta-
bolic and cardiovascular adjustment to work in air and
water at 18, 25, and 33 degrees C. J Appl Physiol.
1976;40(1):85–90.
85. Noakes TD. Body cooling as a method for reducing
hyperthermia. S Afr Med J. 1986;70(6):373–4.
86. Proulx CI, Ducharme MB, Kenny GP. Effect of water
temperature on cooling efficiency during hyperthermia in
humans. J Appl Physiol (1985). 2003;94(4):1317–23.
87. Cooper KE. Physiology of hypothermia. Br J Anaesth.
1959;31(3):96–105.
88. Proulx CI, Ducharme MB, Kenny GP. Safe cooling limits
from exercise-induced hyperthermia. Eur J Appl Physiol.
2006;96(4):434–45.
89. Wyndham CH, Strydom NB, Cooke HM, Maritz JS,
Morrison JF, Fleming PW, et al. Methods of cooling sub-
jects with hyperpyrexia. J Appl Physiol. 1959;14:771–6.
90. Ferris EB, Blankenhorn MA, Robinson HW, Cullen GE.
Heat stroke: clinical and chemical observations on
44 cases. J Clin Invest. 1938;17(3):249–62.
91. Casa DJ, McDermott BP, Lee EC, Yeargin SW, Arm-
strong LE, Maresh CM. Cold water immersion: the gold
standard for exertional heatstroke treatment. Exerc Sport
Sci Rev. 2007;35(3):141–9.
92. O’Connor JP. Simple and effective method to lower body
core temperatures of hyperthermic patients. Am J Emerg
Med. 2017;35(6):881–4.
93. Costrini A. Emergency treatment of exertional heatstroke
and comparison of whole body cooling techniques. Med
Sci Sports Exerc. 1990;22(1):15–8.
94. Khogali M, Weiner JS. Heat stroke: report on 18 cases.
Lancet. 1980;2(8189):276–8.
95. Khogali M, al Khawashi M. Heat stroke during the Mak-
kah pilgrimage. Saudi Med J. 1981;2:85–93.
96. Al-Aska AK, Abu-Aisha H, Yaqub B, Al-Harthi SS, Sal-
lam A. Simplified cooling bed for heatstroke. Lancet.
1987;1(8529):381.
97. Hee-Nee P, Rupeng M, Lee VJ, Chua WC, Seet B. Treat-
ment of exertional heat injuries with portable body cool-
ing unit in a mass endurance event. Am J Emerg Med.
2010;28(2):246–8.
98. Platt M, Vicario S. Rosen’s Emergency Medicine. 7th ed.
Philadelphia, PA: Mosby; 2009.
99. Kielblock AJ, Van Rensburg JP, Franz RM. Body cooling
as a method for reducing hyperthermia. An evaluation of
techniques. S Afr Med J. 1986;69(6):378–80.
100. Richards D, Richards R, Schofield PJ, Ross V, Sutton
JR. Management of heat exhaustion in Sydney’s the
Sun City-to-Surf run runners. Med J Aust. 1979;2
(9):457–61.
101. Phan S, Lissoway J, Lipman GS. Chemical cold packs may
provide insufficient enthalpy change for treatment of
hyperthermia.Wilderness Environ Med. 2013;24(1):37–41.
102. Lissoway JB, Lipman GS, Grahn DA, Cao VH, Shaheen
M, Phan S, et al. Novel application of chemical cold
packs for treatment of exercise-induced hyperthermia: a
randomized controlled trial. Wilderness Environ Med.
2015;26(2):173–9.
103. Saper CB, Breder CD. Endogenous pyrogens in the CNS:
role in the febrile response. Prog Brain Res. 1992;93:419–28.
discussion 428�9.
104. Downey JA, Darling RC. Effect of salicylates on eleva-
tion of body temperature during exercise. J Appl Physiol.
1962;17:323–5.
105. Johnson SC, Ruhling RO. Aspirin in exercise-induced
hyperthermia. Evidence for and against its role. Sports
Med. 1985;2(1):1–7.
106. Beller GA, Boyd 3rd AE. Heat stroke: a report of 13 conse-
cutive cases without mortality despite severe hyperpyrexia
and neurologic dysfunction.Mil Med. 1975;140(7):464–7.
107. Demartini JK, Casa DJ, Stearns R, Belval L, Crago A,
Davis R, et al. Effectiveness of cold water immersion in
the treatment of exertional heat stroke at the Falmouth
Road Race.Med Sci Sports Exerc. 2015;47(2):240–5.
108. O’Donnell Jr TF. Acute heat stroke. Epidemiologic, bio-
chemical, renal, and coagulation studies. JAMA. 1975;
234(8):824–8.
109. Bouchama A, Dehbi M, Chaves-Carballo E. Cooling and
hemodynamic management in heatstroke: practical rec-
ommendations. Crit Care. 2007;11(3):R54.
110. Hart GR, Anderson RJ, Crumpler CP, Shulkin A, Reed G,
Knochel JP. Epidemic classical heat stroke: clinical char-
acteristics and course of 28 patients. Medicine (Balti-
more). 1982;61(3):189–97.
111. Gagnon D, Lemire BB, Casa DJ, Kenny GP. Cold-water
immersion and the treatment of hyperthermia: using 38.6˚C
ARTICLE IN PRESS
WMS Practice Guidelines for Heat-Related Illness 13

as a safe rectal temperature cooling limit. J Athl Train.
2010;45(5):439–44.
112. Newsham KR, Saunders JE, Nordin ES. Comparison of
rectal and tympanic thermometry during exercise. South
Med J. 2002;95(8):804–10.
113. Smith JE. Cooling methods used in the treatment of exer-
tional heat illness. Br J Sports Med. 2005;39(8):503–7.
discussion 507.
114. Horowitz BZ. The golden hour in heat stroke: use of iced
peritoneal lavage. Am J Emerg Med. 1989;7(6):616–9.
115. Yokobori S, Koido Y, Shishido H, Hifumi T, Kawakita K,
Okazaki T, et al. Feasibility and safety of intravascular
temperature management for severe heat stroke: a pro-
spective multicenter pilot study. Crit Care Med. 2018;46
(7):e670–6.
116. Bouchama A, Cafege A, Devol EB, Labdi O, el-Assil K,
Seraj M. Ineffectiveness of dantrolene sodium in the
treatment of heatstroke. Crit Care Med. 1991;19
(2):176–80.
ARTICLE IN PRESS
14 Lipman et al

WILDERNESS MEDICAL SOCIETY CLINICAL PRACTICE GUIDELINES
Wilderness Medical Society Clinical Practice Guidelines forthe Treatment and Prevention of Drowning: 2019 UpdateAndrew C. Schmidt, DO, MPH1; Justin R. Sempsrott, MD2; Seth C. Hawkins, MD3; Ali S. Arastu, MD4;Tracy A. Cushing, MD, MPH5; Paul S. Auerbach, MD, MS6
1Department of Emergency Medicine, University of Florida College of Medicine-Jacksonville, Jacksonville, FL; 2Department of Emergency Medicine,TeamHealth, West Valley Medical Center, Caldwell, Idaho; 3Department of EmergencyMedicine, Wake Forest University, Winston Salem, NC; 4Divisionof Pediatric Critical Care, Stanford University School ofMedicine, Palo Alto, CA; 5Department of EmergencyMedicine, University of ColoradoHospital,Aurora, CO; 6Department of Emergency Medicine, Stanford University School of Medicine, Palo Alto, CA
The Wilderness Medical Society convened a panel to review available evidence supporting practices foracute management and treatment of drowning in out-of-hospital and emergency medical care settings. Lit-erature about definitions and terminology, epidemiology, rescue, resuscitation, acute clinical management,disposition, and drowning prevention was reviewed. The panel graded available evidence supporting prac-tices according to the American College of Chest Physicians criteria and then made recommendations basedon that evidence. Recommendations were based on the panel’s collective clinical experience and judgmentwhen published evidence was lacking. This is the first update to the original practice guidelines published in2016.
Keywords: submersion, immersion, cold water submersion, hypothermia
Introduction
Approximately 360,000 deaths globally are attributed todrowning every year.1 Drowning often affects youngvictims and can have dire personal, emotional, and finan-cial consequences for patients, families, and society. Thegoal of these practice guidelines is to reduce the burdenof drowning through improvements in treatment andprevention. We present accepted drowning terminologyas part of a review and evaluation of literature regardingacute care for the drowning patient, in both out-of-hospital and emergency medical care settings, with parti-cular focus on the wilderness context. The authors reliedupon the experience and knowledge of a panel of wilder-ness and emergency medicine practitioners to makerecommendations where little or unreliable evidenceis available.2 This is the first update of the originalpublication from 2016.3
Methods
The authors of this update reviewed each section of theoriginal document to determine relevance and need forupdating. Articles were identified through PubMed,MEDLINE, and Google Scholar using a keyword searchappropriate to each topic. Randomized controlled trials,observational studies, case series, and review articleswere reviewed and evidence assessed. Abstracts forwhich the full article could not be obtained wereexcluded. If no relevant studies were identified, recom-mendations were based on the panel’s clinical experienceand judgment. Recommendations were graded using theAmerican College of Chest Physicians classificationscheme (see online Supplemental Table 1), in accordancewith prior versions of the Wilderness Medical SocietyPractice Guidelines.4
Epidemiology
The highest-risk age group for drowning worldwide is chil-dren ages 1 to 4 y, primarily owing to unintentional fallsinto water; the next highest-risk group is adolescents and
WILDERNESS & ENVIRONMENTAL MEDICINE XXXX; XXX(XXX): 1e17
Corresponding author: Andrew C. Schmidt, DO, MPH, Department ofEmergency Medicine, 655 W 8th Street, Jacksonville, FL 32209.; e-mail:[email protected].
Submitted for publication December 2018.Accepted for publication June 2019.

young adults in natural bodies of water. In the UnitedStates, there was on average 3536 drowning deaths peryear from 2005 to 2014, plus an additional 679 boating-related deaths, 75% of which were from drowning.5,6
More than 90% of the world’s drowning deaths occur inlow- and middle-income countries.1 In the context of low-and middle-income countries, natural sources of water areoften ubiquitous and used for transportation, cleaning,food, and hydration and lack barriers. Based on WorldHealth Organization and Centers for Disease Control andPrevention systems for classifying drowning statistics,these numbers exclude deaths occurring during floods andother natural disasters. In 2010, there were 12,900 emer-gency department (ED) visits in the United States fordrowning, with 20.3% of patients admitted to the hospital.Drowning deaths were 48% more likely to occur on week-ends compared to weekdays. Fifty-three percent of all maleand 26% of all female drowning deaths occurred in naturalbodies of water.5
The burden of drowning is underreported because moststudies address the issue of fatal drowning. In the UnitedStates, a conservative estimate is that for every fatal drown-ing, another 5 persons seek emergency care for nonfataldrowning.5 Internationally, the burden of nonfatal drown-ing is more difficult to estimate because many patientsmay not present to an emergency medical system or hospi-tal, where data collection typically occurs.5,7,8 In Bangla-desh, a large population-based study showed fatal andnonfatal drowning rates of 15.8 per 100,000 and 318.4per 100,00 compared to 1.17 per 100,000 and 10 per100,000 in the United States.9,10 Risk factors for nonfataldrowning are similar to those for fatal drowning.9,11e15
Terminology
The standard definition for drowning, as defined by theWorld Congress on Drowning in 2002, is “the process ofexperiencing respiratory impairment due to submersion orimmersion in liquid.” Inspired by the Utstein Style forreporting cardiac arrest data, the standard definition allowsfor only 3 outcomes after drowning: 1) morbidity; 2) nomorbidity; and 3) mortality. This definition is based on theunderstanding that “respiratory impairment occurs as theperson’s airway goes below the surface of the liquid (sub-mersion) or water splashes over the face (immersion).”16
However, the inclusion of both submersion and immersionin this definition may cause confusion with the large bodyof work on survival and rescue related specifically to coldwater immersion, which focuses more on hypothermiathan on drowning. For the purposes of these guidelines,which could include cold water conditions, a further dis-tinction is necessary. “Immersion” refers to situations inwhich airways are above water, whereas “submersion”
refers to situations in which airways are under water.Thus immersion (in cold water) may lead to hypothermia,and submersion at any water temperature may lead todrowning. The following modifiers should not be used inassociation with drowning: near, wet, dry, active, passive,saltwater, freshwater, or secondary. Sufficient data relatedto human drowning pathophysiology show that none ofthese modifiers is valid because the final commonpathway is hypoxemia and eventual cardiopulmonaryarrest.2,16,17 By understanding and using the standarddefinition for drowning and abstaining from using incorrectterminology, communication among medical practitioners,data collection agencies, researchers, and policymakershas become more consistent. Accurate communication bet-ter reflects the true incidence, prevalence, and sequelae ofdrowning and should improve clinical dialogue andmanagement.18e20
Rescue of the Drowning Patient
REACHING THE PATIENT
Rescuer safety is paramount during rescue operations; inthe aquatic environment, specific skills, training, and physi-cal capabilities are required. The physical characteristics ofaquatic environments vary widely, with a spectrum includ-ing pools, lakes, rivers, ocean, swift river water, and ice sce-narios, each requiring different sets of equipment andtraining for technical rescue. Few studies objectively mea-sure effectiveness of in-water rescue techniques. Much ofthe literature on this topic is based on experiences and poli-cies of the writers or organizational authorities. There is ahigh prevalence of fatal and nonfatal drowning of untrainedpersons attempting to perform in-water rescues, with 1study revealing 114 rescuer deaths during a 3-y period inTurkey alone.21e23 Hazardous water conditions that led tothe initial person drowning often persist and place thewell-intentioned rescuer at risk for becoming an additionaldrowning patient.24 Rescue by untrained persons shouldbe attempted without entering hazardous conditions byreaching out to the drowning patient with a paddle orbranch; throwing a rope, buoy, cooler, or any floatingobject; or rowing a boat, canoe, or paddleboard to thepatient. Trained rescue personnel should operate accordingto their level of training, expertise, equipment, and comfortlevel. Entering the water to perform a rescue should beattempted only by persons with specific training to operatein that dangerous environment. Few studies have been con-ducted on the effectiveness of different water safety devices(eg, rescue tubes, rescue cans, throw bags, life rings), butwhat has been demonstrated is that proper and effectiveuse of these devices requires basic knowledge of their func-tion combined with regular practice.25
Schmidt et al2

Recommendation. Persons without formal water rescuetraining should attempt rescues from a safe location byreaching, throwing, or rowing to the drowning patient.Persons with formal water rescue training should performin-water rescues according to their level of training andwith personal protective and safety equipment. There isinsufficient evidence to recommend specific rescue devices.If specialized rescue equipment is available, participantsshould be familiar with the location and purpose of thisequipment, and designated rescue personnel with propertraining should be tasked with its use in the event of awater rescue. Recommendation Grade: 1C26e28
PATIENTS IN SUBMERGED VEHICLES
Death from entrapment and drowning in submerged vehi-cles is often not classified as a drowning death, confoundingattempts to accurately track the epidemiology of this type ofdrowning.29 Studies suggest that 10% of drowning deathsmay be due to entrapment in submerged vehicles and thatin the case of inland flooding as much as 10% of motorvehicle crashes result in a drowning death.30e33 There is asmall body of medical and rescue literature on the topic ofvehicle submersions.31,34e39 A formal review of educa-tional and public service information identified “three prob-able significant contributors to [the] high fatality rate [ofdrowning in submerged vehicles]: 1) ‘authorities’ providean inadequate description of vehicle sinking characteristics;2) contradictory and inadequate advice is often provided;and 3) a poor public perception of how to escape.”34 Sev-eral sources recommend questionable escape practiceswithout supporting evidence for efficacy. These practicesinclude allowing the passenger compartment to fill withwater so that it will be easier to open doors, waiting untilthe vehicle sinks to the bottom of a body of water to main-tain orientation, relying on kicking out the windshield oropening doors after the vehicle has fully sunk, and relyingon breathing trapped air in the passenger compartment. Ina formal survey, more than half of the general public iden-tify an option that involves staying in a vehicle while itsinks to the bottom as being the safest option when trappedin a submerging vehicle; this advice often appears in thepopular media.38 Research data derived from 35 vehiclesubmersions conducted in diverse locations and seasonssuggest that this advice is erroneous. Evidence suggeststhe best time to escape from a submerging vehicle is imme-diately during the initial floating phase, ideally during theinitial 30 s to 2 min after water entry when most vehiclesremain partially above the surface.38 An algorithm, usingthe acronym SWOC, has been developed to advise thoseentrapped in water how to sequence escape actions. TheSWOC algorithm recommends the following sequencingof actions: Seatbelts off, Window open, Out immediately,
Children first.39 In 2008, a US-based proprietary out-of-hospital emergency medical dispatcher system added anaddendum to its standardized protocols that instructedemergency medical dispatchers not to persist in getting alocation for a caller in a submerging vehicle. Instead, itrecommends that a caller exit the vehicle immediately if itis submerging, before using precious time to determinelocation, and using the SWOC protocol.40,41
Recommendation. The safest time to escape from asubmerging vehicle is immediately after it enters thewater, during the initial floating phase. If the vehicleremains floating, persons should climb out and remainon top of the vehicle. If it is sinking, they shouldmove away from the vehicle and toward safety afterexiting. Recommendation Grade: 2C
IN-WATER RESUSCITATION
The primary physiologic insult in a drowning patient is cer-ebral hypoxia; its rapid reversal is the primary objective ofdrowning resuscitation. For the purpose of these guidelines,in-water resuscitation (IWR) is defined as an attempt to pro-vide ventilations to a drowning patient who is still in thewater. This does not apply to chest compressions. It isimpossible to perform adequate chest compressions whilethe victim and rescuer are in the water, and so they shouldnot be attempted.42 Successful use of IWR was firstdescribed in 1976, with a manikin-based feasibility studyreported in 1980; however, the first clinical study to showa positive patient outcome was not published until2004.43e45
Available outcome data for IWR are based on a singleretrospective analysis of lifeguard rescues in Brazil andshow significant improvement in survival and neurologicoutcome in persons receiving IWR. These rescues wereperformed by trained, professional lifeguards in the oceanenvironment. Lifeguards would frequently tow the patientbeyond breaking waves and perform mouth-to-mouth ven-tilations while awaiting helicopter pickup.45 Subsequentstudies, primarily using manikins, evaluated ease of per-forming this task in controlled aquatic environments andfound that IWR increases overall rescue time, subjectiverescue difficulty, number of submersions, and wateraspiration.46,47 A single study comparing lifeguards to layrescuers when using IWR found that lifeguards showedimproved rescue times and decreased estimated pulmonaryaspiration.48 Consensus statements from the InternationalLifesaving Federation, United States Lifesaving Associa-tion, American Red Cross, and the Young Men’s ChristianAssociation recommend IWR by trained rescuers when apatient is rescued in shallow water or in deep water whena flotation device is present.49,50
Drowning Treatment and Prevention 3

Rescuer safety and prevention of communicable diseasesare of utmost importance, so consideration should be givento the use of barrier devices during IWR. Food and DrugAdministrationeapproved, IWR-specific devices are avail-able that use a self-purging mechanical one-way valveinstead of the paper valve on standard CPR masks.51,52
Recommendation. IWR should only be considered by arescuer with adequate training, ability, and equipment tosafely and effectively perform the skill in the aquaticenvironment. The aquatic conditions must be sufficientlysafe for the rescuer to perform IWR, and the point ofextrication from the water must be sufficiently distant towarrant an attempt of this technically difficult task.If conditions are too hazardous to safely perform thetask, rapid extrication is indicated without a delay forIWR. Chest compressions should not be attempted in thewater; all drowning patients without a pulse should beextricated as quickly and safely as possible so that early,effective chest compressions and ventilations can beinitiated. Recommendation Grade: 1C
Initial Resuscitation
HYPOTHERMIA
Water is thermally neutral at approximately 33�C (91�F).Because most patients drown in water at a lower tempera-ture than this, concomitant hypothermia is common.30
The main physiologic problem with drowning is brainhypoxia. Current practice suggests that the brain can with-stand longer periods of hypoxia if the body is cooler thanthe normal physiologic range. On one hand, leaving apatient moderately cool, or warming them to a moderatelycool degree, could be beneficial or at least innocuous. Onthe other hand, moderate to severe hypothermia should becorrected, with the understanding that warming may beoperationally difficult in some drowning situations. Beyondinitiation of basic warming measures, the details ofhypothermia treatment, including augmented advancedlife support measures, are beyond the scope of these guide-lines. Readers are encouraged to review the most currentversion of the Wilderness Medical Society PracticeGuidelines for the Out-of-hospital Evaluation and Treat-ment of Accidental Hypothermia.53
Recommendation. Suspect and treat hypothermia.Recommendation Grade: 1C
CARDIOPULMONARY RESUSCITATION ANDPRIORITIZATION OF AIRWAY
Because of the central role of hypoxemia in the pathophy-siology of drowning, initial resuscitation should focus on
establishing and maintaining a patent airway and providingoxygen. Recent updates to cardiopulmonary resuscitation(CPR) algorithms, specifically for the lay rescuer, includerecommendations for compression-only CPR and prioriti-zation of compressions before airway maneuvers.54,55
Compression-only CPR is likely to be of little to no benefitin drowning resuscitation, and its use is limited to untrainedbystanders. Bystander CPR for infants and childrenincludes compressions and ventilations, regardless ofwhich is started first. Professional rescuer CPR shouldemphasize prioritization of airway and breathing beforeinitiation of chest compressions. If the airway is overlookedin initial resuscitation, ongoing hypoxemia leads todecreased survival and worse neurologic outcomes. Incor-rect application of rescue breaths can delay care and causegastric insufflation and pulmonary aspiration. For layresponders or persons without current training in rescuebreathing, compression-only CPR is still the preferredmethod of resuscitation. All persons who may respond toa drowning person (eg, parents, trip leaders, lifeguards)should take CPR classes that include training on properuse of chest compressions and rescue breathing.
Recommendation. Supplying oxygen to the brain is criticalto successful resuscitation of the drowning patient.Establishing an airway and providing oxygen are prioritiesin initial resuscitation. For the patient in cardiac arrest,provide positive pressure ventilations in addition to chestcompressions using the traditional Airway-Breathing-Circulation model of resuscitation. If an advanced airwayis available and properly placed, provide breaths at specifiedtime intervals (every 6 to 8 s) while continuouscompressions are administered. For lay people withouttraining in rescue breathing, compression-only CPR is apreferred alternative to no intervention. RecommendationGrade: 1C
OXYGENATION
Few large-scale studies have evaluated different airwayadjuncts applied to drowning patients. Although ideal res-cue breathing includes supplemental oxygen and a positivepressure delivery device, any amount of oxygen delivery(eg, mouth-to-mouth, bag-valve-mask [BVM] with ambi-ent air) is better than none if supplemental oxygen is notavailable. Manikin studies of supraglottic airways haveshown that lifeguards can successfully insert them, butthere is concern that this does not replicate real worldusage.56,57 Additional concern is that because of pulmonaryedema from drowning, certain supraglottic airway devicesmay perform poorly for oxygenation based on leakpressures.58,59 If the supraglottic airway fails to achieve
Schmidt et al4

adequate chest rise, a BVM or other method to oxygenateand ventilate the patient should be used.
Recent resuscitation data have brought into question thebenefit of providing high oxygen concentrations in theacute setting of out-of-hospital cardiac arrest and stroke,primarily based on data correlating hyperoxemia afterreturn of spontaneous circulation (ROSC) with increasedmortality. Most of these data focus on the period afterROSC in the intensive care unit setting; no studies focusspecifically on cardiac arrest associated with drowning orother primary respiratory events. A single retrospectivecase-control study involving arterial blood analysis duringCPR provides support for using high levels of supplementaloxygen. This study showed a significant increase in survi-val to hospital discharge with increasing levels of arterialoxygenation in all cardiac arrest patients, even at levelsthat would be considered hyperoxemic.60
Recommendation. When resuscitating a drowning patient,oxygen should initially be delivered at the highestconcentration available. For the patient in respiratorydistress or arrest, positive pressure is preferred over passiveventilation. If multiple modalities are available, themethod that most effectively delivers the highestconcentration of oxygen should be used. If a modality ordevice fails, BVM or mouth-to-mouth ventilation shouldbe attempted. Recommendation Grade: 1C
AUTOMATED EXTERNAL DEFIBRILLATOR
Although cerebral hypoxia is the primary cause of morbid-ity in the drowning patient, hypoxic myocardial injurymight also occur. Drowning patients initially typicallyexperience sinus tachycardia, followed by bradycardia, pul-seless electrical activity, and then asystole, owing to thehypoxic nature of the event.61 In drowning patients, ventri-cular fibrillation (VF) is rare, occurring in less than 10% ofpatients; thus, reversal of hypoxemia with ventilations andcompressions should not be delayed in an attempt toapply an automated external defibrillator (AED).61e67
Once resuscitation is established, early application of anAED might be beneficial, given the possibility of VF asthe cause or result of drowning. In the drowning patient,if global myocardial hypoxia persists, attempts at defibrilla-tion may be unsuccessful without concomitant oxygenationand ventilation.
Experimental animal models have shown that as long asAED pads are placed firmly on a patient’s chest and a res-cuer is not in direct contact with that patient, use of anAED in a wet environment does not pose increased risk tothe patient or rescuers.68e70 AEDs have been tested andnoted to correctly detect simulated arrhythmias and delivershocks on moving boats.71
Recommendation. VF is rare in drowning, soincorporation of an AED in the initial minutes of drowningresuscitation should not interfere with oxygenation andventilation. If available, an AED should be used duringresuscitation of a drowning patient; its use is notcontraindicated in a wet environment. RecommendationGrade: 1A
HEIMLICH MANEUVER
Drowning involves water obstructing the airway and caus-ing cerebral hypoxia; in some cases, small amounts ofwater are aspirated into the lungs. This can cause atelecta-sis, direct cellular injury, and pulmonary edema. Evenafter unconsciousness, reflex swallowing of water fromthe hypopharynx into the stomach may occur. Dr HenryHeimlich advocated use of abdominal thrusts in initial treat-ment of the drowning patient, claiming that aspirated watermust first be cleared from the airway to allow properventilations.72e74 In the 30 y since his original report, con-cern has been raised about this recommendation, resultingin an Institute of Medicine report and a systematic literaturereview by the American Red Cross.75,76 All of these inves-tigations failed to identify quality data to support use of theHeimlich maneuver before providing ventilations. Its useduring initial resuscitation delays delivery of ventilationsand prolongs hypoxemia.75
Recommendation. Owing to the possibility ofdelaying ventilations, the Heimlich maneuver is notrecommended for resuscitation of the drowning patient.Recommendation Grade: 1B
CERVICAL SPINE PRECAUTIONS
Recent discussions and research in the field of out-of-hospi-tal medicine have brought in to question the utility, safety,and clinical benefit of what has been called routine spineimmobilization. The most current published review of thistopic specific to austere environments is the WildernessMedical Society Clinical Practice Guidelines for SpinalCord Protection: 2019 Update.77 We recommend review-ing the updated guidelines for current evidence on theutility of this procedure.
Retrospective studies of drowning patients found theincidence of cervical spine injuries was low (0.5e5%)and that most injuries were related to diving from a height.In patients without obvious signs of trauma or a known fallor diving event, the risk of spine injury is low.78,79 In thesepatients, treatment maneuvers focused on restricting spinemotionmay distract rescuers from the critical role of oxyge-nation and ventilation.
Drowning Treatment and Prevention 5

Recommendation. The most current Wilderness MedicalSociety Practice Guidelines concerning the field treatmentof possible spinal injuries should be reviewed whendeveloping or reviewing agency protocols. Drowningpatients who display evidence of spine injury, such asfocal neurologic deficit, have a history of high-risk activity,or exhibit altered mental status are considered to be at ahigher risk for spine injury. This does not include patientswith altered mental status who were witnessed to have notrauma as an inciting event. Treatment considerations forthis population should be carried out in accordance withthe most current version of Wilderness Medical SocietyClinical Practice Guidelines for Spinal Cord Protection.Recommendation Grade: 1C
Postresuscitation Management
OXYGENATION/VENTILATION
Mechanical ventilation
No literature is available comparing out-of-hospital or in-hospital mechanical ventilation strategies for the drowningpatient. Current practice recommends a lung protective ven-tilation strategy similar to that used for patients with acuterespiratory distress syndrome (ARDS), on the premise thatthe lung injury pattern after drowning is similar.16,80,81
This includes mechanical ventilation starting with a tidalvolume (VT) of 6 to 8 mL$kg-1, augmentation of VT andrespiratory rate to maintain plateau pressure <30 mm Hg,and augmentation of positive end expiratory pressure andfraction of inspired oxygen (FIO2) to maintain partial pres-sure of arterial oxygen (PaO2) at 55 to 80 mm Hg.82
Recommendation. Mechanical ventilation for thedrowning patient should follow ARDS protocols.Recommendation Grade: 1C
Noninvasive positive pressure ventilation
Noninvasive positive pressure ventilation (NIPPV) hasbeen used successfully in the out-of-hospital setting.There are case reports describing its successful use indrowning.83e86 Similar to invasive ventilation, the additionof airway pressure to prevent atelectasis and supportrespiratory muscle use while preventing hypoxemia canbe achieved with NIPPV. However, caution should beused with NIPPV in the drowning patient with altered men-tal status because there may be increased risk of vomitingand aspiration. Drowning patients who havemild to moder-ate hypoxemia and are being treated in out-of-hospital andemergency medical systems using NIPPV might benefitfrom this therapy. One small retrospective study showed
similar neurologic outcomes and correction of hypoxemiaand acidosis between patients treated with early endotra-cheal intubation versus NIPPV after drowning; in addition,patients receiving NIPPV had a lower incidence of infec-tion and decreased hospital and intensive care unit lengthof stay.87
Recommendation. NIPPV may be usd in the alertdrowning patient with mild to moderate respiratorysymptoms. Caution should be taken with any patientdisplaying altered mental status and/or active emesisowing to the potential for aspiration. RecommendationGrade: 2C
Diagnostics
RADIOLOGIC TESTING
Several retrospective ED studies of drowning patientsfound that the initial chest radiograph did not correlatewith arterial blood gas levels, outcome, or disposition.88e90
A study of admitted drowning patients showed that thosewho went on to develop acute lung injury or ARDS hadabnormal chest radiograph findings within the first fewhours, but not necessarily on arrival to the ED.80 Head com-puted tomography (CT) has been studied in an attempt toquantify anoxic brain injury in drowning patients. Retro-spective studies have found that patients with abnormalinitial CT all went on to develop severe brain injury ordie, whereas initially normal head CT had no prognosticvalue.91
Recommendation. Initial chest radiograph findings do notcorrelate with arterial blood gas measurements or outcome;x-rays may be useful in tracking changes in patientcondition, but not for determining prognosis if obtained atthe time of presentation. A normal initial head CT doesnot have prognostic value in the drowning patient. Routineuse of neuroimaging in the awake and alert drowningpatient is not recommended unless dictated by a change inclinical status. Recommendation Grade: 1C
LABORATORY TESTING
Canine studies performed in the 1960s showed clinicallysignificant hemodilution and red blood cell lysis associatedwith salt, chlorine, and freshwater drowning.92e94 Thesestudies were based on instilling up to 44 mL$kg-1 of fluidinto the trachea of anesthetized dogs, far greater than the 1to 3 mL$kg-1 typically aspirated by human drowningpatients. Electrolyte abnormalities and hemodilution onlyoccurred in dogs that had 11 mL$kg-1 or more instilled.No studies have identified clinically significant electrolyte
Schmidt et al6

or hematologic abnormalities in drowning patients that helpguide initial therapy or provide prognostic information. Inpatients with altered mental status or decreased level of con-sciousness, laboratory evaluation for alternative causes thatmight have led to the drowning event, such as hypoglyce-mia or intoxication, can be helpful. Arterial blood gas ana-lysis in symptomatic patients can be used to help guiderespiratory resuscitation.
Recommendation. Routine use of complete blood count orelectrolyte testing in the drowning patient is notrecommended. Arterial blood gas testing in patients withevidence of hypoxemia or respiratory distress (eg, cyanosis,low oxygen saturation, tachypnea, persistent tachycardia)may be indicated to guide respiratory interventions. Forpatients whose mental status fails to respond toresuscitation or in whom the initial cause of submersion isunknown, laboratory testing for causes of altered mentalstatus or any inciting event should be considered.Recommendation Grade: 1C
Other Treatments
ANTIBIOTICS
Although microorganisms present in aspirated watermay eventually cause pneumonia, no study to date hasshown benefit from empiric administration of antibio-tics in drowning patients. This is in part because micro-organisms found in drowning-associated pneumonia areatypical bacteria or fungi and often are resistant to stan-dard empiric treatments.95e97 Aspiration of even smallvolumes of water can produce abnormalities on chest radio-graph that can mimic pneumonia. The trauma of the drown-ing event and hypoxemia can cause leukocytosis from stressdemargination aswell as fever from inflammation and irrita-tion caused by water in the airways, making it difficult todifferentiate inflammatory from infectious pneumonitis.98
The decision to administer antibiotics should be madeafter initial resuscitation and ideally be based on expecto-rated sputum or endotracheal aspirate bacterial culture,blood cultures, or urinary antigen tests.95e97 Becausethese tests are not available in the wilderness setting, treat-ment should be initiated for symptoms consistent with pul-monary infection (eg, fever, increased sputum, abnormallung auscultation) that continue after initial resuscitationand treatment phases.
Recommendation. There is no evidence to support empiricantibiotic therapy in the initial treatment of drowningpatients. After initial resuscitation, if pneumonia is present,treatment should be guided by expectorated sputum or
endotracheal aspirate bacterial culture, blood cultures, orurinary antigen tests. In the absence of these tests, decisionto treat should be based on clinical examination focusing onphysical evidence of pulmonary or systemic infection (eg,fever, increased sputum, abnormal lung auscultation).Recommendation Grade: 1A
CORTICOSTEROIDS
Corticosteroids were historically used in drowningpatients to facilitate pulmonary recovery and surfactantproduction. However, there is not sufficient evidence tosupport empiric corticosteroid administration for drown-ing patients.99
Recommendation. Given limited data, corticosteroidsshould not be routinely administered specifically fortreatment of drowning patients. RecommendationGrade: 1C
THERAPEUTIC HYPOTHERMIA
Mild therapeutic hypothermia (TH) has been shown todecrease cerebral oxygen utilization and improve neurolo-gically intact survival in patients with witnessed VF cardiacarrest.81 Current American Heart Association/InternationalLiaison Committee on Resuscitation guidelines recom-mend targeted temperature management for adults after car-diac arrest, at a temperature between 32 and 34�C for atleast 24 h.100 Many institutions have extrapolated thesedata to include non-VF causes of cardiac arrest.
The 2002World Congress onDrowning provided a con-sensus statement recommending TH of 32 to 34�C(90e93�F) for patients achieving ROSC after cardiac arrestdue to drowning.101 Our literature search yielded multiplecase reports and retrospective reviews supporting neurolo-gically intact survival in hypothermic patients, but severalolder studies showed no benefit.102e114 There is no pro-spective study comparing TH to normothermia afterROSC in drowning patients. There might be benefit to dis-continuing rewarming interventions after a hypothermicdrowning patient has reached TH temperature range, butthis has been insufficiently studied to support an evi-dence-based recommendation.
Recommendation. Although current literature recommendtargeted temperature management in postcardiac arrestcare, there is insufficient evidence to either support ordiscourage induction or maintenance of TH in drowningpatients. Recommendation Grade: 2C
Drowning Treatment and Prevention 7

Disposition in the Wilderness
DECISION TO EVACUATE
If a patient survives a drowning event in the wilderness,objective physical examination findings may assist in thedecision to evacuate the patient to advanced medical care.A single large retrospective study of nearly 42,000 oceanlifeguard rescues serves as the primary evidence for on-scene decision-making.115 This study found that patientswho experienced a drowning event but had no symptomsother than mild cough and who did not have abnormallung sounds had 0% mortality. As symptoms worsenedand abnormal lung sounds appeared, mortality increased.Hypotension (systolic blood pressure <90 mm Hg ormean arterial pressure <60 mm Hg) accounted for thenext largest increase in mortality (Table 1). In a retrospec-tive study of children who experienced nonfatal drowning,any clinical deterioration occurred within the first 4 h inpatients presenting with mild symptoms and GlasgowComa Scale score �13.88 These findings are similar tothose from another retrospective study of pediatric patientsin which new symptom development after arrival to thehospital occurred within 4.5 h in all but 1 patient; the 1 out-lier developed symptoms in 7 h and had a good outcome.116
Additional recent emergency department studies are dis-cussed in theDisposition in Emergency Department sectionof these guidelines. These studies revealed similar results inthe fact that clinical decompensation, if present, occurred inthe first few hours of observation.26
Recommendation:1. Any patient with abnormal lung sounds, severe cough,
frothy sputum, foamy material in the airway, depressedmentation, or hypotension warrants immediate evacua-tion to advanced medical care if risks of evacuation donot outweigh potential benefit.
2. Any patient who is asymptomatic (other than a mildcough) and displays normal lung auscultation may beconsidered for release from the scene. Ideally, anotherindividual should be with them for the next 4 to 6 h to
monitor for symptom development or the patient shouldbe advised to seek medical assistance if symptomsdevelop.
3. If evacuation is difficult or may compromise the overallexpedition, patients with mild symptoms and normalmentation should be observed for 4 to 6 h. Any evidenceof decompensation warrants prompt evacuation if therisks of evacuation do not outweigh the potential benefit.
4. If evacuation of a mildly symptomatic patient has begunand the patient becomes asymptomatic for 4 to 6 h, can-celing further evacuation and continuing previous activ-ity may be appropriate.Recommendation Grade: 1C
CEASING WATER-BASED RESCUE ANDRESUSCITATION EFFORTS
Awilderness search and rescue team can range from a smallgroup of untrained participants with no equipment to ahighly trained team with extensive resources. In the wilder-ness setting, available resources, risk to rescuers, and teamsafety must be considered when deciding how long tosearch for a submerged patient. Although each drowningepisode has unique patient and environmental factors, themost important predictor of outcome is duration ofsubmersion.67,117,118 Available evidence shows that prog-nosis is poor with submersion times greater than 30 min,regardless of water temperature.119 There are also casereports of survival with good neurologic outcome despiteprolonged submersion, predominantly in children aged�6 y in water<6�C (43�F) and with use of advanced treat-ment modalities, such as extracorporeal membraneoxygenation.120e125 For the purpose of these guidelines,recommendations are based on available evidence relevantto a typical drowning patient and on the probability of neu-rologically intact survival in specific conditions. A literaturereview of 43 cases serves as the evidence for water-basedrescue.126 The report concludes that there is minimalchance of neurologically intact survival with submersiontime >30 min in water >6�C (43�F) or >90 min in water
Table 1Out-of-hospital management and classification of drowning patients
Grade Pulmonary exam Cardiac exam Mortality (%)
0 Normal auscultation, without cough Radial pulses 01 Normal auscultation, with cough Radial pulses 02 Rales, small foam in airway Radial pulses 0.63 Acute pulmonary edema Radial pulses 5.24 Acute pulmonary edema Hypotension 195 Respiratory arrest Hypotension 446 Cardiopulmonary arrest 93
Adapted from Semprsott et al.25
Schmidt et al8

<6�C (43�F). It is important to note that “submersion time”was defined as beginning upon arrival of emergency ser-vices personnel; total submersion time is often unknown.
If a drowning patient is removed from the water andresuscitation takes place, it might be necessary to decidewhen to cease resuscitation efforts if no signs of life return.Based primarily on retrospective studies, submersion timesof >10 min appear to correlate with increased mortality orsurvival with severe neurologic dysfunction.67,118,127 Inaddition, more than 25 min of resuscitation or prolongedtime to advanced medical care also correlate with negativeoutcomes, but without the statistical significance ofsubmersion time. In a Dutch retrospective review of 160hypothermic drowning patients under the age of 16 y, 98children received CPR for more than 30 min, with only11 surviving to discharge, all of whom were neurologicallydevastated.119,127e129
Recommendation:1. Based on resources, it might be reasonable to cease res-
cue and resuscitation efforts when there is a known sub-mersion time of greater than 30 min in water >6�C(43�F), or greater than 90 min in water <6�C (43�F),or after 25 min of continuous cardiopulmonaryresuscitation.
2. If at any point during search and rescue efforts the safetyof the rescue team becomes threatened, rescue effortsshould be ceased.
3. If resources are available and recovery team safety ismaintained, body recovery efforts may continue beyondthe search and rescue period with the understanding thatresuscitation attempts will likely be futile.Recommendation Grade: 1C
Disposition in the Emergency Department
Although many studies have addressed prognostic factorsfor neurologic survival at hospital discharge, only a fewhave addressed the question of which patients can besafely discharged from the ED. The first, a prospectivestudy of primarily pediatric patients, included follow-upphone interviews with 33 patients who were eitherreleased on the scene or discharged from the ED within1 to 6 h of arrival and found that none of these patientsexperienced delayed effects.130 A retrospective reviewof 48 pediatric drowning patients who presented to a sin-gle ED with Glasgow Coma Scale score �13 studiedwhether factors predicting safe ED discharge could beidentified.88 Initial chest radiograph did not correlatewith severity of disease, and all patients who deteriorateddid so within 4 h of ED arrival. The authors concludedthat patients could be safely discharged home if normal-ized and if there was no deterioration in respiratory
function after 4 to 6 h of observation in the ED. A retro-spective review of hospitalized pediatric patients foundthat in all patients who were initially asymptomatic, butwho went on to develop symptoms during their stay,these symptoms developed within 4.5 h in all but 1 patientand did so within 7 h in the final patient.116 In the 2 y pre-ceding this current guideline update, 3 more pertinent ret-rospective studies investigating safe discharge ofpediatrics patients were published.90,131,132 The findingsof these articles are in line with the aforementioned stu-dies in that patients who initially presented as normal orwith minimal symptoms, with normal mentation, andwith no need for airway support generally could be safelydischarged. Patients in this group who had a clinicaldecline did so within the first few hours and had subse-quent safe discharge. One of the studies derived and vali-dated a clinical score to assist in determining whichpatients may be safely discharged after 8 h of ED observa-tion. The study found that the presence of 4 or more of thefollowing factors predicted safe discharge: normal menta-tion, normal respiratory rate, absence of dyspnea, absenceof need for airway support, and absence ofhypotension.132
Recommendation. After an observation period of 4 to 6 h,it is reasonable to discharge a drowning patient with normalmental status in whom respiratory function is normalizedand no further deterioration in respiratory function hasbeen observed. Recommendation Grade: 2C
Prevention
Prevention has the potential to save far more lives than res-cue or treatment of a drowning person. A comprehensiveprevention program includes participant screening for med-ical diseases that increase risk of drowning, swimming abil-ity, use of safety devices, and use of safe practices when inand around water.
PARTICIPANT SCREENING
Retrospective studies have linked coronary artery disease,prolonged QT syndrome, autism, and seizure disorderswith higher than normal rates of drowning and drowningdeaths.62,133e140 Preparticipation screening should focuson uncovering any medical or physical condition that maypotentially impair decision making, physical abilities, andthus swimming ability. These include a history of sponta-neous syncope, exertional syncope, and family history ofsudden cardiac death. There remains no reliable screeningtool for evaluation of cardiac conduction disorders, butscreening electrocardiogram and family history of suddencardiac death can help clinicians differentiate which
Drowning Treatment and Prevention 9

patients might benefit from further evaluation or genetictesting if indicated.
Recommendation. All patients with coronary arterydisease, prolonged QT syndrome or other ion channeldisorder, autism, seizure disorders, or other medical andphysical impairments should be counseled about theincreased risk of drowning and about steps to mitigate therisk, such as buddy swimming and rescue devices, shouldthey choose to participate in water activities. Given theextremely high rate of drowning in patients with epilepsy,patients should be counseled to never swim without directsupervision. Recommendation Grade: 2C
SWIMMING ABILITY
Common sense dictates that an individual who is a compe-tent swimmer and has the neurocognitive ability to makeappropriate decisions about water safety has a decreasedlikelihood of drowning. However, the best ages to learntechnique and specific swimming skills that reduce a per-son’s chance of drowning are not well established. Most lit-erature evaluates infant and pediatric populations for theeffects of swimming and the effects of infant survival les-sons on drowning and mortality.26,141 There is concernthat by providing swim lessons to young children, parentsmay develop a false sense of security in their child’s swim-ming ability, which might lead to increased drowningincidents.27,28,142
The American Academy of Pediatrics has always main-tained that children should learn to swim at some point intheir life. Previous recommendations were against formalswim lessons for all children age 4 y and under. The mostrecent review by the American Academy of Pediatricsacknowledges a lack of evidence surrounding pediatricswimming lessons and so does not formally recommendfor or against lessons for children under age 4 y.141
There is considerable debate regarding the definition of“swimming” or “survival-swimming” and what constitutesthe most protective approach to swim instruction. Althoughthe ability to swim farther distances can be perceived asincreased swim ability, for the purpose of swimming as atool for drowning prevention, the distance of 25 m (82 ft)has been adopted by international lifesaving agencies anda large population-based study in Bangladesh.143,144
Despite the lack of definitive evidence showing clearbenefit to formal swim lessons, panel members agree thatfamiliarity with and, more importantly, confidence in anaquatic environment would be beneficial in the event ofaccidental immersion or submersion. In addition, uniqueaquatic environments, such as whitewater, should beapproached only after focused instruction on swimmingtechniques specific to that environment.
Recommendation. All persons who participate in activitiesconducted in or around water should have, at a minimum,enough experience and physical capability to maintaintheir head above water, tread water, and make forwardprogress for a distance of 25 m (82 ft). RecommendationGrade: 2C
PERSONAL FLOTATION DEVICES
Within the category of personal flotation devices, devicessuch as lifejackets,manually or automated inflation systems,and neoprene wetsuits are available. Currently, lifejacketsare the only devices with injury prevention data availableand will, therefore, be used as the prototypical model forthis category. In 2017, according to United States CoastGuard data, drowning was the cause of death in more than76% of fatal boating accidents.5 In addition, 85% of thesefatalities were notwearing lifejackets. Three other retrospec-tive studies have found an association between lifejacket useand decreased mortality in boating accidents.145e147 One ofthese studies compared drowning deaths before and afterincreased lifejacket regulations, revealing improved survi-val rates after regulations went into effect. These data sug-gest that activities in and around water, especially whileboating, should include lifejacket use.145
Recommendation. Properly fitted lifejackets that meet localregulatory specifications should be worn by participantswhen boating or engaging in any water sports forwhich lifejackets are recommended. RecommendationGrade: 1C
ALCOHOL USE
Alcohol is a known contributing factor to drowning deaths.Data obtained primarily from telephone studies likely under-represents the true burden of alcohol in drowning causation.In 2017, alcohol was a leading factor in boating-relateddeaths.5 A 2004 review found that 30 to 70% of drowningfatalities have a measurable blood alcohol level, with 10 to30% of deaths being directly attributed to alcohol use.148
Recommendation. Alcohol and other intoxicatingsubstances should be avoided before and during wateractivities. Recommendation Grade: 1C
LIFEGUARDS
There are no specific peer-reviewed studies on the utility oflifeguards on expeditions or wilderness trips.149 A 2001Centers for Disease Control and Prevention workinggroup report recommends the presence of lifeguards fordrowning prevention in open water settings. In 2017, the
Schmidt et al10

United States Lifesaving Association reported over 8 mil-lion preventative actions and over 75,000 water rescuescovering a population of almost 386 million beachgoers.There were 17 reported drowning deaths at guarded bea-ches compared with 131 deaths at beaches withoutlifeguards.150 Among nationally recognized lifeguard certi-fying agencies (Ellis & Associates, American Red Cross,Starfish Aquatics Institute, and National Aquatic SafetyCompany) there are no specific guidelines or recommenda-tions for the number of lifeguards per number of partici-pants in an event or at an aquatic facility.
Recommendation.Despite a lack of definitive evidence, allgroups operating in or near aquatic environments,regardless of size, should consider water safety duringplanning and execution of excursions. This includescontingencies for prevention, rescue, and treatment ofdrowning persons. In high-risk environments or largegroups, consider including personnel with technical rescuetraining and appropriate rescue equipment.Recommendation Grade: 1C
Special Situations
COLD WATER SURVIVAL
No single recommendation can address all possible scenar-ios in a water setting. An unintentional fall into a swift mov-ing river, deep offshore ocean, inland waterways, backyardswimming pool, or through ice into static or moving waterare all treated according to the skill level, preparation, andequipment available to patient and rescuer. Immediateattention must always be given to self-rescue and extricat-ing oneself from a hazardous environment. After immer-sion in cold water, a person has a limited amount of timebefore fatigue and incapacitation render self-rescue impos-sible. Likelihood of survival is increased by having appro-priate gear and training and by dressing for watertemperature, not just air temperature, in the event ofimmersion.
Extensive controlled trials of cold-water survival arelacking, and the available literature is not generalizable toall scenarios. For example, presence of a lifejacket, seastate, weather, physical fitness, clothing, and mental prepa-redness all contribute to survivability in cold water. White-water is different from still water or the ocean in polarregions. A single large literature review serves as the sourcefor recommendations about cold water survival under idealconditions and must be interpreted according to the level oftraining, preparation, and situation presented to thepatient.151
After immersion, the most important decisions a personmust make are: 1) assessment of the presence of any
potential immediate threats to life and 2) whether to swimto safety or await rescue. Should a person choose to awaitrescue, preventing loss of body heat becomes paramount.By positioning the body to protect major areas of heatloss, a patient may lengthen immersion survival time. Aposition that has been proven in a laboratory setting todecrease heat loss is the heat escape lessening position.The goal of this position is to decrease heat loss fromareas such as the arm pits, groin, and, to a lesser extent,neck. This position is achieved by pressing the arms againstthe sides of the chest and squeezing the legs together. Ifpossible, additional protection may be obtained by flexingthe hips and knees and shrugging the shoulders. In somecases, it may be possible to pull the knees to the chestwith the hands. Some individuals will be unstable in thisposition; in this case the arms can simply be folded acrossthe chest. In the event of group immersion, the huddle for-mation has been recommended to lessen heat loss, assistinjured or weak persons, and improve group morale.Although this position has been shown to decrease coolingin participating individuals in a controlled environment, theeffort needed to assist debilitated individuals in an actualemergency may result in increased heat loss (Figures 1and 2).152
Swimming or treading water should be limited to mini-mize heat loss. Life jackets should be worn to aid insulationand flotation. If possible, the ideal location to await rescueis out of the water, even if only partially, to reduce heatloss and delay onset of hypothermia. Prolonged cold-water exposure eventually results in motor disabilities,which can appear within 10 min of immersion, makingadvanced maneuvers difficult. For this reason, it may bebeneficial to affix one’s body or clothing to a floating objectusing rope, or freezing clothing to the ice surface if exit isnot possible. Prolonged immersion will also eventuallylead to cognitive disabilities, rendering decision-makingdifficult.
Should a person decide to swim to safety, some impor-tant physiologic changes may occur. The initial coldshock, which lasts seconds to a few minutes, may promptgasping and hyperventilation and can have a disorientingeffect, making self-rescue attempts difficult. Uponimmersion in cold water, if no immediate life threatsare present, a person should focus on remaining calmand controlling breathing by taking slow, deep breaths.Once a person is able to obtain his or her bearings, heor she may have far less than 10 m of effective swim-ming, and up to 1 h of consciousness, before succumbingto hypothermia. All of these statements assume the per-son is wearing an appropriate lifejacket. Further detaileddiscussion of the science behind cold water immersion isavailable in chapter 8 of Wilderness Medicine (7thedition).30
Drowning Treatment and Prevention 11
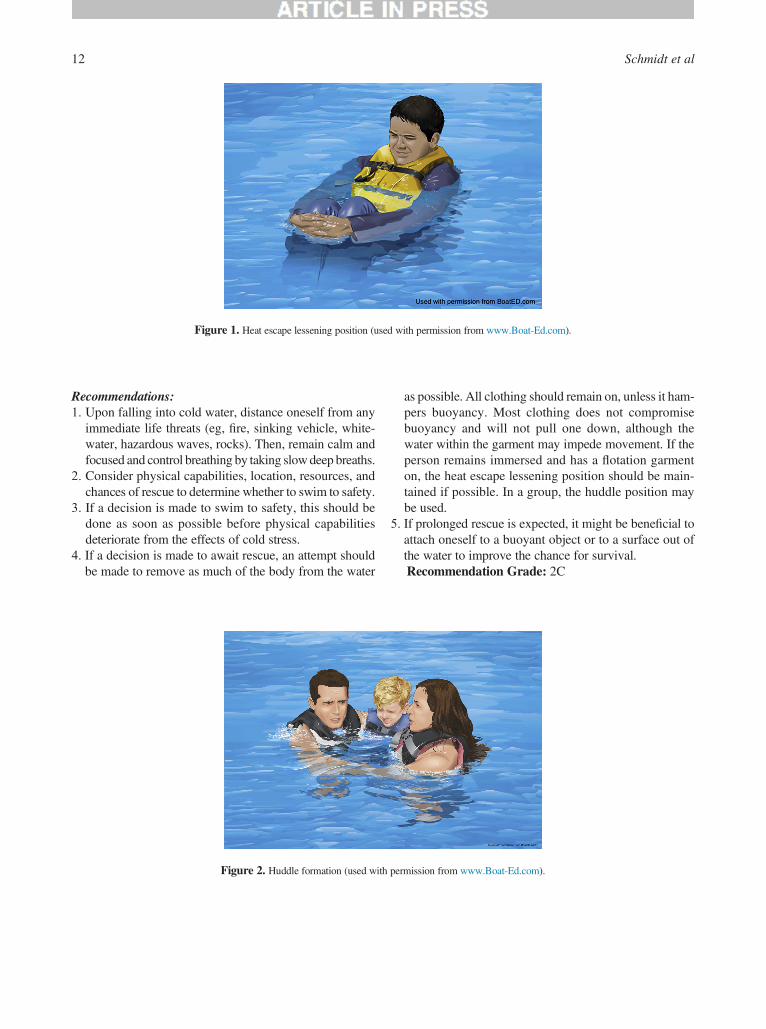
Recommendations:1. Upon falling into cold water, distance oneself from any
immediate life threats (eg, fire, sinking vehicle, white-water, hazardous waves, rocks). Then, remain calm andfocused and control breathing by taking slowdeep breaths.
2. Consider physical capabilities, location, resources, andchances of rescue to determine whether to swim to safety.
3. If a decision is made to swim to safety, this should bedone as soon as possible before physical capabilitiesdeteriorate from the effects of cold stress.
4. If a decision is made to await rescue, an attempt shouldbe made to remove as much of the body from the water
as possible. All clothing should remain on, unless it ham-pers buoyancy. Most clothing does not compromisebuoyancy and will not pull one down, although thewater within the garment may impede movement. If theperson remains immersed and has a flotation garmenton, the heat escape lessening position should be main-tained if possible. In a group, the huddle position maybe used.
5. If prolonged rescue is expected, it might be beneficial toattach oneself to a buoyant object or to a surface out ofthe water to improve the chance for survival.Recommendation Grade: 2C
Figure 1. Heat escape lessening position (used with permission from www.Boat-Ed.com).
Figure 2. Huddle formation (used with permission from www.Boat-Ed.com).
Schmidt et al12

Conclusions
Drowning is a process with outcomes ranging from nomor-bidity to severe morbidity to death. The most importantaspect of treatment is to reverse cerebral hypoxia by provid-ing oxygen to the brain. Drowning prevention can be effec-tive and should be thoroughly deployed.
Author Contributions: All authors contributed to drafting, revision, andapproval of final manuscript.
Disclosures: The authors report the following disclosures. AS, JS, andSH are directors of LifeguardsWithout Borders. SH isMedical Director forLandmark Learning, Starfish Aquatics, and North Carolina State Parks aswell as owner of Hawk Ventures. TC is Section Editor for WMS PracticeGuidelines. AA and PA have no disclosures to report.
Financial/Material Support: None.
Supplementary materials
Supplementary data to this article can be found online athttps://doi.org/10.1016/j.wem.2019.06.007.
References
1. World Health Organization. Preventing drowning: an imple-mentation guide. Geneva. 2017.
2. van Beeck EF, Branche CM, Szpilman D, Modell JH. Bie-rens JJ. A new definition of drowning: towards documenta-tion and prevention of a global public health problem. BullWorld Health Organ. 2005;83(11):853e6.
3. Schmidt AC, Sempsrott JR, Hawkins SC, Arastu AS,Cushing TA, Auerbach PS. Wilderness Medical Societypractice guidelines for the prevention and treatment ofdrowning. Wilderness Environ Med. 2016;27(2):236e51.
4. Guyatt G, Gutterman D, Baumann MH, Addrizzo-Harris D,Hylek EM, Phillips B, et al. Grading strength of recommen-dations and quality of evidence in clinical guidelines: reportfrom an American college of chest physicians task force.Chest. 2006;129:174e81.
5. Centers for Disease Control and Prevention (CDC). Uninten-tional drowning: get the facts. Available at: https://www.cdc.gov/homeandrecreationalsafety/water-safety/waterinjuries-factsheet.html. Accessed November 7, 2017.
6. United States Coast Guard. 2017 recreational boatingstatistics. Available at: http://uscgboating.org/library/accident-statistics/Recreational-Boating-Statistics-2017.pdf.Accessed November 7, 2018.
7. Alonge O, Agrawal P, Talab A, Rahman QS, Rahman AF,Arifeen SE, et al. Fatal and non-fatal injury outcomes: resultsfrom a purposively sampled census of seven rural subdis-tricts in Bangladesh. Lancet Glob Health. 2017;5(8):e818e27.
8. Abdullah SA, Flora MS. Risk factors for nonfatal drowningin children in rural Bangladesh: a community-based case-control study. WHO South East Asia J Public Health.2013;2(2):88e95.
9. Felton H, Myers J, Liu G, Davis DW. Unintentional, non-fatal drowning of children: US trends and racial/ethnic dispa-rities. BMJ Open. 2015;5(12):e008444.
10. Rahman A, Alonge O, Bhuiyan AA, Agrawal P, Salam SS,Talab A, et al. Epidemiology of drowning in Bangladesh:an update. Int J Environ Res Public Health. 2017;14(5):488.
11. Reijnen G, van de Westeringh M, Buster MC, Vos PJE,Reijnders ULJ. Epidemiological aspects of drowning andnon-fatal drowning in the waters of Amsterdam. J ForensicLegal Med. 2018;58:78e81.
12. Byard RW. Drowning and near drowning in rivers. ForensicSci Med Pathol. 2017;13(3):396.
13. Matthews BL, Andrew E, Andronaco R, Cox S, Smith K.Epidemiology of fatal and non-fatal drowning patientsattended by paramedics in Victoria, Australia. Int J Inj Con-trol Saf Promot. 2017;24(3):303e10.
14. Irwin CC, Irwin RL, Ryan TD, Drayer J. The legacy of fear:is fear impacting fatal and non-fatal drowning of AfricanAmerican children? J Black Stud. 2011;42(4):561e76.
15. MaWJ, Nie SP, XuHF, Xu YJ, Song XL, Guo QZ, et al. Ananalysis of risk factors of non-fatal drowning among childrenin rural areas of Guangdong province, China: a case-controlstudy. BMC Public Health. 2010;10:156.
16. Szpilman D, Bierens JJ, Handley AJ, Orlowski JP. Drown-ing. N Engl J Med. 2012;366:2102e10.
17. Idris AH, Berg RA, Bierens J, Bossaert L, Branche CM,Gabrielli A, et al. Recommended guidelines for uniformreporting of data from drowning: The “Utstein Style”.Circu-lation. 2003;108:2565e74.
18. Hawkins S, Semprott J, Schmidt A. ‘Drowning’ in a sea ofmisinformation. Emergency Medicine News. 2017;39(8):39e40.
19. Schmidt A, Semprott J, Hawkins S. Special report: the mythof dry drowning remains at large. Emergency MedicineNews. 2018;40(6):22.
20. Szpilman D, Sempsrott J, Webber J, Hawkins SC, Barcala-Furelos R, Schmidt A, et al. ‘Dry drowning’ and othermyths. Cleve Clin J Med. 2018;85(7):529e35.
21. Franklin RC, Pearn JH. Drowning for love: the aquatic vic-tim-instead-of-rescuer syndrome: Drowning fatalities invol-ving those attempting to rescue a child. J Paediatr ChildHealth. 2011;47(1e2):44e7.
22. Turgut A. A study onmultiple drowning syndromes. Int J InjControl Saf Promot. 2012;19:63e7.
23. Turgut A, Turgut T. A study on rescuer drowning and multi-ple drowning incidents. J Saf Res. 2012;43(2):129e32.
24. Moran K, Stanley T. Bystander perceptions of their capacityto respond in a drowning emergency. Int J Aquatic Res Educ.2013;7(4):290e300.
25. Pearn J, Franklin R. “Flinging the squalor” lifeline rescuesfor drowning prevention. Int J Aquatic Res Educ. 2009:315e21.
26. Brenner RA, Taneja GS, Haynie DL, Trumble AC, Qian C,Klinger RM, et al. Association between swimming lessonsand drowning in childhood: a case-control study. ArchPediatr Adolesc Med. 2009;163(3):203e10.
Drowning Treatment and Prevention 13

27. Morrongiello BA, Sandomierski M, Schwebel DC, Hagel B.Are parents just treading water? The impact of participationin swim lessons on parents’ judgments of children’s drown-ing risk, swimming ability, and supervision needs. AccidAnal Prev. 2013;50:1169e75.
28. Morrongiello BA, Sandomierski M, Spence JR. Changesover swim lessons in parents’ perceptions of children’ssupervision needs in drowning risk situations: “his swim-ming has improved so now he can keep himself safe”.Health Psychol. 2014;33(7):608e15.
29. Semprsott J, Schmidt A, Hawkins S, Cushing T. Submersioninjuries and drowning. In: Auerbach P, ed.Wilderness Med-icine. 7th ed. Philadelphia: Elsevier; 2017:1530e49.
30. Giesbrecht G, Steinman A. Immersion into cold water. In:Auerbach P, ed. Wilderness Medicine. 7th ed. Philadelphia:Elsevier; 2017:162e97.
31. Wintemute GJ, Kraus JF, Teret SP, Wright MA. Deathresulting from motor vehicle immersions: the nature of theinjuries, personal and environmental contributing factors,and potential interventions. Am J Public Health. 1990;80:1068e70.
32. Yale JD, Cole TB, Garrison HG, Runyan CW, Ruback JK.Motor vehicle-related drowning deaths associated withinland flooding after Hurricane Floyd: a field investigation.Traffic Inj Prev. 2003;4:279e84.
33. Smith GS, Brenner RA. The changing risks of drowning foradolescents in the US and effective control strategies. Ado-lesc Med. 1995;6(2):153e70.
34. Lunetta P, Penttila A, Sajantila A. Drowning in Finland:“external cause” and “injury” codes. Inj Prev. 2002;8(4):342e4.
35. French J, Ing R, Von Allmen S, Wood R. Mortality fromflash floods: a review of national weather service reports,1969e81. Public Health Rep. 1983;98(6):584e8.
36. Agocs MM, Trent RB, Russell DM. Activities associatedwith drownings in imperial county, CA, 1980e90: implica-tions for prevention. Public Health Rep. 1994;109(2):290e5.
37. Lobeto A. Engine company operations: vehicle accidents inwater. Fire Eng. 2003;156.
38. McDonald G, Giesbrecht G. Vehicle submersion: a reviewof the problem, associated risks, and survival information.Aviat Space Environ Med. 2013;84(5):498e510.
39. Giesbrecht GG, McDonald GK. My car is sinking: automo-bile submersion, lessons in vehicle escape. Aviat SpaceEnviron Med. 2010;81(8):779e84.
40. Priority Dispatch Corporation. Medical priority dispatch sys-tem ProQA, v5.1.1.23. Current v13.1; last. update. January12, 2018.
41. Giesbrecht GG. The evidence base for a new “vehicle infloodwater” emergency dispatch protocol. Ann Emerg Dis-patch Response. 2016;4(2):7e11.
42. Orlowski JP, Szpilman D. Drowning. Rescue, resuscitation,and reanimation. Pediatr Clin North Am. 2001;48(3):627e46.
43. Ghaphery JL. In-water resuscitation. JAMA. 1981;245(8):821.
44. March NF, Matthews RC. New techniques in external car-diac compressions. Aquatic cardiopulmonary resuscitationJAMA. 1980;244(11):1229e32.
45. Szpilman D, Soares M. In-water resuscitationdis it worth-while? Resuscitation. 2004;63(1):25e31.
46. Perkins GD. In-water resuscitation: A pilot evaluation.Resuscitation. 2005;65(3):321e4.
47. Winkler BE, Eff AM, Eff S, Ehrmann U, Koch A, K€ahlerW,et al. Efficacy of ventilation and ventilation adjuncts duringin-water-resuscitationda randomized cross-over trial.Resuscitation. 2013;84:1137e42.
48. Winkler BE, Eff AM, Eff S, Eff S, Koch A, Kaehler W, et al.Effectiveness and safety of in-water resuscitation performedby lifeguards and laypersons: a crossover manikin study.Prehosp Emerg Care. 2013;17:409e15.
49. The United States Lifeguard Standards Coalition. UnitedStates lifeguard standards. Available at: http://www.lifeguardstandards.org/. Updated 2011. Accessed November10, 2018.
50. International Life Saving Federation. Medical position state-ment: in water resuscitation. Available at: http://www.ilsf.org/about/position-statements. Updated 2001. AccessedNovember 15, 2018.
51. Water Safety Products. BigEasy rescue breathing maskkit. Available at: http://www.watersafety.com/store/lifeguard-equipment/bigeasy-rescue-breathing-mask-kit.html. Updated 2015. Accessed November 20, 2018.
52. The Lifeguard Store. Seal rite mask kit. Available at:https://thelifeguardstore.com/seal-rite-mask-kit-22961.html.Accessed November 10, 2018.
53. Zafren K, Giesbrecht GG, Danzl DF, Brugger H,Sagalyn EB, Walpoth B, et al. Wilderness medical societypractice guidelines for the out-of-hospital evaluation andtreatment of accidental hypothermia: 2014 update. Wilder-ness Environ Med. 2014;25(4 Suppl):S66e85.
54. Truhl�a�r A, Deakin CD, Soar J, Khalifa GE, Alfonzo A,Bierens JJ, et al. European Resuscitation Council guidelinesfor resuscitation 2015: section 4. cardiac arrest in special cir-cumstances. Resuscitation. 2015;95:148e201.
55. Lavonas EJ, Drennan IR, Gabrielli A, Heffner AC,Hoyte CO, Orkin AM, et al. Part 10: Special circumstancesof resuscitation: 2015 American Heart Association guide-lines update for cardiopulmonary resuscitation and emer-gency cardiovascular care. Circulation. 2015;132(18 Suppl2):S501e18.
56. Adelborg K, Al-Mashhadi RH, Nielsen LH, Dalgas C,Mortensen MB, Lofgren B. A randomised crossover com-parison of manikin ventilation through Soft Seal, i-gel andAuraOnce supraglottic airway devices by surf lifeguards.Anaesthesia. 2014;69(4):343e7.
57. McKenna M, Davies M. Supraglottic airway use by life-guards. Anaesthesia. 2014;69(8):928.
58. Baker P, Webber J. Should supraglottic airway devices beused by lifeguards at all? Anaesthesia. 2014;69(8):928e9.
59. Baker PA, Webber JB. Failure to ventilate with supraglotticairways after drowning. Anaesth Intensive Care. 2011;39:675e7.
Schmidt et al14

60. Spindelboeck W, Schindler O, Moser A, Hausler F,Wallner S, Strasser C, et al. Increasing arterial oxygen partialpressure during cardiopulmonary resuscitation is associatedwith improved rates of hospital admission. Resuscitation.2013;84(6):770e5.
61. Eich C, Br€auer A, Timmermann A, Schwarz SK, Russo SG,Neubert K, et al. Outcome of 12 drowned children withattempted resuscitation on cardiopulmonary bypass: an ana-lysis of variables based on the “Utstein Style for drowning”.Resuscitation. 2007;75(1):42e52.
62. Papadodima SA, Sakelliadis EI, Kotretsos PS,Athanaselis SA, Spiliopoulou CA. Cardiovascular diseaseand drowning: autopsy and laboratory findings. Hell J Car-diol. 2007;48(4):198e205.
63. Grmec S, Strnad M, Podgorsek D. Comparison of the char-acteristics and outcome among patients suffering from out-of-hospital primary cardiac arrest and drowning victims incardiac arrest. Int J Emerg Med. 2009;2(1):7e12.
64. Ballesteros MA, Gutierrez-Cuadra M, Munoz P,Minambres E. Prognostic factors and outcome after drown-ing in an adult population. Acta Anaesthesiol Scand.2009;53(7):935e40.
65. Nitta M, Kitamura T, Iwami T, Nadkarni VM, Berg RA,Topjian AA, et al. Out-of-hospital cardiac arrest due todrowning among children and adults from the UtsteinOsaka project. Resuscitation. 2013;84(11):1568e73.
66. Claesson A, Lindqvist J, Herlitz J. Cardiac arrest due todrowningdchanges over time and factors of importancefor survival. Resuscitation. 2014;85(5):644e8.
67. Suominen P, Baillie C, Korpela R, Rautanen S, Ranta S,Olkkola KT. Impact of age, submersion time and water tem-perature on outcome in near-drowning. Resuscitation.2002;52(3):247e54.
68. Lyster T, Jorgenson D,Morgan C. The safe use of automatedexternal defibrillators in a wet environment. Prehosp EmergCare. 2003;7(3):307e11.
69. Schratter A, Weihs W, Holzer M, Janata A, Behringer W,Losert UM, et al. External cardiac defibrillation duringwet-surface cooling in pigs. Am J Emerg Med. 2007;25(4):420e4.
70. Klock-Frezot JC, Ohley WJ, Schock RB, Cote M,Schofield L. Successful defibrillation in water: a preliminarystudy.Conf Proc IEEE EngMed Biol Soc. 2006;1:4028e30.
71. de Vries W, Bierens JJ, Maas MW. Moderate sea states donot influence the application of an AED in rigid inflatableboats. Resuscitation. 2006;70(2):247e53.
72. Heimlich HJ, Spletzer EG. Drowning. N Engl J Med.1993;329(1):65.
73. Heimlich HJ, Patrick EA. Using the Heimlich maneuver tosave near-drowning victims. Postgrad Med. 1988;84(2):62e7, 71.
74. Heimlich HJ. Subdiaphragmatic pressure to expel waterfrom the lungs of drowning persons. Ann Emerg Med.1981;10:476e80.
75. Rosen P, Stoto M, Harley J. The use of the Heimlich maneu-ver in near drowning: Institute of Medicine report. J EmergMed. 1995;13(9):397e405.
76. Francesco P, Fielding R, Wernicki PG, Markenson D.Sub-diaphragmatic thrusts and drowned persons. Int J Aqua-tic Res Educ. 2010;4:81e92.
77. Hawkins SC, Williams J, Bennett BL, Islas A, Kayser DW,Quinn R. Wilderness Medical Society clinical practiceguidelines for spinal cord protection: 2019 update. Wilder-ness Environ Med. In press.
78. Watson RS, Cummings P, Quan L, Bratton S, Weiss NS.Cervical spine injuries among submersion victims.J Trauma. 2001;51(4):658e62.
79. Hwang V, Shofer FS, Durbin DR, Baren JM. Prevalence oftraumatic injuries in drowning and near drowning in childrenand adolescents. Arch Pediatr Adolesc Med. 2003;157(1):50e3.
80. Gregorakos L, Markou N, Psalida V, Kanakaki M,Alexopoulou A, Sotiriou E, et al. Near-drowning: clinicalcourse of lung injury in adults. Lung. 2009;187(2):93e7.
81. Topjian AA, Berg RA, Bierens JJ, Branche CM, Clark RS,Friberg H, et al. Brain resuscitation in the drowning victim.Neurocrit Care. 2012;17(3):441e67.
82. ARDS Clinical Network. Mechanical ventilation protocolsummary. Available at: http://www.ardsnet.org/. Updated2008. Accessed November 2, 2018.
83. Thompson J, Petrie DA, Ackroyd-Stolarz S, Bardua DJ.Out-of-hospital continuous positive airway pressure ventila-tion versus usual care in acute respiratory failure: a rando-mized controlled trial. Ann Emerg Med. 2008;52(3):232e41.
84. Dottorini M, Eslami A, Baglioni S, Fiorenzano G,Todisco T. Nasal-continuous positive airway pressure inthe treatment of near-drowning in freshwater. Chest.1996;110(4):1122e4.
85. Nava S, Schreiber A, Domenighetti G. Noninvasiveventilation for patients with acute lung injury or acuterespiratory distress syndrome. Respir Care. 2011;56(10):1583e8.
86. Ruggeri P, Calcaterra S, Bottari A, Girbino G, Fodale V.Successful management of acute respiratory failure withnoninvasive mechanical ventilation after drowning, in anepileptic-patient. Respir Med Case Rep. 2016;17:90e2.
87. Michelet P, Bouzana F, Charmensat O, Tiger F, Durand-Gasselin J, Hraiech S, et al. Acute respiratory failure afterdrowning: a retrospective multicenter survey. Eur J EmergMed. 2017;24(4):295e300.
88. Causey AL, Tilelli JA, SwansonME. Predicting discharge inuncomplicated near-drowning. Am J Emerg Med.2000;18(1):9e11.
89. Modell JH, Graves SA, Ketover A. Clinical course of 91consecutive near-drowning victims. Chest. 1976;70(2):231e8.
90. Brennan CE, Hong TKF, Wang VJ. Predictors of safe dis-charge for pediatric drowning patients in the emergencydepartment. Am J Emerg Med. 2018;36(9):1619e23.
91. Rafaat KT, Spear RM, Kuelbs C, Parsapour K, Peterson B.Cranial computed tomographic findings in a large group ofchildren with drowning: diagnostic, prognostic, and forensicimplications. Pediatr Crit Care Med. 2008;9(6):567e72.
Drowning Treatment and Prevention 15

92. Modell JH, Davis JH. Electrolyte changes in human drown-ing victims. Anesthesiology. 1969;30(4):414e20.
93. Modell JH, Moya F. Effects of volume of aspirated fluid dur-ing chlorinated fresh water drowning. Anesthesiology.1966;27(5):662e72.
94. Modell JH, Moya F, Newby EJ, Ruiz BC, Showers AV. Theeffects of fluid volume in seawater drowning. Ann InternMed. 1967;67(1):68e80.
95. WoodC. Towards evidence based emergencymedicine: bestBETs from the Manchester royal infirmary. BET 1: prophy-lactic antibiotics in near-drowning. Emerg Med J.2010;27(5):393e4.
96. Ender PT, Dolan MJ. Pneumonia associated with near-drowning. Clin Infect Dis. 1997;25(4):896e907.
97. Tadi�e JM, Heming N, Serve E, Weiss N, Day N, Imbert A,et al. Drowning associated pneumonia: a descriptive cohort.Resuscitation. 2012;83:399e401.
98. van Berkel M, Bierens JJ, Lie RL, de Rooy TP, Kool LJ, vandeVelde EA, et al. Pulmonary oedema, pneumonia andmor-tality in submersion victims; a retrospective study in 125patients. Intensive Care Med. 1996;22(2):101e7.
99. Foex BA, Boyd R. Towards evidence based emergencymedicine: best BETs from the Manchester royal infirmary.Corticosteroids in the management of near-drowning.Emerg Med J. 2001;18(6):465e6.
100. Callaway CW, Donnino MW, Fink EL, Geocadin RG,Golan E, Kern KB, et al. Part 8: post-cardiac arrest care:2015 American Heart Association guidelines update for car-diopulmonary resuscitation and emergency cardiovascularcare. Circulation. 2015;132(18 Suppl 2):S465e82.
101. World Congress on Drowning. Recommendations of theWorld Congress on Drowning. Available at: http://www.ilsf.org/drowning-prevention/report. Updated 2002.Accessed November 10, 2018.
102. Batra RK, Paddle JJ. Therapeutic hypothermia in drowninginduced hypoxic brain injury: a case report. Cases J.2009;2:9103.
103. Varon J, Marik PE. Complete neurological recovery follow-ing delayed initiation of hypothermia in a victim of warmwater near-drowning. Resuscitation. 2006;68(3):421e3.
104. Williamson JP, Illing R, Gertler P, Braude S. Near-drowningtreated with therapeutic hypothermia. Med J Aust.2004;181(9):500e1.
105. de Pont AC, de Jager CP, van den Bergh WM, Schultz MJ.Recovery from near drowning and postanoxic status epilep-ticus with controlled hypothermia. Neth J Med. 2011;69(4):196e7.
106. Rudolph SS, Barnung S. Survival after drowning with car-diac arrest and mild hypothermia. ISRN Cardiol.2011;2011:895625.
107. Choi SP, Youn CS, Park KN,Wee JH, Park JH, Oh SH, et al.Therapeutic hypothermia in adult cardiac arrest because ofdrowning. Acta Anaesthesiol Scand. 2012;56(1):116e23.
108. Kawati R, Covaciu L, Rubertsson S. Hypothermia afterdrowning in paediatric patients. Resuscitation.2009;80(11):1325e6.
109. Mizobuchi M, Nakamura S, Muranishi H, Utsunomiya M,Funatsu A, Kobayashi T, et al. Hypothermia with extracor-poreal membrane oxygenation for sudden cardiac deathand submersion. Am J Emerg Med. 2010;28(1):115.e1ee4.
110. Baldursdottir S, Sigvaldason K, Karason S, Valsson F,Sigurdsson GH. Induced hypothermia in comatose survivorsof asphyxia: a case series of 14 consecutive cases. ActaAnaesthesiol Scand. 2010;54(7):821e6.
111. Oude Lansink-Hartgring A, Ismael F. Controlled hypother-mia and recovery from postanoxic encephalopathy in near-drowning victim. Neth J Med. 2011;69(7):351.
112. Guenther U, Varelmann D, Putensen C,Wrigge H. Extendedtherapeutic hypothermia for several days during extracorpor-eal membrane-oxygenation after drowning and cardiac arresttwo cases of survival with no neurological sequelae.Resusci-tation. 2009;80(3):379e81.
113. Hein OV, Triltsch A, von Buch C, Kox WJ, Spies C. Mildhypothermia after near drowning in twin toddlers. CritCare. 2004;8(5):R353e7.
114. Bohn DJ, Biggar WD, Smith CR, Conn AW, Barker GA.Influence of hypothermia, barbiturate therapy, and intracra-nial pressure monitoring on morbidity and mortality afternear-drowning. Crit Care Med. 1986;14(6):529e34.
115. Szpilman D. Near-drowning and drowning classification: aproposal to stratify mortality based on the analysis of 1,831cases. Chest. 1997;112(3), 66e5.
116. Noonan L, Howrey R, Ginsburg CM. Freshwater submer-sion injuries in children: a retrospective review of seventy-five hospitalized patients. Pediatrics. 1996;98(3 Pt 1):368e71.
117. Quan L, Mack CD, Schiff MA. Association of water tem-perature and submersion duration and drowning outcome.Resuscitation. 2014;85(6):790e4.
118. Suominen PK, Vahatalo R. Neurologic long term outcomeafter drowning in children. Scand J Trauma Resusc EmergMed. 2012;20:55.
119. Kieboom JK, Verkade HJ, Burgerhof JG, Bierens JJ,Rheenen PF, KneyberMC, et al. Outcome after resuscitationbeyond 30 minutes in drowned children with cardiac arrestand hypothermia: Dutch nationwide retrospective cohortstudy. BMJ. 2015;350:h418.
120. Orlowski JP. How much resuscitation is enough resuscita-tion? Pediatrics. 1992;90(6):997e8.
121. Modell JH, Idris AH, Pineda JA, Silverstein JH. Survivalafter prolonged submersion in freshwater in Florida. Chest.2004;125(5):1948e51.
122. Hasibeder WR. Drowning. Curr Opin Anaesthesiol.2003;16(2):139e45.
123. Martin TG. Neardrowning and cold water immersion. AnnEmerg Med. 1984;13(4):263e73.
124. Gilbert M, Busund R, Skagseth A, Nilsen PA, Solbo JP.Resuscitation from accidental hypothermia of 13.7 degreesC with circulatory arrest. Lancet. 2000;355(9201):375e6.
125. Wanscher M, Agersnap L, Ravn J, Yndgaard S, Nielsen JF,Danielsen ER, et al. Outcome of accidental hypothermiawith or without circulatory arrest: experience from the
Schmidt et al16

Danish Praesto fjord boating accident. Resuscitation.2012;83(9):1078e84.
126. Tipton MJ, Golden FS. A proposed decision-making guidefor the search, rescue and resuscitation of submersion(head under) victims based on expert opinion. Resuscitation.2011;82(7):819e24.
127. Quan L, Kinder D. Pediatric submersions: prehospital pre-dictors of outcome. Pediatrics. 1992;90(6):909e13.
128. Youn CS, Choi SP, Yim HW, Park KN. Out-of-hospital car-diac arrest due to drowning: an Utstein Style report of 10years of experience from St. Mary’s hospital. Resuscitation.2009;80(7):778e83.
129. Claesson A, Svensson L, Silfverstolpe J, Herlitz J. Charac-teristics and outcome among patients suffering out-of-hospi-tal cardiac arrest due to drowning. Resuscitation.2008;76(3):381e7.
130. Pratt FD, Haynes BE. Incidence of “secondary drowning”after saltwater submersion. Ann Emerg Med. 1986;15(9):1084e7.
131. Cantu RM, Pruitt CM, Samuy N, Wu CL. Predictors ofemergency department discharge following pediatric drown-ing. Am J Emerg Med. 2018;36(3):446e9.
132. Shenoi RP, Allahabadi S, Rubalcava DM, Camp EA. Thepediatric submersion score predicts children at low risk forinjury following submersions. Acad Emerg Med.2017;24(12):1491e500.
133. Ackerman MJ, Tester DJ, Porter CJ, Edwards WD. Molecu-lar diagnosis of the inherited long-QT syndrome in a womanwho died after near-drowning. N Engl J Med. 1999;341(15):1121e5.
134. Tester DJ, Medeiros-Domingo A, Will ML, Ackerman MJ.Unexplained drownings and the cardiac channelopathies: amolecular autopsy series. Mayo Clin Proc. 2011;86(10):941e7.
135. Bell GS, Gaitatzis A, Bell CL, Johnson AL, Sander JW.Drowning in people with epilepsy: how great is the risk?Neurology. 2008;71(8):578e82.
136. Albertella L, Crawford J, Skinner JR. Presentation and out-come of water-related events in children with long QT syn-drome. Arch Dis Child. 2011;96:704e7.
137. SoRelle R. Genetic drowning trigger. Circulation.2000;101(3):E36.
138. Choi G, Kopplin LJ, Tester DJ, Will ML, Haglund CM,Ackerman MJ. Spectrum and frequency of cardiac channeldefects in swimming-triggered arrhythmia syndromes. Cir-culation. 2004;110(15):2119e24.
139. Lunetta P, Levo A, Laitinen PJ, Fodstad H, Kontula K,Sajantila A. Molecular screening of selected long QT
syndrome (LQTS) mutations in 165 consecutive bodiesfound in water. Int J Legal Med. 2003;117(2):115e7.
140. Tester DJ, Kopplin LJ, Creighton W, Burke AP,Ackerman MJ. Pathogenesis of unexplained drowning:new insights from a molecular autopsy. Mayo Clin Proc.2005;80(5):596e600.
141. Weiss J. American Academy of Pediatrics Committee onInjury, Violence. Prevention of drowning Pediatrics.2010;126(1):e253e62.
142. Moran K, Stanley T. Parental perceptions of toddler watersafety, swimming ability and swimming lessons. Int J InjControl Saf Promot. 2006;13(3):139e43.
143. Mecrow TS, Linnan M, Rahman A, Scarr J, Mashreky SR,Talab A, et al. Does teaching children to swim increaseexposure to water or risk-taking when in the water? Emer-ging evidence from Bangladesh. Inj Prev. 2015;21(3):185e8.
144. Australian Council for the Teaching of Swimming andWater Safety. Audit of national water safety programs.Available at: http://www.watersafety.com.au/Reports.aspx.Updated 2013. Accessed November 20, 2014.
145. Bugeja L, Cassell E, Brodie LR, Walter SJ. Effectiveness ofthe 2005 compulsory personal flotation device (PFD) wear-ing regulations in reducing drowning deaths among recrea-tional boaters in Victoria, Australia. Inj Prev. 2014;20(6):387e92.
146. Cummings P, Mueller BA, Quan L. Association betweenwearing a personal floatation device and death by drowningamong recreational boaters: a matched cohort analysis ofUnited States Coast Guard data. Inj Prev. 2011;17(3):156e9.
147. O’Connor PJ, O’Connor N. Causes and prevention of boat-ing fatalities. Accid Anal Prev. 2005;37(4):689e98.
148. Driscoll TR, Harrison JA, SteenkampM. Review of the roleof alcohol in drowning associated with recreational aquaticactivity. Inj Prev. 2004;10(2):107e13.
149. Branche CM, Stewart S. Lifeguard effectiveness: a report ofthe working group. Centers for Disease Control and Preven-tion, National Center for Injury. Prev Control. 2001.
150. United States Lifesaving Association. 2017 national lifesav-ing statistics. Available at: http://arc.usla.org/Statistics/public.asp. Updated 2013. Accessed November 20, 2018.
151. Ducharme MB, Lounsbury DS. Self-rescue swimming incold water: the latest advice. Appl Physiol Nutr Metab.2007;32(4):799e807.
152. Hayward JS, Eckerson JD, Collis ML. Effect of behavioralvariables on cooling rate of man in cold water. J Appl Phy-siol. 1975;38(6):1073e7.
Drowning Treatment and Prevention 17

WILDERNESS MEDICAL SOCIETY CLINICAL PRACTICE GUIDELINES
Wilderness Medical Society Clinical Practice Guidelines forWater Disinfection forWilderness, International Travel, andAustere SituationsHoward D. Backer, MD, MPH 1,*; Robert W. Derlet, MD, MPH 2; Vincent R. Hill, PhD 3
1California Emergency Medical Services Authority, Racho Cordova, CA; 2Emergency Department, University of California, Davis, Sacramento, CA;3Division of Foodborne, Waterborne and Environmental Diseases, Waterborne Disease Prevention Branch, Centers for Disease Control and Prevention,Atlanta, GA
To provide guidance to clinicians, the Wilderness Medical Society convened experts to develop evidence-based guidelines for water disinfection in situations where the potability of available water is not ensured,including wilderness and international travel, areas affected by disaster, and other areas without adequatesanitation. The guidelines present the available methods for reducing or eliminating microbiologic contam-ination of water for individuals, groups, or households; evaluation of their effectiveness; and practical con-siderations. The evidence evaluation includes both laboratory and clinical publications. The panel graded therecommendations based on the quality of supporting evidence and the balance between benefits and risks orburdens, according to the criteria published by the American College of Chest Physicians.
Keywords: drinking water, water purification, water microbiology, disaster planning, pasteurization,halogens
Introduction
Safe and efficient treatment of drinking water is among themajor public health advances of the last century. Withouttreatment, waterborne diseases can spread rapidly, resultingin large-scale disease and death.1,2 In industrialized nations,the population generally is protected from waterborne dis-ease by sophisticated water supply systems that disinfectwater and provide continuous monitoring. In contrast, tra-velers to wilderness and recreational areas anywhere inthe world and to underdeveloped regions of some countriesmay be confronted with untreated or contaminated waterthat poses a risk of acquiring enteric disease. In addition,disaster situations, such as the 2017 hurricanes that affectedHouston, Texas, and Puerto Rico, may result in a break-down of municipal water systems, exposing victims to non-potable water. These situations necessitate knowledge ofhow to disinfect water at the point-of-use, prior to drinking.
Methods of water treatment that can be applied in the fieldinclude the use of heat, ultraviolet light, clarification, filtra-tion, and chemical disinfection. The choices for the wilder-ness hiker or international traveler are increasing as newtechnology is applied to field applications. Different microor-ganisms have varying susceptibilities to these methods. Therisk of waterborne illness depends on the number and typeof organisms consumed, host factors, and the efficacy ofthe treatment system.
Methods
To develop these guidelines, specialists with expertise inwilderness medicine, travel medicine, public health, andmicrobiology were chosen on the basis of their clinical orresearch experience. Relevant articles were identifiedthrough the PubMed database using the following keywordsor phrases: water disinfection, waterborne illness, wildernesswater, water filtration, emergency or disaster drinking watertreatment. This was supplemented by a hand search of arti-cles from references in the initial PubMed search. Conclu-sions from review articles were cited in an effort to providebackground information and to augment reference selection.
WILDERNESS & ENVIRONMENTAL MEDICINE XXXX; XXX(XXX): 1e21
Corresponding author: Howard D. Backer, MD, MPH, 109 Bonita Ave,Piedmont, CA, 94611; e-mail: [email protected].
Submitted for publication November 2018.Accepted for publication June 2019.

The evidence base for water disinfection has substantialdifferences from other clinical guidelines. Most of the lit-erature concerning the effectiveness of specific disinfec-tants and methods against various waterbornemicroorganisms is laboratory based. Evidence on the bene-fits of disinfection is either population-based public healthresearch of disease outbreaks or randomized householdtrials of water disinfection that are influenced by compli-ance and hygiene. Therefore, the evidence grade is a combi-nation of laboratory, population, and household- orcommunity-level studies.
The authors used a consensus approach to developrecommendations for the disinfection of water. Water treat-ment techniques and recommendations were not evaluatedfor the removal of chemicals or toxins. Evidence gradeswere assigned according to methodology stipulated by theAmerican College of Chest Physicians for grading of evi-dence and recommendations3 (online SupplementaryTable 1). These recommendations are graded on the basisof the totality of supporting evidence and balance betweenthe benefits and risks or burdens for each modality.
Etiology and Risk of Waterborne Infection
WILDERNESS SETTINGS
Millions of people enter wilderness areas each year anddrink surface water. Even in developed countries with lowrates of diarrheal illness, regular waterborne disease out-breaks indicate that the microbiologic quality of the water,especially surface water, is not ensured.4e7 Public healthagencies regularly report outbreaks of disease associatedwith surface water from backcountry and parks as well asfrom campground water systems. The environment andactivity upstream from the travelers’ surface water sourcedefines the risk. Side streams draining springs, snowmelt,and glaciers where there is no human or animal activityare lower risk. In contrast, upstream usage by humans,farm animals, or wildlife pose a major risk. Cattle excretepathogenic strains of Escherichia coli and Salmonella andhave been found in multiple studies to be the major animalspecies contributing to waterborne disease in NorthAmerica.8,9 Giardiasis is a zoonotic infection with numer-ous host species, including farm animals, deer and otherwild ungulates, beavers, and even household animals; how-ever, the extent of transmission to humans is less defined.10
Nonalpine wilderness areas in the United States mayhave streams and rivers that are contaminated with animalwaste, including farm animal runoff, or may be contami-nated with incompletely treated sewage from towns andurban areas. In many countries, wilderness areas are co-occupied by local populations and domesticated animalsthat pollute water sources. Because it is very difficult to
exclude animal and human activity in the watershed, theCenters for Disease Control recommend treating surfacewater before ingestion as a precaution to protect health.
INTERNATIONAL TRAVEL
Substantial progress has been made in the past 20 yearstoward the goal of safe drinking water and sanitation world-wide, particularly in Asia and Latin America11; however,780 million people (11% of world population) still lack asafe water source, and 2.5 billion people lack access toimproved sanitation. Africa and Oceania are the regionswith the greatest need for improvement.More than 890mil-lion persons still practice open defecation, the largest num-ber being in India and Africa.11e13 Studies inunderdeveloped regions around the world show high levelsof microbes in the environment and water sources.14e18
Contamination of tap water commonly occurs because ofantiquated and inadequately monitored waste disposal,water treatment, and distribution systems.19,20
In both developed and developing countries, after nat-ural disasters such as hurricanes, tsunamis, and earth-quakes, one of the most immediate public health problemsis a lack of potable water. Wilderness visitors and interna-tional travelers have no reliable resources to evaluate localwater system quality. Less information is available forremote surface water sources. Appearance, smell, andtaste are not reliable indicators to estimate water safety.
Infectious agents with the potential for waterborne trans-mission include bacteria, viruses, protozoa, and nonpro-tozoan parasites. The list of microbial agents is similar tothe list of microorganisms that can cause travelers’ diarrhea,most of which can be waterborne as well as foodborne.Although the primary reason for disinfecting drinkingwater is to destroy microorganisms from animal andhuman biologic wastes, water may also be contaminatedwith toxins and chemical pollutants from industrial sourcesor from the environment. Escherichia coli and Vibrio cho-lerae may be capable of surviving indefinitely in tropicalwater. Enteric bacterial and viral pathogens survive in tem-perate water generally only several days; however, somespecies such as E coli O157: H7 can survive 12 weeks at25�C.21 Most enteric organisms, including Shigella spp,Salmonella enterica serotype Typhi, hepatitis A, and Cryp-tosporidium spp, can retain viability for long periods in coldwater and can even survive for weeks when frozen in water.
The risk of waterborne illness depends on the number oforganisms consumed, which is in turn determined by thevolume of water, concentration of organisms, and treatmentsystem efficiency.22,23 Additional factors include virulenceof the organism and defenses of the host. Microorganismswith a small infectious dose (eg,Giardia, Cryptosporidium,Shigella spp, hepatitis A, enterohemorrhagic E coli, and
Backer et al2

norovirusdthe leading viral disease risk in water contami-nated with human waste) may cause illness even from inad-vertent drinking during water-based recreationalactivities.10 Most diarrhea among travelers is probablyfoodborne; however, the capacity for waterborne transmis-sion should not be underestimated. Because long-lastingimmunity does not develop for most enteric pathogens,reinfection may occur.
The combined roles of safe water, hygiene, and adequatesanitation in reducing diarrhea and other diseases are clearand well documented. The World Health Organization(WHO) estimates that 94% of diarrheal cases globally arepreventable through modifications to the environment,including access to safe water.1 Recent studies of simplewater interventions in households of developing countriesclearly document improved microbiological quality ofwater, a 30 to 60% reduced incidence of diarrheal illness,enhanced childhood survival, and reduction of parasitic dis-eases, many of which are independent of other measures toimprove sanitation.24
General recommendations for drinking waterdisinfection:
� Treat water when traveling in developing countries.Evidence grade: 1A
� Treat water in wilderness areas with nearby agriculturaluse, animal grazing, or upstream human activity.Evidence grade: 1A
� Treat water in wilderness settings without evidence ofdomestic animal and little to no wildlife or human activ-ity. Evidence grade: 2B
� Treat water in disaster situations affecting municipal orprivate drinking water sources. Evidence grade: 1A
Water Treatment Methods
Multiple techniques for improving the microbiologic qual-ity of water are available to individuals and small groupswhile hiking or traveling. Bottled water may be a conveni-ent and popular solution but creates ecologic problems.Furthermore, in underdeveloped countries, the quality ofbottled water may not meet the standards of developedcountries and may contain pathogenic microbes.25
The term disinfection, the desired result of field watertreatment, is used here to indicate the removal or destruc-tion of harmful microorganisms, which reduces the risk ofillness. This is sometimes used interchangeably with purifi-cation, but the latter term more accurately indicates theremoval of organic or inorganic chemicals and particulatematter to improve color, taste, and odor. Unless specificallydesigned to remove chemical contaminants, disinfectiontechniques may not make water safe from chemical expo-sures. Potable implies drinkable water, but it technically
means that a water source, on average, over a period oftime, contains a minimal microbial hazard so that the statis-tical likelihood of illness is acceptably low. All standards,including water regulations in the United States, acknowl-edge the impracticality of trying to eliminate all microor-ganisms from drinking water. Generally, the goal is a 3 to5 log reduction (99.9e99.999%), allowing a small risk ofenteric infection. Newer standards from the US Environ-mental Protection Agency (US EPA) and the WHO set tar-get goals to reduce some organisms to zero; however, allenforceable standards allow a small risk for entericinfection.26
Product Testing and Rating
Filters are rated by their ability to retain particles of a certainsize, which is described by 2 terms. Absolute rating meansthat 100% of a certain size of particle is retained by the filter(ie, filtered-out). Nominal rating indicates that >90% of agiven particle size will be retained. Filter efficiency is gen-erally determined with hard particles (beads of known dia-meter), but microorganisms are soft and compressibleunder pressure. The US EPA and NSF International arethe primary agencies that set standards for disinfection pro-ducts and protocols for testing to meet these standards.
The US EPA does not endorse, test, or approve mechan-ical filters; it merely assigns registration numbers that dis-tinguish between 2 types of filters: those that usemechanical means only and those that use a chemical desig-nated as a pesticide. Portable water treatment device claimsfor microbiologic reduction are based on consensus perfor-mance standards that serve as a guideline for testing.27
Testing is done or contracted by the manufacturer; the USEPA neither tests nor specifies laboratories. Testing mustbe done with bacteria (Klebsiella), viruses (poliovirus androtavirus), and protozoa (Cryptosporidium has replacedGiardia). A 3-log reduction (99.9%) is required for proto-zoan cysts, 4-log reduction (99.99%) for viruses, and 5- to6-log reduction for bacteria. To be called a microbiologicwater purifier, the unit must remove, kill, or inactivate alltypes of disease-causing microorganisms from the water,including bacteria, viruses, and protozoan cysts, so as torender the processed water safe for drinking. An exceptionfor limited claims may be allowed for units removing speci-fic organisms to serve a definable environmental need, forexample, removal of protozoan cysts.27
Clarification Techniques
Clarification refers to techniques that reduce the turbidity orcloudiness of water caused by natural organic and inorganicmaterial. (Turbidity is measured in nephelometric turbidityunits [NTU].) These techniques can markedly improve the
Water Treatment Clinical Practice Guidelines 3

appearance and taste of water. Theymay reduce the numberof microorganisms, but not enough to ensure potable water;however, clarifying the water facilitates disinfection by fil-tration or chemical treatment. Cloudy water can rapidlyclog filters designed to remove microorganisms. Moreover,cloudy water requires increased levels of chemical treat-ment, and the combined effects of the water contaminantsplus chemical disinfectants results in unpleasant taste.
Adsorption
Granular activated carbon (GAC) is widely used in watertreatment. When activated, charcoal’s regular array of car-bon bonds is disrupted, making it highly reactive foradsorbing dissolved chemicals.28,29 GAC is the bestmeans to remove toxic organic and inorganic chemicalsfrom water (including disinfection byproducts) and toimprove odor and taste.30,31 Thus, it is widely used inmuni-cipal disinfection plants, in household under-sink devices,and in portable water filters. In field water treatment,GAC is best used after chemical disinfection to makewater safer and more palatable by removing disinfectionbyproducts and pesticides, as well as many other organicchemicals and some heavy metals. It removes the taste ofchemical disinfectants such as iodine and chlorine.
GAC does not kill microorganisms and is not designedfor microbial removal; in fact, bacteria attach to charcoal,where they are resistant to chlorination because the chlorineis adsorbed by the GAC.30e32
Sedimentation
Sedimentation is the separation of suspended particles suchas sand and silt that are large enough to settle rapidly bygravity. Most microorganisms, especially protozoan cysts,also settle eventually, but this takes much longer.33 Simplyallowing the water to sit undisturbed for about 1 h or untilsediment has formed on the bottom of the container andthen decanting or filtering the clear water from the topthrough a coffee filter or finely woven cloth will removemany larger particles from the water. A second method ofdisinfection must then be used to obtain potable water.
Coagulationeflocculation
Coagulationeflocculation (C-F) is a technique that hasbeen in use since 2000 BC and remains a routine step inmunicipal water treatment.34,35 C-F can remove smallersuspended particles and chemical complexes too small tosettle by gravity (colloids). Coagulation is achieved withthe addition of a chemical that causes particles to sticktogether by electrostatic and ionic forces. Flocculation is aphysical process that promotes the formation of larger par-ticles by gentle mixing. Alum (an aluminum salt), lime
(alkaline chemicals principally containing calcium or mag-nesium with oxygen), or iron salts are commonly used coa-gulants. Alum is nontoxic and used in the food industry forpickling. It is readily available in most chemical supplystores and some grocery stores. C-F removes 60 to 98%of microorganisms, heavy metals, and some chemicalsand minerals.36,37 The tendency of microorganisms toclump with small particles or clump together to form largeraggregates enhances their removal by C-F. C-F also has thebenefit of reducing the amount of chemical disinfectantneeded because turbidity increases demand for disinfectantssuch as hypochlorite.37e39
The amount of alum added in the field, approximately 1large pinch (1 mL or 1/8 tsp) per 4 L (approximately 1 gal)of water, need not be precise. Stir or shake briskly for 1 minto mix, and then agitate gently and frequently for at least 5min to assist flocculation. If the water is still cloudy, addmore flocculent and repeat mixing. After at least 30 minfor settling, pour the water through a fine-woven cloth orpaper filter. Although most microorganisms are removedwith the floc, a final process of microbiologic filtration orchemical disinfection (below) should be completed toensure disinfection. Several products combine C-F withhalogen disinfection, which allows a single-stepprocess.40e43
Improvisational techniques for clarification
Many inorganic and organic compounds can be used as acoagulant, including lime (calcium oxide) or potash (fromwood ash).44 In an emergency, bleaching powder, bakingpowder, or even the fine white ash from a campfire can beused.45 Other C-F agents used traditionally by native peo-ples include seed extracts from the nirmali plant in southernIndia, moringa plants in Sudan, crushed almonds, dried andcrushed beans, and rauwaq (a form of bentonite clay).46
Adsorbents such as charcoal, clay, and other types oforganic matter have been used for water treatment sincebiblical times.32 These substances are used as the filtermedia and also can act as coagulants.47 Clays can decreaseturbidity and microbes in water by about 90% to 95%, butadsorption is not the main action of ceramic or clay filters.
Assessment of supporting evidence:
� Clarification reduces cloudiness, particulate matter, andwaterborne microorganisms; improves the taste andesthetics of water; and improves the effectiveness of che-mical disinfectants, filtration, and ultraviolet disinfection.However, it does not reliably disinfect if used alone.Evidence grade: 1A
� GAC is highly effective at removing taste and odorcompounds but is not adequate for microbial removal.Evidence grade: 1A
Backer et al4

� Sedimentation is effective for removing large particlessuch as sand and dirt but will not remove suspended ordissolved substances (see C-F). Evidence grade: 2B
� C-F removes most microorganisms, but it does not reli-ably disinfect if used alone. Evidence grade: 1A
� Traditional or improvisational C-F techniques (otherthan alum or those used in municipal disinfectionplants) have empiric evidence but do not have robustscientific evidence or practical use guidance andshould be used with caution to protect the health ofconsumers. Evidence grade: 2C
Disinfection Methods
HEATHeat is the oldest and most reliable means of water disinfec-tion. Heat inactivation of microorganisms is a function oftime and temperature (exponential function of first-orderkinetics). Thus, the thermal death point is reached in ashorter time at higher temperatures, whereas lower tem-peratures are effective if applied for a longer time. Pasteur-ization uses this principle to kill food pathogens andspoiling organisms at temperatures well below boiling, gen-erally between 60�C (140�F) and 70�C (158�F). Flash pas-teurization occurs within 30 s at 70 to 72�C(158e162�F).48,49
All common enteric pathogens are readily inactivated byheat at pasteurization temperatures, although microorgan-isms vary in heat sensitivity, with protozoan cysts beingthe most sensitive to heat, bacteria intermediate, and virusesless sensitive (Table 150e62).50,51 Only bacterial spores aremore resistant, but they are not generally entericpathogens.52
As enteric pathogens are killed within seconds by boil-ing water rapidly at temperatures>60�C (140�F), the tradi-tional advice to boil water for 10 min to ensure potablewater is excessive. The time required to heat water from55�C (131�F) to a boil works toward disinfection; therefore,any water brought to a rapid boil should be adequatelydisinfected.63 Boiling for 1 min is recommended by theUS CDC to account for user variability in identifying boil-ing points and adds a margin of safety. The boiling pointdecreases with increasing altitude, but this is not significantcompared with the time required for thermal death at thesetemperatures (Table 2).
Improvisational techniques
In wilderness or travel environments, the main limita-tion for using heat is availability of fuel. Althoughattaining boiling temperature is not necessary to killmicroorganisms, boiling is the only easily recognizableendpoint without use of a thermometer. Based on
microbiologic testing, hot tap water has been proposedas a means of heat disinfection.64,65
Most water from hot water taps measured in countriesoutside the United States measured 55 to 60�C (131 to140�F).51 As a rule of thumb, water too hot to touch fellwithin the pasteurization range, but tolerance to touch istoo variable to be reliable.66
If no reliable method of water treatment is available, tapwater that has been kept hot in a tank for at least 30 min andis too hot to keep a finger immersed for 5 s (estimated 55 to65�C; 131 to 149�F) is a reasonable alternative. However,this improvisational measure is less useful for hotels thatuse on-demand water heaters without a hot water tank. Tra-velers with access to electricity can boil water with either a
Table 2. Boiling temperatures at various altitudes
Altitude (ft) Altitude (m) Boiling point
5000 1524 95�C (203�F)10,000 3048 90�C (194�F)14,000 4267 86�C (187�F)19,000 5791 81�C (178�F)
Table 1. Heat inactivation of microorganisms
Organism Lethaltemperature/Time
Reference
Protozoan cysts,including Giardia,Entamoebahistolytica
50�C (122�F) for 10min55�C (131�F) for 5 min100�C (212�F)immediately
53e55
Cryptosporidiumoocysts
55�C (131�F) warmedover 20 min64�C (148�F) within2 min
50,56
Parasitic eggs, larvae,and cercariae
50�Ce55�C(122e131�F)
57
Common bacterialenteric pathogens (Ecoli, Salmonella,Campylobacter,Shigella)
55�C (131�F) for30 min or 65�C (149�F)for less than 1 min(standard pasteurizationtemperatures)
48,51
Viruses 56�Ce60�C(133e140�F) in lessthan 20e40 min
52,58,59
Hepatitis A virus 98�C (208�F) for 1 min75�C (167�F) for lessthan 0.5 min85�C (185�F) for 1 minor less (in various foodproducts)
60e62
Water Treatment Clinical Practice Guidelines 5

small electric heating coil or a lightweight electric beveragewarmer brought from home. In austere and desperate situa-tions with hot, sunny climate, pasteurization temperaturecan be achieved with a solar oven or simple reflectors67,68
(see the Solar UV Disinfection [UVeSODIS] section).Assessment of supporting evidence:
� Bringing water to boil (100�C/212�F) will kill pathogenicmicroorganisms. Evidence grade: 1A
� Bringing water at 5000 m (16,000 ft) elevation toboil (83�C/181�F) will kill pathogenic organisms.Evidence grade: 1B
� Tap water that has been tanked for 30 min or longer and istoo hot to touch (60�C) has a significantly reduced num-ber of pathogenic microorganisms, but this cannot berelied on as the sole means of disinfection. Such watermay contain increased amounts of lead or other chemicalsfrom the water heater and piping. Evidence grade: 2B
� Pasteurization temperatures can be achieved with a solaroven. Evidence grade: 2B
ULTRAVIOLET LIGHTUltraviolet (UV) radiation and UV lamp disinfection sys-tems are widely used to disinfect drinking water at the com-munity and household levels. At sufficient doses, allwaterborne enteric pathogens are inactivated by UV radia-tion (UVR). UVC light in the range of 200 to 280 nm isthe most effective. The germicidal effect of UV light isthe result of action on the nucleic acids of microorganismsand depends on light intensity and exposure time. In suffi-cient doses of energy, all waterborne enteric pathogensare inactivated by UVR.69 The UV waves must strike theorganism, so the water must be free of particles that couldact as a shield.70 The UV waves do not alter the water,but they also do not provide any residual disinfectingpower.71 Bacteria and protozoan parasites generally requirelower doses than do enteric viruses and bacterial spores.However, all viruses, including hepatitis A and norovirus,are susceptible, with relatively minor differences, and fol-low similar kinetics. The vegetative cells of bacteria are sig-nificantly more susceptible to UVR than are bacterialspores or viruses.Giardia andCryptosporidium are suscep-tible to practical doses of UVR and may be more sensitivebecause of their relatively large size.72e74 Both largehigh-volume units and portable, lightweight battery-oper-ated units are available for disinfection of small quantitiesof water.
Improvisational technique: UV-SODIS
UV irradiation by sunlight can substantially improve themicrobiologic quality of water and reduce diarrheal illnessin developing countries.75e85 The optimal procedure forthe SODIS technique is to use transparent bottles (eg,
clear plastic beverage bottles), preferably lying on a darksurface and exposed to sunlight for a minimum of 4 hwith intermittent agitation.86 UV and thermal inactivationare strongly synergistic for the solar disinfection of drinkingwater.67,87,88
Assessment of supporting evidence:
� UV light is an effective means of water disinfection.Evidence grade: 1A
� Full sunlight exposure of clear water in a clear plasticbottle for at least 4 h significantly reduces andpossibly eliminates microorganism contamination(Evidence grade: 1B); however, studies evaluatingthis technique for reduction of childhood diarrheashow mixed results. Evidence grade: 2B
FILTRATIONFilters are appealing because of their simplicity and suit-ability for commercial production. Portable water treatmentproducts are the third highest intended purchase of outdoorequipment, after backpacks and tents.89 Filtration is a stan-dard step in municipal water treatment and widely used inthe food and beverage industry and in many other industrialprocesses. Many different types of media, from sand tovegetable products to fabric have been used for water filtra-tion throughout history in various parts of the world.90 Fil-ters have the advantages of being simple and requiring noholding time. They do not add any unpleasant taste andmay improve taste and appearance of water. All filters even-tually clog from suspended particulate matter (present evenin clear streams), requiring cleaning or replacement of thefilter. As a filter clogs, it requires increasing pressure todrive the water through it, which can force microorganismsthrough the filter or damage the filter. A crack or erodedchannel in a filter will allow passage of unfiltered water.Bacteria can grow on filter media and potentially result insome bacteria in filtered water, but pathogenic bacteriaand illness have not been demonstrated.91 Silver is oftenincorporated into the filter media to prevent this growth,but it is not totally effective.
The primary determinant of a microorganism’s suscept-ibility to filtration is its size (Table 3; Figure 1). Portable fil-ters for water treatment can be divided into microfilters withpore sizes down to 0.1 mm, ultrafilters that can remove par-ticles as small as 0.01 mm, nanofilters with pore sizes assmall as 0.001 mm or less, and reverse osmosis filters withpore sizes of 0.0001 mm or less.69 All filters require pres-sure to drive the water through the filter element. The smal-ler the pore size, the more pressure required. Waterbornepathogens often adhere to larger particles or clumptogether, making them easier to remove by physical pro-cesses. Therefore, observed reductions are often greaterthan expected based on their individual sizes.
Backer et al6

Most portable filters are microfilters that can readilyremove protozoan cysts and bacteria but may not removeall viruses, which are much smaller than the pore size ofmost field filters.92,93 Viruses often clump together and toother larger particles or organisms, resulting in an aggregate
large enough to be trapped by the filter; in addition, electro-chemical attraction may cause viruses to adhere to the filtersurface.47,94,95 Through these mechanisms, mechanical fil-ters using ceramic elements with a pore size of 0.2 mm canreduce viral loads by 2 to 3 logs (99e99.9%), but they arenot adequate for complete removal of viruses.96 Ultrafiltra-tion membranes are required for complete microbialremoval, including viruses; they can also remove colloidsand some dissolved solids.97
Recently, hollow-fiber technology has been adapted forfield use; this technology uses bundles of tube fiberswhose pore size can be engineered to achieve ultrafiltrationwith viral removal.98 The large surface area allows thesehollow-fiber filters to have relatively high flow rates atlow pressure. Small group and individual gravity or handpump filters are available through several vendors.
Some filters on the market combine the porous filtermaterial with other substances to help the disinfectionprocess. This may include activated charcoal, iodine,silver, and other substances. Iodine molecules can bebound in a resin engineered into field products, but theeffectiveness of the resin is highly dependent on theproduct design and function. Most companies haveabandoned iodine resinecontaining portable hand-pump filters due to excess iodine or viral breakthroughin the effluent. Only one drink-through bottle remainson the US market, but other products may still be avail-able outside the United States. (GAC was discussed ear-lier, and silver is addressed later.)
Several factors influence the decision of which filter tobuy: 1) flow volume sufficient for the number of personsrelying on the filter; 2) whether the filter functional claims
Table 3. Microorganism susceptibility to filtration
Organism Approximatesize (mm)
Recommended filterrating (mm)
Virusesa 0.03 Ultrafilter, nanofilter,reverse osmosis
Escherichia coli 0.5 by 3e8 0.2e0.4 (microfilter)Campylobacter 0.2e0.4 by
1.5e3.5V cholerae 0.5 by
1.5e3.0Cryptosporidiumoocyst
2e6 1 (microfilter)
Giardia cyst 6e10 by8e15
3e5 (microfilter)
Entamoebahistolytica cyst
5e30(average 10)
Nematode eggs 30e40 by50e80
20 (microfilter)
Schistosomecercariae
50 by 100 Coffee filter or fine cloth,or double thicknessclosely woven clothDracunculus
larvae20 by 500
a Microfilters (includes most filters with pore size of 0.1e0.2 mm) canfilter bacteria and protozoan cysts, but are not effective for virus removalunless designed to rely on electrostatic trapping of viruses. Hollow fiber fil-ters with 0.02 mm pores and reverse osmosis filters are capable of filteringviruses.
Figure 1. Levels of filtration and susceptibility of common microbial pathogens and other contaminants. Adapted from Backer H. Waterdisinfection for international travelers. In: Keystone JS, Kozarsky PE, Connor BA, eds. Travel Medicine. 4th ed. Philadelphia, PA: Elsevier;2019:31e41. Copyright 2019, reprinted with permission from Elsevier.
Water Treatment Clinical Practice Guidelines 7

matches the microbiologic demands that will be put on thefilter; 3) the preferred means of operation (eg, hand pump orgravity); and 4) cost.
Improvisational filtration techniques
Filtration using simple, available products, such as rice hullash filters, crushed charcoal, sponges, and various fabricsand paper, have all been used in developing countries andin emergency situations. Typically, bacteria and virusescan be reduced by as much as 50 to 85% and larger para-sites by 99%, depending on the media. The effectivenessfor decreasing turbidity may be used as an indicator that afilter material will reduce microbiologic contamination.38,99,100
Ceramic filters are a common component in portablewater pump filters, but they are also a cost-effectivemeans of household disinfection in developing countries.Ceramic clay is widely available and very inexpensive tolocally manufacture in the shape of a sink or flower potthat is set into a larger container that collects the filteredwater.101e107
Biosand filters use a technology that has been usedover centuries and is still used widely in municipalplants and at the household and community level.-108e111 Sand filters can be highly effective at removingturbidity (in 1 study, from 6.2 NTU to 0.9 NTU) andimproving microbiologic quality (99% efficacy),depending on their design and operation.112,113 Sandfilters are constructed by forming layers of aggregateincreasing in size from the top to the bottom. The toplayer is very fine sand and the bottom layer consists oflarge gravel. The container needs an exit port on the bot-tom. The top layer forms a biolayer that is important forthe function of the filter. The optimum depth of a com-munity or household sand filter is 2 m, with diameterdetermined by the volume of water needed. An emer-gency sand filter can be made in a 20 L (5.3 gal) bucket,composed of a 10 cm (3.9 in) layer of gravel beneath a23 cm (9.1 in) layer of sand; a layer of cotton cloth,sandwiched between 2 layers of wire mesh, separatesthe sand and gravel layers.38 A sand filter also can beimprovised with stacked buckets of successive filterlayers with holes in the bottom to allow water passage.Many websites provide design and assembly instruc-tions, but there are no data for comparative function.
Assessments of supporting evidence:
� Filtration is effective as a primary or adjunctive means ofwater treatment. Evidence grade: 1A
� Standard commercially available microfilters with a poresize of 0.2 microns are effective in removing protozoaand bacteria. Evidence grade: 1A
� Ultrafiltration with pore size of less than 0.01 isneeded to completely remove pathogenic viruses.Evidence grade: 1A
� Filters may clog, so users should know how to clean themor consider carrying a backup method of disinfection.Evidence grade: 1C
� Biosand filters are a reasonable improvised technique forfiltration. Evidence grade: 1B
CHEMICAL DISINFECTION: HALOGENS (IODINEAND CHLORINE)Worldwide, disinfection with chemicals, chiefly chlor-ine, is the most commonly used method for improvingand maintaining the microbiologic quality of drinkingwater and can be used by individuals and groups in thefield.114 The germicidal activity of chlorine and otherhalogens is well established and results from oxidationof essential cellular structures and enzymes.115,116 Dis-infection effectiveness is determined by characteristicsof the microorganism, the disinfectant, contact time,and environmental factors. Both chlorine and iodineare widely available worldwide in multiple formula-tions. The most commonly available form of chlorineis hypochlorite (household bleach [5e8%] or concen-trated swimming pool granules or tablets [70%]).
Both chlorine and iodine have been used for water disin-fection for more than a century. Hypochlorite, the majorchlorine disinfectant, is currently the preferred means ofmunicipal water disinfection worldwide. Both calciumhypochlorite (Ca[OCl]2) and sodium hypochlorite(NaOCl) readily dissociate in water to form hypochlorite,the active disinfectant.
Iodine is also effective in low concentrations for killingbacteria, viruses, and some protozoan cysts; in higher con-centrations, it is effective against fungi and even bacterialspores. However, it is a poor algaecide. Elemental iodine(I2) and hypoiodous acid (HOI) are the major germicidesin an aqueous solution. Iodine is the only halogen that is asolid at room temperature.
Given adequate concentrations and contact times, bothiodine and chlorine are effective disinfectants with similarbiocidal activity under most conditions.117 Taste preferenceis individual. Of the halogens, iodine reacts least readilywith organic compounds and is less affected by pH, indicat-ing that low iodine residuals should be more stable and per-sistent than corresponding concentrations of chlorine.Despite these advantages, because of its physiologic activ-ity, WHO recommends iodine only for short-term emer-gency use.
Chlorine is still advocated by the WHO and the CDC asa mainstay of large-scale community, individual household,and emergency use.118,119 There are extensive data oneffectiveness of hypochlorite in remote settings.69,120e122
Backer et al8

The CDC/WHO safe water system for household disinfec-tion in developing countries provides a dosage of 1.875 or3.75 mg$L-1 of sodium hypochlorite with a contact timeof 30 min, which is sufficient to inactivate most bacteria,viruses, and some protozoa that cause waterborne diseases.-123 Another advantage of hypochlorite is the ease of adjust-ing the dose for large volumes of water.45,99
Vegetative bacteria (nonspore forming) are very sensitiveto halogens.116,124 Viruses, including hepatitis A, have inter-mediate sensitivity, requiring higher concentrations or longercontact times.125e130 Protozoan cysts are more resistant thanenteric bacteria and enteric viruses but some cysts (eg,Giar-dia) can be inactivated by field doses of halogens.131e135
Cryptosporidium oocysts, however, are much more resistantto halogens, and inactivation is not practical with commondoses of iodine and chlorine used in field water disinfection.-136,137 Little is known aboutCyclospora, but it is assumed tobe similar to Cryptosporidium. Certain parasitic eggs, suchas those of Ascaris, are also resistant, but these are not com-monly spread by water. (All of these resistant cysts and eggs
are susceptible to heat or filtration.) Bacterial spores, such asBacillus anthracis, are relatively resistant to halogens. Withchlorine, however, spores are not much more resistant thanare Giardia cysts; furthermore, they do not normally causewaterborne enteric disease. Relative susceptibility betweenorganisms is similar for iodine and chlorine (Table 4).
Understanding factors that influence the disinfectionreaction allows flexibility with greater reassurance. The pri-mary factors of the first-order chemical disinfection reac-tion are concentration and contact time.133 To achievemicrobial inactivation in aqueous solution with a chemicalagent, a residual concentration must be present for a speci-fied contact time. Lower concentrations can be used withlonger contact times. In field disinfection, this can be usedto minimize halogen dose and improve taste or, conversely,to minimize the required contact time.
Cold water slows chemical reactions; the reaction ratecan be adjusted by longer contact times or higher concentra-tion of disinfectant chemical. Another important factor inchemical disinfection is the presence of organic and
Table 4. Disinfection data for chlorine and iodine to achieve 99.9% kill or inactivationa of select microorganisms
Organism Concentration(mg$L-1)
Time(min)
pH Temp Disinfectionconstant(Ct)a
Reference
ChlorineEscherichia coli 0.1 0.16 6.0 5�C (41�F) 0.016 116
Campylobacter 0.3 0.5 6.0e8.0 25�C (77�F) 0.15 124
20 enteric virus 0.5 60 7.8 2�C (36�F) 30 138
6 enteric viruses 0.5 4.5 6.0e8.0 5�C (41�F) 2.5 125
Norovirus 15
1020sec
6.0 5�C 101.66
126
Hepatitis A virus 0.5 1 6.0 25�C (77�F) 0.5 127
Amebic cysts 3.5 10 25�C (77�F) 35 139
Giardia cysts 2.5 60 6.0e8.0 5�C (41�F) 150 140
Giardia lambliacysts
0.85 90 8.0 2e3�C(36e37�F)
77 135
Giardia muriscysts
3.05 50 7.0 5�C (41�F) 153 134
Cryptosporidium(2 strains)
2020
755501
7.57.5
23�C23�C
15,30010,400
141
IodineEscherichia coli 1.3 1 6.0e7.0 2e5�C
(36e41�F)1.3 31
Hepatitis Az 8 .4 7.0 25�C 3 142
Coxsackie virus 0.5 30 7.0 5�C (41�F) 15 143
Amebic cysts 3.5 10 25�C (77�F) 35 139
Giardia cysts 4 15 5.0 30�C (86�F) 60b 131
Giardia cysts 4 45 5.0 15�C (59�F) 170b 131
Giardia cysts 4 120 5.0 5�C (41�F) 480b 131
a 99.9% is for comparison of disinfection potency and microorganism susceptibility. The standard for potable water is 99.99% kill for viruses and99.999% for bacteria. This would be achieved in each example with a higher concentration of disinfectant or a longer contact time.b 100% kill; viability tested only at 15, 30, 45, 60, and 120 min.
Water Treatment Clinical Practice Guidelines 9

inorganic contaminants, mainly nitrogen compounds fromdecomposition of organisms and their wastes, fecal matter,and urea. These contaminants react, especially with chlor-ine, to form compounds with little or no disinfecting ability,effectively decreasing the concentration of availablehalogen.26,115 Halogen demand is the amount of halogenreacting with impurities. Residual concentration is theamount of active disinfectant remaining after demand ofthe water is met. Halogen demand is associated with turbid-ity (cloudiness).39 Typical recommendations for field treat-ment double the amount of chlorine or iodine in cloudywater; however, it is preferable to use clarification
techniques prior to chemical disinfection in cloudy waterto improve efficacy and taste.144,145
Because of the difficulty of estimating halogen demand, itis prudent to use 3 to 4 mg$L-1 as a target halogen concentra-tion range for clear surface water. Lower concentrations (eg,2 mg$L-1) can be used for back-up treatment of questionabletap water or high-quality well water (Tables 5 and 6).
Halogen toxicity
Chlorine has no known toxicity at the concentrations usedfor water disinfection. Sodium hypochlorite is not
Table 5. Halogen disinfection products and recommended doses
Add to 1 L or qt of water
Iodination techniquesa Amount to achieve 4 mg$L-1 Amount to achieve 8 mg$L-1
Iodine tabsb 0.5 tab (or 1 tab in 2 L) 1 tabTetraglycine hydroperiodideEmergency drinking water germicidal tabletPotable aquaGlobaline
2% iodine solution (tincture) 0.2 mL 0.4 mL5 dropsc 10 drops
10% povidone-iodine solutiond 0.35 mL 0.70 mL8 drops 16 drops
Saturated solution: iodine crystals in watere 13 mL 26 mLChlorination techniquesf Amount to achieve 2 mg$L-1 Amount to achieve 5
mg∙L-1
Sodium hypochlorite (household bleach 5%) 1 drop 0.1 mL2 drops
Sodium hypochlorite (household bleach 8.25%) 1 drop (in 2 L) 1 drop1% bleach (CDC-WHO Safe Water System)g 4e5 drops 8e10 dropsCalcium hypochloriteh (Redi Chlor [0.1-g tab]) Cannot use in small quantities for low
concentrations0.25 tab
Sodium dichloroisocyanurate (NaDCC)i
(Aquatab, Kintab)0.25 tab of 8.5 mg NaDCC (may beimpractical)
0.5 tab (8.5 mg NaDCC)
Chlorine plus flocculating agent (Chlor-Floc) Not practical for small volumes 0.5 tablet per gal yields 5mg∙L-1
a World Health Organization recommends only for short-term emergency use.b Iodine tablets were developed by themilitary with the criteria that theywill disinfect water, including forGiardia, with a short contact (holding) time of
10 min because troops in the field may not wait longer. This high concentration is not necessary for field disinfection of clear water; it is preferable to target4 mg∙L-1 andwait longer. Additionally, the recommendation to use 8mg∙L-1 for cloudy water will result in poor taste, so it is recommended to clarify thewater first.c Measure of a drop varies from 16e24 gtt$mL-1, standard 20 gtt$mL-1 is used here.d Povidone-iodine solutions release free iodine in levels adequate for disinfection, but scant data are available (see text).e A small amount of elemental iodine goes into solution (no significant iodide is present); the saturated solution is used to disinfect drinkingwater. Water
can be added to the crystals hundreds of times before they are completely dissolved.f Can easily be adapted to large or small quantities of water. Simple field test kits or swimming pool test kits with color strips are widely available to
ensure adequate residual chlorine. In usual situations, EPA recommends a target residual of 4 mg$L-1. For household use, the CDC recommends <2 mg∙L-1. Many of the recommended emergency doses exceed this threshold.97 For treatment of large volumes, see formula to calculate in Lantagne (2008).20g Safe water system for long-term routine household point-of-use water disinfection recommends a hypochlorite dose of about 2 mg∙L-1 in clear water
and 4 mg∙L-1 in slightly turbid water. This results in a low yet effective target residual concentration but requires testing in a particular water source toensure sufficient residual.h Stable, concentrated (70%), dry source of hypochlorite that is used for chlorination of swimming pools. Multiple products available in various size
tablets or granular form. Best formulation for large quantities of water.i Available in different strengths to treat different volumes of water. Check packaging to determine proper dose.
Backer et al10

carcinogenic; however, reactions of chlorine with certainorganic contaminants yield chlorinated hydrocarbons,chloroform, and other trihalomethanes, which are consid-ered to have carcinogenic potential in animal models.Nevertheless, the risk of severe illness or even death frominfectious diseases if disinfection is not used far exceedsany risk from byproducts of chlorine disinfection.146
Despite several advantages over chlorine disinfection,iodine has not gained general acceptance because of concernfor its physiologic activity. Some older data indicate thatiodination of water with a low residual concentration of �1to 2 mg$L-1 appears safe, even for long periods of time, inpeople with normal thyroid function.147,148 This is not thecurrent recommendation of major agencies. Recently, theEuropean Union stopped the sale of iodine products usedfor water disinfection. The WHO did not set a guidelinevalue for iodine in drinking water because of a paucity ofdata and because it is not recommended for long-term disin-fection. If the typical wilderness or international traveler dis-infected 3 L of water a day using 2 to 4 mg$L-1 of iodine, theingested amount of iodine would be 6 to 12 mg∙d-1, wellabove US Institute of Medicine recommended dietary allow-ance levels. Levels produced by the recommended doses ofiodine tablets are even higher (16e32 mg∙d-1). Therefore,the use of iodine for water disinfection should be limited toshort periods of �1 mo. Individuals planning to use iodinefor prolonged periods should have their thyroid examinedand thyroid function tests done to ensure they are initiallyeuthyroid. Certain groups should not use iodine for watertreatment: pregnant women (because of concerns of neonatalgoiter); those with known hypersensitivity to iodine; personswith a history of thyroid disease, even if controlled on med-ication; persons with a strong family history of thyroid dis-ease (thyroiditis); and persons from countries with chroniciodine deficiency.149
Improving halogen taste
Objectionable taste and smell limit the acceptance of halo-gens, but taste can be improved by several means. Onemethod is to use the minimum necessary dose with a longercontact time, as in the CDC safe water system. Another
method is to use higher doses and remove the taste throughchemical reduction of chlorine to chloride and iodine toiodide; these have no color or taste. The best andmost readilyavailable agent is ascorbic acid (vitamin C), available in crys-talline or powder form. A small pinch in a liter, mixed afterthe required contact time, will usually suffice. Ascorbicacid is a common ingredient of flavored drink mixes,accounting for their effectiveness in removing the taste ofhalogens. GAC (see above) adsorbs organic and inorganicchemicals, including iodine and chlorine byproducts, therebyimproving odor and tastedthe reason for its common inclu-sion in field filters.
Improvisational techniques
There is no comparable substitute for proven chemical disin-fectants, but there are many common substances that containhalogens. Household bleach is available in most parts of theworld. The active disinfectant is sodium hypochlorite. Pro-ducts for disinfection of swimming pools and spas generallycontain calcium hypochlorite that provides much higher con-centrations than bleach. Hypochlorite is readily releasedfrom different products formulated in liquid, powder, gran-ules, and tablets. Iodine is also available in liquid or tablets;a common household source is tincture of iodine or similartopical disinfectants with an iodine concentration of 2 to8%. These products also contain iodide, which has no disin-fecting power but does contribute to iodine toxicity. Color-less iodine solution contains only iodide and should not beused. Povidone-iodine, a topical disinfectant commonlyused in medical settings, contains active iodine bound to aneutral polymer of high molecular weight that gives theiodine greater solubility and stability. In dilute aqueous solu-tion, povidone-iodine provides a sustained-release reservoir,releasing free iodine in a concentration of 2 to 10 mg$L-1.150
MIXED SPECIES DISINFECTANT (ELECTROLYSIS)
Passing a current through a simple brine salt solution gener-ates free available chlorine and other mixed species disin-fectants that have been shown to be effective againstbacteria, viruses, Cryptosporidium, and bacterialspores.151,152 The process is well described and can be
Table 6. Recommendations for contact time using halogen disinfection in the field
Concentration of halogen Contact time (min) at various water temperatures
5�C (41�F) 15�C (59�F) 30�C (86�F)
2 ppm 240 180 604 ppm 180 60 458 ppm 60 30 15
Concentration and contact time are based on the most resistant organism, which is theGiardia cyst. These are well beyond the time needed to kill bacteriaand viruses. These contact times have been extended from the usual recommendations in cold water to account for the extended inactivation time requiredin very cold water and for the uncertainty of residual concentration.
Water Treatment Clinical Practice Guidelines 11

used on both large and small scales. The main disinfectanteffect is probably attributable to a combination of chlorinedioxide, ozone, superoxides, and hypochlorous acid, givingthe resulting solution greater disinfectant ability than a sim-ple solution of sodium hypochlorite. Small units are nowavailable commercially that use salt, water, and a 12-voltdirect current (automobile) battery to create 60 mL of a0.75% chlorine solution over a 5-min operation cycle thatwill treat up to 200 L of water.
Other common substances, including hydrogen perox-ide and citrus juice that have some disinfectant activity,are discussed later.
Assessments of supporting evidence:
� Halogens chlorine and iodine are an effective means ofdisinfecting water of bacteria, viruses, and Giardia inthe field or household when using appropriate contacttime and halogen concentration. Evidence grade: 1A
� Usual field concentrations of iodine and chlorine are noteffective for other protozoa including Cryptosporidiumand Cyclospora. Evidence grade: 2A
� Extended use of iodine should be weighed against risks ofiodine toxicity. Evidence grade: 1B
� Simple techniques for improving taste of halogenatedwater are available for field use. Evidence grade: 1B
� Mixed species electrolytic disinfection techniques areeffective for water disinfection of microbes that are sus-ceptible to halogens. Evidence grade: 1B
MISCELLANEOUS DISINFECTANTS
Chlorine dioxide
Chlorine dioxide (ClO2), a potent biocide, has been used formany years to disinfect municipal water and in numerousother large-scale applications. Until recently, the benefitsof chlorine dioxide have been limited to large-scale applica-tions because standard formulations must be made on-siteand are associated with a risk for producing volatile gas.Newer methods enable cost-effective and portable ClO2
generation and distribution for use in an ever-wideningarray of small-scale applications. ClO2-production tabletscontain 6.4% sodium chlorite as the active ingredient.After a tablet is added to water, a series of complex chemi-cal reactions occurs, generating chlorine dioxide. Some ofthe intermediary chemical compounds may also have anti-microbial activity.
ClO2 has no taste or odor in water. It is capable of inac-tivating most waterborne pathogens, including Cryptospor-idium parvum oocysts.153e155 It is at least as effective abactericide as chlorine and far superior for virus and para-site inactivation. Several commercial point-of-use applica-tions use ClO2 in liquid or tablet form, but relatively few
data are available on product testing these products.137 Amajor disadvantage for field use of tablets is the long reac-tion or contact time required, with upward of 2 to 4 hneeded to achieve dependable disinfection. ClO2 does notproduce a lasting residual, and water undergoing chlorinedioxide disinfection must be protected from sunlight.
Assessment of supporting evidence:
� Chlorine dioxide is a widely used and potent water disin-fectant, including efficacy against the protozoan parasitesCryptosporidium. Evidence grade: 1A
� Individual use products have limited data demonstrat-ing effective concentration and contact time.Evidence grade: 2B
Silver
Silver ion has bactericidal effects in low doses and someattractive features, including absence of color, taste, andodor. Scant data for disinfection of viruses and proto-zoan cysts indicate limited effect, even at high doses.Moreover, the concentrations are strongly affected byadsorption onto the surface of any container. Silver isphysiologically active but not likely to cause a problemin concentrations found in drinking water. The EPA hasnot approved silver for primary water disinfection in theUnited States, but silver is approved as a water preser-vative to prevent bacterial growth in previously treatedand stored water. In Europe, silver tablets are sold forfield water disinfection. One rational combination pro-duct combines silver with hypochlorite for both disin-fection and preservation. There is some promise insteady release products and incorporation intonanoparticles.156
Assessment of supporting evidence:
� Use of silver in wilderness settings should be limitedto water preservation and not as a primary disinfectant.Evidence grade: 1B
Hydrogen peroxide
Hydrogen peroxide is a strong oxidizing agent that iswidely used as a preservative in food, as a sterilant for med-ical and food equipment, and in many other applications.Although hydrogen peroxide can sterilize water, it is notwidely used as a field water disinfectant, perhaps becausehigh concentrations known to be effective are very caustic,and there is a lack of data for protozoal cysts and quantita-tive data for dilute solutions. It can be used to remove thetaste of hypochlorite and in combination with otherprocesses.157
Assessment of supporting evidence:
� Hydrogen peroxide in typical concentration of 3% cannotbe used as a primary drinking water disinfectant, and
Backer et al12

effective concentrations are not practical for field use.Evidence grade: 1B
Citrus and potassium permanganate
Both citrus juice and potassium permanganate have somedemonstrated antibacterial effects in an aqueous solution.-158 However, data are few and not available for effect oncysts. In municipal water disinfection, potassium perman-ganate is used primarily for reducing contaminants toimprove taste and odor.159 Either substance could be usedin an emergency to reduce bacterial and viral contaminationor as an adjunct in combination with another technique, butthey cannot be recommended as a primary means of waterdisinfection.
Assessment of supporting evidence:
� Citrus juice and potassium permanganate have limitedapplications for drinking water disinfection.Evidence grade: 1C
Nanoparticles: solar photocatalytic disinfection
Several nanomaterials have been shown to have strong anti-microbial properties and are being evaluated for use inwater disinfection and purification.160,161 The metals areof particular interest for water disinfection applicationsbecause they can be activated byUV light to produce potentoxidizers that are excellent disinfectants for microorgan-isms and can break down complex organic contaminantsand even most heavy metals into nontoxic forms. Titanium
Table 7. Summary of field water disinfection techniques
Bacteria Viruses Giardia/Ameba Cryptosporidium Nematodes/Cercarea
Heat þ þ þ þ þFiltration þ þ/�a þ þ þHalogens þ þ þ � þ/�b
Chlorine dioxide and photocatalytic þ þ þ þ DNAb
DNA, data not available.a Most filters make no claims for viruses. Ultrafiltration with hollow fiber technology and reverse osmosis is effective.b Eggs are not very susceptible to halogens but have very low risk of waterborne transmission. No data available for photocatalytic disinfection.
Table 8. Efficacy and effectiveness of point-of-use technologies for developing world households
Treatment process Pathogen Optimal log reductiona Expected log reductionb Diarrheal disease reduction (%)c
Ceramic filters Bacteria 6 2 63 (51e72) for candle filters46 (29e59) for bowl filtersViruses 4 0.5
Protozoa 6 4Free chlorine Bacteria 6 3 37 (25e48)
Viruses 6 3Protozoa 5 3
Coagulation/Chlorination Bacteria 9 7 31 (18e42)Viruses 6 2e4.5Protozoa 5 3
Biosand filtration Bacteria 3 1 47 (21e64)Viruses 3 0.5Protozoa 4 2
SODIS Bacteria 5.5 3 31 (26e37)Viruses 4 2Protozoa 3 1
SODIS, solar disinfection.Data from multiple studies, analyzed and summarized by Sobsey et al (2008).165
Data also from references47,166e168 and Table 7.8 in WHO (2011).26a Skilled operators using optimal conditions and practices (efficacy); log reduction: pretreatment minus posttreatment concentration of organisms (eg, 6
log ¼ 99.999% removal).b Actual field practice by unskilled persons (effectiveness) depends on water quality, quality, and age of filter or materials, following proper procedure,
and other factors.c Summary estimates from published data vary with consistency and correct use of technique, integrity of techniques (eg, cracked filter), and other
household sanitation measures.
Water Treatment Clinical Practice Guidelines 13

dioxide (TiO2) is the most effective photocatalytic sub-stance identified to date. Recent work demonstrated inacti-vation of Cryptosporidium by titanium dioxide.161,162
These methods are widely used in industry, but few pro-ducts have incorporated the technology into individual orsmall group point of use products.163,164
Assessment of supporting evidence:
� New technology using nanoparticles and photocatalyticdisinfection is highly promising for translation intopoint-of-use water disinfection. Evidence grade: 2A
PREFERRED TECHNIQUE
The optimal water treatment technique for an individual orgroup will depend on the number of persons to be served,space and weight accommodations, quality of sourcewater, personal taste preferences, and fuel availability.Because halogens are not effective for killing Cryptospori-dium at drinking water concentrations and common micro-filters are not reliable for virus removal, optimal protectionfor all situations may require a 2-step process of 1) filtrationor C-F, followed by 2) halogenation. Heat (boiling) is effec-tive as a 1-step process in all situations but will not improvethe esthetics of the water. Table 7 summarizes effects ofmajor water disinfection methods on categories of microor-ganisms. Persons living or working in communities wheresanitation and water treatment are lacking are at higherrisk than the average international traveler. Sobsey et alreviewed data for point-of-use methods for household dis-infection in developing countries165 (Table 8).
In disaster situations such as floods, hurricanes, andearthquakes, sanitation and water treatment facilities arefrequently damaged or inundated, so household or point-of-usewater disinfection is advised. Chlorine is the simplestmethod, similar to household water disinfection wherethere is no sanitation or improved water sources.20,99,169
Cloudy water should first be clarified before usinghypochlorite.
On long-distance ocean-going boats where water mustbe desalinated as well as disinfected during the voyage,only reverse osmosis membrane filters are adequate.Water storage also requires consideration. Iodine willwork for short periods only (ie, weeks) because it is apoor algaecide. For prolonged storage, water should bechlorinated and kept in a tightly sealed container to reducethe risk of contamination. For daily use, narrow-mouthedjars or containers with water spigots prevent contaminationfrom repeated contact with hands or utensils.170
Relatively few studies compare multiple techniques ordevices.28,92,96,168,171e179 For more detailed discussion ofdisinfection techniques and available devices, see Backer.180
For reviews of water disinfection techniques and
effectiveness and efficacy data, see the following additionalreferences.69,168,181,182
Sanitation
Sanitation and water treatment are inextricably linked. Stu-dies in developing countries have demonstrated a clear ben-efit of safe drinking water, hygiene, and adequate sanitationin the reduction of diarrheal illness and other infections.-183e188 The benefit is greater when all are applied together,especially with appropriate education.24,189 Personalhygiene, particularly handwashing, prevents spread ofinfection from food contamination during preparation ofmeals.190,191 Disinfection of dishes and utensils is accom-plished by rinsing in water containing enough householdbleach to achieve a distinct chlorine odor. Use of halogensolutions or potassium permanganate solutions to soakvegetables and fruits can reduce microbial contamination,especially if the surface is scrubbed to remove dirt orother particulates, but neither method reaches organismsthat are embedded in surface crevices or protected byother particulate matter.192 Travelers to remote villages,wilderness areas, and persons in disaster situations shouldensure proper waste disposal to prevent additional contam-ination of water supplies. Human waste should be buried 20to 30 cm (8 to 12 in) deep, at least 30 m (100 ft) from anywater, and at a location from which water run-off is notlikely to wash organisms into nearby water sources. Groupsof 3 persons or more should dig a common latrine to avoidnumerous individual potholes and inadequate disposal.
Conclusion
Wilderness and international travelers should carry aneffective means of disinfecting water. It is important for dis-aster and medical relief workers to understand the commonmethods of water treatment and improvisational methods. Itis not possible for travelers to judge the microbiologic qual-ity of water, and it is prudent to assume that even tap wateris nonpotable in many locations. Simple and effective fieldtechniques to improve microbiologic water quality areavailable to travelers. It is important to understand thebasic principles and limitations of heat, filtration, and UVand chemical disinfection and then to become familiarwith at least one technique appropriate for the destination,water source, and needs of the travelers.
Author Contributions: Study concept and design (HDB, RWD, VRH);obtaining funding: N/A; acquisition of the data: N/A; analysis of the data:N/A; drafting of the manuscript (HDB, RWD, VRH); critical revision ofthe manuscript (HDB, RWD, VRH); approval of final manuscript (HDB,RWD, VRH).
Financial/Material Support: None.
Disclosures: None.
Backer et al14

Disclaimer
Use of trade names and commercial sources is for identifi-cation only and does not imply endorsement by the Centersfor Disease Control and Prevention (CDC), the US Depart-ment of Health and Human Services (HHS), or the State ofCalifornia. The findings and conclusions in this report arethose of the authors and do not necessarily represent thoseof CDC or HHS or the State of California.
Supplementary materials
Supplementary material associated with this article canbe found in the online version at https://doi.org/10.1016/j.wem.2019.06.006.
References
1. World Health Organization. Combating waterborne diseaseat the household level. Geneva, Switzerland. Available at:https://www.who.int/water_sanitation_health/publications/combating-waterborne-disease/en/; 2007. Accessed Febru-ary 25, 2019.
2. Schoenen D. Role of disinfection in suppressing the spreadof pathogens with drinking water: possibilities and limita-tions. Water Res. 2002;36(15):3874e88.
3. Guyatt G, Gutterman D, Baumann MH, Addrizzo-Harris D,Hylek EM, Phillips B, et al. Grading strength of recommen-dations and quality of evidence in clinical guidelines: reportfrom an american college of chest physicians task force.Chest. 2006;129(1):174e81.
4. Yoder J, Roberts V, Craun GF, Hill V, Hicks LA,Alexander NT, et al. Surveillance for waterborne diseaseand outbreaks associated with drinking water and water notintended for drinkingdUnited States, 2005e2006. MMWRSurveill Summ. 2008;57(9):39e62.
5. Colford Jr JM, Hilton JF, Wright CC, Arnold BF, Saha S,Wade TJ, et al. The Sonoma water evaluation trial: a rando-mized drinking water intervention trial to reduce gastroin-testinal illness in older adults. Am J Public Health.2009;99(11):1988e95.
6. Reynolds KA, Mena KD, Gerba CP. Risk of waterborne ill-ness via drinking water in the United States. Rev EnvironContam Toxicol. 2008;192:117e58.
7. McClung RP, Roth DM, Vigar M, Roberts VA, Kahler AM,Cocley LA, et al. Waterborne disease outbreaks associatedwith environmental and undetermined exposures to waterd-United States, 2013e2014.MMWRMorb Mortal Wkly Rep.2017;66(44):1222e5.
8. Derlet RW, Carlson JR. An analysis of wilderness water inKings Canyon, Sequoia, and Yosemite national parks forcoliform and pathologic bacteria. Wilderness Environ Med.2004;15(4):238e44.
9. Derlet RW, Ger KA, Richards JR, Carlson JR. Risk factorsfor coliform bacteria in backcountry lakes and streams in
the Sierra Nevada mountains: a 5-year study. WildernessEnviron Med. 2008;19(2):82e90.
10. Feng Y, Xiao L. Zoonotic potential and molecular epide-miology of Giardia species and giardiasis. Clin MicrobiolRev. 2011;24(1):110e40.
11. WHO-UNICEF. Progress on drinking water, sanitation andhygiene: 2017 update and SDG baselines. Geneva: WorldHealth Organization (WHO) and the United Nations Chil-dren’s Fund (UNICEF). Available at: https://www.unicef.org/publications/files/Progress_on_Drinking_Water_Sanitation_and_Hygiene_2017.pdf; 2017. AccessedFebruary 25, 2019.
12. Ngwenya N, Ncube EJ, Parsons J. Recent advances in drink-ing water disinfection: successes and challenges. RevEnviron Contam Toxicol. 2013;222:111e70.
13. WHO-UNICEF. Progress on Sanitation and DrinkingWatere2015 update and MDG assessment. Geneva:World Health Organization (WHO) and the United NationsChildren’s Fund (UNICEF; 2015.
14. Clasen TF, Bastable A. Faecal contamination of drinkingwater during collection and household storage: the need toextend protection to the point of use. J Water Health.2003;1(3):109e15.
15. Gil AI, Lanata CF, Hartinger SM, Mausezahl D, Padilla B,Ochoa TJ, et al. Fecal contamination of food, water, hands,and kitchen utensils at the household level in rural areas ofPeru. J Environ Health. 2014;76(6):102e6.
16. Kravitz JD, Nyaphisi M, Mandel R, Petersen E. Quantitativebacterial examination of domestic water supplies in theLesotho Highlands: water quality, sanitation, and villagehealth. Bull World Health Organ. 1999;77(10):829e36.
17. Rai SK, Ono K, Yanagida JI, Ishiyama-Imura S,Kurokawa M, Rai CK. A large-scale study of bacterial con-tamination of drinking water and its public health impact inNepal. Nepal Med Coll J. 2012;14(3):234e40.
18. Haramoto E. Detection of waterborne protozoa, viruses, andbacteria in groundwater and other water samples in the Kath-manduValley, Nepal. IOPConference Series.Earth EnvironSci. 2018;120:1e7.
19. Wright J, Gundry S, Conroy R. Household drinking water indeveloping countries: a systematic review ofmicrobiologicalcontamination between source and point-of-use. TropicalMed Int Health. 2004;9(1):106e17.
20. Lantagne D. Sodium hypochlorite dosage for household andemergency water treatment. J Am Water Works Assoc.2008;100(8):106e19.
21. Wang G, Doyle M. Survival of enterohemorrhagic Escheri-chia coli O157:H7 in water. J Food Prot. 1998;61(6):662e7.
22. Ford TE. Microbiological safety of drinking water: UnitedStates and global perspectives. Environ Health Perspect.1999;107(suppl 1):191e206.
23. Hurst C, Clark R, Regli S. Estimating the risk of acquiringinfectious disease from ingestion of water. In: Hurst C, ed.Modeling Disease Transmission and its Prevention by Disin-fection. Melbourne: Cambridge University Press; 1996:99e139.
Water Treatment Clinical Practice Guidelines 15

24. Sobsey M, Handzel T, Venczel L. Chlorination and safe sto-rage of household drinking water in developing countries toreduce waterborne disease. Water Sci Technol. 2003;47(3):221e8.
25. Murphy JL, Kahler AM, Nansubuga I, Nanyunja EM,Kaplan B, JothikumarN, et al. Environmental survey of drink-ing water sources in Kampala, Uganda, during a typhoid feveroutbreak. Appl Environ Microbiol. 2017;83(23):1e11.
26. World Health Organization. Guidelines for drinking waterquality. Geneva: WHO; 2011.
27. US Environmental Protection Agency. Report to TaskForce: Guide Standard and Protocol for Testing Microbio-logical Water Purifiers. Cincinnati: USEPA; 1987(Revision).
28. Geldreich E, Reasoner D. Home treatment devices and waterquality. In: McFeters G, ed. Drinking Water Microbiology.New York: Springer-Verlag; 1990:147e68.
29. Rosen A, Booth R. Taste and odor control. In: AmericanWater Works Association, ed. Water Quality and Treat-ment: A Handbook of Public Water Supplies. New York:McGraw Hill; 1971.
30. US Environmental Protection Agency Drinking Water HealthEffects Task Force. Health Effects of Drinking Water Treat-ment Technologies. Michigan: Lewis Publisher; 1989.
31. National Academy of Sciences Safe Drinking Water Com-mittee. The disinfection of drinking water. In: DrinkingWater and Health. 2;1980:5e139.
32. Le Chevallier M, McFeters G. Microbiology of activatedcarbon. In: McFeters G, ed. Drinking Water Microbiology.New York: Springer-Verlag; 1990:104e20.
33. Medema GJ, Schets FM, Teunis PF, Havelaar AH. Sedimen-tation of free and attached Cryptosporidium oocysts andGiardia cysts in water. Appl Environ Microbiol.1998;64(11):4460e6.
34. AWWA Coagulation Committee. Committee report: coagu-lation as an integrated water treatment process. J Am WaterWorks Assoc. 1989:74.
35. Cohen J, Hannah S. Water Quality and Treatment: A Hand-book of Public Water Supplies. New York: McGraw-Hill;1971.
36. Crump JA, Okoth GO, Slutsker L, Ogaja DO, Keswick BH,Luby SP. Effect of point-of-use disinfection, flocculationand combined flocculation-disinfection on drinking waterquality in western Kenya. J Appl Microbiol. 2004;97(1):225e31.
37. Preston K, Lantagne D, Kotlarz N, Jellison K. Turbidity andchlorine demand reduction using alum andmoringa floccula-tion before household chlorination in developing countries.J Water Health. 2010;8(1):60e70.
38. Kotlarz N, Lantagne D, Preston K, Jellison K. Turbidity andchlorine demand reduction using locally available physicalwater clarification mechanisms before household chlorina-tion in developing countries. J Water Health. 2009;7(3):497e506.
39. LeChevallier MW, Evans T, Seidler RJ. Effect of turbidityon chlorination efficiency and bacterial persistence in drink-ing water. Appl Environ Microbiol. 1981;42(1):159e67.
40. Crump JA, Otieno PO, Slutsker L, Keswick BH, Rosen DH,Hoekstra ROM, et al. Household based treatment of drinkingwater with flocculant-disinfectant for preventing diarrhoea inareas with turbid source water in rural western Kenya: clusterrandomised controlled trial. BMJ. 2005;331(7515):478e84.
41. Reller ME, Mendoza CE, Lopez MB, Alvarez M,Hoekstera RM, Olson CA, et al. A randomized controlledtrial of household-based flocculant-disinfectant drinkingwater treatment for diarrhea prevention in rural Guatemala.Am J Trop Med Hyg. 2003;69(4):411e9.
42. Powers E. Efficacy of Flocculating and Other EmergencyWater Purification Tablets. In: Report Natick/TR-93/033.Natick, MA: United States ArmyNatick Research, Develop-ment and Engineering Center; 1993.
43. Powers E, Boutros C, Harper B. Biocidal efficacy of a floc-culating emergency water purification tablet. Appl EnvironMicrobiol. 1994;60:2316e23.
44. Islam MS, Ansaruzzaman M, Mahmud ZH, Marin MA,Malik AK, Neogi SB, et al. A novel and simple mixtureas point-of-use water treatment agent to produce safedrinking water. Trans R Soc Trop Med Hyg.2014;108(5):290e6.
45. US Army. Sanitary control and surveillance of field watersupplies. In: Dept. of Army Technical Bulletin (TB Med577). Washington, DC: Departments of the Army, Navy,and Air Force; 2005. Available at: https://armypubs.army.mil/epubs/DR_pubs/DR_a/pdf/web/tbmed577.pdf. AccessedFebruary 25, 2019.
46. Chaudhuri M, Sattar S. Domestic water treatment for devel-oping countries. In: McFeters G, ed. Drinking Water Micro-biology. New York: Springer-Verlag; 1990.
47. Sobsey M.Managing water in the home: accelerated healthgains from improved water supply. Geneva: WHO/SDE/WSH/02.07; 2002. Available at: https://www.who.int/water_sanitation_health/dwq/WSH02.07.pdf. AccessedFebruary 25, 2019.
48. Frazier W, Westhoff D. Preservation by Use of High Tem-peratures. New York: McGraw-Hill; 1978.
49. Islam MF, Johnston RB. Household pasteurization of drink-ing-water: the chulli water-treatment system. J Health PopulNutr. 2006;24(3):356e62.
50. Fayer R. Effect of high temperature on infectivity of Cryp-tosporidium parvum oocysts in water. Appl Environ Micro-biol. 1994;60(8):273e5.
51. Bandres J, Mathewson J, DuPont H. Heat susceptibility ofbacterial enteropathogens. Arch Intern Med. 1988;148(10):2261e3.
52. Alder V, Simpson R. Sterilization and disinfection byheat methods. In: Russel A, Hugo W, Ayliffe G, eds.Principles and Practice of Disinfection, Preservation,and Sterilization. 2nd ed. Oxford: Blackwell Scientific;1992:483.
53. Aukerman R, Monzingo D. Water treatment to inactiveGiardia. J Forestry. 1989;87(11):18e21.
54. Ongerth J, Johnson R, MacDonald S, Frost F, Stibbs H.Backcountry water treatment to prevent giardiasis. Am JPublic Health. 1989;79:1633e7.
Backer et al16

55. Bingham A, Jarroll E, EAM. Physical factors of excystationin vitro and excystation vs eosin exclusion as determinants ofviability. Exp Parasitol. 1979;47(2):284e91.
56. Anderson B. Moist heat inactivation of Cryptosporidium.Am J Public Health. 1985;75:1433e4.
57. Shephart M. Helminthological aspects of sewage treatment.In: Feachem R, McGarry M, Mara D, eds. Water, Wastes,and Health in Hot Climates. New York: John Wiley andSons; 1977:299e310.
58. Perkins J. Thermal destruction of microorganisms: Heatinactivation of viruses. In: Thomas C, ed. Principles andMethods of Sterilization in Health Sciences. Springfield;1969:63e94.
59. Tuladhar E, Bouwknegt M, Zwietering MH, Koopmans M,Duizer E. Thermal stability of structurally different viruseswith proven or potential relevance to food safety. J ApplMicrobiol. 2012;112(5):1050e7.
60. Baert L, Debevere J, Uyttendaele M. The efficacy of preser-vation methods to inactivate foodborne viruses. Int J FoodMicrobiol. 2009;131(2e3):83e94.
61. Bidawid S, Farber JM, Sattar SA, Hayward S. Heat inactiva-tion of hepatitis A virus in dairy foods. J Food Prot.2000;63(4):522e8.
62. Krugman S, Giles J, Hammond J. Hepatitis virus: effect ofheat on the infectivity and antigenicity of the MS-1 andMS-2 strains. J Infect Dis. 1970;122:432e6.
63. World Health Organization. Boil water. Available at: http://www.who.int/water_sanitation_health/dwq/Boiling_water_01_15.pdf?ua¼1; 2015. Accessed February 25, 2019.
64. Neumann H. Alternatives to water chlorination (Correspon-dence). Rev Infect Dis. 1981;3(6):1255e7.
65. Neumann H. Bacteriological safety of hot tapwater indeveloping countries. Public Health Rep. 1969;84(9):812e4.
66. Groh C, MacPherson D, Groves D. Effect of heat on the ster-ilization of artifically contaminated water. J Travel Med.1996;3(1):11e3.
67. McGuigan KG. Solar disinfection: use of sunlight to decon-taminate drinking water in developing countries. J MedMicrobiol. 1999;48(9):785e7.
68. Ciochetti DA, Metcalf RH. Pasteurization of naturally con-taminated water with solar energy. Appl Environ Microbiol.1984;47(2):223e8.
69. LeChevallier M, Kwok-Keung A. Water Treatment andPathogen Control. London: UK. 2004.
70. Abd-Elmaksoud S, Naranjo JE, Gerba CP. Assessment of aportable handheld UV light device for the disinfection ofviruses and bacteria in water. Food Environ Virol.2013;5(2):87e90.
71. Reygadas F, Gruber JS, Ray I, Nelson KL. Field efficacyevaluation and post-treatment contamination risk assessmentof an ultraviolet disinfection and safe storage system.WaterRes. 2015;85:74e84.
72. Hijnen WA, Beerendonk EF, Medema GJ. Inactivationcredit of UV radiation for viruses, bacteria and proto-zoan (oo)cysts in water: a review. Water Res.2006;40(1):3e22.
73. Linden KG, Shin GA, Faubert G, Cairns W, Sobsey MD.UV disinfection of Giardia lamblia cysts in water. EnvironSci Technol. 2002;36(11):2519e22.
74. Zimmer JL, Slawson RM, Huck PM. Inactivation and poten-tial repair of Cryptosporidium parvum following low- andmedium-pressure ultraviolet irradiation. Water Res.2003;37(14):3517e23.
75. McGuigan KG, Conroy RM, Mosler HJ, Preez du M,Ubomba-Jaswa E, Fernandez-Iba~nez P. Solar water disinfec-tion (SODIS): a review from bench-top to roof-top. J HazardMater. 2012;235e236:29e46.
76. Berney M, Weilenmann HU, Simonetti A, Egli T. Efficacyof solar disinfection of Escherichia coli, Shigella flexneri,Salmonella typhimurium and Vibrio cholerae. J Appl Micro-biol. 2006;101(4):828e36.
77. Cervantes DXF. Feasibility of semi-continuous solar disin-fection system for developing countries at the householdlevel. Massachusetts Institute of Technology; 2003. Avail-able at: http://hdl.handle.net/1721.1/29551. Accessed Febru-ary 25, 2019.
78. Joyce T, McGuigan K, Elmore-Meegan M, Conroy R. Inac-tivation of fecal bacteria in drinking water by solar heating.Appl Environ Microbiol. 1996;62(2):399e402.
79. Conroy RM, Meegan ME, Joyce T, McGuigan K, Barnes J.Solar disinfection of drinking water protects against cholerain children under 6 years of age. Arch Dis Child.2001;85(4):293e5.
80. King BJ, Hoefel D, Daminato DP, Fanok S,Monis PT. SolarUV reduces Cryptosporidium parvum oocyst infectivity inenvironmental waters. J Appl Microbiol. 2008;104(5):1311e23.
81. Tedeschi C, Barsi C, Peterson S, Carey K. A pilot study ofsolar water disinfection in the wilderness setting. J WildEnviron Med. 2014;25(3):340e5.
82. Mausezahl D, Christen A, Pacheco GD, Tellez FA, InarteM,Zapata ME, et al. Solar drinking water disinfection (SODIS)to reduce childhood diarrhoea in rural Bolivia: a cluster-ran-domized, controlled trial. PLoS Med. 2009;6(8), e1000125.
83. Du Preez M, McGuigan KG, Conroy RM. Solar disinfectionof drinking water in the prevention of dysentery in SouthAfrican children aged under 5 years: the role of participantmotivation. Environ Sci Technol. 2010;44(22):8744e9.
84. du Preez M, Conroy RM, Ligondo S, Hennessy J, Elmore-Meegan M, Soita A, et al. Randomized intervention studyof solar disinfection of drinking water in the prevention ofdysentery in Kenyan children aged under 5 years. EnvironSci Technol. 2011;45(21):9315e23.
85. Conroy RM, Elmore-Meegan M, Joyce T, McGuigan KG,Barnes J. Solar disinfection of drinking water and diarrhoeain Maasai children: a controlled field trial. Lancet (LondEngl). 1996;348(9043):1695e7.
86. Meierhofer R, Wegelin M. SODIS Manual. Gallen: depart-ment of water and sanitation in developing countries, Swissfederal institute of envirnomental science and technology;2002. Available at: https://www.sodis.ch/methode/anwendung/ausbildungsmaterial/dokumente_material/sodismanual_2016.pdf. Accessed February 25, 2019.
Water Treatment Clinical Practice Guidelines 17

87. McGuigan K, Joyce T, Conroy R, Gillespie J, Elmore-Meegan M. Solar disinfection of drinking water containedin transparent plastic bottles: characterizing the bacterialinactivation process. J Appl Microbiol. 1998;84(6):1138e48.
88. Rijal GK, Fujioka RS. Synergistic effect of solar radiationand solar heating to disinfect drinking water sources. WaterSci Technol. 2001;43(12):155e62.
89. Jenkins M. What's in the water?. In: Backpacker. 1996:56.90. Larson KL, Hansen C, Ritz M, Carreno D. Acceptance and
impact of point-of-use water filtration systems in rural Gua-temala. J Nurs Scholarsh. 2017;49(1):96e102.
91. Zhang Y, Wang Q, Lou W, Wang Y, Zhu X. Microbiologi-cal safety of household membrane water filter. J EnvironBiol. 2013;34(2 Spec No):481e7.
92. Environmental Health Directorate Health Protection Branch.Assessing the Effectiveness of Small Filtration Systems forPoint-of-Use Disinfection of Drinking Water Supplies.Ottawa: Department of National Health and Welfare; 1980,80-EHD-54.
93. Schlosser O, Robert C, Bourderioux C, Rey M, deRoubin MR. Bacterial removal from inexpensive portablewater treatment systems for travelers. J Travel Med.2001;8(1):12e8.
94. Clasen T, Brown J, Suntura O, Collin S. Safe householdwater treatment and storage using ceramic drip filters: a ran-domised controlled trial in Bolivia. Water Sci Technol.2004;50(1):111e5.
95. Rao V, Symons JM, Ling A, Wang P, Metcalf TG, Hoff JC,et al. Removal of hepatitis A virus and rotavirus by drinkingwater treatment. J Am Water Works Assoc. 1988;80(2):59e67.
96. Horman A, Rimhanen-Finne R, Maunula L, vonBonsdorff CH, Rapala J, Lahti K, et al. Evaluation of thepurification capacity of nine portable, small-scale water pur-ification devices. Water Sci Technol. 2004;50(1):179e83.
97. Mull B, Hill VR. Recovery of diverse microbes in high tur-bidity surface water samples using dead-end ultrafiltration.J Microbiol Methods. 2012;91(3):429e33.
98. Lindquist ED, George CM, Perin J, Neiswender de Calari K,Norman WR, Davis TP, et al. A cluster randomized con-trolled trial to reduce childhood diarrhea using hollow fiberwater filter and/or hygiene-sanitation educational interven-tions. Am J Trop Med Hyg. 2014;91(1):190e7.
99. Lantagne D, Person B, Smith N, Mayer A, Preston K,Blanton E, et al. Emergency water treatment with bleach inthe United States: the need to revise EPA recommendations.Environ Sci Technol. 2014;48(9):5093e100.
100. Kozlicic A, Hadzic A, Bevanda H. Improvised purificationmethods for obtaining individual drinking water supplyunder war and extreme shortage conditions. Prehosp Disas-ter Med. 1994;9(2 Suppl):S25e8.
101. Morris JF, Murphy J, Fagerli K, Schneeberger C, Jarohn P,Moke F, et al. A randomized controlled trial to assess theimpact of ceramic water filters on prevention of diarrheaand Cryptosporidiosis in infants and young children-Wes-tern Kenya, 2013.Am J TropMedHyg. 2018;98(5):1260e8.
102. Moropeng RC, Budeli P, Mpenyana-Monyatsi L,Momba MNB. Dramatic reduction in diarrhoeal diseasesthrough implementation of cost-effective household drink-ing water treatment systems in Makwane Village, LimpopoProvince, South Africa. Int J Environ Res Public Health.2018;15(3):410.
103. Kirby MA, Nagel CL, Rosa G, Umupfasoni MM,Iyakeremye L, Thomas EA, et al. Use, microbiologicaleffectiveness and health impact of a household water filterintervention in rural Rwanda-A matched cohort study. Int JHyg Environ Health. 2017;220(6):1020e9.
104. du Preez M, Conroy RM, Wright JA, Moyo S, Potgieter N,Gundry SW. Use of ceramic water filtration in the preventionof diarrheal disease: a randomized controlled trial in ruralSouth Africa and Zimbabwe. Am J Trop Med Hyg.2008;79(5):696e701.
105. Clasen TF, Brown J, Collin S, Suntura O, Cairncross S.Reducing diarrhea through the use of household-based cera-mic water filters: a randomized, controlled trial in rural Boli-via. Am J Trop Med Hyg. 2004;70(6):651e7.
106. Clasen T, Garcia Parra G, Boisson S, Collin S. Household-based ceramic water filters for the prevention of diarrhea: arandomized, controlled trial of a pilot program in Colombia.Am J Trop Med Hyg. 2005;73(4):790e5.
107. Brown J, Sobsey MD, Loomis D. Local drinking water fil-ters reduce diarrheal disease in Cambodia: a randomized,controlled trial of the ceramic water purifier. Am J TropMed Hyg. 2008;79(3):394e400.
108. Tiwari SS, Schmidt WP, Darby J, Kariuki ZG, Jenkins MW.Intermittent slow sand filtration for preventing diarrhoeaamong children in Kenyan households using unimprovedwater sources: randomized controlled trial. Tropical MedInt Health. 2009;14(11):1374e82.
109. Stauber CE, Ortiz GM, Loomis DP, Sobsey MD.A randomized controlled trial of the concrete biosand filterand its impact on diarrheal disease in Bonao, DominicanRepublic. Am J Trop Med Hyg. 2009;80(2):286e93.
110. Stauber CE, Kominek B, Liang KR, Osman MK,SobseyMD. Evaluation of the impact of the plastic BioSandfilter on health and drinking water quality in rural Tamale,Ghana. Int J Environ Res Public Health. 2012;9(11):3806e33.
111. Fabiszewski de Aceituno AM, Stauber CE, Walters AR,Meza Sanchez RE, Sobsey MD. A randomized controlledtrial of the plastic-housing BioSand filter and its impact ondiarrheal disease in Copan, Honduras. Am J Trop MedHyg. 2012;86(6):913e91.
112. Duke WF, Nordin RN, Baker D, Mazumder A. The use andperformance of BioSand filters in the Artibonite Valley ofHaiti: a field study of 107 households. Rural Remote Health.2006;6(3):570.
113. Regli S. Regulations on filtration and disinfection. Confer-ence on current research in drinking water treatment.1987. Cincinnati, OH.
114. Fagerli K, Trivedi KK, Sodha SV, Blanton E, Ati A,Nguyen T, et al. Comparison of boiling and chlorinationon the quality of stored drinking water and childhood
Backer et al18
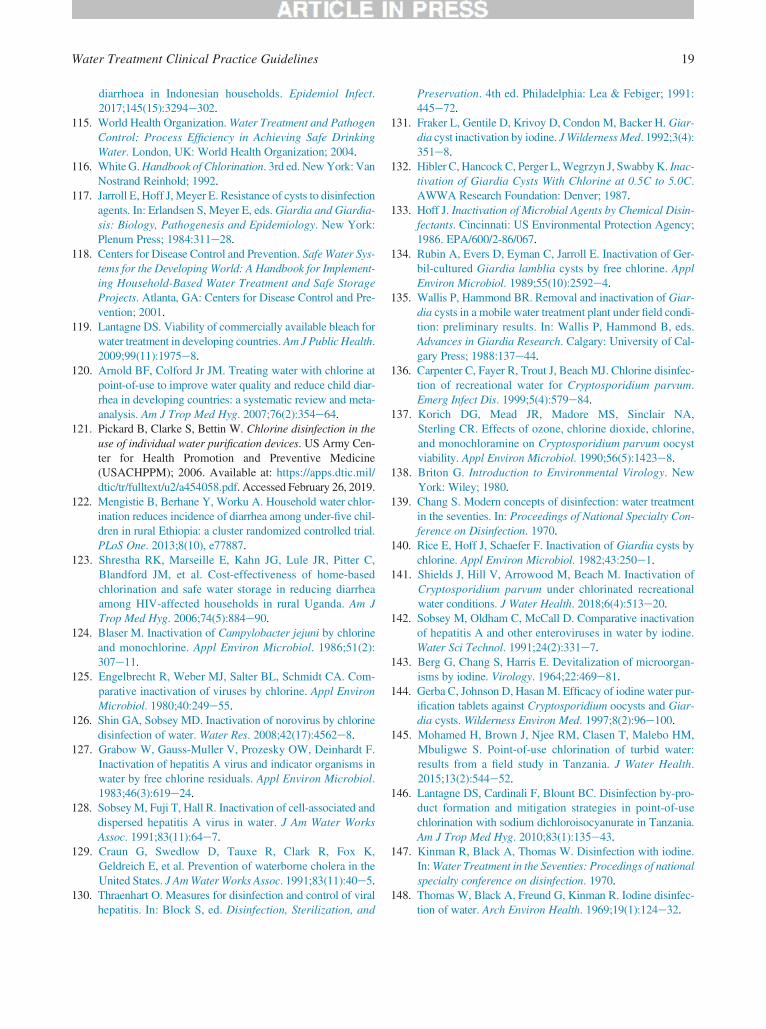
diarrhoea in Indonesian households. Epidemiol Infect.2017;145(15):3294e302.
115. World Health Organization.Water Treatment and PathogenControl: Process Efficiency in Achieving Safe DrinkingWater. London, UK: World Health Organization; 2004.
116. WhiteG.Handbook of Chlorination. 3rd ed. NewYork: VanNostrand Reinhold; 1992.
117. Jarroll E, Hoff J, Meyer E. Resistance of cysts to disinfectionagents. In: Erlandsen S, Meyer E, eds.Giardia and Giardia-sis: Biology, Pathogenesis and Epidemiology. New York:Plenum Press; 1984:311e28.
118. Centers for Disease Control and Prevention. Safe Water Sys-tems for the Developing World: A Handbook for Implement-ing Household-Based Water Treatment and Safe StorageProjects. Atlanta, GA: Centers for Disease Control and Pre-vention; 2001.
119. Lantagne DS. Viability of commercially available bleach forwater treatment in developing countries.Am J Public Health.2009;99(11):1975e8.
120. Arnold BF, Colford Jr JM. Treating water with chlorine atpoint-of-use to improve water quality and reduce child diar-rhea in developing countries: a systematic review and meta-analysis. Am J Trop Med Hyg. 2007;76(2):354e64.
121. Pickard B, Clarke S, Bettin W. Chlorine disinfection in theuse of individual water purification devices. US Army Cen-ter for Health Promotion and Preventive Medicine(USACHPPM); 2006. Available at: https://apps.dtic.mil/dtic/tr/fulltext/u2/a454058.pdf. Accessed February 26, 2019.
122. Mengistie B, Berhane Y, Worku A. Household water chlor-ination reduces incidence of diarrhea among under-five chil-dren in rural Ethiopia: a cluster randomized controlled trial.PLoS One. 2013;8(10), e77887.
123. Shrestha RK, Marseille E, Kahn JG, Lule JR, Pitter C,Blandford JM, et al. Cost-effectiveness of home-basedchlorination and safe water storage in reducing diarrheaamong HIV-affected households in rural Uganda. Am JTrop Med Hyg. 2006;74(5):884e90.
124. Blaser M. Inactivation of Campylobacter jejuni by chlorineand monochlorine. Appl Environ Microbiol. 1986;51(2):307e11.
125. Engelbrecht R, Weber MJ, Salter BL, Schmidt CA. Com-parative inactivation of viruses by chlorine. Appl EnvironMicrobiol. 1980;40:249e55.
126. Shin GA, Sobsey MD. Inactivation of norovirus by chlorinedisinfection of water. Water Res. 2008;42(17):4562e8.
127. Grabow W, Gauss-Muller V, Prozesky OW, Deinhardt F.Inactivation of hepatitis A virus and indicator organisms inwater by free chlorine residuals. Appl Environ Microbiol.1983;46(3):619e24.
128. SobseyM, Fuji T, Hall R. Inactivation of cell-associated anddispersed hepatitis A virus in water. J Am Water WorksAssoc. 1991;83(11):64e7.
129. Craun G, Swedlow D, Tauxe R, Clark R, Fox K,Geldreich E, et al. Prevention of waterborne cholera in theUnited States. J AmWater Works Assoc. 1991;83(11):40e5.
130. Thraenhart O. Measures for disinfection and control of viralhepatitis. In: Block S, ed. Disinfection, Sterilization, and
Preservation. 4th ed. Philadelphia: Lea & Febiger; 1991:445e72.
131. Fraker L, Gentile D, Krivoy D, Condon M, Backer H. Giar-dia cyst inactivation by iodine. JWilderness Med. 1992;3(4):351e8.
132. Hibler C, Hancock C, Perger L,Wegrzyn J, Swabby K. Inac-tivation of Giardia Cysts With Chlorine at 0.5C to 5.0C.AWWA Research Foundation: Denver; 1987.
133. Hoff J. Inactivation of Microbial Agents by Chemical Disin-fectants. Cincinnati: US Environmental Protection Agency;1986. EPA/600/2-86/067.
134. Rubin A, Evers D, Eyman C, Jarroll E. Inactivation of Ger-bil-cultured Giardia lamblia cysts by free chlorine. ApplEnviron Microbiol. 1989;55(10):2592e4.
135. Wallis P, Hammond BR. Removal and inactivation of Giar-dia cysts in a mobile water treatment plant under field condi-tion: preliminary results. In: Wallis P, Hammond B, eds.Advances in Giardia Research. Calgary: University of Cal-gary Press; 1988:137e44.
136. Carpenter C, Fayer R, Trout J, Beach MJ. Chlorine disinfec-tion of recreational water for Cryptosporidium parvum.Emerg Infect Dis. 1999;5(4):579e84.
137. Korich DG, Mead JR, Madore MS, Sinclair NA,Sterling CR. Effects of ozone, chlorine dioxide, chlorine,and monochloramine on Cryptosporidium parvum oocystviability. Appl Environ Microbiol. 1990;56(5):1423e8.
138. Briton G. Introduction to Environmental Virology. NewYork: Wiley; 1980.
139. Chang S. Modern concepts of disinfection: water treatmentin the seventies. In: Proceedings of National Specialty Con-ference on Disinfection. 1970.
140. Rice E, Hoff J, Schaefer F. Inactivation of Giardia cysts bychlorine. Appl Environ Microbiol. 1982;43:250e1.
141. Shields J, Hill V, Arrowood M, Beach M. Inactivation ofCryptosporidium parvum under chlorinated recreationalwater conditions. J Water Health. 2018;6(4):513e20.
142. Sobsey M, Oldham C, McCall D. Comparative inactivationof hepatitis A and other enteroviruses in water by iodine.Water Sci Technol. 1991;24(2):331e7.
143. Berg G, Chang S, Harris E. Devitalization of microorgan-isms by iodine. Virology. 1964;22:469e81.
144. Gerba C, Johnson D, Hasan M. Efficacy of iodine water pur-ification tablets against Cryptosporidium oocysts and Giar-dia cysts. Wilderness Environ Med. 1997;8(2):96e100.
145. Mohamed H, Brown J, Njee RM, Clasen T, Malebo HM,Mbuligwe S. Point-of-use chlorination of turbid water:results from a field study in Tanzania. J Water Health.2015;13(2):544e52.
146. Lantagne DS, Cardinali F, Blount BC. Disinfection by-pro-duct formation and mitigation strategies in point-of-usechlorination with sodium dichloroisocyanurate in Tanzania.Am J Trop Med Hyg. 2010;83(1):135e43.
147. Kinman R, Black A, Thomas W. Disinfection with iodine.In:Water Treatment in the Seventies: Procedings of nationalspecialty conference on disinfection. 1970.
148. Thomas W, Black A, Freund G, Kinman R. Iodine disinfec-tion of water. Arch Environ Health. 1969;19(1):124e32.
Water Treatment Clinical Practice Guidelines 19

149. Backer H, Hollowell J. Use of iodine for water disinfection:iodine toxicity and maximum recommended dose. EnvironHealth Perspect. 2000;108(8):679e84.
150. Gottardi W. Iodine and iodine compounds. In: Block S, ed.Disinfection, Sterilization, and Preservation. 4th ed. Phila-delphia: Lea & Febiger; 1991:152e67.
151. Rutala WA, Weber DJ. New disinfection and sterilizationmethods. Emerg Infect Dis. 2001;7(2):348e53.
152. Venczel L, ArrowoodM, HurdM, SobseyM. Inactivation ofCryptosporidium parvum oocysts and Clostridium perfrin-gens spores by a mixed-oxidant disinfectant and by freechlorine. Appl Environ Microbiol. 1997;63(4):1598e601.
153. Clark RM, Sivagnesan M, Rice EW, Chen J. Developmentof a Ct equation for the inactivation of Cryptosporidiumoccysts with chlorine dioxide. Water Res. 2003;37(11):2773e83.
154. Murphy JL, Haas CN, Arrowood MJ, Hlavsa MC,Beach MJ, Hill VR. Efficacy of chlorine dioxide tablets oninactivation of cryptosporidium oocysts. Environ Sci Tech-nol. 2014;48(10):5849e56.
155. Pereira JT, Costa AO, de Oliveira Silva MB, Schuchard W,Osaki SC, de Castro EA, et al. Comparing the efficacy ofchlorine, chlorine dioxide, and ozone in the inactivation ofCryptosporidium parvum in water from Parana State, South-ern Brazil. Appl Biochem Biotechnol. 2008;151(2e3):464e73.
156. Marchin G. Fina L Contact and demand-release disinfec-tants. Crit Rev Environ Control. 1989;19:227e90.
157. Fisher MB, Keenan CR, Nelson KL, Voelker BM. Speedingup solar disinfection (SODIS): effects of hydrogen peroxide,temperature, pH, and copper plus ascorbate on the photoi-nactivation of E. coli. J Water Health. 2008;6(1):35e51.
158. D’AquinoM, Teves SA. Lemon juice as a natural biocide fordisinfecting drinking water. Bull Pan Am Health Organ.1994;28(4):324e30.
159. United States Environmental Protection Agency. AlternativeDisinfectants and Oxidants Guidance Manual. In: EPA 815-R-99-014. US EPA; 1999. Available at: https://nepis.epa.gov. Accessed February 26, 2019.
160. ChongMN, Jin B, ChowCW, Saint C. Recent developmentsin photocatalytic water treatment technology: a review.Water Res. 2010;44(10):2997e3027.
161. Li Q,Mahendra S, Lyon DY, Brunet L, LigaMV, Li D, et al.Antimicrobial nanomaterials for water disinfection andmicrobial control: potential applications and implications.Water Res. 2008;42(18):4591e602.
162. Sunnotel O, Verdoold R, Dunlop PS, Snelling WJ,Lowery CJ, Dooley JS, et al. Photocatalytic inactivation ofCryptosporidium parvum on nanostructured titanium diox-ide films. J Water Health. 2010;8(1):83e91.
163. Blanco-Galvez J, Fernandez-Ibanez P, Malato-Rodriguez S.Solar photocatalytic detoxification and disinfection of water:recent overview. J Solar Energy Eng. 2006;129(1):4e15.
164. Alrousan DM,Dunlop PS,McMurray TA, Byrne JA. Photo-catalytic inactivation of E. coli in surface water using immo-bilised nanoparticle TiO2 films. Water Res. 2009;43(1):47e54.
165. Sobsey MD, Stauber CE, Casanova LM, Brown JM,Elliott MA. Point of use household drinking water filtration:a practical, effective solution for providing sustained accessto safe drinking water in the developing world. Environ SciTechnol. 2008;42(12):4261e7.
166. Bielefeldt AR, Kowalski K, Summers RS. Bacterial treat-ment effectiveness of point-of-use ceramic water filters.Water Res. 2009;43(14):3559e65.
167. Mwabi JK, Mamba BB, Momba MN. Removal of Escheri-chia coli and faecal coliforms from surface water andgroundwater by household water treatment devices/systems:a sustainable solution for improving water quality in ruralcommunities of the Southern African development commu-nity region. Int J Environ Res Public Health. 2012;9(1):139e70.
168. Clasen T, Menon S. Microbiological performance of com-mon water treatment devices for household use in India.Int J Environ Health Res. 2007;17(2):83e93.
169. Brunkard JM, Ailes E, Roberts VA, Hill V, Hilborn ED,Craun GF, et al. Surveillance for waterborne disease out-breaks associated with drinking waterdUnited States,2007e2008. MMWR Surveill Summ. 2011;60(12):38e68.
170. Sobel J, Mahon B, Mendoza C, Passaro D, Cano F, Baier K,et al. Reduction of fecal contamination of street-vended bev-erages in Guatemala by a simple system for water purifica-tion and storage, handwashing, and beverage storage. Am JTrop Med Hyg. 1998;59(3):380e7.
171. Cullimore D, Jacobsen H. The efficiency of point of usedevices for the exclusion of Giardia muris cysts from amodel water supply system. In: Wallis P, Hammond B,eds. Advances in Giardia Research. Calgary: University ofCalgary Press; 1988:107e12.
172. Hutton P, Ongerth J. Performance evaluation for portablewater treatment filters. Seattle,WA:Department of Environ-mental Health, University of Washington; 1995.
173. Hutton P, Ongerth J. Performance evaluation of ten com-mercially available portable water filters. Sydney, Austalia:Department of Water Engineering, University of New SouthWales; 1997.
174. Jarroll E, Bingham A, Meyer E. Giardia cyst destruction:effectiveness of six small water disinfection methods. Am JTrop Med Hyg. 1980;29(1):8e11.
175. Logsdon G, Symons J, Hoye R, Arozarena M. Alternativefiltration methods for removal of Giardia cysts and cystmodels. J Am Water Works Assoc. 1981;73(2):111e8.
176. Naranjo J, Gerba C. Evaluation of portable water treatmentdevices by a condensed version of the guide of standard pro-tocol for microbiological purifiers (USEPA, 1987). Tucson,AZ: University of Arizona; 1995.
177. Powers E, Boyd C, Harper B, Rubin A. Removal of biologi-cal and chemical challenge from water by commercial freshand salt water purification devices. In: Technical ReportNatick/TR-91-042. Natick, MA: United States Army NatickResearch, Development and Engineering Center; 1991.
178. Tobin R. Performance of point-of-use water treatmentdevices. In: Proceedings of the first conference on coldregions environmental engineering. 1983. Fairbanks, AK.
Backer et al20

179. Tobin R. Testing and evaluating point-of-use treatmentdevices in Canada. J Am Water Works Assoc. 1987;79(10):42e5.
180. Backer H. Field water disinfection. In: Auerbach P, ed.Wild-erness Medicine. 7th ed. Philadelphia: Elsevier; 2017.
181. McDonnell GE. Antisepsis, Disinfection, and Sterilization.Washington, DC: ASM Press; 2007.
182. Bielefeldt AR. Appropriate and sustainable water disinfec-tion methods for developing communities. In:Buchanan K, ed. Water Disinfection. New York City, NY:Nova Science Publishers; 2011:45e75.
183. Clasen T, Roberts I, Rabie T, Schmidt W, Cairncross S.Interventions to improve water quality for preventing diar-rhoea. Cochrane Library: John Wiley & Sons; 2006.
184. OpryszkoMC,Majeed SW, Hansen PM,Myers JA, Baba D,Thompson RE, et al. Water and hygiene interventions toreduce diarrhoea in rural Afghanistan: a randomized con-trolled study. J Water Health. 2010;8(4):687e702.
185. Jung S, Doh YA, Bizuneh DB, Beyene H, Seong J, KwonH,et al. The effects of improved sanitation on diarrheal preva-lence, incidence, and duration in children under five in theSNNPR State, Ethiopia: study protocol for a randomizedcontrolled trial. Trials. 2016;17(1):204.
186. Garrett V, Ogutu P, Mabonga P, Ombeki S, Mwaki A,Aluoch G, et al. Diarrhoea prevention in a high-risk ruralKenyan population through point-of-use chlorination, safewater storage, sanitation, and rainwater harvesting. Epide-miol Infect. 2008;136(11):1463e71.
187. Dreibelbis R, Freeman MC, Greene LE, Saboori S,Rheingans R. The impact of school water, sanitation, andhygiene interventions on the health of younger siblings ofpupils: a cluster-randomized trial in Kenya. Am J PublicHealth. 2014;104(1):e91e7.
188. Cha S, Lee J, Seo D, Park BM, Mansiangi P, Mernard K,et al. Effects of improved sanitation on diarrheal reductionfor children under five in Idiofa, DR Congo: a cluster rando-mized trial. Infect Dis Poverty. 2017;6(1):137e49.
189. Quick RE, Kimura A, Thevos A, Tembo M, Shamputa I,Hutwagner L, et al. Diarrhea prevention through house-hold-level water disinfection and safe storage in Zambia.Am J Trop Med Hyg. 2002;66(5):584e9.
190. Luby SP, Agboatwalla M, Painter J, Altaf A, Billhimer WL,Hoekstra RM, et al. Effect of intensive handwashing promo-tion on childhood diarrhea in high-risk communities in Paki-stan: a randomized controlled trial. JAMA. 2004;291(21):2547e54.
191. Hashi A, Kumie A, Gasana J. Hand washing with soap andWASH educational intervention reduces under-five child-hood diarrhoea incidence in Jigjiga District, Eastern Ethio-pia: a community-based cluster randomized controlled trial.Prev Med Rep. 2017;6:361e8.
192. Ortega YR, Roxas CR, Gilman RH, Miller NJ, Cabrera L,Taquiri C, et al. Isolation of Cryptosporidium parvum andCyclospora cayetanensis from vegetables collected in mar-kets of an endemic region in Peru. Am J Trop Med Hyg.1997;57(6):683e6.
Water Treatment Clinical Practice Guidelines 21